
The birth of the e-clinic. Continuity or transformation in the UK governance of pharmaceutical...
25
1 The Birth of the E-Clinic. Continuity or Transformation in the UK Governance of Pharmaceutical Consumption? Nick Fox, Katie Ward and Alan O’Rourke University of Sheffield Address for correspondence: Dr Nick Fox ScHARR University of Sheffield Regent Court 30 Regent Street Sheffield S1 4DA Word Count: 7995 Key Words: Consumption, Governance, Internet, Internet Pharmacy, Pharmaceutical Drugs, Pharmacy
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of The birth of the e-clinic. Continuity or transformation in the UK governance of pharmaceutical...

1
The Birth of the E-Clinic. Continuity or Transform ation
in the UK Governance of Pharmaceutical Consumption?
Nick Fox, Katie Ward and Alan O’Rourke
University of Sheffield
Address for correspondence:
Dr Nick Fox
ScHARR
University of Sheffield
Regent Court
30 Regent Street
Sheffield S1 4DA
Word Count: 7995
Key Words: Consumption, Governance, Internet, Internet Pharmacy, Pharmaceutical Drugs,
Pharmacy

2
Abstract
Traditional arrangements for the prescription and dispensing of pharmaceuticals have been
challenged by the rise of Internet services enabling consumers to acquire these products
online, without a face-to-face contact with a professional. This paper considers three
moments in the emergence of the ‘e-clinic’ as an alternative route to prescription drugs in the
UK. We examine the phenomenon in relation to issues of governance, considering the legal
and voluntary frameworks that govern prescribing. Documentary and interview data suggest
that the Internet has the potential to transform the relations between prescribers, dispensers
and consumers, but that stakeholders seek continuity by applying existing governance
frameworks and codes of conduct. This continuity can be explained by Rosenau’s (1997)
model of a contested and fragmenting process of technology governance.

3
The Birth of the E-Clinic. Continuity or Transform ation in the
Governance of Pharmaceutical Consumption?
Introduction
Consumers in the United Kingdom (UK) and elsewhere traditionally have accessed
pharmaceuticals in two ways. Medication has fallen into broad categories: those requiring a
doctor’s prescription (prescription-only medicines or POMs) and those available over-the-
counter in the presence of a qualified pharmacist (pharmacy medicines or PMs). In both
cases, most pharmaceuticals can only be accessed by consumers via a healthcare professional. 1
In this paper, we examine how this familiar landscape of pharmaceutical consumption has
been affected by the arrival of the Internet as a medium both for information access and for
global consumption (Armstrong et al 1999, Eysenbach et al 1999, Eysenbach 2000). Driven
in part by commercial pressures in North America, where pharmaceuticals are regulated
within a context of private health care rather than a socialised public system such as the UK’s
NHS, Internet or ‘e-pharmacy’ has developed alongside traditional community pharmacies.
While such e-pharmacies have been aimed at nationals, the global nature of the Internet has
meant that national boundaries have become far more permeable as far as the marketing of
pharmaceuticals is concerned (Pines 2000). More recently, the online doctor’s surgery or ‘e-
clinic’ has emerged, in which an Internet consultation with a qualified medical practitioner is
a precursor to prescription and sale of prescription-only medications.
Drawing on findings from a wider ESRC study 2 into the dynamics of pharmaceutical
consumption in the Internet age and consequences for governance, we describe here a range
of initiatives concerning prescribing that have been facilitated by electronic networks. These
contribute to the ‘birth of the e-clinic’ as a consumption medium in modern healthcare, and in
this paper we examine challenges for the governance of pharmaceuticals in this form of
consumption. Elsewhere (Authors 2005, in press), we have explored some of the social
relations of Internet-enabled pharmaceutical consumption, as patients become consumers and
the credit card substitutes for the patient record.

4
A Framework for Studying Changes in Governance
Governance may be understood as the management of diverse concerns of state and
individual, to sustain both the continuity, security and integrity (and on occasions, cultural,
ethical or religious precepts) of the former and the liberty and rights to self-actualisation of
the latter (Loader 1997: 12, Shore and Wright 1997: 30-31). It is a matter of law and
regulation, but also of responsibility and accountability that goes to the heart of how modern
democratic states and organisations seek to govern themselves and individuals (Rose 1990:
10, Rosenau 1997: 145). At the level of the nation-state and international relations, these
issues have fallen within the purview of political science. However, from a sociological
perspective, governance may be seen more generally as the application of guidance or control
over an activity, in order to achieve a specified outcome (Jewson and Macgregor 1997: 6,
Rosenau 1997: 146).
This paper draws upon the analysis of governance developed by James Rosenau (1995, 1997),
and we have fully developed the application of this approach to the study of technology
governance elsewhere (Authors, submitted a). Rosenau (1997: 14-15) suggests that
governance emerges when those who would control an activity (‘sources of authority’)
achieve a degree of compliance from those who are to be controlled, thereby establishing a
‘system of rule’ that regularises activity. Systems of rule can become established even in the
absence of legal or political authority, and in late modern society, governance is often
voluntaristic, consensual and collaborative (ibid: 147).
In this model, governance is not a final outcome. Rather, environmental changes (for
example, the development of new information technologies) continually challenge systems of
rule, as sources of authority are empowered or disabled (Barry 2001, Cashore 2002). Sources
of authority vie for control, forming coalitions that may range from the relatively stable to ad
hoc alliances that circumvent traditional sources of authority (Rosenau 1997: 171-2).
Moreover, individual or community values, behaviours and prejudices (for example,
individual greed, an increase in people’s analytical skills or a rise in religious bigotry) affect
the stability of systems of rule, and governance is achieved only within highly unstable and
complex cultural contexts (Rosenau 1995: 15). To give an example: the regulation of new
reproductive technologies continue to evolve within a mix of ethical and religious precepts in
a secularising society, falling birth rates and shortage of children for adoption, economic

5
prosperity, idealisation of childhood, concepts of human rights, trust in science and so forth,
as well as from technological advances and global variations in regulation (Jones and Salter
2003). The emergent system of rule achieves compliance only so long as these environmental
factors are stable: if one factor strengthens or weakens in intensity, the system of rule must
adapt accordingly.
This dynamic conception of systems of rule suggests that governance is forever in the process
of breaking down and being re-invented to address environmental (societal, economic,
technological, political and cultural) changes (Rosenau 1995: 17-18). In this paper, we apply
this approach to governance to map the effects of a specific environmental change: the rise of
the ‘networked’, information society, specifically, the Internet. Our proposition is that
governance emerges within a nexus of power relations and that the shape of governance
reflects the on-going struggles and conflicts between stakeholders, including states, social
groups, commercial and other interests and individuals.
Global access to information and communication technologies has changed many traditional
relations, opening up possibilities for new social relations and creating new patterns of
inclusion and exclusion (Holderness 1998, Lenk 1997), enhancing participation for some
while creating new systems of surveillance and control (Baym 1995, Freeman 2002: 752,
Queau 2002). Information technologies render government open to scrutiny and promote
democratisation (Kedzie 2002), human rights and transparency (Richards 2002).
Information networks are themselves governance networks. They allow for different
forms of authority to emerge, for concerted action to take place, and for institutional
creation or reinforcement. … Information (makes) governance less hierarchical and
more plural and democratic (Singh 2002: 18)
Our research examined the extent to which information technology has transformed the
system of rule governing pharmaceutical consumption, and how sources of authority adapt to
meet the changed environmental conditions. What happens when an Internet user has the
power to self-prescribe and consume drugs without face-to-face contact with health
professionals? We have considered elsewhere the social role that consumption is playing in
defining doctor-patient relations, notions of being ‘a patient’, and the de-hegemonising of
expertise in relation to diagnosis and treatment of disease (Authors 2005, in press), and

6
changes in the governance of consumer advertising of pharmaceuticals (Authors, submitted).
Here we explore the emergence of e-pharmacy and the e-clinic. While governance is
increasingly globalised (Singh 2002), the nation-state retains important legal and regulatory
functions: for this reason, we focus specifically on UK governance, although the findings are
generalisable internationally.
The structure of the paper is as follows. Having briefly described the methods used in our
research, we consider the frameworks within which the prescription of medications are
governed, and explore how stakeholders have responded to the challenges of information
technology for pharmaceutical governance. We then examine the birth of the e-clinic through
three ‘moments’ 3 that demonstrate how the Internet has facilitated new methods of supplying
pharmaceutical drugs to consumers:
• the UK electronic transfer of prescriptions pilot;
• an example of a global ‘e-pharmacy’;
• an example of a UK-based ‘e-clinic’.
In a discussion, we examine the findings within a sociological framework that assesses the
part that a technology such as the Internet can play in transforming governance relations.
Research Objectives, Methods and Contexts
The data reported in this paper emerge from a two-year project within the ESRC Innovative
Health Technologies (IHT) programme. The study addressed the impact of the Internet on
purchasing and use of prescription pharmaceuticals, people’s motivations to seek medication
via Internet pharmacies and the regulation of online pharmacies. It applied a range of
qualitative approaches including in-depth face-to-face and telephone interviews, ethnography,
content analysis of paper- and web-based materials including web sites and discussion fora,
and review of documentary sources including governmental and other publications. The
strand of data collection reported in this paper was based on reviews of published reports and
other literature, and interviews with ‘stakeholders’.
The literature and documentary evidence reviewed included governmental reports, relevant
policy documents, documentation published on official web sites including commercial sites,
advertising materials and other grey literature. We summarised these in a series of working
7
papers that informed the data collection with respondents and provided trhe basis for our
understanding of the emerging technological developments in e-enabled pharmacy.
We conducted interviews with a range of stakeholders including government agencies,
professional and commercial organisations and consumers. : This was an exploratory study:
our data provided a mix of background and contextual material and the opportunity to analyse
the perspectives of the different stakeholder organisations and individuals interviewed.
Respondents were selected iteratively to provide a theoretical sample and to enable data
saturation. Thirteen representatives of organisations were recruited directly or by contact with
external relations departments in organisations, and interviewees were senior members of
their organisation with relevant knowledge or responsibility. Eight interviews were with a
single respondent, and two were with two representatives of an organisation interviewed
together. Consumers were recruited via three health discussion forums, 4 usually by asking
questions on a message board followed by private in-depth online interviews. All interviews
were recorded and fully transcribed. The respondents are summarised in Table 1
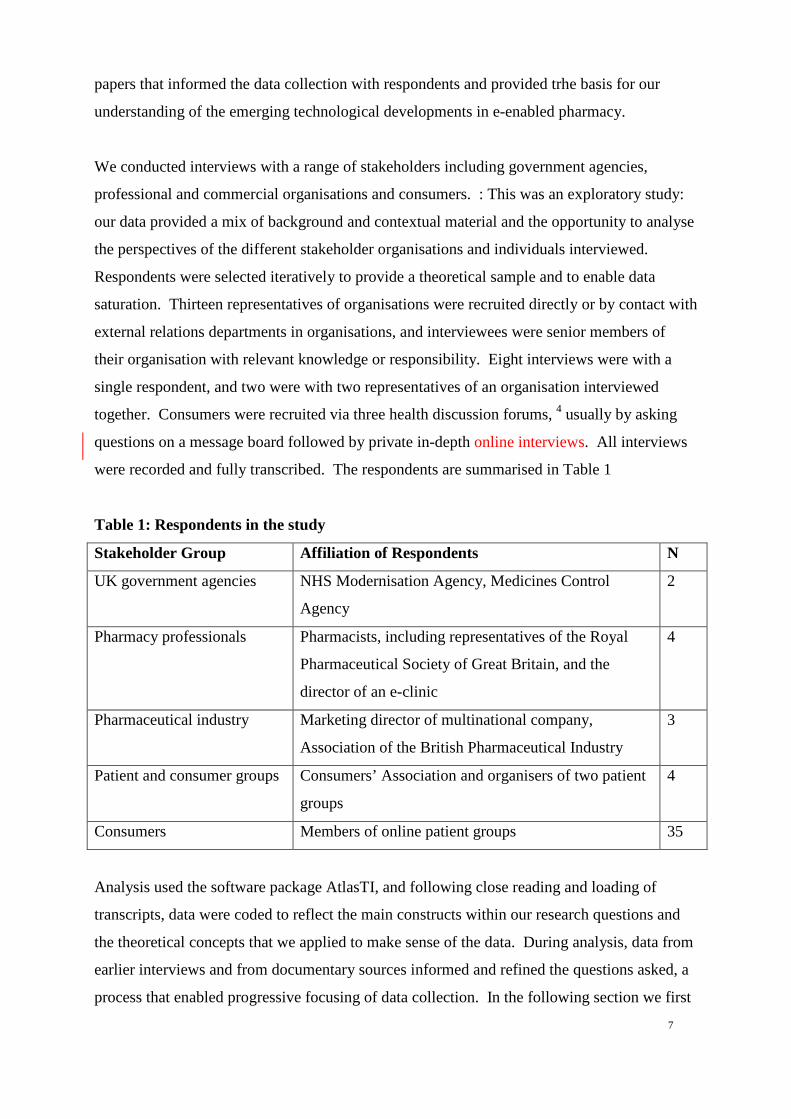
Table 1: Respondents in the study
Stakeholder Group Affiliation of Respondents N
UK government agencies NHS Modernisation Agency, Medicines Control
Agency
2
Pharmacy professionals Pharmacists, including representatives of the Royal
Pharmaceutical Society of Great Britain, and the
director of an e-clinic
4
Pharmaceutical industry Marketing director of multinational company,
Association of the British Pharmaceutical Industry
3
Patient and consumer groups Consumers’ Association and organisers of two patient
groups
4
Consumers Members of online patient groups 35
Analysis used the software package AtlasTI, and following close reading and loading of
transcripts, data were coded to reflect the main constructs within our research questions and
the theoretical concepts that we applied to make sense of the data. During analysis, data from
earlier interviews and from documentary sources informed and refined the questions asked, a
process that enabled progressive focusing of data collection. In the following section we first

8
describe the contexts of pharmaceutical governance, then look at the emergence of e-enabled
prescribing, before finally reporting data from stakeholders.
E-clinics: the Governance Context
To understand the legal and regulatory framework within which the birth of the e-clinic has
emerged, it is helpful to highlight the tension between pharmaceuticals as potentially
dangerous substances and a consumerist perspective that considers medications as
commodities that can be traded on the Internet in much the same way as books, CDs or
refrigerators. Unlike these consumer goods, pharmaceuticals are potent biochemical agents
that may poison or kill. Governments and the scientific community have mediated consumer
demands for effective pharmaceutical treatments for disease in various ways, imposing
safeguards to minimise the risk of inappropriate use.
Most national governments have legal and regulatory frameworks to govern pharmaceutical
use, and the nation-state has traditionally performed this role, although some supra-national
agencies also govern usage (for example, the European Union Drug Regulatory Authorities,
Pan American Network for Drug Regulatory Harmonization). The jurisdiction of such
governance regimes may thus be limited to national or geopolitical boundaries: both
consumers and global pharmaceutical companies operate within the complexities of
regulatory frameworks that vary from nation to nation. In the UK, regulation is under the
auspices of the Medicines and HealthCare Products Regulatory Authority, established under
the Medicine Act 1968 as the executive arm of the Drug Licensing Authority. The licensing
of medicines for use on humans is strictly regulated, and all new drugs must undergo lengthy
trials before they may become available for prescription. The Committee on Safety of
Medicines, an independent committee of experts, advises the Government on the safety,
quality and effectiveness of medicines, and investigates suspected adverse reactions to
medicines already on the market.
Traditionally, medications have been dispensed by pharmacy professionals, within a
regulation framework encompassing a mix of legislation and a self-regulatory code of ethics
to which all UK pharmacists must adhere (RPSGB 2003). In addition to POMs, which
require a prescription by a doctor or nurse-prescriber, PMs can only be dispensed in the
presence of a qualified pharmacist, while the general sales list (GSL) of proprietary

9
compounds, herbal remedies and food supplements can be obtained from a variety of other
outlets in addition to pharmacies. Which drugs have been designated for retail without
prescription has been determined largely by evidence on potency, safety and risk of adverse
side effects (Department of Health 1999), or to encourage self-medication for short-term
illnesses (Bosch 2001). Recently in the UK, a prescription statin (cholesterol-lowering
medication) was re-classified from POM to PM to encourage widespread prophylactic use
(Department of Health website 12 May 2004: press release 0186). Such categorisations vary
from nation to nation, and anomalies occur, so that drugs available in one country as
pharmacy medicines or GSL supplements (for example, melatonin) are POMs in others
(Childs et al 1998).
While the 1968 Medicines Act prohibits both the sale on UK territory of unlicensed drugs and
POMs without a prescription, the same Act permits individuals to import medicinal products
other than controlled substances for their own use (Bynoe 1999). There remains little control
over transactions with providers in foreign countries (Henney et al 1999), and travellers and
others have exploited this right to obtain medicines overseas, with or without professional
sanction. However, the UK and EU explicitly ban direct-to-consumer advertising (DTCA) of
POMs, and before the advent of the Internet, UK consumers were limited in the information
they could access on POMs to the technical information provided with drugs and advertising
in media aimed at health professionals. Proposals to permit DTCA have been criticised as
creating a market in pharmaceuticals that may pressure prescribers to meet patient requests for
specific medications (Shaw and Baker 2004).
The governance of pharmaceuticals addresses the following objectives of various parties:
• a need for control over the supply of potentially dangerous chemicals to protect the public,
through licensing and regulation of prescription;
• regulating the supply of pharmaceuticals possessing significant risks on the basis of
judgements by designated professionals including doctors, nurse-prescribers and
pharmacists, rather than by market forces;
• encouraging pharmaceutical innovation by commercial industry, including protection of
inventions and other intellectual property, to improve the public health, combat disease and
enhance the social and economic well-being of the nation;
• enabling individuals opportunities to access pharmaceuticals other than controlled
substances according to national and international legal frameworks;

10
This suggests that governing pharmaceutical consumption must balance the interests of a
range of stakeholders, including the government (in its various duties to protect the public,
maximise health, encourage technological innovation and account for its expenditure),
medical and pharmacy professions, patients and consumers (including support and interest
groups) and the pharmaceutical industry. This must be done within a broader environment
that acknowledges frameworks of national and international law and human rights legislation
and convention, the dynamics of the trans-national pharmaceutical market, as well as
scientific and technological innovation and social changes, and contingent of course upon
compliance by the general population including special interests such as patient support
groups. Governance is achieved in a partnership involving a mix of government agencies,
professional bodies and scientific advisory groups. In addition to legal requirements, there is
a strong element of professional and industrial self-regulation and what might be called a
‘fudge-factor’ that allows a light touch where appropriate. We now examine how the
development of the Internet as an information and commercial medium affects the system of
rule governing pharmaceutical consumption, before exploring stakeholder views on these
developments.
Three Moments in the Birth of the E-Clinic
Internet-enabled pharmacy is a relatively new phenomenon, but by 2002, Bessell et al had
been able to survey 104 websites offering medications over the Internet to members of the
public. Since then, the exponential rise in outlets has meant that, internationally, obtaining
both PMs and POMs from sources other than local pharmacists has become straightforward.
In North America and elsewhere, pharmacy chains diversified into online sales, and US e-
pharmacies are now accredited through the National Association of Boards of Pharmacy
(Sellers 2000). E-pharmacy has developed alongside traditional community pharmacies in the
US, and while e-pharmacies primarily target domestic consumers, an Internet user in
possession of a credit card can purchase many prescription drugs such as Viagra, Prozac, anti-
cancer drugs and weight loss drugs from these sites and have them sent internationally by
post. In the UK, ‘home-grown’ Internet-enabled pharmacy has developed within national and
EU governance frameworks. Since we began research in 2002, the shape of UK Internet-
enabled pharmacy has continued to develop, and the three ‘moments’ documented below

11
reflect differing degrees of continuity with, and transformation of existing patterns of
pharmaceutical consumption.
Moment 1: Electronic Transfer of Prescriptions
As part of a ‘Pharmacy in the Future’ initiative (DoH 2000) to modernise pharmacy, the UK
Department of Health commissioned a pilot scheme to evaluate electronic transfer of
prescriptions (ETP) between prescribers, pharmacists and the Prescriptions Pricing Authority
(PPA). Previously, POMs could only be legally dispensed against a hand-signed prescription,
however the ETP pilot was justified as a technical advance not prejudicial to public safety.
The Government believes the law permits the distance sale and supply of medicines,
provided that normal safeguards are met. … (I)f proper safeguards and professional
standards are in place, there is no reason in principle why medicines should not be
sold or dispensed electronically, or by other forms of distance sale and supply, like
mail order or home delivery (ibid: 12).
Under the pilot, GPs sent prescriptions electronically to one of three pharmacies in the
scheme, while remuneration of these pharmacies by the PPA (following dispensing of a
prescribed medicine to a patient) was also based on e-communication. In two of the pilot
organisations, patients collected drugs from the pharmacy premises, while a third was a ‘mail-
order’ pharmacy using a courier service to dispense prescriptions. The pilot study evaluation
(Sugden 2003) was broadly positive, although it did not appear to significantly free up
pharmacist or prescriber time (ibid: 10), and indeed required additional GP input to
electronically ‘sign’ repeat prescriptions (ibid: 11). Subject to the findings of the pilot, the
roll-out of ETP in the UK is planned for the near future (DoH 2000).
ETP is a technical solution to reduce paperwork and the need for multiple keying of patient
information during the prescribing process, and its implementation will overturn the legal
requirement for a ‘signature’ on a paper prescription (ibid: 12). However, ETP retains a
traditional model for prescribing pharmaceutical drugs, assuming doctors and other licensed
prescribers remain as exclusive gate-keepers to POMs, a principle strongly supported by
European Union member states (Stanberry 2002: 605) and the US (Charatan 2000).

12
Moment 2: E-Pharmacy and the ‘virtual’ pharmacist
While ETP exploits Internet technology to facilitate dispensing of POMs, the establishment of
online pharmacies enables consumers to purchase PM and GSL pharmaceuticals from a web-
site, for delivery by mail or courier service. Some traditional pharmacies have established
web-sites enabling online purchase of PMs, subject to a short questionnaire assessed by a
qualified pharmacist. These include Boots in the UK, Amcal in Australia and Walgreens in
the US. Other pharmacies without a high-street presence, including Pharmacy2U, also
operate online in a way analogous to a traditional pharmacist. These pharmacies also permit
consumers to purchase POM medicines on submission of a valid, signed prescription either in
person or by mail, and also enable repeat prescriptions to be ordered.
This model of e-pharmacy moves beyond a technical solution to transferring information, to
establish a ‘virtual’ pharmacist as a legitimate alternative to a face-to-face professional
contact. Thus, for example, Pharmacy2U asserts on its website that it
… has developed unique procedures and protocols that allow our pharmacists to check
the suitability of a medicine for a particular patient and ensure its safe delivery.
Qualified pharmacists supervise our service and we are members of the Royal
Pharmaceutical Society of Great Britain and the National Pharmaceutical Association.
Typically, customers purchasing PMs will be asked to complete a product-specific
questionnaire. According to Pharmacy2U, this is ‘checked by a registered pharmacist prior to
dispatch’ to assess the suitability of the drug for the profile elicited by the questionnaire.
The e-pharmacy marks a break from tradition by establishing the legitimacy of the e-
pharmacist, and of creating a market-place for PM drugs via internet promotional materials.
As will be seen in the next section, this virtual model of patient/pharmacist interaction has
been defended as acceptable by pharmacy professionals, and has been incorporated within
self-regulation codes of conduct. However, as with the electronic transfer of prescription
data, this second moment does not challenge the basic assumption that, in relation to POMs,
prescriptions are originated from a face-to-face consultation between patient and prescriber.
Moment 3: the E-clinic and the virtual prescriber

13
The third moment in the birth of the e-clinic establishes the online of virtual medical
consultation as an alternative mode of accessing POMs. In the market-driven US pharmacy
business, there has been a proliferation of websites offering access to prescription medicines.
Following federal regulation (Charatan 2000), most now offer these medications subject to an
online consultation with a registered physician. For UK residents, it is possible to obtain
POMs from e-pharmacies retailing internationally such as AmerimedRX or Epharmacist.com
based in the US, Canada and elsewhere. Typically, a physician employed by the pharmacy or
acting as a consultant reviews an online order. Thus for example, customers of AmerimedRX
must
… complete an online medical questionnaire which is thoroughly reviewed by a
licensed AmeriMedRx physician, and if found suitable for treatment, the prescription
will be dispensed and shipped by our licensed pharmacy. If the consulting physician
has any questions or concerns regarding your medical history or needs more
information, he or she will contact you … (extract from web site)
Most of these e-pharmacies promote a limited range of pharmaceuticals, predominantly ‘life-
style’ drugs such as sildenafil (Viagra), the weight-loss drug orlistat (Xenical), adjunct
therapies such as the pain relief drug celecoxib (Celebrex), and anti-virals such as acyclovir.
Many sites are consumer-orientated, promoting products according to US regulatory
frameworks that permit direct-to-consumer advertising (DTCA). Some US websites will not
retail to overseas consumers, but it is easy to access e-pharmacies that will ship
pharmaceuticals to any address: UK citizens may import POMs other than controlled
substances for personal use. The quality and authenticity of products available from some
sites has been questioned by commentators, as has the safety of trading POMs without
medical advice (Burgermeister 2004).
The ban on consumer advertising of POMs in the UK has been the constraining factor in the
emergence of UK equivalents to these outlets. We interviewed the director of one
organisation that operates legally within the UK as a self-styled ‘online clinic’, offerings a
small number of ‘lifestyle’ treatments for obesity, impotence and male pattern baldness (with
an aspiration to extend this range in the future). It operates as one of three ‘compliant sites’ in
the UK under the Medicines (Advertising) Regulations 1994 and European Directive
2001/83/EC. Unlike US websites, these regulations prevent UK e-clinics from giving details

14
of treatments or costs prior to a free online consultation with a UK-registered doctor. Their
mode of operation was negotiated in discussions with the Medicines and HealthCare
Regulatory Authority (MHRA) during 2003. According to the online clinic director
… their main concern was that you cannot mention POM names on your website as
this is considered advertising. They define a website as an advertising mechanism.
Also, they required a period of consideration for the doctor - they described this as
being similar to going to see your own doctor. For example, you would not go to your
doctor and say 'I would like Viagra please' instead, you would go and discuss your
condition, the doctor considers the facts before selecting a drug or range of drugs.
This principle is one that they feel would need to be replicated and considered
acceptable on the web.
Accordingly, it is only after an online consultation that consumers are e-mailed details of their
diagnosis and suggested treatments, and provided with a web address from which to buy the
treatment from the range of those recommended by the consultant, while repeat orders are
subject to confirmation by the consumer of their medical details. In an interview, the director
of the e-clinic suggested their service offered the security of a UK-regulated and compliant
website and genuine UK-licensed drugs, in contrast with overseas suppliers of POMs that
may be counterfeit or not manufactured to UK standards.
This third moment marks the most radical break with traditional modes of accessing POMs in
the UK, and by branding itself as an online clinic establishes a new model for consultation
with the medical profession. From a governance perspective, it was the issue of promoting
POMs to consumers that was a major stumbling block in the creation of a fully-fledged e-
clinic, rather than the need for face-to-face contact with a medical professional. In terms of
the social relations of prescribing, the e-clinic establishes a consumer model of POM
dispensing, bolstered by a subtle use of language that avoids the term ‘patient’ and an un-
moderated forum that allows consumers to discuss treatments directly with each other,
independent of medical intervention.
Stakeholder Responses to the Birth of the E-Clinic
15
The data from documentary evidence and interviews with stakeholder groups explored the
ways in which UK regulatory frameworks have been applied to address changing patterns of
supply and consumption of prescription medicines. Interviews with those tasked with
regulation and other stakeholders suggested a mix of reliance on established frameworks and
a hint of complacency concerning the extent of the emerging trends.
In the UK, no new legislation has been passed to regulate e-pharmacy, and developments
have been managed within codes of conduct developed by professional bodies (Anonymous
1999, Hansard 2000). Both documentary and interview data suggest a conservative response
to e-pharmacy, with the 1968 Medicines Act (which sets out the requirement for POMs to be
obtained only by valid prescription) judged adequate to address e-pharmacy developments. A
European Commission report on the electronic sale of pharmaceuticals (Muscardini 2001: 57)
assumes that ‘… prescription-only medicines are delivered to patients who can provide a
prescription that reflects meaningful contact with a qualified medical professional’. A
respondent from the Medicines and HealthCare Products Regulatory Agency (MHRA)
confirmed in an interview that in the UK, this has been interpreted to encompass ‘online
consultations’.
… on the question of … the need for a doctor to consult with a patient prior to issuing
a prescription, there is no requirement under medicines legislation for this to be face-
to-face. Therefore, there is nothing to prevent a doctor prescribing or supplying a
medicine on the basis of for example, an on-line questionnaire. That said, we would
take the view that it should contain sufficient information for the doctor to make a
decision about whether or not any proposed treatment was appropriate.
Concerning the ETP initiative, stakeholder reactions saw this as a technical advance in
communication (as one pharmacist respondent commented: ‘its just e-mailing prescriptions in
a secure system, isn’t it?’). Similarly, on the potential for POMs to be acquired from overseas
e-pharmacies, a member of the NHS Modernisation Board felt
… It’s a small problem, but it’s this debate as to whether it’s going to become a bigger
one. And, I wouldn’t like to say actually. I mean it’s probably going to slowly
increase but I’m not sure it’s going to suddenly expand exponentially. Because, if you
think that fifty per cent of medicines are for the over 75s … we’re really talking about

16
more than half of this being for older people and you know, it’s a limited market at the
moment.
The reaction of the MHRA has been to ensure that e-pharmacies based in the UK do not flout
DTCA legislation. This has had consequences for the emergence of fully-fledged e-clinics.
According to the director of an e-clinic, compliance with MHRA guidelines has cost it
business in the global Internet market, but has benefits as
‘… our customers appreciate being on the right side of the law … fraud is reduced and
people buy with more confidence therefore resulting in buying more quantity. … We
are disadvantaged, but there is not much we can do about it as the laws on the
promotion of POMs is different from country to country. We now see it as an
opportunity to establish ourselves in the knowledge that we will not be shut down.
This suggests pragmatism in the face of challenges to governance of e-pharmacy. Wherever
possible, new legislation is to be avoided, and voluntary consensus achieved to manage
environmental changes. In response to the development of e-pharmacy, the Royal
Pharmaceutical Society of Great Britain (RPSGB) updated its code-of-practice to
accommodate new practices, including the potential future use of electronic prescriptions
(RPSGB 2003). An editorial in the profession’s Pharmaceutical Journal reflects a view that
nothing has really changed:
As with all professional services, online pharmacy services must be provided
within the legislative framework for pharmacy and in compliance with existing
professional requirements detailed in the code of ethics. … all requirements of the
Medicines Act 1968 and Regulations must be complied with, including the
requirements for the supplying pharmacy to hold a valid prescription (Anonymous
2000: 9).
The RPSGB argue that the ‘remote patient’ is not new or unique: pharmacists are often
required to dispense medicines to family and friends on a patient’s behalf, and this way of
working can be replicated online using questionnaires and emailed advice as modes of
communication. Many aspects of e-pharmacy such as compliance with marketing

17
regulations, provision of drug information, record keeping and accountability transfer directly
from traditional to online environments (Appelbe and Wingfield 2001).
Thus the Royal Society’s approach is to work within existing legislation and regulatory
guidelines where possible, but to acknowledge that in a developing information-oriented
environment, there was a need for new alliances between government, professional and
patient organisations and the industry in order to govern the technology effectively and
appropriately. A pharmacist respondent voiced anxieties about the constraints that the use of
communication technology for ETP might place on patients.
The idea sounds brilliant in practice, but I would dread to think what would happen if
technology failed. (At present), quite often, the prescription generated is wrong, or
missing the odd item - through the fault of the practice … pharmacy staff spend a lot
of time chasing the surgeries for missing items - I wonder what would happen if this
happened via the internet? … It may mean that patients have to agree to staying with
one pharmacy, and at present this is something that isn't allowed, as patients should be
free to choose where they go.
The pharmaceutical industry is in a position to benefit commercially from environmental
changes that will enable a closer engagement between provider and consumer, including
direct advertising and opening up markets for non—NHS prescription. However, as our
respondents from the Association of the British Pharmaceutical Industry (ABPI) noted, the
pharmaceutical industry is one of the most regulated industries in the UK, and in such a
climate, companies are cautious about overstepping the line. Some multinational
pharmaceutical companies have adapted their web presence to avoid any implication that they
are advertising directly to consumers in countries in which DTCA is illegal. While web
surfers can access US pharmaceutical company sites, many companies provide separate web
sites for US and other visitors and point non-US citizens to web-pages where product
information is couched in language that reduces the sense of marketing.
Respondents from the pharmaceutical industry offered a cautious response to e-pharmacy.
The ABPI supported government efforts to establish electronic prescription transfer as an
example of how the Internet could be used to enhance the development of pharmaceutical
practice. The three respondents from the industry that we interviewed expressed concern over
18
e-pharmacy, which they perceived primarily as a means to market counterfeit products,
undercutting legitimate sales. Illegal selling of pharmaceuticals was a major risk for the
industry as it creates mistrust and potential misuse of drugs such as sildenafil and orlistat. In
addition, they argued that while many drugs sold without prescription on the Internet are
counterfeit, people seem willing to take risks. These responses suggest a stakeholder that is
keen to embrace developments arising from e-technology, but aware that they must work in
collaboration with more influential stakeholders if a more liberal governance regime is to be
realised, and to ensure that their livelihood is not undermined by deregulating intellectual
property and patent rights over products, or by challenging consumer trust in POMs.
While members of the public do not constitute a source of authority concerning
pharmaceutical governance, clearly their compliance with governance is critical to its success.
During our research, we interviewed consumers of a range of pharmaceuticals including
lifestyle drugs such as Viagra and Xenical, as well as correspondents to health chat rooms
(Authors, 2005, in press). Some of these respondents had used e-pharmacy to obtain
pharmaceuticals and other products, while others were strongly opposed, citing safety and
lack of knowledge as hazards of e-pharmacy. One respondent argued against the use of an e-
clinic:
There is a danger of someone ordering the drugs because they might have similar
symptoms to their next-door neighbour, relative, friend and thinking the same drugs
would cure them. A wide number of illnesses and conditions have symptoms which
are very similar but the drugs which would treat one condition won't necessarily treat
another condition even though they have similar or even the same symptoms. …
Prescription drugs should only be prescribed by a doctor after he/she has given a good
examination of the patient.
However, another respondent disagreed, but only for repeat prescriptions.
I think that if a patient knows the medication they should take (based on their own past
experience with the drug) then they should be allowed to purchase the drug over the
Internet without having to wait for a prescription from the GP. For example, women
who take oral contraceptives, people who are on long-term treatment, when an allergy
flares up, etc. … It is a great idea to have an Internet Pharmacy if the patient gets their

19
prescription (for the first time) from their GP and then can obtain the medicine via the
web instead of having to find the time to get to the (pharmacy).
These consumer perspectives must be acknowledged in managing governance of
pharmaceuticals in the Internet age. Elsewhere we have described the ways in which
consumers of POMs have subverted the traditional model of pharmaceutical consumption in
the quest to acquire drugs that can assist in achieving lifestyle objectives (Authors 2005, in
press, submitted b). In an international market-place, governance must balance the demands
for drugs against the need for public safety and the protection of business interests.
Discussion
We have documented three changes to pharmaceutical consumption in the UK that emerge
from the exploitation of Internet technologies. The first, ETP, is primarily a technical fix to
enable more efficient management of pharmaceutical dispensing, while the second and third
are more radical consequences of commercial exploitation of these technologies. These latter
two moments mark changes in the consumer-pharmacist and consumer-prescriber relationship
respectively, replacing face-to-face interaction with virtual encounters. The governance
issues are summarised in Table 2
Table 2: Challenges and Responses to Changes in Prescribing
Challenge to Governance Governance Response
ETP Legal requirement for a physical
prescriber signature on a prescription
Existing law amended to permit
electronic signatures
E-pharmacy No face-to-face opportunity for a
pharmacist to check that a patient is
suitable for a medication; direct-to-
consumer advertising of PMs
Pharmacy code of conduct on
acceptability of pharmacist advice by
phone or to a relative adapted to
cover Internet communication;
similarly for advertising PMs
E-clinic Non-UK
POMs available without prescription
from some websites
UK
Non-UK
Non-UK business lies beyond UK
jurisdiction, and consumers can
import for their own personal use
UK

20
No face-to-face consultation between
prescriber and patient; potential for
direct-to-consumer advertising of
POMs
Following negotiation between
regulator and business, e-
consultation with a GMC-registered
doctor deemed acceptable, but
available POM treatments and prices
not available to consumers until after
diagnosis.
The emergence of global e-pharmacy and the e-clinic has the potential to change the way in
which pharmaceuticals are considered by the public, equating these products with other goods
to be marketed and consumed, and reducing the gate-keeper role of a professional to that of an
online reviewer of a consumer and their self-reported ‘symptoms’. Health care consumers
perceive pharmaceutical technology as an adjunct in the pursuit of a better lifestyle and
experience of embodiment (Authors, 2005), and in a nation where the National Health Service
(NHS) has dominated the way in which POMs are used, the e-clinic provides a new route for
private prescription of drugs, circumventing the evidentially-based guidance provided to NHS
clinicians by the National Institute for Clinical Excellence (NICE). Together, these
developments affect some fundamental power relations between consumers, commerce and
professionals, and may upset a precarious balance between the objectives of ensuring public
safety and freedom of choice and autonomy (Walley et al 2000). The role of professional
expertise in sustaining this balance has been a key component of pharmaceutical governance,
and the e-pharmacy and e-clinic have the potential to undermine the extent to which this
expertise is exerted in the prescribing of pharmaceuticals (Bessell et al 2003: 90).
However, our research suggested a highly conservative response by UK regulators to these
innovations, depending upon established legislation to cover emergent technological changes
to pharmaceutical consumption and online consulting. Data from interviews and
documentary analysis suggest that in the view of regulators and professionals, minor changes
to data protection legislation and modifications to voluntary codes of conduct by professional
bodies and industry can address the emergence of e-prescribing. Thus, for example, Internet
media are to be included in DTCA codes, with online communication confirmed as an
adequate and legitimate method to assess patient suitability for POMs. Our data suggests a
strong tendency towards continuity, despite transformational pressures, with the impact of

21
new communication technology is down-played, and managed ‘at the margins’. How can we
understand this low-key reaction?
We would suggest that, following Rosenau’s (1995) model of governance, the under-stated
response to the birth of the e-clinic may be best understood as efforts by stakeholders to
sustain an existing system of rule in the face of an environmental change (the emergence of
global Internet commerce) rather than overturn existing systems and begin from scratch.
This, we have suggested elsewhere (Authors, forthcoming), is a feature of technology
governance: stakeholders manage environmental change incrementally, until pressure from
one quarter (for example, from consumers or from commercial interests, public morals and so
forth) is so significant that the system of rule must adapt. Governance is a process that is
continually breaking down, and must balance stakeholder interests. This explains the
emphasis on self-regulation in many systems of rule, and efforts to retain a lightness of touch
in terms of legal coercion.
Successful governance depends upon compliance, and with the emergence of the e-clinic, the
motor of change in pharmaceutical use comes from consumers. Given the right of the UK
citizen to import pharmaceuticals for personal consumption, UK regulators have no control
over consumer rights to obtain non-controlled medications from overseas, nor can they
regulate the advertising activities of non-UK companies, except in relation to EU legislation
that applies regulatory controls across member-states. We found a consensus of opinion
among government regulators, industry and professionals, and sustaining this consensus may
be more important than a radical response to alter governance arrangements. Only in the non-
controversial area of electronic prescription transfer have Parliamentary statutory instruments
(2001/2887-2890) been effected to ensure the legality of e-prescriptions. In the radical case
of the e-clinic, negotiations have established the online consultation as valid, so long as it
precedes any discussion or promotion of treatment options.
Currently, we observe the emergence in the UK of an e-clinic managed within existing
systems of rule. A mixture of fudge, strategic alliances between industry, professionals and
government and slightly modified codes of conduct has allowed the UK e-clinic to develop as
a distinct phenomenon, different from its overseas counterparts in terms of scale of operation,
and mimicking a traditional model of patient-prescriber interaction despite the lack of face-to-
face contact. While elsewhere, different cultures of prescribing and pharmaceutical

22
commerce, and of course, differing governance arrangements have led to a burgeoning
provision of online clinics, the analysis of governance applied in this paper suggests that for
the time being, the UK e-clinic will develop as a curiosity. UK e-clinics will subsist within
the interstices of established governance, meeting the demands for some lifestyle treatments
and ensuring a medical overview of pharmaceutical consumption is sustained, albeit at a
distance. Whether these governance arrangements can be maintained will depend upon the
success of the system of rule in balancing consumer demand and commercial enterprise
against public safety and consumer protection.
Notes
1. PMs can only be retailed in the presence of a qualified pharmacist. A general sales (GSL)
that includes proprietary compounds, herbal remedies and food supplements can be obtained
from a variety of other outlets in addition to pharmacies.
2. ESRC project L218252057, funded within the Innovative Health Technologies
programme.
3. We have used the notion of the sociological ‘moment’ to give a sense of development as
the opportunities to exploit Internet technology are recognised and operationalised.
4. Twenty interviews were with respondents in an anorexia forum, 12 in a weight loss forum
and three from a BBC health discussion forum. We followed ethical guidelines that prohibit
covert online data collection (Marx 1998; Reid 1996): all interviewees were fully aware that
their responses to the researcher’s questions were to be used in research.

23
References
Anonymous (1999) Britain’s first internet pharmacy opens. The Pharmaceutical Journal, 263
(7073): 849.
Anonymous (2000) ‘Council sets standards for internet pharmacy’, Pharmaceutical Journal,
264 (7077): 9. Accessed at
http://www.pharmj.com/Editorial/20000101/society/internetpharmacy.html
Appelbe, G.E and Wingfield, J (2001) Dale and Appelbe’s Pharmacy Law and Ethics, 7th
Edition, London: Pharmaceutical Press
Armstrong K, Schwartz JS, Asch DA. (1999) Direct sale of Sildenafil (Viagra) to consumers
over the Internet. New England Journal of Medicine, 341 (18): 1389-1392
Authors (2005) ‘The ‘Expert Patient’: Empowerment or Medical Dominance? The Case of
Weight Loss, Pharmaceuticals and the Internet,’ Social Science & Medicine, 60 (6) 1299-
1309.
Authors (submitted) ‘A Sociology of Technology Governance for the Information Age. The
Case of Pharmaceuticals, Consumer Advertising and the Internet’. Submitted to Sociology.
Authors (in press) ‘Pro-anorexia, Weight-loss Drugs and the Internet: Anti-Medical
Resistance and the Subversion of Technology’. Sociology of Health & Illness.
Barry, A. (2001) Political Machines: Governing a Technological Society. London:
Continuum.
Baym, N.K (1995) ‘The Emergence of Community in Computer Mediated Communication,’
in Jones, S (ed.) Cybersociety: Computer Mediated Communication and Community, pp. 138-
164. Thousand Oaks: Sage.
Bessell, T.L., Anderson, J.N., Silagy, C.A., Sansom, L.N.and Hiller, J.E. (2003) ‘Surfing,
self-medicating and safety: buying non-prescription and complementary medicines via the
Internet’. Quality and Safety in Health Care, 12: 88-92.
Bosch, X. (2001) ‘Spanish pharmacists fight plans to increase sale of over the counter drugs’,
British Medical Journal, 322: 1018.
Burgermeister, J. (2004) ‘UN warns of dangers of drugs sold on internet’, British Medical
Journal, 328: 603.
Bynoe R. (1999) M’Learned Web: Drugs on the Net – Viagra. ZDNet, 6 April 1999.
Accessed at http://news.zdnet.co.uk/story/0,,t269-s2071446,00.html
Cashore, B. (2002) ‘Legitimacy and the privatization of environmental governance’,
Governance, 15 (4) 503-29.

24
Charatan, F. (2000) ‘Clinton to regulate internet prescription drug sales’, British Medical
Journal, 320: 75.
Childs, M., Ellison, L. and Prayle, D. (1998) Drugs and the Internet. New Law Journal, 148
(6868): 1840.
Department of Health (1999) Review of Prescribing, Supply and Administration of
Medicines. Final Report. London: Department of Health.
Department of Health (2000) Pharmacy in the Future – Implementing the NHS Plan. London:
Department of Health.
Eysenbach, G. (2000) ‘Recent advances: Consumer health informatics’, British Medical
Journal, 320: 1713-1716.
Eysenbach, G., Sa, ER. and Diepgen, TL. (1999) ‘Shopping around the internet today and
tomorrow: towards the millennium of cybermedicine,’ British Medical Journal, 319: 1294.
Freeman, J. (2002) ‘The health care state in the information age’, Public Administration, 80
(4) 751-67.
Hansard (2000) House of Commons Debates for 11 Jul 2000: Column 154-9WH.
Henney, JE., Shuren, JE., Nightingale, SL. and McGinnis, TJ. (1999) ‘Internet Purchase of
Prescription Drugs: Buyer Beware [Editorial]. Annals of Internal Medicine, 131 (11): 861-2.
Holderness, M (1998) ‘Who are the World’s Information Poor?’ in Loader, B.D. (ed.)
Cyberspace Divide, pp. 35-57. London: Routledge.
Jewson, N. and MacGregor, S. (1997) ‘Transforming Cities: Social Exclusion And The
Reinvention of Partnership’, in Jewson, N. and MacGregor, S. (eds.) Transforming Cities, pp.
1-15. London: Routledge.
Jones, M. and Salter, B. (2003) ‘The Governance of Human Genetics: Policy Discourse and
Constructions of Public Trust’, New Genetics and Society, .22 (1): .21-41
Loader, B.D. (1997) ‘The governance of cyberspace: politics, technology and global
restructuring’, in Loader, B.D. (ed.) The Governance of Cyberspace. pp. 1- 19. London:
Routledge.
Marx, G. (1998) ‘An ethics for the new surveillance’, Information Society, 14 (3): 171-186.
Muscardini, C. (2001) ‘Written Question: Electronic Sales of Drugs,’ European Union
Commission Official Journal C151E (22/05/2001): 56-7.
Pines WL (2000) Direct-to-consumer advertising. Annals of Pharmacotherapy, 34:1341-4.
Queau, P. (2002) ‘Global governance and knowledge societies’, Development, 45 (4): 10-16.
Reid, E. (1996) ‘Informed consent in the study of online communities: a reflection on the

25
effect of computer-mediated social research’, Information Society, 12: 169-74.
Richards, D.L. (2002) ‘Making the National International: Information Technology and
Government Respect for Human Rights’, in Allison, J.E. (ed.) Technology, Development and
Democracy. Albany: State University of New York Press.
Rosenau, J.N. (1995) ‘Governance for the twenty-first century’, Global Governance, 1: 13-43.
Rosenau, J.N. (1997) Along the Domestic-Foreign Frontier. Cambridge: Cambridge
University Press.
Royal Pharmaceutical Society of Great Britain (2003) Code of Ethics and Standards.
Accessed at http://www.rpsgb.org.uk/pdfs/MEP27s2.pdf.
Sellers J. (2000) Internet pharmacies [Editorial]. American Journal of Health Systems
Pharmacy, 57 (7): 643.
Shaw, J. and Baker, M. (2004) ‘Expert patient: dream or nightmare?’ British Medical Journal,
328: 723-724.
Shore C and Wright S (1997) ‘Policy: a new field of anthropology’, in Shore C and Wright S
(eds.) Anthropology of Policy, pp. 3-39. London: Routledge.
Singh, J.P. (2002) ‘Introduction: Information Technologies and the Changing Scope of Global
Power and Governance’. In Rosenau J.N. and Singh, J.P. (eds.) Information Technologies
and Global Politics, pp 1-38. Albany: State University of New York Press.
Stanberry, B. (2002) ‘Commentary: Legal aspects of health on the internet: a European
perspective. British Medical Journal, 324: 605-6.
Sugden, B. (2003) Electronic Transmission of Prescriptions Evaluation of Pilots. Newcastle:
Sowerby Centre for Health Informatics.
Walley T, Earl-Slater A, Haycox A, Bagust A (2000) An integrated national pharmaceutical
policy for the United Kingdom? British Medical Journal, 321: 1523-1526.




















