Temperature-controlled slow pathway ablation for treatment of ...
11
European Heart Journal (1996) 17, 1092-1102 Temperature-controlled slow pathway ablation for treatment of atrioventricular nodal reentrant tachycardia using a combined anatomical and electrogram guided strategy S. Willems, H. Shenasa, H. Kottkamp, X. Chen, G. Hindricks, S. Yli-Mayry, W. Haverkamp, T. Wichter, B. Rotman, G. Breithardt and M. Borggrefe Hospital of the Weslfdlische Wilhelms University of Munster, Department of Cardiology and Angiology and Institute for Research in Arteriosclerosis, Munster, Germany Alms Anatomical and electrogram-guided techniques have been used separately for slow pathway ablation in atrio- ventricular nodal reentrant tachycardia. The aims of the present study were to analyse electrogram characteristics of target sites and biophysical parameters using a com- bined anatomical and electrogram-guided technique for temperature-controlled radiofrequency catheter ablation of the slow pathway. Methods and results Using a temperature-controlled (pre-selected 60 °C) catheter system, 53 patients with atrio- ventricular nodal reentrant tachycardia underwent slow pathway radiofrequency ablation. Mapping was started posteroseptally near the coronary sinus ostium and continued towards the midseptal area if needed. The longest and latest atrial electrograms with an atrioventricular ratio of <,0-5 were targeted. After a median of two pulses (mean 236 ±1-33), atrioventricular nodal reentrant tachycardia was rendered non-inducible in all patients without compli- cations. Successful sites had longer atrial electrograms (78-8 ± 9-8 vs 67-6 ± 13-3 ms, /><0003) and larger ventricu- lar electrogram amplitudes (92-4 ±51-2 vs 631 ± 28-8 mV, P<0-05) than the failed sites, but had a similar atrio- ventricular ratio, P-A interval and atrial electrogram am- plitude. Overall, an atrial electrogram duration of ^ 70 ms was associated with effective radiofrequency delivery, with 86% sensitivity and 62% specificity. The achieved tem- perature maximum was 62-3 ± 9-8 °C at successful and 58-8 ± 90 °C at unsuccessful sites (ns). There was no significant difference between successful and unsuccessful applications with respect to power output, impedance and total delivery energy. During a pre-discharge study, three patients with inducible atrioventricular nodal reentrant tachycardia underwent a repeat ablation. During 12-3 ± 2-5 (6-15) months of follow-up, three others had a clinical recurrence of atrioventricular nodal reentrant tachycardia. Conclusions The combined approach for slow pathway ablation is highly effective, requiring a low number of radiofrequency pulses. Long atrial activation time seems to be the most powerful predictor of success. Similar catheter tip temperature levels during successful and unsuccessful radiofrequency applications indicate that suboptimal selec- tion of target sites rather than ineffective heating due to poor catheter tissue coupling is responsible for unsuccessful energy delivery. (Eur Heart J 1996; 17: 1092-1102) Key Words: Catheter ablation, atrioventricular nodal reentrant tachycardia, slow pathway, supraventricular tachycardia, temperature control. Introduction Radiofrequency catheter modification of the atrioven- tricular node targeting the fast or slow pathway has been Revision submitted 12 December 1995 and accepted 5 January 1996. In part supported by the Franz-Loogen-Foundation, Dusseldorf, Germany. Correspondence Stephan Willems, MD, Martin Borggrefe, MD, Innere Median C, Uni KJinik Munster, D-48129 Munster, Germany. introduced as a curative approach for atrioventricular nodal reentrant tachycardia 11 " 12 '. Modification of the anteroseptally located fast pathway has been demon- strated to be effective, but carries the risk of complete atrioventricular block' 1 " 81 . However, sequential mapping strategies and titration of energy delivery may decrease the incidence of this complication' 1314 '. Slow pathway modification seems to have a lower risk of inadvertent atrioventricular block, since radiofrequency current is applied to posteroseptal or midseptal areas further 0195-668X/96/071092+11 $18.00/0 1996 The European Society of Cardiology Downloaded from https://academic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Temperature-controlled slow pathway ablation for treatment of ...
European Heart Journal (1996) 17, 1092-1102
Temperature-controlled slow pathway ablation fortreatment of atrioventricular nodal reentrant
tachycardia using a combined anatomical andelectrogram guided strategy
S. Willems, H. Shenasa, H. Kottkamp, X. Chen, G. Hindricks, S. Yli-Mayry,W. Haverkamp, T. Wichter, B. Rotman, G. Breithardt and M. Borggrefe
Hospital of the Weslfdlische Wilhelms University of Munster, Department of Cardiology and Angiology andInstitute for Research in Arteriosclerosis, Munster, Germany
Alms Anatomical and electrogram-guided techniques havebeen used separately for slow pathway ablation in atrio-ventricular nodal reentrant tachycardia. The aims of thepresent study were to analyse electrogram characteristicsof target sites and biophysical parameters using a com-bined anatomical and electrogram-guided technique fortemperature-controlled radiofrequency catheter ablation ofthe slow pathway.
Methods and results Using a temperature-controlled(pre-selected 60 °C) catheter system, 53 patients with atrio-ventricular nodal reentrant tachycardia underwent slowpathway radiofrequency ablation. Mapping was startedposteroseptally near the coronary sinus ostium andcontinued towards the midseptal area if needed. The longestand latest atrial electrograms with an atrioventricular ratioof <,0-5 were targeted. After a median of two pulses (mean236 ±1-33), atrioventricular nodal reentrant tachycardiawas rendered non-inducible in all patients without compli-cations. Successful sites had longer atrial electrograms(78-8 ± 9-8 vs 67-6 ± 13-3 ms, /><0003) and larger ventricu-lar electrogram amplitudes (92-4 ±51-2 vs 631 ± 28-8 mV,P<0-05) than the failed sites, but had a similar atrio-ventricular ratio, P-A interval and atrial electrogram am-plitude. Overall, an atrial electrogram duration of ^ 70 mswas associated with effective radiofrequency delivery, with
86% sensitivity and 62% specificity. The achieved tem-perature maximum was 62-3 ± 9-8 °C at successful and58-8 ± 90 °C at unsuccessful sites (ns). There was nosignificant difference between successful and unsuccessfulapplications with respect to power output, impedance andtotal delivery energy. During a pre-discharge study, threepatients with inducible atrioventricular nodal reentranttachycardia underwent a repeat ablation. During 12-3 ± 2-5(6-15) months of follow-up, three others had a clinicalrecurrence of atrioventricular nodal reentrant tachycardia.
Conclusions The combined approach for slow pathwayablation is highly effective, requiring a low number ofradiofrequency pulses. Long atrial activation time seems tobe the most powerful predictor of success. Similar cathetertip temperature levels during successful and unsuccessfulradiofrequency applications indicate that suboptimal selec-tion of target sites rather than ineffective heating due topoor catheter tissue coupling is responsible for unsuccessfulenergy delivery.(Eur Heart J 1996; 17: 1092-1102)
Key Words: Catheter ablation, atrioventricular nodalreentrant tachycardia, slow pathway, supraventriculartachycardia, temperature control.
Introduction
Radiofrequency catheter modification of the atrioven-tricular node targeting the fast or slow pathway has been
Revision submitted 12 December 1995 and accepted 5 January 1996.
In part supported by the Franz-Loogen-Foundation, Dusseldorf,Germany.
Correspondence Stephan Willems, MD, Martin Borggrefe, MD,Innere Median C, Uni KJinik Munster, D-48129 Munster, Germany.
introduced as a curative approach for atrioventricularnodal reentrant tachycardia11"12'. Modification of theanteroseptally located fast pathway has been demon-strated to be effective, but carries the risk of completeatrioventricular block'1"81. However, sequential mappingstrategies and titration of energy delivery may decreasethe incidence of this complication'1314'. Slow pathwaymodification seems to have a lower risk of inadvertentatrioventricular block, since radiofrequency current isapplied to posteroseptal or midseptal areas further
0195-668X/96/071092+11 $18.00/0 1996 The European Society of Cardiology
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022

Combined approach for slow pathway ablation 1093
away from the central body of the atrioventricularnode13"5-9"12151. To date, strategies for slow path-way ablation have been anatomical or electrogram-guided'3"5'9"12'151. The electrogram-guided method isprimarily oriented on detection of specific slow pathwaypotentials19''01. Nevertheless, several studies have shownthat the recording of distinct slow pathway potentials isnot a prerequisite for successful ablation sites'3'11'12'151.In contrast to previous reports, in this study, mappingwas oriented on both anatomical landmarks and electro-gram criteria, but not focused on the detection ofspecific slow pathway potentials.
So far, modification of the atrioventricular nodehas been performed using power-regulated radio-frequency current1'"151. Experimental findings havedemonstrated that only monitoring of the catheter-tissue interface temperature can accurately predict lesionsize1161. Furthermore, formation of potentially thrombo-genic coagula is critically dependent on abrupt changesin impedance and the catheter tip temperature'1?|181.Overheating of the catheter tip and coagulum formationcan be prevented by closed loop temperature controland thus might improve the procedure's safety1'91.
Reviewing our early experience with radio-frequency catheter ablation of the slow pathway andpreviously described reports regarding the electrogramcharacteristics of successful and failed sites during sinusrhythm'9'10'151, we hypothesized that electrograms at thesuccessful target sites, at the posteroseptal to midseptalregions, should have the following characteristics: (1)later timing of the atrial electrogram when compared tothe onset of the atrial electrogram recorded at the Hisbundle region or the high right atrium, (2) a prolongedand fractionated atrial electrogram with or without apossible slow pathway potential, since this area presum-ably behaves like a zone of slow conduction during sinusrhythm and atrioventricular nodal reentrant tachycar-dia, and (3) a critical ratio of the atrial to ventricularelectrogram amplitude at the target site (atrioventricularratio of ^0-5).
The present study was conducted to test thishypothesis and to assess the feasibility of a new com-bined stepwise anatomical and electrogram-guidedapproach for temperature-controlled catheter ablationof the slow pathway in patients with atrioventricularnodal reentrant tachycardia.
Methods
Patient data
Fifty-three consecutive patients with a history of recur-rent paroxysmal sustained atrioventricular nodal re-entrant tachycardia were prospectively enrolled inthe present study. There were 39 females and 14 males,aged 45-2 ± 17 years (range 15-74). A history of syn-cope was present in 11 cases. Previous antiarrhythmictherapy (2-5 ± 1-3 agents) was discontinued either due
to inefficacy or intolerable side-effects. No patients hadother cardiac abnormalities.
Electrophysiological study
Electrophysiological studies were performed in a fasting,lightly sedated state after written informed consent hadbeen obtained. Antiarrhythmic therapy had been discon-tinued for at least five half-lives. The investigations wereperformed using a conventional method of intracardiacrecording and stimulation'201. Multipolar electrode cath-eters with an inter-electrode spacing of 5 or 10 mm wereintroduced from the femoral veins and positioned intothe right atrium, His bundle region and right ventricularapex under fluoroscopic guidance. Continuous anti-coagulation was maintained throughout the procedurewith an initial bolus injection of 5000 units of heparin,followed by 1000 units i.v. hourly.
When sustained atrioventricular nodal reentranttachycardia could not be reproducibly induced, isopro-terenol was administered, and titrated to achieve a sinusrate increment of 25%. The diagnosis of atrioventricularnodal reentrant tachycardia was made according topreviously published criteria'21'221.
Endocardial mapping
Either a conventional 7F or a 5F deflectable electrodecatheter (Osypka 'Cereblate' Dr P. Osypka, Grenzach-Whylen, Germany) with a thermistor embedded into the4 mm catheter tip was introduced via a femoral vein andused for endocardial mapping and ablation. Bipolarelectrograms of the distal pair of the mapping catheterwere recorded simultaneously at a paper speed of 100and 200 mm . s ~ '. The band pass filter setting was 40to 500 Hz. Since an additional coronary sinus catheterwas not routinely inserted, the coronary sinus ostiumwas transiently intubated with the ablation catheter fordirect localization. Endocardial mapping was guided byboth anatomical landmarks and electrophysiological par-ameters. Initially, the electrode catheter was positionedposteroseptally using biplane fluoroscopic control withLAO 30° and RAO 60° standard views.
At each site, the local bipolar electrograms offive sinus beats prior to energy delivery were analysed.Timing of the atrial electrograms were determined withregard to the onset of surface P, atrial electrogramrecorded on the right atrial and/or His catheter, theamplitude and duration of atrial and ventricular electro-grams and the atrioventricular ratio. Because there is nouniversal definition of slow pathway potentials, we con-sidered both previously described morphologies'9'101 aspossible slow pathway potentials. Therefore, either arapid high frequency signal'91 or a low frequency broaddeflection located after or within the terminal portion ofthe atrial electrogram'101 was labelled as possible slowpathway potential. Distinct slow pathway potentialswere not specifically targeted, although all electrograms
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
1094 S. Willems etal
Figure 1
were evaluated for the presence of a possible slowpathway potential. Electrogram stability was assessedduring sinus rhythm and constant atrial pacing. Theelectrograms were categorized as stable if there was lessthan 10% beat-to-beat variation of the atrial and ven-tricular potential and no new or loss of major deflectionwas observed.
Criteria for selection of electrograms at target siteElectrograms at target sites recorded at the posterosep-tal to midseptal regions were accepted for energy deliv-ery if the following characteristics were present: (1) latertiming of the atrial electrogram when compared to theonset of the atrial electrogram recorded on the His orhigh right atrial catheter, (2) fractionated and longerduration of atrial electrograms than those of the His orhigh right atrial catheter with or without possible slowpathway potential, and (3) an atrial electrogram ampli-tude of half or less of the ventricular electrogram whenrecorded on the same mapping catheter (atrioventricularratio ^0-5).
Measurements of timing of local electrogramsMeasurements were based on their onset with the excep-tion of a few cases where the onset of a local electrogram
could not be reliably determined, in which case the firstrapid deflection crossing the baseline was used. Like-wise, the duration of the local atrial electrogram wasmeasured by determining the interval from its onsetto the beginning of an isoelectric line located precedingthe ventricular electrogram, or to the beginning of theearliest ventricular activity if such an isoelectric line wasnot present. Any possible slow pathway potential wasincluded for the duration of the atrial electrogram.
Electrogram characteristics of de novo (first)successful target sites were also compared to those of denovo (first of four or more) unsuccessful sites, becauseeven unsuccessful energy delivery may add to tissuedamage and thus contribute to the final impulse success.Furthermore, unsuccessful impulses may change localelectrograms. To minimize these influences, we havechosen the first failed sites of those patients who receivedmultiple energy applications. In this subanalysis, the cutoff of four pulses was selected to minimize the aforemen-tioned influences. Radiofrequency application was in-itiated during sinus rhythm. However, when ectopicjunctional rhythms were observed, in order to unmaskradiofrequency-induced atrioventricular block, atrialpacing at cycle lengths of 500 to 400 ms was performedthroughout the energy delivery. Impulse delivery was
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022

Combined approach for slow pathway ablation 1095
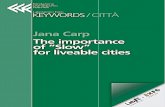
Figure 1 Radiograms show left anterior oblique (60°) and right anterior oblique (30°)views with the ablation catheter (MAP) and additional intracardiac catheters located inthe high right atrium (HRA), His bundle region (HIS) and right ventricular apex (RVA).A representative mapping sequence demonstrates the ablation catheter initially intubatingthe coronary sinus (panel (a)). The estimated area of the coronary sinus os is indicated byan arrow. The mapping electrode is then positioned posteroseptally (panel (b)) and atlower (panel (c)) and upper midseptal (panel (d)) areas.
started posteroseptally close to the ostium of the cor-onary sinus where the most suitable local electrogramrecording was obtained. The mapping procedurewas continued and the catheter was slightly movedtowards more midseptally located sites when the firstpulse was not successful. The electrode catheter waspositioned more superiorly and anteriorly along theinter-atrial septum in a stepwise manner if needed.Figure 1 gives an example of a typical mapping sequenceduring the ablation procedure, where the left andright anterior oblique views with the mapping catheterpositioned in the coronary sinus posteroseptally andat lower and upper mid septal areas, are depicted. Itshould be emphasized that due to induction ofjunctional and atrial ectopic beats by energy delivery,occasionally slight dislocation of the catheter tipwas observed. Therefore, the presence or absence of
slow pathway potentials immediately following appli-cation of energy at these sites was not systematicallyassessed.
Radio frequency catheter ablation
Using the radiofrequency generator HAT 200S (DrOsypka, Grenzach-Whylen, Germany), energy (500 kHzunmodulated current) was delivered during sinusrhythm or atrial pacing between the tip electrode of theablation catheter and the indifferent patch electrodepositioned at the mid-posterior chest wall. Actual poweroutput, impedance, energy delivery and catheter tiptemperature were continuously measured and displayedvia an interface with a microcomputer. Catheter-tip-tissue interface temperature was pre-selected to 60 °C.
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
1096 S. Willems et a\.
Power output was adjusted automatically by the genera-tor (0-50 watt) in order to achieve and maintain thepre-selected tip temperature. Energy delivery (pre-settime 60-90 s) was discontinued automatically when sud-den rises in impedance occurred. A sudden impedancerise of more than 50 Ohm was considered a significantimpedance 'jump'. Subsequently, the catheter was with-drawn to exclude coagulum formation at the electrodetip. Additionally, energy application was stopped im-mediately on catheter dislocation, atrioventricular nodalreentrant tachycardia, Wenckebach periodicity or atrio-ventricular block. Inducibility of atrioventricular nodalreentrant tachycardia and anterograde and retrogradeatrioventricular conduction capabilities were assessedfollowing the delivery of each impulse. Non-inducibilityof atrioventricular nodal reentrant tachycardia at base-line and during isoproterenol infusion was defined as theendpoint of the ablation session. Persisting longitudinaldissociation of the atrioventricular node or the induci-bility of only one atrioventricular nodal reentrant beatwas an acceptable endpoint. Anticoagulation with i.v.heparin was continued for 24 h. All patients underwentechocardiographic investigation within 48 h to excludethrombus formation or pericardial effusion.
Follow-up
All patients underwent a pre-discharge electrophysi-ological study 2-4 days after the ablation procedure andwere regularly followed in the outpatient clinic. Aspirin(100 mg daily) was prescribed for 3 months.
Data analysis
Continuous data are expressed as mean ± SD or asmedian. Variables were compared by Student's t-test orMann-Whitney U test as appropriate. P values <005were considered significant. Statistical analysis was per-formed using a commercially available computer soft-ware (SPSS; SPSS Inc., U.S.A.). Multivariate analysiswas performed to compare electrogram characteristicsof effective and ineffective catheter ablation sites. Atwo-tailed Fisher's exact test was used for two by twocontingency table measurements (GraphPAD InStatInc. 1990, U.S.A.) when required.
Results
Immediate outcome
Atrioventricular nodal reentrant tachycardia was repro-ducibly inducible with or without additional applicationof isoproterenol in all patients prior to the initial abla-tion attempt. The cycle length of the tachycardia was326 ± 61 ms. The common type of atrioventricular nodal
Table 1 Electrophysiological parameters of all patientsbefore ablation and at a control study 2—4 days after slowpathway ablation
PR intervalAH intervalHV interval1AP-CLIVP-CL
Beforeablation
152 ±2079 ±2140±7
308 ±60284 ±56
2-4 daysafter ablation
152 ± 1878 ±2141 ± 8
373 ±94298 ± 63
Pvalue
nsnsns
/><001ns
IAP = Wenckebach point during incremental atrial pacing.IVP = Wenckebach point during incremental ventricular pacing.Values are expressed as mean values ± standard deviation. Allintervals in msec.
reentrant tachycardia was induced in all but one patientwith the uncommon form. Both types were present inanother patient.
A median of two radiofrequency pulses (mean2-36 ± 1 -3) was required to eliminate tachycardia in all53 patients. In 23 patients, only a single energy deliverywas necessary for slow pathway modification. One tofive pulses, delivered to the right posteroseptal to mid-septal area, were required in all but one patient whoreceived 14 pulses. In this patient, 12 ineffective pulseswere delivered to the posteroseptal and midseptal re-gion. Thereafter, two pulses were applied to the anterioraspect of the inter-atrial septum. Subsequently, thetachycardia was no longer inducible. The electrophysi-ological findings (unaltered PR interval, persistent dualatrioventricular nodal physiology) were consistentwith selective modulation of the slow pathway. Themean fluoroscopy time was 27-0 ± 19 min. No completeatrioventricular block or other procedure-relatedcomplications occurred.
Electrophysiological findings
Electrophysiological parameters at the baseline studyand after the ablation session are summarized in Table1. The cycle length at which anterograde atrioventricularblock occurred during incremental atrial pacing in-creased significantly from 308 ± 60 to 373 ± 94 ms fol-lowing the ablation procedure (Z'<001). Retrogradeventriculo-atrial Wenckebach point was not influencedby radiofrequency delivery (284 ± 56 vs 298 ± 63 ms; ns).The duration of PR, AH, and HV interval did notchange significantly after slow pathway ablation. In 36patients (64%), longitudinal dissociation of the atrioven-tricular node, as evidenced by sudden AH prolongationduring premature atrial stimulation, was found beforeablation. This finding persisted in 24 patients (43%) afterthe procedure. Atrioventricular nodal reentrant tachy-cardia was rendered non-inducible in all patients. Asingle retrograde atrioventricular nodal echo beat via thepresumed fast pathway with subsequent block in the
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
Combined approach for slow pathway ablation 1097
Table 2 Electrogram characteristics of successful and unsuccessful target sites forslow pathway ablation
Duration A (ms)Amplitude A (mV)Amplitude V (mV)P-A interval (mV)AV ratioSP potential
All effectivesites
(n = 53)
78-8 ±9-822-5 ± 15-692-4 ±51-256-5 ± 13-20-30 ±0-22
30%
All ineffectivesites
(n = 72)
67-6 ±13-322-7 ± 17-363-1 ±28-854-4 ± 1 8 00-41 ±0-37
12%
p
value
/><0-003ns
/><0-05nsns
/><002
Duration A = duration of atrial electrogram; Amplitude A = maximal amplitude of atnal electro-gram; Amplitude V = maximal amplitude of ventricular electrogTam; P-A interval = intervalbetween P wave of surface ECG and onset of local atrial electrogram; AV ratio = ratioof atrioventricular electrogram; SP potential = incidence of presumed slow pathway potential.Depicted are mean values ± standard deviation.
slow pathway was inducible with or without isoproter-enol infusion in 22 cases (39%) following the ablationsession.
Local electrogram characteristics
Successful versus unsuccessful sitesTable 2 depicts local electrogram characteristics of allsuccessful and all unsuccessful ablation sites. The dur-ation of the local atrial electrogram at effective sites(78-8 ± 9-8 ms) was significantly longer than at ineffec-tive sites (67-6± 13-3 ms, /><0003). There was a higheramplitude of the ventricular electrogram at successfulsites (92-4 ±51-2 mV vs 63-1 ± 28-8 mV, P<005). Poss-ible slow pathway potentials were more frequently ob-served at effective (30%) than at ineffective (12%) targetsites (/><002). At effective sites electrograms were morefrequently classified as stable than at ineffective sites(79% vs 49%). There was no significant difference be-tween successful and unsuccessful ablation sites withrespect to the amplitude of the atrial electrogram, theinterval between surface P-wave and the onset of localatrial activation, and the atrioventricular ratio (Table 2).Multivariate analysis demonstrated that the atrial elec-trogram duration was the only variable with a significantdifference between effective and ineffective target sites. Alocal atrial electrogram duration of 70 ms or morewas predictive of successful ablation site, with 86%sensitivity and 62% specificity.
Successful first versus failed first siteThe electrogram characteristics of 23 patients with only asingle successful radiofrequency application (group 1)were compared to the first unsuccessful target site in 10patients who required four or more pulses (group 2) forslow pathway ablation (Table 3). Local atrial electro-gram duration at target sites of group 1 was significantlylonger when compared to group 2 patients (76-3 ± 9-2 msvs 600 ± 11-6 ms, P<0006). The local atrial electrogrammeasured 70 ms or more in 90% of group 1 patients, but
Table 3 Electrogram characteristics of the successfulfirst site in patients who required only a single radiofre-quency pulse (group 1) and the first failed site in patientswith four or more radiofrequency pulses (group 2)
Duration A (ms)Amplitude A (mV)Amplitude V (mV)P-A interval (ms)AV ratioSP potential
Group 1(n = 23)
76-3 ±9-218-4± 10-573-8 ±53-158-9 ± 11-30-32 ± 0-20
22%
Group 2(n=10)
600 ± 11-616-9 ±20-7410 ±27-953-6 ± 19-90-48 ± 0-40
10%
Pvalue
P<0006nsnsnsnsns
Duration A = duration of atrial electrogram; Amplitude A =maximal amplitude of atrial electrogram; Amplitude V = maximalamplitude of ventricular electrogram; P-A interval = interval be-tween P-wave of surface ECG and onset of local atrial electrogram;AV ratio = ratio of atrioventricular electrogram; SP potential =incidence of presumed slow pathway potential. Depicted are meanvalues ± standard deviation.
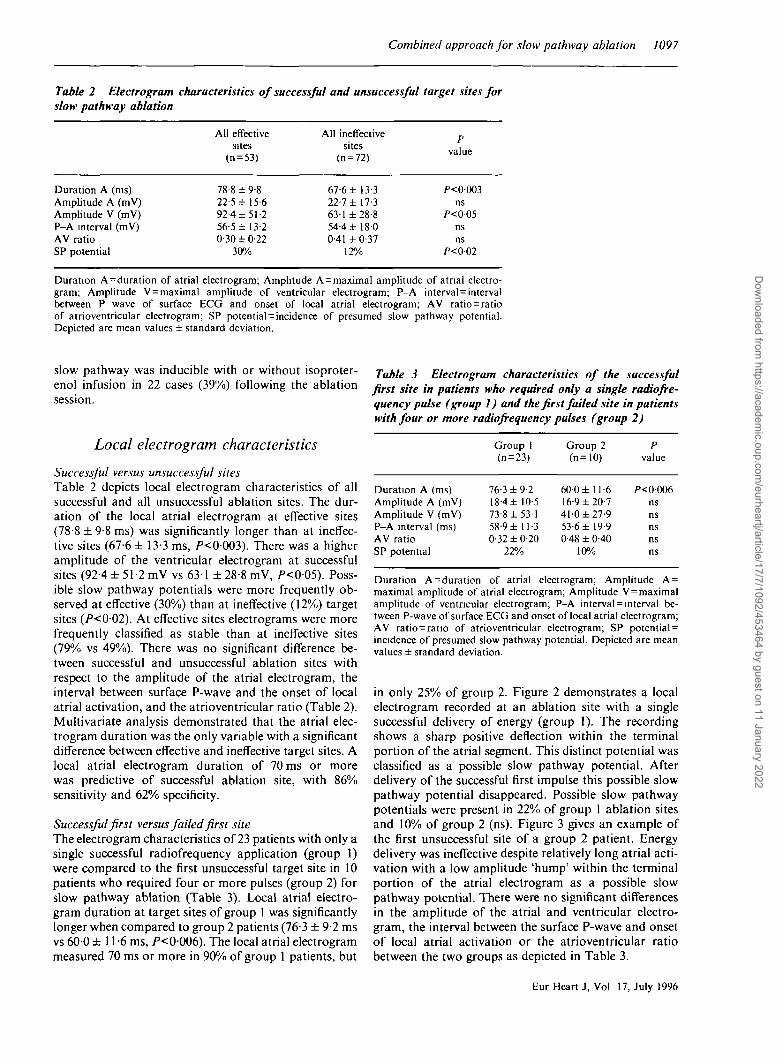
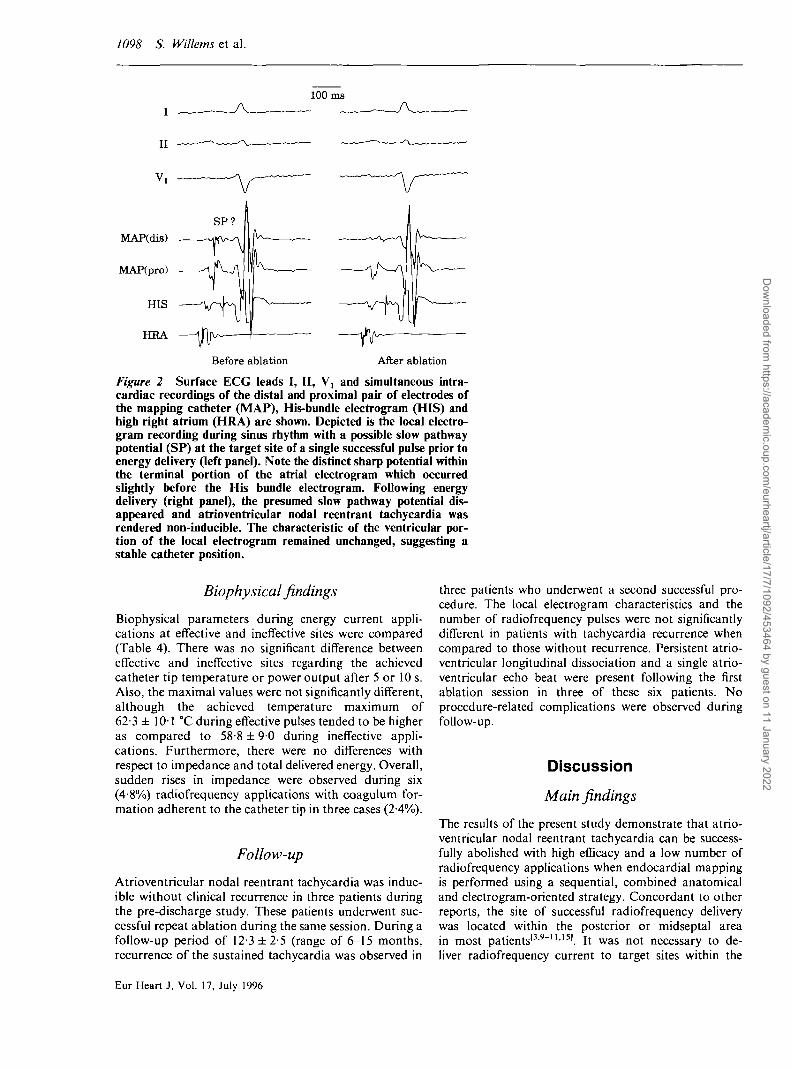
in only 25% of group 2. Figure 2 demonstrates a localelectrogram recorded at an ablation site with a singlesuccessful delivery of energy (group 1). The recordingshows a sharp positive deflection within the terminalportion of the atrial segment. This distinct potential wasclassified as a possible slow pathway potential. Afterdelivery of the successful first impulse this possible slowpathway potential disappeared. Possible slow pathwaypotentials were present in 22% of group 1 ablation sitesand 10% of group 2 (ns). Figure 3 gives an example ofthe first unsuccessful site of a group 2 patient. Energydelivery was ineffective despite relatively long atrial acti-vation with a low amplitude 'hump' within the terminalportion of the atrial electrogram as a possible slowpathway potential. There were no significant differencesin the amplitude of the atrial and ventricular electro-gram, the interval between the surface P-wave and onsetof local atrial activation or the atrioventricular ratiobetween the two groups as depicted in Table 3.
Eur Heart J, Vol 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
1098 S. Willems et al.
100 msI
II
MAP(difi)
MAP(pro)
HIS
HRA
Before ablation After ablation
Figure 2 Surface ECG leads I, II, V, and simultaneous intra-cardiac recordings of the distal and proximal pair of electrodes ofthe mapping catheter (MAP), His-bundle electrogram (HIS) andhigh right atrium (HRA) are shown. Depicted is the local electro-gram recording during sinus rhythm with a possible slow pathwaypotential (SP) at the target site of a single successful pulse prior toenergy delivery (left panel). Note the distinct sharp potential withinthe terminal portion of the atrial electrogram which occurredslightly before the His bundle electrogram. Following energydelivery (right panel), the presumed slow pathway potential dis-appeared and atrioventricular nodal reentrant tachycardia wasrendered non-inducible. The characteristic of the ventricular por-tion of the local electrogram remained unchanged, suggesting astable catheter position.
Biophysical findings
Biophysical parameters during energy current appli-cations at effective and ineffective sites were compared(Table 4). There was no significant difference betweeneffective and ineffective sites regarding the achievedcatheter tip temperature or power output after 5 or 10 s.Also, the maximal values were not significantly different,although the achieved temperature maximum of62-3 ± 101 °C during effective pulses tended to be higheras compared to 58-8 ± 90 during ineffective appli-cations. Furthermore, there were no differences withrespect to impedance and total delivered energy. Overall,sudden rises in impedance were observed during six(48%) radiofrequency applications with coagulum for-mation adherent to the catheter tip in three cases (2-4%).
Follow-up
Atrioventricular nodal reentrant tachycardia was induc-ible without clinical recurrence in three patients duringthe pre-discharge study. These patients underwent suc-cessful repeat ablation during the same session. During afollow-up period of 12-3 ±2-5 (range of 6-15 months,recurrence of the sustained tachycardia was observed in
three patients who underwent a second successful pro-cedure. The local electrogram characteristics and thenumber of radiofrequency pulses were not significantlydifferent in patients with tachycardia recurrence whencompared to those without recurrence. Persistent atrio-ventricular longitudinal dissociation and a single atrio-ventricular echo beat were present following the firstablation session in three of these six patients. Noprocedure-related complications were observed duringfollow-up.
Discussion
Main findings
The results of the present study demonstrate that atrio-ventricular nodal reentrant tachycardia can be success-fully abolished with high efficacy and a low number ofradiofrequency applications when endocardial mappingis performed using a sequential, combined anatomicaland electrogram-oriented strategy. Concordant to otherreports, the site of successful radiofrequency deliverywas located within the posterior or midseptal areain most patients13-9""'151. It was not necessary to de-liver radiofrequency current to target sites within the
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
Combined approach for slow pathway ablation 1099
100 ms
MAP
HIS
HRA
Figure 3 Surface ECG leads I, II, V, and simultaneousintracardiac recordings of the distal pair of electrodes ofthe mapping catheter (MAP), His-bundlc electrogram(HIS) and high right atrium (HRA) are depicted. Thisgraph gives an example of an ablation site with ineffectiveenergy delivery. Atrial activation was relatively long andthe presence of a slow pathway potential was assumed.There was no sharp deflection but a small 'hump' visiblewithin the terminal part of the atrial electrogram.(A=atrium, SP=possible slow pathway potential, V=ventricle.)
Table 4 Biophysical parameters of effective and ineffec-tive ablation sites
All effectivesites
(n = 53)
All ineffectivesites
(n = 72)
Pvalue
Temp 5 s (*C)Temp 10 s (°C)Temp max (*QPower 5 s (W)Power 10 s (W)Power max (W)Total energy (J)Impedance max (ii)
45-1 ±3-3510±4-562-3 ±9-822-4 ±7-936-2 ±12-245-3 ±9-22145 ±1521
113 ± 36
45-3 ±4-650-3 ±5-758-8 ± 9 022-6 ±8-634-3 ± 13-543-5 ±13-22195 ± 1510
108 ± 16
nsnsnsnsnsnsnsns
coronary sinus, as previously described19'151. In onepatient 14 impulses were applied to the anterior aspectof the inter-atrial septum to achieve elimination ofslow pathway conduction. This location outside thecommon boundary demonstrates the potential anatomi-cal variability of slow pathway conduction1251.
Previous strategies for slow pathway ablationwere mainly based on either local electrogram cri-
teria'9101 or anatomical landmarks'3'll>231. When theanatomical-guided strategy was applied, radiofre-quency current was usually delivered unguided tothe posterior aspect of the inter-atrial septum in astepwise manner. Several reports have shown thatthis technique is effective in eradicating atrioventricu-lar nodal reentrant tachycardia'3'""231. The electrogram-guided technique uses endocardial mapping fordetection of distinct slow pathway potentials. Thus,this method is dependent on a high incidence of slowpathway potentials at successful target sites, whichhas not been observed uniformly in other studies'3'111.Using both anatomical- and electrogram-guidedstrategies, tachycardia can be abolished with ahigh success rate. However, unintended ablation ofthe fast pathway and induction of complete heartblock has been observed with both techniques'3'9'111.In some instances, multiple radiofrequency deliverieswere necessary. When the anatomical approachwas applied, the mean number of required radio-frequency pulses ranked between 6 and 20, with amaximum of up to 56 delivered pulses'3'5'11>23]. Oc-casionally, slow pathway conduction could not beabolished and the fast pathway had to be targetedsubsequently13'41. A relatively broad region or net-work of fibres capable of slow conduction and partici-pation in reentrant tachycardia may contribute tothese findings.
Anatomical studies have suggested that fibrescovering the area near the coronary ostium in thedirection of the compact node represent the posteriorinput to the atrioventricular node1241. In addition clinicalobservations during intra-operative ice mapping ofatrioventricular nodal reentrant tachycardia havepointed to the possible variation of fast and slowpathway locations. In that study, slow pathway conduc-tion was interrupted in two patients when cryolesionswere applied not to the posterior or inferior inter-atrialseptum but more superiorly along the tendon ofTordaro[25].
On the basis of these findings, anatomical- andelectrogram-guided strategies were combined in thepresent study to avoid the possible disadvantages de-scribed above. The local electrogram during sinusrhythm was characterized by its detection of the longestand latest fractionated atrial activation. Sequentialmapping was started posteroseptally near the coronarysinus ostium, targeting an ablation site characterizedby the above mentioned criteria and proceeding step-wise to more midseptal sites if required. Recently,the anatomical- and electrogram-guided techniquehas been compared in a randomized study1'51. Four of25 patients assigned for the anatomical approachsubsequently underwent successful electrogram-guidedablation after the initial attempt had been unsuccessful.The cross-over from the anatomical to the electrogram-guided approach in these patients and the average sixto seven radiofrequency applications, respectively,may signify the value of both criteria for slow pathwayablation.
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022
1100 S. Willems et al.
Electrophysiological findings
The electrophysiological findings after the ablationprocedure were suggestive of a selective slow pathwaymodification in all of our patients. Prolongation of thePR interval and unintended ablation of the fast pathwaycould be avoided with the combined stepwise approach.In previous studies, inadvertent ablation of the fastpathway has been observed with an incidence of 1 -3%[91
up to 14%[4] using either the anatomical or electrogram-guided technique1151. This might be due to the previouslydescribed anatomical variability of the location ofthe fast and slow pathways'251. The atrioventricularWenckebach point was prolonged after ablation. Thisfinding, and the unaltered retrograde conductioncapacity, is consistent with previous results followingslow pathway ablation13'9""1.
Following ablation, dual atrioventricular nodalphysiology and single echo beats were observed in 43%and 39% of all patients, respectively. This was acceptedas an endpoint of the procedure if no more than oneecho beat or sustained tachycardia was inducible withor without isoproterenol. This concept is concordantto previous studies with a comparable incidence ofpersistent slow pathway conduction following theprocedure13'10'151.
Local electrogram characteristics
Analysis of all local bipolar electrograms during sinusrhythm demonstrated a significantly longer atrial elec-trogram duration at successful compared to unsuccessfultarget sites. A long duration of local atrial activation of;>70 ms was associated with success with 86% sensitivityand 62% specificity. Long or fractionated local atrialactivation may also be due previous applications ofradiofrequency energy at this site. To exclude this pos-sibility, we also assessed the first target site in patientswith a single successful pulse and the first failed sitein patients who required four or more radiofrequencypulses. Atrial electrogram duration was also significantlylonger at effective compared to ineffective sites whenonly the initial ablation attempts were compared in thesepatients. These data strongly support the notion thatprolonged atrial electrogram duration is indeed an im-portant criterion for identifying the target site, as sug-gested by our approach. The findings are consistent withresults reported by Kalbfleisch and coworkers[l51. Intheir study, local atrial electrograms were significantlylonger and more fractionated at successful compared tounsuccessful target sites. Interestingly, this differencewas also present when target sites were exclusivelyselected on the basis of anatomical criteria.
In all likelihood, the reason for the low numberof radiofrequency impulses required for slow path-way modification in this study may not only be the useof the combined method of mapping but also in thepre-selection and initial screening of local electro-grams. The fact that only very late (later than atrial
electrograms recorded on the high right atrium and Hiscatheter), prolonged and fractionated atrial electro-grams with low atrioventricular ratio were targeted,may have markedly facilitated the ablation procedures.There has been a wide range in the correlation be-tween successful radiofrequency ablation and therecording of slow pathway potentials using a slowpathway-guided mapping approach13'9""'151. The rangeextends from a 100% incidence19''01 to studies thathave reported no evidence for any specific slow path-way potentials despite effective radiofrequency appli-cation'3'"1. This might be due to different electrogramrecording techniques and the fact that mapping wasnot focused solely on the detection of slow path-way potentials in all studies. Nevertheless, previousreports'3'1''12'151 and the present study have shown thatthis is not a prerequisite for the selection of successfulsites for slow pathway ablation.
Biophysical parameters
In the present study, primarily the temperature-controlled mode of radiofrequency current applicationfor transcatheter modulation of the atrioventricularnode was introduced and analysed. Temperature re-sponse, power output level, impedance and the overalldelivered energy did not differ between effective andineffective radiofrequency applications. The almostsimilar temperature response at effective compared toineffective sites indicates that suboptimal target siteselection rather than poor tissue heating is responsiblefor failed radiofrequency application. The catheter tiptemperature levels determined were concordant to re-sults recently reported by Calkins and coworkers'191. Intheir multicentre study, the average temperature levelmeasured 59 °C. However, the comparison with thepresent data might be influenced by the fact that fast andslow pathway ablation were not assessed separately intheir study.
In our study, sudden rises in impedance occurredin 4-8% of all pulses. Experimental in vivo studies havedemonstrated that temperature control but not regu-lation of power output alone accurately predicts lesionsize'161. Abrupt changes in impedance are associatedwith overheating and formation of a carbonized layeradherent to the catheter tip'17'18'. Consequently, sud-den rises in impedance are potentially hazardous andmay cause thromboembolic complications. In the clini-cal setting, thromboembolic events represent a sub-stantial amount of procedure-related complications'261.Furthermore, procedure duration and fluoroscopy ex-posure are prolonged because following each imped-ance rise, the ablation catheter has to be withdrawn inorder to exclude carbonization and thrombus for-mation at the catheter tip. It has been shown that theincidence of sudden rises in impedance is markedlyreduced using a closed-loop feedback temperature-controlled mode compared to power-regulated radio-frequency delivery1191.
Eur Heart J, Vol. 17, JuJy 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022

Combined approach for slow pathway ablation 1101
Limitations
The criteria used to select target sites were only tested inone group as all patients underwent the same approachfor mapping and ablation of slow pathways. Themethod tested was not compared to other methods suchas the anatomical approach alone. Since endocardialmapping was not focused on presence or absence ofpossible slow pathway potentials, no further pacinginterventions or drug administrations, i.e. application ofadenosine, were performed to confirm the evidence forsuspected slow pathway potentials. There was no sys-tematic attempt to record local electrograms at targetsites immediately following energy delivery to assess thepresence or absence of possible slow pathway potentialsbecause the recording of target electrograms was influ-enced by catheter movements caused by junctionalescape beats or extrasystoles.
ConclusionThe present study demonstrates that anatomical andelectrogram criteria are helpful to guide catheterablation of the slow pathway. The combined approachusing prolonged, fractionated and late atrial activationto guide endocardial mapping is highly effective andselective in eliminating atrioventricular nodal reentranttachycardia with a low number of radiofrequency pulses.Successful target sites are characterized by a longeratrial activation compared to unsuccessful slow pathwayablation sites. Strategies for slow pathway ablationshould be based on both criteria using a temperature-controlled mode of radiofrequency delivery.
The authors wish to thank Anke Schwinning for secretarialassistance during preparation of the manuscript.
References[1] Lee MA, Morady F, Kadish A el al. Catheter modification of
the atrioventricular junction with radiofrequency energy forcontrol of atrioventricular nodal reentry tachycardia. Circu-lation 1991; 83: 827-35.
[2] Calkins H, Sousa J, El-Atassi R et al. Diagnosis and cure ofthe WolflF-Parkinson-White syndrome or paroxysmal supra-ventricular tachycardias during a single electrophysiologictest. N Engl J Med 1991; 324: 1612-18.
[3] Jazayeri MR, Hempe SL, Sra JS et al. Selective transcatheterablation of the fast and slow pathways using radiofrequencyenergy in patients with atrioventricular nodal reentrant tachy-cardia. Circulation 1992; 85: 1318-28.
[4] Langberg JJ, Leon A, Borganelli M. A randomized, prospec-tive comparison of anterior and posterior approaches toradiofrequency catheter ablation of atrioventricular tachy-cardia. Circulation 1993; 87: 1551-6.
[5] Chen SA, Chiang CE, Tsang WP et al. Selective radio-frequency catheter ablation of fast and slow pathways in 100patients with atrioventricular nodal reentrant tachycardia.Am Heart J 1993; 125: 1-10.
[6] Mitrani R, Klein LS, Hackett K, Zipes D, Miles W. Radio-frequency ablation for atrioventricular nodal reentranttachycardia: comparison between fast (anterior) and slow(posterior) pathway ablation. J Am Coll Cardiol 1993; 21:432-41.
[7] Langberg JJ. Radiofrequency catheter ablation of AV nodalreentry: The anterior approach. PACE 1993; 16: 615-22.
[8] Willems S, Chen X, Hindricks G et al. Radiofrequencycatheter ablation of AV nodal reentry tachycardia: experiencewith selective fast pathway ablation. Z Kardiol 1994; 83:165-72.
[9] Jackman WM, Beckman KJ, McClelland JH et al. Treatmentof supraventricular tachycardia due to atrioventricular reentryby radiofrequency catheter ablation of slow-pathway conduc-tion. N Engl J Med 1992; 327: 313-18.
[10] Haissaguerre M, Gaita F, Fischer B et al. Elimination ofatrioventricular nodal reentrant tachycardia using discreteslow potentials to guide application of radiofrequency energy.Circulation 1992; 85: 2162-75.
[11] Kay GN, Epstein AE, Dailey SM, Plump VJ. Selectiveradiofrequency ablation of the slow pathway for the treatmentof atrioventricular nodal reentrant tachycardia: evidence forinvolvement of perinodal myocardium within the reentrycircuit. Circulation 1992; 85: 1675-88.
[12] Moulton K, Miller B, Scott J, Woods WT. Radiofrequencycatheter ablation for AV nodal reentry tachycardia: A tech-nique for rapid transection of the slow AV nodal pathway.PACE 1993; 16: 760-8.
[13] Kottkamp H, Hindricks G, Willems S el al. An anatomicallyand electrogram guided approach for effective and safecatheter ablation of the fast pathway for elimination ofatrioventricular nodal reentrant tachycardia. J Am CollCardiol 1995; 25: 974-81.
[14] Langberg JJ, Harvey M, Calkins H, El-Atassi R, KalbfleischSJ, Morady F. Titration of power output during radio-frequency catheter ablation of atrioventricular reentranttachycardias. PACE 1993; 16: 465-70.
[15] Kalbfleisch SJ, Strickberger SA, Williamson B et al. Rand-omized comparison of anatomic and electrogram mappingapproaches to ablation of the slow pathway of atrioventncu-lar node reentrant tachycardia. J Am Coll Cardiol 1994; 23:716-23.
[16] Hindricks G, Haverkamp W, Giilker H et al. Radiofrequencycoagulation of ventricular myocardium: improved predictionof lesion size by monitoring catheter tip temperature. EurHeart J 1989; 10: 972-84.
[17] Haines DE, Verow AF. Observations on electrode-tissueinterface temperature and effect on electrical impedanceduring radiofrequency ablation of ventricular myocardium.Circulation 1990; 82: 1034-8.
[18] Kottkamp H, Hindricks G, Haverkamp W et al. Biophysicalaspects of radiofrequency catheter ablation — significance ofsudden rise of impedance. Z Kardiol 1992; 81: 145-51.
[19] Calkins H, Prystowski E, Carlson M, Klein LS, Saul JP,Gilette P. Temperature monitoring during radiofrequencycatheter ablation procedures using closed loop control. Circu-lation 1994; 90: 1279-86.
[20] Chen X, Borggrefe M, Hindricks G, Haverkamp W,Breithardt G. Radiofrequency catheter ablation of accessorypathways: characteristics of transiently and permanentlyeffective pulses. PACE 1992; 15: 1122-30.
[21] Josephson ME. Supraventricular tachycardias. In: JosephsonME (Hrsg). Clinical Cardiac Electrophysiology. London/Philadelphia: Lea and Febiger, 1990: 182-224.
[22] Jazayeri MR, Sra JS, Deshpande SS et al. Electrophysiologicspectrum of atrioventricular nodal behavior in patientswith atrioventricular nodal reentrant tachycardia undergoingselective fast or slow pathway ablation. J Cardiovasc Electro-physiol 1993; 4: 99-111.
[23] Wathen M, Natale A, Wolfe K, Yee R, Newman D, Klein G.An anatomically guided approach to atrioventricular nodeslow pathway ablation. Am J Cardiol 1992; 70: 886-9.
[24] Becker AE, Anderson RH. Morphology of the human atrio-ventricular junctional area. In: Wellens HJJ, Lie KJ, JanseMJ, eds. The conduction system of the heart: structure,function and clinical implications. The Hague: MartinusNijhoff, 1978: 263-76.
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022

1102 S. Willems etal
[25] Keim S, Werner P, Jazayeri M, Akhtar M, Tchou P. Localiz- [26] Hindricks G and the MERFS investigators. The Multicentreation of the fast and the slow pathways in atrioventricular European Radiofrequency Survey (MERFS): Complicationsnodal reentrant tachycardia by intraoperative ice mapping. of radiofrequency catheter ablation of arrhythmias. Eur HeartCirculation 1992; 86: 919-25. J 1993; 14: 1644-53.
Eur Heart J, Vol. 17, July 1996
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/17/7/1092/453464 by guest on 11 January 2022