The Epidemiology of Narcolepsy - Oxford Academic
14
SLEEP, Vol. 30, No. 1, 2007 13 NARCOLEPSY INTRODUCTION THIS REVIEW CONCERNS THE EPIDEMIOLOGY OF NAR- COLEPSY. AFTER SOME BRIEF INTRODUCTORY COM- MENTS, WE WILL SUMMARIZE WHAT IS KNOWN from descriptive studies about measures of disease frequency in vari- ous populations. We will then turn to analytic studies that attempt to identify risk factors for narcolepsy. Finally, we will review the types of analytic epidemiologic studies that could be considered in exploring further hypotheses about the cause of narcolepsy. History In 1880, Gélineau applied the term narcolepsy to a sleep dis- order characterized by excessive daytime sleepiness and episodic weakness triggered by strong emotions. 1 Subsequently, the term cataplexy was adopted to describe the episodic weakness. 2,3 Di- agnostic criteria evolved emphasizing the clinical tetrad of ex- cessive daytime sleepiness, cataplexy, sleep paralysis, and hyp- nagogic hallucinations. 4 In the 1950s and 1960s, the duality of sleep with rapid eye movement (REM) and non-REM sleep was recognized in normal people, 5 and sleep-onset REM was de- scribed in patients with narcolepsy. 6 In the 1970s, the multiple sleep latency test (MSLT) was added to the polysomnogram as a way to document sleepiness and episodes of sleep-onset REM periods (SOREMP). 5 The recognition that obstructive sleep apnea syndrome was a common treatable cause of sleepiness and that diagnostic tests were reimbursable led to a proliferation of sleep medicine centers with expertise in diagnosing sleep-related con- ditions including narcolepsy. 5 Diagnosis Key to the diagnosis of narcolepsy is the combination of a common symptom, excessive daytime sleepiness, and an uncom- mon symptom, cataplexy. Formal sleep studies with polysom- nography and the MSLT can be used to document the sleepiness and SOREMPs. Caution must be exercised in making a diagnosis of narcolepsy in the absence of cataplexy because formal sleep studies fall short of 100% sensitivity or specificity. 7-9 Diagnos- tic criteria have been recently updated to define narcolepsy with cataplexy, narcolepsy without cataplexy, and narcolepsy due to another underlying medical condition (Table 1). 10 Criteria for nar- colepsy with cataplexy have changed little since the first recogni- tion of the disease. Although encouraged, formal sleep studies are not required for a diagnosis of narcolepsy with cataplexy. The new classification scheme also incorporates knowledge about genetics and hypocretins (orexins) to create clinical and pathophysiologic subtypes of narcolepsy. These aspects of the disease have been extensively reviewed. 11 The association of nar- colepsy with HLA, especially HLA DQB1*0602, has been recog- nized for decades. 12 Because of studies in twins and families, this HLA type is not thought sufficient in itself for the development The Epidemiology of Narcolepsy W.T. Longstreth, Jr., MD, MPH 1-3 ; Thomas D. Koepsell, MD, MPH 1,3,4 ; Thanh G. Ton, PhD 1,3 ; Audrey F. Hendrickson, MPH 1,2 ; Gerald van Belle, PhD 1,5,6 1 The Neuroepidemiology Research Group at the University of Washington, 2 Department of Neurology, School of Medicine, and Departments of 3 Epidemiology, 4 Health Services, 5 Biostatistics, and 6Environmental and Occupational Health Sciences, School of Public Health and Community Medicine, Seattle, WA Epidemiology of Narcolepsy—Longstreth et al Disclosure Statement Dr. Koepsell has received research support from Robert Wood Johnson Foundation, Centers for Disease Control and Prevention, National Institute on Aging, and the Department of Veterans Affairs. Dr. van Belle is on the Sci- entific Advisory Board for Washington University St. Louis Alzheimer Disease Research Center, the University of California San Diego, the University of California at Davis, and the Lovelace Research Foundation; is on the Mock Advisory Panel for Prestwick Pharmaceuticals and Novartis Pharmaceuti- cals; and is an advisor for BIATECH Institute and Blood Cell Storage, Incor- porated. Drs. Ton, Longstreth, and Hendrickson have indicated no financial conflicts of interest. Submitted for publication April 27, 2006 Accepted for publication September 3, 2006 Address correspondence to: WT Longstreth, Jr, MD, Department of Neurol- ogy, Box 359775, Harborview Medical Center, 325 Ninth Avenue, Seattle, WA 98104-2420; Tel: (206) 731-3251; Fax: (206) 731-8787; E-mail: wl@u. washington.edu Abstract: Much has been learned about the pathophysiology of narco- lepsy over the last several decades. It is likely that hypocretin-producing cells in the lateral hypothalamus are selectively destroyed in genetically susceptible individuals carrying 1 or more alleles of HLA DQB1*0602. De- spite advances, the causes of narcolepsy and how to prevent it remain elusive. Classic epidemiology aims not only to enumerate occurrence of disease in populations, but also to identify etiologic risk factors. This re- view details what the application of classic epidemiology has taught us so far about narcolepsy and suggests directions for future studies to clarify its etiology. The prevalence of narcolepsy with cataplexy has been examined in many studies and falls between 25 and 50 per 100,000 people. Infor- mation on incidence is limited, with 1 study finding the incidence of nar- colepsy with cataplexy to be 0.74 per 100,000 person-years. The search for etiologic risk factors has yet to yield important associations. Factors most thoroughly examined include body mass index, immune responses, and stressful life events. Such associations may reflect a consequence rather than a cause of disease. As with other diseases characterized by selective cell loss, such as Parkinson disease or type 1 diabetes mellitus, narcolepsy is likely caused by environmental exposures before the age of onset in genetically susceptible individuals. Matching efforts in these other diseases and using large well-designed epidemiologic studies of narcolepsy, investigators must intensify the search for these exposures, focusing on the first 2 decades of life. Identification of modifiable risk fac- tors will help to prevent this disease. Keywords: Narcolepsy, epidemiology, prevalence, incidence, epidemio- logic factors, risk factors Citation: Longstreth WTJr; Koepsell TD; Ton TG et al. The epidemiology of narcolepsy. SLEEP 2007;30(1):13-26. Downloaded from https://academic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of The Epidemiology of Narcolepsy - Oxford Academic

SLEEP, Vol. 30, No. 1, 2007 13
NARCOLEPSY
INTRODUCTION
THIS REVIEW CONCERNS THE EPIDEMIOLOGY OF NAR-COLEPSY. AFTER SOME BRIEF INTRODUCTORY COM-MENTS, WE WILL SUMMARIZE WHAT IS KNOWN from descriptive studies about measures of disease frequency in vari-ous populations. We will then turn to analytic studies that attempt to identify risk factors for narcolepsy. Finally, we will review the types of analytic epidemiologic studies that could be considered in exploring further hypotheses about the cause of narcolepsy.
History
In 1880, Gélineau applied the term narcolepsy to a sleep dis-order characterized by excessive daytime sleepiness and episodic weakness triggered by strong emotions.1 Subsequently, the term cataplexy was adopted to describe the episodic weakness.2,3 Di-
agnostic criteria evolved emphasizing the clinical tetrad of ex-cessive daytime sleepiness, cataplexy, sleep paralysis, and hyp-nagogic hallucinations.4 In the 1950s and 1960s, the duality of sleep with rapid eye movement (REM) and non-REM sleep was recognized in normal people,5 and sleep-onset REM was de-scribed in patients with narcolepsy.6 In the 1970s, the multiple sleep latency test (MSLT) was added to the polysomnogram as a way to document sleepiness and episodes of sleep-onset REM periods (SOREMP).5 The recognition that obstructive sleep apnea syndrome was a common treatable cause of sleepiness and that diagnostic tests were reimbursable led to a proliferation of sleep medicine centers with expertise in diagnosing sleep-related con-ditions including narcolepsy.5
Diagnosis
Key to the diagnosis of narcolepsy is the combination of a common symptom, excessive daytime sleepiness, and an uncom-mon symptom, cataplexy. Formal sleep studies with polysom-nography and the MSLT can be used to document the sleepiness and SOREMPs. Caution must be exercised in making a diagnosis of narcolepsy in the absence of cataplexy because formal sleep studies fall short of 100% sensitivity or specificity.7-9 Diagnos-tic criteria have been recently updated to define narcolepsy with cataplexy, narcolepsy without cataplexy, and narcolepsy due to another underlying medical condition (Table 1).10 Criteria for nar-colepsy with cataplexy have changed little since the first recogni-tion of the disease. Although encouraged, formal sleep studies are not required for a diagnosis of narcolepsy with cataplexy.
The new classification scheme also incorporates knowledge about genetics and hypocretins (orexins) to create clinical and pathophysiologic subtypes of narcolepsy. These aspects of the disease have been extensively reviewed.11 The association of nar-colepsy with HLA, especially HLA DQB1*0602, has been recog-nized for decades.12 Because of studies in twins and families, this HLA type is not thought sufficient in itself for the development
The Epidemiology of NarcolepsyW.T. Longstreth, Jr., MD, MPH1-3; Thomas D. Koepsell, MD, MPH1,3,4; Thanh G. Ton, PhD1,3; Audrey F. Hendrickson, MPH1,2; Gerald van Belle, PhD1,5,6
1The Neuroepidemiology Research Group at the University of Washington, 2Department of Neurology, School of Medicine, and Departments of 3Epidemiology, 4Health Services, 5Biostatistics, and 6Environmental and Occupational Health Sciences, School of Public Health and Community Medicine, Seattle, WA
Epidemiology of Narcolepsy—Longstreth et al
Disclosure StatementDr. Koepsell has received research support from Robert Wood Johnson Foundation, Centers for Disease Control and Prevention, National Institute on Aging, and the Department of Veterans Affairs. Dr. van Belle is on the Sci-entific Advisory Board for Washington University St. Louis Alzheimer Disease Research Center, the University of California San Diego, the University of California at Davis, and the Lovelace Research Foundation; is on the Mock Advisory Panel for Prestwick Pharmaceuticals and Novartis Pharmaceuti-cals; and is an advisor for BIATECH Institute and Blood Cell Storage, Incor-porated. Drs. Ton, Longstreth, and Hendrickson have indicated no financial conflicts of interest.
Submitted for publication April 27, 2006Accepted for publication September 3, 2006Address correspondence to: WT Longstreth, Jr, MD, Department of Neurol-ogy, Box 359775, Harborview Medical Center, 325 Ninth Avenue, Seattle, WA 98104-2420; Tel: (206) 731-3251; Fax: (206) 731-8787; E-mail: [email protected]
Abstract: Much has been learned about the pathophysiology of narco-lepsy over the last several decades. It is likely that hypocretin-producing cells in the lateral hypothalamus are selectively destroyed in genetically susceptible individuals carrying 1 or more alleles of HLA DQB1*0602. De-spite advances, the causes of narcolepsy and how to prevent it remain elusive. Classic epidemiology aims not only to enumerate occurrence of disease in populations, but also to identify etiologic risk factors. This re-view details what the application of classic epidemiology has taught us so far about narcolepsy and suggests directions for future studies to clarify its etiology. The prevalence of narcolepsy with cataplexy has been examined in many studies and falls between 25 and 50 per 100,000 people. Infor-mation on incidence is limited, with 1 study finding the incidence of nar-colepsy with cataplexy to be 0.74 per 100,000 person-years. The search for etiologic risk factors has yet to yield important associations. Factors
most thoroughly examined include body mass index, immune responses, and stressful life events. Such associations may reflect a consequence rather than a cause of disease. As with other diseases characterized by selective cell loss, such as Parkinson disease or type 1 diabetes mellitus, narcolepsy is likely caused by environmental exposures before the age of onset in genetically susceptible individuals. Matching efforts in these other diseases and using large well-designed epidemiologic studies of narcolepsy, investigators must intensify the search for these exposures, focusing on the first 2 decades of life. Identification of modifiable risk fac-tors will help to prevent this disease. Keywords: Narcolepsy, epidemiology, prevalence, incidence, epidemio-logic factors, risk factorsCitation: Longstreth WTJr; Koepsell TD; Ton TG et al. The epidemiology of narcolepsy. SLEEP 2007;30(1):13-26.
The Sleep Research Society was established in 1961 and now includes over 1200 members from a broad range of disciplines. The SRS is strategically placed to take the lead in promoting and understanding the processes of sleep and its disorders. At the core of the SRS activity is the promotion and facilitation of sleep research and development of new cadres of sleep researchers.
Grant Opportunities:The Sleep Research Foundation (SRSF) was established to award two grants: The Gillin Grant intended for beginning investigators for the purpose of gathering pilot data to be used for future grant applications. The Weitzman Grant intended for researchers to gather additional pilot data for NIH or other federal grants that are scored but not funded.
Training: Student opportunities include travel awards to help trainees in the early stages of postgraduate education attend the SLEEP Annual Meeting. Along with workshops, conferences, and websites that are all geared toward assisting students in their career development, the SRS has also created a trainee manual. This essential manual lists potential mentors and training laboratories, and includes information on grant mechanisms and current job/career opportunities.
Education: A Primer of Sleep Research course covers techniques, core knowledge, and emerging questions in sleep research. The SRS also published the Basics of Sleep Guide intended to serve as a study aid for sleep science, providing information about aspects of sleep while indicating potential areas for further exploration.
Research: Sleep & Public Task Force was created to respond to media articles and public issues, and make recommendations to the legislature concerning sleep and public safety.
The most effective way you can address public health and professional issues facing sleep medicine today is by joining the leading medical specialty society representing your field – THE AMERICAN ACADEMY OF SLEEP MEDICINE
When you become a part of the AASM, you join with other professionals as one strong, collective voice. Together we transform our passion for sleep medicine into meaningful action on behalf of our patients and our profession.
Stay Informed: Professional Publications & Educational Opportunities• Order any of the more than 70 discounted AASM products and services• Enjoy the peer-reviewed journals SLEEP and
Journal of Clinical Sleep Medicine which offer up to 32 CME credit opportunities
• Benefit from discounted fees and sign up for educational opportunities such as the SLEEP Annual
Meeting, Board Review Course, and many more
Practice Smarter:Practice Management Tools• Access the AASM web site, an indispensable resource containing important and up-to-date news, information, and initiatives• Participate in a section and interact with your colleagues through online discussion forums• Explore the members’ only section on the AASM web site that includes the NEW Online Learning Center, Sleep Medicine Advo-cate, Sleep Medicine Question Bank and much more!
Be Heard:Powerful National Advocacy Efforts• Leading the campaign to fix the Medicare Physician Fee Schedule • Promoting fair reimbursement for sleep medicine services• Advocating for patient awareness and monitoring “drowsy driving”
Contact the Membership Department at [email protected] or (708) 492-0930 for the AASM and (708) 492-1093 for the SRS with additional questions about membership.
Apply online at www.aasmnet.orgApply online at www.sleepresearchsociety.org
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 14
of the disease. Most people with this HLA DQB1*0602 do not have and will never develop narcolepsy. Familial forms of narco-lepsy are known but represent a distinct minority. The frequency of HLA DQB1*0602 in patients with narcolepsy depends upon how the disease is defined but is highest among those who have cataplexy.
More recently, a remarkable series of studies have suggested that narcolepsy results from the selective loss of cells in the lateral hypothalamus that secrete a neurotransmitter called hypocretin or orexin. Hypocretin-1 (orexin A) can be measured in the cerebro-spinal fluid (CSF) and has been found to be low in most patients diagnosed with narcolepsy with cataplexy, especially those with DQB1*0602 positivity.13-16 The sensitivity is around 90%, with specificity even higher.17 Nonetheless, about 10% of patients with typical narcolepsy with cataplexy will have normal levels, and, conversely, some patients with narcolepsy without cataplexy will have low levels. Heterogeneity of the disease is further suggested by DQB1*0602 positive monozygotic twin pairs. One pair con-cordant for narcolepsy with cataplexy had normal levels in both twins,18 whereas another pair discordant for narcolepsy had low levels only in the twin with narcolepsy.19 Experiments in animals suggest that symptoms of narcolepsy may not appear until a criti-cal number of hypocretin-producing cells are lost and that the remaining cells may increase their output to compensate for the loss.20,21
Epidemiology
Epidemiology comprises the study of distribution, determi-nants, and outcomes of illness in human populations with the goal of improving people's health.22 Epidemiology can be divided into 2 broad areas of study, classic and clinical.23 Classic epidemiology begins with descriptions of the occurrence and distribution of dis-ease in a population, through descriptive studies. But the power of its methods lies in the attempt to discover determinants of dis-ease, through analytic studies. The identification of etiologic risk factors opens the possibility of preventing disease by controlling
modifiable risk factors. Importantly, prevention is possible even when the pathophysiology of disease is unknown, and, converse-ly, prevention does not always follow as the pathophysiology or pathomechanism of disease starts to be clarified. Clinical epide-miology uses the techniques of classic epidemiology but applies them to populations of patients rather than populations of healthy people. The key question is not who will develop disease but who will experience a particular outcome from disease. Here the drive is to identify modifiable prognostic factors whose control through treatments improves outcomes. This review is limited to the clas-sic epidemiology of narcolepsy and starts with descriptive studies measuring prevalence, which is the proportion of people with nar-colepsy in a population at a particular time, and incidence, which is the rate at which people in a population develop narcolepsy over time.
Descriptive Studies
Prevalence
Putting aside case reports, which characterized much of the earliest literature, the beginnings of epidemiologic research on narcolepsy can be tracked to large case series, especially reports from physicians at the Mayo Clinic detailing their experience with the disease. The first patient given this diagnosis was seen at the Mayo Clinic in 1919; 35 patients, all with cataplexy, were seen between 1919 and 192824 and 33 patients were seen just in 1931.25 Although interesting for the increasing numbers seen at a single referral center, these studies do not provide useful esti-mates of the prevalence of narcolepsy in any defined population or time period. Given the different study designs, disease defini-tions, age groups and geographic regions used in investigations on the prevalence of narcolepsy—not surprisingly—estimates of prevalence have differed. Studies are summarized in the excellent work by Partinen and Hublin26 and in Table 2A, which is broken into sections that attempt to explain some of the differences in estimates.
Some of the highest estimates of prevalence come from studies in which subjects report having been diagnosed with narcolepsy, ranging in four studies from 168 to 799 per 100,000, with broad and overlapping 95% confidence intervals (Table 2a).27-30 The results strain credibility given how often participants had never heard of narcolepsy in a 1997 survey of 1001 adults in the United States conducted by the Gallup Organization.29 Only 53% had heard of narcolepsy, and only 28% of those participants felt they knew what it was.
Estimates are also high from studies based solely on an initial symptom screen without more in-depth evaluations (Table 2a). If the initial screen has a low threshold, which may enhance sen-sitivity but can compromise specificity, the number who screen positive can be inflated by many false positives. In several such surveys, prevalence has ranged from 10% to 30%.31-34 In one of these studies,34 10% of customers in Swiss pharmacies met crite-ria for narcolepsy based on their responses on the Stanford Sleep Disorders Questionnaire.35 When more strict screening criteria are used, estimates are lower, ranging from 160 to 660 per 100,000 people (Table 2a).36-41
Estimates from other studies are lower still. For some, the exact methods used to derive the estimate are unclear or involve many assumptions (Table 2a).42-46 For others, the methods are clearer, and the estimates are fairly consistent, except for those from the
Epidemiology of Narcolepsy—Longstreth et al
Table 1—Diagnostic Criteria for Narcolepsy
Narcolepsy With Cataplexy A. Excessive daytime sleepiness B. Definite history of cataplexy C. MSLT optional but advised D. Hypersomnia not better explained by another disorderNarcolepsy Without Cataplexy A. Excessive daytime sleepiness B. Typical cataplexy is not present C. Abnormal MSLT required D. Hypersomnia not better explained by another disorderNarcolepsy Due to Medical Condition A. Excessive daytime sleepiness B. Definite history of cataplexy, abnormal MSLT, or low CSF hypocretin-1 levels C. Underlying medical or neurological disorder accounts for daytime sleepiness D. Hypersomnia not better explained by another disorder
From The International Classification of Sleep Disorders: Diagnostic and Coding Manual. Westchester, IL: American Academy of Sleep Medicine; 2005. MSLT refers to Multiple Sleep Latency Test; CSF, cerebrospinal fluid.
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 15
Table 2a—Studies on the Prevalence of Narcolepsy
Study yeara Location and population
Diagnosis Number diagnosed/
number screened
Prevalence per 100,000(95% CI)b
Comments
Self-reported diagnosis199227 Tampere, Finland
Random stratified sample of adults
Questionnaire 2/1,190 168 (20 - 606)
199328 Wisconsin, United States
Random sample of state employees
aged 30-60 y
Questionnaire physician-di-agnosis of narcolepsy
13/4,931 264(140 - 450)
Investigators provided ad-ditional information to allow
estimates to be calculated
199729 United StatesNational sample aged 18 y and
older
Telephone survey with physician diagnosis of
narcolepsy
8/1,001 799 (346 - 1569)
Gallup Organization provided additional information to al-
low estimates to be calculated.
200030 SwitzerlandPostal clerks aged
19-65 y
Questionnaire 3/668 449 (93 - 1,307)
Initial symptom screen without follow up testing
200131 Kuwaiti adoles-cents aged 14 to
18 y
Symptoms from question-naire
336/2,574 13,054 (11,775
- 14,417)
Sudden attacks of irresistible sleep
200332 Wisconsin, United States Random sample of state employees aged
30-60 y
Symptoms from questionnaire 790/3,023 26,133 (24,574 - 27,738)
At least 1 of the major symptoms of narcolepsy besides
excessive daytime sleepiness.
200533 Sivas, TurkeyRandom sample of
adults
Interview using standard questionnaire
1,633/5,339 30,586 (29,352 - 31,842)
Answering “yes” to 3 of 14 questions related to narcolepsy
200634 Customers at Swiss pharmacies
Stanford Sleep Disorders Questionnaire35
493/4,901 10,059 (9,231 - 10,935)
Using published cut-off values
197936 Fujisawa City, Japanaged 12-16 y
Screening questionnaire 20/12,469 160 (98 - 248)
198237 FinlandMale military
recruits with mean age 20 y
Questionnaires 8/2,537 315 (136 - 620)
“Symptoms indicating narcolepsy”
199238 JapanAged 17-59 y
Questionnaire 27/4,559 592 (390 - 860)
Answered yes to excessive daytime sleepiness and
cataplexy199439 Finland
White twins aged 33 – 60 y
Screen 75/11,354 660 (520 - 827)
Using prespecified cut-off on Ullanlinna Narcolepsy Scale
31/11,354 273 (186 - 387)
Second screen but not yet second interview
199840 Population in south of France 15 years
and older
Questionnaire screen 29/14,195 204 (137 - 293)
Questionnaires displayed and distributed in waiting rooms of
physicians. 200241 China, Hong Kong
Chinese residentsaged 18-65 y
Phone screen, interview 28/9,851 284 (188 - 410)
Chinese version of the Ullanlinna Narcolepsy Scale
Studies with many or unknown assumptions196242,43 Czechoslovakia ? ? 20 - 30
(?)Investigator’s estimate
197244 San Francisco Bay Area, United States
Uncertain age
Newspaper advertisements and phone interviews
All with cataplexy
? 50(?)
Many assumptions and estimates
197345 Los Angeles area, United StatesUncertain age
Television show ? 67(?)
Many assumptions and estimates
198546 ? ? ? 40 “A reasonable guess”
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022
SLEEP, Vol. 30, No. 1, 2007 16
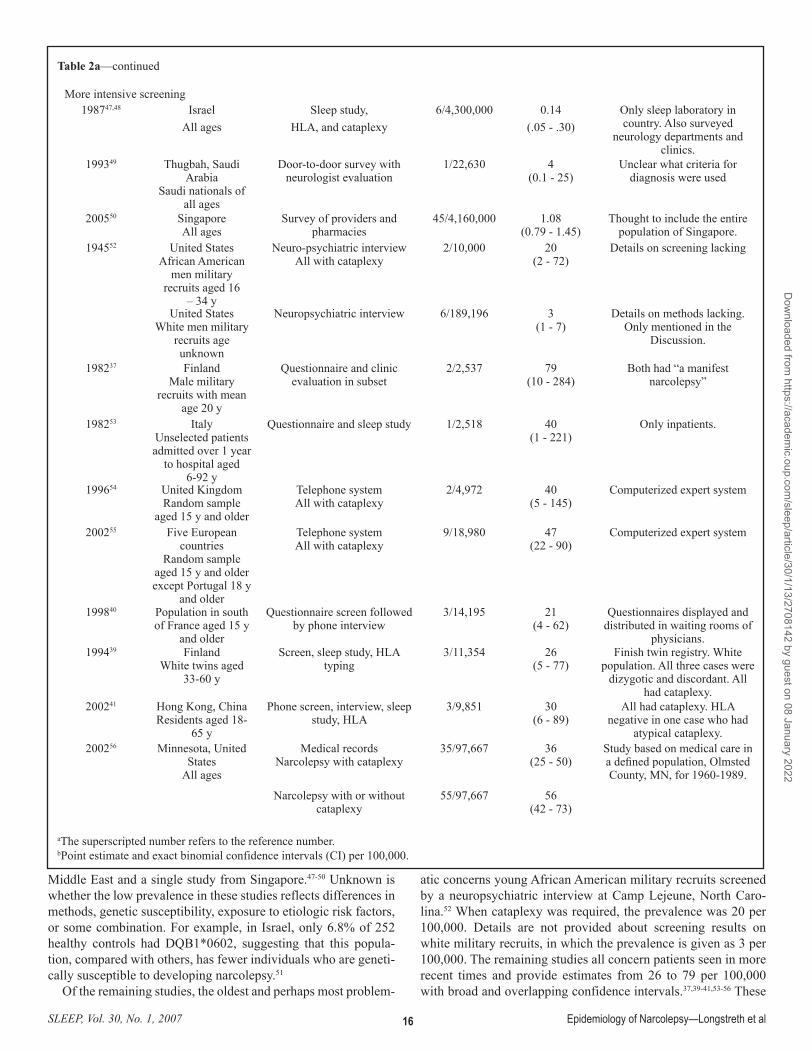
Middle East and a single study from Singapore.47-50 Unknown is whether the low prevalence in these studies reflects differences in methods, genetic susceptibility, exposure to etiologic risk factors, or some combination. For example, in Israel, only 6.8% of 252 healthy controls had DQB1*0602, suggesting that this popula-tion, compared with others, has fewer individuals who are geneti-cally susceptible to developing narcolepsy.51
Of the remaining studies, the oldest and perhaps most problem-
atic concerns young African American military recruits screened by a neuropsychiatric interview at Camp Lejeune, North Caro-lina.52 When cataplexy was required, the prevalence was 20 per 100,000. Details are not provided about screening results on white military recruits, in which the prevalence is given as 3 per 100,000. The remaining studies all concern patients seen in more recent times and provide estimates from 26 to 79 per 100,000 with broad and overlapping confidence intervals.37,39-41,53-56 These
Table 2a—continued
More intensive screening198747,48 Israel
All agesSleep study,
HLA, and cataplexy6/4,300,000 0.14
(.05 - .30)Only sleep laboratory in country. Also surveyed
neurology departments and clinics.
199349 Thugbah, Saudi Arabia
Saudi nationals of all ages
Door-to-door survey with neurologist evaluation
1/22,630 4(0.1 - 25)
Unclear what criteria for diagnosis were used
200550 SingaporeAll ages
Survey of providers and pharmacies
45/4,160,000 1.08(0.79 - 1.45)
Thought to include the entire population of Singapore.
194552 United StatesAfrican American
men military recruits aged 16
– 34 y
Neuro-psychiatric interviewAll with cataplexy
2/10,000 20 (2 - 72)
Details on screening lacking
United StatesWhite men military
recruits age unknown
Neuropsychiatric interview 6/189,196 3 (1 - 7)
Details on methods lacking. Only mentioned in the
Discussion.
198237 FinlandMale military
recruits with mean age 20 y
Questionnaire and clinic evaluation in subset
2/2,537 79(10 - 284)
Both had “a manifest narcolepsy”
198253 ItalyUnselected patients admitted over 1 year
to hospital aged 6-92 y
Questionnaire and sleep study 1/2,518 40(1 - 221)
Only inpatients.
199654 United KingdomRandom sample
aged 15 y and older
Telephone system All with cataplexy
2/4,972 40 (5 - 145)
Computerized expert system
200255 Five European countries
Random sample aged 15 y and older except Portugal 18 y
and older
Telephone systemAll with cataplexy
9/18,980 47 (22 - 90)
Computerized expert system
199840 Population in south of France aged 15 y
and older
Questionnaire screen followed by phone interview
3/14,195 21 (4 - 62)
Questionnaires displayed and distributed in waiting rooms of
physicians. 199439 Finland
White twins aged 33-60 y
Screen, sleep study, HLA typing
3/11,354 26 (5 - 77)
Finish twin registry. White population. All three cases were
dizygotic and discordant. All had cataplexy.
200241 Hong Kong, ChinaResidents aged 18-
65 y
Phone screen, interview, sleep study, HLA
3/9,851 30(6 - 89)
All had cataplexy. HLA negative in one case who had
atypical cataplexy. 200256 Minnesota, United
StatesAll ages
Medical recordsNarcolepsy with cataplexy
35/97,667 36(25 - 50)
Study based on medical care in a defined population, Olmsted County, MN, for 1960-1989.
Narcolepsy with or without cataplexy
55/97,667 56(42 - 73)
aThe superscripted number refers to the reference number.bPoint estimate and exact binomial confidence intervals (CI) per 100,000.
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 17
studies begin with a screen of symptoms followed up by more detailed testing, with the exception being the study from Mayo Clinic investigators.56 Despite other studies suggesting that many patients with narcolepsy do not come to medical attention or that narcolepsy is not diagnosed if they do,39,57 the estimates from Olm-sted County are remarkably similar to those based on multistaged screening of particular populations. Perhaps residents of Olmsted County differ from those living elsewhere in their access to medi-cal care and likelihood of their narcolepsy being diagnosed. One advantage of such studies includes identifying a larger number of people with narcolepsy, with the resulting estimate of prevalence having narrower 95% confidence intervals than in studies with multistaged screening of a population. The most methodologi-cally sound studies seem consistent with the findings from Olm-sted County,56 suggesting that the prevalence of narcolepsy with cataplexy is in the range of 25 to 50 per 100,000.
The prevalence of narcolepsy is higher when cataplexy is not required: 56 per 100,000 with the 95% confidence interval 42 to 73 in the study from Olmsted County.56 In the community-based Wisconsin Sleep Study, nocturnal polysomnograms and MSLTs were performed in 556 people.9 Criteria for narcolepsy without cataplexy (Table 1) were met in 13 (2.3%), of whom 5 (0.9%) were also positive for HLA DQB1*0602. These findings sug-gest that current criteria for narcolepsy without cataplexy (Table 1) will identify many false positives, that many more people are affected by narcolepsy than would be suggested by considering only those symptomatic with typical cataplexy, or that a combina-tion of these explanations is present.9
Incidence
Investigators at the Mayo Clinic also used the records-linkage system of the Rochester Epidemiology Project to estimate the in-cidence of narcolepsy. The average incidence between 1960 and 1989 was 0.74 per 100,000 person-years for narcolepsy with cata-plexy and 1.37 per 100,000 person-years for narcolepsy with or without cataplexy (Table 2b),56 putting it in the range of what has been described for multiple sclerosis and motor neuron disease. If the incidence and time course of illness remain stable over time, prevalence should approximately equal incidence times dura-tion of illness.22 Applying this relation with results from Olmsted County suggests that the estimated duration of narcolepsy with cataplexy would be about 48.6 years (36/0.74).
Demographics
Sex, race, ethnicity, and geographic distribution have not been
studied beyond what has already been described in the studies of prevalence and incidence. In Olmsted County, narcolepsy was more common in men than women,56 as suggested in an early case series from the Mayo Clinic.25 Considering all patients with narcolepsy, the relative risk was 1.6:1, and prevalence ratio was 1.8:1. Considering patients with narcolepsy with cataplexy, the relative risk was 1.2:1, and prevalence ratio was 1.4:1. These findings and those from the Wisconsin Sleep Cohort Study9 sug-gest that the sex difference is greater in those without cataplexy. Although a case series had suggested a bimodal distribution of onset with 1 peak around age 15 and a second peak around age 35,58 the Mayo Clinic study did not.59 In Olmsted County, the me-dian age of onset was 16 year old with a range from 4 to 56. The 25th percentile for onset was 12.5 years; the 75th percentile, 25.7 years; and the 90th percentile, 33.4 years. Onset did not differ by sex or HLA type.
Analytic Studies
Several etiologic hypotheses for narcolepsy have been sug-gested. Over a decade ago, Guilleminault wrote,60 “Clearly, at this time, one must conclude that some combination of genetic and environmental factors is probably involved in the development of human narcolepsy.” We now summarize findings on studies examining a number of factors possibly related with the risk of narcolepsy.
Lifestyle
Little has been reported about lifestyle and behavioral risk factors such as exercise, alcohol use, tobacco use, or illicit drug use. One study suggested that excessive alcohol use may be more common in patients with narcolepsy.61
Obesity
Many studies have indicated an association between narcolep-sy and obesity (Table 3), as was suggested in early case series.24,25 In small studies from the 1970s, narcoleptic cases reported eating more snacks than controls62-64 but, in a subsequent study, were found to consume fewer kilojoules of food per day than controls.65 The early studies also demonstrated that narcoleptic cases were more likely to be overweight than were controls,62-64 an observa-tion subsequently confirmed by others.14,66-73 Using oral glucose tolerance tests, Honda and associates identified definite non–in-sulin-dependent diabetes mellitus in 6 of 48 (12.5%) patients with narcolepsy in Japan and argued that this prevalence was higher than reported in other populations in Japan.66
Table 2b—Studies on the Incidence of Narcolepsy
Study yeara
Location and population
Diagnosis Number diag-nosed by num-ber screened
Incidence per 100,000 person-years (95% CI)b
Comments
200256 Minnesota, United States
All ages
Medical records Narco-lepsy with cataplexy
19/2,558,169 0.74(0.47 - 1.16)
Study based on medical care in a defined population, Olmsted County, MN, for 1960-1989.
Narcolepsy with or with-out cataplexy
35/2,558,169 1.37(0.95 - 1.90)
aThe superscripted number refers to the reference number.bPoint estimate and exact binomial confidence intervals (CI) per 100,000.
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 18
Table 3—Studies of Factors Potentially Associated With Narcolepsy Study yeara
Number of Cases
Diagnosis of Narcolepsy
Number of controls
Source Factors examined Comments
Obesity197562 24 Unknown cata-
plexy14 Community Eating habits Cases more likely over-
weight and more snacks than controls
197663,64 42 Unknown cata-plexy
16 Unknown Eating habits Cases more likely over-weight and more snacks
than controls199665 12 All with cataplexy 12 Matched on sex
and social classSpontaneous food
choiceCases consumed fewer
kilojoules of food per day than controls
198666 197 All with cataplexy 96 General psychia-try patients
Weight Obesity more common in cases than controls
200168 132 All but 3 with cataplexy
5,236 Sample of general Swiss and Ger-man population
BMI Greater in cases than controls
132 All but 3 with cataplexy
104 Psychiatric inpa-tients
BMI Greater in cases than controls
200114 38 All with cataplexy 34 Healthy and neu-rologic controls
BMI and CSF leptin
BMI greater in cases than controls. CSF leptin
higher in cases than controls
200370 138 With and without cataplexy
10,696 Sample of general Dutch population
BMI and waist circumference
Obesity and excess body fat more common in cases than controls
138 With and without cataplexy
33 Patients with idiopathic hyper-
somnia
BMI and waist circumference
Obesity and excess body fat more common in cases than controls
200371 124 Newly diagnosed 120 Newly diagnosed with other condi-
tions
BMI Greater in cases than controls
200472 31 Children 31 Age and gender matched
BMI Greater in cases than controls
200573 157 75% with cata-plexy
164 Spouses of pa-tients with sleep
disorders
BMI Greater in cases than controls even controlling
for age and gender200074 15 All with cataplexy 30 Psychiatric and
neurologic pa-tients matched on age, sex, and BMI
Serum and CSF leptin
Serum levels lower in cases than controls
200275 6 All with cata-plexy, HLA
DQB1*0602, and low CSF hypocre-
tin 1
6 Matched on age, sex, BMI
Plasma leptin levels
Decreased in cases com-pared to controls
Migraine200380 96 From approved
sleep clinicsWith and without
cataplexy
96 Matched on age and sex
Formal evaluation for headache
Migraine not more com-mon (OR 1.13; 95% CI
0.56-2.27) but other types of headaches were (OR 2.23, 95% CI 1.38-3.61)
Genetic issues200187 420 All with cataplexy
in 3 ethnic groups1,087 Unknown in 3
ethnic groupsOther HLA class II
allelesSix increased and three
decreased risk.Also increased risk with DQB1*0602 homozy-
gosity200188 149 All DQB1*0602
positive83 All DQB1*0602
positiveTNF and its recep-
tor-2 genesIncreased risk with the combination of both.
Also Decreased risk with DRB1*1501
200689 370 All with cataplexy and DQB1*0602
positive
735 DQB1*0602 posi-tive in 125
Genomewide search with 23,244
microsatellite markers
In series of case-control studies, new resistance gene found on chromo-
some 21
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 19
Table 3—continuedImmune issues198994 52 Unknown cataplexy 49 Unknown Serologic reac-
tions to bacterial and viral agents
Cases with significantly more elevated antibodies to streptolysin O, 42%
vs. 2%198995 31 All with cataplexy 18 Idiopathic hyper-
somniaAntibodies to streptolysin O
Elevated in both groups, 23% in cases and 33% in
controls199098 100 All with cataplexy 107 Unknown Antibodies to
streptolysin ONot significantly differ-
ent, 48% vs. 36%. 200599 63 All with cataplexy 63 Unrelated family
and community members
Infectious diseases Flu infections and unex-plained fevers before age 20 more common in cases
than controls1988100 11 Unknown cataplexy 10 Sleep apnea Many autoimmune
screensNo differences
2002102 41 With and without cataplexy
0 Multiple autoanti-bodies
No support for autoim-mune hypothesis
2003103 28 With and without cataplexy
0 Antiganglioside antibodies
No support for autoim-mune hypothesis
2004104 39 With and without cataplexy
40 Family and friends
TNF-α, IL-6, human growth
hormone
All elevated in cases
2005105 41 All with cata-plexy and HLA
DQB1*0602
55 Patient with OSA
IgG reactive to prepro-hypocretin, hypocretin-1 & 2
No support for autoim-mune hypothesis
19 All with cata-plexy and HLA
DQB1*0602
13 Patients under-going lumbar
punctures
IgG reactive to prepro-hypocretin, hypocretin-1 & 2
No support for autoim-mune hypothesis
2005106 34 All with cata-plexy and HLA
DQB1*0602
49 Patients with OSA and psychiatric
problems
Various hypocretin antibodies
No support for autoim-mune hypothesis
2005107 45 All with cata-plexy and HLA
DQB1*0602
57 Unknown Serum tests seek-ing reactivity to rat hypothalamic
extract
No support for autoim-mune hypothesis
2005108 76 Unknown cataplexy 111 Unknown Autoantibodies against human lat-eral hypothalamic
neurons
No support for autoim-mune hypothesis
2006109 76 Cataplexy in 88%, HLA DQB1*0602 in 93% of 59 tested
63 Without any medical condition
Autoantibodies against human lat-eral hypothalamic
neurons
No support for autoim-mune hypothesis
2006110 181 All but 10 with cataplexy and HLA
DQB1*0602
101 Healthy controls and 10 with other
hypersomnias
Serum autoan-tibodies against
hypocretin and its 2 receptors
No support for autoim-mune hypothesis
2004111 9 With and with-out cataplexy
but all with HLA DQB1*0602
9 Unknown Functional autoan-tibodies enhancing
postganglionic cholinergic neuro-
transmission
Support for autoimmune hypothesis, antibodies in
cases not controls
2005107 20 All with cata-plexy and HLA
DQB1*0602
20 Unknown IgG in CSF reac-tive to rat hypotha-
lamic protein extract
Support for autoimmune hypothesis, significantly more common in cases
than controlsStress1994114 50 Unknown cataplexy 50 Matched Life-stress events
in year before onset
Cases with more events than controls
200599 63 All with cataplexy 63 Unrelated family and community
members
Psychological stressors
Major change in sleeping habits and childbirth
more common in cases than controls
aSuperscripted numbers refer to the reference numbers.BMI refers to body mass index; CSF, cerebrospinal fluid, TNF, tumor necrosis factor; IL, interleukin; OSA, obstructive sleep apnea; IgG, im-munoglobulin G.
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 20
In a comprehensive study, Kok and associates compared an-thropometric data in 138 patients with narcolepsy to similar mea-surements made in a population survey of 10,696 people and to a group of 33 patients with idiopathic hypersomnia.70 Excess body mass index and excess body fat, as reflected in waist circumfer-ence, were more common in case patients with narcolepsy than those in the 2 control groups. The findings did not seem to depend upon the drugs used by the patients with narcolepsy, an observa-tion also made by others.71 The differences with patients affected by idiopathic hypersomnia suggested that the findings did not simply reflect sleepiness and inactivity but, rather, reflected hypo-cretin levels, which was documented in the CSF of a subgroup of the patients with narcolepsy and idiopathic hypersomnia. In another study, body mass index was higher in narcoleptic patients with lower CSF hypocretin-1 levels, compared with those with higher CSF hypocretin-1 levels.14 Although 1 study documented higher CSF leptin levels in cases than controls,14 another study did not.74 Two studies showed serum leptin levels lower in cases than in controls.74,75 Whether a problem with leptin production, resis-tance, or some combination plays a role in narcolepsy and obesity is unresolved by these studies.
Although obesity seems to be present from the early stages of the disease, even in disease with onset in childhood,72 whether it predates the onset of symptoms of narcolepsy is unknown. Obesity in patients with narcolepsy may be related to some other substance produced by hypocretin-containing cells in that mice lacking these cells have obesity whereas those lacking just hypo-cretin do not.76 Whether obesity provides clues about etiology or is simply a manifestation of narcolepsy cannot be resolved by these case-control studies, none of which examined weight before the onset of disease, for example, at birth.
Associated Diseases
Given these considerations about obesity, patients with nar-colepsy may be at greater risk than the general population for conditions that can complicate abdominal obesity, including type 2 diabetes mellitus and cardiovascular disease. Given that HLA-DQB1*0602 is protective for type 1 diabetes mellitus,77 one would expect fewer narcoleptics to be affected with type 1 as opposed to type 2 diabetes mellitus, but such studies are yet to be done.
A high prevalence of migraine in patients with narcolepsy was suggested by initial case series: 54% of 68 patients in 1 study78 and 37% of 100 patients in another.79 In a follow-up case-con-trol study including 96 patients with narcolepsy and 96 healthy matched controls, a significant association was not found with migraine but was found with other types of headaches, which in all but 2 subjects met criteria for tension-type headaches.80 The investigators suspected that these headaches were most likely a consequence of the sleep disorder or its treatment. Narcolepsy is also said to be associated with other sleep disorders,11 which may reflect in part the bias of being cared for by sleep medicine spe-cialists.
Timing of Birth
A preliminary study on narcolepsy from France suggested peaks for births of patients destined to develop narcolepsy in March and August, with a valley in November.81 An increase in March and a decrease in September was described in a study from the Unit-ed States82 and in a larger overlapping study with patients from
France, Canada, and the United States.83 An increase in the first half of year, especially in the spring, and a decrease in the second half of the year, especially in September, was described in a Ger-man study.84 Using data from the randomized trial of modafinil, investigators found an overall excess of births in March and defi-cit in September in patients with narcolepsy with cataplexy.85 The differences were not significant except in the subgroup whose cataplexy was moderate or severe. Such studies suggest that an exposure in utero may increase risk of disease, in which case con-cordance in monozygotic and dizygotic twins would be expected to be greater than has been described.12,86 Alternatively, an infec-tion in the first few months following birth could affect subse-quent risk of narcolepsy.
Genetics
Although the association of narcolepsy with HLA-DQB1*0602 is well established12 and will not be reviewed further, investiga-tors have attempted to define other genetic contributors to disease risk. In a large case-control study involving 420 case patients with narcolepsy and cataplexy and 1,087 control subjects, inves-tigators examined the risk associated with other HLA class II al-leles.87 They found 6 alleles increased and 3 alleles decreased the risk. Also, risk was increased with DQB1*0602 homozygosity. In another case-control study—in which all subjects, cases and controls, were HLA-DQB1*0602 positive—investigators looked at tumor necrosis factor and its receptor-2 genes in 149 cases and 83 controls.88 Results showed associations with certain combina-tions of tumor necrosis factor and its receptor-2 genes. Finally, in a series of recent case-control studies, investigators used genome-wide association studies starting with 23,244 microsatellite mak-ers to identify a novel resistance gene on chromosome 21.89 They proposed the name narcolepsy candidate-region gene (NLC1-A) and found it to be expressed in the human brain, including the hypothalamus. Confirmation of these findings and investigations of other regions is pending.
Immune Considerations
Given that genetic susceptibility to narcolepsy is linked to a specific HLA type, many investigators have suspected an immu-nologic basis for the disease,90-93 either by an autoimmune mecha-nism or in response to some external antigen, possibly an infec-tious agent. Two studies have suggested a role for streptococcal infections.94,95 Streptococcal disease has long been associated with brain dysfunction thought to be based on an immunologic response, such as with Sydenham chorea and, more recently, pe-diatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS).96,97 Unfortunately, results from these initial studies could not be confirmed in a subsequent large study.98 Infections in general were addressed in another case-control study, in which 63 patients with narcolepsy with cataplexy were recruited from the Stanford Center for Narco-lepsy.99 An equal number of controls frequency matched on age were recruited from unrelated family members of cases and lo-cal community members. Using a mailed self-administered ques-tionnaire, information was collected about events prior to age 20 years old. Flu infections (odds ratio 1.8, p < .05) and unexplained fevers (odds ratio 3.9, p < .05) were more common in cases than in controls.
Several case-control studies have examined a variety of labora-
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 21
tory tests that could support an immunologic basis for narcolepsy. In an early study, investigators looked for markers of autoimmune process but found none, including rheumatoid factor, antinuclear antibodies, antibodies to rodent brain and primate brain stem, and neurocytotoxic antibodies.100 In case series without controls, in-vestigators studied blood and CSF but found little support for an immune-mediated etiology.101-103 In another study, tumor necro-sis factor-α and interleukin-6 and human growth hormone were found to be higher in narcoleptics (n = 39) than in controls (n = 40), who were nonnarcoleptic family members and friends.104
Nonetheless, multiple other efforts have failed to find differences between cases with narcolepsy and controls in a variety of mea-sures, as detailed in Table 3.105-110
Some studies have provided support for an immune-mediated etiology. Comparing 9 cases and 9 controls, investigators identi-fied functional autoantibodies in immunoglobulin G fraction of patients with narcolepsy but not controls.111 The autoantibodies enhanced postganglionic cholinergic neurotransmission. Other investigators have found significant differences when they com-pared CSF of 20 patients with narcolepsy and 20 controls.107
The patients with narcolepsy all had cataplexy, carried HLA DQB1*0602, and had low CSF hypocretin-1 concentrations. The narcoleptic patients but not the controls had immunoglobulin G in their CSF that reacted to a rat hypothalamic protein extract, presumably containing hypocretin-secreting cells. Difficult in all of these studies is knowing if positive findings represent a cause or effect of the disease.
Stress
Case series initially suggested a role for stress,112,113 and sub-sequently 2 case-control studies found associations with stressful events prior to the onset of disease.99,114 In the more recent case-control study, major changes in sleeping habits (odds ratio = 2.0, p < .01) and childbirth (odds ratio = 2.7, p < .05) were more com-mon in cases than in controls.99 Total stressors before age 10 years old were also associated (odds ratio 1.2, p < .05). In a small case series of 9 patients, closed head injury was suggested as another possible stress.115 Such studies are challenging because patients with narcolepsy may be more motivated to recall stressful events than control subjects who lack a dramatic event such as the onset of a chronic disease.
Hypothesis and Epidemiologic Study Designs
Hypothesis
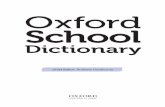
Analytic studies begin with an etiologic hypothesis or model. For narcolepsy, such a model might posit that genetically sus-ceptible individuals, as defined by having 1 or more alleles of HLA DQB1*0602, are exposed to an environmental agent that selectively and irreversibly affects the neurotransmitter systems involved in REM-sleep regulation by destroying hypocretin-pro-ducing cells in the hypothalamus. The system either fails at the time of the exposure or at some later date, possibly following some event that brings the patient to medical attention, at which time symptoms may be recognized as due to narcolepsy (Figure 1). Given that most individuals have the onset of their symptoms of narcolepsy in late adolescence, the exposures responsible for most cases would need to have occurred during or before late ado-lescence. Lack of concordance of narcolepsy in twins makes less
likely an exposure prior to birth, namely in utero.12,86 Analytic studies use a variety of epidemiologic study designs
to address an etiologic hypothesis, with the 2 main observa-tional study designs being the case-control study and the cohort study.22,23 Each has its advantages and disadvantages. Regardless of which is used, design considerations should always include the number of subjects needed to ensure that important associations are not missed due to inadequate statistical power. Investigators must also be alert to the possibility of confounding and effect modification and accept that more than a strong association is needed to establish causality.
Case-Control Studies
For investigations of uncommon diseases like narcolepsy, case-control studies may have advantages, especially when hy-potheses include gene-environment interactions. Investigators begin by identifying patients with narcolepsy. To reduce the risk of bias, ideally, patients with narcolepsy comprise all of the cases in a defined population, not just those seen at specialty clinics. Identification of control subjects is then simplified in that they are recruited from the same population. If gene-environment in-teractions are suspected and a marker for genetic susceptibility is known, the search for environmental risk factors is facilitated if cases and controls are chosen to be similar on this marker. Infor-mation on past exposures is then collected from cases and con-trols in an identical fashion, concentrating on exposures occur-ring before the onset of the disease, say for narcolepsy before the age of 20. To make sure that strong associations are not missed, analyses must consider the genetic marker and seek gene-envi-ronment interactions (Table 4).
Cohort Studies
Rather than starting with a group of cases with the disease, the investigator begins a cohort study by assembling a cohort of people who are free of the disease of interest. The exposures of interest are documented, and both exposed and nonexposed in-dividuals are followed over time for the occurrence of disease. Study cohorts can be assembled prospectively or retrospectively. Although the cohort design is a powerful tool for epidemiologic investigations of etiology, prospective cohort studies may not be practical with uncommon diseases such as narcolepsy, and retro-spective cohort studies depend on having good preexisting data on quite a large population. The study from Olmsted County,
Etiology ofNarcolepsy
ENVIRONMENTALEXPOSURE
CLINICALONSET
DISEASE
PRE-DISEASE
GENETICPREDISPOSITIONHLA DQB1*0602
INJURY TO CRITICAL CELLS
PRODUCINGHYPOCRETIN
MA
SS
OF
CE
LLS
TIME
Figure 1—Model for the etiology of narcolepsy, modified from a similar model proposed for type 1 diabetes.122
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 22
Minnesota, represents an example of a retrospective cohort study, in which patients with narcolepsy were identified between 1960 and 1995 in Olmsted County using the record-linkage system of the Rochester Epidemiology Project.56 A total of 72 patients with narcolepsy were identified and used to calculate prevalence and incidence that are reported in Table 2a and b. To the extent that information on a particular risk factor was available on the entire population in Olmsted County, it could be evaluated in this retro-spective cohort study. Small numbers of patients with narcolepsy, especially those with cataplexy, would limit the statistical power of such studies. Also, without a screen of the entire population, some patients with narcolepsy, especially those without cataplexy, would never be identified or included in such studies.
Given the estimates on incidence and prevalence of narcolepsy, huge numbers of people would need to be screened for the diag-nosis of narcolepsy in a prospective cohort study. In the classical cohort study design, information on potential etiologic risk fac-
tors would have to be collected on the entire cohort. Although such studies may seem impossible, they have been done for other chronic neurologic diseases, such as multiple sclerosis116 and Par-kinson disease,117,118 although not as a primary goal of the origi-nal study, which typically concerns more common diseases, such as vascular disease and cancer. An example would be the cohort study of multiple sclerosis in female registered nurses living in the United States.116 The investigation included combining re-sults from 2 prospective studies, 1 recruiting 121,700 nurses in 1976, and the other, 116,671 nurses in 1989, for a total of 238,371 nurses. On follow-up, consisting of 2,349,356 person-years, 173 women were diagnosed with multiple sclerosis and were eligible for the study of vitamin D, which was found to be protective.116
To date, etiologic questions in narcolepsy have not been ad-dressed in such cohort studies. Even assuming that all participants with prevalent narcolepsy with cataplexy could be identified among the 238,371 nurses in this study and given the estimate above from Olmsted County of prevalence of narcolepsy with cataplexy of 36 per 100,000,56 investigators would anticipate finding only 86 nurses with prevalent narcolepsy. Also, the ex-posure of interest would have had to have been collected as part of the original study. Otherwise, information on the past exposure would need to be collected from everyone in the cohort. Alterna-tively, a nested case-control or case-cohort design could be used, getting exposure data on just a sample of noncases or a sample of the full cohort. Either design would offer major advantages in efficiency. One can even still estimate exposure-specific preva-lences, albeit with somewhat wider confidence limits than if ex-posure data were available on everyone.
DISCUSSION
Compared with other chronic disabling diseases of the nervous system, relatively few epidemiologic studies of narcolepsy have been performed, especially analytic studies addressing etiologic hypotheses. The prevalence of narcolepsy with cataplexy lies be-tween 25 and 50 per 100,000 people. In 1 study, the incidence of narcolepsy with cataplexy was estimated to be 0.74 per 100,000 person-years (95% confidence interval 0.47-1.16).56 With respect to risk factors, the association with HLA DQB1*0602 is well established and makes a gene-environment interaction likely to play a role in the etiology of narcolepsy with cataplexy. Studies showing associations with obesity are consistent but may reflect a consequence rather than a cause of the disease. Evidence to sup-port an immune mechanism of disease has been sought but has not yet pointed to the inciting event, avoidance of which could prevent the disease.
Other diseases with selective cell loss may provide useful les-sons for investigators seeking risk factors for narcolepsy. Parkin-son disease results from a selective loss of dopamine-secreting cells in the substantia nigra. Parkinson disease is an example in which gene-environment interaction is strongly suspected but not yet been established despite substantially more effort than has been devoted to narcolepsy.119-121 Both diseases result from imbalances in neurotransmitter systems. Both are improved by medications that act through these systems to try to restore bal-ance. Suspicions that neurotoxins could cause parkinsonism have been confirmed by observations in patients and animals exposed to certain chemicals, but especially to the meperidine derivative 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP).119 This
Table 4—Hypothetical Example of Gene-Environment Interaction in a Case-Control Study of Narcolepsy
Assume that cases are all patients having narcolepsy with cataplexy in some defined population. Controls are from that same population and do not have narcolepsy. Exposure to some putative risk factor be-fore age 20 years is documented in cases and controls. Table A shows only a weak association with exposure when HLA DQB1*0602 status is not considered. The 95% confidence interval includes 1, and the association is not statistically significant.
A. Case-Patients Control-SubjectsExposed 21 72Not exposed 41 178 62 250Odds ratio (21*178)/(41*72) = 1.3 (95% Confidence interval 0.7 - 2.4)
HLA DQB1*0602 alleles sought and found in 80% of cases and 20% of controls. Anticipating such a difference, investigators had recruited proportionately more controls than cases to obtain comparable num-bers of cases and controls in the following analysis. Only those with 1 or more alleles are included in subsequent analyses and in Table B. The association is stronger. The 95% confidence interval does not include 1, and the association is statistically significant.
B. Case-Patients Control-SubjectsExposed 17 6Not exposed 33 44 50 50Odds ratio (17*44)/(33*6) = 3.8 (95% Confidence interval 1.2 - 12.9)
In those without any HLA DQB1*0602 alleles, Table C shows no association with exposure.
C. Case-Patients Control-SubjectsExposed 4 66Not exposed 8 134 12 200Odds ratio (4*134)/(8*66) = 1.0 (95% Confidence interval 0.2 - 3.9)
Conclusion: A gene-environment interaction is present. Exposure to the putative risk factor only confers risk in those who carry 1 or more HLA DQB1*0602 alleles.
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 23
toxin is very selective in irreversibly damaging a neurotransmit-ter system that employs dopamine. An intensive epidemiologic search continues to identify a xenobiotic that, in susceptible indi-viduals, could act like MPTP to selectively injure neurotransmit-ter systems and result in Parkinson disease. Such an ecogenetic hypothesis may explain other chronic nervous system diseases.
The selective cell loss need not be in the brain to carry potential lessons. Type 1 diabetes mellitus has some remarkable similarities to narcolepsy. Both involve selective loss of cells that secrete an essential chemical, in the case of type 1 diabetes, the beta cells in the pancreatic islets of Langerhans that secrete insulin.122,123 Like narcolepsy, the disease typically starts in childhood, in a geneti-cally susceptible individual defined by certain HLA types. Figure 1 is actually modified from a figure included in a review of type 1 diabetes.122 Curiously, the HLA haplotype associated with suscep-tibility to narcolepsy is found to be protective in type 1 diabetes mellitus. An autoimmune disease is suspected, and autoantibod-ies have been identified to islet cells, insulin, and glutamic acid decarboxylase (GAD). Whether they are a cause or effect of the process that destroys islet cells is uncertain.
Much remains to be learned about the etiology of narcolepsy using the techniques of epidemiology, and the search for etiologic risk factors for narcolepsy should be intensified, as has occurred with many other diseases that affect the nervous system. One ad-vantage with narcolepsy is that the genetic predisposition and the critical period of exposure in the environment are both well de-fined. Prospective cohort studies specifically about narcolepsy are not likely to be done for reasons discussed above. Retrospective cohort studies are possible, as the investigators from the Mayo Clinic have demonstrated, and should be used to seek etiologic risk factors. On the other hand, case-control studies may be the most efficient means to address etiologic hypotheses, especially those including a gene-environment interactions. Finally, case-control studies can be nested in cohort studies if cases can be identified within the cohort study and some assessment is needed, such as blood or CSF test, which would not be appropriate to perform on all members of the cohort. The case patients could be identified and matched to control subjects on factors such as demographics and HLA type and then assessed in a similar fashion. Information prospectively collected as part of the cohort study could be used, or new information could be collected. Such a nested design often requires fewer resources than the cohort design.
Given the similarities between narcolepsy and type 1 diabetes, a search for some of the risk factors suggested for type 1 diabetes, including viral infections, toxins, and certain foods.123 Although investigators have already begun the search for evidence to sup-port an immunologic basis for narcolepsy, little has been done to investigate a neurotoxin as has also been suggested with Parkin-son disease. Genetic susceptibility to a neurotoxin could be con-ferred in a number of ways.124 Whether an HLA gene or another in genetic disequilibrium with the HLA haplotype, the genetic factor could make the sleep-regulatory system or its development more susceptible to injury from a toxin. The genetic factor could also alter the way in which a potential toxin is metabolized, resulting in failure to break down a toxin or in excess production of a toxin from a pro-toxin.
With respect to neurotoxins, a chemical that has the potential to affect brain function seems most likely. Such a substance could include medications or illicit drugs. Exposure to environmental neurotoxins, such as heavy metals, pesticides, and solvents could
happen with certain behaviors such as pica, with certain activi-ties such as playing outdoor sports, or with certain hobbies such as those involving glues and paints. Although most work histo-ries before adulthood will be limited, certain jobs likely done by children and adolescents such as gardening and lawn work could involve exposures to pesticides and fertilizers. Parents' work his-tory could also be important in this regard as a source for a po-tential neurotoxin.
The funding of epidemiologic studies of narcolepsy will remain a challenge. Given the relative scarcity of the disease, multisite collaborative efforts may be needed. Having narcolepsy advocacy groups involved in the design and implementation of such studies will be useful but in proportion to the strength of the group. Us-ing lessons learned from other advocacy groups such as for type 1 diabetes mellitus may also be important. Perhaps partnerships would be useful for diseases whose etiologic pathways may be similar, such as is the case for narcolepsy and type 1 diabetes. The task of finding the etiology for narcolepsy will always depend on a partnership with the basic sciences, but epidemiologic studies can have an important role to play in elucidating how pathophysi-ologic mechanisms ultimately impact the public’s health.
ACKNOWLEDGMENT
This work was supported by a grant from the National Institute of Neurological Disorders and Stroke (NS038523).
REFERENCES
1. Gélineau J. De la narcolepsie. Gaz Hop (Paris) 1880;53:626-8, 54:735-7.
2. Henneberg R. Über genuine Narkolepsie. Neurol Zbl 1916;30:282-90.
3. Adie WJ. Idiopathic narcolepsy: a disease sui generis; with remarks on mechanism of sleep. Brain 1926;49:257-306.
4. Yoss RE, Daly DD. Criteria for the diagnosis of narcoleptic syn-drome. Proc Staff Meet Mayo Clin 1957;32:320-8.
5. Dement WC. History of sleep physiology and medicine. In: Kryger MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. Philadelphia: Elsevier/Saunders; 2005:1-12.
6. Vogel G. Studies in psychophysiology of dreams. III. The dream of narcolepsy. Arch Gen Psychiatry 1960;3:421-8.
7. Aldrich MS. Diagnostic aspects of narcolepsy. Neurology 1998;50(suppl 1):S2-S7.
8. Silber MH, Krahn LE, Slocumb NL. Clinical and polysomnograph-ic findings of narcolepsy with and without cataplexy: a population-based study (abstract). Sleep 2003;26:A282.
9. Mignot E, Lin L, Finn L, et al. Correlates of sleep-onset REM pe-riods during the Multiple Sleep Latency Test in community adults. Brain 2006;129:1609-23.
10. The International Classification of Sleep Disorders: Diagnostic and Coding Manual. Westchester, IL: American Academy of Sleep Medicine; 2005.
11. Overeem S, Mignot E, van Dijk JG, Lammers GJ. Narcolepsy: clin-ical features, new pathophysiologic insights, and future perspec-tives. J Clin Neurophysiol 2001;18:78-105.
12. Chabas D, Taheri S, Renier C, Mignot E. The genetics of narco-lepsy. Annu Rev Genomics Hum Genet 2003;4:459-83.
13. Nishino S, Ripley B, Overeem S, Lammers GJ, Mignot E. Hypo-cretin (orexin) deficiency in human narcolepsy (letter). Lancet 2000;355:39-40.
14. Nishino S, Ripley B, Overeem S, et al. Low cerebrospinal fluid hypocretin (orexin) and altered energy homeostasis in human nar-colepsy. Ann Neurol 2001;50:381-8.
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 24
15. Ripley B, Overeem S, Fujiki N, et al. CSF hypocretin/orexin lev-els in narcolepsy and other neurological conditions. Neurology 2001;57:2253-8.
16. Mignot E, Lammers GJ, Ripley B, et al. The role of cerebrospinal fluid hypocretin measurement in the diagnosis of narcolepsy and other hypersomnias. Arch Neurol 2002;59:1553-62.
17. Baumann CR, Bassetti CL. Hypocretins (orexins) and sleep-wake disorders. Lancet Neurol 2005;4:673-82.
18. Khatami R, Maret S, Werth E, et al. Monozygotic twins concordant for narcolepsy-cataplexy without any detectable abnormality in the hypocretin (orexin) pathway. Lancet 2004;363:1199-200.
19. Dauvilliers Y, Maret S, Bassetti C, et al. A monozygotic twin pair discordant for narcolepsy and CSF hypocretin-1. Neurology 2004;62:2137-8.
20. Gerashchenko D, Kohls MD, Greco M, et al. Hypocretin-2-saporin lesions of the lateral hypothalamus produce narcoleptic-like sleep behavior in the rat. J Neurosci 2001;21:7273-83.
21. Gerashchenko D, Murillo-Rodriguez E, Lin L, et al. Relationship between CSF hypocretin levels and hypocretin neuronal loss. Exp Neurol 2003;184:1010-6.
22. Koepsell TD, Weiss NS. Epidemiologic Methods: Studying the Oc-currence of Illness. Oxford: Oxford University Press; 2003.
23. Nelson LM, Tanner CM, Van Den Eeden SK, Mcguire VM. Neuro-epidemiology: From Principles to Practice. Oxford: Oxford Univer-sity Press; 2004:385.
24. Cave HA. Narcolepsy. Arch Neurol Psychiatry 1931;26:50-101.25. Daniels LE. Narcolepsy. Medicine 1934;13:1-122.26. Partinen M, Hublin C. Epidemiology of sleep disorders. In: Kryger
MH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. Philadelphia: Elsevier Saunders; 2005:626-47.
27. Martikainen K, Hasan J, Urponen H, Vuori I, Partinen M. Day-time sleepiness: a risk factor in community life. Acta Neurol Scand 1992;86:337-41.
28. Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The oc-currence of sleep-disordered breathing among middle-aged adults. N Engl J Med 1993;328:1230-5.
29. Sleepiness in America. Princeton, NJ: The Gallup Organization; 1997.
30. Schmitt BE, Gugger M, Augustiny K, Bassetti C, Radanov BP. Prev-alence of sleep disorders in an employed Swiss population: results of a questionnaire survey. Schweiz Med Wochenschr 2000;130:772-8.
31. Abdel-Khalek AM. Epidemiologic study of sleep disorders in Ku-waiti adolescents. Percept Mot Skills 2001;93:901-10.
32. Szklo-Coxe M, Young T, Mignot E. Narcolepsy-related symptoms in a population-based sample (abstract). Sleep 2003;26:A285.
33. Özdemir L, Akkurt I, Sumer H, et al. The prevalence of sleep related disorders in Sivas, Turkey. Tuberk Toraks 2005;53:20-7.
34. Schwegler K, Klaghofer R, Nirkko AC, Mathis J, Hersberger KE, Bloch KE. Sleep and wakefulness disturbances in Swiss pharmacy customers. Swiss Med Wkly 2006;136:149-54.
35. Douglass AB, Bornstein R, Nino-Murcia G, et al. The Sleep Disor-ders Questionnaire. I: Creation and multivariate structure of SDQ. Sleep 1994;17:160-7.
36. Honda Y. Census of narcolepsy, cataplexy, and sleep life among teen-agers in Fujisawa City (abstract). Sleep Res 1979;8:191.
37. Partinen M. Sleeping habits and sleep disorders of Finnish men be-fore, during, and after military service. Ann Med Milit Fenn 1982;57 (Suppl 1):1-96.
38. Tashiro T, Kanbayashi T, Iijima S, Hishikawa Y. An epidemiologi-cal study of narcolepsy in Japanese (abstract). J Sleep Res 1992;1 (suppl 1):228.
39. Hublin C, Kaprio J, Partinen M, et al. The prevalence of narcolepsy: an epidemiological study of the Finnish Twin Cohort. Ann Neurol 1994;35:709-16.
40. Ondzé B, Lubin S, Lavandier B, Kohler F, Mayeux D, Billiard M. Frequency of narcolepsy in the population of a French “Départ-
ment” (abstract). J Sleep Res 1998;7(suppl 2):193.41. Wing YK, Li RH, Lam CW, Ho CK, Fong SY, Leung T. The prev-
alence of narcolepsy among Chinese in Hong Kong. Ann Neurol 2002;51:578-84.
42. Roth B. Narkolepsie und Hypersomnie von Standpunkt der Physi-ologie des Schlafes. 1962.
43. Roth B. Narcolepsy and Hypersomnia. New York: Karger; 1980.44. Dement W, Zarcone V, Varner V, et al. The prevalence of narcolepsy
(abstract). Sleep Res 1972;1:148.45. Dement WC, Carskadon M, Ley R. The prevalence of narcolepsy II
(abstract). Sleep Res 1973; 2:147.46. Parkes JD. Daytime drowsiness. Sleep and its Disorders. Philadel-
phia: WB Saunders; 1985:275-314.47. Peled R, Lavie P. Narcolepsy-cataplexy: an extremely rare disorder
in Israel (abstract). Sleep Res 1987;16:404.48. Lavie P, Peled R. Narcolepsy is a rare disease in Israel (letter). Sleep
1987;10:608-9.49. al Rajeh S, Bademosi O, Ismail H, et al. A community survey of
neurological disorders in Saudi Arabia: the Thugbah study. Neuro-epidemiology 1993;12:164-78.
50. Seneviratne U, Puvanendran K. Narcolepsy in Singapore: Is it an Elusive Disease? Ann Acad Med Singapore 2005;34:90-3.
51. Kwon OJ, Peled N, Miller K, et al. HLA Class II analysis in Jewish Israeli narcoleptic patients. Hum Immunol 1995;44:199-202.
52. Solomon P. Narcolepsy in Negroes. Dis Nerv System 1945;6:179-83.
53. Franceschi M, Zamproni P, Crippa D, Smirne S. Excessive daytime sleepiness: a 1-year study in an unselected inpatient population. Sleep 1982;5:239-47.
54. Ohayon MM, Priest RG, Caulet M, Guilleminault C. Hypnagogic and hypnopompic hallucinations: Pathological phenomena? Br J Psychiatry 1996;169:459-67.
55. Ohayon MM, Priest RG, Zulley J, Smirne S, Paiva T. Prevalence of narcolepsy symptomatology and diagnosis in the European general population. Neurology 2002;58:1826-33.
56. Silber MH, Krahn LE, Olson EJ, Pankratz VS. The epidemiology of narcolepsy in Olmsted County, Minnesota: a population-based study. Sleep 2002;25:197-202.
57. Hublin C, Partinen M, Kaprio J, Koskenvuo M, Guilleminault C. Epidemiology of narcolepsy. Sleep 1994;17:S7-S12.
58. Dauvilliers Y, Montplaisir J, Molinari N, et al. Age at onset of nar-colepsy in two large populations of patients in France and Quebec. Neurology 2001;57:2029-33.
59. Silber MH, Krahn LE, Slocumb NL. Distribution of age of onset of narcolepsy (abstract). Sleep 2005;28:A222.
60. Guilleminault C. Narcolepsy. In: Chokroverty S, ed. Sleep Disor-ders Medicine: Basic Science, Technical Considerations, and Clini-cal Aspects. Boston: Butterworth-Heinemann, 1994:241-54.
61. Esther MS, Fredrickson PA, Richardson JW. Association of pos-sible or probable alcoholism in patients with narcolepsy (abstract). Sleep Res 1990;19:222.
62. Bell IR, Guilleminault C, Dement WC. Questionnaire survey of eating habits of narcoleptics versus controls (abstract). Sleep Res 1975;4:208.
63. Bell IR, Hawley CD, Guilleminault C, Dement WC. Diet and symp-tom histories in food allergics versus narcoleptics and normals (ab-stract). Sleep Res 1976;5:155.
64. Bell IR. Diet histories in narcolepsy. Adv Sleep Res 1976;3:221-7.65. Lammers GJ, Pijl H, Iestra J, Langius JA, Buunk G, Meinders AE.
Spontaneous food choice in narcolepsy (letter). Sleep 1996;19:75-6.
66. Honda Y, Doi Y, Ninomiya R, Ninomiya C. Increased frequency of non-insulin-dependent diabetes mellitus among narcoleptic pa-tients. Sleep 1986;9:254-9.
67. Schuld A, Hebebrand J, Geller F, Pollmacher T. Increased body-mass index in patients with narcolepsy. Lancet 2000;355:1274-5.
68. Dahmen N, Bierbrauer J, Kasten M. Increased prevalence of obesity
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 25
in narcoleptic patients and relatives. Eur Arch Psychiatry Clin Neu-rosci 2001;251:85-9.
69. Schuld A, Beitinger PA, Dalal M, et al. Increased body mass index (BMI) in male narcoleptic patients, but not in HLA-DR2-positive healthy male volunteers. Sleep Med 2002;3:335-9.
70. Kok SW, Overeem S, Visscher TL, et al. Hypocretin deficiency in narcoleptic humans is associated with abdominal obesity. Obes Res 2003;11:1147-54.
71. de Groen J. Body mass index and narcolepsy (abstract). Sleep 2003;26:A281-2.
72. Kotagal S, Krahn LE, Slocumb N. A putative link between child-hood narcolepsy and obesity. Sleep Med 2004;5:147-50.
73. Ohayon MM, Ferini-Strambi L, Plazzi G, Smirne S, Castronovo V. How age influences the expression of narcolepsy. J Psychosom Res 2005;59:399-405.
74. Schuld A, Blum WF, Uhr M, et al. Reduced leptin levels in human narcolepsy. Neuroendocrinology 2000;72:195-8.
75. Kok SW, Meinders AE, Overeem S, et al. Reduction of plasma leptin levels and loss of its circadian rhythmicity in hypocretin (orexin)-deficient narcoleptic humans. J Clin Endocrinol Metab 2002;87:805-9.
76. Hara J, Yanagisawa M, Sakurai T. Difference in obesity phenotype between orexin-knockout mice and orexin neuron-deficient mice with same genetic background and environmental conditions. Neu-rosci Lett 2005;380:239-42.
77. Siebold C, Hansen BE, Wyer JR, et al. Crystal structure of HLA-DQ0602 that protects against type 1 diabetes and confers strong sus-ceptibility to narcolepsy. Proc Natl Acad Sci U S A 2004;101:1999-2004.
78. Dahmen N, Querings K, Grun B, Bierbrauer J. Increased frequency of migraine in narcoleptic patients. Neurology 1999;52:1291-3.
79. Dahmen N, Kasten M, Wieczorek S, Gencik M, Epplen JT, Ullrich B. Increased frequency of migraine in narcoleptic patients: a confir-matory study. Cephalalgia 2003;23:14-9.
80. The DMKG Study Group. Migraine and idiopathic narcolepsy—a case-control study. Cephalalgia 2003;23:786-9.
81. Carlander B, Tafti M, Billiard M. Season of birth in narcolepsy (ab-stract). Sleep Res 1993;22:180.
82. Okun ML, Lin L, Pelin Z, Hong S, Mignot E. Clinical aspects of narcolepsy-cataplexy across ethnic groups. Sleep 2002;25:27-35.
83. Dauvilliers Y, Carlander B, Molinari N, et al. Month of birth as a risk factor for narcolepsy. Sleep 2003;26:663-5.
84. Dahmen N, Tonn P. Season of birth effect in narcolepsy. Neurology 2003;61:1016-7.
85. Picchioni D, Mignot EJ, Harsh JR. The month-of-birth pattern in narcolepsy is moderated by cataplexy severity and may be indepen-dent of HLA-DQB1*0602. Sleep 2004;27:1471-5.
86. Mignot E. Genetic and familial aspects of narcolepsy. Neurology 1998;50(suppl 1):S16-S22.
87. Mignot E, Lin L, Rogers W, et al. Complex HLA-DR and -DQ inter-actions confer risk of narcolepsy-cataplexy in three ethnic groups. Am J Hum Genet 2001;68:686-99.
88. Hohjoh H, Terada N, Nakayama T, et al. Case-control study with narcoleptic patients and healthy controls who, like the patients, pos-sess both HLA-DRB1*1501 and -DQB1*0602. Tissue Antigens 2001;57:230-5.
89. Kawashima M, Tamiya G, Oka A, et al. Genomewide association analysis of human narcolepsy and a new resistance gene. Am J Hum Genet 2006;79:252-63.
90. Nepom GT. MHC and autoimmune diseases. In: Bach J-F, ed. Monoclonal Antibodies and Peptide Therapy in Autoimmune Dis-eases. New York: Marcel Dekker; 1993:143-64.
91. Carlander B, Eliaou JF, Billiard M. Autoimmune hypothesis in nar-colepsy. Neurophysiol Clin 1993;23:15-22.
92. Mignot E, Tafti M, Dement WC, Grumet FC. Narcolepsy and im-munity. Adv Neuroimmunol 1995;5:23-37.
93. Black JL 3rd. Narcolepsy: a review of evidence for autoimmune
diathesis. Int Rev Psychiatry 2005;17:461-9.94. Billiard M, Laaberki C, Reygrobellet C, Seignalet J, Brissaud L,
Besset A. Elevated antibodies to streptococcal antigens in narcolep-tic subjects. Sleep Res 1989;18:201.
95. Montplaisir J, Poirier G, Lapierre O, Montplaisir S. Streptococcal antibodies in narcolepsy and idiopathic hypersomnia (abstract). Sleep Res 1989;18:271.
96. Snider LA, Swedo SE. PANDAS: current status and directions for research. Mol Psychiatry 2004;9:900-7.
97. Dale RC. Post-streptococcal autoimmune disorders of the central nervous system. Dev Med Child Neurol 2005;47:785-91.
98. Mueller-Eckhardt G, Meier-Ewart K, Schiefer HG. Is there an in-fectious origin of narcolepsy? (letter) Lancet 1990;335:424.
99. Picchioni D, Hope CR, Barry MW, Harsh JR. A case-control study of the environmental risk factors for narcolepsy (abstract). Sleep 2005;28:A217.
100. Rubin RL, Hajdukovich RM, Mitler MM. HLA-DR2 association with excessive somnolence in narcolepsy does not generalize to sleep apnea and is not accompanied by systemic autoimmune ab-normalities. Clin Immunol Immunopathol 1988;49:149-58.
101. Fredrikson S, Carlander B, Billiard M, Link H. CSF immune vari-ables in patients with narcolepsy. Acta Neurol Scand 1990;81:253-4.
102. Black JL 3rd, Krahn LE, Pankratz VS, Silber M. Search for neuron-specific and nonneuron-specific antibodies in narcoleptic patients with and without HLA DQB1*0602. Sleep 2002;25:719-23.
103. Overeem S, Geleijns K, Garssen MP, Jacobs BC, van Doorn PA, Lammers GJ. Screening for anti-ganglioside antibodies in hypocre-tin-deficient human narcolepsy. Neurosci Lett 2003;341:13-6.
104. Okun ML, Giese S, Lin L, Einen M, Mignot E, Coussons-Read ME. Exploring the cytokine and endocrine involvement in narcolepsy. Brain Behav Immun 2004;18:326-32.
105. Black JL 3rd, Silber MH, Krahn LE, et al. Studies of humoral immu-nity to preprohypocretin in human leukocyte antigen DQB1*0602-positive narcoleptic subjects with cataplexy. Biol Psychiatry 2005;58:504-9.
106. Black JL 3rd, Silber MH, Krahn LE, et al. Analysis of hypocretin (orexin) antibodies in patients with narcolepsy. Sleep 2005;28:427-31.
107. Black JL 3rd, Avula RK, Walker DL, et al. HLA DQB1*0602 posi-tive narcoleptic subjects with cataplexy have CSF lgG reactive to rat hypothalamic protein extract. Sleep 2005;28:1191-2.
108. Overeem S, Verschuuren JJ, Schreurs L, et al. Screening for autoan-tibodies against lateral hypothalamic neurons in human narcolepsy (abstract). Sleep 2005;28:A214.
109. Overeem S, Verschuuren JJ, Fronczek R, et al. Immunohistochemi-cal screening for autoantibodies against lateral hypothalamic neu-rons in human narcolepsy. J Neuroimmunol 2006;174:187-91.
110. Tanaka S, Honda Y, Inoue Y, Honda M. Detection of autoantibod-ies against hypocretin, hcrtrl, and hcrtr2 in narcolepsy: anti-Hcrt system antibody in narcolepsy. Sleep 2006;29:633-8.
111. Smith AJ, Jackson MW, Neufing P, McEvoy RD, Gordon TP. A functional autoantibody in narcolepsy. Lancet 2004;364:2122-4.
112. Orellana C, Villemin E, Tafti M, Billiard M. Is clinical onset of narcolepsy related to environmental factors? (abstract) Sleep Res 1991;20:310.
113. Billiard M, Orellana C, Villemin E, Tafti M. Environmental stress factors in human narcolepsy (abstract). Sleep Res 1991;20A:290.
114. Orellana C, Villemin E, Tafti M, Carlander B, Basset A, Billiard M. Life events in the year preceding the onset of narcolepsy. Sleep 1994;17(Suppl):S50-S3.
115. Lankford DA, Wellman JJ, O’Hara C. Posttraumatic narcolepsy in mild to moderate closed head injury. Sleep 1994;17:S25-8.
116. Munger KL, Zhang SM, O’Reilly E, et al. Vitamin D intake and incidence of multiple sclerosis. Neurology 2004;62:60-5.
117. Chen H, Zhang SM, Hernan MA, et al. Nonsteroidal anti-inflam-matory drugs and the risk of Parkinson disease. Arch Neurol
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022

SLEEP, Vol. 30, No. 1, 2007 26
2003;60:1059-64.118. Chen H, Zhang SM, Schwarzschild MA, Hernan MA, Ascherio
A. Physical activity and the risk of Parkinson disease. Neurology 2005;64:664-9.
119. Tanner CM, Langston JW. Do environmental toxins cause Parkin-son’s disease? A critical review. Neurology 1990;40(suppl 3):17-30.
120. Greenamyre JT, Betarbet R, Sherer TB. The rotenone model of Par-kinson’s disease: genes, environment and mitochondria. Parkinson-ism Relat Disord 2003;9 Suppl 2:S59-64.
121. Di Monte DA. The environment and Parkinson’s disease: is the ni-grostriatal system preferentially targeted by neurotoxins? Lancet Neurol 2003;2:531-8.
122. Devendra D, Liu E, Eisenbarth GS. Type 1 diabetes: recent develo-pments. BMJ 2004;328:750-4.
123. Daneman D. Type 1 diabetes. Lancet 2006;367:847-58.124. Williams A. Hypersusceptibility to chemicals: Risk factors for neu-
rological disease? J Neurol Neurosurg Psychiatry 1993;56:943-6.
Epidemiology of Narcolepsy—Longstreth et al
Dow
nloaded from https://academ
ic.oup.com/sleep/article/30/1/13/2708142 by guest on 08 January 2022