Development of Telemedicine and Telecare over Wireless Sensor Network
8
Development of Telemedicine and Telecare over Wireless Sensor Network Shuo-Jen Hsu 1 , Hsin-Hsien Wu 1 , Shih-Wei Chen 2 , Tsang-Chi Liu 3 , Wen-Tzeng Huang 3 , Yuan- Jen Chang 4 , Chin-Hsing Chen 4 , You-Yin Chen 1,* 1 Department of Electrical and Control Engineering, National Chiao Tung University, ROC 2 Department of Electrical Engineering, National Taiwan University, ROC 3 Department of Electrical Engineering, National Taipei University of Technology, ROC 4 Department of Management Information Systems, Central Taiwan University of Science and Technology * [email protected] Abstract Telemedicine & Telecare aided by wireless sensor network (WSN) has recently become a health-caring trend in the future. However, the low data rate of WSN limited the acceptable quality of service. Researches [1-6] adopted ZigBee-based WSN to implement a platform and/or a telecare system. However, the capacity problem due to low data rate characteristic has not been addressed. Our research proposed an arrhythmia-aware telecare system and a new DSP- based WSN platform, enabling good digital signal processing performance in ZigBee-based WSN. Proved by simulations and several real tests, combination of the proposed platform and system can provide a more bandwidth-conserving and reliable telecare system, with lower wireless traffic jam and higher stability. Keywords: Telemedicine, Wireless Sensor Network, ZigBee, DSP, Discrete Wavelet Transform 1. Introduction Telecare has recently become a health-caring trend in the future. People can receive instant healthcare services, such as according advice abnormal vital signals were detected in a hospital, rest home, or at home, where a telecare system is provided. Aided with WSN technologies, the ubiquitous and flexibility of telecare systems can be strengthened with the network configuration. WSN facilitates the telecare system with a center-control feature, which is suitable to deliver the service to a group of people, and to control the delivering of packets well-ordered. IEEE 802.15.4 and ZigBee, proposed to be the standard of WSN by IEEE and ZigBee alliance, gained much attention because of the low power consumption, low cost, easy deployment, and various network topologies. However, the low data rate has become the limitation of the service’s acceptable quality. In [7], for example, 24 kbps was taken as the required data rate for ECG monitoring application, but IEEE 802.15.4 could at most provide 240 kbps. That indicated a maximum of 10 devices could be connected to telecare system to provide ECG monitoring. Such estimation is far behind the goal of WSN-based telecare system, which aimed to deliver the service to an unknown amount of users. Moreover, ECG monitoring service is the least requirement of a well-designed telecare system since ECG is the major vital signal which strongly reflects human body status in an emergency. In [8], evaluation of ECG monitoring traffic in WSN showed that the traffic of a node with no data processing was 4 times larger than one with source coding to data. Furthermore, reduced traffic also lowered the probability of packet collision. As ECG generates more data than other vital signals, a low delay, low computational complexity, and low distortion ECG compression algorithm is required for a telecare system using ZigBee-based WSN. However, compression algorithms have to deal with many digital signal processes, resulting in unacceptable delay that affects the real-time application with a microcontroller- based platform. Meanwhile, many powerful ECG compression algorithms [9-12] were wavelet-based, requiring longer computation time when performed by a microcontroller. Moreover, no evaluations of these algorithms have been conducted on any embedded platform to prove the real-time characteristics. Resent researches [1-6] have adopted a ZigBee- based WSN to implement a telecare system. In these researches, the development of a platform and/or a telecare system was proposed and tested. Nevertheless, none studied the bandwidth problem in WSN with system design, which was related to low data rate. The platforms designed/used in [1-6] were all microcontroller-based. 2008 International Conference on Multimedia and Ubiquitous Engineering 978-0-7695-3134-2/08 $25.00 © 2008 IEEE DOI 10.1109/MUE.2008.105 597
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Development of Telemedicine and Telecare over Wireless Sensor Network

Development of Telemedicine and Telecare over Wireless Sensor Network
Shuo-Jen Hsu1, Hsin-Hsien Wu
1, Shih-Wei Chen
2, Tsang-Chi Liu
3, Wen-Tzeng Huang
3, Yuan-
Jen Chang4, Chin-Hsing Chen
4, You-Yin Chen
1,*
1Department of Electrical and Control Engineering, National Chiao Tung University, ROC 2Department of Electrical Engineering, National Taiwan University, ROC
3Department of Electrical Engineering, National Taipei University of Technology, ROC 4Department of Management Information Systems, Central Taiwan University of Science and
Technology *[email protected]
Abstract
Telemedicine & Telecare aided by wireless sensor network (WSN) has recently become a health-caring trend in the future. However, the low data rate of WSN limited the acceptable quality of service. Researches [1-6] adopted ZigBee-based WSN to implement a platform and/or a telecare system. However, the capacity problem due to low data rate characteristic has not been addressed. Our research proposed an arrhythmia-aware telecare system and a new DSP-based WSN platform, enabling good digital signal processing performance in ZigBee-based WSN. Proved by simulations and several real tests, combination of the proposed platform and system can provide a more bandwidth-conserving and reliable telecare system, with lower wireless traffic jam and higher stability. Keywords: Telemedicine, Wireless Sensor Network,
ZigBee, DSP, Discrete Wavelet Transform
1. Introduction
Telecare has recently become a health-caring trend
in the future. People can receive instant healthcare
services, such as according advice abnormal vital
signals were detected in a hospital, rest home, or at
home, where a telecare system is provided.
Aided with WSN technologies, the ubiquitous and
flexibility of telecare systems can be strengthened with
the network configuration. WSN facilitates the telecare
system with a center-control feature, which is suitable
to deliver the service to a group of people, and to
control the delivering of packets well-ordered. IEEE
802.15.4 and ZigBee, proposed to be the standard of
WSN by IEEE and ZigBee alliance, gained much
attention because of the low power consumption, low
cost, easy deployment, and various network topologies.
However, the low data rate has become the limitation
of the service’s acceptable quality. In [7], for example,
24 kbps was taken as the required data rate for ECG
monitoring application, but IEEE 802.15.4 could at
most provide 240 kbps. That indicated a maximum of
10 devices could be connected to telecare system to
provide ECG monitoring. Such estimation is far behind
the goal of WSN-based telecare system, which aimed
to deliver the service to an unknown amount of users.
Moreover, ECG monitoring service is the least
requirement of a well-designed telecare system since
ECG is the major vital signal which strongly reflects
human body status in an emergency.
In [8], evaluation of ECG monitoring traffic in
WSN showed that the traffic of a node with no data
processing was 4 times larger than one with source
coding to data. Furthermore, reduced traffic also
lowered the probability of packet collision. As ECG
generates more data than other vital signals, a low
delay, low computational complexity, and low
distortion ECG compression algorithm is required for a
telecare system using ZigBee-based WSN. However,
compression algorithms have to deal with many digital
signal processes, resulting in unacceptable delay that
affects the real-time application with a microcontroller-
based platform. Meanwhile, many powerful ECG
compression algorithms [9-12] were wavelet-based,
requiring longer computation time when performed by
a microcontroller. Moreover, no evaluations of these
algorithms have been conducted on any embedded
platform to prove the real-time characteristics.
Resent researches [1-6] have adopted a ZigBee-
based WSN to implement a telecare system. In these
researches, the development of a platform and/or a
telecare system was proposed and tested. Nevertheless,
none studied the bandwidth problem in WSN with
system design, which was related to low data rate. The
platforms designed/used in [1-6] were all
microcontroller-based.
2008 International Conference on Multimedia and Ubiquitous Engineering
978-0-7695-3134-2/08 $25.00 © 2008 IEEEDOI 10.1109/MUE.2008.105
597

This paper established a prototype of a DSP
platform which enables a good digital signal
processing performance in ZigBee-based WSN, and an
arrhythmia-aware telecare system. Discrete wavelet
transform (DWT) and enhanced set partitioning in
hierarchical tree (ESPIHT) [12] were adopted and
modified as the ECG compression algorithm while
transmitting ECG, since it showed excellent
performance and low computational complexity. Our
system reduced the possibility of traffic jam and packet
collision in the WSN. Compared with previous works
[1-6], simulation and testing with several indices, our
system provided a solution for a more bandwidth-
conservable, stable, and reliable WSN-based telecare
system.
2. System Architecture
Figure 1 showed the system architecture of our
proposed system. The hierarchical tree protocol was
adopted. ECG signal of a man which carried a ZigBee
end device would be continuously analyzed by the end
device. If abnormal ECG signals were detected, the
device would immediately locate a wireless channel,
and send the ECG signal to the ZigBee coordinator via
routers. Once the alarm was received, the operator
would respond by sending a telecare service agent for
rescue or check his status for further information. Note
that the ECG detection was designed to be self-
activated, while posture detection was an auxiliary
information to be activated passively.
2.1. Functionality
When an end device was turned on, it would
automatically search an existed WSN to find a suitable
router to join the WSN. If more than one router was
detected, the end device would choose the one with the
highest received signal strength index (RSSI) as its
parent, and send request to joining. Once the end
device receive a network address, indicating the
request was accepted, the end device would send an
authentication packet with the network address and a
pre-loaded authentication key to the coordinator of the
WSN. The end device would be kept in pending until
the coordinator authenticated the key, and a permission
command is sent back to the end device. Before the
new device has been approved, the parent router
would not respond to any request from the end device.
Upon receiving the permission packet, the end device
would sample the ECG sensor every second at 256 Hz.
The QRS/RR detection based on Pan-Tompkins
algorithm would then begin to calculate the QRS, RR,
and average RR width, which would be used to
indicate any occurrence of an arrhythmia. The
Bradycardia, Tachycardia, Asystole, Ventricular
Fibrillation, Skipped Beat, Premature Ventricular
Contraction (PVC), R-on-T Phenomenon, Bigeminy,
Trigeminy, and Interpolated PVC arrhythmias or
normal beat would be determined by the criterions
composed by the three indices [13]. After the QRS/RR
detection, if one of the arrhythmias were detected, a
buzzer on the end device would sound and the sampled
ECG would be transmitted. The ECG would be first
compressed at compression ratio (CR) 8 by our
modified ECG compression algorithm, and then
transmitted to the coordinator via routers. If the
posture query command was received by the end
device, the end device would locate one byte from
each axis and transmit it to the coordinator. Combining
the three values, the posture of the end device could be
Figure 1: System Architecture
598
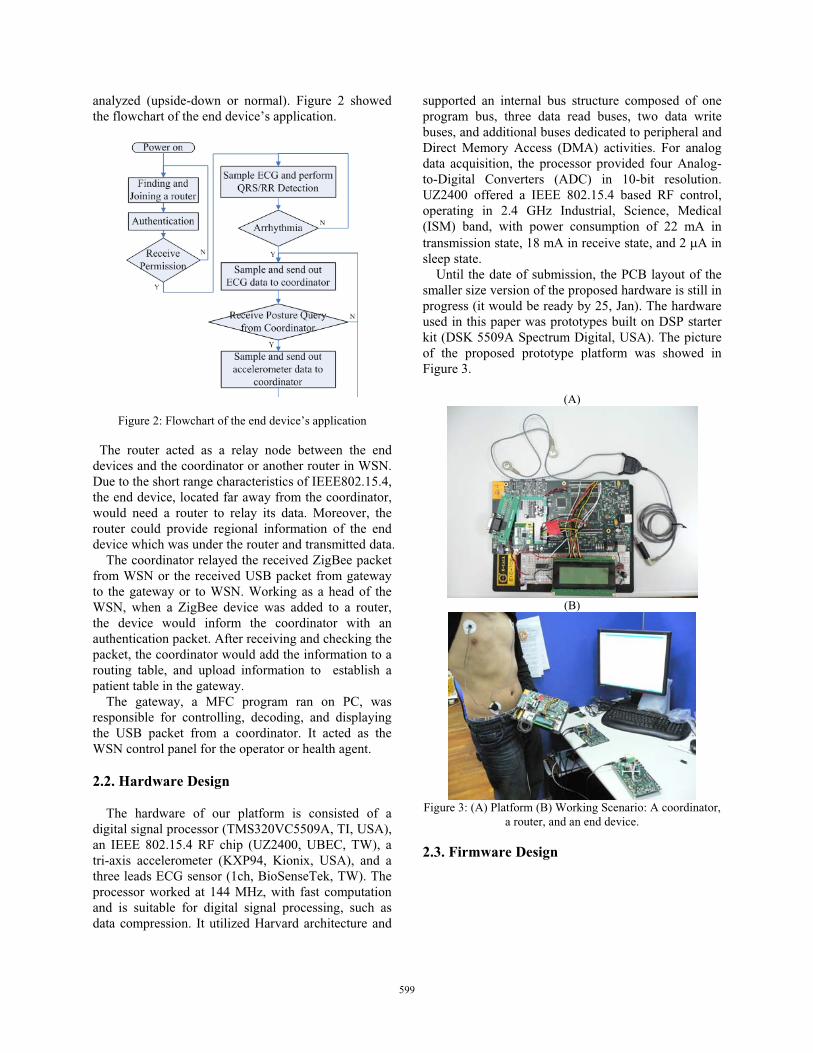
analyzed (upside-down or normal). Figure 2 showed
the flowchart of the end device’s application.
Figure 2: Flowchart of the end device’s application
The router acted as a relay node between the end
devices and the coordinator or another router in WSN.
Due to the short range characteristics of IEEE802.15.4,
the end device, located far away from the coordinator,
would need a router to relay its data. Moreover, the
router could provide regional information of the end
device which was under the router and transmitted data.
The coordinator relayed the received ZigBee packet
from WSN or the received USB packet from gateway
to the gateway or to WSN. Working as a head of the
WSN, when a ZigBee device was added to a router,
the device would inform the coordinator with an
authentication packet. After receiving and checking the
packet, the coordinator would add the information to a
routing table, and upload information to establish a
patient table in the gateway.
The gateway, a MFC program ran on PC, was
responsible for controlling, decoding, and displaying
the USB packet from a coordinator. It acted as the
WSN control panel for the operator or health agent.
2.2. Hardware Design
The hardware of our platform is consisted of a
digital signal processor (TMS320VC5509A, TI, USA),
an IEEE 802.15.4 RF chip (UZ2400, UBEC, TW), a
tri-axis accelerometer (KXP94, Kionix, USA), and a
three leads ECG sensor (1ch, BioSenseTek, TW). The
processor worked at 144 MHz, with fast computation
and is suitable for digital signal processing, such as
data compression. It utilized Harvard architecture and
supported an internal bus structure composed of one
program bus, three data read buses, two data write
buses, and additional buses dedicated to peripheral and
Direct Memory Access (DMA) activities. For analog
data acquisition, the processor provided four Analog-
to-Digital Converters (ADC) in 10-bit resolution.
UZ2400 offered a IEEE 802.15.4 based RF control,
operating in 2.4 GHz Industrial, Science, Medical
(ISM) band, with power consumption of 22 mA in
transmission state, 18 mA in receive state, and 2 �A in
sleep state.
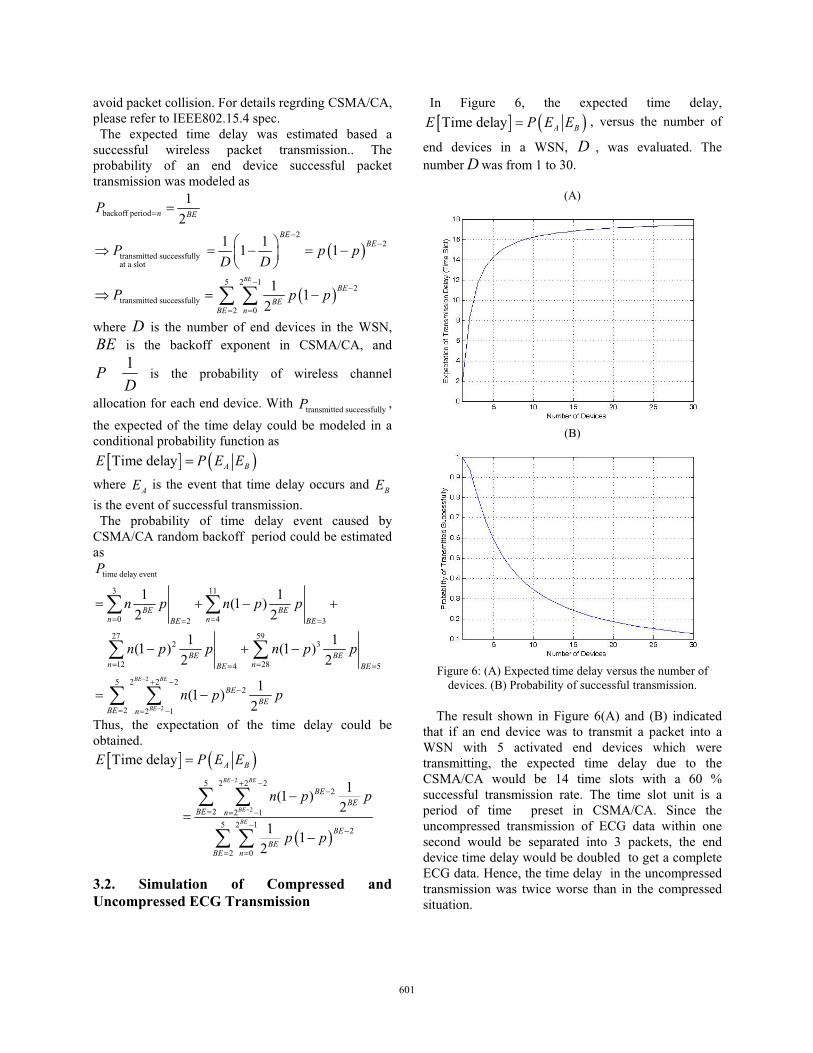
Until the date of submission, the PCB layout of the
smaller size version of the proposed hardware is still in
progress (it would be ready by 25, Jan). The hardware
used in this paper was prototypes built on DSP starter
kit (DSK 5509A Spectrum Digital, USA). The picture
of the proposed prototype platform was showed in
Figure 3.
(A)
(B)
Figure 3: (A) Platform (B) Working Scenario: A coordinator,
a router, and an end device.
2.3. Firmware Design
599

Figure 4: Firmware Architecture on Each Device
ZigBee, an ultra-low power and low data-rate
wireless personal area network standard, was proposed
based on IEEE802.15.4 medium access control (MAC)
and physical (PHY) layers in 2003 and was revised in
2006. The MAC, network (NWK), and application
service (APS) layers were implemented on every
device, providing a wireless communication feature. A
real time operation system (RTOS) (OSEck 3.2.1,
ENEA, UK) was ported on the board. It controlled the
context-switch of each layer, and managed memory
and interruptions. Figure 4 showed the firmware
architecture on each device.
2.4. ECG Compression Algorithm
Low-band coefficients subtraction was proposed to
be an adjusting component in the ECG compression
algorithm composed by DWT and ESPIHT [12]. It was
suitable for embedded systems because of its low
computational complexity and excellent performance.
The block diagram of the proposed modification was
showed in Figure 5.
Figure 5: ECG Compression Algorithm Diagram
After ECG went through the fourth level DWT, we
observed the absolute value of the approximation
coefficients were always about 10 times bigger than
the first level’s detail coefficients, and about 100 times
bigger than other levels’ detail coefficients. These
large approximation coefficients would dominant the
output bitstream, since ESPIHT gave more bits for
large number. In this case, the minimum value of the
absolute value of the sixteen approximation
coefficients was subtracted from the approximation
coefficients, and was directly passed to the packetize
procedure. Thus, the dominant wavelet approximation
coefficients would be reduced before being sent into
ESPIHT,generating shorter output bitstreams. For
reconstruction, the value was simply added back to the
approximation coefficients after depacketizing and
invers ESPIHT procedures. In addition, , if the same
CR was fixed, ESPIHT would be more sensitive on the
smaller thresholds/coefficients and would encode
much smaller changes of the ECG waveform, which
resulting in less distortion after reconstruction.
Compared without the non-modified compression
algorithm, the bitstream sent between decomposition
and reconstruction side was shorter and conserved
more channel bandwidth. For details of the DWT and
ESPIHT, please refer to [12].
3. Mathematical Model and Simulation of Transmission Time Delay
In consideration of realistic situations, we tried to
build a mathematical model and simulate the average
transmission time delay of ECG data within one
second that would be suffered by an end device which
transmits the data either in compressed ECG
transmission or in uncompressed ECG transmission.
The relation between the expected time delay and the
number of end devices in a WSN was evaluated. The
following were the assumptions before mathematical
modeling:
(1). ACK frames were out of considering for simple.
(2).The probability of successful wireless channel
allocation for each device is the same, i.e., uniform
distribution model was used as the probability density
function of each device while transmitting a frame.
3.1. Math Model of Transmission Time Delay
The mathematical modeling began at CSMA/CA,
which is used in wireless communication system to
600
avoid packet collision. For details regrding CSMA/CA,
please refer to IEEE802.15.4 spec.
The expected time delay was estimated based a
successful wireless packet transmission.. The
probability of an end device successful packet
transmission was modeled as
� �
� �
backoff period
22
transmitted successfully at a slot
5 2 12
transmitted successfully
2 0
1
2
1 11 1
11
2
BE
n BE
BEBE
BE
BEBE n
P
P p pD D
P p p
�
��
��
� �
�
� � � � � � ��
� �� �where D is the number of end devices in the WSN,
BE is the backoff exponent in CSMA/CA, and
1P
D is the probability of wireless channel
allocation for each end device. With transmitted successfully
P ,
the expected of the time delay could be modeled in a
conditional probability function as
� � � �Time delay A BE P E E�
where AE is the event that time delay occurs and BEis the event of successful transmission.
The probability of time delay event caused by
CSMA/CA random backoff period could be estimated
as
2
2
time delay event
3 11
0 42 3
27 592 3
12 284 5
5 2 2 22
2 2 1
1 1(1 )
2 2
1 1 (1 ) (1 )
2 2
1(1 )
2
BE BE
BE
BE BEn nBE BE
BE BEn nBE BE
BEBE
BE n
P
n p n p p
n p p n p p
n p p�
�
� �� �
� �� �
� ��
� � �
� � � �
� � �
� �
� �
� �
� �Thus, the expectation of the time delay could be
obtained.
� � � �
� �
2
2
5 2 2 22
2 2 1
5 2 12
2 0
Time delay
1(1 )
2
11
2
BE BE
BE
BE
A B
BEBE
BE n
BE
BEBE n
E P E E
n p p
p p
�
�
� ��
� � ��
�
� �
�
��
�
� �
� �
3.2. Simulation of Compressed and Uncompressed ECG Transmission
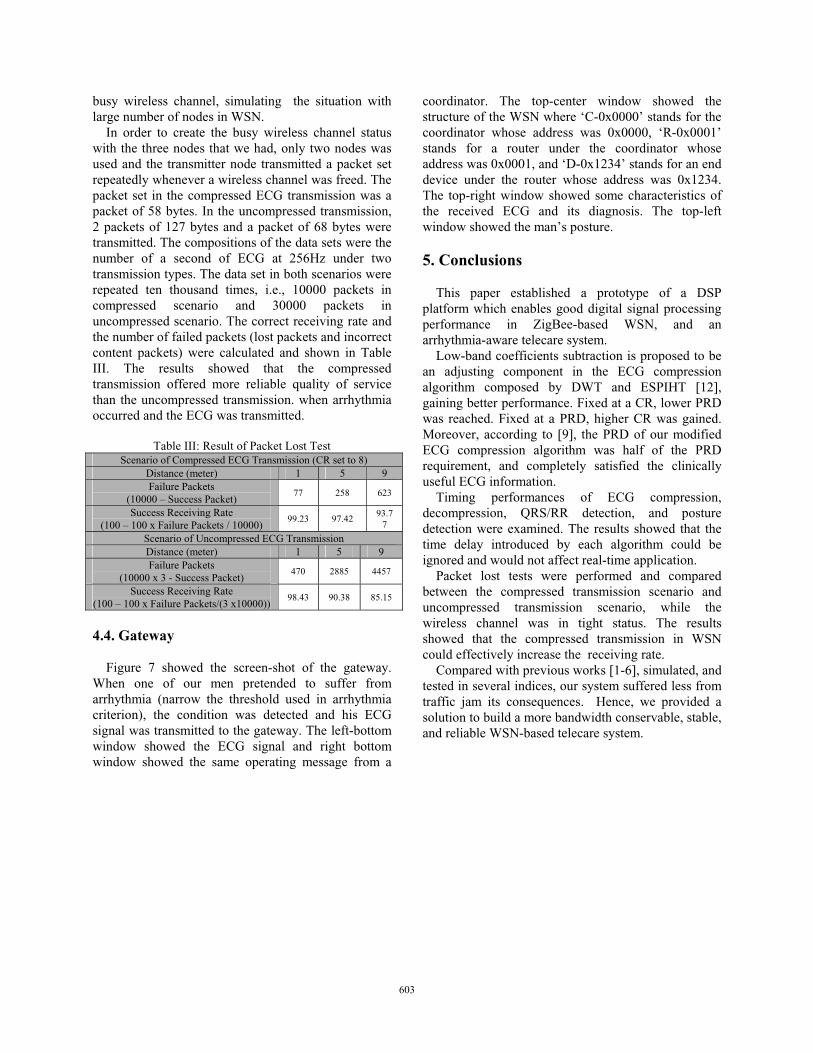
In Figure 6, the expected time delay,
� � � �Time delay A BE P E E� , versus the number of
end devices in a WSN, D , was evaluated. The
number D was from 1 to 30.
(A)
(B)
Figure 6: (A) Expected time delay versus the number of
devices. (B) Probability of successful transmission.
The result shown in Figure 6(A) and (B) indicated
that if an end device was to transmit a packet into a
WSN with 5 activated end devices which were
transmitting, the expected time delay due to the
CSMA/CA would be 14 time slots with a 60 %
successful transmission rate. The time slot unit is a
period of time preset in CSMA/CA. Since the
uncompressed transmission of ECG data within one
second would be separated into 3 packets, the end
device time delay would be doubled to get a complete
ECG data. Hence, the time delay in the uncompressed
transmission was twice worse than in the compressed
situation.
601

4. Results and Discussions
The following results were examined using our three
prototype platforms, which took each role of end
device, router, and coordinator. The extensive, on-the-
spot deployment experiment will be conducted upon
the arrival of the new version platform (25, Jan).
4.1. Timing Performance of ECG Compression Algorithm, QRS/RR Detection Algorithm, and Posture Detection
Table I: Time Performance of ECG Compression
Input
Bytes
Output
Bytes CR
Compression
Time (ms)
Decompression
Time (�s)
51 5.02:1 8.28 240
42 6.09:1 8.12 179
36 7.11:1 8.01 133
32 8.00:1 7.92 126
28 9.14:1 7.87 114
25 10.24:1 7.8 110
21 12.19:1 7.75 99
18 14.22:1 7.7 96
16 16.00:1 7.59 94
14 18.29:1 7.61 91
256
13 19.69:1 7.60 89
Table II: Time Performance of QRS/RR Detection Algorithm
and Posture Detection
Average Time Consumption (�s)
QRS/RR Detection 972
Posture Detection 1
In Table I, the timing performance of ECG
compression, which began when arrhythmia occurs,
and decompression algorithm, were examined on
TMS320VC5509A at 144 MHz and on PC, AMD
Sempron 2800+ at 1.61 GHz respectively. Table I
showed that the time consumed in compression was
approximately 7-8 ms. Since the sampling rate of ECG
of an end device was 256 Hz, a 7-8 ms delay between
two sample periods due to compression algorithm
would result in losing 2 sample points of ECG.
However, it would not affect ECG analysis on the
gateway. Table II showed the time spent on QRS/RR
detection and posture detection.
4.2. CR versus PRD of ECG Compression
Figure 6: Comparison between the compression algorithms which
utilized lowest subband subtraction and non-utilized one
Figure 6 showed the comparison between the
compression algorithms which utilized lowest subband
subtraction and non-utilized one. CR and PRD is
formulated as
sidencompressioofbytesOutput
sidencompressioofbytesInputCR �
� � � �� �
� �%100
ˆ
ˆ
PRD1
0
2
1
0
2
��
�
�
��
�
�
�L
i
L
i
ix
ixix
where )(ix is the output bytes of the decoder in the
gateway, )(ˆ ix is the original sampled data in an end
device, and L is the length of a sample .
The comparison was done offline and evaluated
from one hundred seconds of ECG data. Fixed at a CR,
lower PRD was reached. Fixed at a PRD, higher CR
was gained. About 20-30 bits of output bits can be
omitted. According to [9], CR in 8:1 and 16:1 while
PRD at about 4-5% and 10-15% were suggested to be
clinically useful ECG information by cardiologists. In
Figure 6, CR at 8, chosen in our system, resulted in
PRD less than 2.5 %, which satisfied the criteria
mentioned in [9]. Furthermore, CR at 8 showed good
performance. The time delay was of less than 8, The
length of encoded bytes at 32 bytes was only about 1/4
maximum ZigBee packet length, while the
uncompressed ECG needed 2 and a half maximum
ZigBee packet length.
4.3. Packet Loss Tests
Packet loss tests for compressed ECG transmission
(CR set to 8) and uncompressed ECG transmission
were performed. The goal of the tests was to compare
the reliability of the two transmission types under the
602
busy wireless channel, simulating the situation with
large number of nodes in WSN.
In order to create the busy wireless channel status
with the three nodes that we had, only two nodes was
used and the transmitter node transmitted a packet set
repeatedly whenever a wireless channel was freed. The
packet set in the compressed ECG transmission was a
packet of 58 bytes. In the uncompressed transmission,
2 packets of 127 bytes and a packet of 68 bytes were
transmitted. The compositions of the data sets were the
number of a second of ECG at 256Hz under two
transmission types. The data set in both scenarios were
repeated ten thousand times, i.e., 10000 packets in
compressed scenario and 30000 packets in
uncompressed scenario. The correct receiving rate and
the number of failed packets (lost packets and incorrect
content packets) were calculated and shown in Table
III. The results showed that the compressed
transmission offered more reliable quality of service
than the uncompressed transmission. when arrhythmia
occurred and the ECG was transmitted.
Table III: Result of Packet Lost Test
Scenario of Compressed ECG Transmission (CR set to 8)
Distance (meter) 1 5 9
Failure Packets
(10000 – Success Packet) 77 258 623
Success Receiving Rate
(100 – 100 x Failure Packets / 10000) 99.23 97.42
93.7
7
Scenario of Uncompressed ECG Transmission
Distance (meter) 1 5 9
Failure Packets
(10000 x 3 - Success Packet) 470 2885 4457
Success Receiving Rate
(100 – 100 x Failure Packets/(3 x10000)) 98.43 90.38 85.15
4.4. Gateway
Figure 7 showed the screen-shot of the gateway.
When one of our men pretended to suffer from
arrhythmia (narrow the threshold used in arrhythmia
criterion), the condition was detected and his ECG
signal was transmitted to the gateway. The left-bottom
window showed the ECG signal and right bottom
window showed the same operating message from a
coordinator. The top-center window showed the
structure of the WSN where ‘C-0x0000’ stands for the
coordinator whose address was 0x0000, ‘R-0x0001’
stands for a router under the coordinator whose
address was 0x0001, and ‘D-0x1234’ stands for an end
device under the router whose address was 0x1234.
The top-right window showed some characteristics of
the received ECG and its diagnosis. The top-left
window showed the man’s posture.
5. Conclusions
This paper established a prototype of a DSP
platform which enables good digital signal processing
performance in ZigBee-based WSN, and an
arrhythmia-aware telecare system.
Low-band coefficients subtraction is proposed to be
an adjusting component in the ECG compression
algorithm composed by DWT and ESPIHT [12],
gaining better performance. Fixed at a CR, lower PRD
was reached. Fixed at a PRD, higher CR was gained.
Moreover, according to [9], the PRD of our modified
ECG compression algorithm was half of the PRD
requirement, and completely satisfied the clinically
useful ECG information.
Timing performances of ECG compression,
decompression, QRS/RR detection, and posture
detection were examined. The results showed that the
time delay introduced by each algorithm could be
ignored and would not affect real-time application.
Packet lost tests were performed and compared
between the compressed transmission scenario and
uncompressed transmission scenario, while the
wireless channel was in tight status. The results
showed that the compressed transmission in WSN
could effectively increase the receiving rate.
Compared with previous works [1-6], simulated, and
tested in several indices, our system suffered less from
traffic jam its consequences. Hence, we provided a
solution to build a more bandwidth conservable, stable,
and reliable WSN-based telecare system.
603
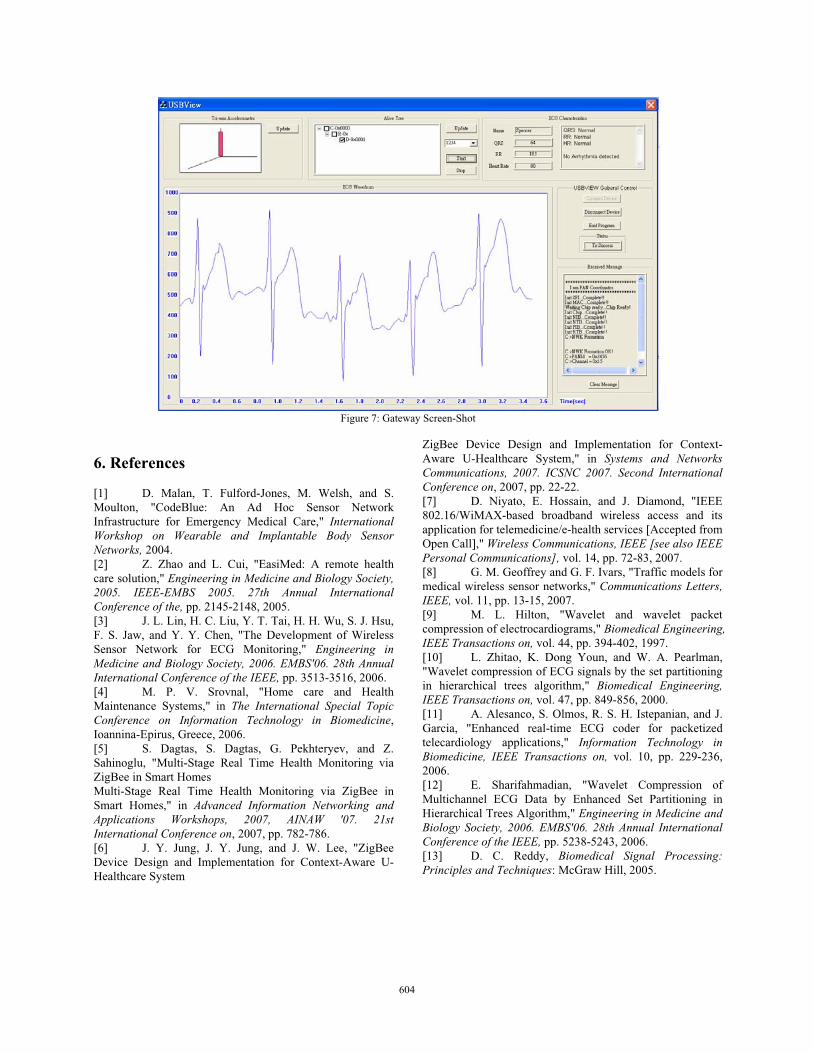
Figure 7: Gateway Screen-Shot
6. References
[1] D. Malan, T. Fulford-Jones, M. Welsh, and S.
Moulton, "CodeBlue: An Ad Hoc Sensor Network
Infrastructure for Emergency Medical Care," InternationalWorkshop on Wearable and Implantable Body Sensor Networks, 2004.
[2] Z. Zhao and L. Cui, "EasiMed: A remote health
care solution," Engineering in Medicine and Biology Society, 2005. IEEE-EMBS 2005. 27th Annual International Conference of the, pp. 2145-2148, 2005.
[3] J. L. Lin, H. C. Liu, Y. T. Tai, H. H. Wu, S. J. Hsu,
F. S. Jaw, and Y. Y. Chen, "The Development of Wireless
Sensor Network for ECG Monitoring," Engineering in Medicine and Biology Society, 2006. EMBS'06. 28th Annual International Conference of the IEEE, pp. 3513-3516, 2006.
[4] M. P. V. Srovnal, "Home care and Health
Maintenance Systems," in The International Special Topic Conference on Information Technology in Biomedicine,
Ioannina-Epirus, Greece, 2006.
[5] S. Dagtas, S. Dagtas, G. Pekhteryev, and Z.
Sahinoglu, "Multi-Stage Real Time Health Monitoring via
ZigBee in Smart Homes
Multi-Stage Real Time Health Monitoring via ZigBee in
Smart Homes," in Advanced Information Networking and Applications Workshops, 2007, AINAW '07. 21st International Conference on, 2007, pp. 782-786.
[6] J. Y. Jung, J. Y. Jung, and J. W. Lee, "ZigBee
Device Design and Implementation for Context-Aware U-
Healthcare System
ZigBee Device Design and Implementation for Context-
Aware U-Healthcare System," in Systems and Networks Communications, 2007. ICSNC 2007. Second International Conference on, 2007, pp. 22-22.
[7] D. Niyato, E. Hossain, and J. Diamond, "IEEE
802.16/WiMAX-based broadband wireless access and its
application for telemedicine/e-health services [Accepted from
Open Call]," Wireless Communications, IEEE [see also IEEE Personal Communications], vol. 14, pp. 72-83, 2007.
[8] G. M. Geoffrey and G. F. Ivars, "Traffic models for
medical wireless sensor networks," Communications Letters, IEEE, vol. 11, pp. 13-15, 2007.
[9] M. L. Hilton, "Wavelet and wavelet packet
compression of electrocardiograms," Biomedical Engineering, IEEE Transactions on, vol. 44, pp. 394-402, 1997.
[10] L. Zhitao, K. Dong Youn, and W. A. Pearlman,
"Wavelet compression of ECG signals by the set partitioning
in hierarchical trees algorithm," Biomedical Engineering, IEEE Transactions on, vol. 47, pp. 849-856, 2000.
[11] A. Alesanco, S. Olmos, R. S. H. Istepanian, and J.
Garcia, "Enhanced real-time ECG coder for packetized
telecardiology applications," Information Technology in Biomedicine, IEEE Transactions on, vol. 10, pp. 229-236,
2006.
[12] E. Sharifahmadian, "Wavelet Compression of
Multichannel ECG Data by Enhanced Set Partitioning in
Hierarchical Trees Algorithm," Engineering in Medicine and Biology Society, 2006. EMBS'06. 28th Annual International Conference of the IEEE, pp. 5238-5243, 2006.
[13] D. C. Reddy, Biomedical Signal Processing: Principles and Techniques: McGraw Hill, 2005.
604