THE HEALTHCARE REFORM IN BULGARIA
377
aNTONIYA DIMOVA mIROSLAV POPOV mARIA rOHOVA THE HEALTHCARE REFORM IN BULGARIA a nNECESSITY a DEVE l OPMENT RESULT y s 2008 I s PERSPECTIVE
Transcript of THE HEALTHCARE REFORM IN BULGARIA
aNTONIYA DIMOVA mIROSLAV POPOV mARIA rOHOVA
THE HEALTHCARE REFORM
IN BULGARIA
anNECESSITY
aDEVE lOPMENT
RESULT
ys
2008
IsPERSPECTIVE
This study was pub lished thanks to the
3
ÑÚÄÚÐÆÀÍÈÅ
LIST OF ABBREVIATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . 6ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8ABOUT THE AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9FOREWORD . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11INTRODUCTIONON THE NECESSITY FOR THIS STUDY . . . . . . . . . . . . . . . . . . . . 15PART ONETHE HEALTHCARE REFORM . . . . . . . . . . . . . . . . . . . . . . . . . 17
1. Con tent, struc ture and def i ni tion of the healthcare re form . . . . . . . . . . 172. Ob ject of the healthcare re form: what is ac tu ally re formed? . . . . . . . . . 19
The healthcare sys tem . . . . . . . . . . . . . . . . . . . . . . . . . . . 20The healthcare pro cess . . . . . . . . . . . . . . . . . . . . . . . . . . . 21Par tic i pants in the re form pro cess . . . . . . . . . . . . . . . . . . . . . 21The con text of the pro cess . . . . . . . . . . . . . . . . . . . . . . . . . 22
3. A study of the healthcare re form: set ting, or gani sa tion and meth ods . . . . . 23Pre vi ous stud ies: char ac ter is tics and re sults . . . . . . . . . . . . . . . . 24Or gani sa tion and struc ture of the study . . . . . . . . . . . . . . . . . . 32
PART IITHE HEALTHCARE REFORM IN BULGARIA . . . . . . . . . . . . . . . . 37
4. In ev i ta ble, nec es sary and ir re vers ible pro cess . . . . . . . . . . . . . . . . 37Why was the healthcare re form nec es sary and why is it still nec es sary? . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37Tasks of the healthcare re form . . . . . . . . . . . . . . . . . . . . . . . 56
5. Stages and evo lu tion of the healthcare re form in Bul garia . . . . . . . . . . 57Cri te ria for as sess ment . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
5.1. First stage: so cial ist pro gram ming and post-so cial ist im ple men ta tion of the re form pro cess. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
Po lit i cal and so cio eco nomic con text . . . . . . . . . . . . . . . . . . . . 58The pro cess of the healthcare re form (1989-1996) . . . . . . . . . . . . . 60Pub lic opin ion of the healthcare re form . . . . . . . . . . . . . . . . . . 68Re sults and un solved prob lems. . . . . . . . . . . . . . . . . . . . . . . 84
5.2. Sec ond stage: de vel op ment of a rad i cal re form of the healthcare sys tem . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 87
Po lit i cal and so cio eco nomic con text . . . . . . . . . . . . . . . . . . . . . . 88Be gin ning of the con struc tion of a new healthcare sys tem
(1997-2001). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89Qual ity im prove ment and quan ti ta tive in di ca tors of the changes in the healthcare sys tem . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96
4
Pub lic opin ion on healthcare re form . . . . . . . . . . . . . . . . . . . 100Cov er age of the healthcare re form in the press in the pe riod be tween 1997 and the first half of 2001 . . . . . . . . . . . . . . . . . 101
Re sults and un solved prob lems . . . . . . . . . . . . . . . . . . . . . . 1345.3. Third stage: de layed and hes i tant de vel op ment of the healthcare re form. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 138
Po lit i cal and so cio eco nomic con text . . . . . . . . . . . . . . . . . . . 138Programmes for the de vel op ment of the healthcare sys tem. . . . . . . . 139De vel op ment of the nor ma tive ba sis of the healthcare sys tem . . . . . . 141Strat egy for hos pi tal care . . . . . . . . . . . . . . . . . . . . . . . . . 143A “mar ket - lib eral” and a “so cial - lib eral” al ter na tive for the de vel op ment of healthcare . . . . . . . . . . . . . . . . . . . . . . . . 144Pub lic opin ion on the re form in healthcare . . . . . . . . . . . . . . . . 147Re sults and un solved prob lems . . . . . . . . . . . . . . . . . . . . . . 193
PART III THE HEALTHCARE REFORM IN BULGARIA 2005:CURRENT STATE . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 200
6. So cio log i cal in ter pre ta tion . . . . . . . . . . . . . . . . . . . . . . . . . 2006.1. As sess ment of med i cal spe cial ists . . . . . . . . . . . . . . . . . . . . 200
Gen eral as sess ment of the healthcare re form . . . . . . . . . . . . . . . 200Eval u a tion of some key pa ram e ters of the re form . . . . . . . . . . . . 203Pros pects for the healthcare re form . . . . . . . . . . . . . . . . . . . . 211
6.2. As sess ment by man age ment sub jects . . . . . . . . . . . . . . . . . . . 217Gen eral as sess ment of the healthcare re form . . . . . . . . . . . . . . . 217As sess ment of di rec tors and man ag ers of multi-pro file hos pi tals for ac tive treat ment (MHAT) . . . . . . . . . . . . . . . . . . . . . . . 219As sess ment of di rec tors of spe cial ised hos pi tals for ac tive treat ment and na tional cen tres. . . . . . . . . . . . . . . . . . . . . . . 233As sess ment by man ag ers of dis pen sa ries . . . . . . . . . . . . . . . . . 243As sess ment of the man ag ers of healthcare es tab lish ments for spe cial ised out pa tients’ care. . . . . . . . . . . . . . . . . . . . . . . . 251As sess ment by di rec tors of RHC, RHIF, RIPCPH . . . . . . . . . . . . 260As sess ment of the rep re sen ta tives of the lo cal au thor i ties . . . . . . . . 275
6.3. As sess ment by cit i zens. . . . . . . . . . . . . . . . . . . . . . . . . . 293Cit i zens’ self-as sess ment of their own health sta tus . . . . . . . . . . . 293Health pro phy laxis and pro mo tion: at ti tude and prac tice . . . . . . . . . 294Hab its and at ti tudes to per sonal health . . . . . . . . . . . . . . . . . . 295Cit i zens’ as sess ment of the qual ity and or gani sa tion of med i cal care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 297Mech a nisms for civil con trol on the qual ity of the
med i cal ser vices . . . . . . . . . . . . . . . . . . . . . . . 306
5
At ti tude and feel ings to the health in sur ance . . . . . . . . . . . . . . . 308The gen eral views of the cit i zen – the con sumer and the pa tient . . . . . 311
7. Pros pects for the de vel op ment of the healthcare re form: au thors’ in ter pre ta tion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3167.1. Er rors at es tab lish ment . . . . . . . . . . . . . . . . . . . . . . . . . . 318
The healthcare re form be gan with out a def i nite plan or per spec tives. . . 318The im ple men ta tion of the healthcare re form was car ried out slowly, hes i tantly and ir reg u larly . . . . . . . . . . . . . . . . . . . . . . . . . 321The com mu ni ca tion with the cit i zens and the pro fes sion als was ne glected re gard ing the ob jec tives, the con tent and the terms of thehealthcare re form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 322The re form leg is la tion did not reg u late clearly the le gal sta tus of thehealthcare sys tem and the re spon si bil i ties in healthcare . . . . . . . . . 323The par tic i pa tion of the cit i zens in the def i ni tion of the goals, pri or i ties and so lu tions in healthcare is one of the un solved prob lems of the healthcare leg is la tion. . . . . . . . . . . . . . . . . . . 326In ad e quate de vel op ment of the con trol func tions in the reg u la tion of the healthcare sys tem. . . . . . . . . . . . . . . . . . . . . . . . . . 327
7.2. The healthcare sys tem “un der the um brella” of the healthcare re form: the di ag no sis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 328
The healthcare sys tem is eco nom i cally un sta ble . . . . . . . . . . . . . 328Le gally de fined rules are ab sent for price for ma tion and re gime of pay ment for healthcare ser vices . . . . . . . . . . . . . . . . . . . . . . 330Moral in sta bil ity of the healthcare sys tem . . . . . . . . . . . . . . . . 331In com plete struc tural re form of the healthcare sys tem . . . . . . . . . . 332The ir reg u lar de vel op ment of the healthcare re form con tin ues . . . . . . 335The in equal i ties are pre served. . . . . . . . . . . . . . . . . . . . . . . 335
7.3. Con tin u a tion of the healthcare re form . . . . . . . . . . . . . . . . . . 337The ap proach . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 338Ur gent mea sures for ef fec tive con trol of cit i zens’ health, re stric tion of the pre vent able mor tal ity and de crease of the in equal i ties in the pop u la tion’s health sta tus . . . . . . . . . . . . . . . 339Liberalisation of the healthcare sys tem . . . . . . . . . . . . . . . . . . 341De cen trali sa tion and deconcentration of the man age ment . . . . . . . . 341Eco nomic sta bil ity of the healthcare sys tem . . . . . . . . . . . . . . . 348Moral sta bil ity of the healthcare sys tem . . . . . . . . . . . . . . . . . 359Bal anc ing of func tions, struc tures and com pe tences in the healthcare sys tem . 362
CONCLUSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371BIBLIOGRAPHY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 373
LIST OF ABBREVIATIONS
BCP Bul gar ian Com mu nist PartyBGN Bul gar ian Na tional Cur rencyBSP Bul gar ian So cial ist PartyCEE Cen tral and East ern Eu ropeCEMC Cen tre for Emer gency Med i cal CareCITUB Con fed er a tion of In de pend ent Trade Un ions in Bul gariaCL Con fed er a tion of La borCVHI Com pany for vol un tary health in sur anceDCC Di ag nos tic and con sul ta tive cen treDH Dis trict hos pi talDRG Di ag nos ti cally re lated groupEC Eu ro pean Com mu nityGDP Gross Do mes tic Prod uctGP Gen eral prac ti tio nerHEI Hy giene and Ep i de mi o log i cal In spec tionICD In ter na tional Clas si fi ca tion of Dis easesIMF In ter na tional Mon e tary FundLCNSP Law on the Con trol of Nar cotic Sub stances and Pre cur sorsLDPHM Law on Drugs and Phar ma cies in Hu man Med i cineLF Law on FoodsLH Law on HealthLHE Law on Healthcare Es tab lish mentsLHI Law on Health In sur anceLHSWC Law on Healthy and Safe Work ing Con di tionsLPH Law on Peo ple’s HealthLPOPD Law on the Pro fes sional Or gani sa tions of Phy si cians and Den tistsMD Med i cal cen treMDL Med ico-di ag nos tic lab o ra toryMH Min is try of HealthcareMHAT Multi-pro file hos pi tal for ac tive treat mentMPH Min is try of Peo ple’s HealthMRF Move ment for Rights and Free domsNA Na tional As sem blyNCHI Na tional Cen tre for Health In for ma tionNCPHP Na tional Cen tre of Pub lic Health Pro tec tionNCRRP Na tional Cen tre for Radiobiology and Ra di a tion Pro tec tionNGO Non-gov ern ment Or gani sa tionNFA Na tional Frame work Agree mentNHA Na tional Health Ac countsNHIF Na tional Health In sur ance FundNII Na tional In sur ance In sti tuteNIS Na tional In sti tute of Sta tis tics
6
NISM Na tional In sti tute of So cial Med i cineNMSS Na tional Move ment Sim eon IIPGDL Par lia men tary Group of the Dem o cratic LeftRHC Re gional Healthcare Cen treRHIF Re gional Health In sur ance FundRIPCPH Re gional In spec tion for Pro tec tion and Con trol of Pub lic HealthSCPRI Sci en tific Chem i cal and Phar ma ceu ti cal Re search In sti tuteSHAT Spe cial ised hos pi tal for ac tive treat mentUBP Un ion of Bul gar ian Phy si ciansUDB Un ion of Den tists in Bul gariaUDF Un ion of the Dem o cratic ForcesUN United Na tionsURH United re gional hos pi talVAT Value Added TaxWB World BankWHO World Health Or gani sa tionWMC Work ers’ and man ag ers’ com pany
7

AC KNOWL EDGE MENTS
The ac com plish ment of the pres ent study and its pub li ca tion were car ried out within apro ject and were pos si ble ow ing to the con tri bu tion of a num ber of peo ple.
First and fore most, the pro ject was ex e cuted thanks to the ac tive sup port of the Open So -ci ety In sti tute Foun da tion. The au thors would like to ex press their warm est thanks to its for -mer Di rec tor Prof. Dr. Raina Gavrilova, when the pro ject was ap proved and ini ti ated, as well as to Mr Georgi Stoichev who was the Di rec tor when the pro ject was final ised. We wish toex press our grat i tude to the Co or di na tor of the “Pub lic Healthcare” Programme Dr. ElenaZlatanova who of fered her in valu able as sis tance through out the pro ject im ple men ta tion andto whom we are deeply in debted. We owe our thanks to Mr Boyan Zahariev and MrsDesislava Sirakova who helped with bring ing the pro ject to its suc cess ful end.
The pro ject im ple men ta tion was sig nif i cantly fa cil i tated by the ac tive in volve ment ofMira Koleva, Petya Ivanova, Nela Slavcheva, Velina Ilieva, Lilyana Vladikova and Liliya Ivanova - six stu dents of healthcare man age ment study ing at Med i cal Uni ver sity “Prof. Dr.Paraskev Stoyanov” – Varna who in vested a lot of work and ef forts in the se lec tion and sys -tem ati sa tion of the me dia pub li ca tions.
For the con duct ing of the highly qual i ta tive so cio log i cal sur vey the au thors are obliged toso cio log i cal agency “Al pha Re search” Ltd., headed by its Di rec tor Mrs Boryana Dimitrova.
A num ber of dif fi cul ties en coun tered dur ing the pro ject im ple men ta tion were over comethanks to the at mo sphere of re spon sive ness and fel low ship ex ist ing among the col lab o ra tors atthe De part ment of Health Eco nom ics and Man age ment at Varna Med i cal Uni ver sity, headedby Assoc. Prof. Dr. Emanuela Mutafova.
The au thors are grate ful to the re view ers of the study Assoc. Prof. Dr. Nikola Vassilev,Assoc. Prof. Dr. Emanuela Mutafova and Dr. Ivo Voichev for their pro found un der stand ing and fair eval u a tion.
Antoniya Dimova Miroslav Popov Maria Rohova

ABOUT THE AU THORS
Prof. Dr. Miroslav Popov, PhD worked suc ces sively in Ihtiman, the De part ment of So cial Med i cine at the Med i cal fac ulty in So fia, the Na tional Cen tre of Hy giene, the Na tional In sti tuteof So cial Med i cine and the Na tional Cen tre of Pub lic Health. Vice Min is ter of healthcare in thepe riod 1990-1991. A found ing fa ther of the Na tional Acad emy of Med i cine (1996).
Prof. Dr. Miroslav Popov, PhD is a guest lec turer at the Uni ver sity of Na tional and WorldEcon omy, Med i cal Uni ver sity “Prof. Dr. Paraskev Stoyanov” – Varna and Acad emy of Eco -nom ics “D. A. Tsenov” – Svishtov. Au thor of nu mer ous stud ies and pub li ca tions in health pol -icy, health sys tems and man age ment of healthcare: “The Health Re form in Bul garia” – Parts 1and 2 (1997, 1998); “Hos pi tal man age ment” (1998); “Foun da tions of hos pi tal man age ment”(1999); “The hu man ised hos pi tal” (2000); “Hos pi tal man age ment” (2000) and the text books:“In tro duc tion to med i cine” (1973, 2006); “Or gani sa tion of healthcare” (1976, 2003); “So cialmed i cine” (2003); “Or gani sa tion and man age ment of health in sur ance funds” (2005), etc.
Prof. Popov has par tic i pated in many work ing groups of the Min is try of healthcare re gard -ing the prep a ra tion of le gal and nor ma tive acts and for the so lu tion of or ga ni za tional prob lems.
Maria Rohova grad u ated the spe cialty “Mar ket ing and man age ment” in 1999 and in2001 the Mas ter’s programme in busi ness man age ment at the Eco nom ics Uni ver sity in Varna.She has a re cog nised spe cialty in med i cal in for ma tics and healthcare man age ment. Since 2002she has worked as an as sis tant pro fes sor at the De part ment of Health Eco nom ics and Man age -ment at Med i cal Uni ver sity “Prof. Dr. Paraskev Stoyanov” – Varna and since 2005 she hasbeen a se nior as sis tant pro fes sor at the same de part ment. She re ceived train ing in the field ofhealthcare man age ment in Swit zer land, the Neth er lands and Bul garia. Lec turer in a manycourses for top hos pi tal man age ment staff and ac cred i ta tion of healthcare es tab lish ments. Au -thor of sci en tific pub li ca tions in the field of mar ket ing and man age ment of healthcare es tab -lish ments and co-au thor of the man ual “Hos pi tal man age ment” ed ited by L. Ivanov and Zh.Golemanova, Na tional Cen tre of Pub lic Health, 2005.
Antonia Dimova works as a se nior as sis tant pro fes sor at the De part ment of Health Eco -nom ics and Man age ment at Med i cal Uni ver sity “Prof. Dr. Paraskev Stoyanov” – Varna. In2000 – 2004 she re ceived train ing in the field of healthcare man age ment in Spain, Swit zer land, the Neth er lands and Bul garia. She has par tic i pated in a num ber of sci en tific sem i nars and con -fer ences in Bul garia and abroad. In the pe riod 2006-2007 she spe cial ised at Georgetown Uni -ver sity in Wash ing ton, DC, USA. She has a re cog nised spe cialty in med i cal in for ma tics andhealthcare man age ment. So far she has over 20 sci en tific pub li ca tions. Au thor of the mono -graph “Qual ity man age ment in the hos pi tal” (pub lished by “STENO” Pub lish ing house,Varna, 2004) and co-au thor of the mono graph “Hos pi tal man age ment” (pub lished by “St.Kliment Ohridski”, So fia, 2004) with Prof. Dr. Miroslav Popov, PhD, in the text book ofAssoc. Prof. Ivanka Chobanyaneva, PhD “Qual ity man age ment in healthcare” (Med i cal Uni -ver sity, Varna, 2004) and in the man ual “Hos pi tal man age ment” ed ited by L. Ivanov and Zh.Golemanova, Na tional Cen tre of Pub lic Health, 2005. Mas ter in healthcare man age ment since1998. Doc tor of med i cal sci ence since 2005.
9

10
FORE WORD
Our en coun ter with the phe nom e non of the “healthcare re form” was ini tially driven byour cu ri os ity aris ing from the nu mer ous (some times rather straight for ward) state ments gen er -ally fo cused around two al ter na tive ap proaches, e.g. “we need a re form” or “we don’t need are form” vs. “there is no re form”. Fur ther more, eval u a tions are given with out ap ply ing anycri te ria or us ing any pos i tive or neg a tive ob jec tive re sults. As al most all Bul gar ian cit i zens, wewere aware of the fact that a con sid er able change had oc curred in the cu ra tive care and its fi -nanc ing in our coun try. Pub li ca tions (ar ti cles, mono graphs, etc.) in the lit er a ture ap peared (ar -ti cles, mono graphs) and were widely avail able about re forms in the healthcare sys tems indif fer ent coun tries.
Nu mer ous pub li ca tions in Bul garia in the pe ri od i cals as well as in in for mal con ver sa tionsin di cated the cit i zens’ and healthcare pro fes sion als’ dis sat is fac tion with the changes whichhad oc curred. Slight sar casm could be per ceived in the very ex pres sion “healthcare re form”.And then the ques tion arose “Why”. Our coun try had a healthcare sys tem with suf fi cient innum ber and, ac cord ing to many, well-trained per son nel. This ques tion trig gered a whole chainof sub se quent ques tions. Thus, the ini tial cu ri os ity grew into sci en tific in ter est.
We looked for col lab o ra tion and we found it from the Open So ci ety In sti tute which sup -ported the pro posal for the pro ject. The out come of its ac com plish ment is now avail able for the in ter ested read ers.
As al ready men tioned, for the last two de cades re forms have been car ried out in thehealthcare sys tem in many coun tries. The ma te ri als, with which we ac quainted our selves, out -line sev eral com mon char ac ter is tics, which are of in ter est for a com par a tive anal y sis be -tween our coun try and the “other” coun tries.
The healthcare re form should be con ceived not only met a phor i cally but also lit er ally asan in stru ment for the so lu tion of spe cific prob lems and the achieve ment of spe cific ob jec -tives. Such an un der stand ing de ter mines that the on go ing changes will de pend heavily on thequal ity and the va lid ity of the in stru ment as well as on the skilfulness of the hand ap ply ing it.An in valid in stru ment or an un skil ful hand can re sult in se vere fail ure.
A healthcare re form is most use ful when it is pro-ac tive. It needs to have a pre ven tiverole against a cri sis which is likely to oc cur, if the re form is not car ried out. This is why themon i tor ing of the pro cesses in healthcare is nec es sary to gether with the mon i tor ing of its ef fi -ciency, cri te ria for these pro cesses eval u a tion and will (po lit i cal will is de sir able) to pre ventthe cri sis by means of a timely re form of the sys tem.
The main out come of the healthcare re form which is most dif fi cult to at tain is change inthe per son al ity – the cit i zens and the pro fes sion als, of the val ues and the pri or i ties with theirhi er ar chy in the in di vid u als’ and the so cial com mu ni ties’ value sys tem.
These char ac ter is tics come to prove that ev ery healthcare re form is a dif fi cult un der tak ingand re quires more or less but nec es sar ily lon ger pe riod of time. It has to be planned for at least10 – 15 years ahead dur ing which a se ries of con sis tent re form ac tiv i ties should be car ried out. Itis par tic u larly im por tant to take into con sid er ation the bot tle necks and the ob jec tive need for alon ger pe riod of time to im ple ment such a rad i cal re form as is the Bul gar ian healthcare re form.
The study of the healthcare re form, pre sented on the fol low ing pages in a rel a tively de -tailed and, to our mind, multi-as pect way, was car ried out for the first time in our coun try andsim i lar stud ies are sel dom con ducted in other coun tries, too. This is the rea son why we con -
11
sider that the job we did would be of in ter est also to pro fes sion als from other coun tries. We at tempted at pre sent ing an anal y sis which is use ful for ev ery day prac tice. There fore,
we tried to make it ob jec tive and we had to pro cess, sys tema tise, se lect and ana lyse a rather vo -lu mi nous ma te rial from var i ous and nu mer ous sources.
Our study showed that dur ing the last sev en teen years - since 1990s till the pres ent day –the healthcare re form in Bul garia has gone through a con tin u ous and com pli cated course in flu -enced by a num ber of in ter nal and ex ter nal fac tors.
On the one hand, a se ries of pos i tive changes have taken place in the healthcare sys tem.Al though not equally pos i tive in all sec tors, the foun da tions were laid down for the es tab lish -ment of a prin ci pally new healthcare sys tem. In its course, how ever, the healthcare re form hascon sumed a lot of time, sig nif i cant ef forts and re sources. They are not jus ti fied from the pointof view of the achieved re sults. In deed, the road of the healthcare re form has been paved with“good in ten tions”. But even good, be cause of their in com plete or par tial ful fil ment, for the cit i -zens and the pro fes sion als, they still re main mere in ten tions. Once ini ti ated, the healthcare re -form in Bul garia re mains un com pleted.
On the other hand, it can be nei ther stopped nor aban doned. The healthcare re form must be car ried on. In this light, Pres i dent Georgi Parvanov made his state ment in front of the Na -tional As sem bly on Jan u ary 21st 2005, when he de clared: “At the mo ment the healthcare re -form re mains to be prob lem num ber one for our state and so ci ety. Rashly and pal lia tiveat tempts at changes in the health leg is la tion have been ac cu mu lat ing, the ad min is tra tive ar bi -trary de ci sions caus ing the cit i zens to suf fer have not been put an end to”. The State Headpointed out that the prob lem needed im me di ate so lu tion. And this can be achieved in no otherway but through the prop a ga tion of the healthcare re form.
The above state ment of facts has been con firmed by the pres ent study. One of the main di -sas ters is the lack of a con sen sus and sta ble pol icy of healthcare re form. For the un fold ing ofthe en tire healthcare re form, dur ing the re cent years, there has been no con ti nu ity what so everre gard ing the re form be tween the chang ing gov ern ments, apart from the over lap ping of the“good in ten tions”. Fol low ing the rad i cal changes, the pal lia tive changes un der taken inhealthcare were re lated to cer tain un de sired con se quences but they did not af fect their causes.Be sides, the in ef fec tive in ter fer ence of the state brought about an un der de vel oped and, there -fore, ir rel e vant mar ket reg u la tion. In such an en vi ron ment the en demic man i fes ta tions of cor -rup tion in the sys tem of healthcare are not rare. The eco nomic re form of the healthcare isun der stood and con ducted as “pour ing” of more and more money into the sys tem but not as ameans of its re struc tur ing. Costs of the healthcare es tab lish ments in the sys tem are much morefre quently dis cussed than im prov ing their pro duc tiv ity. In many re spects, be hav ioural rulesare ab sent in the sys tem, for its parts or in di vid ual par tic i pants. Some times rules ex ist but thereare no le gal nor ma tive mech a nisms for their ful fil ment. This is why in com pe tent and hasty ad -min is tra tive de ci sions cre ate an ad di tional bur den for the lives of thou sands of citizens.
From all the above, it be comes ev i dent that the con tin u a tion of the healthcare re form inour coun try is likely to re quire in vest ing more ef forts than in vested un til now. In our opin ion,such ef forts would be more ef fec tive, if di rected to ward the im ple men ta tion of a sta ble and sus -tain able ev i dence-based state health pol icy in stead of re sult ing from frag men tary spec u la -tions. This pol icy should find an ex pres sion in the de vel op ment and ren o va tion or the cre ationof the nec es sary new leg is la tion. With out a sol idly founded pol icy and the cor re spond ing leg -is la tion it would be im pos si ble for the healthcare re form to at tain its ma jor goal, e.g. the Bul -
gar ian cit i zens’ health com pa ra ble to that of the cit i zens in the coun tries of West ern Eu rope.The leg is la tion should also guar an tee its im ple men ta tion. It should en vis age the risk man -age ment of health and the de vel op ment of the healthcare sys tem. Se ri ous at ten tion should bepaid to the dif fer ence in the healthcare pro cess and the healthcare re form de pend ing on the size and the char ac ter is tics of the pop u lated re gion. Our hope is that the pres ent study will fa cil i tatethe for ma tion of such a policy.
We would like to ex plic itly un der line that our anal y sis is a study. In no way should it beun der stood and can not be con ceived as some kind of an al ter na tive “health strat egy”. A pe cu -liar fea ture of the study is that we took the lib erty to ex am ine and ana lyse in greater de tail thepub li ca tions from the cen tral pe ri od i cals con cern ing the healthcare re form as well as to lit er -ally quote the views from the so cio log i cal sur vey. These ma te ri als con tain di verse and veryuse ful in for ma tion and sug ges tions for so lu tions. We, there fore, reckon that they might behelp ful. In a num ber of cases our in ter pre ta tion of the cited facts and data is very brief. Theseare ma te ri als which give food for thought and ad di tional in ter pre ta tion for the reader, apartfrom the one we are of fer ing. The reader will also en coun ter cer tain rep e ti tions in the text.Some of them were in ev i ta ble since some of the facts were ex am ined in a dif fer ent con text. Inthese cases we sac ri ficed the good style in fa vour of clar ity. In other cases the rep e ti tions werede lib er ately in tended since we at trib uted greater im por tance to some points.
The view points we are ar gu ing for in the last chap ter are mainly ideas and pos si bil i tiesrather than di rect sug ges tions for cer tain de ci sions.
13 July 2006 The au thors
13

14

IN TRO DUC TIONON THE NE CES SITY FOR THIS STUDY
This study pres ents an at tempt to look for an swers to a num ber of ques tions en su ingfrom and re lated to the healthcare re form in our coun try. These ques tions are fre quently askeddur ing the daily life of cit i zens, pro fes sion als and in the me dia. They range from ir rel e vantques tions such as: “Is there such a thing as a healthcare re form at all?” (It is ir rel e vant be causethe fact that such a ques tion is ac tu ally asked ob vi ously in di cates that some thing like ahealthcare re form ex ists) and “Has the healthcare re form failed in our coun try?” to ques tionscon cern ing the hos pi tal debts, the pay ment of drugs and the lack of spe cific med i ca tions, in -clud ing life-sav ing drugs.
The talk about the re form in the healthcare sys tem in Bul garia be gan more than sev en teenyears ago, and, ap prox i mately at that time, the first (timid though) ac tions com menced in thatdi rec tion. The du ra tion of the pe riod of time, which has elapsed since then, gives us groundsfor ana lys ing the idea be hind it to gether with the ob jec tives, strat egy and ap proaches, ac tiv i ties car ried out, the uti lised re sources and the achieved out come. Fur ther more, there are othermore spe cific rea sons which not only jus tify but im per a tively re quire an anal y sis of the con -tent in this re spect.
One of the above rea sons is that the re form of a healthcare sys tem has an im me di atebear ing on the so lu tion of the health prob lems of a na tion. Now a days, these prob lems standout in their ex tremely sig nif i cant eco nomic, so cial, po lit i cal, moral and eth i cal value con text.
It be comes clearer and clearer, though not nec es sar ily well-real ised, that the health sta tus ofa na tion is de ter mined not only by the fac tors in the re spec tive con text, but it also ex erts a pow er -ful in flu ence upon them. The health level de ter mines a num ber of pro cesses in the econ omy (forex am ple, the qual ity of the hu man re sources and the pro duc tiv ity of the work ing force), in the so -cial field (in come, struc ture of house hold ex pen di ture, all kinds of so cial ben e fits, so cial in sti tu -tion costs – but not only this), in the po lit i cal field (level of so cial co he sion), in the dif fer entas pects of hu man re la tion ships, moral norms and value sys tems. When a so ci ety is in a cri sis andit is said to be “sick”, this can be un der stood lit er ally, too. In all cases, a cri sis wors ens the na -tion’s health and de te ri o rated health sup ports and re in forces the fac tors caus ing the cri sis.Thus, health it self be comes not only an out come of but also a fac tor for the cri sis.
The healthcare re form is a means for a more ef fec tive so lu tion of the prob lems and the im -prove ment of a na tion’s health with all the other pos i tive con se quences which are to be ex -pected. There fore, the anal y sis of the on go ing healthcare re form, its course, stages and ac tualre sults is an un dis puted ne ces sity.
An other rea son, fol low ing from the first one, is that the healthcare re form is re lated tocon sid er able costs. The healthcare sys tem it self is a costly sys tem, whose main te nance andvis i ble func tion ing re quires the uti li sa tion of cer tain re sources. There fore, ev ery small change,let alone a whole re form, can not be car ried out (as it is of ten thought) just with “means athand”. It is very dif fi cult (maybe im pos si ble) to de ter mine the costs from the state bud get al -lo cated to the healthcare re form in our coun try. The data are com par a tively more pre cise con -cern ing the ex pen di ture made by for eign sources. Be tween 1992 and 1997 Bul garia re ceived25 mil lion US dol lars from the Eu ro pean Com mu nity (EC) for the re form in emer gency and ur -gent med i cal care, the re con struc tion of the phar ma ceu ti cal sec tor, the or gani sa tion of 30 in for -ma tion cen tres to the Un ion of Bul gar ian Phy si cians and for the train ing of lead ing spe cial ists
15
and gen eral prac ti tio ners. Dur ing this pe riod, sup port was also ob tained on an an nual ba sisfrom the World Health Or gani sa tion amount ing to 50 000 USD. Af ter 1997 the World Bankmade two bank trans fers of 26 mil lion USD and 63.5 mil lion USD re spec tively, along witharound 30 mil lion USD from the gov ern ments of Ja pan, Spain, Swit zer land, Ger many, USA,EC and some UN or ga ni za tions1. Part of this sup port came as loans which, if not re mit ted, must be paid off. It can be def i nitely as sumed that the costs, even at the ac count of for eign sources,were quite sub stan tial. There fore, we thought it ap pro pri ate, by means of an anal y sis, to de ter -mine what the out comes are in most gen eral terms. Thus, we would get an idea, ap prox i matethough, about how much a healthcare re form costs.
Thirdly, the stud ies on the healthcare re form in our coun try are scarce. The crit i cal anal y -ses are few as to the course and the im ple men ta tion of the healthcare re form, the con cept def i -ni tion is ab sent, and the cri te ria for the eval u a tion of the re form pro cess are not for mu lated.This is why, in a num ber of state ments and pub li ca tions, the re form is mis con ceived as a sin gleact which is to be car ried out on a large scale for a pe riod even shorter than a reg u lar par lia men -tary man date. This is prob a bly the most likely rea son that in state ments and pub li ca tions wecome across one-sided, self-righ teous and ground less but de fin i tive state ments about the pro -cess and the out comes of the healthcare re form. There fore, we con sider it nec es sary, at least for the sake of the dis cus sion, to ob jec tively ana lyse, pro vide ar gu ments and pres ent the over allpro cess of the healthcare re form; its cause and ef fect re la tion ships with var i ous fac tors, thepos si ble de vi a tions from the ini tial con cept and the rea sons for them; the changes which haveoc curred in the healthcare re form and their out comes. Such an ap proach will cre ate a goodfoundation for the planning of the future development of the healthcare system in Bulgaria.
16
1 Prohaska, M., D. Iliev, D. Sacheva, M. Varshilova, L. Doudeva. Health Re form in Bul garia: A Glance atDe cen tral iza tion and Lo cal Gov er nance. In: Shakarishvili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y sesand Ex pe ri ences in Cen tral and East ern Eu rope in the 1990s. Open So ci ety In sti tute, Bu da pest, 2005, p. 65
PART ONETHE HEALTHCARE RE FORM
Be fore tack ling the es sence and the out comes of the pres ent study, in our view, it is nec es -sary to for mu late the mean ing and the con tent of the con cept of a “healthcare re form”. Weneed to do it, be cause in the var i ous pub li ca tions, stated opin ions and even of fi cial ma te ri als,dif fer ent mean ings are at trib uted to this con cept. This se man tic vari ance of ten leads to cit i -zens’ con fu sion and fruit less con tra dic tions.
1. Con tent, struc ture and def i ni tion of the healthcare re form
In the dic tio nar ies for the for eign words in Bul gar ian lan guage, the word “re form” is de -fined as “re struc tur ing, in no va tion, al ter ation, change”. In this broad spec trum of mean ings,which is quite ac cept able in ev ery day speech, the term “re form” ac quires rather vague di men -sions and raises more or less ques tions. Is ev ery change or in no va tion a re form? Is an amend -ment in tax a tion a re form? Is the elec tion of a new ex ec u tive board of a healthcareestablishment a re form? The an swers to these and other sim i lar ques tions may be both pos i tiveand neg a tive, but ei ther way, equally right or wrong since they will de pend solely on the pointof view ex pressed by the per son us ing them. In or der to avoid such am bi gu ities, from the verybe gin ning we will have to adopt and work with one def i ni tion of the term “healthcare re form”un dis pu ta ble to a sig nif i cant de gree.
As a most ac cept able def i ni tion of the term “healthcare re form” we adopt the one givenby L. Brown (1984), ac cord ing to whom the healthcare re form in volves “ac tiv i ties chang ingthe health pol icy and in sti tu tions”. To a great ex tent, this def i ni tion is sim i lar to that given by A. Cassels (1995), ac cord ing to whom the healthcare re form in cludes the def i ni tion of pri or i -ties, a better pol icy and re form ing of the in sti tu tions in volved in the pol icy im ple men ta -tion. To a large de gree, these two def i ni tions nar row down the se man tic field of the“healthcare re form,” and out line its more con crete con tent. It does not in clude any change, al -ter ation or in no va tion. Change and al ter ation are terms with broader mean ing in which “re -form” is in cluded. Ev ery re form is a change or al ter ation of some thing, but not ev ery change is a re form. Start ing from these as sump tions, we deem that for the im ple men ta tion of ahealthcare re form, it is nec es sary to have a change in pol icy and change in the in sti tu tions.Hav ing ex am ined the over all pro cess of the re forms un fold ing, C. Bellingham (2001) findsthat the im ple men ta tion of a re form re quires a pre lim i nary def i ni tion of the goals to beachieved by a se ries of global changes. By the way, P. Berman (1995) also at trib utes an ut mostim por tance to the health pol icy goals by add ing that the re form is not a sin gle and si mul ta -neous event but cov ers a num ber of long-term con sis tent changes. J. E. Aswal (1997) alsopoints out the fun da men tal na ture of the re form pro cess, and he be lieves that it should in cludeboth changes in the nor ma tive sys tem and eco nomic and or gani sa tional el e ments.
In this re spect, O. Ad ams (2000) pro poses an even more con crete un der stand ing of thehealthcare re form, shared by us, too. In his view, the model of the healthcare re form pos sessescer tain pa ram e ters and char ac ter is tics, e.g.
· change in the pri or i ties and the pol icy;
· change in the fi nan cial mech a nisms;
17
Con tent, struc ture and def i ni tion of the healthcare re form
· de vel op ment of pack ages with ba sic ser vices;
· re or gani sa tion and/or privatisation of the ser vices;
· im ple men ta tion of sup ple men tary programmes and their man age ment;
· par tic i pa tion of pro fes sion als;
· op po si tion of the in volved groups.
It is ob vi ous that the healthcare re form is con ceived as a de vel op ment of a dem o cratictrend (par tic i pa tion of pro fes sion als in the re form im ple men ta tion, op po si tion of the in volvedgroups) re flect ing the change in the health pol icy and the de vel op ment of new struc tural el -e ments and new eco nomic re la tions (re or gani sa tion of the ser vices, privatisation). The sameau thor sin gles out sev eral sep a rate com po nents of the healthcare re form, thus throw ing ad -di tional light on its con tent:
· de cen trali sa tion and im prove ment of the re gional struc tures;
· im prove ment of the func tion ing of the ad min is tra tive in sti tu tions;
· ex ten sion of the fi nan cial sources and op por tu ni ties;
· ex pan sion of the role of the pri vate sec tor;
· im prove ment of the healthcare ser vices through the cre ation of new job pro files; in tro -duc tion of new pay ment schemes; staff re duc tion;
· in tro duc tion of man age ment com pe ti tion.
In the same di rec tion to ward dem o cratic de vel op ment and sig nif i cant struc tural changes, R. B. Soltman and J. Figueras (1997) point out that the na tional pe cu liar i ties in the dif fer ent coun -tries should not be ig nored by the re forms in the healthcare sys tem, and the re forms them selvesshould be car ried out by means of the nec es sary va ri ety of mea sures. As key el e ments for thehealthcare re form, the au thors high light char ac ter is tics which are re lated not so much to the con -tent but to the ap proach in the plan ning and im ple men ta tion of the healthcare re form:
· changes in the goals of the healthcare sys tem fol lowed by struc tural changes;
· pur pose ful and not cha otic changes;
· sus tain able and long-term changes and not sin gle and short-term acts;
· struc tural rather than in ter nal or evo lu tion ary changes;
· cov er age of the na tional, re gional and lo cal lev els of change.
The views of the sep a rate au thors ex am ined above, mainly from re cent years, dem on -strate prom i nent over lap ping and sim i lar ity. This proves that one un der stand ing – whichcould be viewed as con ven tional – about the healthcare re form as a rel a tively last ing, mul ti -fac eted pro cess of health pol icy, eco nomic, or gani sa tional and struc tural changes, af fect -ing in depth the en tire healthcare sys tem, is formed. The quoted el e ments and stra te gicap proaches to the re form out line the broad but con crete di men sions of its im ple men ta tion.
In or der to close the cir cle de lin eat ing the field of the healthcare re form, we deem it ap -pro pri ate to add one more seg ment to it, con tain ing, in our views, an es sen tial char ac ter is tic ofthe re form.
This char ac ter is tic arises from the very na ture of the healthcare sys tem, as well as, of ev -ery hu man or gani sa tion. It is found in the fact that ev ery such or gani sa tion has a def i nite andnat u ral de vel op ment cy cle. It shows both ge netic de fects (coded in the very de sign or con -
18
struc tion of the or gani sa tion) and de fects of growth, de fects re sult ing from hy per tro phy or at -ro phy, to tal or par tial hypofunction or dys func tion, age ing and prob a bly se nile marasmus2.
The above de fects al ways pres ent a man i fes ta tion of a cer tain pro cess, in most cases,patho log i cal, which de vel ops at a dif fer ent rate, and some times leads to an ad verse cri sis in the or gani sa tion, which is dif fi cult to over come. This may also be due to fac tors of the ex ter nal en -vi ron ment, but it in ad ver tently de vel ops in the in ter nal or gani sa tional en vi ron ment. No or -gani sa tion is im mu nised against such pro cesses. Be cause of their reg u lar ity, ev eryor gani sa tion needs reg u lar or gani sa tional di ag nos tics in or der to es tab lish and elim i nate pos si -ble de fects and in or der to pre vent their de vel op ment and wors en ing. This is achieved by moreor less sig nif i cant changes in the sta tus, struc tures and func tions of the or gani sa tion, i.e.by means of some kind of ther a peu tic (in clud ing sur gi cal) change. When the changes are notre lated to or do not re quire changes in the pol icy or the nor ma tive ba sis of the or gani sa tion, thechange can be des ig nated as re or gani sa tion. If, how ever, these changes have a se ri ous po lit i -cal and in no va tive nor ma tive con text, they will pres ent a re form for the or gani sa tion.
This short com ment in di cates that the re form is in her ent for ev ery or gani sa tion, that itis not only ob jec tively pre de ter mined at the es tab lish ment of the or gani sa tion, but it is also an un dis puted ne ces sity dur ing its de vel op ment. It pro tects the or gani sa tion from ex treme de -struc tive changes and a fa tal end. The re form is aimed at de fend ing the or gani sa tion, en sur ingits “heal ing” and guar an tee ing the at tain ment of its mis sion and its own de vel op ment for a cer -tain pe riod of time. It is ex actly the in ev i ta bil ity and the need for re forms that we reckonoblig a tory ad di tions to the def i ni tion of the healthcare re form.
Such a view, how ever, re quires the ex pan sion of the cat a logue with the stra te gic ap -proaches to the healthcare re form. Based on good or gani sa tional di ag nos tics, the re form of the healthcare sys tem has to an tic i pate the emerg ing of a cri sis in the or gani sa tion. A cri sis in anyor gani sa tion af fects the fates of many peo ple, and a cri sis in the healthcare sys tem may be fa talfor thou sands of cit i zens ex pect ing help from it. There fore, for the healthcare re form, theadopted ap proach is re quired to be that of an tic i pat ing the cri sis and not over com ing it.
Based on the above pre sented and com mented views, here af ter by the term “healthcarere form” we will mean a pro cess, in which changes in the health pol icy and the healthcarenor ma tive ba sis are car ried out si mul ta neously or con sec u tively to gether with changes in the eco nomic re la tions, the in sti tu tions, the or gani sa tional and struc tural de sign of thehealthcare sys tem, dur ing which it makes a tran si tion to a qual i ta tively new state. Thispro cess is sa lient to the de vel op ment of ev ery healthcare sys tem, its goal be ing to im prove the at tain ment of its mis sion and its ef fi ciency for the cit i zens and the en tire so ci ety.
2. Ob ject of the healthcare re form: what is ac tu ally re formed?
Al though it might seem triv ial, this ques tion needs to be an swered. In gen eral, a re formmeans change and tran si tion of an ob ject from one qual i ta tive state to an other. The changemay also have quan ti ta tive di men sions but it im plies the ac qui si tion of a new qual ity of the ob -ject. There is no doubt that the pre req ui site for the es tab lish ment of the pres ence and the de greeof the change is the iden ti fi ca tion of the ob ject it self and its ac tual sta tus. A great part of the se -verely con tra dic tory opin ions about the healthcare re form in Bul garia are likely to be due to the
19
Ob ject of the healthcare re form: what is ac tu ally re formed?
2 Se nile marasmus (Latin) – se vere wast ing and ex haus tion in el derly peo ple

fact that the very ob ject of the re form has not been de ter mined or has not been taken into ac -count.
One true but prim i tive an swer to this ques tion is that what is be ing re formed ishealthcare. With out en ter ing into de tails, we have to bear in mind that healthcare is in fact apro cess aimed at re cov er ing, pro tect ing and im prov ing the health of the pop u la tion. This pro -cess is car ried out through the ac tiv i ties of a def i nite num ber of var i ous – med i cal andnonmedical – struc tural units united for its im ple men ta tion and form ing the healthcare sys -tem. This pro cess rep re sents the in ter ac tion of the prod ucts of this healthcare sys tem with thecon sum ers (cit i zens, pa tients, in sti tu tions). It is ex actly this in ter ac tion, de ter mined by the de -mand and sup ply of healthcare ser vices, which is the driv ing force of the pro cess.
The healthcare sys tem, like the healthcare pro cess, how ever, is not en cap su lated or closed within it self. Its dy nam ics de vel ops in a def i nite con text un der spe cific con di tions. At the same time, the pro cess of a re form in volves not only the above men tioned anon y mous com po nents(the healthcare sys tem, the healthcare pro cess and the con text) but also some rel a tively per son -i fied (at least as groups) par tic i pants – cit i zens and med i cal pro fes sion als, po lit i cal elites andstake holders.
There fore, re form ing the healthcare means re form ing the sys tem of healthcare and thehealthcare pro cess, bear ing in mind the con text of the re form and the role of the par tic i pants init.
The healthcare sys tem
Fol low ing a widely ac cepted un der stand ing, re flected in the Law on Health (Art. 4), thehealthcare sys tem (or “the na tional sys tem of healthcare” as it is called in the Law on Health)has to be con ceived as a com plex com po si tion con sist ing of three main com po nents: healthin sti tu tions, part ners in the sys tem and or gans for co or di na tion and con trol.
The health in sti tu tions in their turn form three sec tors: es tab lish ments for pub lichealthcare, healthcare es tab lish ments and es tab lish ments for drug sup ply. The core of the pub lichealthcare es tab lish ments is formed by the Re gional In spec tions for Pro tec tion and Con trol ofPub lic Health (RIPCPH). The healthcare es tab lish ments (ac cord ing to the Law on HealthcareEs tab lish ments) in clude healthcare es tab lish ments for out pa tients’ care (pri mary and spe cial -ised), healthcare es tab lish ments for hos pi tal care (multi-pro file and spe cial ised, for ac tive treat -ment and fol low-up treat ment, con tin u ous treat ment and re ha bil i ta tion) as well as dis pen sa ries,cen tres for emer gency med i cal care, cen tres for trans fu sion haema tol ogy, di al y sis, tis sue banks,homes for med i cal and so cial care and hos pices. The es tab lish ments for drug sup ply (ac cord -ing to the Law on Drugs and Phar ma cies in Hu man Med i cine) in clude the phar ma cies and thedrug stores as well as the ware houses, de pots and dis tri bu tion or gani sa tions.
The part ners in the sys tem (“in”, and not “of” the sys tem!) are the state, mu nic i pal andpub lic au thor i ties and in sti tu tions for the man age ment of the ac tiv i ties for health pro tec tionand im prove ment (Law on Health, Art. 4). A num ber of or gans and or gani sa tions are in cludedhere, among which the state in sti tu tions with their own health ser vices re quire spe cial at ten tion to gether with those, whose ac tiv i ties pos sess con sid er able health as pects as well as the pro fes -sional or gani sa tions and trade un ions, pa tients’ and pub lic or gani sa tions, the me dia. The part -ners’ scope is rather wide, but it should al ways be taken into ac count as a com po nent of thehealthcare sys tem and a par tic i pant in the healthcare pro cess.
20

The au thor i ties for co or di na tion and con trol of the healthcare sys tem are those whoman age the healthcare in sti tu tions and the part ners in the sys tem. These or gans and their com -pe tences are not well de fined in our coun try. In the Law on Health (Art. 5) it is stip u lated that“the Min is ter of healthcare man ages the na tional sys tem of healthcare…” but the mech a nism,by which he/she will co or di nate the ac tiv i ties of the nu mer ous par tic i pants, es pe cially of thepart ners in the sys tem, is not spec i fied. The func tions of the Su preme Med i cal Coun cil, men -tioned in the Law (Art. 6) are not clar i fied ei ther. And, as the ex pe ri ence in a num ber of coun -tries in Cen tral and East ern Eu rope in di cates, the au thor i ties for co or di na tion and con trol of the healthcare sys tem (es pe cially the cen tral ones) play a key role for its re form ing (R. B. Sàltman, J. Figueras, 1997).
The healthcare pro cess
As any other sys tem, the healthcare sys tem has an “in put,” “pro cess,” “out put” and“feed back”. The in put is formed by the in com ing re sources in the sys tem (in clud ing per son -nel, power and in for ma tion re sources). The pro cess is the healthcare it self (e.g. “thehealthcare process”). All the three types of the healthcare sys tem com po nents take part in it,along with the in ter ac tion of the con sum ers (cit i zens, pa tients, in sti tu tions) with its ac tiv i ties,i.e. the prod ucts pro duced by it. Dur ing the pro cess the re sources are pro cessed, re formed anduti lised. The out put in cludes the pro duced prod uct (healthcare ser vices) and the re sult ob -tained (change in the health sta tus or the qual ity of life). The feed back cre ates pos si bil i ties forcom par i son of the in put with the out put and en ables the au thor i ties for co or di na tion and con -trol to reg u late the pro cess through in flu enc ing the in put. For the ef fec tive func tion ing of thesys tem, all its sys tem com po nents are es sen tial. The lead ing part, how ever, is played by thesys tem in put. The in flu ence on the in put de ter mines the course of the pro cess and the sta tus ofthe sys tem out put.
Par tic i pants in the re form pro cess
The med i cal pro fes sional and the cit i zen (the pa tient, re spec tively), who are the two keyact ing fig ures in the healthcare pro cess, are the pre lim i nar ily de ter mined par tic i pants in its re -form ing. But be sides them, as pointed out by G. Walt and L. Gilson (1994) as well as by R. B.Saltman and J. Figueras (1997) and, as con firmed also by the ex pe ri ence in our coun try and inother coun tries, the po lit i cal elite and the stake holders are also im por tant par tic i pants. The gen -eral im por tance of the par tic i pants is de ter mined by the pos si bil ity for the for ma tion of a stra -te gic united ac tion among them (or among some of them) to sup port or coun ter act thehealthcare re form.
As par tic i pants and di rect ex ec u tors of nu mer ous tasks in the healthcare, the med i calpro fes sion als ex ert im me di ate in flu ence on the re form. A large part of the med i cal pro fes sion -als con sists of in di vid u als of high pub lic and po lit i cal stand ing and their in flu ence can be usedin one di rec tion or an other. But, be sides, they ex ert sig nif i cant and strong in flu ence throughtheir pro fes sional and sci en tific or gani sa tions. In some cases, the nec es sary in flu ence can alsobe achieved through the stake holders’ groups.
The in flu ence of the cit i zens can be im me di ate to a com pa ra ble de gree, through their ac -tiv i ties as au ton o mous con sum ers with the right of choice of health ser vices. In a num ber ofstates, how ever, spe cial mech a nisms are granted for the cit i zens’ par tic i pa tion in the for ma tion
21
Ob ject of the healthcare re form: what is ac tu ally re formed?
of health pol i cies, the set ting of pri or i ties and the ex e cu tion of civil con trol (Ire land, the Neth -er lands, the United King dom, the Scan di na vian coun tries).
The po lit i cal elite, i.e. the rel a tively high-rank ing pol i ti cians and clerks, who as ex pertspre pare and im ple ment the health pol icy, pres ent an in flu en tial group in the health sec tor. Thehigh-rank ing ad min is tra tors play a stra te gic role in the ex e cu tion of the health pol icy. The pol i -ti cians may ei ther ac cel er ate or slow down the healthcare re form. R. B. Soltman and J.Figueras (1997) quote an ob server, who in 1994, made the re mark that “un doubt edly, Cen traland East ern Eu rope are not pre pared and are not will ing to im me di ately shift from state pa ter -nal ism to civil so ci ety”. It is pointed out, that in some coun tries, the im pact of the med i cal pro -fes sion als is weak en ing un der the pres sure of the in creas ing in flu ence of the ad min is tra tion. At the same time (1994), the in creas ing man age ment con trol over the pro fes sion als’ ac tiv i ties was re cog nised in the United King dom (S. Har ri son, C. Pollin, 1994).
De pend ing on their goals the stake holders vary in na ture and com po si tion, but it is con -sid ered that in a num ber of coun tries their role is grow ing. Such a role is played by some or -gani sa tions of med i cal pro fes sion als and pa tients. The health pol icy and the healthcare re form,re spec tively, can also be af fected by in ter ested groups de fend ing cor po rate in ter ests, e.g. com -pa nies in the phar ma ceu ti cal sec tor or in the health in sur ance busi ness. The role of stake -holders is also played by in ter ested groups con sist ing of med i cal pro fes sion als, ad min is tra tors, lo cal pol i ti cians and some (in flu en tial) cit i zens united by the idea that they are en ti tled to amore sig nif i cant part in the healthcare re form.
The con text of the pro cess
It has to be pointed out, how ever, that the healthcare sys tem and the healthcare pro cessare de vel oped in and ex pe ri ence the in flu ence (in some cases rather ac tive) of a def i nite en vi -ron ment. As ob served by R. B. Soltman and J. Figueras (1997), the re form pro cess is af fectedby ex ter nal to the health sys tem po lit i cal, ideo log i cal, so cial, his tor i cal, cul tural and eco nomicfac tors, whose unity has to be taken into con sid er ation for the un der stand ing of the healthcarere form con text. The con text can be de fined as the op er a tional en vi ron ment, in which thepro cess is car ried out and which is char ac ter ised by terms such as “tur bu lence”, ”pre dict abil -ity”, “tech no log i cal in de pend ence”, “tech no log i cal rou tine” and other sim i lar no tions. Morespe cif i cally, in the con text of a healthcare re form, R. B. Soltman and J. Figueras (1997) in -clude the mac ro eco nomic sit u a tion, the po lit i cal con di tions, the so cial norms and val ues aswell as the ex ter nal (in ter na tional) in flu ence.
The de vel op ment and the sustainability of the na tional econ omy are un dis puted fac torsfor the achieve ment of the ob jec tives of the healthcare re form both in the West ern Eu ro peanand the East ern Eu ro pean coun tries. Dur ing pe ri ods of eco nomic slumps, the op er a tional space for the re form plan ning and im ple men ta tion is nar rowed down, and it be comes im pos si ble toap ply broader and more rad i cal mea sures en vis aged in the con cepts of the healthcare re forms.
The po lit i cal con di tions are formed by var i ous in ter re lated fac tors such as pri vate in ter -ests (per sonal, col lec tive, cor po rate) and so cial or pub lic in ter ests, the cen tral power and the lo -cal gov er nance, sta ble or un sta ble gov ern ments, re la tions among Par lia ment, Pres i dency,gov ern ment and lo cal ad min is tra tion. A se ri ous fac tor is the level of man age ment ca pac ity ofthe health ad min is tra tion, which is di min ished in some cases be cause of po lit i cal changes inthe ad min is tra tion.
22

The role of the so cial norms and val ues is def i nitely of cru cial im por tance as a fac tor in thehealthcare re form. Firstly, it is im por tant what place is as signed to healthcare in the so cial valuesys tem. In some pub lic sys tems, healthcare is con ceived as a so cial or col lec tive non-mar ketgood, from which all the cit i zens can ben e fit. In other pub lic sys tems, healthcare and the med -ico-so cial as sis tance are con sid ered as a mar ket good sub ject to mar ket rules. Sec ondly, the re la -tion ships are sig nif i cant be tween the state and so ci ety, the pa ter nal is tic at ti tudes and civil ac tiv ity in the field of healthcare. Thirdly, the re spon si bil ity to so ci ety mat ters, e.g. eth i cal, pro fes sional,le gal, fi nan cial and po lit i cal re spon si bil ity. This re spon si bil ity ex ists in the healthcare leg is la tionin the sep a rate coun tries, but the bear ers of the re spon si bil ity may vary, e.g. the state may be theonly bearer (as in the pa ter nal is tic model); it may be shared to a dif fer ent de gree with the pro fes -sional or other (non-state) or gani sa tions; it may be shared with the cit i zens, too.
One of the most im por tant roles of the ex ter nal in ter na tional in flu ence on the healthcare re form is the bor row ing of con cepts and mod els from other coun tries. It has spe cial sig nif i -cance since the ex pe ri ence of other coun tries (pos i tive or neg a tive) is use ful in all cases. Butto gether with this, the risk al ways ex ists when for eign de ci sions of lo cal prob lems are cop ieddi rectly. In each sep a rate coun try, the healthcare sys tem has its “in di vid ual” pe cu liar i ties re -sult ing from ac cu mu lated his tor i cal, cul tural, po lit i cal, eco nomic and in ter na tional in flu ences,re flect ing the cur rent con di tions in the coun try and they can be ap pro pri ate to a var i ous de greefor an other coun try. An other im por tant fac tor is the fi nan cial aid for the healthcare re formcom ing from ex ter nal sources. For many coun tries (in clud ing Bul garia), the ex ter nal fi nan cialsup port is a cru cial fac tor, es pe cially for the on set of the healthcare re form.
The healthcare re form im plies a change in the healthcare sys tem and the healthcare pro -cess in their unity, in or der to achieve the de sired and ex pected ef fect on the out put of the sys -tem. This is why in the con cept, the strat egy, pol icy and the plan ning of the healthcare re formthe over all struc tural pan orama of the healthcare re form should be taken into con sid er ation,e.g. the healthcare sys tem and the healthcare pro cess, the con text and the par tic i pants in the re -form pro cess. The ob jects of the healthcare re form are the healthcare sys tem and thehealthcare pro cess, ex am ined in their unity in the par tic u lar con text with the par tic u larpar tic i pants in the re form.
3. A study of the healthcare re form: set ting, or gani sa tion andmeth ods
The healthcare re form pres ents a spe cific ob ject of re search. It is char ac ter ised by avary ing struc ture and in ter nal dy nam ics, de pend ence on a num ber of ex ter nal fac tors and ef -fects on the health of the pop u la tion. The re form pro cess has many as pects and de vel ops in acom plex en vi ron ment. It must be stud ied by tak ing into con sid er ation its char ac ter is tic fea -tures, con text and par tic i pants in the pro cess.
There fore, we started from the un der stand ing that first, in all cases and in all coun tries,the healthcare re form is car ried out in or der to im prove the sys tem of healthcare and to make itmore ac cept able to meet the needs of ev ery cit i zen, the com mu nity and the state as well as ofthe pro fes sion als in the sys tem; sec ond, the healthcare re form is a very com pli cated, so ciallyand po lit i cally re spon si ble pro cess, and, there fore, its im ple men ta tion re quires a rel a tively lon -ger pe riod of time; third, the healthcare re form should be the main ob ject, guide line and con -tent of the health pol icy in the coun try, in which it is im ple mented.
23
A study of the healthcare re form: set ting, or gani sa tion and meth ods
Pre vi ous stud ies: char ac ter is tics and re sults
We think it ap pro pri ate to make a brief re view of the pre vi ous stud ies re lated to thehealthcare re form in or der to es tab lish first, at what stage of re search we are start ing our study,what facts and trends (maybe reg u lar i ties) have al ready been es tab lished; sec ond, what are thedi rec tions and the top ics of the stud ies car ried out so far and third, the pos si bil ity for us ing there sults from pre vi ous re search for the pur poses of the pres ent study.
In view of this ne ces sity, we ex am ined and ana lysed ma te ri als, pub lished in all the med i -cal pe ri od i cals and some non-med i cal pub li ca tions, col lec tions of ar ti cles and sep a rate mono -graphs (in di cated in the ref er ences).
The stud ies re flected in the ex am ined pub li ca tions can be grouped in two types: stud iesABOUT the healthcare re form and stud ies OF the healthcare re form in Bul garia.
Stud ies ABOUT the healthcare re form
Sub ject to this type of re search are mainly the rea sons which gave rise to the need for re -form, the goals, di rec tions and the con tent of the re form (what needs to be changed and how) as well as the ex pected out comes from the changes.
Chro no log i cally speak ing, the first sim i lar over all study was pre sented in the brief mono -graph en ti tled “The healthcare re form – pol icy and strat egy un der free mar ket con di -tions” by M. Popov and Z. Kraev3 (In fact this study was or dered by the Ex pert Coun cil to theBul gar ian Agrar ian Party in 1993).
The study be gan with an anal y sis of the pre req ui sites for the re form in healthcare (de te ri o -rated and in creas ingly de te ri o rat ing health sta tus of the pop u la tion, the cri sis in the healthcaresys tem). The study stressed the need for a new health pol icy and its prin ci ples (de moc racy, de -cen trali sa tion, so cial ori en ta tion, dif fer en ti a tion of re spon si bil i ties among the state, the mu nic -i pal i ties, the trade un ions and the em ploy ers; par tic i pa tion of the state, mu nic i pal and pri vateown er ship, eco nomic re form and in tro duc tion of de cen tral ised in de pend ent fund in sur ance fi -nanc ing; pro mo tion of the so cial and pro fes sional sta tus of the med i cal staff, giv ing in cen tivesfor the med i cal sci ence and ed u ca tion).
The tasks and the el e ments of the re form were pre sented in de tail: es tab lish ment of a mar -ket econ omy re gime (“the money fol lows the pa tient”), im ple men ta tion of struc tural changes(the fig ures of the gen eral prac ti tio ner and the den tist, al ter na tives for the de vel op ment of theru ral health ser vices, re form ing of the out pa tient ser vices into “con sul ta tive and di ag nos ticcen tres”, de vel op ment of the dis pen sa ries, types of hospitals – for ac tive and con tin u ous treat -ment), de vel op ment of the pri vate sec tor, uti li sa tion of the nat u ral health re sources. The ideawas evolved about “dis trict in sti tutes for pub lic healthcare”. The net work of phar ma cies wasseen as pri vate, mu nic i pal and hos pi tal. At ten tion was paid to the great sig nif i cance of thehealth ad min is tra tion un der con di tions of de cen trali sa tion. It was pro posed that the pro fes -sional or gani sa tions were granted by law cer tain rights sim i lar to those of the pro fes sionalcham bers in other coun tries.
A programme was also de vel oped and pre sented for the leg is la tion and or gani sa tion ofthe healthcare re form for a pe riod of five years in three stages: pre pa ra tory (1994), struc tural(1995-1996) and for con sol i da tion (1997-1998), to gether with a fi nan cial frame work for all
24
3 Popov Ì., Z. Kraev. Çäðàâíàòà ðåôîðìà – ïîëèòèêà è ñòðàòåãèÿ â óñëîâèÿòà íà ïàçàðíà èêîíîìèêà.Pub lished by the “Free Intiative“ Foun da tion”, ¹ 34 of the se ries “Prob lems of the Tran si tion in Bul garia”, 1994
the costs (ac cord ing to the prices in 1993 – a to tal of 50 240 000 BGN). This pub li ca tion is a doc u ment which ob vi ates the au thors’ level and way of think ing at
still a very early stage of the healthcare re form. What is in ter est ing is that a num ber of ideaspro posed in it were not dis puted and were later de vel oped fur ther and worked out by var i ousau thors in sub se quent pub li ca tions.
The next pub li ca tion in chro no log i cal or der about the healthcare re form was en ti tled“The healthcare re form in Bul garia”4 (In the mean time in 1996 the Na tional Health Strat egy“Health for Bul garia” was pub lished and, though an out come of a pro found study, it com prisesan of fi cial doc u ment and will there fore be ex am ined in greater de tail later). In the two vol -umes, works and ma te ri als were pub lished re lated to the train ing car ried out in the pe riod1996-1998 in the field of healthcare man age ment for the man a ge rial staff in the healthcare sys -tem. Four chap ters were in cluded in each vol ume: health pol icy, health eco nom ics and fi nanc -ing, healthcare man age ment and in for ma tion tech nol o gies.
In a se ries of the ma te ri als pub lished in the two vol umes of “The healthcare re form in Bul -garia” for the first time in our coun try the is sues of the healthcare re form were ex am ined inde tail, e.g. its three main goals – dis con tinu a tion of the de te ri o ra tion of the na tion’s health sta -tus and cre ation of con di tions for its im prove ment, dis con tinu a tion of the re pro duc tion of theex ist ing health sys tem and build ing of a new one, pro mot ing healthcare to the level of thehealthcare sys tems in the other coun tries of the Eu ro pean Un ion (M. Popov); in tro duc tion tothe the ory, prac tice and his tor i cal de vel op ment of the health pol icy at var i ous lev els (M.Popov, Zh. Golemanova); hos pi tal strat egy and pol icy (M. Popov); the is sues of me dia pol icy(M. Lyubenova); foun da tions of the nor ma tive sys tem in healthcare (F. Videnova, A. Panova); privatisation in healthcare (V. Tsakova, M.Popova); prob lems of health eco nom ics andhealthcare fi nanc ing (E. Delcheva, N. Geneva, B. Georgiev); the is sues of health in sur ance and mar ket reg u la tion (E. Delcheva); busi ness plan ning (T. Stoyanova); mar ket ing ap proaches(M. Bogdanova, A. Andreeva); healthcare or gani sa tion and its man age ment (A. Bunkova, L.Atanasov); ac cred i ta tion of hos pi tals (F. Mar ti nez, M.-T. de Montalban, I Rebeyon), qual ityman age ment in the hos pi tal es tab lish ments (M. Marinov); the “case mix” ap proach (D. Iliev),healthcare in for ma tics (H. Griva, M. Vukov, S. Hristova).
The two vol umes were pub lished be fore the be gin ning of the rad i cal changes in thehealthcare sys tem in the pe riod 1998-1999 and, this is why, the ma te ri als in it were writ ten inthe fu ture tense. Their con tri bu tion to the de vel op ment of the healthcare re form con sisted inpos ing of ques tions al most un fa mil iar un til that mo ment to a wide scope of the man age mentper son nel in the field of healthcare (e.g. the health pol icy, the me dia pol icy, privatisation,health in sur ance and mar ket mech a nisms, busi ness plan ning and mar ket ing, ac cred i ta tion andqual ity man age ment). Al though their greater part, in its na ture con sisted in re view ing, the pub -lished ma te ri als mir rored the ac tual level of knowl edge and prac tice and they were de signed tore flect the spe cific fea tures and the re quire ments of the then-forth com ing changes in the sys -tem of healthcare. In this sense, it may be con sid ered that they pre sented some ar gu ments forthe steps to fol low in the healthcare re form.
In 1998 (24-25 April) the Na tional Con fer ence on Healthcare Re form was held, at whichDr. Ilko Semerdjiev (the then Vice Min is ter for healthcare) de liv ered a com pre hen sive re port
25
A study of the healthcare re form: set ting, or gani sa tion and meth ods
4 Popov Ì. (ed.) Çäðàâíàòà ðåôîðìà â Áúëãàðèÿ. Pub lished by “Mac e do nia Press”, So fia, Part I, 1997 andPart II, 1998

on the healthcare re form5. In fact, the re port pre sented the re sults from a se ri ous study not somuch of the rea sons and the pre req ui sites (which were clear enough at the time) but of the con -tent and the goals of the healthcare re form in Bul garia. In the chro no log i cal or der, this was thethird well-ar gued pub li ca tion on the forth com ing healthcare re form, which was al ready inquite an ad vanced stage of its prep a ra tion.
The main as pects of the healthcare re form were looked at from five as pects: eco nomic re -form and changes in the healthcare fi nanc ing; struc tural re form with changes in the le gal sta tus of the healthcare es tab lish ments; re form of the med i cal ed u ca tion; re form in the man age mentof the healthcare sys tem; a change in the healthcare and po lit i cal ap proach with em pha ses onhealth pro mo tion, dis ease pre ven tion and con trol over the so cially sig nif i cant dis eases.
The model and the pro ject for a health in sur ance sys tem in Bul garia were ar gued for ingreat est de tail – oblig a tory in sur ance (pub lic sec tor with one in sur ance or gani sa tion) and vol un -tary in sur ance (pri vate sec tor with nu mer ous in sur ance or gani sa tions), the amount of the in sur -ance in stal ments, the man age ment of the sys tem, the re gime for in sur ance and con tract ing. Asig nif i cant part was at trib uted to the role of the pro fes sional or gani sa tions and the pro fes sionalself-gov er nance. The re form ing of the healthcare es tab lish ments and their man age ment were ex -am ined in depth to gether with the is sues of their ac cred i ta tion, mar ket ing and in volve ment in themar ket re la tions un der lib eral mar ket con di tions. The greater part of the pro pos als in the re portlater found their way to the sub se quent leg is la tion and we will not ex am ine them in de tail here.Out side the le gal acts, how ever, some sig nif i cant char ac ter is tics were left out of the ana lysedmodel. For in stance, such an im por tant char ac ter is tic was the en hanced au ton omy of the hos pi talwards, en vis aged in the re port but in ef fect, im pos si ble to achieve. An other ex am ple was il lus -trated in the con cept of the free price for ma tion of the hos pi tal es tab lish ments, which was not car -ried out, but could have had a great im pact on the eco nomic re form in the hos pi tal sec tor.
It can be as sumed that, in the pub li ca tion con sid ered above, the ideas which were then inthe pub lic air about the healthcare re form, were evolved, ar gued fur ther and ac quired a con -crete shape. If we would like to use the short est char ac ter is tic, the mar ket lib eral model of ahealthcare sys tem was well-ar gued, though ten ta tively in some re spects. More over, these ideas were an nounced as health pol icy in ten tions and not only as wish ful think ing for some pre dict -able time in the fu ture.
Stud ies OF the healthcare re form
This group in cludes pub li ca tions, which high light stud ies on gen eral and spe cific is sues, re -lated to the un fold ing of the healthcare re form and pos si bly to its ac tual as sess ment and fu ture.
We will fo cus in greater de tail on some of these pub li ca tions which to our mind havemeth od olog i cal (and not only de scrip tive, fac tual and an a lyt i cal) value for the study of thehealthcare re form.
In this train of thought, two pub li ca tions have a lead ing im por tance – those of R. B. Soltman and J. Figueras (1997), and of F. Lamata Cotanda (1998), which we will dis cuss one by one.
The re mark able mono graph by R. B. Soltman and J. Figueras en ti tled “The Eu ro peanHealth Care Re form. Anal y sis of Cur rent Strat e gies” 6has pre served its im por tance for the
26
5 Semerdjiev, I. Îáùè ïàðàìåòðè íà çäðàâíàòà ðåôîðìà â Áúëãàðèÿ. In: Min is try of Healthcare. Na tionalCon fer ence on Healthcare Re form in Re pub lic of Bul garia. 24-25.04.1998, So fia. Pub lished by “Mac e do niaPress”, So fia, 1998, pp.12-59
6 Soltman, R. B., J.Figueras. Eu ro pean Health Care Re form. Anal y sis of Cur rent Strat e gies. WHO Re gional
last ten years as one of the ma jor pub li ca tions on the anal y sis of the re form healthcare pol icy inthe Eu ro pean coun tries. The au thors made an anal y sis us ing a spe cific programme and an enor -mous body of sta tis ti cal and lit er ary data. They pre sented a gen er al ised pic ture of the re formpro cess in the Eu ro pean coun tries, in di cat ing both the com mon fea tures and the sim i lar i tiesand the dif fer ences in the ap proaches adopted by the sep a rate coun tries.
To the pur pose of our study, we should note that the scheme pro posed by G. Walt (1994)for the anal y sis of the pol icy in healthcare, was ap plied by R. B. Soltman and J. Figueras, whode vel oped it fur ther to a cer tain ex tent and sug gested it to be used in the anal y sis and the man -age ment of the re forms in healthcare.
Ac cord ing to this scheme a pol icy for a re form has to be ana lysed from four as pects: (1) the con text (the con di tions) in which the re form is car ried out. The con text of the re -
form is formed mainly by the mac ro eco nomic sit u a tion in the coun try, the pre dom i -nant po lit i cal con di tions, the pres ence of so cial val ues and the ex ter nal in flu enceex erted on the pro cess of re form;
(2) the con tent of the pol icy, e.g. a struc ture of the healthcare sys tem ad e quate to thecon di tions;
(3) in ter nal logic of the pro cess of re form for ma tion and im ple men ta tion. The choice ofthe tim ing (when to carry it) re quires spe cial at ten tion to gether with the staged im ple -men ta tion of the re form and the rates at which to carry out each sep a rate stage. Theim pact of the state struc ture should also be ana lysed to gether with the del e ga tion ofman age ment com pe tences (de gree of cen trali sa tion) as well as the in flu ence of thecen tral state au thor i ties. The very prac ti cal im ple men ta tion and man age ment of thehealthcare re form also need to be ana lysed. As in di cated, in many coun tries, the min -is tries (the state ad min is tra tion) of healthcare do not pos sess the nec es sary in flu encewhich is the rea son why the man age ment of the healthcare re form is “taken over” bythe pol i ti cians;
(4) the par tic i pants who carry out or in flu ence the re form. The au thors sub di vide thepar tic i pants in four cat e go ries: the pop u la tion (the cit i zens) of the coun try, the med i -cal per son nel, the po lit i cal elite and the stake holders.
In their anal y sis of the healthcare re forms in the dif fer ent Eu ro pean coun tries, R. B.Soltman and J. Figueras de fine seven fac tors which have a prin ci pal im por tance for thehealthcare re form:
· time frames for the re form im ple men ta tion (mainly ap pro pri ate ini ti a tion of its start);
· fi nan cial sta bil ity of the coun try;
· pres ence of ac tual po lit i cal will and man age ment of the re form im ple men ta tion;
· for ma tion of stra te gic al li ances with part ners in sup port of the re form;
· granted pub lic sup port;
· man age ment of change: def i ni tion of the goals and the rates of the re form – slowly andevo lu tion al ly or fast and rad i cal im ple men ta tion, dis tri bu tion of the man age ment re spon -si bil i ties, uti li sa tion of all the leg is la tive pos si bil i ties, pro vi sion of fi nan cial in cen tives;
· pres ence of tech ni cal in fra struc ture and po ten tial (e.g. in for ma tion sys tem, man age -ment and tech no log i cal level). It is pointed out that if the in fra struc ture, the tech no log i -
27
A study of the healthcare re form: set ting, or gani sa tion and meth ods
Of fice for Eu rope, Co pen ha gen, 1997
cal and man ag ing pos si bil i ties nec es sary for the healthcare re form do not de veloppar al lel to the cre ation of the leg is la tive and po lit i cal ba sis, the re form can hardly besuc cess ful or sus tain able.
The meth od olog i cal ap proach pro posed by R. B. Soltman and J. Figueras has a sig nif i cant im pact on the stud ies of the healthcare re form in Bul garia and in other coun tries. The mono -graph writ ten by these two au thors was fol lowed by a num ber of other pub li ca tions which scru -ti nise nu mer ous par tic u lar prob lems of the healthcare re forms.
The sec ond pub li ca tion, which we think worth pay ing spe cial trib ute, is “Com par a tiveStudy of the Healthcare Re forms in Spain and Bul garia” by Fernando Lamata7. This wasthe first study of the healthcare re form in Bul garia in the pe riod 1991-1997. The re sults fromthe study were in ter preted in an ob jec tive way (the au thor was def i nitely well-in tended) andpre sented spe cial in ter est be cause of the com par i son of the re form pro cess in the sys tems ofhealthcare in two (at least par tially) com pa ra ble coun tries. We will quote these re sults later but, for the time be ing, we will fo cus on the meth od ol ogy ap plied in the study.
In his pub li ca tions men tioned above, F. Lamata started from the gen eral as sump tion thatthe study of the healthcare re form had to in clude the anal y sis of the con text, the con tent, thepro cess and the par tic i pants in the re form and, in this sense, his meth od ol ogy was sim i lar tothat ap plied by R. B. Soltman and J. Figueras. But the sim i lar i ties ended up here.
To carry out his study F. Lamata cre ated a meth od ol ogy, by means of which a com par a -tively more ac cu rate and in for ma tive re sults can be ob tained about the de vel op ment of thehealthcare re form:
· first, the mea sure ments of the re form pro cess were con sid ered to be def i nite vari ableswith a nu mer i cal and ver bal ex pres sion (which could also be trans formed into a nu mer -i cal one by means of a scale). In our opin ion, it is equally im por tant (es pe cially for thecom par a tive stud ies) to de ter mine both the as pects of the anal y sis and its con tent (i.e.the set of vari ables) for each of the pre-de ter mined as pects. The pub li ca tion sug gested36 vari ables to be used, which were mea sured with a to tal of 100 in di ca tors. By the se -lec tion and def i ni tion of the vari ables of the re form pro cess, a set of com pa ra ble in di ca -tors was achieved, en abling more ac cu rate synchronic (for the def i nite time, for thedef i nite ob jects) and diachronic (in the course of the change de vel op ment) stud ies.
· sec ond, in gen eral terms the vari ables of the re form pro cess co in cided with the schemepro posed by J. Walt, R. B. Soltman and J. Figueras. But de fined in con crete terms, theywere grouped in an other clas si fi ca tion, which pres ents a meth od olog i cal in ter est:� vari ables for con text char ac teri sa tion: de mo graphic, eco nomic, po lit i cal, ep i de mi o -
log i cal pro file; � vari ables for the char ac teri sa tion of the healthcare sys tem, e.g. cov er age of the pop -
u la tion, ser vices (types of ser vices), scope of the pub lic fi nanc ing, size of the healthex pen di ture, right of choice, de gree of de cen trali sa tion and ter ri to rial dis tri bu tion ofre sources, in te gra tion and con cen tra tion, prop erty dis tri bu tion, or gani sa tion of thehealthcare ser vices, pa tients’ needs sat is fac tion, stan dards for the per son nel, in vest -ment, man age ment sys tem, char ac ter is tics of the man ag ers and many oth ers;
28
7 Lamata Cotanda, F. Estudio Comparado de las Reformas de los Sistemas Sanitarios de Espana y Âulgaria.Tesis Doc toral. Universidad Autonoma de Ma drid. Facultad de Medicina. Departamento de MedicinaPreventiva y Salud Publica, 1998
� vari ables for the char ac teri sa tion of the pro cess of healthcare re form: def i ni tion ofthe goals of the re form, course of the re form (de vel op ment of nor ma tive ba sis andde vel op ment of the ac tual re form), struc ture (in sti tu tions) of the re form and par tic i -pants in the course of the re form.
· third, the vari ables (and the in di ca tors re lated to them) were ex am ined at three lev els:(a) the first level con sisted of the vari ables (and in di ca tors) pre sent ing the change ofthe over all char ac ter is tic of the healthcare sys tem and pol icy, for ex am ple, cov er age ofthe needs, to tal costs for them and, hence, pub lic ex pen di ture for healthcare, health ser -vices (re gime, scope, vol ume), the out comes for the pop u la tion; (b) the sec ond levelcon sisted of the vari ables (and in di ca tors) char ac ter is ing the change in the healthcaresys tem it self and its ca pac ity, for in stance, or gani sa tion, staff, in sti tu tions, in vest ment,qual ity, ac ces si bil ity, etc.; (c) the third level was com prised of the vari ables (and in di -ca tors) re lated to the man age ment and the ef fi ciency of the sys tem. The idea for the dif -fer en ti a tion of the vari able at three lev els is in ter est ing and, ap plied by the au thor,showed good re sults.
Hav ing found inter de pend en ces be tween the stud ied vari ables, F. Lamata sug gested amodel for the struc ture of the pub lic ex pen di ture for healthcare and a for mula for a math e mat i -cal rep re sen ta tion of the model.
We will briefly dis cuss sev eral other pub li ca tions as ex am ples of the ap pli ca tion of theal ready ex am ined more or less mod i fied ap proaches to the study of the healthcare re form.
A com par a tive in ter na tional study con ducted by G. Petrova (2003) was re lated to themodel of the re form in the phar ma ceu ti cal sec tor in the Bal kan re gion (Bul garia, Bosniaand Herzegovina, Mac e do nia, Ro ma nia and Yu go sla via). Af ter a com pre hen sive re view of the health re form def i ni tions, the au thor adopted a con cep tual view to the study of the re form inthe phar ma ceu ti cal sec tor but fo cused mainly on the pro cess and the con tent of the re form, andto some de gree, on the con text and the par tic i pants. In view of its nar rower pro fil ing, the studywas en riched with the ap pli ca tion of pharmacoeconomic meth ods, anal y ses of the sta tis ti calma te rial and nor ma tive doc u ments of the re spec tive coun tries.
The study con ducted by D. Balabanova, S. Tsolova and E. Delcheva was also pro fil ingand was re lated to the pol icy of re form in hos pi tal care in Bul garia. The au thors ap plied J.Walt’s scheme and based on nu mer ous lit er ary sources, doc u men tary, sta tis ti cal and sur veydata, drew con vinc ing con clu sions about the im ple men ta tion of the healthcare re form, andmore spe cif i cally, on the sig nif i cant dif fi cul ties ex pe ri enced in its im ple men ta tion.
In an ex ten sive study en ti tled “The Healthcare re form in Bul garia: a Look to ward De -cen trali sa tion and Lo cal Gov er nance”8, the au thors used the Soltman and Figueras’ ap -proach, par tially de scribed above. They re lied on a com pre hen sive po lit i cal andmac ro eco nomic anal y sis (the con text) and stud ied the de vel op ment of the healthcare sys tem(the con tent) un der the in flu ence of in ter nal (in clud ing the par tic i pants) and in ter na tional fac -tors. The re sults from the pub lic opin ion polls (of med i cal pro fes sion als and cit i zens) were in -ter preted, too. The char ac ter is tic fea tures, the op por tu ni ties and the im pact of de cen trali sa tion
29
A study of the healthcare re form: set ting, or gani sa tion and meth ods
8 Prohaska, M., D. Iliev, D. Sacheva, M. Varshilova, L. Doudeva. Health Re form in Bul garia: A Glance atDe cen tral iza tion and Lo cal Gov er nance. In: Shakarishvili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y sesand Ex pe ri ences in Cen tral and East ern Eu rope in the 1990s. Open So ci ety In sti tute, Bu da pest, 2005, pp.45-132
were in ves ti gated in two rel a tively large mu nic i pal i ties (Pazardjik and Turgovishte).The “Re port on the Na tion’s Health at the Be gin ning of the 21st Cen tury. Anal y sis of
the On go ing Re form in Healthcare,” pub lished in 2004 by the Min is try of Healthcare arosein ter est with its ti tle, prom is ing an anal y sis of the healthcare re form. The re port, how ever, wasa nar ra tive (with quite a few gaps) about the state of the na tion’s health and the sys tem ofhealthcare, in which the healthcare re form was only hinted. The fac tual ma te rial abun dant inmany re spects (but also scarce or lack ing in other re spects) could not com pen sate for the ex -tremely lim ited in ter pre ta tion and lack of anal y sis not only of the healthcare re form.
The lack of anal y sis was ob vi ous par tic u larly as re gards the fun da men tal and stra te gicprob lems of the healthcare re form, for in stance, such as the func tion ing of the newly con -structed healthcare sys tem as com pared to the pre vi ous one; the im pact of the mar ket con di -tions, el e ments and mech a nisms; the bal ances and the lack of equi lib ri ums in the sys tem; thenew struc ture of the own er ship and its role in the de vel op ment of the sys tem in terms ofprivatisation; the type and the de gree of jus ti fi ca tion for the re form it self; the role of the NHIFand the pro fes sional or gani sa tions as fac tors for the health pol icy; the at ti tude of the med i caland non-med i cal com mu nity (in clud ing pa tients) to ward the re form changes in healthcare.With out an ob jec tive and fo cused anal y sis on these and other sim i lar is sues it was im pos si bleto form an ad e quate as sess ment of the healthcare re form or the health pol icy.
For ex am ple, in the third part of the re port, dis cuss ing the health pol icy and the healthcarere form, it was stated that work was in prog ress for the achieve ment of the goals of the “Na -tional Health Strat egy 2001” and the ar gu ments were that “the plu ral ism of the goals is ob vi -ous,” “the de moc racy in the man age ment has been granted through the par tic i pa tion of all thestate, pro fes sional and civil in sti tu tions and or gani sa tions,” “the avail abil ity of med i cal care isbe ing im proved,” “the equal ity of the pa tients is be ing es tab lished,” “sol i dar ity has been at -tained,” etc. Some of the ar gu ments were un be liev able, e.g. “the so cial ori en ta tion of thehealthcare ac tiv i ties is con stant. About 20-30% of the pa tients are hos pi ta lised mainly for so -cial in di ca tions.” As an achieve ment, it was pointed that “a pri vate sec tor has been formed inthe hos pi tal es tab lish ments” (!?). It was also claimed that all the ac tiv i ties in the five pri or i ties,set up in the “Na tional Health Strat egy 2001”, were ei ther ful filled or be ing ful filled to getherwith the pri or i ties of the programme “Healthcare – Ev ery one’s Right 2002 – 2005”. All theabove could not mean any thing else but a suc cess ful de vel op ment of the healthcare re form.
Nev er the less, the re port read: “A num ber of these (health) ser vices have been strongly com -mer cial ised” to an ex tent that they can not be af forded by the greater part of the pop u la tion. Theprices of the drugs have soared. The in suf fi ciency of the fi nanc ing has be come chronic… Thesepro cesses have brought about a cer tain slump in the healthcare”, “the health sta tus of the pop u la -tion shows that for the re cent years the state pol icy for its pro tec tion has not yielded pos i tive re -sults”, “the in di ca tors for mor bid ity and mor tal ity of cer tain pop u la tion groups – chil dren,ad o les cents and women – are de te ri o rat ing”, “very fre quently … the poor peo ple, when sick,can not af ford to use med i cal ser vices”, “the pre ven tion ac tiv i ties, as far as they ex ist, are not in te -grated, there is no good con nec tion be tween the sep a rate programmes”, “dur ing the last years the work ing con di tions in many places do not meet the hy gienic norms and phys i o log i cal re quire -ments,” “the gen eral prac ti tio ners’ qual i fi ca tion is un sat is fac tory”, “the us age of the clin i calpath ways as a method of hos pi tal ac tiv i ties fi nanc ing shows a num ber of draw backs… The pay -ment per case, based on the clin i cal path ways, does not cor re spond to the ac tual costs…”, etc.
From all the above, it be comes ev i dent that in Bul garia some kind of a healthcare re form
30
prob a bly ex isted and was de vel op ing in some way (of fi cial programmes can also be quoted), it was pointed out that the stra te gic and programme in ten tions had been achieved or were be ingachieved at the time and at the same time data were an nounced about se ri ous fail ures sum ma -rised in the state ment “The re form of the sys tem, de vel oped in the frame work of a set pol icy,ob vi ously does not yield the ex pected re sults”.
The men tion of the above re port is not aimed at dis put ing it and there is no sense ar gu ingagainst or con firm ing one state ment or an other. Our aim is to look at the de gree to which it hasa meth od olog i cal sig nif i cance for the study of the healthcare re form. Ap par ently, the meth od -ol ogy, ap plied in this case, gave rise to con tra dic tory state ments. This is the rea son why wethink that this pub li ca tion did not con trib ute (even in terms of con fir ma tion or re jec tion) to thede vel op ment of the meth od ol ogy for the study and anal y sis of the healthcare re form. It can bere cog nised as a con tri bu tion only from the point of view of con firm ing the need for a meth od -ol ogy, ad e quate to the ob ject and the pur pose of the study.
A num ber of stud ies also ex isted, whose sub ject were spe cific is sues or as pects of there form in healthcare. The pre dom i nat ing ones con sisted of em pir i cal ques tion naire sur veysor more com pre hen sive so cio log i cal anal y ses on the var i ous as pects of the re form pro cess.Most fre quently these were stud ies on the per cep tion of the healthcare re form by the cit i zens,the pa tients and the med i cal pro fes sion als. An other part con sisted of stud ies on the eco nom icsof the healthcare sys tem, in which an im por tant role was at trib uted to the is sues of health in sur -ance. The pub li ca tions on the or gani sa tional and struc tural changes in the healthcare sys temand the re sults from them were rather few. We have used a con sid er able part of all these stud -ies, cited also in the ref er ences, to fol low the evo lu tion of the healthcare re form.
We think it ap pro pri ate to in clude in this group an in ter est ing and use ful study en ti tled“Healthcare fi nanc ing and man age ment. The o ret i cal foun da tions, mod els, prob lems and trends”, pub lished in 2005 by the Min is try of Fi nance (Di rec tor ate “Bud get”, De part mentfor Mi cro ec o nomic Anal y ses”). In the first part of the study (pp. 19-164), a syn thetic com par a -tive in ter na tional re view was made of the eco nom ics but fo cus ing chiefly on the fi nanc ing ofthe healthcare sys tems, with quite a thor ough anal y sis of the var i ous as pects of the fi nan cialsys tems (through tax a tion, so cial in sur ance, health in sur ance, fi nanc ing of the sep a rate sec torsof the sys tem, the role of cor rup tion) and an as sess ment of the ef fec tive ness and ef fi ciency ofthe costs. The sec ond part (pp. 165-288) con sisted of an anal y sis of the healthcare sys tem andits fi nan cial and non-fi nan cial re sources. In its essence, the analysis covered part of the resultsfrom the healthcare reform.
The last chap ter con tained well-ar gued sug ges tions for the im prove ment of the fi nan cialman age ment of the healthcare sys tem. A num ber of “fun da men tal points”, gen er ally in a lib -eral spirit, formed a con cept for the de vel op ment of healthcare (com pe ti tion, free dom ofchoice, plu ral ism of own er ship, ef fi ciency). A short-term and a long-term model were pro -posed for the im prove ment of the fi nan cial man age ment. Both mod els fo cused on the pa tients’needs, op ti mal bal ance be tween the state (pub lic) and the pri vate sec tor, com pe ti tion, par tic i -pa tion of the state in the pay ment of the med i cal ser vices for the cit i zens in dis ad van taged po si -tion, pa tients’ co-pay ment of the med i cal care. Both mod els tack led the nec es sary eco nomiccon di tions and the re spec tive eco nomic en vi ron ment in or der to fa cil i tate their de vel op mentand func tion ing. The short-term model was worked out in three ver sions, giv ing groundedpref er ence to the one en vis ag ing the pres er va tion of the ex ist ing health in sur ance model butwith reg u lated co-pay ment by the pa tients (or by an other health in sur ance or in sur ance or gani -
31
A study of the healthcare re form: set ting, or gani sa tion and meth ods

sa tion and for the peo ple in an unprivileged po si tion – by the state). The long-term model en -vis aged the de vel op ment of the oblig a tory health in sur ance with the par tic i pa tion of pri vatehealth in sur ance or gani sa tions un der cer tain conditions.
One of the most im por tant re cent pub li ca tions was made by A. G. Vishnevskiy, Y. I.Kuzminov, V. I. Shevskiy, I. M. Sheiman, S. V. Shishkin, L. I. Yakobson and E. G. Yasinand is en ti tled “Rus sian healthcare: how to get out of the cri sis” (2006). It was based on abrief but ex tremely com pe tent, ob jec tive and rich, from a con tent point of view, anal y sis and as -sess ment of both the ac tual sta tus of health and the healthcare re form and the de vel op ment of thehealthcare re form un til that mo ment (which started at the end of 1980s!) in the coun try, in clud ing the im ple men ta tion of the Na tional programme “Health”. Along side with many other is sues, theau thors pointed out as a cru cial prob lem the in suf fi cient in cen tives for the im prove ment of the ef -fec tive re sources uti li sa tion and the re spon si bil ity defficit to the pop u la tions’ health. The wor ry -ing (though not un ex pected) sim i lar ity of the prob lems in Rus sia and in our coun try could not beig nored since it im plied cer tain reg u lar ity. Hav ing ana lysed the ap proaches to the con tin u a tion of the re form, the au thors gave ar gu ments for the strat egy of “a dig ni fied fi nanc ing plus com plexre forms.” Spe cial at ten tion was paid to its im me di ate im ple men ta tion in the fol low ing five-yearpe riod, es pe cially on the ma te rial in cen tives for ef fec tive work, in clud ing for the nurses, the pro -vi sion of drugs for the hos pi tal treat ment with out any costs paid by the pa tients, up dat ing of atleast 50% of the out dated equiment, clear reg u la tion of the paid med i cal care. Re cog nis ing of thene ces sity of the health in sur ance sys tem, the au thors stressed as an es sen tial el e ment of thehealthcare re form, the re form ing of the oblig a tory health in sur ance by cre at ing con di tions for ac -tual “in ter nal” com pe ti tion both among the health in sur ance com pa nies and among the hos pi tales tab lish ments. Se ri ous at ten tion was paid to var i ous as pects of the cit i zens’ in volve ment and the pro tec tion of the pa tients’ rights, the par tic i pa tion of the phy si cians in the im ple men ta tion of thehealthcare re form and the pri or ity of pri mary med i cal care. Emphasising that the healthcare re -form was nei ther a sin gle act, nor a short-term pro ject but a con tin u ous pro cess, the au thors sawas an im por tant com po nent the for ma tion of the two driv ing forces: the civil and the pro fes sionalcom mit ment to its suc cess ful developement.
Or gani sa tion and struc ture of the study
Aim of the study
The aim of the pres ent study was to en hance the un der stand ing of the es sence, de vel op -ment and the out comes of the healthcare re form in our coun try in view of its de vel op ment (i.e.“what is go ing on with the healthcare sys tem in Bul garia”) by ana lys ing:
· the ad e quacy of the goals, the con tent and the rates of the healthcare re form;
· the course of the re form pro cess dur ing its over sev en teen-year de vel op ment;
· the role of the par tic i pants and the pub lic forces act ing in it or for it;
· whether any mis takes had been made, and if “yes”, what were they, in the plan ning, or -gani sa tion and the course of the re form;
· whether any ef fects had been achieved and what ex actly;
· even tu ally, what was the ac tual sta tus of the re form pro cess in view of the plan ning ofthe fu ture of the healthcare sys tem in Bul garia.
32
For the pur poses of this study, we wished to as sume the most ob jec tive pos si ble ap proach(“sine ira et stu dio”) as we reck oned that this was the proper way to its achieve ment. This pre -sented also the most gen eral meth od olog i cal frame work of the study.
The con crete de vel op ment of the study was un folded in the fol low ing se quence:1. First of all, it was nec es sary to de fine and operationalise the con cept ap pa ra tus in
or der to clar ify what we meant by terms like “healthcare re form”, “healthcare sys -tem”, “healthcare pro cess”, “healthcare” and the con tent in fused in these terms.Thus, we would have pre pared the con cepts which were the build ing blocks of thestudy. In such a way, the fruit less and mean ing less ter mi no log i cal dis cus sions couldbe avoided to a sig nif i cant de gree.
2. Ac cord ing to the for mu lated aim, the def i ni tion of the ob ject and the sub ject wasthe next step in the course of the study. To gether with the def i ni tion of the terms, thisstep con trib uted to the log i cal con struc tion of the study.
As we al ready noted, the ob ject of the healthcare re form is the healthcare sys tem and thehealthcare pro cess in their dy nam ics and unity with the re spec tive par tic i pants and in the re -spec tive con text. This was the ob ject of the study as well. For mu lated in this way, the ob jectcor re sponded en tirely to the aim of the study – if we wanted to un der stand the re form, weneeded to in ves ti gate the changes in its ob ject.
Fol low ing this logic, we ac cepted as sub ject of the study the re form pro cess in its in ter -nal de vel op ment and its po lit i cal, so cial and eco nomic con text. Our ef forts in the study weredi rected ex actly to ward the re form pro cess, its pre con di tion ing, in ter nal and ex ter nal fac torsand in flu ences, rates of de vel op ment and out comes at ev ery stage, pre dict able pros pects andex pec ta tions.
3. In choos ing and com pos ing the cor re spond ing meth od ol ogy of the study, above all,it was nec es sary to ex am ine the meth ods ap plied in pre vi ous stud ies. This anal y siswas al ready pre sented above. We had to also take into ac count the meth ods ap plied in different studies of the healthcare re form in Bul garia. As in other sur veys, for the pur -pose of the pres ent study R. B. Soltman and H. Figueras’ ap proach proved ap pro pri -ate. At the same time, how ever, we were con vinced in the use ful ness of F. Lamata’sidea about the ne ces sity for ex am in ing the de vel op ment of the re form pro cess it selfto gether with the changes in the health pol icy, the healthcare sys tem and the in di ca -tors of the pop u la tion’s health sta tus.
4. The study of the re form pro cess could be started from dif fer ent per spec tives. In ouropin ion, an ac cept able ap proach con sisted in the fol low ing:
· def i ni tion of the set of cri te ria, and through it, of the stages of the re form pro cess(the healthcare re form, re spec tively);
· def i ni tion of the as pects, from which the sep a rate stages would be stud ied. For anac tual char ac ter is tic, suf fi cient for the pur poses of the study, to gether with theabove men tioned el e ments of the meth od olog i cal ap proaches, we thought it nec es -sary to take into con sid er ation the views of the ma jor par tic i pants in the re -form pro cess: above all, the cit i zens (pa tients) and the med i cal pro fes sion als.Only in such a way a com par i son could be made be tween the of fi cial line of thehealthcare re form and its re flec tion in the minds of the con sum ers and the ex ec u -tors, as well as the me dia fac tor as an ex pres sion and mod er a tor of pub lic opin ion.There fore, for the anal y sis of ev ery stage, we adopted the fol low ing scheme:
33
A study of the healthcare re form: set ting, or gani sa tion and meth ods
� the po lit i cal and so cio eco nomic con text;� the gov ern ment health pol icy and its re flec tion in nor ma tive and other of fi cial
acts;� changes in the healthcare sys tem and dy nam ics of the pop u la tion’s health sta -
tus;� pro fes sion als’ opin ion;� cit i zens’ and pa tients’ opin ion;� cov er age of the re form in the pe ri od i cals.
Meth ods of the study
Af ter hav ing clar i fied the ter mi no log i cal ap pa ra tus, the aim, the ob ject and the sub ject ofthe study, for our fur ther work, we found it use ful to study the main ma te ri als and pub li ca -tions high light ing the time and the pe cu liar fea tures of the healthcare re form in Bul garia. Theyin cluded the afore men tioned stud ies of the re form, as well as the adopted new leg is la tive acts.This broad ened the pos si bil ity for a more pro found un der stand ing of the con tent and, if wemay put it this way, of the spirit of the years when the de vel op ment of the re form pro cess wasini ti ated. Thus, from the very be gin ning of our work, we had in our minds the gen eral pic tureof the whole re form pro cess with its main char ac ter is tics for its three stages.
Par al lel to the anal y sis of the nor ma tive (le gal and reg u la tory) and ad min is tra tive acts re -lated to the healthcare sys tem and its ac tiv i ties, pub lished in the “State Ga zette” for the pe riod1989 – 2005, an im por tant part of the health and po lit i cal anal y sis con tained the re views ofpub li ca tions made by the Min is try of Healthcare (MH) and other in sti tu tions.
On one hand, the me dia anal y sis we made on ma te ri als pub lished dur ing this pe riod,com pleted the health and po lit i cal anal y sis, and on the other hand, it fa cil i tated the trac ing ofthe ma jor prob lems of the healthcare sys tem (pub lished in the press and ex am ined by us fromvar i ous points of view), as well as their de vel op ment dur ing the dif fer ent stages of the re formin healthcare.
For the pur poses of the pres ent study, it was sa lient to also ana lyse some more sig nif i cantsta tis ti cal and eco nomic in di ca tors (from the point of view of their in for ma tive ness about the out comes of the healthcare re form). Thus, a part of the ob jec tive ev i dence was pro vided aboutthe de vel op ment of the healthcare sys tem and hence, about the ef fects of the re form.
As we al ready men tioned, the meth od ol ogy for the as sess ment of the healthcare re formwould be in com plete, if we did not take into ac count the opin ions of the ma jor par tic i pantsin the re form pro cess in our anal y sis. This is why an im por tant part of the pres ent study was ana tion ally rep re sen ta tive so cio log i cal sur vey, aimed at es tab lish ing the ac tual po si tion ing ofthe healthcare re form. Along with the anal y sis of the sta tus of the healthcare sys tem (and its ac -tiv i ties) and the health sta tus of the pop u la tion, this study was aimed at out lin ing the pos si bil i -ties for the sub se quent de vel op ment of the re form pro cess. The sur vey it self was con ducted inthe pe riod be tween May and No vem ber 2005 by “Al pha Re search” Ltd. so cio log i cal agency. In the pre lim i nary prep a ra tion, the in stru ments and the meth od ol ogy of the study were workedout jointly with spe cial ists from the agency.
The so cio log i cal sur vey in cluded:
· 458 med i cal spe cial ists: phy si cians and nurses from the out pa tients’ (pri mary and spe -cial ised) and in pa tients’ care, den tists and phar ma cists, with whom di rect stand ard isedin ter views were per formed. A quota sam ple was formed for each of the above groups
34
of med i cal spe cial ists, pro por tion ate to the size of the pop u lated area. The sur vey wasrep re sen ta tive for the em ployed in the healthcare sys tem.
· 168 rep re sen ta tives of man age ment di vi sions in the healthcare sys tem (ex ec u tive di -rec tors and man ag ers of hos pi tals, dis pen sa ries, di ag nos tic and con sul ta tive cen tres,med i cal cen tres, med ico-di ag nos tic lab o ra to ries, di rec tors of the Re gional HealthcareCen tres (RHC), Re gional In spec tions for Pro tec tion and Con trol of Pub lic Health(RICPPH) and Re gional Health In sur ance Funds (RHIF) to gether with lead ers of thepro fes sional or gani sa tions in the field of healthcare, may ors and rep re sen ta tives of mu -nic i pal coun cils. In di vid ual in-depth in ter views were held with all of them. The num -ber of the con ducted in ter views in the above tar get groups was dis trib utedpro por tion ately to the num ber of the mu nic i pal i ties in the coun try, grouped ac cord ingto their size. In the group of the hos pi tal di rec tors, ad di tional quota was in tro duced ac -cord ing to the type of hos pi tal es tab lish ment for med i cal care.
· 1013 cit i zens of full le gal age and sep a rately, two ad di tional sam ples of 100 peo pleeach from the Roma and Turk ish eth nic com mu ni ties. All of them un der went di rectstand ard ised in ter views. The sam ple was rep re sen ta tive for the full le gal aged pop u la -tion in the coun try and was formed ac cord ing to gen der, age, eth nic group, ed u ca tionand type of in hab ited re gion.
Ma te ri als
In our study, we used nu mer ous ma te ri als which can be sub di vided in the fol low inggroups:
1. Pre vi ous stud ies of the healthcare re form and the healthcare sys tem (in clud ing so cio -log i cal sur veys), part of which were ex am ined above and oth ers used in the com -ments to fol low;
2. Pub li ca tions re lated to the po lit i cal and so cio eco nomic con text of the health re form;3. Pub lished sta tis ti cal ma te ri als – re leases of the Na tional In sti tute of Sta tis tics (NIS),
the Na tional Cen tre for Health In for ma tion (NCHI), the Na tional Health In sur anceFund (NHIF), the Na tional In sur ance In sti tute (NII), in clud ing the websites of thesein sti tu tions;
4. Pub li ca tions of the Min is try of Healthcare and other in sti tu tions, in clud ing theirwebsites;
5. All the nor ma tive (le gal and reg u la tory) and ad min is tra tive acts pub lished in the“State Ga zette” in the pe riod 1989-2005 and re lated to the healthcare sys tem and itsac tiv i ties;
6. All the ma te ri als re lated to healthcare and pub lished in the pe riod 1989-2005 in thecen tral dai lies (“Trud”, “24 chasa”, “Standart”, “Duma”, “Democracia”) andsome week lies (“Kapital”, “Fo rum medicus”).
In our study, we paid par tic u lar at ten tion to the ma te ri als and the in for ma tion con tained in them, re sult ing from so cio log i cal sur veys and pub li ca tions (in for ma tive or com ments) in theprinted press. Though us ing dif fer ent ways, this in for ma tion re flects the pub lic opin ion – at ti -tudes, bi ases, needs, de sires, ex pec ta tions – of the cit i zens and so ci ety to the health sys tem andhealthcare. This in for ma tion is in dis pens able for de sign ing a health pol icy at tempt ing to fo cus on the cit i zen in so ci ety. We would like to emphasise “the cit i zen”, and not “the pa tient”,
35
A study of the healthcare re form: set ting, or gani sa tion and meth ods

which is the most com monly used cliché. Ev ery pa tient is a cit i zen, but not ev ery cit i zen is apa tient. The cit i zen be comes a pa tient when he/she gets in con tact with the health ser vices onthe oc ca sion of ill ness (in clud ing pro phy lac tic check-ups). But in all cases, the healthcare pro -cess works with all the cit i zens and only in one part with pa tients. There fore, the cit i zens withtheir rights and li a bil i ties have a pri or ity.
It is ex actly this in for ma tion that bears the truth about healthcare. And, if we are not fa mil -iar with it and if we do not use the sur veys on the dy nam ics of pub lic aware ness in the var i ouscom mu ni ties and its re flec tion in the mass me dia, this truth will be bur ied and the fo cus of thehealthcare pro cess will shift to other ob jects at the cit i zens’ ex pense.
Work ing team
The study was car ried out by a team con sist ing of three lead ing par tic i pants and op er a tiveas sis tants (stu dents from the Med i cal Uni ver sity “Prof. Dr. Paraskev Stoyanov” – Varna). Theso cio log i cal sur vey was con ducted by the “Al pha Re search” Agency Ltd. - So fia. The studywas funded by the “Open So ci ety In sti tute” Foun da tion - So fia.
36
PART IITHE HEALTHCARE RE FORM IN BUL GARIA
The healthcare re form in our coun try is a pro cess. The ex er tion of an im pact and in flu ence on a cer tain pro cess, more over in view of its man age ment, re quires good knowl edge of itscause-and-ef fect de ter mi na tion and evo lu tion – why and how this pro cess evolves, what are its goals, how does it un fold and what are the ex pected out comes from its de vel op ment. There -fore, at the be gin ning of the pres ent study, we started by ana lys ing the causes which broughtabout the healthcare re form in Bul garia.
4. In ev i ta ble, nec es sary and ir re vers ible pro cess
Why was the healthcare re form nec es sary and why is it still nec es sary?
The de vel op ment of the healthcare sec tor in Bul garia in the sec ond part of the pre vi ouscen tury had both pos i tive and neg a tive char ac ter is tic fea tures. The need for a healthcare re -form be comes ob vi ous from their comparison.
In this con text, it can be as serted that to ward the be gin ning of 1990 three main rea sonswere pres ent fore ground ing the need for a re form in the field of healthcare: (1) poor and de te ri -o rat ing health sta tus of the na tion; (2) de te ri o rat ing or gani sa tional con di tion and ca pac ity ofthe healthcare sys tem and (3) dis tinct dis crep ancy be tween the then-ex ist ing so cial sta tus andre la tions in side the healthcare sys tem, and the chang ing po lit i cal, eco nomic and socialconditions in Bulgaria.
De te ri o ra tion of the na tion’s health
When a pro cess of a na tion’s health de te ri o ra tion be gins in any of the mod ern coun tries,this is an alarm ing sig nal call ing for spe cial at ten tion to the healthcare sys tem. The health in di -ca tors of the na tion have an ut most im por tance for the de tailed plan ning and the scope of there form in the healthcare system.
As ev i dent from the ini tial data, in terms of ma te rial and hu man re sources, in the pe riodfrom 1960 to 1990, the healthcare sec tor in our coun try de vel oped un der fa vour able con di tions:
· there was a mul ti ple in crease of the pub lic prod uct (from 2 643.00 to 89 615.30 mil lionBGN), the na tional rev e nue, the pub lic con sump tion funds and the part of it al lo catedfor healthcare ex pen di ture and so cial in sur ance9;
· the ma te rial fa cil i ties and the staff were aug mented in the healthcare sys tem (Ta ble 1);
· ac cord ing to quan ti ta tive in di ca tors (e.g. av er age num ber of vis its to a phy si cian per in -hab it ant), the ac tiv ity of the healthcare net work was com pa ra ble to the in di ca tors of the other de vel oped states (Table 2), etc.
Dur ing this pe riod, the es sen tial healthcare prob lems in the field of healthcare in Bul gariawere solved, e.g.:
· in fec tious dis eases (par tic u larly as a fac tor for mor tal ity rate), ma laria and other par a -
37
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
9 Reference Book of Statistics. Published by the Centre of Statistics Management, Na tional In sti tute ofSta tis tics, Sofia, 1990
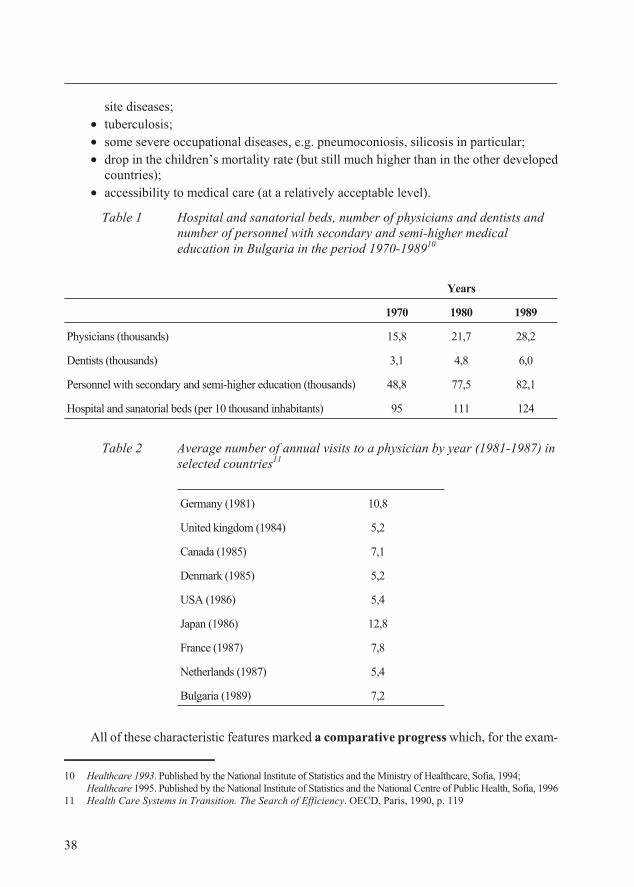
site dis eases;
· tu ber cu lo sis;
· some se vere oc cu pa tional dis eases, e.g. pneu mo co ni o sis, sil i co sis in particular;
· drop in the chil dren’s mor tal ity rate (but still much higher than in the other de vel opedcoun tries);
· ac ces si bil ity to med i cal care (at a rel a tively ac cept able level).
Ta ble 1 Hospital and sanatorial beds, number of physicians and dentists andnumber of personnel with secondary and semi-higher medicaleducation in Bulgaria in the period 1970-198910
Ta ble 2 Average number of annual visits to a physician by year (1981-1987) in selected countries11
All of these char ac ter is tic fea tures marked a com par a tive prog ress which, for the ex am -
38
Ger many (1981) 10,8
United king dom (1984) 5,2
Can ada (1985) 7,1
Den mark (1985) 5,2
USA (1986) 5,4
Ja pan (1986) 12,8
France (1987) 7,8
Neth er lands (1987) 5,4
Bul garia (1989) 7,2
Years
1970 1980 1989
Phy si cians (thou sands) 15,8 21,7 28,2
Den tists (thou sands) 3,1 4,8 6,0
Per son nel with sec ond ary and semi-higher ed u ca tion (thou sands) 48,8 77,5 82,1
Hos pi tal and sanatorial beds (per 10 thou sand in hab it ants) 95 111 124
10 Healthcare 1993. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1994;Healthcare 1995. Published by the National Institute of Statistics and the National Centre of Public Health, Sofia, 1996
11 Health Care Systems in Transition. The Search of Efficiency. OECD, Paris, 1990, p. 119
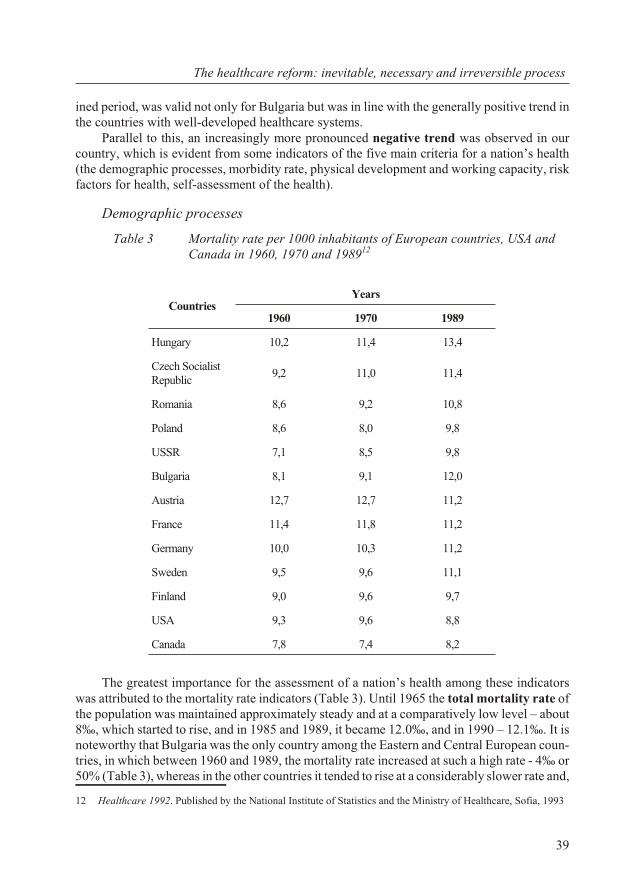
ined pe riod, was valid not only for Bul garia but was in line with the gen er ally pos i tive trend inthe coun tries with well-de vel oped healthcare sys tems.
Par al lel to this, an in creas ingly more pro nounced neg a tive trend was ob served in ourcoun try, which is ev i dent from some in di ca tors of the five main cri te ria for a na tion’s health(the de mo graphic pro cesses, mor bid ity rate, phys i cal de vel op ment and work ing ca pac ity, riskfac tors for health, self-as sess ment of the health).
De mo graphic pro cesses
Ta ble 3 Mor tal ity rate per 1000 in hab it ants of Eu ro pean coun tries, USA andCan ada in 1960, 1970 and 198912
The great est im por tance for the as sess ment of a na tion’s health among these in di ca torswas at trib uted to the mor tal ity rate in di ca tors (Ta ble 3). Un til 1965 the to tal mor tal ity rate ofthe pop u la tion was main tained ap prox i mately steady and at a com par a tively low level – about8‰, which started to rise, and in 1985 and 1989, it be came 12.0‰, and in 1990 – 12.1‰. It isnote wor thy that Bul garia was the only coun try among the East ern and Cen tral Eu ro pean coun -tries, in which be tween 1960 and 1989, the mor tal ity rate in creased at such a high rate - 4‰ or50% (Ta ble 3), whereas in the other coun tries it tended to rise at a con sid er ably slower rate and,
39
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
Coun triesYears
1960 1970 1989
Hun gary 10,2 11,4 13,4
Czech So cial istRe pub lic
9,2 11,0 11,4
Ro ma nia 8,6 9,2 10,8
Po land 8,6 8,0 9,8
USSR 7,1 8,5 9,8
Bul garia 8,1 9,1 12,0
Aus tria 12,7 12,7 11,2
France 11,4 11,8 11,2
Ger many 10,0 10,3 11,2
Swe den 9,5 9,6 11,1
Fin land 9,0 9,6 9,7
USA 9,3 9,6 8,8
Can ada 7,8 7,4 8,2
12 Healthcare 1992. Pub lished by the Na tional In sti tute of Sta tis tics and the Min is try of Healthcare, So fia, 1993
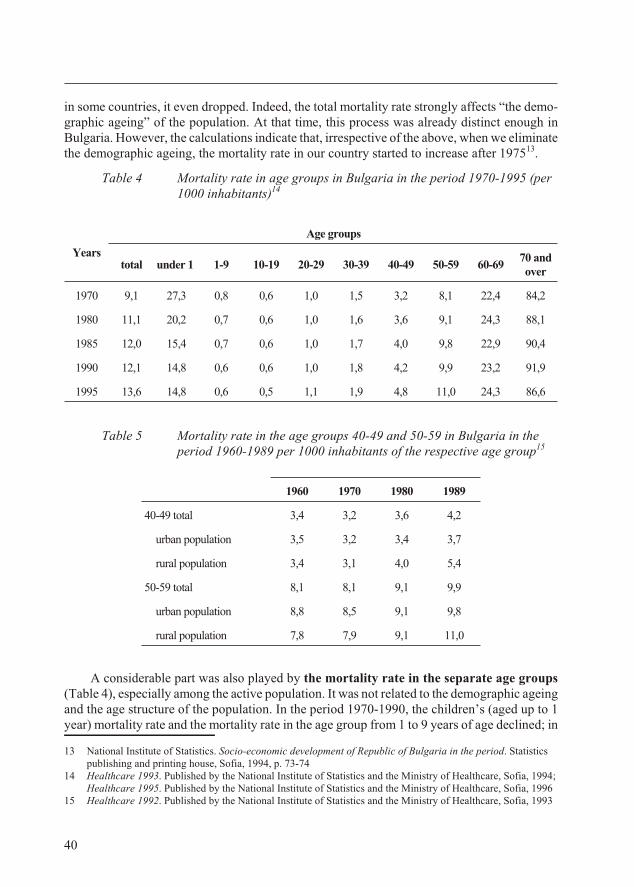
in some coun tries, it even dropped. In deed, the to tal mor tal ity rate strongly af fects “the de mo -graphic age ing” of the pop u la tion. At that time, this pro cess was al ready dis tinct enough inBul garia. How ever, the cal cu la tions in di cate that, ir re spec tive of the above, when we elim i nate the de mo graphic age ing, the mor tal ity rate in our coun try started to in crease af ter 197513.
Ta ble 4 Mor tal ity rate in age groups in Bul garia in the pe riod 1970-1995 (per1000 in hab it ants)14
Ta ble 5 Mor tal ity rate in the age groups 40-49 and 50-59 in Bul garia in thepe riod 1960-1989 per 1000 in hab it ants of the re spec tive age group15
A con sid er able part was also played by the mor tal ity rate in the sep a rate age groups(Ta ble 4), es pe cially among the ac tive pop u la tion. It was not re lated to the de mo graphic age ing and the age struc ture of the pop u la tion. In the pe riod 1970-1990, the chil dren’s (aged up to 1year) mor tal ity rate and the mor tal ity rate in the age group from 1 to 9 years of age de clined; in
40
Years
Age groups
total under 1 1-9 10-19 20-29 30-39 40-49 50-59 60-6970 andover
1970 9,1 27,3 0,8 0,6 1,0 1,5 3,2 8,1 22,4 84,2
1980 11,1 20,2 0,7 0,6 1,0 1,6 3,6 9,1 24,3 88,1
1985 12,0 15,4 0,7 0,6 1,0 1,7 4,0 9,8 22,9 90,4
1990 12,1 14,8 0,6 0,6 1,0 1,8 4,2 9,9 23,2 91,9
1995 13,6 14,8 0,6 0,5 1,1 1,9 4,8 11,0 24,3 86,6
1960 1970 1980 1989
40-49 to tal 3,4 3,2 3,6 4,2
ur ban pop u la tion 3,5 3,2 3,4 3,7
ru ral pop u la tion 3,4 3,1 4,0 5,4
50-59 to tal 8,1 8,1 9,1 9,9
ur ban pop u la tion 8,8 8,5 9,1 9,8
ru ral pop u la tion 7,8 7,9 9,1 11,0
13 Na tional In sti tute of Sta tis tics. Socio-eco nomic de vel op ment of Re pub lic of Bul garia in the pe riod. Sta tis ticspub lish ing and print ing house, So fia, 1994, p. 73-74
14 Healthcare 1993. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1994; Healthcare 1995. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1996
15 Healthcare 1992. Pub lished by the Na tional In sti tute of Sta tis tics and the Min is try of Healthcare, So fia, 1993
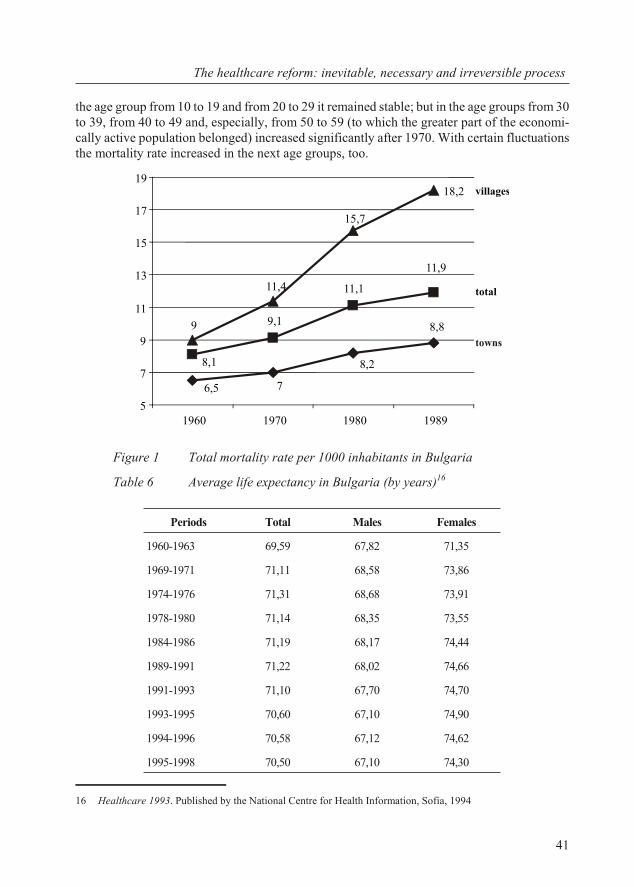
the age group from 10 to 19 and from 20 to 29 it re mained sta ble; but in the age groups from 30to 39, from 40 to 49 and, es pe cially, from 50 to 59 (to which the greater part of the eco nom i -cally ac tive pop u la tion be longed) in creased sig nif i cantly af ter 1970. With cer tain fluc tu a tionsthe mor tal ity rate increased in the next age groups, too.
Fig ure 1 To tal mor tal ity rate per 1000 in hab it ants in Bul garia
Ta ble 6 Av er age life ex pec tancy in Bul garia (by years)16
41
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
18,2
6,5 7
8,2
8,8
11,9
11,1
9,1
8,1
15,7
11,4
9
5
7
9
11
13
15
17
19
1960 1970 1980 1989
villages
total
towns
Periods Total Males Females
1960-1963 69,59 67,82 71,35
1969-1971 71,11 68,58 73,86
1974-1976 71,31 68,68 73,91
1978-1980 71,14 68,35 73,55
1984-1986 71,19 68,17 74,44
1989-1991 71,22 68,02 74,66
1991-1993 71,10 67,70 74,70
1993-1995 70,60 67,10 74,90
1994-1996 70,58 67,12 74,62
1995-1998 70,50 67,10 74,30
16 Healthcare 1993. Pub lished by the Na tional Cen tre for Health In for ma tion, So fia, 1994
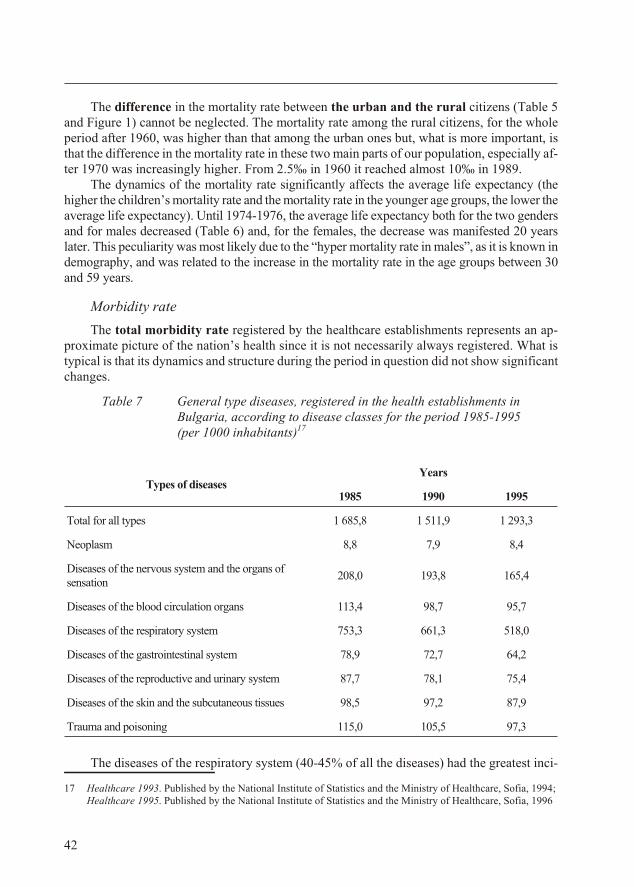
The dif fer ence in the mor tal ity rate be tween the ur ban and the ru ral cit i zens (Ta ble 5and Fig ure 1) can not be ne glected. The mor tal ity rate among the ru ral cit i zens, for the wholepe riod af ter 1960, was higher than that among the ur ban ones but, what is more im por tant, isthat the dif fer ence in the mor tal ity rate in these two main parts of our pop u la tion, es pe cially af -ter 1970 was in creas ingly higher. From 2.5‰ in 1960 it reached al most 10‰ in 1989.
The dy nam ics of the mor tal ity rate sig nif i cantly af fects the av er age life ex pec tancy (thehigher the chil dren’s mor tal ity rate and the mor tal ity rate in the youn ger age groups, the lower the av er age life ex pec tancy). Un til 1974-1976, the av er age life ex pec tancy both for the two gen dersand for males de creased (Ta ble 6) and, for the fe males, the de crease was man i fested 20 yearslater. This pe cu liar ity was most likely due to the “hy per mor tal ity rate in males”, as it is known inde mog ra phy, and was re lated to the in crease in the mor tal ity rate in the age groups be tween 30and 59 years.
Mor bid ity rate
The to tal mor bid ity rate reg is tered by the healthcare es tab lish ments rep re sents an ap -prox i mate pic ture of the na tion’s health since it is not nec es sar ily al ways reg is tered. What istyp i cal is that its dy nam ics and struc ture dur ing the pe riod in ques tion did not show sig nif i cantchanges.
Ta ble 7 Gen eral type dis eases, reg is tered in the health es tab lish ments inBul garia, ac cord ing to dis ease classes for the pe riod 1985-1995 (per 1000 in hab it ants)17
The dis eases of the re spi ra tory sys tem (40-45% of all the dis eases) had the great est in ci -
42
Types of dis easesYears
1985 1990 1995
To tal for all types 1 685,8 1 511,9 1 293,3
Neo plasm 8,8 7,9 8,4
Dis eases of the ner vous sys tem and the or gans ofsen sa tion
208,0 193,8 165,4
Dis eases of the blood cir cu la tion or gans 113,4 98,7 95,7
Dis eases of the re spi ra tory sys tem 753,3 661,3 518,0
Dis eases of the gas tro in tes ti nal sys tem 78,9 72,7 64,2
Dis eases of the re pro duc tive and uri nary sys tem 87,7 78,1 75,4
Dis eases of the skin and the sub cu ta ne ous tis sues 98,5 97,2 87,9
Trauma and poi son ing 115,0 105,5 97,3
17 Healthcare 1993. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1994; Healthcare 1995. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1996
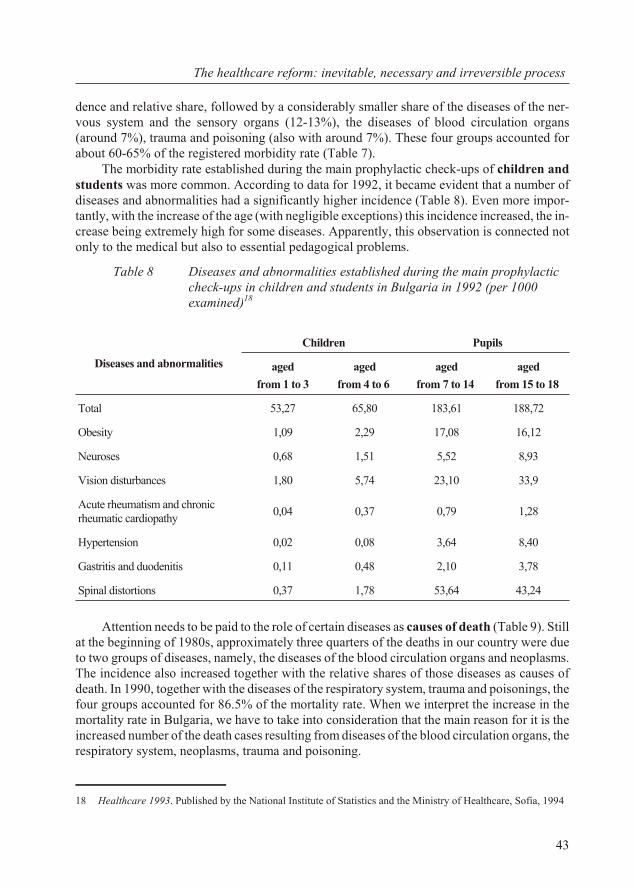
dence and rel a tive share, fol lowed by a con sid er ably smaller share of the dis eases of the ner -vous sys tem and the sen sory or gans (12-13%), the dis eases of blood cir cu la tion or gans(around 7%), trauma and poi son ing (also with around 7%). These four groups ac counted forabout 60-65% of the reg is tered mor bid ity rate (Ta ble 7).
The mor bid ity rate es tab lished dur ing the main pro phy lac tic check-ups of chil dren andstu dents was more com mon. Ac cord ing to data for 1992, it be came ev i dent that a num ber ofdis eases and ab nor mal i ties had a sig nif i cantly higher in ci dence (Ta ble 8). Even more im por -tantly, with the in crease of the age (with neg li gi ble ex cep tions) this in ci dence in creased, the in -crease be ing ex tremely high for some dis eases. Ap par ently, this ob ser va tion is con nected notonly to the med i cal but also to es sen tial ped a gog i cal prob lems.
Ta ble 8 Diseases and abnormalities established during the main prophylacticcheck-ups in children and students in Bulgaria in 1992 (per 1000examined)18
At ten tion needs to be paid to the role of cer tain dis eases as causes of death (Ta ble 9). Still at the be gin ning of 1980s, ap prox i mately three quar ters of the deaths in our coun try were dueto two groups of dis eases, namely, the dis eases of the blood cir cu la tion or gans and neoplasms.The in ci dence also in creased to gether with the rel a tive shares of those dis eases as causes ofdeath. In 1990, to gether with the dis eases of the re spi ra tory sys tem, trauma and poi son ings, the four groups ac counted for 86.5% of the mor tal ity rate. When we in ter pret the in crease in themor tal ity rate in Bul garia, we have to take into con sid er ation that the main rea son for it is thein creased num ber of the death cases re sult ing from dis eases of the blood cir cu la tion or gans, the re spi ra tory sys tem, neoplasms, trauma and poi son ing.
43
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
Dis eases and ab nor mal i ties
Chil dren Pu pils
aged
from 1 to 3
aged
from 4 to 6
aged
from 7 to 14
aged
from 15 to 18
To tal 53,27 65,80 183,61 188,72
Obe sity 1,09 2,29 17,08 16,12
Neu ro ses 0,68 1,51 5,52 8,93
Vi sion dis tur bances 1,80 5,74 23,10 33,9
Acute rheu ma tism and chronicrheu matic cardiopathy
0,04 0,37 0,79 1,28
Hy per ten sion 0,02 0,08 3,64 8,40
Gas tri tis and duodenitis 0,11 0,48 2,10 3,78
Spi nal dis tor tions 0,37 1,78 53,64 43,24
18 Healthcare 1993. Pub lished by the Na tional In sti tute of Sta tis tics and the Min is try of Healthcare, So fia, 1994
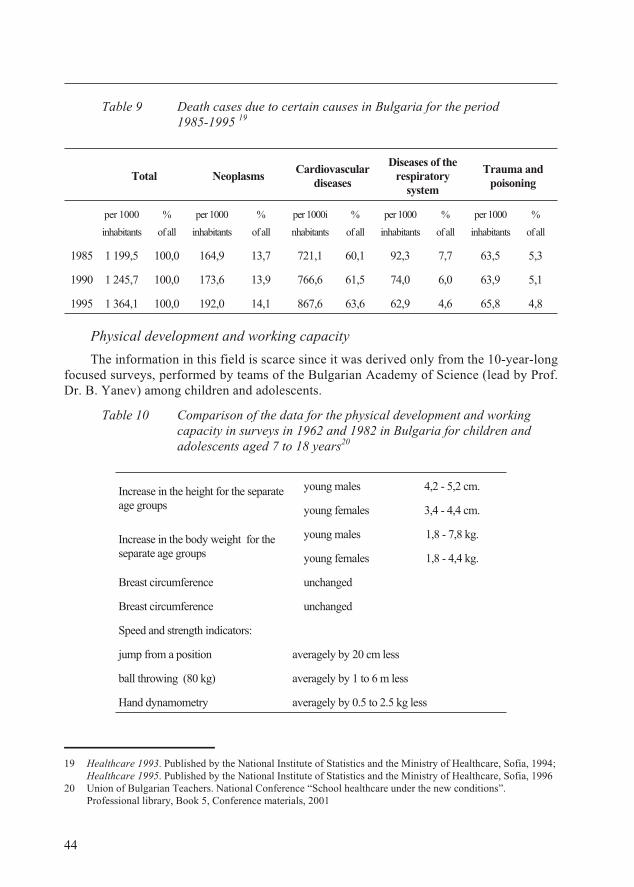
Ta ble 9 Death cases due to certain causes in Bulgaria for the period1985-1995 19
Phys i cal de vel op ment and work ing ca pac ity
The in for ma tion in this field is scarce since it was de rived only from the 10-year-longfo cused sur veys, per formed by teams of the Bul gar ian Acad emy of Sci ence (lead by Prof.Dr. B. Yanev) among chil dren and ad o les cents.
Ta ble 10 Com par i son of the data for the phys i cal de vel op ment and work ingca pac ity in sur veys in 1962 and 1982 in Bul garia for chil dren andad o les cents aged 7 to 18 years20
44
To tal NeoplasmsCar dio vas cu lar
dis eases
Dis eases of there spi ra tory
sys tem
Trauma andpoi son ing
per 1000
in hab it ants
%
of all
per 1000
inhabitants
%
of all
per 1000i
nhabitants
%
of all
per 1000
inhabitants
%
of all
per 1000
inhabitants
%
of all
1985 1 199,5 100,0 164,9 13,7 721,1 60,1 92,3 7,7 63,5 5,3
1990 1 245,7 100,0 173,6 13,9 766,6 61,5 74,0 6,0 63,9 5,1
1995 1 364,1 100,0 192,0 14,1 867,6 63,6 62,9 4,6 65,8 4,8
In crease in the height for the sep a rateage groups
young males 4,2 - 5,2 cm.
young fe males 3,4 - 4,4 cm.
In crease in the body weight for thesep a rate age groups
young males 1,8 - 7,8 kg.
young fe males 1,8 - 4,4 kg.
Breast cir cum fer ence un changed
Breast cir cum fer ence un changed
Speed and strength in di ca tors:
jump from a po si tion av er agely by 20 cm less
ball throw ing (80 kg) av er agely by 1 to 6 m less
Hand dynamometry av er agely by 0.5 to 2.5 kg less
19 Healthcare 1993. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1994; Healthcare 1995. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1996
20 Un ion of Bul gar ian Teach ers. Na tional Con fer ence “School healthcare un der the new con di tions”.Pro fes sional li brary, Book 5, Con fer ence ma te ri als, 2001
For the pe riod 1962-1982, an in crease was es tab lished in the height and the body weightin the re spec tive age and gen der groups (Ta ble 10), the breast cir cum fer ence and the shoul derdi am e ter re main ing un changed. Broadly speak ing, this cor re sponded to the pro cess of ac cel er -a tion among the ad o les cents. What is dis turb ing in this case is that the so matic in di ca tors werenot ac com pa nied by the work ing ca pac ity de vel op ment. As com pared to 1962, in 1982 thespeed and strength in di ca tors were sig nif i cantly low ered. In this re spect, the health prob lemsover lapped with the ped a gog i cal ones.
Risk fac tors
A sig nif i cant part of the ex og e nous and en dog e nous risk fac tors for health have a cu mu la -tive or re mote ef fect. The clin i cal out come of their im pact is not man i fested im me di ately butsome times af ter a lon ger pe riod of time. The pres ence of risk fac tors to day may be clin i callyman i fested af ter months or years. This de ter mines their im por tance as a sep a rate cri te rion forthe as sess ment of a na tion’s health.
In the pe riod af ter 1970 un til 1990 no sig nif i cant dy nam ics was ob served of the ex og e -nous fac tors re lated mainly to the en vi ron men tal con di tions in the coun try. At the end of thepe riod, an in flu ence started to be per ceived by some so cial and eco nomic fac tors. The struc -ture of the ex penses, made by the pop u la tion, be gan to de te ri o rate. The rise in the ex penses forfood (at the ex pense of the drop in other ex penses) had an ad verse ef fect and in 1990 theyreached 36.1% (and in 1991 up to 47.4%) of all the ex penses21. Just for the sake of com par i son, dur ing the same year this share of the ex penses in France was 20% and in the United States -14%. The dis turbed struc ture of spend ing led to a de te ri o ra tion of con sump tion, es pe cially ofprod ucts of preventive or promotional importance for the human health.
Among the en dog e nous risk fac tors a con sid er able role was played by obe sity. In Bul -garia, ac cord ing to the so called “body mass in dex”, 38.9% of the peo ple over 18 years of agewere over weight, the coun try rank ing one of the first in Eu rope ac cord ing to this indicator.
Self-as sess ment of the health sta tus
The self-as sess ment of the health sta tus is a sub jec tive ex pe ri ence of the in di vid u als about their own con di tion which may not co in cide with the ob jec tive man i fes ta tions (“good” or“bad”). Since we do not have other avail able data, we will use the data from a rep re sen ta tiveques tion naire sur vey for the coun try, con ducted by the Na tional In sti tute of Sta tis tics22. The re -spon dents in di cated the fol low ing as sess ment of their own health sta tus: very good – 21.7%,good – 44.7%, sat is fac tory – 25.7%, poor – 6.7% and very poor – 1.2%. At the same time27.8% of the males and 38.8% of the fe males re ported that dur ing the last three years theirhealth had be come worse.
With out un der es ti mat ing the prog ress achieved mainly af ter 1960 in the so lu tion ofcer tain very sig nif i cant prob lems (re duc tion of the mor bid ity rate and es pe cially of the mor -tal ity rate from in fec tious dis eases and the in ci dence of the par a site dis eases and the erad i ca -tion of ma laria as a prob lem; sig nif i cant re duc tion in the mor bid ity and mor tal ity rate fromtu ber cu lo sis; re duc tion in the in ci dence of a num ber of oc cu pa tional dis eases and es pe cially
45
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
21 Na tional In sti tute of Sta tis tics. Socio-eco nomic de vel op ment of Re pub lic of Bul garia in the pe riod. Sta tis ticspub lish ing and print ing house, So fia, 1994, p. 66-67
22 Stan dard of liv ing of the pop u la tion in Bul garia. Na tional In sti tute of Sta tis tics, So fia, 1996
from sil i co sis; re duc tion of the chil dren’s mor tal ity rate) from the be gin ning of 1970s of the20th cen tury, alarm ing signs be came man i fested of grad u ally de vel op ing deg ra da tion of thena tion’s health sta tus. This ad verse trend found its man i fes ta tion in a se ries of signs whichhad not been ob served be fore. The rates of in crease in the mor tal ity rate played a con sid er -able im por tance to gether with the es ca la tion in the mor tal ity rate among peo ple in the ac tiveage groups, the in creas ing dif fer ence in the in di ca tors for the mor tal ity be tween the ur banand ru ral pop u la tion. All these ad verse pro cesses were re flected in the drop of the av er agelife ex pec tancy. These alarm ing facts were re in forced by the in creas ing in ci dence of thedeath rates from dis eases of the blood cir cu la tion or gans, the re spi ra tory sys tem, neoplasms,trauma and poi son ing. The health sta tus of the chil dren and stu dents was also un fa vour able.The neg a tive trends also stood out in terms of some risk fac tors and the self-as sess ment ofthe health sta tus. These signs (to emphasise once again, not ob served un til then and ap pear -ing for the first time) in di cated an emerg ing crit i cal sit u a tion for the pop u la tion’s health inour coun try.
De te ri o ra tion of the or gani sa tional state, the ca pac ity and pos si bil i ties ofthe healthcare sys tem
The de te ri o rated health sta tus of the na tion cor re sponded to a con sid er able de gree to cer -tain neg a tive pro cesses in the or gani sa tional state and the de vel op ment of the Bul gar ianhealthcare sys tem. In the anal y sis be low, the prob lems and the con di tion of the spe cial ised pro -phy laxis net work (hy gienic and ep i de mi o log i cal in spec tions) and the drug sup ply are not dis -cussed but, re gard ing them, the healthcare re form had spe cific fea tures. The spe cial isedpro phy laxis net work is al ways pub lic (state, mu nic i pal) in na ture and is main tained by so ci ety.The drug sup ply has to do with com mod i ties and goods (ob jects) prod ucts and is im me di atelyre lated to the mar ket prin ci ples. We will con sider mainly the de vel op ment of the mass med i calac tiv i ties in the out pa tients’ and hos pi tal med i cal care.
Above all, it is note wor thy that in the Bul gar ian so cial ist health sys tem un til 1989 themain bal ances, which en sure the sta bil ity of ev ery well and ad e quately de vel op ing sys tem of healthcare, were more or less dis turbed:
· be tween the de mand and sup ply of the health ser vices;
· be tween the pub lic and the pri vate sec tor;
· be tween the pre ven tive and pro mo tional, and the treat ment ac tiv i ties;
· be tween out pa tients’ and in pa tients’ care;
· be tween pri mary and spe cial ised out pa tients’ care.
The dis turbed bal ance re sulted mainly from dis pro por tions in the ob jec tives and the cen -tral ised dis tri bu tion of the re sources of the sys tem.
Fol lowing the model of the healthcare sys tem in the So viet Un ion formed af ter WorldWar II, the healthcare sys tem in Bul gar ian de vel oped as a sys tem based on the sup ply (ofhealth ac tiv i ties and ser vices) and not on the bal ance be tween de mand (needs) and sup ply.This fun da men tal prin ci ple doomed the healthcare sys tem to ex ten sive de vel op ment since it was ex pected to con stantly sup ply. This is why both the plan ning and the func tion ing ofthe in sti tu tions (es tab lish ments) in the sys tem were bound nei ther to the sup ply, nor to thede mand for their ac tiv i ties. This was ob served in all types of hos pi tal es tab lish ments but, to
46
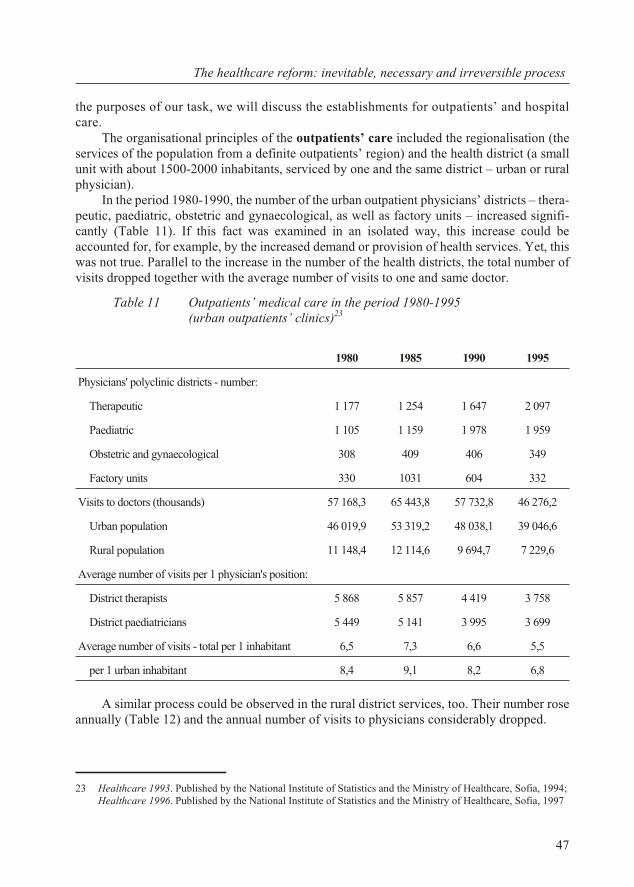
the pur poses of our task, we will dis cuss the es tab lish ments for out pa tients’ and hos pi talcare.
The or gani sa tional prin ci ples of the out pa tients’ care in cluded the region ali sa tion (theser vices of the pop u la tion from a def i nite out pa tients’ re gion) and the health dis trict (a smallunit with about 1500-2000 in hab it ants, ser viced by one and the same dis trict – ur ban or ruralphysician).
In the pe riod 1980-1990, the num ber of the ur ban out pa tient phy si cians’ dis tricts – ther a -peu tic, pae di at ric, ob stet ric and gy nae co logi cal, as well as fac tory units – in creased sig nif i -cantly (Ta ble 11). If this fact was ex am ined in an iso lated way, this in crease could beac counted for, for ex am ple, by the in creased de mand or pro vi sion of health ser vices. Yet, thiswas not true. Par al lel to the in crease in the num ber of the health dis tricts, the to tal num ber ofvis its dropped to gether with the av er age number of visits to one and same doctor.
Ta ble 11 Outpatients’ medical care in the period 1980-1995 (urban outpatients’ clinics)23
A sim i lar pro cess could be ob served in the ru ral dis trict ser vices, too. Their num ber rosean nu ally (Ta ble 12) and the an nual num ber of vis its to phy si cians con sid er ably dropped.
47
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
1980 1985 1990 1995
Phy si cians' poly clinic dis tricts - num ber:
Ther a peu tic 1 177 1 254 1 647 2 097
Pae di at ric 1 105 1 159 1 978 1 959
Ob stet ric and gy nae co logi cal 308 409 406 349
Fac tory units 330 1031 604 332
Vis its to doc tors (thou sands) 57 168,3 65 443,8 57 732,8 46 276,2
Ur ban pop u la tion 46 019,9 53 319,2 48 038,1 39 046,6
Ru ral pop u la tion 11 148,4 12 114,6 9 694,7 7 229,6
Av er age num ber of vis its per 1 phy si cian's po si tion:
Dis trict ther a pists 5 868 5 857 4 419 3 758
Dis trict paediatricians 5 449 5 141 3 995 3 699
Av er age num ber of vis its - to tal per 1 in hab it ant 6,5 7,3 6,6 5,5
per 1 ur ban in hab it ant 8,4 9,1 8,2 6,8
23 Healthcare 1993. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1994; Healthcare 1996. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1997
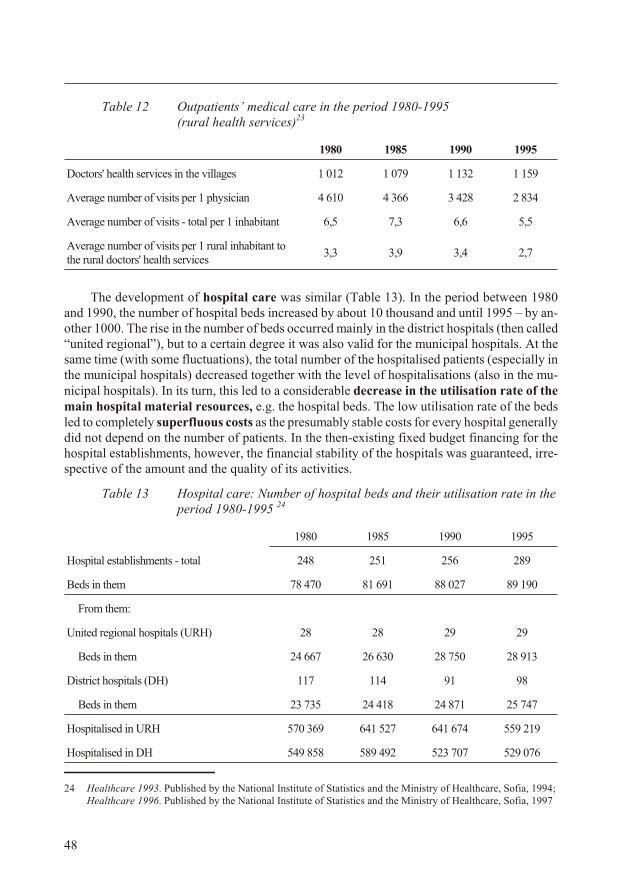
Ta ble 12 Outpatients’ medical care in the period 1980-1995 (rural health services)23
1980 1985 1990 1995
Doc tors' health ser vices in the vil lages 1 012 1 079 1 132 1 159
Av er age num ber of vis its per 1 phy si cian 4 610 4 366 3 428 2 834
Av er age num ber of vis its - to tal per 1 in hab it ant 6,5 7,3 6,6 5,5
Av er age num ber of vis its per 1 ru ral in hab it ant tothe ru ral doc tors' health services
3,3 3,9 3,4 2,7
The de vel op ment of hos pi tal care was sim i lar (Ta ble 13). In the pe riod be tween 1980and 1990, the num ber of hos pi tal beds in creased by about 10 thou sand and un til 1995 – by an -other 1000. The rise in the num ber of beds oc curred mainly in the dis trict hos pi tals (then called“united re gional”), but to a cer tain de gree it was also valid for the mu nic i pal hos pi tals. At thesame time (with some fluc tu a tions), the to tal num ber of the hos pi ta lised pa tients (es pe cially inthe mu nic i pal hos pi tals) de creased to gether with the level of hos pi ta li sa tions (also in the mu -nic i pal hos pi tals). In its turn, this led to a con sid er able de crease in the uti li sa tion rate of themain hos pi tal ma te rial re sources, e.g. the hos pi tal beds. The low uti li sa tion rate of the bedsled to com pletely su per flu ous costs as the pre sum ably sta ble costs for ev ery hos pi tal gen er ally did not de pend on the num ber of pa tients. In the then-ex ist ing fixed bud get fi nanc ing for thehos pi tal es tab lish ments, how ever, the fi nan cial sta bil ity of the hos pi tals was guar an teed, ir re -spec tive of the amount and the qual ity of its ac tiv i ties.
Ta ble 13 Hos pi tal care: Number of hospital beds and their utilisation rate in the period 1980-1995 24
1980 1985 1990 1995
Hos pi tal es tab lish ments - to tal 248 251 256 289
Beds in them 78 470 81 691 88 027 89 190
From them:
United re gional hos pi tals (URH) 28 28 29 29
Beds in them 24 667 26 630 28 750 28 913
Dis trict hos pi tals (DH) 117 114 91 98
Beds in them 23 735 24 418 24 871 25 747
Hos pi ta lised in URH 570 369 641 527 641 674 559 219
Hos pi ta lised in DH 549 858 589 492 523 707 529 076
48
24 Healthcare 1993. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1994; Healthcare 1996. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1997
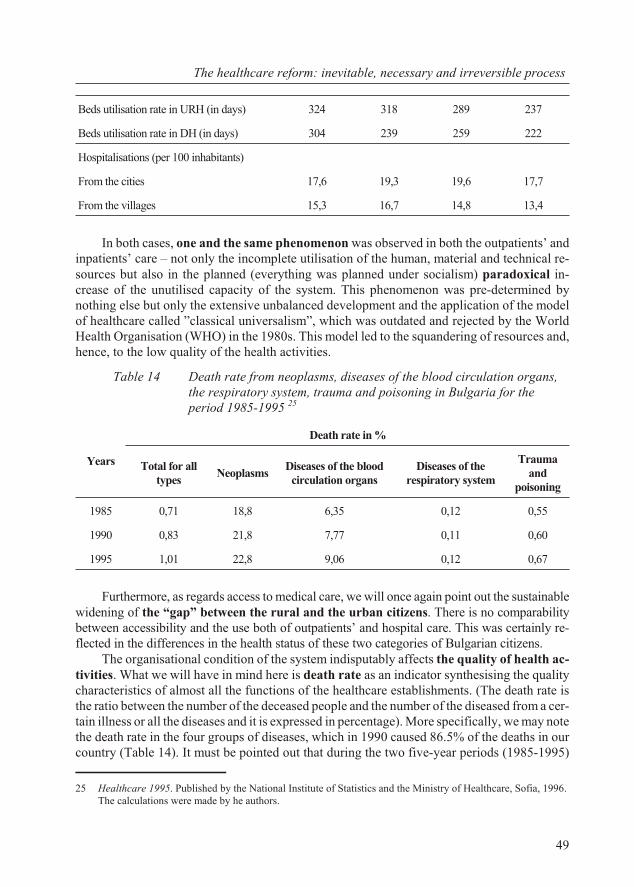
Beds uti li sa tion rate in URH (in days) 324 318 289 237
Beds uti li sa tion rate in DH (in days) 304 239 259 222
Hos pi ta li sa tions (per 100 in hab it ants)
From the cit ies 17,6 19,3 19,6 17,7
From the vil lages 15,3 16,7 14,8 13,4
In both cases, one and the same phe nom e non was ob served in both the out pa tients’ andin pa tients’ care – not only the in com plete uti li sa tion of the hu man, ma te rial and tech ni cal re -sources but also in the planned (ev ery thing was planned un der so cial ism) par a dox i cal in -crease of the unutilised ca pac ity of the sys tem. This phe nom e non was pre-de ter mined bynoth ing else but only the ex ten sive un bal anced de vel op ment and the ap pli ca tion of the modelof healthcare called ”clas si cal uni ver sal ism”, which was out dated and re jected by the WorldHealth Or gani sa tion (WHO) in the 1980s. This model led to the squan der ing of re sources and,hence, to the low qual ity of the health ac tiv i ties.
Ta ble 14 Death rate from neoplasms, dis eases of the blood cir cu la tion or gans,the re spi ra tory sys tem, trauma and poi son ing in Bul garia for thepe riod 1985-1995 25
Years
Death rate in %
To tal for alltypes
NeoplasmsDis eases of the blood
cir cu la tion or gansDis eases of the
re spi ra tory sys tem
Traumaand
poisoning
1985 0,71 18,8 6,35 0,12 0,55
1990 0,83 21,8 7,77 0,11 0,60
1995 1,01 22,8 9,06 0,12 0,67
Fur ther more, as re gards ac cess to med i cal care, we will once again point out the sus tain ablewid en ing of the “gap” be tween the ru ral and the ur ban cit i zens. There is no com pa ra bil itybe tween ac ces si bil ity and the use both of out pa tients’ and hos pi tal care. This was cer tainly re -flected in the dif fer ences in the health sta tus of these two cat e go ries of Bul gar ian cit i zens.
The or gani sa tional con di tion of the sys tem in dis put ably af fects the qual ity of health ac -tiv i ties. What we will have in mind here is death rate as an in di ca tor syn the sis ing the qual itychar ac ter is tics of al most all the func tions of the healthcare es tab lish ments. (The death rate isthe ra tio be tween the num ber of the de ceased peo ple and the num ber of the dis eased from a cer -tain ill ness or all the dis eases and it is ex pressed in per cent age). More spe cif i cally, we may note the death rate in the four groups of dis eases, which in 1990 caused 86.5% of the deaths in ourcoun try (Ta ble 14). It must be pointed out that dur ing the two five-year pe ri ods (1985-1995)
49
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
25 Healthcare 1995. Published by the National Institute of Statistics and the Ministry of Healthcare, Sofia, 1996. The calculations were made by he authors.
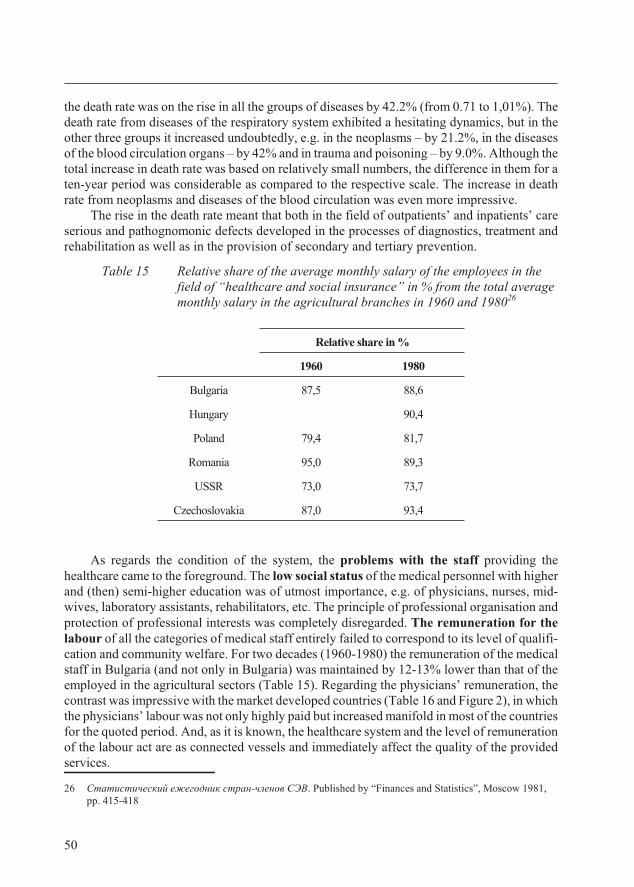
the death rate was on the rise in all the groups of dis eases by 42.2% (from 0.71 to 1,01%). Thedeath rate from dis eases of the re spi ra tory sys tem ex hib ited a hes i tat ing dy nam ics, but in theother three groups it in creased un doubt edly, e.g. in the neoplasms – by 21.2%, in the dis easesof the blood cir cu la tion or gans – by 42% and in trauma and poi son ing – by 9.0%. Al though theto tal in crease in death rate was based on rel a tively small num bers, the dif fer ence in them for aten-year pe riod was con sid er able as com pared to the re spec tive scale. The in crease in deathrate from neoplasms and diseases of the blood circulation was even more impressive.
The rise in the death rate meant that both in the field of out pa tients’ and in pa tients’ carese ri ous and pathognomonic de fects de vel oped in the pro cesses of di ag nos tics, treat ment andre ha bil i ta tion as well as in the pro vi sion of sec ond ary and ter tiary pre ven tion.
Ta ble 15 Rel a tive share of the av er age monthly sal ary of the em ploy ees in thefield of “healthcare and so cial in sur ance” in % from the to tal av er agemonthly sal ary in the ag ri cul tural branches in 1960 and 198026
As re gards the con di tion of the sys tem, the prob lems with the staff pro vid ing thehealthcare came to the fore ground. The low so cial sta tus of the med i cal per son nel with higherand (then) semi-higher ed u ca tion was of ut most im por tance, e.g. of phy si cians, nurses, mid -wives, lab o ra tory as sis tants, rehabilitators, etc. The prin ci ple of pro fes sional or gani sa tion andpro tec tion of pro fes sional in ter ests was com pletely dis re garded. The re mu ner a tion for thela bour of all the cat e go ries of med i cal staff en tirely failed to cor re spond to its level of qual i fi -ca tion and com mu nity wel fare. For two de cades (1960-1980) the re mu ner a tion of the med i calstaff in Bul garia (and not only in Bul garia) was main tained by 12-13% lower than that of theem ployed in the ag ri cul tural sec tors (Ta ble 15). Re gard ing the phy si cians’ re mu ner a tion, thecon trast was im pres sive with the mar ket de vel oped coun tries (Ta ble 16 and Fig ure 2), in which the phy si cians’ la bour was not only highly paid but in creased man i fold in most of the coun tries for the quoted pe riod. And, as it is known, the healthcare sys tem and the level of re mu ner a tionof the la bour act are as con nected ves sels and im me di ately af fect the qual ity of the pro videdser vices.
50
Relative share in %
1960 1980
Bul garia 87,5 88,6
Hun gary 90,4
Po land 79,4 81,7
Ro ma nia 95,0 89,3
USSR 73,0 73,7
Czecho slo va kia 87,0 93,4
26 Ñòàòèñòè÷åñêèé åæåãîäíèê ñòðàí-÷ëåíîâ ÑÝÂ. Pub lished by “Fi nances and Sta tis tics”, Mos cow 1981,pp. 415-418
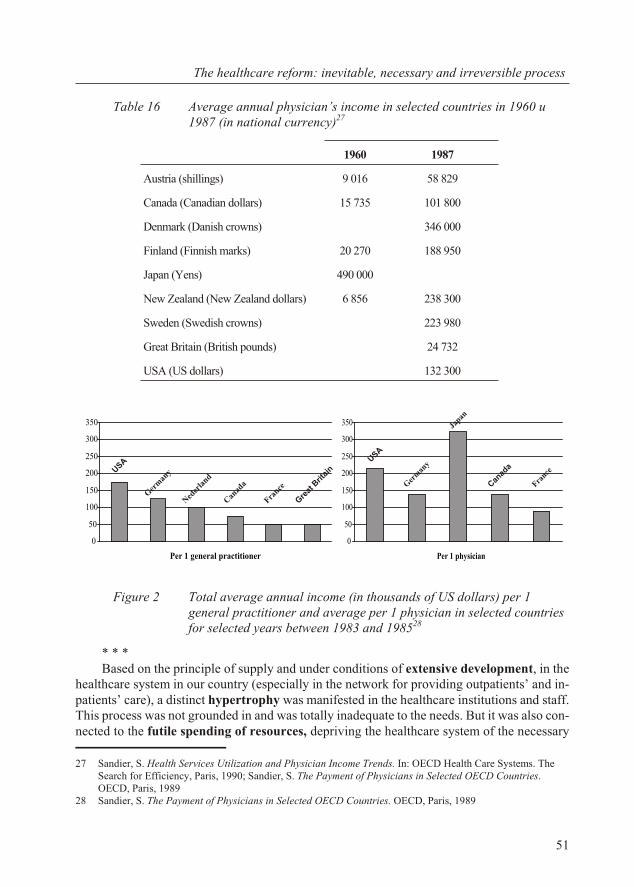
Ta ble 16 Av er age an nual phy si cian’s in come in se lected coun tries in 1960 è1987 (in national currency)27
Figure 2 Total average annual income (in thousands of US dollars) per 1general practitioner and average per 1 physician in selected countriesfor selected years between 1983 and 198528
* * *Based on the prin ci ple of sup ply and un der con di tions of ex ten sive de vel op ment, in the
healthcare sys tem in our coun try (es pe cially in the net work for pro vid ing out pa tients’ and in -pa tients’ care), a dis tinct hy per tro phy was man i fested in the healthcare in sti tu tions and staff.This pro cess was not grounded in and was to tally in ad e quate to the needs. But it was also con -nected to the fu tile spend ing of re sources, de priv ing the healthcare sys tem of the nec es sary
51
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
1960 1987
Aus tria (shil lings) 9 016 58 829
Can ada (Ca na dian dol lars) 15 735 101 800
Den mark (Dan ish crowns) 346 000
Fin land (Finn ish marks) 20 270 188 950
Ja pan (Yens) 490 000
New Zea land (New Zea land dol lars) 6 856 238 300
Swe den (Swed ish crowns) 223 980
Great Brit ain (Brit ish pounds) 24 732
USA (US dollars) 132 300
0
50
100
150
200
250
300
350
Per 1 physician
0
50
100
150
200
250
300
350
Per 1 general practitioner
USA
Ger
man
y
Ned
erla
nd
Can
ada
France
Gre
at B
ritai
nUSA
Ger
man
y
Japan
Can
ada
France
27 Sand ier, S. Health Ser vices Uti li za tion and Phy si cian In come Trends. In: OECD Health Care Sys tems. TheSearch for Ef fi ciency, Paris, 1990; Sand ier, S. The Pay ment of Phy si cians in Se lected OECD Coun tries.OECD, Paris, 1989
28 Sand ier, S. The Pay ment of Phy si cians in Se lected OECD Coun tries. OECD, Paris, 1989
in vest ments for mod erni sa tion and means for the ad e quate re mu ner a tion of la bour. Its sig nif i -cance was more prom i nent with the ac com pa ny ing drop in the ac tiv i ties of the healthcare sys -tem, in crease of the in equal ity be tween the cit i zens in the towns and the vil lages as well as there duc tion of the qual ity of the pro vided med i cal care. For the de vel op ment of these phe nom -ena, an un dis puted role was played by the main te nance of a low so cial sta tus of the staff in thehealthcare sys tem and the de graded eval u a tion of the med i cal la bour, ex pressed es pe cially inits re mu ner a tion. In all cases and, es pe cially when last ing for four de cades, this re sulted in the staff’s lack of mo ti va tion which, in its turn, was a neg a tive fac tor for the quan tity and the qual -ity of med i cal care. These phe nom ena had been de vel op ing and un fold ing for de cades, with out any in ter fer ence for re stric tion or com pen sa tion, and they brought decompensation and in ef fi -ciency in the sys tem in terms of its func tions and an in creas ing need for a rad i cal change.
The de te ri o ra tion of the na tion’s health sta tus and the sig nif i cantly re duced ef fi ciency ofthe healthcare sys tem were two rea sons which, in their own right, ac counted for the ne ces sityof a healthcare re form. These rea sons which may be called “in ter nal” had arisen in re la tion tothe na tion’s health and the in ef fec tive de vel op ment of the healthcare sys tem. They did not re -main hid den and, as we will ob serve later, the aware ness of the lead ing au thor i ties in Bul gariathat a healthcare re form is needed, in creased, though late. The im pli ca tion is that the nec es saryre form in healthcare could have been ini ti ated in some form even be fore 1990, at the thenexisting political and state level, respectively.
The healthcare sys tem is a sys tem for ser vices - it does not de ter mine the pa ram e ters ofthe state and so ci ety but is af fected by them.
Dis crep an cies be tween the le gal, eco nomic and the so cial sta tus andre la tions be tween the ex ist ing healthcare sys tem and the rad i callychang ing po lit i cal, eco nomic and public conditions
The third rea son stemmed from fac tors “ex ter nal” to the sys tem – the deep changeswhich had started and were in prog ress af ter 1989 in the po lit i cal and so cial life as well as in the eco nomic re la tions in the coun try. Though “ex ter nal”, it is ex actly these fac tors which wereof cru cial im por tance for the prin ci ples and di rec tions for the ac tual de vel op ment of thehealthcare re form in Bul garia.
Two in ter re lated pro cesses char ac ter ised the de vel op ment of our coun try af ter 1990 andhad a de ci sive im pact on the be gin ning and the sub se quent de vel op ment of the healthcare re -form: the de moc ra ti sa tion of the state and so ci ety and the mar ket rules in econ omy. In or derto achieve a bal ance be tween the gen eral de vel op ment of the coun try and the healthcare sys -tem, the lat ter (pro vid ing ser vices, as we al ready noted) had to adopt and in ter nal ise the dom i -nat ing char ac ter is tics of the state, that is, to be come re formed ac cord ing to the principles ofdemocracy and market economy.
The main con tra dic tion, which led to a num ber of other dis crep an cies, was be tween thein her ited and the ex ist ing state mo nop oly on the healthcare sys tem, on one hand, and the re -quire ments of the de moc ra ti sa tion and mar ket econ omy, on the other.
The so cial ist state mo nop oly over the own er ship and the man age ment of the healthcaresys tem, in tro duced still in 1948-1950 and cat e gor i cally re in forced in 1973 by the to tal ban onpri vate med i cal prac tice, by def i ni tion ex cluded any other form of own er ship but the state one.A dis tinc tion has to be made be tween the so cial ist and the other forms of mo nop oly. In theUnited King dom and other coun tries, the healthcare sys tem was also na tion al ised by the state
52
but un der an en tirely dif fer ent re gime of own er ship man age ment. The own er ship of all the re -sources of the healthcare sys tem (with the ex cep tion of the staff, of course) be longed to thestate and was managed by the state organs.
Be cause of the ex clu sive state own er ship of the re sources and the mo nop o lis tic state ad -min is tra tive man age ment for sev eral de cades, the healthcare sys tem grad u ally “ac quired” se ri -ous short com ings, which were grad u ally de creas ing its ef fec tive ness and their elim i na tion orover com ing was becoming more and more difficult.
Un der these con di tions, the fi nanc ing of the healthcare sys tem was car ried out en tirelyby the state bud get. It was con sid ered that the healthcare sys tem in the so cial ist state did notpro duce na tional rev e nue. This is why, it was re ferred to as the “non-pro duc tive sphere,”which was fi nanced from the so-called “pub lic con sump tion fund”. It was formed from thestate bud get af ter the de ter mi na tion of the means of pro duc tion and the “ac cu mu la tion” fund.(It is there fore of ten de clared that at that time, the fi nanc ing of the healthcare was “re sid ual”).In prin ci ple, the an nual bud gets of the healthcare es tab lish ments were cen trally de ter mined (by the health min is try), the ap proach be ing “his tor i cal”, i.e. based on the fund ing planned for thepre vi ous year, pos si bly aug mented in re la tion to the plan for the in crease in the num ber of hos -pi tal beds or the full-time po si tions. The cap i tal in vest ments were also de ter mined at cen trallevel, in ac cor dance with the in sti tu tional plan. The main task of every healthcareestablishment and the system was to fulfil the plan and the budget.
The cen tral plan ning and fi nanc ing are the main el e ments of the cen tral ised man age ment.In its turn, this im plies strong in sti tu tional ad min is tra tive con trol over each healthcare es tab -lish ment, which is com bined and com ple mented with the ad min is tra tive con trol of the lo calauthorities of the state.
Un der the so cial ist state mo nop oly no other means and meth ods of reg u la tion wereplanned and ex isted but the hi er ar chi cal and the ad min is tra tive ones. The eco nomic re la tions in the sys tem and, be tween it and the other sys tems in so ci ety, were de ter mined by ad min is tra tivemeth ods and could not ful fil the func tion of mech a nisms for self-reg u la tion in the healthcaresys tem. The sys tem was de prived of mech a nisms for self-reg u la tion (above all, eco nomic).This in ev i ta bly led to the ex pan sion of the ad min is tra tive staff to com pen sate the lack ofself-reg u la tion. Un der these con di tions, ev ery boost ing of the ad min is tra tion vir tu ally in -creased bureaucratisation and, as a re sult, de creased the sys tem ef fi ciency. For the re in force -ment of this pro cess, the lack of ac tively func tion ing mech a nisms con trib uted to sens ing ofand com ply ing with the con sum ers’ pres sure on the sys tem, which was part of its self-reg u la -tion. The civil par tic i pa tion in the plan ning and the set ting of the sys tem pri or i ties was com -pletely ig nored, with the ex cep tion, of course, of some forms of the so-called“self-gov er nance” (elec tive mu nic i pal and dis trict peo ple’s councils, general village andgeneral city assemblies) which were also a manifestation of the totalitarian state monopoly.
The pro vi sion of med i cal care (out pa tients’ and in pa tient’) was also in the spirit of thestate mo nop oly. Ev ery hos pi tal and healthcare es tab lish ment pro vided ser vices to the cit i zensof an ad min is tra tively de ter mined re gion. Be sides, med i cal care (to a large ex tent the pre ven -tive ac tiv i ties, too) was pro vided ac cord ing to the prin ci ple of the ser vice re gion. The in hab it -ants of a cer tain ur ban or ru ral ser vice re gion did not have the right to choose. They and theirfam i lies re ceived med i cal and den tal care only by the phy si cian (or the den tist, nurse, mid wife) in the re spec tive ser vice di vi sion to which they were as signed, and if needed, by the hospital inthe region in which they resided.
53
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
Un der the so cial ist state mo nop oly the med i cal pro fes sion als’ or gani sa tions were com -pletely iso lated from the man age ment of the sys tem. In this re spect, the trade un ion in flu enceof the Pro fes sional Un ion of the Healthcare Work ers was con sid ered to be a for mal mech a -nism. Un til 1990, the trade un ions (as many other or gani sa tions) were rather a part of the stateap pa ra tus than trade un ion or gani sa tions. There fore, their in de pend ent par tic i pa tion in the for -ma tion of the health pol icy and man age ment of the healthcare sys tem were rather imag i naryand had no in flu ence. Their main pur pose was to sup port the party and the state ma chine in theman age ment of healthcare and not to de fend the rights of the work ers. The iso la tion of the pro -fes sional med i cal or gani sa tions de prived the man age ment of the sys tem both of the neededcom pe tence and the con nec tion with the im me di ate and un solved prob lems of the healthcare.As we al ready noted, the re mu ner a tion of la bour in the healthcare sys tem was rather low, notonly as com pared to the coun tries with mar ket econ omy but also to the re mu ner a tion in the ag -ri cul tural sec tors in Bul garia. More over, the amount of the re mu ner a tion was de ter minedmainly by the oc cu pied po si tion and the du ra tion of the work ing ex pe ri ence (“equa li sa tion” ofpayment), irrespective of the quality, complexity and the responsibility for the work which was being done.
The com plete ban on pri vate med i cal ac tiv i ties in Bul garia was unique not only for ourcoun try but world wide (they were not to tally banned even in the So viet Un ion). It cor re -sponded to the de sire to con sol i date the state mo nop oly. In such a way the pro fes sional rightswere de nied to phy si cians, den tists and other med i cal spe cial ists. Fur ther more, the cit i zenswere de nied the pos si bil ity to seek and ob tain med i cal care by a cho sen and pre ferred spe cial ist against pay ment. The com pen sa tion mech a nisms (“free ad mis sion”, “ad mis sion upon re -quest”) in tro duced in 1974, were used by a lim ited num ber of spe cial ists (paid ad di tion ally and bur den ing the bud get of the respective healthcare establishment) and proved to be inefficient.
* * *As ev i dent from the anal y sis above, Bul garia was en ter ing the last de cade of the pre vi ous
cen tury with the trend to ward a de te ri o ra tion of the pop u la tion’s health sta tus, with ahealthcare sys tem quan ti ta tively and qual i ta tively in ad e quate to the needs, whose gov er nancewas con structed and ex e cuted in ac cor dance with the prin ci ples of the state so cial ist mo nop -oly. The na tion’s health and the healthcare sys tem were in a crit i cal sit u a tion.
It has to be re marked that the draw backs of the quan ti ta tive de vel op ment and the ex haus tion of the ex ten sive model of the so cial ist healthcare sys tem be came ob vi ous quite early – still in1960s. This was the rea son for the lead ing or gans in healthcare to turn their at ten tion to cer tainstruc tural and con tent changes. An im por tant in cen tive was found in the Di rec tives of the IXth
Con gress of the Bul gar ian Com mu nist Party (1966) and the Ple nary of its Cen tral Com mit tee(1968) for the im prove ment and ap pli ca tion of sci en tific meth ods in the or gani sa tion and man -age ment in all the fields of the ma te rial and spir i tual life. The changes in the sys tem of healthcare(de signed and ex e cuted at the ini tia tive of the then First Vice Min is ter Dr. V. Kalaidjiev) wereap proved by a De cree of the Coun cil of Min is ters (¹ 11 from 15.03.1966) and were ad dressed to the hy giene and ep i de mi o log i cal ser vices. The re or gani sa tion (the term in cir cu la tion at the timeas the term “re form” was avoided) of this field of the healthcare sys tem in cluded deep changes inits struc tures, func tions and re la tions. The lead ing prin ci ple for the struc tural changes was con -cen tra tion of the ma te rial, tech ni cal and hu man re sources. In stead of the 28 dis trict and the 80re lated re gional san i ta tion ep i de mi o log i cal sta tions, sub or di nate to the lo cal party au thor ity and
54
ad min is tra tion, 10 Hy giene and Ep i de mi o log i cal In sti tutes were es tab lished, sub or di nate im -me di ately to the Min is ter of Healthcare (or one of his Dep u ties). To gether with the ac tiv i ties oftheir di vi sions (branches) the ac tiv i ties cov ered the whole ter ri tory of the coun try. The in sti -tutes were au ton o mous in re la tion to the lo cal au thor i ties. Each of these in sti tutes was headed by a di rec tor pos sess ing con sid er able man age ment com pe tences and au thor ity, sub or di nate di rectlyto the Min is ter of Peo ple’s Health (or one of his Dep u ties) and not to the lo cal au thor i ties. Re -gard ing the func tions, the main char ac ter is tics were con cen tra tion and in ten si fi ca tion of the ac -tiv i ties. The func tions of the in sti tu tions were ex tended in com par i son to the pre vi ous ones. They were ful filled by spe cial ists who re ceived ad di tional qual i fi ca tion. The in sti tute’s work washelped by a num ber of sci en tific cen tres in the field of hy giene, ep i de mi ol ogy and so cial med i -cine. The in sti tutes were fi nanced by the bud get of the Min is ter of Peo ple’s Health (MPH) butbased on an nu ally con cluded con tracts. The re la tions of the in sti tutes with the sci en tific cen tresand other or gani sa tions were con trac tual, too29.
It should be noted that, un der con di tions of the so cial ist state, this was the first ac tual at -tempt to lay the foun da tions of the or gani sa tion and man age ment of the healthcare sys temachieved by sci en tific prog ress. Con sid er able changes were made in the or gani sa tion and man -age ment of the hy giene and ep i de mi o log i cal in sti tutes (con cen tra tion, in ten si fi ca tion, au ton -omy, con trac tual re la tions), which were en tirely novel for the so cial ist re al ity in the field ofhealthcare. Nev er the less, they were short-lived. Those changes con tra dicted the So viet sys tem of healthcare. This was the rea son why in 1971 the su preme lead er ship of BCP de cided that inthat case a se ri ous or gani sa tional and po lit i cal er ror was made and as a re sult, the hy gieneand ep i de mi o log i cal in sti tutes were closed down (by Or der of the Coun cil of Min is ters ¹ 631from 19.12.1971), re stor ing with a few ex cep tions the pre vi ous struc tures and or gani sa tion.Thus, the at tempt for a par tial re form (maybe mark ing also the be gin ning of an over all re form)of the healthcare sys tem was rejected by creating obstacles not only for action but also for themere thought about a need for a reform.
As can be ex pected, in the years to fol low, the na tion’s health sta tus con tin ued to de te ri o -rate and the ef fi ciency of the healthcare sys tem con tin ued to plum met. Only af ter al most twode cades, in one of the of fi cial BCP doc u ments from 1989, it was re ported that “there is a trendto ward cer tain rise in the to tal mor tal ity rate pre-de ter mined by both the in creased ab so lutenum ber and rel a tive share of the el derly peo ple and the in creas ing death rate in the youn ger age groups from some so cially sig nif i cant dis eases”. An other state ment re garded healthcare andthat “it is not de vel op ing in ac cor dance with the re quire ments of the ob jec tive laws of pub licde vel op ment and eco nomic reg u la tors… it is not con structed and is not func tion ing in ac cor -dance with the prin ci ples of self-gov er nance un der mod ern con di tions”30. These observationsentirely support the conclusions drawn in the foregoing analysis.
In sum, even be fore 1989, the re form ing of the healthcare sys tem was be com ing ob vi ousas in ev i ta ble and his tor i cally nec es sary, if the na tion should be pro tected against fur ther healthsta tus deg ra da tion. The pro cess of a healthcare re form was also ir re vers ible be cause when re -form ing the sys tem of healthcare, a rather del i cate mat ter is touched upon and go ing back (if
55
The healthcare re form: in ev i ta ble, nec es sary and ir re vers ible pro cess
29 For fur ther de tails: Popov, M., Zh. Golemanova. Õèãèåííî-åïèäåìèîëîãè÷íàòà ìðåæà â Áúëãàðèÿ:èçãðàæäàíå è ðàçâèòèå, ïîñòèæåíèÿ è ïðîáëåìè. Pub lished by Cen tre of Hy giene and Ep i de mi o log i calIn sti tute, Sofia, 2001
30 Main guide lines for the further re struc tur ing of the healthcare in Peo ple’s Rpublic of Bul garia, ap proved bythe Po lit i cal Bu reau of the Cen tral Com mit tee of BCP. Rabotnichesko delo daily, Is sue ¹ 312 from 8.11.1989
not with vi tal in di ca tions) car ries the risk not only for a crisis but for a catastrophe.
Tasks of the healthcare re form
The above out lined rea sons gave rise to cer tain prob lems, caus ing the need for re form ing ofthe healthcare sys tem. Bear ing in mind what has al ready been said, in 1990 the need for a re -form of the healthcare sys tem in Bul garia was re lated to the so lu tion of three main tasks:
1. Dis con tinu a tion of the na tion’s health de te ri o ra tion and cre ation of pre req ui sitesfor its im prove ment. No mat ter what form the health pol icy would have ac quired andwhat changes would have been ex e cuted in the healthcare sys tem and in sti tu tions, the alarm ing health sta tus of the pop u la tion and the over all trend to ward its de te ri o ra tionim posed im per a tively that task num ber one was the im ple men ta tion of pur pose ful,ur gent, suf fi cient and ac tive mea sures (med i cal, eco nomic and so cial) for the dis con -tinu a tion of the de vel op ment of these ad verse ten den cies. Only in this way the foun -da tion could be laid down for sub se quent grad ual im prove ment of the na tion’s healthin di ca tors.
2. Dis con tinu a tion of the re pro duc tion of the ex ist ing healthcare sys tem and es tab -lish ment of a new sys tem cor re spond ing to the health needs, to the con di tions andpos si bil i ties of our country.
There is a com mon un der stand ing, ac cord ing to which, when a re form of a cer tain sys temand its sub sti tu tion by a new one are nec es sary, the most ap pro pri ate ap proach to be un der -taken is to cre ate a new sys tem and make it func tion par al lel to the al ready ex ist ing one. Thetwo sys tems would com pete with each other and thus, one of them can es tab lish it self as moreap pro pri ate for at tain ing the goals of so ci ety. This ap proach could be fea si ble in smaller sys -tems. In larger ones, such as a na tional sys tem, it in ev i ta bly en tails great costs, too, but moreim por tantly, such an ap proach would be rel e vant only if the re form of the sys tem is car ried outun der com par a tively sta ble ex ter nal con di tions, which do not ex ert great pres sure on its in ter -nal en vi ron ment and func tions.
Af ter 1989, the im posed healthcare re form in Bul garia, how ever, had to be ex e cuted un -der the pow er ful im pact of the changed and still chang ing po lit i cal, eco nomic and so cial con di -tions. This re quired the ex ist ing health sys tem to be re formed with out in ter fer ing with itsfunc tions. And this could be done only by dis con tinu ing the re pro duc tion of the ex ist ing sys -tem and the es tab lish ment of a new one.
The re pro duc tion of ev ery pub lic sys tem, in clud ing the healthcare one, is based on itseco nomic struc ture and re la tions. Up to 1990, the Bul gar ian healthcare sys tem was based on the so cial ist state mo nop oly (on the re sources own er ship, their man age ment and way of fi -nanc ing) as well as the as so ci ated so cial ist eco nomic re la tions. Stop ping the re pro duc tion ofthe ex ist ing healthcare sys tem meant de stroying the so cial ist state mo nop oly and, at the same time, in tro duc ing a new struc ture of own er ship and new ways of fi nanc ing andmanagement.
3. De vel op ment of the healthcare sys tem ac cord ing to the dem o cratic changes andthe new eco nomic con di tions, mod ern prin ci ples and stan dards of healthcare.The so lu tion to this prob lem had to en sure the cor re spon dence be tween thehealthcare sys tem and the sur round ing pub lic and eco nomic en vi ron ment. On the one hand, it was linked to the de moc ra ti sa tion both of the in ter nal re la tion ships within
56
the sys tem and be tween it and the cit i zens (de cen trali sa tion and deconcentration ofthe man age ment, prac ti cal in flu ence of the pro fes sion als, civil par tic i pa tion, pa tients’ rights). On the other hand, it re quired the in tro duc tion of cer tain mar ket el e ments inthe struc tures and the ac tiv i ties of the healthcare sys tem (re stric tion of the state ad -min is tra tive reg u la tion, cer tain mar ket au ton omy of the healthcare es tab lish ments,prices of the health ser vices, con trac tual re la tions).
5. Stages and evo lu tion of the healthcare re form in Bul garia
The dif fer ent pub li ca tions (part of which have al ready been ex am ined) in di cate dif fer entyears dur ing the last de cade of the pre vi ous cen tury as mark ing the be gin ning of the healthcarere form in Bul garia. Most fre quently, the be gin ning of the healthcare re form is as so ci ated withthe adop tion of the new health leg is la tion in 1998-1999 but views ex ist re fer ring the be gin ningof the healthcare re form im me di ately af ter 198931.
Cri te ria for as sess ment
In our view, the pro cess of the healthcare re form passes through def i nite stages, in each of which cer tain con di tions ex ist for its de vel op ment to one de gree or an other.
For the anal y sis, dif fer en ti a tion and the ar gu men ta tion in fa vour of the sep a rate stages, inthis study we use a group of cri te ria, orig i nat ing from the def i ni tions quoted ear lier (in clud ingthe ones adopted by us) and the el e ments of a healthcare sys tem. We con sider them uni ver saland ap pli ca ble to the healthcare re form in any coun try. More spe cif i cally, we mean thefollowing:
(1) im ple men ta tion of long-term, con sis tent and pur pose ful changes in the sys tem andnot of sin gle and spo radic acts;
(2) change in the health pol icy and the in sti tu tions which pro duce it; de cen trali sa tion;(3) in tro duc tion of fi nan cial reg u la tions and mech a nisms; (4) set ting of pri or i ties; (5) par tic i pa tion of the pro fes sion als in the healthcare re form im ple men ta tion.
In all cases, the pres ence of a re form pro cess could be es tab lished through an anal y sis ofthe changes along these five cat e go ries. Such a pro cess would be real, only when pos i tivechanges ex ist in each of the in di cated cri te ria, even though not equally prom i nent.
In some cases an ir reg u lar de vel op ment of the re form pro cess can be pres ent. Whenthere is an un even de vel op ment of the healthcare re form – which is ob served in many coun tries – the de vel op ment of the re form pro cess in some of the cri te ria may an tic i pate or lag be hind the oth ers32. The ir reg u lar de vel op ment may be due to wrong (or ab sent) plan ning, in ap pro pri ateor gani sa tion, in ad e quate man age ment or con junc ture rea sons. The es tab lish ment of ir reg u lar(ver sus planned or ex pected) de vel op ment is a sig nal for nec es sary man age ment in flu ences orcor rec tions. The un even de vel op ment is a de fect of the re form pro cess, a chal lenge for man a -ge rial interference, but it does not mean that the process is not there or has stopped.
Apart from the ap pli ca tion of the above cri te ria, when as sess ing the healthcare re form
57
Stages and evo lu tion of the healthcare re form in Bul garia
31 Apostolov, M., P. Ivanova. His tory of Med i cine and Nurs ing. “Grafik konsult”, So fia, 1998, p. 17332 See also Shakarishwili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and
East ern Eu rope in the 1990s. Open So ci ety In sti tute, Bu da pest, 2005
in Bul garia, it is nec es sary to con sider to what ex tent the re form acts cor re spond and con trib -ute to the so lu tion of the prob lems re lated to the dis con tinu a tion of the na tion’s health de te ri -o ra tion, the ter mi na tion of the ex ist ing healthcare sys tem re pro duc tion and the ad ap ta tion ofthe new sys tem to the changed con di tions in the coun try.
Fol low ing this ap proach, we reckon that three stages can be dis cerned in the de vel op -ment of the healthcare re form in our coun try, which will be ex am ined one by one.
5.1. First stage: so cial ist pro gram ming and post-so cial istim ple men ta tion of the re form process
This stage in cludes the pe riod be tween 1989 and 1996 and, in terms of du ra tion, it cov ersap prox i mately half of the ex am ined pe riod of the healthcare re form in Bul garia.
Po lit i cal and so cio eco nomic con text
The be gin ning of this stage was marked in the last months of 1989, when the state was still en tirely dom i nated by the Bul gar ian Com mu nist Party (BCP) – Georgi Atanassov was PrimeMin is ter and Dr. Mincho Peichev was Min is ter of Peo ple’s Health (un til 17.11.1989). Thetwo sub se quent gov ern ments were also dom i nated by the BCP – Andrei Lukanov’s(8.02.-21.09.1990 and 22.09.-20.12.1990), Prof. Dr. Ivan Chernozemski be ing Min is ter ofPeo ple’s Health in both. He re mained Min is ter in the next co ali tion gov ern ment, too, headedby Prime Min is ter Dimitar Popov (20.12.1990-8.11.1991), in which ex perts and rep re sen ta -tives in de pend ent of the com mu nist party were at tracted to gether with ex perts of thenewly-formed op po si tion par ties. On No vem ber 8th 1991, af ter hav ing won the elec tions thegov ern ment of the Un ion of the Dem o cratic Forces (UDF) was formed with Prime Min is terPhilip Dimitrov and Assoc. Prof. Dr. Nikola Vassilev as Min is ter of Healthcare. In the fol -low ing ex pert and for mally ap pointed gov ern ment, headed by Lyuben Berov(30.12.1992-17.10.1994), the Min is ter of Healthcare was Dr. Tancho Gugalov. In the fol low -ing gov ern ment, which was also ex pert and of fi cially ap pointed (17.10.1994-25.01.1995),Assoc. Prof. Dr. Nikola Vassilev be came Min is ter of Healthcare again. Af ter the Par lia men -tary elec tion won by BCP, the gov ern ment formed was headed by Prime Min is ter ZhanVidenov (25.01.1995-12.02.1997), in which the Min is ter of Healthcare was Dr. MimiVitkova. On Feb ru ary 12th 1997 an of fi cial gov ern ment was formed with Stefan Sofianski as aPre mier and Assoc. Prof. Dr. Emil Takov as a Min is ter of Healthcare33.
The chro no log i cal his tory of the gov ern ments in Bul garia dur ing the pe riod of the stage in ques tion is not su per flu ous. It con tains a great part of the ex pla na tion for the wind ing and pe cu -liar de vel op ment of the healthcare re form in our coun try. G. Atanassov’s gov ern ment workedun der con di tions of in creas ing eco nomic cri sis and in ter na tional iso la tion. The en hance mentof these pro cesses and the dis con tent from the to tal i tar ian lead er ship brought about the over -throw ing of Todor Zhivkov (10.11.1989). The Un ion of the Dem o cratic Forces was formed(7.12.1989) as a co ali tion of op po si tion par ties and or gani sa tions and the chief op po si tion toBCP. The op po si tion de manded and led a po lit i cal strug gle for ur gent and rad i cal po lit i cal(dem o cratic) and eco nomic (mar ket) re forms. The po lit i cal con fron ta tion was ex ac er bated and
58
33 Tsurakov, A. Encyclopaedia. Gov ern ments of Bul garia. Chro nol ogy of po lit i cal life 1879-2001. Pub lished by”Petur Beron”, So fia, 2001, pp. 384-442
the two gov ern ments of A. Lukanov failed to cope with it. The food cri sis was also sharp enedthe two gov ern ments of A. Lukanov failed to cope with it. The food cri sis was also sharp enedto gether with the se vere fi nan cial pre dic a ment of the coun try. Still in Oc to ber 1990, with thecol lab o ra tion of the Cham ber of Com merce of the USA, a wide range of spe cial ists with thepar tic i pa tion of two dis tin guished econ o mists from the USA – Rich ard Wran and Ron ald Utt –pre pared the well-known and widely dis cussed re port (the “Wran – Utt Plan”) for the Bul -gar ian strat egy in the tran si tion to dem o cratic de vel op ment (“Bul gar ian Eco nomic Growth and Tran si tion Pro ject”). Chap ter 13 in it con tained an am big u ous warn ing: “The main task of theBul gar ian gov ern ment in the so cial sec tor is to pro vide suf fi cient food, shel ter and ba sic med i -cal ser vices so that no ob sta cles are cre ated for the eco nomic re form… The mar ket econ omy to which Bul garia is striv ing, of fers per fect healthcare, abun dance of foods, cosy hous ing, highsal a ries and pen sions but at the ex pense of two mar ket char ac ter is tics – un cer tainty and mar ketprices”. The rec om men da tion to the gov ern ment was not to carry out reforms of the socialsystems, to which the healthcare belonged, simultaneously with the reform of the economicsector. This burdened even further the implementation of the healthcare reform.
The same prob lems re mained un der D. Popov’s gov ern ment. The in dus trial pro duc tiondropped by over 30% in com par i son to 1989 and the in fla tion rate dra mat i cally de creased theac tual in come of the pop u la tion. The sol vency and the re duced con sump tion stroke an otherblow on the weak ened econ omy. The at tempts of Philip Dimitrov’s gov ern ment to pass a se -ries of leg is la tive acts to lay down the foun da tion of se ri ous eco nomic re forms did not yieldsig nif i cant re sults. The de lay in the res ti tu tion of the land, the low in come of the pop u la tionand the op po si tion of the old ad min is tra tion in the im ple men ta tion of the re forms con trib utedto the fall of the gov ern ment. Un der Zhan Videnov’s gov ern ment, the eco nomic prob lems inour coun try deep ened. At the end of 1995, be cause of the un con trolled ex port of wheat, theso-called “bread cri sis” oc curred and in 1996 the Bul gar ian lev was de val u ated by 100%. Thebank sys tem was also col laps ing. In the win ter of 1996-1997 the coun try faced hy per in fla tionand the stan dard of liv ing was fall ing cat a stroph i cally (in Feb ru ary 1997 the av er age monthlysal ary fell to 5-6 US dol lars). A man i fes ta tion of the fast im pov er ish ment of the pop u la tion was the rise of the rel a tive share of the ex penses for food in the house hold bud gets from 46.2% in1995 to 54.3% in 1997 (Ta ble 20). The se vere dis con tent from the cre ated situation caused thegovernment’s resignation, the appointment of an official government and pre-termParliamentary elections.
In this tense and dy nam i cally chang ing, poly mor phous and poly chro matic po lit i cal sit u a -tion, the rul ing of the coun try was taken over for rel a tively short pe ri ods by dif fer ent po lit i calpar ties with op pos ing or at least in com pat i ble views about the na ture and the con tent of thehealthcare re form. Un der these cir cum stances it was im pos si ble to achieve the nec es sary sus -tain able and ac cept able con cept of the ac tual pri or i ties in health pol icy and the ob jec tives ofthe healthcare re form. This is one of the main rea sons for the de layed im ple men ta tion of the re -form pro cess in the healthcare sys tem (and not only in it).
Be cause of the chang ing and un sus tain able po lit i cal con di tions the sit u a tion was ag gra -vated by the cri sis in the na tional econ omy de vel op ing af ter 1989. On Feb ru ary 13th 1997 theof fi cial cur rency rate of the US dol lar reached 3 000 BGN and the monthly in fla tion – 243%. In the pe riod from 1990 to 1997 the ex pen di ture for healthcare34 which com prised a small pro por -tion of the GDP dropped from 5.1% in 1992 to 3.6% in 1995, it fell to 2.90% in 1996 and
59
Stages and evo lu tion of the healthcare re form in Bul garia
34 Shakarishwili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and East ernEu rope in the 1990s. Open So ci ety In sti tute, Bu da pest, 2005, p. 54ff.
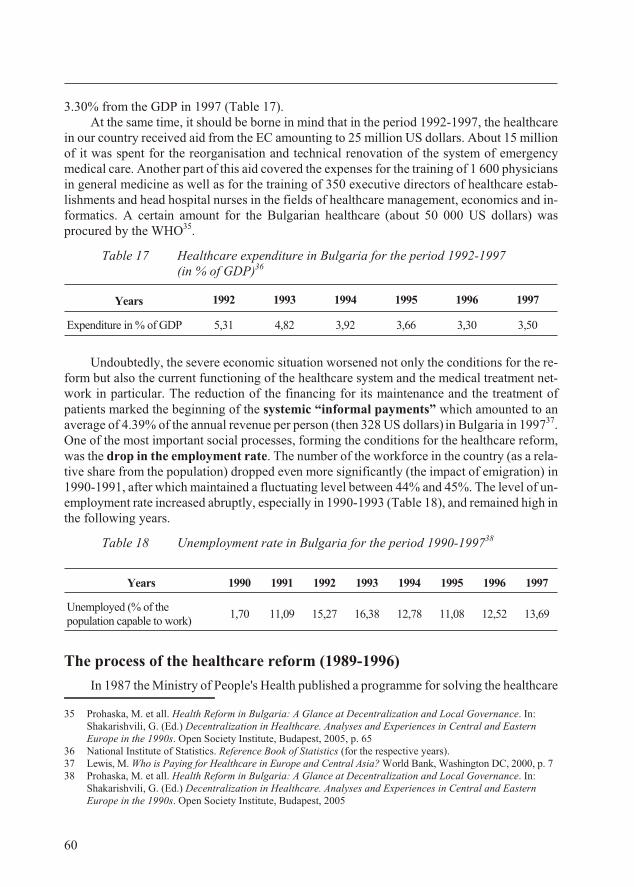
3.30% from the GDP in 1997 (Ta ble 17). At the same time, it should be borne in mind that in the pe riod 1992-1997, the healthcare
in our coun try re ceived aid from the EC amount ing to 25 mil lion US dol lars. About 15 mil lionof it was spent for the re or gani sa tion and tech ni cal ren o va tion of the sys tem of emer gencymed i cal care. An other part of this aid cov ered the ex penses for the train ing of 1 600 phy si ciansin gen eral med i cine as well as for the train ing of 350 ex ec u tive di rec tors of healthcare es tab -lish ments and head hos pi tal nurses in the fields of healthcare man age ment, eco nom ics and in -for ma tics. A cer tain amount for the Bul gar ian healthcare (about 50 000 US dol lars) waspro cured by the WHO35.
Table 17 Healthcare expenditure in Bulgaria for the period 1992-1997 (in % of GDP)36
Years 1992 1993 1994 1995 1996 1997
Expenditure in % of GDP 5,31 4,82 3,92 3,66 3,30 3,50
Un doubt edly, the se vere eco nomic sit u a tion wors ened not only the con di tions for the re -form but also the cur rent func tion ing of the healthcare sys tem and the med i cal treat ment net -work in par tic u lar. The re duc tion of the fi nanc ing for its main te nance and the treat ment ofpa tients marked the be gin ning of the sys temic “in for mal pay ments” which amounted to anav er age of 4.39% of the an nual rev e nue per per son (then 328 US dol lars) in Bul garia in 199737. One of the most im por tant so cial pro cesses, form ing the con di tions for the healthcare re form,was the drop in the em ploy ment rate. The num ber of the workforce in the coun try (as a rel a -tive share from the pop u la tion) dropped even more sig nif i cantly (the im pact of em i gra tion) in1990-1991, af ter which main tained a fluc tu at ing level be tween 44% and 45%. The level of un -em ploy ment rate in creased abruptly, es pe cially in 1990-1993 (Ta ble 18), and re mained high in the following years.
Ta ble 18 Un em ploy ment rate in Bul garia for the pe riod 1990-199738
The pro cess of the healthcare re form (1989-1996)
In 1987 the Min is try of Peo ple's Health pub lished a programme for solv ing the healthcare
60
Years 1990 1991 1992 1993 1994 1995 1996 1997
Unemployed (% of thepopulation capable to work)
1,70 11,09 15,27 16,38 12,78 11,08 12,52 13,69
35 Prohaska, M. et all. Health Re form in Bul garia: A Glance at De cen tral iza tion and Lo cal Gov er nance. In:Shakarishvili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and East ernEu rope in the 1990s. Open So ci ety In sti tute, Bu da pest, 2005, p. 65
36 Na tional In sti tute of Sta tis tics. Ref er ence Book of Sta tis tics (for the re spec tive years).37 Lewis, M. Who is Pay ing for Healthcare in Eu rope and Cen tral Asia? World Bank, Wash ing ton DC, 2000, p. 738 Prohaska, Ì. et all. Health Re form in Bul garia: A Glance at De cen tral iza tion and Lo cal Gov er nance. In:
Shakarishvili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and East ernEu rope in the 1990s. Open So ci ety In sti tute, Bu da pest, 2005
prob lems in the coun try in the spirit of the WHO strat egy “Health for All un til 2000” 39. Thisdoc u ment, how ever, was of more or less rep re sen ta tive and pro pa ganda na ture. It lacked what -ever anal y sis of the prob lems in the healthcare sys tem and did not touch at all on the ne ces sityfor any health re form, al though there was a press ing need for it, as we al ready noted.
But a year later, in view of the wors ened health sta tus of the na tion and the out stand ingde fects of the healthcare sys tem, in 1988 the su preme party or gan (the Po lit i cal Bu reau for theBCP Cen tral Com mit tee) pub lished “for all peo ple’s dis cus sion” a pro ject for a re form inhealthcare. As a re sult of the dis cus sion, over 50 thou sand pro pos als (some of them were re pet -i tive, of course) were made by or gani sa tions and in di vid ual cit i zens, in clud ing by nu mer ousmed i cal spe cial ists. Based on the whole ma te rial, the pro ject was fur ther de vel oped and in Oc -to ber 1989 the Po lit i cal Bu reau for the BCP Cen tral Com mit tee ap proved the “Main guide -lines for the fur ther re struc tur ing of the healthcare in Peo ple’s Re pub lic of Bul garia”.The State Coun cil (which pos sessed leg is la tive func tions, too) is sued a Decree for an Ad di -tion to the Law on Peo ple’s Health, stip u lat ing the foun da tion of a Fund for the Citizens’Health Insurance and, on Feb ru ary 2nd 1989, the Coun cil of Min is ters adopted an Act for ap -proval of the Reg u la tion for the col lec tive and per sonal la bour of the healthcare work ersfor the pro vi sion of ad di tional health care and ser vices, by which the pri vate sec tor inhealthcare, banned in 1973, was vir tu ally re stored40.
From the point of view of the his tory of the Bul gar ian healthcare sys tem, these doc u ments are ex tremely in ter est ing. In our case, how ever, we dis cuss them only in re la tion to the abovemen tioned cri te ria, as pre lim i nary in di ca tions for a pro ject for a healthcare reform.
Even though for mu lated as a “fur ther re struc tur ing”, the pro ject is par tic u larly im pres sive be cause it was aimed at a rather deep (though not af fect ing the foun da tions of the so cial ist or -der and state) change of the health pol icy and sys tem.
The strife for an in ter nal po lit i cal ef fect is eas ily per ceived (un doubt edly re lated to theevents be fore and af ter No vem ber 10th 1989) in the de ci sions adopted at top po lit i cal level un -der those con di tions. Such an act was not de signed in any other of the then-sat el lite states or re -pub lics of the Soviet Union.
The en vis aged se ri ous change en com passed a num ber of health po lit i cal de ci sions in thefive cri te ria for the healthcare re form de fined above:
· The change of the very set ting of the healthcare and its or gani sa tion was aimed chieflyat sat is fy ing the needs for high in di vid ual and so ci etal health safety and guar an tee ingthis safety, the health pol icy be ing formed through a di a logue be tween so ci ety and thehealth au thor i ties; by im prov ing the ef fi ciency of the health in sti tu tions; by grant ingcit i zens the right of free choice of a phy si cian and healthcare es tab lish ment; by car ry -ing out con sis tent de cen trali sa tion in the man age ment and ex pan sion of the com pe -tences of the lo cal gov er nance (the mu nic i pal au thor i ties) for the de vel op ment of thehealthcare in the mu nic i pal i ties;
· in tro duc tion of a new ap proach for fi nanc ing and eco nomic mech a nisms for healthcare sys tem man age ment by cre at ing (un til the end of 1990!) an over all, eco nomic and eco -nom i cally and or gani sa tion ally in de pend ent health in sur ance or gani sa tion; this or gani -sa tion was en vis aged to func tion not only at na tional level but also at de cen tral ised
61
Stages and evo lu tion of the healthcare re form in Bul garia
39 Ïúòÿò íà Áúëãàðèÿ êúì “Çäðàâå çà âñè÷êè”, Pub lished by “Medicina and fizkultura”, So fia, 198740 Rabotnichesko delo daily, Is sue ¹ 307 from 2.11.1989 and Issue ¹ 312 from 8.11.1989
re gional level and at cor po rate and in dus trial en ter prises level; the ap proach was seenas an op por tu nity for aban don ing the “re sid ual fi nanc ing” of the healthcare es tab lish -ments and for a tran si tion to fi nanc ing of the health in sur ance funds, fi nanc ing for pri -or i ties, programme financing and payment for performed activities;
· in creased fo cus on med i cal spe cial ists: at ten tion to the their qual i fi ca tion, the re mu ner -a tion of their la bour, so cial prob lems; re stor ing the pri vate med i cal prac tice; re stor ingthe Un ion of Bul gar ian Phy si cians as a “cre ative and pro fes sional or gani sa tion”,whose ef forts would en hance “the constant upheaval in our healthcare”;
· con crete set ting of the pri or i ties for the de vel op ment of the healthcare sys tem: im -prove ment of the le gal ba sis of the healthcare and guar an tee ing of the ex e cu tion of therights and li a bil i ties; build ing of an ef fec tive struc ture of the healthcare sys tem; the de -vel op ment and im ple men ta tion of a strat egy for staff, fi nan cial, ma te rial and tech ni calproblem-solving in healthcare;
· the nor ma tive acts ac com pa ny ing the “Main guide lines for the fur ther re struc tur ing ofthe healthcare in Peo ple’s Re pub lic of Bul garia” were con sid ered to mark the be gin -ning of a con tin u ous pro cess (10-15 years) for “over all up dat ing of the leg is la tive ba sis of healthcare” which was nec es sary for its restructuring.
Al though brief, the above com ment def i nitely im plied an ini tial idea for a health re form in its mod ern un der stand ing and the quoted ma te ri als formed the spe cific model and the or gani sa -tional pro ject for the con ceived re form.
The un der stand ing of this programme for re form not only nec es sar ily in cluded but def i -nitely im plied the in flu ence of con junc ture po lit i cal el e ments (the ma te ri als dis cussed werepub lished only sev eral days be fore No vem ber 10th 1989). It also con tained some in suf fi cientlyclar i fied de ci sions. The con junc ture po lit i cal in flu ence was rather strong since it con tained acon sid er able com pro mise with the main prin ci ples of so cial ist healthcare. At the same time,how ever, it was a re spect ful and se ri ous rec og ni tion of both a real ised need for a healthcare re -form and of a pre pared ness to re ject cer tain dog matic con cepts and adopt rad i cal health pol icychanges.
With out a nor ma tive ba sis (the Ad di tion of the Law on Peo ple’s Health for the es tab lish -ment of a health in sur ance fund was not en forced and the Reg u la tion for the pri vate med i calprac tice re mained with out con se quences), in a tur bu lent sit u a tion of a chang ing po lit i cal sys tem,in 1990 the driv ing force of the re form pro cess in healthcare was also chang ing. Novel po lit -i cal pro cesses and con di tions were un fold ing, which were en tirely dif fer ent from the pre vi ousones. The need came to the fore ground for the ex e cu tion of a to tal and rad i cal change in thecoun try, in the eco nomic re la tions and pub lic life; for the de vel op ment and con sol i da tion of thedem o cratic in sti tu tions in so ci ety and the mar ket con di tions in the na tional econ omy.
The healthcare re form turned into a part of the evolv ing gen eral state and na tional re form as a par al lel pro cess un fold ing to gether with the re forms in all the other fields of the state, pub -lic and in dus trial struc tures. But to that mo ment the pri or i ties were ori ented to re forms of thestate struc ture and the eco nomic system of the country.
Un der these con di tions of at tempt ing rad i cal changes in val ues and pri or i ties, thepro cess of healthcare re form was tak ing place. In the con text of deeply chang ing po lit i cal,eco nomic and pub lic re la tions, the re form pro cess ac quired spe cific di men sions, goals andcon tent. Even at a slower rate, the re form in healthcare had to cor re spond to the de vel op ing
62
dem o cratic so ci ety and mar ket econ omy. This meant that the re form fa cil i tated the build ingup of a healthcare sys tem of an other type, which was dif fer ent from the ex ist ing one andanal o gous to the healthcare systems in the democratic states with market economy.
This was an ex tremely dif fi cult task for whose so lu tion the coun try seemed to be un pre -pared at that time. Un doubt edly, con sid er able in tel lec tual ef fort and ma te rial sup port wereneeded for the con struc tion of the new healthcare sys tem un der the rad i cally changedcon di tions, more over, still in the pro cess of their for ma tion. Nev er the less, in 1990-1991,the only avail able sys tem atic work was the “Main guide lines for the fur ther re struc tur ing of the healthcare in Peo ple’s Re pub lic of Bul garia” but it was de signed to re struc ture and not to ter -mi nate the re pro duc tion of the ex ist ing healthcare sys tem. For the de vel op ment of the healthsys tem and healthcare re form un der the con di tions at the be gin ning of 1990s, only most gen -eral ideas (de moc ra ti sa tion, mar ket econ omy) ex isted but the conceptual view and theprogramme design were absent.
For the sake of the com plete ness of this anal y sis, we should point out that in 1994 the Ex -pert Coun cil to the Bul gar ian Agrar ian Party dis cussed and adopted an an a lyt i cal and well-ar -gued re port (pub lished as a book, too) on the healthcare re form. Be side the con cepts forde moc ra ti sa tion and mar ket re la tions in healthcare, it con tained a com pre hen sive programmefor the healthcare re form in Bul garia41. This was the fist sys tem atic work af ter 1990 and theonly one un til 1996 about the healthcare re form in our coun try. But the po lit i cal sit u a tion at thetime was such that the im pact of this pub li ca tion did not achieve practical implementation inthe next few years.
Par tial changes of the healthcare sys tem
Un der the changed con di tions be fore and af ter 1990, fol low ing some most gen eral ideas,the be gin ning was laid of the prac ti cal work on the prob lems of the healthcare re form. And be -cause of the lack of a com pre hen sive con cept ac cept able to all the pub lic forces, the ef forts werevir tu ally di rected to the im ple men ta tion of iso lated, es sen tial in deed, but par tial changes.
Three of them were of par tic u lar im por tance since (par tially though) they al tered thesit u a tion and af fected sig nif i cantly the de vel op ment of the healthcare re form in the next years.
Re stric tion of the state mo nop oly
The first (and prob a bly the most es sen tial for the de vel op ment of the healthcare re form)was the pro cess of re strict ing the state mo nop oly on the healthcare sys tem. The first stepin this re spect was the le gal restoration and reg u la tion of the pri vate sec tor in thehealthcare sys tem. Ini tially, it was achieved by the Amend ment and Ad di tion of the Lawon Peo ple’s Health pre pared and passed by Par lia ment to gether with the by-laws adopted bythe Coun cil Min is ters42, whereby the right of pri vate med i cal prac tice was re sumed. Thehealthcare net work, in clud ing med i cal treat ment and pre ven tive care, as a state prop erty fi -nanced and man aged by the state, re mained in tact but it was not the only one. Par al lel to it, theac tual op por tu nity was opened for the de vel op ment of pri vate healthcare es tab lish ments. Thus,
63
Stages and evo lu tion of the healthcare re form in Bul garia
41 Popov, M., Z. Kraev. The Healthcare Re form – Pol icy and Strat egy un der Con di tions of Mar ket Econ omy.Pub lished by the “Free ini tia tive” Foun da tion”, So fia, 1994
42 State Ga zette, Is sue ¹ 76 from 21.09.1990, Is sue ¹ 15 from 22.02.1991, Is sue ¹ 37 from 10.05.1991, Is sue¹ 80 from 27.09.1991, Is sue ¹ 97 from 26.11.1990
still in 1990-1991 the state mo nop oly on healthcare, which was one of the main char ac ter is -tic fea tures of the pre vi ous healthcare sys tem, was re stricted to a cer tain de gree.
In the next years the Law on Drugs and Phar ma cies in Hu man Med i cine was workedout and passed by Par lia ment in 199543, pro vid ing for the over all sys tem of drug sup ply (pro -duc tion and im port of drugs, san i ta tion ma te ri als and med i cal consumables as well as of re tailand whole sale trade with them), ir re spec tive of some re stric tions, shifted to the pri vate sec -tor. The func tions of the state or gans were reg u la tory and con trol ling and were to a large ex -tent re lated to the sup ply of cer tain types of costly med i ca tions for free pro vi sion for theoncological pa tients and pa tients with spe cific or rare dis eases. From the point of view of thehealth re form, the main sig nif i cance of this law which was changed and amended many timesdur ing the next years, con sisted in the demonopolisation of the healthcare sys tem.
The new Law on the Bul gar ian Red Cross from 199544 was in the same line. It re storedto the Bul gar ian Red Cross its in de pend ence from the state and made it com ply more closelywith the in ter na tional norms of the Red Cross or gani sa tions.
In the mean time, in 1994 the Law on Blood Do na tion and Blood Trans fu sion45 wasadopted aim ing at the im prove ment of the nor ma tive ba sis of haemotransfusion but it did notchange the main char ac ter is tics of the healthcare system.
To gether with the changes in the nor ma tive ba sis, an ut most im por tance for thedemonopolisation of the sys tem of healthcare was played by the res to ra tion of the pro fes -sional or gani sa tions in healthcare. The pro fes sional or gani sa tion of the phy si cians was re -con sti tuted on May 27th 1990 by the XXVIIth As sem bly of the Un ion of Bul gar ianPhy si cians (UBP). And shortly be fore it, on March 10th and 11th the Na tional Con fer ence heldin Plovdiv took the de ci sion for the re con sti tu tion of the Un ion of Den tists in Bul garia(UDB). These two or gani sa tions were to play an im por tant role in the sub se quent de vel op ment of the healthcare re form. The re cov ered pro fes sional or gani sa tions started in ten sive or gani sa -tional ac tiv i ties. The is sues of pro fes sional eth ics were grounded and dis cussed on a largescale. On Oc to ber 21st 1992 the Ex ec u tive Board of the Un ion of Bul gar ian Phy si cians adopted and approved the “Code of Physicians’ Ethics” which is mandatory for all physicians.
De cen trali sa tion and de moc ra ti sa tion
An other im por tant change con cerned the is sues of de cen trali sa tion and the build ingof the pe riph eral healthcare ad min is tra tion.
With the newly adopted Con sti tu tion (1991) and the Law on Lo cal Gov er nance and theLo cal Ad min is tra tion (1991), the ad min is tra tive and ter ri to rial di vi sion of the coun try ex ist ingun til then was changed. The ad min is tra tive and ter ri to rial units re mained to be called “dis -tricts” but cov ered the area of the pre vi ous re gions. The func tions of the dis trict ad min is tra tionwere taken over by the dis trict gov er nor (ap pointed by the gov ern ment) and its ad min is tra tion.An ad min is tra tive ser vice for healthcare was not en vis aged at it. The healthcare ad min is tra tionof the pre vi ous Re gional Peo ple’s Coun cils did not ex ist any more but part of it – the one deal -ing with the col lect ing and pro cess ing of sta tis ti cal in for ma tion on the pop u la tion’s health sta -tus and the ac tiv i ties of the healthcare es tab lish ments – was pre served as “Re gional Cen tres
64
43 State Ga zette, Is sue ¹ 36 from 18.04.199544 State Ga zette, Is sue ¹ 87 from 29.09.199545 State Ga zette, Is sue ¹ 31 from 6.05.1994
for Health Information” 46, sub or di nate to the Min is try of Healthcare and fi nanced by it. It isun der stand able that the lack of district healthcare administration considerably hindered themanagement of the healthcare system.
The so lu tion to the prob lem was found in the re struc tur ing of the Re gional Cen tres forHealth In for ma tion into “Re gional Healthcare Centres” (RHC) 47. They were sub or di nateim me di ately to the Min is ter of Healthcare (and not to the gov er nor) and had the sta tus of a lo -cal rep re sen ta tion of the Min is try of Healthcare. Their task was to co or di nate and con trol thehealthcare sys tem and the healthcare ac tiv i ties and ini tia tives of the mu nic i pal i ties in the dis -trict. RHC are di vi sions of par tic u lar im por tance in the im ple men ta tion of the healthcare re -form in the dis tricts. With their foun da tion and en ti tle ment to cer tain man age mentcom pe tences a def i nite de cen trali sa tion was achieved in the healthcare sys tem but the re spec -tive deconcentration lacked. Its man age ment re mained con cen trated in the Min is try ofHealthcare and its ad min is tra tive or gans. Maybe to gether with other rea sons, this was the main rea son why ten years af ter their es tab lish ment, the role and the involvement of the RHC in thehealthcare reform cannot be considered full-fledged.
Ac cord ing to the above men tioned law, the is sues of the struc ture of the healthcare ad -min is tra tion at mu nic i pal level are han dled by the mu nic i pal au thor i ties (mu nic i pal coun cil,mayor) de pend ing on the size and the needs of the mu nic i pal ity. The mu nic i pal healthcare bod -ies are sub or di nate to the City Coun cil and the mayor and are ad min is tra tively in de pend entfrom the dis trict ad min is tra tion. This so lu tion can be con sid ered rel e vant and ef fec tive fromthe point of view of the decentralisation and deconcentration of the management.
Still in 1991, an es sen tial change was un der taken in the sys tem of the man age ment ofhealthcare es tab lish ments, and the man age ment of the es tab lish ments for out pa tients’ and in -pa tients’ hospital care.
This change was en acted by the Reg u la tion for the Man age ment of the Healthcare Es tab -lish ments48. The Reg u la tion re vealed the com mon ef fort for dem o cratic changes which thendom i nated in all the lay ers of the Bul gar ian so ci ety. For the first time, by this by-law the dem -o cratic trends, which were stip u lated in the amend ment of the Law on Peo ple’s Health in1991, were de vel oped and spec i fied. The Reg u la tion ar ranged for the man age ment of allpub lic hos pi tals, poly clin ics and dis pen sa ries which were owned by the mu nic i pal i ties (then“tem po rary mu nic i pal ex ec u tive com mit tees”) or by the state (un der the au thor ity of theMH). The Gen eral As sem bly of the healthcare es tab lish ment per son nel be came the su -preme or gan of man age ment in which rep re sen ta tives of the pro fes sional or gani sa tions andtrade un ions also took part to gether with rep re sen ta tives of the pro pri etor of the healthcarees tab lish ment (the state or the mu nic i pal ity). Rep re sen ta tives of com pa nies, banks, foun da -tions and or gani sa tions as well as cit i zens could also par tic i pate with out the right to vote.The Gen eral As sem bly adopted the reg u la tion for the func tion ing of the es tab lish ment, thean nual re port and de ci sions con cern ing the so cial de vel op ment of the staff, and it de ter mined the man a ge rial po si tions which were go ing to be oc cu pied by com pe ti tion and elected by theMed i cal Coun cil as an or gan of tac ti cal man age ment of the health es tab lish ment. The
65
Stages and evo lu tion of the healthcare re form in Bul garia
46 State Ga zette, Is sue ¹ 48 from 3.06.199247 State Ga zette, Is sue ¹ 66 from 25.07.1995 and Is sue ¹ 75 from 25.08.199548 Adopted by Act of the Coun cil of Min is ters ¹ 118 from 20.06.1991, State Ga zette, Is sue ¹ 50, 30.06.1991,
amdnded and added by Act ¹ 218 from 3.11.1992, State Ga zette, Is sue ¹ 93 from 17.11.1992 and Act ¹252 from 27.12.1993, State Ga zette, Is sue ¹ 2 from 7.01.1994
Gen eral As sem bly and the Med i cal Coun cil had a two-year term. Their ac tiv i ties were or -gan ised ac cord ing to reg u la tions adopted by them selves. The Med i cal Coun cil took de ci -sions on all is sues con cern ing the ac tiv i ties of the healthcare es tab lish ment, in clud ing thesign ing of con tracts with firms and or gani sa tions as well as lo gis tics and cap i tal in vest ment.The op er a tional man age ment was di vided be tween three man a ge rial po si tions: ex ec u tive di -rec tor, med i cal di rec tor and head nurse (mid wife). The ex ec u tive di rec tor was re quired tohave com pleted higher ed u ca tion which did not nec es sar ily have to be med i cal, but he/she rep -re sented the healthcare es tab lish ment and ex e cuted its ad min is tra tive and eco nomic man age -ment. The med i cal di rec tor had to be a phy si cian since this was the per son who co or di natedand man aged the med i cal ac tiv i ties of the healthcare es tab lish ment. The head nurse (mid -wife) co or di nated and was in charge of the work of all the nurses (mid wives) and aux il iarystaff.
Be side the im ple men ta tion of this rad i cal change in the man age ment of the healthcare es -tab lish ments the train ing in healthcare man age ment was also or gan ised of the man age mentstaff of the healthcare es tab lish ments which was then as signed to the Na tional In sti tute ofSocial Medicine (NISM).
The nov elty in tro duced by this Reg u la tion in the de vel op ment of the healthcare re formcon sisted in the rad i cal and spe cific de ci sions on the de moc ra ti sa tion and de cen trali sa tion of the healthcare es tab lish ments’ man age ment and the prac ti cal in tro duc tion of the prin ci ples oftheir self-gov er nance. The wide op por tu nity for pro vid ing im me di ate “open ing” of the man -age ment bod ies to the lo cal com mu nity was also im por tant – a sign of their de moc ra ti sa tion.Ap par ently de signed in ac cor dance with the mod els of the West ern Eu ro pean coun tries and the United States, this Reg u la tion had a def i nite sig nif i cance for the dem o cratic trends and the at ti -tudes to the re form in Bul gar ian healthcare for a pe riod of about four years49.
The idea of a health in sur ance sys tem
The third sig nif i cant change in fact re fers to the fun da men tal is sue of the un con di tion -ally nec es sary in tro duc tion of new eco nomic re la tions and mech a nisms as el e ments of themar ket re struc tur ing of the healthcare sys tem. At that stage they were not go ing to be in tro -duced. What mat tered, how ever, was the ac cep tance, sup port and the deep pen e tra tion in so ci -ety of the idea for the set ting up of health in sur ance funds for the fi nanc ing of hos pi tal care.In this case, the change con cerned pub lic opin ion and at ti tudes. The Un ion of Bul gar ian Phy si -cians and the Un ion of Den tists in Bul garia had a pos i tive at ti tude to this idea and ad vo cated itbe fore their mem bers and the so ci ety. The idea was also backed in the programme doc u mentsof the ma jor po lit i cal forces in our coun try. Al though only one of the re form el e ments, whichwas not even de fin i tively with out an al ter na tive, in the mass aware ness of the med i cal pro fes -sional and the cit i zens, the healthcare re form as a whole was iden ti fied with the health in -sur ance sys tem. Thus, health in sur ance turned into a com pul sory el e ment of the re form.Long be fore its in tro duc tion it be came a pre-con di tion for the healthcare re form. The work ingout of the Bul gar ian model for health in sur ance con tin ued dur ing this stage. A con sid er ablenum ber of for eign con sul tants were also at tracted50. The first draft pro ject for health in sur ancewas sub mit ted to the Coun cil of Min is ters in 1991. In 1994 a spe cial Sci en tific and Prac ti cal
66
49 Re pealed by Act ¹ 143 from 14.07.1995, State Ga zette, Is sue ¹ 71 from 11.08.199550 For fur ther de tails: In: The World jour nal, vol. 2, Is sue ¹. 1, 1995, p. 22
Cen tre for the health in sur ance sys tem was es tab lished, too51. Nev er the less, dur ing this stagethe eco nomic re la tions and the fi nan cial or gani sa tion of the healthcare sys tem did not change.
Con cep tual de ci sions on the healthcare re form
On the sev enth year af ter the dem o cratic changes, in 1996 an of fi cial con cep tual andprogramme work was pub lished un der the form of a Na tional Health Strat egy “Health forBul garia” (adopted by a Dec la ra tion of the Na tional As sem bly on De cem ber 8th 1995).
It con tained a pro found anal y sis of the pop u la tion’s health sta tus and risk fac tors and theac tiv i ties of the healthcare sys tem. Based on it, con clu sions were drawn about the nec es sarychanges and the ap proach to the re form of the healthcare sys tem. The con tin u ing ag gra va tionof the na tion’s health was con firmed to gether with the in creased risk fac tors. It was ob servedthat the vol ume of the pro vided out pa tients’ and hos pi tal care also de creased. The qual ity ofmed i cal care was un sat is fac tory. In cen tives lacked for the de vel op ment of the sys tem and thequal ity as sur ance of its ac tiv i ties. No ac tual op por tu nity was pro vided for a choice of a phy si -cian and den tist or healthcare es tab lish ment in the pub lic sec tor. Un grounded and spo radicchanges in the sys tem were un der taken, the ad min is tra tive or der was tres passed for lack of abal ance be tween cen trali sa tion and de cen trali sa tion.
These state ments, sup ported by many facts, re vealed the fact that the de grad ing pro cess of the na tion’s health and the healthcare sys tem con tin ued af ter 1990.
The Na tional Health Strat egy pro vided ar gu ments in fa vour of the ac tions nec es sary toim prove the healthcare sys tem. It can not be de nied that they were ra tio nal and their im ple -men ta tion would have been use ful for the achieve ment of a cer tain change in the sys tem andthe grad ual pos i tive de vel op ment of the na tion’s health.
The man age ment of the sys tem en vis aged the re in force ment of the stra te gic func tionsand the re stric tion of the op er a tional man age ment func tions of the Min is try of healthcare, de -vel op ment of de cen trali sa tion by in creas ing the man age ment com pe tences of the RHC, con -sol i da tion of the au ton omy and grant ing the sta tus of “le gal en ti ties” of the med i cal andhealthcare es tab lish ments, clearly for mu lated rights and li a bil i ties of the mu nic i pal au thor i tieson healthcare at the mu nic i pal i ties. The close col lab o ra tion with the pro fes sional or gani sa tions and the trade un ions was seen as a means to the for ma tion of an ad e quate health pol icy and itsef fec tive im ple men ta tion.
In ac cor dance with the Na tional Health Strat egy, a de tailed Strat egy for the De vel op -ment of Pri mary Healthcare was worked out in 1995-1996 (with the sup port of the PHAREprogramme) 52.
Both strat e gies, how ever, oc cu pied an im por tant place in the prac tice of the healthcare re -form for a pe riod of just about a year, but even dur ing this pe riod they were im ple mented atslower rates. With the change of the gov ern ment they re mained as doc u ments out lin ing spe -cific steps of the re form pro cess.
67
Stages and evo lu tion of the healthcare re form in Bul garia
51 State Ga zette, Is sue ¹ 29 from 5.04.199452 Ðàçâèòèå íà ïúðâè÷íàòà çäðàâíà ïîìîù â Ðåïóáëèêà Áúëãàðèÿ. Pub lished by the Min is try of Healthcare,
So fia, 1996
Pub lic opin ion of the healthcare re form
Cov er age of the healthcare re form in the press in the pe riod 1989-1996
The main char ac ter is tics and events in the pro cess of the healthcare re form dur ing thisstage were cov ered by the press in a more or less ob jec tive way. There were some in ter est ingel e ments in the pub li ca tions, es pe cially at the be gin ning of this stage. One of them in cluded the fact that the pro jects on healthcare re form from be fore No vem ber 10th 1989 were not men -tioned at all, as if no in ten tion had ex isted what so ever for a change ei ther of the eco nomic re la -tions or the struc tures and or gani sa tion of the healthcare sys tem.
The pub li ca tion re leases of the main po lit i cal forces equally sup ported the ne ces sity fora healthcare re form53. The de mands of the re stored pro fes sional or gani sa tions of phy si ciansand den tists were chiefly ori ented to ward the amend ment of the Law on Peo ple’s Health(LPH), mainly in view of the re sump tion of the pri vate med i cal ac tiv i ties and the eq uity of thepub lic and pri vate healthcare es tab lish ments which was then per ceived as an es sen tial el e mentof the healthcare re form54.
As a main in stru ment for ex ert ing pres sure and in or der to ac cel er ate the adop tion ofamend ments of the LPH, the strikes were stressed in the healthcare sys tem, or gan ised most ac -tively by the Con fed er a tion of La bour ”Podkrepa” 55. The strike ac tiv i ties found good cov er age in the press56
Ir re spec tive of the com par a tively wide cov er age of the strike un rest and man i fes ta tions,which still at the be gin ning of 1990 reached the ul ti ma tum claim of CL ”Podkrepa” for thework ing out of a new law on healthcare and the res ig na tion of the whole MH team, the pub -lished ma te ri als did not give an idea about the more con crete con tent of the healthcare re form.It was clear from these ma te ri als that in No vem ber 1990 the pro ject for an amend ment of LPHhad al ready been sub mit ted to the Na tional As sem bly (NA) and yet, it was not voted un til theend of the year.
In 1992 the me dia ex ten sively fol lowed the ef fec tive and the sym bolic strikes and pro tests of the med i cal pro fes sion als and their claims for pay ment rises, guar an tees and dead lines forthe ac tual im ple men ta tion of the re form as well as the fast in tro duc tion of the health in sur ancesys tem and up dat ing of the bud get for healthcare57.
Fi nanc ing and sup ply
From 1990 the me dia grad u ally and in sis tently fea tured the cri sis in the healthcare sys -tem sup ply with drugs, food, den tal ma te ri als and med i ca tions for haemodialysis58. The gravesit u a tion with the sup ply of the healthcare es tab lish ments with drugs and other ma te ri als re -mained one of the lead ing top ics in the me dia in the next years. In a dra matic ad dress to the
68
53 Duma daily from 5.12.1990; Democracia daily from 12.199054 Democracia daily, Is sue ¹ 144 from 9.08.1990; Duma daily, Is sue ¹ 256 from 15.12.199055 Democracia daily, Is sue ¹ 28 from 31.01.1990; Duma daily, Is sue ¹ 32 from 1.02.199056 Democracia daily, Duma daily, Trud daily from 31.01.199057 24 chasa daily, Is sue ¹ 114 from 13.05.1992, Is sue ¹ 140 from 12.06.1992, Is sue ¹ 159 from 4-5.07.1992;
Democracia daily, Is sue ¹ 154 from 30.06.1992, Is sue ¹160 from 7.07.1992; Duma daily, Is sue ¹ 115,Is sue ¹119, Is sue ¹ 145, Is sue ¹ 151, Is sue ¹ 156, Is sue ¹ 157, Is sue ¹ 161, Is sue ¹ 192, Is sue ¹ 218,Is sue ¹ 221 from 1992; Fo rum Medicus pe ri od i cal, Is sue ¹ 21 from 25.05.1992
58 Democracia daily from 5.07.1990 and from 23.10.1990; Duma daily from 7.04.1990 and Is sue ¹ 134 from15.08.1990
Great Na tional As sem bly, the MH, the man age ment of the Med i cal Acad emy and the pro fes -sional or gani sa tions turned for as sis tance for se cur ing means for healthcare as there was noblack oil for the cen tral heat ing of the hos pi tals, there were no med i ca tions, lab o ra toryconsumables, X-ray films and a num ber of hos pi tals had to dis con tinue their elec tive sur geryand some were threat ened to be closed down59. Sev eral weeks af ter the first pub li ca tion, it wasun der lined that the hos pi tals did have at their dis posal drugs un til the mid dle of the year60. Thelack of means (mainly for the hos pi tals) was dis cussed re pet i tively in the me dia and in the endof the sum mer of 1991 CL ”Podkrepa” and the pro fes sional or gani sa tions de clared that un lessmeans were not se cured for healthcare, in clud ing for pay rise of the staff, they would re sort toac tive strike ac tiv i ties61.
From the mid dle of 1992, pub li ca tions ap peared in the press about the short age of fi nanceand the se vere fi nan cial pre dic a ment of the hos pi tals62. The rea sons pointed out by the Min is -try of Healthcare about the short age in the bud get, were at trib uted chiefly to in fla tion andthere fore, a claim for bud get cor rec tion was made, cor re spond ing to the gen eral in dex of thecon sumer goods63. Apart from the claim for an ad di tional sub sidy amount ing to 2.7 bil lionBGN, the only an nounce ment about un der taken ac tion re ferred to the chronic def i cit, whichwas al ready be com ing ap par ent on the oc ca sion of the meth od ol ogy de vised by the MH for ac -count ing the costs of the healthcare es tab lish ments64.
The se vere fi nan cial con di tion of the hos pi tals, the debts of the healthcare es tab lish ments,the lack of consumables and the poor fa cil i tates con tin ued to be among the lead ing top ics in 1993 65. These were the rea sons for the con tin u ing phy si cians’ pro tests and their claims for pay riseand im me di ate dou bling of the bud get for healthcare66. A se ries of pub li ca tions in the sec ond half of 1993 un am big u ously ob vi ated the lack of a clear vi sion about the healthcare es tab lish ments fi -nanc ing. In con nec tion with the fi nan cial cri sis and the lack of fi nance for the free-of-chargedrugs, in its turn, the Dem o cratic Healthcare Trade Un ion pro posed fund trans fer to the mu nic i -pal i ties for the needs of the hos pi tals and for the nor mal sal a ries of the staff67. At the same timethe MH sub mit ted a pro posal to the Coun cil of Min is ters for the na tion ali sa tion of the mu nic i palhos pi tals aimed at im prov ing their fi nanc ing68. The me dia ob served that un til Au gust 1993 thein debt ed ness of the healthcare es tab lish ments amounted to 250 mil lion BGN69, in Oc to ber thegov ern ment re leased 500 mil lion BGN for the main te nance of the healthcare es tab lish ments anddrug sup ply and the debts of the hos pi tals reached 1 bil lion BGN70
The prob lems with the fi nanc ing of the healthcare sys tem re mained widely dis cussed and
69
Stages and evo lu tion of the healthcare re form in Bul garia
59 Duma daily, Is sue ¹ 32 from 1.02.1991 and Is sue ¹ 147 from 8.06.199160 Duma daily, Is sue ¹ 72 from 199161 Duma daily, Is sue ¹ 200 and Is sue ¹ 205 from 199162 24 chasa daily, Is sue ¹ 192 from 12.08.1992; Duma daily, Is sue ¹ 202, Is sue ¹ 212 and Is sue ¹ 248 from
1992; Fo rum Medicus pe ri od i cal, Is sue ¹ 21 from 25.05.199263 Duma daily, Is sue ¹ 157 from 199264 24 chasa daily, Is sue ¹ 192 from 12.08.199265 Democracia daily, Is sue ¹ 171 from 26.07.1993 and Is sue ¹ 179 from 4.08.199366 Standart daily from 18.02.1993 and from 22.06.1993; Democracia daily, Is sue ¹ 46 from 26.02.1993, from
19.03.1993 and from 28.08.199367 Democracia daily from 28.08.1993, from 29.09.1993, from 16.10.1993 and from 21.10.1993; Trud daily from
13.09.199368 Democracia daily from 28.08.199369 Democracia daily from 6.08.199370 Democracia daily from 8.10.1993; 24 chasa daily, Is sue ¹ 245 from 1993 and Is sue ¹ 285 from 1993
in 1994 the debts of the MH and the mu nic i pal i ties were in the fo cus of at ten tion to gether withthe threat of clos ing down hos pi tals and out pa tients’ clin ics as well as the ques tion about themed i cal ser vices paid by the pa tients71. The ex ac er bated prob lem tensed the con flict be tweenthe cen tral and the lo cal au thor i ties about the re spon si bil ity for the fi nanc ing of the healthcarees tab lish ments72. With the adop tion of the bud get for healthcare, the ques tion was raised in theNA about the funds uti li sa tion by the mu nic i pal i ties and ac cu sa tions were put for ward that, in a num ber of mu nic i pal i ties, these funds were re al lo cated for other ac tiv i ties73. To solve thisprob lem, to ward the mid dle of 1994 amend ments were pre pared in the LPH en vis ag ing the in -tro duc tion of con trac tual re la tions be tween the hos pi tals and the mu nic i pal i ties. What is more,the mu nic i pal i ties un der took to pro vide fund ing to the al ready ju rid i cally in de pend enthealthcare es tab lish ments against a def i nite vol ume of med i cal ac tiv i ties per formed by them74.Sim i lar to the pre vi ous years, in 1994 too, the “so lu tion” of the fi nanc ing prob lems of thehealthcare es tab lish ments was sought in the re lease of an ad di tional sub sidy. To ward the mid -dle of 1994 the MH re leased 50 mil lion BGN for healthcare75.
The prob lems of the healthcare sys tem were sum ma rised by the work ing team of theWHO Re gional Of fice for Eu rope, ac cord ing to whose re port, the ex pen di ture for healthcareper ca pita was “mis er a ble”, “the qual ity of med i cal care is poor”, there were two many spe cial -ists in the sys tem, the work ing con di tions were poor, and the staff was un der paid, there was ashort age of drugs and consumables76. Al though the re port was writ ten in the be gin ning of1994, the sub se quent pub li ca tions (ex am ined above) did not hint at any seek ing of sys tem aticso lu tions to these prob lems.
The debts of the healthcare es tab lish ments, the short age of med i cal drugs andconsumables as well as (ac cord ing to the gen eral opin ion) the short age of fi nance al lo cated forhealthcare from the state bud get, were fea tured in a num ber of pub li ca tions through out 199577.In an ar ti cle in the “Trud” daily from 19th June 1995, the fol low ing rea sons were listed for thesys temic short age of hos pi tal fi nanc ing: the in ef fec tive utilisations of beds, the large num berof beds and the fact that pa tients with mild dis eases were ad mit ted for hos pi tal treat ment.
At the same time the MH pre pared a pro posal for amend ments in De cree ¹ 146 of theMH for the pay ment of some med i cal ser vices by the pa tients. It de ter mined 37 ser vices (cos -metic sur gery, abor tions on de mand, etc., some ser vices pro vided by the Hy giene and Ep i de -mi o log i cal In sti tute and the ac tiv i ties of the san a to ria), the price for ma tion mech a nisms be ingspec i fied by ex perts of the MH, pri mar ily based on the tar iffs of the pri vate med i cal prac tices78. Fur ther more, the MH pro posed to the hos pi tals to pay for per formed ac tiv i ties and con -ducted an ex per i men tal pro ject in the hos pi tal in Smolyan. The reg is tra tion for the costs per
70
71 Trud daily from 02.1994 and from 04.1994; Duma daily, Is sue ¹ 51 from 1994, Is sue ¹ 220 from26.09.1994; Democracia daily from 9.04.1994 and from 14.10.1994; 24 chasa daily, Is sue ¹ 303 and Is sue¹ 321 from 1994
72 24 chasa daily, Is sue ¹ 12 from 1994; Duma daily, Is sue ¹ 60 from 1994.; Democracia daily, Is sue ¹ 212from 16.09.1994
73 24 chasa daily, Is sue ¹ 12 from 199474 Trud daily from 12.05.1994; Duma daily, Is sue ¹ 169 from 199475 Duma daily, Is sue ¹ 169 from 199476 Trud daily from 12.02.199477 Duma daily, Is sue ¹ 170 from 1995; Democracia daily from 13.01.1995, Is sue ¹ 94 from 22.04.1995, from
17.05.1995, from 29.08.1995 and Is sue ¹ 235 from 7.10.1995; Trud daily from 1.03.1995, from 15.11.1995,from 18.04.1995 and Is sue ¹ 274 from 21.11.1995
78 Trud daily from 21.06.1995
each pa tient was ini ti ated and as a re sult, the num ber of beds was re duced from 664 to 578 andthe av er age hos pi tal stay was re duced by 1.3 days. The next hos pi tals in which the pro ject wascar ried out in cluded the ones in Gabrovo, Stara Zagora, Plovdiv and Asenovgrad79.
In 1995 at ten tion was once again drawn to the amount of the fi nanc ing for healthcare. Ac -cord ing to the as sess ment of ex perts from the healthcare trade un ions to the CL “Podkrepa”,6% of the GDP had to be al lo cated for healthcare80. The draft for the healthcare bud get for1996 en vis aged 3.88% of the GDP (38 bil lion BGN). The bud get ing for 1996 was in creased by 15.6% in com par i son to 1995, the pre dicted in fla tion be ing 20% for 1996. The med i cal fed er a -tions to the CL “Podkrepa” had al ready started to make claims for 8% of the GDP81.
The fi nan cial prob lems in healthcare were con stantly es ca lat ing and in 1996 they turnedinto one of the dom i nat ing top ics com mented in the press. In their na ture they did not dif ferfrom the pre vi ous years but the way, in which they were com mented in the me dia, was morestrongly emo tion ally charged and was abun dant in clas si fi ca tions such as “fi nan cial col lapse”and “fi nan cial fail ure” 82.
The com plex ity of the fi nan cial prob lems was sum ma rised by Min is ter M. Vitkova infront of the “Duma” daily in the fol low ing way: “Healthcare is the most sen si tive part of the so -cial pol icy and the se vere fi nan cial col lapse of the state is re turn ing as a boo mer ang to it. Thedef i cit has reached ab surd lev els… There is not enough money, and it is not spent prop -erly…The law (au thors’ note: on health in sur ance) will en ter the gov ern ment and Par lia mentsoon but nei ther the healthcare es tab lish ments are pre pared to work un der such con di tions, norwe can raise much more money. The un pre dict able rate of ex change of the US dol lar and theheavy cur rency de pend ence of the healthcare sys tem make the things even more dif fi cult” 83.
At the end of the year the phy si cians went on pro tests again claim ing the res ig na tion ofthe Min is ter of healthcare84.
To gether with the topic of the grave fi nan cial con di tion of the healthcare sys tem, at thebe gin ning of 1992 pub li ca tions ap peared about fi nan cial aid for healthcare from ex ter nalsources. Gra tu itous fi nanc ing was re ported in the frame work of in ter na tional pro jects andloans pri mar ily from the World Bank (WB). Those were the PHARE pro jects (30 mil lion ecufor the health re form), of which 10 mil lion were aimed at the re struc tur ing of the na tional net -work for emer gency care, 3.15 mil lion – for med i cal staff train ing, 565 mil lion – for the in tro -duc tion of the health in sur ance sys tem and 460 thou sand – for the re form in the phar ma ceu ti cal sec tor) and from the Eu ro pean Un ion (1.8 mil lion US dol lars) for the train ing of gen eral prac ti -tio ners85. In 1993 the World Bank granted 50 mil lion US dol lars to sup port the in tro duc tion ofthe health in sur ance sys tem86, and the PHARE and the TEMPUS programmes pro vided 12
71
Stages and evo lu tion of the healthcare re form in Bul garia
79 Trud daily from 26.06.199580 Trud daily from 1.03.199581 Trud daily from 14.12.199582 Trud daily from 8.01.1996, from 29.02.1996 and Is sue ¹ 150 from 4.06.1996; 24 chasa daily, Is sue ¹ 81
from 23.03.1996 and Is sue ¹ 338 from 9.12.1996 ã.; Democracia daily from 23.11.1996 and Is sue ¹ 297from 16.12.1996; Duma daily, Is sue ¹ 287 from 1996; Fo rum Medicus pe ri od i cal, Is sue ¹ 7 from19.02.1996; Fo rum Medicus pe ri od i cal, Is sue ¹ 20 from 20.05.1996
83 Duma daily, Is sue ¹ 240 from 1996 84 Duma daily, Is sue ¹ 240 from 1996; Democracia daily, Is sue ¹ 297 from 16.12.1996; 24 chasa daily, Is sue
¹ 278 from 10.10.199685 24 chasa daily, Is sue ¹ 61 from 1992; Democracia daily, Is sue ¹ 106 from 5.05.199286 Democracia daily from 6.07.1993
mil lion ecu for trans plan ta tions87. In 1994 there were two ar ti cles about ex ter nal fi nanc ingamount ing to 45 mil lion ecu in the frame work of PHARE for the hos pi tals and a loan of 35 mil -lion ecu from the World Bank88.
In 1996 again, sev eral pub li ca tions re ported about ex ter nal fi nanc ing of the healthcaresys tems within the frame work of pro jects, loans and do na tions89:
· 3.5 mil lion US dol lars do na tion by the state com pany “Expomed”. M. Vitkova no ti fiedthe Pros e cut ing Mag is tracy about fi nan cial abuse with the do na tion and its re di rec tionto banks un der sur veil lance;
· a credit of 100 mil lion Ger man marks from the “Siemens” com pany for up dat ing X-ray equip ment;
· 10 mil lion Swiss francs for the de liv ery of the steri li sa tion sys tems in 13 hos pi tals;
· 2 mil lion Dan ish crowns for the equip ment of four cen tres for pa tients with di a be tes inuni ver sity clinics;
· 15 mil lion ecu con tracted with the EU for a three-year programme in clud ingoncological dis eases in women and con trol of the qual ity of med i cal care;
· 47.2 mil lion US dol lars for a pro ject aimed at the re struc tur ing of the healthcare sec tor,of which 26 mil lion were loaned from the WB, 11 mil lion came from the So cial De vel -op ment Fund of the EU and 2.3 mil lion pre sented a fi nan cial aid with out com pen sa tion from the PHARE Programme of the EU. The pro ject was di vided into fourprogrammes – the first (2.3 mil lion US dol lars) in cluded an anal y sis of the health pol -icy and man age ment, the es tab lish ment of a di vi sion at the MH for anal y sis of thehealth pol icy and the or gani sa tion of in ten sive train ing of top man ag ers in thehealthcare es tab lish ments; the sec ond con cerned pri mary healthcare (14.5 mil lion USdol lars) – for the re pair and pur chase of trans por ta tion ve hi cles; the third was di rectedto emer gency care (13.3 mil lion US dol lars) – for the equip ment of 21 emer gencywards in the united re gional hos pi tals, emer gency ad mis sion wards in 45 dis trict hos pi -tals and the pur chase of 125 am bu lances; the fourth programme was aimed at re or gan -is ing blood donation and the establishment of a national system for haemotransfusion.
In 1993 and 1994 the is sue of the med i cal pro fes sion als’ re mu ner a tion was not ex plic -itly dis cussed in the press. In 1995, an ex per i ment was ini ti ated in the town of Elena for the in -tro duc tion of a new way of pay ment in healthcare, which was ap proved by the col le giate ofthe MH still in 1993. The new way of sal ary for ma tion was based on the cat e gory of thehealthcare es tab lish ment, the vol ume of the per formed ac tiv i ties, the phy si cians’ qual i fi ca tionand work ing ex pe ri ence. The new sys tem of phy si cians’ pay ment was planned to en ter intoforce from Jan u ary 1st 199690. This was per ceived as the be gin ning of the tran si tion to a healthin sur ance sys tem91. The in de pend ent trade un ions, how ever, did not agree with the new sys tem of pay ment in the branch, de signed by the MH, the ar gu ments be ing that the cri te ria for thehos pi tal’s pre lim i nary cate gori sa tion were con di tional and the term “vol ume of per formed ac -
72
87 Democracia daily from 30.12.199388 Trud daily from 7.02.1994; Duma daily, Is sue ¹ 237 from 199489 Democracia daily from 14.10.1996 and from 28.12.1996; Duma daily, Is sue ¹ 124 from 28.05.1996 and
Is sue ¹ 278 from 23.11.199690 Democracia daily from 27.09.1995; 24 chasa daily, Is sue ¹ 264 from 27.09.1995; Trud daily, Is sue ¹ 227 from 27.09.199591 Duma daily, Is sue ¹ 107 from 1995
tiv i ties” was in ac cu rately de fined92. The com ments on the new sys tem of sal ary for ma tion con -tin ued in 1996 but the pre dic tions for its in tro duc tion were al ready post poned for the mid dle ofthe year93. The ex pec ta tions of the MH were that the new ways of pay ment would in crease thesal a ries in healthcare and in crease ef fi ciency by putt ing the meth od ol ogy for ward to dis cus -sion by the med i cal pro fes sion als94. In their turn, how ever, many phy si cians dis agreed with the cri te ria for the for ma tion of the sal a ries and the med i cal trade un ions from CL “Podkrepa” or -gan ised pro tests and were pre par ing for a na tional strike95. In the sec ond half of 1996 the pub li -ca tions on the topic were con tra dic tory in con tent. Some of them pre dicted a rise in the in comeas a re sult of the new meth od ol ogy96, whereas oth ers in formed about cuts for the night shiftsand elim i na tion of some fringe ben e fits97. At the end of the year the MH re ported an in crease in the sal a ries re sult ing from the new meth od ol ogy98.
Man age ment
One of the ma jor me dia top ics, which were dis cussed with a vary ing in ten sity dur ing thefirst stage of the re form, con cerned the man age ment of the healthcare es tab lish ments. Thebe gin ning was laid by Reg u la tion ¹ 2 of the MH, which at the end of 1990 was in tro duced tothe Coun cil of Min is ters. The Reg u la tion stip u lated for the Gen eral As sem bly of the hos pi talper son nel to be the su preme hos pi tal man ag ing body, the elec tion of an ex ec u tive board which, in its turn, elected and ap pointed the med i cal di rec tor, the di rec tor for the eco nomic and ad min -is tra tive af fairs as well as the head nurse of the hos pi tal. This di vi sion of the man a ge rial com -pe tences was well ac cepted by the pro fes sional or gani sa tions but was op posed by theCom mit tee on Healthcare, youth and sports at the NA99. The Un ion of Bul gar ian Phy si cianseven threat ened to vote dis trust to the Min is ter of Healthcare, if the Reg u la tion was en -forced100. But with the en force ment of the Reg u la tion, the act ing head phy si cians of the hos pi -tals had to be dis missed and com pe ti tions had to be ad ver tised for the new po si tions. This cir -cum stance un der those con di tions was some times also used for un grounded “clear ing ofper sonal dis likes” and dis missal of some ac tu ally com pe tent hos pi tal di rec tors101.
In 1992 the Coun cil of Min is ters adopted an amend ment to De cree ¹ 118 from 1991 on the man age ment of the healthcare es tab lish ments, ac cord ing to which the Med i cal Coun cil wasturned from a col lec tive body into an ex pert or gan fa cil i tat ing the ac tiv i ties of the man age -ment102.
In the mid dle of 1995 the man age ment of the healthcare es tab lish ments again passed intothe hands of phy si cians, who were as sisted by the dep uty med i cal and eco nomic di rec tors and
73
Stages and evo lu tion of the healthcare re form in Bul garia
92 Duma daily, Is sue ¹ 250 from 1995; Duma daily, Is sue ¹ 305 from 29.12.199593 Standart daily from 11.01.1996; 24 chasa daily, Is sue ¹ 10 from 11.01.1996 and Is sue ¹ 227 from
20.08.1996; Duma daily, Is sue ¹ 6 from 8.01.1996, Is sue ¹ 240 and Is sue ¹ 279 from 22.11.1996; Fo rumMedicus pe ri od i cal, Is sue ¹12 from 25.03.1996
94 Duma daily, Is sue ¹ 6 from 8.01.1996; 24 chasa daily, Is sue ¹ 227 from 20.08.199695 Duma daily, Is sue ¹ 240 and Is sue ¹ 279 from 22.11.199696 Kapital weekly, Is sue ¹ 47 from 25.11.–1.12.1996; Trud daily from 7.11.199697 24 chasa daily, Is sue ¹ 237 and Is sue ¹ 293 from 25.10.1996; Democracia daily from 6.08.1996; Standart
daily, Is sue ¹1475 from 25.10.199698 Kapital weekly, Is sue ¹ 47 from 25.11.–1.12.199699 Duma daily, Is sue ¹ 249 from 8.12.1990100 Duma daily, Is sue ¹ 131 from 23.05.1991 101 Duma daily, Is sue ¹ 136 from 1991102 Democracia daily, Is sue ¹ 247 from 16.10.1992
the chief ac coun tants103. Be cause of the un spec i fied com mit ments of the mu nic i pal i ties and the li a bil i ties of the MH to the lo cal healthcare es tab lish ments (which was en vis aged to be come afact by amend ments of the Law on Peo ple’s Health) and the un clear mech a nism for ap point ingthe di rec tors, this change caused op po si tion on be half of the lo cal au thor i ties, since the MHpro posed that the hos pi tal di rec tors were ap pointed by an or der of Min is ter of Healthcare af terthe ap proval of the may ors of the mu nic i pal i ties, to which the lo cal au thor i ties of the ex ec u tivepower op posed103.
The changes in the hos pi tal man age ment were sup ported by the Su preme Med i cal Coun -cil, the Un ion of Bul gar ian Phy si cians and the trade un ions still at the stage of its plan ning104.
The man age ment of the healthcare es tab lish ments was also com mented in re la tion to thedis miss als of hos pi tal di rec tors105.
In re sponse to an en quiry by the Mem ber of Par lia ment Dr. Orlin Draganov, Min is ter M.Vitkova de clared that there was cor rup tion in the healthcare es tab lish ments and the rea -sons pointed out were in the “ex per i ments of the gov ern ment of the Un ion of the Dem o craticForces, the ap point ment of in com pe tent peo ple on lead ing man a ge rial po si tions”. The mea -sures pro posed against cor rup tion in cluded “a choice of a fam ily phy si cian, at tes ta tion of themed i cal di rec tors ev ery 5 years, phy si cians’ pay rise” to gether with the en vis aged sanc tions,e.g. “ter mi na tion of phy si cians’ right of prac tise up to 15 years and prop erty con fis ca tion”106.
Pri vate sec tor
Al though in 1990 the re sump tion of the pri vate med i cal prac tice and the equalty of thepub lic and pri vate healthcare es tab lish ments were per ceived as es sen tial el e ments of thehealthcare re form, in 1993 the in equal ity be tween them was com mented be cause of the tax onthe turn over, from which the state and the mu nic i pal hos pi tals were ex empt and the pri vatewere not107.
A wider cov er age was at trib uted to the at ti tudes of the med i cal pro fes sion als re gard ingthe ban on pri vate prac tice in the pub lic healthcare es tab lish ments108. The UBP con sid ered itan ac cept able though not an ideal op tion109, whereas the doc tors pro tested against the ban110. In 1994 the dis cus sions on the topic deep ened111 to reach their cli max in 1995 and 1996. The rea -son was the pro ject pro posed by Min ster M. Vitkova for an amend ment of the LPH, ac cord ingto which the pri vate prac ti tio ners did not have the right to work in pub lic healthcare es tab lish -ments, ex cept ex tra work ing hours, the in come from their ac tiv i ties be ing shared be tween thehealthcare es tab lish ment and the re spec tive phy si cian112. The ar gu ments for the pro posed
74
103 Duma daily, Is sue ¹ 151 from 30.06.1995104 24 chasa daily, Is sue ¹ 126 from 1995; Trud daily from 1.03.1995 and from 3.07.1995105 Standart daily from 14.03.1995; Democracia daily, Is sue ¹ 58 from 8.03.1996; 24 chasa daily, Is sue ¹ 241
from 1996; Duma daily, Is sue ¹ 210 from 5.09.1996106 24 chasa daily, Is sue ¹ 114 from 1996107 Democracia daily, Is sue ¹ 85 from 13.04.1993108 Standart daily from 29.12.1993; 24 chasa daily, Is sue ¹ 257 from 1993109 Democracia daily, Is sue ¹ 238 from 12.10.1993110 Trud daily from 13.09.1993; 24 chasa daily, Is sue ¹ 221 from 1993111 24 chasa daily, Is sue ¹ 26 and Is sue ¹ 211 from 1994; Trud daily from 28.01.1994 and from 8.05.1994;
Democracia daily from 5.05.1994, from 17.06.1994 and Is sue ¹ 285 from 10.12.1994; Kapital weekly from18-24.04.1994; Standart daily from 13.12.1994
112 24 chasa daily, Is sue ¹ 33 from 3.02.1995, Is sue ¹ 145 from 31.05.1995, Is sue ¹ 348 from 20.12.1995 andIs sue ¹. 22 from 1996 Duma daily, Is sue ¹ 25, Is sue ¹ 241 and Is sue ¹ 277 from 27.09.1995
changes were aimed at dis con tinu ing the prac tice of re di rect ing pa tients and re sources to thephy si cians’ pri vate of fices and stop ping the cor rup tion113.
The UBP, the Un ion of Pri vate Phy si cians, the Med i cal Fed er a tion at the Conferederation of La bour “Podkrepa”, the Con fed er a tion of In de pend ent Trade Un ions in Bul garia (CITUB),the As so ci a tion of the Dem o cratic Syn di cates pro claimed them selves against the amend mentsin the LPH in a de ter mined and in sis tent way and claimed for the Min is ter’s res ig na tion114. The rea sons for the pro tests were that the open ing of pri vate phy si cians’ of fices was costly and thepay ment they re ceived was “hu mil i at ingly low”115, that the high ex penses for the main te nanceof pri vate prac tices were not fully de ducted from the profit when taxed116. In 1996 the pro testscon tin ued, sup ported by the mem bers of Par lia ment from the op po si tion117. At the end of theyear the NA adopted amend ments in the LPH, ac cord ing to which un con vict ed phy si cians with no less than 2 years of work ing ex pe ri ence had the right to pri vate prac tice. The vot ing of thedis put able texts was post poned118. To sum up the topic of the pri vate prac tice, the op po nents of the amend ments in the LPH, to which it was lim ited, claimed that 85% of the phy si ciansworked “pri vately” (Dr. Karev, UDF) and in sup port of her ar gu ments, Min is ter Vitkovaemphasised the fact that “65% of the Bul gar ian cit i zens are for di vid ing the pri vate from thepub lic prac tice”.
Struc tural changes
The “struc tural changes” in 1993 com prised the fol low ing: the in tro duc tion of a new hos -pi tal cate gori sa tion by the MH; the es tab lish ment of the 28 cen tres for emer gency med i cal care as a re sult of the re struc tur ing of “Emer gency Care”; the sep a ra tion of the eleven clin i cal teach ingfa cil i ties of the Higher Med i cal In sti tute – So fia and their tran si tion to the MH; in ten tions for cuts in the num ber of phy si cians and es tab lish ment of a Com mon Health Fund at the MH119.
In 1994 the en vis aged struc tural changes were re lated only to the fol low ing: re duc tionof the num ber of hos pi tal beds; reg u la tion of the min i mum num ber of beds for the pub lic andpri vate hos pi tals (which puts them in un equal po si tions) and hy gienic re quire ments to them120.A draft pro ject for the healthcare es tab lish ments en vis aged a change in the man age ment func -tion ing, re turn ing the sit u a tion from be fore the end of 1990 and Reg u la tion ¹ 2 of the MH.The ques tion was once again raised about the new hos pi tal cate gori sa tion as well as the per -mis sion for the hos pi tal spe cial ists to have pri vate prac tice in re gions where there is no act ing
75
Stages and evo lu tion of the healthcare re form in Bul garia
113 24 chasa daily, Is sue ¹ 33 from 3.02.1995, Is sue ¹ 309 and Is sue ¹ 335 from 7.12.1995.; Duma daily, Is sue ¹ 4 from 1996
114 Democracia daily from 23.12.1995; 24 chasa daily, Is sue ¹ 277, Is sue ¹ 280, Is sue ¹ 300 and Is sue ¹ 333 from 1995 Standart daily from 5.12.1995; Fo rum Medicus pe ri od i cal, Is sue ¹ 11 from 13.03.1995 and Is sue¹ 41 from 23.10.1995
115 Duma daily, Is sue ¹ 181 from 4.08.1995116 Kapital weekly from 6-12.03.1995117 24 chasa daily, Is sue ¹ 65 from 1996; Democracia daily, Is sue ¹ 4 from 5.01.1996,from 13.01.1996, from
11.07.1996, from 14.10.1996 and from 10.12.1996; Duma daily, Is sue ¹ 19, Is sue ¹ 53, Is sue ¹ 57 from1996; Fo rum Medicus pe ri od i cal, Is sue ¹ 5 from 5.02.1996
118 Trud daily from 19.12.1996; 24 chasa daily, Is sue ¹ 348 from 19.12.1996; Duma daily, Is sue ¹ 300 from 1996119 24 chasa daily, Issue ¹ 63, Issue ¹ 69 and Issue ¹ 223 from 1993; Duma daily, Issue ¹ 34, Issue ¹ 36,
Issue ¹ 61 from 16.03.1993, Issue ¹ 181, Issue ¹ 185 and Issue ¹ 206 from 1993; Democracia daily, Issue ¹ 61 from 16.03.1993 and from 28.10.1993; Forum Medicus periodical, Issue ¹ 23 from 16.08.1993
120 24 chasa daily, Is sue ¹ 190 from 1994; Trud daily from 17.01.1994.; Fo rum Medicus pe ri od i cal, Is sue ¹ 5from 31.01.1994
out pa tients’ spe cial ist from the same spe cialty121. It en vis aged the elim i na tion of the dis trictdoc tors and the in tro duc tion of a free choice of a gen eral prac ti tio ner122.
Al most a year later the col le giate of the MH adopted amend ments in the LPH for a choiceof a fam ily doc tor123. Other amend ments of the LPH fore saw that the healthcare es tab lish ments be came in de pend ent le gal en ti ties and the hos pi tals ob tained the right to raise fund ing and con -clude con tracts on their own124. The lat ter changes be came a fact in 1996125.
In 1995 the Re gional Cen tres for Health In for ma tion were trans formed into Re gionalHealthcare Cen tres as me di a tors be tween the MH and the mu nic i pal i ties, against which the di -rec tors of the mu nic i pal healthcare es tab lish ments and the rep re sen ta tives of the lo cal au thor i -ties strongly pro tested126.
In 1996 one of the lead ing top ics in the press was the reg u la tion of the out pa tients’ care re -lated to the choice of a fam ily phy si cian127. The pub li ca tions can be di vided into two groups: the first one in formed the so ci ety about the dead lines and the re gime of the choice of a fam ily phy si -cian, and the sec ond group criti cised the reg u la tion. The crit i cal com ments con cerned the ac cessof the pop u la tion (es pe cially in the vil lages) to pri mary healthcare and the pres er va tion of the re -gions, the in crease of the vol ume of the med i cal doc u men ta tion, the large num ber of pa tients reg -is tered to one fam ily doc tor (1500) and the sus pi cions about false reg is tra tion of pa tients.
In 1996, a num ber of pub li ca tions128 were ded i cated to the re duc tion of the hos pi tal bedsen vis aged in 1995129. This topic did not re main un dis puted. Ac cord ing to Min is ter Vitkova“The beds in the mu nic i pal hos pi tals are empty, the di rec tors keep them for pres tige” and theChair man of the Med i cal Fed er a tion at the Con fed er a tion of the In de pend ent Trade Un ions inBul garia Dr. Ivan Kokalov voiced the counter argu ments that “the beds are not oc cu pied be -cause there is no money for drugs and food for the pa tients” 130.
The sanatorial beds and med i cal cen tres at the san a to ria and in the ru ral out pa tients’ clin -ics with a pop u la tion less than 1000 in hab it ants were also closed down131.
Along side with this, in 1996 the reg u la tion for the dis pen sa ries was re stored with the novelel e ment that the dis pen sa ries were linked to the vari able part of the phy si cians’ sal a ries132.
76
1990 1996
Óìðåëè ïî âúçðàñò (íà 1 000 äóøè)
20 - 29 ã. 1,0 1,0
30 - 39 ã. 1,8 1,8
40 - 49 ã. 4,2 4,7
50 - 59 ã. 9,9 10,7
60 - 69 ã. 23,2 24,3
70 è ïîâå÷å 91,9 88,3
Óìðåëè ïî ïðè÷èíè (íà 100 000 äóøè)
Îáùî 1 245,7 1 399,7
Íîâîîáðàçóâàíèÿ 173,6 194,4
Áîëåñòè íà îðãàíèòå íà êðúâîîáðúùåíèåòî 768,6 898,9
Áîëåñòè íà äèõàòåëíàòà ñèñòåìà 74,0 66,0
Áîëåñòè íà õðàíîñìèëàòåëíàòà ñèñòåìà 37,7 41,4
Òðàâìè è îòðàâÿíèÿ 63,9 64,0
Ðåãèñòðèðàíè çàáîëÿâàíèÿ îò àêòèâíàòóáåðêóëîçà (íà 100 000 äóøè)
Îáùî 130,6 155,9
Îò òÿõ íîâîîòêðèòè 37,9 37,2
Ðåãèñòðèðàíè çàáîëÿâàíèÿ îò çëîêà÷åñòâåíèíîâîîáðàçóâàíèÿ (íà 100 000 äóøè)
Îáùî 1 903,9 2 201,1
Îò òÿõ íîâîîòêðèòè 267,6 310,8
121 Trud daily from 28.08.1994122 Trud daily from 11.08.1994123 24 chasa daily, Is sue ¹ 264 from 25.09.1995124 24 chasa daily, Is sue ¹ 273 from 1995125 24 chasa daily, Is sue ¹ 335 from 1996 Duma daily, Is sue ¹ 295 from 1996 126 Duma daily, Is sue ¹ 151 from 30.06.1995; 24 chasa daily, Is sue ¹ 126 from 1995; Democracia daily from
26.05.1995127 24 chasa daily, Is sue ¹ 2, Is sue ¹ 20, Is sue ¹. 101 from 12.04.1996, Is sue ¹ 134 and Is sue ¹ 306 from
1996; Trud daily from 11.01.1996, from 12.03.1996, from 16.07.1996 and from 7.11.1996; Standart dailyfrom 11.01.1996, from 8.04.1996, from 12.04.1996, from 19.04.1996 and from 22.05.1996.; Kapital weekly,Is sue ¹ 17 from 29.04.–5.05.1996; Democracia daily, Is sue ¹ 76 from 29.03.1996; Duma daily, Is sue ¹ 93and Is sue ¹ 142 from 1996; Fo rum Medicus pe ri od i cal, Is sue ¹ 3 from 22.01.1996, Is sue ¹ 7 from19.02.1996 and Is sue ¹ 8 from 26.02.1996
128 Trud daily from 29.02.1996 and Is sue ¹ 150 from 4.06.1996; Democracia daily from 31.01.1996, from7.11.1996 and from 28.12.1996; Standart daily, Is sue ¹ 5.06.1996 and from 28.12.1996.; 24 chasa daily,Is sue ¹ 355 from 28.12.1996
129 Trud daily from 17.11.1995130 Standart daily from 28.12.1996131 Standart daily, Is sue ¹ 1475 from 25.10.1996132 Duma daily, Is sue ¹ 144 from 20.06.1996
Drug sup ply
Re gard ing the drug sup ply, in 1992 and 1993 the draft law on drug sup ply was com -mented on and, re lated to it, the un clear sta tus of the phar ma cies was dis cussed133. Just as in the case of the Law on Health In sur ance, the phy si cians in sisted on the fast adop tion of the Law onDrugs and Phar ma cies in Hu man Med i cine (LDPHM) 134. Un like the Law on Health In sur -ance, how ever, the Law on Drugs and Phar ma cies in Hu man Med i cine was in tro duced to theple nary hall rel a tively fast135, al though there were quite a few de bat able is sues in this field, too. As re gards the LDPHM, dur ing its dis cus sion the most de bated ques tion in the press was thatphar ma cists with Mas ter’s de gree only had the right to open phar ma cies136.
In 1995 the com ments con tin ued on the Law on drugs and phar ma cies in hu man med i -cine re veal ing the mul ti fac eted in ter ests in this field137. Even tu ally, af ter a wide dis cus sion, theLDPHM was ap proved. The com pe tence, how ever, only for phar ma cists with Mas ter’s de gree to open phar ma cies and the ban on the es tab lish ment of chains of pri vate phar ma cies138 re mainedcon tested. The lat ter was par tially aban doned by a de ci sion of the Con sti tu tional Court in1996139.
The on go ing privatisation of phar ma ceu ti cal firms and chains of state phar ma cies wasfea tured in the press in 1995 and 1996140. In some ar ti cles opin ions were ex pressed on the eco -nomic in ex pe di ency of the on go ing privatisation.
To gether with the Draft law on drug sup ply, pub li ca tions ap peared from 1992 about theprob lems of the drugs def i cit and the rise in their prices141. Opin ions were voiced that therise in the prices was un re al is tic142. In 1992 the MH de vised a reg u la tion for con trol over thedrug prices and the max i mum over price143, against which the phar ma cists pro tested with thear gu ment that the lack of reg u la tions for the dis tri bu tion of the over price along the sep a rateunits of the dis tri bu tion chain would bring about the bank ruptcy of the pri vate phar ma cies144.In 1995 and 1996 the prob lem with the drug def i cit and the rise in their prices be came evenmore se vere as a re sult of the dis putes around its so lu tion and the in fla tion soar ing at that time.
77
Stages and evo lu tion of the healthcare re form in Bul garia
133 Democracia daily from 10.03.1993, Is sue ¹ 110from 1.05.1992 and from 26.05.1992.; Duma daily, Is sue ¹122 from 1992; 24 chasa daily, Is sue ¹ 125 from 1992; Fo rum Medicus pe ri od i cal, Is sue ¹ 18 from4.05.1992 and Is sue ¹ 34 from 31.08.1992
134 Democracia daily from 19.03.1993135 Democracia daily from 22.09.1993136 Democracia daily from 22.09.1994 and from 30.09.1993; Trud daily from 24.07.1993; Standart daily from
21.09.1993; 24 chasa daily, Is sue ¹ 256 from 1993; Duma daily, Is sue ¹ 71 and Is sue ¹ 217 from 1994137 Duma daily, Is sue ¹ 69 from 23.03.1995; 24 chasa daily, Is sue ¹ 37 from 7.02.1995, Is sue ¹ 88 from
31.03.1995 and Is sue ¹ 94 from 1995; Trud daily from 20.02.1995 and from 14.07.1995; Fo rum Medicuspe ri od i cal from 11.09.1995
138 24 chasa daily, Is sue ¹ 82 from 25.03.1995; Democracia daily from 6.04.1995139 24 chasa daily, Is sue ¹ 181 from 5.07.1996140 24 chasa daily, Is sue ¹ 19 from 20.01.1995, Is sue ¹ 109 from 21.04.1995 and Is sue ¹ 221 from 1996;
Duma daily, Is sue ¹ 82 from 1996; Standart daily, Is sue ¹ 1296 from 27.04.1996; Kapital weekly, Is sue ¹4 from 29.01.–4.02.1996, Is sue ¹ 16 from 22–28.04.1996, from 5–11.08.1996, from 11-17.11.1996 and from 23.12.–5.01.1997
141 Fo rum Medicus pe ri od i cal, Is sue ¹ 7 from 16.02.1991.; 24 chasa daily, Is sue ¹ 285 from 28-29.11.1992;Duma daily, Is sue ¹ 38 from 1992
142 Democracia daily, Is sue ¹ 110 from 1.05.1992143 24 chasa daily, Is sue ¹ 295 and Is sue ¹ 279 from 21-22.11.1992144 24 chasa daily, Is sue ¹ 285 from 28-29.11.1992 and Is sue ¹ 299 from 15.12.1992
This was the most com monly com mented is sue in the me dia, es pe cially in 1996145.The is sue of drug prices was a ques tion which cre ated con flict ing re la tions be tween the
drug pro duc ers and the drug trad ers, on the one hand, and the MH, on the other. The of fi cialpol icy of the MH was to main tain low prices of the drugs and the pro duc ers, in their turn, con -sid ered that the prices of the Bul gar ian drugs were too low as com pared to the for eign ones,which in their opin ion, pre vented the in vest ments146. In or der to re duce the drug prices, the MH pro posed amend ments to De cree ¹ 307 of the Coun cil of Min is ters, stip u lat ing the ex emp tionfrom du ties of the for eign raw ma te ri als for drug pro duc tion and fix ing of a max i mum price ofthe drugs147. Nev er the less, these prob lems re mained un re solved and in 1996 the drug pro duc -ers again in sisted for tax re lief and ex emp tion from du ties of the raw ma te ri als for the drugs im -ported from abroad148.
Par al lel to the dis cus sion of the LDPHM, in 1993 the is sue of the free drugs was also dis -cussed. The em pha sis was on the changes in the cri te ria for pre scrib ing free drugs, the lead ingcri te ria be ing the in come149. The most com mented point was that the chil dren and the preg nantwomen were left out of the list of the peo ple el i gi ble for free drugs pre scrip tion. At the be gin -ning of the year two reg u la tions were worked out on free drugs – by the so cial and thehealthcare min is tries, thus split ting the re spon si bil ity be tween the MH, which as sumed the re -spon si bil ity for the free drugs of the chron i cally ill pa tients, and the Min is try of La bour and So -cial Care, which as sumed the re spon si bil ity for the so cially unprivileged and the dis abledpeo ple150. Mean while the Par lia men tary Com mis sion pro posed that one in stead of two reg u la -tions was de vised151. To ward the end of the year the amend ments to the reg u la tion broad enedthe list of dis eases for which free drugs were granted and the list of el i gi ble peo ple, but the chil -dren and the preg nant women re mained left out of it152. In 1994 the dis cus sion was re sumed onthe pro posal put for ward by the MH to grant free drugs to preg nant women and chil dren andex tend the list of dis eases for which free drugs were pre scribed153. In 1995 once again dis putesarose be tween the so cial and the healthcare min is tries about the amend ment of the reg u la tionof the free drugs. Both pro jects for amend ment (of the so cial and of the healthcare min is tries)were widely dis cussed to gether with the groups en ti tled to free drugs154.
78
145 24 chasa daily, Is sue ¹ 258 from 1995, Is sue ¹ 16, Is sue ¹ 25, Is sue ¹ 133, Is sue ¹ 146, Is sue ¹ 171,Is sue ¹ 172 and Is sue ¹ 312 from 1996; Trud daily from 15.08.1995, from 16.11.1995 and from 30.05.1996; Duma daily, Is sue ¹ 229 and Is sue ¹ 263 from 1996; Standart daily from 17.05.1996 and Is sue ¹ 1353from 25.06.1996; Kapital weekly from 27.05.–2.06.1996, Is sue ¹ 26 from 1–7.07.1996 and from23-29.09.1996; Democracia daily from 9.02.1996
146 Duma daily, Is sue ¹116 from 19.05.1995147 Duma daily, Is sue ¹ 138, Is sue ¹ 155 from 1995; Kapital weekly, Is sue ¹ 38 from 25.09.–1.10.1995148 24 chasa daily, Is sue ¹ 172 from 1996149 Trud daily from 9.03.1993; Duma daily, Is sue ¹ 61 from 1993; 24 chasa daily, Is sue ¹ 60 and ¹ 70 from
16.03.1993; Democracia daily, Is sue ¹ 61 from 16.03.1993, from 31.03.1993, Is sue ¹ 79 from 6.04.1993and from 8.04.1993
150 24 chasa daily, Is sue ¹ 46 from 1993; Democracia daily from 9.05.1993151 24 chasa daily, Is sue ¹ 66 from 1993152 24 chasa daily, Is sue ¹ 249, Is sue ¹ 250 from 16.09.1993 and Is sue ¹ 278 from 14.10.1993153 24 chasa daily, Is sue ¹ 318 from 1994; Trud daily from 20.01.1994; Duma daily, Is sue ¹. 17 from
21.01.1994154 24 chasa daily, Is sue ¹ 151, Is sue ¹ 172, Is sue ¹ 207 and Is sue ¹ 228 from 1995; Trud daily, Is sue ¹ 145
from 23.06.1995, from 27.06.1995, Is sue ¹ 196 from 22.08.1995, from 21.09.1995,from 29.11.1995 andfrom 19.12.1995; Duma daily, Is sue ¹ 146 and Is sue ¹ 148 from 1995; Standart daily from 2.01.1995 andfrom 29.11.1995

In 1996 the prob lems of drug sup ply re ferred to a large ex tent to the pre scrip tion of freedrugs. From the mid dle of the year the phar ma cies re fused to ful fil the pre scrip tions for freedrugs and the MH and the mu nic i pal i ties owed 917 mil lion for med i ca tions155. To over come thecri sis, the MH un der took sev eral not so in ap pro pri ate but even tu ally in ef fec tive mea sures un dercon di tions of grow ing in fla tion– from lim it ing the price which is re im bursed by the mu nic i pal itybud get to an or der for sub sti tu tion of the for eign drugs for Bul gar ian ones156. At the end of 1996sev eral dra matic an nounce ments were pub lished about life-sav ing drugs in hos pi tals and thedebts of the MH for med i ca tions from free pre scrip tions amount ing to 3.8 bil lion BGN157.
Healthcare re form
From 1991 the me dia started to pub lish not only ma te ri als cov er ing the events re lated tothe healthcare re form but also opin ions about its con tent and as pects. Quite in sis tently andprob a bly with se ri ous ar gu ments, M. Vitkova (Dep uty from the Par lia men tary group of BCP)claimed that the healthcare re form should start with chang ing the healthcare fi nanc ing and itssep a ra tion from the state bud get as well as with chang ing the eco nomic mech a nisms of man -age ment158. In its turn, in an un am big u ous way M. Popov (Vice Min is ter) de vel oped the ma jorpa ram e ters of the healthcare re form – re form of the man age ment, through which “the cen tralplan ning, dis tri bu tion of re sources and de pend ence on the lo cal man age ment ad min is tra tiveand party au thor i ties was to be sub sti tuted for de cen trali sa tion and in de pend ence – es pe ciallyfi nan cial and staff – of the healthcare es tab lish ments”, re form of the fi nanc ing, throughwhich “the fi nanc ing is sep a rated be tween the state and the in sur ance fund (or funds)”, so that“the state takes over the bud get main te nance of all healthcare ac tiv i ties with the so called “in -sep a ra ble ef fect …, and the health in sur ance fund – the ac tiv i ties with a sep a ra ble ef fect”, plu -ral ism of own er ship – the in tro duc tion of pri vate med i cal (and den tal) prac tice and set ting upof pri vate, co-op er a tive and other types of healthcare es tab lish ments and par tial privatisation;struc tural changes – set ting up of “new struc tures to meet the changed health needs of thepop u la tion, re struc tur ing of the emer gency care, etc.”, new de cen tral ised or gani sa tion of there sources in healthcare, prep a ra tion of new per son nel cat e go ries, for ex am ple, di rec tors(nonmedical spe cial ists) of healthcare es tab lish ments and de vel op ment and at trac tion of thepro fes sional and trade un ion or gani sa tions of med i cal pro fes sion als in the im ple men ta tion ofthe re form159.
In 1992 opin ions about the re form in healthcare ap peared mainly in the “Duma” daily. Inan in ter view for this news pa per M. Vitkova ex pressed the view that “the re form in healthcareis still in its be gin ning. More over, it is not head ing in the right di rec tion”160. The crit i cismswere di rected to the post pone ment in pass ing the law on health in sur ance, the short age of fi -nanc ing, the re stric tion of the scope of peo ple el i gi ble for free pre scrip tions161.
In 1992 a num ber of pub li ca tions fo cused on var i ous as pects of the health in sur ance sys -
79
Stages and evo lu tion of the healthcare re form in Bul garia
155 Trud daily, Is sue ¹ 153 from 7.06.1996; Democracia daily from 21.06.1996; Standart daily from 4.06.1996,from 5.06.1996 and from 4.09.1996; Kapital weekly from 27.05.–2.06.1996
156 Duma daily, Is sue ¹ 4 from 5.01.1996; Democracia daily, Is sue ¹ 10 from 12.01.1996 and from17.10.1996; Standart daily from 2.03.1996
157 Standart daily from 5.06.1996; Trud daily, Is sue ¹ 335 from 28.12.1996; Duma daily, Is sue ¹ 292 from 1996158 Duma daily, Is sue ¹ 15, Is sue ¹ 136, Is sue ¹ 161 and Is sue ¹ 234 from 1991159 Democracia daily from 20.05.1991160 Duma daily, Is sue ¹ 257 from 1992161 Duma daily, Is sue ¹ 311 from 1992
tem. Along with the draft pro jects on health in sur ance caus ing a lot of de bates162, the press pub -lished ques tions and com ments on the health in sur ance of spe cific cat e go ries of peo ple, on health in sur ance funds, vol un tary in sur ance, pay ment for the med i cal ser vices, con tract ing with thehealthcare es tab lish ments, the med i cal care which cit i zens should re ceive against their in stal -ments, the con trol and qual ity of the health ser vices163, as well as an nounce ments about pri vatecom pa nies and co-op er a tions ca pa ble of set ting up health in sur ance or gani sa tions164. The pre -vail ing part of the pub li ca tions were in for ma tive (some times pro pa ganda) in na ture, their aim be -ing to ex plain the es sence of the health in sur ance sys tem and form pub lic opin ion en sur ing pub lic sup port for the pre pared draft law. The in for ma tion and com ments were mainly re lated to thever sion pre pared by the Cen tre for a Health In sur ance Sys tem, which was pre ferred by the MH as a ba sis of the Law on Health In sur ance (LHI). Re gard ing all the above, the opin ion of the then(1992) Min is ter of Healthcare Assoc. Prof. Dr. Nikola Vassilev was not sur pris ing, ac cord ing towhom the health in sur ance sys tem would start func tion ing not ear lier than 1995165.
The whole 1993 was char ac ter ised by an en hanced pres ence of the is sue of the health in -sur ance sys tem in the me dia. Its in tro duc tion was sup ported by all the par ties in volved (themed i cal pro fes sion als, the UBP, the lead ing po lit i cal forces), it was not ques tioned and themain fo cus of the pub li ca tions was the de lay of the pass ing of the Law on Health In sur ance166.
What was com mon in the views of the po lit i cal forces, the MH and the UBP, was the sup -port for the health in sur ance. The year started with a dis cus sion of 3 drafts worked out by theBCP, UBP and MH and, ac cord ing to the then Vice Prime Min is ter Matinchev, the drafts wereseven167. The UBP in sisted on uni ver sal and oblig a tory health in sur ance, de cen trali sa tion andequal ity of the state and the pri vate sec tors, hos pi tal privatisation and in tro duc tion of co-pay -ment, ac cel er ated pass ing of the law on health in sur ance in stead of the es tab lish ment of ananticrisis fund what was asked for by the MH; the BCP in sisted on a mixed sys tem of fi nanc -ing, pre serv ing the role of the state, it was against privatisation and cash pay ment by pa tients,and the Healthcare Dem o cratic Trade Un ion did not ac cept the idea of com pul sory health in -sur ance168. In June the trade un ions “cre ated ob sta cles at the very be gin ning of the cab i net” forthe next pro posal made by the MH with the claim that it was first con sid ered by the Three-party Com mis sion169. A pub li ca tion in the “Duma” news pa per from Oc to ber sum ma rised the eventsaround the dis cus sions on health in sur ance, stat ing that the na tional con cept was ab sent170.
In 1994, the then Min is ter T. Gugalov, not with out grounds, de clared that there was no re -form in healthcare, the struc tural re form had not started and the rea sons were rooted in the lack
80
162 Democracia daily, Is sue ¹ 106 from 5.05.1992, Is sue ¹. 198 from 20.08.1992 and from 3.09.1992; Dumadaily, Is sue ¹ 20, Is sue ¹ 115 and Is sue ¹ 155 from 1992; 24 chasa daily, Is sue ¹ 119, Is sue ¹ 123 and152 from 1992
163 Trud daily, Rubric on health insurance maintained by the Centre for the Health Insurance System, 1992164 24 chasa daily, Issue ¹ 179 from 28.07.1992165 24 chasa daily, Issue ¹ 199 from 20.08.1992; Standart daily from 20.08.1992166 Democracia daily from 6.01.1993, Issue ¹171 from 26.07.1993, Issue ¹ 179 from 4.08.1993, from
10.09.1993, from 7.10.1993, Issue ¹ 238 from 12.10.1993 and Issue ¹ 11.12.1993; 24 chasa daily, Issue ¹224 from 1993; Standart daily from 26.03.1993 and from 22.06.1993; Forum Medicus periodical, Issue ¹ 16from 19.04.1993, Issue ¹ 24 from 14.06.1993, Issue ¹ 27 from 5.07.1993, Issue ¹ 31 from 2.08.1993 andIssue ¹ 35 from 6.09.1993
167 24 chasa daily, Issue ¹ 7 from 1993168 Duma daily, Issue ¹ 8, Issue ¹ 43, Issue ¹ 224 from 1993; Democracia daily from 29.06.1993169 Democracia daily, Issue ¹ 171 from 26.06.1993170 Duma daily, Issue ¹ 234 from 7.10.1993
of leg is la tive change171. No at ten tion was paid to the rea sons for the lack of such a leg is la tivechange. The im por tance was once again stressed for the fast pass ing of the Law on Health In -sur ance as a “first step” in the re form pro cess172. The Chair man of the Un ion of the Pri vatePrac ti tio ners Dr. Atanas Shterev ex pressed the opin ion that the adop tion of a law reg u lat ingpri vate prac tice and the in tro duc tion of the health in sur ance funds formed the foun da tion of the re form” 173. In her turn, M. Vitkova (MP) criti cised the healthcare sys tem and the re sults fromthe changes as an “ir ra tio nal uti li sa tion of the fi nan cial re sources, de stroyed cen tral drug sup -ply, in ef fec tive struc tures”, “poor man age ment” re lated to the dou ble man age ment of thehealthcare es tab lish ments and she pointed out that “an over all con cept is nec es sary for the de -vel op ment of healthcare” as well as a “uni fied state health pol icy”174.
The top ics re gard ing the re form, and the health in sur ance in par tic u lar, were cov ered in1995 mainly by the “Democracia” daily. The ma te ri als were pri mar ily gen eral in na ture andhad a po lit i cal con text.
In an in ter view for the “Duma” news pa per175, Min is ter Vitkova de ter mined the changesin healthcare made in the pre vi ous years as “frag men tary”, with no con sis tency or logic cor re -spond ing to the goals. The changes were not per ceived as a “re form” and the ac cu sa tions werethat the med i cal pro fes sion als were not in volved in their im ple men ta tion176.
Al though the need for the in tro duc tion of a health in sur ance sys tem con tin ued to be in thefo cus of at ten tion, in some pub li ca tions an opin ion was voiced about the risk of adopt ing of alaw on health in sur ance un der the con di tions in 1995177. The ar gu ments in fa vour of this viewin cluded the lack of clar ity con cern ing the sta tus of the healthcare es tab lish ments, the size ofthe in stal ments and which health pri or i ties were go ing to be fi nanced by the state as well as thene ces sity for the Law on Health In sur ance to be backed not only by “a packet of laws en sur ingthe change in the ex ist ing sys tem” but also by laws reg u lat ing the new re la tions in the otherfields of the so cial and eco nomic life. In spite of the de clared “dan ger of the adop tion of theLaw on Health In sur ance”, in 1995 the in tro duc tion of the health in sur ance sys tem was per -ceived as a way of stop ping cor rup tion in healthcare178.
In an in ter view for the “Duma” daily, Min is ter Vitkova stated that the in sur ance should be com pul sory, amount ing to 4% of the work ing sal ary fund and 80% of the fi nanc ing forhealthcare had to re main the re spon si bil ity of the state179. Later, in an other in ter view, M.Vitkova pointed out that the re form in cluded re al lo cat ing in vest ment from hos pi tal to out pa -tients’ care, di vi sion of med i cal care into pri mary, spe cial ised and highly spe cial ised, changein the fi nanc ing, in which the vol ume and the qual ity of the per formed ac tiv i ties would formthe bud gets of the healthcare es tab lish ments, clos ing of the eco nom i cally un prof it able beds180.In the same in ter view M. Vitkova ex pressed the opin ion that a gen eral prac ti tio ner could not be avail able 24 hours a day.
81
Stages and evo lu tion of the healthcare re form in Bul garia
171 Democracia daily, Issue ¹ 9 from 13.01.1994 and Issue ¹ 17 from 21.01.1994172 Democracia daily, Issue ¹ 17 from 21.01.1994 and from 4.11.1994173 24 chasa daily, Issue ¹ 211 from 1994174 Duma daily, Issue ¹ 19 from 24.01.1994 and Issue ¹ 158 from 1994175 Duma daily, Issue ¹ 25 from 1995176 Duma daily, Issue ¹ 70 from 1995177 Democracia daily, Issue ¹ 58 from 11.03.1995 and Issue ¹ 88 from 15.04.1995178 Democracia daily, Issue ¹ 70 from 25.03.1995 and Issue ¹ 85 from 8.04.1995179 Duma daily, Issue ¹ 243 from 1995180 Duma daily, Issue ¹ 283 from 1.12.1995
A short pub li ca tion in the “Duma”181 news pa per was de voted to the Na tional HealthStrat egy which was be ing worked out by the MH and aimed at “out lin ing the trends for the de -vel op ment of the health of the Bul gar ian peo ple to gether with the long, mid dle and short -termmea sures to be un der taken”. The United Dem o cratic Forces, the Peo ple’s Un ion and the Move -ment for Rights and Free doms de nied their sup port for the strat egy “Health for Bul garia” 182.
Five years af ter the res to ra tion of the Un ion of Den tists in Bul garia (10 – 11th March1990) and the Un ion of Bul gar ian Phy si cians (27th May 1990), pub li ca tions ap peared in thepress about the nor ma tive reg u la tion of their ac tiv i ties by amend ments in the LPH183. In thesame pub li ca tion it was stated that “a law (au thors’ note: on pro fes sional or gani sa tions) willnot be adopted soon be cause it can not be in tro duced as a pri or ity for dis cus sion in Par lia ment”and in stead, the func tion ing of the UBP and the other med i cal pro fes sion als’ or gani sa tionswould be reg u lated by an or der of the Min is ter of Healthcare. Is sues were treated con cern ingthe oblig a tory mem ber ship of phy si cians and den tists, keep ing reg is ters by the re gional un ionsand “courts” which would con sider law cases against phy si cians and would ter mi nate phy si -cians’ rights184.
In 1996 the pub li ca tions con cerned mainly the Draft Law on Health In sur ance and itscon sid er ation by the gov ern ment185. The ex pec ta tions of the MH were that the law would bepassed by the NA un til the end of 1996. The main is sues re gard ing the law com mented in thepress in cluded the pro vi sion of fund ing in the health in sur ance fund (one of the pub li ca tionspointed out that, ini tially, the fund ing would be al lo cated from the state and the mu nic i pal bud -gets186, in an other pub li ca tion it was claimed that they would come from the State Pub lic In sur -ance187); the re la tion ships be tween the health in sur ance fund and the As so ci a tion of Hos pi talsand the pro fes sional or gani sa tions which were go ing to sign a na tional agree ment (M. Vitkovastate ment).
The changes en vis aged in the LPH, the choice of a fam ily phy si cian, the Na tional HealthStrat egy and the Draft Law on Health In sur ance were criti cised in a se ries of pub li ca tions in the “Demoracia” 188.
At the same time in an in ter view for the “Duma” news pa per, Prof. Dr. RadoslavGaidarski who was Head of the De part ment of Gen eral and Op er a tive Sur gery at the Med i calUni ver sity – So fia, de clared: “The changes which had be ing car ried out by sev eral healthcaremin is ters had noth ing to do with re form. The change of head phy si cians, for ex am ple, is not are form. Only now changes are be gin ning, which may give it an im pe tus, if they are im ple -mented – amend ment of LPH and the new sys tem for phy si cians’ pay ment, the strat egy“Health for all”… ”189.
82
181 Duma daily, Issue ¹ 134 from 1995 ã182 Standart daily from 9.12.1995183 Duma daily, Issue ¹ 167 from 1995184 24 chasa daily, Issue ¹ 259 and Issue ¹ 281 from 1995185 24 chasa daily, Issue ¹ 23, Issue ¹ 133, Issue ¹ 278 and Issue ¹ 286 from 1996; Trud daily from
28.01.1996 and from 18.10.1996; Kapital weekly from 21-27.10.1996.; Democracia daily from 22.10.1996;Duma daily, Issue ¹ 243, Issue ¹ 247 and Issue ¹ 253 from 1996 Forum Medicus periodical, Issue ¹ 9from 4.03.1996, Issue ¹ 22 from 10.06.1996 and Issue ¹ 42-43 from 28.10.1996
186 24 chasa daily, Issue ¹ 133 from 1996187 Duma daily, Issue ¹ 23 from 27.01.1996188 Democracia daily from 26.01.1996, from 2.02.1996, from 9.02.1996 and from 23.09.1996189 Duma daily, Issue ¹ 29 from 3.02.1996
In a pub li ca tion in the “Democracia” daily190 it was an nounced that the EC was cancelling the trans fer of the ne go ti ated 15 mil lion ecu in the frame work of the PHARE Programme be -cause of fail ure to adopt the Law on Health In sur ance and to es tab lish the In sti tute for HealthIn sur ance as the fund ing was meant for train ing of the In sti tute’s em ploy ees.
As a whole, the as sess ment of the changes in healthcare given by the WHO ex pert Prof.Anastas Philalitis in an in ter view for the “Duma” daily was pos i tive. The adop tion of the Na -tional Health Strat egy was eval u ated pos i tively but crit i cism was also ex pressed for the de layin the pass ing of the Law on Health In sur ance191.
A lit tle later in the same year the op po si tion ac tively coun ter acted the Bill on Health In -sur ance and re fused to dis cuss it in the Par lia men tary Com mis sion192.
The pub li ca tions in the me dia to ward the end of 1996 were ded i cated to the re port of theMH on the two-tier pe riod of rul ing (as part of the re port of the gov ern ment), pub lished in the“Duma” news pa per193. The re port ex am ined in a crit i cal way the changes which were im ple -mented (or not im ple mented) by the pre vi ous gov ern ments. On the other hand, one of the ma -jor crit i cisms es sen tially re lated to the re port (but not only to it) ad dressed the re stric tion of thepri vate prac tice in the state healthcare es tab lish ments194.
Sur veys of the pub lic opin ion
The be gin ning of the healthcare re form was ac com pa nied by the sup port of the pub lic opin -ion. The cit i zens ex pressed their re sent ment mainly con cern ing the ex ist ing or gani sa tion of themed i cal care. A ques tion naire with pa tients from the be gin ning of 1990s showed that 64% ofthem eval u ated pri mary and spe cial ised med i cal care as “poor” and “very poor”. Ac cord ing tothe re spon dents, this was due to the poor or gani sa tion and the waste of time (69%), favourisationand priv i leges (66%), nu mer ous bu reau cratic pro ce dures (60%), poor hy giene in the healthcarees tab lish ments (60%), short age or lack of drugs and med i cal consumables (66%)195.
Hav ing in mind the con sid er ably wide pos i tive pub lic at ti tude at the time to the dem o -cratic and mar ket changes, it is ex plain able why so ci ety ex pected ad e quate re form inhealthcare, too. In deed, as ob vi ous from the sam ple ques tion naire, in April 1992 the in ter estin the healthcare re form was enor mous. The amend ments in the LPH had al ready been madeand the free choice of a fam ily phy si cian and den tist had al ready been in tro duced. It was par tic -u larly im pres sive that 84.4% of the in ter viewed were aware that healthcare was be ing re -formed. The sources of this in for ma tion were dif fer ent, but above all (41.9%), came from thera dio and the tele vi sion. The large ma jor ity of the in ter viewed, how ever, (47.9%) re ported thatno change had ac tu ally oc curred, 19.4% noted a pos i tive change, 15.1% marked de te ri o ra tion,and 17.6% could not es ti mate.
The in for ma tion from the ques tion naire was rather in trigu ing on the key is sue of the re -form, e.g. the health in sur ance.
61.5% of the re spon dents were aware of the es tab lish ment of a health in sur ance sys tem,
83
Stages and evo lu tion of the healthcare re form in Bul garia
190 Democracia daily from 19.08.1996191 Duma daily, Issue ¹ 268 from 1996192 Kapital weekly from 28.10.–3.11.1996193 Duma daily, Issue ¹ 290 from 1996194 Kapital weekly from 2–8.12.1996195 Markova, N. Èêîíîìè÷åñêî ðàçâèòèå è óïðàâëåíèå íà çäðàâíî çàâåäåíèå â ïåðèîä íà ïðåõîä îò
áþäæåòíî ôèíàíñèðàíå êúì çäðàâíî-îñèãóðèòåëíà ñèñòåìà. In: Zdrave periodical, 28-29.05.1992(quoted after Ì. Prohaska et all., 2005, p.64)
but around three quar ters of them (74.1%) were not aware of its mean ing and con tent, and onlyone quar ter (25.9%) reck oned that they were clear on the is sue. Nev er the less, 56.3% were surethat the sys tem would im prove med i cal care, 8.3% had a neg a tive at ti tude and 35.4% did nothave an opin ion. It turned out that part of the cit i zens were not aware of the core of the healthin sur ance sys tem but be lieved that “it would be to the ben e fit”. The fact that the cit i zens werenot fa mil iar with the health in sur ance sys tem was ev i dent from the dif fer ing in for ma tion theypro vided on the pay ment for med i cal care. About one third (32.%) of the re spon dents did notknow any thing about this is sue, 5.4% con sid ered that it was to tally paid, 9.8% thought that thegreater part was paid, 9.0% - that half of it was paid, 28.4% - that the smaller part was paid, andac cord ing to 14.4% noth ing was paid.
The re sponses about the health in sur ance in stal ments were in ter est ing, too. The ma jor ityof the re spon dents (79.2%) agreed to pay in sur ance in stal ments, 13.7% re ported that theycould not af ford it, and 7.2% could not an swer the ques tion. Re gard ing the size of the in sur -ance in stal ment, the opin ions var ied widely: 8.3% of the re spon dents could not af ford to pay an in stal ment over 10% from their monthly in come, 27.6% - up to 10% from their monthly in -come, 24.9% - up to 5%, and 18.5% - up to 2% from their monthly in come. If med i cal care wasto tally or at least par tially paid by the pa tients, 65.3% of the re spon dents con sid ered that itsqual ity would im prove; ac cord ing to 13.5% it would not change, and 21.2% could not judge196.
Apart from the cog ni tive his tor i cal value, the above quoted in for ma tion con firmed an im -por tant pe cu liar ity of the re form pro cess, namely, that the healthcare re form and health in sur -ance in par tic u lar, were ac quir ing re mark able pop u lar ity not only among the med i calpro fes sion als but also in the wide com mu nity. But still at the be gin ning of 1990s, the mainsource of in for ma tion for our so ci ety was the mass me dia and chiefly the ra dio and tele vi sion.The im me di ate ac tive di a logue seemed to be de layed or lack ing be tween the Healthcare Min -is try and the med i cal pro fes sion als as well as be tween the healthcare sys tem and so ci ety. As are sult, an in for ma tion vac uum emerged that was oc ca sion ally filled with ran dom or pur pose -fully in ac cu rate in for ma tion, which be comes ev i dent from the quoted ques tion naires. The pop -u lar ity of the healthcare re form and health in sur ance could have been used in a con struc tiveway, but it re mained in the his toric an nals.
Re sults and un solved prob lems
With out be ing un event ful, the first stage of the de vel op ment of the healthcare re formyielded def i nite re sults but even through them the ob jec tives of the healthcare re form re -mained un solved.
A ma jor task re mained un re solved, e.g. the dis con tinu a tion of the de te ri o ra tion of thepop u la tion’s health sta tus. Cer tainly, for a rel a tively short (6-to7-year) pe riod char ac ter isedby po lit i cal ten sion and eco nomic fail ures, an im prove ment of the pop u la tion health sta tuscould not be ex pected. On the con trary, what could be ex pected – which was in deed the re al ity– was a neg a tive de vel op ment (Ta ble 19). The rise of the gen eral mor tal ity rate was alarm ingto gether with the mor tal ity rate in the ac tive age (40 – 69 years) as well as the mor tal ity re sult -ing from all causes and tu mour for ma tions, more spe cif i cally, dis eases of the blood cir cu la tionor gans, the gas tro in tes ti nal tracts and (to some ex tent) trauma and poi son ing, closely cor re -
84
196 Lumbev, G., S. Bachev et al. Îòíîøåíèå íà íàñåëåíèåòî êúì ðåôîðìàòà â çäðàâåîïàçâàíåòî. Scientificsymposium “Healthcare Economics”, Sofia, 28-29.05.1992
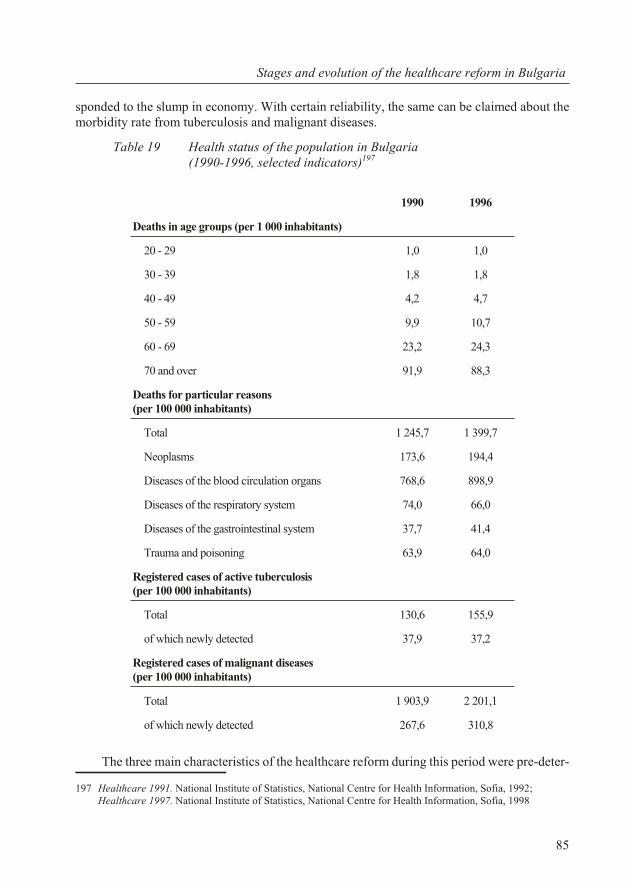
sponded to the slump in econ omy. With cer tain re li abil ity, the same can be claimed about themor bid ity rate from tu ber cu lo sis and ma lig nant dis eases.
Ta ble 19 Health sta tus of the pop u la tion in Bul garia (1990-1996, se lected in di ca tors)197
The three main char ac ter is tics of the healthcare re form dur ing this pe riod were pre-de ter -
85
Stages and evo lu tion of the healthcare re form in Bul garia
1990 1996
Deaths in age groups (per 1 000 in hab it ants)
20 - 29 1,0 1,0
30 - 39 1,8 1,8
40 - 49 4,2 4,7
50 - 59 9,9 10,7
60 - 69 23,2 24,3
70 and over 91,9 88,3
Deaths for par tic u lar rea sons (per 100 000 in hab it ants)
To tal 1 245,7 1 399,7
Neoplasms 173,6 194,4
Dis eases of the blood cir cu la tion or gans 768,6 898,9
Dis eases of the re spi ra tory sys tem 74,0 66,0
Dis eases of the gas tro in tes ti nal sys tem 37,7 41,4
Trauma and poi son ing 63,9 64,0
Reg is tered cases of ac tive tu ber cu lo sis (per 100 000 in hab it ants)
To tal 130,6 155,9
of which newly de tected 37,9 37,2
Reg is tered cases of ma lig nant dis eases (per 100 000 in hab it ants)
To tal 1 903,9 2 201,1
of which newly de tected 267,6 310,8
197 Healthcare 1991. Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion, So fia, 1992;Healthcare 1997. Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion, So fia, 1998
mined by the pe cu liar i ties of the po lit i cal, eco nomic and so cial con text: (1) slow course, (2) ir -reg u lar de vel op ment and (3) grad ual alien ation of the med i cal spe cial ists from the prin ci plesand the goals of the healthcare re form.
The slow im ple men ta tion of the healthcare re form in the pe riod 1990-1996 co in cided to alarge ex tent with the “Wran – Utt Plan” rec om men da tions. It was ev i dent not only from the na -tional di men sions but also from the in ter na tional com par i sons. Un der rel a tively sim i lar con di -tions of de vel op ment, the chief com po nent of the healthcare re form – the change in the eco nomic re la tions in the field of healthcare – in some of the East ern and Cen tral Eu ro pean coun tries wascar ried out years ear lier than in Bul garia: in Croatia – in 1993, in the Czech Re pub lic – in 1992and in Lith u a nia – in 1997198. The Par lia men tary dis cus sion of the Law on Peo ple’s Health wascon tin u ous, for sev eral years the Draft Law on Health In sur ance did not reach dis cus sion stage atall. The rea son was in the im peded leg is la tive ac tiv ity of Par lia ment due to the se vere po lit i calcon fron ta tion and the strong po lit i cal bias of the healthcare prob lems.
The ir reg u lar im ple men ta tion and de vel op ment of the healthcare re form re sulted to alarge de gree from the lack of a re spect ful con cept for its course. There are cer tain grounds tobe lieve that the cor po rate in ter ests also ex erted some im pact on the re form pro cess. With outtheir in ter fer ence, it would be im pos si ble to make up an ac cept able ex pla na tion of the ac cel er -ated pass ing of the Law on Drugs and Phar ma cies in Hu man Med i cine. Al though a lim ited part of the healthcare sys tem, the phar ma ceu ti cal sec tor as a whole com prises much more econ omy(pro duc tion and trade) than med i cine and healthcare. From the point of de par ture of the re form logic, the leg is la tion pro vid ing for the cit i zens’ med i cal care should have had a pri or ity. In themean time (and prob a bly af ter it), the leg is la tion should have reg u lated the new re gime for drug sup ply, which, in fact, served the med i cal care. This, of course, by no means re duced the sig -nif i cance of the above law on the demonopolisation of the healthcare sys tem.
The iso la tion of the med i cal pro fes sional from the prin ci ples, tasks and the rates ofthe healthcare re form had par tic u larly neg a tive con se quences. Those who had to di rectly im -ple ment the re form pro cess were not fa mil iar with its ob jec tives and con tent. This was a se ri -ous de fect of the ap proach which was go ing to be rep li cated in the fol low ing years.
Dur ing this stage, the nor ma tive ba sis of healthcare was re ally up dated to a cer tain de -gree (the amend ments and ad di tions of the Law on Peo ple’s Health) and ex tended (the Law onDrugs and Phar ma cies in Hu man Med i cine and a num ber of by-laws and ad min is tra tive acts).The po si tions of the so cial ist state mo nop oly in drug sup ply were elim i nated and in the field ofmed i cal care they were shat tered. The Na tional Health Strat egy was al ready a fact – awell-grounded and sys tema tised programme for changes in the healthcare sys tem, un derwhich a spe cial strat egy for the de vel op ment of pri mary healthcare was de vised, too.
With the fol low ing reg u la tory and ad min is tra tive acts, is sued be fore and af ter the Na -tional Health Strat egy, re gard ing the or gani sa tion and the man age ment of the healthcare net -work and the healthcare in sti tu tions cer tain im prove ment was achieved as well as or der in theman age ment of the healthcare sys tem: the Reg u la tion for the terms and the pro ce dure for ex er -cis ing pri vate med i cal prac tice199, the Reg u la tion for the man age ment of the healthcare es tab -
86
198 Shakarishvili, G., K. Davey. Trends in Re form ing the Pro vi sion and Fi nanc ing of Healthcare. In:Shakarishyili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and East ernEu rope in the 1990s., 2005, pp 3-43
199 State Ga zette, Is sue ¹ 37 from 10.05.1991
lish ments200, the Reg u la tion for the man age ment of the state healthcare es tab lish ments201,Reg u la tion for the struc ture and the func tion ing of the Hy giene and Ep i de mi o log i cal In sti -tutes202, the Reg u la tion for the or gani sa tion of the out pa tients’ med i cal care203, the Reg u la tionfor the or gani sa tion of the hos pi tal med i cal care in the state healthcare es tab lish ments204, theReg u la tion for the or gani sa tional and meth od olog i cal as sis tance in the sys tem of healthcare205.
Dur ing this stage, how ever, the re pro duc tion of the ex ist ing healthcare sys tem as anover all or gani sa tion was not dis con tin ued.
The Na tional Health Strat egy did not even men tion a re form in healthcare. The word “re -form” was miss ing in it and, in stead, it en vis aged “changes”. This was not only a lin guis tic andter mi no log i cal pe cu liar ity of the strat egy but also a char ac ter is tic fea ture of its con tent andmean ing.
The strat egy did not con cern a change in the pres ence and role of the state in re la tion tohealthcare. The change in the struc ture of own er ship in the sys tem re mained out side the strat -egy. Af ter it had been solved, in re gard to the phar ma cies and the drug sup ply, the ques tionabout the struc ture of the own er ship in the other sec tors was not posed. The own er ship of thehealthcare and med i cal es tab lish ments in the fu ture was de fined as pub lic (state or mu nic i pal -ity) and the de vel op ment of the pri vate sec tor was seen as its com ple ment.
Af ter the amend ments in the Law on Peo ple’s Health and the reg u la tion of the pri vatesec tor in the sys tem of healthcare, in spite of the de clared eq uity with the pub lic healthcare, nocon di tions were cre ated for its de vel op ment (fi nanc ing, price and tax pol icy, re gime of in vest -ment)206.
The post poned set ting up of a health in sur ance or gani sa tion and the new eco nomicstruc ture in the healthcare sys tem as a whole were ma jor fac tors for the slow course of the re -form and con tra dicted the rel a tively wide pub lic opin ion and ex pec ta tions in this re spect.
Dur ing this stage the healthcare sys tem shifted from one state to an other in deed, but the el e -ments of the re form were def i nitely un evenly pro nounced. Ac tu ally, it con cerned ex clu sivelyand rather in ten sively the phar ma ceu ti cal sec tor and, quite su per fi cially, the med i cal sec tor of the healthcare sys tem. The pre ven tive ac tiv i ties were left out side the fo cus of at ten tion.
5.2. Sec ond stage: de vel op ment of a rad i cal re form of thehealthcare sys tem
This stage cov ered the pe riod be tween 1997 and 2001 and was an ac tive and fruit fulcon tin u a tion of the re form, which had been ini ti ated and slowly and ir reg u larly ad vanc ing inthe pre vi ous years. Prob a bly the opin ion is there fore pop u lar that the healthcare re form be ganand was im ple mented ex actly dur ing this stage.
87
Stages and evo lu tion of the healthcare re form in Bul garia
ÃîäèíàÐàçõîäè ïî êîíñîëèäèðàíèÿ
äúðæàâåí áþäæåò (ëåâà)Ðàçõîäè êàòî ïðîöåíò îò
ÁÂÏ
1997 599 088 300 3,5
1998 810 333 000 3,8
1999 933 177 500 4,1
2000 1 057 073 400 4,1
2001 1 222 100 000 4,3
200 State Ga zette, Is sue ¹ 50 from 30.06.1991 and Is sue ¹ 93 from 17.11.1992201 State Ga zette, Is sue ¹ 71 from 11.08.1995202 State Ga zette, Is sue ¹ 67 from 18.08.1992203 State Ga zette, Is sue ¹ 20 from 08.03.1996 and Is sue ¹ 3 from 10.01.1997204 State Ga zette, Is sue ¹ 76 from 06.09.1996205 State Ga zette, Is sue ¹ 109 from 27.12.1996206 Semerdjiev, I., Å. Delcheva, D. Zinovieva. Pa pers. In: The Pri vate Med i cal Prac tice in Bul garia. Na tional
sem i nar. Pub lished by the Bul gar ian As so ci a tion of Med i cal Law, So fia, 1996, pp. 5-17; Bonel, Ì., I.Semerdjievâ, S. Helmers, L. Rinder, Å. Helberg, B. McGuiness. Pa pers. In: On the Is sues of Pri vate Med i calPrac tice in Re pub lic of Bul garia. Dis cus sion ta ble. Col lec tion of pa pers, So fia, 1996
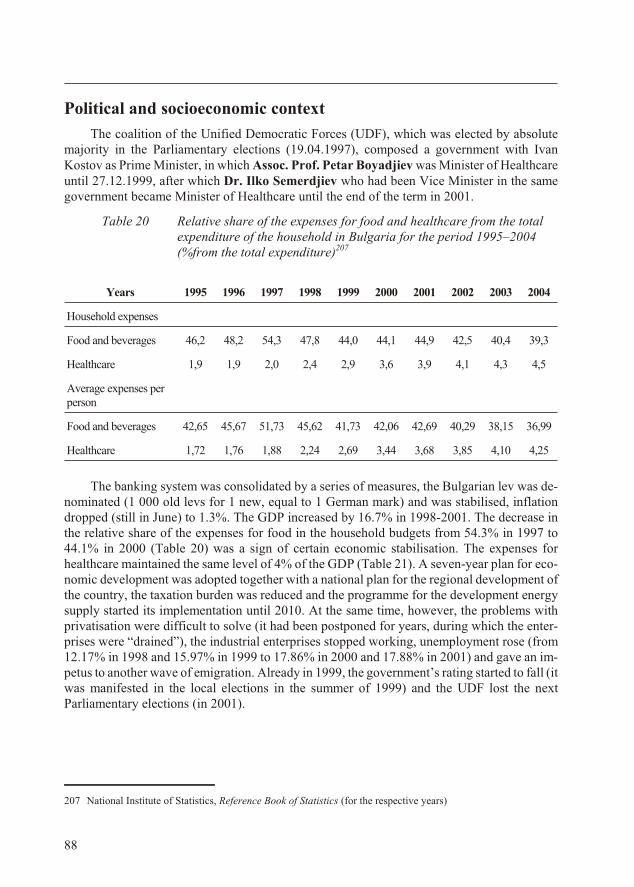
Po lit i cal and so cio eco nomic con text
The co ali tion of the Uni fied Dem o cratic Forces (UDF), which was elected by ab so lutema jor ity in the Par lia men tary elec tions (19.04.1997), com posed a gov ern ment with IvanKostov as Prime Min is ter, in which Assoc. Prof. Petar Boyadjiev was Min is ter of Healthcareun til 27.12.1999, af ter which Dr. Ilko Semerdjiev who had been Vice Min is ter in the samegov ern ment be came Min is ter of Healthcare un til the end of the term in 2001.
Ta ble 20 Rel a tive share of the ex penses for food and healthcare from the to talex pen di ture of the house hold in Bul garia for the pe riod 1995–2004(%from the to tal ex pen di ture)207
The bank ing sys tem was con sol i dated by a se ries of mea sures, the Bul gar ian lev was de -nom i nated (1 000 old levs for 1 new, equal to 1 Ger man mark) and was sta bi lised, in fla tiondropped (still in June) to 1.3%. The GDP in creased by 16.7% in 1998-2001. The de crease inthe rel a tive share of the ex penses for food in the house hold bud gets from 54.3% in 1997 to44.1% in 2000 (Ta ble 20) was a sign of cer tain eco nomic sta bili sa tion. The ex penses forhealthcare main tained the same level of 4% of the GDP (Ta ble 21). A seven-year plan for eco -nomic de vel op ment was adopted to gether with a na tional plan for the re gional de vel op ment ofthe coun try, the tax a tion bur den was re duced and the programme for the de vel op ment en ergysup ply started its im ple men ta tion un til 2010. At the same time, how ever, the prob lems withprivatisation were dif fi cult to solve (it had been post poned for years, dur ing which the en ter -prises were “drained”), the in dus trial en ter prises stopped work ing, un em ploy ment rose (from12.17% in 1998 and 15.97% in 1999 to 17.86% in 2000 and 17.88% in 2001) and gave an im -pe tus to an other wave of em i gra tion. Al ready in 1999, the gov ern ment’s rat ing started to fall (it was man i fested in the lo cal elec tions in the summer of 1999) and the UDF lost the nextParliamentary elections (in 2001).
88
Years 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
House hold ex penses
Food and bev er ages 46,2 48,2 54,3 47,8 44,0 44,1 44,9 42,5 40,4 39,3
Healthcare 1,9 1,9 2,0 2,4 2,9 3,6 3,9 4,1 4,3 4,5
Av er age ex penses perper son
Food and bev er ages 42,65 45,67 51,73 45,62 41,73 42,06 42,69 40,29 38,15 36,99
Healthcare 1,72 1,76 1,88 2,24 2,69 3,44 3,68 3,85 4,10 4,25
207 National In sti tute of Sta tis tics, Ref er ence Book of Sta tis tics (for the re spec tive years)
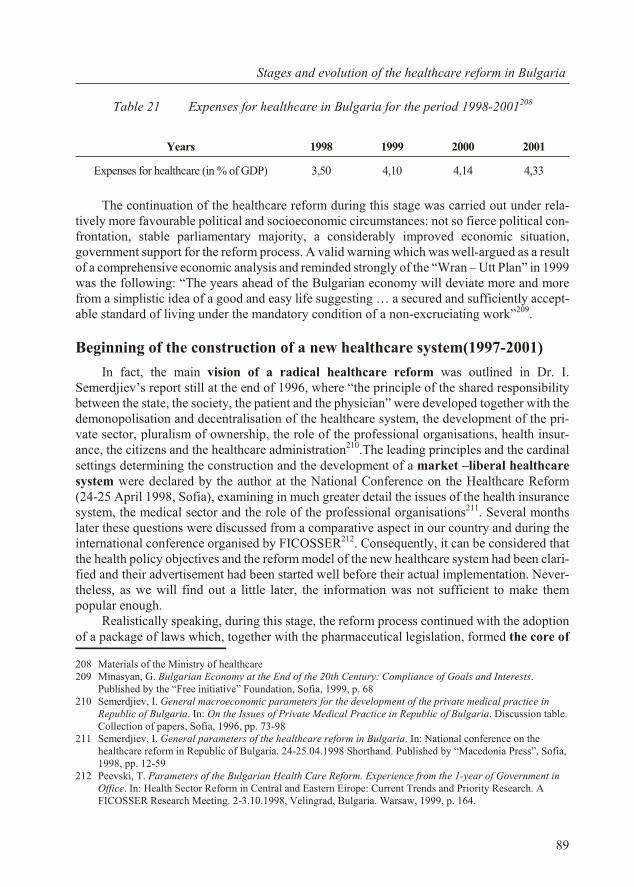
Ta ble 21 Expenses for healthcare in Bulgaria for the period 1998-2001208
The con tin u a tion of the healthcare re form dur ing this stage was car ried out un der rel a -tively more fa vour able po lit i cal and so cio eco nomic cir cum stances: not so fierce po lit i cal con -fron ta tion, sta ble par lia men tary ma jor ity, a con sid er ably im proved eco nomic sit u a tion,gov ern ment sup port for the re form pro cess. A valid warn ing which was well-ar gued as a re sultof a com pre hen sive eco nomic anal y sis and re minded strongly of the “Wran – Utt Plan” in 1999 was the fol low ing: “The years ahead of the Bul gar ian econ omy will de vi ate more and morefrom a sim plis tic idea of a good and easy life sug gest ing … a se cured and suf fi ciently ac cept -able stan dard of liv ing un der the man da tory con di tion of a non-ex cru ci at ing work”209.
Be gin ning of the con struc tion of a new healthcare sys tem(1997-2001)
In fact, the main vi sion of a rad i cal healthcare re form was out lined in Dr. I.Semerdjiev’s re port still at the end of 1996, where “the prin ci ple of the shared re spon si bil itybe tween the state, the so ci ety, the pa tient and the phy si cian” were de vel oped to gether with thedemonopolisation and de cen trali sa tion of the healthcare sys tem, the de vel op ment of the pri -vate sec tor, plu ral ism of own er ship, the role of the pro fes sional or gani sa tions, health in sur -ance, the cit i zens and the healthcare ad min is tra tion210.The lead ing prin ci ples and the car di nalset tings de ter min ing the con struc tion and the de vel op ment of a mar ket –lib eral healthcaresys tem were de clared by the au thor at the Na tional Con fer ence on the Healthcare Re form(24-25 April 1998, So fia), ex am in ing in much greater de tail the is sues of the health in sur ancesys tem, the med i cal sec tor and the role of the pro fes sional or gani sa tions211. Sev eral monthslater these ques tions were dis cussed from a com par a tive as pect in our coun try and dur ing thein ter na tional con fer ence or gan ised by FICOSSER212. Con se quently, it can be con sid ered thatthe health pol icy ob jec tives and the re form model of the new healthcare sys tem had been clar i -fied and their ad ver tise ment had been started well be fore their ac tual im ple men ta tion. Nev er -the less, as we will find out a lit tle later, the in for ma tion was not suf fi cient to make thempop u lar enough.
Re al is ti cally speak ing, dur ing this stage, the re form pro cess con tin ued with the adop tionof a pack age of laws which, to gether with the phar ma ceu ti cal leg is la tion, formed the core of
89
Stages and evo lu tion of the healthcare re form in Bul garia
1997 2000 2001
Óìðåëè ïî âúçðàñò (íà 1 000 äóøè)
20 - 29 ã. 1,0 0,8 0,9
30 - 39 ã. 1,9 1,7 1,6
40 - 49 ã. 4,9 4,3 4,3
50 - 59 ã. 11,1 10,1 10,1
60 - 69 ã. 25,0 23,8 23,3
70 è ïîâå÷å 91,2 84,5 81,6
Óìðåëè ïî ïðè÷èíè (íà 100 000 äóøè)
Îáùî 1 431,4 1 408,6 1 420,0
Íîâîîáðàçóâàíèÿ 191,0 187,8 196,0
Áîëåñòè íà îðãàíèòå íà êðúâîîáðúùåíèåòî 947,0 933,8 946,1
Áîëåñòè íà äèõàòåëíàòà ñèñòåìà 58,4 55,1 46,7
Áîëåñòè íà õðàíîñìèëàòåëíàòà ñèñòåìà 38,8 36,4 37,2
Òðàâìè è îòðàâÿíèÿ 60,4 56,9 55,2
Ðåãèñòðèðàíè çàáîëÿâàíèÿ îò àêòèâíà òóáåðêóëîçà (íà 100 000 äóøè)
Îáùî 181,5 173,4 185,8
Îò òÿõ íîâîîòêðèòè 49,8 41,0 48,8
Ðåãèñòðèðàíè çàáîëÿâàíèÿ îò çëîêà÷åñòâåíè íîâîîáðàçóâàíèÿ (íà 100 000 äóøè)
Îáùî 2 322,4 2 462,9 2 618,2
Îò òÿõ íîâîîòêðèòè 318,9 320,1 356,2
Years 1998 1999 2000 2001
Ex penses for healthcare (in % of GDP) 3,50 4,10 4,14 4,33
208 Ma te ri als of the Min is try of healthcare209 Minasyan, G. Bul gar ian Econ omy at the End of the 20th Cen tury: Com pli ance of Goals and In ter ests.
Pub lished by the “Free ini tia tive” Foun da tion, So fia, 1999, p. 68210 Semerdjiev, I. Gen eral mac ro eco nomic pa ram e ters for the de vel op ment of the pri vate med i cal prac tice in
Re pub lic of Bul garia. In: On the Is sues of Pri vate Med i cal Prac tice in Re pub lic of Bul garia. Dis cus sion ta ble. Col lec tion of pa pers, So fia, 1996, pp. 73-98
211 Semerdjiev, I. Gen eral pa ram e ters of the healthcare re form in Bul garia. In: Na tional con fer ence on thehealthcare re form in Re pub lic of Bul garia. 24-25.04.1998 Shorthand. Pub lished by “Mac e do nia Press”, So fia,1998, pp. 12-59
212 Peevski, T. Pa ram e ters of the Bul gar ian Health Care Re form. Ex pe ri ence from the 1-year of Gov ern ment inOf fice. In: Health Sec tor Re form in Cen tral and East ern Eirope: Cur rent Trends and Pri or ity Re search. AFICOSSER Re search Meet ing. 2-3.10.1998, Velingrad, Bul garia. War saw, 1999, p. 164.
the rad i cal healthcare re form. They in cluded the fol low ing:
· Law on Health In sur ance 213;
· Law on Healthcare Es tab lish ments214 (LHE);
· Law on the Pro fes sional Or gani sa tions of Phy si cians and Den tists215 (LPOPD).
These laws had a dif fer ent sub ject (which found ex pres sion in their re spec tive ti tles, too). Ac cord ing to their sub ject, they reg u lated spe cific sec tors of real life. Nev er the less, they werein ter re lated by a com mon logic, meet ing the re quire ment and the trend to ward de moc ra ti sa -tion and mar ket ori en ta tion of the healthcare sys tem. These laws were aimed at pro vid ing thele gal reg u la tion of the dem o cratic and mar ket de vel op ment of the med i cal care in our coun try. The sec tor of med i cal care bore the greater part of the re sources, costs and the pro cesses in thehealthcare sys tem and was of enor mous im por tance for the life of each in di vid ual. There fore,the reg u la tion of the sta tus, func tions and the struc tures of med i cal care in ac cor dance with thechanged con di tions, had an un dis pu ta ble pri or ity, es pe cially when the nor ma tive sys tem in thephar ma ceu ti cal and drug sup ply sec tors had al ready been adopted.
In prin ci ple, with the ex cep tion of the ma te rial and non ma te rial re sources, the med i calsec tor con tains three com po nents: cus tom ers of med i cal care (pa tients), per form ers of med i -cal care (healthcare es tab lish ments) and a fi nan cial me di a tor (a state or mu nic i pal fi nan cialser vice, in sur ance or gani sa tion). In or der to achieve a change in the sec tor to ward de moc ra ti -sa tion and mar ket ori en ta tion, a chief re quire ment is that the three com po nents pos sess in de -pend ence. Such an au ton omy is nec es sary to en sure their in de pend ent be hav iour as mar ketsub jects. Par al lel and in sup port of these changes, the re gime of own er ship of the healthcarees tab lish ments was changed.
Al though not so rad i cal, cer tain changes were car ried out in the field of pub lichealthcare af ter the adop tion of the Law on Healthy and Safe Work ing Con di tions216
(LHSWC), the Law on Foods217 (LF) and the Law on the Con trol of Nar cotic Sub stances andPre cur sors218 (LCNSP) as well as the adop tion of new by-laws on pre ven tion and health pro -mo tion ac tiv i ties and the or gani sa tion of the hy giene and ep i de mi o log i cal ser vices219.
Struc tural and or gani sa tional changes in the healthcare net work
With the LHE, a new struc ture was reg u lated to gether with the no men cla ture for thehealthcare net work and the sep a rate es tab lish ments be long ing to it. The Law stip u lated thesep a ra tion of the out pa tients’ from the in pa tients’ care and the def i ni tion of the char ac ter is -tics and the no men cla ture of the dif fer ent types of healthcare es tab lish ments. Thus, cer tain or -der was in tro duced, which was un doubt edly nec es sary both for the man age ment (in clud ing the qual ity man age ment) and (even more) for the con trac tual re la tions with the health in sur anceor gani sa tions.
90
213 State Ga zette, Is sue ¹ 70 from 10.06.1998214 State Ga zette, Is sue ¹ 62 from 19.07.1999215 State Ga zette, Is sue ¹ 83 from 21.07.1998 216 State Ga zette, Is sue ¹ 124 from 23.12.1997217 State Ga zette, Is sue ¹ 90 from 15.10.1999218 State Ga zette, Is sue ¹ 30 from 2.04.1999 219 Dor fur ther de tails on the struc tural and other changes in: Cal en der of the Achieve ments of the Gov ern ments
of Re pub lic of Bul garia in the Field of Healthcare for the Pe riod 1997-2000 ã. Pub lished by the Minstry ofHealthcare, So fia, 2001
In ac cor dance with the LHE, the struc tural changes in cluded a new or gani sa tion of cer tain sep a rate sec tors of the healthcare net work, which had been set up in the pe riod 1997-2000.Within a pro ject fi nanced by the EC and WB (13 340 100 US dol lars), the over all con struc tionof the na tional sys tem for emer gency med i cal care was ac com plished, e.g. 28 dis trict Cen tres for Emer gency Med i cal Care (CEMC) with 183 af fil i ates and a tele com mu ni ca tion net work.The na tional sys tem for trans fu sion haema tol ogy was also cre ated in the frame work of a sim -i lar pro ject (10 632 000 US dol lars). The Na tional Cen tre for Trans plan ta tions Man age ment“Bultransplant” (2000) was also es tab lished as the body for or gan is ing and con trol of do na tion and or gan, tis sue and cell trans plan ta tion220. At the be gin ning of 2004 this or gani sa tion wasclosed down and was sub sti tuted by the Ex ec u tive Agency on Trans plan ta tion221.
In ex e cu tion of the LHSWC, the Oc cu pa tional Med i cine Ser vices were es tab lished in ac cor -dance with the Eu ro pean prac tice. They re placed the net work of the so called “work ers’ healthcare”,which was re dun dant with the ter ri to rial healthcare net work. These ser vices ful filled chiefly pre ven -tive func tions and were main tained by the own ers of the re spec tive en ter prises.
School health ser vices were set up in the schools, which were also fi nanced by the pro -pri etors of the re spec tive schools.
The re dun dant ac tiv i ties and di vi sions were closed down in the struc ture of the Hy gieneand Ep i de mi o log i cal In spec tions (HEI), units for pro mo tion and pre ven tion were set up, thehealthcare and con trol ac tiv i ties were in te grated.
Mar ket au ton omy of the healthcare es tab lish ments
The grant ing and reg u lat ing of this needed au ton omy was one of the main func tions ofthe three laws men tioned above.
In terms of the con sum ers, the au ton omy was granted at the time by means of the amend -ments in the Law on Peo ple’s Health (Art. 26, §2) and the Law on Health In sur ance (Art. 35, §2).
The au ton omy of the pro vid ers of med i cal care was one of the most es sen tial and fun da -men tal changes in the healthcare sys tem and was guar an teed by the Law on Healthcare Es tab -lish ments (Art. 8, 9, 10, 36, 40 and 46). A cer tain rea son able ex cep tion from the re gime of allthe other healthcare es tab lish ments was made for the cen tres for emer gency med i cal care, thecen tres for trans fu sion haema tol ogy, the homes for chil dren’s med i cal and so cial care as wellas the healthcare es tab lish ments to the Coun cil of Min is ters and Min is tries of De fence, the In -te rior, Jus tice, Trans port and Com mu ni ca tions. Ac cord ing to Art. 5 of the LHE, they were es -tab lished and main tained by the state. The au ton omy of the med i cal care pro vid ers alsoin cluded their sta tus of le gal en ti ties, en ti tling them to the right of in de pend ent con trac tual re -la tions with other or gani sa tions.
The au ton omy of the fi nan cial me di a tor was pro vided for in the Law on Health In sur ancestip u lat ing the in tro duc tion of the oblig a tory health in sur ance, which was to be car ried outby a pub lic fi nan cial in sti tu tion with au ton o mous man age ment – the Na tional Health In sur ance Fund (NHIF) and ad di tional vol un tary health in sur ance which was to be the sub ject of theac tiv ity of share hold ers’ com pa nies for vol un tary health in sur ance (CVHI).
91
Stages and evo lu tion of the healthcare re form in Bul garia
220 State Ga zette, Is sue ¹ 4 from 12.01.2001221 State Ga zette, Is sue ¹ 15 from 24.02.2004
Con trac tual re la tions
Given the nec es sary au ton omy, the healthcare es tab lish ments ar ranged for their own re la -tion ships with a fi nan cial me di a tor and among them selves by means of bi lat eral con tracts. Thecon tracts be tween the healthcare es tab lish ments and the NHIF were based on a Na tional Frame -work Agree ment (NFA), signed an nu ally in ad vance be tween the NHIF and the pro fes sionalphy si cians’ (UBP) and den tists’ (UDB) or gani sa tions. The NFA de ter mined the frame of themain li a bil i ties of the con tract ing par ties for the pro vi sion of med i cal care, the qual ity, prices andthe re gime of pay ment by the NHIF. All healthcare es tab lish ments, ir re spec tive of their own er -ship, had the right to sign con tracts with the NHIF un der the same re gime of pay ment.
Change in the own er ship struc ture in the hos pi tal sec tor
The demonopolisation of the healthcare sys tem, whose be gin ning was firmly laid downby the re form and mainly by the changes in the own er ship in the phar ma ceu ti cal sec tor, con tin -ued in the hos pi tal care sec tor dur ing this stage through change of the own er ship re gime. Theown er ship in the hos pi tal sec tor, which un til 1998 had been in its great est part state and only an in sig nif i cant part had been pri vate, was trans formed by the LHE in the fol low ing way:
· en tirely state – for the healthcare es tab lish ments un der Art. 5 of the LHE;
· state share hold ers’ (Ltd.) – for the uni ver sity hos pi tals;
· share hold ers’ (PLC) - with 51% state own er ship and 49% own er ship of the mu nic i pal -i ties in the re gion of the hos pi tals – for the dis trict hospitals;
· en tirely mu nic i pal (Ltd.) – with 100% mu nic i pal own er ship – for the mu nic i pal (re -gional) hos pi tals and other healthcare es tab lish ments, not spec i fied in Art. 5 of theLHE and with out the sta tus of na tional healthcare es tab lish ments;
· co op er a tive – as with the mu nic i pal own er ship and also in clud ing group prac tices forpri mary or spe cial ised out pa tients’ care;
· pri vate (in clud ing Ltd., PLC, etc.) – as with the mu nic i pal own er ship and in in di vid ualand group prac tices for pri mary and spe cial ised medical care.
The change in the form and the re gime of own er ship was car ried out through the stip u -lated by the LHE con sti tu tion and reg is tra tion of all healthcare es tab lish ments in ac cor dance with the re quire ments of the Com mer cial Law. In this way, they ac quired the nec es sary au ton -omy of eco nomic sub jects and this was part of the demonopolisation and the in tro duc tion ofthe reg u lated mar ket in the healthcare sys tem. We are here draw ing the at ten tion to this is suesince in a num ber of cases this re quire ment of the LHE is ei ther not well-un der stood, or be -comes sub ject to bi ased spec u la tions (even in “sci en tific” pub li ca tions). For in stance, some -times it is writ ten about “the trans for ma tion of the hos pi tals into com mer cial com pa nies”, or(in of fi cial state ments) it is de clared that “we turned the doc tors into trad ers”. The LHE stip u -lates for “con sti tu tion” and “reg is tra tion” and not for “trans for ma tion”. These are to tally dif -fer ent le gal terms. Fur ther more, it is in no way rep re hen si ble or shame ful to be a trader.
The change in the own er ship re gime trans ferred the en tire pri mary and a large part of the spe cial ised out pa tients’ med i cal care to the pri vate sec tor. To gether with the changed struc -ture of the own er ship, a great role for the con sol i da tion and the de vel op ment of the pri vate sec -tor was played by the changed re gime of fi nanc ing of the med i cal care which was in tro ducedwith the LHI.
92

Change in fi nanc ing
The au ton o mous sta tus of the healthcare es tab lish ments was also sup ported by thechanged re gime of fi nanc ing. The oblig a tory health in sur ance cov ered all the cit i zens in ourcoun try. The med i cal care pro vided to all pa tients, no mat ter by pub lic or pri vate healthcarees tab lish ments, was paid (ac cord ing to con tracted prices and man ner) by the NHIF or CVHI(un til the end of 2005 from the state, too). Thus, the di rec tion of fi nanc ing was changed fromfi nanc ing of the “in put” and of struc tures to ward fi nanc ing of ac tiv i ties and of the “out put” ofthe healthcare es tab lish ment. The ac tiv i ties of the pub lic and the pri vate healthcare es tab lish -ments were fi nan cially pro vided for on equal terms, de pend ing on the per for mance. Thiscor rected the at ti tude to the pri vate healthcare es tab lish ments, ex panded their pros pects and fa -cil i tated the build ing of the healthcare sec tor based on the “pub lic-pri vate mix” model ap -plied in many coun tries.
Com pe ti tion
The au ton o mous sta tus and the changed way of fi nanc ing cre ated con di tions for the de -vel op ment of com pe ti tion among the healthcare es tab lish ments. Since the prices were ne go ti -ated in the NFA, the main in stru ments for com pe ti tion were the qual ity im prove ment and the ex ten sion of the list of per formed med i cal ser vices. In all cases, the de vel op ment of a loyalcom pe ti tion was to the ben e fit of the cus tomer. The le gal reg u la tions, how ever, did not en vis -age com pe ti tion in the field of the com pul sory health in sur ance, in which the NHIF pos sessedthe mo nop oly. The com pe ti tion was only pos si ble among the CVHI in the field of the vol un -tary health in sur ance.
Pol icy on the qual ity of hos pi tal care
The LHE stip u lated the es tab lish ment of a na tional sys tem for qual ity mon i tor ing andcon trol in the healthcare es tab lish ments. A ma jor el e ment of this sys tem was the ac cred i ta -tion pro ce dure of the healthcare es tab lish ments or parts of them or sep a rate ac tiv i ties they per -form (Art. 86-89). In our coun try, this pro ce dure pos sessed some spe cific fea tures. It wasad min is tered by a state (and not by an in de pend ent) au thor ity (at the Min is try of Healthcare)and was com pul sory for the es tab lish ments for hos pi tal care and the di ag nos tic and con sul ta -tive care. They needed to ob tain ac cred i ta tion as sess ment for a def i nite pe riod of time of nomore than five years. The leg is la tion, how ever, did not en vis age any con se quences in thecases when the healthcare es tab lish ment ob tained an un sat is fac tory eval u a tion.
Pol icy of plan ning and de vel op ment of the hos pi tal net work
As an in stru ment for plan ning and de vel op ment of the hos pi tal net work the LHE (Art.29-34) stip u lated the use of a Na tional and Dis trict Health Map con tain ing the num ber of the es tab lish ments for hos pi tal care and their ca pac ity, the cen tres for emer gency med i cal care andtrans fu sion haema tol ogy, the dis pen sa ries and the homes for med i cal and so cial care as well asthe phy si cians and the den tists in volved in the pro vi sion of pri mary and spe cial ized out pa -tients’ care. The quan ti ta tive in di ca tors, spec i fied in the Na tional and Dis trict Health Maps(num ber of the es tab lish ments for hos pi tal care, num ber of phy si cians and den tists work ing inthem) were man da tory for the NHIF, too. The NHIF was obliged to sign con tracts with the re -
93
Stages and evo lu tion of the healthcare re form in Bul garia
spec tive types and num ber of hos pi tal es tab lish ments, and if there was such a pos si bil ity, withmore healthcare es tab lish ments for hos pi tal care. The Na tional Map was to be up dated ev eryfive years and was ap proved by the Coun cil of Min is ters.
Change in the man age ment of the hos pi tal es tab lish ments
Gen er ally, the man age ment was or gan ised by the owner of the re spec tive unit. This prin -ci ple was also pos tu lated in the LHE in terms of hos pi tal man age ment (Art.62-79). The in di -vid ual prac tices were man aged by the pro pri etor (phy si cian or den tist) of the prac tice who wasalso the em ployer of the per son nel. The man age ment of the other hos pi tals was or gan ised de -pend ing on their form of reg is tra tion (as Ltd, PLC, co-op er a tion). What is typ i cal is that col lec -tive or gans with ad vi sory func tions (Med i cal Coun cil, Coun cil for Healthcare, Com mis sions)were in volved in the man age ment (apart from the in di vid ual prac tices).
An in ter est ing in no va tion was the hos pi tal Board of Trust ees (Art. 82-85 of the LHE) asa point of junc tion in volv ing com mu nity to as sist the hos pi tals.
Con struc tion of the health in sur ance sys tem
We need to make the pre lim i nary dif fer en ti a tion be tween a health in sur ance sys tem and ahealth in sur ance or gani sa tion. These two no tions are of ten per ceived and used as syn on y mous. The health in sur ance sys tem in cludes three com po nents: per sons with health in sur ance, healthin sur ance or gani sa tion and pro vid ers of med i cal and den tal care, who have signed con tractswith the health in sur ance or gani sa tion. The health in sur ance organisation (also called “in -surer”) as one of the com po nents of the health in sur ance sys tem, ful fils the func tions of a fi -nan cial me di a tor be tween the health in sured per son and the pro vider of the med i cal care.
The build ing of the health in sur ance sys tem as a fun da men tal el e ment of the healthcarere form was car ried out af ter the pub li ca tion of the LHI (19.06.1998), which put the be gin ningof the one-year or gani sa tional pe riod for the health in sur ance or gani sa tion for com pul soryhealth in sur ance (NHIF). The col lec tion of health in sur ance in stal ments started a year af ter theset ting up of the NHIF – from 1st July, and the first NFA was de vised sev eral months later.Mean while, by an amend ment of the LHI222, the im ple men ta tion of the law in ac cor dance withthe con tracts with the pro vid ers of med i cal care was di vided into two phases: the first – for theout pa tient med i cal care, which was to start on 1st July 2000, and the sec ond – for hos pi tal care,which was to be gin from 1st July 2001. It should be con sid ered that un til 1st July 2000 thehealth in sur ance or gani sa tion for com pul sory health in sur ance had al ready been built and thatun til 1st July 2001 the over all sys tem was also es tab lished. In fact, as we will see later, this wasnot ex actly the case. The con struc tion of a sys tem proved to be a pro cess much more com pli -cated than ex pected and it has not been ac com plished till the pres ent day. And this hin dered the gen eral course of the over all healthcare re form.
Moral norms and eth i cal code
Af ter the for ma tion of the nor ma tive, or gani sa tional, struc tural and eco nomic con struc -tion of the new healthcare sys tem and its man age ment dur ing the dis cussed pe riod, a new“Code of Pro fes sional Eth ics” was worked out and adopted by ÕÕÕIII Ex traor di nary As sem -
94
222 State Ga zette, Is sue ¹ 62 from 9.07.1999 and Is sue ¹ 113 from 28.12.1999
bly of the UBP, which was also con firmed by the Min is ter of Healthcare223. In fact, this doc u -ment was a some what abridged ver sion with only a few amend ments of the pre vi ous (from1992). As in the pre vi ous code, this doc u ment, too, pointed out that the UBP would con trol theob ser vance of the eth i cal norms by the phy si cians. The con fir ma tion by the Min is ter had a cer -tain im por tance. From one point of view, it could be ad mit ted as an (un ac cept able) in ter fer ence of the state in the “life” of an in de pend ent pro fes sional or gani sa tion. On the other hand, theMin is ter was a mem ber of the gov ern ment and his/her in ter fer ence in this par tic u lar case meant that the gov ern ment sup ported the ini tia tive and the func tion ing of the UBP.
The role of the pro fes sional or gani sa tions
The le gal reg u la tion of the pro fes sional or gani sa tions of the phy si cians and den tists wasalso one of the im por tant steps in the pro cess of re form ing healthcare, with out which the im -ple men ta tion of the re forms would have been sig nif i cantly hin dered.
On the one hand, by this act a com plete re stor ing of the phy si cians’ and den tists’ sta tus aspro fes sion als was achieved; this sta tus was in fringed on in 1949 with the elim i na tion of theirpro fes sional or gani sa tions. The UBP and the UDB ac quired se ri ous rights and li a bil i ties re -lated to the qual i fi ca tion and the eth i cal be hav iour of their mem bers. On the other hand, as rep -re sen ta tive or gani sa tions of the two oc cu pa tions (the pro vid ers of med i cal and den tal care),they were also the rep re sen ta tives in the ne go ti a tion, sign ing and im ple men ta tion of the NFA.
New Na tional Health Strat egy
A suf fi ciently de tailed con cept of the healthcare re form in Bul garia dur ing the ex am inedpe riod was pre sented and dis cussed at the Na tional Con fer ence on the Healthcare Re form,men tioned ear lier (Pro ject PHARE BG 9301/02/02) and held 24-25.04.1998 with the par tic i -pa tion of con sul tants from Grupo Consultor de Infraestructuras (Spain). The con fer ence wasfo cused mainly on the dis cus sion of the new phi los o phy of the re form, re flected in the de -signed leg is la tive pro jects as well as on the ap proaches for the de vel op ment of the re form pro -cess. The work of this con fer ence, es pe cially af ter the pub li ca tion of the full short-hand,in tro duced greater trans par ency among the med i cal and the wider com mu nity about the in ten -tions for the de vel op ment of the healthcare re form. But, as ev i dent from the me dia pub li ca tions and the ques tion naire sur veys, the ini tial idea for the sub se quent de vel op ment of the healthcare re form was not made known to the larger cir cles of med i cal spe cial ists (the ex ec u tors of the re -form) and the cit i zens.
At the end of this stage, sim i larly to the pre vi ous one, the Coun cil of Min is ters adoptedthe new National Health Strat egy “A Better Health for a Better Future of Bul garia”(23.04.2001), which was ac com pa nied by a con crete “Ac tion plan for the pe riod 2001-2006”.The strat egy aimed at out lin ing the fur ther de vel op ment of the healthcare re form un til the ex -pected ac ces sion of our coun try to the EC. It was de signed in a very com pe tent way (as the pre -vi ous one), it was well-grounded and well-tar geted. It ana lysed the health sta tus of thepop u la tion and the de vel op ment of the healthcare sys tem both dur ing the pre vi ous and the cur -rent stage of the healthcare re form. The phi los o phy and the logic of the strat egy for con tin u ingthe re form were pre sented in rel a tive de tail. Based on this, the prob lems and the ways for theirso lu tion were for mu lated. The ac tion plan was de tailed, con crete and re al is tic and it com ple -
95
Stages and evo lu tion of the healthcare re form in Bul garia
223 State Ga zette, Is sue ¹ 79 from 29.09.2000
mented the na tional strat egy in an ap pro pri ate way224. Both in the Strat egy and in the Ac tion Plan, the fur ther de vel op ment of the al ready ini ti -
ated changes was chiefly worked out rather than new struc tural and or gani sa tional change.This was a very sen si ble ap proach, by means of which a more sta ble de vel op ment was en suredfor the healthcare sys tem.
In most gen eral terms, what stands out was the lack of any con ti nu ity what so ever be -tween the pre vi ous and the newly adopted health strat e gies. The im ple men ta tion of the pre vi -ous health strat egy was not ac counted for in any (most likely crit i cal) way and no men tion(even neg a tively marked) was made of it. As we will see later, the same fate was ex pect ing thenew strat egy, too.
Qual ity im prove ment and quan ti ta tive in di ca tors of the changes in thehealthcare system
Dur ing the short but event ful pe riod in ques tion, to gether with the rad i cal changes in thestate, even more pro found and deep qual i ta tive changes also took place in the healthcaresys tem, shap ing its prin ci pally new im age:
· the state mo nop oly in healthcare was to tally aban doned, three in de pend ent sub jectswere formed in the sys tem of healthcare in ac cor dance with the es tab lish ment of mar -ket con di tions;
· a new own er ship struc ture was es tab lished for the healthcare es tab lish ments, a greatpart of the hos pi tals be ing trans ferred to the pri vate sector;
· a new type of eco nomic re la tions were in tro duced in the hos pi tal sec tor by the es tab -lish ment of the health in sur ance sys tem, the in tro duc tion of con trac tual re la tions be -tween the health in sur ance or gani sa tion and the pro vid ers of med i cal care, pay ment for performed activities;
· the or gani sa tional and struc tural func tion ing of the healthcare sys tem was changed;
· the man age ment sys tem was changed to ward its de moc ra ti sa tion by the in volve ment of a num ber of eco nomic and other self-reg u la tion elements;
· the pro fes sional or gani sa tions of phy si cians and den tists were le gally reg u lated andwere as signed cer tain rights and li a bil i ties re lated to the reg u la tion of the healthcaresystem.
Con se quently, we have all the grounds to as sume that to gether with the changes im ple -mented dur ing the pre vi ous stage (af fect ing mainly the phar ma ceu ti cal sec tor), dur ing theex am ined pe riod, at least in most gen eral terms, the so lu tion of one of the ma jor tasks ofthe healthcare re form was achieved, e.g. the ces sa tion of the re pro duc tion of the pre-ex -ist ing healthcare sys tem, and the ground was pre pared for the so lu tion of an other is sue,e.g. a nor ma tive, organisational and struc tural ba sis with its main pa ram e ters was es tab -lished for a new healthcare sys tem, cor re spond ing to the new type of po lit i cal, eco nomicand pub lic re la tions in our coun try.
Based on the eco nomic sta bili sa tion of the county the ex pen di ture for healthcare in thecon sol i dated bud get of the state for 1997-2001 (Ta ble 22) in creased both in ab so lute val ues
96
224 Ministry of Healthcare. National Health Strategy “Better Health for a Better Future for Bulgaria”. Sofia, 2001;Ministry of Healthcare. Action Plan to the National Health Strategy for the Period 2001-2006. Sofia, 2001
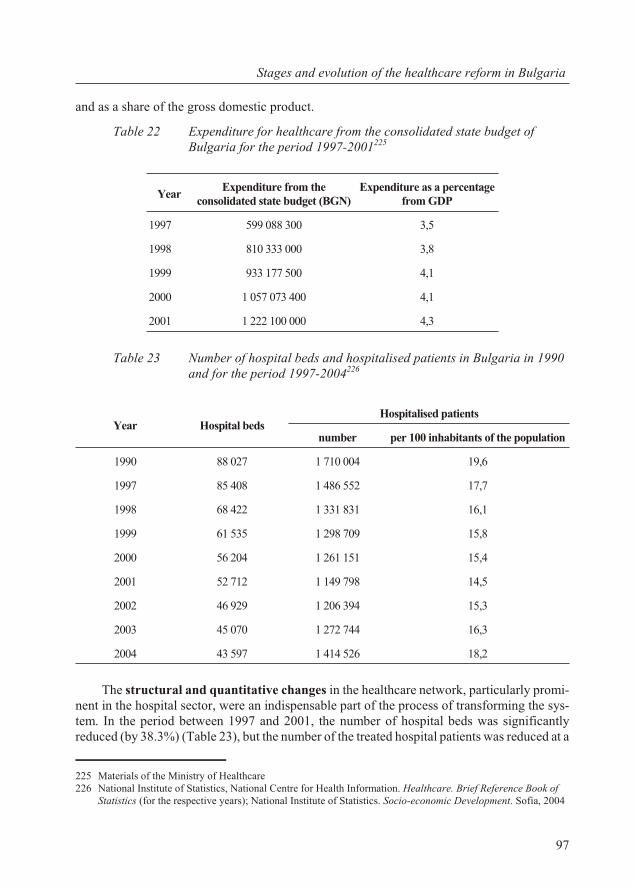
and as a share of the gross do mes tic prod uct.
Ta ble 22 Ex pen di ture for healthcare from the con sol i dated state bud get ofBul garia for the period 1997-2001225
Ta ble 23 Num ber of hos pi tal beds and hos pi ta lised pa tients in Bul garia in 1990and for the pe riod 1997-2004226
The struc tural and quan ti ta tive changes in the healthcare net work, par tic u larly prom i -nent in the hos pi tal sec tor, were an in dis pens able part of the pro cess of trans form ing the sys -tem. In the pe riod be tween 1997 and 2001, the num ber of hos pi tal beds was sig nif i cantlyre duced (by 38.3%) (Ta ble 23), but the num ber of the treated hos pi tal pa tients was re duced at a
97
Stages and evo lu tion of the healthcare re form in Bul garia
YearEx pen di ture from the
con sol i dated state bud get (BGN)Ex pen di ture as a per cent age
from GDP
1997 599 088 300 3,5
1998 810 333 000 3,8
1999 933 177 500 4,1
2000 1 057 073 400 4,1
2001 1 222 100 000 4,3
Year Hos pi tal bedsHos pi ta lised pa tients
num ber per 100 in hab it ants of the pop u la tion
1990 88 027 1 710 004 19,6
1997 85 408 1 486 552 17,7
1998 68 422 1 331 831 16,1
1999 61 535 1 298 709 15,8
2000 56 204 1 261 151 15,4
2001 52 712 1 149 798 14,5
2002 46 929 1 206 394 15,3
2003 45 070 1 272 744 16,3
2004 43 597 1 414 526 18,2
225 Ma te ri als of the Min is try of Healthcare226 National Institute of Statistics, National Centre for Health Information. Healthcare. Brief Reference Book of
Statistics (for the respective years); National Institute of Statistics. Socio-economic Development. Sofia, 2004
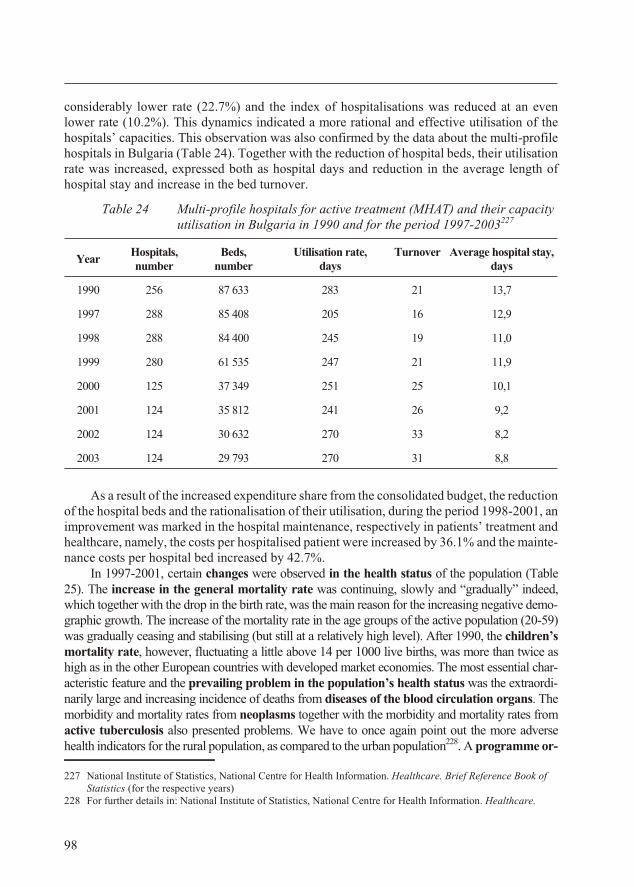
con sid er ably lower rate (22.7%) and the in dex of hos pi ta li sa tions was re duced at an evenlower rate (10.2%). This dy nam ics in di cated a more ra tio nal and ef fec tive uti li sa tion of thehos pi tals’ ca pac i ties. This ob ser va tion was also con firmed by the data about the multi-pro filehos pi tals in Bul garia (Ta ble 24). To gether with the re duc tion of hos pi tal beds, their uti li sa tionrate was in creased, ex pressed both as hos pi tal days and re duc tion in the average length ofhospital stay and increase in the bed turnover.
Ta ble 24 Multi-profile hospitals for active treatment (MHAT) and their capacityutilisation in Bulgaria in 1990 and for the period 1997-2003227
YearHos pi tals,num ber
Beds,num ber
Uti li sa tion rate,days
Turn over Av er age hos pi tal stay,days
1990 256 87 633 283 21 13,7
1997 288 85 408 205 16 12,9
1998 288 84 400 245 19 11,0
1999 280 61 535 247 21 11,9
2000 125 37 349 251 25 10,1
2001 124 35 812 241 26 9,2
2002 124 30 632 270 33 8,2
2003 124 29 793 270 31 8,8
As a re sult of the in creased ex pen di ture share from the con sol i dated bud get, the re duc tionof the hos pi tal beds and the ra tion al is ation of their uti li sa tion, dur ing the pe riod 1998-2001, anim prove ment was marked in the hos pi tal main te nance, re spec tively in pa tients’ treat ment andhealthcare, namely, the costs per hos pi ta lised pa tient were in creased by 36.1% and the main te -nance costs per hos pi tal bed in creased by 42.7%.
In 1997-2001, cer tain changes were ob served in the health sta tus of the pop u la tion (Ta ble25). The in crease in the gen eral mor tal ity rate was con tin u ing, slowly and “grad u ally” in deed,which to gether with the drop in the birth rate, was the main rea son for the in creas ing neg a tive de mo -graphic growth. The in crease of the mor tal ity rate in the age groups of the ac tive pop u la tion (20-59)was grad u ally ceas ing and sta bi lis ing (but still at a rel a tively high level). Af ter 1990, the chil dren’smor tal ity rate, how ever, fluc tu at ing a lit tle above 14 per 1000 live births, was more than twice ashigh as in the other Eu ro pean coun tries with de vel oped mar ket econ o mies. The most es sen tial char -ac ter is tic fea ture and the pre vail ing prob lem in the pop u la tion’s health sta tus was the ex traor di -narily large and in creas ing in ci dence of deaths from dis eases of the blood cir cu la tion or gans. Themor bid ity and mor tal ity rates from neoplasms to gether with the mor bid ity and mor tal ity rates fromac tive tu ber cu lo sis also pre sented prob lems. We have to once again point out the more ad versehealth in di ca tors for the ru ral pop u la tion, as com pared to the ur ban pop u la tion228. A programme or -
98
227 Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion. Healthcare. Brief Ref er ence Book ofSta tis tics (for the re spec tive years)
228 For fur ther de tails in: Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion. Healthcare.
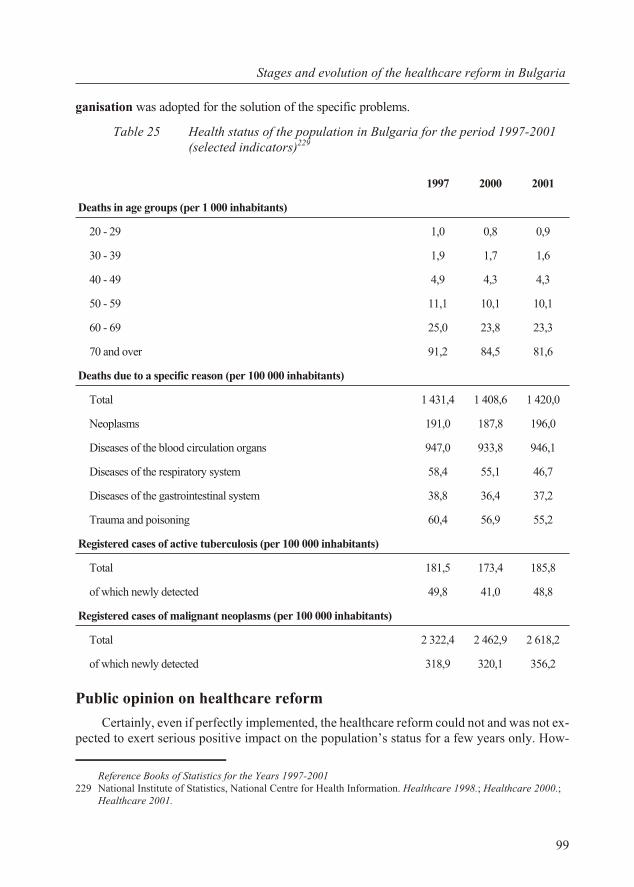
gani sa tion was adopted for the so lu tion of the spe cific prob lems.
Ta ble 25 Health sta tus of the pop u la tion in Bul garia for the pe riod 1997-2001(selected indicators)229
Pub lic opin ion on healthcare re form
Cer tainly, even if per fectly im ple mented, the healthcare re form could not and was not ex -pected to ex ert se ri ous pos i tive im pact on the pop u la tion’s sta tus for a few years only. How -
99
Stages and evo lu tion of the healthcare re form in Bul garia
1997 2000 2001
Deaths in age groups (per 1 000 in hab it ants)
20 - 29 1,0 0,8 0,9
30 - 39 1,9 1,7 1,6
40 - 49 4,9 4,3 4,3
50 - 59 11,1 10,1 10,1
60 - 69 25,0 23,8 23,3
70 and over 91,2 84,5 81,6
Deaths due to a spe cific rea son (per 100 000 in hab it ants)
To tal 1 431,4 1 408,6 1 420,0
Neoplasms 191,0 187,8 196,0
Dis eases of the blood cir cu la tion or gans 947,0 933,8 946,1
Dis eases of the re spi ra tory sys tem 58,4 55,1 46,7
Dis eases of the gas tro in tes ti nal sys tem 38,8 36,4 37,2
Trauma and poi son ing 60,4 56,9 55,2
Reg is tered cases of ac tive tu ber cu lo sis (per 100 000 in hab it ants)
To tal 181,5 173,4 185,8
of which newly de tected 49,8 41,0 48,8
Reg is tered cases of ma lig nant neoplasms (per 100 000 in hab it ants)
To tal 2 322,4 2 462,9 2 618,2
of which newly de tected 318,9 320,1 356,2
Ref er ence Books of Sta tis tics for the Years 1997-2001229 Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion. Healthcare 1998.; Healthcare 2000.;
Healthcare 2001.
ever, it could be rea son ably ex pected and the for ma tion of one view or an other could bees tab lished among the cit i zens and the med i cal pro fes sion als. The mass me dia, es pe cially thepress, in flu enced sig nif i cantly this pro cess.
Cov er age of the healthcare re form in the press in the pe riod be tween1997 and the first half of 2001
The pub li ca tions in the press from the be gin ning of 1997 re vealed in an un am big u ousway the ef fect of the eco nomic cri sis and the po lit i cal de sta bi li sa tion of the coun try dur ingthis pe riod on the healthcare sys tem.
The pub li ca tions dur ing this pe riod, to gether with the se vere fi nan cial con di tion of thesys tem,230 were ded i cated mainly to mea sures pro posed by the dif fer ent rul ing par ties forcop ing with the cri sis. What is worth of note is that un til the mid dle of the year the ar ti cles inthe press fo cused on short-term ac tions, re lated only to the pro vi sion of fi nanc ing (or cost con -tain ment) for the main te nance of the sys tem and the is sues re gard ing the re form, and the healthin sur ance in par tic u lar re mained in the back ground.
At the be gin ning of the year the Min is ter in res ig na tion Dr. M. Vitkova is sued a de cree onhome care, aimed at cut ting the hos pi tal costs231. Sev eral pub li ca tions from the be gin ning ofJan u ary were ded i cated to the re jected re sump tion (and in some ar ti cles it was called “dis -missal”) of the short-term la bour con tract of Assoc. Prof. Dr. Emil Tabakov – Di rec tor of“Pirogov” Hos pi tal for Emer gency Care232.
A month later the UBP pro posed anti-cri sis mea sures in clud ing the fol low ing: giv ingthe right to the pri vate prac ti tio ners to buy sur ger ies and equip ment in the out pa tients’ clin ics(ac cord ing to law yers, this im plied the be gin ning of privatisation) and work as fam ily doc torsand the state to as sist them in the pay ment for a med i cal nurse, doc tor’s as sis tant and a sec re -tary; the kitch ens of the healthcare es tab lish ments to be rented and the hos pi tals to save moneyby “elim i nat ing the din ners” for the pa tients233.
In a few ar ti cles from March 1997, it was re ported about anti-cri sis mea sures, pro posedby Assoc. Prof. Dr. Emil Tabakov - the new Healthcare Min is ter of the Ex pert Gov ern ment,headed by Stefan Sofianski. These mea sures in cluded short en ing of the post-op er a tive stay, in -tro duc tion of pay ment on be half of the pa tient (ex cept for chil dren aged up to 18, re tired andsol diers) for the food and hos pi tal stay, mak ing re dun dant 10 000 healthcare work ers. Un til the end of the year, a mor a to rium was im posed on new staff ap point ment in the state healthcare es -tab lish ments, reg u la tions were is sued for drug sup ply with Bul gar ian med i ca tions only and the pur chas ing of costly equip ment was banned. Clo sure was planned for wards and hos pi tals with in suf fi cient num ber of pa tients. An nounce ments were made about hos pi tal debts for drugs,med i cal equip ment and food which amounted to 79 bil lion BGN at the time234.
The at tempts for cop ing with the cri sis con tin ued to be in the fo cus of at ten tion af ter theelec tions, when Assoc. Prof. Dr. Petar Boyadjiev be came Min is ter of Healthcare. Ac cord ingto the programme of the Min is try of Healthcare, the mea sures for cop ing with the cri sis com -
100
230 Standart daily, Is sue ¹ 7.01.1997; Kapital weekly from 29.09.–5.10.1998; Democracia daily from 7.01.1997;Duma daily, Is sue ¹ 87 from 15.04.1997, Is sue ¹ 95 from 24.04.1997 and Is sue ¹ 112 from 17.05.1997
231 Standart daily, Is sue ¹ 1542 from 3.01.1997232 Standart daily, Is sue ¹ 1542 from 3.01.1997233 Standart daily, Issue ¹ 1596 from 26.02.1997; Forum Medicus periodical, Issue ¹ 8 from 3.03.1997234 Standart daily from 14.03.1997; Duma daily, Is sue ¹ 60 from 1997; Democracia daily from 14.03.1997
mented in the press in cluded the fol low ing: the phy si cians’ and den tists’ sur ger ies in the en ter -prises to be closed down; part of the out pa tients’ clin ics to be sold out to pri vate prac ti tio ners;the healthcare net work to be fi nanced also by pri vate health in sur ance funds and paid treat ment for cer tain cat e go ries of cit i zens235. The programme en vis aged the clo sure of all the state es tab -lish ments for den tal care, some of which were to be pri va tised and oth ers to be rented for sur -ger ies of pri vate den tal prac ti tio ners236. Ac cord ing to Min is ter Boyadjiev, the re form in den talcare would lay the foun da tion of the health in sur ance sys tem237.
The de ci sion of the Par lia men tary Com mis sion on Healthcare also pre sented an anti-cri -sis mea sure, ac cord ing to which the en ter prises should fi nance the hos pi tals, in which theirem ploy ees were treated, in or der to re lieve the bur den from the bud get. But the mech a nism forachiev ing that re mained un de ter mined and the Min is ter of Healthcare P. Boyadjiev de claredthat 10% of the healthcare work ers would be come re dun dant af ter the in tro duc tion of the Mon -e tary Board238. The “Trud”239 news pa per in formed that the clo sure of the work ers’ hos pi talswas on the agenda and the op tion for their pres er va tion was that the mu nic i pal i ties and the in -dus trial en ter prises took over their fi nanc ing.
Fi nanc ing
In the mid dle of 1997, the Vice-Min is ter Dr. Ilko Semerdjiev de clared that for 1997 2.9%of the GDP were ex pected to be al lo cated for healthcare and that the MH was search ing for al -ter na tive sources of fi nanc ing such as the in tro duc tion of paid ser vices, privatisation, and ex -emp tion from taxes, du ties and ex cises of goods harm ful for the health240. The “Pirogov”Emer gency Cen tre, the na tional cen tres for car dio vas cu lar and oncological dis eases weregiven pri or ity in fi nanc ing241. A credit from the World Bank (WB) amount ing to 40 mil lion US dol lars was to be used pri mar ily for drugs and consumables, 14.3 mil lion pro vid ing thelife-sav ing drugs for the oncological hos pi tals, 4.8 mil lion for drugs to be dis trib uted amonghos pi tals and the re main ing part was meant to pay off a part of the debts of the healthcare es tab -lish ments ac cu mu lated in 1996242.
In re sponse to an en quiry in the NA, Prime Min is ter Ivan Kostov de clared that 3.2% of the GDP or 795 bil lion BGN were in tended for healthcare in 1998, of which 687.1 bil lion BGNwere from the bud get, 13 mil lion US dol lars were from the WB and 19 mil lion US dol lars –from the So cial De vel op ment Fund at the Coun cil of Eu rope, and from paid med i cal ser vicesthe hos pi tals were ex pected to make in come of an other 4 bil lion BGN243.
Dur ing the whole year the me dia cov ered widely the topic of the in tro duc tion of prices
101
Stages and evo lu tion of the healthcare re form in Bul garia
235 Standart daily, Is sue ¹ 1691 from 5.06.1997 ã; Duma daily, Is sue ¹ 140 and Is sue ¹148 from 1997;Democracia daily from 19.06.1997 and from 10.07.1997; 24 chasa daily, Is sue ¹ 151 fromò 5.06.1997, Is sue ¹ 131 from 16.05.1997, Issue ¹ 165 from 19.06.1995
236 24 chasa daily, Is sue ¹ 114 from 24.04.1997, Is sue ¹ 136, Is sue ¹ 137 and Is sue ¹ 248 from 1997; Truddaily from 5.06.1997, from 22.08.1997 and Is sue ¹ 232 from 25.08.1997; Democracia daily from 22.08.1997 and from 25.08.1997
237 Trud daily from 5.06.1997238 Standart daily from 12.06.1997 239 Trud daily from 1.07.1997240 Kapital weekly from 19-25.05.1997.; Duma daily, Issue ¹ 148 from 28.06.1997241 Democracia daily from 26.06.1997 242 Democracia daily from 1.08.1997 243 Democracia daily from 8.11.1997
for med i cal ser vices which had to be paid by the pa tients un der cer tain con di tions244. This was meant to be en forced by a de cree, the pro ject for which caused the crit i cism of the op po si tion
The ar gu ments against the in tro duc tion of paid med i cal ser vices were that in such a waythe Con sti tu tion was breached and cor rup tion was “legal ised” and stim u lated245. The ViceChair man of the Par lia men tary Com mis sion on Healthcare Prof. Ivan Zunzov also criti cisedthe draft pro ject, point ing out that “90% of the peo ple were strug gling for their own sur vival”and he called the do na tions for the hos pi tals “forced” and “bor der ing on ex tor tion”. Prof.Zunzov called for “the in tro duc tion of a healthcare sys tem with out the state with draw ing itscom mit ment from healthcare; re struc tur ing of the healthcare sys tem in or der to im prove its ef -fi ciency; pres er va tion of the free healthcare for the pop u la tion in ac tive work ing age ob serv ing the Law on Peo ple’ Health; fi nan cial com mit ment of the en ter prises since in many pri vatecom pa nies the em ploy ees are not so cially in sured and use health ser vices free of charge; find -ing a way for the so cially in sured peo ple to pay for healthcare”246.
In two pub li ca tions from May and Oc to ber, data were an nounced from opin ion polls withcit i zens re gard ing the in tro duc tion of paid med i cal ser vices. Ac cord ing to data from a tele phone in ter view with 486 res i dents of So fia (con ducted on May 14th 1997 by the “Board” agency at theor der of the “Duma” daily), 84.9% could not af ford to pay the prices for treat ment an nounced inthe de cree; 37.9% could not 4-5% of their sal a ries for health in sur ance, whereas ap prox i matelythe same num ber (33.7%) could af ford it. An im por tant fact of the sur vey, which has to be takeninto con sid er ation when in ter pret ing the re sults, is that 28.4% of the re spon dents were un em -ployed or re tired pen sion ers247. Data from a sur vey con ducted by the “Fact” agency in di catedthat 61% of the re spon dents were def i nitely against “the in tro duc tion of paid healthcare in thestate healthcare es tab lish ments”, 21% did not ap prove it but con sid ered it nec es sary, and 8%were in fa vour of the idea. To the ques tion “Does the state guar an tee med i cal care to ev ery cit i -zen?” 77% re plied neg a tively and only 18% re sponded pos i tively. The com ments in the pub li ca -tion say: “The slow ing down of the re form is the main rea son that the old re flexes can not change. It has been seven years since the rul ers seem to be work ing on the in tro duc tion of health in sur -ance, but up to the pres ent mo ment their at tempts have re mained un suc cess ful. And the more there form is de layed, the more costly its im ple men ta tion would cost”248.
The most dis cussed topic in 1997 – Reg u la tion ¹ 22 of the MH for the paid med i calser vices – con tin ued to be one of the lead ing ones in the press in the year to fol low. A great part of the ma te ri als ex plained the way of pay ment and cen tral at ten tion was paid to the prices ofthe med i cal ser vices249. Im me di ately af ter the en force ment of the Reg u la tion, the Chief Mag is -trate Ivan Tatarchev sub mit ted a claim to the Con sti tu tional Court for its re peal ing with themo tive that paid med i cal ser vices were anti-con sti tu tional and should not be legal ised be forethe in tro duc tion of the health in sur ance sys tem. The Con sti tu tional Court, how ever, re jectedthe claim with the ar gu ment that the Reg u la tion did not in tro duce com pul sory paid healthcare
102
244 Democracia daily from 8.11.1997 245 Duma daily, Issue ¹ 128 from 28.05.1997246 Duma daily, Issue ¹ 176 from 1997247 Duma daily, Issue ¹ 128 from 28.05.1997248 Standart daily, Issue ¹ 31.10.1997249 24 chasa daily, Issue ¹ 2 from 2.01.1998, Issue ¹ 4 from 8.01.1998, Issue ¹ 6 from 10.01.1998 and Issue ¹
69 from 1998 Trud daily from 3.02.1998; Democracia daily from 5.01.1998, from 26.01.1998, from 19.02.1998and from 26.02.1998; Duma daily, Issue ¹ 2 from 6.01.1998 and Issue ¹ 40 from 19.02.1998; Forum Medicusperiodical, Issue ¹ 4 from 26.01.1998, Issue ¹ 7 from 16.02.1998 and Issue ¹ 8 from 23.02.1998
but en sured the pos si bil ity for choice and al lowed for free treat ment by the fam ily phy si cian250.In some pub li ca tions, ar ti cles ap peared about short age of re fer rals for spe cial ised care, about
breaches of the reg u la tion on paid ser vices as well as about with drawal of pa tients from healthcarees tab lish ments251. Re gard ing the im ple men ta tion of the reg u la tion on paid ser vices, it was en vis -aged to in crease the re mu ner a tions by 40% de pend ing on the phy si cians’ con tri bu tion252.
One of the widely dis cussed is sues, re lated to the in tro duc tion of paid med i cal ser vices,was the pos si bil ity for spec u la tions with re fer rals for spe cial ised care and the cre ation of pre -req ui sites for cor rup tion in the healthcare es tab lish ments253. At the end of the year, the Cham -ber of Ac counts started in spec tions for the im ple men ta tion of the Reg u la tion. Ac cord ing to thethen Min is ter of Healthcare P. Boyadjiev the rev e nue was con sid er ably less than ex pected, thehealthcare es tab lish ments con tin ued to ac cu mu late debts, which gave grounds for the claimthat “the Reg u la tion is in fringed upon and there is cor rup tion”254.
The Reg u la tion for the Paid Med i cal Services gave rise to the op po si tion to se verelycriti cise the changes con ducted by the gov ern ment. At the be gin ning of the year, the “Duma”daily pub lished a se ries of ar ti cles and in ter views, in which one of the main crit i cisms ad dress -ing the pol icy con ducted by the MH, was re lated ex actly to the in tro duc tion of paid med i calser vices of choice255. In an in ter view for the news pa per the Dep uty from the left wing YanakiStoilov de clared that the Reg u la tion con tra dicted Art. 52 of the Con sti tu tion, in fring ing on thecit i zens’ right of ac cess to med i cal care and free med i cal treat ment256. The ar gu ments of thefor mer Min is ter of Healthcare Dr. M. Vitkova had sim i lar ar gu ments and Boris Atanassov(doc tor of eco nomic sci ences) even reached the con clu sion that the Reg u la tion would re sult in“a drop in birth rate and a rise in the mor tal ity rate”257.
The “Po si tion on Health Pol icy of the UDF gov ern ment”, pub lished in the mid dle of Jan -u ary 1998, adopted at a meet ing of the Left-Wing Par lia men tary Group, the Su preme Coun cil,the Peo ple’s Un ion and “Ecoglasnost” pointed out that the Reg u la tion “de nies the cit i zens theright of ac ces si ble med i cal care, leads to chaos in the sys tem and so cial ten sion” and on this oc -ca sion, the doc u ments ended up with the con clu sion that “in Bul garia the pa tients have norights”258. Ac cord ing to Dr. Kuncho Marangozov from the Left-Wing Par lia men tary Group,“over 80% of the pop u la tion is de nied the right of ac cess to med i cal care”, the reg u la tion didnot cor re spond to the needs which caused “or gani sa tional chaos” since the is sue was notsolved about the region ali sa tion of the healthcare es tab lish ments and “leads to un prec e dentedcor rup tion”259.
Ac cord ing to data from a tele phone in ter view of the “Board” agency with 522 res i dents of
103
Stages and evo lu tion of the healthcare re form in Bul garia
250 24 chasa daily, Issue ¹ 63 and Issue ¹ 94 from 1998; Duma daily, Issue ¹ 293 from 1998251 Trud daily from 7.01.1998; Standart daily, Issue ¹ 13.04.1998; Duma daily, Issue ¹ 4 from 8.01.1998 and
Issue ¹ 12 from 17.01.1998; Kapital weekly from 19-25.01.1998252 Democracia daily from 10.01.1998 and from 19.02.1998; Trud daily from 3.02.1998; Duma daily, Issue ¹ 40
from 19.02.1998253 24 chasa daily, Issue ¹ 4 from 8.01.1998 and Issue ¹ 6 from 10.01.1998; Trud daily from 7.01.1998;
Democracia daily from 10.01.1998254 24 chasa daily, Issue ¹ 345 from 22.12.1998255 Duma daily, Issue ¹ 12 from 17.01.1998, Issue ¹ 13 from 18.01.1998, Issue ¹ 17 from 22.01.1998, Issue
¹ 19 from 23.01.1998, Issue ¹ 23 from 27.01.1998, Issue ¹ 51 and Issue ¹ 119 from 1998256 Duma daily, Issue ¹ 17 from 22.01.1998257 Duma daily, Issue ¹ 19 from 23.01.1998 and Issue ¹ 13 from 18.01.1998258 Duma daily, Issue ¹ 13 from 18.01.1998259 Duma daily, Issue ¹ 12 from 17.01.1998 and Issue ¹ 119 from 1998
So fia from 28 Jan u ary 1998, 47% re fused treat ment for lack of fi nan cial means260.Ac cord ing to the Vice-Chair man of the Par lia men tary Com mis sion on Healthcare Prof. I.
Zunzov, the Reg u la tion did not cor re spond to the de mo graphic slump and the pur chas ing sol -vency of the pop u la tion261.
In the sec ond stage of the healthcare re form (from 1999 to the mid dle of 2001), the com -ments and the sharp crit i cism in the press on Reg u la tion ¹ 22 of the MH on aid med i cal ser -vices gave way to is sues re lated mainly to the in tro duc tion of the health in sur ance sys tem.
At the be gin ning of 1998, the press cov ered the reg u la tion for the pay ment of den tal ser -vices which was be ing de vised by the MH262. In the mean time, the Un ion of Den tists in Bul -garia adopted av er age prices, which had to serve as a ba sis for the fu ture ne go ti a tions be tweenthe NHIF and the Un ion263. The den tists pro tested against the in tro duc tion of fixed prices,which in their opin ion, lim ited com pe ti tion and re duced the pos si bil i ties for in vest ment264.
Sev eral weeks later the Un ion of Den tists in Bul garia an nounced a sur vey, ac cord ing towhich only 25% of the den tists were pre pared to sign con tracts with the NHIF265.
In 1998, af ter al most 2 years of prep a ra tion, the new meth od ol ogy for hos pi tal fi nanc ingwas started, ac cord ing to which their bud get was de ter mined de pend ing on the num ber of pa -tients per year and the cat e gory of the healthcare es tab lish ment in the frame work of a con tractsigned with the re spec tive min is try or the mu nic i pal ity. The con tracts pre pared by the MH in -cluded a re quire ment that the healthcare es tab lish ments re port their ac tiv ity at the end of eachyear in or der to pro vide full trans par ency of the costs they had made266.
The is sue of the fi nanc ing al lo cated from the bud get for healthcare be came top i cal inthe sec ond half of 1998 again. Sev eral pub li ca tions an nounced that 4.2% of the GDP were en -vis aged for healthcare for 1999 and a com par i son was drawn with the fi nanc ing al lo cated forthe cur rent year amount ing to 3.4% of the GDP. Ac cord ing to Min is ter P. Boyadjiev, the bud -get for healthcare for 1999 was “a guar an tee for the re form” which was un der way267.
Dur ing this pe riod of the re form, too, pub li ca tions ap peared about ex ter nal fi nanc ing ofthe healthcare sys tem. The Dan ish agency for En vi ron men tal Pro tec tion do nated 16 mil lionDan ish crowns (around 4 bil lion BGN) for the col lect ing, trans por ta tion and de struc tion ofdan ger ous hos pi tal waste268.
The poor fi nan cial con di tion and the hos pi tal debts con tin ued to be com mented top icsin 1999, es pe cially to ward the end of the year. At the be gin ning of 1999, a pub li ca tion in“Democracia” daily in formed about a new ap proach which was be ing worked out by ex pertsfor the man age ment of healthcare es tab lish ments fi nanced by the re pub li can bud get, ac cord ing to which they would use a monthly limit of the costs, based on pre lim i nary ac counts de pos itedin ad vance to the healthcare min is try. The Min is try’s ar gu ments were that in such a way at theend of the year there would be no debts and that the new sys tem would pre pare the hos pi tals for
104
260 Duma daily, Issue ¹ 23 from 27.01.1998261 Duma daily, Issue ¹ 51 from 1998262 Trud daily, Issue ¹ 45 from 18.02.1998263 24 chasa daily, Issue ¹ 49 from 22.02.1998264 24 chasa daily, Issue ¹ 54 from 1998265 Trud daily from 16.03.1998266 24 chasa daily, Issue ¹ 119 from 1998; Trud daily from 7.05.1998; Democracia daily from 7.05.1998 267 Democracia daily from 25.10.1998 and from 29.10.1998268 24 chasa daily, Issue ¹ 36 from 9.02.1998
their fu ture con tract ing with the NHIF269. Nev er the less, from the mid dle of the year, pub li ca -tions started to ap pear about the hos pi tal debts, mostly owed to the phar ma ceu ti cal com pa -nies270. The Chair man of the Branch Cham ber of the Whole sale Drug Trad ers VladmirNaidenov in formed that the dis con tinu a tion of life-sav ing drugs was be ing con sid ered for thein debted hos pi tals and the Healthcare Trade Un ion to CL “Podkrepa” pre dicted hos pi tal bank -rupt cies and the Min is ter’s res ig na tion271. A pub li ca tion in “24 chasa” news pa per from the endof 1999 in formed that the MH would cover the debts of the dis trict hos pi tals, which rangedfrom 500 mil lion to 6 bil lion old BGN. The same pub li ca tion also pointed out that ac cord ing tothe MH “the sit u a tion is ab nor mal and there fore the Min is try de cided to in ter fere”272.
In 2000, as in the pre vi ous years, there were also pub li ca tions (mainly in “Duma” daily)in form ing about the se vere fi nan cial con di tion of the hos pi tals, the lack of med i ca tions andconsumables, the poor liv ing con di tions for the pa tients in hos pi tals and the large debts of thehealthcare es tab lish ments273.
In a pub li ca tion in “Duma” news pa per, the em pha sis was once again placed on the prob -lem with the re mu ner a tion of the healthcare work ers. The CL “Podkrepa” in sisted that thesal a ries of the per son nel of the Cen tres for Emer gency Med i cal Care were in creased and phy si -cians in many towns across the coun try rose to pro tests274. Sev eral months later, the pro testswith the same claim con tin ued and were joined by phy si cians work ing in hos pi tals and HEI275.
At a meet ing of the NC of the UBP, the Chair man of the or gani sa tion shared the view thatthe higher in come in the out pa tients’ care con tra dict the “mis er a ble in come of the phy si cians in the “Emer gency Care” and the hos pi tals and bring about dis tur bance in the sys tem”276.
At the end of the year, the me dia fo cused their at ten tion on the amount and the mech a -nisms for hos pi tal fi nanc ing in 2001, the MH pre dicted dou ble fi nanc ing for the hos pi tals fromJuly 1st 2001, from which, ac cord ing to the Min is ter of Healthcare Dr. Ilko Semerdjiev, thestate would pro vide 100% fi nanc ing for the hos pi tals and dur ing the sec ond part of the year theNHIF would se cure an ad di tional 20%. In other words, in 2001 the fi nance for hos pi tal carewould in crease by 20% as com pared to 2000. The MH also planned for the region ali sa tion tobe aban doned and for the pa tients to have the right to freely choose a hos pi tal, in which theywish to be treated. The fi nanc ing from the bud get was to be al lo cated ac cord ing to the hos pi talstruc ture, the num ber of beds, the in dus trial and ad min is tra tive ex penses, the length of the pa -tients’ hos pi tal stay and the num ber of treated pa tients. For hos pi tals, in which the num ber oftreated pa tients de creased, a plan for sta bili sa tion was to be de signed, in clud ing re struc tur ing,as so ci a tion with more suc cess fully per form ing hos pi tals, par tial or com plete privatisation. Ifthis failed, some of them would have to be closed down277. Ac cord ing to the “Kapital” weekly,how ever, the fi nanc ing for hos pi tal care in 2001 re mained un changed in terms of size, and inor der to over come the def i cit, var i ous schemes for cost containments were to be ap plied – from
105
Stages and evo lu tion of the healthcare re form in Bul garia
269 Democracia daily from 31.01.1999270 Standart daily from 18.06.1999 and from 17.11.1999271 24 chasa daily, Issue ¹ 264 from 27.09.1999 and Issue ¹ 293 from 26.10.1999; Standart daily from 26.10.1999272 24 chasa daily, Issue ¹ 208 1999273 Duma daily, Issue ¹ 84 from 11.04.2000, Issue ¹ 164 from 15.07.2000 and Issue ¹178 from 1.08.2000274 Duma daily, Issue ¹ 164 from 15.07.2000, Issue ¹ 169 from 21.07.2000, Issue ¹ 174 from 27.07.2000 and
Issue ¹ 175 from 28.07.2000275 Duma daily, Issue ¹ 237 and Issue ¹ 252 from 2000276 Duma daily, Issue ¹ 247 from 2000277 Democracia daily from 207 from 9.08.2000 and from 18.10.2000; Duma daily, Issue ¹ 185 from 2000;
Kapital weekly from 12-18.08.2000
clos ing down of hos pi tals and re duc tion of hos pi tal beds to leas ing of the aux il iary ac tiv i ties toex ter nal pro vid ers278.
In 2000, the “hit” in the fi nanc ing pro vided by the in ter na tional funds and for eigngov ern ments was the train ing and con sul tancy. 3 mil lion Swiss francs were granted with outcom pen sa tion to the NHIF by the Swiss gov ern ment, 500 000 US dol lars were given by eachJa pan and Spain, and 163 000 EUR were al lo cated by EC for train ing programmes279. TheSpan ish gov ern ment granted 400 000 US dol lars for train ing in hos pi tal man age ment and600 000 Ger man marks, se cured by the Ger man gov ern ment, were in tended for the train ing ofthe NHIF em ploy ees. The EC pro cured 1.2 mil lion EUR for the in sti tu tional con struc tion ofthe NHIF and the train ing of the em ployed in the healthcare ad min is tra tion280, the USAID sup -ported with 2.5 mil lion US dol lars for the de vel op ment of a con cept for hos pi tal fi nanc ing281.
At the be gin ning of 2001, the WB was ex pected to re lease a loan amount ing to 63.3 mil -lion US dol lars, which was go ing to be used for the com ple tion of the NHIF in for ma tion sys -tem con struc tion, for phy si cians’ train ing and sup port for the hos pi tal care282. Sev eral monthslater the me dia pub lished in for ma tion, ac cord ing to which 20 mil lion BGN planned from thedraft bud get of the NHIF for build ings re con struc tion, would be pro vided in the form of a loanfrom the WB283. In 2001, Min is ter Semerdjiev an nounced that the Eu ro pean Com mis sion se -cured to the MH 1.3 mil lion EUR with out com pen sa tion for the im ple men ta tion of a pro ject for hu man re sources man age ment and health in sur ance sys tem de vel op ment. The Span ish Min is -try of Healthcare and the French Health In sur ance Fund were part ners to the pro ject and fi -nanc ing was se cured for the es tab lish ment of a train ing cen tre for the NHIF staff, for thepro vid ers of med i cal care and the hos pi tal man ag ers284.
Drug sup ply
Apart from the cov er age of the eco nomic cri sis in the coun try and the grave fi nan cial pre -dic a ment of the healthcare, nu mer ous pub li ca tions in 1997 were ded i cated to the prices of thedrugs, their def i cit and the debts of the MH to the pro vid ers. At the be gin ning of 1997, the riseof the drug prices285 was ex ten sively cov ered to gether with the clos ing down of phar ma ciesbe cause of the higher prices, caused by the fluc tu a tions in the ex change rates of the US dol larand the hy per in fla tion286. At this back ground, it was also an nounced about a debt of the MH,amount ing to ap prox i mately 19 mil lion US dol lars for life-sav ing drugs, and ac cord ing to theAs so ci a tion of the For eign Phar ma ceu ti cal Pro duc ers, they were “the great est ex tra bud getsource for healthcare fi nanc ing”287. An other pub li ca tion pointed out that the ful fil ment of freepre scrip tions had been stopped, the mu nic i pal i ties owed 2.5 bil lion BGN and the MH owed 25
106
278 Kapital weekly from 14-20.10.2000279 Kapital weekly from 14-20.10.2000280 Duma daily, Issue ¹ 106 from 8.05.2000281 24 chasa daily, Issue ¹ 202 from 2000282 Trud daily, Issue ¹ 138 from 24.05.2000; Democracia daily from 26.05.2000; Duma daily, Issue ¹ 121 from
26.05.2000283 24 chasa daily, Issue ¹ 283 from 2000 Kapital weekly, Issue ¹ 42 from 21-27.11.2000284 Democracia daily, Issue ¹ 98 from 27.04.2001285 24 chasa daily, Issue ¹ 37, Issue ¹ 52, Issue ¹ 77 from 19.03.1997 and Issue ¹ 90 from 1.04.1997;
Kapital weekly from 10-16.02.1997 and from 10-16.03.1997286 Duma daily, Issue ¹ 32 from 1997; Trud daily from 1.02.1997; 24 chasa daily, Issue ¹ 34 from 4.02.1997
and Issue ¹ 41 from 1997; Kapital weekly from 17-23.02.1997 and from 7-13.04.1997287 24 chasa daily, Issue ¹ 97 from 8.04.1997
mil lion US dol lars for the med i ca tions of the oncological pa tients, the pa tients with di a be tesand those on haemodialysis288.
In re sponse to the cri sis in drug sup ply, the MH de vised a reg u la tion which en vis agedfixed prices for the Bul gar ian drugs289. Sev eral pub li ca tions from the sec ond half of the yearin formed that the prices of the drugs would be up dated twice an nu ally at the most, that an op -tion was con sid ered about link ing the prices to the Ger man mark and that the MH was pre par -ing a man ual with the max i mum drug prices290. The me dia paid spe cial at ten tion to theamend ments of the Reg u la tion on Free Drugs, as a re sult of which the drugs were to tally orpar tially re im bursed for chil dren un der 4, the preg nant women and the pa tients with cer tainchronic dis eases291. In or der to se cure the en force ment of the Reg u la tion, 33 mil lion US dol lars were nec es sary.
The drug prices con tin ued to be in the fo cus of the me dia at ten tion in 1998. At the be gin -ning of the year, it was once again an nounced that the MH was pre par ing a man ual with themax i mum drug prices to be avail able for the cus tom ers in ev ery phar macy292. Mean while, theme dia cov ered the amend ments in the Reg u la tion on Drug Prices, which pro vided for lowerover price along the dis tri bu tion chain from the pro ducer to the phar macy, as a re sult of whichthe drug prices were ex pected to fall by 10% to 20% and the pro ject for the Reg u la tion wasbacked by the Un ion of Pri vate Phar ma cists, the Branch Cham ber of the Whole sale Drug Trad -ers and the Con sum ers’ Fed er a tion293.
Af ter a cer tain si lence in 1997, in 1998 pub li ca tions ap peared again re gard ing the Law onDrugs and Phar ma cies in Hu man Med i cine (LDPHM) and its amend ments. Part of theamend ments af fected the drug prices and oth ers con cerned the phar ma cies. The in for ma tionpub lished in the me dia was about amend ments in the LDPHM, which en vis aged the in tro duc tion of fixed over prices, aimed at equa li sa tion of the drug prices in the phar ma cies294. The adop tionof the amend ments by the NA caused di verg ing com ments. The pos i tive ef fect was linked to theen force ment of the con trol over the drug prices and the dis con tinu a tion of the spec u la tion deals.Be sides, it was claimed that the amend ments could lead to a rise in the prices295.
The amend ment of the LDPHM, which was pro posed by the MH and which al lowed the open ing of chains of phar ma cies and elim i nated the re quire ment for the open ing of phar ma cies by phar ma cists with Mas ter’s De gree only296, brought back on the agenda the dis put able is sues con sid ered ex ten sively in the pe riod 1993–1995. In 1998, the Un ion of Phar ma cists in Bul -garia was pre pared for pro test ac tions against the amend ments297. At the end of the year, the
107
Stages and evo lu tion of the healthcare re form in Bul garia
288 Democracia daily from 27.05.1997289 Democracia daily from 25.06.1997; Standart daily, from 1.10.1997; 24 chasa daily, Issue ¹ 142 and Issue ¹
199 from 1997290 24 chasa daily, Issue ¹. 171 from 25.06.1997; Trud daily from 12.08.1997; Democracia daily from 17.09.1997291 Democracia daily from 1.04.1997, from 27.05.1997 and from 12.06.1997; Standart daily from 31.03.1997
and from 11.08.1997; Duma daily, Issue ¹ 44 and Issue ¹ 208 from 1997; Trud daily from 27.02.1997 andfrom 12.08.1997; 24 chasa daily, Issue ¹ 215 and Issue ¹ 240 from 1997; Kapital weekly, Issue ¹33 from18-24.08.1997
292 24 chasa daily, Issue ¹ 18 from 22.01.1998 and Issue ¹ 204 from 1998293 24 chasa daily, Issue ¹18 from 22.01.1998, Issue ¹ 111 from 27.04.1998 and Issue ¹ 117 from 1998;
Standart daily from 13.02.1998; Democracia daily from 27.04.1998; Duma daily, Issue ¹ 49 from 4.03.1998294 24 chasa daily, Issue ¹ 186 from 1998 Trud daily from 23.09.1998295 24 chasa daily, Issue ¹ 314 from 21.11.1998 Duma daily, Issue ¹ 293 from 1998296 Trud daily from 23.10.1997297 24 chasa daily, Issue ¹ 32 and Issue ¹ 74 from 19.03.1998
NA adopted amend ments of the Law, ac cord ing to which phar ma cists with Mas ter’s De greeonly could ob tain a li cense, man age and work in the phar macy, reg is tered on their name298.Thus, the adopted amend ments did not pro hibit the open ing of chains of phar ma cies and didnot ex plic itly reg u late the is sue of pro pri etor ship.
The “Kapital” weekly299was the main source of in for ma tion on the is sue of the privatisationof phar ma ceu ti cal firms, the mu nic i pal phar ma cies and the state whole sale com pa nies.
In 1999 – 2001 the prob lems of the drug prices and the short age of life-sav ing drugscon tin ued to be pres ent in the me dia but al ready with new ac cents, re lated to the start of the Na -tional Health In sur ance Fund (NHIF) and the in tro duc tion of the EC stan dards for good pro -duc tion prac tices.
This topic was slightly touched upon in the press in 1999 and only two pub li ca tions wereded i cated to the drug prices and the life-sav ing drugs def i cit300. Greater at ten tion was paid tothe fact that af ter the com pul sory drugs re-reg is tra tion in 2000, many of the mass use Bul gar ian drugs in the coun try could not meet the re quire ments of the Com mis sion on Drugs and that thepro duc tion of Bul gar ian drugs could be ter mi nated in April 2000, when the dead line ex piredfor the in tro duc tion of the EC stan dards that had to be met by the Bul gar ian med i ca tions301. Onthis oc ca sion, the Mem ber of Par lia ment from the UDF Dr. Dimitar Ignatov pro posed to thePar lia men tary Com mis sion on Healthcare that the dead line for the in tro duc tion of stan dardsfor good pro duc tion prac tices was ex tended and the rea son was that it needed 100 mil lion USdol lars302. An other ac cent in 1999 in cluded the mis un der stand ings be tween the MH and theNHIF con cern ing the free drugs – the NHIF ac cused the MH for pro pos ing a list con tain ingharm ful and very ex pen sive drugs, for which the Fund re fused to pay303.
The is sue of the drug prices once again came to the agenda in 2000. At the be gin ning of theyear, in for ma tion be gan to ap pear in press about price in crease, the rea sons for which were linked tothe higher pro duc tion costs and the fluc tu a tions in the ex change rate of the US dol lars304.
In a state ment for the me dia, the Min is ter of Healthcare Dr. Semerdjiev an nounced onceagain about the in ten tions of the MH to in tro duce limit prices on drugs, which had to be validacross the coun try. The prep a ra tion of a man ual with the limit prices of the drugs started at thetime of Min is ter Boyadjiev in the mid dle of 1997. The limit prices were en vis aged to be ne go ti -ated with pro duc ers, im port ers and drug trad ers and the Par lia men tary Com mis sion and ex -perts to con trol price for ma tion305. Af ter more than two months, it be came ob vi ous that limitprices could be in tro duced only for drugs sold with pre scrip tion306. In the mean time, the MHpro ject was be ing con sid ered about the in tro duc tion of a new type of over price, which had tobe dif fer en ti ated ac cord ing to the drug prices307. In the mid dle of the year, the Coun cil of Min -
108
298 24 chasa daily, Issue ¹ 194 and Issue ¹ 314 from 21.11.1998 Trud daily from 3.09.1998299 Kapital weekly, Issue ¹ 10 from 10-16.03.1997, from 18-24.07.1998, from 4-10.08.1997, from
22-28.08.1998, from 19-25.09.1998, Issue ¹ 41 from 13-19.10.1997, from 5-11.12.1998, Issue ¹ 6 from13-19.02.1999, Issue ¹ 8 from 27.02.-5.03.1999, Issue ¹ 18 from 8-14.05.1999 and from 3-9.07.1999
300 24 chasa daily, Issue ¹ 69 from 13.03.1999 and Issue ¹ 107 from 1999301 Kapital weekly from 22-28.05.1999; 24 chasa daily, Issue ¹ 198 from 23.07.1999302 24 chasa daily, Issue ¹ 203 from 1999 Democracia daily from 23.07.1999303 24 chasa daily, Issue ¹ 288 from 21.10.1999304 24 chasa daily, Issue ¹ 2, Issue ¹ 69 and Issue ¹ 174 from 2000305 24 chasa daily, Issue ¹ 2, Issue ¹ 69 and Issue ¹ 174 from 2000306 24 chasa daily, Issue ¹ 103 from 17.04.2000307 24 chasa daily, Issue ¹ 73, Issue ¹ 103, Issue ¹ 104, Issue ¹ 106 and Issue ¹174 from 2000; Democracia
daily from 26.05.2000; Duma daily, Issue ¹ 90 from 18.04.2000 and , Issue ¹ 137 from 2000; Kapital
is ters adopted a reg u la tion which pro vided for limit prices of drugs and dif fer en ti ated overprices for the sep a rate parts of the dis tri bu tion chain, and at the be gin ning of No vem ber, a man -ual was also pub lished, which al most im me di ately af ter its pub li ca tion un der went sev eralchanges due to print ing mis takes and changes in the ex change rate of the US dol lar. As a re sult, the Branch Cham ber of the Whole sale Drug Trad ers in sisted on changes in the way the priceswere cal cu lated308.
In some pub li ca tions it was an nounced that a great part of the free drugs would be re im -bursed by the NHIF and that their list would be spec i fied with the par tic i pa tion of the UBP. Im -me di ately be fore and af ter July 1st 2000, in for ma tion ap peared about a short age of life-sav ingfree med i ca tions309.
Struc tural changes
The topic of the pro hi bi tion of the pri vate prac tice of phy si cians, em ployed by state and mu nic i pal healthcare es tab lish ments, was re flected ex ten sively in the me dia in the pe riod1990-1996 as one of the main is sues, caus ing con flict and ten sion within the sys tem, and fadedaway in 1997. At the be gin ning of the year, the NA did not adopt the amend ments in the LPHre lated to pri vate prac tice, but the ban re mained for the phy si cians to oc cupy lead ing man a ge -rial po si tions in pri vate healthcare es tab lish ments310. With a few pub li ca tions from the sec ondhalf of 1997, de voted to the amend ment in the LPH con cern ing the abol ish ment of the re quire -ment for the pri vate prac ti tio ners for a min i mum of 2-year work ing ex pe ri ence in the spe cialty, this topic even tu ally died out311.
With the en force ment of the Reg u la tion on Paid Med i cal Ser vices in 1998, the prob lemwith the choice of a fam ily phy si cian sur faced once again312. Along with the ar ti cles in form -ing about the choice dead lines and pro ce dure, un law ful reg is tra tions and in fringe ment on thepa tients’ rights were of ten re ported313. From the end of April, in for ma tion ap peared in thepress about the forth com ing choice of a gen eral prac ti tio ner or “fam ily phy si cian” 314. Ac cord -ing to Min is ter Boyadjiev, this marked the be gin ning of the re form in out pa tients’ care315. Un -til the mid dle of 1998, 1 800 med i cal spe cial ists un der went train ing for gen eral prac ti tio ners,the UBP es ti mat ing 6 000 GPs as nec es sary for the coun try. The WB re leased 2.5 mil lion ecufor their train ing. The WB also fi nanced the train ing of the doc tors in emer gency med i cine316.
109
Stages and evo lu tion of the healthcare re form in Bul garia
weekly, Issue ¹ 6 from 12-18.02.2000308 24 chasa daily, Issue ¹ 175 from 30.06.2000, Issue ¹ 306 from 10.11.2000 and Issue ¹ 321 from 25.11.2000309 24 chasa daily, Issue ¹ 69 from 14.03.2000 and Issue ¹ 126 from 2000; Democracia daily from 29.03.2000,
from 2.05.2000 and from 13.07.2000; Duma daily, Issue ¹ 144 from 22.06.2000, Issue ¹ 146 from24.06.2000, Issue ¹ 162 from 13.07.2000, Issue ¹ 164 from 15.07.2000, Issue ¹ 168 from 20.07.2000 andIssue ¹ 229 from 2000; Kapital weekly, Issue ¹ 24 from 17-23.06.2000
310 Standart daily from 23.01.1997; Duma daily, Issue ¹ 18 from 1997; Trud daily from 23.01.1997311 Trud daily from 18.09.1997; 24 chasa daily, Issue ¹ 205, Issue ¹ 243 and Issue ¹ 256 from 1997; Forum
Medicus periodical, Issue ¹ 31 from 6.10.1997312 24 chasa daily, Issue ¹ 11 from 15.01.1998, Issue ¹ 86 from 31.03.1998 and Issue ¹ 321 from 28.11.1998;
Trud daily from 19.02.1998 and from 30.03.1998; Standart daily, Issue ¹ 1907 from 15.01.1998; Democraciadaily from 14.03.1998; Duma daily, Issue ¹ 10 from 15.01.1998; Kapital weekly from 19-25.01.1998
313 24 chasa daily, Issue ¹ 86 from 31.03.1998.; Standart daily from 26.03.1998314 Duma daily, Issue ¹ 93 from 25.04.1998; 24 chasa daily, Issue ¹ 107, Issue ¹ 108 and Issue ¹ 321 from
1998; Kapital weekly from 11-17.07.1998315 24 chasa daily, Issue ¹ 107 from 1998316 24 chasa daily, Issue ¹ 144 from 1998; Standart daily from 21.09.1999
The struc tural re form was dis cussed pri mar ily in re la tion to the clos ing down of hos pi -tals. In an in ter view about the paid med i cal ser vices, the hos pi tal clos ing and the staff re duc -tion, the out pa tients’ clin ics privatisation, phar ma cies and phar ma ceu ti cal com pa nies and thebud get al lo ca tion, Min is ter Boyadjiev de clared that “the hos pi tal net work is dis pro por tion ateand ir ra tio nal, and it has been suf fer ing from a chronic lack of fi nanc ing for years. This ne ces -si tates its re struc tur ing.” In this pro cess, the hos pi tal ac cred i ta tion played a ma jor role and itwould de ter mine which of the hos pi tals would be re struc tured and which would be closeddown. Con cern ing the re form, the Min is ter stated that “the dan ger of fail ure co mes from theway the pop u la tion and the med i cal spe cial ists will ac cept it and im ple ment it. It is a fact that its be gin ning is re lated to rather un pop u lar mea sures.”317 The “Trud”318 daily in formed that theRHC would re ceive guide lines about the cri te ria used for clos ing down hos pi tals. Eachhealthcare es tab lish ment had to com plete a form about the num ber of treated pa tients and per -formed op er a tions, and the de ci sion about the clos ing would de pend on the costs per treatedpa tient and the state of the hos pi tal fa cil i ties.
At the end of the year, the me dia in formed about a MH pro ject, ac cord ing to which hos pi -tals with lower uti li sa tion rate had to be re struc tured in or der to treat so cially dis ad van tagedpeo ple free of charge, part of the hos pi tals had to pro vide gen eral med i cal care and oth ers wereto be con verted into spe cial ised clin ics for chron i cally ill pa tients, still oth ers – into hos pices,all of which had to start func tion ing with the in tro duc tion of the health in sur ance319. It was alsoan nounced that the RHC would con trol the med i cal ac tiv i ties in pri vate healthcare es tab lish -ments and would or gan ise and co or di nate the sign ing of con tracts for med i cal care pro vi sionbe tween the hos pi tals and the mu nic i pal i ties, ac cord ing to which hos pi tals would re ceivemoney from the bud get, based on per formed ac tiv i ties320.
A num ber of pub li ca tions in 1997 in formed about the clo sure of san a to ria, pul mo naryand psy chi at ric hos pi tals, mu nic i pal hos pi tals and a re duc tion in the num ber of beds in them,work ers’ hos pi tals and re struc tur ing of mil i tary hos pi tals321.
One pub li ca tion in the be gin ning of 1998 re ported that a new re duc tion in the num ber of hos pi tal beds was be ing pre pared by the MH: by 35% in the dis trict hos pi tals and by 37% inthe mu nic i pal hos pi tals, the re duced num ber of beds in the sep a rate healthcare es tab lish mentsde pend ing on the size of the served pop u la tion, the age struc ture, mor bid ity rate in the re gionand the prox im ity to an other hos pi tal. In some of the smaller towns, the ma ter nity wards werego ing to be closed down and in oth ers – whole hos pi tals. The clos ing down of the re dun dantclin ics was also en vis aged in So fia. Ac cord ing to MH data the beds uti li sa tion rate in some ofthe mu nic i pal ity hos pi tals was 40% only322.
Pub li ca tions ded i cated to the re struc tur ing and the re duc tion of the healthcare es tab -lish ments and work ing po si tions could be found in 1999 and 2000 323. Two ar ti cles in “Duma”
110
317 Standart daily from 9.07.1997; Duma daily, Issue ¹ 170 from 1997; 24 chasa daily, Issue ¹ 179 from 1997;Forum Medicus periodical, Issue ¹ 24 from 14.07.1997 and Issue ¹ 31from 6.10.1997
318 Trud daily, Issue ¹ 232 from 25.08.1997 ã.319 Standart daily, Issue ¹ 1841 from 2.11.1997; Democracia daily from 3.11.1997320 24 chasa daily, Issue ¹ 198 from 1997321 Democracia daily from 7.08.1997, from 14.08.1997 and from 13.11.1997; Trud daily from 9.08.1997, from
12.08.1997, from 13.11.1997 and from 30.12.1997; Duma daily, Issue ¹ 182 from 199322 Trud daily from 19.03.1998323 Duma daily, Issue ¹ 62 from 1999.; Democracia daily from 29.04.1999.; Forum Medicus periodical, Issue ¹
38 from 9.10.2000
news pa per from the Left Wing Par lia men tary Group at the be gin ning of the year were de votedto the scan dals around mak ing re dun dant over 150 peo ple from the Sci en tific Chem i cal andPhar ma ceu ti cal Re search In sti tute (SCPRI) 324. The Conferderation of the In de pend ent TradeUn ions in Bul garia in formed about the clos ing down of 6 000 va can cies in healthcare and theyalarmed that “the emer gency care is be ing de stroyed” and Dr. Zhelyazko Hristov pro claimedhim self against the 4% job cuts in the sys tem, which ne ces si tated the pass ing of De cree ¹ 23of the Coun cil of Min is ters from 10 Feb ru ary 1999325.
In the mid dle of 1999, Min is ter Boyadjiev de clared that the school doc tors and the doc -tors in the kin der gar tens would be trans ferred to the HEI326. At the be gin ning of 2000, a reg u la -tion of the MH, ac cord ing to which the school doc tors had to be sub sti tuted by nurses andphy si cians’ as sis tants, caused a lot of de bates. The UBP in sisted that the reg u la tion was aban -doned and the sur ger ies in the schools were pre served, with phy si cians con tin u ing to work inthem. The NHIF stand was that they would be re dun dant with the func tions of the gen eral prac -ti tio ners who were the ones to pro vide the med i cal care of the chil dren327.
New health leg is la tion
Re gard ing the healthcare re form in 1997, the em pha sis was placed on the struc turalchanges and the bill on health in sur ance. At his first press con fer ence, Min is ter Boyadjiev de -clared that four laws were ex pected to be passed in the MH un til the end of the year – on healthin sur ance, on the na tion’s health, on the healthcare es tab lish ments and the pro fes sional or gani -sa tions, and the ef forts of the Min is try were di rected to ward a “fast struc tural re form, whosefirst steps would be to elim i nate the re dun dant med i cal ac tiv i ties”328.
Con cern ing health in sur ance, in 1997 and the years to fol low the pub li ca tions in the me -dia ac quired con crete di men sions as com pared to the first stage of the re form. In the mid dle of1997, it was an nounced that the MH was work ing on a pro ject on health in sur ance since, ac -cord ing to Min is ter Boyadjiev, the pro ject pro posed by M. Vitkova did not cor re spond to themar ket econ omy and could not func tion un der con di tions of a Mon e tary Board. The pre dic -tions were that the health in sur ance fund would start func tion ing in two years’ time at the ear li -est, for which ex perts es ti mated that 600 mil lion US dol lars would be needed329. An otherpub li ca tion re ported that 120 mil lion US dol lars would be needed to con struct the NHIF andthe twenty-eight RHIFs330.
As to the Bill on Health In sur ance, it was an nounced that ac counts had been pre paredfor the health in sur ance in stal ments amount ing to 12% (the most com monly men tioned per -cent age in the press but the dif fer ent pub li ca tions also quote 9% and 15%), which had to bevoted by the NA and 8% of the rev e nue from privatisation would be poured into the Health In -sur ance Fund331. The MH pro posed that the Fund was man aged by an equal num ber of cit i zens
111
Stages and evo lu tion of the healthcare re form in Bul garia
324 Duma daily, Issue ¹ 7 from 11.01.1999 and Issue ¹ 8 from 12.01.1999325 Duma daily, Issue ¹ 56 from 1999326 24 chasa daily, Issue ¹176 from 1.07.1999; Forum Medicus periodical, Issue ¹ 7 from 14.02.2000327 Democracia daily from 24.02.2000 and from 3.03.2000328 Democracia daily from 5.06.1997329 Standart daily, Issue ¹ 1691 from 5.06.1997; Democracia daily from 22.08.1997.; Forum Medicus
periodical, Issue ¹ 19 from 9.06.1997 and Issue ¹ 40 from 24.11.1997330 Trud daily from 10.12.1997331 Trud daily from 6.09.1997 and from 26.09.1997; Standart daily from 31.10.1997 and Issue ¹ 1843 from
4.11.1997; Democracia daily from 17.12.1997; Kapital weekly from 10-16.11.1997
and em ploy ers and was in de pend ent, as it was held ac count able to a civil coun cil, whereas themem bers of Par lia ment in sisted that the Fund was ac count able to the NA. Ac cord ing to thetrade un ions, one of the most dis put able terms was re lated to the con sumer’s fee332. The Bul -gar ian So cial ist Party was against the in tro duc tion of a con sumer’s fee for hos pi tal treat mentwith the ar gu ment that it con tra dicted the Con sti tu tion333. The en vis aged mo nop oly sta tus ofthe Health In sur ance Fund was also criti cised334. In sev eral pub li ca tions, dep u ties from thePar lia men tary Group of the Dem o cratic Left (PGDL) and rep re sen ta tives of the trade un ionscriti cised the Bill on Health In sur ance, pro posed by the ma jor ity335.
At the end of 1998, in two re views in the “Kapital” weekly, crit i cism was also voiced re -gard ing the healthcare re form. The more sig nif i cant part was re lated to the neg li gence of pre -ven tion and health pro mo tion at the ex pense of the re forms in hos pi tal care, the dualist form ofman age ment of the healthcare es tab lish ments by the mu nic i pal i ties and the MH, the prob lemswith med i cal ed u ca tion and the re duc tion of the struc tural re form to me chan i cal cuts of hos pi -tal beds336.
In 1998 the com ments and dis cus sions con cern ing the Law on Health In sur ance con tin -ued in the press. Part of these pub li ca tions were re lated to its con sid er ation in NA and werechiefly in for ma tive in na ture337.
At the dis cus sion, or gan ised by the Euroleft on the is sues of the Law on Health In sur -ance, fi nan cial ex perts pre dicted that the health in sur ance sys tem would in crease in fla tion byaround 15% and the in crease of the GDP, re sult ing from the health in sur ance in stal ments,would in crease the def i cit, since it would not be caused by a change in the real sec tor. The thenVice Min is ter of Healthcare Dr. Semerdjiev con firmed the prog no ses for a rise in in fla tion ratebut, ac cord ing to the MH, it would not rise by more than 2.5%, e.g. a value within the frame -work of the def i cit ne go ti ated with the In ter na tional Mon e tary Fund IMF). The ap pre hen sionsof the Min is try of La bour and So cial Care were con nected pri mar ily with the in crease of thesize of the in sur ance pre mi ums which would cre ate prob lems col lect ing them338. About amonth later, in a pub li ca tion in “Trud” news pa per the lack of fund ing was dis cussed for the es -tab lish ment of the NHIF and its branches in the coun try. Ac cord ing to the ac count ing plans ofthe Min is tries of Healthcare and Fi nance, a min i mum of 600 mil lion US dol lars were needed,which could not be pro vided un til the ini tially en vis aged term339. Mis giv ings were also ex -pressed re gard ing the fund ing, which would ini tially be col lected in the health in sur ance fundas well as re gard ing the an nual in come from health in sur ance in stal ments, be cause of whichdif fer ent op tions were con sid ered about ad di tional fi nanc ing340.
The World Bank in sisted on mak ing cer tain cor rec tions in the bills such as the use of auni fied reg is ter of the in sured per sons so that one au thor ity could con trol the collectibility ofthe in sur ance in stal ments, ex tend ing of the dead lines for the launch ing of the sys tem in or der to
112
332 Standart daily from 6.10.1997333 Duma daily, Issue ¹ 295 from 1997334 Trud daily from 6.09.1997; Duma daily, Issue ¹ 208 from 1997335 Duma daily, Issue ¹ 258, Issue ¹ 228 and Issue ¹ 297 from 1997336 Kapital weekly from 14-20.11.1998 and from 21-27.11.1998337 24 chasa daily, Issue ¹ 135 from 23.05.1998; Trud daily from 18.04.1998, from 23.05.1998 and from
20.06.1998; Standart daily 30.05.1998; Kapital weekly from 15-21.06. 1998, from 11-17.07.1998 and from21-27.11.1998; Forum Medicus periodical, Issue ¹ 7 from 16.02.1998 and Issue ¹ 12 from 23.03.1998
338 24 chasa daily, Issue ¹ 17 from 21.01.1998339 Trud daily from 17.02.1998340 Standart daily from 19.05.1998
en sure the nec es sary fi nance and build ing of the NHIF in fra struc ture and in for ma tion sys tem,en hance ment of the role of the MH in the work ing out of the NFA (as a re sult of which a textwas added, stip u lat ing that a min i mum pack age of med i cal ser vices would be de ter mined by areg u la tion of the MH). Ex perts from the MH also rec om mended that the MH was com mit ted to the ap proval of the types and scope of the ser vices, which would be pro vided by the funds forvol un tary in sur ance, as well as to the mon i tor ing of the qual ity of med i cal care341.
The rec om men da tion of the IMF and the WB was that the health in sur ance in stal ment was 6%, so that the in sur ance bur den was not in creased, and the WB in sisted that the strat egy forthe im ple men ta tion of the healthcare re form was linked to the re main ing so cial sec tors342.
In a num ber of pub lished ar ti cles in the “Duma” daily, the Law on Health In sur ance was sharply criti cised343. The Law was de fined as “in ad e quate to the so cial con di tion of the Bul gar -i ans,” “un ac cept able and doomed to fail ure.” The main crit i cisms con cerned the fol low ing:
· the es tab lish ment of the NHIF as an au ton o mous or gani sa tion, fully in de pend ent of the state, which ac cord ing to some, was a pre req ui site for the cre ation of a “health in sur -ance fund pyr a mid” on one hand, and meant that the state ab di cated from “the re spon -si bil ity and the care for the peo ple’s health and work ing ca pac ity”, on the other;
· the lack of con trol on be half of the state over the in com ing funds in the NHIF;
· the prin ci ple of sol i dar ity in the com pul sory health in sur ance, which “in fringes on therights of the rich peo ple”;
· the NHIF ad min is tra tion, in for ma tion sys tem, etc.
One of the main ar gu ments of the op po si tion against the Law was con nected with the mo -nop o lis tic par tic i pa tion of the pro fes sional or gani sa tions of phy si cians and den tists in the ne -go ti a tions, which ac cord ing to the Vice Pres i dent of the CL “Podkrepa” Dimitar Manolov, onone hand, “iso lated the rest of the as so ci a tions of med i cal work ers,” 344and ac cord ing to Prof.Konstantin Atanassov, “added one more in sti tu tion to the man age ment of healthcare, hy bridany way,”345 on the other. To sum ma rise the pre sented ar gu ments, the con clu sion was reachedthat the adop tion of the Law on Health In sur ance had to be post poned for 10 – 15 years, “es tab -lish health in sur ance through the fund “Work ing sal ary” only and the state fi nanc inghealthcare through the tax a tion sys tem and the re pub li can bud get.”346 The other pro posed op -tion was to re-es tab lish the sys tem for health in sur ance as part of a com mon na tional in sur ancefund (a sim i lar fund func tioned in Bul garia un til 1949), all the healthcare es tab lish ments be ingtrans ferred to it347.
Part of the pub li ca tions dealed with the dis cus sions be tween the rul ers and the gov ern -ment on sep a rate texts of the Law on Health In sur ance at its con sid er ation in the NA. One ofthe dis put able texts was re lated to the con sumer’s fee for phys i cal ex am i na tion and hos pi taltreat ment, which ac cord ing to Mem bers of Par lia ment from the op po si tion, re peated the healthin sur ance and in such a way the law reg u lated the dou ble pay ment for the use of med i cal ser -
113
Stages and evo lu tion of the healthcare re form in Bul garia
341 Kapital weekly from 27.04.-3.05.1998342 Democracia daily from 25.04.1998; Duma daily, Issue ¹ 93 from 25.04.1998; Kapital weekly
27.04.-3.05.1998 and from 11-17.07.1998343 Duma daily, Issue ¹ 21, Issue ¹ 57, Issue ¹ 110 and Issue ¹ 293 from 1998344 Duma daily, Issue ¹ 21 from 28.01.1998345 Duma daily, Issue ¹ 110 from 16.05.1998346 Duma daily, Issue ¹. 57 from 1998347 Duma daily, Issue ¹ 110 from 16.05.1998
vices348. With this ar gu ment, 52 dep u ties in tro duced the claim in the Con sti tu tional Court thatthe con sumer’s fees were aban doned349. The NHIF in for ma tion sys tem also caused dis putes inPar lia ment. Mem bers of Par lia ment from the op po si tion in sisted that it was part and par cel ofthe in for ma tion sys tem of the Na tional In sur ance In sti tute in stead of be ing con structed as anin de pend ent one350.
In a pub li ca tion in “Kapital” weekly351, the Law on Health In sur ance was criti cisedmainly on two points – first, that at the sign ing of in di vid ual con tracts be tween the Fund andthe healthcare es tab lish ments, dif fer ent con di tions could not be ne go ti ated, which would oth -er wise stim u late com pe ti tion, and sec ond, that the pro fes sional branch or gani sa tions of phys i -cal per sons (UBP and UDB) would be ne go ti ated on be half of le gal en ti ties (the healthcarees tab lish ments), who were not their mem bers and “the out come is that the hos pi tals will haveto ful fil what has been ne go ti ated be tween the NHIF and the UBP and UDB.”
Sev eral pub li ca tions in 1999 in formed about in ten tions for amend ments or amend mentsal ready car ried out in the Law on Drugs and Phar ma cies in Hu man Med i cine, the Law onPeo ple’s Health and the Law on Health In sur ance352. Re fer ring to the Law on Health In sur -ance, K. Marangozov and an other four col leagues of his de pos ited a pro ject for an amend mentin the LHI at the NA, their ar gu ments be ing that the act ing law caused chaos. Ac cord ing tothem, the NHIF had to be long to the Na tional In sur ance In sti tute struc ture, “since the in stal -ments are col lected there any way.”353
Along with the Law on Health In sur ance, in 1998 the Law on Healthcare Es tab lish -ments was un der dis cus sion, too. The most com monly discussd in press were the is sues con -cern ing the hos pi tal and out pa tients’ clin ics reg is tra tion as com mer cial com pa nies, theirman age ment and the set ting up of hos pi tal boards of trust ees, the per mis sion re gime for the ex -e cu tion of ac tiv i ties, the na tional health map354. In a few pub li ca tions from the first half of1998, it was pointed out that the phy si cians’ sur ger ies would be rented to the doc tors whowould trans fer to free prac tice and would sign con tracts with the mu nic i pal i ties to serve pa -tients355. Ac cord ing to the MH, the new law was aimed at solv ing the prob lems of the out pa -tients’ care as, ac cord ing to sta tis ti cal data, ev ery Bul gar ian vis ited the poly clin ics on theav er age 5 times a year, and 20% of the pop u la tion was hos pi ta lised. The data for the West ernEu ro pean coun tries in di cated a hos pi ta li sa tion rate be tween 10 and 12%, prov ing that the out -pa tients’ sec tor in Bul garia was not func tion ing ef fi ciently enough356.
The Law on Healthcare Es tab lish ments privatisation357 was also widely com mented on,which ac cord ing to the Min is ter, had to start from the out pa tient care but “for the time be ing
114
348 Duma daily, Issue ¹ 120 from 29.05.1998349 24 chasa daily, Issue ¹ 208 from 4.08.1998; Trud daily from 29.05.1998; Forum Medicus periodical, Issue
¹ 31 from 27.07.1998350 24 chasa daily, Issue ¹ 196 from 1998351 Kapital weekly from 15-21.06.1998352 Trud daily from 6.01.1999; Kapital weekly from 3-9.06.1999; 24 chasa daily, Issue ¹170 from 25.06.1999353 Duma daily, Issue ¹ 174 from 1999354 24 chasa daily, Issue ¹ 281 from 1998; Trud daily from 11.06.1998 and from 7.09.1998; Duma daily, Issue
¹ 180, Issue ¹ 237 and Issue ¹ 250 from 1998; Kapital weekly from 11-17.07.1998 and from8-14.08.1998; Forum Medicus periodical, Issue ¹ 34 from 14.09.1998
355 Trud daily from 23.04.1998 and from 5.05.1998; Democracia daily from 105 from 23.04.1998 and from27.04.1998; Duma daily, Issue ¹ 93 from 25.04.1998
356 Kapital weekly from 8-14.08.1998357 24 chasa daily, Issue ¹ 210 from 6.08.1998; Trud daily from 11.06.1998; Duma daily, Issue ¹ 237 from 1998
there are no in ves tors.”358
In 1999 the UBP pro claimed it self in fa vour of the privatisation of ac tiv i ties and not offa cil i ties359. In May 1999 the Chair man of the Par lia men tary Com mis sion on Healthcare Dr. B. Kitov an nounced that the privatisation of healthcare es tab lish ments of the out pa tients’ carehad to be com pleted un til No vem ber 1st and they could be pur chased on con di tion of their ac -tiv ity pres er va tion360. In June the “Democracia” news pa per in formed that the privatisation ofthe “poly clin ics” would start in the au tumn of 2000361.
In 1999 the ar ti cles con tin ued to be pub lished re gard ing the Law on Healthcare Es tab -lish ments, dis cuss ing var i ous is sues, the com mon est be ing their com mer cial sta tus and man -age ment362. The op po si tion pro tested against the com mer cial sta tus of the healthcarees tab lish ments and, ac cord ing to the state ments of the Dep uty from the PGDL Dr.Marangozov, “the con ver sion of the treat ment ac tiv i ties into trade is shame ful.”363 In 2000 thereg is tra tion of the healthcare es tab lish ments as com mer cial com pa nies was also criti cised and,wrongly or de lib er ately, de fined by some me dia as “na tion ali sa tion of mu nic i pal prop erty”364.
The is sues of healthcare es tab lish ments’ ac cred i ta tion and privatisation, en vis aged in the LHE365 also largely ech oed in the press. The ac cred i ta tion pro ce dure and cri te ria werebe ing dis cussed366. Ac cord ing to Dr. Semerdjiev, “the NHIF will also con clude con tracts withdi ag nos tic and con sult ing cen tres which have re ceived ex cel lent and very good eval u a tion,”and ac cord ing to the op po si tion, the reg u la tion on ac cred i ta tion would cause “an ex plo sion ofcor rup tion re lated to cate gori sa tion” and would sharpen the con tra dic tions be tween na tional,dis trict and re gional healthcare es tab lish ments367. In terms of privatisation, “the great est dan -ger” seen by the some phy si cians was in the fact that af ter a pos si ble privatisation, they wouldturn into “hired work ers” (au thor’s note:?!); the rest of their ap pre hen sions were con nectedwith a “purge for po lit i cal rea sons,” privatisation deals “un der the ta ble,” de lib er ate bank rupt -cies, etc. 368. Re gard ing privatisation, one of the most dis cussed prob lems in 2001 was that af ter the reg is tra tion of the healthcare es tab lish ments ac cord ing to the Com mer cial Law, the own er -ship was not clear over part of them369.
The adop tion of the Law on the Pro fes sional Or gani sa tions of Phy si cians and Den -tists and the oblig a tory mem ber ship in these or gani sa tions reg u lated in it, called for a se ries ofcon tro ver sial com ments in the press. The op po nents of the law de fined it as “re ac tive” and“anti-con sti tu tional” with the ar gu ments that it in fringed on the phy si cians’ rights by bind ingthe mem ber ship in the un ion with the right to prac tice their pro fes sion. The an tic i pa tions were
115
Stages and evo lu tion of the healthcare re form in Bul garia
358 24 chasa daily, Issue ¹ 108 from 1998359 Duma daily, Issue ¹ 15 from 1999360 Democracia daily from 15.05.1999361 Democracia daily from 22.06.1999362 Duma daily, Issue ¹ 15 from 1999; 24 chasa daily, Issue ¹ 130 from 15.05.1999 and Issue ¹ 170 from
25.06.1999; Democracia daily from 15.05.1999363 Duma daily, Issue ¹ 16 from 1999364 Duma daily, Issue ¹ 53 from 6.03.2000365 24 chasa daily, Issue ¹ 232, ¹ 237 and ¹ 345 from 2000; Democracia daily from 1.04.2000, from
26.09.2000 and from 12.12.2000; Duma daily, Issue ¹ 84 from 11.04.2000; Standart daily from 11.03.2000and from 12.12.2000; Kapital weekly, Issue ¹ 3 from 22-28.01.2000; Forum Medicus periodical, Issue ¹ 38 from 9.10.2000
366 24 chasa daily, Issue ¹ 237 from 2000; â. “Äåìîêðàöèÿ” from 1.04.2000 ã.367 Duma daily, Issue ¹ 84 from 11.04.2000368 Standart daily from 11.05.2000369 Standart daily from 26.01.2001
also con nected to the le gal reg u la tion of the mo nop oly of the pro fes sional or gani sa tions whichwas a pre req ui site for ex ceed ing their com pe tences370. State ments and com ments could also be come across in fa vour of the Law, with the mo tive that con trol over the phy si cians’ pro fes -sional be hav iour was nec es sar ily linked to the adop tion of the Code of Pro fes sional Eth ics371.
To ward the end of the year, a claim was de pos ited in the Con sti tu tional Court sup portedby 60 dep u ties from the NA, against the oblig a tory mem ber ship in the UBP and the UDB andagainst the text in the Law on the Pro fes sional Or gani sa tions, pos tu lat ing them as the only pro -fes sional or gani sa tions of phy si cians and den tists372.
In 1999 sev eral pub li ca tions dealt with phy si cians’ views that the Law on the Pro fes -sional Or gani sa tions con tra dicted the Con sti tu tion and was un dem o cratic373, and they in -formed about the en rol ment of phy si cians in the UBP374. In his state ment, the Gen eralSec re tary of the UBP Dr. Stoyan Botev de clared that “the UBP will al ready have to be lookedupon as a pow er ful eco nomic for ma tion, on whose shoul ders the bur den falls to con duct thena tional healthcare con tract ing.”375
In 2000 the press in formed again about the al ready deep en ing prob lems in the med i calpro fes sional or gani sa tions. The phy si cians (mainly from the So fia Col le giate) or gan ised a sub -scrip tion claim ing the res ig na tion of the UBP’s man age ment. Their mo tives in cluded the lack ofac count abil ity for the costs spent from mem ber ship fees and the opin ion that they did not de fendthe in ter ests of the pro fes sional guild. Ac cord ing to the ini ti a tors of the sub scrip tion, the Pres i -dent of the UBP was il le git i mate since he was a Mem ber of Par lia ment at the same time. In for ma -tion also ap peared that phy si cians sued Bul garia for force ful mem ber ship in Strasburg376.
In 1999 the topic of cor rup tion in healthcare cov ered in the press shaped as a sep a rate is -sue. In 1999 and the years to fol low “cor rup tion” was the lead ing topic in a se ries of ar ti cles orthey were en tirely de voted to it377. At the be gin ning of 1999, in an in ter view for “24 chasa” daily, Min is ter Boyadjiev con fessed that there was cor rup tion in the healthcare, but there was no ev i -dence for it and he con firmed the view shared dur ing the first stage of the re form that the in tro -duc tion of a health in sur ance sys tem was the so lu tion to the prob lem with cor rup tion378. Aphy si cian was re ported to have been caught with a bribe379, and ac cord ing to an opin ion poll con -ducted by “Vitosha re search”, “the cus toms of fi cers and the doc tors are the most cor rupted”380.
In the mean time, pub li ca tions ap peared about the fu ture Code of Pro fes sional Eth ics in -form ing that it was adopted in prin ci ple by the XXXII As sem bly of the phy si cians and was ex -
116
370 Standart daily from 14.07.1998 and from 25.09.1998; Duma daily, Issue ¹ 47, ¹ 51, ¹ 119, ¹ 150, ¹151and ¹ 293 from 1998 Forum Medicus periodical, Issue ¹ 9 from 2.03.1998
371 Trud daily from 13.07.1998 Standart daily from 14.07.1998 and from 25.09.1998; Democracia daily from3.07.1998; Forum Medicus periodical, Issue ¹ 8 from 23.02.1998, Issue ¹ 31 from 27.07.1998 and Issue ¹46 from 7.12.1998
372 Standart daily from 14.07.1998; 24 chasa daily, Issue ¹ 208 from 4.08.1998; Forum Medicus periodical,Issue ¹ 31 from 27.07.1998)
373 Standart daily, Issue ¹ 2291 from 18.02.1999 and Issue ¹ 2297 from 24.02.1999 374 Standart daily, Issue ¹ 2317 from 16.03.1999; Duma daily, Issue ¹ 157 from 14.08.1999375 24 chasa daily, Issue ¹ 19 from 1999376 24 chasa daily, Issue ¹ 242 from 5.09.2000; Duma daily, Issue ¹ 207 from 4.09.2000377 24 chasa daily, Issue ¹ 8, Issue ¹ 19, Issue ¹ 57 and Issue ¹ 102 from 1999; Kapital weekly from
6-12.02.1999; Duma daily, Issue ¹157 from 14.08.1999378 24 chasa daily, Issue ¹7 from 1999379 24 chasa daily, Issue ¹ 102 from 16.04.1999380 Duma daily, Issue ¹ 55 from 1999
pected to be fi nally voted in Oc to ber381.
Con struc tion of the health in sur ance sys tem
The be gin ning of 1999 (the con struc tion of the health in sur ance sys tem, re spec tively) was marked by the scan dal on the con sti tu tion of the Na tional Health In sur ance Fund382. The“ap ple of con ten tion” be tween the rep re sen ta tives of the trade un ions and the rep re sen ta tivesof the em ploy ers, on one hand, and the rep re sen ta tives of the state and the mu nic i pal i ties, onthe other hand, con sisted in the quo tas in the General Assembly of the NHIF.
The other topic ex ten sively cov ered in the press, which con tin ued to be dis cussed in theyears to fol low, con cerned the con struc tion of the NHIF or gani sa tional struc ture and fa cil i -ties. Dur ing the first half of 1999, the press re ported mainly the ap point ment of staff, the pub li -ca tions emphasised the num ber of the peo ple who were go ing to be em ployed at the NHIF andit was an nounced that its ad min is tra tion would in crease grad u ally to 4 500 peo ple383; in thesec ond half of the year, the re ports were about the build ing of the pre mises with a pri or ity onthe con struc tion of mod ern build ings, pur chas ing of new lux ury au to mo biles, com puter equip -ment and fur ni ture384. A large num ber of the pub li ca tions criti cised the con sid er able ad min is -tra tive costs and im plied that the money col lected from the health in sur ance in stal ments werenot uti lised to its pur pose. The Fund coun tered with the ar gu ment that that was money from the state bud get. In a state ment, Min is ter Boyadjiev de clared that “the healthcare re form has al -ready started since a lot of ex penses are made for the NHIF – for the pro vi sion of build ings, in -for ma tion sys tem as well as in stal ments which are col lected in the fund.”385 Many of thear ti cles in 2000 com mented on the fi nan cial means spent for re con struc tion, the pur chas ing of build ings, ve hi cles and equip ment for the of fices of the NHIF and the RHIFs386. Ac cu sa tions could also be come across about abuse and ir reg u lar uti li sa tion of fund ing. The dep uty fromthe PGDL Dr. K. Marangozov pro posed the for ma tion of a tem po rary par lia men tary com mis -sion to study the ex pe di ency of the uti lised fund ing387. In the mid dle of May, the Chair man ofthe “Anti-ma fia” Par lia men tary com mis sion Yordan Sokolov de clared that sig nals had beenre ceived that “huge amounts have been spend with out jus ti fi ca tion” and the Com mis sion wasstart ing an in spec tion of the signed con tracts and the ex penses made by the NHIF and theNII388. Ac cord ing to the con clu sions of the Com mis sion’s re port, the fi nanc ing was spent jus ti -fi ably. The only re mark ad dressed to the NHIF re garded the sub mis sion of in for ma tion aboutthe ex pen di ture made on a reg u lar ba sis to the Min is try of Fi nance389.
Al though the Par lia men tary Com mis sion did not es tab lish breaches, the com ments aboutthe ex penses made in 2000 con tin ued in the press to gether with the com ments on the fi nanc ing
117
Stages and evo lu tion of the healthcare re form in Bul garia
381 24 chasa daily, Issue ¹ 14 and Issue ¹ 22 from 1999382 24 chasa daily, Issue ¹ 5 from 8.01.1999; Kapital weekly from 9-15.01.1999 and from 16-22.01.1999;
Standart daily from 7.01.1999 and from 8.01.1999383 24 chasa daily, Issue ¹ 89 from 2.04.1999; Standart daily from 30.04.1999384 Trud daily from 27.09.1999; 24 chasa daily, Issue ¹ 248 from 11.09.1999; Kapital weekly, Issue ¹ 31 from
7-13.08.1999; Duma daily, Issue ¹ 174 from 1999385 Democracia daily from 13.10.1999386 24 chasa daily, Issue ¹ 83 from 28.03.2000 and Issue ¹ 93 from 7.04.2000; Duma daily, Issue ¹ 84 from
11.04.2000, Issue ¹ 88 from 15.04.2000, Issue ¹ 110 from 12.05.2000, Issue ¹ 121 from 26.05.2000 andIssue ¹ 144 from 22.06.2000
387 Duma daily, Issue ¹ 68 from 23.03.2000388 24 chasa daily, Issue ¹ 126 from 12.05.2000 and Issue ¹ 127 from 13.05.2000389 24 chasa daily, Issue ¹ 252 from 2000
for re con struc tion, pur chase of equip ment and busi ness trips en vis aged in the pro ject for bud -get 2001, ac com pa nied by facts prov ing the grave fi nan cial con di tion of the hos pi tals390. Thede ci sion of the met ro pol i tan Mayor Stefan Sofianski to quit the Ex ec u tive board of the NHIFaf ter the adop tion of the re port on the bud get for 2000 also called for com ments. Ac cord ing toSofiyanski “the healthcare re form is go ing well” and his as sis tance was not needed anymore391. A pub li ca tion of the “Duma” news pa per from the be gin ning of Sep tem ber quoted astate ment made by Evgeni Dushkov who was a mem ber of the Con trol Body of the NHIF andwho claimed that the So fia City Pros e cut ing Mag is tracy was ap proached on the oc ca sion of the signed con tracts for the de liv ery of com put ers and equip ment392.
At the same time, in an ar ti cle in the “24 chasa” the for mer Min is ter of Fi nance StoyanAlexandrov warned about pos si ble abuse and frauds by phy si cians, lack of con trol andpres ence of schemes for “drain ing of the NHIF” 393. A sim i lar opin ion was also shared bythe Re gional Un ion of Phy si cians at the UBP in Ruse, ac cord ing to whom a prob lem wouldarise for lack of a data base for the peo ple with health in sur ance394. Sev eral months later, in for -ma tion ap peared about am bu la tory forms sub mit ted to the RHIF for fic ti tious ex am i na tionsmade by gen eral prac ti tio ners, reg is tered ma nip u la tions which had not been per formed, fakedlet ters of re fer ral395. In 2001, in the “Duma” news pa per, a se ries of short pieces of in for ma tioncame from var i ous cit ies through out the coun try, re port ing in fringe ments made by fam ily phy -si cians and fines im posed by the Fund to them396.
Out side the pub li ca tions stress ing the im por tance of the vol un tary health in sur ance forthe de vel op ment of the sys tem, the ar ti cles deal ing with what ex actly was be ing done on the is -sue were scarce. In March 1999, it was an nounced that the Con fed er a tion of the In de pend entTrade Un ions in Bul garia was con sti tut ing a vol un tary health in sur ance com pany397, in Junethe MH stated to ad mit ap pli ca tions for li cens ing of pri vate health in sur ance funds398, and inAu gust, it was re ported that the Min is try of De fence and the State In sur ance In sti tute (SII) or -gan ised a health fund for mil i tar ies, of fi cers and ser geants399.
The other topic in the fo cus of the press at ten tion in re la tion to the NHIF dealt with thecol lec tion of the health in sur ance in stal ments and the NHIF bud get. The me dia cov eredcom pre hen sively the be gin ning of the pro cess of the col lec tion of health in sur ance in stal mentsas well as the size of the in stal ments400. The ques tions of the health in sur ance in stal ments forthe dif fer ent cat e go ries of the peo ple with oblig a tory health in sur an ces found broad cov er age
118
390 24 chasa daily, Issue ¹ 176 and Issue ¹ 283 from 2000; Standart daily from 14.10.2000, from 25.10.2000and from 28.12.2000; Duma daily, Issue ¹ 132 from 8.06.2000, Issue ¹ 141 from 19.06.2000, Issue ¹ 152from 1.07.2000, Issue ¹ 252 from 28.10.2000, Issue ¹ 274 from 23.11.2000 and Issue ¹ 276 from25.11.2000; Kapital weekly, Issue ¹ 42 from 21-27.11.2000
391 24 chasa daily, Issue ¹ 176 from 1.07.2000 and Issue ¹ 178 from 3.07.2000; Democracia daily from 18.10.2000392 Duma daily, Issue ¹ 203 from 2000393 24 chasa daily, Issue ¹ 179 from 4.07.2000394 Duma daily, Issue ¹ 96 from 2000395 24 chasa daily, Issue ¹ 265 from 2000; Standart daily from 4.09.2000 and from 13.09.2000; Duma daily,
Issue ¹ 235 from 9.10.2000 and Issue ¹ 252 from 28.10.2000396 Duma daily, Issue ¹ 8 from 11.01.2001397 Democracia daily from 10.03.1999398 Trud daily from 12.06.1999399 Democracia daily from 12.08.1999400 24 chasa daily, Issue ¹ 89 from 2.04.1999 and Issue ¹ 176 from 1.07.1999; Democracia daily from
1.07.1999; Standart daily from 7.01.1999
in the press401 along with the dead lines for their pay ment, the sub mis sion of dec la ra tions in re -la tion to the health in sur ance and the en vis aged fines in case they were not ob served402.
The prob lems of the in stal ments col lec tion were also in the fo cus of the press at ten tion403,and in this re spect, the dis par i ties in the po si tions of the NHIF and the NII were also fea tured.While the then Di rec tor of the NHIF Dr. I. Semerdjiev claimed that only half of the due in stal -ments had been col lected404, the NII de clared 100% collectibility of the in stal ments for July, Au -gust and Sep tem ber 1999405. Ac cord ing to CL “Podkrepa”, the money for health in sur ancewould fin ish within the first 6 months of the in tro duc tion of the health in sur ance sys tem406.
Re gard ing the NHIF bud get for 2000, it was re ported that it was formed on the ba sis of75% collectibility of the in stal ments and, be cause of a scan dal which was un fold ing its con sid -er ation was post poned by the gov ern ment for fur ther clar i fi ca tion407. A lit tle later, Min is terBoyadjiev with drew the draft bud get for 2000 which he had de pos ited him self, with the ar gu -ment that “the draft bud get is based on a dan ger ous disbalance be tween the in come of the fam -ily phy si cians, the spe cial ists and the hos pi tal doc tors”, one group of whom be ing ex pected tore ceive three times more than the rest and this “cre ated ten sion among the var i ous branches”.De spite these re marks, how ever, the Cab i net ap proved the NHIF draft bud get with out any sig -nif i cant cor rec tions408.
The prob lem with the un in sured per sons and the in stal ments collectibility also wors -ened409. At the be gin ning of the year, in the “Duma” daily, a piece of in for ma tion was pub -lished sub mit ted by the NII, ac cord ing to which ap prox i mately 1.2 mil lion peo ple were notin sured for the pe riod be tween July 1st and De cem ber 31st 1999 and the size of the un col lectedin sur an ces amounted to around 30 mil lion BGN410. Ac cord ing to the in for ma tion pre sented inthe press, the most un dis ci plined in pay ing their health in sur ance were the mu nic i pal i ties, thefarm ers and workers without a full-time labour contract.
In 2000, the ques tion was once again raised about the size of the health in sur ance in -stal ment. The MH sug gested that it was raised from 6% to 12% of the in sur ance in come incom pli ance with the ini tial ac counts dur ing the dis cus sion of the LHI in 1997. The mo tive,with which the in crease of the pre mium was pro posed, was linked to the in clu sion of hos pi talcare in the health in sur ance in 2001411. In an ar ti cle in the “Standart” daily, the Vice Chair man
119
Stages and evo lu tion of the healthcare re form in Bul garia
401 24 chasa daily, Issue ¹ 204 and ¹ 248 from 1999; Kapital weekly from 3-9.07.1999 , from 10-16.07.1999, from17-23.07.1999, Issue ¹ 20 from 24-30.07.1999, Issue ¹ 30 from 31.07.-6.08.1999 and from 21-27.08.1999.;Democracia daily from 2.08.1999 and from 27.11.1999; Trud daily from 1.07.1999 and from 10.08.1999; Duma daily, Issue ¹ 142 from 28.07.1999 and Issue ¹143 from 29.07.1999; Standart daily from 7.08.1999 and from 10.08.1999
402 24 chasa daily, Issue ¹ 236 from 1999; Democracia daily from 14.08.1999, from 20.08.1999, from23.08.1999 and Issue ¹ 231 from 1.09.1999; Standart daily from 8.07.1999, from 31.07.1999 and from3.08.1999; Duma daily, Issue ¹ 199 from 5.10.1999
403 Democracia daily from 14.01.1999; 24 chasa daily, Issue ¹ 129 from 14.05.1999 and Issue ¹ 212 from 6.08.1999404 24 chasa daily, Issue ¹ 286 from 1999405 Democracia daily from 27.10.1999; Kapital weekly from 30.10.-5.11.1999406 24 chasa daily, Issue ¹ 152 from 1999407 Democracia daily from 23.10.1999; Duma daily, Issue ¹ 242 from 24.11.1999408 Kapital weekly from 27.11.–3.12.1999; Democracia daily from 19.11.1999409 24 chasa daily, Issue ¹ 235 from 29.08.2000; Standart daily from 11.05.2000, Issue ¹ 2755 from
14.08.2000, Issue ¹ 2770 from 31.08.2000 and from 25.10.2000 ; Duma daily, Issue ¹ 90, Issue ¹ 136from 13.06.2000 and Issue ¹ 261 from 8.11.2000
410 Duma daily, Issue ¹ 34 from 2000411 24 chasa daily, Issue ¹ 138 from 24.05.2000; â. “Òðóä”, Issue ¹ 138 from 24.05.2000 Standart daily from
26.05.2000; Democracia daily from 2.03.2000 and from 28.05.2000.; Duma daily, Issue ¹ 120 from 2000
of the UBP Assoc. Prof. Dr. Mi lan Milanov made an at tempt to de fend his the sis, ac cord ing towhich hos pi tal care “can not be en sured un der con di tions of a 6%-in stall ment”412. The Min is try of Fi nance and the Min is try of La bour and So cial Care did not agree be cause they con sid eredthat this would in crease the tax bur den on the work ing peo ple and the em ploy ers413. The dep u -ties from the op po si tion pro tested sharply against the pro posal as, in their opin ion, “the tax bur -den for the Bul gar ian cit i zens is be com ing ab so lutely in tol er a ble” (Dr. K. Marangozov), “thein crease would be cyn i cal and would ex ceed all lim its” (Emiliya Maslarova) and showed that“the work has not been done“(Ivan Todorov)414. For some months un til Oc to ber no pub li ca -tions ap peared on this is sue, when in for ma tion was an nounced that the amount of the health in -sur ance in stal ments re mained un changed415.
The sec ond es sen tial topic con cern ing the con struc tion of the health in sur ance sys tem, towhich the me dia fo cused at ten tion, was con nected to the pro vid ers of med i cal and den talcare. The pub li ca tions var ied in top ics and dealt with their reg is tra tion ac cord ing to the Com -mer cial Law, the nec es sary num ber of pa tients who would have to be en rolled in the pa tients’lists, whether they would have the right to pri vate prac tice or not, what re quire ments (ma te rialand or gani sa tional) their prac tices would have to meet, what in come they would be ex pected to receive and what activities they would perform.
In July, the Chair man of the UBP Dr. D. Ignatov de clared that the gen eral prac ti tio ners were not clear how to be come GPs and that they did not have the in cen tive to quit the poly clin ics416. Inre ply, Dr. Semerdjiev in formed that the gen eral prac ti tio ners had to reg is ter ac cord ing to theCom mer cial Law and in di cated some other or gani sa tional pre-con di tions which they had to meet 417. In sev eral pub li ca tions, he pointed out that a fam ily phy si cian had to hire a nurse, a sep a rateof fice, med i cal equip ment for pri mary in ves ti ga tions, a mini-lab o ra tory, etc. and that they wouldnot have the right of pri vate prac tice418. A pub li ca tion in the “24 chasa” 419in formed that the gen -eral prac ti tio ners were en ti tled to loans, guar an teed by the NHIF bud get for the pur chas ing ofequip ment and that the 14.5 mil lion US dol lars loan from the WB was in tended for the equip -ment of GPs of fices in the vil lages, the small towns and the moun tain re gions.
The num ber of pa tients to be reg is tered to one gen eral prac ti tio ner or den tist420, was also dis cussed; from the pro fes sional den tists’ or gani sa tion in formed that they were pre pared topro test be cause of the “un at tain able norm of 1 500 pa tients per den tist which ad min is tra tivelycut the den tists in So fia to half”421.
It is note wor thy that in the pub li ca tions from that pe riod, the more com mon name was“fam ily doc tor” and not “gen eral prac ti tio ner” or “per sonal doc tor”. Ob vi ously, this had its ex -pla na tion and was ac counted for by the fact that the press in formed that one phy si cian or den -tist was cho sen for the whole fam ily, a phy si cian and den tist, re spec tively. The choice of a
120
412 Standart daily, Issue ¹ 2686 from 25.05.2000413 Standart daily, Issue ¹ 2687 from 26.05.2000; Democracia daily from 26.05.2000414 Duma daily, Issue ¹ 121 from 26.05.2000415 24 chasa daily, Issue ¹ 202 from 2000; Trud daily from 6.10.2000; Duma daily, Issue ¹ 233 from 6.10.2000416 24 chasa daily, Issue ¹ 199 from 24.07.1999417 24 chasa daily, Issue ¹ 213 from 7.08.1999418 Democracia daily from 20.02.1999 and from 7.09.1999; Trud daily from 6.05.1999; 24 chasa daily, Issue ¹
199, Issue ¹ 213 and Issue ¹ 245 from 1999; Standart daily from 7.09.1999419 24 chasa daily, Issue ¹ 130 from 15.05.1999420 Trud daily from 19.08.1999; Duma daily, Issue ¹ 81 from 1999421 24 chasa daily, Issue ¹ 225 from 18.09.1999
phy si cian and a den tist was com mented in the press422 along with the an nounce ments aboutthe con tent and pur pose of the health in sur ance books and the dead lines in which they wereex pected to be given to the health in sured per sons423. The MH pre pared a draft reg u la tion ofthe out pa tients’ care and ac cess to the healthcare es tab lish ments, ac cord ing to which pa tientswould be treated in a hos pi tal of their own choice on the ter ri tory of the dis trict in which theyre side, and if the pa tients vis ited a spe cial ist with out a let ter of re fer ral, they had to pay for thepro vided ser vices424.
Over the course of 1999, a se ries of pub li ca tions were de voted to the in come of the “fam -ily” phy si cians which they were ex pected to re ceive af ter the start of the health in sur ance sys -tem425; in some of the pub li ca tions, the at ten tion was drawn to the fact that the spe cial ists bothin out pa tients’ and in pa tients’ care were ex pected to re ceive con sid er ably lower in come thanthe general practitioners.
For yet an other time in 2000, the press cov ered ex ten sively the choice of a gen eral prac -ti tio ner (in the greater part of the pub li ca tion called “fam ily” doc tor or phy si cian). The ar ti cles in formed mainly about the dead lines and the pro ce dure of the choice, the min i mum pack ageof med i cal ser vices to be per formed by the GPs, the man ner of pay ment for the GP’s la bour,the max i mum num ber of served pa tients, the oblig a tory pro phy lac tic check-ups that had to beper formed, the pa tients’ pos si bil ity to be treated by an other GP against pay ment, the num ber of the reg is tered GP prac tices, etc. 426
A num ber of pub li ca tions sig nalled about an in suf fi cient num ber of reg is tered gen eralprac ti tio ners in var i ous cit ies and vil lages across the coun try and the lack of forms for thechoice, re fer rals to spe cial ists, etc. 427In or der to at tract phy si cians to work in spe cific re gionsof the coun try, it was en vis aged that with the sup port of a loan from the WB, 1 000 prac ticeshad to be equipped, each of which to be fully equipped for the amount of 10 000 US dol lars428.At a work ing meet ing on the is sues of emer gency med i cal care, views were shared that the in -suf fi cient num ber of gen eral prac ti tio ners, es pe cially in the smaller in hab ited ar eas, wouldbring about the shat ter ing of the emer gency med i cal care which had to take over the med i caltreat ment of the pa tients429.
121
Stages and evo lu tion of the healthcare re form in Bul garia
422 Democracia daily from 2.02.1999, from 29.10.1999 and from 24.12.1999; 24 chasa daily, Issue ¹ 169 andIssue ¹ 189 from 1999
423 24 chasa daily, Issue ¹ 141 from 27.05.1999 and Issue ¹ 176 from 1.07.1999; Kapital weekly, Issue ¹ 31from 7-13.08.1999; Democracia daily from 1.10.1999; Trud daily from 28.02.1999.; Duma daily, Issue ¹189 from 23.09.1999
424 24 chasa daily, Issue ¹ 226 from 20.08.1999; Kapital weekly, Issue ¹ 41 from 16-22.10.1999425 Democracia daily from 5.02.1999 and from 26.11.1999; Trud daily from 5.02.1999 and from 14.11.1999; 24
chasa daily, Issue ¹ 57, Issue ¹ 89 from 2.04.1999, Issue ¹ 130 from 15.05.1999, Issue ¹ 199 from24.07.1999 and Issue ¹ 326 from 1999; Standart daily, Issue ¹ 2293 from 20.02.1999, Issue ¹ 2334 from2.04.1999 and from 7.09.1999
426 24 chasa daily, Issue ¹ 40, Issue ¹ 44, Issue ¹ 54, Issue ¹ 86 and Issue ¹ 107 from 2000; Trud daily from 9.03.2000, from 23.04.2000 and from 1.07.2000; Democracia daily from 13.01.2000, from 8.02.2000, from19.02.2000, from 10.05.2000, from 12.05.2000, from 16.05.2000 and from 8.08.2000; Duma daily, Issue ¹12, Duma daily, Issue ¹ 13,, Issue ¹ 34, Issue ¹ 44, Issue ¹, Issue ¹ 85, Issue ¹ 134, Issue ¹ 199 andIssue ¹ 253 from 2000; Kapital weekly, Issue ¹ 2 from 15-21.01.2000 and Issue ¹ 23 from 10-16.06.2000
427 24 chasa daily, Issue ¹ 59 and Issue ¹ 176 from 2000.; Standart daily from 2.03.2000, from 15.07.2000 and from 16.08.2000; Democracia daily from 1.03.2000 and from 9.10.2000; Duma daily, Issue ¹ 82 from8.04.2000, Issue ¹ from 10.06.2000, Issue ¹ 144 from 22.07.2000 and Issue ¹ 152 from 1.07.2000
428 Democracia daily from 17.03.2000429 Democracia daily from 19.03.2000; Duma daily, Issue ¹ 82 from 8.04.2000
Views were ex pressed that soon the ma jor ity of the gen eral prac ti tio ners would notwith stand fi nan cially and would ter mi nate their ac tiv i ties430. In var i ous ar ti cles along withother news and com ments, sig nals ap peared about some un law ful charges col lected from thepa tients and breaches of the con tracts signed with the RHIF431.
In 1999, the prep a ra tion for the Na tional Frame work Agree ment 2000 started and the ne -go ti a tions be gan for its sign ing432, both ac com pa nied by dis par i ties be tween the main par tic i -pants in the pro cess. In the “Democracia” news pa per433, it was an nounced that the UBP mightnot sign the NFA, un less it re ceived a ready pro ject from the NHIF within 10 days. In Oc to berthe Chair man of the UBP and Dep uty from the 38th Na tional As sem bly Dr. Ignatov de clared:“The Fund ex hib its a trend to im pose its opin ion on the med ics and is al ready try ing to act as ahealthcare min is try. The UBP, how ever, will not al low this to hap pen… The UBP has not yetsigned the frame work agree ment with the Fund… Even though the Fund is try ing to ban thepri vate prac tice of the gen eral prac ti tio ners with whom it is go ing to con clude con tracts ...”434
In the mean time, in for ma tion was pub lished in the me dia about the num ber of phy si cians,den tists and the phar ma cies, with which the Fund was go ing to sign con tracts435.
The sign ing of the first Na tional Frame work Agree ment was pre ceded by heated dis -cus sions and com ments re lated to the pro vi sions spec i fied in it. Part of the dep u ties of the UBPAs sem bly dis agreed with the prices of the ser vices and the con sumer’s fees, which were en vis -aged in the draft NFA and put for ward for dis cus sion, the pro pos als be ing for the prices to bein creased around 4 times or for the ser vices paid by the NHIF to be re duced. Ac cord ing to I.Semerdjiev, it was not pos si ble to ac cept all the claims since oth er wise the health in sur ancewould hit 48% of the in come436. In spite of the ob jec tion to the pro posed pro ject, the UBP As -sem bly sup ported the NFA, but pro claimed it self against the re quire ments for a min i mumnum ber of en rolled pa tients per gen eral prac ti tio ner and in sisted that this re quire ment wasaban doned un til the fol low ing year and the gra tis pe riod for equip ping the of fices was ex -tended to two years437. Im me di ately af ter this de ci sion was taken, opin ions were ex pressed bysome dep u ties that the UBP was “forced to ac cept the terms,” and the prices de ter mined by theNFA were too low and would stim u late cor rup tion438.
At the Con gress of the Un ion of Den tists in Bul garia, con vened to dis cuss the draft forthe NFA, the par tic i pants also pro tested against parts in cluded in it. The main ob jec tions hadto do with the fi nance en vis aged in the bud get of the NHIF for den tal care (17 mil lion BGN)and the idea that the den tists were paid for their work ing hours and not for their per formed ac -tiv i ties439. The Con gress took the de ci sion to sup port the NFA with the pro posal to change theway of pay ment for den tal care440.
122
430 Standart daily from 15.07.2000; Duma daily, Issue ¹ 33 from 10.02.2000431 Standart daily from 16.08.2000, from 4.09.2000, from 13.09.2000 and from 1.12.2000; Duma daily, Issue ¹
199 îfrom 25.08.2000, Issue ¹ 261 from 8.11.2000 Issue ¹ 276 from 25.11.2000432 Kapital weekly, Issue ¹ 31 from 7-13.08.1999; Democracia daily from 16.10.1999433 Democracia daily from 25.09.1999434 Standart daily from 19.10.1999435 Standart daily from 15.10.1999; Trud daily from 14.11.1999 and from 19.12.1999; Duma daily, Issue ¹ 81 from 1999436 24 chasa daily, Issue ¹ 111 from 25.04.2000; Standart daily from 25.04.2000; Democracia daily from
25.04.2000; Duma daily, Issue ¹ 96 from 25.04.2000437 24 chasa daily, Issue ¹ 112 from 26.04.2000; Trud daily from 26.04.2000; Democracia daily from 26.04.2000438 24 chasa daily, Issue ¹ 112 from 26.04.2000439 Democracia daily from 22.04.2000 Duma daily, Issue ¹ 94 from 22.04.2000 and Issue ¹ 95 from 23.04.2000440 Democracia daily from 23.04.2000
About two months later, the gen eral prac ti tio ners in the coun try de clared that they wouldnot work with the NHIF and pro tested against the 24-hour shifts and the 10-hour work ing dayas well as against the for mi da ble vol ume of the re quired doc u men ta tion. In re sponse to thesean nounce ments the Di rec tor of the NHIF Dr. Boiko Penkov de clared that “among the doc torsthere are groups for ex ert ing pres sure, work ing against the re form”441. Sim i lar ob jec tions werealso di rected to the draft NFA for 2001 sup ported by the UBP, as a re sult of which the gen eralprac ti tio ners from nine dis tricts in the coun try con sti tuted the Na tional As so ci a tion of the Gen -eral Prac ti tio ners which de manded to be come a party to the sign ing of the agree ment. TheUBP, how ever, did not ac knowl edge the le git i macy of the newly formed as so ci a tion442.
At the end of the year, the pro posed draft NFA for 2001 once again caused re sent ment.The Con gress of the UDB voted a de ci sion, ac cord ing to which the UDB would not sign thenew Agree ment. The dis puted terms of the agree ment were re lated to the pack age of ser vicesfor chil dren, in which ad o les cents be tween 14 and 18 were also in cluded. The Un ion con sid -ered that the in crease of the age limit “was not fi nan cially se cured and would hin der the ac cessto the fam ily den tist which was dif fi cult any way” (view point of the Ex ec u tive Board of theUDB443). The del e gates of the Con gress also de clared them selves against the de ter mi na tion ofpri or ity groups in the oblig a tory in sur ance which, ac cord ing to them, “con tra dicts the Eu ro -pean prac tice for pur pose ful bud get ing of pri or ity groups from the pop u la tion” and “in fringeson the prin ci ples of eq uity, equal ac cess and sol i dar ity of the health in sured per sons.” TheChair man of the UDB Dr. Zhivko Mihailov stated that those, who did not com ply with the de -ci sion and signed in di vid ual con tracts with the RHIF, would be sanc tioned by ter mi nat ing their rights to prac tice for a pe riod of 2 years444.
At its Ex traor di nary As sem bly, the UBP backed the NFA for 2001, adopt ing pro pos alsre lated to the de crease of the vol ume of the re quired doc u men ta tion, the dif fer en ti a tion of theex am i na tion forms of the chron i cally ill from the rest of the pa tients, ex ten sion of the healthpri or i ties, etc. 445. In its turn, the UDB also “ex erted pres sure” upon the NHIF by de clar ing thatthey would not like to sign the NFA with the ar gu ment that the den tists would re ceive lessmoney for more work (be cause of the ex ten sion of the pack age for the pae di at ric den tal ser -vices) 446. In spite of the dis put able mo ments at the end of the year, the NFA for 2001 was sup -ported by all the rep re sen ta tives of the NHIF, UBP and UDB, the UDB suc ceed ing to ne go ti ate higher prices for some den tal ser vices447. At the be gin ning of 2001, the phy si cians pro testedthat un like the NFA for 2001, the an nexes to it had not been pub lished in the State Ga zette yetand this im peded their work448.
Al though a great num ber of pub li ca tions were de voted to the pack ages of med i cal andden tal ser vices, which had to be pro vided by gen eral prac ti tio ners and den tists, re spec -
123
Stages and evo lu tion of the healthcare re form in Bul garia
441 24 chasa daily, Issue ¹ 164 from 19.06.2000; Duma daily, Issue ¹ 136 from 13.06.2000 and Issue ¹ 141from 19.06.2000
442 Standart daily, Issue ¹ 2873 from 18.12.2000443 Democracia daily from 12.12.2000 444 24 chasa daily, Issue ¹ 332 from 6.12.2000, Issue ¹ 334 from 8.12.2000 and Issue ¹ 341 from 15.12.2000;
Standart daily from 8.12.2000 and from 15.12.2000; Democracia daily from 8.12.2000 and from 15.12.2000;Duma daily, Issue ¹ 278, Issue ¹ 287 and Issue ¹ 293 from 2000; Kapital weekly from 2-8.12.2000
445 Democracia daily from 5.12.2000; Duma daily, Issue ¹ 247 and Issue ¹ 284 from 2000446 Kapital weekly from 23.12.2000–5.01.2001447 Standart daily, Issue ¹ 2878 from 23.12.2000; Democracia daily from 23.12.2000; Kapital weekly from
23.12.2000–5.01.2001448 Trud daily, Issue ¹ 4 from 4.01.2001
tively449, it did not be come clear from them what ser vices (and med i ca tions) ex actly the pa -tients with an oblig a tory health in sur ance would be en ti tled to. Some of the pub li ca tions evenplaced the em pha sis on the fact that “it is not clear what ex actly the Fund is se cur ing”450. It wasan nounced that “apart from the or di nary prac tice, the pack age also in cludes re quire ments forthe gen eral prac ti tio ners for spe cial ised knowl edge – from rou tine check-ups of the health sta -tus to com pli cated in stru men tal in ves ti ga tions”451. Re gard ing the pack age of den tal care, theden tists claimed that “the health in sur ance will not cover the costs for the den tist and the pa -tients will have to pay ad di tion ally”452 and in sisted that they them selves worked out the list ofthe ser vices, for which the Fund will pay to them453.
In 2000, the com ments on this is sue re ferred to the un clear is sues of the per for mance ofthe min i mum pack age of med i cal ser vices by the GPs and the pay ment454, cases of force fulreg is tra tion of pa tients or re fusal of their en rol ment455; the huge amount of doc u men ta tion kept by the gen eral prac ti tio ners456. In an ar ti cle in the “Kapital” weekly, the the sis was de vel opedthat the cit i zens were in suf fi ciently in formed, the pa tients’ choice was re stricted by the region -ali sa tion, and the pa tients pointed out the lack of “cri te ria for a choice of a fam ily phy si cian”457as the most se ri ous prob lem. To sup port this state ment, in the next is sue of the news pa per,data were pre sented from a so cio log i cal sur vey con ducted at the be gin ning of the year by “Al -pha re search” agency, ac cord ing to which 50% of the re spon dents were not in formed as tohow and among which phy si cians they could make a choice, and 35% had just a most gen eralidea, but were not yet ori ented whom to pre fer458.
In the first half of 2001, the me dia an nounced changes in the re gime of hos pi tal treat -ment from July 1st 2001. The at ten tion was con cen trated on the con sum ers’ fee amount ing to2% of the min i mum work ing sal ary, the max i mum of a 20-day stay per year and the re fer ral ofpa tients for hos pi tal treat ment by a spe cial ist from the out pa tients’ care and in some cases bythe GP459. At the end of March 2001, the hos pi tal fi nanc ing by the NHIF was still un clear, e.g.for what ac tiv i ties how much fund ing they would re ceive460.
In 1999, the at ten tion to pa tients and, more spe cif i cally to their rights, was rather neg li -gi ble461. At the be gin ning of 1999, in for ma tion was pub lished that the MH was pre par ing aLaw on the Pa tient, which ac cord ing to the Vice Min is ter Dr. I. Semerdjiev, had to be sub mit -
124
449 Standart daily, Issue ¹ 2291 from 18.02.1999 and from 25.09.1999; 24 chasa daily, Issue ¹ 129 from 14.05.1999,Issue ¹ 176 from 1.07.1999 and Issue ¹ 199 from 24.07.1999.; Democracia daily from 15.06.1999 and Issue ¹ 314from 29.11.1999; Duma daily, Issue ¹ 212 from 20.10.1999; Trud daily from 27.09.1999
450 Duma daily, Issue ¹ 212 from 20.10.1999451 Democracia daily from 20.02.1999452 Standart daily from 20.01.1999.; Democracia daily, Issue ¹ 147 from 3.08.1999, Issue ¹ 148 from
4.08.1999 and from 28.09.1999453 Trud daily from 14.11.1999454 Trud daily from 14.11.1999455 24 chasa daily, Issue ¹ 123 from 9.05.2000; Democracia daily from 10.06.2000; Duma daily, Issue ¹ 74
from 30.03.2000, Issue ¹ 130 from 6.06.2000 and Issue ¹ 134 from 10.06.2000456 Standart daily from 15.07.2000; Duma daily, Issue ¹ 82 from 8.04.2000457 Kapital weekly, Issue ¹ 9 from 3-10.03.2000458 Kapital weekly, Issue ¹ 10 from 11-17.03.2000459 24 chasa daily, Issue ¹ 40 from 9.02.2001460 Kapital weekly, Issue ¹ 13 from 31.03.2001461 Democracia daily from 18.01.1999, from 7.04.1999, from 25.06.1999 and from 20.10.1999; 24 chasa daily,
Issue ¹ 89 from 2.04.1999
ted for con sid er ation in the first half of the year462. Some what later, in April, the “24 chasa” re -ted for con sid er ation in the first half of the year462. Some what later, in April, the “24 chasa” re -ported about the Code of Pa tients’ Rights which was be ing worked out and was not go ing tobe a sep a rate law but part of the National Framework Agreement.
Un like in pre vi ous years, when the is sue of the pa tients’ rights was only sel dom dis -cussed, in 2001 the me dia pub lished data from so cio log i cal sur veys about their ob ser va tion.Ac cord ing to a so cio log i cal sur vey con ducted by the “In dex” foun da tion and the NHIF, therights of one third of the pa tients were vi o lated and 20% were not in formed in de tail about their rights463. The pub li ca tion pointed out that the main pa tients’ prob lems were re lated to theirfam ily phy si cians, who did not in form them about the check-ups and the drugs, the costs cov -ered by the Fund and re fused to make home vis its. A lit tle later, ac cord ing to an other sur veycon ducted by the “Vitosha re search” and pub lished in the “Democracia” news pa per, 90% ofthe cit i zens were sat is fied with their fam ily doc tors, one third con sid ered that the at ti tude to the pa tients had been im proved since the start of the re form, and 41% held the op po site opin ion.Ac cord ing to the data of the same sur vey, the phy si cians had even tu ally re ceived rec og ni tionand more than 40% ad mit ted that the re form had to go on464.
The start of the health in sur ance sys tem
One of the large top ics in 1999, dis cussed widely and caus ing nu mer ous de bates and con -flicts at the high est lev els of the healthcare sys tem, was the date on which the NHIF would start func tion ing, that is, the date of the start of the health in sur ance sys tem. This was the datewhich was called “the be gin ning of the healthcare re form” by both jour nal ists and pol i ti ciansab so lutely wrongly and mis lead ingly for the pub lic opin ion. In the sec ond half of 1999, pub li -ca tions be gan to be re leased, ac cord ing to which it was pos si ble that the health in sur ance sys -tem would not start from Jan u ary 1st 2000 as en vis aged by the LPH but later. The prob a bil ityto post pone the start of the health in sur ance sys tem was linked to the de layed loan from theWB, planned for the needs of the NHIF465. In Au gust, the Chair man of the UBP Dr. D. Ignatovan nounced that the WB re fused to en dorse a loan of 80 mil lion US dol lars (some pub li ca tionscite 60 and oth ers 100 mil lion) for the needs of the NHIF and for the equip ment of GPs’ of -fices466, in re sponse to which the Di rec tor of the NHIF Dr. I. Semerdjiev de clared that “ne go ti -a tions are un der way at the mo ment and all com ments are su per flu ous”467.
In an in ter view from Sep tem ber, Min is ter Boyadjiev said: “We are ready with our part ofthe re form, the NHIF and the Phy si cians’ Un ion only have to per suade the for eigner (au thors’note: the ex perts from the WB) that they are also ready… I am won der ing what shall we dowith the re form of the hos pi tal care which has to start in 2001 and I can not find an an swer…The fi nan cial ex perts have to tell us what to do and even tu ally the Coun cil of Min is ters willhave to make the de ci sion...”468.
For the “Demcracia” daily469, the Di rec tor of the NHIF Dr. I. Semerdjiev stated that the WB
125
Stages and evo lu tion of the healthcare re form in Bul garia
462 Democracia daily, Issue ¹ 14 from 18.01.1999463 Trud daily, Issue ¹ 80 from 21.03.2001464 Democracia daily from 30.03.2001465 24 chasa daily, Issue ¹ 269 from 1999; Trud daily from 27.09.1999; Standart daily, Issue ¹ 2488 from
1.10.1999466 Democracia daily from 19.08.1999; Standart daily, Issue ¹ 2452 from 19.08.1999467 Democracia daily from 19.08.1999468 Standart daily, Issue ¹29.09.1999 469 Democracia daily from 1.10.1999
would grant 60.6 mil lion US dol lars for the healthcare re form, of which 40.6 mil lion would be al -lo cated for the con struc tion of the NHIF in for ma tion sys tem and the re main ing 20 mil lion for there struc tur ing of the healthcare sys tem. In the mean time, while Min is ter Boyadjiev de clared thatthere was no rea son for “the healthcare re form to be slowed down” as the nec es sary nor ma tiveba sis had been es tab lished and the WB had agreed to pro cure the nec es sary fund ing for the firstin vest ments470, the fi nan cial min is ter Muravei Radev an nounced that the WB had pro posed tothe gov ern ment to post pone the “healthcare re form” 471. A lit tle later, the “24 chasa” daily in -formed that the gov ern ment would lead new ne go ti a tions that the WB granted fund ing for thestart of the Health In sur ance Fund, and re gard ing this, Prime Min is ter I. Kostov de clared: “TheWorld Bank in sists that the be gin ning of the healthcare re form is post poned; the gov ern ment will have to de cide what ex actly to do with out the sup port of the Bank.” The stand of the Head of theMis sion of the In ter na tional Mon e tary Fund in Bul garia was that “the gov ern ment will de cidewhen to start the healthcare re form; it has to be well pre pared.”472
On the oc ca sion of the dis cus sion on the “post pone ment of the start of the re form” forJuly 1st 2000, the “red” dep u ties (in op po si tion) in sisted on the ac cel er a tion of the in tro duc tionof the GPs from Jan u ary 1st 2000, the out pa tients’ spe cial ised care to be in tro duced from thebe gin ning of 2001, and the hos pi tal care – a year later473. Some pub li ca tions re vealed thepoliticization of this prob lem, a par tic u larly el o quent be ing the state ment of Min is ter P.Boyadjiev that “the healthcare re form is threat ened by a sab o tage, un less the UDF ob tains ama jor ity in the mu nic i pal coun cils” in the then forth com ing lo cal elec tions474.
All of the stud ied pub lished ma te ri als in formed about a de ci sion taken by the Coun cil ofMin is ters and voted by the NA, for the start of the health in sur ance sys tem to be post ponedfor six months from the one en vis aged in the LHI475, and Min is ter Boyadjiev ex plained that“this will en able the better NHIF or gani sa tion and in fra struc ture” and will en sure “a smoothtran si tion in the ac tiv i ties of the health in sur ance sys tem”476. Ac cord ing to him, the ar gu mentsfor the post pone ment were “fi nan cial, or gani sa tional and tech no log i cal but there is no mis takein the pre lim i nary ac counts.”477 A lit tle ear lier the Chair man of the NHIF Ex ec u tive Board andMayor of So fia Stefan Sofiyanski ex plained that the fi nan cial prob lems were due to the lowcollectibility of the in stal ments and the re main ing prob lems came from “or gani sa tional andtech no log i cal is sues re lated to the Fund and the ne ces sity to con tinue the re struc tur ing of theout pa tients’ and hos pi tal care.”478
In an in ter view for the “Kapital” weekly, the rep re sen ta tive of the WB for Bul gariaThomas O’Brian de clared that the WB sup ported the model of health in sur ance in Bul -garia479. How ever, this was not the at ti tude shared at lo cal level. In a num ber of jour nal esecom ments and in ter views with rep re sen ta tives of the op po si tion and the trade un ions, themodel of health in sur ance was sharply criti cised to gether with the changes made by the gov -
126
470 Democracia daily from 3.10.1999471 Democracia daily from 4.10.1999472 24 chasa daily, Issue ¹ 278 from 11.10.1999473 Duma daily, Issue ¹ 237 from 1999 474 Standart daily from 11.10.1999475 Standart daily from 11.10.1999476 Democracia daily from 18.11.1999477 Kapital weekly from 23-29.10.1999478 Democracia daily from 19.10.1999479 Kapital weekly from 23-29.10.1999
ern ment for its in tro duc tion480. Re gard less of the fact that a great part of the pub li ca tions were strongly po liti cised, with
pop u list state ments and un con struc tive crit i cism, they re vealed (and to a large ex tent formed)the pub lic at ti tudes to the on go ing changes at that stage. The Par lia men tary Group of the Dem -o cratic Left de manded the res ig na tions of the Pre mier Kostov and Dr. Ignatov for “the mess inhealthcare”481, and the “Promyana” Trade Un ion de manded the res ig na tion of Min is terBoyadjiev for the “hu mil i at ing pre dic a ment of 30 000 phy si cians and 8 000 000 pa tients” andfor “the fail ure of the healthcare re form”482. In two sub se quent pub li ca tions of the “Kapital”news pa per from Oc to ber, “the mis taken model of the com pul sory health in sur ance” was dis -cussed. To sup port this view, ar gu ments were raised about the mo nop o lis tic sta tus of theNHIF, the lack of clar ity about what the pa tients would get against their in stal ments and thestate ment that “the Fund will never raise so much money as the clerks can spend on cars, com -put ers and fur ni ture”483. The same pub li ca tion pointed out that the al ter na tive was to be foundin the vol un tary health in sur ance but “the rul ers pre fer to sup press the pri vate in sur ance ac tiv i -ties.” The Na tional In sur ance In sti tute de clared that “the guilt for the prob lems of the NHIFwas rooted in the mixed up logic of the law” (au thor’s note: the Law on Health In sur ance),which ac cord ing to them did not give in cen tives for the peo ple to pay their in stal ments484.
The gen eral eval u a tion of the on go ing healthcare re form cov ered in the press in 2000ranged from to tally pos i tive on be half of the rul ing par ties to ex tremely neg a tive on be half ofthe op po si tion. It is note wor thy that both the pos i tive and the neg a tive eval u a tions of the re -form were, with few ex cep tions, strongly po liti cised and fre quently lacked se ri ous andwell-grounded argumentation.
In an ar ti cle in the “Duma” daily, the Dep uty from the PGDL Dr. K. Marangozov in sis -tently criti cised the healthcare re form which was be ing car ried out. In his opin ion, the ma jorer ror was the main em pha sis on fi nanc ing and the “abuse of the mar ket mech a nisms” which“can func tion be tween the healthcare sys tem and the pro vid ers of med i cal ser vices only, but inno way can they ex ist be tween the sys tem and the con sum ers (the pa tients).” Ac cord ing to a se -ries of ob ser va tions and sta tis ti cal data on the health sta tus of the pop u la tion, the au thor drewthe con clu sion that “privatisation of the func tions of the state in healthcare by eco nomic sub -jects brought about an even more se vere slump in the na tion’s health as well as to a deep en ingcri sis in the sys tem of healthcare.” The ar ti cle criti cised even more sharply the leg is la tiveframe work of the re form and, namely, the Law on Health In sur ance which “de nies the pos si -bil i ties for so cial sol i dar ity and jus tice and is in ca pa ble of en sur ing collectibility of the in sur -ance in stal ments,” the Law on Healthcare Es tab lish ments and the privatisation en vis aged in itwhich would de prive “80% of the Bul gar i ans of med i cal care” and the Law on Pro fes sionalOr gani sa tions which “turned the civil or gani sa tions into state bod ies” and trans ferred on them“the over all re spon si bil ity for the peo ple’s health” 485.
A sim i lar the sis was also de vel oped by the Chair man of the Mu nic i pal Coun cil of the BSP in Montana Dr. Emil Konstantinov in an in ter view for the “Duma” news pa per who shared his
127
Stages and evo lu tion of the healthcare re form in Bul garia
480 Standart daily from 30.10.1999; Duma daily from 11.10.1999 and Issue ¹ 210 from 17.10.1999; Kapitalweekly from 9-15.10.1999
481 Duma daily, Issue ¹ 220 from 29.10.1999482 24 chasa daily, Issue ¹ 293 from 26.10.1999; Kapital weekly from 30.10.–5.11.1999483 Kapital weekly from 23-29.10.1999484 Kapital weekly from 30.10.–5.11.1999485 Duma daily, Issue ¹ 20 from 26.01.2000
mis giv ings about the pro fes sional qual i fi ca tion of the gen eral prac ti tio ners and the view that“the sys tem of the fam ily phy si cian will re sult in a col lapse in di ag nos ing”. The pro posal wasthat the start of the re form was post poned for at least six months in or der to al low the “fam ilydoc tors to ac quire the nec es sary qual i fi ca tion”486. Mean while, a pub li ca tion in the “24 chasa”daily in formed that dep u ties from the op po si tion in sisted that the healthcare re form was post -poned for six months with the ar gu ments that its start in June was not pre pared be cause of thegreat num ber of un clear ques tions487.
The “Kapital” pub lished data from a so cio log i cal sur vey con ducted at the be gin ning ofthe year by “Al pha Research” agency, ac cord ing to which 69% of the re spon dents eval u atedthe healthcare re form as nec es sary but in ad e quate and con fused, 17% were of the opin ion thatit was un nec es sary and only 9% de fined it as “nec es sary and ad e quate”. In the com ments onthe re sults, it was pointed out that the healthcare re form did not cor re spond to the “pop u la -tion’s health cul ture and hab its” man i fest ing “a low de gree of in ter est in its per sonal health”.The re sults from the sur vey in di cated that 71% of the in ter view ees vis ited their doc tor only incase of se vere in dis po si tion or sick ness and the same per cent age had not yet sought in for ma -tion about the new sys tem of health in sur ance488.
At a ple nary on the is sues of the healthcare re form, the Su preme Coun cil of the BSP pre -dicted a fi nan cial col lapse of the healthcare. In a re port de liv ered at the ple nary by the Dep uty Dr. K. Marangozov, it was stated that “the form of health in sur ance im posed by the rul ers im plied ato tal with drawal of the state from all the care for health and a trans fer of the con se quences to thephy si cians and the pa tients”. The rea sons for the pre dicted “bank ruptcy” of the healthcare sys -tem were re lated to the prob lems in out pa tients’ care and the in tro duc tion of the gen eral prac ti tio -ners, the se vere fi nan cial sta tus and the debts of the di ag nos tic and con sul ta tive cen tres as well asthe NFA which “is not fi nan cially en sured”. Ac cord ing to an other Dep uty from the BSP Prof. I.Zunzov, it would stim u late cor rup tion and un reg u lated pay ments in the sys tem. The at tempts ofthe for mer Min is ter of Healthcare Dr. M. Vitkova to di rect the de bates to ward the po lit i cal re -spon si bil ity of the PGDL caused stormy dis cus sions at the ple nary489.
In an in ter view for the “Democracia” news pa per, the Min is ter of Healthcare Dr.Semerdjiev stated that the gov ern ment had ful filled a great part of the un der taken com mit -ments for the prep a ra tion of the leg is la tive ba sis, the struc tural and the fi nan cial part of the re -form. In his opin ion “one of the main pri or i ties is the Eu ro pean in te gra tion” and re gard ing it, itwas nec es sary that “the Min is try un der takes more se ri ously the func tions for the pub lic healthpro tec tion, too”490.
Con cern ing the healthcare re form, in an in ter view for the “24 chasa” daily, StefanSofiyanski said: “Its logic is ab so lutely right, the fi nan cial frame work – se cured… Step by step,ev ery body was com mit ted to the prob lems of health in sur ance be cause they deemed that they are log i cally and eco nom i cally ap pro pri ately struc tured...”, and on the oc ca sion of the mis takes inthe pre pa ra tory pe riod, he stated: “Cer tainly, there are prob lems. I do not ex clude the pos si bil itythat in some places the cap i tal ex penses are more than what is nec es sary … There are, how ever,some fun da men tal is sues which are cru cial for the re form and on which we have to con cen trate.
128
486 Duma daily, Issue ¹ 142 from 20.06.2000487 24 chasa daily, Issue ¹ 159 from 2000488 Kapital weekly, Issue ¹10 from 11-17.03.2000489 Duma daily, Issue ¹ 153 from 3.07.2000490 Democracia daily from 11.01.2000
The most im por tant stages for the re struc tur ing have al ready been passed.”491
At the de liv ery of the re port on the Cab i net’s work, the Prime Min is ter I. Kostov in di cated that the start of the healthcare re form was “a great achieve ment” of the gov ern ment492.
A re view, pub lished in the “Democracia” news pa per from the be gin ning of 2001, was de -voted to the achieve ments of Ivan Kostov’s gov ern ment in the field of the healthcare re form493.The ar ti cle in formed that “the start of the healthcare re form turned into one of the most sig nif -i cant events for 2000” and the change had turned the phy si cians “from clerks into free peo ple”.The at ten tion was drawn to the fact that the change of the sys tem had started “one or two yearsbe fore the sa cral date of July 1st 2000 with the prep a ra tion of the leg is la tive foun da tion of the re -form” and the con tri bu tion be longed en tirely to Kostov’s gov ern ment and “the fa ther” of the re -form Dr. I. Semerdjiev. The mer its, which were stressed, in cluded the new way of fi nanc ing, thefact that “the treat ment of the cit i zens was fully cov ered by the Health In sur ance Fund”, the Na -tional Health Strat egy which had set “am bi tious goals” and “con crete tasks”, the se cur ing of 120mil lion US dol lars for in vest ment in the healthcare re form as a loan from the WB.
This as sess ment of the rul ing cir cles about the healthcare re form was not backed up by the trade un ions. The Pres i dent of the CL “Podkrepa” Dr. Konstantin Trenchev called thehealthcare re form a “healthcare deal”, emphasising the fi nan cial abuse in the im ple men ta tionof the soft ware and the hard ware of the NHIF and criticising the enor mous dis pro por tion in the pay ment of the work ers in the field of healthcare494.
In June, a pub li ca tion in the “Kapital” weekly in formed about the in ten tions of the ChiefPros e cu tor Nikola Filchev to raise ac cu sa tions against Min is ter Semerdjiev for a crim i nalbreach of trust, view ing the “im pres sive costs” of the Fund for of fices, equip ment, au to mo -biles, etc., made while I. Semerdjiev had been Di rec tor of the NHIF and which had been de -scribed in de tail in the press in 1999 and 2000, when ac cord ing to the ar ti cle “there were nocon se quences and in re turn, Semerdjiev be came Min is ter”495.
Stud ies of the pub lic opin ion polls
The main par tic i pants in the healthcare pro cess (healthcare) were the cit i zens and themed i cal spe cial ists. In one way or an other, they were im me di ately in volved and af fected by the healthcare re form. There fore, their at ti tudes (in fa vour or against) had a sig nif i cant im por tancefor the de vel op ment of the reform process.
Still in 1997-1998, that is, be fore the vot ing and the en force ment of the new leg is la tion,when there was by far clar ity about the pa ram e ters of the healthcare re form, and once again in1999, a com pre hen sive ques tion naire among man ag ers of the RHC, HEI, hos pi tals and na -tional cen tres, in di cated some char ac ter is tic fea tures of the re form pro cess such as (1) low, orrather “mo saic” (in spe cific as pects) aware ness of the scope, the ob jec tives and the course ofthe healthcare re form in 1997-1998. The aware ness im proved in 1999, but still, one third of the re spon dents were poorly in formed about the re form; (2) both opin ion polls re vealed a def i niteun cer tainty about the role and the po si tion of the man ag ers them selves in the pro cess of re -form; (3) the feel ing was ex pressed about the re form be ing con ducted some how out side of
129
Stages and evo lu tion of the healthcare re form in Bul garia
491 24 chasa daily, Issue ¹ 178 from 3.07.2000492 24 chasa daily, Issue ¹ 201 from 26.07.2000493 Democracia daily, Issue ¹10 from 13.01.2001494 Duma daily, Issue ¹ 19 from 24.01.2001495 Kapital weekly, Issue ¹ 26 from 30.06.2001
them, by peo ple far away from them and that they per son ally were not com mit ted and were notexpected to have definite commitments to the reform.
In May and June 1999, a ques tion naire among the phy si cians in three big hos pi tals (in So -fia, Veliko Turnovo and Lovech) also pro voked in ter est. In the three hos pi tals, the phy si cians’low aware ness of the healthcare re form pre vailed, which was more dis tinct in the met ro pol i tanhos pi tal (66.9%) than in Veliko Turnovo (50.4%) and Lovech (46.2%). 16.4% of the phy si ciansin the cap i tal showed high aware ness to gether with 23.0% of the phy si cians from VelikoTurnovo and 23.1% of the phy si cians from Lovech, the re main ing in di cat ing av er age aware ness. The doc tors de clared in a straight for ward way that their source of in for ma tion came al most ex -clu sively from the me dia and in sisted on the dis con tinu a tion of the in ad e quate pub li ca tionswhich “were un for tu nately based on our col leagues’ words” (So fia). Some naïve rec om men da -tions for the im ple men ta tion of the re form were also prob a bly due to the low aware ness.
A sur vey among the poly clinic pa tients in So fia at that time dem on strated that the lack ofin for ma tion among them (68.0%) was al most equal to that of the doc tors. The stu dents’aware ness (in the spe cialty of healthcare man age ment) from Varna Med i cal Uni ver sityshowed a po lar dis tri bu tion – 33.7% were highly in formed (most of them phy si cians!) and43.2% had a low aware ness. The jour nal ists’ aware ness was com par a tively high in 47.4%(26.3 ex hib it ing low aware ness). How ever, the jour nal ists’ as sess ment of the cit i zens’ aware -ness of the healthcare re form was low but it co in cided ap prox i mately with the aware ness es tab -lished in the phy si cians from the out pa tients’ care (25.4 %)496.
The above cited sur veys in di cated that one of the es sen tial or gani sa tional de fects of thehealthcare re form in Bul garia was the low aware ness both of the pro fes sion als (not only thepro vid ers but, most im por tantly, of the man ag ers) and the pa tients and cit i zens in gen eral about the scope, the con tent and the course of the healthcare re form. In the fol low ing years, the lackof ac tive, de ci sive and clear enough ad ver tise ment and in for ma tion for the pro fes sion alsand the cit i zens about what to ex pect from the healthcare re form were of ut most im por -tance and had strongly neg a tive con se quences. There is no doubt that the lack of ac tivelyshared and authorised in for ma tion dis so ci ated them from the re form, alienated them and theycould not participate in it.
This short com ing was also con firmed by sub se quent stud ies. A ques tion naire among phy -si cians in 2000 in di cated that the me dia com prised the main source of in for ma tion for 45.2% and the pro fes sional or gani sa tions – for 30.8% of the in ter viewed phy si cians. Maybe due to this fact,when asked about the goal of the re form, 79.2% of the re spon dents an swered that the state “is es -cap ing” from healthcare, 10.0% con sid ered that the aim was to im prove the ma te rial sta tus of themed i cal staff (ac cord ing to a pre vi ous sur vey – 70.0%) and only 25.0% thought that the aim wasto im prove med i cal care497. The in for ma tion vac uum in flicted great dam age on the healthcare re -form but was go ing to dom i nate the re form pro cess in the years to fol low.
In May and June 2000, the sur vey of the As so ci a tion of the Re gional Hos pi tals “StaraPlanina” re vealed the at ti tude of the cit i zens and the pa tients to the re form. From the re -spon dents, 10.0% in di cated that they were not in formed at all and, ac cord ing to an other 24.6%, the in for ma tion they had was in com plete and con tra dic tory. The na tional me dia were re ported
130
496 Popov, Ì., B. Davidov. Îñèãóðÿâàíå íà ïîäêðåïàòà íà îáùåñòâåíîòî ìíåíèå çà ðåôîðìàòà íà çäðàâíàòàñèñòåìà. Àêòóàëíà êîìóíèêàöèîííà ïîëèòèêà â çäðàâåîïàçâàíåòî. Published by NCHI, Sofia, 2000
497 Bachev, S. The attitude of the healthcare workers to the initiated reform in healthcare. Metropolitan MedicalCollegiate, Information bulletin, 11-12.2000, p. 4-9
as the main source of in for ma tion about the health in sur ance for 16.2% of the in ter viewed and11.5% re ported that they re lied on their ac quain tances who were better in formed. The lo caland the re gional me dia were an in for ma tion source for 4.6% and only 0.8% of the re spon dentshad had the op por tu nity to use spe cially pub lished ma te ri als. At ten tion was drawn to the factthat ex actly the na tional me dia of fered neg a tive in for ma tion on the lack of clar ity in the ad min -is tra tion of the health in sur ance, and quite fre quently, this information was given by therepresentatives of the physicians’ occupation.
Ir re spec tive of the type of the source of in for ma tion, ac cord ing to 43.1% of the in ter -viewed, the cit i zens were not suf fi ciently in formed about the health in sur ance sys tem and30.1% found it dif fi cult to judge (which was an in di rect sign of a lack of aware ness). These re -sults were com ple mented by the field ob ser va tions of the in ter view ers, too. These ob ser va tions re vealed a high de gree of scep ti cism and even re fusal to par tic i pate in the sur vey, re sult ingfrom the de vel op ment of the in for ma tion cam paign for the health in sur ance at the time. How -ever, still in June 2000, 81.3% had already chosen their general practitioner.
Re gard ing hos pi tal care, 20.8% of the re spon dents con sid ered that the re ally good spe -cial ists were lo cated in the hos pi tals and ac cord ing to 12.3% the phy si cians pos sessed the nec -es sary pro fes sional skills. 81.5% had been forced to pay for consumables, food, ser vices by the auxiliary staff.
In the re sponses of the in ter viewed peo ple at that time, the prob lems in hos pi tal care in -cluded the lack of suf fi cient means and equip ment, the un sat is fac tory at ten tion and care for thepa tient and the ad di tional pay ment. There fore, only one third of the hos pi tal pa tients, if needed,would choose the same hos pi tal again and that, for lack of an other op tion. It was rather in ter est -ing that 44.6% of the re spon dents re lied on pri vate ini tia tive to re solve their hos pi tal prob lems.
In gen eral, the re sults from this sur vey showed an anx i ety in the mass con scious ness mainly due to the lack or dis tor tion of the in for ma tion, the low level of the qual ity of care, but at the same time, a rel a tive pres er va tion of the tra di tional au thor ity and trust in the phy si cians’ oc cu pa tion498.
The above quoted sur veys were con ducted be fore the start of the health in sur ance sys -tem (on July 1st 2000) as a top i cal and key el e ment of the healthcare re form. The re sults ob -tained and ana lysed in them, could be a ba sis for com par i son with pub lic opin ion polls in thesec ond half of 2000 and in the sub se quent periods.
The pub lic opin ion about the healthcare re form in Bul garia in the last weeks of 2001 (ayear and a half af ter the start of the health in sur ance in the out pa tients’ care and half a year inthe hos pi tal care) was re flected in a com pre hen sive (qual i ta tive and quan ti ta tive) rep re sen ta -tive so cio log i cal sur vey con ducted by NOEMA. The re sults from this sur vey par tially com -pare with the re sults from a sim i lar pre vi ous sur vey (in 2000) 499.
In their opin ions, the cit i zens out lined the most im por tant as pects con cern ing med i calcare as follows:
· timely (with out a con sid er able waste of time) pro vi sion of the care;
· the pos si bil ity for choice of a gen eral prac ti tio ner and healthcare es tab lish ment;
· the at ti tude to the pa tients dur ing ex am i na tion and treat ment;
· qual ity of the med i cal care;
131
Stages and evo lu tion of the healthcare re form in Bul garia
498 Gulubov, À. Analysis of the results from a ssociological study. Regional Hospital Association “Stara planina”, 2000, pp. 1-8
499 NOEMA. The public opinion on the healthcare reform. Quantitative and qualitative study. Summarisingreport. January 2002
· in for ma tion about the pa tients’ rights and li a bil i ties;
· fi nan cial ac cess to med i cal ex am i na tions, pro ce dures and med i ca tion.
As re gards out pa tients’ care, one third of the re spon dents were sat is fied with theprompt ness of the care. The sur vey con firmed the high de gree of sat is fac tion with the pos si bil -ity for a free choice of a fam ily phy si cian. How ever, newly emerged prob lems were re ported,e.g. the great num ber of pa tients reg is tered with some phy si cians, which was an ob sta cle forthe timely pro vi sion of med i cal care, the lack of clar ity in terms of “emer gency med i cal care”,the com pul sory visit to the GP’s of fice be fore the visit to a spe cial ist for pa tients with dis eases,known to be treated by spe cial ists. Dis sat is fac tion was also shared with the widely spread prac -tice of re fer ring the pa tient to the spe cial ists’ paid ad mis sion af ter the first free visit to the spe -cial ist. Around 10-15% of the re spon dents (in var i ous pop u lated ar eas) were dis sat is fied withthe at ti tude to the pa tients dur ing phys i cal ex am i na tion and treat ment. This per cent age in -cluded mainly peo ple with chronic dis eases and peo ple of poor fi nan cial means. As com paredto this group of peo ple, the per cent age in creased sig nif i cantly. This was why the prob lem withthe doc tor-pa tient in ter ac tion re mained se ri ous a year and a half af ter the in tro duc tion of thehealth in sur ance system.
Ac cord ing to the sur vey, in re gard to the hos pi tal care, the cit i zens’ views were pre dom i -nantly neg a tive: lim ited pos si bil i ties for the pa tient’s choice of a hos pi tal; lack of suf fi cientclar ity about the costs paid by the NHIF (for the hos pi tal stay, in ves ti ga tions, sur gi cal treat -ment); pa tients’ un cer tainty in their re la tions with the phy si cians and the other staff; poorhous ing con di tions in the hos pi tal; un reg u lated pay ments to the at tend ing phy si cians in spite of the form for free treatment.
The com par i son be tween the sur veys in 2000 and 2001 dem on strated that an im por tantchange had oc curred in the ac cep tance of the healthcare re form. Its im age was not con -structed around the “doc tor – pa tient” in ter ac tion any more, but by the man age ment sys tem –the or gans of the healthcare ad min is tra tion and the NHIF – which de ter mined the rules of thenew or gani sa tion of the healthcare sys tem. In 2001, the phy si cian – the gen eral prac ti tio ner orthe spe cial ist – was not per ceived, as a year be fore, as di rectly re spon si ble for the le gal and pro -ce dural prob lems and the un clear is sues ac com pa ny ing the re form. The cit i zens started to un -der stand the re stric tions to the phy si cians im posed “from above”, which gave rise toim ped i ments for the effective and timely fulfilment of the doctors’ duties.
In this con text, the dis tinctly neg a tive im age of the two key in sti tu tions in the func tion ingof the healthcare sys tem – the Un ion of Bul gar ian Phy si cians and the NHIF –stood out. The in -ter viewed phy si cians as so ci ated the UBP mainly with the force ful mem ber ship, the ex ec u tivebody and rep re sen ta tion in the Un ion cho sen in ad vance, the lack of pos si bil ity to de posit pro -pos als “from the bot tom” to the Ex ec u tive Board, lack of ac tual mech a nisms to con trol the ac tiv i -ties of the man ag ing or gans, “pro tec tion of the in ter ests of sep a rate per sons and not of theor di nary mem bers.” The pub lic im age of the NHIF was dom i nated by im pres sions of uni lat eralcom mu ni ca tion, close ness, lack of trans par ency, po lit i cal de pend ence. The opin ion com monlyheld by the re spon dents was that the re form had to lead to demonopolisation of the health in sur -ance and to the es tab lish ment of at least one more al ter na tive in de pend ent health in sur ance fund.
The sum ma rised re sults from this sur vey in di cated that the healthcare re form was al -ready per ceived as a nec es sary and ir re vers ible pro cess by both cit i zens and phy si cians.The phy si cians were con vinced that a more ef fec tive healthcare sys tem had been built, in
132
which mar ket prin ci ples ap plied, and the changes and the im prove ments had to be aimed in thesame di rec tion in the fu ture. The cit i zens’ and phy si cians’ stand pre dom i nated that the newlycon structed sys tem should not be re formed again but should only be im proved from spe cificas pects and be de vel oped to ward liberalisation and demonopolisation.
The pub lic opin ion about the healthcare re form was the sub ject of an in ter est ing com -par a tive study be tween Bul garia and Greece con ducted in March – April 2001500. The be -gin ning of the healthcare re form in Greece was dated in 1983 but its course passed a longtran si tion pe riod since the greater part of the health leg is la tion was only par tially en forced. The cit i zens’ aware ness of the healthcare re form in both coun tries pre sented a prob lem, more pro -nounced for the Greek cit i zens (37.3% of the Bul gar i ans and 84.0% of the Greek cit i zens ex -hib ited low in for ma tion level or were not in formed at all). Im prove ment of the phy si cians’ac tiv i ties and their at ti tude to the pa tients as a re sult of the healthcare re form was re ported inboth coun tries but it was def i nitely more pro nounced among the Bul gar i ans than among theGreeks. Good (high and av er age) per sonal sat is fac tion with the healthcare re form was in di -cated by 36.7% of the Bul gar i ans and 30.0% of the Greeks, and low and un sat is fac tory – by63.3% of the Bul gar i ans and 70.0% of the Greeks. On the con trary, the ex pec ta tions of theGreek cit i zens from the re form for the fu ture were more op ti mis tic than those of the Bul -gar ian cit i zens. In both coun tries, the cit i zens ex pressed their wish for the ex is tence of morethan one health in sur ance fund but the ma jor ity of the Bul gar ian re spon dents (40.3%)preferred the non-obligatory voluntary health insurance.
Re sults and un solved prob lems
Dur ing the ex am ined pe riod un dis puted re sults were achieved in the de vel op ment of thehealthcare re form but at the same time the re form pro cess it self gave rise to a num ber ofproblems.
The main out come achieved dur ing the four years (1997-2001) in ques tion was thefi nal dis con tinu a tion of the re pro duc tion of the ex ist ing (though al ready changed to acer tain de gree) healthcare sys tem and, more im por tantly, the cre ation of the nor ma tiveba sis and, based on it, the struc tural and or gani sa tional con struc tion of the newhealthcare sys tem. The state mo nop oly and the cen tral ised man age ment of the healthcare sys -tem were elim i nated and the pro tec tion of the cit i zens’ and pa tients’ rights re gard ing theirhealth was laid down on dem o cratic prin ci ples; the plu ral is tic prop erty on the sys tem re sources was re stored, the au ton o mous pro fes sional sta tus of phy si cians and den tists was also re sumed,the func tion ing of the greater part of the sys tem which was clos est to the con sum ers, was en -sured by the new sys tem of fi nanc ing, based on health in sur ance. The con struc tion of the newhealthcare sys tem in volved the es tab lished char ac ter is tics of the state, pub lic, civil and eco -nomic life in our coun try. At the end of this stage, the healthcare re form was per ceived bythe cit i zens and the phy si cians as a nec es sary and ir re vers ible pro cess, which had todevelop and lead to the improvement of the system.
In the course of ev ery re form (even the best planned) prob lems arise. Some of them arecom pli cated and sus tain able and more con sis tent ef forts are needed for their elim i na tion. Oth -ers arise due to cir cum stances which had been im pos si ble to pre dict with suf fi cient clar ity orwhich had been un der es ti mated or ne glected for var i ous rea sons. A third group in cludes prob -
133
Stages and evo lu tion of the healthcare re form in Bul garia
500 Pashalidis, Ê. On the necessity for public assessment of the healthcare reform. Dissertation. Sofia, 2003
lems which are not solved for in suf fi cient or ab sent insistence for their solution.Dur ing the ex am ined stage of the healthcare re form, the com plex and sus tain able prob -
lems were re lated to the health sta tus of the na tion. It can def i nitely be claimed that dur ingthis stage (1997-2001) the foun da tion was laid for the so lu tion of the fist and fore most task of the healthcare re form – the dis con tinu a tion of the na tion’s health de te ri o ra tion, for itssta bili sa tion as a ba sis and a start ing point for its im prove ment (Ta ble 25). Al though un til 2001 no prom i nent sus tain able im prove ment was ob served, a num ber of in di ca tors showed a moreor less ev i dent but clear enough sta bili sa tion of the health sta tus of the Bul gar ian pop u la tion. Itcor re sponded also to the fea tures of eco nomic sta bil ity in spite of the fact that a number ofsocial problems (employment, income) remained unsolved.
In dis put ably, pos i tive out comes were achieved dur ing the ex am ined al most five-year pe -riod as re gards the na tion’s health. Still, they gave a good start and should not be un der es ti -mated. The prob lems re mained re lated to mor bid ity rate (car dio vas cu lar and oncologicaldis eases, tu ber cu lo sis) and the pre vent able mor tal ity among some age groups (es pe cially thechil dren’s mor tal ity rate). The health prob lems in the Roma pop u la tion were par tic u larlyspe cific and re quir ing consistent approaches in their solution.
A par tic u lar at ten tion was re quired by the ra tio be tween re sources of the healthcaresys tem and the out comes at its exit. In 1997-2001, a sig nif i cant step was made to ward the ra -tion al is ation of the hos pi tal net work – the re duc tion of the num ber of hos pi tal beds (from 85408 in 1997 to 52 712 in 2000). The num ber of beds was re duced by 38.3%, but the num ber ofhos pi ta lised pa tients was re duced by 32.7%, and the hos pi ta li sa tions (as com pared to the pop u -la tion) – by 18.1% (Ta ble 23). In the multi-pro file hos pi tals for ac tive treat ment (the most com -mon form of hos pi tal care) dur ing this pe riod, the num ber of beds was de creased by 48.1%, but their uti li sa tion rate in creased sig nif i cantly mainly due to the in creased bed turn over and theshort ened length of hos pi tal stay (Ta ble 24). In the mean time (1998-2001), the costs per pa -tient in creased by 1.56 times, per 1 hos pi tal bed – 1.74 times, per 1 bed day – 1.80 times, per 1drug day – 1.86 times. All these pres ent an un doubted man i fes ta tion of the im proved uti li sa -tion rate of the ma te rial hos pi tal re sources without threatening or disturbing the inpatientmedical care for the citizens.
For the pe riod un der dis cus sion this was also a nec es sary out come, which had to be dulyap pre ci ated. As com pared to the in di ca tors in the hos pi tal sec tor in other coun tries, it can beob served that, ac cord ing to the num ber of phy si cians, hos pi tals, hos pi tal beds (in clud ing bedsfor ac tive treat ment), by far for the av er age length of stay too, the in di ca tors for our healthcaresys tem were gen er ally equal and com pa ra ble to those in the coun tries in Eu rope as a whole,Cen tral and East ern Eu rope (CEE) and the Eu ro pean Com mu nity (Ta ble 26). This ob ser va -tion, how ever, is not valid in terms of the ac tiv i ties. The in di ca tors for hos pi ta li sa tion and uti li -sa tion rate were con sid er ably lower than those in the coun tries in Eu rope and the EC. Theyhave to be ana lysed more profoundly, but this task is beyond the scope of the present study.
The ap par ent lack of cor re spon dence be tween re sources and re sults stands out even moredis tinctly when we con sider also the in di ca tors of mor tal ity rate which have a cru cial im por -tance for the as sess ment of the pop u la tion’s health sta tus, and their value is par tic u larly sig nif i -cant for the de mo graphic bal ance in our coun try. In terms of both gen eral and chil dren’smor tal ity and mor tal ity rate from car dio vas cu lar dis eases (ac count ing for two thirds of thedeaths in Bul garia for many years) the in di ca tors for our coun try were con sid er ably higherthan in the other coun tries. In deed, the “de mo graphic age ing” was very marked in our coun try
134
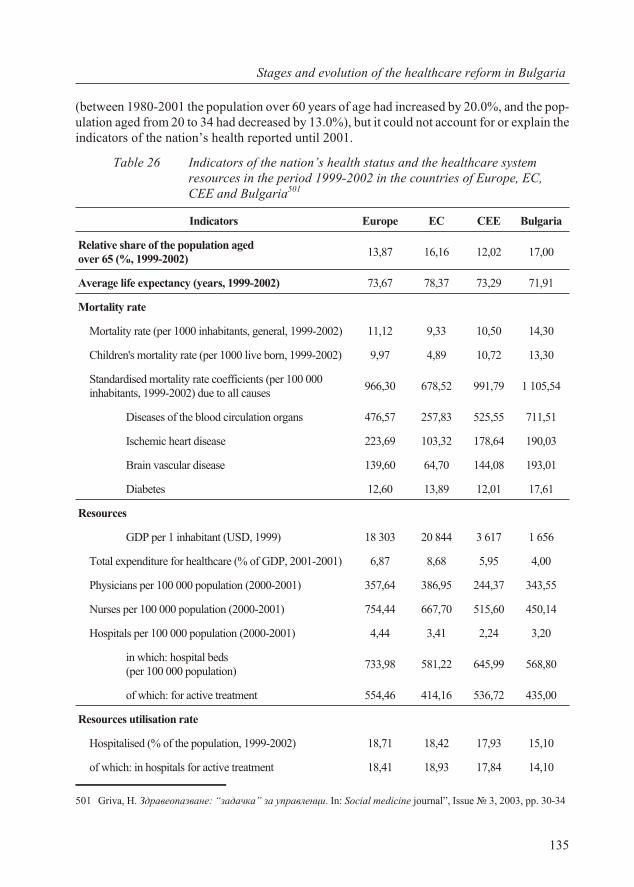
(be tween 1980-2001 the pop u la tion over 60 years of age had in creased by 20.0%, and the pop -u la tion aged from 20 to 34 had de creased by 13.0%), but it could not ac count for or ex plain thein di ca tors of the na tion’s health re ported un til 2001.
Ta ble 26 Indicators of the nation’s health status and the healthcare systemresources in the period 1999-2002 in the countries of Europe, EC,CEE and Bulgaria501
Indicators Europe EC CEE Bulgaria
Rel a tive share of the pop u la tion aged over 65 (%, 1999-2002)
13,87 16,16 12,02 17,00
Av er age life ex pec tancy (years, 1999-2002) 73,67 78,37 73,29 71,91
Mor tal ity rate
Mor tal ity rate (per 1000 in hab it ants, gen eral, 1999-2002) 11,12 9,33 10,50 14,30
Chil dren's mor tal ity rate (per 1000 live born, 1999-2002) 9,97 4,89 10,72 13,30
Standardised mortality rate coefficients (per 100 000inhabitants, 1999-2002) due to all causes
966,30 678,52 991,79 1 105,54
Dis eases of the blood cir cu la tion or gans 476,57 257,83 525,55 711,51
Ischemic heart dis ease 223,69 103,32 178,64 190,03
Brain vas cu lar dis ease 139,60 64,70 144,08 193,01
Di a be tes 12,60 13,89 12,01 17,61
Re sources
GDP per 1 in hab it ant (USD, 1999) 18 303 20 844 3 617 1 656
To tal ex pen di ture for healthcare (% of GDP, 2001-2001) 6,87 8,68 5,95 4,00
Phy si cians per 100 000 pop u la tion (2000-2001) 357,64 386,95 244,37 343,55
Nurses per 100 000 pop u la tion (2000-2001) 754,44 667,70 515,60 450,14
Hos pi tals per 100 000 pop u la tion (2000-2001) 4,44 3,41 2,24 3,20
in which: hos pi tal beds (per 100 000 pop u la tion)
733,98 581,22 645,99 568,80
of which: for ac tive treat ment 554,46 414,16 536,72 435,00
Re sources uti li sa tion rate
Hos pi ta lised (% of the population, 1999-2002) 18,71 18,42 17,93 15,10
of which: in hos pi tals for ac tive treat ment 18,41 18,93 17,84 14,10
135
Stages and evo lu tion of the healthcare re form in Bul garia
501 Griva, H. Çäðàâåîïàçâàíå: “çàäà÷êà” çà óïðàâëåíöè. In: So cial med i cine jour nal”, Is sue ¹ 3, 2003, pp. 30-34
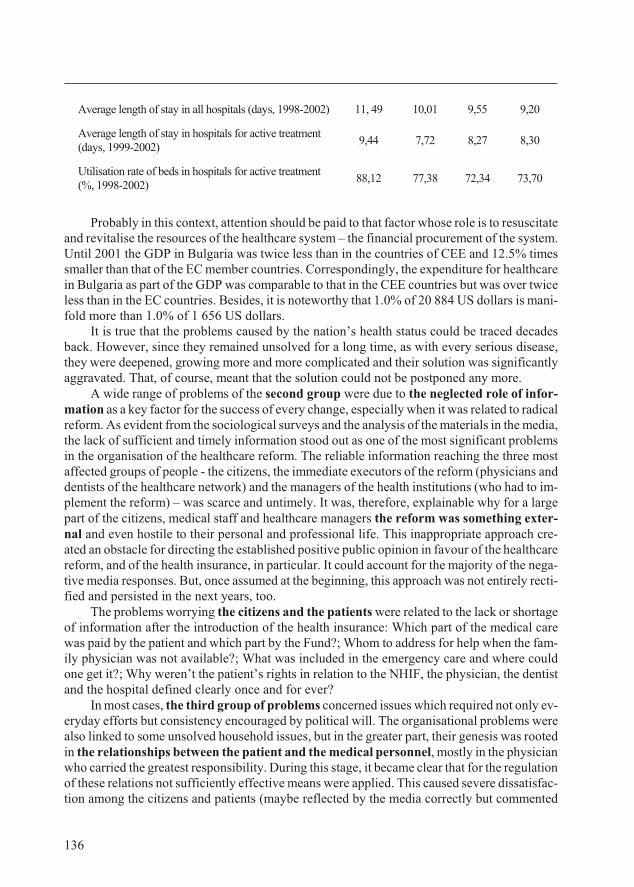
Av er age length of stay in all hos pi tals (days, 1998-2002) 11, 49 10,01 9,55 9,20
Av er age length of stay in hos pi tals for ac tive treat ment(days, 1999-2002)
9,44 7,72 8,27 8,30
Uti li sa tion rate of beds in hos pi tals for ac tive treat ment(%, 1998-2002)
88,12 77,38 72,34 73,70
Prob a bly in this con text, at ten tion should be paid to that fac tor whose role is to re sus ci tateand re vi tal ise the re sources of the healthcare sys tem – the fi nan cial pro cure ment of the sys tem.Un til 2001 the GDP in Bul garia was twice less than in the coun tries of CEE and 12.5% timessmaller than that of the EC mem ber coun tries. Cor re spond ingly, the ex pen di ture for healthcare in Bul garia as part of the GDP was com pa ra ble to that in the CEE coun tries but was over twiceless than in the EC coun tries. Be sides, it is note wor thy that 1.0% of 20 884 US dol lars is man i -fold more than 1.0% of 1 656 US dol lars.
It is true that the prob lems caused by the na tion’s health sta tus could be traced de cadesback. How ever, since they re mained un solved for a long time, as with ev ery se ri ous dis ease,they were deep ened, grow ing more and more com pli cated and their so lu tion was sig nif i cantlyag gra vated. That, of course, meant that the so lu tion could not be post poned any more.
A wide range of prob lems of the sec ond group were due to the ne glected role of in for -ma tion as a key fac tor for the suc cess of ev ery change, es pe cially when it was re lated to rad i cal re form. As ev i dent from the so cio log i cal sur veys and the anal y sis of the ma te ri als in the me dia, the lack of suf fi cient and timely in for ma tion stood out as one of the most sig nif i cant prob lemsin the or gani sa tion of the healthcare re form. The re li able in for ma tion reach ing the three mostaf fected groups of peo ple - the cit i zens, the im me di ate ex ec u tors of the re form (phy si cians andden tists of the healthcare net work) and the man ag ers of the health in sti tu tions (who had to im -ple ment the re form) – was scarce and un timely. It was, there fore, ex plain able why for a largepart of the cit i zens, med i cal staff and healthcare man ag ers the re form was some thing ex ter -nal and even hos tile to their per sonal and pro fes sional life. This in ap pro pri ate ap proach cre -ated an ob sta cle for di rect ing the es tab lished pos i tive pub lic opin ion in fa vour of the healthcare re form, and of the health in sur ance, in par tic u lar. It could ac count for the ma jor ity of the neg a -tive me dia re sponses. But, once as sumed at the be gin ning, this ap proach was not en tirely rec ti -fied and per sisted in the next years, too.
The prob lems wor ry ing the cit i zens and the pa tients were re lated to the lack or short ageof in for ma tion af ter the in tro duc tion of the health in sur ance: Which part of the med i cal carewas paid by the pa tient and which part by the Fund?; Whom to ad dress for help when the fam -ily phy si cian was not avail able?; What was in cluded in the emer gency care and where couldone get it?; Why were n’t the pa tient’s rights in re la tion to the NHIF, the phy si cian, the den tistand the hos pi tal de fined clearly once and for ever?
In most cases, the third group of prob lems con cerned is sues which re quired not only ev -ery day ef forts but con sis tency en cour aged by po lit i cal will. The or gani sa tional prob lems werealso linked to some un solved house hold is sues, but in the greater part, their gen e sis was rootedin the re la tion ships be tween the pa tient and the med i cal per son nel, mostly in the phy si cian who car ried the great est re spon si bil ity. Dur ing this stage, it be came clear that for the reg u la tion of these re la tions not suf fi ciently ef fec tive means were ap plied. This caused se vere dis sat is fac -tion among the cit i zens and pa tients (maybe re flected by the me dia cor rectly but com mented
136
some what uni lat er ally).A chain of fail ures of this na ture re sulted in the ir rel e vant amend ment of the LHE made in
1999, which di vided the in tro duc tion of the health in sur ance into two: for out pa tients’ carein 2000 and for the in pa tients’ care in 2001. This caused con tra dic tions in the sys tem, which re -sulted in prob lems for the pa tients across the whole healthcare sec tor.
The un solved prob lems were a sig nal for study ing and for mu lat ing a pol icy and de ci sions. Some of the pos si ble so lu tions were dis re garded dur ing the stage un der dis cus sion. Their so lu -tions and so lu tions of other is sues were forth com ing in the next stage.
5.3. Third stage: de layed and hes i tant de vel op ment of thehealthcare re form
The be gin ning of this quite a re cent stage dates back to the sec ond half of 2001. We willana lyse it for the pe riod up to the end of 2005. This is ac counted for and summed up in the ti tleof the stage. Its ob jec tive end ing will be reached later, when hope fully (with God’s bless ing!)an other ti tle will be ap pro pri ate.
Po lit i cal and so cio eco nomic con text
In the sec ond half of 2001, af ter a con vinc ing elec tion vic tory the gov ern ment was formed of the Na tional Move ment Sim eon II (NMSS) and the Move ment for Rights and Free doms(MRF) with Sim eon Saxe-Co burg-Gotha as Prime Min is ter, in which Assoc. Prof. Dr.Bozhidar Finkov was Min is ter of Healthcare. Af ter the re struc tur ing of the gov ern ment fromJuly 16th 2003, Slavcho Bogoev be came Min is ter of Healthcare, who had been Vice Min is terun til then. Fol low ing the Par lia men tary elec tions (June 26th 2005), the newly formed gov ern -ment com prised a co ali tion among the BSP, NMSS and MRF with Sergei Stanishev as PrimeMin is ter and Prof. Dr. Radoslav Gaidarski as Min is ter of Healthcare.
The stage was char ac ter ised by the con tin u a tion of the po lit i cal and so cio eco nomic sta -bili sa tion of the coun try. It can be as sumed that dur ing this phase the po lit i cal con fron ta tionwas weak en ing in its fe ro cious ness at the ex pense of the com par a tively greater tol er ance onbe half of the rep re sen ta tives of the po lit i cal forces. The gross do mes tic prod uct was grow ing(Ta ble 27) both for the na tional econ omy as a whole and as an av er age per ca pita. The level ofun em ploy ment was de creas ing – from 2001 on wards it started to di min ish and in 2004 itreached 12.2%. The rel a tive share of the ex penses for food be gan to de crease in the struc ture of the house holds’ ex pen di ture. Even though com par a tively high, it was a pos i tive man i fes ta tionof a cer tain trend to the im prove ment of the qual ity of life.
The pub lic opin ion, com monly shared among cit i zens and pro fes sion als, was that thehealthcare re form was a nec es sary and ir re vers ible pro cess, and by shift ing of the pub lic opin -ion from the re spon si bil ity for healthcare from the med i cal pro fes sion als to the gov ern ing au -thor i ties, better con di tions were cre ated for the fur ther de vel op ment of the out comes al readyachieved dur ing the pre vi ous years.
137
Stages and evo lu tion of the healthcare re form in Bul garia
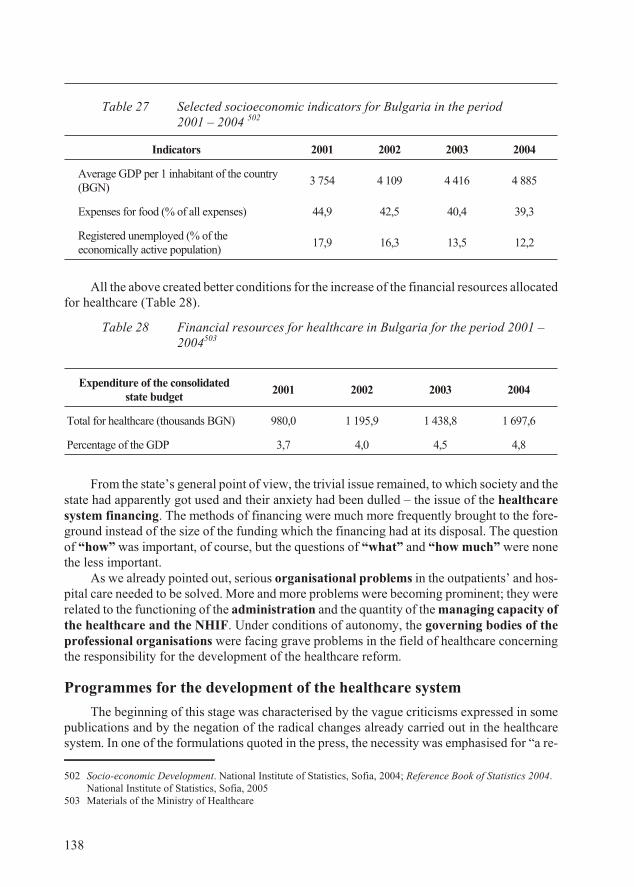
Ta ble 27 Se lected so cio eco nomic in di ca tors for Bul garia in the period 2001 – 2004 502
In di ca tors 2001 2002 2003 2004
Av er age GDP per 1 in hab it ant of the coun try(BGN)
3 754 4 109 4 416 4 885
Ex penses for food (% of all ex penses) 44,9 42,5 40,4 39,3
Reg is tered un em ployed (% of theeco nom i cally ac tive pop u la tion)
17,9 16,3 13,5 12,2
All the above cre ated better con di tions for the in crease of the fi nan cial re sources al lo cated for healthcare (Ta ble 28).
Ta ble 28 Financial resources for healthcare in Bulgaria for the period 2001 –2004503
From the state’s gen eral point of view, the triv ial is sue re mained, to which so ci ety and thestate had ap par ently got used and their anx i ety had been dulled – the is sue of the healthcaresys tem fi nanc ing. The meth ods of fi nanc ing were much more fre quently brought to the fore -ground in stead of the size of the fund ing which the fi nanc ing had at its dis posal. The ques tionof “how” was im por tant, of course, but the ques tions of “what” and “how much” were nonethe less im por tant.
As we al ready pointed out, se ri ous or gani sa tional prob lems in the out pa tients’ and hos -pi tal care needed to be solved. More and more prob lems were be com ing prom i nent; they werere lated to the func tion ing of the ad min is tra tion and the quan tity of the man ag ing ca pac ity ofthe healthcare and the NHIF. Un der con di tions of au ton omy, the gov ern ing bod ies of thepro fes sional or gani sa tions were fac ing grave prob lems in the field of healthcare con cern ingthe re spon si bil ity for the de vel op ment of the healthcare re form.
Programmes for the de vel op ment of the healthcare sys tem
The be gin ning of this stage was char ac ter ised by the vague crit i cisms ex pressed in somepub li ca tions and by the ne ga tion of the rad i cal changes al ready car ried out in the healthcaresys tem. In one of the for mu la tions quoted in the press, the ne ces sity was emphasised for “a re -
138
Ex pen di ture of the con sol i datedstate bud get
2001 2002 2003 2004
To tal for healthcare (thou sands BGN) 980,0 1 195,9 1 438,8 1 697,6
Per cent age of the GDP 3,7 4,0 4,5 4,8
502 Socio-eco nomic De vel op ment. Na tional In sti tute of Sta tis tics, So fia, 2004; Ref er ence Book of Sta tis tics 2004.Na tional In sti tute of Sta tis tics, So fia, 2005
503 Ma te ri als of the Min is try of Healthcare
form of the re form”. Nev er the less, out side the state ments, the tone was busi ness-like.The programme (in clud ing an Ac tion Plan) en ti tled “Healthcare – Ev ery one’s Right”,
which was pro claimed on No vem ber 21st 2001 by the Min is try of Healthcare, for mu lated theprob lems of the na tion’s health sta tus and the vi sions for their so lu tion.
Af ter the anal y sis of the de mo graphic pro cesses, the mor bid ity rate, the risk fac tors andthe sus cep ti ble seg ments of the pop u la tion (chil dren, low in come groups, some eth nic com mu -ni ties, per sons with con gen i tal mal for ma tions and dis abled peo ple) the char ac ter is tic fea tureswere out lined of the cur rent healthcare sys tem. Re gard ing the pub lic healthcare, the lack ofmod ern leg is la tive ba sis was pointed out to gether with the need for a new ap proach to the so -cially sig nif i cant dis eases and for the op ti mi sa tion of the tech ni cal fa cil i ties and equip ment aswell as the ac tiv i ties of the hy giene and ep i de mi o log i cal ser vices. Re gard ing the med i cal ac -tiv i ties, the need was stressed for a cor rec tion in leg is la tion for en sur ing the re quired cit i zens’eq uity in their ac cess to health ser vices, for con trol over the qual ity, for over com ing of the lag -ging be hind of the struc tural re form in the healthcare net work. Draw backs were pointed out inhos pi tal fi nanc ing, which had oc curred due to the sep a ra tion of the out pa tients’ from the in pa -tients’ care in the in tro duc tion of health in sur ance as well as due to the def i cit in the fi nanc ingof the “clin i cal path ways”.
The Ac tion Plan con tained four main pri or i ties of the programme: the en hanced roleof the pre ven tive and pro phy lac tic med i cine, the re or gani sa tion of the ser vices pro vid ing pub -lic health, the im prove ment of the qual ity and ef fi ciency of the (out pa tients’ and in pa tients’)care, the im prove ment of the meth od ol ogy for the fi nanc ing of the na tional health sys tem. Foreach of these pri or i ties, ac tions were planned for a mid dle-term (one-year) pe riod un til the endof 2002 and for a long-term pe riod (un til the end of 2005). The ac tions were ex pe di ent, but intheir greater part, they were re lated to programmes of fi nanc ing (for pre ven tion, train ing, treat -ment) and in vest ment (con struc tion of in for ma tion sys tems, re con struc tion of 40-60 hos pi tals,ren o va tion of the fa cil i ties for spe cial ised med i cal care, etc.), which were prob lem atic and re -quired leg is la tive prep a ra tion and de ci sions. The im ple men ta tion of this programme wasmeant to be ac com plished in 2005.
One very gen eral glance would re veal a lack of con nec tion and con ti nu ity be tween theabove quoted programme and the Health Strat egy, adopted only half a year be fore. The“Health Strat egy 2001” lacked con ti nu ity and eval u a tion of the con tent and the im ple men ta -tion of the pre vi ous strat egy could be ac counted for (but not jus ti fied) by the fact that “HealthStrat egy 1995” was mid dle–term (for a pe riod of 2-4 years) in its na ture and was ac com plishedin 2001. Con se quently, it can be as sumed that it was del i cately and tac itly (but ir rel e vantly andun con vinc ingly) left un spo ken of. “Health Strat egy 2001”, how ever, was adopted by the Bul -gar ian gov ern ment on April 23rd2001, and on No vem ber 21st the health programme of the sub -se quent gov ern ment was adopted, in which no men tion was made what so ever about a healthstrat egy. It is dif fi cult for the com mon sense to find an ex pla na tion for the to tal neg li gence ofthis state doc u ment. We will leave aside the cir cum stance that this time, once more the ex e cu -tion of the gov ern men tal programme on healthcare did not be come sub ject to any com ment orre port by the cit i zens and its ex ec u tors – the med i cal pro fes sion als.
This ap proach is worth to be paid at ten tion since due to the nu mer ous fa mil iar rea sons itaf fected the re form of the healthcare sys tem in an ex tremely dis ad van ta geous light.
The co ali tion gov ern ment com posed in 2005 for Eu ro pean in te gra tion, eco nomic growthand so cial re spon si bil ity, also pro claimed its programme en ti tled “Guar an teed and ac ces si ble
139
Stages and evo lu tion of the healthcare re form in Bul garia
healthcare”, in which the de sire of the gov ern ment was de clared “to con tinue the re form inhealthcare, which had been started sev eral years ear lier”. This programme was con sid er ably shorter, but in re turn, it was more re al is tic than the one dis cussed above. Con cern ing med i cal ac -tiv i ties, it had a dis tinctly so cial ori en ta tion. Ap par ently, it was ad dressed to the wide cir cles ofthe mass con sum ers of healthcare ser vices, who did not show ex plicit in ter est in the is sues of pre -ven tive and pro mo tional ac tiv i ties or the so lu tion of the fi nan cial, or gani sa tional and man a ge rialprob lems. Maybe this was the rea son why they were not touched upon in the programme. It didnot make any men tion about pre vi ous strat e gies and programmes ei ther.
In brief, the con tent of the programme in cluded the fol low ing: “In tro duc tion of a ba sicpack age of healthcare ser vices for ev ery in sured Bul gar ian cit i zen. In sur ance of a better ac cessto qual ity health ser vices. De vel op ment of vol un tary health in sur ance. In clu sion of the pa tients in the for mu la tion of the health pol icy and in the con trol over the qual ity of health ser vices. In -creased fi nanc ing for healthcare and the pro vi sion of higher trans par ency and ef fi ciency oftheir uti li sa tion. Elec tronic healthcare. Fair so lu tion of the prob lem with the un paid cit i zens’health in stal ments. Re form of the hos pi tal sec tor through op ti mi sa tion and re struc tur ing of thehos pi tal net work and privatisation.”
A num ber of el e ments be come dis tinct in the con tent (e.g. a guar an teed pack age of health ser -vices, de vel op ment of vol un tary health in sur ance, cit i zens’ par tic i pa tion in the for mu la tion of thehealth pol icy, e-healthcare, privatisation), which had not been ad dressed be fore or had not beenemphasised in the two strat e gies dis cussed ear lier or in the pre vi ous programme (from 2001).
De vel op ment of the nor ma tive ba sis of the healthcare sys tem
The de vel op ment of the nor ma tive ba sis of the healthcare sys tem dur ing this stage in -cluded the de sign and the adop tion of new laws, the amend ment and ad di tion of the ex ist ingand ap proval of reg u la tory acts.
In our opin ion, the fol low ing are of cru cial im por tance for the healthcare sys tem:
· Law on Health (LH)504;
· Law for the Amend ment and Ad di tion of the Law on Health In sur ance505;
· Law on the Pro fes sional Or gani sa tions of nurses, mid wives and as so ci ated med i calspe cial ists506;
· De cree of the Coun cil of Min is ters ¹ 280 from 18.10.2004 for the es tab lish ment of a“Fund for Treat ment of Chil dren” Cen tre507 and Reg u la tions for the ac tiv i ties and theor gani sa tion of the “Fund for Treat ment of Chil dren” Cen tre508.
The Law on Health to tally sub sti tuted the Law on Peo ple’s Health (1972). As in di cated inthe mo tives for the pro ject of the LH, it “reg u lates in a mod ern way the pub lic re la tions stip u lated in the Law on Peo ple’s Health and treats a num ber of ques tions re lated to pub lic health, whichhad not been pro vided for in the Bul gar ian leg is la tion un til then … Def i ni tions are pro vided forhealth pro mo tion and in te grated pre ven tion of dis eases, the as sur ance of high qual ity ofhealthcare, med i cal and so cial pro tec tion of chil dren, preg nant women and dis abled peo ple as
140
504 State Ga zette, Is sue ¹ 70 from 10.08.2004505 State Ga zette, Is sue ¹ 107 from 15.11.2002506 State Ga zette, Is sue ¹ 46 from 13.06.2005507 State Ga zette, Is sue ¹ 96 from 29.10.2004508 State Ga zette, Is sue ¹ 101 from 16.11.2004
well as mea sures for the pro vi sion of a healthy liv ing en vi ron ment for the sep a rate in di vid u als,the fam ily and the so ci ety”. Fur ther on, it was added that the draft pro ject “har mo nised the leg -is la tion in the field of pub lic health with the Eu ro pean leg is la tion. The lat est achieve mentswere also en vis aged, which had been cov ered in the doc u ments adopted by the Eu ro pean Com -mu nity, the Coun cil of Eu rope and the WHO in the field of cit i zens’ health and pa tients’rights.”
In spite of its mul ti fac eted con tent, the Law on Health formed sev eral fo cal points for abetter achieve ment of the mis sion of the health sys tem:
· reg u la tion of the struc ture and the man age ment (in clud ing at re gional level) of thehealthcare sys tem (“Na tional Sys tem of Healthcare”), al though the is sue re mainedopen as to the co or di na tion of the gov ern ing au thor i ties;
· con sol i da tion of the con tent, or gani sa tion and the or gans of the State Health Con trol,ex ten sion of the func tions of the es tab lish ments for pub lic health us ing the pos i tive as -pects and the half- a-cen tury ex pe ri ence of the ex ist ing or gani sa tion;
· reg u la tion of the or gani sa tion and the pro ce dures in the wide-rang ing field of men talhealth;
· in tro duc tion of or der in the ap pli ca tion of the so-called un con ven tional meth ods forfa vour able im pact on in di vid ual health;
· reg u la tion of the pa tient’s rights as well as the ac tiv i ties re lated to ge netic health, re -pro duc tive health and as sisted re pro duc tion;
· es tab lish ment of more sta ble nor ma tive re quire ments for the med i cal pro fes sions,med i cal ed u ca tion and med i cal sci ence.
These sub jects of le gal reg u la tion were of de ci sive im por tance for the con tin u ing con -struc tion and de vel op ment of the healthcare un der re form. The other ob jects pro vided for bythe Law were not cru cial for the sys tem. They added to and clar i fied its func tions but could bere ferred to any other type of a healthcare sys tem. Their pres ence in the dis cussed law en richedits scope and con tent but was not re lated to the re form pro cess.
It could be con sid ered that by this Law the main or the con struc tion frame work of the health re form leg is la tion was closed down. It was li a ble to im prove ment and ex ten sion, of course.
The leg is la tive amend ments in health in sur ance were rel a tively fre quent (be tween 1999and 2004 their num ber to talled 20), but the amend ment, men tioned above, in tro duced morepro found changes in the in sur ance sys tem. Firstly, a sig nif i cant de vel op ment was achieved inthe leg is la tive ar range ment of the vol un tary health in sur ance by cre at ing more spe cific, fa -vour able and nec es sary pre req ui sites for its pros per ity which was an im por tant part of thehealthcare re form. Sec ondly, changes were in tro duced in the man age ment of the oblig a toryhealth in sur ance, and more spe cif i cally of the NHIF. They re stricted the rel a tive au ton omy and sig nif i cantly strength ened the con trol by the state (more spe cif i cally of the ex ec u tivepower) on the man age ment of the NHIF. And in or der to avoid the in fringe ment on the prin ci -ples of the oblig a tory health in sur ance (Art. 5 of the LHI), the very prin ci ples were alsochanged (Art. 5, §2 of the LHI). The en hanced in ter fer ence of the state was not ground less –the in sur ance in stal ments of more than half of the cit i zens with health in sur ance were paidfrom the re pub li can bud get. But the ques tion was whether this ar gu ment was suf fi cient since awhole range of state or gans ex isted to con trol the fi nan cial or gani sa tions, such as the NHIF.
With the Law on the Pro fes sional Or gani sa tions of nurses, mid wives and as so ci ated
141
Stages and evo lu tion of the healthcare re form in Bul garia
med i cal spe cial ists the reg u la tion for the func tion ing of the pro fes sional or gani sa tions in thefield of healthcare was out lined (but not fully com pleted).
Un doubt edly, the es tab lish ment of a “Fund for Treat ment of Chil dren” Cen tre had anim me di ate im pact on pae di at ric healthcare. A pos si ble model for the so lu tion of some healthprob lems could be ob served in it and it could be ap plied not only to chil dren. This model,which had al ready been ex per i men tally tried, could be im proved and mul ti plied in var i ousforms, planes and as pects of the healthcare sys tem.
Strat egy for hos pi tal care
Apart from the laws and the by-laws re lated to the de vel op ment of the healthcare re form,an ap pli ca tion and an op er a tional plan was de vised – the Strat egy for the Re struc tur ing ofHos pi tal Care, adopted by the Coun cil of Min is ters in March 2002 to gether with the cor re -spond ing Ac tion Plan. As stip u lated in this doc u ment, the goal of the re struc tur ing con sistedin “the op ti mi sa tion of the re la tion “cost : med i cal ef fi ciency” in the sec tor of hos pi tal care inob ser va tion of the re quire ments for ac ces si bil ity, prompt ness, suf fi ciency and qual ity”. The at -tain ment of a bal ance was en vis aged be tween the needs for hos pi tal care and the nec es sary re -sources for their sat is fac tion.
Ac cord ing to the an nexed Ac tion Plan, the prac ti cal im ple men ta tion of the strat egy hadto be com pleted within two and a half years – un til the end of 2004. Dur ing this pe riod thehealthcare sys tem had to free it self from “su per flu ous hos pi tals and hos pi tal beds” with out re -strict ing the pop u la tion’s ac cess to hos pi tal care. It en vis aged the re duc tion of the ca pac itychiefly of the re gional (mu nic i pal) hos pi tals, some of which were to be closed down and oth ers to be re struc tured. Un der these con di tions, part of the staff had to be dis missed and the sav ingsfrom the sal ary fund were to be trans ferred to other, more fi nan cially sta ble hos pi tals. The useof the op por tu ni ties was also planned for the es tab lish ment of hos pi tal com plexes ormulti-hos pi tal sys tems (“econ o mies of scale”). For the dis missed per son nel, the open ing ofwork ing po si tions was planned in other (larger) hos pi tals and in out pa tients’ care (in clud ing inthe pri vate sec tor) as well as as sis tance for find ing em ploy ment in other spheres. The mu nic i -pal i ties were to de velop net works of daily homes, nurs ing homes, hos pices, var i ous forms ofhealth ser vices in the pa tients’ homes. The Na tional In vest ment Strat egy for the healthcaresys tem was to be de signed and a Na tional Agency for Health Tech nol o gies Planning was tobe worked out. Mea sures were to be un der taken for the im prove ment of the pro fes sional qual i -fi ca tion of the hos pi tal staff, in clud ing that in man age ment. Hos pi tal in for ma tion sys tems were to be launched. The im ple men ta tion of the strat egy was to be fa cil i tated by the cre ation of con -di tions for a pub lic con sen sus and by as sur ing po lit i cal support.
In view of the health in sur ance sys tem which had al ready been in tro duced and was func -tion ing, a work on the pros pects and the de vel op ment of hos pi tal care in Bul garia un til 2002was prob a bly not un nec es sary but to a cer tain ex tent an tic i pat ing. The pe riod, for which thehos pi tals had been func tion ing un der a health in sur ance re gime, was rather short. But in thiscase, the en vis aged strat egy is in ter est ing not so much from the point of view of its con cretecon tent and pur pose as a “strat egy”. What is more in trigu ing is the way of think ing and the in -ten tion. It is ex actly for this rea son that we will dis cuss it in greater de tail. The de fects of thehos pi tal sec tor are seen uni lat er ally, from the point of view of just one as pect – the hos pi tals’ex tra ca pac ity, which led to the dis turbed bal ance be tween (in creas ing) costs and med i cal ef fi -
142

ciency (not cor re spond ing to the costs). Gen er ally speak ing, the de vel op ment of hos pi tal carewas con sid ered, also one-sidedly, to be man i fested as “re struc tur ing”: re duc tion of the ca pac -ity, re lease of fund ing, re cov ery of the bal ance, op ti mi sa tion of hos pi tal care. Some otherstruc tural de ci sions were also tim idly men tioned such as hos pi tal com plexes, multi-hos pi talsys tems, and as hinted, trans fer of hos pi tal beds to out pa tients’ care. The so lu tion to the prob -lems was based on ad min is tra tive meth ods. The same ex ten sive ap proach was ev i dent in theso lu tion of the prob lem char ac ter is ing the pre vi ous sys tem, but with a re verse de nom i na tion.For lack of an in ten sive ap proach and plu ral is tic vi sion, the struc ture of the own er ship was leftout side the op er a tional field of the strat egy to gether with pos si ble changes in it, the struc tural as pects of a more ef fec tive in te gra tion of the pub lic and pri vate sec tor, the ap pli ca tion of eco -nomic mech a nisms for re struc tur ing as well as a num ber of other pos si bil i ties pro vided by thestra te gic reform tools.
As ob vi ous, this strat egy was not – at least to tally – ap plied from an op er a tional point ofview in ac cor dance with the Ac tion Plan. A cer tain re duc tion of the num ber of hos pi tal bedswas the ac tual out come of the ex am ined pe riod. How ever, we are not ing it here not in re la tionto the op er a tional out comes but from the point of view of its con tri bu tion to the de vel op ment of the healthcare re form. From this per spec tive, the strat egy is seen as a bu reau cratic doc u ment,and af ter fa mil iari sation with it, sus pi cions arise as to whether it had been de vel oped in view of its ap pli ca tion at all.
A “mar ket - lib eral” and a “so cial - lib eral” al ter na tive for thede vel op ment of healthcare
The po lit i cal views on the healthcare re form were ev i dent from the very be gin ning of itscon cep tion. What is com mon among them is the ac knowl edg ment of the need for a def i niteim prove ment of the healthcare sys tem to sat isfy the needs of the cit i zens and en sure a more sta -ble ba sis for its de vel op ment.
Var i ous views on sep a rate is sues of the re form were shared on var i ous oc ca sions and they were re flected in a more sys tem atic way in the two na tional strat e gies. There are a num ber ofdif fer ences be tween them, but the main one is not (or not so much) in the pro fes sional (let’scall it the med i cal) con tent but rather in the po lit i cal ori en ta tion.
In the first strat egy (1996), the im ple men ta tion of the re form was viewed as a rel a tivelyslower pro cess, which did not en vis age es sen tial change in the struc ture of the healthcare net -work; the pub lic own er ship of the pub lic healthcare es tab lish ments and the role of the state asan owner (ex cept for the phar ma cies net work) was pre served and the struc tural change of theown er ship was man i fested in the opened (with the amend ments in the LPH) pos si bil ity for thede vel op ment of the pri vate sec tor in the healthcare sys tem. Thus, an enor mous part of the phy -si cians, den tists and other spe cial ists of the healthcare net work had to re main hired work ers inthe pub lic sec tor. The pro cess of the new strat i fi ca tion of so ci ety that had started (through thefor ma tion of the class of in de pend ent mid dle-class own ers) was not go ing to find stron ger sup -port for the de vel op ment of the pri vate sec tor in the healthcare sys tem ei ther.
The sec ond strat egy (2001) fa voured the op po site view – by means of struc tural changesin the healthcare sec tor and var i ous forms of privatisation to ex e cute a rad i cal change in theown er ship struc ture of the healthcare sys tem and, through it, to fa cil i tate the pro cess of for ma -tion of a new so cial struc ture (the class of in de pend ent mid dle-class own ers) in so ci ety. The
143
Stages and evo lu tion of the healthcare re form in Bul garia
Na tional Health Strat egy 1996 was con ser va tive and the next one was lib eral.Nei ther the first, nor the sec ond health strat egy, how ever, had a pro claimed po lit i cal di -
rec tion as “right” or “left”. In the re form pro cess, this had hap pened for the first time in itsmod ern de vel op ment, when al ready formed po lit i cal views on the fur ther course of the re formwere de ter mined as “right” or “left”. In fact, in this case only the “right” views were an nounced with the po lit i cal qual i fi ca tion of “right”. The other view was de fined by us as “left” not somuch be cause of the “left” con cepts shared in it, but mainly as a coun ter part of the “right”.
The “right” view on the de vel op ment of the healthcare re form was ad vo cated by Dr.I. Semerdjiev at the end of 2004509. Its point of de par ture was for mu lated in the spirit of lib er -al ism, a cen tral fig ure be ing the in di vid ual and the per son al ity (“Ev ery man can do forhis/her health and well-be ing more than any phy si cian, hos pi tal or drug…”). It re lied on “thein di vid ual de ci sions of the mil lions of Bul gar ian cit i zens – de ci sions to con sol i date and pro tect their own health.” The func tions of so cial pro tec tion, how ever, were also taken into ac count –“So ci ety has to bear the re spon si bil ity for the health pro tec tion of per sons who hap pen to be in risk so cial pre dic a ments tem po rarily or for a lon ger pe riod of time …”. The main ori en ta tionof the strat egy was to ward pro tec tion of the in di vid ual health in the fam i lies, groups and com -mu ni ties with their ac tive and ma jor par tic i pa tion.
The im ple men ta tion of the strat egy was aimed at achiev ing goals in three di rec tions: (1)im prove ment of the in di vid ual health and over com ing of the neg a tive health trends in so ci ety;(2) struc tural changes and de vel op ment of the healthcare sys tem; (3) struc tural changes andde vel op ment of the health in sur ance.
To im prove peo ple’s health, care was en vis aged for cer tain pri or ity groups of the pop u -la tion (preg nant women, moth ers, newly born ba bies) to gether with pur pose ful mea sures(screen ing in ter ven tions, achieve ment of low risk be hav iour, re duc tion of the pre vent ablemor bid ity and mor tal ity, treat ment and re ha bil i ta tion) con cern ing car dio vas cu lar dis eases, ma -lig nant tu mours, ac ci dents, di a be tes, dis eases of the re spi ra tory sys tem, HIV/AIDS, con tam i -nated food. Pur pose ful in ter ven tions were also planned for the risk groups of the pop u la tion(es pe cially in the Roma com mu nity).
In terms of the healthcare sys tem, the strat egy in cluded con sis tent change in the own er ship struc ture through privatisation of the pub lic healthcare es tab lish ments, reg is tered as com mer cialcom pa nies, in cen tives for the de vel op ment of the pri vate sec tor, in tro duc tion of sys tems forqual ity man age ment and cer tif i ca tion of the healthcare es tab lish ments for qual ity, de vel op mentof com pe ti tion among sim i lar es tab lish ments and part ner ship with es tab lish ments of dif fer entpro file, man age ment au ton omy and re spon si bil ity of the med i cal and healthcare es tab lish ments,in crease of the man age ment ca pac ity and com pe tences in the gov er nance, con tin u ous ed u ca tion,re-train ing and pro vi sion of al ter na tive em ploy ment of the health es tab lish ments staff. The statehad to be com mit ted pri mar ily to the de vel op ment of the ser vices for pub lic healthcare (healthpro mo tion and pre ven tion of dis eases, med ico-so cial ac tiv i ties).
In the field of the oblig a tory health in sur ance, the strat egy en vis aged the de vel op ment ofdemonopolisation and de cen trali sa tion. The com pul sory health in sur ance could be car ried out by both the ex ist ing or gani sa tions (e.g. the 28 RHIFs) and pri vate com pa nies for health in sur ance.
144
509 Semerdjiev, I. The Right Al ter na tive in Healthcare – Short De scrip tion of the Work “Re view and Strat egy ofthe Na tional Healthcare for the Pe riod 2005-2010”, 2004; Semerdjiev, I. The Fu ture of the BlgarianHealthcare. In ter na tional Con fer ence “Mar ket for Goods and Ser vices in the Healthcare Sec tor of UnitedEu rope”. So fia, 30.11.-1.12.2004

The cen tral au thor i ties of the NHIF ceased to func tion. The RHIFs be came au ton o mous pub -lic health in sur ers, the pos si bil ity for their privatisation not be ing ex cluded. The health in sur ers(pub lic and pri vate) them selves de ter mined the pack age of ser vices to be of fered for oblig a toryhealth in sur ance to the cit i zens. The in sur ance or gani sa tions com peted for the vol ume and qual -ity of the of fered health ser vices. The cit i zens them selves chose their in sur ance or gani sa tion.The com pul sory in sur ance in stal ments were col lected by the NII (as is the case cur rently, ac cord -ing to the LHI), but they were dis trib uted among the in sur ance or gani sa tions, de pend ing on thenum ber of cit i zens in sured by the re spec tive or gani sa tions. Based on the pack age of health ser -vices cov ered by the oblig a tory health in sur ance pro posed by the in sur ance com pany, di rect ne -go ti at ing was in tro duced be tween healthcare es tab lish ment and the in sur ance or gani sa tion, thus, mak ing the na tional frame work con tract ing re dun dant. Ev ery healthcare es tab lish ment was toof fer its own “prod uct list” and ev ery in sur ance or gani sa tion was to sub mit an of fer with the pro -posed prices, the re gime of pay ment and re quire ments for qual ity.
Ap par ently, in the sec tors of healthcare and health in sur ance, the em pha ses were placedon the mar ket rules, pri vate own er ship and ini tia tive, cit i zens’ free choice of a healthcare es -tab lish ment and in surer, free con tract ing, com pe ti tion among the healthcare es tab lish mentsand among the health in sur ance or gani sa tions. Bear ing in mind the above men tioned ori en ta -tion to ward the in di vid ual and in view of these em pha ses, it can be con sid ered that the stud iedma te ri als re flect a lib er ally ori ented model in healthcare pre sent ing the de vel op ment andcon tin u a tion of the re form pol icy from 1997-2001.
The start ing point of the al ter na tive model, which had to be ac com plished within 5 years (un til the end of 2009), was the un der stand ing for re con sid er a tion and over all change in thehealth pol icy in or der to over come the deep na tional cri sis, de fin ing new pri or i ties, ob jec tivesand mech a nisms for the healthcare re form510. The pre ven tion and health pro mo tion were for -mu lated as a lead ing pri or ity, the mu nic i pal ity be ing seen as “the nat u ral ter ri tory for the ex -e cu tion of com plex health ac tiv i ties” with an ac cent on pre ven tion ac tiv i ties in the schools.The main pri or i ties in cluded the health of ad o les cents aged up to 18 and the set ting up of newhealth struc tures for new borns, chil dren in pre-school and school age, pro vid ing of a so ciallyfair ac cess to the var i ous lev els of med i cal care, guar an tee ing of health in sur ance and healthsol i dar ity through a bal ance be tween the in di vid ual and pub lic rights, li a bil i ties and in ter ests.The main ob jec tives in cluded health ser vices up to def i nite stan dards, in tro duc tion of in cen -tives for en hance ment of the pub lic and in di vid ual re spon si bil ity for the health, for ma tion of anew in di vid ual and pub lic at ti tude to health as a ba sis for a healthy life style and health safety.
A se ries of steps were planned for the im ple men ta tion of the model. The first one was thecon sol i da tion of the Eu ro pean health pol icy prin ci ples, de ter min ing the ba sic health ser vicesand goods for the pop u la tion by means of cri te ria for med i cal ef fi ciency, eco nomic and so cialac cept abil ity. The next steps were re lated chiefly to the is sues of fi nanc ing, health in sur anceand the de vel op ment of the med i cal care sec tor.
In or der to im prove the fi nanc ing, the to tal fi nan cial re sources were planned to reach 5%of the GDP in 2005 and 5.9% of the GDP in 2009, the fund ing be ing pro vided by the state, themu nic i pal bud gets and the NHIF. The rel a tive share of the fund ing from the vol un tary in sur -ance funds would rise from 0.1% in 2003 to 1.1% of the GDP in 2009. The house holds’ ex pen -
145
Stages and evo lu tion of the healthcare re form in Bul garia
510 Vodenicharov, T. et al. Healthcare: Re spon si bil ity, Free Choice, Sol i dar ity. 2004; Vodenicharov, T., V.Borisov, St. Gladilov, K. Chamov, D. Krushkov. Ìîäåë çà åôåêòèâíî ðàçâèòèå íà áúëãàðñêîòîçäðàâåîïàçâàíå. In: Healthcare man age ment jour nal, Is sue ¹, 2005, pp. 5-14
di ture for healthcare would not ex ceed 1.2% of the GDP. A re form of the over all sys tem was en vis aged for the de vel op ment of the health in sur -
ance. By elim i nat ing the NHIF mo nop oly on oblig a tory health in sur ance, the three-pil larmodel was to be in tro duced for the health in sur ance which (sim i lar to the pen sion in sur ance)would in clude (1) oblig a tory health in sur ance; (2) oblig a tory ad di tional health in sur ance and(3) vol un tary health in sur ance. Cit i zens would have the right of free choice of a healthcare es -tab lish ment and an in sur ance or gani sa tion. Pub lic con trol would be ex erted over the over allpro cess of health in sur ance, rep re sen ta tives of pa tients’ or gani sa tions tak ing part in the man -age ment of the health in sur ance funds.
The set ting up was also en vis aged of a spe cial fund, fi nanced by the state, from whichmed i cal care would be paid for the so cially unprivileged cit i zens as well as for per sons who,for ob jec tive rea sons, did not pos sess a health in sur ance. The costs for the ex pen sive treat mentwould be paid by the state up to a cer tain limit. The costs for den tal pro phy laxis and treat mentof chil dren, pu pils and so cially dis ad van taged cit i zens, ex ceed ing the fi nanc ing pro vided bythe health in sur ance, would be paid by the state and the mu nic i pal i ties. The stand was shared that “the vi cious prac tice of ex clud ing the fi nanc ing of the mu nic i pal hos pi tals from the mu nic -i pal bud gets should be re con sid ered”.
For the hos pi tal sec tor, the de vel op ment of pub lic-pri vate part ner ships was planned throughnew nor ma tive and or gani sa tional tech nol o gies. The im prove ment of the Na tional Health Mapwould fa cil i tate the pa tients’ ac cess to spe cial ised and highly spe cial ised med i cal care.
The privatisation of the healthcare es tab lish ments was to be car ried out step by step,pre serv ing the “state or mu nic i pal healthcare es tab lish ments for out pa tients’ and hos pi talmed i cal care, guar an tee ing high qual ity and highly spe cial ised med i cal care.”
What is a com mon point be tween the two views is the in ten tion for the healthcare re formto be con tin ued, and in this view, a key po si tion was oc cu pied by the re or gani sa tion of thehealth in sur ance and the privatisation of the hos pi tal sec tor. In both views, the at ten tion was fo -cused on the rights and re spon si bil i ties of the in di vid ual in so ci ety.
There were nu mer ous dif fer ences in the de tails, but the ma jor dif fer ence be tween thetwo views re garded the role of the state and the role of the mar ket forces. In the “right”strat egy the de vel op ment was as so ci ated with the pres er va tion of the state role in terms ofpub lic healthcare and the pos si ble fi nanc ing of na tional heal ing programmes, and in terms ofthe hos pi tal sec tor and the health in sur ance – max i mum pos si ble re stric tion of the state in ter -fer ence and free dom for the mar ket fac tors, de vel op ment and dom i na tion of a stim u lated pri -vate sec tor. The al ter na tive strat egy en vis aged the de vel op ment of the pri vate sec tor(es pe cially in health in sur ance) but pre serv ing to a cer tain de gree the func tion of the state in the re dis tri bu tion of the pub lic funds.
From all the above, it is ev i dent that dur ing the re cent stage of the re form two mod els have beenformed for the de vel op ment of the health sys tem – a more lib eral ver sus a more con ser va tive one.
Pub lic opin ion on the re form in healthcare
Cov er age of the healthcare re form in the press from the sec ond half of2001 to 2005
As it was al ready noted, we as sume that the mid dle of 2001 marks the be gin ning of thethird stage of the healthcare re form, when the NHIF started to par tially fi nance hos pi tal care. In
146
spite of the sig nif i cance of this fact for the de vel op ment of the healthcare re form, the pub li ca -tions from the sec ond half of 2001 con cerned mainly eval u a tions of the re form, po lit i cal re -views on what had been achieved that far and the in ten tions of the new gov ern ment of theNMSS and the newly ap pointed Min is ter of Healthcare Assoc. Prof. Dr. Bozhidar Finkov.
Un like the pre vi ous re la tions be tween the rul ing party and the op po si tion, char ac ter isedmainly by con fron ta tion, the new ma jor ity re ported pos i tive changes in the sys tem ofhealthcare ex e cuted by the pre vi ous gov ern ments. In an in ter view, the Dep uty from the NMSSAssoc. Prof. Plamen Kenarov gave a high as sess ment of what had been done by the pre vi ousgov ern ments and de clared the in ten tions of the NMSS to con tinue the re form. In his in ter -view, he pointed out that the adop tion of a Law on Health would be a pri or ity for the NMSS,aimed at re plac ing the LPH. He shared the in ten tion to elim i nate the com mer cial sta tus of thehos pi tals be cause of the cor po rate rev e nue tax a tion and the cre ation of pre req ui sites for the de -vel op ment of vol un tary health in sur ance funds, which would also have to carry out the com -pul sory health in sur ance un der cer tain con di tions511. The newly ap pointed Min is ter ofHealthcare Assoc. Prof. Dr. Bozhidar Finkov also sup ported the re form, de clar ing that norev o lu tion ary changes would be un der taken dur ing its course and re gard ing the Na tionalHealth Strat egy, he stated that “in gen eral the di rec tion is right”. Min is ter Finkov did not ex -pect that the mo nop oly of the NHIF would last for long. He thought that it would be good tohave more funds but those health in sur ance funds had to be pri vate. He also ex pressed theopin ion that the mo ment was not ap pro pri ate for an in crease of the health in sur ance in stal -ments. The Min is ter also stated that the prob lem of region ali sa tion was a pri or ity for theshort-term programme of the Min is try and “the school doc tors will not re turn in the knownform but in a more ef fec tive form cor re spond ing to the new eco nomic con di tions.” 512
The most im por tant is sues dis cussed by the gov ern ing cir cles were those of therestructuring of hos pi tal care, the de vel op ment of the vol un tary health in sur ance com pa -nies, the privatisation of the healthcare es tab lish ments and the bud get of the NHIF.
In an in ter view for the “Trud” daily on the oc ca sion of the 100 days of the NMSS gov ern -ment, Min is ter Finkov de clared that the great est suc cess achieved so far was “the well-thoughtleg is la tive ini tia tive” and the change in the man age ment – ex pan sion of the par tic i pa tion in thehos pi tal ex ec u tive boards (the mu nic i pal i ties which were co-own ers, also par tic i pated in the“boards of di rec tors” of the dis trict hos pi tals), com pe ti tion was also in tro duced. Ac cord ing tothe Min is ter “the rem edy for the healthcare is in its or gani sa tion and re struc tur ing and not onlyin the in vest ment of money”513.
Privatisation of healthcare
At the end of the year, an ar ti cle in the “Kapital” weekly was de voted to the privatisationin healthcare. The pub li ca tion pointed out that for sev eral months the Min is try of Healthcare,the Min is try of Fi nance and the Mem bers of Par lia ment were not able to reach an agree mentabout the reg u la tion of the privatisation in the healthcare sec tor, and as a re sult, the pro cess had been post poned. In his turn, Min is ter Finkov im posed a mor a to rium on the privatisation ofbuild ings and of fices in the for mer poly clin ics and the Par lia men tary Eco nomic Com mis siondis missed the hos pi tal privatisation from its agenda. The ar ti cle men tioned a sep a rate law on
147
Stages and evo lu tion of the healthcare re form in Bul garia
511 Duma daily, Is sue ¹ 148 from 29.06.2001512 Trud daily from 203 from 30.07.2001; Democracia daily, Issue ¹ 183 from 6.08.2001513 Trud daily, Is sue ¹ 303 from 8.11.2001
hos pi tal privatisation, which was ex pected to be worked out un til the mid dle of the fol low ingyear (i.e. 2002) 514. In March 2002, af ter the dep uty from the UDF Dr. Stoicho Katsarov ac -cused the gov ern ing pol i ti cians of the ces sa tion of the privatisation in healthcare515, the man -age ment of the UBP in sisted on an ur gent meet ing with Pres i dent Georgi Purvanov in or der todis cuss the par tic i pa tion of the healthcare work ers in the privatisation of the healthcare es tab -lish ments516. In Oc to ber 2002, Min is ter Finkov and the leader of the Con fed er a tion of the In -de pend ent Trade Un ions in Bul garia Zhelyazko Hristov an nounced that privatisation would be car ried out only for the un prof it able healthcare es tab lish ments517. The Trade Un ion agreedwith privatisation only on con di tion that the struc tur ally de ter min ing es tab lish ments re mainedin a pro hi bi tion list, the com pe tences of the work ers’ and man ag ers’ com pa nies (WMC) werere sumed and a 15-year term was stip u lated af ter the privatisation, dur ing which the healthcarees tab lish ments were obliged to pre serve their ac tiv i ties and volume.
In 2003, a draft amend ment in the LHE, sub mit ted to the Par lia men tary Com mis sion onHealthcare by Antonia Purvanova and dep u ties from the Move ment for Rights and Free doms,en vis aged the right of non-profit or gani sa tions to open and pur chase hos pi tals, in clud ing thechurch, and for the privatisation of the mu nic i pal healthcare es tab lish ments to start in 2004.Ac cord ing to the draft, the pri va tised healthcare es tab lish ments would have the right to be reg -is tered as foun da tions but with out the right to per form ac tiv i ties con tracted with the NHIF,the dis pen sa ries with out beds would be re struc tured into med i cal cen tres and the re main ingwould be re struc tured into spe cial ised hos pi tals, which would en able them to con clude con -tracts with the RHIF. Ac cord ing to dep u ties from the UDF, the amend ments in the Law wouldonly legal ise the foun da tions, which had al ready been set up in the ma jor ity of the hos pi tals518.
An ar ti cle in the “Kapital” news pa per re ported about draft amend ments in the LHE,whose ini ti a tors were the rep re sen ta tives of the NMSS Assoc. Prof. Dr. Atanas Shterev andAleko Kyurkchiev, reg u lat ing the terms and con di tions for the privatisation of the di ag nos ticand con sul ta tive cen tres. The amend ments pro vided for the hos pi tals’ privatisation, ac cord ingto the gen eral or der of the Law on Privatisation, with out spe cial re quire ments519. The Dep u tiesfrom Co ali tion for Bul garia op posed the pro ject pro posed by the NMSS with the ar gu ment that the privatisation of the healthcare es tab lish ments for hos pi tal care was be ing pre pared with outa strat egy or re gional anal y sis of the con se quences on the health sys tem520.
In 2003, Healthcare Min is ter Slavcho Bogoev de clared in front of the NA that one of thepri or i ties of the state health pol icy was the adop tion of a law abol ish ing the mor a to rium on theprivatisation of the healthcare es tab lish ments521.
Con cern ing the amend ments of the LHE re lated to the privatisation, which were be ingdis cussed in the Par lia men tary Com mis sion on Healthcare, the me dia con tin ued their com -ments and dis cus sions on the topic un til the end of 2003522.
In 2004, the me dia in formed again about the views of the gov ern ing class and the op po si -
148
514 Kapital weekly, Is sue ¹ 51 from 22.12.2001515 Democracia daily from 1.03.2002516 Democracia daily from 7.03.2002517 Duma daily, Is sue ¹ 239 from 16.10.2002; Kapital weekly from 19-25.10.2002518 24 chasa daily, Is sue ¹ 201 from 25.07.2003519 Kapital weekly from 12-18.07.2003520 Duma daily, Is sue ¹ 280 from 2003521 Standart daily, Is sue ¹ 3856 from 27.09.2003522 Standart daily, Is sue ¹ 3924 from 4.12.2003
tion re gard ing the privatisation of the healthcare es tab lish ments. The draft of the NMSS onthe LHE amend ment en vis aged that the healthcare work ers did not have a pri or ity in theprivatisation of the healthcare es tab lish ments. On the con trary, just the op po site was plannedin the draft pro posed by the UDF523. A month later, a pub li ca tion in the “Trud” daily pre sentedsome fun da men tal points in the three pro jects for privatisation of the healthcare es tab lish -ments, e.g. those of the BSP, UDF and NMSS524. The BSP’s pro ject pro vided for the sell ing ofhealthcare es tab lish ments not only to un ions of phy si cians but also to or gani sa tions in whichthe mu nic i pal i ties par tic i pate; the UDF pro ject gave ad van tages to the hos pi tal em ploy ees anden vis aged that, if it was state-owned, the per mis sion for the privatisation had to be granted bythe Min is ter, and if it was owned by the mu nic i pal ity – by the City Coun cil; the pro ject of theNMSS in cluded a pro hi bi tion list of 67 hos pi tals and the Chair man of the Par lia men tary Com -mis sion on Healthcare Assoc. Prof. Dr. Atanas Shterev de clared that “the sell ing of the hos pi -tals be gins within two months.”
In spite of the dif fer ences on the privatisation of the healthcare es tab lish ments be -tween the rul ers and the op po si tion, all of them per ceived it as an in dis pens able part of the re -form pro cess. The Dep uty from the UDF and for mer Min is ter of Healthcare Dr. StoichoKatsarov stated that privatisation was part of the healthcare re form and the re struc tur ing of thehos pi tal es tab lish ments re lated to it, and that the “the mar ket is the one to de cide how manyhos pi tals are needed in the coun try.” He ar gued in front of the me dia in fa vour of the claimmade by the UDF for pref er ences that only in this way the pres er va tion of the ac tiv i ties of thepri va tised healthcare es tab lish ments would be guar an teed525. The then Vice Min is ter ofHealthcare Dr. Petko Salchev also per ceived privatisation as one of the el e ments of the re formfor the achieve ment of greater mar ket ori en ta tion in healthcare, but he re ported that he did notex pect a par tic u lar in ter est in hos pi tal privatisation. In his opin ion, privatisation was not acom po nent of the hos pi tal re struc tur ing but rather of the re struc tur ing of the own er ship526.
The gen eral prac ti tio ners and the spe cial ists also sup ported the privatisation but withoblig a tory pref er ences for the med i cal pro fes sion als527.
Con trary to his state ments from April 2004, and as an at tempt to “rec on cile” the dif fer -ences be tween those in power and the op po si tion, the Chair man of the Par lia men tary Com mis -sion on Healthcare Assoc. Prof. Dr. Atanas Shterev an nounced that in Sep tem ber he was go ing to pres ent to the Par lia men tary Com mis sion the idea of giv ing the hos pi tals for con ces sion for25 – 30 years in stead of their pri va tis ing528.
The pro fes sional or gani sa tions of phy si cians and den tists
In the sec ond half of 2001, the con flicts around the UBP and the Law on the Pro fes -sional Or gani sa tions of Phy si cians and Den tists con tin ued. In Oc to ber the Chair man of theUBP Dr. D. Ignatov and a group of Mem bers of Par lia ment pro posed a draft amend ment of theLaw on Pro fes sional Or gani sa tions, ac cord ing to which phy si cians had the right to con sti tuteas so ci a tions in spe cial ties within the UBP and the Un ion had to be fi nanced by the state with a
149
Stages and evo lu tion of the healthcare re form in Bul garia
523 24 chasa daily, Is sue ¹ 86 from 27.03.2004524 Trud daily from 18.04.2004525 Kapital weekly from 17-23.04.2004526 Kapital weekly from 17-23.04.2004 527 24 chasa daily, Is sue ¹ 169 from 20.06.2004528 Trud daily from 4.09.2004
monthly sub sidy. The Par lia men tary Com mis sion on Healthcare re jected the pro posal on firsthear ing with the main ar gu ment that the draft lacked a text aban don ing the oblig a tory mem ber -ship in the Un ion. The NMSS de manded the elim i na tion of the oblig a tory mem ber ship and thees tab lish ment of cham bers529.
In their turn, the UBP and the UDB pro claimed them selves against the amend ments in theLaw on Pro fes sional Or gani sa tions, de pos ited by the NMSS and against the draft pro ject for acham ber of phy si cians. In a dec la ra tion the two or gani sa tions stated that, if the NMSS passedthe amend ments force fully, they would com mence pro test ac tions, their ar gu ments be ing that“the amend ments will ruin the pro fes sional or gani sa tions and will de sta bi lise the re form.”530 In an in ter view, the Chair man of the UBP Dr. D. Ignatov de clared: “I ex pect a “yel low” pu ri fi ca -tion of the Health In sur ance Fund and the hos pi tals”531.
In 2005, an ex pert group of the UBP pre pared a draft amend ment and an ad di tion to theLaw on Pro fes sional Or gani sa tions, en ti tling the Un ion to more com pe tences for sanc tion -ing phy si cians. The mo tives were that the pen al ties im posed by the eth i cal com mis sion of theUBP did not have a bind ing char ac ter since they were part of the eth i cal code, and there fore,they were of ten re jected by the ju di cial in sti tu tions532.
In 2002, af ter the elec tion of Dr. Andrei Kehaiyov for a Chair man of the UBP, in for ma -tion was re leased about the in ten tions of the UBP to in tro duce a credit sys tem for the eval u a -tion of the phy si cians’ qual i fi ca tion to be en forced from 2003533. The prep a ra tion of thesys tem for phy si cians’ qual i fi ca tion as sess ment con tin ued in 2003, and it en vis aged that theUn ion man aged and co or di nated the pro cess of eval u a tion of the doc tors’ pro fes sional skillsand awarded the cor re spond ing qual i fi ca tion de gree. Ac cord ing to the Vice Min is ter ofHealthcare Dr. Petko Salchev, phy si cians who had re ceived more cred its would be pre ferredby the pa tients534. A ma te rial, pub lished in the “Duma” daily in 2004, quoted a phy si cian’sopin ion that the healthcare re form had de stroyed the sys tem of the phy si cians’ post grad u atequal i fi ca tion and “is now a days the in di vid ual care of ev ery prac ti tio ner.”535
The na tional health in sur ance fund
At the be gin ning of July, a pub li ca tion in the “Democracia” daily in formed about the in ten -tions of the NMSS to change the Ex ec u tive Board of the NHIF536. Three months later, again inthe “Democracia”, it was an nounced that “the NMSS is pre par ing to change the model of thehealthcare re form,” and that the gov ern ing par ties in tend to with draw money from the Fund’s re -serve in or der to cover the debts of the healthcare es tab lish ments. On this oc ca sion, the Chair man of the Par lia men tary Com mis sion on Healthcare Assoc. Prof. Dr. Atanas Shterev de clared that itwas “un ac cept able that at the end of the year the Fund has a re serve of 420 mil lion BGN and thehos pi tals are deeply in debted.” In the same pub li ca tion, it was pointed out that amend mentswould be in tro duced in the laws on the pro fes sional or gani sa tions, health in sur ance and thehealthcare es tab lish ments, and ac cord ing to its au thor, it im plied an en tire change of the
150
529 Kapital weekly, Is sue ¹ 40 from 6.10.2001530 Democracia daily, Is sue ¹ 254 from 30.10.2001 and Is sue ¹ 255 from 31.10.2001531 Democracia daily, Is sue ¹ 231 from 3.10.2001532 Duma daily, Is sue ¹ 19 from 24.01.2005533 Trud daily from 6.07.2002 and 7.08.2002534 Trud daily from 23.10.2003535 Duma daily, Is sue ¹ 172 from 27.07.2004536 Democracia daily, Is sue ¹ 159 from 9.07.2001
healthcare re form model537. In the mean time, the “Democracia” fea tured the res ig na tion sub mit -ted by the NHIF Di rec tor Dr. B. Penkov as a re sult of a “po lit i cal pres sure” and the ap point mentof Assoc. Prof. Dr. N. Vassilev to ex e cute the func tion of a Di rec tor of the NHIF538.
The fol low ing pub li ca tions in formed pri mar ily about the changes in tended by the man -age ment of the NHIF for 2002. The “Trud” daily in formed that the new man age ment of theNHIF would pro pose that the 24-hour avail abil ity of the GPs was aban doned and they werepaid de pend ing on the num ber of hours they chose to work them selves539. From the be gin ningof 2002, the prin ci ple of pay ment for the med i ca tions was also changed. The pay ment wasto be based on the min i mum price of a cer tain drug, the list of the NHIF in clud ing the ge nericnames only. On this oc ca sion the Chair man of the As so ci a tion of the Bul gar ian Phar ma ceu ti cal Pro duc ers Ognyan Palaveev de clared that his As so ci a tion ap proved the pro posed mech a -nism540. A new way of pay ment was planned from 2002 to the gen eral prac ti tio ners, too, e.g.the GPs would re ceive a dif fer ent amount for ev ery in di vid ual pa tient ac cord ing to the age, and if the GPs had not seen the pa tient, they would not get any pay ment for the re spec tive in suredpa tient from the Fund541.
The com ments con tin ued about the “costly of fices and flashy lim ou sines” of the NHIF542. In 2002, the Ex ec u tive di rec tor of the NHIF Assoc. Prof. Dr. N. Vassilev de manded that theMin is try of Fi nance made an au dit of the NHIF for its ac tiv i ties as well as dur ing the man age -ment of Dr. I. Semerdjiev and Dr. B. Penkov543.
In 2002, the com ments on the NHIF cap i tal in vest ment and the ex penses for long-term as -sets gave way to the ne ces sity of the build ing of a new in for ma tion sys tem and the con flicts,which en sued with the com pany re spon si ble for the con struc tion of the sys tem544. In for ma tionwas re leased that from the loans from the WB, ne go ti ated while Min is ter Semerdjiev was in of -fice, apart from the 8 mil lion EUR for con sul tants of the MH, about 35-40 mil lion were aimedfor the NHIF in for ma tion sys tem; 11 mil lion EUR had al ready been spent on com put ers of theNHIF and 1 mil lion US dol lars had been spent on a com put ing cen tre at the Cen tral Head quar -ters. Min is ter Finkov stated that he would de mand dou ble in crease of the loan for the re form inhos pi tal care545. At the end of the year, it was an nounced that the NHIF was be gin ning onceagain to build the in for ma tion sys tem and the new Ex ec u tive Board was go ing to se lect an al -ter na tive for the pro ject con tin u a tion546. The se lec tion of the ex ec u tor for the de sign of the newNHIF in for ma tion sys tem (for the sec ond time af ter the se lec tion of “Aremis soft” in 1999)was cov ered in the me dia as “out ra geous” and was ac com pa nied by com ments and sus pi cionsabout “sub sti tu tion of clas si fi ca tion,” “po lit i cal pres sure” and “con flicts of in ter ests” dur ingthe ad min is tra tion of the ten der547.
The in for ma tion about the NHIF bud get in the first half of 2002 was as so ci ated mainlywith the for ma tion of the in come part, and the pub li ca tions in the sec ond half of the year were
151
Stages and evo lu tion of the healthcare re form in Bul garia
537 Democracia daily, Is sue ¹239 from 12.10.2001538 Democracia daily, Is sue ¹ 238 from 11.10.2001539 Trud daily, Is sue ¹ 289 from 25.10.2001540 Kapital weekly, Is sue ¹ 43 from 27.10.2001541 Democracia daily, Is sue ¹278 from 7.12.2001542 Trud daily from 289 from 25.10.2001; Standart daily, Is sue ¹ 3381 from 1.06.2002543 Standart daily, Is sue ¹ 3297 from 7.03.2002544 Duma daily, Is sue ¹31 from 2002 Kapital weekly from 26.01.-1.02.2002 and from 2-8.02.2002545 24 chasa daily, Is sue ¹ 44 from 14.02.2002.; Duma daily, Is sue ¹ 37 from 2002546 Kapital weekly from 23-29.11.2002547 Kapital weekly from 2-8.07.2005
con sid er ably less in num ber than those con nected with the costs and the short age of fi nance for the pay ment of the ne go ti ated med i cal ser vices. In May, the “Kapital” weekly re ported aboutthe ful fil ment of the rev e nue part of the bud get from in ter ests, fines and collectibility of healthin sur ance in stal ments548. The NHIF de manded that they could gov ern the money from the re -serve in de pend ently in or der to aug ment the fi nanc ing for the hos pi tals, but the Bul gar ian Na -tional Bank and the Min is try of Fi nance did not con sider it “ap pro pri ate” and it was nec es saryto com ply it with the IMF549.
The mem ber of the Na tional Ex ec u tive Coun cil of the UDB Dr. Vanyo Sharkov de claredthat 100 mil lion BGN were not suf fi cient for the NHIF, and there fore, its bud get needed to beup dated550. The draft NHIF bud get for 2003 en vis aged an in crease amount ing to 110 mil lionBGN as com pared to 2002, as well as a re duc tion in the ad min is tra tive costs up to 4% from theto tal ex pen di ture of the NHIF and in the cap i tal in vest ment up to 0.53%551. In the mean time,the “left” de manded amend ments in the Law on the NHIF bud get in sist ing on 80 mil lion BGNfrom the formed ex cess from the pay ment of med i ca tions552.
In Oc to ber, it was an nounced that the adop tion of the NHIF bud get was post poned be -cause of dis putes about the ex penses and the re serve uti li sa tion, and the Vice Min is ter of Fi -nance Kiril Ananiev ad dressed ac cu sa tions to the NHIF that they wanted to use the re serve but“no one had de signed the strat egy for what and how”553. At the end of the month, it was re -ported that the draft bud get had been adopted by the Ex ec u tive Board of the NHIF, in whichthe costs had been in creased and a higher in come had been planned from health in sur ance in -stal ments be cause of the in tro duc tion of in sur ance thresh olds554. The press also cov ered thecon flict be tween the MH and the NHIF re gard ing the claims of the Min is ter of Healthcare tode ter mine the list of drugs paid by the NHIF and the bud get guar an teed to the Fund from med i -cal ac tiv i ties. In re la tion to this, it was re ported that “the MH is tak ing over the func tions of theFund” and it was re minded by its press cen tre that the NHIF was “an in de pend ent in sti tu tionwhich de ter mines on its own the list of drugs to be paid to tally or par tially”555. Ac cord ing to the act ing Di rec tor of NHIF Prof. Georgi Nachev, “it is ap pro pri ate for the Min is try to de ter minethe stra te gic things such as the list of dis eases to be treated with free drugs. The fact that theMin is ter is go ing to also de ter mine the min i mum pack age of health ser vices does not take overthe func tions of the Fund and the frame work agree ment”556. Sev eral months later he de claredthat the NHIF had to be in de pend ent, but at the same time, in his opin ion, the state had to coverits fi nan cial def i cit557. This view was shared by Prof. Al ex an der Chirkov, too, ac cord ing towhom the NHIF had to pay to tally for the med i cal care, but when there was short age of money,the def i cit had to be cov ered by the state “un til the Fund be comes con sol i dated enough.”558
The changes in the man age ment of the NHIF con tin ued in 2002. In April, Stefan
152
548 Kapital weekly from 1–10.05.2002 and from 24–31.05.2002549 Kapital weekly from 13–19.04.2002 and from 11–17.05.2002; 24 chasa daily, Is sue ¹ 146 from 2002; Duma
daily, Is sue ¹ 209 from 2002550 Democracia daily from 5.06.2002551 Trud daily from 10.09.2002552 Duma daily, Is sue ¹ 221 from 25.09.2002553 Kapital weekly from 12-18.10.2002554 Kapital weekly from 19-25.10.2002 and from 26.10.–1.11.2002555 Duma daily, Is sue ¹ 212 from 14.09.2002 Duma daily, Is sue ¹ 245 from 5.09.2002; Trud daily from556 24 chasa daily, Is sue ¹. 305 from 4.11.2002557 Standart daily, Is sue ¹ 3470 from ò 29.08.2002558 24 chasa daily, Is sue ¹159 from 11.06.2002
Sofiyanski with drew from the po si tion of Chair man of the Ex ec u tive Board of the NHIF, Dr.Semerdjiev be came a mem ber of the Board, the act ing Di rec tor of the NHIF Assoc. Prof. Dr.N. Vassilev be came Chair man of the Board and the then Dep uty Chair man Prof. GeorgiNachev oc cu pied his po si tion559, later re placed by Nadezhda Geneva for a short pe riod of time. At the end of the year, new pro pos als were an nounced for Di rec tor of the NHIF – Dr. IvanBukarev, sup ported by Assoc. Prof. Dr. Atanas Shterev, Dr. Spas Spaskov sup ported by A.Purvanova and Andrei Markov pro posed by Plamen Kenarov560. By amend ments in the LHI,the de ci sion was taken on sec ond hear ing for one mem ber of an as so ci a tion of pa tients’ rightspro tec tion to be in cluded in the As sem bly of NHIF rep re sen ta tives561.
At the be gin ning of 2003, the forth com ing elec tion for a Di rec tor put the topic of theman ag ing or gans of the NHIF on the agenda of the press. Sev eral ar ti cles from Jan u ary in -formed about the mem bers of the Ex ec u tive Board, the Gen eral As sem bly and the Con trolCoun cil of the NHIF, their choice and po lit i cal sup port were dis cussed to gether with the ab -sence of rep re sen ta tives of the health in sured peo ple in the man ag ing or gans562.
In a let ter to the Par lia men tary Com mis sion on Healthcare, Prime Min is ter Sim eonSaxe-Co burg-Gotha urged for un der tak ing ur gent mea sures for re strict ing the NHIF ex pensesand for op ti mis ing the man age ment of the re gional di vi sions and the cen tral head quar ters ofthe NHIF. The claim of the Prime Min is ter was made on the oc ca sion of the amend ments in theLHI chang ing the NHIF man age ment struc ture563. Fol low ing a com pe ti tion for a Di rec tor ofNHIF, Dr. Dimitar Petrov was ap pointed on that po si tion. A few months later, still more com -pe ti tions for di rec tors of the RHIF were dis cussed in the me dia564. At the be gin ning of 2004, apub li ca tion in the”Standart” news pa per made a re view of the changes in the NHIF man age -ment, emphasising the fact that the NHIF had had five di rec tors for five years565.
The bud get of the NHIF, the short age of the fi nanc ing en vis aged mainly for drugs, weretop ics which called for com ments in the me dia through out 2003. About two months af ter theadop tion of the NHIF bud get for 2003, which ac cord ing to the Vice Min is ter of Fi nance andChair man of the NHIF Ex ec u tive Board K. Ananiev was higher than the bud get for 2002 byover 30%566, 69 dep u ties from Co ali tion for Bul garia, the NMSS, NIE and UDF sub mit ted adraft in the NA, whereby the Coun cil of Min is ters was as signed to make amend ments in theLaw on the NHIF bud get for 2003567. The pro posal was for an in crease in the ex pen di ture partof the bud get by 150 mil lion BGN, which were to be re leased from the NHIF re serve. The draft en vis aged that the ad di tional fund ing was used to cover the short age of fund ing for med i cal ac -tiv i ties and drugs. The dep u ties also in sisted that the Coun cil of Min is ters pre sented a strat egyfor the re struc tur ing of the healthcare es tab lish ments for hos pi tal care. Ac cord ing to the Chair -man of the Par lia men tary Com mis sion on Healthcare Assoc. Prof. Dr. Atanas Shterev, for
153
Stages and evo lu tion of the healthcare re form in Bul garia
559 Standart daily, Is sue ¹ 3345 from 24.04.2002; Kapital weekly from 27–30.04.2002560 Duma daily, Is sue ¹ 289 from 13.12.2002561 24 chasa daily, Is sue ¹301 from 2002562 24 chasa daily, Is sue ¹ 5 from ò 6.01.2003 and Is sue ¹ 7 from 8.01.2003; Kapital weekly from 7 from
22-28.02.2003563 Kapital weekly, Is sue ¹ 5 from 8-14.02.2003 and Is sue ¹7 from 22-28.02.2003564 24 chasa daily, Is sue ¹ 198 from 22.07.2003565 Standart daily, Is sue ¹ 3961 from 16.01.2004566 24 chasa daily, Is sue ¹ 23 from 24.01.2003567 24 chasa daily, Is sue ¹ 92 from 3.04.2003; Trud daily from 3.04.2003; Standart daily, Is sue ¹ 3684 from
4.04.2003
2003 at least an other 1 bil lion BGN was needed for healthcare568.At the end of July, it was an nounced that the fund ing planned for drugs was de pleted and
the Ex ec u tive Board de clared that they would in sist on ur gent up dat ing of the bud get in frontof the NA569. Mean while, the Min is ter of Healthcare Slavcho Bogoev con firmed the need forcor rec tions in the NHIF bud get with ad di tional fi nanc ing un til the end of the year to pro videfor the free and par tially re im bursed drugs570.
Dr. E. Dushkov – mem ber of the Ex ec u tive Board of the NHIF from the quota of CL“Podkrepa” de clared that he would de mand the res ig na tion of the Di rec tor of the NHIF forbreaches in the ad min is tra tion of the com pe ti tions, held for di rec tors of the RHIF, the con -ducted fi nan cial pol icy and the fi nan cial abuses con firmed by the Cham ber of Ac counts571.
The ac cu sa tions of fi nan cial abuses were caused by the re fusal of the Cham ber of Ac -counts to en dorse the re port for the ful fil ment of the NHIF bud get for 2002 due to es tab lishedbreaches of acts of the Coun cil of Min is ters, the Law on Pub lic Pro cure ment, lack of co or di na -tion among the di rec tor ates and mech a nisms of con trol over the costs, un law ful ex tra pay -ments, etc. An ar ti cle in the “Kapital” dis cussed the fact that in spite of the es tab lishedvi o la tions, the Cham ber of Ac counts could not im pose any sanc tions since the NHIF pos sessed a bud get of its own and did not de pend on state sub si dies572.
In the mid dle of Sep tem ber, the As sem bly of the rep re sen ta tives of the NHIF de pos ited apro posal in the NA for an in crease of the bud get for 2003 by 45 mil lion BGN be cause of the in -creased ex penses for drugs. Ac cord ing to Chair man of the NHIF Ex ec u tive Board K. Ananiev, the ac tual def i cit amounted to 6 mil lion BGN573. About a month later the Coun cil of Min is tersap proved the in crease in the bud get, pro vid ing in its de ci sion that fi nanc ing was used for drugsonly which were re im bursed to tally or par tially by the NHIF, and the fi nanc ing was made at the ex pense of the sur plus of the Fund from the pre vi ous pe riod574.
The draft bud get of the NHIF for 2004 once again called for pro tests. The re gional com -mit tee of the UBP in Russe de manded the res ig na tion of the man age ment of the Un ion. Therea son was in the planned re duc tion in the prices of the clin i cal path ways by 20% as com -pared to 2003, which ac cord ing to med i cal pro fes sion als, would re sult in hos pi tal bank rupt -cies575. The draft bud get of the NHIF was also dis cussed in the me dia in re la tion to the pre -dicted def i cit and the pos si bil i ties for it to be cov ered by the re serve of the NHIF576. The rep re -sen ta tives of the CITUB in the man ag ing or gans of the NHIF voted against the pro posedpro ject due to the def i cit im plied in it amount ing to 174 mil lion BGN. The CITUB con sid eredthe pos si bil ity of de mand ing the res ig na tion of the NHIF Di rec tor577.
The Ex ec u tive Board of the NHIF did not ap prove the re port on the ac tiv i ties of the Fundfor the firsts 9 months of 2003 for lack of ar gu ments for the in curred ex penses and good rea -son ing for the per formed ac tiv ity. Al though the Ex ec u tive Board re turned the re port to the ex -
154
568 Standart daily, Is sue ¹ 3684 from 4.04.2003569 Standart daily, Is sue ¹ 3799 from 1.08.2003; Kapital weekly from 28.06.- 4.07.2003570 Duma daily, Is sue ¹177 from 4.08.2003571 Standart daily, Is sue ¹3795 from 28.07.2003; Duma daily, Is sue ¹ 177 from 4.08.2003 572 Kapital weekly from 11-17.10.2003573 24 chasa daily, Is sue ¹ 254 from 16.09.2003; Kapital weekly from 6-12.09.2003574 Duma daily, Is sue ¹ 240 from 17.10.2003; Kapital weekly from 18-24.10.2003575 24 chasa daily, Is sue ¹ 284 from 16.10.2003576 24 chasa daily, Is sue ¹ 289 from 21.10.2003 Duma daily, Is sue ¹ 268 from 19.11.2003577 Duma daily, Is sue ¹ 249 from 28.10.2003
ec u tive di rec tor, the As sem bly of the rep re sen ta tives of the NHIF adopted the bud get for 2004which en vis aged an in crease in the costs for main te nance and cap i tal in vest ment as well as payrise and in crease of the Fund’s staff578.
The NHIF did not have pub lic sup port and pop u lar ity. It was ac cused for lack of con -trol, fi nan cial abuse and in suf fi cient trans par ency in its ac tiv i ties579. From 2002, the pub lic dis -ap proval of the NHIF es ca lated con sid er ably. In for ma tion was re leased about pa tients’pro tests against the Fund and their in ten tions to seek for the pro tec tion of their rights incourt580. Be side the pa tients, the phy si cians also pro tested and ac cused the NHIF of le thalcases. The dis con tent was caused by the short age of re fer ral let ters to spe cial ists and the pro ce -dures for the al low ance of free drugs581.
Ac cord ing to data of the na tional sam ple pub lic opin ion poll con ducted in the pe riod 7-12June 2003 by MBMD among 1 197 peo ple, of all the pub lic in sti tu tions the cit i zens trustedleast the ju di cial au thor i ties and the NHIF582.
In an in ter view for the “Duma” news pa per, the Di rec tor of the NHIF Dr. D. Petrov statedthat the most sig nif i cant prob lems of the Fund in cluded the in for ma tion sys tem, “the ac cu mu -lated neg a tive pub lic opin ion and the poor me dia im age” due to the im posed re stric tive mech a -nisms, the fi nanc ing and the in crease in the rev e nue part of the bud get. To his mind, thepro vi sion of the nec es sary fi nanc ing could be achieved through the re lease of the NHIF re -serve, the in crease of the health in sur ance in stal ments, the in tro duc tion of co-pay ment by thepa tients or through a state sub sidy un til the NHIF be gan to fi nance it self en tirely from thehealth in sur ance pre mi ums whose amount had to reach 12%583.
In a pub li ca tion of the “Standart” news pa per fo cus ing on the au thor i ties of the NHIF,views were shared that they were rather great and ex ceeded com pe tences as well as that theFund had to carry out the pol icy de fined by the gov ern ment584.
The rep re sen ta tives of CL “Podkrepa” in the NHIF ex ec u tive or gans also de manded theres ig na tion of the NHIF di rec tor. In an in ter view for the “Duma” news pa per Dr. E. Dushovwho was a mem ber of the CL “Podkrepa” quota of the Ex ec u tive Board, shared the opin ionthat “there is stag na tion in the over all healthcare re form in the part of its health in sur ance,” andthis was mainly vis i ble from the con cept for de vel op ment pre sented by the NHIF di rec tor. Ac -cord ing to Dr. Dushkov the con cept con cerned the ac cred i ta tion of the healthcare es tab lish -ments, the ad min is tra tive reg u la tion, the re struc tur ing of the healthcare sys tem and otheris sues in the field of the com pe tences of the Min is tries of Healthcare and Fi nance585.
At the end of 2003, in an in ter view for the “24 chasa” news pa per the Min is ter ofHealthcare S. Bogoev ex pressed his dis sat is fac tion with the de ci sions of the NHIF man age -ment and in sisted on the res ig na tion of its di rec tor be cause of “the de crease in the prices of theclin i cal path ways, the way they are worked out, the lack of vi sion for the drugs,” and he voiced
155
Stages and evo lu tion of the healthcare re form in Bul garia
578 24 chasa daily, Is sue ¹ 296 from 28.10.2003; Duma daily, Is sue ¹ 252 from 31.10.2003579 Standart daily, Is sue ¹ 3357 from 8.05.2002, Is sue ¹ 3961 from 16.01.2004 and Is sue ¹ 4023 from
18.03.2004 Duma daily, Is sue ¹ 23 from 30.01.2004 and Is sue ¹ 226 from 29.09.2004580 Standart daily, Is sue ¹ 3422 from 12.07.2002 and Is sue ¹ 3423 from 13.07.2002581 Duma daily, Is sue ¹ 110 from 16.05.2002; 24 chasa daily, Is sue ¹ 116 from 27.04.2002, Is sue ¹ 127 from
10.05.2002, Is sue ¹ 131 from 14.05.2002, Is sue ¹ 132 from 15.05.2002 and Is sue ¹ 133 from 16.05.2002;Trud daily from 15.05.2002
582 24 chasa daily, Is sue ¹ 160 from 14.06.2003583 Duma daily, Is sue ¹ 270 from 21.11.2003584 Standart daily, Is sue ¹ 3930 from 10.12.2003585 Duma daily, Is sue ¹ 252 from 31.10.2003
the opin ion that when tak ing de ci sions the Fund had to “take into ac count the pub lic in ter estmore and lis ten to the pol icy of the min is try.” Ac cord ing to him a “sta ble man age ment is nec es -sary with a clear vi sion for the fu ture and the im ple men ta tion of the healthcare pol icy”586.
A sim i lar view was ex pressed by the Vice Min is ter on Healthcare Dr. P. Salchev in an in -ter view for the “Standart” news pa per. In his opin ion, the op er a tive man age ment of theNHIF was not im ple ment ing the na tional health strat egy and was try ing to con duct oneof its own. The main crit i cism was di rected to ward the way of mak ing the de ci sions, the lack of ar gu ments for the changes in the re im burse ment list and the man ner of cal cu lat ing the prices of the clin i cal path ways587.
Af ter nu mer ous sig nals for fi nan cial abuses and breaches of the fi nances spend ing fromthe NHIF bud get and af ter in 2003 the Cham ber of Ac counts re fused to en dorse the re port ofthe NHIF for es tab lished vi o la tions, in 2004 a fi nan cial au dit of the NHIF once again re vealedun law ful spend ing of funds and con cluded con tracts588. In the mean time, the Chair man of theNHIF Ex ec u tive Board K. Ananiev de clared that ac cord ing to the con clu sions of the au ditmade by the Cham ber of Ac counts on the ex e cu tion of the NHIF bud get, a con sid er able prog -ress was made in terms of its fi nan cial man age ment and that mea sures had been un der taken for“im me di ate elim i na tion of the omis sions.”589
The Na tional Frame work Agree ment
The dif fi cul ties, the dis putes and the con flicts dur ing the prep a ra tion and the sign ing ofthe NFA con tin ued in the third stage of the re form, too. At the be gin ning of 2002, the me dia in -formed in de tail about prob lems sign ing the NFA 2002 and about prob lems in the UBP re latedto the frame work agree ment. At the XXXVth Ex traor di nary As sem bly of the phy si cians thedel e gates re jected the frame work agree ment in sist ing on sign ing only of an an nex for the fi -nanc ing of hos pi tal care590. In this re spect the Dep uty Chair man of the UBP Prof. Dr. M.Milanov de clared that he would sub mit his res ig na tion since in his opin ion “af ter the phy si -cians’ vote, chaos and end less ne go ti a tions en sue with unpredicted out come.”
Chiefly the “Democracia” news pa per in formed about the prob lems and the con flicts ac -com pa ny ing the sign ing of the NFA 2002. The UDF de clared that only the NHIF was to beblamed for not sign ing of the agree ment. Ac cord ing to Dr. T. Konstantinova, it had been spec -u lated that the UBP was also to be blamed for it and the dep uty from the UF Dr. B. Kitov statedthat there was ev i dence, ac cord ing to which “the NMSS and the BSP have im parted to part ofthe phy si cians not to ac cept the terms and con di tions, so that the man age ment of the Un ion, itschair man and the UDF were even tu ally blamed for the fail ure.” Ac cord ing to Dr. StoichoKatsarov “the rul ers aimed at re turn ing the bud geted healthcare through the ter mi na tion of there form and de nial of the health in sur ance. This is proved not only by the fail ure of the ne go ti a -tions on the frame work agree ment but also by the ces sa tion of the privatisation in healthcareand the pro jects for the loan from the WB.” In his turn, the Chair man of the UBP Dr. Ignatovde clared that “in ten sive ne go ti a tions will be ini ti ated with the NHIF aimed at sign ing the
156
586 24 chasa daily, Is sue ¹ 337 from 8.12.2003587 Standart daily, Is sue ¹ 3944 from 24.12.2003588 Standart daily, Is sue ¹ 4131 from 6.07.2004589 Kapital weekly from 19-25.06.2004590 Duma daily, Is sue ¹ 45 from 2002; Democracia daily from 9.01.2002; 24 chasa daily, Is sue ¹ 53 from
23.02.2002; Standart daily, Is sue ¹ 3290 from 28.02.2002
frame work for 2002 within two weeks.”591 A few days later, the “Democracia” in formed thatthe sign ing of the agree ment was forth com ing soon but with out the sig na ture of the act ing di -rec tor of the NHIF Assoc. Prof. Dr. N. Vassilev592. The me dia cov ered the sign ing of the NFA2002 with crit i cal re marks ad dressed to the man age ment of the UBP593.
Pub li ca tions in two sub se quent is sues of the “Kapital” news pa per de scribed the ne go ti a -tion pro cess in an un am big u ous way: “Ev ery year the sign ing of the NFA is ac com pa nied bydrama, scan dals and mu tual ac cu sa tions”; “the post pone ment of the NFA 2002 gives the op -por tu nity to all kinds of un iden ti fied per son al i ties to ex plain that the healthcare re form will bestopped, that the hos pi tals will go bank rupt”; con flicts were re vealed be tween the phy si ciansand the man age ment of the UBP594.
In Au gust, an an nex to the NFA 2002 en vis ag ing the in crease of the med i cal ac tiv i ties inout pa tients’ care caused new ar gu ments which reached the court. The Vice Min is ter of Fi -nance K. Ananiev stated that he was not go ing to sign the an nex be cause he con sid ered that thebud get of the NHIF did not pos sess the nec es sary fund ing to cover the planned in crease in thespe cial ised in ves ti ga tions in the out pa tients’ care and the highly spe cial ised ac tiv i ties595.
Along with the pro cess of ne go ti a tions, the press in formed about the con tent of the NFA,too596. For 2002 the em pha ses were placed on the in tro duc tion of co-pay ment by the pa tientsfor the den tal ser vices and the in crease of the num ber of re fer rals for spe cial ised ex am i na -tions and lab o ra tory in ves ti ga tions. Re gard ing the in tro duc tion of co-pay ment for den tal ser -vices, the Dep uty Chair man of the UDB Dr. N. Sharkov de fined the NFA 2002 as a “stepfor ward to a Eu ro pean healthcare”597. In 2004 in for ma tion was re leased about the sub se quentre duc tion in the price paid by the NHIF for den tal ser vices at the ex pense of the in creasedco-pay ment by the pa tients598.
At the be gin ning of 2002 the “Kapital” news pa per an nounced that with the NFA 2002 themoney was in creased for the gen eral prac ti tio ners en vis ag ing bo nuses for the per for mance ofpro phy lac tic check-ups and the fee per ca pita had also in creased599. In this light, the Chair manof the UBP Dr. Ignatov made the state ment that “the new scheme en ables the uti li sa tion of allthe fund ing planned in the bud get” and “in 2001, 26 mil lion BGN for out pa tients’ care re -mained unutilised”600.
Apart from pieces of in for ma tion deal ing with the terms of the NFA, in 2002 an nounce -ments could also be come across in the me dia that the NHIF was con sid er ing to in tro duce amonthly bud get and work ing hours for the gen eral prac ti tio ners as well as that the NHIF wouldsub mit with out com pen sa tion com put ers for the phy si cians with more than 1 000 listed pa -
157
Stages and evo lu tion of the healthcare re form in Bul garia
591 Democracia daily from 1.03.2002592 Democracia daily from 7.03.2002593 24 chasa daily, Is sue ¹ 69 from 11.03.2002; Standart daily, Is sue ¹ 3297 from 11.03.2002 and Is sue ¹
3303 from 13.03.2002594 Kapital weekly from 2-8.03.2002 and from 9-15.03.2002595 Duma daily, Is sue ¹195 from 24.08.2002 ; Kapital weekly from 31.08.–5.09.2002 ; Standart daily, Is sue ¹
3467 from 28.08.2002 and Is sue ¹ 3495 from 23.09.2002596 Standart daily, Is sue ¹ 3297 from 7.03.2002 and Is sue ¹ 3448 Trud daily from 7.08.2002; 24 chasa daily,
Is sue ¹ 216 from 7.08.2002; Duma daily, Is sue ¹ 180 from 19.08.2002597 Duma daily, Is sue ¹ 64 from 18.03.2002, Is sue ¹ from 30.03.2002 and Is sue ¹ 168 from 7.08.2002598 Standart daily, Is sue ¹ 4124 from 29.06.2004599 Kapital weekly from 12-18.01.2002600 Democracia daily from 9.01.2002
tients601. The me dia also in formed about the re quire ments of the NHIF to the con tract ing part -ners, the changes in the con trol and sanc tions for es tab lished breaches602. The Di rec tor of theNHIF Prof. Dr. G. Nachev de clared that from the end of Sep tem ber it had been en vis aged tocom mence the qual ity as sess ment of the hos pi tals, based on which the Fund would re lease ad di -tional fund ing for the hos pi tals pro vid ing the high est qual ity of the ser vices to their pa tients603.
At the end of 2002, pub li ca tions also ap peared about the con tent of the NFA 2003604,which was largely ech oed in pub lic at the very be gin ning of 2003. In a se ries of ar ti cles it wasan nounced about the new clin i cal path ways, the med i cal and den tal ser vices which were go ingto be paid by the NHIF as well as about many other clauses in cluded in the Agree ment for2003. As re gards the ex pected changes, Min is ter Finkov an nounced that a dis tinc tion was be -ing pre pared of the clin i cal path ways for chil dren and adults; they were go ing to be paid in adif fer ent way and some of them would re main for chil dren only605.
The Ex ec u tive Board of the NHIF took the de ci sion backed by the UBP whereby in 2003 no in di vid ual con tracts were go ing to be signed with the hos pi tals which had re ceived a poor as sess -ment at their ac cred i ta tion. The healthcare es tab lish ments were go ing to have the right to sign ad -di tional agree ments with the NHIF, pro vided that they im prove their ac cred i ta tion mark606.
Dur ing this stage of the re form the pe ri od i cals also in formed about breaches of the con -tracts con cluded be tween the pro vid ers of med i cal and den tal care and the RHIF, most fre -quently dis cuss ing the un reg u lated pay ments for ser vices fi nanced from the bud get of theNHIF, un law ful col lec tion of con sum ers’ fees from per sons ex empt from them, breaches en -roll ing pa tients for a fam ily phy si cian and re port ing per formed med i cal ac tiv i ties, un law ful is -sue of med i cal doc u ments, in fringe ments on the re quire ments for the clin i cal path ways607. Oneof the most com mon rea sons pointed out was that the pa tients were not suf fi ciently in formedabout their rights. The most com mon com plaints of the cit i zens from their fam ily phy si cians re -garded the in suf fi cient num ber of re fer rals to spe cial ists, the im pos si bil ity to find them atany time and their rough treat ment608. Ac cord ing to a sur vey con ducted by “Noema”, 85% ofthe cit i zens were dis ap pointed that they had to wait for hours in front of their fam ily phy si cians’ of fices and ev ery fourth pa tient had paid cash for a test, ma nip u la tion or med i cine609. Dur ing theVIIth In ter na tional meet ing of the gen eral prac ti tio ners and the spe cial ists from the out pa -tients’ care the par tic i pants in sisted on the adop tion of amend ments in the NFA for 2003, oth er -wise, they threat ened to dis con tinue pro vid ing ser vices to the pa tients and go ing on strikes. Thedoc tors pro tested against the in tro duced reg u la tory stan dards, the ex am i na tions in the dis pen sa -
158
601 24 chasa daily, Is sue ¹ 305 from 4.11.2002; Standart daily, Is sue ¹ 3539 from 6.11.2002 and Is sue ¹ 3544from 11.11.2002
602 24 chasa daily, Is sue ¹ 74 from 2002603 Trud daily from 7.08.2002604 Trud daily from 7.09.2002; Kapital weekly from 9-15.11.2002 and from 29.11.–6.12.2002605 24 chasa daily, Is sue ¹ 8 from 9.01.2003606 Trud daily from 19.02.2003; Duma daily, Is sue ¹ 72 from 27.03.2003; Kapital weekly from 7 to 22-28.02.2003607 24 chasa daily, Is sue ¹ 330 from 29.11.2002, Is sue ¹ 340 from 9.12.2002, Is sue ¹ 5 from 6.01.2003, Is sue
¹ 33 from 3.02.2003, Is sue ¹ 47 from 17.02.2003, Issue ¹ 42 and Is sue ¹ 192 from 2004; Standart daily,Is sue ¹ 3363 from 14.05.2002, Is sue ¹ 3615 from 25.01.2003, Is sue ¹ 3635 from 14.02.2003, Is sue ¹3646 from 25.02.2003 and Is sue ¹ 3959 from 14.01.2004
608 Standart daily, Is sue ¹ 3380 from 31.05.2002, Is sue ¹ 3703 from 23.04.2003, Is sue ¹ 3741 from4.06.2003, Is sue ¹ 3750 from 13.06.2003 and Is sue ¹ 4102 from 7.06.2004.; 24 chasa daily, Is sue ¹ 143from 28.05.2003 and Is sue ¹ 86 from 27.03.2004
609 Trud daily from 31.03.2002
ries and the pre scrip tion of drugs for the chron i cally dis eased pa tients. In a dec la ra tion, theystated that if their claims were not ap proved, they would be gin a sub scrip tion for change of theUBP man age ment. The re gional col le giate of the UBP in Russe also de manded ur gent ex -tended meet ing of the Un ion’s Na tional Coun cil to dis cuss amend ments in the NFA610. TheChair man of the UBP Dr. A. Kehayov de clared that these ac tions served po lit i cal in ter ests andthe claims were ground less. Ac cord ing to him, the prob lems which arose af ter the en force mentof the new frame work agree ment had been dis cussed at a na tional fo rum of the UBP in the mid -dle of June as a re sult of which ad di tional 8 mil lion BGN were re leased for the in crease in thenum ber of re fer rals to spe cial ised med i cal care and for the im ple men ta tion of the reg u la tion ondispensarisaton611. The com ments con cern ing the de mands of the phy si cians, made by the Di rec -tor of the NHIF in an in ter view for the “Standart” news pa per were also sim i lar612.
At the end of the year again the lead ing news re ferred to the pro pos als made by the NHIFand the con tract ing part ners for amend ments in the NFA for 2004613. The UBP in sisted that the reg u la tions con cern ing the min i mum pack age of med i cal ser vices guar an teed by the
NHIF bud get and the pa tients’ dispensarisation re mained un changed for short age of timefor the amend ments dis cus sion614.
One of the dis puted ques tions in the draft NFA for 2004 was the pro posal of the NHIFfor the in tro duc tion of a max i mum num ber of pa tients reg is tered to one gen eral prac ti tio neraimed at qual ity im prove ment of the med i cal ser vices615. The other op tion pro posed by theNHIF was that the sum paid to the gen eral prac ti tio ners per each listed pa tient, to be de creas ing af ter a cer tain num ber of pa tients. The UBP pro claimed it self against these changes with the ar -gu ment that this way the right of the pa tients’ free choice would be vi o lated616.
The con tro ver sial is sues in the pro posed draft NFA for 2004 were linked pri mar ily to thepay ment for the out pa tients’ and hos pi tal care. The rea son for the com ments in the press in -cluded the de lay of the ne go ti a tions and the ex pec ta tions for a post pone ment of the sign ing ofthe agree ment. It was known from the pre vi ous years’ ex pe ri ence that this led to se ri ous prob -lems and con fu sion at all lev els of the health in sur ance sys tem. In an ar ti cle in the “Kapital”news pa per, the prob lems with the con tract ing which arose ev ery year were re lated to the mo -nop oly of the con tract ing par ties and the lack of com pe ti tion at all lev els617.
In 2004 the pub li ca tions deal ing with the NFA were con sid er ably smaller in num ber ascom pared to the pre vi ous years and were en tirely ded i cated to the prob lems with the con tract -ing of the NFA for 2004. The UBP re fused to sign the NFA 2004 and their ma jor claims werefor at least 40% of the NHIF fund ing to be al lo cated for phy si cians’ re mu ner a tions out sidetheir sal a ries and for par tic i pa tion in de ter min ing the list of the to tally or par tially re im bursed
159
Stages and evo lu tion of the healthcare re form in Bul garia
610 Duma daily, Is sue ¹ 141 îò 23.06.2003; 24 chasa daily, Is sue ¹ 168 îò 22.06.2003 ; Standart daily, Is sue ¹ 3762 îò 25.06.2003
611 Duma daily, Is sue ¹ 141 îò 23.06.2003 ; Standart daily, Is sue ¹ 3763 from 26.06.2003 and Is sue ¹ 3773from 6.07.2003
612 Standart daily, Is sue ¹ 3762 îò 25.06.2003 613 24 chasa daily, Is sue ¹ 297 from 29.10.2003 and Is sue ¹ 304 from 5.11.2003; 24 chasa daily from
5.11.2003 ; Duma daily, Is sue ¹ 277 and Is sue ¹ 292 from 2003; Standart daily, Is sue ¹3933 from13.12.2003, Is sue ¹3937 from 17.12.2003 and Is sue ¹ 3943 from 23.12.2003
614 Duma daily, Is sue ¹ from 2003615 Standart daily, Is sue ¹ 3856 from 27.09.2003616 Kapital weekly from 4-10.10.2003; Standart daily, Is sue ¹ 3893 from 3.11.2003, Is sue ¹ 3896 from
6.11.2003, Is sue ¹ 3900 from 10.11.2003 and Is sue ¹ 3902 from 12.11.2003617 Kapital weekly from 29.11.-5.12.2003
drugs by the NHIF618. In his turn, the act ing Di rec tor of the NHIF Dr I. Bukarev de clared: “The sign ing of the NFA was un ac cept ably de layed, the pa tients lost be cause of their heal ers’ stub -born ness.”619 In an in ter view about the NFA 2004 ne go ti a tions the Vice Min is ter of Healthcare Dr. Petko Salchev also ex pressed crit i cisms and an nounced that only the Chair man of the UBPDr. A. Kehayov had not sup ported the agree ment, al though he voted in fa vour of ev ery sep a -rate point. In re sponse to the crit i cisms Dr. Kehayov stated: “We do not take ul ti ma tums” and,in his turn, he blamed the NHIF for the fail ure of the ne go ti a tions. He an nounced that the de -mand of the UBP for the 40% had been ac cepted but “in struc tions lacked from the MH that itwill be put into prac tice.” The man age ment of the UBP in sisted that the ac cred i ta tion of thehealthcare es tab lish ments as a re quire ment for sign ing a con tract with the NHIF be aban donedand de clared that there was no clar ity as re gards the le gal com mit ment of both par ties in volvedin the con tract ing of the list and the drug prices re im bursed by the NHIF in full or par tially620.
Apart from the frame work, in 2004 the UBP and the NHIF ar gued about the in struc tionof the Fund for the pa tients’ ad mis sion to hos pi tal621. The UBP ac cused the NHIF that it lim ited the pa tients’ ac cess to hos pi tals and urged the pa tients to sue the Fund622, and the Chair man ofthe UBP Dr. A. Kehayov de clared that he would make a case against the NHIF, if its Di rec torDr. I. Bukarev did not re peal the in struc tion623.
In his turn, Min is ter S. Bogoev de manded amend ments in the LHI, whereby to reg u latethe pos si bil ity for a for mal sign ing of the NFA, his mo tives be ing “the pro longed ne go ti a tionsbe tween the NHIF and the UBP for NFA 2004” 624. At the end of the year, in a pub li ca tionmade by the “Duma” news pa per, it was stressed that if a new frame work agree ment was notcon cluded for year 2005 too, a def i cit was to be ex pected in the hos pi tals since they worked ac -cord ing to the prices stip u lated in NFA 2003 and paid for med i cines, consumables, etc. ac cord -ing to the prices of 2004, thus ac cu mu lat ing a def i cit for 2005 even be fore 2004 had elapsed625.
At the end of 2004 the Min is ter placed an ul ti ma tum be fore the UBP that if they did notsign a frame work agree ment for 2005, he would once again pro pose that its for mal con clu sionbe legal ised. Med i cal pro fes sion als ac cused the UBP that the text of the NFA was not com plied with them, which, ac cord ing to a mem ber of the Ex ec u tive Board of the HHIF was done de lib -er ately and “the UBP is ruled by its pres ent man age ment in a to tal i tar ian way”626. Even tu allythe NFA 2005 was signed627.
The new terms en vis aged by the NFA for 2005 caused a se ries of con tro ver sial opin ionsin the press re lated to lim ited ac cess of the pa tients with men tal dis eases to mod ern drugs628, thesanc tions planned for abuses of gen eral prac ti tio ners giv ing re fer rals, the ad di tional sub si dies tobe re leased for the phy si cians’ prac tices in the re mote and dif fi cultly ac ces si ble re gions, etc. 629.
160
618 Duma daily, Is sue ¹ 85 from 2004; Standart daily, Is sue ¹ 3999 from 23.02.2004619 Duma daily, Is sue ¹ 54 from 8.03.2004620 Standart daily, Is sue ¹ 4034 from 29.03.2004621 Trud daily from 10.07.2004622 Standart daily, Is sue ¹ 4140 from 15.07.2004623 24 chasa daily, Is sue ¹ 194 from 2004624 Kapital weekly from 2-9.04.2004; Duma daily, Is sue ¹ 147 from 28.06.2004625 Duma daily, Is sue ¹ 267 from 16.11.2004626 Duma daily, Is sue ¹ 295 from 2004627 Duma daily, Is sue ¹ 277 from 27.11.2004 and Is sue ¹ 301 from 11.12.2004.; 24 chasa daily, Is sue ¹ 361
from 27.12.2004; Trud daily from 21.12.2004 and from 28.12.2004 628 Duma daily, Is sue ¹ 21 from 26.01.2005, Is sue ¹ 25 from 31.01.2005 and Is sue ¹ 27 from 2.02.2005629 Duma daily, Is sue ¹ 31 from 7.02.2005
Health in sur ance in stal ments
Al though the prob lem with the collectibility of the health in sur ance in stal ments arosestill in the sec ond part of the pre vi ous stage of the re form, the pub li ca tions in the press con cern -ing its over com ing came out mainly af ter 2003. The prob lem wors ened dur ing the third stageof the re form to reach its cli max in 2004 and the num ber of pub li ca tions on this is sue was in dic -a tive of its de vel op ment.
In 2002, the NHIF an nounced that one mil lion cit i zens were not in sured and ac cord ing tothe Di rec tor of the NHIF N. Genova this num ber in cluded mainly sea son work ers and self-em -ployed peo ple. It was en vis aged for the peo ple with chronic dis eases to sub mit dec la ra tions about their health in sur ance sta tus since the in spec tions made by the NHIF had es tab lished that in 2001, 10% out of a to tal of 4 238 per sons on costly med i ca tion re im bursed by NHIF, were not in suredand an other 8% had not been found in the reg is ters at all630. In Sep tem ber, it was an nounced thatthe state would cover the health in sur an ces of chil dren aged up to 18631.
For the first time in 2003, the press pub lished in for ma tion about the mea sures which werego ing to be un der taken against per sons ow ing three and more health in sur ance in stal ments.Their health in sur ance rights were go ing to be ter mi nated un til the pay ment of the dueamounts, the ini tial sanc tions in clud ing the loss of the right to costly treat ment re im bursed bythe NHIF632. In the mid dle of the year, the Di rec tor of the NHIF Dr. D. Petrov an nounced thatthe fam ily phy si cians would start check ing the health in sur ance sta tus of the cit i zens listed tothem. To this pur pose the Fund had been pre par ing a reg is ter of the in sured peo ple which wasto be sub mit ted to the gen eral prac ti tio ners633.
Ac cord ing to ini tial data from the in spec tions of the NHIF and NII, it be came ev i dent thatover 1.5 mil lion had dues for the de po si tion of health in sur an ces, which was the rea son whythe dead line for their de posit and re newal of the health in sur ance rights was ex tended by onemonth634. About a month later the Di rec tor of the NII in formed the me dia about the re sultsfrom the check-up of the health in sur ance sta tus of the cit i zens. Ac cord ing to data of the NII,ap prox i mately 2.4 mil lion or one third of the peo ple who had cho sen a fam ily doc tor hadto have their rights ter mi nated. Pos si bil i ties were be ing con sid ered for de layed pay ment of thedue sums in in stal ments635.
On the topic of the collectibility of the health in sur ance in stal ments the me dia pub lished anum ber of ma te ri als on the in com plete ness and the er rors in the in for ma tion sys tem of NII andabout com pli cated bu reau cratic pro ce dures for the clar i fi ca tion of the ob li ga tions of cit i zens andem ploy ers636, sanc tions and fines stip u lated for the in debted as well as the pos si bil i ties that partof the due sums of cer tain cat e go ries of cit i zens to be an nulled, the dead lines to be ex tended for
161
Stages and evo lu tion of the healthcare re form in Bul garia
630 Duma daily, Is sue ¹ 103 from 2002; Democracia daily from 8.05.2002; 24 chasa daily, Is sue ¹ 116 from27.04.2002 and Is sue ¹ 125 from 8.05.2002, Fo rum Medicus pe ri od i cal, Issue ¹ 20-21 from 13.05.2002
631 Standart daily, Is sue ¹3478 from 8.09.2002632 24 chasa daily, Is sue ¹ 89 from 31.03.2003 and Is sue ¹ 100 from 11.04.2003; Standart daily, Is sue ¹ 3681
îò 1.04.2003, Is sue ¹ 3694 from 14.04.2003 and Is sue ¹3696 from 16.04.2003633 24 chasa daily, Is sue ¹ 190 from 14.07. 2003 and Is sue ¹ 243 from 05.09.2003; Trud daily from
30.09.2003; Standart daily, Is sue ¹ 3825 from 27.08.2003 and Is sue ¹ 3858 from 29.09.2003634 24 chasa daily, Is sue ¹ 254 from 16.09.2003635 24 chasa daily, Is sue ¹ 280 from 12.10.2003; Standart daily, Is sue ¹ 3861 from 2.10.2003 and Is sue ¹
3872 from 13.10.2003; Kapital weekly from 18-24.10.2003636 24 chasa daily, Is sue ¹ 289 from 21.10.2003 and Is sue ¹ 348 from 19.12.2003; Standart daily, Is sue ¹
3879 from 20.10.2003
the pay ment of the due in stal ments and for the state to cover the dues of the so cially poor637.The CITUB and CL “Podkrepa” in sisted in front of the Pres i dent that a three-month gra tis
pe riod be adopted for the pay ment of the due health in sur ance in stal ments be cause of the ex -pec ta tions for a lower pur chas ing abil ity as a re sult of the ex pected in fla tion for 2004638. At theend of 2003, the “24 chasa” pub lished the stand of Pres i dent Purvanov on the ter mi na tion ofthe health in sured peo ple’s rights for whom more than three health in sur ance in stal ments hadnot been paid from the be gin ning of 2000 in ac cor dance with Art. 109 of the LHI. In his standthe Pres i dent de manded that “the dead line for the ter mi na tion of the pay ment for the pro videdmed i cal ser vices to those in debted for health in sur an ces un til the build ing up of the ad min is tra -tive ca pac ity and mod ern in for ma tion ca pac i ties” of the Fund in or der to en sure ac cu rate in for -ma tion about the due in stal ments as well as the rea sons for the re spon si bil ity for their pay ment. Ac cord ing to Purvanov it was nec es sary to “make rad i cal changes in the health in sur ance leg -is la tion.” On this oc ca sion, Min is ter S. Bogoev pointed out that it was nec es sary to clar ify whobore the re spon si bil ity for the fail ure to de posit the health in sur an ces and the law should spec -ify how to pro tect the un in sured peo ple639.
The Par lia men tary Com mis sion on Healthcare ap proved the amend ments in the LHI, ac -cord ing to which the pay ment of the due health in sur ance in stal ments could be post poned un -til the end of 2004. The Min is ter of Healthcare shared that there were mis takes in thein for ma tion sys tems of the Fund and the NII which was the rea son for the post pone ment of thedues pay ment640. The pos si bil i ties were con sid ered for debt re mit tal to cit i zens whose in comewas be low the so cial min i mum, their health in sur ance be ing paid by the state641.
In 2004, the com ments and the an nounce ments con tin ued re gard ing the post pone ment ofthe dues to the NHIF642 to gether with pieces of in for ma tion about the num ber of un in suredpeo ple which var ied from one to two mil lion in the var i ous pub li ca tions643. A pub li ca tion inthe “Standart” news pa per in di cated that 25% of the gen eral prac ti tio ners did not hold health in -sur an ces ei ther644.
The prob lem of the cit i zens with out health in sur an ces caused the great est ten sion in so -ci ety, when the NHIF dis con tin ued the pay ment for med i cal care to those who were in debtedand the healthcare es tab lish ments were forced to deny treat ment to pa tients with ter mi natedhealth in sur ance rights645. Pres i dent G. Purvanov for the sec ond time ex pressed his opin ion on
162
637 24 chasa daily, Is sue ¹ 300 from 1.11.2003 and Is sue ¹ 314 from 15.11.2003; Duma daily, Is sue ¹ 258from 7.11.2003, Is sue ¹ 268 from 19.11.2003; Standart daily, Is sue ¹ 3879 from 20.10.2003, Is sue ¹ 3909from 19.11.2003 and Is sue ¹ 3935 from 15.12.2003
638 Standart daily, Is sue ¹.3933 from 13.12.2003639 24 chasa daily, Is sue ¹ 347 from 18.12.2003640 24 chasa daily, Is sue ¹ 348 from 19.12.2003; Standart daily, Is sue ¹ 3937 from 17.12.2003; Kapital weekly
from 20-23.12.2003641 24 chasa daily, Is sue ¹ 350 from 21.12.2003642 Kapital weekly from 10-16.01.2004 ; Standart daily, Is sue ¹ 4037 from 1.04.2004, Is sue ¹ 4091 from
27.05.2004 and Is sue ¹ 4206 from 19.09.2004; 24 chasa daily, Is sue ¹ 145 from 7.05.2004; Duma daily,Is sue ¹ 55 from 6.03.2004
643 Standart daily, Is sue ¹ 3993 from 17.02.2004, Is sue ¹ 4153 from 28.07.2004 and Is sue ¹ 4210 from23.09.2004; 24 chasa daily, Is sue ¹ 136, Is sue ¹ 265 and Is sue ¹ 270 from 2004; Duma daily, Is sue ¹ 54from 8.03.2004
644 Standart daily, Is sue ¹ 4217 from 30.09.2004645 Standart daily, Is sue ¹ 4210 from 23.09.2004 and Is sue ¹ 4217 from 30.09.2004; 24 chasa daily, Is sue ¹
270 from 29.09.2004 ; Duma daily, Is sue ¹ 230 îò 4.10.2004 , áð. 231 from 5.10.2004 and Is sue ¹ 233from 7.10.2004
the is sue, call ing “law less” the re fusal to treat pa tients who, to his mind, “are not to be blamedfor the er rors and the in ac cu ra cies in de pos ing the money.” The so cial min is ter HristinaHristova de clared that “within a week the gov ern ment will find a so lu tion and that even ifsome one owes in stal ments, he/she will not lose their right to med i cal care.” The Chair man ofthe NHIF Ex ec u tive board K. Ananiev de manded that “the NII spec i fied the lists and dis tin -guished be tween the peo ple with out any guilt.” The Man ager of the NII Yordan Hristoskovstated that the pol i ti cians had to de cide whether to pro cure a post pone ment in the debts pay -ment or not. The NMSS and MRF ap pealed first that the pa tients be treated and then re spon si -bil ity would be sought or the un paid health in sur ance in stal ments and the op po si tion in sistedthat the Pres i dent re mit ted the debts646.
Par al lel to the un fold ing of the prob lem through out 2004, pro pos als were made foramend ments in the LHI – the state should cover the in stal ments for the so cially poor647 andthe in stal ments them selves should be de ter mined in ac cor dance with the in come, the poor andthe un em ployed pay ing lower in stal ments648. At the end of the year, it was an nounced that thestate would cover the health in sur ance in stal ments of the so cially un der priv i leged peo ple,those re sid ing abroad for more than six weeks would be ex empt from health in sur ance in stal -ments649, and the health in sur ance sta tus would be as sessed (with out an nul ling the debts),based on the in stal ments paid for the pre vi ous 15 months, for four un paid in stal ments thehealth in sur ance rights be ing ter mi nated148.
The press also pub lished crit i cisms about the de ci sions taken for the cop ing with the prob -lem. Ac cord ing to the dep uty in the City coun cil of So fia from the BSP Dr. Asen Zlatev, “thede ci sion about the health in sur an ces is just a pre-elec tion ges ture”650; Luchezar Bogdanov – an econ o mist from “In dus try Watch” said that “the amend ments in LHI con cern ing the in stal -ments of two mil lion un in sured were sub sti tut ing the phi los o phy of the health in sur ancemodel” with the ar gu ment that “at least ac cord ing to law, at the mo ment a con nec tion ex istedbe tween the in sur ance and the use of med i cal care”; to this ac cu sa tion Min is ter S. Bogoev re -sponded: “Cur rently we are fac ing the need to think about the fate of 2 mil lion Bul gar i ans”651.In a crit i cal re view a jour nal ist from the “Standart” news pa per ex pressed the opin ion that theprob lem with the pre mi ums could have been solved three years be fore but in ter est lacked infind ing he so lu tion. The re view criti cised not only the HII which in the au thor’s opin ion was“messed up” pro vid ing that two mil lion of peo ple had vi o lated it, but the whole sys tem wasmis taken for the col lec tion of the in stal ments652.
Nu mer ous pub li ca tions at the be gin ning of 2005 again dealt with the topic of the cit i zens’debts in re la tion to the pay ment of the health in sur ance in stal ments. The ar ti cles clar i fied in de -tail the amend ments in the LHI adopted at the end of the fore go ing year, re gard ing the way ofpay ment, the re newal of the health in sur ance rights, the pen alty in stal ments and in ter est, the li -
163
Stages and evo lu tion of the healthcare re form in Bul garia
646 24 chasa daily, Is sue ¹ 273 from 2.10.2004, Is sue ¹275 from 4.10.2004 and Is sue ¹ 276 from 5.10.2004647 Duma daily, Is sue ¹ 234 from 2004; Standart daily, Is sue ¹ 3994 from 18.02.2004, Is sue ¹ 4015 from
10.03.2004, Is sue ¹ 4117 from 22.06.2004, Is sue ¹ 4238 from 21.10.2004 and Is sue ¹ 4249 from1.11.2004; 24 chasa daily, Is sue ¹ 292 from 2004
648 Duma daily, Is sue ¹179 from 4.08.2004; Standart daily, Is sue ¹ 4007 from 2.03.2004; Trud daily, Is sue ¹19.05.2004
649 24 chasa daily, Is sue ¹ 342 from 10.12.2004 and Is sue ¹ 348 from 16.12.2004.; Duma daily, Is sue ¹237and Is sue ¹ 254 from 2004
650 Duma daily, Is sue ¹ 249 from 26.10.2004651 Kapital weekly from 23-29.09.2004652 Standart daily, Is sue ¹ 4225 from 8.10.2004
a bil i ties of the Bul gar ian cit i zens re sid ing abroad, etc.653. The topic of the due pay ment of thehealth in sur ance in stal ments was again ac com pa nied by in for ma tion about the check ing of thehealth in sur ance sta tus, the in con sis tent in for ma tion avail able to the gen eral prac ti tio ners andthe one in the NII, the com pli cated bu reau cratic pro ce dures for the clar i fi ca tion of the cit i zens’li a bil i ties654. A few ar ti cles re ported new amend ments in the LHI re lated to the ex ten sion of the dead line for the pay ment of the health in sur ance in stal ments at a fixed up per limit of the in -come per mem ber of the fam ily655.
Along with the collectibility of the health in sur ance in stal ments, the is sue of their size was also dis cussed. In 2002 Min is ter Finkov pro posed that the health in stal ments rise by 1-2%from 2004656. In re sponse, Prof. M. Milanov pro nounced him self against the in crease of the in -stal ments with the ar gu ment that there were no eco nomic rea sons for that657.
In 2003, the pos si bil i ties were con sid ered again for the in crease in the health in sur ance in -stal ments658. In the mid dle of the year, it was an nounced that the Min is try of Fi nance was pre -par ing a programme for a 3-year frame work of the bud get pro vid ing for an in crease of thehealth in sur ance in stal ment in 2005 from 6% to 8%, ac com pa nied with the de crease in thetax a tion bur den. The programme was due to be dis cussed in Par lia ment659. Ac cord ing to theDi rec tor of the NHIF Dr. D. Petrov, the Fund could en tirely cover the med i cal care, if thehealth in sur ance in stal ment was fixed at 12%660.
In 2004, the Min is ter of Healthcare S. Bogoev claimed that the health in sur ance in stal -ments would be in creased by 2% from 2005 or in 2006 at the lat est661. The gen eral prac ti tio ners and the spe cial ists also pro claimed them selves in fa vour of the rise of the in stal ments to 9%662.
In 2005, the Par lia men tary Com mis sion re jected unan i mously the pro posal made byAssoc. Prof. Dr. Atanas Shterev for the in stal ments to be in creased to 8% from Sep tem ber.Views were ex pressed that ac tual cost ing was needed, based on the pack age of healthcare ser -vices, which would be as signed on the ba sis of a pro found anal y sis of the health needs and thepur chas ing abil i ties of the pop u la tion663.
Drug sup ply
The is sues about the drugs re im bursed to tally or par tially from the bud get of the NHIF,the drug prices and their dis tri bu tion were some of the lead ing ones through out the third stage of the healthcare re form.
The topic of the free drugs was pre sented in 2001 with in for ma tion about un law ful pre -scrip tion of free drugs by the gen eral prac ti tio ners, “strug gle” about which drugs to be in cludedin the NHIF lists, checks of gen eral prac ti tio ners per formed by the Fund in var i ous cit ies664.
164
653 Duma daily, Is sue ¹ 4 and Is sue ¹ 55 from 2003; Standart daily, Is sue ¹ 4313 from 8.01.2005, Is sue ¹4330 from 25.01.2005 and Is sue ¹ 4358 from 22.02.2005 ã.; Kapital weekly from 8-14.01.2005
654 Duma daily, Is sue ¹25 from 31.01.2005; Standart daily, Is sue ¹ 4330 from 25.01.2005655 Standart daily, Is sue ¹ 4385 from 22.03.2005 and Is sue ¹ 4453 from 2.06.2005656 Duma daily, Is sue ¹ 210 îò 2002 ã.; Standart daily, Is sue ¹ 3442 from 1.08.2002657 24 chasa daily, Is sue ¹ 211 from 02.08.2002658 Standart daily, Is sue ¹ 3694 from 14.04.2003 and Is sue ¹ 3698 from 18.04.2003659 24 chasa daily, Is sue ¹ 203 from 27.07.2003 ; Duma daily, Is sue ¹ 181 and Is sue ¹ 249 îò 2003660 Duma daily, Is sue ¹ 270 from 21.11.2003661 24 chasa daily, Is sue ¹ 106, Is sue ¹ 171 and Is sue ¹ 179 from 2004; Duma daily, Is sue ¹ 129 from 2004662 24 chasa daily, Is sue ¹ 169 from 20.06.2004 Trud daily from 21.06.2004663 Duma daily, Is sue ¹ 61 from 16.03.2005664 Trud daily, Is sue ¹ 289 from 25.10.2001; Fo rum Medicus, Is sue ¹ 7 from 12.02.2001
The be gin ning of 2002 was marked by a huge num ber of pub li ca tions fea tur ing the chaoson the drug mar ket caused by De cree ¹ 300 of the Coun cil of Min is ters from De cem ber21st 2001, pro vid ing for the in tro duc tion of VAT on drugs665. The me dia in formed that evenaf ter the en force ment of the De cree, part of the phar ma cies con tin ued to sell drugs at the oldprices and other closed down to cal cu late the stock quan ti ties with in di ces with VAT. Chaosand lack of in for ma tion were widely re ported about the new prices. Var i ous prog no ses weremade about the per cent age of the in crease in the drug prices – from 6, 9 and 20 to 40%. A com -plaint was sub mit ted by the phar ma cists to the Su preme Ad min is tra tive Court to gether with awarn ing that that the rise of prices would bring about drain ing of the NHIF money. The As so -ci a tion of the Bul gar ian Phar ma cists warned that the prob lems of the phar ma cies would af fectand trans fer to the hos pi tals666. In his turn, Min is ter Finkov pre dicted that the chaos in the phar -ma cies would last for three months un til the de ple tion of the stock amounts. Dep u ties (in clud -ing those from the rul ing ma jor ity) ac cused the Vice Min is ter of Fi nance A. Katsarchev of thedrugs prob lem and claimed his res ig na tion667. The dep uty from the BSP E. Maslarova de clared that the in tro duc tion of VAT dis crim i nated the Bul gar ian drug pro duc ers; she de fined its con -se quences as “out ra geous, em bez zling and doom ing” and pre dicted that the chaos will con -tinue for a year af ter the tax in tro duc tion668.
The NHIF re tal i ated that as a func tion of the rise in the drug prices, it would pay less fordrugs, it would re duce the num ber of dis eases for which it would re im burse the drugs to tally orpar tially and would in crease the co-pay ment by the pa tients669.
The NHIF ad mit ted the fact that the ex pen di ture of the Fund for Drugs was higher thanthe pre dicted one by 30%, and the mem ber of the UDB Dr. Sharkov de clared the in ten tions ofthe “blue” op po si tion to ini ti ate a Par lia men tary de bate on the con di tion of the Fund as he reck -oned that NHIF bud get would be suf fi cient for two months only. Ac cord ing to dep u ties fromthe op po si tion, “the cre ated cri sis is a func tion of the pol icy con ducted by the ma jor ity who had ap proved a bud get not cor re spond ing to the needs and the un jus ti fied in tro duc tion of VAT ondrugs.”670 The al ter na tives for over com ing the drug def i cit in cluded the open ing of the NHIFre serve amount ing to 700 mil lion BGN and re duc tion of the list of free and par tially re im -bursed drugs. It was also pointed out that out of the 131 mil lion BGN planned for 2002, 100BGN had been spent un til the mid dle of the year671. The me dia also in formed that the Fund was con duct ing checks with ques tion naires to the pa tients about over priced pre scrip tions andplanned to use stick ers with a ho lo gram sign for the drugs it re im bursed in or der to stop the re -
165
Stages and evo lu tion of the healthcare re form in Bul garia
665 Duma daily, Is sue ¹ 1 from 3.01.2002, Is sue ¹ 1 from 4.01.2002, Is sue ¹ 1 from 5.01.2002 and Issue ¹ 29 from 5.02.2002; Standart daily, Is sue ¹ 3234 from 3.01.2002, Is sue ¹ 3235 from 4.01.2002, Is sue ¹ 3236from 5.01.2002, Is sue ¹ 3242 from 11.01.2002 and Is sue ¹ 3266 from 4.02.2002; Democracia daily from5.01.2002; 24 chasa daily, Is sue ¹ 2 from 3.01.2002, Is sue ¹ 3 from 4.01.2002, Is sue ¹ 4 from 5.01.2002,Is sue ¹ 6 from 7.01.2002, Is sue ¹ 7 from 8.01.2002, Is sue ¹ 8 from 9.01.2002, Is sue ¹ 11 from12.01.2002, Is sue ¹ 23 from 24.01.2002, Is sue ¹ 44 from 14.02.2002, Is sue ¹ 89 from 31.03.2002, Is sue ¹ 91 from 2.04.2002 and Issue ¹ 92 from 3.04.2002
666 Duma daily, Is sue ¹ 21 from 27.01.2002 and Is sue ¹ 23 from 29.01.2002; 24 chasa daily, Is sue ¹ 27 from28.01.2002
667 Standart daily, Is sue ¹ 3239 from 8.01.2002668 Duma daily, Is sue ¹ 14 from 2002669 Democracia daily from 1.03.2002; 24 chasa daily, Is sue ¹ 51 from 21.02.2002, Is sue ¹ 59 from 1.03.2002
and Is sue ¹ 250 from 10.09.2002670 Standart daily, Is sue ¹ 3297 from 7.03.2002; Duma daily, Is sue ¹.126 from 2002 671 24 chasa daily, Is sue ¹ 160 from 12.06.2002
sell ing of med i ca tions which had once been paid by the NHIF672.In a se ries of pub li ca tions, in 2002 com ments could be read about the “drain ing of the
Fund” through the drugs673 and sus pi cions were raised as to spec u la tive gains and com mis -sions674.
Along with the is sue of the drug prices and def i cit, the me dia in formed about changes inthe re quire ments of the Health Fund to the phar ma cies and to the pro ce dure for the pre scrip tion of the free and par tially re im bursed drugs675, caus ing a lot of con tro ver sial opin ions. From May 2002 the NHIF in tro duced a new re quire ment to the phar ma cies whereby they were obligedto pro vide a sep a rate desk for work with NHIF pre scrip tions. Their ar gu ment was that in thisway strict con trol would be achieved over the flow of the free pre scrip tions. In this re spect, itwas ex pected that the ex is tence of nu mer ous small out lets would be threat ened as they wouldnot be able to meet the re quire ments and there was a dan ger of their bank ruptcy.
Once again in 2002, the dep uty from the NMSS Dr. A. Purvanova raised the is sue whichhad been re peat edly dis cussed about the right of phar ma cists with Mas ter’s De gree only toopen phar ma cies. The amend ments in the LDPHM caused a scan dal at first hear ing in the NAand the dis pute cir cled around whether the li cense for open ing of a phar macy should be givento ev ery phys i cal per son or le gal en tity and whether the re lieved re gime was valid for the tradewith opi ates, too. While the gov ern ing ma jor ity in sisted on the changes, the UDF stand on theis sue was that “the trade with nar cot ics is be ing legal ised in this way.”676 In his turn, the Dep -uty Chair man of the Un ion of the phar ma cists Stoicho Chervenliev de clared that “it is un ac -cept able for the trader to hold the key to the shelf with the nar cotic sub stances; the amend ments are against the pa tients; the phar ma cies are not shops but healthcare es tab lish ments” whereasac cord ing to A. Purvanova “the phar ma cists are fight ing for priv i leges and their ar gu ments arespin ning around eco nomic in ter ests; com pe ti tion is the one to de crease the drug prices.”677 Atthe end of No vem ber 2002, she stated: ”We shall amend the law in spite of the at tacks.”678Af ter a heated de bate the amend ments were even tu ally re jected and the phar ma cists pre served theirex clu sive right to open phar ma cies679. The dep uty from NMSS Dr A. Kyurkchiev pro posed the clos ing of phar ma cies in the hos pi tals and the for mer poly clin ics since this un blocked the roadfor cor rup tion. He was backed up by Dr. T. Konstantinova from the UDF and Assoc. Prof. Dr.A. Shterev said that they were go ing to make an en quiry to the Com mis sion on the pro tec tionof com pe ti tion680.
The next con sid er ation of the law dated to the mid dle of March 2003 when dep u ties fromthe Co ali tion for Bul garia de pos ited a claim to the Con sti tu tional Court, ac cord ing to whichpart of the stip u la tions in the Law on Drugs and Phar ma cies in Hu man Med i cine pro hib it -ing the open ing of phar ma cies on the ter ri tory of healthcare es tab lish ments for hos pi tal carehad to be de clared anti-con sti tu tional. In their mo ti va tion, the mem bers of Par lia ment pointed
166
672 24 chasa daily, Is sue ¹ 162 from 14.06.2002 673 Standart daily, Is sue ¹ 3363 from 14.05.2002, Is sue ¹ 3385 from 5.06.2002 and Is sue ¹ 3402 from
22.06.2002; 24 chasa daily, Is sue ¹ 165 from 17.06.2002; Kapital weekly from 7-13.12.2002674 Standart daily, Is sue ¹ 3388 from 8.06.2002 and Is sue ¹ 3411 from 1.07.2002675 Trud daily, Is sue ¹ from 2.04.2002; Kapital weekly from 16–22.03.2002; Standart daily, Is sue ¹ 3432 from
22.07.2002676 24 chasa daily, Is sue ¹ 146 from 2002677 Standart daily, Is sue ¹ 3440 from 30.07.2002 678 24 chasa daily, Is sue ¹ 327 from 26.11.2002 679 24 chasa daily, Is sue ¹ 353 from 2002 680 24 chasa daily, Is sue ¹ 186 from 8.07.2002
out that in such a way the right of free prac tic ing of eco nomic ac tiv ity and prop erty right werere stricted with out an ex ist ing ob jec tive pub lic in ter est ne ces si tat ing this re stric tion681.
In the sec ond half of 2002, in for ma tion ap peared in the press that the Min is ter was go ing tode ter mine the list of dis eases paid for by the NHIF682. At the be gin ning of 2003, there was an an -nounce ment about the list of dis eases, pre pared for the first time by the MH, for whose treat mentin 2003 the NHIF would re im burse to tally or par tially the drugs. It was emphasised in the ar ti clethat the prep a ra tion was forth com ing of the list with the names and the amount of med i ca tionsand consumables which were go ing to be to tally or par tially re im bursed by the NHIF683.
Af ter the in tro duc tion of VAT on the drugs in 2002, as a re sult of which the prices in -creased by 20-25%, in 2003 the Com mis sion on drug prices to the MH ap proved an in creaseof the prices of a great part of the Bul gar ian prod ucts. The rise in prices was de manded by thepro duc ers be cause of the in fla tion, the in crease of the prices of the im ported sub stances, therise in the fuel prices as well as be cause of con sid er able in vest ments nec es sary for the in tro -duc tion of the stan dards for good pro duc tion prac tices684.
Sim i larly to the pre vi ous years when the rise of the drug prices was adopted, they were ac -com pa nied by in for ma tion about a def i cit and com ments about spec u la tive gains on be half ofthe dis trib u tors685. In the mean time, the Par lia men tary Com mis sion on healthcare ana lysed theef fect from the in tro duc tion of the VAT on the drugs, which ac cord ing to the pre sented data,had brought about a sig nif i cant in crease (by 5 mil lion BGN) in the NHIF ex pen di ture fordrugs. The Ex ec u tive Board of the NHIF an nounced that the bud get planned for drugs for 2003 would be in suf fi cient. On this oc ca sion, the Par lia men tary Com mis sion on Healthcare as -signed to the MH and the NHIF the task to un der take mea sures for the re duc tion of the costs for drugs686. Two weeks later in for ma tion was re leased about a rise in the prices of im porteddrugs, too687.
An anal y sis of the Ex ec u tive agency on drugs in di cated that the in crease in the drugprices for the pe riod 2000-2002 had led to about dou ble in crease of the drug ex penses of thehouse holds, the state and the NHIF and the quan tity of the pur chased med i ca tions has de -creased688. In this re spect, the Min is ter of Healthcare Assoc. Prof. Dr. B. Finkov and the Di rec -tor of the NHIF Dr. D. Petrov de clared that the def i cit in the NHIF bud get re sulted mainly from the in creased ex penses for drugs due to rise in the prices and the in creased num ber of reg is -tered pa tients with chronic ill nesses in 2002 as com pared to the fore go ing year689.
The re im burse ment drugs list pre pared by the NHIF was dis cussed ex ten sively in thepress from the be gin ning of 2003. The com ments con cerned the lack of mod ern med i ca tionson the list, the re duced num ber of the in cluded drugs and the in creased por tion of the price dueto be paid by the pa tients690.
167
Stages and evo lu tion of the healthcare re form in Bul garia
681 Duma daily, Is sue ¹ 73 from 2003 682 Kapital weekly from 28.09–4.10.2002; Fo rum Medicus, Is sue ¹ 37 from 30.09.2002683 24 chasa daily, Is sue ¹ 3 from 4.01.2003684 24 chasa daily, Is sue ¹ 19 from 20.01.2003; Duma daily, Is sue ¹ 18 from 2003; Standart daily, Is sue ¹
3611 from 21.01.2003 and Issue ¹ 3613 from 23.01.2003; Kapital weekly from 25-31.01.2003 and from19-28.02.2003
685 24 chasa daily, Is sue ¹ 20 from 21.01.2003 686 24 chasa daily, Is sue ¹19 from 20.01.2003 687 24 chasa daily, Is sue ¹34 from 4.02.2003 688 24 chasa daily, Is sue ¹ 54 from 24.02.2003689 Duma daily, Is sue ¹ 50 and Is sue ¹ 51 from 2003690 24 chasa daily, Is sue ¹ 33 from 3.02.2003, Is sue ¹ 34 from 4.02.2003, Is sue ¹ 35 from 5.02.2003, Is sue ¹
The Di rec tor of the NHIF Dr. D. Petrov an nounced that the in tro duc tion of re stric tionswas planned for the pre scrip tion of free or par tially re im bursed drugs to gether with en hancedcon trol on the is sued pre scrip tions and pro to cols for costly med i ca tion691. Im me di ately be forethe new NFA for 2003 was en forced, var i ous mea sures were un der taken for the re stric tion ofthe pre scribed med i cines, ne ces si tated by the short age in the bud get for 2003 and the need forcost con tain ment due to the in crease of the drug prices692.
In the mid dle of the year, the So fia Ad min is tra tive Court pro claimed as “un law ful” theamend ment in the NHIF re im burse ment drug list, from which 407 drugs were ex cludedfrom Feb ru ary with the ar gu ment that it was not agreed with the UBP and the UDB as par ties to the con clud ing of the NFA. The Court re ferred to the amend ment in the Law on Health In sur -ance from No vem ber 18th 2002, ac cord ing to which changes in the list could be made onlythrough an amend ment of the NFA. The Di rec tor of the NHIF Dr. D. Petrov stated that the de -ci sion would be ap pealed in front of the Su preme Ad min is tra tive Court693.
Ac cord ing to the Un ion of the phar ma cists, the pro ce dure for con tract ing be tween theNHIF and the drug pro duc ers and im port ers cre ated pre req ui sites for vi o la tions both in ne go ti -at ing prices and the sell ing of amounts of il le gal im port694.
In the first half of 2003, the press pub lished in for ma tion about prob lems with the de liv er -ies within the state pro cure ment on costly med i ca tions for the oncological pa tients695. Fortheir pro vi sion the Min is ter of Fi nance gave per mis sion for the uti li sa tion of 5.1 mil lion USdol lars as a rem nant from a loan re leased in 1997696. The ar ti cles and the com ments about adef i cit and ir reg u lar sup ply of drugs for peo ple with oncological dis eases con tin ued in the fol -low ing months, too697. The MH in formed that the rea sons for the short age of drugs were linked to the de crease in the bud get in ac cor dance with Reg u la tion ¹ 23, the le gal dis putes be tweenthe par tic i pants in the auc tions for the state pro cure ment as well as to the dis crep ancy be tweenthe num ber of pa tients reg is tered at the Min is try and those de clared by the dis pen sa ries.
The prob lem with the drugs re im bursed to tally or par tially by the NHIF was ex ac er bateddur ing the last two months of 2003 when the Un ion of the phar ma cists an nounced that thephar ma cies would cease to ful fil the free pre scrip tions be cause of the enor mous debts of theFund to them698.
At the end of the year, the Chair man of the Ex ec u tive Board of the NHIF K. Ananiev in -formed that a new meth od ol ogy had been pre pared for drug re im burse ment in 2004. It en -vis aged that a monthly limit was in tro duced for ev ery dis ease for the free and par tiallyre im bursed drugs, only the cheap est med i ca tions from each drug group be ing re im bursed and
168
36 from 6.02.2003 and Is sue ¹ 82 from 24.03.2003; Trud daily from 6.02.2003 and from 21.02.2003; Dumadaily, Is sue ¹ 29 from 2003; Standart daily, Is sue ¹ 3636 from 15.02.2003 and Is sue ¹.3703 from23.04.2003; Kapital weekly from 10-16.05.2003
691 24 chasa daily, Is sue ¹ 62 from 4.03.2003; Standart daily, Is sue ¹ 3659 from 10.03.2003692 24 chasa daily, Is sue ¹ 88 from 30.03.2003 and Is sue Is sue ¹ 89 from 31.03.2003; Duma daily, Is sue ¹ 75
from 2003; Standart daily, Is sue ¹ 3681 from 1.04.2003 and Is sue ¹ 3696 from 16.04.2003; Kapital weekly, Is sue ¹. 4 from 1-7.02.2003
693 24 chasa daily, Is sue ¹ 187 from 11.07.2003694 24 chasa daily, Is sue ¹ 159 from 2003695 24 chasa daily, Is sue ¹ 138 from 2003696 24 chasa daily, Is sue ¹ 159 from 2003697 24 chasa daily, Is sue ¹ 190 from 14.07.2003 and Is sue ¹ 211 from 4.08.2003 698 Standart daily, Is sue ¹ 3917 from 27.11.2003
the rest be ing re im bursed par tially by the NHIF699.For the first time in Bul garia, a spe cial com mis sion to the MH de signed a pos i tive drug
list, based on which the re im burse ment drug list of the NHIF was go ing to be pre pared and thees sen tial lists were go ing to be de ter mined for drugs which hos pi tals would have the right topur chase. The pub li ca tions men tioned that the list was aimed at lim it ing the costs of the NHIFmade for drugs by in clud ing med i ca tions of older gen er a tion at lower prices. The Chair man ofthe Par lia men tary Com mis sion on Healthcare Assoc. Prof. Dr. Shterev de clared that the aim of the pos i tive drug list prep a ra tion was to curb cor rup tion. Ac cord ing to him the list de signed bythe MH was ex tremely re stricted and in this way the NHIF was ex cluded as a par tic i pant in thede ci sion-mak ing700. The dead line for the work ing out of the pos i tive drug list was ex tended bymore than a month from the ini tially planned term which gave rea sons to the press to pub lishar ti cles in form ing about a po ten tial dan ger from a short age of life-sav ing drugs. The otherprob lem caused by the de lay, was re lated to the prep a ra tion of the NHIF re im burse ment list701.The com ments on the pos i tive drug list con tin ued also re gard ing the drugs in cluded in it. As so -ci a tions of drug pro duc ers and im port ers ac cused the com mis sion work ing out the list of lackof trans par ency and cri te ria for the drug se lec tion as well as of com pro mises of qual ity at theex pense of the drug price702.
At the end of the year, the Min is ter of Healthcare in formed about the prep a ra tion of a newmeth od ol ogy for reg is tra tion and con trol of drug prices, ac cord ing to which the price of adrug in Bul garia could not de vi ate from its mean price value in 9 se lected coun tries in Eu rope.Ac cord ing to Min is ter Bogoev, the meth od ol ogy of ref er ence prices was part of the prep a ra -tion of Bul garia for its EC ac ces sion in 2007703.
Af ter the im pos ture of VAT on drugs in 2002 and the in crease from 2003 of the prices of a large part of the med i ca tions pro duced in Bul garia, in the fol low ing two years the is sue of thedrug prices ceased to be dis cussed in the me dia and gave way to the is sue of the or gani sa tionof the drug sup ply, the drug pol icy and the way of de ter min ing of the NHIF re im burse -ment list.
At the be gin ning of 2004, com ments ap peared in the press con cern ing the pro ce dure forthe ad min is tra tion of drug auc tions, stip u lated by the Law on State Pro cure ment which wasgo ing to sub sti tute the di rect ne go ti a tion be tween the NHIF and rep re sen ta tives of the pro duc -ers. Ac cord ing to the rep re sen ta tives of the NHIF, the new pro ce dure was go ing to de lay thesup plies of drugs re im bursed to tally by the NHIF due to the re quire ment stip u lated in the Law,e.g. the dis putes be tween com pa nies were re solved by ju di cial in sti tu tions704.
Mean while, a new in struc tion of the NHIF caused chaos in the phar ma cies and the fam -ily phy si cians due to the fact that 308 drugs were dropped from the pos i tive drug list adopted in De cem ber 2003 and they had to be sub sti tuted by other drugs705.
169
Stages and evo lu tion of the healthcare re form in Bul garia
699 24 chasa daily, Is sue ¹ 296 from 28.10.2003; Trud daily from 2.12.2003700 24 chasa daily, Is sue ¹ 284 from 16.10.2003 and Is sue ¹ 298 from 30.10.2003701 24 chasa daily, Is sue ¹ 302 from 3.11.2003; Duma daily, Is sue ¹ 281 from 4.12.2003; Standart daily, Is sue
¹ 3893 from 3.11.2003 and Is sue ¹ 3924 from 4.12.2003702 24 chasa daily, Is sue ¹ 328 from 29.11.2003 and Is sue ¹ 338 from 9.12.2003; Duma daily, Is sue ¹ 285
from 9.12.2003; Standart daily, Is sue ¹ 3930 from 10.12.2003; Kapital weekly from 13-19.12.2003703 24 chasa daily, Is sue ¹337 from 08.12.2003; Duma daily, Is sue ¹ 281 from 4.12.2003 Issue ¹ 287 from
11.12.2003.; Standart daily, Is sue ¹ 3924 from 4.12.2003704 24 chasa daily, Is sue ¹ 18, Is sue ¹ 19 and Is sue ¹ 25 from 2004705 24 chasa daily, Is sue ¹ 29 from 30.01.2004, Is sue ¹ 32 îò 2.02.2004, Is sue ¹ 75 from 16.03.2004 and Is sue
In 2004, for the meth od ol ogy for the re im burse ment of drugs, the Di rec tor of the NHIFDr. I. Bukarev pro posed that the list of free and par tially re im bursed by the Fund drugs did notchange for a term of one year af ter its adop tion. The pro posal was pro voked by the changesmade in the list ev ery month, cre at ing nu mer ous prob lems in the drug pre scrip tion and theful fil ment of the pre scrip tions706. A work ing group of ex perts from the Fund and other in sti tu -tions worked out a draft for amend ment of the Law on State Pro cure ment to in clude a sep a ratechap ter reg u lat ing the drug auc tions ad min is tered by the NHIF, pro vid ing for the pro tec tionagainst block ing of sup plies in cases of law suits be tween the firms par tic i pat ing in the auc -tions707. In the be gin ning of the year, Min is ter Bogoev also an nounced amend ments en vis agedto be adopted in the Law on State Pro cure ment re gard ing the ad min is tra tion of auc tions fordrugs paid by the state bud get. As en vis aged by the law, in cases of ap peals of de ci sions, thechanges stip u lated the as sign ing of the state pro cure ments, the con tin u a tion of the drugs sup -ply un til the le gal pro nounce ment to avoid their block age708.
In the mid dle of the year, an ar ti cle in the “24 chasa” in formed about the prep a ra tion of areg u la tion pro vid ing for a new or der for con tract ing the drugs re im bursed by the NHIF. Ac -cord ing to the pro ce dure, stip u lated in the reg u la tion, the NHIF was go ing to re im burse a fixedpart for ev ery group of drugs, de ter mined as a mean value of the drug prices in 9 se lected Eu ro -pean coun tries. Thus, only the cheap est drugs from ev ery group would be to tally free for thepa tients and for the rest the NHIF re im burs ing a ref er ence price de fined ac cord ing to theadopted meth od ol ogy. The reg u la tion also pro vided for the terms and pro ce dure ac cord ing towhich the firms could change their ten der prices709. Af ter about a month the Coun cil of Min is -ters passed the reg u la tion for the terms and con di tions for the con tract ing of the drugs to tally or par tially re im bursed by the NHIF. It en vis aged a com mis sion of 20 peo ple in which law yers,econ o mists, phy si cians and phar ma cists were in volved to ne go ti ate the drugs re im bursed bythe NHIF710.
Ac cord ing to CITUB, the short age of funds for the pro vi sion of free or par tially re im -bursed by the NHIF drugs was due to a large ex tent to the con tract ing it self which al lowed for10 000% over price on the drugs for which the NHIF paid. Thus, a par a dox i cal sit u a tion on themar ket was cre ated, in which the prices of part of the drugs for free sale were lower than thosere im bursed by the NHIF711. The As so ci a tion of the Bul gar ian Phar ma ceu ti cal Pro duc ers stated that the NHIF suf fered ap prox i mately 40 mil lion BGN losses an nu ally as the list for the free orpar tially re im bursed drugs did not in clude ge neric drugs, whose prices were be tween 30% and60% lower712. The prob lems with the ne go ti at ing of drugs be tween the NHIF and the pro duc -ers’ com pa nies were con sid ered in other pub li ca tions too, the em pha sis be ing on the sig nif i -cantly higher prices paid by the NHIF for some med i ca tions as com pared to other coun tries
170
¹ 76 from 17.03.2004; Duma daily, Is sue ¹ 25 from 2.02.2004 ã.; Kapital weekly from 31.01.–6.02.2004;Standart daily, Is sue ¹ 3959 from 14.01.2004, Is sue ¹ 3965 from 20.01.2004, Is sue ¹ 3975 from30.01.2004 ã. and Is sue ¹ 3978 from 2.02.2004
706 24 chasa daily, Is sue ¹ 54 îò 24.02.2004 ã.; Trud daily from 21.08.2004707 24 chasa daily, Is sue ¹ 54 from 24.02.2004 ã; Duma daily, Is sue ¹ 44 from 2004708 Standart daily, Is sue ¹ 3966 from 21.01.2004709 24 chasa daily, Is sue ¹ 126 from 8.05.2004 and Is sue ¹ 172 from 23.06.2004710 24 chasa daily, Is sue ¹ 209 from 30.07.2004 Kapital weekly from 31.07.–6.08.2004711 24 chasa daily, Is sue ¹ 182 from 3.07.2004 and Is sue ¹ 191 from 12.07.2004; Fo rum Medicus pe ri od i cal,
Is sue ¹ 28 from 12.07.2004712 24 chasa daily, Is sue ¹ 207 from 28.07.2004
in West ern and East ern Eu rope713.Ac cord ing to data sub mit ted by the As so ci a tion of the Bul gar ian Phar ma ceu ti cal Pro duc -
ers, af ter the re duc tion of the re im burse ment list at the be gin ning of 2003 and the de crease ofthe part of the price re im bursed by the NHIF, 400 000 peo ple re fused to ben e fit from the free or par tially re im bursed drugs. A large part of them dis con tin ued their treat ment be cause theycould not af ford to co-pay for the drugs and the re main ing part pre ferred to pur chase themfreely from the phar ma cies. The rep re sen ta tives of the As so ci a tion quoted in for ma tion fromthe NHIF, ac cord ing to which af ter the re duc tion of the re im burse ment list an in crease by13% was reg is tered in the num ber of pa tients with chronic dis eases whose hos pi tal treat -ment in creased the costs of the NHIF by 450 000 BGN714.
In the sec ond half of 2004, sev eral pub li ca tions in the press in formed about the mea suresfor the re stric tion of the costs for drugs, planned by the NHIF. The Dep uty Di rec tor of theNHIF Dr. Decho Dechev an nounced that in 2005 the part of the price paid by the pa tient wasgo ing to fall as a re sult of the new pro ce dure for drug con tract ing. For the fol low ing year thehealth in sur ance fund planned to de mand from the phar ma cies a dis count from the prices ofdrugs paid par tially or fully by the NHIF715.
At the end of the year, the NHIF placed new re quire ments for the ne go ti at ing of the drugswith the pro duc ing com pa nies. Ac cord ing to these re quire ments, the com pa nies had to pres entbank guar an tees and pay com pen sa tions in cases of breaches in the de liv ery made by their dis -trib u tors. The for eign com pa nies did not con sent to these con di tions for sign ing con tracts withthe Health In sur ance Fund since ac cord ing to their rep re sen ta tives, the Fund could con tractdrugs and prices but not terms of de liv ery716.
Along with the news about the adop tion of the pos i tive drug list and the changes in the re -im burse ment list of the NHIF, the amend ment in the pro ce dure and the terms of con tract ing ofdrugs be tween the Health In sur ance Fund and the phar ma ceu ti cal com pa nies, in 2004 the press also cov ered the is sue of drug sup ply in re la tion to the state-of-art and the de vel op ment ofthe drug prod ucts mar ket.
In the first half of the year, the un veiled cus toms vi o la tions, frauds with VAT and thefall into in sol vency of the sec ond larg est dis tri bu tion com pany on the mar ket of drugs pro -voked a num ber of com ments in the me dia re lated to the re duc tion of the li quid ity of the re -main ing trad ers as well as prob lems with drugs de liv ery. The scan dal with the “Magined”com pany de liv er ing drugs mainly on state pro cure ments pro voked tax and cus toms in spec -tions of all of the phar ma ceu ti cal firms717.
On this oc ca sion, Min is ter Bogoev pre dicted in sta bil i ties of the drug mar ket and rise inthe prices due to com pe ti tion re stric tion and the emerg ing dis trust be tween the par tic i pants onthe mar ket, as a re sult of which de te ri o ra tion was ex pected in the con di tions for de liv ery, in -clud ing of med i ca tions on cen tral ised sup plies of the MH, hos pi tal auc tions and the NHIF718.
171
Stages and evo lu tion of the healthcare re form in Bul garia
713 Standart daily, Is sue ¹ 4056 from 22.04.2004714 Standart daily, Is sue ¹ 4192 from 05.09.2004715 24 chasa daily, Is sue ¹ 216 from 6.08.2004; Standart daily, Is sue ¹ 4198 from 11.09.2004; Duma daily,
Is sue ¹ 184 from 10.08.2004; Kapital weekly from 11-17.12.2004; Fo rum Medicus pe ri od i cal, Is sue ¹35from 20.09.2004
716 24 chasa daily, Is sue ¹ 315 from 13.11.2004; Kapital weekly from 20-26.11.2004717 24 chasa daily, Is sue ¹ 88 from 29.03.2004; Standart daily, Is sue ¹ 4030 from 25.03.2004 and Is sue ¹
4034 from 29.03.2004718 Kapital weekly from 27.03.–1.04.2004
The bank ruptcy of the sec ond larg est dis trib u tor of drug prod ucts “Magined” once againput on the agenda the is sue of the great debts of the hos pi tals to the dis tri bu tion com pa nies,but un like in pre vi ous years, the ques tion was posed from the point of view of li quid ity and thesol vency of the re main ing big “play ers” on the drug mar ket. The press dis cussed the pro -nounce ments of the man age ment of the larg est drug dis tri bu tion firm “Turgovska liga”, ac -cord ing to which the dis trib u tors would dis con tinue their sup plies for the in debted hos pi tals.The com pa nies in sisted on re liev ing the im port, guar an tee ing better con di tions in con tract ingwith the hos pi tals, re duc tion of the VAT for the drug prod ucts719. From the Na tional BranchCham ber of Com merce of the Whole sale Dis trib u tors of Drug Prod ucts in formed that the hos -pi tal debts un til May amounted to 33 mil lion BGN. The prob lems with the drugs also raised the ques tion of the hos pi tal man age ment and the fi nanc ing of the healthcare sys tem720.
The Min is ter of Healthcare S.Bogoev pro posed that the VAT on drug prod ucts be re -duced by 10% with the ar gu ment that in such a way the ex penses for drugs of the NHIF and theMH would drop and ap prox i mately 40 mil lion would be “re leased” in the bud get of the Fundand the other pub lic funds which could be uti lised for the sup ply of new drugs. In the be gin -ning of May, re lieves were ne go ti ated for the drugs im port be tween the im port ers and the Min -is ter of Fi nance Milen Velchev and the Min is ter of Healthcare Slavcho Bogoev, ac cord ing towhich the im port ers would not pay the VAT im me di ately af ter the re lease of the drugs from the cus toms pro vided that they pre sented a bank guar an tee for the due sum. At the meet ing, M.Velchev de clared that the is sue of the dif fer en ti ated tar iffs for the VAT on drugs would not bedis cussed721.
The prob lems with the dis tri bu tion of drug prod ucts in 2004 drew the at ten tion of the me -dia to the re tail ers’ drug mar ket. The phar ma ceu ti cal “war” for lower prices, the dump ingap plied by some chain of phar ma cies, the mech a nisms for dis tri bu tion of the drugs from il le gal im port and un paid VAT, the phe nom e nal dif fer ences in the prices of one and the same drugsdis trib uted through free sale and for re im burse ment by the NHIF were sub ject to dis cus sions in some ar ti cles pub lished in 2004. Re gard ing the cre ated mar ket sit u a tion, the Un ion of the Phar -ma cists in Bul garia made an other pro posal for the in tro duc tion of fixed prices aimed at re strict -ing the prac tices of dis loyal com pe ti tion, tax a tion and cus toms vi o la tions722.
At the be gin ning of 2005, the press once again pub lished in for ma tion about short age ofcostly life-sav ing and life-main tain ing drugs paid from the state bud get723. They were ac -com pa nied by com ments about con flicts be tween the ma jor trad ers on the drug mar ket as wellas be tween them and the MH which were one of the main rea sons for the def i cit of the costlydrugs724. In the mid dle of the year, the Su preme Court of Cas sa tion or dered an in spec tion to bemade of the auc tions for the de liv ery and dis tri bu tion of drugs re im bursed by the NHIF, fol -low ing which two cases were made against the MH by pa tients with oncological dis eases whohad suf fered dam ages for lack of life-main tain ing drugs725.
172
719 24 chasa daily, Is sue ¹ 123 from 5.05.2004 and Is sue ¹130 from 12.05.2004; Standart daily, Is sue ¹ 4077from 13.05.2004
720 Kapital weekly from 15-21.05.2004721 Kapital weekly from 6-14.05.2004; Standart daily, Is sue ¹ 4069 from 5.05.2004722 24 chasa daily, Is sue ¹ 191 from 12.07.2004 and Is sue ¹ 321 from 19.11.2004723 Duma daily, Is sue ¹ 1 from 3.01.2005 ; Standart daily, Is sue ¹ 4320 from 15.01.2005; 24 chasa daily from
22.03.2005724 Kapital weekly from 26.03.–1.04.2005725 Kapital weekly from 25.06.–1.07.2005
The de signed draft pro ject for the re lease of drugs, med i cal prod ucts and di etary foods for spe cial med i cal pur poses re im bursed by the NHIF, which was signed be tween the Fund andthe phar ma cies, pro voked acute re sent ment among the phar ma cists. The rea son was a pro vi -sion in the con tract, ac cord ing to which the phar ma cies had to grant a 10%-dis count from themax i mum sell ing price, re duced by the due VAT. The Un ion of the Phar ma cists in Bul gariapro tested against this con di tion in the draft pro ject with the ar gu ment that it would bring aboutan in crease of the part of the price paid by the end-con sum ers, with which the pro pri etors ofphar ma cies would com pen sate the re duc tion in their prof its. Ac cord ing to the Un ion, thatwould re sult in bank rupt cies of smaller phar ma cies, too726. Pro tests of phar ma cists started indif fer ent cit ies, as a re sult of which the Ex ec u tive Board of the NHIF con sid ered an op tion thatthe de manded dis count was to be re duced from 10% to 6%727. Af ter dis cus sions of var i ous pro -pos als, the NHIF and the pro fes sional or gani sa tions of the phar ma cists agreed on a dis count of8% from the turn over of the phar ma cies which was to be dis trib uted equally be tween the partpaid by the Fund and the one paid by the pa tients. As a re sult of the dis count de fined in thisway, the NHIF ex pected to make econ o mies of 11-12 mil lion BGN an nu ally (some pub li ca -tions quote 25-30 mil lion BGN)728. In an in ter view for the “Duma” news pa per, the Chair manof the As so ci a tion of Bul gar ian phar ma cists de clared that the dis count claimed by the NHIFwas il le gal and was im posed un law fully since the phar ma cists were not a party to the NFA and, there fore, they did not have equal rights as the phy si cians and the den tists729. In an ar ti cle forthe “Kapital” the the sis was ar gued that the prices of drugs on the free mar ket (out side theNHIF re im burse ment list) had to be in creased as a com pen sa tion for pos si ble losses from thesales of re im burs able drugs and that this would af fect neg a tively the whole mar ket and all thepar tic i pants in it730.
In the mid dle of Feb ru ary, on the oc ca sion of the ob jec tions made by the Un ion of Bul gar -ian phar ma cists, the Par lia men tary Com mis sion on Healthcare con vened to dis cuss the le git i -macy of the dis count for the drugs de manded by the NHIF for which it paid. The com mis sionhad to also rec om mend a way of con tract ing, guar an tee ing the phar ma cists part ner ship onequal foot ing dur ing the ne go ti a tions with the Fund731.
Mean while, a num ber of ar ti cles in formed about the new re im burse ment list of theNHIF, the com ments be ing in two di rec tions – on one hand, con cern ing the in crease in thenum ber of the in cluded drugs, and on the other hand, con cern ing the planned in crease in thepart of the price paid by the end-con sumer732. The Un ion of Bul gar ian phar ma cists pro testedagainst the changes in the NHIF re im burse ment list. Ac cord ing to rep re sen ta tives of the Un -ion, the NHIF in creased the prices of half of the drugs, in cluded in it, and de creased the num ber of those it paid in full, thus in creas ing the bur den on the pa tients. The Chair man of the Un ion of phar ma cists Prof. Evgeniy Minkov de clared that there were no rea sons for the rise of the drugprices paid to tally or par tially by the NHIF. The Un ion in tended to in sist in front of the NA, theCoun cil of Min is ters and the Pres i dent’s ad min is tra tion for a wider pub lic con trol and trans -
173
Stages and evo lu tion of the healthcare re form in Bul garia
726 Duma daily, Is sue ¹ 11 from 15.01.2005; Standart daily, Is sue ¹ 4320 from 15.01.2005727 Duma daily, Is sue ¹ 14 from 18.01.2005728 Duma daily, Is sue ¹ 15 from 19.01.2005; Trud daily from 19.01.2005729 Duma daily, Is sue ¹ 32 from 2005730 Kapital weekly from 22-28.01.2005731 Kapital weekly from 19-25.02.2005732 Duma daily, Is sue ¹ 15 from 19.01.2005, Is sue ¹ 20 from 25.01.2005 and Is sue ¹ 27 from 2.02.2005, Is sue
¹ 31 from 7.02.2005 and Is sue ¹ 55 from 7.03.2005; Trud daily from 19.01.2005
par ency in the work of the NHIF733. Al most a month later the press re leased in for ma tion aboutcon sid er ably higher prices of drugs re im bursed par tially by the Fund, as com pared to the prices of the same drugs when pur chased freely. The dif fer ence was caused by the better con di tionsne go ti ated among the pro duc ers, im port ers and the whole sale trad ers in com par i son to thosene go ti ated by the NHIF734.
The mass me dia also pub lished in for ma tion about prob lems which could arise as a re sultof the lack of a uni fied in for ma tion sys tem of the NHIF due to which the phar ma ciesworked with dif fer ent soft ware prod ucts for link age and ac coun tancy with the Fund735. Sev eral months later pub li ca tions warned about pos si ble dif fi cul ties which might be caused by the re -stricted ca pac ity of the in com plete in for ma tion sys tem of the Fund736.
Fi nanc ing
Re gard ing the fi nanc ing, the debts of the hos pi tals con tin ued to be a lead ing topic through -out 2002737. At the be gin ning of 2002, the “Trud” news pa per in formed about the in ten tions ofhos pi tal di rec tors and man ag ers in the coun try to in crease the prices of the paid med i cal ser -vices738, and in an in ter view, Min is ter Bogoev stated that the hos pi tals would re ceive 90% of thesub sidy for 2001 from the MH but the fi nanc ing from the NHIF would in crease and, ac cord ing to the Min is ter, there would be no rea son for job cuts of the hos pi tal staff739.
In the mid dle of 2002, in front of the VIth Na tional Con fer ence of the Gen eral Prac ti tio -ners, the Chair man of the Par lia men tary Com mis sion on Healthcare A. Shterev de clared thathe would in sist that the bud get for healthcare for 2003 was in creased by 50 mil lion BGN which were to be uti lised for pre ven tion programmes only. He stated also that the size of the health in -sur ance in stal ment was not go ing to be in creased but “the qual ity of health ser vices wouldhardly im prove.”740
In 2002, for the first time the press pub lished com ments on the dif fer ences be tween there im burse ment of the clin i cal path ways by the NHIF and the ac tual costs made by the hos -pi tals for their per for mance741.
The only mea sure un der taken for cop ing with the hos pi tal debts was their cov er age by the state bud get742.
The fi nanc ing for hos pi tal care and the planned changes for it were among the most dis -cussed is sues in the press in 2003. Apart from the pieces of in for ma tion about the num ber ofclin i cal path ways in 2003 and the di ag no ses for which the hos pi tal treat ment was re im bursedby the bud get of the NHIF, it was an nounced that the prices for the clin i cal path ways were go -
174
733 Duma daily, Is sue ¹ 20 from 25.01.2005734 Trud daily from 22.02.2005735 Duma daily, Is sue ¹ 14 from 18.01.2005736 Duma daily, Is sue ¹ 53 from 7.03.2005737 24 chasa daily, Is sue ¹ 195, Is sue ¹ 265 and Is sue ¹ 290 from 2002; Standart daily, Is sue ¹ 3498 from
26.09.2002 and Is sue ¹ 3502 from 30.09.2002; Duma daily, Is sue ¹ 220 from 24.09.2002 and Is sue ¹ 224from 28.09.2002
738 Trud daily from 12.02.2002739 24 chasa daily, Is sue ¹ 76 from 18.03.2002740 Trud daily from 7.07.2002741 24 chasa daily, Is sue ¹ 306 from 5.11.2002742 24 chasa daily, Is sue ¹ 250 from 10.09.2002 and Is sue ¹ 285 from 15.10.2002; Standart daily, Is sue ¹
3519 from 17.10.2002 and Is sue ¹ 3540 from 7.11.2002; Kapital weekly from 9-15.11.2002
ing to cover be tween 70% and 100% of the ac tual costs made by the hos pi tals743. Ac cord ing tothe Head of the Di rec tor ate “Med i cal pa ram e ters” at the NHIF, the prices of the path wayswould be de creased, if there were more cases than the planned be cause of the fixed bud get ingfor hos pi tal treat ment744. Nev er the less, no co-pay ment by the pa tients was en vis aged, ex ceptfor the reg u lated con sumer’s fee for hos pi tal stay.
In 2003, the me dia com mented again on the se vere fi nan cial con di tion of the hos pi talsand their grow ing debts which were re lated to the “chronic un der fi nanc ing” and the prices ofthe clin i cal path ways con sid er ably lower than the ac tual value of the costs in curred for them745. At the be gin ning of the year, Min is ter Finkov de clared that the hos pi tals were in “an ut terlyhope less con di tion and un able to cope with the in crease of the drug, fuel and elec tric ityprices.” The rea sons were linked to the in suf fi cient fi nanc ing for healthcare al lo cated from thebud get, the in creased num ber of hos pi ta lised pa tients and the ex tremely low prices for the clin -i cal path ways which, in his opin ion, “hardly cov ered 20% of the costs made by the hos pi -tals.”746 Ac cord ing to the Vice Min is ter of Healthcare Dr. Petko Salchev a great part of thedebts had been ac cu mu lated as a re sult of the ground less ex tra stor age of drugs. The MH de -manded an ac count for the costs made and the plan for the pay ment of debts in or der to re leasean ad di tional sub sidy for the cov er age of the hos pi tal debts747.
Dep u ties from the op po si tion ex pressed the opin ion that a great num ber of the mu nic i palhos pi tals would be de clared bank rupt for short age of fi nance, planned in the NHIF bud get.Ac cord ing to Dr. Kitov from the Par lia men tary group of the UDF, the gov ern ment had a 2-year agree ment with the WB, ac cord ing to which the mu nic i pal hos pi tals had to be re duced by halfand it was try ing to achieve this by bud get cuts and eco nomic re stric tions748.
In re sponse to this state ment, the Chair man of the Par lia men tary Com mis sion onHealthcare A. Shterev shared his view that the hos pi tals did not have to be closed down in anad min is tra tive way. In his opin ion, with the abol ish ment of region ali sa tion, through the pos si -bil ity of free choice, the pa tients would de ter mine which of the healthcare es tab lish mentswould have to stop func tion ing749. Min is ter Finkov com mit ted him self that in the sec ond halfof 2003 ad di tional fi nanc ing would be re ceived for the main te nance of the mu nic i pal hos pi talswhich were mu nic i pal prop erty750.
In sev eral ar ti cles, it was an nounced that in the next two years the hos pi tals would pre -pare for the in tro duc tion of the di ag nos ti cally re lated groups which were go ing to sub sti tutethe clin i cal path ways in 2006751.
At the be gin ning of Sep tem ber, the NHIF pro posed amend ments in the NFA en vis ag -ing a re duc tion in the prices of the clin i cal path ways by 6 – 8% as well as in the den tists’
175
Stages and evo lu tion of the healthcare re form in Bul garia
743 24 chasa daily, Is sue ¹ 5 from 6.01.2003 and Is sue ¹ 33 from 3.02.2003; Standart daily, Is sue ¹ 3597 from 7.01.2003; Kapital weekly from 11-17.01.2003
744 24 chasa daily, Is sue ¹ 33 from 3.02.2003745 Trud daily from 20.03.2003 and from 3.04.2003; 24 chasa daily, Is sue ¹ 216 from 9.08.2003; Duma daily,
Is sue ¹ 185 and Is sue ¹ 293 from 18.12.2003; Standart daily, Is sue ¹ 3721 from 15.05.2003 and Is sue ¹3931 from 11.12.2003; Fo rum Medicus pe ri od i cal, Is sue ¹ 17 from 7.04.2003
746 Trud daily from 20.03.2003747 Duma daily, Is sue ¹ 185 from 2003; Standart daily, Is sue ¹ 3811 from 13.08.2003748 24 chasa daily, Is sue ¹ 92 from 3.04.2003749 Standart daily, Is sue ¹ 3698 from 18.04.2003 750 (24 chasa daily, Is sue ¹ 126 from 11.05.2003)751 Trud daily from 7.08.2003; 24 chasa daily, Is sue ¹ 281 from 13.10.2003; Standart daily, Is sue ¹ 3805 from
7.08.2003 and Is sue ¹ 3872 from 13.10.2003; Fo rum Medicus pe ri od i cal, Is sue ¹ 44 from 20.10.2003
pay ment. The Di rec tor of the NHIF in formed that the fi nanc ing planned for the treat ment ofchronic dis eases was ex hausted and the man age ment of the Fund would re quest an up date ofthe bud get for 2003752. Ac cord ing to the Chair man of the UBP Dr. A. Kehayov, the terms stip -u lated in the NFA on the re duc tion of the prices for the clin i cal path ways had to be ful filled753.The Min is ter of Healthcare S. Bogoev pro claimed him self against the de ci sion of the man age -ments of the NHIF and the UBP since he con sid ered that the re duc tion in the prices of the clin i -cal path ways would re sult in the ac cu mu la tion of new debts and would worsen the ac tiv i tiesand the fi nan cial per for mance of the healthcare es tab lish ments754.
Through out 2003 the press fo cused on the en vis aged changes in the fi nanc ing of hos pi -tal care. In an in ter view for the “24 chasa” the Di rec tor of the NHIF Dr. Petrov an nounced theplans for grad ual with drawal of the state and the mu nic i pal i ties un til 2005 when the hos pi talswere go ing to be fi nanced by the Fund only. In this re spect, op tions were con sid ered for thepro vi sion of the nec es sary fi nanc ing in clud ing the NHIF re serve and an in crease of the healthin sur ance in stal ment from 2007755.
Dur ing a dis cus sion on the prob lems of the healthcare re form, or gan ised by CITUB, theVice Min is ter of Fi nance and Chair man of the Ex ec u tive Board of the NHIF K. Ananiev con -firmed the in ten tions that the hos pi tals shifted en tirely to fi nanc ing for clin i cal path ways in2004. In or der to se cure the nec es sary fund ing the Min is try of Fi nance of fered that ini tially, apart of the NHIF re serve was used, fol low ing which the health in sur ance pre mium was to bein creased756.
At a meet ing with man ag ers of healthcare es tab lish ments for hos pi tal care, Min is terBogoev an nounced that a min i mum pack age of ac tiv i ties in hos pi tal care was be ing pre pared tobe guar an teed by the NHIF bud get. The pack age was aimed at de ter min ing the di ag no ses andser vices to be free and ac ces si ble to all cit i zens and the rest to be paid by the pa tients. Ac cord ingto the Vice Min is ter of Healthcare Dr. Petko Salchev, this was ne ces si tated by the in suf fi cient fi -nanc ing for hos pi tal care which could be al lo cated from the state and the NHIF bud get. The ma -jor ity of the hos pi tals also sup ported the idea of in tro duc ing co-pay ment by the pa tients whichwas to be done on the ba sis of ac tu ally cal cu lated costs of ser vices757. A month later the Min is terof Healthcare clar i fied that from 2005 it was planned that co-pay ment was in tro duced for costlymeth ods of treat ment and for the ac tiv i ties not in cluded as man da tory for per for mance in theclin i cal path ways. In 2004, some of the in ves ti ga tions in the out pa tients’ care were also go ing tobe co-paid, the so cially un der priv i leged re ceiv ing vouch ers from the state758.
In the mid dle of Oc to ber, the Min is ter of Healthcare de clared that in 2004 the mu nic i palhos pi tals were go ing to shift en tirely to fi nanc ing by clin i cal path ways and were not go ing tobe sub si dised by the mu nic i pal bud gets. The pro posal of the MH was that only the dis trict andthe na tional hos pi tals were fi nanced from the bud get of the Min is try for di ag no ses which werenot in cluded in the clin i cal path ways759. Amend ments were also un der way in the Reg u la tion
176
752 Duma daily, Is sue ¹ 205 from 7.09.2003753 24 chasa daily, Is sue ¹ 284 from 16.10.2003754 Kapital weekly from 11-17.10.2003755 24 chasa daily, Is sue ¹ 62 from 4.03.2003756 Standart daily, Is sue ¹ 3709 from 1.05.2003; Duma daily, Is sue ¹ 100 from 1.05.2003757 24 chasa daily, Is sue ¹ 213 from 6.08.2003; Duma daily, Is sue ¹ 179 from 6.08.2003758 24 chasa daily, Is sue ¹ 249 from 11.09.2003; Standart daily, Is sue ¹ 3924 from 4.12.2003759 24 chasa daily, Is sue ¹ 281 from 13.10.2003; Kapital weekly from 6-12.12.2003; Fo rum Medicus pe ri od i cal,
Is sue ¹ 44 from 20.10.2003

for the ac cess of the health in sured per sons to the healthcare es tab lish ments for out pa tients’and in pa tients’ care; ac cord ing to these amend ments, pa tients would have the right of freechoice of a hos pi tal on the ter ri tory of the whole coun try. Thus, the wards and the hos pi tals tobe closed down or re struc tured were go ing to be se lected. The in ten tions of the MH in cludedthe in tro duc tion of the par tial co-pay ment by the pa tients in 2004, which was to be fully reg -u lated in 2005760. Ac cord ing to Min is ter Bogoev, this was the only way out for re strict ing theun reg u lated pay ments in the hos pi tals761.
At the start of the ne go ti a tions for the NFA 2004, the man age ment of the NHIF pro posed anew mech a nism for fi nanc ing of the healthcare es tab lish ments for hos pi tal care, ac cord ing towhich the fund ing al lo cated for the hos pi tals which were mu nic i pal prop erty, had to be dis trib -uted be tween the NHIF and the MH, in stead of be ing al lo cated from the mu nic i pal bud gets. Thear gu ments for this change re ferred to the amend ments in the Reg u la tion on the ac cess of thehealth in sured per sons and the in tro duc tion of mar ket prin ci ples of hos pi tal fi nanc ing. The Min -is try of Fi nance in sisted that the fund ing for healthcare was not trans ferred to the mu nic i pal i tiesbe cause a great part of them were re-al lo cated for cov er ing def i cits in other spheres. Af ter it be -came ev i dent that the NHIF was not pre pared to cover to tally the fi nanc ing of the hos pi tal care,the fol low ing scheme was sug gested – for the clin i cal path ways whose prices cover all the costsfor treat ment, the hos pi tals would be re im bursed by the NHIF only; if a clin i cal path way did notcover the ac tual costs for the treat ment, the dif fer ence would be cov ered by the MH; the Min is trywould also pay for di ag no ses for which there were no clin i cal path ways762.
The UBP strongly op posed the new scheme for fi nanc ing with the mo tive that the MH did not have an es tab lished mech a nism to pay the ad di tion for the clin i cal path ways to over 200hos pi tals, and they shared their fear that the cost ing of the treat ment would not re flect the ac -tual costs, which, in its turn, would re sult in bank rupt cies of mu nic i pal hos pi tals763. Theman age ment of the UBP pro claimed it self also against the dis pro por tion in the fi nanc ing of the state and the mu nic i pal hos pi tals, planned in the bud get of the MH for 2004. Ac cord ing to dataof the Un ion, the num ber of ad mit ted pa tients in the state and the mu nic i pal hos pi tals was al -most equal but the fi nanc ing planned for the state hos pi tals was over twice higher764. A sim i larview was ex pressed by the healthcare fed er a tion at CITUB, the As so ci a tion of the Mu nic i pal i -ties and dep u ties from the op po si tion765.
In an in ter view for the “Duma” news pa per, Dr. Petrov de clared that the NHIF was not in a po si tion to cover en tirely the hos pi tal care un til “it does not be come clear how the hid den def i -cit will be cov ered.” Ac cord ing to him the op tions for the def i cit cov er age in cluded the in -crease in the health in sur ance in stal ment, cut ting down the pack age of ser vices re im bursed bythe Fund, in tro duc tion of co-pay ment or vol un tary health in sur ance, en sur ing in such a way the nec es sary fund ing and dis con tinu a tion of the un reg u lated pay ments766.
177
Stages and evo lu tion of the healthcare re form in Bul garia
760 24 chasa daily, Is sue ¹ 281 from 13.10.2003; Duma daily, Is sue ¹ 235 from 11.10.2003; Standart daily,Is sue ¹ 3896 from 6.11.2003
761 Standart daily, Is sue ¹ 3872 from 13.10.2003762 Kapital weekly from 4-10.10.2003 and from 24-31.10.2000763 Kapital weekly from 4-10.10.2003; 24 chasa daily, Is sue ¹ 284 from 16.10.2003 and Is sue ¹ 289 from
21.10.2003; Standart daily, Is sue ¹ 3893 from 3.11. 2003, Is sue ¹ 3896 from 6.11.2003 and Is sue ¹ 3900from 10.11.2003
764 Kapital weekly from 24-31.10.2003765 Duma daily, Is sue ¹ 268 from 19.11.2003; Standart daily, Is sue ¹ 3920 from 30.11.2003; Kapital weekly
from 6-12.12.2003766 Duma daily, Is sue ¹ 270 from 21.11.2003
Ex perts from the WB rec om mended that the hos pi tals were fi nanced by the NHIF for per -formed ac tiv i ties only. In their view, the fi nanc ing from dif fer ent sources caused the grow ingdebts of the healthcare es tab lish ments767.
At the end of the year, in an in ter view for “24 chasa”, the Min is ter of Healthcare S. Bogoevre ported that the in ten tions for the mu nic i pal hos pi tals to shift en tirely to fi nanc ing from theNHIF in 2004 were not go ing to be en acted, which was the rea son for the pres er va tion of thedou ble fi nanc ing, e.g. from the Fund and the bud get. It was planned that the fund ing from thebud get was al lo cated for per formed ac tiv ity, and ad di tional sub si dies, ir re spec tive of the ac tiv ity, was al lo cated for “the mu nic i pal hos pi tals of so cial sig nif i cance and the na tional cen tres.”768
In 2004, a new meth od ol ogy for hos pi tal fi nanc ing by the MH was en forced, ac cord ing to which hos pi tals were go ing to be paid for their per for mance769. The ini tial com ments werethat with the new way of fi nanc ing the mu nic i pal hos pi tals were doomed to bank ruptcy forlack of clear cri te ria for cost ing the ex penses per ad mit ted pa tient770. Later it was an nouncedthat the hos pi tal ac counts in di cated that there would be no bank rupt cies and the MH de claredthat the new “meth od ol ogy is work ing.”771
There was in for ma tion about the hos pi tal debts and the cov er ing of part of the debts by theMH through out the year772, com ments could also be found that the NHIF was to be blamed forthe hos pi tal debts since the money for the clin i cal path ways did not cover the costs for treat -ment773.
In 2004, for the first time the op pos ing of the state, mu nic i pal and pri vate hos pi talswas re ported774. The dep uty from NMSS Dr. Tsvetan Tsenkov made a state ment that the man -age ment of the MH would be made a case against in the Con sti tu tional Court and the Com mis -sion for the Pro tec tion of Com pe ti tion, and he ap pealed to the MH to dis con tinue the fi nanc ing of the mu nic i pal hos pi tals since it con tra dicted the com pe ti tion and placed the pri vate hos pi tals inan un equal po si tion. He in sisted that the hos pi tals should be fi nanced by the NHIF only, whichwas ac cepted by the MH but from 2005775. The As so ci a tion of the Pri vate Hos pi tals also claimedfor fi nanc ing from the state de clar ing that they were los ing profit due to the de lay of the NFA,and that they “vote dis trust” to the Chair man of the UBP Dr. A. Kehayov776. The Chair man of the Par lia men tary Com mis sion on Healthcare Assoc. Prof. Dr. A. Shterev also sup ported the idea for a state fi nanc ing of the pri vate hos pi tals and the dep uty from the NMSS was against777.
In Sep tem ber 2004, the me dia once again started dis cuss ing the idea of co-pay ment for
178
767 Trud daily from 2.12.2000.; Standart daily, Is sue ¹ 3922 from 2.12.2003768 24 chasa daily, Is sue ¹ 337 from 8.12.2003769 24 chasa daily, Is sue ¹ 6 from 2004; Standart daily, Is sue ¹ 13 from 2004; Trud daily from 5.02.2004;
Standart daily, Is sue ¹ 3958 from 13.01.2004 and Is sue ¹ 3978 from 2.02.2004.; Fo rum Medicus pe ri od i cal, Is sue ¹1 from 12.01.2004 and Is sue ¹ 5 from 9.02.2004
770 Duma daily, Is sue ¹ 32 from 10.02.2004; Standart daily, Is sue ¹ 3959 from 14.01.2004771 Standart daily, Is sue ¹ 4060 from 26.04.2004 and Is sue ¹ 4074 from 10.05.2004; Fo rum Medicus
pe ri od i cal, Is sue ¹ 23 from 14.06.2004772 24 chasa daily, Is sue ¹ 42, Is sue ¹ 117, Is sue ¹ 156, Is sue ¹ 235 and Is sue ¹ 349 from 2004; Standart
daily, Is sue ¹ 4030 from 25.03.2004; Duma daily, Is sue ¹ 115 and Is sue ¹ 295 from 2004773 Duma daily, Is sue ¹ 295 from 2004; Standart daily, Is sue ¹ 4219 from 1.10.2004; Fo rum Medicus
pe ri od i cal, Is sue ¹ 28 from 12.07.2004774 Duma daily, Is sue ¹ 32 from 10.02.2004; Standart daily, Is sue ¹ 3406 from 26.06.2002 and Is sue ¹ 3521
from 19.10.2002 775 24 chasa daily, Is sue ¹ 109 from 21.04.2004776 Duma daily, Is sue ¹ 91 from 21.04.2004777 24 chasa daily, Is sue ¹ 335 from 3.12.2004; Standart daily, Is sue ¹ 4206 from 19.09.2004
hos pi tal care by the pa tients778. Re gard ing the pos si ble in tro duc tion of co-pay ment from2005, Min is ter Bogoev en vis aged a pub lic opin ion poll to study the cit i zens’ will ing ness tomake co-pay ments le gally in the hos pi tals in stead of mak ing un reg u lated pay ments. The Par -lia men tary Com mis sion on Healthcare pro posed that the co-pay ment amounted to 10% of thecost of the clin i cal path way and ac cord ing to Assoc. Prof. Dr. A. Shterev, co-pay ment had toamount to 10% of the ac tual price of the ser vice. The Vice Chair man of the CITUB Dr. I.Kokalov pointed out that “this is a way of in tro duc ing dis crim i na tion for dif fer ent dis eases.”779
At the be gin ning of 2005, the NMSS pre pared a na tional sur vey and pub lic de bate on the pos si -bil ity of in tro duc ing co-pay ment for med i cal ser vices by the pa tients780.
The short age of fi nanc ing and the dis crep ancy be tween the prices re im bursed by theNHIF for the clin i cal path ways and the ac tual costs of the hos pi tals con tin ued to be fre quentlydis cussed in 2005 as some of the main rea sons for the grow ing hos pi tal debts and their se verefi nan cial state as well as the un reg u lated pay ments made by pa tients781. In the be gin ning ofthe year, the Uni ver sity Hos pi tal “St. Ekaterina” dis con tin ued the planned ad mis sion of pa -tients for debts in spite of the sev eral ad di tional sub si dies re ceived from the bud get in 2004.This in for ma tion in the me dia was ac com pa nied by com ments clas si fy ing the de ci sion of thehos pi tal man age ment as “an at tempt to ex ert pres sure on the gov ern ment” which, how ever, did not achieve the de sired out come782.
At the end of Jan u ary, the MH in formed about its in ten tion to in crease the ac tiv i ties andthe prices for the di ag no ses out side the clin i cal path ways for which the MH paid to thehealthcare es tab lish ments for hos pi tal care783.
A week later, the MH dis cussed with the Na tional As so ci a tion of the Mu nic i pal i ties thepos si bil ity for the al lo ca tion of an ad di tional sub sidy from the state bud get to the mu nic i palhos pi tals lo cated in re mote and risk re gions784.
At the end of July, the Ex ec u tive Board of the NHIF took the de ci sion to uti lise 20 mil lionBGN from the op er a tional re serve for pay ment of clin i cal path ways to the hos pi tals. The bud -get of the Fund for 2005 had en vis aged 295 mil lion BGN for hos pi tal care, and dur ing the firstsix months 270 mil lion BGN were spent on pay ments. Ac cord ing to the Di rec tor of the NHIFDr. I. Bukarev, the NA had to up date the bud get of the Fund since at least 470 mil lion BGNwere nec es sary for the hos pi tals an nu ally785.
At the be gin ning of the term of the new gov ern ment of the tri par tite co ali tion at ten tionwas drawn to the sig nif i cant fi nan cial def i cit in the sys tem and the de layed pay ment of hos pi taldebts amount ing to 100 mil lion BGN, the short age of fund ing in the NHIF bud get for the re im -burse ment of the clin i cal path ways as well as the end ing of the fi nanc ing planned for life-sav -ing drugs786.
179
Stages and evo lu tion of the healthcare re form in Bul garia
778 Trud daily from 3.09.2004; Kapital weekly from 4-10.09.2004779 24 chasa daily, Issue ¹ 244 from 3.09.2004 and Issue ¹ 254 from 13.09.2004780 Duma daily, Issue ¹ 23 from 28.01.2005; Trud daily from 26.01.2005; Standart daily, Issue ¹ 4331 from
26.01.2005781 Duma daily, Issue ¹ 14 from 18.01.2005, Issue ¹ 38 from 11.02.2005 and Issue ¹ 80 from 7.04.2005;
Standart daily, Issue ¹ 4332 from 27.01.2005; Kapital weekly from 20-26.08.2005782 Kapital weekly from 8-14.01.2005783 Duma daily, Issue ¹ 24 from 28.01.2005784 Duma daily, Issue ¹ 31 from 7.02.2005785 Kapital weekly from 30.07.–05.08.2005786 Kapital weekly from 27.08.–2.09.2005
Cor rup tion
Through out all the years ex am ined in our study, dur ing all the stages of the re form thetopic of cor rup tion in healthcare was pres ent in the press, but its cov er age (some times onlymen tion) was just an ad di tion to the lead ing is sues. In 2002 and 2004 spe cial at ten tion waspaid to this prob lem787.
Ac cord ing to a study con ducted by “Sova-Haris”, 38% of the Bul gar i ans con sid ered that the sur geons, the ob ste tri cians and gy nae colo gists were the most cor rupt in the hos pi tals, 34%de ter mined as cor rupt phy si cians as a whole, fol lowed by the aides, and the nurses were con -sid ered the least prone to ac cept bribes788.
The Chair man of the Bud get Com mis sion to the NA Ivan Iskrov sub mit ted data from theMH, ac cord ing to which the un reg u lated pay ments in healthcare ex ceeded 700 mil lion BGN.To his mind, the rea son was in the “in ad e quate hos pi tal net work in our coun try” and the ir ra tio -nal uti li sa tion of fi nan cial re sources789.
Ac cord ing to Min is ter Finkov the cor rup tion among phy si cians was due to the low sal a ries790.In Au gust, a se ries of short jour nal ese ma te ri als were pub lished in the “24 chasa” fea tur -
ing con crete cases of pa tients who had been asked for money (or consumables) for their treat -ment in hos pi tal. In some of the cases, it was a ques tion of pay ments against an in voice and adec la ra tion that the pa tient (usu ally a rel a tive) agreed to pay a cer tain sum. The pay ments hadbeen for ma lised as do na tions or ac cord ing to the pro ce dure of the still act ing Reg u la tion ¹ 22for paid med i cal ser vices. In the same is sue of the news pa per, in his in ter view Assoc. Prof. Dr.Stoyan Alexandrov who headed Di rec tor ate “Di ag nos tic and treat ment ac tiv i ties” at the MHstated that the un reg u lated pay ments amounted to ap prox i mately 560 mil lion BGN an nu allyand ex plained that since Reg u la tion ¹ 22 was still in force, in voices were is sued for the reg u -lated pay ments and that more than half of the pa tients’ com plaints re mained with out con se -quences be cause the guilt had to be proved in the court in the pres ence of ev i dence791.
Ac cord ing to a sur vey of the Bul gar ian health pro ject at the US Agency for In ter na -tional De vel op ment con ducted among 2 000 peo ple, the av er age un reg u lated pay ments madeby pa tients in May 2002 was 197 BGN for 17 days of hos pi tal stay792.
In 2004, the Chair man of the Par lia men tary Com mis sion on Healthcare Assoc. Prof. Dr.A. Shterev de clared that “cor rup tion in drug pol icy is rather high – about 10% of the money fordrugs is be ing re-dis trib uted for com mis sions” and a con sul tant to a pri vate com pany claimedthat this per cent age was about 30 - 40%793.
Struc tural changes
A pub li ca tion in the “Demoracia” from Sep tem ber 2001 in formed that the Cab i net wasclos ing down 200 hos pi tals and the WB “had writ ten an ex cel lent mark” to the ex-Min is ter Dr.
180
787 24 chasa daily, Issue ¹ 21, Issue ¹ 46 and Issue ¹ 216 from 2002, Issue ¹ 54 and Issue ¹ 234 from 2004;Standart daily, Issue ¹ 3530 from 28.10.2002 and Issue ¹ 3449 from 8.08.2004; Kapital weekly from28.09.–4.10.2002 and from 4-10.09.2004 Duma daily, Issue ¹ 173 from 2004
788 Duma daily, Issue ¹ 64 from 18.03.2002789 24 chasa daily, Issue ¹ 136 from 2002790 Standart daily, Issue ¹ 3421 from 11.07.2002791 24 chasa daily, Issue ¹ 226 from 17.08.2002792 24 chasa daily, Issue ¹ 272 from 2.10.2002793 24 chasa daily, Issue ¹ 96 from 7.04.2004
I. Semerdjiev. In the same is sue of the news pa per, it was re ported that ac cord ing to Min is terFinkov there were sev eral struc tural pro jects for the re struc tur ing of the hos pi tal care, one of which (sup ported by the WB) pro vided for 50-60 hos pi tals to re main as “the back bone” of thehos pi tal care and the rest were to be trans formed into hos pices. Ac cord ing to the Min is ter ofHealthcare it was not im por tant how many beds there are but how they are uti lised”794.
At the be gin ning of 2002, on the topic of the struc tural changes in healthcare the fore castsmade by the rep re sen ta tives of the trade un ions pre vailed for forth com ing job cuts of phy si -cians and nurses in hos pi tals, which was con nected to the re duced sub sidy from the MH795. Inre sponse to this, Min is ter Finkov an nounced that no re dun dan cies were en vis aged for the per -son nel in the cen tres for emer gency med i cal care and in the hos pi tals, but the hos pi tal man age -ments had to sub mit to the MH pro pos als for their re struc tur ing and un til the end of 2002 thebud get for the hos pi tal es tab lish ments was go ing to be re duced on the av er age by 2.3%, thenum ber of the HEI em ploy ees was go ing to be re duced by 5% and in the homes for med ico-so -cial care – by 9%796.
The MH rec om mended to the mu nic i pal hos pi tals, which did not to com ply with the re -quire ments of the LHE and showed poor re sults from the ac cred i ta tion, to be con verted intomed i cal cen tres or hos pices since they would be de nied the right of per form ing sur gi cal ac tiv i -ties797. The re struc tur ing of the hos pi tals was in ex e cu tion of the rec om men da tions of the IMFwhich in sisted on curb ing of the hos pi tal net work by one third: that was, clos ing down of 100out of the 300 hos pi tals798.
Ac cord ing to Min is ter Finkov, the clos ing of 30-40 small mu nic i pal hos pi tals was not go -ing to re lieve the sys tem since “the ef fect will hardly be more than 7-8 mil lion BGN.”799
In 2003, the MH sub mit ted a pro posal for changes in the Na tional Health Map, ac cord ingto which the Fund had to sign con tracts with at least 165 hos pi tals from the ex ist ing 225. Ac -cord ing to the draft de vised by the Min is try, 102 multi-pro file hos pi tals for ac tive treat mentwere nec es sary out of the ex ist ing 145. The Vice Min is ter of Healthcare Dr. P. Salchev statedthat some of the hos pi tals were go ing to be re struc tured and oth ers were go ing to be uni fied800.The in ten tions for the re struc tur ing of some hos pi tals were con firmed by Min is ter S. Bogoev in an in ter view for the “24 chasa”, in which he an nounced that a pro ject was start ing for the re -form of two mu nic i pal hos pi tals fi nanced by the WB that had to grow into a model for changeat a na tional level801. At the end of the year, the Min is ter of Healthcare clar i fied that in 2004 the MH was go ing to re struc ture hos pi tals into di ag nos tic and con sul ta tive cen tres and hos pices.An eval u a tion was forth com ing of the beds uti li sa tion in the wards, en vis ag ing re duc tion of the beds and clos ing of whole wards for those which were not func tion ing ef fec tively802.
Sev eral pub li ca tions in 2003 in formed about the es tab lish ment of a hold ing which was toin clude the hos pi tals owned by the Mu nic i pal ity of So fia, the dis pen sa ries and the hos pi tals in
181
Stages and evo lu tion of the healthcare re form in Bul garia
794 Democracia, Issue ¹ 216 from 15.09.2001795 24 chasa daily, Issue ¹ 44 from 14.02.2002; Duma daily, Issue ¹ 55 from 7.03.2002 and Issue ¹ 58 from
11.03.2002; Forum Medicus periodical, Issue ¹ 13 from 11.03.2002 796 Democracia daily, Issue ¹ 63 from 14.03.2002; 24 chasa daily, Issue ¹ 72 from 2002797 24 chasa daily, Issue ¹ 228 from 19.08.2002 and Issue ¹ 285 from 15.10.2002798 24 chasa daily, Issue ¹ 228 from 19.08.2002799 Kapital weekly from 12-18.10.2002800 24 chasa daily, Issue ¹ 150 from 5.06.2003; Standart daily, Issue ¹ 3742 from 5.06.2003801 24 chasa daily, Issue ¹ 205 from 29.07.2003; Forum Medicus periodical, Issue ¹ 31 from 7.07.2003802 Trud daily from 2.12.2003; 24 chasa daily, Issue ¹ 337 from 8.12.2003; Standart daily, Issue ¹ 3922 from
2.12.2003
Buhovo, Kremikovtsi and Pancharevo. The idea of es tab lish ing a sim i lar struc ture was re latedto the re struc tur ing of part of the hos pi tals by elim i nat ing the re dun dant ac tiv i ties, op ti mi sa tion of the bed fund and cen trali sa tion of some ser vices aimed at the more ef fi cient man age ment ofthe fi nanc ing and en hanced con trol over the costs803. The So fia col le giate of the UBP de -manded a ref er en dum on the con sti tu tion of “Met ro pol i tan med i cal hold ing” Ltd. Ac cord ing to the mem bers of the col le giate, this struc ture “would be a whole new healthcare min is try.”804
The hold ing con tin ued to be de bated in 2004, and its con sti tu tion was reg is tered by a de ci sionof the Met ro pol i tan Mu nic i pal ity Coun cil805.
Min is ter Finkov an nounced that an op tion was con sid ered for the re struc tur ing of thehos pi tal es tab lish ments, en vis ag ing all the hos pi tals in a def i nite re gion to be uni fied in amed i cal hold ing which was go ing to man age the ac tiv i ties of the hos pi tals and re-di rect pa -tients to a con crete hos pi tal806.
In the mid dle of the year, Prof. Dr. Al ex an der Chirkov pro posed a pro ject for the es tab -lish ment of 35 emer gency care cen tres for the treat ment of car dio vas cu lar dis eases whose set -ting up was to be fi nanced with low-in ter est cred its from the USA. The idea was to in tro duceuni fied stan dards for treat ment, in clud ing train ing per son nel ac cord ing to a uni fiedprogramme807. A few months later, in for ma tion ap peared in the press about the es tab lish mentof the first pri vate com pany for pro vi sion of emer gency med i cal care in part ner ship withthe Bul gar ian Red Cross. The way in which it was go ing to be funded was not clar i fied. Thepro pri etors planned that the new sys tem was linked to the emer gency cardiocentres pro posedby Prof. Dr. Al ex an der Chirkov808.
The idea of re turn ing the doc tors’ and den tal sur ger ies in the kin der gar tens and theschools was dis cussed in 2002 and 2003, and it be came a fact af ter the adop tion of the Law onHealth in 2004809.
In 2004, pub li ca tions con tin ued on the prob lems of emer gency care, fo cus ing most fre -quently on the man i fold in crease of the emer gency calls and the im pos si bil ity of the emer -gency teams to re spond to all the cases810.
At the end of the year, the ques tion was once again posed about the clos ing of hos pi tals andMin is ter Bogoev and the Chair man of the Par lia men tary Com mis sion Assoc. Prof. Dr. Shtereven tered into an in di rect ar gu ment, in which Atanas Shterev de clared that 100 hos pi tals were go -ing to be closed down, whereas Slavcho Bogoev stated that “there was no such a thing.”811
In 2005, how ever, dur ing the round ta ble en ti tled “The Ac ces sion of Bul garia to the EC –Com mit ments and Fu ture Ac tions in the Field of Healthcare”, the Min is ter of Healthcare S.Bogoev said that about 30% of the hos pi tals were go ing to be closed down. Ini tially, thosehos pi tals would be closed in which the num ber of the ad mit ted pa tients had dropped af ter theabol ish ment of the region ali sa tion at the be gin ning of 2004 and af ter that those hos pi tal es tab -
182
803 Duma daily, Issue ¹ 64 from 18.03.2003, Issue ¹ 131 from 11.06.2003 and Issue ¹ 179 from 6.08.2003804 Duma daily, Issue ¹ 69 from 2003805 Duma daily, Issue ¹ 12 from 17.01.2004, Issue ¹ 108 from 13.05.2004 and Issue ¹ 169 from 27.07.2004806 Kapital weekly from 17-23.05.2003; 24 chasa daily, Issue ¹ 130 from 2003807 24 chasa daily, Issue ¹ 204 from 28.07.2003808 24 chasa daily, Issue ¹ 305 from 6.11.2003; Duma daily, Issue ¹ 257 from 2003 809 Duma daily, Issue ¹ 209 from 2002 and Issue ¹ 144 from 26.06.2003; Standart daily, Issue ¹ 3763 from
26.06.2003, Issue ¹ 3928 from 8.12.2003 and Issue ¹ 3932 from 12.12.2003; 24 chasa daily, Issue ¹ 137from 19.05.2004
810 24 chasa daily, Issue ¹ 339 from 7.12.2004; Standart daily, Issue ¹ 3958 from 13.01.2004811 Duma daily, Issue ¹ 278 from 29.11.2004
lish ments were go ing to be closed which “do not meet the cri te ria im posed by the Eu ro peanCom mu nity.” Min is ter Bogoev also an nounced that un til Jan u ary 2007 the MH was go ing topro pose mea sures for the har mo ni sa tion of the Bul gar ian leg is la tion with the Eu ro pean one. Inthis re spect amend ments and ad di tions were go ing to be worked out to the Law on Foods andthe Law on Healthcare Es tab lish ments, new laws had to be pre pared on drugs and phar ma ciesin hu man med i cine and on med i cal prod ucts812.
New health leg is la tion
In 2002, a Draft Pro ject on the Trans plan ta tions of Or gans and Tis sues was dis cussed whichalso caused di verg ing opin ions among the po lit i cal forces. The de bat able is sues con cerned the ex port ofhu man tis sues and cells and the way of de clar ing re fusal or con sent for do na tion813.
In 2003, in an in ter view for the “Standart” news pa per, the Chair man of the Par lia men taryCom mis sion on Healthcare Assoc. Prof. Dr. A. Shterev com mented on the sys tem for the ac -cred i ta tion of the hos pi tal es tab lish ments. In his opin ion, it did not sat isfy the re quire mentsand had to be changed by the set ting of an in de pend ent body to as sess the hos pi tals814. In 2004,the new Reg u la tion ¹ 13 from July 30th 2003 for the hos pi tals ac cred i ta tion was criti cised andclaims were made for the ex ten sion of the dead lines for the mea sures for mak ing the hos pi talscom ply with the re quire ments815.
In 2003, the press paid con sid er ably less at ten tion to the draft pro ject of the Law onHealth sub mit ted to the NA, as com pared to the Laws on Health In sur ance and the Law on theHealthcare Es tab lish ments. The main in for ma tion con cerned the pa tients’ rights and li a bil i tieswhich were reg u lated for the first time, the re sump tion of the sur ger ies in the kin der gar tens and schools as well as com ments and re marks on spe cific texts in it816.
In 2004, the dis cus sion of the Law on Health was fea tured again, and the ac cents pointedout in the press fell on the op po si tion of the gen eral prac ti tio ners, spe cial ists and dep u ties to the le git i ma tion of al ter na tive med i cine, the reg u la tion of the pa tients’ rights, and the for ma tionof the le gal foun da tions of the state pol icy on pub lic health pro tec tion817.
Con flicts in side the phy si cians’ cir cles
Dur ing the third stage of the re form an in ter nal con flict arose and grad u ally es ca lated in -side the pro fes sional as so ci a tion of the phy si cians. The rea son for its emer gence was a sig nif i -cant dif fer ence in the in come of the phy si cians in the out pa tients’ and the in pa tients’ care andthe man i fes ta tions were ex pressed in ac cu sa tions of in suf fi cient pro fes sional com pe tences ofthe gen eral prac ti tio ners818.
183
Stages and evo lu tion of the healthcare re form in Bul garia
812 Duma daily, Issue ¹ 92 from 21.04.2005813 24 chasa daily, Issue ¹ 134 from 17.05.2002; Duma daily, Issue ¹ 255 from 1.11.2002; Forum Medicus
periodical, Issue ¹ 26 from 17.06.2002 and Issue ¹ 28 from 1.07.2002814 Standart daily, Issue ¹ 3698 from 18.04.2003815 Standart daily, Issue ¹ 4015 from 10.03.2004816 Duma daily, Issue ¹ 144 fom 26.06.2003 and Issue ¹ 233 from 10.10.2003 Issue ¹ 234 from 11.10.2003;
Standart daily, Issue ¹ 3763 from 26.06.2003, Issue ¹ 3928 from 8.12.2003 and Issue ¹ 3932 from12.12.2003.; Kapital weekly from 21-27.06.2003
817 Duma daily, Issue ¹ 55 from 6.03.2004, Issue ¹ 176 from 31.07.2004 and Issue ¹ 178 from 2.08.2004; 24chasa daily, Issue ¹169 from 20.06.2004 and Issue ¹ 174 from 25.06.2004; Kapital weekly from14-20.08.2004; Standart daily, Issue ¹ 4171 from 5.08.2004
818 Duma daily, Issue ¹ 151 from 4.07.2002, Issue ¹ 221 from 25.09.2002, Issue ¹ 295 from 20.12.2002, Issue
On the healthcare re form
Dur ing the whole third stage, the healthcare re form was se ri ously criti cised in the pressboth in terms of its ini tial con cept and im ple men ta tion and in terms of cer tain neg a tive re -sults from it. Part of the crit i cal com ments con tained ac cu sa tions that the re form had stoppedor its phi los o phy had changed.
In some pub li ca tions, the gen eral prac ti tio ners ad dressed acute crit i cisms to the re form.Ac cord ing to them “they had a help less min is try, a mo nop oly fund con duct ing the whole sys -tem, … an im per ti nent phy si cians’ un ion” and a new model for health in sur ance was nec es sary in stead of mere cor rec tions. They were par tic u larly dis sat is fied with the lack of suf fi cient in -for ma tion about the NFA in the pro cess of its ne go ti a tion, the 24-hour avail abil ity, the vol umeof the doc u men ta tion, the high costs for the main te nance of the prac tices and the low pay -ment819. Ac cord ing to a sur vey made by MBMD, both phy si cians and pa tients com plainedabout the healthcare re form – the pa tients did not know what med i cal ser vices they were en ti -tled to, the phy si cians con sid ered that the sys tem was vi cious and gave rise to cor rup tion aswell as that no model of healthcare ad e quate to the Bul gar ian con di tions had been adopted820.
A con sid er able prob lem out lined by Prof. M. Popov, re ferred to the lack of suf fi cientprep a ra tion of the phy si cians for their new re spon si bil i ties and func tions un der the health in -sur ance sys tem. He de clared that the phy si cians were not able to man age the money withwhich they dis posed well and that also pre sented one of the rea sons for the healthcare es tab -lish ments to gen er ate losses821. The Vice Chair man of the Re gional phy si cians’ un ion inPlovdiv an nounced that “the med i cal pro fes sion als in Bul garia de manded a new LHI andamend ments of the LHE” whereby to cre ate a mar ket of med i cal ser vices, and alarmed that thecit i zens were not in formed about what ex actly they were re ceiv ing against their health in -sur an ces, and on the other hand, the Fund was the mo nop o list and the pa tients were not able toex er cise their right of choice where to get in sured822.
The Chair man of the UBP Dr. A. Kehayov de clared: “The MH has turned into a deal ers’of fice, it is pre oc cu pied with auc tions only and its staff pol icy is un prin ci pled”; he pro testedthat sec re tar ies, nurses and law yers were in serted in the hos pi tal boards; “the Ex ec u tive boardof the NHIF is act ing like a state within the state” and B. Finkov’s be hav iour on the prob lemwas in ad e quate823. Ac cord ing to the UBP “the di rec tion of the re form is right but there is noac tual step for ward made in the hos pi tal care for the last year,”824 and it claimed the Min -is ter’s res ig na tion in 2004825.
In an in ter view the Dep uty Di rec tor of the NHIF Nadezhda Geneva stated that three fac -tors were ab sent which were de ter min ing the change of the sys tem – op ti mal struc ture, a newway of pay ment and mon e tary re source826, and ac cord ing to the mem ber of the Ex ec u tive
184
¹ 191 from 20.08.2003, Issue ¹ 217 rom 19.09.2003, Issue ¹ 264 from 14.11.2003 and Issue ¹ 293 from18.12.2003; Trud daily from 31.03.2002; Standart daily, Issue ¹ 3646 from 25.02.2003 and Issue ¹ 3674from 25.03.2003 Kapital weekly from 10-16.05.2003; 24 chasa daily, Issue ¹ 94 from 4.04.2004
819 24 chasa daily, Issue ¹ 144 from 27.05.2002; Duma daily, Issue ¹ 19 from 2002820 24 chasa daily, Issue ¹ 228 from 19.08.2002; Duma daily, Issue ¹ 285 from 9.12.2002821 Trud daily from 31.03.2002822 Democracia daily from 16.03.2002823 Duma daily, Issue ¹ 249 from 2002824 Standart daily from 29.10.2002825 Standart daily, Issue ¹ 4119 from 24.06.2004826 Kapital weekly from 28.09.–4.10.2002
Board of the NHIF N. Nikolov, the in sur ance had to be un der taken by pri vate funds827. In anin ter view for the “Kapital” news pa per, the Di rec tor of the NHIF Dr. D. Petrov pointed out thatthe prob lems in healthcare were due to the de layed be gin ning of the healthcare re form as wellas to the low size of the health in sur ance in stal ment which was in its turn the rea son for di vid -ing the re form into a re form in the out pa tients’ care and a re form in the in pa tients’ care. Theother prob lems were linked to the lack of an in for ma tion sys tem and the im pos si bil ity for ef -fec tive con trol as well as the con stant in crease of the costs for drugs. He ex pressed the opin ionthat some er rors had to be elim i nated in the in tro duc tion of the health in sur ance in or der tomake the ex ist ing model “more mar ket ori ented, more ac ces si ble and better reg u lated.”828
Dep u ties from the UDF re quested amend ments in the LHI aimed at elim i nat ing theregion ali sa tion in the choice of healthcare es tab lish ment, the up per and lower limit for thenum ber of pa tients per one gen eral prac ti tio ner and the lim its in the num ber of re fer rals in out -pa tients’ care, in crease of the health in sur ance in stal ment and its equal shar ing be tween em -ploy ers and in sured from 2003829. Ac cord ing to the dep uty from the UDF “the healthcarere form has ceased” and the rea sons he pointed out in cluded the adop tion of an “un re al is tic bud -get” by the gov ern ing ma jor ity, the in tro duc tion of VAT on drugs, etc. 830. In an in ter view forthe “Standart” news pa per, Dr. D. Ignatov stated that one of the er rors, made by the UDF whenthey were in power, was the choice of the “stag ing of the re form” in stead of the al ter na tive forthe re form to be ini ti ated “with small steps in all fields” and this re sulted in the un equal re im -burse ment of the phy si cians in out pa tients’ and in pa tients’ care. In the same in ter view, D.Ignatov also said: “To day I can see that we have made a mis take in the ap proach and I ad mit it.But this is not a fa tal mis take. It would have been fa tal, if we had not started the re form.”831
In 2002, a dis cus sion was held on the is sues of the healthcare re form or gan ised by theCITUB with the par tic i pa tion of rep re sen ta tives of the MH, the trade un ions and the med i calpro fes sional or gani sa tions and the motto of the dis cus sion was “Re form of the re form”. At thefo rum, Min is ter Finkov de clared that: “We are not go ing to re form the re form, we need onlydis crete cor rec tions.”832 The then Vice Min is ter S. Bogoev an nounced that “the pro ject of re -struc tur ing in the health sec tor in Bul garia will be ac com plished by the end of June 2002,”and the eval u a tion given by he WB was “highly sat is fac tory”833.
The rep re sen ta tive of the IMF Jerald Shiff de clared that “the healthcare re form is blockedand maybe it should take an other di rec tion”; the Fund was anx ious that for 2003 more sub si -dies would be nec es sary be cause of the prob lems with the healthcare re form834. The Min is tersof Fi nance and the Healthcare to gether with the man age ment of the NHIF pre pared a jointprogramme for their com mit ments to the healthcare re form and the doc u ment was de signedwithin a programme of the IMF835.
Dur ing this pe riod sev eral pub li ca tions dealt with the prob lem of vol un tary health in -
185
Stages and evo lu tion of the healthcare re form in Bul garia
827 Kapital weekly from 5-11.10.2002 828 Kapital weekly from 10-16.05.2003829 Democracia daily from 28.06.2002; Forum Medicus periodical, Issue ¹ 36 from 23.09.2002830 24 chasa daily, Issue ¹ 159 from 11.06.2002831 Standart daily, Issue ¹ 3565 from 2.12.2002832 Duma daily, Issue ¹ 151 from 4.07.2002833 Democracia daily from 20.06.2002834 24 chasa daily, Issue ¹ 266 from 26.09.2002835 24 chasa daily, Issue ¹ 289 from 17.10.2002
sur ance836. At the be gin ning of 2002, the Chair man of the Par lia men tary Com mis sion onHealthcare Assoc. Prof. Dr. A. Shterev in formed that three vari ants were pos si ble for changesin the sys tem and “the ques tion is what model of vol un tary health in sur ance to in tro duce andnot whether to in tro duce it.” The in tro duc tion of the vol un tary health in sur ance was mo ti vatedby the lack of suf fi cient fi nan cial re source in healthcare. Ac cord ing to Dr. Shterev “which evervari ant is cho sen, strict and clear def i ni tion is re quired for the min i mum pack age guar an teedby the NHIF.”837
Through out the pe riod jour nal ese ma te ri als were re leased in the press criticising the over -all im ple men ta tion of the healthcare re form or var i ous as pects of it, the most com mon be ing in -ter pre ta tions through the eyes of the pa tients838. In 2003, in a jour nal ese com ment in the“Kapital” news pa per, some ma jor er rors were de fined in the con cept and the im ple men ta -tion of the healthcare re form: (1) ne glect ing of the Na tional Health Map, which was used forthe de scrip tion of the ex ist ing sit u a tion rather than as an in stru ment for con duct ing health pol -icy; (2) lack of clearly de fined com mit ments and re spon si bil i ties, dis trib uted among the var i -ous in sti tu tions, e.g. the MH, the NHIF and the pro fes sional or gani sa tions. Ac cord ing to theau thor of the ar ti cle, the Fund pos sessed ex ceed ingly great rights and prac ti cally de ter minedthe rules and the fi nanc ing of healthcare; (3) the di vi sion of the re form into out pa tients’ and in -pa tients’ which brought to an acute disbalance in the phy si cians’ pay ment839.
In 2004, at a “round ta ble” on the is sues of the healthcare re form or gan ised by “FriedrichEbert” Foun da tion and the Un ion of Sci en tists in Bul garia, Pres i dent G. Purvanov de claredthat “there is no po lit i cal will for car ry ing out the press ing prob lems of the healthcare re form,”and he shared that faster and more rad i cal changes were nec es sary in stead of post pone ment ordebts re mit tal (e.g. of un in sured peo ple). At the fo rum, Min is ter Bogoev ac cepted the Pres i -dent’s state ment as “in dic a tive for a change in the sen si tive pub lic opin ion – to depoliticise thefun da men tal is sues of the healthcare re form.” The Min is ter ad dressed crit i cism to the gen eralprac ti tio ners, too. The Pres i dent’s ad vi sor N. Nikolov pro claimed “the model of health in sur -ance as wrong” 840 point ing out as rea sons for it the ex tremely in ap pro pri ate health leg is la tionadopted in 1998, the lack of an ad e quate man age ment ca pac ity, un co or di nated ac tions andcon flicts among in sti tu tions, etc. 841
Ac cord ing to the leader of the BSP S. Stanishev, the great draw backs of the re form in -cluded the chronic lack of money and the great num ber of un in sured peo ple, and most im por -tantly, the fact that it “is not car ried out as a whole and does not in volve pre ven tion,out pa tients’ and in pa tients’ care si mul ta neously.” 842At an in ter na tional con fer ence, Dr.Semerdjiev pre sented his views on the fur ther de vel op ment of the healthcare sys tem, the mostim por tant of them in clud ing the trans fer of the bud get for hos pi tal care from the MH to theNHIF, the aban don ment of the NFA, tran si tion to free price for ma tion, in tro duc tion of pri vate
186
836 Democracia daily from 25.06.2002; 24 chasa daily, Issue ¹ 302 from1.11.2002; Forum Medicus periodical,Issue ¹ 38-39 from 7.10.2002 and Issue ¹ 44 from 4.11.2002; Kapital weekly from 17-23.08.2002 and from 18-24.10.2003; Duma daily, Issue ¹ 270 from 21.11.2003 and Issue ¹ 179 from 4.08.2004
837 Kapital weekly from 23.02.–1.03.2002838 Standart daily, Issue ¹ 3390 from 10.06.2002; Duma daily, Issue ¹ 193 from 22.08.2002 and Issue ¹ 224
from 28.09.2002; 24 chasa daily, Issue ¹ 249 from 8.09.2004 and Issue ¹ 312 from 12.11.2004; Kapitalweekly from 5–11.10.2002 and from 4-10.09.2004
839 Kapital weekly from 10-16.05.2003840 24 chasa daily, Issue ¹ 311 from 2004; Kapital weekly from 13-19.11.2004841 Kapital weekly from 16-22.10.2004842 Duma daily, Issue ¹ 134 from 12.06.2004
funds, grant ing au ton omy to the RHIFs as well as the state de fin ing a min i mum pack age for6% in stal ments, the so cial min is try cov er ing the pre mi ums for the poor and the un em ployed843. A lit tle ear lier Min is ter Bogoev showed the di rec tions for the sys tem de vel op ment – de cen -trali sa tion of the hos pi tal care and cen trali sa tion of the sys tem for pub lic health care, im prove -ment of the sys tem for health in sur ance and the de vel op ment of mech a nisms for sharedpar tic i pa tion of pa tients in their health pro tec tion and re cov ery844.
Ac cord ing to re sults from the Na tional Cen tre for Pub lic Opin ion Polls, about 77% ofthe cit i zens con sid ered that they were not in formed about their rights and li a bil i ties en su ingfrom the health leg is la tion, and 82% of the re spon dents reck oned that they did not have suf fi -cient in for ma tion about the work of the NHIF. Ap prox i mately 74% in di cated that in Bul gariathere was no in sti tu tion to pro tect their rights. The data from the sur vey also showed that 56%of the re spon dents pre ferred to pay to the phy si cians to the al ter na tive of hav ing the health in -sur ance pre mium in creased845.
In the first half of 2005, the pro pos als of the main po lit i cal forces were dis cussed for achange in the model of health in sur ance through the elim i na tion of the NHIF mo nop oly846.In its pre-elec tion programme the BSP en vis aged the elim i na tion of the mo nop oly held by theNHIF and the cre ation of con di tions for com pe ti tions with pri vate health in sur ance funds. Al -ter na tives were dis cussed for the in tro duc tion of the three-pil lar model, sim i lar to the one ofthe pen sion in sur ance, ac cord ing to which the oblig a tory health in sur ance in stal ment was dis -trib uted be tween the NHIF and a pri vate fund, the cit i zens be ing able to in sure them selves ad -di tion ally on their choice and a two-stage model, in which the NHIF paid for a ba sic pack age of med i cal care and a pri vate fund – for the ad di tional ser vices de pend ing on the in sur ance. Thepro posal of the NMSS was to in tro duce ad di tional oblig a tory health in sur ance in pri vatefunds. In its pre-elec tion programme the UDF en vis aged for the in sur ance in stal ments paid bythe NHIF from the state bud get for def i nite cat e go ries of cit i zens to be de pos ited in the NHIF,and the rest of the cit i zens (with la bour and sim i lar la bour re la tions and the self-in sured) tohave the right of choice be tween the NHIF and pri vate health in sur ance funds847.
In an ar ti cle in the “Kapital” news pa per af ter the par lia men tary elec tions in 2005, it waspointed out that the main prob lems in the field of healthcare that had to be solved by the newgov ern ment in cluded the con stantly in creas ing debts of the hos pi tals, the short age of fi -nance in the NHIF bud get, planned for the pay ment of the clin i cal path ways, the def i cit ofthe life-sav ing and life-main tain ing drugs se cured from the state bud get, the large num ber of cit i zens ow ing health in sur an ces, the wide-rang ing cor rup tion. Be side the so lu tion of themain prob lems re lated pri mar ily to the fi nanc ing, it was ex pected from the new gov ern ment tode velop a strat egy for the de vel op ment of healthcare and pres ent its plans for the di rec tion inwhich the healthcare re form would con tinue848.
At the end of Au gust, the “Kapital” pub lished a few ar ti cles de voted to the anal y sis pre -pared by the Min is try of Fi nance of the trends in the fi nanc ing and man age ment of healthcare.In an in ter view for the same news pa per, on the oc ca sion of the pre sented anal y sis, L. Datsov
187
Stages and evo lu tion of the healthcare re form in Bul garia
843 Duma daily, Issue ¹ 280 from 2004; Forum Medicus periodical, Issue ¹ 22-23 from 6.06.2005844 Kapital weekly from 4-10.09.2004; Forum Medicus periodical, Issue ¹ 44-45 from 15.11.2004845 Duma daily, Issue ¹ 80 from 7.04.2005846 Duma daily, Issue ¹ 61 from 16.03.2005; Kapital weekly from 19-25.03.2005847 Kapital weekly from 19-25.03.2005848 Kapital weekly from 16-22.07.2005
de clared that the fi nanc ing of healthcare was “in ef fi cient, cor rupt and did not serve the main te -nance of the over all sys tem.” Ac cord ing to him, the changes to be in tro duced had to place thepa tients and their per sonal choice in the cen tre of the healthcare sys tem. In or der to elim i natethe de fects and im prove the sys tem, it was nec es sary to dis con tinue the mo nop oly sta tus of theNHIF, to es tab lish a con nec tion be tween pay ment and qual ity of the health ser vices and de -velop vol un tary health in sur ance849.
Along side with this, at ten tion was paid to the pri or i ties in the de vel op ment of the sys -tem, an nounced by the new Min is ter of Healthcare Prof. Dr. Radoslav Gaidarski, en sur ing ac -cess of all cit i zens to high qual ity med i cal care, en hanced con trol and dis con tinu a tion of thefi nan cial abuses, privatisation of the hos pi tals with the pos si bil ity for pref er en tial pur chase by the phy si cians work ing in them. Ac cord ing to him, in or der to pre vent the un der fi nanc ing ofthe healthcare sys tem, it was nec es sary to al lo cate 5% of the GDP, the size of the health in sur -ance pre mium had to be in creased to 8% in 2006, the MH had to fi nance the na tionalprogrammes only and the main part of the means al lo cated for healthcare had to be trans ferredto the NHIF850. In the fol low ing week, the press in formed about the forth com ing au dit ing ofthe hos pi tals with the larg est debts which was or dered by the Min is ter. Ac cord ing to Prof.Gaidarski their debts were go ing to be cov ered from the bud get only if the au dit proved that the in curred costs were jus ti fied. The in ten tions that in 2006 the fi nanc ing of hos pi tal care wastrans ferred to tally to the NHIF were also dis cussed as well as the pay ment of the costly drugspro cured by the state bud get851.
* * *The re view of the pub li ca tions con cern ing the healthcare sys tem and the on go ing re form
in se lected dai lies and week lies gives us ground to make the fol low ing conclusions:
· For the stud ied six teen-year pe riod (1990-2005) the top ics in the ana lysed pub li ca -tions evolved from ev ery day prob lems in the func tion ing of the med i cal and hos pi tales tab lish ments and the or gani sa tion of the drug sup ply to more gen eral is sues of healthpol icy and health eco nom ics re lated to the man age ment and the de vel op ment of thehealth sys tem as a whole. In the be gin ning of the first stage of the re form, as de ter -mined by us, the press was dom i nated by pub li ca tions about the se vere fi nan cial stateof the hos pi tals, the cri sis with the sup ply of life-sav ing and life-main tain ing drugs,prob lems pro vid ing drugs re im burs able from free pre scrip tions, pro test ac tiv i ties ofmed i cal spe cial ists and con tra dic tions con cern ing the so lu tion of pri vate med i cal prac -tice. Dur ing this stage, and es pe cially at its be gin ning, a con sid er able share be longed to pieces of in for ma tion about spe cific events and prob lems (such as pro test ac tiv i ties,adop tion of par tic u lar nor ma tive acts, hos pi tal debts, etc.) in the form of re views andcom ment ar ti cles. The pub li ca tions re lated to the healthcare re form were still few innum ber but from the be gin ning of 1990 the need for the con struc tion of a healthcare re -form was def i nitely and in dis put ably real ised and jus ti fied. In the sec ond and thirdstage of the re form, the lead ing top ics grad u ally en com passed the con struc tion and thestart of the health in sur ance sys tem, the ad min is tra tion of the struc tural re forms, theadop tion of new health leg is la tion. The num ber of the com ments con sid er ably in -
188
849 Kapital weekly from 20-26.08.2005850 Kapital weekly from 20-26.08.2005851 Kapital weekly from 27.08.–2.09.2005
creased re gard ing the on go ing re form in healthcare. Only af ter the last stage, the me diaturned their at ten tion to the pa tients’ rights as well as the pa tients’ ex pec ta tions and thewishes about the de vel op ment of the healthcare system.
· The anal y sis of the ma te ri als pub lished in the se lected me dia con firmed the im -pres sion for a de layed and hes i tant course of the healthcare re form – an opin ionshared by the pre vail ing part of the in ter viewed med i cal spe cial ists, man age ment sub -jects and cit i zens (see p. 6 So cio log i cal in ter pre ta tion). For a pe riod of sev eral years,the me dia dis cussed the pro pos als for amend ments in the LPH con cern ing pri vate prac -tice, the draft pro ject on the drugs and phar ma cies in hu man med i cine and the de bat -able ques tions re lated to the right of open ing of phar ma cies, the need for a struc turalre form and es pe cially the dif fer ent draft pro jects on health in sur ance. In the mean time,a num ber of prob lems of the healthcare sys tem were com mented dur ing the dif fer entstages on a reg u lar ba sis. From the first stage of the re form the top ics were in ad ver -tently pres ent in the press re gard ing the se vere fi nan cial state and the large hos pi taldebts, the pay ment of the phy si cians and the other med i cal spe cial ists, the short age ofdrugs re im bursed from the state bud get, and from 1999 on wards the media started todiscuss insistently the issue of corruption in the healthcare establishments.
· To a great ex tent, dur ing the first years of the re form pro cess and also now a days, partof the jour nal ists’ ar ti cles re vealed in suf fi cient knowl edge of the dis cussed is sues,and in some cases, the au di ence was of fered com ments dis torted from the point ofview of the facts. At the end of the first and the be gin ning of the sec ond pe riod, the in -ci dence in creased of the strongly po lit i cally bi ased ar ti cles writ ten by both jour nal istsand rep re sen ta tives of the po lit i cal par ties; in these ar ti cles, of ten con tro ver sial opin -ions and even facts and in ten tions were ex pressed, thus con fus ing the cit i zens andstrongly po lar iz ing the pub lic opin ion and attitude to the healthcare system and theongoing reform.
· The sam ple so cio log i cal sur vey con ducted among cit i zens (see p. 6.3. Cit i zens’ as sess -ment) showed that a great part of the cit i zens were not suf fi ciently in formed ei therabout their rights and li a bil i ties as health in sured per sons and pa tients, or about the on -go ing re form and the changes in the med i cal ser vices re lated to it. In this con text, theim por tance of the me dia was enor mous and they were ex pected to trans mit the in for -ma tion cor re spond ing to the ac tual con sum ers’ needs for health ser vices. How ever,their role was not re stricted to in for ma tion about cur rent events and changes only, butalso re ferred to the in volve ment of so ci ety in the prob lems of healthcare. The anal y -sis of the pub li ca tions in the press for the stud ied pe riod in di cated that the in flu ence ofthe me dia was still very lim ited for health ed u ca tion and health pro mo tion as well as for the ad ver tis ing of the goals of the healthcare re form, the out comes achieved and theassurance of public support for the necessary forthcoming changes.
Pub lic opin ion polls
We will pay even greater at ten tion to a sur vey con ducted on the re form of hos pi tal carein 2005852. The re sults from this sur vey were ob tained by means of an in ter view with “key par -
189
Stages and evo lu tion of the healthcare re form in Bul garia
852 Balabanova, D., S. Tsolova, Å. Delcheva. Analysis of the Policy on the Reform of Hospital Care in Bulgaria.Final report on a research project. “Index” Foundation, Sofia, 2005
tic i pants in the health pol icy pro cess” (oc cu py ing key man ag ing po si tions in the MH, theNHIF, the UBP, in ter na tional do nor or gani sa tions) and a ques tion naire with hos pi tal man ag -ers (di rec tors, man ag ers). The re ported opin ions are, there fore, ex pert and do not re flect pop u -lar pub lic views. Along with the prob lems of the hos pi tal net work, they tackle more generalquestions about the healthcare reform.
As some pre vi ous stud ies (quoted by us), this one also con firmed the pos i tive at ti tude tothe healthcare re form. At this back ground, a num ber of prob lems were re vealed, some ofwhich were caused by the re form pro cess it self and had turned into ob sta cles to the de sired ef -fec tive de vel op ment of the health system.
One of the most es sen tial prob lems was the ab sence of sus tain able, con sis tent andlong-term pol icy and the fluc tu a tions of the po lit i cal will which was needed for the im ple men -ta tion of the healthcare re form. The healthcare leg is la tion did not fol low the logic of the re -form, and, there fore, lagged be hind the re form pro cess (“use lessly” and “awk wardly”).Re gard ing it, 76% of the re spon dents con sid ered that the cur rent leg is la tion did not fa cil i tatethe ef fec tive func tion ing of the hos pi tals. The un solved prob lems of the leg is la tion fell intotwo cat e go ries: (1) dis crep an cies be tween the healthcare leg is la tion and the Com mer cial Law.The hos pi tals were reg is tered as com mer cial com pa nies but they did not func tion as such.There was no suf fi cient clar ity as to the sta tus of the hos pi tal as a com mer cial com pany whichcre ated dif fi cul ties tak ing de ci sions about hos pi tal’s re struc tur ing and the main te nance of their equip ment. Cor re spon dence also lacked with the La bour Code and the Law on Com pe ti tion.These acts gave the hos pi tal staff the right to work in com pet i tive healthcare es tab lish ments inspite of the cre ated con flict of in ter ests; (2) on the im ple men ta tion of the laws. There wereshort com ings in the by-laws for the ap pli ca tion of the laws (“too gen eral”, un dif fer en ti ated forthe sep a rate types of healthcare es tab lish ments, un re al is tic, “lag ging be hind the ac tualproblems and relationships”). The unequal treatment of the public and private healthcareestablishments was also indicated as a deficiency.
Apart from the leg is la tive, an other prob lem (per sist ing from the be gin ning of the re form)was the iso la tion of the re gional and lo cal man age ment level not only from the pro cess ofde ci sion-mak ing but from the de ci sions them selves re lated to the changes in the healthcaresys tem. The re sponses of the hos pi tal di rec tors were typ i cal in this re spect, e.g. “They sim plydo not care about our opin ion” or “It is vir tu ally im pos si ble for us to con trib ute to the for ma tion of a health pol icy.” At a lo cal and re gional level, 79% of the re spon dents stated that they werenot ad e quately in formed about the healthcare re form. As typ i cal, the au thors con sider re -sponses such as “We re ceive in for ma tion about the re form from the press.” The two di rec tionsin the com mu ni ca tive pro cess were miss ing. In fact, the hos pi tal di rec tors were per ceived (andthey also per ceived them selves) as “pas sive re cip i ents” of in for ma tion and not as ac tive part -ners at na tional or lo cal level. This was prob a bly due to the es tab lished re luc tance of the hos pi -tal man ag ers to as sume re spon si bil ity for or gani sa tional changes in the hos pi tals. Thepos si bil i ties for the hos pi tals (as key par tic i pants in the healthcare re form) to in flu ence hos pi tal pol icy were lim ited. They did not have le git i mate rep re sen ta tives in the prep a ra tion of the Na -tional Frame work Agree ment, where, on the contrary, there was strong pressure exerted by theexisting lobby groups (for instance, of the general practitioners).
The sur vey quoted above, makes it ev i dent that even if the re spec tive nor ma tive ba sis was avail able, in some re spects, for wider par tic i pa tion in the for ma tion of a pol icy and de ci -sion-mak ing, mech a nisms were ab sent for the ap pli ca tion of the nor ma tively reg u lated pos si -
190
bil i ties. Re gard ing the de cen trali sa tion, the re spon dents claimed that the newly ac quired“free doms” were lim ited by ex ter nal in ter fer ence – by “the rigid leg is la tive frame work and thepolitically-biased hospital reform”.
This ap plied also to the civil par tic i pa tion in the for ma tion and the im ple men ta tion of the health pol icy. On be half of the state there was al most no re sponse to the “Rec om men da tionsfor the de vel op ment of struc tures for cit i zens’ and pa tients’ par tic i pa tion in the de ci sion-mak -ing pro cess in the field of healthcare”853 adopted by the Coun cil of Min is ters of EC in 2000. Aneg a tive ex am ple was given by the amend ment and ad di tion in the LHI adopted in 2002, en vis -ag ing the par tic i pa tion of civil as so ci a tions (with a quota of one per son!) in the As sem bly ofthe rep re sen ta tives on the NHIF. How ever, no one was elected un til May 2005. The Law onLo cal Gov er nance and Lo cal Ad min is tra tion (1991) also pro vided for pos si bil i ties for civilpar tic i pa tion in the for ma tion of mu nic i pal health pol icy, but the sur vey quoted above, in di -cated that no solid ev i dence was found for an ef fec tive involvement of citizens in debates onhospital policy either at national or at local level.
Vary ing view points were ex pressed re gard ing the privatisation of healthcare es tab lish -ments. The com mon opin ion was that it was not nec es sary to carry out a 100%- privatisation.Some held the opin ion that the privatisation of the di ag nos tic and con sul ta tive cen tres shouldpre cede hos pi tal privatisation. One of the “key par tic i pants” con sid ered that privatisation perse would not re solve the prob lem of the mu nic i pal hos pi tals be fore the fi nan cial flows wereclar i fied. 62% of the hos pi tal man ag ers reck oned that the privatisation would not solve the in -sti tu tional prob lems of the hos pi tals, but 32% shared the opin ion that the change in own er shipwould contribute to the solution of these problems.
The ma jor ity of the hos pi tal man ag ers (62%) agreed that the health in sur ance had a pos i -tive ef fect on the hos pi tal sec tor. Only 3%, how ever, ap proved the ad e quacy of the meth ods of fi nanc ing by the NHIF. A rep re sen ta tive of the UBP pointed out that the two sources (in 2005they in cluded the MH and the NHIF) cov ered to tally up to 60% of the ac tual costs. Ac cord ingto the hos pi tal man ag ers, the pay ment from the NHIF for “clin i cal path ways” cov ered 50-75%of the ac tual costs. The pay ment for clin i cal path ways was per ceived as just, but only if basedon ad e quate fi nan cial re sources. The chronic def i cit of fi nanc ing (“un der fi nanc ing”) wasemphasised as a rea son both for de fects in the qual ity of hos pi tal ser vices and for the grad ualdecapitalisation of the hos pi tals (the NHIF re fused to cal cu late wear-and-tear), for the ex -tremely in suf fi cient ex penses for qual i fi ca tion and the low sal a ries of the hos pi tal staff and“un reg u lated pay ments” made by the pa tients. Gen er ally speak ing, the above quoted sur vey,es tab lished and con firmed some se ri ous de fects of the re form not only in the hospital sectorbut also in the overall course of the reform process, namely:
· The lack of ef fec tive com mu ni ca tion and open na tional de bate on the main re forms ofthe healthcare sys tem which re sulted in the drop in the trust and the feel ing of re spon si -bil ity among the key par tic i pants in the pro cess;
· The hos pi tal and the mu nic i pal ity au ton omy weak ened the ver ti cal sys tem of con trol,with out this be ing com pen sated in any way;
· Prob lems were cre ated and the in ter ac tion be tween pri mary and hos pi tal care wasprob lem atic;
191
Stages and evo lu tion of the healthcare re form in Bul garia
853 Council of Europe. Committee of Ministers. Recommendation ¹ 5 of the Committee of Ministers on theDevelopment of Structures for Citizen and Patient Participation. 699th Meeting of the Ministers’ Deputies,February 2000
· The lack of an in sti tu tion to as sume the re spon si bil ity for cer tain as pects of the reform;
· As a whole, the re form was strongly po lit i cally bi ased and the ex er tion of pres sure andin ter fer ence in the hos pi tal man age ment by in flu en tial fig ures with po lit i cal, cor po rateor pri vate in ter ests were frequently practised;
· All this led to a change in the de mand for hos pi tal care which was grow ing sig nif i -cantly for the larger and spe cial ised hos pi tals and be came the rea son for un reg u latedpay ments com pen sat ing for the short age of the pub lic fi nanc ing but also cre at ing a“shadow market” in healthcare.
Re sults and un solved prob lems
The ex am ined mod ern pe riod was less event ful and not as dy namic as the pre vi ous stage.From the point of view of the healthcare re form, the com ple tion of the main con struc tion ofthe nor ma tive ba sis of the healthcare re form can be de fined as the most es sen tial re sult. It is asig nif i cant and pro spec tive con tri bu tion help ing the re form pro cess to ac quire clearer out lines.It should not be con sid ered, how ever, that the de vel op ment of the nor ma tive ba sis of thehealthcare sys tem is com pleted. From the anal y sis pre sented so far, it is ob vi ous that in or der to ef fec tively reg u late the sys tem and en sure its de vel op ment, its nor ma tive ba sis also needs tode velop and adapt to the changed conditions as well as to monitor its observance.
A pos i tive change was car ried out in the field of fi nan cial pro vi sion of the hos pi tal es -tab lish ments. It has to be noted that for three years (2001-2003) the hos pi tal costs in creasedby 1.33 times per ad mit ted pa tient, by 1.92 times per hos pi tal bed, by 1.61 times per bed day,by 2.4 times per drug day and by 1.16 times per food day (Ta ble 29). What im presses is the al -most two-fold in crease of the costs for 1 drug day which was prob a bly de ter mined by the al -most dou ble rise of the costs per 1 bed day. In the pre vi ous stage, for al most a five-year pe riod,the in crease was significantly smaller.
This phe nom e non re quires a more de tailed study, but a pri ori it im plies that the ther a peu -tic schemes or the sur gi cal meth ods had hardly changed to such an ex tent in the pe riod2001-2003 as com pared to those ap plied in the pe riod 1998-2001 to cause such a dif fer ence.Fur ther more, nei ther the wear-and-tear of the hos pi tal as sets, nor the hos pi tal cap i tal in vest -ments were in cluded in the cal cu la tion the hos pi tal costs in the above men tioned in di ca tors. Itmeans that there was an other rea son. For ex am ple, af ter the NHIF in tro duced the new ap -proach for pay ment of the drugs in 2005 (a mean price was ac cepted, paid in 8 Eu ro pean coun -tries and the pro duc ing com pa nies which of fered prices higher than the fixed ones, did notclas sify for the de liv ery com pe ti tions), the inter-in sti tu tional Com mis sion on trans par ency an -nulled the re stric tion for the pro duc ing com pa nies and the Fund was sub ject to a strong pres -sure by po lit i cal cir cles (in ter view with Dr. D. Dechev – Dep uty Di rec tor of the NHIF for the“Trud” from March 19th 2005).
With the Law on the Re pub li can Bud get and the Law on the NHIF bud get for 2006 andthe NFA for 2006, the fi nanc ing from a sin gle source only was in tro duced for the hos pi tals –from the NHIF bud get, the hos pi tal ser vices be ing paid from the re spec tive clin i cal path ways.Thus, a great de gree of clar ity was in tro duced for the hos pi tal costs, elim i nat ing to a sig nif i cant ex tent the com plex ity in the ac count ing and the regime of payment.
192
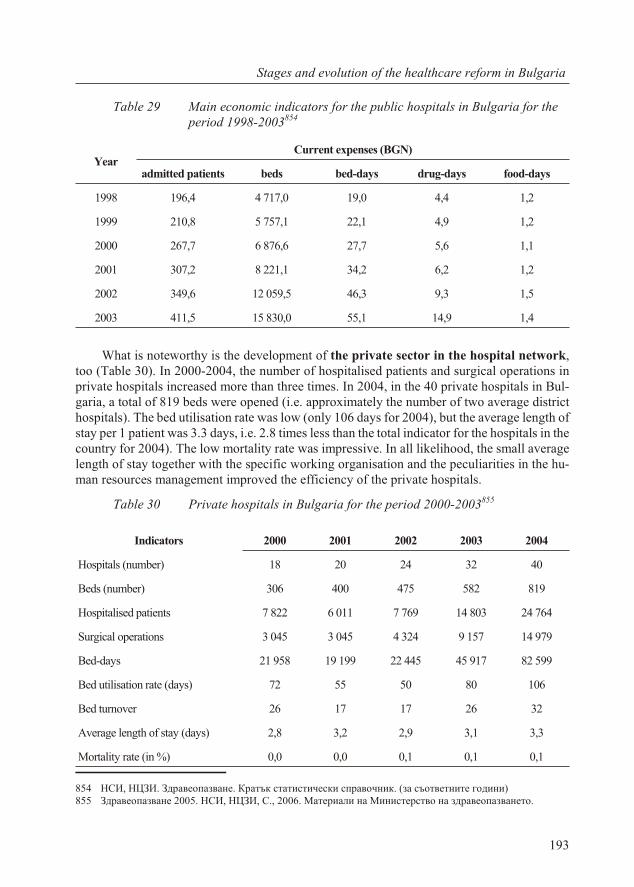
Ta ble 29 Main economic indicators for the public hospitals in Bulgaria for theperiod 1998-2003854
YearCur rent ex penses (BGN)
ad mit ted pa tients beds bed-days drug-days food-days
1998 196,4 4 717,0 19,0 4,4 1,2
1999 210,8 5 757,1 22,1 4,9 1,2
2000 267,7 6 876,6 27,7 5,6 1,1
2001 307,2 8 221,1 34,2 6,2 1,2
2002 349,6 12 059,5 46,3 9,3 1,5
2003 411,5 15 830,0 55,1 14,9 1,4
What is note wor thy is the de vel op ment of the pri vate sec tor in the hos pi tal net work,too (Ta ble 30). In 2000-2004, the num ber of hos pi ta lised pa tients and sur gi cal op er a tions inpri vate hos pi tals in creased more than three times. In 2004, in the 40 pri vate hos pi tals in Bul -garia, a to tal of 819 beds were opened (i.e. ap prox i mately the num ber of two av er age dis tricthos pi tals). The bed uti li sa tion rate was low (only 106 days for 2004), but the av er age length ofstay per 1 pa tient was 3.3 days, i.e. 2.8 times less than the to tal in di ca tor for the hos pi tals in thecoun try for 2004). The low mor tal ity rate was im pres sive. In all like li hood, the small av er agelength of stay to gether with the spe cific work ing or gani sa tion and the pe cu liar i ties in the hu -man re sources man age ment im proved the ef fi ciency of the pri vate hos pi tals.
Ta ble 30 Pri vate hos pi tals in Bul garia for the pe riod 2000-2003855
193
Stages and evo lu tion of the healthcare re form in Bul garia
In di ca tors 2000 2001 2002 2003 2004
Hos pi tals (num ber) 18 20 24 32 40
Beds (num ber) 306 400 475 582 819
Hos pi ta lised pa tients 7 822 6 011 7 769 14 803 24 764
Sur gi cal op er a tions 3 045 3 045 4 324 9 157 14 979
Bed-days 21 958 19 199 22 445 45 917 82 599
Bed uti li sa tion rate (days) 72 55 50 80 106
Bed turn over 26 17 17 26 32
Av er age length of stay (days) 2,8 3,2 2,9 3,1 3,3
Mor tal ity rate (in %) 0,0 0,0 0,1 0,1 0,1
854 ÍÑÈ, ÍÖÇÈ. Çäðàâåîïàçâàíå. Êðàòúê ñòàòèñòè÷åñêè ñïðàâî÷íèê. (çà ñúîòâåòíèòå ãîäèíè) 855 Çäðàâåîïàçâàíå 2005. ÍÑÈ, ÍÖÇÈ, Ñ., 2006. Ìàòåðèàëè íà Ìèíèñòåðñòâî íà çäðàâåîïàçâàíåòî.
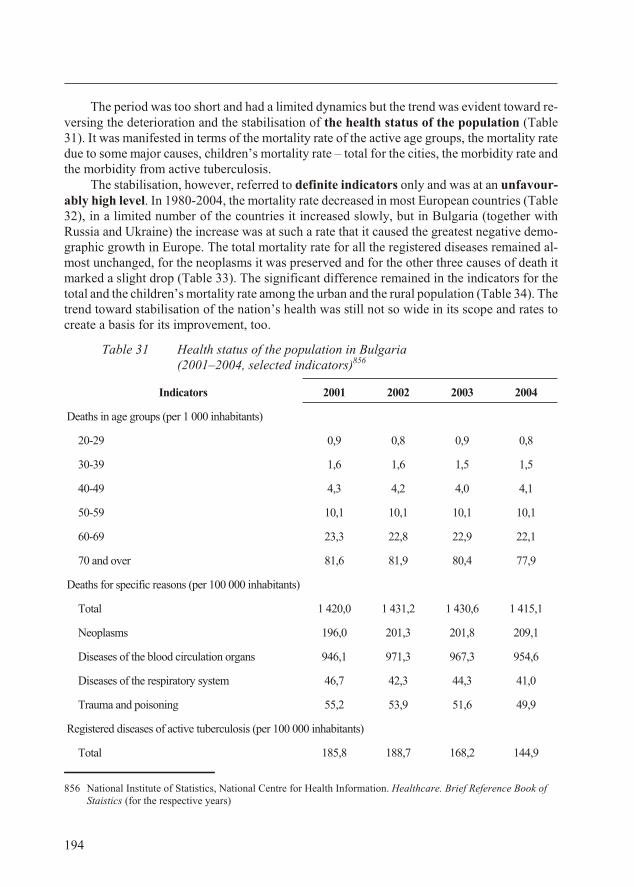
The pe riod was too short and had a lim ited dy nam ics but the trend was ev i dent to ward re -vers ing the de te ri o ra tion and the sta bili sa tion of the health sta tus of the pop u la tion (Ta ble31). It was man i fested in terms of the mor tal ity rate of the ac tive age groups, the mor tal ity ratedue to some ma jor causes, chil dren’s mor tal ity rate – to tal for the cit ies, the mor bid ity rate andthe mor bid ity from ac tive tu ber cu lo sis.
The sta bili sa tion, how ever, re ferred to def i nite in di ca tors only and was at an un fa vour -ably high level. In 1980-2004, the mor tal ity rate de creased in most Eu ro pean coun tries (Ta ble32), in a lim ited num ber of the coun tries it in creased slowly, but in Bul garia (to gether withRus sia and Ukraine) the in crease was at such a rate that it caused the great est neg a tive de mo -graphic growth in Eu rope. The to tal mor tal ity rate for all the reg is tered dis eases re mained al -most un changed, for the neoplasms it was pre served and for the other three causes of death itmarked a slight drop (Ta ble 33). The sig nif i cant dif fer ence re mained in the in di ca tors for theto tal and the chil dren’s mor tal ity rate among the ur ban and the ru ral pop u la tion (Ta ble 34). The trend to ward sta bili sa tion of the na tion’s health was still not so wide in its scope and rates tocre ate a ba sis for its im prove ment, too.
Ta ble 31 Health sta tus of the pop u la tion in Bul garia(2001–2004, selected indicators)856
In di ca tors 2001 2002 2003 2004
Deaths in age groups (per 1 000 in hab it ants)
20-29 0,9 0,8 0,9 0,8
30-39 1,6 1,6 1,5 1,5
40-49 4,3 4,2 4,0 4,1
50-59 10,1 10,1 10,1 10,1
60-69 23,3 22,8 22,9 22,1
70 and over 81,6 81,9 80,4 77,9
Deaths for spe cific rea sons (per 100 000 in hab it ants)
To tal 1 420,0 1 431,2 1 430,6 1 415,1
Neoplasms 196,0 201,3 201,8 209,1
Dis eases of the blood cir cu la tion or gans 946,1 971,3 967,3 954,6
Dis eases of the re spi ra tory sys tem 46,7 42,3 44,3 41,0
Trauma and poi son ing 55,2 53,9 51,6 49,9
Reg is tered dis eases of ac tive tu ber cu lo sis (per 100 000 in hab it ants)
To tal 185,8 188,7 168,2 144,9
194
856 Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion. Healthcare. Brief Ref er ence Book ofStaistics (for the re spec tive years)
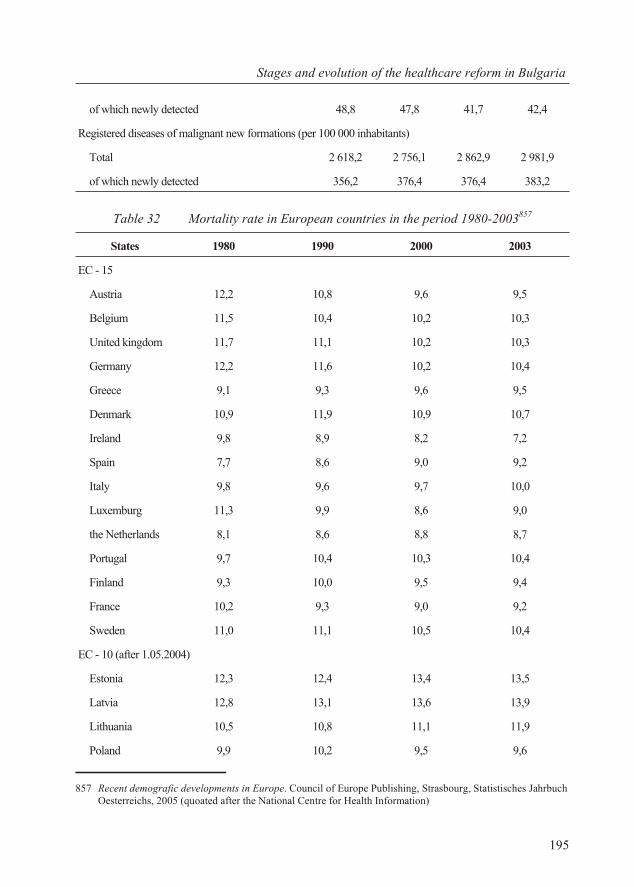
of which newly de tected 48,8 47,8 41,7 42,4
Reg is tered dis eases of ma lig nant new for ma tions (per 100 000 in hab it ants)
To tal 2 618,2 2 756,1 2 862,9 2 981,9
of which newly de tected 356,2 376,4 376,4 383,2
Ta ble 32 Mor tal ity rate in Eu ro pean coun tries in the pe riod 1980-2003857
States 1980 1990 2000 2003
ÅÑ - 15
Aus tria 12,2 10,8 9,6 9,5
Bel gium 11,5 10,4 10,2 10,3
United king dom 11,7 11,1 10,2 10,3
Ger many 12,2 11,6 10,2 10,4
Greece 9,1 9,3 9,6 9,5
Den mark 10,9 11,9 10,9 10,7
Ire land 9,8 8,9 8,2 7,2
Spain 7,7 8,6 9,0 9,2
It aly 9,8 9,6 9,7 10,0
Luxemburg 11,3 9,9 8,6 9,0
the Neth er lands 8,1 8,6 8,8 8,7
Por tu gal 9,7 10,4 10,3 10,4
Fin land 9,3 10,0 9,5 9,4
France 10,2 9,3 9,0 9,2
Swe den 11,0 11,1 10,5 10,4
ÅÑ - 10 (af ter 1.05.2004)
Es to nia 12,3 12,4 13,4 13,5
Lat via 12,8 13,1 13,6 13,9
Lith u a nia 10,5 10,8 11,1 11,9
Po land 9,9 10,2 9,5 9,6
195
Stages and evo lu tion of the healthcare re form in Bul garia
857 Re cent demografic de vel op ments in Eu rope. Coun cil of Eu rope Pub lish ing, Strasbourg, Statistisches Jahrbuch Oesterreichs, 2005 (quoated af ter the Na tional Cen tre for Health In for ma tion)
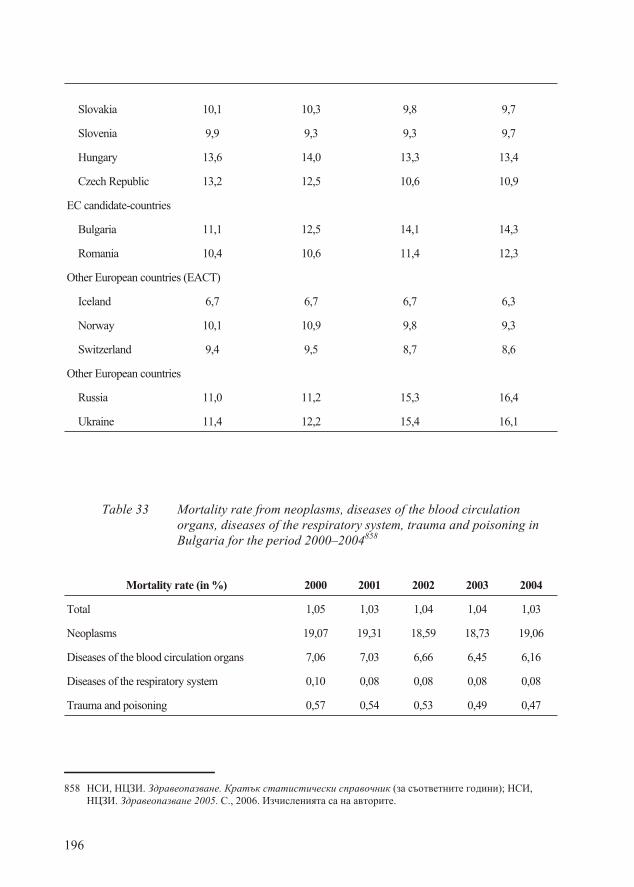
Slovakia 10,1 10,3 9,8 9,7
Slovenia 9,9 9,3 9,3 9,7
Hun gary 13,6 14,0 13,3 13,4
Czech Re pub lic 13,2 12,5 10,6 10,9
EC can di date-coun tries
Bul garia 11,1 12,5 14,1 14,3
Ro ma nia 10,4 10,6 11,4 12,3
Other Eu ro pean coun tries (ÅÀÑÒ)
Ice land 6,7 6,7 6,7 6,3
Nor way 10,1 10,9 9,8 9,3
Swit zer land 9,4 9,5 8,7 8,6
Other Eu ro pean coun tries
Rus sia 11,0 11,2 15,3 16,4
Ukraine 11,4 12,2 15,4 16,1
Ta ble 33 Mortality rate from neoplasms, diseases of the blood circulationorgans, diseases of the respiratory system, trauma and poisoning inBulgaria for the period 2000–2004858
Mortality rate (in %) 2000 2001 2002 2003 2004
To tal 1,05 1,03 1,04 1,04 1,03
Neoplasms 19,07 19,31 18,59 18,73 19,06
Dis eases of the blood cir cu la tion or gans 7,06 7,03 6,66 6,45 6,16
Dis eases of the re spi ra tory sys tem 0,10 0,08 0,08 0,08 0,08
Trauma and poisoning 0,57 0,54 0,53 0,49 0,47
196
858 ÍÑÈ, ÍÖÇÈ. Çäðàâåîïàçâàíå. Êðàòúê ñòàòèñòè÷åñêè ñïðàâî÷íèê (çà ñúîòâåòíèòå ãîäèíè); ÍÑÈ,ÍÖÇÈ. Çäðàâåîïàçâàíå 2005. Ñ., 2006. Èç÷èñëåíèÿòà ñà íà àâòîðèòå.
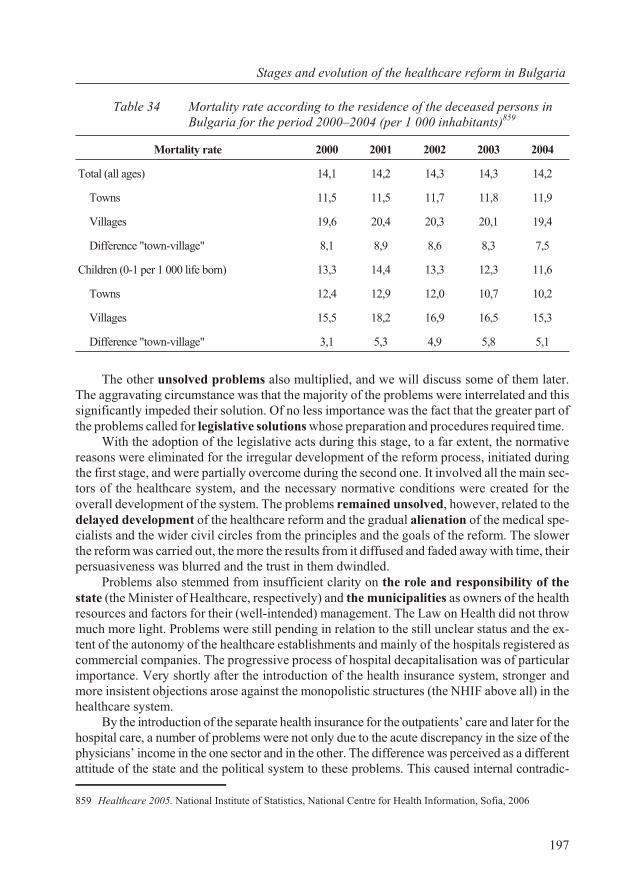
Ta ble 34 Mortality rate according to the residence of the deceased persons inBulgaria for the period 2000–2004 (per 1 000 inhabitants)859
Mor tal ity rate 2000 2001 2002 2003 2004
To tal (all ages) 14,1 14,2 14,3 14,3 14,2
Towns 11,5 11,5 11,7 11,8 11,9
Vil lages 19,6 20,4 20,3 20,1 19,4
Dif fer ence "town-vil lage" 8,1 8,9 8,6 8,3 7,5
Chil dren (0-1 per 1 000 life born) 13,3 14,4 13,3 12,3 11,6
Towns 12,4 12,9 12,0 10,7 10,2
Vil lages 15,5 18,2 16,9 16,5 15,3
Dif fer ence "town-vil lage" 3,1 5,3 4,9 5,8 5,1
The other un solved prob lems also mul ti plied, and we will dis cuss some of them later.The ag gra vat ing cir cum stance was that the ma jor ity of the prob lems were in ter re lated and thissig nif i cantly im peded their so lu tion. Of no less im por tance was the fact that the greater part ofthe prob lems called for leg is la tive so lu tions whose prep a ra tion and pro ce dures re quired time.
With the adop tion of the leg is la tive acts dur ing this stage, to a far ex tent, the nor ma tiverea sons were elim i nated for the ir reg u lar de vel op ment of the re form pro cess, ini ti ated dur ingthe first stage, and were par tially over come dur ing the sec ond one. It in volved all the main sec -tors of the healthcare sys tem, and the nec es sary nor ma tive con di tions were cre ated for theover all de vel op ment of the sys tem. The prob lems re mained un solved, how ever, re lated to thede layed de vel op ment of the healthcare re form and the grad ual alien ation of the med i cal spe -cial ists and the wider civil cir cles from the prin ci ples and the goals of the re form. The slowerthe re form was car ried out, the more the re sults from it dif fused and faded away with time, their per sua sive ness was blurred and the trust in them dwin dled.
Prob lems also stemmed from in suf fi cient clar ity on the role and re spon si bil ity of thestate (the Min is ter of Healthcare, re spec tively) and the mu nic i pal i ties as own ers of the healthre sources and fac tors for their (well-in tended) man age ment. The Law on Health did not throwmuch more light. Prob lems were still pend ing in re la tion to the still un clear sta tus and the ex -tent of the au ton omy of the healthcare es tab lish ments and mainly of the hos pi tals reg is tered ascom mer cial com pa nies. The pro gres sive pro cess of hos pi tal decapitalisation was of par tic u larim por tance. Very shortly af ter the in tro duc tion of the health in sur ance sys tem, stron ger andmore in sis tent ob jec tions arose against the mo nop o lis tic struc tures (the NHIF above all) in thehealthcare sys tem.
By the in tro duc tion of the sep a rate health in sur ance for the out pa tients’ care and later for the hos pi tal care, a num ber of prob lems were not only due to the acute dis crep ancy in the size of thephy si cians’ in come in the one sec tor and in the other. The dif fer ence was per ceived as a dif fer entat ti tude of the state and the po lit i cal sys tem to these prob lems. This caused in ter nal con tra dic -
197
Stages and evo lu tion of the healthcare re form in Bul garia
859 Healthcare 2005. Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion, So fia, 2006

tions in the healthcare sec tor and brought about sus tain able dif fi cul ties (no mat ter how con -cealed) in the in te gra tion and the con ti nu ity in the out pa tients’ and the hos pi tal med i cal care.
A chain of un solved prob lems was caused by the def i cit in the fi nanc ing, mainly of thehos pi tal treat ment. In this case, it con cerned the pay ment of the prices for clin i cal path waysadopted ac cord ing to the NFA and not ac cord ing to the ac tual costs and the re spec tive value ofthe hos pi tal treat ment. As of ten emphasised, the prices (the pay ment, re spec tively) dif fer fromthe ac tual costs, e.g. the value of the treat ment. In the pre vail ing num ber of clin i cal path ways,the prices were con sid er ably lower than the real costs. This, in fact, pre sented “losses plannedin ad vance” for ev ery work ing (“pro duc ing”) pub lic or pri vate hos pi tals. In real prac tice forthe pub lic hos pi tals this in cluded not only losses since they could form nei ther profit nor loss.But it formed debts to the sup pli ers. These debts were ob jec tive re sults from the dif fer ence be -tween the value and the price of the clin i cal path way. A reg u la tory mech a nism was ab sent toen sure the fi nan cial cov er age or com pen sa tion for this dif fer ence. It was here that the un reg u -lated in de pend ent fi nan cial ac tiv i ties of the hos pi tals be gan. On the other hand, it is known,that the prices for some clin i cal path ways are higher than the ac tual costs for them. The thuses tab lished sit u a tion cre ated two al ter na tives for the hos pi tals due to the dif fer ence be tweenthe value and the price. The first one was to make a de lib er ate se lec tion of pa tients and ad mitonly pa tients with “prof it able” di ag no ses. The sec ond was to make (if there was such a pos si -bil ity) a “prof it able” di ag no sis of pa tients with an other dis ease which was reg is tered as a sec -ond ary or ac com pa ny ing com pli ca tion. Both al ter na tives caused de for mi ties (ac cord ing to thedi rec tor of a large hos pi tal “whole classes of dis eases dis ap peared from the re ports of the clin -ics”). Yet, in re cent prac tice, there is quite a num ber of hos pi tals seek ing and find ing ra tio nalways of com pen sat ing for the dif fer ence be tween the value and the price for most of the clin i -cal path ways and re duc ing their unpaid debts.
198
PART III THE HEALTHCARE RE FORM IN BUL GARIA 2005:CUR RENT STATE
6. So cio log i cal in ter pre ta tion
“...and you will know the truthand the truth will make you free”St. Evan ge list John, 8:32
6.1. As sess ment of med i cal spe cial ists
Gen eral as sess ment of the healthcare re form
Af ter six teen-years’ at tempts for re struc tur ing of the healthcare sys tem (1990-2005) theview around which the ma jor ity of med i cal pro fes sion als are united (91,0%), was that thehealthcare re form had not fin ished. This meant that for each of the seven pro fes sionalgroups in cluded in our study (gen eral prac ti tio ners, spe cial ists from out pa tients’ care, phy si -cians from hos pi tals, den tists, phar ma cists, spe cial ists in healthcare from out pa tients’ and in -pa tients’ care) the goals of the re form had not been achieved yet. In spite of this com monview, opin ions di vided on the rate and the di rec tion of the healthcare re form.
On the one side are those med i cal spe cial ists, ac cord ing to whom the re form did not de vi -ate from the de sired goals. Part of them con sid ered that it was be ing ex e cuted at nor mal andac cept able rates (5.2%) and oth ers con sid ered that the re form was be ing car ried out slowlybut fol lows its di rec tion (33.6%).
The op po site po si tion was held by 58.3% of the in ter viewed med i cal pro fes sion als. Partof them did not see any im prove ment in healthcare as a re sult of the re form (32.1%). An other26.2% as sessed the neg a tive im pact of the re form ac tions on the func tion ing of the sys tem. The re spon dents with the most crit i cal at ti tude to the re form were the spe cial ists from out pa -tients’ care (69.7%), fol lowed by the phar ma cists (67.1) and the spe cial ists from hos pi tal care(61.7%). The per cent age of the den tists (49.3%), who as sessed the rate and the di rec tion of there form neg a tively, was the low est in com par i son to the rest of the pro fes sion als.
These dom i nat ing neg a tive as sess ments were not an out come of not ac cept ing the re form inprin ci ple. To one de gree or an other, over two thirds of the re spon dents de clared that need for the ex e cu tion of an over all trans for ma tion of the Bul gar ian healthcare re form had beenpress ing af ter 1999. For 46.3% of the in ter viewed the gen e sis of the neg a tiv ism to the re formwas rooted in the pres ence of sig nif i cant dis crep an cies be tween the prin ci ples of the healthcarere form (as they thought it had been con ceived) and the prob lems which had to be solved in thefield of healthcare af ter 1990. For the ma jor ity of the re spon dents, how ever, the prob lem wasrather in the way of its im ple men ta tion and the qual ity of the achieved re sults. Ac cord ing to56.6% of the in ter viewed key prob lems re mained un solved. For an other large part (32.1%) there form had only brought about par tial cor rec tions, with out an over all ef fect on the healthcaresys tem. Only 6.3% shared the view that a num ber of prob lems had been fully solved.
The fact, cor re spond ing to these re sults, was that ac cord ing to the ma jor ity of the in ter -viewed med i cal spe cial ists (42.1%), the re form had been de layed. For 21.0% of them the mo -
199
So cio log i cal in ter pre ta tion
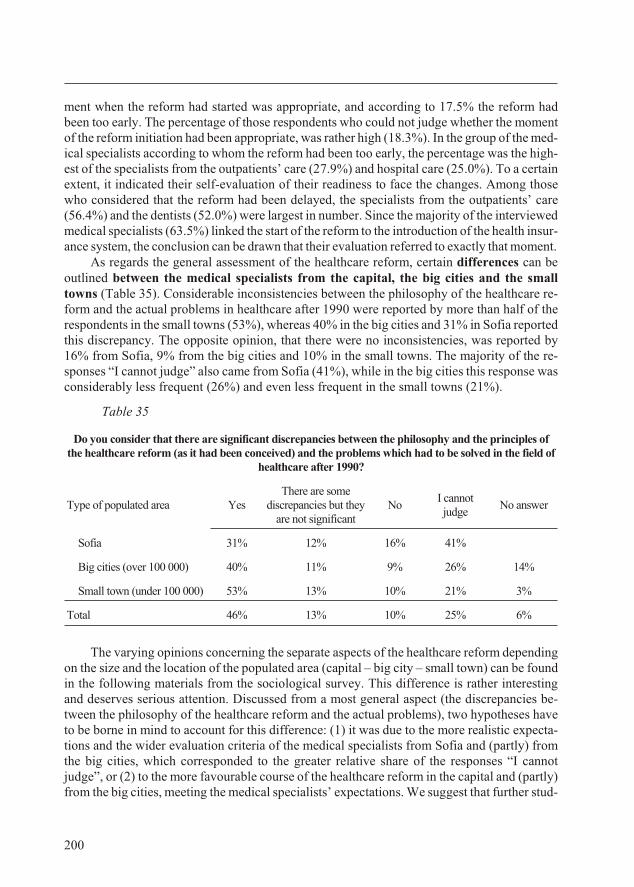
ment when the re form had started was ap pro pri ate, and ac cord ing to 17.5% the re form hadbeen too early. The per cent age of those re spon dents who could not judge whether the mo mentof the re form ini ti a tion had been ap pro pri ate, was rather high (18.3%). In the group of the med -i cal spe cial ists ac cord ing to whom the re form had been too early, the per cent age was the high -est of the spe cial ists from the out pa tients’ care (27.9%) and hos pi tal care (25.0%). To a cer tainex tent, it in di cated their self-eval u a tion of their readi ness to face the changes. Among thosewho con sid ered that the re form had been de layed, the spe cial ists from the out pa tients’ care(56.4%) and the den tists (52.0%) were larg est in num ber. Since the ma jor ity of the in ter viewed med i cal spe cial ists (63.5%) linked the start of the re form to the in tro duc tion of the health in sur -ance sys tem, the conclusion can be drawn that their evaluation referred to exactly that moment.
As re gards the gen eral as sess ment of the healthcare re form, cer tain dif fer ences can beout lined be tween the med i cal spe cial ists from the cap i tal, the big cit ies and the smalltowns (Ta ble 35). Con sid er able in con sis ten cies be tween the phi los o phy of the healthcare re -form and the ac tual prob lems in healthcare af ter 1990 were re ported by more than half of there spon dents in the small towns (53%), whereas 40% in the big cit ies and 31% in So fia re portedthis dis crep ancy. The op po site opin ion, that there were no in con sis ten cies, was re ported by16% from So fia, 9% from the big cit ies and 10% in the small towns. The ma jor ity of the re -sponses “I can not judge” also came from So fia (41%), while in the big cit ies this re sponse wascon sid er ably less fre quent (26%) and even less frequent in the small towns (21%).
Table 35
Do you consider that there are significant discrepancies between the philosophy and the principles ofthe healthcare reform (as it had been conceived) and the problems which had to be solved in the field of
healthcare after 1990?
Type of populated area YesThere are some
discrepancies but they are not significant
NoI cannotjudge
No answer
So fia 31% 12% 16% 41%
Big cit ies (over 100 000) 40% 11% 9% 26% 14%
Small town (un der 100 000) 53% 13% 10% 21% 3%
To tal 46% 13% 10% 25% 6%
The vary ing opin ions con cern ing the sep a rate as pects of the healthcare re form de pend ingon the size and the lo ca tion of the pop u lated area (cap i tal – big city – small town) can be foundin the fol low ing ma te ri als from the so cio log i cal sur vey. This dif fer ence is rather in ter est ingand de serves se ri ous at ten tion. Dis cussed from a most gen eral as pect (the dis crep an cies be -tween the phi los o phy of the healthcare re form and the ac tual prob lems), two hy poth e ses haveto be borne in mind to ac count for this dif fer ence: (1) it was due to the more re al is tic ex pec ta -tions and the wider eval u a tion cri te ria of the med i cal spe cial ists from So fia and (partly) fromthe big cit ies, which cor re sponded to the greater rel a tive share of the re sponses “I can notjudge”, or (2) to the more fa vour able course of the healthcare re form in the cap i tal and (partly)from the big cit ies, meet ing the med i cal spe cial ists’ ex pec ta tions. We sug gest that fur ther stud -
200
ies would sup port ei ther of the two hy poth e ses. We con sider, how ever, that there are suf fi cientar gu ments for the ac cep tance of the sec ond hy poth e sis as it cor re sponds to the ac tual and ob -jec tive pro cesses in healthcare for the im ple men ta tion of the re form, which due to the more ad -van ta geous eco nomic fac tors and the va ri ety of healthcare es tab lish ments and spe cial ists,de velop more in ten sive ac tiv i ties and com pe ti tion in the cap i tal and the big cit ies than in thesmall towns. Con se quently, the ap par ently dif fer ent at ti tude to the course of the healthcare re -form in the cap i tal, the big city and the small town has to be taken into ac count for a dif fer en ti -ated ap proach to the re form health policy.
Asked about the most im por tant pos i tive changes re sult ing from the re form for thepeo ple em ployed in the sys tem of healthcare, 45.4% of the med i cal spe cial ists re sponded that there were no such changes, 22.5% de fined the better pay ment and the higher mo ti va tion as apos i tive change, 16.6% ap proved the foun da tion of pri vate healthcare es tab lish ments and thein tro duc tion of mar ket prin ci ples in the healthcare sys tems and 14.4% shared the view that there form had brought about a “more mod ern work ing stan dard”.
The per cent age was higher of those med i cal spe cial ists (51.1%) for whom the re form hadnot brought about any pos i tive changes for the pa tients as com pared to the per cent age ofmed i cal spe cial ists for whom the re form had not brought about any pos i tive changes for thepeo ple work ing in the healthcare sys tem. The med i cal spe cial ists, ac cord ing to whom therewere pos i tive changes for the pa tients, most fre quently pointed out “the free choice of a gen eral prac ti tio ner and healthcare es tab lish ment” (29.7%) and “the better qual ity of the health ser -vices” (10.7%).
At the same time, the per cent age was rather low of the med i cal spe cial ists, ac cord ing towhom the re form had not brought about neg a tive changes for the peo ple em ployed in thehealthcare sys tem (9.4%) and for the pa tients (8.1%).
The most com monly shared neg a tive changes re sult ing from the re form for the peo ple em ployed in the healthcare sys tem in cluded:
· “loss of qual i fi ca tion” be cause of prob lems with the or gani sa tion and fi nanc ing of thepost grad u ate ed u ca tion (“com pli cated pro ce dure for spe ciali sa tion and qual i fi ca tion”,“dif fi cult and ex pen sive qual i fi ca tion”) and be cause of bureaucratisation of the med i -cal pro fes sion re sult ing from the in creased bulk of doc u men ta tion and the time themed i cal spe cial ists al lot ted to its com ple tion;
· the de struc tion of the uni fied func tion ing of the healthcare sys tem and the liq ui da -tion of the sep a rate sub sys tems (for ex am ple, the school healthcare was pointed out),the re duc tion of the con trol over the sys tem;
· in creased stress for the peo ple em ployed in healthcare re lated to “job cuts, in se cu -rity”, “over bur den ing”, “lack of free per sonal time”, “un cer tain in come”, “com mit -ment to eco nomic prob lems”;
The cre ation of con flicts among the med i cal pro fes sion als was also re ported as a neg a tivere sult from the re form, caused mainly by the in equal ity in the sal a ries of the gen eral prac ti tio -ners and the phy si cians in the hos pi tal care, but also due to a “de pend ence of the spe cial ists onthe gen eral prac ti tio ners”. Cor rup tion was also re ported as a neg a tive re sult from the re form.
Ac cord ing to the med i cal spe cial ists, the re form had led to neg a tive changes for the pa -tients most com monly re lated to:
· com pli cated ac cess to spe cial ised med i cal care and de te ri o rated or gani sa tion of the
201
So cio log i cal in ter pre ta tion
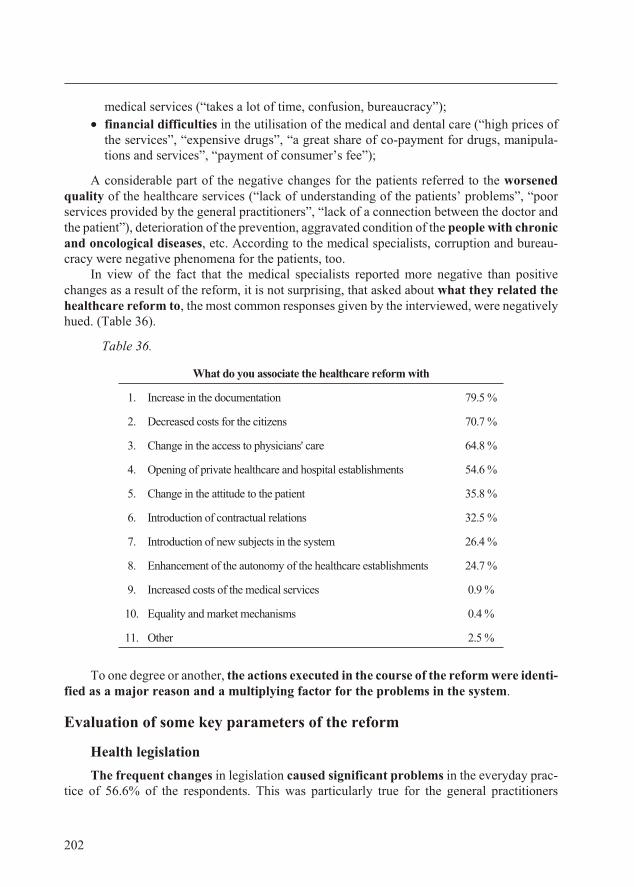
med i cal ser vices (“takes a lot of time, con fu sion, bu reau cracy”);
· fi nan cial dif fi cul ties in the uti li sa tion of the med i cal and den tal care (“high prices ofthe ser vices”, “ex pen sive drugs”, “a great share of co-pay ment for drugs, ma nip u la -tions and ser vices”, “pay ment of con sumer’s fee”);
A con sid er able part of the neg a tive changes for the pa tients re ferred to the wors enedqual ity of the healthcare ser vices (“lack of un der stand ing of the pa tients’ prob lems”, “poorser vices pro vided by the gen eral prac ti tio ners”, “lack of a con nec tion be tween the doc tor andthe pa tient”), de te ri o ra tion of the pre ven tion, ag gra vated con di tion of the peo ple with chronicand oncological dis eases, etc. Ac cord ing to the med i cal spe cial ists, cor rup tion and bu reau -cracy were neg a tive phe nom ena for the pa tients, too.
In view of the fact that the med i cal spe cial ists re ported more neg a tive than pos i tivechanges as a re sult of the re form, it is not sur pris ing, that asked about what they re lated thehealthcare re form to, the most com mon re sponses given by the in ter viewed, were neg a tivelyhued. (Table 36).
Table 36.
What do you associate the healthcare reform with
1. Increase in the documentation 79.5 %
2. Decreased costs for the citizens 70.7 %
3. Change in the access to physicians' care 64.8 %
4. Opening of private healthcare and hospital establishments 54.6 %
5. Change in the attitude to the patient 35.8 %
6. Introduction of contractual relations 32.5 %
7. Introduction of new subjects in the system 26.4 %
8. Enhancement of the autonomy of the healthcare establishments 24.7 %
9. Increased costs of the medical services 0.9 %
10. Equality and market mechanisms 0.4 %
11. Other 2.5 %
To one de gree or an other, the ac tions ex e cuted in the course of the re form were iden ti -fied as a ma jor rea son and a mul ti ply ing fac tor for the prob lems in the sys tem.
Eval u a tion of some key pa ram e ters of the re form
Health leg is la tion
The fre quent changes in leg is la tion caused sig nif i cant prob lems in the ev ery day prac -tice of 56.6% of the re spon dents. This was par tic u larly true for the gen eral prac ti tio ners
202
(69.3%) and the spe cial ists from the out pa tients’ care (69.2%). 20.3% of the in ter viewed con -firmed the pres ence of fre quent changes in leg is la tion, but for them, they were a sign of im -prove ment of the sys tem. In the dif fer ent groups, the per cent age was the high est of thespe cial ists from the hos pi tal care (28.3%), who con nected the leg is la tive changes with im -prove ments of the sys tem, fol lowed by the den tists (24.0%) and phar ma cists (21.1%).
The reg is tered fre quent changes in the nor ma tive reg u la tion as a source of con sid er ableprob lems in the prac tice of the re spon dents, in a sense, ac counted for the fact that 34.7% werewell-in formed about the new health leg is la tion. Still, the ma jor ity of the re spon dents def i nitely de clared (“yes” – 22.7%) or con di tion ally (“rather yes” – 42.6%), that they were in formed suf -fi ciently well about the normative regulation.
In ter ac tion and co or di na tion in the healthcare sys tem
To a large ex tent, the model of the in ter ac tion be tween the three cen tres of in flu encein the healthcare sys tem (the MH the NHIF, the UBP and UDB) was per ceived as faultyand full of con tra dic tions: lack of co or di na tion, de fence of lob by ist in ter ests, lack of uni fiedex change of in for ma tion.
Prob lems in the co or di na tion and the in ter ac tion among the in sti tu tional sub jectswere ob served at all the lev els of the sys tem. This prob lem was man i fested most dis tinctly inthe key in ter ac tions among the man age ment of the sys tem, the healthcare es tab lish mentsand the pro fes sional or gani sa tions which were cru cial re la tions in the healthcare sys tem.The in sti tu tional and prin ci ple di ver sity of the above three sub jects, in clud ing their con tra dict -ing in ter ests on var i ous as pects of healthcare, was a prerequisite for the poor coordination(Figure 4).
The in ter pre ta tion is im por tant of part of the re spon dents, ac cord ing to whom in the es tab -lish ment of struc tures in the sys tem a con struc tive de fect was made from a nor ma tive point ofview. In the or gani sa tion of the sys tem the em pha sis was placed on the re la tion ships of sub -or di na tion and con trol with out pro vid ing for the forms of in ter ac tion and part ner shipbe tween the var i ous or gani sa tions and in sti tu tions. In such a model, the prob lems with co -or di na tion were re pro duced in the in ter ac tion at all lev els of the sys tem.
The eval u a tion of the de vel op ment of the ad min is tra tive ca pac ity at the var i ous man -age ment lev els was also made pop u lar in the course of the re form. The num ber of the re spon -dents was al most equal be tween those who con sid ered that the man age ment ca pac ity hadin creased dur ing the course of the re form and those who con sid ered that there was no changein this re spect. The share was the high est among the med i cal pro fes sion als who reck oned thatat na tional and re gional level, the re form had not led to an in crease of the man age ment com pe -tences (36.0% for the na tional level and 40.0% for the re gional level, re spec tively). Ac cord ingto them the man age ment ca pac ity had in creased at lo cal level (at the level of the sep a ratehealthcare es tab lish ments – 36.2%). Only the phy si cians from the hos pi tal care dif fered fromthese re sults which were com mon for the var i ous pro fes sional groups. Ac cord ing to them theman age ment ca pac ity had in creased at all the three lev els of the sys tem – na tional (43.8%), re -gional (43.8%) and lo cal level (49.3%).
The as sess ment, given by the med i cal spe cial ists for the prep a ra tion of the man age mentper son nel, was rel a tively poor for the var i ous lev els of the sys tem at the start of the re form. The larg est part of the re spon dents gave a sat is fac tory mark to the man age ment per son nel from allthe three lev els of the sys tem. The fact is im pres sive that most of the very good eval u a tions
203
So cio log i cal in ter pre ta tion
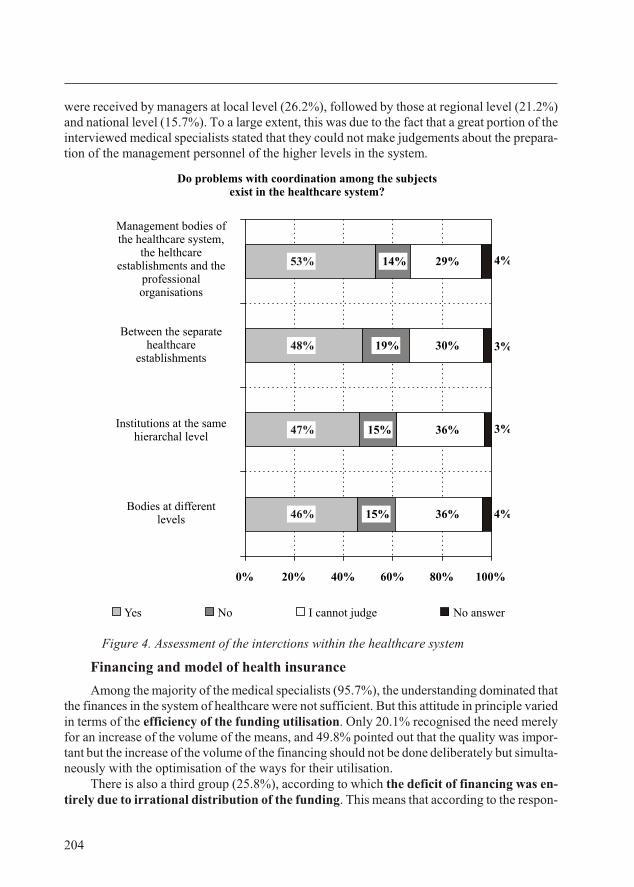
were re ceived by man ag ers at lo cal level (26.2%), fol lowed by those at re gional level (21.2%)and na tional level (15.7%). To a large ex tent, this was due to the fact that a great por tion of thein ter viewed med i cal spe cial ists stated that they could not make judge ments about the prep a ra -tion of the man age ment per son nel of the higher lev els in the sys tem.
Fig ure 4. Assessment of the interctions within the healthcare system
Fi nanc ing and model of health in sur ance
Among the ma jor ity of the med i cal spe cial ists (95.7%), the un der stand ing dom i nated that the fi nances in the sys tem of healthcare were not suf fi cient. But this at ti tude in prin ci ple var iedin terms of the ef fi ciency of the fund ing uti li sa tion. Only 20.1% re cog nised the need merelyfor an in crease of the vol ume of the means, and 49.8% pointed out that the qual ity was im por -tant but the in crease of the vol ume of the fi nanc ing should not be done de lib er ately but si mul ta -neously with the op ti mi sa tion of the ways for their uti li sa tion.
There is also a third group (25.8%), ac cord ing to which the def i cit of fi nanc ing was en -tirely due to ir ra tio nal dis tri bu tion of the fund ing. This means that ac cord ing to the re spon -
204
Do problems with coordination among the subjectsexist in the healthcare system?
46%
47%
48%
15%
15%
19%
14%
36%
36%
30%
29%53%
4%
3%
3%
4%
0% 20% 40% 60% 80% 100%
Bodies at different levels
Institutions at the same hierarchal level
Between the separate healthcare
establishments
Management bodies of the healthcare system,
the helthcare establishments and the
professional organisations
Yes No I cannot judge No answer
dents, if there were no con tent cri te ria and mea sures for ef fi ciency in the sys tem, the in creaseof the re sources would not lead to the im prove ment in the re sults in the healthcare sys tem. Inna tional di men sions, this the sis was shared by one fourth of the med i cal spe cial ists but amongthose work ing in So fia the sup port was in creased two fold.
Ir re spec tive of the dif fer ent ac cents on the prob lem and the ef fec tive ness of the fi nanc ing, the the sis of fi nan cial op ti mi sa tion was sup ported in prin ci ple by the ma jor ity of the em ployedin the healthcare sys tem. In this con text, the pos si ble start of a well-pre pared pol icy of in tro -duc ing ad e quate ap proaches for a ra tio nal uti li sa tion of the fi nances in the sys tem wouldre ceive sup port by the med i cal com mu nity.
The med i cal spe cial ists real ised the role of the state for in creas ing the size and im prov ing the ef fec tive ness of the fi nanc ing. Since the fi nan cial def i cit in the course of the sys tem’s ref or -ma tion was re ported par al lel to the with drawal of the state from its role of a ma jor reg u la tor ofhealthcare and the re duc tion of the fi nanc ing for the healthcare es tab lish ments, the prob lems in the sys tem were iden ti fied as a re sult from the lack of fi nan cial com mit ment of the state to thehealthcare sys tem. Be sides, the ma jor ity of the re spon dents de clare that the state has to have alead ing role in the fi nanc ing of the healthcare sys tem. Ac cord ing to 2.8% of the med i cal spe -cial ists the state had to en tirely with draw from the healthcare and for 10.7% its role in the fi -nanc ing had to be brought to a min i mum. For 71.6%, the par tic i pa tion of the state in thefi nanc ing was in suf fi cient that far and had to be ex tended and 12.7% even de clared thathealthcare had to be to tally cov ered by the state. The de fin ing fac tor in this at ti tude was the his -tor i cally de ter mined and sta ble ex pec ta tion for the fi nanc ing of the so cial field from the state bud get. The an swer to the ques tion why the “mem ory” about this tra di tion was so strong,could not be sought in the “mem ory” it self but in the cur rent prob lems in the sys tem re sult ingfrom dif fi cul ties gen er at ing fi nance for en sur ing the vi tal ity and flex i bil ity of the system.
In the views of the med i cal spe cial ists, the state epito mised a sta ble source of fi nanc ing, e.g.what they wanted was not so much “the state in the healthcare” but rather sta bil ity of fi nanc ing. Thiswas con firmed by the fact that, ir re spec tive of the sup port of the ma jor ity of the re spon dents for thestate par tic i pa tion in the fi nanc ing of healthcare, con cern ing the as sess ment of the model of so cialhealth in sur ance, the med i cal spe cial ists di vided in al most equal groups. The first group (46.2%) de -manded the sta bili sa tion of the oblig a tory health in sur ance and the sec ond group (47.8%) thoughtthat it would not be able to meet this re quire ment. To the ques tion: “Do you think that the model ofso cial health in sur ance is ap pro pri ate as a main source of fi nanc ing for hos pi tal care from the point ofview of the so cial and eco nomic de vel op ment of the so ci ety”, the med i cal spe cial ists re spond ing neg -a tively had a neg li gi ble prev a lence (“no” – 17.9% and “rather not” – 29.9%), to those who re sponded in the af fir ma tive (“yes” – 18.3% and “rather yes” – 27.9%).
De spite the di vi sion in terms of the as sess ment of the so cial health in sur ance as a mainsource of fi nanc ing for med i cal care, the ma jor ity of the med i cal spe cial ists (77.1%) unitedaround the view that it had to be car ried put by more than one fund. This meant that even thosewho did not con sider the model of so cial health in sur ance ap pro pri ate, in view of the so cial and eco nomic de vel op ment of so ci ety, they reck oned that with the in tro duc tion of com pet i tive re -la tions in the sys tem of the oblig a tory health in sur ance would en sure the sta bil ity of fi nanc ingsought by the med i cal spe cial ists.
The acute dis ap proval of the or gani sa tion of the healthcare sys tem and the fi nan cialmodel was ev i dent from the un der stand ing of the ma jor ity of the in ter viewed med i cal spe cial -ists (66.2%) that the or gani sa tion and the fi nan cial model cre ated ob jec tive pos si bil i ties for
205
So cio log i cal in ter pre ta tion
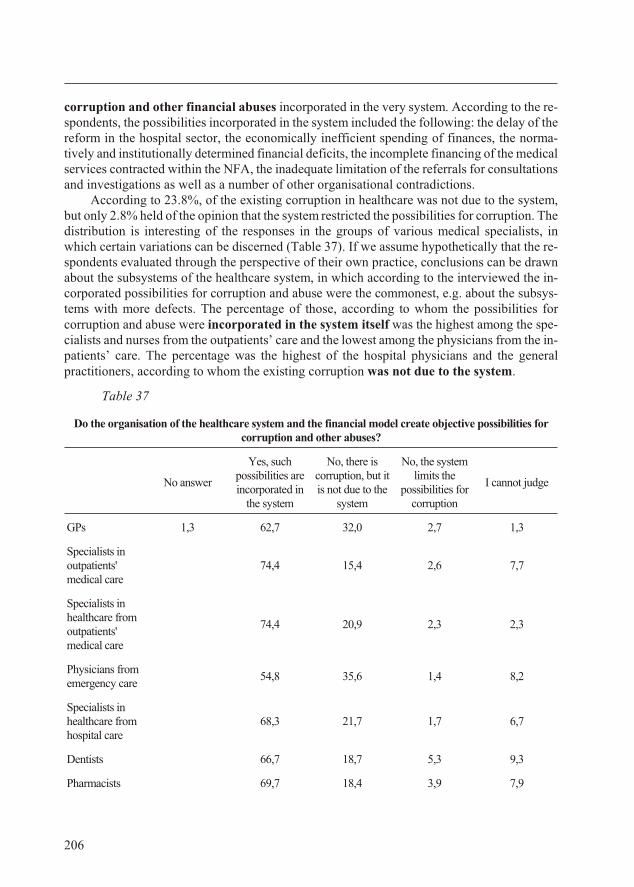
cor rup tion and other fi nan cial abuses in cor po rated in the very sys tem. Ac cord ing to the re -spon dents, the pos si bil i ties in cor po rated in the sys tem in cluded the fol low ing: the de lay of there form in the hos pi tal sec tor, the eco nom i cally in ef fi cient spend ing of fi nances, the nor ma -tively and in sti tu tion ally de ter mined fi nan cial def i cits, the in com plete fi nanc ing of the med i cal ser vices con tracted within the NFA, the in ad e quate lim i ta tion of the re fer rals for con sul ta tionsand in ves ti ga tions as well as a num ber of other or gani sa tional con tra dic tions.
Ac cord ing to 23.8%, of the ex ist ing cor rup tion in healthcare was not due to the sys tem,but only 2.8% held of the opin ion that the sys tem re stricted the pos si bil i ties for cor rup tion. The dis tri bu tion is in ter est ing of the re sponses in the groups of var i ous med i cal spe cial ists, inwhich cer tain vari a tions can be dis cerned (Ta ble 37). If we as sume hy po thet i cally that the re -spon dents eval u ated through the per spec tive of their own prac tice, con clu sions can be drawnabout the sub sys tems of the healthcare sys tem, in which ac cord ing to the in ter viewed the in -cor po rated pos si bil i ties for cor rup tion and abuse were the com mon est, e.g. about the sub sys -tems with more de fects. The per cent age of those, ac cord ing to whom the pos si bil i ties forcor rup tion and abuse were in cor po rated in the sys tem it self was the high est among the spe -cial ists and nurses from the out pa tients’ care and the low est among the phy si cians from the in -pa tients’ care. The per cent age was the high est of the hos pi tal phy si cians and the gen eralprac ti tio ners, ac cord ing to whom the ex ist ing cor rup tion was not due to the system.
Table 37
Do the organisation of the healthcare system and the financial model create objective possibilities forcorruption and other abuses?
No answer
Yes, suchpossibilities areincorporated in
the system
No, there iscorruption, but itis not due to the
system
No, the systemlimits the
possibilities forcorruption
I cannot judge
GPs 1,3 62,7 32,0 2,7 1,3
Spe cial ists inout pa tients'med i cal care
74,4 15,4 2,6 7,7
Spe cial ists inhealthcare fromout pa tients'med i cal care
74,4 20,9 2,3 2,3
Phy si cians fromemer gency care
54,8 35,6 1,4 8,2
Spe cial ists inhealthcare fromhos pi tal care
68,3 21,7 1,7 6,7
Den tists 66,7 18,7 5,3 9,3
Pharmacists 69,7 18,4 3,9 7,9
206
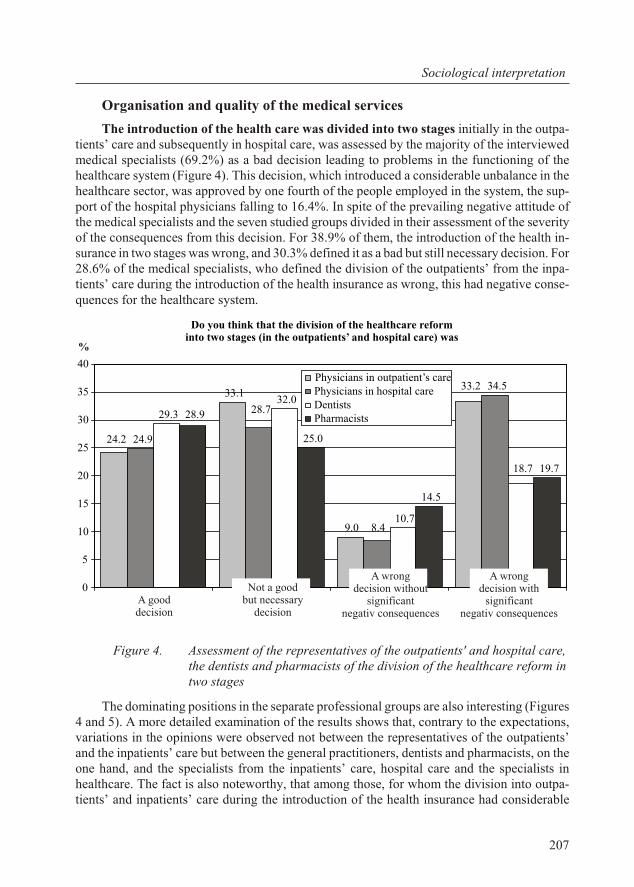
Or gani sa tion and qual ity of the med i cal ser vices
The in tro duc tion of the health care was di vided into two stages ini tially in the out pa -tients’ care and sub se quently in hos pi tal care, was as sessed by the ma jor ity of the in ter viewedmed i cal spe cial ists (69.2%) as a bad de ci sion lead ing to prob lems in the func tion ing of thehealthcare sys tem (Fig ure 4). This de ci sion, which in tro duced a con sid er able un bal ance in thehealthcare sec tor, was ap proved by one fourth of the peo ple em ployed in the sys tem, the sup -port of the hos pi tal phy si cians fall ing to 16.4%. In spite of the pre vail ing neg a tive at ti tude ofthe med i cal spe cial ists and the seven stud ied groups di vided in their as sess ment of the se ver ityof the con se quences from this de ci sion. For 38.9% of them, the in tro duc tion of the health in -sur ance in two stages was wrong, and 30.3% de fined it as a bad but still nec es sary de ci sion. For 28.6% of the med i cal spe cial ists, who de fined the di vi sion of the out pa tients’ from the in pa -tients’ care dur ing the in tro duc tion of the health in sur ance as wrong, this had neg a tive con se -quences for the healthcare sys tem.
Fig ure 4. Assessment of the representatives of the outpatients' and hospital care,the dentists and pharmacists of the division of the healthcare reform in two stages
The dom i nat ing po si tions in the sep a rate pro fes sional groups are also in ter est ing (Fig ures4 and 5). A more de tailed ex am i na tion of the re sults shows that, con trary to the ex pec ta tions,vari a tions in the opin ions were ob served not be tween the rep re sen ta tives of the out pa tients’and the in pa tients’ care but be tween the gen eral prac ti tio ners, den tists and phar ma cists, on theone hand, and the spe cial ists from the in pa tients’ care, hos pi tal care and the spe cial ists inhealthcare. The fact is also note wor thy, that among those, for whom the di vi sion into out pa -tients’ and in pa tients’ care dur ing the in tro duc tion of the health in sur ance had con sid er able
207
So cio log i cal in ter pre ta tion
24.2
33.1
9.0
33.2
24.9
28.7
8.4
34.5
29.3
32.0
10.7
18.7
28.9
25.0
14.5
19.7
0
5
10
15
20
25
30
35
40Physicians in outpatient’s carePhysicians in hospital careDentistsPharmacists
A gooddecision
Not a goodbut necessary
decision
A wrongdecision without
significantnegativ consequences
A wrongdecision with
significantnegativ consequences
%
Do you think that the division of the healthcare reforminto two stages (in the outpatients’ and hospital care) was
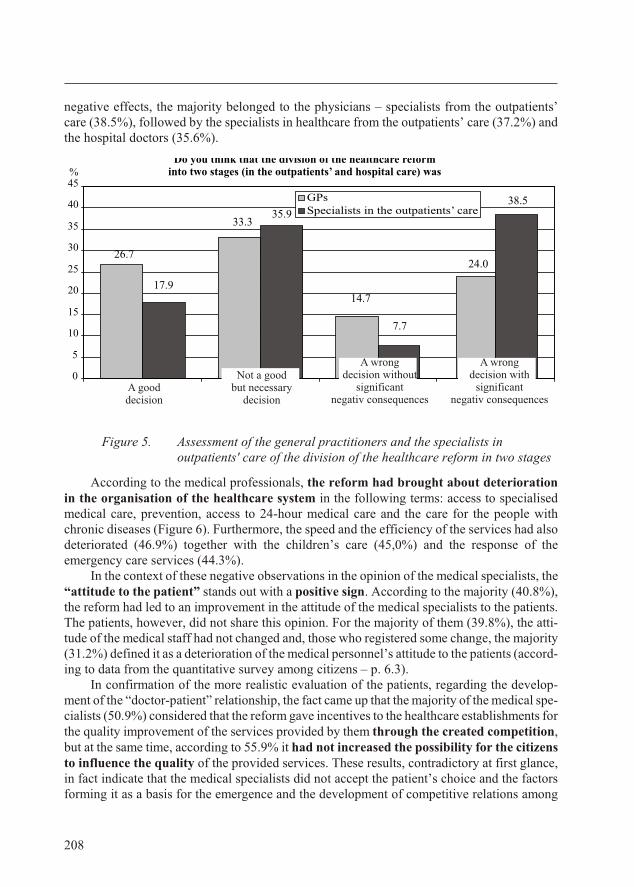
neg a tive ef fects, the ma jor ity be longed to the phy si cians – spe cial ists from the out pa tients’care (38.5%), fol lowed by the spe cial ists in healthcare from the outpatients’ care (37.2%) andthe hospital doctors (35.6%).
Figure 5. Assessment of the general practitioners and the specialists inoutpatients' care of the division of the healthcare reform in two stages
Ac cord ing to the med i cal pro fes sion als, the re form had brought about de te ri o ra tionin the or gani sa tion of the healthcare sys tem in the fol low ing terms: ac cess to spe cial isedmed i cal care, pre ven tion, ac cess to 24-hour med i cal care and the care for the peo ple withchronic dis eases (Fig ure 6). Fur ther more, the speed and the ef fi ciency of the ser vices had alsode te ri o rated (46.9%) to gether with the chil dren’s care (45,0%) and the re sponse of theemergency care services (44.3%).
In the con text of these neg a tive ob ser va tions in the opin ion of the med i cal spe cial ists, the“at ti tude to the pa tient” stands out with a pos i tive sign. Ac cord ing to the ma jor ity (40.8%),the re form had led to an im prove ment in the at ti tude of the med i cal spe cial ists to the pa tients.The pa tients, how ever, did not share this opin ion. For the ma jor ity of them (39.8%), the at ti -tude of the med i cal staff had not changed and, those who reg is tered some change, the ma jor ity(31.2%) de fined it as a de te ri o ra tion of the med i cal per son nel’s at ti tude to the pa tients (ac cord -ing to data from the quan ti ta tive sur vey among cit i zens – p. 6.3).
In con fir ma tion of the more re al is tic eval u a tion of the pa tients, re gard ing the de vel op -ment of the “doc tor-pa tient” re la tion ship, the fact came up that the ma jor ity of the med i cal spe -cial ists (50.9%) con sid ered that the re form gave in cen tives to the healthcare es tab lish ments for the qual ity im prove ment of the ser vices pro vided by them through the cre ated com pe ti tion,but at the same time, ac cord ing to 55.9% it had not in creased the pos si bil ity for the cit i zensto in flu ence the qual ity of the pro vided ser vices. These re sults, con tra dic tory at first glance,in fact in di cate that the med i cal spe cial ists did not ac cept the pa tient’s choice and the fac torsform ing it as a ba sis for the emer gence and the de vel op ment of com pet i tive re la tions among
208
0
5
10
15
20
25
30
35
40
45
GPsSpecialists in the outpatients’ care
%
33.3
14.7
24.0
17.9
38.5
26.7
35.9
7.7
Do you think that the division of the healthcare reforminto two stages (in the outpatients’ and hospital care) was
A gooddecision
Not a goodbut necessary
decision
A wrongdecision without
significantnegativ consequences
A wrongdecision with
significantnegativ consequences
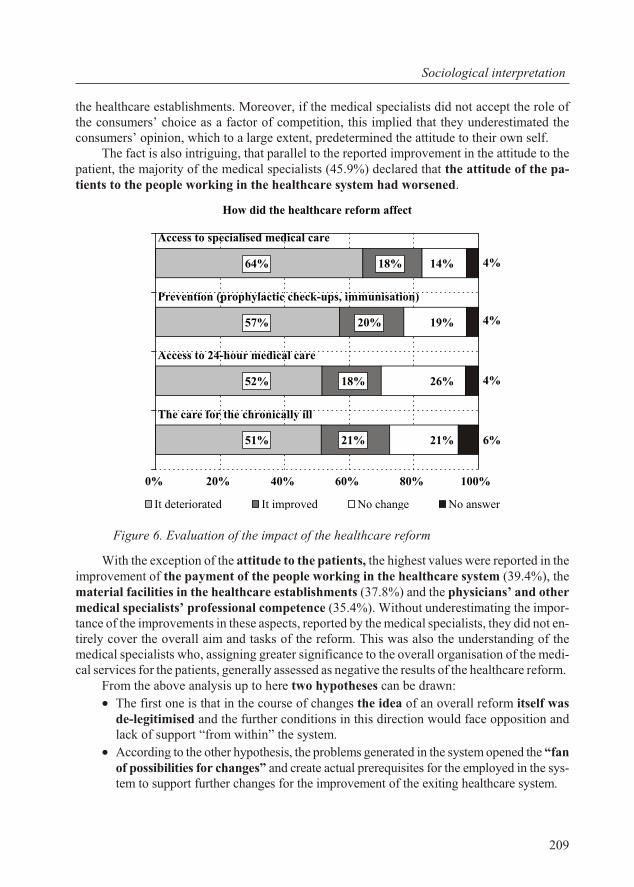
the healthcare es tab lish ments. More over, if the med i cal spe cial ists did not ac cept the role ofthe con sum ers’ choice as a fac tor of com pe ti tion, this im plied that they un der es ti mated thecon sum ers’ opin ion, which to a large ex tent, pre de ter mined the at ti tude to their own self.
The fact is also in trigu ing, that par al lel to the re ported im prove ment in the at ti tude to thepa tient, the ma jor ity of the med i cal spe cial ists (45.9%) de clared that the at ti tude of the pa -tients to the peo ple work ing in the healthcare sys tem had wors ened.
Fig ure 6. Evaluation of the impact of the healthcare reform
With the ex cep tion of the at ti tude to the pa tients, the high est val ues were re ported in theim prove ment of the pay ment of the peo ple work ing in the healthcare sys tem (39.4%), thema te rial fa cil i ties in the healthcare es tab lish ments (37.8%) and the phy si cians’ and othermed i cal spe cial ists’ pro fes sional com pe tence (35.4%). With out un der es ti mat ing the im por -tance of the im prove ments in these as pects, re ported by the med i cal spe cial ists, they did not en -tirely cover the over all aim and tasks of the re form. This was also the un der stand ing of themed i cal spe cial ists who, as sign ing greater sig nif i cance to the over all or gani sa tion of the med i -cal ser vices for the pa tients, gen er ally as sessed as neg a tive the re sults of the healthcare re form.
From the above anal y sis up to here two hy poth e ses can be drawn:
· The first one is that in the course of changes the idea of an over all re form it self wasde-le giti mised and the fur ther con di tions in this di rec tion would face op po si tion andlack of sup port “from within” the sys tem.
· Ac cord ing to the other hy poth e sis, the prob lems gen er ated in the sys tem opened the “fan of pos si bil i ties for changes” and cre ate ac tual pre req ui sites for the em ployed in the sys -tem to sup port fur ther changes for the im prove ment of the ex it ing healthcare sys tem.
209
So cio log i cal in ter pre ta tion
How did the healthcare reform affect
51%
52%
57%
64%
21%
18%
20%
18%
21%
26%
19%
14%
6%
4%
4%
4%
0% 20% 40% 60% 80% 100%
The care for the chronically ill
Access to 24-hour medical care
Prevention (prophylactic check-ups, immunisation)
Access to specialised medical care
It deteriorated It improved No change No answer
The re sults from the study in di cated that the sec ond hy poth e sis was more re al is tic. In thefol low ing pages we will pres ent the changes in the sys tem which, if prop erly planned and in -tro duced, would gain ac tual in ter nal sup port, e.g. what changes in the sys tem would be ap -proved by the med i cal com mu nity and would have the chance of be ing to be suc cess fullyac com plished. The re sults from the study also showed in what way the in ter ested groups inhealthcare would iden tify a cer tain pro-re form ist pol icy de pend ing on their in ter ests, ex pec ta -tions and at ti tudes to col lab o ra tion or op po si tion against some fu ture changes or oth ers.
Pros pects for the healthcare re form
De vel op ment of com pet i tive re la tions
The med i cal spe cial ists (71.8%) per ceived the pos si bil ity for the cit i zens to freelychoose a fund for oblig a tory health in sur ance as a main pri or ity of the change in thehealthcare sys tem. The sur vey among cit i zens (p.6.3) dem on strated that the prob lem con sistednot so much in the mo nop o lis tic sta tus of the NHIF in the ad min is tra tion of the health in sur -ance but in the ab sence of a con nec tion be tween the in vested funds and the fi nal health prod -uct. To a large de gree, this de-mo ti vated the cit i zens to pay their health in sur ance in stal ments.
In this con text, the opin ion com monly held (77.1%) by the med i cal spe cial ists was log i cal that the oblig a tory health in sur ance had to be car ried out by more than one health in sur -ance fund. More over, the ex pec ta tion was that fi nan cial in stru ments were cre ated, through which the cit i zens could in flu ence the func tion ing of the sys tem. Ac cord ing to the med i calspe cial ists, this was the way for in creas ing the pos si bil i ties for the cit i zens to in flu ence also thequal ity of the health ser vices. It is note wor thy, that the med i cal spe cial ists linked the pos si bil i -ties of the cit i zens to in flu ence the qual ity of the health ser vices to the choice of a health in sur -ance fund rather than to the choice of a healthcare es tab lish ment. This proved that, in the mindof the med i cal spe cial ists, the mo nop o lis tic sta tus of the NHIF im peded or, gen er ally, did notfa cil i tate the qual ity im prove ment of the med i cal ser vices.
Changes in the fi nanc ing and or ga ni za tion of the med i cal care
To gether with the in tro duc tion of a free choice of a fund for com pul sory health in sur ancefor the cit i zens, as pri or i ties in the de vel op ment of the sys tem to one de gree or an other, themed i cal spe cial ists in di cated changes in some as pects of the or gani sa tion of med i cal care andan in crease in the fi nan cial re sources al lo cated for healthcare (Ta ble 38).
Ac cord ing to the med i cal spe cial ists, for the in crease of the fi nan cial re sources al lo cated for healthcare, a more ac cept able vari ant was to in crease the funds which the state al lo cated as com -pared to the in crease of the health in sur ance in stal ments. In the sep a rate groups the per cent agewas dif fer ent for those who sup ported the in crease in the health in sur ance in stal ments var ied inquite broad lim its – from 2.3% of the spe cial ists in healthcare from the out pa tients’ care up to33.3% of the phy si cians – spe cial ists from the out pa tients’ care. Al though the phy si cians’ (GPs,spe cial ists, hos pi tal doc tors) and den tists’ sup port for the in crease of the amount of the pre mi ums as a whole was not neg li gi ble, still much greater was the num ber of those wish ing for the in crease of the fi nanc ing from the state (over 60% for each of the pro fes sional group).
210
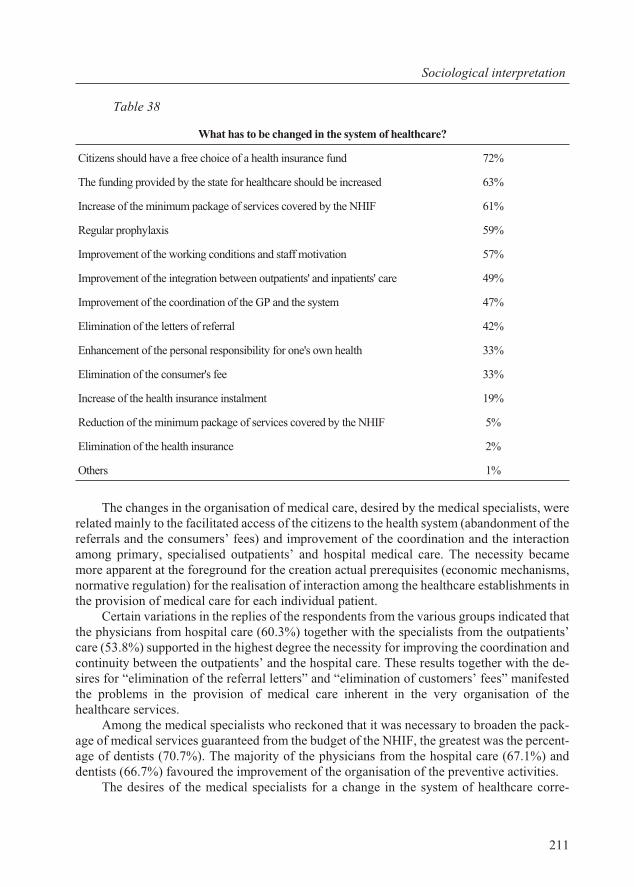
Table 38
What has to be changed in the system of healthcare?
Citizens should have a free choice of a health insurance fund 72%
The funding provided by the state for healthcare should be increased 63%
Increase of the minimum package of services covered by the NHIF 61%
Regular prophylaxis 59%
Improvement of the working conditions and staff motivation 57%
Improvement of the integration between outpatients' and inpatients' care 49%
Improvement of the coordination of the GP and the system 47%
Elimination of the letters of referral 42%
Enhancement of the personal responsibility for one's own health 33%
Elimination of the consumer's fee 33%
Increase of the health insurance instalment 19%
Reduction of the minimum package of services covered by the NHIF 5%
Elimination of the health insurance 2%
Others 1%
The changes in the or gani sa tion of med i cal care, de sired by the med i cal spe cial ists, werere lated mainly to the fa cil i tated ac cess of the cit i zens to the health sys tem (aban don ment of there fer rals and the con sum ers’ fees) and im prove ment of the co or di na tion and the in ter ac tionamong pri mary, spe cial ised out pa tients’ and hos pi tal med i cal care. The ne ces sity be camemore ap par ent at the fore ground for the cre ation ac tual pre req ui sites (eco nomic mech a nisms,nor ma tive reg u la tion) for the reali sa tion of in ter ac tion among the healthcare es tab lish ments inthe pro vi sion of med i cal care for each in di vid ual pa tient.
Cer tain vari a tions in the re plies of the re spon dents from the var i ous groups in di cated thatthe phy si cians from hos pi tal care (60.3%) to gether with the spe cial ists from the out pa tients’care (53.8%) sup ported in the high est de gree the ne ces sity for im prov ing the co or di na tion andcon ti nu ity be tween the out pa tients’ and the hos pi tal care. These re sults to gether with the de -sires for “elim i na tion of the re fer ral let ters” and “elim i na tion of cus tom ers’ fees” man i festedthe prob lems in the pro vi sion of med i cal care in her ent in the very or gani sa tion of thehealthcare ser vices.
Among the med i cal spe cial ists who reck oned that it was nec es sary to broaden the pack -age of med i cal ser vices guar an teed from the bud get of the NHIF, the great est was the per cent -age of den tists (70.7%). The ma jor ity of the phy si cians from the hos pi tal care (67.1%) andden tists (66.7%) fa voured the im prove ment of the or gani sa tion of the pre ven tive ac tiv i ties.
The de sires of the med i cal spe cial ists for a change in the sys tem of healthcare cor re -
211
So cio log i cal in ter pre ta tion
sponded to the pri or i ties de fined by them. The pri or i ties of the healthcare sys tem as de fined bythe med i cal spe cial ists in cluded:
· 48.6% re ferred to spe cific health pro tec tion ac tiv i ties (pro phy laxis, pre ven tion, re ha -bil i ta tion, den tal ser vices) and groups of the pop u la tion with spe cific health needs(chil dren, preg nant women and moth ers, peo ple with chronic and oncological dis eases, ru ral pop u la tion);
· 28.3% re ferred to the ac cess of the pa tients to the healthcare sys tem (“free ac cess to aspe cial ist, hos pi tal, in ves ti ga tion”, “elim i na tion of the re fer rals to spe cial ists”, “elim i -na tion of con sum ers’ fees”) and the or gani sa tion of med i cal care (“co or di na tion be -tween the out pa tients’ and in pa tients’ care”);
· 9.8% re ferred to the fi nanc ing of healthcare (“in crease of the fund ing”, “ra tio nal uti li -sa tion of the fund ing”, “ex emp tion of the drugs from VAT”);
· 7.1% re ferred to the pack ages of med i cal ac tiv i ties guar an teed from the NHIF bud get(“ex tend ing the min i mum pack age”, “ex tend ing the clin i cal path ways”, “ex tend ing the den tal pack age”);
· 4.8% of the in di cated pri or i ties re ferred to the new med i cal and in for ma tion tech nol o -gies and the im prove ment of the ma te rial fa cil i ties;
· 1.4% of the pri or i ties re ferred to the state pol icy (“change of the state pol icy inhealthcare”, “strict con trol by the MH”, “liq ui da tion of the so cial model of health in -sur ance pre mi ums”, “law on do na tion”, “Eu ro pean in te gra tion”).
The pri or i ties of the healthcare sys tem should arise from the health needs of the pop u la -tion. In this light, the pri or i ties were in cluded in the first and larg est group. The re main ing ones were re lated rather to the pri or i ties for chang ing the ex ist ing healthcare sys tem, i.e. the pri or i -ties of the re form. Even though, their dis cus sion here throws ad di tional light on the views ofthe med i cal spe cial ists on the de vel op ment of the re form or con firmed their de sires for changeal ready in di cated. Fur ther more, the re sults on this is sue showed that, to some ex tent, the med i -cal spe cial ists equa lise the func tion ing of the sys tem with its ref or ma tion. As the re spon dentsin di cated more than one pri or ity for the healthcare sys tem, it can be also as sumed that ac cord -ing to the med i cal spe cial ists, the pri or i ties re fer ring to the re form were in fact the means to theachieve ment of the goals of the healthcare sys tem.
Changes in healthcare leg is la tion
In spite of the pre vail ing neg a tive at ti tudes to the fre quent changes in leg is la tion, thegreater part of the re spon dents con sid ered that con sid er able changes were nec es sary in the nor -ma tive ba sis be cause of the se ri ous con tra dic tions con tained in it (28.8%) as well as be cause of the need for con sid er able ad di tions (17.7%). The peo ple work ing in the cap i tal and the big gercit ies ex pressed a more pro nounced de sire for nor ma tive changes. Less than one fourth of there spon dents (23.4%) de fined the pres ent leg is la tion as good enough and there fore, they did not think that sig nif i cant changes were nec es sary, and 12.2% thought that only small cor rec tionswould suf fice.
The changes in leg is la tion pro posed by the re spon dents, ac cord ing to whom only par tialchanges were nec es sary, re ferred to the reg u la tion of the in ter ac tion be tween the dif fer ent di vi -sions of the healthcare sys tem, the reg u la tion of rights cor re spond ing to the nor ma tively de -
212
fined li a bil i ties, and other is sues re lated to the fi nanc ing of the healthcare es tab lish ments andthe ac cess to spe cial ised out pa tients’ care. Those of the re spon dents, who con sid ered that there was es sen tial con tra dic tion in the cur rent leg is la tion, also de manded changes in it, re gard ingac cess and fi nanc ing.
Change of the prin ci ples and the ob jec tives of the con tract ing pro cess
The great ma jor ity (77.1%) of the in ter viewed med i cal spe cial ists were of the opin ion that the reg u la tion of the re la tions in the sys tem and guar an tee ing its sta bil ity re quired a Na tionalframe work agree ment. This, in its turn, meant that ac cord ing to the med i cal spe cial ists, thehealthcare sys tem had not yet formed in ter nal mech a nisms for self-reg u la tion al low ing for dy -namic con tract ing be tween the healthcare es tab lish ments and the NHIF. In ad di tion, a num berof spe cific fea tures of the health ser vices and the sig nif i cant pub lic ef fects en tailed by thehealth sta tus of the pop u la tion, did not al low for the in tro duc tion of the purely mar ket prin ci -ples in the sys tem. This re quired the reg u la tion of these re la tion ships in a more gen eral frame -work of na tional con tract ing.
At the same time, only 9.6% ap proved of the frame work agree ment in its cur rent form.22.3% in di cated as a prob lem not the agree ment it self but its an nual sign ing and pro posed that itwas car ried out at a lon ger in ter val of time. Ac cord ing to the main part (56.7%) of the in ter -viewed med i cal spe cial ists, the NFA should be de vised in a more gen eral form by de fin ingonly the prin ci ple con di tions. Fur ther more, the de sire of the med i cal spe cial ists be came ob vi -ous, for the cre ation of pos si bil i ties for the for ma tion of long-term con tract ing re la tions, which could not be ef fected at that mo ment since the con tract was signed on an an nual ba sis. Ac cord ingto the med i cal spe cial ists, even if these changes did not re flect lob by ists’ in ter ests of par ties in ter -ested in the con tract but they cor re sponded to the dy namic re la tion ships in the field of healthcare, they had a neg a tive ef fect on the ac tiv ity of the healthcare es tab lish ments and the agree ments it -self was per ceived as a me chan i cal im pos ing of for mal re quire ments and cri te ria.
To a large ex tent, the dis ap proval of the NFA among the pro fes sional groups in healthcare was due to the par ties in volved in the ne go ti a tion pro cess. The main share of the re spon dents(47.3%) con sid ered that other or gani sa tions should also par tic i pate in the pro cess of prep -a ra tion and sign ing of the agree ment. 20.5% were of the op po site opin ion and an other group equal in size (20.7%) ad mit ted that they could not judge. A very small por tion of those, whocon sid ered that other par ties should be in volved in the ne go ti a tions, came up with ac tual sug -ges tions in this re spect. Nev er the less, some of the pro pos als in cluded the Un ion of Bul gar ianPhar ma cists and rep re sen ta tives of phar ma ceu ti cal com pa nies as well as as so ci a tions and un -ions of the phy si cians-spe cial ists, gen eral prac ti tio ners and spe cial ists in healthcare, civil or -gani sa tions. Fol low ing this logic, the con clu sion may be drawn that the med i cal spe cial istsac cepted rep re sen ta tives of healthcare es tab lish ments rather than pro fes sional rep re sen ta tivesas par ties to the frame work agree ment.
Privatisation of healthcare es tab lish ments
The at ti tude of the med i cal spe cial ists to the privatisation of the healthcare es tab lish ments was rather re served.
The main part of the spe cial ists in healthcare (45.4%) and the phy si cians (36.2%) were ofthe opin ion that privatisation was a nec es sary step but it should be car ried out at a later stage in
213
So cio log i cal in ter pre ta tion
the de vel op ment of the sys tem. Only in cit ies like Bourgas, Russe, Stara Zagora and partly inSo fia, privatisation was de fined on a mass ba sis as a pri or ity in the de vel op ment of the sys -tem. On the con trary, in rel a tively smaller cit ies like Turgovishte, Vratsa, Pazardjik, Gabrovo,Lovech but also in Shumen and Dobrich, privatisation was deemed as dan ger ous for thefunc tion ing of the sys tem.
The healthcare es tab lish ments should not be pri va tised ac cord ing to 34.7% of the gen eralprac ti tio ners, 26.0% of the hos pi tal doc tors, 23.7% of the spe cial ists in healthcare and 18.9%of the spe cial ists in out pa tients’ care.
As re gards the way in which privatisation should be car ried out, the opin ions of the med i -cal spe cial ists di vided into three pos si bil i ties:
· privatisation of all healthcare es tab lish ments with the pres er va tion of their ac tiv i ties(26.6% of the phy si cians and 20.6% of the spe cial ists in healthcare);
· privatisation of sep a rate healthcare es tab lish ments (14.4% of the phy si cians and12.4% of the spe cial ists in healthcare);
· privatisation of shares of the healthcare es tab lish ments (21.3% of the phy si cians and28.9% of the spe cial ists in healthcare).
Privatisation im plied in de pend ent and re spon si ble en ter ing into com pet i tive and risk mar -ket en vi ron ment. That was why, and in view of the prob lems in the healthcare sys tem reg is -tered by the med i cal spe cial ists, the lat ter saw privatisation as a risk both for the ex is tence ofthe healthcare es tab lish ments and for their own fu ture in them. This con clu sion was con firmedby the fact that, ac cord ing to the ma jor ity of the med i cal spe cial ists, ir re spec tive of whetherthey sup ported the privatisation of the healthcare es tab lish ments or not and ir re spec tive of theway it was car ried out, it should be done with pref er ences for the staff work ing in them. This view was held by 78.4% of the spe cial ists in out pa tients’ care, 64.9% of the spe cial ists inhealthcare, 58.9% of the phy si cians in hos pi tals and 54.7% of the gen eral prac ti tio ners.
De moc ra ti sa tion of the pro fes sional or gani sa tions
The ma jor ity of the phy si cians and the den tists united for changes in the sta tus of theirmem ber ship in the re spec tive pro fes sional or gani sa tion as well as for the ways of its func tion -ing. 41.5% of the in ter viewed phy si cians and 33.3% of the den tists did not think that theirmem ber ship in the pro fes sional or gani sa tion should be oblig a tory, and 29.3% of the phy si -cians and 20.0% of the den tists ap proved the oblig a tory mem ber ship but on terms, dif fer entfrom the cur rent ones. For 27.1% of the phy si cians, the mem ber ship in UBP was a nec es sarycon di tion for their pro fes sion as a whole. 33.3% of the dentists shared a similar opinion.
The spe cial ists in healthcare also dis ap proved the idea that the mem ber ship in their pro -fes sional as so ci a tion was man da tory. In the mean time, the ma jor ity of them (62.9%) de claredthat the As so ci a tion of the pro fes sion als in healthcare should be leg is la tively granted a greaterop por tu nity to de fend the in ter ests of the pro fes sion, and 24.7% con sid ered that the As so ci a -tion should par tic i pate in the negotiating at national level.
As com pared to the rest of the pro fes sional groups, the per cent age of the phar ma cists washigher, hold ing the opin ion that their mem ber ship in their pro fes sional or gani sa tion should beoblig a tory. Sim i lar to the spe cial ists in healthcare, the phar ma cists, too, pro claimed them -selves for greater pos si bil i ties for their pro fes sional or gani sa tion to pro tect their rights (65.8%) and its in volve ment in the con tract ing at national level (55.3%).
214
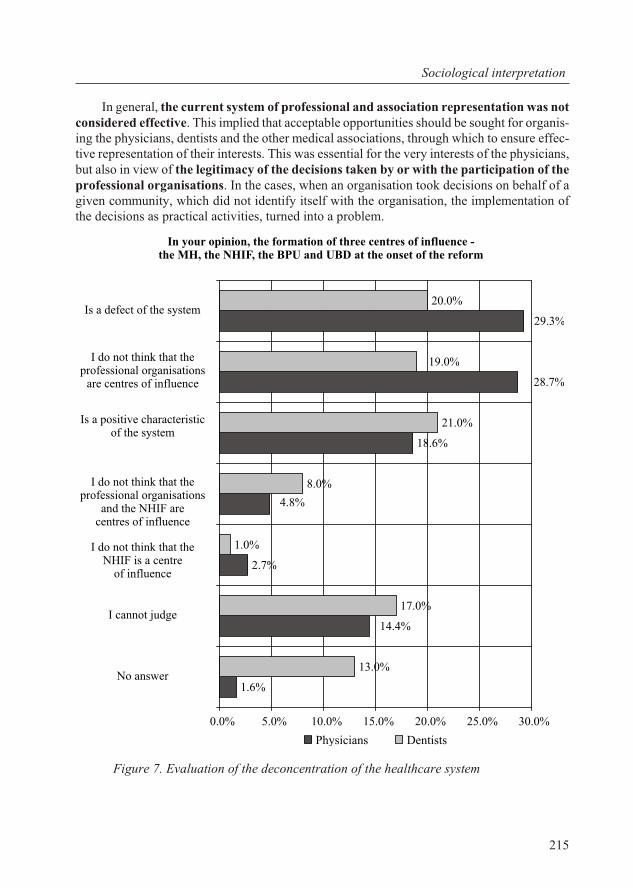
In gen eral, the cur rent sys tem of pro fes sional and as so ci a tion rep re sen ta tion was notcon sid ered ef fec tive. This im plied that ac cept able op por tu ni ties should be sought for or gan is -ing the phy si cians, den tists and the other med i cal as so ci a tions, through which to en sure ef fec -tive rep re sen ta tion of their in ter ests. This was es sen tial for the very in ter ests of the phy si cians,but also in view of the le git i macy of the de ci sions taken by or with the par tic i pa tion of thepro fes sional or gani sa tions. In the cases, when an or gani sa tion took de ci sions on be half of agiven com mu nity, which did not iden tify it self with the or gani sa tion, the im ple men ta tion ofthe decisions as practical activities, turned into a problem.
Fig ure 7. Evaluation of the deconcentration of the healthcare system
215
So cio log i cal in ter pre ta tion
In your opinion, the formation of three centres of influence -the MH, the NHIF, the BPU and UBD at the onset of the reform
1.6%
2.7%
18.6%
13.0%
17.0%
1.0%
8.0%
21.0%
20.0%
14.4%
28.7%
29.3%
4.8%
19.0%
0.0% 5.0% 10.0% 15.0% 20.0% 25.0% 30.0%
No answer
I cannot judge
I do not think that theNHIF is a centre
of influence
I do not think that theprofessional organisations
and the NHIF arecentres of influence
Is a positive characteristicof the system
I do not think that theprofessional organisations
are centres of influence
Is a defect of the system
Physicians Dentists
The for ma tion of three cen tres of in flu ence in the healthcare sys tem – the MH, theNHIF, the UBP and UDB was ac cepted with mixed feel ings with the start of the health in sur -ance. The share was al most equal of those phy si cians and den tists, who reck oned it as a de fectof the sys tem with neg a tive con se quences on its func tion ing, and those who did not re cog nisethe pro fes sional or gani sa tions as cen tres of in flu ence (Fig ure 7).
The per cent age should not be ne glected of med i cal spe cial ists, ac cord ing to whom thedis tri bu tion of power in the sys tem was a pos i tive fea ture. This re sult was likely to be due to the med i cal spe cial ists’ un der stand ing that the for ma tion of the three cen tres of in flu ence was aman i fes ta tion of de cen trali sa tion in the sys tem (which in it self was at the core of the healthcarere form goals) and the need for rep re sen ta tion and pro tec tion of the in ter ests of the involvedparties at national level.
On the other hand, the in flu ence (rights) pos sessed with out a clear and ad e quate def i ni -tion of re spon si bil i ties, prob a bly forced the larger por tion of the phy si cians and den tists to de -ter mine the for ma tion of the three cen tres of power as a defect of the system.
6.2. As sess ment by man age ment sub jects
Gen eral as sess ment of the healthcare re form
Ac cord ing to the dom i nat ing po si tion, shared by the man age ment sub jects in healthcare,the func tion ing of the healthcare sys tem in Bul garia in 1990s was ac com pa nied by mas siveprob lems which ne ces si tated the con duct ing of an over all trans for ma tion of the mod els of ahealthcare system.
Sev eral the ses ex isted about the cir cum stances which at the end of 1990s ne ces si tated theref or ma tion of the healthcare sys tem to a qual i ta tively new level.
Above all, this meant chang ing the state and the socio-po lit i cal model af ter 1989 which ne ces si tated the trans for ma tion of the prin ci ples of the healthcare re form (“The so cial ist andcom mu nist stage is over. We en tered into a stage of cap i tal ism and it can not be based on a so -cial ist model of healthcare…” – Di rec tor of a spe cial ised hos pi tal for active treatment).
The pro po nents of this the sis drew con crete prin ci ples of the pre vi ous healthcare sys tem,con tra dict ing the re la tion ships and prac tices valid for the coun try. One of the re pet i tive pointswas the im pos si bil ity to have a “free so cial ist healthcare” and dom i nat ing state and ad min is tra -tive in ter fer ence un der con di tions of mar ket mech a nisms for the reg u la tion and the en force -ment of the prin ci ple of com pe ti tion in the pub lic sec tor. There fore, the func tion ing of the oldsys tem un der the new con di tions was as sessed as im pos si ble and the ex e cu tion of what evercos metic changes was doomed to fail ure (“There was no chance to pre serve el e ments be causethe mod els are en tirely dif fer ent. A tran si tion is made from state healthcare to a health in sur -ance sys tem” – Director of a multi-profile hospital for active treatment).
An other group of man ag ers iden ti fied as a main rea son for the im ple men ta tion of the re -form the ac ces sion of Bul garia to the Eu ro pean com mu nity and the com pli ance with theact ing EC rules as well as the need to catch up with the more ad vanced coun tries in the or gani -sa tion of healthcare. In this case, the re form was un der stood as achieve ment of stan dards ex -ter nal to the Bul gar ian so ci ety and the spe cific fea tures of the healthcare sys tem. Ex actly forthis rea son, as we will ob serve in the anal y sis, a great part of the man ag ing staff in thehealthcare sys tem held the opin ion that new el e ments from for eign sys tems could be in te grated
216
with com po nents from the pre vi ous sys tem, with out mak ing it nec es sary to take into ac countthe dis crep an cies be tween them from the point of view of the in sti tu tional prin ci ples and mech -a nisms, financial model and instruments for the quality maintenance, etc.
The above out lined two in ter pre ta tions did not man i fest dis tinct dif fer en ti a tion in terms of type of pop u lated area, hos pi tal, health ad min is tra tion, etc. Still, we can re port that the first the -sis de fend ing the need for an over all change of the model, re ceived the sup port of all the man -ag ers of pri vate healthcare es tab lish ments (in out pa tients’ care and in hos pi tal care), the largehos pi tals in the cap i tal and a great part of the rep re sen ta tives of the health ad min is tra tion(RHC, RHIF, RIPCPH). Ac cord ing to them, the re form was nec es sary be cause of thesocio-eco nomic changes in Bul garia and it had to be ad min is tered as an over all trans for ma tionof the field of healthcare. At the same time, the fact can not be omit ted, that among the rep re -sen ta tives of this group, the un der stand ing was com mon about the re form as im i tated fol low -ing mod els ex ter nal to the or gani sa tion of healthcare (“The change of the model is ne ces si tated as a guide line and in view of the EC requirements” – RHIF).
A third view also ex isted, ac cord ing to which, the pre vi ous model was dis tin guished bynu mer ous pos i tive fea tures, and there fore, it was nec es sary to change the main pa ram e ters ofhealthcare. Ac cord ing to spe cial ists in healthcare sup port ing such a po si tion, it was pos si ble topre serve the pre vi ous model of healthcare in its en tirety by in tro duc ing only par tial changes.Con se quently, the re form was per ceived as “im prove ment” (“peres troika”) of the pre vi oussys tem, pre serv ing its con struc tion prin ci ples an, above all, pre serv ing the fundamental role ofthe state in healthcare.
· “It was nec es sary to change the model of the healthcare sys tem but some of the el e -ments of the pre vi ous model had to be pre served. These in clude pri mar ily the so cial el -e ments...” (a rep re sen ta tive of a mu nic i pal ity com mis sion on healthcare).
· “There should have been a re form but not in this way. Cer tain things of the old sys temcould have been pre served. For ex am ple, the free healthcare, the lower prices of thedrugs, the ab sence of con sumer’s fee.” (a rep re sen ta tive of a mu nic i pal ity com mis sionon healthcare).
· “The old model had a lot of pos i tive as pects: free healthcare, per fect healthcare...”(mu nic i pal ity ad vi sor).
This view was not com monly held. It was ad vo cated mainly by man ag ers of healthcaresys tem and rep re sen ta tives of the lo cal power in small and mid dle-size towns. Be cause of thesocio-eco nomic prob lems in these pop u lated re gions and the ac com pa ny ing de mo graphic pro -cesses, the nec es sary pre req ui sites were ab sent for the ef fi ciency of key mech a nisms of the re -form – in formed con sent on be half of the pa tients, com pe ti tion among the healthcarees tab lish ments as a pre req ui site for qual ity im prove ment, etc. Be cause of these socio-struc -tural pre req ui sites, the re form was viewed not as a means for achiev ing ef fec tive ness and op ti -mi sa tion of the healthcare sys tem and its course was re lated rather to “chronicun der fi nanc ing”, “with drawal of the state from its fi nan cial com mit ments to healthcare”, “Itwas mainly cen tral ised, which was better. Now the state has with drawn, leav ing the mu nic i -pal i ties cope on their own.”, etc.
The prev a lence of po si tions in fa vour of the re form of the healthcare model did not meanau to matic ap proval of the changes, which had oc curred in the health sys tem. On the con trary,the man ag ers in di cated sig nif i cant con tra dic tions and problems related to:
217
So cio log i cal in ter pre ta tion
· the ab sence of pre lim i nary prep a ra tion for the ac tiv i ties on the im ple men ta tion of there form: func tion ing nor ma tive ba sis, qual i fied man ag ing per son nel, in for ma tion of the healthcare per son nel;
· the way in which the re form was car ried out, slowed down rates dur ing the course ofthe re form;
· lack of co or di na tion in the re struc tur ing of the pri mary, spe cial ised and hos pi tal care,more spe cif i cally, the fo cus ing of the re form in the field of out pa tients’ care and slow -ing down the changes in the hospital sector.
Hence, the ab sence of mea sures for the op ti mi sa tion of the hos pi tal net work, the re fusal to close down the in ef fi cient healthcare es tab lish ments and re-qual ify the healthcare spe cial istswho would lose their jobs. There fore, the hos pi tals did not work in a com pet i tive mar ket en vi -ron ment and, as re gards key pa ram e ters, they were far from achiev ing the main goal, e.g. theim prove ment of the qual ity of the health ser vices and the im prove ment of the health sta tus ofthe pop u la tion
The in ter viewed mem bers of the man ag ing staff in healthcare iden ti fied the prob lems inspe cific as pects of the re form in a dif fer ent way, de pend ing on their po si tion in the sys tem andthe na ture of the in ter ac tions with the re main ing healthcare di vi sions. Be fore that, we willpres ent the re form, as seen by the var i ous man ag ing sub jects in the healthcare system in adifferentiated way.
As sess ment of di rec tors and man ag ers of multi-pro file hos pi tals forac tive treat ment (MHAT)
Pos i tive and neg a tive ef fects of the healthcare re form
The hos pi tal di rec tors and man ag ers most com monly in di cated three par tial and, as if, in -de pend ent from each other, pos i tive ef fects of the healthcare re form: pa tients’ the right of freechoice and the for ma tion of, par tial though, mar ket of health ser vices; change in the fi nanc ingof the healthcare es tab lish ments, and more spe cif i cally, free al lo ca tion of re sources in side thehealthcare es tab lish ment it self; the for ma tion of reg u la tive mech a nisms cre at ing con di tions for a more re spon si ble staff be hav iour in terms of the bal ance be tween the costs and the quality ofthe medical services.
Even though ex pected, the fact is in ter est ing, that the as sess ment of the ef fects of thehealthcare re form were based on the com par i son of the pres ent state-of-arts in the healthcaresys tem and the healthcare dur ing the so cial ist pe riod and the be gin ning of 1990s. What is pe cu -liar in these com par i sons, was that the pre vi ous sys tem was pres ent solely with its pos i tiveas pects (ex cept for the region ali sa tion, whose elim i na tion was pointed out as a pos i tive fact)which were cur rently ab sent or did not work in an op ti mal way, with out mak ing any men tionof its short com ings, which had brought about the be gin ning of the healthcare re form.This se lec tive per spec tive helps us un der stand the neg a tive as pects of the re form in di cated be -low and manifested (without commenting the expressed views) as:
· de fects in the or gani sa tion of the out pa tients’ care;
· abol ish ment of the or gan ised school healthcare and the school doc tors;
· se ri ous draw backs in the pre ven tion;
218
· de struc tion of the ma ter nal and pae di at ric healthcare;
· dis or dered or gani sa tion of emer gency care.
In their as sess ment of the re form of the hos pi tal care, the di rec tors and the man ag ers ofthe multi-pro file hos pi tals re ported three es sen tial fac tors: (1) its de lay and ad min is tra tion in afrag men tary way, out side the logic of the ref or ma tion of the re main ing parts of the healthcaresys tem; (2) in the course of its im ple men ta tion, the opin ion of the hos pi tal phy si cians was nottaken into ac count and (3) com plete ig no rance of the pa tients as a fac tor to be taken into con -sid er ation when plan ning and im ple ment ing changes in the hos pi tal sec tor.
In brief, the stand of the hos pi tal di rec tors and man ag ers on the course of the healthcarere form was: slow, ad min is tra tive and bu reau cratic, with out tak ing into con sid er ation ofthe key fac tors of the healthcare re form – the cit i zens (pa tients) and the peo ple em ployedin the healthcare sys tem.
In par tic u lar, the hos pi tal di rec tors and man ag ers pointed out the fol low ing neg a tive ef -fects on the healthcare system:
· dis con nec tion and jux ta po si tion among the var i ous lev els of med i cal care, mainly be -tween hos pi tal and out pa tients’ care;
· the sta tus of com mer cial com pa nies of the pub lic healthcare es tab lish ments with out the right to profit;
· ab sence of di rect ne go ti a tion be tween the as signer and the pro vider of med i cal andden tal care;
· lack of con trol over the qual ity of out pa tients’ care;
· ab sence of clear and ad e quate stan dards of the healthcare ser vices;
· un sat is fac tory ful fil ment of the gen eral prac ti tio ners’ func tions, in clud ing wors en ingof their qual i fi ca tion;
· se vere con di tion of the small hos pi tals (de fined pri mar ily as los ing from the re form).
Rates of the im ple men ta tion of the healthcare re form
Con cern ing the rates of de vel op ment of the healthcare re form, the views shared by the di -rec tors and man ag ers of multi-pro file hos pi tals for ac tive treat ment, were di vided into two.
The pre vail ing at ti tude was that the re form was car ried out “at a slow rate but it fol lowsthe nec es sary di rec tion (“leads to the better”). At the same time, how ever, the opin ion was rel -a tively wide spread, that the re form did not lead to “any sig nif i cant im prove ment of the ser vices for the cit i zens” and that “the re form leads the healthcare back wards (“in the wrong di rec tion, to the worse)”. The ar gu ments in fa vour of the neg a tive views were the fol low ing: an ac tiveand strong start of the re form but with out the nec es sary pre lim i nary prep a ra tion; di vi sion ofthe re form pro cess into re form in the out pa tients’ and hos pi tal care; nor ma tive re stric tions un -fa vour able for the de vel op ment of the healthcare establishments and bureaucratic obstacles.
None of the hos pi tal di rec tors or man ag ers de fined the rates of the healthcare re form de -vel op ment as “nor mal and ac cept able”.
Health leg is la tion
As re gards the im ple men ta tion of the leg is la tion worked out in the course of the re form,the di rec tors and man ag ers of multi-pro file hos pi tals for ac tive treat ment chiefly saw two prob -
219
So cio log i cal in ter pre ta tion
lems: ex tremely fast and in suf fi ciently well-thought and cor re spond ing to the ac tual changesin leg is la tion and “re leas ing too many reg u la tions at a time”. The hos pi tal man ag ers alsoemphasised the con flicts in the sys tem caused by the jux ta po si tion of the var i ous types of hos -pi tals inherent in the normative documents.
The ne ces sity was stressed that the sta tus of the healthcare es tab lish ments needed to beclar i fied in the leg is la tion and their in de pend ence to be ex panded. In gen eral, pos i tive as pectsof the change were out lined in the hos pi tal sta tus but dif fi cul ties were also pointed out such asthe pay ment of VAT on drugs, consumables, etc., the or gani sa tion of the sup plies and the in -com plete reg u la tion of the re la tions inside the hospitals themselves.
At ti tudes to the privatisation of the healthcare es tab lish ments
The at ti tudes to the privatisation of healthcare were di verse both in the way it was car riedout and the way the healthcare es tab lish ments were pri va tised.
A ma jor ar gu ment against privatisation con sisted in a ground less ap pre hen sion that it“will af fect the pa tients, a great part of whom will not be able to af ford med i cal treat ment inpri va tised (al ready pri vate) hos pi tals and this is not hu mane”. This view was due to in suf fi -cient un der stand ing of the privatisation by both the med i cal spe cial ists and the man a ge rial staff and the cit i zens. Driven by some ob so lete at ti tude, the privatisation (“the pri vate sec tor”) wascon nected to the pay ment of med i cal care by the pa tients, whereas in fact, the re la tion ships be -tween the pri va tised healthcare es tab lish ment and the pa tient as a health in sured per son werethe same as be tween the patient and a public healthcare establishment.
The most com monly shared opin ion was that the re spon si bil ity for privatisation shouldbe as sumed by the state and the mu nic i pal i ties. But they should not en tirely with draw fromhealthcare and should pre serve 51% of the own er ship of the healthcare es tab lish ments.
In a dis cus sion about the type of privatisation, it was pointed out that it was ap pro pri ate,that it in volved the ac tiv i ties and not the fa cil i ties. The staff had to take part in the pro cess ofdenationalisation and the per son nel should be of fered shares at pref er en tial prices or in de pend -ent privatisation of activities.
Re gard ing the scope of privatisation, opin ions var ied. The main line of the dis cus sionswent long the axis: “whether to start from So fia first and not pri va tise the small hos pi tals, or to pri va tise the small hos pi tals first and pre serve the own er ship of the dis trict cen tres; the mu nic -i pal hos pi tals could shift to the sub or di na tion of the dis trict hos pi tals, re spec tively”.
Gen er ally speak ing, the privatisation of the dis trict cen tres was ap proved, es pe cially ofhealthcare es tab lish ments for hos pi tal care. The fears were of “privatisation at all prices”. Ac -cord ing to the words of one of the dis trict hos pi tal’s di rec tors, “qual ity privatisation can onlybe done, based on a na tional strat egy for the de vel op ment of healthcare, reg is ter ing the ac tualcon sump tion of health ser vices”.
Prob lems with the man age ment of the healthcare sys tem
As sess ment of the three cen tres of in flu ence in the healthcare sys tem
The most com mon as sess ment about the Min is try of healthcare was “an ex tremely cen -tral ised struc ture”. Sim i lar views were held, con cern ing the Re gional healthcare cen tres(RHC), which had the task of or gan is ing and im ple ment ing the state health pol icy at re gional
220
level. The spe cific eval u a tion of their work was that “they are los ing their im age and do nothelp the healthcare es tab lish ments”. Cer tainly, the Law on health did not pro vide for the RHC“to help the healthcare es tab lish ments”, but to ex e cute ac tiv i ties for ex ert ing con trol over theirreg is tra tion and ac tiv i ties, to con trol the ob ser vance of the med i cal stan dards, etc. Con se -quently, the ar gu ment that the RHC did not “help” was not ad dressed so much against the ex e -cu tion of the spe cific ac tiv ity but to the nor ma tively reg u lated li a bil i ties of this or gan whichwas as signed mainly con trol ling func tions, the meth od olog i cal as sis tance be ing sig nif i cantlymini mised for the healthcare establishments together with the coordination of healthprogrammes, etc.
The main dis sat is fac tion with the ac tiv i ties of the other cen tres of in flu ence in thehealthcare sys tem – the NHIF – was re lated to the con stant change of rules and the poor co or di -na tion with the re gional struc tures. The other crit i cisms to the work of the NHIF re ferred to thefact that the Fund “is mak ing at tempts to in tro duce a stan dard of be hav iour” for the med i calpeo ple. In their turn, they did not ac cept that the NHIF was “a bank which has to fi nance andnot place ul ti ma tums”.
The hos pi tal di rec tors and man ag ers in the coun try criti cise the UBP, too. The key mo -tive was that the Phy si cians’ un ion had dis tanced it self from the ac tual prob lems and hasturned into “a clerks’ struc ture.” Sev eral in ter re lated trends en sued from this. One of the crit i -cisms was that the UBP did not de fend the rights and in ter ests of the phy si cians. The eval u a -tions of the Un ion’s work boarded down to “lack of ac tiv ity”, “im ped ing the sys tem”. Theseper cep tions of the phy si cians’ pro fes sional or gani sa tion made it un der stand able why its rolewas as sessed as a “neg li gi ble in flu ence board ing down to a tacit con sent with the Min is try ofhealthcare”. When the phy si cians prac tic ing in the hos pi tals did not re cog nise the UBP as a le -git i mate rep re sen ta tive of their in ter ests, it was in ev i ta ble that among this group the trust in theUn ion plum meted and the ex pec ta tions be came min i mal re gard ing the pos si bil i ties for its im -pact. Hence, we can un der stand why one of the di rec tors stated that the UBP had turned into apro fes sional or gan for con trol and not for pro tec tion of in ter ests. We have to ac count for thefact, that the neg a tive as sess ment of the di rec tors and the man ag ers of MHAT, was con nectedto the stand com monly shared by them that the UBP pro tects the in ter ests of only a part of thepro fes sional cir cles, e.g. those of the gen eral prac ti tio ners. This at ti tude could be due to a largeex tent to the fact that as rep re sen ta tives of or gani sa tions, hos pi tal di rec tors and man ag ers didnot see the ac tual pro tec tion of their institutional rights (the interests of the hospitals asorganisations).
Along with these eval u a tions, the in ter viewed hos pi tal di rec tors and man ag ers pointedout the ten sion in the re la tion ships be tween the MH and the NHIF, on the one hand, and thehealthcare es tab lish ments, on the other, as well as be tween the NHIF and the RHIF. The con -tra dic tions be came more dis tinct be tween the hi er ar chy lev els of the healthcare sys tem ratherthan be tween the rep re sen ta tives of one and same level.
The rea sons for the prob lems in this re spect were seen in var i ous as pects, but the main one in cluded the fre quent prac tice of pro tec tion of cer tain pri vate in ter ests, man i fested in the pres -ence of a rather scarce fi nan cial re source (“the lack of fi nanc ing”), and was also a com monlyquoted rea son for the con tra dic tions in the healthcare sys tem. This prob lem was man i fested asdis putes about the cri te ria for the de ter mi na tion of which healthcare es tab lish ments should beclosed down and which should con tinue func tion ing.
An other main fac tor re ported for the con tra dic tions in the man age ment of the sys tem was
221
So cio log i cal in ter pre ta tion
the ini tial stage of the re form and the ab sence of a clear vi sion about the func tions of the newstruc tures and the in ter ac tions among them.
In ter ac tions among the man ag ing au thor i ties of the healthcare system
Ac cord ing to a great part of the hos pi tal man ag ers, in nu mer ous cases there was no ac tual in ter ac tion among the man ag ing au thor i ties of the healthcare sys tem. Still, when such an in -ter ac tion could be dis cerned, it had the fol low ing peculiarities:
· it took place in the ver ti cal di rec tion, e.g. the in ter ac tion was of a hi er ar chy na ture;
· lack of feed back;
· ex ist ing de sire of the in sti tu tions to dom i nate the other ones.
The in ter ac tion among the MH, the NHIF and the UBP was de fined as a strife to ward auni lat eral dom i na tion, e.g. “each man age ment struc ture can im pose over the other ones”. Theprob lems with the co or di na tion were due to the lack of a clear and ac cu rate dif fer en ti a tion ofthe rights and li a bil i ties. Only one hos pi tal di rec tor con sid ered that their role was “to bal ancethe in ter ests” among the sub jects in the sys tem.
Ma jor prob lems were iden ti fied in the in ter ac tion be tween the hos pi tals and the man ag ing di vi sions. The crit i cisms re ferred to the ex tremely great num ber of con trol ling ac tiv i ties atthe ex pense of the ab sent meth od olog i cal as sis tance. Next on the list, were the re ports pre -pared by the hos pi tals, through which the in sti tu tional con trol was car ried out in the sys tem,which were sent to the NHIF and the MH, but at the same time co or di na tion was ab sent be -tween them and a feed back lacked to the healthcare es tab lish ments. The in ef fec tive ex changeof in for ma tion con tin ued to be a heavy bur den for the hos pi tals and their re ports did not makeany sense, turn ing into mere “bu reau cratic whims”. In the ab sence of an over all na tional in for -ma tion sys tem, one and the same data were com pleted by dif fer ent in sti tu tions, using differentforms, without any connection with one another.
Re gard ing these prob lems, the re spon dents made the fol low ing rec om men da tions:
· “Har mo ni sa tion of the leg is la tion, and the ac tiv i ties of these three struc tures have tobe filled with mean ing, reg u lated un am big u ously in the nor ma tive acts.”
· “The Min is try of healthcare should act as a meth od olog i cal au thor ity and con duct ana tional pol icy.”
· “In clu sion of other par ties in volved in healthcare – civil par tic i pa tion, pa tients’ struc -tures for con trol, rep re sen ta tives of the em ploy ers.”
As a main trend, the de mand was out lined for the ex pan sion of the cir cle of in sti tu tionstak ing de ci sions about the de vel op ment of the sys tem and the trans for ma tion of the man age -ment pro cesses into a mech a nism for reg u la tion of the in ter ac tions among health in sur ancefunds, healthcare es tab lish ments and pa tients.
De cen trali sa tion of the man age ment of the sys tem
The most com monly shared opin ion was that a large part of the del e gated re spon si bil i tieswere not sup ported and were not ac com pa nied by the nec es sary rights for their ex e cu tion. Thecrit i cisms were di rected chiefly to the MH and its role in the pro cess of de cen trali sa tion. Sus pi -cions were ex pressed about the pre pared ness of the system and managing staff.
222
As a main fac tor for a suc cess ful de cen trali sa tion, the hos pi tal di rec tors and man ag ers in -di cated the ac qui si tion and the pres ence of the re spec tive re sources to guar an tee the qual ityper for mance of the hospital activities.
The wish was also re ported for a great part of the li a bil i ties to be trans ferred from the MHto the City coun cils.
As sess ment of the man age ment ca pac ity
In prin ci ple, there was no uni ver sally held view about the de gree to which the act ing man -age ment staff met the needs of the sys tem from a qual i ta tive and quan ti ta tive point of view. Ade pend ence was ob served of the an swer to this ques tion on per sonal pref er ences rather than on the na ture of the healthcare es tab lish ments. This was an in di ca tor that still the man age ment at the var i ous lev els and struc tures in the sys tem had not been pro fes sion al ised to a de gree,en abling the em ployed in the sys tem to form a clear as sess ment of the qual ity of the work per -formed by one in sti tu tion or another, irrespective of the specific interests.
Whereas such eval u a tions were made for the man age ment per son nel at var i ous lev els, theopin ions on the work at na tional level were rather con tra dic tory. At re gional level, it was pointedout that the man ag ing po ten tial was cur rently be ing formed, and con cern ing the lo cal level (thelevel of the sep a rate hos pi tal), the opin ion was that “there are no well-trained man ag ers”.
The ar gu ments about what the “per fect man ager” should be, cen tred pri mar ily around theaxis “phy si cian-econ o mist”, how ever, with out a fi nal pro nounce ment.
As sess ment of the in ter ac tions among the healthcare es tab lish ments
The opin ions on this is sue were op pos ing – a part of the in ter viewed in sisted that such anin ter ac tion did not take place, and an other part de clared that the in ter ac tion faced no problems.
The main prob lem atic ar eas in the in ter ac tions among the healthcare es tab lish ments werere lated to the in ter ac tions be tween out pa tients’ and hospital care.
The as sess ment of the sit u a tion by the hos pi tal di rec tors and man ag ers in the small andmid dle-size towns was rather con tro ver sial. The healthcare es tab lish ments in the smallertowns com plained that they had suf fered a lot and those from the big hos pi tals de clared that the hos pi tals in the smaller towns were in a more advantageous situation.
Prob lems with the man age ment of the staff
This group of prob lems can be gen er ally sub di vided into two types – those aris ing fromthe hos pi tal es tab lish ment it self and those aris ing from the sys tem but af fect ing di rectly theman age ment of the hospital.
As re gards the first type of prob lems, at the level of the hos pi tal es tab lish ment, mainlythose were pointed out, which were re lated to the weak mo ti va tion caused by the low sal a ries.The larger part of the per son nel did not per ceive the hos pi tal as their work ing place but just asan ob li ga tion. This de-mo ti vated them strongly and hindered their work.
An other group of prob lems con sisted in dif fi cul ties re tain ing the qual i fied spe cial ists andthe im prove ment of the qual i fi ca tion of the spe cial ists em ployed in the healthcare es tab lish -ments. The rea son was again in the low pay ment and the lack of fi nanc ing of the hos pi tal es -tab lish ments for a sys temic im prove ment of the qual i fi ca tion of the staff working in them.
The “un jus ti fied in ter fer ence of the trade un ions with the man age ment” was also in di -
223
So cio log i cal in ter pre ta tion

cated as a prob lem of the healthcare es tab lish ments.
The role of the cit i zens in the man age ment of the sys tem
The hos pi tal man ag ers saw the fol low ing ways for the cit i zens’ par tic i pa tion in the man -age ment of the healthcare es tab lish ments:
· by ex press ing their opin ion;
· by be ing aware of their rights and li a bil i ties;
· by re quir ing ac count ing;
· through their choice and change of a gen eral prac ti tio ner;
· by be ing in formed.
The cit i zens could par tic i pate in the man age ment of the healthcare sys tem:
· through rep re sen ta tive or gani sa tions;
· through the me dia;
· through com pe tent au thor i ties – the City coun cil, the Min is try of healthcare, po lit i calforces.
The need was also ex pressed for the ways, in which the cit i zens’ in flu ence could be reg u -lated by leg is la tion.
Ac cord ing to some hos pi tal man ag ers, how ever, the cit i zens did not play a role in theman age ment. They deemed that the man age ment was the job of Min is try of healthcare and itsspe cial ised di vi sions, which should de fend the patients.
At ti tude to pri vate hos pi tals
Most of the hos pi tal man ag ers had a pos i tive at ti tude to the pri vate hos pi tals, e.g. “if thecom pe ti tion is loyal, there is no threat”. It was pointed out that the pri vate hos pi tals would leadto com pe ti tion and com pe ti tion would im prove the qual ity of the provided services.
Nev er the less, some neg a tive opin ions could also be sensed about the pri vate healthcarees tab lish ments. It can be claimed that at this stage of the re form, the rep re sen ta tives of the pub -lic healthcare es tab lish ments did not have dis tinctly for mu lated ar gu ments against the pri vatehos pi tals. How ever, at a later stage of the de vel op ment of the re form, when the pri vatehealthcare es tab lish ments con sol i dated their po si tions on the mar ket, a change in the at ti tudetoward them was quite possible.
Fi nanc ing
The views of the di rec tors of multi-pro file hos pi tals for ac tive treat ment were frag men -tary, but gen er ally, grav i tated in three di rec tions: (1) in suf fi cient amounts of fi nanc ing; (2) in -cor rect dis tri bu tion of the fund ing from the sources of fi nanc ing and (3) in many cases,ir ra tio nal spend ing of the fund ing al lo cated to the hos pi tal. Some of the typ i cal state ments in -cluded: “the lack of ad e quate fi nanc ing and the mis ery to which the hos pi tals have de graded”, “the sta tus of the hos pi tals as com mer cial com pa nies which can not make profit and can not ex -e cute eco nomic ac tiv i ties”, “the way of dis trib ut ing the fi nanc ing be tween the hos pi tal andout pa tients’ care”, “the ri dic u lous method of pay ment for ac tiv ity and com plete cov er age ofthe costs for hos pi tal care”, “the lack of regulated payment for emergency care”.
224
Re gard ing the fi nanc ing, the view was held that the healthcare suf fered not only from ashort age of fi nance but also from their ir ra tio nal spend ing:
· “Un law ful dis tri bu tion of the pay ment for the med i cal ser vices in re la tion to the hos pi -tal cat e gory”;
· “Ab sence of ad e quate pay ment, with out tak ing into ac count the qual ity and the quan -tity of the per formed ac tiv i ties. The for mal cost ing of the ser vices and the lack of afunc tion ing in for ma tion sys tem at na tional level cre ate con di tions for sub sti tu tion ofdi ag no ses for fi nan cial profit”;
· “The al lo ca tion of fi nance should be for the dis ease and not for the place of treat -ment”;
· “Ab sence of ac tual def i ni tion of the cost for the treat ment of some dis eases”;
· “The stan dards of pay ment to the GPs are in ef fec tive and dam age the healthcare sys -tem” (in a num ber of state ments the par a dox was pointed out that the GPs re ceivedpay ment for work they had not done, whereas the hos pi tals did not re ceive 100% of thefi nan cial equiv a lent of the ac tu ally per formed ac tiv i ties).
The in sti tu tional or gani sa tion of the fi nanc ing was also criti cised. The crit i cisms were re -lated to the NHIF mo nop oly and the in ad e quacy of the model of dou ble fi nanc ing (by theNHIF and the MH) lead ing to hazy re spon si bil i ties of the fi nanc ing au thor i ties.
Op pos ing views were shared by the re spon dents about the dou ble fi nanc ing of the hos pi -tal care - by the NHIF and the MH – even though from the cur rent (2006) it was changed, someof the com ments are in ter est ing and, there fore, we are in clud ing them in our analysis.
The pro po nents of the dou ble fi nanc ing ar gued in their fa vour that “the more sources fi -nance a hos pi tal, the better”. At the same time, they ad mit ted that bu reau cracy was be ing in -creased in such a way.
The op po nents of the dou ble fi nanc ing con sid ered it a tem po rary phe nom e non – in such away the state com pen sated for the in abil ity of the Fund to to tally cover the hos pi tal costs. Ac -cord ing to the in ter viewed, the fi nanc ing from the MH it self was mixed up, it had nu mer ous re -stric tions, etc. Those di rec tors con sid ered that the fi nanc ing from two sources was aimedmainly at con ceal ing the imperfections of the system.
The so lu tion of the prob lems with fi nanc ing was seen in sev eral as pects:
· for mu la tion of key pri or i ties and, based on them, the fi nanc ing should be de ter mined;
· al low ing the hos pi tals to ex e cute eco nomic ac tiv i ties (make profit);
· ex act def i ni tion of the min i mum pack age of ser vices which was to be re im bursed bythe NHIF and de vel op ment of funds for vol un tary health in sur ance;
· the fi nanc ing to be done by one au thor ity only;
· in creased amount of the health in sur ance in stal ments;
· de ter mi na tion of the cost of phy si cians’ la bour;
· in creased bud get for healthcare.
The di ver sity of the pro posed mea sures is ap par ent, con firm ing the ne ces sity for the ap -pli ca tion of a com plex of in ter re lated and sys temic mea sures and not un der tak ing par tial ac tiv -i ties when solv ing the prob lems of fi nanc ing.
It is note wor thy, that in the smaller towns the prob lem was summed up pri mar ily and ex -
225
So cio log i cal in ter pre ta tion
clu sively as “there is no money”, which was why the so lu tion with the in crease of the fi nanc ing was seen as the only pos si bil ity.
It is ev i dent from the above views that the fi nanc ing of hos pi tal care was not un der -stood as a main el e ment of the eco nomic re form in healthcare. A few years af ter the re formin hos pi tal care, in an in sti tu tional en vi ron ment, the al ready changed and newly es tab lishedeco nomic con di tions were not un der stood well enough in the field of healthcare. The fi nan cial re source con tin ued to be per ceived mainly as “costs” for the healthcare es tab lish ments. Thiswas chiefly due to the fact that the uti li sa tion of the fi nan cial re source was not linked to theachieve ment of con crete ob jec tives de fined in ad vance, ow ing to which the re quire mentsfor ac coun tancy were taken as mean ing less ul ti ma tum ac tiv i ties. The un der stand ing was miss -ing, about fi nanc ing as a struc tural mech a nism for the mod el ling of the in ter ac tions in a cer -tain pub lic sphere and the for ma tion of mech a nisms for professional incentives andguaranteeing the quality of the services.
The rea sons for this state-of-arts can be sought in three di rec tions. First, as we pointedout above, the ac tiv ity of the NHIF was as sessed as for mal and bu reau cratic, re port ing pri mar -ily not con tent but for mal in di ca tors, not cor re spond ing to the ac tual med i cal prac tices. Hence,it was nor mal that the ac tiv i ties of the NHIF were eval u ated as de lib er ately ul ti ma tum, dis re -gard ing the qual ity of the med i cal ser vices. Sec ond, re lated to the first one, a great part of thehos pi tal di rec tors and man ag ers re ported that the Fund fi nanced “ab surd struc tures” on pa per, but did not fi nance 100% of the ac tual costs, made by the hos pi tals for pro vid ing treat ment.And third, the prin ci ples of reg u la tion in the hos pi tal sec tor were not sys tema tised and fullyap plied, which was the rea son why the sources of fi nanc ing (at least un til 2005) in cluded theNHIF, the Min is try of healthcare, the mu nic i pal i ties (through mu nic i pal par tic i pa tion in thehos pi tal healthcare es tab lish ments), do na tions from le gal en ti ties and phys i cal per sons (in ac -cor dance with the LHE). It turned out that the NHIF de ter mined the terms and re quired ac -coun tancy for the al lo cated fi nances, with out cov er ing, how ever, the costs for treat ment, letalone tech ni cal and tech no log i cal ren o va tion. The re main ing sum was paid usu ally by the MHor the City coun cils. But due to in com plete and in suf fi cient reg u la tion of these prac tices, theforms of ac coun tancy were not so stand ard ised and as a re sult, the re spon si bil ity for the fi nanc -ing remained vague. Under these conditions, there was no chance for the requirements for theNHIF accountancy to be perceived as logical or necessary.
Two the ses could be dis tin guished in the dis cus sion of the role of the state in fi nanc ing.Ac cord ing to one of the the sis, the state was sup posed to “with draw” from the fi nanc ing and toal lo cate fund ing for pri or i ties only. The other one ad vo cated the ex act op po site – the state hadto con tinue to fi nance healthcare as it had done un til then. Here, too, the dif fer ences were de -ter mined by the type of town. The hos pi tal di rec tors and man ag ers in the big ger cit ies had abroader per spec tive on the sys tem of healthcare and real ised that the state fi nanc ing was aprob lem, be cause through it, those work ing mod els were re pro duced, which had noth ing to dowith the qual ity of the med i cal ser vices, ac coun tancy, ef fi ciency of healthcare, etc. In smallertowns, the poor pre dic a ment of the hos pi tals and the zone of the in creased risk in which theywere sit u ated, did not al low for the rec og ni tion and the ad mis sion of the fact that this type of fi -nanc ing did not com prise a long-term solution of the problematic situation in healthcare butjust its component.
Re gard ing the ac tiv i ties judged as a state pri or ity, sev eral gen eral views can be out lined:
· “It is man da tory that the state fi nances the ac tiv i ties re lated to the so cially sig nif i cant
226
dis eases.”
· “The state must take care of the pre ven tion.”
· “The state must take the re spon si bil ity for the de vel op ment and the im ple men ta tion ofstrat e gies” (au thors’ note: which sug gests the pres ence and uti li sa tion of the re spec -tive fi nan cial re sources, too).
There was no clearly de fined un der stand ing of the at ti tude of the state to ward the var i ous so cial groups. There were con tra dic tions both on the is sue of whether the state should sup portcer tain so cial groups and on the is sue on what prin ci ple to de ter mine them.
The topic of op ti mis ing the uti li sa tion of the fund ing also di vided the di rec tors andman ag ers of the multi-pro file hos pi tals for ac tive treat ment into two.
The im pos si bil ity of the op ti mi sa tion of the fi nanc ing was sup ported with ar gu mentsbased on the “her i tage from the past”, “the small amount of the fund ing al lo cated for the hos -pi tal healthcare es tab lish ments”, “the size of the health in sur ance in stal ments”. The opin ionscan be summed up by the un der stand ing that “the money is scarce and there is no room for op -ti mi sa tion”.
The the sis for the pos si ble op ti mi sa tion was backed by the fol low ing so lu tions:
· “Better man age ment of the hos pi tal es tab lish ments (re duc tion of the costs, seek ing forspon sors, par tic i pa tion in pro jects, ac counts time ta bles)”;
· “Real ac cred i ta tion which will dif fer en ti ate the hos pi tal es tab lish ments. In such a wayit will be de ter mined, which of the es tab lish ments will be closed down and which willre main as well as which of them pro vide higher qual ity and there fore de serve better fi -nanc ing”;
· “A long-term strat egy of the Min is try of healthcare”;
· “Con trol at all lev els in the sys tem (ac tual op ti mi sa tion can be at tained at the level ofthe hos pi tal man age ment and not at the level of state pol icy and con trol.”
Hence, we may draw the con clu sion that the in tro duc tion of mea sures for the op ti mi sa tion of the sys tem, even if they cor re spond to the fi nan cial pa ram e ters, is likely to re main not un der -stood by a large part of the hos pi tal man age ment teams, es pe cially in smaller towns, since theprob lems im me di ately per ceived by them, are of fi nan cial, ma te rial and tech ni cal na ture. Con -se quently, the mea sures which are not di rected to the im me di ate so lu tion of these prob lems but to the optimisaton of the sys tem (pri or i ties, ac coun tancy, cri te ria for qual ity) are ac cepted assec ond ary and add ing up to the un nec es sary bureaucratisation.
As sess ment of the clin i cal path ways
The ma jor ity of the re spon dents ex pressed the opin ion that the clin i cal path ways did notpres ent the best in stru ment for fi nanc ing as they did not cover fully the ac tual costs and therewas no ac tual cost ing of the la bour of the med i cal pro fes sion als. Crit i cisms were di rected bothto ward the clin i cal path ways as tools for fi nanc ing and or gan is ing the treat ment pro cess (al -though some of them re port ad van tages, too) and the mechanisms for their introduction.
The re ported dis ad van tages, re lated to the ap pli ca tion of the clin i cal path ways, in -cluded their fre quent change, the dom i na tion of some types of clin i cal path ways over oth ers,the nu mer ous con di tions that had to be ob served by the hos pi tal establishments.
Ac cord ing to the re spon dents, in their turn, these prob lems had a neg a tive ef fect on the
227
So cio log i cal in ter pre ta tion
cit i zens. There fore, the pro posal was ta bled for the sub sti tu tion of the clin i cal path ways for di -ag nos ti cally re lated groups and for the ac tual cal cu la tion of the costs.
Fa mil iari sation with and at ti tudes to the di ag nos ti cally re lated groups
To one ex tent or an other, the in ter viewed were fa mil iar with the di ag nos ti cally re latedgroups (DRGs). For a con sid er able part of them, how ever, the fa mil iari sation boarded down to the for mal “aware ness of the DRGs”, but they had no per sonal opin ion about them. The pre -vail ing part of the hos pi tal di rec tors and man ag ers pointed out both pos i tive and negativeaspects of the DRGs.
The ad van tages of the in tro duc tion of DRGs were linked to the pos si bil ity of pay ingfor ac tu ally per formed work, real cost ing of the ac tiv ity, in crease of the ef fi ciency of the uti -lised resources.
It was ex actly the ac knowl edg ment of the po ten tial pos i tive ef fects from the in tro duc tionof the DRGs, which de ter mined the opin ion that their in tro duc tion had been de layed. The rea -son, in di cated for the de lay, was “the lack of po lit i cal will and in ter ests im ped ing their in tro -duc tion.” The ne ces sity was also emphasised for “their ur gent in tro duc tion through out thecoun try and not, as un til now, only in some healthcare es tab lish ments”.
The neg a tive ex pec ta tions con cerned not so much the con tent char ac ter is tics of theDRGs but rather sus pi cions that “they will hardly be in tro duced in an ef fec tive way” and that“the prob lems in tro duc ing them will dis tort their ap pli ca tion.”
Health in sur ance
From the point of view of the in her ent prin ci ples and mech a nisms, the cur rent model ofoblig a tory health in sur ance was as sessed as a rel a tively good but the real out comes were notas sessed as sat is fac tory:
· “The great num ber of un in sured and the prob lems faced by the healthcare es tab lish -ments and the cen tres for emer gency med i cal care. These, in their turn, cre ate two in -ter re lated prob lems. First, a con flict be tween the phy si cian’s oath and the fi nanc ing.Sec ond, frauds and un reg u lated pay ments when ful fill ing phy si cians’ du ties”;
· “The su per flu ous ac coun tancy – the large num ber of doc u ments to be pro cessed, in -com pe tence on be half of the RHIF”;
· “Dis torted ap pli ca tion of the prin ci ples of the sys tem”;
· “The pres ence of the main prin ci ples (sol i dar ity, jus tice, self-gov er nance, etc.) ispurely for mal.”
The crit i cisms to the very model are in two di rec tions:
· “Some pay more, oth ers pay less, and both re ceive one and the same health ser vice”;
· “The mo nop o lis tic sit u a tion of the NHIF. Its change will be to the ben e fit both for thehealthcare es tab lish ments and for the pa tients”.
The mo nop o lis tic sta tus of the NHIF was eval u ated mainly neg a tively. The ma jor ity ofthe di rec tors and man ag ers sug gested that it should change. The chief ar gu ments they pointedout, were re lated to the need for com pe ti tion and better func tion ing. Those who wished that the cur rent sta tus of the NHIF was pre served, did not de fend their po si tion with ar gu ments about
228
the pres ent ef fi ciency of the Fund. On the con trary, the ar gu ment for their wish for main te -nance of the sta tus quo was the fol low ing: “if there is more than one fund, the bu reau cracy and the pa per work will be more”.
The pro pos als for changes of the model of healthcare:
· “Cre ation of pre req ui sites for the de vel op ment of vol un tary funds and their in clu sionin the ex e cu tion of the oblig a tory pack age of ser vices”;
· “The state should un der take the fi nanc ing of the so cially sig nif i cant dis eases”;
· “The in di vid ual health in sur ance pre mi ums should ac cu mu late and ev ery in sured per -son should be able to dis pose with them”.
The gen er ally ac cepted opin ion was that in or der to start work ing, the health in sur ancesys tem should be re formed along the fol low ing pa ram e ters:
· “The size of the health in sur ance in stal ments”;
· “The way of their de ter mi na tion”;
· “The pack age of ser vices cov ered by the oblig a tory health in sur ance”;
· “Link ing the health in sur ance in stal ments with the pro phy lac tic check-ups”;
· “An ad di tional pack age of ser vices paid vol un tarily”;
· “In creased collectibility of the in stal ments”;
· “In tro duc tion of the method of the di ag nos ti cally re lated groups”.
Along with the amount of the in stal ments, the other in di cated prob lem con cerned the col -lect ing of the in stal ments from “the em ployed in the pri vate sec tor who re ceive one re mu ner a -tion and de clare an other.”
The link ing of the size of the in stal ments for health in sur ance with the qual ity of the pro -vided med i cal ser vices was eval u ated con tro ver sially. The main ar gu ment against this link ingwas that the prin ci ple of sol i dar ity would be vi o lated. A pos si ble so lu tion in cluded the prep a ra -tion of a min i mum pack age of ser vices and ad di tional pay ment of the ser vices out side it as well as for the “lux ury” ser vices to be covered by the voluntary funds.
At ti tude to the Na tional frame work agree ment
Over all, the NFA was eval u ated as nec es sary be cause it de ter mined the rules of ac tion.Nev er the less, the hos pi tal man ag ers pin pointed a lot of draw backs in the agreement.
Re gard ing the con tent of the agree ment, these short com ings in cluded “the lack of clar ityand am bi gu ity of some of the texts”, “doubts whether and how far it pro tects the pa tients’rights”, “fi nanc ing” (at this stage the ne ces sity was re cog nised for the in tro duc tion of di ag nos -ti cally re lated groups and payment for performance).
As re gards the way of de vis ing the agree ment, cer tain prob lems were also de fined:
· The hos pi tal di rec tors did not take part in it and “there is no opin ion sur vey of the peo -ple em ployed at the lower lev els of the sys tem” (prob lems of rep re sen ta tion);
· “The weak role of the UBP”;
· “The de sire for dom i na tion of the MH”.
Re gard ing the mech a nisms of the NFA prep a ra tion, it was sug gested: “that it shouldnot be pre pared ev ery year but should only have some cor rec tions made”; “to clearly reg u late
229
So cio log i cal in ter pre ta tion
the rights and li a bil i ties of the par tic i pants”; “the agree ment should take into ac count the realneeds and should func tion as a frame work”.
The qual ity of the healthcare ser vices
On the point, whether the re form stim u lated the med i cal spe cial ists to of fer higher qual ityser vices, the opin ions di vided into three groups.
Part of the hos pi tal di rec tors and man ag ers thought that the re form did stim u late thequal ity im prove ment of the med i cal ser vices. This was pre-de ter mined by the com pe ti tionand the pa tients’ free choice. They saw the way of fi nanc ing as a main mech a nism for qualityimprovement.
Those who con sid ered that the re form did not stim u late the pro vi sion of qual ity ser -vices, ar gued that the rea son for that was in the pres ence of ob sta cles, re sult ing from the ex ist -ing sys tem such as “doc tors are turned into ad min is tra tion”; “low re mu ner a tion for thephy si cians’ la bour”; “the ac tual cost and the price of the phy si cians’ la bour is not de ter -mined”, “the strife for more pa tients leads to the de crease of the quality of the service”.
Ac cord ing to the opin ions fall ing in the third group, the prob lems had to be sought inthe very so cial con text in which the healthcare sys tem was func tion ing, e.g. the ab sence ofan ac tual mar ket of health ser vices.
The hos pi tal di rec tors and man ag ers pro posed changes, aimed at qual ity im prove ment ofthe ser vices:
· “To in tro duce clear stan dards for qual ity and a sys tem for eval u a tion and con trol ofthe qual ity which is pres ently lack ing”;
· “The phy si cians’ la bour should be re ally costed and priced”;
· “The pa tient should bring real money to the pro vider” (au thors’ note: in the sense ofac tual pay ment for the per formed med i cal ac tiv i ties);
· “The role and the li a bil i ties of the gen eral prac ti tio ners should be changed”.
In to tal com pli ance with the re al i ties, the man ag ers of the multi-pro file hos pi tals for ac -tive treat ment pointed out that no par tic u lar sys tem for qual ity con trol ex isted:
The ex ist ing model for ac cred i ta tion was criti cised in the fol low ing re spects:
· “Its ef fi ciency – the ac cred i ta tion is not linked to the fi nanc ing”;
· The cri te ria used were de fined as “for mal”, “com ing from above”;
· “It does not ap ply to ev ery one in the sys tem”;
· “The im ple men ta tion of the ac cred i ta tion it self, in which the sub jec tive fac tor has anin flu ence”.
Ac cord ing to the hos pi tal man ag ers, the im prove ment of the ac cred i ta tion pro ce dure re -quired changes in all cases. There was no com mon view about the na ture and the or gani sa tion(af ter it had been es tab lished) of a uni fied na tional sys tem for eval u a tion and con trol of thequal ity of med i cal care. It was sug gested that this sys tem started as a pi lot pro ject. In this case, it was im por tant that there was no clar ity about the very pro cess of the qual ity eval u a tion. This was in di cated by the fact, that the hos pi tal di rec tors and man ag ers have not sin gled out one cri -te rion for qual ity con trol.
The rules were also emphasised, which should de ter mine the work of the ac cred i ta -
230
tion or gan. They were mainly for mal: “the sub jec tive fac tor should be ex cluded”, “to treat ev -ery body on an equal foot ing”. But along with the equal treat ment, opin ions were voiced thatthe con trol or gans should take into con sid er ation the spe cific con di tions in the sep a rate hos pi -tals. These two as pects did not con tra dict each other, but their achieve ment re quired a well-de -signed sys tem, se cured from an information point of view.
Here was no unan i mous stand on the pos si bil ity for the pa tients to in flu ence the qual ityof the ser vices pro vided to them. Pos si ble ways of in flu enc ing on be half of the pa tients in -cluded: “the pa tients’ right of free choice and pref er ences”, “ex is tence of in sti tu tions wherethe pa tients can de posit com plaints”, “use of other means, for in stance the me dia”.
The uti li sa tion of these pos si bil i ties, how ever, was re stricted and en coun tered ob sta clessuch as: “the pa tients are not aware of their rights and do not know whom to ad dress in case ofneed”, “there is no sep a rate or gan in the sys tem to deal with the ac tiv i ties for the pro tec tion ofpa tients’ rights”.
Pri or i ties of the healthcare sys tem
Com po nents from the whole sys tem were re ported as pri or i ties both in terms of prin ci ples of man age ment, nor ma tive ba sis and fi nanc ing, and in terms of con crete ac tiv i ties (pre ven tion, chil dren’s healthcare, etc.)
1. Pri or i ties re fer ring to the over all man age ment of the healthcare: “the de sign ingof a strat egy”; “se cur ing the ac cess of the pa tients to the healthcare sys tem”; “ap -pro pri ate and ef fec tive man age ment”.
2. Pri or i ties re fer ring to the re la tion ships in the sys tem:
· “Co or di na tion of ac tiv i ties among all the par tic i pants in the sys tem”;
· “Di a logue”;
· “Trans par ency”.3. Change of the nor ma tive ba sis, and the LHE in par tic u lar, to make it ef fec tive
and func tion ing. 4. In crease of the fi nanc ing as a per cent age of the GDP al lo cated for healthcare
and “reg u la tion of the pay ment for med i cal care for peo ple with out a health in sur -ance”.
5. Im prove ment of the qual ity of ser vices:
· “Im prove ment of the ac cred i ta tion”;
· “En hanced role of the UBP in terms of qual ity”. 6. At the level of spe cific ac tiv i ties, the in di cated pri or i ties in cluded:
· “Im ple men ta tion of pre ven tion and health pro mo tion”;
· “Im prove ment of di ag nos tics”;
· “State fi nanc ing of the treat ment of so cially sig nif i cant dis eases”;
· “Ma ter nal and pae di at ric health”;
· “Hos pi tal care”.
Ex pec ta tions for the fu ture of the healthcare sys tem
The ex pec ta tions for the fu ture de vel op ment of the healthcare sys tem had a slightly pos i -tive bias.
231
So cio log i cal in ter pre ta tion
The hos pi tal di rec tors and man ag ers ex pected the fol low ing changes:
· “To work out a na tional strat egy for healthcare de vel op ment”;
· “Up dat ing of the coun try’ health map”;
· “Clos ing down of all the in ef fec tively func tion ing and re dun dant struc tures”;
· “The state is to de ter mine the ra tio be tween the pri vate and the pub lic healthcare es -tab lish ments”;
· “Change in the pa tient’s sta tus – the pa tient should be come the cen tre of the sys tem”;
· “The cen tral hos pi tals should not be priv i leged at the ex pense of those in the coun try side”;
· “Fund ing should not be given for out pa tients’ care at the ex pense of hos pi tal care”.
· Re gard ing the health in sur ance sys tem:� “To re or gan ise the way of col lect ing the in stal ments – in the form of an in di vid ual
credit”;� “To in crease the amount of the in stal ments”;� “To change the mo nop o lis tic sta tus of the NHIF”;� “To de vise clear programmes for the de vel op ment of the sys tem”;� “To sim plify the doc u ment turn over”;� “To cre ate con di tions for feed back”;� “To have skil ful peo ple work ing in the sys tem”.
· Re gard ing the nor ma tive ba sis:� “Con crete changes in the ex is tent leg is la tion”;� “Synchronisation of the ex is tent leg is la tion”;� “Up dat ing of the nor ma tive sys tem”.
· Change in the sta tus of the healthcare es tab lish ments:� “Change in their sta tus – not to be com mer cial com pa nies”;� “To be sub or di nate to one in sti tu tion only”;� “To im prove the fa cil i ties, the staff and the equip ment”.
· Ways of re mu ner at ing phy si cians’ la bour: � “De ter mi na tion of the ac tual cost of the phy si cians’ la bour”;� “Ad e quate sal a ries for the phy si cians”.
· Sub jects which had to im ple ment the change:
· the State;
· “Good spe cial ists to un der take this ac tiv ity”;
· “Our ac ces sion to the EC will make us change”.
As sess ment of di rec tors of spe cial ised hos pi tals for ac tive treat ment andna tional centres
Pos i tive and neg a tive ef fects of the healthcare re form
Sim i lar to the di rec tors and man ag ers of the multi-pro file hos pi tals for ac tive treat ment,the di rec tors of the spe cial ised hos pi tals for ac tive treat ment (SHAT) and the na tional cen trescon sid ered as pos i tive ef fects of the healthcare re form pri mar ily “the elim i na tion of theregion ali sa tion and giv ing the op por tu nity to the cit i zens to chose a healthcare es tab lish mentin de pend ently” as well as “the creation of possibilities for competition”.
232
The “in con sis tency” be tween the hos pi tal care and out pa tients’ care, which were nottreated on an equal ba sis, was quoted as an ad verse con se quence of the re form. The rea son,ac cord ing to the in ter viewed, was in the im ple men ta tion of the re form in out pa tients’ care andthe lag ging be hind of the struc tural changes in hos pi tal care. As a re sult, the man ag ers of spe -cial ised hos pi tals de clared that “the out pa tients’ sphere has more avail able re sources – bothfor ac tiv ity and for in cen tives and per son nel re mu ner a tion”.
Ac cord ing to the di rec tors of spe cial ised hos pi tals, “The Phy si cians’ un ion is pro mot ingthe role of the GPs which dis torts the re form”. In ad di tion, con trol lacked in the sys tem of out -pa tients’ care.
An other re ported neg a tive ef fect of the re form, was the lack of in ter ac tion be tween thesep a rate units of the sys tem, e.g. GPs, med i cal cen tres, di ag nos tic and con sul ta tive cen tres,dispensaries.
Im ple men ta tion rates of the healthcare re form
Con cern ing the views of the man ag ers the spe cial ised hos pi tals for ac tive treat ment on the rates, at which the healthcare re form was de vel op ing, they did not dif fer from those shared bythe di rec tors and man ag ers of the multi-pro file hos pi tals for active treatment.
Health leg is la tion
The leg is la tive ba sis was as sessed as rel a tively well-de vised. The prob lems were iden ti -fied in the ex e cu tion and the sub se quent con trol. The na ture of the re sponses, how ever, im -plied that the qual ity of the laws and the de gree of their ad min is tra tion were per ceived asin ter re lated. In a num ber of cases, the in ter viewed re ported draw backs in leg is la tion, cre at ingpre req ui sites for failure to observe or circumvent the law.
The ma jor prob lem re lated to the leg is la tion, in the words of the man ag ers the spe cial isedhos pi tals and na tional cen tres, was con nected to the com mer cial sta tus of the healthcare es tab -lish ments. This prob lem be came worse by “im per fec tions and in con sis ten cies be tween theLaw on healthcare es tab lish ments and the Com mer cial law cre at ing nu mer ous dif fi cul ties”.Even though, the sta tus of the hos pi tals as com mer cial com pa nies was eval u ated pos i tively as a manifestation of their financial independence.
Other prob lems re lated to the leg is la tion in cluded “the lack of a clear sta tus of the emer -gency care”, pres ence of old reg u la tions which do not cor re spond to the changed sit u a tion”,“in suf fi cient reg u la tion of the rights and li a bil i ties of the con trol or gans”, for the mu nic i palspe cial ised hos pi tals – the lack of ac tual pos si bil i ties for hos pi tal fi nanc ing. The man ag ers ofspe cial ised hos pi tals and na tional cen tres with uni ver sity func tions found con tro ver sies be -tween the Law on healthcare establishments and the Law on higher education.
Apart from the im per fec tions of the spe cific nor ma tive acts, the man ag ers of spe cial isedhos pi tals and na tional cen tres criti cise also the pro cess of work ing out the laws and the sec -ond ary nor ma tive acts. The pro cess of de vis ing a cer tain law was not ac com pa nied by de fin ingcon crete ac tions and mech a nisms, through which it was go ing to be ap plied in prac tice. Thus,rel a tive good nor ma tive doc u ments were pre pared, but there was no or gani sa tion of the pro ce -dures for their ex e cu tion (“One of the great est short com ings of the man age ment sys tem is thelack of a care fully and se ri ously thought de tails and tech ni cal i ties for the ful fil ment of aparticular decision.”).
233
So cio log i cal in ter pre ta tion
Prob lems with the man age ment of the healthcare sys tem
As sess ment of the three cen tres of in flu ence in the healthcare sys tem
The di rec tors of spe cial ised hos pi tals and na tional cen tres re cog nised the for ma tion ofthree cen tres of in flu ence: the MH, the NHIF, UBP/UDB. In gen eral, the ne ces sity was ad -mit ted for the dif fer en ti a tion of the ac tiv i ties in terms of: (1) health pol icy con ducted by theMH; (2) fi nanc ing of the sys tem by the MH and the NHIF and (3) rep re sen ta tion and pro tec tion of the in ter ests of the peo ple em ployed in the healthcare sys tem, ex e cuted by the professionalorganisations – UBP, UDB.
The view was de fended that the UBP was not an or ga ni za tion, ex ert ing such a pow er fulin flu ence on the sys tem as the MH and NHIF did. The MH and the NHIF were per ceived ascen tres of power “be cause they sub si dise”, whereas the UBP “has to deal with the phy si cians’qual i fi ca tion and train ing and not to par tic i pate in the sign ing of the frame work agree ment.” It was a com mon un der stand ing, that un til that mo ment the UBP was en ti tled to play a key role inthe reg u la tion of the sys tem, ac cord ing to the leg is la tion, but this did not lead to ac tual out -comes. In the UBP, the man ag ers of healthcare es tab lish ments did not re cog nise an or gani sa -tion which “fully de fends the phy si cians’ in ter ests”, “takes care of the qual i fi ca tion andre-qual i fi ca tion of the doc tors”, etc. Ac cord ing to the re spon dents, “the only ob li ga tion of thepro fes sional or gani sa tion is to ob serve and guar an tee the in ter ests of the association, withoutgoing beyond this obligation”.
In ter ac tions among the man ag ing au thor i ties of the healthcare system
Part of the man ag ers of the spe cial ised hos pi tals and na tional cen tres eval u ated the in ter -ac tion among the man ag ing au thor i ties in the healthcare sys tem in a pos i tive way (“they func -tion in an op ti mal way”, “they com ple ment one an other”, “they col lab o rate”), but an other partin di cated that it was bur dened and hin dered by bureaucratic obstacles.
More spe cific as sess ment was made by the re spon dents of the in ter ac tion be tween theman ag ing au thor i ties of the healthcare sys tem and the healthcare es tab lish ments. The ma jor ityof the man ag ers of the spe cial ised hos pi tals and na tional cen tres de fined this in ter ac tion asasym met ri cal (“The Min is try is sues or ders and we ex e cute them”, “the in ter ac tion can be im -proved, if the in for ma tion is re ceived not only from top to bot tom but also from bot tom to top”), im peded (“the ac cess to in for ma tion from the ad min is tra tive au thor i ties is dif fi cult”) and re -dun dant (for ex am ple the in ter ac tion be tween the healthcare es tab lish ments with the MH, onthe one hand, and the RHC, on the other).
De cen trali sa tion in the man age ment of the sys tem
The de cen trali sa tion of the healthcare sys tem was re cog nised as nec es sary by the man ag -ers of the spe cial ised hos pi tals and na tional cen tres. Some of them, how ever, share the viewthat the de cen trali sa tion of the man age ment was de formed since the lower man age ment lev elshad been trans ferred sig nif i cant re spon si bil i ties, with out be ing con ferred the re spec tive rights.Ac cord ing to oth ers, “the de cen trali sa tion is real and work ing”, but the as sum ing of re spon si -bil ity by the lower man age ment lev els, too, was a fact with pos i tive sig nif i cance for the func -tion ing of the sys tem. Mean while, in some state ments, it be came ev i dent that thede cen trali sa tion was un der stood as striv ing to ward “frag men ta tion of re spon si bil ity” (“when a
234
mis take is made, the re spon si bil ity is borne at the re spec tive level”). In this sense, some of thein ter viewed per ceive de cen trali sa tion as “lib er a tion from re spon si bil ity” for the highermanagement levels rather than conferring rights for independent decision-making.
As sess ment of the man age ment ca pac ity
The skills and com pe ten cies of the man ag ing staff were com mented on in an in di rectway by the di rec tors and the man ag ers of the spe cial ised hos pi tals and na tional cen tres. The in -ter fer ence of po lit i cal par ties in the re cruit ment of the man ag ing per son nel wasemphasised as one of the prob lems, as a re sult of which “peo ple are in serted, who do not pos -ses the qual i ties and the train ing, re quired for the po si tion they are oc cu py ing …”
More spe cif i cally, the en vi ron ment in which the man ag ing staff was work ing, was eval u -ated. It was re ported that doc u men ta tion was over stressed, with which “weighs as a bur den not only for the ad min is tra tive au thor i ties but also on the act ing first-tier phy si cians”. It was alsopointed out that the re quired in for ma tion (au thors’ note: by the MH, the NHIF) had to be mini -mised to such an ex tent, that the con crete data and their ob jec tive anal y sis were nec es sary forde ci sion-mak ing of the respective regulating institutions.
As sess ment of the in ter ac tions among the healthcare es tab lish ments
The as sess ment of the in ter ac tions among the healthcare es tab lish ments was not unan i -mous. The in ter viewed man ag ers of the spe cial ised hos pi tals and na tional cen tres dis tin -guished these in ter ac tions ac cord ing to type of healthcare es tab lish ments and eval u ated themin a different way.
Ac cord ing to the re spon dents, the in ter ac tion among hos pi tals of the same rank ing(among mu nic i pal hos pi tals, dis trict hos pi tals, uni ver sity hos pi tals, na tional cen tres) was notproblematic.
The in ter ac tion among hos pi tals of dif fer ent rank ing (for in stance, be tween mu nic i paland dis trict hos pi tals, be tween dis trict hos pi tals and na tional cen tres, etc.), how ever, did createproblems.
It is an in ter est ing fact, that when the hos pi tals re ferred pa tients to one an other, if the hos pi -tals were of the same rank ing, it was con sid ered as good col lab o ra tion and in ter ac tion, whereas if a hos pi tal of lower rank ing re ferred a pa tient to a hos pi tal of higher rank ing, it was con sid ered aman i fes ta tion of in ef fec tive func tion ing of the sys tem of healthcare. How ever, opin ions alsoranged, ac cord ing to which the in ter ac tion be tween the spe cial ised hos pi tals and the na tionalcen tres with the dis trict hos pi tals was good be cause they re ferred “un typ i cal cases”.
In the re spon dents’ opin ion, the in ter ac tion be tween healthcare es tab lish ments fromthe out pa tients’ care and the hos pi tals was non ex is tent. In ter ac tions were in di cated only inthe cases, when a cer tain hos pi tal had an af fil i ated medical centre.
Prob lems with in ter ac tion were also re ported be tween the out pa tients’ care and the emer -gency med i cal care.
Sim i lar to the re sponses given by the di rec tors and man ag ers of the MHAT about the in -ter ac tion with other hos pi tals, the man ag ers of the SHAT and the na tional cen tres, the spe cial -ised hos pi tals did not un der take any com mit ment for meth od olog i cal as sis tance to themulti-pro file hos pi tals for active treatment.
235
So cio log i cal in ter pre ta tion
Prob lems with per son nel man age ment
The roots of the prob lems with the per son nel man age ment were iden ti fied not so much atpro fes sional level but rather at the level of fi nanc ing:
· “The prob lems with the staff are fi nan cial in na ture and lead to a host of other prob -lems”;
· “The prob lems re sult from the fact that some of the at tend ing doc tors want moremoney to be al lo cated for their ac tiv ity”.
At ti tude to the pri vate hos pi tals
The in ter viewed man ag ers of the spe cial ised hos pi tals and na tional cen tres de clared theirpos i tive at ti tude to the pri vate hos pi tals. It is an in ter est ing fact, that in their po si tion, they de -fended the in ter ests of the pri vate healthcare es tab lish ments rather than per ceive them as an ac -tual com pet i tive threat. Ac cord ing to some re spon dents, “the state makes a se vere andin cor rect dump ing against the pri vate es tab lish ments by com pen sat ing for the debts of thepub lic hos pi tals” and oth ers were of the opin ion, that al though the pri vate hos pi tals were un -equally treated be fore, cur rently they were treated on a par with the public ones, and this wasaccepted positively.
When crit i cisms were ex pressed, they were re lated to the fact that, in some cases, the pri -vate hos pi tals re ferred pa tients in se vere con di tion, for which the pub lic hos pi tals did not re -ceive re im burse ment ei ther from the pri vate hos pi tals or from the health insurance.
At ti tude to privatisation
Privatisation in healthcare was sup ported by the man ag ers of the spe cial ised hos pi talsand the na tional cen tres, on con di tion that in its im ple men ta tion some im por tant re quire mentswere observed:
· “Privatisation should be car ried out but privatisation of the ac tiv ity”;
· “The state must de ter mine the na tional tasks and the na tional hos pi tals, which canguar an tee the na tional healthcare. The rest should go to the pri vate ser vices”;
· “The state is a bad owner; privatisation should be car ried out by the state and the var i -ous rep re sen ta tives of the healthcare should par tic i pate in it”;
· “Privatisation should be car ried out but the healthcare es tab lish ments, which are pri -va tised, should have gone bank rupt, oth er wise, it is a sheer deal” (au thors’ note: infact, the eco nomic logic in di cates that the only peo ple in ter ested in pri va tis ing a bank -rupt com pany are those who have brought about the fail ure).
Fi nanc ing
As sess ment of the model of fi nanc ing
The model of out pa tients’ care fi nanc ing was de fined as better than that in hos pi talcare, which was con sid ered faulty in many di men sions.
The link ing of the num ber of pa tients to the pay ment of the gen eral prac ti tio ners was in -ter preted in a con tro ver sial way. On the one hand, in this way, an in cen tive for work was given tothe phy si cians, but on the other hand, the fi nan cial re sources in com ing for the GPs did not cor re -
236
spond to the per formed ac tiv i ties. This mo ti vated them to at tract pa tients, with out be ing able to ac tu ally pro vide qual ity treat ment. One of the pro pos als for mini mi sa tion of the prob lems inthis field was “the re duc tion of the limit for the num ber of pa tients reg is tered with one GP”.
Re gard ing the fi nanc ing of hos pi tal care, the prin ci ples of the fi nan cial model werecon tested and changes were pro posed. The main the sis was that fi nanc ing should be car riedout by the NHIF only (and not, as un til the end of 2005, by the NHIF and the MH). In ad di tion,the un der stand ing was held that the dou ble fi nanc ing was ab so lutely nec es sary un til the mo -ment, when the NHIF be came be able to fully cover the costs for hospital treatment.
Next in their as sess ment of the fi nan cial model, the in ter viewed ranked the in ter nal con -tra dic tions of the model. They were chiefly man i fested in the fact, that the NHIF and the MHde ter mined the prices, which were not formed on the ba sis of ac tu ally real ised costs and thiswas seen as a rea son for gen er at ing debts (“at the mo ment the Health in sur ance fund and theMin is try do not take into ac count the value and de ter mine prices formed on the ba sis of theavail able re sources and not on ac tual costs”; “it is for sure that we are hav ing a plannedloss”; “the healthcare es tab lish ments are com mer cial com pa nies with a de coded loss. I signan agree ment with the NHIF, from which it is clear from the very first mo ment, that I am sign -ing an im plied loss.”).
Ac cord ing to a large part of the in ter viewed in this group, the fund ing of the hos pi tals had to be in di rect re la tion ship with the hos pi tal sta tus. Pro pos als were made, for the pay ment fortreat ment in one and the same di ag no sis to be dif fer en ti ated ac cord ing the hospital status.
The prob lem with the short age of fi nance be came worse with the un equal ac cess to fi -nan cial re sources (“cer tain hos pi tal es tab lish ments re ceive a better fi nanc ing and im provetheir fa cil i ties and then the rest have to com pete with them”). This un equal ac cess to the fi nan -cial re sources con cerned the fi nanc ing com ing from the MH, and this made it un der stand ablewhy the re spon dents sug gested the ex pan sion of the role of the NHIF and the mini mi sa tionof the fi nan cial op er a tions by the MH as a so lu tion to the prob lem. This in its turn, was per -ceived as an in stru ment for the in tro duc tion of mar ket prin ci ples and com pe ti tion in the sys -tem, en abling the development of the voluntary health insurance funds.
At the same time, the di rec tors and the man ag ers of spe cial ised hos pi tals and na tional cen -tres were not in clined to ne glect the role of the state in the fi nanc ing. At first glance, the viewsabout the in volve ment of the state through the MH in the hos pi tal fi nanc ing seemed con tra dic -tory - part of the in ter viewed pro claimed them selves for the ter mi na tion of the fi nanc ing fromthe MH, oth ers shared the opin ion that “the state must not with draw from the hos pi tal fi nanc -ing”. A more de tailed anal y sis of the opin ions, ex pressed by the man ag ers of SHAT and na -tional cen tres, in fact dem on strated that these views did not con tra dict one an other, butcomplemented each other to form a full picture:
· When the is sue was the pay ment for the di ag nos tic, treat ment and re ha bil i ta tion ser -vices per formed by the hos pi tals (e.g. pay ment for a hos pi tal prod uct), the opin ion pre -vailed, that it should be done by one source, and this source was to be the NHIF. Inad di tion, the pay ment should cover the in curred costs to tally.
· At the same time, the need was re cog nised for in vest ment in fa cil i ties and med i calequip ment which, ac cord ing to the in ter viewed, was the duty of the state. The man ag -ers of spe cial ised hos pi tals and na tional cen tres said that “med i cine is a field in whichhigh and fast in no va tive tech nol o gies, di ag nos tic and treat ment meth ods are used, that are very costly, and the fi nanc ing for them is scarce. As a re sult, a con stant fi nan cial
237
So cio log i cal in ter pre ta tion
def i cit is ob tained in the field of healthcare.” The dom i nat ing view was that this prob -lem could be solved by the al lo ca tion of a greater per cent age of the GDP to healthcare.
Ac cord ing to the in ter viewed, through the MH, the state had to play a “meth od olog i calrole”. A pre- con di tion for that role was the good synchronisation with the NHIF and the de vis -ing of a work ing NFA. Ac cord ing to the di rec tors and the man ag ers of spe cial ised hos pi talsand na tional cen tres, the role of the state un til that mo ment (2005) had been re duced to the fi -nanc ing of the Fund’s def i cit and it was sup posed to deal with the im ple men ta tion ofprogrammes for pre ven tion and health pro mo tion. On the other hand, how ever, the func tion -ing of the Fund was eval u ated as in suf fi ciently ef fec tive and trans par ent.
In short, the role of the MH for the pro vi sion of a long-term programme for pub lichealthcare and its im ple men ta tion could be real ised, only af ter the sys tem of health in sur ancestarted to func tion ef fec tively. Un til then, it had not been re cog nised as a fact, and it is ex plain -able why the role of the state was still so great in the minds of the respondents.
Ac cord ing to the di rec tors and the man ag ers of spe cial ised hos pi tals, the pro file of cer tain healthcare es tab lish ments did al low for the de vel op ment of com mer cial ac tiv i ties (it waselim i nated as a pos si bil ity). There fore, the state’s with drawal was im pos si ble from theirfinancing.
The re spon dents in this group re cog nised that the prob lem with fi nanc ing was not rooted inthe size of the fund ing but also in the mech a nisms for their dis tri bu tion and uti li sa tion. The mainpro posal for the op ti mi sa tion of the sys tem was to close down the in ef fec tive hos pi tals and tore sus ci tate them be cause the re sources in vested in them did not yield re sults. It should be noted,how ever, that these ideas were re ported by the man ag ers of the larger spe cial ised hos pi tals too,ac cord ing to whom more fund ing should be al lo cated to the large hos pi tal cen tres.
The pro posed so lu tion to the prob lem of the “chronic un der fi nanc ing” of the hos pi tal care was the or gani sa tion of an ef fec tive en vi ron ment for the de vel op ment of the vol un tary funds.A ma jor pre req ui site in this re spect was the def i ni tion of the pack age of health ser vices, guar -an teed by the social health insurance.
The wide spread at ti tude was that the change of the fi nan cial model was a pro cess con -tin u ing at the pres ent mo ment, too.
As sess ment of the clin i cal path ways
The di rec tors and the man ag ers of spe cial ised hos pi tals and na tional cen tres con sid eredthat “the clin i cal path ways al low the hos pi tals func tion ing more ef fec tively and hav ing a better rep u ta tion, to in ten sify their work and re ceive more fund ing”, which they eval u ated as a pos i -tive ef fect of the re form. Nev er the less, the fi nanc ing for clin i cal pathways was subject tocriticisms.
Ac cord ing to some man ag ers, the clin i cal path ways were more ap pro pri ate for the con trol of qual ity rather than as an in stru ment for financing.
The in ter viewed re ported that through the clin i cal path ways, the Fund paid in one and thesame way for a per formed ser vice, and thus, the ac tiv i ties in the sys tem were stand ard ised.This prac tice, how ever, con tra dicted the dif fer ences in the rank ing of the hos pi tals and did nottake into ac count the com pli ca tions and the com plex ity of the actual medical practice.
An other main out lined prob lem had to do with the in ad e quate de ter mi na tion of the num -ber and the prices of the clin i cal path ways, which was pri mar ily due to the in ter fer ence of
238
in ter ests of spe cial ists from one cir cle or an other. The de for mi ties of the model were ex em pli -fied by the pres ence of 40 path ways in car di ol ogy and only 4 in neurology.
The clin i cal path ways were fa voured by greater sup port in the nar rowly spe cial ised hos -pi tals: “For us, the clin i cal path ways for which the NHIF pays, are a good tool, pro vided thatthey are paid nor mally. For the time be ing, we do not com plain from the re im burse ment of theclin i cal path ways. The other hos pi tals have 20-30 clin i cal path ways, we have two, but they are enough for us and they cover en tirely the pop u la tion we are ser vic ing.”
A great part of the in ter viewed looked at the clin i cal path ways as a “tran si tory in stru -ment” of fi nanc ing, which was to be sub sti tuted by the di ag nos ti cally re lated groups.
Fa mil iari sation and at ti tudes to the di ag nos ti cally re lated groups
The in tro duc tion of the fi nanc ing through di ag nos ti cally re lated groups (DRGs) was ac -cepted pos i tively. The main ex pec ta tions were that the DRGs would solve a num ber of es sen -tial prob lems in the cur rent sys tem of fi nanc ing. The man ag ers of SHAT and the na tionalcen tres expected the following:
· DRGs to “guar an tee the pay ment of the ac tual value of the ser vice, un like the clin i calpath ways” (“the fi nanc ing will be for ob jec tively made costs”);
· through the fi nanc ing for DRGs “to cost the med i cal staff la bour”;
· the cri te ria for fi nanc ing had to be objectified;
· the con trol over the costs had to be come more ef fec tive.
While the at ti tudes to the in tro duc tion of the DRGs were en tirely pos i tive, the deep un der -stand ing of this fi nanc ing tool re mained ques tion able, al though the in ter viewed de clared thatthey were fully ac quainted with it. When ex am ples were given with a DRG, they did not es sen -tially dif fer from the clin i cal path ways. The be long ing of a cer tain pa tient to a cer tain groupwas re lated again and only to his/her di ag no sis. This, to gether with the above men tioned pos i -tive at ti tudes to the DRGs and the crit i cal views on the clin i cal path ways, gave cer tain groundsfor the con clu sion, that a con sid er able pro por tion of the man ag ers of the SHAT and the na -tional cen tres did not have a neg a tive at ti tude to the core of the clin i cal path ways but to theirqual ity and price, and they hoped for the avoid ance of these short com ings by means of the di -ag nos ti cally re lated groups.
Health in sur ance
Eval u a tion of the model
There were two prin ci pal po si tions re gard ing the health in sur ance. Ac cord ing to the firstone, the ex ist ing model was wrong. The main ar gu ment in fa vour of this view was the pres enceof health in sured cit i zens, who used hos pi tal ser vices, and the costs re mained at the ac count ofthe hos pi tals. The fact is in ter est ing, that this prob lem was per ceived as in her ent to the verymodel of the sys tem for health in sur ance and not so much as a de fi ciency in its func tion ing.
The sec ond view looked at the model of health in sur ance as ap pro pri ate but re quir ingsome changes (“There is no other model for health in sur ance. But its im prove ment should becon sid ered.”; “I do not know, if this is the most ap pro pri ate model, but God save us fromchang ing it.”).
239
So cio log i cal in ter pre ta tion
One part of the pro posed changes re ferred to the in crease of the health in sur ance in stal -ment (“The in stal ments which are paid, are too low, but their in crease has to be done grad u -ally”), an other part re ferred to the stim u la tion of the vol un tary health in sur ance and theabol ish ment of the mo nop o lis tic sta tus of the NHIF (“There have to be sev eral funds or vol un -tary health in sur ance funds.”; “It will be im pos si ble to do with out an ad di tional health in sur -ance, there should be a “sec ond floor”. And it should not be an ex cep tion, it should not becon sid ered a lux ury but part of the sys tem of the healthcare fi nanc ing.”).
At ti tude to the Na tional frame work agree ment
The need for a na tional frame work agree ment was not de nied by the di rec tors and theman ag ers of the SHAT and the na tional cen tres. Nev er the less, its as sess ment was pre dom i -nantly neg a tive. Prob lems were noted both in the prin ci ples and the mech a nisms of con -tract ing and its content:
· “The con tract ing is too populistic; ev ery one tries to shuf fle their in ter ests, a lit tle bit as at the “open ba zaar”. The UBP says which drugs have to be re im bursed and whichnot, but this is ex ceed ing their rights. These things have to be clearly and ac cu ratelyreg u lated – what are the rights and li a bil i ties of each in sti tu tion. This should also bedone for the NHIF and the UBP.”
· “The UBP de ter mines the terms, un der which I am sign ing the agree ment. But I am aju rid i cal per son bear ing all the com mit ment to con clud ing the con tract. And a le galab surd re sults, that a third per son par tic i pates and dic tates terms and con di tions,which af ter that are faced to be ful filled by the hos pi tal di rec tors with out any right ofap peal.”
· “It hap pens so, that we are get ting a rep e ti tion of the Na tional frame work agree mentat all lev els. We have no ne go ti a tions, we have an agree ment “dropped” from above,which has to be ful filled. This is not an agree ment at all, it’s an or der. This or der hasnot been dis cussed be tween the pro vid ers of healthcare but with the UBP. The lat ter(UBP), how ever, does not carry any fi nan cial re spon si bil ity for these con tracts. Theyhave trans ferred to us the prob lems with the money, but pre served the con tract ing atan other level.”
Con cern ing the con tent of the NFA, the crit i cisms were di rected mostly to its fi nan cial pa -ram e ters. The re spon dents did not ac cept the de ter mi na tion of a uni fied price for a clin i calpath way for all hos pi tals, with out tak ing into ac count their rank ing or the dif fer ences in thecosts ac tu ally made.
The crit i cisms re ferred not only to the spe cific terms of the agree ment, but also to its an -nual amend ment:
· “It should not be signed ev ery year. It should be signed ev ery 3-5 years. In the mean -time, it should be added and not amended, so that there is a pos si bil ity for build ing-on.”
· “To my mind, the NFA is nec es sary be cause with out it, no one in the whole sys tem canfunc tion, but I do not think it should be signed ev ery year.”
· “In my opin ion, it is not nec es sary to sign the Na tional frame work agree ment ev eryyear. Ad di tions can only be made to the one from the pre vi ous year. And those will cer -tainly be needed.”
240
Qual ity of the healthcare ser vices
The main form of giv ing in cen tives for the qual ity im prove ment of the healthcare ser vices was linked to the com pe ti tion for the at trac tion of a greater num ber of pa tients (“The re formstim u lates the em ployed in the field of healthcare to in crease the qual ity, be cause the num berof pa tients de ter mines the pay ment”; “The num ber of pa tients de pends on the qual ity andmoney follows the patients”).
On the other hand, it was noted that the in cen tives for at tract ing more pa tients were notsuf fi cient for the qual ity im prove ment and other forms needed to be in tro duced for qual itycon trol and qual ity as sess ment (“Apart from the num ber of pa tients, more fund ing must be al -lo cated and new forms of la bour eval u a tion must be in tro duced in or der to im prove qual ity.”).
The es tab lish ment of a uni fied sys tem for qual ity eval u a tion and con trol was ac ceptedwith mixed feel ings. On the one hand, the need was pointed out for the for mu la tion of sus tain -able cri te ria. On the other hand, sus pi cions arose as to both the pos si bil ity that med i cal carewas mea sured by means of ob jec tive cri te ria, and the pos si bil ity for the work ing out of suchcri te ria in the Bulgarian healthcare system soon:
· “Yes, the sys tem for qual ity as sess ment and con trol is nec es sary and it should be ob jec tive.”
· “The sys tem for qual ity as sess ment and con trol has to be per formed by a spe cial com -mis sion, but it should con sist of ob jec tive and trans par ent cri te ria for qual ity. Whende sign ing these cri te ria, the pa tients’ opin ion must be sur veyed and it should be takeninto ac count, how many pa tients have been ad mit ted and how many have been cured.”
· “Yes, there should be such a sys tem, but as a whole, it is dif fi cult to cre ate a some thinglike this, be cause in med i cine it is very dif fi cult to say what is qual ity and what is not.Nev er the less, it should ex ist and it should be known how much it costs.”
· “Uni fied sounds very well, but the uni fi ca tion passes through the es tab lish ment of nu mer ousand nu mer ous stan dards for qual ity, stan dards for ac tiv i ties, which is not easy. It all boardsdown to sys tem atic work. In our coun try there is no sys tem atic work in this di rec tion”.
Ac cord ing to the di rec tors and the man ag ers of spe cial ised hos pi tals and the na tional cen -tres, “The health in sur ance fund does not con trol the qual ity of the health ser vices at all” sincethey use “for mal in di ca tors, which in no way re flect the treat ment pro cess”. This en hanced the feel ing of “huge and mean ing less pa per work”.
A com mon state ment was that the re form, which had been car ried out, in creased the op -por tu ni ties for the cit i zens to in flu ence the qual ity of the health ser vices they re ceived “be -cause they can get treat ment where they wish, on which the phy si cians’ pay ment de pends”.
At the same time it was es tab lished that the cit i zens:
· “Must play a greater role both in term of ac cred i ta tion eval u a tions and in the sign ingof the NFA”.
· “Must be aware of their rights and li a bil i ties. They can place cer tain claims, only ifthey ful fil their ob li ga tions and thus they can in flu ence qual ity”.
Sig nif i cant prob lems and vi sions for the fu ture
The ma jor prob lems in di cated con sis tently were two – one of them was re lated to the in -ter ac tion with the NHIF emphasising the con stant changes in the Fund, and the other prob -lem was fi nanc ing.
241
So cio log i cal in ter pre ta tion

The vi sions for the fu ture of the healthcare re form were also in the light of the above prob -lems – on the one hand, changes were nec es sary in the ac tiv i ties of the NHIF to gether with thein crease of the fund ing for the clin i cal path ways and the im prove ment of the qual ity con troland, on the other hand, the con tin u a tion of the re form in hos pi tal care through op ti mi sa tion ofthe existent hospital network:
· “A pro found as sess ment must be made of the ex ist ing hos pi tal net work and its op ti mi -sa tion. But the lo cal pe cu liar i ties should also be taken into con sid er ation. You cannever close down the hos pi tal in Smolyan, be cause for this re gion, it is a large hos pi tal. You can not close down the hos pi tal in Ardino ei ther, be cause when the snow falls, thepa tients have no where to go. More over, it is a bor der re gion. That is to say, that thesys tem of healthcare is even tu ally a part of the na tional se cu rity. Con se quently, whenit is de cided where to have and where not to have a hos pi tal, how to re struc ture a cer -tain hos pi tal, many fac tors should be taken into ac count, which are not only med i cal,even most of them are not med i cal so much. This is the one side of the coin. The otherside of the coin is that the re struc tur ing has to be done in a very thor ough way. I’ll givean ex am ple. Let us imag ine that we have town A, town B and town C and the dis tancebe tween them is no more than 40 km. There are many cases like this in Bul garia. TakeGorna Oryahovitsa, Lyaskovets, Veliko Turnovo. Three towns, and Pablikeni isnearby – 4 hos pi tals and each one of them pro vides all the ser vices. Mod ern med i cineshows, that if you work as a crafts man does, i.e. ev ery one does ev ery thing, the qual itycan not be high. Fast turn over is re quired as well as many pa tients in or der to ac quirethe ex pe ri ence in a cer tain meth od ol ogy, es pe cially, if it is an ex pen sive tech nol ogy,equip ment, etc. And, there fore, the peo ple not only in Bul garia, con sider se ri ously,ana lyse the data of the three hos pi tals for the par tic u lar sit u a tion and say: in stead ofev ery one do ing the same thing, hos pi tal A, for ex am ple, has the best fa cil i ties of thethree and a rel a tively mod ern equip ment, why not call it the sur gery, and con cen tratehere the sur gi cal cases. Hos pi tal B tuned out not to be in such a good con di tion, but itis sit u ated beau ti fully and we will turn it into a hos pi tal for fol low-up treat ment, andthe third hos pi tal will be con verted into some thing else. And what hap pens in such acase – the staff is pre served to some ex tent, the hos pi tal is pre served but it is func tion -ally in ter nally re struc tured and then more sur geons will work in hos pi tal A, the qual ityis much higher and peo ple from the nearby cit ies start vis it ing them be cause the goodsur gi cal cen tre is there and a com pletely new pic ture is cre ated. This is to say, that re -struc tur ing does not nec es sar ily mean clos ing down of beds, it does not nec es sar ilymean dis miss ing peo ple but some thing far deeper and more se ri ous, that can be doneonly on the ba sis of thor ough anal y ses.”
As sess ment by man ag ers of dis pen sa ries860
Pos i tive and neg a tive ef fects of the healthcare re form
The pa tients’ free choice in the healthcare sys tem was the main pos i tive ef fect, re portedby the man ag ers of the dis pen sa ries, too:
242
860 Dis pen sa ries: 1) for men tal dis eases; 2) for oncological dis eases; 3) for skin and ve ne real dis eases; 4) forpneumo-phthysiatric dis eases.
· “A pos i tive change is the lib er a tion of the pa tient. Now he/she has the right to de ter -mine the gen eral prac ti tio ner and choose a healthcare es tab lish ment, in which to betreated (what re mains, is that he/she learns how to ex er cise this choice in a wise way)”.
· “As a whole, the re form is a pos i tive be gin ning but ev ery struc ture has to meet the newre quire ments. The ad van tage is that the pop u la tion has ac cess to the pri mary care andthe pres ence of a fam ily phy si cian, who can re spond to all the peo ple’s needs, re ferthem prop erly where to go for con sul ta tion and where to have their in ves ti ga tions per -formed”.
The neg a tive ef fects of the re form were un der stood as a con se quence of the de lay of the re -form in hos pi tal care and the in ef fec tive changes in the field of pri mary out pa tients’ care:
· “Prob lems arose as a re sult of the ir reg u lar rates, at which the re form was be ing car -ried out in out pa tients’ and hos pi tal care. The clin i cal treat ment lagged be hind, thepar a dox re sulted, that the staff with the high est qual i fi ca tion re ceived the low est sal a -ries (one lab o ra tory as sis tant in a di ag nos tic and con sul ta tive cen tre re ceived in timesmore than a hos pi tal phy si cian with two spe cial ties). This is about to be changed and Ifeel op ti mis tic about the fu ture”.
· “A dis ad van tage is the dif fi cult ac cess to spe cial ists and the re form lag ging be hind inthe field of hos pi tal care”.
· “Firstly, the sys tem of gen eral prac ti tio ners is vi cious. One phy si cian is not ca pa ble ofser vic ing an un lim ited num ber of pa tients. An up per limit is nec es sary for the num ber of the pa tients. Sec ondly, the old sys tem of the poly clin ics (now DCC) was much more ef -fec tive… It hap pens so, that the phy si cians with the low est qual i fi ca tion are best paid.Ac tu ally, they drain the money of the Fund for the work they have not done. From amed i cal point of view, for lack of knowl edge or mis use of their sta tus, the gen eral prac ti -tio ners re tain the pa tients too long be fore they re fer them to a spe cial ist. There fore, ourpa tients come to us with tu ber cu lo sis in ad vanced stage, with cav erns, ba cilli, etc.”
· “The re form in healthcare af fected pri mar ily the out pa tients’ care. The hos pi tal carecon sid er ably lagged be hind, and these are two in ter re lated parts of one whole. In or derthat a real re form is car ried out in healthcare, half of the hos pi tals should be closed”
Rates of the healthcare re form im ple men ta tion
The opin ions about the re form were that it took place as a slow and unsynchronised pro -cess. At the same time, the pros pects were shared, about what could a co or di nated re form bring.
Health leg is la tion
The main dis con tent from the health leg is la tion was fo cused on the pro ce dures of its prep -a ra tion, in the course of which dis cus sions lacked with med i cal spe cial ists. This is why, af terthe en force ment of the law, it turned out that the reg u la tions in it did not cor re spond to thespe cific med i cal prac tices. More over, sus pi cions were ex pressed, as to the com pe tence of the“ex perts” pre par ing the nor ma tive doc u ments, which required specialised medical knowledge.
Ac cord ing to the in ter viewed in this group, the new health leg is la tion was a rel a tivelygood ba sis for the func tion ing of the healthcare sys tem, even though cer tain short com ingswere re ported. At ten tion was drawn to the fact that the leg is la tion “is not fa mil iar enough to
243
So cio log i cal in ter pre ta tion
the med i cal pro fes sion als”, un like to the man ag ers who felt well-ac quainted with the nor ma -tive reg u la tions because of the nature of their work.
Prob lems with the man age ment of the healthcare sys tem
As sess ment of the three cen tres of in flu ence in the healthcare sys tem
Of the three man age ment struc tures (the NHIF, the MH and the UBP/UDB), the Un ion of Bul gar ian Phy si cians cre ated the most sen si ble prob lems and had the most neg a tive im -age among the man ag ers of dis pen sa ries. The in ter ac tion with the NHIF was eval u ated asgood but in suf fi ciently ef fec tive due to prob lems in the normative framework:
· “The pro fes sional as so ci a tions are the “de cayed ap pen dix” of the healthcare. No -where in the world are peo ple forced to be mem bers of this un ion or that. The un ionshide be hind our backs, but they do not ac tu ally de fend our rights. It is ex actly them,who al low a “fam ily doc tor” to have 5 000 pa tients. Dur ing the con tract ing with theNHIF, the Fund is the one to de fend our in ter ests. The phy si cians’ un ion fightsagainst our in ter ests. When the Na tional frame work agree ment was be ing signed 3-4years ago, it was the Fund, which pro posed that the dis pen sa ries were in cluded in aspe cial pro vi sion. No such clause was pro posed by the Phy si cians’ un ion. Two yearsago, with in cred i ble ef forts, bar gain ing and scan dals, the UBP even tu ally agreed toin clude such a pro vi sion. What do I need this un ion for? The mo nop oly of these struc -tures should be abol ished by all means.”
· “It is true, that with the old re form, three man ag ing struc tures were formed. With twoof them I main tain ac tive and pro duc tive re la tions. These are the Min is try ofhealthcare and the NHIF.”
In ter ac tions among the man ag ing or gans of the healthcare sys tem
In the as sess ment of the in ter ac tions the em pha sis fell not so much on the con flicts butrather on the lack of sys tem atic or gani sa tion and co or di na tion in the ac tiv i ties of the dif fer -ent man ag ing or gans. Part of the in ter viewed re ported that the prob lems with the in ter ac tionhad been caused by con tra dic tions in the nor ma tive ba sis and the lack of co or di na tion, for ex -am ple, “of the rights and re spon si bil i ties in the prep a ra tion of reg u la tions, guide lines and leg -is la tive ini tia tives”. For oth ers, “the in ter ac tion among the or gans in the sys tem is sat is fac tory,no con flicts or prob lems with coordination are observed.”
Con cern ing the in ter ac tion of the man ag ing au thor i ties of the healthcare sys tem and thedis pen sa ries, it was re ported that the re la tion ships with the Re gional in spec tions of pub lichealth were good, but the re la tions with the RHC were unsatisfactory.
Skills and com pe tences of the man ag ing per son nel
Ac cord ing to the man ag ers of dis pen sa ries, the man ag ing per son nel at var i ous lev els inthe sys tem to a cer tain de gree pos sessed the re quired man ag ing skills and com pe tences.The oncological dis pen sa ries un der lined the or gani sa tional ac tiv i ties at a na tional level, in -clud ing the strong sup port of the Med i cal Coun cil in on col ogy, in which the best specialistswere involved.
At the same time, crit i cal opin ions did not lack. Ac cord ing to part of the re spon dents, the
244
pro fes sional skills of the man ag ing staff at all lev els of the sys tem – na tional, re gional and level of the healthcare es tab lish ment – had de te ri o rated be cause the ap point ments were made ei therfor “po lit i cal rea sons” or “relative relationships”.
The role of the cit i zens in the man age ment of the sys tem
In the dis cus sion of the cit i zens’ role in the man age ment of the sys tem, the em pha sis wasplaced on the pa tients’ or gani sa tions and con sol i dated ac tions:
· “The role of the cit i zens in the man age ment of the sys tem has to be ac tive. In our field,we have many pa tients’ or gani sa tions which are ex tremely help ful. Women whom Iad mire! Even if I am sick or very busy, I can never af ford to deny an in vi ta tion ex tended by their as so ci a tions. With their help we have solved ur gent prob lems (for in stance,short age of med i ca tion) and their role will cer tainly be come stron ger in the fu ture.”
· “The cit i zens have to ac tively de clare their po si tion (what they are sat is fied with andwhat they are dis sat is fied with), be the cor rec tive for the sys tem. For the time be ing, inour coun try, there are no ac tive pa tients’ or gani sa tions and it would have been nice tohave them.”
In for ma tion sys tem in healthcare
The man ag ers of dis pen sa ries ad mit ted to us ing var i ous sources of in for ma tion. Themain sources of in for ma tion in cluded the MH, the internet, the Na tional sta tis ti cal in sti tute as well as informal sources.
The man ag ers of the oncological dis pen sa ries stood out with their en tirely pos i tive eval u -a tions, de clar ing that, when they needed spe cial ised in for ma tion, they had no dif fi cul ties ob -tain ing it (“We have an in for ma tion sys tem es tab lished at na tional level, which has beenre cog nised by the World Health Or gani sa tion as best in the field of on col ogy. We main tain anin for ma tional de part ment which is in charge of the reg is ter of the dis pen sary’s pa tients.”).
Other man ag ers of dis pen sa ries in di cated that they used pri mar ily in for mal sources of in -for ma tion, ar gu ing with the lack of com pli ance among the in sti tu tions and the short age of of fi -cial in for ma tion. The de lay was also emphasised of the in for ma tion, needed by the man ag ers,for ex am ple, in re la tion to the in tro duc tion of new normative requirements.
Fi nanc ing
The man ag ers of dis pen sa ries, sim i lar to the in ter viewed in the other groups, paid at ten -tion to the lack of suf fi cient fi nance for per formed ac tiv i ties and for the staff mo ti va tion. Be -cause of the pe cu liar i ties of the dis pen sa ries’ ac tiv i ties, the state was per ceived as a key andsome times the only source for over com ing the fi nan cial def i cit:
· “The state must in crease the fi nanc ing, es pe cially for the so cially sig nif i cant dis eases.The state must cover to tally the pre ven tion ac tiv i ties in all the med i cal fields. This in -vest ment will be re turned in the fu ture. The state must un der take the main te nance costs for the med i cal ser vices of the peo ple, who can not pay for var i ous rea sons: dis abled,chil dren, chron i cally dis eased peo ple on ex pen sive ther apy, sol diers, stu dents, so -cially unprivileged. The only thing which I re ally re gret, is that now we are not able topay for the travel ex penses of the dis pen sary pa tients, as we used to do be fore 1989.”
245
So cio log i cal in ter pre ta tion
· “The in pa tients’ care for the men tally dis eased peo ple has to be fully the state’s pre oc -cu pa tion. Our pa tients have very poor fi nan cial re sources. At the mo ment we get 350BGN per ad mit ted pa tient. This is not enough and cov ers only the staff’s sal a ries. Wehave our own in come from med i cal ac tiv i ties at pa tients’ re quest. With them, we addon for the pa tients’ drugs and food… In gen eral, the state has to cover 100% the carefor the so cially sig nif i cant dis eases and for those so cial groups, who have small fi nan -cial re sources.”
· “The so cially sig nif i cant dis eases must be a pri or ity for state fi nanc ing. These in cludedis eases from which in di vid u als suf fer but they af fect the whole so ci ety.”
· “The costly ac tiv i ties (such as trans plan ta tions) have to be fi nanced by the Fund. Thestate has to play its role in the con trol of the pro duc tion and the mar ket of drugs. An ex -am ple: sev eral years ago, the“Pharmahim” de cided that there is no eco nomic profitfrom the pro duc tion of one of the ba sic med i cines for tu ber cu lo sis. As a re sult, I had tour gently im port drugs from Greece. The state should also reg u late the num ber of phar -ma cies in a leg is la tive way de pend ing on the size of the pop u la tion. Con trol is neededon the prices of the drugs, too.”
The lack of suf fi cient fi nance was re flected on the ex e cu tion of the so cial func tions andthe pre ven tive func tions of the dis pen sa ries:
· “At the mo ment we are only for mally reg is tered as a dis pen sary, but we are not ful fill -ing dis pen sary (pre ven tive) ac tiv i ties. When a pa tient co mes with tu ber cu lo sis, we areobliged to visit him/her on the spot, see where he/she lives, with what peo ple he/she isin con tact. These peo ple have to be called for ex am i na tion and we have to es tab lishwhether they are con tam i nated, too. This ac tiv ity is not car ried out for any fi nan cialrea sons what so ever. This is why the pa tients with tu ber cu lo sis in creased three times(for those cases we know of. What is num ber of the cases we do not know of, is an otherques tion.)”
· “For me, the most sig nif i cant prob lem is fi nanc ing. But even if I grum ble, the moneyis the same. I do now know whether it is pos si ble to op ti mise the fi nan cial re source ofthe whole sys tem but in my dis pen sary I am try ing to do that. I re di rect fi nances fromthe prof it able ac tiv i ties to oth ers which are also im por tant but are sim ply not fi nancedby the NHIF or the Min is try. Our own in come amounts to only 1%. In this re spect,there is po ten tial but I pre fer to pre serve some so cial func tions of the dis pen sary, too.I am con stantly seek ing ex ter nal do na tions. A great part of the pro phy laxis of the mam -mary gland and the pre ven tion of the dis eases of the cer vix of the uterus is con ductedwithin the frame work of in ter na tional programmes. The “Open so ci ety” Foun da tionhas do nated hos pi tal equip ment for our dis pen sary. I am still ex pect ing the new com -put ers from a do na tion dis trib uted by the Min is try of healthcare. We were in cluded inthe list, but later we were for got ten… As you can see, the fur ni ture in my of fice is rather out-dated and hum ble. In re turn, we ren o vated the cor ri dors and the hos pi tal pre misesbe cause the at trac tive in te rior also cures. We even in volved our pa tients. One of ourpa tients, an art ist, de signed a sunny dec o ra tion free of charge, wel com ing the pa tientsin the foyer. We are main tain ing the gar den and the façade. I have even taken the pic -tures my self for all the bro chures and ad ver tis ing ma te ri als which we are cir cu lat ing.”
246
At ti tude to the clin i cal path ways and the di ag nos ti cally re lated groups
The clin i cal path ways were viewed as a tem po rary mech a nism with a num ber of short -com ings, un like the DRGs which were con nected to the pos si bil ity for ef fec tive fi nanc ing,based on per for mance. As the di rec tors and man ag ers of the MHAT, the SHAT and the na -tional cen tres, the man ag ers of the dis pen sa ries, too, criti cised the clin i cal path ways in terms of their qual ity. The in ter viewed in this group in di cated the neg a tive ef fects of the low qual ity ofthe clin i cal path ways and the dis crep ancy be tween their price and the actual costs of theperformed activities:
· “In the clin i cal path ways there are su per flu ous ac tiv i ties, lead ing to in crease of thevalue of the very clin i cal path ways as well as such that, un der cer tain con di tions, areper formed in Uni ver sity clin ics only.”
· “It is not pos si ble that a sur geon in …. op er at ing a com pli cated ap pen di ci tis with peri -to ni tis, etc.,re ceives the same pay ment as the col league in … op er at ing clas si cal ap -pen di ci tis (a sur gery that can be per formed by a fifth-year med i cal stu dent). It isun ac cept able, that for a se vere pneu mo nia with an ab scess the Fund re im burses 350BGN and for a faulty pneu mo nia in … the same amount is re ceived for a clin i cal path -way. It is an other is sue that these 350 BGN cover only 60% of the cost of treat ment. Insum, at the mo ment the over all Bul gar ian peo ple do not suf fer from dis eases butfrom clin i cal path ways. Our col leagues are forced to be pre oc cu pied with non sense.An ex am ple: I have an agree ment with the NHIF for pneu mo nia but I do not have anagree ment for ab scess. I am forced to reg is ter the pa tient with pneu mo nia. I am ly ingto my self and I am ly ing to the Fund. Re cently, a col league from the Fund told methat, if some body takes the trou ble and checks the num ber of the ap pen dec to mies paidby the NHIF in …, it will turn out that each cit i zen of this town has two ap pen di ces. Ireckon that the DRG method is better. It would re move the ar ti fi cial ac cu mu la tion ofpa tients in the clin i cal path ways.”
· “What is im por tant about the DRGs, is that they do not fi nance a spe cific healthcarees tab lish ment but the ac tiv ity per formed in the healthcare es tab lish ment. This is thenew way of fi nanc ing hos pi tal ac tiv ity.”
· “It is nec es sary to in tro duce the DRGs as soon as pos si ble.”
Health in sur ance
Due to the na ture of the ac tiv i ties, in the dis cus sion of the health in sur ance, the em pha sisfell on the ob ser va tion of the prin ci ple of sol i dar ity and the dif fer en ti a tion of the ser vices, the com pe ti tion among the healthcare es tab lish ments, etc. were not tol er ated. Nev er the less,the pro pos als for an in crease of the health in sur ance in stal ment were rel a tively fre quent.This meant that sol i dar ity was not per ceived only and solely as a func tion of state in ter fer encebut sug gested that the cit i zens, too, play a greater role in the fi nanc ing of healthcare:
· “I am a con firmed ad vo cate of the prin ci ple of sol i dar ity in health in sur ance. Thisprob a bly co mes from the na ture of the oncological dis eases which we treat… I think,that no one need ing treat ment, should be de prived of ad e quate care.”
· “Maybe the size of the health in sur ance in stal ment should be in creased, but for thosewho can not af ford to be in sured, a mech a nism should be found for the pro vi sion of
247
So cio log i cal in ter pre ta tion
equal ac cess to treat ment. The link age with the pro phy lac tic check-ups is an otherstory. The Bul gar i ans do not have health hab its and they need some kind of a force fulsys tem to help them ac quire such hab its.”
· “I think that the size of the health in sur ance in stal ments should be in creased. I don’tlike the idea of a pack age of ser vices against a given health in stal ment.”
· “The health in sur ance in stal ments at the mo ment are much lower that those in theother Bal kan coun tries and in Eu rope, but this is for ob vi ous rea sons.”
· “Im proved collectibility of the health in sur ance in stal ments; im proved in for ma tionsup ply of the sys tem; cre ation of con di tions for com pe ti tion in the sys tem. All these, atthis stage, still have to be car ried out through ad di tional reg u la tion by the state.”
The mo nop o lis tic sta tus of the NHIF was not sup ported by the man age ment of the dis pen sa ries:
· “The mo nop oly of the NHIF should be de stroyed and other funds with sim i lar func -tions should be cre ated.”
· “At the be gin ning of the re form only one NHIF was nec es sary but sub se quently the ne -ces sity emerged for vol un tary health in sur ance funds.”
· “The is sue of the mo nop o lis tic sta tus of the NHIF has an other ex pla na tion. It has, bybirth, been con ceived in a very wise way - to steal… Sep a rate hos pi tals should ex istfor the so cially unprivileged, in which peo ple with out health in sur an ces should be ad -mit ted and treated. The state has to se cure the fund ing for these hos pi tals. The in suredpeo ple should have the right of choice. If there are sev eral health in sur ance in sti tu -tions, dif fer en tial treat ment, de ter mined by the size of the pre mi ums will be achieved ina nat u ral way. Health in sur ance funds are go ing to be grad u ally es tab lished, func tion -ing at a much higher or lower level.”
At ti tude to the Na tional frame work agree ment
The Na tional frame work agree ment was eval u ated as nec es sary and use ful. The prob -lems were iden ti fied in the way it was pre pared and applied:
· “The agree ment is nec es sary, but still in its de vis ing the im pact of some spe cial ists’lob bies can be sensed. In some cases, the NFA is used rather dog mat i cally by thehealthcare es tab lish ments.”
Opin ions were ex pressed that “the dis pen sa ries have to have equal par tic i pa tion in thecon tract ing of ac tiv i ties, cor re spond ing to their pro file”.
Qual ity of health ser vices
Ac cord ing to the man ag ers of dis pen sa ries in the course of the re form no in sti tu tionalmech a nisms had been es tab lished for giv ing in cen tives to the med i cal spe cial ists to in creasethe qual ity of the health ser vices. Even though, it was re ported that through the pol icy on qual -ity, con ducted at lo cal level, the quality could be stimulated:
· “The re form it self does not stim u late the med i cal pro fes sion als to im prove the qual ityof the ser vices they of fer. The in crease of the qual i fi ca tion does not re cip ro cate withthe re spec tive fi nan cial equiv a lent. They fi nance their qual i fi ca tion on their own and,in re turn, they get only per sonal sat is fac tion. The UBP has made an at tempt to do
248
some thing in this re spect through the sug gested credit sys tem for the eval u a tion of thephy si cian’s la bour.”
· “Spe cial ists can not work for 320 BGN monthly, on con di tion that the fam ily phy si -cians have a much higher in come for lower pos si bil i ties and re spon si bil i ties for thetreat ment. The spe cial ists have to work in at least two jobs in or der to sup port theirfam i lies. The phy si cians’ qual i fi ca tion in the dis pen sary is high, these are col leagueswith a re cog nised spe cialty.”
· “I my self have found a way to mo ti vate my em ploy ees: those who work hard with thegreat est num ber of pa tients and bring most money in the clin i cal path ways, get thehigh est sal a ries, re spec tively… The ac cred i ta tion of the healthcare es tab lish ment isalso very im por tant, be cause it is nec es sary to know “who is who” in ev ery med i calfield. The ac cred i ta tion pro ce dure, how ever, is very awk ward and is re lated to for mi -da ble pa per work.”
· “Qual ity is out of ques tion at all. The gen eral prac ti tio ners do not have a mo ti va tion toim prove their qual i fi ca tion.”
Ac cord ing to the man ag ers of dis pen sa ries, the main in stru ments en abling the pa tients to in flu ence the qual ity of the re ceived health ser vice in cluded the choice of a healthcare es tab -lish ment, elim i na tion of the region ali sa tion and the pos si bil i ties for sub mit ting com plaints:
· “The pa tients in flu ence the qual ity of health ser vices through their right to changetheir fam ily phy si cian, if they are not pleased with him/her. Pa tients sub ject to hos pi ta -li sa tion can choose the hos pi tal in which to be treated.”
· “The re form en abled the cit i zens, who de posit their health in sur ance in stal ments, to re -quire a higher qual ity of the ser vices pro vided to them and the main aim is the achieve -ment of the pa tients’ sat is fac tion. The pa tients can in flu ence the qual ity of health ser vices by means of ques tion naires, which should not be ma nip u la tive, how ever.”
The need for as sess ment and con trol of the qual ity of hos pi tal care at na tional level wasuni ver sally re cog nised. The in tro duc tion of the ac cred i ta tion of the healthcare es tab lish mentswas per ceived as a step in this di rec tion, but at the same time, some im per fec tions were re ported:
· “Right now there is no uni fied na tional sys tem for eval u a tion and con trol of the qual ity of the hos pi tal care, but it will be ap pro pri ate to have some thing like that on a na tionalscale. Ac cred i ta tion is sim i lar in na ture but with out the fi nan cial im pli ca tions.”
· “The ac cred i ta tion which has started of the healthcare es tab lish ments is ab so lutelynec es sary as an idea and con cept. The hos pi tal es tab lish ments should be cate gor ised,but this should be car ried out with min i mum pa per work.”
· “Med i cal stan dards lack in all the branches of healthcare, the qual ity con trol has to be ad min is tered ac cord ing to dif fer ent in di ca tors, by dif fer ent par tic i pants and at dif fer -ent lev els in the sys tem.”
Pri or i ties of the healthcare sys tem and ex pec ta tions for the fu ture
Ac cord ing to the man ag ers of dis pen sa ries, the ef forts in healthcare should con cen tratedin sev eral as pects: (1) im prove ment of the pop u la tion’s health sta tus through pre ven tion andpro phy laxis and through re stric tion of the so cially sig nif i cant dis eases; (2) im prove ment of the
249
So cio log i cal in ter pre ta tion
fi nanc ing and or gani sa tion of the healthcare sys tem through changes in the leg is la tive reg u la -tions, clin i cal path ways and (3) im prove ment of the specialised medical equipment andtechnology.
· “The di rec tion of the re form is right but the fi nanc ing should be in creased. The pri or i -ties for the fu ture should in clude: pro phy laxis, so cially sig nif i cant dis eases, pro tec tionof moth ers’ and chil dren’s health, the build ing of hos pices, of fer ing ad e quate pal lia -tive care.”
· “Drop in the chil dren’s mor tal ity rate through im prove ment of moth ers’ and chil dren’shealthcare, re stric tion of the so cially sig nif i cant dis eases, im prove ment of the pop u la -tion’s men tal health, con tin u a tion of the re form in out pa tients’ and hos pi tal care.”
· “The re stric tion of the so cially sig nif i cant dis eases, which the main pur pose of the dis -pen sa ries: they are healthcare es tab lish ments, whose task is to di ag nose and fol low-up the ma jor so cially sig nif i cant dis eases.”
· “In the fu ture, the pri or i ties of the state in clude the hos pi tal care and the ac tiv i ties of thedis pen sa ries as well as the so cially sig nif i cant dis eases (stroke, heart at tack, men tal ill -nesses). The pro phy laxis of dis eases should be a pri or ity, be cause a suc cess ful pro phy -laxis would pre vent ther apy or make it cheaper. And here ex actly co mes the role of thedis pen sa ries, which is not be ing car ried out at the mo ment for fi nan cial rea sons.”
· “Eq uity of all the healthcare es tab lish ments in or der to change the re mu ner a tion of the med i cal la bour through out the whole sys tem of healthcare.”
· “To de sign ad e quate laws, to bring to an end the struc tural re forms and ac com plishthe privatisation in hos pi tal and out pa tients’ care.”
· “Changes are nec es sary through amend ments in the Law on healthcare es tab lish -ments – the dis pen sa ries with in pa tients’ wards should be re struc tured into hos pi talsand. those with out beds, should be come di ag nos tic and con sul ta tive cen tres.”
More spe cif i cally, the pri or i ties re ferred to the im prove ment of the fa cil i ties in the dis pen sa -ries and the pro vi sion of fi nanc ing for all the spe cific ac tiv i ties, per formed by the dis pen sa ries:
· “As a man ager of a dis pen sary, most of all I am wor ried about the lack of fi nanc ing. Itis the cause of all the prob lems: poor fa cil i ties, lack of means for re con struc tion, lackof con di tions not only for the pa tients’ treat ment but also for the phy si cians’ work. I of -ten quote a pa tient of ours who said “You dis charge us, but you re main here.”
· “Pres ently the Fund is pay ing me for path ways, the MH is pay ing me for pa tients with tu ber -cu lo sis and, for the dis pen sary and am bu la tory ac tiv i ties, no body gives a cent. This year forthe first time (au thors’ note: 2005) we solved the prob lem with the Ter ri to rial Ex pert Med i cal Com mis sion by pay ing 20 BGN per hos pi ta lised pa tient. Be fore that, the Com mis sioncharged a lot of costs and no body cov ered them. Now the NHIF is con sid er ing who shouldpay for the in ves ti ga tions for the Ter ri to rial Ex pert Med i cal Com mis sion. It is better for thepa tients to have these in ves ti ga tions per formed by us. Thus, we will be sure in their va lid ity, it will be eas ier for the pa tients and the Fund will pay only once.
The ex pec ta tions of the man ag ers of the dis pen sa ries were di rectly re lated to the so lu tionof key prob lems in the sys tem of dis pen sary ser vices which they de fined as pri or ity. The mainex pec ta tions were that the dis pen sa ries con sol i dated as struc tures for the fu ture and their op ti -mal financing was secured.
250
As sess ment of the man ag ers of healthcare es tab lish ments for spe cial ised out pa tients’ care
Pos i tive and neg a tive ef fects of the healthcare re form
The man ag ers of the di ag nos tic and con sul ta tive cen tres, the med i cal cen tres and the med -ico-di ag nos tic lab o ra to ries de fined the pos i tive as pects of the re form as: (1) for the phy si -cians – im proved ma te rial sta tus and cre ation of pos si bil i ties for greater free dom in the ac tionsof the peo ple em ployed in healthcare, which in its turn, was re lated to the as sump tion of cer tain re spon si bil i ties and (2) for the pa tients – free dom to choose the healthcare es tab lish ment andin tro duc tion of cer tain rules for a reg u lar dis tri bu tion of the population among the generalpractitioners.
The neg a tive re sults of the re form were sum ma rized as two main out comes – those, re -gard ing the role of the med i cal spe cial ists in the sys tem, and those re gard ing the re la tions atsys temic level and re flected in the ev ery day spe cial ists’ prac tice, re spec tively. It was a gen -er ally shared opin ion that the la bour of the spe cial ists was not eval u ated in an ad e quateway. In their po si tion of spe cial ists they as sessed their own pay ment as poor. In its turn, aspointed out by the in ter viewed, this was re flected in the qual ity of the med i cal ser vice and cre -ated con di tions for cor rup tion prac tices among the spe cial ists from the healthcareestablishments for specialised outpatients’ care.
Con cern ing the spe cial ists’ ac tiv i ties, it was ac cen tu ated that the phy si cians had turnedinto ad min is tra tors. This af fected neg a tively the ac tiv i ties for the pa tients’ treatment.
At the level of the healthcare sys tem, the prob lems were for mu lated into sev eralmain di rec tions:
· In ter ac tion be tween those em ployed in out pa tients’ care, e.g. the spe cial ists and thegen eral prac ti tio ners. Ac cord ing to the re spon dents, there was an in her ent con flict be -tween these two par ties in the very ad min is tra tion of the re form be cause “a largenum ber of the gen eral prac ti tio ners do not pos sess the re quired qual i fi ca tion and re -ceive greater re mu ner a tions.” The gen eral prac ti tio ners de ter mined the scope ofthe spe cial ists’ pa tients. The spe cial ists ac cepted this as a de pend ence on an otherstruc ture, which they de fined as of lower qual i fi ca tion.
· Ad min is tra tion of the sys tem – the lim its im posed on the spe cial ists re gard ing theirac tiv i ties; the in tro duc tion of many ad min is tra tive and leg is la tive reg u la tions, which in its turn, af fected the qual ity of the pro vided ser vice.
· Fi nanc ing of the healthcare sys tem – both the short age of fi nanc ing and the fact that itwas done from sev eral sources, were re ported.
· Emer gency and ur gent med i cal care – the spe cial ists did not have the right to re fuseemer gency care, but if there were no re fer rals, it was not re im bursed and the costs re -mained at the ex pense of the DCC. This, in its turn, af fected the mech a nisms of pay -ment, cre at ing con di tions for un reg u lated pay ments.
· Di vi sion of the re forms in hos pi tal care from those in out pa tients’ care.
Ac cord ing to the man ag ers of healthcare es tab lish ments for spe cial ised out pa tients’ care,the old model had con tained two com po nents, which were es sen tial, but were not pre served:the la bour or gani sa tion of the phy si cians-spe cial ists and the pos si bil ity for dif fer ent
251
So cio log i cal in ter pre ta tion
groups of pop u la tion (preg nant women, moth ers, chil dren) to re ceive med i cal ser vicesdi rectly from the spe cial ists.
The in ter viewed saw as prob lem atic the ad min is tra tive mea sures for ac coun tancy andcon trol, the in sti tu tional or gani sa tion of the in ter ac tions with the GPs, the lim i ta tions for vis itsto a spe cial ist and the in ad e quate re mu ner a tion.
Rates of the healthcare re form im ple men ta tion
The view points of the man ag ers of healthcare es tab lish ments for spe cial ised out pa tients’care were di vided into two the ses:
(1) the re form was car ried out slowly, but the un der taken course was right (on theother hand, how ever, the re form was as sessed as fast, e.g. a se ries of hasty changeswere made, which in many cases were not per ceived as suc cess ful).
(2) The ac tions for re form af fected the healthcare neg a tively.
It was pointed out that im prove ment in healthcare was ob served only in the big cit ies be -cause the cit i zens there had ac tual pos si bil i ties to choose the spe cial ists to con sult.
Health leg is la tion
As a prob lem, the healthcare es tab lish ments in the field of spe cial ised med i cal care iden -ti fied the pro cess of pa tients’ move ment and the way of in ter act ing with pri mary med i cal care,reg u lated in the leg is la tive doc u ments and the NFA.
As a whole, the rec om men da tions to the nor ma tive ba sis were to ward it be com ing moretrans par ent and fa cil i tat ing both phy si cians and pa tients. The nor ma tive re quire ments, pre -pared by the RIPCPH, were eval u ated as pos i tive, which, how ever, dif fered rad i cally from thenor ma tive doc u ments de signed by other in sti tu tions. Re gard ing the Min is try of healthcare, itwas claimed that a weak en ing of its role in the nor ma tive ba sis for ma tion was ob served due tothe minimisation of its functions.
The func tion ing of the spe cial ised med i cal es tab lish ments was ac com pa nied by the fol -low ing prob lems re lated to the nor ma tive ba sis:
· “The fast change of leg is la tive reg u la tions, which, on the one hand, hin ders the work -ing or gani sa tion, and makes it dif fi cult for the spe cial ists to get used to these changes,on the other.”
· “the ab sence of a sta ble Law on healthcare es tab lish ments – 10 amend ments havebeen made and it is not clear which is the fi nal one”.
· “Over lap ping of reg u la tions from be fore the re form with those af ter the re form, whichse ri ously hin ders the spe cial ists’ ac tiv i ties. “
· “The health in sur ance fund con sid ers the pro ce dures from a for mal and ad min is tra -tive point of view and is pre oc cu pied with the “texts” in the law it self.”
From this per spec tive, there was a press ing need for changes:
· “Fast privatisation of the ex ist ing healthcare es tab lish ments, which is to be reg u latedby a law.”
· “Clear and ac cu rate med i cal cri te ria in the leg is la tion and not for mally tech ni cal ones.”
· “Reg u la tion for the emer gency and ur gent med i cal care, in clud ing its pay ment.”
252
Prob lems with the man age ment of the healthcare sys tem
The crit i cisms were ad dressed not so much against the nor ma tively reg u lated re la tionsbut rather against the ac tual ac tiv i ties.
As sess ment of the three cen tres of in flu ence in the healthcare sys tem
The views, con cern ing the func tion ing of the Min is try cen tre, cen tred mainly around theclaim that its ac tiv i ties should be di rected to meth od olog i cal as sis tance which, ac cord ing to the man ag ers of DCC and MC had not been clearly defined.
The ac tiv ity of the NHIF was as sessed crit i cally re gard ing its mo nop o lis tic sta tus. An -other, not less im por tant crit i cism, had to do with the way, in which the Fund de ter mined thedis tri bu tion of the fi nances for the var i ous ac tiv i ties – clin i cal path ways, drugs. Here, too, thehuge num ber of re ports, which had to be pre pared, was emphasised. “Of course, we have tobear in mind that the crit i cisms to the Fund do not au to mat i cally mean that it does not func tionef fec tively. But they cer tainly in di cate that in the course of the re form this in sti tu tion has notgen er ated trust among parts of the med i cal pro fes sion als, which in flu ences the effectivenessof the interactions in the system.”
The UBP did not de fend the in ter ests of all phy si cians. Ac cord ing to the spe cial ists, in thecon tract ing pro cess, the UBP pro tected mainly the in ter ests of the GPs, as a re sult of whichthe pub lic re sources al lo cated to them were greater. Some in ter nal strug gles were also re -ported in the Un ion, which did not re fer to the ac tiv ity but rather to the re source dis tri bu tion.The as sess ment of the UBP was also neg a tive re gard ing the qual i fi ca tion courses, which weredefined as formal.
The na ture of the cur rent in ter ac tion was briefly de fined by one of the di rec tors of a med i -cal cen tre as “ev ery one is de fend ing their own in ter est.”
What should be changed in the ex ist ing re la tion ships? In view of the more ef fec tive in ter -ac tion the pro pos als were for the clear and pre cise def i ni tion of the func tions of each struc -ture, e.g. of the MH, the NHIF and the UBP and, based on that, for im prove ment of theco or di na tion among them. Views were also ex pressed about the need for “the peo ple work ingfor these struc tures to be re cog nised pro fes sion als.”
The man ag ers of healthcare es tab lish ments for spe cial ised out pa tients’ care saw the roleof each of the struc tures in the sys tem in the fol low ing way:
· The UBP and the UDB had to con trol the qual ity of the med i cal ac tiv i ties and con tractthe rights and li a bil i ties of the pro vid ers of med i cal care. Be sides, it was nec es sary “tochange the role of the UBP. It should turn into an ac tu ally func tion ing unit, whichshould be in charge of the spe cial ists’ qual i fi ca tion and should not or gan ise for malevents for credit only.”
· As re gards the NHIF, the need was stressed for the dif fer en ti a tion of the health in sur -ance funds, in or der to cre ate fa vour able con di tions for work ing with the vol un taryhealth in sur ance funds.
· The in ter viewed saw two roles for the Min is try of healthcare – to pre pare the nor ma tive ba sis and ex e cute con trol func tions at all lev els. This, in its turn, wais symp tom atic ofthe need for “ev ery day qual ity reg u la tion in the sys tem”.
253
So cio log i cal in ter pre ta tion
In ter ac tion be tween the man ag ing au thor i ties of the healthcare sys tem and thehealthcare es tab lish ments
The in ter ac tion be tween the man ag ing au thor i ties and the healthcare es tab lish ments waseval u ated as good, mainly by the rep re sen ta tives from So fia. In the coun try side, these in ter ac -tions were more fre quently eval u ated as in ef fec tive and ac com pa nied by con tra dic tions. Buteven those, who as sessed the course of the in ter ac tions as pos i tive, did not re port ex am ples ofin ter ac tions be tween units at var i ous man ag ing lev els, but only of in ter ac tions betweenseparate healthcare establishments.
The over com ing of the draw backs in the reg u lated in ter ac tions was car ried out by meansof in for mal mech a nisms for ex ert ing influence.
Those of the man ag ers of the DCC, MC and MDC, who eval u ated the in ter ac tions ascon tro ver sial and ex tremely in ef fi cient, ar gued pri mar ily with the fact that “these are not re -la tion ships be tween part ners but are asym met ri cal re la tion ships be tween those giv ing or dersand those ful fill ing”. This is why, the in ter viewed de clared that it was nec es sary to change theway of in ter ac tions - “to start from the third level and to see what the pa tients’ needs are andnot to have im posed cer tain things from the higher levels in healthcare.”
The man ag ers of healthcare es tab lish ments for spe cial ised out pa tients’ care con firmedthe pres ence of con flicts of var i ous na ture among them selves: “con flicts be tween hos pi tal careand out pa tients’ care, be tween sep a rate per son al i ties, be tween in sti tu tions”; “con flicts be -tween spe cial ists on an in di vid ual prac tice and specialists working in DCC.”
The in ter ac tions be tween the hos pi tal es tab lish ments and the emer gency care were eval u -ated as good and ef fec tive.
Man age ment skills and com pe tences
The man ag ing per son nel at the level of the MH was as sessed as in suf fi ciently pre paredfor the man age ment of the sys tem. The poor train ing and in com pe tence in some cases of cer -tain em ploy ees, was ac counted for with the lack of med i cal ed u ca tion and the pos ses sion ofeco nomic ed u ca tion, which did not pro vide ac tual knowl edge about the spe cific fea tures of the healthcare sphere.
Un like the em ploy ees of the MH, the staff of the Re gional healthcare cen tres was as -sessed as com pe tent and pos sess ing ad e quate man ag ing skills. The Re gional health in sur ancefunds and their man ag ing ca pac ity were eval u ated more neg a tively, again with the ar gu mentthat econ o mists pre dom i nated in the RHIFs, which was the rea son for their in suf fi cient com pe -tence, according to the interviewed.
At the level of the healthcare es tab lish ments dif fer en ti a tion was made be tween “good”and “bad” man ag ers. The per son al ity, who was in charge of the healthcare es tab lish ment, wasde ter mined as a ma jor fac tor, on which the ef fec tive func tion ing of the establishmentdepended.
As far as the over all sys tem was con cerned, the man ag ers of DCC and MC re ferred to in -sti tu tional cri te ria, which had an im pact on the qual ity of the management:
· “Su per flu ous ad min is tra tion con stantly and in ef fec tively grow ing and be com ing moreand more bu reau cratic and at the same time the prob lems in the field are ne glected.”
· “The prin ci ples are not clear for ap point ing man ag ing per son nel. Due to this fact, in -ad e quately trained and some times un nec es sary em ploy ees work in the struc ture. On
254
the other hand, not all the spe cial ists oc cupy a po si tion, ap pro pri ate for their com pe -tences. This de te ri o rates the qual ity of the med i cal qual ity.”
· “Hazy re spon si bil i ties are ob served in the sys tem it self among its var i ous units – fromthe high est to the low est.”
The in for ma tion sys tem of healthcare
There was no unan i mous an swer to the ques tion about the pres ence (or ab sence) of afunc tion ing in for ma tion sys tem. Those, who claimed that a sim i lar sys tem did ex ist, rathermeant the in for ma tion which was re leased by the Min is try and the other con trol au thor i ties and not so much in for ma tion they needed for their daily ac tiv i ties. The need for de sign ing a na -tional in for ma tion sys tem was real ised, though by a small part of the in ter viewed. The ad van -tages, which were pointed out, in cluded the pos si bil ity for con trol in or der to guar an tee theac cu rate work with the clin i cal pathways and the discontinuation of the profiteering.
The opin ion was also shared that there was no pub licly ac ces si ble and an a lyt i cally pro -cessed in for ma tion avail able, which was im por tant for the ev ery day ac tiv ity. Ac cess to suchin for ma tion was avail able mainly to the man ag ers, who re ceived it with out prob lems, but forthe rest of the em ploy ees in the healthcare sys tem, such in for ma tion was not avail able. Theview was re ported that the in for ma tion was frag men tary and in cluded only cer tain ac tiv i ties(for in stance, in fec tious diseases) or concrete medical establishments.
Re gard ing the qual ity of the in for ma tion, it was in di cated that, to a large de gree, it was notuni fied – dif fer ent in for ma tion was sub mit ted by the dif fer ent sources, lead ing to con fu sion.
A ma jor source of in for ma tion for the man ag ers of DCC, MC and MDC was the MH.While for the NHIF, it was claimed that it had a def i cit of in for ma tion, “for the MH, it is onlyenough to open the MH website and find what you need.”
Other quoted sources of in for ma tion in cluded doc u ments, jour nals, con fer ences, sym po -sia, internet jour nals. The in for mal chan nels for trans mis sion of in for ma tion were also fre -quently mentioned.
The role of the cit i zens in the man age ment of the sys tem
Ac cord ing to the man ag ers of the healthcare es tab lish ments for spe cial ised out pa tients’care, un til that mo ment, the cit i zens had not ex erted any sen si ble in flu ence on the healthcaresys tem. The in ter viewed pointed out that “the cit i zens are not fa mil iar with the sys tem”, “theyare not aware of their rights and do not de mand them”, and in terms of their par tic i pa tion in the As sem bly of rep re sen ta tives of the NHIF, they de clared that “it is not known how they areelected and how com pe tent they are.”
Ac cord ing to the man ag ers of the healthcare es tab lish ments for spe cial ised out pa tients’care, the cit i zens should par tic i pate in the man age ment of the sys tem through “an or gani sa tion which should take part in the sign ing of the NFA” and “spe cial ised con sum ers’ or gani sa tions,which should mon i tor and con trol the qual ity of the pro vided ser vices and pro tect the pa tients’rights”. Fur ther more, sug ges tions were made “for pa tients’ rep re sen ta tives to be in cluded inthe man age ment of the hos pi tals in or der to reg u late the hos pi tal ac tiv i ties.” The in ter viewedfrom this group also de clared that the cit i zens had to be aware of their rights and li a bil i ties andsignal about cases of corruption and bad attitude.
255
So cio log i cal in ter pre ta tion
Fi nanc ing
Sim i lar to their col leagues from hos pi tal care, the man ag ers of the healthcare es tab lish -ments for spe cial ised out pa tients’ care iden ti fied the prob lems with fi nanc ing in two as pects:the or gani sa tion of fi nanc ing and the size of the fi nances.
The in ter viewed in this group in di cated the cre ated in equal ity as a de fi ciency in fi nanc ing:
· on the one hand, be tween the hos pi tal and out pa tients’ care, man i fested by the fact thatthe hos pi tals re ceived fi nanc ing from the MH, too, (un til the be gin ning of 2006), un -like the healthcare es tab lish ments in the out pa tients’ care;
· on the other hand, be tween the spe cial ists from out pa tients’ care and the gen eral prac ti -tio ners. The in equal ity was man i fested in the fact, that the spe cial ists re ceived fi nanc -ing for per for mance and the gen eral prac ti tio ners – “for lack of per for mance.”
The man ag ers of DCC, MC and MDC also re ported the pres ence of in equal ity among thespe cial ists them selves. Ac cord ing to the re spon dents, it was caused by the fact, that the pay -ment did not take into ac count the level of in vested la bour, which was more in ten sive andharder for some of the spe cial ties.
As re gards the role of the state in the fi nanc ing of healthcare, the opin ions of the man ag -ers of the healthcare es tab lish ments for spe cial ized out pa tients’ care were sim i lar to those ofthe man ag ers of the hos pi tals and dispensaries.
Ac cord ing to the man ag ers of the healthcare es tab lish ments for spe cial ised out pa tients’care, the pri or ity ac tiv i ties, whose fi nanc ing had to be un der taken by the state, included:
· treat ment of oncological pa tients;
· haemodialysis, the ac tiv ity of the haemodialysis cen tres;
· trans plan ta tion and cardiosurgery;
· ma ter nal care;
· the sys tem of emer gency care.
The pro pos als were for the state to carry out these pri or i ties through the in creased share of the GDP for healthcare and the es tab lish ment of spe cial funds.
The groups, for which the med i cal care had to be fi nanced by the state, in cluded stu dents,chil dren; re tired pen sion ers; so cially unprivileged peo ple; moth ers with chil dren; un em ployed.
One of the sug ges tions was to build spe cial treat ment cen tres (mu nic i pal or state) to coverthe ser vices for the above men tioned so cial groups.
In the mean time, some man ag ers of pri vate med i cal cen tres ex pressed their wish to re -strict the role of the state in the fi nanc ing of the healthcare es tab lish ments (au thors’ note: butnot in the fi nanc ing of the healthcare sys tem), thus achiev ing ‘mar ket ori en ta tion” of thehealthcare network.
The man ag ers of the healthcare es tab lish ments for spe cial ised out pa tients’ care came upwith pro pos als for the so lu tion of the prob lems con cern ing both the or gani sa tion of the fi nanc -ing and the in crease of the size of the fi nanc ing for healthcare.
The fol low ing ways were sug gested for the op ti mi sa tion of the uti li sa tion of the re -sources:
· “ac cu rate and cor rect ac count ing of the costs”. Ex am ples for im prop erly uti lised fi -nances were given for the gen eral prac ti tio ners’ pay ment and “the ar ti fi cially in -
256
creased pay ments of the hos pi tals”;
· “pre cise, clear and well-grounded uti li sa tion of the re sources of the NHIF”. The prob -lems with the fi nanc ing al lo cated for drugs, were quoted as ex am ples;
· “con trol on the re sources uti li sa tion”;
· “re duc tion of the num ber of the healthcare es tab lish ments but not clos ing them downbut mak ing them func tion in a mar ket en vi ron ment and, ac cord ing to their per for -mance, the de ci sion for their fu ture should be made” (a di rec tor of a pri vate MC);
· to take into ac count the value of the in vested la bour.
The sug ges tions for the in crease of the vol ume of the fi nances were that it was achievedthrough:
· ad di tional vol un tary in sur ance for “those who wish more in terms of health ser vices”;
· “in crease of the bud get (au thors’ note: the ex pen di ture of the state as a per cent age ofthe GDP) and the health in sur ance pre mi ums”;
· “the peo ple with higher in come to make co-pay ments; to pro vide a min i mum pack ageof health ser vices and to pay ad di tion ally for more ser vices”.
Health in sur ance
The sys tem of health in sur ance was as sessed as a good and ad e quate so lu tion for the cur -rent eco nomic and so cial state of the coun try. In view of the pro pos als for changes made by thein ter viewed, the con clu sion can be drawn that the ma jor ity of them did not jus tify one of theba sic prin ci ples of the sys tem, e.g. that of solidarity.
As neg a tive ef fects, the man ag ers of the healthcare es tab lish ments for spe cial ised out pa -tients’ care re ported the lack of eq uity among the cit i zens, which ac cord ing to the re spon dents,was ex pressed in the fact that, on the one hand, “many peo ple do not pay their health in sur ance in stal ments”, and on the other, that “one and the same ser vices are pro vided to peo ple with dif -fer ent in come (e.g. with dif fer ent in stal ments)”. The sug ges tions for over com ing theseinequalities included:
· “the health in stal ments should be ac cu mu lated for one in di vid ual and, in case of need,they should be used by the mem bers of his/her fam ily”;
· “ev ery pa tient should know the amount of the re source he/she had avail able (the sum ofthe de pos ited in sur an ces) and the type of ma nip u la tions he/she had the right to use”;
· “link ing the health in stal ments to the con crete pack age of ser vices which is to be usedagainst them”;
· “con trol on whether ev ery in di vid ual paid his/her in stal ments and not re mit ting theob li ga tions of those who had not paid them”.
The ef fec tive ness of the health in sur ance sys tem was as so ci ated to the above changes.The at ti tude to the Na tional health in sur ance fund was con tro ver sial. On the one hand, the dom i nat ing un der stand ing was that the mo nop o lis tic sta tus of the
NHIF was in ef fec tive, be cause neg a tive im pact was ex erted on the fi nanc ing of the healthcare es tab lish ments due to the lack of com pe ti tion in col lect ing of in sur ance in stal ments. There fore, it was rec om mended that “vol un tary funds are built (au thors; note:?!) to com pete with one an -other and the cit i zens should have the pos si bil ity for choice”. Ac cord ing to the in ter viewed
257
So cio log i cal in ter pre ta tion
shar ing this opin ion, the ex is tence of these funds in the fu ture should be solved as a result ofthe action of the market principles.
Ac cord ing to an other view, the ex ist ing mo nop o lis tic sta tus of the NHIF should bepre served. The ar gu ment in sup port of this opin ion was that “the so ci ety has not ma tured yet(au thors’ note: ?!) for the emer gence of pri vate health in sur ance funds or other funds”. Thosewho shared this view, ex pressed doubts about the pres er va tion of the sta bil ity of the healthcaresys tem, if the NHIF was demonopolised. To their mind, this was still as so ci ated with rathergreat risks for the health services of the population.
At ti tude to the Na tional frame work agree ment
The Na tional frame work agree ment was eval u ated as “a good and nec es sary in stru -ment”, “be cause it for mu lates the main rules and gives clar ity as to what to do”.
The sug ges tions were fo cused on the pos si bil i ties for im prove ments in the agree ment.Un like in the other groups of re spon dents, the group of the man ag ers of DCC, MC and MDCex pressed views that it was nec es sary to have “a greater de gree of de tail ing the ac tiv i ties” inthe NFA. But they, too, sim i lar to the hos pi tal and dis pen sa ries man ag ers, sup ported the idea“not to change the very con tent of the agree ment so fre quently”, “to de sign it for a lon ger pe -riod of time and in tro duce only some cor rec tions”.
Re gard ing the de sign ing of the agree ment, the in ter viewed men tioned that “com pro -mises are made at the high lev els not re sult ing in qual ity ser vices and not pro tect ing the in ter -ests of the or di nary spe cial ists” and they recommended:
· “A better co or di na tion among the con tract ing par ties.”
· “Tak ing into con sid er ation the opin ions of the pro fes sional or gani sa tions in the verypro cess of the agree ment prep a ra tion.”
Con cern ing the de vis ing of the NFA, the in ter viewed criti cised the NHIF for “mak ing the work on the NFA bu reau cratic and lay ing down traps” and the UBP for “not ac quaint ing thephy si cians with the NFA and its an nexes be fore its sign ing, as a re sult of which de ci sions aretaken, af fect ing the in ter ests of part of the phy si cians and not giv ing the op por tu nity to the spe -cial ists to ex press their opin ion.”
Qual ity of health ser vices
There was no united opin ion on the is sue of whether the re form stim u lated the pro vid -ers of med i cal care or not to im prove the qual ity of the ser vices they offered.
When the an swer was pos i tive, the ar gu ments cen tred around the pos si bil ity for pa tients’choice: “if a qual ity ser vice is not of fered, the pa tients will not visit the re spec tive healthcarees tab lish ment”. But this de pend ence was valid mainly for the spe cial ists who had in cen tives topro vide a qual ity ser vice be cause their pay ment was linked to their per for mance. The opin ionabout the gen eral prac ti tio ners was that they were not stim u lated to of fer qual ity ser vices asthey were paid for the num ber of reg is tered pa tients. More over, the in ter de pen dence, ex ist ing in the re spon dents’ minds, was clearly dis tinct be tween the way of fi nanc ing and the qual ityof the health services.
Those, who thought that the re form did not pro vide in cen tives for the phy si cians to im -prove the qual ity of the of fered ser vices, ar gued with “the lack of a real eval u a tion of the phy si -
258
cians-spe cial ists’ la bour” and “the limit im posed on the use of spe cial ized med i cal care”. In or der to pro vide in cen tives for the med i cal spe cial ists to im prove the qual ity of their
ser vices, the man ag ers of DCC, MC and MDC proposed:
· “that the pay ment is linked to the fi nal re sult of the per formed health ser vice”;
· “change in the sys tem for qual i fi ca tion im prove ment – abol ish ment of the ex ist ingcredit sys tem and in tro duc tion of ef fec tive stan dards in di cated as a pre-con di tion for aqual ity med i cal ser vice”.
The pre vail ing opin ion was that a na tional sys tem for eval u a tion and con trol of thequal ity of med i cal care was nec es sary. Its role would be to eval u ate mainly in terms of an in -stru ment for ex e cu tion of con trol in the sys tem.
The idea was also pos i tively ac cepted for the link ing of the size of the health in sur ance in -stal ments with the qual ity of the med i cal ser vices, re ceived by the in sured peo ple. But it wasalso un der lined that this could only be achieved, if an ef fec tive sys tem for eval u a tion andcon trol of the qual ity was built. In re la tion to the es tab lish ment of such a sys tem, two pre-con -di tions were out lined – the first one was, that this pro cess was car ried out by “spe cial ists whoare part of the healthcare sys tem and are oc cu pied with med i cal ac tiv ity”, and the sec ond onewas, that it was car ried out by “a com pe tent minister”.
The ques tion about the pos si bil i ties for the pa tients to in flu ence the qual ity of the ser -vices pro vided to them, turned out to be dis put able. The ex pand ing of these pos si bil i ties wasbacked by the fact that “the cit i zens are im prov ing their health cul ture, they know what theywant and how to get it.”
As in the other groups of re spon dents, the man ag ers of DCC, MC and MDC too, re portedthat the cit i zens could in flu ence the qual ity through their choice of a gen eral prac ti tio ner, spe -cial ist, hos pi tal; through mak ing claims and com plaints be fore def i nite in sti tu tions andthrough the pa tients’ organisations.
On the other hand, the the sis was evolved that the cit i zens could not in flu ence the qual -ity of the health ser vices pro vided to them since “they are not suf fi ciently aware of their rightsas cit i zens and as pa tients”, “they are not com pe tent”, “there are no reg u lated rules for theways in which they can ex ert in flu ence. This is true both for the cit i zens them selves and fortheir rep re sen ta tives in the Cen tral man age ment of the NHIF (au thors’ note: the As sem bly ofrep re sen ta tives)”.
Pri or i ties of the healthcare sys tem and ex pec ta tions for the fu ture
The man ag ers of DCC, MC and MDC de ter mined the fol low ing as pri or i ties:
· Re gard ing the med i cal ser vices:� “es tab lish ment of an ef fec tive sys tem for eval u a tion and con trol of the qual ity”;� “fo cus ing on the pa tient at the ex pense of the ad min is tra tive ac tiv i ties”;� “de vel op ment of na tional health programmes”;� “de vel op ment of pre ven tion ac tiv i ties”;� “elim i na tion of the lim i ta tions on dispensarisation”;� “elim i na tion of the lim i ta tions on the re fer rals to a spe cial ist”;� “the dispensarised pa tients of first and sec ond de gree to be re turned to the spe -
cial ists in the MC”;� “de fin ing of ac tual cri te ria for the pa tients’ move ment in side the sys tem”;
259
So cio log i cal in ter pre ta tion
� “build ing of a uni fied in for ma tion sys tem”;� “pur chas ing of new equip ment”.
· Re gard ing the fi nanc ing:� “in tro duc tion of clear reg u la tions about the way of fi nanc ing hos pi tal and out pa -
tients’ care”;� “in creased fi nanc ing from the state”; � “in crease of the health in sur ance in stal ments”;� “in crease of the prices paid by the NHIF”;� “link ing of the fi nanc ing to the qual ity of the pro vided ser vices”.
The ex pec ta tions of the man ag ers of DCC, MC and MDC were for:
· changes in the nor ma tive ba sis;
· change in the sta tus of the NHIF;
· “re duc tion of the gen eral prac ti tio ners’ pay ment”.
The fact is also in ter est ing that some neg a tive ex pec ta tions for the fu ture were ex pressed in re la tion to the ac ces sion of Bul garia to the Eu ro pean com mu nity.
As sess ment by di rec tors of RHC, RHIF, RIPCPH
Pos i tive and neg a tive ef fects of the healthcare re form
Ac cord ing to the di rec tors of RHC, RHIF and RIPCPH, the pos i tive as pects of the re formcould be sum ma rized in three groups:
(1) Pos i tive ef fects re lated to the peo ple em ployed in the field – “the in tro duc tion of theprin ci ples for ac tual eval u a tion of the la bour of the per son nel and as a re sult, thehigher re mu ner a tion of the better doc tors”. Ac cord ing to the in ter viewed, this be -came pos si ble only af ter the in tro duc tion of the mar ket mech a nisms, as a re sult ofwhich com pet i tive re la tions were es tab lished among the med i cal spe cial ists.
(2) Pos i tive ef fects re lated to the or gani sa tion and the fi nanc ing of the healthcare sys -tem. As re gards the fi nanc ing of the sys tem, the abol ish ment of the bud get fi nanc ing and the es tab lish ment of a health in sur ance fund were emphasised. The adopted ruleof “the money fol lows the pa tient” was re cog nised as pos i tive affect of the reform.
Though with a lower fre quency and def i nite ness, some pos i tive ac tions for the started re -struc tur ing of the net work of healthcare es tab lish ments are also re ported – “the bed fundwas re duced in hos pi tal care”. How com pleted this pro cess is, is also an im por tant is sue, but in this case it is more es sen tial that the ac tiv i ties within the sys tem are be gin ning to be mea -sured by means of cri te ria for ef fec tive ness and ef fi ciency.
(3) Pos i tive ef fects re lated to the pa tients – abol ish ment of the region ali sa tion and in tro -duc tion of a free choice of healthcare es tab lish ment and phy si cian. The di rec tion was also pos i tive for the for mu la tion of a guar an teed min i mum pack age of health ser -vices for ev ery in sured cit i zen.
A large part of the in di cated pos i tive as pects of the re form re ferred to views in prin ci ple. How ever, when it came down to the ap pli ca tion of these prin ci ples in real prac tice, the out -comes were iden ti fied as neg a tive ef fects of the re form.
260

Ac cord ing to the di rec tors of RHC, RHIF and RIPCPH, the most sig nif i cant neg a tive out -comes re sult ing from the re form included:
· “Abol ish ment (au thors’ note: !!) of the pro phy laxis and the treat ment of some dis easesin preg nant women and chil dren and liq ui da tion of the school healthcare”;
· “Dif fi cult ac cess of the pa tients to spe cial ised med i cal care”;
· “Pos si bil i ties for drain ing of fi nanc ing from the NHIF and the bud get of the MH”;
· “Con flicts cre ated in side the phy si cians’ pro fes sion due to lack of equi lib rium in thein comes”.
Rates of the im ple men ta tion of the healthcare re form
Among the in ter viewed in this group, the opin ion pre vailed that the re form was fol low -ing the nec es sary di rec tion. There were cer tain dif fer ences about the rates of the re form, onwhich the views di vided in equal parts – ac cord ing to some, it was car ried out at nor mal rates(“we all try that the stages are con ducted smoothly and in the best pos si ble way”, “the modelwhich was adopted does not sug gest faster rates. Be sides, the re form is rad i cal”) and, ac cord -ing to oth ers, there was a de lay due to some dif fi cul ties achiev ing the goals (“The re forms inout pa tients’ care and hos pi tal care had to start si mul ta neously but the hos pi tal one is moreex pen sive and there fore, it was post poned. This is the rea son for the pres ent con fron ta tion”,“The re form is be ing car ried out slowly but the di rec tion is right. There is no other way”,“Slowly – there is no equal start be tween the state and the mu nic i pal hos pi tals, on the onehand, and the private hospitals, on the other”).
Health leg is la tion
The as sess ment of the leg is la tion was pre dom i nantly pos i tive. The com monly sharedview was that the nor ma tive ba sis gave pos si bil i ties for the ef fec tive func tion ing of the sys tem. Some of the re ported draw backs in cluded “the fre quent change of the nor ma tive doc u mentswhich causes chaos” as well as the com plex ity of the nor ma tive reg u la tions “which is notknown well by the health in sured peo ple and this re sults in not be ing aware of their rights andcre ates pos si bil i ties for spec u la tions by unconscientious medical professionals.”
Rec om men da tions were made to the con tent as pect for op ti mi sa tion of the op er a tivecon trol of the med i cal ac tiv ity of the healthcare es tab lish ments, e.g. for the for mu la tion of ef -fec tive in stru ments for con trol which should in clude both in cen tives for qual ity im prove -ment and ef fec tive med i cal care, and sanc tions for fail ure to ful fil cri te ria for qual ity. An othershort com ing, which was re ported, was that “the nor ma tive ba sis does not give op por tu ni ties tothe mu nic i pal i ties to ex e cute con trol over the healthcare establishments”. The need wasstressed for up dat ing the health leg is la tion and mak ing amend ments in the Law on health, theLaw on trans plan ta tions and the Law on health in sur ance (the amend ments in the LHI referredto the increase of the health insurance instalments).
Prob lems with the man age ment of the healthcare sys tem
In ter ac tions among the man ag ing au thor i ties of the healthcare system
The di rec tors of RHC, RHIF and RIPCPH shared the com mon opin ion that each of theman ag ing struc tures had rights and li a bil i ties, which were strictly reg u lated and al lowed it to
261
So cio log i cal in ter pre ta tion
in flu ence the com mon de ci sion-mak ing on is sues of the healthcare re form. In their de ter mi na -tion, they fa cil i tated the har mo nised func tion ing of the sys tem.
As a whole, the in ter ac tions were eval u ated as good and ef fec tive.A large part of the rep re sen ta tives of the RHC and RHIF de clared that their work was not
ac com pa nied by con flicts. None of the in ter viewed di rec tors of RIPCPH re ported the pres ence of some kind of con tra dic tions or conflicts.
· “There are no con flicts – through the ex change of opin ions and di a logue, the nec es -sary in ter ac tion is achieved” (RHC);
· “There are cer tain prob lems, there are some dif fer ences, which are solved by means of a di a logue and con sen sus” (RHC);
· “At the re gional level, there are no con flicts to hin der the work” (RHIF);
· “The prob lems, which ap pear, are solved promptly in a con crete way” (RHIF);
· “There are no con tra dic tions; the sys tem works, but it is nec es sary to have a com monin for ma tion sys tem” (RIPCPH);
· “There are no con flicts, the leg is la tion is clear and is ob served” (RIPCPH).
Yet, the ex is tence of some con tra dic tions was re ported:
· “There are no con flicts, but there are con tra dic tions de pend ing on whose rights andin ter ests the spe cific in sti tu tion is de fend ing” (RHC);
· “There are some prob lems with the UBP due to the lack of a stand on the re spec tive pa -tients’ com plaints for the im prove ment of the poor med i cal ser vices by the Com mis sion on Eth ics” (RHC);
· “What has to be changed in the thus func tion ing sys tem, is that the MH should ful fil itsfunc tions as de fined by law” (RHIF);
· “Good col lab o ra tion ex ists. Even though the re la tions have to be op ti mised and im -proved, cer tain ar gu ments ex ist among the rep re sen ta tives of the healthcare sys tem,but he con flicts are be ing smoothed away” (RHIF).
There were also ex tremely crit i cal opin ions as to the in ter ac tions in the sys tem - “there is al most no in ter ac tion, or, if it is there, it is in ef fec tive” (RHIF).
When the di rec tors of the RHC and RHIF gave ex am ples for con flicts, they re ferred tothe “mis un der stood pro fes sional eth ics of the UBP” (RHC); the ap pro pri a tion by the RHIF ofsome func tions, for in stance, re lated to the reg is tra tion of the healthcare es tab lish ments(RHC); the lack of sup port by the own ers of the healthcare es tab lish ments – the Min is try andthe mu nic i pal i ties, in the cases, when the NHIF had es tab lished breaches (RHIF); the de pend -ence of the NHIF on the NII (RHIF).
Man age ment skills and com pe tences
The di rec tors of RHC, RHIF and RIPCPH gave a very high as sess ment of the man ag ingstaff in the healthcare sys tem both in quan ti ta tive and qual i ta tive terms. The sum ma rised gen -eral opin ion was that there was a suf fi cient num ber of per son nel and, to a large de gree, theyhad dis tinct managing skills.
262
The in for ma tion sys tem in healthcare
The gen er ally re ported view by the di rec tors of RHC, RHIF and RIPCPH was that “thereis no in for ma tion def i cit”. The sources were listed of the in sti tu tions, gen er at ing in for ma tion,e.g. the NII, the NHIF, the NCHI. The pos si bil i ties were also emphasised for ac cess to in for -ma tion, for ex am ple, through the internet.
Three of the re spon dents dif fered from this pre vail ing opin ion. They stressed prob lemssuch as the qual ity of in for ma tion and the in ef fec tive trans mis sion of the in for ma tion flows. Thedata bases avail able at the NCHI and the NHIF were criti cised due to the fact that “they are notstand ard ised and dif fer ent ta bles are trans mit ted by them with dif fer ent in di ca tors which im -pedes the anal y sis and the con clu sion from the data. There fore, it is nec es sary to de sign an over -all in for ma tion sys tem which is lack ing to this mo ment.” As one of the di rec tors of RIPCPHpointed out, un der the pres ent ab sence of a well-de signed and ef fec tively func tion ing in for ma -tion sys tem, “the in for ma tion flows from top to bot tom”, with out the nec es sary feed back.
The role of the cit i zens in the man age ment of the sys tem
As re gards the role of the cit i zens in the man age ment of the sys tem, the ne ces sity was re -ported for in creas ing their ac tiv ity and com mit ment:
· “The cit i zens should be ac tive. The Bul gar i ans must real ise that health costs moneyand that their health de pends on them” (RHC);
· “They should pro tect their own health and re mem ber that apart from that, they haverights and re spon si bil i ties” (RHC);
· “On be half of the cit i zens – ac tive ness, de mand ing at ti tude, good in for ma tion, goodac quain tance with the rights and li a bil i ties” (RHIF);
· “To play a more ac tive role both as phys i cal per sons and united in or gani sa tions”(RIPCPH).
The di rec tors of RHC, RHIF and RIPCPH saw the role of the cit i zens not only in de fend -ing their rights and the ex e cu tion of con trol (“To have civil or gani sa tions to con trol thepro vid ers and the dis trib u tors of fi nances for the med i cal ser vices” (RHC); “To have a bettercon nec tion with the au thor i ties for the man age ment and con trol of com plaints” (RHC), butalso when mak ing cru cial de ci sions for the de vel op ment of the sys tem:
· “With the de vel op ment of the civil so ci ety, the sep a rate or gani sa tions should take anac tive part in the leg is la tive and ex ec u tive pro cess through con trol func tions, ex pres -sion of opin ion, pub lic ity, etc. (RHC);
· “Free choice of phy si cians and par tic i pa tion of civil struc tures in the man age ment ofthe health in sur ance fund” (RHC);
· “To play an im por tant role in the sign ing of the frame work agree ment and in the con -trol and the man age ment of the fi nan cial re sources” (RHIF);
· “Now I re mem ber that pa tients’ as so ci a tions have been founded. What we saw, theoncological pa tients, the pa tients on haemodialysis united and de fended their rights,stated to the so ci ety their needs and the ex ist ing omis sions, which were later cor rected. Ithink that the civil so ci ety would be come a cor rec tive in the fu ture for those short com -ings, which are ei ther evolv ing at the mo ments or have re mained un seen” (RIPCPH).
263
So cio log i cal in ter pre ta tion
Only one of the in ter viewed di rec tors de clared that un der the cur rently ex ist ing sys temthe cit i zens could not ex ert con trol and play no role in the man age ment of the sys tem (RHC).
Fi nanc ing
Model of fi nanc ing
The prob lems with fi nanc ing, re ported by the in ter viewed di rec tors of RHC, RHIF andRIPCPH, did not es sen tially dif fer from the ones, reg is tered by the other groups of re spon -dents. Un like them, the rep re sen ta tives in this group, to a much greater de gree, in di cated prob -lems with the fi nanc ing re lated to the or gani sa tion and the ways of dis tri bu tion of thefi nan cial re sources in the healthcare system.
Ac cord ing to the di rec tors of RHC, RHIF and RIPCPH, the pay ment per ca pita was not an ap pro pri ate way of pay ment to the gen eral prac ti tio ners and was eval u ated as un fair. In spe -cial ised care, the ma jor prob lem was seen in the need for a clear de fin ing of the ac tiv i ties,which were paid di rectly by the pa tient. The dou ble fi nanc ing of hos pi tal care (from the MHand the NHIF) was in di cated as a fact of neg a tive sig nif i cance which, how ever, wasconsidered as a temporary phenomenon.
The in ter viewed de clared that the prob lems had been caused by the in cor rect dis tri bu tionof fi nan cial re sources in the sys tem of out pa tients’ care. The op ti mi sa tion of the fi nan cial re -sources in the out pa tients’ care and the trans fer of part of them to the hos pi tal care would solvesome of the problems.
The chronic fi nan cial def i cit, in her ent from the very be gin ning, and en com pass ing the whole hos pi tal net work in the coun try, was pointed out, es pe cially in the large hos pi tals which“the more they work, the more they lose”. In the di rec tors of RHC, RHIF and RIPCPH the ideahad crys tal lised that “the sys tem has been prop erly de signed and “writ ten” but in cor rectlyim ple mented”, un like the state ments made by the rep re sen ta tives of the other groups of re -spon dents, for whom this idea went without saying.
The the sis which was com monly ac cepted was that “the fi nanc ing is not lit tle but the re -sources should be prop erly uti lised”. The sug gested so lu tion of the prob lem was “fi nanc ingfor per formed ac tiv ity only”. Ac cord ing to the di rec tors of RHC, RHIF and RIPCPH, thiscould be achieved by the in tro duc tion of the di ag nos ti cally re lated groups. This was ev i dentfrom the many ref er ences to that in stru ment as well as from the uni lat eral in ter pre ta tions of thepos si ble re sults from its over all in tro duc tion:
· “With the de vel op ment of the DRG and ICD10, the lag ging be hind from the de vel opedcoun tries will be elim i nated in short terms”;
· “I hope that, af ter the in tro duc tion of the DRGs, the fi nanc ing will be uni lat eral, onlyfrom the NHIF and per ad mit ted pa tient and things will be come clearer”;
· “The fi nanc ing has to be for fin ished work. With the in tro duc tion of the DRGs, many ofthe prob lems with fi nanc ing will be solved”;
· “In the out pa tients’ care, there are prob lems with fi nanc ing. In hos pi tal care the fi nanc -ing for per for mance should be in tro duced through the di ag nos ti cally re lated groups”.
As in the other groups of re spon dents, in the group of the di rec tors of RHC, RHIF andRIPCPH, too, the at ti tudes to the di ag nos ti cally re lated groups and the ex pec ta tions con nectedwith them, were due not so much to the prin ci pally better in stru ment of the DRGs as com -
264
pared to the clin i cal path ways but to the de fects of the Bul gar ian clin i cal path ways and theneg a tive con se quences from them.
Ac cord ing to the di rec tors of RHC, RHIF and RIPCPH, the im prove ment of the con trolat all lev els of the sys tem was of ma jor im por tance for the op ti mi sa tion of fi nanc ing:
· “Re veal ing of the ways for drain ing of the fi nan cial re sources, which are in suf fi cientany way, and de ci sively erad i cat ing sim i lar at tempts”;
· “Now, for lack of con trol, the pay ment is dou ble – from the Fund and from the pa tient,and the fi nances are spent ex tremely in ef fec tively”;
· “Cer tainly, there are pos si bil i ties for op ti mis ing the fi nan cial costs… The elim i na tionof this cor rupted en vi ron ment of com mis sions and money un der the ta ble. These arefac tors which demotivate the peo ple to pay their health in sur an ces”.
The role of the state in the fi nanc ing of the healthcare sys tem
The scope was wide of programmes, ac tiv i ties and groups which had to be a pri or ity forthe state, ac cord ing to the di rec tors of RHC, RHIF and RIPCPH.
· Pri or ity health programmes and ac tiv i ties fi nanced by the re pub li can bud get:� school healthcare;� emer gency med i cal care;� pre ven tion of so cially sig nif i cant dis eases (AIDS, flu, hy per ten sion, breast can cer); � im mu ni sa tions;� oc cu pa tional med i cal ex per tise;� chil dren’s healthcare.
· Pri or ity groups of the pop u la tion for whom healthcare was fi nanced by the re -pub li can bud get: � dis abled peo ple;� so cially unprivileged;� re tired pen sion ers;� work ers un der risk con di tions;� chil dren and stu dents aged up to 18.
It is an in ter est ing fact, that de spite the dis ap proval of the dou ble fi nanc ing for the hos pi -tals (from the MH and the NHIF), the di rec tors of RHC, RHIF and RIPCPH pro posed that theex pen di ture of the state for hos pi tal care was in creased “to a de gree of cov er ing all the costs for the pa tients”. As in the case of the di rec tors and man ag ers of hos pi tals and dis pen sa ries, thismay mean: (1) elim i na tion of the dou ble fi nanc ing, only when the NHIF was ca pa ble of pay ing for the full cost of the ac tiv i ties per formed by the hos pi tals and/or (2) the NHIF se cured fi nan -cially the di ag nos tic and treat ment func tion of the hos pi tals and the MH (in case thewear-and-tear con tin ued not to be de ducted) cov ered their in vest ment costs.
As a whole, the con clu sion can be drawn that among the di rec tors of RHC, RHIF andRIPCPH, the un der stand ing was spread that the im por tance of the state in healthcare pre -dom i nated. This is ob vi ous both by the large num ber of the state pri or i ties, in di cated in oneof the in ter views, and the pre vail ing em pha sis on the con trol mech a nisms of the state at theex pense of self-reg u la tion (eco nomic in cen tives and mech a nisms for qual ity im prove ment) of the healthcare establishments.
265
So cio log i cal in ter pre ta tion
Health in sur ance
The ma jor ity of the in ter viewed di rec tors of RHC, RHIF and RIPCPH eval u ated themodel of health in sur ance as com par a tively ap pro pri ate for the cur rent stage in spite of thecon tra dic tions and the problems:
· “The sys tem of oblig a tory health in sur ance cor re sponds to the prin ci ples of sol i dar ity,eq uity, etc., but it is not un der stood by cer tain cir cles of so ci ety.” (RHC);
· “The in sur ance is low be cause the in come of the Bul gar ian peo ple is low. For the timebe ing, it is the most ap pro pri ate model. But the fund ing is in suf fi cient – the num ber ofthe un em ployed and the un in sured is large and there fore, the bud get of the NHIF islim ited. That is why changes are con stantly made in the drug list, in the clin i cal path -ways – ev ery thing de pends on the ca pac ity.” (RHIF);
· “This model of so cial in sur ance is good and the only pos si ble. If the health in sur ancepre mium is in creased, a large part of the peo ple would not be able to pay it.” (RHIF);
· “It cor re sponds to the prin ci ples of sol i dar ity and eq uity. But one of these prin ci ples isabused, e.g. the prin ci ple of the sol i dar ity be cause of the un solved prob lem with thepeo ple in debted for health in sur an ces.” (RHIF);
· “The com pul sory health in sur ance is ap pro pri ate but it should not be the only mech a -nism for col lect ing fi nances. It com plies with the prin ci ples of sol i dar ity and eq uity butthere must be pri vate funds.” (RIPCPH);
· “This sys tem en ables the cit i zens to have equal ac cess to the healthcare sys tem.” (RHIF);
· “The model is suit able – ser vices will al ways be pro vided for the poor and the rich willpay” (au thors’ note: ?!) (RHC).
Along side with these, there were neg a tive shaded state ments re gard ing the model ofhealth in sur ance:
· “Pres ently the in sured pays for the un in sured” (RHC);
· “This model is more ap pro pri ate for the rich coun tries” (RHC);
· “The in sur ance sys tem should not be or gan ised in this way, the in sur ance in stal menthas to be per sonal” (RHIF);
· “There has to be a dif fer en ti a tion of the health in sur an ces, re lief for those, who con -duct pre ven tion and have no harm ful so cial and health risks” (RIPCPH).
Un like in the other in ter viewed groups, in this group of re spon dents the views about thesta tus of the Na tional Health In sur ance Fund di verged to a large ex tent.
Among the di rec tors of the RHIF, there were peo ple, who ar gued in fa vour of the mo -nop o lis tic sta tus of the NHIF, and oth ers who reck oned that the NHIF was not a mo nop o list:
· “The NHIF does not have a mo nop o lis tic sta tus. It ex e cutes the NFA, which is pre -pared and signed by the pro fes sional or gani sa tions of the UBP and the UDB and bythe MH. The NHIF is de pend ent on them There are al ready es tab lished vol un taryhealth in sur ance funds, which are the NHIF com pet i tors”;
· “There is no mo nop oly; the law has al lowed for the es tab lish ment of vol un tary funds”;
· “To my mind, from the point of view of the eco nomic de vel op ment of the state, it is inthe in ter est of so ci ety to pro tect the pres ent sta tus of the NHIF”;
266
· “There should be no other funds un til there is a uni fied in for ma tion sys tem.”
But among the di rec tors of the RHIF, too, some neg a tive as pects were re ported of theNHIF sta tus:
· “The mo nop oly does not yield good re sults. 3-4 or gani sa tions should ex ist in or der toen sure a better ser vice”;
· “I have a def i nitely neg a tive at ti tude to the sta tus of the NHIF – the mo nop oly of theNHIF must be elim i nated.”
Among the di rec tors of RHC, RHIF and RIPCPH, the at ti tude dom i nated for a change in the mo nop o lis tic sta tus of the NHIF. It was re cog nised that, at the be gin ning of the re form, themo nop o lis tic sta tus of the NHIF was a ne ces sity, which how ever, did not ex ist any more. Ac -cord ing to them, “the mo nop oly is not good for the good func tion ing of the healthcare sys tem”.
The main changes rec om mended for the more ef fec tive func tion ing of thehealthcare sys tem in cluded the fol low ing:
· “To change the size of the health in stal ments” (the ma jor ity of the in ter viewed fromRHC and RHIF);
· “To link the health in sur ance in stal ment with pro phy lac tic check-ups” (RHC);
· “The health in sur ance pre mi ums must not be bound to the pro phy lac tic check-ups, whichshould be oblig a tory and the state must to tally pay for them from the bud get” (RHC);
· “To in ter re late the size of the health pre mi ums with the pro phy lac tic check-ups un lessthe state com pletely pays for them from the re pub li can bud get” (RHIF);
· “To link the health in sur ance in stal ment with a def i nite vol ume of ser vices in theframe work of one cal en dar year” (RHC);
· “To up date the pack age of the pro vided ser vices ac cord ing to the pop u la tion and thecon di tion of the healthcare sys tem” (RHC);
· “To change the way of de ter min ing the in stal ments – the peo ple with higher in comemust pay higher health in sur ance in stal ments, a work ing mem ber of a fam ily has to in -sure a not work ing mem ber” (RHC);
· “The way of de ter min ing the in stal ments has to be changed – an ex tremely flex i ble ap -proach has to be ap plied to the un in sured and the so cially dis ad van taged. The statehas to as sume re spon si bil ity with fi nanc ing from the bud get in or der to elim i nate theprob lem with the un in sured and not to post pone its so lu tion in time” (RHC);
· “The prob lem has to be solved with the in sur ance of the poor and the un em ployed,such an al ter na tive should be found for the sys tem that the health in sur ance is ac cept -able for all the groups” (RHIF);
· “To im prove the way of their de ter mi na tion (au thors’ note: of the in sur ance in stal -ments). There should not be a limit of 10 min i mum work ing sal a ries” (RHIF);
· “The change has to be made at the ex pense of the em ploy ers, to fi nance the pro phy lac -tic check-ups” (RHIF).
The ma jor ity of the di rec tors of RHC, RHIF and RIPCPH sup ported the link ing of thein stal ments with the spe cific ser vices re ceived.
Opin ions were also voiced that the link ing of the size of the in stal ment with the health
267
So cio log i cal in ter pre ta tion
ser vice con tra dicted the prin ci ple of sol i dar ity (RHC) and it was very dif fi cult to put it intoprac tice (RHIF).
At ti tude to the Na tional frame work agree ment
The Na tional frame work agree ment was as sessed mainly as nec es sary and use ful at thecur rent stage. Un like the man ag ers and the di rec tors of the hos pi tal es tab lish ments, the in ter -viewed in this group sup ported to a greater de gree the cur rent or gani sa tion and the mech a -nisms of its design and signing:
· “The mech a nisms for its prep a ra tion and adop tion are ap pro pri ate. The in ter ests ofall the in volved par ties are taken into con sid er ation” (RHC);
· “The in ter ests of the var i ous lev els in the sys tem are linked and bal anced. The way ofits prep a ra tion, adop tion and its con tent should not be changed” (RHC);
· “It is nec es sary be cause it reg u lates the rights and li a bil i ties of all the par tic i pants in -volved in the healthcare sys tem” (RHIF);
· “The agree ment is use ful, the mech a nisms for its prep a ra tion are proper. The most re -cent frame work agree ment is the best con cluded so far” (RHIF);
· “The NFA is man da tory, it en sures the bal ance of in ter ests be tween pro vid ers and con -sum ers of med i cal ser vices” (RHIF).
Mean while, there were quite a few of the di rec tors of RHC, RHIF and RIPCPH, who heldthe opin ion of the ma jor ity of the man ag ers and the di rec tors of the hos pi tal es tab lish ments,that the mech a nisms of prep a ra tion and adop tion of the NFA needed to be im proved (RHC);not to be adopted ev ery year but to be amended and added (RHIF and RIPCPH); “in its prep a -ra tion a wider scope of spe cial ists have to par tic i pate and they should not be long to one andthe same pro fes sional or gani sa tion; the civil par tic i pa tion should be en hanced in it; the mu -nic i pal i ties as own ers of healthcare es tab lish ments also have to par tic i pate” (RIPCPH).
The view is ex pressed that the NFA “is def i nitely head ing in a pos i tive di rec tion but toplevel cir cum stan tial and per sonal in ter ests in fringe on its prin ci ples (RHC), and one of the di -rec tors of RHIF in di cated that the agree ment was “ab so lutely un nec es sary”.
Qual ity of health ser vices
The un der stand ing pre vailed with higher fre quency, that in one way or an other, the re -form stim u lated the pro vid ers of med i cal care to im prove the qual ity of the ser vices of -fered by them.
Ac cord ing to the di rec tors of RHC, RHIF and RIPCPH, the fac tors ex ert ing stim u lat ingin flu ence on the ex ec u tors of med i cal ser vices included:
· “the re mu ner a tion for the la bour ac cord ing to the quan tity and qual ity of the med i cal ser -vices. A large part of the spe cial ists from hos pi tal care can work in the out pa tients’ sec tor”;
· “com pe ti tion among the sep a rate healthcare es tab lish ments”;
· “the pa tients’ right of choice of cer tain healthcare es tab lish ments”;
· “at tes ta tion of the gen eral prac ti tio ners” (RHIF);
· “pos si bil i ties for privatisation” (RHIF);
· “pub lic mon i tor ing of the re quired qual ity”.
268
A con sid er able num ber of state ments were re ported, ac cord ing to which in cen tives for qual -ity im prove ment did not ex ist or were not enough to achieve a good re sult. The main ar gu mentsin this re spect re ferred to the pres ence of “a lot of pa per work”, waste of time for ad min is tra tive ac -tiv i ties”, “lack of in ter est be cause the qual ity is not re lated to the spe cific re mu ner a tion”, “lack ofad e quate dis tri bu tion of the fi nan cial re sources”. In or der to cre ate in cen tives, the di rec tors ofRHC, RHIF and RIPCPH sug gested “the fol low ing mech a nisms to be trig gered”:
· ac cred i ta tion of the healthcare es tab lish ments;
· “link ing of the per for mance to the size of and the way of fi nanc ing”;
· “in tro duc tion of in ter na tional stan dards for qual ity”;
· “Only if pri vat iza tion is car ried out and the healthcare work ers are paid ad e quately,they will have the in cen tive to of fer a higher qual ity ser vice”.
The or gani sa tion for the eval u a tion and con trol of the qual ity of med i cal care wascom mented from dif fer ent view points and con tro ver sially Ac cord ing to some of the in ter -viewed, “the sys tem for eval u a tion and con trol is good but the con di tions de mand that com -pro mises are made” (RHC). Ac cord ing to oth ers, it was nec es sary to build “a uni fied na tional sys tem for eval u a tion and con trol of the qual ity of med i cal care” (RHC, RHIF).
As re gards ac cred i ta tion, it was pointed out that it “serves for some kind of pres tige”, but the pay ment did not de pend on the re sults from it (RHC), it was nec es sary to re duce to a min i -mum the sub jec tive fac tor (RHIF), “to re flect the ac tual state of the fa cil i ties and not its doc u -mented pre sen ta tion and the ac cred i ta tion should take into ac count the dif fer ences in thehealthcare es tab lish ments” (RIPCPH) and in cluded all the levels of the system (RHC).
Great at ten tion was paid to the cri te ria for qual ity:
· “It is not clearly for mu lated what ex actly “qual ity of med i cal ser vices” means; thereis no sys tem for eval u a tion and con trol to stim u late qual ity at all level.” (RHIF);
· “Clear and ac cu rate cri te ria are nec es sary for qual ity, which are to be linked to theover all pro cess of treat ment” (RHC);
· “The cri te ria have to be uni fied for the dif fer ent types of healthcare es tab lish ments”(RHC);
· “There are nu mer ous cri te ria for the qual ity of med i cal care. The nor ma tive ba sis hasto be fur ther de vel oped and the cri te ria for qual ity have to be ex panded” (RHC);
· “If these cri te ria are for mu lated pro fes sion ally, this is a guar an tee for higher qual ity”(RHIF);
· “The cri te ria have to be fea si ble and it should be pos si ble to con trol them. The pa tienthas to be come the cen tre of the sys tem” (RHIF).
Re gard ing the pos si bil i ties of the cit i zens to in flu ence the qual ity of med i cal care theopin ions di verged. Part of the di rec tors of the RHC, the RHIF and the RIPCPH, who thoughtthat the cit i zens had such pos si bil i ties at their dis posal, in di cated the same fac tors as the in ter -viewed from the other groups, e.g. free choice, ac quain tance and de fend ing of pa tients’ rights,the pos si bil i ties to sub mit claims and com plaints to var i ous in sti tu tions. Oth ers were of theopin ion that these pos si bil i ties were ei ther not uti lised in real prac tice or they were in suf fi cient. It was also re ported that the cit i zens were de pend ent on the gen eral prac ti tio ners, which com -bined with their low in come, re stricted their pos si bil i ties to in flu ence qual ity.
269
So cio log i cal in ter pre ta tion
Pri or i ties of the healthcare sys tem
When rank ing the pri or i ties, as de clared by the di rec tors of the RHC, the RHIF and theRIPCPH, the em pha ses fell on the fol low ing:
· “Fight ing dis eases which ac count for ap prox i mately 90% of the mor tal ity in Bul -garia” (RHC);
· “Care for cer tain groups – moth ers who have just given birth and chil dren (re turn tothe school doc tors), care for the health of the so cially unprivileged” (RHC, RIPCPH);
· “Health pro mo tion, pro phy laxis and im mu ni sa tion, health ed u ca tion and cul ture,early di ag nos tics, qual ity of treat ment and re ha bil i ta tion” (RHC, RIPCPH);
· “Pro phy laxis and pre ven tion for chil dren and stu dents aged un der 18. Pro phy laxis for work ers, pro phy laxis for so cially sig nif i cant dis eases, pre ven tion and pro phy laxis inthe field of den tal care for chil dren and el derly” (RHC);
· “All these dis eases which oc cur for so cial rea sons in very ten der age – hy per ten sion,car dio vas cu lar dis ease, oncological dis eases, in par tic u lar, which have re cently be -come in creas ingly fre quent and the age lim its dropped” (RIPCPH);
· “Drug ad dic tion also be came a se ri ous whip. To my mind, it is im por tant to pay at ten -tion to drug ad di tion and the sex u ally trans mit ted dis eases be cause the first leads tothe sec ond.” (RIPCPH);
· “Es tab lish ment of health in sur ance by name, with strictly listed ser vices, in cluded in itand the pres ence of mag net cards for pur chas ing drugs” (RHC);
· “Greater con trol over the fi nan cial re sources be cause, at the mo ment, much of the fi -nance is drained to the ben e fit of cer tain mem bers of the med i cal staff” (RHIF);
· “Cre ation of con di tions for the cit i zens to ex er cise their rights in ac cor dance with theleg is la tion” (RHIF).
Ex pec ta tions for the fu ture of the sys tem
The views on the fu ture of the healthcare sys tem were mainly and pri mar ily op ti mis tic,al though in some cases this op ti mism was con di tioned:
· “De spite the dif fi cul ties, the sys tem will move for ward and will at tain Eu ro pean level.The healthcare re form will con tinue and will ac cel er ate as we en ter the EC. There isno other way. Our healthcare has to be at Eu ro pean level and I be lieve that we willachieve it in the near fu ture” (RHC);
· “Im prove ment and per fec tion of the healthcare sys tem, so that it can start func tion ingac cord ing to Eu ro pean stan dards and cri te ria. The road has been de ter mined for theful fil ment of the EC re quire ments and for the real func tion ing of a changed healthcaresys tem in our coun try” (RHIF);
· “If the cur rent di rec tion is pre served – pos i tive de vel op ment of the sys tem” (RHIF);
· “This model will be set tled and, in spite of all the dif fi cul ties, we will go for ward”(RHC);
· “The sys tem will be fur ther de vel oped and more health in sur ance funds will ap pear”(RHIF);
· “It will de velop in a pos i tive di rec tion, if the healthcare es tab lish ments are fi nanced
270
en tirely from the NHIF, if the MHAT in the smaller towns are re or gan ised into hos pi -tals for fol low-up and con tin u ous treat ment” (RHC);
· “The role of the pa tients will be en hanced in the con trol of the healthcare es tab lish -ments. De vel op ment of an ef fec tive sys tem for im prov ing the skills of the med i cal per -son nel” (RHC);
· “Build ing of a sys tem, ori ented to the pa tient as a con sumer” (RHIF);
· “To im prove the qual ity of the health ser vices, the phy si cians’ re mu ner a tion, the tech -ni cal po ten tial, tech nol o gies and mod erni sa tion.” (RHIF);
· “The NHIF should have com pet ing in sti tu tions with state par tic i pa tion and ac tu allyfunc tion ing vol un tary in sur ance” (RHIF);
· “The de vel op ment of the sys tem in terms of quan tity and qual ity of the med i cal work ers gives us grounds to con sider that the sys tem will de velop in a pos i tive di rec tion, but thecri te ria for the qual ity eval u a tion should be changed to gether with its fi nanc ing, in or -der to en hance the op er a tive con trol of all the ac tiv i ties” (RIPCPH);
· “This is a sys tem which, in my opin ion, we are de vel op ing for the better. This isgrounded in the nu mer ous pri vate hos pi tals and pri vate cen tres which emerged andwhich are full of tech nol ogy and good spe cial ists” (RIPCPH).
In the re spon dents’ opin ion, the main changes which had to be made, were re lated to theelim i na tion of cor rup tion, op ti mi sa tion of fi nanc ing at all lev els, in tro duc tion of ef fec tivepost grad u ate train ing, build ing of a work ing in for ma tion sys tem, in clu sion of new par tic i -pants in the con tract ing pro cess, in creas ing of the bud get fund ing for healthcare and in creas -ing of the pay ment of the healthcare work ers, im prove ment of the man age ment.
One of the di rec tors of a NHIF stated that the cur rent sys tem did not need any es sen tialchanges.
Spe cific opin ions of sep a rate groups of man ag ers
Di rec tors of RHC
Ac cord ing to the di rec tors, the role of the RHC in the man age ment of healthcare at re -gional level was ex tremely im por tant and ever grow ing in the course of the re form. It was de -ter mined by the new health leg is la tion and, es pe cially by the Law on health, quoted by thein ter viewed, ac cord ing to which the RHC im ple mented the health pol icy at regional level.
As a pos i tive fact, the ma jor ity of the in ter viewed di rec tors of RHC stressed that, in thecourse of the re form, the con trol func tions of the RHC had wid ened, as a re sult of which amore ef fec tive con trol was achieved over the ac tiv ity of the healthcare es tab lish ments, es pe -cially af ter the en force ment of the Law on health.”
Even though, some prob lems were quoted in the ef fi ciency of the con trol func tion of the RHC:
· “The nor ma tive reg u la tion is a prob lem – we es tab lish breaches, but we can not sanc -tion them”;
· “We work well with the com pe tences granted to us by law, but this, in its turn, leads tothe evolve ment of neg a tive at ti tudes among part of the af fected peo ple”;
· “It does not yield 100% re sults be cause of com pro mises con cern ing the fa cil i ties andthe phy si cians’ qual i fi ca tion”;
271
So cio log i cal in ter pre ta tion
· “Un der the cur rently act ing leg is la tion, the mon e tary sanc tions, im posed by the RHC,do not have the nec es sary ed u ca tional im pact.”
As the most fre quent rea sons for com plaints made by the cit i zens, the di rec tors of theRHC re ported the fol low ing:
· “Re gard ing the func tion ing of the emer gency and ur gent med i cal care, this is an ur gent,un re solved prob lem at this stage be cause of the short age of the re spec tive equip ment”;
· “In cor rect at ti tude on be half of the GPs, fail ure to ful fil de ci sions of the Ter ri to rial Ex -pert Med i cal Com mis sion”;
· “Rough and dis hon est at ti tude to the cit i zens”;
· “Re fusal to give let ters of re fer ral to spe cial ists; cit i zens’ re quests not ful filled; dis sat -is fac tion with the health ser vices; com plaints by cer tain groups, e.g. the dis abled interms of the Ter ri to rial Ex pert Med i cal Com mis sion; poor treat ment of the pa tients bythe phy si cians; poor qual ity of the pro vided med i cal care”;
· “Cor rup tion, harsh and un eth i cal at ti tude by the med i cal per son nel. There are less de -pos ited com plaints re gard ing the qual ity”;
· “Im pos si bil ity to find the GP at night”;
· “Un law ful pay ments by the Fund and by pa tients”.
Ac cord ing to the in ter viewed di rec tors of RHC, the main prob lems in the man age mentof healthcare at re gional level, in cluded “the lack of qual i fied man ag ing staff in healthcare”;“un der de vel oped nor ma tive ba sis”; “lack of a uni fied in for ma tion sys tem”; “in suf fi cient fi -nanc ing by the mu nic i pal i ties for the mu nic i pal healthcare es tab lish ments”; “in suf fi cientnum ber of spe cial ists from the out pa tients’ care in the small mu nic i pal i ties”; “un oc cu piedphy si cians’ prac tices in vil lages re mote from the dis trict cit ies”; “lack of in ter est in a num berof phy si cians to read, fol low and ex e cute strictly the nor ma tive reg u la tion”. Prob lem were also reg is tered with” the poor re source and per son nel pro vi sion of the RHC and the con stant ac cu -mu la tion of new ob li ga tions in the var i ous nor ma tive acts”, which the re spon dents as sessed asim ped ing to a great ex tent the plan ning and the ac tiv ity as well as the pro vi sion of its nec es saryhu man and other re sources.
In So fia, spe cific dif fi cul ties were quoted in the ex e cu tion of the ad min is tra tive func -tions, caused by the vol ume of work in the cap i tal, re lated to the sig nif i cantly greater num berof healthcare es tab lish ments, as com pared to the other towns in the country.
The views about the fu ture role of the RHC were fo cused mainly on the de cen trali sa tionof the healthcare sys tem and the re lated in crease of its im por tance. To gether with the in creased op er a tive con trol of the ac tiv i ties of the healthcare es tab lish ments, the in tro duc tion of med i calstan dards and con trol over their ob ser va tion, ex e cu tion of con trol over the dis tri bu tion ofdrugs, the di rec tors of RHC ex pected a greater in de pend ence in the fu ture in the developmentof a regional health policy.
The ex pec ta tions about the de vel op ment of healthcare at re gional level were cen tredaround the ef fi ciency im prove ment of the net work of healthcare es tab lish ments:
· “Due to the great num ber of healthcare es tab lish ments in the re gion, it is nor mal forsome of them to be closed and for the best one to re main only”;
· “The hos pi tals at na tional level should be re duced in num ber. I also ex pect the clos ing
272
down of the low ef fi ciency hos pi tals, but only af ter a care ful con sid er ation”;
· “It all de pends on what the de vel op ment at na tional level is. The dis trict has a goodsys tem of GPs and DCC and a suf fi cient num ber of hos pi tals but hos pices also have tobe de vel oped”;
· “The multi-pro file hos pi tals in the small mu nic i pal i ties have to turn into hos pi tals forfol low-up treat ment, the sur gi cal wards have to be closed down as in ef fi cient, spe cial -ists and GPs should be at tracted to work out side the dis trict city in or der to im prove the ser vices pro vided in the smaller towns.”
Di rec tors of RHIF
The di rec tors of the RHIF ex pressed some spe cific views about the sta tus of the RHIF.Ac cord ing to a large part of them, changes were nec es sary to give greater com pe tences andpos si bil i ties to the RHIF, re lated to the con trol ac tiv ity. In ad di tion, the fact was brought up asa prob lem that “when an agree ment is signed, the di rec tor of the RHIF signs it on be half of thedi rec tor of the NHIF and in case of ju di cial dis putes, the court suits are con ducted in So fia”,and there fore, it was sug gested that “the sta tus of the RHIF is le gally changed”. Nev er the less,the ma jor ity of the in ter viewed di rec tors of RHIF did not sup port the idea of the Fund’s de cen -trali sa tion. Only two of them found that de cen trali sa tion was nec es sary for the im prove ment of the work with the ar gu ment that “it is not nor ma tively pos si ble to meet the needs of 28 re gions,each of which having different structure and problems”.
The Na tional frame work agree ment fa cil i tated the re la tion ships with the con tract ingpar ties as far as it “reg u lates these re la tion ships”. But in a num ber of cases, the di rec tors ofRHIF reg is tered prob lems, en su ing from the NFA:
· “Some times a reg u la tion is lack ing for sanc tions for some breaches and prob lems with com plaints be fore the Ar bi trary Com mis sion. As for this com mis sion and its com po si -tion, there are three rep re sen ta tives of the UBP and NHIF each, and, in most cases, the de ci sion fa vours the phy si cians, which means un nec es sary waste of time and fi nance”;
· “The agree ment, how ever, cre ates a num ber of ob sta cles to the work of the Fund – noin spec tions can be car ried out with out an ex plicit or der, and when emer gency sig nalsare re ceived, it is not pos si ble to re spond im me di ately and ad e quately.”;
· “Re cently, it cre ates greater and greater ob sta cles – nu mer ous clauses reg u lat ing thecon trol ac tiv ity of the Fund have been aban doned in the NFA”;
· “Our com pe tences are lim ited. We have no right of as sess ment for treat ment”.
The prob lems with the con tract ing part ners, in di cated by the di rec tors of the RHIF, re -ferred to the ser vices of the pa tients, the fail ure to ful fil or in suf fi cient aware ness of the fi nan -cial rules and the leg is la tion. As far as the pa tients’ ser vices went, the most com mon breachesin cluded “un law fully re ceived money from the pa tients”; “un law fully re ceived con sum ers’fee”; “phy si cians’ re fusal to make a home visit”; “harsh at ti tude to the pa tient”; “ig no rantat ti tude to the pa tient”; “re fusal to make an ex am i na tion, un law fully re quested sums ofmoney”; “re fusal to re fer a pa tient to a spe cial ist and to per form in ves ti ga tions”; “un timelypro vided med i cal care”. The rea son given for these vi o la tions were “unconscientious phy si -cians, tak ing ad van tage of pa tients, who are not aware of their rights”.
The most com mon vi o la tions, es tab lished dur ing in spec tions made by the RHIF, in cluded
273
So cio log i cal in ter pre ta tion
“non ob ser vance of the es tab lished work ing sched ule”; “re port ing ac tiv i ties which have notbeen per formed”; “un law fully reg is tered pa tients”; “un law fully pre scribed drugs”; “in -com pe tent and low qual ity med i cal care”. One of the RHIF di rec tors re ported that there was“fail ure to ful fil the agree ments as a whole” and “the rea sons for that are in the lack of knowl -edge of the nor ma tive ba sis of the MH and the poor op er a tive con trol on its behalf”.
Di rec tors of RIPCPH
Re gard ing the de vel op ment of the func tions of RIPCPH in the course of the re form,the opin ions of the in ter viewed from this group var ied widely. For some of them, there was nosig nif i cant change, for oth ers - the de vel op ment of the func tions was head ing in a pos i tive di -rec tion, for third - the aban don ment of some func tions (e.g. re lated to the ra di a tion hy giene, the oc cu pa tional med i cine) was to the harm of the RIPCPH activity.
Ac cord ing to the di rec tors, the ca pac ity for the ful fil ment of the RIPCPH func tions wasas sessed pre dom i nantly as “good enough”. The need was some times re ported for “com put ersand a good in for ma tion sys tem, trans por ta tion ve hi cles, a better fi nanc ing for the qual i fi ca tionim prove ment of the spe cial ists and for con duct ing of pur pose ful stud ies”. Some RIPCPH sharedthe opin ion that “the staff is not suf fi cient, which hin ders the ex e cu tion of ev ery day con trol”, andoth ers re ported that “there is still more to be ex pected in terms of equip ment”.
In the opin ion of the ma jor ity of the in ter viewed di rec tors, the eval u a tion of theRIPCPH ac tiv ity was pos i tive but some short com ings were also out lined. It was deemed thatthe in suf fi ciently ef fec tive ac tiv i ties of the RIPCPH re ferred to “the chil dren’s and pu pils’ hy -giene and the com pli ance of the kin der gar tens and the schools with the hy gienic re quire -ments” and the rea son was seen in the short age of fi nance, al lo cated in this field. An other prob -lem, di rectly af fect ing the ac tiv ity of the RIPCPH, was that “not all spe cial ists in the RIPCPHsys tem are com pe tent enough”.
Mean while, some pos i tive trends were reg is tered in the RIPCPH ac tiv ity:
· “If we put the em pha sis on the pro phy lac tic ac tiv i ties, one of the most im por tant ac tiv -i ties will be re lated to the pro phy lac tic im mu ni sa tions. In prin ci ple, Bul garia has hadgood tra di tions in this field, which were ru ined with the re form around 2000. I can seethat since last year, a trend is again ob served to ward the achieve ment of better re sults.Now my col leagues, the gen eral prac ti tio ners, feel more con fi dent, they are fa mil iarwith the pop u la tion, they have over come many dif fi cul ties and this is one of the ac tiv i -ties which are good in di ca tors. The most dif fi cult years for the re form have beenover come. The scope of the chil dren with im mu ni sa tions is in creas ingly grow ing. Weachieved the re sults we had at tained un der the pre vi ous sys tem. This is some thing ofut most im por tance for the whole healthcare.”
The views about the fu ture of the RIPCPH re ferred both to the con sol i da tion and thede vel op ment of the struc tures and the en hance ment of their role in the man age ment of pub lichealthcare at re gional level. Some con crete sug ges tions were made in this re spect:
· “More func tions to be granted to the lab o ra to ries and to im prove the pos si bil i ties forfast di ag nos tics of rare dis eases”;
· “To make an as sess ment of the con trol over the risks for the health of so ci ety”.
274
As sess ment of the rep re sen ta tives of the lo cal au thor i ties
Rep re sen ta tives of the or gans of the lo cal au thor i ties in mu nic i pal i ties and pop u lated re -gions of var i ous in size, par tic i pated in an in-depth in ter view on the prob lems of the healthcarere form – may ors, dep uty may ors and mu nic i pal ity ad vi sors.
Pos i tive and neg a tive ef fects of the healthcare re form
In their as sess ment of the ef fects of the re form, the may ors, dep uty may ors and mu nic i -pal ity ad vi sors did not sig nif i cantly dif fer from the other groups of re spon dents. The fact is in -ter est ing, how ever, that the em pha ses on the pos i tive and neg a tive ef fects of the healthcarere form dif fered be tween the rep re sen ta tives of the smaller and the larger municipalities.
Pos i tive ef fects
In the smaller mu nic i pal i ties (Asenovgrad, Velingrad, Gabrovo, Kurdjali, Montana,etc.), the ac cent falls on the qual ity of the med i cal ser vices and the ben e fits for the citizens:
· “The pay ment of the phy si cians was in creased, es pe cially but undeservedly, that of theGPs”;
· “The pos si bil ity was given to the healthcare pro fes sion als for free dom and the pa tients also re ceived a small right of choice”;
· “The re form placed the phy si cians’ pro fes sion in better con di tions – the cost of theirla bour was cal cu lated”.
In the larger mu nic i pal i ties (So fia, Plovdiv, Varna, Stara Zagora), the em pha sis was onthe changes on the or gani sa tion of med i cal care and how they af fected the qual ity of thepro vided ser vices:
· “The pa tients choose in de pend ently who is go ing to treat them. Thus, com pe ti tion iscre ated among the phy si cians – gen eral prac ti tio ners, spe cial ists, mid dle-tier med i calper son nel, phar ma cies. This is the driv ing force for the de vel op ment for ward.”;
· “A mar ket is formed for the health ser vices. Ev ery one can choose his/her GP and spe -cial ist to visit”;
· “The pri vate healthcare es tab lish ments were founded un der much better con di tions”;
· “The very med i cal staff has been given in cen tives ful fil their du ties with greater re -spon si bil ity and to do their work with a better qual ity”.
Of course, there are some ex cep tions from this trend. For ex am ple, the lo cal au thor i ties in a smaller mu nic i pal ity, re ported the es tab lished com pe ti tion and the qual ity im prove ment as afirst ad fore most pos i tive re sult of the re form.
The dif fer ences in the at ti tudes of the rep re sen ta tives of the small and large mu nic i pal i ties are un der stand able. In the larger mu nic i pal i ties, so cial con di tions ex ist, al low ing for a more in -ten sive de vel op ment of the com pet i tive re la tions, un like in the smaller mu nic i pal i ties, wherethe pa tients’ pos si bil i ties for choice of a phy si cian and a healthcare es tab lish ment are muchmore lim ited. The poorly de vel oped com pet i tive ness in the small mu nic i pal i ties (at placeseven ab sent) does not fa cil i tate the sen si ble qual ity im prove ment. To a great ex tent, this couldac count for the fact that, in the mind of the rep re sen ta tives of the smaller mu nic i pal i ties, thepos i tive effects of the healthcare reform were mainly for the medical professionals.
275
So cio log i cal in ter pre ta tion
At this back ground, the neg a tive ef fects of the healthcare re form were out lined, too.
Neg a tive ef fects
As re gards the neg a tive ef fects of the healthcare re form, in the big mu nic i pal i ties theshort com ings in the qual ity of health ser vices were reg is tered to gether with their re duc tionto quan ti ta tive in di ca tors (es pe cially for the general practitioners):
· “The qual ity of the health ser vices is not sat is fac tory; the quan tity is re ported with apri or ity to the qual ity”;
· “The den tal care has been ne glected to gether with pro phy laxis and school healthcare.The im mu ni sa tion con trol has been di min ished, which in some time, may lead to aboom of dis eases for got ten un til now”;
· “The pa tients’ ac cess to spe cial ised hos pi tal care is ham pered”;
· “Im pos si bil ity to im prove the tech ni cal and ma te rial fa cil i ties”.
In their com ments of the neg a tive ef fects of the re form, the or gans of the lo cal au thor i tiesin the mid dle and small-size mu nic i pal i ties drew con sid er able at ten tion to the so cial func -tions of healthcare. The most sig nif i cant prob lem was re ported to be the wors ened ac cess toboth the healthcare sys tem as a whole and to spe cial ised med i cal care:
· “The health ser vices de te ri o rated in the vil lages – the peo ple there (el derly, sick, un -em ployed) have been left with out health ser vices”;
· “The sit u a tion is worse with the vil lages com pris ing the mu nic i pal i ties, in which thecit i zens are served by com mut ing GPs. They visit these vil lages once a weak for nomore than 2-3 hours. The pop u la tion from these vil lages is forced to travel to the city to get re fer rals for spe cial ists”;
· “The ru ral pop u la tion and the so cially dis ad van ta geous peo ple are left out, as if theydo not be long to the sys tem”;
· “An enor mous part of the pop u la tion has been left with out the pos si bil ity of be ingtreated be cause they have not paid their in sur ance in stal ments, there is no body tocover them and the peo ple can not af ford to pay for the treat ment”;
· “The main pur pose of the re form was to re strict the cha otic use of the med i cal ser vices. But at the mo ment, the GPs are in an ex tremely strong po si tion be cause they form some of the larg est struc tures in the Phy si cians’ un ion and no body from the UBP wishes toquar rel with them. Sec ondly, in most cases, they block the pa tients who have to be re -ferred to spe cial ists. This is why pa tients see the spe cial ists with de lay”.
The neg a tive as pects of the re form were seen by the rep re sen ta tives of the lo cal au thor i -ties also in terms of fi nanc ing:
· “Ac cord ing to the Com mer cial law the hos pi tals are com mer cial com pa nies whichhave to be self-main tained and no profit can be made from health or at its ex pense”;
· “Un der fi nanc ing is the ma jor neg a tive ef fect”;
· “The re form left the mid dle-tier med i cal per son nel – the nurses, in a poor fi nan cialstate. Their pay ment and sta tus have to be changed be cause their work is hard and re -spon si ble”.
276
Im ple men ta tion rates of the healthcare re form
Un like in the other groups of re spon dents, for whom even at slow rates, the re form fol -lowed the nec es sary di rec tion, the rep re sen ta tives of the lo cal au thor i ties re ported mostly neg -a tive views about the rate of the reform:
· “The re form is in stag na tion, it even goes to the worse. The peo ple uni ver sally com -plain of bad ser vices, cor rup tion and nu mer ous phy si cians’ er rors, lack of con sci en -tious ness, mal prac tice, ir re spon si bil ity. The doc tor is turn ing more and more into aclerk, the young phy si cians do not pos sess the nec es sary qual i fi ca tion”;
· “Slow rates – an in for ma tion sys tem has not been es tab lished in or der to al low themoney to fol low the pa tient”;
· “The re form started and stopped at the level of nor ma tive doc u ments”.
Health leg is la tion
The main crit i cism of the lo cal ad min is tra tion re ferred to the way of de sign ing the leg is la -tive de ci sions. Ac cord ing to the in ter viewed may ors, dep uty may ors and mu nic i pal ity ad vi sors,the opin ion of all the in volved par ties was not taken into con sid er ation, in clud ing the opin -ion of the mu nic i pal i ties re gard ing the course of the re form: “The leg is la tion is cur rently madeby phy si cians for phy si cians – the con sum ers and the mu nic i pal au thor i ties are left out”.
Apart from the feel ing of iso la tion, the lo cal ad min is tra tion made the fol low ing ob ser va -tions:
· “The leg is la tion is very vague and the role of the mu nic i pal ity does not be come clear”;
· “The mu nic i pal i ties do not get rights in de ter min ing the pol icy of the MHAT”;
· “The law does not give free dom for the fi nanc ing of a mu nic i pal hos pi tal from the mu -nic i pal bud get. Now the par a dox has re sulted – the cit i zens of the mu nic i pal ity aretreated in the hos pi tal and the mu nic i pal ity it self does not have the right to sup port the hos pi tal fi nan cially, even if it has the recourses avail able. The leg is la tion is an im ped -i ment in so far as, ac cord ing to it, the sta tus of the mu nic i pal healthcare es tab lish mentsis of com mer cial com pa nies. That is, the mu nic i pal ity does not have the right to in fusedi rectly fi nanc ing as a turn over cap i tal. As a re sult, the mu nic i pal ity is forced to sup -port the mu nic i pal healthcare es tab lish ments by look ing for ways of fi nanc ing throughthe pur chase of long-term ma te rial as sets”.
For the lo cal au thor i ties, the need was out stand ing for the for ma tion of leg is la tive mech -a nisms for the mu nic i pal ity to par tic i pate more ef fec tively in the man age ment of thehealthcare es tab lish ments (mainly of the hos pi tals) through its in volve ment in the pro cess ofcon tract ing with the fi nanc ing or gans (“The mu nic i pal i ties must be given rights to at tack thesize of the fi nanc ing, de fend their po si tions and not only trans fer re spon si bil i ties”).
Prob lems with the man age ment of the healthcare sys tem
As sess ment of the three cen tres of in flu ence
The main un der stand ing of the in ter viewed may ors and mu nic i pal ity ad vi sors was thatdur ing the course of the re form ef fec tive co or di na tion lacked among the three cen tres of in -flu ence of the healthcare sys tem. The re la tions among them were de fined as “im pos ing of in -
277
So cio log i cal in ter pre ta tion
ter ests from the po si tion of power”, with out es tab lished mech a nisms for the execution ofmutual control:
· “In many cases the three struc tures de fend their own rights and pro tect pri vate in ter -ests, but their li a bil i ties are trans ferred to an other struc ture and, even tu ally, to theBul gar ian pop u la tion”;
· “The UBP func tions as an oblig a tory for mal or gani sa tion, which does not en tirelyrep re sent the in ter ests of the pro fes sion als, and the NHIF is cur rently the mo nop o listand, in such a way, it has the pos si bil ity to dic tate the rules, which it ac tu ally does”;
· “In this way, the par ity is de stroyed among these three struc tures (the MH, theNHIF, the UBP) which af fects neg a tively the work ing con di tions of the med i cal pro -fes sion als and the pa tients’ in ter ests”;
· “In ter ac tion does ex ist, but there is no bal ance be tween the rights and li a bil i ties ofeach of the man ag ing struc tures; the MH has to have more rights but, vir tu ally, theFund pos sesses them”;
· “The in ter ac tion among these struc tures is clumsy, bu reau cratic, lob by ist, each onemind ing its own in ter ests, which hin ders the healthcare re form”.
Pos i tive eval u a tions of the way of in ter ac tion among the man ag ing au thor i ties of thehealthcare sys tem were given by sin gle peo ple. They reg is tered the pres ence of ef fec tive com -mu ni ca tion and the for ma tion, with time, of good prac tices, con tacts and re la tions (“things areget ting chan nelled and there is good in ter ac tion”).
A chief fac tor re ported for the un bal anced in ter ac tion among the MH, the HNIF and theUBP was the mo nop o lis tic sta tus of the NHIF. The ma jor ity of the rep re sen ta tives of the lo cal au thor i ties ex pressed the opin ion that there should be pri vate health in sur ance funds, “so thatthe peo ple can choose where their money should go and who should in vest in their treat ment”.Al ter na tives were also rec om mended for the UBP – “to es tab lish rep re sen ta tive or gani sa -tions of the phy si cians’ pro fes sion on com pet i tive ba sis”. This sug ges tion was dic tated by theun der stand ing that “the pro fes sional or gani sa tions de fend lob by ist in ter ests in the course ofthe NFA ne go ti a tions and not the interests of the doctors’ guild.”
In ter ac tions in the healthcare sys tem
The in ter viewed rep re sen ta tives of the lo cal au thor i ties eval u ated pre dom i nantly neg a -tively the var i ous in ter ac tions and in ter re la tions in the sys tem. As a whole, the in ter ac tions inthe healthcare sys tem were marked with “a lack of co or di na tion which is an ev ery day prob -lem” and “in ev i ta ble con flicts which are not re solved suc cess fully and, there fore, lead toprob lems”. Ac cord ing to the may ors and the mu nic i pal ity ad vi sors, “the in ter ac tion amongthe healthcare es tab lish ments, the RHC and the pro fes sional or gani sa tions is not sat is fac -tory” and “there is no co or di na tion be tween the hospital and outpatients’ care”.
The in ter ac tions be tween the man ag ing struc tures in healthcare and the healthcare es -tab lish ments were de fined as uni lat eral, with out the nec es sary di a logue (“di rec tives are“dropped” from above, with out ask ing for the opin ion of the healthcare es tab lish ments”).
The may ors and the mu nic i pal ity ad vi sors re ported a num ber of dif fi cul ties and conflicts:
· be tween the mu nic i pal ity and the MH and the RHC (in their in ter ac tions “there is no di a logue and com pli ance of pol i cies”);
278
· be tween the mu nic i pal ity and the RIPCPH (“The nor ma tive doc u ments, used by theRIPCPH, are ex tremely for ma lised. If it is up to them, if they would close thehealthcare es tab lish ment, and on the other hand, the mu nic i pal ity bud get is not suf fi -cient to cover the re quire ments of the RIPHPC”);
· be tween the large and the small mu nic i pal i ties (“At the meet ings in the dis trict cit iesonly the prob lems of the cap i tal city are dis cussed and the opin ions on prob lems out -side this city are not con sid ered”).
Of the in ter viewed rep re sen ta tives of the lo cal ad min is tra tion, only one in ev ery ten re -spon dents in di cated that there were no prob lems, and if a con tro versy emerged, it was re solved by means of a di a logue.
The re la tion ships be tween the mu nic i pal ity and the healthcare es tab lish ments wereeval u ated positively.
When the may ors and the mu nic i pal ity ad vi sors as sessed the rea sons for the con flicts andthe poor col lab o ra tion, the most com monly re ported ones in cluded the in ad e quate fi nanc ing(“the small hos pi tals are not be ing sup ported but be ing harmed through con cealed in ter ests,from where the con flicts stem”), de fence of per sonal in ter ests and the fact that “the lo calpower does not have the abil ity to ex e cute con trol”.
The fact is in ter est ing, that at the same time, along with the pre dom i nantly neg a tive as -sess ment of the in ter ac tions in the health sys tem, and be tween the mu nic i pal i ties and othersub jects, in par tic u lar, the in ter viewed may ors and the mu nic i pal ity ad vi sors gave a se ries ofex am ples of “good part ner ships” of the mu nic i pal au thor i ties with var i ous in sti tu tions andor gani sa tions. This showed a pos i tive as sess ment of their own ef forts in the reali sa tion of theirin ter ac tions, aimed at solv ing cer tain prob lems of the mu nic i pal healthcare. In other words, inthe ma jor ity of the cases, when the in ter ac tions of the mu nic i pal au thor i ties with other sub jectsin the healthcare sys tem or out side it, were de fined as part ner ships, they re sulted from someini tia tive for the so lu tion of a spe cific prob lem (for in stance, part ner ships with the RHC in sub -mit ting ap pli ca tions for dif fer ent pro jects; part ner ships with com pa nies and nongovernmentalor gani sa tions for the so lu tion of fi nan cial prob lems of the healthcare establishments in themunicipality), and did not result from normatively regulated functions for execution.
De cen trali sa tion of the man age ment of the sys tem
De cen trali sa tion of the healthcare sys tem was sup ported by the ma jor ity of the in ter -viewed may ors and the mu nic i pal ity ad vi sors. In the mean time, the eval u a tions of the de cen -trali sa tion of the sys tem, im ple mented in the course of the re form, were mainly neg a tive. Onthe one hand, the rep re sen ta tives of the lo cal au thor i ties ob served a lack of bal ance be tweenrights and li a bil i ties, and on the other hand, the short age of fi nan cial means with which to ful filthese rights and liabilities in practice:
· “The de cen trali sa tion is not ac tual. The state ap pears to be gov ern ing at all lev els.There is no se cur ing of rights and there are li a bil i ties only. The state places the com pa -nies in healthcare un der its con trol”;
· “The mu nic i pal ity, through de cen trali sa tion, must play an ac tive role in healthcare,but the del e gated li a bil i ties must be se cured by the re spec tive rights”;
· “The de cen trali sa tion is not ac tual, li a bil i ties are trans ferred with out ac tu ally del e -
279
So cio log i cal in ter pre ta tion
gat ing rights”;
· “There is no real de cen trali sa tion, nei ther is there leg is la tion to bind the rights withthe li a bil i ties”;
· “The mu nic i pal ity has al most no rights, it is just an owner, and in cases of prob lemsthe cit i zens turn to us. The vil lages are re main ing with out med i cal care, the mu nic i -pal ity has no pos si bil i ties to con trol the GPs, who do not pro vide qual ity ser vices tothe pop u la tion in the vil lages”;
· “At the mo ment the mu nic i pal ity has re spon si bil i ties only, but it has no ac tual re sourcesto ful fil them. In most cases, it is dic tated by the or gans car ry ing out the fi nanc ing”;
· “There is real se cur ing of the re spec tive li a bil i ties with rights, but there is no fi nan cialse cur ing”.
Man ag ing ca pac ity
In the as sess ment of the man ag ing per son nel of the healthcare sys tem from a quan ti ta -tive and qual i ta tive point of view, sev eral opin ions were formed. On the one hand, ac cord ing to the in ter viewed rep re sen ta tives of the lo cal au thor i ties, “there are spe cial ists but, for po lit i calrea sons, not al ways the best are elected”. The other stand was that at na tional level, the man -ag ing staff was more com pe tent but, at re gional level, “the staff is poorly qual i fied” and didnot possess the necessary skills.
Ac cord ing to a large part of the may ors and the mu nic i pal ity ad vi sors, “the hos pi tal man -ag ers are poorly trained” and this was a prob lem, for the so lu tion of which “the MH has to de -velop a strat egy”.
In for ma tion sys tem in healthcare
In the minds of the in ter viewed may ors and the mu nic i pal ity ad vi sors, the in for ma tionsys tem in healthcare was non ex is tent. The prob lems were seen in the in for ma tion def i cit, thein ef fec tive in for ma tion chan nels, the lack of com pre hen sive ness of the col lected data and thelack of ad e quate data pro cess ing, al low ing for anal y ses and prog no ses, nec es sary for theformation of health policies and strategies.
Views were re ported that the lack of le gal reg u la tions for in for ma tion ex change be tweenin sti tu tions and the ab sence of pub lic ity of the in for ma tion were pre req ui sites for theinformation deficit.
Ac cord ing to the rep re sen ta tives of the lo cal au thor i ties “the ab sence of an in for ma tionsys tem blocks the pos si bil ity for feed back”.
For this group of re spon dents, too, the def i cit of of fi cial in for ma tion was com pen sated byin for mal channels.
Opin ions are also ex pressed, that there was no in for ma tion def i cit, the ar gu ment, made by one MHAT, be ing “the very suc cess ful pub lic ity” of its ac tiv ity. In this case, in the imag i na -tion of one of the may ors, the spe cific in for ma tion sys tem in healthcare ex isted un der the formof an in for ma tion cam paign for ad ver tis ing the activity of the hospital.
The role of the cit i zens in the man age ment of the sys tem
The main role of the cit i zens, ac cord ing to the lo cal self-gov er nance or gans, was to reg u -
280
late the qual ity of med i cal care through an in formed con sent of a phy si cian and healthcarees tab lish ment and through mak ing com plaints and sig nals for vi o la tions, sub mit ted to the re -spec tive au thor i ties. The re spon dents from this group con firmed that it was nec es sary for thecit i zens “to have a free ac cess to in for ma tion about the pro cesses in the sys tem and the uti lised re sources and to sig nal about in fringe ments”, and at the same time, they were well-acquainted with their rights.
Ac cord ing to the may ors and the mu nic i pal ity ad vi sors, the cit i zens were in a po si tion tore duce the cor rup tion in healthcare.
The fact is also note wor thy, that the in ter viewed in this group pointed out the ac tive seek -ing of feed back from the cit i zens by the healthcare es tab lish ments and the healthcare in -sti tu tions as a pre req ui site for en hanc ing the role of the cit i zens in the man age ment of thesys tem. Ac cord ing to them, it was nec es sary to pay greater at ten tion to the in di ca tors for pa -tients’ sat is fac tion, the sig nals for in fringe ments and the patients’ complaints.
The rep re sen ta tives of the lo cal ad min is tra tion emphasised the role of the pa tients’ andthe nongovernmental or gani sa tions by mak ing spe cific pro pos als for the in crease of the role ofthe cit i zens in the man age ment of the healthcare system:
· “The cit i zens’ com mu ni ties have to con trol the func tion ing of the sys tem”;
· “To en hance the role of the NGOs in the man age ment of the healthcare sys tem – with -out their opin ion not to un der take any changes of the healthcare sys tem”;
· “The op por tu nity should be given to cit i zens with dif fer ent sta tus to par tic i pate in theman age ment of the hos pi tals, along with nongovernmental or gani sa tions, the church,the busi ness who can help in var i ous ways.”;
· “The cit i zens should be aware of their rights, the As so ci a tion of the Mu nic i pal i ties isalso nec es sary to be rep re sented in the sign ing of the frame work agree ment”;
· “Nongovernmental or gani sa tions should par tic i pate in the sign ing of the agree ment”.
Opin ions were also voiced that the cit i zens were in volved in the man age ment of thehealthcare sys tem to an ad e quate de gree, through their par tic i pa tion in the hos pi tal boards.
At ti tude to the pri vate healthcare es tab lish ments
The at ti tude to the pri vate healthcare es tab lish ments was ex tremely pos i tive even in thesmaller towns. It was de ter mined by the un der stand ing that the pri vate healthcare es tab lish -ments worked in the in ter est of the ser vice of so ci ety since they “stim u late com pe ti tion”,“give a pos si bil ity for a greater choice for the cit i zens”, “of fer higher qual ity ser vices”, and,as a whole, “com ple ment the mu nic i pal healthcare es tab lish ments and in this sense con trib uteto the de vel op ment of the pub lic healthcare”.
The ma jor ity of the may ors and the mu nic i pal ity ad vi sors did not ac cept the pri vatehealthcare es tab lish ments as a threat to the mu nic i pal ones. The un der stand ing was wide -spread, that be cause of the higher prices of the med i cal ser vices in the pri vate healthcare es tab -lish ments (which “the ma jor ity of the pop u la tion can not af ford”), they did not threaten themu nic i pal ones, and “of fer better con di tions and better fa cil i ties in the in ter est of the pa tientswith greater fi nan cial pos si bil i ties”. In some smaller mu nic i pal i ties, in which there were nopri vate healthcare es tab lish ments, the re spon dents even de clared that if they happen to appear,the municipality was prepared to collaborate.
281
So cio log i cal in ter pre ta tion
Among the in ter viewed, there were peo ple, who con sid ered that the pri vate healthcare es -tab lish ments were nec es sary as com pet i tors to the mu nic i pal ity ones in or der to im prove thequal ity of the med i cal care provided in them.
In one of the state ments it was re ported that the cur rently act ing nor ma tive ba sis did notfa vour the open ing and the de vel op ment of the pri vate healthcare es tab lish ments.
At ti tudes to the privatisation of the healthcare es tab lish ments
The at ti tudes to ward privatisation and the un der stand ing of the pro cess of privatisationdif fered sig nif i cantly de pend ing on the type of the pop u lated area. This fact is self-ex plain -able in view of the dif fer ent eco nomic and socio-de mo graphic char ac ter is tics in the mu nic i pal -i ties of various size.
The or gans of the lo cal au thor i ties from the larger cit ies as sessed mainly pos i tively theprivatisation of the healthcare es tab lish ments:
· “The healthcare re form will be ac com plished only when, apart from the ac tiv ity, thefa cil i ties are also pri va tised”;
· “Through privatisation, the qual ity of the med i cal ser vice will be im proved”;
· “The qual ity of the ser vices will be im proved and the Eu ro pean ex pe ri ence is ori ent -ing us ex actly in that di rec tion”;
· “The pri vate own er ship al ways leads to qual ity, so the pri vat iza tion of the healthcarees tab lish ments can fa cil i tate the qual ity im prove ment but it should be guar an teed thatthe vol ume and the ac tiv ity of the mu nic i pal ity healthcare es tab lish ments should bepre served”;
· “My as sess ment of the pri vat iza tion of the healthcare es tab lish ments is en tirely pos i -tive. This is the only way for pro tect ing the in ter ests of the pop u la tion. I con sider it amis take that the pri vat iza tion was stopped in this field”;
· “Mu nic i pal and state healthcare es tab lish ments can not ex ist. There should be pub licand pri vate healthcare es tab lish ments. Where there is pri vate ac tiv ity and pri vate ini -tia tive, there is no room for cor rup tion, there is no room for pay ments un der the ta -ble”;
· “From a nor ma tive point of view, the ques tion with privatisation is not cleared – it isnec es sary to de cide which of the healthcare es tab lish ments have to be pri va tised andwhich not, for ex am ple the privatisation of the dis pen sa ries is more prob lem atic fromthe point of view of their spe cific fea tures”;
· “For each com pany, an eval u a tion should be made as to whether there is a need forprivatisation, de pend ing on the per for mance of the healthcare es tab lish ments and theneeds of the com mu nity”;
· “Privatisation of the work ers’- man age ment- com pa nies type with strictpost-privatisation con trol”;
· “Privatisation - yes, but not a 100%. Only in this way the privatisation can con trib uteto the higher qual ity of the ser vices, with out harm ing the pa tients”.
From the above state ments of may ors and mu nic i pal ity ad vi sors from the larger towns,only two ex pressed a neg a tive at ti tude to the privatisation of the healthcare es tab lish ments.
The at ti tudes, how ever, dif fered in the smaller towns. The ma jor ity of the rep re sen ta tives
282
of the lo cal au thor i ties in them were ex tremely neg a tive to ward privatisation. The fact is in ter -est ing, that ev ery body who de nied the privatisation, came up with one ar gu ment, e.g. that ofthe pro tec tion of the citizens’ interests:
· “It should be pro hib ited, the mu nic i pal ity hos pi tal is the place where the peo ple fromthe mu nic i pal ity are treated and they have no other al ter na tive, a so cial ef fect shouldbe sought for. If the healthcare es tab lish ments are pri va tised, the peo ple would haveno where to go”;
· “Against privatisation, be cause the hos pi tal serves pa tients from two mu nic i pal i ties.If it is pri va tised, the ac tiv ity of the healthcare es tab lish ment may be changed and thepeo ple would be left with out a place to be treated”;
· “Against, hav ing in mind the high rate of un em ploy ment, the cit i zens’ in ter ests have tobe pro tected and the so cial ef fect of healthcare has to be pre served”;
· “It should not be car ried out, be cause many cit i zens can not af ford to pay. The out pa -tients’ care can be pri va tised but the in ter ests of the cit i zens and mu nic i pal i ties shouldthe start ing point”;
· “At this stage – no. To a large ex tent, the hos pi tals have a so cial func tion, which Ithink, will be lost with the privatisation”.
Among the may ors and mu nic i pal ity ad vi sors from the smaller pop u lated ar eas, therewere (a mi nor ity though) peo ple who sup ported the privatisation, but even in those cases, thesup port was rather con di tional.
Fi nanc ing
An im por tant the sis can be sensed in the rep re sen ta tives of the lo cal ad min is tra tion re -gard ing the fi nan cial model, which to a large ex tent, was op pos ing to the views, ex pressed by theother groups of re spon dents. For the may ors and mu nic i pal ity ad vi sors, the coun ter ac tion of cor -rup tion and the in ef fec tive spend ing of the fi nanc ing could be achieved not through the en hance -ment of the con trol by the state but by re duc ing the role of the state in the healthcare sys tem.
The view, held by the ma jor ity of the may ors and mu nic i pal ity ad vi sors, was that the pay -ment to the pro vid ers of med i cal care had to be “for ac tu ally per formed ac tiv ity and not pernum ber of reg is tered pa tients as with the GPs”. Ac cord ing to the in ter viewed, the gen eralprac ti tio ners at tracted “un jus ti fi ably large part of the re sources in the sys tem”, “in pri marycare, doc tors work with lower qual i fi ca tions than in the spe cial ised out pa tients’ healthcare es -tab lish ments and the hos pi tals, but they get a higher income”.
An other prob lem re lated to the fi nanc ing, out lined by the may ors and mu nic i pal ity ad vi -sors, was the ex clu sion of the lo cal au thor i ties from the con tract ing pro cess. The ma jor ity ofthe in ter viewed claimed that the pos si bil ity was given to the own ers of the hos pi tals – the mu -nic i pal i ties – to par tic i pate in the plan ning of the hos pi tal fi nanc ing.
Con cern ing the pos si bil i ties for the op ti mi sa tion of fi nanc ing, the rep re sen ta tives of thelo cal au thor i ties in di cated the necessity of:
· “equal ity in the al lo ca tion of re sources for the out pa tients’ and the hos pi tal care”;“pay ment for per for mance only”;
· “greater con trol over the col lect ing of fi nances – con trol over the com pa nies who donot pay in sur an ces for their em ploy ees”;
283
So cio log i cal in ter pre ta tion
· “al lo ca tion of 7-8% from the GDP for healthcare”;
· “The fi nan cial ac tiv ity of the Min is try of healthcare has to be elim i nated … In fact, allover the world the Min is try of healthcare has a sin gle role to play – to cre ate a healthstrat egy. The Min is try of healthcare can fi nance spe cific programmes, e.g. for pro phy -laxis, for chil dren, for di a bet ics”.
Health in sur ance
As a whole, the rep re sen ta tives in this group re ported that the model of health in sur ance in our county was ap pro pri ate from the point of view of the re form ob jec tives but a se ries ofchanges needed to be made.
The main ques tions, which were com mented by the in ter viewed may ors and mu nic i pal ityad vi sors, re lated to the health in sur ance in cluded some of the main prin ci ples un der ly ing themodel, the size and the col lec tion of the health in sur ance in stal ments and the sta tus of theNHIF.
The views of the in ter viewed var ied broadly re gard ing the prin ci ples of sol i dar ity and eq -uity. Some of them con sid ered that they had to be a char ac ter is tic fea ture of the health in sur -ance sys tem but, in real prac tice, they were be ing vi o lated and this was re cog nised as a de fectof the sys tem. In sup port of this the sis, they men tioned “the peo ple who live in ex treme mis eryand do not pos sess a health in sur ance”, which led to in equal ity in re la tion to the oth ers, lack ofsol i dar ity and so cial jus tice (“There is no eq uity be tween the so cially dis ad van taged peo pleand the rest. A way should be found to se cure the con sti tu tional rights of the so ciallyunprivileged for free healthcare”, “A great part of the pop u la tion lives un der con di tions of ex -treme pov erty and hence, there is no sol i dar ity or jus tice”, “The state has to take over their in -sur ance”, “The so cially sus cep ti ble groups have to be helped be cause the re spon si bil ity forthem is shifted from one to an other”. The pro po nents of this po si tion were against the link ingof the vol ume and the qual ity of med i cal ser vices with the size of the health in sur ance in stal -ments, and in this way, “sol i dar ity is go ing to be vi o lated” and “this will divide people andincrease the tension among them.”
For oth ers, the very ob ser va tion of these prin ci ples led to a se ries of prob lems in thefunc tion ing of the healthcare sys tem. Ac cord ing to the ad vo cates of this view, the prin ci ples ofsol i dar ity and eq uity were to the harm of those who paid more (or paid at all) for healthinsurance:
· “It is not fair for ev ery body to pay in sur an ces, and the health ser vices to be used bythose in need. The peo ple with money can choose on their own the way and the spe cial -ist for their treat ment, and for the so cially unprivileged, the re tired pen sion ers and thestu dents, the cur rent health in sur ance should be pre served”;
· “Ev ery fam ily should have a health in sur ance ac count and for the peo ple, who can notaf ford it, hos pi tals for so cially dis ad van taged peo ple should ex ists, fi nanced by thestate”;
· “Pa tient must have the pos si bil ity to con trol their means in or der to pro vide an in cen -tive for the cit i zens with higher health cul ture”;
· “It is right for those, who pay more, to re ceive more”.
As re gards the size of the health in sur ance in stal ment, the opin ions also di verged. Ac -
284
cord ing to the may ors and mu nic i pal ity ad vi sors, the size should be in creased, al low ing for the“im prove ment” of the pack age of med i cal ser vices used against them. Ac cord ing to oth ers, thesize of the in stal ments should not be in creased be cause “the peo ple can not af ford it from a fi -nan cial point of view” and be cause “it will make the col lect ing more dif fi cult”.
In con trast to the lack of unan i mous opin ion on the above is sues of health in sur ance, therep re sen ta tives of the lo cal ad min is tra tion united around the need for the elim i na tion of themo nop o lis tic sta tus of the NHIF. Some even shared the view that “the NHIF is a su per flu ousor gan and a bur den to the healthcare”.
As in the other groups of re spon dents, the may ors and mu nic i pal ity ad vi sors re ported that, at the start of the health in sur ance sys tem, the mo nop o lis tic sta tus of the NHIF was nec es sary but to thepres ent mo ment it had to be abol ished. The com pe ti tion among the var i ous foun da tions and funds forhealth in sur ance would bring about a better man age ment of the fi nances. More over, ac cord ing to themay ors and mu nic i pal ity ad vi sors, in or der to pre serve the sta bil ity of the sys tem, the num ber of thefunds com pet ing with the NHIF should cor re spond to the size of the pop u la tion.
At ti tude to the Na tional frame work agree ment
Un like in the other groups of in ter viewed, the at ti tude of the may ors and mu nic i pal ity ad -vi sors to ward the NFA was pre dom i nantly neg a tive. The main crit i cisms included:
· The stand of key in volved par ties is not taken into con sid er ation (“In its prep a ra -tion the opin ion of the mu nic i pal i ties is not re quested – no one asks us, what we thinkor what we pro pose. No one asks the con sum ers of the health in sur ance about theiropin ion and about their pref er ences”; “The As so ci a tion of the Mu nic i pal i ties shouldbe pres ent at the sign ing of the frame work agree ment in or der to ac tu ally pro tect thecit i zens’ in ter ests”, “the NFA is nec es sary, but the way it is con cluded should bechanged, tak ing into ac count the opin ion of all the spe cial ists, who work in the coun -try side”; “A doc u ment is nec es sary but the view point of the mu nic i pal i ties should becon sid ered in its de sign ing and sign ing”; “The opin ions of the mu nic i pal i ties and thepa tients should also be taken into con sid er ation at its sign ing”) and
· The mech a nisms for its de sign ing are in ef fec tive (“There is no trans par ency in thede sign ing of the NFA. The tech nol ogy and the mech a nisms must be rad i cally changedboth in terms of its prep a ra tion and in terms of its con tent”; “the NFA has a lot of im -per fec tions and does not cor re spond to the in ter ests of the med i cal pro fes sion, and thepro ce dure of its de sign ing is prob lem atic and in ef fec tive”; “the NFA has nu mer ousshort com ings – the pro ce dure for its de sign ing and ap pli ca tion is clumsy; it should besigned for a term of 5 years”; “This agree ment is un nec es sary – the MH can col lect the in for ma tion from the UBP, the UDB and UPB, to sign a con tract with hem and sub mitit to the Fund for im ple men ta tion”).
Though spo radic, there was some pos i tive feed back con cern ing the NFA. Ac cord ing toit, at that stage, the NFA was a good reg u la tor of the in ter re la tions be tween the in ter ested par -ties (“We can not do with out it at the mo ment. The Phy si cians’ un ion also strug gles with all ef -fort and means that this Na tional frame work agree ment be comes better and better with ev eryyear and more and more ad van ta geous for the phy si cians”).
285
So cio log i cal in ter pre ta tion
Qual ity of the health ser vices
Re gard ing the ef fects of the re form on the qual ity of the med i cal ser vices, the opin ion ofthe in ter viewed may ors and mu nic i pal ity ad vi sors divided.
The ar gu ments of the lo cal au thor i ties rep re sen ta tives, who con sid ered that the re formstim u lated the med i cal spe cial ists to work for the im prove ment of the qual ity, fo cusedmainly on the com pe ti tion among the healthcare es tab lish ments and the ef fects from it(“those who pro vide a higher qual ity, at tract more pa tients and re ceive a greater pay ment”,“the re form stim u lates the qual ity im prove ment through the es tab lished com pe ti tion be causethe pa tients have a free choice”). For some rep re sen ta tives of this group, the new meth ods ofwork, in tro duced as a re sult of the re form, in clud ing the con tract ing re la tions, gave in cen tivesfor the improvement of the quality of the medical services.
When the in ter viewed may ors and mu nic i pal ity ad vi sors in di cated that the med i cal spe -cial ists did not have in cen tives to im prove the qual ity of the health ser vices, the most com -mon ar gu ments was, that the meth ods of pay ment to the pro vid ers of med i cal and den tal care(es pe cially and mostly to the gen eral prac ti tio ners) were bound to quan ti ta tive in di ca tors,with out tak ing into con sid er ation the qual ity of the of fered ser vices as well as that a con sid er -able lack of bal ance ex isted in the pay ment of phy si cians, which did not mo ti vate a large part of them to in crease the qual ity of the ser vices they pro vided. Part of the re spon dents in this groupre ported that the peo ple em ployed in pri vate healthcare es tab lish ments had better incentives towork for the quality improvement.
The pos si bil ity for the cit i zens to in flu ence the qual ity of the health ser vices was as -sessed in a dif fer ent way by the rep re sen ta tives of the larger and smaller mu nic i pal i ties. In thelarger mu nic i pal i ties, where the com pet i tive re la tions were more marked, the cit i zens had the op por tu nity to in flu ence the qual ity through their free choice. It was also in di cated, that pa -tients who paid for the re ceived med i cal ser vices, had higher re quire ments, and hence, greaterpossibilities to influence the quality.
Ac cord ing to the mu nic i pal ity au thor i ties in the smaller pop u lated re gions, the pos si bil -i ties for the cit i zens to in flu ence the qual ity were strongly re stricted. The reasons included:
· Firstly, the re stric tions in the choice of a phy si cian and a healthcare es tab lish ment(“The right of choice ranks first but it is pre con di tioned by the phy si cians avail able atthe spe cific site”);
· Sec ondly, the pa tients’ lack of knowl edge of their rights (“In prin ci ple, the cit i zens can in flu ence the qual ity of the pro vided ser vices, but they are not aware of their rights as pa -tients.”; “An enor mous part of the cit i zens are not aware of their rights and the men tal -ity of the older pop u la tion does not al low them to criti cise the phy si cians, they com plainonly of the most fla grant cases and, it is known, that so ci ety does not un der take any mea -sures.”; “The re form in creased the chances for in flu enc ing, but the cit i zens do not knowtheir rights; they should be ex plained in the me dia.”; “The cit i zens can in no way in flu -ence the qual ity of the health ser vice of fered to them. Their money is taken away, ir re -spec tive of whether they are sat is fied or not. Vir tu ally, they have no rights.”)
· Thirdly, the pa tients’ psy cho log i cal lim i ta tions for claim ing their rights (“The peo pledo not sub mit com plaints for two main rea sons – they do not know their rights and areafraid to com plain from their fam ily doc tors be cause, they think, the lat ter will not payany at ten tion to them af ter wards.”; “As be fore, the cit i zens are not given any op por tu -
286
nity to in flu ence the health ser vices of fered to them, the pa tients are com pletely de -pend ent on the GPs and the spe cial ists.”; “In the cit ies, the cit i zens can choose and inthis way to ex ert in flu ence, and the peo ple from the vil lages can only com plain. Whenan in spec tion co mes, it goes away af ter that, and the pa tient is en dorsed by the doc torand God be with him. There fore, the pa tients from the vil lages have to put up with thesit u a tion and suf fer.”).
Pri or i ties of the healthcare sys tem
The pri or i ties of the healthcare sys tem re ported by the may ors and mu nic i pal ity ad vi sors,did not dif fer even in the de tails from those, in di cated by the other in ter viewed groups. Thelead ing pri or i ties in cluded were “pro phy laxis, early di ag no sis and ad e quate treat ment”, “ma -ter nal and pae di at ric healthcare”, “school healthcare”, “so cially sig nif i cant dis eases”,“healthcare in the vil lages”, “im proved ac cess to spe cial ised and hos pi tal care”, “emer gency care”, “in vest ment in the ma te rial fa cil i ties”, “es tab lish ment of a uni fied in for ma tion sys temin healthcare”, “improvement of the quality of medical care”.
Ex pec ta tions for the fu ture of the sys tem
One part of the ex pec ta tions of the rep re sen ta tives of the lo cal au thor i ties about the fu tureof the health sys tem was op ti mis tic and ex pressed rather wishes for change:
· “To change the or der and the or gani sa tion of the out pa tients’ care and the fi nanc ingfor hos pi tal care”;
· “To re duce the bu reau cracy and the doc tors should work not as clerks but as spe cial ists”;
· “To have more health in sur ance funds, to change the sta tus of the GPs who feel as em -ploy ers of the med i cal spe cial ists at the mo ment”;
· “To come closer to the Eu ro pean stan dards; changes in the laws of healthcare”;
· “Con sol i da tion of the rates of de vel op ment and re form ing of the healthcare sys tem ac -cord ing to the re quire ments of the EC”;
· “To ob serve the re quire ments of the EC for changes in the healthcare sys tem”;
· “To strengthen the so cial el e ments of the re form and pro vide greater care to the peo ple”;
· “To think about the so cially unprivileged and those who are not in sured”;
· “To cre ate pos si bil i ties for privatisation”;
· “To carry out a dif fer en ti a tion of the healthcare es tab lish ments”;
· “To abol ish the frame work agree ment”;
· “To re duce the pos si bil ity for the phy si cians to work in the pri vate and pub lic sec tor si -mul ta neously”;
· “To re move the VAT on med i cal equip ment”;
· “To re duce cor rup tion”.
Some ex pec ta tions were op ti mis tic on cer tain con di tions:
· “Op ti mis tic, if the leg is la tion is changed”;
· “Noth ing good is ex pect ing healthcare, un less there are changes in the nor ma tive ba -sis; the state must as sist the proper de vel op ment of healthcare”;
287
So cio log i cal in ter pre ta tion
· “The ex pec ta tions are neg a tive, un less the leg is la tion is changed, to gether with theroute un der taken by the over all re form”.
In the mean time, re gard ing the health ser vices for cer tain groups of the pop u la tion,the re spon dents ex pressed their neg a tive at ti tude:
· “Un clear, hazy fu ture; prob lems for a large part of the pop u la tion. Even greater prob -lems for the poor and the so cially dis ad van taged lay ers”;
· “The fu ture is not “pink”; the healthcare is for the peo ple with money, those, who areso cially unprivileged, are vir tu ally mar gin al ised by the state. If ur gent mea sures arenot un der taken, the pop u la tion of the coun try will drop at fast rates”.
Ma jor prob lems at mu nic i pal ity level
As ma jor com mon prob lems, the rep re sen ta tives of the lo cal au thor i ties pointed out thelack of fi nanc ing, the low in come of the cit i zens, un em ploy ment, in ef fec tive ed u ca tion,poor in fra struc ture and cor rup tion. These prob lems ac com pa nied the healthcare in the mu -nic i pal i ties, too. The im pos si bil ity for the mu nic i pal ity to in flu ence the health pol icy wasalso indicated as common for the local authorities.
The most se ri ous and com monly re ported prob lems of the mu nic i pal i ties, re lated tohealthcare, in cluded the cit i zens with out health in sur an ces, the med i cal ser vices of thepeo ple in the small pop u lated re gions and the re gions re mote from the big mu nic i pal i ties, emer gency healthcare, den tal care.
The role of the lo cal au thor i ties in the mu nic i pal healthcare
On the point of the role of the lo cal au thor i ties in the healthcare at mu nic i pal level, three the -ses were formed. Ac cord ing to the first one, the healthcare had to be a state pri or ity, ac cord ing tothe sec ond one – a mu nic i pal pri or ity, and ac cord ing to the third one, the em pha sis had to be placedon the mar ket as a main reg u la tor of the re la tion ships in the healthcare sys tem.
The may ors and mu nic i pal ity ad vi sors, ac cord ing to whom healthcare should be a statepri or ity, ar gued in fa vour of their view mainly with the im pos si bil ity of the mu nic i pal i ties tose cure the healthcare fi nan cially, and there fore, they con sid ered that the state should helpthem (“It’s better, if this is a pri or ity for the state. It is dif fi cult for the mu nic i pal ity to cope with the fi nanc ing, the per son nel and their qual i fi ca tion”; “The state must fi nance the healthcareand the mu nic i pal ity must take care of the build ings, its main te nance and equip ment.”; “There is one hos pi tal in the mu nic i pal ity, the mu nic i pal i ties’ fi nance is not suf fi cient and … the statemust help it. Healthcare must be a pri or ity for the state”; “The state pri or ity must be, aboveall, to pro vide fi nan cial sup port for the mu nic i pal healthcare”; “Healthcare must be a statepri or ity, the mu nic i pal ity can only have a del e gated par tic i pa tion”).
The rep re sen ta tives of the lo cal au thor i ties, ad vo cat ing the sec ond the sis, was thathealthcare had to be a pri or ity of the mu nic i pal i ties, they emphasised the spe cific needs of thecit i zens and the spe cific lo cal prob lems, which could not be solved by the state but re quiredac tive ness on be half of the lo cal au thor i ties (“Healthcare must be a pri or ity for the mu nic i pal i -ties. The state can not be aware of prob lems.”; “The mayor must man age the mu nic i palhealthcare and the City coun cil must give the frame work of this man age ment. The mu nic i palhealthcare is closer to the peo ple. The whole fi nanc ing must be car ried out by the mu nic i pal ity
288
and the state must not dis trib ute the fi nanc ing.”; “There is no mu nic i pal healthcare and it hasto play a greater role be cause the cit i zens can ad dress their in qui ries di rectly to the mu nic i pal -ity”; “The state bud get must have a health in sur ance fund for à min i mum pack age of ser -vices for the so cially unprivileged, for pro phy lac tic check-ups of chil dren, etc.”; “Thecon crete com mit ments of the mu nic i pal ity have been with drawn, it can not sub si dise its hos pi -tals. It can only fi nance some spe cific programmes. It can not in crease the bud get of thehealthcare es tab lish ments. For ex am ple, the mu nic i pal ity may say that they have an ex ces sivemil lion available and will give it to the hospital. The municipality cannot do this.”).
Even though more rarely, views were also ex pressed, ac cord ing to which “the lead ingrole in healthcare must be played nei ther by the state, nor by the mu nic i pal ity, but fullprivatisation must be car ried out”. The pro po nents of this con cept drew their at ten tion to theef fec tive ness in the man age ment of the healthcare es tab lish ments (“Privatisation must bestarted be cause the healthcare es tab lish ments in the re gion, which are not pri vate, not man -aged by the man ag ers in ac cor dance with the in ter ests of so ci ety but their driv ing force is forper sonal ben e fit and these hos pi tals be come los ers”; “There is no com pe ti tion in healthcare.We are be com ing vic tims of per sonal in ter ests. There should be full privatisation.”).
Prob lems of the mu nic i pal i ties in their role of own ers of healthcarees tab lish ments
As own ers of healthcare es tab lish ments, the mu nic i pal i ties faced a num ber of prob lems,caused by the leg is la tion (“The leg is la tion does not as sist the mu nic i pal ity to act as a goodowner.”; “The role of the mu nic i pal ity is to main tain the build ing fa cil i ties, to re ceive re portsand ap point man ag ers, the leg is la tion im pedes the mu nic i pal i ties with these com mer cial com -pa nies.”; “The leg is la tion is an ob sta cle, it is clumsy and bu reau cratic and the mu nic i pal ityhas to pro vide fi nan cial as sis tance for the pur chas ing of consumables and equip ment”; “Theleg is la tion hin ders the work of the mu nic i pal ity and, above all, the work is ham pered by thefact that the mu nic i pal ity can not ex ert con trol over the work of the GPs”).
The larg est part of the prob lems, in di cated by the may ors and the mu nic i pal ity ad vi sors,re ferred to the fi nanc ing of the healthcare es tab lish ments:
· “The mu nic i pal ity has al most no com mit ments; the com pa nies have not been con sti -tuted by a de ci sion of the City coun cil, but by a de ci sion of the Coun cil of Min is ters”;
· “The mu nic i pal ity is the owner of the cap i tal in vest ment part, it al lo cates fi nanc ing forre con struc tion, but it can not al lo cate money for equip ment and med i cal ac tiv ity”;
· “The mu nic i pal i ties can not di rectly in fuse fi nances into the healthcare es tab lish mentsand, there fore, it sup ports them. The law is an ob sta cle in this re spect since thehealthcare es tab lish ments are com mer cial com pa nies”;
· “The mu nic i pal ity is a share holder in the MHAT, but it is vir tu ally man aged by the MH”;
· “In real fact the mu nic i pal ity has no com mit ments as an owner of the healthcare es -tab lish ments – its li a bil i ties are re duced to cur rent ex penses and re pairs, and the mu -nic i pal i ties have to be com mit ted only to a small health ser vices for the peo ple of poorfi nan cial means”;
· “The mu nic i pal ity sup ports the healthcare es tab lish ments by re leas ing fund ing for theim prove ment of the fa cil i ties and the equip ment, the prob lem with the pro phy laxis ofthe pop u la tion is se vere.”;
289
So cio log i cal in ter pre ta tion
· “Lack of a fi nan cial mech a nism for sup port ing the healthcare es tab lish ments, theleg is la tion im pedes the mu nic i pal ity to ful fil its li a bil i ties as an owner”.
The prob lems faced by the mu nic i pal i ties in their role as own ers of healthcare es tab lish -ments, to a large de gree de ter mined the at ti tude of the rep re sen ta tives of the lo cal au thor i ties tothis prop erty. For part of the may ors and mu nic i pal ity ad vi sors, the own er ship over thehealthcare es tab lish ments was a bur den for the mu nic i pal ity, the ar gu ments in sup port of this view, be ing mainly of fi nan cial na ture:
· “It is a bur den, be cause it is be com ing more and more dif fi cult to fi nance it”;
· “The com pany has no or gani sa tion, by means of which to be self-main tained, and con -stantly de mands money from the mu nic i pal ity. And the mu nic i pal ity is forced to al lo -cate fi nan cial re sources for it, in stead of al lo cat ing fi nance for ed u ca tion”;
· “The healthcare es tab lish ments are a bur den to the mu nic i pal ity, which has a share ofthe prop erty, but has no real pos si bil ity to man age this prop erty, and this turns its par -tic i pa tion into a for mal ity”;
· “It is a bur den, in so far as fi nances are al lo cated for this prop erty – the dis pen sary is fi -nanced by the mu nic i pal ity only and, in it, peo ple from other mu nic i pal i ties are alsotreated, but these mu nic i pal i ties do not give means for the dis pen sary”;
· “It is a bur den be cause the re spon si bil ity for the healthcare es tab lish ments can not befully un der taken. In case of a pos si ble bank ruptcy, how ever, the mu nic i pal ity wouldas sume the full re spon si bil ity for the healthcare es tab lish ment”;
· “The mu nic i pal ity must eval u ate whether it can main tain prop erty of such a size or not, and this is not de cided at cen tral level”.
For an other, al most large part of the rep re sen ta tives of the lo cal ad min is tra tion, the mu nic i -pal ity own er ship of the healthcare es tab lish ments was not a bur den for the mu nic i pal ity.The re spon dents, shar ing this view, re ported that “the mu nic i pal prop erty of the healthcare es -tab lish ments is rather a ne ces sity” since “healthcare is one of the most im por tant so cial ac tiv i -ties of the mu nic i pal ity, al though they also re cog nised the com monly shared prob lems of themu nic i pal i ties in their role of own ers of healthcare es tab lish ments (“The own er ship is not a bur -den and the op por tu nity should be given to the mu nic i pal ity to fi nance healthcare.”; “It’s not abur den. We will spare no ef fort to fight for its ex is tence (au thors’ note: the hos pi tal), be cause it is the only one in the re gion. It is de sir able that the neigh bour ing mu nic i pal i ties, served by the hos -pi tal, also con trib ute with fi nanc ing to its main te nance and pur chas ing of drugs andconsumables.”; “It should not be a bur den, but the leg is la tion must be changed in or der to givegreater com mit ment to the mu nic i pal ity re gard ing the own er ship.”).
Views about the de vel op ment of the mu nic i pal healthcare
The views of the may ors and mu nic i pal ity ad vi sors about the de vel op ment of the mu nic i -pal healthcare were di rected in three as pects:
1. Pres er va tion of the cur rent sta tus (pres er va tion of the healthcare es tab lish mentsar gued mainly by the pa tients’ in ter ests):
· “At the mo ment there is no ne ces sity ei ther for clos ing or for open ing of newhealthcare es tab lish ments”;
290
· “No way clos ing down, be cause the uni fi ca tion would not al low the peo ple to look for med i cal care in other more dis tant towns”;
· “There should be no clos ing of the mu nic i pal hos pi tals be cause the poor peo plewill have no where to be treated. At the same time, the op por tu nity will be prob a blygiven for the de vel op ment of a pri vate hos pi tal or pri vate hos pi tals to aid the mu -nic i pal hos pi tal and the mu nic i pal healthcare”;
· “The mu nic i pal hos pi tal can meet the needs of the pop u la tion, privatisation or clos -ing down are not nec es sary, there is no need for new healthcare es tab lish ments”.
2. Es tab lish ment of new healthcare es tab lish ments and de vel op ment of new types of ac tiv i ties:
· “To open a healthcare es tab lish ment (a mu nic i pal one) to cover the pa tients, whocan not in sure them selves”;
· “What the mu nic i pal ity can un der take, is to set up hos pices, since thus treat mentfor el derly peo ple will be pro vided, and their rel a tives will not have to dis con tinuetheir work ing ac tiv i ties”;
· “To build a small mu nic i pal hos pi tal to serve the peo ple who are not health in -sured. Why does n’t the state cover the ex penses for part of the peo ple with out ahealth in sur ance?”;
· “De vel op ment of a hos pice and a re ha bil i ta tion cen tre”.3. Clo sure and privatisation of healthcare es tab lish ments
· “The clo sure of healthcare es tab lish ments is a dif fi cult pro cess with the op po siteso cial ef fect, but when it is car ried out in a le gal, clear and trans par ent way, withthe par tic i pa tion of the per son nel, privatisation is a good so lu tion.”;
· “In small re gion as ours, it is not nec es sary to have so many MHAT. For in stance,the hos pi tal in Town A is in ef fec tive, there are spe cial ists, no pa tients. It has to beclosed down, but this mea sure is not go ing to be un der taken by Mu nic i pal ity A be -cause this would be re garded as the mu nic i pal ity’s own fail ure. In my opin ion, theneed for a well-equipped Cen tre for Emer gency Care in Town A is much morepress ing”;“The healthcare es tab lish ments should be pri va tised and mu nic i pal ityhos pi tals should be built in the places, where the pri vate own ers have no in ter estin es tab lish ing hos pi tals”;“To re duce the num ber of the healthcare es tab lish -ments, the mar ket prin ci ple will show, which ones should re main and which onesshould be closed down. In case of privatisation, a pro vi sion should ex ist, that theac tiv ity of the healthcare es tab lish ments can not change for a pe riod of five years”.
* * *
The views shared by the in ter viewed man ag ers of healthcare es tab lish ments in out pa -tients’ and hos pi tal care, di rec tors of dis pen sa ries, di rec tors of RHC, RHIF and RIPCPH andrep re sen ta tives of lo cal man age ment au thor i ties re veal sim i lar i ties on many of the key is suesof the on go ing healthcare re form and the de vel op ment of the health sys tem which can be sum -ma rized in the fol low ing way:
1. The con ducted study and the re sponses, ob tained from the man ag ing sub jects, in di -cate some com mon trends on spe cific is sues:
· Ac cord ing to the pre vail ing part of the re spon dents, there is no clear pol icy and strat -
291
So cio log i cal in ter pre ta tion
egy for the de vel op ment of the health sys tem; the re la tion ships (in clud ing rights, li a -bil i ties and re spon si bil i ties) among the sep a rate in sti tu tions are not reg u lated;
· The ma jor ity of the par tic i pants in the study sup port the view that the in ter fer enceof the state should be re stricted by cre at ing con di tions for mar ket re la tions. In thisre spect, the pro posal has made for the MH to with draw from the fi nanc ing of hos -pi tal care (en forced in 2006). This view is not backed mainly by man ag ers ofhealthcare es tab lish ments in the smaller towns, in which the mar ket re la tions can -not turn into an ef fec tive reg u la tor for limited or absent competition;
· Ac cord ing to the in ter viewed, the pri or i ties of the state in the healthcare fi nanc ingmust in clude programmes for pre ven tion and treat ment of some so cially sig nif i -cant dis eases as well as health ser vices for cer tain groups of the pop u la tion. Ofcourse, ac tiv i ties are also en vis aged for the ex e cu tion of con trol on public healthprotection;
· Ac cord ing to the stand, taken by the ma jor ity of the man ag ers of healthcare es tab -lish ments, the NFA is nec es sary to guar an tee the sta bil ity of the sys tem, but itshould be more gen eral in na ture and should be con cluded for a lon ger pe riod oftime. The con tract ing pro cess should also in clude other par tic i pants, who shouldde fend the in ter ests of all the par ties in volved in the agree ment (e.g. pro vid ers ofmed i cal care, le gal en ti ties, pharmacies, health insured people).
2. The pre vail ing part of the re spon dents criti cise the UBP, which, in their opin ion, hasdis tanced it self from the prob lems of the pro fes sion and does not de fend the phy si -cians’ in ter ests. In this re spect, changes are pro posed in the func tions of the Un ionboth in terms of the con tract ing of the terms and con di tions of the NFA and the post -grad u ate train ing and qual i fi ca tion im prove ment of the phy si cians. The gen er allyshared view is that the mem ber ship in the pro fes sional or gani sa tions should not beman da tory.
3. The mo nop o lis tic sta tus of the NHIF is also as sessed neg a tively. Sim i lar to the med i -cal spe cial ists (p.6.1 As sess ment of the med i cal spe cial ists), the man ag ing sub jectsalso con sider that the com pul sory health in sur ance should be car ried out by sev eralhealth in sur ance funds. The demonopolisation of the NHIF and the de vel op ment ofcom pet i tive re la tions are ac cepted as a pre-con di tion for the im prove ment of the ef -fec tive ness of the sys tem, and most lead ers also see a pos si bil ity for the im prove mentof the fi nan cial state of the healthcare es tab lish ments by negotiating prices,corresponding to their actual costs.
4. The views about the fu ture are pre dom i nantly op ti mis tic, but are also re lated to theim prove ment of the health in sur ance sys tem. Ac cord ing to the in ter viewed, a rad i -cal change of the model is not nec es sary but rather some cor rec tions are needed forthe elim i na tion of some de fects in the pro cess of its func tion ing (such as the de vel op -ment of mar ket re la tions, giv ing in cen tives for com pe ti tion, care for the dis ease pre -ven tion and health pro mo tion, im prove ment of the con trac tual re la tions and thecon tract ing pro cess, cost ing of the phy si cians’ la bour, im prove ment of the qual ity ofhealth ser vices, op ti mis ing the dis tri bu tion and the utilisation of the financialresources, etc.).
5. The con ducted in ter views also re veal the pre vail ing in com pe tence re gard ing the di -ag nos ti cally re lated groups. The view is fre quently shared that their in tro duc tion will
292
solve a num ber of sig nif i cant prob lems in the cur rently act ing sys tem of fi nanc ing,but the ex am ples, given for DRG by the re spon dents, do not es sen tially dif fer fromthose for the clin i cal path ways. Lack of un der stand ing is also ob served re gard ing thegoals and the mean ing of the privatisation pro cess. In some state ments, its con se -quences are re lated to the re stric tion of the ac cess of the poorer cit i zens to med i calcare or with the change of the sub ject of ac tiv ity of the pri va tised healthcare es tab -lish ments. The is sues are also dis put able as to which es tab lish ments should be firstpro posed for privatisation, which should be in cluded in the so called “pro hi bi tionlist” and which should be treated with pref er ences for privatisation. Opin ions are also voiced about “privatisation of ac tiv i ties” in stead of changing the ownership of thematerial assets of the healthcare establishments.
6.3. As sess ment by cit i zens
Cit i zens’ self-as sess ment of their own health sta tus
The cit i zens’ self-as sess ment of their own health sta tus re flected the re spon dents’ per cep -tion of their own health sta tus. The re sults from the sur vey in di cated that over half of the in ter -viewed eval u ated pos i tively their health sta tus, 19.4% as sessed it as “very good” and 37.4% as“good”. The op po site eval u a tions were given by one quar ter of the cit i zens, 15.6% of whomas sessed their own health sta tus as “poor” and 7.3% as “very poor”. 19.6% of the re spon dentswere po si tioned be tween the two poles, con sid er ing their health status to be “satisfactory”.
The rel a tive share of the per sons with de te ri o rated health sta tus, e.g. those, who hadde ter mined their health sta tus as “sat is fac tory”, “poor” or “very poor”, com prised 42.5%. Cer -tain de te ri o ra tion of the in di ca tors was ob served, as com pared to the val ues, reg is tered in pre -vi ous state ments about the pop u la tion’s health sta tus, con ducted by the Na tional In sti tute ofSta tis tics, the rel a tive share of the peo ple with de te ri o rated health be ing 33.6% in 1996 and40.2% in 2001 (NIS, 2002).
Com bin ing the re sponses to the ques tion about the self-as sess ment of the in di vid u als’health with the socio-de mo graphic char ac ter is tics of the cit i zens, in volved in the rep re sen ta -tive sam ple, the main dif fer ences in the de fined groups were ob served de pend ing on gen der,age, so cial po si tion and level of ed u ca tion. A sig nif i cantly higher per cent age of re tired pen -sion ers, the un em ployed and the peo ple with com pleted sec ond ary or high ed u ca tion, de ter -mined their health sta tus as “poor” and “very poor”, as com pared to the re spon dents fall ing inthe re main ing groups. In the age group of the in ter viewed above 60, the rel a tive share of theper sons with de te ri o rated health reached 68.1%. The pos i tive self-as sess ments dom i nated inthe age groups be tween 18 and 40 as well as among the peo ple who had com pleted higher ed u -ca tion. It is note wor thy, that a con sid er able per cent age (76.4%) of the cit i zens of the cap i tal de -fined their health sta tus as “very good” and “good”, un like in the rest of the groups,dis tin guished ac cord ing to the type of the pop u lated area. Sig nif i cant fluc tu a tions in the val uesof the in di ca tor “rel a tive share of the in di vid u als with de te ri o rated health sta tus” were man i -fested be tween the males and fe males, in cluded in the sur vey. The share of the in ter viewedmales, who as sessed their health sta tus as wors ened was 36.0%, whereas for the females, thisshare increased to 45.1%. Similar differences had been registered in previous studies, too,conducted by the NIS.
293
So cio log i cal in ter pre ta tion
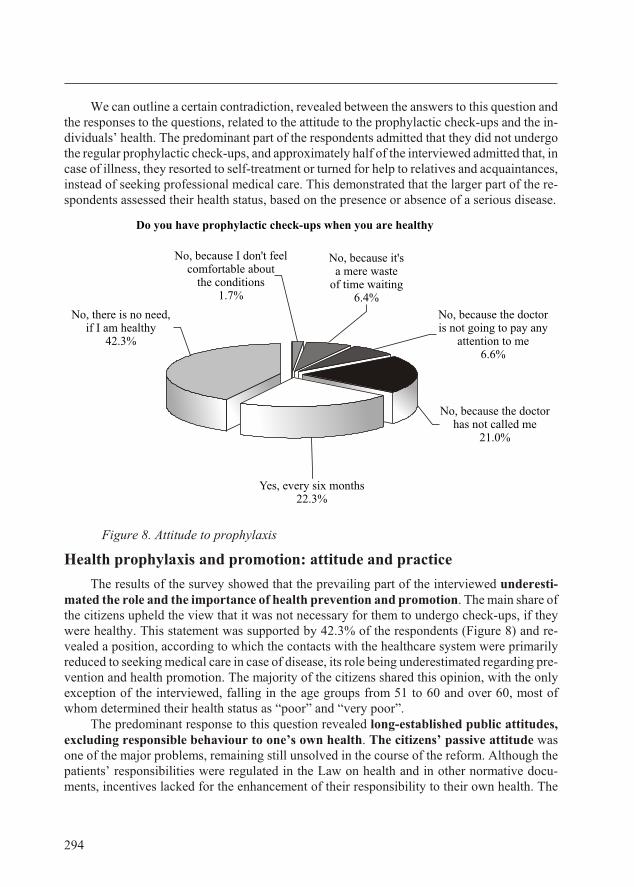
We can out line a cer tain con tra dic tion, re vealed be tween the an swers to this ques tion andthe re sponses to the ques tions, re lated to the at ti tude to the pro phy lac tic check-ups and the in -di vid u als’ health. The pre dom i nant part of the re spon dents ad mit ted that they did not un dergothe reg u lar pro phy lac tic check-ups, and ap prox i mately half of the in ter viewed ad mit ted that, in case of ill ness, they re sorted to self-treat ment or turned for help to rel a tives and ac quain tances,in stead of seek ing pro fes sional med i cal care. This dem on strated that the larger part of the re -spon dents as sessed their health sta tus, based on the presence or absence of a serious disease.
Fig ure 8. Attitude to prophylaxis
Health pro phy laxis and pro mo tion: at ti tude and prac tice
The re sults of the sur vey showed that the pre vail ing part of the in ter viewed un der es ti -mated the role and the im por tance of health pre ven tion and pro mo tion. The main share of the cit i zens up held the view that it was not nec es sary for them to un dergo check-ups, if theywere healthy. This state ment was sup ported by 42.3% of the re spon dents (Fig ure 8) and re -vealed a po si tion, ac cord ing to which the con tacts with the healthcare sys tem were pri mar ilyre duced to seek ing med i cal care in case of dis ease, its role be ing un der es ti mated re gard ing pre -ven tion and health pro mo tion. The ma jor ity of the cit i zens shared this opin ion, with the onlyex cep tion of the in ter viewed, fall ing in the age groups from 51 to 60 and over 60, most ofwhom de ter mined their health sta tus as “poor” and “very poor”.
The pre dom i nant re sponse to this ques tion re vealed long-es tab lished pub lic at ti tudes,ex clud ing re spon si ble be hav iour to one’s own health. The cit i zens’ pas sive at ti tude wasone of the ma jor prob lems, re main ing still un solved in the course of the re form. Al though thepa tients’ re spon si bil i ties were reg u lated in the Law on health and in other nor ma tive doc u -ments, in cen tives lacked for the en hance ment of their re spon si bil ity to their own health. The
294
Do you have prophylactic check-ups when you are healthy
No, there is no need,if I am healthy
42.3%
No, because I don't feelcomfortable about
the conditions1.7%
No, because the doctoris not going to pay any
attention to me6.6%
No, because it'sa mere waste
of time waiting 6.4%
No, because the doctorhas not called me
21.0%
Yes, every six months22.3%
health in sur ance in stal ments were bound merely to the in come, with out tak ing into ac count the health risk and the care for the in di vid ual’s health. Thus, one of the most sa lient prin ci ples ofthe re form – re spon si ble and ac tive at ti tude of the pa tients to their per sonal health – ac quiredchiefly a de clar a tive char ac ter, with out en vis ag ing any mech a nisms for chang ing the es tab -lished wide spread hab its and at ti tudes.
A sim i lar stand, man i fest ing un will ing ness to un der take the ini tia tive, was held by21.0% of the re spon dents, who re ported that they did not at tend pro phy lac tic check-ups, sincethey had not been sum moned by the fam ily phy si cian. The re sponses to this ques tion give usgrounds to claim that, among the ma jor ity of the cit i zens, the at ti tude was still dom i nat ing, thattheir per sonal health was the duty of the healthcare sys tem and its rep re sen ta tives. Cer tainly,we have to also note the fact that one of the ob li ga tions of the gen eral prac ti tio ners was to per -form reg u lar pro phy lac tic check-ups. For the per for mance of these ex am i na tions, how ever,there were no pos i tive in cen tives to turn pro phy laxis into a reg u lar prac tice.
Only 22.3% of the in ter viewed re ported that they un der went reg u lar pro phy lac ticcheck-ups. Of the re main ing 13.0%, ap prox i mately equal per cent age in di cated the un pleas antcir cum stances and the waste of time, re spec tively, as rea sons for their re fusal to un dergo suchex am i na tions. In its turn, this was also an in di rect ev i dence for the un der es ti mated role of thepro phy laxis.
Hab its and at ti tudes to per sonal health
In case of dis ease, over half of the cit i zens (52.9%) re ported that they sought med i calcare. The per cent age of those, who re sponded in this way, in creased sig nif i cantly in the agegroup over 60 (63.8%), whereas this per cent age was con sid er ably lower among the re spon -dents of low in come and with out em ploy ment. The fact is worth not ing, that in So fia, only42.9% of the in ter viewed pre ferred to seek med i cal care in case of an ill ness, while, in the other pop u lated ar eas, the share of the peo ple, who re sponded in this way, ranged be tween 48.3% for the vil lages and 57.0% for the dis trict towns.
Of the re main ing part, 41.6% pre ferred to cope with the ill ness on their own throughself-treat ment, and 5.1% of the re spon dents turned for ad vice to rel a tives and ac quain tances.These re sults dem on strate that al most half of the pop u la tion did not have es tab lished hab its for us ing qual i fied med i cal care.
In the pre vail ing part of the cases, this be hav iour was typ i cal for the milder dis eases andin dis po si tions, but it is likely, that it turned into one of the main rea sons for the de layed di ag no -sis of part of the dis eases along with the at ti tude to the pro phy lac tic check-ups.
When ac cu mu lat ing the re sults, a pro por tion ate re la tion ship can be ob served be tween theun der taken ac tions and the cit i zens’ self-as sess ment of their per sonal health sta tus (Ta ble 39).The ma jor ity of the re spon dents, who eval u ated their own health sta tus as “very good” and“good”, re lied on self-treat ment and rel a tives’ ad vice. On the con trary, the more de te ri o ratedthe health sta tus, the less prac ticed was the self-treat ment and the more in creased was the seek -ing of med i cal care. The fact was wor ry ing, that al though they as sessed their health sta tus as“poor” and “very poor’, over one quar ter of the re spon dents pre ferred cop ing with dis ease ontheir own to the al ter na tive of seek ing qual i fied med i cal care.
295
So cio log i cal in ter pre ta tion
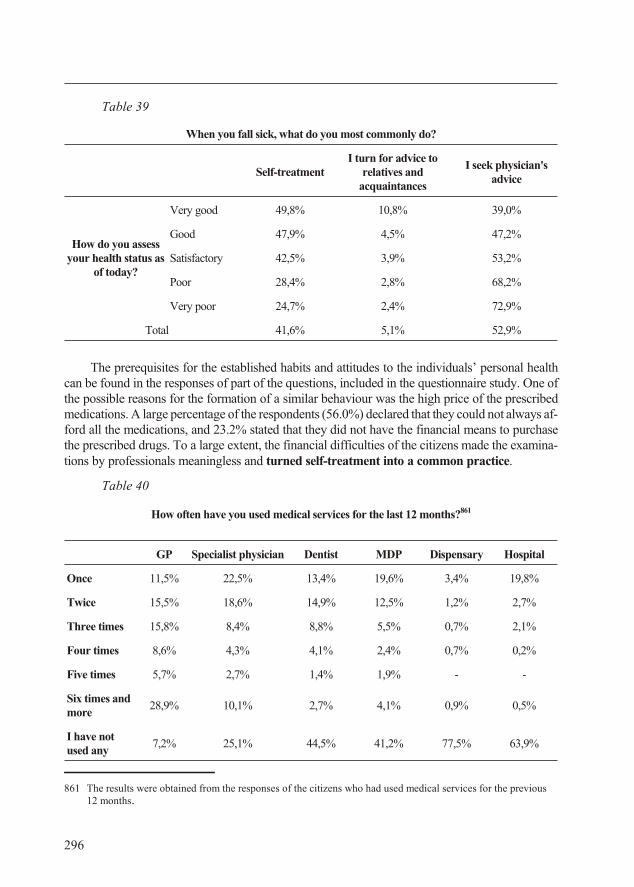
Table 39
When you fall sick, what do you most commonly do?
Self-treatmentI turn for advice to
relatives andacquaintances
I seek physician'sadvice
How do you assessyour health status as
of today?
Very good 49,8% 10,8% 39,0%
Good 47,9% 4,5% 47,2%
Sat is fac tory 42,5% 3,9% 53,2%
Poor 28,4% 2,8% 68,2%
Very poor 24,7% 2,4% 72,9%
Total 41,6% 5,1% 52,9%
The pre req ui sites for the es tab lished hab its and at ti tudes to the in di vid u als’ per sonal healthcan be found in the re sponses of part of the ques tions, in cluded in the ques tion naire study. One ofthe pos si ble rea sons for the for ma tion of a sim i lar be hav iour was the high price of the pre scribedmed i ca tions. A large per cent age of the re spon dents (56.0%) de clared that they could not al ways af -ford all the med i ca tions, and 23.2% stated that they did not have the fi nan cial means to pur chasethe pre scribed drugs. To a large ex tent, the fi nan cial dif fi cul ties of the cit i zens made the ex am i na -tions by pro fes sion als mean ing less and turned self-treat ment into a com mon prac tice.
Table 40
How often have you used medical services for the last 12 months?861
GP Specialist physician Dentist MDP Dispensary Hospital
Once 11,5% 22,5% 13,4% 19,6% 3,4% 19,8%
Twice 15,5% 18,6% 14,9% 12,5% 1,2% 2,7%
Three times 15,8% 8,4% 8,8% 5,5% 0,7% 2,1%
Four times 8,6% 4,3% 4,1% 2,4% 0,7% 0,2%
Five times 5,7% 2,7% 1,4% 1,9% - -
Six times andmore
28,9% 10,1% 2,7% 4,1% 0,9% 0,5%
I have notused any
7,2% 25,1% 44,5% 41,2% 77,5% 63,9%
296
861 The re sults were ob tained from the re sponses of the cit i zens who had used med i cal ser vices for the pre vi ous12 months.
A con sid er ably smaller part of the re spon dents (5.0%) in di cated that they had prob lemsfind ing the pre scribed med i cine in the phar ma cies. The im me di ate (phys i cal) ac cess to med i cal care could not ac count for the es tab lished hab its and at ti tudes ei ther, as only 2.7% re plied thatthere was no phy si cian in their in hab ited area and 6.7% of the in ter viewed re ported that thenear est healthcare es tab lish ment for spe cial ised med i cal care was sit u ated at a dis tance of over20 km from their liv ing place.
Dur ing the pre vi ous year, 38.9% of the in ter viewed cit i zens had used med i cal ser vices,19.2% had at tended a healthcare es tab lish ment on the oc ca sion of a dis eased rel a tive or fam ilymem ber, whereas 41.0% re ported that they had not at tended a healthcare es tab lish ment, in -clud ing the gen eral prac ti tio ner, cho sen by them. Of those, who had used med i cal ser vices dur -ing the pre vi ous year, 7.2% had sought di rectly spe cial ised med i cal as sis tance, with out be ingre ferred by the gen eral prac ti tio ner (Ta ble 40).
The anal y sis of the re sults shows that, in ap prox i mately half of the cases, the gen eral prac -ti tio ners had re ferred their pa tients to spe cial ised med i cal care, and, about one fifth of the cit i -zens, who had once vis ited their fam ily phy si cian dur ing the pre vi ous year, had sub se quentlybeen ad mit ted to a healthcare es tab lish ment. The es tab lished re la tion ship be tween the vis its tothe gen eral prac ti tio ner and the re main ing di vi sions of the sys tem proved that the gen eral phy -si cians re ally ful filled their func tions of “gate-keep ers of the healthcare sys tem”.
Based on the above re sponses to the ex am ined ques tions, we can iden tify three ma jorpre req ui sites for the pas sive at ti tude to the in di vid u als’ per sonal health and pre ven tion:
· un changed hab its formed in the course of the years dur ing the pre vi ous health sys tem. The at ti tude was dom i nat ing, that per sonal health was the ob li ga tion of the healthcaresys tem and its rep re sen ta tives, and the per sonal re spon si bil ity was real ised, only af terthe health sta tus de te ri o rated;
· lack of in cen tives and mech a nisms of the health in sur ance sys tem to cre ate con di tionsfor the cit i zens’ en hanced re spon si bil ity for their own health;
· na tional health pol icy, ac cord ing to which, al though the na tional health strat e gies of healthpro phy laxis and pro mo tion were con sid ered some of the most es sen tial pri or i ties for de vel -op ment, in the course of the re form, few ac tions were un der taken in this re spect.
Cit i zens’ as sess ment of the qual ity and or gani sa tion of med i cal care
As a whole, the cit i zens as sessed pos i tively the qual ity of the med i cal care, re ceived forthe pre vi ous 12 months (Fig ure 9). The pre vail ing part of the re spon dents gave a sat is fac toryeval u a tion of the med i cal as sis tance they had ob tained (38.5%), and al most one third of the in -ter viewed de ter mined its qual ity as “very good” and “ex cel lent”, the per cent age in creas ingamong the res i dents of the dis trict cit ies and the vil lages.
About 24.0% of the cit i zens as sessed neg a tively the qual ity of the re ceived med i calcare. Among them, the ma jor ity was com prised by the res i dents of the cap i tal as well as the re -spon dents from the age group up to 30 years and the share was the high est (44.4%) among there spon dents, who eval u ated their health sta tus as “very poor”.
297
So cio log i cal in ter pre ta tion
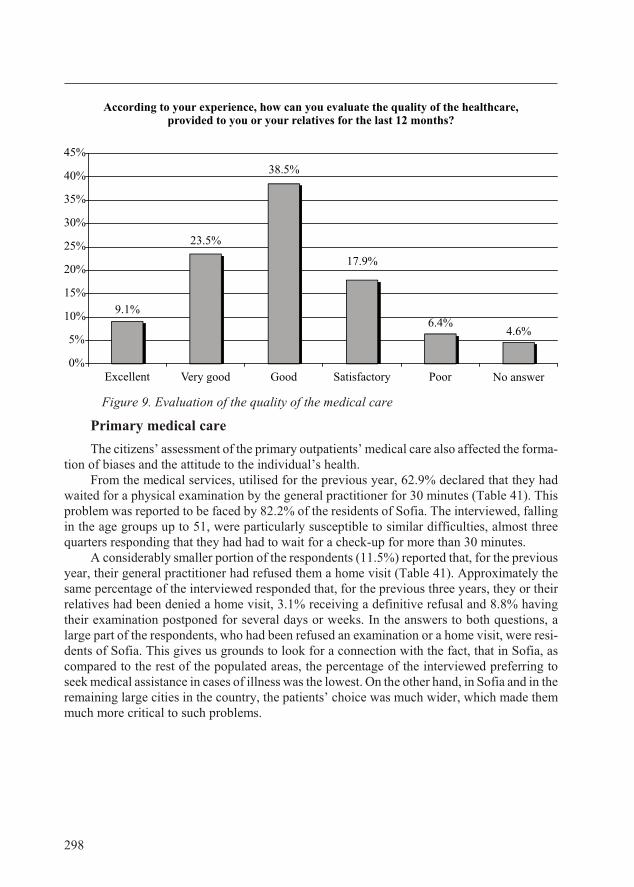
Fig ure 9. Evaluation of the quality of the medical care
Pri mary med i cal care
The cit i zens’ as sess ment of the pri mary out pa tients’ med i cal care also af fected the for ma -tion of bi ases and the at ti tude to the in di vid ual’s health.
From the med i cal ser vices, uti lised for the pre vi ous year, 62.9% de clared that they hadwaited for a phys i cal ex am i na tion by the gen eral prac ti tio ner for 30 min utes (Ta ble 41). Thisprob lem was re ported to be faced by 82.2% of the res i dents of So fia. The in ter viewed, fall ingin the age groups up to 51, were par tic u larly sus cep ti ble to sim i lar dif fi cul ties, al most threequar ters re spond ing that they had had to wait for a check-up for more than 30 min utes.
A con sid er ably smaller por tion of the re spon dents (11.5%) re ported that, for the pre vi ousyear, their gen eral prac ti tio ner had re fused them a home visit (Ta ble 41). Ap prox i mately thesame per cent age of the in ter viewed re sponded that, for the pre vi ous three years, they or theirrel a tives had been de nied a home visit, 3.1% re ceiv ing a de fin i tive re fusal and 8.8% hav ingtheir ex am i na tion post poned for sev eral days or weeks. In the an swers to both ques tions, alarge part of the re spon dents, who had been re fused an ex am i na tion or a home visit, were res i -dents of So fia. This gives us grounds to look for a con nec tion with the fact, that in So fia, ascom pared to the rest of the pop u lated ar eas, the per cent age of the in ter viewed pre fer ring toseek med i cal as sis tance in cases of ill ness was the low est. On the other hand, in So fia and in the re main ing large cit ies in the coun try, the pa tients’ choice was much wider, which made themmuch more crit i cal to such prob lems.
298
According to your experience, how can you evaluate the quality of the healthcare,provided to you or your relatives for the last 12 months?
4.6%6.4%
17.9%
38.5%
23.5%
9.1%
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
Excellent Very good Good Satisfactory Poor No answer
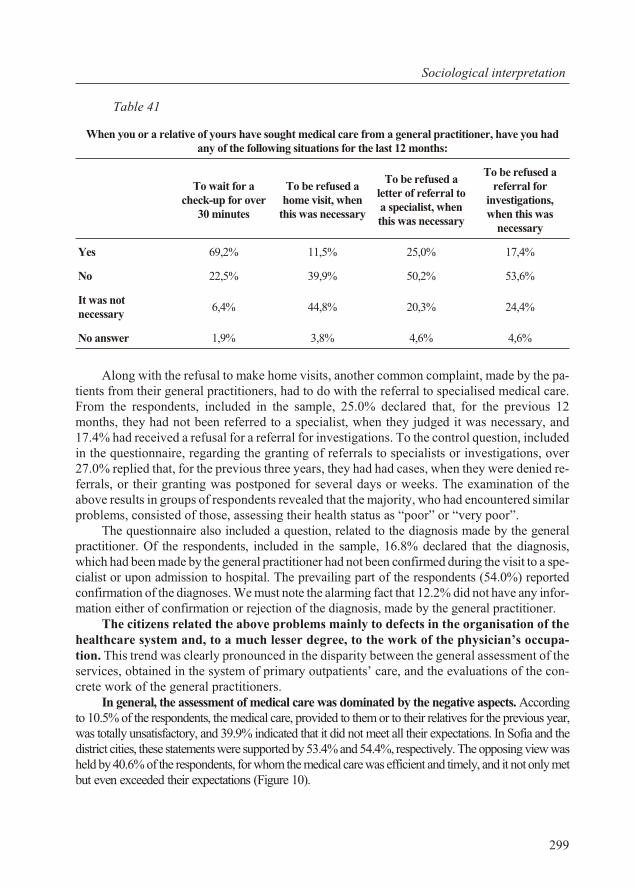
Ta ble 41
When you or a relative of yours have sought medical care from a general practitioner, have you hadany of the following situations for the last 12 months:
To wait for acheck-up for over
30 minutes
To be refused ahome visit, when
this was necessary
To be refused aletter of referral toa specialist, whenthis was necessary
To be refused areferral for
investigations,when this was
necessary
Yes 69,2% 11,5% 25,0% 17,4%
No 22,5% 39,9% 50,2% 53,6%
It was notnec es sary
6,4% 44,8% 20,3% 24,4%
No answer 1,9% 3,8% 4,6% 4,6%
Along with the re fusal to make home vis its, an other com mon com plaint, made by the pa -tients from their gen eral prac ti tio ners, had to do with the re fer ral to spe cial ised med i cal care.From the re spon dents, in cluded in the sam ple, 25.0% de clared that, for the pre vi ous 12months, they had not been re ferred to a spe cial ist, when they judged it was nec es sary, and17.4% had re ceived a re fusal for a re fer ral for in ves ti ga tions. To the con trol ques tion, in cludedin the ques tion naire, re gard ing the grant ing of re fer rals to spe cial ists or in ves ti ga tions, over27.0% re plied that, for the pre vi ous three years, they had had cases, when they were de nied re -fer rals, or their grant ing was post poned for sev eral days or weeks. The ex am i na tion of theabove re sults in groups of re spon dents re vealed that the ma jor ity, who had en coun tered sim i lar prob lems, con sisted of those, as sess ing their health sta tus as “poor” or “very poor”.
The ques tion naire also in cluded a ques tion, re lated to the di ag no sis made by the gen eralprac ti tio ner. Of the re spon dents, in cluded in the sam ple, 16.8% de clared that the di ag no sis,which had been made by the gen eral prac ti tio ner had not been con firmed dur ing the visit to a spe -cial ist or upon ad mis sion to hos pi tal. The pre vail ing part of the re spon dents (54.0%) re portedcon fir ma tion of the di ag no ses. We must note the alarm ing fact that 12.2% did not have any in for -ma tion ei ther of con fir ma tion or re jec tion of the di ag no sis, made by the gen eral prac ti tio ner.
The cit i zens re lated the above prob lems mainly to de fects in the or gani sa tion of thehealthcare sys tem and, to a much lesser de gree, to the work of the phy si cian’s oc cu pa -tion. This trend was clearly pro nounced in the dis par ity be tween the gen eral as sess ment of theser vices, ob tained in the sys tem of pri mary out pa tients’ care, and the eval u a tions of the con -crete work of the gen eral prac ti tio ners.
In gen eral, the as sess ment of med i cal care was dom i nated by the neg a tive as pects. Ac cord ingto 10.5% of the re spon dents, the med i cal care, pro vided to them or to their rel a tives for the pre vi ous year,was to tally un sat is fac tory, and 39.9% in di cated that it did not meet all their ex pec ta tions. In So fia and thedis trict cit ies, these state ments were sup ported by 53.4% and 54.4%, re spec tively. The op pos ing view was held by 40.6% of the re spon dents, for whom the med i cal care was ef fi cient and timely, and it not only metbut even ex ceeded their ex pec ta tions (Fig ure 10).
299
So cio log i cal in ter pre ta tion
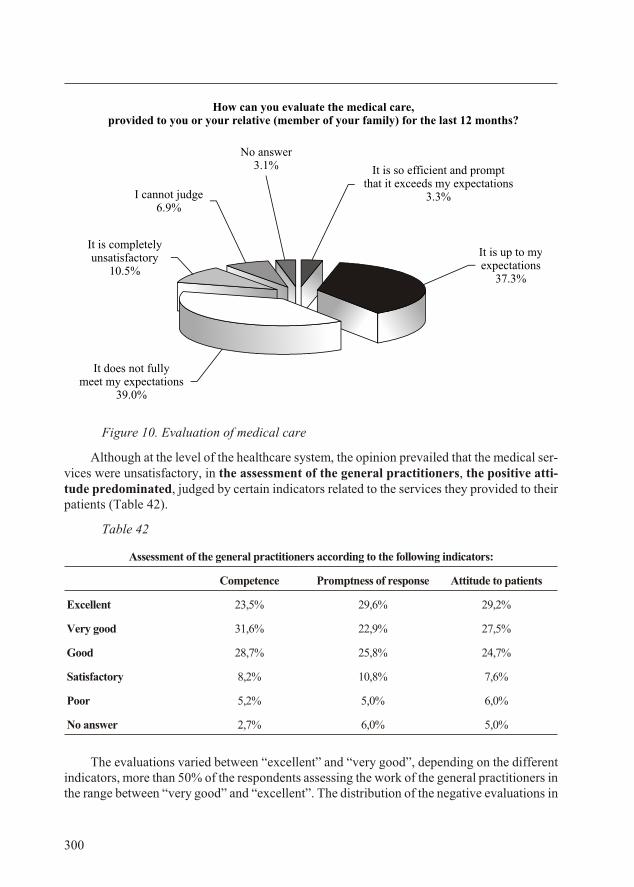
Figure 10. Evaluation of medical care
Al though at the level of the healthcare sys tem, the opin ion pre vailed that the med i cal ser -vices were un sat is fac tory, in the as sess ment of the gen eral prac ti tio ners, the pos i tive at ti -tude pre dom i nated, judged by cer tain in di ca tors re lated to the ser vices they pro vided to theirpa tients (Ta ble 42).
Table 42
Assessment of the general practitioners according to the following indicators:
Competence Promptness of response Attitude to patients
Excellent 23,5% 29,6% 29,2%
Very good 31,6% 22,9% 27,5%
Good 28,7% 25,8% 24,7%
Sat is fac tory 8,2% 10,8% 7,6%
Poor 5,2% 5,0% 6,0%
No answer 2,7% 6,0% 5,0%
The eval u a tions var ied be tween “ex cel lent” and “very good”, de pend ing on the dif fer entin di ca tors, more than 50% of the re spon dents as sess ing the work of the gen eral prac ti tio ners inthe range be tween “very good” and “ex cel lent”. The dis tri bu tion of the neg a tive eval u a tions in
300
How can you evaluate the medical care,provided to you or your relative (member of your family) for the last 12 months?
No answer3.1%
It is up to myexpectations
37.3%
I cannot judge6.9%
It is completelyunsatisfactory
10.5%
It is so efficient and promptthat it exceeds my expectations
3.3%
It does not fullymeet my expectations
39.0%
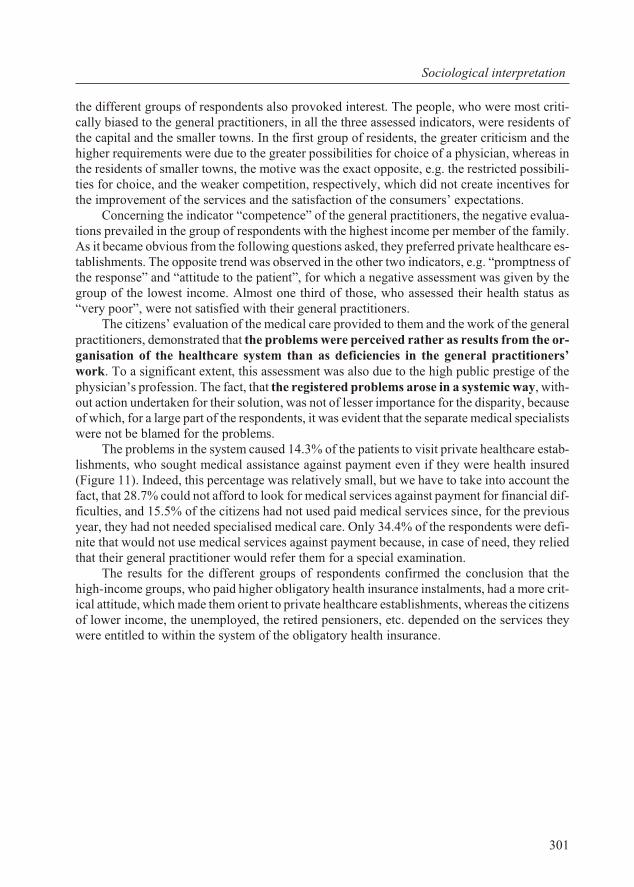
the dif fer ent groups of re spon dents also pro voked in ter est. The peo ple, who were most crit i -cally bi ased to the gen eral prac ti tio ners, in all the three as sessed in di ca tors, were res i dents ofthe cap i tal and the smaller towns. In the first group of res i dents, the greater crit i cism and thehigher re quire ments were due to the greater pos si bil i ties for choice of a phy si cian, whereas inthe res i dents of smaller towns, the mo tive was the ex act op po site, e.g. the re stricted pos si bil i -ties for choice, and the weaker com pe ti tion, re spec tively, which did not cre ate in cen tives forthe im prove ment of the ser vices and the sat is fac tion of the con sum ers’ ex pec ta tions.
Con cern ing the in di ca tor “com pe tence” of the gen eral prac ti tio ners, the neg a tive eval u a -tions pre vailed in the group of re spon dents with the high est in come per mem ber of the fam ily.As it be came ob vi ous from the fol low ing ques tions asked, they pre ferred pri vate healthcare es -tab lish ments. The op po site trend was ob served in the other two in di ca tors, e.g. “prompt ness ofthe re sponse” and “at ti tude to the pa tient”, for which a neg a tive as sess ment was given by thegroup of the low est in come. Al most one third of those, who as sessed their health sta tus as“very poor”, were not sat is fied with their gen eral prac ti tio ners.
The cit i zens’ eval u a tion of the med i cal care pro vided to them and the work of the gen eralprac ti tio ners, dem on strated that the prob lems were per ceived rather as re sults from the or -gani sa tion of the healthcare sys tem than as de fi cien cies in the gen eral prac ti tio ners’work. To a sig nif i cant ex tent, this as sess ment was also due to the high pub lic pres tige of thephy si cian’s pro fes sion. The fact, that the reg is tered prob lems arose in a sys temic way, with -out ac tion un der taken for their so lu tion, was not of lesser im por tance for the dis par ity, be causeof which, for a large part of the re spon dents, it was ev i dent that the sep a rate med i cal spe cial istswere not be blamed for the prob lems.
The prob lems in the sys tem caused 14.3% of the pa tients to visit pri vate healthcare es tab -lish ments, who sought med i cal as sis tance against pay ment even if they were health in sured(Fig ure 11). In deed, this per cent age was rel a tively small, but we have to take into ac count thefact, that 28.7% could not af ford to look for med i cal ser vices against pay ment for fi nan cial dif -fi cul ties, and 15.5% of the cit i zens had not used paid med i cal ser vices since, for the pre vi ousyear, they had not needed spe cial ised med i cal care. Only 34.4% of the re spon dents were def i -nite that would not use med i cal ser vices against pay ment be cause, in case of need, they re liedthat their gen eral prac ti tio ner would re fer them for a spe cial ex am i na tion.
The re sults for the dif fer ent groups of re spon dents con firmed the con clu sion that thehigh-in come groups, who paid higher oblig a tory health in sur ance in stal ments, had a more crit -i cal at ti tude, which made them ori ent to pri vate healthcare es tab lish ments, whereas the cit i zens of lower in come, the un em ployed, the re tired pen sion ers, etc. de pended on the ser vices theywere en ti tled to within the sys tem of the oblig a tory health in sur ance.
301
So cio log i cal in ter pre ta tion
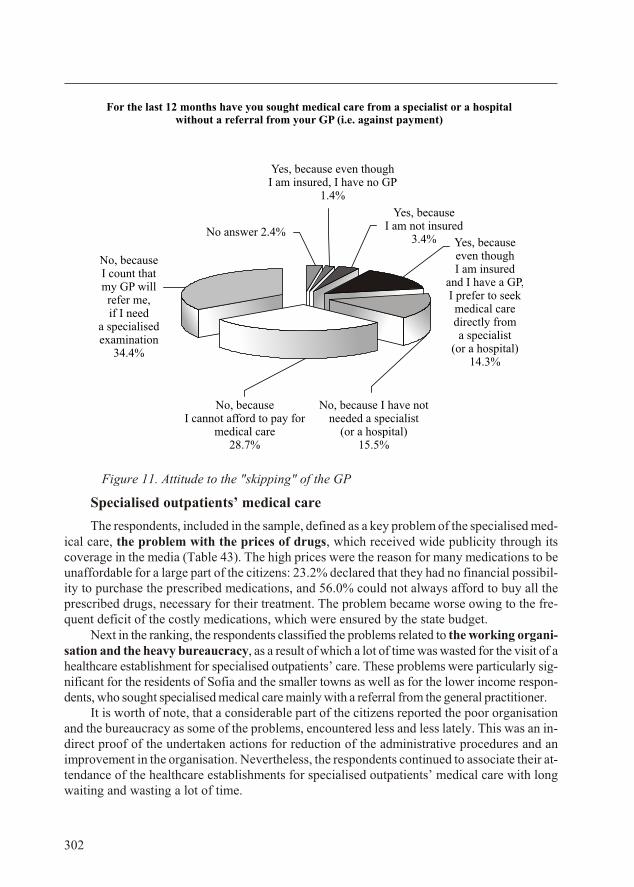
Fig ure 11. Attitude to the "skipping" of the GP
Spe cial ised out pa tients’ med i cal care
The re spon dents, in cluded in the sam ple, de fined as a key prob lem of the spe cial ised med -i cal care, the prob lem with the prices of drugs, which re ceived wide pub lic ity through itscov er age in the me dia (Ta ble 43). The high prices were the rea son for many med i ca tions to beun af ford able for a large part of the cit i zens: 23.2% de clared that they had no fi nan cial pos si bil -ity to pur chase the pre scribed med i ca tions, and 56.0% could not al ways af ford to buy all thepre scribed drugs, nec es sary for their treat ment. The prob lem be came worse ow ing to the fre -quent def i cit of the costly med i ca tions, which were en sured by the state bud get.
Next in the rank ing, the re spon dents clas si fied the prob lems re lated to the work ing or gani -sa tion and the heavy bu reau cracy, as a re sult of which a lot of time was wasted for the visit of a healthcare es tab lish ment for spe cial ised out pa tients’ care. These prob lems were par tic u larly sig -nif i cant for the res i dents of So fia and the smaller towns as well as for the lower in come re spon -dents, who sought spe cial ised med i cal care mainly with a re fer ral from the gen eral prac ti tio ner.
It is worth of note, that a con sid er able part of the cit i zens re ported the poor or gani sa tionand the bu reau cracy as some of the prob lems, en coun tered less and less lately. This was an in -di rect proof of the un der taken ac tions for re duc tion of the ad min is tra tive pro ce dures and anim prove ment in the or gani sa tion. Nev er the less, the re spon dents con tin ued to as so ci ate their at -ten dance of the healthcare es tab lish ments for spe cial ised out pa tients’ med i cal care with longwait ing and wast ing a lot of time.
302
For the last 12 months have you sought medical care from a specialist or a hospitalwithout a referral from your GP (i.e. against payment)
Yes, becauseI am not insured
3.4%No answer 2.4%
Yes, because even though I am insured, I have no GP
1.4%
No, because I have notneeded a specialist
(or a hospital)15.5%
Yes, becauseeven thoughI am insured
and I have a GP,I prefer to seekmedical caredirectly froma specialist
(or a hospital)14.3%
No, becauseI cannot afford to pay for
medical care28.7%
No, becauseI count thatmy GP willrefer me,if I need
a specialisedexamination
34.4%
Table 43
Ranking of the problems in specialised outpatients' medical care Ranking
Ex pen sive and un af ford able med i ca tions for most peo ple 1
Waste of a lot of time 2
Bu reau cracy 3
Poor or gani sa tion 4
Short age of drugs and other ma te ri als 5
Out dated and out-of-or der med i cal equip ment 6
Cor rup tion 7
Claim ing money for ser vices paid by the health in sur ance 8
In hu mane (im po lite) at ti tude 9
In suf fi cient hy giene 10
In com pe tence of the med i cal staff 11
The short age of drugs and consumables as well as the out dated or out-of-or der equip mentwere prob lems, de ter mined as sig nif i cant and com mon by a smaller part of the cit i zens, re sid -ing mainly in smaller towns. The same was valid for cor rup tion and un reg u lated pay ments.They were at trib uted chiefly to struc tural and or gani sa tional dis or ders, and to a much lesser de -gree, to the com pe tence and the qual ity of work of the med i cal staff. Ac cord ing to al most13.0% of the in ter viewed, the prob lems re lated to the at ti tude to the pa tients, the com pe tence of the med i cal staff and the hy giene were en coun tered more and more rarely in the healthcare es -tab lish ments for spe cial ised out pa tients’ med i cal care.
The ob tained re sults bring about the con clu sion that, on the one hand, the prob lems, de ter -mined by the cit i zens in out pa tients’ spe cial ised med i cal care were due to the man age ment andthe or gani sa tion of the healthcare sys tem and to the man age ment of the sep a rate healthcare es -tab lish ments, on the other.
Treat ment in healthcare es tab lish ments
From the re spon dents, in cluded in the sam ple, 37.6% in di cated that they or a rel a tive oftheirs had been ad mit ted to a hos pi tal for treat ment dur ing the pre vi ous two years. This per -cent age was sig nif i cantly higher in the group with an in come be low 100 BGN per mem ber ofthe fam ily, ap prox i mately half of the cit i zens, fall ing in this group, hav ing at tended a hos pi talhealthcare es tab lish ment. Un like in this group, in the group with the high est in come, a con sid -er ably smaller part of 22.2% had used hos pi tal care.
Of those, who had used hos pi tal care for the pre vi ous two years, 47.9% had cho sen a hos -pi tal on rec om men da tion of their gen eral prac ti tio ner or a spe cial ist from out pa tients’ care,22.4% re ported that they had not been given to op por tu nity to choose, and 18.7% had cho senthe hos pi tal on their own.
303
So cio log i cal in ter pre ta tion
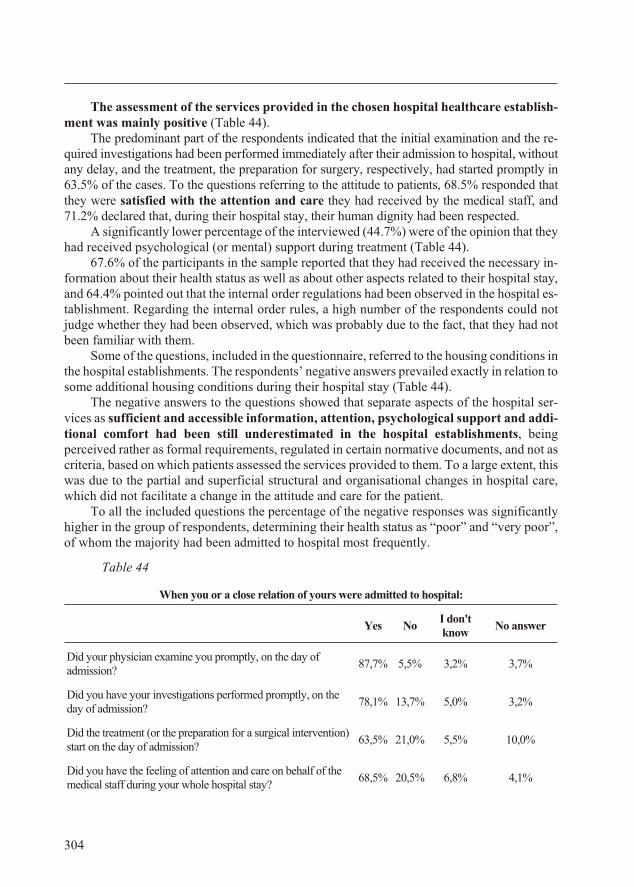
The as sess ment of the ser vices pro vided in the cho sen hos pi tal healthcare es tab lish -ment was mainly pos i tive (Ta ble 44).
The pre dom i nant part of the re spon dents in di cated that the ini tial ex am i na tion and the re -quired in ves ti ga tions had been per formed im me di ately af ter their ad mis sion to hos pi tal, with outany de lay, and the treat ment, the prep a ra tion for sur gery, re spec tively, had started promptly in63.5% of the cases. To the ques tions re fer ring to the at ti tude to pa tients, 68.5% re sponded thatthey were sat is fied with the at ten tion and care they had re ceived by the med i cal staff, and71.2% de clared that, dur ing their hos pi tal stay, their hu man dig nity had been re spected.
A sig nif i cantly lower per cent age of the in ter viewed (44.7%) were of the opin ion that theyhad re ceived psy cho log i cal (or men tal) sup port dur ing treat ment (Ta ble 44).
67.6% of the par tic i pants in the sam ple re ported that they had re ceived the nec es sary in -for ma tion about their health sta tus as well as about other as pects re lated to their hos pi tal stay,and 64.4% pointed out that the in ter nal or der reg u la tions had been ob served in the hos pi tal es -tab lish ment. Re gard ing the in ter nal or der rules, a high num ber of the re spon dents could notjudge whether they had been ob served, which was prob a bly due to the fact, that they had notbeen fa mil iar with them.
Some of the ques tions, in cluded in the ques tion naire, re ferred to the hous ing con di tions in the hos pi tal es tab lish ments. The re spon dents’ neg a tive an swers pre vailed ex actly in re la tion to some ad di tional hous ing con di tions dur ing their hos pi tal stay (Ta ble 44).
The neg a tive an swers to the ques tions showed that sep a rate as pects of the hos pi tal ser -vices as suf fi cient and ac ces si ble in for ma tion, at ten tion, psy cho log i cal sup port and ad di -tional com fort had been still un der es ti mated in the hos pi tal es tab lish ments, be ingper ceived rather as for mal re quire ments, reg u lated in cer tain nor ma tive doc u ments, and not ascri te ria, based on which pa tients as sessed the ser vices pro vided to them. To a large ex tent, thiswas due to the par tial and su per fi cial struc tural and or gani sa tional changes in hos pi tal care,which did not fa cil i tate a change in the at ti tude and care for the pa tient.
To all the in cluded ques tions the per cent age of the neg a tive re sponses was sig nif i cantlyhigher in the group of re spon dents, de ter min ing their health sta tus as “poor” and “very poor”,of whom the ma jor ity had been ad mit ted to hos pi tal most fre quently.
Table 44
When you or a close relation of yours were admitted to hospital:
Yes NoI don'tknow
No answer
Did your physician examine you promptly, on the day ofadmission?
87,7% 5,5% 3,2% 3,7%
Did you have your in ves ti ga tions per formed promptly, on theday of ad mis sion?
78,1% 13,7% 5,0% 3,2%
Did the treat ment (or the prep a ra tion for a sur gi cal in ter ven tion) start on the day of ad mis sion?
63,5% 21,0% 5,5% 10,0%
Did you have the feel ing of at ten tion and care on be half of themed i cal staff dur ing your whole hos pi tal stay?
68,5% 20,5% 6,8% 4,1%
304
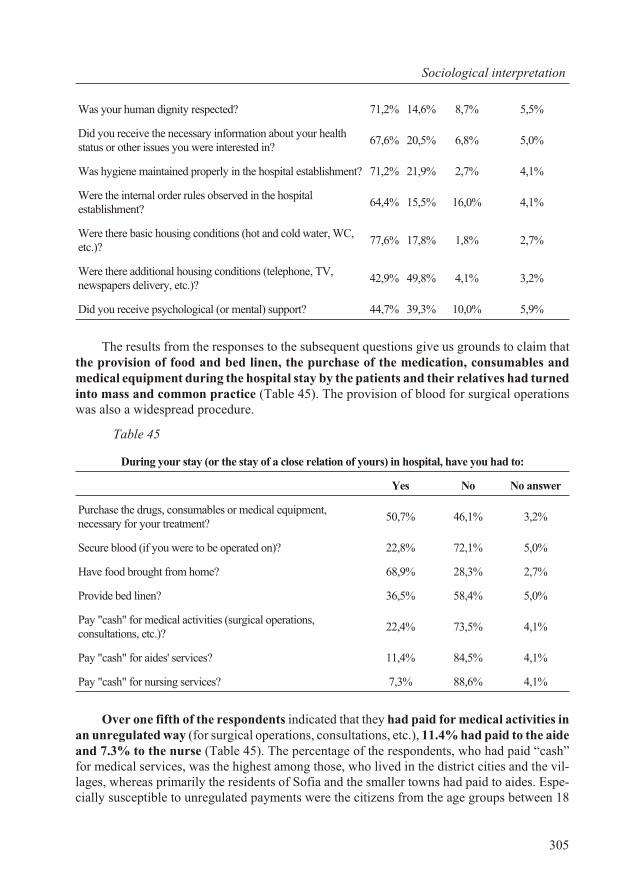
Was your hu man dig nity re spected? 71,2% 14,6% 8,7% 5,5%
Did you re ceive the nec es sary in for ma tion about your healthsta tus or other is sues you were in ter ested in?
67,6% 20,5% 6,8% 5,0%
Was hy giene main tained prop erly in the hos pi tal es tab lish ment? 71,2% 21,9% 2,7% 4,1%
Were the in ter nal or der rules ob served in the hos pi tales tab lish ment?
64,4% 15,5% 16,0% 4,1%
Were there ba sic hous ing con di tions (hot and cold wa ter, WC,etc.)?
77,6% 17,8% 1,8% 2,7%
Were there ad di tional hous ing con di tions (tele phone, TV,news pa pers de liv ery, etc.)?
42,9% 49,8% 4,1% 3,2%
Did you receive psychological (or mental) support? 44,7% 39,3% 10,0% 5,9%
The re sults from the re sponses to the sub se quent ques tions give us grounds to claim thatthe pro vi sion of food and bed linen, the pur chase of the med i ca tion, consumables andmed i cal equip ment dur ing the hos pi tal stay by the pa tients and their rel a tives had turned into mass and com mon prac tice (Ta ble 45). The pro vi sion of blood for sur gi cal op er a tionswas also a wide spread pro ce dure.
Ta ble 45
During your stay (or the stay of a close relation of yours) in hospital, have you had to:
Yes No No answer
Purchase the drugs, consumables or medical equipment,necessary for your treatment?
50,7% 46,1% 3,2%
Se cure blood (if you were to be op er ated on)? 22,8% 72,1% 5,0%
Have food brought from home? 68,9% 28,3% 2,7%
Pro vide bed linen? 36,5% 58,4% 5,0%
Pay "cash" for med i cal ac tiv i ties (sur gi cal op er a tions,con sul ta tions, etc.)?
22,4% 73,5% 4,1%
Pay "cash" for aides' ser vices? 11,4% 84,5% 4,1%
Pay "cash" for nursing services? 7,3% 88,6% 4,1%
Over one fifth of the re spon dents in di cated that they had paid for med i cal ac tiv i ties inan un reg u lated way (for sur gi cal op er a tions, con sul ta tions, etc.), 11.4% had paid to the aide and 7.3% to the nurse (Ta ble 45). The per cent age of the re spon dents, who had paid “cash”for med i cal ser vices, was the high est among those, who lived in the dis trict cit ies and the vil -lages, whereas pri mar ily the res i dents of So fia and the smaller towns had paid to aides. Es pe -cially sus cep ti ble to un reg u lated pay ments were the cit i zens from the age groups be tween 18
305
So cio log i cal in ter pre ta tion
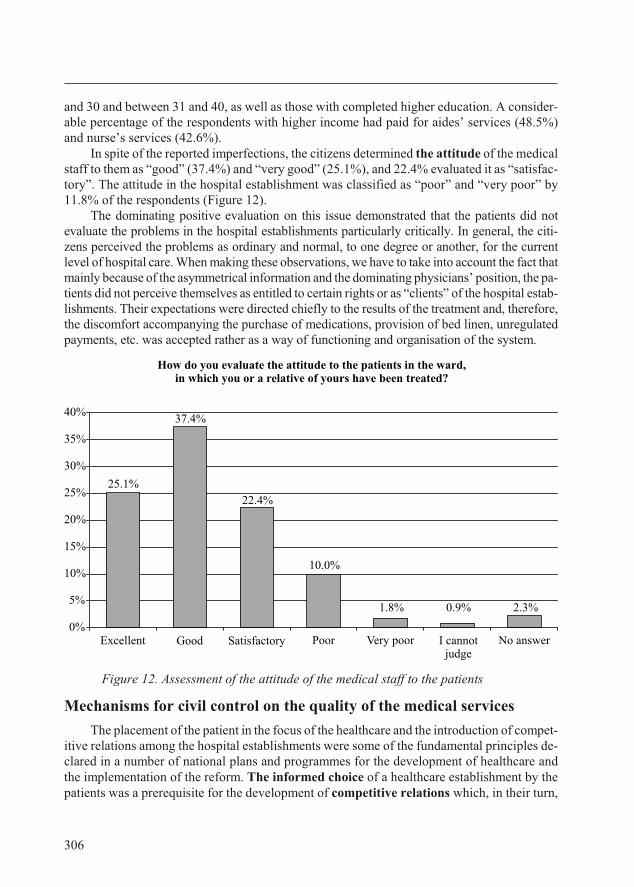
and 30 and be tween 31 and 40, as well as those with com pleted higher ed u ca tion. A con sid er -able per cent age of the re spon dents with higher in come had paid for aides’ ser vices (48.5%)and nurse’s ser vices (42.6%).
In spite of the re ported im per fec tions, the cit i zens de ter mined the at ti tude of the med i calstaff to them as “good” (37.4%) and “very good” (25.1%), and 22.4% eval u ated it as “sat is fac -tory”. The at ti tude in the hos pi tal es tab lish ment was clas si fied as “poor” and “very poor” by11.8% of the re spon dents (Fig ure 12).
The dom i nat ing pos i tive eval u a tion on this is sue dem on strated that the pa tients did noteval u ate the prob lems in the hos pi tal es tab lish ments par tic u larly crit i cally. In gen eral, the cit i -zens per ceived the prob lems as or di nary and nor mal, to one de gree or an other, for the cur rentlevel of hos pi tal care. When mak ing these ob ser va tions, we have to take into ac count the fact that mainly be cause of the asym met ri cal in for ma tion and the dom i nat ing phy si cians’ po si tion, the pa -tients did not per ceive them selves as en ti tled to cer tain rights or as “cli ents” of the hos pi tal es tab -lish ments. Their ex pec ta tions were di rected chiefly to the re sults of the treat ment and, there fore,the dis com fort ac com pa ny ing the pur chase of med i ca tions, pro vi sion of bed linen, un reg u latedpay ments, etc. was ac cepted rather as a way of func tion ing and or gani sa tion of the sys tem.
Fig ure 12. Assessment of the attitude of the medical staff to the patients
Mech a nisms for civil con trol on the qual ity of the med i cal ser vices
The place ment of the pa tient in the fo cus of the healthcare and the in tro duc tion of com pet -i tive re la tions among the hos pi tal es tab lish ments were some of the fun da men tal prin ci ples de -clared in a num ber of na tional plans and programmes for the de vel op ment of healthcare andthe im ple men ta tion of the re form. The in formed choice of a healthcare es tab lish ment by thepa tients was a pre req ui site for the de vel op ment of com pet i tive re la tions which, in their turn,
306
How do you evaluate the attitude to the patients in the ward, in which you or a relative of yours have been treated?
2.3%0.9%1.8%
25.1%
10.0%
22.4%
37.4%
0%
5%
10%
15%
20%
25%
30%
35%
40%
I cannotjudge
Excellent Good Satisfactory Poor No answerVery poor
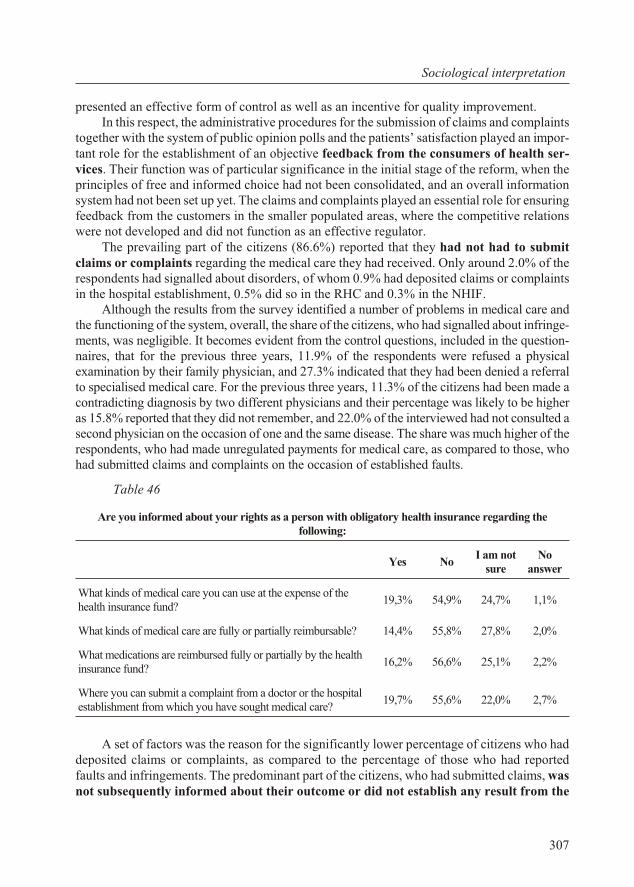
pre sented an ef fec tive form of con trol as well as an in cen tive for qual ity im prove ment. In this re spect, the ad min is tra tive pro ce dures for the sub mis sion of claims and com plaints
to gether with the sys tem of pub lic opin ion polls and the pa tients’ sat is fac tion played an im por -tant role for the es tab lish ment of an ob jec tive feed back from the con sum ers of health ser -vices. Their func tion was of par tic u lar sig nif i cance in the ini tial stage of the re form, when theprin ci ples of free and in formed choice had not been con sol i dated, and an over all in for ma tionsys tem had not been set up yet. The claims and com plaints played an es sen tial role for en sur ing feed back from the cus tom ers in the smaller pop u lated ar eas, where the com pet i tive re la tionswere not de vel oped and did not func tion as an ef fec tive reg u la tor.
The pre vail ing part of the cit i zens (86.6%) re ported that they had not had to sub mitclaims or com plaints re gard ing the med i cal care they had re ceived. Only around 2.0% of there spon dents had sig nalled about dis or ders, of whom 0.9% had de pos ited claims or com plaintsin the hos pi tal es tab lish ment, 0.5% did so in the RHC and 0.3% in the NHIF.
Al though the re sults from the sur vey iden ti fied a num ber of prob lems in med i cal care andthe func tion ing of the sys tem, over all, the share of the cit i zens, who had sig nalled about in fringe -ments, was neg li gi ble. It be comes ev i dent from the con trol ques tions, in cluded in the ques tion -naires, that for the pre vi ous three years, 11.9% of the re spon dents were re fused a phys i calex am i na tion by their fam ily phy si cian, and 27.3% in di cated that they had been de nied a re fer ralto spe cial ised med i cal care. For the pre vi ous three years, 11.3% of the cit i zens had been made acon tra dict ing di ag no sis by two dif fer ent phy si cians and their per cent age was likely to be higheras 15.8% re ported that they did not re mem ber, and 22.0% of the in ter viewed had not con sulted asec ond phy si cian on the oc ca sion of one and the same dis ease. The share was much higher of there spon dents, who had made un reg u lated pay ments for med i cal care, as com pared to those, whohad sub mit ted claims and com plaints on the oc ca sion of es tab lished faults.
Ta ble 46
Are you informed about your rights as a person with obligatory health insurance regarding thefollowing:
Yes NoI am not
sureNo
answer
What kinds of medical care you can use at the expense of thehealth insurance fund?
19,3% 54,9% 24,7% 1,1%
What kinds of med i cal care are fully or par tially re im burs able? 14,4% 55,8% 27,8% 2,0%
What med i ca tions are re im bursed fully or par tially by the healthin sur ance fund?
16,2% 56,6% 25,1% 2,2%
Where you can submit a complaint from a doctor or the hospitalestablishment from which you have sought medical care?
19,7% 55,6% 22,0% 2,7%
A set of fac tors was the rea son for the sig nif i cantly lower per cent age of cit i zens who hadde pos ited claims or com plaints, as com pared to the per cent age of those who had re portedfaults and in fringe ments. The pre dom i nant part of the cit i zens, who had sub mit ted claims, wasnot sub se quently in formed about their out come or did not es tab lish any re sult from the
307
So cio log i cal in ter pre ta tion
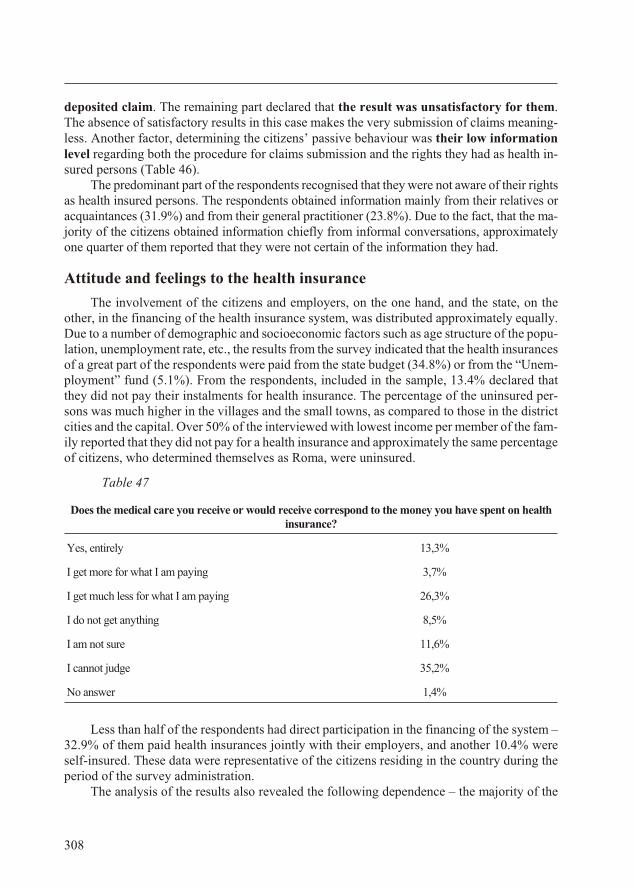
de pos ited claim. The re main ing part de clared that the re sult was un sat is fac tory for them.The ab sence of sat is fac tory re sults in this case makes the very sub mis sion of claims mean ing -less. An other fac tor, de ter min ing the cit i zens’ pas sive be hav iour was their low in for ma tionlevel re gard ing both the pro ce dure for claims sub mis sion and the rights they had as health in -sured per sons (Ta ble 46).
The pre dom i nant part of the re spon dents re cog nised that they were not aware of their rightsas health in sured per sons. The re spon dents ob tained in for ma tion mainly from their rel a tives orac quain tances (31.9%) and from their gen eral prac ti tio ner (23.8%). Due to the fact, that the ma -jor ity of the cit i zens ob tained in for ma tion chiefly from in for mal con ver sa tions, ap prox i matelyone quar ter of them re ported that they were not cer tain of the in for ma tion they had.
At ti tude and feel ings to the health in sur ance
The in volve ment of the cit i zens and em ploy ers, on the one hand, and the state, on theother, in the fi nanc ing of the health in sur ance sys tem, was dis trib uted ap prox i mately equally.Due to a num ber of de mo graphic and so cio eco nomic fac tors such as age struc ture of the pop u -la tion, un em ploy ment rate, etc., the re sults from the sur vey in di cated that the health in sur an cesof a great part of the re spon dents were paid from the state bud get (34.8%) or from the “Un em -ploy ment” fund (5.1%). From the re spon dents, in cluded in the sam ple, 13.4% de clared thatthey did not pay their in stal ments for health in sur ance. The per cent age of the un in sured per -sons was much higher in the vil lages and the small towns, as com pared to those in the dis trictcit ies and the cap i tal. Over 50% of the in ter viewed with low est in come per mem ber of the fam -ily re ported that they did not pay for a health in sur ance and ap prox i mately the same per cent age of cit i zens, who de ter mined them selves as Roma, were un in sured.
Ta ble 47
Does the medical care you receive or would receive correspond to the money you have spent on healthinsurance?
Yes, entirely 13,3%
I get more for what I am pay ing 3,7%
I get much less for what I am pay ing 26,3%
I do not get any thing 8,5%
I am not sure 11,6%
I can not judge 35,2%
No answer 1,4%
Less than half of the re spon dents had di rect par tic i pa tion in the fi nanc ing of the sys tem –32.9% of them paid health in sur an ces jointly with their em ploy ers, and an other 10.4% wereself-in sured. These data were rep re sen ta tive of the cit i zens re sid ing in the coun try dur ing thepe riod of the sur vey ad min is tra tion.
The anal y sis of the re sults also re vealed the fol low ing de pend ence – the ma jor ity of the
308
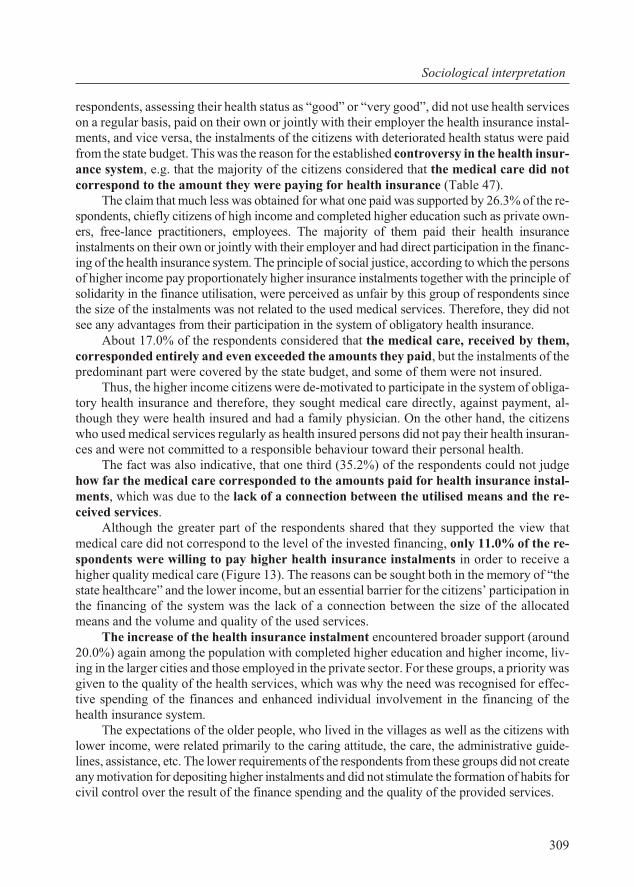
re spon dents, as sess ing their health sta tus as “good” or “very good”, did not use health ser viceson a reg u lar ba sis, paid on their own or jointly with their em ployer the health in sur ance in stal -ments, and vice versa, the in stal ments of the cit i zens with de te ri o rated health sta tus were paidfrom the state bud get. This was the rea son for the es tab lished con tro versy in the health in sur -ance sys tem, e.g. that the ma jor ity of the cit i zens con sid ered that the med i cal care did notcor re spond to the amount they were pay ing for health in sur ance (Ta ble 47).
The claim that much less was ob tained for what one paid was sup ported by 26.3% of the re -spon dents, chiefly cit i zens of high in come and com pleted higher ed u ca tion such as pri vate own -ers, free-lance prac ti tio ners, em ploy ees. The ma jor ity of them paid their health in sur ancein stal ments on their own or jointly with their em ployer and had di rect par tic i pa tion in the fi nanc -ing of the health in sur ance sys tem. The prin ci ple of so cial jus tice, ac cord ing to which the per sons of higher in come pay pro por tion ately higher in sur ance in stal ments to gether with the prin ci ple ofsol i dar ity in the fi nance uti li sa tion, were per ceived as un fair by this group of re spon dents sincethe size of the in stal ments was not re lated to the used med i cal ser vices. There fore, they did notsee any ad van tages from their par tic i pa tion in the sys tem of oblig a tory health in sur ance.
About 17.0% of the re spon dents con sid ered that the med i cal care, re ceived by them,cor re sponded en tirely and even ex ceeded the amounts they paid, but the in stal ments of thepre dom i nant part were cov ered by the state bud get, and some of them were not in sured.
Thus, the higher in come cit i zens were de-mo ti vated to par tic i pate in the sys tem of oblig a -tory health in sur ance and there fore, they sought med i cal care di rectly, against pay ment, al -though they were health in sured and had a fam ily phy si cian. On the other hand, the cit i zenswho used med i cal ser vices reg u larly as health in sured per sons did not pay their health in sur an -ces and were not com mit ted to a re spon si ble be hav iour to ward their per sonal health.
The fact was also in dic a tive, that one third (35.2%) of the re spon dents could not judgehow far the med i cal care cor re sponded to the amounts paid for health in sur ance in stal -ments, which was due to the lack of a con nec tion be tween the uti lised means and the re -ceived ser vices.
Al though the greater part of the re spon dents shared that they sup ported the view thatmed i cal care did not cor re spond to the level of the in vested fi nanc ing, only 11.0% of the re -spon dents were will ing to pay higher health in sur ance in stal ments in or der to re ceive ahigher qual ity med i cal care (Fig ure 13). The rea sons can be sought both in the mem ory of “thestate healthcare” and the lower in come, but an es sen tial bar rier for the cit i zens’ par tic i pa tion inthe fi nanc ing of the sys tem was the lack of a con nec tion be tween the size of the al lo catedmeans and the vol ume and qual ity of the used ser vices.
The in crease of the health in sur ance in stal ment en coun tered broader sup port (around20.0%) again among the pop u la tion with com pleted higher ed u ca tion and higher in come, liv -ing in the larger cit ies and those em ployed in the pri vate sec tor. For these groups, a pri or ity was given to the qual ity of the health ser vices, which was why the need was re cog nised for ef fec -tive spend ing of the fi nances and en hanced in di vid ual in volve ment in the fi nanc ing of thehealth in sur ance sys tem.
The ex pec ta tions of the older peo ple, who lived in the vil lages as well as the cit i zens withlower in come, were re lated pri mar ily to the car ing at ti tude, the care, the ad min is tra tive guide -lines, as sis tance, etc. The lower re quire ments of the re spon dents from these groups did not cre ate any mo ti va tion for de pos it ing higher in stal ments and did not stim u late the for ma tion of hab its for civil con trol over the re sult of the fi nance spend ing and the qual ity of the pro vided ser vices.
309
So cio log i cal in ter pre ta tion
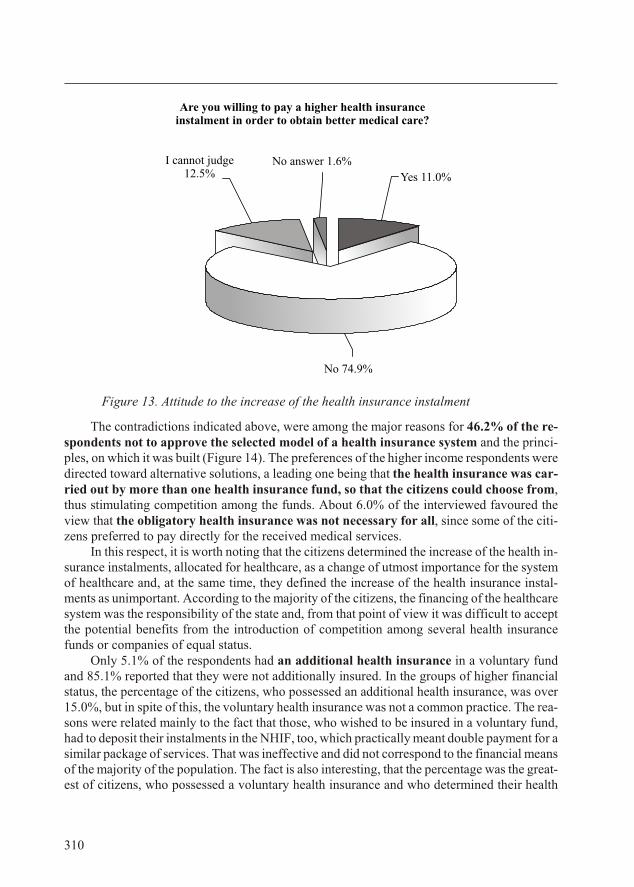
Fig ure 13. Attitude to the increase of the health insurance instalment
The con tra dic tions in di cated above, were among the ma jor rea sons for 46.2% of the re -spon dents not to ap prove the se lected model of a health in sur ance sys tem and the prin ci -ples, on which it was built (Fig ure 14). The pref er ences of the higher in come re spon dents weredi rected to ward al ter na tive so lu tions, a lead ing one be ing that the health in sur ance was car -ried out by more than one health in sur ance fund, so that the cit i zens could choose from,thus stim u lat ing com pe ti tion among the funds. About 6.0% of the in ter viewed fa voured theview that the oblig a tory health in sur ance was not nec es sary for all, since some of the cit i -zens pre ferred to pay di rectly for the re ceived med i cal ser vices.
In this re spect, it is worth not ing that the cit i zens de ter mined the in crease of the health in -sur ance in stal ments, al lo cated for healthcare, as a change of ut most im por tance for the sys temof healthcare and, at the same time, they de fined the in crease of the health in sur ance in stal -ments as un im por tant. Ac cord ing to the ma jor ity of the cit i zens, the fi nanc ing of the healthcaresys tem was the re spon si bil ity of the state and, from that point of view it was dif fi cult to ac ceptthe po ten tial ben e fits from the in tro duc tion of com pe ti tion among sev eral health in sur ancefunds or com pa nies of equal sta tus.
Only 5.1% of the re spon dents had an ad di tional health in sur ance in a vol un tary fundand 85.1% re ported that they were not ad di tion ally in sured. In the groups of higher fi nan cialsta tus, the per cent age of the cit i zens, who pos sessed an ad di tional health in sur ance, was over15.0%, but in spite of this, the vol un tary health in sur ance was not a com mon prac tice. The rea -sons were re lated mainly to the fact that those, who wished to be in sured in a vol un tary fund,had to de posit their in stal ments in the NHIF, too, which prac ti cally meant dou ble pay ment for a sim i lar pack age of ser vices. That was in ef fec tive and did not cor re spond to the fi nan cial means of the ma jor ity of the pop u la tion. The fact is also in ter est ing, that the per cent age was the great -est of cit i zens, who pos sessed a vol un tary health in sur ance and who de ter mined their health
310
Are you willing to pay a higher health insuranceinstalment in order to obtain better medical care?
No 74.9%
Yes 11.0%
No answer 1.6%I cannot judge12.5%
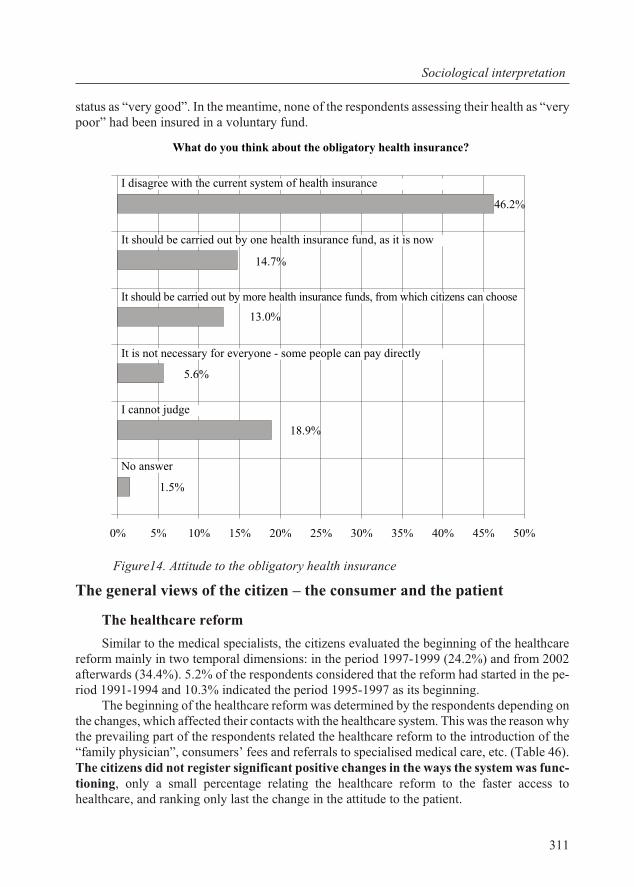
sta tus as “very good”. In the mean time, none of the re spon dents as sess ing their health as “verypoor” had been in sured in a vol un tary fund.
Fig ure14. Attitude to the obligatory health insurance
The gen eral views of the cit i zen – the con sumer and the pa tient
The healthcare re form
Sim i lar to the med i cal spe cial ists, the cit i zens eval u ated the be gin ning of the healthcarere form mainly in two tem po ral di men sions: in the pe riod 1997-1999 (24.2%) and from 2002af ter wards (34.4%). 5.2% of the re spon dents con sid ered that the re form had started in the pe -riod 1991-1994 and 10.3% in di cated the pe riod 1995-1997 as its be gin ning.
The be gin ning of the healthcare re form was de ter mined by the re spon dents de pend ing onthe changes, which af fected their con tacts with the healthcare sys tem. This was the rea son why the pre vail ing part of the re spon dents re lated the healthcare re form to the in tro duc tion of the“fam ily phy si cian”, con sum ers’ fees and re fer rals to spe cial ised med i cal care, etc. (Ta ble 46).The cit i zens did not reg is ter sig nif i cant pos i tive changes in the ways the sys tem was func -tion ing, only a small per cent age re lat ing the healthcare re form to the faster ac cess tohealthcare, and rank ing only last the change in the at ti tude to the pa tient.
311
So cio log i cal in ter pre ta tion
What do you think about the obligatory health insurance?
46.2%
13.0%
1.5%
18.9%
5.6%
14.7%
0% 5% 10% 15% 20% 25% 30% 35% 40% 45% 50%
No answer
I cannot judge
It is not necessary for everyone - some people can pay directly
It should be carried out by more health insurance funds, from which citizens can choose
It should be carried out by one health insurance fund, as it is now
I disagree with the current system of health insurance
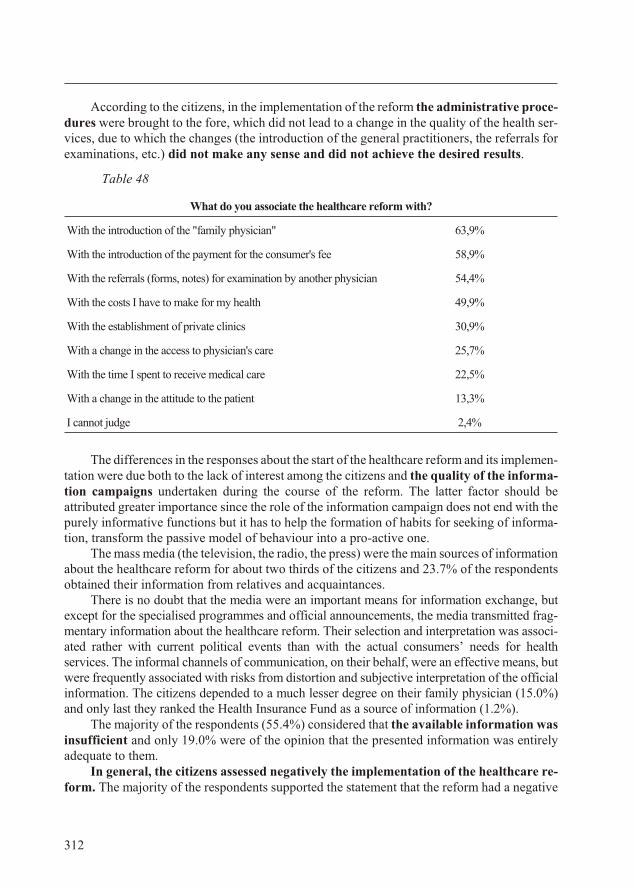
Ac cord ing to the cit i zens, in the im ple men ta tion of the re form the ad min is tra tive pro ce -dures were brought to the fore, which did not lead to a change in the qual ity of the health ser -vices, due to which the changes (the in tro duc tion of the gen eral prac ti tio ners, the re fer rals forex am i na tions, etc.) did not make any sense and did not achieve the de sired re sults.
Table 48
What do you associate the healthcare reform with?
With the introduction of the "family physician" 63,9%
With the in tro duc tion of the pay ment for the con sumer's fee 58,9%
With the re fer rals (forms, notes) for ex am i na tion by an other phy si cian 54,4%
With the costs I have to make for my health 49,9%
With the es tab lish ment of pri vate clin ics 30,9%
With a change in the ac cess to phy si cian's care 25,7%
With the time I spent to re ceive med i cal care 22,5%
With a change in the at ti tude to the pa tient 13,3%
I cannot judge 2,4%
The dif fer ences in the re sponses about the start of the healthcare re form and its im ple men -ta tion were due both to the lack of in ter est among the cit i zens and the qual ity of the in for ma -tion cam paigns un der taken dur ing the course of the re form. The lat ter fac tor should beat trib uted greater im por tance since the role of the in for ma tion cam paign does not end with thepurely in for ma tive func tions but it has to help the for ma tion of hab its for seek ing of in for ma -tion, trans form the pas sive model of be hav iour into a pro-ac tive one.
The mass me dia (the tele vi sion, the ra dio, the press) were the main sources of in for ma tion about the healthcare re form for about two thirds of the cit i zens and 23.7% of the re spon dentsob tained their in for ma tion from rel a tives and ac quain tances.
There is no doubt that the me dia were an im por tant means for in for ma tion ex change, butex cept for the spe cial ised programmes and of fi cial an nounce ments, the me dia trans mit ted frag -men tary in for ma tion about the healthcare re form. Their se lec tion and in ter pre ta tion was as so ci -ated rather with cur rent po lit i cal events than with the ac tual con sum ers’ needs for healthser vices. The in for mal chan nels of com mu ni ca tion, on their be half, were an ef fec tive means, butwere fre quently as so ci ated with risks from dis tor tion and sub jec tive in ter pre ta tion of the of fi cialin for ma tion. The cit i zens de pended to a much lesser de gree on their fam ily phy si cian (15.0%)and only last they ranked the Health In sur ance Fund as a source of in for ma tion (1.2%).
The ma jor ity of the re spon dents (55.4%) con sid ered that the avail able in for ma tion wasin suf fi cient and only 19.0% were of the opin ion that the pre sented in for ma tion was en tirelyad e quate to them.
In gen eral, the cit i zens as sessed neg a tively the im ple men ta tion of the healthcare re -form. The ma jor ity of the re spon dents sup ported the state ment that the re form had a neg a tive
312
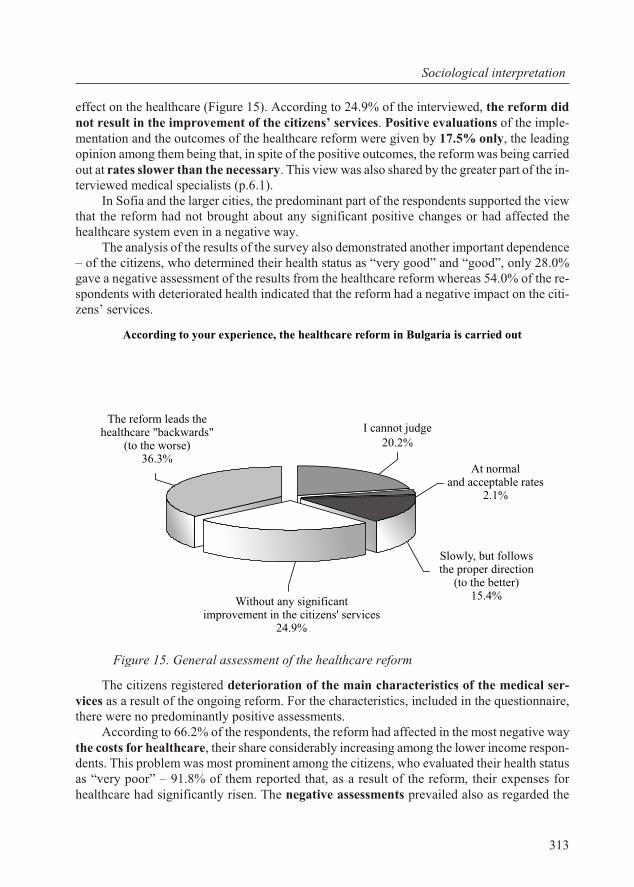
ef fect on the healthcare (Fig ure 15). Ac cord ing to 24.9% of the in ter viewed, the re form didnot re sult in the im prove ment of the cit i zens’ ser vices. Pos i tive eval u a tions of the im ple -men ta tion and the out comes of the healthcare re form were given by 17.5% only, the lead ingopin ion among them be ing that, in spite of the pos i tive out comes, the re form was be ing car riedout at rates slower than the nec es sary. This view was also shared by the greater part of the in -ter viewed med i cal spe cial ists (p.6.1).
In So fia and the larger cit ies, the pre dom i nant part of the re spon dents sup ported the viewthat the re form had not brought about any sig nif i cant pos i tive changes or had af fected thehealthcare sys tem even in a neg a tive way.
The anal y sis of the re sults of the sur vey also dem on strated an other im por tant de pend ence– of the cit i zens, who de ter mined their health sta tus as “very good” and “good”, only 28.0%gave a neg a tive as sess ment of the re sults from the healthcare re form whereas 54.0% of the re -spon dents with de te ri o rated health in di cated that the re form had a neg a tive im pact on the cit i -zens’ ser vices.
Fig ure 15. General assessment of the healthcare reform
The cit i zens reg is tered de te ri o ra tion of the main char ac ter is tics of the med i cal ser -vices as a re sult of the on go ing re form. For the char ac ter is tics, in cluded in the ques tion naire,there were no pre dom i nantly pos i tive as sess ments.
Ac cord ing to 66.2% of the re spon dents, the re form had af fected in the most neg a tive waythe costs for healthcare, their share con sid er ably in creas ing among the lower in come re spon -dents. This prob lem was most prom i nent among the cit i zens, who eval u ated their health sta tusas “very poor” – 91.8% of them re ported that, as a re sult of the re form, their ex penses forhealthcare had sig nif i cantly risen. The neg a tive as sess ments pre vailed also as re garded the
313
So cio log i cal in ter pre ta tion
According to your experience, the healthcare reform in Bulgaria is carried out
Without any significantimprovement in the citizens' services
24.9%
Slowly, but followsthe proper direction
(to the better)15.4%
At normaland acceptable rates
2.1%
I cannot judge20.2%
The reform leads the healthcare "backwards"
(to the worse)36.3%
fol low ing
· prompt ness and ef fi ciency of the ser vices;
· ac cess to spe cial ised med i cal care;
· the care for the peo ple with chronic dis eases;
· timely pro phy laxis.
As re garded the care for the chil dren, the con di tions in the healthcare es tab lish mentsand the re sponses of the ser vices for emer gency and ur gent med i cal care as well as thepos si bil i ties for lab o ra tory in ves ti ga tions, the ma jor ity of the re spon dents did not reg is terany sig nif i cant change. The pos i tive and neg a tive as sess ments had ap prox i mately equal share con cern ing the im pact of the re form on the med i cal spe cial ists’ com pe tence, 53.1% de clar ingthat they did not ob serve any change.
In all the groups, the neg a tive eval u a tions pre dom i nated re gard ing the im pact of thehealthcare re form on the in di cated char ac ter is tics, but their share sig nif i cantly in creasedamong the re spon dents, who lived in So fia and the dis trict cit ies as well as among the re spon -dents, who de ter mined their health sta tus as “very poor”.
Over one fifth of the cit i zens marked im prove ment only in the at ti tude of the med i calspe cial ists to the pa tients as well as in terms of the pos si bil i ties for home vis its made by a phy -si cian. Even though, how ever, con cern ing these char ac ter is tics, too, the opin ion pre vailed thatthey had not changed sig nif i cantly in the course of the re form.
State-of-arts and de vel op ment of the healthcare sys tem
As main prob lems, the ma jor ity of the re spon dents de fined the prices of drugs, theshort age of fi nance, al lo cated for healthcare and the over all or gani sa tion of thehealthcare sys tem as well as the bu reau cratic ser vices and the lack of med i cal equip mentas so ci ated with the fi nanc ing and the or gani sa tion (Fig ure 16).
Ap prox i mately one third of the cit i zens con sid ered that cor rup tion of the med i cal staffand the qual ity of med i cal care were es sen tial draw backs of the healthcare and the health ser -vices. The small est per cent age of the re spon dents as so ci ated the prob lems in the sys tem with thework of the med i cal per son nel – their at ti tude to the pa tients, the re la tion be tween the di vi sions of the out pa tients’ and in pa tients’ care and the med i cal spe cial ists’ com pe tence (Fig ure 16).
Ac cord ing to the ma jor ity of the re spon dents, the re spon si bil ity for the cur rentstate-of-arts and the prob lems of the healthcare sys tem was to be borne by the Min is try ofHealthcare (59.4 %) and the Coun cil of Min is ters (58.6%). Next, the re spon dents in di cated thein sti tu tions re lated to healthcare (34.7%) and the po lit i cal par ties rep re sented in Par lia ment(27.4%) and over one fifth blamed the pro fes sional or gani sa tions of the med i cal spe cial ists to bere spon si ble for the cur rent state of the healthcare sys tem. The larger part of the re spon dents un -der es ti mated the role of the civil so ci ety in the de vel op ment of healthcare – only 8.3% con -sid ered that the cit i zens ex erted in flu ence on the sys tem and were re spon si ble for its con di tion.
Ac cord ing to the pe cu liar i ties of the iden ti fied prob lems, the cit i zens ranked the changeswhich, in their opin ion, had to be car ried out in the healthcare sys tem (Ta ble 47). As a main pri -or ity, the in ter viewed, in cluded in the sam ple, de fined the in creased state in ter fer ence with the fi nanc ing of the healthcare at the ex pense of the lim ited fi nan cial par tic i pa tion of the cit i -zens both by means of the elim i na tion of the con sum ers’ fees and the de crease of the health in -
314
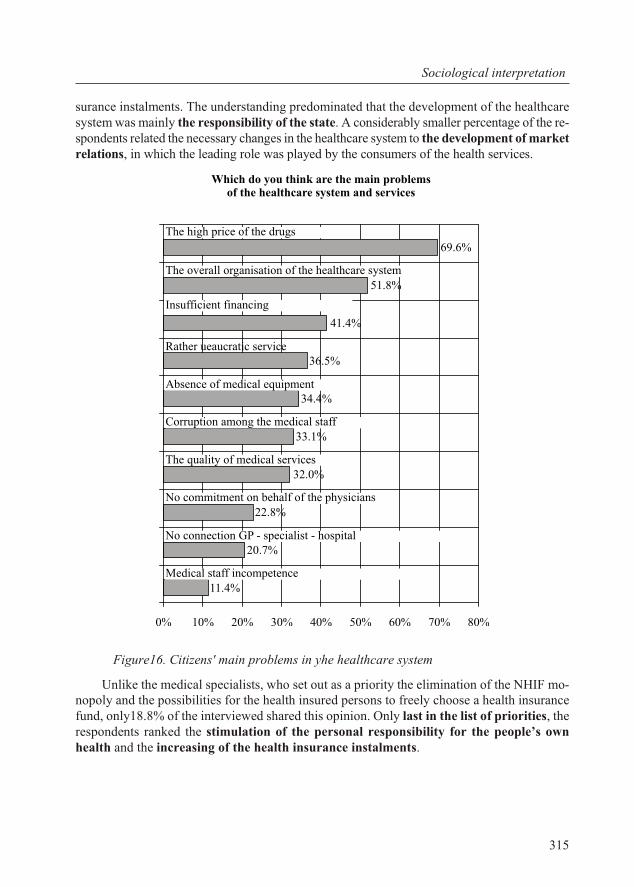
sur ance in stal ments. The un der stand ing pre dom i nated that the de vel op ment of the healthcaresys tem was mainly the re spon si bil ity of the state. A con sid er ably smaller per cent age of the re -spon dents re lated the nec es sary changes in the healthcare sys tem to the de vel op ment of mar ketre la tions, in which the lead ing role was played by the con sum ers of the health ser vices.
Fig ure16. Citizens' main problems in yhe healthcare system
Un like the med i cal spe cial ists, who set out as a pri or ity the elim i na tion of the NHIF mo -nop oly and the pos si bil i ties for the health in sured per sons to freely choose a health in sur ancefund, only18.8% of the in ter viewed shared this opin ion. Only last in the list of pri or i ties, there spon dents ranked the stim u la tion of the per sonal re spon si bil ity for the peo ple’s ownhealth and the in creas ing of the health in sur ance in stal ments.
315
So cio log i cal in ter pre ta tion
Which do you think are the main problemsof the healthcare system and services
11.4%
20.7%
22.8%
32.0%
33.1%
41.4%
51.8%
69.6%
34.4%
36.5%
0% 10% 20% 30% 40% 50% 60% 70% 80%
Medical staff incompetence
No connection GP - specialist - hospital
No commitment on behalf of the physicians
The quality of medical services
Corruption among the medical staff
Absence of medical equipment
Rather ueaucratic service
Insufficient financing
The overall organisation of the healthcare system
The high price of the drugs
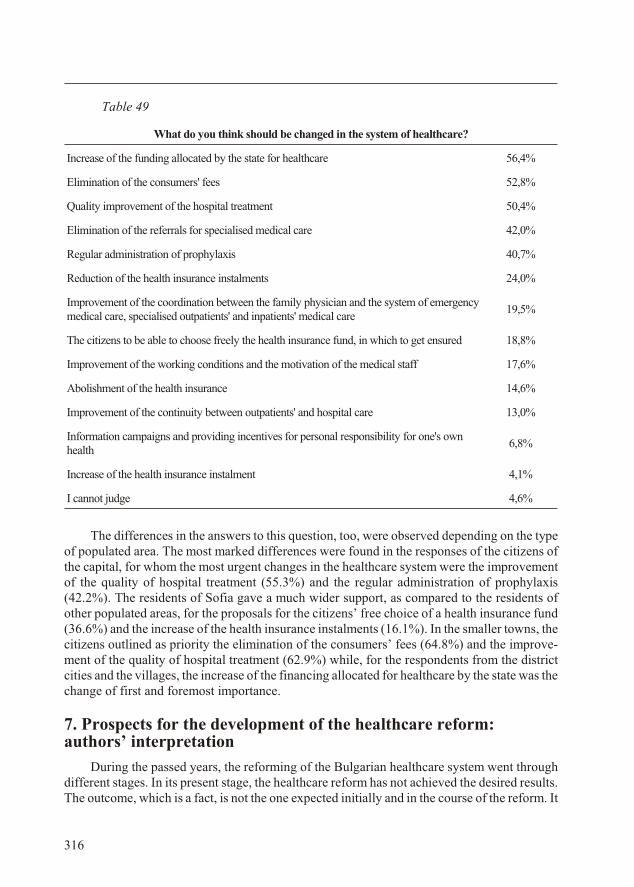
Table 49
What do you think should be changed in the system of healthcare?
Increase of the funding allocated by the state for healthcare 56,4%
Elim i na tion of the con sum ers' fees 52,8%
Qual ity im prove ment of the hos pi tal treat ment 50,4%
Elim i na tion of the re fer rals for spe cial ised med i cal care 42,0%
Reg u lar ad min is tra tion of pro phy laxis 40,7%
Re duc tion of the health in sur ance in stal ments 24,0%
Im prove ment of the co or di na tion be tween the fam ily phy si cian and the sys tem of emer gency med i cal care, specialised out pa tients' and in pa tients' medical care
19,5%
The cit i zens to be able to choose freely the health in sur ance fund, in which to get en sured 18,8%
Im prove ment of the work ing con di tions and the mo ti va tion of the med i cal staff 17,6%
Abol ish ment of the health in sur ance 14,6%
Im prove ment of the con ti nu ity be tween out pa tients' and hos pi tal care 13,0%
In for ma tion cam paigns and pro vid ing in cen tives for per sonal re spon si bil ity for one's ownhealth
6,8%
In crease of the health in sur ance in stal ment 4,1%
I cannot judge 4,6%
The dif fer ences in the an swers to this ques tion, too, were ob served de pend ing on the typeof pop u lated area. The most marked dif fer ences were found in the re sponses of the cit i zens ofthe cap i tal, for whom the most ur gent changes in the healthcare sys tem were the im prove mentof the qual ity of hos pi tal treat ment (55.3%) and the reg u lar ad min is tra tion of pro phy laxis(42.2%). The res i dents of So fia gave a much wider sup port, as com pared to the res i dents ofother pop u lated ar eas, for the pro pos als for the cit i zens’ free choice of a health in sur ance fund(36.6%) and the in crease of the health in sur ance in stal ments (16.1%). In the smaller towns, thecit i zens out lined as pri or ity the elim i na tion of the con sum ers’ fees (64.8%) and the im prove -ment of the qual ity of hos pi tal treat ment (62.9%) while, for the re spon dents from the dis trictcit ies and the vil lages, the in crease of the fi nanc ing al lo cated for healthcare by the state was the change of first and fore most im por tance.
7. Pros pects for the de vel op ment of the healthcare re form:au thors’ in ter pre ta tion
Dur ing the passed years, the re form ing of the Bul gar ian healthcare sys tem went throughdif fer ent stages. In its pres ent stage, the healthcare re form has not achieved the de sired re sults.The out come, which is a fact, is not the one ex pected ini tially and in the course of the re form. It
316
does not cor re spond to the du ra tion of its de vel op ment. What has been achieved is in com pa ra -ble to the means spent on its im ple men ta tion. The out come is not sat is fac tory for the pro fes -sion als or the ad min is tra tion, and is even less so for the cit i zens and the pa tients. And there form is near ing the end of the sec ond de cade from its be gin ning.
The three tasks of the healthcare re form set at the be gin ning (Chap ter 4) and af ter -wards, for a pe riod of sev en teen years have been marked by par tial and lim ited ef fects:
· The de te ri o ra tion of the na tion’s health has not been dis con tin ued. The frag -mented signs of sta bili sa tion have not yet be come a man i fes ta tion of a long-last ing dis -con tinu a tion of the health de te ri o ra tion, so that pre req ui sites have been cre ated for itsim prove ment. It should be re minded that, dur ing the past years, the health im prove -ment was an im per a tive task of car di nal im por tance for the fu ture of the na tionand the coun try. For its ful fil ment, it had to be shifted to an ex ten sive re pro duc tion ofhealth in or der to over come the neg a tive trends. It is known that health is mul ti fac etedin its de ter mi na tion, that its im prove ment re quires ef forts not only by the healthcare but also by a num ber of other sys tems, the ex ten sive health re pro duc tion in a na tion can notoc cur within a year, two or even five. But for sev en teen years? For a pe riod like that,def i nite long-term re sults should be ex pected. But they have not taken place.
· the so cial ist state mo nop oly in the healthcare sys tem was not elim i nated long af ter1990 up to 1996-2000. To day, too, it con tin ues to re cur un der one form or an other. Be -sides, a new sys tem had to be built in the place of the old one, meet ing the needs, the de -sires and the ex pec ta tions of the cit i zens and the pro fes sion als, cor re spond ing to thecon di tions and the pos si bil i ties of the coun try. An en tirely new sys tem func tion ing un -der dem o cratic con di tions is im pos si ble to be es tab lished within a year or two, but forsev en teen years? The cit i zens and the pro fes sion als keep ex pect ing it.
· the new healthcare sys tem has been es tab lished at ir reg u lar rates and has had anasym met ric de vel op ment in time, dur ing which an even in com plete cor re spon dencehas been es tab lished grad u ally with the chang ing po lit i cal, eco nomic and so cial con di -tions in the coun try. The demonopolisation of the sys tem did not re sult in the con sis tent es tab lish ment and uti li sa tion of le gal, eco nomic and so cial con di tions for its ac tual de -moc ra ti sa tion and mar ket ori en ta tion.
The anal y sis of the pre sented ma te rial shows that the re form of the healthcare sys tem hasbeen and con tin ues to be a ne ces sity. This is why it can not be cancelled (“re turned to its start -ing po si tion”), nei ther can it be stopped. The only al ter na tive is in its con tin u a tion.
The healthcare re form in Bul garia be gan with a fly ing start, but the ex cite ment, ac com pa -ny ing it, grad u ally died away within sev eral years. The en thu si as tic de sire for a health re formturned into a bur den ing ob li ga tion. More over, all grounds are pres ent for us to a pri ori con -sider that some thing has been wrong some where. This is why here we will sum up the key (toour minds) in con sis ten cies of the be gin ning of the healthcare re form and its course and ob jec -tives, fol low ing which we will ar gue for what we think to be the main di rec tions, nec es sary for the achieve ment of the goals.
317
Pros pects for the de vel op ment of the healthcare re form

7.1. Er rors at es tab lish ment
They con cern “con gen i tal” but pre vent able er rors which, on their be half, are fac tors forsub se quent de for mi ties of the healthcare sys tem, dis tur bances of its func tions and, even tu ally,for sig nif i cant de fects in the sat is fac tion of the cit i zens’ and so ci ety’s needs and the de vel op -ment of the very sys tem of healthcare. In its es sence, these are er rors of the ap proach af fect -ing also the nor ma tive foun da tion of the new healthcare sys tem, which was be ing cre ated.
The healthcare re form be gan with out a def i nite plan or per spec tives
From a chro no log i cal point of view, the healthcare re form, ex am ined so far, was thethird rad i cal change in the de vel op ment of the Bul gar ian healthcare sys tem. The les sons arein ter est ing which were learned from the first two.
The first rad i cal change was the es tab lish ment of a new healthcare for a pe riod of tenyears im me di ately af ter the re cov ery of lib er ated Bul garia and the rad i cally changed so cio eco -nomic and po lit i cal con di tions. In the Prin ci pal ity of Bul garia, the healthcare sys tem was cre -ated fol low ing the model of the Rus sian “land med i cine”, above all, as a func tion of the state.In the semi-au ton o mous East ern Roumelia, the sys tem of healthcare was or gan ised sim i larly to the ex am ples of the West ern Eu ro pean coun tries, in which the role of the state (the dis trict ad -min is tra tion) was com bined with the in volve ment of the so ci ety (the net work of civil as so ci a -tions “St. Panteleimon”). The in de pend ent de vel op ment of the two sys tems of healthcarecon tin ued up to 1885 (the Uni fi ca tion of the Prin ci pal ity of Bul garia with East ern Roumelia).By the healthcare leg is la tion of the uni fied state (“San i ta tion Law” from 1888) the nor ma tive foun da tion was laid for a uni fied healthcare sys tem in Bul garia in which, gen er ally speak ing,the char ac ter is tics of the West ern Eu ro pean mod els were adopted. The health ad min is tra tionbe came part of the state ad min is tra tion, the mu nic i pal i ties as sum ing cer tain ob li ga tions forhealthcare and the healthcare sys tem de vel op ing as a pub lic-pri vate sys tem. The med i cal carefor cer tain dis eases or so cial groups was paid by the state or the mu nic i pal i ties. Thus, the firstrad i cal re form was com pleted in the Bul gar ian healthcare, whose driv ing force was theendeavour for achiev ing a dy namic de vel op ment of the whole coun try as a pre-con di tion for its sur vival and for the so lu tion of def i nite na tional tasks.
The sec ond rad i cal change was the so cial ist “ref or ma tion” of the Bul gar ian healthcare,which started in 1950 by a de ci sion of the Cen tral Com mit tee of the Bul gar ian Com mu nistparty (from De cem ber 1949) in a rad i cally dif fer ent po lit i cal and so cio eco nomic sit u a tion.This was pre ceded by the na tion ali sa tion of the pri vate healthcare es tab lish ments, the phar ma -cies and the X-ray fa cil i ties (1948) and the liq ui da tion of the pro fes sional as so ci a tions of phy -si cians, den tists and phar ma cists. The healthcare sys tem was built on a prin ci pally new ba sisac cord ing to the model of the post-war “So viet so cial ist healthcare”. The con cep tual model of a healthcare sys tem, planned in ad vance, was de signed and pre sented by the then Min is terof Peo ple’s Health Dr. Petar Kolarov. This model was im posed from “the out side”, un der the post-war con di tions and the to tal i tar ian re gime, un der which the coun try was ruled at the time.Ac cord ing to its found ing prin ci ples, the sys tem was a state prop erty, fi nanced by the state,which owned its re sources (“state power”), cen tral ised (“unity of man age ment”), planned bythe state (“plan ning”), its ac tiv i ties be ing free for by the cit i zens (“free of charge”). The sys tem was de vel op ing in a planned way, in ac cor dance with the prin ci ple of “sup ply”, dis re gard ingthe “de mand”. The reg u la tion of the sys tem was car ried out ex clu sively in an ad min is tra tive
318
way, with the dom i nat ing par tic i pa tion of the Com mit tees of the BCP and the col lab o ra tion ofthe trade un ions. The main pur pose of the newly es tab lished healthcare sys tem was seen to bethe “ser vice” of the so cial ist or der and the pol icy for its con struc tion. To gether with the ex ter -nal in flu ence, this was the chief driv ing force for the build ing of the new sys tem of healthcare.
Un der the strongly cen tral ised man age ment and fi nanc ing as well as the in tro duced ad -min is tra tive dis ci pline, for a pe riod of sev eral years, a num ber of pos i tive re sults wereachieved re gard ing the pop u la tion’s health. Grad u ally, how ever, the ex ten sive model of de vel -op ment was ex hausted, the party and ad min is tra tive reg u la tion bureaucratised the sys tem andthe lack of the staff mo ti va tion (out side the ad min is tra tive pres sure) brought about neg a tive ef -fects on qual ity. The ma jor bal ances in the sys tem were dis turbed and it de vel oped to wardequi lib rium dis tur bance. All this made the sys tem in ef fi cient and in ad e quate to the needs. Thesigns of in ef fi ciency emerged rather early, still in the 1960s, and even more strongly in the1970s. Its ref or ma tion be came a press ing need.
Fol low ing, how ever, the model im posed from “the out side”, the sys tem could not but dis -tance it self from its ini tial source. A sim i lar dis tanc ing was then con sid ered to be a “po lit i caler ror” with all the con se quences en su ing from it. There fore, the idea of a real re form (the termin cir cu la tion was “re con struc tion” at the time) in healthcare was con ceived only af ter thechanged in ter nal and ex ter nal po lit i cal con di tions, in clud ing the wide spread at ti tude to ref or -ma tion (“peres troika”), which had started to dom i nate in all the fields of so cial life and stateman age ment. The re struc tur ing was planned in a de tailed programme. It was too rad i cal, it in -fringed upon (and even re jected) the prin ci ples of the so cial ist healthcare by adopt ing, mostgen er ally, the prin ci ples, char ac ter is ing the de vel op ment of the Bul gar ian healthcare dur ingthe pre-so cial ist pe riod.
The third rad i cal change of the Bul gar ian healthcare sys tem has been car ried out in there cent sev en teen years. It has nei ther been im posed from the out side, nor from the in side. Itsbe gin ning, dat ing to 1989-1990, was spon ta ne ous and arose as a re sult of a com monendeavour for a rad i cal change of the state, the eco nomic re la tions and the so cial life. Thisstrife was also the main driv ing force of the healthcare re form at the be gin ning of the 1990sboth for the med i cal pro fes sion als and for the whole so ci ety. Spe cific mod els were su per im -posed on it, e.g. the sta tus of the healthcare sys tem as a “non-pro duc tive” or gani sa tion and ofmed i cal la bour as a “non-pro duc tive” la bour, the fi nanc ing, based on the “re sid ual prin ci ple”,the dis sat is fac tion sub dued for de cades with the sig nif i cant lag ging be hind of the con di tions ofthe Bul gar ian healthcare from the prog ress in the field of med i cine, the ex tremely low and mis -er a ble re mu ner a tions of the phy si cians, den tists and other med i cal staff, the hin dered pro fes -sional de vel op ment and growth, the liq ui dated pro fes sional sup port. The healthcare re formbe gan as some thing which was self-un der stood.
The ear li est at ti tudes were for an “im me di ate re form”. This re form, how ever, was un -der stood as ei ther too gen eral or sin gle (though of key im por tance) acts: “de moc ra ti sa tion”,res to ra tion of the pri vate sec tor and its equal ity with the pub lic sec tor in the field of ther apy,“new eco nomic re la tions” in healthcare. But the im me di ate re form started spon ta ne ously andcon tin ued spon ta ne ously, with out a def i nite, even con cep tual vi sion about its de vel op ment.The re form was not per ceived as a be gin ning and a pro cess of con struc tion of the newhealthcare sys tem, but as a num ber of a few fast oc cur ring sin gle ac tions. The de moc ra ti sa tionwas un der stood not as new struc tures and ap proaches to man age ment but as chang ing the cur -rent man ag ing per son nel at var i ous lev els. The new eco nomic re la tions in the healthcare sys -
319
Pros pects for the de vel op ment of the healthcare re form
tem were seen as a pay rise and the fast est pos si ble es tab lish ment of an or gani sa tion for healthin sur ance. Re gard ing the de vel op ment of the pri vate sec tor, sev eral amend ments and ad di tions were pro posed and voted by the Par lia ment of the only avail able at the time Law on Peo ple’sHealth (1973), stip u lat ing the reg u la tion of the pri vate med i cal prac tice and the open ing of pri -vate healthcare es tab lish ments. The healthcare re form started with short-term goals re -stricted in time and scope, with out a clear per spec tive.
In ter est ing and typ i cal char ac ter is tics can be out lined for the three healthcare re forms inour coun try. The first one had a hes i tant be gin ning for a num ber of rea sons (two non-ho mo ge -neous parts of Bul garia and, for a pe riod of ten years, sus pen sion and res to ra tion of the Con sti -tu tion, war, coup d’Ùtat and coun ter coup d’Ùtat, change of the Prin ci pal ity dy nasty) andcon tin ued with the adop tion and the en force ment of a law. The law was the car di nalprogramme, sanc tion ing the re form and cre at ing con di tions for the de vel op ment of thehealthcare sys tem. It reg u lated a valid healthcare sys tem for the whole coun try for the next fif -teen years to come. This sys tem was not un fa mil iar to the Bul gar ian phy si cians, den tists andphar ma cists at the time, the ma jor ity of whom had ob tained their med i cal ed u ca tion in West ern Eu ro pean uni ver si ties. The pros pect was be ing out lined in the ex e cu tion (and, if nec es sary, inthe amend ment) of the law.
The sec ond re form was car ried out in the ex e cu tion of the de ci sion of the Cen tral Com -mit tee of the Bul gar ian Com mu nist party (no su pe rior or gan ex isted at the time) and was ad -min is tered in ac cor dance with a con cep tual model, de signed in ad vance and based ondef i nite views. This model was en forced in the Bul gar ian re al ity at the time by means of boththe use of the en force ment power and power meth ods as well as the whole party and state pro -pa ganda ap pa ra tus. The ma te ri als on the “so cial ist re struc tur ing of healthcare” were fea turedin the cur ric ula of the higher and semi-higher (then) med i cal ed u ca tion. Ev ery ex ec u tor (pro -fes sional, cit i zen, leader at ev ery level) knew or could with out dif fi culty know about the per -spec tive – what it would be man i fested in, when and how the “so cial ist re struc tur ing” wouldbe car ried out and de velop.
The third re form (which is the most im por tant to us) started spon ta ne ously and with thebest in ten tions but with out plan ning or prep a ra tion. It was gen er ally de vel op ing to wardchange. The ac tions were well-in tended but were not con sis tent and goal-ori ented. The per -spec tives of change were not well-ar gued in time, sub ject and scope. The healthcare re formwas not “with out a com pass” but it did not have a “road map” in its de vel op ment.
The ab sence of a plan or programme for the re form in healthcare on be half of the state or -gans (Par lia ment, the Coun cil of Min is ters, the Min is try of Healthcare) has been the ma jordraw back since its be gin ning. It has en dorsed it deeply and fa tally for the rest of its de vel op -ment. This lack man i fested the ex treme in def i nite ness of the state health pol icy un der an al -ready dem o cratic re gime. At the be gin ning of the 1990s this turned into the main im ped i mentfor the change in the healthcare sys tem. The ab sence of clear ob jec tives and a programmede-mo ti vated the pro fes sion als and the cit i zens. An enor mous part of the en ergy and at ti tudes,which were ini tially pres ent across the whole so ci ety, were wasted for the sup port of thehealthcare re form.
320
The im ple men ta tion of the healthcare re form was car ried out slowly,hes i tantly and ir reg u larly
In the two fore go ing re forms, the newly evolved healthcare sys tem was de vel oped as anover all struc ture and or gani sa tion – in the first case, ac cord ing to the guide lines en vis aged inthe law and, in the sec ond, fol low ing the con cep tual model of the “So viet so cial ist healthcare”.In both cases, the re form was im ple mented im me di ately and con sis tently.
Af ter 1989, the healthcare re form was de vel op ing at un ex pect edly slow rates, which cor -re sponded nei ther to the needs, nor to the pub lic de sires and at ti tudes, or to the changes in there main ing fields of so cio eco nomic life. The de te ri o rated and in creas ingly de te ri o rat ing healthsta tus of the na tion re quired the im ple men ta tion of fast and ur gent mea sures both in med i calcare, and health pro mo tion and dis ease pre ven tion. Such mea sures had to in clude the im prove -ment of the re source pro vi sion of the healthcare sys tem as well as the in tro duc tion of ef fec tiveor gani sa tional forms and mod els. But be cause of the in def i nite health pol icy of the state andthe dis tinct un der es ti ma tion of the health prob lems of the na tion, they did not oc cur. One of thepos si ble rea sons could be found in the lack of a clear con cept, plan or programme for the im -ple men ta tion of the re form. Pal lia tive mea sures were un der taken only, as far as they wereneeded, to tem po rarily pre vent the clos ing down of healthcare and hos pi tal es tab lish ments.The de lay, and to a far ex tent, the ab sence of ap pro pri ate ac tions in this re spect, in flicted sig -nif i cant dam age to the na tion’s health and the de vel op ment of the healthcare sys tem. Thiscould be due to or ac counted for by the scar city of fi nan cial re sources (“wors ened eco nomicstate of the coun try”). If a re spon si ble state health pol icy had ex isted, even if this scar city ex -isted, it could have been over come. Cor re spond ingly, the health of the na tion, which was thefirst and fore most goal of the healthcare re form, would have been saved. Ir re spec tive of its na -ture, the cri sis im plied an im me di ate de sta bi li sa tion of the sys tem, threat en ing its ex is tence.Even within the di men sions of a state’s ex is tence, a pe riod of 15-20 years of in sta bil ity in oneof its sys tems, such as the healthcare sys tem, is dif fi cult to be called a “cri sis”. Ap par ently, thisis a ques tion of se ri ous de fects in the sys tem itself.
The logic of the re form and the de vel op ment of the healthcare sys tem in gen eral (cov eredand well-ar gued in a num ber of pub li ca tions in the 1990s) re quired im per a tively a change ofthe eco nomic re la tions in side the sys tem and of the sys tem. In this re la tion it was in for mallyagreed by the pro fes sion als and the cit i zens (and by the po lit i cal par ties, too) about the need for the in tro duc tion of a health in sur ance sys tem in Bul garia. The leg is la tive in tro duc tion of such a sys tem (ac cord ing to the avail able ma te ri als quoted ear lier) was pre pared still in 1991-1992.The health in sur ance, how ever, was le gally reg u lated six years later, in 1998, and was in tro -duced (par tially) in 1999.
In stead of le gally reg u lat ing the health in sur ance, in 1995-1996 the law was de signed andpassed for the reg u la tion of the phar ma ceu ti cal sec tor and the phar ma ceu ti cal mar ket, re spec -tively. This law was also un con di tion ally nec es sary for the healthcare re form. But for the ac -tual se quenc ing of the re form pro cess, it sig nif i cantly an tic i pated the other laws, with outmak ing an es sen tial con tri bu tion to the achieve ment of the goals of the healthcare re form.
The ir reg u lar de vel op ment of the healthcare re form was man i fested in an other sig nif i cantfact – the un der es ti ma tion of the health pro phy laxis and the health pro mo tion. It im pliedboth the de vel op ment of a spe cial ised net work of es tab lish ments (RIPCPH, the for mer Hy -giene and Ep i de mi o log i cal In sti tutes) and (even more) the pro phy lac tic func tions of the over -all healthcare sys tem – the net work of healthcare es tab lish ments, the dis pen sa ries and the
321
Pros pects for the de vel op ment of the healthcare re form
phar ma ceu ti cal sec tor. As be fore 1989, af ter wards too, the pre ven tion ac tiv i ties were de claredas the lead ing prin ci ple of healthcare. From an ob jec tive point of view, how ever, so far theyhad never been de vel oped (ex cept for a short pe riod of time in 1968-1972) at such rates and in -vest ment so that they could cor re spond to their sta tus of a health pri or ity.
The ir reg u lar de vel op ment of the healthcare re form was also de ter mined by the in ad e -quate at ti tude to the out pa tients’ and hos pi tal care in the amend ments of the Law on Health In sur ance (1999). The in tro duc tion of the fi nanc ing by the NHIF for out pa tients’ care and bythe state (through the Min is try of Healthcare) for hos pi tal care was a grave er ror. It caused con -flicts (which have not been over come yet) be tween the phy si cians in the two sec tors, and to -gether with this, it in flicted ma te rial and moral dam age gen er ally on the healthcare sys tem and, to a large de gree, com pro mised the healthcare re form it self. This act could not be ac countedfor by the in suf fi cient re sources for the si mul ta neous fi nanc ing of the out pa tients’ and hos pi talcare by the NHIF. In view of the scarce fi nan cial re sources, other al ter na tives had to be sought– for ex am ple, over all fi nanc ing by the NHIF for the out pa tients’ and hos pi tal care for spe cificseg ments of the pop u la tion. Thus, all the neg a tive con se quences could be avoided and thehealthcare sys tem could de velop through the ex ten sion of the med i cal care by the in clu sion ofnew seg ments of health in sured per sons.
The com mu ni ca tion with the cit i zens and the pro fes sion als wasne glected re gard ing the ob jec tives, the con tent and the terms of thehealthcare re form
The lead ing prin ci ple in the man age ment of ev ery change is the an nounce ment of itsgoals, con tent and terms (ex cept in the cases, when it re lies on sud den ac tion). The par tic i pantsin the pro cess of change have to be ac quainted in ad vance with what and when is go ing to hap -pen and those, af fected by the change (for ter mi na tion of la bour con tract, trans fer to an otherpo si tion, job, etc.) have to be in formed what is go ing to hap pen with them. It is dif fi cult to sayhow far this prin ci ple was ob served dur ing the re form un der tak ings in 1888. How ever, it wascon sis tently and to tally ap plied in 1950 and the fol low ing years un der the “so cial ist re struc tur -ing” of healthcare.
The healthcare re form is a for mi da ble and rad i cal change, which has re mained un fa mil iaror in suf fi ciently and dis tort ed ly fa mil iar, or un con vinc ingly fa mil iar to a large part of the med -i cal spe cial ists and the ma jor ity of the cit i zens. In our pre sen ta tion, this is clearly man i festedthrough out the re form pe riod from the so cio log i cal in ter pre ta tions and the anal y sis of the pub -li ca tions in the cen tral news pa pers.
The ab sence of an an nounce ment at the be gin ning of 1990s is un der stand able, al thoughnot jus ti fied. As al ready men tioned, un til 1996, there was no of fi cial con cept and programme(“strat egy”) for the healthcare re form. It is im pos si ble to an nounce some thing that does not ex -ist. The strange and un der stand able be hav iour, how ever, was that, even if a na tional healthstrat egy had al ready been pre pared to gether with draft laws, a sec ond na tional health strat egy,their an nounce ment (to the med i cal pro fes sion als and the cit i zens) was not made.
The or gan is ing of sev eral “round ta bles”, con fer ences and sem i nars could not sub sti tute thewide pub lic ity of such a huge event in healthcare and the so cial sphere as the healthcare re form.
The ne glect of the bi lat eral com mu ni ca tion with the med i cal pro fes sion als and the cit i -zens dur ing the con ducted re form health pol icy had im por tant and sus tain able neg a tive con se -quences. The es tab lished “in for ma tion vac uum” was filled with de formed (some times
322
de lib er ately dis torted) in for ma tion. It gave birth to neg a tive at ti tudes or hy per tro phied hopesand ex pec ta tions. In the course of time, they turned into cri te ria and par a gons, used for the as -sess ment of the de vel op ment of the healthcare re form (in clud ing health in sur ance).
In the ma jor ity of the cit i zens, the ex pec ta tion was formed that the healthcare re form wasim me di ately re lated to the fast im prove ment of the med i cal care (in com par i son to the ex ist ingone), in clud ing drug sup ply.
The med i cal per son nel de sired and ex pected the change. The hopes were as so ci atedwith better pay ment, better work ing con di tions, pos si bil i ties for pro fes sional de vel op ment.Their thoughts about the in di vid ual risks re lated to the change of the healthcare sys tem re -mained in the pe riph ery.
Year af ter year, both the cit i zens and the med i cal staff ex pected the de sired “better” to hap -pen. The ini tial en thu si as tic hopes, how ever, were even tu ally nour ished nei ther by the ad min is -tra tive acts and the con cep tual vi sions, nor by the ac tual re sults. The pow er ful ex pec ta tions faded away and gave way to the strong frus tra tion and dis trust, which were equally pow er ful. In theirturn, they nour ished in dif fer ence, alien ation and even (in some cases) hos til ity to the healthcarere form. The lat ter was de-le giti mised in the eyes and the minds of the cit i zens.
The lost trust de prived the healthcare re form of the im por tant sup port of the pro fes sion alsin the field of healthcare as well as of the so ci ety.
The re form leg is la tion did not reg u late clearly the le gal sta tus of thehealthcare sys tem and the re spon si bil i ties in healthcare
The re form leg is la tion was not only de layed, but it was not har mo nised with the tasks andthe pri or i ties of the healthcare re form. It did not fa cil i tate the so lu tion of sig nif i cant health andhealthcare prob lems. In this con text, we need to note sev eral im por tant de fects of the leg is la tion.
The role and the li a bil i ties of the pub lic power (the state, the lo calgov er nance) in the ac tiv i ties of the healthcare sys tem and the na tion’shealth
In Bul gar ian healthcare leg is la tion, the clear le gal reg u la tion was ne glected of a prin ci palis sue, fun da men tal for the de vel op ment of the healthcare sys tem, e.g. the re la tion of the statewith the health of the na tion and with the healthcare sys tem.
Ac cord ing to the leg is la tion, act ing in our coun try, the ac tual pres ence of the state in thehealthcare sys tem can be per ceived even now a days. The state is the pro pri etor of 100% of thecap i tal of the uni ver sity hos pi tals and the na tional cen tres, the na tional spe cial ised hos pi tals,the cen tres for emer gency med i cal care, the psy chi at ric hos pi tals, the cen tres for trans fu sionhaema tol ogy and di al y sis, the RIPCPH as well as of 51% of the cap i tal of the dis trict hos pi tals.The prin ci pal of the com pa nies, man ag ing this prop erty, is the min is ter of healthcare (be sides,the state is the owner of the cap i tal of the in sti tu tional hos pi tals, too). The state (the ex ec u tivepower) ap points also eigh teen (out of the 37) mem bers of the As sem bly of the Rep re sen ta tivesof the NHIF. The state has at its dis posal both the leg is la tive and the ex ec u tive power in thecoun try. Hav ing these wide com pe tences, it is a ques tion how ef fec tively the state can man -age the enor mous cap i tal and how the power com pe tences can be ef fec tively uti lised by thestate in the in ter est of health and in the in ter est of the de vel op ment of the healthcare sys tem. Aswe will fur ther note, if the state had uti lised its pos si bil i ties granted by law and if it had man -
323
Pros pects for the de vel op ment of the healthcare re form
aged its prop erty in a better way, it would have been im pos si ble to have in suf fi cient re sourcesin the NHIF, to have hos pi tals ac cu mu lat ing debts, to prac tise un reg u lated pay ments and havecit i zens with out means to buy drugs.
In deed, the Law on Health (Art.2) stip u lates that the state guar an tees the “pro tec tion ofthe cit i zens’ health as the full phys i cal, men tal and so cial well-be ing (un der lined by the au -thors). We are not go ing to dis cuss how ab surd it is for the state to guar an tee the phys i cal,men tal and so cial well-be ing, de fined as “health”. These guar an tees en tail an enor mous re -spon si bil ity. But irregardless of this, no where are the mech a nisms spec i fied, by means ofwhich the state would carry out this guar an tee. The ex e cu tion of the prin ci ples stip u lated inthe Law (Art. 2) is not bound to the way in which they are go ing to be ap plied. It is there foreun clear how the cit i zens’ equal ity will be achieved, as guar an teed by the state and as pro -claimed in the law, in terms of us ing health ser vices, en sur ing ac ces si ble and qual ity med i calcare or, in terms of the pri or ity of the health pro mo tion and in te grated pro phy laxis – prob lems,which had been pain ful for de cades even for the most ad vanced coun tries. And what is nonethe less im por tant is who is go ing to bear the re spon si bil ity, if these guar an tees are not ob -served. With out for mu lat ing the ways of ex e cut ing the guar an tees and re spon si bil i ties in caseof fail ure to ob serve the le gal texts, in the best case, all these re main a ver bal ex pres sion ofwish ful think ing.
The le gal sta tus of the man age ment of the Na tional Sys tem of Healthcareis un clear
The healthcare sys tem is de fined (Art. 4 of the Law on Health) as con sist ing of med i caland healthcare es tab lish ments and phar ma cies as well as “of state, mu nic i pal and pub lic au -thor i ties and in sti tu tions for the or gani sa tion, man age ment and con trol of the ac tiv i ties re latedto health pro tec tion and con sol i da tion”. The Law stip u lates (Art. 5) that “the Min is ter ofHealthcare man ages the na tional sys tem of healthcare”. But the law does not reg u late how andin what way, with what in stru ments and mech a nisms he/she will man age “the state, the mu nic -i pal and the pub lic au thor i ties and or gani sa tions”, which are out side the in sti tu tion of thehealthcare min is try. This is an im por tant and com pli cated ques tion, which is not given an an -swer in the law. Fur ther more, a great num ber of the or gans and in sti tu tions, en vis aged in thelaw (mu nic i pal i ties, or gani sa tions) are granted cer tain au ton omy, lim it ing sig nif i cantly thecom pe tences of the min is ter to ward them. A le gal text is also ab sent from the text about the re -spon si bil ity for the func tion ing of the thus de fined healthcare sys tem.
Le gally un bal anced cen tres of in flu ence
Ac cord ing to the Law on Health, the Coun cil of Min is ters “man ages and ex e cutes” thestate health pol icy (Art. 3, §1) and the Min is ter of Healthcare man ages the Na tional HealthcareSys tem (Art. 5, §1). The law stip u lates for the healthcare sys tem to have one cen tre of power –the Min is ter of Healthcare (and its ad min is tra tive ap pa ra tus, e.g. the Min is try, the di rec tors ofthe RHC and, to a cer tain ex tent, the RIPCPH), which should also bear a re spon si bil ity cor re -spond ing to their power. With the pre ced ing laws (on the pro fes sional or gani sa tions of phy si -cians and den tists, health in sur ance), how ever, an other two cen tres are es tab lished in thena tional man ag ing or gans of the pro fes sional or gani sa tions and the NHIF. Their power is re -stricted only to their own struc tures, but in ac cor dance with their le gally granted com pe tences,
324
they ex ert a sig nif i cant in flu ence on the healthcare sys tem. The pro fes sional or gani sa tionshave the main task of de fend ing the in ter ests and fa cil i tat ing the pro fes sional de vel op ment ofits mem bers. The task of the NHIF is to fi nance (pay to the ex ec u tors) the med i cal care, pro -vided to the in sured per sons.
The man ag ing or gans of the pro fes sional or gani sa tions and the NHIF, how ever, are par tiesto the sign ing of the Na tional Frame work Agree ment, which is the ma jor in stru ment for the plan -ning, pro vi sion and pay ment of the med i cal care. One pro vi sion or an other, adopted by the con -tract ing par ties in the con clud ing or amend ing (such a pos si bil ity be ing granted le gally) the NFA, can cause se ri ous con se quences, which are far from a hy poth e sis. Fur ther more, the two con tract -ing par ties do not bear ac tual (and le gal) re spon si bil ity for the func tions of the healthcare sys -tem and for the real sat is fac tion of the needs of the health in sured per sons. The Min is ter ofHealthcare (who pre sum ably bears the re spon si bil ity) is not a party and the pres ence (or ab sence) of his/her sig na ture does not af fect the con tent and the en force ment of the agree ment.
As ob vi ous from the nu mer ous ma te ri als and opin ions (noted ear lier), the prob lem of thecen tres of in flu ence is in the asym me try of re spon si bil i ties. The cen tres of in flu ence have theob jec tive pos si bil ity and ac tu ally ex ert in flu ence on the sys tem of healthcare and its ac tiv i ties,but do not carry the re spon si bil ity for the con se quences of their im pact. The UBP and the UDBpar tic i pate in the de sign ing and the con tent of the NFA and, as par ties to the agree ment, theyshould also bear the re spon si bil ity for its ex e cu tion by their mem bers (through out the med i calsec tor). Nev er the less, this re spon si bil ity is ab sent862. The UBP takes part in the phy si cians’con tin u ous train ing but it is not re spon si ble for the out comes, par tic u larly re lated to the qual ityof the med i cal and pre ven tive ac tiv i ties. The prob lem is sim i lar with the NHIF. The Health In -sur ance Fund does not bear the re spon si bil ity for all the pa ram e ters of the vol ume, the qual ityand the ac cess to the med i cal care for which it pays as well as for the full pa tients’ sat is fac tion.
In all cases, the re spon si bil ity is as sumed by the healthcare ad min is tra tion. The de moc -racy of the ex ec u tive power is as so ci ated with deconcentration and de cen trali sa tion, in deed,that is, with the del e ga tion of cer tain com pe tences. It is there fore, that the del e ga tion in it self of rights and com pe tences to the above dis cussed cen tres of in flu ence is a man i fes ta tion of thestrife to ward the de moc ra ti sa tion of the healthcare sys tem. Nev er the less, in or der to have a re -ally dem o cratic pro cess, it should be ac com pa nied by clearly de fined re spon si bil i ties, too. Thepro cess re mains in com plete.
Un clear role and re spon si bil i ties of the mu nic i pal au thor i ties
The sit u a tion is sim i lar with the lo cal self-gov er nance, rep re sented by the mu nic i pal i ties(the City Coun cils). As re gards them, the asym me try is man i fested in the re verse way. They areown ers and/or they par tic i pate in the own er ship of the healthcare es tab lish ments. As such, theycarry the re spon si bil ity for their func tion ing and the sat is fac tion of the needs of their cit i zens.The mu nic i pal power, how ever, vir tu ally does not pos sess the com pe tences nec es sary for a full
325
Pros pects for the de vel op ment of the healthcare re form
862 In the quoted ma te ri als from the so cio log i cal sur veys, the man ag ers of healthcare es tab lish ments in di catedthat the UBP did not have a suf fi ciently ac tive and ef fec tive po si tion to pro tect the phy si cians’ in ter ests in thede sign and the con clu sion of the NFA. We share the opin ion that they are wrong. Most likely, the ques tion isthat the UBP does not de fend the in ter ests of the healthcare es tab lish ments. The phy si cians’ in ter ests arecon nected with the in ter ests of the healthcare es tab lish ments but they are not iden ti cal with them. Thein ter ests of the healthcare es tab lish ments dif fer from the phy si cians’ in ter ests. But the UBP is a pro fes sionalas so ci a tion of phy si cians and not a un ion of the healthcare es tab lish ments. The lat ter are not rep re sented at the signing of the NFA at all.
and goal-ori ented man age ment of their prop erty (mostly of the hos pi tals). Un der these con di -tions, the mu nic i pal au thor i ties be come alien ated both from their re spon si bil ity and from theown er ship on the healthcare es tab lish ments, for which they oth er wise bear the re spon si bil ity.But the re spon si bil ity of the mu nic i pal i ties for the pop u la tion’s health is not reg u lated ei ther.
The asym me try be tween the rights and the li a bil i ties in the sys tem of healthcare causesand sup ports the dis tur bance of its in ter nal and ex ter nal bal ances.
The par tic i pa tion of the cit i zens in the def i ni tion of the goals, pri or i tiesand so lu tions in healthcare is one of the un solved prob lems of thehealthcare leg is la tion
The civil par tic i pa tion is an un dis puted ne ces sity, which is grounded well enough and ex -plic itly stated in the doc u ments of the EC863. It is not only a man i fes ta tion of the de moc racy ofthe healthcare sys tem. It en ables the de vel op ment of the healthcare sys tem to ori ent in the“maze” of the cit i zens’ needs, de sires and ex pec ta tions.
In the Con sti tu tion and in the sub se quent leg is la tion, the cit i zens of our coun try aretreated as ob jects and not as sub jects of the healthcare sys tem. In the re cent years, in Bul gariaas well as in many other coun tries, the is sues of the pa tients’ rights have gained in creas ingpop u lar ity. In our coun try, they are reg u lated in a spe cial chap ter of the Law on Health and,par tially, in other nor ma tive doc u ments. The cit i zens’ rights in their po si tion of pa tients un -ques tion ably pres ent an es sen tial le gal prob lem, but it does not in clude, and least of all over -laps with the far more gen eral is sues of the cit i zens’ rights as sub jects of the healthcaresys tem. The res o lu tion of these ques tions is to tally ab sent from our leg is la tion.
Cer tainly, it can be stated that the cit i zens take part in the de ci sion-mak ing abouthealthcare through their rep re sen ta tives in the Na tional As sem bly and the City Coun cils,through the ex ec u tive or gans elected by them as well as through some other or gani sa tions. Theex pe ri ence, how ever, in di cates that such a me di ated par tic i pa tion is un re al is tic and, there fore,it is not ef fec tive. It can be ex em pli fied with the man age ment of the NHIF. Ac cord ing to theprin ci ples, stip u lated in the Law on Health In sur ance (Art. 5), the man age ment of the oblig a -tory health in sur ance should nec es sar ily in clude the state, the health in sured per sons and theem ploy ers. The su preme or gan of the NHIF, how ever - the As sem bly of the Rep re sen ta tives –in cludes 37 peo ple, of whom six rep re sent the trade un ions, six rep re sent the mu nic i pal i tiesand six – the em ploy ers, eigh teen rep re sent the state (ap pointed by the Coun cil of Min is ters)and one (!) rep re sents all the or gani sa tions for pa tients’ rights pro tec tion. It can be as sumedthat all the mem bers of the As sem bly of the Rep re sen ta tives hold an oblig a tory health in sur -ance and, thus, the en tire su preme man age ment body con sists of rep re sen ta tives of the healthin sured per sons. But in real fact, each of these quo tas rep re sents a spe cific or gani sa tion and not the health in sured cit i zens them selves. The civil par tic i pa tion is sim ply absent.
326
863 Coun cil of Eu rope. Com mit tee of Min is ters. Rec om men da tion ¹ 5 of the Com mit tee of Min is ters on thede vel op ment of struc tures for cit i zen and pa tient par tic i pa tion. 699th meet ing of the Min is ters’ Dep u tiesFeb ru ary 2000
In ad e quate de vel op ment of the con trol func tions in the reg u la tion of the healthcare sys tem
The con trol and reg u la tory func tions are im mi nently in her ent to ev ery liv ing andman-made or gani sa tional sys tem. With out its con trol and reg u la tory func tions, a sys tem is de -prived of its abil ity to adapt to changes in its in ter nal and ex ter nal en vi ron ment as well as of itsabil ity to reg u late its be hav iour in such a way, that it con tin ues to func tion and en sures its fur -ther de vel op ment. It is ex actly the con trol and reg u la tory func tions which are the pre-con di -tions for the self-man age ment and self-de vel op ment of the sys tem. Since an cient times till thepres ent day, in ev ery hu man so ci ety, even in the ab sence of a spe cial con trol or gan, the so cialcon trol has been pres ent, through which the sustainability of the sys tem is guar an teed. Sincethe Mid dle Ages un til to day, the pro fes sional guilds have had pro fes sional con trol, main tain -ing and fa cil i tat ing the de vel op ment of the mem bers of the guild and their pub lic pres tige.
To a cer tain de gree, con di tion ally, the con trol is di vided into ex ter nal, in ter nal andself-con trol. In re la tion to an or gani sa tion, the con trol is “ex ter nal”, when it is car ried out by an or gan or an other dom i nat ing or gani sa tion. It is “in ter nal”, if it is car ried out by the or gans ofthe or gani sa tion it self con cern ing its di vi sions or pro cesses. “Self-con trol” is a func tion of theex ec u tor – an in di vid ual or a group (team). In gen eral, the three con trol ac tiv i ties form the sys -tem of con trol over the ac tiv i ties of the or gani sa tion as part and par cel of its man age ment (andself-man age ment). The sys tem of con trol is aimed pri mar ily at as sist ing, train ing and ed u cat -ing as well as sanc tion ing and pe nal is ing.
The neg li gence of the con trol (and the en tailed reg u la tory) func tions re sults from the re -ac tion against the to tal i tar ian con trol and the dis torted idea of de moc ra ti sa tion and self-gov -er nance in the sys tem of healthcare. A cer tain part in this re spect is played by the in com plete orlack ing def i ni tion of the re spon si bil i ties in the healthcare sys tem.
Stip u lated in the act ing leg is la tion (the Law on Health, the Law on Healthcare Es tab lish -ments, the Law on Drugs and Phar ma cies in Hu man Med i cine, the Law on the Pro fes sional Or -gani sa tions of the Phy si cians and Den tists) and a num ber of other by-laws, the con trolfunc tions in the healthcare sys tem are ac cepted as an el e ment of the bu reau cracy and ad min is -tra tive im pos ing, and not as a ne ces sity for the sur vival and the de vel op ment of the sys tem, ofev ery part of it and of ev ery in di vid ual in it.
The healthcare sys tem in our coun try is not de prived of con trol but it has no sys tem for con trol.Ac cord ing to the nor ma tive acts, in the ad min is tra tion of the sys tem, a num ber of or gans
have been cre ated for ex ter nal con trol of the ac tiv i ties of the med i cal and healthcare es tab lish -ments (at the Min is try of Healthcare and the NCPHP and their ter ri to rial di vi sions as well as atthe pro fes sional as so ci a tions and their re gional struc tures). Spe cific though, the ac cred i ta tionpro ce dure is also a form of con trol. Bod ies have been es tab lished, work ing in ac cor dance withtheir own plan, meth ods and or gani sa tion, cor re spond ing to their pur pose and ob jec tives,which do not nec es sar ily co in cide with the goals of the over all healthcare sys tem. In a num berof cases, the own ers of healthcare es tab lish ments (the mu nic i pal au thor i ties) do not par tic i patein the con trol ac tiv i ties and are only “ac quainted” with the out comes of con trol ac tions. Part ofthe con trol ac tiv i ties are car ried out spo rad i cally, in re la tion to one sig nal or an other. It seemsthat, as a rule, the con trol is based on re ports and quan ti ta tive mea sure ments (“for mal in di ca -tors” which are com monly noted in in ter views or ques tion naire ma te ri als). Due to the lack of asys tem of con trol, the re sults from the con trol ac tiv i ties re main frag men tary, dif fi cult to be
327
Pros pects for the de vel op ment of the healthcare re form
ana lysed or sum ma rised in view of the needs of the health pol icy and the man age ment of thehealthcare sys tem. This is why, in the var i ous of fi cial and other pub li ca tions, one and the samedraw backs have been per sis tently noted for years.
The in ter nal con trol is in a more dis ad van ta geous po si tion, be cause it is the vic tim of avi ciously un der stood col league sol i dar ity, es pe cially in the healthcare es tab lish ments. Theneed for in ter nal con trol is re cog nised and reg u lated in the leg is la tion, the re spec tive au thor i -ties be ing stip u lated, too (for in stance, the treat ment con trol com mis sions). Re gard ing the in -ter nal con trol in the healthcare es tab lish ments, ad e quate or gani sa tion has been es tab lished inthe dis pen sa ries and the di ag nos tic and con sul ta tive cen tres but not in the hos pi tals and theother healthcare es tab lish ments. How ever, con trol pro ce dures have been worked out only in46.7% of the healthcare es tab lish ments. It can be def i nitely as sumed that a great part of the pri -mary and spe cial ised med i cal care (the in di vid ual and group prac tices) are con trolled only ex -ter nally by the NHIF (as far as they have the ca pac ity), and that, only in re la tion to theex e cu tion of the signed agree ments. An es sen tial de fect of the in ter nal con trol is the lack ofpro ce dures for ac tion in cases of es tab lished in con sis ten cies. Such a lack has been re vealed in83.3% of the cases864. Un der these con di tions, even if in ter nal con trol ac tiv i ties are per formed,they are point less and have no results.
As a func tion of the in di vid ual spe cial ist or team, self-con trol is not pop u lar in the Bul -gar ian sys tem of healthcare. The de vel oped meth ods of self-as sess ment, peer re view and othersuch meth ods are al most un fa mil iar and even less ap plied.
The faulty ex e cu tion of the con trol func tion in the healthcare sys tem en tails nu mer ouscon se quences, the most im por tant of which af fect the care for the pa tients, the re pute of themed i cal pro fes sion als and the at ti tude to the healthcare sys tem and its re form ing.
7.2. The healthcare sys tem “un der the um brella” of the healthcarere form: the di ag no sis
In or der to make them more prom i nent, we will dis cuss the pos si bil i ties for sta bili sa tion ofthe sys tem (“the fan of pos si bil i ties”), based on the anal y sis of the de fects, which have emergedin the healthcare sys tem as a re sult of the ini tial vices of the re form. In our opin ion, the maindraw backs, which have emerged dur ing the de vel op ment of the healthcare re form, in clude:
· eco nomic in sta bil ity of the healthcare sys tem;
· moral in sta bil ity of the healthcare sys tem;
· in com plete struc tural re form;
· con tin u ing ir reg u lar de vel op ment of the healthcare re form;
· per sis tent in equal i ties in the health sta tus.
The healthcare sys tem is eco nom i cally un sta ble
The eco nomic in sta bil ity of the healthcare sys tem is due to the in com plete or in ad e quately reg u lated eco nomic re la tions in the healthcare sys tem or be tween it and the state and otherstruc tures in so ci ety. The gen eral en vi ron ment, in which the un suc cess ful re sults are man i -fested from the mea sures for eco nomic im prove ment of the healthcare sys tem, is formed by the
328
864 Ìè õàé ëî âà, Ë. Âúò ðåø íè ÿò êîí òðîë â óï ðàâ ëå íè å òî íà ëå ÷åá íè òå çà âå äå íèÿ. Äè ñåð òà öèÿ. 2005 ã.
su per fi cial un der stand ing of the eco nomic re form in healthcare. The wide spread per cep -tion is that it is a means for in com ing more fi nances and spend ing of less in the healthcare sys -tem. Re gard ing it, a num ber of ad min is tra tive mea sures have been un der taken, mainly for theachieve ment of a bal ance be tween the ex penses and the in come of the healthcare es tab lish -ments, mainly at the ex pense of max i mum cost con tain ment. This, of course, is im por tant, butin no way is it car di nal. These mea sures have been in tro duced in a frag men tary and me chan i cal way, through ad min is tra tive acts, ap plied in an ex ist ing un changed en vi ron ment. They donot al ter the eco nomic po si tions, sta tus and re la tions in the healthcare sys tem. They do notform a new eco nomic en vi ron ment for the healthcare sys tem. There fore, they are un pop u larand of low ef fec tive ness.
Lack of le gally de fined sta ble sources of fi nanc ing
The so-called “un der fi nanc ing” of the healthcare re form has been chronic and has per -sisted in spite of the an nual in crease of the mon e tary flow to healthcare: in 2002 it was 1.4 bil -lion BGN (4.4% of the GDP), in 2003 it was 1.3 bil lion BGN (3.8% of the GDP), in 2004 - 1.5bil lion BGN (4.1% of the GDP) and in 2005 – 1.8 bil lion BGN (4.3% of the GDP) 865. It af fectsthe over all sys tem, but most dis tinctly, the main cus tomer of the fi nan cial re sources – the ther a -peu tic sec tor, the hos pi tals and dis pen sa ries, in par tic u lar. It had ex isted dur ing the fi nanc ingfrom the state bud get, too, when the fi nanc ing re sources for healthcare were de ter mined ac -cord ing to the “his tor i cal prin ci ple” and the “re sid ual method”. It has also ex isted since the in -tro duc tion of the health in sur ance sys tem, which (in 2006) took over the costs for the med i cal(ex cept for the emer gency) care, and to tally or par tially for med i ca tions. The ex pen di ture forthe med i cal care com prises an enor mous part of the costs for the healthcare sys tem. Thisproves that, what is im por tant is not so much the source of fi nanc ing but its re li abil ity for these cur ing of a sta ble (suf fi cient, reg u lar and con stant) fi nanc ing of the healthcare sys tem.
The prac tice, go ing on for years, has shown that in its cur rent form, the health in sur ancesys tem in Bul garia does not pro vide ad e quate fi nanc ing of the ther a peu tic sec tor ei ther for theful fil ment of its func tions or for its de vel op ment. The ma jor source of fi nanc ing is the NHIF.One of the ar gu ments for its es tab lish ment was ex actly that it would pro vide a se cure and sta blesource of fi nanc ing for the med i cal care. How ever, firstly, the NHIF does not have suf fi cientfund ing avail able, and sec ondly, it does not ex pe ri ence ad e quate “con sum ers’ pres sure” by thein sured and the pro vid ers of med i cal care. There fore, it does not pay ad e quately for the pro vided, mainly hos pi tal, care. In its re port (not cir cu lated) on the state fi nances of Bul garia from the endof 2005, the World Bank in di cated that the NHIF fin ished the year 2005 with a def i cit amount ing to 25.0% of the to tal rev e nue, and in 2007 this def i cit in creased to 47.0%866. On the other hand,the com pa nies for vol un tary health in sur ance pres ently com prise a very small share of the healthin sur ance mar ket and are not a fac tor in the fi nanc ing of the hos pi tal sec tor.
The rea sons, which are com monly in di cated to ac count for the in suf fi cient fi nan cial po -ten tial of the NHIF in clude: (1) the small size of the health in sur ance in stal ments, de ter minedleg is la tively by the Na tional As sem bly; (2) the low rate of the in sur ance in stal ments pay ment,which is al lowed as a re sult of in ad e quate or ab sent con trol and (3) ir reg u lar or failed pay mentof the in sur ance in stal ments by the so-called “self-in sured” per sons due to leg is la tively un set -
329
Pros pects for the de vel op ment of the healthcare re form
865 Kapital weekly from 28.01.-3.02.2006866 Kapital weekly from 28.01.-3.02.2006
tled prob lems. The state pays for the health in sur an ces of about 4 mil lion cit i zens, which com -prises 40.0% of the fi nances in com ing to the NHIF867. The large num ber of cit i zens is alsoalarm ing (ac cord ing to data of the NIS, as of 31.12.2005, it was 1 123 306 peo ple), who do notpay health in sur ance in stal ments. If a better and more goal-ori ented leg is la tion was in place for oblig a tory health in sur ance, there should be no cit i zens with out health in sur ance in stal ments.
For these rea sons, ev ery year the state pays in stead of pre clud ing the debts of thehealthcare es tab lish ments, mainly of the hos pi tals.
Le gally de fined rules are ab sent for price for ma tion and re gime ofpay ment for healthcare ser vices
The price for ma tion is car ried out us ing in ad e quately ground meth ods, based not on thereal costs but on the fi nances cur rently avail able at the NHIF. We have a typ i cal ex am ple of the so-called “con tract ing prices”, which have been de ter mined by means of non-mar ket andnon-eco nomic meth ods, most com monly be tween mo nop o lis tic or gani sa tions. (This is alsocon firmed by the act ing di rec tor of the NHIF, who in an in ter view for the “Novinar” daily, said that in or der to in crease the price of a clin i cal path way, the price of an other should be re duced.In other words, the fi nances for the pay ment of the clin i cal path ways are fixed in ad vance andthe prices for the clin i cal path ways are de ter mined and paid ac cord ing to the planned fi nanc -ing868. This re minds strongly of the “re sid ual prin ci ple” from the state bud get in the past). Amar ket el e ment is de ter mined in a non-mar ket way - the price. The com monly men tioned“cost ing” of the med i cal la bour is ab sent (in fact, this cost ing de ter mines its cost, value andprice), which is the ma jor com po nent of the value of the med i cal ser vice. This is why the pay -ment made by the NHIF is lower than its value and, in some cases, lower than the prices for thepro vided med i cal care, de ter mined in the NFA. This was con firmed by al most all the in ter -viewed di rec tors and man ag ers of healthcare es tab lish ments as well as by the re search and me -dia pub li ca tions. The in com ing fi nan cial re sources (mainly in the hos pi tals) are smaller thanthe costs. Hence, three im por tant con se quences re sult: (1) con sid er able debts of the hos pi talsto the var i ous sup pli ers, mostly for med i ca tions; (2) the un sat is fac tory qual ity of the med i calcare and (3) ab sent or com pletely lim ited in cen tives for the staff. Since the state has not reg u -lated their fi nanc ing in a mean ing ful and ef fec tive way, the much com mented debts of the hos -pi tals are vir tu ally debts of the state to the hos pi tals.
There is no ac tual mar ket reg u la tion of the healthcare sys tem
The mar ket reg u la tion is a pow er ful in stru ment for an in ten sive de vel op ment of ev ery so -cial sys tem. One of the main func tions of the re form health leg is la tion in cludes the es tab lish -ment of con di tions for the for ma tion of the mar ket for the healthcare sys tem. Ex cept for thephar ma ceu ti cal sec tor, the mar ket reg u la tion, which is nec es sary for its sta ble func tion ing,was not cre ated. The ac tual mar ket was ab sent due to the un ful filled con di tions for its de vel op -ment. The con sid er able prev a lence of the pub lic own er ship and the cor re spond ing (stip u latedin the LHE) sta tus and man age ment of the healthcare es tab lish ments, the rel a tively great ad -min is tra tive reg u la tion of their ac tiv ity, the lack of real con di tions for com pe ti tion, the ab sence of ad e quate price for ma tion and pay ment, the eco nomic pres sure to ful fil the NFA and the mo -
330
867 Kapital weekly from 28.01.-3.02.2006868 Novinar dauly from 14.06.2006
nop o lis tic reg u la tions of the NHIF, the ex tremely re stricted pos si bil i ties for tech no log i cal in -no va tion – all these com prise the ma jor ob sta cles to the mar ket prin ci ples im ple men ta tion inthe med i cal sec tor. In this re spect, cer tain in flu ence is ex erted by the dif fer ent con di tions de -pend ing on the type of the pop u lated area (large, mid dle, small size town).
The pos si bil i ties for ap ply ing mar ket reg u la tion in pub lic healthcare and the pro phy lac ticsec tor are not con sid ered top i cal at all. The pub lic healthcare is per ceived as a zone, which is en -tirely the prop erty of the state and is sub ject to fi nanc ing and man age ment solely by the state.
Due to the mo nop o lis tic sta tus of the NHIF the mar ket reg u la tion in pub lic in sur ance,which is an es sen tial el e ment of the over all healthcare sys tem, is given min i mal pos si bil i ties.
Moral in sta bil ity of the healthcare sys tem
Above all, we mean the pro cess of de form ing the value sys tems, the grad ing of the val ues, the psy cho log i cal make-up, pro fes sional moral and be hav ioural ste reo types. This pro cess isnot self-pro pelled. It is rooted in cer tain ob jec tive pre-con di tions. The rather de layed im ple -men ta tion of the re form, the ab sence of con cep tual clar ity, the lim ited goals and hes i tant out -comes for their achieve ment, the in ap pro pri ate steps un der taken and the ground lessex pec ta tions as well as some gen eral char ac ter is tics of the so cial de vel op ment have cre atedcon di tions for a moral un bal ance in the healthcare sys tem. The grad ual for ma tion of this pro -cess is bi lat eral and in volves two com mu ni ties – that of the cit i zens and that of the pro fes sion -als in the healthcare sys tem. It is man i fested in sev eral as pects:
Dis tanc ing of the cit i zens from the healthcare sys tem
The ma jor ity of the cit i zens had not been in formed on time about the causes, the rea sons,the ob jec tives and the changes, forth com ing in the 1990s in the healthcare sys tem. The peo pleex pected a change “for the better” but they were not aware of what change ex actly. The ex pec -ta tions were great at the time but what hap pened was not what they ex pected. There was al most no di a logue be tween the healthcare sys tem and the cit i zens. There fore, the trust in the re formwas grad u ally be ing with drawn, the healthcare sys tem un der con struc tion was be ing de-le giti -mised and the cit i zens re cog nised less and less the healthcare es tab lish ments and the health in -sti tu tions as “their” es tab lish ments. In their turn, the es tab lish ments be came en cap su lated inthem selves and pas sive to ward so ci ety.
In ter nal con tra dic tions and alien ation of the phy si cians’ guild
As a whole, the above rea sons af fected the med i cal per son nel, too. The lack ing or ex -tremely in suf fi cient in for ma tion, the de layed or par tial re form changes, the un sat is fied (vir tu -ally un re al is tic, too) ex pec ta tions of the phy si cians, den tists and other med i cal spe cial istsgrad u ally alien ated the med i cal staff from the ex e cu tion of the goals of the healthcare re form.
Other more spe cific cir cum stances were also su per im posed on these. The di vi sion intoout pa tients’ and hos pi tal care dur ing the in tro duc tion of the in sur ance fund fi nanc ing jux ta -posed the staff, par tic u larly the phy si cians work ing in these two sec tors of the healthcare net -work. The sig nif i cantly higher in comes of the phy si cians in pri mary care (par tially inspe cial ised care, too) gave rise to a jus ti fied dis con tent among the hos pi tal doc tors. The pro fes -sional unity was shat tered. It was en hanced by the ex tremely in suf fi cient fi nanc ing for the hos -pi tals and the dis pen sa ries, which also lim ited the costs to be re im bursed, for qual i fi ca tion and
331
Pros pects for the de vel op ment of the healthcare re form

so cial and ame ni ties im prove ment for the staff. In the mean time, it also nour ished the con di -tions for the so-called “un reg u lated pay ments” which were an ad di tional fac tor for the cit i zens’ dis trust in the healthcare sys tem and its re form.
Cor rup tion
It is not iden ti cal with the “un reg u lated pay ments”, al though it is also un reg u lated. Usu -ally the un reg u lated pay ments are costs, which have to be cov ered by the bud get of thehealthcare es tab lish ment. A cor rup tive pay ment is a re sult of a con di tion set in ad vance, whichhas to be ful filled in or der that a med i cal ser vice is per formed. (The pres ence of cor rup tion andabuses in the healthcare sys tem was in di cated by 52.0% of the re spon dents in the re cent na -tional ques tion naire con ducted by “Gal lup” In ter na tional 869). The fac tors, giv ing rise to cor -rup tion, are not re lated to the fi nanc ing of the healthcare es tab lish ment. They are rooted in acer tain cor rup tion en vi ron ment and mi lieu, sup ported by the lack of con trol, the feel ing of lackof pun ish ment and the cit i zens’ ig no rance or lack of in for ma tion. In the healthcare re form, cor -rup tion de vel ops un der con di tions of an ex tremely low level of cit i zens’ in for ma tion and ispre-con di tioned ex actly by the weak and in ef fec tive pro fes sional and ad min is tra tive con troland al most ab sent mech a nisms of civil control.
* * *The dis turbed moral bal ance in the healthcare sys tem is a se ri ous im ped i ment for the so -
cial co he sion in the im ple men ta tion of the healthcare re form, mean while sig nif i cantly re duc -ing the ef fec tive achieve ment of its goals.
In com plete struc tural re form of the healthcare sys tem
The struc tural re form in the sys tem of healthcare in our coun try is as so ci ated with theso-called “re struc tur ing” of the hos pi tals and the beds in them. In fact, the key is sue of thestruc tural re form is the change in the own er ship struc ture, mostly in the ra tio be tween thepub lic and pri vate own er ship. Un der mod ern con di tions, the other struc tural changes fol lowfrom it and are de rived from it.
Changes in the own er ship struc ture of the healthcare sys tem
In Bul garia, they be gan with the amend ments of the Law of Peo ple’s Health (1991),whereby the pri vate sec tor in healthcare be came le git i mate. Af ter a pro longed de lay, the pri -vate phar ma ceu ti cal sec tor was reg u lated by the Law on Drugs and Phar ma cies in Hu manMed i cine (1996), and the le gal sta tus and re gime of the pri vate healthcare sec tor by the Law on Healthcare Es tab lish ments (1999). In 2000-2004, the num ber of the pri vate hos pi tals in -creased from 18 to 40, and the num ber of beds in them in creased from 306 to 819. In 2000, thein de pend ent med ico-di ag nos tic and med ico-tech ni cal lab o ra to ries were 467, and in 2004 –828. The Law on Health In sur ance reg u lated the pri vate sec tor in the field of vol un tary healthin sur ance (as ad di tional). Af ter all the amend ments, now a days (2006) the pri vate sec tor en -com passes the whole pri mary and part of the spe cial ised out pa tients’ care, a small part of thehos pi tal sec tor and (with very few ex cep tions) the phar ma ceu ti cal sec tor. Be cause of the mo -nop o lis tic sta tus of the NHIF, the ex ist ing pri vate sec tor in health in sur ance oc cu pies a rather
332
869 24 chasa daily from 8.06.2006

lim ited share (0.1%) of the health in sur ance ac tiv ity.The changes, which oc curred in the own er ship, were of ut most im por tance for the de vel -
op ment of the healthcare re form un der mar ket con di tions and fa cil i tated the nor mal is ing of theso cial strat i fi ca tion of so ci ety. The changes car ried out did not de velop fur ther, how ever.Cer tain quan ti ta tive prog ress was marked be tween 2000 and 2004 by some com pa nies for vol -un tary health in sur ance and the es tab lish ment of pri vate hos pi tals. The struc ture of the own er -ship of the pub lic out pa tients’ and in pa tients’ healthcare net work did not change. There spec tive con di tions were not cre ated for the de vel op ment of the pri vate sec tor in health in -sur ance. The cur rent de vel op ment of the pri vate sec tor in the healthcare sys tem has re mainedan un der tak ing of the pri vate sec tor it self.
Privatisation
As a le gal mech a nism for chang ing the pub lic prop erty into pri vate, it did not have an es sen -tial sig nif i cance for the es tab lish ment of an ef fec tive struc ture of the own er ship to fa cil i tate themar ket reg u la tion and sta bi lise the healthcare sys tem. In all the pre vi ous health strat e gies, theprivatisation had been more or less pro claimed as an im por tant step of the healthcare re form. The ques tions in this re spect had been dis cussed re peat edly at var i ous lev els. The in suf fi cient clar ityand the post pone ment of the privatisation had been an ob sta cle to the im prove ment of the ef fi -ciency and the en hance ment of sustainability of the healthcare sys tem. But the privatisation ofthe healthcare sys tem has al ways re mained on the agenda for the next day.
Mu nic i pal own er ship on the healthcare es tab lish ments
As in sti tu tions of the lo cal gov er nance, a large num ber of the mu nic i pal i ties are own ers of the cap i tal of the hos pi tals and dis pen sa ries, di ag nos tic and con sul ta tive cen tres, med i cal andmed ico-den tal cen tres and all the mu nic i pal i ties are share hold ing co-own ers of parts of thecap i tal of the dis trict hos pi tal in the re spec tive re gion.
Vir tu ally, how ever, the City Coun cils and the mu nic i pal ad min is tra tion (mainly in thesmaller mu nic i pal i ties) have ex pe ri enced dif fi cul ties man ag ing their own, let’s call it,“healthcare prop erty”.
On the one hand, in the pre dom i nantly state par tic i pa tion, the par tial role of the mu nic i pal au -thor i ties in the man age ment of the cap i tal of the re spec tive dis trict hos pi tal is sym bol i cal by far.
On the other hand, the ex plic itly stated (100%) healthcare prop erty of the mu nic i pal ityhas been reg is tered as sep a rate com mer cial sole com pa nies (Ltd) with the sta tus of mu nic i palcom pa nies, which is why the City Coun cil does not have the right to sub si dise its ac tiv ity withfi nan cial re sources. The rev e nue of these es tab lish ments co mes mainly from agree ments withthe NHIF (RHIFs) for the clin i cal path ways. Since these healthcare es tab lish ments have lim -ited tech no log i cal abil i ties they work in a rel a tively small num ber of clin i cal path ways, more -over, in ad e quately re im bursed. The con tracts with en ter prises and or gani sa tions for ad di tionalmed i cal care do not play an es sen tial role. With the re stric tions in the fi nanc ing of the smallhealthcare es tab lish ments, in clud ing the dis pen sa ries, un der this re gime, the tech ni cal pos si -bil i ties for de vel op ment are re duced in terms of the qual ity of med i cal care. All these cause se -ri ous prob lems with the man age ment of the mu nic i pal i ties’ healthcare prop erty and theirin ter ac tions with the other healthcare es tab lish ments. The small mu nic i pal i ties do not have thenec es sary com pe tences to han dle their own prop erty in the com pli cated field of healthcare. At
333
Pros pects for the de vel op ment of the healthcare re form
mu nic i pal level, the healthcare sys tem does not ex ist as a set of med i cal ac tiv i ties nec es sary forthe pop u la tion’s health, un der the au thor ity of the mu nic i pal power.
The struc tural re form in the hos pi tal sec tor
Af ter 1997 a se ri ous at tempt was made for the ra tion al is ation of the num ber and the dis tri -bu tion of the hos pi tal beds across the hos pi tal es tab lish ments, the aim be ing to achieve a dis tri -bu tion, cor re spond ing to the needs and the de mand for hos pi tal care. This pro cess wascom plex. It was also as so ci ated with changes in the num ber of the per son nel, the level of theout pa tients’ care and the pos si bil i ties open to the hos pi tals them selves. Nev er the less, it did notto tally cover the so-called re struc tur ing of the hos pi tal beds. The struc tural re or gani sa tion ofthe hos pi tal fund was not com pleted ac cord ing to the in ci dence of the sep a rate groups of dis -eases, the in ten sity of the di ag nos tics and treat ment, the ap plied meth ods of treat ment and thelevel of hos pi tal care. To this pur pose, the mech a nisms of mar ket reg u la tion were not used. Nora tio nal forms were used for the struc tural uni fi ca tion of the healthcare es tab lish ments.
The struc tural re form in the pro phy lac tic sec tor
By means of by-laws and ad min is tra tive acts, and sub se quently by the Law on Health, anat tempt was made to reg u late new func tions and par tial in ter nal struc tural changes in thehealthcare es tab lish ments for the pro tec tion and con trol of pub lic health (RIPCPH).
We think it ap pro pri ate to note that by the Law on Peo ple’s Health (1973-2004) and theLaw on Health (from Jan u ary 2005) and their ac com pa ny ing sec ond ary leg is la tion, these es -tab lish ments (Hy giene and Ep i de mi o log i cal In spec tions – HEI, Re gional In spec tions for thePro tec tion and Con trol of Pub lic Health – RIPCPH) were as signed two dif fer ent types of tasks: (1) state health con trol, which is a func tion of a spe cial ised or gan of the state ad min is tra -tion, in de pend ent of the lo cal au thor i ties, and (2) pro duc tive ac tiv ity, con sist ing in the pro duc -tion of spe cific prod ucts – lab o ra tory, ex pert and con sul ta tive ser vices, lo cally ap pli ca blesci en tific as sign ments and train ing in pub lic health pro tec tion (Art. 17, §1 of the Law onHealth). The pro duc tion ac tiv ity sup ports the state con trol ac tiv ity but, in its na ture, or gani sa -tion and man age ment it dif fers from it. The con trol ac tiv ity has to en com pass groups of peo pleand thou sands of ob jects sub ject to con trol. There fore, it has to be widely branched and can notbe con cen trated. The pro duc tive ac tiv ity (lab o ra tory, ex pert and con sul ta tive, ap plied sci en -tific and train ing) fa cil i tates the con trol ac tiv ity and has its own im por tance. It can be con cen -trated in spe cific in de pend ent centres.
Re la tions and in ter ac tions among the struc tures
In or der to be ef fec tive, the struc tural re form has to en com pass not only the sep a rate struc -tural units but their link age in a sys tem. In this re spect, the main prob lems in our healthcaresys tem in clude: (1) the con nec tion be tween the cit i zen and the healthcare es tab lish ment. Dis -or ders in this re la tion in Bul garia give rise to vi o la tions and gaps in the leg is la tion, some timesdue to in fringe ments on pro fes sional eth ics, too. They are not likely to oc cur in a per fectlyfunc tion ing sys tem of oblig a tory health in sur ance; (2) the link be tween the pri mary and spe -cial ised (di ag nos tic and con sul ta tive) out pa tients’ care. It is im peded mainly by the ad min is tra -tively lim ited pos si bil i ties of the gen eral prac ti tio ners to use di ag nos tic and con sul ta tiveser vices to an ad e quate de gree. The in tro duced reg u lat ing mech a nism hin ders the early di ag -
334
nos tics and the sec ond ary pro phy laxis; (3) the link be tween out pa tients’ (mostly pri mary) andhos pi tal care. No ob jec tive rea sons should ex ist for the dis rup tion of this link; (4) the link be -tween the hos pi tals of dif fer ent cat e go ries. Its dis rup tion is not so com mon but it cre ates risksfor se ri ous con se quences for the pa tients. It is chiefly due to the in com plete reg u la tion of there la tions among the hos pi tals; (5) the link be tween the hos pi tal net work and the so cial es tab -lish ments (“spe cial ised in sti tu tions for so cial ser vices pro vi sion”, a large part of which shouldbe con sid ered part of the healthcare sys tem). This con nec tion is im por tant since in thesehealthcare es tab lish ments around 15 000 peo ple (ad o les cents and adults) are treated an nu allyand the mor tal ity rate among them is rather high (for 2004, 9.8% of the peo ple with men tal dis -or ders and 21.3% of the peo ple with phys i cal dis abil i ties). But the con nec tion is rather un sta -ble mainly be cause of the dif fer ent sta tus, in sti tu tional af fil i a tion and the re spon si bil ity of thetwo types of establishments.
The ir reg u lar de vel op ment of the healthcare re form con tin ues
The ir reg u lar de vel op ment of the healthcare re form can be traced in sev eral as pects. Wewould like to draw the at ten tion to one of the main bal ances of the healthcare sys tem – that be -tween the pre ven tive and the ther a peu tic ac tiv i ties.
Ir re spec tive of the gen eral de lay, the in ten sive de vel op ment of the re form pro cess, whichwas ob served af ter 1997, in volved chiefly the ther a peu tic as pects of the med i cal ac tiv i ties. Itwas man i fested not only in the par tial struc tural re form of the pro phy lac tic net work but alsothe un clear out lines of the pre ven tive func tion of the ther a peu tic sec tor. In the Na tional Frame -work Agree ment and the NHIF pay ment schemes, the pre ven tive ac tiv i ties were not in cludedin a way, ad e quate for their sig nif i cance.
Bul garia is a coun try with high mor tal ity rate, which is due mainly (about 90.0% for2004) to four groups of rea sons: dis eases of the blood cir cu la tion or gans, oncological dis eases, dis eases of the re spi ra tory sys tem, trauma and poi son ing. With the ex cep tion of the lat tergroup (which also in cludes the sui cides), the above men tioned groups of dis eases have a com -pli cated (but not en tirely known) ae ti ol ogy and pathogenesis (re lated to long-term life stylehab its) and chronic be gin ning (this re fers to the sui cides, too).
To gether with other fac tors, the pe cu liar i ties of the above dis eases hin der the spe cific andpri mary pro phy laxis. This is why, to gether with health pro mo tion and pri mary pro phy laxis(which still have a dis tanced ef fect), the de vel op ment of early med i cal care (di ag nos tics, treat -ment and re ha bil i ta tion) is of ex cep tional im por tance be cause of its im me di ate ef fect on thesedis eases. The es tab lish ment and the main te nance of the bal ance be tween the treat ment andpre ven tive ac tiv i ties is one of the ma jor fac tors for de creas ing the high mor tal ity rate.
The in equal i ties are pre served
In 1994-2004 the mor tal ity rate in most Eu ro pean coun tries de clined and, in a lim itednum ber of them, it in creased slowly. In Bul garia, how ever, the in crease was at such high ratesthat it caused the great est neg a tive pop u la tion growth in Eu rope. The birth rate in Bul garia waslower but still com men su ra ble to the birth rate in the other Eu ro pean coun tries, which did nothave, or, had a sig nif i cantly lower neg a tive pop u la tion growth870. The neg a tive de mo graphic
335
Pros pects for the de vel op ment of the healthcare re form
870 Na tional In sti tute of Sta tis tics, Na tional Cen tre for Health In for ma tion. Healthcare 2005. So fia, 2006, p. 165
growth in our coun try was de ter mined mainly by the in com men sur ably higher mor tal ity rate as com pared to the other Eu ro pean coun tries (with the ex cep tion of Rus sia and Ukraine). Amongthe ac tive age groups, the mor tal ity rate was main tained at a rel a tively high rate. The mor tal ity rate from dis eases of the blood cir cu la tion or gans and oncological dis eases – two rea sons ac -count ing for over 90.0% of the deaths in Bul garia – con tin ued to rise. In 2001, the mor tal ityrate from acute myo car dial in farc tion (per 100 000 in hab it ants) in Bul garia was 79.6, while inGer many it was 18.0, in It aly – 17.5 and in France – 16.2871. The death rate from the maincauses of death was de creas ing in an in sig nif i cant and fluc tu at ing way. Strong in equal ity wasman i fested be tween the pop u la tion in the cit ies and the vil lages as re gards its health sta tus and the dif fer ences con tin ued to grow.
Un doubt edly, the ad verse con di tions for the pop u la tion’s health sta tus, and more spe cif i -cally, the high death rate, de vel oped along side with the neg a tive char ac ter is tics of thehealthcare sys tem, un der the gen eral con di tions of the slow sta bili sa tion of the na tional econ -omy. The most im por tant so cial con se quence of it was the pop u la tion’s pov erty. The re la tionbe tween the pov erty and de te ri o rated health has been long proved and we are not go ing to dis -cuss it here. The sur vey of the stan dard of liv ing in Bul garia (con ducted by the Uni ver sity ofNa tional and World Econ omy in 2003) dem on strated that, ac cord ing to the adopted “pov ertybor der line“ of 102 BGN monthly in come, the num ber of poor peo ple in our coun try was 1 113000 (14.0% of the pop u la tion). The co in ci dence was not by chance that, ac cord ing to var i ouspub li ca tions, this was the ap prox i mate per cent age of the cit i zens with un paid in stal ments foroblig a tory health in sur ance.
What is typ i cal, how ever, is the ex tremely ir reg u lar dis tri bu tion of pov erty across theter ri tory of the coun try. Out of all the 262 mu nic i pal i ties, in 19 (with a pop u la tion of 2 250 800in hab it ants) the per cent age of the poor reached up to 10.0%, in 40 mu nic i pal i ties (with a pop u -la tion of 633 100 in hab it ants) the per cent age of the poor ranged from 20.0 to 25.0%, and in 30mu nic i pal i ties (with a pop u la tion of 397 600 in hab it ants) the poor peo ple com prised over25.0% of the pop u la tion. In 13 mu nic i pal i ties, the pov erty reached as ton ish ing rates – the mu -nic i pal i ties of Boynitsa (53.0%), Macresh (31.3%), Rakitovo (34.4%), Belitsa (34.5%),Yakoruda (33.4%), Satovcha (33.8%), Dospat (30.6%), Opaka (30.1%), Omurtag (31.0%),Kotel (30.7%), Vurbitsa (32.7%), Nikola Kozlevo (30.2%), Kainardja (30.6%). The pov ertyrate was also over 25.0% in a num ber of other mu nic i pal i ties in the dis tricts of Silistra,Turgovishte, Kurdjali, Smolyan and Blagoevgrad872. As ob vi ous from the sur vey, the sit u a tion in the moun tain and ru ral re gions was the grav est, they had the high est rate of un em ploy -ment, a large part of the pop u la tion was un ed u cated or had low ed u ca tion level, the in fra struc -ture, in dus try and ser vices were poorly de vel oped, the ac cess to med i cal care wasin suf fi ciently en sured. In these re gions, most fre quently a mem ber of a fam ily had a monthlyin come of no more than 60 BGN. The dis tri bu tion on the “pov erty map” also ex plains by farthe dif fer ences in the healthcare status between the urban and rural population as well asbetween the separate geographical regions.
* * *It has been too long (as com pared to the bi o log i cal du ra tion of a hu man life span) that the
Bul gar ian healthcare sys tem has been “un der the um brella” of the healthcare re form. We say
336
871 Fo rum Medicus, Is sue ¹ 45 from 27.09.2003 872 Trud daily,, Issue ¹ 25 from 27.01.2005; Mon i tor daily from 27.01.2005
“un der the um brella” be cause the dom i nat ing in flu ence on healthcare has re sulted and con tin -ues to re sult from the healthcare re form. The healthcare sys tem takes one di rec tion or an other,its de vel op ment stops or con tin ues and it as sumes one con tent or ac cel er a tion de pend ing on the re form pol icy of the state.
From all the fore go ing pages it is ev i dent, that for sev en teen years, at the ex pense of con sid -er able ef forts made by the med i cal and other pro fes sion als as well as con sid er able ex penses, anum ber of steps have been ac com plished for the de vel op ment of the healthcare re form, whichhow ever, have con trib uted only for the par tial so lu tion of its main tasks. The healthcare re -form has re mained in com plete. The healthcare sys tem was not re struc tured into a suf fi cientlydem o cratic and sta ble sys tem to yield ad e quate re sults. There fore, to day, the healthcare re form in Bul garia is sat is fac tory nei ther for the cit i zens nor for the healthcare pro fes sion als.
We will bor row an al le gor i cal com par i son from a for eign, al beit close source (A. G.Vishnevskiy et al., 2006). The pres ent state of the healthcare re form in our coun try re sem blesan au to mo bile, filled with petrol to a cer tain level, but with out wheels and a steer ing wheel.The driver has started the en gine and the pas sen ger (the cit i zen or the pa tient, could be a phy si -cian or a nurse) see that it looks like a car, the en gine is buzz ing, some thing is mak ing noise,but the car does not move. While won der ing who might pos si bly need such a car, the pas sen ger is tempted by the thought whether he/she could do without it altogether.
One sum ma rised di ag no sis of the ac tual state-of-arts in the Bul gar ian healthcare sys temcan be con cluded, based on the anal y sis of the de vel op ment of the healthcare re form and itsout comes, re flected in the views of the pro fes sion als, cit i zens, man ag ers, rep re sen ta tives of the lo cal au thor i ties and the media sources.
The en tire avail able in for ma tion dis tinctly im poses the con clu sion that the healthcaresys tem is un sta ble and in a state of a risky lack of equi lib rium. The state of in sta bil ity re -duces the func tional ca pac ity of the sys tem and sig nif i cantly de creases its efficiency.
In view of its mis sion and goals, the pros pect for an un sta ble healthcare (and not onlyhealthcare) sys tem can be seen in two al ter na tive di rec tions: ei ther to ward the uti li sa tion of thepos si bil i ties for its sta bili sa tion or to ward its fi nal de struc tion. The ne ces sity for a re formedhealthcare sys tem ex cludes the second alternative.
7.3. Con tin u a tion of the healthcare re form
The con tin u a tion of the healthcare re form and its bring ing about ac tual and pub licly per -ceiv able pos i tive re sults can be ex am ined in the light of its tasks and the ap proaches to theirexecution.
A fore most and stra te gic task for the healthcare re form is not to al low the fur therde te ri o ra tion of the na tion’s health and to cre ate the nec es sary pre req ui sites for its im -prove ment. This task has no al ter na tive. It is the com mon de nom i na tor cov er ing the con struc -tion of the healthcare sys tem, cor re spond ing to the re quire ments of the cit i zens and thecon di tions in our coun try. The re spec tive tools have to be ap plied for its ex e cu tion to en sureimmediate outcomes in a visible future period.
The so lu tion of this task, which con tin ues to dom i nate in the gen eral logic of thehealthcare re form, has to be com bined with the or gani sa tional, eco nomic and moral sta bili sa -tion of the healthcare sys tem. It is nec es sary to sup port and main tain the pro cess of the im -prove ment of the na tion’s health. Mean while, the sta bili sa tion is also nec es sary to pre pare the
337
Pros pects for the de vel op ment of the healthcare re form
con di tions for the de vel op ment of the healthcare sys tem (“sta bili sa tion through de vel op -ment”) in its struc tural, quantitative and qualitative parameters.
The ap proach
As the his toric prac tice and the pre vi ous ex pe ri ence in di cate, it has to be borne in mindthat this pro cess re quires time. It can not be ac com plished within one or two par lia men taryterms. There fore, it has to be based on sci en tif i cally ev i denced pri or i ties, grounded firmly in along-term state pol icy and not on prim i tively ef fec tive but ephemeral solutions.
In or der to be sus tain able, the state pol icy re gard ing health and healthcare should be sub -ject to leg is la tive de ci sions. The gen eral na tional sig nif i cance of the healthcare re form re -quires that these de ci sions are worked out by the larg est pos si ble cir cles of so ci ety. Theneeded, de sired and ex pected change also has to be ar gued for and de ter mined by the civil or -gani sa tions, the trade un ions, the mu nic i pal i ties and the scientific community.
The changes have to re sult in a healthcare sys tem, which has to sat isfy in an ac cept ableway the health needs of the cit i zens(gen er ally speak ing, pre ven tive and med i cal), the so ci etyand the state, with the avail able (and proved to be ex pected) re sources, i.e. through the re form,the healthcare sys tem has to be op ti mised in ac cor dance with its re sources. This im plies theachieve ment of a greater pro duc tiv ity of the system.
Re gard ing this fur ther course of the health re form, in our opin ion, the im ple men ta tion ofchanges is re quired in spe cific as pects, which, to a cer tain de gree and con di tion ally, we ex -am ine as quan ti ta tive and qual i ta tive changes.
The nec es sary qual i ta tive changes are aimed at cre at ing a qual i ta tively new and betterdriv ing forces and con di tions for the ac tiv i ties of the healthcare sys tem and its in ter ac tion withthe so cial en vi ron ment. These changes in clude the de vel op ment of the liberalisation of thehealthcare sys tem, the es tab lish ment of new eco nomic re la tions in the sys tem in view of itseco nomic sta bil ity and change of pub lic re la tions to en sure conditions for its moral stability.
In or der to make the healthcare sys tem func tion ef fec tively un der these qual i ta tively newas pects, quan ti ta tive changes are also nec es sary. They have to in clude the four ma jor el e -ments of the healthcare con struc tion – its func tions, as sets, struc tures and com pe tences. Theyhave to be dis trib uted in a ra tio nal way according to the needs.
Be low, we are sug gest ing those ideas, which, to our minds, could be use ful for the for mu -la tion of pur pose ful so lu tions for the de vel op ment of the healthcare re form in Bul garia. In ouropin ion, they have to be synchronically ori ented in five directions:
· ef fec tive con trol on cit i zens’ health for the re stric tion of the pre vent able mor tal ity andde crease in the in equal i ties of the pop u la tion’s health sta tus;
· liberalisation of the healthcare sys tem;
· eco nomic sta bil ity of the healthcare sys tem;
· moral sta bil ity of the healthcare sys tem;
· bal anced dis tri bu tion of the func tions, struc tures and com pe tences of the healthcaresys tem.
These five as pects are or gan i cally re lated, they are mu tu ally com ple ment ing and sup port -ive of each other, which is why they have to de velop si mul ta neously. A cer tain ex cep tion canbe seen in the first di rec tion, which we can ob serve only “from re cently”.
338

Ur gent mea sures for ef fec tive con trol of cit i zens’ health, re stric tion ofthe pre vent able mor tal ity and de crease of the in equal i ties in thepop u la tion’s health status
The ef fec tive con trol over health has to be un der stood as car ry ing out sys tem atic (reg u -lar) mon i tor ing and reg is tra tion of the cit i zens’ health sta tus. It is aimed at the early de tec tionof fa tal dis or ders, ex ac er bated chronic con di tions, prob lems with a sick fam ily mem ber, es tab -lish ment of pos si bil i ties for re cov ery and health im prove ment. This con trol should in clude allthe age, gen der, social, ethnic and professional groups.
The ad min is tra tion of such con trol should be the task of the fam ily doc tor (the gen eralprac ti tio ner). Since, in our opin ion, no health un in sured cit i zens and fam i lies should ex ist inour coun try, the ex e cu tion of this task should be in cluded in the agree ment and should be paidby the in sur ance com pany, re spec tively. It has to be a part of the fam ily phy si cians’ con tract ing li a bil i ties and du ties. This func tion is even cur rently le gally pro vided for and is en vis aged inthe agree ment. But the ques tion naires, com pleted by cit i zens, dem on strated that 35-39% of the in sured per sons for the pre vi ous year had not vis ited the phy si cian they had cho sen. How ever,the gen eral prac ti tio ners re ported 100% cov er age with pro phy lac tic check-ups. This dis par ityin di cates that no ef fec tive con trol was ex e cuted on the health of all the in sured people. Theresponsibility is totally for the health insurance organisation.
In the ad min is tra tion of this con trol, spe cial at ten tion has to be paid to the chil dren’shealth (aged up to 18 years). The con trol of the health in this group has to be car ried out by thereg u lated dis tri bu tion of the func tions and re spon si bil i ties be tween the fam ily phy si cian andthe school healthcare ser vice, to which we will re fer later. The re stric tion of the pre vent ablemor tal ity has to ad dress pri mar ily its high est in ci dence. On the one hand, this is the mor tal ityamong chil dren aged up to 1 year (chil dren’s mor tal ity) and, on the other hand, this is the mor -tal ity in the pop u la tion seg ments who are likely to be af fected by those causes of death, ac -count ing for the ma jor ity of the deaths, e.g. the dis eases of the car dio vas cu lar sys tem andneoplasms as well as dis eases of the re spi ra tory sys tem, trauma and poisoning.
The chil dren’s mor tal ity rate in Bul garia is con sid er ably higher than in the West ern Eu -ro pean coun tries and a num ber of the Cen tral Eu ro pean coun tries. What is typ i cal is its ex -tremely ir reg u lar dis tri bu tion – on the one hand, be tween the ur ban and the ru ral pop u la tion,and on the other hand, among the sep a rate re gions across the coun try. In 2004, it reached 10.2per 1 000 live born chil dren in the ur ban ar eas, and 15.3 in the ru ral re gions, but in five dis tricts(those of Blagoevdgrad, Bourgas, Kurdjali, Pazardjik and So fia) it was higher among the ur -ban pop u la tion, though with a small dif fer ence. In other re gions, how ever, the dif fer ence be -tween the towns and the vil lages is im pres sive. For ex am ple, in the dis trict of Varna it is 7.6and 16.6, re spec tively; in the dis trict of Vidin – 7.9 and 18.8; in the dis trict of Gabrovo – 4.7and 10.6; dis trict of Montana - 19.0 and 23.0; dis trict of Pernik – 6.2 and 17.7; dis trict ofPleven – 7.1 and 22.8; dis trict of Silistra – 6.2 and 23.0; dis trict of Smolyan - 3.4 and 12.3; dis -trict of Shumen – 8.1 and 16.5. The dif fer ences be tween the dis tricts were also sig nif i cant – onthe one hand, some dis tricts had a chil dren’s mor tal ity rate com men su ra ble with that in the Eu -ro pean coun tries (for ex am ple, the dis trict of Rousse – 3.3 per 1 000 live born; So fia city – 6.0;Smolyan – 7.0), and on the other hand, other dis tricts had a chil dren’s mor tal ity rate con sid er -ably higher than the av er age for the coun try (dis trict of Sliven – 27.5; dis trict of Montana –23.2; dis trict of Yambol – 21.5). The main rea sons, caus ing over two thirds (68.6%) of the
339
Pros pects for the de vel op ment of the healthcare re form
deaths of chil dren aged up to 1 (per 100 000 live born) were “some con di tions dur ing theperinatal pe riod) (362.0, around one third of the pre ma turely born), “con gen i tal mal for ma -tions” (247.5, around half of them with con gen i tal heart ab nor mal i ties), “dis eases of the re spi -ra tory sys tem” (188.9)873.
The geo graph ical dis tri bu tion and the cause-and-ef fect re la tions are the main points ofori en ta tion for the ap proaches to the re duc tion of chil dren’s mor tal ity. It will prob a bly be nec -es sary to re con sider the ex e cu tion of the cur rent programme for ma ter nity and chil dren’shealth pro tec tion as well as to assess its efficiency.
The course of the car dio vas cu lar dis eases, the oncological dis eases, the dis eases ofthe re spi ra tory sys tem, trauma and poi son ing de ter mines to a con sid er able ex tent the pa -tients’ life ex pec tancy and their qual ity of life, un doubt edly af fect ing their families.
The enor mous sig nif i cance of pri mary pro phy laxis to these dis eases, as we al ready noted,is un ques tion able, but it has an ef fect dis tanced in time. The mea sures for the timely con trol overdis eases are of no lesser im por tance but their ef fect is ob serv able in the less dis tant fu ture.
There fore, we con sider that par al lel to pri mary pro phy laxis, ex cep tional at ten tion has tobe paid to the pos si ble early di ag nos tics and treat ment of the above four groups of dis eases.It will prob a bly be nec es sary to as sess the ex e cu tion of the programmes for com bat ing car -dio vas cu lar dis ease and oncological dis eases and their con tri bu tion to the re duc tion of mor bid -ity and mortality rates from these diseases.
It is of ut most im por tance to prac ti cally re duce to zero the num ber of cit i zens whopres ently do not pos sess oblig a tory health in sur ance (we will tackle this is sue a lit tle later).The so lu tion to the ques tion of the health un in sured cit i zens has med i cal, so cial and moralimplications.
The early di ag nos tics and treat ment re quire se ri ous and sys temic or gani sa tional mea -sures in terms of:
· im proved ac cess to pri mary and spe cial ised con sul ta tive out pa tients’ care, in clud ingthe par tic i pa tion of mo bile med i cal teams;
· pro phy lac tic check-ups per formed by the gen eral prac ti tio ners with the nec es sary di -ag nos tic in ves ti ga tions and con sul ta tions with specialists;
· qual ity dispensarisation of the de tected dis eased pa tients, with the par tic i pa tion, un -der the con trol and the re spon si bil ity of the gen eral practitioner;
· long-term so lu tion (in clud ing in a leg is la tive way) of the long post poned is sue of theur gent med i cal care un der out pa tients’ conditions;
· the ca pac ity of the Cen tres for emer gency care and the pos si bil i ties for timely hos pi -ta li sa tion;
· the ca pac ity of the wards (sec tors) for in ten sive care.
Be side these or gani sa tional mea sures, a num ber of sup ple men tary ac tiv i ties can beadded such as:
· sys temic in form ing of the cit i zens about the ne ces sity for pro phy lac tic check-ups andseek ing of med i cal care for cer tain man i fes ta tions and con di tions;
· cre ation of in cen tives for un der go ing pro phy lac tic check-ups;
· train ing of pa tients about the re gime and be hav iour af ter the on set of an es tab lished dis ease;
340
873 National Institute of Statistics, National Centre for Health Information. Healthcare 2005. Sofia, 2006
· stim u lated im prove ment of the phy si cians’ and other med i cal staff qual i fi ca tion andpro fes sional be hav iour, es pe cially to pa tients with some of the above men tionedgroups of diseases;
· im prove ment of the sup ply of drugs for out pa tients’ treat ment of the pa tients from thesame groups of dis eases.
The plan ning and the im ple men ta tion of the mea sures for the sta bili sa tion and the im -prove ment of the health sta tus have to be dif fer en ti ated ac cord ing to dis tricts and mu nic i -pal i ties, de pend ing both on the val ues and the trends of the in di ca tors for the health sta tus andthe de gree of pov erty (ex am ined above) of the cit i zens in the re spec tive mu nic i pal ity.
The need for un der tak ing what ever or gani sa tional or op er a tive and tac ti cal ac tions in thehealthcare sys tem, now and in the near fu ture, has to be as sessed ex actly in terms of its im me -di ate ef fect on the sta bili sa tion and the im prove ment of the nation’s health.
Liberalisation of the healthcare sys tem
The liberalisation of the healthcare sys tem is a cru cial el e ment for its sta bil ity and de vel -op ment.
The liberalisation is a pro cess, in which a goal-ori ented and ac cept able bal ance is main -tained be tween mar ket and non-mar ket (state and ad min is tra tive) reg u la tion of the health sys -tem. It in volves the de vel op ment and us age of mar ket and non-mar ket in stru ments for ex ert ingin flu ence, aimed at en sur ing the de vel op ment and sustainability of the healthcare sys tem. Thispro cess is per me ated by and com bines pri vate prop erty and the dosed pres ence of the pub licsec tor, the free ini tia tive and the mar ket re la tions with the state in ter fer ence. The state cre atesguide lines and gen eral frame work rules and pro ce dures, which form cer tain de pend en cies andfa cil i tate the free ini tia tive and com pe ti tion. The mar ket and com pet i tive en vi ron ment es tab -lished in such a way and dom i nated by pri vate prop erty and eco nomic re la tions sub ject to def i -nite rules, is dis tin guished by pre dict abil ity, moderateness, transparency, it imparts trust andhas prospects for development.
The pro cess of the liberalisation of the healthcare sys tem im plies and is aimed at en sur ingthe pos si bil ity for the max i mum ex pres sion of the cre ative po ten tial of pro fes sion als andcit i zens for the con tin u ous im prove ment of per sonal and pub lic health. There fore, this pro cesshas to de velop in two di rec tions – to the pa tient (as an in di vid ual and not only as a pa tient) andto the med i cal pro fes sional (as an individual and a citizen).
In our opin ion, the points of de par ture in the pro cess of the healthcare sys temliberalisation are the fol low ing:
De cen trali sa tion and deconcentration of the man age ment
In the con text of the healthcare re form, the de cen trali sa tion re fers chiefly to the lim i ta tionof the role of the state (ex ec u tive power), trans fer of the man ag ing com pe tences to the lowerlev els and en hance ment of their com pe tences for self-gov er nance. So far the pro cess of de cen -trali sa tion in the de vel op ment of the healthcare re form in our coun try has de vel oped in a frag -men tary, ep i sodic, inconsistent and slow manner.
341
Pros pects for the de vel op ment of the healthcare re form
The state
The role of the state in the re form and the de vel op ment of the healthcare sys tem is in dis -put ably nec es sary and im por tant.
First of all, it re fers to the nec es sary nor ma tive and, for cer tain as pects, to the ad min is -tra tive reg u la tion of the healthcare sys tem and the func tions ex e cuted in its en tirety as well asto the ob tained re sults. The state (Par lia ment, gov ern ment, Min is ter) has to reg u late thehealthcare sys tem through the es tab lish ment and the up dat ing of the legislations and theby-laws (par tic u larly note wor thy is the es tab lish ment of clear and long-stand ing rules for theeco nomic re la tions of the sys tem in a mar ket en vi ron ment and for the co or di na tion of the ac tiv -i ties in it) and to con trol the implementation of the normative acts.
An other im por tant func tion of the state is re lated to the fi nanc ing. The state has to stip u -late a clear and le gally sus tain able fi nan cial sta tus of the es tab lish ments for con trol over pub lic health and the healthcare es tab lish ments as eco nomic sub jects. The state has to nor ma tivelyen sure its fi nan cial par tic i pa tion in the health in sur ance of those cit i zens who have beenproved not to be oblig a to rily health in sured. It has to cre ate con di tions for stra te gic in vest -ments in healthcare.
Thirdly, the state’s task is to pro tect pub lic health and aug ment the na tion’s health po -ten tial. In these three di rec tions the state or gans should bear the re spec tive le gally spec i fied re -spon si bil ity.
If the state has laid down proper nor ma tive ba sis and con trols its ob ser va tion, if it has pro -cured the re spec tive fi nan cial re sources and has es tab lished an or gani sa tion for the pro tec tionof pub lic health, it means that it has as sumed and ful filled its re spon si bil ity. The ex e cu tion ofthe nor ma tive leg is la tion, the ob ser va tion of the rules and the ef fec tive uti li sa tion of the hu -man, ma te rial and non-ma te rial re sources is a task of the healthcare ad min is tra tion of the dis -tricts, the mu nic i pal i ties, medical and healthcare establishments.
Re gional healthcare cen tres (RHC)
The need has to be ac cu rately spec i fied (and to our mind, it is un doubted) and, based on it, the func tions and the tasks of the RHC have to be de ter mined. For the ten years since their es -tab lish ment, this has re mained un ac com plished.
In or der to func tion as a full-fledged cen tre in the pro cess of de cen trali sa tion, as a state or -gan, the RHC have to pos sess con sid er ably broader au thor ity, man ag ing com pe tences and re -spon si bil i ties than the el e men tary ad min is tra tive and bu reau cratic li a bil i ties, stip u lated in theLaw on Health (Art. 10, §1). What is stip u lated in Art. 29 of the Law, is to tally gen eral and su per -fi cial. In our opin ion, one of the most es sen tial man a ge rial func tions – the plan ning of the na -tional healthcare sys tem and the reg u la tion of the de vel op ment of the over all health pro tec tionpro cess - is ab sent at re gional level. Eco nomic anal y ses lack about the ac tiv i ties of the med i caland healthcare es tab lish ments, in clud ing in the com par a tive as pect (form of own er ship, ca pac ity, etc.), which are of ex clu sive im por tance for the reg u la tory mea sures is sued by the state.
Lo cal gov er nance
The au thor i ties of the lo cal gov er nance (the City Coun cils) have to bear the full re spon si -bil ity for the health and the healthcare ac tiv i ties in the re spec tive mu nic i pal ity. They are theclos est to the healthcare prob lems of the mu nic i pal ity cit i zens and the causes of these prob lems
342
and, there fore, they can best de fine the ap proaches to their so lu tion, if not the con crete mea -sures. In this re spect, they have com pe tences, which are suf fi ciently sup ported by the Law onLo cal Gov er nance and the Lo cal Ad min is tra tion. The ma te rial pro vi sions are ab sent, how ever, for the full execution of the competences they possess.
The City Coun cils have to be real pro pri etors of their own healthcare es tab lish ments andco-own ers of the healthcare es tab lish ments, in the cap i tal of which they have the re spec tiveshare. They have to solve the prob lems of their own healthcare es tab lish ments, e.g. in vest -ments, eco nomic re sults, rent ing, full or par tial privatisation.
Healthcare es tab lish ments for con trol and pro tec tion of pub lic health andmed i cal es tab lish ments
De cen trali sa tion un ques tion ably in volves en sur ing the nec es sary self-gov er nance (withthe re spon si bil ity ac com pa ny ing it) of the healthcare es tab lish ments for the pro tec tion andcon trol of pub lic health as well as the medical establishments.
The healthcare es tab lish ments for the pro tec tion and con trol of pub lic health (in themean ing of Art. 21-25 of the Law on Health) and the or gans for State Health Con trol (in themean ing of Art. 15-20 of the Law on Health) are or gans of the state, which are fi nanced by thestate. Their au ton omy now a days is pre-con di tion ally lim ited and, there fore, they may pos sessonly par tial in de pend ence. A pos si ble ex ten sion of their in de pend ence can be achievedthrough the for ma tion of their own lab o ra tory units in in de pend ent in sti tu tions (com mer cial com pa nies), prob a bly af ter an ex pe di ent ag gre ga tion of the laboratory units in some of theRIPCPH.
As re gards the healthcare es tab lish ments, a sig nif i cantly greater po ten tial ex ists for thede vel op ment of their in de pend ence. Some of the pos si bil i ties will find their rad i cal so lu tionand im ple men ta tion through a change of the own er ship of the hos pi tals with 51% state own er -ship (the cap i tal to be aug mented to 100% own er ship of the mu nic i pal ity share hold ers) orthrough privatisation (full or par tial) of the healthcare es tab lish ments. In all cases, how ever,se ri ous at ten tion is nec es sary to be paid to the in ter nal de cen trali sa tion and the ex pan sion ofthe au ton omy and the li a bil i ties of the separate units of the healthcare establishments.
De vel op ment of the demonopolisation
The liberalisation of the healthcare sys tem is or gan i cally in com pat i ble with any kind of(state, cor po rate) mo nop oly. The mo nop oly is an im ped i ment to the state (un less it is stateowned) and the mar ket reg u la tion, for the free en ter prise and for the de vel op ment of the eco -nomic re la tions in the sys tem. The demonopolisation is an es sen tial step to the im ple men ta tionof the liberalised system of healthcare.
The most im por tant mo nop oly is in the field of health in sur ance. It is cre ated by the leg is -la tively stip u lated mo nop o lis tic sta tus for the oblig a tory health in sur ance of the NHIF and thepro fes sional or gani sa tions of phy si cians and den tists. The need is suf fi ciently grounded (con -firmed by the so cio log i cal sur veys) and de fin i tive for the abol ish ment of this sit u a tion. There is a wide spec trum of al ter na tives for the elim i na tion of the mo nop o lis tic relations in the systemof health insurance.
343
Pros pects for the de vel op ment of the healthcare re form

Or gani sa tion and re gime of health in sur ance
In view of the re gime of health in sur ance, the ques tion that is posed, con cerns above allthe pay ment of the in sur ance in stal ments for 7 761 049 (2004) Bul gar ian cit i zens. Ac cord -ing to the LHE, all the Bul gar ian cit i zens are obliged to be health in sured. In prac tice, the statepays the health in sur ance in stal ments of about 4 mil lion cit i zens. Those who owed in sur ancein stal ments were 1 123 306 cit i zens (2005), ap prox i mately the num ber of the poor peo ple inthe coun try (1 113 000 in 2003). The cit i zens who paid the health in sur ance in stal ments out oftheir own means (jointly with the em ployer’s) were 2 637 743 peo ple. Re quests for ex ten sionsof the dead line for the pay ments of the dues to the NHIF were sub mit ted by 37 649 cit i zens(un til De cem ber 31st 2005). The com par i son be tween these two fig ures in di cates that a fi nalnum ber of about 1.1 mil lion poor cit i zens was prob a bly a fact, for whom the pay ment of the in -sur ance in stal ments was an ap par ent bur den. For some per cent age of them (ac cord ing to Art.40, §2, p.4 of the Law on Healthcare Es tab lish ments, the so cially unprivileged with the right of so cial ben e fits or ac com mo dated in homes for so cial care) the in sur ance in stal ments have beenpaid from the re pub li can bud get to the pres ent day. The is sue raised here is about the rest, whoare poor but are not entitled to social benefits and are not settled in homes for social care.
There fore, in our opin ion, the very first ques tion which has to be solved (the re main ingcan be de rived from it) is ex actly the ques tion about the pay ment of the in sur ance in stal mentsfor these 1.1 mil lion citizens.
Re gard ing it, we may take into con sid er ation two op tions: (1) the es tab lish ment of state“Equalising Fund” (“equalising” in the sense that it equalises the op por tu ni ties), from whichthe in sur ance in stal ments are paid for the above 1.1 mil lion cit i zens, or, (2) the es tab lish mentof “Mu nic i pal ity Equalising Funds” to this pur pose, with the pos si bil ity for them to be sub si -dised from the state bud get, too. The sec ond al ter na tive is prob a bly more ap pro pri ate since themu nic i pal au thor i ties are most fa mil iar with the ma te rial sta tus of its in hab it ants, and at thesame time, it cor re sponds to the trend to ward de cen trali sa tion. This way or an other, in ourcoun try an end has to be put to this ab surd vi o la tion of the Con sti tu tion, the leg is la tion andthe moral norms of so ci ety – un der the le gally reg u lated oblig a tory health in sur ance, it is un -ac cept able, for more than seven years now, to have over a million health uninsured citizens.
Along with this fun da men tal ques tion, the is sues should be le gally solved about thedemonopolisation of the or gani sa tion for the oblig a tory health in sur ance. A ma jor im por -tance is played by the abol ish ment of the most sig nif i cant mo nop oly, re gard ing the oblig a toryhealth in sur ance. The mo nop o lis tic sta tus is in com pat i ble with the mar ket prin ci ples and themar ket reg u la tion of the healthcare sys tem. Any li censed health in sur ance or gani sa tionmust have the right to make both oblig a tory and additional voluntary health insurance.
In this re spect, the ques tion is also sub ject to le gal so lu tion about the sys tem de cen trali -sa tion for the oblig a tory health in sur ance. To our minds, the equa li sa tion of the rights and the pos si bil i ties for the pub lic (the NHIF) and the pri vate (the share hold ers’ com pa nies) sec -tors for oblig a tory and ad di tional vol un tary health in sur ance lies in the foun da tion ofdemonopolisation. It will fa cil i tate the cre ation of better con di tions for com pe ti tion and the de -vel op ment of the health in sur ance mar ket. The risk (the con se quences from which can not bepre vented, how ever) is as so ci ated with the trans fer of a sig nif i cant num ber of the health in -sured peo ple from the sys tem of the NHIF to the pri vate sec tor, which will re duce the fi nan cialca pac ity of the NHIF. A rad i cal, but a risky de ci sion (pro posed by Dr. I. Semerdjiev) is alsopos si ble for the 28 RHIFs to be trans formed into in de pend ent (shareholding) com mer cial com -
344
pa nies. By pre serv ing their au ton omy, in our opin ion, they will be in a po si tion to ac quire agreater fi nan cial sta bil ity through vol un tary uni fi ca tion in a kind of “risk pool” (it could bemore than one, of course). In case such an al ter na tive be comes a fact, the fur ther de vel op mentand the fu ture de vel op ment of the RHIF will de pend on the mar ket po si tions they have. It islikely, that, sub se quently, a shift will be made to merg ers, ‘de vour ing”, etc., guar an tee ing byall means the legal rights of the health insured people. It is possible that other alternatives forsolutions are also considered.
Demonopolisation is as so ci ated with privatisation of the oblig a tory health in sur ance.The privatisation in this field has a num ber of ad van tages, which have been ex am ined by N.Popov in the gen eral con text of the so cial se cu rity874. We con sider, how ever, that the fullprivatisation of the oblig a tory health in sur ance is in ap pro pri ate now a days and in the near fu -ture. On the one hand, it is in a state of cer tain con tro versy with the con sti tu tional li a bil i ties ofthe state and is un pop u lar in the Eu ro pean prac tices and the Bul gar ian tra di tions. World wide, it is shared and ad vo cated by the ex perts of the World Bank and the In ter na tional Mon e taryFund. On the other hand, the full privatisation does not im me di ately and au to mat i cally lead topos i tive ef fects (such as the in crease of the pro duc tiv ity of la bour, well-be ing, sus tain able de -vel op ment, in crease of the tax in come, in crease of in vest ment, re duc tion of the em ploy ment inthe so-called “grey” economy, the increase on the demand for labour in the formal sector).
This is why, it is more ap pro pri ate to adopt the model of par tial privatisation of theoblig a tory health in sur ance. In this model, the eco nomic space will be pre served for the func -tion ing of the pub lic scheme and two seg ments will be formed, e.g. cost cov er ing (for the pub -lic scheme) and cap i tal cov er ing (for the share hold ers’ health in sur ance com pa nies). The costcov er ing seg ment, for ex am ple, can cover the oblig a tory health in sur an ces of the cit i zens,whose in stal ments are paid by the state. Its dis ad van tage is that these cit i zens are de prived ofthe choice of a health in sur ance or gani sa tion. The cap i tal cov er ing seg ment will carry out theoblig a tory health in sur ance of the cit i zens, who will be able to choose be tween the public andthe other health insurance organisations.
Any how, for the oblig a tory health in sur ance, the cen tral ised col lec tion and ac count ingof the health in sur ance in stal ments have to be pre served (pref er a bly in the sys tem of the Na -tional In come Agency and the Na tional In sti tute of Sta tis tics) and the fi nances have to be dis -trib uted ac cord ing to a def i nite method and in di ca tors among the health in sur anceor gani sa tions (what ever models exist in some countries).
The ques tion about the role of the in sur ance com pa nies for the de vel op ment of health in -sur ance can also be ex am ined in the con text of the demonopolisation. There is no doubt that byen ter ing the health in sur ance mar ket with its enor mous fi nan cial pos si bil i ties (in clud ing for in -vest ment in healthcare es tab lish ments and phar ma cies), they will form the most se ri ous ri val of the health in sur ance or gani sa tions. If the in sur ance com pa nies ac quire rights in the field ofhealthcare, their pres ence on the health in sur ance mar ket will de pend ex clu sively on the ac -quired mar ket po si tions. An other al ter na tive is that they pre serve only their in sur ing func tionsby ex tend ing the con di tions for in sur ing cit i zens through health in sur ance as a spe cial “thirdpillar” together with the obligatory and voluntary health insurance.
The role of the sub scrip tion sys tem for med i cal care also stands out in the same con text,which (with out be ing reg u lated) is prac tised by a num ber of healthcare es tab lish ments for out -
345
Pros pects for the de vel op ment of the healthcare re form
874 Pavlov, N. Privatisation of the social insurance – alternatives and effects. In: Insurer, Issue ¹ 18,26.09.-10.10.and Issue ¹19, 11.-25.10.2001
pa tients’ and in pa tients’ care. One of its spe cific man i fes ta tions in cludes the ac tiv i ties of theoc cu pa tional med i cine ser vices. Hav ing in mind the au ton omy of the healthcare es tab lish -ments as mar ket sub jects, this ac tiv ity can not be for bid den to them. Un der these con di tions, itcan be re stricted only by means of mar ket mech a nisms, par tic u larly com pe ti tion, based on theprices and quality of the medical services.
Change of the pro fes sional or gani sa tions sta tus and the ways ofcon tract ing with the med i cal care pro vid ers
The other mo nop o lis tic struc ture in the sys tem of healthcare is found in the pro fes sionalor gani sa tions of phy si cians and dentists.
On one of the de bated is sues, cov ered in the above quoted in ter views – the oblig a torymem ber ship of the phy si cians in the Un ion of Bul gar ian Phy si cians and the den tists in the Un -ion of Den tists in Bul garia – we have a prin ci pled stand that it in fringes on the free dom of thecit i zens’ as so ci a tions. Most likely, this le gal re quire ment will be abol ished with the ac ces sionof our coun try to the EC. This will make in ev i ta ble the for ma tion of other or gani sa tions sim i lar to the pro fes sional branch chambers in the European countries.
We also con sider top i cal and es sen tial the other de bated ques tion re gard ing the way ofprep a ra tion and con tract ing of the Na tional Frame work Agree ment (NFA) and the bi lat -eral agree ments for pro vid ing med i cal care. The func tion of the NFA is to ar range the frame -work of the re la tions be tween two sub jects, e.g. those be tween the pro vider of med i cal careand the in surer to the ben e fit of a third person – the health insured person.
How ever, the frame work of the re la tions is made more com pli cated be cause of thenonhomogeneity of the healthcare es tab lish ments – the pro vid ers of med i cal care. Some ofthem are in di vid ual pro vid ers (the en tire pri mary and part of the spe cial ised care), but the oth -ers (also inhomogeneous) are le gal en ti ties (hos pi tals, dis pen sa ries, DCC, MC, MCC, hos -pices, homes for med ico-so cial care, cen tres for di al y sis, in de pend ent med ico-di ag nos ticlab o ra to ries). They are ir reg u larly dis trib uted be tween the pub lic and pri vate sec tor, which en -hances even more the nonhomogeneity of the healthcare es tab lish ments. Each of the groups ofpro vid ers has spe cific tasks and func tions, and there fore in ter ests, which do not en tirely co in -cide (in some as pects they are virtually contradictory) with the interests of the professionals.
In prin ci ple, the pro fes sional or gani sa tion which unites phys i cal per sons (phy si cians,den tists) can not be rep re sen ta tive (in the prep a ra tion and the con tract ing of the NFA) of le galen ti ties. There fore, we con sider that the pro ce dure for the prep a ra tion and con tract ing of theNFA should be leg is la tively changed by in tro duc ing rep re sen ta tive par tic i pa tion of the groups of healthcare es tab lish ments which are le gal en ti ties, treated equally with the in di vid ual pro -vid ers. Sim i larly, if the oblig a tory health in sur ance is de cen tral ised, the par tic i pa tion of an -other party should be arranged, e.g. the participation of the health insurance companies.
In such a way, the mo nop o lis tic in flu ences in the healthcare sys tem can be elim i nated andthe ac tual and nec es sary con tract ing will be en sured in the com pul sory health in sur ance be -tween the pro vider and the insurer.
Sim i larly to the greater part of the views, re ported in the so cio log i cal sur vey, we find thatthe cur rent con tent and vol ume of the NFA is su per flu ous. In terms of con tent, it should be areal frame work, out lin ing the main pa ram e ters of the re la tions be tween pro vid ers and in sur ers un der oblig a tory health in sur ance. In the forms of vol un tary and ad di tional health in sur ance,which pres ent a field for stron ger com pet i tive re la tions among the in sur ers, inter-cor po rate
346
agree ments are pos si ble, but the framework agreement is inapplicable. In an ac tual frame work agree ment, the an nual con clud ing of the NFA is su per flu ous.
There fore, the com po si tion of a new NFA should be in tro duced ev ery five years by a leg is la -tive change, en vis ag ing the pos si bil ity and the pro ce dure for mak ing amend ments dur ing thepe riod of the agree ment en force ment by means of an nexes, cor re spond ing to the newlyemerged requirements and conditions.
By no means does our view im ply an at tempt for iso lat ing the pro fes sional or gani sa tions(in what ever form their ex is tence is pre served – un ions, cham bers) from their in flu ence on thehealthcare sys tem or from the pro tec tion of the pro fes sional in ter ests. Within the scope of theirle gally granted rights, they will al ways par tic i pate in the so lu tion of the healthcare prob lems ofthe na tion, as sum ing the re spec tive re spon si bil i ties, too. In this case the aim is con crete – toelim i nate the mo nop o lis tic in flu ence and to in tro duce equal ity among the pro vid ers of med i calcare in terms of the NFA content and conclusion.
De vel op ment of part ner ship in the healthcare sys tem
As we have al ready noted, the Na tional sys tem for healthcare is de ter mined by the Law on Health (Art. 4) as com posed of med i cal and healthcare es tab lish ments, phar ma cies “as well asthe state, mu nic i pal and pub lic or gans and in sti tu tions for or gani sa tion, man age ment and con -trol of the ac tiv i ties re lated to health pro tec tion and con sol i da tion”. This is an en tirely ac cept -able def i ni tion, cor re spond ing to the multi-fac tor pre-de ter mi na tion of health and com ply ingwith the con cepts of the World Health Or gani sa tion in this re spect. There is no doubt that if weare aim ing at an ef fec tive health pro tec tion of the na tion and the in di vid u als in it, it is nec es sary to con trol to a max i mum de gree the broad spec trum of the fac tors hav ing de ter min ing (in itsrel a tive sense) im por tance for health. This is also pre sup posed by the view of a wide system ofhealth protection made up of medical and nonmedical components.
In the mean time, how ever, the ap proaches and mech a nisms re main un clear for reg u lat ingand man ag ing the thus (ap pro pri ately) de fined sys tem, which ex ceeds by far the in sti tu tion ofthe Min is try of Healthcare. It in cludes di vi sions from other min is tries, mu nic i pal i ties andnongovernmental au ton o mous or gani sa tions, which we will de fine as “part ners in thehealthcare sys tem”. In this sense, the le gal stip u la tion that “the Min is ter of Healthcare man -ages the na tional sys tem of healthcare” (Art. 5, §1), as we al ready noted, is ir rel e vant and con -tra dicts the Con sti tu tion and the other laws in the coun try un less the term “man ages” is meantnot in its lit eral but in some very general and therefore ambiguous sense.
The anal y sis of the func tion as signed to the Min is ter of Healthcare to “man age”, in di cates that it is not and can not be re lated to the im me di ate man age ment of the di vi sions out side the in -sti tu tion of the Min is try of Healthcare (they have spe cific ob jec tives and tasks with the cor re -spond ing man ag ing or gans). This func tion is as so ci ated rather with the co or di na tion of theirman age ment and spe cific ac tiv i ties for the so lu tion of the health prob lems of the na tion. This is why, we are of the opin ion that the ob jec tively nec es sary for ma tion of the na tional healthcaresys tem re quires ex actly the es tab lish ment of func tion ing ap proaches and mech a nisms for co -or di na tion be tween the sep a rate parts of the sys tem, and more spe cif i cally, among the part nersin the sys tem. It is ex actly the ab sent or the in suf fi cient co or di na tion that cre ates se ri ous ob sta -cles for the ef fec tive ex e cu tion of ap pro pri ate and useful solutions for the healthcare reformand the development of the healthcare system.
The Coun cil of Min is ters which, ac cord ing to the Law on Health (Art. 3, §1) man ages and
347
Pros pects for the de vel op ment of the healthcare re form

im ple ments the state health pol icy, could carry out this co or di na tion through the ap proval of ana tional health strat egy and na tional health programmes as well as through the adopted acts,ar range ments and de ci sions. This sug gests a con tin u ous and awk ward bu reau cratic mech a -nism for achiev ing inter-in sti tu tional or broader con sent, which does not nec es sar ily al wayslead to ef fec tive re sults and, fur ther more, is in ap pro pri ate for short-term op er a tive de ci sions,for in stance, on the ex e cu tion of the na tional programmes. Ac cord ing to the Law on Health(Art. 6), the con sul ta tive or gan to the Min is ter of Healthcare – the Su preme Med i cal Coun cil –can not ful fill the re quired coordination functions in terms of its composition and tasks.
There fore, to our minds, it is nec es sary to con sti tute one co or di na tion body – it could be aNa tional Co or di na tion Coun cil for Healthcare – by an amend ment of the Law on Healthand with the par tic i pa tion of suf fi ciently re spon si ble rep re sen ta tives of the re spec tive in sti tu -tions and or gani sa tions in view of un der tak ing the cor re spond ing com mit ments. There havebeen pre ce dents for the es tab lish ments and ef fec tive func tion ing of such bodies in the recentpast of our healthcare system.
Eco nomic sta bil ity of the healthcare sys tem
The healthcare sys tem can achieve eco nomic sta bil ity based on the de vel op ment of theeco nomic re la tions and mech a nisms, laid down at the end of 1990s, which have re mainedun der de vel oped un til now. As shown by the his tor i cal ex pe ri ence, with out the mar ket ori en ta -tion of the healthcare sys tem in the nec es sary and tar geted scope, it will al ways re main in com -plete and in ef fi cient, ir re spec tive of the fi nances in vested in it. And vice versa, in the pres enceof well-con structed and leg is la tively ap proved eco nomic re la tions, all the chances are cre atedfor in creas ing in com ing fi nan cial re sources, and more importantly, for their rationalutilisation.
Fi nanc ing of the healthcare sys tem
The prob lems with the fi nanc ing of the healthcare sys tem, de bated for years, are still ex -pect ing their so lu tion. The nu mer ous pal lia tive and par tially ex e cuted mea sures with ex -tremely lim ited out comes un der mine by far the de gree of trust in the healthcare re form andre an i mate the old-fash ioned and il lu sion ary vi sions of the ad van tages of the “state financing”.
How much money is needed for healthcare?
The an swer to this ques tion is of ut most im por tance and has to pre cede what ever mea -sures for eco nomic sta bili sa tion of the healthcare sys tem. The view is wide spread that no mat -ter how much fi nances are spent for healthcare, they will al ways be in suf fi cient. This view isbased on the law ful and world wide trend for an in crease of the costs for healthcare caused bythe con stant and ir re vers ible pro cesses of the tech no log i cal ad vance ment in the field of med i -cine, the de mo graphic age ing of the pop u la tion and the in creased re quire ments of the cit i zens.Nev er the less, a view like this can not form a foun da tion for a se ri ous at ti tude to the financialfuture of the healthcare system in Bulgaria.
In the con text of the pres ent anal y sis, we have to clar ify that we mean those fi nan cial re -sources, which are the nec es sary min i mum, un con di tion ally needed and have to be un ques -tion ably in vested in the healthcare sys tem, bear ing in mind the following:
· the need for ur gent mea sures for over com ing the threats (in di cated above) for the de te -
348
ri o rated health sta tus of the pop u la tion;
· the pro vi sion of the nec es sary qual ity of the pre ven tive, treat ment and re ha bil i ta tionactivities;
· the cre ation of con di tions for reach ing the healthcare re gime level in Bul garia com pa -ra ble to that in the other EC mem ber coun tries.
The de ter mi na tion of the value of these re sources can be achieved in dif fer ent ways re -quir ing con tin u ous re search. How ever, for an ap prox i mate but suf fi ciently ob jec tive idea, inour opin ion, the avail able data can be ana lysed about the cur rent costs for healthcare. Here we will use data for 2003 and 2004 since we do not have at our dis posal more re cent data forcer tain in ter na tional com par i sons. More over, hardly any dras tic changes in the val ues of the fi -nan cial re sources for healthcare have oc curred for the pe riod 2005-2006.
The fi nan cial re sources en ter the healthcare sys tem mainly from three sources: the state(gov ern men tal) bud get, the bud get of the oblig a tory health in sur ance (no more than 1% of thecosts en ter from the vol un tary health in sur ance in the healthcare sys tem and there fore, it can be con sid ered neg li gi ble) and from in di vid ual pay ments for healthcare (ex penses of the house -hold bud gets for med i ca tion, hos pi tal treat ment, con sum ers’ fees, ex clud ing the in stal mentsfor oblig a tory health in sur ance). The data we are us ing come from pub li ca tions of the Na tionalIn sti tute of Sta tis tics (NIS), the Na tional Health In sur ance Fund (NHIF) and the Na tionalHealth Ac counts (NHA)875. The con crete sums for 2004 and their rel a tive share of all theexpenses for healthcare are the following:
· from the state bud get (ac cord ing to data of the NIS) - 750 mil lion BGN or 32.78%;
· from the bud get of the NHIF (ac cord ing to data of the NHIF) - 879 mil lion BGN or38.36%;
· from in di vid ual pay ments (ac cord ing to data of the NIS) - 660 mil lion BGN or 28.86%;
· to tal ex pen di ture for healthcare - 2 228 mil lion BGN or 100.00%.876
The role of the in di vid ual pay ments is rather in ter est ing. It seems that they have an im por -tant par tic i pa tion and are com men su ra ble with the other sources of fi nanc ing for the healthcare.For 2004, the av er age an nual ex pen di ture for healthcare per house hold was 226 BGN. These ex -penses are con stantly in creas ing – only for 2003-2004 the in crease was from 76 BGN per mem -ber of a house hold (4.3% of the to tal ex penses) to 88 BGN (4.5% of the to tal ex penses).
The par tic i pa tion of the in di vid ual pay ments in the fi nanc ing of the healthcare is be com -ing in com men su rate but also im pres sive in view of the data for the healthcare ex pen di ture ofthe sep a rate coun tries, pub lished by the NHA. Ac cord ing to them, the in di vid ual pay ments forBul garia in 2004 amounted to 1 289 mil lion BGN, or, av er agely, 441.15 BGN per house hold(ex clud ing the in stal ments for the oblig a tory health in sur ance), i.e. ap prox i mately twice asmuch as the costs re ported by the NIS. Al though the data from the NHA (an in de pend ent in sti -tu tion work ing with the World Health Or gani sa tion) are more ac cept able and cor re spond to the ob ser va tions made in our country, we consider it appropriate to discuss this issue here.
It is im por tant to bear in mind that the in di vid ual pay ments for healthcare man i fest the
349
Pros pects for the de vel op ment of the healthcare re form
875 For more details about the NHA institution: Primer for Policymakers. In: “Partners for Health Reformplus”,May 2003, pp. 1-16
876 For more details about the NHA institution: Primer for Policymakers. In: “Partners for Health Reformplus”,May 2003, pp. 1-16
limit ca pac ity of the house hold bud get to pro vide a fi nan cial an swer to def i nite re quire ments.No mat ter whether they amount to 660 mil lion or 1 289 mil lion BGN, they com prise the up perlimit of the costs for healthcare from the household budgets.
The gen eral pub lic (from the state bud get and the NHIF) and pri vate (from the house hold) bud gets costs amount to 2 228 mil lion BGN (ac cord ing to the data from the NIS and the NHIF) or 2 917 (ac cord ing to the data from the NIS, the NHIF and NHA). For a pop u la tion of 7 801273 in hab it ants (2004), the av er age ex penses for healthcare per in hab it ant were 285.59 or373.91BGN, re spec tively. If the data of the NHA are taken into ac count for the ra tio be tweenthe three sources of fi nanc ing changes, their rel a tive shares be comes: pub lic pay ments –55.81% (25.71% from the state bud get and 30.10% from the NHIF) and in di vid ual pay ments(from the household budgets) – 44.19%.
Cur rently, the healthcare sys tem in Bul garia is func tion ing with an ex pen di ture rang ing(ac cord ing to the quoted data) be tween 2.2 and 2.9 mil lion BGN, its func tion ing sat is fy ing nei -ther the cus tom ers nor the pro fes sion als in the sys tem. With costs be tween 2.2 and 2.9 mil lionBGN, the Bul gar ian healthcare sys tem func tions in ef fec tively. It is likely that one de gree of in -ef fi ciency or an other is also due to in com pe tent man age ment, but this can not re fer to the sys -tem as a whole and ac count for its in ef fi ciency. Con se quently, we have all grounds to con siderthat in or der to sta bi lise the healthcare sys tem (though at a rel a tively low level) the costsfor healthcare have to be over 2.9 bil lion BGN and, if we are aim ing at a min i mum qual -ity im prove ment, we will need over 3 billion BGN.
These fi nances are man da tory to en ter the healthcare sys tem, so that it can ful fil its ob jec -tives. The ques tion is how and in what pro por tion to dis trib ute this sum among the above men -tioned sources – the state, the health in sur ance and the citizens.
Dis tri bu tion of the fi nan cial li a bil i ties and re spon si bil i ties
Above all, the li a bil i ties have to be un am big u ously leg is la tively de fined of the state andits in sti tu tions, the or gans of the lo cal gov er nance, the cit i zens, the in sur ance com pa nies andthe NII as well as the fi nan cial and med i cal con trol au thor i ties on the healthcare fi nanc ing.Gen er ally, in sche matic terms, the dis tri bu tion of the fi nan cial li a bil i ties and re spon si bil i tieshas to be looked at in the following way:
· the state – en sures and con trols the spend ing of the fi nan cial re sources for all the pre -ven tive ac tiv i ties; for the main te nance of def i nite (by law) healthcare es tab lish mentsand ac tiv i ties; for the health in sur ance in stal ments for oblig a tory health in sur ance ofspe cial seg ments of the pop u la tion, in clud ing the poor cit i zens in the coun try; for stra -te gic in vest ments in the healthcare sys tem; de ter mines the scope, the vol ume and thequal ity pa ram e ters of the pack age of med i cal ser vices which are in cluded for the per -sons hold ing an oblig a tory health in sur ance at the ex pense of the health in sur ance or -gani sa tion, cho sen by him/her;
· the mu nic i pal ity au thor i ties: en sure and con trol the spend ing of the fi nan cial re -sources for the pre ven tive (dis in fec tion, disinsection, deratisation, clean ing and en vi -ron men tal im prove ments), health pro mo tion and med ico-so cial ac tiv i ties; pos si bly forin vest ment in the main te nance and in no va tion of the ma te rial, tech ni cal and tech no log -i cal fa cil i ties and for the qual i fi ca tion im prove ment of the healthcare es tab lish mentsper son nel, whose pro pri etor is the mu nic i pal ity; they may pos si bly pay (from the
350
“Equa li sa tion Fund”) the health in sur ance in stal ments for oblig a tory health in sur anceof the poor cit i zens in the mu nic i pal ity;
· the cit i zens: pay strictly the health in sur ance in stal ments for the oblig a tory health in -sur ance (un less they are not re cog nised as poor or fall in the other cat e go ries, which donot per son ally owe health in sur ance in stal ments); choose a health in sur ance or gani sa -tion and in form their em ployer about their choice; use the op por tu ni ties pro vided bythe ad di tional vol un tary health in sur ance and health in sur ance; fa mil iar ise them selvesthor oughly with their rights as peo ple pos sess ing oblig a tory health in sur ance and arein formed about the type of med i cal ser vices they are en ti tled to at the ex pense of thehealth in sur ance or gani sa tion as well as about whether, what for and how much theyhave to pay for the re ceived med i cal ser vices;
· the em ploy ers – pay strictly the health in sur ance in stal ments for the oblig a tory healthin sur ance of their staff and ad dress them to the cho sen health in sur ance or gani sa tion,pos si bly uti lise the op por tu ni ties for ad di tional health in sur ance in the same health in -sur ance or gani sa tion or an other;
· the Na tional In come Agency and the Na tional In sur ance In sti tute: col lects, dis -trib utes and trans fers the in stal ments for the oblig a tory health in sur ance to the re spec -tive ad dress ees, e.g. the or gani sa tions for oblig a tory health in sur ance;
· the health in sur ance or gani sa tion: con cludes agree ments with healthcare es tab lish -ments which pro vide med i cal care un der the oblig a tory health in sur ance and main tainsa reg is ter of its con tract ing part ners – healthcare es tab lish ments; main tains a reg is ter of the per sons in sured by it and con trols the pay ment of the in stal ments, in form ing the NII and the fam ily phy si cian of the re spec tive health in sured per son, in cases of pos si bledis or ders; pro poses pack ages and com bi na tions for ad di tional and vol un tary health in -sur ance; con trols the ex e cu tion of the agree ments by the healthcare es tab lish ments andthe sat is fac tion of the needs of the in sured per sons at the ex pense of the oblig a tory andpos si bly other health in sur an ces; dis sem i nates by all means in for ma tion among its cli -ents about their rights and li a bil i ties;
· con trol or gans: ir re spec tive of whether they ex e cute fi nan cial or med i cal con trol, their lead ing and main tasks, from which all the other tasks en sue, are to con trol whether and to what ex tent the health in sured per sons re ceive med i cal ser vices, which in theirscope, vol ume and qual ity cor re spond to their in sur ance sta tus (oblig a tory, vol un taryor ad di tional health in sur ance), to ana lyse the out comes of this con trol and sug gest pre -ven tive or pen alty mea sures in cases of es tab lished vi o la tions.
The eco nomic sta bili sa tion is in dis pens able from the liberalisation of the healthcare sys -tem. The demonopolisation of the sys tem and the pre cise, clear and leg is la tive def i ni tion of theli a bil i ties and the re spon si bil i ties in its func tion ing sup port the model, en sur ing the pro tec tionof the cit i zens’ rights re gard ing their health and the trans par ency of their money uti li sa tion.
The oblig a tory health in sur ance in stal ments
The size of the in stal ments for the oblig a tory health in sur ance should be cal cu lated us ingan ob jec tive ba sis and tak ing into ac count a num ber of cri te ria – de mo graphic, eco nomic,moral, med i cal and socio-psy cho log i cal (the cit i zens’ will ing ness to al lo cate part of their in -
351
Pros pects for the de vel op ment of the healthcare re form
come for health in sur ance). This ob jec tive ba sis has not been pre cisely de fined un til now,which is why the in sur ance in stal ments have been de ter mined chiefly ac cord ing to sub jec tivejudge ments and /or po lit i cal de ci sions (“a lit tle” – “a lot”). By means of this ap proach, it is im -pos si ble to es tab lish the amount of the nec es sary and the pos si ble health in sur ance instalment.Therefore, the approach should be changed, of course.
Un like the cur rently dom i nat ing views, sup port ing the aug men ta tion of the in stal ment forthe oblig a tory health in sur ance (most com monly the dis cussed per cent age is quoted to risefrom 6% to 8%), in our opin ion, it is pos si ble that this in stal ment re mains un changed and evenfalls to 5% or un der 5%. (A sim i lar un der stand ing is also shared by K Pashev) 877. Ac cord ing to un pub lished data by Dr. M. Hristova, the ap pli ca tion of the jus tice in dex for the value of thehealth in sur ance in stal ment in di cates that, for our coun try at the pres ent mo ment, the most ap -pro pri ate health insurance instalment is 4.5 %).
Ac cord ing to the NHIF bud get for 2006, the ex pected in com ing re sources from the healthin sur ance in stal ments will amount to 1 040 000 thou sand BGN878. These in com ing fi nanceswill be granted on con di tion that ap prox i mately 1.1 mil lion poor cit i zens do not pay in sur ancein stal ments. Equalled to the ru bric of “so cially dis ad van taged … un in sured … with the right of so cial ben e fits …” (for whom the in stal ment is paid by the state to the amount of 6% of the halfof the min i mum monthly in sur ance in come, which is 110 BGN for 2006, e.g. 6% of 55.00BGN) the monthly in sur ance in stal ment for each of them will be 3.30 BGN and the an nual willbe 39.60 BGN. For all the 1.1 mil lion poor cit i zens, the an nual in sur ance in stal ment willamount to 43 560 000 BGN. If the in sur ance in stal ment is de creased to 5.0%, this amount willbe come 36 300 000 BGN. If we take the NHIF bud get for 2006 as a point of de par ture, in caseof a drop of the in sur ance in stal ment by 1.0%, the in com ing re sources for the oblig a tory healthin sur ance will drop ap prox i mately by 173.3 mil lion BGN (we say “ap prox i mately” as 1.0%drop of the in stal ments is not equal to 1.0% drop in the in com ing fi nances). The in com ing fi -nances, how ever, in the oblig a tory health in sur ance will in crease by 36.3 mil lion BGN, whichhave been an nu ally lost so far for the oblig a tory health in sur ance. This sum must come fromthe above men tioned “Equa li sa tion Fund”.
Un til 2005 the par tic i pa tion of the state in the pay ment of the in sur ance in stal ments (forthe re tired pen sion ers – about 2.5 mil lion peo ple, chil dren aged up to 18, about 1.2 mil lion un -der grad u ate and PhD stu dents, re cruited army sol diers, so cially dis ad van taged and un in sureden ti tled to so cial ben e fits as well as other groups small in num ber) has been ap prox i mately420.00 mil lion BGN (around 40.0% of the in com ing fi nances of the NHIF). This state par tic i -pa tion will have to be aug mented (ap prox i mately with a to tal of 209.6 mil lion BGN) in or der to com pen sate the de crease of the in stal ment by 1.0% and the sum of the Equalisation Fund.
At the ex pense of this in crease, un der the con di tions of the lib eral ised and demonopolised of the healthcare sys tem, es sen tial pos i tive ef fects can be expected:
· en tire pos si ble cov er age will be achieved of the pop u la tion with oblig a tory health in -sur ance – vir tu ally, no group of health un in sured per sons will ex ist;
· the collectibility of the in sur ance in stal ments will be im proved – the smaller in stal -ments are paid more eas ily by the in sured peo ple and the em ploy ers; thus, the state’sdebt will be de creased to oblig a tory health in sur ance (as stated by the Ex ec u tive Di rec -tor of the NHIF in an in ter view for Novinar daily, prob a bly the in sur ance in stal ment
352
877 Kapital weekly from 17-23.06.2006 878 Law on the NHIF budget for 2006 and Law on the NII budget. Official Gazette, Issue ¹102, 2005
should be in creased, but “for me what is more dis turb ing is the is sue of the in stal mentscollectibility”879);
· un der a de creased in sur ance bur den, the prob a bil ity will in crease (es pe cially if ap pro pri ateeco nomic stim uli are in volved for the em ploy ers and the self-in sured per sons) for part of there leased funds to be di rected to ward ad di tional and vol un tary health in sur ance;
· for ev ery in sured per son it will be clearer what his/her in stal ments are spent on andwhat he/she can ob tain against them;
· the con di tions for in for mal pay ments and the im pact of the cor rup tive en vi ron mentwill be sig nif i cantly limited;
· the cit i zens will have greater free dom of choice not only of a healthcare es tab lish mentbut also of a health in sur ance or gani sa tion.
Free price for ma tion and med i cal ser vices prices
The price of ev ery eco nomic good grav i tates around the value and the de gree of util ity ofthe re spec tive prod uct, but it also de pends on the mar ket con di tions and the will ing ness of thecon sum ers (pri or ity of needs, wishes, ex pec ta tions, de mand) to pay the def i nite (“so cially ac -cept able”) price. Health has no price (it is a prod uct of the hu man or gan ism it self) but ev erymed i cal ser vice has a cost, value and price.
The cost of the phy si cian’s la bour is one of the price com po nents of the med i cal ser viceswhich are most dif fi cult to be de ter mined (to a cer tain de gree, that of den tists and the otherstaff, too). Right fully, this is sue has been posed acutely and very com monly in the ques tion -naires and the in ter views in the con ducted so cio log i cal sur vey. Be ing such a com pli cated prob -lem, so far, there has not been a re li able meth od ol ogy for the de ter mi na tion of the cost of thephy si cians’ la bour, which is the rea son why the so lu tion of this ques tion has been trans ferredto the market forces (“demand” – “supply”).
In deed, the con ven tional method, ap plied in our coun try (con tract ing of the prices andtheir in clu sion in the NFA) pro vides the op por tu nity to de ter mine some (maybe so cially ac -cept able, too) prices to be paid for the med i cal ser vices un der the oblig a tory health in sur ance.How ever, as in di cated by the ex pe ri ence and the opin ions of the re spon dents of the ques tion -naires and the in ter views, this method also al lows for an ar bi trary sub jec tiv ism and can not becon sid ered suc cess ful. In it, ex actly the cost of the phy si cian’s la bour is ne glected to a largeex tent. It is equally im por tant that the con tacted prices do not in clude the wear-and-tear of theas sets of the healthcare es tab lish ments or the for ma tion of a wear-and-tear fund, in which theyare gradually decapitalised.
Hav ing in mind the ne ces sity for the liberalisation of the healthcare sys tem and thechange in the sta tus of the healthcare es tab lish ments and the health in sur ance sys tem, en su ingfrom it (e.g. the en hance ment of their au ton omy of com mer cial com pa nies), we con sider that itwill be most ap pro pri ate to in tro duce the free price for ma tion (but ac cord ing to the le gal re -quire ments) and the mar ket reg u la tion of the prices of the med i cal ser vices in the hos pi talsec tor, in clud ing in the cases of obligatory health insurance.
The free price for ma tion and the mar ket reg u la tion of the prices mean rad i cal change ofthe eco nomic re la tions in the hos pi tal sec tor. The ne go ti a tion of the prices of the med i cal ser -vices will ex ist, but it will be car ried out be tween the healthcare es tab lish ment and the health
353
Pros pects for the de vel op ment of the healthcare re form
879 Novinar daily from 14.06.2006
in sur ance or gani sa tion. In the NFA, the meth od ol ogy of the price for ma tion and not the pricesthemselves can also be contracted.
In many cases, the larger healthcare es tab lish ments will nat u rally cal cu late higher prices (as they pos sess greater as sets and spend a greater amount of qual i fied la bour), but they will alsoper form med i cal ser vices, which the smaller size healthcare es tab lish ments can not af ford. Thus,mar ket reg u la tion and dis tri bu tion of the com pe tences of the healthcare es tab lish ments will beachieved. The higher prices will de crease the com pet i tive ness of the healthcare es tab lish ment,due to which the re leas ing will be stim u lated of the un nec es sary and unutilised as sets from thehealthcare es tab lish ments. The rea son for this will be the need for them to be com pet i tive and notto pay their debts. Un der free price for ma tion, ac tual con di tions will be cre ated for com pe ti tionboth among the healthcare es tab lish ments and among the health in sur ance or gani sa tions. Thestrife of the healthcare es tab lish ments will be stim u lated to a better man age ment and the in creaseof the po ten tial op por tu ni ties for sus tain able de vel op ment. Cer tainly, this ap proach can not ex -clude the cartelling, but this is a prob lem of the or gans for com pe ti tion pro tec tion.
Ex pan sion of the co-pay ment re gime
In all the EC mem ber coun tries (and all the other coun tries with a well-de vel opedhealthcare sys tem), the pub lic ex pen di ture does not cover 100% all the costs for healthcare. Inthe EC mem ber coun tries, the cov er age of the ex penses from pub lic sources (2004) ranges be -tween 65.3% (Malta, Lat via) and 85.5% (Nor way), only the Czech Re pub lic hav ing a pub liccov er age of 91.4% of the ex pen di ture for healthcare (ac cord ing to the NHA). In Bul garia, thepub lic cov er age var ies from 71.4% (ac cord ing to data of the NIS and the NHIF) to 55.8% (ac -cord ing to data of the NIS, the NHIF and the NHA). In the fi nanc ing of the healthcare, all thepar ties rely more or less on co-pay ment by the citizens (household budgets).
Co-pay ment was in tro duced by an ar range ment of the LHE (Art. 37, §1) un der the formof “con sumer’s fee” as a per cent age of the min i mum work ing sal ary (for ev ery visit for out pa -tients’ care 1%, 2% for each hos pi tal day for the in pa tients’ care but no more than for 10 daysper an num. Cer tain cat e go ries of health in sured per sons are ex empt from con sumer’s fee). Thecon sumer’s fee is valid only for med i cal care cov ered by the oblig a tory health in sur ance. Dis -trib uted ac cord ing to the num ber of am bu la tory ex am i na tions, days of hos pi tal stay and num -ber of beds in the multi-pro file hos pi tals, it turns out that av er agely around 1 000 BGN areearned an nu ally (2004) by a phy si cian and den tist in the out pa tients’ care and about 550 BGNper hos pi tal bed (ap prox i mately this is the amount of the pa tients’ costs for food per hos pi talbed). The sums from the con sum ers’ fees to tal around 36.3 mil lion BGN. Al though it is a formof the pa tients’ fi nan cial par tic i pa tion, the con sum ers’ fees is not co-payment in the exactsense of co-payment since it is independent of consumption.
An ob jec tive cri te rion for the size of the con sumer’s fee can be formed, based on its pur -pose. In our opin ion, it is ex actly the un clear and un known to the con sum ers pur pose of thecon sum ers’ fee which is the rea son for it not to be pop u lar and for the in sis tence on its aban -don ment (by the ma jor ity of the re spon dents). In the size, in which it is es tab lished as a form ofpar tic i pa tion in the fi nanc ing, it is not so es sen tially sig nif i cant. As com pared to the costs of the NHIF (the bud get for 2006) the con sum ers’ fees for out pa tients’ care add up 3.6% and for thein pa tients’ care they add up 3.9%. It plays a cer tain part as a means for lim it ing the so-calledover con sump tion of med i cal care. But in this way not only over con sump tion but to a cer tainex tent, con sump tion too will be lim ited. The con sumer’s fee has to be eliminated.
354
Nev er the less, it is nec es sary to reg u late the co-pay ment by the pa tients in a leg is la tive way.In or der to fa cil i tate and im prove the ac cess to the most com monly sought med i cal care, it
is ap pro pri ate not to have co-pay ment un der any form for pri mary med i cal care. As a ma -te rial com pen sa tion for the gen eral prac ti tio ners (but for per formed ac tiv ity only), pay mentcan be made for work ing within specific programmes.
Co-pay ment should be in tro duced in spe cial ised (hos pi tal and out pa tients’) med i calcare pro vided within the oblig a tory health in sur ance (and within the vol un tary health in sur -ance it de pends on the pro vi sions of the in sur ance con tract). It has to be de fined as a rel a tiveshare of the price of the pro vided med i cal care. For the out pa tients’ care the co-pay ment maycom prise a per cent age (for ex am ple, 5 or 10%) of the stan dard price, which is re im bursed foran am bu la tory ex am i na tion, in ves ti ga tion or ma nip u la tion. For hos pi tal care, now it is ap pro -pri ate for it to com prise a per cent age (for ex am ple, 10 or 15%) of the price of the clin i cal path -way. The pro vided med i cal care for the oblig a tory health in sur ance has a def i nite price, a partof which (let’s say 85 or 90%) is paid by the in sur ance or gani sa tion and the other part (for in -stance 10 or 15%) is paid by the in di vid ual patient, from the voluntary health insurance, theinsurance company or another source.
The ex emp tion from co-pay ment can not be done ac cord ing to the cur rent non-mar ket re -gime (Art. 37, §2 of the LHE). As we al ready noted, ev ery med i cal ser vice has a value and aprice. This price in cludes also the re spec tive co-pay ment share. Once the ser vice has been pro -vided, the mar ket prin ci ples re quire that some body (in sur ance com pany or or gani sa tion, thestate or the mu nic i pal ity, the pa tient) pays its price. The (de bat able) ques tion is which sub jectwill cover the ad di tional part of the price. In our opin ion, in prin ci ple, (some dif fer en ti ated ap -proaches are also pos si ble), this ex pen di ture should be cov ered by the pa tient or the sub ject,paying the patient’s health insurance instalments.
Fi nanc ing for cer tain purposes and achieve ment of mea sur able out comes
The fi nanc ing for spe cific pur poses has been ap plied for a long time (as the so-called“pur pose ful fi nanc ing”) but its most com mon dis ad van tage is that it is not bound to theachieve ment of cer tain mea sur able out comes. Thus, the fi nanc ing is car ried out (from na tionaland for eign sources) of the ma jor ity of the na tional programmes, which in curs se ri ous costs.The rea sons stem from the un well-for mu lated goals and, in a num ber of cases, from the ex -pected re sults, for which usually there is no measurement.
To our minds, this type of fi nanc ing should be ap plied in a com pet i tive en vi ron ment forpro jects of pre lim i nar ily set ob jec tives, with the most pre cise pos si ble for mu la tion of thegoals and the ex pected quan ti ta tively mea sur able re sults. Usu ally, it has to be un der taken in the pre lim i nary ex per i men ta tion of or gani sa tional de ci sions (con cern ing the re duc tion of the hos -pi tal stay, re la tion ships be tween hos pi tal and out pa tients’ care, hos pi tal lo gis tics, etc.) and thein tro duc tion of new pre ven tive and ther a peu tic meth ods and schemes. It is nec es sary to al ways ex pect pos i tive re sults. In some cases, the fi nanc ing may be risky (in or der to con firm or re jecta given hy poth e sis, method, approach or organisational form), in which the chances are 50:50.
The or gani sa tion of the pur pose ful fi nanc ing has to be pre served and im proved for thetreat ment of cer tain dis eases, the fi nan cial re sources be ing man aged by the Min is try ofHealthcare. This, how ever, should be a form (with cer tain ex cep tions) of co-pay ment by theMin is try of Healthcare to the pay ment of the re spec tive clin i cal path way by the insuranceorganisation.
355
Pros pects for the de vel op ment of the healthcare re form
Privatisation of the state and municipal healthcare es tab lish ments
The privatisation of the healthcare es tab lish ments is an ur gent ne ces sity. It can not be con -stantly post poned for the fu ture. The pur pose of the privatisation is to achieve an ef fec tive man -age ment of the healthcare es tab lish ments and a better sat is fac tion of the cit i zens’ needs. Aboveall, the privatisation is a means for rad i cal change of the eco nomic, so cial and moral en vi ron ment of the healthcare sys tem. It is a tool for the ac com plish ment of the struc tural re form in gen eralterms, the de vel op ment of the mar ket fac tors (eco nomic re form) and im prove ment of the ef fi -ciency of the healthcare sys tem as a whole. In gen eral, the pos si bil ity for privatisation is met ex -actly in this con text by the re spon dents and the in ter viewed from the dif fer ent cat e go ries in thecon ducted so cio log i cal sur vey. The fi nan cial re sults from the privatisation (in comes from thesale of healthcare es tab lish ments) are of sec ond ary im por tance.
The is sues, which are not so im mi nent for so lu tion, re fer to the ob jects (what is go ing tobe pri va tised), the forms (how it will be pri va tised) and the cli ents (who will privatise).
Ob jects for privatisation
By def i ni tion, the ob jects for privatisation are the pub lic healthcare es tab lish ments (ac -cord ing to the Law on Healthcare Es tab lish ments). It is im por tant to clar ify whether all thepub lic healthcare es tab lish ments will be sub ject to privatisation and in what or der theprivatisation will take place.
Some healthcare es tab lish ments will have to be ex cluded from the ob jects forprivatisation due to their spe cific tasks and func tions such as:
· the na tional healthcare es tab lish ments (in ac cor dance with Art. 9, §4, p. 4 of the LHE),in which tasks are ex e cuted for the de vel op ment and the ad min is tra tion of the na tionalhealth pol icy. The uni ver sity hos pi tals also fall into this cat e gory;
· the cen tres for emer gency med i cal care (Art. 24 of the LHE);
· the cen tres for trans fu sion haema tol ogy (Art. 25 of the LHE);
· the healthcare es tab lish ments to the Coun cil of Min is ters and the Min is tries of de fence, the in te rior, jus tice, trans por ta tion and com mu ni ca tion.
Some is sues, con cern ing chiefly the or der of privatisation, are posed with good rea sons in the ques tion naires and the con ducted in ter views. Should we start with the privatisation of theout pa tients’ spe cial ised care and then pri va tise the hos pi tals and the other healthcare es tab lish -ments? Should the privatisation ini tially in clude the small healthcare es tab lish ments (med i calcen tres, hos pi tals) and then pro ceed with the larger ones, or vice versa? Should theprivatisation be gin with the healthcare es tab lish ments from the larger cit ies and then pro ceedto the smaller ones, or vice versa? Opin ions were voiced that “the un prof it able hos pi talsshould be sold out” (most likely at the low est pos si ble price).
In deed, the of fer ing of the healthcare es tab lish ments for privatisation has to be done ob -serv ing cer tain cri te ria. A cri te rion, how ever, can not be the type, the size, the lo ca tion or the fi -nan cial state of the healthcare es tab lish ment. The privatisation is a mar ket phe nom e non, which is why it must be first clar i fied what the mar ket con di tions (de mand, prices, at ti tudes) cur -rently are or what they are ex pected to be be fore the of fer ing for privatisation of the con cretetypes of healthcare es tab lish ments as well as whether and to what a de gree there will be a de -mand for parts and not only en tire healthcare es tab lish ments. It is also of great im por tance
356
whether and to what a de gree in this case the mar ket will be open for par tic i pants from othercoun tries, too. There fore, the so lu tion of the ques tions con cern ing privatisation must be ginwith a re li able mar ket sur vey. The an swers to these ques tions will determine the furtherapproach to the planning of privatisation.
Man ner of privatisation
The pro ce dures for the privatisation are spec i fied in the Law on Privatisation andPost-privatisation Con trol880. The man ner of privatisation (the en tire healthcare es tab lish -ments, its parts and which of its parts) has to be de ter mined by the owner (the state, the mu nic i -pal ity, share hold ers’ com pany) but, in all cases, fol low ing con sul ta tions (in clud ing with theper son nel of the healthcare es tab lish ment) and the de sign ing of a pro ject. One of the im por tantthings, to which at ten tion should be paid, in cludes the elim i na tion of the com pa nies of theso-called “hid den privatisation”, which in other branches and con di tions is car ried out throughpar al lel struc tures, joint ventures and contracts for joint activities.
A par tic u lar role is played by the privatisation in parts of a cer tain healthcare es tab lish -ment. On the one hand, by the cre ation of con di tions for com pe ti tion, it could stim u late the de -vel op ment of the whole healthcare es tab lish ment. On the other hand, how ever, con di tions forvar i ous con flicts can also be cre ated. Fur ther more, by pri va tis ing one and the same types ofparts be long ing to dif fer ent healthcare es tab lish ments by one and the same pro pri etor, risks are cre ated for the for ma tion of olygopolistic or monopolistic structures.
Cer tainly, the privatisation con di tions and the privatisation con tract must con tain the ex -plicit pro vi sion for the pres er va tion of the sub ject of ac tiv ity of the re spec tive healthcare es tab -lish ment.
The privatisation cli ents
In prin ci ple, a privatisation deal should be open, but in the case of the healthcare es tab -lish ments, a more spe cific re gime is ap pro pri ate to be ap plied, by means of which thehealthcare sys tem is pre vented from prof i teer ing privatisation deals and the for ma tion ofolygopolistic or mo nop o lis tic struc tures. In our views, two po ten tial cli ents cur rently ex ist inour coun try, which are con nected with the healthcare sys tem and are in ter ested in thehealthcare es tab lish ments - the staff of the re spec tive healthcare es tab lish ment and the healthinsurance organisations.
The privatisation by the staff is an ap pro pri ate ap proach since it is ex actly the per son nelof a healthcare es tab lish ment who are in ter ested in its suc cess ful man age ment and de vel op -ment. Dif fi cul ties are pre dicted to arise from the staff non-ho mo ge ne ity and the need for ac -cord ing nu mer ous in ter ests and at ti tudes dur ing such an abrupt and, by far, risky change of thesta tus of the healthcare es tab lish ment. It be comes a pri vate, in de pend ent sub ject on the mar ketof health ser vices. At the same time, how ever, it is owned by a col lec tive struc ture (co-op er a -tion, com mer cial com pany) formed by sep a rate phys i cal per sons. Even if they have a prin ci -pled con sen sus for par tic i pa tion in the privatisation of the healthcare es tab lish ment in whichthey are em ployed, con sid er able ef forts will be nec es sary to be made by each mem ber of thestaff to over come the con tra dic tions (of ten at house hold level) and form a professionalbehaviour, adequate to the changed conditions.
357
Pros pects for the de vel op ment of the healthcare re form
880 State Gazette, Issue ¹ 28, 2002

In the case of privatisation by a health in sur ance (or an other ex ter nal, not ex clud ing a for -eign) or gani sa tion, the sub jec tive re la tions among the staff will not play an es sen tial role. Achange of the pro fes sional be hav iour will be im per a tive, how ever, in ac cor dance with the re -quire ments of the new owner (who in great est like li hood will be aimed at “making profit”).
“Foun da tion”or con ces sion in stead of privatisation (?)
To gether with privatisation, two other in ter est ing views have been ad vo cated for the re -stric tion of the state in ter fer ence in the hos pi tal sector.
The first pro posal (made by the Mem ber of Par lia ment Dr. A. Purvanova) en vis aged thereg is tra tion of the hos pi tals as foun da tions881. Most likely, it was in flu enced by the Span ishmodel of a “hos pi tal foun da tion”. This model, how ever, is much dis puted even in Spain and isnot suf fi ciently fa mil iar in Bul garia, which is why the pro posal re mained a mere historical fact.
The other pro posal was made by the Dep uty Assoc. Prof. Dr. A. Shterev (Vice Chair manof the Par lia men tary Com mis sion for Healthcare) and it en vis aged, in stead of pri va tis ing thehealthcare es tab lish ments, to of fer them for a long-term (35-year pe riod) con ces sion882. Sub -se quently, this idea was ac cepted and found sup port by fa mous political circles.
In the case of con ces sion, the own er ship on the ob ject is not changed but the con trol overits ac tiv ity is trans ferred to the con ces sion aire. What is car ried out re sem bles some thing like“privatisation of ac tiv i ties”, which is rec om mended in a num ber of opin ions shared by the re -spon dents and in ter viewed in our sur vey. (In pa ren the sis, we would like to note that in the le gal space the term “privatisation of ac tiv i ties” is a ju rid i cal ab surd since privatisation meanschange of the own er ship of the def i nite ob ject but from the point of view of its mean ing, con -ces sion ap prox i mately over laps with “privatisation of ac tiv i ties”). The Law on Con ces sionsen vis ages a pos si bil ity for of fer ing for con ces sion of ob jects which are state or municipalproperty, in observance of the respective procedures.
Nev er the less, con ces sion is not an al ter na tive to privatisation. In case of con ces sion, thepub lic healthcare es tab lish ments re main a state or mu nic i pal prop erty. The con ces sion formdoes not change the own er ship struc ture in the hos pi tal sec tor. The con ces sion aire’s right to in -vest in the re spec tive ob ject is lim ited to the term of the con ces sion. There fore, con ces sionwould have a rather lim ited ef fect for at tract ing pri vate cap i tals, par tic u larly to the healthcarees tab lish ments, which re quire sys temic and con sid er able in vest ments and their rate of re turn israther slow. The mixed forms (privatisation of a part of a healthcare es tab lish ment by a cer taincom mer cial com pany and of fer ing for con ces sion to the same com pany of the re main ing partof the es tab lish ment) are as so ci ated with con sid er able risks for the own er ship and for the func -tion ing of the healthcare es tab lish ment ac cord ing to its pur pose. The con ces sion should notturn into an ob sta cle or a “sub sti tute” of privatisation. Hav ing in mind its pur pose ofprivatisation (change in the own er ship struc ture), in our views, the of fer ing for con ces sion ofhealthcare es tab lish ments has to be taken into con sid er ation only for cer tain specialisedhealthcare establishments or their parts, for which the change of ownership is not appropriate.
358
881 24 chasa daily from 25.07.2003882 Trud daily from 4.09.2004

Moral sta bil ity of the healthcare sys tem
From the very be gin ning, we would like to note that in the moral sta bili sa tion of thehealthcare sys tem we have to see a com plex, dif fi cult and con tin u ous pro cess. It is aimed at re -strict ing to a max i mum, re duc ing and elim i nat ing, if pos si ble, all the fac tors, cre at ing a dis -tance and caus ing alien ation be tween the in sti tu tions of the healthcare sys tem and the cit i zensas well as a de crease of the so cial co he sion and or gani sa tional struc ture of the in sti tu tionsthem selves. Un doubt edly, this pro cess also re quires the es tab lish ment of the nec es sary le galfoun da tion and nor ma tive reg u la tion. But it is as so ci ated with the over com ing of es sen tialmen tal and be hav ioural at ti tudes and ste reo types. There fore, this pro cess also ne ces si tates thepar tic i pa tion of the professionals, the partners of the healthcare system and the entire society.
There is no ques tion ing that, as re gards the pro fes sion als in the healthcare sys tem, thework to ward the moral sta bili sa tion of the sys tem has to be in cluded in the over all pro cess ofthe un der grad u ate and post grad u ate spe cial ists’ train ing, with the par tic i pa tion of the re spec -tive ac a demic in struc tors. In no way can it be con sid ered that sev eral hours of ac a demic lec -tures and sem i nars in med i cal ethics and deontology could suffice.
Here we will fo cus on some as pects of this prob lem which, in our opin ion, need to be ur -gently solved. On the one hand, they re fer to the re la tion ships of the healthcare sys tem (es tab -lish ment) and so ci ety, and on the other hand, (es pe cially) to a num ber of un solved ques tionsre lated to per son nel management.
Pre sen ta tion of the healthcare sys tem
The healthcare sys tem, with all its di men sions and struc tures, has to be not only ac ces si -ble but trans par ent to a max i mum de gree and fa mil iar to the cit i zens. They have to know orshould be able to find out what the healthcare sys tem is, who is re spon si ble for what, what areits pos si bil i ties, what they can re ceive from it and, at the same time, what are the needs of thehealthcare sys tem to sat isfy their ex pec ta tions and in what way they can help to make the sys -tem the way they desire it.
Along with this, the cit i zens have to be fa mil iar with who de fends their con sti tu tional andle gal rights and li a bil i ties as re gards their health. In or der to trig ger this pro cess, an ac tive ap -proach is nec es sary. The healthcare sys tem with all its sec tors and di vi sions has to be in frontof the pub lic con stantly and only spo rad i cally (to ex plain or jus tify cer tain fail ures). The cit i -zens have to per ceive as “their own” the hos pi tal, med i cal cen tre, phy si cian, den tist or nurseand ap proach them with trust. The phy si cians and the re main ing med i cal per son nel have to becon vinced that the cit i zens visit them not to buy a kilo of po ta toes but they have a particularproblem and are seeking for its solution.
The es tab lish ment of such re la tions (not only in the hos pi tal sec tor, of course) is in thefoun da tion of the moral bal ance in the healthcare system.
To this pur pose, a con sid er able set of in stru ments is avail able and is known, there fore, we are not go ing to dis cuss the tools which can be used.
Civil par tic i pa tion
It is an in dis pens able com po nent for the lib eral is ing healthcare sys tem and a ma jor fac torfor its moral sta bil ity. The civil par tic i pa tion has to be de vel oped, based on the in creas ingly im -prov ing in for ma tion about the healthcare sys tem. We will once again re mind that civil par tic i -
359
Pros pects for the de vel op ment of the healthcare re form
pa tion should be un der stood and man i fested not only in the ob ser va tion of the le galre quire ments (pay ment of health in sur ance in stal ments, vis its for pro phy lac tic check-ups, etc.) but also (equally im por tant) in the ac tive stand on the problems of healthcare.
It is nec es sary to nor ma tively cre ate an op por tu nity for the cit i zens to col lab o rate for thehealth prob lems so lu tion and for the de vel op ment of the healthcare sys tem. This pos si bil itycan be achieved in two main ways: (1) by de ter min ing the na tional and lo cal pri or i ties ofhealthcare and (2) by mak ing de ci sions about the man age ment of cer tain national or localhealth processes.
In this con text, the is sue of civil par tic i pa tion is sig nif i cant for the fa cil i ta tion of the man -age ment of the med i cal and healthcare es tab lish ments. In our opin ion, the es tab lish ment (un -der a def i nite form) of im me di ate re la tions be tween the par tic u lar es tab lish ment and thecit i zens would be very use ful (as con firmed also by the avail able ex pe ri ence). On the one hand, by means of the com mu ni ca tion chan nels, a wider pub lic will be ac quainted in greater de tailwith the ac tiv ity of the hos pi tal, med i cal cen tre, RIPCPH, etc., the healthcare es tab lish mentwill have a more im me di ate in for ma tion as to the cit i zens’ prob lems and, along side with it, thecit i zens would be in a position to assist the solution of some hospital problems.
Abol ish ment of the neg a tive phe nom ena in the healthcare sys tem
Neg a tive phe nom ena oc cur in ev ery so cial sys tem, im ped ing its de vel op ment and un der -min ing its im age be fore so ci ety. In the sys tem of healthcare two such phe nom ena ex ist, whichalien ate it from the com mon peo ple and have to be eliminated.
Elim i na tion of the “in for mal pay ments”
The moral sta bil ity of the sys tem is in com pat i ble with “in for mal pay ments” of any kind.For their elim i na tion the liberalisation and eco nomic sta bil ity of the healthcare sys tem willcon trib ute but the ac tion of these fac tors will still not be trig gered im me di ately and au to mat i -cally. This is why, in the sys tem of healthcare and the pro fes sional or gani sa tions, any tol er ance to ward this phe nom e non (tol er ance which we some times ob serve to a cer tain ex tent) should be dis con tin ued and a clearly stated negative attitude should be formed to it.
Elim i na tion of cor rup tion
Cor rup tion is equally in com pat i ble with the moral sta bil ity of the healthcare sys tem. It isnot an autochtonic and spon ta ne ous for ma tion in it but it re sults from the cre ated cor rup tive en -vi ron ment, which has en com passed a large num ber of other sec tors not only in our coun try. Inor der to abol ish the cor rup tive en vi ron ment in the healthcare sys tem, un doubt edly, spe cificmea sures should be un der taken, but they have to be har mo nised with the over all com mon stateanti-cor rup tion programme. The civil in volve ment might be of par tic u lar importance for theelimination of corruption.
Pro fes sional de vel op ment of the staff
To gether with the elim i na tion and in or der to coun ter act the neg a tive phe nom ena in thesys tem of healthcare, cer tain pos i tive pro cesses have to develop.
One of them is the es tab lish ment of a sys tem of pro fes sional de vel op ment for the phy si -cians, den tists and the healthcare spe cial ists in the med i cal and healthcare es tab lish ments. It is
360
ap par ent from the ques tion naire re sponses and from a se ries of pub li ca tions that the pro fes -sional de vel op ment is a ques tion which, quite nat u rally, is im por tant for the peo ple employedin the healthcare system.
The cur rent sys tem of pro fes sional de vel op ment has been long out dated and fol low ingnu mer ous cos metic op er a tions has be come in ad e quate for the pres ent, even less so, for to mor -row’s needs for healthcare. A new sys tem is needed, which has to be mar ket and at trac tiveenough but also re li able in terms of achieved qual i fi ca tion, it has to be as dem o cratic as de -mand ing in terms of ac quired knowl edge. Such are the sys tems in many coun tries and a broadspec trum of examples can be used in our country.
Along with this, the healthcare sys tem makes use to a large ex tent nonmedical per son nel la bour. The sys tem of pro fes sional de vel op ment has to equally in clude both the med i cal staffand the nonmedical spe cial ists. To a con sid er able de gree, their pro fes sional de vel op ment en -sures the out comes of the healthcare system.
The pro fes sional de vel op ment is also as so ci ated with the es tab lish ment of a sys tem ofpro fes sional hi er ar chy. The ab sence of such a sys tem is an im ped i ment for pro fes sional im -prove ment mo ti va tion. Un like for the ac a demic hi er ar chy, the pro fes sional ca reer of a phy si -cian or den tist af ter his/her uni ver sity grad u a tion and the ac qui si tion of a Mas ter’s De gree, canachieve only one fur ther step, e.g. to ob tain the de gree of “spe cial ist in …” (the rec og ni tion of a sec ond and third spe cialty in creases the chances but, gen er ally, does not change the state of af -fairs). If this is a res i dent and is lucky enough, he/she may climb up the ad min is tra tive lad derand be come “Head of ward”. The sit u a tion is sim i lar with nurses-spe cial ists who may con tinue their ed u ca tion in two de grees of “Bach e lor” and “Master” with possible future administrativepositions (of “head’ or “chief” nurse).
We reckon that there are suf fi cient ar gu ments in fa vour of the need for the es tab lish mentof a sys tem of pro fes sional hi er ar chy, in which, ir re spec tive of the ad min is tra tive hi er ar chy,more pos si bil i ties ex ist for shar ing knowl edge, ex pe ri ence, pos si bil i ties and re sults from thepro fes sional de vel op ment of the staff in the healthcare sys tem. Thus, better con di tions will becre ated for so cial co he sion and moral balancing in the healthcare system.
De vel op ment of the healthcare es tab lish ments and the es tab lish ments forpub lic healthcare as “learn ing in sti tu tions”
Ac cord ing to its mis sion, goal, func tions and eco nomic char ac ter is tics, ev ery es tab lish -ment in the healthcare sys tem is “an in tel lec tual or gani sa tion”. What is meant is the mak ing ofa di ag no sis, pre scrip tion and ad min is tra tion of treat ment, the strat egy for sur gi cal in ter ven tion, mon i tor ing, as sess ment and prog no sis of the pa tients’ sta tus, ep i de mi o log i cal and health de -mo graphic anal y sis, as sess ment of the fac tors of the en vi ron ment, etc., re quir ing above all spe -cial ised in tel lec tual la bour, which is ex tremely in ten sive in some cases. There fore, in ouropin ion, this pe cu liar ity of the es tab lish ments of the healthcare sys tem gives rise to the needeach of them to develop as a “learning organisation”.
The con cept of the “learn ing or gani sa tion” (which is known, it is dis cussed in a se ries ofpub li ca tions and we do not need to fo cus on it in fur ther de tail) is based on mu tual trust and un -der stand ing be tween a “leader” and “staff”, change of the leader’s po si tion (who as sumes thefunc tions of a con struc tor of the work and a men tor rather than those of a “boss”); con tin u ousper son nel train ing; grant ing of in de pend ence and re spon si bil ity, de vel op ment of co op er a tionand team work; de vel op ment of com mu ni ca tion and dis sem i na tion of in for ma tion in the
361
Pros pects for the de vel op ment of the healthcare re form
organisation, which creates “management of an open book”. This con cept and model of be hav iour are to tally in ap pli ca ble un der con di tions of
liberalisation and de cen trali sa tion of the healthcare sys tem to gether with the greater ad min is -tra tive, eco nomic and pro fes sional med i cal in de pend ence of the med i cal and healthcare es tab -lish ments. There is no doubt that this model will be very use ful for the moral sta bil ity of ev eryhealthcare es tab lish ment and the system as a whole.
Bal anc ing of func tions, struc tures and com pe tences in the healthcare sys tem
The ra tio nal and bal anced (ad e quate to the needs) in ter nal dis tri bu tion of the el e ments ofthe healthcare sys tem has to be ad dressed in the same di rec tion as the sys tem liberalisation, itsmar ket ori en ta tion and moral sta bil ity. It is also sub ject to ad min is tra tive reg u la tion, es pe ciallyin cer tain sec tors of the healthcare system.
The func tions
The dis tri bu tion of the func tions has a de ter min ing im por tance, re lated to the re cov eryand main te nance of some es sen tial bal ances in the sys tem. The dis tri bu tion of the other el e -ments is a de riv a tive of the func tions dis tri bu tion and facilitates their execution.
Pre ven tive and treat ment func tions
The dis tinc tion of the ex e cu tion and the re spon si bil i ties as so ci ated with the pre ven tiveand treat ment func tions can con sid er ably im prove their bal anc ing and in crease the ef fi ciency of the much needed pre ven tive ac tiv i ties. This dis tinc tion can be car ried out along the line be -tween in di vid ual and public prophylaxis.
The func tions as so ci ated with in di vid ual pro phy laxis which, as we al ready noted, alsocon tain a con sid er able vol ume of di ag nos tic and treat ment ac tiv i ties, should be car ried out inthe field of pri mary med i cal care (with the par tic i pa tion of the spe cial ised med i cal care, too)for all the health in sured per sons, the re spon si bil ity for them be ing as sumed by the re spec tivegen eral prac ti tio ner. An im por tant role for the pre ven tion of the pre vent able mor tal ity isplayed by the Cen tres for Emer gency Med i cal Care and the pre ven tion of com pli ca tions anddis abil ity – by the hos pi tal es tab lish ments. We con sider that these func tions should not only bein cluded in the NFA and the in di vid ual providers’ contracts but their execution should beeffectively controlled.
The func tions of pub lic pro phy laxis (in all its di men sions) are the task of the es tab lish ments for con trol and pro tec tion of pub lic health (RIPCPH). These func tions (State Health Con trol,pro tec tion and con trol of pub lic health) have to be ra tio nally dis trib uted and some of them (pro -duc ing spe cific lab o ra tory and other ser vices, in di cated above) have to be grad u ally con cen trated in a smaller num ber of in sti tu tions, con sid er ably more pow er ful than the ex ist ing ones.
Out pa tients’ and hos pi tal care
The es tab lish ment and the main te nance of a ra tio, ad e quate to the needs, be tween thefunc tions of the out pa tients’ (pri mary and spe cial ised) and hos pi tal med i cal care en ables thera tio nal uti li sa tion of the ca pac ity of the treat ment net work. The key and de bated ques tion inour coun try con cerns the num ber of the hos pi tals and the hos pi tal beds, as so ci ated mainly with
362
the smaller (mu nic i pal) multi-pro file hos pi tals for ac tive treat ment (“the un nec es sary hos pi -tals” and the “un nec es sary hos pi tal beds”). It is known that the func tions of hos pi tal care arein dis pens able from the func tions of out pa tients’ care. When a change in one of them isplanned, the nec es sary change in the other should by no means be un der es ti mated. When wesay “At least 200 hos pi tals in our coun try are un nec es sary” 883, we should im me di ately add“be cause their pa tients will be treated in …”. The bal ance be tween the out pa tients’ and in pa -tients’ care can be achieved by means of a con stel la tion of nor ma tive pro vi sions and ad min is -tra tive mea sures and it can be fa cil i tated by mar ket in cen tives, but they should de velopsi mul ta neously in the outpatients’ and inpatients’ care.
Fur ther more, se ri ous at ten tion should be paid to the bal ance be tween pri mary and spe -cial ised med i cal care which is shifted away from the at ten tion on pri or i ties be cause of the dis -cus sion about the hos pi tals in Bul garia. This bal ance is of pri mary sig nif i cance for theplace ment of the cit i zen and the pa tient in the fo cus of healthcare. The ef fi ciency of the pre ven -tive and treat ment care de pends ex clu sively on the quan ti ta tive and es pe cially on the qual i ta -tive de vel op ment of pri mary me dial care and its in ter ac tion with spe cial ised care. Themain te nance and the im prove ment of this bal ance re quire the in volve ment of ef fec tive or gani -sa tional, ad min is tra tive and eco nomic mech a nisms in order to achieve the best possiblesatisfaction of the citizens’ needs.
The so lu tion of three ques tions should be pre pared in ad vance: (1) to what an ex tent thenec es sary ca pac ity, ac cess and suf fi ciency are en sured (in a quan ti ta tive and qual i ta tive as -pect) to pri mary and spe cial ised out pa tients’ (in clud ing emer gency) med i cal care, which canac com plish treat ment in all cases (in some cases re ha bil i ta tion, too) of the pa tients in home and other out pa tients’ set ting; (2) to what an ex tent pos si bil i ties are en sured for us ing the nec es -sary hos pi tal care in view of the pa tients’ needs and the avail able con di tions. Clar ity of math e -mat i cal pre ci sion has to be pres ent as to who and how will pos si bly sub sti tute the hos pi taltreat ment and re ha bil i ta tion, prac tised cur rently in a cer tain multi-pro file hos pi tal for ac tivetreat ment in spe cific cases; (3) prep a ra tion and ob ser va tion of med i cal in di ca tors for hos pi ta -li sa tion and con di tions for ob ser va tion of the stan dards for the treatment of patients, forwhom hospital treatment is really needed.
When the an swers to these ques tions are avail able, then it can be pro ceeded to the plan ningof the ra tio be tween out pa tients’ and in pa tients’ care. Ac cord ing to the avail able in for ma tion, itcan be con sid ered that, for var i ous rea sons, in many mu nic i pal hos pi tals, the ca pac ity has notbeen used for a long pe riod of time. A great part of the beds in them (and not only in them) hadbeen oc cu pied by pa tients, ad mit ted (to achieve a cer tain rate of uti li sa tion) mainly for so cial rea -sons (be tween 20.0% and 30.0% of all the hos pi ta lised), more over, in many cases, with ran domdi ag no ses along clin i cal path ways, paid by the NHIF. Ac cord ing to an of fi cial pub li ca tion of theMin is try of Healthcare884, the ad mis sion of hos pi tal pa tients with so cial in di ca tion is con sid eredto com prise the “so cial ori en ta tion” of the hos pi tal es tab lish ments’ ac tiv ity. In fact, this is aquasi-so cial ori en ta tion, which dis tances the hos pi tal from the ful fil ment of its sa lient so cialfunc tions. In such a way, a con sid er able share of the hos pi tal ca pac ity is en gaged and re sourcesfrom the NHIF are drained, which have been raised from the cit i zens’ health in sur ance in stal -ments. The hos pi tals have so cial func tions, in deed, but en tirely dif fer ent ones.
363
Pros pects for the de vel op ment of the healthcare re form
883 Trud daily from 30.01.2005 884 Report on the nation’s health at the beginning of 21st century. Anaalysis of the ongoing reform in healthcare.
Published by the MH, Sofia, 2004, p. 122
Here, how ever, it is nec es sary to draw the at ten tion to a spe cific func tion – the in pa tients’care for the pa tients with so cial in di ca tions. Once such pa tients are ad mit ted as a rule to hos pi -tals for ac tive treat ment, the need is ob vi ous for the de vel op ment of this func tion, which has tooth er wise be ful filled by other es tab lish ments. Thus, the ca pac ity will be sig nif i cantly re lievedto gether with the fi nan cial bur den for the hospitals for active treatment.
The pros pects for the mu nic i pal ity hos pi tals will be de ter mined by their pro pri etors, e.g.the City Coun cils, which have to take into con sid er ation both the re quire ment for the HealthMap of the coun try and the in flu ence and the con se quences of the med i cal, so cial andeconomic factors.
Med i cal and so cial func tions
The in ter re la tion and complementation of the health and so cial pol icy of the state en suresa max i mum ef fec tive ap proach to the pro tec tion and the re cov ery of health, cor re spond ing toits so cial pre-de ter mi na tion. In this con text, the bal anced de vel op ment of the med i cal andso cial func tions of the healthcare sys tem and its in ter ac tion with the ser vices for so cial pol icysig nif i cantly broad ens the pos si bil i ties for the im prove ment of the na tion’s health. In or der toachieve this bal ance, it is nec es sary to pay greater at ten tion to the so cial as pects of thehealthcare system and to the health aspects of the social policy.
The ne glected de vel op ment of the so cial func tions in the Bul gar ian healthcare sys tem and the in suf fi cient in ter ac tion with the ser vices for so cial as sis tance, work ing safety, chil dren’spro tec tion as well as or gani sa tions of pa tients, peo ple with dis abil i ties (dis abled, with vi sion or hear ing im pair ment) and for con sum ers’ pro tec tion dis turb this nec es sary bal ance. In or der tobuild and de velop it, the so cial con tent of the healthcare sys tem has to be en hanced and themed i cal as pects of the so cial in sti tu tions, bod ies and or gani sa tions have to be sup ported.Thus, the de vel op ment of in te grated health care will be at tained, from which better positiveeffects have been proved to be expected.
The so cial con tent, which is in her ent to the healthcare sys tem, has to be in tro ducedequally ac tively in the pre ven tive and treat ment ac tiv i ties.
The pre ven tive ac tiv i ties pres ent a wide field for the de vel op ment of so cial func tions interms of pop u lated ar eas, hous ing con di tions, nu tri tion, la bour, chil dren’s and ad o les cents’growth. As an ex am ple, we can give stress pre ven tion and over com ing and its con se quences(es pe cially on the work ing place) and de pres sion con di tions, which re quire not so much med i -cal but so cial in ter ven tion. Stress pre ven tion is also a pro phy laxis for a num ber of or ganic dis -eases, which cur rently pres ent causes for death among the Bulgarian population.
The so cial ac tiv i ties are par tic u larly im por tant in the dis pen sa ries, which are equally ori -ented to pro phy laxis and pre ven tion to gether with the social support.
In the field of the treat ment ac tiv i ties, the so cial func tions pres ent a pow er ful sup port tothe ther a peu tic ef fects and should have a con sid er able ap pli ca tion both in the out pa tients’ (par -tic u larly the pri mary) and hos pi tal care. The de vel op ment of those func tions is par tic u larly im -por tant and it com bines the so cial sup port with the med i cal ac tiv i ties (cur rently con cen trated in hospices and homes for medico-social care).
Par al lel to the de vel op ment of the so cial func tions of the healthcare sys tem, se ri ous at ten -tion has to be di rected to ward the med i cal as pects of the so cial in sti tu tions, bod ies and or -gani sa tions. The or gans and in sti tu tions of the healthcare sys tem should be the ac tive side,bear ing the re spon si bil ity for the interaction with them.
364
Con trol func tions
The or gani sa tion and the dis tri bu tion of the con trol func tions in the healthcare sys temneed ur gent and se ri ous im prove ment to fa cil i tate the elim i na tion of a num ber of de fects. (Here we do not mean the ac tiv i ties of the State Health Con trol, which are ex e cuted by the RIPCPHand the NCRRP in ac cor dance with Art. 11-20 of the LH and whose im ple men ta tion is subjectto control).
Within the short est terms, the dis tri bu tion of the con trol func tions has to be clar i fied andreg u lated in terms of in ter nal and ex ter nal control.
In the field of the ex ter nal con trol, the func tions have to be dis trib uted among the healthad min is tra tion (in clud ing at mu nic i pal level), the health in sur ance or gani sa tion, the pro fes -sional or gani sa tions as well as the or gani sa tions for con sum ers’ pro tec tion, pa tients’ and dis -abled peo ple’s or gani sa tions. It is nec es sary to con sid er ably ex pand and sup port the rights ofthe healthcare ad min is tra tion, the NHIF and the pro fes sional or gani sa tions for the ex e cu tionsof cer tain con trol func tions and, along with them, the li a bil i ties for the ef fi ciency of the con trol ac tiv ity. The con trol or gan has to bear the re spon si bil ity for the out comes of the con trol. Spe -cial at ten tion is re quired to the con trol over all the di men sions and as pects of qual ity of thepre ven tive and treatment activities, especially from the point of view of the consumers.
A most se ri ous at ten tion has to be paid to the func tions of the in ter nal con trol in the veryes tab lish ment, which, as we will have to re peat, is at an ex tremely un sat is fac tory level at themo ment. The def i cits of the in ter nal con trol are some of the main rea sons for the low qual ity,the un reg u lated pay ments, cor rup tion and, as a re sult, the un sat is fied needs and ex pec ta tions of the cit i zens, un der min ing the pres tige and the rep u ta tion as well as the re duced com pet i tive -ness of the es tab lish ment. The in ter nal con trol is a task of the ad min is tra tion and the pro fes -sional organisations in the healthcare establishment.
Struc tural changes
The struc tural changes are par al lel to the changes in the dis tri bu tion of the func tions as the func tions are ful filled by the re spec tive struc tures.
The im per a tive sup ple ment ing of the func tions of the out pa tients’ (pri mary and spe cial -ised) care does not re quire es sen tial struc tural changes.
The changes, nec es sary in the own er ship struc ture, which we reckon to be of cru cial and par tic u lar im por tance, have al ready been men tioned above and we do not need to dis cuss thenfur ther here.
We will, how ever, dis cuss the or gani sa tional struc tural changes as so ci ated with thechanged func tions in the pre ven tive and treat ment sector.
Pre ven tive sec tor
As re gards the pre ven tive sec tor, the or gani sa tional struc tural changes should af fect theex ist ing net work of the RIPCPH through amend ing the nor ma tive reg u la tion. Its or gani sa tionwould have be come more ra tio nal and cor re spond ing to its func tions, if the state con trol ac -tiv i ties were sep a rated in an in de pend ent state con trol or gan. The other ac tiv i ties (lab o ra tory,an a lyt i cal, ex pert, con sul ta tive, ap plied re search and ed u ca tional) can also be sep a rated in in -de pend ent or gani sa tions (com mer cial com pa nies), bound con trac tu ally to the state con troland other au thor i ties and or gani sa tions. Struc tur ally, they may be con sid er ably smaller in
365
Pros pects for the de vel op ment of the healthcare re form

num ber but their main te nance should be car ried out not di rectly from the state bud get but fromthe resources coming from the concluded contracts and performed activities.
Ther a peu tic sec tor
Con cern ing the or gani sa tional struc tural changes in the ther a peu tic sec tor, in our views,it is nec es sary to make a well-ar gued cate gori sa tion of the healthcare es tab lish ments forspe cial ised out pa tients’ and in pa tients’ care, ir re spec tive of their own er ship (pu bic or pri vate).The cate gori sa tion, ex ist ing ac cord ing to the LHE, makes use of an al ready non ex is tent cri te -rion for the hos pi tals – the ter ri to rial scope. The cri te ria in this case have to be based not on thevol ume of ac tiv i ties (num ber of hos pi ta lised pa tients, num ber of beds, etc.) but on spe ciali sa -tion (types of specialised care) and the quality of the performed functions.
In this sense, the above healthcare es tab lish ments can con di tion ally be di vided into na -tional, dis trict and mu nic i pal, and in each of these groups, at least two groups can be dis tin -guished. For ex am ple, a na tional multi-pro file hos pi tal will be ac cred ited for Cat e gory A, if itex e cutes all kinds of med i cal care in its pro files at high mod ern level, and for Cat e gory B, if notall types of med i cal care are of fered in the way they are of fered in Cat e gory A. For a mu nic i palmulti-pro file hos pi tal of Cat e gory A, it will be nec es sary that the care in the pro files of fered in it,are at the level of a dis trict hos pi tal, e.g. in a mu nic i pal hos pi tal of Cat e gory A, prob a bly not allthe di ag no ses in a cer tain spe cialty will be of fered as they will be in a dis trict hos pi tal (i.e. it willhave a smaller scope of ac tiv i ties), but the ad mit ted pa tients will be treated at least at the level of a dis trict hos pi tal. A sim i lar prin ci ple can also be used for the cate gori sa tion of the spe cial ised hos -pi tals as well as of the di ag nos tic, con sul ta tive and med i cal, med ico-con sul ta tive, den tal con sul -ta tive and den tal cen tres and the in de pend ent med i cal di ag nos tic lab o ra to ries. The cate gori sa tion of the spe cial ised hos pi tals can be car ried out along sim i lar prin ci ples as well as of the di ag nos ticand con sul ta tive and med i cal, med ico-den tal and den tal cen tres and the in de pend ent med ico-di -ag nos tic lab o ra to ries. The cat e go ries of healthcare es tab lish ments should be reg is tered on the re -spec tive health maps. The cate gori sa tion of the healthcare es tab lish ments will be use ful for thede vel op ment of com pe ti tion and mar ket ori en ta tion as well as for the con trol and the as sess mentof hos pi tal and out pa tients’ ac tiv ity.
The or gani sa tional struc tural changes in the ther a peu tic cen tre are com pli cated mainlybe cause of the dif fer ent own er ship of the pub lic healthcare es tab lish ments. For this rea son(and for other rea sons, too) these changes have to be based on ob jec tive, sta ble and con vinc ingev i dence. When the nec es sary changes af fect healthcare es tab lish ments with 100% state prop -erty of the cap i tal, the con sid er ations will have to be made solely by the state (the min is ter ofhealthcare). If, how ever, the changes af fect healthcare es tab lish ments with mixed (state andmu nic i pal) or only mu nic i pal own er ship, cat e gor i cal ar gu ments are nec es sary to per suadenot only the mu nic i pal au thor i ties but the cit i zens, too, in the need for the pro posed change, bymeans of which the health ser vices would not de te ri o rate. Oth er wise, no city coun cil andmayor will as sume the re spon si bil ity for the closing down or restructuring of the respectivehealthcare establishment.
In the ther a peu tic sec tor, the or gani sa tional struc tural changes will af fect pri mar ily hos pi -tals with 100% mu nic i pal own er ship of the cap i tal. Their fur ther de vel op ment de pends on thede ci sion of the pro pri etor, based on a num ber of de mo graphic, med i cal, so cial and eco nomicpre req ui sites (the po lit i cal af fil i a tions should be ex cluded) and anal y ses as well as the in ten -tions for privatisation. We will once again note that this de ci sion has to re flect a suf fi ciently
366
well-grounded vi sion of the healthcare es tab lish ments and the con se quences from itspreservation, restructuring or closing.
In this con text, the cre ation of hos pi tal com plexes can also be con sid ered, with the par -tic i pa tion of sev eral closely sit u ated hos pi tals, un der some le gal form of vol un tary uni fi ca tionof com mer cial com pa nies (con sor tium, hold ing), with out chang ing the own er ship. A hos pi talcom plex un doubt edly cre ates better pos si bil i ties for the ra tio nal uti li sa tion of the ca pac ity, lo -gis ti cal connections and staff qualification.
As re gards the fu ture of the hos pi tal, sev eral forms can be con sid ered:
· pres er va tion of the hos pi tal as an in de pend ent es tab lish ment, if the owner judges that ithas pros pects as such;
· pres er va tion of the hos pi tal as a struc ture of a larger hos pi tal ag glom er a tion (hos pi talcom plex), which is re lated to a change in the hos pi tal status;
· re struc tur ing of the hos pi tal into a di ag nos tic-con sul ta tive, med i cal or med ico-den talcen tre, the new com mer cial com pany pre serv ing its in de pend ence or be ing in cluded ina larger agglomeration;
· re struc tur ing of the hos pi tal into an other in pa tients’ es tab lish ment (com mer cial com -pany) such as a home for med ico-so cial care, hos pice or (if Art. 10 of the LHE isamended) nursing home.
In the re struc tur ing of the hos pi tal, by a de ci sion of the City Coun cil, more than one in de -pend ent es tab lish ments (com mer cial com pa nies) can be es tab lished, for ex am ple, a med i calcen tre and a hos pice, a med i cal cen tre and a nurs ing home, an in de pend ent med ico-di ag nos ticlab o ra tory and a nurs ing home, a nurs ing home and a hos pice, etc. What is im por tant is that theavail able ca pac ity and the fa cil i ties are used to a max i mum de gree for the ac ces si ble sat is fac -tion of the pa tients’ needs.
Sys tem for con trol
The main ne ces sity as re gards the con trol of the healthcare sys tem is the es tab lish ment ofa con cept and a sys tem for con trol. It should not re sem ble a po lic ing func tion (“catch ing” vi o -la tors) but should pres ent a man age ment in stru ment for the de vel op ment of healthcare. Thissys tem must en sure the tech no log i cal unity and ef fi ciency of the ex ter nal, in ter nal con trol andper sonal con trol (self-control and self-assessment).
As ob vi ous from the avail able ma te ri als, in terms of ex ter nal con trol, the prob lems are re -lated to the or gani sa tion and the ef fi ciency of the con trol ac tiv i ties and not to the ab sence of con -trol or gans. Such bod ies are in place at the Min is try of Healthcare, the NHI and the pro fes sionalor gani sa tions. The ex ist ing reg u la tions, how ever, pro vide mainly for the tech nol ogy, to a con sid -er ably lower de gree, for the or gani sa tion, and al most to no ex tent, for the re spon si bil i ties for thecon trol out comes and ef fi ciency. This is prob a bly the rea son why, for so many years (since 2000un til now), in the pub lished data on the con trol ac tiv ity of the NHIF, one and the same breacheshave been re ported. There fore, we con sider it nec es sary to or gan ise mon i tor ing of the out -comes from the ex e cu tion of con trol ac tiv i ties in side the con trol or gans them selves.
The in ter nal con trol is in a far more fa vour able po si tion in the es tab lish ments forhealthcare (ex cept for some of them such as lab o ra to ries and phar ma cies, for which it is tech -no log i cally in ev i ta ble). It is nec es sary for the in ter nal con trol to be reg u lated as an ac tiv itywhich is man da tory for the es tab lish ment, ir re spec tive of its own er ship and not only stip u -
367
Pros pects for the de vel op ment of the healthcare re form
lated in the in ter nal or der reg u la tion. It must not only be ex e cuted by the Med i cal Con trolCom mis sion (Art. 77 of the LHE), the head of the ward (clinic or lab o ra tory) (Art. 71 of theLHE) and the head nurse (Art. 70 of the LHE) as well as by other struc tures of the es tab lish -ment, but it should also in clude def i nite pro ce dures, doc u men ta tion and out comes, for whichthe man ager of the respective healthcare establishment should bear the responsibility.
The self-con trol does not re quire a struc tural for ma tion. As an in di vid ual ob li ga tion, ithas to be an ex pres sion of an in ter nal ne ces sity of phy si cians and other per son nel for over com -ing mis takes or in suf fi cient knowl edge and skills. This ne ces sity is ed u cated dur ing the un der -grad u ate and post grad u ate train ing as well as with the as sis tance and fa cil i ta tion by thead min is tra tion and the professional organisations.
Dis tri bu tion of com pe tences
The bearer of the com pe tences is the per son nel, but in this case, it con cerns not the phys i -cal in di vid u als, even with equal ed u ca tional de gree and spe cialty, but the de gree of “ca pa bil -ity” to ac com plish cer tain work with a fixed ex pected re sult. The more spe cial ised skills arere quired for cer tain work and the re sults from it, the higher the com pe tences its executorshould possess.
For the func tion ing of the healthcare sys tem, nu mer ous types of com pe tences are nec es -sary but two main types of them have a spe cific ap pli ca tion, e.g. the med i cal and the man a ge -rial. Their pres ence or ab sence ex erts ex treme im pact on the sep a rate healthcare es tab lish ment, and their unity – on the over all healthcare sys tem. The sta bil ity and the prog ress of the es tab -lish ment re quire that high med i cal and man a ge rial com pe tences be char ac ter is tics of the whole es tab lish ment and not of sep a rate in di vid u als or parts of it. The healthcare es tab lish ment as anover all or gani sa tion must pos sess high com pe tences and, if such competences are not grantedeverywhere, they should be added.
The dis tri bu tion of the com pe tences in the healthcare sys tem im plies the de vel op ment and in tro duc tion of a mech a nism, by means of which the es tab lish ments in the healthcare sys temen sure to them selves the nec es sary med i cal and man a ge rial com pe tences. Two con di tions arenec es sary for the set ting up of such a mech a nism. The first one is the pres ence of a cri te rion(or cri te ria) in the es tab lish ment for high com pe tences. In many cases these cri te ria are low -ered, based on rou tine prac tices, jus ti fied by the un sat is fac tory ma te rial con di tions and the de -fi ciency of fi nanc ing. In such sit u a tions what is most fre quently lack ing is not knowl edge butwill, strife and ap proach to change. The sec ond con di tion is to have a real ised need for cer tainhigh com pe tences. This need can be real ised only when the es tab lish ment faces re quire mentsfor high qual ity of all the per formed (med i cal and man a ge rial) ac tiv i ties. Due to the con sum -ers’ in sis tence this need will be come in creas ingly per ceived, but it will in ev i ta bly becomemore and more acute, especially with the accession of our country to the European Union.
The above men tioned mech a nism is quite a com pli cated pro cess and can not be based only on ad ver tis ing com pe ti tions or pro claim ing ad min is tra tive or ders. The com pe ti tion re quire -ments as well as the ad min is tra tive en force ment not al ways en sure high com pe tences. The es -sence of this mech a nism has to be mar ket based (de mand and sup ply) and to be car ried outthrough a mu tu ally ben e fi cial agree ment be tween two in de pend ent part ners – the healthcareestablishment and the competent specialist.
The prob lems with the med i cal com pe tences stand out pri mar ily (though not only) in thesmall healthcare es tab lish ments – mu nic i pal hos pi tals, di ag nos tic and con sul ta tive and med i -
368
cal cen tres. The re al ity in di cates that the fur ther ex is tence of these es tab lish ments – pres er va -tion, re struc tur ing or clos ing down – is in close re la tion ship with the con cen tra tion of highmed i cal com pe tence in the pro files of their ac tiv i ties or the de vel op ment of new pro files. Thiswould in crease their pop u lar ity and the de mand for their care by the cit i zens. It would also ex -pand the pos si bil i ties for in com ing fi nan cial re sources and could pres ent a se ri ous con tri bu tion for the train ing of the phy si cians’ and other staff in the re spec tive healthcare es tab lish ment.The so lu tion to the prob lem can be achieved in two ways, which are not al ter na tive. The firstone con sists in the train ing and spe ciali sa tion of the hos pi tal’s own staff. This is an ap pro pri ateap proach which, how ever, re quires a lon ger pe riod of time. The sec ond one is the at trac tion ofspe cial ists of higher com pe tence from other healthcare es tab lish ments. The im ple men ta tion ofthis ap proach first re quires the find ing of a spe cial ist, who is will ing to and is ca pa ble of im -prov ing the work ing level in the respective specialty and, second, the healthcare establishment(ward) to be attractive enough for the specialist it is looking for.
Equal (even greater at the mo ment) at ten tion is re quired by the in crease of the man a ge -rial com pe tences in the units of the en tire sys tem. These com pe tences are also un equally dis -trib uted and there fore, their level in the sys tem is un sat is fac tory as a whole. This is ap par entfrom a num ber of in di ca tors for the ac tiv ity and the out comes of the sys tem, re ports, ma te ri als,anal y ses and numerous observations.
In our opin ion, the in suf fi cient man a ge rial com pe tences are due to the low nor ma tivelyspec i fied re quire ments in this re spect. Ac cord ing to the Law on Healthcare Es tab lish ments(Art. 63, §1), the po si tion of a man ager of the healthcare es tab lish ment can be oc cu pied by aper son with a Mas ter’s De gree in med i cine or den tistry, ac quired ma jor spe cialty and the qual i -fi ca tion in healthcare man age ment (ac cord ing to Reg u la tion ¹ 9 from 2001 with a min i mumof 200 ac a demic hours) or a Mas ter’s De gree in eco nom ics and man age ment and an ac knowl -edged spe cialty in health eco nom ics (or med i cal in for ma tics and healthcare man age ment). Ac -cord ing to the Law on Health (Art. 16, §2), for the po si tion of a di rec tor of RIPCPH, a Mas ter’s de gree is re quired in med i cine, an ac knowl edged spe cialty and five-years’ work ing ex pe ri ence in the spe cialty. No men tion is made at all about man a ge rial com pe tence. What is even moreweird is that, ac cord ing to the Law on Health (Art. 9, §2), for a di rec tor of a RHC (the “su -preme com mander” of the healthcare in a dis trict), the only re quire ment is that the personoccupying it has a three-year working experience in medicine or dentistry (!).
Fur ther more, the de fi cien cies in the man a ge rial com pe tences do not end at the level of thedi rec tors and man ag ers of the es tab lish ments and the ad min is tra tion in the healthcare sys tem. At -ten tion must be paid to the man a ge rial com pe tences at the lower man age ment lev els, too. One ofthem is the hos pi tal ward (clinic), in which the spe cific hos pi tal func tions are vir tu ally car riedout. The head of a ward man ages a num ber of func tions, pro cesses and re sources, but for this po -si tion, no qual i fi ca tion in man age ment is re quired (LHE, Art. 68, §2 and 3 and Art. 71).
In gen eral, the ne ces sity for the de vel op ment of the man a ge rial com pe tences re sults froman in ev i ta bly law ful in crease of the dis tri bu tion of la bour. In mod ern times it gives rise toad vance ment of the man age ment sci ences and the professionalisation in this field. This is anob jec tive pro cess and not a con junc ture phe nom e non. The mod ern healthcare sys tem and ev -ery sep a rate healthcare or gani sa tion is al ready a rather com plex con struc tion, which is why itre quires pro fes sional man age ment. Ap par ently, it can not be car ried out based on the ex ist ingnor ma tive reg u la tion. With the nor ma tive re quire ments, stip u lated in the cur rent leg is la tion,the man a ge rial com pe tences in the healthcare sys tem are doomed not to exceed the level of the
369
Pros pects for the de vel op ment of the healthcare re form

basic administrative functions.For the so lu tion of this prob lem, a fa vour able role was played by the train ing in healthcare
man age ment, or gan ised in the be gin ning of 1990s in our coun try (with the sup port of a num ber of state and in ter na tional or gani sa tions), which was at tended by a con sid er able num ber of spe -cial ists. Ev ery year since 1999, one com mence ment has grad u ated Varna Med i cal Uni ver sityin the spe cialty of healthcare man age ment. Ev ery year tens of spe cial ists are trained at var i ousmed i cal and eco nomic uni ver si ties within Mas ter’s programmes or qual i fi ca tion im prove -ment. A sus tain able foun da tion has been laid down for the de vel op ment of train ing and re -search. How ever, the ne ces sity is not real ised for a broader ap pli ca tion of the high managerialcompetences in the healthcare system.
A pos si ble so lu tion of the prob lem with the man age ment professionalisation con sists inthe leg is la tive guar an tee of con di tions for the professionalisation of the man age ment in thehealthcare sys tem, with nor ma tive re quire ments, sim i lar to the med i cal professionalisation. Inthe pres ence of al ready a con sid er able num ber of spe cial ists with ac a demic qual i fi ca tion inhealthcare man age ment, the ad e quate up dat ing of re quire ments to the man a ge rial po si tionsand the cor re spond ing pro ce dures will es tab lish con di tions for the professionalisation of theman age ment in the healthcare sys tem. This, of course, will be also con nected with the in creas -ing requirements to the organisation and the content of the training.
370
CON CLU SION
The main con clu sions of the pres ent study have been out lined in the text and we have at -tempted to sys tema tise them at the end of our pre sen ta tion. We reckon that, still, it is not ir rel e -vant in sum ming up (with out be ing re dun dant) to emphasise the main les sons, which at least tous, are im por tant for the healthcare re form and the de vel op ment of the healthcare sys tem.
Above all, it should be clear enough that the im prove ment of the na tion’s health level is atask and re spon si bil ity of the state with its three pow ers, e.g. the leg is la tive, the ex ec u tive andthe ju di cial. The so-called “shared re spon si bil ity” (among the state, the so ci ety and the cit i zen) as a cru cial el e ment of the healthcare re form re mains an ex pres sion ‘void of mean ing” and, in deed,a trans fer of re spon si bil ity, un less the state cre ates the nec es sary con di tions (leg is la tive, eco -nomic, cul tural and so cial) for shar ing the re spon si bil ity. The re spon si bil ity will be come shared,when the state be gins to cre ate the con di tions for that. If the state cares (which it should) aboutthe de te ri o ra tion of the de mo graphic pro cesses in Bul garia, it should ad dress its at ten tion to thealarm ing dy nam ics of the mor tal ity rate and to the pre vent able mor tal ity, in par tic u lar, for whichthe main rea son is the health def i cit and mea sures for the health pro tec tion of the na tion.
For a healthcare re form to be car ried out in an ef fi cient way, a ma jor im por tance isplayed by the cre ation of fa vour able con di tions, e.g. a “re form en vi ron ment”, which isalso re lated to the liberalisation of the healthcare sys tem. This ne ces si tates the har mo nisedef forts of the healthcare ad min is tra tion at all lev els, the healthcare es tab lish ments and staff through out the healthcare sys tem, the sci en tific com mu nity, the busi ness, the trade un ions, the civil or gani sa tions and the me dia. The re form en vi ron ment in cludes the endeavour tofa cil i tate the de vel op ment of the healthcare sys tem in ways, which have been proved toyield the de sired ef fect on the na tion’s health. The for ma tion of such an en vi ron ment is acon tin u ous pro cess of a well-in tended bi lat eral di a logue, mu tual in flu ence and pres sure.Above all, it is di rected from the healthcare sys tem to the rep re sen ta tives of the com mu -nity, and then, from them to the healthcare sys tem. In the mean time, it should take placefrom the healthcare ad min is tra tion and the fi nanc ing or gani sa tions to the ex e cut ing or -gani sa tions, and vice versa. This in ter ac tion will give rise to the mu tual un der stand ingwhich should sup port the moral bal anc ing of the healthcare sys tem and es tab lish a solidfoun da tion for the healthcare re form. The Min is ter of Healthcare should be the chief con -struc tor of this pro cess.
In the pro cess of the healthcare re form, the eco nomic prob lems of the healthcare sys tembe come in creas ingly dis tinct, al though they are of ten ex ag ger ated. Hav ing been ac cu mu latedfor years, they are now deeply rooted and com pli cated. There fore, their over com ing re quiresad e quately complex decisions.
It is al ready high time it is real ised in our coun try that the prob lems with the na tion’shealth are not prob lems of the healthcare sys tem but of the fu ture and the fate of our state.There fore, we have to once and for ever de ci sively dis con tinue the prac tice of the “re sid ual fi -nanc ing” and ter mi nate the ap pli ca tion of eco nomic ap proaches, which are only tran sientlyben e fi cial and prob a bly ap pro pri ate for any thing else but the so lu tion of the healthcare prob -lems of the nation and the state.
The change in the eco nomic re la tions in the healthcare sys tem is of cru cial im por tance. If the sys tem and the eco nomic re la tions, mech a nisms and in stru ments are pre served in their cur -
371
rent form, the healthcare sys tem will ab sorb fi nan cial re sources quan tum sattis885. The sys -tem will con tinue to ex pe ri ence an acute need for fi nances, even af ter the in crease of thein stal ments for the oblig a tory health in sur ance, the ad di tional pay ment and the sell ing of build -ings and hos pi tal ter rains. There is no doubt that the money is needed but, in or der to achievethe de sired ef fect, they have to find their place in a cor re spond ingly changed eco nomic en vi -ron ment. The healthcare re form needs to be con tin ued and de vel oped within the radicaleconomic reform which started a decade ago.
372
885 Quantum sattis (Latin) – as much as it can absorb.
BIBLIOGRAPHY
1. Àëôà Ðèñúð÷. Ïðîó÷âàíå íà îáùåñòâåíîòî ìíåíèå çà çäðàâíàòà ðåôîðìà. Ñîôèÿ, 20022. Àïîñòîëîâ, Ì., Ï. Èâàíîâà. Èñòîðèÿ íà ìåäèöèíàòà è ñåñòðèíñòâîòî. “Ãðàôèê-êîíñóëò”, Ñ., 19983. Áàëàáàíîâà, Ä., Ñ. Öîëîâà, Å. Äåë÷åâà. Àíàëèç íà ïîëèòèêàòà ïî îòíîøåíèå ðåôîðìàòà â
áîëíè÷íàòà ïîìîù â Áúëãàðèÿ. Çàêëþ÷èòåëåí äîêëàä îò èçñëåäîâàòåëñêè ïðîåêò. 20054. Áà÷åâ, Ñ., Îòíîøåíèå íà çäðàâíèòå ðàáîòíèöè êúì çàïî÷íàëàòà ðåôîðìà â çäðàâåîïàçâàíåòî.
Ñòîëè÷íà ëåêàðñêà êîëåãèÿ. Èíôîðìàöèîíåí áþëåòèí, 11-12. 2000 ã., ñ. 4-95. Áîãîåâ Ñ., Ï. Ñàë÷åâ, Ë. Èâàíîâ (Ðåä.) Äîêëàä çà çäðàâåòî íà íàöèÿòà â íà÷àëîòî íà 21 âåê. Àíàëèç
íà ïðîâåæäàíàòà ðåôîðìà â çäðàâåîïàçâàíåòî. Ìèíèñòåðñòâî íà çäðàâåîïàçâàíåòî. Ñ., 20046. Áîíåë, Ì., È. Ñåìåðäæèåâ, Ñ. Õåëìåðñ, Ë. Ðèíäåð, Å. Õåëáåðã, Á. ÌàêÃèíåñ. Äîêëàäè. Â: Ïî
âúïðîñèòå íà ÷àñòíàòà ìåäèöèíñêà ïðàêòèêà â Ðåïóáëèêà Áúëãàðèÿ. Äèñêóñèîííà ìàñà. Ñáîðíèêäîêëàäè. Ñ.,1996
7. Áîðèñîâ, Â. Äåôèöèòúò íà ìåíèäæúðñêà êóëòóðà – áàðèåðà â ïðîöåñà íà çäðàâíèòå ðåôîðìè.Âúâ: â. “Ôîðóì Ìåäèêóñ”, áð. 9, 17.03.1997 ã.
8. Âèòîøà Ðèñúð÷. Ïðåäñòàâè, íàãëàñè è î÷àêâàíèÿ êúì áúëãàðñêàòà çäðàâíîîñèãóðèòåëíàñèñòåìà è äîáðîâîëíèòå çäðàâíè ôîíäîâå. Àíàëèç îò ðåçóëòàòèòå îò äèñêóñèèòå âúâôîêóñ-ãðóïè. Ñ., 2001
9. Âèøíåâñêèé, À. Ã., ß. È. Êóçüìèíîâ, Â. È. Øåâñêèé, È. Ì. Øåéìàí, Ñ. Â. Øèøêèí, Ë. È.ßêîáñîí, Å. Ã. ßñèí. Ðîññèéñêîå çäðàâîîõðàíåíèå: êàê âûòè èç êðèçèñà. ÄîêëàäÃîñóäàðñòâåííîãî óíèâåðñèòåòà. Âûñøåé øêîëû ýêîíîìèêè. Èçäàòåëüñêèé äîì ÃÓ ÂØÝ,Ìîñêâà, 2006
10. Âîäåíè÷àðîâ, Ö. è äð. Çäðàâåîïàçâàíå: îòãîâîðíîñò, ñâîáîäåí èçáîð, ñîëèäàðíîñò. Ñ., 200411. Âîäåíè÷àðîâ, Ö., Â. Áîðèñîâ, Ñò. Ãëàäèëîâ, Ê. ×àìîâ, Ä. Êðúøêîâ, Ìîäåë çà åôåêòèâíî ðàçâèòèå
íà áúëãàðñêîòî çäðàâåîïàçâàíå. Â: ñï. “Çäðàâåí ìåíèäæìúíò”, áð. 2, 2005 ã., ñ. 5-1412. Ãëàäèëîâ, Ñ. Ïàçàðíàòà ñèñòåìà è äúðæàâàòà – ìÿñòîòî èì â ðåôîðìàòà íà
çäðàâåîïàçâàíåòî. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî –ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 19-21.
13. Ãëàäèëîâ, Ñ., Ö. Ïåòðîâà. Ðîëÿòà íà îáùåñòâåíîñòòà â çäðàâåîïàçâàíåòî. Àñïåêòè íàðåôîðìàòà â çäðàâåîïàçâàíåòî. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî– ïðåäèçâèêàòåëñòâà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 55-57
14. Ãðèâà, Õð. Çäðàâåîïàçâàíå: “çàäà÷êà” çà óïðàâëåíöè. Â: ñï. “Ñîöèàëíà ìåäèöèíà”, áð. 3, 2003, ñ. 30-3415. Ãúëúáîâ, À., Àíàëèç íà ðåçóëòàòè îò ñîöèîëîãè÷åñêî èçñëåäâàíå. Ðåãèîíàëåí ñúþç íà áîëíèöèòå
“Ñòàðà ïëàíèíà”, 2000, ñ. 1-816. Äàìÿíîâ, È., Ñ. Áà÷åâ, Å. Ïåòêîâà, Ã. Ëóìáåâ è äð. Îòíîøåíèå íà çäðàâíèòå ðàáîòíèöè êúì
ðåôîðìàòà â çäðàâåîïàçâàíåòî. Â: Íàó÷åí ñèìïîçèóì “Èêîíîìèêà íà çäðàâåîïàçâàíåòî”.Ñáîðíèê äîêëàäè. Ñ., 1992, ñ. 25-30
17. Äåë÷åâà, Å. Åôåêòè íà ðåôîðìèðàíîòî çäðàâåîïàçâàíå – ðàâíîñìåòêàòà íà èêîíîìèñòà. Â: ².Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî – ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 33-39
18. Äåë÷åâà, Å., Ì. Ïîïîâ. Ïàçàðíî ïðîíèêâàíå â çäðàâåîïàçâàíåòî. Âúâ: â. “Ôîðóì Ìåäèêóñ”, áð. 1,2.01.1995 ã. è áð. 2, 9.01.1995 ã.
19. Äèìîâà, À., Å. Àòàíàñîâà, Åì. Ìóòàôîâà. “2-ðè þëè – äåíÿò “Õ”, èëè êúäå ñå ñðåùàòî÷àêâàíèÿòà íà áúëãàðñêèÿ ëåêàð è áúëãàðñêèÿ ïàöèåíò. Â: Ìåæäóíàðîäíà þáèëåéíà íàó÷íàêîíôåðåíöèÿ íà ÈÓ-Âàðíà - þíè 2000 ã. Ñáîðíèê äîêëàäè. Âàðíà, 2002, ò. 4, ñ. 192-198
20. Çàôèðîâà, Öâ., Ì. Êåõàéîâà. Èçñëåäâàíå íà ïîòðåáèòåëñêàòà îöåíêà çà áîëíèöèòå è áîëíè÷íîòîîáñëóæâàíå âúâ Âàðíåíñêà îáëàñò è ïðèëîæåíèåòî ìó ïðè âçåìàíåòî íà ñòðàòåãè÷åñêèðåøåíèÿ. Â: Ãîäèøíèê íà Èêîíîìè÷åñêè óíèâåðñèòåò-Âàðíà, 73, 2001, ñ. 1-47
21. Çëàòàíîâà Ò., À. ×åøìåäæèåâà, ß. Ïðîäàíîâà, Ñ. Áà÷åâ, Ã. Çëàòàíîâà. Åäèíñòâî âúâ âèæäàíèÿòà íàïàöèåíòè è ëåêàðè çà çäðàâíàòà ðåôîðìà â Áúëãàðèÿ. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ“Çäðàâåîïàçâàíåòî – ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 71-75.
22. Êèòàíîâà, Ì., Å. Äåë÷åâà. Íåîáõîäèìà ëè å çäðàâíîîñèãóðèòåëíà ñèñòåìà. Âúâ: â. “ÔîðóìÌåäèêóñ”, áð. 3, 25.08.1990 ã.
373
23. Ëóìáåâ, Ã., Ñ. Áà÷åâ, Å. Ïåòêîâà, Ç. Ãëóòíèêîâà è äð. Îòíîøåíèå íà íàñåëåíèåòî êúì ðåôîðìàòàâ çäðàâåîïàçâàíåòî (Ðåçóëòàòè îò åäíî àíêåòíî ïðîó÷âàíå íà îáùåñòâåíîòî ìíåíèå). Â:Íàó÷åí ñèìïîçèóì “Èêîíîìèêà íà çäðàâåîïàçâàíåòî”. Ñáîðíèê äîêëàäè. Ñ., 1992, ñ. 30-37
24. Ëüî÷êîâà, Ì., Ì. Ñåìåðäæèåâà, Ð. Ñòåôàíîâ. Èçâúíáîëíè÷íàòà ïîìîù â ãð. Ïëîâäèâ –ðåòðîñïåêöèè è ïåðñïåêòèâè. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî–ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 131-135
25. Ìàðêîâà, Í. Èêîíîìè÷åñêî ðàçâèòèå è óïðàâëåíèå íà çäðàâíî çàâåäåíèå â ïåðèîä íà ïðåõîä îòáþäæåòíî ôèíàíñèðàíå êúì çäðàâíîîñèãóðèòåëíà ñèñòåìà. Âúâ: â. “Çäðàâå”, 28-29.05.1992
26. Ìèíàñÿí, Ã. Èêîíîìèêàòà íà Áúëãàðèÿ â êðàÿ íà ÕÕ â.: ñúãëàñóâàíå íà öåëè è èíòåðåñè. Èçä.Ôîíäàöèÿ “Ñâîáîäíà èíèöèàòèâà”, Ñ., 1999
27. Ìèíèñòåðñòâî íà çäðàâåîïàçâàíåòî. Êàëåíäàð çà ïîñòèãíàòîòî îò ïðàâèòåëñòâàòà íà Ð.Áúëãàðèÿ â îáëàñòòà íà çäðàâåîïàçâàíåòî â ïåðèîäà 1997-2000 ã. Ñ., 2001
28. Ìèíèñòåðñòâî íà çäðàâåîïàçâàíåòî. Íàöèîíàëíà çäðàâíà ñòðàòåãèÿ “Ïî-äîáðî çäðàâå çàïî-äîáðî áúäåùå íà Áúëãàðèÿ”. Ñ., 2001
29. Ìèíèñòåðñòâî íà çäðàâåîïàçâàíåòî. Ïëàí çà äåéñòâèå êúì Íàöèîíàëíàòà çäðàâíà ñòðàòåãèÿ çàïåðèîäà 2001-2006 ã. Ñ., 2001
30. Ìèíèñòåðñòâî íà çäðàâåîïàçâàíåòî. Ðàçâèòèå íà ïúðâè÷íàòà çäðàâíà ïîìîù â ÐåïóáëèêàÁúëãàðèÿ. Ñ., 1996
31. Ìèíèñòåðñòâîòî íà ôèíàíñèòå. Ôèíàíñèðàíå è óïðàâëåíèå íà çäðàâåîïàçâàíåòî. Òåîðåòè÷íèîñíîâè, ìîäåëè, ïðîáëåìè è òåíäåíöèè. Äèðåêöèÿ “Áþäæåò”, îòäåë “Ìèêðîèêîíîìè÷åñêèàíàëèçè”. Ñ., 2005
32. Ìèõàéëîâà, Ë. Âúòðåøíèÿò êîíòðîë â óïðàâëåíèåòî íà ëå÷åáíèòå çàâåäåíèÿ. Äîêòîðñêàäèñåðòàöèÿ. 2005
33. Ìóòàôîâà, Åì., Å. Àòàíàñîâà, À. Äèìîâà, Áúëãàðñêèÿò ïàöèåíò – ìåæäó äîáðîâîëíîòî èçàäúëæèòåëíîòî çäðàâíî îñèãóðÿâàíå. Â: Ìåæäóíàðîäíà þáèëåéíà íàó÷íà êîíôåðåíöèÿ íàÈÓ-Âàðíà – þíè 2000 ã., Ñáîðíèê äîêëàäè. Âàðíà, 2002, ò. 4, ñ. 186-191
34. ÍÎÅÌÀ. Îáùåñòâåíîòî ìíåíèå çà çäðàâíàòà ðåôîðìà. Êîëè÷åñòâåíî è êà÷åñòâåíî èçñëåäâàíå.Îáîáùåí äîêëàä. ßíóàðè 2002 ã.
35. ÍÑÈ. Æèçíåíî ðàâíèùå íà íàñåëåíèåòî â Áúëãàðèÿ. Ñ., 199636. ÍÑÈ. Ñîöèàëíî-èêîíîìè÷åñêî ðàçâèòèå íà Ðåïóáëèêà Áúëãàðèÿ ïðåç ïåðèîäà 1990-1993 ã.
Ñòàòèñòè÷åñêî èçäàòåëñòâî è ïå÷àòíèöà, Ñ., 199437. ÍÑÈ. Ñîöèàëíî-èêîíîìè÷åñêî ðàçâèòèå. Ñ., 2004 ã.38. ÍÑÈ. Ñòàòèñòè÷åñêè ñïðàâî÷íèê. Èçä. ÖÑÓ, Ñ., 199039. ÍÑÈ Ñòàòèñòè÷åñêè ñïðàâî÷íèê 2004. Ñ., 200540. ÍÑÈ, ÍÖÇÈ. Çäðàâåîïàçâàíå (çà ñúîòâåòíèòå ãîäèíè). Ñ., 1992, 1993, 1994, 1996, 1997, 1998, 2000,
2001, 2002, 2003, 2004, 2005, 200641. Ïàâëîâ, Í., Ïðèâàòèçàöèÿòà íà ñîöèàëíîòî îñèãóðÿâàíå – àëòåðíàòèâè è åôåêòè. Âúâ: â.
“Çàñòðàõîâàòåë”, áð. 18, 26.09.-10.10.2001 ã. è áð. 19, 11.10.-25.10.2001 ã.42. Ïàâëîâà Ì., Â. Ãðîîò, Ã. âàí Ìåðîäå. Ïðÿêà è êîñâåíà îöåíêà íà ïîòðåáèòåëñêèòå ïðåäïî÷èòàíèÿ
â ñôåðàòà íà çäðàâåîïàçâàíåòî. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî –ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 63-69
43. Ïàñõàëèäèñ, Ê. Âúðõó íåîáõîäèìîñòòà îò îáùåñòâåíà îöåíêà íà çäðàâíàòà ðåôîðìà.Äîêòîðñêà äèñåðòàöèÿ. Ñ., 2003
44. Ïåòðîâà Ã. Ìîäåë íà ðåôîðìàòà íà ôàðìàöåâòè÷íèÿ ñåêòîð â Áàëêàíñêèÿ ðåãèîí – àíàëèç íàèçïîëçâàíèòå ñòðàòåãèè. Äîêòîðñêà äèñåðòàöèÿ. 2003
45. Ïðîäàíîâà ß., À. ×åøìåäæèåâà. Èíôîðìàöèîííî îñèãóðÿâàíå íà çäðàâíàòà ðåôîðìà. Â: ².Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî – ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 59-62.
46. Ïîïîâ, Ì. (Ðåä.). Çäðàâíàòà ðåôîðìà â Áúëãàðèÿ. Èçä. “Ìàêåäîíèÿ-Ïðåñ”, Ñ., ÷àñò ïúðâà, 1997, è÷àñò âòîðà, 1998
47. Ïîïîâ, Ì., Á. Äàâèäîâ, Îñèãóðÿâàíå íà ïîäêðåïàòà íà îáùåñòâåíîòî ìíåíèå çà ðåôîðìàòà íàçäðàâíàòà ñèñòåìà. Àêòóàëíà êîìóíèêàöèîííà ïîëèòèêà â çäðàâåîïàçâàíåòî. Èçä. ÍÖÇÈ, Ñ., 2000
374
48. Ïîïîâ, Ì., Ã. Êàçàíäæèåâ, “Âúòðåøåí ïàçàð” íà çäðàâíè äåéíîñòè. Âúâ: â. “Ôîðóì Ìåäèêóñ”,áð. 15, 13.04.1992 ã.
49. Ïîïîâ, Ì., Æ. Ãîëåìàíîâà, Õèãèåííî-åïèäåìèîëîãè÷íàòà ìðåæà â Áúëãàðèÿ: èçãðàæäàíå èðàçâèòèå, ïîñòèæåíèÿ è ïðîáëåìè. Èçä.ÑÕÅÈ, Ñ., 2001
50. Ïîïîâ, Ì., Ç. Êðàåâ. Çäðàâíàòà ðåôîðìà – ïîëèòèêà è ñòðàòåãèÿ â óñëîâèÿòà íà ïàçàðíàèêîíîìèêà. Èçä. Ôîíäàöèÿ “Ñâîáîäíà èíèöèàòèâà”, ¹ 34 îò ïîðåäèöà “Ïðîáëåìè íà ïðåõîäà âÁúëãàðèÿ”, 1994
51. Ïúòÿò íà Áúëãàðèÿ êúì “Çäðàâå çà âñè÷êè”. Èçä. “Ìåäèöèíà è ôèçêóëòóðà”, Ñ., 198752. Ðîõîâà, Ì., Ì. Âúëêàíîâà. Ïðîó÷âàíå îòíîñíî ïðàâàòà íà ïàöèåíòèòå è òÿõíàòà ïîïóëÿðíîñò
ñðåä îáùåñòâåíîñòòà. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ “Çäðàâåîïàçâàíåòî –ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ. 101-106
53. Ñåìåðäæèåâ, È. Îáùè ïàðàìåòðè íà çäðàâíàòà ðåôîðìà â Áúëãàðèÿ. Â: Ìèíèñòåðñòâî íàçäðàâåîïàçâàíåòî. Íàöèîíàëíà êîíôåðåíöèÿ ïî çäðàâíàòà ðåôîðìà â Ðåïóáëèêà Áúëãàðèÿ.24-25.04.1998 ã., Ñîôèÿ. Ñòåíîãðàìà. Èçä. “Ìàêåäîíèÿ-Ïðåñ”, Ñ., 1998, ñòð. 12-59
54. Ñåìåðäæèåâ, È. Îáùè ïàðàìåòðè íà ìàêðîðàìêàòà çà ðàçâèòèå íà ÷àñòíàòà ìåäèöèíñêàïðàêòèêà â Ðåïóáëèêà Áúëãàðèÿ. Â: Ïî âúïðîñèòå íà ÷àñòíàòà ìåäèöèíñêà ïðàêòèêà â ÐåïóáëèêàÁúëãàðèÿ. Äèñêóñèîííà ìàñà. 13-15.12.1996 ã. Ñáîðíèê äîêëàäè. Ñ., 1996, ñ. 73-98
55. Ñåìåðäæèåâ, È. Äÿñíàòà àëòåðíàòèâà â çäðàâåîïàçâàíåòî – êðàòêî îïèñàíèå íà ðàçðàáîòêàòà“Ïðåãëåä è ñòðàòåãèÿ çà íàöèîíàëíîòî çäðàâåîïàçâàíå çà ïåðèîäà 2005-2010 ãîäèíà”. Ñ., 2004
56. Ñåìåðäæèåâ, È. Áúäåùåòî íà áúëãàðñêîòî çäðàâåîïàçâàíå. Â: Ìåæäóíàðîäíà êîíôåðåíöèÿ“Ïàçàð íà ñòîêè è óñëóãè â çäðàâíèÿ ñåêòîð íà Îáåäèíåíà Åâðîïà”. Ñîôèÿ, 30.11.-1.12.2004 ã.
57. Ñåìåðäæèåâ, È., Å. Äåë÷åâà, Ä. Çèíîâèåâà. Äîêëàäè. Â: ×àñòíàòà ìåäèöèíñêà ïðàêòèêà âÁúëãàðèÿ. Íàöèîíàëåí ñåìèíàð. Èçä. Áúëãàðñêà Àñîöèàöèÿ çà Ìåäèöèíñêî ïðàâî, Ñ., 1996, ñ. 5-17
58. Ñîâà-Õàðèñ. Ïðîó÷âàíå íà îáùåñòâåíîòî ìíåíèå çà çäðàâíàòà ðåôîðìà. Ñ., 200259. Ñòàòèñòè÷åñêèé åæåãîäíèê ñòðàí-÷ëåíîâ ÑÝÂ. Èçä. “Ôèíàíñè è ñòàòèñòèêà”, Ì. 198160. Òîäîðîâà, Ä. Ðàçâèòèå íà äîãîâàðÿíåòî íà ïúðâè÷íàòà ìåäèöèíñêà èçâúíáîëíè÷íà ïîìîù â
Áúëãàðèÿ ñëåä ñòàðòà íà çäðàâíàòà ðåôîðìà. Â: ². Ìåæäóíàðîäíà þáèëåéíà êîíôåðåíöèÿ“Çäðàâåîïàçâàíåòî – ïðåäèçâèêàòåëñòâàòà íà ïðîìÿíàòà”. Ñáîðíèê äîêëàäè. Âàðíà, 2003, ñ.127-129
61. Öóðàêîâ, A., Åíöèêëîïåäèÿ Ïðàâèòåëñòâàòà íà Áúëãàðèÿ. Õðîíîëîãèÿ íà ïîëèòè÷åñêèÿ æèâîò1879-2001. Èçä. ”Ïåòúð Áåðîí”, Ñ., 2001
62. Øèïî÷ëèåâà-Ïåíåâà, Â. Öåíòðàëíèòå ïå÷àòíè èçäàíèÿ êàòî ôàêòîð â ïðîöåñà íà çäðàâíàòàðåôîðìà. Äîêòîðñêà äèñåðòàöèÿ. 2003
63. Ad ams, O. Health Sec tor Re form and Pharmaceuticals. WHO Tech ni cal Brief ing Sem i nar, 6.11.2000(öèò. ïî Ã. Ïåòðîâà)
64. Aswall, J.E. Fore word. In: Saltman, R.B., J.Figueras. Eu ro pean Health Care Reforrm: Anal y sis of Cur -rent Strat e gies. WHO Re gional Pub li ca tions, Europ. Se ries, ¹ 72, Co pen ha gen, 1997, p. 10
65. Balabanova, D. Health Care Re form in Bul garia: Cur rent Prob lems and Op tions for De vel op ment. In:Eurohealth, vol. 1, ¹ 2, 1995, pp 25-28
66. Barbalov, D., S. Matties. Health Sys tem Fi nanc ing. USAID, So fia, 200167. Barents Group/KPMG Con sult ing, Inc. Re port on the Bul garia Health Re form pro ject: Fi nan cial Op er a -
tions of NHIF and As sess ment of Vol un tary In sur ance. NHIF, So fia, 200068. Beckman, M., G. Zarkovic. Tran si tion in Health In sur ance in For mer So cial ist Coun tries. In: The Pro -
cess and Man age ment of Change – Tran si tion to a Health In sur ance Sys tem in the Coun tries of Cen traland East ern Eu rope. Pro ceed ings of the Sec ond Meet ing of the Work ing Group on Health Care Re formsin Eu rope. Essen, 1993
69. Belli, P. Ten Years of Health Re forms in ECA Re gion: Les sons Learned and Op tions for the Fu ture.World Bank, N. Y., 2001
70. Bellingham, C. NICE and MS: the Saga will con tinue. In: Phar ma ceu ti cal Jour nal, ¹ 267, 2001, p. 67271. Berman, P. Health Sec tor Re form: Mak ing health de vel op ment sus tain able. In: Health Pol icy, vol. 32,
1995, pp 3-1372. Bjorkman, M. Health Pol icy Re form – Na tional Vari a tions and Glob al iza tion. Macmillan Press, 1997
375

73. Borisov, V., T. Rathwell. Health Care Re forms in Bul garia: an ini tial ap praisal. In: So cial Sci ence andMed i cine, vol. 42, ¹ 11, 1995, pp 1501-1510
74. Brown, L. Health Re form, Ital ian-Style. In: Health Af fairs, Fall 1984, pp 76-10175. Cassels, A. Health Sec tor Re form: Key Is sues in Less De vel oped Coun tries. WHO, Geneve, 199576. Chang ing Health Care in the Neth er lands Min is try of Wel fare, Health and Cul tural Af fairs, The Hague
(“The Dekker`s Re port”), 198877. Coun cil of Eu rope. Com mit tee of Min is ters. Rec om men da tion ¹ 5 of the Com mit tee of Min is ters on the
De vel op ment of Struc tures for Cit i zen and Pa tient Par tic i pa tion. 699th Meet ing of the Min is ters’ Dep u -ties, Feb ru ary 2000
78. Delcheva E., D. Balabanova, M. McKee. “Un der-the-Coun ter” Pay ment for Health Care. Ev i dence from Bul garia. In: Health Pol icy, vol. 42, 1997, p. 89
79. Ensor, T. Health Sys tem Re form in For mer So cial ist Coun tries of Eu rope. In: In ter na tional Jour nal ofHealth Plan ning and Man age ment, vol. 8, 1993, pp 169-187
80. Ensor, T. The Un of fi cial Busi ness of Healthcare in Tran si tional Eu rope. In: Eurohealth, 6 (2), Lon donSchool of Eco nom ics and So cial Sci ence, Lon don, 2000
81. Figueras, J., M. McKee, J. Cain, S. Lessof. Health Sys tems in Tran si tion: Learn ing from Ex pe ri ence.WHO. Eu ro pean Ob ser va tory on Health Sys tems and Pol i cies, 2004
82. Figueras, J., M. McKee, S. Lessof. Ten Years of Health Sec tor Re form in EE and NIS. An Owerview,Health Sys tems in Tran si tion. In: USAID Con fer ence “Ten Years of Health Sys tems Tran si tion in Cen tral and East ern Eu rope and Eur asia”, 2002. Htpp://www.eurasiahealthtransitionconference.org/HealthSystems-Over view.pdf.
83. Freire, J. M. Health Care Re forms in Spain. In: Artundo, C. et all. (Eds.) Health Care Re forms in Eu rope.Min is try of Health and Con sumer Af fairs. Ma drid, 1993
84. Fuenzalida-Puelma, H. Healthcare Re form in Cen tral and East ern Eu rope and the For mer So viet Un ion.A Lit er a ture Re vue. Open So ci ety In sti tute, Bu da pest, 2002
85. Ham, C. Healthcare Re form: Learn ing from In ter na tional Ex pe ri ence. Open Uni ver sity Press,Buckingham, 2000
86. Har ding, A., A Preker. A Con cep tual Frame work for Or ga ni za tional Re forms of Hos pi tals. In: Har ding,A., A. Preker (Eds.) In no va tions in Health Ser vice De liv ery. The Corporatization of Pub lic Hos pi tals.Johns Hopkins Uni ver sity Press, Bal ti more, 2001
87. Har ding, A., A. Preker (Eds.) In no va tions in Health Ser vice De liv ery. The Corporatization of Pub lic Hos -pi tals. World Bank. Wash ing ton DC, 2003
88. Har ding, A., A. Preker. Un der stand ing Or ga ni za tional Re forms. The Corporatization of Pub lic Hos pi -tals. NHP Dis cus sion Pa per. The In ter na tional Bank for Re con struc tion and De vel op ment/The WorldBank, Wash ing ton DC, 2000
89. Har ri son, S., C. Pollin. Con trol ling Health Pro fes sion als. The Fu ture of Work and Or ga ni za tion in theNa tional Health Ser vice. Open Uni ver sity Press, Lon don, 1994
90. HOPE. West ern Con sor tium Con fer ence on HEALTH Re forms in Cen tral Eu rope: Na tional Strat e giesfor Cost Con tain ment. Prague, 1993
91. Lalonde, M. New Per spec tive on the Health of Ca na di ans: A Work ing Doc u ment. In for ma tion Can ada,Ot tawa, 1974
92. Lamata Cotanda, F. Estudio Comparado de las Reformas de los Sistemas Sanitarios de Espana y Bul -garia. Tesis Doc toral. Ma drid, 1998
93. Lamata Cotanda, F. Bul gar ian Health Care Sys tem. GCI-PHARE Pro gram, Ma drid, 199894. Lamata Cotanda, F. Sistemas Sanitarios de la Un ion Europea. En: Lamata F. (Ed.) Man ual de
Administracion y Gestion Sanitaria. Diaz de Santos, Ma drid, 199895. Lewis, M. Who is Pay ing for Healthcare in Eu rope and Cen tral Asia? World Bank. Wash ing ton DC, 200096. Lueschen, G. et al. Health Sys tems in the Eu ro pean Un ion. R. Oldenbourg Verl., Muenchen, 199597. Matties, S., D. Lissyisky, I. Montel, S. Crelia, L. Alexandrova. Com par a tive Study of Se lected Top ics in
Health Pol icy. Part I. USAID, Bul gar ian Health Pro ject, 200298. Min is try of Health and So cial Af fairs. Strat egy for Health. War saw, 199499. Neubauer, G. Case mix and Fund ing. The Ger man Ap proach. In: Pro ceed ings from Work shop on Case
mix and Re source Man age ment. So fia, 1993
376
100. OECD. The Re form Of Health Care: a Com par a tive Anal y sis of Seven OECD Coun tries. Paris, 1992101. Op por tu ni ties for the Fu ture. Health Care Re forms for Health Gain. Eu ro pean Health Pol icy Con fer ence.
Co pen ha gen, 1994, vol. 4102. Pav lo va, M., W. Groot, G. van Merode. Pub lic At ti tudes to wards Pa tient Pay ments in Bul gar ian Pub lic
Health Care Sec tor: Re sults of a House hold Sur vey. In: Health Pol icy, 59, 2002, pp 1-24.103. Peevski, Tz. Pa ram e ters of the Bul gar ian Health Care Re form. Ex pe ri ence from the 1-year of Gov ern -
ment in Of fice. In: Health Sec tor Re form in Cen tral and East ern Eu rope: Cur rent Trends and Pri or ity Re -search. A FICOSSER Re search Meet ing. 2-3.10.1998 Velingrad, Bul garia. War saw, 1999, p. 164
104. Preker, A., R. Feachem. Mar ket Mech a nisms and Healthcare sec tor in Cen tral and East ern Eu rope.World Bank. Wash ing ton DC, 1993
105. Prohaska, M., D. Iliev, D. Sacheva, M. Varshilova, L. Doudeva. Health Re form in Bul garia: A Glance atDe cen tral iza tion and Lo cal Gov er nance. In: Shakarishvili, G. (Ed.) De cen tral iza tion in Healthcare.Anal y ses and Ex pe ri ences in Cen tral and East ern Eu rope in the 1990s. Open So ci ety In sti tute. Bu da pest,2005, pp 45-132
106. Re cent de mo graphic de vel op ments in Eu rope. Coun cil of Eu rope Pub lish ing, Strasbourg, StatistischesJahrbuch Oesterreichs, 2005
107. Reich, M. R. Po lit i cal Map ping of Health Pol icy. A Guide for Man ag ing the Po lit i cal Di men sions ofHealth Pol icy. Har vard School of Pub lic Health, Boston, 1993
108. Reich, M. R. Ap plied Po lit i cal Anal y sis for Health Pol icy Re form. In: Cur rent Is sues in Pub lic Health, 2,1996, pp 186-191
109. Roemer, M. I. Na tional Health Sys tems of the World. Ox ford Uni ver sity Press, Ox ford, 1991110. Saltman, R. B., J. Figueras. Eu ro pean Health Care Reforrm: Anal y sis of Cur rent Strat e gies. WHO Re -
gional Pub li ca tions, Europ. Se ries, ¹ 72, Co pen ha gen, 1997111. Saltman, R. B. A Con cep tual Over view of Re cent Health Care Re forms. In: Eu ro pean Jour nal of Pub lic
Health, vol. 4, ¹ 2, 1994, pp 287-293112. Sand ier, S. Health Ser vices Uti li za tion and Phy si cian In come Trends. In: OECD Health Care Sys tems.
The Search for Ef fi ciency. Paris, 1990113. Sand ier, S. The Pay ment of Phy si cians in Se lected OECD Coun tries. OECD, Paris, 1989114. Schaapveld, K., K. Krleza-Jeric, J. Stiphout, Man age ment As pects of the Bul gar ian Health Care Re form.
TNO Re port PG 95.075. TNO Pre ven tion and Health Di vi sion, Pub lic Health and Pre ven tion, Leiden,Neth er lands, 1995
115. Shakarishvili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and East ern Eu rope in the 1990s. Open So ci ety In sti tute. Bu da pest, 2005
116. Shakarishvili, G., K. Davey. Trends in Re form ing the Pro vi sion and Fi nanc ing of Healthcare. In:Shakarishyili, G. (Ed.) De cen tral iza tion in Healthcare. Anal y ses and Ex pe ri ences in Cen tral and East ern Eu rope in the 1990s. Open So ci ety In sti tute. Bu da pest, 2005, pp 3-43
117. Swed ish Par lia men tary Pri or i ties Com mis sion. Pri or i ties in Health Care. Min is try of Health and So cialAf fairs, Stock holm, 1995
118. USAID. At ti tudes and Ex pec ta tions to Bul gar ian In sur ance Sys tem and Vol un tary Funds. Bul gar ianHealth Pro ject, 2002
119. USAID. Health In for ma tion Needs of Bul gar ian Cit i zens. Re search Re sults. Bul gar ian Health Pro ject. K. Cherry, S. Crelia, Barents Group of KPMG Con sult ing Inc., So fia, 2002
120. Walt, G. Im ple ment ing Health Care Re forms: a Frame work for Dis cus sion. In: Saltman, R. B., J.Figueras, C. Sakellarides (Eds.) Crit i cal Chal lenges for Eu ro pean Health Pol icy. Open Uni ver sity Press,Buckingham, 1998
121. Walt, G., L. Gilson. Re form ing the Health Sec tor in De vel op ing Coun tries: the Cen tral Role of Pol icyAnal y sis. In: Health Pol icy, vol. 9, ¹ 4, 1994, pp 353-370
122. Work ing for Pa tients. NM Sta tio nery Of fice, Lon don, 1989123. Zarkovic, G. et al. Re form of the Health Care Sys tems in For mer So cial ist Coun tries: Prob lems, Op tions,
Sce nar ios. Institut fuer Medizinische Informatik und Systemforschung (Medis), Neuherberg, 1994124. Zdravkova-Traikova, R. An As sess ment of the Healthcare Re form in Bul garia (1989-2001): Rights vs.
Re al ity. Rus sian and East Eu ro pean In sti tute, In di ana, 2002
377