Development of Telemedicine and Telecare over Wireless Sensor Network

The Journal onInformation Technology
in Healthcare
HTI J
Volume 2 Issue 22004
ISSN 1479-649X
EDITOR
Clyde Saldanha
EDITORIAL BOARD
Lodewijk Bos (Netherlands)Jimmy Chan (Hong Kong)
Stephen Chu (New Zealand)Charles Doarn (USA)
Syed Haque (USA)Robert Istepanian (UK)Chien-Tsai Liu (Taiwan)Valentin Masero (Spain)Jeannette Murphy (UK)
Dean Sittig (USA)Roger Tackley (UK)

The Journal on Information Technology in Healthcare
Aims and ScopeThe Journal on Information Technology in Healthcare aims to improve the quality and safety ofpatient care, by encouraging and promoting the use of Information Technology (IT) in healthcare.The journal acts as a medium for the international exchange of knowledge and experience of thebenefits of IT in healthcare. It publishes papers that educate healthcare professionals on the use ofIT in clinical practice, and particularly papers that provide objective evidence of the benefits of IT inhealthcare.
SubscriptionsThe Journal on Information Technology in Healthcare is published 6 times a year.2004 subscription prices (6 issues) are :
Institutional Individual
Great Britain £120 £100Europe €200 €180USA US$220 US$180Rest of the world £135 £115
Payment can be made by cheque or banker’s draft. Cheques should be made payable to The Journal onInformation Technology in Healthcare. Subscription orders and requests for sample copies should besent to: JITH, 72 Churston Drive, Morden, Surrey, SM4 4JQ, UK. E-mail: [email protected] : +44 (0)870 130 1572.Claims for issues not received should be made within 3 months of publication of the issue.
Copyright© The Journal on Information Technology in Healthcare. All rights reserved.The Journal on Information Technology in Healthcare is protected by copyright. Apart from fairdealing for the purposes of research, private study, criticism or review, no part of this publicationmay be reproduced, stored or transmitted in any form or by any means without the prior writtenpermission of the Editor.
DisclaimerAll papers are published in good faith. Authors are responsible for the scientific content andaccuracy of their papers. Although every effort is made to ensure accuracy and avoid mistakes, noliability on the part of the Editor, publisher or their agents is accepted for the consequences of anyinaccurate or misleading information. The opinions, data and statements that appear in articlespublished in the journal are those of the authors, and not necessarily those of the Editor orpublisher. The Editor and publisher disclaim any responsibility or liability for such material and donot guarantee, warrant or endorse any product or service described in this publication.
Publisher: Health Technology Press, 72 Churston Drive, Morden, Surrey, SM4 4JQ, UK.
Advertising: To advertise in this journal, please contact William D’Sa, 25 Oxford Avenue, London,SW20 8LS, UK.Tel +44 (0)20 8543 1230. Fax +44 (0)870 130 1572.E-mail: [email protected]
Typeset by Toby Matthews, Oxford.Printed by Saleh Aldossry, KSA.

HTI J
The Journal on Information Technologyin Healthcare
Volume 2 Issue 2
CONTENTS
TeleCARE for the ElderlyClyde Saldanha 69
TeleCARE: Collaborative Virtual Elderly Care Support CommunitiesLuis Camarinha-Matos, Hamideh Afsarmanesh 73
Management of Federated Information in Tele-assistance EnvironmentsHamideh Afsarmanesh, Victor Guevara-Masis, Louis Otto Hertzberger 87
Tele-assistance Services to Improve the Quality of Life for Elderly Patientsand their Relatives: The Tele-CARE Approach
José María Aguilar, Javier Cantos, Guillermo Expósito, Pedro José Gómez 109
TeleCARE Time Bank: A Virtual Community for Elderly Care Supportedby Mobile Agents
Octavio Castolo, Filipa Ferrada, Luis Camarinha-Matos 119


69
TeleCARE for the Elderly
HTI J © The Journal on Information Technology in Healthcare 2004; 2(2): 69–71
People over 65 years of age are the fastest growing population segment in manycountries in the world. In the USA, for example, it is projected that their numberswill increase to almost 60 million by the year 20251. This increase in the numberof elderly people will place an enormous burden on healthcare resources. De-mand for services will exceed those that can be delivered by current healthcaresystems and consequently a new infrastructure and system of delivering health-care will be necessary.
Design of such a system should aspire to the goals and vision of a 21st centuryhealthcare system. Whenever possible elderly people should be able to lead full,active, independent lives. Care should be delivered pro-actively, be patient-centred and readily accessible. In addition it should be multi-disciplinary andcoordinated.
Developments in information and communication technology have made thesegoals a reality. The papers in this issue illustrate their use in the TeleCARE projectto create a virtual elderly support community. This enables elderly people toremain in their homes with the reassurance of appropriate aid in the event of anaccident or emergency. In addition their quality of life can be improved by theprovision of other services.
The first paper elaborates on the TeleCARE platform that has been developedfor the project. This consists of a basic platform and a specialised services plat-form. The basic platform supports:
• Communications • Interfacing to external devices • Storage and manipulation of data and information • Provision of a catalogue of all devices and services
The specialised services platform provides: • Functionalities such as interfaces for the elderly and Web access • Individual services, e.g. Living Status Monitoring and Agenda Reminder
The first paper gives details of the individual technologies employed in theplatform. In addition, the authors elaborate on how these technologies help toconfer fundamental characteristics such as robustness, flexibility, adaptability,scalability, extensibility and inter-operability.
The second paper gives a detailed account of how information is stored andretrieved in the collaborative network of the TeleCARE project. The approachadopted is similar to that described for the Regional Information System in Fin-land2; namely to keep information in the database of the original institution and

Saldanha
70 The Journal on Information Technology in Healthcare 2004; 2(2): 69–71
to search for it when required. However, unlike the Finnish system in which aseparate Reference database is created to provide links to the original information,in the TeleCARE system information is searched for using mobile software agents.This confers the possibility of combining intelligent decision-making with theinformation retrieval tasks. For example, the searcher may choose to search allinstitutions to retrieve all possible answers, or choose to search only until acondition is satisfied, and then terminate the search.
The third paper describes two of the specialised services that have been devel-oped for the TeleCARE project. These are:
• Agenda Reminder • Living Status Monitoring
Forgetfulness is a common problem in old age. Mild cognitive impairmentaffects approximately 17%3 of the older population and the prevalence of demen-tia in the community is estimated to be between 10–20%4. The problem willincrease in the future as the incidence of Alzheimer’s disease is increasing and lifeexpectancy for Alzheimer and multi-infarct patients is also increasing5,6. TheAgenda Reminder service is designed to help elderly people remember the dailytasks they have to do, and also to remind them of appointments and meetings. Anindividual agenda is created by a carer but can be modified on the instruction ofthe elderly person or a relative.
A major fear for elderly people living alone is the inability to summon aid inthe event of an accident or medical emergency. The Living Status Monitoring(LSM) service is designed to address this concern. The LSM uses special devices tomonitor a patient in their home. When the devices sense something abnormal,e.g. a loud noise followed by absence of movement, they alert the Care Centre.Personnel at the centre can then obtain additional information from other de-vices, e.g. a web camera, and by conversing with the elderly person. This helpsthem to establish the exact nature of the problem, and to ensure appropriatedeployment of emergency services. The system also allows the patient to activelycontact the centre whenever they feel the need to.
Loneliness is one of the biggest problems facing the elderly. This is not merelya social problem. Loneliness is a recognised risk factor for a number of medicalconditions including depression, alcohol abuse and suicide7,8. There is also someevidence to suggest that loneliness increases the risk of cardiovascular disease9.The last paper in this issue describes the Tele Bank service of the TeleCAREproject. This is a service that has been designed to allow elderly people to play anactive role in their community and to remain socially integrated.
Although the TeleCARE platform has been developed specifically for elderlypeople, the principles underlying its development are applicable to other areas ofhealthcare. In addition the platform is generic enough to be adapted for otheruses, for example, mental health patients or children with disabilities.

TeleCARE for the Elderly
71
HTI J
© The Journal on Information Technology in Healthcare 2004; 2(2): 69–71
Clyde Saldanha MD FRCSEdEditor
REFERENCES
1 Martin LG. Population aging policies in East Asia and the United States. Science 1991; 251:527–31.
2 Itälä T. Invited commentary. The Journal on Information Technology in Healthcare 2003; 1:120–24.
3 Di Carlo A, Baldereschi M, Amaducci L, et al. Cognitive impairment without dementia inolder people: prevalence, vascular risk factors, impact on disability; the Italian Longitudi-nal Study on Aging. J Am Geriat Soc 2000; 48: 775–82.
4 Graham JE, Rockwood K, Beattie BL et al. Prevalence and severity of cognitive impairmentwith and without dementia in an elderly population. Lancet 1997; 349: 1793–96.
5 Gruenberg EM. Epidemiology of senile dementia. Adv Neurol 1978; 19: 437–57.6 Alva G, Potkin SG. Alzheimer disease and other dementias. Clin Geriatr Med 2003; 19:
763–76.7 Alpass FM, Neville S. Loneliness, health and depression in older males. Aging Ment Health
2003; 7: 212–216.8 Waern M, Rubenowitz E, Wilhelmson K. Predictors of suicide in the old elderly. Gerontol-
ogy 2003; 49: 328–34.9 Olsen RB, Olsen J, Gunner-Svensson F, Waldstrom B. Social networks and longevity: a 14
year follow-up study among elderly in Denmark. Soc Sci Med 1991; 33: 1189–95.


73
HTI J © The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
TeleCARE: Collaborative Virtual Elderly Care SupportCommunities
Luis Camarinha-Matos, Hamideh Afsarmanesh*
New University of Lisbon/Uninova, Quinta da Torre, Portugal and * University of Amsterdam, Kruislaan,The Netherlands.
ABSTRACT
The growth in the elderly population imposes an urgent need to develop new approachesto care provision. Integration of a number of technologies such as multi-agent systems,federated information management, safe communications, hypermedia interfaces, rich sen-sorial environments and increased intelligence in home appliances represents an importantenabling factor for the design and development of virtual elderly support community envi-ronments. In this paper, a platform based on mobile agents combined with federated infor-mation management mechanisms is introduced as a flexible infrastructure on top of whichspecialised care services are built.
INTRODUCTION
One of the key challenges facing modern societies is the increasing speed at whichthe population is aging1. In Europe, for example, during the last three decades thenumber of people aged 60 years or more has risen by about 50%. This inevitablyplaces a considerable strain on resources and finances. To deal with this challenge,new ways of providing elderly assistance and care must be found, including thecreation of a new technological infrastructure.
Although a new technological infrastructure will not be the solution to allproblems, it will play a fundamental role in the creation of a new concept ofan integrated elderly care system. This system will consist of a number oforganisations such as care centres, day centres, healthcare institutions and socialsecurity institutions acting in cooperation with relevant personnel, e.g. health-care professionals, social care assistants, elderly people and their relatives. Whenbased on computer networks and adequate supporting tools, collaborationamong care institutions may evolve towards operating as a long-term virtual
Correspondence and reprint requests: Professor Luis M. Camarinha-Matos, New University of Lisbon/Uninova, Quinta da Torre, 2829-516 Monte Caparica, Portugal. E-mail: [email protected].

Camarinha-Matos & Afsarmanesh
74 The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
organisation and the various involved humans will become part of a virtualcommunity (VC).
The potential for technological solutions to increase care services and reducecosts has been demonstrated by various research projects. One example is ‘socialalarm’ systems2, developed for people living in remote and hard-to-access areas.Such systems comprise a portable alarm trigger and an alarm telephone that dialsa social alarm control centre in the event of an emergency. More recent work hasfocused on mobile social alarm systems and online monitoring systems based onelectronic sensors and other devices. To enhance applicability and ease of use,recent projects have focused on the development of smart home appliances andspecialised user interfaces3,4. Advances in computer networks and ubiquitouscomputing offer not only the opportunity for more advanced care approachesincluding comprehensive status monitoring and other forms of assistance such asagenda reminders, but also the creation of the opportunity for the elderly tobecome involved in the community and thus reduce their feelings of loneliness.
To enable elderly people to stay at home and live an independent, activelifestyle, new support services are necessary. These are particularly required toaddress the following problems:
• Loneliness. This is one of the most serious problems affecting the elderlypopulation. The development of applications to enrich an elderly person’ssocial life and to avoid the problem of loneliness is of great importance.Fieldwork data show that today the elderly hardly participate in activitiesrelating with others and 16% of them express dissatisfaction with theirsocial lives5. According to family members, 28% of the elderly have little orno contact with other people.
• Interconnection between the homes of the elderly and the homes orworkplaces of family members caring for them. Such a connection is im-portant to provide access to loved ones. According to a survey carried outwith relatives caring for an elderly person, 31% of them stated the need tobe in contact with the elderly person (currently done either by phone orpersonal visits) at times when they are alone5.
• Interconnections to entities dedicated to providing different services forthe elderly. Connections to care centres, social centres, and social services,will also bring potential benefits to the elderly. It will reduce their lonelinessand make it easier and quicker for them to obtain help and advice. Theconnection is also likely to benefit healthcare workers. By enabling continu-ous contact with the elderly person, without the need for being physicallypresent, it is likely to reduce the number of visits they have to make to theelderly.
To achieve these objectives, the TeleCARE project6–8 has aimed to design anddevelop a configurable framework focused on virtual communities for elderlysupport. The proposed solution is seen as complementary to other initiatives for
TeleCARE
The Journal on Information Technology in Healthcare 2004; 2(2): 73–86 75
the integration of the elderly into society and reduction of their isolation. Withdifferent organisations developing different products and services in a variety ofdifferent areas, it was felt an important consideration was the need for a commonplatform into which all these developments could be plugged so thatinteroperability was possible. The TeleCARE project proposes such a commonand extendable platform as a common infrastructure.
A crucial issue when developing a system to provide care and assistance toelderly people living independent lives in their own homes is the assurance ofprivacy. Consequently special care must be devoted to establishing mechanismsthat will protect the elderly person’s privacy.
THE TELECARE PLATFORM
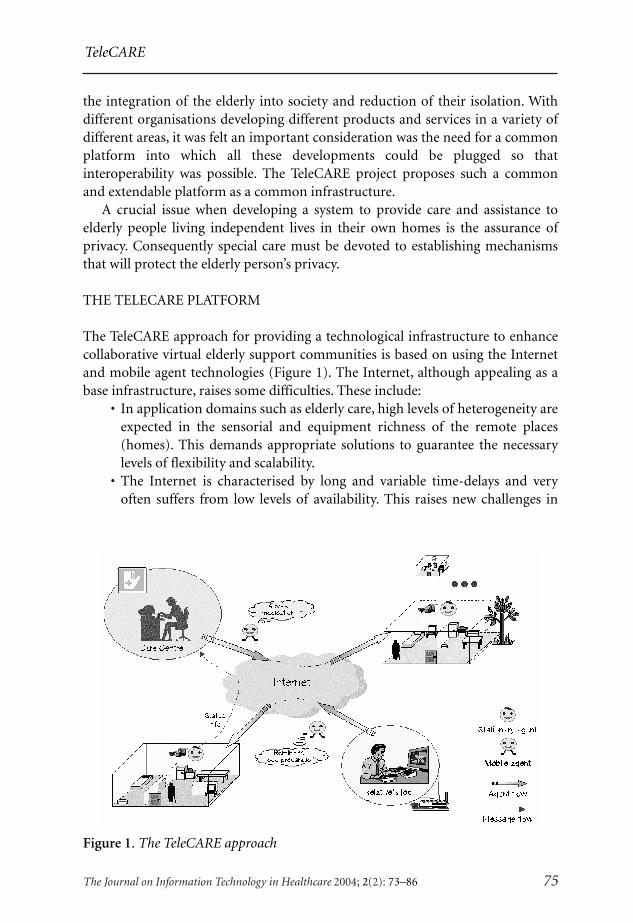
The TeleCARE approach for providing a technological infrastructure to enhancecollaborative virtual elderly support communities is based on using the Internetand mobile agent technologies (Figure 1). The Internet, although appealing as abase infrastructure, raises some difficulties. These include:
• In application domains such as elderly care, high levels of heterogeneity areexpected in the sensorial and equipment richness of the remote places(homes). This demands appropriate solutions to guarantee the necessarylevels of flexibility and scalability.
• The Internet is characterised by long and variable time-delays and veryoften suffers from low levels of availability. This raises new challenges in
Figure 1. The TeleCARE approach

Camarinha-Matos & Afsarmanesh
76 The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
assuring the reliability of the implemented system and its dependence onthe characteristics of the network.
• The emergence of mobile and ubiquitous computing raises the importanceof wireless connections where the actual connection to the network mayhave to be reduced to short periods.
• The execution environments, involving legacy components, are potentiallyunstructured and uncertain. This means that it is difficult to cope withthese environments by resorting to deterministically programmed systems.
The mobile agents paradigm offers interesting characteristics that in fact di-rectly address several of the above issues9:
• Moving the code to the place where actions are required enables real-timeresponse, autonomy and continuity of service provision with reduced de-pendency on network availability and delays.
Figure 2. The TeleCARE platform architecture
Vertical Services LevelVertical Services Level
Core MAS Platform LevelCore MAS Platform Level
External Enabler LevelExternal Enabler Level
Virtual CommunitySupport
Web-accessSupport
SpecialisedInterfaces
Time Bankservice
StatusMonitoring
service
Enter-tainmentservice
Agendaservice
Platform Manager
Basic Multi-Agent Platform
Resource Catalogue Mgnt.
Inter-platform mobility
Federated InformationManagement
Safe CommunicationInfrastructure
Device Abstraction Layer
Inter-agent Communication
PersistenceSupport
OntologyManagement
System
InferenceEngine
AgentExit
Control
AgentReception &Registration
AgentFactory
Device/Vertical Service Registry
ResourceManagers
FederatedQuery
Processor
Ontology-baseddata Structure
Generator
Sp
ecia
lised
Co
mp
on
ents
Tel
eCA
RE
Bas
ic P
latf
orm

TeleCARE
The Journal on Information Technology in Healthcare 2004; 2(2): 73–86 77
• Since new mobile agents can be built and sent for remote execution when-ever needed, higher levels of flexibility and scalability are achieved.
Figure 2 shows a block diagram of the TeleCARE infrastructure to supportcollaboration in the elderly care virtual organisation8,10. The Basic Platform isintended to be installed at each node of the TeleCARE network. The SpecialisedComponents (vertical services) have a distributed implementation over the Tel-eCARE network. The three-level infrastructure comprises:
• External Enabler Level: This supports the communication over the net-work and interfacing to the external (local) devices. Specifically it includes:a) A safe communications infrastructure provides safe communications, sup-
porting both agent mobility and inter-agent message passing. A virtualprivate network (VPN) approach is adopted. In critical cases wherecommunications reliability is mandatory, redundant channels, in addi-tion to the Internet, may be supported and hidden by this layer.
b) A device abstraction layer interfaces to the sensors and monitoring de-vices and other hardware (home appliances, environment controllers,etc.). These interfaces represent the bridge to any ‘intelligent home’ or‘local domotics network’, hiding aspects such as low-level protocols,wire-based or wireless communications, etc. Universal Plug and Play(UPnP) is one of the approaches adopted to interface devices11.
• Core Multi-Agent System (MAS) Platform Level: This is the main compo-nent of the basic platform. It supports the creation, launching, reception(authentication and some rights verification) and execution of stationaryand mobile agents as well as their interactions. It supports the storage andmanipulation of data and information to be handled within TeleCARE. Itprovides a catalogue of all devices and services supported in TeleCARE. Asintelligent agents are envisaged, an inference engine is included. Main mod-ules in this layer are:a) Basic multi-agent system (MAS) platform (based on Aglets).b) Inference engine (based on a Prolog interpreter).c) Ontology support (based on Protégé). A facility is developed providing
the basic mechanisms for dynamic schema description by TeleCAREservice developers.
d) Persistence support as an extension to the MAS platform to provide somebasic recovery mechanisms in case one node goes down.
e) Inter-platform mobility is an extension to the basic MAS platform andsupports generalised mobility of agents, including security mechanisms.This module includes the Agent Reception and Registration component(for incoming mobile agents) and the Agent Exit Control component(for outgoing mobile agents).
f) Inter-agent communication is another extension to the basic MAS plat-form and supports communication between and coordination of agents

Camarinha-Matos & Afsarmanesh
78 The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
independent of their current location, via FIPA ACL (Foundation forIntelligent Physical Agents – Agent Communication Language) messages.
g) Platform manager specifies and configures the operating conditions ofthe platform in each site. It assists in recovery from errors, monitoringthe operation status, etc. It includes:– An agent factory: a module that supports the creation/specification
and launching of new agents.– Resource manager agents: to provide a common and abstract way of
dealing with devices and appliances in TeleCARE.h) Federated information management supports the necessary management
of information while preserving information privacy and careful con-trol of access rights to local data for external users. This module, installedin each site, is the local component of the Federated Information Man-agement Architecture (FIMA), which includes:– Federated query processing which provides the ability to retrieve in-
formation from a number of TeleCARE nodes.– Federated access control to assist with querying and providing access
to the stored information.– Automatic ontology-based schema generation which generates data-
base schemas from the ontology definitions provided by TeleCAREsoftware developers.
i) Resource catalogue management to manage the catalogue of resourcesincluding support for their specification, discovery and access proxies ofall devices and services available at each site.
• Services Level: This is the application level and consists of two sets ofspecialised services:a) Base horizontal services – This is a set of specialised base services that
provide specific functionality for the other (vertical) services, includingthe following:❑ Specialised interfaces for elderly – Specialised interfaces are required
to enable elderly people to use the system in their homes as many ofthem are not skilled in the use of computers. The ultimate goal is tomake the usage of the system pleasant and easy, and thus the Tel-eCARE infrastructure ‘invisible’ to the elderly.
❑ Virtual Community Support – To support and facilitate the creationand operation of community-based services designed for the elderly.For this purpose, specific virtual community management function-alities are supported within the service development environment ofTeleCARE.
❑ Web service access – To allow remote access to some services via a webbrowser. This functionality is particularly useful to allow relatives of

TeleCARE
The Journal on Information Technology in Healthcare 2004; 2(2): 73–86 79
elderly people to have access to the TeleCARE network from theirworkplaces or their own homes.
b) Vertical Services – A set of specialised vertical services can be imple-mented on top of the horizontal TeleCARE infrastructure defined in theprevious levels to support different interactions with the system. Takinginto account the priorities identified through extensive fieldwork, thefollowing initial services have been developed by the TeleCARE consor-tium:❑ Living Status Monitoring. This service represents an advance regard-
ing the more traditional ‘social alarm’ systems, as it allows not onlybilateral interactions and some semi-automatic supervisionfunctionalities, but also the collection of additional information whenhelp is needed or requested. The availability of assistance 24 hours aday significantly increases the elderly’s quality of life and relatives’peace of mind.
❑ Agenda Reminder. The daily activities related to the welfare of theelderly can be easily scheduled in order to improve their quality oflife and wellbeing. This service, implemented through a number ofagents, is able to remind the elderly of a number of activities, rangingfrom medication to exercise guidance or appointments made withthe care centre.
❑ Time Bank. This service provides a mechanism for collaborative com-munity building/re-enforcement, i.e. a way for people to cometogether and help each other. At the same time it represents one ofthe mechanisms to support the ‘active aging’ concept.
❑ Entertainment. The Entertainment Services are designed to ease thesense of isolation the elderly feel and provide light entertainmentapplications to improve their sense of wellbeing. This also helps tocontribute to the maintenance of a social life and active aging. As afirst demonstration a combination of games, music and educationprogrammes are offered.
TELECARE PLATFORM IMPLEMENTATION
A TeleCARE prototype platform was developed in Java that integrates and resortsto various open source or freeware supporting technologies, e.g. Aglets mobileagents platform12, Protégé ontology manager, SAP DB management system, andCastor.
In order to support the requirements of this application domain, a number ofinnovative technical features and components were developed as the middlewareon top of the base development environment. The following is a list of thesefeatures and components, with some details about their implemented capabilities:

Camarinha-Matos & Afsarmanesh
80 The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
❑ Inclusion of agents’ persistence support. Persistency is a mechanism thatallows the storage of information about the running activities of the agents,and whenever a system crashes to allow them to be resumed when thesystem is restarted. Aglets provides a method called snapshot, which saves asnapshot of an agent into a secondary/non-volatile storage. For persistencypurposes, every TeleCARE agent can invoke the tcSave method, which doesa call to snapshot, for storing information about its execution status whennecessary. If there is a system failure, the last snapshot of the agent isrestored and its execution can be resumed with the information stored inthat snapshot. In the current version, automatic support for persistency isprovided on three events: (i) at the creation of the agent, (ii) just after theagent arrives at a new location, and (iii) when the agent is activated. It is upto the developer to decide where he/she wants to make additional snap-shots of his/her agent, calling the tcSave method.
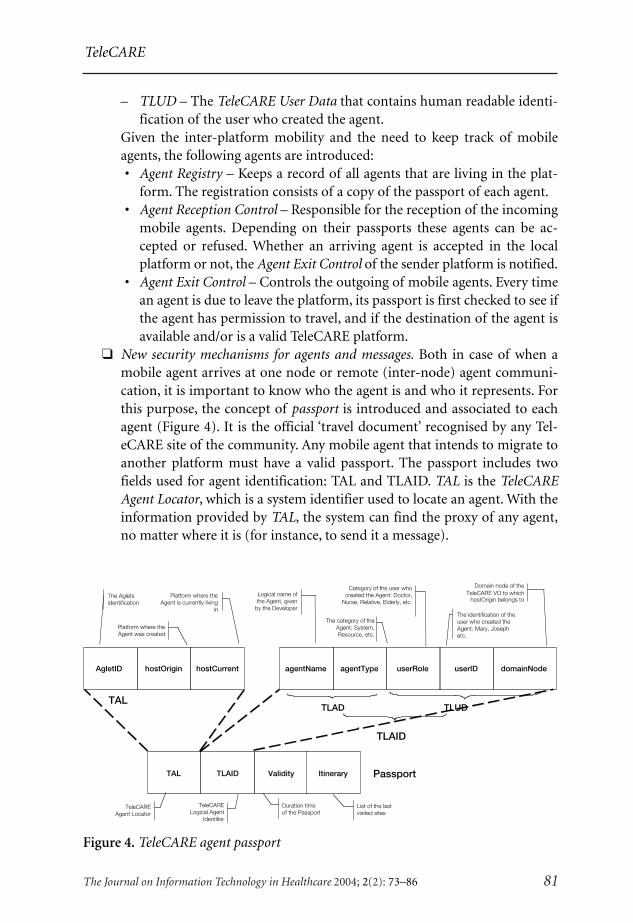
❑ High-level agent identification and localisation. A TeleCARE Logical AgentIdentification (TLAID) structure was introduced, which is used to vali-date an agent at any platform and to locate an agent (using humanunderstandable data). With the information provided by the TLAID, thedevelopers can identify any TeleCARE agent given its name, type, role oruser ID, and/or domain node of the TeleCARE Virtual Organisation thatthe origin host (or platform) of the agent belongs to. TLAID is composedof two substructures:– TLAD – The TeleCARE Agent Data that contains specific human read-
able identification of the agent.
Figure 3. The TeleCARE interface for the Care Centre
TeleCARE
The Journal on Information Technology in Healthcare 2004; 2(2): 73–86 81
– TLUD – The TeleCARE User Data that contains human readable identi-fication of the user who created the agent.
Given the inter-platform mobility and the need to keep track of mobileagents, the following agents are introduced: • Agent Registry – Keeps a record of all agents that are living in the plat-
form. The registration consists of a copy of the passport of each agent. • Agent Reception Control – Responsible for the reception of the incoming
mobile agents. Depending on their passports these agents can be ac-cepted or refused. Whether an arriving agent is accepted in the localplatform or not, the Agent Exit Control of the sender platform is notified.
• Agent Exit Control – Controls the outgoing of mobile agents. Every timean agent is due to leave the platform, its passport is first checked to see ifthe agent has permission to travel, and if the destination of the agent isavailable and/or is a valid TeleCARE platform.
❑ New security mechanisms for agents and messages. Both in case of when amobile agent arrives at one node or remote (inter-node) agent communi-cation, it is important to know who the agent is and who it represents. Forthis purpose, the concept of passport is introduced and associated to eachagent (Figure 4). It is the official ‘travel document’ recognised by any Tel-eCARE site of the community. Any mobile agent that intends to migrate toanother platform must have a valid passport. The passport includes twofields used for agent identification: TAL and TLAID. TAL is the TeleCAREAgent Locator, which is a system identifier used to locate an agent. With theinformation provided by TAL, the system can find the proxy of any agent,no matter where it is (for instance, to send it a message).
Figure 4. TeleCARE agent passport
TAL Passport
The Agletsidentification
Platform where the Agent was created
TAL
TLAID
TLAID Validity Itinerary
AgletID hostOrigin hostCurrent agentName agentType userRole userID
The identification of the user who created the Agent: Mary, Joseph etc.
Duration time of the Passport
List of the last visited sites
domainNode
TLAD TLUD
Platform where the Agent is currently living
in
Logical name of the Agent, given
by the Developer
Category of the user whocreated the Agent: Doctor,
Nurse, Relative, Elderly, etc.
The category of theAgent: System,Resource, etc.
Domain node of theTeleCARE VO to which
hostOrigin belongs to
TeleCARELogical Agent
Identifier
TeleCAREAgent Locator

Camarinha-Matos & Afsarmanesh
82 The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
❑ Generalised communication mechanisms. The Aglets system provides a sim-ple mechanism for inter-agent communication. However, this mechanismis not sufficient for reliable communication for highly mobile agents13 orwhen persistence mechanisms based on cloning are implemented, namelydue to changes in the AgletID. Therefore, the platform implements addi-tional communication services: • Extended message exchange mechanisms, which allow reliable inter-
agent communication. • Handling FIPA ACL messages.
❑ Integration and management of resources in TeleCARE. Two kinds of re-sources are considered in TeleCARE including the hardware devices and thesoftware services. The Universal Plug and Play (UPnP) specification is anarchitecture for pervasive peer-to-peer network connectivity of intelligentappliances, wireless devices and personal computers (PCs). Home appli-ances and sensors are connected to the TeleCARE platform following UPnP.The Web Services Definition Language (WSDL) provides the frameworkfor definition of service specifications and their interfaces. The horizontaland vertical services of TeleCARE are defined and provided through theTeleCARE platform using WSDL.
The Resource Catalog Management (RCAM) component supports theorganisation, storage and access to the UPnP (for devices) and WSDL (forservices) definitions of the TeleCARE resources.
Furthermore, in order to facilitate the access to and invocation of Tel-eCARE resources an Abstract Resource Manager Agent (ARMA) template isprovided. ARMA is instantiated and customised for each resource, becomingits actual Resource Manager. Application services can access a resource’sfunctions through its corresponding Resource Manager that also checks andenforces the access rights of the requesting agents on the requested resource.
❑ Integration of Federated Information Management and mobile agents. Feder-ated Information Management (FIMA) is a key component of the CoreMulti-Agent System Platform Level. FIMA enables applications to distrib-ute data transparently across multiple machines within the TeleCAREnetwork. The design of FIMA is based on the federated databases approach,in order to support cooperation and information sharing, while reinforcingthe required level of autonomy and heterogeneity among individual datasources (e.g. elderly home, care centre, leisure centre, etc.) within a Tel-eCARE network. The federated query processing is implemented by MIRA(Mobile Information Retrieval Agent) in such a way that applications canrequest to execute queries in: • Parallel mode, e.g. accessing data from several remote sources simulta-
neously. • Serial mode, e.g. accessing data from different nodes one after the other.
TeleCARE
The Journal on Information Technology in Healthcare 2004; 2(2): 73–86 83
• Sequential mode, similar to the serial mode but in which the processcan be stopped once the client is satisfied with the result, providing ahigh user interactivity to control the information processing overhead.
❑ Ontology-based database schema generator. The Dynamic Ontology-basedSchema Generation (DOSG) component of the core platform of TeleCAREsupports and assists service developers with their direct definition of data-base schemas for the data that needs to be stored and processed by theircode. It can thus eliminate the need for database experts to define andmodify these schemas as it provides facilities for dynamic and automaticdefinition of the database schemas (relational and XML schemas) and the(Java source) code for the structures defined by users, so that they can beautomatically stored in a database and processed by application programs.As such, the service developers of TeleCARE, can use the Protégé ontologysystem as the interface for their structure definitions, and do not need tohave database expertise to define these database schemas.
❑ Integration of Web services. In order to provide access to TeleCARE servicesfor relatives having access to the Internet, a mechanism is implemented toprovide a bridge between the multi-agent platform and a web browser.
❑ Integration of biometric security. A fingerprint identification device is inte-grated with the platform providing a mechanism to implement safer useridentification. This is particularly useful in care centres, where differentusers (e.g. nurses, doctors, care workers) with different information accessrights can have access to the system. A taxonomy of users and roles istherefore associated with the biometric-based login process.
❑ Variety of user interfaces. People using the system will possess a diverserange of computer skills. Consequently access to the TeleCARE platformand services has to be made accessible through a variety of user interfaces.In particular, specialised interfaces have to be provided to make the systemeasy to use for elderly people with little or no computer skills. For userswith good computer skills (e.g. care centre workers or relatives havingaccess through a web browser) the interface can be Windows-based.
TELECARE SERVICES IMPLEMENTATION
In the TeleCARE environment each vertical service can be implemented in differ-ent ways as a set of distributed stationary and/or mobile agents. For instance, amonitoring service might involve a stationary agent in the care centre (interactingwith the care worker), a number of stationary agents in the elderly home (agentsin charge of monitoring local sensors, e.g. temperature sensor, presence sensor),and some mobile agents sent from the care centre to the elderly home (Figures 5and 6). The mobile agents might carry a mission, for instance MIRAs sent tocollect information from different sensors and to report back to the care centre.

Camarinha-Matos & Afsarmanesh
84 The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
The stationary agents in one platform can also communicate, via ACL mes-sages, with other mobile or stationary agents residing at another platform. Since aTeleCARE message includes extended agent identification, (as described in thepassport section above), the receiver of a message can check the identity and rightsof the sender, no matter at which location it is running at that moment.
The use of mobile agents facilitates the remote deployment of the servicefunctionalities according to the services required by each elderly person. As differ-ent elderly people have different needs, such flexibility is required. With thismechanism it is also easier to install updated versions of services.
An integrated prototype system including the TeleCARE platform and a set ofdemonstration services was developed, showing the feasibility of the suggestedapproach. This integrated system was partially validated through a field assess-ment phase that took place in southern Spain, and involving four classesof potential users: (i) the elderly and their relatives; (ii) care providers/care workers;
Figure 6. Example of monitoring service interfaces at an elderly person’s home and acare centre
CARE4U
loud
Figure 5. Example of service implementation
Care Centre Elderly Person’s Home
Internet
MonitoringApplication agent
Care worker
SpecificMonitoragents
Mobile agentwith monitoring mission
TeleCAREPlatform
TeleCAREPlatform
ACL

TeleCARE
The Journal on Information Technology in Healthcare 2004; 2(2): 73–86 85
(iii) decision-makers (on social policies); and (iv) software developers.The TeleCARE concept and its functionalities were well accepted by these poten-tial users, although it is clear that the system is at a research prototype stage andsubstantial engineering work is still necessary in order to make it a robust product.
CONCLUSIONS
The growing elderly population imposes an urgent need to develop new ap-proaches to care provision. Recent developments in a number of technologies,such as multi-agent systems, federated information management, safe communi-cations, hypermedia interfaces, rich sensorial environments and increasedintelligence of home appliances represent important enabling factors for thedesign and development of virtual elderly support community environments. Inparticular, a platform based on mobile agents combined with federated informa-tion management mechanisms provide a flexible infrastructure on top of whichspecialised care services can be built. Nevertheless, the specific characteristics ofthe elderly population, who are not very open to new technologies, necessitatescareful integration of the infrastructure with traditional home appliances includ-ing television sets. Furthermore, the fine tuning and eventual acceptance of thetechnology can only be determined when reliable prototypes are tested in thefield with real users. This field trial constitutes the next phase in the TeleCAREproject.
ACKNOWLEDGEMENTS
This work was funded in part by the IST programme of the European Commission. Theauthors would like to acknowledge the contribution of the TeleCARE consortium members(Uninova, University of Amsterdam, SKILL, RoundRose Associates, Camera de Comercio deNavarra, and Synkronix).
REFERENCES
1 Saranummi N, Kivisaari S, Sarkikoski T, Graafmans J. Ageing and Technology: State of theArt. Report for the European Commission, Institute for Prospective Studies, Seville,Spain, 1996.
2 Vlaskamp F. Social Alarms Go Mobile: Emergency Assistance for Mobile Users, www.fernuni-hagen.de/FTB/aaate99/paper/99_67.htm, 1999.
3 Dutta-Roy A. Networks for homes, IEEE Spectrum 1999; 36: 32–38.4 Hampicke M. Smart home: Speech based user interfaces for smart home applications.
COST 219 Seminar on Speech and Hearing Technology, Cottbus, Germany, 2002.5 Pascual A. TeleCARE final report on users’ requirements. TeleCARE Deliverable D1.3, 2002.6 Camarinha-Matos LM, Afsarmanesh H. Design of a virtual community infrastructure
for elderly care. In Proceedings of PRO-VE ’02 – 3rd IFIP Working Conference on

86
HTI J
© The Journal on Information Technology in Healthcare 2004; 2(2): 73–86
Camarinha-Matos & Afsarmanesh
Infrastructures for Virtual Enterprises. Dordrecht, The Netherlands: Kluwer AcademicPublishers, 2002.
7 Camarinha-Matos LM, Afsarmanesh H. Virtual communities and elderly support. In KluevVV, D’Attellis CE, Mastorakis NE (eds.), MIV ’01 in “Advances in Automation, Multimediaand Video Systems, and Modern Compuuter Science”. WSES, 2001.
8 Camarinha-Matos LM, Castolo O, Rosas J. A multi-agent based platform for virtual com-munities in elderly care. In Proceedings of ETFA ’03 – 9th International Conference onEmerging Technologies and Factory Automation. Lisbon, Portugal, 2003.
9 Camarinha-Matos LM, Vieira W. Intelligent mobile agents in elderly care. Journal of Robot-ics and Autonomous Systems 1999; 27: 59–75.
10 Camarinha-Matos LM, Afsarmanesh H. A multi-agent based infrastructure to supportvirtual communities in elderly care. Accepted for publication in International Journal ofNetworking and Virtual Organisations.
11 Universal Plug and Play Device Architecture. Universal Plug and Play Forum, http://www.upnp.org/.
12 Java Aglet Community. Aglets API Documentation, v. 2.0.2. http://aglets.sourceforge.net/.13 Murphy A, Picco GP. Reliable communication for highly mobile agents. In Autonomous
Agents and Multi-Agent Systems. Dordrecht, The Netherlands: Kluwer Academic Publish-ers, 2002.

87
HTI J
Correspondence and reprint requests: Hamideh Afsarmanesh, University of Amsterdam, Faculty ofScience, Kruislaan 403, 1098 SJ Amsterdam, The Netherlands. E-Mail: [email protected].
© The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
INTRODUCTION
Tele-assistance services and remote supervision applications are progressively in-creasing to improve the efficiency and availability of care services (e.g. remotelyoperated appliances, remote homecare services, etc.). Ongoing advances in tele-communications, networking, artificial intelligence, safe communication facilitiesand information management provide the groundwork for emerging services,based on collaborative networked environments dedicated to tele-assistance. Acollaborative environment as such, is usually a highly distributed network com-posed of heterogeneous and autonomous nodes that are interested in providingorganised support and care provision to the clients. Each node individually playsan assisting role, however, many organisations involved in the collaborative net-work need to maintain their autonomy and their rights to both their proprietarydata and local resources. Thus, the collaboration among different active organisa-tions (e.g. care centres and leisure centres) in the network forms a Virtual
Management of Federated Information in Tele-assistance Environments
Hamideh Afsarmanesh, Victor Guevara-Masis,Louis Otto Hertzberger
University of Amsterdam, Faculty of Science, The Netherlands.
ABSTRACT
An advanced tele-assistance environment for elderly care is being developed by the re-search carried out in the context of the TeleCARE project. This environment is a highly dis-tributed collaborative network composed of heterogeneous and autonomous nodes. Theanalysis of information management requirements has identified both the modelling andfunctionality requirements at each node, as well as the information exchange/integrationnecessary for interoperation within the network. Based on the examination of these require-ments, three key and innovative components were identified that together support the man-agement of all information related to the TeleCARE environment. These components, namelythe Federated Information Management component (FIMA), the Resources Catalogue Man-agement component (RCAM), and the Dynamic Ontology-based data Structure Generator(DOSG) are introduced, and their implementation details are discussed.
Afsarmanesh, Guevara-Masis & Hertzberger
88 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
Organisation (VO)1, while the collaboration among active individuals (e.g. rela-tives’ and friends’ nodes) in the network forms a Virtual Community (VC)2.
Interest in deploying tele-assistance services is global, with the perceived ad-vantages of using emerging technologies to provide remote access at low cost.However, the development of tele-assistance services is extremely complex. Due tothe growing number of technologies under development, new hardware (sensorialdevices, appliances, etc.) are being deployed in a fragmented and non-interoperableway. Furthermore, a number of other advanced capabilities and features are re-quired by the software managing the remote operation/access to resources. Forinstance, the secure transfer, reliability, safety and privacy of the informationexchanged within the network should be assured. The design and development ofan affordable infrastructure for tele-assistance is, therefore, a crucial requirementfor the effective deployment of applications in such collaborative networks.
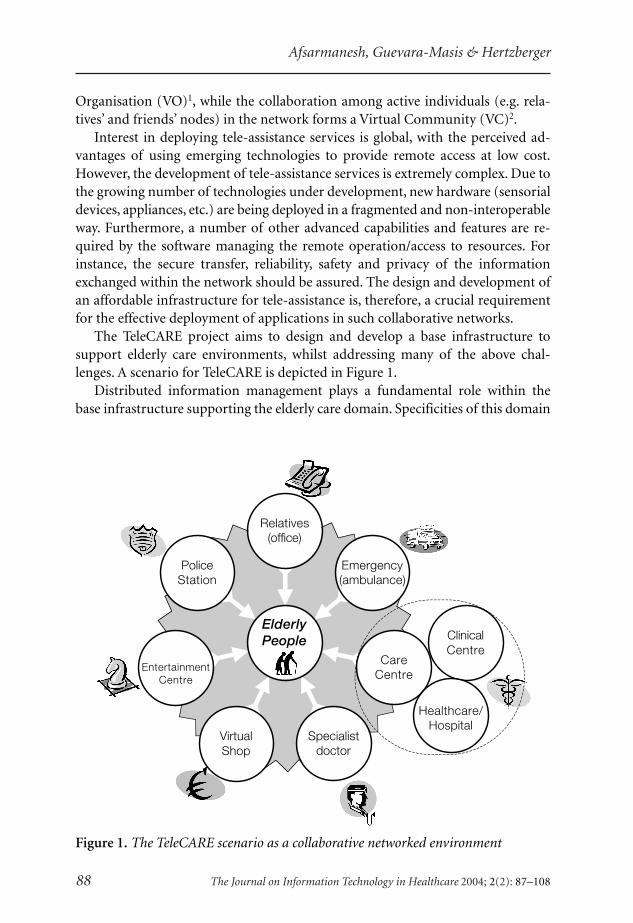
The TeleCARE project aims to design and develop a base infrastructure tosupport elderly care environments, whilst addressing many of the above chal-lenges. A scenario for TeleCARE is depicted in Figure 1.
Distributed information management plays a fundamental role within thebase infrastructure supporting the elderly care domain. Specificities of this domain
Figure 1. The TeleCARE scenario as a collaborative networked environment
Relatives(office)
Emergency(ambulance)
CareCentre
Specialistdoctor
VirtualShop
EntertainmentCentre
PoliceStation
ClinicalCentre
Healthcare/Hospital
ElderlyPeople

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 89
include the autonomy and independence of its involved personnel, the criticaldata that is handled about individuals, and the variety of hardware/softwareresources supporting the elderly care environment. Considering the independ-ence and autonomy of the network nodes, many challenges are involved inhandling their information. These challenges include the organisation, manage-ment and provision of retrieval facilities for both the heterogeneous data that isstored at the nodes, as well as the information regarding its hardware and softwareresources (i.e. devices and services), while preserving users access rights andauthorisation.
In addition, considering the incremental development of the support servicesto be made available within the elderly care network, developers of such servicesrequire assistance to make their services interoperate with other existing systemsand resources. One problematic issue here is that in order for services to beconnected to the elderly care network, their developers must structure and storeall their data within the network’s database. To avoid the need for expertise indatabase modelling, it should be sufficient for developers to use an editor throughwhich they can define their data by its ontology, which in turn can be automati-cally translated into proper database structures and stored in the network'sdatabase.
This article first briefly describes the TeleCARE platform architecture and itsmain elements. It then presents the three main components developed in theTeleCARE project to support and facilitate the management of all the informationrelated to tele-assistance for elderly persons in the tele-care environment. Thesecomponents are:
• FIMA — Federated Information Management • RCAM — Resource Catalogue Management • DOSG — Dynamic Ontology-based data Structure Generation
Although the above components are currently developed to benefit the area ofelderly care networks, these components are generic enough to enable a very largenumber of the designed and developed components to be applied to any ad-vanced emerging collaborative network.
RELATED TECHNOLOGIES
Before describing the information management itself, it is pertinent to reviewsome of the TeleCARE technologies that are most closely related to informationmanagement.
Multi-Agent Systems (MAS)During the last decade, MAS together with agent mobility have advanced to thelevel that they can offer many potential advantages including robustness, effi-ciency, flexibility, adaptability, scalability, inter-operation of multiple existing

Afsarmanesh, Guevara-Masis & Hertzberger
90 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
systems, reliability and extensibility. The emerging field of mobile software hasstarted to gain widespread acceptance, and nowadays is used for building applica-tions in the area of collaborative networks, and to feature interactions amongmembers3,4. A mobile agent is a program that acts on behalf of its user or anotherprogram creating it and is able to migrate from host to host within a networkfollowing its own itinerary. The mobile agent can choose when and where it willmigrate and may interrupt its own execution and continue elsewhere within thenetwork. Depending on its software implementation, a mobile agent can returnresults and messages in asynchronous fashion. Mobile agents can perform com-plex information gathering strategies autonomously; while stationary agents cancollect and digest the information of interest and assemble a result report. Agentscan be either reactive in performing services by responding to changes in theirenvironment, or pro-active, by performing tasks to fulfil their goals. A mobileagent is also able to travel, searching for specific information across the networkand retrieving it. As it performs these actions, a mobile agent can also deploy newapplications or upgrade the software running at different sites. Key elements of anagent’s mobility are autonomy and behaviour. Once goals are established, themobile agent is guided by its own capacities to fulfil the action. Mobile agents canalso hold some decision-making control. Thus, while searching its itinerary it canrun independently from the interventions of the user who created it.
The TeleCARE infrastructure is based on Aglets5,6, a multi-agent system, thatsupports agent mobility based on Java. The designed platform supports seamlessinteractions among stationary and mobile intelligent agents, with planning, errordiagnosis, and recovery capabilities. Agents are able to recognise and self-adapt todiverse environments. At the same time, the mobile agent technology provides arich base for information brokerage in networked environments7 and a possibleapproach for implementing distributed/federated information managementsystems8.
Ontology SystemAn ontology refers to the set of logical definitions that express the meaning ofterms for a particular domain. These conceptual definitions make use of explicitassumptions and may include semantics as well. Ontologies are based on theunderstanding of the members of a particular domain, such as biomedicine, andhelp to reduce ambiguity in human and computer interactions.
An ontology definition constitutes a collection of concepts and interconnec-tions that describe the information units of particular applications. For theirapplication plan, the platform and vertical service developers, who are the expertson the semantics of data required, first design all information units that need tobe shared in a collaborative environment. The semantic heterogeneity among theshared information is resolved by mapping it into an ontological definition. Thisontology can be understood and consulted by both humans and software agents9.

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 91
Essentially, developers describe their shared information through the use ofontologies. The ontology management system in the TeleCARE architecture sup-ports this process, and the developers can transparently define their conceptualmodel. The ontology management system preferred for TeleCARE is Protégé10.
Protégé-2000, or Protégé for short, is an ontology system developed by Stan-ford Medical Informatics Laboratory that can be used by software systemdevelopers and domain experts to develop their knowledge-based systems. Thissystem assists its users with the creation of their knowledge base, since it supportsthe definition of structured classes and information storage. Originally, Protégéwas designed specifically for the medical domain but it grew as a general-purposeset of tools for building knowledge-based systems in any domain. In TeleCARErelated domains such as clinical medicine and the biomedical sector, where com-plex concepts need to be modelled, Protégé is already being used to define classhierarchies and to provide semantics on concepts11. A number of applications andontologies in the particular domain of medical care have been developed withProtégé and used in problem-solving and decision-making. Examples of ontologiesdeveloped with Protégé include: Health Level Seven (HL7) Data Types, Top-LevelReference Information Model (RIM) classes, Biological Processes Ontology, GeneOntology (GO), and GuideLine Interchange Format (GLIF) Ontology.
Federated Information ManagementThe federated information management and federated database mechanisms ad-dress the sharing and exchange of distributed information in a highlyheterogeneous environment12–14. The federated approach to information manage-ment in networks of independent cooperative nodes is well suited to managementof all local and distributed information handled in TeleCARE, while preservingthe node autonomy and information privacy. The federated query processingmechanisms allow access to distributed information according to their definedaccess rights, where TeleCARE sites represent autonomous nodes in the federa-tion. Namely, TeleCARE sites run independent of each other, and may evolveindependently in terms of applications, devices, services and data models.
The establishment of federated schemas is a critical task during the set up andimplementation of the federated information management. Information sharingis generally performed based on those schemas, and any misinterpretation ofdata during communication between information systems is called semantic het-erogeneity. In TeleCARE, to avoid misinterpretations of data, the federatedinformation system uses explicit data structures specified from ontologicaldefinitions.
The TeleCARE platform applies the results gained in previous research anddevelopment projects for federation of autonomous and heterogeneous expertsystems. Federated information management has also been applied to virtualorganisations to support the cooperation between the nodes in the federation to
Afsarmanesh, Guevara-Masis & Hertzberger
92 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
accomplish a common or global task, while the local autonomy and independenceof every node is preserved and reinforced.
TELECARE AS A TELE-ASSISTANCE PLATFORM
The overall goal of the TeleCARE project is the design and development of aconfigurable framework solution for tele-supervision and tele-assistance, to sup-port the elderly. The proposed solution has been seen as complementary to otherinitiatives, focused on the integration of the elderly into society to reduce theirisolation15. The TeleCARE solution benefits from the merging of a number oftechnologies and paradigms in order to provide an open architecture supportingseamless future expansion. Specifically, it is based on the integration of:
• Multi-agent systems, including both stationary and mobile intelligentagents
• Federated database systems • Secure communications • Services likely to be offered by emerging ubiquitous computing and intelli-
gent home appliances.In essence, the core horizontal platform developed for TeleCARE provides the
MAS, mobility, safe communications and the federated information managementservices. The TeleCARE consortium has further developed some vertical serviceson top of this platform, including status monitoring, as well as other forms ofassistance such as agenda reminders, entertainment services and Time Bank. Inaddition a few base services for supporting virtual communities, Web access and aspecialised elderly user-interface are also provided.
THE TELECARE REFERENCE ARCHITECTURE
The reference architecture for TeleCARE nodes provides cooperation/federationamong different nodes of the elderly care network as depicted in Figure 2.
The designed architecture of the TeleCARE node is composed of a three-levelplatform. At the bottom, the External Enabler Level provides support for theexternal communication of the TeleCARE node and the interfaces with externalresources. The Core MAS Platform Level is the major component of this architec-ture, and includes essential support for software agents. Finally, at the top, theVertical Services Level is the open component where a variety of services can begradually added to the node.
External Enabler LevelThis level supports the remote communication with other nodes and providesinterfacing mechanisms to the external devices. This level comprises two segments:

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 93
• A safe communications infrastructure to provide safe communicationsand support both secure and reliable agent/messages passing among differ-ent nodes.
• A device abstraction layer that interfaces the sensors, monitoring devices,and other hardware (home appliances, environment controllers, etc.) to theTeleCARE environment.
Core MAS Platform Level The platform level is the main component of the environment and offers funda-mental services for agents as well as for their interactions. These services includethe creation, launching, reception, user authentication, access rights verification,and execution of stationary and mobile agents. The main modules at this levelinclude:
Figure 2. The TeleCARE platform reference architecture
Vertical Services LevelVertical Services Level
Core MAS Platform LevelCore MAS Platform Level
External Enabler LevelExternal Enabler Level
Virtual CommunitySupport
Web-accessSupport
SpecialisedInterfaces
Time Bankservice
StatusMonitoring
service
Enter-tainmentservice
Agendaservice
Platform Manager
Basic Multi-Agent Platform
Resource Catalogue Mgnt.
Inter-platform mobility
Federated InformationManagement
Safe CommunicationInfrastructure
Device Abstraction Layer
Inter-agent Communication
PersistenceSupport
OntologyManagement
System
InferenceEngine
AgentExit
Control
AgentReception &Registration
AgentFactory
Device/Vertical Service Registry
ResourceManagers
FederatedQuery
Processor
Ontology-baseddata Structure
Generator
Sp
ecia
lised
Co
mp
on
ents
Tel
eCA
RE
Bas
ic P
latf
orm

Afsarmanesh, Guevara-Masis & Hertzberger
94 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
• The Basic Multi-Agent Platform that provides the essential multi-agent sup-port, and is based on the Aglets framework5 with the following extensions:
i. Ontology management system — The Protégé 200010 is used in theplatform for the definition of the ontologies.
ii. Inference engine — For intelligent agent interpretation using a Prologinterpreter.
iii. Persistence support — For basic recovery mechanisms. • Inter-platform Mobility is an extension to the basic MAS platform to sup-
port generalised mobility of agents, including agent security mechanisms.This module includes the Agent Reception and Registration component, andthe Agent Exit Control component, for administration of stationary andmobile agents.
• Inter-agent Communication is an extension to support credentials andcoordination of agent communication, independent of the agent location.
• The Federated Information Management supports the management of in-formation at TeleCARE nodes and provides the infrastructure for flexibleprocessing of federated queries, data structure generation based on onto-logical definitions and preserving information privacy through access rightsmanagement. This component was developed using Java in conjunctionwith free and open source software, namely the SAP DB relational databasesystem16 and the Castor data binding middleware for Java17.
• The Resource Catalogue Management manages the catalogue of resources,and registers the descriptions of all device and vertical services available atthe site as well as their access rights.
• The Agent Factory supports the creation and specification of new agents. • The Platform Manager configures and specifies the operating conditions of
the platform at each site, including user administration and nodemanagement.
Vertical Services LevelThe applications and Vertical Services Level focuses on the actual support for theelderly (who require specialised user interfaces), care providers, and relatives ofthe elderly (assuming that they are able to interact with normal computer inter-faces). It is composed of two layers.
• Base Services that provide specific support to other value-added services.i. Virtual Community Support to assist the management of the Virtual
Community (VC) for the elderly care environment.ii. Specialised interfaces for the elderly are designed to be easily used by
people who are unfamiliar with computers, and also for assistingpeople with diminished physical abilities, such as poor hearing oreyesight.
Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 95
iii. Web-access support enables Web-based mechanisms to interface withthe TeleCARE environment.
• Vertical Services — A number of specialised vertical services are imple-mented as specific TeleCARE applications, including a VC-based Time Bank,a living status monitoring service, an agenda reminder service, and anentertainment service.
MANAGEMENT OF INFORMATION IN TELECARE
The analysis of information management requirements for the TeleCARE net-work has identified both the modelling and functionality required to be supportedlocally at each node, as well as for the information exchange/integration andnecessary interoperation among the sites. Based on the analysis of these require-ments, the necessity of three main components was identified that together supportboth the management of all information related to the TeleCARE network. Thesecomponents, namely FIMA, RCAM and DOSG are described below.
FIMA — FEDERATED INFORMATION MANAGEMENT
The Federated Information Management component of TeleCARE supports ap-plications that may require a variety of data models and large numbers of usersand agents accessing and retrieving its data, while supporting the pre-definedvisibility rights to physically distributed and heterogeneous data. The federateddatabase architecture of FIMA does not require any centralisation of data orcontrol and thus supports the flexibility and extensibility aspects required forfuture use of the TeleCARE system. The database architecture can also support avariety of application architectures that may be used for development of differentvertical services for TeleCARE, including both the client/server and the agent-based systems. The database repository of FIMA is developed using the SAP DB asthe base. The SAP DB provides an open source and freeware database manage-ment system, and was one of the main reasons for selecting it for the TeleCAREproject.
The two key functionalities offered by FIMA include: • Federated Data and Schema Management. This handles all the data and
schemas defined in the network while supporting the definition of ad-equate levels of information privacy for access by authorised agents andusers.
• Federated Query Processing. This supports the collection of all necessarydata from different distributed heterogeneous and autonomous nodes,through a single query issued by the user, as if all data distributed amongdifferent nodes are in fact available at the local site.

Afsarmanesh, Guevara-Masis & Hertzberger
96 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
Figure 3 shows a high level architecture of FIMA and its main software com-ponents. These components, depending on their role and functionality, are allimplemented as stationary and/or mobile agents. Detailed description of all theseagents is outside the scope of this paper. Below we focus on the Federated QueryProcessing (FQP) of FIMA and provide details on the stationary and mobileagents supporting this functionality, and how the query processing performanceis improved in comparison to other agent-based approaches8.
The processing of federated queries is a complex task, and it is briefly detailedas follows. First, the requester sends a query (which is in high-level format) to theFIMA interface, which generates an agent designed to handle this request. Thequery is then translated considering the internal structures of the stored data, anda set of sub-queries is established. These sub-queries are one by one assigned tomobile agents with the proper itinerary. After this step, these mobile agents aredispatched to the remote nodes to accomplish their mission, to perform the localquery and to send the results back to the original node. Finally, the received resultsare merged at the node and returned back to the requester, see Figure 4.
What should be appreciated is that the main goal of the federated query proces-sor component in FIMA is to enable TeleCARE agents and end-users to query theauthorised information, without concern for all the details about database connec-tions, agents creation, their travelling among nodes and processing of the data.
Figure 3. Federated Information Management Architecture – FIMA
Otherinternal
componentsz
TeleCARE node
Deviceabstraction layer
- DIMA -Data Interface Mapping Access
- AIMS -Agent Information
Management System
FIMS
Age
nt
- MIRA -Mobile Information
Retrieval Agent
Base Service
Service A
Service B
Service C
VerticalServices Level
Core MASPlatform Level
External Enabler Level
DBMS - IAMA -Information
Access Manager
FIMA
F I M S
M I R A

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 97
Below are the main agents involved in federated query processing of FIMA: • FIMS Agent: Federated Information Management Server Agent, acting as
the FIMA interface agent. • FQP Agent: Federated Query Processor Agent, acting as the query supervi-
sor. • MIRA Agent: Mobile Information Retrieval Agent, acting as the mobile
component, transferring the jobs to other nodes, for this process.
FEDERATED INFORMATION MANAGEMENT SERVER AGENT
The Federated Information Management Server Agent (FIMS Agent) managesthe interface to access the information in FIMA. It must be continuously avail-able and running. It supports multi-users and thus can fulfil requests fromnumerous agents simultaneously that may have different purposes other thanjust executing a single query. However, in order to speed up the data retrievalprocess FIMS Agent does not handle all the query processing related operations.Whenever FIMS receives a request for a federated query, it generates anotheragent (FQP Agent) in a different execution thread, thus allowing it to maintainits primary operation. This mechanism provides the highest performance forquery processing, since the new FQP Agent will focus only on the task ofperforming the query.
Figure 4. Main agent components of Federated Query Processing
FQP instruction(XML specification)
Queryexecution
FIMS Agent- Agent interface
FQP Agent- Query handling
MIRAs- Access to remote
information
Requesteragent
FQP Agentcreation
M I R A
F I M S
M I R A
M I R A
M I R A
F Q P

Afsarmanesh, Guevara-Masis & Hertzberger
98 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
When the FIMS Agent summons the FQP Agent it also includes the credentialsof the requester into this new FQP Agent. As a result, from that point on all queryoperations are bound to that FQP Agent, i.e. it will supervise the processing of afederated query, and thus the FIMS Agent is freed from the responsibility of thefederated query execution.
FEDERATED QUERY PROCESSOR AGENT
The Federated Query Processor Agent (FQP Agent) is at the heart of the federateddata processing in FIMA. It implements several advanced features particularlyuseful in the collaborative TeleCARE environment. Some of the mechanisms usedfor federated query processing of FIMA are also integral to the TeleCARE infra-structure (e.g., the multi-agent and the Java object oriented programmingenvironments).
A number of techniques are used to improve the performance of the queryprocessing, for example: (1) special multi-thread processing; (2) simultaneousexecution of several queries and (3) reduction of communication costs by reduc-ing the size (i.e. content) of the mobile agents involved during the query execution.
Table 1. Processing of federated queries
Query translation The query that arrives in high level functional format in XML is first trans-lated into internal handling structures.
MIRA creation Depending on the type of federated query and on the targeted itinerary,appropriate Mobile Information Retrieval Agents (MIRAs) are created,e.g. if the query type is ‘parallel’ then multiple MIRAs will be created,one per target node.
Query decomposition The original query is divided into a number of sub-queries according tothe number of target nodes, and these sub-queries are assigned to thecorresponding MIRA agents.
MIRA transmission Each MIRA is sent to a remote node carrying the corresponding sub-query.
Query evaluation The MIRA agent performs the MIRA-to-FIMS Agent communication ofthe remote node in order to execute and retrieve the requested infor-mation from that node.
Result transmission The MIRA transmits the information resulted from the sub-query to theFQP Agent.
Information merge Once all results arrive from the MIRA to the FQP Agent, the FQP mergesthe sub-results and sends the final results to the requester.
Resource release When the execution of the query completes, the requester can agree torelease resources generated by the FQP Agent, disposing all the MIRAagents involved in the query evaluation as well as the FQP itself. Notethat disposing the FQP Agent at any stage of the query execution willeffectively close the processing of the federated query.

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 99
All these mechanisms focus on the internal operations for the processing offederated queries. The number of these internal operations is large and they aregrouped in several task categories, which are summarised in Table 1.
MOBILE INFORMATION RETRIEVAL AGENT
The Mobile Information Retrieval Agent (MIRA) is a mobile agent that transmitsthe federated query to other nodes. Being a software agent, it also guarantees thepossibility of combining intelligent decision-making with the information re-trieval tasks. Therefore, it can support a range of federated queries. For example:
• Gathering information from several specific nodes at once and merging theresults at the originating node
• Searching all nodes one by one in an attempt to retrieve all possible an-swers, or to find the best answer
• Searching all nodes one by one until a certain condition is satisfied. Forexample, finding the first possible answer, or finding a satisfactory answer.In the latter case the answer is sent to the originator node and a ‘satisfac-tion’ response is required from the originator node to decide whether tocontinue the search or to stop. The search may also be modified to allow forfinding a specific number of answers and then quitting.
Handling of MIRA agents is solely performed by the FQP Agent and it iscompletely transparent to the requester. Clearly, from the requester point of view,the proper execution of the query and its results is what really matters, and nothow the query mechanism was implemented. This transparency noticeably re-duces the system complexity since the TeleCARE application designers anddevelopers are not concerned about internal details of the processing mechanism.
As part of the strategy to enforce the visibility levels and access rights on theinformation, FIMS Agent will also “borrow (from the TeleCARE platform system)and check the credentials” of the requester agent for creating the FQP Agent. TheFQP agent in turn uses those credentials to create authorised MIRA agents. Ingeneral, this strategy is used in FIMA to validate the access rights to the informa-tion for requesters, no matter if the requester is local or remote. Visibility levelsand access rights are further described later in this paper.
PROCESSING OF QUERY TYPES
The federated query processing mechanism of FIMA supports access and retrievalof data from multiple TeleCARE nodes, so that the data can be retrieved eitherfrom the same or different remote nodes. Three types of federated queries aresupported in FIMA to allow retrieval from remote data stored in different nodeson the network.

Afsarmanesh, Guevara-Masis & Hertzberger
100 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
• Parallel query type, where speed of performance is the key consideration. • Serial query type, where optimisation of resource usage is the focus. • Sequential query type, which requires interactivity with the requester to
control the information-processing overhead (see Figure 5).One advantage of providing different types of query and access methods is
that the requester can choose which of the three options to use. This allows him tocontrol the general performance and overhead of the process and thus optimiseperformance of the federated queries for specific purposes.
The design of the architecture of FIMA carefully considers necessary data andagent traffic among the TeleCARE nodes. Two communication mechanisms be-tween the nodes are properly supported. These are (1) inter-agent message passingand (2) agent mobility. They are respectively considered for supporting the casesof ‘information push’ and ‘information pull’ among the agents:
• Information push: A simple TeleCARE information exchange case is consid-ered where a Care Centre site requires periodic sending of the sensed datafrom the home sites. In this case, the data collected at the home site ispushed from the home site to the Care Centre. The ‘push’ action is per-formed as ‘messages’ sent from one agent to another.
• Information pull: To illustrate the information pull, assume that an elderlyperson wishes to plan a special fun activity in his/her community and startsthis planning through an ‘entertainment service’ at home. The correspond-ing ‘elderly entertainment service’ at the home site searches for relevant
Figure 5. Sequential query type in FIMA
query
FQP Agent- Query Processing
Requesteragent
Agent transmission
Partial results
Msg. Continue!
Node – 2
Sap DB - database
F Q P
Node – 3
Node – 1
M I R A
M I R A
M I R A
F I M S
F I M S
F I M S

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 101
data to be collected from the Virtual Community. Then, a MIRA agent thatmay contain a parallel, serial, or sequential federated query (depending onthe kind of request, if it is to all, or, for instance, a specific number ofpeople), can pull names from one or more leisure centres.
VISIBILITY LEVELS IN TELECARE
In federated information management networks, different autonomous nodescan have different visibility levels and access rights to other nodes’ information.Thus, every node in the federation can decide what part of its local informationshould be available to each member in the federation13,14.
In other federated database environments the approach for visibility levels iseither based on individual export schema definitions, on the local schema forevery external ‘user’, or based on the definition of a complete hierarchy of exportschemas. However, due to the highly dynamic nature of the TeleCARE environ-ment, where users and nodes are added and removed regularly, a differentapproach is adopted for defining the visibility levels. This approach is based onthe credential of every agent, and specifically of the agent type, that also repre-sents the role of the user generating the agent.
DOSG — DYNAMIC ONTOLOGY-BASED DATA STRUCTURE GENERATION
Typically, for building large systems and applications, the assistance of a databaseexpert is required to define the structure for concepts and entities of the environ-ment, namely the database schema. The DOSG component supports and assistsboth the TeleCARE component developers as well as its service developer, withtheir direct definition and modification of database schemas, for the data thatneeds to be processed by their code, while eliminating the need for databaseexpertise. Namely, DOSG provides facilities for dynamic and automatic definitionand modification of database schemas, so that they can be automatically stored inthe database. As a consequence, the service developers of TeleCARE, can simplyuse the user friendly interface provided for the ‘Protégé’ ontology system to pro-vide their data structure definitions.
The main focus of DOSG in TeleCARE is transforming the ontology definitionprovided for some information into the underlying information managementmodel (based on the relational database system), as well as the Java objects specifi-cation. DOSG provides a highly innovative mechanism to leverage the objectknowledge model in ways that vertical service developers can use to store, retrieveand manipulate information seamlessly through the federated information man-agement layer of the TeleCARE platform.
DOSG is designed as a plug-in to Protégé. It extends Protégé’s ontology editorwith an interface that allows users to parameterise the automatic data structure
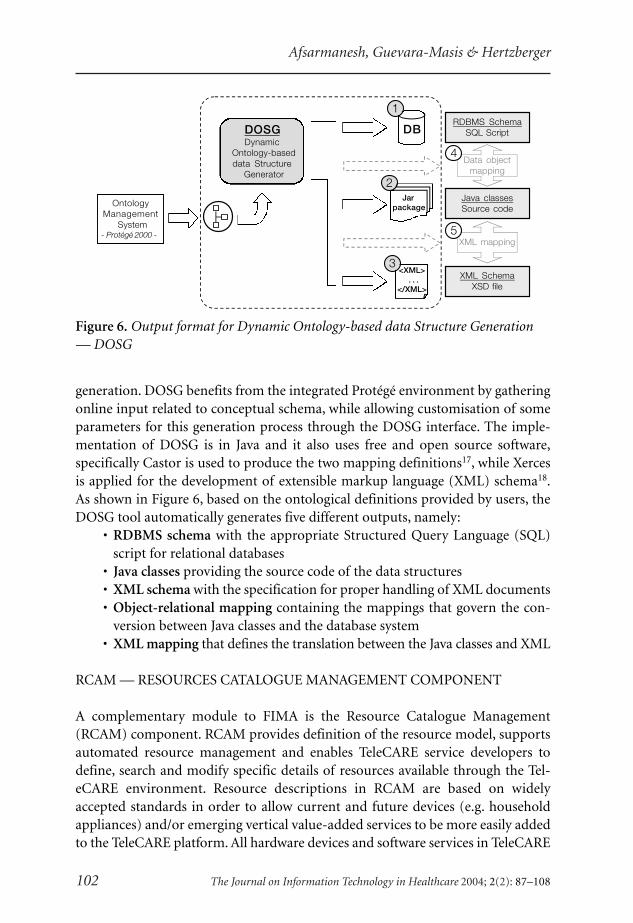
Afsarmanesh, Guevara-Masis & Hertzberger
102 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
generation. DOSG benefits from the integrated Protégé environment by gatheringonline input related to conceptual schema, while allowing customisation of someparameters for this generation process through the DOSG interface. The imple-mentation of DOSG is in Java and it also uses free and open source software,specifically Castor is used to produce the two mapping definitions17, while Xercesis applied for the development of extensible markup language (XML) schema18.As shown in Figure 6, based on the ontological definitions provided by users, theDOSG tool automatically generates five different outputs, namely:
• RDBMS schema with the appropriate Structured Query Language (SQL)script for relational databases
• Java classes providing the source code of the data structures • XML schema with the specification for proper handling of XML documents • Object-relational mapping containing the mappings that govern the con-
version between Java classes and the database system • XML mapping that defines the translation between the Java classes and XML
RCAM — RESOURCES CATALOGUE MANAGEMENT COMPONENT
A complementary module to FIMA is the Resource Catalogue Management(RCAM) component. RCAM provides definition of the resource model, supportsautomated resource management and enables TeleCARE service developers todefine, search and modify specific details of resources available through the Tel-eCARE environment. Resource descriptions in RCAM are based on widelyaccepted standards in order to allow current and future devices (e.g. householdappliances) and/or emerging vertical value-added services to be more easily addedto the TeleCARE platform. All hardware devices and software services in TeleCARE
Figure 6. Output format for Dynamic Ontology-based data Structure Generation— DOSG
XML SchemaXSD file
RDBMS SchemaSQL Script
Java classesSource code
DB
Data objectmapping
XML mapping
Jarpackage
<XML> . . .
</XML>
OntologyManagement
System- Protégé 2000 - 5
4
DOSGDynamic
Ontology-baseddata Structure
Generator2
3
1

Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 103
are treated as resources. Basically, RCAM acts like a registry for all resources, theirinternal service descriptions and interfaces. Namely, for every resource of theTeleCARE environment, RCAM manages three types of information:
i. The catalogue entry representing a definition of the resourceii. The entries for the resource’s internal services definitions
iii. The access rights to the resourceIn order to support current and future devices, and emerging vertical services,
TeleCARE resource definitions in RCAM are based on widely accepted standards.The hardware device definitions are based on the Universal Plug and Play (UPnP)specification19, while the software vertical service definitions are based on WebService Definition Language (WSDL) specification20. Furthermore, RCAM resourcesdefinition has been extended to better support users’ access rights to resources,based on agent identification, part of the TeleCARE passport definition21.
The RCAM Agent provides basic operations on the TeleCARE resource model.These operations can be grouped into the following categories: resource adver-tisement and publishing, resource discovery, resource access rights management(see Figure 7).
The suggested TeleCARE resource model involves the following actors: re-source provider, resource broker, and resource requester. RCAM Agent acts as anautomated resource broker. This resource broker provides a searchable (catalogue)repository of resource definitions through which resource providers can advertiseand publish the functionality of their resources. Additionally, resource requesterssearch for appropriate resource services and obtain the necessary information touse them.
Furthermore, RCAM can store information about the access rights to Tel-eCARE resources based on the TeleCARE passport definition. As such, for everyresource, related information regarding the Agent-type, User-role and User-id of
Figure 7. Resource handling operations
ResourceBroker
Resource Catalogue
ResourceRequester
Request Description
Advertisement /Publishing
Resource/serviceinformation
Discovery
Invocation andExecution
Description
ResourceProvider
- Device and Vertical Services-
Resource Description
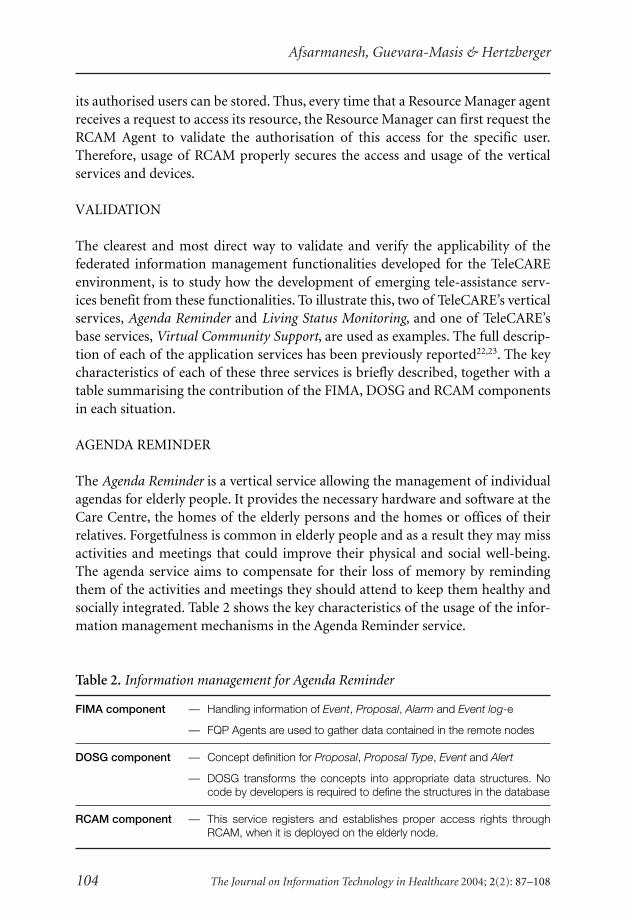
Afsarmanesh, Guevara-Masis & Hertzberger
104 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
its authorised users can be stored. Thus, every time that a Resource Manager agentreceives a request to access its resource, the Resource Manager can first request theRCAM Agent to validate the authorisation of this access for the specific user.Therefore, usage of RCAM properly secures the access and usage of the verticalservices and devices.
VALIDATION
The clearest and most direct way to validate and verify the applicability of thefederated information management functionalities developed for the TeleCAREenvironment, is to study how the development of emerging tele-assistance serv-ices benefit from these functionalities. To illustrate this, two of TeleCARE’s verticalservices, Agenda Reminder and Living Status Monitoring, and one of TeleCARE’sbase services, Virtual Community Support, are used as examples. The full descrip-tion of each of the application services has been previously reported22,23. The keycharacteristics of each of these three services is briefly described, together with atable summarising the contribution of the FIMA, DOSG and RCAM componentsin each situation.
AGENDA REMINDER
The Agenda Reminder is a vertical service allowing the management of individualagendas for elderly people. It provides the necessary hardware and software at theCare Centre, the homes of the elderly persons and the homes or offices of theirrelatives. Forgetfulness is common in elderly people and as a result they may missactivities and meetings that could improve their physical and social well-being.The agenda service aims to compensate for their loss of memory by remindingthem of the activities and meetings they should attend to keep them healthy andsocially integrated. Table 2 shows the key characteristics of the usage of the infor-mation management mechanisms in the Agenda Reminder service.
Table 2. Information management for Agenda Reminder
FIMA component — Handling information of Event, Proposal, Alarm and Event log-e
— FQP Agents are used to gather data contained in the remote nodes
DOSG component — Concept definition for Proposal, Proposal Type, Event and Alert
— DOSG transforms the concepts into appropriate data structures. Nocode by developers is required to define the structures in the database
RCAM component — This service registers and establishes proper access rights throughRCAM, when it is deployed on the elderly node.
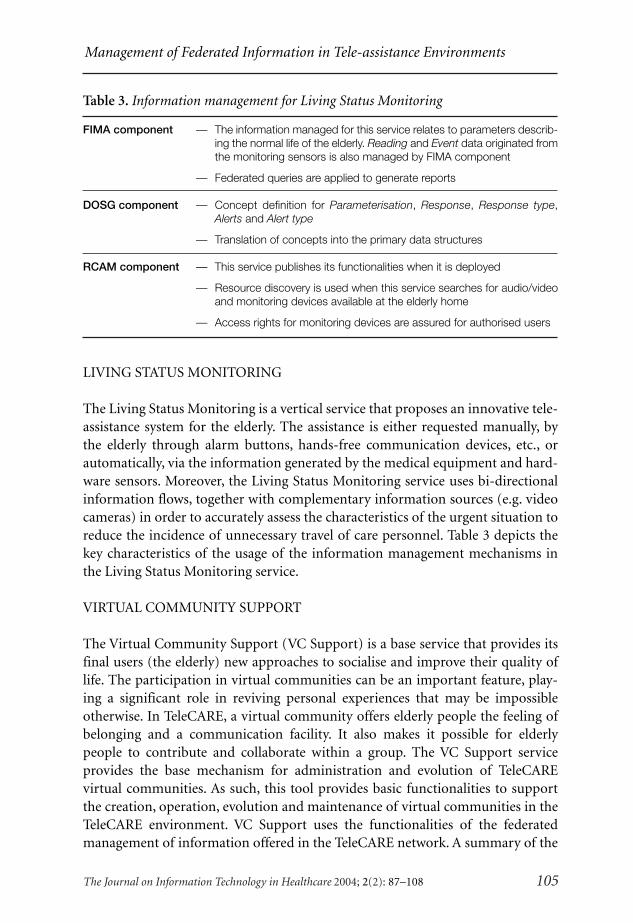
Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 105
LIVING STATUS MONITORING
The Living Status Monitoring is a vertical service that proposes an innovative tele-assistance system for the elderly. The assistance is either requested manually, bythe elderly through alarm buttons, hands-free communication devices, etc., orautomatically, via the information generated by the medical equipment and hard-ware sensors. Moreover, the Living Status Monitoring service uses bi-directionalinformation flows, together with complementary information sources (e.g. videocameras) in order to accurately assess the characteristics of the urgent situation toreduce the incidence of unnecessary travel of care personnel. Table 3 depicts thekey characteristics of the usage of the information management mechanisms inthe Living Status Monitoring service.
VIRTUAL COMMUNITY SUPPORT
The Virtual Community Support (VC Support) is a base service that provides itsfinal users (the elderly) new approaches to socialise and improve their quality oflife. The participation in virtual communities can be an important feature, play-ing a significant role in reviving personal experiences that may be impossibleotherwise. In TeleCARE, a virtual community offers elderly people the feeling ofbelonging and a communication facility. It also makes it possible for elderlypeople to contribute and collaborate within a group. The VC Support serviceprovides the base mechanism for administration and evolution of TeleCAREvirtual communities. As such, this tool provides basic functionalities to supportthe creation, operation, evolution and maintenance of virtual communities in theTeleCARE environment. VC Support uses the functionalities of the federatedmanagement of information offered in the TeleCARE network. A summary of the
Table 3. Information management for Living Status Monitoring
FIMA component — The information managed for this service relates to parameters describ-ing the normal life of the elderly. Reading and Event data originated fromthe monitoring sensors is also managed by FIMA component
— Federated queries are applied to generate reports
DOSG component — Concept definition for Parameterisation, Response, Response type,Alerts and Alert type
— Translation of concepts into the primary data structures
RCAM component — This service publishes its functionalities when it is deployed
— Resource discovery is used when this service searches for audio/videoand monitoring devices available at the elderly home
— Access rights for monitoring devices are assured for authorised users
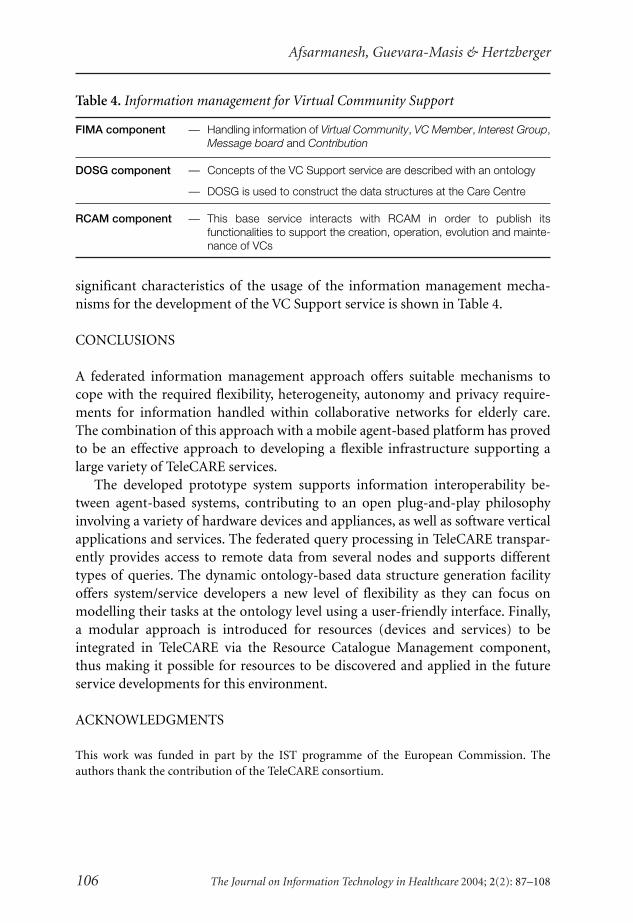
Afsarmanesh, Guevara-Masis & Hertzberger
106 The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
significant characteristics of the usage of the information management mecha-nisms for the development of the VC Support service is shown in Table 4.
CONCLUSIONS
A federated information management approach offers suitable mechanisms tocope with the required flexibility, heterogeneity, autonomy and privacy require-ments for information handled within collaborative networks for elderly care.The combination of this approach with a mobile agent-based platform has provedto be an effective approach to developing a flexible infrastructure supporting alarge variety of TeleCARE services.
The developed prototype system supports information interoperability be-tween agent-based systems, contributing to an open plug-and-play philosophyinvolving a variety of hardware devices and appliances, as well as software verticalapplications and services. The federated query processing in TeleCARE transpar-ently provides access to remote data from several nodes and supports differenttypes of queries. The dynamic ontology-based data structure generation facilityoffers system/service developers a new level of flexibility as they can focus onmodelling their tasks at the ontology level using a user-friendly interface. Finally,a modular approach is introduced for resources (devices and services) to beintegrated in TeleCARE via the Resource Catalogue Management component,thus making it possible for resources to be discovered and applied in the futureservice developments for this environment.
ACKNOWLEDGMENTS
This work was funded in part by the IST programme of the European Commission. Theauthors thank the contribution of the TeleCARE consortium.
Table 4. Information management for Virtual Community Support
FIMA component — Handling information of Virtual Community, VC Member, Interest Group,Message board and Contribution
DOSG component — Concepts of the VC Support service are described with an ontology
— DOSG is used to construct the data structures at the Care Centre
RCAM component — This base service interacts with RCAM in order to publish itsfunctionalities to support the creation, operation, evolution and mainte-nance of VCs
Management of Federated Information in Tele-assistance Environments
The Journal on Information Technology in Healthcare 2004; 2(2): 87–108 107
REFERENCES
1 Camarinha-Matos LM, Afsarmanesh H. The virtual enterprise concept. In Camarinha-Matos LM, Afsarmanesh H (eds.), Infrastructures for Virtual Enterprises. Dordrecht, TheNetherlands: Kluwer Academic Publishers, 1999: 3–14.
2 Rheingold H. The Virtual Community: Homesteading on the Electronic Frontier. Reading,MA: Addison-Wesley, 1993.
3 Camarinha-Matos LM, Afsarmanesh H. Virtual enterprise modeling and support infra-structures: applying multi-agent systems approaches. In Luck M, Stpankova V, Trappl R(eds.), Multi-Agent Systems and Applications. Lecture Notes in Artificial Intelligence.Berlin: Springer Verlag, 2001: 335–64.
4 Li Y, Huang B, Liu W, Wu C, Gou H. Multi-agent system for partner selection of virtualenterprise. In Gan R (ed.), Proceedings of the World Computer Congress 2000, Track onInformation Technology for Business Management. Beijing: Publishing House of Electron-ics Industry, 2000: 287–94.
5 IBM Tokyo Research Laboratory. Aglets Workbench, IBM Japan. http://www.trl.ibm.com/aglets/, 2002.
6 Aglets.org. The Aglets Portal. http://aglets.sourceforge.net/, 2002.7 Wang AI, Liu C, Conradi RA. Multi-agent architecture for cooperative software engineer-
ing. International Conference on Software Engineering and Knowledge Engineering (SEKE’99), Kaiserslautern, 1999: 1–22.
8 Papastavrou S, Samaras G, Pitoura E. Mobile agents for WWW distributed database access.International Conference on Data Engineering (ICDE ’99). Sydney, 1999: 228–37.
9 Huhns MN, Singh MP. Ontologies for agents. IEEE Internet Computing 1996; 1: 81–83.10 Stanford Medical Informatics. The Protégé Project. Stanford University School of Medicine,
http://protege.stanford.edu/, 2003.11 Noy NF, Sintek M, Decker S, Crubezy M, Fergerson RW, Musen MA. Creating semantic
Web contents with Protégé-2000. IEEE Intelligent Systems 2001; 16: 60–71.12 Afsarmanesh H, Camarinha-Matos LM. Federated information management for coopera-
tive virtual organizations. 8th International Conference on Databases and Expert SystemsApplications, DEXA ’97, Toulouse, 1997: 561–72.
13 Busse S, Kutsche RD, Leser U, Weber H. Federated information systems: concepts, termi-nology and architectures. Computergestutzte Informationssysteme CIS. Berlin: TechnischeUniversität Berlin, 1999.
14 Sheth A, Larson J. Federated database systems for managing distributed, heterogeneous,and autonomous databases. ACM Computing Surveys 1990; 22: 183–36.
15 TeleCARE. A Multi-Agent Tele-Supervision System for Elderly Care. http://www.uninova.pt/~telecare, 2003.
16 SAP AG. SAP DB, http://www.sapdb.org/, 2003.17 ExoLab Group. Castor, http://www.castor.org/, 2004.18 Apache Software Foundation. Xerces2 Java Parser, http://xml.apache.org/xerces2-j/
index.html, 2004.19 UPnP Forum. Universal Plug and Play, http://www.upnp.org/, 2002.20 W3C Consortium. Web Services Description Language (WSDL), http://www.w3.org/TR/
wsdl, 2001.21 Camarinha-Matos LM, Afsarmanesh H. A multi-agent based infrastructure to support
virtual communities in elderly care. International Journal of Networking and VirtualOrganizations, forthcoming, 2004.
108
HTI J
© The Journal on Information Technology in Healthcare 2004; 2(2): 87–108
Afsarmanesh, Guevara-Masis & Hertzberger
22 Aguilar JM, Cantos J, Expósito G, Gómez P. Agenda reminder and living status monitoring:the telecare approach. 1st International Workshop on Tele-Care and Collaborative VirtualCommunities in Elderly Care (TELECARE-2004), Porto, 2004.
23 Afsarmanesh H, Guevara-Masis V, Hertzberger O, Virtual community support in Tel-eCARE. 4th IFIP working conference on Virtual Enterprises PRO-VE ’03, Lugano,Switzerland, 2003, Dordrecht, The Netherlands: Kluwer Academic Publishers, 2003:211–20.

109
HTI J © The Journal on Information Technology in Healthcare 2004; 2(2): 109–117
INTRODUCTION
Tele-assistance is a set of services which, with the aid of new technologies incomputing and telecommunications enables elderly people to be connected toone or more specialised care centres. These are staffed by qualified personnel whoin response to an emergency can provide appropriate action either by themselvesor by mobilising other resources. A major perceived advantage of the provision ofsuch services is that they allow elderly people to lead an independent life with thereassurance that in the event of a crisis, e.g. an accident or medical emergency,they will be able to immediately obtain appropriate help. In addition the servicesalso help them to deal with lesser problems such as anxiety and loneliness.
By enabling vulnerable people to remain in their habitual surroundings, tele-assistance offers elderly people the following benefits1,2:
• Improved quality of life • Increased confidence, well-being and safety • Avoidance of personal, social and economic costs associated with leaving
familiar surroundings
Tele-assistance Services to Improve the Quality of Lifefor Elderly Patients and their Relatives: The Tele-CAREApproach
José María Aguilar, Javier Cantos, Guillermo Expósito,Pedro José Gómez
InnovaTD – Grupo Skill, Tecnologia, Spain.
ABSTRACT
Tele-assistance services based on information and communications technologies (ICT) havethe potential to improve the quality of life for both elderly people and their relatives. In par-ticular they can increase their peace of mind, confidence and security. This paper describestwo of the services, Agenda Reminder and Living Status Monitoring, that have been devel-oped for the TeleCARE platform. Functional aspects of these services, and how they workin practice, to improve patients’ quality of life and security are illustrated with examples.
Correspondence and reprint requests: J Aguilar, InnovaTD – Grupo Skill, Tecnologia 9 41120 Gelves(Sevilla), Spain. E-mail :[email protected].

Aguilar, Cantos, Expósito & Gómez
110 The Journal on Information Technology in Healthcare 2004; 2(2): 109–117
• Facilitates contact with social and family members • Ensures immediate intervention in the event of personal, social or medical
crisesTo be able to offer an effective and efficient tele-assistance service, the Tel-
eCARE project3–6 has developed the model shown in Figure 1.The model consists of a basic platform that supports fundamental functions
such as communication and information management, and a specialised platformwhich provides a range of services. Two of these are:
• Agenda Reminder • Living Status Monitoring
AGENDA REMINDER SERVICE
The ‘Agenda Reminder’ service of the TeleCARE platform aims to provide elderlypeople with a better well-being by reminding them of activities they have to do in
Figure 1. The TeleCARE platform reference architecture
Vertical Services LevelVertical Services Level
Core MAS Platform LevelCore MAS Platform Level
External Enabler LevelExternal Enabler Level
Virtual CommunitySupport
Web-accessSupport
SpecialisedInterfaces
Time Bankservice
StatusMonitoring
service
Enter-tainmentservice
Agendaservice
Platform Manager
Basic Multi-Agent Platform
Resource Catalogue Mgnt.
Inter-platform mobility
Federated InformationManagement
Safe CommunicationInfrastructure
Device Abstraction Layer
Inter-agent Communication
PersistenceSupport
OntologyManagement
System
InferenceEngine
AgentExit
Control
AgentReception &Registration
AgentFactory
Device/Vertical Service Registry
ResourceManagers
FederatedQuery
Processor
Ontology-baseddata Structure
Generator
Sp
ecia
lised
Co
mp
on
ents
Tel
eCA
RE
Bas
ic P
latf
orm

Tele-assistance Services to Improve Quality of Life
The Journal on Information Technology in Healthcare 2004; 2(2): 109–117 111
order to keep them healthy and socially integrated 7. A common problem experi-enced by elderly people is forgetfulness. Consequently they frequently missappointments and activities that could enhance their social and physical well-being.
The ‘Agenda Reminder’ service requires the co-operation and input of theelderly person, their relatives and carers (Table 1). An agenda is created for theelderly person by the carer which can be modified in response to instructionsfrom the elderly person, relatives or on the initiative of the carer. For the system tofunction properly, appropriate software and hardware has to be installed in theCare Centre, in the homes of elderly people and the homes of their relatives.
To enhance flexibility and functionality, the service is structured in three sub-systems.
• Agenda Management: This centralises all the management and mainte-nance activities of the elderly person. It has the tools8 to allow the CareCentre staff to deal with proposals for updates, and, based on these, tocreate, modify or delete an entry in the agenda. In addition, the Care Centrewill directly enter all appointments or events it deems appropriate for thebenefit of the elderly person.
• Proposal Management: This allows the elderly person or his/her relativesto make proposals for creating, modifying and deleting events from theagenda.
• Reminder Management: This generates automatic reminders of events andsends them to the elderly person. The system is designed to assure receiptof the reminder, and whenever possible confirmation that the person hasattended the event. If the person does not attend the event an alert isgenerated and sent to the Care Centre. A staff member at the Care Centrethen directly contacts the elderly person or a relative to establish a cause forthe non attendance.
Although the Agenda service is initiated in the Care Centre, it then utilisesthe mobile agent technology9–12 of the basic multi-agent platform as shown inFigure 2.
Table 1. Functionalities, target users and topology of the Agenda Reminder Service
Functionalities Target users Topology
– Start new agenda Care professionals Care Centre (coordinator)– Edit agenda entries: exercises, or Tele-assistance Centres appointments, medication reminder, etc.– Send reminder & get confirmation Elderly people Elderly homes– Generate alert to Care Centre Elderly people’s– Generate alert to relative(s) relatives Relatives’ homes/work
places

Aguilar, Cantos, Expósito & Gómez
112 The Journal on Information Technology in Healthcare 2004; 2(2): 109–117
At the Care Centre an Agenda Reminder Server Manager Agent is responsiblefor the entire management and control of the service. This includes tasks such asmanagement of proposals, events and alerts, and the registration of new elderlypeople for the service. Incoming and outgoing data flow and the Windows-basedinterface of the care staff is managed by a Server Interface Agent. A Web Connec-tor Agent may be used to set up a bridge to the Internet through a web server. Thisagent does not really belong to the Agenda, but forms part of the Web Accessmodule that is used by relatives from their home or office.
Whenever an elderly person is registered with the Agenda service, an AgendaReminder Client Manager agent is created in the Centre. This agent will travel(with the data on the elderly person) to the node installed in his or her house, todeploy the service there. All communications between the two nodes pass throughthis agent. It is also responsible for managing proposals in the home, generatingnotifications and generating service-related alerts in the home.
This is a clear example of how agent mobility works. This deployment consistsof creating the other two component agents of the service in the elderly person’shome, the Clock Agent and the Client Interface Agent, that are also shown inFigure 2. The Clock Agent is responsible for launching the events at the appropri-ate time. The Client Interface Agent manages the interface with the elderly person,controlling the information which appears on the specialised interface13,14 and theincoming and outgoing data, all of which are always oriented towards the elderlyperson. Once the deployment has been carried out, the Agenda is active in theelderly person’s home.
Figure 2. Agenda Reminder deployment
CARE CENTRE
WEB SERVER
ELDERLY PERSON’S HOME
Clock Agent
Agenda Reminder Client Manager
Agenda Reminder Server Manager
Server Interface Agent
Web Connector
Agent
Client Interface Agent
Tele-assistance Services to Improve Quality of Life
The Journal on Information Technology in Healthcare 2004; 2(2): 109–117 113
Agenda Reminder ScenarioJuan and Ana are 72 and 68 years old respectively. They live in their own home inan agricultural village 50 kilometres from the city centre. Juan is in the early stagesof Alzheimer’s disease and has memory problems. Ana suffers with arthritis in herhands and also frequently forgets to do daily tasks. They have one daughter wholives and works in the city. Both of them prefer to stay in their home instead ofgoing to live in an elderly persons care centre.
The Agenda system reminds them every morning of the tasks and appoint-ments they have to do that day, e.g. the groceries they need to buy, or anymedical appointments they have. For example, one morning the system remindsthem that Ana has an appointment that evening at the health centre. When Anagoes to the health centre, Juan stays alone at home and watches a TV pro-gramme. During the programme the system reminds him that he has to take hisevening medication.
LIVING STATUS MONITORING SERVICE
The Living Status Monitoring (LSM) service is designed to provide assistanceeither on the demand of the user (requested assistance), e.g. by pressing an alertbutton, or automatically (automatic assistance) via information provided by spe-cial sensing devices. To enable staff at the Care Centre to more accurately assessthe situation, bi-directional information flow and complementary informationfrom other sources, e.g. cameras, are also provided. These measures help to reducethe incidence of false alarms.
Key perceived benefits of the system are3: • Enabling the elderly and their relatives to enjoy a higher peace of mind, and
thus improve their quality of life • Cost savings by ensuring that assistance provided is both necessary and
appropriateThe LSM service basically consists of monitoring and supervising the activities
of the elderly person in his/her own home, by means of a number of deviceswhich, upon detecting any irregular behaviour, inform the Care Centre so thatappropriate action can be taken (Table 2).
In its operational state, the system has the following functional subsystems: • Behaviour Profile Management: This subsystem makes it possible to define
standard behaviour profiles for each elderly person. Once these are estab-lished, monitoring devices installed in the home will enable the system todistinguish between normal and irregular behaviour
• Monitoring Management: This subsystem is the heart of the LSM. It isresponsible for:– Carrying out the entire process of analysing the information collected by
the devices

Aguilar, Cantos, Expósito & Gómez
114 The Journal on Information Technology in Healthcare 2004; 2(2): 109–117
– Correlating this data with the profile of the elderly person– Generating pertinent notifications and/or alarms
All of the situations that occur are stored in a log which can be used asfeedback for the system, and to generate reports.
• Communication Management: This subsystem allows direct communica-tion with the elderly person by means of devices such as loudspeakers and/or the web camera installed in the home. The elderly person may contactthe Care Centre directly whenever he/she wishes, and the Care Centre andthe relative may establish communication and/or view the images from thecamera installed in the elderly person’s home.
Table 2. Functionalities, target users and topology of the Living Status Monitoringvertical service
Functionalities Target users Topology
– Define monitoring conditions Care professionals Care Centre (coordinator)– Collect information from sensors or Tele-assistance Centres– Call for assistance (alarm button)– Access elderly people’s file– Locate elderly people– Contact/advise elderly people Elderly people Elderly persons’ homes– Generate alert/warning to Care Centre Elderly people’s Relatives homes/work– Generate alert/warning to relatives relatives places (notification only)– Call emergency services
Figure 3. Living Status Monitoring deployment
WEB SERVER
LSM Server Manager
Server Interface Agent
< ELDERLY PERSON’S HOME
Web Connector Agent
CARE CENTRE
HomeWatchAgent
LSM Client Manager
Resource Manager
(Device 1)
Resource
Manager
(Device 3)
Resource Manager
(Device n)
LSM Device Agent 1
LSM Device Agent 2
LSM Device Agent 3
LSM Device Agent n
Resource
Manager
(Device 2)
Client Interface
Agent

Tele-assistance Services to Improve Quality of Life
The Journal on Information Technology in Healthcare 2004; 2(2): 109–117 115
The LSM works in a similar way to the Agenda service8–12, but in this casedifferent agents are involved. Figure 3 shows the set of agents involved in both theCare Centre and the elderly person’s home. As with the Agenda, the service isinitiated in the Centre, and services are launched from there to the homes ofelderly people registered with the LSM.
In this case two agents once again make up the service in the Centre, and aWeb connector agent provides access via the Internet.
The service interface agent and the web connector agent perform the sametasks as in the Agenda service. The LSM Server Manager Agent is in charge of themanagement and control of the service at the Care Centre. However, its tasks aredifferent to those performed in the Agenda service. Its tasks include the registra-tion of new elderly people in the service, inputting and managing the elderlyperson’s lifestyle pattern according to the system’s parameters, management ofalerts, direct connection to the home and the temporary activation or deactiva-tion of the service.
The deployment of the service is the same as for the Agenda service once a newelderly person subscribes to the LSM. However, in this case, as shown in Figure 3,once the LSM Client Manager agent travels to the home, a greater number ofagents are created to form the service.
The LSM Client Manager Agent is a bridge that stores all the informationrelated to the Centre and the elderly person. All communications between the twonodes pass through this agent.
The Home Watch Agent is the brain of the service and is in charge of analysingwhat is happening inside the home. It collects and analyses all the informationfrom the sensors, using the information on the elderly person’s lifestyle andeverything that has happened previously in the home. This analysis will bringabout a response if an anomalous situation is detected. This response may takethe form of an automatic call to the elderly person requesting a confirmation thathe or she is well, or an alert sent to the Care Centre for the initiation of theappropriate action, which may include a direct connection with the home.
The Client Interface Agent manages the interface with the elderly person. Itcontrols the information which appears on the specialised interface13–14 and theincoming and outgoing data, all of which are always oriented towards the elderlyperson.
For each of the devices located in the home, a device agent is created as a go-between. The LSM Device Agents interrogate the resource catalogue to find outwhether such a device exists, and if not will notify the system of the non-existenceof the device.
As with the Web agent, Resource Managers do not form part of the service, butappear in the diagram for the sake of completeness. They are created in the elderlyperson’s home when the device they manage is installed. They are the agents inclosest contact with the devices, and can even implement, when necessary, the

Aguilar, Cantos, Expósito & Gómez
116 The Journal on Information Technology in Healthcare 2004; 2(2): 109–117
proprietary code for the device. They constitute a device abstraction layer, makingthe devices transparent to the remainder of the system.
Once again, when the deployment is complete, Living Status Monitoring canbe considered to be active in the elderly person’s home.
Living Status Monitoring ScenarioMrs. Dolores Fernández is a 74 year old widow who lives alone. One morning shefeels unwell and contacts the Care Centre by pressing the panic button. A memberof staff at the Centre checks her personal information and learns that she is a non-insulin dependent diabetic taking glicazide tablets. On questioning he discoversthat she has taken her medication that morning but not eaten any breakfast. Headvises her to take a sugary drink or eat a chocolate bar. He then checks back 30minutes later to find that she is feeling much better. Three weeks later, sensorsinstalled at Mrs Fernández’s home send an alert to the Care Centre since nomovement was detected in the home between 6 and 7pm. A member at the CareCentre rings her home to check that she is all right, but obtains no response. Thestaff member then alerts the emergency services and her relatives. He is able togive the medical emergency services details of her medical history. The emergencyservices enter her house and find that she has suffered a stroke. The immediatelytransport her to hospital.
CONCLUSION
This paper describes the functions of the Agenda Reminder and Living StatusMonitoring Services of the TeleCARE project. It demonstrates the suitability ofthe technologies selected for the TeleCARE platform to achieve the objectives ofhelping elderly people lead high quality, independent life-styles with security andpeace of mind.
The mobile multi-agent platform appears to be the best option for establishinga network of nodes which are heterogeneous, autonomous and with a wide physi-cal distribution. The federated information management is well-suited to thepurpose intended. Agents can be sent to collect information from each node, andat no time is there any centralisation of data, which would be highly inappropriatein this type of situation. As regards security, both with respect to the communica-tions infrastructure and management of information, privacy is maintained at alltimes and access to information is controlled using both roles and user identifica-tion. Finally, all of the aspects added to the system, such as the modular design,making use of abstraction layers at several levels, plug and play support and theuse of standards or common practices where viable, have made it possible for thearchitecture to be generic, open and flexible, thus fulfilling the initial aim of theproject.

117
HTI J
© The Journal on Information Technology in Healthcare 2004; 2(2): 109–117
Tele-assistance Services to Improve Quality of Life
ACKNOWLEDGEMENTS
This work was funded in part by the IST programme of the European Commission. Theauthors thank the contribution of the TeleCARE consortium members.
REFERENCES
1 UNIGES Tele-assistance Magazine. http://www.uniges.com/type/mod/pl02.asp?p01=teleasistencia.
2 Compliance with G8 Commitments: From Birmingham 1998 to Köln 1999: – ComplianceStudies by Issue Area: Active Aging. http://www.g7.utoronto.ca/g7/evaluations/1999koln/compliance/aging.htm. http://www.sodexho.com/sodexhoAnglais/site/LiensSite/Lien_Com_Library.cfm.
3 Camarinha-Matos LM, Castolo O, Vieira W. A mobile agents approach to virtual laborato-ries and remote supervision. Journal of Intelligent and Robotic Systems 2002; 35: 1–22.
4 Camarinha-Matos LM, Afsarmanes H. Virtual communities and elderly support. Proceed-ings of MIV ’01 in Advances in Automation, Multimedia and Video Systems, and ModernComputer Science, September 2001. Kluev VV, D’Attellis CE, Mastorakis NE (eds.), WSES:279–84.
5 Camarinha-Matos LM, Afsarmanes H. Design of a virtual community infrastructure forelderly care. Proceedings of PRO-VE 2002 – 3rd IFIP Working Conference on Infrastructuresfor Virtual Enterprises, Sesimbra, Portugal, 1–3 May 2002. Amsterdam: Kluwer: 439–50,
6 Camarinha-Matos LM, Castolo O. A multi-agent based platform for virtual communitiesin elderly care. Rosas in Proceedings of ETFA ’03 – 9th International Conference on Emerg-ing Technologies and Factory Automation, Lisboa, Portugal, 16–19 September 2003: 421–28.
7 Sodexho. From “Old Folks” to the “Power Age” – The changing role of seniors in the newmillennium, Report ICC / CMA – 03/09/99, Sodexho Research Institute on the Quality ofDaily Life, 1999.
8 Falasconi S, Lanzola G, Stefanelli M, Using ontologies in multi-agent systems. Proceedingsof the Knowledge Acquisition For Knowledge-Based Systems Workshop (KAW ’96), Banff,Canada, 1996.
9 Hurst L, Cunnigham P, Somers F. Mobile agents – smarts messages. Proceedings of the FirstInternational Workshop on Mobile Agents, MA ’97. Berlin: Springer Verlag, 1997.
10 Lange DB, Oshima M. Programming and Deploying Java Mobile Agents with Aglets. Addison-Wesley, 1998.
11 FIPA Content Language Library Specification; Foundation for Intelligent Agent Systems,2001. http://www.fipa.org/.
12 Murphy AL, Pico GP. Reliable Communication for Highly Mobile Agents. AutonomousAgents and Multi-Agent Systems, 2002; 5: 81–100.
13 Stephanidis C. Universal Access in the Information Society: Methods, Tools, and InteractionTechnologies, Published online: 23 May 2001. Berlin: Springer Verlag, 2001.
14 Oakley I, Adams, A. Brewster S, Gray P. Guidelines for the Design of Haptic Widgets.Proceedings of BCS HCI 2002, London, UK. Berlin: Springer Verlag: 195–212.


119
HTI J © The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
INTRODUCTION
Participation in a community is an important aspect of life for most people. Infact most humans have a natural affinity for living in communities. The structuralprocess that is associated with community building is communication. Withoutcommunication there can be no action to organise social relations1. Today’s fastemerging information and communication technologies have stimulated the crea-tion of virtual communities through use of the Internet.
Virtual communities have been defined as “social aggregations that emerge fromthe Net when people carry on public discussions long enough, with sufficient humanfeeling to form webs of personal relationships”2. A virtual community is also seen as“a community of people sharing interests, ideas, and feelings over the Internet”3.Virtual communities can also be regarded as distributed online services connect-ing a group of people that gather to keep in touch, focused on some commoninterest or purpose4.
An important application context for virtual communities is elderly care. Tra-ditional approaches to care provision are based on support from either relatives,or elderly care centres. However, these two solutions have become increasinglyinsufficient for the following reasons:
TeleCARE Time Bank: A Virtual Community forElderly Care Supported by Mobile Agents
Octavio Castolo, Filipa Ferrada, Luis Camarinha-Matos
New University of Lisbon/Uninova, 2829-516 Monte Caparica, Portugal.
ABSTRACT
The virtual community concept when supported by adequate information and communica-tions technology (ICT) and organisational infrastructures, represents a very promising ap-proach for a new philosophy in elderly care and active aging. A mobile agents-basedapproach to implementing services to support a Time Bank virtual community in elderlycare is described and a prototype system developed in the context of the TeleCARE projectis presented.
Correspondence and reprint requests: Professor Luis M. Camarinha-Matos, New University of Lisbon/Uninova, 2829-516 Monte Caparica, Portugal. E-mail: [email protected].
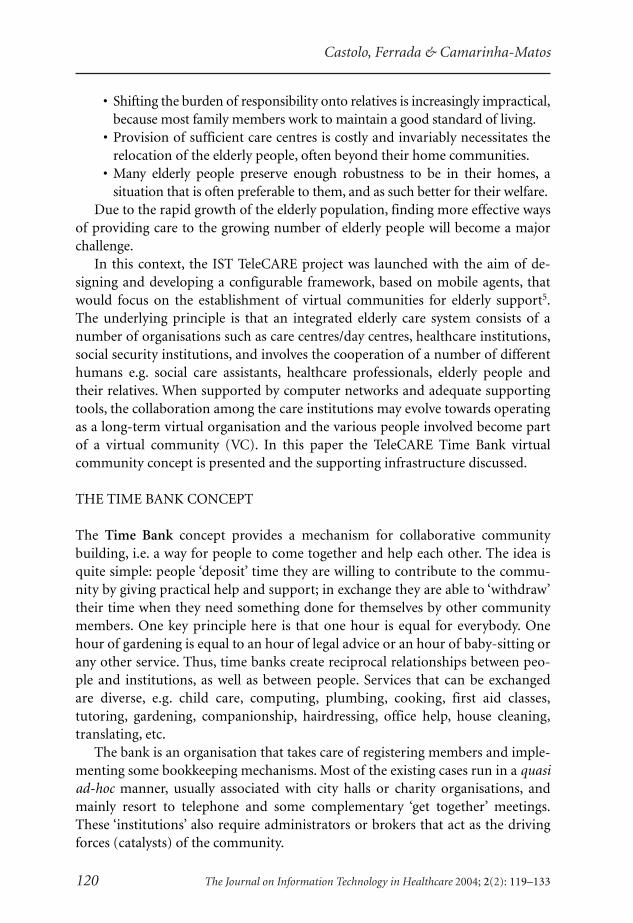
Castolo, Ferrada & Camarinha-Matos
120 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
• Shifting the burden of responsibility onto relatives is increasingly impractical,because most family members work to maintain a good standard of living.
• Provision of sufficient care centres is costly and invariably necessitates therelocation of the elderly people, often beyond their home communities.
• Many elderly people preserve enough robustness to be in their homes, asituation that is often preferable to them, and as such better for their welfare.
Due to the rapid growth of the elderly population, finding more effective waysof providing care to the growing number of elderly people will become a majorchallenge.
In this context, the IST TeleCARE project was launched with the aim of de-signing and developing a configurable framework, based on mobile agents, thatwould focus on the establishment of virtual communities for elderly support5.The underlying principle is that an integrated elderly care system consists of anumber of organisations such as care centres/day centres, healthcare institutions,social security institutions, and involves the cooperation of a number of differenthumans e.g. social care assistants, healthcare professionals, elderly people andtheir relatives. When supported by computer networks and adequate supportingtools, the collaboration among the care institutions may evolve towards operatingas a long-term virtual organisation and the various people involved become partof a virtual community (VC). In this paper the TeleCARE Time Bank virtualcommunity concept is presented and the supporting infrastructure discussed.
THE TIME BANK CONCEPT
The Time Bank concept provides a mechanism for collaborative communitybuilding, i.e. a way for people to come together and help each other. The idea isquite simple: people ‘deposit’ time they are willing to contribute to the commu-nity by giving practical help and support; in exchange they are able to ‘withdraw’their time when they need something done for themselves by other communitymembers. One key principle here is that one hour is equal for everybody. Onehour of gardening is equal to an hour of legal advice or an hour of baby-sitting orany other service. Thus, time banks create reciprocal relationships between peo-ple and institutions, as well as between people. Services that can be exchangedare diverse, e.g. child care, computing, plumbing, cooking, first aid classes,tutoring, gardening, companionship, hairdressing, office help, house cleaning,translating, etc.
The bank is an organisation that takes care of registering members and imple-menting some bookkeeping mechanisms. Most of the existing cases run in a quasiad-hoc manner, usually associated with city halls or charity organisations, andmainly resort to telephone and some complementary ‘get together’ meetings.These ‘institutions’ also require administrators or brokers that act as the drivingforces (catalysts) of the community.

TeleCARE Time Bank
The Journal on Information Technology in Healthcare 2004; 2(2): 119–133 121
The Time Bank idea was conceived in the mid-80s by Edgar Cahn who set upthe Time Dollar movement in the United States6. The following principles formu-lated by Cahn are the fundamental basis for the Time Bank7:
• Assets: the real wealth of our society is its people. • Redefining work: to include all those things that support healthy individu-
als and communities and the work that is not currently valued in themarket economy.
• Reciprocity: we need each other. • Social capital: humans need social networks as much as they need roads
and utility lines.The main goals for Time Banks are8: • To promote people participating actively in their daily lives. • To offer opportunities to give and receive services. • To act as instruments of mutual aid based on interchanges of time.
The TeleCARE Time Bank aims to apply this concept to the elderly care do-main by providing adequate information communication technology (ICT)support tools to facilitate the establishment and operation of such communities.The aim is to provide elderly people with a way to feel useful in society by givingthem an opportunity to share their skills and experiences with others. At the sametime, it enables elderly people to fill their days and to integrate into a communityto obtain better support for their own needs.
In fact, the current paradigm of aging as a ‘dependent’ stage of life does notmatch either current realities for elderly people or likely scenarios for the 21stcentury. Aging is less and less synonymous with dependency, because not allelderly people suffer from chronic illnesses, and even persons with chronic condi-tions and functional limitations retain other significant capabilities9.
The active aging concept reflects the desire and ability of many elderly peopleto remain engaged in economically and socially productive activities. Active agingmeans more than simply encouraging paid employment among elderly people.Societies should foster socially important activities such as volunteering, house-hold and child-care help, care-giving to the disabled elderly, and support for socialservice organisations, as envisaged in the Time Bank concept.
There are not many tools for supporting Time Bank activities reported in theliterature. One tool described is Timekeeper10 which provides simple administra-tive services for Time Banks based on Microsoft Access 97. However, it onlysupports administration for Time Bank members’ accounts. It does not providesupport for virtual communities, as the concept is understood in the literature.
THE TELECARE TIME BANK
The TeleCARE Time Bank is one of the vertical (application) services that run ontop of the TeleCARE platform (Figure 1). This platform provides an infrastruc-

Castolo, Ferrada & Camarinha-Matos
122 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
ture for the implementation of distributed Internet-based systems in elderly care11.The infrastructure is based on multi-agent technology (mobile and stationaryagents), federated information management, and safe communications (virtualprivate network). The TeleCARE multi-agent system (MAS) platform is installedat each site (elderly persons’ homes, care centres, etc.) creating a flexible infra-structure that supports the idea of plug-and-play vertical services which can beprogressively added to the system.
The TeleCARE Time Bank service supports the following macro-functionalities: • Creating and managing the Time Bank virtual community. • Performing the matching process between a service required by a member
and the potential provider members that could accomplish it. • Supporting the negotiation process between members. • Providing member account management including account statements.
The Time Bank is managed by a Coordinator/Administrator who is in chargeof the members’ accounts, promotes active participation of members and assistsin finding the best provider for a requested service. Participants in the TeleCARETime Bank virtual community include: (i) elderly people, (ii) their relatives and(iii) a care centre (that performs the coordination role). A Unified ModelingLanguage (UML) use case diagram of the main activities of the participants in theTeleCARE Time Bank is depicted in Figure 2.
Typically, a transaction between members in a time bank includes the follow-ing main phases: service request, service performance and confirmation of aservice accomplishment. In the TeleCARE Time Bank this process can be furtherdetailed in the following steps:
Figure 1. The TeleCARE architecture
Vertical Services Level
TeleCARE MAS TeleCARE MAS PlatformPlatform
Virtual Community Support
Time Bank service
Specialised Interfacesfor Elderly
Web Access Support
Status Monitoring
service
Enter-tainment service
Agenda service

TeleCARE Time Bank
The Journal on Information Technology in Healthcare 2004; 2(2): 119–133 123
A. Request a service:a) A member, the Requester, needs a service.b) The Requester contacts the Time Bank agency (Administrator) to request
the service.c) The Administrator matches the requested service with the available po-
tential provider member(s) and sends a list of the potential Providers tothe Requester.
d) The Requester selects one of the potential Provider(s).e) The Administrator contacts the selected potential Provider.f) The potential Provider receives the service requirement.g) The potential Provider confirms acceptance or refusal to provide the
service.h) Once the Provider agrees to provide the requested service, the Adminis-
trator confirms service acceptance to the Requester.i) If necessary, Requester and Provider interact directly to negotiate terms
and conditions for service accomplishment.B. The service is performed.C. Service accomplishment:
a) The Requester issues a cheque to the Provider corresponding to the serv-ice, indicating how much time (in hours) the task took to accomplish.
Figure 2. Unified Modeling Language (UML) use case diagram of participants’activities of the TeleCARE Time Bank service
Time Bank
management
requesting services
account statement
matching member’s servicerequest to potential /available providers
Elderly people
Relatives
Administrator
requesting accountstatements
account statementmanagement
provision ofservices
request forsubscription
account(s) creationand maintenance
log access
Member
Care Centre
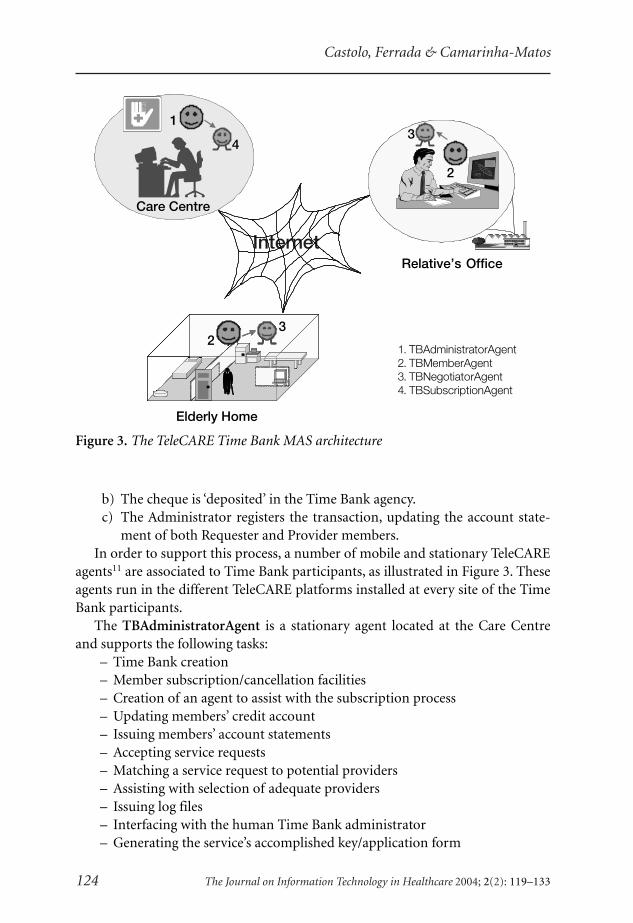
Castolo, Ferrada & Camarinha-Matos
124 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
b) The cheque is ‘deposited’ in the Time Bank agency.c) The Administrator registers the transaction, updating the account state-
ment of both Requester and Provider members.In order to support this process, a number of mobile and stationary TeleCARE
agents11 are associated to Time Bank participants, as illustrated in Figure 3. Theseagents run in the different TeleCARE platforms installed at every site of the TimeBank participants.
The TBAdministratorAgent is a stationary agent located at the Care Centreand supports the following tasks:
– Time Bank creation– Member subscription/cancellation facilities– Creation of an agent to assist with the subscription process– Updating members’ credit account– Issuing members’ account statements– Accepting service requests– Matching a service request to potential providers– Assisting with selection of adequate providers– Issuing log files– Interfacing with the human Time Bank administrator– Generating the service’s accomplished key/application form
Figure 3. The TeleCARE Time Bank MAS architecture
1. TBAdministratorAgent2. TBMemberAgent3. TBNegotiatorAgent4. TBSubscriptionAgent
InternetRelative’s Office
2
3
Elderly Home
32
Care Centre
1
4
2
3
2
3
32
32
32
Care Centre
1
4
Care Centre
1
4

TeleCARE Time Bank
The Journal on Information Technology in Healthcare 2004; 2(2): 119–133 125
The TBMemberAgent is a stationary agent that represents the members (eld-erly persons and/or their relatives) of the Time Bank. It assists members inperforming the following tasks:
– Requests for member subscription– Filling out application forms for requesting services– Creating an agent for negotiation process– Filling out application forms for services accomplished– Requesting member statement accounts– Interfacing with other human Time Bank members
The TBNegotiatorAgent is an agent created by the TBMemberAgent in orderto execute the negotiation process whenever a member requests a service. Eachtime a service is requested, a TBNegotiatorAgent is created. This is a mobile agentthat has the following characteristics:
Figure 4. A service transaction in the TeleCARE Time Bank
TBMemberAgent:Requester
TBNegotiatorAgent
TBAdministratorAgent TBMemberAgent:Provider
request a service
travels toAdministrator
place /platformrequest for a service
return list of potential providerssend list of potential providers
select pot. provider
inform selected provider
matching w potential providers
Accept?->Yesreturn response
return "ok"
inform acceptance of the service
inform acceptance of the service
update account statement & store data
inform selected provider
send email to selected provider
generates a key & store data
creates aTBNegotiatorAgent
The requested service is being realised .
acknowledges service accomplishment (generating a cheque )
send cheque to Administrator
travels to[selected]Provider
place /platform
request for a service (a window's request is displayed at Provider )

Castolo, Ferrada & Camarinha-Matos
126 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
– Capacity to migrate to other platforms (Administrator and potential pro-vider Member(s) sites).
– Capacity for interaction with the agent TBAdministratorAgent at the Ad-ministrator’s site, and the TBMemberAgent located at the potentialproviders’ sites.
The TBSubscriptionAgent is a mobile agent created by theTBAdministratorAgent when a subscription process is solicited. It has the follow-ing features:
– Capacity to migrate to other platforms (Administrator and/or Member).– Capacity to interact with the member who requests a subscription, when
the subscription is requested from the member’s location.– Capacity to interact with the Time Bank administrator who realises the
subscription of a member, when the subscription is requested from theAdministrator’s location.
– Fills out the application form for the Time Bank subscription.It should be noted that a subscription can be requested remotely (from the
potential member’s home) or in the Care Centre.The participants of the Time Bank interact either with the
TBAdministratorAgent, in case of the Care Centre, or the TBMemberAgent, in thecase of elderly people and/or their relatives, in order to realise the various tasks ofthe Time Bank activity. An AUML sequence diagram12 is depicted in Figure 4showing some of the Time Bank agents’ activities in the process of requesting aservice, and notification of service accomplishment.
Taxonomy of the ServicesIn order to facilitate the searching for a service and matching with the potentialproviders, a taxonomy of services is maintained (see Table 1). The initial tax-onomy was defined based on information provided by GRAAL, a Portuguesenongovernmental organisation that promotes the Time Bank concept in Portugal.
The services to be offered by an operational Time Bank are specified accordingto the skills and needs of its members. Therefore, new categories and services canbe defined (or removed) if necessary.
Time Bank OntologyOntologies play a key role in supporting proper interaction among the variouscomponents of this (geographically) distributed multi-agent system. The TimeBank ontologies are modelled using the Protégé13 system and Java classes areautomatically generated from these ontologies by the Dynamic Ontology-baseddata Structure Generator tool developed by a TeleCARE partner, the University ofAmsterdam. The UML diagram of the Java classes and relations corresponding tothe Administrator side ontology is shown in Figure 5.

TeleCARE Time Bank
The Journal on Information Technology in Healthcare 2004; 2(2): 119–133 127
Table 1. The TeleCARE Time Bank services’ taxonomy
Category Services
A. Baby-minding A01 – Baby-sitting
A02 – Taking children to school/looking after them
A0x – …
B. Leisure B01 – Bicycling (bicycle)
B02 – Walking
B0x – …
C. Housekeeping C01 – Washing the car
C02 – Washing dishes
C0x – …
D. Animals and plants D01 – Gardening
D02 – Looking after animals or plants when person is away e.g.vacation
D03 – Helping bathe animals (dogs, cats, etc.)
E. Bricolage (do-it-yourself) E01 – Minor domestic repairs
E02 – Carpentry
E03 – Electrical repairs
F. Accompany (accompanying) F01 – Accompanying to the doctor
F02 – Talking
F0x – Taking to Church
G. Cooking G01 – Cooking a special meal
G02 – Cooking food for freezing
H. Crafts H01 – Seam adjustments
H02 – Embroidering/embellishment
H03 – Knitting
I. Lessons I01 – Tutoring
I02 – Language teaching
I0x – …
J. Secretarial J01 – Proofreading
J02 – Word processing
J0x – …
K. Time Bank collaboration K01 – Supporting bureaucratic activities
K02 – Helping at meetings

Castolo, Ferrada & Camarinha-Matos
128 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
Figu
re 5
. The
Adm
inis
trat
or s
ide
onto
logy
Acc
oun
tDet
ails
-des
crip
tion :
Str
ing
-cre
dits
: Int
eger
-dat
e : S
trin
g-h
our :
Str
ing
Acc
oun
t
-bal
ance
: In
tege
r-a
ccou
ntD
etai
lsLi
st :
Acc
ount
Det
ails
-mem
ber :
Mem
ber
Ava
ilab
ility
-day
: Str
ing
-beg
inH
our :
Str
ing
-end
Hou
r : S
trin
gSki
lls
-Ski
llsTo
Offe
rLis
t : S
kills
TB-S
kills
ToR
eque
stLi
st :
Ski
llsTB
-ava
ilabi
lityL
ist
: Ava
ilabi
lity
-mem
ber :
Mem
ber
Mem
ber
-mem
berN
umbe
r : In
tege
r-u
ser :
Use
r-p
hoto
: Pho
toTB
-ref
Peo
pleL
ist :
Ref
Peo
ple
1
1
1
0..*
depe
nds
1
1
1
1..*de
pend
s
1
1
Ref
Peo
ple
-isM
embe
rTB
: B
oole
an-p
erso
n : P
erso
n
1
1..*
Ski
llsT
B
-cod
e : S
trin
g-c
odeD
escr
iptio
n : S
trin
g-s
kills
Cat
egor
y : S
kills
Cat
egor
y
Ad
min
istr
ato
r
-UR
L : S
trin
g-u
sern
ame
: Str
ing
-pas
swor
d : S
trin
g-la
stM
embe
rNum
ber :
Inte
ger
-em
ailT
empl
ate
: Em
ailT
empl
ate
Em
ailT
emp
late
-em
a ilF
rom
: S
trin
g-e
ma i
lSub
ject
: S
trin
g-h
ostS
MTP
: S
trin
g
1
1de
pend
s
Ser
vice
-cod
e : S
trin
g-d
ate :
Str
ing
-beg
inH
our :
Str
ing
-end
Hou
r : S
trin
g
Ser
vice
Req
uest
ed
-ser
vice
ToA
ccom
plis
h : S
ervi
ce-m
embe
rReq
uest
er :
Inte
ger
-mem
berP
rovi
der :
Inte
ger
1
1
depe
nds
Ski
llsC
ateg
ory
-cat
egor
y : S
trin
g-c
atD
escr
iptio
n : S
trin
g-s
kills
TBLi
st :
Ski
llsTB
-ena
bleC
ateg
ory
: Boo
lean
11.
.*
1
1..*
1
1..*
Per
son
-firs
tNam
e : S
trin
g-la
stN
ame
: Str
ing
-gen
der :
Sym
bol
-birt
hdat
e : S
trin
g-ID
Doc
umen
t : S
trin
g-n
atio
nalit
y : S
trin
g-p
rofe
ssio
n : S
trin
g-a
ddre
ssLi
st :
Add
ress
-nod
eLis
t : N
ode
-tel
epho
neLi
st :
Tele
phon
e-e
lect
roni
cAdd
ress
List
: E
lect
roni
cAdd
ress
Ad
dre
ss
-add
ress
Text
: S
trin
g-p
osta
lCod
e : S
trin
g-c
ity : S
trin
g-s
tate
: Str
ing
-cou
ntry
: Str
ing
-add
ress
Type
: S
ymbo
l
No
de
-UR
L : S
trin
g-lo
gica
lNam
e : S
trin
g-s
ubsc
riptio
nDat
e : S
trin
g-p
hysi
calA
ddre
ss :
Add
ress
1..*
0..*
1..*
1..*
1..*
1
Eld
erly
-per
son :
Per
son
-eld
erly
Dat
a : S
trin
g-d
isab
ilityL
ist :
Dis
abilit
y-p
hysi
cian
: P
erso
n
1
1..*
Rel
atio
nTyp
e
-rel
atio
nKin
d : S
ymbo
l-e
lder
lyP
erso
n : E
lder
ly-r
elat
ive
: Per
son
Ro
le
-rol
eNam
e : S
trin
g-d
escr
iptio
n : S
trin
g
1
1..*
1
1..*
1..*
1
Tel
epho
ne
-tel
epho
neN
umbe
r : S
trin
g-t
elep
hone
Exte
nsio
nNum
ber :
Str
ing
-tel
epho
neN
umbe
rTyp
e : S
ymbo
l
Ele
ctro
nicA
dd
ress
-ele
ctro
nicA
ddre
ssTe
xt : S
trin
g-e
lect
roni
cAdd
ress
Type
: Sym
bol
Use
r
-per
son :
Per
son
-use
rnam
e : S
trin
g-p
assw
ord :
Str
ing
-sub
scrip
tionD
ate
: Str
ing
-rol
eLis
t : R
ole
-pic
ture
: Pho
to
1
0..*
1
0..*
1 1
1
1
Pho
to
-imag
e : b
yte
1
1
Dis
abili
ty
-des
crip
tion :
Str
ing
-car
eToT
ake
: Str
ing
10.
.*
1
1
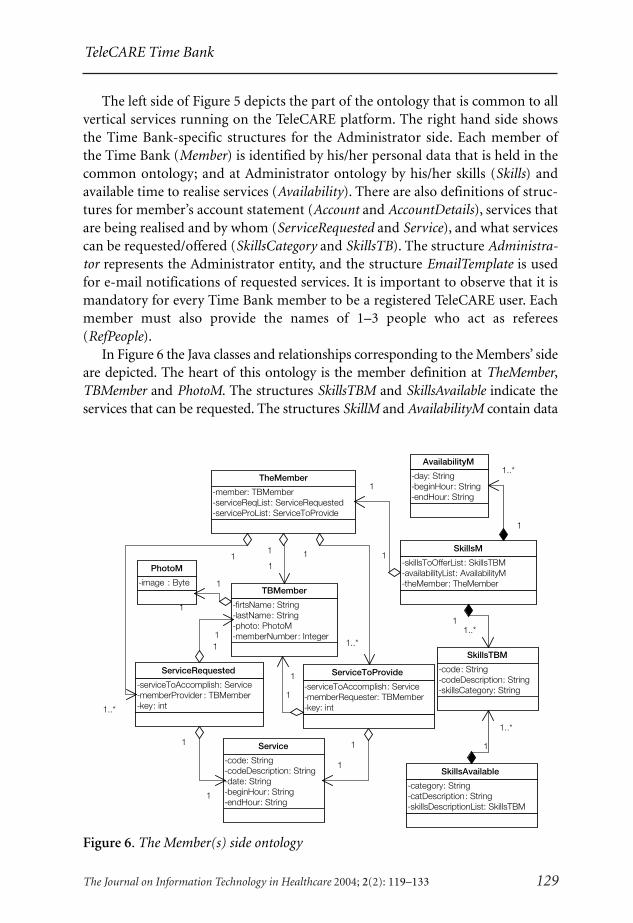
TeleCARE Time Bank
The Journal on Information Technology in Healthcare 2004; 2(2): 119–133 129
The left side of Figure 5 depicts the part of the ontology that is common to allvertical services running on the TeleCARE platform. The right hand side showsthe Time Bank-specific structures for the Administrator side. Each member ofthe Time Bank (Member) is identified by his/her personal data that is held in thecommon ontology; and at Administrator ontology by his/her skills (Skills) andavailable time to realise services (Availability). There are also definitions of struc-tures for member’s account statement (Account and AccountDetails), services thatare being realised and by whom (ServiceRequested and Service), and what servicescan be requested/offered (SkillsCategory and SkillsTB). The structure Administra-tor represents the Administrator entity, and the structure EmailTemplate is usedfor e-mail notifications of requested services. It is important to observe that it ismandatory for every Time Bank member to be a registered TeleCARE user. Eachmember must also provide the names of 1–3 people who act as referees(RefPeople).
In Figure 6 the Java classes and relationships corresponding to the Members’ sideare depicted. The heart of this ontology is the member definition at TheMember,TBMember and PhotoM. The structures SkillsTBM and SkillsAvailable indicate theservices that can be requested. The structures SkillM and AvailabilityM contain data
Figure 6. The Member(s) side ontology
SkillsTBM
-code : String-codeDescription : String-skillsCategory : String
AvailabilityM
-day : String-beginHour : String-endHour : String
SkillsM
-skillsToOfferList : SkillsTBM-availabilityList : AvailabilityM-theMember : TheMember
1
1..*
11..*
PhotoM
-image : Byte
TheMember
-member : TBMember-serviceReqList : ServiceRequested-serviceProList : ServiceToProvide
1
1
Service
-code : String-codeDescription : String-date : String-beginHour : String-endHour : String
TBMember
-firtsName : String-lastName : String-photo : PhotoM-memberNumber : Integer
ServiceRequested
-serviceToAccomplish : Service-memberProvider : TBMember-key : int
1
1..*
11
1
1
1
1
SkillsAvailable
-category : String-catDescription : String-skillsDescriptionList : SkillsTBM
1
1..*
1
1
ServiceToProvide
-serviceToAccomplish : Service-memberRequester : TBMember-key : int
1
1..*
1
1
1
1

Castolo, Ferrada & Camarinha-Matos
130 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
Figure 7. Requesting a service
Figure 8. Identifying a service provider

TeleCARE Time Bank
The Journal on Information Technology in Healthcare 2004; 2(2): 119–133 131
Figure 9. Issuing a cheque after a service is accomplished
Figure 10. Example of the Time Bank web interface: list of potential providers for arequested service

Castolo, Ferrada & Camarinha-Matos
132 The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
of skills and availability time of the local member, respectively. Finally the structuresService, ServiceRequested and ServiceToProvide track the service accomplishment.
Implementation AspectsThe Time Bank service prototype was developed in Java, on top of the TeleCAREmulti-agent platform14 that extends AGLETS (a multi-agent software develop-ment system) and integrates a distributed/federated information managementsubsystem. In Figures 7, 8 and 9 some of the user interfaces of the developedsystem are illustrated.
The functionalities provided can be accessed both via the TeleCARE userinterfaces (running in the multi-agent platform) or via a web browser. The latterneed to use the component Web Access Support of the TeleCARE architecture (seeFigure 1) developed by the TeleCARE partner Skill, Consejeros de Gestión. Theweb interface is shown in Figure 10.
For the implementation of this particular service other implementation ap-proaches (not necessarily agent-based) could have been adopted. It was, however,felt to be preferable to take advantage of the functionalities provided by theTeleCARE platform. The goal was also to have this service integrated with otherservices provided to the elderly care community. Thinking in terms of futuredevelopments, the use of agents and the underlying TeleCARE platform willalso facilitate the development of more intelligent matching and negotiationprocesses.
CONCLUSIONS
The Time Bank model seems particularly suitable to support the ‘active aging’concept and represents a good example of a virtual community. It is now com-monly accepted that while there is no simple solution to successfully living a longlife in a healthy manner, the concepts of active aging and remaining active andengaged in society are critical components in maintaining quality of life. Activelyengaged older persons are more likely to remain cognitively and physically stimu-lated, to nurture healthy interpersonal relationships and remain involved ascontributing members of their societies. The integration of a Time Bank supportservice within an elderly care system thus seems a promising contribution to:
– Encourage the sense of ‘being involved in/part of society’ and being useful.– Allowing elderly people to share and use their valuable experiences for the
benefit of the community.– Facilitate inter-generation interaction.
The mobile agents-based prototype system developed in the framework of theTeleCARE project illustrates a good set of functionalities to support such virtualcommunities. Nevertheless, it shall be noted that the actual success of field imple-mentation of the system depends on further progress on the elderly user interfaces,
133
HTI J
© The Journal on Information Technology in Healthcare 2004; 2(2): 119–133
TeleCARE Time Bank
namely its integration with TV sets and other home appliances, as well as thecreation of a new attitude towards elderly care by the various personnel andinstitutions involved in this domain.
ACKNOWLEDGEMENTS
This work was funded in part by the IST program of the European Commission. The authorsthank the contribution of the TeleCARE consortium members.
REFERENCES
1 Fernback J, Thompson B. Computer-mediated Communication and the American Collectivity:The Dimensions of Community within Cyberspace. Albuquerque, New Mexico: Interna-tional Communication Association, 1995.
2 Rheingold H. The Virtual Community. Boston: Addison-Wesley, 1993.3 Whatis?com, part of the TeachTarget Network of Enterprises IT Web Site. http://
whatis.techtarget.com/.4 Afsarmanesh H, Guevara-Masís V, Hertzberger LO. Virtual community support in Tel-
eCARE. PRO-VE ’03, 4th IFIP Working Conference on Virtual Enterprises. Lugano,Switzerland, 2003: 211–20.
5 Camarinha-Matos LM, Afsarmanesh H. Design of a virtual community infrastructure forelderly care. PRO-VE ’02, 3rd IFIP Working Conference on Infrastructures for VirtualEnterprises. Sesimbra, Portugal, 2002: 439–50.
6 Robinson J. The UK time bank movement. Transnational Seminar of the Banco de Tempo.Lisbon, Portugal, 2003.
7 Cahn E. No More Throw-Away People: The Co-production Imperative. Washington DC:Essential Books, 2000.
8 Méndez E. Public Policies on Conciliation of Working and Family Life & Time Banks.Transnational Seminar of the Banco de Tempo. Lisbon, Portugal, 2003.
9 U.S. Department of Health and Human Services. Active Aging: A Shift in the Paradigm.http://aspe.hhs.gov/daltcp/reports/actaging.htm.
10 Gordon K. Timekeeper for Time Dollars. http://www.timekeeper.org/timekeeper/.11 Camarinha-Matos LM, Castolo O, and Rosas J. A Multi-agent based Platform for Virtual
Communities in Elderly Care. ETFA-2003, 9th IEEE International Conference on EmergingTechnologies and Factory Automation. Lisbon, Portugal, 2003.
12 Bauer B, Müller JP, and Odell J. Agent UML: a formalism for specifying multiagent interac-tion. In Ciancarini P, Wooldridge M (eds.), Agent-Oriented Software Engineering. Berlin:Springer-Verlag, 2001: 91–103.
13 Stanford Medical Informatics. The Protégé Project. http://protege.stanford.edu/.14 Camarinha-Matos LM, Afsarmanesh H. A multi-agent based infrastructure to support
virtual communities in elderly care. Accepted for publication in International Journal ofNetworking and Virtual Organisations, forthcoming.

Call for Papers
The medical industry and healthcare service systems are increasingly having to rely on HealthInformation Standards to achieve the aims of providing efficient, high quality, evidence-based care. Standards are necessary to link regional healthcare core knowledge and for creatingElectronic Health Records to enable healthcare professionals to easily and readily accesspatient information. The 3rd Cross-Strait and Asia-Pacific HL7 Conference will focus on therole of Embracing Health Information Standards in the Commitment to Creating ElectronicHealth Records. The Conference will promote the development of the medical and healthcareindustry of the Asia-Pacific Region through the participation of physicians, scientists andexperts from government and industry. The unique Conference atmosphere will facilitatemulti-disciplinary exchange of ideas, discussion and the creation of effective strategies tomeet the demands and needs of future healthcare.
Topics covered will include, but are not limited to, the following
1 Healthcare Information Standards and Applications2 Electronic Health Insurance Claims3 Healthcare Smart Cards4 Mobile Healthcare Transmission5 Disease Surveillance6 Electronic Medical Records7 Clinical Document Architecture8 Healthcare Information Security and Privacy9 Clinical Decision Support10 Knowledge Management and e-Learning11 Cross-Strait Health Information Development12 Medical Information Management13 Healthcare Information Management14 Other Related Fields
Key Dates
• Submission Deadline: May 1, 2004• Notification of Acceptance: May 24, 2004• Submission of Final Version: June 6, 2004• Conference: July 9–11, 2004

Instructions for Preparation and Submission of Papers
1. Submitted papers should be in English and structured under the following headings:Topic of Paper, Introduction, Materials and Methods, Results, Discussion and Conclu-sion. Papers should be typed and accompanied by an Abstract not exceeding 500 words.The paper itself should not exceed 12 A4 pages (Times New Roman size 12 font, doublespaced), including tables, graphs and references. Detailed instructions and sample papersmay be downloaded from http://www.hl7.org.tw.
2. The affiliated institutes of all authors should be stated. The corresponding author shouldbe identified and an e-mail address provided for contact.
3. Papers must not have been previously published.4. Accepted papers will be posted at http://www.hl7.org.tw on May 24, 2004. Notification of
Acceptance, Scheduled Presentation Time and Detailed Contents of the Conference will besent to the corresponding author by e-mail and Registered Mail on May 31, 2004.
5. Authors are responsible for the accuracy of their papers and will be required to sign a“Publication Confirmation and Authorization” form. This should be returned to theConference Secretariat by fax together with the final version of the paper before June 6,2004.
6. To avoid interruptions in the proceedings due to withdrawal of presentations, acceptedpapers will only be placed in the Conference Program after presenters have paid theregistration fee for the Conference.
Presentation of Accepted Papers
The time allocated for individual presentations is 20 minutes (15 minutes for the presentationitself and 5 minutes for discussion). The Conference organizers will provide all necessary audio-visual equipment. Selected papers from the Conference will be published in The Journal onInformation Technology in Healthcare.
Paper Submission
The deadline for submission of papers is May 1, 2004. All papers should be submittedelectronically via email to the Conference Secretariat at [email protected] or throughthe online paper submission system at http://www.hl7.org.tw. Manuscripts must be submittedin Microsoft Word format, files submitted in other formats will not be accepted.

The Health Informatics Society of Australia (HISA) extends a warm invitation to the 12th annualHIC2004 conference. The conference attracts key delegates and vendors involved in all health sectors.
HIC 2004’s theme of Let’s Make a Difference relates to the question of value.
� How can we work together to increase the positive impacts that health ICT canmake in both health practice and patient care?
� How do we ensure those improvements are achievable and sustainable both inpractice and management?
The theme is action orientated and improvement focused. The following table identifies the sub-themes that will feature in the conference program design.
The theme applies at many levels, e.g. for individual workers in health, your profession, yourorganization, your region, your state, your country, etc, as well as at the consumer, practice,management, research and educational levels.
Building the Case Making IT Happen Gaining the Value
� Research � Design and Planning � Realising Benefits� Concept Development � Partnering Options � Managing Change� Business Case � Project/Program � Governance� Cost/Benefit Analysis Management � Accountability� Stakeholder Buy-in � Technology Selection � Evaluation
� Proving the Concept� Integration
For all Conference information please visit www.hic.org.au.Inquiries to: [email protected]

HINZ Conference and Exhibition 2004
“TOWARDS A HEALTHY NATION”Population Health ���� Primary Care ���� Workforce
Management
27th-29th July, 2004
Wellington Convention Centre
Call for Papers
You are invited to submit a paper for consideration by the Scientific Program Committee for
inclusion in the HINZ 2004 conference program, and to be published in the conference
proceedings.
Closing date – 30 April 2004.
There are five possible submission types:
• Scientific Papers
These papers report on research, development, and leading edge application of informatics
in health care, addressing the theme of the Conference. Scientific papers length is limited
to 4 to 8 pages long.
• Future Vision Papers
These papers address the future role of information and communication technologies in
supporting knowledge management and organizational learning in healthcare. Future Vision
papers length is limited to 4 to 8 pages long.
• Review Papers
These papers highlight the current state-of-the-art of some aspect dealing with the main
theme of the Conference, and present a thorough synthesis of key research and application
issues. Review papers length is limited to 4 to 8 pages long.
• Short Papers
These papers report on current experiences in Health IT development, procurement,
implementation and evaluation. They serve as medium for interchange of personal and
organisational experiences with Health IT. Short papers length is limited to 3-4 pages long.
• Posters
Posters are intended as a medium for presenters to report new or novice Health IT ideas
and experiences. Authors are required to submit a one-page description of the themes and
contents of the poster presentation. If accepted, authors are required to prepare poster
size presentation materials for presentation during the conference. Authors will have the
opportunity to discuss their presentations and ideas with delegates during coffee and lunch
breaks. The one-page poster theme and content will be published in the poster section of
the conference proceedings.
Conference papers considered highly relevant by the scientific program committee will be
submitted, on behalf of author(s) to the editorial board of both the Health and Informatics
Online, and the Journal on Information Technology in Healthcare for consideration in a special
2004 edition publication.
Author's Kit
Everything you need know to prepare you paper submission is explained at
www.hinz.org.nz/hinz2004/authorguide
On the site you will find instructions for authors and a paper template.
All submissions need to be made electronically, either in Word or “rtf” formats. Submissions
not following the HINZ 2004 template or not submitted electronically will be rejected.
Enquiries should be made by contacting HINZ – [email protected]

CALL FOR PAPERS
The journal aims to educate healthcare pro-fessionals on the use of IT in healthcare,and to provide them with objective evi-dence of the benefits of IT in clinical prac-tice. To achieve these aims the journal seeksto publish the following types of papers:
(i) Articles that educate healthcare pro-fessionals on the principles and prac-tice of the use of IT in healthcare.Articles should be written in a formatthat can be understood and appreci-ated by readers without in-depthknowledge of computers or medicalinformatics.
(ii) Articles that provide practical advicefor selecting and implementing IT so-lutions into clinical practice and/oroptimising use of existing IT systems.
(iii) Papers that provide objective evidenceof the benefits of IT in clinical prac-tice.
All articles submitted to the journal un-dergo peer review. To ensure their interna-tional relevance, and that they can beunderstood and appreciated by an interna-tional readership, at least 2 reviewers foreach article are not from the same countryas the author(s). In addition, for researchpapers, at least 2 reviewers are clinicians.
If you would like to submit an article orpaper to the journal, please see the ‘Instruc-tions for Authors’.
ONLINE COMMUNITY
http://www.communityzero.com/JITH
An online community has been created forreaders of the journal to enable them toexchange ideas, knowledge and experience.Among its features members can:
Access papers published in the journalParticipate in discussionsVote in pollsPost notices of meetings
Membership to the community is free. Thewebsite can be explored by clicking on thePreview button and following the instruc-tions.
If you have any questions or would likefurther information about the online com-munity, please e-mail [email protected].
REVIEWERS
The journal is dependent on reviewers toensure the quality and originality of thepapers it publishes. If you would like to actas a reviewer for papers submitted to thejournal, please e-mail your details and areasof interest to [email protected].
HTI J
HTI J

INSTRUCTIONS FOR AUTHORS
Aims and Scope: The Journal on Information Technology in Healthcare aims to im-prove the quality and safety of patient care, by encouraging and promoting the use ofInformation Technology (IT) in healthcare. The journal acts as a medium for theinternational exchange of knowledge and experience of the benefits of IT in health-care. It principally publishes papers that objectively demonstrate clinical and costbenefits of IT in healthcare. It also publishes papers that offer practical advice forselecting and implementing IT systems.
Submission of Papers: Papers in keeping with the aims of the journal should besubmitted to the Editor. The journal will accept papers submitted by e-mail [email protected]. Manuscripts submitted by post should be typed, with double spac-ing, on one side of A4. One copy of the typescript and illustrations, together with anexact matching copy on floppy disk or CD-ROM should be sent to:
Clyde Saldanha, Editor, The Journal on Information Technology in Healthcare, 72Churston Drive, Morden, Surrey, SM4 4JQ, UK.
A copy of the manuscript should be retained as insurance against loss in the mail.
Acknowledgements of Submissions: All submissions will be acknowledged on receiptby e-mail to the corresponding author. Further correspondence will be made asappropriate.
Abstract: Research papers should have a structured abstract with the following head-ings: Objective, Design, Setting, Methods, Results, Conclusion.
Style and Content of Manuscript: Papers should be set out under the headings:Introduction, Methods, Results and Discussion. They should as far as possible bewritten in a format that can be understood by readers who do not have in-depthknowledge of computers or medical informatics. Papers should ideally contain suffi-cient information for interested readers to be able to evaluate the feasibility andcost-effectiveness of implementing a described system into their practice. Studiesshould abide by high ethical standards, and if appropriate, should have receivedethical approval from the local institutional human research committee.
Use British rather than American spelling throughout the manuscript.
References: References should be identified by Arabic superscripts in the text andnumbered in the order in which they appear in the paper. They should be listed at theend of the paper in the order that they are first cited in the text. Give the full namesand initials of all authors, unless there are more than six, when only the first three
The Journal onInformation Technology
in HealthcareHT
I J

should be given, followed by et al. Names should be followed by the title of the article;the title of the journal; the year of publication; the volume number and the first andlast page numbers. Journal titles should be given in full or abbreviated according tothe style of Index Medicus. Titles of books should be followed by the place of publica-tion; the publisher and the year.
Peer Review: All papers submitted to The Journal on Information Technology in Health-care undergo a peer review process. On the basis of the reviewers’ responses, paperswill be rejected, accepted subject to revision or accepted unconditionally. Rejectedmanuscripts will not be returned to authors unless expressly requested.
Acceptance of Papers: On acceptance the Editor retains the right to make stylisticchanges, decide on the date of publication and shorten material if necessary.
Final versions of all accepted manuscripts must be submitted in electronic format.
Proofs: Authors are sent one copy of the proofs. Corrections should be confined totypographical errors or matters of accuracy. Extensive amendments are not permissi-ble. Authors should return proofs as soon as possible and not later than the date givenin the covering letter.
Reprints: These are available if ordered at the time of returning the proofs. Details ofcharges will be sent with the proofs.
Copyright: All material received by The Journal on Information Technology in Health-care are assumed to be submitted exclusively and not to have been previously publishedin the English language.
The author(s) bear(s) the responsibility for checking whether material submittedis subject to copyright or ownership rights; for example in the use of diagrams ortables. If a submission is finally published the copyright becomes that of The Journalon Information Technology in Healthcare, and permission for any reproduction mustbe sought from the Editor.
Dual Publication: A paper is accepted for publication on the understanding that it hasnot been submitted simultaneously to another journal in the English language.
Accuracy and Liability: A contribution is accepted on the strict understanding that itsauthor(s) is (are) responsible for the accuracy of all information contained in thecontribution and that references to named people and/or organisations are bothaccurate and without libelous implications.
Conflict of Interest: If authors have received payment/substantial gifts from compa-nies whose products are featured in the paper, or have a commercial interest in thehardware and/or software used for the study, this must be acknowledged in a state-ment at the end of the text.
HTI J
❏ Please enter my 2004 subscription toThe Journal on Information Tech-nology in Healthcare (ISSN 1479-649X), for Volume 2 (6 issues).
SUBSCRIPTION RATES
Institutional Individual
Great Britain £120 £100Europe €200 €180USA US$220 US$180Rest of the world £135 £115
❏ I enclose cheque/ banker’s draftmade payable to The Journal onInformation Technology inHealthcare.
❏ Please invoice me.
❏ I have arranged payment by BankersAutomated Credit Service (BACS) toBarclays Bank, 8 Alexandra House,Wimbledon, London SW19 7LA.Sort Code 20-96-89Account Number 00728837Name of account: The Journal onInformation Technology inHealthcare
Name:
Address:
Postcode:
Country:
Tel:
Fax:
E-mail:
PLEASE POST TO:
SubscriptionsThe Journal on Information Technologyin Healthcare72 Churston DriveMordenSurreySM4 4JQUnited Kingdom
E-mail : [email protected] : +44 (0)870 130 1572
The Journal onInformation Technology
in HealthcareHT
I JSubscription To


Copyright © 2022 FDOKUMEN