
The cost-effectiveness ratio of a managed protocol for severe sepsis
6
The cost-effectiveness ratio of a managed protocol for severe sepsis ☆ , ☆☆ Murillo Santucci Cesar Assuncao, MD, MSC a, ⁎, Vanessa Teich, BSc b , Sandra Christina Pereira Lima Shiramizo, RN a , Denizart Vianna Araújo, MD c , Renato Melli Carrera, MD a , Ary Serpa Neto, MD, MSC a , Eliezer Silva, MD, PhD a, ⁎ a Department of Critically Ill Patient, Intensive Care Unit, Hospital Israelita Albert Einstein, Av Albert Einstein, 627/701, Sao Paulo (SP), Brazil 05652-000 b MedInsight, Decisions in Health Care, Rio de Janeiro, Baazil c Department of Internal Medicine, Medical Sciences School, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, Brazil abstract article info Keywords: Sepsis Severe sepsis Septic shock Cost-effectiveness analysis Outcome Protocol Purpose: Severe sepsis is a time-dependent disease, and implementation of early treatment has been associated with mortality rate reduction. However, the literature is controversial regarding cost-effectiveness analysis of this intervention. The aim was to assess the cost-effectiveness of a managed protocol for the treatment of severe sepsis. Materials and methods: This is a prospective cohort study involving a historical comparison (before and after the implementation of the protocol) of patients who had been hospitalized with severe sepsis and septic shock. The group of patients who were treated before the assistance routine was implemented was considered to be the control. The case-managed nurse involved with assistance protocol performed the data collection. This nurse received special training to ensure the quality of the data and to measure the intervention throughout the implementation process. Results: A total of 414 patients were analyzed. The mortality rates were 57% in the control group and 38% in the protocol group (P = .002). After the implementation of the protocol, the absolute risk reduction was 18%; and the relative risk reduction was 31.8%. There was a tendency for a reduction in the cost of the full hospitalization, but this trend did not reach statistical significance. Nevertheless, the cost of hospitalization in the intensive care unit was reduced significantly from US $138,237 ± $202,418 in the control group to US $85,484 ± $127,471 in the protocol group (P = .003). The managed protocol for sepsis resulted in an average gain of 3.2 life-years after being discharged from the hospital (8.8 ± 13.3 years in the control group and 12.0 ± 14.0 years in the protocol group, P = .01). Conclusions: Given that the incremental cost was lower than or equal to zero, the effectiveness of the protocol was justified by the significant increase in the life-years saved and the reduced mortality. © 2014 Elsevier Inc. All rights reserved. 1. Introduction Sepsis is a common disease that is associated with high morbidity and mortality rates, especially in developing countries. In Brazil, there are an estimated 500,000 new cases of severe sepsis every year; and the sepsis mortality rate, ranging between 40% and 60%, is one of the highest in the world [1,2]. The direct costs associated with sepsis treatment have reached approximately 17 billion dollars per year [3]. In Brazil, Sogayar et al conducted an elegant study that found that the median total cost of sepsis treatment in the intensive care unit (ICU) was US $9632 per patient, which corresponds to a daily cost of US $934. Furthermore, nonsurvivors exhibited significantly higher costs than survivors [2]. Delays in recognition and treatment onset increase mortality risk of severe sepsis patients. A recent study showed that physicians’ ability to recognize severe sepsis is unsatisfactory, which may impact the clinical outcome [4]. In addition, several studies have showed an association with lower mortality rate and implementation of the 6- and 24-hour bundles recommended by the Surviving Sepsis Campaign (SSC) [3,5–8]. Nevertheless, the expenses that are associated with these bundles and the direct costs that are related to the treatments have been only partially assessed [9–12]. Therefore, an assessment of the incremental costs and benefits of the SSC implementation is crucial, especially in developing countries such as Brazil. The primary aim of the present study was to assess the cost- effectiveness ratio of a managed protocol for severe sepsis that was Journal of Critical Care xxx (2014) xxx–xxx Abbreviations: ICU, intensive care unit; SSC, Surviving Sepsis Campaign. ☆ Competing interests: The authors declare that they have no competing interests. ☆☆ Nonfinancial competing interests: Murillo Santucci Cesar Assuncao is a member of the Latin American Institute of Sepsis; Eliezer Silva is a member of the Steering Committee of the Global Sepsis Alliance, member of the Board of Sepsis Surviving Campaign, and former President of the Latin American Sepsis Institute. ⁎ Corresponding author. Hospital Israelita Albert Einstein, Av Albert Einstein, 627/ 701, Sao Paulo (SP), Brazil 05652-000. Tel/fax: +55 11 2151 1521. E-mail addresses: [email protected] (M.S.C. Assuncao), [email protected] (V. Teich), [email protected] (S.C.P.L. Shiramizo), [email protected] (D.V. Araújo), [email protected] (A. Serpa Neto), [email protected] (E. Silva). http://dx.doi.org/10.1016/j.jcrc.2014.03.008 0883-9441/© 2014 Elsevier Inc. All rights reserved. Contents lists available at ScienceDirect Journal of Critical Care journal homepage: www.jccjournal.org Please cite this article as: Assuncao MSC, et al, The cost-effectiveness ratio of a managed protocol for severe sepsis, J Crit Care (2014), http:// dx.doi.org/10.1016/j.jcrc.2014.03.008
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The cost-effectiveness ratio of a managed protocol for severe sepsis

Journal of Critical Care xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Critical Care
j ourna l homepage: www. jcc journa l .org
The cost-effectiveness ratio of a managed protocol for severe sepsis☆,☆☆
Murillo Santucci CesarAssuncao,MD,MSC a,⁎, Vanessa Teich, BSc b, SandraChristinaPereira LimaShiramizo, RN a,Denizart Vianna Araújo, MD c, Renato Melli Carrera, MD a, Ary Serpa Neto, MD, MSC a, Eliezer Silva, MD, PhD a,⁎a Department of Critically Ill Patient, Intensive Care Unit, Hospital Israelita Albert Einstein, Av Albert Einstein, 627/701, Sao Paulo (SP), Brazil 05652-000b MedInsight, Decisions in Health Care, Rio de Janeiro, Baazilc Department of Internal Medicine, Medical Sciences School, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, Brazil
a b s t r a c ta r t i c l e i n f o
Abbreviations: ICU, intensive care unit; SSC, Survivi☆ Competing interests: The authors declare that they
☆☆ Nonfinancial competing interests: Murillo Santuccithe Latin American Institute of Sepsis; Eliezer SilvaCommittee of the Global Sepsis Alliance, member of tCampaign, and former President of the Latin American S⁎ Corresponding author. Hospital Israelita Albert Ein
701, Sao Paulo (SP), Brazil 05652-000. Tel/fax: +55 11E-mail addresses: [email protected] (M.S.C. Assu
[email protected] (V. Teich), sandralima@[email protected] (D.V. Araújo), aryserpa@[email protected] (E. Silva).
http://dx.doi.org/10.1016/j.jcrc.2014.03.0080883-9441/© 2014 Elsevier Inc. All rights reserved.
Please cite this article as: Assuncao MSC, etdx.doi.org/10.1016/j.jcrc.2014.03.008
Keywords:
SepsisSevere sepsisSeptic shockCost-effectiveness analysisOutcomeProtocolPurpose: Severe sepsis is a time-dependent disease, and implementation of early treatment has beenassociated with mortality rate reduction. However, the literature is controversial regarding cost-effectivenessanalysis of this intervention. The aim was to assess the cost-effectiveness of a managed protocol for thetreatment of severe sepsis.Materials and methods: This is a prospective cohort study involving a historical comparison (before and afterthe implementation of the protocol) of patients who had been hospitalized with severe sepsis and septic
shock. The group of patients who were treated before the assistance routine was implemented wasconsidered to be the control. The case-managed nurse involved with assistance protocol performed the datacollection. This nurse received special training to ensure the quality of the data and to measure theintervention throughout the implementation process.Results: A total of 414 patients were analyzed. The mortality rates were 57% in the control group and 38% inthe protocol group (P= .002). After the implementation of the protocol, the absolute risk reduction was 18%;and the relative risk reduction was 31.8%. There was a tendency for a reduction in the cost of the fullhospitalization, but this trend did not reach statistical significance. Nevertheless, the cost of hospitalization inthe intensive care unit was reduced significantly from US $138,237 ± $202,418 in the control group to US$85,484 ± $127,471 in the protocol group (P = .003). The managed protocol for sepsis resulted in anaverage gain of 3.2 life-years after being discharged from the hospital (8.8 ± 13.3 years in the control groupand 12.0 ± 14.0 years in the protocol group, P = .01).Conclusions: Given that the incremental cost was lower than or equal to zero, the effectiveness of the protocolwas justified by the significant increase in the life-years saved and the reduced mortality.© 2014 Elsevier Inc. All rights reserved.
1. Introduction
Sepsis is a common disease that is associated with high morbidityand mortality rates, especially in developing countries. In Brazil, thereare an estimated 500,000 new cases of severe sepsis every year; andthe sepsis mortality rate, ranging between 40% and 60%, is one of thehighest in the world [1,2]. The direct costs associated with sepsistreatment have reached approximately 17 billion dollars per year [3].
ng Sepsis Campaign.have no competing interests.Cesar Assuncao is a member ofis a member of the Steeringhe Board of Sepsis Survivingepsis Institute.stein, Av Albert Einstein, 627/2151 1521.ncao),instein.br (S.C.P.L. Shiramizo),.com.br (A. Serpa Neto),
al, The cost-effectiveness rat
In Brazil, Sogayar et al conducted an elegant study that found that themedian total cost of sepsis treatment in the intensive care unit (ICU)was US $9632 per patient, which corresponds to a daily cost of US$934. Furthermore, nonsurvivors exhibited significantly higher coststhan survivors [2].
Delays in recognition and treatment onset increase mortality riskof severe sepsis patients. A recent study showed that physicians’ability to recognize severe sepsis is unsatisfactory, which mayimpact the clinical outcome [4]. In addition, several studies haveshowed an association with lower mortality rate and implementationof the 6- and 24-hour bundles recommended by the Surviving SepsisCampaign (SSC) [3,5–8]. Nevertheless, the expenses that areassociated with these bundles and the direct costs that are relatedto the treatments have been only partially assessed [9–12]. Therefore,an assessment of the incremental costs and benefits of the SSCimplementation is crucial, especially in developing countries suchas Brazil.
The primary aim of the present study was to assess the cost-effectiveness ratio of a managed protocol for severe sepsis that was
io of a managed protocol for severe sepsis, J Crit Care (2014), http://

2 M.S.C. Assuncao et al. / Journal of Critical Care xxx (2014) xxx–xxx
implemented at a private institution in Brazil. The secondary aimsincluded assessments of morbidity before and after the implementa-tion of the severe sepsis and septic shock treatment routine and theimpact of the SSC’s 6- and 24-hour bundles on the mortality ofpatients with severe sepsis and septic shock.
2. Materials and methods
2.1. Design and setting
The present study was a prospective cohort study involving ahistorical comparison (before and after the implementation of theprotocol). The study included all patients with severe sepsis andseptic shock who had been admitted to the ICU at the HospitalIsraelita Albert Einstein, São Paulo, Brazil, between July 2005 andDecember 2008. The hospital is a 600-bed private institution thatannually assists approximately 100,000 patients in the emergencydepartment and 3000 patients in the ICU.
Fig. 1. Algorithm of the assistance routine in the treatm
Please cite this article as: Assuncao MSC, et al, The cost-effectiveness ratdx.doi.org/10.1016/j.jcrc.2014.03.008
A managed protocol that was based on the SSC recommendationswas implemented in April 2006 [13]. The protocol included lectures,e-learning modules for themultidisciplinary team, and the distributionof explanatory brochures about sepsis. The regular clinical staff and allof the physicians in the emergency department and ICUwere includedin the campaign. The group of patients who were treated before theassistance routinewas implemented was considered to be the control.The data collection was performed by the nurse who managed theassistance protocol. This nurse received special training to ensure thequality of the data and to measure the intervention throughout theimplementation process.
The diagnosis of sepsis was established according to the 1992criteria of the American College of Chest Physicians/Society of CriticalCareMedicine [14]. In the present study, the initial presentation of thepatients was assessed as a function of the departments in which thediagnoses were performed, including the emergency department,wards, ICU, step-down unit, and operating room.
The approach for treating patients with severe sepsis and septicshock was assessed according to the SSC guidelines for 6-hour
ent of patients with severe sepsis and septic shock.
io of a managed protocol for severe sepsis, J Crit Care (2014), http://

3M.S.C. Assuncao et al. / Journal of Critical Care xxx (2014) xxx–xxx
management (serum lactatemeasurement, blood cultures, antibiotics,and “Early Goal-Directed Therapy,” which includes the measurementof central venous or mixed oxygen saturation and the maintenance ofcentral venous and mean arterial pressure) and 24-hour management(glucose control, low doses of corticoids, protective strategy ofmechanical ventilation, and drotrecogin alfa). The algorithm of theinstitutional assistance routine is summarized in Fig. 1. The AcutePhysiological and Chronic Health Evaluation II score was used toassess the severity of the populations for both study periods [15]. Thein-hospital status was assessed on 30, 60, and 90 days and 5 yearsafter admission.
The cost of each patient’s treatment was calculated from thedata that were provided by the hospital charging system, whichcorresponded to the expenses associated with the full hospitalizationand the ICU stay. The price index of the Brazilian Medical Association(AssociaçãoMédicaBrasileira)wasused as a reference for the cost of themedical procedures, and the BRASINDICE price index was used toestimate the costs of medications, solutions, and hospital consumables[16]. These costs were estimated based on the 2010 value of theUS dollar. The costs were calculated for the entire hospitalization andfrom the moment that severe sepsis/septic shock was diagnosed, ascertain patients had been admitted to the hospital for diseases otherthan sepsis. However, to compare the sepsis treatment costs, only theperiod after sepsis diagnosis was considered. To account for the impactof inflationonhealth, the costs between thedata collectionperiodswereupdated using the inflation rate index that was calculated by theEconomic Research Institute Foundation (Fundação Instituto dePesquisas Econômicas) [17]. The daily cost was calculated by dividingthe average total sepsis hospitalization cost by the average length ofhospitalization after sepsis was diagnosed.
2.2. Cost-effectiveness analysis
A cost-effectiveness analysis involves the calculation of theincremental cost of a new technology or intervention and the healthgain that is afforded by the new intervention [18]. The health gain istypically measured as life-years saved. The ratio between the costsand outcomes is known as the incremental cost-effectiveness ratio,
Table 1Demographic data for the investigated population.
General(n = 414)
Control(n = 92)
Protocol(n = 322)
P⁎
Age, y 66 ± 19 66 ± 19 67 ± 19 .500APACHE II 24.1 ± 7.5 25.2 ± 7.6 23.7 ± 7.4 .500Male, n (%) 240 (58) 56 (61) 184 (57) .520Number of organ dysfunctions 3 ± 1.3 3.6 ± 1.2 2.8 ± 1.2 b .001Type of dysfunction, n
Cardiovascular 84 86 84 .681Renal 51 50 52 .732Hematologic 33 53 28 b .001Respiratory 51 64 47 .005Neurological 33 37 32 .351Metabolic 49 71 43 b .001
Diagnosis, n (%)Septic shock 294 (71) 60 (65) 235 (73) .150Severe sepsis 120 (29) 32 (35) 87 (27) .150
Diagnosis site, n (%)ER 161 (39) 19 (21) 142 (44) b .001ICU 101 (25) 53 (58) 48 (15) b .001Ward 89 (21) 15 (16) 74 (23) .190SDU 39 (9) 4 (4) 35 (11) .050OR 8 (2) 1 (1) 7 (2) .500Other hospital 16 (4) 0 (0) 16 (5) .030
Data presented as mean ± standard deviation or n (%).ER, emergency room; SDU, step-down unit; OR, operating room; APACHE, AcutePhysiological and Chronic Health Evaluation.⁎ Difference between control and protocol groups.
Please cite this article as: Assuncao MSC, et al, The cost-effectiveness ratdx.doi.org/10.1016/j.jcrc.2014.03.008
which expresses the incremental cost per additional outcome that isattained by the new technology or intervention.
As previously described, the costs for the patients were calculatedwith the hospital price list; the survival of each patient was estimatedbased on the average age and sex life expectancy at the time of hospitaldischarge, which is estimated by the Brazilian Institute of GeographyandStatistics (Instituto BrasileirodeGeografiae Estatística) [19]. The lifeexpectancy of the patients who died during hospitalizationwas rated aszero. To estimate the life-years that were saved by the sepsismanagement protocol, the average survivals of each group werecalculated and compared.
2.3. Statistical analysis
The descriptive data were expressed as frequencies andpercentages, and the continuous data were expressed as the means(± standard deviation). Independent Student t test was used for thecomparison of continuous variables, and χ2 was used for thecomparison between categorical variables between the 2 groups.Time-to-event was defined as time from the ICU admission to the lastfollow-up in years. In the model, the categorical outcomevariables were tested for trend with the control group as reference.A Kaplan-Meier curve was constructed, and log-rank test was used todetermine the univariate significance of the study variable.
The software R was used to perform the statistical analysis, andsignificance was set at P b .05.
3. Results
A total of 414 patients were assessed, including 92 in the controlgroup and 322 in the protocol group. The primary characteristics ofthe analyzed patients and the departments in which the diagnoseswere performed are described in Table 1.
The global mortality rate for the 414 patients was 42%; mortalityrates were significantly higher in the control group compared to theprotocol group (57% vs 38%, P = .002) (Table 2 and Fig. 2). Theprotocol resulted in an absolute risk reduction of 18% and a relativerisk reduction of 31.8% with a needed number to treat of 5 patients.The average life expectancies after discharge from the hospital werelower in the control group compared to the protocol group (8.8± 13.3vs 12.0 ± 14.0 years, P = .01). The sepsis management protocolresulted in an average gain of 3.2 life-years.
Although not statistically significant, there were a reduction in thecost of in-hospital treatment and a reduction in hospitalization afterdiagnosis of severe sepsis or septic shock at the hospital and ICU(Table 3). There was a significant reduction in the cost of treatmentduring the ICU stay (US $138,237 ± $202,418 in the control group vsUS $85,484 ± $127,471 in the protocol group; P = .003). Before andafter the protocol was implemented, the daily costs of hospitalizationwere US $6223 and US $3893, respectively (P b .001). An estimation ofthe incremental cost-effectiveness ratio was not relevant, as theincremental cost was lower than or equal to zero. The effectiveness ofthe protocol was justified by the significant increase in the life-yearssaved and the reduced mortality.
The average length of hospitalization exhibited a significantincrease after the protocol implementation (54 ± 130 vs 37 ± 44
Table 2Mortality rates in control and protocol groups.
Mortality (%) Control Protocol P
General (in-hospital) 56.5 38.4 .002Within 30 d 34 22 .02Within 60 d 14 7 .03Within 90 d 7 4 .032
io of a managed protocol for severe sepsis, J Crit Care (2014), http://
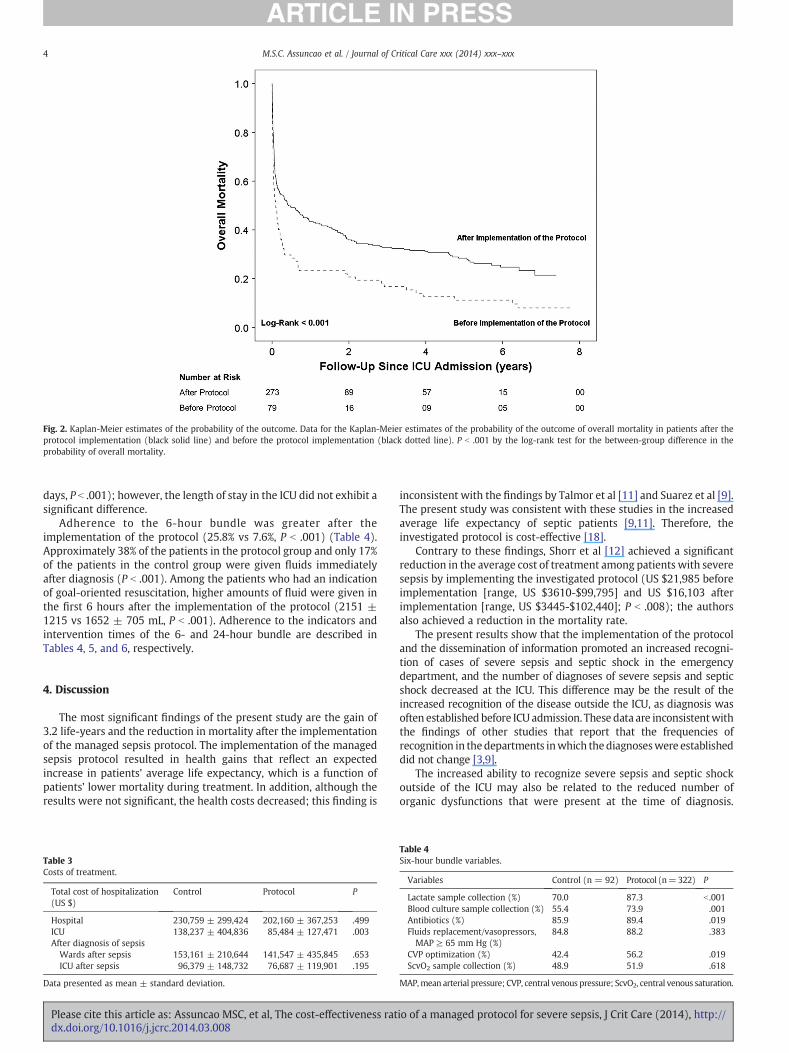
Fig. 2. Kaplan-Meier estimates of the probability of the outcome. Data for the Kaplan-Meier estimates of the probability of the outcome of overall mortality in patients after theprotocol implementation (black solid line) and before the protocol implementation (black dotted line). P b .001 by the log-rank test for the between-group difference in theprobability of overall mortality.
4 M.S.C. Assuncao et al. / Journal of Critical Care xxx (2014) xxx–xxx
days, P b .001); however, the length of stay in the ICU did not exhibit asignificant difference.
Adherence to the 6-hour bundle was greater after theimplementation of the protocol (25.8% vs 7.6%, P b .001) (Table 4).Approximately 38% of the patients in the protocol group and only 17%of the patients in the control group were given fluids immediatelyafter diagnosis (P b .001). Among the patients who had an indicationof goal-oriented resuscitation, higher amounts of fluid were given inthe first 6 hours after the implementation of the protocol (2151 ±1215 vs 1652 ± 705 mL, P b .001). Adherence to the indicators andintervention times of the 6- and 24-hour bundle are described inTables 4, 5, and 6, respectively.
4. Discussion
The most significant findings of the present study are the gain of3.2 life-years and the reduction in mortality after the implementationof the managed sepsis protocol. The implementation of the managedsepsis protocol resulted in health gains that reflect an expectedincrease in patients’ average life expectancy, which is a function ofpatients’ lower mortality during treatment. In addition, although theresults were not significant, the health costs decreased; this finding is
Table 3Costs of treatment.
Total cost of hospitalization(US $)
Control Protocol P
Hospital 230,759 ± 299,424 202,160 ± 367,253 .499ICU 138,237 ± 404,836 85,484 ± 127,471 .003After diagnosis of sepsisWards after sepsis 153,161 ± 210,644 141,547 ± 435,845 .653ICU after sepsis 96,379 ± 148,732 76,687 ± 119,901 .195
Data presented as mean ± standard deviation.
Please cite this article as: Assuncao MSC, et al, The cost-effectiveness ratdx.doi.org/10.1016/j.jcrc.2014.03.008
inconsistent with the findings by Talmor et al [11] and Suarez et al [9].The present study was consistent with these studies in the increasedaverage life expectancy of septic patients [9,11]. Therefore, theinvestigated protocol is cost-effective [18].
Contrary to these findings, Shorr et al [12] achieved a significantreduction in the average cost of treatment among patients with severesepsis by implementing the investigated protocol (US $21,985 beforeimplementation [range, US $3610-$99,795] and US $16,103 afterimplementation [range, US $3445-$102,440]; P b .008); the authorsalso achieved a reduction in the mortality rate.
The present results show that the implementation of the protocoland the dissemination of information promoted an increased recogni-tion of cases of severe sepsis and septic shock in the emergencydepartment, and the number of diagnoses of severe sepsis and septicshock decreased at the ICU. This difference may be the result of theincreased recognition of the disease outside the ICU, as diagnosis wasoften established before ICU admission. These data are inconsistentwiththe findings of other studies that report that the frequencies ofrecognition in thedepartments inwhich thediagnoseswere establisheddid not change [3,9].
The increased ability to recognize severe sepsis and septic shockoutside of the ICU may also be related to the reduced number oforganic dysfunctions that were present at the time of diagnosis.
Table 4Six-hour bundle variables.
Variables Control (n = 92) Protocol (n=322) P
Lactate sample collection (%) 70.0 87.3 b .001Blood culture sample collection (%) 55.4 73.9 .001Antibiotics (%) 85.9 89.4 .019Fluids replacement/vasopressors,MAP ≥ 65 mm Hg (%)
84.8 88.2 .383
CVP optimization (%) 42.4 56.2 .019ScvO2 sample collection (%) 48.9 51.9 .618
MAP,mean arterial pressure; CVP, central venous pressure; ScvO2, central venous saturation.
io of a managed protocol for severe sepsis, J Crit Care (2014), http://

Table 5Average time between diagnosis and performance of the six-hour bundle elements.
6-h bundle variable Control Protocol P
Average time between diagnosis and (h)Lactate sample collection 1.52 ± 1.46 1.44 ± 1.48 .517Blood culture sample collection 1.34 ± 1.74 0.70 ± 0.96 .371Antibiotics 1.66 ± 1.56 1.17 ± 1.23 .026CVP measurement 1.98 ± 1.88 3.28 ± 1.92 .002ScvO2 sample collection 1.60 ± 1.70 2.73 ± 1.89 .002
Data presented as mean ± standard deviation.
5M.S.C. Assuncao et al. / Journal of Critical Care xxx (2014) xxx–xxx
Although the present study found a reduction in respiratory,hematologic, and metabolic dysfunction after the protocol wasimplemented, only the reduction in respiratory dysfunction is consis-tent with other studies [3,9]. This finding is interesting becauseincreased respiratory dysfunctionmay be a function of more aggressivefluid infusion to correct hypovolemia and tissue hypoperfusion.
The length of stay in the ICUwas lower in the protocol group, whichis likely related to the speed of intervention. A shorter length of stayallows dysfunctions to be resolved early and prevents the progressionand appearance of new dysfunctions. Curiously, other studies have notreported reductions in the length of stay in the ICU [3,9,11]. The timingof the intervention is also related to favorable clinical outcomes forsepsis. Several studies have shown that early intervention in patientswith severe sepsis and septic shock reduces both morbidity andmortality, whereas intervention delays can increase the risk of deathamong patients with severe sepsis [20,5,21]. The reduction in mortalityin the present study is likely related to the early prescription ofantibiotics and appropriate resuscitation, which are consistent withstricter adherence to the 6-hour bundle; this hypothesis has also beenreported by previous studies [3,9–11,5,22]. The adherence to the initialresuscitation bundle in the present study after the implementation ofthe protocolwas higher than the adherence thatwas recently publishedwith the SSC data [22].
The present study was conducted at a single center. The relativerisk reduction of 31.8% is consistent with the findings of Talmor et al[11], who also performed their study at a single center and onlyincluded patients with septic shock. Along with the remainder ofstudies on this subject, the present study was based on anobservational (nonrandomized) design. This aspect may be consid-ered to be an advantage, as it is closer to real-life conditions withregard to the everyday treatment of severe sepsis and septic shock.Different from previous studies, we performed a longer patientfollow-up after hospital discharge. The recommended study modelinvolves a cost-utility design that assesses quality of life and the gainin life-years among survivors of the investigated protocol [18].Nevertheless, the present study corroborates the cost-effectivenessratio of this protocol that was previously reported by other authors
Table 6Compliance with the 24-hour bundle variables.
24-h bundle variables Control Protocol P
Protective strategy of mechanical ventilation⁎ 55.4 46.3 .121Glucose control 100 99.0 .354
Glucose control b150 mg/dL 58.9 54.2 .427Hypoglycemia 0.0 5.7 .020
Use of corticoids † 52.2 68.0 .005Use of drotrecogin alfa (activated) 10.9 46.9 b .001
‡Patients inwhomdrotrecogin alfawas contraindicatedare consideredashavingcompliedwith this 24-hour bundle criterion.⁎ Plateau pressure b 30 cm H2O.† Patients in whom corticoids were contraindicated are considered as having complied
with this 24-hour bundle criterion.
Please cite this article as: Assuncao MSC, et al, The cost-effectiveness ratdx.doi.org/10.1016/j.jcrc.2014.03.008
[9–12]. In addition, although the sample size was small, it was largerthan in other studies [9–12]. The recommended study model couldnot be performed because of the lack of data on the quality of life ofeach patient on long-term follow-ups.
5. Conclusions
The present study showed that the investigated managed protocolfor severe sepsis and septic shock management is cost-effective. Theprotocol can be compared with other protocols that apply tointerventions for acute situations [23–26], and it resulted in a gainof life-years in this population of patients with severe sepsis.Therefore, managed protocols for the treatment of patients withsevere sepsis are fully indicated.
Key messages
• The managed protocol for sepsis is cost-effective because itincreases patient life expectancy.
• Training in the systematization of sepsis assistance is effective.• Theapproach to sepsis bymeansof aprotocol reducespatientmortality.• A reduction in the time to intervention is the key to reducingsepsis mortality.
• Early recognition and a rapid approach to sepsis by means of amanaged protocol potentially reduce mortality.
References
[1] Silva E, Pedro Mde A, Sogayar AC, et al. Brazilian Sepsis Epidemiological Study(BASES study). Crit Care 2004;8:R251–60.
[2] Sogayar AM, Machado FR, Rea-Neto A, et al. A multicentre, prospective study toevaluate costs of septic patients in Brazilian intensive care units. Pharmacoeco-nomics 2008;26:425–34.
[3] Ferrer R, Artigas A, Levy MM, et al. Improvement in process of care and outcomeafter a multicenter severe sepsis educational program in Spain. JAMA2008;299:2294–303.
[4] Assuncao M, Akamine N, Cardoso GS, et al. Survey on physicians' knowledge ofsepsis: do they recognize it promptly? J Crit Care 2010;25:545–52.
[5] Westphal GA, Koenig A, Caldeira Filho M, et al. Reduced mortality after theimplementation of a protocol for the early detection of severe sepsis. J Crit Care2011;26:76–81.
[6] Gao F,Melody T, Daniels DF, et al. The impact of compliancewith 6-hour and 24-hoursepsis bundles on hospital mortality in patients with severe sepsis: a prospectiveobservational study. Crit Care 2005;9:R764–70.
[7] Nguyen HB, Corbett SW, Steele R, et al. Implementation of a bundle of qualityindicators for the earlymanagement of severe sepsis and septic shock is associatedwith decreased mortality. Crit Care Med 2007;35:1105–12.
[8] Castellanos-Ortega A, Suberviola B, Garcia-Astudillo LA, et al. Impact of theSurviving Sepsis Campaign protocols on hospital length of stay and mortality inseptic shock patients: results of a three-year follow-up quasi-experimental study.Crit Care Med 2010;38:1036–43.
[9] Suarez D, Ferrer R, Artigas A, et al. Cost-effectiveness of the Surviving SepsisCampaign protocol for severe sepsis: a prospective nation-wide study in Spain.Intensive Care Med 2011;37:444–52.
[10] Jones AE, Troyer JL, Kline JA. Cost-effectiveness of an emergency department-based early sepsis resuscitation protocol. Crit Care Med 2011;1:1306–12.
[11] Talmor D, Greenberg D, Howell MD, et al. The costs and cost-effectiveness of anintegrated sepsis treatment protocol. Crit Care Med 2008;36:1168–74.
[12] ShorrAF,MicekST, JacksonWL, et al. Economic implicationsof anevidence-basedsepsisprotocol: canwe improve outcomes and lower costs? Crit CareMed2007;35:1257–62.
[13] Pereira AJ, Fernandes Jr CJ, Sousa AG, et al. Improving performance and outcome(mortality) after implementation of a change-bundle approach for managementof septic patients. Einstein 2008;6:395–401.
[14] Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure andguidelines for the use of innovative therapies in sepsis. The ACCP/SCCM ConsensusConference Committee. American College of Chest Physicians/Society of CriticalCare Medicine. Chest 1992;101:1644–55.
[15] Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity of diseaseclassification system. Crit Care Med 1985;13:818–29.
[16] Brasindice price index: Brasindice price index. http://www.brasindice.com.br . [AndreiPublicações Médicas, Farmacêuticas e Técnicas Ltda].
[17] Fundação Instituto de Pesquisas Econômicas. http://www.fipe.org.br/web/index.asp . [Fipe é uma entidade de direito privado, sem fins lucrativos, criada em 1973para apoiar o Departamento de Economia da Faculdade de Economia,Administração e Contabilidade da Universidade de São Paulo (FEA-USP), comdestacada atuação nas áreas de pesquisa e ensino., p site].
[18] Coughlin MT, Angus DC. Economic evaluation of new therapies in critical illness.Crit Care Med 2003;31:S7–S16.
io of a managed protocol for severe sepsis, J Crit Care (2014), http://
6 M.S.C. Assuncao et al. / Journal of Critical Care xxx (2014) xxx–xxx
[19] Instituto Brasileiro de Geografia e Estatística, www.ibge.gov.br/ .[20] Ferrer R, Artigas A, Suarez D, et al. Effectiveness of treatments for severe sepsis: a
prospective, multicenter, observational study. Am J Respir Crit Care Med2009;180:861–6.
[21] Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation ofeffective antimicrobial therapy is the critical determinant of survival in humanseptic shock*. Crit Care Med 2006;34:1589–96.
[22] LevyMM, Dellinger RP, Townsend SR, et al. The Surviving Sepsis Campaign: resultsof an international guideline-based performance improvement program targetingsevere sepsis*. Crit Care Med 2010;38:367–74.
Please cite this article as: Assuncao MSC, et al, The cost-effectiveness ratdx.doi.org/10.1016/j.jcrc.2014.03.008
[23] Shorr AF, Susla GM, Kollef MH. Linezolid for treatment of ventilator-associatedpneumonia: a cost-effective alternative to vancomycin*. Crit CareMed 2004:137–43.
[24] Micek ST, Roubinian N, Heuring T, et al. Before-after study of a standardizedhospital order set for the management of septic shock. Crit Care Med2006;34:2707–13.
[25] Guzauskas GF, Boudreau DM, Villa KF, et al. The cost-effectiveness of primarystroke centers for acute stroke care. Stroke 2012;43:1617–23.
[26] Awissi DK, Begin C, Moisan J, et al. I-SAVE study: impact of sedation, analgesia, anddelirium protocols evaluated in the intensive care unit: an economic evaluation.Ann Pharmacother 2012;46:21–8.
io of a managed protocol for severe sepsis, J Crit Care (2014), http://




















