
Atypical Antipsychotics as Augmentation Therapy in Anorexia Nervosa
Upload
independentCategory
view
1download
0
The Experience and Impact of Pregnancy in Bulimia Nervosa: A Series of Case Studies
Linda Lewis and Daniel le Grange
The aim of the present study was to investigate the impact of pregnancy on women suffering from bulimia nervosa. Six mothers completed several rating scales and participated in a semi-structured interview. These were used to construct a case study of the subjects with regard to their emotional experiences during pregnancy and their eating pathology during and following the pregnancy. Fears commonly experienced during the course of pregnancy included losing control of their eating and weight, causing damage to the unborn child by engaging in bulimic practices and not being able to cope with a newborn infant. With regard to eating patholoo during pregnancy, subjects did not experience an amelioration in bulimic symptoms. In the puerperium there was a resurgence of bulimic symptoms for all women either at a level of severity equal to or worse than before conception. Albeit tentative, pregnancy does not seem to provide women with an opportunity for recovery from bulimia newosa and pregnancy may, in some cases, result in an exacerbation of bulimic symptoms.
INTRODUCTION
Pregnancy and parenthood in patients with an eating disorder have received relatively little attention. Recruiting large numbers of mothers with an eating disorder is difficult as relatively few bulimic and anorexic women become pregnant (Glassman et al., 1991), and even smaller numbers report their eating disorder to their physician (Frank0 and Walton, 1993; Hollifield and Hobdy, 1990; Lemberg and Phillips, 1989). Notwithstanding, case reports (Feingold et al., 1988; Hollifield and Hobdy, 1990; Ramchandani and Whedon, 1988; Willis and Rand, 1988) as well as larger retrospective studies (Lacey and Smith, 1987; Lemberg and Phillips, 1989; Mitchell et al., 1991) investigating pregnancy in eating disorders, have been reported. Few of these studies, though, have yielded conclusive results, either in terms of the health outcome of the infant or the effect of the pregnancy on the eating disorder.
Some studies have alluded to the ameliorating effects of the pregnancy on the eating disorder (Blinder and Hagman, 1984; Brinch et al., 1988;
CCC 10724133/94/020093-13 01994 by John Wiley & Sons, Ltd. and Eating Disorders Association
European Eating Disorders Review Vol. 2 No. 2 (1994)

L. Lewis and D. le Grange
Fairburn et al., 1992; Lacey and Smith, 1987; Lemberg and Phillips, 1989; Rarnchandani, 1984; Ramchandani and Whedon, 1988; Willis and Rand, 1988), whilst others comment on the extent to which bulimic symptoms are maintained or exacerbated during pregnancy (Feingold et al. , 1988; Hollifield and Hobdy, 1990; Stewart et al., 1987). After delivery, though, bulimic symptoms have been reported to recur either at the same intensity (Edelstein and King, 1992; Lemberg and Phillips, 1989; Ramchandani, 1984; Ramchandani and Whedon, 1988; Willis and Rand, 1991) or worse than before (Brinch et al., 1988; Lacey and Smith, 1987; Woodside and Shekter-Wolfson, 1990). Those who experience a resurgence of bulimic symptoms also tend to suffer from interpersonal difficulties and a sense of failure as women, and are inclined to use the pregnancy as an attempt to combat these problems (Lacey and Smith, 1987). Others attribute the regression in symptomatology to feeling fat and wanting to lose weight, the stress of motherhood and, in some cases, the added responsibility of a career outside the home (Lemberg and Phillips, 1989). For those women in whom symptoms improve or remit, pregnancy seemed to have a beneficial effect on body-image (Lemberg and Phillips, 1989) and also provide them with increased meaning and purpose in life (Lacey and Smith, 1987).
While most studies on bulimia nervosa and pregnancy have focused on the effects of active eating pathology on the fetus's well-being or the effects of the pregnancy on eating pathology, little attention has been paid to the emotional experiences of pregnant women suffering from eating disorders. Fears of incompetence in mothering and of congenital malformations of the unborn child are common amongst normal pregnant women (e.g. Drake et al., 1988; Istvan, 1986; Jones, 1990; Raskin et al., 1990). Edelstein and King (1992) argue that these fears are exacerbated when the pregnant woman suffers or has suffered from an eating disorder. They have found that women who continue to engage in bulimic behaviours during pregnancy experience considerable fear, guilt and shame with regard to the potential damage this may cause the unborn child. Yet, the fear of losing control of eating patterns and gaining weight during pregnancy habitually overrides concerns for the well-being of the fetus (Feingold et al., 1988; Franko and Walton, 1993; Hollifield and Hobdy, 1990; Lemberg and Phillips, 1989).
Women who do experience a remission of bulimic symptoms during pregnancy explain this either in terms of concern for the health of the unborn child (Lacey and Smith, 1987; Ramchandani and Whedon, 1988), concern about their own competence as caretakers (Blinder and Hagman, 1984) or seeing pregnancy as a legitimate reason to take care of themselves (Lemberg and Phillips, 1989). No study to date, however, has systematically examined the affective experience of bulimic women during pregnancy.
The aims of the present study were to investigate retrospectively (i) the emotional experience of pregnancy by women suffering from bulimia nervosa,
94

Pregnancy in Bulimia Nervosa
and (ii) whether pregnancy has an ameliorating, neutral or exacerbating effect on bulimic symptoms during, and/or following, pregnancy.
METHOD Subjects
The sample comprised of six mothers who were diagnosed with bulimia nervosa (DSM-III-R, APA, 1987) at the time of index pregnancy. Three subjects had a concurrent diagnosis of anorexia nervosa (DSM-111-R, APA, 1987). Subjects were recruited from an eating disorders support group and an outpatient eating disorders clinic, and gave informed consent. At present half the sample remains bulimic, one woman is anorexic while the remaining two fulfil the criteria for what is proposed to be classified as binge eating disorder in the DSM-IV (cf. Spitzer et al., 1991).
Measures
All subjects completed a 7-item Personal Details Questionnaire and participated in a semi-structured interview enquiring about the Experience of Pregnancy and the Impact of Pregnancy on the Eating Disorder. These measures were designed specifically for the purposes of this study and were administered by one of us (L. L.).
Personal details questionnaire This inventory was used to obtain demographic information concerning issues such as age, number of children, and current or previous diagnoses.
Semiestructured interview This interview was divided into two parts. In the first part information pertaining to the subject’s experience of the index pregnancy was elicited and, in the second part, information regarding the impact of the pregnancy on the eating disorder was explored.
(i) Experience of pregnancy. This part of the interview explored different areas relating to the subjects’ experience of pregnancy. For example, questions, regarding previous miscarriages or abortions were asked, as well as details about the delivery, health and weight of the infant at index pregnancy. In addition to this, information regarding the subjects’ emotional experiences during the pregnancy was obtained including whether they felt anxious, depressed or excited about the prospect of mothering.
95

L. Lewis and D. le Grange
(ii) Impact of pregnancy on the eating disorder. The second part was designed to elicit information pertaining to the subjects’ eating behaviour during the index pregnancy and the period following delivery. Questions were asked regarding the extent to which the subjects continued, if at all, to binge, purge, take laxatives, exercise during the course of the pregnancy and the reasons why, if at all, they endeavoured to change their eating behaviour during this period.
The eating attitude test (EAT) The EAT (Garner and Garfinkel, 1979) is a widely used 40-item screening test. A cut-off score reliably differentiates eating and non eating-disordered populations.
The Morgan.Russe1 assessment schedule Changes in the subjects’ clinical status, personal and social adjustment were quantified by the use of the Morgan-Russell Assessment Schedule (Morgan and Hayward, 1988; Morgan and Russell, 1975). These scales can be used to produce a global measure of outcome and facilitate a threefold categorization: (1) Good outcome, weight is within 15 per cent of average body weight (ABW), regular menstrual cycles. (2) Intermediate outcome, body weight is within 15 per cent of ABW, amenorrhoea persists. (3) Poor outcome, weight is below 15 per cent ABW or bulimic symptoms are present.
Procedure
Four of the subjects were interviewed in their homes while the remaining two were interviewed at their place of work. First, the Personal Details Questionnaire was administered. This was followed by the interview exploring the Experience of Pregnancy and the Impact of the Pregnancy on the Eating Disorder. The Morgan-Russell Assessment Schedule and the EAT were then administered.
RESULTS
Characteristics of the subjects
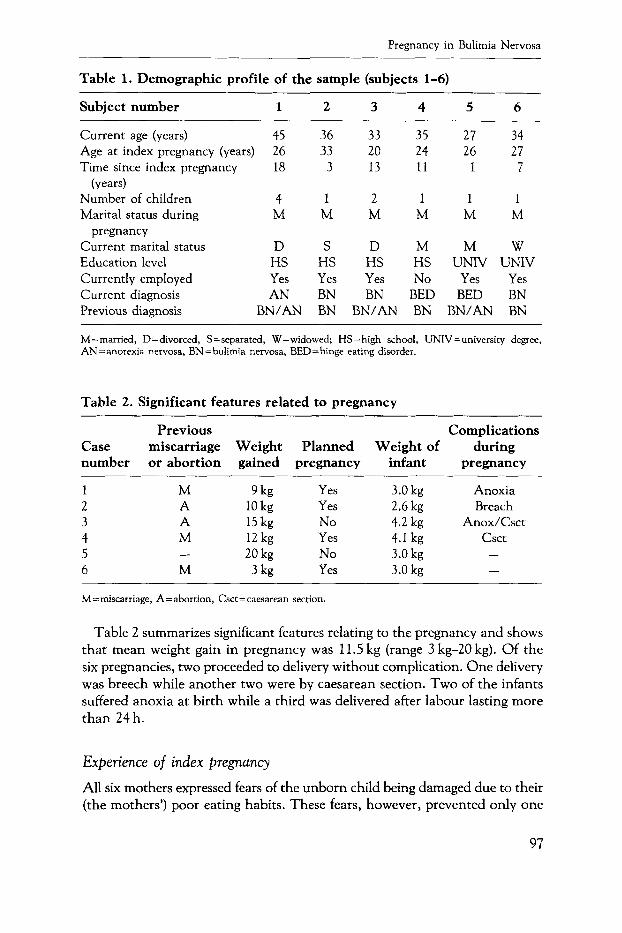
Demographic information of the subjects is presented in Table 1. Mothers’ mean age at index pregnancy was 26 years (range 20-33 years). O n average, nine years (range 1-18 years) have lapsed between index pregnancy and interview. Of the six subjects, three had previous miscarriages and two had a previous abortion. All subjects were married at the time of conception. Only two subjects are married at present. Of the remainder, one is separated, one is widowed and two are divorced.
96
Pregnancy in Bulimia Nervosa
Table 1. Demographic profile of the sample (subjects 1-6)
Subject number 1 2 3 4 5 6
Current age (years) 45 Age at index pregnancy (years) 26 Time since index pregnancy 18
Number of children 4 Marital status during M
Current marital status D Education level HS Currently employed Yes Current diagnosis AN Previous diagnosis BN/AN
(years)
pregnancy
36 33 3
1 M
S HS Yes BN BN
33 20 13
2 M
D HS Yes UN
BN/AN
35 24 11
1 M
M HS No
BED BN
27 34 26 27
1 7
1 1 M M
M W UNIV UNIV
Yes Yes BED BN
UN/AN BN
M = married, D=divorced, S = separated, W = widowed; HS = high school, UNIV = university degree, AN =anorexia nervosa, BN= bulimia nervosa, BED=binge eating disorder.
Table 2. Significant features related to pregnancy
Case number
1 2 3 4 5 6
Previous miscarriage or abortion
M A A M
M -
Weight gained
Planned pregnancy
9kg 10 kg 15 kg 12 kg 20 kg 3 kg
Yes Yes No Yes No Yes
Complications Weight of during
infant pregnancy
3.0 kg Anoxia 2.6 kg Breach 4.2 kg Anox/Csct 4.1 kg Csct 3.0 kg - 3.0 kg -
M= miscarriage, A= abortion, Csct = caesarean section.
Table 2 summarizes significant features relating to the pregnancy and shows that mean weight gain in pregnancy was 11.5 kg (range 3 kg-20 kg). Of the six pregnancies, two proceeded to delivery without complication. One delivery was breech while another two were by caesarean section. Two of the infants suffered anoxia at birth while a third was delivered after labour lasting more than 24 h.
Experience of index pregnancy
All six mothers expressed fears of the unborn child being damaged due to their (the mothers’) poor eating habits. These fears, however, prevented only one
97

L. Lewis and D. le Grange
woman from abstaining from bulimic behaviour. All six women expressed fear of losing control of their weight during pregnancy and this motivated two women to follow a restricting diet throughout their pregnancies. Another fear reported by two of the women was that of not being able to mother the child properly. The remainder of the subjects felt confident about their abilities in this regard. Notwithstanding, all six mothers were excited at the prospect of mothering.
In terms of the emotional experiences of the women during the course of the pregnancy, none indicated that they felt depressed for extensive periods during the pregnancy. Four out of the six women, though, said they felt depressed at least three times per week. With regard to anxiety, all of the women reported to experience some anxiety during the pregnancy with two women experiencing anxiety most of the time. This anxiety related to fears about the health of the fetus and their ability to cope with their responsibilities once the baby was born. For most of the women this anxiety was exacerbated by the fact that they received little, if any, support from spouses, family and friends during the pregnancy.
Effects of index pregnancy on eating disorder symptoms
Table 3 provides a summary of bulimic symptoms experienced by subjects during index pregnancy. All of the women, except for one who was vague about the history of her eating behaviour, were bulimic at conception. As Table 3 illustrates, four of the six women continued to binge, and three continued to purge and use laxatives during the pregnancy. Of the three women who stopped purging or using laxatives, two substituted this method of weight control with daily exercise.
None of the women experienced an improvement in their bulimic symptoms following pregnancy. While one woman in the sample reported no change in the intensity of her eating disorder after her pregnancy, the remaining five women experienced a deterioration in bulimic symptoms. For all of the women, anxiety over weight gained during the pregnancy precipitated the deterioration
Table 3. Bulimic symptoms during pregnancy
Case number Exercise Bingeing Purging Laxatives
1 Daily Yes Yes Yes 2 Alternate days No Yes Yes 3 None Yes Yes Yes 4 None Yes No No 5 Daily Yes No No 6 Daily No No No
98
Pregnancy in Bulimia Nervosa
Table 4. Bulimic symptoms before and after pregnancy, and current diagnosis
~ ~ ~~ ~~~~
Case Binge-purge episodes Binge-purge episodes Current number before (per week) after (per week) diagnosis
1 3 7 A N 2 28 35 BN 3 4 7 BN 4 * 4 BED 5 7 7 BED 6 2 2 BN
*Vague, AN= anorexia nervosa, BN = bulimia nervosa, BED = binge eating disorder.
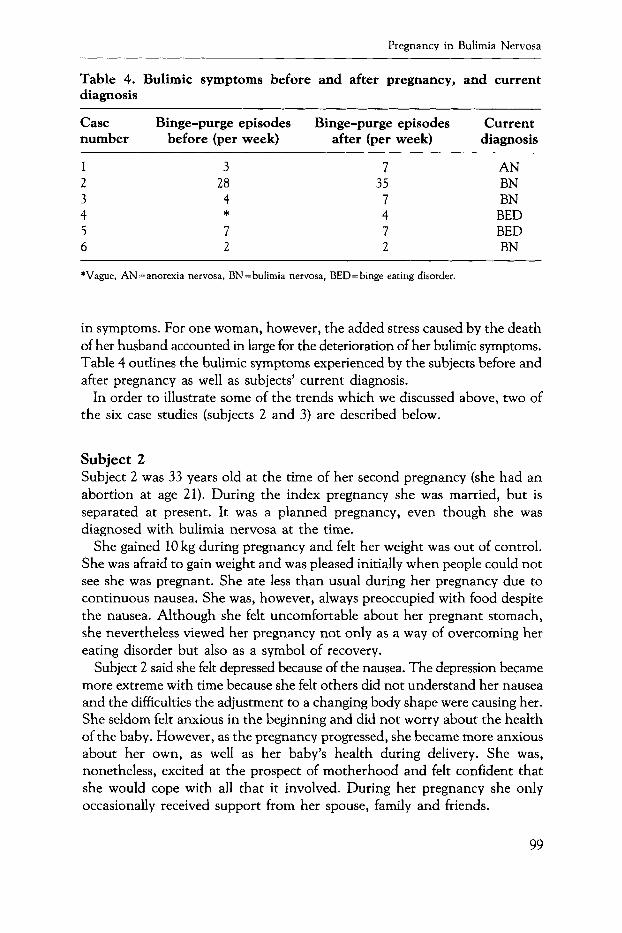
in symptoms. For one woman, however, the added stress caused by the death of her husband accounted in large for the deterioration of her bulimic symptoms. Table 4 outlines the bulimic symptoms experienced by the subjects before and after pregnancy as well as subjects’ current diagnosis.
In order to illustrate some of the trends which we discussed above, two of the six case studies (subjects 2 and 3) are described below.
Subject 2 Subject 2 was 33 years old at the time of her second pregnancy (she had an abortion at age 21). During the index pregnancy she was married, but is separated at present. It was a planned pregnancy, even though she was diagnosed with bulimia nervosa at the time.
She gained 10 kg during pregnancy and felt her weight was out of control. She was afraid to gain weight and was pleased initially when people could not see she was pregnant. She ate less than usual during her pregnancy due to continuous nausea, She was, however, always preoccupied with food despite the nausea. Although she felt uncomfortable about her pregnant stomach, she nevertheless viewed her pregnancy not only as a way of overcoming her eating disorder but also as a symbol of recovery.
Subject 2 said she felt depressed because of the nausea. The depression became more extreme with time because she felt others did not understand her nausea and the difficulties the adjustment to a changing body shape were causing her. She seldom felt anxious in the beginning and did not worry about the health of the baby. However, as the pregnancy progressed, she became more anxious about her own, as well as her baby’s health during delivery. She was, nonetheless, excited at the prospect of motherhood and felt confident that she would cope with all that it involved. During her pregnancy she only occasionally received support from her spouse, family and friends.
99

L. Lewis and D. le Grange
When her pregnancy was confirmed, she reduced her bingeing episodes from four times a day to not bingeing at all. She continued to purge up to four times a week mainly because she felt this would help her get rid of the nausea. She stopped using laxatives and diuretics immediately. She was motivated to change her eating behaviour for fear of the health of the fetus and because of the anticipated guilt she knew she would feel if she had continued bingeing.
Subject 2 had a breech delivery and her son, weighing 2.6 kg, was born healthy. Following the birth her bulimic symptoms deteriorated to levels worse than before her pregnancy, bingeing and purging on average four times a day.
At present, she is 86 per cent of ABW and still suffers from bulimia nervosa. Although her Morgan-Russell Outcome Score indicates a good outcome, its significance is tempered by her continuing bulimic symptoms. Her high EAT score also indicates some degree of eating pathology. Therefore, although in some ways this subject can be considered to have improved, her clinical status is evidence of a poor outcome.
Subject 3 Subject 3 was 20 years old when she became pregnant with her first child (she had an abortion at age 18). During her index pregnancy she was married but at present, 13 years later, is divorced. Before her pregnancy she suffered from both bulimia and anorexia nervosa. Her pregnancy was unplanned, but she was pleased that she could fall pregnant again after having had an abortion. During the index pregnancy she gained 15 kg and felt that throughout this period her eating and her weight were out of control. She did not exercise at all during the pregnancy.
She felt uncomfortable about her pregnant stomach and did not view the pregnancy as a way of overcoming her eating disorder nor as a symbol of her recovery. During her pregnancy, subject 3 felt depressed at least three times a week because she was uncomfortable with her body, her marriage ‘was a disaster’ and ‘food was and is a constant depression’. With regard to anxiety she says that ‘as per usual’ she was anxious most of the time. She was excited about the prospect of motherhood and saw it as a way of relieving herself of the guilt she experienced over her abortion. She did not worry that she would not be competent as a mother. During her pregnancy she hardly ever received support from family and friends mainly because she had recently moved to another city and did not know people there. She was unable to share her experiences with her husband.
When her pregnancy was confirmed, subject 3 tried to alter her eating behaviour of bingeing and purging four times a week. However, she continued to binge and purge at least once a week, took laxatives daily and used diuretics periodically. She felt guilty about her eating behaviour and worried about the harm it was causing the fetus. In particular, she was worried about the damage
100

Pregnancy in Bulimia Nervosa
that would be caused by her misuse of laxatives but coped with this by denying that there was a problem.
Subject 3 had a caesarean section delivery. Her son, who weighed 4.2 kg at birth, suffered anoxia during delivery which resulted in minimal cerebral palsy. Following the birth, her eating disorder symptoms deteriorated to levels worse than before her pregnancy. She says, ‘I just starved completely or binged and purged daily-after being such a heffalump I wanted to. A lot of people said “God you are huge” and that was hard’.
She is currently 85 per cent of ABW with a diagnosis of bulimia nervosa. Her severe eating pathology and poor outcome is reflected in her Morgan-Russell Outcome Score of 3.3, an EAT score of 83 and persistent bulimic symptoms.
DISCUSSION
The results of this study must be regarded as preliminary for a number of reasons. In the first place, the sample size is small and thus the findings have restricted applicability beyond the subjects under investigation. Second, the study is limited in so far as it relies on retrospective information pertaining to the pregnancies which, in some cases, were a considerable time prior to this investigation. In addition, information was collected solely on the basis of self-report and thus problems of bias and recall cannot be ignored when analysing the data. Loftus and Loftus (1980), for instance, point to several possible pitfalls in this regard, such as memory fabrication or memory corruption. Also, being pregnant has significant social meaning, and what they refer to as ‘anticipation schematas’, can have a significant impact on what one remembers, e.g. only bad or only good experiences. Third, sample selection in this study, as in most other studies of this nature, may have introduced a further limitation in the generalizability of the results in that subjects recruited were all receiving some form of treatment, either from a clinician or a support group. It is thus possible that this particular group of women suffer from more chronic and severe bulimic symptoms than those who chose not to seek help.
Despite the small number of subjects and a considerable amount of variation in their experiences, some meaningful trends have emerged from this study. Similar to an earlier report (Woodside and Shekter-Wolfson, 1990), high levels of marital difficulties were experienced by the subjects in our study. All six women were married at the time of conception, whilst only two remain as such at present. Moreover, those women who had the most severe eating pathology during pregnancy also seem to be the women who subsequently divorced or separated from their spouses. In other words, it could be hypothesized that those women who enjoyed stable relationships were better able to control their bulimic behaviour during pregnancy than those who tended to have interpersonal problems. This finding is similar to that of Lacey and
101
L. Lewis and D. le Grange
Smith (1987) who report that women who stopped binge-eating completely, tend to have stable and meaningful relationships whereas those who continued their bulimic behaviour during pregnancy and afterwards tend to have interpersonal problems and a sense of failure as women. O n the basis of these findings it can be speculated at this stage that pregnancy does not provide women with an opportunity for recovery from bulimia nervosa. In some cases, it may also have serious ramifications for their interpersonal relationships.
All of the women feared losing control of their eating and weight during pregnancy although, as Lemberg and Phillips (1989) found, this proved to be unfounded in that subjects reported normal weight gains. The greatest fear experienced by all of the women was that of damaging their unborn child as a result of their unhealthy eating behaviour. This finding has also been reported in a number of recent studies (Hollifield and Hobdy, 1990; Lacey and Smith, 1987; Lemberg and Phillips, 1989). However, on the whole, it would appear as if this fear did not prevent them from engaging in bulimic behaviour. Although Lemberg and Phillips (1989) did not find evidence to support the notion that poor eating behaviour resulted in complications to the fetus, Lacey and Smith (1987) indicate that abnormal eating behaviour could damage the unborn child. In the present study it was found that those women who continued to purge during pregnancy also presented with complications at birth (e.g. anoxia, caesarean-section and breech delivery). According to two of the mother’s reports, their children suffered permanent damage in the form of ‘learning difficulties’ and ‘mild cerebral palsy’. The small number of cases in our study, however, prevents us from commenting more conclusively about the relationship between bulimic practices during pregnancy and resultant damage to the unborn child.
Although the entire sample of women were excited at the prospect of motherhood, most of them were anxious about their ability to cope when the baby was born. This, along with the high levels of anxiety experienced by all of the women in terms of the health of the unborn child, may possibly have accounted for the continuation of bulimic symptoms during pregnancy. Indeed, the two women who experienced the greatest anxiety during pregnancy were also the only two women who continued to binge, urge and take laxatives throughout the course of the pregnancy.
Contrary to Lacey and Smith’s (1987) findings that bulimic symptoms are not worsened by pregnancy and that pregnancy may even be curative, the current study found that during the course of pregnancy only one woman stopped bingeing and purging, whilst the remainder continued to binge and/or purge. Half the sample also continued to misuse laxatives. The subject who abstained in total from binge-purge behaviour did, however, engage in daily excercise as an alternative means of weight control which, in itself, has been found to be potentially dangerous to the fetus (Carpenter et al., 1988).
102

Pregnancy in Bulimia Nervosa
Following pregnancy the severity of bulimic symptoms remained the same as it was before pregnancy for one woman, whereas the remaining women experienced an exacerbation in symptoms following delivery. As in other studies of this sort (Lacey and Smith, 1987; Lemberg and Phillips, 1989; Willis and Rand, 1988; Woodside and Shekter-Wolfson, 1990) the resurgence of symptoms in the puerperium period was attributed to anxiety over weight gained during pregnancy and the attendant desperation to return to prepregnancy weight. As Willis and Rand (1988) state, perhaps it is when the constraint of potential fetal injury is removed that women feel they are ‘allowed’ to engage in their abnormal eating behaviour again, to an extent even worse than prior to pregnancy. Thus, although in some studies women have been found to experience an amelioration in bulimic symptoms following pregnancy (Blinder and Hagman, 1984; Brinch et al., 1988; Fairburn et af., 1992; Lacey and Smith, 1987; Lemberg and Phillips, 1989; Ramchandani, 1984; Ramchandani and Whedon, 1988; Willis and Rand, 1988), the present study, along with others (Feingold et al., 1988; Hollifield and Hobdy, 1990; Stewart et al., 1987), add weight to the contrary finding that pregnancy has, at best a neutral, or even an exacerbating effect on bulimic behaviour.
While some researchers see pregnancy as providing the necessary motivation to let go of one’s eating disorder (Lacey and Smith, 1987), others recommend a delay in pregnancy until the eating disorder is in remission (Edelstein and King, 1992; Stewart et al., 1987). The inconsistent results emerging from studies in this area point to the requirement for increased research efforts in which prospective and longitudinal measures are used to ascertain the impact of pregnancy on eating disorders in larger samples of bulimic women. Our study also points to the need for more controlled experimental investigations in which such factors as chronicity of the eating disorder, age since giving birth, participation in treatment, among others, are controlled for.
Finally, attention should be directed towards informing mental health clinicians and obstetricians as well as bulimic women of the complications that may arise during pregnancy if symptoms continue. From this study it seems clear that bulimic women who are pregnant require extra attention and monitoring by their obstetrician and, if possible, therapeutic support. Since most women are secretive about their bulimia nervosa, obstetricians should be alert to all possible reasons for lack of weight gain in their pregnant patients as well as be informed about the nutritional practices of these patients.
REFERENCES
AMERICAN PSYCHIATRIC ASSOCIATION (1987). Diagnostic and Statistical Manual of Mental Disorders, 3rd edn, revised. Washington D.C.: American Psychiatric Association.
103

L. Lewis and D. le Grange
BLINDER, B. J., and Hagman, J. 0. (1984). Pregnancy and eating disorders. Papers presented at the First International Conference on Eating Disorders, New York, NY.
BRINCH, M., Isager, T. and Tolstrup, K. (1988). Anorexia nervosa and motherhood: Reproductional pattern and mothering behaviour of 50 women. Acta Psychiatrica Scandinawica, 7 7, 98-104.
CARPENTER, M. W., Sady, S. P., Hoegsberg, B., Sady, M. A., Haydon, B., Cullinane, E. M., Coustan, D. R. and Thompson, P. D. (1988). Fetal heart rate response to maternal exertion. J o u m l of the American Medical Association, 259, 3006-3009.
DRAKE, M. L., Verhulst, D. and Fawcett, B. (1988). Physical and psychological symptoms experienced by Canadian women and their husbands during pregnancy and postpartum. Journal of Advanced Nursing, 13, 436-440.
EDELSTEIN, C. K. and King, B. H. (1992). Pregnancy in eating disorders. In: Special Problems in Managing Eating Disorders (eds. J. Yager, H. E. Gwirtsman and C. K. Edelstein). Washington D.C.: American Psychiatric Press.
FAIRBURN, C. G., Stein, D. M. and Jones, R. (1992). Eating habits and eating disorders during pregnancy. Psychosomatic Medicine, 54, 665-672.
FEINGOLD, M., Kaminer, Y., Lyons, K., Chaudhury, A. K., Costigan, K. and Cetrulo, C. L. (1988). Bulimia nervosa in pregnancy: A case report. Obstetrics and Gynecology, 71 part 2, 1025-1027.
FRANKO, D. L. and Walton, B. E. (1993). Pregnancy and eating disorders: A review and clinical implications. International Journal of Eating Disorders, 13, 41-45.
GARNER, D. M. and Garfinkel, P. E. (1979). The Eating Attitudes Test: and index of the symptoms of anorexia nervosa. Psychological Medicine, 9, 273-279.
GLASSMAN, J. N., Rich, C. L., Darko, D. and Clarkin, A. (1991). Menstrual dysfunction in bulimia. Annals of Clinical Psychiatry, 3, 161-165.
HOLLIFIELD, J. and Hobdy, J. (1990). The course of pregnancy complicated by bulimia. Psychotherapy, 27, 249-255.
ISTVAN, J. (1986). Stress, anxiety and birth outcomes: A critical review of the evidence. Psychological Bulletin, 100, 33 1-348.
JONES, K. (1990). Expectant fears. Nursing Times, 86, 36-38. LACEY, J. H. and Smith, G. (1987). Bulimia nervosa: The impact of pregnancy on
mother and baby. British journal of Psychiatry, 150, 777-781. LEMBERG, R. and Phillips, J. (1989). The impact of pregnancy on anorexia nervosa
and bulimia. lnternational Journal of Eating Disorders, 8, 285-295. LOFTUS, E. S. and Loftus, J. R. (1980). On the permanence of stored information
in the human brain. American Psychologist, 35, 409-420. MITCHELL, J. E., Seim, H. C., Glotter, D., SOU, E. A. and Pyle, R. L. (1991). A
retrospective study of pregnancy in bulimia nervosa. International Journal of Eating Disorders, 10, 209-214.
MORGAN, H. G. and Hayward, A. E. (1988). Clinical assessment of anorexia nervosa. British journal of Psychiatry, 152, 367-371.
MORGAN, H. G. and Russell, G. F. M. (1975). Value of family background and clinical features as predictors of long-term outcome in anorexia nervosa: Four- year follow-up study of 41 patients. Psychological Medicine, 5, 355-371.
104

Pregnancy in Bulimia Nervosa
RAMCHANDANI, D. (1984). Hypothalamic factors and bulimia. American Journal of Psychiatry, 141, 1311.
RAMCHANDANI, D. and Whedon, B. (1988). The effect of pregnancy on bulimia. lnternational Journal of Eating Disorders, 7, 845-848.
RASKIN, V. D., Richman, J. A. and Gaines, C. (1990). Patterns of depressive symptoms in expectant and new parents. American Journal of Psychiatry, 147, 658-660.
SPITZER, R. L., Devlin, M. J., Walsh, B. T., Hasin, D., Wing, R., Marcus, M. D., Stunkard, A. J., Wadden, T., Yanovski, S., Agras, W. S., Mitchell, J. and Nonas, C. (1991). Binge eating disorder: To be or not ro be in DSM-IV! International Journal of Eating Disorders, 10, 627-630.
STEWART, D. E., Raskin, J., Garfinkel, P. E., MacDonald, 0. L. and Robinson, G. E. (1987). Anorexia nervosa, bulimia, and pregnancy. American Journal of Obstetrics and Gynecology, 157, 1194-1198.
WILLIS, D. C. and Rand, C. S. W. (1988). Pregnancy in bulimic women. Obstetrics and Gynecology, 7 1, 708-7 10.
WOODSIDE, D. B. and Shekter-Wolfson, L. F. (1990). Parenting by patients with anorexia nervosa and bulimia nervosa. International Journal of Eating Disorders, 9, 303-309.
Linda Lewis, BSocSc (Hons) (Graduate student, Department of Psychology) University of Cape Town, Rondebosch 7700, South Africa.
Daniel le Grange, MA (ClinPsych), PhD, CPsychol (Addressee for correspondence) (Senior Lecturer, Department. of Psychology) University of Cape Town, Rondebosch 7700, South Africa.
105
Copyright © 2022 FDOKUMEN




















