BELLUM PERSICUM (171-168 V.CHR). QUELLEN UND MODERNE HISTORIOGRAPHIE
Upload
independentCategory
view
1download
0
CLINICAL STUDY – PATIENT STUDY
Surgical treatment of high-grade gliomas in motor areas.The impact of different supportive technologies: a 171-patientseries
Andrea Talacchi • Sergio Turazzi • Francesca Locatelli • Francesco Sala •
Alberto Beltramello • Franco Alessandrini • Paolo Manganotti •
Paola Lanteri • Roberta Gambin • Mario Ganau • Vincenzo Tramontano •
Barbara Santini • Massimo Gerosa
Received: 30 October 2009 / Accepted: 13 April 2010 / Published online: 14 May 2010
� Springer Science+Business Media, LLC. 2010
Abstract In the last few years much has been published
to validate new technology in brain mapping for clinical
purposes, but there have been few clinical results. In this
report we describe our five-year experience in the surgical
management of malignant gliomas around motor areas with
an evaluation of the impact of functional magnetic reso-
nance imaging (fMRI) plus navigator and intraoperative
neurophysiology (IN). End-points were extent of removal,
morbidity, and survival. Variables describing patient and
tumor characteristics and treatment modalities were sta-
tistically weighted in relation to treatment outcome. Tumor
depth (P = 0.01), midline shift C1 cm. (P = 0.05), and
insular location (P = 0.001) negatively affected extent of
removal, whereas IN (P \ 0.001) and fMRI plus navigator
(P = 0.02) contributed to increasing the rate of total
removal (73%, 71% vs. 40%). Postoperative motor
impairment was mild and transient in a minority of cases
(20%). General complications, as defined by the Glioma
Outcome Project, occurred in 23% of cases. IN was the
only factor associated with acute postoperative motor
deterioration (P \ 0.001). IN and age [65 years (P =
0.01) were associated with the occurrence of complica-
tions. Overall survival was significantly higher in patients
operated with IN or fMRI plus navigator (P \ 0.01).
Comparing different surgical strategies used in the same
period, we observed that supportive technologies in glioma
surgery have their primary impact on the quality of
resection and survival. IN led to transient motor impair-
ment and some additional complications which did not
affect functional outcome.
Keywords Brain tumors � Surgical treatment �Motor pathways � Functional magnetic resonance �Intraoperative neurophysiology
Introduction
Most clinical series on gliomas seek to establish prognostic
factors, especially for survival [1–4]. Location has seldom
been considered a variable. Few studies have investigated
specific tumor locations, in line with the hypothesis that,
because eloquent areas are a risk factor for higher mor-
bidity, the extent of removal will be necessarily limited
[5–8]. Although what precisely constitutes residual tumor
is still controversial [9, 10], thus restricting the possibility
A. Talacchi � F. Sala � M. Ganau � V. Tramontano �B. Santini � M. Gerosa
Section of Neurosurgery, Department of Neurological Sciences
and Vision, University Hospital, Verona, Italy
S. Turazzi � R. Gambin
Division of Neurosurgery, University Hospital, Verona, Italy
F. Locatelli
Section of Epidemiology and Medical Statistics, Department of
Hygiene and Public Health, University of Verona, Verona, Italy
P. Manganotti
Section of Neurology, Department of Neurological Sciences
and Vision, University Hospital, Verona, Italy
A. Beltramello � F. Alessandrini
Division of Neuroradiology, University Hospital, Verona, Italy
P. Lanteri
Division of Neurology, ‘‘Sacro Cuore’’ Hospital, Negrar,
Verona, Italy
A. Talacchi (&)
Section of Neurosurgery, Department of Neurological Sciences
and Vision, University Hospital, P. Stefani 1, 37126 Verona,
Italy
e-mail: [email protected]
123
J Neurooncol (2010) 100:417–426
DOI 10.1007/s11060-010-0193-x

of defining the role of removal, every effort should be
undertaken to differentiate and properly define subgroups
of cases in which prognosis could be significantly
improved if specific surgical treatment were given.
Surgical planning is evolving continuously with advan-
ces in surgical technology (high magnetic field MRI, MR
spectroscopy, IN including awake surgery, intraoperative
MRI, etc.) applied to current treatment modalities [11–14].
And although numerous recent papers have addressed the
validation of these techniques, their impact on clinical
practice is yet to be determined [15–17].
We report our experience with the surgical treatment of
malignant gliomas around supratentorial motor areas. The
objectives of this study were to determine the results of
treatment and the role of the supportive technology—IN
and fMRI-guided surgery. Because the extent of tumor
removal and functional outcome are so closely interrelated,
we considered a pool of outcome variables—extent of
removal, postoperative change in motor grading, compli-
cations, and follow-up—all of which, because of their
reciprocal influence, help to give complete results.
Materials and methods
We retrospectively reviewed all supratentorial malignant
gliomas operated on since January 2002 at the Department
of Neurosurgery, University of Verona, shortly after the
introduction of IN: 171 patients with preoperative motor
impairment or with tumors 1 cm or less from motor path-
ways as determined at MRI. Patients with recurrences or
multifocal tumors were excluded from the study.
Records included clinical history, neurological exami-
nation, MRI, and operative notes in all cases. fMRI was
usually performed as an alternative to intraoperative map-
ping, with or without the aid of frameless stereotactic image-
guided surgery. Preoperative and postoperative MRI studies
were performed within 48 h of the operation in all but 18
cases, in which computed tomography (CT) was carried out
postoperatively with the same timing. The latest technology
for brain surgery, including microscopy and cavitron, were
available. All four surgeons who operated had done more
than 100 operations for gliomas before this series. Surgical
strategy was discussed by the team, but the choice and
application of additional technology to surgical planning was
an individual decision. Follow-up (four-month, functionally
independent survival, and overall survival) was possible for
most patients. Functionally independent survival was the
period of survival with Karnofski score (KPS) C80. All
patients underwent radiotherapy and most (n = 131)
received chemotherapy with temozolamide (TMZ). TMZ
treatment schedules varied as did the number of cycles and
combination with radiotherapy (concomitant or adjuvant).
Patient characteristics
Table 1 lists age, sex, motor grading (MRC scale), symp-
toms and signs, KPS, and symptom duration. Note that our
interpretation of the MRC scale emphasized even slight
modifications in strength. Accordingly, we considered 4?, 4,
and 4- to be single points on the scale, in addition to 1–3 and
5, because of the functional gap between 3 (movements
against gravity) and 5 (normal). Thus, patients who were able
to maintain a static position for a few seconds only were
classified as 4-, those with slow drooping of one arm as 4,
and those with some impairment evident only against resis-
tance as 4?.
Tumor characteristics
Table 1 reports side, size, location, MRI T2-weighted
alterations, midline shift, tumor depth, and histology.
Characteristics of treatment
Retrospectively, three types of supportive treatment modal-
ity were recognized: null (a), fMRI and navigator (b), and
intraoperative neurophysiologic monitoring (c). Each
modality was used alone in 101, 19, and 51 cases, respec-
tively (Table 1) based on single-case evaluation and sur-
geon’s choice. Because of uncertainties about some of the
methodological issues in the intraoperative use of these
techniques, some surgeons do not trust them or prefer only
one of them.
fMRI and navigator
The MR imaging data were acquired with a Siemens 1.5
Tesla and 3.0 Tesla scanner (Siemens, Erlangen, Germany)
and a standard birdcage radiofrequency coil. The functional
images were acquired using gradient echo-planar imaging
(EPI) (TR/TE 3000/30; 36 axial slices; 128 9 128 matrix;
3.2-mm slice thickness with no gap, 220 mm FOV). With
two dumping scans, the total acquisition time for both tasks
(finger tapping and toe flexing contralateral to the affected
side) was 6 min and 36 s. Three-dimensional T1-weighted
anatomic images were acquired with a spoiled gradient recall
sequence (MPRAGE, TR/TE 2300/3.93; 256 9 256 image
matrix; 1-mm slice thickness with no gap; 230 mm FOV).
The fMRI data were analyzed using Brain Voyager QX
1.8 software. Data processing included slice time correc-
tion and 3D motion correction; 3D rigid-body registration
was used to align the reconstructed fMRI data against a
reference image, and spatial smoothing (Gaussian filtering:
full width of half maximum 6 mm) was applied. The vol-
ume of activation of the primary motor cortex was deter-
mined using a cross-correlation technique. A statistical
418 J Neurooncol (2010) 100:417–426
123
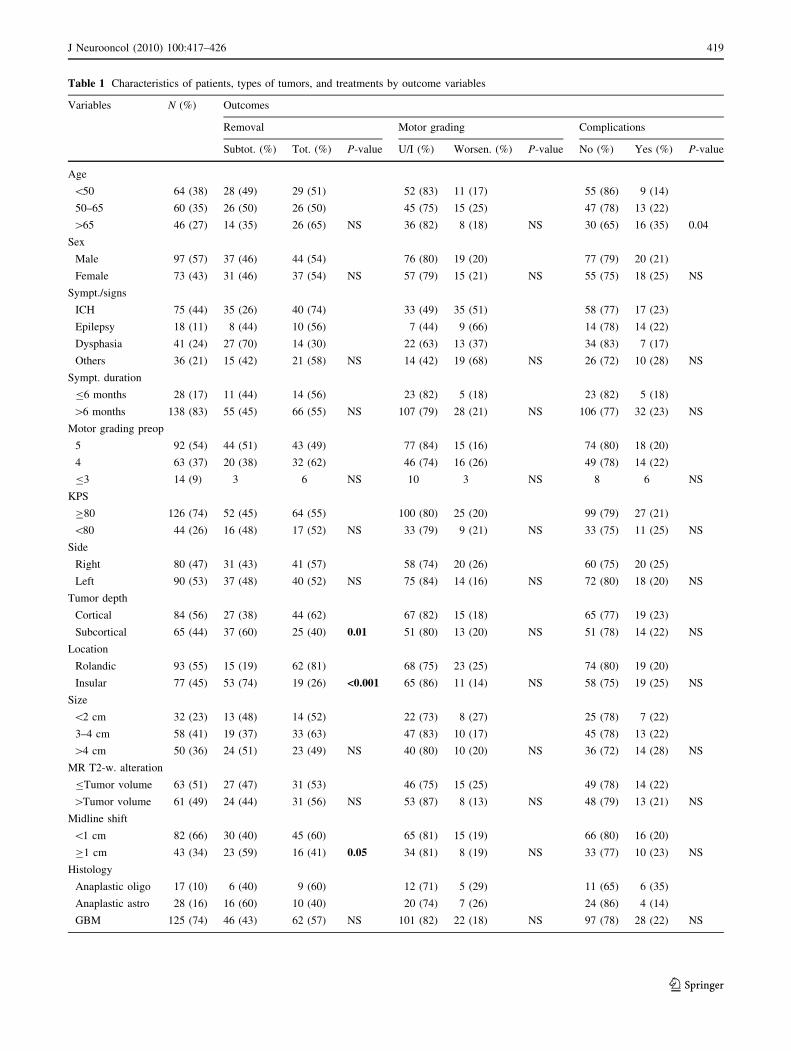
Table 1 Characteristics of patients, types of tumors, and treatments by outcome variables
Variables N (%) Outcomes
Removal Motor grading Complications
Subtot. (%) Tot. (%) P-value U/I (%) Worsen. (%) P-value No (%) Yes (%) P-value
Age
\50 64 (38) 28 (49) 29 (51) 52 (83) 11 (17) 55 (86) 9 (14)
50–65 60 (35) 26 (50) 26 (50) 45 (75) 15 (25) 47 (78) 13 (22)
[65 46 (27) 14 (35) 26 (65) NS 36 (82) 8 (18) NS 30 (65) 16 (35) 0.04
Sex
Male 97 (57) 37 (46) 44 (54) 76 (80) 19 (20) 77 (79) 20 (21)
Female 73 (43) 31 (46) 37 (54) NS 57 (79) 15 (21) NS 55 (75) 18 (25) NS
Sympt./signs
ICH 75 (44) 35 (26) 40 (74) 33 (49) 35 (51) 58 (77) 17 (23)
Epilepsy 18 (11) 8 (44) 10 (56) 7 (44) 9 (66) 14 (78) 14 (22)
Dysphasia 41 (24) 27 (70) 14 (30) 22 (63) 13 (37) 34 (83) 7 (17)
Others 36 (21) 15 (42) 21 (58) NS 14 (42) 19 (68) NS 26 (72) 10 (28) NS
Sympt. duration
B6 months 28 (17) 11 (44) 14 (56) 23 (82) 5 (18) 23 (82) 5 (18)
[6 months 138 (83) 55 (45) 66 (55) NS 107 (79) 28 (21) NS 106 (77) 32 (23) NS
Motor grading preop
5 92 (54) 44 (51) 43 (49) 77 (84) 15 (16) 74 (80) 18 (20)
4 63 (37) 20 (38) 32 (62) 46 (74) 16 (26) 49 (78) 14 (22)
B3 14 (9) 3 6 NS 10 3 NS 8 6 NS
KPS
C80 126 (74) 52 (45) 64 (55) 100 (80) 25 (20) 99 (79) 27 (21)
\80 44 (26) 16 (48) 17 (52) NS 33 (79) 9 (21) NS 33 (75) 11 (25) NS
Side
Right 80 (47) 31 (43) 41 (57) 58 (74) 20 (26) 60 (75) 20 (25)
Left 90 (53) 37 (48) 40 (52) NS 75 (84) 14 (16) NS 72 (80) 18 (20) NS
Tumor depth
Cortical 84 (56) 27 (38) 44 (62) 67 (82) 15 (18) 65 (77) 19 (23)
Subcortical 65 (44) 37 (60) 25 (40) 0.01 51 (80) 13 (20) NS 51 (78) 14 (22) NS
Location
Rolandic 93 (55) 15 (19) 62 (81) 68 (75) 23 (25) 74 (80) 19 (20)
Insular 77 (45) 53 (74) 19 (26) <0.001 65 (86) 11 (14) NS 58 (75) 19 (25) NS
Size
\2 cm 32 (23) 13 (48) 14 (52) 22 (73) 8 (27) 25 (78) 7 (22)
3–4 cm 58 (41) 19 (37) 33 (63) 47 (83) 10 (17) 45 (78) 13 (22)
[4 cm 50 (36) 24 (51) 23 (49) NS 40 (80) 10 (20) NS 36 (72) 14 (28) NS
MR T2-w. alteration
BTumor volume 63 (51) 27 (47) 31 (53) 46 (75) 15 (25) 49 (78) 14 (22)
[Tumor volume 61 (49) 24 (44) 31 (56) NS 53 (87) 8 (13) NS 48 (79) 13 (21) NS
Midline shift
\1 cm 82 (66) 30 (40) 45 (60) 65 (81) 15 (19) 66 (80) 16 (20)
C1 cm 43 (34) 23 (59) 16 (41) 0.05 34 (81) 8 (19) NS 33 (77) 10 (23) NS
Histology
Anaplastic oligo 17 (10) 6 (40) 9 (60) 12 (71) 5 (29) 11 (65) 6 (35)
Anaplastic astro 28 (16) 16 (60) 10 (40) 20 (74) 7 (26) 24 (86) 4 (14)
GBM 125 (74) 46 (43) 62 (57) NS 101 (82) 22 (18) NS 97 (78) 28 (22) NS
J Neurooncol (2010) 100:417–426 419
123
threshold of P-value \ 0.5 for each patient was considered
significant.
Anatomic and functional imaging were simply fused,
resliced with DICOM format and then transferred via fast
Ethernet to a navigation data set (StealthStation; Medtronic
Sofamor-Danek, Memphis, TN, USA).
Intraoperative neurophysiology
Neurophysiological techniques for motor-evoked potentials
(MEPs) are described elsewhere [18]. The same monopolar
multipulse stimulation technique used for MEPs monitoring
was also used for cortical and subcortical mapping. In this
case, the same stimulation conditions were used to map the
cortex with a handheld monopolar probe. Subsequently,
especially when approaching the tumor–brain interface,
functional motor mapping was repeated subcortically to
identify and spare the white matter motor tracts. Threshold
intensities up to 20 mA were reached in a stepwise manner,
starting from low thresholds, to obtain indications about
proximity to subcortical motor pathways. As far as we could
distinguish tumor from healthy tissue, we continued to
remove it, even if IN showed we were very closely
approaching the motor pathways (until 1–2 mA); we were
more cautious in cases of infiltrated brain and stopped
resection at 4–5 mA.
Outcome
Extent of tumor removal, morbidity (variation in motor
score and complications), four-month outcome, and sur-
vival were considered. Extent of tumor removal (total
versus subtotal and partial) was determined postoperatively
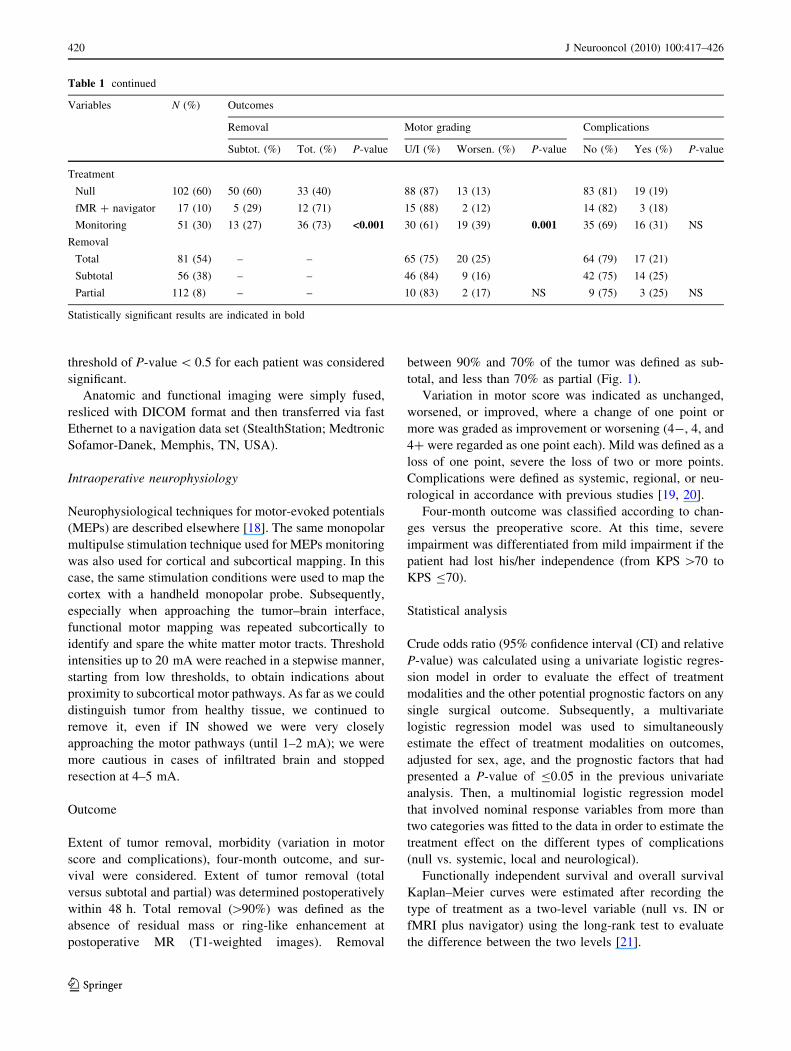
within 48 h. Total removal ([90%) was defined as the
absence of residual mass or ring-like enhancement at
postoperative MR (T1-weighted images). Removal
between 90% and 70% of the tumor was defined as sub-
total, and less than 70% as partial (Fig. 1).
Variation in motor score was indicated as unchanged,
worsened, or improved, where a change of one point or
more was graded as improvement or worsening (4-, 4, and
4? were regarded as one point each). Mild was defined as a
loss of one point, severe the loss of two or more points.
Complications were defined as systemic, regional, or neu-
rological in accordance with previous studies [19, 20].
Four-month outcome was classified according to chan-
ges versus the preoperative score. At this time, severe
impairment was differentiated from mild impairment if the
patient had lost his/her independence (from KPS [70 to
KPS B70).
Statistical analysis
Crude odds ratio (95% confidence interval (CI) and relative
P-value) was calculated using a univariate logistic regres-
sion model in order to evaluate the effect of treatment
modalities and the other potential prognostic factors on any
single surgical outcome. Subsequently, a multivariate
logistic regression model was used to simultaneously
estimate the effect of treatment modalities on outcomes,
adjusted for sex, age, and the prognostic factors that had
presented a P-value of B0.05 in the previous univariate
analysis. Then, a multinomial logistic regression model
that involved nominal response variables from more than
two categories was fitted to the data in order to estimate the
treatment effect on the different types of complications
(null vs. systemic, local and neurological).
Functionally independent survival and overall survival
Kaplan–Meier curves were estimated after recording the
type of treatment as a two-level variable (null vs. IN or
fMRI plus navigator) using the long-rank test to evaluate
the difference between the two levels [21].
Table 1 continued
Variables N (%) Outcomes
Removal Motor grading Complications
Subtot. (%) Tot. (%) P-value U/I (%) Worsen. (%) P-value No (%) Yes (%) P-value
Treatment
Null 102 (60) 50 (60) 33 (40) 88 (87) 13 (13) 83 (81) 19 (19)
fMR ? navigator 17 (10) 5 (29) 12 (71) 15 (88) 2 (12) 14 (82) 3 (18)
Monitoring 51 (30) 13 (27) 36 (73) <0.001 30 (61) 19 (39) 0.001 35 (69) 16 (31) NS
Removal
Total 81 (54) – – 65 (75) 20 (25) 64 (79) 17 (21)
Subtotal 56 (38) – – 46 (84) 9 (16) 42 (75) 14 (25)
Partial 112 (8) – – 10 (83) 2 (17) NS 9 (75) 3 (25) NS
Statistically significant results are indicated in bold
420 J Neurooncol (2010) 100:417–426
123
Statistical analysis was performed using STATA soft-
ware, release 7.0 (Stata Corporation, College Station, TX,
USA) [22].
Results
Extent of removal
Total removal was achieved in 54% of cases overall. Age,
sex, preoperative motor grading, KPS, symptoms and
signs, symptom duration, side, size, location, tumor depth,
MRI T2-weighted alterations, histology, and treatment
were entered into the univariate analysis in order to find
variables possibly associated with the extent of resection
(total vs. subtotal and partial) (Table 1).
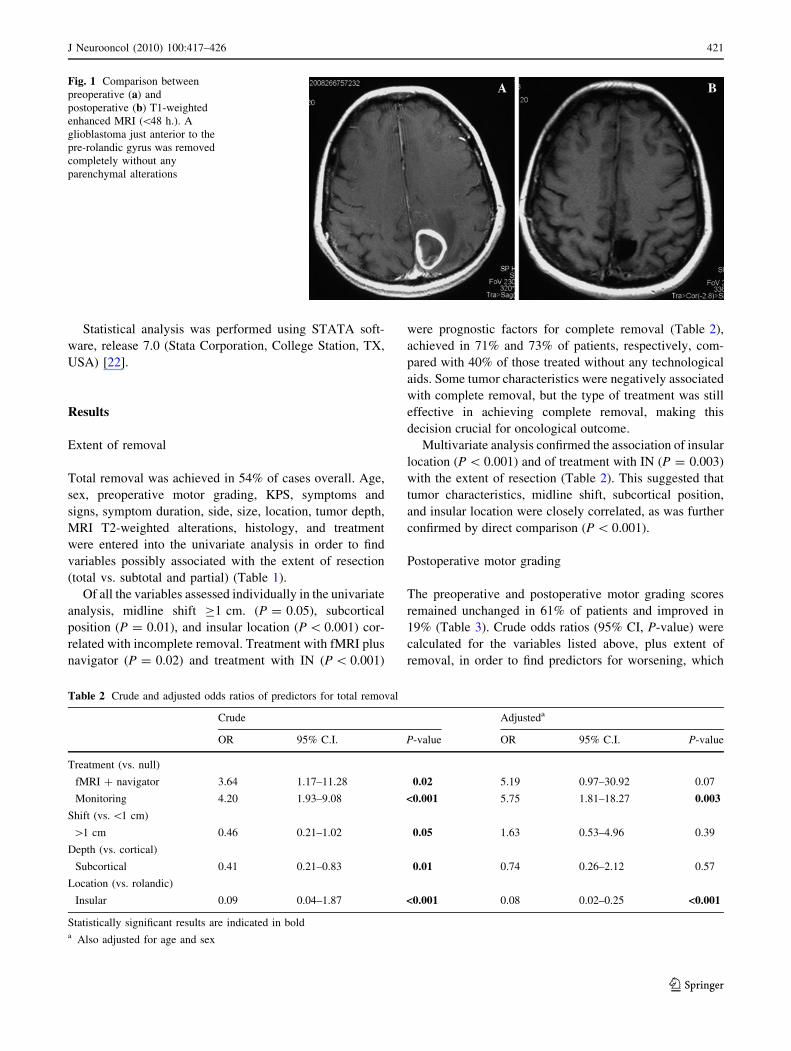
Of all the variables assessed individually in the univariate
analysis, midline shift C1 cm. (P = 0.05), subcortical
position (P = 0.01), and insular location (P \ 0.001) cor-
related with incomplete removal. Treatment with fMRI plus
navigator (P = 0.02) and treatment with IN (P \ 0.001)
were prognostic factors for complete removal (Table 2),
achieved in 71% and 73% of patients, respectively, com-
pared with 40% of those treated without any technological
aids. Some tumor characteristics were negatively associated
with complete removal, but the type of treatment was still
effective in achieving complete removal, making this
decision crucial for oncological outcome.
Multivariate analysis confirmed the association of insular
location (P \ 0.001) and of treatment with IN (P = 0.003)
with the extent of resection (Table 2). This suggested that
tumor characteristics, midline shift, subcortical position,
and insular location were closely correlated, as was further
confirmed by direct comparison (P \ 0.001).
Postoperative motor grading
The preoperative and postoperative motor grading scores
remained unchanged in 61% of patients and improved in
19% (Table 3). Crude odds ratios (95% CI, P-value) were
calculated for the variables listed above, plus extent of
removal, in order to find predictors for worsening, which
Fig. 1 Comparison between
preoperative (a) and
postoperative (b) T1-weighted
enhanced MRI (\48 h.). A
glioblastoma just anterior to the
pre-rolandic gyrus was removed
completely without any
parenchymal alterations
Table 2 Crude and adjusted odds ratios of predictors for total removal
Crude Adjusteda
OR 95% C.I. P-value OR 95% C.I. P-value
Treatment (vs. null)
fMRI ? navigator 3.64 1.17–11.28 0.02 5.19 0.97–30.92 0.07
Monitoring 4.20 1.93–9.08 <0.001 5.75 1.81–18.27 0.003
Shift (vs. \1 cm)
[1 cm 0.46 0.21–1.02 0.05 1.63 0.53–4.96 0.39
Depth (vs. cortical)
Subcortical 0.41 0.21–0.83 0.01 0.74 0.26–2.12 0.57
Location (vs. rolandic)
Insular 0.09 0.04–1.87 <0.001 0.08 0.02–0.25 <0.001
Statistically significant results are indicated in bolda Also adjusted for age and sex
J Neurooncol (2010) 100:417–426 421
123
occurred in 20% of cases (mild in 13%, severe in 7%). IN
was the only variable that was significantly associated with
postoperative worsening (39% vs. 13%; P \ 0.001), which
was confirmed after adjusting for the other variables
(P \ 0.001) (Table 4).
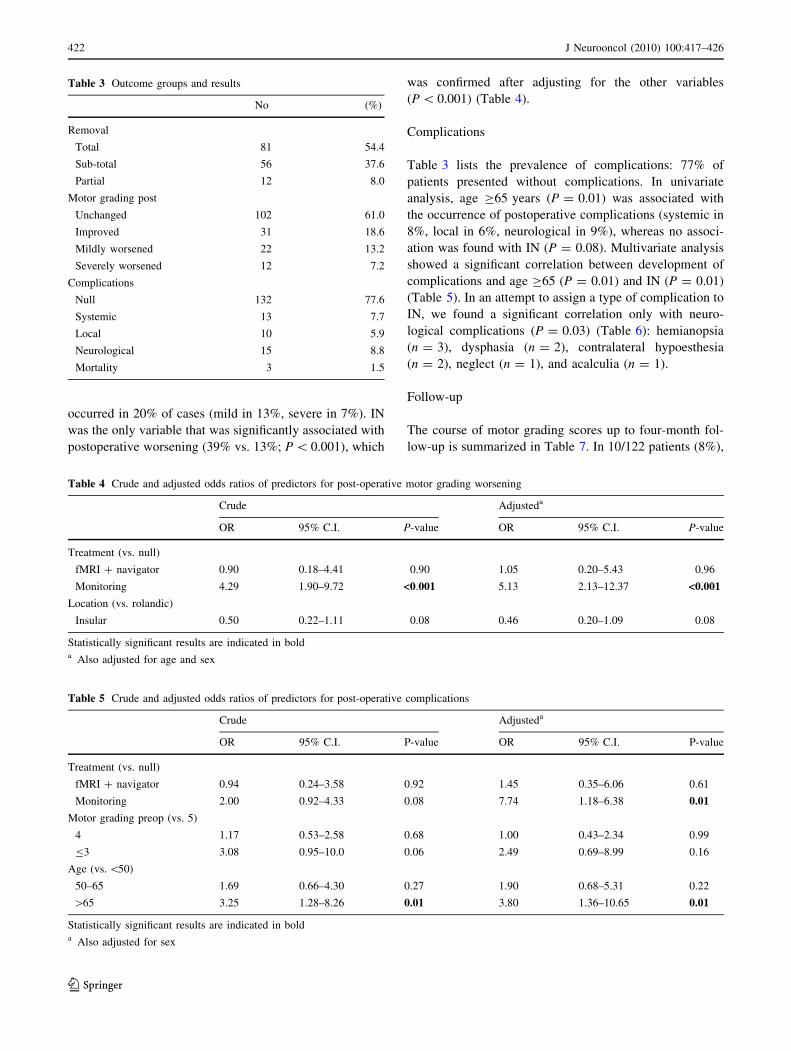
Complications
Table 3 lists the prevalence of complications: 77% of
patients presented without complications. In univariate
analysis, age C65 years (P = 0.01) was associated with
the occurrence of postoperative complications (systemic in
8%, local in 6%, neurological in 9%), whereas no associ-
ation was found with IN (P = 0.08). Multivariate analysis
showed a significant correlation between development of
complications and age C65 (P = 0.01) and IN (P = 0.01)
(Table 5). In an attempt to assign a type of complication to
IN, we found a significant correlation only with neuro-
logical complications (P = 0.03) (Table 6): hemianopsia
(n = 3), dysphasia (n = 2), contralateral hypoesthesia
(n = 2), neglect (n = 1), and acalculia (n = 1).
Follow-up
The course of motor grading scores up to four-month fol-
low-up is summarized in Table 7. In 10/122 patients (8%),
Table 5 Crude and adjusted odds ratios of predictors for post-operative complications
Crude Adjusteda
OR 95% C.I. P-value OR 95% C.I. P-value
Treatment (vs. null)
fMRI ? navigator 0.94 0.24–3.58 0.92 1.45 0.35–6.06 0.61
Monitoring 2.00 0.92–4.33 0.08 7.74 1.18–6.38 0.01
Motor grading preop (vs. 5)
4 1.17 0.53–2.58 0.68 1.00 0.43–2.34 0.99
B3 3.08 0.95–10.0 0.06 2.49 0.69–8.99 0.16
Age (vs. \50)
50–65 1.69 0.66–4.30 0.27 1.90 0.68–5.31 0.22
[65 3.25 1.28–8.26 0.01 3.80 1.36–10.65 0.01
Statistically significant results are indicated in bolda Also adjusted for sex
Table 3 Outcome groups and results
No (%)
Removal
Total 81 54.4
Sub-total 56 37.6
Partial 12 8.0
Motor grading post
Unchanged 102 61.0
Improved 31 18.6
Mildly worsened 22 13.2
Severely worsened 12 7.2
Complications
Null 132 77.6
Systemic 13 7.7
Local 10 5.9
Neurological 15 8.8
Mortality 3 1.5
Table 4 Crude and adjusted odds ratios of predictors for post-operative motor grading worsening
Crude Adjusteda
OR 95% C.I. P-value OR 95% C.I. P-value
Treatment (vs. null)
fMRI ? navigator 0.90 0.18–4.41 0.90 1.05 0.20–5.43 0.96
Monitoring 4.29 1.90–9.72 <0.001 5.13 2.13–12.37 <0.001
Location (vs. rolandic)
Insular 0.50 0.22–1.11 0.08 0.46 0.20–1.09 0.08
Statistically significant results are indicated in bolda Also adjusted for age and sex
422 J Neurooncol (2010) 100:417–426
123

motor grading score worsened and should therefore be
considered to reflect persistent deficits. Of these 10
patients, six had received treatment without any additional
technical aids, one with the aid of fMRI plus navigator, and
three with IN. Of these 10 patients, two presented with
severe impairment, because they changed functional per-
formance status group (from KPS [70 to KPS B70); both
had been operated on without any additional technical aids.
The remaining eight patients had mild deficits which did
not affect their functional status.
Neurological deficits due to complications subsided
within a few weeks in most cases (6/9 cases) and did not
change functional outcome. Later in the follow-up, 15% of
patients underwent reoperation for tumor recurrence.
Globally, 106 (62%) patients were traced for the follow-
up. No difference was found between traced and untraced
subjects with regard to histology, age, KPS, reoperation, or
TMZ treatment, but the rate of total removal differed sig-
nificantly (62% vs. 40%, respectively; P \ 0.01) as did
treatment modality (IN or fMRI plus navigator in 36% vs.
20%, respectively; P \ 0.05)
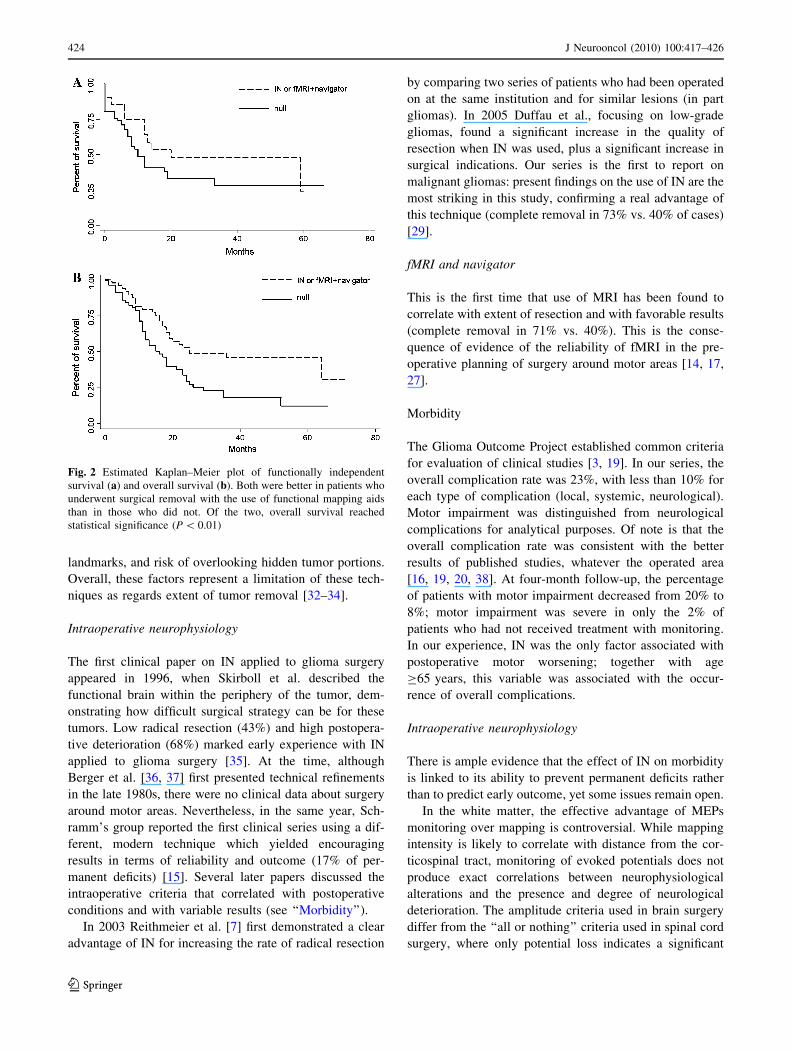
Overall, the univariate analysis showed that treatment
modality was significantly associated with overall survival
(P \ 0.01) but not with functionally independent survival
(Fig. 2). No further statistical analysis of the currently
available population can be made.
Discussion
With improvements in surgical techniques, nervous and
vascular structures can be safely manipulated and ever
greater proportions of tumor removed. The choice of
approach to subcortical diffuse glioma and the decision to
resect the infiltrated brain surrounding an enhanced mass
are the cornerstones of modern aggressive surgical strategy
and require knowledge of brain functions at the tumor
margin in individual cases [17, 23–25]. In malignant gli-
omas, because of the patient’s short life expectancy, the
cost–benefit balance is even more unfavorable than in any
other tumor. The risk of postoperative neurological dete-
rioration is present for all eloquent areas, but correlative
investigation of anatomy and function in motor areas has
provided the most reliable test to date, opening an oppor-
tunity for informed decisions about the implementation of
surgical treatment and a rationale for further extension of
these techniques to other eloquent areas [13, 26]. Intraop-
erative neurophysiological mapping and monitoring is the
gold standard for this purpose, and fMRI with the aid of
frameless stereotactic image-guided devices is almost as
reliable, especially for superficial lesions [11, 14, 27–29].
These techniques can have additional and unexplored value
when combined with techniques which improve the intra-
operative definition of tumor margins (5-ALA, infrared
spectroscopic imaging, etc.) [30, 31].
Extent of removal
In our experience, some tumor characteristics (insular
location, midline shift C1 cm and subcortical position) still
limit the extent of removal, but IN, and fMRI plus navi-
gator to a lesser extent, have an important impact on the
extent of total removal. Insular gliomas have infiltrative
behavior and intimate cohabitation with brain vascular
supply, making intraoperative mapping only a minor part
of a strategy aimed at safe removal. Similarly, deep tumors
may present additional problems: lack of functional infor-
mation about non-motor areas, paucity of anatomical
Table 7 Time course of motor grading in the postoperative period
Motor grading pre-op Motor grading post-op Motor grading 4 months
= : ; = : ;
5 53 (82%) 0 12(18%) 62 (95%) 0 3 (5%)
4 18 (38%) 14 (30%) 15(32%) 12 (25%) 30 (64%) 5 (11%)
B3 6 2 2 4 4 2
Total 77 (63%) 16 (13%) 29 (24%) 78 (64%) 34 (28%) 10a (8%)
a Treatment null n = 6 (10%); treatment fMRI ? navigator n = 1 (11%); treatment monitoring n = 3 (10%)
: Improved, ; worsened, = unchanged, compared with pre-op
Table 6 The effect of treatment, univariate multinomial odds ratios
(mOR), on type of complications
Complications Treatment mOR 95% CI P-value
Systemic fMRI ? navigator NE* NE* NE*
Monitoring 1.05 0.30–3.65 0.93
Local fMRI ? navigator 1.13 0.12–10.40 0.91
Monitoring 1.34 0.30–5.90 0.70
Neurological fMRI ? navigator 2.37 0.42–13.44 0.33
Monitoring 3.80 1.16–12.41 0.03
* No subjects with systemic complications in treatment with
fMRI ? navigator
Statistically significant results are indicated in bold
J Neurooncol (2010) 100:417–426 423
123
landmarks, and risk of overlooking hidden tumor portions.
Overall, these factors represent a limitation of these tech-
niques as regards extent of tumor removal [32–34].
Intraoperative neurophysiology
The first clinical paper on IN applied to glioma surgery
appeared in 1996, when Skirboll et al. described the
functional brain within the periphery of the tumor, dem-
onstrating how difficult surgical strategy can be for these
tumors. Low radical resection (43%) and high postopera-
tive deterioration (68%) marked early experience with IN
applied to glioma surgery [35]. At the time, although
Berger et al. [36, 37] first presented technical refinements
in the late 1980s, there were no clinical data about surgery
around motor areas. Nevertheless, in the same year, Sch-
ramm’s group reported the first clinical series using a dif-
ferent, modern technique which yielded encouraging
results in terms of reliability and outcome (17% of per-
manent deficits) [15]. Several later papers discussed the
intraoperative criteria that correlated with postoperative
conditions and with variable results (see ‘‘Morbidity’’).
In 2003 Reithmeier et al. [7] first demonstrated a clear
advantage of IN for increasing the rate of radical resection
by comparing two series of patients who had been operated
on at the same institution and for similar lesions (in part
gliomas). In 2005 Duffau et al., focusing on low-grade
gliomas, found a significant increase in the quality of
resection when IN was used, plus a significant increase in
surgical indications. Our series is the first to report on
malignant gliomas: present findings on the use of IN are the
most striking in this study, confirming a real advantage of
this technique (complete removal in 73% vs. 40% of cases)
[29].
fMRI and navigator
This is the first time that use of MRI has been found to
correlate with extent of resection and with favorable results
(complete removal in 71% vs. 40%). This is the conse-
quence of evidence of the reliability of fMRI in the pre-
operative planning of surgery around motor areas [14, 17,
27].
Morbidity
The Glioma Outcome Project established common criteria
for evaluation of clinical studies [3, 19]. In our series, the
overall complication rate was 23%, with less than 10% for
each type of complication (local, systemic, neurological).
Motor impairment was distinguished from neurological
complications for analytical purposes. Of note is that the
overall complication rate was consistent with the better
results of published studies, whatever the operated area
[16, 19, 20, 38]. At four-month follow-up, the percentage
of patients with motor impairment decreased from 20% to
8%; motor impairment was severe in only the 2% of
patients who had not received treatment with monitoring.
In our experience, IN was the only factor associated with
postoperative motor worsening; together with age
C65 years, this variable was associated with the occur-
rence of overall complications.
Intraoperative neurophysiology
There is ample evidence that the effect of IN on morbidity
is linked to its ability to prevent permanent deficits rather
than to predict early outcome, yet some issues remain open.
In the white matter, the effective advantage of MEPs
monitoring over mapping is controversial. While mapping
intensity is likely to correlate with distance from the cor-
ticospinal tract, monitoring of evoked potentials does not
produce exact correlations between neurophysiological
alterations and the presence and degree of neurological
deterioration. The amplitude criteria used in brain surgery
differ from the ‘‘all or nothing’’ criteria used in spinal cord
surgery, where only potential loss indicates a significant
Fig. 2 Estimated Kaplan–Meier plot of functionally independent
survival (a) and overall survival (b). Both were better in patients who
underwent surgical removal with the use of functional mapping aids
than in those who did not. Of the two, overall survival reached
statistical significance (P \ 0.01)
424 J Neurooncol (2010) 100:417–426
123

new permanent paresis. This difference suggests a more
complex pathophysiology of injury to the motor system
during brain surgery as compared with spinal cord surgery,
for which there is no a full explanation [28].
Nevertheless, continuous MEPs monitoring remains a
valid indicator of motor pathway function and can detect
ischemic derangements which would be likely to go
unrecognized with mapping techniques alone [39]. In ret-
rospective studies, patients who showed intraoperative
deterioration of muscle MEPs (e.g. amplitude decreased by
50% or more and/or transient loss of potentials) presented
with postoperative motor deficits [26, 28]. Other authors,
using the bipolar 60-Hz technique, showed a correlation
between positive subcortical mapping and a higher risk of
postoperative motor deficit. In all these series, most motor
deficits were transient and patients recovered within
3–4 months. With either modality, persistent deficits were
rare but remained in around 10% of cases in all clinical
series [5, 40].
Follow-up
The reversibility of most postoperative motor deficits at
follow-up is critical, because it suggests that better tumor
resection can be achieved without leaving the patients with
permanent neurological deterioration. On the other hand,
contrary to the often-repeated claim that IN prevents per-
manent impairment, we did not find a significant difference
between the functional outcomes in patients operated on
using IN, fMRI plus navigator, or nothing, at early follow-
up. At least in this preliminary analysis, these results were
confirmed at long-term follow-up: there was no difference
in functionally independent survival, whereas overall sur-
vival was significantly better for the patients operated on
with functional mapping aids. This finding compares
favorably with prospective studies which showed that
survival is prolonged by improving the quality of resection
[41, 42]. Moreover, these results may be further improved
when surgical treatment is combined with traditional and
new chemotherapeutic agents (i.e. signal transduction
inhibitors) [43].
Conclusions
Although our study has the limitations of any retrospective
study, some important findings emerged about malignant
gliomas, which have never been studied using uniform
criteria in large clinical series in modern intraoperative
settings. While our perioperative data are comprehensive,
including statistical analysis, the number of patients
decreased over the follow-up period, preventing further
analysis. Outcome analysis showed that both IN and fMRI
plus navigator had an important effect on the surgical
treatment of high-grade gliomas in motor areas. Both these
techniques significantly improved the quality of resection,
which is the main reason why these techniques are rec-
ommended. IN was associated with a higher risk of mild
transient postoperative motor deficits and other types of
neurological deficits, although their incidence and severity
compared favorably with those reported in other published
series. Further prospective studies are needed to confirm
the effect of these techniques, in combination with che-
motherapeutic agents, on survival.
References
1. Berger MS, Deliganis AV, Dobbins J et al (1994) The effect of
extent of resection on recurrence in patients with low grade
cerebral hemisphere gliomas. Cancer 74:1784–1791
2. Lacroix M, Abi-Said D, Fourney DR et al (2001) A multivariate
analysis of 416 patients with glioblastoma multiforme: prognosis,
extent of resection, and survival. J Neurosurg 95:190–198
3. Laws ER, Parney IF, Huang W, The Gliomas Outcome Investi-
gators et al (2003) Survival following surgery and prognostic
factors for recently diagnosed malignant glioma: data from the
glioma outcomes project. J Neurosurg 99:467–473
4. Quingley MR, Maroon JC (1991) The relationship between sur-
vival and the extent of the resection in patients with supratentorial
malignant gliomas. Neurosurgery 29(3):385–389
5. Duffau H, Capelle L, Denvil D et al (2003) Usefulness of intra-
operative electrical subcortical mapping during surgery for low-
grade gliomas located within eloquent brain regions: functional
result in a consecutive series of 103 patients. J Neurosurg
98:764–778
6. Ebeling U, Schmid UD, Ying H et al (1992) Safe surgery of
lesions near the motor cortex using intra-operative mapping
techniques: a report on 50 patients. Acta Neurochir 119:23–28
7. Reithmeier T, Krammer M, Gumprecth H et al (2003) Neuro-
navigation combined with electrophysiological monitoring for
surgery of lesions in eloquent brain areas in 42 cases: a retro-
spective comparison of the neurological outcome and the quality
of resection with a control group with a similar lesions. Minim
Invasive Neurosurg 46:65–71
8. Russell SM, Elliott R, Forshaw D et al (2005) Resection of parietal
lobe gliomas: incidence and evolution of neurological deficits in 28
consecutive patients correlated to the location and morphological
characteristics of the tumor. J Neurosurg 103:1010–1017
9. Dumas-Duport C, Monsaingeon V, Szikla G (1982) Serial ste-
reotactic biopsies: a double histological code of gliomas
according to malignancy and 3-D configuration, as an aid to
therapeutic decision and assessment of results. Appl Neuro-
physiol 45:431–437
10. Kelly PJ, Daumas-Duport C, Scheithauer BW et al (1987) Ste-
reotactic histological correlations of computed tomography- and
magnetic resonance imaging-defined abnormalities inpatients
with glial neoplasms. Mayo Clin Proc 62:450–459
11. Gumprecht H, Ebel GK, Auer DP et al (2002) Neuronavigation
and functional MRI for surgery in patients with lesion in eloquent
brain areas. Minim Invasive Neurosurg 45:151–153
12. Kamada K, Todo T, Masutani J et al (2005) Combined use of
tractography-integrated functional neuronavigation and direct
fiber stimulation. J Neurosurg 102:664–672
J Neurooncol (2010) 100:417–426 425
123
13. King RB, Schell GR (1987) Cortical localization and monitoring
during cerebral operations. J Neurosurg 67:210–219
14. Roessler K, Donat M, Lanzerberger R et al (2005) Evaluation of
preoperative high magnetic field motor functional MRI (3 Tesla)
in Glioma patients by navigated electrocortical stimulation and
postoperative outcome. J Neurol Neurosurg Psychiatry 76:1152–
1157
15. Cedzich C, Taniguchi M, Schafer S et al (1996) Somatosensory
evoked potential phase reversal and direct motor cortex stimu-
lation during surgery in and around the central region. Neuro-
surgery 38(5):962–970
16. Fadul C, Wood J, Thaler H et al (1988) Morbidity and mortality
of craniotomy for excision of supratentorial gliomas. Neurology
38:1374–1379
17. Lehericy S, Duffau H, Cornu P et al (2000) Correspondence
between functional magnetic resonance imaging somatotopic and
individual brain anatomy of the central region: comparison with
intraoperative stimulation in patients with brain tumors. J Neu-
rosurg 92:589–598
18. Sala F, Lanteri P (2003) Brain surgery in motor areas: the
invaluable assistance of intraoperative neurophysiological moni-
toring. J Neurosurg Sci 47:79–88
19. Chang SM, Parney IF, McDermott M, The Gliomas Outcome
Investigators et al (2003) Perioperative complications and neu-
rological outcomes of first and second craniotomies among
patients enrolled in the glioma outcome project. J Neurosurg
98:1175–1181
20. Sawaya R, Hammoud M, Schoppa D et al (1998) Neurological
outcomes in a modern series of 400 craniotomies for treatment of
parenchymal tumors. Neurosurgery 42:1044–1056
21. Kaplan EL, Meier P (1958) Non-parametric estimation from
incomplete observations. J Am Stat Assoc 53:457–481
22. McCullagh P, Nelder JA (1989) Generalized linear models.
Chapman and Hall, London
23. Black PM, Ronner SF (1987) Cortical mapping for defining the
limits of tumor resection. Neurosurgery 20(6):914–919
24. Keles GE, Berger MS (2004) Advances in neurosurgical tech-
nique in the current management of brain tumors. Semin Oncol
31:659–665
25. Meyer FB, Bates LM, Goerss SJ et al (2001) Awake craniotomy
for aggressive resection of primary gliomas located in eloquent
brain. Mayo Clin Proc 76:677–687
26. Kombos T, Suess O, Ciklatekerlio O et al (2001) Monitoring of
intraoperative motor evoked potentials to increase the safety of
surgery in and around the motor cortex. J Neurosurg 95:608–614
27. Krishnan R, Raabe A, Hattingen E et al (2004) Functional
magnetic resonance imaging- integrated Neuronavigation: cor-
relation between lesion-to-motor cortex distance and outcome.
Neurosurgery 55(4):904–915
28. Neuloh G, Pechstein U, Cedzich C et al (2004) Motor evoked
potential monitoring with supratentorial surgery. Neurosurgery
54:1061–1072
29. Duffau H, Lopes M, Arthuis F et al (2005) Contribution of
intraoperative electrical stimulation in surgery of low gliomas: a
comparative study between two series without (1985–96) and
with (1996–2003) functional mapping in the same institution. J
Neurol Neurosurg Psychiatry 76:845–851
30. Sobottka SB, Geiger KD, Salzer R et al (2009) Suitability of
infrared spectroscopic imaging as an intraoperative tool in cere-
bral glioma surgery. Anal Bioanal Chem 393:187–195
31. Stummer W, Pichlmeier U, Meinel T et al (2006) Fluorescence-
guided surgery with 5-aminolevulinic acid for resection of
malignant glioma: a randomised controlled multicentre phase III
trial. Lancet Oncol 7:392–401
32. Jeremic B, Milicic B, Gruijcic D et al (2004) Clinical prognostic
factors in patients with malignant glioma treated with combined
modality approach. Am J Clin Oncol 27:195–204
33. Devaux BC, O’Fallon JR, Kelly PJ (1993) Resection, biopsy, and
survival in malignant glial neoplasms. A retrospective study of
clinical parameters, therapy, and outcome. J Neurosurg 78:767–
775
34. Vecht CJ, Avezaat CJJ, van Putten WLJ et al (1990) The influ-
ence of the extent of surgery on the neurological function and
survival in malignant glioma. A retrospective analysis in 243.
J Neurol Neurosurg Psychiatry 53:466–471
35. Skirboll SS, Ojemann GA, Berger MS et al (1996) Functional
cortex and subcortical white matter located within gliomas.
Neurosurgery 38(4):678–685
36. Berger M (1995) Functional mapping-guided resection of low-
grade gliomas. Clin Neurosurg 42:437–456
37. Berger MS, Ojemann GA (1991) Intraoperative brain mapping
techniques in neuro-oncology. Epilepsy 58:153–161
38. Brell M, Ibanez J, Caral L et al (2000) Factors influencing
complications of intra-axial brain tumours. Acta Neurochir 142:
739–750
39. Neuloh G, Pechstein U, Schramm J (2007) Motor tract moni-
toring during insular glioma surgery. J Neurosurg 106:582–592
40. Keles GE, Lundin DA, Lamborn KR et al (2004) Intraoperative
subcortical stimulation mapping for hemispherical periolandic
glioma located within or adjacent to the descending motor
pathways: evaluation of morbidity and assessment of functional
outcome in 294 patients. J Neurosurg 100:369–375
41. Mc Girt MJ, Chaichana KL, Gathinji M et al (2009) Independent
association of extent of resection with survival in patients with
malignant brain astrocytoma. J Neurosurg 110:156–162
42. Stummer W, Reulen HJ, Meinel T et al (2008) Extent of resection
and survival in glioblastoma multiforme: identification of and
adjustment for bias. Neurosurgery 62:564–576
43. Van den Bent MJ, Hegi ME, Stupp R (2006) Recent developments
in the use of chemotherapy in brain tumors. Eur J Cancer 42:
582–588
426 J Neurooncol (2010) 100:417–426
123
Copyright © 2022 FDOKUMEN