Surgical Therapy for Heart Failure - Critical Care Medicine
14
Surgical Therapy for Heart Failure Craig H Selzman, MD, FACS, Rajendra S Bhati, MD, Brett C Sheridan, MD, FACS, William E Stansfield, MD, Michael R Mill, MD, FACS After a meeting of the American College of Cardiol- ogy in 2003, the cover of US News and World Report boldly proclaimed: “The end of heart disease.” 1 The media frenzy after one of the national cardiology meetings is always interesting to observe. The late- breaking trials of pharmacology, drug-eluting coro- nary stents, and percutaneous heart valves conspire to make even the busiest cardiothoracic surgeon think of his or her own professional future. But amid our car- diologic colleagues’ excitement over the “vanishing scalpel” 1 are some sobering statistics ( Table 1). Car- diovascular disease remains the leading cause of death in the US. Ischemic heart disease accounts for a large portion of these deaths. Although the number of pa- tients dying acutely from myocardial infarction has decreased nearly 30% in the last 2 decades, the num- ber of patients dying from heart failure (HF) has dou- bled. Despite improving medical therapy, many of these patients continue to have functional decline and ultimately die. Management of HF, as such, has evolved into a steadily growing discipline. This review will discuss the role of surgical therapy for treating the enlarging population of patients with HF. HEART FAILURE—THE MODERN EPIDEMIC The American Heart Association’s latest update esti- mates that nearly 5,000,000 Americans suffer from HF. Over 500,000 patients are newly diagnosed each year. HF does not discriminate by gender, race, or age. It is increasingly prevalent in men and women, Caucasian and non-Caucasian, and young and old. At age 40, the lifetime risk of HF developing is 20%. 2 Importantly, because of an aging population and better medical ther- apy, patients with advanced HF are now much older, with more attendant comorbidities. 3 HF is associated with staggering costs to society—estimated to be more than $30 billion last year—that are related to repeat hospitalizations, loss of work potential, and prescription medicines. 3 Although medical therapy has greatly in- creased the quality and length of life for these patients, diagnosis of HF has traditionally carried a mortality rate of 20% within 1 year and 50% within 2 years. 4 HF is the clinical end point for a number of diseases resulting in myocardial dysfunction. Ischemic cardio- myopathies (from coronary artery disease) and dilated cardiomyopathies (either idiopathic or familial) make up the majority of cases. Many other diseases can also lead to end-stage heart failure, including valvular, con- genital, metabolic, and inflammatory disorders. Patho- logically, cardiac remodeling is characterized by myocyte hypertrophy, chamber dilation, and changes in matrix composition. Ultimately, the fibrotic heart becomes more spherical and, subsequently, a less-efficient pump. An important goal is to identify and favorably intervene before onset of terminal myocardial remodeling. Patients present with a variety of symptoms related to both systolic (poor antegrade pump function) and dia- stolic (poor ventricular relaxation and compliance) dys- function. Descriptions of patients with HF have been noted as early as 1600 BC in the Ebers papyrus. Other references to “dropsy” (accumulation of lymph fluid) and cardiac cachexia were noted by Hippocrates.Typical symptoms of HF include dyspnea on exertion, orthop- nea, paroxysmal nocturnal dyspnea, fatigue, and ab- dominal symptoms related to right heart congestion. These symptoms are often associated with several phys- ical findings, including elevated jugular venous pressure, a third heart sound, pulmonary congestion, and periph- eral edema. Traditionally, the New York Heart Association (NYHA) Classification has been used to define the func- tional limitations of patients with HF. Recent guidelines have suggested a new classification system that empha- sizes its evolution, progression, and structural deteriora- tion (Table 2). 5 This staging system encourages the same Competing Interests Declared: None. Supported by the Franklin H Martin, MD, FACS, American College of Surgeons Faculty Research Grant (CHS). Received January 20, 2006; Revised April 20, 2006; Accepted April 24, 2006. From the Division of Cardiothoracic Surgery, Department of Surgery, Uni- versity of North Carolina, Chapel Hill, NC. Correspondence address: Craig H Selzman, MD, Division of Cardiothoracic Surgery, University of North Carolina at Chapel Hill, 3040 Burnett Womack Bldg, CB #7065, Chapel Hill, NC 27599-7065. email: selzman@med. unc.edu 226 © 2006 by the American College of Surgeons ISSN 1072-7515/06/$32.00 Published by Elsevier Inc. doi:10.1016/j.jamcollsurg.2006.04.022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Surgical Therapy for Heart Failure - Critical Care Medicine

SCW
Aobmmbnmhdsdiptdbbtuewe
HTmOHialb
CSS
RFvCSBu
©P
urgical Therapy for Heart Failureraig H Selzman, MD, FACS, Rajendra S Bhati, MD, Brett C Sheridan, MD, FACS,
illiam E Stansfield, MD, Michael R Mill, MD, FACSawwthmcdo
rmculglhcmAb
bsfnrasndTiae
(ths
fter a meeting of the American College of Cardiol-gy in 2003, the cover of US News and World Reportoldly proclaimed: “The end of heart disease.”1 Theedia frenzy after one of the national cardiologyeetings is always interesting to observe. The late-
reaking trials of pharmacology, drug-eluting coro-ary stents, and percutaneous heart valves conspire toake even the busiest cardiothoracic surgeon think of
is or her own professional future. But amid our car-iologic colleagues’ excitement over the “vanishingcalpel”1 are some sobering statistics (Table 1). Car-iovascular disease remains the leading cause of death
n the US. Ischemic heart disease accounts for a largeortion of these deaths. Although the number of pa-ients dying acutely from myocardial infarction hasecreased nearly 30% in the last 2 decades, the num-er of patients dying from heart failure (HF) has dou-led. Despite improving medical therapy, many ofhese patients continue to have functional decline andltimately die. Management of HF, as such, hasvolved into a steadily growing discipline. This reviewill discuss the role of surgical therapy for treating the
nlarging population of patients with HF.
EART FAILURE—THE MODERN EPIDEMIChe American Heart Association’s latest update esti-ates that nearly 5,000,000 Americans suffer from HF.ver 500,000 patients are newly diagnosed each year.F does not discriminate by gender, race, or age. It is
ncreasingly prevalent in men and women, Caucasiannd non-Caucasian, and young and old. At age 40, theifetime risk of HF developing is 20%.2 Importantly,ecause of an aging population and better medical ther-
ompeting Interests Declared: None.upported by the Franklin H Martin, MD, FACS, American College ofurgeons Faculty Research Grant (CHS).
eceived January 20, 2006; Revised April 20, 2006; Accepted April 24, 2006.rom the Division of Cardiothoracic Surgery, Department of Surgery, Uni-ersity of North Carolina, Chapel Hill, NC.orrespondence address: Craig H Selzman, MD, Division of Cardiothoracicurgery, University of North Carolina at Chapel Hill, 3040 Burnett Womackldg, CB #7065, Chapel Hill, NC 27599-7065. email: selzman@med.
tnc.edu
2262006 by the American College of Surgeons
ublished by Elsevier Inc.
py, patients with advanced HF are now much older,ith more attendant comorbidities.3 HF is associatedith staggering costs to society—estimated to be more
han $30 billion last year—that are related to repeatospitalizations, loss of work potential, and prescriptionedicines.3 Although medical therapy has greatly in-
reased the quality and length of life for these patients,iagnosis of HF has traditionally carried a mortality ratef 20% within 1 year and 50% within 2 years.4
HF is the clinical end point for a number of diseasesesulting in myocardial dysfunction. Ischemic cardio-yopathies (from coronary artery disease) and dilated
ardiomyopathies (either idiopathic or familial) makep the majority of cases. Many other diseases can also
ead to end-stage heart failure, including valvular, con-enital, metabolic, and inflammatory disorders. Patho-ogically, cardiac remodeling is characterized by myocyteypertrophy, chamber dilation, and changes in matrixomposition. Ultimately, the fibrotic heart becomesore spherical and, subsequently, a less-efficient pump.n important goal is to identify and favorably interveneefore onset of terminal myocardial remodeling.Patients present with a variety of symptoms related to
oth systolic (poor antegrade pump function) and dia-tolic (poor ventricular relaxation and compliance) dys-unction. Descriptions of patients with HF have beenoted as early as 1600 BC in the Ebers papyrus. Othereferences to “dropsy” (accumulation of lymph fluid)nd cardiac cachexia were noted by Hippocrates. Typicalymptoms of HF include dyspnea on exertion, orthop-ea, paroxysmal nocturnal dyspnea, fatigue, and ab-ominal symptoms related to right heart congestion.hese symptoms are often associated with several phys-
cal findings, including elevated jugular venous pressure,third heart sound, pulmonary congestion, and periph-ral edema.
Traditionally, the New York Heart AssociationNYHA) Classification has been used to define the func-ional limitations of patients with HF. Recent guidelinesave suggested a new classification system that empha-izes its evolution, progression, and structural deteriora-
ion (Table 2).5 This staging system encourages the sameISSN 1072-7515/06/$32.00doi:10.1016/j.jamcollsurg.2006.04.022

lctwaH
twvnptftmof
HMa1(5ovtfcfsv
p
iusAtrsp
anmucuDtdatnnwri
SDoaocpttai
T1847$
*A
227Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
evels of care of HF patients that we would use for can-er: identify and treat patients at risk for HF (ie, hyper-ension), with early disease (ie, diastolic dysfunction),ith established disease (ie, medically managed HF),
nd with advanced disease (ie, medically refractoryF).4
A host of diagnostic studies are available to studyhese patients. Transthoracic echocardiography with orithout pharmacologic stress is inexpensive and pro-ides functional and anatomic information. Radio-ucleotide scans can evaluate ejection fraction (EF), es-ecially of the right ventricle. MRI has recently provedo be a valuable resource in assessment of myocardialunction and viability. Right and left heart catheteriza-ion assesses presence of coronary artery disease and pul-onary vascular disease. Finally, measurement of peak
xygen consumption with exercise can help stratify theunctional limitation of patients with HF.
EART FAILURE—MEDICAL THERAPYedical therapy, including preventive measures, serves
s the first-line strategy for treating patients with HF. In997, the Systolic Hypertension in the Elderly ProgramSHEP) Cooperative Research Group followed over,000 patients with isolated systolic hypertension. HFccurred more than twice as often in the placebo groupersus those treated with antihypertensive agents. Addi-ionally, treated patients with an earlier myocardial in-arction had an 80% risk reduction in HF developmentompared with those not treated.6 Control of other riskactors, including diabetes, coronary artery disease, andtructural valve disease, similarly prevents pathologicentricular remodeling and HF development.
Once diagnosis of HF is established, a number of
Abbreviations and Acronyms
AF � atrial fibrillationCABG � coronary artery bypass graftingCHF � congestive heart failureEF � ejection fractionHF � heart failureLV � left ventricleLVAD/RVAD � left/right ventricular assist deviceMR � mitral regurgitationNYHA � New York Heart AssociationTAH � total artificial heartVAD � ventricular assist device
harmacologic strategies exist to limit and reverse man- c
festations of congestive heart failure (CHF). In partic-lar, blocking the renin-angiotensin and �-adrenergicystems improves mortality among patients with HF.ngiotensin-converting enzyme inhibitors, and angio-
ensin receptor blockers, increase survival and decreaseepeat hospitalizations.7 These benefits are also found ineveral types of �-adrenergic blockers, including meto-rolol and carvedilol.8,9
Patients often have difficulty tolerating eitherngiotensin-converting enzyme inhibitors or �-blockers. Aumber of additional medication regimens are also used inanaging these patients, including loop and thiazide di-
retics and aldosterone antagonists. Diuretic therapy de-reases ventricular diastolic pressure, which reduces ventric-lar wall stress, and maximizes subendocardial perfusion.igoxin, a cardiac glycoside, is used to help improve symp-
oms associated with CHF through improvement in car-iac contractility. Although use of digoxin does not confersurvival benefit, it has reduced the number of hospitaliza-
ions from worsening HF.10 Recently, there has been re-ewed enthusiasm for vasodilator therapy using a combi-ation of hydralazine and isosorbide dinitrate.11 Finally,hen patients are refractory to standard therapy, they often
equire hospitalization for IV diuretics, vasodilators, andnotropic agents.
URGICAL ALTERNATIVES FOR ADVANCED HFespite considerable improvements in medical therapy,
verall death rates for HF patients have failed to dropppreciably. And, with nearly 10% of the populationver 75 years old diagnosed with HF, a more compli-ated set of patients is emerging and growing. Typically,atients over 65 years of age are not candidates for heartransplantation. Older patients can successfully receiveraditional approaches to heart operation,12 but resourcellocation and increased morbidity and mortality raisemportant societal issues.13 A number of innovative surgi-
able 1. 2005 Cardiovascular Disease Statistics*3,000,000 Prevalence of coronary heart disease65,000 Number of first or recurrent myocardial infarctions94,382 Deaths from coronary heart disease,600,000 Number of patients who have survived a heart attack142billion Annual cost of caring for coronary heart disease
Data from Heart Disease and Stroke Statistics—Updates 2005. Dallas, TX:merican Heart Association; 2005.
al approaches have evolved to service these diverse, refrac-

tf
HWttpsorfmm(e(soloSrniictammair
pd
pahd1tcbot
CHfmCtrbme3secro5(
i“rUpt
TN
I
I
I
I
A ion; H
228 Selzman et al Surgical Therapy for Heart Failure J Am Coll Surg
ory medical patients, with aims of enhancing ventricularunction, quality of life, and, ultimately, survival (Fig. 1).
eart transplantationith progressive end-stage HF despite maximal medical
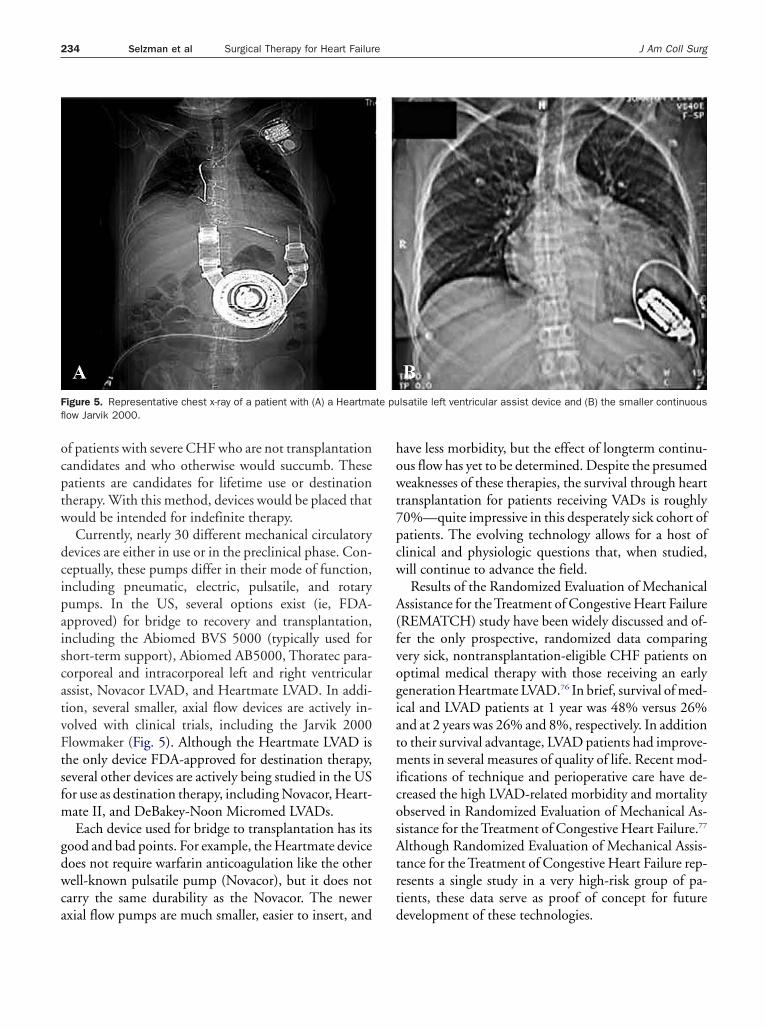
herapy, the “gold standard” therapy has been heartransplantation. Since the first orthotopic heart trans-lantation in 1967 by Christiaan Barnard, the world haseen tremendous progress and advancement in the fieldf cardiac transplantation. Compared with patients whoeceive only medical therapy, transplant recipients haveewer rehospitalizations, marked functional improve-ents, enhanced quality of life, more gainful employ-ent, and longer lives, with 50% surviving to 10 years
Fig. 2).14 Careful selection of donors and recipients andfforts to minimize potential perioperative dangersischemic times, pulmonary hypertension, mechanicalupport, cardiogenic shock) are critical to ensure goodutcomes.15 The single largest advancement in ensuringongterm allograft function is attributed to developmentf immunologic modulators. Pioneered by Dr Normanhumway at Stanford University,16 steroids and antipu-ine metabolites, including azathioprine and mycophe-olate mofetil, have been widely used. Central to current
mmunosuppressive regimens are the calcineurin inhib-tors, cyclosporine, and tacrolimus. These drugs inhibitellular pathways responsible for interleukin-2 produc-ion and subsequent T-cell activation. “Triple drug ther-py,” consisting of steroids, calcineurin inhibitors, andycophenolate mofetil, has become standard initial im-unotherapy after heart transplantation.17 Additional
gents, such as antithymoctye globulin, rapamycin, andnterleukin-2 receptor antagonists, also have importantoles in modern immunosuppression protocols.18
Although heart transplantation is a viable solution foratients with end-stage HD, use is limited by inadequate
able 2. Heart Failure Classificationsew York Heart Association
No symptoms
I Symptoms with substantial activity
II Symptoms with minimal activity
V Symptoms at rest
CC, American College of Cardiologists; AHA, American Hospital Associat
onor supply. In the US, fewer than 2,500 heart trans- w
lantations are performed each year.14,19 Unfortunately,n estimated 10% to 20% of patients die annually on theeart transplant waiting list.19,20 Of the 5 million peopleiagnosed with HF, it is estimated that 30,000 to00,000 patients suffer from such advanced disease thathey would benefit from transplantation or mechanicalirculatory support.21,22 This disparity between the num-ers of patients needing transplants and the availabilityf heart donors has refocused efforts to find other wayso support the severely failing heart.
oronary artery bypassistorically, studies of medical versus surgical therapy
or coronary artery disease focused on patients with nor-al left ventricle (LV) function. The Veterans Affairsooperative Study of Surgery demonstrated a substan-
ially higher survival rate in a subset of patients witheduced left ventricular EFs (� 50%) after coronaryypass operation versus those who were randomized toedical therapy. This survival benefit was particularly
vident at the 11-year followup period (50% versus8%).23 The Coronary Artery Surgery Study (CASS)howed that in patients with left main equivalent dis-ase, operative revascularization prolonged life in mostlinical and angiographic subgroups versus those whoeceived medical therapy. Importantly, this study dem-nstrated that surgical therapy markedly improved the-year cumulative survival in patients with EF � 50%80% versus 47%).24
These earlier randomized trials are limited by theirnclusion of patients with what is currently consideredgood” EF. That is, many patients referred for coronaryevascularization live with EF � 35%. Both the Yale andniversity of Virginia groups, among many others, haveublished their results of coronary artery bypass opera-ions in patients with extremely poor LF function who
ACC/AHA guidelines
A No structural damageHigh risk for developing HF
B Structural abnormalityNo symptoms
C Structural abnormalityPrevious or current symptoms
D Refractory symptoms
F, heart failure.
ere on the transplant waiting list. Elefteriades and col-
le8cru
gwturnerLltms
ttlofmt
ptnmc
Hichgmbeamg
ADaokasddCitLmsg
Futv
FfsfiLapw
229Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
eagues25 demonstrated that coronary artery bypass op-ration in patients with EF � 30% had a survival rate of0% at 4.5 years, which remarkably approaches that ofardiac transplantation. Likewise, Kron and colleagues26
eported a 3-year survival rate of 83% in patients whonderwent coronary bypass with EF � 20%.Pathophysiologically, patients who stand to gain the
reatest benefit from surgical revascularization are thoseho possess hibernating myocardium. This term is used
o describe regions of the heart that are dysfunctionalnder ischemic conditions but retain the capacity toegain normal function after blood flow is restored.27 Aumber of studies demonstrate that patients with isch-mic HF and substantial areas of viable myocardium caneduce mortality, improve NYHA class, favorably alterV geometry, and increase LV EF after surgical revascu-arization.28 MRI has become particularly useful for de-ermining both wall motion abnormalities and viableyocardium and has been demonstrated to predict the
uccess of low-EF revascularization.29
Many surgeons have evolved their practices to meethe demands of higher-risk patients and adopt measureso strive for better graft patency. The former is high-ighted by adoption of off-cardiopulmonary bypass andn-cardiopulmonary bypass, beating heart techniquesor revascularization.30 The latter, “preventive” strategy isanifest by increased use of bilateral mammary and ar-
erial grafting.31
Although the Coronary Artery Surgery Study, Euro-ean, and Veterans Affairs studies established many ofhe standards for treatment of coronary artery disease,o such large studies address similar questions in theodern medical era, especially in patients with ischemic
igure 1. Contemporary management of the patient with heart fail-re is multimodal and multidisciplinary. CRT, chronic resynchroniza-ion therapy; ICD, implantable cardioverter-defibrillator; LVAD, leftentricular assist device; TAH, total artificial heart.
ardiomyopathies. The Surgical Treatment of Ischemic p
eart Failure (STICH) trial is a prospective, random-zed trial currently underway to determine the role oforonary artery bypass in patients with HF. The firstypothesis will test whether coronary artery bypassrafting (CABG) with intensive medical therapy versusedical therapy alone confers an additional survival
enefit in patients with EF � 35%. End points of inter-st will be morbidity and mortality rates, quality of life,nd economic impact of the treatment strategies. Enroll-ent for this arm of the study is expected to reach its
oal of 1,000 patients by the end of 2006.32,33
ortic valve replacementiseases of the aortic valve can frequently lead to onset
nd progression of CHF. Although the natural historiesf both aortic stenosis and aortic regurgitation are wellnown, patients are frequently followed conservativelyfter presenting with considerable HF. Of the three clas-ic symptoms of aortic stenosis—syncope, angina, andyspnea—the latter is the most robust risk factor foreath, with only 50% of patients alive within 2 years.34
onversely, age-corrected survival of patients undergo-ng aortic valve replacement for aortic stenosis is similaro the normal population.35 Unfortunately, once severeV dysfunction develops, results of aortic valve replace-ent are more guarded.36 Because of poor LV function,
ubstantial transvalvular gradients (ie, low output, lowradient aortic stenosis) are not able to develop in these
igure 2. Kaplan-Meier survival for heart transplantations per-ormed between January 1982 and June 2003. Conditional half-lifeignifies the time to 50% survival for those recipients surviving therst year posttransplantation. Reprinted from Taylor DO, EdwardsB, Boucek MM, et al. Registry of the International Society for Heartnd Lung Transplantation: twenty-second official adult heart trans-lant report—2005. J Heart Lung Transplant 2005;24:945�955,ith permission.14
atients. Critical in the preoperative decision process is

d(fpPccosoditttpta
csettac5
r1oss
MMCdoitimmlnicewrpvv
03:1
230 Selzman et al Surgical Therapy for Heart Failure J Am Coll Surg
etermining if ventricular dysfunction is truly valvularwhich would improve with replacement) versus otherorms of cardiomyopathy, such as ischemia or restrictiverocesses (which would not improve with replacement).recise measurement of aortic valve area is difficult be-ause the calculated valve area is directly proportional toardiac output. Also, the Gorlin constant varies at lowerutputs. In this situation, the valve areas might be con-idered critically small when, at operation, the valve isnly moderately diseased. Preoperative evaluation withobutamine (increase contractile reserve) or vasodilator-
nduced stress echocardiography (using continuity equa-ion rather than the Gorlin formula) can be helpful withhis distinction and can guide candidacy for this rela-ively high-risk procedure.37 Nevertheless, because of theossibility of ventricular recovery and lengthened pa-ient survival, most patients with HF and aortic stenosisre offered valve replacement.38
Timing of surgical intervention for aortic insuffi-iency is more challenging than with patients with aortictenosis. Similarly, once symptoms occur and there isvidence of LV structural changes, morbidity and mor-ality for aortic insufficiency increases.39 In a retrospec-ive review from the Mayo Clinic, 450 patients receivingortic valve replacement for aortic insufficiency wereompared by ranges of EF (� 35%, 35% to 50%, �
Figure 3. Pathophysiology of mitral regurgitaannular dilation impede the mitral leaflets frothe heart fails). Changes in ventricular geomleaflet tenting, additionally restricting their mtransplant surgical options for heart failure. Inthe adult. 2nd ed. New York: McGraw-Hill; 20
0%). Although the group with severe dysfunction car- r
ied an operative mortality of 14%, EF improved and0-year survival was 41%.40 Earlier intervention, beforenset of severe LV dysfunction, is crucial to improvingurvival of patients with this lesion,41 as seen with aortictenosis.
itral valve repairitral valve regurgitation can both cause and result fromHF. Its presence is an independent risk factor for car-iovascular morbidity and mortality.42 The pathophysi-logy of mitral regurgitation (MR) is generally a result ofts etiology. In addition to frank papillary muscle rup-ure associated with acute myocardial infarction, chronicschemic cardiomyopathies result in papillary muscle
igration as the ventricle dilates, causing tenting of theitral leaflets, restricting their coaptation (Fig. 3). Di-
ated cardiomyopathies can have similar issues and an-ular dilation. In addition to mitral MR, this alteration
n the LV geometry contributes to volume overload, in-reases LV wall tension, and leaves patients susceptible toxacerbations of HF.43 Mitral valve operation in patientsith HF has gained enthusiasm because it abolishes the
egurgitant lesion and decreases symptoms. The patho-hysiologic rationale for repair or replacement is to re-erse the cycle of excessive ventricular volume, allow forentricular unloading, and promote myocardial
ssociated with heart failure. Ventricular andequately meeting (ZC, zone of coaptation asith papillary muscle displacement results in. Reprinted from Badhar V, Bolling SF. Non-n LJ, Edmunds LH Jr, eds. Cardiac surgery in515�1526, with permission.94
tion am adetry wotion: Coh
emodeling.

vawHhpatmbicipsrstwtlwlm
ildectctIrvloftspptct
VAmasasrpcdtchsflfreTTSrwimoSsirC
rstamnakseStn
231Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
Among others, the Michigan group has been an ad-ocate for mitral repair in the HF population. Bollingnd colleagues44 demonstrated that mitral valve repairas associated with an increased EF, an improvement inF class from 3.9 to 2.0, and a decrease in the number of
ospitalizations. Additional effects with repair in theseatients is the increase in coronary blood flow reservefforded by reduction in LV volume.45 Despite the po-ential benefits of mitral reconstruction operation, aore recent retrospective review showed no demonstra-
le decrease in longterm mortality in patients undergo-ng mitral valve repair for patients with severe MR andonsiderable LV dysfunction.46 This most recent analysiss not overly surprising. HF in the majority of theseatients is not because of flail leaflets, for example, but isecondary to ventricular dysfunction. Most commonly,epair for cardiomyopathy-associated MR involves in-ertion of either a complete or partial band attached tohe annulus of the mitral valve. Mitral repair only dealsith one aspect of the overall pathophysiologic condi-
ion, ie, annuloplasty rings can assist with tenting of theeaflet, but do not address papillary muscle displacementith ventricular scarring.47 In many patients, the under-
ying problem continues unabated (ie, primaryyopathy).In evaluating studies of HF with MR, it will be
mportant to separate causes (ie, ischemic versus di-ated) and surgical approaches. Future trials must beesigned to distinguish differences among various op-rative strategies, such as annuloplasty, papillary mus-le resuspension, secondary chordal transection, ven-ricular reconstruction, passive restraints, andhordal-sparing valve replacement. Paramount inhese procedures is to have little or no residual MR.48
f feasibility of repair is deemed improbable, mitraleplacement should be performed. Traditional mitralalve replacement includes complete resection of theeaflets and the chordal attachments. This destructionf the subvalvular apparatus results in ventricular dys-unction. Preservation of the chordal attachments tohe ventricle with valve replacement might provideimilar or even better results than annuloplasty inatients with MR and HF.49,50 Although it might notortend an increased survival in these high-risk pa-ients,51,52 the beneficial effects on quality of life (de-reased HF) will likely keep low EF mitral valve in-
erventions in the armamentarium of HF surgeons. ventricular restorationfter transmural myocardial infarction, the ventricle re-odels pathologically from its normal elliptical shape tospherical shape and this change in geometry is respon-
ible, in part, for the constellation of symptoms associ-ted with CHF and decreased survival.53,54 There areeveral ventricular restoration techniques, all aim to cor-ect this pathologic alteration in geometry. Most ap-roaches involve incising and excluding nonviable myo-ardium with either patch or primary reconstruction,ecreasing ventricular volume. Although the initial en-husiasm of ventricular resection in nonischemic dilatedardiomyopathies (“the Batista procedure”) has faded, itas long been established that resection of dyskineticegments associated with LV aneurysm can increaseunctional status and prolong life.55,56 Success of earlyytic and percutaneous therapy for acute myocardial in-arctions has decreased the incidence of true LV aneu-ysms. Ventricular restoration as such, now focuses onxcluding more subtle regions of akinetic myocardium.he Reconstructive Endoventricular Surgery returningorsion Original Radius Elliptical shape to the LV (RE-TORE) group reported in 2004 that after ventricularestoration using the technique described by Dor, thereas an increase in EF from 29.6% to 39.5%, a decrease
n end-systolic volume index, and considerable improve-ent in NYHA function class (67% NYHA III/IV pre-
peratively versus 85% NYHA I/II postoperatively).57
imilarly, Yamaguchi and colleagues58 demonstrated aubstantially improved 5-year survival in patients withschemic cardiomyopathy who underwent ventricularestoration and CABG versus those who underwentABG alone, 90% versus 53.5%, respectively.Much enthusiasm currently exists to use ventricular
emodeling operation for HF patients. Most studies out-ide of the Reconstructive Endoventricular Surgery re-urning Torsion Original Radius Elliptical investigatorsre single-institution, retrospective analyses. Althoughany believe that this therapy is warranted for dyski-
etic and large akinetic segments of myocardium, somere beginning to perform this procedure even on hypo-inetic regions. The major study of ventricular recon-truction is the NIH-funded Surgical Treatment of Isch-mic Heart Failure trial. In its second hypothesis, theurgical Treatment of Ischemic Heart Failure investiga-ors are prospectively randomizing patients with aki-etic, low EF ventricles to CABG versus CABG and
entricular reconstruction. Enrollment for this aim will
blri
PFlatwaiawtwtio
(tistcsaPNftrrvdtcdcsid
EPn
1nmpsrtalvttvbtdcc(mIrfi(sdFtirp5gamAit
dfottre
232 Selzman et al Surgical Therapy for Heart Failure J Am Coll Surg
e met within the next year and, after prolonged fol-owup, should shed light on the importance of bothevascularization and ventricular geometry in these veryll patients.32
assive restraintsundamental principles in hemodynamics (ie, Laplace’s
aw) hint as to the progression of structural deteriorationssociated with HF. A cycle exists with increasing ven-ricular volume resulting in increased wall tension,hich is compensated with thickening of the ventricle
nd its dilation. Historically, dynamic cardiomyoplasty,e, wrapping the latissmus dorsi muscle around the heartnd entraining it to beat synchronously with the heart,as intended to augment systolic function. Although
his technique was somewhat cumbersome and not over-helmingly successful, investigators learned that this ex-
ernal fixation of the heart prevented its dilation andmproved HF. Recent enthusiasm, as such, has focusedn devices that restrain the heart.
The most studied product is the CorCap deviceAcorn Cardiovascular), which is a mesh-like supporthat is sewn circumferentially around the ventricle. An-mal studies have demonstrated its downregulation oftretch response proteins, attenuation of myocyte hyper-rophy, and improvement of sarcoplasmic-reticulum cal-ium cycling.59 Early reports in humans have demon-trated a decrease in ventricular chamber dimensionsnd improvement in EF and NYHA class.60 The Acornivotal Trial was completed recently. Patients withYHA class III/IV disease were randomized to one of
our groups: optimal medical therapy, optimal medicalherapy with the cardiac support device, mitral valveepair/replacement alone, or mitral valve repair/eplacement with cardiac support device. Results re-ealed that patients who received the cardiac supportevice required fewer major cardiac procedures (eg,ransplantation, left ventricular assist device [LVAD])ompared with controls after implantation, a greater re-uction in LV end diastolic and systolic volumes, andonsiderable improvement in quality of life.61 Wide-pread use is not available, but the FDA recently deniedts approval, citing need for additional statistical evi-ence to demonstrate its efficacy.62
lectrophysiologyatients with HF and interventricular conduction ab-
ormalities (roughly defined as a QRS interval � 120 to t30 ms) are potential candidates for chronic resynchro-ization therapy by insertion of a biventricular pace-aker. Chronic resynchronization therapy aims to im-
rove cardiac performance by restoring interventriculareptal electrical and mechanical synchrony of the heart,educing presystolic MR, and optimizing diastolic func-ion by reducing mismatch between cardiac contractilitynd energy expenditure.63 Technically, three cardiaceads are placed transvenously: an atrial lead, a rightentricular lead, and a LV lead, which is threadedhrough the coronary sinus and out one of its lateral wallributaries. Surgeons have assisted on difficult trans-enous LV placements by epicardial insertion of LV leadsy a number of techniques, including minithorocotomy,horocoscopy, or robotically. Several prospective, ran-omized trials have been performed evaluating the effi-acy of chronic resynchronization therapy. The Multi-enter InSync Randomized Clinical EvaluationMIRACLE) Study Group demonstrated an improve-ent in NYHA functional class, quality of life, and EF.64
n addition to augmenting functional capacity, chronicesynchronization therapy also appears to favorably af-ect mortality effect. Although the Comparison of Med-cal Therapy, Pacing, and Defibrillation in Heart FailureCOMPANION) trial only demonstrated an increase inurvival when biventricular pacing was placed with aefibrillator,65 the Cardiac Resynchronization in Heartailure (CARE-HF) trial recently showed a 36% reduc-ion in death with biventricular pacing alone.66 Mortal-ty in both studies was usually sudden death. Indeed, theole of the implantable cardioverter defibrillator has ex-anded rapidly over the last decade. Patients with HF areto 10 times more likely to die of sudden death than theeneral population. Sudden death from both ischemicnd nonischemic sustained ventricular tachyarrhyth-ias has been remarkably reduced, such that currentmerican Heart Association guidelines recommend an
mplantable cardioverter defibrillator in virtually all pa-ients with EF � 35%.
Interestingly, prophylactic use of an implantable car-ioverter defibrillator at the time of low-EF CABGailed to improve survival compared with those patientsnly revascularized.67 This study speaks to the impor-ance of the independent influence of CABG on reduc-ion of mortality in ischemic cardiomyopathies. We haveecently adopted an approach of placing prophylactic LVpicardial leads on patients with conduction delays at
he time of high-risk HF operation. These leads are tun-
naTp
impgnvpcwpccc
aidtpplatMmtfttswsteatt
MVIuw
mDippaSr(
bIomscaDadsaopacfmo
FveiitsI
233Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
eled for future connection to a traditional transvenoustrial and right ventricle biventricular pacer-defibrillator.he benefit of this strategy remains to be provedrospectively.
Atrial fibrillation (AF), with or without HF, is anndependent risk factor for increased cardiovascular
orbidity and mortality. In a large retrospective study ofatients with LV dysfunction, patients with AF hadreater all-cause mortality (34% versus 23%) and greaterumber of deaths attributed to pump failure (16.7%ersus 9.4%).68 Aggressive management of AF in HFatients is receiving greater attention. Compared withontrols, HF patients with concurrent AF who under-ent catheter ablation demonstrated considerable im-rovement in LV function (increased EF by 21%), de-rease in LV dimensions, and improvements in exerciseapacity, symptoms, and quality of life as compared withontrols.69
The cardiac surgical community has increasinglydopted an aggressive approach to treatment of AF dur-ng concurrent operations. The Cox-Maze procedure,eveloped in the early 1990s, involves creation of mul-iple incisions to prevent atrial reentry and allow forropagation of normal sinus impulses. This techniqueroved successful in curing AF, but is technically chal-
enging and time-intensive, lessening its widespreaddoption.70 A number of variations from this originalechnique have evolved throughout the past decade.
ost use a host of adjunct ablation devices to replaceany of the “cut and sew” lesions, including cryo-
hermy, radiofrequency, microwave, and high-intensityocused ultrasonography. The ease and efficacy of theseechnologies have allowed their adoption in combina-ion with other procedures performed for HF. Indeed,ome evidence exists that LV function can be improvedith concomitant ablation of AF during operations for
tructural (usually valvular) heart disease.71,72 Althoughhe conceptual advantages of restoring atrial functionxist, no study has looked at the role of surgical AFblation in impacting the natural history of these pa-ients. To date, surgical ablation for lone AF in HF pa-ients remains anecdotal.73
ECHANICAL CIRCULATORY SUPPORTentricular assist devicesn 1963, Dr Michael DeBakey reported the first clinicalse of a ventricular assist device (VAD) in an individual
ho suffered a cardiac arrest after an aortic valve replace- fent. Unfortunately, the patient died. Three years later,eBakey successfully implanted a newer device in an
ndividual who was unable to be weaned from cardio-ulmonary bypass. This patient was mechanically sup-orted for 10 days, allowing for myocardial recovery,nd was successfully discharged from the hospital.74
ince this early era, VAD development has progressedapidly and is now an invaluable tool in treatment of HFFig. 4).
A number of devices are currently available to supportoth the acutely and chronically decompensated heart.n some cases of extreme cardiopulmonary failure, thenly recourse is complete support with extracorporealembrane oxygenation. Despite some encouraging re-
ults with extracorporeal membrane oxygenation forardiogenic shock,75 most patients requiring circulatoryssistance can be helped with ventricular support alone.epending on the particular device used, both the right
nd LVs can be assisted (LVAD, right ventricular assistevice [RVAD], and biVAD). Conceptually, they are allimilar: blood is removed from the failing ventricle intopump, which delivers blood to either the aorta (LVAD)r pulmonary artery (RVAD). Often these devices can belaced temporarily to allow myocardial recovery (ie,cute viral myocarditis, postcardiotomy). The mostommon use of these devices is to bridge the acutelyailing heart to eventual heart transplantation. Thisethod allows patients to recover end-organ damage,
btain rehabilitation, and possibly go home before de-
igure 4. Mechanical circulatory assist devices. A number of de-ices are currently available in the US (many more are in preclinicalvaluation or in feasibility testing clinical trials) for three mainndications. Bridge to eligibility is a term used to describe devicemplantation in patients initially thought to be poor candidates forransplantation. If conditions improve (eg, resolution of renal failure)uch that they are suitable for transplantation, the patient is listed.f not, the ventricular assist device is used as terminal therapy.
initive heart transplantation. Finally, there are a group
ocptw
dcipaiscatvFtsfm
gdwca
howt7pcw
A(fvogiatmicosAtrt
Ffl
234 Selzman et al Surgical Therapy for Heart Failure J Am Coll Surg
f patients with severe CHF who are not transplantationandidates and who otherwise would succumb. Theseatients are candidates for lifetime use or destinationherapy. With this method, devices would be placed thatould be intended for indefinite therapy.Currently, nearly 30 different mechanical circulatory
evices are either in use or in the preclinical phase. Con-eptually, these pumps differ in their mode of function,ncluding pneumatic, electric, pulsatile, and rotaryumps. In the US, several options exist (ie, FDA-pproved) for bridge to recovery and transplantation,ncluding the Abiomed BVS 5000 (typically used forhort-term support), Abiomed AB5000, Thoratec para-orporeal and intracorporeal left and right ventricularssist, Novacor LVAD, and Heartmate LVAD. In addi-ion, several smaller, axial flow devices are actively in-olved with clinical trials, including the Jarvik 2000lowmaker (Fig. 5). Although the Heartmate LVAD ishe only device FDA-approved for destination therapy,everal other devices are actively being studied in the USor use as destination therapy, including Novacor, Heart-ate II, and DeBakey-Noon Micromed LVADs.Each device used for bridge to transplantation has its
ood and bad points. For example, the Heartmate deviceoes not require warfarin anticoagulation like the otherell-known pulsatile pump (Novacor), but it does not
arry the same durability as the Novacor. The newer
igure 5. Representative chest x-ray of a patient with (A) a Heartmaow Jarvik 2000.
xial flow pumps are much smaller, easier to insert, and d
ave less morbidity, but the effect of longterm continu-us flow has yet to be determined. Despite the presumedeaknesses of these therapies, the survival through heart
ransplantation for patients receiving VADs is roughly0%—quite impressive in this desperately sick cohort ofatients. The evolving technology allows for a host oflinical and physiologic questions that, when studied,ill continue to advance the field.Results of the Randomized Evaluation of Mechanical
ssistance for the Treatment of Congestive Heart FailureREMATCH) study have been widely discussed and of-er the only prospective, randomized data comparingery sick, nontransplantation-eligible CHF patients onptimal medical therapy with those receiving an earlyeneration Heartmate LVAD.76 In brief, survival of med-cal and LVAD patients at 1 year was 48% versus 26%nd at 2 years was 26% and 8%, respectively. In additiono their survival advantage, LVAD patients had improve-ents in several measures of quality of life. Recent mod-
fications of technique and perioperative care have de-reased the high LVAD-related morbidity and mortalitybserved in Randomized Evaluation of Mechanical As-istance for the Treatment of Congestive Heart Failure.77
lthough Randomized Evaluation of Mechanical Assis-ance for the Treatment of Congestive Heart Failure rep-esents a single study in a very high-risk group of pa-ients, these data serve as proof of concept for future
lsatile left ventricular assist device and (B) the smaller continuous
te puevelopment of these technologies.

TToiCabdnorsstptt
tsiIbttawalcmitufrp
sthdeawsiogivuv
TAsipmIp
ctfrlttta(a
T
NMMMPVWF (brid
235Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
otal artificial hearthe creation of a suitable total artificial heart (TAH) forrthotopic implantation has been the subject of intensenvestigation for the past 40 years.78 In 1969, Dr Dentonooley implanted the Liotta TAH in a high-risk patient
fter failing to wean the patient off cardiopulmonaryypass after LV aneurysm repair. He was sustained for 3ays until a donor heart became available. Unfortu-ately, the patient died from pneumonia and multiplergan failure.79 The historic development of the TAH isich with technologic genius, device failure, and per-onal intrigue.78 Compared with LVADs, the TAH haseveral potential advantages, including assisting the pa-ient with severe biventricular failure, lack of deviceocket and lessened risk of infection, and treating pa-ients with systemic diseases who are not otherwiseransplantation candidates (amyloidosis, malignancy).
To date, there are two TAHs receiving the most atten-ion (Table 3). The Cardiowest (Syncardia Systems) is atructural cousin of the original Jarvik-7 TAH that wasmplanted in Barney Clark with great publicity in 1982.nvestigators have recently reported data allowing it toecome the only FDA-approved TAH for use as a bridgeo transplantation. Nearly 80% of patients survived toransplantation versus only 46% in the control, medicalrm. Survival rates at 1 and 5 years in device patientsere 86% and 64%, respectively, compared with 69%nd 34% in the control group.80 The Cardiowest’s mainimitation is its external power source and large controlonsul. The Abiocor TAH (Abiomed) uses a novelethod of transcutaneous transmission of energy, free-
ng the patient of any external drive lines. External bat-ery packs are exchanged by the patient and can last forp to 4 hours. The first clinical implantation was per-ormed in July 2001. Currently, only 14 patients haveeceived the device, as part of a trial that includes only
able 3. Comparison of Cardiowest and Abiocor Total Artific
o. of implants � 5echanism Pneaximum stroke volume (mL) 70aximum cardiac output (L/min) 9
ower source Extealves Meceight (g) 160
DA-approved Yes
atients with less than 30 days to live. Although all have m
ubsequently died, four patients were ambulatory afterhe operation, two patients were discharged from theospital to a transitional care setting, and one of theischarged patients was discharged to home on postop-rative day 209.81 The Abiocor is limited by its large size,llowing implantation in only 50% of men and 20% ofomen. The next TAH to emerge clinically will be the
econd-generation TAH from Abiomed. The Abiocor IIs designed to be 35% smaller and durable to pump forver 5 years. Despite over 40 years of effort, the emer-ence of artificial heart technology into clinical practices still immature. With approval of the Cardiowest de-ice, and new efforts with smaller pumps, TAHs willltimately be a routine component of HF operation forery sick HF patients with biventricular failure.
RANSLATIONAL APPROACHESlthough many therapies are time-tested, such as bypass
urgery and aortic valve replacement, others are matur-ng, waiting for longterm followup and well-designedrospective studies. The future is filled with advance-ents in mechanical devices and translational strategies.
ndeed, biologic approaches to HF are actively beingursued, both experimentally and clinically.Hottest on this list is use of stem cells to augment
ardiac function.82,83 Cellular transplantation is based onhe theory that a cardiac progenitor cell can progress intoully differentiated cardiac myocytes and subsequentlyeplace damaged myocardium.84 Conversely, some be-ieve that these cells play more of a supportive role, ratherhan a regenerative role, by optimizing conditions forhe heart to recover from ischemia.85,86 Multiple cellypes are currently being studied both experimentallynd clinically; these include bone marrow stem cellsboth mesenchymal and hematopoetic), dendritic cells,dipocytes, endothelial progenitor cells, and skeletal
eartCardiowest Abiocor
14ic Hydraulic
608Internal
cal Trileaflet plastic900
ge to transplantation) No
ial H
70umat
rnalhani
yoblasts.

crcdeucstsUmrbwbis3its
fitafoip
tdaursuTmst
asi
Tostp
R
1
1
1
1
1
1
236 Selzman et al Surgical Therapy for Heart Failure J Am Coll Surg
To date, clinical trials are performed mostly in singleenters with limited patient numbers. Some intriguingesults have been reported. Intracoronary infusion ofardiac progenitor cells in patients with acute myocar-ial infarctions have demonstrated improved LV EF andnd-systolic volumes.87 In a recent phase I clinical trialsing autologous skeletal myoblasts at the time of surgi-al revascularization, Menasché and colleagues88 demon-trated increased NYHA functional class (2.7 preopera-ively to 1.6 postoperatively), EF (24% to 32%), andystolic thickening by echo at the site of implant in 63%.nfortunately, ventricular arrhythmias developed inany of these patients. Recently, Patel and colleagues89
andomized 20 patients to receive off-cardiopulmonaryypass revascularization in HF patients (EF � 35%)ith or without subepicardial injection of autologousone marrow stem cells. Compared with the revascular-zation group, the stem cell-treated patients were ob-erved to have increased EF at 6 months (46% versus7%).89 Many variations on the stem cell theme exist,ncluding angiogenic therapy to increase vascularity athe site of infarct and growth factors to increase nativetem cell homing to injured myocardium.90,91
More questions than answers exist in this growingield, including optimal cell type, optimal cell density,dentification of correct patients, frequency of adminis-ration, and adjuncts for revascularization. Most avail-ble clinical trials vary tremendously in many of theseeatures and are nonrandomized, making interpretationf the results difficult. Although use of biologic therapys in its infancy, these early results show its potentialromise.In conclusion, the modern paradigm of treating pa-
ients with HF is truly multidisciplinary, including car-iologists, cardiac surgeons, nurses, social workers, ther-pists, and basic scientists. Thematically, these patientsniformly have multiple comorbidities and are at highisk with any intervention. Their ultimate outcomes, asuch, depend on the constellation of preoperative eval-ation, intraoperative conduct, and postoperative care.hese patients, as to the latter point, require meticulousultiorgan attention to ensure their success. Indeed, a
olid working relationship among caregivers is essentialo an effective HF surgery program.92,93
Management of HF is truly multifaceted in naturend is constantly evolving. Clinically and scientifically,urgeons are uniquely positioned to have a considerable
mpact on treatment strategies for these sick patients.he number of options—ranging from bypass and valveperations to transplantation and mechanical assist—uggest that the so-called “vanishing scalpel” will be cen-ral to the longevity and quality of life for our aging HFopulation.
EFERENCES
1. Comarow A, Healy B. The future is now. US News World Rep2003;135(19):41–70.
2. Lloyd-Jones DM, Larson MG, Leip EP, et al. Lifetime risk fordeveloping congestive heart failure: the Framingham HeartStudy. Circulation 2002;106:3068–3072.
3. Heart Disease and Stroke Statistics—Updates 2005. Dallas, TX:American Heart Association; 2005.
4. Jessup M, Brozena S. Heart failure. N Engl J Med 2003;348:2007–2018.
5. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines forthe evaluation and management of chronic heart failure in theadult: executive summary. A report of the American College ofCardiology/American Heart Association Task Force on PracticeGuidelines (Committee to revise the 1995 Guidelines for theEvaluation and Management of Heart Failure). J Am Coll Car-diol 2001;38:2101–2113.
6. Kostis JB, Davis BR, Cutler J, et al. Prevention of heart failure byantihypertensive drug treatment in older persons with isolatedsystolic hypertension. SHEP Cooperative Research Group.JAMA 1997;278:212–216.
7. Garg R, Yusuf S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality and morbidity inpatients with heart failure. Collaborative Group on ACE Inhib-itor Trials. JAMA 1995;273:1450–1456.
8. Effect of metoprolol CR/XL in chronic heart failure: MetoprololCR/XL Randomised Intervention Trial in Congestive HeartFailure (MERIT-HF). Lancet 1999;353(9169):2001�2007.
9. Packer M, Coats AJ, Fowler MB, et al. Effect of carvedilol onsurvival in severe chronic heart failure. N Engl J Med 2001;344:1651–1658.
0. The Digitalis Investigation Group. The effect of digoxin onmortality and morbidity in patients with heart failure. N EnglJ Med 1997;336:525�533.
1. Elkayam U, Bitar F. Effects of nitrates and hydralazine in heartfailure: clinical evidence before the African American heart fail-ure trial. Am J Cardiol 2005;96(7B):37i–43i.
2. Fruitman DS, MacDougall CE, Ross DB. Cardiac surgery inoctogenarians: can elderly patients benefit? Quality of life aftercardiac surgery. Ann Thorac Surg 1999;68:2129–2135.
3. Scott BH, Seifert FC, Grimson R, Glass PS. Octogenariansundergoing coronary artery bypass graft surgery: resource utili-zation, postoperative mortality, and morbidity. J CardiothoracVasc Anesth 2005;19:583–588.
4. Taylor DO, Edwards LB, Boucek MM, et al. Registry of theInternational Society for Heart and Lung Transplantation:twenty-second official adult heart transplant report. J HeartLung Transplant 2005;24:945–955.
5. Cimato TR, Jessup M. Recipient selection in cardiac transplan-tation: contraindications and risk factors for mortality. J Heart
Lung Transplant 2002;21:1161–1173.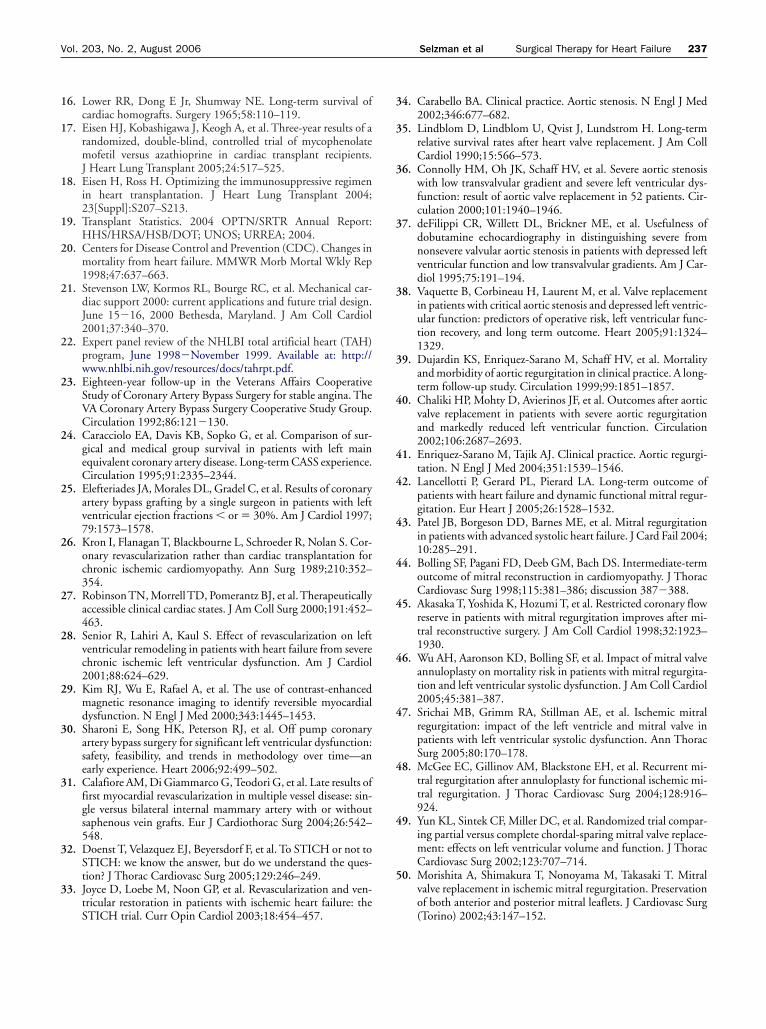
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
237Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
6. Lower RR, Dong E Jr, Shumway NE. Long-term survival ofcardiac homografts. Surgery 1965;58:110–119.
7. Eisen HJ, Kobashigawa J, Keogh A, et al. Three-year results of arandomized, double-blind, controlled trial of mycophenolatemofetil versus azathioprine in cardiac transplant recipients.J Heart Lung Transplant 2005;24:517–525.
8. Eisen H, Ross H. Optimizing the immunosuppressive regimenin heart transplantation. J Heart Lung Transplant 2004;23[Suppl]:S207–S213.
9. Transplant Statistics. 2004 OPTN/SRTR Annual Report:HHS/HRSA/HSB/DOT; UNOS; URREA; 2004.
0. Centers for Disease Control and Prevention (CDC). Changes inmortality from heart failure. MMWR Morb Mortal Wkly Rep1998;47:637–663.
1. Stevenson LW, Kormos RL, Bourge RC, et al. Mechanical car-diac support 2000: current applications and future trial design.June 15�16, 2000 Bethesda, Maryland. J Am Coll Cardiol2001;37:340–370.
2. Expert panel review of the NHLBI total artificial heart (TAH)program, June 1998�November 1999. Available at: http://www.nhlbi.nih.gov/resources/docs/tahrpt.pdf.
3. Eighteen-year follow-up in the Veterans Affairs CooperativeStudy of Coronary Artery Bypass Surgery for stable angina. TheVA Coronary Artery Bypass Surgery Cooperative Study Group.Circulation 1992;86:121�130.
4. Caracciolo EA, Davis KB, Sopko G, et al. Comparison of sur-gical and medical group survival in patients with left mainequivalent coronary artery disease. Long-term CASS experience.Circulation 1995;91:2335–2344.
5. Elefteriades JA, Morales DL, Gradel C, et al. Results of coronaryartery bypass grafting by a single surgeon in patients with leftventricular ejection fractions � or � 30%. Am J Cardiol 1997;79:1573–1578.
6. Kron I, Flanagan T, Blackbourne L, Schroeder R, Nolan S. Cor-onary revascularization rather than cardiac transplantation forchronic ischemic cardiomyopathy. Ann Surg 1989;210:352–354.
7. Robinson TN, Morrell TD, Pomerantz BJ, et al. Therapeuticallyaccessible clinical cardiac states. J Am Coll Surg 2000;191:452–463.
8. Senior R, Lahiri A, Kaul S. Effect of revascularization on leftventricular remodeling in patients with heart failure from severechronic ischemic left ventricular dysfunction. Am J Cardiol2001;88:624–629.
9. Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhancedmagnetic resonance imaging to identify reversible myocardialdysfunction. N Engl J Med 2000;343:1445–1453.
0. Sharoni E, Song HK, Peterson RJ, et al. Off pump coronaryartery bypass surgery for significant left ventricular dysfunction:safety, feasibility, and trends in methodology over time—anearly experience. Heart 2006;92:499–502.
1. Calafiore AM, Di Giammarco G, Teodori G, et al. Late results offirst myocardial revascularization in multiple vessel disease: sin-gle versus bilateral internal mammary artery with or withoutsaphenous vein grafts. Eur J Cardiothorac Surg 2004;26:542–548.
2. Doenst T, Velazquez EJ, Beyersdorf F, et al. To STICH or not toSTICH: we know the answer, but do we understand the ques-tion? J Thorac Cardiovasc Surg 2005;129:246–249.
3. Joyce D, Loebe M, Noon GP, et al. Revascularization and ven-tricular restoration in patients with ischemic heart failure: the
STICH trial. Curr Opin Cardiol 2003;18:454–457.4. Carabello BA. Clinical practice. Aortic stenosis. N Engl J Med2002;346:677–682.
5. Lindblom D, Lindblom U, Qvist J, Lundstrom H. Long-termrelative survival rates after heart valve replacement. J Am CollCardiol 1990;15:566–573.
6. Connolly HM, Oh JK, Schaff HV, et al. Severe aortic stenosiswith low transvalvular gradient and severe left ventricular dys-function: result of aortic valve replacement in 52 patients. Cir-culation 2000;101:1940–1946.
7. deFilippi CR, Willett DL, Brickner ME, et al. Usefulness ofdobutamine echocardiography in distinguishing severe fromnonsevere valvular aortic stenosis in patients with depressed leftventricular function and low transvalvular gradients. Am J Car-diol 1995;75:191–194.
8. Vaquette B, Corbineau H, Laurent M, et al. Valve replacementin patients with critical aortic stenosis and depressed left ventric-ular function: predictors of operative risk, left ventricular func-tion recovery, and long term outcome. Heart 2005;91:1324–1329.
9. Dujardin KS, Enriquez-Sarano M, Schaff HV, et al. Mortalityand morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation 1999;99:1851–1857.
0. Chaliki HP, Mohty D, Avierinos JF, et al. Outcomes after aorticvalve replacement in patients with severe aortic regurgitationand markedly reduced left ventricular function. Circulation2002;106:2687–2693.
1. Enriquez-Sarano M, Tajik AJ. Clinical practice. Aortic regurgi-tation. N Engl J Med 2004;351:1539–1546.
2. Lancellotti P, Gerard PL, Pierard LA. Long-term outcome ofpatients with heart failure and dynamic functional mitral regur-gitation. Eur Heart J 2005;26:1528–1532.
3. Patel JB, Borgeson DD, Barnes ME, et al. Mitral regurgitationin patients with advanced systolic heart failure. J Card Fail 2004;10:285–291.
4. Bolling SF, Pagani FD, Deeb GM, Bach DS. Intermediate-termoutcome of mitral reconstruction in cardiomyopathy. J ThoracCardiovasc Surg 1998;115:381–386; discussion 387�388.
5. Akasaka T, Yoshida K, Hozumi T, et al. Restricted coronary flowreserve in patients with mitral regurgitation improves after mi-tral reconstructive surgery. J Am Coll Cardiol 1998;32:1923–1930.
6. Wu AH, Aaronson KD, Bolling SF, et al. Impact of mitral valveannuloplasty on mortality risk in patients with mitral regurgita-tion and left ventricular systolic dysfunction. J Am Coll Cardiol2005;45:381–387.
7. Srichai MB, Grimm RA, Stillman AE, et al. Ischemic mitralregurgitation: impact of the left ventricle and mitral valve inpatients with left ventricular systolic dysfunction. Ann ThoracSurg 2005;80:170–178.
8. McGee EC, Gillinov AM, Blackstone EH, et al. Recurrent mi-tral regurgitation after annuloplasty for functional ischemic mi-tral regurgitation. J Thorac Cardiovasc Surg 2004;128:916–924.
9. Yun KL, Sintek CF, Miller DC, et al. Randomized trial compar-ing partial versus complete chordal-sparing mitral valve replace-ment: effects on left ventricular volume and function. J ThoracCardiovasc Surg 2002;123:707–714.
0. Morishita A, Shimakura T, Nonoyama M, Takasaki T. Mitralvalve replacement in ischemic mitral regurgitation. Preservationof both anterior and posterior mitral leaflets. J Cardiovasc Surg
(Torino) 2002;43:147–152.
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
7
7
8
8
8
8
8
8
8
8
238 Selzman et al Surgical Therapy for Heart Failure J Am Coll Surg
1. Miller DC. Ischemic mitral regurgitation redux—to repair or toreplace? J Thorac Cardiovasc Surg 2001;122:1059–1062.
2. Gillinov AM, Wierup PN, Blackstone EH, et al. Is repair pref-erable to replacement for ischemic mitral regurgitation? J Tho-rac Cardiovasc Surg 2001;122:1125–1141.
3. Yamaguchi A, Ino T, Adachi H, et al. Left ventricular volumepredicts postoperative course in patients with ischemic cardio-myopathy. Ann Thorac Surg 1998;65:434–438.
4. Buckberg GD. Ventricular restoration—a surgical approach toreverse ventricular remodeling. Heart Fail Rev 2004;9:233–239;discussion 347�351.
5. Mickleborough LL, Carson S, Ivanov J. Repair of dyskinetic orakinetic left ventricular aneurysm: results obtained with a mod-ified linear closure. J Thorac Cardiovasc Surg 2001;121:675–682.
6. Ott DA, Parravacini R, Cooley DA, et al. Improved cardiacfunction following left ventricular aneurysm resection: pre- andpostoperative performance studies in 150 patients. Tex HeartInst J 1982;9:267–273.
7. Athanasuleas CL, Buckberg GD, Stanley AW, et al. Surgicalventricular restoration in the treatment of congestive heart fail-ure due to post-infarction ventricular dilation. J Am Coll Car-diol 2004;44:1439–1445.
8. Yamaguchi A, Adachi H, Kawahito K, et al. Left ventricularreconstruction benefits patients with dilated ischemic cardiomy-opathy. Ann Thorac Surg 2005;79:456–461.
9. Sabbah HN, Sharov VG, Gupta RC, et al. Reversal of chronicmolecular and cellular abnormalities due to heart failure by pas-sive mechanical ventricular containment. Circ Res 2003;93:1095–1101.
0. Oz MC, Konertz WF, Kleber FX, et al. Global surgical experi-ence with the Acorn cardiac support device. J Thorac CardiovascSurg 2003;126:983–991.
1. Blom AS, Mukherjee R, Pilla JJ, et al. Cardiac support devicemodifies left ventricular geometry and myocardial structure af-ter myocardial infarction. Circulation 2005;112:1274–1283.
2. Advisory Panel Does Not Recommend Approval for New HeartFailure Therapy Researchers and Company Representatives Re-main Optimistic. Acorn cardiovascular. Available at: http://www.acorncv.com/about_acorn/documents/FINAL-June222005AcornNewsRelease_001.pdf; 2005.
3. Rosanio S, Schwarz ER, Ahmad M, et al. Benefits, unresolvedquestions, and technical issues of cardiac resynchronizationtherapy for heart failure. Am J Cardiol 2005;96:710–717.
4. Abraham WT, Fisher WG, Smith AL, et al. Cardiac resynchro-nization in chronic heart failure. N Engl J Med 2002;346:1845–1853.
5. Bristow MR, Saxon LA, Boehmer J, et al. Cardiac-resynchronization therapy with or without an implantable defi-brillator in advanced chronic heart failure. N Engl J Med 2004;350:2140–2150.
6. Cleland JG, Daubert JC, Erdmann E, et al. The effect of cardiacresynchronization on morbidity and mortality in heart failure.N Engl J Med 2005;352:1539–1549.
7. Bigger JT Jr. Prophylactic use of implanted cardiac defibrillatorsin patients at high risk for ventricular arrhythmias aftercoronary-artery bypass graft surgery. Coronary Artery BypassGraft (CABG) Patch Trial Investigators. N Engl J Med 1997;337:1569–1575.
8. Dries DL, Exner DV, Gersh BJ, et al. Atrial fibrillation is asso-ciated with an increased risk for mortality and heart failure pro-
gression in patients with asymptomatic and symptomatic left 8ventricular systolic dysfunction: a retrospective analysis of theSOLVD trials. Studies of Left Ventricular Dysfunction. J AmColl Cardiol 1998;32:695–703.
9. Hsu LF, Jais P, Sanders P, et al. Catheter ablation for atrial fibril-lation in congestive heart failure. N Engl J Med 2004;351:2373–2383.
0. Cox JL, Schuessler RB, D’Agostino HJ Jr, et al. The surgicaltreatment of atrial fibrillation. III. Development of a definitivesurgical procedure. J Thorac Cardiovasc Surg 1991;101:569–583.
1. Schaff HV, Dearani JA, Daly RC, et al. Cox-Maze procedure foratrial fibrillation: Mayo Clinic experience. Semin Thorac Car-diovasc Surg 2000;12:30–37.
2. Gillinov AM, Sirak J, Blackstone EH, et al. The Cox mazeprocedure in mitral valve disease: predictors of recurrent atrialfibrillation. J Thorac Cardiovasc Surg 2005;130:1653–1660.
3. Brizzio ME, Navia JL, Atik FA, et al. Combined minimallyinvasive pulmonary vein isolation, left atrial appendage excisionand cardiac resynchronization therapy for heart failure: case re-port. Heart Surg Forum 2005;8:E249–E252.
4. DeBakey ME. Development of mechanical heart devices. AnnThorac Surg 2005;79:S2228–S2231.
5. Pagani FD, Lynch W, Swaniker F, et al. Extracorporeal life sup-port to left ventricular assist device bridge to heart transplant: astrategy to optimize survival and resource utilization. Circula-tion 1999;100[Suppl]:II206–II210.
6. Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term mechan-ical left ventricular assistance for end-stage heart failure. N EnglJ Med 2001;345:1435–1443.
7. Park SJ, Tector A, Piccioni W, et al. Left ventricular assist devicesas destination therapy: a new look at survival. J Thorac Cardio-vasc Surg 2005;129:9–17.
8. Gray NA, Selzman CH. Current status of the total artificialheart. Am Heart J. In press.
9. Cooley DA, Liotta D, Hallman GL, et al. Orthotopic cardiacprosthesis for two-staged cardiac replacement. Am J Cardiol1969;24:723–730.
0. Copeland JG, Smith RG, Arabia FA, et al. Cardiac replacementwith a total artificial heart as a bridge to transplantation. N EnglJ Med 2004;351:859–867.
1. Dowling RD, Gray LA Jr, Etoch SW, et al. Initial experiencewith the AbioCor implantable replacement heart system. J Tho-rac Cardiovasc Surg 2004;127:131–141.
2. Nagy RD, Tsai BM, Wang M, et al. Stem cell transplantation asa therapeutic approach to organ failure. J Surg Res 2005;129:152–160.
3. Raeburn CD, Zimmerman MA, Arya J, et al. Stem cells andmyocardial repair. J Am Coll Surg 2002;195:686–693.
4. Orlic D, Kajstura J, Chimenti S, et al. Bone marrow cells regen-erate infarcted myocardium. Nature 2001;410(6829):701–705.
5. Ziegelhoeffer T, Fernandez B, Kostin S, et al. Bone marrow-derived cells do not incorporate into the adult growing vascula-ture. Circ Res 2004;94:230–238.
6. Beltrami AP, Barlucchi L, Torella D, et al. Adult cardiac stemcells are multipotent and support myocardial regeneration. Cell2003;114:763–776.
7. Schachinger V, Assmus B, Britten MB, et al. Transplantation ofprogenitor cells and regeneration enhancement in acute myocar-dial infarction: final one-year results of the TOPCARE-AMITrial. J Am Coll Cardiol 2004;44:1690–1699.
8. Menasché P, Hagege AA, Vilquin JT, et al. Autologous skeletal

8
9
9
9
9
9
239Vol. 203, No. 2, August 2006 Selzman et al Surgical Therapy for Heart Failure
myoblast transplantation for severe postinfarction leftventricular dysfunction. J Am Coll Cardiol 2003;41:1078–1083.
9. Patel AN, Geffner L, Vina RF, et al. Surgical treatment for con-gestive heart failure with autologous adult stem cell transplanta-tion: a prospective randomized study. J Thorac Cardiovasc Surg2005;130:1631–1638.
0. Kang HJ, Kim HS, Zhang SY, et al. Effects of intracoronaryinfusion of peripheral blood stem-cells mobilised withgranulocyte-colony stimulating factor on left ventricular systolicfunction and restenosis after coronary stenting in myocardialinfarction: the MAGIC cell randomised clinical trial. Lancet
2004;363(9411):751–756.1. Grines CL, Watkins MW, Helmer G, et al. Angiogenic GeneTherapy (AGENT) trial in patients with stable angina pectoris.Circulation 2002;105:1291–1297.
2. Trouillet JL, Scheimberg A, Vuagnat A, et al. Long-term out-come and quality of life of patients requiring multidisciplinaryintensive care unit admission after cardiac operations. J ThoracCardiovasc Surg 1996;112:926–934.
3. Roche RJ, Farmery AD, Garrard CS. Outcome for cardiotho-racic surgical patients requiring multidisciplinary intensive care.Eur J Anaesthesiol 2003;20:719–725.
4. Badhar V, Bolling SF. Nontransplant surgical options for heartfailure. In: Cohn LJ, Edmunds LH Jr., eds. Cardiac surgery in
the adult. 2nd ed. New York: McGraw-Hill; 2003:1515–1526.Member Benefit
CME-1 Program OnlineTo date: 76,300 CME-1 Credits
www.jacscme.facs.org