SARSA BB: Un algoritmo on policy para Sistemas Clasificadores

The BsmI Vitamin D Receptor Restriction FragmentLength Polymorphism (bb) Influences the Effect of
Calcium Intake on Bone Mineral Density
DOUGLAS P. KIEL,1 RICHARD H. MYERS,2 L. ADRIENNE CUPPLES,3 XIANG F. KONG,4
XUE H. ZHU,4 JOSE ORDOVAS,5 ERNEST J. SCHAEFER,5 DAVID T. FELSON,6 DAVID RUSH,5
PETER W.F. WILSON,7 JOHN A. EISMAN,8 and MICHAEL F. HOLICK4
ABSTRACT
Previous studies of the vitamin D receptor (VDR) polymorphisms and bone mineral density (BMD) have suggestedthat there may be differences in calcium absorption among groups of women with different VDR genotypes, andthat the association may be stronger in younger women. To investigate the association between the VDRpolymorphisms and BMD, this study was undertaken in the Framingham Study Cohort and a group of youngervolunteers. Subjects from the Framingham Study (ages 69–90 years) included those who underwent BMD testingand who had genotyping for the VDR alleles (n 5 328) using polymerase chain reaction methods and restrictionfragment length polymorphisms with BsmI (B absence, b presence of cut site). A group of younger volunteersubjects (ages 18–68) also underwent BMD testing and VDR genotyping (n 5 94). In Framingham Cohortsubjects with the bb genotype, but not the Bb or BB genotypes, there were significant associations between calciumintake and BMD at five of six skeletal sites, such that BMD was 7–12% higher in those with dietary calcium intakesgreater than 800 mg/day compared with those with intakes <500 mg/day. The data also suggested that BMD washigher in persons with the bb genotype only in the group with calcium intakes above 800 mg/day. No significantdifferences were found in the Framingham Cohort for age-, sex-, and weight-adjusted BMD at any skeletal sitebetween those with the BB genotype and those with the bb genotype regardless of 25-hydroxyvitamin D levels orcountry of origin. In the younger volunteers, BMD of the femoral neck was 5.4% higher (p < 0.05) in the bbgenotype group compared with the BB group and 11% higher (p < 0.05) in males with the bb genotype comparedwith the BB group. There were no significant differences at the lumbar spine. In this study, the association betweencalcium intake and BMD appeared to be dependent upon VDR genotype. The finding of an association betweendietary calcium intake and BMD only in the bb genotype group suggests that the VDR genotype may play a rolein the absorption of dietary calcium. Studies that do not consider calcium intake may not detect associationsbetween VDR genotype and BMD. In addition, the association between VDR alleles and BMD may become lessevident in older subjects. (J Bone Miner Res 1997;12:1049–1057)
1Hebrew Rehabilitation Center for Aged Research and Training Institute and Harvard Medical School, Division on Aging, Boston,Massachusetts, U.S.A.
2Boston University Department of Neurogenetics and Neurology, Boston University School of Medicine, Boston, Massachusetts,U.S.A.
3Department of Epidemiology and Biostatistics, Boston University School of Public Health, Boston, Massachusetts, U.S.A.4Boston University Vitamin D, Skin and Bone Research Laboratory and Department of Medicine, Boston, Massachusetts, U.S.A.5USDA Human Nutrition Research Center, Tufts University, Boston, Massachusetts, U.S.A.6Boston University Arthritis Center and Department of Medicine, Boston University School of Medicine, Boston, Massachusetts,
U.S.A.7Framingham Heart Study, NHLBI, Framingham, Massachusetts, U.S.A.8Garvan Institute of Medical Research and St. Vincent’s Hospital, Sydney, Australia.
JOURNAL OF BONE AND MINERAL RESEARCHVolume 12, Number 7, 1997Blackwell Science, Inc.© 1997 American Society for Bone and Mineral Research
1049

INTRODUCTION
THE GENETIC BASIS for the observed familial concordanceof osteoporosis has been intensively examined(1–15)
since the first report of an association between the vitaminD receptor (VDR) gene polymorphisms and bone mineraldensity (BMD).(1) Considerable controversy has arisen withregard to the role that the VDR gene polymorphisms playin the determination of adult BMD.(16,17) Parfitt suggestedthat the reason for the divergent findings from Australiaand England compared with the United States might relateto the fact that patterns of migration to Australia and theU.S. differed, with a higher proportion from Britain inAustralia, and a higher proportion from continental Europein the U.S.(18) However, recently Keen reported no associ-ation of VDR alleles and BMD in a large British popula-tion, and other studies have reported positive associationsin Japanese(6,14) and U.S. populations.(8,19) Riggs et al.suggested that the VDR association with BMD might beage dependent.(9,10)
Recently, Dawson-Hughes and colleagues identified dif-ferences in fractional calcium absorption between groupswith different VDR genotypes, such that women with theBB genotype were less able to increase the fractional ab-sorption of calcium during a period with no calcium sup-plementation than were women in the bb genotypegroup.(20) During the period of no calcium supplementa-tion, the 45Ca absorption index was significantly lower inthe BB group than in the bb group. These findings sug-gested that there may be a functional defect in the intestinalVDR, associated with the BB genotype, resulting in re-duced calcium absorption efficiency on low calcium intake.These findings were consistent with previous findings fromthe same group that genotype differences in femoral neckbone loss depend on the calcium intake level.(10) The find-ings from several previous studies have been conflictingwith regard to the role of dietary calcium intake in therelation between the VDR genotypes and BMD.(10,11)
To examine further the association between VDR poly-morphisms and BMD, we used data from the FraminghamCohort, a population-based sample of elderly persons, andcompared these results with a group of younger volunteers.The use of these two groups permitted us to define furtherthe effects of age, calcium intake, vitamin D status, andethnic origin on the relation between VDR genotype andBMD.
MATERIALS AND METHODS
Framingham Study sample
The Framingham Study began in 1948 with the primarygoal of evaluating risk factors for heart disease. The partic-ipants, initially ages 30–60 years, have been examined every2 years since that time, and by 1988, over half the originalcohort had died. The Framingham Osteoporosis Study, acomponent of the biennial examination performed in 1988–1989, involved 1164 surviving subjects (448 men and 716women), aged 68–98 years, 98% of whom were white.(21)
All subjects underwent bone densitometry of the hip and
spine (L2-L4) using a Lunar DP-3 (Lunar Corp. Madison,WI, U.S.A.), and the one-third and ultra-distal radius usinga Lunar SP-2. Coefficients of variation (CVs) were consis-tent with other studies using dual-photon absorptiometryand single-photon absorptiometry.(21) Standard protocolsand quality assurance were employed as previously de-scribed.(21) Subjects eligible for the VDR component of thisstudy included those with available samples of DNA andwith BMD results from 1988–1989. These individuals weredivided into quintiles according to their femoral neck BMD,and 60 subjects (30 men and 30 women) within each quin-tile were randomly selected for DNA analysis. This wasdone to derive a sample with a wide range of BMDs.Additional random samples were added according to theavailability of DNA, for a total sample of 328.
Younger volunteer sample
By advertising, word of mouth, and recruitment from thestudents, staff, and Boston Medical Center patients withother medical disorders not related to calcium and bonemetabolism, a convenience sample of 94 subjects under theage of 70 years underwent bone densitometry testing andhad blood drawn for genetic analysis. The subjects that wereseen at Boston Medical Center were either volunteers (i.e.,medical students, residents, or staff with no medical condi-tions) or patients with psoriasis who had no other medicalconditions and who were not taking any medications (ste-roids, anticonvulsants) that would affect their bone health.All volunteers underwent dual-energy X-ray absorptiom-etry scanning of the hip and spine using a Norland XR-26densitometer (Norland Corp., Fort Atkinson, WI. U.S.A.).The precision for the hip and spine using this device is 1%.
VDR polymorphisms
For Framingham subjects, DNA was extracted fromwhole blood specimens collected at the time of the bonedensitometry visit (1988–1989). DNA was extracted by phe-nol chloroform extraction and stored at 220°C. For medicalcenter volunteers, blood was drawn and subjects’ genomicDNA isolation was performed using a QIAamp Blood Kit(Qiagen, Inc., Chatsworth, CA, U.S.A.). All samples ofgenomic DNA were mixed with sequence-specific primersto amplify the region of the gene from exon 7 to the 39untranslated region by PCR (GIBCO BRL, Gaithersburg,MD, U.S.A.). Two primers from cDNA nucleotide se-quence 1021 to intron 8 produce one BsmI (Promega,Madison, WI, U.S.A.) restriction endonuclease site.(1) Sub-jects homozygous for the absence of the BsmI site weredesignated as genotype BB.
Other variables
In the VDR analyses, age, and weight were measured atthe time of bone densitometry for all subjects. For theFramingham sample only, calcium intake was estimatedusing the Willett food frequency questionnaire.(22) Thisfood frequency questionnaire permits the estimation ofnutrient intake for ranking or categorizing subjects, but it
1050 KIEL ET AL.

does not provide precise quantitative measures of nutrientintake. Calcium from supplement use was included in thedaily intake estimate. The serum 25-hydroxyvitamin D(25(OH)D) concentration was determined by a competitiveprotein-binding assay.(23) Inter- and intra-assay CVs for the25(OH)D assay were 10 and 7%, respectively. At an exam-ination prior to the bone density determinations, all sub-jects were queried as to the country of origin of theirfamilies. Most Framingham subjects were first generation
Americans whose parents came from Europe. Country oforigin was dichotomized into those subjects whose familiescame from England or Ireland, versus those subjects whosefamilies came from Italy, Eastern Europe, or Western Eu-rope. Subjects with families listed as having come fromCanada (n 5 5) or subjects coded as “other” or “missing”(n 5 5) were excluded from analyses employing this vari-able. For the young volunteer sample, only age and weightwere available as covariates.
Analysis of VDR polymorphisms and BMD
We used multiple regression analysis to assess the asso-ciation of VDR genotype with BMD at different sites,adjusting for potential confounding factors. The contribu-tion of the group variable, genotype (BB, Bb, or bb), wasquantified using the least-squares means option of thePROC GLM program in SAS software (SAS Institute,Cary, NC, U.S.A.).(24) In this case, the mean BMDs for theBB and Bb genotype groups, adjusted for other covariatesin the regression model, were compared with the adjustedmean BMD of the bb genotype group. Ninety-five percentconfidence intervals (95% CIs) around the adjusted meanswere calculated by adding and subtracting to these adjustedmeans, 1.963 the standard error of the adjusted mean.
To examine the effect of calcium intake, 25(OH)D level,and country of origin on the relation between VDR geno-type and BMD, the Framingham data were further ana-lyzed because of the availability of these variables for thissample. Interaction terms between genotype group (bb, Bb,
TABLE 1. CHARACTERISTICS OF THE TWO STUDY POPULATIONS
Characteristic*
Framinghamsubjects
Medicalcenter
volunteers
(n 5 328) (n 5 94)
Age (years) 6 SD 76 6 5 47 6 12Weight (lbs) 6 SD 155 6 31 159 6 43Calcium intake (mg/day) 6 SD† 827 6 432 —25(OH)D (ng/ml) 6 SD† 30 6 13 —Percent female 52 57Genotype
BB (%) 46 (14) 20 (21)Bb (%) 161 (49) 45 (48)bb (%) 121 (37) 29 (31)
* Continuous variables are means 6 standard deviations.† Data on calcium intake and vitamin D level were not available
in medical center volunteers.
TABLE 2. ADJUSTED MEAN BMDS (95% CI) BY VITAMIN D RECEPTOR GENOTYPE FOR MEMBERS
OF THE FRAMINGHAM COHORT*
Skeletal site BB Bb bb
Males and females n 5 46 n 5 161 n 5 121Femoral neck 0.781 (0.748–0.813) 0.771 (0.754–0.788) 0.795 (0.775–0.815)Ward’s area 0.601 (0.563-0.638) 0.599 (0.579-0.618) 0.622 (0.594–0.644)Trochanter 0.708 (0.667–0.749) 0.717 (0.695–0.738)† 0.752 (0.727–0.777)1/3 radius 0.627 (0.603–0.651) 0.593 (0.580–0.606) 0.606 (0.591–0.621)Ultra-distal radius 0.301 (0.281–0.320) 0.295 (0.284–0.306) 0.306 (0.294–0.319)Lumbar spine 1.179 (1.125–1.232) 1.160 (1.131–0.189) 1.202 (1.168–1.235)
Males n 5 24 n 5 85 n 5 46Femoral neck 0.856 (0.803–0.909) 0.862 (0.835–0.889) 0.880 (0.844–0.916)Ward’s area 0.667 (0.604–0.731) 0.674 (0.641–0.706) 0.691 (0.647–0.734)Trochanter 0.826 (0.759–0.893) 0.851 (0.816–0.885) 0.884 (0.838–0.930)1/3 radius 0.727 (0.693–0.761) 0.717 (0.698–0.735) 0.720 (0.696–0.744)Ultra-distal radius 0.360 (0.327–0.392) 0.366 (0.348–0.383) 0.388 (0.364–0.411)Lumbar spine 1.294 (1.211–1.377) 1.330 (1.286–1.374) 1.353 (1.293–1.413)
Females n 5 22 n 5 17 n 5 74Femoral neck 0.714 (0.673–0.754) 0.690 (0.668–0.711) 0.718 (0.696–0.740)Ward’s area 0.543 (0.500–0.585) 0.531 (0.508–0.554) 0.559 (0.536–0.582)Trochanter 0.602 (0.553–0.651) 0.598 (0.572–0.624)† 0.635 (0.608–0.661)1/3 radius 0.538 (0.504–0.572) 0.480 (0.462–0.499) 0.500 (0.482–0.519)Ultra-distal radius 0.249 (0.226–0.272) 0.229 (0.216–0.242) 0.233 (0.220–0.246)Lumbar spine 1.076 (1.007–1.144) 1.005 (0.969–1.042)† 1.062 (1.024–1.099)
* Adjusted for age and weight and sex for population as a whole, and for age and weight for men and women.†p # 0.05 compared with bb (referent).
VDR GENOTYPES AND BMD: EFFECT OF AGE AND CALCIUM 1051

BB) and either calcium intake (,500, 500–800, and .800mg/day, respectively), 25(OH)D level (,20, 20–30, and.30 ng/ml, respectively), or country of origin (United King-dom/Ireland, European) were included in the regressionmodels. For the specific analysis involving calcium intake, asignificant association between calcium intake and BMDwas observed at the hip and forearm (but not the spine) foronly one of the three genotype groups, suggesting an inter-action. Therefore, we performed another regression onBMD for all hip and forearm sites measured (five sites),evaluating the interaction between calcium intake andVDR genotype while accounting for the correlation ofBMD among the five skeletal sites that we measured. Thiswas accomplished using the PROC MIXED procedure inSAS, which accounts for the correlation between the BMDsof five skeletal sites measured in the same individual.(25)
The analysis was repeated within men and womenseparately.
RESULTS
Table 1 reveals the characteristics of the two study pop-ulations. The mean age of the Framingham subjects was 76years (range 69–90) compared with 47 years (range 18–68)for the Medical Center volunteers. The percent of females
was comparable between the two groups as was the meanweight. In the Framingham subjects, mean dietary calciumintake and serum 25(OH)D levels were at a sufficient level,although there was large variability. There were slightlygreater percentages of the BB genotype in the volunteerpopulation than in the Framingham sample.
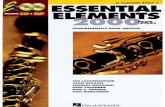
As shown in Table 2, for the Framingham sample, therewere no significant differences in age- and weight-adjustedBMD between those with the BB genotype and those withthe bb genotype. The results were unchanged without ad-justment for age and weight. At some sites, such as thefemoral neck, radius, and spine, the heterozygotes hadslightly lower BMD than either homozygous group, butthese small differences were not statistically significant. Incontrast, among the younger Medical Center volunteers(Fig. 1), age-, weight-, and sex-adjusted BMD of the fem-oral neck was lower in the BB genotype group comparedwith the bb group. The unadjusted results were the same.When examined separately for males and females (data notshown), the difference in BMD between the “bb” and “BB”genotypes was 11.4% in the males and 3.2% in the females.There were no significant differences at the lumbar spine.
We then examined in the Framingham subjects whetherthe association between VDR genotype and BMD differedaccording to dietary calcium intakes or serum 25(OH)Dlevels. As shown in Table 3 and Fig. 2a, BMD was higher in
TABLE 3. AGE-, SEX-, AND WEIGHT-ADJUSTED MEAN BMD (95% CI) IN SUBJECTS FROM THE FRAMINGHAM STUDY BY
VITAMIN D RECEPTOR GENOTYPE ACCORDING TO DAILY CALCIUM INTAKE (MG/DAY)*
n BB (n 5 41) Bb (n 5 138) bb (n 5 104)
Femoral neck,500 63 0.781 (0.718–0.844) 0.748 (0.708–0.788) 0.766 (0.723–0.808)500–800 99 0.769 (0.709–0.830) 0.804 (0.774–0.833) 0.770 (0.736–0.805).800 118 0.792 (0.740–0.845) 0.763 (0.736–0.791)† 0.831 (0.799–0.863)‡
Ward’s area,500 63 0.591 (0.518–0.664) 0.577 (0.530–0.623) 0.582 (0.532–0.631)500–800 99 0.576 (0.506–0.646) 0.640 (0.606–0.674) 0.599 (0.559–0.640).800 118 0.624 (0.564–0.685) 0.587 (0.555–0.619)† 0.663 (0.626–0.700)‡
Trochanter,500 63 0.704 (0.628–0.779) 0.723 (0.675–0.771) 0.717 (0.666–0.768)500–800 99 0.716 (0.643–0.788) 0.741 (0.706–0.777) 0.732 (0.690–0.774).800 118 0.695 (0.632–0.758)† 0.715 (0.682–0.748)† 0.788 (0.749–0.826)‡
1/3 radius,500 64 0.657 (0.610–0.703)† 0.566 (0.535–0.597) 0.582 (0.550–0.615)500–800 100 0.627 (0.581–0.673) 0.603 (0.580–0.625) 0.601 (0.575–0.628).800 114 0.616 (0.578–0.655) 0.599 (0.578–0.621) 0.627 (0.602–0.652)‡
Ultra-distal radius,500 60 0.295 (0.257–0.333) 0.300 (0.273–0.326) 0.281 (0.253–0.308)500–800 95 0.308 (0.270–0.346) 0.300 (0.281–0.319) 0.303 (0.281–0.325).800 113 0.304 (0.273–0.336) 0.289 (0.272–0.307)† 0.320 (0.300–0.341)‡
Lumbar spine,500 64 1.253 (1.147–1.358) 1.118 (1.047–1.188) 1.205 (1.130–1.279)500–800 98 1.107 (1.001–1.213)‡ 1.158 (1.107–1.209) 1.203 (1.140–1.265).800 119 1.169 (1.080–1.258) 1.188 (1.140–1.236) 1.220 (1.164–1.276)
* Number of subjects is less than previous analyses because of missing data on calcium intake.† p # 0.05 compared with bb (referent).‡ p # 0.05 compared with Ca , 500 (referent) within given genotype group.
1052 KIEL ET AL.

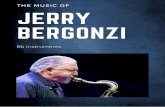
those with the bb genotype compared with the BB genotypeonly when calcium intakes were above 800 mg/day, althoughthese differences were only statistically significant at thetrochanter. In the group with calcium intakes below 500
mg/day, individuals with the bb genotype actually had lowerradial BMD than those with the BB genotype ( p , 0.05). Inthe same way that calcium intake influenced the associationbetween genotype group and BMD, VDR genotype influ-enced the relation between calcium intake and BMD. Over-all, regardless of skeletal site, there were no significantassociations between calcium intake and BMD (all p-values.0.10); however, there were consistently higher BMDs atall skeletal sites (7–12% higher) except the spine in thosewith calcium intake .800 mg/day compared with those withcalcium intake .500 mg/day among those with the bb ge-notype. This is shown graphically in Figs. 2a and 2b. Inter-action terms (calcium intake by genotype) were included inmodels of BMD for all skeletal sites except the spine, andthese were statistically significant ( p , 0.05) for men andwomen combined and when analyzed separately.
To explore further the hypothesis that the VDR andBMD association might depend on the vitamin D status, ormight be limited to families who had come to the U.S. fromBritain versus other European countries, we examined inthe Framingham subjects the VDR genotype as it related toBMD in those persons whose families had come from eitherEngland or Ireland versus those whose families had comefrom Eastern or Western Europe. As shown in Tables 4 and5, there were no significant BMD differences between theBB and bb genotypes regardless of 25(OH)D level or coun-try of origin. Levels of 25(OH)D were not associated withBMD at any skeletal site (all p-values .0.10).
DISCUSSION
In this study of a large population-based cohort of ad-vanced age, the Framingham Study Cohort, we detected aneffect of the BsmI vitamin D receptor restriction fragmentlength polymorphism (RFLP) bb, on the association be-tween calcium intake and BMD, but not between the levelof serum 25(OH)D, or country of origin and BMD. Dietarycalcium intake was positively associated with BMD onlyamong those with the bb genotype. In the younger volun-teer sample, femoral neck BMD was significantly loweramong individuals with the BB genotype compared with thebb genotype, especially in men.
The finding of an interaction between calcium intake,VDR genotype, and BMD in postmenopausal women hasbeen described by other investigators(10,11); however, theresults appear to be conflicting, with one study demonstrat-ing an interaction between the BB genotype and the calci-um/BMD association,(10) and the other an interaction in-volving the Bb genotype.(11) The current study implicates aninteraction involving the bb genotype group. These findingsmay not be “conflicting” if the gene–environment interac-tion were dependent on the level of dietary calcium intake.In fact, the level of dietary calcium intake varied consider-ably between the current study (calcium intake averaged827 mg/day), the study by Krall and colleagues (274–530mg/day),(10) and the study by Ferrari and colleagues (calci-um intake 1226–1235 mg/day).(11) Salamone and colleaguesrecently described an interaction between VDR genotypeand calcium intake in healthy premenopausal women in
FIG. 1. Age-, weight-, and sex-adjusted BMD (means695% CI) at two skeletal sites in younger volunteer sampleaccording to BsmI genotype.
VDR GENOTYPES AND BMD: EFFECT OF AGE AND CALCIUM 1053

which the BB and Bb genotype groups demonstrated anassociation between higher calcium intake and greater fem-oral BMD; however, the cut point for high and low calciumintake was 1036 mg/day.(26) The gene–environment inter-actions between the VDR and calcium intake are likely tobe complex and may depend on the level of calcium intakebeing examined.
Compared with previous studies, the mean age of ourolder population was greater than any of the previouslypublished positive(3,6,8–11,14,27) or negative(2,4,5,7,12,13,15)
studies and population-based, rather than a volunteer sam-
ple. By performing analyses stratified by calcium intake andvitamin D status, we were able to describe the influence ofthese factors on the association between VDR genotypeand BMD.
The results from our Framingham population representsone of the largest population-based samples studied to date,and the reported genotype frequencies are based on apopulation-based sample of mostly European origin, com-pared with previous studies which used volunteer or conve-nience samples. The finding of such an association for thefermoral neck among the younger volunteers adds further
FIG. 2. (A) Age-, sex-, and weight-adjusted BMD of the trochanter according to calcium intake (mg/day) and VDRgenotype group. (B) Age-, sex-, and weight-adjusted BMD of the ultradistal radius according to calcium intake (mg/day)and VDR genotype group. †p # 0.05 compared with bb in calcium group .800 mg/day; ‡p # 0.05 compared with Ca ,500in bb group.
1054 KIEL ET AL.

support to the hypothesis of others(9) that the VDR poly-morphism may be more highly associated with BMD of thehip in younger populations. With advancing age, the rela-tion between VDR genotype and BMD may not beapparent.
There may be several limitations to the current study.First, it is cross-sectional, which limits the investigation ofcausal relationships. Second, the number of persons withthe BB genotype was small, limiting the power to detect arelationship between calcium intake and BMD in thisgroup. If the younger volunteer population was healthierthan the general population, this sample may have hadmore favorable BMDs for any specific genotype than thegeneral population. This would have tended to obscure arelationship between genotype and BMD, suggesting thatour results may have underestimated the true association.
Other studies which have failed to find increased BMDamong persons with the bb genotype may contain a largerproportion of individuals with low calcium intake, therebymasking the association. These results, if confirmed byothers, may also be of clinical significance. If persons withthe Bb and BB genotypes do not respond to calcium re-placement, such therapies may be of less benefit to theseindividuals. Alternatively, the bb genotype may provide aninitial indication that calcium replacement therapy is of
importance. Indeed, persons with the bb genotype who hadlow calcium intake actually had lower radial BMD than didthose with the BB and Bb genotype, further suggesting theimportance of intervention in this group.
The BsmI RFLP is in an intron of the VDR gene and isnot known to alter the protein product; however, there isearly evidence that the rate of VDR gene transcription orstability of the transcript may differ according to geno-type.(28) While post-transcriptional modification related tothe BsmI RFLP is possible, additional work is needed toidentify the mechanism to explain the finding that calciumsupplementation was associated with greater BMD only forthose with the bb genotype. At present, one likely interpre-tation is that the b allele is in disequilibrium with a mutationwithin the VDR gene which promotes calcium absorption.Further understanding of the biologic mechanisms under-lying these genetic differences will help define the role ofthe VDR gene in the inheritance of BMD.
ACKNOWLEDGMENTS
We wish to acknowledge Clorinda Cali Hoffman for hercontributions to the tracking of specimens and for data anal-ysis. Supported by NIH grants AG13645 and AR/AG41398.
TABLE 4. AGE-, SEX-, AND WEIGHT-ADJUSTED MEAN BMD (95% CI) IN SUBJECTS FROM THE FRAMINGHAM STUDY BY VITAMIN
D RECEPTOR GENOTYPE ACCORDING TO LEVEL OF 25(OH)D LEVEL (NG/ML)*
Skeletal site andvitamin D groups n BB (n 5 42) Bb (n 5 151) bb (n 5 111)
Femoral neck,20 75 0.749 (0.675–0.822) 0.747 (0.712–0.781)† 0.809 (0.771–0.846)20–30 85 0.824 (0.764–0.884) 0.791 (0.757–0.826) 0.781 (0.746–0.816).30 141 0.776 (0.730–0.823) 0.775 (0.751–0.798) 0.807 (0.775–0.839)
Ward’s area,20 75 0.550 (0.468–0.631) 0.597 (0.559–0.635) 0.621 (0.580–0.662)20–30 85 0.658 (0.592–0.724)‡ 0.599 (0.561–0.637) 0.607 (0.569–0.646),30 141 0.597 (0.546–0.649) 0.599 (0.573–0.625)† 0.649 (0.613–0.684)
Trochanter,20 75 0.644 (0.551–0.737) 0.702 (0.658–0.745) 0.735 (0.688–0.782)20–30 85 0.752 (0.677–0.828) 0.724 (0.681–0.767) 0.750 (0.706–0.794).30 141 0.712 (0.653–0.771) 0.724 (0.694–0.754)† 0.779 (0.739–0.820)
1/3 radius,20 75 0.625 (0.567–0.682) 0.579 (0.552–0.606) 0.609 (0.580–0.638)20–30 86 0.619 (0.574–0.664) 0.605 (0.578–0.632) 0.592 (0.565–0.620).30 139 0.637 (0.601–0.673) 0.601 (0.582–0.620) 0.622 (0.596–0.647)
Ultra-distal radius,20 71 0.299 (0.251–0.347) 0.287 (0.264–0.310) 0.301 (0.276–0.327)20–30 80 0.304 (0.267–0.341) 0.298 (0.275–0.321) 0.297 (0.273–0.320).30 139 0.300 (0.270–0.329) 0.299 (0.283–0.315) 0.320 (0.299–0.341)
Lumbar spine,20 76 1.199 (1.068–1.330) 1.189 (1.128–1.249) 1.210 (1.144–1.277)20–30 85 1.232 (1.130–1.334) 1.145 (1.084–1.206) 1.155 (1.092–1.218).30 141 1.149 (1.068–1.230)† 1.162 (1.120–1.205)† 1.245 (1.188–1.303)
* Numbers of subjects is less than previous analyses because of missing data on 25(OH)D level.† p # 0.05 compared with bb (referent).‡ p # 0.05 compared with vitamin D , 20 (referent).
VDR GENOTYPES AND BMD: EFFECT OF AGE AND CALCIUM 1055

REFERENCES
1. Morrison NA, Qi JC, Tokita A, Kelly PJ, Crofts L, Nguyen TV,Sambrook PN, Eisman JA 1994 Prediction of bone densityfrom vitamin D receptor alleles. Nature 367:284–287.
2. Hustmyer FG, Peacock M, Hui S, Johnston CC, Christian J1994 Bone mineral density in relation to polymorphism at thevitamin D receptor gene locus. J Clin Invest 94:2130–2134.
3. Spector TD, Keen RW, Arden NK, Morrison NA, Major PJ,Nguyen TV, Kelly PJ, Baker JR, Sambrook PN, Lanchbury JS,Eisman JA 1995 Influence of vitamin D receptor genotype onbone mineral density in postmenopausal women: A twin studyin Britain. Br Med J 310:1357–1360.
4. Looney JE, Yoon H, Fischer M, Farley SM, Farley JR,Wergedal JE, Baylink DJ 1995 Lack of high prevalence of theBB vitamin D receptor genotype in severely osteoporoticwomen. J Clin Endo Metab 80:2158–2162.
5. Melhus H, Kindmark A, Amer S, Wilen B, Lindh E, LjunghallS 1994 Vitamin D receptor genotypes in osteoporosis. Lancet344:949–950.
6. Yamagata Z, Miyamura T, Iijima S, Asaka A, Sasaki M, KatoJ, Koizumi K 1994 Vitamin D receptor gene polymorphism andbone mineral density in healthy Japanese women. Lancet344:1027.
7. Kroger H, Mahonen A, Ryhanen S, Turunen AM, Alhava E,Maenpaa P 1995 Vitamin D receptor genotypes and bonemineral density. Lancet 345:1238.
8. Fleet JC, Harris SS, Wood RJ, Dawson-Hughes B 1995 theBsmI vitamin D receptor restriction fragment length polymor-phism (BB) predicts low bone density in premenopausal blackand white women. J Bone Miner Res 10:985–990.
9. Riggs BL, Nguyen TV, Melton LJ, III, Morrison NA, O’FallonWM, Kelly PJ, Egan KS, Sambrook PN, Muhs JM, Eisman JA1995 The contribution of vitamin D receptor gene alleles to thedetermination of bone mineral density in normal and osteopo-rotic women. J Bone Miner Res 10:991–996.
10. Krall EA, Parry P, Lichter JB, Dawson-Hughes B 1995 VitaminD receptor alleles and rates of bone loss: Influences of yearssince menopause and calcium intake. J Bone Miner Res10:978–984.
11. Ferrari S, Rizzoli R, Chevalley T, Slosman D, Eisman JA,Bonjour JP 1995 Vitamin-D-receptor-gene polymorphisms andchange in lumbar-spine bone mineral density. Lancet 345:423–424.
12. Keen RW, Major PJ, Lanchbury JS, Spector TD 1995 Vitamin-D-receptor-gene polymorphism and bone loss. Lancet 345:990.
13. Garnero P, Borel O, Sornay-Rendu E, Delmas PD 1995 Vita-min D receptor gene polymorphisms do not predict boneturnover and bone mass in healthy premenopausal women.J Bone Miner Res 10:1283–1288.
14. Tokita A, Matsumoto H, Morrison N, et al. 1996 Vitamin Dreceptor alleles, bone mineral density and turnover in pre-menopausal Japanese women. J Bone Miner Res 11:1003–1009.
15. Garnero P, Borel O, Sornay-Rendu E, Arlot ME, Delmas PD1996 Vitamin D receptor gene polymorphisms are not relatedto bone turnover, rate of bone loss, and bone mass in post-menopausal women: The OFELY Study. J Bone Miner Res11:827–834.
16. Eisman JA 1995 Vitamin D receptor gene alleles and osteo-porosis: An affirmative view. J Bone Miner Res 10:1289–1293.
17. Peacock M 1995 Vitamin D receptor gene alleles and osteo-porosis: A contrasting view. J. Bone Miner Res 10:1294–1297.
18. Parfitt AM 1994 Vitamin D receptor genotypes in osteoporo-sis. Lancet 344:1580.
19. Cooper G, Umbach DM 1996 Are vitamin D receptor poly-morphisms associated with bone mineral density? A meta-analysis. J Bone Miner Res 11:1841–1849.
20. Dawson-Hughes B, Harris SS, Finneran S 1995 Calcium ab-sorption on high and low calcium intakes in relation to vitaminD receptor genotype. J Clin Endocrinol Metab 80:3657–3661.
21. Hannan MT, Felson DT, Anderson JJ 1992 Bone mineral
TABLE 5. AGE-, SEX-, AND WEIGHT-ADJUSTED BMD IN SUBJECTS FROM THE FRAMINGHAM STUDY ACCORDING TO VDRGENOTYPE AND COUNTRY OF ORIGIN*
Skeletal site andcountry of origin n BB (n 5 42) Bb (n 5 151) bb (n 5 111)
Femoral neckU.K./Ireland 92 0.767 (0.707–0.828) 0.761 (0.729–-0.793) 0.792 (0.753–0.830)Europe 209 0.786 (0.746–0.827) 0.775 (0.754–0.797) 0.793 (0.769–0.817)
Ward’s areaU.K./Ireland 92 0.582 (0.513–0.651) 0.591 (0.555–0.627) 0.612 (0.569–0.656)Europe 209 0.606 (0.560–0.652) 0.607 (0.583–0.632) 0.621 (0.593–0.649)
TrochanterU.K./Ireland 92 0.705 (0.628–0.782) 0.692 (0.651–0.732) 0.749 (0.700–0.798)Europe 209 0.709 (0.658–0.761) 0.730 (0.702–0.758) 0.749 (0.717–0.780)
1/3 radiusU.K./Ireland 91 0.656 (0.610–0.702) 0.590 (0.566–0.614) 0.607 (0.578–0.636)Europe 208 0.611 (0.580–0.641) 0.594 (0.577–0.610) 0.605 (0.586–0.623)
Ultra-distal radiusU.K./Ireland 88 0.305 (0.269–0.341) 0.287 (0.267–0.307) 0.311 (0.288–0.334)Europe 201 0.296 (0.273–0.320) 0.298 (0.285–0.312) 0.298 (0.283–0.313)
Lumbar spineU.K./Ireland 92 1.252 (1.149–1.355) 1.162 (1.108–1.216) 1.182 (1.117–1.248)Europe 211 1.148 (1.081–1.214) 1.160 (1.124–1.197) 1.207 (1.165–1.249)
* Numbers of subjects is less than previous analyses because of missing data on country of origin.
1056 KIEL ET AL.

density in elderly men and women: Results form the Framing-ham osteoporosis study. J Bone Miner Res 7:547–553.
22. Willett WC, Sampson L, Stampfer MJ, Rosner B, Bain C,Witschi J, Hennekens CH, Speizer FE 1985 Reproducibilityand validity of a semiquantitative food frequency question-naire. Am J Epidemiol 122:51–65.
23. Preece MA, O’Riordan JLH, Lawson DEM, Kodicek E 1974 Acompetitive protein-binding assay for 25-hydroxycholecalcif-erol and 25-hydroxyergocalciferol in serum. Clin Chim Acta54:235–242.
24. SAS Institute, Inc. 1990 SAS/STAT Users Guide. Version 6.09;GLM Procedure, Vol 2. SAS Institute, Cary, NC, U.S.A., pp.893–908, 948.
25. SAS Institute, Inc. 1992 SAS Technical Report P-229 SAS/STAT Software: Changes and Enhancements. Release 6.07;The MIXED Procedure. SAS Institute, Cary, NC, U.S.A., pp.289–366.
26. Salamone LM, Glynn NW, Black DM, Ferrell RE, Palermo L,Epstein RS, Kuller LH, Cauley JA 1996 Determinants of pre-
menopausal bone mineral density: The interplay of genetic andlifestyle factors. J Bone Miner Res 11:1557–1565.
27. Matsuyama T, Ishii S, Tokita A, Yabuta K, Yamamori S,Morrison NA, Eisman JA 1995 Vitamin D receptor genotypesand bone mineral density. Lancet 345:1238–1239.
28. Crofts LA, Morrison NA, Dudman N, Eisman JA 1996 Differ-ential expression of VDR gene alleles. J Bone Miner Res 11(Suppl 1):S208.
Address reprint requests to:Douglas P. Kiel, M.D., M.P.H.
Hebrew Rehabilitation Center for AgedResearch and Training Institute
1200 Centre StreetBoston, MA 02131 U.S.A.
Received in original form October 23, 1996; in revised form Jan-uary 10, 1997; accepted January 22, 1997.
VDR GENOTYPES AND BMD: EFFECT OF AGE AND CALCIUM 1057
Copyright © 2022 FDOKUMEN