
Gang-rape of mentally challenged woman triggers YSRCP-TD ...
Upload
leidenunivCategory
view
0download
0
The Independent Living Skills Survey: AComprehensive Measure of the Community
Functioning of Severely and PersistentlyMentally 111 Individuals
by Charles J. Wallace, Robert Paul Liberman, Robert Tauber,and Jeannie Wallace
Abstract
The research reported in this article investigated thepsychometric characteristics of the IndependentLiving Skills Survey (ILSS), a comprehensive, objec-tive, performance-focused, easy-to-administer measureof the basic functional living skills of individuals withsevere and persistent mental illness (SPMI). Two ver-sions were developed, one for informants and one forself-report. Data from three research projects wereanalyzed to determine the versions' internal consis-tency, stability, interrater reliability, sensitivity to theeffects of skills training, and concurrent and predictivevalidity. The results indicated that the two versionshave acceptable psychometric characteristics, and sug-gestions are offered for their use in planning individu-alized treatment, evaluating programmatic services,and determining eligibility for benefits.
Keywords: Severe and persistent mental illness,assessment, community functioning, self-report, infor-mant.
Schizophrenia Bulletin, 26(3):631-658,2000.
Within the past two decades, the standard of treatment ofindividuals with SPMI has expanded from reducing theirsymptoms to improving their social and instrumental rolefunctioning (National Institute of Mental Health [NIMH]1991). This expanded treatment—variously labeledbiopsychosocial treatment, psychoeducational treatment,or psychiatric rehabilitation—is based on the premise thatrole functioning is a product of an individual's skills andmotivation and of the environment's rewards, opportuni-ties, and demands. Functioning can be.improved by acombination of enhancing the individual's skills, increas-ing the environment's opportunities and rewards, andreducing the environment's demands (Liberman 1992).
Psychiatric rehabilitation begins with a comprehen-sive and detailed assessment of the individual's currentfunctioning. The assessment is focused on the "degree to
which the individual's abilities and performance matchthe demands of his or her home, work, school, family, andsocial situations. By comparing the functional skills andresources possessed by the individual to those required tomaintain community tenure, one gleans information aboutfunctional areas of strengths and deficits. Treatment is tar-geted at deficit areas" (Bedell et al. 1997, p. 219).
As treatment progresses, the assessment is repeated andthe changes in functioning measure the treatment's efficacy.On the basis of these changes, the plan is modified by alter-ing the mix of services, the functional areas to be treated, orboth. Because the assessment is a continuing guide for allo-cating often scarce treatment resources, it must be psycho-metrically sound and its results must be easily and unam-biguously interpreted by a wide range of practitioners.
In addition to its role in planning individualized treat-ment, the assessment could be used to evaluate the effectsof a program of services on role functioning. The resultsof the assessment would be aggregated across a program'sparticipants, and the summary statistics would describethe program's case mix and its participants' typical levelof functioning. Changes in these summary statistics acrossrepeated administrations would measure the efficacy of itsservices for improving functioning and point to pro-gramwide revisions to accommodate new needs of achanging case mix. Were the assessment to be adminis-tered across programs, payers could compare the resultsand select programs that produce a desired balancebetween costs and improvement (Smith et al. 1997).Paying for services based on achieving outcomes such asimproved functioning has been advocated by a number ofstakeholders, including the providers themselves (Meyer1997; Outcomes Roundtable, Smith et al. 1997).
The assessment could also provide a standardizedmeans of collecting, recording, and summarizing the
Send reprint requests to Dr. C.J. Wallace, Psychiatric RehabilitationConsultants, Box 2867, Camarillo, CA 93010-2867; e-mail:[email protected].
631
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
information needed to determine individuals' eligibilityfor disability benefits. The Social Security Administration(SSA) defines eligibility, in part, as inadequate perfor-mance of basic instrumental roles. Performance is typi-cally assessed by an interviewer who makes the subjectivedecision that the applicant meets eligibility criteria.Pincus et al. (1991) found that almost 25 percent of 732applicants were classified inconsistently when well-trained psychiatrists used both the SSA's criteria and theirown clinical judgment to determine eligibility. An objec-tive measure of functioning might increase the consis-tency and efficiency of the process, identifying applicantswhose scores clearly indicate eligibility and referringthose with questionable scores for further evaluation.
Although a systematic assessment of role functioningmay be useful in theory for planning treatment, evaluatingprograms, and determining eligibility, implementing aspecific instrument, or even providing a list of recom-mended instruments from which to choose, is no meanfeat. The differences and potential conflicts among thevarious stakeholders are heightened by the process. Forexample, if outcomes-based payment is to be the rule, allproviders must use a common set of outcome measures(NIMH 1986; Smith et al. 1997), even though this levelstheir playing field and severely limits their opportunitiesto claim superiority over one another. Clearly this limita-tion is fraught with controversy for all stakeholders, notjust the providers.
To encourage cooperation among stakeholders and tobegin the process of implementing outcome measures,various committees, task forces, and organizations ofstakeholders have been formed to specify the criteria thecommon measures must fulfill to reflect everyone's needsand values (NIMH 1986; Newman and Ciarlo 1994;Kaufmann and Manderscheid 1997; Smith et al. 1997).Three criteria discussed in the reports of these ad hocgroups are relevant to the research reported in this article.
First, most stakeholders agree that role functioning isonly one, albeit an important one, of several dimensionsthat define outcomes. Other dimensions include symp-toms, quality of life, satisfaction with treatment, andaccess to services.
Second, no stakeholder opposes the criterion that allmeasures must be psychometrically sound. The OutcomesRoundtable report (Smith et al. 1997), for example, statesthat the "tools for assessing outcomes should havedemonstrated validity and reliability, and must be sensi-tive to clinically important change over time" (p. 1034).Vieweg et al. (1997) note that three of the ten "lessons"they learned from the State of Missouri's implementationof an outcomes measurement system highlighted theimportance of the measures' psychometric soundness,including "measuring anything poorly is not better than
measuring nothing at all....Keep the process simple, butnot so simple that you don't get meaningful information"(p. 33). The implication is that the measures must havesufficient length to be reliable and breadth to be valid, andthat resources must be allotted to carefully develop andpilot the measures. Assessors must be thoroughly trained,and the accuracy of their procedures must be continuouslymonitored.
The third criterion, comprehensiveness, is somewhatcontroversial. Some stakeholders have strongly endorsedbrevity, suggesting that "administrators require brief user-friendly outcome measures that can be used repeatedlyover time to monitor program quality" (Srebnik et al.1997, pp. 903-904). The typical measure advocated bythese stakeholders is a consumer-completed report cardthat consists of a few questions surveying access to ser-vices, satisfaction, and current functioning (e.g., MentalHealth Statistics Improvement Program report card,Kaufmann and Manderscheid 1997).
Other stakeholders have countered that brevity in thiscontext risks psychometric soundness and is synonymouswith incomplete and useless results. This seems to be theprevailing view, as exemplified by the report issued by thenumerous consumer, family, payer, and provider organiza-tions participating in the Outcomes Roundtable (Smith etal. 1997). The report recommends that outcome measuresbe comprehensive, include the perspectives of all stake-holders, focus on areas of personal functioning affectedby the specific disorder of interest, and be capable of rep-etition at clinically meaningful intervals (Smith et al.1997). The decade-earlier NIMH report (1986) even moreexplicitly recommended a comprehensiveness that thor-oughly integrated program evaluation and individualizedtreatment assessment. The NIMH report noted that out-come measures should include the perspectives of all rele-vant participants and should produce scores with clear andobjective referents that are understandable by a wide audi-ence and are useful in designing and providing clinicalservices.
Since the 1986 NIMH report, several articles havebeen published (e.g., Wallace 1986; Goldman et al. 1992;Dickerson 1997) reviewing a wide range of measures ofrole functioning. Dickerson's recent review is particularlythorough and informative; she selected nine widely dis-tributed measures, summarized the published informationabout their psychometric adequacy, and then comparedtheir comprehensiveness, specificity, and inclusion ofmultiple perspectives. Like all previous reviewers, sheconcluded that none fulfills all the criteria.
Some of the measures (e.g., Social Adjustment Scale-II (SAS-II), Schooler et al. 1979; New York Level of CareSurvey, Fabisiak et al. 1983) assess role functioning thatis irrelevant to many individuals with SPMI. The SAS-II
632
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
assesses individuals' performance in major instrumentalroles such as spouse, parent, and wage earner. Becausemost individuals with SPMI are unemployed, have neverbeen married, and interact with a very limited network ofacquaintances, they score near the floor of the S AS-II, andthe results are marginally useful at best. The New YorkLevel of Care Survey assesses individuals' performanceof basic behaviors such as ambulating, toileting, and self-dressing. Because all but the most profoundly disabledindividuals with SPMI perform all of these behaviors,they score at the ceiling and the results are again margin-ally useful.
Other measures assess an adequate range of roles, butnot in sufficient detail to pinpoint the skills to beimproved (Colorado Client Assessment Record [CCAR],Ellis et al. 1991; Role Functioning Scale [RFS],McPheeters 1984 and Goodman et al. 1993). The CCARand the RFS use a single item to assess each of nine areasand five areas, respectively, of community behaviors.
Still other measures provide a detailed assessment ofan adequate range of roles but use response scales thatconfound several variables (e.g., Behavioral andSymptom Identification Scale-32 [BASIS-32], Eisen etal. 1994; Life Skills Profile [LSP], Rosen et al. 1989). TheBASIS-32, for example, asks respondents to indicate thedegree of difficulty they have experienced during the pastweek in 32 areas of functioning such as "managing day-to-day life," "leisure time and recreation," and "role func-tioning." Although having difficulty in an area mightidentify it as a potential target for intervention, the diffi-culty may be the result of several causes (e.g., lack offunds to engage in recreation activities), only some ofwhich are amenable to treatment. The LSP asks an infor-mant to rate an individual as "incapable of budgeting,""incapable of food preparation," and "incapable of work."Although an individual might not currently budget, pre-pare food, or have a job, the causes may be "the lack of alearned skill, the lack of opportunity to perform the skill,amotivation, or other factors" (Dickerson 1997, p. 899).Including "incapable" in the item stem precludes endors-ing causes other than a lack of skills, and the LSP doesnot include items to assess these other possible causes.
Other measures use response scales that primarilyreflect the idiosyncratic judgments of the respondents(e.g., CCAR; Multnomah Scales, Barker et al. 1994). TheCCAR asks an informant to rate an individual's role per-formance on a 50-point scale anchored by the terms"above average, average, slight dysfunction, moderatedysfunction, severe/extreme dysfunction." TheMultnomah Scales ask an informant to rate performanceas "effective" or "ineffective." Both reflect the infor-mant's idiosyncratic norms for the terms "average," "dys-functional," "effective," and "ineffective." These norms
may not be comparable across informants and are likelyto be different across settings.
Finally, except for a very few measures (e.g., SAS-II;Psychiatric Status Schedule, Spitzer et al. 1970; KatzAdjustment Scales, Katz and Lyerly 1963), the informa-tion is gathered from only one source, typically an infor-mant such as a case manager. Unfortunately, this makesthe results subject to the limitations of that source, and"each stakeholder may have a different point of view.. .allof which are legitimate from the vantage points of the var-ious stakeholders" (Dickerson 1997, p. 898). The implica-tion is that including only one source may miss informa-tion that might alter the design and course of anintervention.
Given these limitations, the purpose of the researchreported in this article was to develop a comprehensivemeasure that would (1) assess role functioning in thelifestyles relevant to the majority of individuals withSPMI, (2) include information from multiple sources, and(3) use a simple and objective response scale focused onthe performance of specific skills. The focus on perfor-mance would separate functioning from its immediatecauses and stimulate a systematic appraisal of the individ-ual's skills and motivation and the environment's opportu-nities and rewards in order to identify the causes of defi-cient performance.
This measure of functioning, the ILSS, has now beenadministered in three clinical research projects with morethan 300 participants, and the purpose of this article is toextend the previous reports about its psychometric charac-teristics (Wallace 1986; Cyr et al. 1994). Since the 1986report, a scale has been added to assess interpersonalskills, and a self-report version has been developed. Thisarticle will describe the psychometric characteristics ofboth the informant and the self-report versions.
MethodsILSS. Two versions of the ILSS were developed andevaluated: one for informants' reports and one for self-report. Each is described below, followed by brief sum-maries of the three projects that supplied the psychometricdata. Both versions are presented in the appendix.
Informant version. As described in Wallace (1986),development of the informant version (ILSS-I) beganwith an inspection of 15 widely available measures ofsocial and independent living skills such as thePsychiatric Status Schedule, the Katz Adjustment Scale,the Personal Adjustment and Role Skills test, and theAmerican Association on Mental Deficiency's AdaptiveBehavior Scale. Nine areas of social and independent liv-ing skills seemed to be routinely assessed across the 15instruments. The relevant items on each instrument were
633
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
reviewed, and an initial pool of 102 items was generatedto assess the nine areas.
The 102 items were submitted to a panel of fivesocial workers and five operators of board and carehomes, who were asked to comment on the comprehen-siveness of the nine areas and the acceptability, clarity,and importance for overall community adjustment of eachitem. On the basis of their comments, 10 items werereplaced or revised and 5 were added, for a total of 107items. The 107 items were then submitted to five moreoperators and three more social workers, who suggestedrevisions to 10 of the items. Thirteen items were laterdeleted after comments by respondents that they wereconfusing, vague, or not applicable, and 9 more wereadded to assess interpersonal interactional skills for a finaltotal of 103 items.
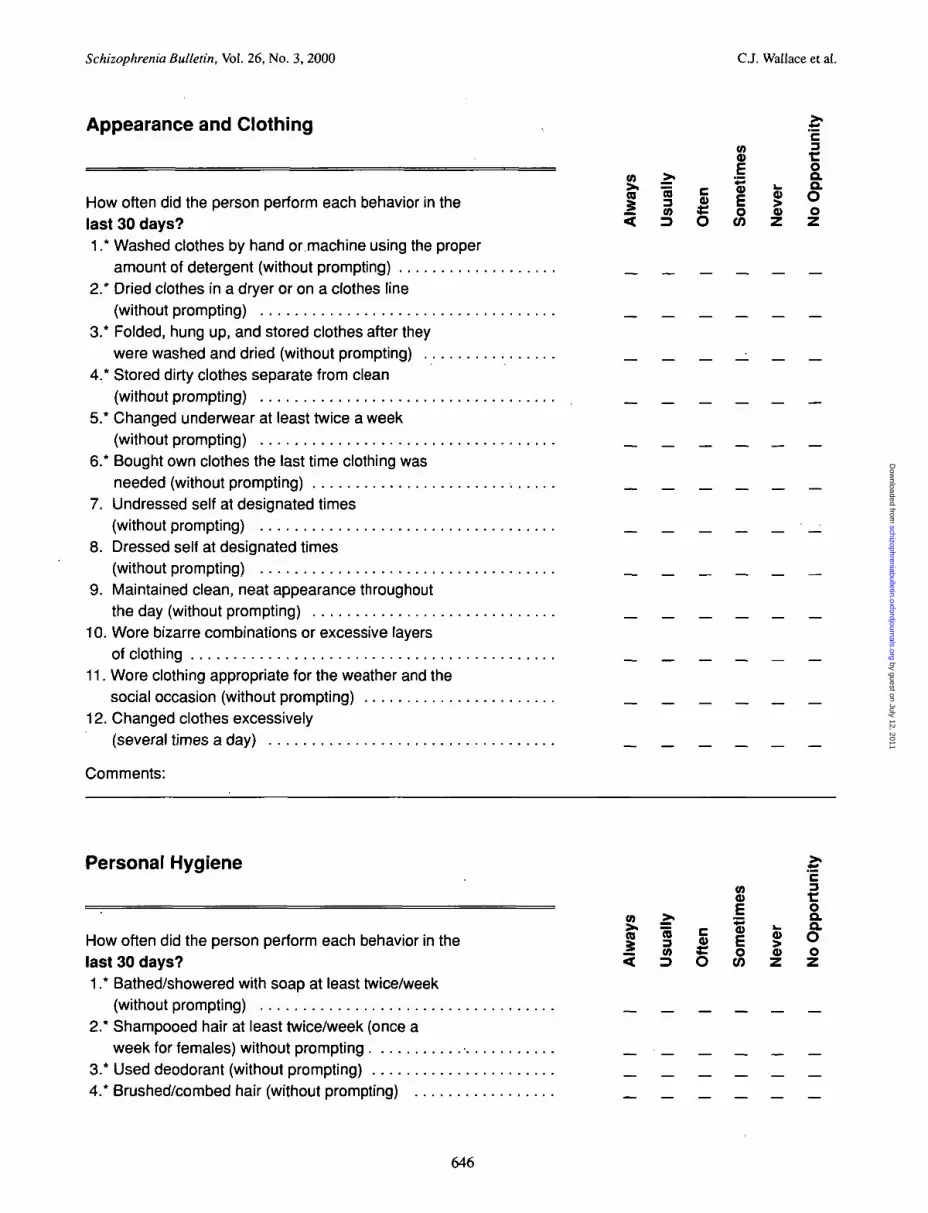
The 103 items assess performance in 12 areas ofbasic community living skills: personal hygiene (6 items),appearance and care of clothing (12 items), care of per-sonal possessions and living space (9 items), food prepa-ration (9 items), care of one's own health and safety (10items), money management (10 items), transportation (7items), leisure and recreational activities (13 items), jobseeking (6 items), job maintenance (3 items), eatingbehaviors (9 items), and social interactions (9 items). Theitems describe relatively specific behaviors and skills suchas "washes hair twice a week," "stores money in a safeplace," "cleans and stores dishes and utensils after ameal," and "reads the want ads." Informants indicate howfrequently an individual has performed each skill withinthe past month on the five-point scale (never, sometimes,often, usually, and always) used in the Nurses 'Observation Scale for Inpatient Evaluation (NOSIE), afrequently administered measure of inpatients' function-ing. To accommodate the possibility that an individual inthe community facilities for which the ILSS-I is intendedmay have only limited opportunities to perform a skill(e.g., prepare one's meals in a facility in which the staffprepare and serve meals), a sixth response option wasadded, "no opportunity."
The ILSS-I can be conveniently administered in per-son, by phone, or by mail, because completion requiresonly a brief oral or written explanation of the responsescale and 20—35 minutes of the informant's time. Theanswers are scored from 0 (never) to 4 (always), thensummed and averaged per functional area; itemsanswered "no opportunity" are ignored. An area is notscored, however, if three or fewer items are answeredwith other than the "no opportunity" option.
Self-report version. The self-report version(ILSS-SR) was developed to offer a simplified version ofthe ILSS—I suitable for administration in typically busyclinical settings. Additionally, many individuals have only
limited contact, if any, with an informant who is suffi-ciently knowledgeable to complete the ILSS-I. In thatcase, the only source of information is self-report.
To develop this version, a panel of clinicians andindividuals with SPMI selected 51 items from the ILSS-Ias particularly relevant for daily living and treatmentplanning. The 51 items were rephrased for self-report(e.g., "wash your hair twice a week" and "store yourmoney in a safe place" versus "washes his/her hair twiceper week" and "stores his/her money in a safe place"),and the response scale was simplified to a Yes or Noanswer about performance of each skill within the pastmonth. A response option, "not apply," was added toaccount for the variations presented by individuals' livingsituations in the opportunities to perform a skill, and 10items were added to increase coverage of several areas.
The test was formatted as a questionnaire thatrequires from 20-30 minutes to complete. For individualswho have reading difficulties, an interview format wasdeveloped that requires the interviewer to read the ques-tions to the respondent and, if necessary, to ask therespondent to answer by pointing to one of the threeresponse options, all of which are written on a large card.The advantage of the interview format is that it can beadministered during an individual's routine visit to a prac-titioner and may provide opportunities for the practitionerto ask about significant events pertaining to the individ-ual's living environment. The research reported in thisarticle was conducted with the interview format only, toavoid any inaccurate assumptions about respondents'reading ability.
The interview format includes nine additional itemsthat ask for the interviewer's ratings of various aspects ofthe individual's personal hygiene and appearance. Theresulting 70 items are grouped into 10 areas: personalhygiene (12 items), appearance and care of clothing (9items), care of personal possessions and living space (6items), food preparation (7 items), care of personal healthand safety (7 items), money management (5 items), trans-portation (5 items), leisure and recreational activities (12items), job seeking (4 items), and job maintenance (3items). Scoring is much the same as for the ILSS-I;answers are summed (0 = No, 1 = Yes), and then averagedper functional area; those items answered "not apply" areignored. An area is not scored if three or fewer items areanswered with other than the "not apply" option.
Research Projects. The ILSS was administered as one ofa battery of measures given to participants in three clini-cal research projects. Briefly, the three projects were asfollows.
Veterans Affairs. The project at the West LosAngeles Veterans Affairs (VA) Medical Center was a
634
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
comparison of the effects of skills training "modules" andpsychosocial (expressive) occupational therapy (Libermanet al. 1998). A total of 84 participants with SPMI, all ofwhom were outpatients with a DSM-IIl—R diagnosis ofschizophrenia, were randomly assigned to receive 6months of either skills training or occupational therapy,conducted on an intensive 4-day-per-week, 5-hour-per-day schedule. As part of a battery of dependent measures,participants completed the ILSS-SR at the beginning ofthe project, immediately after the 6 months of skills train-ing or occupational therapy, 6 months later (12 monthsafter enrollment), and then yearly for 2 additional years(24 and 36 months after enrollment).
In addition to the ILSS-SR, the battery of measuresincluded the Brief Psychiatric Rating Scale (BPRS,UCLA expanded version, Lukoff et al. 1986), the Profileof Adaptation to Life-Change version (PAL-C, Ellsworth1979), and the Global Assessment Scale (GAS, Endicottet al. 1976). The expanded BPRS is a 24-item measurethat assesses psychiatric symptoms such as hallucinations,unusual thought content, depression, guilt, anxiety, motorretardation, and withdrawal. The 24 symptoms are ratedon a seven-point scale (absent to extremely severe) basedon verbal responses and nonverbal behaviors elicited dur-ing a semistructured interview. For this and for the SantaBarbara project described below, the interviewers weretrained and their ongoing accuracy monitored by theDiagnostic and Psychopathology Unit of the UCLAClinical Research Center for Schizophrenia andPsychiatric Rehabilitation (Robert P. Liberman, M.D.,principal investigator). All interviewers achieved thetraining standard of a minimum trainee-trainer interraterreliability of a kappa statistic of 0.80 and maintained thatlevel throughout the project's lifetime. The total of the 24ratings was calculated as a measure of overall psy-chopathology; in addition, totals were calculated for thefive factors of thought disorder, anergia, anxiety/depres-sion, hostility, and activation.
The interviewers completed the GAS after adminis-tering the BPRS. The GAS is an overall rating made by arater of an individual's social role, instrumental role, andpsychiatric functioning. The rating is made on a 100-pointscale anchored every decile by a detailed description ofthe functioning to be assigned that value. The Diagnosticand Psychopathology Unit monitored the quality of thequestions asked by the interviewers to elicit informationneeded to complete the GAS, if individuals did not spon-taneously mention that information during their responsesto the BPRS.
The PAL-C was completed by the majority ofrespondents just before or after the BPRS interview; oth-ers completed it at home and returned their responses bymail. The measure is a 43-item self-report questionnairethat assesses five areas: feelings (e.g., good, blue); rela-
tionships with significant others (spouse, children); sub-stance abuse (drugs, alcohol); physical health; and mone-tary difficulties in the past 30-45 days. The measure is amodification of the Personal Adjustment and Role Skillsscale developed by Ellsworth and his colleagues to mea-sure the community functioning of severely mentally illveterans and to compare the outcomes of different typesof treatment programs (Ellsworth et al. 1968). The instru-ment has been used to assess individuals who were func-tioning at a somewhat higher level than those for whomthe ILSS was designed, more akin to the level of those forwhom the SAS-II was designed.
Santa Barbara. The Santa Barbara (SB) project wasconducted in collaboration with the Santa Barbara County(California) Department of Mental Health and was similarto the VA project. A third condition, routine services, wasadded to the comparison of skills training with occupa-tional therapy. A total of 131 individuals with SPMI par-ticipated and were randomly assigned to the three condi-tions. The ILSS-I, ILSS-SR, BPRS, PAL-C, and GASwere administered at the beginning of the project andsemiannually thereafter for up to 42 months of followup.Only a small subset of participants was followed for 42months; the results from just the first 36 months were ana-lyzed to equate and pool the VA and SB ILSS-SR data.
For the ILSS-I, the informant who completed thequestionnaire was not necessarily the same person fromtesting to testing. Most participants lived in sheltered,nonfamilial housing, and the turnover of staff and ownersmeant that the.same informant was generally not availablefor 24 months. Thus, unless the same informant was avail-able, any residence staff member, owner, or other personwho had detailed knowledge of an individual's daily func-tioning was asked to complete the ILSS-I. For those par-ticipants who lived in familial housing at any testing, afamily member was asked to complete the ILSS-I.
Social Security Administration. The SSA projectwas an investigation of the relationship among psychiatricsymptoms, work, and the assessment of eligibility for SSI(Supplemental Security Income) and SSDI (SupplementalSecurity Disability Income) disability benefits. Of the pro-ject's three studies, only one—the validation of Part B cri-teria for assessing disability—is relevant to the investiga-tion of the psychometric characteristics of the ILSS. Atotal of 233 individuals participated: 24 percent with aDSM-III-R diagnosis of a schizophrenia spectrum disor-der, 21 percent with a diagnosis of substance abuse ordependence, and 55 percent with a DSM—III-R diagnosisof a major mood disorder. Participants were recruitedfrom inpatient facilities, board and care homes, and men-tal health outpatient programs in the metropolitan LosAngeles area. A battery of measures was administered,including the ILSS-SR and a "work sample" that con-sisted of tasks and interpersonal interactions commonly
635
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3,2000 C.J. Wallace et al.
encountered in an assembly line job. Participants werefollowed quarterly for 1 year to collect information abouttheir employment status and the decision made by theSSA about their disability status.
Results
Reliability. Three types of reliability were calculated:internal consistency, stability, and, interrater reliability.The ILSS-SR responses of participants in the VA and SBprojects were combined, into one sample, and calculationsof the measure's internal consistency and stability wereconducted with selected programs from Systat 7.01. TheILSS-I responses of informants in the SB project wereused to calculate its internal consistency and stability; theSB participants' and informants' responses were also usedto calculate the two versions' interrater reliability.Responses of the SSA participants were not used to calcu-late reliability because they were negatively skewed. Thenegative skew had been anticipated because the ILSS pro-duces scores "at the ceiling" when administered to indi-viduals who are not severely or persistently ill. Only 24percent of the participants were diagnosed with a schizo-phrenia spectrum disorder, and all were currently or hadrecently been living independently or semi-independentlywith sufficient skill to be considered for competitiveemployment.
Internal consistency. Calculation of the internal con-sistency of both the ILSS-SR and the ILSS-I versionsbegan with inspection of each respondent's answers toidentify any item for which the answer was missing oreither the "not apply" or "no opportunity" option hadbeen selected. Any such item resulted in elimination fromthe calculation of internal consistency of all of the respon-dent's answers for all items in that functional area for thattesting.
Coefficient alpha was then calculated for each func-tional area at each of the five repeated testings. Becauseof the elimination of some respondents' data for somefunctional areas at some testings, the alphas were basedon different sample sizes. For example, 181 participantshad complete data for calculation of alpha for the area"Care of Personal Possessions" at the initial testing, 159at the second testing, 133 at the third testing, 106 at thefourth testing, and 121 at the fifth testing. The smallestsample size for any alpha for any combinations of areaand testing for the ILSS-SR was 80, the largest was 206,and the average was 130.63. For the ILSS-I, the smallestsample size was 45, the largest was 101, and the averagewas 73.72. In the majority of cases, responses were elimi-nated because the "not apply" or "no opportunity"response had been selected. The weighted average coeffi-
cient alphas across the five testings for the ten functionalareas common to the two versions of the ILSS are pre-sented in table 1. Each average was calculated by weight-ing its components by their sample sizes. The weightedaverage coefficient alpha for the two functional areasunique to the ILSS—I, eating and social interactions, were0.821 and 0.829, respectively.
The alphas for the ILSS-SR ranged from marginal togood, while those for the ILSS-I ranged from good toexcellent. There are six possible explanations for the con-sistently higher alphas of the ILSS-I. First, the ILSS-Ihas more items per area, which results in higher alphas,assuming the additional items are correlated with the ini-tial items (De Vellis 1991). Second, the ILSS-I's five-point response scale has a higher ceiling than theILSS-SR's dichotomous scale. This results in more nor-mally distributed totals compared to the somewhat nega-tive skew of the ILSS-SR totals.
Third, the functional areas are less the unidimen-sional "traits" needed to appropriately use and interpretcoefficient alpha than they are convenient groupings ofitems linked by a treatment-relevant characteristic such asthe time or place of their occurrence. The functional area"Leisure and Recreation Activities," for example, includesitems as diverse as watching television, playing a tablegame, attending church and civic events, seeing a movieor play, and participating in a sport such as basketball orfootball. From a clinical and treatment planning perspec-tive, all of these items belong in the same groupingbecause they are activities conducted at times other thanwork that can function as opportunities to build a socialnetwork or as alternatives to using illegal substances oralcohol. From a psychometric perspective, coefficientalpha will be low because the items require far differentbehaviors and opportunities to perform, and engaging inany one results in not doing the others given the limitedtime and money available to most respondents to engagein the entire set of activities. Thus, there is no "trait" ratio-nale for predicting that these items will be correlated andyield a high coefficient alpha, despite the definite clinicalutility of grouping them together.
Fourth, the participants and the informants respondfrom a very different perspective about the frequency withwhich participants perform the very specific behaviorsassessed by the ILSS-SR and ILSS-I. Participants havefar more information about the specific variations in thefrequency and topography of their own behavior, whileinformants typically have a more global impression ofparticipants that may be updated only at irregular inter-vals. Thus, a participant may respond, for example, thathe or she has just started to play tennis or some othersport as the result of changes introduced into the partici-pant's residential facility, while the informant may
636
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
d
ICO
I22.
8I"5
JO
O)
o
1
£(0U
2
CO CD •"*h*. CO ^ "
© d o
inCNJ
o ino oOT OT
s §OT CO
o d d
CM
•* in coCO OT COTt in ri;o d d
s ?•<*d
i nCO
d
CO
d
OTCOCOd
oo
inom
CM CO
°. CMd d
cqd
COCMCO
©
CO OI--- OT
d d
CM
COCO
S 5 O i - OCO •>- COCO CO CO
r-. oo OTCM i - OT i nCD OT I*-; 00© o d d
0 5 OT
m
CM o in^ CM CDh~. OT CD
d o ©
h - OCM CMco ind d
m CM
o o o o o
co in i- oh. f- Ui (Of>- OT in N .
CO
.398
(/> w/ * ^ _ i^^ iu
1 1 | | !8 8 « « £
aler er
nal co co
1rr_ w _
CO gaj eg
g |-^ to
II
I!"DOTCO II
W EO O)
c? ™
11 II
« >•
s i
1 !
si.2 g« ra
if
c3«(D C
S-8CC IIQ-OTllOT
to . .
IIIi
cos
.1d>co_>.co
CO
CD
is
112 So oc cCO CO_ c c£ a. a.
respond from an overall impression that the participanthas been and continues to be uninvolved in leisure andrecreation activities other than watching TV. Hence, morevariation from time to time among a variety of disparateitems might be expected of the participant while the infor-mant maintains an internally coherent, global impression.
Fifth, participants may be responding not so muchfrom detailed knowledge of specific variations in theirown behavior but from a response bias introduced byattending to momentary variations in the environment.Finally, the individuals' responses may simply reflect mis-takes in their responding due to a lack of insight into theirbehavior.
Table 2 presents the correlations among the scales ofthe ILSS-SR (upper diagonal) and the ILSS-I (lowerdiagonal). The correlations closely parallel the internalconsistency coefficients presented in table 1. The I ver-sion's correlations are considerably higher and generallysignificant compared to the SR's lower and generally non-significant correlations.
Stability. Calculation of the stability of the SR and Iversions began by grouping the testings into pairs of lag 1time periods: 1-2, 2-3, 3-4, and 4-5, each lasting sixmonths. Each respondent's answers were then inspectedto identify any item for which the answer was missing orthe "not apply" or "no opportunity" option had beenselected. Any such item resulted in elimination of thatitem from both testings in the lag 1 pair. The remainingitems were scored, and means were calculated per respon-dent for each functional area in which at least three itemsremained after elimination of those with missing data.Means for a respondent were not calculated for areas withfewer than three items.
These means were then correlated for each functionalarea for each lag 1 pair: for example, the mean PersonalHygiene scores of 193 participants at time 1 were corre-lated with their means at time 2; the mean PersonalHygiene scores of 172 participants at time 2 were corre-lated with their means at time 3 (21 of the 193 at time 1had either discontinued their participation or had fewerthan three remaining items at time 3 to calculate a meanfor Personal Hygiene); and so on. Because of the elimina-tion of some data for some areas of functioning for somelag 1 pairs, the correlations in table 1 are based on differ-ent sample sizes. The smallest sample size for any lag 1correlation for the ILSS-SR was 121, the largest was 206,and the average was 160.12. For the ILSS-I, the smallestsample size for any sample was 65, the largest was 113,and the average was 92.86.
The weighted average stability coefficients across thefour lag 1 correlations for the ten functional areas com-mon to the two versions of the ILSS are presented in table1. Each average was calculated by transforming its com-
637
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 CJ. Wallace et al.
1
HL
SS
•oc
oc
2
he IL
Sle
s fo
r tl
CO
£O)JO
UJ
(0(0co•7(0
£
5
|i
oc
V)
Mai
nJo
bIb
See
k
o
Lei
sure
(0c
Tra
0)
Mon
jalt
h
Eou.
Car
e
(5Q.
< •
Q)C0)'5)
I-S
ILS
m ^ c o c o m c M o o i n c oC O C M C 7 > - * T - C M C M C O O
d d d d d d d d d
O O O O C O O O I O C O» O J C D i r ) » j 5d d d d d d d d
oCMCO
O ) O l CO CO O ) COCM co T- o in co
CMoCM
o oo r- o h- inoo en co h~ o oi - 1 - O T - CM CO
d d d d d d
C\J min cod d
inCO 0 0 COi n cq • *o d d
O t-~ CM CM h -m h- co o oCM CM -r- CM CO
d d d d d
CO N CO O)o a> r- coCO • * CO ^ t
d o d o
o > o o o c 7 > r - - . o ) c o ^ —0 > C 0 0 0 O CO IO ^" N CMi - CM o cvi N in ^ co ind d d d d d d d d
ooc\j co
CO
o d d
S CM COr-. in CM T- co co1- Tf CO CO Tt h-cq cq • * -<t co rt
d d d d d d
m inco i-~.CM co
d d
CO N U) « O 00 rin oo CM in m CM mcp in co • * T t cq •*
d d d d d d d
o>cot
inNd
coo
di -~.ooC D td d
c M c o <n c O ' *d d d
d d d d d d d d d
s ii l
alli ^ iCD O O
coCO ^
Is*
o > <o O
ponent correlations to z scores, weighting each componentz by its sample size, averaging them, and then convertingthe average z to r. The weighted average stability coeffi-cient for the two functional areas unique to the ILSS-I,eating and social interactions, were 0.890 and 0.858respectively.
Like the results for internal consistency, the stabilitiesof the functional areas for the ILSS-SR ranged from mar-ginal to good, while the stabilities of the ILSS-I rangedfrom good to excellent. The six differences between theversions that explain the ILSS-SR's lower alphas areequally applicable to explaining its lower stabilities.However, the stabilities of both versions' total scores areequally acceptable.
Interrater reliability. Calculation of interrater relia-bility began with inspection of participants' and infor-mants' answers to the 58 common items to identify thoseat each testing for which one or both of the respondents'answers were missing or for which the "not apply" or "noopportunity" option had been selected. These items wereeliminated from both respondents' answers at that testing.The remaining items were scored, and means were calcu-lated per respondent for each functional area if three itemsin that area remained after the initial culling of missingdata. These means were then correlated for each func-tional area for each testing. Because of the elimination ofsome data for some areas of functioning for some testings,the correlations were based on different sample sizes. Thesmallest sample size for any testing was 67, the largestwas 107, and the average was 96.3.
The weighted average interrater correlation coeffi-cients across the five testings for the ten functional areascommon to the two versions of the ILSS are presented intable 1. Each average was calculated by transforming itscomponent correlations to z scores, weighting each com-ponent z by its sample size, averaging them, and then con-verting the average z to r.
The results indicate that there was moderate agreementbetween respondents and informants. Although it might beargued that the two sources of information should be in rel-atively high to almost perfect agreement, respondents' andinformants' opportunities to observe participants' behaviorswere considerably different, and these differences werelikely magnified by the specificity of the items. As notedpreviously, the participants had more immediate informa-tion about the variations in the frequency and topographyof their own behaviors than informants and were able torespond to the specific questions of the ELSS with the mostrecent information about these changes. In contrast, infor-mants typically had global impressions of participants thatwere updated sporadically at best.
Furthermore, compared to the agreement reportedbetween other types of observer-participant pairings about
638
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
the quantity and quality of participants' behaviors, thesecorrelations are the same or higher. Achenbach et al.(1987), for example, conducted a meta-analysis of thecorrelations between observers and between observersand children about the behaviors of 269 samples of chil-dren who were reported to have emotional and conductdisorders. The average correlation between similar typesof raters such as two teachers or both parents ranged from0.54 to 0.64; the average correlations between differenttypes of informants such as teacher-parent pairings rangedfrom 0.24 to 0.42, and the average correlations betweenchildren and informants ranged from 0.20 to 0.27. The lat-ter correlations are the ones that are the most comparableto those listed in table 1; all of the table 1 correlationsexceeded the 0.20 to 0.27 range.
McCrae and Costa (1992) found that spouses' ratingsof the other spouse's facets of the Neuroticism-Extraversion-Openness Personality Inventory correlatedwith that spouse's self-ratings from 0.22 to 0.37, lowerthan the majority of those listed in table 1 even though, thespouses' accuracy could not be questioned because nonehad SPMI. It should also be noted that the Glazer et al.(1982) study, which concluded that there was "high agree-ment between the reports of 56 schizophrenic patients andtheir significant others" (about global role functioning)(p. 170), found intraclass correlations ranging from 0.27to 0.81 for the nine areas of the SAS-II, with 0.56 for allitems combined. The values in table 1 are similar butsomewhat lower, likely reflecting the greater specificity ofthe ILSS items.
ValidityCorrelations with other tests. The means for each
functional area and the overall score on the ILSS-SRwere correlated with BPRS factor and overall totals, totalson the five scales of the PAL-C, and GAS scores for eachof the five test times. Similarly, informants' ILSS-I meansper functional area and overall score were correlated withBPRS, PAL-C, and GAS scores. Because of the elimina-tion of some data for some respondents for some areas offunctioning at some testings, and because informantsfailed to complete the ILSS-I despite repeated reminders,the correlations were based on different sample sizes. Theaverage sample size was 160.2 for the ILSS-SR and 89.7for the ILSS-I.
The weighted average correlation of the GAS and thetotal BPRS with the ten functional areas common to theILSSs and the two areas unique to the ILSS-I, averagedacross the five testings, are presented in table 3. Eachaverage was calculated by transforming its componentcorrelations to z scores, weighting each component z byits sample size, averaging them, and then converting theaverage z to r. The correlations with the PAL-C are not
Table 3. Validity coefficients for the ILSS-SRand the ILSS-I
Area
HygieneAppearCareFoodHealthMoneyTransLeisureJobSeekJobMainSocialEatingTotal
ILSS-I
GAS
0.1830.2080.2180.2090.274*0.246*0.2250.1630.1340.237*0.2190.1950.268*
BPRStotal
-0.171-0.238*-0.201-0.172-0.252*-0.308*-0.201-0.123-0.208-0.238-0.199-0.202-0.271*
ILSS-SR
GAS
0.265*0.273*0.1400.1330.249*0.231*0.1870.1940.1440.126
NANA
0.375*
BPRStotal
-0.252*-0.257*-0.187-0.141-0.192-0.190-0.118-0.104-0.071-0.196
NANA
-0.318*
Note.—Appear = Personal Appearance; BPRS = BriefPsychiatric Rating Scale; Care = Care of PersonalPossessions; Food = Food Preparation; GAS = GlobalAssessment Scale; Health = Care of Personal Health andSafety; ILSS-I = Independent Living Skills Survey-Informantversion; ILSS-SR = Independent Living Skills Survey-Self-report version; JobMain = Job Maintenance; JobSeek = JobSeeking; Money = Money Management; NA = not applicable;Social = Social Interactions; Trans = Transportation.
*p < 0.0.1
presented because they were, as expected, low and non-significant.
The majority of the correlations listed in table 3, par-ticularly the ones for the ILSS-I, are significant at the0.01 level. The 0.01 level of significance was chosen tobalance compensation for the inflation of alpha across thenumber of analyses with their power. Albeit low, all corre-lations are in the expected direction and are consistentacross the various areas of the ILSS, particularly for theILSS-I. It is important to note that these validity coeffi-cients are consistent despite different methods of gather-ing the information (questionnaire, highly structuredinterview, open-ended interview), different responsescales (frequency scale, intensity scale, dichotomous per-formance scale, single global scale), and different types ofrespondent (self, informant, trained rater).
These coefficients may also indirectly provide infor-mation about the bias that either informants or partici-pants might bring to their reporting. Focusing on theILSS-SR and ILSS-I totals, the approximately equal cor-relations between the ILSS-I total and the GAS andBPRS totals on the one hand, and the ILSS-SR total andthe GAS and BPRS totals on the other, indicate that nei-ther informants nor participants were uniquely biasedreporters.
639
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
Prediction of employment. All SSA participants'ILSS-SR scores were transformed to create a less skeweddistribution. After estimating the few missing scores byassigning them a randomly generated "yes" or "no," thetotal for the test was calculated, converted to a percentageof the total possible, and transformed to the square root ofthe percentage.
After the year-long followup, two measures ofemployment status were calculated, employability andsustained employability. Each was measured with adichotomous variable, the former defined as working atleast 1 month at the SSA's definition of "substantial gain-ful activity" (minimum of $300 of income during themonth), and the latter defined as working at that incomelevel for either 6 continuous months or the last 3 monthsof the followup period. In addition to the ILSS-SR and a3- or 15-day sample of actual work behavior, the BPRS,the SAS-II, and a comprehensive measure of work historywere administered. J
The two measures of employment were analyzed asdependent variables in separate stepwise survival analyses(SAS procedure LIFETEST) to identify the measures thatalone and in combination predicted outcomes. Aftercovarying participants' initial eligibility status (adjudi-cated disabled or not), the transformed ILSS-SR total wasthe one measure that best predicted employability eitheralone or after the other variables had been entered into thestepwise analysis, surpassing even work history. It wasthe second best predictor of sustained employment,exceeded only by the BPRS. Furthermore, the trans-formed ILSS-SR scores were significantly associatedwith initial adjudicated status.
Sensitivity to the effects of treatment. The datafrom the VA and SB projects were analyzed to determineboth the sensitivity of the ILSS to the effects of skillstraining, and the stability of that sensitivity across the fol-lowup testings.
The ILSS-SR overall total and scale totals from theVA project were each analyzed with three separate split-plot factorial analysis of covariance. For each analysis,the pretest score was the covariate, and treatment condi-tion (occupational therapy vs. skills training) was thebetween-subjects variable. During the course of the pro-ject, a number of participants were unavailable for sometestings or terminated prematurely, particularly at the 24-month (after enrollment) followup. Analyzing only partic-ipants who had completed all testings would have ignoreddata from many who had completed some but not all ofthe followup testings. To analyze as much of the data aspossible, the three split-plot factorial analyses of covari-ance included different time periods as the within-subjectsvariable. The period for the first included the immediateposttreatment and 12-month (after enrollment) testings;
the time period for the second included the 12- and 24-month (after enrollment) testings; and the time period forthe third included the 24- and 36-month (after enrollment)testings.
The results of the analyses indicated that the overalltotal and the totals for the Care of Personal Possessions,Food Preparation, and Money Management scales weresignificantly higher (all Fs p < 0.05) for the skills traininggroup at posttest and remained so during all the followuptestings. The totals for the Transportation and HealthMaintenance scales were also significantly higher for theskills training at posttest but did not remain so during thefollowup period.
The ILSS-SR and ELSS-I data from the SB projectwere analyzed similarly to those from the VA project;analyses of covariance using the pretest scores as thecovariates, treatment condition (occupational therapy,skills training, routine services) as the between-subjectsvariable and testing times (post, 12, 18, 24, 30, and 36months after enrollment) as the within-subjects variable,time. The testing times were not paired, however, sincethere were fewer instances of early termination or missingdata. Significant main effects or interactions were furtheranalyzed with Tukey's honestly significant differences testfor the group main effect and a test of simple interactioneffects for the interaction.
The results indicated that the skills training groupreported significantly higher functioning (all Fs < 0.03) onthe ILSS-SR Food Preparation, Money Management, andHealth Maintenance scales than either of the other twogroups at posttest and throughout the followup period. Forthe ILSS-I, informants reported that the functioning ofthe skills training group was significantly higher (all Fs< 0.04) than the other two groups on the FoodPreparation, Money Management, and Social Interactionscales. Functioning remained significantly higher duringthe followup period except for the 12-month followupscores on the Food Preparation and Money Managementscales, at which point the two treatment groups were sig-nificantly higher than routine services but with no signifi-cant difference between the skills training and occupa-tional therapy groups. The two treatment groups were alsoreported to be functioning significantly higher than theroutine services group on the Transportation and HealthMaintenance scales throughout the testing period, with nodifferences between them.
Discussion
Considered in the aggregate, these results suggest that theILSS-SR and ILSS-I are generally reliable, stable, andsensitive measures of basic functional living skills. The
640
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
coefficients of internal consistency and stability of theILSS-I matched or exceeded those reported for similarinstruments such as the LSP, and its scale totals and itsoverall total in particular were correlated with scores fromsimilar measures. The coefficients of internal consistencyand stability of the ILSS-SR, while lower than those of theILSS-I, were generally acceptable; its scale totals and over-all total successfully discriminated between contrastedgroups, were correlated with scores from similar measures,reflected the effects of an intervention designed to improvefunctional living and social skills, and predicted vocationaloutcomes. Furthermore, all of these results were based onreasonably sized samples measured repeatedly over 24months; hence, the values presented in tables 1 and 2 arelikely stable estimates of the characteristics of both ver-sions when they are used with individuals with SPMI livingin a wide range of community facilities.
Two studies have also published results about thepsychometric adequacy of both versions of the ILSS. Theinitial report of the ILSS-I (Wallace 1986) summarizedthe results of a study with operators of 59 board and carehomes who completed the ILSS-I, the NOSIE-30, andthe MACC-II (Mood-Affect-Communication, andCooperation—Revised) for one resident in each home whowas diagnosed with chronic schizophrenia. The diagnoseswere confirmed based on information obtained during asemistructured interview conducted with the resident,using questions selected from the Present StateExamination and scored with the criteria of the NewHaven Schizophrenia Index. The interviews were tape-recorded, and they were rated by an independent raterwho agreed with the diagnosis in all 59 cases.
The coefficient alphas ranged from 0.67 to 0.84, sim-ilar to but slightly lower than those reported in table 1.The four positive assets scores of the NOSIE-30 (socialcompetence, social interest, personal neatness, and total)were correlated with the ILSS-I totals per area and theoverall total. Seventy percent of the correlations were sig-nificant at the 0.01 level, with an additional four signifi-cant at the 0.05 level. As expected, the ILSS-I scale totalsand overall total were not significantly correlated with thenegative factors of the NOSIE-30. For the MACC-II, 18percent were significantly correlated at the 0.01 level,with an additional 18 percent significant at the 0.05 level.
The second study (Cyr et al. 1994) reported the psy-chometric characteristics of a French translation of theILSS-SR. All but the two job scales had acceptable coef-ficients of internal consistency (alpha) and stability; thejob scales were markedly skewed with restricted vari-ances because few of the 145 participants with SPMIwere employed. The scales discriminated between partici-pants as a function of gender, diagnosis, and amount ofsupervision needed in their residences.
However, no matter what these results indicate aboutthe psychometrics of the two versions of the ILSS, theyare of little use in convincing practitioners to integrate theILSS into their routine documentation procedures.Integrating systematic assessments into the brief, idiosyn-cratic questions and observations of overworked andunderpaid practitioners is hardly welcomed. To increasethe probability that the ILSS would become part of rou-tine procedures, its items and scales were specifically con-structed to meet clinicians' suggestions for useful infor-mation. Each item's content was reviewed forapplicability and acceptability by diverse clinicians andindividuals with SPMI. Several items were added withextreme base rates whose "counter base-rate" perfor-mance was a clinically meaningful indicator of a majorchange in an individual's status. Despite the items'skewed distributions, the trade-off between internal con-sistency reliability and clinical utility was consideredworthwhile. A number of items were reworded or droppedto make the assessment less intrusive and offensive forindividuals.
The items were grouped into "clinically coherent"scales that maximized clinicians' and individuals' under-standing of the total scores on each scale. In contrast, thescales of other instruments have been typically con-structed from a factor analysis of the items that maxi-mizes the scales' internal consistency. The disadvantageof this approach is that the items of a scale may be clini-cally unrelated and produce totals that are difficult tointerpret. For example, the LSP groups the items "poorlygroomed" and "incapable of work" in the same scalelabeled "Self-Care"; the items "generally inactive" and"no warmth to others" in the same scale labeled "SocialContact"; and the items "reduced compliance with med-ication" and "takes others' possessions" in the scalelabeled "Responsibility." From a clinical perspective, theitems in each of the three pairs involve rather differentbehaviors despite their common groupings and mayreflect different causes and require different treatments.Thus, the LSP's scale totals provide somewhat confusinginformation despite each one's high internal consistency.
The compromises involved in maximizing the clini-cal utility of the FLSS's scales in relation to their internalconsistency are illustrated by the Recreation and LeisureActivities scale. Clinically, assessing an individual's useof free time to engage in recreational and leisure activitiesis valuable because these activities provide opportunitiesto socialize and avoid drug and alcohol use.Psychometrically, engaging in one activity (which islikely a function of environmental opportunity and per-sonal predilection, which varies substantially fromrespondent to respondent) leads to not engaging in otheractivities. This built-in negative correlation results in a
641
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
low coefficient alpha. On the other hand, scales such asPersonal Hygiene measure the frequency of performanceof behaviors that generally occur at the same time andplace and are performed as part of an internally consistentpattern. Thus, the scale would be both clinically and psy-chometrically acceptable. In all instances, the emphasiswas placed on making the ILSS clinically useful.
Of course, maximizing internal consistency increasesthe power of analyses of the scales' relationships withother clinically meaningful variables such as communitytenure, symptom severity, gender, ethnicity, and medica-tion. Furthermore, inspection of seemingly disparate butinternally consistent items may point to latent variablesthat had not been previously considered as determinantsof community functioning.
This compromise between content-coherent andinternally consistent scales is but one of the limitations ofthe ILSS. The scales' deliberately narrow focus on perfor-mance does not provide information about the personal orenvironmental factors that influence that performance.Designing an effective treatment plan most certainlyrequires information about a client's skills and motivationand about the environment's opportunities and support.Any or all of these factors can be the targets of the plan'sservices.
On the other hand, this narrow focus avoids the con-founds inherent in items such as the LSP's "incapable ofbudgeting," "incapable of food preparation," and "inca-pable of work." Development of the ILSS assumed thatpractitioners' detailed clinical assessments would provideinformation about the relative importance of skills, moti-vation, opportunities, and rewards and suggest which arefavorable targets for services.
The results of the SSA project point to yet anotherlimitation of the ILSS-SR; the ceiling is restricted whenthe test is administered to less severely or persistently illindividuals. This is largely the result of focusing theinstrument on respondents with SPMI, the majority ofwhom are unemployed, have never been married, interactwith a limited network of friends, and live in shelteredresidences. Other instruments such as the SAS-II arewidely available and do provide a ceiling with sufficientroom to assess the functioning of less severely or persis-tently ill respondents.
The ILSS-SR's Yes/No response scale also con-tributes to the lowered ceiling. The test was designed tobe particularly easy to administer and to complete, and thesimplicity of the dichotomous scale was preferred to thegreater complexity of the ILSS-I's five-point frequency ofoccurrence scale. However, four of the five points of theILSS-I's scale (sometimes, often, usually, always) areequivalent to answering Yes on the ILSS-SR's dichoto-mous scale, and only one point (never) is equivalent to
answering No. In effect, the ILSS-SR's simplicity andease sacrifice the ILSS—I's more finely graduated informa-tion and lead to a restricted ceiling. This restricted vari-ance is generally a compromise in using dichotomouscompared to polychotomous response scales, and theILSS-SR version is being revised to determine its charac-teristics and acceptability if it adopted the ILSS-I ver-sion's response scale.
Finally, although the efforts to enhance the ILSS'sclinical utility have been spurred and rewarded by practi-tioners' comments, more is needed to increase the chancethat both versions will be adopted as part of routine proce-dures. Specifically, methods of summarizing the resultsacross items and scales, and of using these summaries toprovide comparisons with various norms (e.g., other indi-viduals with SPMI living in a variety of settings, "suc-cessful" vs. "unsuccessful" individuals, minimum require-ments to live successfully in a class of settings and in alocal exemplar of that class) are clearly needed. Given thedemands on practitioners to make billable every instant oftheir time, efforts to shorten documentation and the timeto complete it are highly valued. Practitioners generallydislike completing "administrative" tasks such as totalingitem scores, graphing the totals, and consulting compari-son tables. The acceptability of the ILSS would be greatlyenhanced by producing relatively automated summariesand even suggesting treatment plans.
Fortunately, the ubiquity of the personal computermakes this a feasible goal, and efforts are currently under-way to devise a PC-based "expert" system that wouldautomate the process but not violate Joint Commission onAccreditation of Healthcare Organizations standards forindividuation of care. Such a system could accommodatevarious groupings of items to use only those that were rel-evant for a particular use, highlight the extreme base rateitems whose answers suggested a change in clinical sta-tus, and assist less experienced clinicians to acquire theknowledge of the experts who established the system'srules.
References
Achenbach, T.M.; McConaughy, S.H.; and Howell, C.T.Child/adolescent behavioral and emotional problems:Implications of cross-informant correlations for situationalspecificity. Psychological Bulletin, 101:213-232,1987.
Barker, S.; Barron, N.; McFarland, B.H.; Bigelow, D.A.;and Carnahan, T. A community ability scale for chroni-cally mentally ill consumers: H Applications. CommunityMental Health Journal, 30:459-472,1994.
Bedell, J.R.; Hunter, R.H.; and Corrigan, P.W. Currentapproaches to assessment and treatment of persons with
642
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
serious mental illness. Professional Psychology: Researchand Practice, 28:217-228, 1997.
Cyr, M.; Toupin, J.; Lesage, A.D.; and Valiquette, C.A.Assessment of independent living skills for psychoticpatients: Further validity and reliability. Journal ofNervous and Mental Disease, 182:91-97, 1994.
De Vellis, R.R. Scale Development: Theory andApplications. Newbury Park, CA: Sage Publishing, 1991.
Dickerson, F.B. Assessing clinical outcomes: The commu-nity functioning of persons with serious mental illness.Psychiatric Services, 48:897-902, 1997.
Eisen, S.V.; Dill, D.L.; and Grob, M.C. Reliability andvalidity of a brief patient-report instrument for psychiatricoutcome evaluation. Hospital and Community Psychiatry,45:242-247, 1994.
Ellis, R.H.; Wackwitz, J.H.; and Foster, M. Uses of anempirically derived client typology based on level offunctioning: Twelve years of the CCAR. Journal ofMental Health Administration, 18:88-100, 1991.
Ellsworth, R.B. Profile of Adaptation to Life-ChangeScale. Palo Alto, CA: Consulting Psychologists Press,1979.
Ellsworth, R.B.; Foster, L.; Childers, B.; Arthur, G.; andKroeker, D. Hospital and community adjustment as per-ceived by psychiatric patients. Journal of Consulting andClinical Psychology Monograph, 32(5, pt. 2), 1968.
Endicott, J.; Spitzer, R.L.; Fleiss, J.L.; and Cohen, J. TheGlobal Assessment Scale: A procedure for measuringoverall severity of psychiatric disturbance. Archives ofGeneral Psychiatry, 33:766-771, 1976.
Fabisiak, S.; Baskin, D.; and Hammer, R. The New YorkState Level of Care Survey in community mental healthcenters and New York State's psychiatric centers.Psychiatric Quarterly, 55:25-34, 1983.
Glazer, W.; Sholomskas, D.; Williams, D.; and Weissman,M.M. Chronic schizophrenics in the community: Are theyable to report their social adjustment? American JournalofOrthopsychiatry, 52:166-171, 1982.
Goldman, H.H.; Skodol, A.E.; and Lave, T.R. RevisingAxis V for DSM-TV: A review of measures of social func-tioning. American Journal of Psychiatry, 149:1148-1156,1992.
Goodman, S.H.; Sewell, D.R.; Cooley, E.L.; and Leavitt,N. Assessing levels of adaptive functioning: The RoleFunctioning Scale. Community Mental Health Journal,29:119-131, 1993.
Katz, M.M., and Lyerly, S.B. Methods for measuringadjustment and social behavior in the community: I.Rationale, description, discriminative validity and scaledevelopment. Psychological Reports, 13:503-535, 1963.
Kaufmann, C , and Manderscheid, R. The consumer-ori-ented mental health report card. Behavioral HealthcareTomorrow, 6:56-57, 1997.
Kennedy, C.S.; Simmens, S.J.; Pincus, H.A.; andGoldman, H.H. The Social Security disability evaluationstudy. New Directions for Mental Health Services,45:29-36, 1990.
Liberman, R.P. Handbook of Psychiatric Rehabilitation.New York, NY: MacMillan, 1992.
Liberman, R.P.; Blackwell, G.A.; Wallace, C.J.; Mintz, J.;Kopelowicz, A.; and Vaccaro, J.V. Skills training vs. psy-chosocial occupational therapy for persons with persistentschizophrenia. American Journal of Psychiatry,155:1087-1091, 1998.
Lukoff, D.; Nuechterlein, K.H.; and Ventura, J. AppendixA. Manual for expanded Brief Psychiatric Rating Scale(BPRS). Schizophrenia Bulletin, 12(4):594-602, 1986.
McCrae, R.R., and Costa, P.T. Discriminant validity of theNEO-PIR facet scales. Educational and PsychologicalMeasurement, 52:229-237, 1992.
McPheeters, H.L. Statewide Mental Health OutcomeEvaluation: A perspective of two southern states.Community Mental Health Journal, 20:44-55, 1984.
Meyer, Z.J. At-risk for results: Guaranteeing performancebased on patient outcomes. Behavioral HealthcareTomorrow, 6:25-31, 1997.
National, Institute of Mental Health. Series FN No. 9,Assessing Mental Health Treatment OutcomeMeasurement Techniques. (DHHS Publication No. ADM86-1301.) Washington, DC: U.S. Government PrintingOffice, 1986.
National Institute of Mental Health. Caring for PeopleWith Severe Mental Disorders: A National Plan ofResearch to Improve Services. (DHHS Publication No.ADM 91-1762.) Washington, DC: US GovernmentPrinting Office, 1991.
Newman, F.L., and Ciarlo, J.A. Criteria for selecting psy-chological instruments for treatment outcome assessment.In: Maruish, M.E., ed. The Use of Psychological Testingfor Treatment Planning and Outcome Assessment.Hillsdale, NJ: Lawrence Erlbaum, 1994. pp. 98-110.
Pincus, H.A.; Kennedy, C ; Simmens, S.J.; Goldman,H.H.; Sirovatka, P.; and Sharfstein, S.S. Determining dis-ability due to mental impairment: APA's evaluation ofSocial Security Administration guidelines. AmericanJournal of Psychiatry, 148:1037-1043, 1991.
Rosen, A.; Hadzi-Pavlovic, D.; and Parker, G. The LifeSkills Profile: A measure assessing function and disabilityin schizophrenia. Schizophrenia Bulletin, 15(2):325-337,1989.
643
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
Schooler, N.; Hogarty, G.; and Weissman, M. SocialAdjustment Scale II (SAS-II). In: Hargreaves, W.A.;Attkinson, C.C.; and Sorenson, J.E., eds. ResourceMaterials for Community Mental Health ProgramEvaluators. (DHHS Publication No. ADM 79-328.)Washington, DC: U.S. Government Printing Office, 1979.pp. 129-131.
Smith, G.R.; Manderscheid, R.W.; Flynn, L.M.; andSteinwachs, D.M. Principles for assessment of patientoutcomes in mental health care. Psychiatric Services,48:1033-1036, 1997.
Spitzer, R.L.; Endicott, J.; Fleiss, J.L.; and Cohen, J. ThePsychiatric Status Schedule: A technique for evaluatingpsychopathology and impairment in role functioning.Archives of General Psychiatry, 23:41-55,1970.
Srebnik, D.; Hendryx, M.; Stevenson, J.; Caverly, S.;Dyck, D.G.; and Cauce, A.M. Development of outcomeindicators for monitoring the quality of public mentalhealth. Psychiatric Services, 48:903-909,1997.
Vieweg, B.W.; Graber, P.S.; Wilson, R.C.; and Won Cho,D.W. Lessons and surprises from the public sector.Behavioral Healthcare Tomorrow, 6:31-37,1997.
Wallace, C.J. Functional assessment in rehabilitation.Schizophrenia Bulletin, 12(4):604-630, 1986.
The Authors
Charles J. Wallace, Ph.D., is Professor of MedicalPsychology; Robert Paul Liberman, M.D., is Professor ofPsychiatry; and Robert Tauber, M.A., is ResearchAssociate, University of California at Los Angeles,Neuropsychiatric Institute, Department of Psychiatry, LosAngeles, CA. Jeannie Wallace, Ph.D., is in private prac-tice in Encino, CA.
Appendix. Independent Living SkillsSurvey
The following are the two versions of Independent LivingSkills Survey: the Informant Questionnaire and the Self-Report Interview. Items with asterisks are common toboth versions. These instruments are available on requestfrom Dr. C.J. Wallace, Psychiatric RehabilitationConsultants, Box 2867, Camarillo, CA, 93010-2867.
644
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
Independent Living Skills Survey
Informant Questionnaire
The purpose of this questionnaire is to obtain your view of the community adjustment of one of your relatives,or one of the consumers of your facility's services. "Community adjustment" means how often your relative orthe consumer performs the tasks needed to live a satisfying, independent life in the community. These taskstypically include taking care of one's personal appearance, money, possessions, residence, and health; find-ing and keeping a job; and interacting with others.
A number of these tasks—e.g., Vacuumed or mopped as needed; Bought own groceries; Budgeted money—are listed on the following pages. Please indicate how often your relative or the consumer you are rating per-formed each of these tasks during the past 30 days. If your relative or the consumer Always performed atask, place a checkmark on the line that is in the Always column next to the task; if your relative or the con-sumer Usually performed a task, place a checkmark on the line that is in the Usually column; if your relativeor the consumer Often performed a task, place a checkmark on the line in the Often column; if your relativeor the consumer Sometimes performed a task, place a checkmark on the line in the Sometimes column; ifyour relative or the consumer Never performed a task, place a checkmark on the line in the Never column.Put ONLY ONE checkmark for each task.
There are some tasks that cannot be performed because there is No Opportunity to do so. For example,using a bus is impossible if public transportation is not available; meals cannot be cooked if the residentialstaff does all the work and limits access to the kitchen; and medication cannot be self-administered if some-one else stores the medication and dispenses it. If a task is never performed because there is NoOpportunity to do so, place a checkmark on the line in the No Opportunity column next to that task.
If you wish to write comments about your answers or provide information that is important for understandingyour relative's or the consumer's adjustment, please feel free to write them in the comments lines and/or onthe back of this questionnaire.
MANY, MANY THANKS FOR YOUR HELP!!
Relative or consumer to be rated:
Your name: Date of completion:
Your relationship to the person you're rating:
645
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from
CO
1>.
sual
ften
O
a>
tim
o(0
Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
Appearance and Clothing
roQ.
i_ Q.
How often did the person perform each behavior in the J 3 « E > Q
last 30 days? ~1 .* Washed clothes by hand or machine using the proper
amount of detergent (without prompting)2.* Dried clothes in a dryer or on a clothes line
(without prompting)3.* Folded, hung up, and stored clothes after they
were washed and dried (without prompting)4.* Stored dirty clothes separate from clean
(without prompting)5.* Changed underwear at least twice a week
(without prompting)6.* Bought own clothes the last time clothing was
needed (without prompting)7. Undressed self at designated times
(without prompting)8. Dressed self at designated times
(without prompting)9. Maintained clean, neat appearance throughout
the day (without prompting)10. Wore bizarre combinations or excessive layers
of clothing11. Wore clothing appropriate for the weather and the
social occasion (without prompting)12. Changed clothes excessively
(several times a day)
Comments:
Personal Hygiene &tn 1
» >• £ 9-How often did the person perform each behavior in the > 3 «> E > ®last 30 days? < => O w z 21 .* Bathed/showered with soap at least twice/week
(without prompting) _ _ _ _ _ _2.* Shampooed hair at least twice/week (once a
week for females) without prompting _ _ _ _ _ _3.* Used deodorant (without prompting) _ _ _ _ _ _4.* Brushed/combed hair (without prompting) __ _ _ _ _ _
646
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3,2000
5.* Brushed teeth with toothpaste at least once/day(without prompting)
6. If needed, got a haircut or had hair styled(without prompting)
Comments:
Care of Personal Possessions
How often did the person perform each behavior in thelast 30 days?1 .* Made the bed (without prompting)2.* Kept room clean (without prompting)3.* Picked up "clutter" and put items back where they
belong (without prompting)4.* Wiped up spills such as coffee
(without prompting)5.* Vacuumed or mopped as needed
(without prompting)6.* Dusted furniture as needed
(without prompting)7. Changed bed linens as needed
(without prompting)8. Performed assigned household tasks
(without prompting)9. Used others' possessions inappropriately and/or
without permission
Comments:
(0
ual
S. en
(0
I §1
Coa.aOo
Food Preparation/Storage
How often did the person perform each behavior in thelast 30 days?1 .* Prepared simple foods such as sandwiches, cold
cereal, etc. that did not require cooking2.* Prepared foods that require some cooking such
as eggs, TV dinners3.* Discarded spoiled foods (without prompting) . . . .
(0
Iway
sual
l
3io
a>UIJ:
o ever
z
roa.a.Ooz
647
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

V)
1 sual
ften
O
COCDE
o(0
Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
4.* Used a dishwasher or washed dishes by handafter meals (without prompting)
5.* Put away dishes after washing them(without prompting)
6.* Had good nutritional choices in foods; that is,didn't live on candy and soda
7.* Bought own groceries—more than just snackfoods (without prompting)
8. Stored foods appropriately (without prompting)9. Cleared table (without prompting)
Comments:
Health Maintenance .~c3roa
i_ Q.
How often did the person perform each behavior in the % 3 | j E > ®last 30 days? < 5 O « z z1 .* Self-administered medication (if not on medication,
when the person last took medication) _ _ _ _ _ _2.* If didn't self-administer medication, cooperated with
the person who administered it (score same as item#1 if person self-administered medication) _ _ _ _,. _ _
3.* Contacted appropriate person (e.g., physician,social worker, residential care operator, parent) torenew a prescription for a medication presentlybeing prescribed _ _ _ _ _ _
4.* When last ill with a minor physical problemsuch as a cold, correctly took care of himself/herself ; _ _ _ _ _ _
5.* Knows proper use of insurance or welfare coverage(e.g., Blue Cross, Medicare, MediCal, Medicaid)for treatment _ _ _ _ _ _
6.* If smokes, did so safely _ _ _ _ _ _7. Reported physical problems appropriately
(neither over- nor underreported) _ _ _ _ _ _8. Obtained help from appropriate public agency
or other resource (fire, police, social worker,doctor, dentist) when needed _ _ _ _ _ _
9. Understands terms guardianship or conservator(if relevant) _ _ _ _ _ _
10. Used telephone inappropriately (i.e., madelong-distance calls charged to another numberwithout permission, called others during the
648
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
middle of the night)
Comments:
Money Management £to ICD C
' ' c * I . II 1 I I I ?How often did the person perform each behavior in the * - « - - -last 30 days? < 3 O w z z1 .* Paid bills such as rent, utilities, phone, and
transportation (without prompting) _ _ _ _ _ _2* Made a deposit or withdrawal at a bank
(without prompting) _ _ _ _ _ _3.* Budgeted money (planned how funds
were to be spent) _ _ _ _ _ _4.* Cashed paycheck or SSI check
(without prompting) _ _ _ _ _ _5.* Purchased essential items prior to spending
money on luxuries (without prompting) _ _ _ _ _ _6. Purchased prescribed medication
(without prompting) _ _ _ _ _ _7. Maintained appropriate identification for
cashing checks _ _ _ _ _ _8. Contacted person responsible for financial
support to ask questions and relay relevantinformation _ _ _ _ _ _
9. Returned or exchanged defective goods(without prompting) _ _ _ _ _ _
10. Counted change in store (without prompting) _ _ _ _ _ _
Comments:
Transportation
How often did the person perform each behavior in the 3 3 £5last 30 days? < = O1 .* Had a valid, current driver's license _ _ _2* Used public buses, trains, or subway
(without prompting) _ _ _3.* When last went to an unfamiliar place, asked others or called
public transportation for directions (without prompting) _ _ _
649
Ulj
CD
0w
1CD
z
c
rtu
0Q.Q.
Oz
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
4.* Read bus schedule the last time the informationwas needed (without prompting)
5. Walked to places in the neighborhood(without prompting)
6. Followed pedestrian rules (without prompting) . .7. Acted appropriately on buses, trains, subways .
Comments:
Leisure and Community .•=en 3
. c o
* f c i fc JfHow often did the person perform each behavior in the § a <B E > °
^ ^ ^ w * : o <i> o
last 30 days? < => O </> z z1 .* Worked regularly on a hobby (without prompting) _ _ _ _ _ _2* Attended religious services (without prompting) _ _ _ _ _ _3.* Wrote letters or visited friends/relatives
(without prompting) _ _ _ _ _ _4.* Attended movies/theater (without prompting) _ _ _ _ _ _5.* Read books, newspapers, or magazines
(without prompting) _ _ _ _ _ _6.* Attended meetings of civic or other organizations
such as VFW (without prompting) _ _ _ _ _ _7.* Listened to radio or watched TV
(without prompting) _ _ _ _ ••_ _8.* Worked in the garden or yard
(without prompting) _ _ _ _ _ _9.* Attended spectator sport (without prompting) _ _ _ _ _ _10.* Bowled, played pool or other sports
(without prompting) _ _ _ _ _ _11.* Played cards/table games (without prompting) _ _ _ _ _ _12.* Was registered to vote _ _ _ _ _ _13. Violated general social etiquette (e.g.,
scratched body parts in public, belched inpublic without apologies) _ _ _ _ _ _
Comments:
650
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
Job Seeking
How often did the person perform each behavior in thelast 30 days?1 .* Read classified ads one or more times per week
to look for jobs (without prompting)2.* Contacted potential employers to determine
possible job openings (without prompting)3.* Contacted friends/peers/social workers/employment
agencies for job leads (without prompting)4.* Participated in a job interview (without prompting)..5. Had realistic job aspirations6. Had realistic interest in and desire to work
Comments:
(A > •
f 1.2 0)< 3
ten
(Ad)LU
I
met
o 13
roQ.aoz
Job Maintenance
How often did the person perform each behavior whenlast employed?1 .* When last employed, arrived at work on time
and followed daily break and work schedule(without prompting)
2* When last employed, got along with coworkers . . .3.* When last employed, got along with supervisors . .
Comments:
(0
< 3 O
0)
o§1Q)
c3
Oa.a.Oo
Eating
How often did the person perform each behavior in thelast 30 days?1. Drank neatly (without prompting)2. Used appropriate utensils and dishes
(without prompting)3. Ate at a reasonable pace (without prompting) . . . .4. Chewed food with mouth closed
(without prompting)
(A
<
lien
(A
Ca)
(AQ)EoS
i 5
Coaa.Oo
651
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from
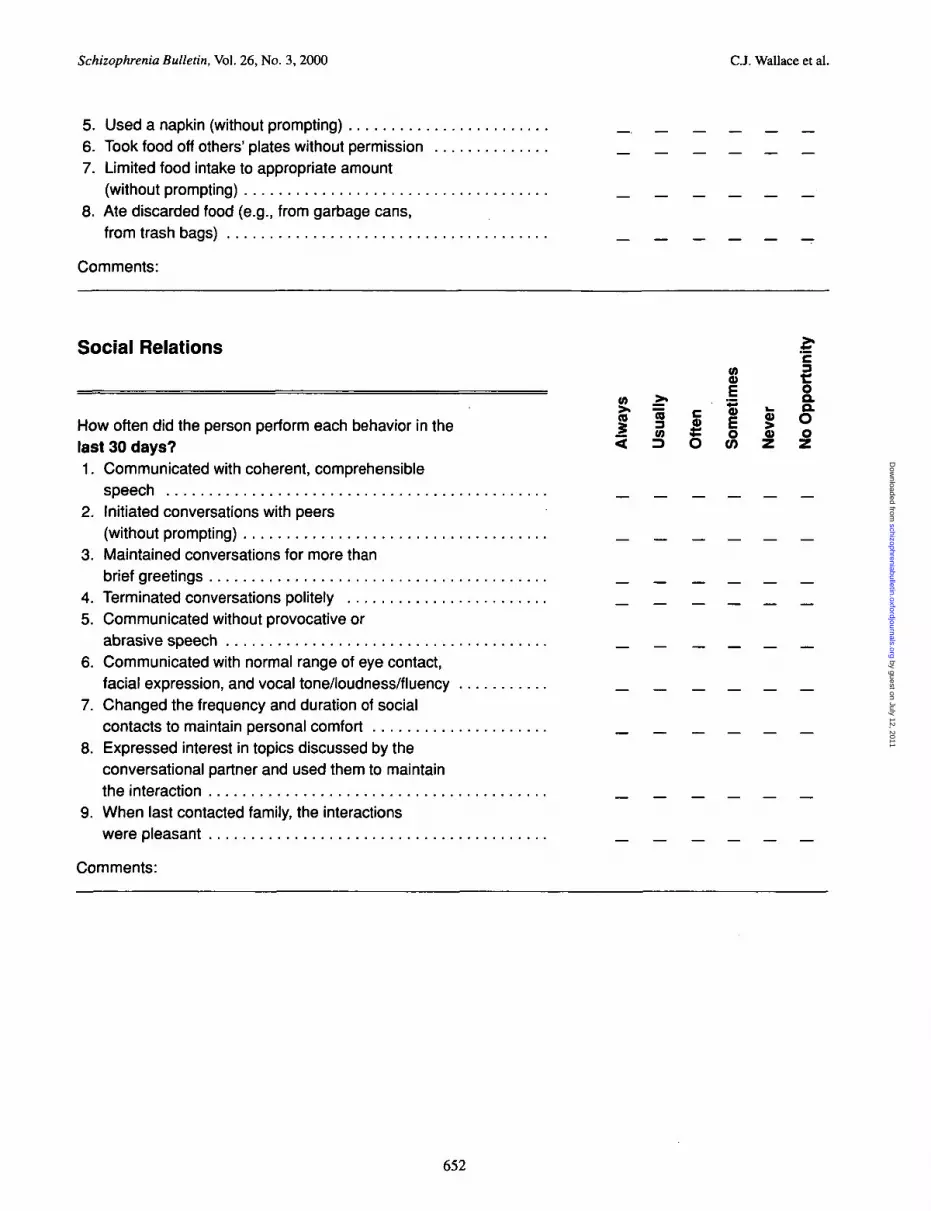
Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
5. Used a napkin (without prompting)6. Took food off others' plates without permission7. Limited food intake to appropriate amount
(without prompting)8. Ate discarded food (e.g., from garbage cans,
from trash bags)
Comments:
Social Relations £(0 I
o) >• . ~ 9->» = c a> i- o .
How often did the person perform each behavior in the J 3 *! | « olast 30 days? < = O « z z1. Communicated with coherent, comprehensible
speech _ _ _ _ _ _2. Initiated conversations with peers
(without prompting) _ _ _ _ _ _3. Maintained conversations for more than
brief greetings _ _ _ _ _ _4. Terminated conversations politely _ _ _ _ _ _5. Communicated without provocative or
abrasive speech _ _ _ _ _ _6. Communicated with normal range of eye contact,
facial expression, and vocal tone/loudness/fluency _ _ _ _ _ _7. Changed the frequency and duration of social
contacts to maintain personal comfort _ _ _ _ _ _8. Expressed interest in topics discussed by the
conversational partner and used them to maintainthe interaction _ _ _ _ _ _
9. When last contacted family, the interactionswere pleasant _ _ _ _ _ _
Comments:
652
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 20OO
Independent Living Skills Survey
Self-Report Interview
The purpose of this questionnaire is to obtain an individual's view of his/her own community adjustment."Community adjustment" means how often the individual performs the tasks needed to live a satisfying, inde-pendent life in the community. These tasks typically include taking care of one's personal appearance, money,possessions, residence, and health; finding and keeping a job; and interacting with others.
A number of these tasks—e.g., Vacuum or mop your floor; Buy your own groceries; Budget your money—arelisted on the following pages. The individual's report of how often he/she performs these tasks will be obtainedduring an interview that should be conducted after a comfortable relationship has been established. Tell theindividual that the interview consists of a comprehensive set of questions about the performance of ALL ofthe skills needed to live in the community. Some of the questions may seem irrelevant or even "babyish," butALL must be asked so that a thorough picture can be drawn about the individual's strengths.
PLEASE DO NOT SKIP ANY QUESTIONS. For each, begin by reading the "time frame" statement (In the last30 days, did you...) followed by a task (vacuum or mop your floor). Ask the individual to respond YES, NO, orNOT APPLY, and, based on that response, place a checkmark in the appropriate column. If the individual hasbeen in an unusually restrictive setting such as a hospital for the past 30 days and the restrictive setting is notthe one in which the individual typically resides, change the time frame statement to When you are living inyour typical residence, NOT the hospital, do you...
Explain that the NOT APPLY response option means a task may not be performed because the setting does-n't allow it. Using a bus is impossible, for example, if public transportation is not available; meals cannot becooked if the residential staff does all the work and limits access to the kitchen; and medication cannot beself-administered if someone else stores the medication and dispenses it. If the individual responds that atask is not performed because there is NOT APPLY to do so, BE SURE TO ASK FOR FOLLOWUP INFOR-MATION THAT VERIFIES THE LACK OF ENVIRONMENTAL OPPORTUNITY.
Write comments about the individual's answers or provide information that is important for understandinghis/her environment in the comments lines and/or on the back of this questionnaire.
Individual:
Your name: Date of completion:
653
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
Appearance and Clothing >,
Q.
2 O O
In the last 30 days, did you? > z z1 .* Wash your clothes by hand or machine using the proper
amount of detergent?2.* Dry your clothes in a dryer or on a clothes line?3.* Fold, hang up, and store your clothes after they were
washed and dried?4.* Store your dirty clothes separate from your clean clothes?5.* Change your underwear at least twice a week?6.* Buy your own clothes the last time you needed some?
INTERVIEWER'S OBSERVATIONS7. Clothing appears neat and clean8. Clothing appears appropriate for the time
of year9. Colors and types of clothing appear
appropriately coordinated
Comments:
Personal Hygiene >.a.Q.
8 o oIn the last 30 days, did you? >- z z1 .* Bathe or shower using soap at least
twice a week?2.* Shampoo your hair at least twice a week
(once a week for females)?3.* Use deodorant daily?4.* Brush or comb your hair daily?5.* Brush your teeth (or dentures) using toothpaste
at least once a day?6. Regularly clean your nails? >
INTERVIEWER'S OBSERVATIONS
7. Face, arms, hands, etc. appear clean8. Hair appears clean9. Hair appears neatly combed10. Hair appears neatly cut11. No body odor12. Nails appear clean
Comments:
654
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3,2000
Care of Personal Possessions
In the last 30 days, did you?1 .* Make your bed daily?2* Keep your room clean?3.* Pick up your "clutter" and put back items where
they belong?4.* Wipe up spills on your furniture or carpet
such as coffee?5.* Vacuum (if you have a carpet) or mop your floor?6.* Dust your furniture?
Comments:
(0
Q.<
O O
Food Preparation/Storage
In the last 30 days, did you?1 .* Prepare simple foods such as sandwiches,
cold cereal, etc., that did not require cooking? . . .2.* Prepare foods that required a small amount
of cooking such as fried eggs, TV dinners?3.* Discard spoiled foods?4.* Wash dishes after meals by hand or in a machine?5.* Put away the dishes after they'd dried?6.* Choose mostly nutritional foods to eat; that is,
you didn't live on candy and soda?7.* Buy your own groceries - more than snacks?
Comments:
Q.Q.
<
o o
Health Maintenance
In the last 30 days, did you?1 .* Administer your own medication? (If you are not
prescribed medication, did you administer your ownmedication when you were last taking it?)
2.* If you take medication now but you do not administerit yourself, cooperate with the person who administers the
Q.<
0)
655
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from
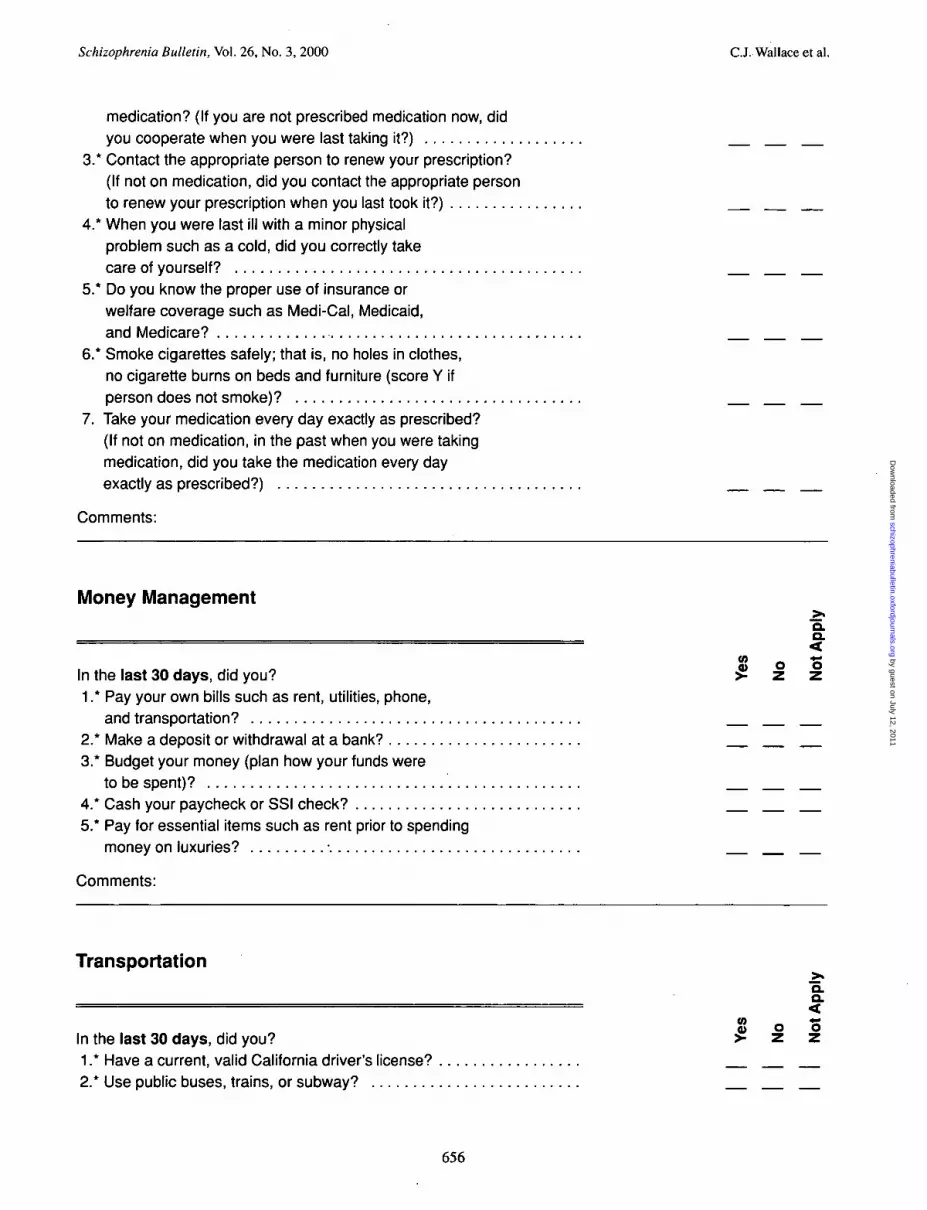
Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
medication? (If you are not prescribed medication now, didyou cooperate when you were last taking it?)
3.* Contact the appropriate person to renew your prescription?(If not on medication, did you contact the appropriate personto renew your prescription when you last took it?)
4.* When you were last ill with a minor physicalproblem such as a cold, did you correctly takecare of yourself?
5.* Do you know the proper use of insurance orwelfare coverage such as Medi-Cal, Medicaid,and Medicare?
6.* Smoke cigarettes safely; that is, no holes in clothes,no cigarette burns on beds and furniture (score Y ifperson does not smoke)?
7. Take your medication every day exactly as prescribed?(If not on medication, in the past when you were takingmedication, did you take the medication every dayexactly as prescribed?)
Comments:
Money ManagementQ.Q.<
W O O
In the last 30 days, did you? £ z z1 .* Pay your own bills such as rent, utilities, phone,
and transportation?2.* Make a deposit or withdrawal at a bank?3.* Budget your money (plan how your funds were
to be spent)?4.* Cash your paycheck or SSI check?5.* Pay for essential items such as rent prior to spending
money on luxuries? \
Comments:
Transportation
Q .
In the last 30 days, did you?1 .* Have a current, valid California driver's license?2* Use public buses, trains, or subway?
656
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

The Independent Living Skills Survey Schizophrenia Bulletin, Vol. 26, No. 3, 2000
3.* When you last went to an unfamiliar place,did you ask others or call public transportationfor directions?
4.* Read a bus schedule the last time youneeded the information?
5. Have and use your own car?
Comments:
Leisure and CommunityQ.Q.<
In the last 30 days, did you?1 .* Have a hobby on which you worked regularly?2.* Attend religious services?3.* Write letters or visit friends/relatives?4.* Attend movies/theater?5.* Read books, newspapers, or magazines? . . . .6.* Attend meetings of civic organizations or
organizations such as VFW?7.* Listen to the radio or watch TV?8.* Work in the garden or yard?9.* Attend a spectator sport?10.* Bowl, play pool, or other sports?11 .* Play cards/table games?12.* Are you currently registered to vote?
Comments:
CO
2
Job SeekingQ.a.<
In the last 30 days, did you?1 .* Read the classified ads one or more times per
week to look for jobs?2.* Contact potential employers to determine
possible job openings?3.* Contact friends and others such as employment
agencies to obtain job leads?4.* Participate in job interviews?
2
657
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from

Schizophrenia Bulletin, Vol. 26, No. 3, 2000 C.J. Wallace et al.
Comments:
Job MaintenanceQ.
a.<
o) - -eOn your current job or when you were last employed, did you? >-1 .* Get along with your coworkers?2.* Get along with your supervisors?3.* Arrive on time for work and follow a daily work
and break schedule?
Comments:
658
by guest on July 12, 2011schizophreniabulletin.oxfordjournals.org
Dow
nloaded from
Copyright © 2022 FDOKUMEN




















