Sunday, 29 August 2010 - Oxford Academic
296
Sunday, 29 August 2010 Downloaded from https://academic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Sunday, 29 August 2010 - Oxford Academic

Sunday, 29 August 2010
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Improved quantitation of valvular heart disease 3
IMPROVED QUANTITATION OF VALVULAR HEARTDISEASE
100 3D color-Doppler echocardiography and chronic aorticregurgitation: a novel approach for severity assessment
L. Perez De Isla, J. Zamorano, C. Fernandez-Golfin, P. Marcos-Alberca,C. Almeria, J.L. Rodrigo, A. Saltijeral, C. Macaya. Hospital Clinic SanCarlos, Madrid, Spain
Background: 3D echocardiography provides a complete evaluation of the aor-tic valve and adjacent structures and it improves the assessment of this cardiacregion. Three-dimensional color-Doppler chocardiography (3DCDE) evaluationmight improve the measurements of the functional regurgitant orifice in patientswith Chronic Aortic Regurgitation (CAR).Objectives: Our aim was to compare the accuracy of current echo-Doppler meth-ods and 3DCDE for the assessment of CAR severity. The reference method usedin this work was the CAR severity determined by means of cardiac magnetic res-onance (CMR)Methods: Thirty two consecutive patients with an established diagnosis of CARrecruited in our institution, comprised our study group. CAR severity was deter-mined by conventional Echo-Doppler methods and by 3DCDE and their resultswere compared with those obtained by means of CMR.Results: Mean age was 63.0±13.5 years. Twenty two patients (68.8%) weremen. Compared with the traditional echo-Doppler methods, 3DCDE evaluationhad the best linear association with CMR results (3D vena contracta cross sec-tional area method: r=0.8; r square= 0.77; p<0.001. 3D vena contracta crosssectional area/left ventricular outflow tract cross sectional area method: r=0.87;r square=0.7; p<0.001). The ROC analysis showed an excellent area undercurve for detection of severe CAR (3D vena contracta cross sectional areamethod=0.97; 3D vena contracta cross sectional area/left ventricular outflow tractcross sectional area method=0.98). Inter and intra-observer variability for the3DCDE evaluation was good (ICC=0.89 and ICC=0.91 for inter and intra observervariability respectively).
Main Results
AUC Cut-off point Sensitivity Specificity PPV NPV
3D vena contracta CSA 0.97 0.50 cm2 100% 92.6% 81.8% 100%3D vena contracta CSA/3D LVOT CSA 0.98 0.19 100% 77.8% 60.0% 100%
AUC: Area under curve; CSA: Cross sectional area; LVOT: Left ventricular outflow tract; NPV:Negtive predictive value; PPV: Positive predictive value.
Conclusions: 3DCDE is an accurate and highly reproducible diagnostic tool forestimating CAR severity. Compared with the traditional echo-Doppler methods,3DCDE has the best agreement with the CMR determined CAR severity. Thus,3DCDE is a diagnostic method that may improve the therapeutic management ofpatients with CAR.
101 3D vs 2D echocardiographic assessment of the leftventricular outflow tract: implications for theassessment of aortic stenosis
S. Gianstefani1, V. Sachpekidis1 , M. Ishida2, A. Chiribiri2, A. Bhan1,M. Paul1, L.A. Smith1, M.J. Monaghan1 . 1King’s College Hospital,
London, United Kingdom; 2St Thomas’ Hospital, London, United Kingdom
Purpose: The echocardiographic assessment of aortic stenosis severity is basedupon the continuity equation, which requires an accurate measurement of theleft ventricular outflow tract (LVOT) cross-sectional area. A 2D estimate of thisarea requires geometric assumptions about LVOT circularity and therefore maybeinaccurate in irregularly shaped LVOTs. The aim of this study is to evaluate theaccuracy of real-time three-dimensional transthoracic echocardiography (RT3DE)in the assessment of LVOT area, by direct measurement, using cardiac magneticresonance (CMR) as a reference method.Methods: 20 patients with a normal aortic valve and in sinus rhythm, undergoinga clinically indicated CMR were prospectively studied. LVOT diameter was mea-sured using 2D transthoracic echocardiography (TTE) in the parasternal long axisview and the LVOT area was calculated in the standard way. For each patient a3D data-set of the LVOT was acquired and direct measurement of LVOT area wasmade off line using dedicated software. These results were compared to LVOTarea obtained by CMR.Results: 2D and 3D LVOT measurements both demonstrated a good correlation
3D LVOT planimetry
with CMR: 4.1±0.8 cm2 for 2D and 4.9±1.0 for 3D vs 5.5±1.4 for CMR (r=0.759and 0.740 respectively, p=0.001 for both). However 2D measurements markedlyunderestimated the LVOT area (Bland-Altman bias -1.34±0.92). There was alsoan underestimation with RT3DE but this was to a much smaller extent (-0.51±0.94cm2).Conclusions: RT3DE is a more accurate method for the assessment of LVOTarea than 2D TTE, when compared to CMR, and may be preferable in the assess-ment of patients with aortic stenosis. This could be because the 3D measurementavoids the potentially incorrect geometrical assumption of circularity of the LVOT.
102 Overestimation of gradients by Doppler is related toseverity of aortic stenosis: an in-vitro study
P. Jiamsripong, J.C. Adams, V. Marupakula, E.M. Mcmahon,M. Belohlavek, H.P. Chaliki. Mayo Clinic, Scottsdale, United States ofAmerica
Background: Doppler echocardiography has been known to overestimate pres-sure gradients when compared to catheter measured gradients in mechanicalaortic valves. However, it is not clear whether the overestimation is related to theunderlying severity of an aortic stenosis. We hypothesize this difference in gradi-ents between Doppler and catheter measurements increases with the severity ofthe stenosis.Methods: Mean gradients were measured simultaneously by Doppler echocar-diography and Millar catheters across disks with known severity (0.5 cm2 and 0.9cm2 orifices). The disks were mounted in the aortic position in a left heart modelthat allowed for a variety of controlled conditions. The stroke volume was changedbetween 50 and 70 ml while the heart rate was altered between 40 bpm and 70bpm. We used normal saline as the test fluid.Results: Doppler measured mean gradients across the most stenotic orifice(0.5 cm2) are highly correlated (r=0.99 and p<0.0001) with those measured bycatheter, but there is significant overestimation by Doppler (Slope of 2.8). Simi-larly, Doppler measured mean gradients across the less stenotic orifice (0.9 cm2)are also highly correlated (r=0.99 and p<0.0001) with catheter measurements,but there is also significant overestimation by Doppler (Slope of 1.9) (Figure, leftpanel). Magnitude of differences between Doppler versus catheter measured gra-dients is higher with the highly stenotic orifice (median 35 mm Hg) when com-pared to the less stenotic orifice (median 5 mm Hg) (p<0.0001) (Figure, rightpanel).
Figure
Conclusions: Overestimation of a gradient across an aortic stenosis by Dopplerwhen compared to a catheter is related to the degree of underlying stenosis invarious hemodynamic conditions. Further in-vivo studies are needed to verify ourfindings.
103 VTI ratio is both more variable and more time-consumingthan peak velocity in calculating aortic valve area
R. Baruah, C. Raphael, S. Rizvi, B. Unsworth, S. Sen, A. Kyriacou,P. Pabari, J. Mayet, N. Sutaria, D.P. Francis. St. Mary’s Hospital andImperial College, International Centre for Circulatory Health, London,
United Kingdom
Aims: The severity of aortic stenosis may be assessed by various methods in-cluding the aortic valve area (AVA), by the application of the continuity equation.VTI ratio is commonly recommended for it’s calculation with the ratios of peakvelocity as an acceptable alternative. We surveyed the choice of method used inclinical practice and investigated if the increased time required calculating the VTIis justified through reduced variability.Method: First, a survey was conducted of echocardiography centres across theUK and cardiology trainees in England to assess the preferred methods for as-sessing severity of AS and reasons for this. Second, 1008 Doppler echocardio-graphic images from 24 patients with AS were obtained from sequential clinicalstudies. 21 operators across 6 centres performed analysis of Doppler traces forVTI and peak velocity. Dimensionless Indices were calibrated and calculated forboth techniques along with the average time.Results: In clinical practice, n=50, the most popular method of assessing severityof AS, was valve area by continuity equation. More operators felt that tracing theVTI is more reproducible and valid than using the peak velocity, even though theybelieved tracing Doppler traces is more time-consuming.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

4 Improved quantitation of valvular heart disease / Vascular access and bleeding complications
Inter-operator variability of VTI Dimensionless Index was 7.5 times greater thanpeak velocity (17±5% versus 2±1%, p<0.01). The majority of the variability oc-curs in tracing the outer edges of the VTI trace. The average time taken for VTIwas 5.3 times greater than peak velocities (23.7±3.5 s, 4.5±1.2 s, p<0.01).
TRacing VTI versus Peak velocity
Conclusions: The measurement of VTI is markedly more variable and time con-suming than peak velocity ratio in the assessment of aortic stenosis.
104 Direct planimetry of mitral valve regurgitation orificearea by real-time 3D transesophageal echocardiography
E. Altiok, S. Hamada, S. Van Hall, M. Hanenberg, E. Grabskaya,M. Becker, N. Marx, R. Hoffmann. University Hospital Aachen, RWTH,Internal Medicine I, Cardiology, Pulmonology & Vascular Medicine,
Aachen, Germany
Background: Quantification of mitral valve regurgitation including calculation ofthe effective regurgitation orifice area (EROA) is performed using proximal isove-locity surface area (PISA) method. However, these methods assume a hemi-spherical convergence zone. In case of non-circular regurgitation orifice quan-tification of mitral valve regurgitation may be incorrect. Direct planimetry of theanatomic regurgitation orifice area (AROA) from 3-dimensional datasets obtainedby (3D) transesophageal echocardiography (TEE) has become possible. We com-pared measurements of AROA by 3D TEE to EROA by the PISA method.Methods: 3D-TEE images were acquired from 54 patients (mean age 71±13years). EROA was determined by PISA method. Anatomic regurgitation orificearea (AROA) was measured with commercially available QLAB Software (Philips)after adjusting the first and the second plane in order to reveal the smallest orificein the third plane where planimetry could take place. Furthermore we classifiedthe AROA in circular and non-circular by calculating the ratio of medial-lateraldistance above anterior-posterior distance (≤1.5 as compared to >1.5).Results: AROA determined by planimetry was 0.30±0.19 cm2 and EROA de-termined by PISA method was 0.31±0.20 cm2. A correlation of r=0.96 (p<0.001)between AROA and EROA was found for all patients (n=54). In patients with a cir-cular regurgitation orifice area (n=9) the correlation was r=0.99 (p<0.001), in pa-tients with non-circular regurgitation orifice area (n=46) it was r=0.94 (p<0.001).When looking at agreement between methods AROA and EROA demonstratedgreater spread of measurements in the non-circular AROA group (average bias:0.002cm2, 95%CI: -0.139 cm2 to 0.134 cm2) when compared to the circular AROAgroup (average bias: -0.023 cm2, 95%CI: -0.084 cm2 to 0.037 cm2). In the non-circular AROA group mean difference of regurgitation orifice area was higher(0.052±0.045 cm2) compared to the circular AROA group (0.028±0.026 cm2).Conclusions: Measurements of regurgitation orifice area by 3D TEE correlatewell with the EROA by PISA method. However, agreement between methods isbetter for patients with a circular regurgitation orifice area compared to patientsshowing a non-circular regurgitation orifice area.
105 3D transesophageal echocardiography: assessment ofmorphology and function of prosthetic valves
A.A. Mohamed, A.S. Omran, A. Arifi. National Guard Hospital, KingAbdulaziz Cardiac Center (KACC), Riyadh, Saudi Arabia
Background: Valve surgery carries substantial risks unique to the im-planted prosthetic device. These complications include prosthetic valve endo-carditis (PVE), obstruction (PVO) and valve dehiscence. Therefore, early detec-tion of prosthetic valve dysfunction (PVD), is crucial for the appropriate manage-ment. Echocardiography has been the main modality for the diagnosis of pros-thetic valve dysfunction. Real-time 3D Transesophageal Echocardiography (RT3D
TEE) represents a significant advance in the field of echocardiography. It providesunique views for mitral valve prosthesis, from Left Atrium (LA) and left ventricu-lar (LV) perspectives. It has also been shown to give high quality 3D images ofprosthetic valves in both the mitral and aortic positions. We present our centerexperience with 3D TEE in assessing the morphology and function of prostheticvalves and comparing the 2D and 3D echo in assessing the prosthetic valve dys-functionMaterial and Methods: From October 2008 till October 2009, a total of 27 casesof suspected prosthetic valves dysfunction, 12 in the mitral position, 9 in aorticposition and 6 in both mitral and aortic positions. Of the 27 cases, 13 cases weresuspected endocarditis, 8 valve obstruction and paravalvular leak/dehiscence in6 cases. We have performed 2 D echo and Real time 3D TEE and off line analysisusing Q lab soft ware, which have increased the accuracy of the diagnosis andthe management planning.
Conclusion: Real-time 3D TEE was superior to 2D TEE in the diagnosis of pros-thetic valve obstruction due to pannus formation or valve thrombosis. 3 D echowas also superior in defining the site of the paravalvular leak and valve dehis-cence as it offers excellent and non conventional views for the prosthetic valveswithout the need for mentally reconstructing 2D images.
VASCULAR ACCESS AND BLEEDING COMPLICATIONSDURING PERCUTANEOUS CARDIOVASCULAR
INTERVENTIONS
126 Heparin bridging or uninterrupted oral anticoagulationduring coronary stenting - data from the AFCAS registry
H. Lahtela1, A. Schlitt2, A. Rubboli3, M. Niemela4, P. Karjalainen5,M. Puurunen6, S. Vikman7, P. Kirchhof8, J. Ehret9, J. Airaksinen1.1Turku University Hospital, Turku, Finland; 2Martin Luther University of
Halle-Wittenberg, Halle, Germany; 3University of Bologna, Bologna, Italy; 4OuluUniversity Hospital, Oulu, Finland; 5Satakunta Central Hospital, Pori, Finland;6Helsinki University Central Hospital, Helsinki, Finland; 7Tampere UniversityHospital, Tampere, Finland; 8University Hospital of Munster, Munster, Germany;9Kerckhoff Clinic, Department of Cardiology, Bad Nauheim, Germany
Purpose: Uninterrupted oral anticoagulation (UAC) is increasingly used duringcoronary stenting, although bridging therapy (BT) is still a common recommenda-tion.Methods: In this interim analysis of the AFCAS multicenter European prospec-tive Registry where patients with atrial fibrillation undergoing coronary stentingare included, two groups were identified for the in-hospital outcome comparisonaccording to whether the procedure was carried out during UAC or BT.Results: In the BT group, warfarin was withdrawn for a mean of 4 (range 1-15) days prior to stenting (mean INR 1.9) and low-molecular weight heparin wasused for BT. In the UAC group, mean procedural INR was 2.2 (p=0,000). Thetwo groups were comparable with respect to the baseline characteristics (meanage 73 years), but glycoprotein inhibitors and femoral access were more oftenused in the BT group. Non-major bleeding and access site complications weremore common in the BT group, but there were no other significant differences inthe other hospital outcome measures (Table 1). Femoral access (p=0.01) and age(p=0.04) were the significant independent predictors for in-hospital complications.
Table 1. In-hospital complications in the study groups
BT (n= 80) UAC (n=205) P value
Cardiac death 1 (0,5%) 1 (1,3%) 0,5Major adverse cardiac events 4 (5%) 5 (2%) 0,3Stroke 0 1 (0,5%) 1,000Major bleeding 1 (1%) 3 (2%) 1,000Non-major bleeding 11 (14%) 6 (3%) 0,001Access site complications 21 (27%) 15 (7%) 0,000All in-hospital complications 27 (34%) 23 (11,4%) 0,000
Conclusion: In our prospective, multicenter, observational registry, coronarystenting appears to be a safe procedure during UAC with no excess bleedingor thrombotic complications as compared to BT.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Vascular access and bleeding complications during percutaneous cardiovascular interventions 5
127 Incidence, predictors and prognostic implications ofbleeding complicating contemporary primarypercutaneous coronary interventions
D. Matic1, I. Mrdovic1, G. Stankovic2, M. Asanin1, N. Antonijevic1,D. Rajic1, M. Srdic1, T. Ivosevic3, N. Brdar1, Z. Vasiljevic1. 1Cardiology
Clinic, Emergency Department, Clinical Center of Serbia, Belgrade, Serbia;2Cardiology Clinic, Clinical Center of Serbia, Belgrade, Serbia; 3Clinic forAnesthesiology and Reanimathology, Clinical Center of Serbia, Belgrade, Serbia
Background: The use of primary percutaneous coronary interventions (PCI) andpotent antiplatelet agents and anticoagulants has increased the risk of majorbleeding complications in pts presenting with ST-elevation myocardial infarction(STEMI). The aim of this study was to investigate the incidence, predictors andprognostic impact of peri-procedural bleeding in a population of unselected ptsundergoing contemporary primary PCI.Methods: All consecutive STEMI pts who underwent primary PCI between1/2005 and 7/2009, were studied. Major bleeding was defined according to theGlobal Use of Strategies to Open Occluded Coronary Arteries (GUSTO) studycriteria.Results: Of the 770 STEMI pts with primary PCI, major bleeding occurred in32 pts (4.2%). Pts with major bleeding were older, more frequently female gen-der, more often had systemic hypertension, chronic renal failure, were at cardio-genic chock, had a higher weight, and less likely to be current smokers (Table).In-hospital mortality was three-fold-higher in pts who developed major bleedingcompared with those who did not (9.4% vs. 2.9%; p<0.03). In multivariate logisticregression analysis, significant predictors of major bleeding were advanced age(≥65 years) (OR=3.40; 95% CI for OR 1.44-8.02; p=0.005) and female gender(OR=3.73; 95% CI for OR 1.72-8.08; p=0.001).
Characteristics and outcomes of patients
Characteristics Major bleeding No major bleeding p value(n=32) (n=738)
Mean age (years) ± SD 67.2±11.3 58.6±11.2 <0.0001Female gender, % 56.3 24.1 <0.0001Systemic hypertension, % 78.1 61.1 0.05Smoking (current), % 40.6 62.5 0.01Chronic renal failure, % 31.1 15.3 0.01Weight (kg) 74.9±12.1 84.8±28.2 0.05Cardiogenic shock, % 9.4 2.7 0.03In-hospital mortality, % 9.4 2.9 0.03
Conclusion: Major bleeding complicating primary PCI occurs relatively fre-quently and is associated with three-fold-higher in-hospital mortality. Women andthose of advanced age are at particularly high risk.
128 Procedural and intermediate term outcomes afterendovascular procedures in cancer patients with chronicthrombocytopenia: first consecutive case series
C. Iliescu1, S. Mukerji2, G. Iliescu1, W. Yusuf1, J.B. Durand1. 1TheUniversity of Texas MD Anderson Cancer Center, Houston, United
States of America; 2The University of Texas Health Science Center at Houston,Houston, United States of America
Background: Thrombocytopenia has been a contraindication for interventionalprocedures due to possible increased risk of bleeding. Thrombocytopenia can bea marker of severity of the disease (i.e. sepsis, bleeding), but can also representa "new normality" for many cancer survivors (i.e. status post bone marrow trans-plant, leukemia, chemo-radiation treatment of solid tumors). The aim of our studywas to assess safety of endovascular interventions in cancer patients with chronicthrombocytopenia.Methods: Between January 2009 and December 2009, 281 consecutive can-cer patients underwent coronary angiography for abnormal cardiovascular stresstest or acute coronary syndrome in a tertiary center. Thrombocytopenia was de-fined as absolute platelet count <100,000. Patients with sepsis or actively bleed-ing where excluded. Left heart catheterization and the subsequent clinically indi-cated procedures, intravascular ultrasound (IVUS), fractional flow reserve (FFR)and coronary stenting where performed preferably through radial approach, un-less patients had history of coronary artery bypass surgery (CABG) and eitherabnormal modified Allen test or abnormal pulse oximetry testing.Results: Procedures were completed in 20 patients with thrombocytopenia (witha mean platelet count of 49, lowest platelet count 9) without major bleeding com-plications through radial (40%) or femoral approach (60%). No platelet transfu-sions were used. A small femoral hematoma was present in 1 patient in thefemoral group (platelet count 14). All patients have received heparin to achieve anACT>270 and were started on single or dual antiplatelet regimen based on theprocedure performed. Survival at 3 months was 95%, with only one death sec-ondary to sepsis. No myocardial infarction, emergent CABG, target lesion revas-cularization or stroke was noted at 3 months follow-up, as well as no evidence ofintracranial bleeding or hemodynamically significant gastrointestinal bleeding.Conclusion: To the best of our knowledge, this is the first consecutive case-series of patients with chronic thrombocytopenia that underwent endovascularprocedures. There was no associated increased major bleeding or major adversecardiovascular events in a tertiary center with expertise in high-risk interventions.As the number of cancer survivors with chronic thrombocytopenia will continue
to increase, further studies will be needed to be conducted to further evaluateoutcomes.
129 High rate of vascular access site complications detectedby routine vascular ultrasound after radial arterycatheterization. Short term results in 182 consecutivepatients
M. Uhlemann1, S. Gielen1, C. Kleinecke1, D. Scheinert2, G. Schuler1.1University of Leipzig, Heart Center, Department of Internal Medicine
and Cardiology, Leipzig, Germany; 2Department of Internal Medicine/Angiology,Parkkrankenhaus, Leipzig, Germany
Objectives: Radial access for coronary procedures is widely recommended to re-duce vascular access site complications compared to femoral access. To assessthe frequency of radial artery complications we started a prospective registry andperformed routine radial artery vascular ultrasound after each procedure in 182consecutive patients (pts).Methods: From 11/2009-02/2010,182pts with the indication for cardiac catheter-ization (64±11.1yrs (range 33-88yrs),56% male) were included in the registry.A6F standard short vascular sheath was used and 2500 IE unfractionated hep-arin were given routinely for a diagnostic angiography.Vascular ultrasound of theaccess site was performed after a mean of 1 day (range 0-34days) after catheter-ization in all pts.Follow-up vascular ultrasound in case of radial artery occlusionwas performed in 79.6% after a mean of 9.8±7.9days (range 1-46days). 11ptswere lost to follow-up. If pts presented with symptoms, they received heparin, ifthey were asymptomatic,no heparin was given. 40pts received LMH over a meantime of 10±7.6days.In case of persistent radial occlusion,a second follow-up wasperformed in 21 of 54pts (39%) after 24.8±15.3days, a third follow-up in 6 ptsafter 22.8±6.5days.Results: The access site was the right radial artery in 177 cases and the leftin 5pts.Vascular complications were detected in 61pts (33.5%), of whom 29pts(47.5%) were symptomatic.No evidence of major/minor bleeding.Occlusion ofthe radial artery in 54pts (29.7%),a pseudoaneurysm in 3pts and av-fistula in2pts.Of the pseudoaneurysms,two could be managed by ultrasound-guided com-pression,one required vascular surgery.Mean occlusion length was 14.4±5.8cm(range 3-25cm).In 22pts undergoing percutaneous coronary intervention with full-dose heparinization,radial occlusion was seen in 5pts (22.7%).At the first follow-up,34pts (79%) were still presenting with radial occlusion,regular flow of the radialartery in 9 pts.At the second follow-up,regular flow of the radial artery was seen in8 of 22pts (36%),a radial occlusion in 13pts.At time of the third follow-up,regularflow of the radial artery was seen in two pts (33%).Altogether,18 of 43pts (42%)in the follow-up-group showed a restoration of flow of the radial artery.Conclusions: Even though radial access for coronary procedures was success-ful in reducing major bleeding, the rate of radial artery occlusions detected byprospective vascular ultrasound examination was higher than expected. The rea-sons for this finding (ineffective anticoagulation, use of sheaths without hydrophiliccoating) need to be evaluated in further controlled studies.
130 Impact of vascular closure devices on vascularcomplications after percutaneous coronaryinterventions
T. Vandendriessche, M. Claeys, J. Bosmans, S. Haine, H. Miljoen,C. Vrints. University of Antwerp Hospital (Edegem), Department ofCardiology, Antwerp, Belgium
Purpose: Complications of vascular access are among the most common ad-verse events after transfemoral percutaneous coronary intervention (PCI). Vas-cular closure devices (VCD) have the potential to reduce the time to hemostasis,facilitate patient mobilization and improve patient satisfaction. However the is-sue of VCD safety compared with conventional manual or assisted compressionwith respect to vascular complications remains controversial. The purpose of thisstudy was to assess femoral arterial access-related vascular outcomes after PCIrelated to the use of VCD.Methods: A total of 4,258 consecutive patients undergoing transfemoral PCI werestudied through a single centre prospective registry from January 2006 to June2007 (period 1; no VCD available; n = 2,181) and from July 2007 to December2008 (period 2;VCD available; n = 2,077). During period 2, 668 (32%) receivedVCD. Decision for use of VCD was based upon clinical and angiographic charac-teristics of the patient, on the location of puncture site and was left to the discre-tion of the operator. Univariate and multivariate logistic regression analyses wereused to determine the predictors of vascular complications.Results: The overall vascular complication rate was 3.43%, and was composedof false aneurysm (76%), arteriovenous fistula (5%), arterial occlusion (3%), arte-rial infection (1%) and unspecified (15%). 13 patients needed emergency vascularsurgery. Vascular complications were as frequent during period 1 as during period2 for the group in which VCD were not used (3.81% versus 3.60%, P=0.74). Pa-tient characteristics of both groups were comparable. Vascular complication rateduring period 2 was significantly lower if VCD were used (1.68% versus 3.60%,P=0.017). However, patients who received a VCD were younger (64.7 year ver-sus 67.0 year, P<0.0001), more frequently male (77% versus 71%, P=0.003), re-ceived less often GPIIbIIIa inhibitors (21% versus 26%, P=0.01) and had less fre-quently ST elevation myocardial infarction (6.5% versus 12%, P=0.003). Multivari-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

6 Vascular access and bleeding complications / Ventricle remodelling at the molecular level
ate logistic regression analysis revealed that VCD use during period 2 was inde-pendently associated with a 48% (95% CI 25%-94%) reduction in the risk of vas-cular complications. The other independent risk factor was older age (P=0.038).Conclusions: In this large single centre contemporary practice, recent use ofVCD was associated with almost 50% reduction in the rate of vascular complica-tions as compared to conventional treatment with manual or assisted compres-sion after transfemoral PCI.
131 Use, patient characteristics and clinical outcome ofarterial access closure devices during percutaneouscoronary interventions (PCI) in clinical practice. Resultsof the ALKK PCI Registry
R. Zahn1, M. Hochadel1 , H. Mudra2, S. Kerber3, K.E. Hauptmann4,A. Elsaesser5, S. Behrens6, J. Senges1, U. Zeymer1. 1Clinical Centerof Ludwigshafen, Ludwigshafen am Rhein, Germany; 2Staedt. Klinikum,Muenchen-Neuperlach, Germany; 3Cardiovascular Clinic Bad Neustadt,Department of Cardiology, Bad Neustadt an der Saale, Germany; 4Krankenhausder Barmherzigen Brüder, Trier, Germany; 5Hospital Oldenburg, Oldenburg,Germany; 6Vivantes Humboldt Hospital, Berlin, Germany
Background: Arterial access closure devices (ACD) are an alternative to manualcompression (MC) to seal the vascular access side after percutaneous coronaryinterventions (PCI). However, there are limited data on the use and clinical out-come associated the use of ACDs in clinical practice of PCI.Methods: We analysed data of the prospective German ALKK PCI Registry.Results: In 2008 17667 PCIs in 16661 patients were performed via the femoralartery at 39 hospitals and included in the ALKK PCI Registry. An ACD was usedin 6936 (41.6%) of patients, whereas 9725 (58.4%) patients were treated by MC.The mean proportion of patients treated with an ACD per participating hospitalwas 37.7±32.1% (Range: 0 – 97.3%). Patient and interventional characteristics,as well as clinical events in relation to the use of an ACD compared to MC aregiven in the table:After adjusting for age, gender, renal failure, ACS and cardiogenic shock compli-cation rates at the access side were still not significantly different for ACD com-pared to MC (OR=0.89, 95%-CI 0.70-1.14).
ACD, n=6936 (100%) MC, n=9725 (100%) p-value
Age (years) 67.2±11.4 67.3±11.5 0.58Women 28.7% 28.1% 0.40Prior PCI 36.3% 34.1% 0.004Prior CABG 11.8% 12.2% 0.47Acute coronary syndrome 41.9% 53.3% <0.001Cardiogenic shock 1.3% 2.8% <0.001Renal failure 15.2% 16.3% 0.060Diabetes mellitus 24.1% 25.0% 0.24Intervention and outcome
Radiation time (minutes) 10.0±7.6 11.1±9.2 <0.001Access side complications 1.6% 1.9% 0.17Myocardial infarction 0.3% 0.5% 0.16Stroke/TIA 0.1% 0.2% 0.088Hospital death 1.3% 3.0% <0.001
Conclusions: In current clinical practice of PCI via the femoral artery in Ger-many ACD were used in 42%, with a large inter-hospital range. We did not find adifference of the access side complication rates between ACD and MC.
VENTRICLE REMODELLING AT THE MOLECULAR LEVEL
171 Mimecan is an essential regulator of cardiacextracellular matrix integrity after myocardial infarction
L.N.L.C. Van Aelst1, M. Swinnen1, M. Schellings2, P. Carai1,P. Carmeliet1, S. Cook3, S. Heymans2. 1Catholic University ofLeuven/Vesalius Research Center, Leuven, Belgium; 2Cardiovascular
Research Institute Maastricht (CARIM), Maastricht, Netherlands; 3ImperialCollege London, London, United Kingdom
Mimecan (or osteoglycin) is a small leucin-rich proteoglycan that belongs to thefamily of matricellular proteins, which are secreted, non-structural proteins of theextracellular matrix (ECM) that mediate cell-matrix interactions during tissue re-pair and tumour growth. Here, we investigated whether mimecan may be impli-cated in cardiac healing and function after myocardial infarction (MI).In the MI-model induced by permanent ligation of the left coronary artery, micewith a targeted inactivation of mimecan (KO) exhibited a 55% mortality (12/21) asopposed to absent mortality in wild-type (WT) mice (0/21) within 14 days (d) afterligation (Fig. A). Mortality resulted from increased cardiac rupture; echocardio-graphic analysis in the surviving KO mice revealed increased cardiac dilatation.Mimecan KO infarcts showed a disorganized granulation tissue 3 d after MI (Fig.B). After 14 d, impaired collagen maturation was obvious in mimecan KO as op-posed to WT infarcts (ratio orange-red to yellow-green birefringent collagen in theinfarct area WT vs. KO, mean ± SEM: 33.3±3.4 vs. 18.2±4.1; P<0.05). Nor af-ter 3 d, nor after 14 d, infarct size, degree of inflammation and capillary growthdiffered between KO and WT infarcts. Importantly, adenoviral overexpression of
mimecan (AdV-Mim) in WT mice via iv injection, resulting in a tenfold increase ofmimecan plasma levels, significantly attenuated cardiac dilatation and dysfunc-tion (Fig. C and D) at 14 d after MI, compared to AdV-R5 control.
In conclusion, These findings indicate that increased mimecan is essential formaintenance of the integrity and maturation of the cardiac ECM after MI. Theprotective effects of mimecan emphasize the potential therapeutic applications ofthis protein to prevent cardiac dilatation and dysfunction after MI.
172 The impact of diabetes mellitus on left ventricularmyocardial structure and function in aortic stenosisbefore valve replacement
I. Falcao-Pires1 , N. Hamdani2, C. Gavina3, J. Van Der Velden2,A. Borbely2, C.G. Schalkwijk2, H.W.M. Niessen2, G. Stienen2,
A.F. Leite-Moreira1 , W.J. Paulus2. 1University of Porto, Faculty of Medicine,Porto, Portugal; 2VU University Medical Center, Amsterdam, Netherlands; 3SaoJoao Hospital, Porto, Portugal
Purpose: Diabetes mellitus (DM) is an independent risk factor for progressionof aortic valve stenosis (AS) and significantly impacts longterm outcome aftervalve replacement. High incidence of residual heart failure may account for thisprognosis. We aimed to assess the impact of DM on diastolic (dys)function of ASpatients.Methods: Patients with severe isolated AS (n=46) and AS plus type-II diabetespatients (AS-DM+, n=16) with preserved left ventricular (LV) ejection fraction andno clinical or angiographic signs of coronary artery disease were studied. Dopplerechocardiographic data was used to compare in vivo LV function. Biopsies wereused to assess fibrosis, cardiomyocyte hypertrophy (MyD), advanced glycationendproducts (AGEs) and phosphorylation of myofilamentary proteins. Cardiomy-ocytes were also isolated and permeabilized to measure active force (Factive),resting force (Fpassive) and calcium sensitivity (pCa50).Results: In isolated AS, LV deceleration time and end-diastolic pressure wereaugmented and the latter significantly correlated with increased fibrosis (r=0.40,p=0.04) and MyD (r=0.60, p<0.001). In AS-DM+ patients, diastolic dysfunctionwas exacerbated in comparison with isolated AS, as fibrosis, cardiomyocytes hy-pertrophy and AGEs were further increased and Fpassive significantly rose. Fur-thermore, AS-DM+ patients presented with a higher PKA-induced drop of pCa50,which was correlated with higher levels of PKA-induced phosphorylation of Tro-ponin I.Conclusions: We characterized the diastolic disturbances associated with ASchronic pressure overload alone and in the presence of diabetes. DM exacerbatesthe existing diastolic dysfunction of AS patients through extracellular matrix alter-ations (fibrosis and AGEs), Fpassive raise and PKA-mediated hyperphosphory-lation status of troponin I. This study highlights the need for earlier therapeuticinterventions in order to prevent the faster progression of diastolic dysfunction indiabetic AS patients.
173 The Eya4/Six1 signalling cascade is crucial in acquiredheart disease
T. Williams, J. Schoenberger, N. Burkard, M. Czolbe, F. Panther,O. Ritter. Department of Internal Medicine I, Molecular Cardiology,wurzburg, Germany
Rationale: We previously identified a mutation in the human transcriptional cofac-tor Eya4 as cause of familial dilated cardiomyopathy (DCM). We now hypothesizethat the Eya4/Six1 signalling cascade also is crucial in acquired heart disease.Hypothesis: We hypothesize that the transcriptional complex Eya4/Six1 regu-lates targets relevant in normal cardiac function. We speculate that Eya4/Six1complexes regulate the expression of p27kip1 (p27), a known inhibitor of hyper-trophy in adult cardiomyocytes, upon hypertrophic stimuli.Methods and results: We examined the correlation of p27 phosphorylation andEya4 in cryosections of failing and normal human hearts. Immunocytochemicalanalysis revealed Eya4 is distributed in the cytoplasm while p27 resides mainly
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
Ventricle remodelling at the molecular level / Pathobiology and pathophysiology of pulmonary hypertension 7
in the nucleus. In sections of failing human hearts, Eya4 was accumulated inthe perinuclear region; nuclear p27 levels were significantly diminished, phos-phorylated p27 was evenly distributed in the cytoplasm. In a murine model of MI,immunofluorescence staining showed Eya4 is translocated to the nucleus in atime-dependent manner. 16 min after experimental MI there is a strong perinu-clear accumulation of Eya4 in cardiomyocytes; translocation to the nucleus wasdetectable 24h post infarction compared to the cytoplasmic distribution in controlheart tissue. We studied the effect of Eya4 overexpression on the nuclear translo-cation in permanent mammalian cell lines and cardiac myocytes by immunofluo-rescence microscopy. 48h post transfection EGFP-tagged WT Eya4 was locatedin the cytoplasm and translocated to the nucleus after co-expression with DsRed-tagged Six1.We also studied the effect of Eya4 overexpression on the expression of p27 incontrast to the cardiac Eya4 mutant E193. Studies using a p27 promoter frag-ment (including Six1 consensus sites) cloned in front of a Luciferase reportergene revealed that Eya4 acts as a suppressor of p27, whereas E193 could notsufficiently inhibit p27 expression. Further transfection experiments demonstratedthat an Eya4 overexpression and subsequent p27 suppression increased the ex-pression of molecular markers for myocardial hypertrophy and increased proteinsynthesis.Conclusion: In summary, we provide evidence that the Eya4/Six1 signalling cas-cade is not only relevant in a rare version of heritable DCM but also in more com-mon forms of acquired heart disease. Eya4/Six1 seems to suppress p27, whichwas shown to be an important inhibitor of hypertrophy in postmitotic cardiomy-ocytes.
174 Strong up-regulation of Runx2 in DCC-susceptibleC3H/He mice after freeze-thaw-injury
A.-K. Sowa, J. Erdmann, H. Schunkert, Z.A. Aherrahrou. Department ofMedicine II, Luebeck, Germany
Introduction: C3H/He mice were used as model for Dystrophic CardiacCalcification (DCC) using freeze-thaw-injury. DCC shares many features with os-teogenesis.Aim: The aim of this study was to analyze the expression-level of transcription-factors involved in osteogenesis and to identify respective target-genes of thesefor a better understanding of initiation and development of DCC.Methods: DCC-susceptible C3H/He and DCC-resistant C57BL/6 mice (n=3)were subjected to freeze-thaw-injury to induce calcification. Early at 24 and 72hours necrotic and healthy myocardium from each mouse were separated. tRNAand cryo-sections from each tissue were prepared for histological analysis andrelative-real-time-PCR quantification using the ��Ct-method.Results: Using Calcein-staining calcification-like deposits appear in resistant andsusceptible mice 1 day after injury. Calcification progresses in C3H/He but not inC57BL/6 mice 2 days later. Among the tested transcription-factors a 30.26-foldup-regulation of Runx2 was detected in calcified tissue of C3H/He. Low expres-sion was found for Sox9,Vdr, Nfkb, Msx1, Smad1, Smad2 and Smad4, none forMsx2, Twist1 and Smad3. Based on this finding we further tested downstream-genes of Runx2: Vdr, Dmp1, Phex, Osterix, Col1a2, IBSP,MMP2, MMP8, MMP9,MMP13, Bglap II, Opn and Akp2. An up-regulationof Col1a2 (4.45-fold ofinduc-tion), of MMP8 (16.55-fold) and of MMP13 (15.17-fold) was observed.Conclusion: Infiltrating cells differentiate into osteoblast-like-cells following injurythrough highexpression of Runx2, which activates in turn the MMPs-pathway tocleave collagen (type-I, -II, -III). The MMPs/collagen-interactions and their con-tribution in repair-processes and tissue-remodelling may explain calcification inmyocardium of susceptible mice.
175 FT23, an orally active anti-fibrotic compound attenuatesstructural and functional dysfunction in an experimentalmodel of diabetic cardiomyopathy
S.M. Tan1, Y. Zhang1, H. Krum2, R.E. Gilbert3, D.J. Kelly1. 1TheUniversity of Melbourne, Department of Medicine, St Vincent’s Hospital,
Melbourne, Australia; 2Monash University, Department of Epidemiology &Preventive Medicine, Melbourne, Australia; 3University of Toronto, Toronto,Canada
Purpose: Diabetic cardiomyopathy (DCM) is characterized by early diastolic dys-function and structural changes such as interstitial fibrosis that are independentof blood pressure or coronary heart disease. We have previously characterised adiabetic (mRen-2)27 rat model that manifests pathological and physiological char-acteristics of human DCM. Using the Ren-2 rat model, we sought to investigatethe effect of FT23 on the structural and functional changes associated with DCM.Methods: Using the [3H]-proline incorporation assay, rat mesangial cells werestimulated with transforming growth factor-β (TGF-β) and FT derivatives werescreened for their anti-fibrotic efficacy compared to tranilast. Among those, FT23displayed activity 2-5 times higher than that of tranilast and can be synthesisedon a 1kg scale, providing the capability to progress into animal model. Heterozy-gous Ren-2 rats were rendered diabetic with streptozotocin by tail-vein injection.Rats were then treated with FT23 (200mg/kg/day bid) or vehicle from week 8to 16 post onset of diabetes. Echocardiography was performed to assess heartfunction before the rats were sacrificed and their hearts collected for histologicalanalyses.
Results: FT23 significantly attenuated the increased heart to body weight ra-tio in treated diabetic rats (0.32±0.01% vs 0.29±0.01%; P=0.03) without mod-ulating blood glucose or blood pressure. Diastolic dysfunction as measured bymitral valve (MV) E/A ratio (1.49±0.06 vs 1.79±0.07; P=0.01) and MV decel-eration time (73.9±7ms vs 57.1±3ms; P=0.01) were also attenuated by FT23when compared to untreated diabetic rats. Histological examination of picrosiriusred-stained heart sections revealed that cardiac fibrosis in the diabetic animalswas attenuated by FT23 when compared to untreated animals (1.54±0.3% vs0.85±0.08%; P=0.0007), with a concomitant reduction in collagen I immunos-taining (2.36±0.4% vs 1.40±0.1%; P=0.02) and the infiltration of macrophages(6.27±0.9 cells/field vs 4.55±0.5 cells/field; P=0.05) as demonstrated by ED1immunostaining. These changes were associated with a reduction in the activityof TGF-β as measured by its immediate downstream signalling molecule, phos-phorylated Smad2 (0.37±0.04% vs 0.24±0.02%; P=0.01).Conclusion: Our results suggest that FT23 inhibits the activity of TGF-β andattenuates the structural and functional manifestations of diastolic dysfunctionobserved in a model of DCM.
176 Combination therapy with ACE-inhibitors andAT1-receptor-blockers has no additional benefit inexperimental cardiac pressure overload despite minordifferences between the two treatments
P. Mueller, A. Kazakov, A. Semenov, P. Jagoda, M. Boehm, U. Laufs.Saarland University Hospital, Homburg, Germany
Purpose: ACE-inhibitors (ACEI) and AT1-receptor-blockers (ARB) are therapeu-tically used in cardiac remodelling processes. We aimed to characterise differentcellular effects of both substances as mono- or combination therapy in cardiacpressure overload.Methods & Results: C57Bl/6 mice received either vehicle, the ACEI ramipril (R,2.5 mg/kg body weight), the ARB telmisartan (T, 20 mg/kg body weight) or thecombination from both substances (RT). The 1:8 dose-ratio of the ACEI in rela-tion to the ARB were used to mimic the doses used in the ONTARGET study.In all mouse groups, pressure overload was induced by transverse aortic con-striction (TAC, 360 μm for 35 d; n=4-12 per group). Cardiac hypertrophy inducedby TAC was reduced in all three treatment groups [heart weight per tibia length;mg/mm; (sham (S) 7.8±0.4, TAC 13.3±0.9, R-TAC 11±0.5, T-TAC 8.8±0.3, RT-TAC 9.3±0.1) with the most pronounced effect in the telmisartan group. The car-diomyocyte short axis parameter was increased by TAC ([μm]; S 10.6±0.3, TAC15.5±0.5) and was reduced similarly by ACEI (10.8±0.1), ARB (10.7±0.3) andthe combination therapy (10.3±0.3). ACEI, ARB and the combination therapy re-duced the extent of TAC-induced cardiac fibrosis significantly (Sirius red staining,[%] S 6.7±0.2, TAC 2.6±0.5, R-TAC 0.5±0.1, T-TAC0.5±0.2, RT-TAC 0.8±0.4).The increased number of proliferating Ki67pos non-cardiomyocytes/mm2 in theTAC-group was reduced more potently by the ARB than by the ACEI (S 3±0.6,TAC 17.5±2.4, R-TAC 4±1.6, T-TAC 0.5±0.2, RT-TAC 3.7±1.5). The same wasobserved for the percentage of Ki67pos cardiomyocytes ([%] TAC 0.11±0.02, R-TAC 0.02±0.007, T-TAC 0±0, RT-TAC 0.005±0.0.002).4 days of drug treatment induced a significant increase of Sca1pos/VEGFR1posendothelial progenitor cells in all animals in the treated SHAM-groups ([%S] R-S146±12, T-S 126±11, RT-S 181±21). After 1 day of TAC, only ramipril increasedEPC ([%S] TAC 134±9, R-TAC 329±61, T-TAC 124±12, RT-TAC 182±11). After 5weeks of TAC, ARB monotherapy did not change EPC-level compared to vehicleor the combination therapy - but raised it compared to ACEI monotherapy ([%S]TAC 137±14, R-TAC 102±5, T-TAC 131±10, RT-TAC 101±23).Neither TAC nor any of the therapies changed the number of cardiac capillariesper cardiomyocytes (podocalyxin immunostaining; S 2.1±0.1, TAC 2.3±0.1, R-TAC 2.2±0.1, T-TAC 2±0.1, RT-TAC 2±0.1).Conclusions: ACE-inhibition and AT1-receptor blockade have beneficial effectsin remodelling processes during cardiac pressure overload. There are small dif-ferences between the two therapeutical approaches, but the combination therapyhas no additional benefit.
PATHOBIOLOGY AND PATHOPHYSIOLOGY OFPULMONARY HYPERTENSION
177 Prognostic value of echocardiographic parameters inpatients with pulmonary arterial hypertension (PAH)treated with targeted therapies
E. Beciani, M. Palazzini, C. Bachetti, F. Sgro, E. Conficoni, E. Gotti,G. Mazzanti, A. Manes, A. Branzi, N. Galie. Institute of Cardiology,
University of Bologna, Bologna, Italy
Purpose: PAH is associated with abnormalities of right heart structure and func-tion that are major determinants of prognosis. Although several echocardio-graphic variables have been associated with outcome in previous studies, theseresults are derived from small cohorts of patients treated with conventional ther-apy or with PAH-targeted drugs as monotherapy. The aim of this study was toprospectively assess the prognostic value of echocardiographic parameters ascompared to clinical and haemodynamic measures in a large cohort of PAH pa-tients treated according to current guidelines.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
8 Pathobiology and pathophysiology of pulmonary hypertension
Methods: Between September 2000 and December 2009 we enrolled 337 pa-tients (mean age 52±17 tears; 62%females) with PAH of different sub-groups(203 idiopathic PAH, 9 heritable PAH, 4 drug-induced PAH, 89 PAH associatedwith connective tissue disease, 31 PAH associated with HIV infection, 1 PAH dueto chronic haemolytic anaemia). At baseline, patients underwent clinical evalua-tion, six minute walk distance (6MWD), right heart catheterization and echocar-diography.Results: After a mean follow-up of 37±31 months, 119 patients died, 4 under-went lung transplantation and 17 were lost to follow-up. Eighty-one percent ofthe patients (n=273) were treated with PAH-targeted treatments and 49% of themwith double or triple combination therapy. Variables associated with poor survivalby univariate Cox life-table analysis were as follows: age (p<0.001); male sex(p 0.006); WHO functional class III/IV (p<0.001); 6 minute walk distance (6MWD)(p<0.001); right atrial pressure (p=0.003); cardiac index (p=0.037); mixed venousoxygen saturation (p<0.001); right atrial area index (RAAI) (p<0.001); tricuspidregurgitation maximal velocity (p=0.011); TR area (p<0.001); right ventricular di-astolic area index (p=0.035); left ventricular diastolic area index (p=0.003); peri-cardial effusion size (p=0.002). In the multivariate analysis age [p=0,004; (HR1.022; CI 1.007-1.037)], male sex [p=0,041; (HR 1.540; CI 1.018-2.330)], 6MWD[p<0.001; (HR 0.995; CI 0.993-0.997)] and RAAI [p=0.010; (HR 1.055; CI 1.013-1.099)] were independently correlated to prognosis.Conclusions: in a large cohort of PAH patients treated with current targeted ther-apies, the RAAI appears to be the strongest independent echocardiographic pa-rameter related to survival.
178 Cardiovascular magnetic resonance measured rightventricular mass influences prognosis in pulmonaryarterial hypertension
W.M. Bradlow1, R.G. Assomull1, F. Williams2, A. Taegtmeyer2 ,W. Gin-Sing2, J. Strange3, M.R. Wilkins2, L.G.E. Howard2,
R.H. Mohiaddin1 , J.S.R. Gibbs2. 1Royal Brompton Hospital, London, UnitedKingdom; 2Hammersmith Hospital, London, United Kingdom; 3Bristol RoyalInfirmary, Bristol, United Kingdom
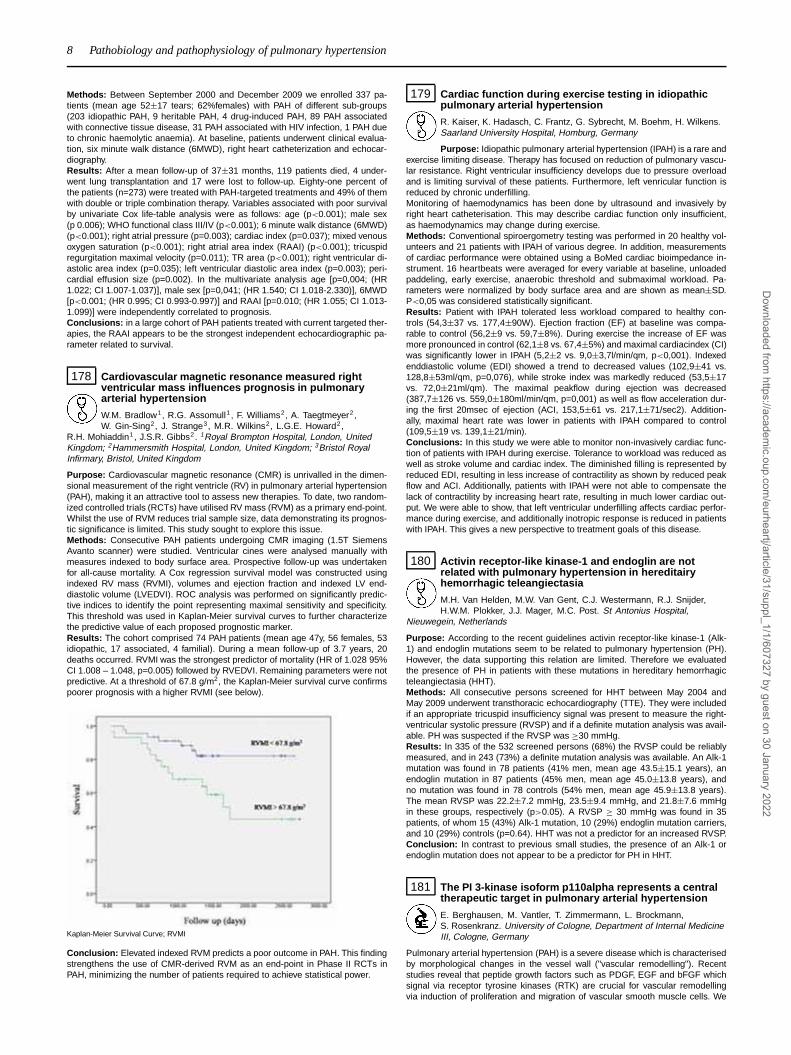
Purpose: Cardiovascular magnetic resonance (CMR) is unrivalled in the dimen-sional measurement of the right ventricle (RV) in pulmonary arterial hypertension(PAH), making it an attractive tool to assess new therapies. To date, two random-ized controlled trials (RCTs) have utilised RV mass (RVM) as a primary end-point.Whilst the use of RVM reduces trial sample size, data demonstrating its prognos-tic significance is limited. This study sought to explore this issue.Methods: Consecutive PAH patients undergoing CMR imaging (1.5T SiemensAvanto scanner) were studied. Ventricular cines were analysed manually withmeasures indexed to body surface area. Prospective follow-up was undertakenfor all-cause mortality. A Cox regression survival model was constructed usingindexed RV mass (RVMI), volumes and ejection fraction and indexed LV end-diastolic volume (LVEDVI). ROC analysis was performed on significantly predic-tive indices to identify the point representing maximal sensitivity and specificity.This threshold was used in Kaplan-Meier survival curves to further characterizethe predictive value of each proposed prognostic marker.Results: The cohort comprised 74 PAH patients (mean age 47y, 56 females, 53idiopathic, 17 associated, 4 familial). During a mean follow-up of 3.7 years, 20deaths occurred. RVMI was the strongest predictor of mortality (HR of 1.028 95%CI 1.008 – 1.048, p=0.005) followed by RVEDVI. Remaining parameters were notpredictive. At a threshold of 67.8 g/m2, the Kaplan-Meier survival curve confirmspoorer prognosis with a higher RVMI (see below).
Kaplan-Meier Survival Curve; RVMI
Conclusion: Elevated indexed RVM predicts a poor outcome in PAH. This findingstrengthens the use of CMR-derived RVM as an end-point in Phase II RCTs inPAH, minimizing the number of patients required to achieve statistical power.
179 Cardiac function during exercise testing in idiopathicpulmonary arterial hypertension
R. Kaiser, K. Hadasch, C. Frantz, G. Sybrecht, M. Boehm, H. Wilkens.Saarland University Hospital, Homburg, Germany
Purpose: Idiopathic pulmonary arterial hypertension (IPAH) is a rare andexercise limiting disease. Therapy has focused on reduction of pulmonary vascu-lar resistance. Right ventricular insufficiency develops due to pressure overloadand is limiting survival of these patients. Furthermore, left venricular function isreduced by chronic underfilling.Monitoring of haemodynamics has been done by ultrasound and invasively byright heart catheterisation. This may describe cardiac function only insufficient,as haemodynamics may change during exercise.Methods: Conventional spiroergometry testing was performed in 20 healthy vol-unteers and 21 patients with IPAH of various degree. In addition, measurementsof cardiac performance were obtained using a BoMed cardiac bioimpedance in-strument. 16 heartbeats were averaged for every variable at baseline, unloadedpaddeling, early exercise, anaerobic threshold and submaximal workload. Pa-rameters were normalized by body surface area and are shown as mean±SD.P<0,05 was considered statistically significant.Results: Patient with IPAH tolerated less workload compared to healthy con-trols (54,3±37 vs. 177,4±90W). Ejection fraction (EF) at baseline was compa-rable to control (56,2±9 vs. 59,7±8%). During exercise the increase of EF wasmore pronounced in control (62,1±8 vs. 67,4±5%) and maximal cardiacindex (CI)was significantly lower in IPAH (5,2±2 vs. 9,0±3,7l/min/qm, p<0,001). Indexedenddiastolic volume (EDI) showed a trend to decreased values (102,9±41 vs.128,8±53ml/qm, p=0,076), while stroke index was markedly reduced (53,5±17vs. 72,0±21ml/qm). The maximal peakflow during ejection was decreased(387,7±126 vs. 559,0±180ml/min/qm, p=0,001) as well as flow acceleration dur-ing the first 20msec of ejection (ACI, 153,5±61 vs. 217,1±71/sec2). Addition-ally, maximal heart rate was lower in patients with IPAH compared to control(109,5±19 vs. 139,1±21/min).Conclusions: In this study we were able to monitor non-invasively cardiac func-tion of patients with IPAH during exercise. Tolerance to workload was reduced aswell as stroke volume and cardiac index. The diminished filling is represented byreduced EDI, resulting in less increase of contractility as shown by reduced peakflow and ACI. Additionally, patients with IPAH were not able to compensate thelack of contractility by increasing heart rate, resulting in much lower cardiac out-put. We were able to show, that left ventricular underfilling affects cardiac perfor-mance during exercise, and additionally inotropic response is reduced in patientswith IPAH. This gives a new perspective to treatment goals of this disease.
180 Activin receptor-like kinase-1 and endoglin are notrelated with pulmonary hypertension in hereditairyhemorrhagic teleangiectasia
M.H. Van Helden, M.W. Van Gent, C.J. Westermann, R.J. Snijder,H.W.M. Plokker, J.J. Mager, M.C. Post. St Antonius Hospital,
Nieuwegein, Netherlands
Purpose: According to the recent guidelines activin receptor-like kinase-1 (Alk-1) and endoglin mutations seem to be related to pulmonary hypertension (PH).However, the data supporting this relation are limited. Therefore we evaluatedthe presence of PH in patients with these mutations in hereditary hemorrhagicteleangiectasia (HHT).Methods: All consecutive persons screened for HHT between May 2004 andMay 2009 underwent transthoracic echocardiography (TTE). They were includedif an appropriate tricuspid insufficiency signal was present to measure the right-ventricular systolic pressure (RVSP) and if a definite mutation analysis was avail-able. PH was suspected if the RVSP was ≥30 mmHg.Results: In 335 of the 532 screened persons (68%) the RVSP could be reliablymeasured, and in 243 (73%) a definite mutation analysis was available. An Alk-1mutation was found in 78 patients (41% men, mean age 43.5±15.1 years), anendoglin mutation in 87 patients (45% men, mean age 45.0±13.8 years), andno mutation was found in 78 controls (54% men, mean age 45.9±13.8 years).The mean RVSP was 22.2±7.2 mmHg, 23.5±9.4 mmHg, and 21.8±7.6 mmHgin these groups, respectively (p>0.05). A RVSP ≥ 30 mmHg was found in 35patients, of whom 15 (43%) Alk-1 mutation, 10 (29%) endoglin mutation carriers,and 10 (29%) controls (p=0.64). HHT was not a predictor for an increased RVSP.Conclusion: In contrast to previous small studies, the presence of an Alk-1 orendoglin mutation does not appear to be a predictor for PH in HHT.
181 The PI 3-kinase isoform p110alpha represents a centraltherapeutic target in pulmonary arterial hypertension
E. Berghausen, M. Vantler, T. Zimmermann, L. Brockmann,S. Rosenkranz. University of Cologne, Department of Internal MedicineIII, Cologne, Germany
Pulmonary arterial hypertension (PAH) is a severe disease which is characterisedby morphological changes in the vessel wall ("vascular remodelling"). Recentstudies reveal that peptide growth factors such as PDGF, EGF and bFGF whichsignal via receptor tyrosine kinases (RTK) are crucial for vascular remodellingvia induction of proliferation and migration of vascular smooth muscle cells. We
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Pathobiology and pathophysiology of pulmonary hypertension / New insights into ischaemia/reperfusion mechanisms 9
compared the effect of the tyrosine kinase inhibitor Imatinib and subtype-specificinhibitors of the PI3K-isoforms p110alpha (PIK75) and p110beta (TGX221) ongrowth-factor induced proliferation and chemotaxis of human pulmonary arterialsmooth muscle cells (hPASMC). Starved cells were pre-incubated with inhibitorsfor 30 min and then stimulated with either PDGF-BB (30ng/ml) or a growth factorcocktail (GFC) containing FBS and different growth factors (EGF, FGF, insulin andPDGF). Proliferation was detected using a BrdU incorporation assay. Chemotaxiswas quantified using a modified Boyden-chamber. PDGF mediated hVSMC pro-liferation and chemotaxis were dose-dependently decreased by Imatinib (IC50:3μM). However, when hPASMCs were stimulated with GFC instead of PDGF,Imatinib did not affect the mitogenic and chemotactic response. In order to tar-get a common central downstream mediator of RTK signalling, we tested PI3Kisoform selective inhibitors. PDGF and GFC- induced proliferation and chemo-taxis were both dose-dependently inhibited by PIK75 (p110alpha-inhibitor: IC50300nM). But were unaffected by TGX211 (p110beta) and IC 87114, which inhibitsp110delta and served as a negative control. These results indicated that growthfactor induced proliferation and chemotaxis of hPASMC are both mediated by thep110alpha isoform of PI3K which therefore represents a promising therapeuticapproach for the reversal of vascular remodelling in PAH.
182 Cell therapy using cardiac-committed human embryonicstem cells improves right ventricular function in aporcine model of chronic overload: first promisingresults
V. Lambert1, A. Capderou2, E. Gouadon2 , E. Le Bret1, C. Rucker-Martin2, S. Dinanian3, B. Stos1, M. Puceat4, A. Serraf1, J.F. Renaud2.
1Centre Chirurgical Marie-Lannelongue, le Plessis Robinson, France; 2INSERMU-999, le Plessis Robinson, France; 3AP-HP - Hospital Antoine-Beclere,Department of Cardiology, Clamart, France; 4INSERM Avenir Program, stem celland cardiogenesis, Evry, France
Purpose: Advances in cardiac surgery have improved short-term prognoses ofpatients with congenital heart diseases but, at long-term, right ventricular (RV)failure may occur, leading to morbidity and mortality. As conventional therapiesgives transitory results, cell therapy may be a therapeutic option for cardiac re-pair. The ability of embryonic stem cells differentiation towards a cardiomyogenicphenotype makes them attractive candidates. Our aim was to evaluate, in a largeanimal model, effects of human cardiac progenitors transplantation on the RVfunction.Methods: RV dysfunction was created in 6 piglets mimicking RV tract sequel-lae of repaired tetralogy of Fallot leading, after 4 months, to a chronic combined,barométric and volumetric, RV overload. 3 pigs received vehicle, 3 others receivedHUES-24 derived human cardiac progenitors injected at multiple sites into thefree wall of RV myocardium. All pigs were immunosuppressed using Tacrolimus.Myocardial function was measured 3 months after cell transplantation by conduc-tance catheter technique using maximal elastance (Emax) slope and ventricularenergetics (stroke work, pression-volume area). The risk of ventricular arrhythmiawas evaluated by programmed ventricular stimulation at the end of the follow-up.Structural remodelling was assessed by histology.Results: All pigs survived; no complication occurred related to myocardial injec-tions or immunosuppression. No ventricular arrhythmia was induced. In all treatedpigs, myocardial contractility was improved as assessed by an increasing Emaxslope relative to baseline (0.61±0.02 vs 0.40±0.01, p<0.001) and to controls atthe follow-up end (0.32±0.02, p<0.05). Stroke work was similar in both groups,pression-volume area tended to increase in the treated group suggesting that thetotal energy output was augmented. In treated pigs, myocardial fibrosis appearedonly in peritrabecular area whereas in both peritrabecular and perimyocyte areain controls.Conclusion: Transmyocardial transplantation of cardiac-committed human em-bryonic stem cells in failed RV secondary to chronic overload is feasible, improvesRV myocardial contractility and allows a better adaptation to chronic overload.
NEW INSIGHTS INTO ISCHAEMIA/REPERFUSIONMECHANISMS
183 The scavenger receptor class B type I-deficient,hypomorphic apolipoprotein E-R61 mouse - a newmouse model exhibiting diet-induced occlusive coronaryatherosclerosis and myocardial infarction
K. Tiemann1, M. Kuhlmann2, M. Muehlmeister1, J. Stypmann1, T. Liu1,L. Ting1, S. Hermann2, M. Schaefers2 . 1University Clinic, Dept. of cardiologyand angiology, Muenster, Germany; 2University of Muenster, Dept. of NuclearMedicine, Muenster, Germany
Transgenic mouse models of atherosclerosis demonstrate plaque developmentin the aorta and its branches without complete coronary occlusion and myocar-dial infarction (MI). At present there is no suitable mouse model mimicking theclinical pathogenesis of MI. Recently, a new k.o. mouse was described, lack-ing the Scavenger Receptor class B type I (SR-BI K.O.) expressing reduced lev-els of an ApoE4-like murine ApoE isoform (ApoE-R61(hypo)), developing occlu-sive coronary atherosclerosis, MI and cardiac dysfunction under a high-fat/high-
cholesterol- (HFC-)diet. Aim of the present study was to further characterize thismouse strain with special focus on molecular imaging techniques. All mice werefed a normal chow diet before starting the experiments. After onset of the HFC-diet SR-BI K.O./ApoE-R61(hypo) mice died within 4 weeks. Histological analysisrevealed massive plaque development in the aorta and the coronary arteries,coronary occlusion, as well as tissue breakup and extensive fibrosis in the my-ocardium. TUNEL staining and immunohistochemistry demonstrated cell death,apoptosis (caspase-3), inflammation (MRP-14; activated macrophages) and my-ocardial remodelling (MMP-9). The massive plaque development in the coro-nary artery system was also visualized by 3D-CT-imaging of explanted heartsperfused with microfil®. Serially performed echocardiography documented a dra-matic drop in myocardial pump function and perfusion deficits in myocardial con-trast echocardiography. In some animals focal wall motion abnormalities as wellas focal edema were found. In F-18-FDG-PET scans in some mice this was ac-companied by focal defects in F-18-FDG-uptake. In most animals myocardial F-18-FDG-uptake was rather inhomogeneous, indicating multiple micro-infarctionevents which were confirmed by histology. In contrast, the hearts of HFC-dietfed SR-BI wildtype/ApoE-R61(hypo) mice appeared histologically and function-ally normal. Interestingly, extensive coronary plaque deposition was found alsoin some homozygous double-transgenic mice which continued with normal chowdiet, however, this resulted not in MI or total occlusion. In conclusion, the presentresults indicate that the SR-BI K.O./ApoE-R61(hypo) mouse-strain seems to be avaluable animal model for the development of new sophisticated molecular probesfor all steps in the course of atherosclerosis, from early plaque development un-til coronary occlusion and MI. In addition, the model has the advantage that theprogression of atherosclerosis can be altered (and therefore adopted to the ex-perimental needs) by modifying the lipid content in the diet.
184 Effect of Frizzled 4/6 double deletion in developmentalvascularisation and post-ischemic angiogenesis
B. Seguy1, R. Chauvel1, C. Allieres1, J.M.D. Lamaziere1, C. Duplaa1,T. Couffinhal2. 1Inserm U828, University Bordeaux 2, Pessac, France;2Cardiovascular Hospital of Haut-Leveque, Pessac, France
sFRP-1, a Wnt/Frizzled modulator, is an in vivo pro-angiogenic agent and wasshown to be a ligand for Frizzled 4 and 6 receptors. Fzd 4-/- mice exhibit severedefects in retinal vascularisation. Fzd 6 -/- mice have no known vascular pheno-typeAim: To explore Fzd 4 -/- and 6 -/- mice developmental and post-ischemicvascularization and, because of possible redundancy, the double deletion 4/6 -/-.Method: 3-D vessels analysis using a microscanner (μCT) (Oses ATVB 2009).Adult mice were injected with a radio-opaque agent and we compared kid-ney, heart, normal and ischemic muscle vascular network after μCT recon-structions. Fzd 4 -/-, 6 -/- and Fzd 4/6-/- mice (n=5/group) were comparedto littermates (n=10) using the following parameters: connectivity/volume, den-sity/volume, mean vessel diameter.Results: Compared to littermates, deleted mice showed a drastic reduction ofvessels density and connectivity of kidneys,heart and normal muscle vascular-ization. I.e.: average littermate kidney connectivity was 800/mm3±40, Fzd 6 -/-352/mm3±32, Fzd 4 -/- 327/mm3±22, Fzd 4/6 -/- 310/mm3±18. Double deletionwas not synergistic in alteration of physiologic vascularization.In hindlimb ischemic model, at D15, clinical or blood flow parameters were notaltered in Fzd 6-/-, whereas Fzd 4-/- displayed a strong alteration, even strongerin Fzd 4/6-/-. As analyzed by μCT, Fzd 6-/- have little alteration of parameters ofneo angiogenesis, whereas Fzd 4-/- exhibit a strong decrease in vessel densityand connectivity. Double deletion 4/6 induced a major defect in post-ischemicangiogenesis.
Micro CT kidneys WT
Conclusion: For the first time, we showed that Fzd 4 and 6 played a role invessel development and angiogenesis. A confocal microscopic analysisis actuallyrealized to further characterize those aspects.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
10 New insights into ischaemia/reperfusion mechanisms
185 Placental growth factor increases regional myocardialblood flow and function in porcine chronic myocardialischemia
X. Liu1, G. Reyns2, P. Verhamme1, P. Pokreisz1, P. Claus3,S. Vandenwijngaert1 , S. Ghysels4, F. Maes5, J. Bogaert4, S. Janssens1 .
1Catholic University of Leuven, Department of Cardiology, Leuven, Belgium;2VIB, Leuven, Belgium; 3Catholic University of Leuven, Dept CardiovascularDis., Division Imaging & Cardiovascular Dynamics, Leuven, Belgium; 4UniversityHospitals (UZ) Leuven, Department of Radiology, Leuven, Belgium; 5ESAT,Leuven, Belgium
Purpose: Placental growth factor (PlGF), a member of the vascular endothelialgrowth factor family, has a distinct biologic phenotype with a predominant proan-giogenic role in disease without affecting quiescent vessels in healthy organs. Wetested whether systemic administration of recombinant human (rh)PlGF improvesregional myocardial blood flow and systolic function recovery in a new porcinechronic myocardial ischemia model.Methods: We implanted a flow-limiting stent in the proximal LAD of pigs and mea-sured systemic hemodynamics, regional myocardial function using 3.0 T mag-netic resonance imaging, and blood flow using colored microspheres injection 4weeks later. Animals were then randomized in a blinded way to receive chronic rh-PlGF infusion (15μg/kg/day, n=11) or PBS (con, n=10) for 2 weeks via a minipumpconnected to the jugular vein. Regional myocardial perfusion and function in theischemic and remote zones were again measured after 8 weeks and neovascu-larization was evaluated on lectin- and smooth muscle (SM) actin-stained sec-tions. Glycogen utilization was evaluated on periodic acid schiff (PAS) stainedsections and tissue extracts by western blot. Oxidative stress was evaluated us-ing 8-hydroxy-2’-deoxyguanosine (8-OHdG) immunohistochemistry. Apoptosis inthe ischemic zone was evaluated using caspase-3 and terminal dUTP nick end-labeling (TUNEL) with the in situ cell death detection kit.Results: Infusion of rhPlGF transiently increased PlGF serum levels more than30 fold (1153±180 vs 33±19 pg/ml at baseline, p<0.001) without affecting sys-temic hemodynamics. Compared to 4 weeks, rhPlGF increased regional myocar-dial blood flow (� RBF (ml/min/g): 0.4±0.11 in PlGF vs 0.04±0.04 in con), re-gional wall motion (� WM (mm): 0.5±0.2 in PlGF vs -0.3±0.3 in con) and systolicwall thickening (� WT (%): 7.0±3.7 in PlGF vs -1.8±3.2 in con) to the ischemicarea at 8 weeks (p<0.05 vs con for all). Functional improvement after rhPlGF wasaccompanied by pathologic evidence of increased myocardial neovascularization,enhanced glycogen utilization and reduced oxidative stress and preserved nucleidensity and apoptosis in the ischemic zone (p<0.05 vs con).Conclusions: Systemic rhPlGF infusion significantly enhances regional bloodflow and contractile function of chronically ischemic myocardium without adverselocal or systemic effects. PlGF-mediated increase in myocardial perfusion andmetabolism during ischemic stress represents an attractive therapeutic strategyfor chronic ischemic cardiomyopathy.
186 Lack of Toll-like receptor 2 promotes survival andpreserves cardiac function and geometry after acute MI
E. Aguor1, F. Arslan2, K. Van De Kolk2, P. Doevendan3 , D.D.E. Kleijn2,G. Pasterkamp2. 1Interuniversity Cardiology Institute of the Netherlands(ICIN), Utrecht, Netherlands; 2University Medical Center Utrecht,
Experimental Cardiology Laboratory, Utrecht, Netherlands; 3University MedicalCenter Utrecht, Division Heart and Lungs, Utrecht, Netherlands
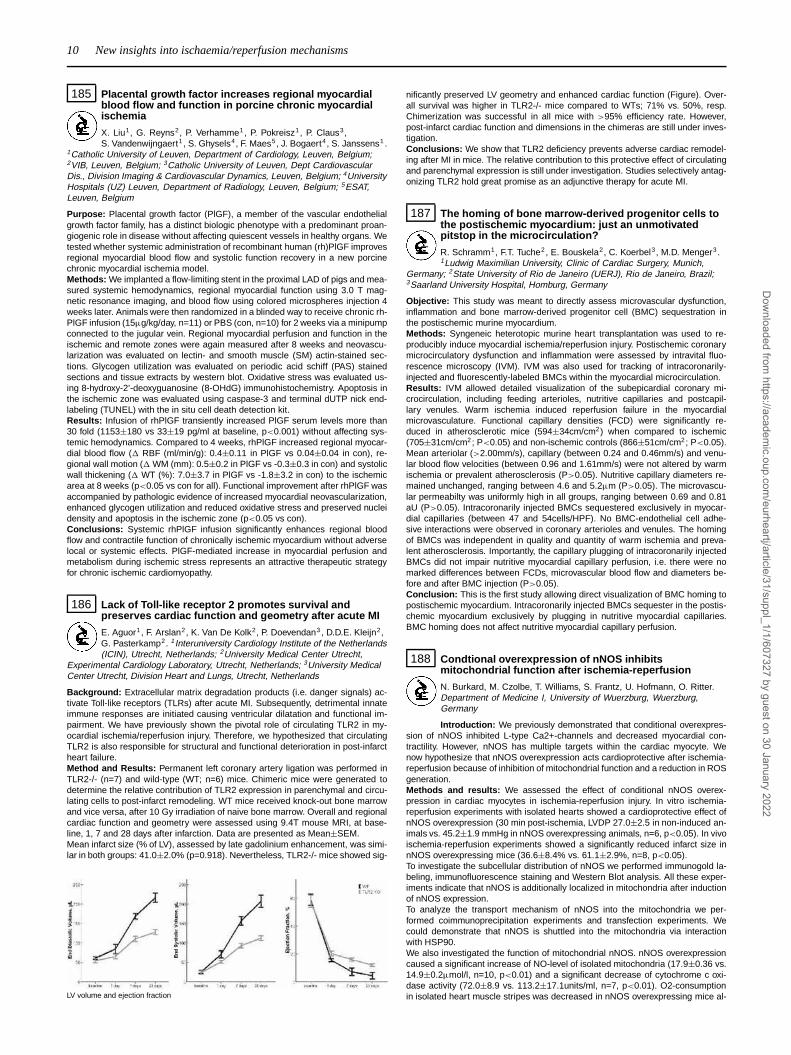
Background: Extracellular matrix degradation products (i.e. danger signals) ac-tivate Toll-like receptors (TLRs) after acute MI. Subsequently, detrimental innateimmune responses are initiated causing ventricular dilatation and functional im-pairment. We have previously shown the pivotal role of circulating TLR2 in my-ocardial ischemia/reperfusion injury. Therefore, we hypothesized that circulatingTLR2 is also responsible for structural and functional deterioration in post-infarctheart failure.Method and Results: Permanent left coronary artery ligation was performed inTLR2-/- (n=7) and wild-type (WT; n=6) mice. Chimeric mice were generated todetermine the relative contribution of TLR2 expression in parenchymal and circu-lating cells to post-infarct remodeling. WT mice received knock-out bone marrowand vice versa, after 10 Gy irradiation of naive bone marrow. Overall and regionalcardiac function and geometry were assessed using 9.4T mouse MRI, at base-line, 1, 7 and 28 days after infarction. Data are presented as Mean±SEM.Mean infarct size (% of LV), assessed by late gadolinium enhancement, was simi-lar in both groups: 41.0±2.0% (p=0.918). Nevertheless, TLR2-/- mice showed sig-
LV volume and ejection fraction
nificantly preserved LV geometry and enhanced cardiac function (Figure). Over-all survival was higher in TLR2-/- mice compared to WTs; 71% vs. 50%, resp.Chimerization was successful in all mice with >95% efficiency rate. However,post-infarct cardiac function and dimensions in the chimeras are still under inves-tigation.Conclusions: We show that TLR2 deficiency prevents adverse cardiac remodel-ing after MI in mice. The relative contribution to this protective effect of circulatingand parenchymal expression is still under investigation. Studies selectively antag-onizing TLR2 hold great promise as an adjunctive therapy for acute MI.
187 The homing of bone marrow-derived progenitor cells tothe postischemic myocardium: just an unmotivatedpitstop in the microcirculation?
R. Schramm1, F.T. Tuche2, E. Bouskela2, C. Koerbel3, M.D. Menger3 .1Ludwig Maximilian University, Clinic of Cardiac Surgery, Munich,
Germany; 2State University of Rio de Janeiro (UERJ), Rio de Janeiro, Brazil;3Saarland University Hospital, Homburg, Germany
Objective: This study was meant to directly assess microvascular dysfunction,inflammation and bone marrow-derived progenitor cell (BMC) sequestration inthe postischemic murine myocardium.Methods: Syngeneic heterotopic murine heart transplantation was used to re-producibly induce myocardial ischemia/reperfusion injury. Postischemic coronarymicrocirculatory dysfunction and inflammation were assessed by intravital fluo-rescence microscopy (IVM). IVM was also used for tracking of intracoronarily-injected and fluorescently-labeled BMCs within the myocardial microcirculation.Results: IVM allowed detailed visualization of the subepicardial coronary mi-crocirculation, including feeding arterioles, nutritive capillaries and postcapil-lary venules. Warm ischemia induced reperfusion failure in the myocardialmicrovasculature. Functional capillary densities (FCD) were significantly re-duced in atherosclerotic mice (594±34cm/cm2) when compared to ischemic(705±31cm/cm2; P<0.05) and non-ischemic controls (866±51cm/cm2; P<0.05).Mean arteriolar (>2.00mm/s), capillary (between 0.24 and 0.46mm/s) and venu-lar blood flow velocities (between 0.96 and 1.61mm/s) were not altered by warmischemia or prevalent atherosclerosis (P>0.05). Nutritive capillary diameters re-mained unchanged, ranging between 4.6 and 5.2μm (P>0.05). The microvascu-lar permeabilty was uniformly high in all groups, ranging between 0.69 and 0.81aU (P>0.05). Intracoronarily injected BMCs sequestered exclusively in myocar-dial capillaries (between 47 and 54cells/HPF). No BMC-endothelial cell adhe-sive interactions were observed in coronary arterioles and venules. The homingof BMCs was independent in quality and quantity of warm ischemia and preva-lent atherosclerosis. Importantly, the capillary plugging of intracoronarily injectedBMCs did not impair nutritive myocardial capillary perfusion, i.e. there were nomarked differences between FCDs, microvascular blood flow and diameters be-fore and after BMC injection (P>0.05).Conclusion: This is the first study allowing direct visualization of BMC homing topostischemic myocardium. Intracoronarily injected BMCs sequester in the postis-chemic myocardium exclusively by plugging in nutritive myocardial capillaries.BMC homing does not affect nutritive myocardial capillary perfusion.
188 Condtional overexpression of nNOS inhibitsmitochondrial function after ischemia-reperfusion
N. Burkard, M. Czolbe, T. Williams, S. Frantz, U. Hofmann, O. Ritter.Department of Medicine I, University of Wuerzburg, Wuerzburg,Germany
Introduction: We previously demonstrated that conditional overexpres-sion of nNOS inhibited L-type Ca2+-channels and decreased myocardial con-tractility. However, nNOS has multiple targets within the cardiac myocyte. Wenow hypothesize that nNOS overexpression acts cardioprotective after ischemia-reperfusion because of inhibition of mitochondrial function and a reduction in ROSgeneration.Methods and results: We assessed the effect of conditional nNOS overex-pression in cardiac myocytes in ischemia-reperfusion injury. In vitro ischemia-reperfusion experiments with isolated hearts showed a cardioprotective effect ofnNOS overexpression (30 min post-ischemia, LVDP 27.0±2.5 in non-induced an-imals vs. 45.2±1.9 mmHg in nNOS overexpressing animals, n=6, p<0.05). In vivoischemia-reperfusion experiments showed a significantly reduced infarct size innNOS overexpressing mice (36.6±8.4% vs. 61.1±2.9%, n=8, p<0.05).To investigate the subcellular distribution of nNOS we performed immunogold la-beling, immunofluorescence staining and Western Blot analysis. All these exper-iments indicate that nNOS is additionally localized in mitochondria after inductionof nNOS expression.To analyze the transport mechanism of nNOS into the mitochondria we per-formed coimmunoprecipitation experiments and transfection experiments. Wecould demonstrate that nNOS is shuttled into the mitochondria via interactionwith HSP90.We also investigated the function of mitochondrial nNOS. nNOS overexpressioncaused a significant increase of NO-level of isolated mitochondria (17.9±0.36 vs.14.9±0.2μmol/l, n=10, p<0.01) and a significant decrease of cytochrome c oxi-dase activity (72.0±8.9 vs. 113.2±17.1units/ml, n=7, p<0.01). O2-consumptionin isolated heart muscle stripes was decreased in nNOS overexpressing mice al-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

New insights into ischaemia/reperfusion mechanisms / Vascular and myocardial effects of oxygen species 11
ready under resting conditions (0.018±0.01 vs. 0.025±0.007ml [O2] x mm-3 xmin-1, n=11, p<0.05). Additionally, we found that the ROS concentration was sig-nificantly decreased in hearts of nNOS overexpressing mice (6.14±0.685μM vs.14.53±1.7μM, n=5, p<0.01) which was caused by inhibition of XOR activity byabundant nNOS expression.Discussion: We demonstrated that conditional transgenic overexpression ofnNOS resulted in myocardial protection after ischemia-reperfusion injury by sup-pression of ROS generation and inhibition of myocardial oxygen consumption inthe mitochondria.
VASCULAR AND MYOCARDIAL EFFECTS OF OXYGENSPECIES
206 Serum adiponectin regulates vascular O2- generationand NO bioavailability in patients with coronaryatherosclerosis
C. Antoniades1, C. Shirodaria1, P. Leeson1 , C. Bakogiannis2,M. Demosthenous2 , A. Antonopoulos2 , D. Tousoulis2 , A. Miliou2,
C. Stefanadis2, K.M. Channon1. 1University of Oxford, Oxford, United Kingdom;2University of Athens, Athens, Greece
Purpose: Evidence suggests that adiponectin, an adipokine produced by adiposetissue, may have an anti-inflammatory and antioxidant role in human atheroscle-rosis. However, very little is known regarding its role in the regulation of vascu-lar function in patients with atherosclerosis. We examined the impact of circulat-ing adiponectin on vascular superoxide (O2-) generation and nitric oxide (NO)bioavailability in human arteries and veins.Methods: The study population consisted of 320 patients with coronaryatherosclerosis (CAD) undergoing elective coronary bypass operation. Endothe-lial function was estimated in the brachial artery by flow mediated dilation (FMD),and adiponectin levels were measured in blood obtained preoperatively. Vascu-lar O2- was measured in saphenous veins (SV) and mammary arteries (IMA) inthe presence or absence of LNAME (an endothelial nitric oxide synthase (eNOS)inhibitor). NO bioavailability was also estimated in SV segments ex vivo, by deter-mining the vasorelaxations in response to acetylcholine (ACh).Results: Circulating adiponectin was positively associated with FMD (r=0.310,p=0.032) and vasorelaxations of SV segments in response to ACh (Fig.A). Impor-tantly, adiponectin was negatively associated with vascular O2- in both SV andIMA (Fig. B), while low adiponectin was associated with more LNAME inhibitableO2- in SV and IMA, suggesting more eNOS uncoupling (Fig. C).
Conclusions: This is the first study demonstrating that adiponectin has a directimpact on NO bioavailability in human vessels, by improving eNOS coupling andsuppressing vascular O2- generation in patients with atherosclerosis. These novelfindings suggest that this adipokine may be directly involved in the regulation ofvascular redox state in humans.
207 NAD-Transhydrogenase regulates mitochondrialformation of reactive oxygen species in cardiacmyocytes
A. Von Hardenberg, M. Kohlhaas, A. Nickel, M. Hohl, J.-A. Saar,M. Bohm, C. Maack. Saarland University Hospital, Department ofInternal Medicine III, Cardiology, Homburg, Germany
Purpose: Oxidative stress is causally linked to the progression of heart failure,and mitochondria are important sources for reactive oxygen species (ROS). Inmitochondria, elimination of H2O2 consumes reduced NADPH. After its oxida-tion, NADP+ is re-reduced to NADPH by NAD-transhydrogenase (Nnt), isocitrate-dehydrogenase (IDHm) and malic enzyme (MEP). C57BL6J mice frequentlyserve as a background for genetic and surgical interventions. Recently, a mu-tation in the Nnt gene of C57BL/6J mice was discovered, accounting for glucoseintolerance of this strain. The role of the Nnt in regulating redox state and ROSformation in cardiac mitochondria, however, has never been assessed.Methods and Results: The loss of exons 7-11 of the Nnt gene (RT-PCR) and lackof Nnt activity (fluorimetric assays) were verified in myocardium of C57BL/6J (J-)mice, whereas in C57/BL6N (N-) mice, the gene and protein were intact. Therewas no compensatory upregulation of IDHm or MEP activity in J-mice. To testthe functional relevance of Nnt deficiency, cardiac myocytes were field-stimulated
at 0.5 Hz, and sarcomere shortening was monitored together with fluorescentindicators (indo-1, SBFI, TMRM, DCF, mitoSOX) or cellular autofluorescence. Atbaseline, the mitochondrial redox state of NAD(P)H/NAD(P)+ was more oxidizedin J- than in N-mice (51±3% vs. 39±2% oxidized NAD(P)+; n=25/36; p<0.01).This was associated with a ∼50% decrease of the amplitude of cytosolic Ca2+transients and ∼30% slowing of Ca2+ decay in J- vs. N-mice (n=22/24; p<0.05).Cytosolic [Na+], diastolic Ca2+, mitochondrial H2O2 and O2- generation weresimilar at 0.5 Hz in both strains. To induce a transition of workload, myocyteswere superfused with isoproterenol (100 nM) and paced at 5 Hz for 3 min. Underthese conditions, similar Ca2+ transient amplitudes and sarcomere shorteningwere achieved. The NAD(P)H redox state, however, was oxidized further in J- thanin N-mice (to 60±4% vs. 46±2% oxidized NAD(P)+; p<0.001). While after thetransition, net formation of H2O2 and O2- remained unchanged in N-mice, H2O2(but not O2-) formation increased in J-mice (H2O2: 1.46±0.06 (J) vs. 1.29±0.04F/F0 (N); p<0.05). The mitochondrial membrane potential was maintained duringthe transition in either strain.Conclusions: By regenerating NADPH during workload transitions in the heart,the Nnt plays a key role in maintaining the antioxidative capacity of the mitochon-drial matrix, preventing H2O2 formation. Nnt deficiency in C57BL/6J mice predis-poses this strain to cardiac oxidative stress, which may influence the phenotypesof genetic and surgical interventions.
208 Concomitant transactivation by AP-1 of miRNAsbelonging to miR-17-5p seed family in response tooxidative stress causes cardiomyocyte apoptosis bytargeting Stat3 and Bcl-2
X. Luo, J. Zhang, J. Xiao, G. Chen, Z. Wang. Montreal Heart Instituteaffiliated with the University of Montreal, Montreal, Canada
The action of miRNAs is critically determined by their 5’end 2-8 nts sequencemotifs called "seed site"; base-pairing of a miRNA seed motif to the complemen-tary site in the 3’UTR of its target gene has been shown to be sufficient to elicitrepression. MiRNAs can be grouped into "seed families" based on their seed mo-tifs. Many of the known miRNAs are expressed as polycistronic transcripts; themiR-17∼92 cluster is a prototypical example of a polycistronic miRNA gene en-coding six miRNAs (miR-17-5p, miR-18, miR-19a, miR-19b, miR-20 and miR-92).This cluster has two paralogs, miR-106a∼363 (miR-106a, miR-18b, miR-19b-2,miR-20b, miR-92a-2 and miR-363) and miR-106b∼25 (miR-106b, miR-93, andmiR-25). These miRNAs are known to act as bona fide oncogenes with their anti-apoptotic effect and are believed to be a new target for cancer therapy. We stud-ied the function of these miRNAs in cardiac cells focusing on apoptosis. In a ratmodel of ischemia/reperfusion injury (I/R-I), the miRNAs belonging to the miR-17-92 seed family (miR-17-5p, miR-20a, miR-20b, miR-106a, miR-106b, and miR-93)were found all upregulated by miRNA microarray analysis and subsequent real-time RT-PCR. Consistently, higher levels of these miRNAs were also observedin the left ventricular tissues from patients with myocardial infarction. Addition-ally, upregulation of these miRNAs were also found in neonatal rat ventricularcells (NRVCs) and H9c2 cells treated with H2O2. Transfection any one of thesemiRNAs into NRVCs did not cause cell death under normal conditions, but pro-moted the apoptosis-induced by H2O2. We experimentally established the sur-vival factors Stat3 and Bcl-2 as the cognate targets for the miR-17-5p seed familymiRNAs, which is likely the mechanism underlying their apoptosis-promoting ac-tion. We further characterized the promoter regions of the three different clustersand found that these miRNAs were all transcriptionally activated by a commontranscription factor AP-1 (c-jun/c-fox), the activity of which was enhanced by ox-idative stress. We conclude that (1) the miR-17-5p seed family miRNAs mediatethe apoptotic signal of oxidative stress and contribute to the I/R-I; (2) concordantupregulation of the miRNAs belonging to the same seed family but different ge-nomic clusters in response to cellular stress indicates that a cell has an intrinsicprogram to convene the miRNAs having the same set of target genes thereby thesame cellular functions to undertake a decision of the cell fate; and (3) precautionshould be taken when using these miRNAs as a target for anti-cancer therapy forthey may cause cardiac complications.
209 Endothelial no synthase and telomerase reversetranscriptase synergize to reduce vascular senescenceand to augment stress resistance by physical exercise
C.M. Werner1 , J. Poess1, J. Haendeler2 , M. Boehm1, U. Laufs1.1Universitätsklinikum des Saarlandes - Klinik für Innere Medizin III,
Homburg, Germany; 2Heinrich-Heine University of Dusseldorf, Institute ofEnvironmental Health Research, Dusseldorf, Germany
Background: Aging accelerates the development of cardiovascular diseases. Onthe cellular level, the complex process of aging is determined by the function oftelomeres and telomere-associated factors, cell cycle regulators and the accumu-lation of oxidative stress-induced damage. Physical activity reduces cardiovascu-lar morbidity and mortality. We studied the molecular effects of physical exerciseon vascular senescence and apoptosis of running and sedentary mice.Methods and Results: C57/Bl6 wild-type, endothelial nitric oxide synthase(eNOS-/-) deficient and telomerase reverse transcriptase (TERT-/-) deficient micewere randomized to voluntary running or no running wheel conditions for threeweeks. Telomere repeat amplification protocol and western blots showed a pro-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

12 Vascular and myocardial effects of oxygen species / Cardiac resynchronisation therapy: the reality
found increase of aortic telomerase activity (303±32%) and TERT protein ex-pression. Furthermore, exercise increased protein levels of telomere-repeat bind-ing factor 2 (254±35%) and reduced protein expression of the senescence- andapoptosis-related factors Chk2, p16 and p53. These exercise-induced changeswere attenuated in eNOS-/- and TERT-/- mice. Aortic telomere length as deter-mined by fluorescence in-situ hybridization in aortic cryosections did not differbetween 3 week and 6 months old sedentary or running mice, but was lower in18 months old control mice. Endothelium-dependent vasodilation markedly im-proved in both wild-type and TERT-/- mice after 3 weeks exercise, but was com-pletely absent in eNOS-/- animals, whereas endothelium-independent vasodilata-tion was comparable in all groups. In addition, B6.129 wild-type and TERT-/-showed a comparable increase in eNOS phosphorylation by physical training.The physiologic relevance of these findings was tested by induction of vascularoxidative stress in-vivo by injection of lipopolysaccharide (LPS, 120ng, i.p.). En-dothelial apoptosis in the thoracic aorta was quantified by hairpin oligonucleotideassays. LPS increased apoptosis to 690±8% of controls which was potently pre-vented in exercised animals (202±12%). This protection was reduced in TERT-/-(450±15%) and abolished in eNOS-/- mice. All experiments n=6-10, values aremean±SEM.Conclusions: Voluntary physical activity up-regulates aortic telomerase activityand the expression of telomere-regulating proteins. Mice preconditioned by vol-untary running exhibit a marked reduction of lipopolysaccharide-induced aorticendothelial apoptosis. Transgenic mouse studies show that endothelial NO syn-thase (eNOS) and telomerase reverse transcriptase (TERT) synergize to conferendothelial stress-resistance following physical activity.
211 Ventricle-specific effects of nitric oxide deficiency onextracellular matrix formation
R. Schreckenberg, M. Rebelo, S. Wenzel, K.D. Schlueter. Justus-LiebigUniversity Giessen, Institute of Physiological, Giessen, Germany
Background: A chronic NO deficiency occurs under several physiologi-cal and pathophysiological conditions. The reduction in NOS activity during heartfailure or chronic renal insufficiency must also be considered, such as the reducedNO levels in postmenopausal women. On the other hand, a chronic decrease inNO is considered responsible for a variety of cardiovascular diseases. There isevidence that chronic NO deficiency contributes to increased matrix depositionand fibrosis. The current study investigates to what extent chronic NO deficit af-fects the cardiac deposition of extracellular matrix in the left (LV) and right (RV)ventricle.Methods: NO deficit was achieved in adult rats by feeding them the NO-synthase-inhibitor L-NAME alone (L) and in combination with hydralazine (L/H) or captopril(L/C) (n=8 each group). The efficiency of the L-NAME substitution was checkedweekly via tail-cuff blood pressure measurement. Heart weight to body weightratio, the expression of fibrotic and hypertrophic genes (RT-PCR, Western Blot)as well as the postmortal ventricular geometry were determined after four weeks.Results: No changes occurred in any parameters in the LV independent of thetreatment scheme. In contrast, RV of the L and L/H group displayed a significantincrease in TGFβ (+87 and 75%) and collagen (+76 and 105%) expression andindicated signs of a dilated cardiomyopathy. These changes could be preventedby additional feeding of captopril (L/C). In isolated cardiomyocytes of untreatedrats L-NAME treatment led to an increased ROS production (+56%) which couldbe blocked by preincubation with captopril. The observation that only RV wereaffected by this mechanism could be explained by an increased expression ofsuperoxide dismutase 2 (SOD2) as an important antioxidant defense in LV only.As a consequence, exclusively in RV TGFβ activity increased, contributed to aworsening of the Decorin/Bigycan ratio and subsequent to an increased collagendeposition.Conclusion: Increased levels of TGFβ are responsible for an upregulation of col-lagen synthesis in RV in chronic NO deficient rats. The cardioprotective effectsof captopril are mediated through a normalization of ROS production and theDecorin/Biglycan ratio independent of blood pressure reducing effects.
MODERATED POSTERSCARDIAC RESYNCHRONISATION THERAPY:
THE REALITY
P229 Cost-effectiveness evaluation of CRT in patients withasymptomatic or mildly symptomatic left ventriculardysfunction based on the 24 month outcomes from theEuropean cohort
C. Linde1, S. Mealing2, N. Hawkins2, J. Eaton2, B. Brown3,C. Daubert4. 1Karolinska Institute, Danderyd Hospital, Stockholm, Sweden;2Oxford Outcomes Ltd, Oxford, United Kingdom; 3Medtronic InternationalTrading Sarl, Tolochenaz, Switzerland; 4University Hospital of Rennes - HospitalPontchaillou, Rennes, France
Introduction: Cardiac resynchronization therapy (CRT) has previously beenshown to be cost-effective for patients with moderate to severe heart failure(NYHA class III/IV). We analysed the effects of CRT in patients with mild heart
failure (NYHA class I/II), based on the results of the REsynchronization reVErsesRemodeling in Systolic left vEntricular dysfunction (REVERSE) trial.Methods: In a pre-specified health care economics sub-study of the REVERSEtrial, 262 European patients were randomised 2:1 to CRT (CRT ON) or to control(CRT switched OFF) for 24 months. After 24 months, all devices were switchedon.An economic model was developed which extrapolated from the trial data to pre-dict the effect of CRT on life years, Quality Adjusted Life Years (QALYs), and costsover various time periods up to 10 years.Weibull survival regression analysis of the REVERSE data was used to predictsurvival over time. Multinomial Logistic regression was used to predict changes inthe mix of NYHA class over time in surviving patients. Predicted NYHA class waslinked to hospitalisation rates using a Poisson regression of the REVERSE dataand to utilities using published evidence. Costs and benefits were discounted at3.5% p.a. Univariate and probabilistic sensitivity analyses were undertaken.Results: At 24 months, time to first heart failure hospitalisation and time to firstheart failure hospitalisation or death were significantly delayed by CRT. The CRTON group gained 0.94 life years or 0.80 QALYs compared to the CRT OFF group,at an additional cost of �11,455. This yielded an incremental cost effectivenessratio of �14.278 per QALY gained. Sensitivity analysis indicated that CRT is costeffective compared to conventional thresholds after approximately 4.5 years. Inaddition, CRT needs only to demonstrate a modest impact on all cause mortality(HR=0.82) in mild heart failure in order to be cost-effective. The results are robustto changes in all other parameters.Conclusions: Based on the results of the REVERSE trial, CRT is a cost-effectivetreatment for patients with mild heart failure compared to conventional thresholdvalues.
P230 To what extent do the characteristics at implantation ofCRT-P and CRT-D patients differ in daily practice?
E. Marijon1, G. Galidie1, L. Trinquart1, M. Chauvin2, J.Y. Le Heuzey1.1AP-HP - European Hospital Georges Pompidou, Paris, France; 2NewCivil Hospital, Cardiovascular Medico-Surgical Activities, Strasbourg,
France
Background: Cardiac resynchronization therapy (CRT) without an implantablecardioverter defibrillator (CRT-P) is an established therapy in selected symp-tomatic patients with systolic heart failure, improving symptoms and reducingmortality. The question whether resynchronization therapy associated with defib-rillation (CRT-D) might add a substantial survival edge, attributable to a reductionin sudden cardiac death, is currently open to debate. The decision to implant aCRT-D versus a CRT-P device is essentially based on clinical sense. The presentstudy reports the baseline characteristics of patients implanted with a CRT-D com-pared those implanted with a CRT-P in daily practice.Methods: CeRtiTuDe, a French National study carried out by the French Soci-ety of Cardiology, has registered CRT implantations in France since 1st January2008. On 1st December 2009, the baseline characteristics of patients who re-ceived a CRT-P were compared to those who received a CRT-D device.Results: Among the 1360 consecutive patients enrolled in the study, 880 receivedCRT-D and 461 patients received CRT-P (CRT-D/CRT-P ratio: 1.9). The most sig-nificant (p<0.001) differences respectively were: age (65.7 vs. 74.5 years), pro-portion of men (83% vs. 68%), functional class NYHA IV (5% vs. 10%), perma-nent atrial fibrillation (20% vs. 36%), and etiology of heart failure (ischemic, 49%vs. 36%). No significant differences were noted regarding ejection fraction (mean26%) and QRS duration (mean 160 ms). Duration of hospitalization (6.2 days)and in-hospital mortality (2.9%) remained equivalent.Conclusion: CRT-P is preferred for older patients with marked advance heartfailure. It is likely that the reason for the choice to implant or not a cardioverterdefibrillator is mainly based on the competing risk of dying from progressive heartfailure or non cardiovascular causes.
P231 Role of age in patients with ICD or CRT implantation:Results from the German Device Registry
H. Rittger1, A.M. Sinha1, K.H. Kuck2, D. Andresen3, E. Hoffmann4,B. Schumacher5 , J. Tebbenjohanns6 , S. Willems7, J. Senges8,J. Brachmann1 . 1Coburg Clinical Center, Coburg, Germany;
2Asklepios Clinic St. Georg, Hamburg, Germany; 3Vivantes Hospital amUrban, Berlin, Germany; 4Hospital Munich-Bogenhausen, Munich, Germany;5Cardiovascular Clinic Bad Neustadt, Department of Cardiology, Bad Neustadtan der Saale, Germany; 6Hospital Hildesheim, Hildesheim, Germany; 7UniversityMedical Center Hamburg-Eppendorf, Center for Cardiology and CardiovascularSurgery, Hamburg, Germany; 8Heart Attack Research Center at the University ofHeidelberg, Ludwigshafen am Rhein, Germany
Purpose: The German Device Registry is designed as multi-centric and prospec-tive for implantation of implantable cardioverter defibrillator (ICD) and cardiacresynchronization therapy (CRT) devices. Patient (pt) characteristics and compli-cations during implantation and follow-up are documented by 68 German centers.This is the first report about data from the German Device Registry.Methods and Results: From 03/07 to 12/09, 3261 pts (2673/82% male, medianage 68.0) were included in the registry. Cardiac diseases were present in 94.6%of pts with coronary artery disease in 62.0%, cardiomyopathy in 35.7%, and
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
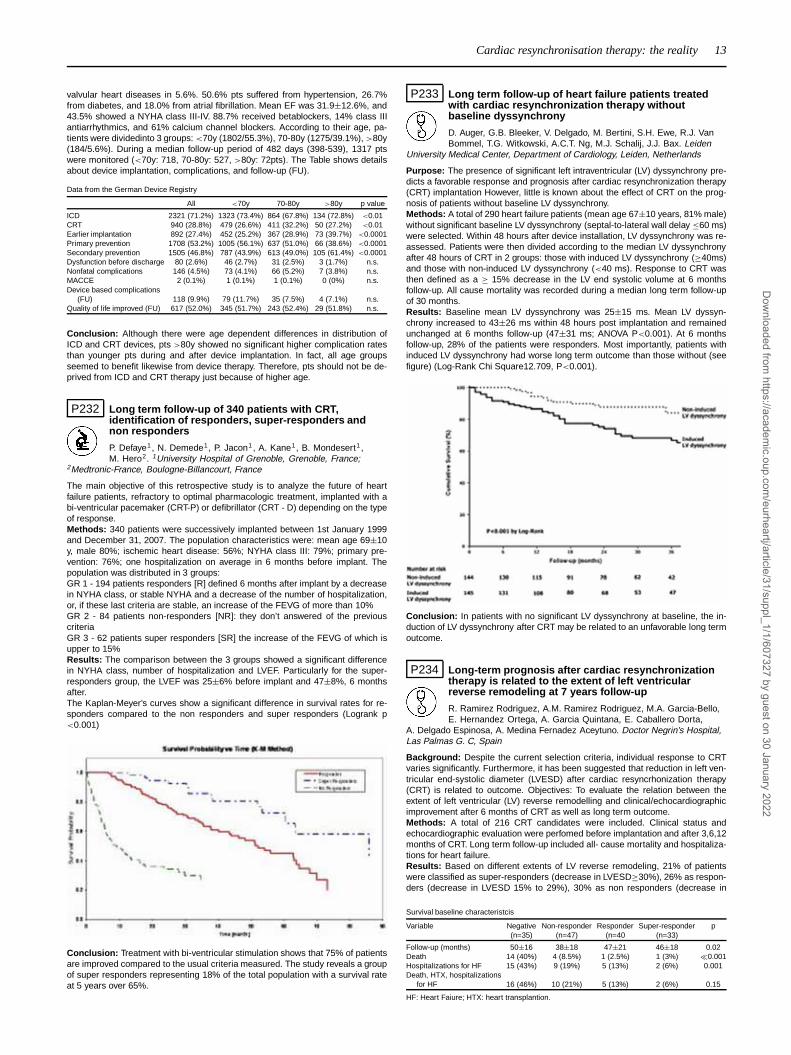
Cardiac resynchronisation therapy: the reality 13
valvular heart diseases in 5.6%. 50.6% pts suffered from hypertension, 26.7%from diabetes, and 18.0% from atrial fibrillation. Mean EF was 31.9±12.6%, and43.5% showed a NYHA class III-IV. 88.7% received betablockers, 14% class IIIantiarrhythmics, and 61% calcium channel blockers. According to their age, pa-tients were dividedinto 3 groups: <70y (1802/55.3%), 70-80y (1275/39.1%), >80y(184/5.6%). During a median follow-up period of 482 days (398-539), 1317 ptswere monitored (<70y: 718, 70-80y: 527, >80y: 72pts). The Table shows detailsabout device implantation, complications, and follow-up (FU).
Data from the German Device Registry
All <70y 70-80y >80y p value
ICD 2321 (71.2%) 1323 (73.4%) 864 (67.8%) 134 (72.8%) <0.01CRT 940 (28.8%) 479 (26.6%) 411 (32.2%) 50 (27.2%) <0.01Earlier implantation 892 (27.4%) 452 (25.2%) 367 (28.9%) 73 (39.7%) <0.0001Primary prevention 1708 (53.2%) 1005 (56.1%) 637 (51.0%) 66 (38.6%) <0.0001Secondary prevention 1505 (46.8%) 787 (43.9%) 613 (49.0%) 105 (61.4%) <0.0001Dysfunction before discharge 80 (2.6%) 46 (2.7%) 31 (2.5%) 3 (1.7%) n.s.Nonfatal complications 146 (4.5%) 73 (4.1%) 66 (5.2%) 7 (3.8%) n.s.MACCE 2 (0.1%) 1 (0.1%) 1 (0.1%) 0 (0%) n.s.Device based complications
(FU) 118 (9.9%) 79 (11.7%) 35 (7.5%) 4 (7.1%) n.s.Quality of life improved (FU) 617 (52.0%) 345 (51.7%) 243 (52.4%) 29 (51.8%) n.s.
Conclusion: Although there were age dependent differences in distribution ofICD and CRT devices, pts >80y showed no significant higher complication ratesthan younger pts during and after device implantation. In fact, all age groupsseemed to benefit likewise from device therapy. Therefore, pts should not be de-prived from ICD and CRT therapy just because of higher age.
P232 Long term follow-up of 340 patients with CRT,identification of responders, super-responders andnon responders
P. Defaye1, N. Demede1, P. Jacon1, A. Kane1, B. Mondesert1 ,M. Hero2. 1University Hospital of Grenoble, Grenoble, France;
2Medtronic-France, Boulogne-Billancourt, France
The main objective of this retrospective study is to analyze the future of heartfailure patients, refractory to optimal pharmacologic treatment, implanted with abi-ventricular pacemaker (CRT-P) or defibrillator (CRT - D) depending on the typeof response.Methods: 340 patients were successively implanted between 1st January 1999and December 31, 2007. The population characteristics were: mean age 69±10y, male 80%; ischemic heart disease: 56%; NYHA class III: 79%; primary pre-vention: 76%; one hospitalization on average in 6 months before implant. Thepopulation was distributed in 3 groups:GR 1 - 194 patients responders [R] defined 6 months after implant by a decreasein NYHA class, or stable NYHA and a decrease of the number of hospitalization,or, if these last criteria are stable, an increase of the FEVG of more than 10%GR 2 - 84 patients non-responders [NR]: they don’t answered of the previouscriteriaGR 3 - 62 patients super responders [SR] the increase of the FEVG of which isupper to 15%Results: The comparison between the 3 groups showed a significant differencein NYHA class, number of hospitalization and LVEF. Particularly for the super-responders group, the LVEF was 25±6% before implant and 47±8%, 6 monthsafter.The Kaplan-Meyer’s curves show a significant difference in survival rates for re-sponders compared to the non responders and super responders (Logrank p<0.001)
Conclusion: Treatment with bi-ventricular stimulation shows that 75% of patientsare improved compared to the usual criteria measured. The study reveals a groupof super responders representing 18% of the total population with a survival rateat 5 years over 65%.
P233 Long term follow-up of heart failure patients treatedwith cardiac resynchronization therapy withoutbaseline dyssynchrony
D. Auger, G.B. Bleeker, V. Delgado, M. Bertini, S.H. Ewe, R.J. VanBommel, T.G. Witkowski, A.C.T. Ng, M.J. Schalij, J.J. Bax. Leiden
University Medical Center, Department of Cardiology, Leiden, Netherlands
Purpose: The presence of significant left intraventricular (LV) dyssynchrony pre-dicts a favorable response and prognosis after cardiac resynchronization therapy(CRT) implantation However, little is known about the effect of CRT on the prog-nosis of patients without baseline LV dyssynchrony.Methods: A total of 290 heart failure patients (mean age 67±10 years, 81% male)without significant baseline LV dyssynchrony (septal-to-lateral wall delay ≤60 ms)were selected. Within 48 hours after device installation, LV dyssynchrony was re-assessed. Patients were then divided according to the median LV dyssynchronyafter 48 hours of CRT in 2 groups: those with induced LV dyssynchrony (≥40ms)and those with non-induced LV dyssynchrony (<40 ms). Response to CRT wasthen defined as a ≥ 15% decrease in the LV end systolic volume at 6 monthsfollow-up. All cause mortality was recorded during a median long term follow-upof 30 months.Results: Baseline mean LV dyssynchrony was 25±15 ms. Mean LV dyssyn-chrony increased to 43±26 ms within 48 hours post implantation and remainedunchanged at 6 months follow-up (47±31 ms; ANOVA P<0.001). At 6 monthsfollow-up, 28% of the patients were responders. Most importantly, patients withinduced LV dyssynchrony had worse long term outcome than those without (seefigure) (Log-Rank Chi Square12.709, P<0.001).
Conclusion: In patients with no significant LV dyssynchrony at baseline, the in-duction of LV dyssynchrony after CRT may be related to an unfavorable long termoutcome.
P234 Long-term prognosis after cardiac resynchronizationtherapy is related to the extent of left ventricularreverse remodeling at 7 years follow-up
R. Ramirez Rodriguez, A.M. Ramirez Rodriguez, M.A. Garcia-Bello,E. Hernandez Ortega, A. Garcia Quintana, E. Caballero Dorta,
A. Delgado Espinosa, A. Medina Fernadez Aceytuno. Doctor Negrin’s Hospital,Las Palmas G. C, Spain
Background: Despite the current selection criteria, individual response to CRTvaries significantly. Furthermore, it has been suggested that reduction in left ven-tricular end-systolic diameter (LVESD) after cardiac resyncrhonization therapy(CRT) is related to outcome. Objectives: To evaluate the relation between theextent of left ventricular (LV) reverse remodelling and clinical/echocardiographicimprovement after 6 months of CRT as well as long term outcome.Methods: A total of 216 CRT candidates were included. Clinical status andechocardiographic evaluation were perfomed before implantation and after 3,6,12months of CRT. Long term follow-up included all- cause mortality and hospitaliza-tions for heart failure.Results: Based on different extents of LV reverse remodeling, 21% of patientswere classified as super-responders (decrease in LVESD≥30%), 26% as respon-ders (decrease in LVESD 15% to 29%), 30% as non responders (decrease in
Survival baseline characteristcis
Variable Negative Non-responder Responder Super-responder p(n=35) (n=47) (n=40 (n=33)
Follow-up (months) 50±16 38±18 47±21 46±18 0.02Death 14 (40%) 4 (8.5%) 1 (2.5%) 1 (3%) �0.001Hospitalizations for HF 15 (43%) 9 (19%) 5 (13%) 2 (6%) 0.001Death, HTX, hospitalizations
for HF 16 (46%) 10 (21%) 5 (13%) 2 (6%) 0.15
HF: Heart Faiure; HTX: heart transplantion.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
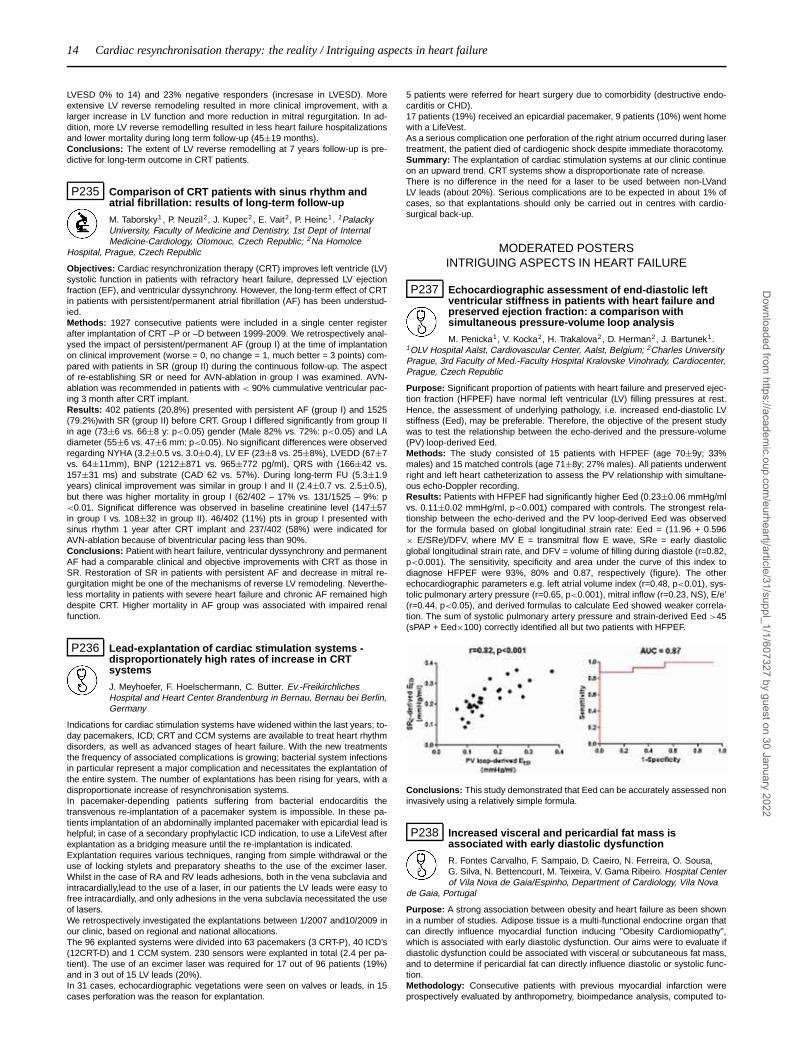
14 Cardiac resynchronisation therapy: the reality / Intriguing aspects in heart failure
LVESD 0% to 14) and 23% negative responders (incresase in LVESD). Moreextensive LV reverse remodeling resulted in more clinical improvement, with alarger increase in LV function and more reduction in mitral regurgitation. In ad-dition, more LV reverse remodelling resulted in less heart failure hospitalizationsand lower mortality during long term follow-up (45±19 months).Conclusions: The extent of LV reverse remodelling at 7 years follow-up is pre-dictive for long-term outcome in CRT patients.
P235 Comparison of CRT patients with sinus rhythm andatrial fibrillation: results of long-term follow-up
M. Taborsky1 , P. Neuzil2, J. Kupec2, E. Vait2, P. Heinc1. 1PalackyUniversity, Faculty of Medicine and Dentistry, 1st Dept of InternalMedicine-Cardiology, Olomouc, Czech Republic; 2Na Homolce
Hospital, Prague, Czech Republic
Objectives: Cardiac resynchronization therapy (CRT) improves left ventricle (LV)systolic function in patients with refractory heart failure, depressed LV ejectionfraction (EF), and ventricular dyssynchrony. However, the long-term effect of CRTin patients with persistent/permanent atrial fibrillation (AF) has been understud-ied.Methods: 1927 consecutive patients were included in a single center registerafter implantation of CRT –P or –D between 1999-2009. We retrospectively anal-ysed the impact of persistent/permanent AF (group I) at the time of implantationon clinical improvement (worse = 0, no change = 1, much better = 3 points) com-pared with patients in SR (group II) during the continuous follow-up. The aspectof re-establishing SR or need for AVN-ablation in group I was examined. AVN-ablation was recommended in patients with < 90% cummulative ventricular pac-ing 3 month after CRT implant.Results: 402 patients (20,8%) presented with persistent AF (group I) and 1525(79.2%)with SR (group II) before CRT. Group I differed significantly from group IIin age (73±6 vs. 66±8 y: p<0.05) gender (Male 82% vs. 72%: p<0.05) and LAdiameter (55±6 vs. 47±6 mm: p<0.05). No significant differences were observedregarding NYHA (3.2±0.5 vs. 3.0±0.4), LV EF (23±8 vs. 25±8%), LVEDD (67±7vs. 64±11mm), BNP (1212±871 vs. 965±772 pg/ml), QRS with (166±42 vs.157±31 ms) and substrate (CAD 62 vs. 57%). During long-term FU (5.3±1.9years) clinical improvement was similar in group I and II (2.4±0.7 vs. 2.5±0.5),but there was higher mortality in group I (62/402 – 17% vs. 131/1525 – 9%: p<0.01. Significat difference was observed in baseline creatinine level (147±57in group I vs. 108±32 in group II). 46/402 (11%) pts in group I presented withsinus rhythm 1 year after CRT implant and 237/402 (58%) were indicated forAVN-ablation because of biventricular pacing less than 90%.Conclusions: Patient with heart failure, ventricular dyssynchrony and permanentAF had a comparable clinical and objective improvements with CRT as those inSR. Restoration of SR in patients with persistent AF and decrease in mitral re-gurgitation might be one of the mechanisms of reverse LV remodeling. Neverthe-less mortality in patients with severe heart failure and chronic AF remained highdespite CRT. Higher mortality in AF group was associated with impaired renalfunction.
P236 Lead-explantation of cardiac stimulation systems -disproportionately high rates of increase in CRTsystems
J. Meyhoefer, F. Hoelschermann, C. Butter. Ev.-FreikirchlichesHospital and Heart Center Brandenburg in Bernau, Bernau bei Berlin,Germany
Indications for cardiac stimulation systems have widened within the last years; to-day pacemakers, ICD, CRT and CCM systems are available to treat heart rhythmdisorders, as well as advanced stages of heart failure. With the new treatmentsthe frequency of associated complications is growing; bacterial system infectionsin particular represent a major complication and necessitates the explantation ofthe entire system. The number of explantations has been rising for years, with adisproportionate increase of resynchronisation systems.In pacemaker-depending patients suffering from bacterial endocarditis thetransvenous re-implantation of a pacemaker system is impossible. In these pa-tients implantation of an abdominally implanted pacemaker with epicardial lead ishelpful; in case of a secondary prophylactic ICD indication, to use a LifeVest afterexplantation as a bridging measure until the re-implantation is indicated.Explantation requires various techniques, ranging from simple withdrawal or theuse of locking stylets and preparatory sheaths to the use of the excimer laser.Whilst in the case of RA and RV leads adhesions, both in the vena subclavia andintracardially,lead to the use of a laser, in our patients the LV leads were easy tofree intracardially, and only adhesions in the vena subclavia necessitated the useof lasers.We retrospectively investigated the explantations between 1/2007 and10/2009 inour clinic, based on regional and national allocations.The 96 explanted systems were divided into 63 pacemakers (3 CRT-P), 40 ICD’s(12CRT-D) and 1 CCM system. 230 sensors were explanted in total (2.4 per pa-tient). The use of an excimer laser was required for 17 out of 96 patients (19%)and in 3 out of 15 LV leads (20%).In 31 cases, echocardiographic vegetations were seen on valves or leads, in 15cases perforation was the reason for explantation.
5 patients were referred for heart surgery due to comorbidity (destructive endo-carditis or CHD).17 patients (19%) received an epicardial pacemaker, 9 patients (10%) went homewith a LifeVest.As a serious complication one perforation of the right atrium occurred during lasertreatment, the patient died of cardiogenic shock despite immediate thoracotomy.Summary: The explantation of cardiac stimulation systems at our clinic continueon an upward trend. CRT systems show a disproportionate rate of ncrease.There is no difference in the need for a laser to be used between non-LVandLV leads (about 20%). Serious complications are to be expected in about 1% ofcases, so that explantations should only be carried out in centres with cardio-surgical back-up.
MODERATED POSTERSINTRIGUING ASPECTS IN HEART FAILURE
P237 Echocardiographic assessment of end-diastolic leftventricular stiffness in patients with heart failure andpreserved ejection fraction: a comparison withsimultaneous pressure-volume loop analysis
M. Penicka1, V. Kocka2, H. Trakalova2, D. Herman2, J. Bartunek1.1OLV Hospital Aalst, Cardiovascular Center, Aalst, Belgium; 2Charles UniversityPrague, 3rd Faculty of Med.-Faculty Hospital Kralovske Vinohrady, Cardiocenter,Prague, Czech Republic
Purpose: Significant proportion of patients with heart failure and preserved ejec-tion fraction (HFPEF) have normal left ventricular (LV) filling pressures at rest.Hence, the assessment of underlying pathology, i.e. increased end-diastolic LVstiffness (Eed), may be preferable. Therefore, the objective of the present studywas to test the relationship between the echo-derived and the pressure-volume(PV) loop-derived Eed.Methods: The study consisted of 15 patients with HFPEF (age 70±9y; 33%males) and 15 matched controls (age 71±8y; 27% males). All patients underwentright and left heart catheterization to assess the PV relationship with simultane-ous echo-Doppler recording.Results: Patients with HFPEF had significantly higher Eed (0.23±0.06 mmHg/mlvs. 0.11±0.02 mmHg/ml, p<0.001) compared with controls. The strongest rela-tionship between the echo-derived and the PV loop-derived Eed was observedfor the formula based on global longitudinal strain rate: Eed = (11.96 + 0.596× E/SRe)/DFV, where MV E = transmitral flow E wave, SRe = early diastolicglobal longitudinal strain rate, and DFV = volume of filling during diastole (r=0.82,p<0.001). The sensitivity, specificity and area under the curve of this index todiagnose HFPEF were 93%, 80% and 0.87, respectively (figure). The otherechocardiographic parameters e.g. left atrial volume index (r=0.48, p<0.01), sys-tolic pulmonary artery pressure (r=0.65, p<0.001), mitral inflow (r=0.23, NS), E/e’(r=0.44, p<0.05), and derived formulas to calculate Eed showed weaker correla-tion. The sum of systolic pulmonary artery pressure and strain-derived Eed >45(sPAP + Eed×100) correctly identified all but two patients with HFPEF.
Conclusions: This study demonstrated that Eed can be accurately assessed noninvasively using a relatively simple formula.
P238 Increased visceral and pericardial fat mass isassociated with early diastolic dysfunction
R. Fontes Carvalho, F. Sampaio, D. Caeiro, N. Ferreira, O. Sousa,G. Silva, N. Bettencourt, M. Teixeira, V. Gama Ribeiro. Hospital Centerof Vila Nova de Gaia/Espinho, Department of Cardiology, Vila Nova
de Gaia, Portugal
Purpose: A strong association between obesity and heart failure as been shownin a number of studies. Adipose tissue is a multi-functional endocrine organ thatcan directly influence myocardial function inducing "Obesity Cardiomiopathy",which is associated with early diastolic dysfunction. Our aims were to evaluate ifdiastolic dysfunction could be associated with visceral or subcutaneous fat mass,and to determine if pericardial fat can directly influence diastolic or systolic func-tion.Methodology: Consecutive patients with previous myocardial infarction wereprospectively evaluated by anthropometry, bioimpedance analysis, computed to-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Intriguing aspects in heart failure 15
mography scan (CT) and echocardiography. Systolic function was assessed bytwo-D and three-D ejection fraction (2D-EF and 3D-EF), and diastolic function bymitral inflow velocity profile (E and A velocities, E/A, DT), tissue Doppler velocity(septal, lateral and mean Ea and E/E’ ratio) and pulmonary vein flow pattern. Weused chest multidetector CT to quantify volume of pericardial fat, and abdominalCT (at L4-L5 level) to measure visceral, subcutaneous and total abdominal fatmass areas.Results: Overall, 94 patients were evaluated, mean age 55±11 years, 85% male,29% obese, mean body mass index (BMI) 27,4±4,4, 3D-EF 54±10% and medianlat E/Ea 7,46±2,9.Diastolic function, but not ejection fraction (p=0,99), was correlated with BMI(p=0,03, with lateral E/E’). No association was found with abdominal perimeter(p=0,08). Increased total abdominal fat mass (visceral+subcutaneous) was asso-ciated with diastolic dysfunction, assessed by septal E/E’ (p=0,07), lateral E/E’(p=0,03) and mean E/E’ (p=0,035). We found a direct association between dias-tolic dysfunction parameters and visceral intra-abdominal fat mass measured byCT (p= 0,02, with lat E/E’), but no correlation with subcutaneous fat area by CT(p=0,1 with lat E/E’).Increased epicardial fat volume was also associated with diastolic dysfunction (p=0,01, with lat E/E’), even after multivariate regression analysis.We found no correlation between systolic function (either measured by 2D or 3Dejection fraction) and total, visceral, subcutaneous or epicardial fat mass mea-surements.Conclusion: Both pericardial and visceral abdominal adipose tissue, but not sub-cutaneous fat, are associated with early diastolic dysfunction, which taken to-gether with previous studies, support the hypothesis that adipose tissue can con-tribute to impaired diastolic function. Also, our study is the first demonstrating anassociation between pericardial fat and diastolic dysfunction.
P239 Impact of nutritional status on middle term mortality ofpatients with heart failure
J.L. Bonilla-Palomas, A.L. Gamez Lopez, M.P. Anguita-Sanchez,J.C. Castillo-Dominguez, M. Crespin-Crespin, D. Garcia-Fuertes,A. Lopez-Granados, M. Ruiz Ortiz, J.M. Arizon Del Prado, J. Suarez
De Lezo. University Hospital Reina Sofia, Cordoba, Spain
Heart failure (HF) is a chronic disease with high morbidity and mortality at shortand long term. Several independent prognostic factors have been described, butit has not been so well studied if nutritional characteristics can play a role in theprognosis of these patients.Purpose: The aim of our study was to evaluate the possible influence on mediumterm mortality of nutritional parameters in patients with HF.Methods: 208 consecutively discharged patients after a heart failure hospitaliza-tion in our center from January 2007 to March 2008 were prospectively analysed.Previous to discharge, and once the patients were stabilised, a complete nutri-tional assessment using anthropometry (body mass index, tricipital skinfold thick-ness and brachial muscular perimeter), biochemical markers (total protein, albu-min, prealbumin, transferrin, cholesterol, vitamins D, B12, folate and lymphocytes)and a global nutritional evaluation by the Mini Nutritional Assessment (MNA) testwere performed. In addition to this, usual demographic, clinical, functional andtreatment variables were studied. Its possible independent association with mor-tality was analyzed by Cox multivariate analysis.Results: The mean age was 73±10 years, 46% were female, left ventricularejection fraction was 45±16%, and the most frequent etiology was ischemicheart disease (41,8%). Overall mortality was 26% (the median of follow-ap was12 months). We found that older age (HR 1.07; 95%CI, 1.02-1.12, p=0,003),lower serum sodium (HR 0.95; 95%CI, 0.9-0.99, p=0,03), hypertensive versusischemic etiology (HR 0.23; 95%CI, 0.08-0.68, p=0,008), lower creatinine clear-ance (MDRD) (HR 0.98; 95%CI, 0.96-0.99, p=0,02), hypoalbuminemia (HR 1.9;95%CI, 1.03-3.6, p=0,04), and the states of malnutrition (HR 4.7; 95%CI, 1.6-13.7, p=0,005) and at risk of malnutrition (HR 2.7; 95%CI, 1.01-7.2, p=0,049)determined by the MNA test, were the only independent predictors of 12 monthsmortality.Conclusions: two nutritional parameters (hypoalbuminemia and the MNA test)not yet studied are independent prognoses factors of mortality in addition to clas-sic prognosis factors like age, ischemic etiology and comorbidity features. Thisseems to indicate that the nutritional status of patients with HF can play an impor-tant role in the evolution of these patients.
P240 Prognostic significance of congestion severity atdischarge in patients hospitalized with heart failure:insights from the EVEREST trial
S. Khan1, M.A. Konstam2, F. Zannad3, P.S. Pang1, A.P. Maggioni4 ,K. Swedberg5, J.E. Udelson2, G. Filippatos6, G. Fonarow7,
M. Gheorghiade1 . 1Northwestern University, Chicago, United States of America;2Tufts Medical Center, Boston, United States of America; 3Inserm - ClinicalInvestigation Centre (CIC), Nancy, France; 4ANMCO Research Center, Florence,Italy; 5Sahlgrenska University Hospital, Gothenburg, Sweden; 6University ofAthens, Athens, Greece; 7University of California Los Angeles (UCLA), LosAngeles, United States of America
Purpose: In patients admitted with heart failure (HF), the presence of congestion
at discharge is associated with high post-discharge morbidity and mortality. How-ever, the outcomes of patients based on the severity of congestion at the timeof discharge, derived from the degree of jugular venous distensions (JVD), rales,and peripheral edema, has not been previously well studied.Methods: The Efficacy of Vasopressin Antagonism in Heart Failure OutcomeStudy (EVEREST) trial randomized 4,133 patients admitted with worsening HFand ejection fraction ≤40% to tolvaptan or placebo within 48 hours of hospitaliza-tion and had a median follow-up of 9.9 months. We studied the 2061 patients inthe placebo arm. Congestion was assessed on a scale of 0-3 for each: orthop-nea (none, seldom, frequent, continuous), JVD (<6, 6-9, 10-15, >15 cm H2O),and edema (absent/trace, slight, moderate, marked). A Cox proportional-hazardmodel was used to assess the correlation of the congestion score with all-causemortality (ACM), CV mortality, and readmission for HF, adjusted for the following:age, EF, previous HF hospitalization, Systolic Blood Pressure, BNP, BUN, base-line diuretics, and beta-blockers at discharge.Results: At randomization, after initial therapy with diuretics, the congestion scorewas 4 (1.8)[mean, (SD)] The mean change during hospitalization was 3 (1.8)resulting in a discharge score of 1 (1.4). Average decrease in body weight was 2.8kg. Mean admission BNP was 1375 (NT-proBNP 7620) and mean discharge BNPwas 948 (NT-proBNP 5354). Medications at discharge included diuretics (85%),ACEI/ARB (87%), and beta-blockers (74%). Approximately 72% of patients atdischarge had a congestion score of 0 or 1, which was associated with a 15%ACM rate and a 29% HF re-hospitalization rate during follow-up. Higher dischargecongestion score correlated with increased risk. The adjusted hazard ratio (aHR)for each additional point was 1.16 (95% CI 1.09-1.24, p<0.0001) for ACM, 1.10(95% CI 1.02, 1.19, p=0.01) for CV mortality, and 1.07 (95% CI 1.01, 1.14, p=0.02)for repeat HF hospitalization.Conclusion: Our results confirmed that the severity of congestion at dischargeis an important predictor of post-discharge outcomes. However, the absence ofcongestion at discharge does not confer a good prognosis, despite a significantdecrease in body weight, treatment with evidence-based therapies, and closefollow-up in the post-discharge period. Optimization of congestion may be insuffi-cient and additional surrogate markers may be needed to guide therapy.
P241 Glycaemic control and the development of heart failureand its importance in diabetic patients with establishedheart failure
A.K.F. Wong, L. Donnelly, A. Doney, M. Pauriah, M. Jabir, R. Libianto,D. Elder, A.M. Choy, A.D. Struthers, C.C. Lang. University of Dundee,
Dundee, United Kingdom
Background: In diabetes, poor glycaemic control, as indexed by haemoglobinA1c (HbA1c), is associated with increased risk of cardiovascular events. The re-lationship between glycaemic control and chronic heart failure (CHF) is less welldefined. There is controversy regarding the importance of glycaemic control inpatients with type 2 diabetes mellitus (T2DM) and CHF with recent evidence sug-gesting that tight glycaemic control may be associated with worse survival.AimThe aim of this study was to examine the relationship between HbA1c and the riskof incident CHF and to examine the relationship between HbA1c and outcome inT2DM with established CHF.Methods: This study was carried out in the population (approximately 400,000) ofTayside in Scotland, using data from the Go-DARTS diabetic population and thedispensed prescribing database maintained by the Health Informatics Centre. Theincidence date of new CHF was determined during the study period (Jan 1991 toJune 2008). CHF was defined as the presence of a hospital discharge code forCHF or the prescription of CHF medication (loop diuretic plus ACE inhibitor) fol-lowing a myocardial infarction. A prospective case control study was performedwith each case of CHF matched with up to 5 controls for gender and age at dateof diagnosis with diabetes. Development of CHF was modeled using conditionallogistic regression using mean HbA1c during the study period, number of HbA1cmeasures, standard deviation, mean arterial pressure and thiazolidinediones pre-scribing as covariates. Subsequently a proportional hazards model was used toconsider the impact of HbA1c on survival of the cases.Results: Out of 9172 diabetic individuals there were 691 incident cases of CHF(mean age at diagnosis of 70.6±9.8 yrs, 60% males). The adjusted HR of de-veloping CHF for each 1% increase in HbA1c was 1.31 (95% CI 1.20-1.44)p=1.43x10-9. In the cases there were subsequently 211 deaths. After adjustment,the HR of death for each 1% increase in HbA1c was 1.24 (95% CI 1.09-1.42)p=0.0013.Conclusions: These data suggest that glycaemic control is an independent riskfactor for incident CHF in persons with T2DM. In diabetic patients with establishedCHF, poor glycaemic control is associated with a worse outcome.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

16 Intriguing aspects in heart failure / Novel nuclear imaging
P242 Worsening renal failure in elderly patients with heartfailure on intense medical therapy: clinical predictorsand prognostic impact
M.T. Maeder1 , H. Rickli1, P. Ammann1, D. Hack1, D. Weilenmann1,T. Dieterle2, S. Kiencke3, W. Estlinbaum4, M. Pfisterer2, H.P. Brunner-
La Rocca5. 1Cantonal Hospital St. Gallen, St. Gallen, Switzerland; 2UniversityHospital Basel, Basel, Switzerland; 3University Hospital, Bruderholz, Switzerland;4Cantonal Hospital Liestal, Liestal, Switzerland; 5Maastricht University MedicalCenter, Department of Cardiology, Maastricht, Netherlands
Purpose: In patients with chronic heart failure (HF), worsening renal failure(WRF) complicates medical therapy and is a predictor of mortality. However, themechanisms underlying WRF in HF are poorly understood. There are concernsthat aggressive HF pharmacotherapy could result in WRF and thereby offset thebeneficial effects of HF treatment. The aim of this study was to assess clinical pre-dictors and the prognostic value of WRF in patients with chronic HF undergoingintense medical therapy.Methods: In 565 patients (age 77±8 years) included in the Trial of IntensifiedMedical versus standard treatment in Elderly patients with Congestive HF (TIME-CHF) surviving at least one month (M), serum creatinine (SCr) was measuredat baseline, M 1, M 3, and M 6 or until a patient died. WRF was defined as anyincrease in SCr by at least 0.5 mg/dl (44 mcmol/l) within the first six months.Clinical predictors and impact of WRF on 18-months outcome were assessed.Results: WRF occurred in 124/565 (22%) patients. Treatment with spironolac-tone (odds ratio [OR]=2.24, p=0.001), history of renal failure (OR=1.70, p=0.03),loop diuretic dose (OR=1.09 per 40mg furosemide aequivalent, p=0.04), higherbaseline NT-proBNP (OR=1.27 per ln of NT-proBNP, p=0.05), history of peripheraloedema (OR=1.23 per grade [0-3], p=0.04), and history of urinary tract infections(OR=2.21, p=0.05) were independently associated with WRF. Other factors in-cluding age and gender, but also allocation to NT-proBNP-guided therapy, andtreatment with and adjustment of betablockers, angiotensin converting enzymeinhibitors (ACEI) and angiotensin receptor blockers (ARB) were not associatedwith WRF. Patients with WRF had higher rates of death (hazard ratio [HR]=1.98,p=0.001), death or hospitalisation (HR=1.49, p=0.002), and death or HF hospital-isation (HR=1.85, p<0.001) compared to those without WRF. After adjustment forbaseline differences, WRF was still predictive of death (HR=1.70, p=0.02), deathor hospitalisation (HR=1.26, p=0.07) and death or HF hospitalisation (HR=1.38,p=0.06).Conclusions: WRF is associated with signs of more severe HF and preexistingrenal failure, particularly if high-doses of loop diuretics or spironolactone are used.In contrast, treatment with betablockers, ACEI, and ARB was not associated withWRF. Since WRF predicts worse outcome independently of other prognostic pa-rameters, it should be monitored carefully particularly in patients at risk.
P243 Impact of heart failure on pulmonary function andclassification of COPD
G. Guder1, S. Brenner1, F. Rutten2, D. Berliner1, B. Jany3, G. Ertl1,C.E. Angermann1 , A.W. Hoes2, S. Stork1. 1Medizinische Klinik I,Kardiologie, Klinikum der Universität Würzburg, Wuerzburg, Germany;
2University Medical Center Utrecht - Julius Centre for Health Sciences andPrimary Care, Utrecht, Netherlands; 3Missionsaerztliche Klinik, Wuerzburg,Germany
Purpose: Heart failure (HF) has substantial impact on pulmonary function, ham-pering the interpretation of pulmonary function testing (PFT). We evaluated PFTparameters in 3 groups of patients; COPD only, COPD+HF, and HF only.Method: Data from a Dutch and a German cohort study were combined; 404 pa-tients suspected of COPD (21% with co-existing HF) and 632 patients with HF(16% with COPD). PFT was performed during an ambulatory visit. COPD wasdiagnosed if the ratio of forced expiratory volume in 1 s and forced vital capacity(FEV1/FVC) was <0.70, and classified as GOLD 1-4 if FEV1 was >80/50-80/30-50/<30. HF was confirmed by echocardiography. In total, 202 patients with COPD(group, G1), 153 with COPD+HF (G2) and 562 patients with HF (G3) were anal-ysed.Results: Patients in G1 were older, more often male and smokers, and displayedclassical hyperinflation (high total lung capacity [TLC] and high residual volume[RV]; Table). In G2, RV levels were as high as in G1, but TLC levels were inbetween G1 and G3. No differences were seen between G1 and G2 if gradedaccording to GOLD 1-4: 23/50/23/4% vs 21/56/21/2%. Of note patients with HF
Characteristics between groups
COPD HF+COPD HF
Age, years 73±5 69±11* 66±12# §
Female sex, % 34 24* 27#
LVEF, % 60±6 43±11* 43±11#
Never-smoker, % 19 31* 47#§
NYHA class I-IV, % — 12/43/44/1 23/54/22/1§
FEV1, % of predicted 65±20 64±19 93±20# §
FVC, % of predicted 90±20 82±19* 91±19§
FEV1/FVC 0.56±0.10 0.61±0.09* 0.81±0.07# §
TLC, % of predicted 117±19 103±23* 93±17# §
RV, % of predicted 149±45 141±41 105±32# §
P<0.05 *COPD vs HF+COPD; #COPD vs HF; §HF+COPD vs HF.
without COPD (G3) also had reduced FEV1 levels, a theoretical "GOLD catego-rization" yielded here 74/24/2/0%.Conclusions: In stable HF patients lung volumes as FEV1 are reduced also inthe absence of COPD. Hence, a relevant proportion of FEV1 reduction appearsto be a consequence of HF and not of COPD. Applying the GOLD classificationin patients with HF and co-existing COPD may cause diagnostic misclassificationand thus pulmonary over-treatment.
P244 Self-rated health during beta-blocker titration in elderlypatients with heart failure: the CIBIS-ELD analysis
M. Lainscak1, S. Inkrot2, J. Farkas3, E. Tahirovic2 , A. Topper2 ,S. Apostolovic4, H. Radlach2, G. Gelbrich5, C.H. Herrmann-Lingen6 ,H.D. Duengen2 . 1University Clinic of Respiratory and Allergic
Diseases Golnik, Department of Cardiology, Golnik, Slovenia; 2Charite - CampusVirchow-Klinikum, Department of Cardiology, Berlin, Germany; 3University ofLjubljana, Faculty of Medicine, Chair of Public Health, Ljubljana, Slovenia;4Clinical Center, Clinic for Cardiology, Nis, Serbia; 5University of Leipzig,Coordination Centre for Clinical Trials Leipzig (KKSL), Leipzig, Germany;6Georg-August-University Gottingen, Department of Cardiology, Gottingen,Germany
Purpose: Self-rated health (SRH) predicts outcome in patients with heart failure(HF). Beta-blockers (BB) improve patients’ quality of life and reduce mortality. Weaimed to evaluate SRH during BB titration in elderly patients with HF.Methods: The Cardiac Insufficiency Bisoprolol Study in Elderly (CIBIS-ELD) wasa multicenter, double-blind trial, which randomized 883 patients ≥65 years withchronic HF (73±6 years, 38% women, LVEF 42±14%) to bisoprolol or carvedilol.SRH was assessed at baseline and after 12 weeks using WHO approved instru-ment with 5-grade descriptive scale: very good, good, fair, poor, very poor.Results: Median SRH at baseline and after 12 weeks was fair but more patientsreported poor or very poor SRH at baseline (36% vs. 30%, p=0.012) - Figure.From baseline to follow-up, SRH improved in 33.6% of the patients and worsenedin 8.4% (p<0.001). Improved SRH was associated with higher rates of improvedNYHA class (41.8% vs. 26.4%, p<0.001), stronger decrease of heart rate (–9.1vs. –6.0 bpm, p=0.003) and higher gain in six-minute walk distance (+27 vs. +12m, p=0.004), regardless of the BB dose achieved at follow-up (p=0.56). Poor orvery poor SRH at baseline was related to higher rates of adverse events dur-ing BB titration (69.7% vs. 55.7%, p<0.001), particularly temporary worseningof HF (27.9% vs. 14.4%, p<0.001), dizziness, drowsiness or fatigue (14.2% vs.8.7%, p=0.02), pulmonary side effects (6.7% vs. 3.0%, p=0.02), and hospitalisa-tion (4.6% vs. 1.2%, p=0.008).
Figure. Distribution of SRH.
Conclusions: SRH improves during BB titration and is associated with heart ratecontrol and clinical improvement. Poor or very poor SRH predicts higher occur-rence of adverse events and may be useful as an additional assessment in clinicalpractice.
NOVEL NUCLEAR IMAGING
262 High speed versus standard SPECT: improveddiagnostic accuracy in patients with coronary arterydisease
A. Gimelli, A. Kusch, A. Giorgetti, D. Genovesi, P. Marzullo. FondazioneToscana Gabriele Monasterio, CNR, Pisa, Italy
Objectives: The purpose of this study was to compare myocardial perfu-sion imaging obtained by high-speed single-photon emission computed tomogra-phy (SPECT) with conventional SPECT imaging for the evaluation of myocardialperfusion in patients with known or suspected coronary artery disease.Background: A novel technology has been developed for high-speed SPECTmyocardial perfusion imaging by employing a bank of independently controlleddetector columns with pin-hole tungsten collimators and multiple cadmium zinctelluride crystal arrays.Methods: A total of 34 patients underwent single-day Tc-99m tetrofosminestress/rest myocardial perfusion imaging. High-speed SPECT images were ob-tained within 10 min before conventional SPECT. Stress and rest acquisition timeswere 20 and 18 min for conventional imaging and 5 and 4 min for high-speed
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Novel nuclear imaging 17
SPECT, respectively. Images were visually analyzed, and the summed stressscore (SSS) and summed rest score (SRS) were calculated.Results: Coronary angiograms showed significant epicardial coronary artery dis-ease in 30/34 (88%) patients. When only patients with significant coronary arterydisease were analysed, SSS was 9±3 versus 7±3 (p=.031 respectively of high-speed and standard images). Sensitivity for detection of coronary artery diseasewas significantly higher for high speed camera as compared to standard camera(94% versus 88%, P<0.019) as well as specificity (88% versus 79%, P<0.032).No differences in terms of ejection fraction and volumes were obtained.Conclusion: High-speed SPECT provides fast myocardial perfusion imaging withhigh image quality. The evaluation of extension and severity of myocardial is-chemia evaluated by high-speed SPECT is higher when compared to conven-tional SPECT.
263 Coronary perfusion reserve versus absolute myocardialblood flow in the detection of significant coronary arterydisease
E. Joutsiniemi, A. Saraste, M. Maki, M. Pietila, S. Kajander, H. Ukkonen,J. Airaksinen, J. Knuuti. University of Turku, Turku, Finland
Background and aims: Coronary perfusion reserve, a ratio of stress and restperfusion, has been widely used with many imaging techniques to detected signif-icant coronary artery disease (CAD). Recently it has become possible to quantifymyocardial perfusion in absolute terms. However, it remains to be studied whetherabsolute stress perfusion alone is sufficient for detection of significant CAD in theclinical practice. We wanted to compare coronary perfusion reserve (CPR) andabsolute perfusion parameters in the detection of CAD.Methods: 104 patients with moderate (30-70%) pretest likelihood of CAD wereenrolled. Regional myocardial perfusion (MBF) was measured using PET withO-15-water at rest and during adenosine (140 ug/min) stress using validatedquantitative model and software. All patients subsequently underwent invasivecoronary angiography (ICA). Hemodynamically significant stenosis was definedas >50% of luminal narrowing (in borderline cases intracoronary FFR <0.80 con-firmed hemodynamic significance). All analysis were done blinded and a ROCanalysis was performed to compare the accuracies of CPR, MBF and also theabsolute MBF increase by adenosine.Results: The PPV, NPV, sensitivity and specificity of CPR were 65%, 94%, 81%and 87% with optimal cut-off value of 2.5 (AUC 0.90). The corresponding valuesfor stress MBF were 74%, 98%, 95% and 90%, respectively, with optimal cut-offvalues of 2.4 ml/min/g (AUC 0.95). Interestingly, the absolute increase of MBFby adenosine resulted also in very accurate results (93% sensitivity and 86%specificity when using 1.5 ml/min/g as a cut-off; AUC 0.95).Conclusions: The absolute quantification of stress perfusion provides alonemore accurate diagnosis of significant CAD than perfusion reserve. Also the in-crease of MBF between stress and rest in absolute terms works better than thereserve. The results indicate that quantification of myocardial perfusion in abso-lute terms is useful and provides additional clinical information.
264 Site of latest mechanical activation, left ventricular leadposition and response to cardiac resynchronizationtherapy
J.M.J. Boogers1, J. Chen2, R.J. Van Bommel1, C.J.W. Borleffs1,P. Dibbets-Schneider3 , M.P. Stokkel3, M.J. Schalij1, E.E. Van Der
Wall1, E.V. Garcia2, J.J. Bax1. 1Leiden University Medical Center, Departmentof Cardiology, Leiden, Netherlands; 2Emory University School of Medicine,Atlanta, United States of America; 3Leiden University Medical Center, Leiden,Netherlands
Purpose: Response to cardiac resynchronization therapy (CRT) has been re-lated to pre-existent mechanical dyssynchrony, location and extent of infarctedmyocardium and left ventricular (LV) lead position. Recently, the importance ofLV lead position and the site of latest mechanical activation have been demon-strated for the prediction of CRT response. To date, echocardiography has beenused extensively to assess the site of delayed mechanical activation in CRT pa-tients. Despite its potential, phase analysis on gated myocardial perfusion SPECT(GMPS) has not been used for assessment of the site of latest mechanical activa-tion in patients referred for CRT. Accordingly, the current study sought to evaluatethe relation between the site of latest mechanical activation, LV lead position andCRT response in patients referred for CRT.Methods: The patient population consisted of consecutive advanced heart failurepatients currently indicated for CRT. Before implantation, 2D echocardiographyand GMPS were performed. 2D echocardiography was performed to assess LVend-systolic volume (LVESV), LV end-diastolic volume (LVEDV) and LV ejectionfraction (LVEF). The site of latest mechanical activation was assessed by phaseanalysis on GMPS and related to LV lead position on fluoroscopy. Echocardio-graphy was repeated after 6 months of CRT. Response to CRT was defined as>15% decrease in LVESV.Results: Fifty-one patients (71% men, 68±9 yrs) with advanced heart failurewere enrolled. In 30 (59%) patients, the LV lead was positioned at the site of lat-est mechanical activation (concordant), whereas the LV lead was positioned out-side the site of latest mechanical activation (discordant) in 21 (41%) of patients.Among all baseline variables, only percentage CRT responders was significantly
higher in patients with concordant LV lead position than patients with discordantLV lead position (83% vs. 33%, p<0.05). After 6 months of CRT, patients with con-cordant LV lead position showed a significant decrease in LVESV (153±33 mL vs.108±35 mL, p<0.05) and LVEDV (210±44 mL vs. 170±44 mL, p<0.05) as wellas a significant improvement in LVEF (27±7% vs. 36±12%, p<0.05). Patientswith discordant LV lead position showed no improvement in echocardiographicvariables.Conclusions: Patients with concordant LV lead position as assessed by phaseanalysis on GMPS showed superior echocardiographic response to CRT as com-pared to patients with discordant LV lead position.
265 Coronary revascularization versus medical therapy toimprove long-term survival - a SPECT-based study
J. Herrmann, T.D. Miller, D.R. Holmes Jr, H.V. Schaff, D.O. Hodge,R.J. Gibbons. Mayo Clinic, Rochester, United States of America
Background: The survival benefit of coronary artery revascularization(Revasc) compared with medical therapy (Med Tx) may depend on the amount ofmyocardial ischemia, but the current data are limited.Methods: Retrospective cohort study of all patients without a history of MI,prior Revasc, cardiomyopathy, significant valve disease undergoing nuclear stressimaging at the Clinic between 3/30/2003-5/8/2008. Mortality status was deter-mined by the Social Security Death Index (median follow-up 3.5 years). Survivalwas stratified on the basis of the extent of myocardial ischemia on exercise orpharmacological SPECT imaging (difference of the summed stress and rest scoredivided by the total maximum score and multiplied by 100) and the treatment (MedTx versus Revasc) received within 90 days of nuclear stress testing.Results: Overall 16,315 patients were included in the study (age 64±12 yrs, 56%male). 323 patients (2%) underwent Revasc within 3 months of nuclear stresstesting. Overall 5-year survival did not differ significantly between Med Tx andRevasc (89 vs. 87%, p=0.07). The rate of revascularization varied directly withthe burden of ischemia, from 0.4% in those patients without detectable ischemiato 33% in those patients with large ischemia burden (p<0.001, Table). A possiblesurvival advantage with Revasc was present in patients with the largest burden ofmyocardial ischemia (> 20% of the left ventricle, Table).
Survival according to extent of ischemia
Ischemic burden Patients Revasc Rate of Revasc 5-year Med Tx 5-year p-value(% myocardium) (n) (n) survival (n) survival
0 12499 48 0.4% 85% 12451 90% 0.071-5 1689 36 2% 84% 1653 85% 0.596-10 1200 59 5% 87% 1141 85% 0.8311-20 686 100 15% 81% 586 83% 0.81>20 241 80 33% 97% 161 82% 0.01
Conclusions: The rate of revascularization in our practice varies directly withthe amount of ischemic burden. These unadjusted data suggest that a survivaladvantage with Revasc was present in patients with a large amount of ischemia.
266 High-speed myocardial perfusion imaging using a noveldetector technique: validation of CT attenuationcorrection
B. Herzog, R.R. Buechel, L. Husmann, A. Pazhenkottil, I.A. Burger,R.N. Nkoulou, I. Valenta, C.A. Wyss, V. Treyer, P.A. Kaufmann.
University Hospital Zurich, Zurich, Switzerland
Purpose: We aimed at validating attenuation correction (AC) using low-dosestandalone CT for myocardial perfusion imaging (MPI) obtained on a novel ul-tra fast gamma camera with cadmium-zinc-telluride (CZT) detector technology.Methods: Sixty-six consecutive patients (BMI: 27.2±3.5 kg/m2; range 19.1-36.0kg/m2) underwent a one-day 99mTc-tetrofosmin adenosine-stress/rest imagingprotocol each with 15 minutes acquisition time on a standard dual-head-SPECT-camera (Ventri, GE Healthcare). All scans were repeated within minutes on theCZT camera (Discovery NN 530c) with 3 minutes acquisition time for stress (lowdose) and 2 minutes acquisition time for rest (high dose) as recently established.Intraclass correlation and Bland-Altman limits of agreement were used to com-pare percent of maximum myocardial uptake (20 segment model) of MPI scansfrom CZT versus those from SPECT, both with and without CT AC, respectively. Inaddition clinical agreement was assessed for each coronary territory for all scansfrom both devices.Results: There was an excellent clinical agreement between MPI without ACfrom CZT and the standard camera at both, stress and rest (96%), underlined byan excellent correlation and narrow BA limits of agreement of segmental traceruptake (stress: r=0.90, p<0.001; BA=-18-15; rest: r=0.91, p<0.001; BA=-15.4-15.5). Similarly, after AC clinical agreement was 96% for stress and 99% for restMPI scans and segmental uptake was highly correlated between the two scannersat stress (r=0.87, p<0.001; BA=-16-14) and at rest (r=0.88, p<0.001; BA=-16-14).Conclusions: Our results support that AC of MPI on the novel CZT camera isfeasible as it provides high correlation of segmental tracer uptake and an excellentclinical agreement compared to conventional SPECT camera.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

18 Novel nuclear imaging / Risk models to guide revascularization strategies
267 The prognostic value of normal stress SPECTmyocardial perfusion imaging
M. Mazzanti1, M. Marini1, G. Ascoli2, G.P. Perna1. 1Cardiology CenterG.M. Lancisi, Ancona, Italy; 2Medicina Nucleare, Ancona, Italy
Background and Purpose: For the reason that stress-only nuclearimaging may save time and should reduce radiation exposure, aim of the study isto validate the prognostic value of normal stress scans in a large group of patients.Methods: Retrospectively, we examined patients at low-to-intermediate pre-testlikelihood of coronary artery disease (CAD) presenting for a Tc-99m SPECT MPIover a 62 months period who underwent a stress-only gated Myocardial PerfusionImaging (so GMPI). In this protocol, if the stress images were normal (SSS ≤ 4),rest imaging was not performed. Stress-only group was compared to those pa-tients who performed a two-days stress/rest protocol during the same time period.Only patients with normal perfusion and normal left-ventricular ejection fraction,no known CAD, and no pre-organ transplantation were included. Mortality for allcauses was determined and survival was analyzed using Kaplan-Meier statistics.Results: Out of 16,729 patients undergoing a Tc-99m gated MPI, 1,977 patientswho had a normal so GMPI and 3,853 who had a normal stress/rest scan with amean follow-up of 41±7 months were analyzed. The so GMPI cohort was 65% F,55±12 yrs and the stress/rest group was 61% F, 63±11 yrs. The 1 year all-causemortality was 1.3% in the so GMPI group and 1.1% in the stress/rest group. Whilethere was a greater proportion of low-to-intermediate pre-test likelihood of CADpatients in the so GMPI (91% vs 73%), there was no significant difference inmortality based on stressor (exercise vs pharmacologic).Conclusions: so GMPI has a very good 1 year prognosis and it is comparable tothat of a standard stress/rest GMPI.
RISK MODELS TO GUIDE REVASCULARIZATIONSTRATEGIES
292 Long term outcomes following percutaneousintervention with multiple DES implantation in patientswith low, intermediate and high SYNTAX scores
R. Al-Lamee1, R. Gerber2, A. Ielasi3, M. Ferraro4 , C. Godino1,M. Mussardo3, A. Latib1, A. Chieffo3, A. Colombo1. 1EMO-GVM Heart
Center Columbus and San Raffaele Hospital, Milan, Italy; 2Imperial College NHSHealthcare Trust, London, United Kingdom; 3San Raffaele Hospital, IRCCS,Milan, Italy; 4EMO-GVM Heart Center Columbus, Milan, Italy
Purpose: To assess the clinical and angiographic outcomes of patients with mul-tiple drug-eluting stent (DES) implantation, and the relationship between theseoutcomes and the SYNTAX score.Methods: This study included all patients with de novo lesions following implan-tation of ≥4 DES at our institutions from April 2002 to April 2004.Results: A total of 407 patients were included with a mean SYNTAX score of23.9±8.5. This was composed of 45% low score (<22), 41% intermediate score(22-33) and 12% high score (>33). The patients were also divided according tothe number of DES implanted: 4 in 35%, 4-6 in 41%, and >6 in 24%. The meannumber of stents was 5.6±1.9), total DES length of 135±49mm, with a significantincrease in length of DES based on SYNTAX score (low vs. high score group,p=0.002), and number of stents implanted (p<0.001). Clinical follow up was ob-tained in 99% (30±16 months) with 73% angiographic follow-up. There was nosignificant difference in the major adverse cardiac event (MACE) rate between the3 SYNTAX subgroups: 34% in low score group, 36% in intermediate score groupand 40% in high score group (p=0.72). There was also no significant differencein the rates of target lesion revascularization (TLR), or target vessel revascular-ization (TVR) between these groups. However, following division according to thenumber of DES implanted, there were significant differences in MACE rates: 17%with 4 DES, 35% with 4-6 DES, and 61% with >6 DES (p<0.001). There was alsoa significant difference in the TLR (p<0.001) and TVR rates (p<0.001) betweenthese groups.
Freedom from MACE according to No of DES
Conclusions: We found that there was no significant difference in outcome basedon SYNTAX score subgroups; however repeat revascularization rates and MACEsignificantly correlated the number of DES implanted.
293 Five year outcomes of percutaneous coronaryintervention compared to bypass surgery in patientswith multi-vessel disease involving the proximal leftanterior descending artery: an ARTS-II sub-study
S. Garg1, G. Sarno1, H.M. Garcia-Garcia2, J. Gomez-Lara1 ,J.L. Gutierrez-Chico1, P.W. Serruys1. 1Erasmus Medical Center, Thoraxcenter,Rotterdam, Netherlands; 2Cardialysis, Rotterdam, Netherlands
Aim: The aim of this study was to compare the long-term outcomes of treatmentwith sirolimus drug eluting stents (SES) to bare metal stents (BMS) and coro-nary artery bypass surgery (CABG) in patients with multi-vessel disease (MVD)involving the proximal left anterior descending (LAD) artery.Methods: The 5-year clinical outcomes were compared between the 682 patientsenrolled in the Arterial Revascularisation Therapies study Part I and II who hadMVD involving the proximal LAD, and were treated with BMS (187, 27.4%), CABG(206, 30.2%), and SES (289, 42.4%).Results: At 5-year follow-up the primary endpoint of major adverse car-diovascular and cerebrovascular events (MACCE) occurred in 33.7%, 18.0%and 24.9% of patients treated with BMS, CABG and SES respectively (BMSvs. SES p=0.04, CABG vs. SES p=0.07). Unadjusted rates of mortality anddeath/stroke/myocardial infarction (safety) were comparable between all threetreatments. Following adjustment of confounding factors a prognostic advantagewas seen with SES compared with CABG (Mortality HR: 3.68, 95%CI:1.23-11.02,p=0.02), however safety and overall MACCE remained similar. Repeat revascu-larisation was significantly reduced following CABG irrespective of adjustment.The absolute difference in MACCE between patients with a logistic EuroSCOREabove and below the mean (i.e. 2.09%) was 18.8% (p=0.001), and 1.9% (p=0.28)for CABG and SES respectively. In patients with a high EuroSCORE, SES wasa significantly safer treatment (p=0.04) whilst repeat revascularisation remainedlower with CABG irrespective of the EuroSCORE.Conclusion: At 5-year follow-up CABG has comparable safety, and superior ef-ficacy in terms of reducing repeat revascularisation compared to BMS and SESin the treatment of patients with MVD involving the proximal LAD however, appro-priate patient selection remains imperative.
294 Impact of diabetes mellitus on multivessel coronaryartery disease treated with sirolimus-eluting stent fromj-Cypher registry
T. Tada1, K. Mitsudo2, T. Kimura1, T. Morimoto1, A. Kawamura3,T. Sone4, A. Miura5, Y. Kazatani6, T. Kawasaki7, M. Nomura8. 1Kyoto
University, Graduate School of Medicine, Kyoto, Japan; 2Kurashiki CentralHospital, Cardiology Department, Kurashiki, Japan; 3National CardiovascularCenter, Suita, Japan; 4Ogaki Municipal Hospital, Ogaki, Japan; 5JapanRed Cross Society Wakayama Medical Center, Wakayama, Japan; 6EhimePrefectural Central Hospital, Matsuyama, Japan; 7Shin-Koga Hospital, Kurume,Japan; 8Fujita Health University, Banbuntane Hotokukai Hospital, Nagoya, Japan
Purpose: To compare clinical outcomes in patients with and without diabetesmellitus (DM) after implantation of sirolimus-eluting stents (SES) for multivesselcoronary artery disease.Methods & Results: In an observational study (The j-Cypher registry), 3-yearclinical outcomes were assessed in consecutive 10778 patients undergoing SESimplantation alone. 2626 patients had de novo multivessel coronary artery dis-ease (MVD) and 1174 (45% of patients with MVD) patients were diagnosed asDM. Event rate of a composite of all cause death, myocardial infarction (MI) andstroke, it was defined as hard endpoint, and Target lesion revascularization (TLR)were estimated by Kaplan-Meier method and compared using log-rank. The inde-pendent predictors of hard endpoint and TLR were determined using Cox propor-tional hazards regression. Cumulative incidence of hard endpoint was similar forpatients with or without DM (18% vs. 16%, p=0.13), whereas TLR rate was muchhigher in patients with DM (17% vs. 11%, p<0.0001). The independent predictorsof hard endpoint were renal insufficiency, previous heart failure, previous stroke,BMI<25, acute coronary syndrome, and peripheral vessel disease, but not dia-betes (Hazard ratio [HR] 1.04; 95% CI 0.93–1.15, p=0.52).
Cumulative incidence of hard event, TLR
Conclusions: In this large, real world study in Japanese patients with SES im-plantation, although diabetes-associated excess risk of TLR, there were no sig-nificant differences in long-term risk of hard endpoint, a composite of all causedeath, MI and stroke, between nondiabetic patients and diabetic patients withMVD.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
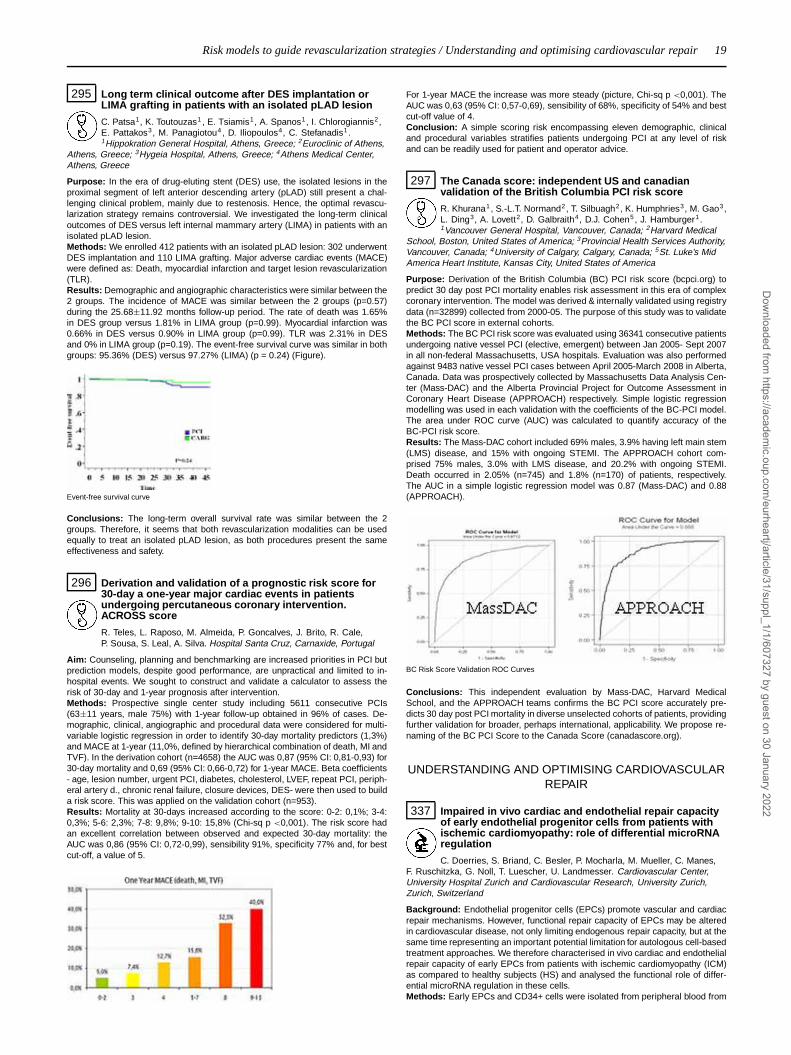
Risk models to guide revascularization strategies / Understanding and optimising cardiovascular repair 19
295 Long term clinical outcome after DES implantation orLIMA grafting in patients with an isolated pLAD lesion
C. Patsa1, K. Toutouzas1 , E. Tsiamis1, A. Spanos1, I. Chlorogiannis2,E. Pattakos3, M. Panagiotou4, D. Iliopoulos4, C. Stefanadis1.1Hippokration General Hospital, Athens, Greece; 2Euroclinic of Athens,
Athens, Greece; 3Hygeia Hospital, Athens, Greece; 4Athens Medical Center,Athens, Greece
Purpose: In the era of drug-eluting stent (DES) use, the isolated lesions in theproximal segment of left anterior descending artery (pLAD) still present a chal-lenging clinical problem, mainly due to restenosis. Hence, the optimal revascu-larization strategy remains controversial. We investigated the long-term clinicaloutcomes of DES versus left internal mammary artery (LIMA) in patients with anisolated pLAD lesion.Methods: We enrolled 412 patients with an isolated pLAD lesion: 302 underwentDES implantation and 110 LIMA grafting. Major adverse cardiac events (MACE)were defined as: Death, myocardial infarction and target lesion revascularization(TLR).Results: Demographic and angiographic characteristics were similar between the2 groups. The incidence of MACE was similar between the 2 groups (p=0.57)during the 25.68±11.92 months follow-up period. The rate of death was 1.65%in DES group versus 1.81% in LIMA group (p=0.99). Myocardial infarction was0.66% in DES versus 0.90% in LIMA group (p=0.99). TLR was 2.31% in DESand 0% in LIMA group (p=0.19). The event-free survival curve was similar in bothgroups: 95.36% (DES) versus 97.27% (LIMA) (p = 0.24) (Figure).
Event-free survival curve
Conclusions: The long-term overall survival rate was similar between the 2groups. Therefore, it seems that both revascularization modalities can be usedequally to treat an isolated pLAD lesion, as both procedures present the sameeffectiveness and safety.
296 Derivation and validation of a prognostic risk score for30-day a one-year major cardiac events in patientsundergoing percutaneous coronary intervention.ACROSS score
R. Teles, L. Raposo, M. Almeida, P. Goncalves, J. Brito, R. Cale,P. Sousa, S. Leal, A. Silva. Hospital Santa Cruz, Carnaxide, Portugal
Aim: Counseling, planning and benchmarking are increased priorities in PCI butprediction models, despite good performance, are unpractical and limited to in-hospital events. We sought to construct and validate a calculator to assess therisk of 30-day and 1-year prognosis after intervention.Methods: Prospective single center study including 5611 consecutive PCIs(63±11 years, male 75%) with 1-year follow-up obtained in 96% of cases. De-mographic, clinical, angiographic and procedural data were considered for multi-variable logistic regression in order to identify 30-day mortality predictors (1,3%)and MACE at 1-year (11,0%, defined by hierarchical combination of death, MI andTVF). In the derivation cohort (n=4658) the AUC was 0,87 (95% CI: 0,81-0,93) for30-day mortality and 0,69 (95% CI: 0,66-0,72) for 1-year MACE. Beta coefficients- age, lesion number, urgent PCI, diabetes, cholesterol, LVEF, repeat PCI, periph-eral artery d., chronic renal failure, closure devices, DES- were then used to builda risk score. This was applied on the validation cohort (n=953).Results: Mortality at 30-days increased according to the score: 0-2: 0,1%; 3-4:0,3%; 5-6: 2,3%; 7-8: 9,8%; 9-10: 15,8% (Chi-sq p <0,001). The risk score hadan excellent correlation between observed and expected 30-day mortality: theAUC was 0,86 (95% CI: 0,72-0,99), sensibility 91%, specificity 77% and, for bestcut-off, a value of 5.
For 1-year MACE the increase was more steady (picture, Chi-sq p <0,001). TheAUC was 0,63 (95% CI: 0,57-0,69), sensibility of 68%, specificity of 54% and bestcut-off value of 4.Conclusion: A simple scoring risk encompassing eleven demographic, clinicaland procedural variables stratifies patients undergoing PCI at any level of riskand can be readily used for patient and operator advice.
297 The Canada score: independent US and canadianvalidation of the British Columbia PCI risk score
R. Khurana1, S.-L.T. Normand2, T. Silbuagh2, K. Humphries3, M. Gao3,L. Ding3, A. Lovett2, D. Galbraith4, D.J. Cohen5, J. Hamburger1 .1Vancouver General Hospital, Vancouver, Canada; 2Harvard Medical
School, Boston, United States of America; 3Provincial Health Services Authority,Vancouver, Canada; 4University of Calgary, Calgary, Canada; 5St. Luke’s MidAmerica Heart Institute, Kansas City, United States of America
Purpose: Derivation of the British Columbia (BC) PCI risk score (bcpci.org) topredict 30 day post PCI mortality enables risk assessment in this era of complexcoronary intervention. The model was derived & internally validated using registrydata (n=32899) collected from 2000-05. The purpose of this study was to validatethe BC PCI score in external cohorts.Methods: The BC PCI risk score was evaluated using 36341 consecutive patientsundergoing native vessel PCI (elective, emergent) between Jan 2005- Sept 2007in all non-federal Massachusetts, USA hospitals. Evaluation was also performedagainst 9483 native vessel PCI cases between April 2005-March 2008 in Alberta,Canada. Data was prospectively collected by Massachusetts Data Analysis Cen-ter (Mass-DAC) and the Alberta Provincial Project for Outcome Assessment inCoronary Heart Disease (APPROACH) respectively. Simple logistic regressionmodelling was used in each validation with the coefficients of the BC-PCI model.The area under ROC curve (AUC) was calculated to quantify accuracy of theBC-PCI risk score.Results: The Mass-DAC cohort included 69% males, 3.9% having left main stem(LMS) disease, and 15% with ongoing STEMI. The APPROACH cohort com-prised 75% males, 3.0% with LMS disease, and 20.2% with ongoing STEMI.Death occurred in 2.05% (n=745) and 1.8% (n=170) of patients, respectively.The AUC in a simple logistic regression model was 0.87 (Mass-DAC) and 0.88(APPROACH).
BC Risk Score Validation ROC Curves
Conclusions: This independent evaluation by Mass-DAC, Harvard MedicalSchool, and the APPROACH teams confirms the BC PCI score accurately pre-dicts 30 day post PCI mortality in diverse unselected cohorts of patients, providingfurther validation for broader, perhaps international, applicability. We propose re-naming of the BC PCI Score to the Canada Score (canadascore.org).
UNDERSTANDING AND OPTIMISING CARDIOVASCULARREPAIR
337 Impaired in vivo cardiac and endothelial repair capacityof early endothelial progenitor cells from patients withischemic cardiomyopathy: role of differential microRNAregulation
C. Doerries, S. Briand, C. Besler, P. Mocharla, M. Mueller, C. Manes,F. Ruschitzka, G. Noll, T. Luescher, U. Landmesser. Cardiovascular Center,University Hospital Zurich and Cardiovascular Research, University Zurich,Zurich, Switzerland
Background: Endothelial progenitor cells (EPCs) promote vascular and cardiacrepair mechanisms. However, functional repair capacity of EPCs may be alteredin cardiovascular disease, not only limiting endogenous repair capacity, but at thesame time representing an important potential limitation for autologous cell-basedtreatment approaches. We therefore characterised in vivo cardiac and endothelialrepair capacity of early EPCs from patients with ischemic cardiomyopathy (ICM)as compared to healthy subjects (HS) and analysed the functional role of differ-ential microRNA regulation in these cells.Methods: Early EPCs and CD34+ cells were isolated from peripheral blood from
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

20 Understanding and optimising cardiovascular repair
patients with heart failure due to ICM and healthy subjects. In vivo cardiac andendothelial repair capacity of EPCs were examined after transplantation into nudemice with myocardial infarction and carotid injury. The microRNA profile of EPCswas characterised using a microRNA array, results of array were confirmed byquantitative RT-PCR. The functional role of microRNAs was examined by trans-fection with antimirs.Results: In vivo cardiac and endothelial repair capacity of EPCs derived from pa-tients with heart failure due to ICM was markedly reduced as compared to HS (LV-ejection fraction: 22.1±3.9 versus 43.4±3.9%, P<0.05; reendothelialized area:16.7±1.1 versus 25.4±2.1%, P<0.05). Cardiac function improved after transplan-tation of EPCs from healthy subjects, but not after transplantation of EPCs frompatients with ICM as determined by cardiac MRI and haemodynamic analyses.MicroRNA profiling indicated a markedly reduced expression of the miR126 andmiR130a in EPCs and CD34+ cells from patients with ICM. Furthermore, lev-els of the respective targets, SRED-1 and HOXA-5, were upregulated in thesecells. Moreover, down-regulation of miR126 impaired the cardiac repair capacityof EPCs from HS, and down-regulation of miR130a, but not of miR126 abolishedendothelial repair capacity of EPCs from HS.Conclusions: In vivo cardiac and endothelial repair capacity of early EPCs aremarkedly impaired in patients with heart failure due to ICM. Down-regulation ofmiR126 impairs the cardiac repair capacity of EPCs, whereas down-regulation ofmiR130a, but not of miR126, abolishes the endothelial repair capacity of EPCs.Altered microRNA regulation may represent an interesting target for the optimisa-tion of cell-based treatment approaches.
338 Dual stem cell comprising administration of G-CSF andsitagliptin improves stem cell homing, cardiac functionand survival after MI in mice
H.D. Theiss, L. Krieg, M. Vallaster, J. Mueller-Hoecker, W.M. Franz.Ludwig-Maximilians University, Munich, Germany
Background: Cardiac homing of stem cells occurs via the SDF-1-CXCR4 axis.Myocardial SDF-1 is cleaved by the extracellular protease CD26. We hypothe-sized that inhibition of CD26 by Sitaglitpin (which is a clinically admitted antidia-betic drug) leads to an increase of myocardial SDF-1 thus improving the homingof G-CSF-mobilized stem cells after myocardial infarction (MI) in a mouse model.Methods: We induced AMI in 10-11 weeks old male C57BL/6 mice using surgicalocclusion of the left descending artery. Mice were then treated either with G-CSFin combination with Sitagliptin ("G-CSF+Sita"), G-CSF ("G-CSF") or Sitagliptin("Sita") alone or saline ("control"). FACS analyses were used to determine cardiacstem cell populations after 6 days. Cardiac function parameters were assessedusing a Millar-Tip catheter system. Histology was performed to examine infarctsize 30 days after AMI. Survival was analyzed by Kaplan-Meier-method for 30days (n=20 in each group).Findings: In the first step, we established the optimal dosage of Sitagliptin ad-ministration using mass spectrometry. As proof of principle, DPP-IV activity wasdecreased in G-CSF+Sita mice. G-CSF + Sitagliptin administration lead to a sig-nificantly improved cardiac homing of several CD34+ stem cell populations anda relevant induction of resident cardiac stem cells in the G-CSF+Sita group. Be-sides, myocardial remodeling was reduced in the G-CSF+Sita group compared tothe other treatment regimes. Cardiac function was almost doubled in G-CSF+Sitamice after 30 days. Finally, G-CSF+Sita mice showed a significant increase ofsurvival after 30 days (80% versus 40% in G-CSF mice and 35% in the salinegroup).Interpretation: This is the first study showing that combined application of G-CSFand Sitagliptin improves cardiac function and survival after myocardial infarctionby an enhanced cardiac homing of stem cells. Since Sitagliptin is a clinically useddrug, our results have immediate impact on the transfer of this therapeutic ap-proach from bench to bedside.
339 Donor age negatively influences the cytoprotectiveparacrine effects exerted by human mesenchymal stemcells
P. Danieli1, E. Cervio1, M.C. Ciuffreda1, F. Pisano1, M. Roccio2,M. Gnecchi1. 1Foundation IRCCS Polyclinic San Matteo, Departmentof Cardiology, Pavia, Italy; 2Foundation IRCCS Polyclinic San Matteo,
Department of Gynecology, Pavia, Italy
Background: In animal models mesenchymal stem cells (MSC) repair infarctedhearts mainly through cytoprotective paracrine mechanisms. For translationalpurposes, it would be important to verify if human MSC also mediate cardio-protection. In particular, since ischemic heart diseases occur mainly in elderly, itis essential to establish if donor age influences the production of cytoprotectivefactors. Accordingly, we compared the paracrine properties of fetal MSC (F-MSC)with adult MSC. Furthermore, we aimed to elucidate through which signallingpathway MSC lead to cytoprotection.Methods: F-MSC were isolated from human placenta and adult MSC fromthe bone marrow of young (yBM-MSC; age<65 years) or old (oBM-MSC;age>65) donors. Rat neonatal cardiomyocytes (H9c2) were exposed to hypoxia(6 hrs)/reoxygenation (18 hrs) (H/R) in the presence of control medium (CTRL-M) or conditioned medium from F-MSC (F-CM), yBM-MSC (y-CM) or oBM-MSC(o-CM). H9c2 viability was evaluated by MTS assay. Apoptosis was measured
by TUNEL staining and by cleaved Caspase 3 (colorimetric assay and Westernblot). We evaluated SAPK/JNK and p38 MAPK activation by Western blot and theexpression of pro- and anti-apoptotic genes by RT-PCR.Results: The H/R protocol reduced H9c2 viability by 55% (p<0.001 CTRL-M vsbasal condition). Compared with CTRL-M, both F-CM and y-CM increased cellviability (+45% and +33% respectively; p<0.017) while o-CM had no effect. F-CMsignificantly reduced the number of TUNEL positive cells (-91% vs CTRL-M and-89% vs o-CM; p<0.001). The y-CM also reduced H9c2 apoptotic nuclei (-67,5%vs CTRL-M, p<0.01; -64% vs o-CM, p<0.01). In contrast, o-CM did not preventapoptosis (-11% vs CTRL-M, p=ns). Both colorimetric assay and Western blotshowed that Caspase-3 activation was prevented by F-CM and y-CM but not byo-CM. The H/R protocol strongly activated both SAPK/JNK and p38 MAPK. Thisactivation was markedly reduced by F-CM while y-CM and o-CM had modest ef-fect on both pathways. Furthermore, compared with CTRL-M and both y-CM ando-CM, F-CM up-regulated the anti-apoptotic genes Bcl-2 and Stat3 and down-regulated the pro-apoptotic genes TNF-α and FasL.Conclusions: We showed that human MSC mediate cardiomyocyte protection byreleasing soluble anti-apoptotic factors. However, donor age negatively influencesthe cytoprotective properties of adult MSC. We also demonstrated that MSC offetal origin exerts powerful cytoprotective effects via inhibition of different pro-apoptotic signalling pathways. Our data suggest that autologous MSC therapy forischemic heart diseases may be less effective in elderly patients.
340 Recruitment of inflammatory and vascular repair cells isselectively regulated by kinin signaling in patients withcoronary disease
N. Kraenkel1 , M. Mueller2, M. Meyer2, C. Templin2, T.F. Luescher2 ,U. Landmesser2 . 1University of Zurich-Irchel, Department of Anatomy
and Physiology, Cardiovascular Research, Zurich, Switzerland; 2UniversityHospital Zurich, Department of Internal Medicine, Division of Cardiology, Zurich,Switzerland
Purpose: Atherosclerosis is associated with increased recruitment of inflamma-tory cells from the blood to the vessel wall, while recruitment of anti-inflammatoryand vascular repair-promoting cells seems to be impaired. As we and othershave shown, kinins are involved in the recruitment of inflammatory as well asangiogenesis-promoting cells. Aim of the present study was to assess whetherendothelial derived kinins affect the selective recruitment of inflammatory versusregenerative cells from the blood to the vessel wall, thereby participating in regu-lation of vascular inflammation/atherosclerosis vs. healing of endothelial injury.Methods: Expression of the B1 and B2 kinin receptors (B1R, B2R) on periph-eral blood mononuclear cell (PBMC) subsets of coronary artery disease patients(CAD) and age- matched healthy subjects (H) was assessed by flow cytometry.Adhesion to and transmigration through an endothelial monolayer was studied invitro after exposure to bradykinin (BK) and selective B1R and B2R blockade.Results: In H subjects, expression of both kinin receptors was virtually absent onlymphocytes and highest in angio-supportive CD14+Tie2+ monocytes and CD45-CD34+KDR+, CD34+CXCR4+ and CD133+CXCR4+ circulating progenitor cells(CPC). In CAD, B1R was consistently upregulated in inflammatory CD14hiCD16-monocytes and in regenerative monocyte and CPC populations (two- to 16-foldvs. H). In contrast, B2R was differentially regulated between cell types, with up-regulation on inflammatory CD14hiCD16- monocytes (2.4-fold vs. H), no changeon CD14+Tie2+ monocytes (1.0-fold vs. H) and downregulation on CPC (0.4- to0.6-fold of H).Adhesion of H CD14hiCD16- monocytes to endothelium was reduced upon BKstimulation together with an induction of transmigration, but BK was ineffectivein CAD. For CD34+ CPC, unstimulated adhesion was reduced in CAD versus H(CAD: 28.3±3.1%, H: 37.0±7.2% of CD34+ CPC adhere). In CAD, BK increasedadhesion of CD34+ CPC via the B2R, but not the B1R.Conclusions: We show for the first time that kinin receptor expression and –signaling are differentially modulated on distinct circulating cell populations inCAD. Interfering with kinin signaling might prove a novel therapeutic opportunityto stimulate recruitment of vascular repair, and limit vascular infiltration of inflam-matory cell types to the vessel wall, thereby delaying the onset of atherosclerosisand promoting vascular healing. In a currently ongoing in vivo study we test theefficacy of ex vivo B1R blockade on recruitment and endothelial regenerative ca-pacity of CAD-derived PBMC in a mouse model of endothelial injury.
341 Efficient gene transfer to cardiomyocytes mediated bysurface-immobilized polyplex
Y.S. Kim, Y. Ahn, H.L. Che, M.H. Hong, M.H. Jeong, I.K. Park. ChonnamNational University Hospital, Gwangju, Korea, Republic of
Purpose: Cardiomyocytes are difficult to transfer therapeutic genes withstandard protocols using commercially available reagents unless viral vectors areused. Surface gene delivery has been used successfully after immobilizing thenanoparticles onto atelocollagen-coated surface to deliver genetic materials intocells. In this study, we have explored a safe and efficient technique for gene trans-fer and expression screening in cardiomyocytes with surface-immobilized poly-plex on atelocollagen-coated layer.Methods and Results: The nanoparticles carrying reporter genes encoding fire-fly luciferase (Fluc), secreted alkaline phosphatase (SEAP) or red fluorescence
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
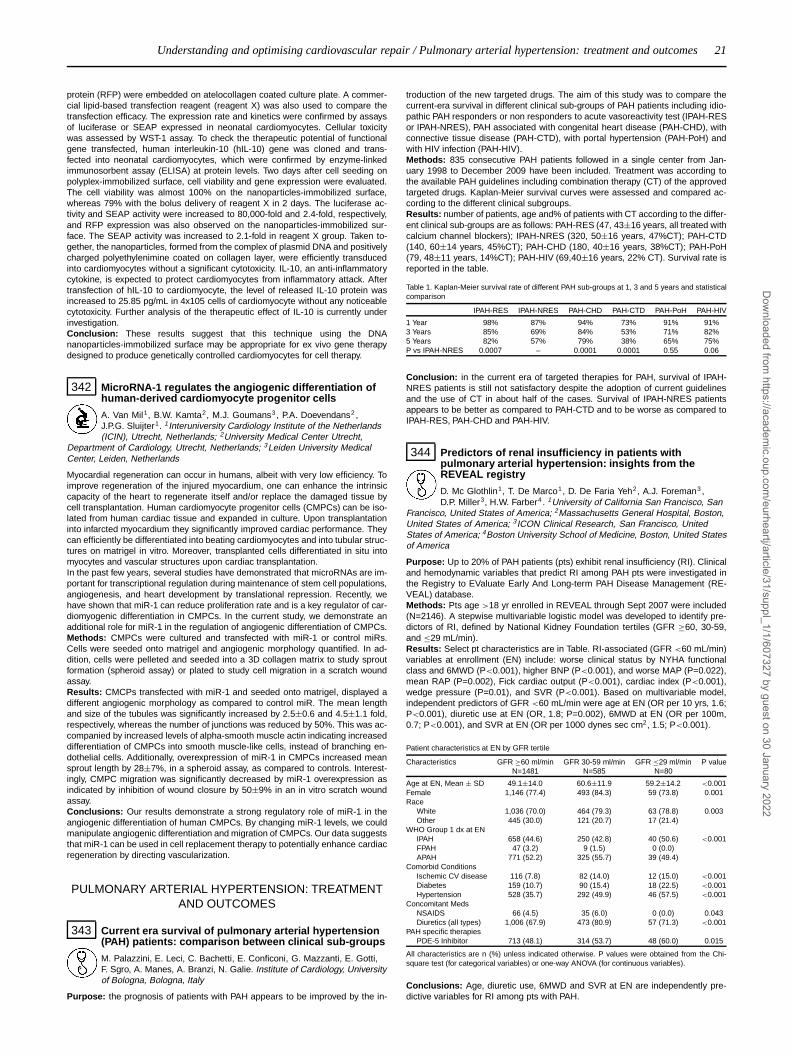
Understanding and optimising cardiovascular repair / Pulmonary arterial hypertension: treatment and outcomes 21
protein (RFP) were embedded on atelocollagen coated culture plate. A commer-cial lipid-based transfection reagent (reagent X) was also used to compare thetransfection efficacy. The expression rate and kinetics were confirmed by assaysof luciferase or SEAP expressed in neonatal cardiomyocytes. Cellular toxicitywas assessed by WST-1 assay. To check the therapeutic potential of functionalgene transfected, human interleukin-10 (hIL-10) gene was cloned and trans-fected into neonatal cardiomyocytes, which were confirmed by enzyme-linkedimmunosorbent assay (ELISA) at protein levels. Two days after cell seeding onpolyplex-immobilized surface, cell viability and gene expression were evaluated.The cell viability was almost 100% on the nanoparticles-immobilized surface,whereas 79% with the bolus delivery of reagent X in 2 days. The luciferase ac-tivity and SEAP activity were increased to 80,000-fold and 2.4-fold, respectively,and RFP expression was also observed on the nanoparticles-immobilized sur-face. The SEAP activity was increased to 2.1-fold in reagent X group. Taken to-gether, the nanoparticles, formed from the complex of plasmid DNA and positivelycharged polyethylenimine coated on collagen layer, were efficiently transducedinto cardiomyocytes without a significant cytotoxicity. IL-10, an anti-inflammatorycytokine, is expected to protect cardiomyocytes from inflammatory attack. Aftertransfection of hIL-10 to cardiomyocyte, the level of released IL-10 protein wasincreased to 25.85 pg/mL in 4x105 cells of cardiomyocyte without any noticeablecytotoxicity. Further analysis of the therapeutic effect of IL-10 is currently underinvestigation.Conclusion: These results suggest that this technique using the DNAnanoparticles-immobilized surface may be appropriate for ex vivo gene therapydesigned to produce genetically controlled cardiomyocytes for cell therapy.
342 MicroRNA-1 regulates the angiogenic differentiation ofhuman-derived cardiomyocyte progenitor cells
A. Van Mil1, B.W. Kamta2, M.J. Goumans3, P.A. Doevendans2 ,J.P.G. Sluijter1. 1Interuniversity Cardiology Institute of the Netherlands(ICIN), Utrecht, Netherlands; 2University Medical Center Utrecht,
Department of Cardiology, Utrecht, Netherlands; 3Leiden University MedicalCenter, Leiden, Netherlands
Myocardial regeneration can occur in humans, albeit with very low efficiency. Toimprove regeneration of the injured myocardium, one can enhance the intrinsiccapacity of the heart to regenerate itself and/or replace the damaged tissue bycell transplantation. Human cardiomyocyte progenitor cells (CMPCs) can be iso-lated from human cardiac tissue and expanded in culture. Upon transplantationinto infarcted myocardium they significantly improved cardiac performance. Theycan efficiently be differentiated into beating cardiomyocytes and into tubular struc-tures on matrigel in vitro. Moreover, transplanted cells differentiated in situ intomyocytes and vascular structures upon cardiac transplantation.In the past few years, several studies have demonstrated that microRNAs are im-portant for transcriptional regulation during maintenance of stem cell populations,angiogenesis, and heart development by translational repression. Recently, wehave shown that miR-1 can reduce proliferation rate and is a key regulator of car-diomyogenic differentiation in CMPCs. In the current study, we demonstrate anadditional role for miR-1 in the regulation of angiogenic differentiation of CMPCs.Methods: CMPCs were cultured and transfected with miR-1 or control miRs.Cells were seeded onto matrigel and angiogenic morphology quantified. In ad-dition, cells were pelleted and seeded into a 3D collagen matrix to study sproutformation (spheroid assay) or plated to study cell migration in a scratch woundassay.Results: CMCPs transfected with miR-1 and seeded onto matrigel, displayed adifferent angiogenic morphology as compared to control miR. The mean lengthand size of the tubules was significantly increased by 2.5±0.6 and 4.5±1.1 fold,respectively, whereas the number of junctions was reduced by 50%. This was ac-companied by increased levels of alpha-smooth muscle actin indicating increaseddifferentiation of CMPCs into smooth muscle-like cells, instead of branching en-dothelial cells. Additionally, overexpression of miR-1 in CMPCs increased meansprout length by 28±7%, in a spheroid assay, as compared to controls. Interest-ingly, CMPC migration was significantly decreased by miR-1 overexpression asindicated by inhibition of wound closure by 50±9% in an in vitro scratch woundassay.Conclusions: Our results demonstrate a strong regulatory role of miR-1 in theangiogenic differentiation of human CMPCs. By changing miR-1 levels, we couldmanipulate angiogenic differentiation and migration of CMPCs. Our data suggeststhat miR-1 can be used in cell replacement therapy to potentially enhance cardiacregeneration by directing vascularization.
PULMONARY ARTERIAL HYPERTENSION: TREATMENTAND OUTCOMES
343 Current era survival of pulmonary arterial hypertension(PAH) patients: comparison between clinical sub-groups
M. Palazzini, E. Leci, C. Bachetti, E. Conficoni, G. Mazzanti, E. Gotti,F. Sgro, A. Manes, A. Branzi, N. Galie. Institute of Cardiology, Universityof Bologna, Bologna, Italy
Purpose: the prognosis of patients with PAH appears to be improved by the in-
troduction of the new targeted drugs. The aim of this study was to compare thecurrent-era survival in different clinical sub-groups of PAH patients including idio-pathic PAH responders or non responders to acute vasoreactivity test (IPAH-RESor IPAH-NRES), PAH associated with congenital heart disease (PAH-CHD), withconnective tissue disease (PAH-CTD), with portal hypertension (PAH-PoH) andwith HIV infection (PAH-HIV).Methods: 835 consecutive PAH patients followed in a single center from Jan-uary 1998 to December 2009 have been included. Treatment was according tothe available PAH guidelines including combination therapy (CT) of the approvedtargeted drugs. Kaplan-Meier survival curves were assessed and compared ac-cording to the different clinical subgroups.Results: number of patients, age and% of patients with CT according to the differ-ent clinical sub-groups are as follows: PAH-RES (47, 43±16 years, all treated withcalcium channel blockers); IPAH-NRES (320, 50±16 years, 47%CT); PAH-CTD(140, 60±14 years, 45%CT); PAH-CHD (180, 40±16 years, 38%CT); PAH-PoH(79, 48±11 years, 14%CT); PAH-HIV (69,40±16 years, 22% CT). Survival rate isreported in the table.
Table 1. Kaplan-Meier survival rate of different PAH sub-groups at 1, 3 and 5 years and statisticalcomparison
IPAH-RES IPAH-NRES PAH-CHD PAH-CTD PAH-PoH PAH-HIV
1 Year 98% 87% 94% 73% 91% 91%3 Years 85% 69% 84% 53% 71% 82%5 Years 82% 57% 79% 38% 65% 75%P vs IPAH-NRES 0.0007 – 0.0001 0.0001 0.55 0.06
Conclusion: in the current era of targeted therapies for PAH, survival of IPAH-NRES patients is still not satisfactory despite the adoption of current guidelinesand the use of CT in about half of the cases. Survival of IPAH-NRES patientsappears to be better as compared to PAH-CTD and to be worse as compared toIPAH-RES, PAH-CHD and PAH-HIV.
344 Predictors of renal insufficiency in patients withpulmonary arterial hypertension: insights from theREVEAL registry
D. Mc Glothlin1, T. De Marco1, D. De Faria Yeh2, A.J. Foreman3 ,D.P. Miller3, H.W. Farber4 . 1University of California San Francisco, San
Francisco, United States of America; 2Massachusetts General Hospital, Boston,United States of America; 3ICON Clinical Research, San Francisco, UnitedStates of America; 4Boston University School of Medicine, Boston, United Statesof America
Purpose: Up to 20% of PAH patients (pts) exhibit renal insufficiency (RI). Clinicaland hemodynamic variables that predict RI among PAH pts were investigated inthe Registry to EValuate Early And Long-term PAH Disease Management (RE-VEAL) database.Methods: Pts age >18 yr enrolled in REVEAL through Sept 2007 were included(N=2146). A stepwise multivariable logistic model was developed to identify pre-dictors of RI, defined by National Kidney Foundation tertiles (GFR ≥60, 30-59,and ≤29 mL/min).Results: Select pt characteristics are in Table. RI-associated (GFR <60 mL/min)variables at enrollment (EN) include: worse clinical status by NYHA functionalclass and 6MWD (P<0.001), higher BNP (P<0.001), and worse MAP (P=0.022),mean RAP (P=0.002), Fick cardiac output (P<0.001), cardiac index (P<0.001),wedge pressure (P=0.01), and SVR (P<0.001). Based on multivariable model,independent predictors of GFR <60 mL/min were age at EN (OR per 10 yrs, 1.6;P<0.001), diuretic use at EN (OR, 1.8; P=0.002), 6MWD at EN (OR per 100m,0.7; P<0.001), and SVR at EN (OR per 1000 dynes sec cm2, 1.5; P<0.001).
Patient characteristics at EN by GFR tertile
Characteristics GFR ≥60 ml/min GFR 30-59 ml/min GFR ≤29 ml/min P valueN=1481 N=585 N=80
Age at EN, Mean ± SD 49.1±14.0 60.6±11.9 59.2±14.2 <0.001Female 1,146 (77.4) 493 (84.3) 59 (73.8) 0.001Race
White 1,036 (70.0) 464 (79.3) 63 (78.8) 0.003Other 445 (30.0) 121 (20.7) 17 (21.4)
WHO Group 1 dx at ENIPAH 658 (44.6) 250 (42.8) 40 (50.6) <0.001FPAH 47 (3.2) 9 (1.5) 0 (0.0)APAH 771 (52.2) 325 (55.7) 39 (49.4)
Comorbid ConditionsIschemic CV disease 116 (7.8) 82 (14.0) 12 (15.0) <0.001Diabetes 159 (10.7) 90 (15.4) 18 (22.5) <0.001Hypertension 528 (35.7) 292 (49.9) 46 (57.5) <0.001
Concomitant MedsNSAIDS 66 (4.5) 35 (6.0) 0 (0.0) 0.043Diuretics (all types) 1,006 (67.9) 473 (80.9) 57 (71.3) <0.001
PAH specific therapiesPDE-5 Inhibitor 713 (48.1) 314 (53.7) 48 (60.0) 0.015
All characteristics are n (%) unless indicated otherwise. P values were obtained from the Chi-square test (for categorical variables) or one-way ANOVA (for continuous variables).
Conclusions: Age, diuretic use, 6MWD and SVR at EN are independently pre-dictive variables for RI among pts with PAH.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
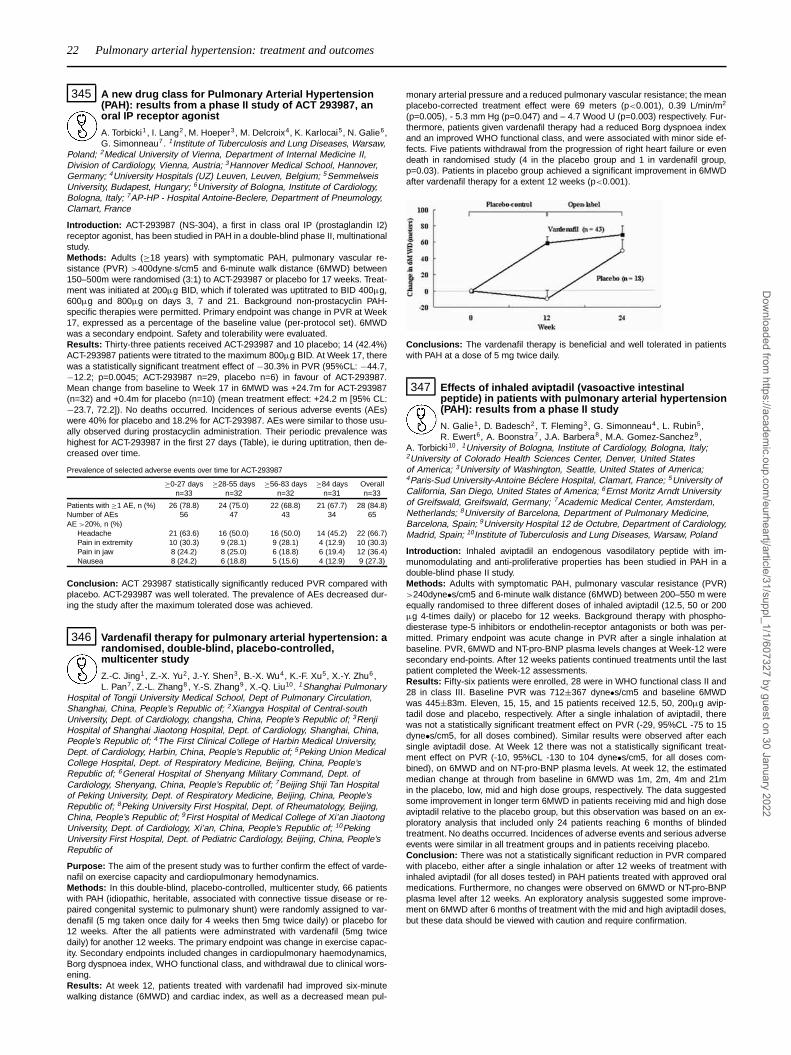
22 Pulmonary arterial hypertension: treatment and outcomes
345 A new drug class for Pulmonary Arterial Hypertension(PAH): results from a phase II study of ACT 293987, anoral IP receptor agonist
A. Torbicki1, I. Lang2, M. Hoeper3 , M. Delcroix4, K. Karlocai5, N. Galie6,G. Simonneau7. 1Institute of Tuberculosis and Lung Diseases, Warsaw,
Poland; 2Medical University of Vienna, Department of Internal Medicine II,Division of Cardiology, Vienna, Austria; 3Hannover Medical School, Hannover,Germany; 4University Hospitals (UZ) Leuven, Leuven, Belgium; 5SemmelweisUniversity, Budapest, Hungary; 6University of Bologna, Institute of Cardiology,Bologna, Italy; 7AP-HP - Hospital Antoine-Beclere, Department of Pneumology,Clamart, France
Introduction: ACT-293987 (NS-304), a first in class oral IP (prostaglandin I2)receptor agonist, has been studied in PAH in a double-blind phase II, multinationalstudy.Methods: Adults (≥18 years) with symptomatic PAH, pulmonary vascular re-sistance (PVR) >400dyne·s/cm5 and 6-minute walk distance (6MWD) between150–500m were randomised (3:1) to ACT-293987 or placebo for 17 weeks. Treat-ment was initiated at 200μg BID, which if tolerated was uptitrated to BID 400μg,600μg and 800μg on days 3, 7 and 21. Background non-prostacyclin PAH-specific therapies were permitted. Primary endpoint was change in PVR at Week17, expressed as a percentage of the baseline value (per-protocol set). 6MWDwas a secondary endpoint. Safety and tolerability were evaluated.Results: Thirty-three patients received ACT-293987 and 10 placebo; 14 (42.4%)ACT-293987 patients were titrated to the maximum 800μg BID. At Week 17, therewas a statistically significant treatment effect of −30.3% in PVR (95%CL: −44.7,−12.2; p=0.0045; ACT-293987 n=29, placebo n=6) in favour of ACT-293987.Mean change from baseline to Week 17 in 6MWD was +24.7m for ACT-293987(n=32) and +0.4m for placebo (n=10) (mean treatment effect: +24.2 m [95% CL:−23.7, 72.2]). No deaths occurred. Incidences of serious adverse events (AEs)were 40% for placebo and 18.2% for ACT-293987. AEs were similar to those usu-ally observed during prostacyclin administration. Their periodic prevalence washighest for ACT-293987 in the first 27 days (Table), ie during uptitration, then de-creased over time.
Prevalence of selected adverse events over time for ACT-293987
≥0-27 days ≥28-55 days ≥56-83 days ≥84 days Overalln=33 n=32 n=32 n=31 n=33
Patients with ≥1 AE, n (%) 26 (78.8) 24 (75.0) 22 (68.8) 21 (67.7) 28 (84.8)Number of AEs 56 47 43 34 65AE >20%, n (%)
Headache 21 (63.6) 16 (50.0) 16 (50.0) 14 (45.2) 22 (66.7)Pain in extremity 10 (30.3) 9 (28.1) 9 (28.1) 4 (12.9) 10 (30.3)Pain in jaw 8 (24.2) 8 (25.0) 6 (18.8) 6 (19.4) 12 (36.4)Nausea 8 (24.2) 6 (18.8) 5 (15.6) 4 (12.9) 9 (27.3)
Conclusion: ACT 293987 statistically significantly reduced PVR compared withplacebo. ACT-293987 was well tolerated. The prevalence of AEs decreased dur-ing the study after the maximum tolerated dose was achieved.
346 Vardenafil therapy for pulmonary arterial hypertension: arandomised, double-blind, placebo-controlled,multicenter study
Z.-C. Jing1, Z.-X. Yu2, J.-Y. Shen3, B.-X. Wu4, K.-F. Xu5, X.-Y. Zhu6,L. Pan7, Z.-L. Zhang8 , Y.-S. Zhang9 , X.-Q. Liu10. 1Shanghai Pulmonary
Hospital of Tongji University Medical School, Dept of Pulmonary Circulation,Shanghai, China, People’s Republic of; 2Xiangya Hospital of Central-southUniversity, Dept. of Cardiology, changsha, China, People’s Republic of; 3RenjiHospital of Shanghai Jiaotong Hospital, Dept. of Cardiology, Shanghai, China,People’s Republic of; 4The First Clinical College of Harbin Medical University,Dept. of Cardiology, Harbin, China, People’s Republic of; 5Peking Union MedicalCollege Hospital, Dept. of Respiratory Medicine, Beijing, China, People’sRepublic of; 6General Hospital of Shenyang Military Command, Dept. ofCardiology, Shenyang, China, People’s Republic of; 7Beijing Shiji Tan Hospitalof Peking University, Dept. of Respiratory Medicine, Beijing, China, People’sRepublic of; 8Peking University First Hospital, Dept. of Rheumatology, Beijing,China, People’s Republic of; 9First Hospital of Medical College of Xi’an JiaotongUniversity, Dept. of Cardiology, Xi’an, China, People’s Republic of; 10PekingUniversity First Hospital, Dept. of Pediatric Cardiology, Beijing, China, People’sRepublic of
Purpose: The aim of the present study was to further confirm the effect of varde-nafil on exercise capacity and cardiopulmonary hemodynamics.Methods: In this double-blind, placebo-controlled, multicenter study, 66 patientswith PAH (idiopathic, heritable, associated with connective tissue disease or re-paired congenital systemic to pulmonary shunt) were randomly assigned to var-denafil (5 mg taken once daily for 4 weeks then 5mg twice daily) or placebo for12 weeks. After the all patients were adminstrated with vardenafil (5mg twicedaily) for another 12 weeks. The primary endpoint was change in exercise capac-ity. Secondary endpoints included changes in cardiopulmonary haemodynamics,Borg dyspnoea index, WHO functional class, and withdrawal due to clinical wors-ening.Results: At week 12, patients treated with vardenafil had improved six-minutewalking distance (6MWD) and cardiac index, as well as a decreased mean pul-
monary arterial pressure and a reduced pulmonary vascular resistance; the meanplacebo-corrected treatment effect were 69 meters (p<0.001), 0.39 L/min/m2
(p=0.005), - 5.3 mm Hg (p=0.047) and – 4.7 Wood U (p=0.003) respectively. Fur-thermore, patients given vardenafil therapy had a reduced Borg dyspnoea indexand an improved WHO functional class, and were associated with minor side ef-fects. Five patients withdrawal from the progression of right heart failure or evendeath in randomised study (4 in the placebo group and 1 in vardenafil group,p=0.03). Patients in placebo group achieved a significant improvement in 6MWDafter vardenafil therapy for a extent 12 weeks (p<0.001).
Conclusions: The vardenafil therapy is beneficial and well tolerated in patientswith PAH at a dose of 5 mg twice daily.
347 Effects of inhaled aviptadil (vasoactive intestinalpeptide) in patients with pulmonary arterial hypertension(PAH): results from a phase II study
N. Galie1, D. Badesch2, T. Fleming3, G. Simonneau4, L. Rubin5,R. Ewert6, A. Boonstra7 , J.A. Barbera8, M.A. Gomez-Sanchez9 ,
A. Torbicki10. 1University of Bologna, Institute of Cardiology, Bologna, Italy;2University of Colorado Health Sciences Center, Denver, United Statesof America; 3University of Washington, Seattle, United States of America;4Paris-Sud University-Antoine Béclere Hospital, Clamart, France; 5University ofCalifornia, San Diego, United States of America; 6Ernst Moritz Arndt Universityof Greifswald, Greifswald, Germany; 7Academic Medical Center, Amsterdam,Netherlands; 8University of Barcelona, Department of Pulmonary Medicine,Barcelona, Spain; 9University Hospital 12 de Octubre, Department of Cardiology,Madrid, Spain; 10Institute of Tuberculosis and Lung Diseases, Warsaw, Poland
Introduction: Inhaled aviptadil an endogenous vasodilatory peptide with im-munomodulating and anti-proliferative properties has been studied in PAH in adouble-blind phase II study.Methods: Adults with symptomatic PAH, pulmonary vascular resistance (PVR)>240dyne•s/cm5 and 6-minute walk distance (6MWD) between 200–550 m wereequally randomised to three different doses of inhaled aviptadil (12.5, 50 or 200μg 4-times daily) or placebo for 12 weeks. Background therapy with phospho-diesterase type-5 inhibitors or endothelin-receptor antagonists or both was per-mitted. Primary endpoint was acute change in PVR after a single inhalation atbaseline. PVR, 6MWD and NT-pro-BNP plasma levels changes at Week-12 weresecondary end-points. After 12 weeks patients continued treatments until the lastpatient completed the Week-12 assessments.Results: Fifty-six patients were enrolled, 28 were in WHO functional class II and28 in class III. Baseline PVR was 712±367 dyne•s/cm5 and baseline 6MWDwas 445±83m. Eleven, 15, 15, and 15 patients received 12.5, 50, 200μg avip-tadil dose and placebo, respectively. After a single inhalation of aviptadil, therewas not a statistically significant treatment effect on PVR (-29, 95%CL -75 to 15dyne•s/cm5, for all doses combined). Similar results were observed after eachsingle aviptadil dose. At Week 12 there was not a statistically significant treat-ment effect on PVR (-10, 95%CL -130 to 104 dyne•s/cm5, for all doses com-bined), on 6MWD and on NT-pro-BNP plasma levels. At week 12, the estimatedmedian change at through from baseline in 6MWD was 1m, 2m, 4m and 21min the placebo, low, mid and high dose groups, respectively. The data suggestedsome improvement in longer term 6MWD in patients receiving mid and high doseaviptadil relative to the placebo group, but this observation was based on an ex-ploratory analysis that included only 24 patients reaching 6 months of blindedtreatment. No deaths occurred. Incidences of adverse events and serious adverseevents were similar in all treatment groups and in patients receiving placebo.Conclusion: There was not a statistically significant reduction in PVR comparedwith placebo, either after a single inhalation or after 12 weeks of treatment withinhaled aviptadil (for all doses tested) in PAH patients treated with approved oralmedications. Furthermore, no changes were observed on 6MWD or NT-pro-BNPplasma level after 12 weeks. An exploratory analysis suggested some improve-ment on 6MWD after 6 months of treatment with the mid and high aviptadil doses,but these data should be viewed with caution and require confirmation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Pulmonary arterial hypertension / Chronic ischaemic heart disease: update on outcome predictors and treatment 23
348 Exploratory modeling of exercise capacity andhemodynamic endpoints in patients with pulmonaryarterial hypertension
J. Wagg1, L. Claret1, R. Bruno1, K. Dykstra1, X. Gao2, L. Harnisch3.1Pharsight, a Certara™ company, St. Louis, MO, United States of
America; 2Clinical Pharmacology, Pfizer Inc, New London, CT, United States ofAmerica; 3Global Pharmacometrics, Pfizer Ltd, Sandwich, UK, United Kingdom
Purpose: The efficacy of the currently registered medications in the manage-ment of pulmonary arterial hypertension (PAH) is mainly based on showing im-provement in exercise capacity (6-minute walk distance [6MWD]). Hemodynamicendpoints (in particular pulmonary vascular resistance [PVR]) may play an impor-tant role in early drug development or in specific patient populations (eg, pediatricpatients). This study aims to assess the relationship between 6MWD and PVR inPAH patients.Methods: 6MWD and PVR data from 2 pivotal sildenafil studies (SUPER-1[n=194], PACES-1 [n=226]) and 1 sitaxentan trial (STRIDE-1 [n=161]) constitutedthe pooled patient-level database. In addition, the treatment responses from 15PAH trials with treprostinil, beraprost, sitaxentan, iloprost, bosentan, sildenafil,and tadalafil (n=2077 overall) were extracted from publications. Exploratory anal-yses were conducted to assess the relationship between 6MWD and PVR re-sponses based on patient-level or summary data using either simple or mixed-effects linear models.Results: Patient-level data showed a linear relationship between change frombaseline in 6MWD and PVR for each of the 3 studies and across the integrateddatabase (slope [SE], –0.039 [0.008] m/dyne·s·cm-5), P<0.001; n=581). The in-tegrated analysis of summary public domain data confirmed this relationship, as-sessing additionally the impact of treatment and drug class as well as disease-defining characteristics, such as functional class, etiology, and population (age,sex). These findings are consistent with results presented in an analysis con-ducted by the US Food and Drug Administration based on 5 pivotal trials. Accord-ing to these models, a 200 dyne·s·cm-5 improvement in PVR would yield a 22- to33-m improvement in 6MWD.Conclusion: The improvement in exercise capacity (6MWD) is a function of im-provement in PVR. PVR might be a suitable endpoint to assess drug effect inearly clinical and pediatric studies.
CHRONIC ISCHAEMIC HEART DISEASE: UPDATE ONOUTCOME PREDICTORS AND TREATMENT
349 Prognostic value of high-sensitivity cardiac troponin T inpatients with stable and unstable coronary arterydisease presenting with lowest limit of detection ofconventional troponin
G. Ndrepepa, S. Braun, I. Ott, K. Hosl, H. Holle, S. Schulz, J. Mehilli,A. Schomig, A. Kastrati. German Heart Center, Clinic at the Technical Universityof Munich, Munich, Germany
Purpose: The prognostic value of high-sensitivity cardiac troponin T (hs-cTnT) inpatients with stable and unstable coronary artery disease (CAD) presenting withlowest limit of detection of conventional cardiac troponin has not been studied. Weundertook this study to assess the 5-year prognostic value of hs-cTnT in patientswith stable and unstable CAD presenting with a conventional cardiac troponinlevel of 0.01 μg/L.Methods: This study included 1057 patients with stable (n=821) and unstable(n=236) CAD presenting with a conventional cardiac troponin level of 0.01 μg/L.The new hs-cTnT (Roche Diagnostics) with an analytical sensitivity of 0.003 μg/Lwas measured. The primary outcome analyis was 5-year mortality.Results: The hs-cTnT level (median, 25-75 percentiles) was 0.008 [0.004-0.013]μg/L. Based on the median value, patients were divided into 2 groups: the groupwith hs-cTnT >median (high hs-cTnT group, n=565) and the group with hs-cTnT≤median (low hs-cTnT group, n=492). There were 63 deaths in the high hs-cTnTgroup and 23 deaths in the low hs-cTnT group (Kaplan-Meier of 5-year mortality17% and 6%, respectively; odds ratio [OR]=2.69, 95% confidence interval [CI]1.68-4.33, P<0.001, Figure).
hs-cTnT-5y-Mortality
Conclusions: In patients with stable and unstable CAD presenting with lowestlimit of detection of conventional cardiac troponin, hs-cTnT further stratifies pa-tients and markedly improves prediction of long-term mortality.
350 Biomarkers in cardiovascular disease: evidence offluctuation in patient with stable coronary artery disease
F. Cocci1, F. Veneziani2 , F. Petrucci2, G. Lazzerini3, A. Papa4,V. Lubrano4 , D. Battaglia4, S. Cerisano2, A. Mazzarisi4, P. Marraccini4.1University of Pisa, Department of Cardiac, Thoracic and Vascular,
Pisa, Italy; 2Hospital of Santa Maria Nuova, Florence, Italy; 3Institute ofClinical Physiology of CNR, Pisa, Italy; 4Institute of Clinical Physiology of CNR,Foundation G. Monasterio, Pisa, Italy
Purpose: Biomarkers are measured for stratify risk and guide clinical manange-ment in patients (pts) with coronary artery disease (CAD). However little is knownabout the fluctuation of biomarkers and its clinical significance in pts with stableCAD.Methods: 104 pts (mean age 72±9 yrs, 21% female) with stable angina gave aninformed consent and entered the study. The pts were followed every month dur-ing 1 year. At each appointement a clinical evaluation and blood sample weredone. The MACE, NYHA and Canadian class were recorded in a database.The following biomarkers were assayed: osteoprotegerin (OPG, pg/mL), sICAM-1(ng/mL), sVCAM-1 (ng/mL), sE-selectin (ng/mL), sCD40L (ng/mL) and C-reactiveprotein (hsCRP, mg/dL).Results: 88 pts completed the study, 8 pts were censored for MACE (1 car-diac death, 2 non-cardiac death, 3 myocardial infarct, 2 non cardiac disease),8 pts were lost to the follow-up. Thus 1056 blood samples were processed and6336 assays were done. A variation of Canadian or NYHA class was recordedin 17 pts and in 1 pt. The mean, SD and variance in the whole population,the intra-pt minimal and maximal variance (Min and Max-variance) for eachbiomarker are shown in Table 1. A significant correlation was found betweensE-selectin and sVCAM-1 (y=9,071+0,01x; R2=0,067, p<0,0001), sE-selectinand sICAM-1 (y=10,59+0,016x; R2=0,062, p<0,0001), sVCAM-1 and sICAM-1(y=743,44+0,275x; R2=0,027, p<0,0001). An inconsistent correlation was foundbetween NHYA and Canadian class and biomarker concentrations.
Table 1
Biomarker Mean SD Variance Min-Variance Max-Variance
hsCRP 0,314 0,72 0,519 0,0001 8,92OPG 112 191 36127 43,12 38550sICAM-1 458 236 55808 359 45619sVCAM-1 869 390 152210 206 445088sE-selectin 17,84 15,11 228 1,32 563sCD40L 5,02 4,72 22,31 0,214 45,83
Conclusion: in pts with stable CAD a wide fluctuation of biomarkers corre-lated with plaque grow (CRP, OPG), plaque instability (sICAM-1, sVCAM-1, sE-selectin), plaque thrombosis (sCD40L) was found. How these fluctuations reflecta dynamic status of atherosclerotic process and a possible variable susceptibilityto acute coronary episodes remain to be ascertained.
351 Differential characteristics of inflammatory response tostent implantation between de novo and in-stentrestenosis lesion in patients with stable angina
H. Hikita1, E. Nakashima1, T. Fujinami1, K. Ohnishi1, T. Kamiishi1,T. Nozato1, A. Sato2, M. Isobe3, A. Takahashi1 . 1Yokosuka
Kyosai Hospital, Cardiovascular Center, Yokosuka, Japan; 2University ofTsukuba, Graduate School of Comprehensive Human Sciences, Divisionof Cardiovascular, Tsukuba, Japan; 3Tokyo Medical and Dental University,Department of Cardiology, Tokyo, Japan
Background: Mechanical coronary plaque rupture during stent implantation hasbeen reported to cause an increase in serum levels of high sensitivity C-reactiveprotein (hs-CRP). The purpose of the study is to evaluate differential inflammatoryresponse to stenting based on target-lesion morphology.Methods and Results: We measured serum hs-CRP in 226 patients (age64.5±8.4 years, mean±SD, men n=161, women n=65) with stable angina pec-toris before elective percutaneous coronary intervention with stent implantation(PCI-stent) and 24 hours after the completion of PCI-stent without complications.Intravascular ultrasound-Virtual Histology (IVUS-VH) identified the area and per-cent area of four types of plaque component at the target lesion before PCI-stent:fibrous, fibro-fatty, dense calcium, and necrotic core. Study patients were dividedinto two groups:186 patients with de novo lesion who underwent PCI-stent (denovo-group) and 40 patients with intrastent restenosis undergoing PCI-stent (ISR-group). The de novo-group had a significant increase in hs-CRP after PCI-stent(0.21±0.27 mg/dl before, 0.69±0.59 after, p<0.001), while the ISR-group showedno significant increase after stenting (0.32±0.35 before, 0.35±0.23 after). IVUS-VH showed that the de novo-group had larger %necrotic core area (19.7±10.4vs 6.4±5.6, p<0.01) and %fibrofatty area (16.4±11.3 vs 7.2±6.7, p<0.01) thanthe ISR-group, while the ISR-group had larger %fibrous area (81.2±15.3 vs60.5±15.4, p<0.01).Conclusions: Differential inflammatory response to stent implantation betweenin de novo plaque and in ISR lesion is related to lesion morphology.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
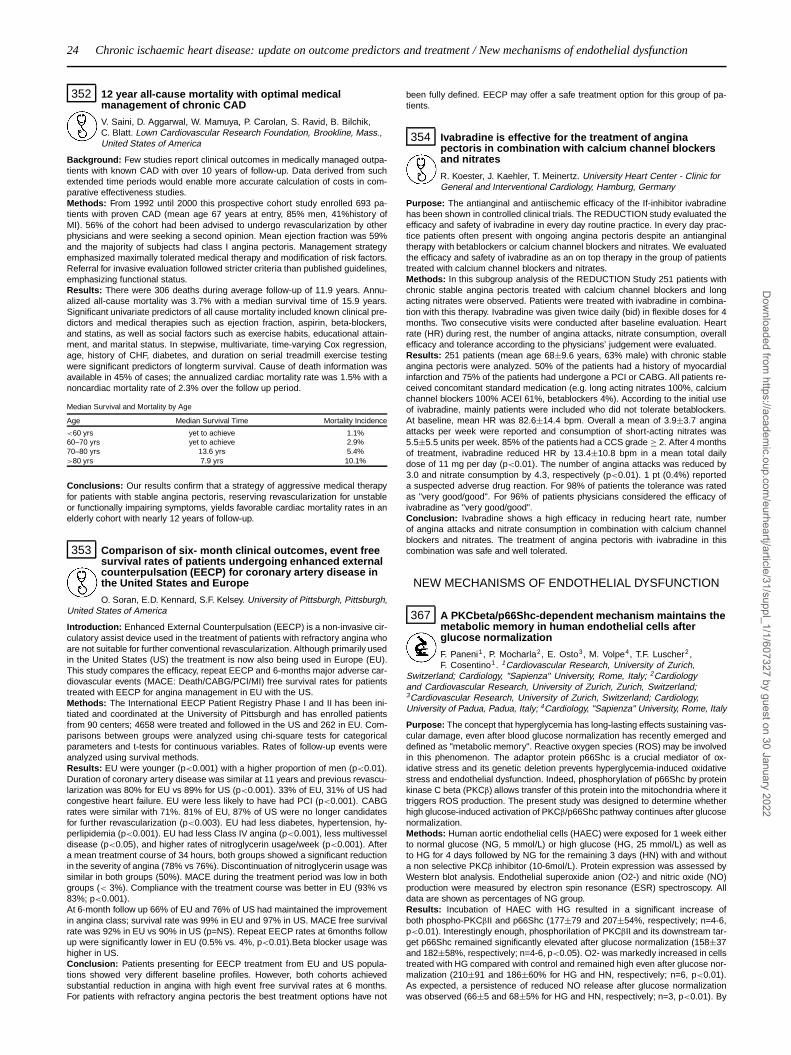
24 Chronic ischaemic heart disease: update on outcome predictors and treatment / New mechanisms of endothelial dysfunction
352 12 year all-cause mortality with optimal medicalmanagement of chronic CAD
V. Saini, D. Aggarwal, W. Mamuya, P. Carolan, S. Ravid, B. Bilchik,C. Blatt. Lown Cardiovascular Research Foundation, Brookline, Mass.,United States of America
Background: Few studies report clinical outcomes in medically managed outpa-tients with known CAD with over 10 years of follow-up. Data derived from suchextended time periods would enable more accurate calculation of costs in com-parative effectiveness studies.Methods: From 1992 until 2000 this prospective cohort study enrolled 693 pa-tients with proven CAD (mean age 67 years at entry, 85% men, 41%history ofMI). 56% of the cohort had been advised to undergo revascularization by otherphysicians and were seeking a second opinion. Mean ejection fraction was 59%and the majority of subjects had class I angina pectoris. Management strategyemphasized maximally tolerated medical therapy and modification of risk factors.Referral for invasive evaluation followed stricter criteria than published guidelines,emphasizing functional status.Results: There were 306 deaths during average follow-up of 11.9 years. Annu-alized all-cause mortality was 3.7% with a median survival time of 15.9 years.Significant univariate predictors of all cause mortality included known clinical pre-dictors and medical therapies such as ejection fraction, aspirin, beta-blockers,and statins, as well as social factors such as exercise habits, educational attain-ment, and marital status. In stepwise, multivariate, time-varying Cox regression,age, history of CHF, diabetes, and duration on serial treadmill exercise testingwere significant predictors of longterm survival. Cause of death information wasavailable in 45% of cases; the annualized cardiac mortality rate was 1.5% with anoncardiac mortality rate of 2.3% over the follow up period.
Median Survival and Mortality by Age
Age Median Survival Time Mortality Incidence
<60 yrs yet to achieve 1.1%60–70 yrs yet to achieve 2.9%70–80 yrs 13.6 yrs 5.4%>80 yrs 7.9 yrs 10.1%
Conclusions: Our results confirm that a strategy of aggressive medical therapyfor patients with stable angina pectoris, reserving revascularization for unstableor functionally impairing symptoms, yields favorable cardiac mortality rates in anelderly cohort with nearly 12 years of follow-up.
353 Comparison of six- month clinical outcomes, event freesurvival rates of patients undergoing enhanced externalcounterpulsation (EECP) for coronary artery disease inthe United States and Europe
O. Soran, E.D. Kennard, S.F. Kelsey. University of Pittsburgh, Pittsburgh,United States of America
Introduction: Enhanced External Counterpulsation (EECP) is a non-invasive cir-culatory assist device used in the treatment of patients with refractory angina whoare not suitable for further conventional revascularization. Although primarily usedin the United States (US) the treatment is now also being used in Europe (EU).This study compares the efficacy, repeat EECP and 6-months major adverse car-diovascular events (MACE: Death/CABG/PCI/MI) free survival rates for patientstreated with EECP for angina management in EU with the US.Methods: The International EECP Patient Registry Phase I and II has been ini-tiated and coordinated at the University of Pittsburgh and has enrolled patientsfrom 90 centers; 4658 were treated and followed in the US and 262 in EU. Com-parisons between groups were analyzed using chi-square tests for categoricalparameters and t-tests for continuous variables. Rates of follow-up events wereanalyzed using survival methods.Results: EU were younger (p<0.001) with a higher proportion of men (p<0.01).Duration of coronary artery disease was similar at 11 years and previous revascu-larization was 80% for EU vs 89% for US (p<0.001). 33% of EU, 31% of US hadcongestive heart failure. EU were less likely to have had PCI (p<0.001). CABGrates were similar with 71%. 81% of EU, 87% of US were no longer candidatesfor further revascularization (p<0.003). EU had less diabetes, hypertension, hy-perlipidemia (p<0.001). EU had less Class IV angina (p<0.001), less multivesseldisease (p<0.05), and higher rates of nitroglycerin usage/week (p<0.001). Aftera mean treatment course of 34 hours, both groups showed a significant reductionin the severity of angina (78% vs 76%). Discontinuation of nitroglycerin usage wassimilar in both groups (50%). MACE during the treatment period was low in bothgroups (< 3%). Compliance with the treatment course was better in EU (93% vs83%; p<0.001).At 6-month follow up 66% of EU and 76% of US had maintained the improvementin angina class; survival rate was 99% in EU and 97% in US. MACE free survivalrate was 92% in EU vs 90% in US (p=NS). Repeat EECP rates at 6months followup were significantly lower in EU (0.5% vs. 4%, p<0.01).Beta blocker usage washigher in US.Conclusion: Patients presenting for EECP treatment from EU and US popula-tions showed very different baseline profiles. However, both cohorts achievedsubstantial reduction in angina with high event free survival rates at 6 months.For patients with refractory angina pectoris the best treatment options have not
been fully defined. EECP may offer a safe treatment option for this group of pa-tients.
354 Ivabradine is effective for the treatment of anginapectoris in combination with calcium channel blockersand nitrates
R. Koester, J. Kaehler, T. Meinertz. University Heart Center - Clinic forGeneral and Interventional Cardiology, Hamburg, Germany
Purpose: The antianginal and antiischemic efficacy of the If-inhibitor ivabradinehas been shown in controlled clinical trials. The REDUCTION study evaluated theefficacy and safety of ivabradine in every day routine practice. In every day prac-tice patients often present with ongoing angina pectoris despite an antianginaltherapy with betablockers or calcium channel blockers and nitrates. We evaluatedthe efficacy and safety of ivabradine as an on top therapy in the group of patientstreated with calcium channel blockers and nitrates.Methods: In this subgroup analysis of the REDUCTION Study 251 patients withchronic stable angina pectoris treated with calcium channel blockers and longacting nitrates were observed. Patients were treated with ivabradine in combina-tion with this therapy. Ivabradine was given twice daily (bid) in flexible doses for 4months. Two consecutive visits were conducted after baseline evaluation. Heartrate (HR) during rest, the number of angina attacks, nitrate consumption, overallefficacy and tolerance according to the physicians’ judgement were evaluated.Results: 251 patients (mean age 68±9.6 years, 63% male) with chronic stableangina pectoris were analyzed. 50% of the patients had a history of myocardialinfarction and 75% of the patients had undergone a PCI or CABG. All patients re-ceived concomitant standard medication (e.g. long acting nitrates 100%, calciumchannel blockers 100% ACEI 61%, betablockers 4%). According to the initial useof ivabradine, mainly patients were included who did not tolerate betablockers.At baseline, mean HR was 82.6±14.4 bpm. Overall a mean of 3.9±3.7 anginaattacks per week were reported and consumption of short-acting nitrates was5.5±5.5 units per week. 85% of the patients had a CCS grade ≥ 2. After 4 monthsof treatment, ivabradine reduced HR by 13.4±10.8 bpm in a mean total dailydose of 11 mg per day (p<0.01). The number of angina attacks was reduced by3.0 and nitrate consumption by 4.3, respectively (p<0.01). 1 pt (0.4%) reporteda suspected adverse drug reaction. For 98% of patients the tolerance was ratedas "very good/good". For 96% of patients physicians considered the efficacy ofivabradine as "very good/good".Conclusion: Ivabradine shows a high efficacy in reducing heart rate, numberof angina attacks and nitrate consumption in combination with calcium channelblockers and nitrates. The treatment of angina pectoris with ivabradine in thiscombination was safe and well tolerated.
NEW MECHANISMS OF ENDOTHELIAL DYSFUNCTION
367 A PKCbeta/p66Shc-dependent mechanism maintains themetabolic memory in human endothelial cells afterglucose normalization
F. Paneni1, P. Mocharla2, E. Osto3, M. Volpe4, T.F. Luscher2 ,F. Cosentino1. 1Cardiovascular Research, University of Zurich,
Switzerland; Cardiology, "Sapienza" University, Rome, Italy; 2Cardiologyand Cardiovascular Research, University of Zurich, Zurich, Switzerland;3Cardiovascular Research, University of Zurich, Switzerland; Cardiology,University of Padua, Padua, Italy; 4Cardiology, "Sapienza" University, Rome, Italy
Purpose: The concept that hyperglycemia has long-lasting effects sustaining vas-cular damage, even after blood glucose normalization has recently emerged anddefined as "metabolic memory". Reactive oxygen species (ROS) may be involvedin this phenomenon. The adaptor protein p66Shc is a crucial mediator of ox-idative stress and its genetic deletion prevents hyperglycemia-induced oxidativestress and endothelial dysfunction. Indeed, phosphorylation of p66Shc by proteinkinase C beta (PKCβ) allows transfer of this protein into the mitochondria where ittriggers ROS production. The present study was designed to determine whetherhigh glucose-induced activation of PKCβ/p66Shc pathway continues after glucosenormalization.Methods: Human aortic endothelial cells (HAEC) were exposed for 1 week eitherto normal glucose (NG, 5 mmol/L) or high glucose (HG, 25 mmol/L) as well asto HG for 4 days followed by NG for the remaining 3 days (HN) with and withouta non selective PKCβ inhibitor (10-6mol/L). Protein expression was assessed byWestern blot analysis. Endothelial superoxide anion (O2-) and nitric oxide (NO)production were measured by electron spin resonance (ESR) spectroscopy. Alldata are shown as percentages of NG group.Results: Incubation of HAEC with HG resulted in a significant increase ofboth phospho-PKCβII and p66Shc (177±79 and 207±54%, respectively; n=4-6,p<0.01). Interestingly enough, phosphorilation of PKCβII and its downstream tar-get p66Shc remained significantly elevated after glucose normalization (158±37and 182±58%, respectively; n=4-6, p<0.05). O2- was markedly increased in cellstreated with HG compared with control and remained high even after glucose nor-malization (210±91 and 186±60% for HG and HN, respectively; n=6, p<0.01).As expected, a persistence of reduced NO release after glucose normalizationwas observed (66±5 and 68±5% for HG and HN, respectively; n=3, p<0.01). By
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

New mechanisms of endothelial dysfunction 25
contrast, glucose normalization in the presence of non selective PKCβ inhibitionabolished p66Shc phosphorilation (108±33%, p=NS) as well as O2- production(107±35%, p=NS) and restored NO availability to control values (92±1%, p=NS).Conclusions: These results demonstrate that PKCβ/p66Shc pathway may playa crucial role in triggering persistence of vascular dysfunction after blood glucosenormalization. Indeed, PKCβ inhibition via blockade of downstream p66Shc abol-ishes ROS-mediated metabolic memory. Our study provides molecular insightsfor understanding the progression of diabetic complications despite tight glycemiccontrol. The use of PKCβ inhibitors may support hypoglycemic therapy in diabeticpatients.
368 Genetic deletion of poly (ADP-ribose) polymerase-1promotes oxidative stress induced endothelialdysfunction
C. Gebhard1, B.E. Stahli1, G.G. Camici2, A. Akhmedov2 , L. Hogger2 ,P.O. Hassa3, M.O. Hottiger3, T.F. Luscher1 , F.C. Tanner1 . 1Cardiology,Cardiovascular Center, University Hospital Zürich, Zürich, Switzerland;
2Cardiovascular Research, Physiology Institute, University of Zürich, Zürich,Switzerland; 3Institute of Veterinary Biochemistry and Molecular Biology,University of Zürich, Zürich, Switzerland
Purpose: Production of reactive oxygen species (ROS) and loss of endothelialNO bioavailability are key features in endothelial dysfunction. The nuclear enzymepoly (adenosine diphosphate [ADP]-ribose) polymerase-1 (PARP-1) is considereda downstream effector of oxidative stress, leading to NAD+ consumption and ATPdepletion. Furthermore, PARP-1 activation is involved in DNA repair. This studywas designed to examine the effect of genetic PARP-1 deletion on oxidative stressinduced vascular dysfunction.Methods: PARP-1(-/-) mice and wild type (WT) control were injected withparaquat (PQ) (10 mg/kg of body weight) or sodium chloride 24 hours prior toexperiment. Thoracic aortae were harvested and suspended in organ chambersfor isometric tension recording.Results: PQ markedly impaired endothelium-dependent relaxations to acetyl-choline in PARP-1(-/-) mice as compared to WT control; maximal relaxation inPQ treated PARP-1 (-/-) mice was 45% as compared to 80% in WT control.Relaxations to sodium nitroprusside did not differ. Basal vascular tone as wellas contractions to norepinephrine were enhanced in PQ treated PARP-1(-/-)mice, while receptor-independent contractions to KCl reached similar levels in allgroups. Untreated PARP-1(-/-) mice did not develop such alterations; moreoverendothelial function remained unaffected in WT mice with or without PQ treat-ment. Indomethacin (10E-5 mol/L) completely reversed impaired relaxations toacetylcholine in PQ treated PARP-1(-/-) mice, and attenuated enhanced nore-pinephrine induced contractions. Both, superoxide dismutase (150 U/ml) andcatalase (150 U/ml), completely restored endothelium-dependent relaxations inPQ treated PARP-1(-/-) mice. After pretreatment with N(omega)-nitro-L-argininemethyl ester (L-NAME), contractions to acetylcholine and basal vascular tonewere enhanced in PQ treated PARP-1(-/-) mice.Conclusions: This study demonstrates that genetic PARP-1 deletion promotesoxidative stress induced endothelial dysfunction. These effects are mediated viaenhanced production of cyclooxygenase derived ROS mediating vasoconstric-tion. Hence, PARP-1 may exert a protective effect on endothelial function underconditions of oxidative stress.
369 Membrane Type I Matrix Metalloproteinase (MT1-MMP)mediates thrombin-induced RhoA/Rac1 activation andtheir downstream signaling in endothelial cells
K. Ando1, T. Ishibashi1, H. Ohkawara1, K. Sugimoto1, N. Sakamoto1,Y. Okamoto2, Y. Takuwa2, Y. Takeishi1. 1Fukushima Medical University,
Fukushima, Japan; 2Kanazawa University Graduate School of Medicine,Kanazawa, Japan
Background: Thrombin induces vascular responses including the molecular ex-pression of tissue factor (TF) and plasminogen activator inhibitor-1 (PAI-1), whichis modulated by RhoA-dependent Ca2+ and Rac1-mediated redox signaling path-ways. Recent studies have shown that membrane type I matrix metalloproteinase(MT1-MMP) functions not only as a protease but also as a signaling molecule.We have shown an integral role of MT1-MMP in oxidized LDL-induced endothe-lial dysfunction. Hypothesis: MT1-MMP may mediate RhoA and Rac1 activationand their downstream events including Ca2+ signaling, reactive oxygen species(ROS) generation and protein expression of TF and PAI-1 in response to thrombinin endothelial cells (ECs).Methods: We used cultured human aortic ECs. MT1-MMP was knockdowned bysmall interfering RNA (siRNA). RhoA was inhibited by C3 exoenzyme, whereasRac1 was inhibited by adenovirus-mediated gene transfection of dominant neg-ative Rac1. RhoA and Rac1 activation was determined by a pull-down assay.Intracellular Ca2+ concentration ([Ca2+]i) was fluorescently measured by fura-2assay. NADPH oxidase activity was determined by a luminescence assay. De-tection of intracellular ROS generation was performed using the ROS-sensitivefluorescent probe 2’,7’-dichlorodihydro-fluorescein-diacetate (H2DCF-DA).Results: Pull-down assay revealed that silencing of MT1-MMP by siRNA atten-uated RhoA and Rac1 activation in thrombin-stimulated ECs. Inhibition of RhoAsuppressed [Ca2+]i increase in response to thrombin in presence or absence of
extracellular Ca2+, whereas the expression of TF and PAI-1 was attenuated bypretreatment of ECs with BAPTA/AM, a Ca2+ chelator or with C3 exoenzyme. In-hibition of Rac1 blocked NADPH oxidsase activity and ROS generation as well asTF and PAI-1 expression, whereas thrombin-activated TF and PAI-1 expressionwas blocked by a NADPH oxidase inhibitor and an antioxidant. Finally, silencing ofMT1-MMP attenuated thrombin-induced intracellular Ca2+ mobilization, NADPHoxidase activity, and ROS generation as well as TF and PAI-1 expression.Conclusions: We show a new insight into the signaling pathways involved inMT1-MMP in thrombin-triggered endothelial responses including RhoA and Rac1activation and their downstream events, indicating a crucial role of MT1-MMPin agonist-induced endothelial responses. The present study suggests that thissignaling axis of MT1-MMP/RhoA·Rac1 may be an attractive target for endothelialdysfunction of coronary artery disease.
370 Asymmetrical dimethylarginine as a mediator ofendothelial dysfunction in acute inflammation atdifferent disease stages
M. Demosthenous1 , C. Antoniades1, A.S. Antonopoulos1, D. Tousoulis1 ,C. Bakogiannis1, C. Vlachopoulos1, K. Petrochilou1, M. Toutouza1 ,
K.M. Channon2 , C. Stefanadis1. 1Hippokration Hospital, University of Athens,Athens, Greece; 2University of Oxford, Oxford, United Kingdom
Purpose: Low grade inflammation is a major determinant of endothelial dysfunc-tion in patients with advanced atherosclerosis, but the exact mechanisms linkinginflammation with endothelial function are unclear. We examined the role of asym-metrical dimethylarginine (ADMA), an endogenous inhibitor of endothelial nitricoxide synthase (eNOS), as a link between acute inflammation and endothelialdysfunction before and after the development of advanced atherosclerosis.Methods: The study population consisted of 20 healthy individuals (Part A) and62 patients with coronary artery disease (CAD, Part B). Subjects in Part A wererandomized to receive vaccination by using Salmonella Typhii vaccine or placebo(n=10 per group) and followed up for 24 hours. Patients in Part B were then ran-domized to receive vaccination (n=54) or placebo (n=8) and followed up for 8hours. Endothelial function was evaluated by brachial artery flow mediated dila-tion (FMD), while interleukin 6 (IL-6) and ADMA were measured by ELISA.Results: Acute inflammation documented by a raise of IL-6 at 8h and 12h (Fig. Afor healthy individuals and Fig. B for CAD) resulted in a simultaneous decrease ofFMD in both healthy (Fig. C) and CAD (Fig. D). However, circulating ADMA wasincreased only in healthy (Fig. E) but not in CAD (Fig. F).
*p<0.05; **p<0.01 vs 0h
Conclusions: Acute inflammation leads to a rapid decline of endothelial functionin both healthy individuals and patients with CAD. Importantly, endothelial dys-function is accompanied by an elevation of ADMA only in healthy but not in CADpatients, suggesting that ADMA may be a mediator of inflammation-induced en-dothelial dysfunction leading to atherogenesis, but its expression after the devel-opment of CAD is regulated by mechanisms other than background inflammation.
371 Chronic hypoxemia alone induces major vasculardysfunction in the absence of additional cardiovascularrisk factors
S.F. Rimoldi1, C. Sartori2, E. Rexhaj2, M. Villena3, U. Scherrer2,Y. Allemann1. 1Swiss Cardiovascular Center Bern, University Hospital
Bern, Bern, Switzerland; 2University Hospital Center Vaudois, Department ofInternal Medicine, Lausanne, Switzerland; 3Bolivian Institute of High AltitudeBiology, La Paz, Bolivia
Objectives: Patients suffering from diseases associated with chronic hypoxemia(such as obstructive sleep apnea or chronic obstructive pulmonary disease) areat increased risk for cardiovascular (CV) morbidity. Because these patients oftenhave several additional CV risk factors such as smoking, hypertension and obe-sity, it is difficult to differentiate the contribution of these risk factors and those ofchronic hypoxemia on the development of systemic vascular dysfunction and CVrisk.Chronic mountain sickness (CMS) is characterized by chronic hypoxemia relatedat least in part to hypoventilation and allows to study the effects of chronic hypoxiaon vascular function in the absence of other confounding CV risk factors.Methods: We assessed endothelium-dependent (flow-mediated vasodilation,FMD) and -independent (glycerin trinitrate, 250 μg, per os) vasodilation, vascular
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
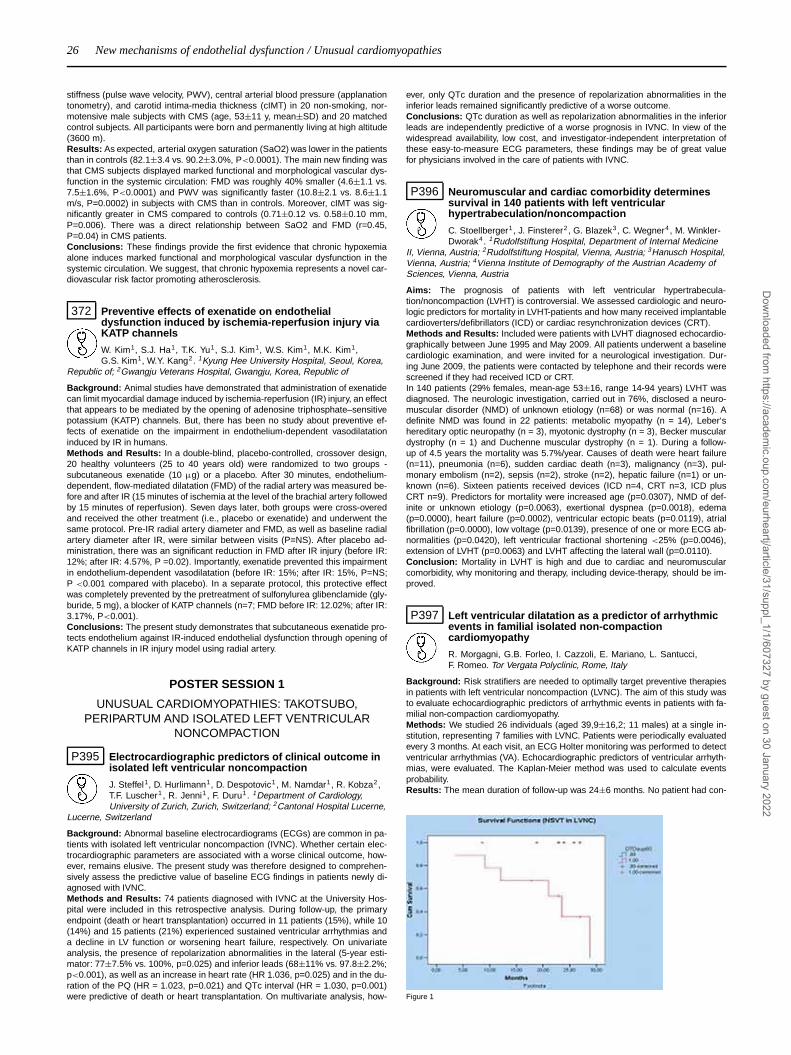
26 New mechanisms of endothelial dysfunction / Unusual cardiomyopathies
stiffness (pulse wave velocity, PWV), central arterial blood pressure (applanationtonometry), and carotid intima-media thickness (cIMT) in 20 non-smoking, nor-motensive male subjects with CMS (age, 53±11 y, mean±SD) and 20 matchedcontrol subjects. All participants were born and permanently living at high altitude(3600 m).Results: As expected, arterial oxygen saturation (SaO2) was lower in the patientsthan in controls (82.1±3.4 vs. 90.2±3.0%, P<0.0001). The main new finding wasthat CMS subjects displayed marked functional and morphological vascular dys-function in the systemic circulation: FMD was roughly 40% smaller (4.6±1.1 vs.7.5±1.6%, P<0.0001) and PWV was significantly faster (10.8±2.1 vs. 8.6±1.1m/s, P=0.0002) in subjects with CMS than in controls. Moreover, cIMT was sig-nificantly greater in CMS compared to controls (0.71±0.12 vs. 0.58±0.10 mm,P=0.006). There was a direct relationship between SaO2 and FMD (r=0.45,P=0.04) in CMS patients.Conclusions: These findings provide the first evidence that chronic hypoxemiaalone induces marked functional and morphological vascular dysfunction in thesystemic circulation. We suggest, that chronic hypoxemia represents a novel car-diovascular risk factor promoting atherosclerosis.
372 Preventive effects of exenatide on endothelialdysfunction induced by ischemia-reperfusion injury viaKATP channels
W. Kim1, S.J. Ha1, T.K. Yu1, S.J. Kim1, W.S. Kim1, M.K. Kim1,G.S. Kim1, W.Y. Kang2. 1Kyung Hee University Hospital, Seoul, Korea,
Republic of; 2Gwangju Veterans Hospital, Gwangju, Korea, Republic of
Background: Animal studies have demonstrated that administration of exenatidecan limit myocardial damage induced by ischemia-reperfusion (IR) injury, an effectthat appears to be mediated by the opening of adenosine triphosphate–sensitivepotassium (KATP) channels. But, there has been no study about preventive ef-fects of exenatide on the impairment in endothelium-dependent vasodilatationinduced by IR in humans.Methods and Results: In a double-blind, placebo-controlled, crossover design,20 healthy volunteers (25 to 40 years old) were randomized to two groups -subcutaneous exenatide (10 μg) or a placebo. After 30 minutes, endothelium-dependent, flow-mediated dilatation (FMD) of the radial artery was measured be-fore and after IR (15 minutes of ischemia at the level of the brachial artery followedby 15 minutes of reperfusion). Seven days later, both groups were cross-overedand received the other treatment (i.e., placebo or exenatide) and underwent thesame protocol. Pre-IR radial artery diameter and FMD, as well as baseline radialartery diameter after IR, were similar between visits (P=NS). After placebo ad-ministration, there was an significant reduction in FMD after IR injury (before IR:12%; after IR: 4.57%, P =0.02). Importantly, exenatide prevented this impairmentin endothelium-dependent vasodilatation (before IR: 15%; after IR: 15%, P=NS;P <0.001 compared with placebo). In a separate protocol, this protective effectwas completely prevented by the pretreatment of sulfonylurea glibenclamide (gly-buride, 5 mg), a blocker of KATP channels (n=7; FMD before IR: 12.02%; after IR:3.17%, P<0.001).Conclusions: The present study demonstrates that subcutaneous exenatide pro-tects endothelium against IR-induced endothelial dysfunction through opening ofKATP channels in IR injury model using radial artery.
POSTER SESSION 1
UNUSUAL CARDIOMYOPATHIES: TAKOTSUBO,PERIPARTUM AND ISOLATED LEFT VENTRICULAR
NONCOMPACTION
P395 Electrocardiographic predictors of clinical outcome inisolated left ventricular noncompaction
J. Steffel1, D. Hurlimann1, D. Despotovic1 , M. Namdar1, R. Kobza2,T.F. Luscher1 , R. Jenni1, F. Duru1. 1Department of Cardiology,University of Zurich, Zurich, Switzerland; 2Cantonal Hospital Lucerne,
Lucerne, Switzerland
Background: Abnormal baseline electrocardiograms (ECGs) are common in pa-tients with isolated left ventricular noncompaction (IVNC). Whether certain elec-trocardiographic parameters are associated with a worse clinical outcome, how-ever, remains elusive. The present study was therefore designed to comprehen-sively assess the predictive value of baseline ECG findings in patients newly di-agnosed with IVNC.Methods and Results: 74 patients diagnosed with IVNC at the University Hos-pital were included in this retrospective analysis. During follow-up, the primaryendpoint (death or heart transplantation) occurred in 11 patients (15%), while 10(14%) and 15 patients (21%) experienced sustained ventricular arrhythmias anda decline in LV function or worsening heart failure, respectively. On univariateanalysis, the presence of repolarization abnormalities in the lateral (5-year esti-mator: 77±7.5% vs. 100%, p=0.025) and inferior leads (68±11% vs. 97.8±2.2%;p<0.001), as well as an increase in heart rate (HR 1.036, p=0.025) and in the du-ration of the PQ (HR = 1.023, p=0.021) and QTc interval (HR = 1.030, p=0.001)were predictive of death or heart transplantation. On multivariate analysis, how-
ever, only QTc duration and the presence of repolarization abnormalities in theinferior leads remained significantly predictive of a worse outcome.Conclusions: QTc duration as well as repolarization abnormalities in the inferiorleads are independently predictive of a worse prognosis in IVNC. In view of thewidespread availability, low cost, and investigator-independent interpretation ofthese easy-to-measure ECG parameters, these findings may be of great valuefor physicians involved in the care of patients with IVNC.
P396 Neuromuscular and cardiac comorbidity determinessurvival in 140 patients with left ventricularhypertrabeculation/noncompaction
C. Stoellberger1, J. Finsterer2, G. Blazek3, C. Wegner4 , M. Winkler-Dworak4. 1Rudolfstiftung Hospital, Department of Internal Medicine
II, Vienna, Austria; 2Rudolfstiftung Hospital, Vienna, Austria; 3Hanusch Hospital,Vienna, Austria; 4Vienna Institute of Demography of the Austrian Academy ofSciences, Vienna, Austria
Aims: The prognosis of patients with left ventricular hypertrabecula-tion/noncompaction (LVHT) is controversial. We assessed cardiologic and neuro-logic predictors for mortality in LVHT-patients and how many received implantablecardioverters/defibrillators (ICD) or cardiac resynchronization devices (CRT).Methods and Results: Included were patients with LVHT diagnosed echocardio-graphically between June 1995 and May 2009. All patients underwent a baselinecardiologic examination, and were invited for a neurological investigation. Dur-ing June 2009, the patients were contacted by telephone and their records werescreened if they had received ICD or CRT.In 140 patients (29% females, mean-age 53±16, range 14-94 years) LVHT wasdiagnosed. The neurologic investigation, carried out in 76%, disclosed a neuro-muscular disorder (NMD) of unknown etiology (n=68) or was normal (n=16). Adefinite NMD was found in 22 patients: metabolic myopathy (n = 14), Leber‘shereditary optic neuropathy (n = 3), myotonic dystrophy (n = 3), Becker musculardystrophy (n = 1) and Duchenne muscular dystrophy (n = 1). During a follow-up of 4.5 years the mortality was 5.7%/year. Causes of death were heart failure(n=11), pneumonia (n=6), sudden cardiac death (n=3), malignancy (n=3), pul-monary embolism (n=2), sepsis (n=2), stroke (n=2), hepatic failure (n=1) or un-known (n=6). Sixteen patients received devices (ICD n=4, CRT n=3, ICD plusCRT n=9). Predictors for mortality were increased age (p=0.0307), NMD of def-inite or unknown etiology (p=0.0063), exertional dyspnea (p=0.0018), edema(p=0.0000), heart failure (p=0.0002), ventricular ectopic beats (p=0.0119), atrialfibrillation (p=0.0000), low voltage (p=0.0139), presence of one or more ECG ab-normalities (p=0.0420), left ventricular fractional shortening <25% (p=0.0046),extension of LVHT (p=0.0063) and LVHT affecting the lateral wall (p=0.0110).Conclusion: Mortality in LVHT is high and due to cardiac and neuromuscularcomorbidity, why monitoring and therapy, including device-therapy, should be im-proved.
P397 Left ventricular dilatation as a predictor of arrhythmicevents in familial isolated non-compactioncardiomyopathy
R. Morgagni, G.B. Forleo, I. Cazzoli, E. Mariano, L. Santucci,F. Romeo. Tor Vergata Polyclinic, Rome, Italy
Background: Risk stratifiers are needed to optimally target preventive therapiesin patients with left ventricular noncompaction (LVNC). The aim of this study wasto evaluate echocardiographic predictors of arrhythmic events in patients with fa-milial non-compaction cardiomyopathy.Methods: We studied 26 individuals (aged 39,9±16,2; 11 males) at a single in-stitution, representing 7 families with LVNC. Patients were periodically evaluatedevery 3 months. At each visit, an ECG Holter monitoring was performed to detectventricular arrhythmias (VA). Echocardiographic predictors of ventricular arrhyth-mias, were evaluated. The Kaplan-Meier method was used to calculate eventsprobability.Results: The mean duration of follow-up was 24±6 months. No patient had con-
Figure 1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Unusual cardiomyopathies: Takotsubo, peripartum and isolated left ventricular noncompaction 27
comitant hypertension, diabetes mellitus or other significant cardiovascular disor-der. Left ventricular (LV) systolic function was depressed in 10 patients (38,5%),with a mean ejection fraction (EF) of 44,0% ± 3,2% at diagnosis. Nine patients(34,6%) had LV dilatation (EDD ≥ 60 mm). Among them only 5 patients (55,5%)had EF < 45%. Two patients (7,7%) had non-sustained ventricular tachycardia on24 h Holter monitoring. Ventricular tachycardia (VT) was evidenced in 6 patients(23,1%), all of them with LV dilatation. Three patients (50%) with VT had LVEF <
45%. By Kaplan Meier analysis, the only echocardiographic predictor of VA wasLV dilatation (p <0.001; Figure1).Conclusions: In families with LVNC, left ventricular dilatation was the onlyechocardiographic predictor factor associated with subsequent development ofVA. This finding might be helpful to optimally target preventive therapies in pa-tients with familial LVNC.
P398 Prognosis of non-compaction cardiomyopathy in thepediatric population
M. Veyrier1, G. Teyssier2 , R. Henaine1, F. Sassolas1, C. Ducreux1,M. Gouton1, J. Ninet1, A. Bozio1, S. Di Filippo1. 1University Hospitalof Lyon - Hospital Louis Pradel, Lyon, France; 2University Hospital of
Saint Etienne - Hospital Nord, Saint Etienne, France
The aim of this study was to determine factors of outcome in children diagnosedwith non-compaction of the myocardium.Material and methods: Patients less than 18years of age with diagnosis of non-compaction of the myocardium (according to echocardiographic criteria) were re-viewed for clinical, ECG and echocardiographic data and outcomes. Cases withstructural congenital heart disease were excluded.Results: From 1996 to 2009, 31 patients (17 males), aged 0 to 207months atdiagnosis (median 7.5months), were followed-up for 0.5 to 99months (median12.5months). Seventeen presented with heart failure (55%), 14 (45%) with syn-copes or chest pain or no symptom. Familial reccurrence was 48%. ECG wasabnormal in all cases, QT>440ms in 22.5%. Non compacted/Compacted indexwas 1.6±3.5 (median 2.3) and >2 in 54.8% (17cases). LV apex was involved in96.7%, with more than 3 locations in 29% and RV involvement in 13%. Shorteningfraction was 24.8±11.6% (median 24%). Six patients died (19.3%) at median age7.7months (3.6 to 43) and median follow-up 2.7months (0.5 to 12.7). Five under-went heart transplantation (16%) at median age 12months (6 to 72) and medianfollow-up 2.8months (1.8 to 27.8). At least one episode of heart failure occurredin 17 (57%), arrhythmic or thromboembolic events in respectively 4 (13%) and3 (9.6%). Freedom from death or transplantation was 70% at 6months and 60%at 1 and 5years follow-up. Age at diagnosis < 1year, low shortening fraction,Non compacted/Compacted index >2, three locations or more, heart failure andthromboembolic events were factors for poor prognosis.Conclusion: Non-compaction cardiomyopathy in children carries on high rate ofmortality and morbidity. Heart loss occurs more frequently within 3months after di-agnosis in infants with severely impaired systolic function and/or thromboembolicevents.
P399 Peripartum cardiomyopathy as a part of familial dilatedcardiomyopathy
K.Y. Van Spaendonck-Zwarts1 , J.P. Van Tintelen1, D.J. VanVeldhuisen2, R. Van Der Werf2, J.D.H. Jongbloed1, W.J. Paulus3,D. Dooijes4, M.P. Van Den Berg2. 1University Medical Center,
Department of Genetics, groningen, Netherlands; 2University Medical Center,Department of Cardiology, groningen, Netherlands; 3VU University MedicalCenter, Department of Physiology, amsterdam, Netherlands; 4Erasmus MedicalCenter, Department of Genetics, rotterdam, Netherlands
Purpose: Anecdotal cases of familial clustering of peripartum cardiomyopathy(PPCM) and familial occurrence of both PPCM and idiopathic dilated cardiomy-opathy (DCM) have been observed, suggesting that genetic factors may play arole in the pathogenesis of PPCM. We hypothesized that some cases of PPCMare part of the spectrum of familial DCM, presenting in the peripartum period.Methods: Firstly, we reviewed our database of 90 DCM families focussing specif-ically on the presence of PPCM patients. Secondly, in a reverse approach, wereviewed 10 PPCM patients observed in our clinic since the early nineties and weperformed cardiological screening of the first degree relatives of three PPCM pa-tients without recovery. Finally, we analyzed the genes most commonly involvedin DCM in the PPCM patients.Results: We identified a substantial number (5/90, 6%) of DCM families withPPCM patients. Secondly, cardiological screening of first degree relatives ofPPCM patients revealed thus far undiagnosed DCM in all three families ofPPCM patients without recovery. Finally, genetic analysis revealed a mutation(c.149A>G, p.Gln50Arg) in the gene encoding cardiac troponin C (TNNC1) seg-regating with disease in a DCM family with a member with PPCM, providing prooffor the genetic nature of disease in this case.Conclusion: These findings strongly suggest that a subset of PPCM is an initialmanifestation of familial DCM. This may have important implications for cardio-logical screening in these families.
P400 Risk factors for disease development and predictors ofoutcome in peripartum cardiomyopathy
N.B.A. Ntusi, B.M. Mayosi. University of Cape Town, Groote SchuurHospital, Cape Town, South Africa
Background: Risk factors for development of peripartum cardiomy-opathy (PPCM) are poorly understood. Reports on outcome of PPCM are con-flicting, with variable mortality rates reported by different authors.Purpose: To define the risk factors for development of PPCM and the predictorsof survival outcome in PPCM.Methods: Retrospective analysis of the medical records of patients diagnosedwith PPCM at the Groote Schuur Hospital Cardiac Clinic, South Africa, betweenFebruary 1 1996 and December 31 2009. Diagnosis of PPCM was based ondevelopment of heart failure between the last month of pregnancy and fifth post-partum month in women without pre-existing heart disease, or any other identi-fiable cause of heart failure, including pregnancy-induced hypertension. Patientsalso needed to fulfill established echocardiographic criteria for diagnosis. Mea-surements from clinical assessment, chest radiography, electrocardiography, two-dimensional and Doppler colour-flow echocardiography and cardiac catheterisa-tion (where available) were reviewed.Results: There were 30 PPCM patients studied, with a mean age of 31.45±7.48years. Ethnicity, gravidity, parity, and unemployment were not associated with in-creased risk of developing PPCM in this study. However, twin pregnancy emergedas a significant risk factor for disease development in PPCM (p<0.001). The me-dian follow-up was 4.33 years (range 0.16 − 13.8). During the study period 5(16.6%) subjects died and 24 (80%) patients remained in chronic heart failure.Complications included intra-cardiac thrombus formation (16.7%), atrial fibrilla-tion (10.0%), stroke (6.7%), and pulmonary hypertension (13.3%). One patienthad cardiac resynchronisation therapy and another patient had orthotopic hearttransplantation. Predictors of increased mortality in the time-to-event analysis in-cluded twin pregnancy (p<0.001), heart rate greater than 120 bpm at first clinicvisit (p=0.017), presence of atrial fibrillation (p=0.023), use of warfarin (p=0.019),and NYHA functional class III and IV symptoms at last visit (p=0.005). On multi-variate logistic regression analysis only NYHA functional class III/IV status at lastvisit was a significant predictor of mortality (OR 3.107 [1.329 − 11.981], p=0.047).Conclusions: PPCM affects young women, with significant morbidity and mortal-ity. Mortality in this study is lower than in many other previously reported studies.Twin pregnancy is a risk factor for development of PPCM. The NYHA functionalclass emerges as a powerful predictor of mortality in this study.
P401 Echocardiographic evaluation of patients with acuteheart failure during pregnancy with or withoutidentifiable precipitating factors
R. Kuperstein, M.J. Simchen, Y. Frenkel, M.S. Feinberg, D. Freimark.Tel Hashomer Hospital, Ramat Gan, Israel
Background: Peripartum cardiomyopathy (PPCM) is defined as the onset of car-diac failure without identifiable cause 1 month pre, to 5 months post-partum. Be-cause it is difficult to distinguish between classical PPCM and acute heart fail-ure (AHF) due to a precipitating factor (PF), most such patients are usually dis-charged with a diagnosis of PPCM, an ominous prognostic factor regarding futurepregnancies.Methods: We studied women diagnosed with PPCM according to Leviev HeartCenter registry between 1998-2009 in order to differentiate between patients withand without PF. Mean follow up time was 39±38 months (1-140).Results: 41 women were diagnosed with PPCM. Seventeen had identifiable PFfor AHF (5 hypertensive crisis or eclampsia, 6 acute blood dyscrasia with massivefluid reposition, 2 sepsis, 4 other causes). Presentation with acute pulmonaryedema was more common in women with PF (58% vs 25%, p=0.05).During the follow up period 83% of the patients with vs. 30% of the patients with-out PF improved their LVEF to ≥50% (p<0.01).
Echocardigraphic characteristics of patients with AHF with and without PF
AHF with PF (n=17) AHF without PF (n=24) p
LVEDD (mm) 51±6 57±7 0.01LVESD (mm) 39±6 46±7 0.03LVEDD/BSA (mm/m2) 29±3 32±4 0.01LVEF (%) 35±9 27±10 0.006SF (%) 23±8 19±6 0.1
LVEF, LV ejection fraction; LVEDD, LV end-diastolic dimension; LVESD, LV end-systolic dimen-sion; BSA, body surface area.
Conclusions: Women who develop AHF with identifiable PF have smaller base-line LV dimensions and better LVEF then patients without PF. Unlike patients withheart failure without PF (PPCM), most of the patients with AHF+PF recover LVfunction allowing positive consideration of future pregnancies.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
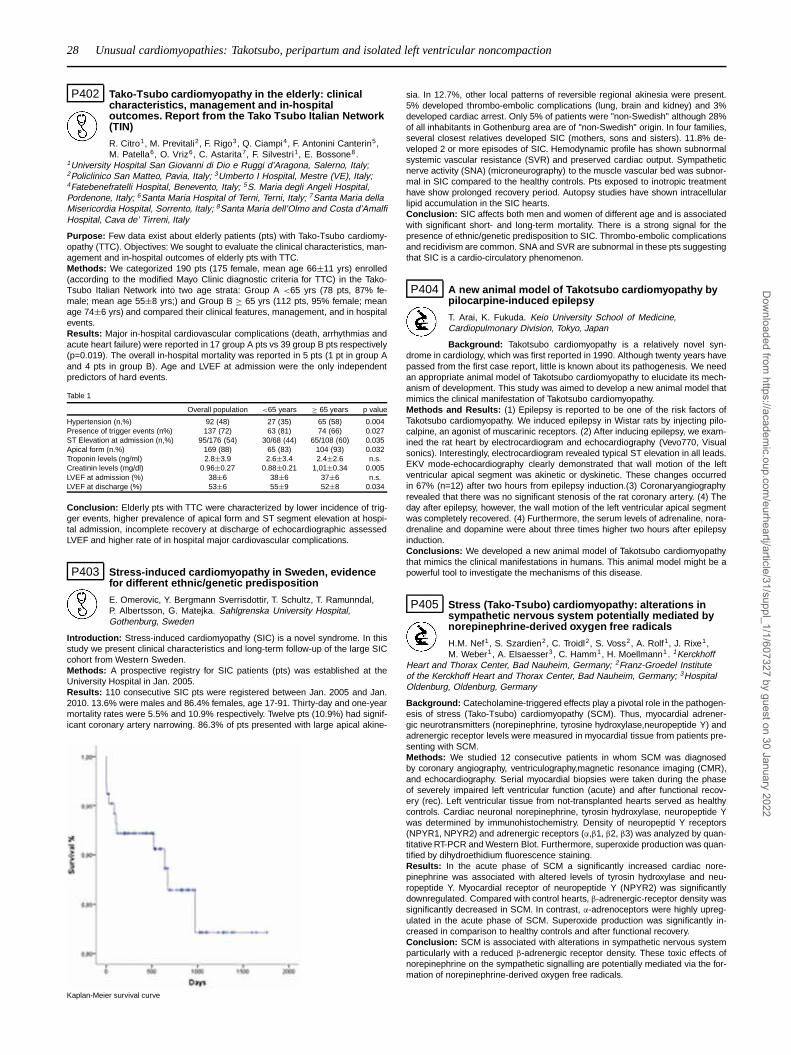
28 Unusual cardiomyopathies: Takotsubo, peripartum and isolated left ventricular noncompaction
P402 Tako-Tsubo cardiomyopathy in the elderly: clinicalcharacteristics, management and in-hospitaloutcomes. Report from the Tako Tsubo Italian Network(TIN)
R. Citro1, M. Previtali2, F. Rigo3, Q. Ciampi4, F. Antonini Canterin5,M. Patella6, O. Vriz6, C. Astarita7, F. Silvestri1, E. Bossone8.
1University Hospital San Giovanni di Dio e Ruggi d’Aragona, Salerno, Italy;2Policlinico San Matteo, Pavia, Italy; 3Umberto I Hospital, Mestre (VE), Italy;4Fatebenefratelli Hospital, Benevento, Italy; 5S. Maria degli Angeli Hospital,Pordenone, Italy; 6Santa Maria Hospital of Terni, Terni, Italy; 7Santa Maria dellaMisericordia Hospital, Sorrento, Italy; 8Santa Maria dell’Olmo and Costa d’AmalfiHospital, Cava de’ Tirreni, Italy
Purpose: Few data exist about elderly patients (pts) with Tako-Tsubo cardiomy-opathy (TTC). Objectives: We sought to evaluate the clinical characteristics, man-agement and in-hospital outcomes of elderly pts with TTC.Methods: We categorized 190 pts (175 female, mean age 66±11 yrs) enrolled(according to the modified Mayo Clinic diagnostic criteria for TTC) in the Tako-Tsubo Italian Network into two age strata: Group A <65 yrs (78 pts, 87% fe-male; mean age 55±8 yrs;) and Group B ≥ 65 yrs (112 pts, 95% female; meanage 74±6 yrs) and compared their clinical features, management, and in hospitalevents.Results: Major in-hospital cardiovascular complications (death, arrhythmias andacute heart failure) were reported in 17 group A pts vs 39 group B pts respectively(p=0.019). The overall in-hospital mortality was reported in 5 pts (1 pt in group Aand 4 pts in group B). Age and LVEF at admission were the only independentpredictors of hard events.
Table 1
Overall population <65 years ≥ 65 years p value
Hypertension (n,%) 92 (48) 27 (35) 65 (58) 0.004Presence of trigger events (n%) 137 (72) 63 (81) 74 (66) 0.027ST Elevation at admission (n,%) 95/176 (54) 30/68 (44) 65/108 (60) 0.035Apical form (n.%) 169 (88) 65 (83) 104 (93) 0.032Troponin levels (ng/ml) 2.8±3.9 2.6±3.4 2.4±2.6 n.s.Creatinin levels (mg/dl) 0.96±0.27 0.88±0.21 1,01±0.34 0.005LVEF at admission (%) 38±6 38±6 37±6 n.s.LVEF at discharge (%) 53±6 55±9 52±8 0.034
Conclusion: Elderly pts with TTC were characterized by lower incidence of trig-ger events, higher prevalence of apical form and ST segment elevation at hospi-tal admission, incomplete recovery at discharge of echocardiographic assessedLVEF and higher rate of in hospital major cardiovascular complications.
P403 Stress-induced cardiomyopathy in Sweden, evidencefor different ethnic/genetic predisposition
E. Omerovic, Y. Bergmann Sverrisdottir, T. Schultz, T. Ramunndal,P. Albertsson, G. Matejka. Sahlgrenska University Hospital,Gothenburg, Sweden
Introduction: Stress-induced cardiomyopathy (SIC) is a novel syndrome. In thisstudy we present clinical characteristics and long-term follow-up of the large SICcohort from Western Sweden.Methods: A prospective registry for SIC patients (pts) was established at theUniversity Hospital in Jan. 2005.Results: 110 consecutive SIC pts were registered between Jan. 2005 and Jan.2010. 13.6% were males and 86.4% females, age 17-91. Thirty-day and one-yearmortality rates were 5.5% and 10.9% respectively. Twelve pts (10.9%) had signif-icant coronary artery narrowing. 86.3% of pts presented with large apical akine-
Kaplan-Meier survival curve
sia. In 12.7%, other local patterns of reversible regional akinesia were present.5% developed thrombo-embolic complications (lung, brain and kidney) and 3%developed cardiac arrest. Only 5% of patients were "non-Swedish" although 28%of all inhabitants in Gothenburg area are of "non-Swedish" origin. In four families,several closest relatives developed SIC (mothers, sons and sisters). 11.8% de-veloped 2 or more episodes of SIC. Hemodynamic profile has shown subnormalsystemic vascular resistance (SVR) and preserved cardiac output. Sympatheticnerve activity (SNA) (microneurography) to the muscle vascular bed was subnor-mal in SIC compared to the healthy controls. Pts exposed to inotropic treatmenthave show prolonged recovery period. Autopsy studies have shown intracellularlipid accumulation in the SIC hearts.Conclusion: SIC affects both men and women of different age and is associatedwith significant short- and long-term mortality. There is a strong signal for thepresence of ethnic/genetic predisposition to SIC. Thrombo-embolic complicationsand recidivism are common. SNA and SVR are subnormal in these pts suggestingthat SIC is a cardio-circulatory phenomenon.
P404 A new animal model of Takotsubo cardiomyopathy bypilocarpine-induced epilepsy
T. Arai, K. Fukuda. Keio University School of Medicine,Cardiopulmonary Division, Tokyo, Japan
Background: Takotsubo cardiomyopathy is a relatively novel syn-drome in cardiology, which was first reported in 1990. Although twenty years havepassed from the first case report, little is known about its pathogenesis. We needan appropriate animal model of Takotsubo cardiomyopathy to elucidate its mech-anism of development. This study was aimed to develop a new animal model thatmimics the clinical manifestation of Takotsubo cardiomyopathy.Methods and Results: (1) Epilepsy is reported to be one of the risk factors ofTakotsubo cardiomyopathy. We induced epilepsy in Wistar rats by injecting pilo-calpine, an agonist of muscarinic receptors. (2) After inducing epilepsy, we exam-ined the rat heart by electrocardiogram and echocardiography (Vevo770, Visualsonics). Interestingly, electrocardiogram revealed typical ST elevation in all leads.EKV mode-echocardiography clearly demonstrated that wall motion of the leftventricular apical segment was akinetic or dyskinetic. These changes occurredin 67% (n=12) after two hours from epilepsy induction.(3) Coronaryangiographyrevealed that there was no significant stenosis of the rat coronary artery. (4) Theday after epilepsy, however, the wall motion of the left ventricular apical segmentwas completely recovered. (4) Furthermore, the serum levels of adrenaline, nora-drenaline and dopamine were about three times higher two hours after epilepsyinduction.Conclusions: We developed a new animal model of Takotsubo cardiomyopathythat mimics the clinical manifestations in humans. This animal model might be apowerful tool to investigate the mechanisms of this disease.
P405 Stress (Tako-Tsubo) cardiomyopathy: alterations insympathetic nervous system potentially mediated bynorepinephrine-derived oxygen free radicals
H.M. Nef1, S. Szardien2, C. Troidl2, S. Voss2, A. Rolf1, J. Rixe1,M. Weber1 , A. Elsaesser3, C. Hamm1, H. Moellmann1. 1Kerckhoff
Heart and Thorax Center, Bad Nauheim, Germany; 2Franz-Groedel Instituteof the Kerckhoff Heart and Thorax Center, Bad Nauheim, Germany; 3HospitalOldenburg, Oldenburg, Germany
Background: Catecholamine-triggered effects play a pivotal role in the pathogen-esis of stress (Tako-Tsubo) cardiomyopathy (SCM). Thus, myocardial adrener-gic neurotransmitters (norepinephrine, tyrosine hydroxylase,neuropeptide Y) andadrenergic receptor levels were measured in myocardial tissue from patients pre-senting with SCM.Methods: We studied 12 consecutive patients in whom SCM was diagnosedby coronary angiography, ventriculography,magnetic resonance imaging (CMR),and echocardiography. Serial myocardial biopsies were taken during the phaseof severely impaired left ventricular function (acute) and after functional recov-ery (rec). Left ventricular tissue from not-transplanted hearts served as healthycontrols. Cardiac neuronal norepinephrine, tyrosin hydroxylase, neuropeptide Ywas determined by immunohistochemistry. Density of neuropeptid Y receptors(NPYR1, NPYR2) and adrenergic receptors (α,β1, β2, β3) was analyzed by quan-titative RT-PCR and Western Blot. Furthermore, superoxide production was quan-tified by dihydroethidium fluorescence staining.Results: In the acute phase of SCM a significantly increased cardiac nore-pinephrine was associated with altered levels of tyrosin hydroxylase and neu-ropeptide Y. Myocardial receptor of neuropeptide Y (NPYR2) was significantlydownregulated. Compared with control hearts, β-adrenergic-receptor density wassignificantly decreased in SCM. In contrast, α-adrenoceptors were highly upreg-ulated in the acute phase of SCM. Superoxide production was significantly in-creased in comparison to healthy controls and after functional recovery.Conclusion: SCM is associated with alterations in sympathetic nervous systemparticularly with a reduced β-adrenergic receptor density. These toxic effects ofnorepinephrine on the sympathetic signalling are potentially mediated via the for-mation of norepinephrine-derived oxygen free radicals.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Unusual cardiomyopathies: Takotsubo, peripartum and isolated left ventricular noncompaction 29
P406 Very long term natural history on TakoTsubocardiomyopathy (Apical transient dyskinesia)
I. Nunez-Gil1, M. Luaces2, J.C. Garcia Rubira1, A. Fernandez Ortiz1,C. Acebal1, M. Del Trigo1, D. Vivas1, J. Alonso2, J. Zamorano1 ,C. Macaya1. 1Hospital Clinic San Carlos, Madrid, Spain; 2Hospital de
Fuenlabrada, Fuenlabrada, Spain
Background: Takotsubo syndrome presents features mimicking acute coronarysyndromes. Althought good prognosis has been previously reported, long termfollow up data are lacking. Our aim was to establish the long term natural historyof this entity.Methods: 80 patients were prospectively studied between January, 2003 tillFebruary, 2010. Inclusion criteria were: presentation mimicking acute coronarysyndrome; Transient dys/akinesis of left ventricular segments by ventriculogram,without significant coronary artery narrowing; ECG abnormalities and elevatedtroponin/CK; Absence of: intracranial disease or pheochromocytoma.Results: Most were women, 86.3%. Mean age was 66.75±13 years. Cardio-vascular risk factors were displayed frequently: hypertension 67.5%, dyslipemia50.0%, diabetes 17.5%, smoking habit 12.5%, family history 18.8% and obesity25% (BMI≥30). Onset emotional stress situation was present in 45.0%. Chestpain was the most frequent onset symptom (92.2%). Elevation in biomarkerswere demonstrated in 100% (Median peak CK 196.00 U/L and Tn I 3.91ng/ml).ECG changes were displayed in 100% (60%, ST segment elevation; mean QTc515±73). Onset mean LVEF was 48.74±11%. Most showed Killip I (71.3%) butII (13.8%), III (5.0%) and IV (10.0%) were also present. Median in-stay was 7.0days. A complete LV recovery was displayed in 100% by echocardiography (LVEF63.52±7%). Median follow-up was 1138 days (inter-quartile range 660.0-1660.5).After discharge (figure), 3.8% suffered a recurrence, 15% patients underwent car-diology readmission during follow up, and 4 died (2 sudden death, 1 sepsis, and1 pneumonia).
Conclusion: Takotsubo cardiomyopathy is not lacking of in-hospital complica-tions, including cardiogenic shock. Conversely, after discharge it seems to carrya good long-term prognostic.
P407 Takotsubo cardiomyopathy has a unique cardiacbiomarker profile - a new approach for non-invasivedifferentiation of acute coronary syndroms and stressinduced cardiomyopathy
G.M. Froehlich, B. Schoch, T.F. Luescher, F. Ruschitzka, F. Enseleit.University Hospital Zurich, Department of Internal Medicine, Division ofCardiology, Zurich, Switzerland
Background: Takotsubo Cardiomyopathy (TC) usually is not recognized untilheart catheterization reveals typical wall motion abnormalities in the absence ofsignificant coronary artery disease. It was the aim of our study to identify TCby its unique cardiac biomarker profile at an early stage and with non-invasiveprocedures only.Methods: We compared the ratios of NT-proBNP/myoglobin and NT-proBNP/Troponin T (TnT) in three study groups: patients with TC (n=32), patientswith ST-elevation myocardial infarction (STEMI, n=48) and patients with non-ST-elevation myocardial infarction (NSTEMI, n=20). Biomarkers were recorded seri-ally at admission and peak levels at day one, two and three. Optimal cut-off valuesto distinguish TC from STEMI and NSTEMI were calculated with ROC-curves.Correlation of NT-proBNP and mortality was calculated in all three groups. In TC,additionally, correlation of NT-proBNP and reoccurrence of Takotsubo events wasdetermined.Results: At admission, NT-proBNP (ng/l)/myoglobin (ug/l) ratio above 4.1 pre-dicted TC at a specificity of 90% and a sensitivity of 85%. Ratio of peak proBNP(ng/l)/peak TnT (ug/l) levels had a 89% sensitivity with a corresponding speci-ficity of 95%. No correlation was found between NT-proBNP levels and mortalityor reoccurrence of Takotsubo events in the TC group, whereas NTproBNP pre-dicted mortality in the STEMI (Spearman coefficient - 0.399 p=0.014) and in theNSTEMI group (Spearman coefficient: - 0.545 p=0.03).Conclusion: Patients with TC can safely be identified by their unique cardiacbiomarker profile among patients presenting with acute coronary syndromes. InTC, NT-proBNP values have no prognostic relevance in terms of mortality or re-currence of Takotsubo episodes.
P408 Haemostatic changes in stress-inducedcardiomyopathy
O. Parkkonen1, P. Mustonen2, M. Puurunen2, M.L. Lokki3,M. Nieminen1, J. Sinisalo1. 1Helsinki University Central Hospital,Department of Medicine, Division of Cardiology, Helsinki, Finland;
2Finnish Red Cross Blood Service, Department of Haemostasis, Helsinki,Finland; 3Haartman Institute, University of Helsinki, Helsinki, Finland
Purpose: Postulated mechanisms for stress-induced cardiomyopathy (SIC) arecoronary artery spasm, microvascular dysfunction and catecholamine excess.Thrombotic occlusion of coronaries has not been convincingly excluded. We com-pared different markers of coagulation and platelet activation among patients withclassic acute coronary syndrome (ACS), acute stress-induced cardiomyopathy(SIC) and elective patients without coronary artery disease (no-CAD).Methods: 5300 consecutive patients signed for coronary angiogram were col-lected for Corogene-registry. ACS patients (n=2104) were angiographed in acutephase, all having standard antiplatelet and anticoagulation medication. Of them58 turned out to have stress-induced cardiomyopathy. From the same registry,equal number of age and sex matched classic ACS and elective patients with-out coronary disease were selected. Blood samples for fibrinogen (Fg), d-dimer,soluble glycoprotein V (sGPV), vonWillebrand factor -antigen (vWF:ag) analyseswere collected just prior angiogram.Results: SIC patients had lower BMI, less hypertension and dyslipidemia thanpatients with ACS (26.3±4.6 vs. 28.6±5.8; p =0,025, 47% vs. 67%; p = 0,025and 50% vs 78%; p = 0,002, consequently). SIC patients had also lower BMI thanpatients with no-CAD (26.3±4.6 vs. 28.1±5.4, p=0,038).Discussion: In SIC markers of platelet activation (sGPV) and fibrin formation (d-dimer) were on equal level than in elective no-CAD, which argues against the roleof platelet activation and thrombus formation in the pathophysiology of SIC.However, in SIC vWF:ag and Fg were significantly higher than in elective no-CAD.vWF:ag in SIC was even markedly higher than in ACS. Fg and vWF:ag are acutephase reactants of which especially vWF:ag is strongly influenced by adrenergicstimulation.
Haemostatic parameters
SIC ACS No CAD p p p(1) (2) (3) (1 vs 2) (1 vs 3) (2 vs 3)
P-vWF:ag, % 172.5 148.0 130.0 0.11 <0.0001 0.031(136.5 to 215.3) (129.0 to 203.0) (100.5 to 171.3)
P-D-Dimer, μg/L 0.3 0.4 0.3 0.038 0.59 0.16(0.2 to 0.6) (0.2 to 1.0) (0.2 to 0.6)
P-Fg, g/L 3.9 4.1 3.5 0.098 0.007 <0.0001(3.2 to 5.0) (3.4 to 5.1) (3.1 to 4.0)
P-sGPV, ng/mL 37.8 42.1 36.6 0.26 0.11 0.011(33.0 to 53.8) (33.8 to 58.4) (25.8 to 47.8)
Conclusions: Changes of the haemostatic parameters support the role of cate-cholamine excess, but not platelet activation and thrombus formation in the patho-physiology of SIC.
P409 Myocardial edema is a major determinant of reversibleleft ventricular dysfunction in Tako-Tsubocardiomyopathy
A. Turco, C. Raineri, R. Camporotondo, A. Repetto, L. OltronaVisconti, M. Previtali. Foundation IRCCS Polyclinic San Matteo,
Department of Cardiology, Pavia, Italy
Purpose: Tako-Tsubo cardiomyopathy (TTC) is characterized by severe re-versible regional myocardial dysfunction whose determinants are as yet uncom-pletely defined. Myocardial edema (ME) has been demonstrated in TTC by car-diac magnetic resonance (CMR) but its characteristics and correlation with theseverity of left ventricular (LV) dysfunction has not been defined. The purposeof the study was to assess the extent of ME and its relation to LV dysfunctionin patients (pts) with TTC studied with CMR during the acute phase and after 1month.Methods: 10 pts, all women, aged 62±14 yrs, with TTC (7 apical and 3 mid-ventricular) underwent CMR at a mean of 3±1 days from admission and after1 month. Peak Troponin I was 3.5±2.2 ng/ml. ME was defined as a hyperen-hanced signal (a signal intensity > 2 SD compared to normal myocardium) ontriple inversion recovery T2-weighted images. Presence and extent of ME wasevaluated semiquantitatively (0= no ME, 1= ME) and quantitatively (mass of ME,grams) on a short axis 16-segment LV model. Delayed enhancement (DE) af-ter gadolinium injection was used to assess the presence of myocardial necrosisor fibrosis; LV end-diastolic (LVEDV) and end-systolic volumes (LVESV), ejectionfraction (EF), wall motion score index (WMSI) and diastolic thickness on a 16-segment (sgs) model were assessed by ecg-gated cine steady state sequencesin short axis.Results: During acute phase mean EF was 43±7%, LVEDV and LVESV 126±23and 72±24 ml respectively. No patients showed DE. ME was present in 58/82(71%) dysfunctional sgs and in 3/78 (3%, p<0.001) normal sgs. Mass of ME was27±17grams, 42±16% of the mass of LV. Both the mass of ME and the numberof sgs with ME were significantly correlated with LVEF (r=0.90, p=0.0005 andr=0.90, p=0.0003) and with WMSI (r=0.85, p=0.0029 and r=0.90, p=0.0003). Nosignificant correlation was found between ME and LVEDV, LVESV and diastolic
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

30 Unusual cardiomyopathies: Takotsubo, peripartum and isolated left ventricular noncompaction
sg thickness. At 1 month control CMR ME resolved in all pts and FE improvedfrom 43±7% to 58±8% (p<0.001).Conclusions: 1) In the acute phase TTC is characterized by an extensive MEwhose distribution corresponds to the disfunctional sgs. 2)The extent of ME isstrongly correlated with the severity of LV disfunction. 3)Resolution of ME is as-sociated with recovery of LV function; thus, ME appears to be a major determinantof myocardial stunning observed in TTC.
P410 Is beta-blocker treatment able to prevent theoccurrence of stress cardiomyopathy?
B. Schneider1, A. Athanasiadis2 , J. Stein1. 1Sana Kliniken, Luebeck,Germany; 2Robert- Bosch Krankenhaus, Stuttgart, Germany
Background: Tako-tsubo cardiomyopathy (TTC) is often preceded byemotional or physical stress. Since sympathetic activation may contribute to thepathogenesis of TTC, beta-blocker (BB) therapy has been recommended. No trialdata, however, are available so far to guide the treatment of "stress cardiomyopa-thy". This study assessed if BB pre-treatment has an influence on the manifesta-tion and the clinical course of TTC.Methods: Over a 9-year period, TTC was diagnosed in 70 pts (63 f, 7 m, age71±12). Of these, 5 pts (7%) had discontinued long term BB therapy 3-14 daysbefore manifestation of TTC which was triggered by physical stress. For the pur-pose of this study, pts with continuous BB therapy on the day of TTC onset werecompared to TTC pts without BB pre-treatment. If there were no contraindications,pts received a BB during the acute event and at hospital discharge.Results: Because of hypertension and atrial fibrillation, 12/70 pts (17%) weretaking a BB at TTC onset (metoprolol n=9; atenolol, propranolol and sotalol n=1,respectively). Age, sex, symptoms, triggering events and time from symptom on-set to hospital admission were not different among pts with and without BB pre-treatment. ECG changes (ST-segment elevation, T-wave inversion, pathologicalQ wave, QTc interval, atrial fibrillation, ventricular tachycardia, time to ECG nor-malization) were similar in both groups. Cardiac markers CK and CK-MB werenot different, but troponin I was significantly less in BB pre-treatment (3.34±2.24vs 7.09±5.9 ng/ml, p=0.02). Time from symptom onset to cardiac catheterization,ejection fraction, left ventricular (LV) end-diastolic pressure, ballooning patternand time to normalization of LV function were comparable. Complications duringthe acute clinical course occurred with similar frequency (7/12 vs 29/58, p=ns),however, major complications (cardiogenic shock, acute mitral regurgitation, LVthrombus, stroke, death) were not seen in pts with BB pre-treatment.All 68 surviving pts received a BB at hospital discharge. During a median follow-up of 54 months, 5/68 pts (7%) had a recurrence of TTC occurring after 2-35months; 4/5 pts were still taking a BB (carvedilol n=3, propranolol n=1).Conclusion: BB therapy is not able to prevent the occurrence of TTC. However,myocardial damage appears to be less, and serious complications such as car-diogenic shock, LV thrombus or death were not observed with BB pre-treatment.Discontinuation of chronic BB therapy in combination with physical stress maytrigger the onset of TTC.
P411 Risk stratification in tako-tsubo cardiomyopathy
R. Proietti1, A. Compare2, E. Grossi3, P. Silva4, A. Dello Russo5,M. Casella5, S. Bartoletti6, L. Daliento7, A. Angelini7. 1Sant’AndreaHospital, Vercelli, Italy; 2University of Bergamo, Bergamo, Italy;3Centro Diagnostico Italiano, Milano, Italy; 4Niguarda Hospital, Milano,
Italy; 5University of Milan, Foundation Monzino (IRCCS), Center Cardiology, Dptof Cardiology, Milan, Italy; 6Catholic University of the Sacred Heart, Rome, Italy;7University of Padua, Department of Cardiology, Padua, Italy
Studies on the long-term follow-up of tako-tsubo cardiomyopathy (TTC) report ahigh mortality and morbidity including TTC recurrence. No report are availableregarding the influence of psychological features on long-term prognosis. We aimto assess the recurrence of symptoms among TTC patients and to verify if theyare connected to peculiar personality traits.We enrolled 37 patients who had been diagnosed with a TTC. The male to fe-male ratio was 1:9, mean age 68 yrs. A psychological assessment was performedon all patients using self-reporting questionnaires on personality risk traits: typeA (TAPB), type D (DS-14), cynism hostility (suscale of the cook-medley scale),anger-in (STAXI subscale) and alexithymia (TAS 20). Cardiovascular risk factorswere distributed as following: 6% had diabetes,36% hyperlipidemia,31% familyhistory,14% smoking and 75% hypertension. After hospital discharge patient ther-apy included:ASA 72%, β-blokers 56%, statins 28% and ACE-inhibitors 50%.In our cohort 24 patients reported recurrence of chest pain (group A) of variableintensity after discharge, while 13 patients did not refer chest pain or other symp-toms (group B). We had no cases of recurrent TTC. All patients referred chestpain to be associated with stressful events. In 14 cases chest pain was so in-tense that it lead to at least once emergency department admission and 2 casesresulted in hospital admission. Most patients referring recurrence of chest painreported other associated symptoms such as tiredness, palpitation and dyspnea.We found no significant differences in home therapy and the distribution of car-diovascular risk factors between groups A and B of our casistica. However, wedid observe significant differences in some psychological variables. Specifically,patients in group A vs B, had a psychological profile characterised by Type Dpersonality (p=.02), Anger-in trait (p=.03) and alexithymia (p=.002).
Our survey shows that most TTC patients continue to refer chest pain recur-rence after the main event; furthermore, home therapy seems not able to pro-vide a useful prevention while a psychological analysis has evidenced differentpsychological characteristic. Particularly, TTC patients with recurrent chest painseems to have more difficulty in identifying and expressing feelings, specificallyanger (anger-in), and in distinguishing between feelings and the bodily sensationsof emotional arousal (alexitimia). Thus, these results suggest that the long-termmanagement of TTC would benefit greatly from a psychological risk stratificationalong with a subsequent psychological intervention.
P412 Incidence and clinical relevance of left ventricularthrombus in patients with tako- tsubo cardiomyopathy:results of the German tako-tsubo registry
B. Schneider1, A. Athanasiadis2, J. Schwab3, W. Pistner4,U. Gottwald5, W. Toepel6 , R. Schoeller7, B. Gerecke8, W. Kasper9,
U. Sechtem2. 1Sana Kliniken, Luebeck, Germany; 2Robert- Bosch Krankenhaus,Stuttgart, Germany; 3Klinikum Nuernberg Süd, Nuernberg, Germany; 4KlinikumAschaffenburg, Aschaffenburg, Germany; 5Allgemeines Krankenhaus Celle,Celle, Germany; 6Klinikum Idar- Oberstein, Idar-Oberstein, Germany; 7DRKKliniken Berlin Westend, Berlin, Germany; 8Klinikum der Stadt Wolfsburg,Wolfsburg, Germany; 9St. Josefs Hospital, Wiesbaden, Germany
Background: Tako-tsubo cardiomyopathy (TTC) is increasingly recognized allover the world. A TTC registry has been initiated in Germany to further charac-terize this syndrome. Left ventricular thrombi (LVT) complicating TTC have beenreported only sporadically. This study evaluated the incidence and clinical rele-vance of LVT in patients (pts) of the German TTC registry.Methods: From 37 hospitals, 324 pts (296 f, 28 m, age 68±12) were includedaccording to the following criteria: 1) acute chest symptoms, 2) ischemic ECGchanges, 3) reversible LV akinesia not corresponding to a single coronary arteryterritory, 4) absence of coronary artery stenoses.Results: Within the first week of symptom onset, 301 pts were studied by echo-cardiography (echo, n=276) and/or cardiac MRI (n=147). In 8 female pts (inci-dence 2.7%), LVT was diagnosed between day 1 and day 5. Apical ballooning waspresent in 7 pts and mid- ventricular ballooning in 1 pt. Multiple mobile thrombiwere seen in 3 pts, and in 1 pt spontaneous echo contrast was present within thedyskinetic apex. In 3 of 4 pts studied by both echo and CMRI, LVT were detectedonly by CMRI. No pt had right ventricular thrombus.Pts with LVT were significantly older (76±12 vs 67±12 years, p<0.05). Symp-toms, triggering events, time from symptom onset to hospital admission and car-diac markers were not different among both groups. The admission ECG in ptswith LVT more frequently displayed negative T-waves (100% vs 66%, p<0.05);heart rate, ST-segment elevation and Q waves were similar. The QTc was longer(491±67 vs 465±52 ms day 1, 539±87 vs 500±64 ms day 3) and ventricu-lar tachycardia (29% vs 8%, p=0.05) occurred more frequently in pts with LVT,whereas atrial fibrillation was similar (14% vs 15%). LV ejection -fraction (48±21%vs 49±14%) was not different, but right ventricular involvement (50% vs 17%,p<0.02) and the need for an intraaortic balloon pump (12.5% vs 0.7%, p<0.001)were significantly more frequent in pts with LVT. Acute medication (ASS, clopi-dogrel, heparin, beta-blocker, ACE-inhibitor, catecholamines) was similar in bothgroups. In 2 of 8 pts (25%) LVT were progressing despite therapeutic doses ofheparin, aspirin and clopidogrel. Both suffered a large stroke, 1 pt died.One additional pt had a stroke on day 2 after TTC onset; echo did not show LVT.CMRI, however, was not performed.Conclusion: LV thrombi occur in 2.7% of pts with TTC and a severe clinicalcourse. CMRI is the imaging method of choice as echo underestimates the inci-dence of LVT. Despite therapeutic anticoagulation, LVT may grow and embolize,resulting in disabling stroke.
P413 Ventricular tachycardia and atrial fibrillationcomplicating the clinical course of tako-tsubo cardio-myopathy: results of the German tako- tsubo registry
B. Schneider1, A. Athanasiadis2, W. Pistner3, J. Schwab4,U. Gottwald5, R. Schoeller6, W. Toepel7 , K.D. Winter8, C. Stellbrink9,
U. Sechtem2. 1Sana Kliniken, Lübeck, Germany; 2Robert- Bosch Krankenhaus,Stuttgart, Germany; 3Klinikum Aschaffenburg, Aschaffenburg, Germany;4Klinikum Nürnberg Süd, Nürnberg, Germany; 5Allgemeines Krankenhaus Celle,Celle, Germany; 6DRK- Kliniken Berlin Westend, Berlin, Germany; 7KlinikumIdar-Oberstein, Idar-Oberstein, Germany; 8Hermann-Josef-Krankenhaus,Erkelenz, Germany; 9Klinikum Bielefeld, Bielefeld, Germany
Background: Tako-tsubo cardiomyopathy (TTC) has increasingly been recog-nized over the past years. Most studies, however, are fairly small. A German TTCregistry has been initiated to further characterize this syndrome in a larger patientpopulation. This study evaluated the incidence and clinical relevance of ventricu-lar arrhythmias (VA) and atrial fibrillation (AF) as complications of TTC.Methods: From 37 heart centres, 324 pts (296 f, 28 m, age 68±12) wereincluded according to the following criteria: 1) acute chest symptoms, 2) ischemicECG changes, 3) reversible LV akinesia not corresponding to a single coronaryartery territory, 4) absence of coronary artery stenoses. During hospitalisation,7/324 pts (2.2%) died (cardiogenic shock n=4; myocardial rupture, stroke andasystole n=1 each).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Unusual cardiomyopathies / Cardiomyopathies associated with cardiotoxicity and with muscular distrophy 31
Results: During the first 48 hours, 209 pts were continuously monitored and haddaily ECG recordings. Ventricular tachycardia and/or ventricular fibrillation wasdocumented in 17 pts (8%) and newly diagnosed AF in 32 pts (15%). TTC ptswith and without arrhythmias were compared.In pts with VA, time from symptom onset to hospital admission was shorter(3.8±3.2 vs 8.7±7.3 hours, p<0.001). Pulmonary oedema (29% vs 12%,p<0.05), need for intraaortic balloon pumping (6% vs 0.5%, p<0.05) or resuscita-tion (18% vs 3%, p<0.002) and left ventricular thrombi (12% vs 3%, p=0.05) wereseen more frequently. The QTc interval was only slightly more prolonged (476±45vs 470±55 ms day 1, 521±80 vs 510±57 ms day 2, 533±93 vs 508±60 ms day 3,all p=ns). Heart rate and other ECG parameters (ST- segment elevation, T- waveinversion, Q waves) were similar. Regarding age, sex, symptoms, trigger events,cardiac markers, ejection fraction, ballooning pattern, pre- and acute medicationand mortality there was no significant difference among pts with and without VA.Pts with AF frequently were on a pre-medication with diuretics (50% vs 12%,p<0.005), had a lower ejection fraction (45±14% vs 52±15%, p<0.02) und pre-sented more frequently with pulmonary oedema (25% vs 11%, p<0.05) and car-diogenic shock (16% vs 5%, p<0.05). Age, sex, symptoms, trigger events, cardiacmarkers, ECG changes, ballooning pattern, pre- and acute medication other thandiuretics, and mortality were not significantly different among pts with and withoutnewly diagnosed AF.Conclusion: During the acute phase of TTC, ventricular arrhythmias are ob-served in 8% and atrial fibrillation in 15%. Patients with arrhythmias have a morecomplicated clinical course, however, mortality is not increased.
P414 Tako-tsubo cardiomyopathy: electrocardiographicchanges in apical ballooning versus mid-ventricularballooning
B. Schneider, K. Peters, J. Stein. Sana Kliniken, Luebeck, Germany
Background: Tako-tsubo cardiomyopathy (TTC) mimics acute my-ocardial infarction. Besides the typical presentation of apical ballooning (AB), avariant form with mid-ventricular ballooning (MB) has been recognized. This studyaimed to assess if there are electrocardiographic differences between these twoTTC variants.Methods: Over a 7.5 years period, we observed 58 TTC patients (51 f, 7m;70±12 years). By angiography, 35 cases (60%) had AB and 23 (40%) MB. Ejec-tion fraction was similar (54±15 vs 51±12%, p=ns). ECG on admission, at thetime of maximal T-wave inversion, before discharge and the daily QTc-intervalwere compared.Results: Median time interval from symptom onset to hospital admission wassimilar (21 [12–42] vs 21 [11–28] hours; p=ns). At presentation, most patientshad ST-segment elevation (AB: 94%, MB: 100%; p=ns). The number of leads withST-segment elevation (4.6±2.3 vs 3.3±2.2 leads; p=0.046) and the magnitude ofST-segment elevation (0.7±0.5 mV vs 0.4±0.3 mV; p=0.008) were significantlygreater in AB. In both groups, ST-segment elevation most frequently occurred inlead V2 and V3 (AB: 89% and 91%, MB: 75% and 70%; both p=ns). ReciprocalST-segment depression was present in a quarter of all patients (AB: 25%, MB:26%; p=ns).During follow-up, AB patients displayed significantly more leads with T-wave inver-sion (8.1±1.1 vs 5.9±2.5 leads; p<0.001), and the magnitude of T-wave inversion(3.3±1.6 vs 1.4±0.9 mV; p<0.001) was significantly larger than in MB. The occur-rence of T-wave inversion was similar in lead I (AB: 77%, MB: 65%; p=ns), II (AB:77%, MB: 65%; p=ns), aVL (AB: 66%, MB: 75%; p=ns) and V2 (AB: 86%, MB:80%; p=ns). AB patients, however, developed more wide spread T-wave inversionin lead aVF (AB: 54%, MB: 25%; p=0.049), V3 (AB: 97%, MB: 65%; p=0.002), V4(AB: 97%, MB: 50%; p<0.001), V5 (AB: 97%, MB: 50%; p<0.001) and V6 (AB:94%, MB: 40%; p<0.001). The maximal QTc interval was not significantly differ-ent (516±43 ms vs. 505±48 ms; p=ns), but occurred earlier in AB (day 2) than inMB (day 4). An abnormal Q wave at presentation (AB: 23%, MB: 35%; p=ns) dis-appeared in all patients. The occurrence of ventricular arrhythmias (AB: 3%, MB:9%; p=ns) and atrial fibrillation (AB: 20%, MB: 17%; p=ns) was not different. ECGnormalization occurred in all patients at 56 (36–88) vs 45 (15–66) days (p=ns).Conclusion: ECG findings in AB are much more pronounced than in MB. The ex-tent of ST-segment elevation at initial presentation and of T-wave inversion duringfollow-up is significantly greater in AB. The maximal QTc interval occurs earlier inAB than in MB.
P415 Myocardial bridging is associated with an apicalballooning pattern and left ventricular thrombusformation - results of the German tako-tsubo registry
A. Athanasiadis1, B. Schneider2, W. Pistner3, R. Schoeller4,C. Stellbrink5, W. Kasper6, J. Schwab7, W. Von Scheidt8,
U. Sechtem1. 1Robert Bosch Hospital, Stuttgart, Germany; 2Sana-KlinikenLuebeck GmbH, Luebeck, Germany; 3Hospital Aschaffenburg, Aschaffenburg,Germany; 4DRK Clinics Berlin/Westend at the Charite-University MedicineBerlin, Berlin, Germany; 5Urban Hospitals Bielefeld, Bielefeld, Germany;6St. Josefs Hospital, Wiesbaden, Germany; 7Nurnberg Hospital, Nuremberg,Germany; 8Hospital Augsburg, Augsburg, Germany
Background: The German tako-tsubo cardiomyopathy (TTC) registry has beeninitiated to further evaluate this syndrome in a western population. We aimed to
assess the influence of coronary abnormalities, especially myocardial bridging(MB) on the pattern of left ventricular involvement and the clinical course of TTCpatients.Methods: Inclusion criteria were: 1) acute chest symptoms (angina, dyspnea) orsyncope, 2) reversible ECG changes (ST-segment elevation ± T-wave inversion),3) reversible left ventricular dysfunction with a wall motion abnormality not cor-responding to a single coronary artery territory, 4) no significant coronary arterystenoses. Myocardial bridging was defined as >15% diameter reduction of thecoronary artery during systole after nitroglycerin application and identification ofa "milking" effect.Results: Of 324 patients (pts) in the registry, 19 pts (5.9%) had a MB in the leftanterior descending coronary artery (LAD). All patients with MB were women witha mean age of 71±12 years. An apical ballooning pattern was found in 73.7%of pts with MB versus 63.3% of pts without MB (n.s.). Left ventricular ejectionfraction was similar (51±16% vs. 48±14%, n.s.). Most pts with MB (79%) hadangina as the leading symptom, 1 pt (5.3%) had a syncope, 1 pt (5.3%) headache,and in the remaining 2 pts (10.4%) no symptoms could be determined. In ptswithout MB, only 71.5% had angina, 2% no symptoms and 3% a syncope (n.s.vs. pts with MB). An emotional triggering event could be detected in 31.6% ofthe pts with MB vs. 36.4% of the pts without MB, a physical trigger in 26.3% vs.32.5% (n.s.) and a combination of both triggering events in 15.8% vs. 8.5% (n.s.).Cardiac markers were not different in pts with or without MB. The frequenciesof ST-segment elevation, T-inversion and Q-wave were similar on the baselineECG and on the follow-up ECGs at day 1 and day 2. Also the QTc intervals werenot different among both groups. There were also no differences regarding theoccurrence of arrhythmias, lung edema and cardiogenic shock. Interestingly, ptswith MB presented more left ventricular thrombi than pts without MB (11.1% vs.2.1%, p=0.02).Conclusion: Myocardial bridging of the LAD was observed in 5.9% of the ptswith TTC. Main symptom in these pts was angina. In most cases with MB, anapical ballooning pattern was identified with a significantly higher frequency ofleft ventricular thrombi.
CARDIOMYOPATHIES ASSOCIATED WITHCARDIOTOXICITY AND WITH MUSCULAR DISTROPHY
P416 Utility of research of the QT/QTc intervals dispersionand cardiac biomarkers for early diagnosis ofanthracycline induced cardiotoxicity in children
A.-G. Dimitriu1, C. Mandric1, I. Miron1, L. Dimitriu2. 1University ofMedicine and Pharmacy, Iasi, Romania; 2Medex Medical Center, Iasi,
Romania
Purpose: To establish the usefulness of research of dispersion QT/QTc intervalsand values of cardiac biomarkers- B natriuretic peptide (BNP) and troponin (cTnI)for early detection of cardiotoxicity in children with malignancies especially typehaematological.Methods: Patients: 46 children (aged 2 months - 18 years), treated with anthra-cyclines ± other drugs with cardiotoxic efects for malignancies. Control group: 20healthy children without cardiovascular history. Patients and controls were eval-uated by clinical exam, surface 12 lead ECG (3 consecutive cycles of measur-ing the QT/QTc intervals and QT/QTc intervals dispersion), Doppler echocardio-graphy for systolic/diastolic functions of LV, determining plasma levels of cardiacbiomarkers BNP and cTnI.Results: Were found some significant changes of the parameters in patients com-parativ with controls: *increasing the dispersion of the QT/QTc intervals in 73% ofpatients especially those with a cumulative dose of anthracyclines> 250 mg/m2
and in patients with echocardiographic changes induced by anthracycline car-diotoxicity, even only with diastolic dysfunction of LV:- the mean of QT dispersion:80 miliseconds in patients and 40 millisec. in controls; - the mean QTc dispersion:87,103 millisec. in patients and 55.47 millisec in controls; ** Increased plasma lev-els of BNP in 45.7% of patients, from a mean baseline of 89 ng/ml (0-117 ng/ml)to value 240 ng/ml (0-810 ng/ml),** increasing cTnI values. plasma at 4.34% ofcases, the initial values <0.04 pg/ml to values> 0.04 pg/ml in 2 cases. Biologicalchanges were correlated in most cases with the presence of clinical manifesta-tions, echocardiografical changes induced cardiotoxicity and increase of disper-sion QT/QTc intervals.Conclusions: Increased levels of cardiac biomarkers: BNP and cTnI and of thedispersion of QT/QTc intervals in children treated with anthracyclines ± otherdrugs with cardiotoxic efects positively correlates with installation of the cardiotox-icity with clinical or infraclinical manifestations, constituing an useful indicator forthe.cardiotoxicity. Changes in this parameters appeared early than echocardio-graphic changes anthracicline induced cardiotoxicity and is necessary to system-atic monitoring these parameters during and after cytostatic treatment
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

32 Cardiomyopathies associated with cardiotoxicity and with muscular distrophy
P417 Multiple biomarkers in detection ofchemotherapy-induced cardiotoxicity in patientstreated for acute leukemia
J.M. Horacek1, M. Vasatova2, R. Pudil3, M. Tichy2, L. Jebavy1,J. Maly4. 1University of Defence, Faculty of Military Health Sciences,Department of Internal Medicine, Hradec Kralove, Czech Republic;
2University Hospital, Institute of Clinical Biochemistry and Diagnostics, HradecKralove, Czech Republic; 3Charles University Prague, Faculty of Medicine inHradec Kralove, 1st Department of Medicine, Hradec Kralove, Czech Republic;4Charles University Prague, Faculty of Medicine in Hradec Kralove, 2ndDepartment of Medicine, Hradec Kralove, Czech Republic
Purpose: Cardiotoxicity is a potentially serious complication of anticancer therapythat can significantly impair patient’s quality of life. The greatest risk for develop-ment of cardiotoxicity represent anthracyclines (ANT) and high-dose chemother-apy (HD-CT). Various methods including cardiac biomarkers have been recom-mended for monitoring of cardiotoxicity in oncology. The aim of the study wasto monitor cardiotoxicity of conventional and HD-CT with multiple biomarkers ofcardiac injury – glycogen phosphorylase BB (GPBB), heart-type fatty acid bind-ing protein (H-FABP), cardiac troponins (cTnT, cTnI), creatine kinase MB (CK-MBmass), myoglobin.Methods: A total of 47 adult acute leukemia patients were studied – 24 patientstreated with conventional CT containing anthracyclines (ANT, mean total cumula-tive dose 463.2±114.3 mg/m2) and 23 patients treated with HD-CT (myeloablativepreparative regimen Bu/Cy2 or Cy/TBI) followed by hematopoietic cell transplan-tation (HCT). All patients had normal liver and renal functions during the study.Cardiac biomarkers were assessed prior to treatment (before CT/HD-CT), afterfirst CT with ANT, after last CT with ANT in the first group, after HD-CT and af-ter HCT in the second group. Cardiac biomarkers were measured on EvidenceRandox (GPBB, FABP, cTnI) and Elecsys Roche (cTnT, CK-MB mass, myoglobin)analyzers. Values above the reference range recommended by the manufacturerswere considered elevated.Results: Before CT/HD-CT, all biomarkers of cardiac injury were below the cut-offvalues in all patients. GPBB increased above the cut-off (7.30 μg/L) in 4 (16.7%)patients after first CT and in 5 (20.8%) patients after last CT with ANT. GPBBincreased above the cut-off in 5 (21.7%) patients after HD-CT and remained ele-vated in 5 (21.7%) patients after HCT. CTnI became elevated (above 0.40 μg/L)in 2 (8.3%) patients after first and last CT with ANT. Both patients with cTnI pos-itivity had elevated GPBB. Other tested biomarkers remained below the cut-offsduring the study.Conclusions: Our results suggest that GPBB could become a sensitivebiomarker for detection of acute cardiotoxicity associated with conventional CTcontaining ANT and HD-CT followed by HCT. The predictive value for develop-ment of cardiomyopathy in the future is not known and will be evaluated duringa prospective follow-up. Based on our data, a larger prospective and multicen-ter study would be most desirable to define the potential role of new circulatingbiomarkers in the assessment of cardiotoxicity in oncology. MO 0FVZ0000503,MZO 00179906, MSM 0021620817.
P418 Anthracycline-induced cardiomyopathy in patients withchronic lymphocytic leukemia: response to carvedilol
B. Samura. Zaporozhye State Medical University, Zaporozhye, Ukraine
Purpose: The aim of this study was to determine the protective ef-fect of carvedilol in anthracycline-induced cardiomyopathy. The natural history ofanthracycline-induced cardiomyopathy, as well as its response to cardiovasculartherapy, remains poorly defined. Hence, evidence-based recommendations formanagement of this form of cardiomyopathy are still lacking. Carvedilol is a nons-elective that also blocks alpha1-adrenergic receptors and is a potent antioxidant.Anthracyclines are commonly used in the treatment of several tumours, but theircardiac toxicity prevents their use at maximum myelotoxic doses, representing animportant problem. In this study, we have evaluated the role of these β-adrenergicreceptor antagonists administered in combination with anthracyclines on a reduc-tion in cardiac toxicity.Methods: Patients with chronic lymphocytic leukemia in whom anthracyclines(daunorubicin, eprirubicin, or doxorubicin) therapy was planned were enrolled inthe study. We included in the study 25 patients in carvedilol and 10 patients incontrol groups. In the carvedilol group, 12.5 mg once-daily oral carvedilol wasgiven during 6 months. The patients were evaluated with echocardiography beforeand after chemotherapy. Left ventricular ejection fraction (EF) and systolic anddiastolic diameters were calculated.Results: At the end of 6 months of follow-up, 1 patient in the carvedilol group and3 in the perindopril group had died. Control EF was below 50% in 1 patient in thecarvedilol group and in 4 in the control group. The mean EF of the carvedilol groupwas similar at baseline and control echocardiography (65.4 vs. 63.1, respectively;p = 0.2), in the control group the mean EF at control echocardiography was sig-nificantly lower (65.1 vs. 48.3; p < 0.001). Both systolic and diastolic diameterswere significantly increased compared with basal measures in the control group.In Doppler study, whereas E velocities in the carvedilol group decreased, E ve-locities and E/A ratios were significantly reduced in the control group.Conclusions: Prophylactic use of carvedilol in patients with chronic lymphocyticleukemia receiving anthracyclines may protect both systolic and diastolic func-tions of the left ventricle.
P419 Investigating the role of nitrosative stress indoxorubicin induced cardiomyopathy in rats. Theprotective effect of the natural olive constituentoleuropein
K. Ioannidis1, I. Andreadou1 , F. Sigala2, S. Kostidis1,L. Skaltsounis1, E. Mikros1, E.K. Iliodromitis3, M. Anastasiou-
Nana3, D.T.H. Kremastinos3. 1University of Athens, Faculty of Pharmacy,Athens, Greece; 2University of Athens Medical School, Hippokration GeneralHospital, Athens, Greece; 3University of Athens, Medical School, SecondUniversity Dept. of Cardiology, Athens, Greece
Introduction: Doxorubicin (DXR) is a commonly used agent but its use is limitedbecause of the induced cardiomyopathy. Whilst there is evidence that oxidative ornitrosative stress is implicated, the whole mechanism that results in heart failureis complex and not fully elucidated. Oleuropein (OLEU) - a polyphenolic con-stituent of the olive and its products - is capable of preventing acute and chronicDXR-induced cardiotoxicity as we have previously shown. Moreover, iNOS andperoxynitrite form nitrotyrosine (NT), a marker of nitrosative stress that is formedin acute DXR-induced toxicity. In the present study we tested: a) whether iNOSand NT are involved in chronic DXR-induced toxicity in parallel with other biomark-ers that are involved in the modulation of nitrosative stress, cardiac remodeling orapoptosis and b) whether OLEU has a protective role by preventing deleteriousintracellular mediators.Methods: Ninety rats were divided into 6 groups and treated as follows: Controlgroup no treatment, OLEU-70 and OLEU-140 groups with 70 and 140 mg/kg-1
of OLEU respectively, given intraperitoneally (i.p.), for 14 consecutive days, DXRgroup with 18mg/kg-1 of DXR i.p., divided into 6 equal doses and given over aperiod of 2 weeks, OLEU-70-DXR and OLEU-140-DXR groups, with combinedOLEU and DXR that were given as previously described. The rats were sacrificedat the end and the hearts were excised for tissue assessment of protein carbonylconcentration (PCs), nitrotyrosine (NT), interleukin-6 (IL-6), Big endothelin-1 (BigET-1) and iNOS by immunohistochemistry and by Western-Blot. NMR spectra oftissue extracts have been also recorded and further analysed with multivariatestatistics.Results: Tissue levels of NT, PCs, IL-6 and Big ET-1 were significantly increasedin the DXR group whereas a significant reduction in these mediators was ob-served in the Control and in both OLEU groups. Increased expression of iNOSwas also detected in the DXR group compared to the Control and OLEU groups.The NMR based metabonomic study, performed through the analysis of spectro-scopic data, depicted differences in the metabolic profile of the various groupswith significant metabolite alterations.Conclusion: Nitrosative stress is involved in NT and iNOS expression beingelevated in chronic DXR-induced toxicity of the heart and it is correlated withinteleukin-6 and Big ET-1. OLEU prevents the DXR-induced toxicity by reduc-ing nitrosative stress and by reversing deleterious intracellular mediators. Thus, itmay be considered as an innovative therapy that eliminates chronic DXR-inducedtoxicity.
P420 High prevalence of myocardial damage evaluated bycardiovascular magnetic resonance in asymptomaticsubject with cocaine addiction
G.D. Aquaro1, A. Gabutti1, M. Meini2, C. Passino3, M. Lombardi1 ,M. Emdin1. 1Gabriele Monasterio Foundation, Pisa, Italy; 2Pisa
Hospital, ASL 5, pisa, Italy; 3Institute of Clinical Physiology of CNR, Pisa, Italy
Background: Cocaine addiction is associated with cardiovascular Complicationsincluding myocardial ischemia and infarction in absence of obstructive coronaryartery disease, accelerated atherosclerosis, coronary vasoconstriction, myocardi-tis, arrhythmias and sudden death. The prevalence of myocardial damage inasymptomatic patients was not evaluated. Cardiovascular magnetic resonance(CMR) allows detection of myocardial damages as oedema and fibrosis. Aim: tocharacterize the presence of myocardial damage in patients with cocaine addic-tion without cardiac manifestations.Methods: Twenty-five consecutive patients (18 males, mean age 40±6 years)without history of heart disease were enrolled within the first 48h of withdrawalof cocaine assumption. Study protocol included: physical examination, electro-cardiogram (EKG), echocardiography, exercise test stress, 24 hours EKG Holtermonitoring, biohumoral markers of cardiac involvement (including natriuretic pep-tides and troponine I assay) and CMR examination. CMR study was performedusing a 1.5 Tesla scanner and included the evaluation of ventricular volumes,mass and ejection fraction by the acquisition of short axis views cine images witha SSFP pulse sequence. Myocardial oedema was evaluated by short axis andlong axis views using a T2-weighted STIR sequence. Myocardial fibrosis/scar wasevaluated by late gadolinium enhancement (LGE) technique by the acquisition ofshort axis images after the injection of gadolinium-based contrast media.Results: Mean duration of previous cocaine addiction was 7±4 years. All sub-jects had a normal resting EKG and a negative exercise stress test. Echocardio-graphic evaluation was normal in all the patients. Relevant arrhythmic events atHolter monitoring were not detected. Biohumoral marker of cardiac involvementwere negative in all the patients. Four patients refused CMR examination due toclaustrophobia. All subjects had normal left ventricular systolic function (averageejection fraction 63±7%), but in 9 regional wall motion abnormalities were found.Left ventricular myocardial oedema was detected in 12 (57%) patients. A pos-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Cardiomyopathies associated with cardiotoxicity and with muscular distrophy 33
itive LGE was found in 17 patients (80.9%). Nine (43%) patients showed bothmyocardial oedema and LGE.Conclusions: At CMR, a high prevalence of myocardial damage was found inpatients with history of cocaine addiction, characterized by presence of eitheroedema/fibrosis or regional dyssinergies, not evident at echocardiographic ex-amination in absence of biohumoral and resting/stress EKG abnormalities.
P421 Myocardium weight increases by an anticancer agentwith cardiac toxicity (the new formula used to calculatethe desirable dose of anti-cancer agent)
M. Arao, Y. Kitahara, K. Setsuta. Tokyo Metropolitan KomagomeHospital, Tokyo, Japan
Purpose: The dosages of anticancer drugs are generally determined based onbody surface area, but there are no indices for dosage that take into accountthe effects of anticancer agents with cardiac toxicity on the heart. We observedchanges in the heart caused by the administration of an anticancer agents withcardiac toxicity, investigated the relationship with the dosage of the agent, andanalyzed the effects on the on the heart at the initial stage.Methods: We selected 167 consecutive breast cancer patients (all females;mean: 51±9.5 years old) who completed adjuvant chemotherapy with 3 drugs(cyclophosphamide, epirubicin hydrochloride, and fluorouracil (5-FU)) (CEF) overa 24-month period. Echocardiography was performed before and after severalcycles of CEF. The LVDd/s, LVEDV, LVESV, IVST, PWT, LVEF, E/A, Tei index(T-I), Relative wall thickness (RWT), left ventricular mass (LVM) and LVM index(LVMI) were calculated. We also analyzed the correlation between total amountof CEF(�CEF)/LVM(I) and the rate of change in the LVM (�LVM) (%).Results: No significant changes were observed in the indices of cardiac func-tion, such as LVEF, Tei-Index, and A/E ratio. On the other hand, after thetreatment with the anticancer drugs, there were significant increases in theLVM (145.2±36.1 vs. 166±40.2; P<0.00000000001), in the LVMI (94.1±21.7vs. 107±23.5; p<0.00000000001) and in the RWT (0.402±0.07;0.424±0.07p<0.001). Moreover, a significant positive correlation was observed between�CEF/LVM and �LVM (r=0.5,P<0.00000000001, y=0.89x-25.4), and between�CEF/LVMI and �LVM (r=0.5, P<0.00000000001,y=0.56x-25.4).Conclusion: After the administration of an anticancer agent with cardiac toxi-city, significant increases were observed in the left ventricle mass. There wasa significant correlation between the change rate and the amount of anticanceragent per LVM. It was indicated that the form of increase in LVM involved a ten-dency toward concentric hypertrophy. The formula used to calculate the desir-able dose of anti-cancer drugs was: "�CEF (mg)=(1.8×�LVM+45.4)×LVMI". Inorder to maintain the LVMI at less than 130g/m2 after the administration of anti-cancer agents, the desirable dose is as follows. �CEF (mg)<23400-134.6×LVMI,cyclophosphamide<(10636-61×LVMI)mg, epirubicin<(2128-12×LVMI)mg. Weexpect that the above phenomena will provide clues for clarifying the clinical con-ditions related to the cardiac toxicity of anticancer agents.
P422 Glycogen phosphorylase BB as a marker of cardiactoxicity during hematopoietic cell transplantation forhematological malignancies
J.M. Horacek1, L. Jebavy1, M. Vasatova2, M. Tichy2, P. Zak3,R. Pudil4, J. Maly3. 1University of Defence, Faculty of Military Health
Sciences, Department of Internal Medicine, Hradec Kralove, Czech Republic;2University Hospital, Institute of Clinical Biochemistry and Diagnostics, HradecKralove, Czech Republic; 3Charles University Prague, Faculty of Medicinein Hradec Kralove, 2nd Department of Medicine, Hradec Kralove, CzechRepublic; 4Charles University Prague, Faculty of Medicine in Hradec Kralove, 1stDepartment of Medicine, Hradec Kralove, Czech Republic
Purpose: Cardiac toxicity is a potentially serious complication of hematooncologytreatment. Preparative regimen (PR) followed by hematopoietic cell transplanta-tion (HCT) represents a high risk for development of cardiotoxicity. Various meth-ods including cardiac biomarkers have been recommended for monitoring of car-diotoxicity. The aim of the study was to assess cardiac toxicity during HCT withmultiple biomarkers of cardiac injury – myoglobin, creatine kinase MB (CK-MBmass), cardiac troponin I (cTnI), heart-type fatty acid binding protein (H-FABP),glycogen phosphorylase BB (GPBB). Experience with new perspective cardiacbiomarkers (GPBB, H-FABP) in this context is very limited.Methods: A total of 53 patients (mean age 49.9±12.3 years, median 54 years, 33males) transplanted for various hematological malignancies were studied. Thirtytransplants were autologous, 23 allogeneic. Cardiac biomarkers were measuredon Randox Evidence analyzer the day after completion of preparative regimen (af-ter PR) and the day after infusion of hematopoietic cell graft (after HCT). Valuesabove the reference range recommended by the manufacturer were consideredelevated. The cut-off values for cardiac injury were as follows: 76.0 μg/L for myo-globin, 4.80 μg/L for CK-MB mass, 0.40 μg/L for cTnI, 4.50 μg/L for H-FABP and7.30 μg/L for GPBB.Results: We found significant elevations in GPBB (above 7.30 μg/L) in 8 (15.1%)patients after PR and in 9 (17.0%) after HCT. H-FABP increased slightly abovethe cut-off after HCT in 1 (1.9%) patient. Other cardiac biomarkers (myoglobin,CK-MB mass, cTnI) remained within the reference range in all patients. We founda significant correlation between elevation in GPBB and diastolic left ventricu-
lar (LV) dysfunction on echocardiography (r=0.603; p<0.0001). No patient mani-fested clinical cardiotoxicity in the peritransplant period.Conclusions: Our results suggest that administration of PR followed by HCTcould be associated with myocardial injury manifested by increased release ofGPBB from cardiomyocytes which could correlate with diastolic LV dysfunctionon echocardiography. In asymptomatic patients, these findings could be consid-ered a sign of acute subclinical cardiotoxicity. Whether these acute changes willhave predictive value for development of treatment-related cardiomyopathy in thefuture is not clear and should be evaluated during a prospective follow-up. Furtherstudies in a larger number of patients will be needed to confirm our preliminaryresults and define the potential role of new biomarkers of cardiac injury in thiscontext. MO 0FVZ0000503, MZO 00179906, MSM 0021620817.
P423 Detection of myocardial damage in female carriers ofDuchenne muscular dystrophy using cardiac magneticresonance
T. Iwase1, S. Takao2, M. Akaike1, K. Adachi3, Y. Ueda1, M. Harada2,H. Nishitani4, M. Sata1. 1Department of Cardiovascular Medicine,
Institute of Health Biosciences, The University of Tokushima, Tokushima, Japan;2Department of Medical Imaging, Institute of Health Biosciences, The Universityof Tokushima Graduate, Toskuhima, Japan; 3Department of Internal Medicineand Neurology, Tokushima National Hospital, Tokushima, Japan; 4Department ofRadiology, Institute of Health Biosciences, The University of Tokushima GraduateSchoo, Tokushima, Japan
Background: Cardiac involvement is a recognized complication in female carriersof Duchenne muscular dystrophy (DMD). Since segmental or global LV wall mo-tion abnormalities in DMD carriers can arise even without apparent muscle weak-ness, it is difficult to differentiate cardiac involvement of a DMD carrier from otherheart diseases in a non-invasive manner. Cardiac magnetic resonance (CMR)with late gadolinium enhancement (LGE) enables assessment of regional wallmotion abnormality and myocardial damage with high spatial resolution.Methods and Results: Gadolinium-enhanced CMR was performed in 7 femaleDMD carriers, and CMR findings were compared with those in 36 patients withLV wall motion abnormalities due to other heart diseases (20 patients with dilatedcaridomyopathy, 10 with significant coronary artery disease, and 6 with cardiacsarcoidosis). LGE was frequently located in lateral segments, consistent with wallmotion abnormalities in DMD carriers. Whereas focal LGE was observed at themidmyocardial layer in DMD carriers, LGE involved the subepicardial or subendo-cardial layer in patients with cardiac sarcoidosis (Figure 1). CMR revealed suben-docardial or transmural LGE in patients with coronary artery disease, and noneof the patients with dilated cardiomyopathy had LGE.
Figure 1
Conclusions: CMR findings of DMD carriers were characterized by midmyocar-dial LGE, which was localized at lateral segments. CMR may be a useful modalityfor detecting cardiac involvement in DMD carriers with LV wall motion abnormali-ties.
P424 Cardiovascular magnetic resonance (CMR)-taggingenables insight into the pathophysiology ofcardiomyopathy in patients with muscular dystrophy
A. Yilmaz1, K.N. Hor2, D.W. Benson2, W. Mazur2, K. Rost1,S. Roesch1, U. Sechtem1, W.M. Gottliebson2. 1Robert Bosch
Hospital, Stuttgart, Germany; 2Cincinnati Children’s Hospital Medical Center,Cincinnati, United States of America
Objectives: The aim of this study was to evaluate whether the analysis ofsegmental circumferential strain based on cardiovascular magnetic resonance(CMR)-tagging may explain the typical pattern of myocardial fibrosis in patientswith Becker muscular dystrophy (BMD).Background: Cardiomyopathy is a frequent finding in BMD patients. Previously,impaired global peak circumferential strain (PCS) as well as progressive myocar-dial fibrosis starting primarily in the lateral free wall of the left ventricle (LV) havebeen described using CMR. However, the segmental distribution of PCS abnor-malities and their association to the distribution pattern of myocardial fibrosis areso far unknown.Methods: 27 patients (median 25yrs; IQR 21-29yrs) with BMD and 11 healthycontrols underwent a comprehensive CMR study (on a 1.5-T system) comprisingcine-CMR for the assessment of functional parameters, CMR-tagging for the as-sessment of segmental PCS and late gadolinium enhancement (LGE)-CMR forthe assessment of myocardial fibrosis.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

34 Cardiomyopathies associated with cardiotoxicity and with muscular distrophy / New frontiers in diseases of the myocardium
Results: In 27 BMD patients, median LV ejection fraction (LV-EF) was 52% (IQR49 to 64%) with 9 (33.3%) patients demonstrating a normal LV-EF (≥ 60%). Pres-ence of LGE was confirmed in 21 (77.8%) patients with a median number ofLGE-positive segments of 6 (IQR 1 to 11) and a typical involvement of (at least)the LV free wall in all of them. Median global PCS was -9.6 (IQR -10.6 to -8.4) inBMD patients and -17.0 (IQR -18.0 to -15.6; p<0.001) in controls. BMD patientswith a reduced LV-EF (n=18) demonstrated a significantly impaired global PCScompared to those patients with normal LV-EF ≥ 60% (-8.8 vs – 10.5; p=0.035).LGE-positive patients (n=21) also demonstrated an impaired global PCS com-pared to those without LGE (-9.0 vs – 10.5; p=0.091). The most severe segmentalimpairment of PCS in LGE-positive BMD patients as well as in those with reducedLV-EF were detected in the (antero-)lateral wall (-8.8 and -8.6, respectively vs. -11.0 in controls; p=0.053). Moreover, BMD patients without LGE as well as thosewith a normal LV-EF again demonstrated the most severe segmental impairmentof PCS in the (infero-)lateral wall (-8.5 and -9.2, respectively vs. -16.1 in controls;p<0.001).Conclusion: Impairment of myocardial strain can be detected using CMR-tagging prior to the occurrence of myocardial fibrosis and/or cardiac systolic dys-function in BMD patients and predominantly occurs in the lateral LV free wall (evenin the absence of myocardial fibrosis and/or systolic dysfunction). This may ex-plain the typical lateral pattern of myocardial damage seen in the disease courseof these patients.
NEW FRONTIERS IN DISEASES OF THE MYOCARDIUM
P425 Asymptomatic arrhythmogenic right ventricularcardiomyopathy mutation carriers have impairedbiventricular function by myocardial strain
K.H. Haugaa1, S.I. Sarvari1, O.G. Anfinsen1, T.P. Leren2,O.A. Smiseth1, J.P. Amlie1, T. Edvardsen1. 1Dept of Cardiology, Oslo
University Hospital, Rikshospitalet, Oslo, Norway; 2Dept of Medical Genetics,Oslo University Hospital, Rikshospitalet, Oslo, Norway
Purpose: Life threatening arrhythmias can occur prior to apparent ventriculardysfunction in arrhythmogenic right ventricular cardiomyopathy (ARVC) mutationcarriers. Myocardial strain by echocardiography is a sensitive tool for assessingventricular function. The purpose of this study was to investigate right (RV) andleft ventricular (LV) function by strain in asymptomatic ARVC mutation carriers notfulfilling current ARVC criteria.Methods: We included 21 individuals (age 39±20 years) positive for an ARVC re-lated mutation (18 Plakophilin2 and 3 Desmoplakin) diagnosed by family geneticscreening. 20 age matched healthy individuals served as control group. Strainmeasurements were assessed by speckle tracking echocardiography. RV strainwas calculated in a 6 segment model and LV global strain in a 16 segment model.Results: ARVC mutation carriers had significantly reduced strain in RV comparedto healthy individuals (-21.8±3.5% vs. -24.5±3.3%, p=0.01). In addition, LV strainwas significantly reduced in mutation carriers compared to healthy individuals (-20.4±1.6% vs. -22.4±2.6%, p<0.01). LVEF did not differ between ARVC mutationcarriers and healthy (63±4% vs. 65±5%, p=0.21).Conclusions: Asymptomatic ARVC mutation carriers with no signs of the diseaseby current diagnostic guidelines had significantly reduced biventricular functionassessed by strain echocardiography although LVEF was normal. Reduced RVand LV strains indicate subclinical cardiac dysfunction in asymptomatic ARVCmutation carriers and that strain echocardiography may be helpful in decisionsregarding preventive treatment.
P426 Troponin T and beta myosin mutations have differentleft ventricular functional effects in patients withhyperthrophic cardiomyopathy and in healthy carriers
S. Ghio1, M. Revera2, L. Van Der Merwe3, P.A. Brink4, M. Buscemi1,J.C. Moolman-Smook5. 1Foundation IRCCS Polyclinic San Matteo,
Department of Cardiology, Pavia, Italy; 2Istituto Auxologico Italiano, Universityof Milano-Bicocca, Milano, Italy; 3Stellenbosch (South Africa) - University ofStellenbosch, Biostatistics Unit, Medical Research Counc, Stellenbosch, SouthAfrica; 4Stellenbosch (South Africa) - University fo Stellenbosch, Department ofMedi, Stellenbosch, South Africa; 5Stellenbosch (South Africa) - University foStellenbosch, Department of biomedical Sciences, Stellenbosch, South Africa
Purpose: Genotype to phenotype correlation studies in patients with hypertrophiccardiomyopathy (HCM) have typically yielded inconsistent results. The aim of thepresent study was to use new echocardiographic techniques for the evaluationof systolic and diastolic left ventricular (LV) function in patients with HCM and inmutation carriers family members.Methods: Standard and tissue Doppler (TDI) echocardiography was performedin 57 index HCM patients with known troponin T or beta myosin mutations (Pts,mean age 47±15 years, 51% males), in 37 healthy carriers (HC, mean age 29±20years, 54% males) and 79 non-carriers (NC, mean age 36±13 years, 44% males)family members (R92W: 18 Pts, 15 HC and 26 NC; A797T: 23 Pts, 12 HC and38 NC; R403W: 16 Pts, 10 HC and 16 NC). TDI was acquired in 2-D mode fromapical views. Off-line analysis was performed in 4 basal and 4 middle LV seg-ments to obtain peak systolic (S) velocity, peak strain (ε) and duration of systole
(Sys) as indicators of systolic LV function and peak early diastolic (E’) velocityand duration of isovolumic relaxation (IVRT) as indicators of diastolic LV function.Statistical analysis was performed comparing Pts vs NC as well as HC vs NCwithin the same mutation group and adjusting (random effects) for age, sex, BSA,corresponding segmental LV wall thickness at standard echocardiography, familymembership of subjects and multiple (regional) observations on each subject.Results: R92W Pts had similar S and ε and lower E’ (-2.2 cm/s, p<0.0001) ascompared to NC; R92W HC showed slightly but non significantly higher S and ε
and significantly higher E’ (+1.4 cm/s, p<0.01) as compared to NC. A797T Ptsshowed lower ε (-2.8, p=0.0102), lower E’ (-1.6 cm/s, p=0.0012) and prolongedIVRT (+20.4 ms, p=0.0004) as compared to NC; A797T HC showed similar S andε, slightly but non significantly lower E’, similar IVRT as compared to NC. R403WPts showed lower S (-0.66 cm/s, p=0.0331), lower E’ (-1.9 cm/s, p=0.0007) andprolonged IVRT (+20 ms, p=0.0008) as compared to NC. R403W HC had lowerS (-0.9 cm/s, p=0.0184) longer Sys (+25 ms, p<0.0056), similar E’ and IVRT ascompared to NC.Conclusions: TDI and strain analysis allows to identify distinct functional effect ofcausal mutations in HCM patients and in HC. Troponin T mutation does not impairLV systolic function in HCM patients; HC show a relative increase in systolic anddiastolic LV function. Beta myosin mutations (in particular R403W mutation) areassociated with an important systolic and diastolic dysfunction in HCM patientsand with early alterations of diastolic and systolic function in HC.
P427 Hypertrophic cardiomyopathy: sleep apnea seems tohave a negative impact on disease progression
C. Prinz, O. Oldenburg, T. Bitter, C. Piper, D. Horstkotte, L. Faber.Department of Cardiology, Heart and Diabetes Center NorthRhine-Westphalia, Ruhr University Bochum, Bad Oeynhausen,
Germany
Introduction: Sleep disordered breathing (SDB) has a high prevalence and prog-nostic impact in patients (pts) with various cardiac diseases. Aim of this study wasto investigate the prevalence and influence of SDB on disease severity in pts withhypertrophic cardiomyopathy (HCM).Patients and methods: In a cohort of roughly 1400 clinically characterizedHCM pts. we identified 63 patients (40 men; mean age 59.5±3.3 years, NYHAclass: 1.9±0.1) who underwent in-hospital unattended cardiorespiratory polygra-phy (Embletta, Embla, NL) in addition to standard diagnostics including echocar-diography. In case the apnea-hypopnea-index (AHI) was >5/h pts were consid-ered to have SDB, if the AHI was >15/h pts were considered to need therapy ofSDB. If thoracic and abdominal inspiration efforts were documented, SDB wasconsidered to be obstructive (OSA), otherwise central sleep apnea (CSA) wasdiagnosed.Results: SDB (AHI>5/h) was observed in 50 pts (79.4%) with an AHI of23.7±5.0/h. OSA was documented in 37 pts (74%; AHI: 22.0±5.5/h), 13 pts(26%) demonstrated CSA (AHI: 28.4±12.6/h; ns). 23 pts (36.5%) had severeSDB (AHI: 38.9±6.7/h) requiring specific therapy. Pts with a larger left atriumon echocardiography (LA >50 mm; 21 pts) had a higher severity of SDB thanthose without atrial dilatation (AHI: 16.2±4.5 vs 26.7±10.1/h, p<0.05). No corre-lations were found between sleep apnea and other parameters like left ventricularoutflow gradients in HOCM or occurrence of SAM.Conclusions: SDB is common in pts with HCM with predominance of OSA.Severity of sleep apnea correlates with LA size as a classical marker for globaldisease severity. It can be speculated that activation of the sympathetic system inuntreated sleep apnea has a negative impact on progression of HCM.
P428 Clinical and genetic comparisons in hypertrophiccardiomyopathy
V.U. Kaplunova, Y.N. Belenkov, E.V. Privalova, A.A. Fomin,A.Y. Suvorov. I.M. Sechenov Moscow Medical Academy, Moscow,Russian Federation
Purpose: identification of genetic markers, which impact the course and progno-sis of hypertrophic cardiomyopathy (HCM).Materials and methods: 61 patients (26 men, 35 women) and the control group(61 people) were subjected to genotyping of 12 polymorphisms of gene-modifiers,that characterize the RAAS, endothelin system, metalloproteinases, and bloodcoagulation system: coagulation factor II (F2), coagulation factor V (proaccelerin)(F5), coagulation factor VII (serum prothrombin conversion accelerator) (F7), en-dothelin 1 (EDN1), endothelin receptor type A (EDNRA), cytochrome P450, fam-ily 11, subfamily B, polypeptide 2 (CYP11B2), nitric oxide synthase 3 (endothelialcell) (NOS3), angiotensinogen (AGT), angiotensin II receptor type 1 (AGTR1),integrin beta 3 (ITG), matrix metalloproteinase 3 (stromelysin 1, progelatinase)(MMP53), chymase 1 (mast cell) (CMA1).Results: The analysis of polymorphisms in HCM and the control group showedthat the presence of combinations of certain genes-modifiers (NOS3 (qa,p<0.001), ATG (tc, p=0.09) and ITG (tt, p=0.10)) is more typical for patients withHCM. It was revealed, that the polymorphism gt (NOS3 gene) is associated withmore frequent atrial fibrillation (p=0.005), stroke (p=0.03) and higher risk of sud-den cardiac death (SCD) (p=0,039), thus determining more severe prognosis ofHCM, compared with gg polymorphism. It was also shown, that the polymorphismgg of NOS3 gene provides a higher value left ventricular mass (LVM) (p=0.05).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

New frontiers in diseases of the myocardium 35
Gt polymorphism is associated with pathology of the Q-wave (p=0,019), morefrequent supraventricular tachycardia (p=0.10), left anterior bundle branch block(p=0.018) and with a lesser extent of supraventricular extrasystole (p=0.068).There is also a tendency for more frequent development of coronary heart dis-ease (CHD) (p=0.08).Conclusions: analysis of polymorphisms of genes-modifiers has revealed theimportance of combination of polymorphisms of genes NOS3 (qa), ATG5 (tc) andITG (tt), typical for patients with HCM. Modification gt and gg of NOS3 gene poly-morphism is a predictor of more severe hypertrophy, more frequent occurrenceof atrial fibrillation, strokes and SCD, thus determining unfavorable prognosis inHCM.
P429 Myocardial damage biomarkers in hypertrophiccardiomyopathy: prognostic role of high sensitivitycardiac troponin I and T
C. Calore1, P. Melacini1, F. Santi1, M. Mion2, V. Pescatore1,A. Padoan2, F. Corbetti3, M. Zaninotto2 , M. Plebani2, S. Iliceto1.
1University of Padua, Department of Cardiac Thoracic and Vascular Sciences,Padua, Italy; 2University Hospital of Padua, Department of Laboratory Medicine,Padua, Italy; 3University of Padua, Department of Radiology, Padua, Italy
Purpose: Hypertrophic cardiomyopathy (HCM) is a primary myocardium diseasecharacterized by heterogeneous clinical presentation and natural history, rangingfrom asymptomatic forms to malignant expressions that may result in prematuredeath or in progressive heart failure through several pathways. Myocardial is-chemia is responsible for myocyte death and replacement fibrosis that play a cru-cial role in disease progression. Aim of this study was to assess cardiac troponinI and T values (hs-cTnI and hs-cTnT, measured using high sensitivity methods)in HCM, and to define their role in management of HCM patients and in outcomeprediction.Methods: hs-cTnI and hs-cTnT concentrations were measured in 67 consecu-tive HCM patients by immunoassay, and the relation between biomarkers andclinical-instrumental parameters was evaluated. Age, gender, symptoms, ECGabnormalities, arrhythmias at Holter monitoring, echocardiographic and cardiacmagnetic resonance data were collected. Patient with evidence of epicardial coro-nary artery disease were excluded. Serum hs-cTnI and hs-cTnT values were con-sidered positive above the 99th percentile of a healthy volunteers population witha coefficient of variation<10%. The cut-off level was 0.045 μg/L and 14 ng/L forhs-cTnI and hs-cTnT, respectively.Results: Patients with positive troponins values (14 pts, 21% and 24 pts, 36% re-spectively for hs-cTnI and hs-cTnT) showed lower ejection fraction (EF) (54±10%vs 60±8%, p= 0.035 for hs-cTnI; 55±11% vs 61±7%, p= 0.05 for hs-cTnT), mostsevere diastolic dysfunction (prevalence of restrictive pattern 21% vs 5%, p= 0.02for hs-cTnI; and 22% vs 0%, p= 0.002 for hs-cTnT), and ischemic ECG abnor-malities, i.e. ST-segment downsloping (57% vs 11%, p= 0.0002 for hs-cTnI; 42%vs 9%, p= 0.002, for hs-cTnT). At multivariate analysis, using models consider-ing also age and gender, inverse-linear relationships were found among ln hs-cTnT, EF and diastolic dysfunction (R2 0.26, adjusted R2 0.23, p= 0.0002), aswell as among ln hs-cTnI, ST-segment downsloping and the presence of ven-tricular tachiarrhythmias (R2 0.33, adjusted R2 0.30, p< 0.0001). During a meanfollow-up of 26±18 months, patients with at least one hs-cTn value above the99th percentile had worse outcome by Kaplan-Meier curves considering com-bined endpoint (progressive severe heart failure, heart-failure related death orcardiac transplantation) (p= 0.04).Conclusions: High-sensitivity cardiac troponins are interesting markers of HCMprogression to advanced heart failure in setting of impaired systolic functionand/or severe diastolic dysfunction and useful predictors of prognosis.
P430 Compromised left ventricular filling time and reducedright ventricular function: potential causes forbreathlessness in HCM
S. Morner1 , Y. Zhao2, P. Lindqvist3, M. Henein2. 1Dept ofCardiology,Heart Center, Umeå University Hospital, Umeå, Sweden;
2Dept of Public Health and Clinical Medicine, Umeå University, Umeå, Sweden;3Umea University Hospital, Department of Clinical Physiology, Umea, Sweden
Background: Exertional symptoms are common in hypertrophic cardiomyopathy(HCM) even in the absence of left ventricular outflow tract (LVOT) obstruction.Restrictive LV filling and arrhythmia can cause symptoms, but some patients haveunexplained breathlessness. We studied such a group of patients to find otherexplanations for their symptoms.Methods: We studied 36 non-obstructive HCM patients, 18 limited by dysp-nea and 18 asymptomatic (Table). Measurements were compared with 50 age-matched controls.Results: Group I were slightly older than group II (p<0.05) and had more fe-males (p<0.05). LV systolic function was not different between groups comparedwith normals (63±7% and 62±7% vs 63±8% (p=NS for all). LV long axis am-plitude was equally reduced in the two patient groups compared with normals(lateral wall 11.5±2.9mm and 11.8±3.0mm vs 14.9±2.5mm,p<0.001 and septalwall (8.6±1.8mm and 10.1±2.5mm vs 13.0±2.6mm, p<0.001).Septal long axiswas more depressed in Group I than Group II (p<0.05). E/A-ratio and E/Em werenot different between groups but relative filling time was significantly shorter only
in Group I, with respect to normals (49.8±5.2% and 55.8±6.7% vs 54.4±7.4%,p<0.01). TAPSE was reduced in both groups (19.5±3.5mm and 22.5±5.0mm vs25.2±4.5mm, p<0.001) and more so in Group I compared to group II (p<0.05).
Table 1. Characteristics of asymptomatic vs. symptomatic HCM patients
Asymptomatic (n=18) Dyspnoea (n=18) P
Age (y) 48±18 60±13 0.02Gender (F/M) 3/15 7/11 0.011E/A 1.6±0.7 1.4±0.7 0.41E/Em 10.3±7.8 8.5±2.7 0.42FT/RR (%) 55.8±6.7 49.8±5.2 0.007AVL 11.8±3.0 11.5±2.9 0.78AVS 10.1±2.5 8.6±1.8 0.05TAPSE 22.5±5.0 19.5±3.5 0.03
Conclusion: In HCM patients with normal LV ejection fraction and no outflow tractobstruction, long axis function is depressed and more so in symptomatic ones. Inthem, filling time is abbreviated suggesting asynchronous cavity function. In ad-dition right ventricular function is compromised too. These two disturbances areknown for their contribution to exercise intolerance in myocardial disease condi-tions.
P431 Type of fibrosis predicts serious events in patientswith obstructive hypertrophic cardiomyopathy
V.M. Almaas1, E. Heyerdahl Strom2, H. Scott2, C.P. Dahl3,T. Edvardsen4, S. Aakhus4, O.R. Geiran5, J.P. Amlie4. 1Dept. ogCardiology, Oslo University Hospital, Rikshospitalet, University of
Oslo, Oslo, Norway; 2Dept. of Pathology, Oslo University Hospital, Rikshospitalet,Oslo, Norway; 3Research Institute for Internal Medicine, Oslo University Hospital,Rikshospitalet, Oslo, Norway; 4Dept. of Cardiology, Oslo University Hospital,Rikshospitalet, Oslo, Norway; 5Dept. of Thoracic and Cardiovascular Surgery,Oslo University Hospital, Rikshospitalet, Oslo, Norway
Purpose: Myocardial scarring (fibrosis) is an established pathophysiological fea-ture associated with markers of sudden cardiac death (SCD) in patients with hy-pertrophic cardiomyopathy (HCM). The aim of this study was to describe the as-sociations between pericellular and replacement-type fibrosis, serious events andrisk factors for SCD in HCM-patients undergoing septal myectomy.Methods: Twenty-four HCM-patients (54.2% men; mean age 58.0±10.4 years)underwent risk stratification for SCD followed by septal myectomy. Risk factorsfor SCD: prior cardiac arrest; family history of SCD; unexplained syncope; non-sustained ventricular tachycardia (nsVT); abnormal blood pressure response; hy-pertrophy ≥ 30 mm. Degree of pericellular and replacement fibrosis was deter-mined (percentage of total specimen) on histopathology of surgical specimen.Patients with earlier myocardial infarction were excluded.Results: Maximal interventricular septal thickness was 1.9±0.3 cm, intraventricu-lar gradient was 57±23 mmHg, NYHA classification was 2.9±0.4 and CCS classi-fication was 1.7±1.1. Patients with events (prior cardiac arrest, nsVT, unexplainedsyncope) had significantly higher median percentage area of pericellular fibrosisthan patients without events (30.0, range 17-62 v. 8.0, range 0-60, P=0.0094,Mann Whitney (Figure)). Patients with one or two risk factors had significantlyhigher mean percentage area of pericellular fibrosis than patients with no riskfactors (26.9±23.8 v. 9.9±6.2, P=0.034, unpaired t-test). Replacement fibrosiswas not associated with events or with risk factors.
Pericellular and replacement fibrosis
Conclusion: There is an association between increased area of pericellular fi-brosis and serious events and risk factors for SCD in patients with obstructiveHCM.
P432 Diffuse late gadolinium enhancement bycardiovascular magnetic resonance predictssignificant intraventricular systolic dyssynchrony inpatients with non-ischeamic dilated cardiomyopathy
K. Tigen1, T. Karaahmet1 , C. Kirma1, C. Dundar1, S. Pala1, I. Isiklar2,C. Cevik3, E. Gurel1, A. Kilicgedik1, Y. Basaran1. 1Kartal Kosuyolu HeartEducation and Research Hospital, Istanbul, Turkey; 2Baskent University, Istanbul,Turkey; 3Texas Tech University Health Sciences Center, Lubbock, Texas, UnitedStates of America
Purpose: Left ventricular dyssynchrony and myocardial fibrosis are common find-ings in patients with non-ischemic dilated cardiomyopathy (NDCM). We inves-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
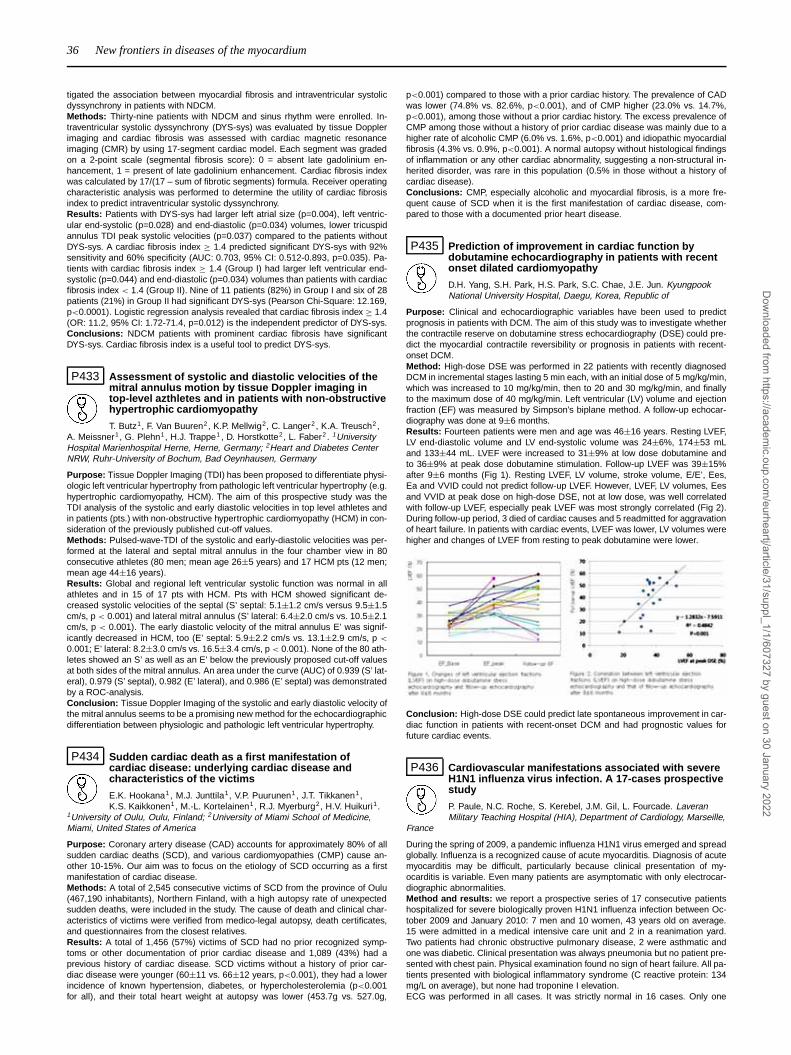
36 New frontiers in diseases of the myocardium
tigated the association between myocardial fibrosis and intraventricular systolicdyssynchrony in patients with NDCM.Methods: Thirty-nine patients with NDCM and sinus rhythm were enrolled. In-traventricular systolic dyssynchrony (DYS-sys) was evaluated by tissue Dopplerimaging and cardiac fibrosis was assessed with cardiac magnetic resonanceimaging (CMR) by using 17-segment cardiac model. Each segment was gradedon a 2-point scale (segmental fibrosis score): 0 = absent late gadolinium en-hancement, 1 = present of late gadolinium enhancement. Cardiac fibrosis indexwas calculated by 17/(17 – sum of fibrotic segments) formula. Receiver operatingcharacteristic analysis was performed to determine the utility of cardiac fibrosisindex to predict intraventricular systolic dyssynchrony.Results: Patients with DYS-sys had larger left atrial size (p=0.004), left ventric-ular end-systolic (p=0.028) and end-diastolic (p=0.034) volumes, lower tricuspidannulus TDI peak systolic velocities (p=0.037) compared to the patients withoutDYS-sys. A cardiac fibrosis index ≥ 1.4 predicted significant DYS-sys with 92%sensitivity and 60% specificity (AUC: 0.703, 95% CI: 0.512-0.893, p=0.035). Pa-tients with cardiac fibrosis index ≥ 1.4 (Group I) had larger left ventricular end-systolic (p=0.044) and end-diastolic (p=0.034) volumes than patients with cardiacfibrosis index < 1.4 (Group II). Nine of 11 patients (82%) in Group I and six of 28patients (21%) in Group II had significant DYS-sys (Pearson Chi-Square: 12.169,p<0.0001). Logistic regression analysis revealed that cardiac fibrosis index ≥ 1.4(OR: 11.2, 95% CI: 1.72-71.4, p=0.012) is the independent predictor of DYS-sys.Conclusions: NDCM patients with prominent cardiac fibrosis have significantDYS-sys. Cardiac fibrosis index is a useful tool to predict DYS-sys.
P433 Assessment of systolic and diastolic velocities of themitral annulus motion by tissue Doppler imaging intop-level azthletes and in patients with non-obstructivehypertrophic cardiomyopathy
T. Butz1, F. Van Buuren2, K.P. Mellwig2, C. Langer2 , K.A. Treusch2,A. Meissner1, G. Plehn1, H.J. Trappe1 , D. Horstkotte2, L. Faber2 . 1UniversityHospital Marienhospital Herne, Herne, Germany; 2Heart and Diabetes CenterNRW, Ruhr-University of Bochum, Bad Oeynhausen, Germany
Purpose: Tissue Doppler Imaging (TDI) has been proposed to differentiate physi-ologic left ventricular hypertrophy from pathologic left ventricular hypertrophy (e.g.hypertrophic cardiomyopathy, HCM). The aim of this prospective study was theTDI analysis of the systolic and early diastolic velocities in top level athletes andin patients (pts.) with non-obstructive hypertrophic cardiomyopathy (HCM) in con-sideration of the previously published cut-off values.Methods: Pulsed-wave-TDI of the systolic and early-diastolic velocities was per-formed at the lateral and septal mitral annulus in the four chamber view in 80consecutive athletes (80 men; mean age 26±5 years) and 17 HCM pts (12 men;mean age 44±16 years).Results: Global and regional left ventricular systolic function was normal in allathletes and in 15 of 17 pts with HCM. Pts with HCM showed significant de-creased systolic velocities of the septal (S’ septal: 5.1±1.2 cm/s versus 9.5±1.5cm/s, p < 0.001) and lateral mitral annulus (S’ lateral: 6.4±2.0 cm/s vs. 10.5±2.1cm/s, p < 0.001). The early diastolic velocity of the mitral annulus E’ was signif-icantly decreased in HCM, too (E’ septal: 5.9±2.2 cm/s vs. 13.1±2.9 cm/s, p <
0.001; E’ lateral: 8.2±3.0 cm/s vs. 16.5±3.4 cm/s, p < 0.001). None of the 80 ath-letes showed an S’ as well as an E’ below the previously proposed cut-off valuesat both sides of the mitral annulus. An area under the curve (AUC) of 0.939 (S’ lat-eral), 0.979 (S’ septal), 0.982 (E’ lateral), and 0.986 (E’ septal) was demonstratedby a ROC-analysis.Conclusion: Tissue Doppler Imaging of the systolic and early diastolic velocity ofthe mitral annulus seems to be a promising new method for the echocardiographicdifferentiation between physiologic and pathologic left ventricular hypertrophy.
P434 Sudden cardiac death as a first manifestation ofcardiac disease: underlying cardiac disease andcharacteristics of the victims
E.K. Hookana1, M.J. Junttila1, V.P. Puurunen1, J.T. Tikkanen1,K.S. Kaikkonen1, M.-L. Kortelainen1, R.J. Myerburg2, H.V. Huikuri1.
1University of Oulu, Oulu, Finland; 2University of Miami School of Medicine,Miami, United States of America
Purpose: Coronary artery disease (CAD) accounts for approximately 80% of allsudden cardiac deaths (SCD), and various cardiomyopathies (CMP) cause an-other 10-15%. Our aim was to focus on the etiology of SCD occurring as a firstmanifestation of cardiac disease.Methods: A total of 2,545 consecutive victims of SCD from the province of Oulu(467,190 inhabitants), Northern Finland, with a high autopsy rate of unexpectedsudden deaths, were included in the study. The cause of death and clinical char-acteristics of victims were verified from medico-legal autopsy, death certificates,and questionnaires from the closest relatives.Results: A total of 1,456 (57%) victims of SCD had no prior recognized symp-toms or other documentation of prior cardiac disease and 1,089 (43%) had aprevious history of cardiac disease. SCD victims without a history of prior car-diac disease were younger (60±11 vs. 66±12 years, p<0.001), they had a lowerincidence of known hypertension, diabetes, or hypercholesterolemia (p<0.001for all), and their total heart weight at autopsy was lower (453.7g vs. 527.0g,
p<0.001) compared to those with a prior cardiac history. The prevalence of CADwas lower (74.8% vs. 82.6%, p<0.001), and of CMP higher (23.0% vs. 14.7%,p<0.001), among those without a prior cardiac history. The excess prevalence ofCMP among those without a history of prior cardiac disease was mainly due to ahigher rate of alcoholic CMP (6.0% vs. 1.6%, p<0.001) and idiopathic myocardialfibrosis (4.3% vs. 0.9%, p<0.001). A normal autopsy without histological findingsof inflammation or any other cardiac abnormality, suggesting a non-structural in-herited disorder, was rare in this population (0.5% in those without a history ofcardiac disease).Conclusions: CMP, especially alcoholic and myocardial fibrosis, is a more fre-quent cause of SCD when it is the first manifestation of cardiac disease, com-pared to those with a documented prior heart disease.
P435 Prediction of improvement in cardiac function bydobutamine echocardiography in patients with recentonset dilated cardiomyopathy
D.H. Yang, S.H. Park, H.S. Park, S.C. Chae, J.E. Jun. KyungpookNational University Hospital, Daegu, Korea, Republic of
Purpose: Clinical and echocardiographic variables have been used to predictprognosis in patients with DCM. The aim of this study was to investigate whetherthe contractile reserve on dobutamine stress echocardiography (DSE) could pre-dict the myocardial contractile reversibility or prognosis in patients with recent-onset DCM.Method: High-dose DSE was performed in 22 patients with recently diagnosedDCM in incremental stages lasting 5 min each, with an initial dose of 5 mg/kg/min,which was increased to 10 mg/kg/min, then to 20 and 30 mg/kg/min, and finallyto the maximum dose of 40 mg/kg/min. Left ventricular (LV) volume and ejectionfraction (EF) was measured by Simpson’s biplane method. A follow-up echocar-diography was done at 9±6 months.Results: Fourteen patients were men and age was 46±16 years. Resting LVEF,LV end-diastolic volume and LV end-systolic volume was 24±6%, 174±53 mLand 133±44 mL. LVEF were increased to 31±9% at low dose dobutamine andto 36±9% at peak dose dobutamine stimulation. Follow-up LVEF was 39±15%after 9±6 months (Fig 1). Resting LVEF, LV volume, stroke volume, E/E’, Ees,Ea and VVID could not predict follow-up LVEF. However, LVEF, LV volumes, Eesand VVID at peak dose on high-dose DSE, not at low dose, was well correlatedwith follow-up LVEF, especially peak LVEF was most strongly correlated (Fig 2).During follow-up period, 3 died of cardiac causes and 5 readmitted for aggravationof heart failure. In patients with cardiac events, LVEF was lower, LV volumes werehigher and changes of LVEF from resting to peak dobutamine were lower.
Conclusion: High-dose DSE could predict late spontaneous improvement in car-diac function in patients with recent-onset DCM and had prognostic values forfuture cardiac events.
P436 Cardiovascular manifestations associated with severeH1N1 influenza virus infection. A 17-cases prospectivestudy
P. Paule, N.C. Roche, S. Kerebel, J.M. Gil, L. Fourcade. LaveranMilitary Teaching Hospital (HIA), Department of Cardiology, Marseille,
France
During the spring of 2009, a pandemic influenza H1N1 virus emerged and spreadglobally. Influenza is a recognized cause of acute myocarditis. Diagnosis of acutemyocarditis may be difficult, particularly because clinical presentation of my-ocarditis is variable. Even many patients are asymptomatic with only electrocar-diographic abnormalities.Method and results: we report a prospective series of 17 consecutive patientshospitalized for severe biologically proven H1N1 influenza infection between Oc-tober 2009 and January 2010: 7 men and 10 women, 43 years old on average.15 were admitted in a medical intensive care unit and 2 in a reanimation yard.Two patients had chronic obstructive pulmonary disease, 2 were asthmatic andone was diabetic. Clinical presentation was always pneumonia but no patient pre-sented with chest pain. Physical examination found no sign of heart failure. All pa-tients presented with biological inflammatory syndrome (C reactive protein: 134mg/L on average), but none had troponine I elevation.ECG was performed in all cases. It was strictly normal in 16 cases. Only one
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

New frontiers in diseases of the myocardium 37
young black woman had T wave negativity in leads V1 to V3. Echocardiographyrevealed neither left ventricular dysfunction nor segmental motion abnormality orpericardial effusion. Cardiac MRI was performed with cine-MRI and T2-weightedsequences, first-pass perfusion of gadolinium and late enhancement sequences.It showed no abnormality. Holter monitoring remained normal. Two months afterthe acute episode, stress ECG showed normalisation of the repolarisation duringexercise, compatible with a particular pattern in a black person.Conclusions: at the time of admission in our series of 17 patients with severeinfluenza H1N1 virus infection, we found no clinical or paraclinical (ECG or tropo-nine I) disorder suggestive of acute myocarditis.
P437 Clinical, electrocardiographic and biochemicaldifferences between acute myocarditis and Tako-Tsubocardiomyopathy
A. Pastor1, J.M. Rubio Campal1, F. Navarro1, A. Pinero1, B. Ibanez2,L. Duarte1, P. Sanchez-Borque1 , H.P. Gaebelt1, J. Hernandez1 ,
J. Farre1. 1Foundation Jimenez Diaz, Madrid, Spain; 2Hospital Clinic San Carlos,Department of Cardiology, Madrid, Spain
Introduction: Acute myocarditis and Tako-Tsubo cardiomyopathy (TTC) are twodifferent entities sharing a similar clinical presentation (chest pain and cardiacenzymes release mimicking an acute myocardial infarction but without any sig-nificant obstructive coronary artery stenosis). Apart of that, they differ in type ofprecipitating factors, clinical and ECG evolution, levels of cardiac enzymes re-lease, left ventricular ejection fraction (LVEF) and angiographic appearance ofthe LV.Methods: We have analyzed the precipitating factors, clinical presentation, ECGat admission and during hospital stay, levels of enzyme release (CK and troponinI) and LVEF in 80 patients with acute myocarditis and in 19 patients with TTC.Results: Most of the TTC patients were female (85% vs. 5% in the myocardi-tis group; p<0.001) and older as compared with myocarditis patients (70±15vs. 32±12 yr, p<0.001). The presence of a previous emotionally stressful eventwas more frequent in the TTC patients (53% vs. 4% p<0.001). Myocarditis pre-sented a seasonal pattern with preference for the winter season (62% vs. 30%in TTC group; p<0.001). TTC patients showed a higher ST-segment elevation atadmission (3±0.7 vs. 1.9±1mm; p<0.001), a significantly lower LVEF (40±11vs. 55±11%; p<0.001) but a significantly lower enzymatic release [(CK peak281±192 vs. 635±416 U/L; p<0,001), (Troponin I peak 6±4 vs. 15±13 ng/ml;p<0,001)].Conclusions: Acute myocarditis has a clear young male preponderance and isassociated generally with a preserved LVEF, a lower ST segment elevation atadmission and a higher enzyme release, whereas Tako-Tsubo cardiomyopathyis related to elder female and presents with a more severe LV dysfunction anda higher elevation of the ST-segment but a lower enzymatic activity. All theseclinical differences reinforce the idea that the TTC and acute myocarditis must beconsidered two different clinical syndromes that affect very different populationgroups.
P438 ISG-15 is crucial in the pathogenesis of enterovirusmyocarditis
A. Voigt1, N.L. Diny1, E. Opitz1, K. Klingel2, A. Riad3, C. Tschoepe3 ,K.P. Knobeloch4, K. Stangl1, P.M. Kloetzel1. 1Charite - UniversityMedicine Berlin, Campus Mitte, Berlin, Germany; 2Medizinische
Universitaetsklinik Tuebingen, Tubingen, Germany; 3Charite - Campus BenjaminFranklin, Berlin, Germany; 4University Medical Center Freiburg, Freiburg,Germany
Type I Interferon signaling is known to play a major role in enterovirus myocarditis.ISG15 (Interferon stimulated gene of 15kDa) is among the downstream effectorsof Interferon. It is crucially involved in antiviral processes: it alters the structure,stability, activity or subcellular localization of key players in innate antiviral re-sponses like JAK1 and STAT1, pattern recognition receptors and antiviral effectorproteins MxA, PKR and RNaseL. Our interest in ISG15 arises from preliminarydata pointing to a differential regulation of ISGylation processes in enterovirus(CVB3)-induced myocarditis. To investigate the role of ISG15 and ISGylation indetail, ISG15-deficient mice were infected with CVB3 and sacrified at differenttime point post infection. ISG15-deficient mice were highly susceptible to CVB3 in-fection: viral load was tremendously increased already at early stages of infection,which was associated with severe inflammation and tissues necrosis. In contrastto the wt littermates, ISG15-deficient mice developed chronic myocarditis with se-vere fibrosis at later stages of the disease. Also, systemic effects were recorded: amajor weight loss was observed in CVB3-infection in ISG15-deficiency. In conclu-sion, the delayed antiviral response with increased inflammation, high viral loadsand chronic fibrosis in ISG15-deficient mice make the ISGylation pathway a cru-cial host factor in the pathogenesis of enterovirus myocarditis and a potentialtarget for antiviral therapeutic strategies.
P439 PQ segment depression in differentiation ofperimyocarditis and STEMI
V. Kyto, P. Porela, K.E. Airaksinen. Turku University Hospital, Turku,Finland, Finland
Differential diagnosis of perimyocarditis and ST-elevation myocardialinfarction (STEMI) is difficult, especially in crowded emergency departmentswhere availability of imaging modalities is limited and diagnosis of STEMI shouldbe made promptly to allow adequate reperfusion treatment. We studied the PQsegment depression in standard ECG as potential tool to differentiate perimy-ocarditis from STEMI.Methods: Patients admitted to Turku University Hospital in 2002-2007 due toperimyocarditis were retrospectively screened and those in sinus rhythm who ful-filled the ESC/AHA guideline ECG criteria for STEMI on admission and were tro-ponin positive were included (n=34). In addition, guideline fulfilling STEMI patientswith angiographically confirmed diagnosis were randomly selected from the sametime period (n=46). Exclusion criteria were II or III degree atrioventricular block,bundle-branch block and prior coronary bypass surgery. Standard 12 lead ECGsrecorded at hospital admission (prior to reperfusion therapy) were analyzed fordeviation of PQ segment ≥0.5 mm from baseline prior to P wave.Results: Depressions of PQ segment were found in at least two leads in 85.3%perimyocarditis patients and in 10.9% STEMI patients (p<0.001). PQ changeswere depressions in all leads except in AVR in which 47.1% of perimyocarditisand 8.7% of STEMI patients showed PQ segment elevation (p<0.001). In per-imyocarditis PQ depressions were most common in leads II and V3 (in 67.6%and 52.9% respectively) and least common in AVL (in 2.9%). Both precordial andlimb leads showed PQ segment depressions in 85.3% of perimyocarditis patientsand in 2.2% of STEMI patients (p<0.001). Sensitivity of PQ depressions in bothprecordial and limb leads to differentiate perimyocarditis from STEMI was 85%,specificity 98%, positive predictive value 0.97 and negative predictive value 0.9.Conclusion: PQ segment depressions in both precordial and limb leads instadard ECG appears to be useful tool for initial differentiation of perimyocarditisfrom STEMI.
P440 Description of the cardiomyopathy associated withfriedreich’s ataxia
J. Finegold1 , P. Giunti2, W. Mckenna1, P. Elliott1, A. Pantazis1. 1TheHeart Hospital, London, United Kingdom; 2University College London,London, United Kingdom
Purpose: Friedreich’s Ataxia (FRDA) is an autosomal recessive spino-cerebellardegenerative disorder associated with GAA trinucleotide repeat expansions in thecausative frataxin gene. Cardiac involvement in the pathogenesis of this diseasehas been noted since the disorder was first described, albeit inadequately char-acterised. Aim: To describe the cardiomyopathy associated with FRDAMethods: We retrospectively studied 47 consecutive patients (mean age at firstcardiac screening 30.9 ± s.d. 12.6 years - 49% male) with a genetic diagnosis ofFRDA followed at a dedicated cardiac unit between 1984 and 2009 (follow-up 0.6to 24.7 years - mean 5.8).Results: 30 of the patients developed neurological symptoms before the age of16 years. 70% of all the patients had repolarisation abnormalities in the infero-lateral ECG leads. 6 patients had left ventricular wall thickness above ≥13mmand 23 patients had increased relative wall thickness. Echocardiographic charac-teristics of the FRDA population different age groups are shown in Table 1. Fourpatients developed heart failure with EF 20% and atrial fibrillation (1 permanent/3paroxysmal) at a mean age of 41 years. These patients all displayed neurologicalsymptoms <16 years of age.
Table 1. Changes in echocardiographic characteristics in the FRDA population with increasingage
Age (years) at first cardiac screening
10-20 20-30 30-40 40-50 >50
Number of patients 10 13 11 10 3LV ejection fraction (%) 60.6 64.1 63.5 68.3 43.7Number of patients in Heart Failure (EF<20%) 1 0 0 2 1Diastolic interventricular septum thickness (cm) 1.33 0.93 0.9 0.87 0.77Relative wall thickness (RWTma) 0.62 0.5 0.37 0.38 0.27Mitral valve E/A ratio 1.63 1.86 1.24 1.11 1.09
Conclusion: Patients with FRDA often have electrocardiographic abnormalities.RWTma is increased in half of the population. Cardiac complications and HFappear to be prevalent in the patients after the fourth decade of life and only withinthe group of patients who had developed neurological symptoms at a young age.
P441 Acute myocarditis presenting as acute coronarysyndrome: diagnostic importance of early cardiacmagnetic resonance imaging
P. Monney, N. Sekhri, A. Wragg, S. Petersen, C. Knight, L.C. Davies,M. Westwood, P.G. Mills, A. Mathur, S.A. Mohiddin. The London Chest
Hospital, London, United Kingdom
Purpose: In about 10% of patients presenting with features of acute coronary
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

38 New frontiers in diseases of the myocardium / Infiltrative and forage diseases: from disease mechanism to management
syndrome (ACS) and elevated serum troponin, acute myocarditis is often sus-pected after normal coronary angiography. Cardiac magnetic resonance imaging(CMR) may help diagnose myocarditis by demonstrating myocardial oedema (T2imaging) and specific patterns of late gadolinium enhancement (LGE). Reportsof CMR’s sensitivity for myocarditis vary widely; we hypothesised early scanningmore frequently detects diagnostic abnormalities.Methods: We compared consecutive CMR’s of 19 patients admitted with featuresof ACS but non-obstructed coronary arteries: an acute scan (<2 weeks after ad-mission), and a convalescent scan (>3 weeks).Results: All patients were referred to a tertiary centre following a diagnosis ofACS. Mean age was 43±11 years and 63% were male. All had elevated serumtroponin. Five were referred with ST elevation and 14 for non-ST elevation; 18with chest pain and 1 with syncope. The acute scan was performed 4±3 days(median=4, range 0-10) after admission. Mean ejection fraction (EF) was 59±9%with preserved systolic function in 74% and mild systolic dysfunction in 26%. Re-gional wall motion abnormalities (RWMA) were present in 42%, and a pericardialeffusion in 26%. T2-weighted imaging was abnormal in 83%, affecting 3.4±3.8myocardial segments. All patients had regional LGE, involving 5.6±5.0 segments(range 1-16). T2 and LGE abnormalities favoured inferior, infero-lateral and apicalsegments. A convalescent scan was performed 78±67 days (median=46, range22-221) after admission. There was no change in LV volumes but EF increasedsignificantly (62±8%, p<0.05). Mild systolic dysfunction was detected in 17%.RWMA persisted in 5 patients and effusion in 4. Frequency of T2 abnormalitiesdecreased to 34% (p<0.01) involving 1.1±2.1 segments (p=0.01). LGE remaineddetectable in most patients (95%), but decreased to 2.9±3.9 segments (p=0.005).Septal LGE decreased from 24 to 8 segments (p<0.005) but persisted for all inbasal inferolateral segment. Abnormal T2 or LGE signals were never detected insegments previously unaffected.Conclusion: CMR’s diagnostic accuracy for myocarditis is extremely high early inthe illness, declining thereafter. There was no evidence of disease progression,though persistent inflammation was detected in a third. The prognostic impor-tance of the distribution, severity and persistence of the acutely detected abnor-malities remain unknown.
INFILTRATIVE AND FORAGE DISEASES: FROM DISEASEMECHANISM TO MANAGEMENT
P442 Diagnostic value of early electrocardiographic changesin fabry disease
M. Namdar, J. Steffel, M. Vidovic, C.B. Brunckhorst, J. Holzmeister,T.F. Luescher, R. Jenni, F. Duru. University Hospital Zurich, Zurich,Switzerland
Background: Fabry disease (FD) is an inherited X-chromosomal lysosomal stor-age disease resulting in intracellular storage of globotriaosylceramide (Gb3). Car-diac involvement is most frequently manifested as left ventricular hypertrophy(LVH). However, patients with FD may also suffer from various conduction ab-normalities before LVH develops. The present study was designed to analyzeconduction abnormalities in FD without LVH and compare them with a group ofhealthy individuals.Methods and Results: Baseline ECG- and echocardiographic measurementsof patients with FD (n = 30) were compared with those of heart rate- and age-matched healthy individuals (n = 50). There were no differences in baseline de-mographic and echocardiographic parameters between the two groups. In con-trast, PQ-interval (131±18 ms vs. 155±20 ms, p<0.000001) and the QRS-width(83±11 ms vs. 90±9 ms, p<0.05) were significantly shorter, and repolarizationdispersion was more pronounced in patients with FD. Moreover, P-wave durationwas significantly shorter (74±16 ms vs. 105±14 ms, p<0.000001) in FD and ac-counted predominantly for the shortening of the PQ-interval. At a cut-off of 80 ms,P-wave duration showed a 92% sensitivity and 80% specificity for the diagnosisof FD.
ROC P vs. PQ
Conclusions: P-wave duration, PQ-interval and QRS-width is shorter and repo-larization dispersion more pronounced in patients with FD as compared to heartrate- and age-matched controls. The significant shortening of the PQ-interval inFD might be due to accelerated intraatrial impulse propagation manifested by amarked shortening of the P-wave duration. Moreover, the latter demonstrated avery high diagnostic value for FD. Our data may therefore have important diag-nostic and therapeutic implications for the treatment of patients with FD.
P443 Two-dimensional speckle-tracking strain imaging formonitoring enzyme replacement therapy in patientswith Anderson Fabry disease
S. Charwat1, G. Sunder-Plassmann2 , M. Zehetgruber3 , J. Bergler-Klein3, S. Graf3, G. Mundigler3. 1Medical University of Vienna,
Department of Internal Medicine II, Division of Angiology, Vienna, Austria;2Medical University of Vienna, Department of Internal Medicine III, Divisionof Nephrology, Vienna, Austria; 3Medical University of Vienna, Department ofInternal Medicine II, Division of Cardiology, Vienna, Austria
Purpose: Anderson-Fabry disease (AFD) is a rare hereditary X-linked lysoso-mal storage disorder. It is characterized by a deficiency of alpha-galactosidase Awith accumulation of globotriaosylceramide in various organs including the heart.Patients frequently develop myocardial hypertrophy with consecutive diastolic andsystolic left ventricular dysfunction. Enzyme replacement therapy (ERT) has beenshown to provide beneficial effects on cardiac manifestations of AFD. Calcula-tion of global longitudinal strain (GLS) derived from echocardiographic imagesby speckle tracking is a new technique, which may allow monitoring of functionalchanges.Methods: We examined 21 patients (12 females with a mean age of 40 years, and9 males with a mean age of 41 years) with genetically confirmed AFD. 5 womenand 3 men were on ERT at study entry with a mean duration of 15.9±10.5 months.5 of these had an echocardiographic follow up (FUP), at 54.9±20.6 months af-ter start of ERT. Echocardiographic analysis was performed from digitally storedloops by a blinded observer. Thickness of the interventricular septum (IVS) andthe posterior wall (PW) was measured using standard criteria. GLS was calcu-lated from apical 4-chamber, 2-chamber- and apical long axis views using internalsoftware.Results: In the total cohort GLS was -16.8% ± 4.2%. In comparison, patientswith IVS <12mm had nonsignificantly better GLS than pts. with IVS >12mm (-17,7% ± 2.2% vs. -15.8% ± 4.0%, p = 0.37). Correlation between GLS valuesand IVS was r = 0.54, p = 0.06 and between GLS and PW r = 0.58, p = 0.05.Female pts. had worse GLS than male pts. (-15.12% ± 2.3% vs. -18.0% ± 5.0%,p = 0.13). Baseline GLS for pts. on ERT did not differ from those without ERT (-16.3% ± 3.8% vs. -17.0% ± 4.6%, p = 0.5). At FUP, the 4 patients showing a GLShigher than -18.0% at baseline had improved under ERT (from -15.0%±3.9% to-18.5%±5.4%, p=0.02).Conclusions: Worse GLS values are associated with left ventricular hypertrophyin patients with Anderson-Fabry disease. GLS improved during ERT and thusmay provide a novel tool for assessment of treatment effects in such patients.
P444 Prominent papillary muscles in Fabry disease: adiagnostic marker?
M. Niemann, D. Liu, K. Hu, S. Herrmann, S. Stoerk, F. Breunig,G. Ertl, C. Wanner, F. Weidemann. Medizinische Klinik I, Wuerzburg,Germany
Background: Fabry disease is often linked with a prominent papillary muscle.It remains unknown if this sign could be used as a diagnostic marker to screenFabry patients.Methods: In 101 consecutive patients with concentric left ventricular hypertrophy(28 Fabry, 30 Friedreich, 34 isolated arterial hypertension, 9 amyloidosis) and20 healthy controls standard echo was performed. In addition, the areas of bothpapillary muscles as well as the left ventricular (LV) endocardial circumferencewere manually circumscribed in short axis views. A ratio of papillary muscle sizeto LV circumference was calculated (PM_LV_ratio).Results: The papillary muscle size was positively correlated to left ventricular wallthickness in this cohort (p<0.001; r=0.51). In all patient subgroups the absolutepapillary muscle size and the PM_LV_ratio were significantly higher compared tocontrols. However, Fabry patients showed a significant larger absolute papillarymuscle size than Friedreich and amyloidosis patients and a higher PM_LV_ratiothan hypertensive and amyloidosis patients. Enlarged absolute papillary musclesize was evidenced in 21 (75%) and higher papillary muscle to LV circumferenceratio was found in 22 (78%) out of 28 Fabry patients. Combining these two pa-rameters yield a satisfactory sensitivity (=75%) and specifity (=86%) for diagnos-ing Fabry disease. Only 10 out of 73 non-Fabry patients (14%) (4 Friedreich, 1amyloidosis and 5 hypertensive patients) showed an increased absolute papillarymuscle size and PM_LV_ratio.Conclusion: This study confirmed the assumption that the prominent papillarymuscle could be an echocardiographic marker for screening Fabry patients withconcentric left ventricular hypertrophy.
P445 Cardiac involvement in Fabry disease
L. Caballero1, V. Climent1, F. Marin2, A. Garcia Honrubia3, S. Heras1,P. Perez Berbel1, J. Sanchez1, M. Moreno1, M.A. Quintanilla1,F. Sogorb1. 1General University Hospital of Alicante, Departmentof Cardiology, Alicante, Spain; 2Hospital Universitario Virgen de la
Arrixaca, Murcia, Spain; 3General Hospital of Elche, Elche, Spain
Introduction: Fabry disease (FD) is an X-linked lysosomal storage disordercaused by the deficit of the enzyme α-galactosidase A and consequently thedeposit of glicosphyingolipids (Gb3) in different tissues. This multisystemic stor-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Infiltrative and forage diseases: from disease mechanism to management 39
age mainly causes in the heart a symmetric hypertrophic cardiomyopathy andatrioventricular (AV) conduction abnormalities. Recently tissue Doppler imaging(TDI) has been introduced as a new method to quantify regional myocardial func-tion and may detect alterations in myocardial function even before left ventricularhypertrophy occurs. We report a case series of Fabry patients, describing theircardiac affectation and the utility of TDI to study the myocardial performance.Method: We studied 22 patients (12 males, age 43±18 years) genetically di-agnosed of FD. We registered different echocardiography parameters: left ven-tricular wall thickness (LVWT), ejection fraction, left ventricular mass, diastolicfunction, TDI parameters, and AV conduction abnormalities in ECG.Results: Eight patients (38%) were with enzyme replacement therapy. Thirteenpatients (61%) had left ventricular hypertrophy (LVH) in the echocardiography(LVWT 14.5±4.5 mm; left ventricular mass index: 148±60 g/m2) and eight of them(38%) had diastolic dysfunction with an E/Ea ratio >15. Seven patients (33%) hadAV conduction abnormalities: 5% first-degree AV block and 3 (14%) completeheart block. Eight patients (38%) showed attenuated systolic wave values (TDI)in basal septum and 13 (61%) had attenuated strain values in the basal septum,without abnormalities in the mid septum. Patients with LVH had minor values ofsystolic wave and strain in the basal septum than patients without LVH (p<0.05).Conclusions: a significant percentage of patients with FD had cardiac affecta-tion, especially LVH and secondly, AV conduction delay and complete heart block.Abnormalities of systolic wave and strain in the basal septum can help to charac-terize patients with HVI and suspicion of Fabry disease.
P446 Interference of cardiac amyloidosis on atrio-ventricularand intraventricular electrical conduction
S. Perlini1, F. Salinaro1, F. Musca1, I. Fracchioni1 , I. Zunino1,E. Demichele1, L. Obici2, G. Palladini2, C. Rapezzi3, G. Merlini2.1Clinica Medica II, Fondaz IRCCS S.Matteo, University of Pavia,
Pavia, Italy; 2Center for Amyloidosis, Biotechnology Laboratories IRCCSSan Matteo, Pavia, Italy; 3University Hospital Polyclinic San Orsola-Malpighi,Department of Cardiology, Bologna, Italy
Background: In cardiac amyloidosis extracellular amyloid deposition leads tomarked increases in myocardial electrical impedance and enhanced anisotropyin impulse conduction. This is associated with different degrees of conduction de-lays and may participate to the development of re-entry circuits, that in turn mayexplain repetitive supraventricular or ventricular arrhythmias.Methods: To assess the prevalence of atrio-ventricular and intra-ventricular con-duction delays, 12-lead electrocardiograms (EKG) were evaluated in 228 consec-utive newly diagnosed patients with cardiac AL amyloidosis and sinus rhythm,who were referred between 2006 and 2009. Patients in whom cardiac involve-ment was excluded served as controls (n=81). EKG tracings were analysed inorder to measure PQ, QRS, and QT intervals, and to annotate the presence of in-traventricular conduction delays (complete or incomplete right/left bundle branchblock, left anterior or posterior hemiblock). Patients with atrial fibrillation or with apacemaker were not included in the present analysis.Results: When compared with patients without myocardial involvement, patientswith cardiac AL showed higher heart rate (75±14 vs 69±13 b/min, p<0.001) anda longer PQ interval (179±31 vs 205±49 msec, p<0.001), without significantchanges in mean QRS interval (83±12 vs 84±11 msec, p=ns) or in QT dura-tion (400±36 vs 400±49 msec, p=ns). The prevalence of intraventricular con-duction delays (ranging from incomplete to complete bundle branch block) wasnot increased in patients with cardiac AL. In contrast, patients with newly diag-nosed cardiac AL showed a much higher prevalence of atrio-ventricular conduc-tion delays (29% vs 3%, p<0.001), ranging from first-degree to third-degree atrio-ventricular block. No difference between the two groups was observed in terms oftreatment with drugs having negative dromotropic effects, such as digoxin, beta-blockers or non-dihydropyridine calcium antagonists.Conclusions: In evaluating patients with cardiac AL amyloidosis at diagnosis,care should be taken to identify atrio-ventricular conduction delays, by a sim-ple 12-lead electrocardiogram. This will help selecting patients in whom furtherdiagnostic steps are needed to warrant a proper cardiological support to AL treat-ment.
P447 The contribution of the EKG/echocardiographic massratio to the diagnosis of cardiac AL amyloidosis
F. Salinaro1, I. Fracchioni1 , I. Zunino1, E. Demichele1, F. Musca1,A. Milan2, F. Veglio2, C. Rapezzi3, G. Merlini4, S. Perlini1. 1ClinicaMedica II, Fondaz IRCCS S.Matteo, University of Pavia, Pavia, Italy;
2Department of Internal Medicine, University of Torino, Torino, Italy; 3UniversityHospital Polyclinic San Orsola-Malpighi, Department of Cardiology, Bologna,Italy; 4Center for Amyloidosis, Biotechnology Laboratories IRCCS San Matteo,Pavia, Italy
Background: In cardiac amyloidosis the increase in wall thickness caused byextracellular amyloid deposition leads to marked increases in left ventricular (LV)mass. At variance with other forms of cardiac hypertrophy, this is often associ-ated with abnormally low electrocardiographic (EKG) voltages, due to the nega-tive effects of amyloid infiltration on intracardiac electrical conduction. Althoughalmost 1/3 of cardiac AL patients do not strictly fulfil the definition of EKG lowvolt-ages (<5 mV in all peripheral leads), such a discrepancy (low EKG "electrical"
LV mass/high echo-derived LV mass) might be a powerful clue suggesting thediagnosis of cardiac amyloidosis.Methods: To evaluate the possible relevance of this finding, we compared anindex of the EKG/echo mass estimate in patients with cardiac AL (n=218), non-cardiac AL (n=69), hypertension with different degrees of LV hypertrophy (n=125),and in normotensive patients withnormal LV mass (n=99). Echo-derived LV masswas estimated via the Devereux’s formula and indexed to body surface area(g/m2), whereas the peripheral lead QRS score (i.e. the sum of QRS voltagesin the conventional peripheral leads, mV) was used as an index of "electrical" LVmass. EKG/Echo ratio was expressed as[mV/(g/m2)]. Care was taken to excludepatients with other possible causes of low EKG voltages, such as large pericar-dial effusions, obesity, chronic obstructive lung disease, and severe peripheraloedema.Results: No difference was observed in the EKG/echo mass ratio when com-paring patients with non-cardiac AL with either normotensive or hypertensivesubjects, indicating a "normal" relationship between LV mass and EKG volt-ages [0.51±0.12, 0.54±0.13, and0.49±0.15 mV/(g/m2), respectively]. In contrast,the EKG/echo mass ratio was markedly depressed in patients with cardiac AL[0.19±0.10 mV/(g/m2), p<0.001]. The area underthe ROC curve for the detec-tion of cardiac AL involvement was high: 0.96 (95%CI, 0.93 to 0.98). The bestcutoff for the diagnosis of heart involvement was 0.33 mV/(g/m2), giving a 93.8%sensitivity and a 91.1% specificity.Conclusions: In patients with unexplained LV hypertrophy, an abnormally lowEKG/echo mass ratio might be a powerful clue suggesting the diagnosis of car-diac amyloidosis.
P448 Patterns of myocardial infiltration in cardiacamyloidosis: a morphometric histologic study
S. Longhi, O. Leone, C. Quarta, G. Galati, C. Gagliardi, C. Villani,M. Lorenzini, F. Lai, C. Rapezzi. University Hospital Polyclinic SanOrsola-Malpighi, Bologna, Italy
Purpose: To define the histologic patterns of myocardial amyloid infiltration (inorder to improve the interpretation of Magnetic Resonance Imaging with LateGadolinium Enhancement (MRI-LGE)).Methods: We analyzed 9 hearts of pts with primary (n=5) or hereditarytransthyretin (n=4) amyloidosis explanted during heart transplant or autopsy. Foreach heart, a histologic macrosection of left ventricle (LV) was obtained at thepapillary muscle level and 6 segments (anterior, posterior, inter-papillary, lat-eral, septal anterior and septal posterior) and 3 concentric layers were identified(Figure). Mallory trichrome staining was used to characterize amyloid. A semi-automatic system (Image Plus Software) was used to identify and quantify musclecells, fibrosis and amyloid infiltration within each segment and layer.Results: Distribution of amyloid deposition among the 6 segments was not uni-form; the percentage of amyloid in each segment was as follows: septal anterior21±7%; septal posterior 17±8%, anterior 21±10%; posterior 11±8%; interpapil-lary 15±10%; lateral 15±8%. Amount of infiltration was highest in subendocardiallayer (49±16%) followed by subepicardial (30±6%) and middle layers (21±11%);however, inter-patients variability was very high. In 8/9 hearts we identified 3 to 6macro-areas of amyloid infiltration (ranging from 3 to 18% of the overall surfaceof LV section and comprising multiple, contiguous segments and layers.
Conclusions: Although amyloid most frequently involves the subendocardiallayer of LV, interindividual variability is high. Myocardial infiltration is not uniformlydistributed but often aggregates in large transmural areas, converging across thevarious ventricular segments. Awareness of this finding is necessary to properlyinterpret MRI-LGE of pts with cardiac amyloidosis.
P450 Can strain by speckle tracking imaging differentiatebetween survivors and non-survivors in primaryamyloid patients with normal left ventricle ejectionfraction?
H.K. Saleh, H.R. Villarraga, D. Bellavia, Y. Yu, Y. Koshino, J.F. Hsiao,G.C. Kane, P.A. Pellikka, F.A. Miller. Mayo Clinic, Rochester,
Minnesota, United States of America
Background: The aim was to assess left ventricular strain (S) and systolic strainrate (SR) by speckle tracking Echocardiography (STE) in survivors and non-survivors of biopsy proven primary amyloid patients with preserved left ventricleejection fraction (LVEF).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

40 Infiltrative and forage diseases: from disease mechanism to management
Methods: 118 patients & 66 controls were studied. Subjects with LVEF <50%,severe valvular disease, arrhythmia, or prior cardiac surgery were excluded. LVglobal (G) longitudinal (L) & circumferential (C) strain (GLS, GCS) and systolicstrain rate (GLSR, GCSR) were measured (Velocity Vector Imaging, SiemensMedical Solutions, Malvern PA). During median follow-up of 4 (2,5) years, 43 pa-tients died.Results: Basic characteristics of survivors vs non survivors included: age 58±9years vs. 60±11 years, p=0.3; BMI 26±5 kg/m2 vs. 25±4 kg/m2, p=0.11; LVMI108±32 g/m2 vs. 140±42 g/m2, p<0.001; left atrial volume index (LAVI) 35±11vs. 42±12 cc/m 2, p=0.005; LVEF 64±6% vs. 65±7%, p=0.6; e’ 0.08±0.11 m/secvs. 0.06±0.02 m/sec, p=0.04; E/e’ 12±7 vs. 19±13, p=0.003; respectively.GLS and GLSR in patients vs control (-13±4% vs. -17±2%, p<0.001 and -0.77±0.23 s-1 vs. -0.96±0.14 s-1, p<0.001) respectively and in non-survivorsvs. survivors (-10±4% vs -14±4%, p<0.001 and -0.67±0.25 s-1 vs -0.82±0.21s-1, p=0.002) respectively.GCS and GCSR were not significant.GLS and GLSR were good differentiators between survivors and non-survivorswith AUC values of 0.84 and 0.78, after adjusting for gender, BMI and LVMI with(HR 1.25, CI [1.09, 1.45], p=.001) for GLS and (HR 1.12, CI [1.03, 1.28], p=.005)for GLSR. (Figure)
Survival Probability By Global L S
Conclusion: In amyloid patients with normal LVEF GLS and GLSR are signifi-cantly reduced in non-survivors. This method could prove useful as a prognostictool.
P451 Effect of myocardial iron removal on right ventricularfunction: insights from a randomized, placebocontrolled, double-blind trial in thalassemia major
F. Alpendurada1, J.P. Carpenter1, G.C. Smith1, M.A. Tanner1 ,W. Banya1, R. Galanello2, D.J. Pennell1. 1Royal Brompton Hospital,
London, United Kingdom; 2Ospedale Regionale per le Microcitemie, Cagliari,Italy
Purpose: Combined therapy with subcutaneous deferoxamine (DFO) and oraldeferiprone is superior to DFO monotherapy in removing cardiac iron and im-proving left ventricular ejection fraction (EF) in thalassemia major (TM) patients.The aim of this study was to assess the effects of combined treatment versusDFO monotherapy on right ventricular (RV) function in TM patients with cardiaciron overload.Methods: 65 TM patients on DFO monotherapy with mild to moderate myocar-dial iron (T2* 8-20ms) were randomized to receive additional oral placebo (DFOgroup) or oral deferiprone (combined group). Cardiac T2*, RV volumes and EFwere evaluated using cardiovascular magnetic resonance at baseline and 12months. Observers were blinded to chelation regime. RVEF and RV volumes werecompared using a paired two-tailed t-test. ANCOVA was used to compare changein T2* and RVEF with treatment and baseline measures as covariates.Results: The combined group was superior to the DFO group for improvementin T2* (ratio of change in geometric means 1.50 vs. 1.24, p=0.02) and improve-ment in RVEF (3.7 vs 0.3%, p=0.01). In the combined group, RVEF increasedfrom 59.1±6.6% at baseline to 62.8±5.7% at 12 months (p<0.001) whereas inthe DFO group, RVEF did not improve significantly (59.9±7.4% vs 60.2±6.7%,p=0.79). The increase in RVEF was greater in patients with baseline T2* below12ms (4.7 vs -0.4%, p=0.005) than those with T2* above 12ms (2.5 vs 0.8%,p=0.41). There was no difference in end-diastolic volume between groups.
Change in RVEF over 12 months
Conclusions: In TM patients with mild to moderate cardiac iron loading, RV func-tion improves with combined treatment, and this is superior to standard chelationwith DFO alone. The improvement in RV function is more significant at higherbaseline levels of iron loading.
P452 Relationship between myocardial iron load asassessed by T2* and left ventricular systolic functionin a large cohort of unselected thalassemia majorpatients on modern therapy
D. Farmakis1 , E. Polymeropoulos1 , A. Giakoumis1, E. Gotsis2,A. Aessopos1. 1Laiko University Hospital, Athens, Greece; 2InstituteEuromedica-Encephalos, Athens, Greece
Aim: Left heart failure, resulting primarily from transfusional iron overload, is theleading cause of mortality in patients with thalassemia major. T2* value, derivedby cardiac magnetic resonance (CMR) imaging, is the most accurate methodto evaluate myocardial iron load; its relationship however with left ventricular (LV)systolic function has not been adequately assessed in large cohorts of unselectedpatients receiving modern therapy.Methods: We studied 610 consecutive thalassemia major patients, aged29±8years (range, 8-59 years), on regular blood transfusions (pre-transfusionhemoglobin ≥9.5 g/dL) and standard iron chelation regimens (deferoxamine, de-feriprone or both). Patients underwent CMR for the assessment of myocardial T2*and LV ejection fraction (LVEF).Results: Mean myocardial T2* was 23±12 ms; 20% of patients had severe ironload (T2* <10 ms), another 20% had mild iron load (T2* 10-20 ms) and the re-maining 60% had no detectable myocardial iron (T2* >20 ms). Mean LVEF was66±7%; 2% of patients had overt LV systolic dysfunction (LVEF <50%) and 12%had slightly impaired LV systolic function (LVEF 50-59%); LVEF was significantlycorrelated with T2* (Spearman’s rho=0.189, p<0.001; Figure, left panel). In thesubgroup with severe iron load, 8% of patients had LVEF<50% and 20% hadLVEF 50-59%. In the subgroup with mild iron load, none of patients had LVEF<50%, but 13% had LVEF 50-59%. Finally, in the subgroup with no detectablecardiac iron, 1 patient had LVEF<50% and 7% of patients had LVEF 50-59%(Figure, right panel).
Conclusion: In unselected thalassemia major patients on modern therapy, LVEFhas a continuous linear relationship with myocardial iron load and even mild ornot detectable iron burden may be associated with LV systolic dysfunction.
P453 Impact of systemic sclerosis on electromechanicalcharacteristics of the heart
T. Karaahmet1 , K. Tigen1, E. Gurel1, M. Takir2, A. Avci1, C. Cevik3,S. Pala1, C. Dundar1, Y. Basaran1. 1Kartal Kosuyolu Heart Educationand Research Hospital, Istanbul, Turkey; 2SB Goztepe Education and
Research Hospital, Istanbul, Turkey; 3Texas Tech University Health SciencesCenter, Lubbock, Texas, United States of America
Purpose: Primary myocardial involvement is common in systemic sclerosis(SSc). We evaluated the atrial and ventricular electromechanical characteristicsby using tissue Doppler echocardiography in patients with SSc with subclinicalcardiac involvement.Methods: Twenty-seven consecutive patients (24 women; mean age ± SD49.9±11.3 years) presenting with SSc without pulmonary arterial hypertensionor symptomatic heart failure were prospectively studied. Electrocardiographic Pwave dispersion (Pd), corrected QT dispersion (QTcd), interatrial, intraatrial, inter-ventricular and intraventricular electromechanical delays were analyzed by tissueDoppler echocardiography and BNP levels were measured. Results were com-pared with 17 healthy controls.Results: There was no difference in conventional and tissue Doppler parame-ters between two groups. However, patients with SSc had higher mean Pd (mean[±SD] 46.8±15 ms, 36±8 ms, respectively, p=0.004) and mean interatrial elec-tromechanical delay time (DT) (mean [±SD] 32.2±9.2 ms, 24.7±9.7 ms, respec-tively, p=0.01), mean electromechanical delay time for all segments (Mean Ts)(mean [±SD] 148.8±18.8 ms, 129.3±13.4 ms, respectively, p<0.001) and intra-ventricular DT (mean [±SD] 27.6±12.5 ms, 16.2±7.2 ms, respectively, p<0.001).Intraventricular DT was the only parameter that correlated significantly with Mean-Ts. BNP levels were within normal limits in both groups, however they were higherin patients with SSc than in controls. (mean [±SD] 37.5±28.5 pg/mL, 23.1±16.0pg/mL, respectively, p=0.03).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Infiltrative and forage diseases: from disease mechanism to management / Experimental studies on ischemia-reperfusion 41
Conclusions: Evaluation of atrial and ventricular electromechanical parametersby using tissue Doppler echocardiography seems to be useful to detect subclinicalcardiac involvement in SSc patients with normal conventional echocardiographicfindings.
P454 Prognostic value and follow-up utility of plasma brainnatreuretic peptide in cardiac sarcoidosis
Y. Yoshikazu1, M. Horigome1, T. Seki1, A. Izawa2, M. Hongo2,U. Ikeda1. 1National Matsumoto Medical Center, Matsumoto, Japan;2SHinshu University, Matsumoto, Japan
Background: Corticosteroid treatment is generally indicated in patients with car-diac sarcoidosis (CS). A reliable heart-specific marker for the monitoring of steroidtreatment remains to be established in CS. Although plasma brain natriuretic pep-tide (BNP) level is related to the severity of heart failure, clinical utility of BNPmeasurement on the follow-up of CS patients treated with corticosteroids is un-known.Methods: We studied 30 CS patients who measured plasma BNP levels, andcompared the values to clinical findings and outcome. Serial measurements werealso performed before and during steroid treatment.Results: At the time of BNP measurement, 8 patients showed abnormal gallium-67 uptake in the myocardium. BNP levels of the 8 patients were significantlyhigher than those of the other patients with negative results (549±515pg/ml ver-sus 104±122pg/ml, p<0.05), although left ventricular ejection fraction was similarbetween the two groups. Plasma BNP levels of 16 patients requiring device thera-pies were significantly higher than those of the other 14 patients (342±459pg/mlversus 43±35pg/ml, p<0.05). All patients received oral prednisone with an ini-tial dose of 30mg/day and a maintenance dose of 5 to 10mg/day. Plasma BNPconcentrations were unchanged within 6 months after starting corticosteroids(221±144pg/ml to 188±124pg/ml, not significant), but significantly decreased un-til 12 months (221±144pg/ml to 118±136pg/ml, p<0.05). During a mean follow-up of 3 years, we clinically detected relapse of cardiac lesions in 8 patients pre-senting with recurrence of abnormal myocardial gallium-67 uptake, conductiondisturbance or arrhythmias, or rapid worsening left ventricular ejection fraction(LVEF) after the long-term stable clinical course. The 8 showed a significantly in-creased BNP level when the relapse occurred (58±53pg/ml to 125±116pg/ml,p<0.05). After an increase in corticosteroid dose or addition of methotrexate,the BNP levels were significantly decreased (125±116pg/ml to 58±68pg/ml,p<0.05). Cardiac event-free survival was significantly worse in patients with BNP>100pg/ml than BNP <100pg/ml (log-rank:11.0, p <0.01).Conclusions: Plasma BNP levels may be related to the disease activity andseverity in CS. Serial measurements of BNP are helpful for the management ofCS patients treated with corticosteroids.
EXPERIMENTAL STUDIES ON ISCHEMIA-REPERFUSION
P455 Sphingolipid levels in transient cardiac ischemia andthe underlying signaling pathway(s) and mechanismsfor the cardioprotective effect of sphingolipid moleculeS1P and its analogue drug FTY720
E. Eroume A Egom1, M.A. Mamas1, M.T.A. Mohamed1, V. Charlton-Menys1, J.K. Cruickshank1, L. Neyses1, E. Cartwright1, F. Fath-Ordoubadi2 ,M. Lei1. 1University of Manchester, Manchester, United Kingdom; 2UniversityHospital of South Manchester, Manchester, United Kingdom
Purpose: Animal studies suggest that sphingolipids are important signalingmolecules produced by cardiac tissue during ischemic stress. We investigatedwhether plasma long chain sphingoid bases (LCSB) concentrations were alteredby transient cardiac ischemia following temporary coronary artery occlusion dur-ing percutaneous coronary intervention (PCI) in humans. In experiments reportedhere, we also investigated the signaling through the S1P cascade by LCSB un-derlying the S1P cardio-protective effect.Methods: Venous samples were collected from either the coronary sinus (n=7)or femoral vein (n=24) of 31 patients aged 40 to 73 years-old at 1, 5 min and 12 h,following induction of transient myocardial ischemia during elective PCI. PlasmaLCSB levels were assessed by spectrophotometry. LDH cytotoxicity assay wasused to assess the cardioprotective effect of LCSB-related compounds on CoCl2-induced hypoxia or global ischemia in neonatal cardiac myocytes. The effect ofFTY720 on activation of Pak1/Akt was assessed by western blot.Results: At 1 min coronary sinus levels of LCSB were increased by 1072% (n=7,all P<0.001), while peripheral blood levels were increased by 579% (n=24). At5 min, coronary sinus LCSB levels were still increased (941%), as were pe-ripheral levels of LCSB (617%, 95% CI). At 12 h, peripheral levels of LCSB re-mained greater than baseline levels in all patients (436%). All these LCSB relatedmolecules displayed protective effects against hypoxic/ischemic cell injury, reduc-ing dramatically LDH release compared with controls. There was a significant in-crease in phospho-Pak1/Akt levels after 15 mins of treatment with 25 nM FTY720compared with control non-treated myocytes. However, there was no significantdifference in the levels non-phospho-Pak1/Akt expression between non-treatedand FTY720 treated. The activation of Pak1/Akt was significantly PTX-sensitive.
Our data also showed that FTY720 triggered the NO release from cardiac my-ocytes through PTX-sensitive PI3K/Akt/eNOS.Conclusions: This study demonstrates, for the first time, the behaviour of plasmaLCBS following transient cardiac ischemia in humans with dramatic and early in-creases in LCBS. Our data also indicate that the cardio-protective effect of LCBSis likely to involve activation of signaling through the Pak1/Akt/eNOS cascade.
P456 Remote postconditioning compared with localpostconditioning in a rat model of myocardialinfarction
N. Ghaboura1 , S. Tamareille1, A. Croue2, V. Mateus1, J. Jeanneteau1 ,D. Henrion3, A. Furber1 , F. Prunier1. 1University Hospital of Angers,UPRES 3860 (LPRM), Angers, France; 2University Hospital of Angers,
Angers, France; 3Inserm U771 CNRS UMR 6214, Angers, France
Background: Remote postconditioning (RIPost), a new concept of applying briefischemic stimulus in a distant organ after onset of the myocardial ischemia butprior to the reperfusion, can offer cardioprotection against ischemic/reperfusion(I/R) injury. The aims of the present study were to examine whether: 1) RIPost isas effective as local myocardial ischemic postconditioning (IPost), 2) the combi-nation of RIPost and IPost may enhance cardioprotection, 3) RIPost involves theRISK pathway activation as known in the IPost.Methods: Forty-three open chest rats were exposed to 40 min ischemia inducedby coronary artery occlusion followed by 2 hours of reperfusion and divided intothe following groups: 1) Control (n=6, no additional intervention); 2) IPost (n=7,LAD was subjected to 3 cycles of 10 sec occlusion/10 sec reperfusion at thebeginning of the reperfusion); 3) RIPost (n=6, limb underwent one cycle of 10min I/10 min R, started at 20 min after LAD ligation); 4) IPost+RIPost (n=6); 5)IPost+PI3K inhibitor wortmanin (Wort 15μg/kg, injected in the femoral vein 15min after LAD ligation) (n=6); 6) RIPost+Wort (n=6), 7) IPost+RIPost+Wort (n=6).Area at risk (AR) and infarct size (INF) were measured using Evans blue and TTCstaining.Results: Both RIPost and IPost reduced INF/AR as compared to Control(24.69±6.02% and 34.25±3.36% vs 54.93±6.46% respectively, p<0.05 for bothgroups). Additional cardioprotection was found in the combined IPost+RIPostgroup in comparison with Control and IPost groups (18.04±4.89%, p<0.05 vsControl and IPost). IPost+RIPost decreased INF/AR as compared with RIPost butthe difference was not significant (p=0.41). The significant decrease in infarct sizewas abolished in IPost, RIPost and combined IPost+RIPost groups when PI3K/Aktsignaling pathway was inhibited by wortmanin.Conclusion: RIPost was effective as IPost to prevent I/R injuries with a trendtoward superiority of RIPost. Similarly to IPost, RIPost involved the activation ofthe RISK pathway. Easier to apply with at least similar cardioprotection than IPost,RIPost seems an attractive strategy to decrease reperfusion injury.
P457 The GSK3-b inhibitor 6-bromoindirubin reduces theinfarct size via suppression of mitochondrial proteinsin anesthetized rabbits
I. Andreadou1, E.K. Iliodromitis2, A. Zoga2, D. Haratsi1, C. Katseli1,K. Vougogiannopoulou1 , M. Anastasiou-Nana2, D.T.H. Kremastinos2.
1University of Athens, Faculty of Pharmacy, Athens, Greece; 2Universityof Athens, Medical School, Second University Dept. of Cardiology, Athens,Greece
Purpose: Ischemic preconditioning (PC) and postconditioning (PostC) protect theischemic heart by limiting the infarct size. Common ligands, receptors and intra-cellular mediators target against lethal reperfusion injury by preventing openingof the mitochondrial permeability transition pores (mPTP). Several studies con-cerning the role of glycogen synthase kinase-3β (GSK-3β) as a common targetproximal to mPTP opening have been conducted so far in cardiac cells, isolatedhearts and transgenic animals with rather controversial findings. However, in vivostudies elucidating the role of GSK-3β are missing and molecules that ultimatelydetermine the level of tolerance against cell death after reperfusion have not beenidentified. Aim: We sought to determine whether pharmacological inhibition ofGSK-3β at reperfusion by the specific inhibitor 6-bromoindirubin (BIO) is essen-tial for cardioprotection in anesthetized rabbits.Methods: Forty four New Zealand white male rabbits were randomly divided into4 groups and were subjected to 30min regional ischemia of the heart and 3hoursreperfusion with the following additional interventions: Control group not otherintervention, PostC group was subjected to 8 cycles of 30sec ischemia/30secreperfusion immediately after the end of the index ischemia, BIO-5 and BIO-10groups treated with 5 and 10 mg/kg-1 of BIO respectively, given intravenously atthe 20th min of sustained ischemia. After the end of reperfusion period, the in-farct size (I) was delineated by TTC staining, the area at risk (R) by fluorescentparticles and the percent (%) I/R ratio was calculated. In a second series of ex-periments, four respective to the first series groups were subjected to the sameprotocol up to the 10th min of reperfusion where the hearts were quickly excisedand immersed in liquid nitrogen for GSK-3β, voltage-dependent anion channel(VDAC) and adenine nucleotide translocator (ANT) assessment.Results: Infarct size was significantly reduced in PostC, BIO-5 and BIO-10 groups(I/R 26.4±2.3%, 34.0±2.6%, 28.9±4.3% respectively, vs 49.5±3.9% in Control,p<0.05). The administration of BIO at both doses inhibited the total GSK3-β level
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

42 Experimental studies on ischemia-reperfusion
(p<0.01) and the levels of total VDAC and ANT (p<0.01) in the ischemic regionof the heart.Conclusion: We conclude that total inhibition of GSK3-β protects the heart atreperfusion by decreasing both VDAC and ANT and possibly preventing mPTPopening. Inhibition of GSK3-β may should be considered as an essential target ofnovel therapy for cardioprotection upon reperfusion.
P458 Carotid remote perconditioning is a strong stimulus forinfarct size reduction in anesthetized rabbitsindependently of PI3-Akt pathway
E. Mastromanolis1 , A. Zoga1, I. Andreadou2 , D. Farmakis1 ,A.R. Vrettou1, E.K. Iliodromitis1, M. Anastasiou-Nana1,
D.T.H. Kremastinos1. 1Attikon University Hospital, Athens, Greece; 2University ofAthens, Faculty of Pharmacy, Athens, Greece
Background: Postconditioning (PostC), consisted of short-lived episodes ofischemia/reperfusion, confers myocardial protection against infarction. Notonly local PostC but also the remote application of short episodes of is-chemia/reperfusion, preferably called perconditioning (PerC), renders the heartmore tolerant to lethal injury. However, the most suitable timing of PerC applica-tion is not known. In the present study, we sought to determine the effectivenessof PerC at different time points in relation to myocardial ischemia in vivo and toevaluate whether PI3K-Akt pathway is involved.Method: We studied 38 open-chest New Zealand, white, male, anesthetized rab-bits. All animals were subjected to 30-min regional myocardial ischemia, by lig-ation of a prominent coronary artery, followed by 3-hour reperfusion. PerC wasaccomplished by ligation of left carotid artery and consisted of 4 cycles of 60-secischemia/60-sec reperfusion. The animals were randomly divided into 6 groups,according to the presence and the timing of PerC: Control group: no PerC; PerC-A group: PerC started at 29.30 min of myocardial ischemia and ended at 6.30 minof reperfusion; PerC-B group: PerC started at 23.30 min of ischemia and endedat 0.30 min of reperfusion; PerC-C group: PerC started at 22.30 min of ischemiaand ended at 29.30 min of ischemia; PerC-D group: PerC started at 0.30 minof reperfusion and ended at 7.30min of reperfusion; Perc-A-Wort group: sameintervention with Perc-A group but treated with the PI3K inhibitor Wortmannin(20μg/kg iv) 30 sec before myocardial reperfusion. The infarct size (I) and areaat risk (R) were delineated with the aid of TTC staining and green fluorescentmicrospheres, respectively, and their ratio was expressed in percent (%I/R).Results: The %I/R was significantly reduced in all study groups subjected to PerC(22.7±2.1% in PerC-A, 23.8±3.2% in PerC-B, 29.3±3.7% in PerC-C, 31.6±3.8%in PerC-D and 22.5±4% in PerC-A Wort vs 47±2.55% in Control group, p< 0.05).Conclusion: The present study confirms that PerC, induced by short-lived occlu-sions of the carotid artery, is a strong stimulus for the reduction of infarct size inanesthetized rabbits, independently of its timing and the PI3K-Akt pathway.
P459 Exercise training restores cardioprotection againstischemia-reperfusion in obese ob/ob mice
O. Bouhidel, B. Ghaleh, V. Martin, R. Zini, D. Morin, A. Berdeaux,S. Pons. INSERM U 955 Equipe 03, Creteil, France
Background: Previous studies using healthy animals have demon-strated cardioprotective effects of physical exercise against ischemia-reperfusioninjury. Among the different mechanisms associated with this cardioprotectivestrategy, up-regulation of the pro-survival signaling pathway so-called the reper-fusion injury salvage kinase (RISK) and the mitochondrial protection have beendemonstrated to play a key role. However, it is well known that obesity, a major riskfactor for cardiovascular diseases, impairs these cardioprotective signaling path-ways (e.g., during postconditioning or pharmacological cardioprotection). There-fore, we examined if so, the cardioprotective effects of exercise are maintained ina context of obesity and the mechanisms implicated.Methods: To address this issue, leptin-deficient obese (ob/ob) and C57BL/6J(WT-used as control) male mice were assigned to four groups at 5 weeks of age:sedentary ob/ob, exercise ob/ob, sedentary WT and exercise WT. Exercise groupswere submitted to a regular muscular exercise (5 days/7 during 3 weeks). A firstgroup of mice underwent 30 min of coronary artery occlusion followed by 24 hof reperfusion for infarct size measurement. Additional mice were sacrificed at 10min of reperfusion for western blot analysis and mitochondrial studies.Results: In WT mice, physical exercise reduced significantly infarct size (-52%,p<0.05) and increased the phosphorylation of kinases such as Akt, ERK 1/2,p70S6K1, AMPK and GSK3β. The level of corresponding phosphatases (PTEN,MKP3 and PP2C) was simultaneously decreased. Oxygraphic and fluorimet-ric studies performed on isolated mitochondria from the infarcted myocardiumshowed that oxidative phosphorylation parameters were improved and calciumconcentration opening mPTP was increased in exercise WT as compared withsedentary WT. Interestingly, exercise induced a similar cardioprotective effect inob/ob mice than in WT mice with a similar reduction in infarct size (-54%, p<0.05),increase in kinase phosphorylation, decrease in phosphatase expression and im-provement of mitochondrial function.Conclusion: These results demonstrate that chronic exercise elicits cardiopro-tection in ob/ob mice and restores normal cardioprotective phenotype and signal-ing pathway despite maintenance of obesity.
P460 Inhalation of hydrogen gas reduced infarct sizefollowing ischemia and reperfusion via mitochondrialKATP channels in canine hearts
A. Yoshida1, H. Asanuma2, H. Sasaki1, S. Sanada1, S. Yamazaki1,S. Takashima3 , T. Minamino3, M. Asakura1, M. Kitakaze1. 1National
Cardiovascular Center, Suita, Osaka, Japan; 2Kinki University, School ofMedicine, Osakasayama, Japan; 3Osaka University Graduate School ofMedicine, Osaka, Japan
Purpose: Inhalation of hydrogen (H2) gas has been demonstrated to limit in-farct size against ischemia-reperfusion injury in rat hearts. H2 gas selectively re-duces the level of hydroxyl radicals, the most cytotoxic of reactive oxygen species.However, the exact cellular mechanism has not been elucidated. We investigatedwhether the inhalation of H2 gas reduces infarct size in canine hearts and mito-chondrial ATP-sensitive K+ channels (mKATP) is attributable to its protection.Methods: After randomization to either H2 (1.3% H2 gas, 30% O2 and 68.7% N2)or control group (30% O2 and 70% N2), the left anterior descending coronaryartery of the open-chest beagle dog was occluded for 90 minutes followed byreperfusion for 6 hours. Either H2 (n=5) or control gas (n=5) was inhaled justbefore reperfusion until 1 hour of reperfusion. In addition, 5-hydroxydecanoate(5-HD, 10 mg/kg), a selective mKATP blocker was infused into a systemic vein for5 min before gas inhalation [H2 gas with 5-HD group (n=5) and control gas with5-HD group (n=5), respectively]. Risk area and infarct size were assessed withEvans Blue and triphenyltetrazolium chloride, respectively.Results: H2 gas reduced infarct size normalized by risk area (16.1±12.9% vs.44.8±16.3%; p<0.05), and 5-HD abolished the effect of H2 gas (48.0±22.4%with H2 gas vs. 45.3±3.4% with control gas; p<0.01). There were no differencesin either area at risk or collateral flow among the four groups.
Myocardial Infarct Size
Conclusions: The inhalation of H2 gas potently reduces infarct size mainly viareduction of reperfusion injury following myocardial ischemia in canine hearts,which is mainly attributable to mitochondrial ATP-sensitive K+ channels. H2 gasmay be an effective adjunctive therapy in acute MI patients with reperfusion ther-apy.
P461 Alteration of RISK/GSK-3beta signaling in diabetic rathearts impairs erythropoietin-induced cardioprotection
N. Ghaboura1 , S. Tamareille1, A. Croue2, D. Henrion3, A. Furber1 ,F. Prunier1. 1University Hospital of Angers, UPRES 3860 (LPRM),Angers, France; 2University Hospital of Angers, Angers, France;
3Inserm U771 CNRS UMR 6214, Angers, France
Purpose: Recent studies have reported cardioprotective effects of erythropoietin(EPO) against ischemic reperfusion (I/R) injury through activation of the RISKpathway. Here, we examined whether EPO-induced cardioprotection is main-tained in streptozotocin (STZ)-induced diabetic rats.Methods: Isolated hearts were obtained from healthy adult rats or STZ-induceddiabetic rats. All hearts underwent 25min ischemia and were assigned to receiveeither 2h reperfusion with no intervention or with one dose of EPO (1000 or 5000IU/kg) injected at the onset of reperfusion.Results: In hearts from healthy rats: 1) EPO 1000 IU/kg was cardioprotective (in-farct size was 14.4±0.6% of the left ventricle in EPO-treated hearts vs 36.2±4.2%in untreated hearts, p<0.05); 2) EPO-induced cardioprotection was associatedwith significant increase in phosphorylated forms of Akt, ERK1/2 and their down-stream target GSK-3β 30min after reperfusion. Four weeks after STZ injection,diabetic rats displayed: 1) inhibition of EPO-induced cardioprotection (infarct sizewas 32.1±2.4% in STZ-rats receiving 1000 IU/kg, 32.66±5.09% in STZ-rats re-ceiving 5000 IU/kg and 31.9±1.9% in untreated STZ-rat hearts, all p=ns); 2) noup-regulation of PI3K/Akt, ERK1/2 and GSK-3β signaling in response to EPO.However, administration of the GSK-3β inhibitor SB216763 was cardioprotectivein both healthy and STZ-rat hearts.Conclusion: Diabetic hearts were refractory to EPO-induced cardioprotectionbecause of the disruption of GSK-3β signaling upstream. Hence, direct inhibitionof GSK-3β may provide a novel strategy to protect diabetic hearts against I/Rinjury.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Experimental studies on ischemia-reperfusion 43
P462 TRO40303 improves left ventricular remodelling afterischemia-reperfusion in mice
H.B. Thibault1, L. Augeul1 , S. Schaller2, C. Chaimbault2,M. Michaud2, J. Afxantidis2, P. Berna2, R. Pruss2, M. Ovize1,G.A. Derumeaux1. 1Inserm U886, University Claude Bernard Lyon 1,
Lyon, France; 2Trophos S.A., Luminy Biotech Entreprise, Marseille, France
Purpose: Left ventricular (LV) remodelling parameters is predictive of adversecardiovascular events after myocardial infarction (MI). TRO40303, a new com-pound that induces cardioprotection at least in part by inhibition of mitochondrialpermability transition, has previsously shown to reduce MI size and improve func-tional recovery 24 hours after ischemia-reperfusion (IR) in mice. We sought toinvestigate the effect of TRO40303 on LV remodelling 1 month after IR.Methods: C57 BL/6 mice underwent 60 min of ischemia induced by left coronaryartery ligation followed by 1 month of reperfusion. Mice were randomly assignedto a control (C; n=13, IR without any intervention), a TRO40303 (TR; n=12 IVbolus of TRO40303 1 mg/kg 5 min before reperfusion) and a TRO40303 vehiclegroup (V; n=20, IV bolus of hydroxyl propyl β cyclodextrine 5 min before reperfu-sion). Echocardiography (13 MHz, Vivid 7, GE) was performed at baseline and af-ter 1 Month of reperfusion to measure left ventricular (LV) end-diastolic (LVEDV),end-systolic volumes (LVESV), LV ejection fraction (LVEF).Results: At baseline, all groups had similar LV volumes and EF. Mortality duringreperfusion was similar in the 3 groups (38% in C, 33% in TR and 30% in V).One month after IR, V and C exhibited a severe LV remodelling characterized bya dramatic increase in LVEDV and LVESV and a decrease in LVEF (Figure, *:p<0.05 vs baseline). No difference was found between these 2 groups. TR micedeveloped an increase in LVEDV and LVESV but no significant decrease of LVEFcompared to baseline. One month after IR, TR mice had a better LVEF than Cand V groups (Figure, †: ANOVA significant between the 3 groups).
LV echocardiographic measurements
Conclusion: TRO40303 improves LV remodelling one month after MI and pre-serves LV function in mice.
P463 Preconditioning and postconditioning alone or incombination in different burdens and models ofischemia
K. Iliodromitis, D. Farmakis, A. Zoga, E. Prokovas, T. Manolaki,A.R. Vrettou, E.K. Iliodromitis, M. Anastasiou-Nana, D.T. Kremastinos.Attikon Hospital, 2nd University Department of Cardiology, Athens,
Greece
Aim: To investigate the effects of preconditioning (PreC) and postconditioning(PostC), alone or in combination, on infarct size in different ischemia (isc) models.Methods: We subjected 81 anesthetized male rabbits to regional myocardial iscfollowed by 3 hours of reperfusion (rep). We applied 3 isc models [a 40-min period(40), a 20-min period (20) and 2 sequential 20-min periods separated by 12-minrep (20-20)] and 3 types of interventions [no intervention (controls, C), 2 cyclesof 5-min isc/10-min rep before index isc (PreC) and 6 cycles of 10-sec isc/10-secrep after index isc and/or between the sequential isc periods (PostC)] (12 groupsin total). Infarct size (I) and area at risk (R) were delineated by TTC staining andfluorescent particles, respectively; I/R ratio was calculated in %.Results: Overall, %I/R differed significantly among groups (p<0.001). In controlgroups, C-40 was more harmful than C-20 (p=0.006). In intervention groups, nodifferences were found in %I/R among the different interventions. When inter-vention and control groups were compared, all interventions groups had signif-icantly lower %I/R compared to C-40group (p<0.001), no intervention renderedsignificantly lower %I/R compared to C-20 group, whereas compared to C-20-20 group, PreC-20-20, 20-PostC-20, 20-PostC-20-PostC and PreC-20-20-PostC
Figure 1
groups had significantly lower %I/R (p=0.001, <0.001, 0.003, 0.011 and 0.036,respectively; Figure: *significantly different vs C-40; † significantly different vs C-20-20).Conclusions: A given isc duration seems to cause the same myocardial injuryindependently whether it is applied continuously or sequentially. PreC and PostC,alone or in combination, are equally effective in continuous or sequential periodsof prolonged isc, but may not be protective in shorter isc periods.
P464 Local arginase inhibition mediates cardioprotectionagainst ischemia/reperfusion via increased nitric oxideproduction
A.T. Gonon1, C. Jung2, P.-O. Sjoquist2, J.O. Lundberg3 , J. Pernow2.1Karolinska University Hospital, Department of Clinical Physiology,
Stockholm, Sweden; 2Karolinska University Hospital, Department of Cardiology,Stockholm, Sweden; 3Karolinska Institute, Department of Physiology andPharmacology, Stockholm, Sweden
Reduced bioavailability of nitric oxide (NO) is critical for the development of is-chemia/reperfusion injury. Arginase is up-regulated during ischemia and reperfu-sion and might consume the NO substrate L-arginine by converting it to urea andornithine resulting in reduced bioavailability of NO. The aim of the study was todetermine whether inhibition of arginase results in increased NO production andthereby confers protection against myocardial ischemia and reperfusion.Method: Twenty anesthetized pigs were subjected to coronary artery (LAD) oc-clusion for 40 min followed by 4 h reperfusion. The pigs were randomized to re-ceive an intracoronary infusion of either vehicle (n=7), the arginase inhibitor N-omega-hydroxy-nor-L-arginine (nor-NOHA, 2 mg/min, n=7) or the combination ofnor-NOHA and the NO-synthase inhibitor NG-monomethyl-L-arginine (L-NMMA,0.4 mg/min, n=6) into the jeopardized area at the end of ischemia and start ofreperfusion.Results: There was no significant difference in hemodynamics between the threegroups. The infarct size of the vehicle group was 78±4% of the area at risk. Nor-NOHA reduced infarct size to 46±5% (P<0.01). Co-adminstration of L-NMMA ab-rogated the cardioprotective effect mediated by nor-NOHA (infarct size 72±6%).The concentrations of the NO metabolite nitrite increased significantly in plasmaof the great coronary vein during early reperfusion in the group receiving nor-NOHA in comparison with the vehicle group (P<0.05).Conclusion: Local inhibition of arginase protects against myocardial ischemiaand reperfusion via a mechanism that is dependent on increased bioavailabilityof NO.
P465 N-2-mercaptopropionyl glycine has a critical role inpreconditioning due to its action on reactive oxygenand nitrogen species
I. Andreadou1 , E.K. Iliodromitis2, V. Souridis2, A. Zoga2,K. Iliodromitis2, T. Fotopoulou1 , M. Demopoulou1,
D.T.H. Kremastinos2, M. Anastasiou-Nana2. 1University of Athens, Fac-ulty of Pharmacy, Athens, Greece; 2Attikon University Hospital, Athens,Greece
Background: The production of reactive oxygen (ROS) and nitrogen (RNS)species before ischemia (isc) is a critical step in preconditioning (PC). However,controversies exist for the role of redox signaling during the first minutes of longreperfusion (rep) as an essential component of PC in vivo. The administrationof the antioxidant compound N-2-mercaptropropionyl glycine (MPG) prior to pro-longed isc has no effect on infarct size, it prevents the protection afforded by 1cycle of PC, but it does not prevent the protection afforded by 4 cycles of PC invivo. The aim of the present study was to evaluate the effect of MPG on PC at thetime of prolonged isc and long rep and to determine the role of ROS productionat that period.Methods: Male rabbits were divided into 6 groups, anesthetized and were sub-jected to 30 min isc of the heart after ligation of a prominent coronary artery and3 h rep with the following interventions before: 1) Control group no intervention,2) PC-1 group to one cycle of PC with 5min isc/10min rep, 3) PC-4 group to fourcycles of PC, 4) MPG group was treated for 60min with MPG (1 mg/kg/min) thatwas infused from the 20th min of isc and continued up to 50th min of rep, 5) MPG-PC-1 and 6) MPG-PC-4 groups were also treated with MPG and subjected to PCwith one or four cycles of PC as described in the respective groups. After the endof the experiments all hearts were harvested and the infarct size (I) and the areaat risk (R) were estimated in % I/R. The antioxidant ability of MPG at the earlyphase of rep was assessed in a second series of experiments consisted from 24rabbits that were subjected to the above interventions up to 10th min of rep. Tis-sue samples were taken from the ischemic and non ischemic regions at that timepoint for tissue analysis of malondialdehyde (MDA) as a lipid peroxidation productand for nitrotyrosine levels as a marker of peroxynitrite and nitrosative stress.Results: Infarct size was smaller in all PC groups and in all MPG groups(16.5±3.9% in the PC-1, 13.7±3.1% in the PC-4, 18.6±5.0% in the MPG,9.7±2.0% in the MPG-PC-1, 15.0±2.8% in the MPG-PC-4, vs 48.0±7.2% in theControl, P<0.05). MPG did not prevent lipid peroxidation and nitrotyrosine forma-tion within the cardiac tissue 10 min after the restoration of flow.Conclusion: MPG given before the end of prolonged isc and during the early
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

44 Experimental studies on ischemia-reperfusion
phase of rep reduces the infarct size and does not negates the protective effectof PC. Intracellular ROS and RNS are important in PC early at rep.
P467 The combination of L-arginine and ischemicpostconditioning at the onset of reperfusion limitsmyocardial injury in the pig
A.T. Gonon1, C. Jung2, J. Yang2, P.-O. Sjoquist2, J. Pernow2.1Karolinska University Hospital, Department of Clinical Physiology,
Stockholm, Sweden; 2Karolinska University Hospital, Department of Cardiology,Stockholm, Sweden
The aim of the study was to investigate whether ischemic postconditioning (IPoC)combined with i.v. infusion of the nitric oxide (NO) substrate L-arginine at the on-set of reperfusion exerts cardioprotective effect that is superior to either treatmentgiven separately.Method: Twenty-six anesthetized pigs were subjected to coronary artery (LAD)ligation for 40 min followed by 4 h reperfusion. The pigs were randomized into fourdifferent groups receiving either i.v. vehicle, i.v. L-arginine, IPoC together with i.v.vehicle or IPoC together with i.v. L-arginine. All infusions were started 10 minbefore reperfusion.Results: The infarct size of the vehicle group was 82±4% of the area at risk. L-arginine together with IPoC significantly reduced infarct size to 59±4% (P<0.01).IPoC alone (86±3%) or L-arginine alone (79±8%) did not influence infarct sizecompared to the vehicle group. Except for higher LAD flow during early reper-fusion in the IPoC L-arginine group, hemodynamic parameters did not differ be-tween the groups. In comparison with the vehicle group, there were no changesin expression of Akt, phosphorylated Akt Ser473, inducible nitric oxide syn-thase (iNOS), endothelial NOS or phosphorylated eNOS Ser1177 in the is-chemic/reperfused myocardium.Conclusion: L-arginine given systemically at the onset of reperfusion protects thepig heart against ischemia and reperfusion injury only when combined with IPoC.These results indicate that IPoC facilitates the protection mediated by L-arginineadministered i.v. before reperfusion.
P468 Coronary microembolisation induces acute andprogressive diastolic heart failure
H. Post1, M. Schwarzl1, P. Steendijk2, S. Huber1, M. Truschnig-Wilders1, H. Maechler1 , B. Pieske1. 1Medical University of Graz,Graz, Austria; 2Leiden University Medical Center, Leiden, Netherlands
At the regional myocardial level, coronary microembolisation (CME) inducesacute and progressive loss of wall thickening related to ischemia and initiationof inflammatory processes. We assessed the effects of CME on global left ven-tricular (LV) performance.In 6 anaesthetized pigs (69±2 kg), LV function was determined by Swan-Ganzand conductance catheters. Polystyrol microbeads (45 μM, n=500.000) were in-fused every 10 min (3-4 times) into the left circumflex coronary to decrease car-diac power output by > 40%. Data are compared between control (Con), after theend of repetitive CME (CME 0h) and at 6h later (CME 6h); *: p<0.05 vs Con, #:p<0.05 vs CME 0h.Heart rate increased from 87±4 to 89±5 and 110±8* bpm. Cardiac output de-creased from 6.5±0.3 to 4.5±0.2* and 4.4±0.2* l/min, LV peak pressure from126±8 to 90±3* and 78±4* mmHg, LV dP/dtmax from 2330±181 to 1436±68*and 1346±71* mmHg/s, and stroke volume from 75±4 to 52±3* and 40±3* ml.In contrast, LV ejection fraction (EF) remained preserved; Con: 58±2, CME 0h:52±3, CME 6h: 55±4%, p=NS. Preservation of EF was related to a progressivereduction of LV end-diastolic volume (LVedV); Con: 129±4 ml, CME 0h: 101±9 ml,CME 6h: 74±5 ml. Pressure-volume analysis during aortic balloon catheter infla-tion demonstrated a profound leftward shift of the end-diastolic pressure-volumerelationship (EDPVR, graph: original tracing), while the position of the end-systolicpressure-volume relationship at physiological pressures remained unchanged.Global LV failure after CME thus comprised an inability of the LV to maintain anadaequate preload, which was not detected by LV ejection fraction.
We conclude that diastolic dysfunction is a predominant mechanism of acute LVfailure induced by coronary microembolisation.
P469 Role of sirt1 in acute myocardial infarction
K. Jores, W. Bielenberg, P. Stieger, J.M. Daniel, H. Tillmanns,D. Sedding. University Hospital Giessen and Marburg, CampusGiessen, Giessen, Germany
Background: The NAD(+)-dependent deacetylase Sirt1, a nicoti-namide adenine dinucleotide (NAD)-dependent histone deacetylase functionsin a wide array of cellular processes, including gene silencing, longevity, pro-tection from oxidative stress, DNA damage repair and apoptosis. Recently,overexpression of Sirt1 has been shown to protect cardiomyocytes from is-chemia/reperfusion injury. However, the endogenous expression and activity ofSirt1 as well as the regulating mechanisms remain elusive.Objective: Here we investigated the mechanisms which regulate Sirt1 expressionand activity in the ischemic heart in vivo.Methods: The left coronary artery (LAD) of C57/Bl6 mice was ligated and micewere euthanized 1, 4, 12, 24 and 48h following induction of ischemia. Ischemicmyocardium was identified by injection of evans blue dye and dissected for furtherevaluation. Following RNA and protein isolation, the mRNA and protein levels aswell as Sirt1 activity were determined.Results: Sirt1 mRNA levels remained unchanged at all time points, but Sirt1 pro-tein levels were significantly upregulated at 24 and 48h. Despite increased proteinlevels, enzymatic Sirt1 activity dramatically decreased in a time-dependent man-ner. We next determined NAD-levels in ischemic myocardium since NAD+ actsnot only as a cofactor for cellular respiration but also as a substrate for NAD(+)-dependent enzymes, such as Sirt1. NAD-levels dramatically decreased in thenon-perfused myocardium in parallel to the decrease in Sirt1 activity. The cellularNAD+ synthesis is regulated by both the de novo and the salvage pathways. Sinceonly the salvage pathway regulates NAD-levels under ischemic conditions, we fo-cused on the molecules of this pathway to elucidate the mechanisms which reg-ulate cellular NAD content under ischemic conditions. Our data now indicate thatthe Nicotinamide phosphoribosyltransferase (Nampt), which is the rate-limitingenzyme in the salvage pathway is significantly downregulated at the mRNA andprotein level at 12, 24 and 48h.Conclusions: Our data indicate that Sirt1 activity, which is critical for cardiomy-ocyte survival, is downregulated in the ischemic myocardium. The reduced activ-ity is due to a downregulation of Nampt, which critically regulates NAD+ contentsin the ischemic myocardium, thereby modulating Sirt1 activity and cardiac my-ocyte survival. Thus, reconstitution of Nampt or NAD-independent activation ofSirt1 may represent a promising strategy to inhibit myocardial injury in responseto myocardial ischemia.
P472 The iron-regulatory peptide hepcidin is upregulated inthe ischemic and in the remote myocardium aftermyocardial infarction
G. Simonis1, K. Mueller2, P. Schwarz2, S. Wiedemann1, G. Adler2,R.H. Strasser1, H. Kulaksiz2. 1Dresden University of Technology,
Dresden, Germany; 2University of Ulm, Ulm, Germany
Background: Recent evidence suggests that iron metabolism is a strong con-tributor to the ischemic damage after myocardial infarction. Hepcidin, a recentlydiscovered peptide hormone, regulates iron uptake and metabolism, protectingthe body from iron overload. In this study we analyzed the regulation of hepcidinin the heart and blood of rats after myocardial infarction.Methods: To induce a myocardial infarction in the rats, left anterior descend-ing coronary artery ligation was performed. After 1-24 hours, biopsies from theischemic and the non-ischemic myocardium were taken. In these biopsies, themRNA levels and the protein expression of hepcidin were analyzed by quantita-tive RT-PCR and immunoblot analysis, respectively. In parallel, the serum levelsof prohepcidin were measured by ELISA.
mRNA of hepcidin, hemojuvelin and IREG-1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Experimental studies on ischemia-reperfusion 45
Results: 6 hours after myocardial infarction, the hepcidin mRNA expression wasupregulated in the ischemic and in the non-ischemic myocardium. The upregula-tion was specific for hepcidin, since other iron-related genes (hemojuvelin, IREG-1) remained unchanged (Figure). Furthermore, the alteration of the hepcidin pro-tein expression in the ischemic area was connected to the level of hepcidin in theserum of the infarcted rats, where hepcidin also raised up. Angiotensin receptorblockade with candesartan did not influence the mRNA regulation of hepcidin.Conclusion: These data show a particular upregulation of the iron-regulatorypeptide hepcidin in the ischemic and the non-ischemic myocardium after myocar-dial infarction. It could be assumed that upregulation of hepcidin may reduce irontoxicity and thus infarct-size expansion in an infarcted heart.
P473 Systolic and postsystolic velocities quantify low grademyocardial ischaemia by a miniaturized epicardialultrasonic sensor
S. Hyler1, S. Pischke1, P.S. Halvorsen1, A. Espinoza1, S. Hestenes1,J. Bergsland1, E. Fosse1, H. Skulstad2. 1University of Oslo,
Faculty Division Rikshospitalet University Hospital, Interventional Centre, Oslo,Norway; 2University of Oslo, Faculty Division Rikshospitalet University Hospital,Department of Cardiology, Oslo, Norway
Background: Early detection of myocardial ischaemia during heart surgery isessential to preserve ventricular function. More sensitive methods for continuousassessment of myocardial function are required. We tested a miniaturized epicar-dial ultrasonic transducer for detection of graded myocardial ischaemia.Methods: Coronary bypass from left internal mammary artery (LIMA) to left an-terior descending coronary artery (LAD) was performed in six pigs to regulatecoronary perfusion. Intermittent ischaemia was induced by reducing LIMA-flow to75%, 50% and 25% for 5 min. Subendocardial peak systolic (Vsys) and postsys-tolic (Vpst) velocities were continuously obtained by two miniaturized epicardialultrasonic transducers (Ø=5mm) in the LAD and circumflex (Cx) area. In addition,radial strain was calculated as 2D strain by echocardiography. Left ventricularpeak (LVP) and end-diastolic pressure (LVEDP) were measured with a micro-manometer. Values are given as median (interquartile range).Results: During all levels of flow reduction Vsys decreased significantly (p<0.05)from baseline, while Vpst increased at 50% and 25% flow (p<0.05) (fig.1A).These findings correlate with systolic (R=0.89, p<0.01) and postsystolic (R=0.64,p<0.01) radial strain. No changes were seen in the Cx area. Moderate flow reduc-tion (75% and 50%) did not affect hemodynamic parameters, but a small decreasein LVP (p<0.05) was seen when flow was reduced to 25% (fig.1B).
Conclusion: Mild and moderate myocardial ischaemia can be quantified by tis-sue velocity measurements from epicardial ultrasonic sensors. The findings arepromising for continuously real-time monitoring of myocardial function duringheart surgery, and with further miniaturizing of the sensor, also in the postop-erative period.
P474 Spinal cord stimulation effects on myocardialischemia, infarct size, ventricular arrhythmia andnon-invasive electrophysiology in a porcineischemia-reperfusion model
J. Odenstedt1 , B. Linderoth2 , L. Bergfeldt1, O. Ekre3,L. Grip1, C. Mannheimer3 , P. Andrell3. 1Dept of Molecular and ClinicalMedicine/Cardiology, Sahlgrenska Academy, Univ. of Gothenburg, Gothenburg,Sweden; 2Dept of Clinical Neuroscience, Section of Neurosurgery, KarolinskaInstitutet and Univ Hospital, Stockholm, Sweden; 3Multidisciplinary Pain Center,Sahlgrenska Univ Hospital/Östra, Gothenburg, Sweden
Purpose: Susceptibility to ventricular arrhythmias and sudden cardiac death canbe reduced via modulation of autonomic tone. Spinal cord stimulation (SCS) pre-sumably affects both the autonomic tone and reduces myocardial ischemia. Theaim was to investigate whether SCS could reduce myocardial ischemia, infarctsize and the occurrence of ventricular arrhythmias as well as repolarisation alter-ations in a porcine ischemia-reperfusion model.Methods: Anaesthetised common land-race pigs were randomised to SCS(n=10) or sham treatment (n=10) before, during and after 45 minutes of coro-
nary occlusion. Area at risk (AAR), infarct size (IS) and the amount of sponta-neous ventricular arrhythmias were analysed. Continuous 3-D vectorcardiography(VCG) was recorded and analysed with respect to ECG intervals, the ST-segment,and the T vector and T vector loop morphology.Results: In the SCS group, ventricular arrhythmias occurred less frequently(p=0.039) and the increase in ST-vector magnitude was less pronounced(p=0.024). However, SCS showed no effect on AAR, IS or IS/AAR. Tamplitudeand Tarea increased in response to ischemia suggesting increased repolarisationgradients, but SCS reduced these changes (p<0.01 for both). No other parame-ters differed between the groups.Conclusions: SCS reduced the accumulated incidence of spontaneous ventric-ular arrhythmias during ischemia-reperfusion in association with a reduction ofrepolarisation alterations. Furthermore, VCG signs of myocardial ischemia werereduced by SCS, but this phenomenon was not accompanied by any effect oninfarct size.
P475 During acute myocardial ischemia, AT-1 receptorantagonism prevents systolic and diastolicdysfunction caused by hemodynamic overload: aneffect partially mediated by AT-2 receptor activation
R. Fontes Carvalho, R. Ladeiras-Lopes, M. Pintalhao, A.L. Pires,R. Ferreira, P. Castro-Chaves, A. Leite-Moreira. University of Porto, Faculty ofMedicine, Department of Physiology, Porto, Portugal
Purpose: Acute hemodynamic overload frequently occurs after myocardial is-chemia and directly contributes to a greater decline in myocardial contractilityand an increase in myocardial stiffness. Both these processes might be partiallymediated by angiotensin II (AngII). Our aim was to evaluate, the importance ofAT-1 and AT-2 receptors antagonists on the systolic and diastolic responses to anhemodynamic overload during acute ischaemia.Methods: Rabbit papillary muscles (modified Krebs solution,0.2Hz,1.8mMCa2+,30°C) were mechanically overloaded by stretching from 92% Lmax to 100%Lmax (length at which maximal force is developed) in 3 situations: 1) during acuteischemia, followed by reperfusion (control,n=7);2) during acute ischemia, in thepresence a selective AT1-receptor antagonist (AT1 group; ZD-7155, 10-6M; n=7);3) during an ischemic insult in the presence of both a AT-1 and a selective AT2-receptor antagonist (AT1+AT2group; ZD-7155,10-6M+PD-123,319,10-6M;n=8).Immediate (1 min) and delayed responses (60 min) to muscle overload were eval-uated. Results as mean±St error (p<0.05).Results: In the control muscles, after the immediate increase in contractility uponstretch, there was a steady decrease in active tension (AT) of 70,4±5,2% at60 min. In the presence of AT-1 antagonist, this contractility reduction was pre-vented (AT decreased only 4,1±11,0% in AT1 group vs 70,4±5,2% in control,p<0,001). This effect was partially blocked when the AT2 receptor antagonistwas also present (AT decreased 35,5±11,0% in AT1+AT2 vs 4,1±11,0% in AT1group,p<0,05).Considering diastolic function, in the control group, immediately after stretch therewas an increase in myocardial stiffness, which was sustained over time. On thecontrary, when the AT1 receptor was selectively blocked, a beneficial effect wasagain observed, leading to a significant decrease in myocardial stiffness (pas-sive tension decreased 28,7±3,7% in AT1 group, p<0,05). The addition of PD-123,319 (AT1+AT2) did not modify this response.Conclusion: During myocardial ischemia, an acute hemodynamic overload di-rectly leads to a decline in contractility and an increase in myocardial stiffness,which can successfully be prevented by selective AT1-receptor antagonist. Thesystolic counterpart of this effect is partially dependent on AT2 receptor activa-tion. Our results highlight the importance of using ARBs early, during the acutephase of myocardial ischemia, which can probably avoid further hemodynamicdeterioration. They also support AT2 stimulation as a potential therapeutic targetin myocardial ischemia.
P476 A new type I angiotensin II receptor blocker,Fimasartan, has cardioprotecive effect by reducingischemia/reperfusion injury in rat ischemic model
D.J. Choi1, E.J. Kim1, M.J. Park1, I.H. Chae1, G.Y. Cho1, E.S. Jeon2,T.J. Yeon1, S.J. Park2, J.W. Seo1. 1Seoul National University, Seoul,
Korea, Republic of; 2Sungkyunkwan University, Seoul, Korea, Republic of
Angiotensin II receptor blocker (ARB) is well known as antihypertensive agentto reduce the blood pressure. In addition, inhibition of rennin-angiotensin system(RAS) is important to protect the cardiovascular system as well. We investigatedthe protective effect of Fimasartan, a newly developed ARB, against myocardialI/R injury and its underlying mechanismsIn male Sprague-Dawley rats (weight of 200-230mg), 3mg/kg of Fimasartan orcontrol buffer was infused intravenously over 30min before coronary occlusion.Area of necrosis (AN by TTC), the area at risk (AAR by Evans blue), and LVsize were measured after 30min of coronary occlusion and 24 hours of reperfu-sion. To determine the mechanisms of Fimasartan, we assessed DNA laddering,TUNEL assay and Western blot was performed with myocardial tissue and cul-ture myocytes in ischemic/reperfusion conditions. Hemodynamic measurementsand blood samples was done after ischemia/reperfusion injury for C-reactive pro-tein, and TNF-a measurement. Fimasartan reduced infarct size in AN/AAR by
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

46 Experimental studies on ischemia-reperfusion
47% (control vs. Fimasartan; 47.3±11.8 vs. 25.2±9.6, p<0.05) and in AN/LV by52.3% (30.4±10.5 vs. 14.5±9.6, p<0.05, respectively), while the size of AAR/LVwas not different. In sham group, IR injury, DNA fragmentation and the numberof apoptotic nuclei in the ischemic area were increased, and this effects wereabolished by Fimasartan. The expression of Bcl-2 in the myocardium was in-creased, while the CRP and TNF-α was decreased by 20.9% (control vs. fimasar-tan; 404.2±44.0 ug/ml vs. 320.0±47.7 ug/ml, p<0.05) and by 22.2% (controlvs. fimasartan; 164.93±18.57 pg/mg protein vs. 127.79±26.78 pg/mg protein,p<0.05) by Fimasartan, respectively.These results suggest that Fimasartan may have a protective effect on myocar-dial ischemia/reperfusion injury. This protective ability is possibly through its anti-inflammation and anti-apoptosis effect. These data imply new clinical applicationof Fimasartan for myocardial protection from ischemia-reperfusion injury conjunc-tion with reperfusion therapy during myocardial salvege.
P477 Acute distension of the ischemic region predictsincreased ventricular fibrillation inducibility followingcoronary occlusion in anesthetized pigs
J.A. Barrabes, J. Inserte, L. Agullo, M.A. Garcia, A. Rodriguez-Sinovas, D. Garcia-Dorado. University Hospital Vall d’Hebron,
Barcelona, Spain
Purpose: The distension of the ischemic region has been related to an increasedincidence of ventricular arrhythmias following coronary occlusion (CO) but themechanisms of this association are unclear. Particularly, the potential influenceof regional distension on ventricular fibrillation (VF) inducibility is unknown. Weaimed to assess whether regional ischemic dilatation is associated with VF in-ducibility by programmed electrical stimulation during acute CO in pigs.Methods: Eighteen thiopental-anesthetized, open-chest pigs were subjected toCO of the mid left anterior descending artery (LAD). Segment length in LAD-dependent and control myocardium was monitored by means of ultrasonic crys-tals. Two stimulation electrodes were implanted in the subepicardial border zone,the preferential site of origin of premature ventricular beats during regional is-chemia. VF inducibility was tested by introducing up to 3 extrastimuli at progres-sively shorter coupling intervals after a drive train of 8 paced beats (S1-S1, 600ms). When VF occurred, the heart was defibrillated. The stimulation protocol wasperformed before CO and then continuously repeated between 10 and 60 min ofCO, allowing 3 min (2 min if no VF occurred) recovery after each defibrillation.Results: Ten minutes after CO, heart rate was 87±5 beats/min, mean arterialpressure was 56±3 mmHg, LV enddiastolic pressure was 11±1 mmHg, and end-diastolic length (EDL) averaged 109.4±0.9% of baseline in LAD myocardium(P<0.001 with respect to baseline value) and 101.1±0.5% in the control zone(P=0.03 with respect to baseline). The area at risk (fluorescein injection at theend of the experiment) averaged 13.2±2.3% of ventricular mass. Twelve animals(67%) had 1.3±0.5 episodes of spontaneous VF during CO. A mean of 6.6±0.5stimulation protocols were completed during the ischemic period. VF was inducedbefore CO in 11 animals (61%) and during CO in all (5.4±0.6 episodes per an-imal). The increase in EDL in the ischemic region 10 min after CO was directlyassociated (r=0.67, P=0.002) with the number of VF episodes subsequently in-duced during CO and inversely associated (r=-0.55, P=0.018) with the number ofextrastimuli needed to induce VF in this period.Conclusion: Regional ischemic expansion predicts an increased VF inducibilityduring acute CO. Whether this association represents a cause-effect relationshipand the underlying mechanisms deserve further investigation.
P478 TRO40303 inhibits mitochondrial permeabilitytransition pore by a new mechanism
S. Schaller1, S. Paradis2, G.A. Ngoh3, C. Gouarne1, B. Buisson1,J.L. Abitbol1, A. Berdeaux2, S. Jones3, D. Morin2, R. Pruss1.1Trophos S.A., Marseille, France; 2INSERM U 955 IMRB, Créteil,
France; 3Institute of Molecular Cardiology, Louseville, KY, United States ofAmerica
Purpose: TRO40303 is a new cardioprotective compound that binds to theouter mitochondrial membrane protein TSPO 18 kDa. TRO40303 reduces in-farct size and promotes functional myocardial recovery in rodent models ofischemia-reperfusion injury. TRO40303 reduces mitochondrial permeability tran-sition (mPT) and release of apoptotic factors from the mitochondria. To investigatefurther the impact of TRO40303 on mPT, we compared the effects of TRO40303and cyclosporine A (CsA) on calcium retention capacity (CRC) of isolated cardiacmitochondria and in a model of oxidative stress-induced mPT in cardiomyocytes.Methods: Left ventricle rat heart mitochondria were used to assess CRC aftertreatments with 3 μM TRO40303, 1 μM CsA or DMSO. Pulses of 10 μM Ca2+were added until mPT was detected by monitoring medium Ca2+ concentrationwith Calcium Green-5N. Primary neonatal rat cardiomyocytes were intoxicatedwith 100 μM H2O2. mPT was evaluated by monitoring the decrease in the stan-dard deviation of calcein fluorescence intensity as a measure of calcein releasefrom mitochondria, while at the same time ROS production was measured withDCF, cytoplasmic and mitochondrial Ca2+ with Fluo-4 and Rhod-2 respectivelyand mitochondrial membrane potential using TMRM.Results: Whereas TRO40303 had no effect on isolated mitochondria, CsA in-creased CRC as expected. However on intact cardiomyocytes both TRO40303
and CsA inhibited mPT in a similar manner. Increased ROS production trig-gered by H2O2 intoxication was an early event that was significantly inhibitedby TRO40303 while CsA had only a slight, non-significant effect. Subsequent tomPT, both TRO40303 and CsA significantly attenuated the rise in cytoplasmicand mitochondrial Ca2+ to a similar extent. Loss of the mitochondrial membranepotential was significantly attenuated by CsA and there was a clear trend of re-duction with TRO40303.Conclusion: Although stress-induced mPT and subsequent calcium rise occur-ring as the result of H2O2 treatment is similarly inhibited by TRO40303 andCsA, the drugs exhibit different mechanism. CsA inhibits mPT by binding to Cy-clophilin D on the inner mitochondrial membrane, decreasing the sensitivity toCa2+-induced mPT as reflected by its effect on CRC of isolated mitochondria.TRO40303 modulates mPT by reducing oxidative stress-induced ROS produc-tion in intact cells possibly via its interaction with TSPO.
P479 Interventricular septum ischemia is critical forcardiogenic shock development during rightventricular infarction
D. Koudoumas, P. Glentis, E. Tseliou, L. Katsaros, I. Pozios, N. Diakos,S. Vakrou, E. Konstantakis, S. Drakos, J. Nanas. University of Athens,
School of Medicine, 3rd Cardiology Dept., Athens, Greece
Objectives: Right ventricular (RV) ischemia occurs in 50% of patients with acuteinferior myocardial infarction and may result in severe hemodynamic compromiseassociated with poor clinical outcome. However, it is not known whether it is thefunction of the inerventricular septum in particular or the size of the infarcted LVmyocardium that, when added to RV ischemia, play major role for hemodynamicdecompensation in this setting. We investigated the role of location and size ofthe infarct of the left ventricle (LV) on the severity of hemodynamic compromiseduring right ventricular infarction.Methods: In 14 anesthetized, open chest pigs right ventricular free wall ischemiawas created by ligating all branches of right and left coronary arteries to the rightventricular free wall (Phase 1). In Group A (RV+LV septum, n=6) the posteriordescending artery was ligated, followed by gradual ligation of the left anteriordescending artery in a proximal to distal fashion (Phase 2). In Group B (RV+LVfree wall, n=8) all branches of circumflex artery were ligated, followed by ligationof all diagonal branches of left anterior descending artery from proximal to dis-tal (Phase 2). Systolic, diastolic and mean arterial pressure, right and left atrialpressure, systolic pulmonary pressure and heart rate were recorded during base-line, phase 1 and phase 2. Cardiac output (CO) was measured with an ultrasonicflowmeter placed around the pulmonary artery. A 50% drop of CO from baselinewas considered as the end-point, where animals were euthanized for infract sizemeasurement.Results: There were no statistical significant differences between the two groups,in all the recorded hemodynamic parameters, at all time phases of the experi-ment. CO (% of baseline) did not differ statistically between the two groups inphase 1 (71.78±2.79% vs 78.09±6.02%, p>0.05) or phase 2 (46.31±6.10%vs 51.29±8.42%, p>0.05). The infract size was significantly smaller in group A(31.19±1.37% vs 42.68±3.35% in group B, p=0.01), despite similar hemodynam-ics. Left ventricular infract size was 21.69±2.0% in group A vs 35.76±3.81% ingroup B (p=0.01).Conclusion: Interventricular septum ischemia plays a critical role in the devel-opment of cardiogenic shock during right ventricular infarction. A significantlysmaller size septal infarct (in comparison to one of the LV free wall) results insevere hemodynamic compromise. The development of LV mechanical dyssyn-chrony may be the reason for this phenomenon.
P480 Remote preconditioning by bilateral carotid arteryocclusion limits myocardial infarct size in in vivo rabbithearts: involvement of extracellular signal-regulatedkinase 1/2 (ERK1/2)
K. Arishiro1, Y. Momota2, M. Miyamae1, C. Okusa2, K. Kaneda2,J. Kotani2, N. Domae1, V.M. Figueredo3. 1Osaka Dental University, Departmentof Internal Medicine, Osaka, Japan; 2Osaka Dental University, Department ofAnesthesiology, Osaka, Japan; 3Albert Einstein Medical Center, Department ofCardiology, Philadelphia, United States of America
Purpose: Ischemia in remote parts of the body, such as a limb or renal artery,can induce a cardioprotective effect (remote ischemic preconditioning or RPC).The purpose of this study was to assess the effect on myocardial infarct sizeof preconditioning at a distance induced by carotid artery occlusion. Further, weinvestigated the involvement of extracellular signal-regulated kinase 1/2 (ERK1/2)and norepinephrine increases in this RPC.Methods: Male Japanese white rabbits weighing 2.2-3.1 kg were anesthetizedwith pentobarbital 25 mg/kg. After tracheostomy ventilation was controlled tomaintain PaCO2 at 32±5 mmHg. Rabbits were subjected to 30 min left ante-rior coronary artery occlusion and 120 min reperfusion (control n=8; RPC n=8).In RPC, preconditioning was elicited by four cycles of bilateral carotid artery oc-clusion for 5 min followed by 5 min reperfusion. The right femoral artery wascannulated for determination of systemic arterial blood pressure and to analyzeblood sampling for determination of plasma norepinephrine levels. The area atrisk (AAR) as a percentage of the left ventricle (LV) was determined by Evans
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Experimental studies on ischemia-reperfusion / Risk protection in acute coronary syndromes 47
blue dye. After experiments, hearts were frozen and cut into 2 mm thick trans-verse slices. The slices were stained in 1.0% triphenyltetrazonium solution andincubated in 10% formalin to identify viable and necrotic tissue. Plasma nore-pinephrine concentration was measured immediately after preconditioning. Tis-sue samples were obtained from LV (AAR and non AAR) and brain at 10 minafter reperfusion to examine phosphorylation of ERK1/2 by Western immunoblot-ting.Results: Blood pressure significantly increased in RPC after preconditioning(systolic: 152±10 to 190±19 mmHg, diastolic: 88±7 to 113±12 mmHg) and re-turned to preischemic value by reperfusion. There was no significant differencein AAR between the two groups (control: 33.0±6.8%, RPC: 31.6±10.7%). Infarctsize was significantly reduced in RPC compared to control (control: 57.3±10.4%,RPC: 35.2±8.5%; p<0.01). Western blot analysis of brain samples revealed anincrease in phosphorylation of ERK1/2 in the RPC group, whereas it was notshown in the myocardium. Plasma norepinephrine increased immediately afterpreconditioning (control: 149±21 pg/ml, RPC: 432±74 pg/ml; p<0.01).Conclusion: Remote preconditioning by bilateral carotid artery occlusion de-creased myocardial infarct size in in vivo rabbit heart. Phosphorylation of ERKwas higher in the brain, but not in the myocardium immediately after precondi-tioning. Blood pressure and plasma norepinephrine levels were higher after RPC.
P481 Temporal and spatial changes in the expression ofCa2+ regulatory proteins in a modified model ofischemic cardiomyopathy
Y. Kawase, D. Ladage, C.W. Kho, A. Lee, S. Shapiro, K. Ishikawa,M. Garcia, R. Hajjar. Mount Sinai Hospital, New York, United States of
America
There is no satisfactory model for chronic ischemic cardiomyopathy in large an-imal. The purpose of this study was to develop and characterize an alternativemodel for chronic ischemic cardiomyopathy (CIM) in Yorkshire pigs. To induceprogressive stenosis, a plastic occluder with fixed diameter (1.0mm) fitted with an18 gauge copper wire was placed around the proximal left anterior descending(LAD) artery. Coronary angiography, hemodynamic measurements and echocar-diography were performed at baseline, one, two, four, eight, and twelve (1W, 2W,4W, 8W, and 12W) weeks follow up (n=14). Mortality rate before 4W was 7.1%(1/14). Mortality rate at 12W was 42.9% (6/14). Total occlusion was not observedat 2W. Incidence of total LAD occlusion was observed in 54% of the pigs at 4W(7/13) and 88% at 12W (7/8). Rich collateral formation was observed in all pigsthat showed total artery occlusion. A severe depression of fractional shorteningarea and (dp/dt) max was also observed in these animals. The expression ofcardiac specific biomarkers were profiled. A significant reduction of sarcoplasmicreticulum ATPase (SERCA2a) and an increase of Na2+-Ca2+ exchanger wasobserved in the ischemic regions of all pigs with total occlusion, but only in thenon-ischemic regions of pigs that showed total occlusion at 4W, implying the de-velopment of cardiac remodeling. The size of scar was 11.4±1.4%. Changes inexpression of these proteins were observed predominantly in the end myocardiumlayer.
In this model, the timing and incidence of total occlusion and onset of mortalityofferssignificant advantages over other CIM models. In addition, the temporal andspatial changes in certain cardiac protein expression were observed both, in theischemic and non-ischemic regions after total coronary occlusion.
P482 Release of bioactive matrix cleavage products duringearly ischemia-reperfusion as indicator of myocardialremodelling
A. Lauten1, A. Gerhard-Garcia2, J. Faraby2 , E. Majos2, C. Jung1,H.R. Figulla1, W. Bloch2. 1Universitaetsklinikum Jena, Jena,
Germany; 2Institute of Cardiovascular Research and Sports Medicine, Cologne,Germany
Purpose: Ischemic injury is a known inductor of myocardial remodelling and re-sults in proteolytic cleavage of extracellular matrix (ECM) proteins. Protein degra-dation may generate fragments with biological activity during vascular develop-ment, function and repair in the postischemic myocardium. Here we investigate
the release of Tumstatin (TUM; 28 kDa fragment of collagen IV alpha 3), Arresten(ARR; 26 kDa fragment of collagen IV alpha 1) and Endorepellin (END, 85kDafragment of perlecan) in an animal model of ischemia-reperfusion (I/R).Methods and Results: In this blinded study, 30 pigs where randomized to 60minof global myocardial ischemia at either 4°C or 37°C or served as control. Fivetransmyocardial tissue samples where collected at baseline prior to ischemia andwithin 150min of reperfusion. Cleavage products of ECM proteins including colla-gen IV (alpha 1 and alpha 3 chain) and perlecan where analyzed by immunoblot-ting with specific antibodies. Within 150min of reperfusion after normothermicischemia an increased release of the proteolytic fragments TUM (2-fold), ARR(3-fold) and END (4-fold) compared to baseline was observed. However releaseof cleavage products remained unchanged after hypothermic I/R and in controls.Creatin Kinase measured in samples from the coronary as maker of myocar-dial injury was elevated after normothermic I/R only, thus correlating to increasedpostischemic matrix processing in this group.Conclusion: The study demonstrates release of Tumstatin, Arresten and En-dorepellin during early reperfusion after myocardial ischemia. Elevated levels ofthese proteolytic fragments with biological activity at this early stage may po-tentially affect vascular growth and blood vessels formation in the postischemicmyocardium. These findings may contribute to a broader understanding of postis-chemic extracellular matrix remodelling and vascular development after ischemiaof the heart.
P483 Assessment of myocardial viability using pressurederived coronary flow reserve in a porcine model ofrecent myocardial infarction
A. Kotsia1, D. Nikas2, N. Papamichail1, K.K. Naka2, C.S. Katsouras2,L.K. Michalis1. 1University Hospital of Ioannina, Ioannina, Greece;
2University of Ioannina, Michaelidion Cardiac Center, Ioannina, Greece
Purpose: Coronary vasodilatory reserve in infarcted myocardium is impaired,despite patency of infarct-related artery (IRA), proportionally to tissue necrosis.Thus coronary flow reserve (CFR) coming of coronary pressure measurementsin patent IRA might correlate with the amount of viable myocardium in the in-fracted area. We aimed to validate pressure-derived CFR as a viability index in aclosed-chest pig animal model of recent myocardial infarction.Methods: Ten pigs sustained myocardial infarction by occluding the left circumflexartery in the mid segment for 45 minutes. 48 hours later the animals underwentcoronary angiography and 27 various degrees of artificial stenoses were createdby inflating balloon catheters at different pressures at the site of the vessel oc-clusion. The stenoses were characterized according the as mild (n=7) moder-ate (n=14) and severe (n=6). Proximal and distal coronary pressures at the tipof the catheter with a fluid-filled transducer system and with a 0.014” pressureguide wire (Wavewire, Endosonics Corp, USA) respectively. Both pressures wererecorded at rest and during hyperemia. Pressure-derived CFR was calculated bythe square root of the pressure gradient across the stenosis during hyperemia di-vided by the square root of the pressure gradient at rest. Viable myocardium wasdelineated by the 2,3,5-Triphenyl Tetrazolium Chloride (TTC) staining techniqueafter extraction of the porcine heart at the end of the protocol. Myocardial viabilitywas defined as a proportion of the viable myocardial area to the area at risk (V/Rratio) in every pig.Results: Pressure-derived CFR correlated well with the amount of viable my-ocardium measured by V/R ratio in stenoses of moderate severity (r=0.660,p=0.01) while no significant correlation was observed in mild (r=-0.318, p=NS)or severe stenoses (r= 0.079, p=NS).Conclusions: Pressure-derived CFR values are correlated well with the amountof viable myocardium as early as 48 hours post MI, when the IRA is moderatelystenosed.
RISK PROTECTION IN ACUTE CORONARY SYNDROMES
P484 Exercise-induced ST-segment elevation in right-sidedchest leads is indicative of right ventriculardysfunction post inferior myocardial infarction
A. Michaelides, C. Liakos, D. Tousoulis, G. Vyssoulis, K. Aggeli,C. Antoniades, L. Raftopoulos, D. Soulis, K. Toutouzas, C. Stefanadis.
1st University Department of Cardiology, Athens Medical School, HippokrationHospital, Athens, Greece
Purpose: The incorporation of right-sided chest leads (V3R–V5R) into the stan-dard exercise testing has been reported to improve its diagnostic accuracy. Thepurpose of this study was to evaluate the ability of exercise testing in detectingright ventricular (RV) dysfunction post myocardial infarction (MI) of the inferiorwall, using additional V3R–V5R leads.Methods: We studied 133 patients (59±5 years, 81 males) with a history of in-ferior MI due to right coronary artery obstruction (affirmed with coronary angiog-raphy). All patients underwent an echocardiographic assessment of RV function4 weeks after discharge and an exercise treadmill test in order to detect possibleRV dysfunction. Recordings during exercise were obtained with the standard 12leads plus V3R–V5R.Results: From 133 patients, 97 (group A) presented with normal right ventricle
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

48 Risk protection in acute coronary syndromes
Figure 1
according to the echocardiographic study while the rest 36 patients (group B) pre-sented with RV dysfunction. Maximal exercise-induced ST-segment deviation (inmm) was similar in the standard 12 leads for the 2 groups (2.1±0.4 vs 1.8±0.3,p=NS) while in V3R–V5R it was greater in group B (0.7±0.3 vs 1.4±0.4, p<0.05).Sensitivity (Se), positive prognostic value (Ppv), negative prognostic value (Npv)and accuracy (Ac) of exercise testing in detecting RV dysfunction were all im-proved (Figure) using V3R–V5R (78 vs 47%, 39 vs 29%, 87 vs 75%, 62 vs 55%respectively, p<0.05 for all) while specificity (Sp) was not deteriorated (56 vs 58%,p=NS).Conclusions: The addition of right-sided chest leads (V3R–V5R) improves thediagnostic ability of standard exercise testing in detecting and especially in ex-cluding RV dysfunction post inferior MI.
P485 Mortality in patients with ST-segment elevationmyocardial infarction treated with percutaneouscoronary intervention. 10-year follow-up
M. Gasior1, D. Pres1, M. Gierlotka1, M. Hawranek1, A. Lekston1,M. Tajstra1, K. Wilczek1, R. Wojnar1, M. Zembala2, L. Polonski1. 1III
Chair and Department of Cardiology, Silesian Centre for Heart Diseases, Zabrze,Poland; 2Department of Cardiac Surgery and Transplantology, Silesian Centrefor Heart Diseases, Zabrze, Poland
The use of percutaneous coronary intervention (PCI) for treatment of ST-segmentelevation myocardial infarction (STEMI) significantly improved prognosis of pa-tients in comparison with fibrinolytic therapy. Multivessel coronary disease wors-ens outcome of patients with STEMI. There are not many evidences in terms oflong-term mortality in patients with STEMI treated with PCI.Purpose: The purpose of this analysis was to assess 10-year mortality in patientstreated in acute phase of STEMI with PCI and to compare outcome of patientswith single-, double- or triple-coronary artery disease.Methods: In the analysis consecutive patients treated in acute phase of STEMIwith PCI in 1999-2008 were included. Patients were divided into three groups independence on number of involved coronary arteries: I group – single-coronaryartery disease, II group - double-coronary artery disease, III group – triple-coronary artery disease. Selected parameters of in-hospital and 10-year obser-vation were compared among groups.Results: A total of 3742 patients with STEMI treated with PCI were included inthe analysis. Number of patients in the selected groups was as follows: group I –1835, group II – 1169 and group III – 592. 10-year mortality in patients treated inacute phase of STEMI with PCI was 28.8%. Long-term mortality was determinedby number of involved coronary arteries. 1-year mortality was 5.9% vs 11.1% vs19.4% (p=0.001), 5-year was 12.5% vs 19.4% vs 31.0% (p=0.0001) and 10-yearwas 15.7% vs 23.0% vs 36.8% (p=0.001), respectively for patients with single-,double- or triple-coronary artery disease. Moreover the multivariate analysis re-vealed that number of significantly diseased vessels was a prognostic factor ofhigher 1-year mortality [per 1 vessel HR=1.28 (1.11-1.47); p=0.0007]] and 5-yearmortality [per 1 vessel HR=1.22 (1.06-1.40); p=0.005] whereas was not indepen-dent factor of higher 10-year mortality [per 1 vessel HR=1.28 (0.78-2.10); p=0.33].The prognostic factors of 10-year mortality were: age [per 1 year HR=1.04 (1.01-1.07); p=0.02], anterior wall myocardial infarction [HR=2.30 (1.14-4.64); p=0.02],smoking [HR=2.62 (1.21-5.65); p=0.01], blood glucose level on admission [per1mmol/L HR=1.24 (1.11-1.39); p=0.0002] and left ventricular ejection fraction [per1% HR=0.95 (0.91-0.99); p=0.03].Conclusions: The higher number of involved coronary arteries in patients treatedin acute phase of STEMI with PCI the higher long-term mortality. PCI is notenough successful method of treatment of patients with STEMI and multivesselcoronary disease.
P486 Temporal trends in the management and outcome ofpatients with STEMI presenting with cardiogenic shock
G. Greenberg, A.A. Assali, V.H. Vaknin-Assa, B.D. Brosh, B.A. Battler,R.K. Kornowski, L.E. Lev. Rabin Medical Center, Sackler Faculty ofMedicine, Tel Aviv University, Dept. of Cardiology, Petah Tikva, Israel
Background: Acute STEMI presenting with cardiogenic shock (CS) is associatedwith dismal prognosis. In recent years significant advances have been made in
catheter-based and pharmacological therapies for STEMI. It is not clear whetherthese advances impacted the prognosis of patients (pts) with STEMI who presentwith CS. We aimed to assess outcomes of these pts in 2 time periods and identifymajor factors that impact prognosis.Methods: We employed our primary PCI registry, which includes all pts withSTEMI who underwent primary PCI between 2001 and 2008 in 2 tertiary medi-cal centers. We identified 131 pts who presented with CS and underwent primaryPCI. Pts were allocated into 2 groups based on the period of presentation: 1st pe-riod: 2001-2004 (n=70); 2nd period: 2005-2008 (n=61). Clinical and angiographiccharacteristics, and outcome up to 6 months were evaluated.Results: Clinical characteristics and outcome are shown in the Table. Despiteyounger age, lower proportion of pts with renal failure and higher rates of stentuse in the 2nd period, mortality did not differ and remained high in both periods(>50% at 6 months). Use of IABP did not differ between the periods (72 vs.77%). In multivariate analysis model, factors which were associated with 1 monthmortality were: diabetes (OR=4, CI 1.3-13, P=0.02), LVEF<40% (OR=1.8, CI 1.2-2.8, P=0.01), GFR<60 ml/min/m2 (OR=1.8, CI 1.2-2.6, P=0.002) and trend for GPIIb/IIIa inhibitor use (OR=0.4, CI 0.1-1.05, P=0.07).
Clinical characteristics and outcomes
Variable 1st Period, n=70 2nd Period, n=61 P value
Age (years) 70±12 64±13 0.002Male (%) 64 72 0.3GFR < 60ml/min/m2 (%) 57 38 0.04Stent Deployment (%) 89 98 0.031 month stent thrombosis (%) 1.4 1.6 0.91 month re-infarction (%) 6 5 0.81 month death (%) 53 43 0.26 month death (%) 59 52 0.4
Conclusion: Despite changes in clinical characteristics and management of ptswith STEMI presenting with CS during the past decade, the prognosis remainspoor. It is possible that further use of measures such as IABP or GP IIb/IIIa in-hibitors may improve outcome.
P487(W) Moderate coffee consumption seems to havebeneficial effect on left ventricular systolic functiononly in normotensive patients after an acutecoronary event
C. Castorini, P. Aggelopoulos, C. Chrysohoou, C. Liontou,E. Christoforatou, A. Aggelis, C. Antoniou, G. Tsitsinakis, C. Pitsavos,C. Stefanadis. University of Athens, Athens, Greece
Background: Hypertension and coronary heart disease are major risk factorsfor the incidence and progression of heart failure, which frequently coexist, hav-ing synergistic effects that promote left ventricular remodelling. Coffee consump-tion and its effects on the cardiovascular system have been widely investigated,however the question whether coffee drinking increases the risk of acute coro-nary syndromes continues to be controversial.The aim of the present work was toevaluate the association between coffee consumption and the development of leftventricular systolic dysfunction (LVSD) in patients who had had an acute coronarysyndrome.Methods: During 2006-2007, 144 male (65±14 years) and 50 female (71±12years) post-acute coronary syndrome patients who developed LVSD (ejectionfraction <40%) after the cardiac event and 129 males (64±12 years) and 51 fe-males (67±10 years) post-acute coronary syndrome patients without LVSD (ejec-tion fraction >50%), were included in the study. Participants were age and sexmatched and consequently selected. Detailed information regarding their medi-cal records, socio-demographic, anthropometric data, and various psychological,and lifestyle characteristics (physical activity, smoking habits etc) were recorded.Particularly, nutritional habits, including coffee consumption, were evaluated usinga semi-quantitative food-frequency questionnaire.Results: Multi-adjusted analysis revealed that in normotensive patients coffeeconsumption of 1-2 cups/day was associated with 89% (95%CI: 0.01-0.82) lowerlikelihood of developing LVSD and consumption of 3-5 cups/day with 92.5%(95%CI: 0.008-0.69) lower likelihood for LVSD, compared with rare consumptionof coffee and after adjusting for various confounders. On the other hand in hyper-tensive patients coffee consumption of 3-5 cups/day was associated with 7-foldhigher likelihood for developing LVSD (95%CI: 1.39-41.10) as compared with rarecoffee consumption.Conclusion: Coffee consumption has opposite effects on the likelihood of devel-oping LVSD in post ACS patients depending on their blood pressure levels, beingprotective in normotensive, but augmenting the likelihood for LVSD in hyperten-sive patients.
P488 Ergonovine-induced coronary artery spasm andlong-term survival in patients with chest pain andnon-significant coronary artery stenosis
A. Ntalianis, E. Puymirat, M. Conte, A. Peace, F. Mangiacapra,O. Muller, C. Trana, G.R. Heyndrickx, E. Barbato, W. Wijns. OLV
Hospital Aalst, Cardiovascular Center, Aalst, Belgium
Purpose: Although coronary artery spasm has been linked to vascular endothe-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Risk protection in acute coronary syndromes 49
lial dysfunction and adverse cardiovascular events it is generally considered arelatively benign disease when treated appropriately. We investigated the impactof ergonovine (E)-induced coronary spasm during coronary angiography on long-term prognosis in patients with chest pain and non-significant coronary arterystenosis.Methods: All consecutive patients with non-significant coronary stenosis under-going an E provocation test because of clinical suspicion of variant angina wererecruited. For all patients, vasoactive medications were withheld for at least 48hours before catheterization. Intravenous E was administered at the end of thediagnostic catheterization and vasoreactivity and coronary artery spasm wereassessed angiographically. By protocol, intracoronary nitrates were administeredafter E in all cases. The primary and secondary end-points were: a) long-termsurvival rates (10 years) and b) long-term survival free of cardiovascular events(stroke, myocardial infarction, revascularization) respectively.Results: In total, 218 patients (mean age: 56±11 years) were enrolled. All pa-tients were on optimal medical treatment. The mean duration of follow-up was:75±51 months. The E test was characterized as positive in 79 patients (43%women). Long-term survival rates were lower in patients with positive E test(84% vs 96%, p=0.04) (figure). Similarly, long-term survival free of cardiovascularevents was also lower in the same group (71% vs 91%, p=0.004).
Long-term survival
Conclusions: Coronary artery spasm induced during ergonovine provocationtest, associates with worse long-term survival and higher incidence of adversecardiovascular events among patients with chest pain and non-significant coro-nary artery stenosis.
P489 Relationship between plasma glucose and mortality innon-diabetic patients with acute coronary syndromeand systolic heart failure: insights from the EPHESUStrial
P. Deedwania1 , R. Desai2, M. Mujib2, B. Pitt3, A. Ahmed2. 1Universityof California San Francisco, School of Medicine, Fresno, Fresno, United Statesof America; 2University of Alabama at Birmingham, Birmingham, United Statesof America; 3University of Michigan Medical School, Ann Arbor, United States ofAmerica
Purpose: Hyperglycemia is associated with poor outcomes in acute coronarysyndrome (ACS). However, it has been suggested that plasma glucose (PG) mayhave a J- or U-shaped association with mortality in ACS patients without diabetesmellitus (DM). Accordingly, we examined the association between baseline PGand mortality in Eplerenone Post-Acute Myocardial Infarction Heart Failure Effi-cacy and Survival Study (EPHESUS) participants without DM.Methods: Of the 6632 EPHESUS ACS patients with systolic HF, 4490 had noDM at baseline. Of these, 4411 had data on random baseline PG. Patients werecategorized into 5 groups based on PG: <80, 80–109, 110–139, 140–179 and>180 mg/dL. Associations between PG and all-cause mortality during 16 monthsof median follow-up were estimated using Cox regression models, with and with-out adjustment for major prognostically important covariates (using PG 110–130as the reference category).Results: Patients with higher PG groups were more likely to be older, smokers,have lower ejection fraction, and receive nitrates, statins, digoxin, loop diuretics,and coronary interventions during index admission. Unadjusted and multivariable-adjusted hazard ratio (HR) and 95% confidence interval (CI) for mortality associ-ated with various PG levels are displayed in the Table.
Baseline plasma glucose (mg/dL) in those without baseline diabetes mellitus (n=4411)
<80 80–109 110–139 140–179 >180(n=380) (n=2418) (n=1059) (n=422) (n=108)
Death (%) 49 (13%) 290 (12%) 157 (15%) 79 (19%) 24 (18%) P=0.001*Unadjusted HR 0.90 0.79 1.00 1.34 1.33
(95%CI) (0.65–1.24) (0.65–0.97) (1.02–1.76) (0.86–2.04)Adjusted HR 0.97 0.80 1.00 1.25 0.95
(95%CI) (0.70–1.36) (0.65–0.98) (0.94–1.65) (0.61–1.48)
*Chi square
Conclusions: In non-DM ACS patients with systolic HF, baseline PG had a linearunadjusted association with mortality, which increased with increasing plasmaglucose.
P490 Increased baseline rho kinase activity is anindependent predictor of adverse cardiovascularoutcome in acute coronary syndrome
M. Dong1, M. Zhang1, R.J. Li1, J.K. Liao2, C.M. Yu1. 1Institute ofVascular Medicine, Prince of Wales Hospital, The Chinese University
of Hong Kong, Hong Kong, China, People’s Republic of; 2Vascular MedicineResearch Unit, Brigham and Women’s Hospital and Harvard Medical School,Boston, Massachusetts, United States of America
Background: Increased Rho kinase (ROCK) activity is associated with endothe-lial dysfunction and vascular inflammation, which might impact on the clinicalcourse of acute coronary syndrome (ACS). This study aimed to investigate if ele-vated ROCK activity is associated with worse outcomes after ACS.Methods: 163 patients admitted for ACS were studied. Baseline ROCK activitywas measured by phosphorylation of myosin binding subunit (MBS) in peripheralleukocytes (measured by ratio of phosphorylation MBS/total MBS). Patients werefollowed up for 12 months or until occurrence of MACE (cardiac death, nonfatalmyocardial infarction, revascularization).Results: There were 33 patients (20.24%) who developed MACE. Patients whohad MACE were older (74.88±11.47 vs 67.68±12.92 years, p=0.003), had higherpeak creatine phosphokinase level (1550±1997 vs 605±1144 U/I, p<0.001),poorer renal function (creatinine: 136±106 vs 250±228 μmol/l, p<0.001; eGFR:42.7±24.7 vs 58.3±34.5 ml/min/1.73m2, p<0.001), heart failure symptom on pre-sentation (45.5% vs 16.8%, p<0.001), did not receive percutaneous coronary in-tervention (PCI) treatment in index admission (70.8% vs 38.5%, p=0.004) andhigher baseline leukocyte ROCK activity (3.57±1.31 vs 3.11±0.84, p=0.003).By ROC analysis, the best cutoff value of baseline ROCK activity for predict-ing 12-month MACE events was 3.1, with a sensitivity of 61% and a speci-ficity of 59%). By multivariate stepwise Cox hazard regression model, creatinine>200μmol/l (OR=5.245, 95% CI=2.230-12.336, P=0.06), PCI treatment on ad-mission (OR=0.258, 95% CI=0.099-0.675, P=0.016) and baseline ROCK activity>3.1 (OR=2.232, 95% CI=1.019-4.890, P=0.034) were independent predictors ofMACE.Conclusion: Increased ROCK activity is an independent predictor of adverseoutcome at 12-month after ACS.
P491 Novel insights into the pathophysiology of unstableangina using a high sensitive troponin assay
T. Reichlin, R. Twerenbold, M. Reiter, W. Hochholzer, J. Meissner,M. Potocki, M. Noveanu, P. Buser, S. Osswald, C.H. Mueller. UniversityHospital Basel, Basel, Switzerland
Background: The pathophysiology and myocardial injury in unstable angina (UA)is poorly understood. Novel high-sensitive troponin assays should allow us todetermine whether UA is characterized by low level acute myocardial injury thatwas not detectable by previous standard troponin assays.Methods: In an international multicenter study, we enrolled 1163 consecutivepatients with a suspected acute coronary syndrome. High-sensitive troponin T(hsTnT) was determined in a blinded fashion at presentation and after 1, 2, 3,and 6 hours. The final diagnosis was adjudicated by two cardiologists using allavailable clinical information including coronary angiography, stress testing, andthe standard troponin levels obtained during clinical care.Results: The adjudicated diagnosis was UA in 164 patients. Changes of hsTnTin patients with UA, acute myocardial infarction (AMI, n=185) and non-cardiacchest pain (NCCP, n=561) were -0.1ng/l (-0.8 to +0.9ng/l) in UA, 15.8 ng/l (2.7to 57.8ng/l) in AMI and 0.0ng/l (-1.1 to 1.2ng/l) in NCCP (p<0.001 and p=0.85for comparison) within the first hour after presentation. Changes within 2 hourswere -0.1ng/l (-0.9 to +1.0ng/l) in UA, 36.6 ng/l (11.7 to 109.3ng/l) in AMI and0.0ng/l (-0.7 to 0.7ng/l) in NCCP (p<0.001 and p=0.97 for comparison). 45% ofUA patients had a hsTnT level above the 99th percentile in healthy volunteers (14ng/l), as compared to 20% in patients with NCCP.
Changes of hs TnT accoring to Diagnosis
Conclusions: UA does not seem to result in relevant acute myocardial injury asquantified by changes in hsTnT in the majority of patients. This important differ-ence between UA and AMI suggests that UA and AMI are different diseases on
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

50 Risk protection in acute coronary syndromes
the myocardial level and highlights the importance of the delta criterion in thecurrent definition of AMI.
P492 Mild heart failure is a mortality marker after a non STsegment elevation acute myocardial infarction
M. Del Trigo, I. Nunez-Gil, J.C. Garcia Rubira, C. Acebal, D. Vivas,A. D Agustin, S. Bordes, B. Ibanez, C. Macaya, A. Fenandez Ortiz.Hospital Clinic San Carlos, Madrid, Spain
Background: The Killip classification is based on heart failure physical examina-tion derived parameters after a myocardial infarction. However, prognostic dataabout its lower degrees are scarce on non ST elevation acute myocardial infarc-tion (NSTEMI), nowadays, a growing form of myocardial infarction. Our objectivewas to assess the prognostic value of mild heart failure after a NSTEMI.Methods: Of 835 consecutively patients admitted with a NSTEMI between 2005and 2007, we selected those on Killip1 (K1=684) or 2 (K2=113), being >K2excluded (38 patients, with pulmonary oedema or cardiogenic shock). Clinical,angiographic, treatment features, and 30-days all cause mortality, together withother cardiovascular outcomes were prospectively recorded.Results: Differences were shown regarding gender (male: K1 72.1% Vs K252.0%, p<0.001), mean age (K1 66.6 years Vs K2 73.8 years, p<0.001), higherfrequency of Diabetes Mellitus (p<0.001) and arterial hypertension (p<0.001) butless were smokers (p=0.003) in the onset heart failure group. Previous recordson infarction/revascularization procedures were similar. Infarction size, assessedby Troponin I and Creatinkinase (p=0.378, p=0.855) did not displayed differenceseither. Multivessel coronary disease was more frequent on K2 patients (p=0.015).Outcomes were worst regarding higher evolutive Killip degrees, combined event,and death (1.8% Vs 14.2%, p<0.001). After multivariate analysis, onset mild heartfailure remained as an adverse prognostic factor (OR=7.00; IC95%:2.69-18.20;p<0,001).
Conclusion: Even milder baseline heart failure degrees are still linked to a worseprognostic, including higher short-term mortality after a NSTEMI. Probably, thisfact should prompt a more aggressive approach and an earlier cardiac catheteri-zation.
P493 Standard ECG to predict culprit left main disease inunselected patients with non ST-segment elevationacute coronary syndrome
N. Taglieri, P. Ortolani, F. Saia, S. Rosmini, L. Cinti, C. Villani, L. Alessi,F. Vagnarelli, A. Branzi, C. Rapezzi. University of Bologna, Institute of
Cardiology, Bologna, Italy
Purpose: To determine the ECG features associated with culprit left main disease(LMD) in patients with non ST elevation acute coronary syndrome (NSTE-ACS).Methods: We included 601 consecutive patients with NSTE-ACS undergoingcoronary catheterization. Inclusion criteria were: chest pain within 24h and oneof the following: 1) ST depression (STD)≥ 0.5 mm in any lead 2) transient STE3) negative T wave ≥ 1mm or T wave pseudonormalization 4) positive cardiacbiomarkers 5) documentation of coronary artery disease. Patients with prior coro-nary bypass were excluded.Results: Patients with culprit LMD (n = 50; 8.3%) were older (mean age 76 vs.70 y; p = 0.002) had a higher prevalence of male gender (78% vs 65%; p = 0.06),prior stroke/TIA (20.0% vs. 6.7%; p = 0.001) peripheral artery disease 38.0% vs15.8%; p < 0.001) and Killip class ≥ 3 (30.0 vs 9.8, p < 0.001) than patientswithout culprit LMD (n =551; 91.7%). No differences were observed in terms ofRBBB or known LBBB.Compared to the other group patients with culprit LMD had a higher rate of STD(58% vs 33.2%, p <0.001), a higher mean value of max and sum STD (1.60±1.6vs. 0.63±1.12mm; 6.16±7.04 vs. 2.05±4.17, respectively) and a lower preva-lence of normal ecg (4.0% vs. 8.0%; p = 0.048) and negative T wave (6.0% vs.19.1). The prevalence of lead aVR-STE≥1mm was significantly higher in patients
Abstract P493 – Table 1
ECG Sensitivity % Specificity % Positive Predictive Value % Negative Predictive Value % Predictive Accuracy % Adjusted OR C-statistic(95% CI) (95% CI) (95% CI) (95% CI) (95% CI) (95% CI)
STD 58 (54-62) 67 (63-71) 14 (11-17) 95 (93-97) 66 (62-70) 2.3 (1.3-4.3) 0.765aVR STE + STD 42 (38-35) 90 (88-92) 27 (23-31) 95 (93-97) 86 (83-89) 5.1 (2.6-9.9) 0.784aVR STE + Max STD≥ 1.5mm 40 (36-44) 92 (90-94) 31 (27-35) 94 (92-96) 88 (85-91) 5.9 (2.9-11.7) 0.790aVR STE + Diffuse STD 42 (38-45) 92 (90-94) 31 (27-35) 95 (93-97) 87 (84-90) 6.2 (3.1-12.1) 0.791
Diffuse = ≥2 peripheral leads + ≥2 precordial leads.
that had culprit LMD than those who had not (42% vs. 10%, P <0.001). This dif-ference was found only in the subgroup with aVR STE + STD. On multivariableanalysis male gender, age, STD and aVR-STE were independent predictors ofculprit LMD.Table 1 shows that the association of STD and lead aVR-STE had a higher pre-dictive accuracy compared to STD. The presence of the former pattern increased>5-fold the risk of culprit LMD. No differences were observed between quantita-tive and qualitative analysis.Conclusions: Combined evaluation of aVR-STE and STD improves the diagnos-tic performance of standard ECG to predict culprit LMD across the whole ECGspectrum of patients with NSTE-ACS.
P494 Plasma aldosterone levels prior to primary PCI forSTEMI are predictive of myocardial reperfusion statusafter PCI and late outcome
F. Beygui, J.P. Labbe, N. Vignolles, A. Bellemain-Appaix, J. Silvain,G. Cayla, O. Barthelemy, D. Brugier, J.P. Collet, G. Montalescot.
AP-HP - Hospital Pitie-Salpetriere, Paris, France
Purpose: Plasma aldosterone levels at presentation and myocardial reperfusionassessed by myocardial blush grade (MBG) after primary PCI are predictors ofoutcome after STEMI.We aimed to assess the whether aldosterone levels at presentation correlate toMBG after primary PCI.Methods: Aldosterone levels at presentation and MBG after primary PCI were as-sessed in 265 consecutive patients presenting within 12 hours after STEMI onsetand followed-up for 6 months. The relationship between baseline characteristicsof the patients as well as plasma aldosterone levels and MBG were assessedin a multivariable model. Aldosterone levels and MBG were also assessed aspotential correlates of 6 month mortality.Results: Patients were 64±14 yo; 21% were female. MBG grades 0, 1, 2, 3 werefound in 39 (15%), 124 (47%), 1 (<1%), and 101 (38%) patients respectively.MBG 3 and 2 were gathered for further analysis. A stepwise significant (globalp=0.002) relationship was found between MBG and aldosterone levels at presen-tation (figure). On multivariable analysis the only correlates of a MBG 2/3 gradewere aldosterone levels at presentation (OR 3.1[1.4-6.8]) and clopidogrel therapyprior to STEMI onset (OR 4.3[1.4-13.2]).At 6 months follow-up 23 deaths were reported. Both aldosterone levels and MBGwere correlated to 6 month mortality on univariable and multivraiable analysis (OR7 [1.3-36.6] and, OR 0.06 [0.01-0.22] and O.1 [0.03-0.28] for aldosterone quartile4 versus 1, and MBG 2/3 and 1 vs 0 respectively.
Conclusions: High aldosterone levels at presentation for STEMI are correlatedto both post primary PCI myocardial reperfusion and late mortality. These findingssupport the hypothesis of a possible aldosterone-related vascular injury and thebenefit of a very early aldosterone blockade in STEMI patients.
P495 Impact of in-hospital delay to invasive treatment ofNSTEMI patients on early and 12-month clinicaloutcomes: analysis from the PL-ACS Registry
M. Gierlotka1, G. Opolski2, L. Polonski1, M.R. Dada2, K. Wilczek1,M. Gasior1, K.J. Filipiak2. 1Medical University of Silesia, Silesian
Center for Heart Diseases, Zabrze, Poland; 2Medical University of Warsaw, 1stDepartment of Cardiology, Warsaw, Poland
Purpose: Although previous clinical trials have shown that invasive strategy im-proves clinical outcomes in patients (pts) with non-ST-segment elevation myocar-dial infarction (NSTEMI), the timing of such procedure remains ambiguous. Wesought to assess the impact of in-hospital delay to invasive treatment on earlyand 12-month clinical outcomes in NSTEMI.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
Risk protection in acute coronary syndromes 51
Methods: PL-ACS registry comprises 467 hospitals in Poland. We assessedbaseline characteristics, and clinical outcomes in 11 433 NSTEMI pts, withoutcardiogenic shock on admission hospitalised between October 2003 and Octo-ber 2008. Patients who underwent intervention within the first 2 hours were ex-cluded. Four groups were analysed based on the time from admission to coro-nary angiography: 2-24h, 24-48h, 48-72h, and >72h, respectively. The primaryoutcomes were: in-hospital MACE (death, MI, stroke or major bleeding), 30-daymortality and 12-month mortality.Results: 61% of NSTEMI pts had coronary angiography performed between 2-24h, 15% between 24-48h, 7% between 48-72h, and 17% of pts later than 72hfrom admission (table). Although there were several differences in baseline char-acteristics between the groups, in-hospital MACE rates, as well as 30-day mor-talities were comparable. The median length of stay (LOS) was significantly pro-longed in >72h group (10 days), compared to 4 days in 2-24h group (p<0.001).The 12-month mortality was relatively low in pts treated within 24-48h when com-pared to the other groups.
Table 1
Door-to-coronary angiography time P value
2-24 h 24-48 h 48-72 h >72 h
N 6994 1729 811 1899Percutaneous Coronary
Intervention 5069 (72.5%) 1116 (64.5%) 511 (63%) 1040 (54.8%) <0.0001Coronary Artery Bypass
Surgery 1228 (17.6%) 334 (19.3%) 181 (22.3%) 403 (21.2%) 0.0001In-hospital MACE 311 (4.4%) 101 (5.8%) 42 (5.2%) 91 (4.8%) 0.099In-hospital death 85 (1.2%) 16 (0.9%) 11 (1.4%) 32 (1.7%) 0.21LOS in days (median) 4 (3-7) 6 (4-8) 6 (5-9) 10 (7-14) <0.00130-day mortality 190 (2.7%) 39 (2.3%) 22 (2.7%) 53 (2.8%) 0.7312-month mortality 578 (8.3%) 131 (7.6%) 66 (8.1%) 195 (10.3%) 0.017
Conclusions: Early invasive strategy within 2-48h from hospital presentation inNSTEMI pts is safe and associated with shorter LOS when compared to catheter-based interventions perfomed later. The delayed intervention after 72h increases12-month mortality.
P496 Electrocardiographic pattern to enhance prediction ofin-hospital cardiovascular death in patients with nonST elevation acute coronary syndrome
N. Taglieri, A. Marzocchi, G. Melandri, L. Cinti, S. Rosmini, C. Villani,F. Vagnarelli, L. Alessi, A. Branzi, C. Rapezzi. University of Bologna,
Institute of Cardiology, Bologna, Italy
Purpose: To investigate the prognostic significance of lead aVR ST elevtion(STE) associated with ST depression in other leads in patients with non STEacute coronary syndrome (NSTE-ACS).Methods: We included NSTE-ACS patients who met the following inclusion crite-ria: chest pain within 24h plus one of the following: 1) ST depression ≥ 0.5 mm inany lead 2) transient ST elevation in two contiguous leads 3) negative T wave ≥1mm 4) positive cardiac biomarkers 5) documentation of coronary artery disease.The study population was divided into two groups according to the presence ornot on admission ECG of simultaneous aVR STE ≥ 1mm and STD (defined ashigh risk ECG pattern). In-hospital cardiovascular (CV) death was the primarystudy endpoint. Secondary end point was the rate of left main disease (LMD) asculprit artery.Results: 888 consecutive patients (mean age 73.4±12.4) were included, 570were male, 764 had NSTEMI. 121 patients had high risk ECG pattern and theydisclosed a worse clinical profile as compared to 575 patients with no high riskECG pattern (median GRACE risk score: 182 vs. 142, respectively). Thirty fivepatients (3.9%) died from cardiovascular cause. Patients with the high risk ECGpattern had a higher rate of primary (13.2% vs. 2.5%, p<0.001) and secondary(24.7% vs. 5.0%, p<0.001) endpoint compared to patients with no high-risk ECGpattern. We further divided the study population into low risk and high risk patientsaccording to the median value of the GRACE risk score. Of note, for each level ofrisk the high risk ECG pattern independently predicted in-Hospital CV death andculprit LMD (Figure).
Conclusions: Lead aVR STE associated with STD in other leads may provide
further prognostic information in patients with NSTE-ACS on top of recommendedscoring system.
P497 Clinical use of a high-sensitive cardiac troponin assayin patients with suspected myocardial infarction
T. Reichlin, R. Twerenbold, W. Hochholzer, M. Reiter, J. Meissner,M. Potocki, M. Noveanu, N. Arenja, S. Osswald, C.H. Mueller.University Hospital Basel, Basel, Switzerland
Background: Novel high-sensitive cardiac troponin (hs-cTn) assays have beenshown to improve the early diagnosis of acute myocardial infarction (AMI). How-ever, the optimal clinical use of hs-cTn tests remains unknown.Methods: In an international multicenter study, we enrolled 1043 patients pre-senting with suspected AMI to the ED. The final diagnoses were adjudicated bytwo independent cardiologists using all available clinical information and hs-cTnTlevels obtained at presentation and after 1, 2, 3 and 6 hours. 74 patients (7%) hadto be excluded due to insufficient clinical work-up.Results: The final diagnoses was AMI in 234 of 969 patients (24%). For the di-agnosis of AMI, the area under the ROC-curve (AUC) for baseline hs-cTnT atpresentation was 0.94 (95% CI 0.93-0.96). This was similar to absolute values ofchanges in hs-cTnT within the first hour (AUC 0.93, 95% CI 0.91-0.96, p=0.63),while relative changes of hs-cTnT within the first hour had a very limited diagnos-tic accuracy (AUC 0.67, 95% CI 0.62-0.72). The combination of baseline levelsof hs-cTnT with absolute changes within the first hour significantly improved di-agnostic accuracy (AUC 0.97, 95% CI 0.96-0.98, p<0.001 for comparisons withbaseline and changes). In patients with a baseline hs-cTnT level ≤12.5 ng/l andwith a change in hs-cTnT ≤2 ng/l within the first hour (in total 57% of patients),AMI was ruled out with a sensitivity and negative predictive value of 100% at aspecificity of 73% and a positive predictive value of 47%.
Conclusions: For the diagnosis of AMI, absolute but not relative changes of hs-cTnT have a very high diagnostic accuracy and should be used in conjunction withbaseline values. The combination of baseline values and early changes within thefirst hour seems to allow a rapid and reliable rule out of AMI.
P498 Early diagnosis of acute myocardial infarction usingthe combination of a high-sensitive cardiac troponinassays and copeptin - insights from a multicenter study
C. Heinisch1, R. Twerenbold1 , M. Reiter1, T. Reichlin1, J. Meissner1,N. Arenja1, T. Socrates1, W. Hochholzer2 , C. Mueller2. 1University
Hospital Basel, Department of Internal Medicine, Basel, Switzerland; 2HarvardMedical School, Boston, United States of America
Purpose: The rapid and reliable diagnosis of acute myocardial infarction (AMI) isa major unmet clinical need. Previously, two novel approaches have been shownto significantly improve early diagnostic accuracy: high-sensitive troponin T (hs-TnT) assays and copeptin, a sensitive marker of endogenous stress. It is un-known, whether the combination of hs-TnT and copeptin would further increasediagnostic accuracy.Methods: We conducted a multicenter study to examine diagnostic accuracy ofthe combination of a new hs-TnT assay and copeptin performed on blood samplesobtained in the emergency department from 1170 consecutive patients present-ing with symptoms suggestive of AMI. Hs-TnT and copeptin levels were deter-mined in a blinded fashion. The final diagnosis was adjudicated by two indepen-dent cardiologists.Results: AMI was the adjudicated final diagnosis in 184 (16%) patients. The di-agnostic accuracy for measurements obtained at presentation, as quantified bythe area under the receiver operating characteristic curve (AUC), was significantlyhigher for the combination of hs-TnT and copeptin (0.956; 95% confidence inter-val (CI) 0.943 to 0.967) as compared to hs-TnT alone (0.947; 95%CI 0.933 to0.959,p=0.006,Figure). In patients presenting within three hours after the onsetof chest pain (n=416,50 patients with AMI), the AUC was 0.920 (95% confidenceinterval 0.890 to 0.944) for the combination with copeptin and 0.907 (95%CI 0.875to 0.933, p=0.133) for hsTnT alone.Conclusions: The additional use of copeptin further increases early diagnosticaccuracy on top of hs-TnT. The incremental benefit is small but may be clinically
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
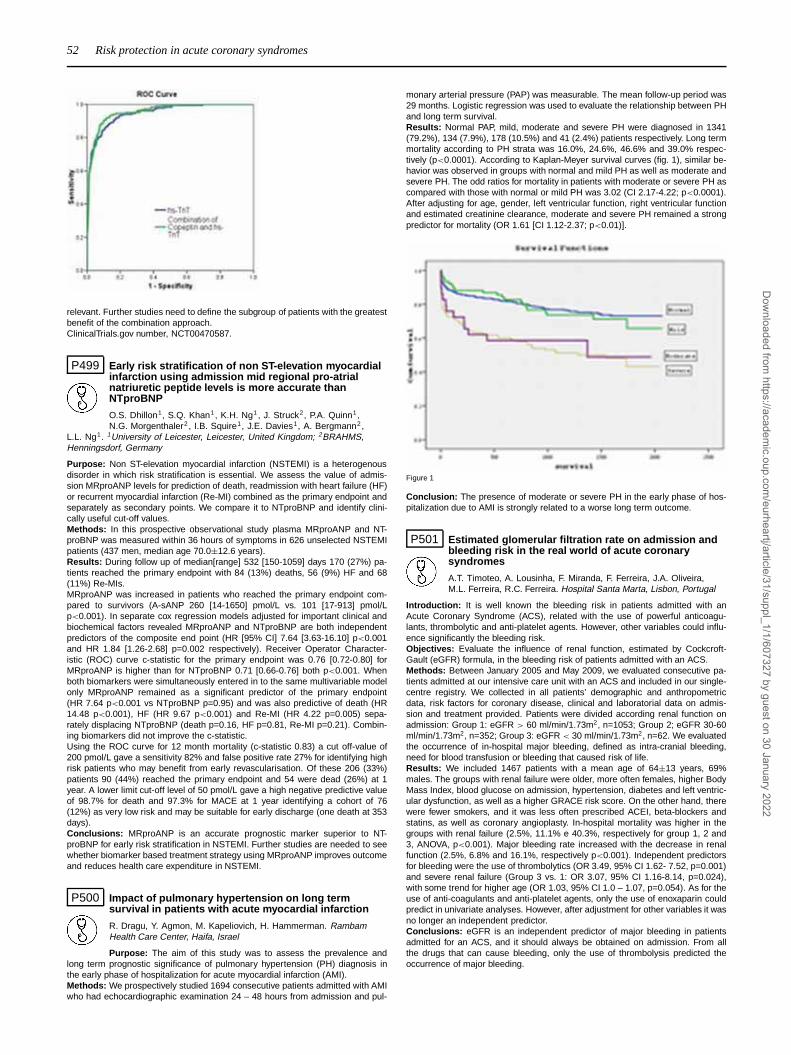
52 Risk protection in acute coronary syndromes
relevant. Further studies need to define the subgroup of patients with the greatestbenefit of the combination approach.ClinicalTrials.gov number, NCT00470587.
P499 Early risk stratification of non ST-elevation myocardialinfarction using admission mid regional pro-atrialnatriuretic peptide levels is more accurate thanNTproBNP
O.S. Dhillon1, S.Q. Khan1, K.H. Ng1, J. Struck2, P.A. Quinn1,N.G. Morgenthaler2 , I.B. Squire1, J.E. Davies1, A. Bergmann2,
L.L. Ng1. 1University of Leicester, Leicester, United Kingdom; 2BRAHMS,Henningsdorf, Germany
Purpose: Non ST-elevation myocardial infarction (NSTEMI) is a heterogenousdisorder in which risk stratification is essential. We assess the value of admis-sion MRproANP levels for prediction of death, readmission with heart failure (HF)or recurrent myocardial infarction (Re-MI) combined as the primary endpoint andseparately as secondary points. We compare it to NTproBNP and identify clini-cally useful cut-off values.Methods: In this prospective observational study plasma MRproANP and NT-proBNP was measured within 36 hours of symptoms in 626 unselected NSTEMIpatients (437 men, median age 70.0±12.6 years).Results: During follow up of median[range] 532 [150-1059] days 170 (27%) pa-tients reached the primary endpoint with 84 (13%) deaths, 56 (9%) HF and 68(11%) Re-MIs.MRproANP was increased in patients who reached the primary endpoint com-pared to survivors (A-sANP 260 [14-1650] pmol/L vs. 101 [17-913] pmol/Lp<0.001). In separate cox regression models adjusted for important clinical andbiochemical factors revealed MRproANP and NTproBNP are both independentpredictors of the composite end point (HR [95% CI] 7.64 [3.63-16.10] p<0.001and HR 1.84 [1.26-2.68] p=0.002 respectively). Receiver Operator Character-istic (ROC) curve c-statistic for the primary endpoint was 0.76 [0.72-0.80] forMRproANP is higher than for NTproBNP 0.71 [0.66-0.76] both p<0.001. Whenboth biomarkers were simultaneously entered in to the same multivariable modelonly MRproANP remained as a significant predictor of the primary endpoint(HR 7.64 p<0.001 vs NTproBNP p=0.95) and was also predictive of death (HR14.48 p<0.001), HF (HR 9.67 p<0.001) and Re-MI (HR 4.22 p=0.005) sepa-rately displacing NTproBNP (death p=0.16, HF p=0.81, Re-MI p=0.21). Combin-ing biomarkers did not improve the c-statistic.Using the ROC curve for 12 month mortality (c-statistic 0.83) a cut off-value of200 pmol/L gave a sensitivity 82% and false positive rate 27% for identifying highrisk patients who may benefit from early revascularisation. Of these 206 (33%)patients 90 (44%) reached the primary endpoint and 54 were dead (26%) at 1year. A lower limit cut-off level of 50 pmol/L gave a high negative predictive valueof 98.7% for death and 97.3% for MACE at 1 year identifying a cohort of 76(12%) as very low risk and may be suitable for early discharge (one death at 353days).Conclusions: MRproANP is an accurate prognostic marker superior to NT-proBNP for early risk stratification in NSTEMI. Further studies are needed to seewhether biomarker based treatment strategy using MRproANP improves outcomeand reduces health care expenditure in NSTEMI.
P500 Impact of pulmonary hypertension on long termsurvival in patients with acute myocardial infarction
R. Dragu, Y. Agmon, M. Kapeliovich, H. Hammerman. RambamHealth Care Center, Haifa, Israel
Purpose: The aim of this study was to assess the prevalence andlong term prognostic significance of pulmonary hypertension (PH) diagnosis inthe early phase of hospitalization for acute myocardial infarction (AMI).Methods: We prospectively studied 1694 consecutive patients admitted with AMIwho had echocardiographic examination 24 – 48 hours from admission and pul-
monary arterial pressure (PAP) was measurable. The mean follow-up period was29 months. Logistic regression was used to evaluate the relationship between PHand long term survival.Results: Normal PAP, mild, moderate and severe PH were diagnosed in 1341(79.2%), 134 (7.9%), 178 (10.5%) and 41 (2.4%) patients respectively. Long termmortality according to PH strata was 16.0%, 24.6%, 46.6% and 39.0% respec-tively (p<0.0001). According to Kaplan-Meyer survival curves (fig. 1), similar be-havior was observed in groups with normal and mild PH as well as moderate andsevere PH. The odd ratios for mortality in patients with moderate or severe PH ascompared with those with normal or mild PH was 3.02 (CI 2.17-4.22; p<0.0001).After adjusting for age, gender, left ventricular function, right ventricular functionand estimated creatinine clearance, moderate and severe PH remained a strongpredictor for mortality (OR 1.61 [CI 1.12-2.37; p<0.01)].
Figure 1
Conclusion: The presence of moderate or severe PH in the early phase of hos-pitalization due to AMI is strongly related to a worse long term outcome.
P501 Estimated glomerular filtration rate on admission andbleeding risk in the real world of acute coronarysyndromes
A.T. Timoteo, A. Lousinha, F. Miranda, F. Ferreira, J.A. Oliveira,M.L. Ferreira, R.C. Ferreira. Hospital Santa Marta, Lisbon, Portugal
Introduction: It is well known the bleeding risk in patients admitted with anAcute Coronary Syndrome (ACS), related with the use of powerful anticoagu-lants, thrombolytic and anti-platelet agents. However, other variables could influ-ence significantly the bleeding risk.Objectives: Evaluate the influence of renal function, estimated by Cockcroft-Gault (eGFR) formula, in the bleeding risk of patients admitted with an ACS.Methods: Between January 2005 and May 2009, we evaluated consecutive pa-tients admitted at our intensive care unit with an ACS and included in our single-centre registry. We collected in all patients’ demographic and anthropometricdata, risk factors for coronary disease, clinical and laboratorial data on admis-sion and treatment provided. Patients were divided according renal function onadmission: Group 1: eGFR > 60 ml/min/1.73m2, n=1053; Group 2; eGFR 30-60ml/min/1.73m2, n=352; Group 3: eGFR < 30 ml/min/1.73m2, n=62. We evaluatedthe occurrence of in-hospital major bleeding, defined as intra-cranial bleeding,need for blood transfusion or bleeding that caused risk of life.Results: We included 1467 patients with a mean age of 64±13 years, 69%males. The groups with renal failure were older, more often females, higher BodyMass Index, blood glucose on admission, hypertension, diabetes and left ventric-ular dysfunction, as well as a higher GRACE risk score. On the other hand, therewere fewer smokers, and it was less often prescribed ACEI, beta-blockers andstatins, as well as coronary angioplasty. In-hospital mortality was higher in thegroups with renal failure (2.5%, 11.1% e 40.3%, respectively for group 1, 2 and3, ANOVA, p<0.001). Major bleeding rate increased with the decrease in renalfunction (2.5%, 6.8% and 16.1%, respectively p<0.001). Independent predictorsfor bleeding were the use of thrombolytics (OR 3.49, 95% CI 1.62- 7.52, p=0.001)and severe renal failure (Group 3 vs. 1: OR 3.07, 95% CI 1.16-8.14, p=0.024),with some trend for higher age (OR 1.03, 95% CI 1.0 – 1.07, p=0.054). As for theuse of anti-coagulants and anti-platelet agents, only the use of enoxaparin couldpredict in univariate analyses. However, after adjustment for other variables it wasno longer an independent predictor.Conclusions: eGFR is an independent predictor of major bleeding in patientsadmitted for an ACS, and it should always be obtained on admission. From allthe drugs that can cause bleeding, only the use of thrombolysis predicted theoccurrence of major bleeding.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Risk protection in acute coronary syndromes 53
P502 B type natriuretic peptide levels predict extent andseverity of coronary disease in non-ST elevationcoronary syndromes and normal left ventricularsystolic function
A. Palazzuoli1, G. Antonelli1, M. Fineschi2 , I. Quatrini1, A. Calabro’1,M.S. Campagna1 , M. Caputo1, C. Pierli2, R. Nuti1, A. Maisel3.
1Department of Internal Medicine and Metabolic Diseases, Siena, Italy; 2SantaMaria Alle Scotte Polyclinic, Invasive Cardiology, Siena, Italy; 3San DiegoVeterans Affairs Medical Center, San Diego, United States of America
Purpose: Recently B type natriuretic peptide (BNP) has been employed in pa-tients with coronary artery disease (CAD) with ST elevation and non-ST elevation.BNP is able to predict systolic dysfunction, adding new prognostic informationwith respect to traditional markers. However it is not known if there is a relationbetween CAD severity and BNP levels.Methods: This study compared BNP levels in patients with stable angina (SA)and acute coronary syndromes (ACS) with non-ST elevation in relation to an-giographic lesions using TIMI and Gensini Scores. We studied 282 patients withCAD without ST elevation and preserved systolic function. BNP samples weremeasured in all recruited patients within 24 hours of hospitalization.Results: BNP values were progressively increased in relation with diagno-sis: SA (52.6±49.4 pg/mL), Unstable angina (UA) (243.3±212 pg/mL), NSTE-ACS (421.7±334 pg/mL) (p< 0.0001 and p< 0.007 respectively). No statisti-cally significant difference was observed between patients with SA and controls(21.2±6.8 pg/mL). Analysis of BNP in relation to number of involved vesselsdemonstrated significantly increased levels in patients with multi-vessel diseasecompared to patients with 1 or 2 vessels disease (1-vessel: 86.2±46.3 pg/mL;2- vessels: 127±297 pg/mL; 3- vessels: 295±318 pg/mL; 4-vessels: 297±347pg/mL; p<0.001 and p<0.003, respectively). BNP evaluation, using GensiniScore showed a strong relation between BNP and coronary disease extension(r=0.38 p<0.0001). This trend was maintained in all CAD groups (SA= r 0.54; UAr = 0.36 NSTE-ACS r= 0.28).Conclusions: Circulating BNP levels appear elevated in ACS with diffuse coro-nary involvement, even in the absence of systolic dysfunction. BNP is also asso-ciated with multi-vessel disease and coronary disease extension.
P503 Comparison mid regional pro-atrial natriuretic peptidelevels and GRACE risk score for prediction of shortand long term events in patients with non ST-elevationmyocardial infarction
O.S. Dhillon1, H.K. Narayan1, K.H. Ng1, J. Struck2,N.G. Morgenthaler2 , P.A. Quinn1, I.B. Squire1, J.E. Davies1, A. Bergmann2,L.L. Ng1. 1University of Leicester, Leicester, United Kingdom; 2BRAHMS,Henningsdorf, Germany
Purpose: Non ST-elevation myocardial infarction (NSTEMI) is a heterogenousdisorder in which early risk stratification should guide management. We assessthe value of admission MRproANP levels for prediction of death, readmission withheart failure (HF) or recurrent myocardial infarction (Re-MI) combined as the pri-mary endpoint and separately as secondary endpoints. We compare it to GRACERisk Score (GRS) for prediction of short and long term adverse events and iden-tify clinically useful cut-off values.Methods: In this prospective observational study plasma MRproANP was mea-sured within 36 hours of symptoms in 631 unselected patients (437 men, medianage 70.0±12.6 years) patients with NSTEMI.Results: During follow up of median[range] 532 [150-1059] days 170 (27%) pa-tients reached the primary endpoint with 84 (13%) deaths, 56 (9%) HF and 68(11%) Re-MIs.In separate Cox regression models after adjustment for important clinical andbiochemical factors both MRproANP and GRS were associated with the primaryendpoint (HR [95% Confidence Interval] 7.64 [3.63-16.10] p<0.001 and HR 1.01[1.00-1.02] p=0.006 respectively). Receiver Operator Characteristic (ROC) curvec-statistic for the primary endpoint was 0.76 [0.72-0.80] for MRproANP higherthan for GRS 0.71 [0.67-0.76] both p<0.001. With both markers entered in to themodel simultaneously MRproANP retained prediction of the primary endpoint HR6.68 p<0.001 as did GRS HR 1.01 p=0.04. For death over the course of followup MRproANP displaces GRS (HR 18.01 p<0.001 vs HR 1.01 p=0.23) and hasa higher c-statistic (0.83 vs 0.75 both p<0.001). The relationship between MR-proANP and GRS and shorter term events were compared, for death at 30 daysand 6 months both markers were predictive (HR 1.02 p=0.02 and HR 1.01p=0.02respectively for GRS, HR 8.50 p=0.03 and HR 10.28 p<0.001 respectively forA-sANP) with similar results for the primary endpoint. Elevated MRproANP waspredictive of re-MI on multivariate analysis (HR 4.22 p=0.005) whereas GRS wasnot (HR 1.01 p=0.20). Combining the markers did not improve the c-statistic.A cut off-value of 200 pmol/L for MRproANP identifies high risk patients with a44% primary endpoint and 26% mortality rate at 1 year. A lower limit cut-off levelof 50 pmol/L identifies a cohort of 76 (12.1%) as very low risk whom may besuitable for early discharge (one death at 353 days).Conclusions: Early risk stratification with MRproANP level is superior to GRACErisk score for prediction of adverse events after NSTEMI. A biomarker based treat-ment strategy using MRproANP needs further assessment.
P504 Smoking during myocardial infarction increases therisk of severe arrhythmic complications
D. Zysko, J. Gajek, M. Obremska, M. Cielecka, A. Hulok,A. Wojnalowicz, E. Staniszewska-Marszalek, W. Mazurek. WroclawMedical University, Wroclaw, Poland
Smoking is a well established risk factor for atherosclerosis. The aim of the studywas to assess arrhythmic complications during myocardial infarction and smokingduring related cardiac pain.The study group consisted of patients admitted with acute myocardial infarction.Only current smokers were included in the study when the time of the last smokedcigarette was known. Patients were divided into groups: Group I consisted of 55pts who were smoking and group II with 107 pts who were not smoking duringchest pain. The medical history, the duration of smoking, the number of cigarettessmoked daily, the time when the last cigarette had been smoked was noted. Theoccurrence of ventricular fibrillation, ventricular tachycardia and atrioventricularblock (analysed together as severe arrhythmic complications) were assessed onthe basis of emergency medical service’s reports or during the hospitalisation.The analysed data are presented in the table:
Table
Group I (n=55) Group II (n=107) p value
Age (years) 57.4±11.9 57.9±11.4 NSMale gender (%) 82 84 NSCigarettes smoked per day (n) 26.3±14.2 19.9±10.1 <0.005Duration of smoking (years) 33.2±13.1 31.2±11.5 NSArterial hypertension (%) 67 60 NSDiabetes mellitus (%) 16.7 9 NSPrevious myocardial infarction (%) 5.6 10.4 NSSTEMI (%) 78 79 NSInferior wall inferction (%) 51 43 NSVF or VT (%) 7.3 1.9 NSAV block (%) 10.9 0.9 <0.005VF or VT or AV block (%) 18.2 2.8 <0.001
The patients in group I reported higher number of cigarettes smoked daily. Severearrhythmic complications occurred more frequently in those smokers. Logistic re-gression analysis revealed that smoking during chest pain was only independentfactor related with severe arrhythmic complication in our group OR 6.8 (CI 1.7-26.5, p<0.01).Conclusion: Smoking during acute myocardial infarction is related with the higherpercentage of severe arrhythmic complications.
P505 Impact of the CRUSADE, ACUITY and TIMI majorbleeding definitions on in-hospital mortality in patientswith non- ST elevation acute myocardial infarction
R.M. Agra Bermejo, E. Abu Assi, S. Raposeiras Roubin, P. CabanasGrandio, J.M. Garcia Acuna, C. Pena Gil, J.R. Gonzalez Juanatey.
University Clinical Hospital of Santiago de Compostela, Department ofCardiology, Santiago de Compostela, Spain
Background: Major bleeding is associated with increased mortality in patientswith non-ST elevation acute myocardial infarction (NSTEMI). Although severalmajor bleeding definitions exist, the predictive accuracy of different scales hasrarely been compared. We assessed the impact of major bleeding (MB), definedby the CRUSADE, ACUITY and TIMI criteria, on in-hospital mortality in patientswith NSTEMI.Methods: Retrospectively, between 2004 and 2009, 794 consecutive patientswith the definitive diagnosis of NSTEMI were evaluated. MB was defined by theCRUSADE scale (intracraneal bleeding, retroperitoneal bleeding, a fall in hema-tocrit ≥12% (baseline to nadir), any red blood cell transfusion in which baselinehematocrit was ≥28%, or any in which this was <28% with overt bleeding), ACU-ITY scale (intracranial, intraocular, or retroperitoneal bleeding; access site bleed-ing with intervention; hematoma 5 cm; hemoglobin drop 3g/dL with source or4g/dL without source; or transfusion, and by the TIMI scale (intracranial bleeding;hemoglobin drop >5g/dL or hematocrit dorp >15%). Separate adjusted modelsassessed the impact of MB established by each scale on the in-hospital mortality.Results: 696 (88%) patients underwent cardiac catheterization (91% via ra-dial approach). 519 (74.5%) were revascularized. 41 (5.2%) died in-hospital.CRUSADE-, ACUITY- and TIMI-MB occurred in 15.4%, 11.8%, and 5.2%, respec-tively. In a covariate-adjusted multivariable model including each scale only, bothCRUSADE and ACUITY-MB was an independent predictor of in-hospital mortality(Odds ratio 3.2, [95% confidence interval: 1.2–5.4] and 2.6 [1.6-4.1], respectively(p<0.01). TIMI-MB was not an independent predictor of in-hospital death (1.6[0.5-5.2] (p=0.3).Conclusions: CRUSADE- and ACUITY- MB are both independent predictors ofin-hospital mortality in NSTEMI patients. Although CRUSADE- and ACUITY-MBare powerfull for predicting in-hospital mortality in NSTEMI patients, CRUSADE-MB is more common and thus identifies more patients at risk from MB.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

54 Risk protection in acute coronary syndromes
P506 Incidence and risk factors for the development ofcardiogenic shock in patients with NSTEMI - data of thedresden myocardial infarction registry
M. Gerlach, K. Foerster, C. Genee, K. Haacke, H. Schroetter,G. Simonis, R. Marquetant, T. Wittlinger, R.H. Strasser. Heart Center
Dresden, University Hospital, Dresden, Germany
Background: Cardiogenic shock (CS) is a major complication in acute coronarysyndroms (ACS) as patients with ACS and CS have a much higher mortality. Forpatients with ST-Elevation myocardial infarction (STEMI), guidelines insist on aquickest possible coronary reperfusion. Little evidence is available for patientswith CS in Non-STEMI (NSTEMI). Objective was to identify risk factors for CS inNSTEMI.Methods: Since September 2005, all patients with ACS were included into theDresden myocardial infarction registry after written consent. All consecutive pa-tients with CS (defined as RR<90mmHg, need of IABP implantation or cate-cholamine therapy >12 hours, and signs of organ malperfusion) between 9/2005and 10/2007 were analyzed and compared to NSTEMI patients without CS.Results: 1517 consecutive patients (NSTEMI: n=670, 44.2%) were included. 165patients (10.9%) developed a CS. Patients with NSTEMI had fewer CS thanpatients with STEMI (5.1% (n=34) vs. 15.5% (n=131)). Patients received cate-cholamines for 50.8 h (NSTEMI) and 51.5 h (STEMI). An intraaortic balloon pump(IABP) was implanted in 65.7% of NSTEMI and in 71.0% of STEMI patients.In comparison to NSTEMI patients without CS, CS patients had a more com-plex cardiovascular risk profile (hypertension 88.2% vs. 75.8% p=0.04; diabetes61.8% vs. 37.3% p=0,002; prior ACS: 35,3% vs. 23.9%, p=0.16; obesity 26.5%vs. 22.1%, p=0.31). There were no differences regarding gender or age. Never-theless, patients with NSTEMI and CS had significant higher ischemic parametersat admission than NSTEMI patients without CS. Further they had a significanly re-duced ejection fraction and there were also significant more cardiac arrests priorto hospital admission in patients with NSTEMI and CS.CS patients with NSTEMI had a lower in-hospital and 12-month mortality com-pared to CS patients with STEMI (in-hospital: 26.5% vs. 43.5%, p=0.05; 12-month: 48.1% vs. 59.1%, p=0.2). However, the 12-month mortality was almost4 times higher for NSTEMI patients with CS in comparison to NSTEMI patientswithout CS (in-hospital: 26.3% vs. 2.4%, p<0.001; 12-month: 48.1% vs. 11.4%,p<0.001). After hospital discharge NSTEMI and STEMI patients with CS had acomparable 12-month mortality (16% vs. 16.6%, NSTEMI vs. STEMI, p=n.s.),though mortality remained still higher than mortality for survivors without CS.Conclusion: In patients with NSTEMI, diabetes mellitus, arterial hypertensionand a reduced ejection fraction are predictors of an increased risk for the devel-opment of CS resulting in a reduced longterm survival.
P507 Mean platelet volume and prognosis in non STelevation acute coronary syndrome
V. Roldan1, A. Lopez Cuenca2, P. Perez-Berbel3, L. Mainar4,A. Tello-Montoliu3, E. Jover2, D. Hernandez-Romero2 , M. Valdes2,V. Vicente1, F. Marin2. 1Hospital Morales Meseguer, Murcia, Spain;
2Hospital Universitario Virgen de la Arrixaca, Murcia, Murcia, Spain; 3GeneralUniversity Hospital of Alicante, Alicante, Spain; 4Hospital General de Requena,Requena, Spain
Mean platelet volume (MPV) reflects platelet size and correlates with the func-tional status of platelets, thus large platelets are metabolically more active thansmall platelets and have greater pro-thrombotic potential. Previous evidence sug-gests that MPV may be a risk factor for recurrent myocardial infarction indepen-dent of established risk factors as hypertension, so it could be considered as anemerging risk marker for atherothrombosis. We hypothesized that patients withnon-ST elevation acute coronary syndromes (nSTEACS) could have large plate-les (elevated MPV) and this proposed biomarker may predict new adverse events.Methods: Patients with the diagnosis of nSTEACS were included from two ter-tiary hospitals. Current therapies following actual guidelines were followed in themanagement of these patients, and all medications were registered in data base.We included 379 consecutive patients with nSTEACS, aged 67±13 years old,64% males, and 87 healthy controls matched for age and sex. TIMI risk scorewas calculated at admittance in all these patients and haematological parame-ters, as well as troponin T (TnT), haemoglobin (Hb), creatinine, platelet count andMPV were collected. After discharge, a 6-month follow-up was performed usingtelephone contact or clinical interview. Cardiovascular adverse events (CAE) wasdefined as cardiovascular death, new ACS (with or without ST elevation), urgentcoronary revascularization, and acute heart failure.Results: 29% patients presented with downsloping ST and 40% with increasedlevels of TnT. TIMI risk score was 3.0±1.6. There was no difference in plateletcount (p=0.208) but patients showed larger platelets, MPV: 11.0 (10.3-11.8) vs9.2 (8.6-10.0) fl; p<0.001. We found statistical correlation with platelet count (r2:-0.24; p<0.001) and TIMI risk score (r2: 0.15, p=0.007). In Cox regression anal-ysis, MPV at admittance, as continuous variable, was a significant predictor ofCAE at univariate analysis, RR 1.26 CI95% (1.02-1.56), p=0.030, but adjustmentwith TIMI risk score, MPV lost its statistical significance.Conclusions: Patients presenting with nSTEACS showed large platelet as-sessed by MPV. Although MPV showed a significant influence in prognosis inthe univeriate analysis, it is lost after adjusting by an established risk score.
P508 Value of admission glucose and glycosylatedhemoglobin as predictors of adverse events in patientswith acute coronary syndrome without ST segmentelevation
M. Kmet1, A. Pernat2, I. Kranjec2, B. Rajer3. 1Novo mesto GeneralHospital, Novo mesto, Slovenia; 2University Medical Centre Ljubljana,
Department of Cardiology, Ljubljana, Slovenia; 3Faculty of Economics, Ljubljana,Slovenia
Background: Glucometabolic status is important predictor of prognosis in pa-tients with acute myocardial infarction. Both, admission glucose, and glycosylatedhaemoglobin A1c (HbA1c) were implicated as predictors of prognosis. However,data mostly obtained in mixed population, including patients with acute coronarysyndrome with and without ST elevation, showed conflicting results. We evaluatedprognostic role of admission glucose and HbA1c in patients with non ST elevationacute coronary syndrome (NSTEACS).Methods: A 106 patients with NSTEACS (55 with unstable angina and 51 withnon-ST elevation myocardial infarction) were included. The average age was 66.1years, 60% were male. HbA1c and blood glucose were measured at admission.The follow-up period lasted for a year. The main combined outcome variable in-cluded death from cardiovascular causes and rehospitalisation due to acute coro-nary sydrome or heart failure. Independent variables were HbA1c, age, sex, bodyweight, cholesterol level, admission glucose, diabetes mellitus, troponin T, arterialhypertension, congestive heart failure, treatment with ACE inhibitors or angioten-sin receptor blockers, Aspirin and smoking, respectively.Results: Combined endpoint occured in 43 (41%) patients during 12 monthfollow-up. Mean HbA1c value was significantly higher in the group of patientswho had complication (7.6±2,6 vs 5,8±1,2, p < 0.05). Logistic regression iden-tified HbA1c (OR 1,6) and male sex (OR 0,25) as independent predictors of ad-verse outcome, but not admission glucose (OR 1,16, p=0.2). This was confirmedby Kaplan Meier analysis which showed significant difference in event rates be-tween patients with HbA1c < 6.5 mmol/l, and > 8 mmol/l.Conclusion: Results from our study indicate that the admission level of HbA1c,but not admission glucose, is predictor of mortality and major adverse events inpatients with NSTEACS.
P509 Effect of data collection method on the hospitalincidence of acute coronary syndrome
A. Torabi, J.G.F. Cleland, H. Panahi, A.L. Clark, P. Atkin, J. Cook.Castle Hill Hospital, Hull, United Kingdom
Background: Acute coronary syndromes (ACS) are common but theirincidence and outcome depend greatly on how data are collected.Aims: To identify, using different survey methods, the incidence of ACS and my-ocardial infarction.Methods: The Hull and East Yorkshire Hospitals serve a population of approx-imately 560,000. Patients admitted with ACS to cardiology or general medicalwards during 2005 were identified prospectively by trained nurses (HIPP). Pa-tients with a death or discharge code of myocardial infarction were also identifiedby the hospital information department (HID) and from Myocardial Infarction Na-tional Audit Project (MINAP) records.Results: The prospective survey identified 1,731 admissions (1,439 patients) withACS during 2005, of which 764 (704 patients) had a myocardial infarction. Thehospital information department reported only 552 admissions (544 patients) withmyocardial infarction and only 206 admissions (203 patients) were reported toMINAP. Using all three data-bases, 934 admissions (873 patients) for myocardialinfarction were identified, for which TnT was >1ug/L in 443, 0.03 to 1.0 in 435,<0.03 in 19 and not recorded in 37. A further 823 patients had plasma troponinT >0.03ug/L but did not have ACS ascertained by any survey method. Of 873patients with myocardial infarction, 146 died during admission and 218 by oneyear.
MI patients identified by HIPP,MINAP,HID
Conclusion: MINAP and hospital statistics grossly underestimate hospital activ-ity. Data collection methods may have a large impact on the reported incidenceof ACS.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Risk protection in acute coronary syndromes 55
P510 The timing of coronary angiography in acute coronarysyndrome- what are the outcome differences beyondsix months?
A.S. Koh, J.K.B. Tan, K.W.Q. Guo, S. Chia, T.S.J. Chua, T.H. Koh,J.W.C. Tan. National Heart Centre, Singapore, Singapore
Background and Aim: Recent studies appear to suggest a correlation betweentiming to coronary angiography and clinical outcome among patients with acutecoronary syndrome (ACS). The efficacy of early invasive strategy over routine ordelayed timing to cardiac catheterization remains controversial. We aim to study6- and 12-month outcomes of ACS patients who are stratified according to early(≤24 hours), intermediate (>24 to <48 hours) and delayed (≥48 hours) coronaryangiography.Methods: This is a prospective observational study of patients with ACS definedas either unstable angina pectoris or non-ST elevation myocardial infarction (MI)admitted between October 2008 and July 2009. Baseline clinical characteristicsof age, gender, cardiovascular risk factors (diabetes mellitus, hypertension, dys-lipidemia) and TIMI score were analyzed and adjusted for outcomes. The primaryoutcome was combined major adverse cardiovascular events (MACE) of death ornon-fatal MI, as well as target vessel revascularization (TVR) up to 12 months.Results: This study consisted of 642 patients (75% males, mean age 60±13)with median follow-up of 7 months and median TIMI score of 4. Over half (50.2%)were categorized as high-risk (TIMI score ≥4). 281 patients (43.5%) had earlyangiography, 170 (26.5%) had angiography between >24 to <48 hours and 191(30%) patients had delayed angiography. Among the three groups, the delayedgroup had reduced overall event-free survival (p=0.001). Compared to the earlyand intermediate groups, patients in the delayed group had higher overall MACEat 6 months (7.7%, 5.9%, 15.7%; p<0.001) and 12 months (8.1%, 7.6%, 16.8%;p=0.001) that was largely related to a higher frequency of death and MI (6.4%,5.9%, 14.7%; p=0.001). In high-risk patients, the primary outcome occurred in10.9% of patients in the early group, as compared with 13.2% in intermediategroup and 23.9% in delayed group (p=0.015). However, in low-risk patients (TIMIscores <4), there was no significant difference between the groups (7.1% vs.3.4% vs. 5.9%, p=0.316). There were no differences in rates of TVR betweenthe groups by unadjusted (3.4%, 4.1%, 6.8%; p=0.098) or adjusted analyses(p=0.22).Conclusions: In this observational analysis, early and intermediate timing tocoronary angiography appear to be superior to the delayed strategy in reducingdeath and non-fatal MI in high-risk patients. Further studies are warranted to un-derstand and better define patient subgroups for which an early invasive strategymay be clinically efficacious.
P511 NT-pro brain natriuretic peptide is a useful diagnostictool in the emergency department for the screening ofpatients with chest pain
R. Della Bona1, L.M. Biasucci1, G. Biasillo1, G. Niccoli1, I. Dato1,M. Gustapane1, M. Leo1, N. Gentiloni Silveri1, M. Zaninotto2 ,
F. Crea1. 1Catholic University of the Sacred Heart, Rome, Italy; 2UniversityHospital of Padua, Department of Laboratory Medicine, Padua, Italy
Purpose: Management of chest pain patients (pts) in Emergency Department(ED) represents a challenging clinical problem. Troponins (I and T) are the refer-ence biomarker for diagnosis of Acute Coronary Syndrome (ACS), but still falsepositive and false negative results can be expected. Several biomarkers havebeen proposed for the management of pts with chest pain in ED, among theseNT-pro Brain Natriuretic Peptide (NT-proBNP) is a well tested biomarkers, withrobust analytical performance and sounding pathophysiological background forearly identification of ACS pts. We evaluated NT-proBNP for early diagnosis ofACS, in comparison with conventional Troponin T assay and EKG.Methods: Six hundred and ninety-six consecutive pts admitted to ED within 12hours from the onset of chest pain were enrolled. Serum levels of NT-proBNPand conventional Roche cTnT (cTnT) were measured from baseline samples.EKG and previous history of ACS were obtained in all pts. NT-proBNP was ana-lyzed as quartiles; diagnostic accuracy of biomarkers was evaluated by construct-ing Receiver-Operating Characteristic (ROC) curve and calculating Area UnderCurve (AUC).Results: Ninety-seven pts (14% of overall population) were discharged with adiagnosis of ACS according to current guidelines. NT-proBNP showed a diag-nostic accuracy similar to cTNT and EKG, being respectively: AUC=0,74 for NT-proBNP; AUC=0,70 for cTnT and AUC 0.71 for EKG. NT-proBNP serum levelsmeasurement improves the diagnostic performance of cTnT and EKG (AUC=0,83for EKG+cTnT; AUC=0,88 for EKG+cTnT+NT-proBNP). In pts with normal EKG atadmission, NT-proBNP showed an AUC=0,78, conversely in pts with EKG abnor-malities at admission NT-proBNP showed an AUC=0,57 (p=0,0007). In pts withnormal cTnT serum levels at admission, NT-proBNP showed an AUC=0,67, con-versely in pts with cTnT≥0,03 at admission NT-proBNP showed an AUC=0,56(p=0,004). Five hundred and ninety out of 696 pts were TnT and EKG negativeat admission, yet 26 of them had ACS. In these pts NT-proBNP remained highlypredictive of ACS with AUC= 0.73.Conclusions: In our population of chest pain pts in ED, NT-proBNP showed adiagnostic performance similar to cTnT and EKG; NT-proBNP serum levels mea-surement in addition to EKG and cTnT evaluation weakly improves the diagnostic
accuracy for ACS. Our data also show that in pts with chest pain and normal TnTand/or EKG, NT-proBNP may represent an excellent diagnostic tool.
P512 Analysis of prognosis according to the timing ofpercutaneous coronary intervention in acute non-STsegment elevation myocardial infarction: based on theKorean acute myocardial infarction registry
T.J. Hong, J.S. Park, H.C. Lee, M.S. Ahn, H.S. Yang, H.W. Lee,J.M. Hwang. Pusan National University Hospital, Pusan, Korea, Republic of
Background: Acute non-ST segment elevation myocardial infarction (NSTEMI)is usually managed according to an early invasive strategy for patients with highclinical risks. However, clinical trials on early intervention in Korea are evidentlylimited. Based on the data enrolled in the KAMIR, authors analyzed the prognosisaccording to the timing of PCI in patientswith acute NSTEMI in Korea.Methods: 2455 patients of high risk NSTEMI in KAMIR from Oct. 2005 and Feb.2008 were classified by the time interval from the onset of chest pain to the PCI(Group I < 24 hr, Group II 24-48 hr, GroupIII > 48hr). The clinical outcomes wereevaluated based on major adverse cardiac events (MACE) during the follow upperiod.Results: Of the 2455 patients enrolled, 329 patients experienced MACE; MI,rePCI, CABG, cardiac death and non-cardiac death. The incidence of MACEin the group I was 113 (15.1%), the group II 83 (14.4%) and the group III132(11.6%), accordingly. The group I showed higher incidence of MACE than thegroup III, with statistical significance (p=0.008, Multivariable adjusted hazard ratio0.551, [95%confidence interval, 0.351-0.865]). The group II had lower incidenceof MACE than the group I, but without statistic significance (p=0.18, Multivariableadjusted hazard ratio 0.74, [95%confidence interval, 0.436-1.256]).
Multivariate Hazard Ratio
Variables Hazard Ratio Confidence Interval
Age 1.011 0.99-1.03Time interval (hrs)
24-47.9 0.740 0.436-1.256≥48 0.551 0.351-0.865
PCI related Complications (+) 2.335 1.45-3.77Multi-vessel coronary arteries 2.157 1.36-3.43
Conclusion: In patients with NSTEMI, the incidence of MACE presented insignif-icant difference when PCI performed within 48 hours of symptom onset. Clinicaloutcome of PCI in patients with NSTEMI seems irrelevant to the timing of PCI,especially in groups undergone PCI within 48hrs.
P513 LDL-cholesterol paradox in patients admitted with anacute coronary syndrome
A.T. Timoteo, F. Ferreira, F. Miranda, J.A. Oliveira, M.L. Ferreira,R.C. Ferreira. Hospital Santa Marta, Lisbon, Portugal
Introduction: In the context of Acute Coronary Syndromes (ACS),there have been several paradoxical relationships with prognosis for known riskfactors for coronary artery disease such as smoking and obesity. Other risk fac-tors remain as important prognostic factors after ACS such as diabetes and hy-perglicemia on admission. As for lipid profile, few studies have addressed theirimpact.Objectives: Evaluate the influence of LDL-cholesterol in short- and medium-termprognosis after ACS.Methods: Between January 2005 and December 2008, we evaluated consec-utive patients admitted at our ICU and included in a single-centre registry. In allpatients, we collected demographic and anthropometric data, risk factors for coro-nary artery disease, clinical and laboratorial data on admission, including lipidprofile. Patients were divided in four quartiles according to LDL-cholesterol lev-els on admission: Q1 (≤96 mg/dl); Q2 (97 – 120 mg/dl); Q3 (121-145 mg/dl); Q4(≥146 mg/dl). We evaluated the occurrence of in-hospital, 30-day and one-yearmortality in the follow-up.Results: We included 1055 patients, with a mean age of 64±13 years, 68%males. In the quartiles progression, there is a reduction in age, previous historyof myocardial infarction, hypertension and diabetes, statins use before admissionand GRACE risk score (ANOVA, p<0.01 for all variables). On the other hand,there was an increase in admission blood pressure, all lipid variables, prevalenceof smoking, presentation as ST-segment elevation myocardial infarction and useof beta-blockers and coronary angioplasty after admission. There were no differ-ences in statins use after admission as well as for in-hospital (8.1%, 6.1%, 4.9%and 3.7%, respectively, p=0.17) or 30-day mortality (9.6%, 8.3%, 5.7% and 4.8%,p=0.115). One-year mortality was significantly higher in the group with lower LDL-cholesterol (11.9%, 9.1%, 8.7% and 4.8%, p=0.037). By multivariate logistic re-gression analysis, quartile 1 and 2 (the last one with a trend) are independentpredictors of mortality in the first year of follow-up in comparison with quartile4 (OR 2.65, 95% CI 1.35-5.19, p=0.004; OR 1.96, 95% CI 0.99-3.93, p=0.059,respectively).Conclusions: We found a paradoxical relationship between LDL-cholesterol lev-els on admission and one-year mortality in the follow-up after ACS.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

56 Risk protection in acute coronary syndromes
P514 Relation between red blood cell distribution width andbleeding risk in patients with non-ST elevation acutecoronary syndromes
S. Goncalves, J. Ferreira Santos, P. Amador, L. Neves Soares. Serviçode Cardiologia, Setubal, Portugal
Introduction: Increased red blood cell distribution width (RDW) has been identi-fied as a risk marker in patients (pts) with heart failure, stable coronary diseaseand acute coronary syndromes. Nevertheless, the relation between RDW andbleeding events in patients with non-ST-segment elevation acute coronary syn-dromes (NSTE-ACS) is not clarified.Aim: Evaluate the relation between RDW and the risk of adverse events, includingmajor bleeding, in pts with NSTE-ACS.Methods: We studied 513 consecutive pts (aged 68±12 years, 68% male sex)admitted to a coronary care unit with NSTE-ACS. Pts were divided into threegroups, according to tertiles of baseline RDW. Clinical and laboratorial charac-teristics were determined and compared between groups. Occurrence of majorbleeding (Crusade definition), in-hospital death and the combined endpoint ofmajor bleeding or in-hospital death were evaluated. The relation between RDWand adverse events was determined.Results: The mean RDW value was 15.1±1.6%. Pts with higher RDW levelswere older, had more frequently a past history of coronary disease (myocardialinfarction or coronary revascularization), a higher heart rate at admission andlower hemoglobin levels. Higher baseline RDW values were related to an increasein risk of major bleeding, in-hospital death and its combination (table). RDW >
15.7% was an independent predictor of hemorrhagic events (OR 3.1 CI 95% 1.4-6.9).
% of Events according to RWD tertiles
Events Tertile 1 Tertile 2 Tertile 3 p(RDW<14.4%) (14.4≤RDW<15.4%) (RDW ≥15.4%)
Major Bleeding (%) 4.3 5.0 11.5 0.017In-hospital death (%) 0.0 1.7 4.0 0.028Major Bleeding or
in-hospital death (%) 4.3 6.7 15.5 0.001
Conclusions: In pts with NSTE- ACS, RDW, an easily assessed laboratorial pa-rameter, was a strong and independent predictor of adverse clinical events, in-cluding in-hospital death and/or major bleeding.
P515 Impact of renal failure on the bleeding risk of patientswith non-ST acute coronary syndromes submitted topercutaneous coronary intervention
S. Goncalves, J. Ferreira Santos, P. Amador, L. Neves Soares. Serviçode Cardiologia, Setubal, Portugal
Background: Renal failure is associated with a worse prognosis in patients (pts)with non-ST-segment elevation acute coronary syndromes (NSTE-ACS). In thispopulation, pursue of a systematic invasive strategy has been questioned due tothe risk of adverse events.Aim: To evaluate the impact of renal dysfunction on the bleeding risk of pts withNSTE-ACS, submitted to percutaneous coronary intervention (PCI).Methods: We studied 514 consecutive pts (aged 68±12 years, 68% male sex)admitted to a coronary unit with NSTE-ACS. Pts were stratified according to crea-tinine clearance (estimated with the Cockroft-Gault formula) and renal dysfunctionwas defined as a creatinine clearance<60ml/min. Occurrence of major bleeding(using Crusade definition) was assessed. The relation between renal dysfunctionand hemorrhagic events in pts submitted to PCI was determined.Results: Renal dysfuncion was present in 264 pts (51.4%) and 36 bleedingevents were recorded. Pts with renal dysfunction had a higher risk profile. Nev-ertheless, they were less frequently submitted to coronariography or PCI. Thepresence of renal clearance < 60ml/min was an independent predictor of bled-ding events. Use of PCI was associated with a higher number of hemorrhagicevents, only in pts with renal dysfunction (see figure).
% Bleeding Events according to CrCl
Conclusions: Renal dysfunction is frequent in pts with NSTE-ACS and is asso-ciated with an increase risk of bleeding events, especially in pts undergoing PCI.
P516 Prognostic value of corrected QT-interval prolongationin hypertensive patients with non-ST-segmentelevation acute coronary syndrome
A. Stachurska, E. Marcos Blanco, R. Bascompte Claret, I. LacambraBlasco, A. Del Rio Ligorit. Hospital Clinico Universitario "Lozano
Blesa", Zaragoza, Spain
Background: The QT-interval on the surface electrocardiogram (ECG) predictscardiovascular complications in acute myocardial infarction (AMI) and in high-risksubjects such as hypertensive or diabetic patients. However its prognostic rolein hypertensive patients who develop non-ST-segment elevation acute coronarysyndrome (NSTEACS) has been understudied. Hypertension is one of the leadingrisk factors for myocardial infarction and cardiovascular death world-wide, andthe analysis of QT interval duration in NSTEACS might contribute to improvecardiovascular risk stratification in the individual hypertensive patients. The aimof this study was to determine the prognostic value of QT interval in hypertensivepatients with NSTEACS.Methods: We studies retrospectively 65 hypertensive subjects from a larger co-hort of patients (n=102) with NSTEACS diagnosed on the basis of preestablishedcriteria (ischemic changes in ECG y/or elevation of troponin y/or creatine kinaseMB isoenzyme levels). Patients with at least one of the following were not in-cluded: angina pectoris not in Braunwald class II or III B (post-AMI angina, severevalvular disease, severe cardiomyopathy, serum potassium levels<3,5 mmol/ml,use of antiarrhytmic drugs, QRS≥120 ms (pacemaker, bandle branch block),Wolff-Parkinson-White syndrome or atrial fibrillation. Standard 12-lead ECG wasrecorded for every patient at admission and two more in the first 24 hours of hos-pitalization. The QT interval was measured manually and corrected using Bazett’sformula (cQT). The ECG with the longest cQT interval was taken for analysis ineach patient. We considered cQT prolongation from ≥0,45 ms for men and from≥0,47 ms for women. The primary end point was the combination of AMI, emer-gency revascularization, death, fatal arrhythmia and implantable cardioverter de-fibrillator implantation up to 6 months after discharge.Results: Of the 34 patients (52,3%) who reached the primary end point, 15(44,1%) had cQT prolongation (p=0,033). Binary logistic regression analysisshowed that cQT prolongation was an independent predictor of the combinedendpoint (OR 3,3; IC (95%) 1,1-10,1; p=0,037). Likewise there were 3 patients(4,6%) who suffered from AMI during the follow up and all of them had cQTprolongation (p=0,01). We found the best cut-off point for AMI complication ina cQT≥0,457 with 67% of sensitivity and 79% of specificity (ROC area 0,85;p=0,042).Conclusion: The study shows that cQT prolongation is an independent predic-tor of cardiovascular risk in hypertensive patients with non-ST-segment elevationacute coronary syndrome.
P517 Clinical Outcomes of Totally Occluded Infarct RelatedArtery in Acute ST segment Elevation MyocardialInfarction are Different from Acute Non-ST segmentElevation Myocardial Infarction in DES era
S. Ramasamy1, S.W. Rha1, K.L. Poddar1 , J.Y. Park1, C.U. Choi1,K.Y. Chen2, C.G. Park1, H.S. Seo1, D.J. Oh1, M.H. Jeong3. 1Korea UniversityGuro Hospital, Seoul, Korea, Republic of; 2Cardiology Department, the SecondHospital of Tianjin Medical University, Tianjin, China, People’s Republic of;3Chonnam National University Hospital, Gwangju, Korea, Republic of
Objectives: Totally occluded infarct related artery (IRA) in acute ST-segment el-evation myocardial Infarction (STEMI) patients (pts) have worse prognosis com-pared with non total occlusion of IRA pts in high risk subsets in the bare metalstent era. However, there are limited data regarding the prognosis of STEMI ptscompared with NSTEMI pts with total occlusion in IRA in the drug-eluting stent(DES) era.Methods: Study population consisted of 3839 consecutive STEMI and NSTEMIpts enrolled in the Korea Acute Myocardial Infarction Registry (KAMIR). We com-pared the clinical outcomes of STEMI pts with total occlusion in IRA (TIMI 0.1,n=2825, 73.58%) to those of pts with NSTEMI with total occlusion in IRA (TIMI0,1, n=1014) who underwent percutaneous coronary intervention (PCI) with DES.Results: Baseline clinical and procedural characteristics were similar betweenthe two groups except NSTEMI pts had more females, dyslipidemia, diabetes,hypertension. Pts with STEMI group were more likely to develop cardiogenicshock and in hospital mortality, recurrent Q-MI and higher cumulative mortalityat 8 months (p=0.004, Odds Ratio, 1.81, 95% CI, 1.21-2.70) but showed similar
Table 1. Eight-Month Clinical outcomes (on Multivariate analysis)
Variables, N (%) STEMI Group (n=2825 pts) NSTEMI Group (n=1159 pts) P value
Cardiogenic Shock 119 (4.2) 20 (2.0) 0.014*Total deaths 170 (6.0) 35 (3.5) 0.004*Cardiac Deaths 98 (3.5) 23 (2.3) 0.081Any Re MI 59 (2.1) 13 (1.3) 0.717Q-MI 51 (1.8) 5 (0.5) 0.001*Non Q-MI 8 (0.3) 8 (0.8) 0.012*Repeat Revascularization 135 (4.8) 59 (5.8) 0.122TLR-PCI 35 (1.2) 17 (1.7) 0.207TVR-PCI 65 (2.3) 25 (2.5) 0.238Total MACE 341 (12.1) 111 (10.9) 0.401
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Risk protection in acute coronary syndromes / Coronary Artery Bypass Surgery 57
midterm repeat revascularization and total major adverse cardiac events (MACE)after the multivariate analysis (Table).Conclusion: The incidence of total occlusion of IRA was higher in STEMI pts(73.58%) at the AMI setting. STEMI group were more likely to have a worse base-line characteristics, short term as well as midterm clinical events as comparedwith those of NSTMI pts with total occlusion group.
P518 Low-dose sodium nitrite provides targetted relief ofmyocardial ischaemia in patients with coronary arterydisease
T.E. Ingram1, R.A. Bleasdale2 , C. Templeton2, C. Williams2,A.G. Fraser1 , P.E. James1. 1Cardiff University, Cardiff, United
Kingdom; 2Royal Glamorgan Hospital, Llantrisant, United Kingdom
Purpose: Inorganic nitrite (NO2-) has traditionally been considered to be a rela-tively inert metabolite of nitric oxide. Recent evidence suggests that its effects areenhanced in hypoxia or ischaemia.Method: A double-blind, placebo-controlled, cross-over study was performed inten subjects with proven myocardial ischaemia documented by exercise toler-ance testing and coronary angiography. Two dobutamine stress echocardiogra-phy (DSE) studies were performed on each subject: with either 0.9% saline orsodium nitrite (NaNO2) 1.5μmol/min for 20 min; a dose previously shown to beinert in normoxia but to vasodilate in hypoxia. Myocardial ischaemia was identifiedby peak systolic velocity (PSV) response during DSE in a six basal-wall segmentmodel of the left ventricle. Using the placebo study results, walls were classifiedinto tertiles: the lower tertile of responders of PSV to heart rate (HR) labelled is-chaemia (n=18) and the upper tertile control (n=18); thus creating four groups:saline/ischaemia (S/I), NO2-/ischaemia (N/I), saline/control (S/C), NO2-/control(N/C).Result: Data from each stage of each DSE was corrected for baseline values andplaced on a scatter plot graph. The linear regression gradient of the S/I group was40% lower than the N/I group; with no overlap in 95% confidence intervals, see fig-ure. The peak-dose dobutamine values of �PSV/�HR (cm/s/s) were different inthe S/I group compared to the three other groups (i.e. mean±SEM: S/I=3.7±0.6,N/I=8.2±1.0, S/C=10.5±1.1, N/C=8.4±0.7; P<0.01, repeated measures ANOVAwith Bonferroni post-test). No difference was present between the three othergroups.
Response of PSV to HR in ischaemic walls
Conclusion: Low-dose NaNO2 provides a therapeutic effect to ischaemic my-ocardium. This is the first study in patients to demonstrate a targeted vasodilatoreffect of NO2- to tissues in need only.
P519 A high carbohydrate meal yields a lower ischemicthreshold than a high fat meal in patients with stablecoronary disease
R. Spoladore, G. Fragasso, C. Montano, F. Arioli, G. Lattuada,A. Salerno, L. Luzi, G. Perseghin, R. D’amato, A. Margonato. San
Raffaele Hospital, IRCCS, Milan, Italy
Background: Previous studies have evidenced a significant reduction of coro-nary flow reserve after ingestion of meals of different composition. A possiblerole of hyper-insulinemia and increased free-fatty acids levels, which are delete-rious during acute myocardial ischemia and reperfusion, has been hypothesized.To our knowledge, no study has assessed the effect of meal composition in thepost-absorptive state in patients with coronary artery disease. Aim of the study isto assess the ischemic threshold and stress-induced left ventricular dysfunctionafter high fat (HFM) and high carbohydrate (HCM) meals in patients with stablecoronary disease, in the post-absorptive state.Methods and Results: Twelve pts (9 males, age 68±7 yrs) underwent stress(treadmill exercise testing-Bruce protocol) echocardiography after fasting (8hrs),after a HFM and HCM (2 hrs). Time to 1mm ST segment depression (time to1mm) and stress wall motion score index (WMSI) were evaluated. Before eatingand just before exercise testing glucose, insulin, triglycerides, total cholesteroland FFA levels were assayed.Results are expressed as medians (Q1-Q3). HFM did not affect exercise variablescompared to fasting, whereas HCM resulted in a reduction of the ischemic thresh-old [time to 1 mm ST-segment depression from 376 (343-493) to 297 (180-420)sec, p=0.003]. Compared to fasting [1.31 (1,14-1.50)], stress WMSI was higher
after both HCM [1.56 (1.44-1.69)] and after HFM [1.56 (1.29-1.63)] (p=0.04 forboth). Blood glucose and insulin levels were significantly higher after HCM, com-pared to fasting and HFM.Conclusions: In pts with coronary disease, exercise testing after a high carbo-hydrate meal results in a lower ischemic threshold compared to high fat meal.However, the magnitude of ischemia appears similar. Hyperglycemia and hyper-insulinemia were the only metabolic determinants that were identified as potentialmetabolic mechanisms of this phenomenon.
P520 Assessing clinical outcomes in percutaneous coronaryintervention: the role of risk adjustment
P. Sousa1, A.S. Uva1, A. Belo2, F.J. Pinto3. 1National School of PublicHealth of the New University of Lisbon, Lisbon, Portugal; 2NationalCenter for Data Collection on Cardiology, Coimbra, Portugal; 3Hospital
Lisbon North, Hospital Santa Maria, Lisbon, Portugal
Purpose: Variation in patient’s baseline clinical risks precludes the direct com-parison of outcomes across operators, hospitals and health care plans. The aimof this study was to develop and test a risk adjustment model for major adversecardiac and cerebrovascular events (MACCE), following PCI procedures, usingrecent data from a national multi-centre registry and, to highlight the use of therisk adjustment methodology when assessing clinical outcomes in PCI.Methods: A multivariate logistic regression model was build in order to identifyindependent risk factors for MACCE. After that the model was tested in the pop-ulation who underwent PCI between January 2008 and January 2010, a total of8129 procedures. The ROC curve and the Hosmer-Lemeshow test were calcu-lated.Results: Factors associated with MACCE, only the ones with statistical signif-icance, are presented in table 1, The ROC curve and the Hosmer-Lemeshowgoodness of fit statistic, for the tested group were 0.78 and 0.21 respectively.
Table 1. Independent risk factors for major adverse cardiac and cerebrovascular events (only theones with statistical significance)
Variable Coefficient Adjusted OR (CI 95%) P value
Age 70 years to 79 years 1.26 2.53 (1.74; 8.77) 0. 001Age > 80 years 1.33 3,91 (1.61; 8.86) 0.002Gender Female 0.54 1.72 (1.13; 2.61) 0.01Acute Myocardial Infarction 0.99 2.68 (1.46; 4.93) 0.001Cardiogenic Shock 1.80 6.05 (2.44; 15.01) <0.001Renal failure 1.09 2.98 (1.28; 6.97) 0.01Ejection fraction severely impaired 1.37 3.94 (2.22; 7.01) <0.001Three or more vessels diseases 0.78 2.18 (1.35; 3.51) 0.001Intra Aortic Balloon Pump 1.44 4.21 (1.53; 11.56) 0.005Non-Stenting 1.07 2.92 (1.72; 4.96) <0.001Priority of procedure (urgent/emergent) 0.74 2.11 (1.13; 3.91) 0.02Constant -6.63 – –
Conclusions: A risk adjustment model for in-hospital MACCE after PCI, was suc-cessfully developed. The model was tested in a "real world" population, showingthat it has discriminative power adequate for genuine clinical utility. This repre-sents a substantial step forward on credible and reliable comparison of clinicalresults among providers (centres/hospitals).
CORONARY ARTERY BYPASS SURGERY
P522 Myocardial NADPH-oxidase and uncoupled NOS aspredictors of post-operative atrial fibrillation inpatients undergoing cardiac surgery
M. Demosthenous1 , C. Antoniades1, M. Margaritis1,A.S. Antonopoulos1, D. Tousoulis1 , C. Bakogiannis1 , C. Triantafyllou1,
S. Reilly2, B. Cassadei2 , C. Stefanadis1. 1Hippokration Hospital, University ofAthens, Athens, Greece; 2University of Oxford, Oxford, United Kingdom
Purpose: Paroxysmal atrial fibrillation (PAF) is a common complication post car-diac surgery. Myocardial redox state is a key feature in the pathogenesis of post-operative PAF. However, the exact mechanisms linking myocardial redox stateand post-operative PAF are still unclear. We examined the impact of myocardialsuperoxide (O2-) and peroxynitrite (ONOO-) on the development of PAF post car-diac surgery, and the mechanisms regulating their generation.Methods: The study population consisted of 98 patients with sinus rhythm (SR)undergoing elective coronary bypass operation. Sixty-nine patients remained inSR and 24 developed PAF post-operatively. Samples of right atrium appendageswere obtained during operation. Myocardial O2- generation was determined bylucigenin-enhanced chemiluminescence while urate-inhibitable luminol chemilu-minescence was used to estimate ONOO- generation. NADPH oxidase activitywas estimated by defining NADPH-stimulated O2- and its apocynin-inhibitablefraction, uncoupled nitric oxide synthase (NOS) contribution by using LNAME andmitochondrial oxidases by using rotenone.Results: Patients who developed PAF had not significantly higher resting O2-(A). However, NADPH-stimulated (B) and apocynin-inhibitable (C) O2- were sig-nificantly greater in PAF compared to SR patients. There was no significant differ-ence in rotenone-inhibitable O2- (D) between the two groups. However, LNAME-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
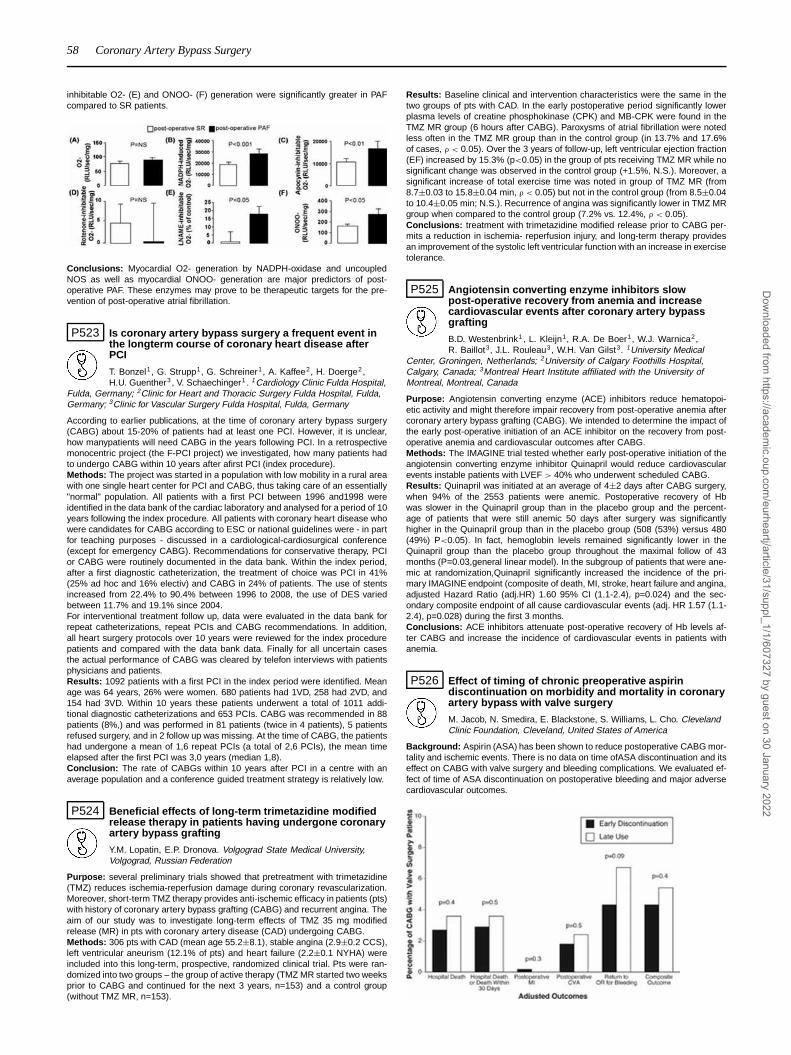
58 Coronary Artery Bypass Surgery
inhibitable O2- (E) and ONOO- (F) generation were significantly greater in PAFcompared to SR patients.
Conclusions: Myocardial O2- generation by NADPH-oxidase and uncoupledNOS as well as myocardial ONOO- generation are major predictors of post-operative PAF. These enzymes may prove to be therapeutic targets for the pre-vention of post-operative atrial fibrillation.
P523 Is coronary artery bypass surgery a frequent event inthe longterm course of coronary heart disease afterPCI
T. Bonzel1, G. Strupp1, G. Schreiner1, A. Kaffee2, H. Doerge2,H.U. Guenther3 , V. Schaechinger1 . 1Cardiology Clinic Fulda Hospital,
Fulda, Germany; 2Clinic for Heart and Thoracic Surgery Fulda Hospital, Fulda,Germany; 3Clinic for Vascular Surgery Fulda Hospital, Fulda, Germany
According to earlier publications, at the time of coronary artery bypass surgery(CABG) about 15-20% of patients had at least one PCI. However, it is unclear,how manypatients will need CABG in the years following PCI. In a retrospectivemonocentric project (the F-PCI project) we investigated, how many patients hadto undergo CABG within 10 years after afirst PCI (index procedure).Methods: The project was started in a population with low mobility in a rural areawith one single heart center for PCI and CABG, thus taking care of an essentially"normal" population. All patients with a first PCI between 1996 and1998 wereidentified in the data bank of the cardiac laboratory and analysed for a period of 10years following the index procedure. All patients with coronary heart disease whowere candidates for CABG according to ESC or national guidelines were - in partfor teaching purposes - discussed in a cardiological-cardiosurgical conference(except for emergency CABG). Recommendations for conservative therapy, PCIor CABG were routinely documented in the data bank. Within the index period,after a first diagnostic catheterization, the treatment of choice was PCI in 41%(25% ad hoc and 16% electiv) and CABG in 24% of patients. The use of stentsincreased from 22.4% to 90.4% between 1996 to 2008, the use of DES variedbetween 11.7% and 19.1% since 2004.For interventional treatment follow up, data were evaluated in the data bank forrepeat catheterizations, repeat PCIs and CABG recommendations. In addition,all heart surgery protocols over 10 years were reviewed for the index procedurepatients and compared with the data bank data. Finally for all uncertain casesthe actual performance of CABG was cleared by telefon interviews with patientsphysicians and patients.Results: 1092 patients with a first PCI in the index period were identified. Meanage was 64 years, 26% were women. 680 patients had 1VD, 258 had 2VD, and154 had 3VD. Within 10 years these patients underwent a total of 1011 addi-tional diagnostic catheterizations and 653 PCIs. CABG was recommended in 88patients (8%,) and was performed in 81 patients (twice in 4 patients), 5 patientsrefused surgery, and in 2 follow up was missing. At the time of CABG, the patientshad undergone a mean of 1,6 repeat PCIs (a total of 2,6 PCIs), the mean timeelapsed after the first PCI was 3,0 years (median 1,8).Conclusion: The rate of CABGs within 10 years after PCI in a centre with anaverage population and a conference guided treatment strategy is relatively low.
P524 Beneficial effects of long-term trimetazidine modifiedrelease therapy in patients having undergone coronaryartery bypass grafting
Y.M. Lopatin, E.P. Dronova. Volgograd State Medical University,Volgograd, Russian Federation
Purpose: several preliminary trials showed that pretreatment with trimetazidine(TMZ) reduces ischemia-reperfusion damage during coronary revascularization.Moreover, short-term TMZ therapy provides anti-ischemic efficacy in patients (pts)with history of coronary artery bypass grafting (CABG) and recurrent angina. Theaim of our study was to investigate long-term effects of TMZ 35 mg modifiedrelease (MR) in pts with coronary artery disease (CAD) undergoing CABG.Methods: 306 pts with CAD (mean age 55.2±8.1), stable angina (2.9±0.2 CCS),left ventricular aneurism (12.1% of pts) and heart failure (2.2±0.1 NYHA) wereincluded into this long-term, prospective, randomized clinical trial. Pts were ran-domized into two groups – the group of active therapy (TMZ MR started two weeksprior to CABG and continued for the next 3 years, n=153) and a control group(without TMZ MR, n=153).
Results: Baseline clinical and intervention characteristics were the same in thetwo groups of pts with CAD. In the early postoperative period significantly lowerplasma levels of creatine phosphokinase (CPK) and MB-CPK were found in theTMZ MR group (6 hours after CABG). Paroxysms of atrial fibrillation were notedless often in the TMZ MR group than in the control group (in 13.7% and 17.6%of cases, ρ < 0.05). Over the 3 years of follow-up, left ventricular ejection fraction(EF) increased by 15.3% (p<0.05) in the group of pts receiving TMZ MR while nosignificant change was observed in the control group (+1.5%, N.S.). Moreover, asignificant increase of total exercise time was noted in group of TMZ MR (from8.7±0.03 to 15.8±0.04 min, ρ < 0.05) but not in the control group (from 8.5±0.04to 10.4±0.05 min; N.S.). Recurrence of angina was significantly lower in TMZ MRgroup when compared to the control group (7.2% vs. 12.4%, ρ < 0.05).Conclusions: treatment with trimetazidine modified release prior to CABG per-mits a reduction in ischemia- reperfusion injury, and long-term therapy providesan improvement of the systolic left ventricular function with an increase in exercisetolerance.
P525 Angiotensin converting enzyme inhibitors slowpost-operative recovery from anemia and increasecardiovascular events after coronary artery bypassgrafting
B.D. Westenbrink1 , L. Kleijn1, R.A. De Boer1, W.J. Warnica2,R. Baillot3, J.L. Rouleau3, W.H. Van Gilst3. 1University Medical
Center, Groningen, Netherlands; 2University of Calgary Foothills Hospital,Calgary, Canada; 3Montreal Heart Institute affiliated with the University ofMontreal, Montreal, Canada
Purpose: Angiotensin converting enzyme (ACE) inhibitors reduce hematopoi-etic activity and might therefore impair recovery from post-operative anemia aftercoronary artery bypass grafting (CABG). We intended to determine the impact ofthe early post-operative initiation of an ACE inhibitor on the recovery from post-operative anemia and cardiovascular outcomes after CABG.Methods: The IMAGINE trial tested whether early post-operative initiation of theangiotensin converting enzyme inhibitor Quinapril would reduce cardiovascularevents instable patients with LVEF > 40% who underwent scheduled CABG.Results: Quinapril was initiated at an average of 4±2 days after CABG surgery,when 94% of the 2553 patients were anemic. Postoperative recovery of Hbwas slower in the Quinapril group than in the placebo group and the percent-age of patients that were still anemic 50 days after surgery was significantlyhigher in the Quinapril group than in the placebo group (508 (53%) versus 480(49%) P<0.05). In fact, hemoglobin levels remained significantly lower in theQuinapril group than the placebo group throughout the maximal follow of 43months (P=0.03,general linear model). In the subgroup of patients that were ane-mic at randomization,Quinapril significantly increased the incidence of the pri-mary IMAGINE endpoint (composite of death, MI, stroke, heart failure and angina,adjusted Hazard Ratio (adj.HR) 1.60 95% CI (1.1-2.4), p=0.024) and the sec-ondary composite endpoint of all cause cardiovascular events (adj. HR 1.57 (1.1-2.4), p=0.028) during the first 3 months.Conclusions: ACE inhibitors attenuate post-operative recovery of Hb levels af-ter CABG and increase the incidence of cardiovascular events in patients withanemia.
P526 Effect of timing of chronic preoperative aspirindiscontinuation on morbidity and mortality in coronaryartery bypass with valve surgery
M. Jacob, N. Smedira, E. Blackstone, S. Williams, L. Cho. ClevelandClinic Foundation, Cleveland, United States of America
Background: Aspirin (ASA) has been shown to reduce postoperative CABG mor-tality and ischemic events. There is no data on time ofASA discontinuation and itseffect on CABG with valve surgery and bleeding complications. We evaluated ef-fect of time of ASA discontinuation on postoperative bleeding and major adversecardiovascular outcomes.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Coronary Artery Bypass Surgery 59
Methods: From January 1, 2002 - January 31, 2008, 1963 patients were on pre-operative ASA and underwent CABG with valve surgery at Cleveland Clinic. Us-ing propensity analysis, outcomes of matched groups were compared. Of those,1404 (72%) discontinued ASA greater than 5 days from the day of surgery (earlydiscontinuation) and 559 (28%) continued ASA use within 5 days of surgery (lateuse).Results: Overall, the two groups were well matched for baseline characteristicsas well as valve surgery. Late ASA use was associated with a trend toward in-creased reoperation for bleeding 37 (6.7%) vs. 24 (4.3%) (p = 0.09). There wasnosignificant difference between the groups with regards to the composite out-come of 30-day mortality, nonfatal MI, and nonfatal stroke or the secondary out-comes as seen in figure 1.Conclusions: Among patients undergoing CABG with valve surgery there wasno difference in outcomes with regards to timing of ASA discontinuation exceptfor a trend toward increased reoperation for bleeding in the late ASA group. Lateuse of ASA in CABG with valve surgery must be weighed against increased riskof bleeding.
P527 Prophylactic magnesium does not prevent atrialfibrillation after cardiac surgery: a meta-analysis andcomprehensive review of randomized trials
M. Yamashita, R. Cook, M. Kearns, K. Ramanathan, K. Gin,K. Humphries. University of British Columbia, Vancouver, Canada
Background: Atrial fibrillation (AF) after cardiac surgery is a common compli-cation that is associated with an increased risk of death and stroke and longerlengths of stay in hospital. Previous trials have shown widely divergent results,while meta-analyses have concluded that magnesium prevents postoperative AF,although with a significant degree of heterogeneity. Recently, the largest random-ized controlled trial (RCT) published to date concluded that magnesium sulphateis not protective against AF following cardiac surgery. The objective of this studywas to conduct a new meta-analysis to include the results of this large RCT, aswell as other trials not previously included, and to investigate the previously doc-umented heterogeneity in the meta-analyses.Methods: The MEDLINE, EMBASE and CENTRAL databases were searched toretrieve relevant studies published up until December 2009. Only RCTs in adultswhich compared magnesium to placebo for the prophylaxis of AF after cardiacsurgery were included. Pooled effect estimates for the odds ratio of incidence ofAF, incidence of stroke and 30 day all-cause mortality were calculated using therandom and fixed effects models. A pooled effect estimate for the weighted meandifference (WMD) of length of hospital stay was also calculated. Heterogeneitywas assessed using the I2 statistic and publication bias was evaluated. Severalsensitivity analyses were performed to examine the effects of study design pa-rameters on outcomes.Results: Nineteen studies were initially included in this analysis. Overall, therewas 43% risk reduction in incidence of AF associated with magnesium (OR=0.57,p=0.001). However, there was a significant amount of heterogeneity (I2=66.6%,p<0.001) and evidence of publication bias. A second analysis of the five double-blind, intention to treat studies, where AF was the primary outcome, revealedmagnesium does not protect against postoperative AF (OR=0.94, p=0.77), with areduced amount of heterogeneity (I2=40.4%, p=0.15). The incidence of postop-erative stroke (OR=0.72, p=0.64), early death (OR=1.07, p=0.86) and length ofhospital stay (WMD=-0.20 days, p=0.14) were not different between the magne-sium and placebo control groups.Conclusions: When the evidence is restricted to high quality RCTs, prophylacticintravenous magnesium is not effective in preventing AF following cardiac surgery.
P528 All-arterial revascularization as a protection factor forin-hospital mortality compared to conventionalcoronary artery bypass surgery
P. Farsky, P.V. Viana, V.L. Amato, J.A. Farran, F. Rinaldi, P. Chaccur,C. Abdulmassih. Institute Dante Pazzanese of Cardiology, Sao Paulo,
Brazil
Background: Arterial grafts have superior long term patency compared to saphe-nous vein graft in coronary artery bypass surgery (CABG). All arterial revascular-ization (AA) is technically more complicated, more demanding, and the use ofbilateral thoracic artery may lead to increase morbidity and radial artery is proneto vasospasm.Objective: The aim of this study is to compare in-hospital results of AA comparedto conventional CABG in a single cardiology teaching hospital.Material and methods: This is a retrospective analysis of a prospective databank of all isolated CABG performed in a single institution 1999 to 2007.Data analysis: For categorical variables the χ2 was used for comparisons, andStudent t test for continuous. We utilized the logistic regression considering mor-tality as the dependent variable.Results: The overall study population consisted in 4388 patients, with 464 AAand 3924 conventional CABG. In the baseline characteristics the AA group wasyounger, had less hypertension, stroke, chronic kidney disease, peripheral arterialdisease, left main disease, three vessel disease and dysfunctional left ventricularcompared to conventional CABG group.Comparing the in-hospital outcomes, the AA group had less atrial fibrillation (8,6%
vs 12.8%; p=0,01), stroke (1,9% vs 2,7%; p=0,003), low cardiac output (6,7% vs14.1%; p<0,001), shorter length of ICU (55.9hs vs 74.3 hs, p<0,001) and lowerincidence of death (1.5% vs 5.0%; p<0,001).In logistic regression analysis, the following characteristics were associated withhigher in hospital mortality: female gender, older age, lower weight, chronic kidneydisease, left ventricular dysfunction, peripheral arterial disease and number ofdisease arteries. The AA group had a protective effect in mortality, as shown inthis analysis.Conclusions: The patients for all-arterial CABG are still highly selected in respectof comorbidies, and have a lower rate of in-hospital morbidity and mortality incomparison to conventional CABG. The all arterial procedure appears to be aprotection factor in this cohort. This procedure should be extended to a broadrange of patients, offering the best in-hospital and long term results.
P529 Perioperative risk factors for serious gastrointestinalcomplications treated by laparotomy aftercardiopulmonary bypass operations
P. Soos1, B. Schmack2, M. Karck2, G. Szabo2. 1SemmelweisUniversity Heart Center, Budapest, Hungary; 2University Hospital of
Heidelberg, Department of Cardiac Surgery, Heidelberg, Germany
Purpose: gastrointestinal (GI) complications are rare but often fatal conse-quences of cardiac surgery, especially after cardiopulmonary bypass (CPB) oper-ations. The therapy can be conservative or - in critical cases - surgical, however anearly and safe diagnosis may prevent the development of life threatening GI com-plications. The aim of our study was to characterize the risk factors and perioper-ative predictors for GI complications treated by laparotomy after CPB operations.Methods: in a retrospective analysis of 12 years CPB operations 13552 patientswere involved in the study. Laparotomy was performed after CPB in 277 (2.0%)cases; heart valve disease 57 (20.6%), coronary bypass 125 (45.1%), bypassand valve 48 (17.3%), aortic aneurism 23 (8.3%), heart transplant 20 (7.2%) andother 4 (1.4%).Results: after logistic regression 6 of 13 risk factors were found to be in-dependent preoperative predictors of laparotomy; age (OR:1.031 (CI:1.019-1.043), p<0.001), NYHA status III-IV, history of myocardial infarct (1.343 (1.054-1.710), p<0.05), history of arterial (1.452 (1.131-1.866), p<0.05) and renaldisease (2.181 (1.686-2.821), p<0.001), history of cardiac reoperation (2.690(1.750-4.134), p<0.001). Lengths of operation- (1.006 (1.005-1.007), p<0.001),bypass- (1.007 (1.006-1.009), p<0.001), aortic cross-clamp- (1.005 (1.002-1.008), p<0.05) and cardiac arrest (1.015 (1.006-1.024), p<0.05) time were pos-itive intraoperative predictors for serious GI events. Postoperative risk factorswere: low output syndrome (13.455 (10.516-17.215), p<0.001), IABP implanta-tion (12.257 (9.604-15.643), p<0.001), CPR (9.595 (7.036-13.085), p<0.001),renal (29.145 (21.322-39.839), p<0.001) and pulmonary complications (18.193(14.171-23.358), p<0.001), arrhythmias (9.387 (6.451-13.660), p<0.001) andinfections (29.659 (22.877-38.452), p<0.001). Mortality after three years washigher (p<0.001) in the laparotomized patient group 181 (64.9%) vs. in the restof the patients 1216 (9.2%).Conclusion: history of preoperative gastrointestinal disease doesn’t seem to de-termine the incidence of serious postoperative GI complications after CPB op-erations. Focusing on preoperative and intraoperative risk factors may improveoutcome of critical postoperative GI comlications.
P530 Coronary artery bypass graft surgery after acutemyocardial infarction: does a delayed approach stillhold?
D.S. Sim1, M.H. Jeong1, Y.K. Ahn1, Y.J. Kim2, S.C. Chae3,T.J. Hong4, I.W. Seong5, J.K. Chae6, M.C. Cho7, K.B. Seung8.1Chonnam National University Hospital, Gwangju, Korea, Republic
of; 2Yeungnam University Hospital, Daegu, Korea, Republic of; 3KyungpookNational University Hospital, Daegu, Korea, Republic of; 4Busan NationalUnversity Hospital, Busan, Korea, Republic of; 5Chungnam National UniversityHospital, Daejon, Korea, Republic of; 6Chonbuk National University Hospital,Jeonju, Korea, Republic of; 7Chungbuk National University Hospital, Cheongju,Korea, Republic of; 8Catholic University Hospital, Seoul, Korea, Republic of
Background: The optimal timing of coronary artery bypass graft surgery (CABG)after acute myocardial infarction (AMI) remains controversial, although it has beencommon practice to wait for days to weeks in non-urgent cases to allow for my-ocardial recovery.Objective: We assessed the effect of CABG timing on short-term clinical out-comes in AMI patients.Subjects and Methods: A total of 387 patients, enrolled in the nationwideprospective Korea Acute Myocardial Infarction Registry between November 2005and January 2008, were grouped into early and late groups based on the me-dian time from admission to CABG. The primary endpoint was in-hospital mor-tality. Regression adjustment with propensity scores was applied to control forfactors associated with clinical urgency before CABG, including ventricular tachy-cardia/fibrillation (VT/VF) on admission, mechanical complications of AMI, intra-aortic balloon counterpulsation (IABP), mechanical ventilation, left ventricularejection fraction (LVEF), location of culprit lesions, and failed percutaneous coro-nary intervention (PCI).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

60 Coronary Artery Bypass Surgery
Results: The median time of CABG was 3 and 6 days in ST-elevation MI (STEMI)and non-ST-elevation MI (NSTEMI), respectively. In STEMI, early CABG group(<3 days, N=80) had significantly higher rates of in-hospital death (17.5% vs.6.0%, p=0.021), failed PCI (19.6 vs. 6.6%, p=0.023), cardiogenic shock (11.3%vs. 1.2%, p=0.007), and IABP (26.3% vs. 8.3%, p=0.002). Late group (≥3 days,N=84) had higher rates of thrombolysis (16.7% vs. 3.8%, p= 0.007) and multi-vessel disease (96.1% vs. 73.2%, p <0.0005). After adjustment, however, in-hospital mortality was similar between early and late groups (p=0.457). Predictorsof mortality were age, Killip class IV, and VT/VF on admission. In NSTEMI, earlygroup (< 6 days, N=113) had higher rates of IABP (15.0% vs. 6.4%, p=0.037)and mechanical ventilation (13.3% vs. 4.5%, p=0.023), compared to late group(≥6 days, N=110). After adjustment, in-hospital mortality was not different be-tween the two groups (11.5% vs. 7.5%, p=0.450). Mechanical ventilation beforeCABG was a predictor of mortality in NSTEMI.Conclusion: In patients with AMI undergoing non-urgent surgical intervention,early CABG within two to five days may be considered without increased mortalityrisk, compared to CABG performed later.
P531 Quality of life in elderly patients after coronary arterybypass grafting
A. Goncalves1, S.M. Oliveira1, R. Almeida1, A. Azevedo2, P. Dias1,P. Pinho1. 1Sao Joao Hospital, Porto, Portugal; 2University of Porto,Faculty of Medicine, Porto, Portugal
Introduction: Improved life expectancy led to an increasing number of elderly pa-tients requiring coronary artery bypass grafting (CABG). These patients presenthigher mortality and morbidity rates and the effects on quality of life are uncertain.In this study we aimed to assess long-term survival and quality of life of elderlypatients undergoing CABG.Methods: We retrospectively analyzed records of all patients with 75 years ofage or older submitted to CABG from January 2002 to December 2006 at our cen-ter. Demographic data, risk factors, postoperative complications and EuroSCOREclassification were analyzed. Follow-up was made by telephone interviews in2008 for the purpose of this study. Functional status was assessed and classi-fied with Barthel Index (BI), assuming autonomous status when scoring ≥ 85.Quality of life was considered as the self perception of well-being. When it wasnot possible to contact the patient herself, vital status was questioned to the nextof kin. Postoperative mortality was compared with that of the general Portuguesepopulation of the same age and gender, using standardized mortality ratio (SMR).Results: We included 115 patients≥75 years. The mean age at time of surgerywas 78±2.3 years, 80 (69.6%) were men and 84 (73%) had a high-risk Eu-roSCORE. Follow-up on vital status was achieved in 113 (98.3%) patients aftera mean period of 3.7±1.9 years. Twenty one (18.3%) patients died (including 7inhospital deaths after surgery). The SMR at 1 year was 2.45 (95% CI, 1.45-3.87) in men and 1.19 (95% CI, 0.25-3.45) in women. We obtained informationon BI score and quality of life for 79 (85.9%) patients. Among these, 70 (88.6%)were autonomous according to BI and 53 (67.9%) considered having had an im-provement in quality of life after surgery. None of the demographic and clinicalcharacteristics at baseline predicted a significantly better quality of life at longterm.Conclusion: After a CABG surgery, elderly men had a 2.5-fold higher risk ofdeath at one year than the general male population of the same age, while womenhad the same death rate than the female general population of the same age.Among those who survived, the majority was functionally autonomous and con-sidered having a better quality of life after surgery than before. These resultssuggest that appropriate selection of elderly patients for CABG brings benefitswith respect to survival, functional status and quality of life.
P532 Short-term preoperative treatment with atorvastatinimproves myocardial redox state in patientsundergoing elective CABG by affecting NADPHoxidase activity and NOS coupling
C. Antoniades1, M. Demosthenous2 , M. Margaritis2, D. Tousoulis2 ,A. Antonopoulos2 , A. Paschalis2, G. Ekonomopoulos2 , S. Reilly1, B. Casadei1,C. Stefanadis2 . 1University of Oxford, Oxford, United Kingdom; 2University ofAthens, Athens, Greece
Purpose: Treatment with statins reduces post-operative complications and im-proves survival of patients undergoing elective CABG, but the exact mechanismsof these effects are unclear. We examined the effect of short-term preoperativetreatment with atorvastatin on myocardial redox of patients with low LDL levels,undergoing elective CABG.Methods: Forty two statin-naïve patients scheduled for elective CABG were ran-domized to either atorvastatin 40mg/d or placebo (n=21 per group) for 3 dayspreoperatively. Blood samples were obtained at baseline and at the morning ofthe operation, while myocardial samples of right atrial appendage were obtainedduring CABG. Myocardial superoxide (O2-) was determined by lucigenin chemi-luminescence while urate-inhibitable luminol chemiluminescence was used to es-timate peroxynitrite (ONOO-) generation. NADPH oxidase activity was estimatedby defining NADPH-stimulated O2-. Uncoupled nitric oxide synthase (NOS) con-tribution to myocardial O2- was estimated by using LNAME, mitochondrial oxi-dases by using rotenone and flavin-containing enzymes by using DPI.
Results: Atorvastatin reduced resting O2- (a), NADPH-stimulated (b) and DPI-inhibitable O2- (c). Although there was no significant effect on rotenone-inhibitableO2- (d), atorvastatin reversed LNAME-inhibitable O2- (e) and reduced ONOO-(f) generation. There was a borderline reduction of serum LDL (p<0.05) aftertreatment, but delta(LDL) was unrelated to myocardial oxidative stress.
Conclusions: Short term atorvastatin treatment reduced myocardial NADPH-oxidase activity and improved NOS coupling, supressing myocardial generationof both O2- and ONOO-. These findings may partly explain the beneficial effectof preoperative statin treatment on post-operative CABG complications.
P533 The total arterial off-pump coronary revascularizationvia antero-lateral mini-thoracotomy in multi-vesseldisease using standard stabilizers
A. Ursulescu1, M. Albert1, R. Nagib1, H. Baumbach1, M. Maedge1,M. Hansen2, U. Franke1 . 1Robert Bosch Hospital Departement
of Cardiovascular Surgery, Stuttgart, Germany; 2Robert Bosch HospitalDepartement of Anesthesiology, Stuttgart, Germany
Purpose: Off-pump myocardial revascularization allows superior results regard-ing mortality and neurological outcome. However, median sternotomy may leadto severe deep sternal wound infection and/or postoperative pain syndromes.Furthermore it represents a major psychological barrier for the decision to sur-gical myocardial revascularization compared to the interventional therapy. Con-sequently, total arterial revascularization avoiding sternotomy should be the aimof developments for the future. We report here a series of consecutive patientswho underwent total arterial myocardial revascularization in off-pump fashion viaantero-lateral mini-thoracotomy using standard stabilizers.Methods: Between January 2009 and January 2010, 81 patients underwentminimally invasive total arterial off-pump myocardial revascularization. All singleLIMA-bypass procedures (MIDCAB) were excluded. In all patients the left internalmammary artery (LIMA) was used. Additionally the radial artery was harvestedendoscopically in all patients for the use as T-grafts. After a mini-thoracotomy(7 cm.) was performed in the fourth and/or fifth intercostal space, the LIMA washarvested under direct vizualisation in a skelttonized fashion. For the exposureof the coronary revascularization areas we used the OPCAB standard stabilizersystems (Maquet Acrobat™, Estech Hercules™ or Medtronic Evolution™) andas well intracoronary shunts. Local intercostal anesthetic infiltration was used forpostoperative pain management.Results: There were no post-operative myocardial infarction and no cerebrovas-cular stroke, respectively. No patient required re-exploration or re-operation. Onepatient died in hospital 8 days after the revascularization by acute pulmonary em-bolism. A mean of 2.2±0.4 anastomoses were performed with access to all coro-nary arteries. Revascularization areas were the anterior wall (n=78), the lateralwall (n=54) and the posterior wall (n=17), respectively. The mean ventilation timewas 4,2 h and 31% (n=25) patients could be extubated post-operatively in theOR. The mean ICU-stay was 1.4±0.9 days and mean hospital-stay was 9.9±3.1days. There were no wound complications.Conclusion: The minimally invasive off-pump myocardial revascularization viaantero-lateral mini-thoracotomy is a safe and feasible procedure. This approachoffers a fast recovery and a reduced ICU-stay.
P534 Cardiac neurostimulation in CABG patients: initialexperience
K. Mischke, M. Schmid, N. Hatam, J. Spillner, C. Eickholt, O. Rana,E. Saygili, R. Autschbach, N. Marx, P. Schauerte. University HospitalAachen, Medical Faculty RWTH, Aachen, Germany
Purpose: Atrial fibrillation is a common rhythm disorder after coronary arterybypass grafting (CABG). Patients with a high ventricular rate due to atrial fibril-lation in the acute postoperative setting frequently require rate or rhythm control.Rate control and amiodarone application might be limited in same patients dueto side effects of the medication. An increase in negative dromotropy und thusdecrease in in ventricular heart rate can also be achieved by electrical stimulationof parasympathetic fibers that innervate the AV-node. Selective vagal stimulationmight thus be a new therapeutic approach for rate control in postoperative atrialfibrillation.Methods: In 7 patients, an epicardial pacemaker lead was implanted in the inter-atrial parasympathetic ganglionated plexus (IAGP) during CABG and connected
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Coronary Artery Bypass Surgery 61
to a stimulator. In addition, epicardial pacemaker leads were implanted implantedin the atrium and ventricle. The effect of neurostimulation was tested introper-ative. In case of postoperative atrial fibrillation with a high ventricular rate, highfrequency stimulation was performed for rate control.Results: The neurostimulation lead could be implanted in all patients. Neurostim-ulation effectively reduced ventricular rate during atrial fibrillation up to completeAV-block. In case of postoperative atrial fibrillation, neurostimulation rapidly re-duced the ventricular rate.Conclusion: Cardiac neurostimulation allows an effective ventricular rate controlin the acute postoperative setting after CABG.
P535 Predictors of long hospital stay after cardiac surgery
S. Kerbage, G.G. Giunta, E.G. Gallucci, H.R. Raffaelli, E.D. Dulbecco,J.A. Abud, G.B. Bozovich, R.F. Favaloro. Favaloro FoundationUniversity Hospital, Buenos Aires, Argentina
Introduction: Long hospital stay (LHS) after cardiac surgery (CS) hasan impact in the costs/effectiveness ratio.Objective: The objective is to describe the population under study and evaluatepredictors of LHS.Materials & Methods: Patients referred to CS were selected. The procedureswere divided into coronary bypass graft (CABG, n=1209), valve replacement orrepair (VRR, n=703) or both (COMB, n=444). Hospitalization data were separatedin tertiles. LHS was defined as an in-hospital stay in the 3rd tertile for each surgery(CABG > 10, VRR > 12 and COMB > 10 days). Independent predictors of LHDwere calculated by multiple logistic regression.Results: Multivariate analysis showed age (p<0.0001), ejection fraction(p<0.01), urgent-emergent (p<0.0001) and chronic renal failure (p<0.005) asindependent predictors of LHS in CABG. In VRR group, independent vari-ables associated with LHS are urgent-emergent (p<0.001), chronic renal fail-ure (p<0.005), diabetes (p<0.05) and tricuspid intervention (p<0.01). Urgent-emergent (p<0.05), ejection fraction (p<0.005), chronic renal failure (p<0.01)and mitral intervention (p<0.01) independently predicted LHS in COMB group.
Groups and In-hospital stay relations
CABG VRR COMB p (Kruskal-Wallis ANOVA)
n 1209 703 444Age (years) 63.9±9.6 58.9±15.2 69.4±9.3 < 0.0001In-hospital stay 11±11.8 13.2±12 16.5±17.8 < 0.0001
Conclusion: The association of independent variables is a useful tool in LHS pre-diction. Score development including a combination of these variables, adjustedto CABG, VRR and COMB may be of use.
P536 Off-Pump vs conventional coronary artery bypassgrafting surgery in Argentina. Characterists of thepopulation, evolution and morbi-mortality
D. Lowenstein Haber, F. Guardiani, P. Pieroni, G. Sayavedra, L. Pfister,S. Donato, S. Trejo, F. Landeta, L. Carrizo, J. Thierer. Conarec,
Buenos Aires, Argentina
Purpose: To compare the epidemiological profile, the postoperative evolution andpredictors of mortality in patients undergoing off-pump vs. conventional coronaryartery bypass grafting (CABG) surgery.Methods: The Argentine Cardiovascular Surgery Registry is a national multi-centre prospective study. From September 2007 to October 2008, 1465 patientsundergoing CABG were included: 851 (58.1%) treated with conventional CABGand 614 (41.9%) with off pump CABG. Both types of procedures are performedin 38 centers (76%).Results: There was no difference between both groups in mean age, sex andventricular function. The off pump group had a higher prevalence of diabetes(33.5% vs. 28.2%, p:< 0.03) and history of stroke (5.2% vs. 3.1%, p<0.04). Theconventional CABG group had more left main disease (31.9% vs. 23.4, p<0.01)and unscheduled surgery (27.5% vs. 22.6%; (p<0.004). Although the averagenumbers of grafts was higher in this group (3.1±0.8 vs. 2.5±0.9, p: <0.001), therewas no difference in the use of internal mammary or radial artery graphts. Theneed for reoperation was lower in off pump CABG (2.44% vs. 5.21%, p=0.004) aswas the incidence of other major complications (kidney failure, low cardiac output,stroke, bleeding, severe arrhythmia and sepsis: 20.52% vs. 28.2%, p=0.001).The conventional CABG group presented a trend to higher mortality (5.17% vs.3.09%, p = 0.053).Conclusion: A high proportion of surgical coronary revascularitation proceduresin Argentina are off pump. Beyond some differences in baseline characteristicsthis technique is associated lower morbidity and trend towards lower mortality.
P537 Strong association of preoperative atrial fibrillationwith hospital mortality in elderly patients undergoingcardiac surgery
B. Frilling1, W. Von Renteln-Kruse1, F.C. Riess2. 1Albertinen Hospitalat University of Hamburg, Center of the Geriatrics and Gerontology,
Hamburg, Germany; 2Albertinen Hospital, Department of Cardiac Surgery,Hamburg, Germany
An increasing number of elderly patients develop cardiac disease requiringsurgery. Assessing operative risk is one of the key aspects of clinical decision-making in these patients. The predictive value of current operative risk scoressuch as the EuroSCORE is disputable in elderly patients. Atrial fibrillation (AFIB)is not included in the calculation of the EuroSCORE.Methods: Prospective cohort study of elderly patients undergoing cardiacsurgery. 490 patients underwent Comprehensive Geraitric Assessment on theday before elecitve or urgent cardiac surgery.Results: Mean EuroSCORE was 16.2%; hospital mortality was 2.9%. 147 pa-tients (30%) had atrial fibrillation before surgery.
Patient characteristics
AFIB No AFIB OR (95% CI)
Age > 80 years 38.8% 25.9% 1.8 (1.2-2.7)Female gender 49.0% 42.9% 1.3 (0.9-1.9)Urgent operation 45.6% 27.1% 2.3 (1.5-3.4)Heart failure (EF < 45%) 34.7% 18.7% 2.3 (1.5-3.6)Recent cardiac decompensation 34.0% 8.5% 5.6 (3.4-9.3)Renal insufficiency 36.7% 23.6% 1.9 (1.2-3.9)Diabetes 37.4% 23.0% 2.0 (1.3-3.0)Acute renal failure postoperatively 16.3% 3.5% 5.4 (2.6-11.1)Pacemaker implantation 10.2% 3.5% 3.1 (1.4-6.6)Stroke 1.4% 1.5% 0.9 (0.2-4.9)Delirium 22.5% 16.0% 1.5 (0.9-2.5)In-hospital death 6.8% 0.9% 8.3 (2.2-30.5)
Conclusion: Preoperative atrial fibrillation is associated with considerable oper-ative mortality and morbidity. Evaluation of heart rhythm before cardiac surgerymay improve risk assessment in elderly patients undergoing cardiac surgery.
P538 The response of endogenous nitric oxide synthaseinhibitor ADMA to open heart surgery
A. Nemeth1, A. Cziraki1, Z. Ajtay1, E. Sulyok2, Z. Lenkey1,S. Szabados1, A. Nasri1, J.M. Lobenhoffer3 , F. Awiszus4, S.M. Bode-Boger3. 1Heart Institute, University of Pecs, Pecs, Hungary; 2Institute
of Public Health and Health promotion, Faculty of Health Sciences, University ofPecs, Pecs, Hungary; 3Otto-von-Guericke University of Magdeburg, Institute ofClinical Pharmacology, Magdeburg, Germany; 4Otto-von-Guericke University ofMagdeburg, Department of Orthopedics, Magdeburg, Germany
Purpose: NO metabolism can be characterized by asymmetric dimethylarginine(ADMA) which is an endogenous competitive inhibitor of nitric oxide synthase.The concentration of ADMA is increased in patients with endothelial dysfunction.Methods: Plasma levels of ADMA, l-arginine and symmetric dimethylarginine(SDMA) were measured by liquid chromatography-tandem mass spectrometry(LC-MS-MS) in both the coronary sinus and peripheral vein of 21 patients un-derwent off-pump CABG surgery (OPCAB) and 20 patients underwent on-pumpsurgery with cardiopulmonary bypass (CPB). The measurements were performed24 h before, 3 times during the operation, on the 1st and 5th day after surgery.Results: ADMA levels remained constant in the OPCAB group both in the coro-nary sinus samples (F=0.416, p<0.685) and in the peripheral blood (F=0.574,p<0.562). However, ADMA concentration increased significantly in patients whounderwent on-pump surgery with CPB in both the coronary sinus (F=14.751,p<0.001) and the peripheral vein (F=30.738, p<0.001), the intersubject time ef-fect, therefore, proved to be markedly different between the two groups (F=6.990,p<0.002). In the present study l-arginine levels did not exhibit significant differ-ences during OPCAB neither in the blood samples from coronary sinus (F=1.006,p<0.362) nor from the peripheral vein (F=0.812, p<0.435). By contrast, l-arginineconcentration increased steadily at periphery (F=6.226, p<0.012), whereas it didnot change in the coronary sinus (F=2.050, p<0.161) during CPB. The time-course of l-arginine was significantly different in the coronary sinus samples(F=3.255, p<0.05) and also in the peripheral blood (F=3.255, p<0.05).Conclusions: Plasma levels of ADMA, SDMA and l-arginine are reliable markersof an early ischaemia-reperfusion injury. The response pattern of the new car-diovascular risk factor, ADMA was significantly different between the two groups.Its long-term follow-up may be suitable to monitor the improvement of coronaryendothelial function after revascularisation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

62 Coronary Artery Bypass Surgery
P539 Surgical coronary revascularization in patients withrecent acute myocardial infarction: long-termcomparison between on-pump and off-pump strategies
S.R.N. Leal1, R. Cale1, R. Rodrigues2, J. Calquinha2, L. Bruges2,M. Abecasis2, J. Pedro Neves2, J. Moradas Ferreira2, J. Aniceto
Silva1, J. Queiroz E Melo2. 1Hospital West Lisbon, Hospital Santa Cruz,Department of Cardiology, Lisbon, Portugal; 2Hospital West Lisbon, HospitalSanta Cruz, Department of Cardiothoracic Surgery, Lisbon, Portugal
Purpose: Off-pump coronary revascularization is gaining preponderance in sur-gical practice, although it’s superiority over on-pump modality hasn’t been showedin all clinical scenarios. Is the aim of our study to compare on-pump and off-pumpstrategies in the context of recent acute myocardial infarction.Methods: Retrospective 1 year analysis of consecutive patients submitted toon-pump or off-pump CABG surgery in the context of AMI≤6 weeks. Com-parative evaluation of prognosis at 30d, 1Y and 2Y (follow-up 729±339d)through multivariate Cox regression for the endpoints (1) death and (2)death+AMI+revascularization+stroke (MACE). Subanalysis of the results by pre-cocity of CABG surgery (0-2 vs 2-6w after AMI).Results: 90 Patients, 73.3% m, 66.1±10.9Y. Presentation: HTA 85.2%, DM38.2%, dyslipidemia 68.8%, tabagism 49.1%, BMI 26.5±3.7, HF 19.8%. CADextension: LMCA 21.8%, 3 vessels 59.1%. Additive EuroSCORE 6.0±2.8. On-pump vs. off-pump revascularization: no differences except previous stroke (6.0vs 18.3%, P=0.03), interval AMI-CABG (19.1 vs 30.9d, p=0.03), complete revas-cularization (74 vs 55%, p=0.05), number of bypasses (2.8±0.7 vs 2.4±0.9,P=0.005) and venous grafts (1.3±0.9 vs 0.9±0.7, P=0.008) and bleeding vol-ume (709±351 vs 511±333cc, P=0.02). Survival analysis: death 30d 2.3 vs 6.4%(P=0.10), 1Y 7.0 vs 10.6% (P=0.41), 2Y 9.3 vs 10.6% (P=0.38); MACE 30d 2.3vs 8.5% (P=0.06), 1Y 14.0 vs 19.1% (P=0.28), 2Y 16.3% vs 21.3% (P=0.37).Adjusted survival curves didn’t show differences for the endpoints through FUP.Subanalysis by precocity of CABG surgery: no FUP differences between strate-gies (CABG 0-2w death P=0.79, MACE=0.48; CABG 2-6w death P=0.52, MACEP=0.38).
Long-term comparison of endpoint MACE
Conclusions: Off-pump revascularization in patients with recent AMI didn’tdemonstrate superiority. It’s aplication must be guided by patient characteristics.
P540 Impact of the SYNTAX score on the referral to coronaryartery bypass graft surgery before and after SYNTAXtrial publication
G. Abounader, L.M. Stevens, N. Noiseux, J.B. Masson, A. Kokis,F. Gobeil, S. Mansour. Montreal University Hospital Center, Montreal,
Canada
Purpose: The Syntax score (SXscore) has been developed as a combination ofseveral validated angiographic classifications aiming to characterize the coronarylesions with respect to their functional impact, location, and complexity. Its prog-nostic value has recently been highlighted in patients with left main (LM) and/ormultivessel (MV) coronary artery disease. The aim of this study was to evaluatethe impact of the SYNTAX trial publication on the referral of this population of pa-tients to coronary artery bypass graft surgery (CABG) in a high volume tertiarycenter.Methods: In a retrospective analysis we review the coronary angiogram of pa-tients referred for isolated non–urgent (CABG) based on physician decision be-cause of a LM and/or MV disease before and after the publication of the SYNTAXtrial. The SXscore was calculated and patients were subsequently divided in threegroups of low (0-22), intermediate (23-32) and high score (>32).Results: Between March and June 2008, 1132 patients had a coronary an-giogram and 114 patients (10%) were referred for CABG (cohort A). BetweenMarch and June 2009, 1095 patients had a coronary angiogram and 126 patients(12%) were referred for CABG (cohort B). No significant difference was foundbetween the cohort A & B in the rate of referred patients with low, intermediateor high Sxscore (13% vs. 17%; 44% vs. 35% and 43% vs. 48%, respectively;p=0.338). In addition, no significant difference was noted between the cohortA & B in the rate of referred patients with a significant LM stenosis (51% vs.38%; p=0.052), chronic total occlusion (42% vs. 53%; p=0.094), calcified lesions(47% vs. 52%; p=0.521), tortuous vessels (43% vs. 43%; p>.999), thrombus (7%vs. 8%; p=0.812), or left dominance (4% vs. 9%; p=0.204). However, cohort Ashowed a significant higher rate of referred patients with bifurcation (90%, vs.
81%; p=0.045), long lesions (84% vs. 71%; p=0.014) and distal LM (91% vs.76%; p=0.047). Finally, in a subgroup analysis of patients older than 65 years wenoticed a significant increase of the rate of referred patients with a low SXscorein the cohort B as compared to the cohort A (19% vs. 7%; p=0.048).Conclusion: The majority of patients referred for CABG based on physician de-cision before and after the SYNTAX trial publication had an intermediate and highSxscore. However, relying on the SXscore in the elderly population could preventreferral and avoid CABG for patients with low Sxscore but elevated surgical risk.
P541 Perioperative hemostasis and bleeding risk indouble-antiplatelet high risk patients undergoingcoronary revascularization procedure. A prospectivecontrolled study
V. Tarzia, C. Paolini, T. Bottio, G. Rizzoli, L. Spiezia, C. Dal Lin,E. Buratto, P. Simioni, G. Gerosa. University of Padua, Department of
Cardiac Thoracic and Vascular Sciences, Padua, Italy
Purpose: Double-clopidogrel-aspirin treatment plays a crucial role in preventingcoronary arteries and stent thrombosis, thus it might reduce early grafts occlusionafter coronary-surgery. Rotation-thromboelastometry (ROTEM) is a well-knowntest to provide information on the contribution of fibrinogen and platelets to clotformation. To determine the risk of perioperative-bleeding induced by the double-treatment, we undertook a prospective study of consecutive patients undergoingsurgery.Methods: There were two groups: patients with double-antiplatelet (n= 50) andpatients (n= 50) with single management. The double and single groups had sim-ilar preoperative demographic, clinical, and biologic characteristics and operativemanagement. Classic coagulation parameters and ROTEM profile were preoper-atively performed in both groups. The same eparin-treatment was administeredin all. Two ROTEM assays, INTEM and EXTEM, were performed and CT, CFT,MCF, alpha-angle and thrombin-generation-potential as expressed by the Area-Under-Curve (AUC) were analyzed.Results: Important bleeding occurred in 8 double-treated and in 6 single-treated(p=NS). Among bleeders classic coagulation parameters were comparable. Onthe contrary we observed that the AUC-value was significantly lower in bleeders(5030±1115 mmX100) than no-bleeders (6568±548 mmX100) (p<0.0001) andthat the double-therapy was not associated to a significantly higher bleeding risk.The bleeding incidence was 16% percent in double-treated as compared with12% percent in the single.Conclusions: We conclude that there is little risk of important bleeding at-tributable to double-treatment after coronary-surgery. Furthermore, we observedthat patients with a low AUC value are at a significantly higher risk of bleeding ascompared to patients with higher AUC.
P542 Preoperative C-reactive protein and atrial fibrillationafter isolated off-pump coronary artery bypass grafting
T. Kinoshita, T. Asai, T. Suzuki, A. Kambara, K. Matsubayashi. ShigaUniversity of Medical Science, Otsu, Japan
Background: We investigated whether elevated preoperative CRPlevel is associated with postoperative atrial fibrillation in a large patient popula-tion undergoing isolated off-pump coronary artery bypass grafting.Methods: The present study included 630 patients undergoing isolated off-pumpcoronary artery bypass grafting without conversion to cardiopulmonary bypass bya single surgeon between 2002 and 2008 after excluding the patients with chronicatrial fibrillation, atrial flutter, and prior pacemaker implantation.Results: Postoperative atrial fibrillation occurred in 141 patients and most often(35%) on postoperative day 2, with 81% occurrences on postoperative day 1,2, or 3. Patients who developed atrial fibrillation had significantly higher pre- andpost-operative CRP (Table). In a multivariate logistic regression including elevatedCRP (≥ 0.3 mg/dL) and the recognized risk factors for postoperative atrial fibril-lation: age, gender, hypertension, diabetes mellitus, chronic heart failure, previ-ous myocardial infarction, ejection fraction, left atrial dimension, and preoperativemedication (statin and beta blocker), elevated CRP was a significant predictor ofpostoperative atrial fibrillation (Odds ratio, 1.71; 95% confidence interval, 1.13 to2.59; p = 0.01).
Time course of changes in CRP
Atrial Fibrillation No Atrial Fibrillation p valuen=141 n=489
Preoperative 0.32 (0.14-1.65) 0.26 (0.11-0.68) 0.01POD1 5.70 (4.01-8.25) 5.23 (3.59-7.85) 0.29POD2 19.00 (14.72-23.63) 17.63 (13.75-27.56) 0.03POD3 17.87 (13.64-23.84) 15.85 (10.83-21.21) 0.04POD4 12.40 (8.56-16.23) 9.94 (7.00-14.25) 0.01POD5 9.14 (6.96-13.41) 7.57 (5.18-11.11) 0.03POD6 6.43 (4.35-9.30) 4.71 (3.27-7.31) 0.01Peak 20.21 (16.63-25.92) 18.20 (13.96-24.21) 0.01
POD denotes postoperative day.
Conclusion: Preoperative CRP is independently associated the occurrence ofpostoperative atrial fibrillation after off-pump coronary artery bypass grafting.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart transplant and aortic surgery 63
HEART TRANSPLANT AND AORTIC SURGERY
P543 Early in-hospital mortality of acute aortic syndromes:results from the French National Multicentric Registry
B. Honton1, E. Berrard2, P. Berthoumieu3, G. Mulak4, J. Roncalli1,C. Mounier-Vehier5, N. Danchin6, E. Bonnefoy7, C. Spaulding8,M. Elbaz1. 1University Hospital of Toulouse - Rangueil Hospital,
Departments of Cardiology, Toulouse, France; 2University Hospital of Toulouse -Rangueil Hospital, Department of Epidemiology, Toulouse, France; 3UniversityHospital of Toulouse - Rangueil Hospital, Department of CardiovascularSurgery, Toulouse, France; 4Department of French Society of Cardiology, Paris,France; 5University Hospital of Lille - Department of Cardiology, Lille, France;6AP-HP, European Hospital Georges Pompidou - Department of Cardiology,Paris, France; 7University Hospital of Lyon - L.Pradel Hospital, Department ofCardiology, Lyon, France; 8AP-HP, Cochin Hospital - Department of Cardiology,Paris, France
Background: Acute Aortic diseases are life threatening syndromes. Despite re-cent improvement in management, data are limited regarding the actual diagnosisaccuracy, therapeutic and mortality of such disease. We aimed to assess deter-minants of in-hospital mortality in patients with acute aortic syndromes.Method: Our analysis was based on data from the French prospective NationalMulticentre Registry (14 referral French Health Care Centers) of acute aortic syn-dromes (Feb 2008 - Dec 2009). Assessment of determinants of in-hospital mor-tality was based on multivariable logistic regression.Results: The study included 278 patients (72% men) mean aged 66 (± 14)years. Aortic syndromes consisted in type A dissection (n=143), type B dissection(n=90), intra mural hematoma (n=21), complicated thoracic aneurysm (n=20) andpenetrating ulcer (n=4). Only 2% patients were suffering from elastic fibers dis-orders. Hypertension and aortic aneurysm histories were noted in 70% (n=194)and 14.3% (n=40) patients respectively. Electrocardiogram abnormality of repo-larization was noted in 48% (n=134) patients. Major aortic complications werecardiogenic shock and visceral malperfusion in 14.3% (n=40) and 13.6% patients(n=38) respectively. Disease management was medical in 35% patients, surgery(45%) or endovascular treatment (13%). Total intrahospital mortality was 21%(n=56) [40% (n=8) in complicated thoracic aneurysm group, 27% (n=37) in typeA dissection group, 16% (n=3) in intra mural hematoma group, (9%) (n=8) in typeB dissection group and none in penetrating ulcer group (p=0.001)]. Determinantsindependently and significantly associated with in-hospital mortality were: typeof acute aortic syndrome (Odds ratio= 0.34 [95% confidence interval: 0.14-0.86]for type B dissection, OR= 1.38 [0.45-4.22] for complicated thoracic aneurysmand OR= 0.46 [0.12-1.79] for intra mural hematoma or penetrating ulcer, versustype A dissection), age above to 65 years (OR: 2.73 [1.33-5.61]), history of hy-pertension (OR: 0.43 [0.21-0.86]), history of aneurysm (OR: 2.47 [1.04 -5.88]),cardiogenic shock (OR=2.71 [1.18-6.24]) and visceral malperfusion syndrome(OR=2.42 [1.01-5.78]).Conclusion: Despite recent progress in diagnostic and therapeutic, acute aor-tic syndromes are still associated with high intrahospital mortality. These resultsidentify higher risk patients of poor in-hospital prognosis. This recent large mul-ticentric study emphasizes the need to still improve the management of patientssuffering from acute aortic diseases.
P544 Prevention of perioperative cardiovascularcomplications in abdominal aneurysm surgery;implemention of new guidelines decreases risk
O. Schouten1, S.E. Hoeks2, W.H. Hoffmann1, I.H. Oei1, P.C. Smit1,J. Koning1, D. Poldermans2. 1Reinier de Graaf Gasthuis, Delft,
Netherlands; 2Erasmus MC, Rotterdam, Netherlands
Background: Patients undergoing open abdominal aortic aneurysm repair are athigh risk for perioperative cardiovascular events. Recently new ESC guidelinesfor the prevention of perioperative events have been issued.Aim: To establish potential benefits of adherence to the new perioperative guide-lines.Methods: Consecutive patients undergoing open abdominal aortic aneurysmrepair between 2004-2009 were included. Cardiac risk factors were noted: MI,angina, CHF, TIA/CVA, diabetes, renal dysfunction, age >70 years. Also medica-tion use, including statins and beta-blockers, was noted. Primary endpoint was theoccurence of perioperative cardiovascular complications including cardiac death,myocardial infarction, myocardial ischemia, new-onset atrial fibrillation, heart fail-ure and stroke.Results: In total 163 patients were included (age 72 yrs, 85% male). Only 36%of patients were on both beta-blocker and statin therapy as recommended by theguidelines, while 16% did not receive either medication. In total 28 patients (17%)experienced a perioperative cardiovascular complication while 6 (3.7%) patientsdied within 30 days after surgery. The risk of cardiovascular complications waslowest in patients on both beta-blocker and statin (12%), patients on either beta-blockers or statins had a 17% risk, and patients without statins and beta-blockershad the highest risk (27%). In multivariate analysis, adjusted for cardiovascu-lar risk factors, adherence to guidelines was associated with a 60% decreasedrisk for perioperative cardiovascular complications (OR 0.38, 95% CI 0.14-0.97,p=0.04).
Conclusions: Adherence to the new ESC guidelines for the prevention of cardio-vascular events indeed seems to be associated with lower incidence of perioper-ative events in patients undergoing aortic aneurysm repair.
P545 Prevalence of mutations of smooth muscle alpha-actin2 (ACTA2) in thoracic aneurysms and dissections andphenotype characterisation
F.I. Gambarin, E. Disabella, R. Dore, M. Grasso, V. Favalli, A. Serio,M. Pasotti, E. Antoniazzi, M. Mosconi, E. Arbustini. Foundation IRCCS
Polyclinic San Matteo - University of Pavia, Pavia, Italy
Purpose: Smooth muscle Alpha-actin (ACTA2) mutations cause non-syndromicthoracic aortic aneurysms and dissections (TAAD), both familial and sporadic.We aimed at estimating the prevalence of mutations of the ACTA2 gene in aconsecutive series of TAAD, both familial and sporadic, and evaluating associatedextravascular traits.Methods: We evaluated the prevalence of mutations of ACTA2 in a consecutiveseries of 100 TAAD, 43 familial and 57 sporadic. The inclusion criteria were di-agnosis of TAAD, exclusion of Marfan Syndrome, Loeys-Dietz and Ehlers-Danlostype IV Syndromes. Probands underwent multidisciplinary clinical and imagingevaluation, genetic counselling, and direct sequencing of ACTA2. Relatives un-derwent clinical and genetic screening.Results: We identified five mutations in the familial TAAD group (12%). Theknown p.Arg149Cys and the novel p.Asp82Glu, p.Glu243Lys and p.Val45Leu mu-tations affected evolutionary conserved residues. The IVS4+1G>A mutation wasnovel. All mutations were absent in 400 controls.Type A dissection was the first manifestation of the aortic aneurysm in 4 probandsand occurred unexpectedly in 5 additional relatives unaware of the familial risk.Of 22 relatives who underwent clinical and genetic screening, 12 were carriersof the mutation identified in the corresponding proband while 2 were affected buthad no genetic testing.The aortic aneurysm and dissection were age-dependant and absent in mutatedchildren. Of the nine patients who suffered acute dissection, 5 died after surgery.At the time of dissection, the size of the aortic aneurysm ranged from 4 to 9.5cm. Extra vascular ocular, skeletal, nervous and pulmonary traits were variablyassociated with the TAAD, being iris flocculi the most common extravasculat trait.Conclusions: Our clinical series documents a prevalence of ACTA2 mutations in12% of familial TAAD. This datum confirms ACTA2 as a major disease gene forTAAD. Timely diagnosis of TAAD in the probands, genetic counselling and familyscreening may identify predisposed relatives and prevent catastrophic aortic dis-sections. An alerting datum in our series is the occurrence of aortic root dissectionat dilatation values <50 mm, which is usually considered the limit for preventivesurgery in Marfan syndrome.
P546 Temporary decline of renal function after vascularsurgery is an independent predictor for chronic kidneydisease
J.P. Van Kuijk1, W.J. Flu1, M. Chonchol2, S.E. Hoeks1, T.A. Winkel1,H.J.M. Verhagen1 , J.J. Bax3, D. Poldermans1. 1Erasmus Medical
Center, Rotterdam, Netherlands; 2University of Colorado Denver, Aurora, UnitedStates of America; 3Leiden University Medical Center, Department of Cardiology,Leiden, Netherlands
Purpose: Acute kidney injury is common in surgical patients and has been iden-tified as an independent predictor of short- and long-term cardiovascular diseaseand mortality. However, data on the relationship between reversible transitory de-cline in kidney function and chronic kidney disease are lacking. Therefore, weassessed the prognostic value of temporary renal function decline on the devel-opment of long-term chronic kidney disease.Methods: The study included 1.308 vascular surgery patients, which were di-vided into 3 groups based on changes in Modification of Diet in Renal Disease-Glomerular Filtration Rate (MDRD-GFR) on days 1, 2, and 3 after surgery, com-pared to baseline. Group 1, improved or unchanged (change in MDRD-GFR±10%); group 2, temporary worsening (worsening >10% at day 1 or 2, followedby complete recovery within 10% to baseline at day 3); and group 3, persistentworsening (>10% decrease). Primary endpoint was the development of incidentchronic kidney disease during a median follow-up of 5.0 years (IQR 2.6-8.5).Results: Perioperative renal function was classified as unchanged, temporaryand persistent decline in 739 (57%), 294 (22%) and 275 (21%) patients, respec-tively. During follow-up, 417 (32%) patients developed chronic kidney disease. In
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
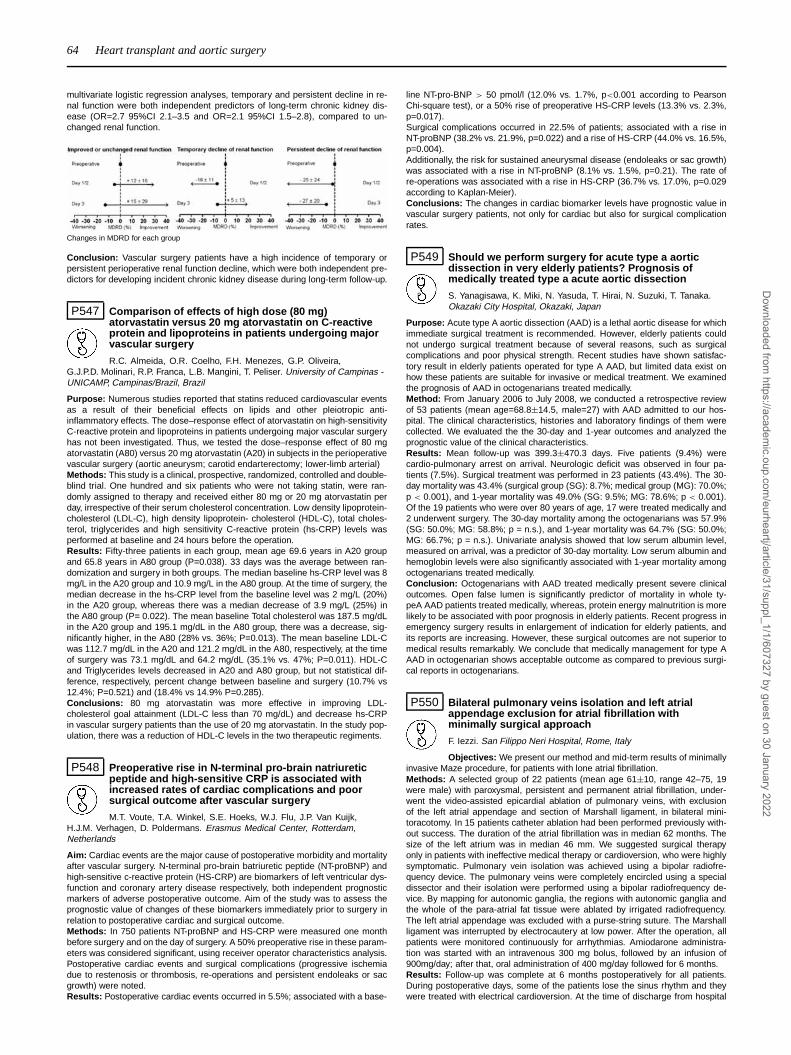
64 Heart transplant and aortic surgery
multivariate logistic regression analyses, temporary and persistent decline in re-nal function were both independent predictors of long-term chronic kidney dis-ease (OR=2.7 95%CI 2.1–3.5 and OR=2.1 95%CI 1.5–2.8), compared to un-changed renal function.
Changes in MDRD for each group
Conclusion: Vascular surgery patients have a high incidence of temporary orpersistent perioperative renal function decline, which were both independent pre-dictors for developing incident chronic kidney disease during long-term follow-up.
P547 Comparison of effects of high dose (80 mg)atorvastatin versus 20 mg atorvastatin on C-reactiveprotein and lipoproteins in patients undergoing majorvascular surgery
R.C. Almeida, O.R. Coelho, F.H. Menezes, G.P. Oliveira,G.J.P.D. Molinari, R.P. Franca, L.B. Mangini, T. Peliser. University of Campinas -UNICAMP, Campinas/Brazil, Brazil
Purpose: Numerous studies reported that statins reduced cardiovascular eventsas a result of their beneficial effects on lipids and other pleiotropic anti-inflammatory effects. The dose–response effect of atorvastatin on high-sensitivityC-reactive protein and lipoproteins in patients undergoing major vascular surgeryhas not been investigated. Thus, we tested the dose–response effect of 80 mgatorvastatin (A80) versus 20 mg atorvastatin (A20) in subjects in the perioperativevascular surgery (aortic aneurysm; carotid endarterectomy; lower-limb arterial)Methods: This study is a clinical, prospective, randomized, controlled and double-blind trial. One hundred and six patients who were not taking statin, were ran-domly assigned to therapy and received either 80 mg or 20 mg atorvastatin perday, irrespective of their serum cholesterol concentration. Low density lipoprotein-cholesterol (LDL-C), high density lipoprotein- cholesterol (HDL-C), total choles-terol, triglycerides and high sensitivity C-reactive protein (hs-CRP) levels wasperformed at baseline and 24 hours before the operation.Results: Fifty-three patients in each group, mean age 69.6 years in A20 groupand 65.8 years in A80 group (P=0.038). 33 days was the average between ran-domization and surgery in both groups. The median baseline hs-CRP level was 8mg/L in the A20 group and 10.9 mg/L in the A80 group. At the time of surgery, themedian decrease in the hs-CRP level from the baseline level was 2 mg/L (20%)in the A20 group, whereas there was a median decrease of 3.9 mg/L (25%) inthe A80 group (P= 0.022). The mean baseline Total cholesterol was 187.5 mg/dLin the A20 group and 195.1 mg/dL in the A80 group, there was a decrease, sig-nificantly higher, in the A80 (28% vs. 36%; P=0.013). The mean baseline LDL-Cwas 112.7 mg/dL in the A20 and 121.2 mg/dL in the A80, respectively, at the timeof surgery was 73.1 mg/dL and 64.2 mg/dL (35.1% vs. 47%; P=0.011). HDL-Cand Triglycerides levels decreased in A20 and A80 group, but not statistical dif-ference, respectively, percent change between baseline and surgery (10.7% vs12.4%; P=0.521) and (18.4% vs 14.9% P=0.285).Conclusions: 80 mg atorvastatin was more effective in improving LDL-cholesterol goal attainment (LDL-C less than 70 mg/dL) and decrease hs-CRPin vascular surgery patients than the use of 20 mg atorvastatin. In the study pop-ulation, there was a reduction of HDL-C levels in the two therapeutic regiments.
P548 Preoperative rise in N-terminal pro-brain natriureticpeptide and high-sensitive CRP is associated withincreased rates of cardiac complications and poorsurgical outcome after vascular surgery
M.T. Voute, T.A. Winkel, S.E. Hoeks, W.J. Flu, J.P. Van Kuijk,H.J.M. Verhagen, D. Poldermans. Erasmus Medical Center, Rotterdam,Netherlands
Aim: Cardiac events are the major cause of postoperative morbidity and mortalityafter vascular surgery. N-terminal pro-brain batriuretic peptide (NT-proBNP) andhigh-sensitive c-reactive protein (HS-CRP) are biomarkers of left ventricular dys-function and coronary artery disease respectively, both independent prognosticmarkers of adverse postoperative outcome. Aim of the study was to assess theprognostic value of changes of these biomarkers immediately prior to surgery inrelation to postoperative cardiac and surgical outcome.Methods: In 750 patients NT-proBNP and HS-CRP were measured one monthbefore surgery and on the day of surgery. A 50% preoperative rise in these param-eters was considered significant, using receiver operator characteristics analysis.Postoperative cardiac events and surgical complications (progressive ischemiadue to restenosis or thrombosis, re-operations and persistent endoleaks or sacgrowth) were noted.Results: Postoperative cardiac events occurred in 5.5%; associated with a base-
line NT-pro-BNP > 50 pmol/l (12.0% vs. 1.7%, p<0.001 according to PearsonChi-square test), or a 50% rise of preoperative HS-CRP levels (13.3% vs. 2.3%,p=0.017).Surgical complications occurred in 22.5% of patients; associated with a rise inNT-proBNP (38.2% vs. 21.9%, p=0.022) and a rise of HS-CRP (44.0% vs. 16.5%,p=0.004).Additionally, the risk for sustained aneurysmal disease (endoleaks or sac growth)was associated with a rise in NT-proBNP (8.1% vs. 1.5%, p=0.21). The rate ofre-operations was associated with a rise in HS-CRP (36.7% vs. 17.0%, p=0.029according to Kaplan-Meier).Conclusions: The changes in cardiac biomarker levels have prognostic value invascular surgery patients, not only for cardiac but also for surgical complicationrates.
P549 Should we perform surgery for acute type a aorticdissection in very elderly patients? Prognosis ofmedically treated type a acute aortic dissection
S. Yanagisawa, K. Miki, N. Yasuda, T. Hirai, N. Suzuki, T. Tanaka.Okazaki City Hospital, Okazaki, Japan
Purpose: Acute type A aortic dissection (AAD) is a lethal aortic disease for whichimmediate surgical treatment is recommended. However, elderly patients couldnot undergo surgical treatment because of several reasons, such as surgicalcomplications and poor physical strength. Recent studies have shown satisfac-tory result in elderly patients operated for type A AAD, but limited data exist onhow these patients are suitable for invasive or medical treatment. We examinedthe prognosis of AAD in octogenarians treated medically.Method: From January 2006 to July 2008, we conducted a retrospective reviewof 53 patients (mean age=68.8±14.5, male=27) with AAD admitted to our hos-pital. The clinical characteristics, histories and laboratory findings of them werecollected. We evaluated the the 30-day and 1-year outcomes and analyzed theprognostic value of the clinical characteristics.Results: Mean follow-up was 399.3±470.3 days. Five patients (9.4%) werecardio-pulmonary arrest on arrival. Neurologic deficit was observed in four pa-tients (7.5%). Surgical treatment was performed in 23 patients (43.4%). The 30-day mortality was 43.4% (surgical group (SG): 8.7%; medical group (MG): 70.0%;p < 0.001), and 1-year mortality was 49.0% (SG: 9.5%; MG: 78.6%; p < 0.001).Of the 19 patients who were over 80 years of age, 17 were treated medically and2 underwent surgery. The 30-day mortality among the octogenarians was 57.9%(SG: 50.0%; MG: 58.8%; p = n.s.), and 1-year mortality was 64.7% (SG: 50.0%;MG: 66.7%; p = n.s.). Univariate analysis showed that low serum albumin level,measured on arrival, was a predictor of 30-day mortality. Low serum albumin andhemoglobin levels were also significantly associated with 1-year mortality amongoctogenarians treated medically.Conclusion: Octogenarians with AAD treated medically present severe clinicaloutcomes. Open false lumen is significantly predictor of mortality in whole ty-peA AAD patients treated medically, whereas, protein energy malnutrition is morelikely to be associated with poor prognosis in elderly patients. Recent progress inemergency surgery results in enlargement of indication for elderly patients, andits reports are increasing. However, these surgical outcomes are not superior tomedical results remarkably. We conclude that medically management for type AAAD in octogenarian shows acceptable outcome as compared to previous surgi-cal reports in octogenarians.
P550 Bilateral pulmonary veins isolation and left atrialappendage exclusion for atrial fibrillation withminimally surgical approach
F. Iezzi. San Filippo Neri Hospital, Rome, Italy
Objectives: We present our method and mid-term results of minimallyinvasive Maze procedure, for patients with lone atrial fibrillation.Methods: A selected group of 22 patients (mean age 61±10, range 42–75, 19were male) with paroxysmal, persistent and permanent atrial fibrillation, under-went the video-assisted epicardial ablation of pulmonary veins, with exclusionof the left atrial appendage and section of Marshall ligament, in bilateral mini-toracotomy. In 15 patients catheter ablation had been performed previously with-out success. The duration of the atrial fibrillation was in median 62 months. Thesize of the left atrium was in median 46 mm. We suggested surgical therapyonly in patients with ineffective medical therapy or cardioversion, who were highlysymptomatic. Pulmonary vein isolation was achieved using a bipolar radiofre-quency device. The pulmonary veins were completely encircled using a specialdissector and their isolation were performed using a bipolar radiofrequency de-vice. By mapping for autonomic ganglia, the regions with autonomic ganglia andthe whole of the para-atrial fat tissue were ablated by irrigated radiofrequency.The left atrial appendage was excluded with a purse-string suture. The Marshallligament was interrupted by electrocautery at low power. After the operation, allpatients were monitored continuously for arrhythmias. Amiodarone administra-tion was started with an intravenous 300 mg bolus, followed by an infusion of900mg/day; after that, oral administration of 400 mg/day followed for 6 months.Results: Follow-up was complete at 6 months postoperatively for all patients.During postoperative days, some of the patients lose the sinus rhythm and theywere treated with electrical cardioversion. At the time of discharge from hospital
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
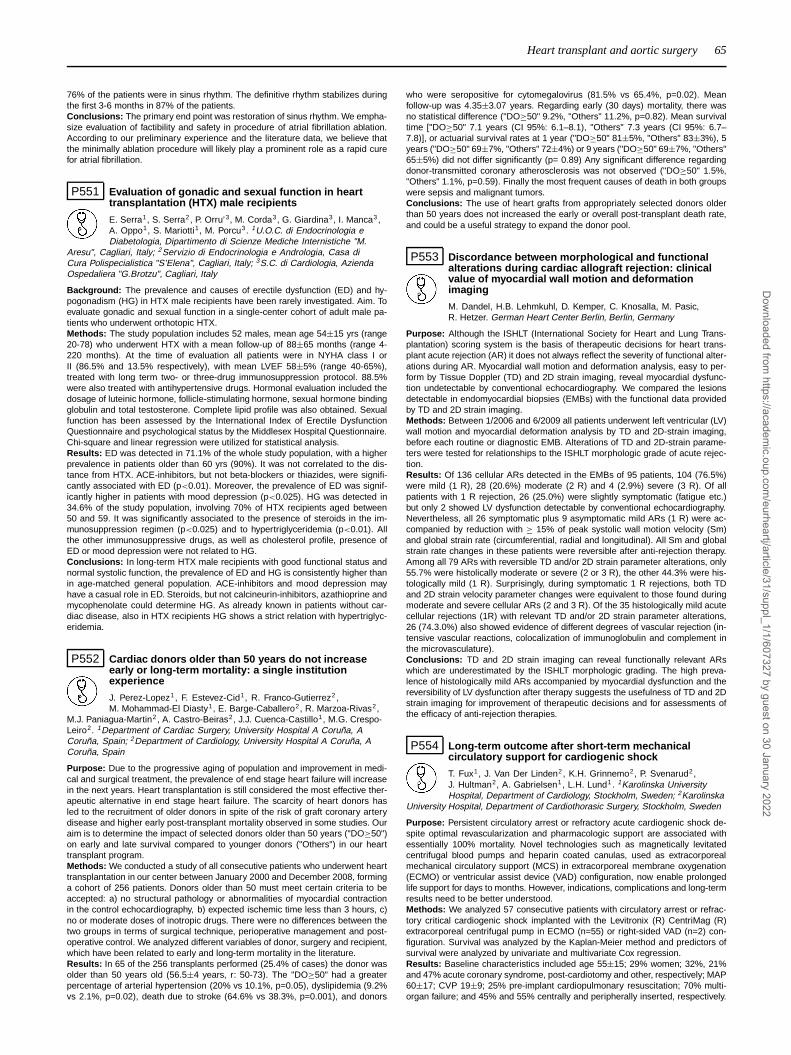
Heart transplant and aortic surgery 65
76% of the patients were in sinus rhythm. The definitive rhythm stabilizes duringthe first 3-6 months in 87% of the patients.Conclusions: The primary end point was restoration of sinus rhythm. We empha-size evaluation of factibility and safety in procedure of atrial fibrillation ablation.According to our preliminary experience and the literature data, we believe thatthe minimally ablation procedure will likely play a prominent role as a rapid curefor atrial fibrillation.
P551 Evaluation of gonadic and sexual function in hearttransplantation (HTX) male recipients
E. Serra1, S. Serra2, P. Orru’3, M. Corda3, G. Giardina3, I. Manca3,A. Oppo1, S. Mariotti1, M. Porcu3. 1U.O.C. di Endocrinologia eDiabetologia, Dipartimento di Scienze Mediche Internistiche "M.
Aresu", Cagliari, Italy; 2Servizio di Endocrinologia e Andrologia, Casa diCura Polispecialistica "S’Elena", Cagliari, Italy; 3S.C. di Cardiologia, AziendaOspedaliera "G.Brotzu", Cagliari, Italy
Background: The prevalence and causes of erectile dysfunction (ED) and hy-pogonadism (HG) in HTX male recipients have been rarely investigated. Aim. Toevaluate gonadic and sexual function in a single-center cohort of adult male pa-tients who underwent orthotopic HTX.Methods: The study population includes 52 males, mean age 54±15 yrs (range20-78) who underwent HTX with a mean follow-up of 88±65 months (range 4-220 months). At the time of evaluation all patients were in NYHA class I orII (86.5% and 13.5% respectively), with mean LVEF 58±5% (range 40-65%),treated with long term two- or three-drug immunosuppression protocol. 88.5%were also treated with antihypertensive drugs. Hormonal evaluation included thedosage of luteinic hormone, follicle-stimulating hormone, sexual hormone bindingglobulin and total testosterone. Complete lipid profile was also obtained. Sexualfunction has been assessed by the International Index of Erectile DysfunctionQuestionnaire and psychological status by the Middlesex Hospital Questionnaire.Chi-square and linear regression were utilized for statistical analysis.Results: ED was detected in 71.1% of the whole study population, with a higherprevalence in patients older than 60 yrs (90%). It was not correlated to the dis-tance from HTX. ACE-inhibitors, but not beta-blockers or thiazides, were signifi-cantly associated with ED (p<0.01). Moreover, the prevalence of ED was signif-icantly higher in patients with mood depression (p<0.025). HG was detected in34.6% of the study population, involving 70% of HTX recipients aged between50 and 59. It was significantly associated to the presence of steroids in the im-munosuppression regimen (p<0.025) and to hypertriglyceridemia (p<0.01). Allthe other immunosuppressive drugs, as well as cholesterol profile, presence ofED or mood depression were not related to HG.Conclusions: In long-term HTX male recipients with good functional status andnormal systolic function, the prevalence of ED and HG is consistently higher thanin age-matched general population. ACE-inhibitors and mood depression mayhave a casual role in ED. Steroids, but not calcineurin-inhibitors, azathioprine andmycophenolate could determine HG. As already known in patients without car-diac disease, also in HTX recipients HG shows a strict relation with hypertriglyc-eridemia.
P552 Cardiac donors older than 50 years do not increaseearly or long-term mortality: a single institutionexperience
J. Perez-Lopez1, F. Estevez-Cid1, R. Franco-Gutierrez2 ,M. Mohammad-El Diasty1, E. Barge-Caballero2, R. Marzoa-Rivas2,
M.J. Paniagua-Martin2 , A. Castro-Beiras2, J.J. Cuenca-Castillo1, M.G. Crespo-Leiro2. 1Department of Cardiac Surgery, University Hospital A Coruña, ACoruña, Spain; 2Department of Cardiology, University Hospital A Coruña, ACoruña, Spain
Purpose: Due to the progressive aging of population and improvement in medi-cal and surgical treatment, the prevalence of end stage heart failure will increasein the next years. Heart transplantation is still considered the most effective ther-apeutic alternative in end stage heart failure. The scarcity of heart donors hasled to the recruitment of older donors in spite of the risk of graft coronary arterydisease and higher early post-transplant mortality observed in some studies. Ouraim is to determine the impact of selected donors older than 50 years ("DO≥50")on early and late survival compared to younger donors ("Others") in our hearttransplant program.Methods: We conducted a study of all consecutive patients who underwent hearttransplantation in our center between January 2000 and December 2008, forminga cohort of 256 patients. Donors older than 50 must meet certain criteria to beaccepted: a) no structural pathology or abnormalities of myocardial contractionin the control echocardiography, b) expected ischemic time less than 3 hours, c)no or moderate doses of inotropic drugs. There were no differences between thetwo groups in terms of surgical technique, perioperative management and post-operative control. We analyzed different variables of donor, surgery and recipient,which have been related to early and long-term mortality in the literature.Results: In 65 of the 256 transplants performed (25.4% of cases) the donor wasolder than 50 years old (56.5±4 years, r: 50-73). The "DO≥50" had a greaterpercentage of arterial hypertension (20% vs 10.1%, p=0.05), dyslipidemia (9.2%vs 2.1%, p=0.02), death due to stroke (64.6% vs 38.3%, p=0.001), and donors
who were seropositive for cytomegalovirus (81.5% vs 65.4%, p=0.02). Meanfollow-up was 4.35±3.07 years. Regarding early (30 days) mortality, there wasno statistical difference ("DO≥50" 9.2%, "Others" 11.2%, p=0.82). Mean survivaltime ["DO≥50" 7.1 years (CI 95%: 6.1–8.1), "Others" 7.3 years (CI 95%: 6.7–7.8)], or actuarial survival rates at 1 year ("DO≥50" 81±5%, "Others" 83±3%), 5years ("DO≥50" 69±7%, "Others" 72±4%) or 9 years ("DO≥50" 69±7%, "Others"65±5%) did not differ significantly (p= 0.89) Any significant difference regardingdonor-transmitted coronary atherosclerosis was not observed ("DO≥50" 1.5%,"Others" 1.1%, p=0.59). Finally the most frequent causes of death in both groupswere sepsis and malignant tumors.Conclusions: The use of heart grafts from appropriately selected donors olderthan 50 years does not increased the early or overall post-transplant death rate,and could be a useful strategy to expand the donor pool.
P553 Discordance between morphological and functionalalterations during cardiac allograft rejection: clinicalvalue of myocardial wall motion and deformationimaging
M. Dandel, H.B. Lehmkuhl, D. Kemper, C. Knosalla, M. Pasic,R. Hetzer. German Heart Center Berlin, Berlin, Germany
Purpose: Although the ISHLT (International Society for Heart and Lung Trans-plantation) scoring system is the basis of therapeutic decisions for heart trans-plant acute rejection (AR) it does not always reflect the severity of functional alter-ations during AR. Myocardial wall motion and deformation analysis, easy to per-form by Tissue Doppler (TD) and 2D strain imaging, reveal myocardial dysfunc-tion undetectable by conventional echocardiography. We compared the lesionsdetectable in endomyocardial biopsies (EMBs) with the functional data providedby TD and 2D strain imaging.Methods: Between 1/2006 and 6/2009 all patients underwent left ventricular (LV)wall motion and myocardial deformation analysis by TD and 2D-strain imaging,before each routine or diagnostic EMB. Alterations of TD and 2D-strain parame-ters were tested for relationships to the ISHLT morphologic grade of acute rejec-tion.Results: Of 136 cellular ARs detected in the EMBs of 95 patients, 104 (76.5%)were mild (1 R), 28 (20.6%) moderate (2 R) and 4 (2.9%) severe (3 R). Of allpatients with 1 R rejection, 26 (25.0%) were slightly symptomatic (fatigue etc.)but only 2 showed LV dysfunction detectable by conventional echocardiography.Nevertheless, all 26 symptomatic plus 9 asymptomatic mild ARs (1 R) were ac-companied by reduction with ≥ 15% of peak systolic wall motion velocity (Sm)and global strain rate (circumferential, radial and longitudinal). All Sm and globalstrain rate changes in these patients were reversible after anti-rejection therapy.Among all 79 ARs with reversible TD and/or 2D strain parameter alterations, only55.7% were histolically moderate or severe (2 or 3 R), the other 44.3% were his-tologically mild (1 R). Surprisingly, during symptomatic 1 R rejections, both TDand 2D strain velocity parameter changes were equivalent to those found duringmoderate and severe cellular ARs (2 and 3 R). Of the 35 histologically mild acutecellular rejections (1R) with relevant TD and/or 2D strain parameter alterations,26 (74.3.0%) also showed evidence of different degrees of vascular rejection (in-tensive vascular reactions, colocalization of immunoglobulin and complement inthe microvasculature).Conclusions: TD and 2D strain imaging can reveal functionally relevant ARswhich are underestimated by the ISHLT morphologic grading. The high preva-lence of histologically mild ARs accompanied by myocardial dysfunction and thereversibility of LV dysfunction after therapy suggests the usefulness of TD and 2Dstrain imaging for improvement of therapeutic decisions and for assessments ofthe efficacy of anti-rejection therapies.
P554 Long-term outcome after short-term mechanicalcirculatory support for cardiogenic shock
T. Fux1, J. Van Der Linden2, K.H. Grinnemo2, P. Svenarud2,J. Hultman2, A. Gabrielsen1, L.H. Lund1. 1Karolinska UniversityHospital, Department of Cardiology, Stockholm, Sweden; 2Karolinska
University Hospital, Department of Cardiothorasic Surgery, Stockholm, Sweden
Purpose: Persistent circulatory arrest or refractory acute cardiogenic shock de-spite optimal revascularization and pharmacologic support are associated withessentially 100% mortality. Novel technologies such as magnetically levitatedcentrifugal blood pumps and heparin coated canulas, used as extracorporealmechanical circulatory support (MCS) in extracorporeal membrane oxygenation(ECMO) or ventricular assist device (VAD) configuration, now enable prolongedlife support for days to months. However, indications, complications and long-termresults need to be better understood.Methods: We analyzed 57 consecutive patients with circulatory arrest or refrac-tory critical cardiogenic shock implanted with the Levitronix (R) CentriMag (R)extracorporeal centrifugal pump in ECMO (n=55) or right-sided VAD (n=2) con-figuration. Survival was analyzed by the Kaplan-Meier method and predictors ofsurvival were analyzed by univariate and multivariate Cox regression.Results: Baseline characteristics included age 55±15; 29% women; 32%, 21%and 47% acute coronary syndrome, post-cardiotomy and other, respectively; MAP60±17; CVP 19±9; 25% pre-implant cardiopulmonary resuscitation; 70% multi-organ failure; and 45% and 55% centrally and peripherally inserted, respectively.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

66 Heart transplant and aortic surgery
Mean MCS duration was 11±11 days and patients were followed for 206±349days post implant. Thirty-day and one-year survival were 42% and 30% respec-tively. From MCS, 64% died, 20% were successfully weaned, 12% received ur-gent heart transplantation and 4% received an LVAD. Bleeding requiring transfu-sion occurred in 87%; pneumonia 50%; renal replacement therapy 46%; sepsis34%; cerebral hemorrhage 14%; and thromboembolism 11%. Causes of deathwere 29% multi-organ failure; 20% other; 14% bleeding; 7% stroke; and 30% re-mained alive at end of follow up. Univariate predictors of death were older age,lower GFR, and lower EF and mean arterial blood pressure on MCS. In multivari-ate analysis only age remained a significant predictor.Conclusion: Short-term extracorporeal MCS is associated with numerous com-plications but achieves reasonable short- and long-term survival in a critically illpopulation that otherwise would not survive. Future efforts should be directed atidentifying patients with the most to gain at the lowest risk and cost.
P555 Time-course of cardiac improvement before theremoval of mechanical circulatory support systems inpatients with chronic non-ischemic cardiomyopathywho were weaned from ventricular assist devices
M. Dandel, Y. Weng, A. Stepanenko, T. Krabatsch, E. Potapov,H. Lehmkuhl, T. Drews, C. Knosalla, R. Hetzer. German Heart Center Berlin,Berlin, Germany
Purpose: Weaning from ventricular assist devices (VADs) after unloading pro-moted cardiac improvement is a clinical option with potentially successful resultsfor >15 years. Echocardiographic (ECHO) data obtained during off-pump trialsare paramount for weaning decisions. Previously we showed that several pre-explantation ECHO parameters allow the distinction between patients with andwithout the potential to maintain cardiac stability for >5 years after weaning. Afterrepeated detection of a partial reversibility of unloading-induced cardiac recov-ery already before VAD explantation, in order to improve weaning decisions, weassessed the predictive value of this phenomenon for patients’ post-weaning out-come.Methods: Among 91 patients weaned from VADs since 1995, a homogenousgroup of 46 with non-ischemic CCM was selected for the evaluation of ECHO-data obtained during serial "off-pump" trials before explantation.Results: In the evaluated patients post-weaning 10-year survival reached65.7±7.6%. Of 16 patients who have died to date, only 5 died due to weaningrelated complications or due to HF recurrence. In patients with LV end-diastolicdiameter (LVEDD) ≤ 55mm and LVEF ≥ 45% at the time of VAD removal, pre-explantation stability of LVEF and/or LVEDD (no or less than 10% alteration incomparison to the best of all off-pump values until VAD removal) showed a 94.1%predictive value for cardiac stability during the first 5 post-weaning years. Pre-explantation alterations of LVEF with >10% of best "off-pump" values or a de-crease with >10% of the LV end-diastolic relative wall thickness (RWT) duringthe final off-pump trials in patients with pre-explantation off-pump LVEF of be-tween 45%-50% showed predictive values of 87.5% and 83.3%, respectively forHF recurrence during the first 5 post-weaning years. The stability of LV systolicwall motion peak velocity (Sm) and strain rate (SR) values, after maximum cardiacimprovement, also appeared predictive for the outcome after VAD removal. "Offpump" Sm values ≥ 8 cm/s without >10% reduction until VAD removal showeda predictive of 90% and 87.5% for 3 and 5 year post-weaning cardiac stability,respectively. No Sm reduction of > 10% during "off pump" trials in pts. with "offpump" LVEF ≥ 45% showed similar predictive values for post-weaning cardiacstability.Conclusions: Pre-explantation time-course of LVEF, LVEDD, Sm and SR, as wellas the RWT and Sm changes during the final off-pump trials before VAD removalare predictive for the long-term stability of unloading-induced cardiac recoveryand can improve weaning decisions in patients with non-ischemic CCM.
P556 Clinical efficacy of anti-thymocyte globulin versusbasiliximab as induction therapy for cardiactransplantation in the last decade - are there short-termdifferences among Asians?
A.S. Koh, D.K.L. Sim, L.K. Ka, L.N. Chia, T.E. Tan, C.H. Lim,C. Sivathasan, B.W.K. Kwok. National Heart Centre, Singapore, Singapore
Aim: Conventional induction therapy regimens involve the use of polyclonal anti-lymphocytes like antithymocyte globulin (ATG) in cardiac transplantation as pro-phylaxis against early rejection. Monoclonal antibodies specific to interleukin-2receptors have been developed in more recent times to selectively target acti-vated T-cells in order to avoid the adverse effects of T-lymphocyte depletion. Weaim to evaluate short-term clinical efficacy of either immunosuppressive inductionregimens based on ATG or basiliximab in a large Asian registry.Methods: We prospectively collected data from a single centre of all consecutivepatients who underwent cardiac transplantation from July 1990 to October 2009.Allograft rejection was assessed by endomyocardial biopsy. Clinical efficacy wasassessed by the incidence of acute rejection (ISHLT Grade ≥ 2), death and oc-currence of bacterial, viral or fungal infections requiring antimicrobial treatment,at 3 and 6 months.Results: Out of 47 cardiac transplant patients, 23 patients received ATG while24 patients received basiliximab as induction therapy combined with triple im-
munosuppression. Baseline characteristics of gender and indication for cardiactransplant were similar between the ATG and the basiliximab group (p=ns). Meanfollow-up duration were similar between the ATG and the basiliximab group(5.20±1.86 vs. 5.11±2.03 months, p=0.89). The ATG group had more acute re-jection episodes than the basiliximab group (49 vs. 5, p<0.001) at 3 months anda trend towards higher incidence of rejection at 6 months (11 vs. 5, p=0.07).There was no difference in the number of biopsies performed at 3 months (170vs. 170, p=0.65) and 6 months (68 vs. 73, p=0.87). By 6 months, the occurrenceof death was no different between the ATG and the basiliximab group (21% vs.17%, p=1.00). At 3 months, there were more viral (65.2% vs. 25%, OR 5.63,95%CI 1.59-19.85, p=0.008) infections in the ATG group than in the basiliximabgroup. Both groups received standard prophylactic anti-viral therapy (p=0.21).Conclusion: Basiliximab appears to be superior over ATG in reducing short-termacute rejection and viral infections among Asians. Further studies are warrantedto evaluate the clinical implications of superior short-term results on overall sur-vival benefit.
P557 Electromechanical interference between left ventricularassist devices and implantable cardioverterdefibrillators
S. Goetze, T. Krabatsch, E. Fleck, R. Hetzer, J. Moeller. GermanHeart Center Berlin, Berlin, Germany
The implantation of ventricular assist devices (VAD) is an inestimable therapeuticoption or bridge to cardiac transplantation for patients (pts) with end stage heartfailure. In accordance with the guidelines, more and more of these pts have un-dergone prior implantation of an implantable cardioverter defibrillator (ICD). Anearlier case report demonstrated an adverse interaction between a Heart MateII-VAD and a St Jude Medical ICD (SJM, type Atlas V 193) in a single patient,where telemetry of the ICD was no longer possible after VAD implantation. To un-derstand, whether other ICD and VAD systems are also affected, it was the aimof our study to systematically investigate potential interactions between differentVADs and ICDs from various manufacturers in a major cardiovascular center. Weexamined 264 pts who received VADs within the last 11 years and evaluated 5different VAD-systems: DeBakey I (39 pts), DeBakey II (2 pts), Incor I (165 pts),Dura Heart (15 pts) and Heart Mate II (43 pts). Of these VAD pts, 70 pts carriedICDs, which included all common systems ranging from single and dual cham-ber ICDs to CRT-D. Of these ICDs, 38% (n= 27) were from Medtronic (3 differentmodels), 37% (n=26) were from Boston Scientific/Guidant/CPI (7 different mod-els), 16% (n=11) were from Biotronik (5 different models), and 10% (n=6) werefrom SJM (3 different models). Throughout all pts examined, only one case withan adverse interaction between the VAD (Heart Mate II) and the ICD (SJM, AtlasVR 193) was observed. In this patient, telemetry with the defibrillator program-mer could not be established while the VAD was in operating mode. However,during VAD-pump-stop telemetry with this ICD was re-established revealing reg-ular ICD function in this patient. Yet in all other Heart Mate II pts carrying otherICD types (n=9), no disturbances during telemetry were recorded. Also, telemetrywith the same ICD type (SJM, Atlas VR 193) was not affected in a patient withan Incor I-VAD. These data demonstrate, that only in a minority of ICD- and VAD-systems significant electromechanical interferences occur, which, however haveto be known prior to VAD implantation.
P558 Changes in regulatory miRNA’s during continuous flowLVAD-support in the failing human heart
S. Lok, M.E.I. Schipper, J. Van Kuik, J. Lahpor, P.A.F. Doevendans,R.A. De Weger, N. De Jonge. University Medical Center Utrecht,Utrecht, Netherlands
Introduction: Left ventricular assist devices (LVAD) are commonly used in pa-tients with end-stage heart failure as a bridge to transplantation. Pulsatile volume-displacement devices (P-LVAD) are being substituted by continuous flow devices(C-LVAD). After LVAD-support, the symptoms of heart failure diminish which isparalleled by morphological and physiological changes. Micro-RNA’s (miR’s) playan important role in the intracellular regulation of gene expression.Purpose: The goal of this study was to investigate the expression of selectedmiR’s before and after C-LVAD support and to compare the miR expression withresults obtained from P-LVAD support.
miR expression during C-LVAD support
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart transplant and aortic surgery 67
Methods: Eleven patients with a C-LVAD and 9 patients with a P-LVAD wereincluded in this study. Alle were diagnosed with a DCM. Myocardial tissue wassnap frozen at time of LVAD implantation (pre LVAD) and compared with tissueof the explanted hearts after HTx (post LVAD). Control myocardial tissue wasobtained from 2 donor hearts declined for HTx because of non-cardiac reasons.miR expression was determined by Q-PCR.Results: Expression of miR1, miR133a and miR133b did not differ between pa-tients with a P-LVAD and C-LVAD. These miR’s showed a tendency to decreaseafter LVAD-support, however, this was not significant. The expression of miRlet-7a, miR151 and miR378 tended to increase (although not significant) after C-LVAD-support. This increase in miR expression was more pronounced in the pa-tients with a previous myocarditis.Conclusion: During LVAD treatment, there are no significant changes in the se-lected miR expression in all DCM patients with a C-LVAD. However, miR’s clearlyshow changes in individual patients, that may indicate that these miR’s may beused as hallmarks for myocardial changes.
P559 Evaluation of left ventricular function by tissue Dopplerand 2D strain imaging can facilitate the decision towean patients with unloading-induced cardiacrecovery from mechanical assist devices
M. Dandel, H.B. Lehmkuhl, A. Stepanenko, T. Krabatsch, E. Potapov,Y. Weng, C. Knosalla, R. Hetzer. German Heart Center Berlin, Berlin, Germany
Purpose: Echocardiographic monitoring of cardiac size and function during "off-pump" trials is useful for detection of myocardial recovery during mechanical un-loading. Previously we showed that in patients with idiopathic dilated cardiomy-opathy as the underlying cause of LVAD implantation, parameters such as leftventricular (LV) diameters and ejection fraction (EF) can predict the outcome af-ter LV assist device (LVAD) removal without transplantation (Tx). However, highinter-observer variability and load dependency of EF measurements are limita-tions. Because parameters measurable by tissue Doppler (TD) and 2D strainimaging are more reliable for estimation of LV systolic function, we assessed theirusefulness for evaluation of LVAD-promoted cardiac recovery.Methods: TD data collection was started in 1999. Pulsed-wave TD (PW-TD)measurements of systolic wall motion peak velocities (Sm) at the basal poste-rior wall were performed during "off-pump" trials before LVAD removal and duringthe follow-up. Since 2005, also strain and strain rate (SR) measurements (radial,circumferential, longitudinal) were performed. Weaning decisions were made in-dependently of PW-TD velocity and 2D strain data.Results: Heart failure recurred after LVAD removal in 9 (25.7%) of 35 patientswith non-ischemic chronic cardiomyopathy (CCM) as the underlying cause ofLVAD implantation who underwent PW-TD monitoring before and after LVAD re-moval. Longitudinal and radial Sm was lower in these 9 patients than in thosewith post-weaning cardiac stability (p < 0.01) Stable patients showed Sm > 8cm/s. Off-pump Sm ≥ 8cm/s showed predictive values of between 87 and 90%for 5 year post-weaning stability. Strain and SR measurements performed in 23patients with non-ischemic CCM as the underlying cause of LVAD implantationrevealed higher systolic values in post-weaning stable patients (p < 0.01). In pa-tients with cardiac stability global systolic strain and SR values were: ≥ 30% and≥ 0.95/s for radial thickening, ≥ 15% and ≥ 0.8/s for circumferential shorten-ing, ≥ 12% and ≥ 0.65/s for longitudinal shortening, respectively. Sm, strain andSR instability before and early after LVAD removal appeared predictive for post-weaning HF recurrence.Conclusion: TD and 2D strain imaging, which are easy to perform and not timeconsuming, are useful for evaluation of unloading-induced cardiac recovery andhelpful for prognostic assessment before and early after LVAD removal. Evalu-ation of ventricular function by PW-TD and 2D Strain imaging can facilitate thedecision to wean patients from mechanical assist devices and remove them fromTx-lists.
P560 Extended donor criteria in heart transplantation withpharmacological stress echocardiography
T. Bombardini1, S. Gherardi2, G. Arpesella3, M. Maccherini4,W. Serra5, E. Pasanisi6, R. Del Bene7, E. Picano6. 1Institute ofClinical Physiology of CNR, Pisa, Italy; 2Cardiology Division, Bufalini
Hospital, Cesena, Italy; 3Dept of Surgery and Transplants, University of Bologna,Bologna, Italy; 4Dept of Surgery and Transplants, Siena, Italy; 5CardiologyDivision, Parma, Italy; 6Fondazione G Monasterio, Pisa, Italy; 7Careggi Hospital,Florence, Italy
Objectives: The aim of this study is to establish the feasibility of an approachbased on pharmacological stress echocardiography as a gatekeeper for extendedheart donor criteria.Background: Because of the shortage of donor hearts, the criteria for accep-tance have been considerably expanded. An abnormal result at pharmacologicalstress echocardiography is associated with significant coronary artery diseaseand/or occult cardiomyopathy at cardio-autoptic verification.Methods: From April 2005 to January 2010, 36 "marginal" candidate donors (age57±5 years, 19 male) were initially enrolled. After legal declaration of brain death,marginal donors underwent rest and, if normal, dipyridamole (0.84 mg/kg in 6’, n= 23) or dobutamine (up to 40 mcg/kg, n=3) stress echocardiography.
Results: We found 16 eligible hearts with normal findings. Of these, 3 were nottransplanted due to lack of a matching recipient, and autoptic verification showedabsence of significant coronary artery disease or cardiomyopathy abnormalities.The remaining 13 eligible hearts were uneventfully transplanted in marginal emer-gency recipients. All showed normal (n = 10) or nearly-normal (minor single- ves-sel disease, in 3) angiographic, intravascular ultrasound, hemodynamic and ven-tricolographic findings at 1 month. At follow-up (median 10, interquartile ranges7-34 months), 11 patients survived and 2 had died, one at 2 months from gen-eral sepsis and one at 32 months from allograft vasculopathy in recurrent multiplemyeloma.
Conclusions: Pharmacological stress echocardiography can safely be per-formed in candidate heart donors with brain death, and shows potential for ex-tending donor criteria in heart transplantation.
P561 Long-term outcomes of heart transplantation in olderrecipients
C.M. Tavares Aguiar, M.J. Rebocho, M. Abecasis, J.P. Neves, J. Melo.Hospital Santa Cruz, Carnaxide, Portugal
Background: Heart transplantation (HTx), the best option for the man-agement of advanced heart failure in selected patients, is increasingly performedin the elderly. We evaluated HTx outcomes with the hypothesis that older recipi-ents may be at higher risk of mortality and major complications.Methods: We analyzed 179 patients, aged 49±11 years (35 female), who un-derwent HTx in an adult age, at a single institution. The study population wasdichotomized according to whether HTx was performed before or after the 1st ofJanuary 2000. Patients transplanted at an age ≥60 years were considered olderrecipients, and were compared to younger recipients with respect to survival.Results: HTx was performed at an age ≥60 years on 31 recipients. The propor-tion of older recipients increased from 13.1% among the 99 patients transplantedbefore the year 2000, to 22.5% among the 80 transplanted thereafter. The olderrecipients’ ages averaged 63.6±3.2 years (maximum 72.5 years). Older recipi-ents more often were male, had ischemic cardiomyopathy as the underlying dis-ease, and were transplanted in a status of hemodynamic instability (on intra-aorticballoonpump). Overall, 110 patients died during follow-up. Patients who under-went HTx before the year 2000 showed significantly lower survival rates at 1-yearand 5-years after HTx (respectively 70.6% and 46.5% versus 76.0% and 71.6%for patients transplanted since 2000; interaction test P=0.009). Recipient age didnot influence these survival rates in patients transplanted before the year 2000.In contrast, for patients transplanted in the year 2000 or later, survival was signif-icantly lower among the older recipients (multivariable adjusted hazard ratio fordeath = 4.26; 95% CI, 1.20-15.16; P=0.025). Older recipients transplanted in theyear 2000 or later more often developed cancer during follow-up; the incidencesof allograft vasculopathy and end-stage renal disease were not affected by recip-ient age at the time of HTx.Conclusions: Long-term outcomes of HTx have improved significantly in the re-cent years, but not for older recipients. High-risk features prior to HTx and a higherincidence of malignancy may impair survival after HTx in older recipients. Tech-nological improvements in ventricular assist devices and other alternatives maybecome particularly relevant for older patients with end-stage heart failure.
P562 Coronary flow velocity pattern by transthoracicechocardiography: a new noninvasive diagnostic andprognostic marker of cardiac allograft vasculopathy
E. Osto, G. Famoso, A. Gambino, G. Tarantini, C. Sarais, G. Feltrin,S. Pontarollo, G. Gerosa, S. Iliceto, F. Tona. University of Padova,
Padova, Italy
Background: Cardiac allograft vasculopathy (CAV) is the main limiting factor inlong-term heart transplant (HT) recipients. We studied the potential role of coro-nary flow velocity pattern by transthoracic echocardiography as diagnostic andprognostic marker in CAV.Methods: Diastolic peak velocity (DPV) and deceleration time of diastolic flowvelocity (DDT) were measured in the left anterior descending coronary artery bytransthoracic echocardiography in 78 HT recipients (65 male, aged 50±12 yearsat HT, at 8.1±4.3 years after HT). DPV and DDT were measured blindly fromangiograms. CAV was defined as any angiographic lesion and significant CAVas a stenosis ≥50%. Follow up was 18±5 months. Combined endpoints werecardiac death, stent implantation and heart failure.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

68 Heart transplant and aortic surgery / Valve and coronary surgery
Results: CAV was diagnosed in 32 patients (pts) (41%) (group A) while 46 ptshad normal coronary angiograms (group B). DPV and DDT were 27±9 cm/s and912±209 ms, respectively. DPV was higher in group A (31±11 vs 25±6 cm/s,p=0.01) and DDT was shorter in group A (822±230 vs 975±170 ms, p=0.001). ADDT cutpoint ≤922 ms, identified by ROC curve analysis (AUC 0.715, p=0.001),was 69% specific and 72% sensitive for detecting CAV, with positive (PPV) andnegative predictive value (NPV) of 62% and 78% respectively (accuracy 70%)(p<0.0001). For significant CAV, DDT ≤922 ms (AUC 0.654, p=0.03) was 61%specific and 68% sensitive with PPV and NPV of 40% and 83% respectively(accuracy 63%) (p=0.02). At multiple logistic regression analysis, independentpredictor of CAV was DDT ≤922 ms (OR 5.8, p=0.001) and of significant CAVDPV >28 cm/s and DDT ≤922 ms (OR 3.1, p=0.03 and OR 3.6, p=0.02, respec-tively). Pts with events had higher CAV prevalence (p=0.002) and shorter DDT(p=0.006). A DDT cutpoint ≤840 ms (AUC 0.797, p=0.01), was 74% specific and86% sensitive for predicting events, with PPV and NPV of 31% and 97%, re-specively (p=0.002). Pts with DDT ≤840 ms had a lower servival free from events(p=0.01).Conclusions: Noninvasive assessment by transthoracic echocardiography re-veals that a shorter DDT is associated with angiographically detectable CAV. ADDT cutoff ≤922 ms proved accurate to rule out the presence of CAV and is anindependent predictor of CAV. Moreover DDT is a reliable surrogate marker forsubsequent events.
P563 Microvasculopathy preceeds and predicts epicardialangiographic cardiac allograft vasculopathy in hearttransplant patients
E. Osto, G. Famoso, G. Gambino, G. Tarantini, C. Sarais, G. Feltrin,S. Pontarollo, G. Gerosa, S. Iliceto, F. Tona. University of Padova,
Padova, Italy
Background: Cardiac allograft vasculopathy (CAV) affects both epicardial coro-nary vessels and microvasculature. We assessed either the presence or the riskof CAV and severe microvascular dysfunction in relationship with time from hearttransplantation (HT) and the validity of coronary flow reserve (CFR) as a predictorof CAV onset.Methods: CFR was assessed in the left anterior descending coronary artery bytransthoracic echocardiography in 120 HT pts (97 male, aged 50±12 years atHT), at 9±6 years post-HT. CAV was defined as any angiographic lesion ≥10%.Microvascular dysfunction was defined as CFR <2.5. The relationship betweentime from HT and CAV or microvascular dysfunction was evaluated by logisticregression. To evaluate CAV new onset, coronary angiography was repeated after3.6±1.2 years.Results: CAV was diagnosed in 75 pts (62%) (group A), 45 (38%) had no CAV(group B). Group A had lower CFR than group B (2.2±0.6 vs 3.1±0.7, p<0.0001).At 5, 10 and 15 years from HT the probability of CFR<2.5 resulted higher thanCAV probability (p<0.0001 for all comparisons) (Figure). In addition, a close cor-relation was observed between the presence of CAV and the evidence of CFR<
2.5 (χ2=21, OR 6.4, p <0.0001). CFR was lower in pts with CAV onset (3.4±0.5vs 2.6±0.8, p=0.002). A CFR<2.5 was 100% specific and 60% sensitive for pre-dicting CAV onset, (PPV= 100%, NPV=61%) (p<0.0001). Pts with CFR<2.5 hada lower survival free from CAV onset (38% vs 100%, p<0.0001) (Figure). ByCox regression a CFR<2.5 predicted CAV onset (HR 6.3, 95% CI 2.5–15.6,p<0.0001).
Conclusions: In HT patients the risk of CAV and microvascular dysfunction in-creases with time from HT. The risk of severe microvascular dysfunction is higherthan that of CAV. Finally, lower CFR is a reliable predictor of CAV onset.
P564 Efficacy and safety of a prothrombin complexconcentrate in patients with oral anticoagulation whoundergo Heart transplantation
R. Franco Gutierrez, M. Crespo Leiro, G. Aldama Lopez,M.J. Paniagua Martin, J.A. Rodriguez Fernandez, R. Campo Perez,
R. Marzoa Rivas, E. Barge Caballero, J.J. Cuenca Castillo, A. Castro Beiras.Complejo Hospitalario Universitario A Coruña, La Coruña, Spain
Purpose: Many patients with terminal heart failure receive oral anticoagulation.The reversal of the anticoagulant effect in patients undergoing cardiac transplan-
tation is traditionally performed with fresh frozen plasma, but this method hasseveral limitations. The use of prothrombin complex concentrate (PCC) could bea solution. The purpose of this study is to evaluate the efficacy and safety of pro-thrombin complex concentrate in patients with oral anticoagulation undergoingheart transplantation.Methods: A prospective study of anticoagulated patients undergoing cardiactransplantation whose effect was reversed with PCC (n = 39) prior to surgery com-pared with a historic cohort reversed with fresh frozen plasma (n = 62). The fol-lowing variables were measured: peri- and postoperative bleeding, redo surgery,mortality at ICU, mortality at one-month and mortality at one year, combined endpoint of death due to hypovolemic shock, redo surgery due to bleeding or trans-fusion, combined end point of redo surgery due to bleeding or transfusion.Results: The percentage of patients in the group receiving fresh frozen plasmatransfusions, transfusion of concentrated red cells, platelets and fresh frozenplasma was 84, 79, 47 and 58% versus 71, 64, 53 y 54% of the PCC group(p = 0.138), (p = 0.154), (p = 0.676), (p = 0.834) respectively. 14 patients werere-operated, 21% (13/62) of the fresh frozen plasma group compared to 2.6%(1/39) of the PCC group. There were no differences in mortality in the ICU, at onemonth and a year. In a multivariate analysis the prothrombin complex concentratewas protective for reinterventions OR 0.0833 (CI 0.0084 - 0.826) p = 0.034. Therewere two skin reactions related to fresh frozen plasma, and none with PCC. Therewas no statistical difference in the combined end points between the two groups.Conclusions: In our experience the administration of PCC for reversal of theanticoagulant effect in patients undergoing cardiac transplantation is safe andappears to be beneficial in terms of reduction in reinterventions; however, therewere no statistical differences in the amount of haem derivative transfusions andin the combined end points.
VALVE AND CORONARY SURGERY
P565 Incidence of deep vein thrombosis after coronaryartery bypass graft surgery
S.K. Hosseini, M. Salarifar, A. Karimi, S.H. Shirani, M. Shirzad,N. Ghafari Marandi. Tehran University of Medical Sciences,Department of Cardiology, Tehran, Iran (Islamic Republic of)
Purpose: We sought to investigate the incidence of deep vein thrombosis (DVT)among patients who have undergone coronary artery bypass grafting (CABG),given the paucity of related data in the literature.Methods: A total of 800 post-CABG patients were registered and examined vialower limb venous ultrasound before discharge from hospital on post-operativedays 6 and 7. Post-operative follow-up was performed through telephone contactsabout 1months after CABG.Results: DVT was detected in 179 (22.4%) patients. Proximal DVT and isolatedcalf DVT rates were 0.5% and 21.6%, respectively. Pulmonary emboli and deathafter hospital discharge occured in 3 patients. The number of clots located in theipsilateral leg to the harvest site was more than that found in the contralateral leg.The predictive risk factors for DVT were age, body mass index, and smoking.Conclusion: The rate of asymptomatic DVT in our post-CABG patients was con-siderable. The results raise the question of should all post-CABG patients be ex-amined by venous ultrasound or should they be prescribed anticoagulants sincethe latter is more cost-effective? Clinical trials comparing these protocols shouldbe conducted.
P566 Epidemiology and new predictors of low cardiac outputsyndrome after isolated coronary artery bypassgrafting
J.M. Arribas Leal, D.A. Pascual, P.L. Tornel, F. Gutierrez, J.J. Garcia-Puente, A. Jimenez, F. Marin, J.A. Ruiperez, R. Arcas, M. Valdes.
University Hospital Virgen De La Arrixaca, Murcia, Spain
Background: Low cardiac output syndrome (LCOS) remains a common compli-cation of CABG. We aimed to study the epidemiology and preoperative predictorsof LCOS in patients undergoing isolated CABG, and to evaluate the role of NT-proBNP levels in LCOS after CABG.Methods: Prospective study of 203 consecutive patients (64±9 years, 74%male), who underwent programmed CABG. NT-proBNP levels were measuredin a blinded fashion. LCOS was defined as the need of postoperative intra-aorticballoon pump (IABP) or inotropic support for more than 30 minutes in the inten-sive care unit (ICU). Operative death and acute myocardial infarction (AMI) wereregistered.Results: A total of 84 (41%) patients had LCOS in the ICU; 77 (38%) neededinotropic support and 29 (14%) needed IABP. Five patients died (2. 5%) and 27suffered AMI (13%); the composite endpoint of death/AMI occurred in 28 patients(14%). Pre-operative NT-proBNP levels did not differ in patients with LCOS vs.patients without LCOS [248 (128-982)] vs. 239 (107-558)] (p = 0.342). Indepen-dent predictors of LCOS were preoperative heart failure (OR: 6.9; CI 95% (1.5-31.25), p = 0.012), recent acute coronary syndrome (ACS) (OR: 11.76; CI 95%(2.36-58.8), p = 0.003) and length of preoperative QRS interval (OR: 1.034; CI95% (1.003-1.066), p = 0.031). NT-proBNP levels did not differ in patients withdeath/AMI vs patients without [292 (165-2450) vs. 241 (103-686)] (p = 0.301)],
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Valve and coronary surgery 69
whereas LCOS was associated with a higher rate of death/AMI (25% vs 6%, p< 0.001). We identified as independent predictors of death/AMI: LCOS (OR: 5.6;CI 95% (2.2-14.5), p<0.001) and lack of statin pre-treatment (OR: 3.8; CI 95%(1.5-9.2), p = 0.003).Conclusions: LCOS was a frequent event after CABG, associated with highermortality and morbidity. LCOS was predicted by QRS length, previous heart fail-ure and recent ACS. Pre-operative NT-prBNP concentration was not predictive ofLCOS.
P567 Optimal timing for surgical myocardialrevascularisation early after acute myocardialinfarction
S. Kacar, M. Stanic, M. Golubovic, V. Torbica, N. Cemerlic-Adjic,K. Pavlovic, S. Nicin, B. Mihajlovic. Institute of CardiovascularDiseases of Vojvodina, Sremska Kamenica, Serbia
Purpose: Until recently, acute myocardial infarction (AMI) was considered asacontraindication to surgical myocardial revascularisation. Nowdays, manyreportssuggest it is necessary to operate some patients in the early periodfrom the be-ginning of AMI with anacceptable risk. The aim of the study: to detect an optimaltiming for coronarysurgery, early after AMI.Methods: From January 2007 to April 2009, 63 pts. with AMI underwent isolated-surgical myocardial revascularisation at our clinic. Eleven patients (17%) werefe-male and 32 pts. (51%) were older than 65 years. ST elevation myocardialinfarc-tion (STEMI) was present in 43%pts. (27/63) while NSTEMI was present in 57%pts. (36/63). A significantleft main aretry stenosis was registered in 35 pts. (56%).Patients weredivided in 5 groups (I-V), according tothe time period from the be-ginning of AMI to operation: I - less than 12 hours (20pts.); II – 12 to 24 hours (9pts.); III – 2 to 7 days (12 pts.); IV – 8 to 15days (10 pts.); V - 15 to 30 days (12pts).Results: The mean number of revascularized coronary arteries was 3.4 (2-7).Thethirthy day postopterative mortality, for the whole group was 1.6%. The post-operative mortality after 3 monthswas 4.8% (3/63) for all 63 patients. Threemonths after surgery the mortality rate according to groups was asfollows: I-0;II – 11.1%; III- 16.7%; IVand V -0.Conclusion: According to our experience AMI is not a contraindication to my-ocardialrevascularisation. On the contrary, it is necessary to operate unstable pa-tientsas early as possible, during the first 12 hours from AIM. In the period from2to 8 days after AMI the risk of surgery is the highest. After that period,accordingto our experience, the risk is similar to the risk in electivecoronary surgery.
P568 Chronic kidney disease is a risk predictor forsymptomatic late saphenous vein graft occlusion inacute coronary syndrome but not in stable coronaryartery disease
P. Rostoff1, J. Nessler1, A. Gackowski1, G. Gajos1, P. Latacz1,B. Nessler1, J. Sadowski2, W. Piwowarska1. 1Dept. of Coronary
Disease CM UJ, Krakow, Poland; 2Dept. of Cardiovascular Surgery andTransplantology CM UJ, Krakow, Poland
There is strong evidence that patients with chronic kidney disease (CKD) consti-tute a high-risk population for cardiovascular morbidity and mortality. The impor-tance of CKD as a risk predictor for symptomatic late saphenous vein graft (SVG)occlusion in post-CABG patients remains unclear.The aim of this study was to evaluate the prevalence and impact of CKD on therisk of symptomatic late SVG occlusion in post-CABG patients.Methods: 124 consecutive post-CABG pts (78 M, aged 43-77 yrs, mean age61.9±7.9 yrs), were enrolled based on the following inclusion criteria: (a) recur-rence of angina, at least 1 year after CABG, confirmed by non-invasive testing;(b) no significant angiographic progression of atherosclerosis (<30% stenosis in-crease) in non-bypassed coronary arteries. ACS was diagnosed in 63 (50.8%)pts. Both, ACS and non-ACS groups had the same number of implanted SVGs(2.3/pt).Results: CKD was found in 104 (83.9%) pts, and was not more frequent in ACSpts, as compared to non-ACS pts (87.3% vs 80.3%; p=NS). Univariate analysisshowed a significant association between moderate to severe CKD (GFR <60mL/min/1.73m2) and late SVG occlusion in ACS population (OR 2.59; 95% CI1.33–5.27). No significant relationship was found between CKD and late SVGocclusion in patients with stable coronary artery disease. Multivariate analysisrevealed five independent predictors of symptomatic late SVG occlusion in ACSpopulation: current smoking (OR 4.01; 95% CI 1.42–11.38), female gender (OR3.19; 95% CI 1.64–6.53), body mass index >30 kg/m2 (OR 2.75; 95% CI 1.92–8.14), plasma fibrinogen >3.5 g/L (OR 2.15; 95% CI 1.01–4.65), and time afterCABG (OR 1.11; 95% CI 1.01–1.23).Conclusions: 1. Moderate to severe chronic kidney disease is a significant, butnot independent predictor of late saphenous vein graft occlusion in post-CABGpatients with acute coronary syndrome. 2. No significant association is appar-ent between chronic kidney disease and symptomatic late saphenous vein graftocclusion in stable coronary artery disease.
P569 Does EuroSCORE overestimate risk in coronarysurgery?
B. Mihajlovic, S. Nicin, N. Cemerlic-Adjic, K. Pavlovic, M. Golubovic,J. Dejanovic, L. Velicki, M. Fabri. Institute of Cardiovascular Diseasesof Vojvodina, Sremska Kamenica, Serbia
Purpose: The European System for Cardiac Operative riskEvaluation (Eu-roSCORE) was developed in order to predict operative risk in cardiac surgeryand to assess the quality of the cardio-surgical care. The aim of the study: toevaluate our results in isolated coronary surgery using the additive EuroSCOREmodel.Methods: The data were collected prospectively andanalyzed retrospectively, bycomparing the predicted operative risk according to the additive EuroSCOREmodel and observed 30 days postoperative mortality in 4,675 consecutive, iso-lated coronary, patients operated on during the last 8 years (2001-2008) at ourClinic. For statistical analyses the Pearson, Chi-square and ANOVA tests wereused.Results: The total postoperative mortality, predictedby the EuroSCORE was2.9±2.25 while the observed one was 2.2% (p=0.554). When the predicted andobserved results were compared over the years, from 2001 to 2008, a consider-ably lower observed mortality was found during the last 4 years (2.1% vs. 3.01%;2.1% vs. 3.06%;1.3% vs. 2.96%; and 1.5% vs. 2.92% in 2005,2006,2007 and2008 respectively).Conclusion: During the last years theresults in isolated coronary surgery haveconsiderably improved. The EuroSCORE overestimates operative risk in coronarysurgery. In order to improve itspredictive value, the model should be recalibrated.
P570 Acute kidney injury after cardiac surgery: report fromthe battlefield
L.S. De Santo1, G.P. Romano2, A. Della Corte3, G.A. Nappi3,C. Bancone3 , F. Grimaldi3, M. De Feo3. 1University of Foggia, Foggia,Italy; 2Dept. Cardiovascular Surgery and Transplant V Monaldi
Hospital, Naples, Italy; 3Second University of Naples, Naples, Italy
Purpose: Acute kidney injury (AKI) after cardiac surgery is highly prevalent andprognostically important. Lacking effective therapies, risk factor modification mayoffer a means of preventing this complication. The aim of the present study wasto identify and determine the prognostic importance of such risk factors.Methods: Data from a single center prospective cohort of 2568 adult patients(mean age 62.4±11.6, 34.7% female, 18.2% urgent/emergent, 40.2% CABG,35.8% Valvular, 16.8% combined, 5,1% complex, 7.1% redo) who underwent car-diac surgery between January 2004 and December 2007 were analyzed (usingmultivariable logistic regression modeling) to determine the independent relation-ships between 3 thresholds of AKI (>25%, >50%, and >75% decrease in esti-mated glomerular filtration rate within 1 week of surgery or need for postoperativedialysis according to RIFLE criteria) with death rates, as well as to identify riskfactors for AKI.Results: The 3 thresholds of AKI occurred in 33.5% (n=859), 6,2% (n=159),and 1,1% (n=29) of the cohort, respectively and were independently associatedeach with a significant increase in the risk of death. AKI was predicted by severalperioperative variables, including age, diabetes, hepatic disorders, pre-operativeuse of warfarin, redo procedure, blood loss and transfusion, perioperative intra-aortic balloon pump use and prolonged cardiopulmonary bypass. Protective effectwas exerted by use of de-leukocitated blood product (OR 0,70; 95%IC 0,51-0.95;p=0,022).Conclusions: Even lesser degrees of AKI implied an increased risk of death.Aetiology is multifactorial and attempts to risk factors modification appear complexand marginal.
P571 Effect of blood transfusion practice in cardiac surgeryon in-hospital mortality: clinical evidences from a42-month single centre experience
L.S. De Santo1, G.P. Romano2, A. Della Corte3, G.A. Nappi3,C. Bancone3 , F. Grimaldi3, N. Galdieri2, M. De Feo3. 1University of
Foggia, Foggia, Italy; 2Dept. Cardiovascular Surgery and Transplant V MonaldiHospital, Naples, Italy; 3Second University of Naples, Naples, Italy
Purpose: This study aimed to identify a high-risk profile associated with in-creased perioperative blood consumption and the effect of transfusion practiceon hospital mortality.Methods: This single centre prospective study investigated 3042 consecutive pa-tients undergoing cardiac surgery procedures between January 2004 and June2007, collecting 100 variables per patient. 2828 patients, who underwent on pumpprocedures, were stratified by propensity-score analysis according to the highestrisk of being transfused. Data from patients in the two highest quintiles of riskwere then pooled to evaluate the effects of transfusion on in-hospital mortality(1131 patients) by multivariate classification tree analysis.Results: Twelve variables stand out as determinants of transfusion risk: age,BSA, diabetes, preoperative creatinine clearance, preoperative anaemia, surgi-cal priority, lowest haemoglobin concentration during ECC, ECC length, 24-hrblood loss volume, resternotomy for bleeding, low cardiac output syndrome andacute kidney injury. As disclosed by the classification model, transfusion of >6
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

70 Valve and coronary surgery
blood units independently predicts in-hospital mortality (4.5% vs 35.1% p<0.001).Acute kidney injury significantly increases this relative risk (23.6% vs 62.2%p<0.001). Mortality in patients receiving <6 blood units is determined by cardiaccomplications, non cardiac morbidity and on-pump oxygen delivery (p<0.001 inall comparisons).Conclusions: Extent and appropriateness of transfusion practice strongly relayon patient profile. The impact of massive blood usage on mortality may be the re-flection of both severity and/or duration of illness and the invasiveness of the peri-operative process of care more than a direct transfusion drawback. Intraoperativefactors and major perioperative complications exert, as expected, an independentrole on outcomes.
P572 Peri-operative assessment of left ventricle bythree-dimensional echocardiography: feasibility andreproducibility
A. Meris, L. Santambrogio, R. Mauri, A. Engeler, G. Casso, T. Cassina.Foundation "Cardiocentro Ticino", Lugano, Switzerland
Purpose: Bi-dimensional trans-oesophageal echocardiography (2D TEE) ispart of the standard monitoring tools during cardiac surgery. Currently, three-dimensional echocardiography (3D echo) is becoming a new promising techniquefor assessing left ventricular (LV) volumes and function. Its routinely applicationin peri-operative settings has still not been systematically evaluated. The aim ofthis study is to assess feasibility, reproducibility and the time consumption for 3Decho during cardiac surgery.Methods: 72 consecutive patients scheduled for elective cardiac surgery under-went peri-operative TEE using an iE33 ultrasound machine equipped with a 3Dmatrix array transducer. TEE images of the LV were acquired before sternotomyand after sternal closure. 2D LV images were recorded at mid-oesophageal levelin 3 different views (four-, two-chamber and long-axis) and the ejection fraction(EF) was calculated online by biplane Simpson’s method. 3D full volume imageswere acquired over seven cardiac cycles. 3D LV volumes and EF were analysedby semi-automatic border detection (Q-lab 3D-Advanced quantification software).LV end-diastolic volume (EDV), end-systolic volume (ESV) and EF evaluated withboth methods, were compared with a t-test and Pearson’s correlation. The timeneeded for 3D and 2D images acquirement were compared as well. In 20 patientsrandomly selected 3D measurements were repeated to test the intra-observer re-producibility by Bland-Altman’s method.Results: 51 patients (71%) underwent coronary artery bypass graft, 11 (15%)valvular or aortic root surgery and 10 (14%) combined surgery. The 3D acquisi-tion time was shorter compared to the 2D (131±39 sec to 151±25 sec, p<0.05).LV volumes analysed by 3D and 2D echo showed a good correlation (r = 0.94for EDV, r = 0.90 for ESV), but volumes measured with 3D echo were slightlyhigher than those obtained from 2D echo (EDV: 91±30 to 84±29 ml, p < 0.05;ESV: 41±22 to 38±22, p=0.11). The limits of agreement for intra-observer repro-ducibility were -3.5 to 5.6 ml for EDV, -3.1 to 3.8 ml for ESV and -2.7 to 3.3% forEF.Conclusions: This study demonstrated that routinely a LV assessment by intra-operative 3D echo is feasible, not time-consuming and with a good reproducibility.The 3D echo seems to be superior to the 2D echo as it provides more LV informa-tion by desired cut-plane from the 3D full-volume data-set. Therefore, employmentof 3D echo during cardiac surgery should be implemented.
P573 The effect of high-dose atorvastatin on a backgroundof standard-dose chronic statin therapy in patientsundergoing cardiac surgery
A.J. Ludman1, D.J. Hausenloy1 , V. Venugopal1 , G. Babu1, E. Boston-Griffiths1, D. Lawrence2, J. Yap2, M. Hayward2, G. Bognolo2,
D.M. Yellon1. 1University College London, London, United Kingdom; 2The HeartHospital, London, United Kingdom
Purpose: The acute administration of atorvastatin reduces myocardial infarct sizein animal studies. Interestingly, this effect is lost with chronic atorvastatin therapy,although it can be recaptured if a high-dose of atorvastatin is given acutely. Wehypothesised that high-dose atorvastatin treatment on a background of chronicstandard-dose statin therapy would reduce myocardial injury during coronaryartery bypass graft (CABG) surgery.Methods: 98 consenting patients undergoing elective CABG surgery were re-cruited as follows: (1) 45 patients were randomised to receive either 160mgof atorvastatin two hours pre-operatively and a further dose 24 hours followingsurgery or their standard ‘statin’ therapy. (2) 53 patients were randomised to re-ceive either 160mg atorvastatin 12 hours pre-operatively and a further dose 24hours following surgery or their standard ‘statin’ therapy. The cardiac surgeonwas blinded to the treatment allocation. Blood samples for Troponin-T were takenprior to surgery and at 6, 12, 24, 48 and 72 hours post-operatively. Serum creatinekinase, renal function and liver enzymes were also monitored.Results: There were no significant differences between treatment groups withrespect to patient characteristics. Specifically, there was no difference in meanEuroScore ((1) Atorva 2.9±2.7, Control 2.8±1.7; (2) Atorva 1.9±1.9, Control2.2±1.7), cross-clamp time ((1) Atorva 48±25 mins, Control 45±16 mins; (2)Atorva 49±21 mins, Control 49±15 mins) or bypass time ((1) Atorva 84±39mins, Control 80±23 mins; (2) Atorva 80±23 mins, Control 83±23 mins). High-
dose atorvastatin therapy was safe with no reported side-effects. There wereno significant differences in either serum Troponin-T at each time point or totalTroponin release over 72 hours, calculated as the Area Under the Curve (Twohours pre-treatment: Atorva 29.6±34.8 μg/L versus Control 25.0±22.0 μg/L.Twelve hours pre-treatment: Atorva 21.8±14.3 μg/L versus Control 21±8.7 μg/L;P>0.05).Conclusions: We report that the administration of high-dose atorvastatin therapyon a background of standard-dose chronic therapy did not reduce peri-operativemyocardial injury in patients undergoing elective CABG surgery. We speculatethat the failure to observe any beneficial effects with high-dose atorvastatin ther-apy was due to the fact that low-risk patients were selected with relatively shortcross-clamp and bypass times, in whom peri-operative myocardial injury is min-imal. Further studies are required to determine the effect of this treatment inter-vention in high-risk patients undergoing CABG±valve surgery with longer cross-clamp and bypass times.
P574 Coronary artery bypass graft surgery in acutemyocardial infarction: preoperative predictors of acuteand one-year mortality
R. Cale, S. Leal, L. Raposo, M.J. Rebocho, M. Abecasis, J. Neves,M. Ferreira, J. Calquinha, J. Aniceto Silva, J. Queiros E Melo. Hospital
de Santa Cruz, Lisbon, Portugal
Purpose: Coronary artery bypass graft surgery (CABG) in the acute phase ofmyocardial infarction (MI) is associated with high operative mortality. The aim ofour study is to assess preoperative predictors of 30 days and one year mortalityin patients undergoing CABG after acute and sub-acute phase of MI.Methods: restrospective analysis of 110 consecutive patients from a single cen-tre (mean age 66±11 years, 30 females, 38% diabetes) who underwent isolatedCABG after MI between January 2007 and December 2007 (43 Q-wave MI). Pre-dictors factors for death at 30-days and 1-year follow-up were assessed by multi-variate analysis, adjusted for baseline characteristics and Euro risk score.Results: Over an average follow-up of 725±341 days, 16 (14,5%) patients died,9 (8,2%) were due to cardiovascular cause. Thirty days and one year mortalitywas 3,8% and 9,2%, respectively. Mean time interval between MI and CABG was25±30 days. Euro risk score, age, glomerular filtration rate (GFR, estimated byCockcroft-Gault equation), anaemia and multivessel disease were identified aspredictors of death at 1-year. On multivariate analysis, GFR (HR 0,958; 95%CI0,930-0,987; p=0,005) and multivessel disease (HR 0,147; 95%CI 0,030-0,714;p=0,017) were the only preoperative predictors of death at 1-year. GFR was theonly independent predictor of death at 30-days (HR 0,961; 95%CI 0,924-1,000;p=0,047). GFR was also a predictor of 30-days (HR 0,960; 95%CI 0,923-0,999,p=0,045) and 1-year mortality (HR 0,960; 95%CI 0,934-0,986, p=0,003), inde-pendent of euro risk score.Conclusion: In our population of patients submitted to CABG after acute or sub-acute phase of MI, lower glomerular filtration rate was predictive of worse prog-nosis at 30-days and 1-year. GFR should be calculated systematically in pre-operative time to avoid underestimation of surgical risk.
P575 Right ventricular, left ventricular and biventricularpacing all fail to impress after coronary artery bypasssurgery
B. Gordon1, K. Morrice1, P. Elliott2, A. Graham2, M. Harbinson3,E.W. Chew1. 1Belfast City Hospital Trust, Belfast, United Kingdom;
2Royal Victoria Hospital, Belfast, United Kingdom; 3Queen’s University, Belfast,United Kingdom
Background: Studies that have evaluated the role of temporary biventricularpacing after cardiac surgery have reported conflicting findings due to differentmethodological reasons. Our aim was to clarify the post-operative value of tem-porary pacing in patients undergoing coronary artery bypass grafting (CABG) byevaluating the haemodynamic effect of multiple different pacing configurations.Methods: 19 (of 26 enrolled) patients (mean left ventricular ejection fraction46.7%) had bipolar pacing wires attached to right atrium, right ventricle (RV),anterior left ventricle (LV) and posterolateral LV walls during CABG. Two hoursafter surgery, periods of 10 minutes pacing separated by 10 minutes of rest wereapplied using 4 biventricular (anterior and lateral using simultaneous and sequen-tial methods to complete the pacing circuit) and 3 univentricular (RV, anterior LVand lateral LV) pacing configurations. Haemodynamic changes were compared toa control period of no pacing. Primary outcome was change in cardiac index af-ter pacing. Secondary outcome variables included cardiac output, systolic bloodpressure, systemic vascular resistance, pulmonary wedge pressure and centralvenous pressure. Comparisons were made using analysis of variance with Dun-nett’s test.Results: Mean cardiac index increased after anterior simultaneous (3.04 to 3.3L/min/m2, p=0.006), lateral simultaneous (3.16 to 3.32 L/min/m2, p=0.043) andlateral sequential (3.08 to 3.34 L/min/m2, p=0.009) biventricular pacing configu-rations. However, when changes were compared to the change observed after acontrol period of no pacing, there was no significant difference in primary or sec-ondary outcome variables with any pacing configuration in the group as a whole.An anterior or lateral simultaneous biventricular configuration resulted in a signif-icant increase, compared to control, in systolic blood pressure only in those with
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Valve and coronary surgery 71
baseline low LV function (n=7, mean LV ejection fraction 29.4%). There were noother differences between normal and low LV groups.Conclusion: Significant observed improvements with biventricular pacing afterCABG are not actually significant when compared to a true control period of nopacing. Such a control period has been lacking in previous studies. In addition,neither right nor left univentricular pacing demonstrated any benefit. Therefore,no temporary pacing configuration can be recommended as a routine means ofimproving post-operative haemodynamics. A repeat study with larger numberswould be welcome in confirming these findings.
P576 Comparison of a clinical score with individual clinicianjudgment for assigning priority for heart valve surgery
R.A.H. Stewart1, A. Hamer2, B. Mahon3, P. Ruygrok4, N. Kang4,A. Sasse3, R. Fischer5 , R. Luke6, A. Barber7, R. Naden7. 1TheUniversity of Auckland, Auckland, New Zealand; 2Nelson Hospital,
Nelson, New Zealand; 3Wellington Hospital, Wellington, New Zealand; 4AucklandCity Hospital, Auckland, New Zealand; 5Hamilton Hospital, Hamilton, NewZealand; 6Hastings Hospital, Hastings, New Zealand; 7Ministry of Health,Wellington, New Zealand
Background: Priority for cardiac surgery is usually based on a clinician’s judg-ment of the degree of urgency. Point systems have the potential to improve theaccuracy and consistency of this assessment. A working group of New ZealandCardiologists and Cardiac Surgeons developed a Clinical Priority Score (CPS) forassigning priority for surgery for heart valve disease based on current guidelinesof the AHA/ACC and ESC. Categories scored include the severity of the valvelesion, symptoms related to the valve lesion, the presence and amount of cardiacdysfunction, risk of progression and the presence of an additional AHA/ACC/ESCclass 1 indication for surgery. Clear definitions relevant to individual valve lesionswere used within each category. Points were assigned using decision analysissoftware which calculates weights based on the consensus ‘expert’ responses toa series of choices. The aim of this study was to compare the CPS with individualclinician judgment for assigning priority for heart valve surgery.Methods: 25 vignettes of cases referred for a broad range of heart valve surgerywere independently ranked for urgency by 8 cardiologists or cardiac surgeons. Aclinical consensus rank (1 to 25) was then agreed by first determining the averagerank then re-ranking cases after group discussion. The final consensus rank wascompared to the rank assigned from the CPS and with the initial rank of eachclinician.Results: There was a close correlation between the CPS score and final consen-sus judgment (r= 0.91), which on average was better than for individual clinicians(mean r=0.74, SD 0.13). For CPS and individual clinicians respectively the pro-portion of cases where agreement was very good (≤2 rank places different) was60% and 37%, good (2.5 to 4) 24% and 28%, modest (4 to 8) 16% and 25%, andpoor (>8 rank places different) 0% and 14.5%, p=0.008.Conclusion: Priority for surgery for heart valve disease assigned by a systematicpoint score was consistent with consensus clinical judgment. In contrast individualclinician judgment was variable and more likely to assign a priority inconsistentwith the consensus judgment.
P577 Clinical evaluation of a percutaneous aortic valvereplacement program: preliminary results andimplications for patient selection
A. Berenguer Jofresa, S. Canovas, O. Gil, I. Marques, R. Paya,J.V. Vilar, F. Pomar, J.L. Perez, J. Estornell, J. Martinez Leon.
University General Hospital of Valencia, Valencia, Spain
Background: Current devices for percutaneous aortic valve replacement (PAVR)have limitations. Data comparing PAVR with conventional surgery (CS) and med-ical treatment (MT) are lacking. Therefore, not every high risk patient with severeaortic stenosis (AS) is a fully candidate for PAVR.Objectives: The role of PAVR with available devices needs to be defined. In thepresent study we analyze the selection process in our institution and the clinicaloutcomes with the Edwards Sapien (ES) valve.Methods: From May 2008 to December 2009, 44 patients (24 women) with se-vere AS were proposed for PAVR. Forty out of them fulfilled at least 2 of the follow-ing criteria: Euroscore (ESC) ≥ 20, previous cardiac surgery, porcelain aorta andage ≥ 80. All patients were studied by cardiac catheterization, transesophagealecho and Angio TC. Aortic annulus (AA) and femoral arteries (FA) were evaluatedfor feasibility of an ES 23 or 26 mm valve. Final decision was obtained individu-ally after evaluation of clinical and anatomical data, and patient wishes. Clinicaloutcomes were evaluated in all patients.Results: 21 (47.7%) had ESC>20%, 7 (16%) porcelain aorta, 7 (16%) previouscardiac surgery and 29 (66%) age>80. Four (10%) patients died during evalu-ation and were excluded from the analysis. In the remaining 36, mean age was79±4 years, ESC 27±16%, aortic valve area 0.57±0.15 mm2, aortic annulus21.6±1.5 mm, right common FA 7.26±1.23 mm, left common FA 7.3±1.23 mmand creatinine 1.2±0.25 mg/dl. Nine (25%) patients had large AA (>24.5 mm)and PAVR was rejected, 4 out of them with a mean ESC 34±13 underwent MTand 5 with a mean ESC 21±13 (p=0.1) underwent CS. In the remaining 27, 16patients (44%) had not femoral access: 6 patients underwent MT, 5 CS and 5were treated by transapical (TA) PAVR. In 11 patients with suitable FA, 4 under-
went MT, 1 with a low ESC (7.5%) CS and 6 transfemoral (TF) PAVR. In summary,CS was performed in 11 (31%) with 30 day-mortality (30dM) 0%, TF-PAVR in 6(16%) with 30dM 0%, TA-PAVR in 5 (14%) with 30dM (2/5) 40% and MT in 14(39%) with 6.2% (1/14) mortality after 261±76 days of follow up.Conclusions: 1) These are high risk patients, as far as 10% of patients diedduring evaluation, 2) Large AA avoided the PAVR with the ES valve in 25% ofpatients, 3) Despite 27 (75%) had AA suitable for an ES valve, only 11 (30%)were selected for PAVR, being unsuitable FA the main cause for rejection. 3)CS is a good option for these patients, particularly in the lower risk patients, 4)Results with the TF-PAVR approach are encouraging whereas the TA-PAVR mightbe improved.
P578 Aortic valve replacement in the elderly: doesconcomitant coronary artery bypass grafting predict aworse short-term outcome?
A.S. Correia, S.M. Oliveira, M. Paiva, A. Goncalves, R. Almeida,M. Pereira, E. Alves, P. Dias, A. Abreu, P. Pinho. Sao Joao Hospital,
Porto, Portugal
Purpose: In this study we aimed to assess the short-term results and recognizethe predictors of in-hospital mortality in elderly patients submitted to aortic valvereplacement (AVR) with or without concomitant coronary artery bypass grafting(CABG).Methods: We retrospectively analyzed records of patients aged ≥75 years con-secutively submitted to AVR, isolated or with CABG, from January 2002 to De-cember 2006. Demographic data, cardiovascular risk factors, postoperative com-plications and additive EuroSCORE classification were analyzed.Results: We included 179 patients (73 men (40.1%)), with a mean age of78.5±2.6 years, who had been submitted to AVR with concomitant CABG (n = 65(36.3%)) or to AVR only (n = 114 (63.7%)). Patients submitted to AVR with CABGwere more likely to be diabetic (40% vs 17.7%, p=0.001) and dyslipidemic (62.5%vs 42.3%, p=0.012); had more frequently extracardiac arteriopathy manifestations(30.8% vs 6.2%, p>0.001), previous history of stroke (26.2% vs 5.3%, p<0.001)and recent myocardial infarction (MI) (32.8% vs 8.9%, p<0.001). Carotid surgery(5 (7.7%) patients) and unstable angina [3 patients (4.7%)] occurred only in com-bined group. Mean EuroSCORE was significantly higher in the combined surgerygroup (6.97 vs. 8.91, p<0.001). Overall in-hospital risk of death was 4.5% and itwas 5.6 (OR: 1.1-29.1, CI 95%) times higher in combined group. No significantdifferences between groups were observed regarding gender and arterial hyper-tension, obesity, renal insufficiency, major bleeding, prolonged orotracheal intuba-tion, time of extracorporeal circulation, critical state and associated aortic surgery.In univariate analysis, predictors of in-hospital mortality for isolated AVR wereacute MI in the previous 90 days (50% vs. 8.2%, p=0.040), major bleeding (100%vs. 3.8%, p<0,001), and previous stroke (50% vs. 4.5%, p=0.004). The predictorsof in-hospital mortality, in the combined surgery group, were major bleeding(20% vs. 1.72%, p=0,025), prolonged orotracheal intubation (100% vs. 1.7%,p<0,001) and duration of extracorporeal circulation (218 vs. 138 min, p<0,001).EuroSCORE was not a predictor of in-hospital mortality in these two populations.Conclusion: AVR only or in combination with CABG in the elderly had a satis-factory short-term outcome, with an in-hospital mortality rate of 4.5% in our pop-ulation. Predictors of in-hospital mortality were different in these two groups withexception of major bleeding. Patients submitted to AVR with concomitant CABGpresented a significantly higher risk of mortality.
P579 Comparison of rivaroxaban, low molecular-weightheparin and unfractionated heparin in preventingthrombus formation on mechanical heart valves:results of an in vitro study
A. Kaeberich1, U. Raaz1, L. Maegdefessel2 , T. Linde3, U. Steinseifer3,E. Perzborn4, B. Hauroeder5 , M. Buerke1, K. Werdan1, A. Schlitt1. 1MartinLuther University of Halle-Wittenberg, Halle, Germany; 2Stanford UniversityMedical Center, Division of Cardiovascular Medicine, Stanford, United States ofAmerica; 3Helmholtz - Institute for Biomedical Engineering of institute of RWTHAachen University, Aachen, Germany; 4Bayer Schering Pharma AG, Berlin,Germany; 5Central Institute of the Federal Armed Forces, Koblenz, Germany
Introduction: Lifelong oral anticoagulation (OAC) is mandatory after mechanicalheart valve implantation to prevent thromboembolic events. However, under theestablished treatment with vitamin K antagonists (VKA) there is a considerablerate of embolic events as well as anticoagulant related bleedings. Therefore theinvestigation of more effective and safer antithrombotic agents is of extraordinaryinterest. Rivaroxaban (riva) is a new orally available direct and selective coagu-lation factor Xa inhibitor. The aim of this in vitro study was to test the hypothesisthat riva is equivalent to enoxaparin (enoxa) and unfractionated heparin (UFH) inpreventing thrombus formation on mechanical heart valves.Materials and Methods: Blood samples (230ml) from male volunteers were an-ticoagulated with therapeutic plasma concentrations of riva 300ng/ml, UFH 0.8IU/l or enoxa 0.7 IU/ml (n=10/condition). Bileaflet mechanical heart valves wereplaced in an in vitro device (THIA II Thrombotester) allowing exposure to anti-coagulated blood samples under pulsatile circulation conditions for a duration of60 min. Overall heart valve thrombus weight and electron microscopic features(deposition of platelets and fibrin on the heart valve surface) were quantified.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

72 Valve and coronary surgery / Controversies on drug eluting stent implantation
Results: Thrombus weight was not significanty different between riva, UFH, andenoxa treated groups (figure 1). Also electron microscopy analysis did not detectdifferences between the specific anticoagulants tested.
Figure 1
Conclusions: Our results indicate that riva is as effective as UFH and LMWHin preventing thrombus formation on mechanical heart valves. Thus we hypothe-size that rivaroxaban is a competitive oral available alternative to VKA, UFH andLMWH, that might overcome the limitations of current OAC in patients after im-plantation of artificial heart valves.
P580 Early outcome after cardiac surgery in the elderly:what can we rely on to predict survival?
S.M. Oliveira1, A.S. Correia1, M. Paiva1, A. Goncalves1, R. Almeida1,M. Pereira2, E. Alves2, P. Dias1, A. Abreu1, P. Pinho1. 1Sao JoaoHospital, Porto, Portugal; 2University of Porto Medical School,
Department of Hygiene and Epidemiology, Porto, Portugal
Introduction: Increase in life expectancy is resulting in more elderly patients re-ferred for cardiac surgery. We aimed to assess short-term outcome and predic-tors of in-hospital mortality of elderly submitted to coronary artery bypass surgery(CABG) with or without aortic valve replacement (AVR).Methods: We analyzed records of patients ≥75years submitted to CABG onlyor with AVR from 2002 to 2006. Clinical data and additive EuroSCORE wereevaluated.Results: We included 180 patients, 65 (36.1%) submitted to CABG with AVRand 115 (63.9%) to CABG only. Mean age was 78±2.5years. Patients submit-ted to CABG only were more likely to be men (69.6% vs. 44.6%,p=0.001), hadsuffered an AMI in the previous 90 days (49.6% vs. 32.8%, p=0.031), haveshorter in-hospital stay (12.6 vs. 17.4 days,p=0,015). Mean EuroSCORE washigher in patients submitted to CABG with AVR (7.2 vs. 8.9, p<0.001). Overall, 13(7.2%) patients died and the risk of dying was not statistically different betweengroups (OR=1.57; 95%CI 0.50-4.88). Predictors of in-hospital mortality (univari-ate analysis) for isolated CABG were left ventricular dysfunction (18.2% vs. 3.3%,p=0.034), combined carotid artery surgery (30% vs. 3.8%, p=0.009), hemodial-ysis after CABG (71.4% vs. 0.9%, p<0.001), major bleeding (40% vs. 3.7%,p=0.012) and orotracheal intubation ≥72h (30% vs. 2.9%, p=0.004); regardingCABG with AVR, predictors were major bleeding, (20.0% vs. 1.7%, p=0.025),orotracheal intubation ≥72h (100% vs. 1.7%, p<0.001) and extracorporeal circu-lation duration (138 vs. 218 min, p<0.001).
Conclusion: CABG in the elderly, with or without AVR, was associated with anin-hospital mortality of 7.2%. Few preoperative factors are available for risk strati-fication. These results highlight the importance of appropriate patient selection inorder to obtain a satisfactory short-term outcome.
P581 Moderate preoperative anemia is not associated withincreasd morbidity and mortality for cardiac surgery
A.R. Hershson, N. Marini, J.I. Olmos, L. Padial, G.E. Bozovich,R.R. Favaloro. Favaloro Foundation University Hospital, Buenos Aires,Argentina
Objectives: To evaluate whether mild or moderate anemia before cardiac surgeryis associated with post operative morbidity and mortality.Methods: Single centre retrospective cohort study including all on pump cardiacsurgeries performed in adults between June 2005 and June 2009. All coronary bypass, valve repair/replacement and combined procedures were analysed, exclud-
ing patients with chronic renal failure (creatinine >2mg/dl) or dialysis, Parsonnetscore >20, severe anemia (Haemoglobin <10 g/dl), or operated on emergency.Anemia was defined as haemoglobin <13 g/dl in men and <12 g/dl in women.The endpoint was a combination of death, stroke, dialysis, or mediastinitis. Rel-ative risks were estimated by means of odds ratios (OR) an the correspondingconfidence limits for an alpha of 0.05. Confounders were controlled through back-wise logistic regression.Results: Cohort n= 1012; mean age 64.38±11.3, male gender 69.96%. The over-all incidence of endpoint was 7.21% (n=73). Mean haemoglobin was 13.75±1.27g/dl, thus 160 (15.81%) qualified as anemic. We observed no association be-tween anemia and complications (OR 1.16, 95% C.I. 0.63-2.16). After adjustingfor age, gender, COPD, and combined surgery OR= 0.95 (95% C.I. 0.50-1.81).There was a trend towards a higher number of units transfused between groups(7.96±10.87 vs 5.88±7.96), while no significant differences were observed in thehospital length of stay (8.15±5.22 vs 8.21±6.85 days).Conclusion: Cardiac surgery can be safely performed in patients with mild ormoderate anemia undergoing all kinds of procedures, without a significant in-crease in hospital length of stay.
CONTROVERSIES ON DRUG ELUTING STENTIMPLANTATION
P582 Malapposed struts in drug-eluting stents entail higherrisk of incomplete tissue coverage at 9-13 monthscompared to well-apposed struts: in-vivodemonstration with optical coherence tomography
J.L. Gutierrez-Chico1, E. Regar1, P. Juni2, H. Garcia-Garcia3,H. Kelbaek4, C. Macaya5, S. Silber6, C. Di Mario7, S. Windecker8,P.W. Serruys1. 1Erasmus Medical Center, Thoraxcenter, Department ofCardiology, Rotterdam, Netherlands; 2University of Bern, Institute of Socialand Preventive Medicine, Bern, Switzerland; 3Cardialysis B.V., Rotterdam,Netherlands; 4Rigshospitalet, Copenhagen University Hospital, Copenhagen,Denmark; 5Hospital Clinic San Carlos, Department of Cardiology, Madrid, Spain;6HKL Dr Mueller Klinik, Munich, Germany; 7Royal Brompton Hospital, London,United Kingdom; 8Bern University Hospital, Swiss Cardiovascular Center, Bern,Switzerland
Introduction: Intravascular ultrasound studies have linked incomplete stent ap-position (ISA) to stent thrombosis. However, it remains uncertain whether ISArepresents per se a handicap for proper healing, or is rather the consequence ofa process causing primarily delayed healing and stent thrombosis, like an inflam-matory reaction. This study is aimed to assess the tissue coverage of ISA strutsin a cohort of patients with drug-eluting stents (DES), using optical coherencetomography (OCT).Methods: 102 DES implanted in 61 patients enrolled in 2 all-comers randomizedtrials, comprising 4 different types of stent (labelled A, B, C and D), were examinedwith OCT at 9-13 months follow-up. The tissue coverage of ISA vs. well-apposedstruts was compared using statistical pooled analysis, that takes into accountbetween- and within-cluster variability.Results: 5 OCT pullbacks were excluded due to poor quality. 97 stents, 16479struts, 1739.5 mm of stented vessel were finally analyzed. In the whole sample734 (4.5%) well-apposed and 34 (20.4%) ISA struts were not covered. In thepooled analysis, 65 stents were totally well-apposed, 25 had complete coverageof all well-apposed and ISA struts, and 30 were suitable for pooled comparison.The effect presented significant heterogeneity (H=1,60; I2=60,82, p<0,0001). Af-ter stratification by type of stent, Stent A still presented heterogeneity, but in all theother strata the effect was homogeneous, with risk-ratios of non coverage for ISAstruts ranging from 5.57 (95% CI: 4.18–7.41) to 76.60 (95% CI: 15.95 – 367.82).
n Magnitude of effect Heterogeneity of the effect
RR 95% CI H I2 p value
Lower Upper
Stent A 14 6,03 4,84 7,50 1,75 67,37 0,0001Stent B 6 5,57 4,18 7,41 1,14 22,85 0,26Stent C 2 76,60 15,95 367,82 1,35 44,87 0,18Stent D 8 13,38 8,42 21,25 1,00 0,00 0,59
Conclusion: Tissue coverage is delayed in ISA compared to well-apposed strutsin DES at 9-13 months. The magnitude of this effect seems influenced by thetype of stent. These findings suggest that ISA represents per se a handicap foradequate healing.
P583 The aftermath of the controversy: Drug-Eluting Stentuse declines; more restenosis is seen
L. Marcoff, C.T. Jurkovitz, D. Murphy, P. Kolm, J.R. Bowen,W.S. Weintraub, E. Rahman. Christiana Care Health System, Newark,United States of America
Background: Reports presented at European Society of Cardiology (ESC) 2006meeting about increased mortality associated with drug-eluting stents (DES),possibly due to late stent thrombosis, sparked controversy and resulted in de-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
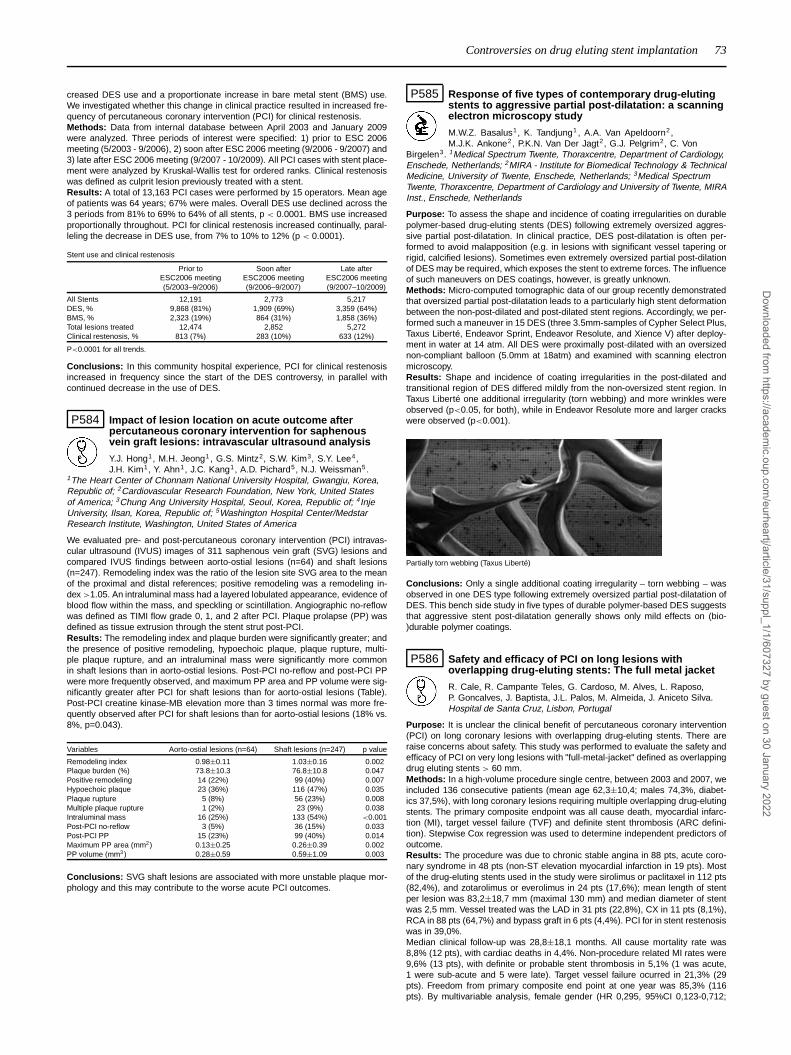
Controversies on drug eluting stent implantation 73
creased DES use and a proportionate increase in bare metal stent (BMS) use.We investigated whether this change in clinical practice resulted in increased fre-quency of percutaneous coronary intervention (PCI) for clinical restenosis.Methods: Data from internal database between April 2003 and January 2009were analyzed. Three periods of interest were specified: 1) prior to ESC 2006meeting (5/2003 - 9/2006), 2) soon after ESC 2006 meeting (9/2006 - 9/2007) and3) late after ESC 2006 meeting (9/2007 - 10/2009). All PCI cases with stent place-ment were analyzed by Kruskal-Wallis test for ordered ranks. Clinical restenosiswas defined as culprit lesion previously treated with a stent.Results: A total of 13,163 PCI cases were performed by 15 operators. Mean ageof patients was 64 years; 67% were males. Overall DES use declined across the3 periods from 81% to 69% to 64% of all stents, p < 0.0001. BMS use increasedproportionally throughout. PCI for clinical restenosis increased continually, paral-leling the decrease in DES use, from 7% to 10% to 12% (p < 0.0001).
Stent use and clinical restenosis
Prior to Soon after Late afterESC2006 meeting ESC2006 meeting ESC2006 meeting(5/2003–9/2006) (9/2006–9/2007) (9/2007–10/2009)
All Stents 12,191 2,773 5,217DES, % 9,868 (81%) 1,909 (69%) 3,359 (64%)BMS, % 2,323 (19%) 864 (31%) 1,858 (36%)Total lesions treated 12,474 2,852 5,272Clinical restenosis, % 813 (7%) 283 (10%) 633 (12%)
P<0.0001 for all trends.
Conclusions: In this community hospital experience, PCI for clinical restenosisincreased in frequency since the start of the DES controversy, in parallel withcontinued decrease in the use of DES.
P584 Impact of lesion location on acute outcome afterpercutaneous coronary intervention for saphenousvein graft lesions: intravascular ultrasound analysis
Y.J. Hong1, M.H. Jeong1, G.S. Mintz2, S.W. Kim3, S.Y. Lee4,J.H. Kim1, Y. Ahn1, J.C. Kang1, A.D. Pichard5, N.J. Weissman5.
1The Heart Center of Chonnam National University Hospital, Gwangju, Korea,Republic of; 2Cardiovascular Research Foundation, New York, United Statesof America; 3Chung Ang University Hospital, Seoul, Korea, Republic of; 4InjeUniversity, Ilsan, Korea, Republic of; 5Washington Hospital Center/MedstarResearch Institute, Washington, United States of America
We evaluated pre- and post-percutaneous coronary intervention (PCI) intravas-cular ultrasound (IVUS) images of 311 saphenous vein graft (SVG) lesions andcompared IVUS findings between aorto-ostial lesions (n=64) and shaft lesions(n=247). Remodeling index was the ratio of the lesion site SVG area to the meanof the proximal and distal references; positive remodeling was a remodeling in-dex >1.05. An intraluminal mass had a layered lobulated appearance, evidence ofblood flow within the mass, and speckling or scintillation. Angiographic no-reflowwas defined as TIMI flow grade 0, 1, and 2 after PCI. Plaque prolapse (PP) wasdefined as tissue extrusion through the stent strut post-PCI.Results: The remodeling index and plaque burden were significantly greater; andthe presence of positive remodeling, hypoechoic plaque, plaque rupture, multi-ple plaque rupture, and an intraluminal mass were significantly more commonin shaft lesions than in aorto-ostial lesions. Post-PCI no-reflow and post-PCI PPwere more frequently observed, and maximum PP area and PP volume were sig-nificantly greater after PCI for shaft lesions than for aorto-ostial lesions (Table).Post-PCI creatine kinase-MB elevation more than 3 times normal was more fre-quently observed after PCI for shaft lesions than for aorto-ostial lesions (18% vs.8%, p=0.043).
Variables Aorto-ostial lesions (n=64) Shaft lesions (n=247) p value
Remodeling index 0.98±0.11 1.03±0.16 0.002Plaque burden (%) 73.8±10.3 76.8±10.8 0.047Positive remodeling 14 (22%) 99 (40%) 0.007Hypoechoic plaque 23 (36%) 116 (47%) 0.035Plaque rupture 5 (8%) 56 (23%) 0.008Multiple plaque rupture 1 (2%) 23 (9%) 0.038Intraluminal mass 16 (25%) 133 (54%) <0.001Post-PCI no-reflow 3 (5%) 36 (15%) 0.033Post-PCI PP 15 (23%) 99 (40%) 0.014Maximum PP area (mm2) 0.13±0.25 0.26±0.39 0.002PP volume (mm3) 0.28±0.59 0.59±1.09 0.003
Conclusions: SVG shaft lesions are associated with more unstable plaque mor-phology and this may contribute to the worse acute PCI outcomes.
P585 Response of five types of contemporary drug-elutingstents to aggressive partial post-dilatation: a scanningelectron microscopy study
M.W.Z. Basalus1, K. Tandjung1 , A.A. Van Apeldoorn2,M.J.K. Ankone2, P.K.N. Van Der Jagt2, G.J. Pelgrim2, C. Von
Birgelen3. 1Medical Spectrum Twente, Thoraxcentre, Department of Cardiology,Enschede, Netherlands; 2MIRA - Institute for Biomedical Technology & TechnicalMedicine, University of Twente, Enschede, Netherlands; 3Medical SpectrumTwente, Thoraxcentre, Department of Cardiology and University of Twente, MIRAInst., Enschede, Netherlands
Purpose: To assess the shape and incidence of coating irregularities on durablepolymer-based drug-eluting stents (DES) following extremely oversized aggres-sive partial post-dilatation. In clinical practice, DES post-dilatation is often per-formed to avoid malapposition (e.g. in lesions with significant vessel tapering orrigid, calcified lesions). Sometimes even extremely oversized partial post-dilationof DES may be required, which exposes the stent to extreme forces. The influenceof such maneuvers on DES coatings, however, is greatly unknown.Methods: Micro-computed tomographic data of our group recently demonstratedthat oversized partial post-dilatation leads to a particularly high stent deformationbetween the non-post-dilated and post-dilated stent regions. Accordingly, we per-formed such a maneuver in 15 DES (three 3.5mm-samples of Cypher Select Plus,Taxus Liberté, Endeavor Sprint, Endeavor Resolute, and Xience V) after deploy-ment in water at 14 atm. All DES were proximally post-dilated with an oversizednon-compliant balloon (5.0mm at 18atm) and examined with scanning electronmicroscopy.Results: Shape and incidence of coating irregularities in the post-dilated andtransitional region of DES differed mildly from the non-oversized stent region. InTaxus Liberté one additional irregularity (torn webbing) and more wrinkles wereobserved (p<0.05, for both), while in Endeavor Resolute more and larger crackswere observed (p<0.001).
Partially torn webbing (Taxus Liberté)
Conclusions: Only a single additional coating irregularity – torn webbing – wasobserved in one DES type following extremely oversized partial post-dilatation ofDES. This bench side study in five types of durable polymer-based DES suggeststhat aggressive stent post-dilatation generally shows only mild effects on (bio-)durable polymer coatings.
P586 Safety and efficacy of PCI on long lesions withoverlapping drug-eluting stents: The full metal jacket
R. Cale, R. Campante Teles, G. Cardoso, M. Alves, L. Raposo,P. Goncalves, J. Baptista, J.L. Palos, M. Almeida, J. Aniceto Silva.Hospital de Santa Cruz, Lisbon, Portugal
Purpose: It is unclear the clinical benefit of percutaneous coronary intervention(PCI) on long coronary lesions with overlapping drug-eluting stents. There areraise concerns about safety. This study was performed to evaluate the safety andefficacy of PCI on very long lesions with "full-metal-jacket" defined as overlappingdrug eluting stents > 60 mm.Methods: In a high-volume procedure single centre, between 2003 and 2007, weincluded 136 consecutive patients (mean age 62,3±10,4; males 74,3%, diabet-ics 37,5%), with long coronary lesions requiring multiple overlapping drug-elutingstents. The primary composite endpoint was all cause death, myocardial infarc-tion (MI), target vessel failure (TVF) and definite stent thrombosis (ARC defini-tion). Stepwise Cox regression was used to determine independent predictors ofoutcome.Results: The procedure was due to chronic stable angina in 88 pts, acute coro-nary syndrome in 48 pts (non-ST elevation myocardial infarction in 19 pts). Mostof the drug-eluting stents used in the study were sirolimus or paclitaxel in 112 pts(82,4%), and zotarolimus or everolimus in 24 pts (17,6%); mean length of stentper lesion was 83,2±18,7 mm (maximal 130 mm) and median diameter of stentwas 2,5 mm. Vessel treated was the LAD in 31 pts (22,8%), CX in 11 pts (8,1%),RCA in 88 pts (64,7%) and bypass graft in 6 pts (4,4%). PCI for in stent restenosiswas in 39,0%.Median clinical follow-up was 28,8±18,1 months. All cause mortality rate was8,8% (12 pts), with cardiac deaths in 4,4%. Non-procedure related MI rates were9,6% (13 pts), with definite or probable stent thrombosis in 5,1% (1 was acute,1 were sub-acute and 5 were late). Target vessel failure ocurred in 21,3% (29pts). Freedom from primary composite end point at one year was 85,3% (116pts). By multivariable analysis, female gender (HR 0,295, 95%CI 0,123-0,712;
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

74 Controversies on drug eluting stent implantation / Cardiovascular research: about contraction and electrical activity
p=0,007) and non-RCA procedure (HR 0,292, 95%IC 0,119-0,716; p=0,007) wereindependent predictors of primary composite end point at one year. First genera-tion drug-eluting stents, its length and reference diameter were not predictors ofevents.Conclusions: The treatment of very long lesions with overlapping drug-elutingstents although efficacious is associated to higher rate of stent thrombosis raisingsafety concerns.
CARDIOVASCULAR RESEARCH: ABOUT CONTRACTIONAND ELECTRICAL ACTIVITY
P587 Gene expression profiling of human extracellularmatrix genes in human myocardial tissue of the rightatrial auricle: differences in cardiac remodellingbetween ischemic and valvular heart disease
M. Franz1 , A. Baldinger1, P. Richter2, K. Gruen3, K. Hekmat3,H. Kosmehl4, H.R. Figulla1, A. Berndt2, B.R. Brehm1. 1University Hospital Jena,Department of Internal Medicine I, Jena, Germany; 2University Hospital Jena,Institute of Pathology, Jena, Germany; 3University Hospital Jena, Department ofCardiothoracic Surgery, Jena, Germany; 4HELIOS Klinikum Erfurt, Institute ofPathology, Erfurt, Germany
Background: Cardiovascular diseases are accompanied by structural and func-tional changes in the cardiac extracellular matrix (ECM) including a variety ofadhesion molecules, proteases or growth factors. The right atrial auricle is easilyavailable during cardiac surgery and might serve as a potential tool for the in-vestigation of cardiac remodelling. Hitherto there is no detailed gene expressionanalysis focussed on ECM and adhesion molecules in myocardial tissue of theright atrial auricle from patients with ischemic (ICM, due to coronary artery dis-ease) compared to valvular (VCM, due to an aortic valve stenosis) heart diseaseboth known to represent main causes of cardiac morbidity and mortality in man.Methods: Therefore, the object of the study was to investigate the ECM remod-elling in right atrial myocardial tissue focussing on differences between ICM andVCM due to an aortic valve stenosis. Tissue samples of the right atrial auriclefrom patients with ICM and VCM showing different grades of histological damagewere analysed by PCR based gene expression profiling of 84 ECM and adhesionmolecules.Results: We could demonstrate dynamic changes in ECM gene expression lev-els between ICM and VCM. In general, there were increased expression-levelsfor the majority of ECM genes in VCM compared to ICM. For 14 genes thesedifferences showed statistical significance including connective tissue growthfactor (CTGF, p=0.007), Collagen I (p=0.017), Collagen VI (p=0.005), Versican(p=0.006), Fibronectin (p=0.030), Laminin-beta 1 (p=0.005), MMP-14 (p=0.013),TIMP-2 (p=0.011) and Tenascin-C (p=0.030). Especially the genes for collagenI, CTGF, Laminin-beta 1, MMP-14 and Tenascin-C showed more than 3.0 foldup-regulations in VCM compared to ICM.Conclusions: Human myocardial tissue from the right atrial auricle can be sug-gested as a valuable model to investigate cardiac ECM remodelling in ischemicand valvular heart diseases. A variety of candidate genes of ECM and adhesionmolecules are significantly up-regulated in VCM compared to ICM even in theright atrial auricle. Thus, a functional important role of these genes in pathogen-esis of cardiac remodelling especially in response to pressure overload can besuggested. Moreover, the changes in the cardiac ECM are not restricted to areasdirectly affected by mechanical stress but occur in the entire heart.
P588 Interleukin 6 is not necessary for beta-adrenergicdependent myocardial hypertrophy
K. Kaminski1, S. Litvinovich2, T. Bonda1, M. Dziemidowicz1,K. Ptaszynska1, M. Kozuch1, W.J. Musial1, M.M. Winnicka1. 1MedicalUniversity of Bialystok, Bialystok, Poland; 2Grodno State Medical
University, Grodno, Belarus
In recent years several reports have suggested involvement of interleukin 6 (IL-6)in effects of catecholamines on myocardium. Moreover, lack of STAT3 (down-stream signal transducer of IL-6) results in severe heart failure after isoproterenolstimulation. Here we present a study of β-adrenergic effects on myocardium ofIL-6 deficient mice.Methods: Thirty male, 12 week old C57Bl6/J mice and 29 age and sex matchedanimals from IL-6 knockout strain (C57Bl6/J IL6-/-) were used in the study.In each genotype there were three groups: placebo, short isoproterenol (3days 60mg/kg/day in ip injections) and long isoproterenol treatment (16 days50mg/kg/day in ip injections). Mice were sacrificed 24 hours after the last isopro-terenol or placebo injection, hearts were dissected, weighed and fixed in isoos-motic formalin. Total heart and left ventricle (LV) weights were related to bodyweight and tibia length. Paraffin embedded samples were cut and stained withhematoxylin and eosin or with sirius red.Results: Both short and long treatment with isoproterenol caused significant in-crease of LV/tibia ratio in both WT and IL-6 KO animals. There were no significantdifferences between genotypes in respect to heart weight. We have found similarextent of fibrosis and no profound changes in myocardial histology between WT
and IL-6 KO mice. We did not find increased mortality nor signs of heart failure inIL-6 KO isoproterenol-treated animals.
Heart/tibia length LV/tibia length RV/tibia length Fibrosis*
WT placebo 6.3±0.7 5.1±0.6 0.7±0.1 1.8±0.13 day iso 7.9±0.7# 6.3±0.6# 1.1±0.2# NA16 day iso 7.6±0.4# 6.2±0.3# 0.9±0.1# 2.1±0.4
IL6 KO placebo 6.6±0.6 5.4±0.4 0.7±0.1 1.9±0.53 day iso 8.4±0.5# 6.8±0.8# 1±0.1# NA16 day iso 7.8±0.9# 6.3±0.5# 1±0.1# 2±0.6
*Semi-quantitative assessment in relative units. #p<0.01 vs respective placebo group.
Conclusion: IL-6 is not necessary for induction of cardiac hypertrophy by beta-adrenergic agonists. Moreover mice devoid of IL-6 gene are not particularly sus-ceptible to heart failure caused by isoproterenol.
P589 Metabolic stress causes early glucose intolerance andmyocardial dysfunction in eNOS partial knockout mice
C. Vecoli1, M. Novelli2, A.I. Corciu3, R. Sicari3, F. Scebba1,F. Coceani1, A. L’abbate1, P. Masiello2, D. Neglia4. 1Scuola SuperioreSant’Anna, Pisa, Italy; 2Universita’ di Pisa, Dipartimento di Patologia
Sperimentale, Biotecnologie Mediche, Infettivologia e, Pisa, Italy; 3CNR-IstitutoFisiologia Clinica, Pisa, Italy; 4Fondazione G. Monasterio CNR - RegioneToscana, Pisa, Italy
Background: eNOS gene deletion as well as long-term high fat diet are ableto induce glucose intolerance and hypertension. It is not known whether theseconditions are synergic. Our aim is to investigate whether a metabolic stress maycause an early impairment of glucose metabolism and myocardial function in micewith a partial deficiency of eNOS gene (eNOS +/- mice).Methods: Wild type (WT) and eNOS +/- mice were fed a standard (chow) diet ora high-fat diet (HF). After 7 weeks, an intraperitoneal glucose tolerance test wasperformed and cardiac function was evaluated by trans-thoracic echocardiogra-phy.Results: eNOS +/- mice showed increased body weight compared to WT(p<0.01) while HF diet induced significant increase in body weight in both groupsof animals. Interestingly, no difference was observed between chow-fed eNOS +/-and WT fed with HF. After 7 weeks of diet, blood glucose levels were not signifi-cantly different in WT and HF-fed WT; conversely, a significant increase occurredin HF-fed eNOS +/- with respect to chow-fed eNOS +/- (193±5.3 versus 165±6.7mg/dl, p<0.01). Glucose tolerance test revealed that while the post-loading bloodglucose profile was only slightly abnormal in HF-fed WT, a clear-cut glucose in-tolerance was present in HF-fed eNOS +/- (AUC was 195±8.0 mg/dl x min in WT,236±19.2 in HF-fed WT, 232±11.0 in eNOS +/-, 329±32.5 in HF-fed eNOS +/-;p<0.05 vs. other groups). At cardiac level, the partial deficiency of eNOS associ-ated with HF diet resulted in significant decrease in percent fractional shortening(%FS) and increase in LVESD (%FS was 52.4±1.2 in eNOS +/- and 48.5±2.9HF-fed eNOS +/-; LVESD was 1.3±0.1 mm in eNOS +/- and 1.5±0.4 HF-fedeNOS +/-; both p<.05). No difference was measured in LV function between WTmice fed with or without HF diet.Conclusion: eNOS +/- mice, when fed with a HF-rich diet, develop an early glu-cose intolerance and myocardial dysfunction. These results suggest that genet-ically abnormal eNOS expression enhances the effects of metabolic stress andpredisposes to myocardial damage.
P590 Effects of cardiac overexpression of the AT1angiotensin II receptor on the mortality in transgenicmice
L.F. Matorra, A. Rey Deutsch, M. Donato, V. Casanova, E. Cicale,C. Lightowler, G. Pidal, C. Morales, N. Basso, R.J. Gelpi. Institute ofCardiovascular Pathophysiology, Buenos Aires, Argentina
Overexpression of the AT1 Angiotensin II receptor (AT1R) induces sudden deathin transgenic mice after 3 weeks of life with ventricular hypertrophy and bradycar-dia. Other authors have shown that AT1R overexpression increases mortality inmice as from day 80 of life with signs of heart failure, and another study showedhypertrophy and 2nd degree atrioventricular block but without mortality. Hence,mortality timing as well as the cause of death in mice with AT1R overexpressionis still controversial. The objective was to assess survival rate, ventricular func-tion and electrocardiographic alterations in two models of transgenic mice with:1) AT1R specific cardiac overexpression (Group 2, G2, n=14); and 2) overex-pression of AT1R mutant lacking Gαq/Gαi coupling (G3, n=15). Non transgenicmice were used as control group (G1,n=8). Kaplan-Meier curves were built withG1,n=92, G2, n=144 and G3, n=30 (see Figure). At 30 days of life electrocardio-gram and left ventricular (LV) function were assessed. The heart rate was 492±29b/min (G1), 300±24 b/min (G2) (p<0,05 vs G1) and 185±5 b/min (G3) (p<0,05vs G1 and G2). The PQ segment was 44±3 msec (G1), 92±3 (G2) (p<0,05 vsG1) but it was not measured in G3 owing to the absence of sinus rhythm. Sec-ond degree atrioventricular block (AVB) was observed in G2 and 3rd degree inG3. Both systolic and diastolic LV function did not show changes and no signs ofheart failure were noted. The heart weight/body weight ratio was G1: 4,69±0,11;G2: 5,83±0,21 (p<0.05 vs. G1); G3: 7.91±0,21 (p<0,05 vs. G1 and G2). Hence,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Cardiovascular research: about contraction and electrical activity 75
Kaplan-Meier curve
AT1R overexpression is associated to bradyarrhythmias and mortality unrelatedto heart failure. G protein uncoupling induces severe hypertrophy and 3rd degreeAVB; however it suppresses early mortality induced by AT1 R overexpression.
P591 Circulating microRNA-208b and miR-499 reflectmyocardial damage in cardiovascular disease
M.F. Corsten1, R. Dennert1, S. Jochems1, T. Kuznetsova2,D.R. Wagner3 , J. Staessen2, L. Hofstra1, S. Heymans1, B. Schroen1.1Maastricht University, Center for Heart Failure Research, Maastricht,
Netherlands; 2Catholic University of Leuven, Department of CardiovascularDiseases, Leuven, Belgium; 3Centre de Recherche Public (CRP) - Santé,Luxembourg, Luxembourg
Purpose: Small RNA molecules, called microRNAs, freely circulate in humanplasma and correlate to varying pathologies, sparking interest in their applicationas novel biomarkers. In this study, we have explored their diagnostic potential ina selection of prevalent cardiovascular disorders.Methods: MicroRNAs were isolated from plasmas from well-characterized pa-tients from databases for the following diseases: acute myocardial infarction (AMI:n=36 versus 36 controls), viral myocarditis (VM): n=14 vs n=20 post-VM patientsand n=20 controls), diastolic dysfunction (4 groups of n=20), and acutely decom-pensated congestive heart failure (CHF: n=33 vs 20 controls). Plasma levels ofselected microRNAs, including heart-associated (miR-1, -133a, -208b and -499),fibrosis-associated (miR-21 and miR-29b) and leukocyte-associated (miR-146, -155 and -223) candidates, were subsequently assessed using real-time PCR.Results: Remarkably, plasma microRNA levels were not affected by a wide rangeof clinical confounders, including age, gender, BMI, kidney function, systolic bloodpressure, and white blood cell count. Most strikingly, in plasma from AMI pa-tients, cardiac myocyte-associated microRNAs were highly elevated (miR-208b:1500-fold, p<0.005, and miR-499: 90-fold, p<0.001), as compared to patientswith atypical chest pain and normal coronary arteries (AUC in ROC-curve: 0.89with p<0.0000001 for both). These levels correlated with levels of troponin T,indicating the release of microRNAs out of injured cardiomyocytes. In VM, weobserved a milder but also significant elevation of these miRs, 30- and 6-fold,respectively. Plasma levels of leukocyte-expressed microRNAs were not signifi-cantly affected in AMI or VM patients, despite elevated white blood cell counts.MiR-1 plasma levels showed only a non-significant trend towards increased levelsin relation to cardiac damage. Finally, in acutely decompensated congestive heartfailure or diastolic dysfunction, no significant changes in all miRs studied could beobserved, though intruigingly, muscle-specific miR-133a levels correlated to NT-proBNP levels (R2 = 0.18, p<0.001) in patients with diastolic dysfunction, but notis the setting of acutely decompensated CHF.Conclusions: Our data show that cardiac damage in AMI and VM initiates therelease of specific microRNAs-208b and -499 into the circulation. Importantly,these plasma microRNA levels are not affected by a range of clinical confounders.Thus, microRNA detection represent a promising novel diagnostic strategy in themanagement of acute cardiovascular disease.
P592 Prophylactic beta-blockade prevents induction ofventricular tachycardia in exercise trained desmoplakinknockout mice - a preventative therapy for ARVC
J. Gomes, A. Tinker, P.D. Lambiase. University College London,Institute of Cardiovascular Science, London, United Kingdom
Purpose: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is responsi-ble for up to 20% of sudden cardiac deaths in the young – especially athletes.Mutations in desmosomal proteins have been linked to ARVC but the mechanismof arrhythmogenesis has not been clearly defined. We have examined the ar-rhythmic substrate and the effect of exercise by performing electrophysiologicalstudies (EP) on a cardiac restricted desmoplakin (DSP) heterozygous knockoutmouse (hetKO), as a model of ARVC.Methods: 8 week old het KO and wild type (WT) DSP mice were allowed toexercise freely on a wheel for 4 weeks and the total distance recorded. Prolongedrelease propranolol pellets (2.5mg/kg/day) were implanted subcutaneously in onegroup of these mice before exercise. ECGs were recorded, a standard EP studywith VT stimulation protocol and echocardiography was performed at the end ofthis period as well as on a control group of mice that did not exercise.Results: No significant differences were seen in ECG parameters (PR, QRS du-ration, QT interval), EP parameters (SNRT, AVNERP, VERP), LV size or distance
run between the exercise and the β blocker group. 5/5 het KO mice in the exer-cise group developed VT during VT stimulation study and only 1/4 het KO miceimplanted with β blocker pellets (p<0.05) (see Fig.1). The duration of VT was alsosignificantly shorter in the β blocked group (p<0.05).
Conclusions: Exercise increases the susceptibility to ventricular arrhythmia inDSP het KO mice and this is reduced by prophylactic β blockade. This suggestsprophylactic β blockade may exert protective effects on adverse electrical remod-eling caused by increased wall stress during exercise in DSP mutation carriers.
P593 Biased agonism/antagonism of beta-arrestin activationby the angiotensin II type 1 receptor: a study of sartansand angiotensin II analogs using aldosterone turnoveras a readout
A. Lymperopoulos1 , G. Rengo2, W.J. Koch2. 1Nova SoutheasternUniversity, Ft. Lauderdale, United States of America; 2Thomas JeffersonUniversity, Philadelphia, United States of America
Introduction: we showed recently that activation of the scaffolding protein β-arrestin-1 (βarr1) by the angiotensin II (AngII) type 1 receptor (AT1R) mediatesAngII-induced aldosterone production in vitro and physiologically in vivo. Herein,we sought to investigate the relative potency of various AT1R antagonist drugs(sartans) at inhibiting βarr vs. G-protein activation and hence aldosterone produc-tion in vitro and in vivo. Additionally, we tested novel AngII "biased" agonist (i.e.that only stimulate βarrs and not G-proteins) analogs at stimulating βarr activityand aldosterone production. Finally, we investigated the alterations in plasma al-dosterone levels conferred by these agents and their impact on cardiac functionof post-myocardial infarction (MI) rats.Methods: for the in vitro tests, the adrenocortical H295R cell line was used, whichproduces aldosterone in response to AngII. For in vivo studies, post-MI rats over-expressing βarr1 in their adrenals received 7-day-long treatments with the agentsof interest.Results: Among the sartans tested, candesartan and valsartan were the mostpotent βarr activation and βarr-mediated aldosterone production inhibitors in vitro,as well as the most "biased" antagonists towards βarr vs. G-protein inhibition.Conversely, losartan and irbesartan were the least potent βarr inhibitors and theleast "biased" antagonists towards βarr inhibition. These in vitro findings werecorroborated in vivo, since candesartan and valsartan, contrary to irbesartan,caused significant plasma aldosterone reductions in post-MI rats. Accordingly,cardiac ejection fraction (EF) and contractility were significantly augmented incandesartan- and valsartan-treated rats (EF: 41.1±1% and 40±1% respectively,vs. 35±0.3% for saline-treated), but further deteriorated in irbesartan-treatedpost-MI rats (EF: 32±1%, n=7 rats/group). Finally, a novel AT1R biased agonisthas been identified, CORET ([Sar1,Cys(Et)5,Leu8]-AngII), which is far more po-tent at stimulating βarr than SII, the standard AT1R biased agonist. CORET pro-duces far greater aldosterone secretion in vitro than SII, and significantly worsenshyperaldosteronism and cardiac function of post-MI rats in vivo.Conclusions: candesartan and valsartan are the most potent sartans at lower-ing aldosterone in vitro and in vivo after MI, thus ameliorating cardiac function inheart failure progression. Losartan and irbesartan appear the least potent sartansat doing so. CORET is a novel, very potent AT1R biased agonist for βarr activa-tion, thus it might prove a very valuable research tool for future studies of AT1R"biased" βarr agonism.
P594 Vardenafil and fasudil treatment affect the heart andkidney
B.K. Huntley, S. Ameenuddin, H.H. Chen. Mayo Clinic, Department ofCardiovascular Disease, Rochester, United States of America
Purpose: Diabetes is a major risk factor for left ventricular dysfunctionwith cardiac and renal fibrosis. Fasudil is a Rho kinase inhibitor that has beenshown to prevent the development of nephropathy in diabetic (DM) rats. Varde-nafil, a phosphodiesterase-5 (PDE V) inhibitor, also impacts the RhoA/Rho Ki-nase pathway and has been shown to improve cardiovascular dysfunction in DMrats. We examined the differential effects of these two treatments on heart andkidney fibrosis and associated Rho Kinase pathway involvement.Methods: DM was induced in male Wistar rats by injecting Streptozotocin (65mg/kg). Four weeks after establishing diabetes, rats were divided into threegroups, one group received no treatment (n-6), one group (n=5) received daily Fa-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

76 Cardiovascular research: about contraction and electrical activity
sudil for two months at 100mg/kg/day and one group received Vardenafil for twomonths at 5mg/kg/day. A non-diabetic control (n=6) was also examined. Myocar-dial and kidney snap frozen tissue were used for quantitative PCR and WesternBlot (WB) analysis. Tissue sections were stained for picrosirius red and collagenIII to assess the infiltration of collagen.Results: As anticipated, DM rats developed fibrosis in both the left ventricle (LV)and kidney medulla (KM) compared to non-diabetic controls. Both Fasudil andVardenafil reduced fibrosis in LV and KM, however Fasudil was more effective inthe LV, while Vardenafil was more effective in the KM. Importantly, this differen-tial effect on fibrosis resulted in a greater improvement of diastolic function byFasudil and a greater improvement of renal function by Vardenafil. Interestingly,Vardenafil more greatly reduced collagen III expression than picrosirius red in KM,while in LV both stainings changed proportionately. To assess Rho kinase path-way involvement, full length Rho-associated, coiled-coil containing protein kinase(ROCK 1) and active C-terminal ROCK 1 were assess by WB and the ratio of fulllength to active forms determined. Fasudil significantly reduced the ROCK 1 ratioin LV tissue, but not in KM. Conversely, Vardenafil did not affect ROCK 1 ratio inLV, but was significantly reduced in KM.Conclusion: We demonstrate that diabetes induces fibrosis in both LV and KM.This fibrosis was more greatly attenuated by Fasudil in LV with a greater improve-ment in diastolic function, and by Vardenafil in KM with a greater improvemention renal function. Our studies suggest that the fibrosis induced in LV by diabetesis different from the fibrosis induced in KM and responds differently to two dif-ferent treatments. Both may involve the RhoA/Rho kinase pathway but at distinctpathway levels.
P595 Early combined therapy with sildenafil and adiposetissue-derived mesenchymal stem cells alleviates leftventricular remodeling and improves heart function inrat dilated cardiomyopathy
H.K. Yip, Y.C. Lin, M. Fu, S. Leu, C.K. Sun, S. Chua. Chang GungMemorial Hospital-Kaohsiung Medical Center, Chang Gung University Collegeof Medicine, Kaohsiung, Taiwan
Purpose: Sildenafil and mesenchymal stem cells (MSC) have been shown toimprove left ventricular (LV) function of dilated cardiomyopathy (DCM). We inves-tigated whether early combined sildenafil and adipose tissue-derived (AD) MSCtherapy offers synergistic benefit in alleviating LV remodeling and preserving LVcontractility in a Fischer rat DCM model which was induced via subcutaneous in-jection of porcine heart myosin mixed with an equal volume of Freund completeadjuvant.Methods and Results: The rats (n=8 per group) were divided into group 1 (nor-mal control), group 2 (saline-treated DCM), group 3 (DCM with 2.0 x 106 ADM-SCs implanted into LV anterior wall), group 4 (DCM with oral sildenafil of 30mg/kg/day), and group 5 (DCM plus combined sildenafil and ADMSCs). ADMSCimplantation and oral sildenafil were given on day 3 after DCM induction. The ratswere sacrificed on day 90 following DCM induction. The results showed systolicblood pressure was similar among 5 groups. Protein expressions of Cx43 and mi-tochondrial Cytochrome-C and mRNA expressions of PGC-1α, eNOS, Bcl-2 andIL-10 were lower in group 2 than in other groups, and lower in groups 3 and 4 thanin groups 1 and 5 (all p<0.05). The mRNA expressions of endothelin-1, MMP-9,Bax and caspase-3 were higher in group 2 than in other groups, and higher ingroups 3 and 4 than in groups 1 and 5 (all p<0.05). The LV ejection fraction waslower in group 2 than in other groups, and lower in groups 3 and 4 than in groups1 and 5, whereas cardiomyocyte apoptosis, mitochondrial oxidative stress, LVsystolic and diastolic dimensions, and fibrosis of LV myocardium were higher ingroup 2 than in other groups, and higher in groups 3 and 4 than in groups 1 and5 (all p<0.005).Conclusion: Early therapy of combined sildenafil and ADMSCs was superior toeither one for preserving LV function and reducing LV remodeling in DCM rats.
P596 Myocardial aging, fibrosis and dysfunction: role ofc-type natriuretic peptide
S.J. Sangaralingham1 , D. Bellavia1, P.M. Mckie1, F.L. Martin1,T. Ichiki1, G.E. Harders1, E.L. Ritman2, H.H. Chen1, J.C. BurnettJr1. 1Mayo Clinic, Department of Cardiovascular Disease, Rochester,
United States of America; 2Mayo Clinic, Department of Physiology andBiomedical Engineering, Rochester, United States of America
Purpose: The aging heart is characterized by myocardial fibrosis with subse-quent myocardial dysfunction which may contribute to the development of heartfailure (HF), particularly in the elderly. C-type natriuretic peptide (CNP) is of en-dothelial cell origin and represents the most potent anti-fibrotic peptide of the na-triuretic peptide family and is pro-angiogenic. The impact of aging on plasma CNPand associated left ventricular (LV) alterations in structure and function are unde-fined. We hypothesized that a decrease in plasma CNP occurs with aging and isassociated with an increase in LV fibrosis and altered LV structure and function.Methods: Studies were performed in 2, 11 and 20 month old male Fischer rats(n=8/group). Left ventricular structure and function was assessed by standardand speckle-derived echocardiography and cardiac microCT imaging. Left ventri-cles were harvested for gross and histopathologic analysis and plasma CNP wasmeasured. *p≤0.05 vs 2 months; # p≤0.05 vs 11 months.
Results: Aging from 2 to 11 to 20 months (equivalent to human aging from ado-lescence to the 6th decade of life) was associated with a significant incrementaldecrease in plasma CNP (from 30±3 to 21+1* to 9±1*# pg/ml) and significantand progressive LV fibrosis (from 9±1 to 15±1* to 21±1*# %). The decrease inplasma CNP, seen with aging, was also associated with a significant reductionsin ejection fraction (88±1 to 80±1*%), circumferential systolic strain (-23±1 to-18±1*%), circumferential systolic (sSR) and diastolic strain rate (SR-E) (-6.1±0.2to -4.8±0.2*1/s and 7.1±0.6 to 5.6±0.2*1/s, respectively) and total coronary mi-crovascular volume (12.6 to 4.4 mm3). Importantly there was a strong negativecorrelation between LV fibrosis and plasma CNP levels (r2 =0.68, p<0.0001)while plasma CNP was a strong predictor of LV fibrosis as were circumferentialsSR and SR-E significant predictors. In bivariate regression models, a reductionin plasma CNP was the only variable that remained a significant predictor of LVfibrosis.Conclusion: We report for the first time that aging is characterized by a progres-sive decline in plasma CNP together with a progressive increase in LV fibrosis,a reduction in coronary microvascular volume and functional LV impairment. Fur-ther studies are warranted to explore the role of the reduction in endogenous CNPas a mechanism of myocardial aging with altered LV structure and function andthe therapeutic potential of novel CNP based peptides to prevent cardiac agingand delay the progression to HF.
P597 Molecular modulation of post-ischemic cardiacremodeling by hindlimb ischemia
G. Esposito1, G.G. Schiattarella1, C. Perrino1, A. Franzone1 ,A. Sannino1, G. Gargiulo1, G. Pironti1, A. Cannavo1, N. Zambrano2 ,M. Chiariello1. 1University Hospital Federico II, Naples,
Italy; 2University of Naples Federico II, Dpt of Biochemistry & Med.Biotechn./CEINGE-Advanced Biotechnology, Naples, Italy
Purpose: Peripheral arterial disease (PAD) is an important clinical manifestationof systemic atherosclerosis, up to 50% of patients with PAD undergoes to death byacute myocardial infarction and ischemic stroke. The release of several bioumoralfactors by chronic ischemic limb has been recently involved in the negative prog-nostic association between PAD and coronary artery disease. In this study we in-vestigated the molecular mechanism(s) whereby chronic hindlimb ischemia mightactivate detrimental signaling pathways involved in ischemic cardiac remodeling.Methods: In order to test the detrimental role of chronic hindlimb ischemia onpost-ischemic cardiac remodeling, we analized cardiac function and molecular al-terations in 4 groups of mice: 1) mice with unilateral hindlimb ischemia (L); 2) micethat after five weeks of hindlimb ischemia underwent myocardial infarction (PL5);3) mice undergoing only myocardial infarction (MI); 4) control mice (SHAM).Results: Seven days after MI, cardiac function was evaluated by transthoracicechocardiography in all the groups. Interestingly, cardiac function was significantlydecreased in PL5 mice compared to MI (% fractional shortening, MI: 47.2±1.9;PL5: 38.5±0.8, p<0.05), and this was associated with a strong increase in %cardiomyocyte apoptotic death as shown by TUNEL assay (MI:10.5±2.2, PL5:54.3±2.5, p<0.05). Consistent with these results, PL5 hearts exhibited a signif-icant activation of p53 compared to MI (p<0.05). To exclude the involvement ofinflammatory mediators in the development of myocardial damage due to chronichindlimb ischemia, left ventricular samples from each of the four experimentalgroups were subjected to multiplex assay for pro-inflammatory cytokines TNF-α,IL-1β and IL-6. Importantly, 5 weeks of hindlimb ischemia did not significantly af-fect pro-inflammatory cytokines levels in PL5 hearts compared to MI (MI:TNF-α 75.3±0.6, IL-1β: 115.4±0.9, IL-6: 149.7±0.4; PL5: TNF-α 83.4±0.3, IL-1β:108.5±0.2, IL-6: 125.6±0.9, not significant). Next, rat neonatal cardiomyocyteswere incubated with serum of PL5 and MI mice for 4 hours in low oxygen condi-tions, and the apoptotic cell death was then evaluated by TUNEL assay. Surpris-ingly, only serum from PL5 mice was able to induce marked positivity to TUNELstaining in cardiomyocytes.Conclusions: Our data show for the first time that chronic hindlimb ischemiaplays an important role in the modulation of post-ischemic cardiac remodeling.This role is independent from atherosclerosis or systemic inflammation, and ismediated by the activation of pro-apoptotic pathways.
P598 Dietary supplementation with docosahexaenoic acid(DHA), but not with eicosapentaenoic acid (EPA),reduces plasma lipids and attenuates pressureoverload induced cardiac dysfunction and hypertrophy
M.K. Duda, U. Mackiewicz, M. Maczewski. The Medical Centre ofPostgraduate Education, Department of Clinical Physiology, Warsaw, Poland
Objective: Recent evidence suggests that supplementation with fish oil rich inboth EPA and DHA lowers circulating triglycerides, cholesterol and free fatty acidsconcentration, and may prevent development of heart failure. The present investi-gation compared effect of EPA and DHA on adaptation of the left ventricular (LV)to chronic pressure overload.Methods: Male Wistar rats were fed either a standard chow or a modified stan-dard chow containing 3% of total energy from DHA, EPA or DHA+EPA (50:50).After 1 week rats underwent pressure overload induced by abdominal aortic band-ing or sham surgery (n=8-10/group). After 12 weeks LV function was assessed byechocardiography and blood samples were obtained.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Cardiovascular research: about contraction and electrical activity 77
Results: On the standard diet banding increased LV mass by 39%, LV enddiastolic volume by 51% and end systolic volume by 149% compared tosham (p<0.05). Serum free fatty acids, triglycerides and cholesterol were low-ered with DHA and DHA+EPA (0.27±0.02, 0.28±0.03 vs. 0.55±0.06mmol/L,0.75±0.5, 0.79±0.05 vs. 1.36±0.15mg/mL and 0.48±0.02, 0.51±0.02 vs.0.66±0.03mg/mL; p<0.05, respectively) and only free fatty acids concentrationwas modestly decreased with EPA (0.39±0.02 vs. 0.55±0.06mmol/L, p<0.05).As shown in Figure, supplementation with DHA or DHA+EPA prevented the in-crease in LV mass, and end diastolic and end systolic volumes, but EPA had noeffect.
Conclusion: DHA from fish oil, but not EPA, attenuated pressure overload in-duced LV hypertrophy, LV remodeling and contractile dysfunction. This beneficialeffect of DHA corresponded with a favorable impact on serum lipids profile.
P599 A cardiac biopacemaker created by acceleration of asubsidiary pacemaker via adenovirus-mediatedexpression of a chimaeric pacemaker channel, HCN212
G.M. Morris1, P.A. Kingston1, H. Dobrzynski1 , M. Lei1,R.B. Robinson2, M.R. Boyett1. 1University of Manchester,
Manchester, United Kingdom; 2Columbia University, New York, United States ofAmerica
Introduction: Sick sinus syndrome (SSS) is common and may require pace-maker implantation, gene therapy (biopacemaking) may be an alternative. Thesinus node (SN) is highly specialised, so repair may be superior to a de novobiopacemaker in the working myocardium. We hypothesised that expression of achimaeric pacemaker channel (HCN212) in a bradycardic subsidiary pacemakerregion of the SN may increase the pacemaker rate.Methods: A SSS model was generated by the removal of the upper two-thirds ofa rat SN. The leading pacemaker site was identified by activation mapping. SomeSSS preparations were injected in this region with adenovirus containing HCN212(Ad-HCN212). Control (intact rat SN) and SSS preparations were maintained intissue culture and electrical activity was monitored.Results: The SSS model displayed a slower rate than the control (Fig. 1). Cellsize in the subsidiary pacemaker (superior aspect of inferior vena cava, IVC) wascomparable to the centre of the SN and smaller than in the working myocardium(P<0.001). The subsidiary pacemaker was responsive to β-adrenergic stimulationand was partially dependent on the pacemaker "funny" current, If. In contrast tocentral SN, HCN4 was undetectable by immunohistochemistry in the subsidiarypacemaker (but connexin43 was). Injection of Ad-HCN212 significantly increasedthe pacemaker rate towards that in the intact SN (Fig. 1).
Figure 1. Mean (±SEM) pacemaker rates of control, SSS, and SSS preparations expressinggreen fluorescent protein (Ad-GFP) or HCN212 (Ad-HCN212). ***P<0.001.
Conclusions: There is a subsidiary pacemaker close to the IVC that shares somecharacteristics of the centre of the SN. Adenovirus-mediated expression of HCNchannels in the subsidiary pacemaker returned the pacemaker rate towards nor-mal.
P600 Genome-wide linkage analysis in a large family withprogressive cardiac conduction disease and suddendeath: a novel lamin A/C complex deletion
R.F.J. Marsman1, A. Bardai1, A.V. Postma2, L. Beekman2,R.H. Lekanne Deprez3, A.A.M. Wilde4, L.J. Jordaens5 ,
C.R. Bezzina1. 1Academic Medical Center, Heart Failure Research Center,Department of Experimental Cardiology, Amsterdam, Netherlands; 2AcademicMedical Center, Heart Failure Research Center, Department of Anatomy,Embryology and Physiology, Amsterdam, Netherlands; 3Academic MedicalCenter, Amsterdam, Netherlands; 4Academic Medical Center, Departmentof Cardiology at the University of Amsterdam, Amsterdam, Netherlands;5Erasmus Medical Center, Thoraxcenter, Department of Cardiology, Rotterdam,Netherlands
Objective: The purpose of this study was to identify the underlying genetic defectin a large Dutch family with progressive conduction disease and sudden cardiacdeath.Methods: We evaluated twenty-three members of a four-generation Dutch fam-ily with conduction disease transmitted in an autosomal dominant fashion. Sub-jects underwent standard 12-lead electrocardiography, 24-hr ambulatory ECGand echocardiography. Twenty-five individuals were genotyped with the use ofthe Illumina Human610-Quad BeadChip. Merlin software was used for multipointlinkage analysis. Standard PCR-based exon-scanning techniques were used aswell as multiplex ligation-dependent probe amplification (MLPA) for mutation de-tection. Fine mapping of the sequences bordering the breakpoints was carriedout using direct sequencing.Results: Nine affected family members were identified, of whom three died sud-denly, five displayed AV conduction abnormalities, four had atrial arrhythmias andtwo experienced documented ventricular tachyarrhythmias. Some family mem-bers showed mild signs of dilated cardiomyopathy. ECG abnormalities oftenpresented in middle adult life (30-50 years of age). Genome-wide genetic link-age analysis identified five chromosomal regions in aggregate spanning approxi-mately 67 cM with a maximum parametric logarithm of odds (LOD) score of 2.3.Sequence analysis of candidate genes, including CACNA1H, GJA5, CASQ2 andLMNA did not reveal any non-synonymous variant. MLPA analysis of the LMNAgene, encoding the nuclear-envelop protein lamin A/C, revealed a novel generearrangement; inversion of 22 bp, flanked by a 3.8-kb and a 7.8-kb deletion,omitting exons 3 to 12. The presence of short direct repeats in the vicinity of thedeletion breakpoints suggest a possible serial replication slippage event.Conclusions: We identified for the first time a complex deletion in the LMNA genein a four-generation Dutch family with progressive conduction system disease,including sinus bradycardia, atrioventricular block and atrial arrhythmias.This research was funded by the NHS grant 2007B010.
P601 Discrepancy between acute and long-term effects ofthe calmodulin/CaMKII/calcineurin pathway onarrhythmogenesis in the CAVB dog
V.J.A. Bourgonje, M. Schoenmakers, H.D.M. Beekman, R. VanDer Nagel, L.J. De Windt, A.A.B. Van Veen, M.A. Vos. University
Medical Center Utrecht, Division Heart and Lungs, Medical Physiology, Utrecht,Netherlands
Introduction: CaMKII & calcineurin activation can lead to arrhythmias via anacute and a chronic pathway (Fig. 1). In the chronic AV-block (CAVB) dog, en-hanced susceptibility for arrhythmias and ventricular remodelling is present. Here,we studied whether 1) cardiac remodelling in the CAVB dog is due to long-termCaMKII/calcineurin activation, and 2) whether blocking of CaMKII at the acutephase is anti-arrhythmic.Methods: To block activation of Calcineurin, cyclosporin A (CSA) was given to 5dogs. 7 non-treated CAVB dogs served as control. Dofetilide was administeredto induce TdP. In another group of 5 TdP-sensitive CAVB dogs, the Calmodulininhibitor W-7 was administered to determine if CaMKII was involved in arrhyth-mogeneity. Left ventricular biopsies were taken at 0, 2, and 9 weeks of AV-block,and expression of (phosphorylated, P) CaMKII and Rcan1-4 (downstream targetof Calcineurin) was determined.Results: CSA treatment in the CAVB dog did not inhibit electrical (QTc +17%in CSA vs. 21% in control) or structural remodelling (heart to body weight ratiowas 9 gr/kg in both groups at 2 weeks AV-block remodelling), nor did it preventTdP-arrhythmias (4 out of 7 dogs in control and 4/5 in CSA). In line with this,expression of Rcan1-4 remained unaltered.At 2 and 9 weeks after AV-block, CaMKII protein and CaMKII-P was not changed.
Figure 1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

78 Cardiovascular research: about contraction and electrical activity
W-7 was nonetheless anti-arhythmic (32±18 before treatment vs. 4±7 TdP per10 minutes after W-7 treatment, P=0.002).Conclusions: Occurrence of remodelling and arrhythmias in the CAVB dog arenot related to chronic activation of CaMKII/Calcineurin. In contrast, arrhythmiascould be efficiently reduced through acute inhibition of Calmodulin, which suggesta differential role of the pathway in acute and chronically induced arrhythmias.
P602 Regulation of B-Adrenergic control of heart rate byGTP-Cycolhydolase 1 and Tetrahydrobiopterin
D. Adlam1, J.P. De Bono1, E. Danson1, A. Tatham1, B. Casadei1,D.J. Paterson2, K.M. Channon1 . 1University of Oxford, Departmentof Cardiovascular Medicine, Oxford, United Kingdom; 2University of
Oxford, Laboratory of Physiology, Oxford, United Kingdom
Purpose: Clinical markers of cardiac autonomic function, such as heart rate andthe response to exercise, are important predictors of cardiovascular risk. Tetrahy-drobiopterin (BH4) is a required cofactor for enzymes with roles in cardiac auto-nomic function, including nitric oxide synthase and tyrosine hydroxylase. Synthe-sis of BH4 is regulated by GTP cyclohydrolase I (GTPCH), encoded by GCH1.Recent clinical studies have reported associations between GCH1 variants andheart rate, but the mechanistic importance of GCH1 and BH4 in autonomic func-tion in vivo remains unclear. We sought to investigate the effect of BH4 defi-ciency on the autonomic regulation of heart rate in a mouse model of BH4 de-ficiency.Methods and Results: In the hph-1 ENU mouse model, reduced cardiac GCH1expression, GTPCH enzymatic activity and BH4 were associated with increasedresting heart rate measured by tail-cuff, whereas blood pressure was not signifi-cantly different. Voluntary wheel exercise training with continuous radiotelemetrydecreased resting heart rate, but hph-1 mice retained a relative tachycardia. Vagalnerve stimulation in vitro induced bradycardia equally in hph-1 and WT mice, bothbefore and after exercise training. Direct atrial responses to carbamylcholine werealso equal. In contrast, propranolol treatment normalized the resting tachycardiain hph-1 mice in vivo. Stellate ganglion stimulation and isoproterenol applicationin vitro induced a greater tachycardic response in hph-1 mice.
Effect of BH4 on sympathetic function
Conclusions: Thus, reduced GCH1 expression causes BH4 deficiency that re-sults in tachycardia through enhanced β-adrenergic sensitivity, with no significanteffect on vagal function. GCH1 expression and BH4 are novel determinants ofcardiac autonomic regulation that may have important roles in cardiovascularpathophysiology.
P603 Recurrence of atrial fibrillation after concomitantablation and mitral valve surgery is associated with leftatrial fibrosis
A. Olasinska-Wisniewska, T. Mularek-Kubzdela, W. Sarnowski,A. Marszalek, W. Seniuk, M. Jemielity, S. Stefaniak, Z. Oko-
Sarnowska, B. Perek, S. Grajek. Poznan University of Medical Sciences, Poznan,Poland
Background: Atrial fibrillation intra-surgical ablation is a procedure which is in-creasingly performed in conjunction with surgery for various heart diseases. Al-though restoration of sinus rhythm is effective initially, atrial fibrillation may recur.We investigated whether the extent of left atrial fibrosis is associated with ablationresults at 1 year follow-up.Methods: Concomitant ablation of AF, lasting 2 to 240 months, was performedin 66 patients (mean age of 60,5±7.1 y, 77,3% female) with paroxysmal (22 pts)or permanent (44 pts) AF undergoing mitral valve operations. Biopsies of theposterior wall of the left atrium were obtained during the operation. The slideswere stained with Azan staines for collagen and the extent of fibrosis in the leftatrium was determined by an automatic image analyzer. Clinical outcome wasevaluated 12 months post surgery.Results: Mean LA fibrosis in study group was 42±11,8%. Pts with perma-nent AF presented higher percentage of fibrosis than pts with paroxysmal AF(45,8%±11,8 vs 34,6%±7,9, p=0,0001). Three patients died perioperatively, and7 during follow-up. One patient was lost to follow-up. The remaining 55 patientswere assessed for AF recurrence at 12 month. AF was present in 21 pts (GroupI) and sinus rhythm in 34 pts (Group II). LA fibrosis was significantly higher in theGroup I with recurrent AF (47,6±12,3% vs 38,7±11,2%, p=0,009). No correla-tions were found between percentage of fibrosis and history of diabetes mellitus,arterial hypertension and age. The ablation success rate was higher in pts withparoxysmal AF than with permanent AF (19 vs 15, p=0,0006).
Conclusion: The higher percentage of LA fibrosis is associated with increasedrisk of recurrent AF after concomitant ablation and mitral valve surgery. Patientswith paroxysmal AF show lower degree of fibrosis and better ablation results.
P604 Atrial structural changes following nicotine exposure:implications for atrial fibrillation
L. Mackenzie1, G. Rangnekar1 , A. Chakrabarty2 , P. Sanders2.1University of Adelaide, Adelaide, Australia; 2Royal Adelaide Hospital,Cardiovascular Research Centre, Adelaide, Australia
Introduction: Smoking has been implicated as one of the new risk factors ac-counting for the burgeoning epidemic of atrial fibrillation (AF). Structural remodel-ing is recognized as an important element forming the AF substrate. We investi-gated whether nicotine, an important element in cigarette smoking, causes atrialstructural remodelling.Methods: 72 adult male Sprague Dawley rats were studied in 3 equal groups:high dose nicotine (6mg/kg/day); low dose nicotine (0.6mg/kg/day); and saline,infused via subcutaneous osmotic pumps. Atria were harvested at 7 or 14 days forhistological analysis. Sections (6μm) were stained for fibrosis (Picro Sirius Red),glycogen and mast cells (Periodic Acid Schiff counterstained with Toluidine Blue).A plasma level of cotinine, the primary metabolite of nicotine, was measured byELISA.Results: The table presents the data for each element evaluated at 7 and 14days in each group. Nicotine treatment resulted in a dose dependent increasesin the levels of collagen (r2=0.809), glycogen (r2=0.789) and mast cell infiltrates(r2=0.722) with the levels of each being correlated with plasma cotinine levels(P<0.001).
Control Low Dose High Dose P value(d7/d14) Nicotine (d7/d14) Nicotine (d7/d14)
% Collagen content 1.7±0.7/2.4±0.9 3.1±1.6/3.9±1.0 5.6±0.8/9.1±1.7 P<0.001% Glycogen accumulation 2.2±0.3/2.7±1.5 2.7±1.5/14.3±3.5 18.9±3.9/20.9±2.2 P<0.001% Mast Cell infiltration 0.1±0.1/0.6±0.2 0.7±0.9/2.5±1.3 3.1±1.3/3.0±0.6 P<0.001
Conclusion: Nicotine exposure results in a dose dependent, progressive atrialstructural remodelling characterized by increased collagen and glycogen depositsand inflammatory cell infiltrates. These abnormalities may account for the asso-ciation between cigarette smoking and AF. In addition, it raises concern of thepotential detrimental effects of nicotine replacement therapies.
P605 Generation of a diet-induced mouse model of obesitywith features of cardiomyopathy and coronarymicrovascular remodelling
C. Kleinert1, M. Mancini2, A. Varela-Carver1, H.T. Parker1,M. Leopizzi2 , G. D’amati2, P.G. Camici1. 1Imperial College London,
London, United Kingdom; 2Sapienza University of Rome, Rome, Italy
Purpose: Different types of primary and secondary cardiomyopathies are char-acterised by interstitial and replacement fibrosis as well as coronary microvas-cular remodelling. The mechanisms of microvascular remodelling remain poorlyunderstood. Animal models are therefore necessary to unravel the pathogeneticmechanisms of coronary microvascular remodelling and test the effect of potentialnew treatments.Methods: A mouse model of diet-induced obesity (DIO) was generated by feed-ing C57BL/6 mice a 45% high-fat diet for a maximum of 14 weeks. Physiologicaldata were recorded throughout this period. After sacrifice, hearts were fixed informalin and paraffin embedded. Multiple 4 μm thick short axis sections were cutfrom each heart and stained with hematoxylin-eosin and Picrosirius red. Imagesof all histological fields were acquired at a magnification of 40x. The number ofintramural coronary arterioles for each heart was recorded. Vessel and lumen di-ameters and the medial area of intramural arteriolar vessels were measured andlumen/vessel area was then derived. Histological and histomorphometric studieswere carried out using Metamorph 6.2 software.Results: Compared to age-matched controls, DIO mice had a significant increasein fasting serum insulin levels (0.59±0.03 vs. 2.79±0.62, p<0.05, n=15 per group)as well as a significant increase in both the body weight/tibia ratio (1.53±0.13 vs.2.23±0.15, p<0.0005, n=15 per group) and the fat weight/tibia ratio (39.63±16.66vs. 158.11±20.94, p<0.0005, n=15 per group). Additionally, a significant in-crease in the heart weight/tibia ratio (6.84±0.19 vs. 7.49±0.17, p<0.05, n=15per group) in high-fat diet fed mice was observed. Histological and histomorpho-metric analysis of DIO mice showed a significant increase in interstitial fibrosis(2891±833.52μ2 vs. 7204±1842.24μ2, p<0.05, n=4 per group) and small ves-sel remodelling with a significant increase in medial area (1325.61±225.77μ2 vs.3384.14±310.28μ2, p<0.0005, n=6 per group) as well as a significant reductionof lumen/vessel area (0.38±0.03 vs. 0.27±0.03, p<0.05, n=6 per group) com-pared to control mice.Conclusions: We have successfully generated a diet-induced mouse model withfeatures of cardiomyopathy and coronary microvascular remodelling. The pheno-type of small vessel remodelling in this mouse model is closer to the phenotypeseen in patients with arterial hypertension or hypertrophic cardiomyopathy com-pared to other mouse or rat models.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Cardiovascular research: about contraction and electrical activity / Basic progress in cardiovascular repair 79
P606 Hemodynamic compromise following high-dosepantoprazole infusion in mice
B. Unsoeld, N. Teucher, M. Didie, S. Sosalla, C. Jacobshagen,T. Seidler, L. Maier, G. Hasenfuss, W. Schillinger. UniversitaetsmedizinGoettingen, Goettingen, Germany
Background: It has been shown that proton pump inhibitors reduce contractileforce in isolated rabbit and human myocardium by reducing calcium transientsand myofilament calcium sensitivity. This study was planned to investigtate thein vivo hemodynamic effects of pantoprazole in healthy myocardium and in thesetting of heart failure.Methods: Pressure volume loops were recorded in sham operated mice and mice4 weeks after myocardial infarction. The hemodynamic effects of intravenous in-fusion of Pantoprazole were recorded.Results: Infusion of 10mg/kg/min pantoprazole induced bradycardia (heart rate82±2% of baseline, n=9, p<0.01), decreased myocardial contractility (dp/dtmaxnormalized to blood pressure 86±4% of baseline, preload adjusted maximalpower 43±7%, n=9, p<0.01 each) and reduced arterial elastance (78±6% ofbaseline, n=9, p<0.01). These changes led to a decrease of systolic blood pres-sure to 84±3% of the value before pantoprazole infusion (n=9,p<0.01).The described effects were fast, beginning immediately with the infusion and usu-ally reaching a plateau after 2 or 3 minutes of infusion. After stopping the contin-uous infusion the effects were at least partially reversible with a relatively fastkinetics. The effects were of comparable size in healty mice and mice with MI.However in 4 out of 13 mice with MI infusion of 3-10mg/kg/min pantozole rapidlylead to pump failure which was lethal in 2 of the animals. The 2 other mice recov-ered after the infusion was stopped immediately.Conclusion: At higher infusion rates pantoprazole is able to induce negativehemodynamic responses. Especially in the setting of heart failure these effectscan lead to significant impairment of cardiac function. Therefore high infusionrates of pantoprazole should be avoided especially in heart failure patients. Asthe observed effects are rate-dependent and reversible lower infusion rates seemto avoid the possible problems.
BASIC PROGRESS IN CARDIOVASCULAR REPAIR
P608 Dual stem cell therapy after myocardial infarctionworks specifically by the cxcr4-sdf1 axis andstimulates myocardial perfusion and resident cardiacstem cells
H.D. Theiss, M. Vallaster, C. Rischpler, S. Brunner, L. Krieg,M. Hacker, J. Mueller-Hoecker, W.M. Franz. Ludwig-Maximilians
University, Munich, Germany
Background: Dual stem cell therapy comprising G-CSF based stem cell mobi-lization and stabilization of cardiac SDF-1 by DPP-IV-inhibition may revolutionizetherapy of myocardial infarction. It finally leads to improved cardiac homing ofstem cells, enhanced heart function and increased survival. However, it remainsunclear, whether this new approach works specifically by the SDF1-CXCR4- axis,stimulation of resident cardiac stem cells and improved myocardial perfusion.Methods: We induced AMI in 10 weeks old male C57BL/6 mice using surgicalocclusion of the left descending artery (LAD). Mice were then treated with G-CSF+/- the DPP-IV inhibitor Diprotin A. Saline treated animals served as controls. An-tagonization of CXCR-4 was performed by application of AMD3100. FACS anal-yses were used to determine stem cell populations in the myocardium after 6days. Histology was performed to examine capillary density after 6 days and in-farct size 30 days after AMI. Cardiac function parameters were assessed using aMillar-Tip catheter system. Survival was analyzed by Kaplan-Meier-method for 30days (n=20 in each group). Myocardial perfusion was measured by single photonemission computed tomography (SPECT).Findings: First, we established in a titration scheme the optimal dosage ofAMD3100 (1,25mg/kg) that is sufficient to block CXCR-4 but is not mobilizingstem cells in a relevant extent. Based on these findings, AMD3100 effectively in-verted the beneficial effect of G-CSF and Diprotin A concerning the homing ofcirculating stem cells, cardiac remodeling (infarct size), heart function and sur-vival (Kaplan-Meier curves). Secondly, G-CSF and Diprotin A application signif-icantly enhanced neovascularization (represented by CD31 positive capillariesin the borderzone). Besides, dual stem cell therapy significantly enhanced my-ocardial blood flow (SPECT) which was antagonized by AMD. Finally G-CSF +Diprotin A administration effectively stimulated the pool of resident cardiac stemcells (FACS) which was reversed by AMD3100 as well.Interpretation: Dual stem cell therapy mainly works by the SDF1-CXCR4-axis.This gives final proof that the extent of stem cell homing which is associated withan increase of myocardial perfusion and enhancement of resident cardiac stemcells is decisive for the success of this new therapeutic approach.
P609 Human embryonic stem cell-derived cardiomyocytesimprove cardiac function after myocardial infarction:paracrine effects outweigh the contribution of activecontractile force
L.W. Van Laake1, R. Passier2, K. Den Ouden1, C. Schreurs2,J. Monshouwer-Kloots2 , D. Ward-Van Oostwaard2, C. Van Echteld1,P.A. Doevendans1 , C.L. Mummery2. 1University Medical Center Utrecht, DivisionHeart and Lungs, Utrecht, Netherlands; 2Leiden University Medical Center,Department of Anatomy and Embryology, Leiden, Netherlands
Purpose: Transplantation of human embryonic stem cell-derived cardiomyocytes(hESC-CM) has been shown to improve function of the rodent heart one month af-ter myocardial infarction. Since the mechanistic basis and optimal delivery strate-gies are unclear, we investigated the influence of the number of injected cells,resulting graft size and possible paracrine mechanisms in this process.Methods: Myocardial infarction was induced in non-obese diabetic severe com-bined immunodeficient (NOD-SCID) mice (n=84) followed by injection of hESC-CM at different dosages, hESC-non-CM derivatives, culture medium or no injec-tion at all. Serial high resolution (9.4 T) magnetic resonance images were ac-quired after 2 days, 4 weeks and 12 weeks to assess cardiac function (n=70).Graft sizes were quantified, identified by epifluorescence of a transgenic GFP-marker and characterized by immunofluorescent co-staining. Possible paracrinecontributions of the donor cells were investigated using (immuno-)histochemicalstaining.Results: Transplantation of either hESC-CM or other differentiated hESC-derivatives improved short, mid- and long term cardiac performance and sur-vival, although cardiomyocyte-containing populations provided additional func-tional benefit above other cells at mid-term (4 weeks). Cardiomyocytes were alsothe only cells present in significant numbers in grafts 12 weeks after injection.The temporary cardiomyocyte-specific enhancement was associated with ele-vated vascular density around the graft and attenuated compensatory remodel-ing. However, increasing the number of hESC-CM for injection failed to enhanceheart function further. Moreover, we observed that small graft size was associatedwith a better functional outcome.Conclusions: Our results showed that hESC-CM increased myocardial vascu-larization and improved heart function in an immunodeficient mouse model ofmyocardial infarction but that their functional advantage over differentiated hESC-non-CM was lost at the long term. Since doubling graft size did not further en-hance cardiac function, active contraction of donor cells is not likely to be themechanism behind the observed functional improvement in this model; paracrineeffects including stimulation of neovascularization appear more important.
P610 Safety and efficacy of autologous mesenchymal stemcells for the treatment of end-stage dilatedcardiomyopathy - a comparison of intracoronary anddirect intramyocardial injection
S.P. Chin1, A.E. Poey2, S.K. Chang2, C.Y. Wong3, K.H. Lam4,S.K. Cheong5. 1International Medical University, Kuala Lumpur, Malaysia;2Penang Adventist Hospital, Penang, Malaysia; 3Cytopeutics, Kuala Lumpur,Malaysia; 4Assunta Hospital, Selangor, Malaysia; 5Universiti Tunku AbdulRahman, Kuala Lumpur, Malaysia
Background: Bone marrow stem cells may improve cardiac function followingheart attack. Mesenchymal stem cells (MSC) from bone marrow can differen-tiate into cardiomyocytes, vascular smooth muscle and endothelial cells. Theyalso exhibit immune-modulatory and paracrine effects to augment cardiac repair.However their safety, optimal cell number and route of administration are not de-termined for patients with severe dilated cardiomyopathy.Objective: To demonstrate the safety and efficacy of autologous MSC treatmentfor patients with ischemic or non-ischemic dilated cardiomyopathy via direct in-tramyocardial and intracoronary injection.Methods: Twenty patients were screened. Eight patients were excluded due topresence of significant viable myocardium amenable to revascularisation whiletwo patients were referred for biventricular pacing instead. Of the remaining pa-tients (all male, mean age 58 years) five had ischemic cardiomyopathy deemedunlikely to benefit from CABG alone. Two patients had previous revascularizationthat remained patent, and three had non-ischemic dilated cardiomyopathy. MSCexpansion using animal-free culture media achieved required numbers withinthree weeks. Patients who had not been revascularised (n=5; IM group) receivedCABG with concurrent intramyocardial injection of 1.0×106 MSC/kg body weightwhile patients with patent vessels (n=5, IC group) received intracoronary injectionof 2.0×106 MSC/kg b.w. via coronary catheterization.Results: All patients tolerated either procedure well (mean follow up 1 year).There were no ventricular arrhythmias, pericardial bleeding or coronary occlu-sion post-treatment. There were significant improvements from baseline to sixand twelve months in functional score (NYHA 3.8;1.5,1.0), left ventricular ejec-tion fraction (26.5%, 50.1%, 63.5%), end diastolic and end systolic volumes anddiameter and interventricular septal wall thickness. IM group showed greater im-provement than IC group. The magnitude of improvement in each group is largerthan that reported for conventional therapy alone. Scar reduction was noted inboth groups by 12 months.Conclusion: Autologous bone marrow mesenchymal stem cells are safe for se-vere dilated cardiomyopathy and appear to be beneficial, whether as adjunctive
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

80 Basic progress in cardiovascular repair
treatment to revascularization in ischemic cardiomyopathy or for non-ischemicdilated cardiomyopathy. The cell number required were appropriate for respec-tive route of administration. Larger randomized multicentre studies are now war-ranted.
P611 Adipose-derived mesenchymal stem cells markedlyattenuate brain infarct size and improve neurologicalfunction in rats
S. Chua, C.M. Yuen, S. Leu, Y.C. Lin, C.K. Sun, H.K. Yip. Chang GungMemorial Hospital-Kaohsiung Medical Center, Chang Gung University
College of Medicine, Kaohsiung, Taiwan
Purpose: This study tested the therapeutic effect of adipose-derived mesenchy-mal stem cells (ADMSCs) on brain infarction area (BIA) and neurological statusin a rat model of acute ischemic stroke (IS).Methods and Results: Acute IS of left middle cerebral artery territory was in-duced by occluding distal left internal carotid artery in adult male Sprague Dawley(SD) rats (n=30) that were then categorized into group 1 (IS only) and group 2 (ISplus intravenous ADMSCs (2.0 x 106 at 0, 12 and 24h after the procedure). Therats were sacrificed and brain tissues were harvested for analysis on day 21 afterthe procedure. The results showed that BIA was larger in group 1 than in group2 (p<0.001). The sensorimotor functional test (corner test) identified a higherfrequency of turning movement to left in group 1 than in group 2 (p<0.05). ThemRNA expressions of Bax, caspase 3, interleukin (IL)-18, toll-like receptor-4 andplasminogen activator inhibitor-1 were higher, whereas Bcl-2 and IL-8/Gro werelower in group1 than in group 2 (all p<0.05). Western blot demonstrated a lowerCXCR4 and stromal-cell derived factor-1 (SDF-1) in group 1 than in group 2 (allp<0.01). IHF staining showed lower expressions of CXCR4, SDF-1, von Wille-bran factor and doublecortin, whereas the number of apoptotic nuclei on TUNELassay was higher in group 1 than in group 2 (all p<0.001). IHC showed that cel-lular proliferation and number of small vessels were lower but glial fibrillary acidprotein was higher in group 1 than in group 2 (all p<0.01).Conclusions: ADMSC therapy significantly limited BIA and improved sensorimo-tor dysfunction after acute IS.
P612 tPA-mediated plasmin generation is crucial for kineticand angiogenesis ability of EPCs in response toischemia through modulating activities of MMP-9 andchemokines
H.K. Yip, S. Chua, S. Leu, C.H. Chai, Y.C. Lin, C.K. Sun. Chang GungMemorial Hospital-Kaohsiung Medical Center, Chang Gung University Collegeof Medicine, Kaohsiung, Taiwan
Purpose: By applying ischemic models to different genetically modified animals,including metalloproteinase knock out (MMP-9-/-) mice and B6 wide-type, thisstudy attempted to clarify the upstream signaling of tissue plasminogen activa-tor (tPA) in manipulating the downstream signaling of chemokine [stromal cell-derived factor (SDF)-1α] and proteolytic enzyme (MMP)-9) to regulate EPC kinet-ics and angiogenesis.Methods and Results: Compared to only culture-medium group, tPA-treated theculturing human umbilical vein endothelial cells (HUVECs) and mouse endothe-lial cells (SVEC 4-10 cell line) markedly enhanced the SDF-1α, KDR and vas-cular endothelial growth factor expressions in both surface of these cells and insupernatant levels (all p values <0.01). After acute limb-ischemic induction (leftfemoral artery and vein to be ligated, cut, and excised), circulating level of SDF-1α, VEGF and EPCs (CD34+, CD133+, KDR+ Sca-1+ and C-kit+ cells) weremarkedly enhanced in B6 mice with then in without tPA treatment (all p values<0.01). Additionally, in the ischemic condition, these EPC chemokine levels wereremarkably higher in B6 mice than in MMP-9-/- mice (all p values < 0.05). Also,in ischemic condition, tPA treatment notably increased circulating level of SDF-1α and EPCs (CD34+, CD133+, KDR+ Sca-1+ and C-kit+ cells), whereas thistreatment significantly decreased bone-marrow levels of SDF-1α and EPCs in B6mice (all p values < 0.001). However, these alternations were less obvious andless consistent in MMP-9-/- than in B6 mice. Moreover, by day 28, the angio-genesis determined by immunohistochemical stain and blood flow assessed bylaser Doppler in ischemia area was substantially higher in B6 than in MMP-9-/-mice.Conclusion: tPA therapy promotes kinetic activity of EPCs in response to is-chemic stimulations though manipulating plasminogen/plasmin-mediated MMP-9and chemokine activity.
P613 Long term functionality and growth oftissue-engineered living, autologous vascular grafts ina large animal model: the final step towards humanapplication?
M.Y. Emmert1, B. Weber2 , D. Schmidt2, J. Kelm2, R. Jenni3,T. Frauenfelder4 , S. Leschka4, V. Falk1, G. Zund2, S.P. Hoerstrup2.
1University Hospital Zurich, Division of Cardiac and Vascular Surgery, Zurich,Switzerland; 2Regenerative Medicine Program at University Hospital Zurich,Zurich, Switzerland; 3University Hospital Zurich, Department of InternalMedicine, Division of Cardiology, Zurich, Switzerland; 4University HospitalZurich, Zurich, Switzerland
Purpose: Living autologous vascular grafts with the capacity for regeneration andgrowth may overcome the limitations of contemporary artificial prostheses. Par-ticularly in congenital cardiovascular surgery, there is an unmet medical need forgrowing replacement materials. Here we investigate long-term growth capacity,functionality and safety of tissue-engineered living pulmonary arteries in a grow-ing lamb model.Methods: Vascular cells were sequentially seeded on biodegradable scaffolds(diameter 18±1mm) and were grown in vitro for 21days using biomimetic condi-tions. Next, the produced tissue-engineered vascular grafts (TEVGs) were surgi-cally implanted as main pulmonary artery (PA) replacements in lambs (n=15) andfollowed up for 220 weeks.Results: All procedures were performed uneventfully. Trans-oesophageal echo-cardiography at 20, 50, 80, 100 and 220 weeks displayed excellent functionalityand CT–angiography did not detect any signs of degeneration such as thrombusformation, calcification, stenosis or aneurysm. In regard to wall tension, shearstress and flow velocity, 3D-CT analysis showed sufficient and stable results overthe whole follow-up period. Functional growth was confirmed by help of CT vol-ume measurements which displayed a significant volume increase of the TEVGfrom an initial volume of 6.4ccm early after implantation up to 13.2ccm after240weeks. Histology showed tissue formation reminiscent of native PA.
Figure 1. 3D-CT analysis displays normal systolic wall pressure (A), low wall shear stress (B)and normal velocity-coded streamlines (C).
Conclusions: Our results provide systematic evidence of growth, functionalityand safety of TEVG in a full growth animal model over a long-term period. Thesefindings provide the experimental basis to enter into future clinical trials.
P615 Caffeine induces endothelial tissue factor expressionthrough inhibition of phosphatidylinositol 3-Kinase
C. Gebhard1, E.W. Holy1, G.G. Camici1, A. Akhmedov1, S. Stampfli1,H. Greutert1, A. Breitenstein1, Z. Yang2, T.F. Luscher1 , F.C. Tanner1 .1University of Zurich-Irchel, Department of Anatomy and Physiology,
Cardiovascular Research, Zurich, Switzerland; 2Vascular Biology, Department ofMedicine, University of Fribourg, Fribourg, Switzerland
Background: Tissue factor (TF) is a key activator of coagulation and involved inacute coronary syndromes. Caffeine is often reported to increase cardiovascularrisk; however, its effect on cardiovascular morbidity and mortality is controversial.Hence, this study was designed to investigate the impact of caffeine on endothe-lial TF expression.Methods and Results: Caffeine concentration-dependently enhanced TF proteinexpression and surface activity of human endothelial cells stimulated by tumornecrosis factor (TNF)-α or thrombin. Tissue factor pathway inhibitor (TFPI) ex-pression was not altered under these conditions. Caffeine inhibited Phosphatidyli-nositol 3-Kinase (PI3K) activity and this effect was comparable to that of theknown PI3K inhibitor LY294002. Consistently, treatment of endothelial cells withLY294002 enhanced TNF-α induced TF expression to a similar extent as caffeine,and adenoviral expression of the active PI3K mutant (p110) reversed the effect ofboth caffeine and LY294002 on TF expression. Caffeine and LY294002 increasedDNA binding capacity of the transcription factor NFkB, whereas the activation pat-tern of mitogen-activated protein kinases (MAPK) remained unaltered. Luciferasereporter assay revealed a caffeine dependent activation of the TF promoter, andRT-PCR revealed a dose dependent increase in TF mRNA levels when stimulatedwith caffeine in the presence of TNF-α. In THP-1 cells and VSMC TF expressionremained unaltered by caffeine.Conclusions: These observations indicate that PI3K signalling mediates caffeineinduced TF expression leading to activation of NFkB and upregulation of TF. Sincethe caffeine concentrations applied in the present study are within the plasmarange measured in humans, our findings indicate that caffeine enhances the pro-thrombotic potential of endothelial cells and underscore the importance of PI3Kin mediating these effects.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Basic progress in cardiovascular repair 81
P616(W) Vascular bradykinin type-2 receptoroverexpression in eNOS knockout mice
O. Kocgirli, S. Valcaccia, V.T. Dao, T. Suvorava, S. Kumpf,M. Floeren, M. Oppermann, G. Kojda. Institute of Pharmacology,düsseldorf, Germany
Purpose: The activation of vascular bradykinin type-2 receptor (BKR-2) producesvasodilatory effects mediated by prostacyclin and NO. In eNOS knockout mice,coronary flow responses to bradykinin are largly increased. These data suggestthat NO might act as a negative feed-back regulator on vascular BKR-2 expres-sion and/or activity.Methods: We used a human head and neck squamous carcinoma cell lineexpressing BKR-2 (UDSCC-2) and another one without BKR-2 expression(UDSCC-3) which were established in our labaratory to confirm the detectionof BKR-2. For in vivo experiments we used eNOS++ mice which has more than2 times higher endothelial NOS, eNOSn (transnegative litter mates) for negativecontrol, eNOS knockout and C57Bl/6 mice. For in vitro experiments we used pri-mary cultured porcine aortic endothelial cells and porcine aortic smooth musclecells which were incubated with 10 μM S-nitroso-N-acetylpenicillamine (SNAP)(NO-Donor) or Ca-Ionophor together with NG-nitro-L-Arginine-Methyl-Ester (L-NAME) (NOS inhibitor). C57Bl/6 mice were fed with NO-donor pentaerythrityl-tetranitrate (PETN, 0mg, 6mg or 60mg kg/KG/d).Results: The expression of BKR-2 in eNOS++ compared to eNOSn mice lung(124.6±28.4%) and heart (114.5±18.1%) have not shown any significant differ-ence. The knockout mice have shown an increase of BKR-2 expression (lung130.7±6.5%, p<0.005, heart 172±26%, p<0.05). The C57Bl/6 mice which weretreated with PETN and the cells which were incubated with SNAP or L-NAMEshowed no significant difference in BKR-2 expession.Conclusion: These data suggest that an increase of BKR-2 expression in knock-out eNOS mice could cause the largely increase of coronary flow mediated bybradykinin. NO does not seem to have any effect on vascular BKR-2 expression,in vitro and in vivo.
P617 Angiotensin II-induced monocyte chemoattractantprotein-1 production in human endothelial cells ismediated by angiotensin receptor-2 and modulated bystatins
B.K. Rodino-Janeiro, M. Gonzalez-Peteiro, R. Ucieda-Somoza,J.R. Gonzalez-Juanatey, E. Alvarez. University Clinical Hospital of
Santiago de Compostela, Santiago de Compostela, Spain
Purpose: Monocyte chemoattractant protein-1 (MCP-1) is the main factor in-volved in the migration of monocytes into the vessel wall and therefore, it playsa crucial role in the atherosclerotic plaque formation. Angiotensin II (ANG) hasdemonstrated to induce MCP-1 production in macrophagues and endothelial cellsin vitro and to promote atherosclerosis formation in animal models. Losartan, anangiotensin receptor-1 (AT1) antagonist, inhibits these effects in vitro. However,neither angiotensin-converting-enzyme inhibitors nor AT blockers modify the el-evated MCP-1 levels observed in human patients after an acute myocardial in-farction. Statins can also modulate MCP-1 expression in endothelial cells in vitro:depending on the stimulating conditions they can down-regulate or up-regulateMCP-1 expression. Taking all together, the objective of this work was to evaluatethe effects of the statins and of the AT antagonists on the ANG-induced MCP-1production in human umbilical vein endothelial cells (HUVEC).Methods: HUVEC were isolated from umbilical cords and cultured under appro-priate conditions. ANG (100 nM) were used as stimuli and the effects of pravas-tatin (1-60 μM), losartan (100 μM) and PD 123319 (10 μM) on MCP-1 accumula-tion in cell culture supernatants were analyzed by enzyme-linked immunosorbentassay.Results: ANG, after 6 hours of treatment, significantly enhanced MCP-1 produc-tion. On the contrary, pravastatin, PD 123319 or losartan alone did not modifiedMCP-1 production. However, pravastatin inhibited, in a concentration dependentmanner (1-60 μM), the ANG-induced MCP-1 production. Interestingly, ANG in-duction was inhibited as well by the AT2 blocker, PD 123319 (10 μM), but not bythe AT1 antagonist, losartan (100 μM)Conclusions: Our results demonstrated that ANG-induced MCP-1 productionin human endothelial cells is mediated by the AT2, not by the receptor type 1.Besides, this stimulation was totally inhibited by pravastatin. Both findings couldhave important clinical implications in atherosclerosis prevention.
P618 Endothelial C-Reactive protein increases plateletadhesion under flow conditions
H. Danenberg, R.M. Pachino, E. Grad. Hadassah-Hebrew UniversityMedical Center, Jerusalem, Israel
Background: While data regarding the pathogenetic role of C- reactiveprotein (CRP) in atherothrombosis is accumulating it is still controversial whetherlocal CRP secretion is of any pathobiological significance. The present study ex-amined whether endothelial-derived CRP modulates an autocrine prothromboticactivity.Methods and Results: Endothelial cells were isolated from hearts of mice trans-genic to human CRP (CRPtg) and grown in primary cultures. Human CRP ex-
pression was confirmed in these cells as compared with no expression in cul-tures derived from wildtype congenes. Adhesion of human platelets to endothe-lial cells was studied in the "cone and plate" flow system. Platelet adhesionto cells expressing CRP was significantly increased as compared with controls(n=6, p<0.01). The pro-adhesive effect of CRP was significantly suppressed inmouse heart endothelial cells and in human umbilical vein endothelial cells fol-lowing treatment with SiRNA for human CRP. Adhesion was modulated by an in-crease in p-selectin; blocking P-selectin with neutralizing antibody significantly de-creased the adhesion of platelets to CRP-expressing cells (40.4±10.5 to 9.4±6.9platelets/high power field, n=5-6, p<0.01).Conclusions: human CRP that is locally produced in endothelial cells increasesplatelet adhesion to endothelial cells under normal shear flow conditions. Thesefindings support the notion that the presence of CRP at the "scene of the crime"can indicate "evidence of guilt"; ie, CRP exerts a local effect on endothelial cells,via p-selectin expression that promotes platelet adhesion and subsequent throm-bus formation.
P619 Experimental target identification and functionalcharacterization of hypoxia-induced miR-210
F. Martelli1, P. Fasanaro1 , G. Zaccagnini1 , S. Greco2, M. Lorenzi3,C. Banfi4, M. Pescatori5, M. Ivan6, M.C. Capogrossi1 . 1DermopaticInstitute of the Immacolata, Rome, Italy; 2IRRCS-Policlinico San
Donato, San Donato Milanese, Milan, Italy; 3INRCA, Ancona, Italy; 4CentroCardiologico Monzino-IRCCS, Milan, Italy; 5Erasmus Medical Center, Rotterdam,Netherlands; 6Indiana University School of Medicine, Indianapolis, United Statesof America
Purpose: MicroRNAs (miRNAs) are small non-protein-coding RNAs that are in-corporated into the RNA-induced silencing complex (RISC) and inhibit gene ex-pression by regulating the stability and/or the translational efficiency of target mR-NAs. Specifically, miR-210 is a key player of cell response to hypoxia, modulatingcell survival, glycolysis, VEGF-driven endothelial cell migration and the ability ofendothelial cells to form capillary-like structures. A crucial step in understandingmiRNA function is the identification of their targets. Thus, we adopted an inte-grated strategy for large-scale identification of new miR-210 targets.Methods and results: A combination of transcriptomics and proteomics withbioinformatic approaches was adopted to identify potential miR-210 targets. Toexperimentally validate these candidate genes, miR-210-loaded RISC complexwas purified by immuno-precipitation along with miR-210 targets. The complexwas significantly enriched in mRNAs of 32 candidate targets, such as BDNF,GPD1L, ISCU, PTPN1, NCAM and the non-coding RNA Xist. A sub-set of thenewly identified targets was further confirmed by 3’UTR-reporter assays, andhypoxia-induced down-modulation of their expression in endothelial cells was res-cued blocking miR-210, providing support for the approach validity.A mouse model of hindlimb ischemia displayed an almost 4 fold increase of miR-210 expression 2 days after femoral artery dissection. Tail vein injection of LNA-anti-miR-210 induced down modulation of both miR-210 and its target mRNAs.Functional consequences of miR-210 blockade are currently being investigated.Finally, Gene Ontology analysis of the targets highlighted known miR-210 im-pact on cell cycle regulation and differentiation, and predicted a new role of thismiRNA in RNA processing, DNA binding, development, membrane trafficking andaminoacid catabolism.Conclusions: we validated a multidisciplinary approach for miRNAs target iden-tification and indicated novel molecular mechanisms underpinning miR-210 rolein endothelial cell response to hypoxia.
P620 Sildenafil limits monocrotaline-induced pulmonaryhypertension in rats through suppression ofpulmonary vascular remodeling
T.H. Tsai1, S. Chua1, M. Fu1, L.T. Chang2, C.J. Wu1, C.J. Wu1,J.J. Sheu1, S.Y. Chung1, H.K. Yip1. 1Chang Gung Memorial
Hospital-Kaohsiung Medical Center, Chang Gung University College of Medicine,Kaohsiung, Taiwan; 2Meiho Institute of Technology, Department of Nursing,Divsion of Basic Medical Science, Pingtung, Taiwan
Purpose: We hypothesize that sildenafil attenuates pulmonary hypertension(PAH) through suppression of pulmonary vascular remodeling.Methods: Thirty male adult Sprague-Dawley rats were randomized to receivesaline injection (group 1), monocrotaline (MCT) (60 mg/kg, subcutaneous) (group2), and MCT plus oral sildenafil (30 gm/kg/day) (group 3) on day 5 after MCTadministration.Results: By day 35, Western blot showed lower connexin43 (Cx43) and mem-branous protein kinase C epsilon expressions, but higher oxidative stress in rightventricle (RV) in group 2 than in other groups (all p values < 0.01). Addition-ally, pulmonary Smad1/5 was lowest, whereas Cx43 and Smad3 were highest ingroup 2 (all p values < 0.05). Pulmonary mRNA expressions of TNF-α, caspase-3, plasminogen activator inhibitor-1, and TGF-β were higher, whereas bone mor-phogenetic protein type II receptor, Bcl-2 and eNOS were lower in group 2 thanin other groups (all p values < 0.01). Similarly, mRNA expressions of TNF-α,caspase-3, and β- myosin heavy chain (MHC) were increased, while Bcl-2, eNOS,and α-MHC in RV were reduced in group 2 compared with other groups (all p val-ues < 0.01). Number of lung arterioles was lowest, whereas number of arterioles
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

82 Basic progress in cardiovascular repair
with muscularization of medial-layer was highest in group 2 (all p values <0.02).RV systolic pressure and RV weight were elevated in group 2 compared with othergroups (all p values < 0.001).Conclusion: Sildenafil effectively alleviates MCT-induced PAH through suppress-ing pulmonary vascular remodeling.
P621 Non-invasive localisation of cellular inflammation inabdominal aortic aneurysms using ultrasmallsuperparamagnetic particles of iron oxide
J.M.J. Richards1, S.I.K. Semple2, C. Gray2, T.J. Macgillivray2,J.P. Langrish1, W. Wallace3, G. Mckillop4, R.T.A. Chalmers5,
O.J. Garden6, D.E. Newby1. 1University of Edinburgh, Centre for CardiovascularScience, Edinburgh, United Kingdom; 2Clinical Research Imaging Centre,University of Edinburgh, Edinburgh, United Kingdom; 3Department of Pathology,Royal Infirmary of Edinburgh, Edinburgh, United Kingdom; 4Departmentof Radiology, Royal Infirmary of Edinburgh, Edinburgh, United Kingdom;5Department of Surgery, Royal Infirmary of Edinburgh, Edinburgh, UnitedKingdom; 6Centre of Clinical and Surgical Sciences (Surgery), University ofEdinburgh, Edinburgh, United Kingdom
Purpose: Abdominal aortic aneurysm (AAA) disease is characterised by focalhotspots of neovascularisation,inflammation and proteolysis. These hotspots rep-resent areas of AAAs at risk of expansion and rupture. We have used magneticresonance imaging (MRI) scanning with ultrasmall superparamagnetic particlesof iron oxide (USPIO) to detect areas of cellular (macrophage) inflammation.Methods: Patients (n=29) with asymptomatic AAA (>4 cm in diameter) wereimaged in a 3T MRI scanner before and 24 h after administration of USPIO.Multi-echo, gradient-echo T2*-weighted and TSE T2-weighted sequences wereacquired. Images were registered and mean per cent change in T2* value wascalculated on a multi-voxel grid. In patients undergoing open surgery, aortic walltissue was obtained and stained for CD68 (macrophages) and iron (Prussianblue).Results: USPIO administration resulted in differential changes in T2* value withinthe AAA. A change in T2* value in the peri-luminal thrombus was seen in the ma-jority of patients. In addition, some patients had focal areas of USPIO uptake else-where within the AAA, consistent with inflammatory hotspots and aneurysm in-stability. Figure 1: Accumulation of USPIO (red) results in a reduction in T2* value(see scale). (A) Patient with an apparent inflammatory unstable aneurysm, and(B) patient with peri-luminal USPIO uptake only suggesting a stable aneurysm.The T2* value of skeletal muscle (control) was unchanged. Histological analysisof AAA wall showed USPIO co-localising with macrophages.
Figure 1. Colour map of % change in T2* value
Conclusion: We have demonstrated for the first time non-invasive, in vivo de-tection of macrophages and inflammation in AAA using MRI and USPIO. Thisrepresents a promising, highly relevant approach to the detection of AAA inflam-mation and the prediction of disease progression and rupture.
P622 Genome-wide gene expression in aneurysmal aorticwalls of patients with Marfan Syndrome andLoeys-Dietz Syndromes with known causativemutations
V. Favalli1, P. Magni2, M. Grasso1, E. Disabella1, B. De Giorgio1,P. Tarantino1, I. Guida1, E. Serafini1, M. Agozzino1, E. Arbustini1.
1Foundation IRCCS Polyclinic San Matteo - University of Pavia, Pavia, Italy;2University of Pavia, dpt of Computer Engineering and Systems Science, Pavia,Italy
Purpose: Aortic aneurysms constitute the most severe clinical complications inboth Marfan Syndrome (MFS) and Loeys-Dietz syndromes (LDS). The diseasesare caused by defects of Fibrillin 1 (FBN1) and Transforming Growth Factor BetaReceptors 1 and 2 (TRGBR1-2) genes and are associated with increased activecirculating and tissue TGFb which causes the arterial wall damage. We aimedat investigating the whole-genome expression of aortic walls obtained at surgeryfrom MFS patients with FBN1mutations and LDS with mutations of TGFBR1-2.Methods: We performed cRNA microarray analysis in 20 aneurysmatic aorticwalls collected immediately after surgery from 8 patients with MFS, 6 with LDS
and 6 with non-FBN1 & TRGBR1-2-related aneurysm (controls). Genome-wideanalysis was performed using Applied Biosystems 1700 Chemiluminescent Mi-croarray Analyzer following manufacturer’s protocol for samples preparation andsignal detection. Statistical significance was determined using the Student’s t-test for unpaired data with FDR correction: a P value <0.05 was regarded assignificant, and a Fold Change difference of ± 4 was considered for over-underexpression between different groups.Results: We determined gene expression differences in aortic samples from MFSand LDS, vs controls. Of 32878 cRNAs, 17503 genes in MFS and 17482 genesin LDS were selected for the further analysis. The gene expression patterns wereclassified into functional groups, based on the Gene Ontology annotation system.In LDS aortas vs. controls the differentially expressed genes (3248 according tocorrected t-test) were in the pathways of VEGF signaling, cell cycle, angiogenesis,methionine biosynthesis, thiamine metabolism, tricarboxylic acid cycle. In MFSaortas vs. controls, the differentially expressed genes (4430) were in the path-ways of integrin signalling, interleuking signalling, insulin/IGF pathway, vitamin B6metabolism, triacyl-glycerol metabolism. The comparative analysis between LDSvs. MFS showed differentially expressed genes (765) of the following pathways:thiamine metabolism, proline biosynthesis, P38, MAPK, integrin, TGFb, ATP syn-thesis cytochome, cytoskeletal regulation by RHO-GTPase. In particular, LDS vs.MFS showed over-expression of genes ACTA2 and MYH11 playing in the cy-toskeletal regulation pathway.Conclusions: These results suggest that the FBN1 and TGFBR1-2 gene defectsaffects the alteration of several pathways, most of them involved in cytoskeletonand extracellular matrix. ACTA2 and MYH11 over-expressed in LDS aneurismalwalls vs MFS, are potential candidates as phenotype modifiers.
P623 microRNA-155 blocks necrotic cell death in humancardiomyocyte progenitor cells by targeting RIP1
J. Liu1, K.R. Vrijsen1, A. Van Mil1, M.I.F. Oerlemans1, M.J. Goumans2,P.A. Doevendans1 , J.P.G. Sluijter1. 1University Medical CenterUtrecht, Department of Cardiology, Utrecht, Netherlands; 2Leiden
University Medical Center, Department of Molecular and Cellular Biology, Leiden,Netherlands
Purposes: Cell transplantation therapy has been put forward for myocardial re-generation upon injury. Although promising results were obtained, many issuesneed to be addressed before fully appreciating their impact. One of the hurdles ispoor graft-cell survival upon injection, thereby limiting potential beneficial effects.Here, we attempt to improve cardiomyocyte progenitor cells (CMPCs) survival byincreasing microRNA-155 (miR-155) levels, thereby potentially improve engraft-ment upon transplantation.Method: CMPCs were stimulated by hydrogen-peroxide in serum-free mediumand cell viability, apoptosis and necrosis were subsequently detected by AnnV/7-AAD staining using flow cytometric analysis. In addition, to improve cell viability,cells were pre-treated with miR-155, RIP1 siRNA, or a RIP1 inhibitor, Necrostatin-1 (Nec-1). Taqman-based RT-PCR was performed for quantification of miR-155levels and qRT-PCR was performed for analyzing genes involved in apoptosis andPI3K-Akt pro-survival pathways. CMPCs, transfected with miR-155,were injectedin infarcted myocardium in SCID-NOD mice. Mice were sacrificed after 2 daysand engrafted cells were quantified by immunochemistry.Results: Upon hydrogen-peroxide stimulation, we observed that necrosis is themain cause of cell death in CMPCs, accompanied by a 4- fold increase of miR-155levels. Over-expressing miR-155 in CMPCs revealed that necrotic cell death wasdiminished by 40±2.3% via down-regulation of RIP1. In addition, inhibiting RIP1via siRNA mediated knockdown or Nec-1 pre-treatment, necrosis was reduced by38±2.5% and 33±1.9%, respectively. Interestingly, miR-155 transfection did notchange other pro-survival and apoptotic related gene expression. Increasing miR-155 levels improved CMPC engraftment with 26±4.9% at 2 days post-injection.Conclusions: Necrotic cell death of CMPCs was repressed via miR-155 by tar-geting RIP1, independent of activation of PI3K-Akt pro-survival pathways. Inject-ing miR-155 transfected cells in the infarcted heart improved cell survival andmight be a potential novel approach to improve cell engraftment for cellular ther-apy.
P624 Protease resistant stromal cell derived factor-1increases blood flow in a hindlimb ischemia mousemodel
V.F.M. Segers1, V. Revin1, W. Wu1, H. Qiu1, Z. Yan1, R.T. Lee2,A. Sandrasagra1 . 1Provasculon, Cambridge, United States ofAmerica; 2Brigham and Women’s Hospital, Harvard Medical School,
Boston, United States of America
Purpose: Peripheral vascular disease is an invalidating disease, which affectsapproximately 25 million individuals in North America, Europe and Japan; how-ever few drug therapies have been designed to specifically address this impor-tant medical condition. Stromal cell derived factor-1 (SDF-1) is a chemokine thatattracts endothelial progenitor cells and promotes angiogenesis and has beenshown to promote therapeutic neovascularization using gene therapy based ap-proaches. However, systemic and local delivery approaches employing SDF-1protein have been less successful in models of hindlimb ischemia, likely becauseof degradation by proteases or rapid diffusion from the sites of intramuscular injec-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Basic progress in cardiovascular repair 83
tion. We hypothesized that protease resistant variants of SDF-1 when deliveredlocally with a self-assembling peptide hydrogel, a sustained release formulation,would increase blood flow in a rodent model of hindlimb ischemia.Methods and Results: We designed and purified a variant of SDF-1, calledSSDF-1(S4V), that is resistant to DPPIV/CD26 and MMP-2 cleavage. SSDF-1(S4V) is active in vitro and induces angiogenesis in a matrigel plug assay in vivo.We made fusion proteins of SSDF-1 and SSDF-1(S4V) with the 16 amino acidsequence of self-assembling peptides (SAP), called SSDF-1-RAD and SSDF-1(S4V)-RAD. In an in vitro binding experiment, 77.7% of SSDF-1-RAD stably in-corporates into a hydrogel of self-assembling peptides. We tested these variantsof SDF-1 in a blinded hindlimb ischemia mouse study. SSDF-1(S4V)-RAD incor-porated in the hydrogel improved blood flow measured as measured by laserdoppler from 23.1±1.9% (untreated control) to 55.1±5.7% 6 weeks after surgery.SAP peptides only or SAP with SSDF-1-RAD did not significantly improve bloodflow. Furthermore, SSDF-1(S4V)-RAD delivered in a self-assembling peptide hy-drogel increased formation of new arterioles.Conclusions: We designed variants of SDF-1 that are resistant to DPPIV/CD26and MMP-2 cleavage and that allow for prolonged delivery with self-assemblingpeptides. We showed that these variants improve blood flow in a model of periph-eral vascular disease in mice.
P625 Ferritin as a reporter gene to track stem cells bycardiac magnetic resonance imaging, in vivo
V. Lionetti1, M. Campan1, G.D. Aquaro2, M. Matteucci1,M. Menicagli3, F. Forini4, A. Pucci3, M. Lombardi2 , M. Pistello5,F.A. Recchia1. 1Sector of Medicine, Scuola Superiore Sant’Anna,
Pisa, Italy; 2MRI Laboratory, Fondazione G.Monasterio CNR-Regione Toscana,Pisa, Italy; 3Division of Surgical, Molecular and Ultrastructural Pathology,University Hospital, Pisa, Italy; 4Institute of Clinical Physiology of CNR, Pisa,Italy; 5Retrovirus Cntr and Virology Section, Dept of Experimental Pathology,Univ of Pisa, Pisa, Italy
Purpose: To date, the reporter gene technology for in vivo detection of stem cellsby magnetic resonance imaging (MRI) has found virtually no application in thecardiological field. We tested the potential of human ferritin heavy chain (hFTH),an iron-binding protein, to function as reporter gene for tracking the fate of stemcells, in intact hearts, by MRI.Methods: Cardiospheres (Cs), i.e. clusters of progenitor and stem cells, were ob-tained from pig hearts and stably transduced with a lentiviral vector to overexpresshFTH. Myocardial infarction (MI) was then induced in male rats by left anterior de-scending artery ligation. Forty five minutes following MI, the rats were subjectedto intramyocardial injection of 200 hFTH-Cs (n=9), or 200 non-transduced Cs(n=6) or sterile saline solution (Control, n=7) in the viable myocardium borderingthe pale infarcted area (border zone). Cardiac 1.5 tesla MRI was performed at1 and 4 weeks following MI in order to localize iron-induced magnetic suscepti-bility artifacts and to assess infarct size as well as global and regional function.Serial histological analysis of excised hearts included Perls’ staining for visuali-sation of iron enrichment and immunohistochemical analysis with a pig specificanti-mitochondrial antibody for identification of the trasplanted cells and for celltype characterisation.Results: We found the presence of iron-enriched tissue only in the border zoneof hearts that received transduced Cs. Importantly, cell transduction did non af-fect their survival and in vivo regenerative potential, as indicated by a better pre-served left ventricular (LV) global function and a smaller infarct size in both groupsof animals that received Cs compared to saline: ejection fraction was 29±4% inMI+FTH-Cs and 27±3% in MI+Cs (N.S.) vs. 15±3% in MI+PBS (P<0.05); in-farct ratio was 27±5% in MI+FTH-Cs and 27±1% in MI+Cs (N.S.) vs. 46±6% inMI+PBS group (P<0.05). Serial LV sections of hFTH-Cs rats showed the pres-ence of iron enrichment mainly in endothelial cells (CD31 positive cells) andmyofibroblasts (αSMA positive cells) of swine origin, and to a lesser extent inmacrophages (CD68 positive cells). On the other hand, we could not detect Cs-derived Troponin I-positive cells (mature cardiomyocytes).Conclusions: We developed a novel method, based on reporter gene transferand standard MRI imaging, that allows tracking of diving and differentiating stemcells combined with quantitative functional assessments of the regenerating my-ocardium.
P626 Overexpression of an Abcc6-encoding protein variantfrom C3H/He enhances calcification in mesenchymalstem cell
A.-K. Sowa, J. Erdmann, S. Wrobel, H. Schunkert, Z. Aherrahrou.Department of Medicine II, Luebeck, Germany
Background: Abcc6 belongs to a gene family encoding for ABC-transporterswith an ATP-binding cassette, specifically for the multidrug-resistance-protein 6(MRP6). In mice, Abcc6 was found to predispose C3H/He strains to dystrophiccardiac calcification (DCC). The sequence of Abcc6 is found to vary in sevenbase pairs leading to amino acids exchanges between DCC-resistant C57BL/6and DCC-susceptible C3H/HeJ mice.The aim of this study is to study the role of these variants in calcification in an invitro cell culture model.Material and methods: Both variants of cDNA encoding for the C3H/HeJ and the
C57BL/6 protein were cloned and inserted in a pSG5 expression vector (pSG5-Abcc6-C3H and pSG5-Abcc6-B6 respectively). We established a calcifying cellculture model using the mesenchymal stem cell line C3H10T1/2. Cells were trans-fected with empty pSG5 vector (pSG5), pSG5-Abcc6-C3H and pSG5-Abcc6-B6.Induction of calcification was first optimized adding 1, 2, 4, and 7 mM inorganicphosphate to the media. Cells were analyzed 3, 7 and 21 daysafter inductionof calcification. Calcium deposits were stained using calcein and Alizarin Red Sstaining and quantified by Randox Ca Kit.Results: Using RT-PCR a very low expression of native Abcc6 was found in mes-enchymal stem cellline C3H10T1/2. Generally, the time course analysis after in-duction of calcification revealed no calcification after 3 days, an initiation of cal-cification after 7 days and a strong calcification after 21 days. Thus, 7 days wasconsidered as a time point for detailed analysis. After transfection, the mean val-ues of calcium deposits were measured to be 9.42 μmol in pSG5 empty vector,13.76 μmol in pSG5-Abcc6-C3H and 9.13 μmol in pSG5-Abcc6-B6 transfectedcells (n=9, 3 independent experiments x 3 samples in each experiment). A sig-nificant increase of 1.55-fold in calcium deposits was found in cells transfectedwith pSG5-Abcc6-C3H compared to those transfected with pSG5 (13.75 vs 9.42,respectively; p=0.0063). However a non significant decrease in calcium depositswas observed in cells transfected with pSG5-Abcc6-B6 compared to pSG5 (9.13μmol vs 9.42 μmol respectively; p=0.7321). At molecular level, the expressionlevel of Osteopontin, a bone marker, was also found high in cells transfected withpSG5-Abcc6-C3H, thus reflecting the results obtained measuring Ca 2+.Conclusion: Using cell culture model, we functionally demonstrate for the firsttime the effect of the amino acid substitutions found in the C3H/HeJ-MRP6 oncalcification in vitro.
P628 High density lipoprotein reduces lipid inducedmacrophage inflammation and enhances insulinmediated glucose uptake in human skeletal muscle
B.A. Kingwell1, A. Natoli1, M. Reddy Luthmoodoo1 , D. Sviridov1,B.G. Drew2. 1Baker IDI Heart and Diabetes Institute, Melbourne,
Australia; 2UCLA, David Geffen School of Medicine, Los Angeles, United Statesof America
Purpose: Recent data from our laboratory and others indicate that HDL reducesblood glucose through multiple actions including enhanced insulin secretion (1,2) and increased glucose uptake into skeletal muscle via the AMP-activated pro-tein kinase (AMPK) signaling pathway (1, 3). We further hypothesized that HDLmay improve insulin sensitivity via lipid removal and anti-inflammatory actions inmacrophages associated with excess adiposity/ectopic lipid deposition.Methods: A variety of macrophage cell models including RAW 264.7 (mouse),THP-1 (human) and primary human macrophages from healthy participants wereincubated separately with lipid challenges including palmitate (0.5mM) and acety-lated LDL (100μg/mL), then co-treated with either HDL (50μg/mL) or vehicle (18hrs). Macrophage cultures were then incubated in fresh media (4 hrs) and theconditioned media (CM) applied (1:10) to primary human skeletal muscle cellcultures derived from unmedicated patients with type 2 diabetes mellitus for 24hours and insulin-mediated glucose uptake (2-deoxy glucose) and insulin signal-ing (pAkt) assessed (n=7, all in triplicate).Results: HDL treatment ameliorated cytokine release (TNFα/IL1β) frommacrophages in response to lipid challenges by 50% through suppression of theJNK pathway (39% reduction in JNK phosphorylation). In skeletal muscle culturestreated with THP-1 CM, acetylated LDL treatment reduced insulin-mediated glu-cose uptake by 31.3±4.1% (p=0.04). Co-treatment with HDL restored insulin me-diated glucose uptake to control levels (51.0±13.4% greater than acetylated LDLtreatment alone; p=0.002). Results from RAW and THP-1 macrophages were re-capitulated in primary human macrophages and demonstrate that HDL mediatedimprovements in skeletal muscle glucose uptake relate to phosphorylation of thekey insulin signaling protein Akt.Conclusion: Macrophage inflammation associated with excess/ectopic adiposityis reduced by HDL and these effects may contribute to improved insulin sensi-tivity and glucose homeostasis. These findings, together with a growing body ofevidence linking HDL to glucose metabolism, suggest that therapeutics aimed atelevating plasma HDL levels may provide efficacy in preventing and treating type2 diabetes.1. Circulation 2009; 119(15):2103-2111.2. Nat Med 2007; 13(3):340-347.3. Diabetologia 2007; 50(9):1960-1968.
P629 Umbilical cord blood-derived mesenchymal stem cellsacquire cardiac phenotype with oxytocin treatment andenhance cardiac recovery after myocardial infarction
Y.S. Kim, Y. Ahn, J.S. Kwon, M.H. Jeong, J.G. Cho, J.C. Park,J.C. Kang. Chonnam National University Hospital, Gwangju, Korea,
Republic of
Purpose: Oxytocin stimulates cardiomyogenesis of embryonic stem cells andadult cardiac stem cells. We previously reported that oxytocin has a promi-gratory effect on umbilical cord blood-derived mesenchymal stem cells (UCB-MSCs). Here we cultured UCB-MSCs with oxytocin and examined their pheno-typic changes in vitro and in vivo.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

84 Basic progress in cardiovascular repair / Improved understanding of coronary artery disease in all its facets
Methods and Results: UCB-MSCs were pretreated with 100 nM oxytocin. Car-diac markers were assessed by immunofluorescent staining. UCB-MSCs ex-pressed connexin43 (Cnx43), cardiac troponin I (cTnI), and α-sarcomeric actin(α-SA) after oxytocin supplementation. Next, oxytocin-supplemented USC-MSCs(OT-USCs) were co-cultured with hypoxia-reoxygenated neonatal rat cardiomy-ocytes, and the expression of Cnx43, cTnI, and α-SA was prominently induced.To examine the effect of OT-USCs in infarcted heart, ischemia-reperfusion wasinduced in rats, and PBS (group 1), 1-day OT-USCs (group 2), or 7-day OT-USCs(group 3) were injected into the infarcted myocardium. Two weeks after injection,histological changes and cardiac function were examined. Cardiac fibrosis andmacrophage infiltration were much lower in group 3 than in group 2. The expres-sion and reorganization of Cnx43 were greater in Group3 than in group 2. Cnx43and cTnI-positive OT-USCs were observed in both groups 2 and 3. The cardiaccontractility of group 3 was greater than that of group 2.Conclusion: Supplementation of UCB-MSCs with oxytocin can contribute to thecardiogenic potentialization for cardiac repair.
P630 Vasoprotective effects of a novel PARP-inhibitor inspontaneously hypertensive rats
K. Magyar1 , Z. Vamos2, K. Bruszt1, I. Solti3, K. Hideg4, B. Sumegi3,A. Koller2, R. Halmosi1, K. Toth1. 1University of Pecs, MedicalSchool, Heart Institute & 1st Dpt of Medicine, Div. of Cardiology, Pecs,
Hungary; 2University of Pecs, Medical School, Department of Pathophysiologyand Gerontology, Pecs, Hungary; 3University of Pecs, Medical School,Department of Biochemistry and Medical Chemistry, Pecs, Hungary; 4Organicand Pharmacological Chemistry, Pecs, Hungary
Purpose: Hypertension elicits remodeling of large vessels and vasomotor dys-function in resistance arteries via increased oxidative stress and consequentpoly(ADP-ribose) polimerase (PARP) activation. Thus we hypothesized that treat-ment of spontaneously hypertensive rat (SHR) with a novel PARP-inhibitor (L-2286) will have vasoprotective effects.Methods: One group of SHRs received no treatment (SHR-C) and the other(SHR-L) received 5 mg/kg/day L-2286 for 32 weeks. Normotensive age-matchedgroups were also included (treated: CFY-L and control: CFY-C). In carotid arter-ies the following were measured: intima-media thickness (IMT), arterial stiffnessindex (ASI), acetylcholine- (ACh) and sodium nitroprusside (SNP) - induced re-laxation and angiotensin II (Ang II) - induced contractions. Blood pressure withtail-cuff method was assessed.Results: L-2286 treatment did not affect the blood pressure of SHR and CFYrats (SHR: 232±2 vs. CFY: 130±1 Hgmm). At the beginning of the study IMT(CFY: 39±2.5 μm, SHR: 40±2.3) and ASI (CFY: 3.79±0.46, SHR: 3.86±0,41)were similar in SHR and CFY rats. However, at the end of the study IMT and ASIvalues were elevated in SHR-C compared to CFY-C (IMT: CFY: 41±2 μm, SHR:78±5 μm; ASI: CFY: 4.1±0.1, SHR: 5.8±0.3, p<0.01), which were decreasedsignificantly by L-2286 treatment (SHR-L: IMT: 63±1 μm, ASI: 4.3±0.4, p<0.05).Relaxation of carotid arteries to ACh was significantly increased in SHR-L groupcompared to SHR-C (22.3±8% vs. 41±5%, p<0.05), but responses to SNP didnot differ. Contractions of carotid arteries to KCl were decreased in SHR-L com-pared to SHR-C (1.2±0.2 mN vs. 6±0.8 mN, p<0.05), similarly the contractionsto Ang II were greater in SHR-C than in SHR-L (2.4 mN±0.8 vs. 1.2 mN±0.2 mN,p<0.05).Conclusions: These data suggest that chronic inhibition of PARP decreases vas-cular remodeling and improves both endothelial and smooth muscle dependentvasomotor function.(Support: PTE ÁOK-KA 34039-21/2009, OTKA K71591, OTKA T67984)
IMPROVED UNDERSTANDING OF CORONARY ARTERYDISEASE IN ALL ITS FACETS
P631 Phosphorylation of syndecan-4 acts as a molecularswitch of the pro-hypertrophic calcineurin-NFATsignalling pathway in the myocardium
I.G. Lunde1 , A.V. Finsen2, H. Jarstadmarken1, H. Kvaloy1, A. Hasic1,I. Sjaastad3, T. Tonnesen4 , S.A. Wilcox-Adelman5, C.R. Carlson1,
G. Christensen1. 1Institute for Experimental Medical Research, UllevaalUniversity Hospital, Oslo, Norway; 2University of Oslo, Faculty DivisionRikshospitalet University Hospital, Department of Cardiology, Oslo, Norway;3University of Oslo, Faculty Division Ulleval University Hospital, Departmentof Cardiology, Oslo, Norway; 4Department of Cardiothoracic Surgery, UllevaalUniversity Hospital, Oslo, Norway; 5Boston Biomedical Research Institute,Watertown, Massachusetts, United States of America
Background: Myocardial hypertrophy and heart failure develop in response topressure overload, however, the signalling processes involved are poorly under-stood. We have previously linked syndecan-4, a transmembrane proteoglycan lo-calized to focal adhesions and costameres in cardiomyocytes, to pathological my-ocardial hypertrophy. In brief, mice lacking syndecan-4 do not develop concentrichypertrophy after aortic banding. In the present study we demonstrate a crucialrole for phosphorylation of syndecan-4 in regulating the central pro-hypertrophic
calcineurin-Nuclear Factor of Activated T-cell (NFAT) signalling pathway in themyocardium.Methods/Results: Pull-down experiments showed that recombinant calcineurinbinds directly to syndecan-4. Immunoprecipitations showed that the associa-tion between endogenous calcineurin, its activator calmodulin and syndecan-4 was stronger in pressure-overloaded murine hearts, compared to sham. Thesyndecan-4 cytoplasmic domain is 28 amino acids long and composed of threeregions; C1 and C2 are conserved between the four syndecans, while the V-region is specific for each of them. Peptide array experiments showed that cal-cineurin interacts with the V-region of syndecan-4 through its autoinhibitory do-main. Phosphorylation of serine 179 (pS179) in C1 has previously been shownto be important for protein associations. We demonstrate that pS179 is reducedin patients with aortic stenosis and in pressure-overloaded murine hearts, com-pared to controls. More calcineurin immunoprecipitated with non-phosphorylatedsyndecan-4 than with pS179, indicating that reduced pS179 in syndecan-4 isinvolved in the hypertrophic response. Similarly, pull-down with pS179 or pep-tides mimicking constitutive pS179 (S179D/E) resulted in reduced binding of cal-cineurin. Activation of NFATc4 occurred in HEK293 cells transfected with a mutantmimicking minimally phosphorylated S179 (S179A) whereas S179D/E mutationsdid not. Finally, we recently found that overexpression of calcineurin in HEK293reduces pS179, indicating that calcineurin regulates its own binding and activa-tion.Conclusions: Our results indicate that in a pressure-overloaded heart, serine179 in syndecan-4 is dephosphorylated by calcineurin, and calcineurin bindsto the intracellular V-region through its autoinhibitory domain. Increased bindingof calcineurin to syndecan-4 results in activation of NFATc4, a well-known pro-hypertrophic transcription factor. Conclusively, these data suggest a crucial rolefor phosphorylation of syndecan-4 and the syndecan-4-calcineurin interaction indevelopment of myocardial hypertrophy.
P632 The association of the chromosome 9p21 locus on riskof coronary artery disease is not mediated by an effecton telomere length
V. Codd1, P. Van Der Harst2, S. Rafelt1, A.S. Hall3, N.J. Samani1.1University of Leicester, Leicester, United Kingdom; 2University
Medical Center, Groningen, Netherlands; 3University of Leeds, Leeds, UnitedKingdom
Background: Recently, genome-wide association (GWA) studies of coronaryartery disease (CAD) and myocardial infarction (MI) have identified a novel lo-cus on chromosome 9p21.3, where a common variant increases risk by 20-30%per copy of the allele. The mechanism by which the locus affects risk of CADis unclear and there is no correlation of the genotype at the locus with tradi-tional cardiovascular risk factors. The region encompasses the genes coding forthe cyclin-dependent kinase inhibitors p15ink4b and p16ink4a and a non-codingRNA, ANRIL. Although any function of ANRIL is not currently understood, thecyclin-dependent kinase inhibitors are regulators of the cell cycle and reducecell proliferation and promote cellular senescence and apoptosis. As we and oth-ers have previously shown an association between shorter telomere length, amarker of senescence, biological ageing and CAD risk, we investigated whetherthe 9p21.3 locus is associated with mean leucocyte telomere length and thusconveys risk of CAD via a mechanism involving biological ageing.Methods: We measured telomere length in a subset (1487 CAD cases and 1430National Blood Service control subjects) from the Wellcome Trust Case ControlConsortium (WTCCC) GWA Study which established the strong association ofchromosome 9p21 with CAD. Mean leucocyte telomere length was measuredusing an established quantitative PCR technique. The association of genotype atthe 9p21 locus (SNP rs1333049) with age and gender corrected telomere lengthwas analysed.Results: The subset of cases and controls showed a strong association (P=8.08x10-11) of the locus with CAD as seen in the full WTCCC sample. Both caseand control groups showed an age related decrease in telomere length (decline inT/S ratio per year of -0.006 and -0.009 respectively, P<0.0001 for both cases andcontrols) and also exhibited a previously reported effect of gender, with femalesshowing longer telomeres after accounting for age (+0.031 T/S ratio, P=0.058in cases and +0.033 T/S, P=0.015 in controls). There was a highly significantdifference in mean telomere length between cases and controls of -0.29 in T/Sratio (p<0.0001). However, despite observing the strong associations of both thechromosome 9p21 locus and shorter telomeres with risk of CAD, we found noassociation of the 9p21 locus with telomere length (P= 0.56).Conclusions/Implications: We therefore conclude that the chromosome 9p21locus does not affect risk of CAD by a mechanism involving telomere length andpremature biological ageing. Further studies are required to elucidate the role ofthis locus on CAD.
P633 The anti-apoptotic signalling by Tissue Factor/FactorVIIa is not dependent on PAR1, PAR2 or GRP-78
M. Aberg, M. Johnell, M. Wickstrom, A. Siegbahn. Uppsala UniversityHospital, Department of Medical Sciences, Clinical Chemistry,Uppsala, Sweden
Purpose: Tissue factor (TF) initiates blood coagulation but is also a signalling
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Improved understanding of coronary artery disease in all its facets 85
receptor involved in the migration and survival of cells. Co-receptors interlinkedwith TF biological functions are the protease activated receptors (PARs) andglucose regulated protein (GRP)-78. These receptors are all expressed withinthe atherosclerotic plaque on inflammatory cells (monocytes/macrophages) andon plaque stabilizing cells (smooth muscle cells, fibroblasts), but also on ma-lignant cells which often serves as model system when studying TF/FVIIa sig-nalling. Death receptor-induced apoptosis may be mediated by monocytes andT-lymphocytes within the plaque and contributes to its destabilization. This studydetermines the impact of PAR1, PAR2, and GRP-78 on anti-apoptotic signalingmediated by the TF/FVIIa complex.Methods: Apoptosis was induced in MDA-MB-231 breast cancer cells using TNF-related apoptosis inducing ligand (TRAIL, 6h). Signalling events were determinedby adding FVIIa (10 or 100 nM), FVIIa/FX (5/130 nM), active site-inhibited FVIIa(FVIIai, 100 nM), the PI3-kinase inhibitor, agonist towards PAR1, PAR2 and GRP-78, and blocking antibodies against TF, PAR1, PAR2, and GRP-78. mRNA levelswere analyzed by real-time PCR and protein expressions by flow cytometry orwestern blot. Caspase-8 and -3 levels, cell size, and nuclear morphology wererecorded using an automated fluorescence imaging microscope.Results: The signalling abilities and functionality of TF- and PARs were deter-mined by analyzing the expression of IL-8 mRNA. Similarly, functional GRP-78signalling was verified by quantifying p44/42 phosporylation. Addition of FVIIa(both 10 and 100 nM) and FVIIa/FX, but not FVIIai, significantly reduced thecaspase-8 and -3 activation, the cell shrinkage, and the nuclear alterations in theTRAIL-treated cells. The effect by TF/FVIIa on TRAIL-induced apoptosis was de-pendent on the PI3-kinase/AKT signalling pathway. TF-blocking antibodies clearlyaffected the pro-survival signalling. However, despite functional receptors, addi-tion of specific agonists or blocking antibodies (+FVIIa) to PAR1, PAR2, and GRP-78 had no effect on the observed apoptosis markers.Conclusions: Death receptor induced apoptosis may be of importance for theatherosclerotic plaque rupture. We hereby report that TF/FVIIa-induced signallinggoverns this pathway of apoptosis independently of PAR1, PAR2, and GRP-78.The TF anti-apoptotic signalling pathway was, however, dependent on the prote-olytic activity of FVIIa which entails the search for another, at present, unknowncell surface component that may interact with the TF/FVIIa complex.
P634 Cardiac fibroblasts secretome protects cardiomyocytesfrom simulated ischemia reperfusion injury
M. Abrial, D. Angoulvant, C. Crola, F. Ivanes, S. Benhabbouche,M. Ovize, R. Ferrera. Inserm U886, University Claude Bernard Lyon1, Lyon, France
Objectives: Cardiac fibroblasts are the most prevalent cell type in the heart andplay a key role in regulating normal myocardial function and in the adverse my-ocardial remodelling following myocardial infarction. We hypothesized that CF andtheir secretome, may be implicated in endogenous cardioprotection against is-chemia reperfusion (I/R) injury.Method: Neonatal rat cardiomyocytes (NRC) and CF were isolated from 2 daysold Wistar rat’s hearts and cultured separately. They were subsequently co cul-tured either with direct cell contact in the same culture dish or indirect cell con-tact using a semi-permeable cell culture insert containing CF in the NRC culturedish. Isolated cell culture and co cultures were subjected to 3 hours of simulatedischemia followed by 20 hours of simulated reperfusion (n=5/group). A dose re-sponse experiment was performed using several co-culture (NRC/CF) ratio. Atthe end of reperfusion, cell viability assay (MTT) and cell death measurements(LDH and Troponin i) were performed to quantify I/R injury. Data are means ±SEM. Group comparison was performed by 1 way ANOVA.Results: Compared to isolated NRC alone, direct co culture groups showed upto 60±10% reduction of cell death. Indirect co culture groups showed the samemagnitude of protection suggesting a paracrine effect (Figure 1). The dose re-sponse experiment showed that the highest protection was obtained with a 1:1 coculture ratio. Both cell viability and cell death assays showed concordant results.
Figure 1
Conclusion: Our data suggest that CF may participate in endogenous cardiopro-tection against ischemia reperfusion injury. They suggest that this protection maybe mediated by paracrine mechanisms triggered by CF secretome with a doseresponse pattern.
P635 Protective effect of the CYP polymorphism withincreased activation of clopidogrel on cardiovascularevents
K. Tiroch, D. Sibbing, W. Koch, T. Roosen-Runge, A. Kastrati. GermanHeart Center, Clinic at the Technical University of Munich, Munich,
Germany
Background: The prodrug clopidogrel requires activation by cytochrome P-450(CYP) enzymes for its antiplatelet effect. The genes encoding CYP enzymes arepolymorphic, leading to reduced or increased function, depending on the respec-tive genotype. Reduced function alleles have been associated with an increase incardiovascular events.Methods: We tested the association between the ABCB1 (C/T) T-allele, leadingto reduced intestinal clopidogrel absorption, and the CYP2C19*17 (C/T) T-allele,leading to increased clopidogrel activation, with the need of clinically-driven targetlesion revascularization (TLR) and the secondary end point of major adverse car-diovascular events (MACE, including death, MI, and TLR) in a high risk populationof 925 patients with acute myocardial infarction (MI).Results: Carriers of the protective CYP2C19*17 T-allele had a 37% relative re-duction in the incidence of the primary end point TLR (14.0% vs. 22.3%, p=0.002),and a 22% relative reduction of the secondary end point MACE (22.0% vs. 28.1%,p=0.04), compared with noncarriers, respectively. The association of the T-allelewith TLR remained significant in the multivariate analysis (P=0.001). Genotypesof the ABCB1 C/T polymorphism were not associated with the incidence of TLRor MACE.
Risk alleles and MACE
ABCB1 CYP Allel *17
CC T allele P value CC T allele P value(n=203) (n=725) (n=565) (n=363)
TLR 42 (20.7) 135 (18.6) 0.580 126 (22.3) 51 (14.0) 0.002Death 17 (8.4) 47 (6.5) 0.337 34 (6.0) 30 (8.3) 0.203Repeat MI 6 (3.0) 16 (2.2) 0.509 15 (2.7) 7 (1.9) 0.480Death or MI 21 (10.3) 56 (7.7) 0.216 42 (7.4) 35 (9.6) 0.255Stent thrombosis 3 (1.5) 7 (1.0) 0.517 6 (1.1) 4 (1.1) 0.964MACE 60 (29.6) 179 (24.7) 0.206 159 (28.1) 80 (22.0) 0.040Stroke 1 (0.5) 7 (1.0) 0.524 5 (0.9) 3 (0.8) 0.930MACE or Stroke 61 (30.0) 183 (25.2) 0.227 162 (28.7) 82 (22.6) 0.042Defect final 14.5±17.0 14.6±16.8 0.960 15.2±16.1 13.6±17.5 0.217
Conclusions: Based on the genetic analysis in a high risk population of acuteMI patients with interventional treatment and long-term clopidogrel, our studyfound for the first time a protective effect for carriers of an increased-functionCYP2C19*17 T-allele with significantly lower rates of TLR and MACE.
P636 A1298C polymorphism in the MTHFR gene predisposesto cardiovascular risk in rheumatoid arthritis
C. Gonzalez Juanatey1, M.A. Gonzalez-Gay2, R. Palomino-Morales3,L. Rodriguez4, B. Fernandez-Gutierrez4 , A. Testa1 , T. Vazquez1,J.A. Miranda1, J. Martin3, J. Llorca5. 1Hospital Xeral Calde, Lugo,
Spain; 2Hospital Marques de Valdecilla, Santander, Spain; 3Consejo Superior deInvestigaciones Cientificas (CSIC), Granada, Spain; 4Hospital Clinic San Carlos,Madrid, Spain; 5University of Cantabria, Santander, Spain
Background: Patients with rheumatoid arthritis (RA) have increased risk of car-diovascular (CV) disease due to accelerated atherosclerosis. Hyperhomocys-teinemia has been found to be an independent non-traditional risk factor for CVdisease, including coronary disease, in the general population. High elevationsmay be seen in uncommon autosomal defects of the metabolizing enzymes cys-tathionine beta-synthase and methylene tetrahydrofolate reductase (MTHFR). Acommon C677T polymorphism in the gene coding for the 5,10-MTHFR enzymehas been found to be a new candidate genetic risk factor for CV disease in thegeneral population.Objective: To determine the contribution of the MTHFR 677 C>T and 1298 A>Cgene polymorphisms to the susceptibility to RA.We also assessed whether these two MTHFR gene polymorphisms may be im-plicated in the development of CV events and subclinical atherosclerosis mani-fested by the presence of endothelial dysfunction in a series of Spanish patientswith RA.Methods: Six hundred and twelve patients fulfilling the 1987 American Collegeof Rheumatology classification criteria for RA, seen at the rheumatology outpa-tient clinics of two Hospitals, were studied. Patients and controls (N= 865) weregenotyped using predesigned TaqMan single nucleotide polymorphism genotyp-ing assays.Results: No significant differences in allele or genotype frequencies for theMTHFR gene polymorphisms between RA patients and controls were found. Also,no association between the MTHFR 677 C>T polymorphism and CV events orendothelial dysfunction was observed. However, RA patients carrying the MTHFR1298 allele C have an increased risk of CV events after 5 (38.7% versus 30.3%;OR: 1.45; 95% CI 1.00- 2.10; p= 0.04) and 10 years’ (42.2% versus 31.0%;OR: 1.62; 95% CI 1.08- 2.43; p= 0.01) followup. Moreover, patients carrying theMTHFR 1298 AC and CC genotypes had a significantly decreased flow-mediatedendothelium-dependent vasodilatation (4.3±3.9%) compared to those carryingthe MTHFR 1298 AA genotype (6.5±4.4%); p= 0.005.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

86 Improved understanding of coronary artery disease in all its facets
Conclusions: Our results show that the MTHFR 1298 A>C gene polymorphisminfer an increased risk for increased subclinical atherosclerosis and CV events inpatients with RA.
P637 Irreversible alterations of miRNA abundance in anischemia/reperfusion model of myocardial infarction inmice
C. Troidl1, H. Moellmann1, J. Wilhelm2, S. Voss1, S. Szardien1,F. Rybinski1, K. Troidl3, C.W. Hamm1, A. Elsaesser4, H. Nef1.1Kerckhoff Clinic, Bad Nauheim, Germany; 2Institute for Biochemistry,
Justus-Liebig-University Giessen, Giessen, Germany; 3Max Planck Institutefor Heart and Lung Research, Bad Nauheim, Germany; 4Dept. of Cardiology,General Hospital Oldenburg, Oldenburg, Germany
Background: miRNAs are important regulators of inflammation and remodellingprocesses of the damaged myocardium after infarction. Aim of the present studywas to identify the transcriptional profile of miRNAs after occlusion of a coronaryartery with special focus on ischemia-reperfusion injury.Methods: In 60 mice ligature of the ramus interventricularis anterior (RIVA)was performed. In 30 mice the ligature was removed after 45 min (is-chemia/reperfusion model; IR-group). The remaining mice (n=30) retained theligature until tissue isolation (MI-group). Infarct area of all mice was isolated after2d, 5d, and 10d (each n=10) and miRNA abundance was investigated using mi-croarrays (EMBL miChip V 9.2 based on miRBase 9.2). 10 sham treated animalsserved as controls. Identified target miRNAs were validated using quantitativereal-time PCR.Results: 7 miRNAs showed significant differences after ligature compared tosham treated controls (miR-21, miR-223, miR-689, miR-499-5p, miR-378, miR-129-5p and miR-149). miR-21 and miR-223 were up-regulated in both groups(IR- and MI-group). miR-21 levels were increased after 2 and 5 days continu-ously, in contrast miR-223 showed highest levels after 2 days and declined to nor-mal values after 7 days. miR-499-5p, miR-378 and miR-149 showed decreasedabundance in the MI-group. In the IR-group miR-499-5p and miR-149 showed adecreased abundance 5 days after ischemia/reperfusion. The qRT-PCR valida-tion revealed no significant differences for miR-689 and 129-5p between the IR-,MI-group and sham group.Conclusion: 5 of 7 miRNAs showed significant alterations after ischemia-reperfusion. Altered levels of miR-21, miR-223, miR-378 and miR-129-5p in bothgroups (IR and MI) might reflect common remodelling mechanisms after disturbedblood supply in the myocardium, whereas even a recovery of blood supply leadsto irreversible changes of miRNA abundance. Furthermore, levels of miR-499-5p,known to influence differentiation of cardiomyocytes, and abundance of miR-149,which might potentially contribute to myocardial fibrosis are decreased in I/R. Thismight account for the special characteristics of reperfusion injury. Whether theseobserved alterations are involved in reperfusion injury mechanisms have to befurther elucidated.
P638 Coronary Artery Disease (CAD) - possible role ofgenetic inflammatory markers in north Indianpopulation
N. Sinha, H. Rai, N. Singh, S. Kumar, S. Agarwal. Sanjay Gandhi PostGraduate Institute of Medical Sciences, Lucknow, India
Background: Different alleles of chemokine receptors (CCR5) and fractalkine re-ceptor (CX3CR1) polymorphisms are found in ethnic populations which are beingstudied to have a possible role in development CAD.Methodology: We studied frequencies of two genetic variants of CC chemokinereceptor 5 (CCR5) namely CCR5-d32 and CCR5-59029 and those of fractalkinereceptors (CX3CR1) namely CX3CR1-V249I and CX3CR1-T280M in 308 provencases of CAD (mean age 52.39±12.81 yrs, 86.36% males) and 300 age and sexmatched controls using genotyping techniques like Polymerase Chain Reaction(PCR) and Restriction Fragment Length Polymorphism analysis (RFLP). Geno-type/allele frequencies were compared using chi-square test.Results: Diabetes was present in 19.4% cases, hypertension in 27.2%, while16.1% were smokers. 26.2% of patients had family history of premature CAD. Themean levels of Total Cholesterol, HDL-C, LDL-C and Triglycerides were statisti-cally more in patients compared to controls (p<0.01). Diagnosis for the patientsstudied stable angina in 4.6%, unstable angina in 6.6%, previous MI in 74.7%,and asymptomatic known CAD 1.6% cases.Genotyping of patient and controls for chemokine and fractalkine receptor mark-ers revealed mixed results; for markers CX3CR1-V249I, revealed II (Mutant)-14 (4.5%), VV and VI (heterozygote & wild allele)- 212 (68.8%)+82 (26.6%),(p=0.001, 95%CI=0.325-0.630, adjusted OR=0.453). Genotyping of CX3CR1-T280M revealed TT (wild allele)-254 (82.5%) and TM and MM (heterozygote&mutant)-13 (4.2%)+41 (13.3%), p=0.001, 95%CI=0.256-0.543 and adjustedOR=0.373 against their controls indicating their protective role in CAD.Analysis of CCR5 del 32 which revealed ++ and +/�32 (wild & heterozygoteallele)-294 (95.5%) and �32/�32 (mutant)-0 (0%) with p=0.05, 95%CI=0.999-7.90, OR=2.81 and for CCR5 59029 revealed AA (Mutant)-75 (24.4%), AG andGG (wild & heterozygote allele)- 136 (44.2%)+97 (31.5%), (p<0.005, CI=1.159-2.345, adjusted OR=1.648) both suggesting increased risk for CAD when com-pared to controls.
Conclusion: In north Indian population the mutant alleles of fractalkine recep-tors (CX3CR5) have been found have a reduced risk of atherosclerosis and andthose of chemokine receptor (CCR) appear to have a higher risk of developingpremature CAD
P639 Overlapping sirolimus- but not zotarolimus-elutingstents have adverse effects on both epicardial andmicrocirculatory endothelial function in porcinecoronary arteries
T. Nakamura, I. Brants, D. Panchal, J. Li, J.P. Chen, J. Singh, S. King,N. Chronos, D. Hou. Saint Joseph’s Translational Research Institute, Atlanta,United States of America
Background: The safety features of Endeavor (ZES) in comparison with Cypher(SES) are reported clinically in long-term follow-up studies, which highlight verylow rate of late thrombosis despite short period of DAPT. We aimed to investigateendothelial function at both epicardial and microvascular coronary levels afteroverlapping ZES and SES in porcine coronary arteries.Methods: Overlapping of bare metal stents (BMS) (n=12), SES (n=12), and ZES(n=13) were implanted into 19 pigs. Each pig received two pairs of identical stents,with S/A ratio of 1.1:1 and overlapping segment of 1/3 to 1
2 of single stent length.Coronary endothelial function 5-10 mm proximal and distal to the stents, as wellas TIMI frame count, was estimated by incremental acetylcholine (Ach, 10-6, 10-5M/ml) and nitroglycerin (NTG, 400μg) infusion at 1 month.Results: Angiographic minimal luminal diameter, as well as percent diameterstenosis was no significantly different among three types of stent (P>0.05).Endothelium-dependent vasomotion at distal non-stented reference segmentswas significantly impaired in SES compared to both ZES and BMS. The meancoronary diameter changes at Ach 10-6 and 10-5 was -3.12±3.63% and -5.39±5.89% for SES, 1.81±7.33% and 3.00±5.46% for ZES, as well as -0.34±9.77% and -0.96±12.16% for BMS (P < 0.07 and 0.002; SES vs both oth-ers, respectively). Similar patterns were seen at proximal sites, but no significantdifference among groups. TIMI frame count following Ach 10-6 M/ml was alsosignificantly increased in SES vs ZES (p<0.05). No differences in NTG-inducedvasodilatation were observed among groups.Conclusions: While profound inhibition of endothelium-dependent vasomotor re-laxation in both distal conduit and far distal micro-coronary arteries was found foroverlapping SES, overlapping ZES demonstrated preserved endothelial vasodi-latation at both macro- and micro- levels in this porcine model.
P640 Inhibition of leukotriene C4 release via the multidrugresistance protein-1 reduces oxidative stress andapoptosis in cardiomyocytes
M.U. Becher, A. Ghanem, G. Nickenig, C. Mueller. University HospitalBonn, Bonn, Germany
Leukotriene C4 is a derivative of arachidonic acid and is associated with oxidativestress and apoptosis. Cellular release of LTC4 is mediated via the multidrug resis-tance related protein-1 (MRP-1). Inhibition of MRP-1 reduces the release of thepro-oxidative LTC4. We hypothesized, that inside-outside transport of LTC4 viaMRP-1 might be a substantial pro-oxidative mechanism in cardiomyocytes andthat inhibition of MRP-1 might affect cardiac function.Incubation of cultured embryonic cardiomyocytes (eCM) with recombined LTC4induced the generation of reactive oxygen species (ROS) and induced apopto-sis. Pharmacologic LTC4 receptor inhibition using the specific Cys-LT1 receptorblocker Montelukast antagonized this effect.The in vivo relevance of this finding was tested in a mouse model. Four groupsof mice (5-7 animals per group) received cryo-injury of the anterior wall. Twogroups (Wildtype, WT) were treated with either the specific CysLT1-receptor-blocker Montelukast or received the specific MRP-1-inhibitor MK571. One groupconsisted of 5 MRP-1-/- mice and one group of 5 untreated WT mice servedas control. Cardiac function was measured via two-dimensional guided M-modeechocardiography 14 days after injury. Left-ventricular-function at rest (WTun-treated vs. MRP-1-/-, WTMontelukast, WTMK571) and under dobutamine stress(WTuntreated vs. WTMontelukast and WTMK571) were assessed before thehearts were excised. The following echocardiographic parameters were analysed:EFrest[%], EFstress[%], scarrest[%], scarstress[%] and myocardial recruitment[%] (scarrest-scarstress).Animals treated with Montelukast (WTMontelukast LV-EFrest 40%, LV-EFstress51%), or MK571 (WTMK571 LV-EFrest 39%, LV-EFstress 47%) had a significantbetter left-ventricular-function than untreated animals (WTuntreated LV-EFrest33%, LV-EFstress 41%). Myocardial recruitment under dobutamine stress (WT-Montelukast scarrest 19%, scarstress 12%, recruitment 7%) was highest in an-imals treated with montelukast compared to treatment with MK571 (WTMK571scarrest 15%, scarstress 10%, recruitment 5%) or untreated animals (WTun-treated scarrest 20%, scarstress 15%, recruitment 5%). Moreover left ventricularfunction was significantly better in MRP-1-/- mice (MRP-1-/- LV-EF: 74,7%) thanWT-mice (WT LV-EF: 58.2%). The rate of apoptotic cardiomyocytes was reducedwithin the periinfarcted space. Concentration of LTC4 within the plasma was sig-nificantly lower in MRP-1-/- animals compared to WT-mice.Potentially, MRP1 inhibition or particularly Cys-LT1R-blockade via Montelukastmay offer therapeutical approaches for treatment of acute coronary syndrome.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Improved understanding of coronary artery disease in all its facets 87
P641 Ovariectomy restores the infarct size-limiting effect ofpostconditioning in female rabbits
E. Demerouti1, I. Andreadou2, A. Zoga1, I.K. Aggeli3,K. Gaitanaki3, I. Beis3, M. Anastasiou-Nana1, D.T.H. Kremastinos1,E.K. Iliodromitis1. 1University of Athens, Medical School, Second
University Dept. of Cardiology, Athens, Greece; 2University of Athens, Faculty ofPharmacy, Athens, Greece; 3University of Athens, School of Biology, Departmentof Animal and Human Physiology, Athens, Greece
Introduction: Whilst ischemic preconditioning (PreC) and postconditioning(Postc) protect the ischemic heart by limiting the infarct size, gender seems tointerfere with the final cardioprotective effect. Several in vivo studies have shownthat the protection from PreC fades and is eventually lost in female animals afterovariectomy. However, the cardioprotective effect of Postc in females is still in dis-pute with rather divergent results and no studies have been performed in femaleanimals after ovariectomy so far.Aim: To test whether Postc is effective in limiting the infarct size in anesthetized fe-male rabbits, to determine whether endogenous estrogens have a role in the finaloutcome and to investigate intracellular alterations in phosphorylation of ERKs,p38-MAPK, and AKT (RISK kinases) in intact or ovariectomized rabbits.Methods: Intact or ovariectomized adult female rabbits were subjected to 30 minregional ischemia of the heart followed by three hours reperfusion. The animalswere divided into 3 groups as follows: A control group (FemC), a Postc group thatwas subjected to 8 cycles of 30sec ischemia/30sec reperfusion applied immedi-ately after the end of index ischemia and a group that was subjected to the samePostc protocol four weeks after surgical ovariectomy (OvxPostc group). After theend of the long reperfusion period, the infarct size (I) was delineated by TTC stain-ing, the area at risk (R) by fluorescent particles and the percent (%) I/R ratio wascalculated. In a second series of experiments, three respective to the first seriesgroups were subjected to the same protocol up to the 10th min of reperfusionwhere the hearts were quickly excised and immersed in liquid nitrogen for ERKs,p38-MAPK, and AKT assessment.Results: Infarct size was reduced only in OvxPostc group (25.3±2.7%, vs48.05±2% in FemC and 55.1±2.7% in Postc groups respectively, p<0.05). Thephosphorylation of ERKs, p38-MAPK, and AKT in the ischemic region of theheart, was significantly higher in the protected OvxPostc group vs the other un-protected groups.Conclusion: We conclude that the ineffectiveness of Postc to reduce the infarctsize in anesthetized female rabbits is restored after ovariectomy probably via theRISK pathway. Hormonal status seems to interfere with alterations in intracellularsignaling.
P642 Sarcoplasmic reticulum induced Ca2+ oscillations butnot ROS are the cause for opening of mitochondrialpermeability transition pores in reperfused cardiacmyocytes
Y. Abdallah, W. Iraqi, T. Shahzad, S.A. Kasseckert, A. Erdogan,D. Sedding, C. Neuhof, K.D. Schlueter, H. Tillmanns, H.M. Piper. Justus LiebigUniversity, Giessen, Germany
Objective: Opening of mitochondrial permeability transition pores (MPTP) isknown induces cell death in reperfused myocardium and pharmacological inhi-bition of MPTP was able to reduce infarct size in patients with acute myocardialinfarction. We showed previously that reperfusion causes hypercontracture andnecrosis of cardiac myocytes due to oscillatory elevations of cytosolic Ca2+ origi-nating from the sarcoplasmic reticulum (SR). We now investigated if SR-triggeredCa2+ oscillations or ROS are causally connected in signalling pathways leadingto MPTP opening and cardiac myocyte death in the early reperfusion.Methods: Isolated cardiac myocytes from adult rats were subjected to 80 min ofsimulated ischemia and for 20 min of simulated reperfusion. MPTP opening wasdetected in whole cells by monitoring the mitochondrial inner membrane potential(��m) with JC-1. Fura-2 was used to monitor cytosolic [Ca2+]i or mitochondrial[Ca2+]m after quenching the cytosolic compartment with manganese. Mitochon-drial ROS were detected by the use of MitoSox Red. Necrosis was determined bypropidium iodide staining.Results: Within the first 10 min, reperfusion induced a collapse of mitochon-drial inner membrane potential (��m) and an increase in Mg2+ concentration,indicating ATP-degradation, after a brief initial recovery. Simultaneously, Ca2+oscillations occurred, [Ca2+]m and [ROS]m increased, cells developed hyper-contracture, and underwent necrosis at the end of reperfusion. Inhibition of SRCa2+ uptake with thapsigargine (100 nmol/L), SR Ca2+ release with ryanodine(5 μmol/L), mitochondrial Ca2+ uptake with Ru 360 (1 μmol/L), or MPTP open-ing with cyclosporine A (0.5 μmol/L) prevented significantly the collapse of �ψ,the increase in [Ca2+]c, [Ca2+]m, [ROS]m; and reduced the frequency of Ca2+oscillations as well as hypercontracture and necrosis.ROS scavengers, 2-MPG (0.5 mmol/L) or N-acetylcysteine (0.1 mmol/L) had noeffect on these parameters, but reduced ROSm. ROSm were also reduced inpresence of thapsigargine, ryanodine, Ru 360 or cyclosporine A.Conclusions: MPTP opening occurs early in reperfusion and is due to the Ca2+oscillations originating primarily from the SR. Mitochondrial ROS are rather a re-sult but not a cause of MPTP opening.
P643 The delayed cellular pHi recovery through inhibition ofglycogen synthase kinase 3-beta protects cardiacmyocytes against reperfusion injury
W. Iraqi, T. Shahzad, S.A. Kasseckert, M. Aslam, A. Erdogan,K.D. Schlueter, D. Sedding, H. Tillmanns, H.M. Piper, Y. Abdallah.
Justus Liebig University, Giessen, Germany
In previous studies we have shown that inhibition of glycogen synthase kinase-3β
(GSK-3β) protects cardiac myocytes against acute reperfusion injury. Inhibitionof GSK-3β significantly reduced the development of hypercontracture and necro-sis in reperfused cardiac myocytes. The aim of our present study is to investi-gate how inhibition of GSK-3β modifies the intracellular pH during ischemia andreperfusion and whether this modification is accompanied by changes of cytosolicCa2+-oscillations during reperfusion.To simulate ischemia and reperfusion, isolated cardiac myocytes of adult ratswere superfused anoxically (60 minutes 100% N2; no glucose; pH 6.4) and thenreperfused with a normoxic buffer (25 minutes 21% O2; 2.5mM glucose; pH 7.4).Cytosolic Ca2+ was measured by the Ca2+-fluorescence indicator Fura-2. Thecellular pH was detected by the fluorescence indicator BCECF. SB216763 (6 μM),a specific inhibitor of GSK-3β was applied in the last 8 minutes of ischemia andduring the whole time of reperfusion.The frequency of cytosolic Ca2+-oscillations during reperfusion was markedly re-duced in presence of SB216763 (10±2.2 vs. 34±4.2 oscillations per minute incontrol). During simulated ischemia, cardiac myocytes developed an acidosis ofpH 6.30±0.07 (pH under normoxic conditions: 7.20±0.08). During reperfusion,cellular pH recovered and achieved a maximal value of 6.68±0.05 within 12 min-utes of reperfusion in control. In presence of SB216763, cellular pH recoveredslower and achieved a maximal value of 6.84±0.05 after 25 minutes of reperfu-sion.The results show that inhibition of GSK-3β significantly reduces the frequency ofthe cytosolic Ca2+-oscillations during reperfusion. In addition, inhibition of GSK-3β delays the cellular alkalisation at the beginning of reperfusion and achievesbetter recovery of pH during further reperfusion.
P644 Effect of sildenafil on sympathetic hyperinnervation inpost-infarcted rat hearts
T.-M. Lee1, N.-C. Chang2. 1Chi Mei Medical Center, Tainan, Taiwan;2Taipei Medical University Hospital, Taipei, Taiwan
Purpose: We assessed whether sildenafil attenuates cardiac sympa-thetic reinnervation after myocardial infarction through activation of ATP-sensitivepotassium (KATP) channels. Sildenafil, a phosphodiesterase-5 inhibitor, has beenshown to provide cardioprotection against ischemia/reperfusion injury via activa-tion of mitochondrial KATP channels. It is unclear whether similar benefits arefound by modulating sympathetic innervation in chronic settings after myocardialinfarction.Methods: Twenty-four hours after ligation of the anterior descending artery, maleWistar rats were randomized to either vehicle, nicorandil (a specific mitochondrialKATP channel agonist), pinacidil (a nonspecific KATP channel agonist), silde-nafil, glibenclamide (a KATP channel blocker), or a combination of nicorandil andglibenclamide, pinacidil and glibenclamide or sildenafil and glibenclamide for 4weeks. To elucidate the role of mitochondrial KATP channels in modulating nervegrowth factor, 5-hydroxydecanoate was assessed in an in vitro model.Results: Myocardial norepinephrine levels revealed a significant elevation invehicle-treated rats at the remote zone compared with sham-operated rats. Im-munohistochemical analysis for tyrosine hydroxylase, growth associated factor 43and neurofilament also confirmed the change of myocardial norepinephrine. Thiswas paralleled by a significant upregulation of nerve growth factor protein expres-sion and mRNA in the vehicle-treated rats, which reduced after administering ei-ther nicorandil, pinacidil or sildenafil. Arrhythmic scores during programmed stim-ulation in the vehicle-treated rats were significantly higher than those treated withsildenafil. In contrast, the beneficial effects of sildenafil-induced were reversed bythe addition of either glibenclamide or 5-hydroxydecanoate, implicating mitochon-drial KATP channels as the relevant target.Conclusions: Chronic use of sildenafil after infarction, resulting in attenuatedsympathetic reinnervation by activation of mitochondrial KATP channels, maymodify the arrhythmogenic response to programmed electrical stimulation.
P645 Cardiomyocytes synthetize several newly discoveredadipokines (chemerin, omentin and nesfatin-1) closelyrelated to metabolic syndrome
F. Sandra, D. Rodriguez-Penas, P.V. Lear, A. Mosquera-Leal,V. Garcia-Rua, J.R. Gonzalez-Juanatey, M.F. Lago. IDIS, University
Clinical Hospital, Santiago de Compostela, Spain
Purpose: Adipokines play an important role as regulators of cardiovascular func-tion. Because of their close relationship with pathological conditions such as obe-sity, diabetes and hypertension, we hypothesised that several newly discoveredadipokines could be part of a paracrine/autocrine regulatory system at the car-diac level. Our aim was to determine the expression of omentin, chemerin andnesfatin-1 at the mRNA and protein levels in cardiomyocytes.Methods: Real-time PCR, western blotting and immunohistochemistry were used
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

88 Improved understanding of coronary artery disease in all its facets
to quantify mRNA and protein levels of chemerin, omentin and nesfatin-1 in hu-man, mouse and rat heart tissue, and in isolated cardiomyocytes. We also studiedthe metabolic effects on cultured neonatal rat cardiomyocytes of the only com-mercially available of these peptide adipokines, nesfatin-1. We assessed fattyacid metabolism with uptake assays, and glucose metabolism using immunohis-tochemistry and confocal analysis of the intracellular distribution of the glucosetransporter Glut-4. In addition, a microarray analysis of the complete rat genomewas performed (Affimetrix, Progenika Biopharma S.A) on cultured rat cardiomy-ocytes treated with nesfatin-1.Results: Chemerin, omentin and nesfatin-1 were expressed at mRNA and pro-tein levels in human, mouse and rat heart tissue, and in isolated cardiomy-ocytes. Following treatments with nesfatin-1 of isolated neonatal rat cardiomy-ocytes: 1) at 0.01μM-1μM for 30min, nesfatin-1 did not modify fatty acid up-take; 2) at 0.1μM for 10min, however, nesfatin-1 mobilised Glut-4 from the nu-cleus/nuclear membrane to the cytoplasm/cytoplasmic membrane; and 3) 1045gene sequences were significantly modified by 3h treatment with 1μM nesfatin-1. Of those genes, 225 have been implicated in primary metabolic process suchas fatty acid metabolism (e.g. Long-chain-fatty-acid-CoA ligase 4; DiacylglycerolO-acyltransferase 1), cholesterol metabolism (e.g. Cholesterol acyltransferase 1;Estradiol 17-beta-dehydrogenase) and glucose metabolism (e.g. Pyruvate kinaseisozymes M1/M2; Phosphoglucomutase-2; L-lactate dehydrogenase A chain).Conclusions: The new adipokines chemerin, omentin and nesfatin-1 are ex-pressed in human, mouse and rat heart tissue, and in isolated cardiomyocytes.Nesfatin-1 induces changes in the expression of genes involved in fatty acid,cholesterol and glucose metabolism, and regulates intracellular Glut-4 mobiliza-tion in isolated cardiomyocytes.
P646 Matrix metalloproteinases 2 an 3 gene polymorphismsand the risk of target vessel revascularisation afterpercutaneous coronary intervention
J.J.W. Verschuren1, M.L. Sampietro2, D. Pons1, S. Trompet1 , P. DeKnijf2, A.H. Zwinderman3, R.J. De Winter4, R.A. Tio5, M.P.M. De
Maat6, J.W. Jukema1. 1Leiden University Medical Center, Department ofCardiology, Leiden, Netherlands; 2Leiden University Medical Center, Departmentof Human Genetics, Leiden, Netherlands; 3Academic Medical Center,Department of Clinical Epidemiology Biostatistics & Bioinformatics, Amsterdam,Netherlands; 4Academic Medical Center, Department of Cardiology at theUniversity of Amsterdam, Amsterdam, Netherlands; 5University Medical Center,Department of Cardiology, Groningen, Netherlands; 6Erasmus Medical Center,Departement of Hematology, Rotterdam, Netherlands
Purpose: Matrix metalloproteinases (MMP) are known to be involved in vascu-lar remodelling and inflammation, important features of restenosis after percuta-neous coronary intervention (PCI). Previous studies showed a significant associ-ation of the 5A/6A polymorphism of MMP3 gene and elevated MMP2 levels withrestenosis after PCI. We examined whether multiple SNPs, covering the full ge-nomic region of MMP2 and MMP3, were associated with restenosis in the GEN-DER study population.Methods: The GENetic Determinants of Restenosis (GENDER) project is a mul-ticenter prospective follow-up study that enrolled 3104 consecutive patients whounderwent successful PCI. Restenosis, defined as target vessel revascularisa-tion (TVR), occurred in 304 (9.8%) of the patients. Polymorphisms of MMP2and MMP3 were selected from the SNPper database, based on the minor allelefrequency (>5%) and their position to provide coverage of all haplotype blocks.Genotyping was performed by MassArray platform (Sequenom). Furthermore, in295 cases and 571 controls a genome-wide association analysis (GWA) was per-formed as well, using Illumina Human 610-Quad Beadchips.Results: No significant association was found in 19 SNPs of the MMP2 gene orin 12 SNPs of the MMP3 gene with regard to TVR.Conclusion: We found no significant association with this SNP-broad gene ap-proach in combination with data from a GWA. Although we did not test all theknown polymorphisms of the MMP2 and MMP3 gene, using tagging analyseswe examined those SNPs covering all known haplotypes of MMP2 and MMP3to conclude no major effects are to be expected from these genes on the riskof coronary restenosis after successful PCI. With this study we merely exclude2 previously proposed candidate genes for involvement in the increased risk forrestenosis, so future research may focus on other targets.
P647 Endovascular non thermal irreversible electroporationattenuates post-angioplasty luminal loss andneointimal formation in New-Zealand white rabbits
E. Maor1, A. Ivorra2, J. Mitchell3, B. Rubinsky4. 1Chaim ShebaMedical Center, Tel Hashomer, Israel; 2University Pompeu Fabra,
Barcelona, Spain; 3Angiodynamics, Queensbury, New-York, United States ofAmerica; 4University of California at Berkeley, Berkeley, United States of America
Using fundamental principles of electroporation and heat transfer simulations wedeveloped a novel endovascular ablation approach - non thermal irreversible elec-troporation (NTIRE), which selectively destroys cellular components of the arterialwall without affecting the extracellular scaffold.Methods: Computer simulations were used to demonstrate that NTIRE does notinduce thermal damage to the arterial wall. Using an endovascular approach, a
custom made device was used in-vivo to apply ninety NTIRE pulses to the rightiliac arteries of eight New-Zealand white rabbits. Evaluation at 7 and 35 days in-cluded H&E, Masson’s trichrome, elastic Von Gieson, smooth muscle actin, pro-liferating cell nuclear antigen, Von Willebrand, and S-100 antigen. In addition, 24iliac arteries of 12 additional animals were used to evaluate the effect of NTIREon luminal loss at 35 days in a rabbit model of balloon angioplasty.Results: One week after NTIRE, normal iliac arteries experienced completetransmural and circumferential cellular ablation, minimal damage to extra-cellularcomponents and re-endothelialization. After five weeks there was no evidence ofvascular smooth muscle cells (VSMC) regeneration and. In angioplasty-damagedarteries, results at 35 days demonstrated the ability of NTIRE to significantly re-duce post-angioplasty luminal loss. Compared with controls, NTIRE-treated arte-rial segments were wider (0.85±0.18 vs. 0.58±0.22 cm2, p = 0.001), experiencedless luminal loss (18%±19% vs. 38%±24%, p<0.001), demonstrated wider pointof maximal stenosis (0.21±0.09 cm vs. 0.11±0.06, p = 0.004), and showed lessneointimal formation (3.91±1.39 vs. 2.64±2.29 mm2, p < 0.001).Conclusions: NTIRE can ablate cells with minimal damage to extra-cellular com-ponents, minor inflammatory response and limited VSMC regeneration. In addi-tion, it holds the potential to prevent post-angioplasty luminal loss, treat arterialrestenosis and ablate cardiac arrhythmia pathways.
P648 Improved renal hemodynamics in diabetic rats treatedwith Telmisartan and Amlodipine
J. Peti-Peterdi, I. Toma, S.L. Vargas, J. Koo. University of SouthernCalifornia (USC), Los Angeles, United States of America
Background: Activation of the intra-renal renin-angiotensin system(RAS) is well established in diabetic nephropathy (DN), the most common causeof end-stage renal disease. Therefore, common strategies for preventing DN pro-gression include angiotensin (ANG) converting enzyme inhibitors (ACEI) andANGII type 1 receptor blockers (ARB). Other effective antihypertensive treat-ments, such as the use of calcium channel blockers (CCBs), have raised ques-tions regarding their effect on renal function especially in a high risk patient pop-ulation (AJH 2007; 20:417–422). In this study we aimed to test the effects ofthe emerging combination treatment with ARB telmisartan and CCB amlodipineon renal/glomerular hemodynamics, and tubular (pro)renin (a recently discoveredkey element of the RAS) in a diabetic rat model with nephrosclerosis using asensitive renal imaging technique.Methods: Submicron resolution deep optical sectioning of the intact kidney wasperformed in streptozotocin (STZ) treated, diabetic, 12 weeks-old Munich-Wistar-Fromter rats using quantitative, in vivo multi-photon fluorescence microscopy.Rats were treated for 28 days after STZ-injection with telmisartan (3mg/kg/day),amlodipine (10mg/kg/day) or both. Another group of rats were treated with telmis-artan (3mg/kg/day) in combination with ramipril (10mg/kg/day) as comparison forthe added blood pressure lowering effect by the ARB+CCB combination.Results: Compared to control (C), Telmisartan (T) ± Amlodipine (A) signifi-cantly reduced mean arterial blood pressure (C=145±7, T=101±6, A=118±12,T+A=97±6 mmHg), glomerular diameter (C=166±2, T=157±2, A=154±4, T+A=147±4 μm), single nephron GFR (C=68±4, T=29±4, A=27±4, T+A =36±3nl/min), and similarly improved red blood cell velocity in peritubular capillaries.The combination caused a 1.4-fold increase in the ratio of efferent/afferent arteri-ole diameter. In addition, the 3-fold increased renal tubular (pro)renin content wascompletely abolished by T±A, but not by T in combination with the ACEI ramipril(T+R) at a similar antihypertensive effect (76±14 mmHg).Conclusion: Combination of telmisartan with amlodipine lowers BP, and pre-serves the beneficial effect of telmisartan on the kidney besides the added benefiton blood pressure control. Telmisartan provides a balance in glomerular hemo-dynamics by effectively dilating the efferent arterioles in the presence of CCBs,which preferentially dilates the afferent arterioles. The net effect leads to improve-ment of renal and glomerular hemodynamics in diabetes, and likely contributes torenal protection during long term treatment.
P649 Preischemic efferent vagal stimulation increasesinfarct size in rabbit hearts by activation of muscarinicreceptors
B. Buchholz, M. Rodriguez, F.C. Ivalde, N.A. Siachoque, M. Donato,R.J. Gelpi. Institute of Cardiovascular Physiopathology, Buenos Aires,
Argentina
It has been shown that vagal stimulation (VS) induces cardioprotective proteinoverexpression, attenuates arrhythmias and improves survival in post myocardialinfarction chronic heart failure. In addition, the administration of exogenous acetyl-choline mimics ischemic preconditioning. However, there are no conclusive datain regards to the effects of in vivo VS on the infarct size induced by ischemia andreperfusion and its interaction with the sympathetic nervous system. The objec-tive of this study was to evaluate the effects of VS on the infarct size performingVS before the ischemia.Methods: Male rabbits subjected to 45 min of regional myocardial ischemia fol-lowed by 4 hours of reperfusion were used (Group 1, G1, n=13). In group 2 (G2,n=9) G1 protocol was repeated but, in addition, right efferent VS was performedduring 10 min to an intensity enough to reduce heart rate (HR) 10-20%. In group3 (G3, n=4) the G2 protocol was repeated but atropine was administered during
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Improved understanding of coronary artery disease in all its facets / Pulse wave velocity and ambulatory blood pressure monitoring 89
the stimulation, at a dose necessary to block the effect of VS on HR. In group4 (G4, n=5) the G2 protocol was repeated but a β1-adrenergic blocker (Esmolol;3 mg/kg bolus followed by 0.5 mg/kg/min infusion) was administered during thestimulation. To eliminate the afferent stimulation, the vagus nerve was sectionedat the cervical level. A catheter was placed in the left ventricle (LV) to measure theleft ventricular systolic pressure (LVSP), the LV end diastolic pressure (LVEDP),the LV +dP/dt and the HR. Risk area and infarct zone were measured with EvansBlue and triphenyl tetrazolium chloride, respectively.Results: In G1, G2 and G3 the LVEDP increased during ischemia and slightlydecreased during reperfusion, but it did not change in G4. No significant changeswere observed in LVSP, LV+dP/dt and HR during ischemia and reperfusion in ei-ther group. The VS increased the infarct size from 43.4±2.9% (G1) to 60.7±4.4%(G2) (p<0.05). The administration of atropine during VS (G3) reverted this effectreducing the infarct size to 41.3±2.4% (p<0.05 vs G2). However, Esmolol onlyreduced the infarct size to 51.8±5.5% (G4).Conclusions: Efferent VS performed before ischemia significantly increased theinfarct size by a muscarinic cholinergic mechanism. This deleterious effect is alsopartially reverted by β1-adrenergic blockade.
P650 Curcumin reduces the cardiac ischemia-reperfusioninjury in cardiomyocytes via inhibition of Toll-likereceptor 2
Y.S. Kim, Y. Ahn, J.S. Kwon, M.H. Jeong, J.G. Cho, J.C. Park,J.C. Kang. Chonnam National University Hospital, Gwangju, Korea,
Republic of
Purpose: Myocardial infarction (MI) is one of the major causes of mortality andinflammation has been implicated in the myocardial cell death. Toll-like receptor 2(TLR2) is a key mediator of the innate immune system, and curcumin, a polyphe-nolic compound derived from turmeric, has antioxidant and anti-inflammatory ac-tivities.Methods and Results: In this study, rat cardiomyocytes (CMs) was stim-ulated with tumor necrosis factor (TNF)-α, peptidoglycan (PGN) or hy-poxia/reoxygenation (H/R) with or without curcumin pretreatment. Sprauge-Dawley rats were fed curcumin (300 mg/kg/day) one week before cardiac is-chemia/reperfusion (I/R) injury. I/R was induced by ligation of left anterior de-scending coronary artery for 30 minutes followed by release. Both mRNA andprotein of TLR2 were upregulated in infarcted myocardium, while TLR4 was re-mained unchanged. In CMs, TLR2 and monocyte chemoattractant protein (MCP)-1 mRNA were increased by TNF-α, PGN, or H/R, whereas blunted by curcumin.Immunofluorescence staining of CMs also showed that TLR2 and MCP-1 wereincreased after H/R, whereas curcumin pretreated CMs were not. In animalstudy, two weeks after I/R TLR2 were increased in infarct zone, whereas stayedunchanged in Cur+I/R group. Macrophage infiltration (CD68) and high-mobilitygroup box (HMGB1) were increased in I/R group, whereas decreased in Cur+I/Rgroup. Connexin43 was reduced in I/R group, while recovered significantly inCur+I/R group. Cardiac contractility in Cur+I/R group was also improved com-pared with in I/R group (max dP/dt in Cur+I/R group; 9660±612 vs. in I/T group;8119±366, p<0.05).Conclusion: These results suggest that selective inhibition of TLR2 by curcumincould be a therapeutic tool for post myocardial infarction.
P651 A translational approach to assess dynamic changesin the immune system following an acute ST-segmentelevation myocardial infarction
M.J. Forteza, V. Bodi Peris, I. Benet, J. Sanchis, J. Nunez, I. Trapero,L. Mainar, F.J. Chorro, C. Gomez, A. Llacer. Hospital Clinico
Universitario, INCLIVA, Universidad de Valencia, Valencia, Spain
Purpose: Preliminary data suggests that in acute ST-segment elevation myocar-dial infarction (STEMI) an uncontrolled immune response occurs. The purpose ofthis study was to analyze the dynamics as well as the mechanisms underlying thelymphocyte-mediated immunity changes in reperfused STEMI.Methods: We studied 18 patients with a first STEMI treated with percutaneousrevascularization. A wide variety of lymphocyte subtypes were serially determinedusing flow citometry, before reperfusion and 24 h, 96 h and 30 days afterwards;values were compared with 18 age- and sex-matched control subjects with nor-mal coronary arteries. In an experimental series of 6 swine with an anterior STEMIinduced by means of angioplasty balloon inflation, lymphocyte subtypes were alsoassessed at baseline, 1 h after balloon inflation, 2 h and 72 h after reperfusion.Results: In comparison with controls, patients displayed a loss of circulatinglymphocytes. The most significant changes in lymphocyte subtypes were de-tected at 24 h and steadily returned to normal values within the following month.CD4+CD25+ FoxP3 regulatory T cells dropped (31±18 vs. 19±10 cells/ml,p=0.05). Lymphopenia affected T cells but not B cells and it was mediated byan increase in lymphocyte apoptosis (26±15 vs. 9±9%, p=0.002). In patients, weobserved a tendency towards a decrease in aggressive pro-inflammatory T lym-phocytes such as less T natural killers (122±112 vs. 194±82 cells/ml, p=0.03),less Thelper1-Thelper2 ratio (1.9±0.8 vs. 3.2±2.3, p=0.02) or more CD4/CD8 ra-tio (3.1±1.6 vs. 2.1±0.9, p=0.03) and an attempt to preserve anti-inflammatoryThelper2 cells (18±8% vs. 14±5%, p=0.05). In swine, in comparison with base-line values, severe ischemia (mediated by 1 h balloon inflation) induced an acute
increase in lymphocyte count and regulatory T cells while serial determinationsfollowing reperfusion paralleled results in patients in terms of lymphopenia, apop-tosis and loss of regulatory T cells.Conclusions: A complex immune response associated with a loss of regulatoryT cells occurs in reperfused STEMI. A self-defensive mechanism mediated by aboost in lymphocyte apoptosis and a decrease in pro-inflammatory T cell takesplace.
P652 Speckle tracking echocardiography for the quantitativeassessment of regional myocardial function in themurine model of myocardial infarction
E. Szymczyk1, P. Lipiec1, K. Kaminski2, M. Kozuch2, T. Bonda2,M. Winnicka2, J. Kasprzak1. 1Medical University of Lodz, 2nd
Department of Cardiology, Lodz, Poland; 2Medical University of Bialystok,Bialystok, Poland
Introduction: Echocardiographic assessment of cardiovascular structure andfunction in murine models has developed into one of the most commonly usednon-invasive technique for serial evaluation of cardiac phenotype in mice.Aim: We aimed to examine feasibility of speckle tracking echocardiography in theregion of scar in comparison to normal myocardium.Material and methods: 30 mice with complete endocardial border delineation ofleft ventricle after myocardial infarction induced by coronary ligation were includedin the study. Parasternal short axis views (greyscale and tissue Doppler imaging)were acquired in all anesthetized subjects with the use of linear transducer. Thedata were analyzed off-line by two independent investigators using 2D speckle-tracking technique with assessment of radial S.Results: Reproducibility of radial strain measurements (S) in the infarct regionwith myocardium thicker than 0,06cm was r=0,63; p<0,05, while reproducibilityof S in the region thinner than 0,06cm and thicker 0,03cm was r=0,49; p<0,05.Reproducibility of S in the region of scar where wall thickness was thinner than0,03cm was r=0,12, p=NS. In normal myocardium the reproducibility of radialstrain was r=0,89; p<0,0001.Conclusions: 2-D speckle tracking is a feasible method in the region of normaland infarcted myocardium unless it is thinner than 3mm.
PULSE WAVE VELOCITY AND AMBULATORY BLOODPRESSURE MONITORING
P653 Effect of computer system using short messagesservice for patient feedback on blood pressure controlin patients with arterial hypertension
O.M. Posnenkova, V.I. Gridnev, A.R. Kiselev, V.I. Schwarz. ResearchInstitute of Cardiology, Saratov, Russian Federation
Purpose: To determine the impact of a computer system using short messagesservice (SMS) for patient feedback on the control of blood pressure (BP) in pa-tients with arterial hypertension (AH) managed in primary care unit.Methods: 199 patients (≥18 years old) with established AH managed in primarycare unit were enrolled in the study. 97 of them (mean age 49±11.3 years) wereoffered to answer to automatically generated SMS requests about their BP levelduring 1 year. The other 102 patients (mean age 51±11.1 years) received usualcare. Their BP records concerned the same year were extracted from ambula-tory cards retrospectively. Three control check points were assigned for the groupof SMS monitoring - 1, 6 and 12 months of follow up. The number of patients,withdrawn from SMS monitoring, and principal causes of withdrawal were de-termined on every checkpoint. A part of patients with goal BP was estimated inthis group over each control period. Goal BP was defined according with ESH-ESC Hypertension Guidelines (2007). In a year of follow up, the percent of goalBP achievement was compared in SMS monitoring group via the group of usualcare.Results: From 97 patients, included in the group of SMS monitoring, 62 (64%)successfully completed one year of follow up. During the first month 15 patients(16%) had left the study. The principal cause in 9 patients (60%, p<0.05) was"difficulties in use of text messaging system". During the period from 1 to 6 monthsof observation 19 patients had else withdrawn. The main cause in 15 of them(79%, p<0.05) was "lost of interest". Patients corresponded, that they felt welland was satisfied by treatment. During the period from 6 to 12 months only 1patient had withdrawn (cause – "lost of interest"). In the group of SMS monitoringgoal BP was achieved in 84% of patients (CI 75% - 93%) after the first month ofstudy, in 77% (CI 67% - 88%) after six months and in 71% (CI 60% - 83%) after12 months of observation. In the group of usual care goal BP was achieved inonly 12% of patients (CI 5% – 18%). Odds ratio was 13 (CI 6.0-29.6).Conclusion: Use of computer system with patient feedback via SMS raisesachievement of goal BP in AH patients as compared with usual care in primaryunit, and facilitate BP maintenance on goal in a long time period.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

90 Pulse wave velocity and ambulatory blood pressure monitoring
P654 Influence of pharmacogenetically determinedtreatment on daily Blood Pressure (BP) profile inhypertensive (EAH) patients depending on fivecandidate genes’ polymorphisms
L. Sydorchuk1, K.M. Amosova2, V.P. Pishak1, I.I. Sydorchuk1,J.V. Ursuliak1, R.I. Sydorchuk1. 1Bukovinian State Medical University, Chernivtsi,Ukraine; 2National State Medical University, Kiev, Ukraine
Purpose: To evaluate the influence of combination antihypertensive therapy ondaily BP profile depending on I/D polymorphism in ACE gene, A1166C in AGTR1gene, T894G in eNOS gene, Pro12Ala in PPAR-G2, Arg389Gly in ADRB1 genein EAH patients.Methods: 249 patients (EAH I – 26.5%; EAH II – 45.8%; EAH III – 27.7%;women – 48.2%, men – 51.8%, mean age 50.5±10.4 yrs) underwent ther-apy modified accordingly to individual genes’ polymorphism (hydrochloroth-iazide (HCTZ)+angiotensin II receptor (ARB) blocker), HCTZ+beta1-blockers(BB), HCTZ+ACE inhibitors (ACEI), calcium antagonists (CA)+ARB, CA+BB,CA+ACEI). BP was assessed with office (BPoffice) and 24h ambulatory moni-toring (BP24h). Efficacy criteria based on ESC/ESH 2007 recommendations.Results: In carriers of D-allele of ACE gene, CC-genotype of AGTR1 gene,T-allele of eNOS gene, Pro-allele of PPAR-G2 gene and ArgArg-genotype ofADRB1 gene normal daily BP profile "dipper" appeared 1.2-2.1 times rarely(p<.05-.001), more often – unfavorable "non-dipper" BP profile (in 12.4-34.3%,p≤.001). In TT-genotype of eNOS gene carriers in 2.2 times more often regis-tered "night-peaker" BP profile (p=.044). After pharmacogenetically determinedtreatment number of patients with daily "dipper" BP profile increased to 75.6% vs65.5% (p<.001): reliably in AGTR1 gene’ CC-genotype carriers (13.1%, p=.005),eNOS gene’ TT-genotype (12.3%, p<.001), AlaAla- and ProPro-genotypes ofPPAR-G2 gene (20.0%, p<.001 and 13.75%, p=.047, accordingly), GlyGly-genotype of ADRB1 gene (25.8%, p<.001). The number of patients with "non-dipper" BP profile decreased to 19.9% vs 26.5% before pharmacogenetic correc-tion (p<.01): reliably in D-allele of ACE gene (in 7.9%, p=.049 and 8.7%, p=.015,accordingly), CC-genotype carriers of AGTR1 gene (in 6.7%, p<.01), T-allele ofeNOS gene (7.0%, p=.035 and 9.8%, p<.001, accordingly), Ala-allele of PPAR-G2 gene (in 13.3%, p<.001 and 8.0%, p=.017, accordingly), GlyGly-genotype ofADRB1 gene (in 6.4%, p<.01). The number of patients with "night-peaker" BPprofile reduced to 4.0% vs 7.2% before pharmacogenetic correction (p=.016), butsignificantly enough only in TT-genotype carriers of eNOS gene (p=.039).Conclusions: Pharmacogenetically determined therapy caused reliable increaseof "dipper" BP profile in EAH patients (p<.001) with significant advantage inI-allele ACE gene carriers combinations of HCTZ+ARB, less HCTZ+BB, thanHCTZ+ACEI (91.7%, 73.5% and 66.0%, accordingly, p<.001). In DD-genotypecarriers more effective were combinations of CA with ARB, BB and ACEI (73.3-70.4%).
P655 The effects of nocturnal hypertension on arterialstiffness and kidney damage in dipper hypertensives:The necessity of estimating absolute nocturnal bloodpressure values along with dipping profile
D. Syrseloudis, C. Tsioufis, M. Selima, C. Thomopoulos, E. Stefanadi,D. Aragiannis, D. Roussos, I. Kallikazaros, C. Stefanadis. First Cardiology Clinic,University of Athens,Hippokration Hospital, Athens, Greece
Purpose: Both blood pressure (BP) non- dipping and nocturnal hypertensionhave been associated with accelerated target organ damage (TOD) hyperten-sion. However the combination of a nocturnal BP reduction within the range ofthe dipping profile with increased absolute nocturnal BP values has never beeninvestigated as regards TOD. We investigated the relationships of nocturnal BPwith indices of vascular and kidney damage in dipper hypertensive subjects.Methods: We studied 402 subjects with stage I -II, newly diagnosed essen-tial hypertension. According to two 24h ambulatory BP recordings 127 dippersubjects were selected and subdivided in nighttime hypertensives (NH, n=75)(nighttime BP ≥120/70) and nighttime normotensives (NN, n=52) (nighttime BP<120/70mmHg). All the participants underwent echocardiographic examination,pulse wave velocity (PWV), albumin to creatinine ratio (ACR), metabolic profileand high sensitivity C- reactive protein (hs-CRP) assessment.Results: NH compared to NN dippers had higher log10(c-f PWV) (0.92±0.07 vs0.87±0.05 m/s p<0.001), higher log10(ACR) values (1.20±0.50 vs 1.02±0.27mg/g, p=0.01) and log10(hs- CRP) levels (0.32±0.33 vs 0.012±0.29 mg/l,p<0.001). Nighttime compared to daytime and 24h systolic BP was correlatedto a higher degree with c-f PWV, while it outweighed daytime BP as an ACR prog-nosticator.Conclusion: Nighttime BP is associated more closely with c-f PWV, compared todaytime and 24h BP, as well as with ACR when compared to daytime BP. Greatervalues of c-f PWV and hs-CRP imply that a greater cardiovascular risk couldbe attributed to nocturnal hypertensive dippers as compared to their nocturnalnormotensive counterparts.
P656 Influence of gender and systolic blood pressure ondevelopment of sustained hypertension in children andadolescents with white coat hypertension
C. Esis, M. Bracho, E. Silva, A. Gonzalez, J. Villasmil, S. Briceno.Instituto de Investigación de Enfermedades Cardiovasculares -
Universidad del Zulia, Maracaibo, Venezuela
Purpose: In previous studies we observed that most children and adoles-cents who progress to sustained hypertension (SH) had white coat hypertension(WCH). Our interest was to determine the variables that predict the developmentof SH in children and adolescents with WCH.Methods: A randomized study was carried out in 184 patients (91 boys and 93girls, aged 10-19 years). At baseline, office blood pressure (BP) and a first am-bulatory BP monitoring (ABPM) were performed to all patients. We included onlypatients with WCH defined as office BP measurements ≥ 95th percentile for sexand age or >140/90 mmHg for those ≥ 18 years, and systolic or diastolic daytimevalues obtained by ABPM < 95yh percentile for sex and height or <135/85 mmHgfor those ≥ 18 years. All subjects with WCH, after follow-up (3.04±1.51 years),were undergoing a second ABPM to identify new SH which was defined as officeBP measurements ≥ 95th percentile for sex and age or >140/90 mmHg for those≥ 18 years, and systolic or diastolic daytime values obtained by ABPM ≥ 95thpercentile for sex and height or > 135/85 mmHg for those ≥ 18 years. A logisticregression model was used to evaluate the effect of age, gender, BMI, and initialoffice BP on the development of SH in patients with WCH.Results: At baseline, we identified 22 patients with WCH (12.0%), of these 16were men (72.72%). After follow-up, 40.9% (n=9) of WCH developed HS (allwere men, mean age 15.00±1.87 years). The patients WCH who developed HShad higher baseline office systolic BP (141.75±6.88 vs. 134.07±6.59 mmHg, P=0.016) and daytime systolic BP for ABPM (128.88±5.01 vs. 123.30±6.30 mmHg,P= 0.039) than those without SH. The only variables that correlated significantlywith SH were baseline office systolic BP and gender. Logistic regression analysisshowed that baseline office systolic BP (OR = 1.191, 95% CI = 1.013-1.401, P =0.034) predicted significantly SH in the follow-up.Conclusions: In this group of children and adolescents with WCH, baseline of-fice systolic BP predicted HS, regardless of age and BMI of the patient. Malewith higher values of systolic blood pressure present an increased risk of HS.The WCH represent a cardiovascular condition prior to the development of SH inchildren and adolescent.
P657 Synergistic effect of ACE D/D polymorphism andadipokines on clinical blood pressure phenotypes
C. Thomopoulos1 , O. Papazachou1, M. Daskalaki1, N. Rodolakis1,A. Komnou1, D. Perrea2, D.P. Papadopoulos3 , T.H. Makris1.1Elena Venizelou General & Maternity Hospital, Department of
Cardiology, Athens, Greece; 2University of Athens Medical School, Laboratory ofExperimental Surgery and Surgical Research, Athens, Greece; 3Departement ofCardiology, Laiko General Hospital, Athens, Greece
Objective: We hypothesized that ACE D/D carriers would demonstrate ad-verse adipokine phenotype with potentially increased pro-atherogenic effects. Weaimed to determine whether there is a synergistic effect between ACE D/D poly-morphism and levels of resistin (Res) and adiponectin (Adp) on diverse bloodpressure (BP) clinical phenotypes.Methods: Among 312 consecutive untreated patients, we studied 232 (120 men,body mass index [BMI] = 26±2.4kg/m2) after having excluded those with a historyof any cardiovascular disease, glucose metabolism abnormalities or other concur-rent medical condition and finally those under any potential vasoactive treatment.Petients underwent to office and ambulatory BP measurements and were classi-fied into: sustained hypertensives (SH, n=80), masked hypertensives (MH, n=33),white-coat hypertensives (WCH, n=51) and normotensives (NT, n=68). Left ven-tricular mass index (LVMI), metabolic profile and Res and Adp determination wasalso performed. DNA was extracted from white blood cells, and participants werefurther divided into those with either non-ACE D/D (ie, ACE I/I and ACE I/D) orACE D/D polymorphism.Results: ACE D/D prevalence was: 40% (n=32) in SH vs. 36% (n=12) in MHvs. 26% (n=13) in WCH vs. 28% (n=19) in NT, p<0.001, whereas the lev-els of log(10)(Res) and log(10)(Adp) were: 1.15±0.08 and 0.81±0.09 in SHvs. 1.1±0.07 and 0.82±0.08 in MH vs. 0.91±0.06 and 0.93±0.07 in WCH vs.0.76±0.09 and 1.04±0.08 ng/mL and mg/mL respectively, p<0.001 for both.Metabolic profile parameters did not differ between the groups, whereas LVMIwas different (p<0.005). A significant correlation was detected between ACE D/Dpolymorphism with log(10)(Res) and log(10)(Adp) respectively (p<0.01 for both).In two different multinomial logistic regression models the interaction terms oflog(10)(Res)xACED/D and log(10)(Adp)xACED/D were determinants (OR, 95%CI) of SH: 1.37 (1.15-1.65) and 0.66 (0.52-0.87) respectively, p<0.001 and MH:1.24 (1.08-1.54) and 0.72 (0.53-0.91).Conclusion: There is a synergistic effect of adipose tissue molecular signals andACE D/D polymorphism on out-of-clinic BP phenotypes. A cross-talk betweenACE genotype and adipose tissue phenotype may contribute to the ameliorationof cardiovascular risk stratification in hypertension.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Pulse wave velocity and ambulatory blood pressure monitoring 91
P658 Diurnal variation pattern in home blood pressuremonitoring was useful predictor of target organdamage
J.S. Ko1, Y.K. Ahn1, J.B. Park2, C.G. Park3, H.J. Youn4, D.J. Choi5,J.H. Shin6, D.W. Kim7, J.H. Bae8. 1The heart center of chonnamnational university hospital, Gwangju, Korea, Republic of; 2Cheil
general hospital, Kwandong university, Gangneung, Korea, Republic of; 3KoreaUniversity Guro Hospital, Seoul, Korea, Republic of; 4Catholic UniversityHospital, Seoul, Korea, Republic of; 5Seoul National University Hospital,Seoul, Korea, Republic of; 6Ajou Univesity Hospital, Suwon, Korea, Republicof; 7Chungbuk National University Hospital, Cheongju, Korea, Republic of;8Konyang University Hospital, Daejeon, Korea, Republic of
Purposes: Pattern of diurnal variation in ambulatory blood pressure mornitoring(ABPM) has established predictive value for target organ damage. Several studiesdemonstrate good correlation between data form home blood pressure monitoring(HBPM) and ambulatory blood pressure monitoring (ABPM). We aimed to clarifyclinical implication of diurnal variation in HBPM focused on predicting target organdamage.Methods: We enrolled 1,087 out patients (mean age 56.8±9.6, male 47.7%) withdiagnosed hypertension who were consistent in antihypertensive medication for6 months. Home blood pressure was checked in every morning and evening for2weeks. Incidence of target organ damage and metabolic syndrome were ana-lyzed according to pattern of diurnal variation in HBPM.Results: We quantified diurnal variation of blood pressure with difference index:(1-mean BP at night/mean BP at morning)x100. When we divided whole patientsinto three groups, difference index was more than 10% in 106 patients (9.8%,exaggerated variation group) and less than 10% in 595 patients (54.7%, modestvariation group). 386 patients (35.5%, reverse variation group) showed negativedifference index value. There was no significant difference in baseline character-istics, life style factors, content of medication and laboratory data among threegroups. We evaluated various target organ damage including heart, kidney, brainand peripheral artery disease according to diurnal variation pattern. Incidenceof brain damage such as stroke and TIA was significant higher in exaggeratedvariation group (5.7%) and reverse variation group (3.4%) than modest variationgroup (1.4%) (p=0.017). After multivariate analysis using logistic regression test,diurnal variation pattern in HBPM remained independent predictor for stroke/TIA(HR=2.127, p=0.018, 95% CI 0.089-0.707)Conclusion: Exaggerated or reverse diurnal variation pattern in HBPM was use-ful predictor of stroke/TIA.
P659 Night-time blood pressure load and left atrium size inthe early stages of essential hypertension
E. Taxiarchou, C. Tsioufis, I. Andrikou, A. Mazaraki, D. Syrseloudis,D. Soulis, T. Papaioannou, C. Stefanadis. First Cardiology Clinic,University of Athens,Hippokration Hospital, Athens, Greece
Purpose: Left atrial (LA) enlargement is a common finding in hypertensive pa-tients and might be an index for future adverse cardiovascular events. Similarly,abnormal diurnal variation patterns of blood pressure (BP) have been associatedwith an excess of target organ damage and adverse cardiovascular outcome. Theaim of this study was to evaluate the relationship between ambulatory BP param-eters and LA size.Methods: 424 consecutive, newly diagnosed subjects (aged 51±10 years), withuntreated stage I-II essential hypertension [office BP =151/97 mmHg] were clas-sified according to their nocturnal BP fall on 24-hour ambulatory BP monitoringto non-dippers (those with<10% nocturnal systolic and diastolic BP fall, n=227)and dippers (the remaining subjects, n=197). All subjects underwent completeechocardiographic study and LA volume was indexed for body surface area toestimate LA volume index (LAVI).Results: Non-dippers compared to dippers did not differ regarding age, sex, of-fice BP, 24-h systolic and 24-h diastolic BP and biochemical profile (p=NS for allcases). However, non-dippers compared to dippers had significantly increased bydefinition night systolic BP (132±15 vs 119±11, p<0.001) and night diastolic BP(80±11 vs 73±9 mmHg, p<0.001), increased 24-h pulse pressure (PP) (52±9 vs50±8 mmHg, p<0.005), and night PP (52±10 vs 47±7 mmHg, p<0.001), as wellas LA diameter (3.90±0.45 vs 3.70±0.47 cm, p=0.001), LA volume (47.2±14.4 vs43.8±14.1 ml, p<0.05) and LAVI (23.7±6.5 vs 22.5±6.6 ml/m2, p<0.05). In theentire population LA diameter and LAVI exhibited positive relationships with 24-h systolic BP (r=168, p<0.001 and r=0.133, p<0.01, respectively), night systolicBP (r=0.216, p<0.001 and r=0.185, p<0.001 respectively), 24-h PP (r=0.181,p<0.001 and r=0.200, p<0.001, respectively), day PP (r=0.150, p<0.005 andr=0.204, p<0.001, respectively) and night PP (r=0.164, p=0.001 and r=0.215,p<0.001, respectively). Multiple regression analysis models revealed that amongcomponents of ambulatory BP, only night systolic BP was an independent pre-dictor of LA diameter (β=0.216, p<0.001) and only night PP was an independentpredictor of LAVI (β=0.215, p<0.001).Conclusions: Circadian BP variation and especially non dipping status seemsto be a determinant of LA enlargement in hypertensive patients. Whether theabovementioned association contributes to the high cardiovascular risk observedin patients with augmented night BP load remains to be determined in futurestudies.
P660 Non-dipping status is accompanied by a state ofhypoadiponectinemia and pronounced arterialstiffness in essential hypertensive subjects
I. Andrikou, C. Tsioufis, K. Dimitriadis, D. Syrseloudis, T. Papaioannou,A. Mazaraki, D. Aragiannis, D. Tousoulis, C. Stefanadis. First
Cardiology Clinic, University of Athens,Hippokration Hospital, Athens, Greece
Purpose: The absence of nocturnal blood pressure (BP) fall is related throughdiverse mechanisms with adverse cardiovascular outcome, while adiponectin isemerging as a marker of atherosclerosis progression. We examined the associ-ation between non-dipping status and plasma concentrations of adiponectin andarterial stiffness in essential hypertensive subjects.Methods: 148 newly diagnosed untreated non-diabetic patients with stage I to IIessential hypertension [98 men, mean age=49 years, office BP=150/97 mmHg]underwent 24-h ambulatory BP monitoring and were classified as dippers andnon-dippers according to the diurnal variation of >10% between mean daytimeand nighttime systolic and diastolic BP. Arterial stiffness was evaluated on thebasis of carotid to femoral pulse wave velocity (PWV), by means of a comput-erized method (Complior SP). Moreover, venous blood samples were drawn forestimation of lipid profile and adiponectin levels.Results: Non-dippers (n=38) compared to dippers (n=110) were older (55±7 vs49±9 years, p<0.0001), and had higher left ventricular mass index (119±12vs 101±18 g/m2, p<0.05). In the total population, plasma adiponectin levelswere negatively related with BMI (r=-0.168, p<0.05), waist to hip ratio, (r=-0.421, p<0.0001), office systolic BP (r=-0.285, p<0.0001), 24-h systolic BP(r=-0.194, p<0.05), total cholesterol (r=-0.220, p<0.005), and PWV (r=-0.280,p<0.001), while it was positively associated with systolic BP fall (r=0.520,p<0.001). Additionally, PWV was associated with BMI (r=0.233, p<0.05), 24-hsystolic BP (r=0.327, p<0.0001) and negatively related to systolic BP fall (r=-0.17,p<0.05). Non-dippers compared to dippers exhibited attenuated adiponectin val-ues (7.9±3.6 vs 9.7±4.4 μg/ml, p<0.05), and higher PWV values (8.6±1.2 vs7.7±4.2 m/sec, p<0.05), while the two groups did not differ regarding metabolicprofile (p=NS). Analysis of covariance revealed that adiponectin and PWV valuesremained statistically different between groups after adjustment for confoundingfactors (p<0.05).Conclusions: Non-dippers hypertensives are characterized by more pro-nounced activation of pro-atherogenic mechanisms, as reflected by low levelsof adiponectin, and arterial stiffening. These findings may partially explain theincreased cardiovascular risk associated with non-dipping status, in this setting.
P661 Association of myocardin and GATA4 gene expressionlevels in peripheral blood mononuclear cells ofpatients with essential hypertension with ambulatoryblood pressure monitoring parameters
J.E. Kontaraki1, M.E. Marketou2, E.A. Zacharis2 , F.I. Parthenakis2,P.E. Vardas2. 1Univ. of Crete, Faculty of Medicine, Molecular Cardiology Lab,Heraklion, Greece; 2Heraklion University Hospital, Department of Cardiology,Heraklion, Greece
AbstractPurpose: Ambulatory blood pressure monitoring (ABPM) is a useful tool for eval-uating 24-hour blood pressure profile and a good predictor of target organ dam-age in hypertensive patients. We evaluated gene expression levels of the tran-scription factors myocardin and GATA4 which are important for cardiomyocyteand smooth muscle cells differentiation and are implicated in vasculogenesis dur-ing embryonic development, in peripheral blood mononuclear cells of patientswith essential hypertension in relation to ABPM parameters.Methods: 24-hour ABPM and blood sampling were obtained in 40 untreated hy-pertensive patients. Gene transcript levels were determined by quantitative realtime reverse transcription PCR.Results: Transcript levels of myocardin (r=0.844, p<0.001) and GATA4 (r=0.654,p<0.001) showed strong positive correlations with 24-hour systolic blood pres-sure as well with 24-hour mean blood pressure (r=0.638, p<0.001) and (r=0.464,p=0.002) respectively. Similarly, we found significant positive correlations of my-ocardin (r=0.597, p<0.001) and GATA4 (r=0.491, p=0.001) with 24-hour pulsepressure. Significant negative correlations of myocardin r=-0.685, p<0.001) andGATA4 r=-0.516, p=0.001) with mean 24-hour dipping status were observed too.Conclusions: Myocardin and GATA4 transcript levels show strong correlationswith parameters derived from 24-hour ABPM defining them as possible candidatebiomarkers in hypertension. The positive correlations with 24h pulse pressureand the negative correlations with dipping might indicate a possible implication ofthese genes in target organ damage.
P662 Early vascular changes preceding morphologicalcardiac changes in hypertensive patients
M.A.K. Abdel Wahab. El Minya univeristy hospital, El Minya, Egypt
Background: Left ventricular hypertrophy (LVH) has been identified asa powerful independent risk factor not only for total and cardiovascular
mortality, but also for sudden cardiac death.Aim: To verify the vascular changes occurring before morphological changes inLV geometry in hypertensive patients.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

92 Pulse wave velocity and ambulatory blood pressure monitoring
Patients and methods: 50 hypertensive patients and 20 normo-tensive subjectswere divided into three groups as follows: normo-tensive subjects with normal LVgeometry (Group I, n=20), hypertensive patients with normal LV geometry (GroupII, n=18); hypertensive patients with abnormal LV geometry (Group III, n= 32). Of-fice and 24h systolic and diastolic blood pressure measurement was done forall groups and from it ambulatory arterial stiffness index (AASI) was calculated.Endothelial function was assessed by endothelium-dependent flow-mediated di-latation (FMD) and -independent vasodilatation (after sublingual administration ofnitroglycerin) of the brachial artery using high-resolution vascular ultrasound. Wealso assessed the intima-media thickness (IMT) of the common carotid, and leftventricular mass index (LVMI).Results: AASI and IMT were significantly increased and FMD is significantly de-creased in hypertensive patients with normal LV geometry (Group II) comparedto normo-tensive subjects with normal LV geometry (Group I) (P = < 0.001, 0.001and 0.046 respectively). These changes were augmented when the LV geometryprogressed into abnormal geometry so AASI and IMT were significantly increasedand FMD is significantly decreased in group III compared to group II (P = 0.011,0.013 and 0.049 respectively.
Comparison between FMD in group 1 and group 2
Group 1 Group 2 P
Mean SD Mean SD
FMD% 16.08 6.48300 10.10 11.01051 0.046Dilatation ratio. 94.8 40.06131 50.28 26.03541 <0.001
Conclusion: early vascular changes in the form of increased IMT, reduced va-sodilator capacity and increased arterial stiffness precedes changes in LV geom-etry. So IMT, FMD and AASI may be useful markers for early detection of high riskhypertensive patients and for assessment of the efficacy of different therapeuticmodalities in prevention of structural and morphological cardiac changes.
P663 Relationship between nocturnal blood pressurepatterns and daytime blood pressure variability in theSpanish ambulatory blood pressure monitoringregistry
G. Bilo1, S. Hoshide2, A. De La Sierra3, J.R. Banegas4, M. Gorostidi5,J. Segura6, L.M. Ruilope6, G. Mancia7, G. Parati1. 1Dept. Cardiology,
Ist. Auxologico Italiano, Dept. of Clin. Med. and Prevention, Univ. Milano-Bicocca,Milan, Italy; 2Jichi Medical University, Department of Cardiology, Tochigi, Japan;3Department of Internal Medicine. Hospital Mutua Terrassa, University ofBarcelona, Barcelona, Spain; 4Department of Epidemiology and Public Health,Autonomous University, Madrid, Spain; 5Department of Nephrology. HospitalSan Agustín, Avilés, Spain; 6Hypertension Unit, 12 de Octubre Hospital, Madrid,Spain; 7University of Milan-Bicocca, Department Clinical Medicine & Prevention,Milan, Italy
Objective: Abnormal nocturnal blood pressure (BP) (nocturnal hypertension, ab-sent or excessive night-time BP fall) and increased short-term BP variability areassociated with an increased cardiovascular risk. Aim: to investigate relationshipbetween nocturnal BP patterns and daytime BP variability in a large number ofsubjects (Spanish Ambulatory Blood Pressure Monitoring Registry).Methods: In 18405 subjects (age 52.7±14.3 years, male 54%) not on antihyper-tensive medication for at least 2 weeks ambulatory BP monitoring was performed(Spacelabs 90207). BP variability was quantified as standard deviation (SD) ofdaytime values. Data were analyzed by subdividing subjects into: (Model 1) cat-egories of day/night systolic (S)BP pattern [risers (R): <0% nocturnal SBP fall,nondippers: 0-5% (ND1) and 5-10% (ND2), dippers (D): 10-20%, extreme dippers(ED): >20%] and (Model 2) quintiles of mean night-time SBP. The differences be-tween categories were adjusted for age, BMI, gender, smoking, diabetes, dyslipi-demia, previous cardiovascular disease, renal insufficiency and mean 24 h SBP(Model 1) or mean awake SBP (Model 2).Results: Significant differences in daytime SBP SD were found betweenday/night SBP fall categories (p<0.0001) and between night-time SBP quintiles(p<0.0001) (see Figure).
Figure 1. *p<0.05; **p<0.01; ***p<0.001
Conclusions: Untreated subjects with very high or very low nocturnal BP, as wellas with "riser" and "extreme-dipper" SBP profile show increased short-term BPvariability during the awake period even after adjustment for major confounders.This relationship may reflect an increased sympathetic activity in these subjects.Studies on the clinical relevance of these ambulatory BP patterns should thus notdisregard such an association.
P664 The effect of diurnal variation patterns of bloodpressure on cardiovascular structural and functionalterations in essential hypertensive patients
E. Taxiarchou, C. Tsioufis, D. Syrseloudis, A. Mazaraki, D. Aragiannis,V. Tzamou, I. Andrikou, L. Lioni, C. Stefanadis. First Cardiology Clinic,
University of Athens,Hippokration Hospital, Athens, Greece
Purpose: Abnormal circadian blood pressure (BP) variation has been associatedwith an excess of target organ damage and adverse cardiovascular outcome. Theaim of our study was to investigate the correlation of ambulatory BP parametersand dipping status with cardiac structural and functional alterations and arterialstiffness in essential hypertensive patients.Methods: A total of 526 consecutive essential hypertensive subjects (aged51±10, office BP=151/97 mmHg) were classified according to their nocturnal BPfall on 24-hour ambulatory BP monitoring into non-dippers (those with<10% noc-turnal systolic and diastolic BP fall, n=421) and dippers (the remaining subjects,n=350). Left atrial (LA) volume and left ventricular (LV) mass were indexed forbody surface area to estimate LA volume index and LV mass index, respectively.LV diastolic function was estimated by means of both conventional and pulsedtissue Doppler imaging echocardiography, averaging diastolic mitral annular ve-locities measurements (Em, Am, Em/Am ratio) from four separate sites (septal,lateral, anterior, inferior). Moreover, aortic stiffness was evaluated on the basis ofthe carotid-femoral pulse wave velocity (c-f PWV) measurement by an automaticdevice (Complior SP).Results: Non-dippers compared to dippers did not differ regarding sex, bodymass index, office systolic and diastolic BP, 24-h systolic and diastolic BP andbiochemical profile (p=NS for all cases) while non-dippers had significantly in-creased 24h pulse pressure (PP) (52±9 vs 50±8 mmHg, p=0.005). In addi-tion non-dippers compared to dippers had significantly increased LV mass in-dex (104±27 vs 97±24 gr/m2, p<0.005), LA diameter (3.89±0.44 vs 3.72±0.46cm p<0.001), LA volume (47.3±14.1 vs 43.8±13.8, p<0.01), LA volume index(23.8±6.4 vs 22.6±6.5 ml/m2, p<0.05), while they did not differ according rel-ative wall thickness, c-f PWV and Em/Am ratio (p=NS, for all cases). Multipleregression analysis models revealed that among components of ambulatory BP,only night systolic BP was an independent predictor of LV mass index (β=0.297,p<0.001) and LA diameter (β=0.216, p<0.001), while night PP was an indepen-dent predictor of LAVI (β=0.215, p<0.001).Conclusions: A blunted reduction in night-time BP seems to be associated withpronounced unfavorable enlargement of cardiac cavities but not with cardiac stiff-ening and impaired aortic elasticity. These results strengthen the evidence aboutthe clinical significance of unmask the non-dipping status in hypertensive patients.
P665 Ventricular-arterial coupling and left ventriculartorsional dynamics in hypertensive heart disease
C.C. Beladan1, B.A. Popescu1, A. Calin1, M. Rosca1, B. Moise2,F. Voinea2, R. Enache1, D. Muraru2, R. Jurcut1, C. Ginghina1.1University of Medicine and Pharmacy Carol Davila, Bucharest,
Romania; 2Institute of Cardiovascular Diseases "Prof. Dr. CC Iliescu", Bucharest,Romania
Background: Patients (pts) with hypertension (HTN) exhibit increased arterialand ventricular stiffness leading to reduced cardiac mechanic efficiency and exer-cise capacity. Ventricular-arterial (V-A) coupling and left ventricular (LV) torsionaldynamics are key determinants of cardiovascular performance and are both re-lated to changes in arterial load and LV contractility.Purpose: To assess the relationship between V-A coupling and LV torsional dy-namics in pts with HTN and normal LV ejection fraction (LVEF).Methods: Forty hypertensive pts (58±10 years, 19 men) with normal ejectionfraction (>50%) were consecutively enrolled. A comprehensive echocardiogramwas performed in all. Basal and apical LV rotation, peak systolic LV twist normal-ized for LV diastolic longitudinal length - LV torsion (LVtor), and peak LV untwist-ing rate were measured by speckle tracking echocardiography using dedicatedsoftware (2D strain, EchoPac). V-A coupling was assessed as the ratio betweenthe arterial elastance (Ea) and the end-systolic ventricular elastance (Ees). Eawas calculated from stroke volume (SV) and end-systolic pressure: Ea = (Sys-tolic BP × 0.9)/SV and Ees was calculated by a modified single-beat method,as previously described, using an estimated normalized ventricular elastance atarterial end-diastole (ENd): Ees = [Diastolic BP – (ENd(est) × Systolic BP ×0.9)]/(ENd(est) × SV).Results: In this cohort LV mass index was 121±45 g/m2, LVEF was 59±7% andE/E’ ratio was 8.8±2.3. Ea/Ees ratio was 0.81±0.27, Ea was 2.6±1.1 mmHg/mland Ees was 3.4±1.4 mmHg/mL. In univariate analyses the Ea/Ees ratio corre-lated significantly with LV mass index (r=0.51, p=0.003) LVtor (r=-0.40, p=0.01),peak LV untwisting rate (r=0.49, p=0.002), peak apical rotation (r=-0.35, p=0.03),peak apical backrotation rate (r=0.43, p=0.007). The correlation between Ea/Eesratio and E/E’ ratio was borderline significant (r=0.33, p=0.05). At multivariateanalysis, LV mass index and peak LV untwisting rate were the only independentcorrelates of Ea/Ees ratio (p<0.001).Conclusions: Ventricular-arterial coupling is directly related to the severity ofLVH in pts with HTN. There is a significant relation between V-A coupling andLV torsional dynamics parameters: the higher the V-A coupling the worse the LVtwisting and untwisting parameters. Further studies are needed to assess theclinical relevance of these findings.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Pulse wave velocity and ambulatory blood pressure monitoring 93
P666 Hypotension load associates with myocardial ischemiain haemodialysis patients with pre-existing ischemicheart disease
V. Dobronravov, J. Vladimirova, E. Borovskaya, A. Smirnov.Saint-Petersburg Pavlov State Medical University, Saint-Petersburg,
Russian Federation
The relationship between arterial blood pressure (ABP) and risk of death in thehaemodialysis (HD) population tended to be U-shaped, as it was suggested, be-cause of pre-existing cardiac disease in patients with the low ABP. Howewer, onecan propose that the lowering of ABP aggravates myocardial ischemia (MI), andthus, has a negative influence on prognosis and survival of HD pts. We nextwanted to ascertain whether arterial hypotension load is associated with MI.48-hour ECG and ABP ambulatory monitoring (AM) including HD session andsubsequent interdialytic period was performed in 61 prevalent stable HD ptswith pre-existing ischemic heart disease (IHD). 35 among them (age 56±11 yr,M:F 21:14, HD vintage 86 (7-288) month) had at least one episode of ST seg-ment depression defined as MI and were entered the study. The number andtotal duration of ST-depressions were correlated to absolute systolic, diastolic,pulse, mean ABP levels and hypertension/hypotension load indices, such as:1) percent/duration of systolic/diastolic ABP readings above upper normal lim-its (>139/89 mmHg at daytime, >119/79 mmHg at nighttime); 2) percent/durationof systolic/diastolic ABP readings below lower normal limits (<101/61 mmHg atdaytime, <86/48 mmHg at nighttime).142 episodes of MI were detected totally: 113 in 1st day of AM and 29 in 2nd. Onthe 1st day, MI number was found to be negatively correlated with mean overnightsystolic ABP (R=-0,462, p=0,008), pulse ABP (R=-0,498, p=0,003) and systolichypertension load indices at nighttime, while the MI number and its total dura-tion had significant positive correlations with systolic/diastolic hypotension loadindices in day- and nighttime (all p<0,05). On 2nd day of AM, number and dura-tion of ST depression episodes correlates negatively with mean value of systolic,pulse ABP and systolic hypertension load indices (all p<0,025) and positively withsystolic (but not diastolic) hypotension load indices (all p<0,025).The mean duration of systolic/diastolic hypotension load during 1st and 2nd 24-hour intervals of AM (1,8 (95%CI 0,6-3,1)/2,6 (95%CI 1,1-4,2) hours, and 1,2(95%CI 0,5-2,9)/2,2 hours (95%CI 0,8-3,6), respectively) were much more thatthe mean duration of MI in both intervals studied (8,5 min (95%CI 4,4 - 12,5) and2,1 min (95%CI 0,6-3,7), respectively).In conclusion, hypotension load is clearly associated with MI in HD patients withIHD, while MI is not likely to be the primary event, causing arterial hypotension inthe group studied. It can be considered that decrease of ABP seems to aggravatepre-existing MI in HD patients.
P667 Maintained increased proximal aortic stiffness 6months after pre-eclamptic pregnancy
M.E. Estensen1, E.W. Remme2, A. Swillens3, P. Segers3,T. Henriksen4, O.A. Smiseth5, L. Gullestad5, S. Aakhus5. 1NationalResource Center for Women‘s Health, Oslo University Hospital,
Rikshospitalet,Norway, Oslo, Norway; 2Institute for Surgical Research, Universityof Oslo, Oslo, Norway; 3IBiTech, Ghent University, Ghent, Belgium, Belgium;4Department of Obstetrics, Oslo University Hospital, Rikshospitalet, Norway,Oslo, Norway; 5University of Oslo, Faculty Division Rikshospitalet UniversityHospital, Department of Cardiology, Oslo, Norway
Purpose: Pre-eclampsia (PE) occurs in 3-10% of all pregnancies.The adaptationof the systemic arterial tree in these patients have not been well described. Weperformed a comparison of systemic arterial properties in women with PE in thirdtrimester and at 6 months postpartum (PP), with women with normal pregnancy(NP) and follow-up as control.Methods: 35 women (33±6 years) with PE and 65 (33±1 years) with NP werestudied. Aortic root pressure and flow were obtained by calibrated right subclavianartery pulse trace, and aortic annular Doppler blood flow recordings. Systemic ar-terial properties were described by total arterial compliance (C), arterial elastance(end systolic pressure/stroke volume, Ea) characteristic impedance (parameterof proximal aortic stiffness, Z0), and peripheral arterial resistance (R). Parame-ters were estimated both by use of a 4-element Windkessel (WK) model and byFourier analysis of central aortic pressure and flow data.Results: In PE pregnancy at term, Z0, Ea and R was higher and C was lower
Results
At termNP 6 mo PPNP At termPE 6 mo PPPE P �
(�NP vs �PE)
Mean arterial pressure(mmHg) 85±7 86±7.3 115±10*# 98±12# <0.001
Heart rate (beats/min) 77±10* 66±7 75±10 70±11# 0.005Cardiac output (L/min) 5.8±1.1* 4.9±0.9 6.4±1.2*# 5.4±1.2# 0.70R (mmHg/(ml/s)) 0.92±0.23* 1.10±0.29 1.13±0.24# 1.13±0.27 0.04Z0 WK (mmHg/(ml/ms)) 65±24 68±22 85±32# 75±21# 0.06Z0 FD (mmHg/(ml/ms)) 45±23* 50±21 64±32# 55±25# 0.003C WK (ml/mmHg) 1.55±0.46* 1.40±0.45 1.34±0.40# 1.38±0.50 0.17C PPM (ml/mmHg) 1.21±0.33 1.14±0.30 0.96±0.25 1.07±0.32# 0.06Ea (mmHg/ml) 1.19±0.28 1.27±0.28 1.48±0.32# 1.43±0.37# 0.30
*p<0.05 vs 6 months, #p<0.05 vs normal pregnancy. FD = frequency domain, PPM = pulsepressure method.
than in NP indicating a higher vascular resistance from the proximal aorta to theperipheral resistance vessels in PE. Although Z0 was significantly reduced and Cwas increased in the PE group at 6 months PP, R was unchanged. Neither Z0, C,nor R attained normal values after PE pregnancy.Conclusion: PE is characterized by a maintained elevated arterial proximal andperipheral resistance and lower compliance during and after pregnancy. The al-terations in blood pressure cannot be explained changes in R, but is likely relatedto changes in Z0 and C.
P668 Role of farnesylpyrophosphate synthase inangiotensin II-induced cardiac hypertrophy
Y. Ye, S.-J. Hu. First Affiliated Hospital of College of Medicine,Zhejiang University, Institute of Cardiology, Hangzhou, China, People’sRepublic of
The Rho guanosine triphosphatase (Rho GTPases) family, including RhoA, playsan important role in angiotensin II (AngII)-mediated cardiac hypertrophy. Farne-sylpyrophosphate synthase (FPPS)-catalyzed isoprenoid intermediates are nec-essary for activation of RhoA. The present study was designed to investigate therole of FPPS in myocardial hypertrophy associated with Ang II. First, we demon-strated that FPPS expression was elevated both in cultured neonatal cardiomy-ocytes (NCMs) following Ang II treatment and in the hypertrophic myocardiumof 18-week-old spontaneously hypertensive rats (SHRs). Then, the importanceof FPPS was assessed by RNA interference against FPPS in NCMs. SuccessfulFPPS silencing in NCMs completely inhibited the hypertrophy marker genes of β-myosin heavy chain (β-MHC) and brain natriuretic peptide (BNP), as well as cellsurface area. Furthermore, FPPS knockdown prevented elevated RhoA activitycompared with non-silenced controls. Similarly, increased-phosphorylation of p-38 and c-Jun N-terminal kinase (JNK) mitogen-activated protein kinases (MAPK)by Ang II was attenuated. In vivo gene transfer also attenuated hypertrophicresponses as indexed by left ventricular weight/body weight, heart weight/bodyweight, and echocardiography, as well as expression of β-MHC and BNP mRNAin SHRs. In conclusion, FPPS with RhoA-associated p-38 and JNK MAPK signal-ing plays an important role in Ang II-induced cardiac hypertrophy.
P669 Body size measures as predictors of increased arterialstiffening in hypertensive subjects: a 6-year follow-upstudy
C. Thomopoulos, C. Tsioufis, E. Andrikou, D. Flessas, I. Andrikou,A. Mazaraki, I. Eleftheriadou, L. Lioni, D. Tousoulis, C. Stefanadis.
First Cardiology Clinic, University of Athens,Hippokration Hospital, Athens,Greece
Objective: To assess whether the progression of aortic stiffening as defined bythe upper quartile of carotid-femoral pulse wave velocity (PWV) at follow-up isinfluenced by body size measures in untreated newly diagnosed hypertensives.Methods: We prospectively studied 163 white hypertensive non-diabetic pa-tients (52±10 years, 98 men, 59 smokers, body mass index=28.8±5.4kg/m2 ,waist circumference=98±12cm) in a 6-year period. All patients underwent 24-hour ambulatory monitoring, and PWV measurement with Complior SP, whereasmetabolic profile, estimated creatinine clearance (eGFR) and echocardiographicmeasurements were also performed at both baseline and last outpatient clinicvisit (follow-up: 4.5±0.89 years). All subjects were under optimal antihyperten-sive therapy complemented by supplementary vasoactive drugs where appropri-ate and the spectrum of drugs implemented within the last 6-month period beforelast visit consisted of: renin-angiotensin system inhibitors RAASI (49%), diuretics(25%), calcium-channel blockers (20%), beta-blockers (13%), statins (16%) andantiplatelet agents (18%).Results: Between baseline and last follow-up visit it was accomplished an in-crease in waist by 5.3±5.6cm, a decrease in BMI by 1.9±4.1kg/m2, while PWVwas increased by 1.83±1.37m/s (7.9±1.5 vs. 9.6±1.5m/s, the upper follow-up quartile for PWV [≥10.3m/sec] had prevalence of 27%). During follow-up,24h systolic and diastolic BP were decreased by 12.7±9.1 and 8.2±6.2mmHg(130±12 vs. 122±12 and 80±9 vs. 75±8mmHg) respectively. In Cox regres-sion models by implementing alternatively baseline BMI and waist, as well astheir respective differences from the last visit determination, the upper quartile ofPWV was predicted by BMI 1.05 (1.01-1.08), p=0.009 and waist 1.037 (1.014-1.061) p=0.001. Common positive predictor in the models remained baselinePWV, whereas baseline 24h diastolic BP and RAASI treatment predicted neg-atively the outcome (p<0.01 for all).Conclusion: Body adiposity measures predict enhanced aortic stiffening in hy-pertensive patients and RAASI treatment had an antistiffening effect in our cohort.
P670 Distinct impact of isolated systolic and isolateddiastolic hypertension in arterial stiffening in newlydiagnosed essential hypertension
D. Tsiachris, C. Tsioufis, D. Syrseloudis, I. Andrikou, D. Aragiannis,E. Stefanadi, H. Tatsis, E. Tsiamis, C. Stefanadis. First Cardiology
Clinic, University of Athens,Hippokration Hospital, Athens, Greece
Purpose: Isolated systolic hypertension (ISH) has been associated with adverse
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

94 Pulse wave velocity and ambulatory blood pressure monitoring
cardiovascular outcome compared to isolated diastolic hypertension (IDH) orsystolic–diastolic hypertension (SDH). Ambulatory arterial stiffness index (AASI),a measure based on the relative behavior of 24-hour systolic and diastolic bloodpressure (BP), has been suggested as a marker of arterial stiffness and a pre-dictor of cardiovascular mortality. Our aim was to investigate the relationship be-tween specific ambulatory hypertensive patterns and arterial stiffness parametersin the early stages of essential hypertension.Methods: We studied 180 consecutive subjects (aged 51±10 years, 363 males)with untreated essential hypertension. All subjects underwent ambulatory BPmonitoring, echocardiography and carotid – femoral PWV measurement by acomputerized device (Complior SP). AASI was defined as 1 minus the regres-sion slope of 24-h ambulatory diastolic and systolic BP. The study population wascategorized by ambulatory BP level into three groups: those with ISH (24h SBP>130 and 24h DBP<80 mmHg, n=36), those with IDH (24h SBP <130 and 24hDBP>80 mmHg, n=21) and those with SDH (24h SBP and DBP>130/80 mm Hg,n=123).Results: Hypertensives with ISH compared to those with IDH were older (53±10vs. 46±9 years, p=0.002) and had by definition greater 24-systolic BP (by 11.6mmHg) and pulse pressure (by 17.2 mmHg) while there was no difference re-garding sex, body mass index, waist circumference and lipid profile (p=NS for allcases). Hypertensives with ISH did not differ also compared to those with IDH withrespect to left ventricular mass index, relative wall thickness and transmitral flowDoppler parameters (p=NS for all). Moreover, hypertensives with ISH comparedto those with IDH exhibited significantly greater values of 24h AASI (0.44±0.14vs. 0.26±0.13 cm/s, p<0.001) and PWV (9.6±1.6 vs 8.6±1.0, p=0.017). Differ-ence in AASI values between the two groups remained significant even afteradjustment for age (p=0.003) in contrast with the difference in PWV (p=0.313).24h AASI was correlated with 24h PP (r=0.483, p<0.001) and 24h systolic BP(r=0.268, p<0.001).Conclusions: Ambulatory ISH compared to IDH is associated by impaired re-gional and systemic arterial stiffness, as reflected by increased aortic PWV and24h AASI in the setting of newly diagnosed essential hypertension. These find-ings may further elucidate the adverse prognostic role of ISH.
P671 Correlation between left ventricular mass (LVM) andambulatory or clinic blood pressure (BP) in very elderlysubjects
S. Carugo1, A. Esposito1, B. Caimi1, A. Pernigotti1, C. Redaelli1,M. Pozzi1, M. Maisaidi1, M. Monti1, G. Mancia2. 1University of Milan,
Pio Albergo Trivulzio, Milan, Italy; 2Università Milano-Bicocca, Ospedale S.Gerardo, Monza, Milano, Italy
Purpose: LVM is positively related to BP and the relationship is closer for ambula-tory (A) as compared to clinic (C) values. Limited information exists as to whetherthis is the case also at a very advanced age.Methods: We studied 82 patients (71 males and 11 females) older than 90 years(age 94±3.6 years, mean ±SD). LVM was assessed by echocardiography andindicized (I) to either body surface area (BSA) or height at -2.7. BP was measuredboth in the clinic environment (via standard methodology) and automatically overthe 24 hours.Results: Clinic BP was 121.42±17.03/70.07.2±9.49 (systolic/diastolic) mmHg;24 h mean BP was 129.0±16.17/65.24±8.56 mmHg, with only little differencebetween day and night values; LVMI/BSA was 121.6±40.8 g/m2 and LVMI/height54.5±18.9 there was a significant (p<0.001) correlation between LVMI valuesand both clinic or ambulatory systolic BP regardless how LVMI was calculated.In both instances the correlation was closer for ambulatory than for clinic val-ues (LVMI/BSA: p<0.0001 r 0.022; LVMI/height: p<0.001 r 0.024). LVMI showeda much weaker correlation with clinic and ambulatory diastolic BP. Systolic butnot diastolic BP correlated also with left atrial dimension (p<0.001) again moreclosely when ambulatory rather than clinic BP was considered (p<0.0001 r0.011).Conclusion: Even in very elderly subjects LVMI is related to and possibly de-pends on BP levels. Like in younger individuals BP load over the 24 hours is abetter determinant of alterations in cardiac structure than BP measured in thedoctor’s office.
P672 Aortic Size Index enlargement is associated to centralhemodynamics in essential hypertension
A. Milan, F. Tosello, D. Naso, C. Magnino, A. Fabbri, A. Vairo, D. Leone,E. Puglisi, E. Avenatti, F. Veglio. Dept. of Medicine and Exp. Oncology,Div. of Int. Med., Hypertension Unit, University of Torino, Torino, Italy
Background: Arterial hypertension is a leading cause of aortic root dilatation(ARD). Mechanical stress in the aortic wall is proportional to blood pressure (BP)and vessel diameter, thus hypertension and aortic dilation are risk factors for aor-tic dissection. Objective of this study was to evaluate the association betweenbrachial and central blood pressure (bBP and cBP) levels and aortic root dilata-tion (ARD) in essential hypertensive patients.Methods: A total of 190 untreated and treated essential hypertensive patients(mean age, 55±11 years) were considered for this analysis. We measured pul-satile hemodynamics and proximal aortic diameter directly using tonometry, ultra-sound imaging (echocardiography), and Doppler.
Results: 91 hypertensive patients had an ARD (defined as Aortic Size Index (ASi)> 2 cm/m2). Central haemodynamic variables were significantly associated toASi. Patients with increased ASi, were significantly older (60±10 vs. 50±11 years;p<0.0001), had higher levels of Augmentation Index (AIx; 28±10 vs. 21±10p<0.0001), Augmentation Pressure (AP; 13±6 vs 8±5 mmHg, p<0.0001), andcentral Pulse Pressure (cPP; 44±10 vs 39±8 mmHg p<0.0001) compared topatients with normal ASi. In a logistic regression analysis Aix resulted the onlysignificant predictor of ASi.
Figure 1
Conclusions: In hypertensive patients Augmentation Index and central BloodPressure were associated to Aortic Root Dilatation, whereas brachial Pulse Pres-sure was not. Patients with increased Aortic Size index may loose part of theelastic properties of the aorta, demonstrating a more strict correlation betweenASi and central haemodynamic indexes, in particular central Pulse Pressure andAugmentation Index.
P673 Arterial Stiffness predicts progression of aorticdisease in marfan syndrome
K. Mortensen1, M. Rybcynski2, M.A. Aydin2, J. Stritzke1, M. Reppel1,T. Meinertz2, H. Schunkert1, Y. Von Kodolitsch2. 1Departmentof Cardiology, Luebeck, Germany; 2University Medical Center
Hamburg-Eppendorf, Center for Cardiology and Cardiovascular Surgery,Hamburg, Germany
Background: Non-invasive applanation tonometry (APT) is useful to measurearterial stiffness. APT is established to predict cardiovascular disease progres-sion in many conditions such as arterial hypertension, coronary artery diseaseand renal disease. We test in this study, whether APT measurements relate toprogression of aortic disease in Marfan syndrome (MFS).Methods: We performed APT in 50 consecutive, medically treated adults withMFS (19 men, 31 women aged 32±13 years), who had not undergone previouscardiovascular surgery.Results: During 22±16 months of follow-up, 26 of these patients developed pro-gression of aortic disease, which we defined as progression of aortic root di-ameters ≥5 mm/annum (18 individuals), aortic surgery ≥3 months after APT (7individuals), or onset of acute aortic dissection any time after APT (1 individual).Univariate Cox regression analysis suggested an association of aortic diseaseprogression with age (P=.001), total cholesterol levels (P=.04), aortic root diam-eter (P=.007), descending aorta diameter (P=.01), aortic root ratio (P=.02), andaugmentation index (AIx@HR75; P<.006). Multivariate Cox regression analysisconfirmed an independent impact on aortic progression exclusively for aortic rootdiameters (HR=1.347; 95% CI 1.104–1.643; P=.003) and AIx@HR75 (HR=1.246;95% CI 1.029–1.508; P=.02). In addition, Kaplan–Meier survival curves analysisillustrated significantly lower rates of aortic root disease progression both withlower AIX@HR75 (P=.025) and with lower PWV values (P=.027).Conclusions: We provide evidence that arterial stiffness relates to aortic diseaseprogression in medically treated patients with MFS. We assume that arterial stiff-ness might improve significantly risk stratification in the clinical management ofMFS patients.
P674 Ambulatory blood pressure variability in normotensionand in white coat, masked and sustained hypertension.Data from the Spanish ambulatory blood pressureregistry
S. Hoshide1, G. Bilo2, A. De La Sierra3, J.R. Banegas4, M. Gorostidi5,J. Segura6, L.M. Ruilope6, G. Mancia7, G. Parati2. 1Jichi Medical University,Dept. of Cardiology, Tochigi, Japan; 2Dept. Cardiology, Ist. Auxologico Italiano,Dept. of Clin. Med. and Prevention, Univ. Milano-Bicocca, Milan, Italy; 3Dept. ofInternal Medicine. Hospital Mutua Terrassa, University of Barcelona, Barcelona,Spain; 4Dept. of Epidemiology and Public Health, Autonomous University,Madrid, Spain; 5Deptt of Nephrology. Hospital San Agustín, Avilés, Spain;6Hypertension Unit, 12 de Octubre Hospital, Madrid, Spain; 7University ofMilan-Bicocca, Dept. Clinical Medicine & Prevention, Milan, Italy
Objective: Based on office and ambulatory blood pressure (BP), subjects canbe classified as normotensive (NT), white coat, masked or sustained hyperten-sive (WCHT, MHT, SHT, respectively). Aim: To assess whether these categories
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Pulse wave velocity and ambulatory blood pressure monitoring / Endothelial function 95
are associated with differences in daily life BP variability (V) in a large group ofsubjects (Spanish Ambulatory Blood Pressure Monitoring Registry).Methods: We analyzed ambulatory BP recordings (Spacelabs 90207) obtainedin 18395 subjects (age: 52.8±14.7 years, 55% males) not on antihypertensivemedication. Based on the accepted cutoffs for office (<140/90mmHg) and 24h(<130/80mmHg) BP normality, subjects were classified as NT, WCHT, MHT andSHT. BPV was quantified as 24h standard deviation (SD), weighted 24h (wSD)and average real variability (ARV: average absolute BP difference between suc-cessive readings) for systolic (S) and diastolic (D)BP. The difference in BPV be-tween BP categories was adjusted for age, BMI, gender, smoking, diabetes, dys-lipidemia, previous cardiovascular diseases, renal insufficiency and average 24hSBP or DBP as appropriate.Results: The distribution of subjects was: 15.8%, 30.0%, 6.4% and 47.8% in NT,WCHT, MHT and SHT groups, respectively. The adjusted estimates of 24h SBPVand DBPV in the four groups are shown in the table. Compared to NT, night-timeSBP SD was similarly elevated in MHT and SHT (p<0.001), but not in WCHT.
NT WCHT MHT SHT
24 h SBP SD 12.5 13.6° 12.8 13.6°24 h DBP SD 10.3 10.9° 10.3 10.8°24h SBP wSD 10.0 10.6° 10.4# 10.7°24h DBP wSD 8.2 8.4° 8.2 8.3*SBP ARV 8.8 9.0° 9.1° 9.0°DBP ARV 7.2 7.3 7.2 7.3
*p<0.05 vs. NT; #p<0.01 vs. NT; °p<0.001 vs. NT.
Conclusions: Compared to NT, after adjusting for mean BP we found an in-creased 24h BPV in WCHT similar to that observed in SHT, with smaller differ-ences in MHT. Conversely, night-time BPV was increased in MHT and in SHTbut not in WCHT. Increased office BP seems thus associated with higher BP re-activity to daily life stimuli, irrespective of differences in average out-of-office BP.These findings may be relevant when considering the higher cardiovascular riskreported by some studies in WCHT.
ENDOTHELIAL FUNCTION
P675 AMP activated protein kinase mediates vascularprotective effects during exercise training
E. Schulz, S. Schuhmacher, P. Wenzel, M. Oelze, A. Daiber,T. Muenzel. University Medical Center of the Johannes GutenbergUniversity Mainz, Mainz, Germany
Background: Regular physical activity is known to protect the vasculature by an-tioxidative effects and upregulation of endothelial nitric oxide synthase. Duringskeletal muscle contraction, the AMP activated protein kinase is being activatedand improves glucose uptake and metabolism. This may explain the positive ef-fects of exercise regarding metabolic control in diabetics. Since the AMP activatedproteinkinase (AMPK) is also an important mediator of angiogenesis and eNOSactivation, we examined the vascular effects of AMPK deletion during chronic ex-ercise training.Methods and Results: Since vascular cells almost exclusively harbour the al-pha1AMPK isoform, alpha1AMPK knockout and corresponding wildtype micewere used to study the effects of decreased vascular AMPK activity. Alpha1AMPKand wildtype mice underwent voluntary exercise training in running wheels. Themean running distance was 4.2 + 0.8 km/d in wildtype mice and 4.0 + 0.9 km/din alpha1AMPK knockout mice (p=ns). Exercise training significantly increasedplasma nitrite production and serum antioxidative capacity in wildtype mice, whileit decreased both parameters in alpha1AMPK knockout mice. In addition, regularphysical activity caused an increased expression of AMPK, which was associatedwith increased aortic eNOS expression and activation-associated eNOS phos-phorylation at serine1177. Knockout of the alpha1AMPK isoforms resulted in anappr. 90% reduction of total aortic AMPK expression. Moreover, exercise trainingdid not longer increase eNOS expression or eNOS phosphorylation at serine1177in mice lacking the alpha1AMPK isoform.Conclusion: Intact AMPK signalling is required for the vascular protective effectsof exercise training. Pharmacological AMPK activation might be a novel approachin the near future to simulate the beneficial effects of physical activity.
P676 LOX-1 cooperates with renin-angiotensin system inmonocyte adhesion-induced redox-sensitive and Ca2+signaling pathways in endothelial cells
N. Sakamoto1, T. Ishibashi1, K. Sugimoto1, H. Ohkawara1, N. Inoue2,T. Sawamura3, Y. Takeishi1. 1Fukushima Medical University,
Fukushima, Japan; 2Japan Labour Health and Welfare Organization Kobe RosaiHospital, Kobe, Japan; 3National Cardiovascular Center Research Institute,Suita, Japan
Purpose: NADPH oxidase is closely associated with renin-angiotensin system(RAS) in the vasculature. Lectin-like oxidized-LDL receptor-1 (LOX-1) is a ma-jor receptor for oxidized LDL. We have recently reported that NADPH oxidase-dependent and Ca2+ signaling pathways are mediated via LOX-1 in endothelial
cells (ECs) by monocyte adhesion independent of oxidized LDL. We hypothesizedthat RAS plays an essential role in redox-sensitive and Ca2+ signaling pathwaysinduced in ECs by monocyte adhesion and LOX-1 mediates RAS-dependentevents in monocyte-EC interaction.Methods: AT1 receptor activation in ECs was evaluated by epidermal growthfactor receptor (EGFR) transactivation. A neutral antibody (TS92) was used forinhibition of LOX-1. Whole peripheral blood was pretreated with or without 10mmol/L ACE inhibitor (temocaprilat) or AT1 receptor antagonist (olmesartan) for 3hours, followed by monocyte isolation and then isolated monocytes were added tocultured human aortic ECs. Rac1 activity was determined by membrane translo-carion, whereas NADPH oxidase activity was determined by lucigenin-enhancedchemiluminescence. MCP-1, ICAM-1 and TF expression and NF-kB phosphory-lation were assessed by Western blotting.Results: Monocyte adhesion increased Rac1 activity, NADPH oxidase activity,and ROS generation within 30 minutes and NF-kB phosphorylation within 1 hour,resulting in upregulation of MCP-1, ICAM-1 and TF expression in ECs. Ca2+signaling including intracellular Ca2+ mobilization and Ca2+ influx was inducedin ECs just after adding monocytes. These redox-sensitive and Ca2+ signalingpathways were blocked by pretreatment of whole blood or ECs with temocaprilatand olmesartan, as well as by inhibition of endothelial LOX-1 by TS92. Impor-tantly, RT-PCR of ACE revealed that monocyte adhesion upregulated endothelialRAS within 6 hours, which was attenuated by inhibition of LOX-1. Furthermore,monocyte adhesion triggered EGFR transactivation within 30 minutes in ECs,which was blocked by inhibition of endothelial LOX-1 by TS92. These findings in-dicated the linkage of LOX-1 with RAS in monocyte-EC interaction independentof oxidized LDL-LOX-1 axis.Conclusions: We show new insights into the regulation of LOX-1/RAS axisin monocyte adhesion-induced redox-sensitive and Ca2+ signaling pathways inECs, which may be an attractive target for treatment of endothelial dysfunction.
P677 oxLDL mediated p66shc activation and ROSproduction goes through LOX-1receptor-1 andmediated by protein kinase C beta and c-JunN-terminal kinase in human aortic endothelial cells
Y. Shi1, F. Cosentino1, G. Camici1, A. Akhmedov1, P. Vanhoutte2 ,F. Tanner1 , T. Luscher1 . 1Institution of Physiology, Cardiovascular Research,Zurich, Switzerland; 2The University of Hong Kong, Department of Pharmacology,Hong Kong, Hong Kong SAR, People’s Republic of China
Background: p66Shc is a mitochondrial adaptor protein mediating oxidativestress and apoptosis. As reactive oxygen species (ROS) are involved in vascu-lar dysfunction, it may represent a promising therapeutic target against. Indeed,p66Shc knockout mice fed high fat diet develop less foam cells and atheroscleroticlesions. The present study was designed to elucidate the molecular pathways me-diating the proatherogenic effects of p66Shc.Methods: The expression of p66Shc protein was measured by western blotting.The production of superoxide anion was measured by electron-spin resonancespectroscopy. Small interference RNA (SiRNA) against p66Shc was added inserum-free medium for four hours.Results: oxLDL increased p66Shc phosphorylation in a dose-dependent man-ner, while leaving total protein levels unchanged. Inhibition or silencing of lectin-like oxidized LDL receptor-1 (LOX-1) prevented p66Shc phosphorylation in cellsstimulated with oxLDL, but not in cells stimulated with lysophosphatidylcholine,indicating that the effect of oxLDL is mediated via the LOX-1 receptor. oxLDL acti-vated protein kinase C beta II (PKCβ II) on both T641 and S660 and inhibitorsof PKCβ II reduced phosphorylated p66Shc, indicating that PKCβ II activatesp66Shc. oxLDL activated c-Jun N-terminal kinase (c-JNK), while inhibitors of JNKreduced phosphorylated p66Shc, indicating that also JNK takes part in its acti-vation. Apocynin reduced the levels of phosphorylated PKCβ II, phosphorylatedJNK, and phosphorylated of p66Shc, suggesting that O2- plays an important rolein these responses. Phosphorylation of JNK was prevented by PKC inhibitors,suggesting that JNK activation is downstream of PKC kinase. In addition, theincreased production of O2- by oxLDL was blunted by PKC inhibitors or JNK in-hibitor, indicating that both PKC and JNK regulate ROS generation. Furthermore,inhibition of p66Shc by SiRNA reduced the production of O2- in cell treated withoxLDL, but not in control condition, suggesting that the p66Shc protein takes partin the oxLDL stimulated ROS production.Conclusion: oxLDL activates endothelial p66Shc through a PKC/JNK-dependent, superoxide-mediated mechanism. This study offers novel mechanis-tic insight into the pro-atherosclerosis properties of p66Shc protein and possiblynovel therapeutic targets.
P678 Ephrin-A1 mediated adhesion of monocytes toendothelial cells is dependent on the Rho signalingpathway - possible implications for atheroscleroticplaque development-
S. Jellinghaus1, G. Ende1, D.M. Poitz1, A. Augstein1, M. Tsurkan2,P. Barthel1, G. Simonis1, R.H. Strasser1. 1University of Technology Dresden,Heart Center University Hospital, Dresden, Germany; 2Leibniz Institute ofPolymer Research, Dresden, Germany
The Eph family of Eph receptors and ephrin ligands represent the largest sub-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

96 Endothelial function
group of tyrosine kinase receptors. Eph/ephrin mediated cell-cell-interactions areessential in processes like developmental biology, tumour biology (growth andneovascularization) and inflammation. It is not known if the Eph-family has spe-cific functions in the pathophysiology of atherosclerosis.The aim of the present study was to investigate the potential role of Eph/ephrininteractions in the development of the atherosclerotic plaque. A crucial processduring the formation and progression of an atherosclerotic plaque is the interac-tion between monocytes/macrophages and endothelial cells.The immunohistochemical analysis of human coronary atheroslerotic plaquesrevealed the expression of ephrinA1- and ephrinB-ligands as well as EphA4-,EphA2- and EphB1-receptor in different cell types within the plaque. The receptorEphA4 is mainly expressed in macrophages and neovessels in the plaque. Stim-ulation of human umbilical vein endothelial cells (HUVEC) with the soluble ligandephrinA1-Fc (8μg/ml) leads to an activation of the receptor EphA4, identified byimmunoprecipitation and tyrosine phosphorylation, and to a fourfold increasedadhesion of human monocytes (THP-1 cells) to the endothelial cells comparedto stimulation with Fc as control. The effect of a specific inhibition of the receptorEphA4 on monocyte adhesion to HUVEC by using small peptides is currently un-der investigation. The ephrinA1-mediated increase in monocyte adhesion to HU-VEC was significantly reduced by inhibitors of the Rho signaling pathway (Y27632as ROCK-inhibitior and C3-Transferase as RhoA-inhibition). Furthermore, an in-duction of the ligand ephrinA1 in HUVEC under hypoxic conditions was identifiedsuggesting a potential ephrinA1 regulation in atherosclerotic plaques.These results demonstrate that the ephrinA1–mediated EphA4 forward signal-ing plays an important role during monocyte adhesion to endothelial cells. TheRho signaling pathway is involved in this effect. The fact that EphA4 is highly ex-pressed in neovessels and ephrinA1 in macrophages within the plaque suggeststhat EphA4/ephrinA1 interactions between monocytes and endothelial cells arefundamentally involved in the development of the atherosclerotic plaque. This no-tion is even more supported by the observation that hypoxia is the potential triggerfor the regulation of Eph receptors or ephrin ligands in atherosclerotic plaque.
P679 Increased cytochrome P4502E1 expression and alteredhydroxyeicosatetraenoic acid formation mediatediabetic vascular dysfunction
A. Schaefer1, D. Fraccarollo1 , P. Galuppo1, J. Widder1, E. Barbosa-Sicard2, I. Fleming2, J. Bauersachs1. 1University of Wuerzburg,
Wuerzburg, Germany; 2University of Frankfurt/Main, Frankfurt, Germany
Background: We investigated the mechanisms underlying endothelial dysfunc-tion and the non-contractile smooth muscle cell (SMC) phenotype in diabetes.Methods: Diabetes was induced by single intravenous injection of streptozotocin(50 mg/ml) in male Wistar rats. After 4 weeks of hyperglycaemia, vascular functionwas assessed by organ bath studies and vascular protein expression was studiedby RNA microarrays and Western Blot.Results: Endothelial function and contractile vasomotor responses were sig-nificantly impaired, while vascular superoxide formation was increased in theaorta from diabetic versus healthy control rats. Cytochrome P4502E1 (CYP2E1)was identified as the highest upregulated gene in diabetic aorta using RNA mi-croarrays. CYP2E1 protein was significantly increased (16-fold) in diabetic aorta.CYP2E1 is the source of the vasomodulators 18- and 19-HETE, which wereboth significantly increased in diabetes and are known to reduce 20-hydroxy-eicosatetraenoic acid (20-HETE), a potent vasoconstrictor. Induction of CYP2E1expression by isoniazide in healthy rats mimicked the diabetic non-contractile vas-cular response. Pre-incubation of aortae from STZ-diabetic rats in vitro with 20-HETE rescued contractile function. cGMP is an endogenous inhibitor of CYP2E1.Since cGMP levels/signalling are dramatically reduced during diabetic endothelialdysfunction, chronic sGC acticvation was performed in vivo for the last 2 weeksusing the novel sGC activator HMR1766. Chronic treatment with HMR1766 im-proved NO sensitivity and endothelial function, reduced CYP2E1 expression andsuperoxide formation, lowered 19-HETE and enhanced 20-HETE levels, and re-versed the contractile deficit observed in placebo-treated diabetic rats.Conclusions: Upregulation of CYP2E1 is essentially involved in diabetic vas-cular dysfunction. Chronic treatment with the sGC activator HMR1766 reducedoxidative stress, decreased CYP2E1 levels, and normalized vasomotor functionin diabetic rats.
P680 Endothelium-dependent vasomotor dysfunctionfollowing overlapping sirolimus- but notzotarolimus-eluting stents is associated local oxidativestress in a porcine coronary model
T. Nakamura, K. Natarajan, J.N. Yue, J. Li, T. Goodchild, J. Singh,N. Chronos, D. Hou. Saint Joseph’s Translational Research Institute, Atlanta,United States of America
Background: The safety features of Endeavor (ZES) in comparison with Cypher(SES) are reported clinically in long-term follow-up studies, which highlight verylow rate of late thrombosis despite short period of DAPT. We investigated coro-nary vasomotor function and local oxidative mediator production after overlappingZES and SES in porcine coronary arteries.Methods: Overlapping of bare metal stents (BMS) (n=12), SES (n=12), and ZES(n=13) were implanted into 19 pigs. Each pig received two pairs of identical stents,
with S/A ratio of 1.1:1 and overlapping segment of 1/3 to 12 of single stent length.
At 28d, endothelial function 5-10 mm distal to the stents was estimated by acetyl-choline (Ach, 10-6, 10-5 M/ml) and nitroglycerin (NTG, 400μg) infusion followedby lucigenin luminometry and western blot measuring of O2
•–, and eNOS, Akt,phosphorylated Akt.Results: Endothelium-dependent vasomotion was significantly impaired in SEScompared to both ZES and BMS. The mean coronary diameter changes at Ach10-6 and 10-5 was -3.12±3.63% and -5.39±5.89% for SES, 1.81±7.33% and3.00±5.46% for ZES, as well as -0.34±9.77% and -0.96±12.16% for BMS (P <
0.07 and 0.002; SES vs both others, respectively). Meanwhile, local O2•– produc-
tion was 64% increased in SES vs ZES (p = 0.05). Densitometry analysis demon-strated significantly decreasing eNOS and pAkt proteins expression in SES ver-sus ZES and BMS (p <0.001 respectively).Conclusions: Elevating local oxidative stress may play a role to contribute ab-normal endothelium-dependent coronary relaxation following overlapping SES.Overlapping ZES showed enhancing anti-oxidative molecules expression in thisporcine model.
P681 Impact of niacin therapy on endothelial vasomotricityin patients with low HDL shortly after an acutecoronary syndrome
T.H. Lhermusier, V. Bataille, V. Bongard, J. Roncalli, A. Bura-Riviere,J. Ferrieres, D. Carrie, M. Galinier, J.P. Cambou, M. Elbaz.
Cardiovascular and Metabolic Pole, Rangueil Hospital„ Toulouse, France
Purpose: Atheroprotective effects of HDL-cholesterol [HDL-C] may be partiallyexplained by its potential role in maintaining or restoring endothelial function.However, the usefulness of niacin, the most effective molecule to increase HDL-C,to restore endothelial function remains controversial. Furthermore, the benefits ofits use shortly after an acute coronary syndrome [ACS] in subjects with low HDL-C and endothelial dysfunction [ED] are unknown.Methods: The EVAN-ACS study is a double-blind randomized placebo-controlledtrial aiming at assessing the potential effects of extended-release niacin on en-dothelial function in subjects with low HDL-C (<40 mg/dL) and ED who recentlysuffered from an ACS. Patients were systematically screened over a period of18 months. Flow Mediated Dilation [FMD] of the brachial artery was measuredwithin 7 days after the ACS in patients matching with inclusion criteria. Subjectswith FMD<7% (ED) were randomized either to the Treatment Group [TG] (niacin1000 mg/d) or to the Placebo Group [PG]. Patients concurrently received the op-timal recommended treatments. After 12 weeks, biological measurements and aFMD assessment were performed again.Results: 93 patients were included and 75 with ED randomized; 68 followed thestudy protocol to the end. Median age was 51 (interquartile range [IR] =45-61)and 92.6% were men. No differences were observed between the two groupsfor age, gender, smoking habits, blood pressure, plasma lipoprotein and CRPlevels or FMD. After 12 weeks, FMD had significantly increased both in the TG(median absolute change: +3.6%, p<0.001) and in the PG (+2.1%, p<0.001),without any difference between the two groups (p=0.87). In the same way, CRP,LDL-C and triglycerides levels decreased and HDL-C level increased significantlyin both groups, but the extent of these changes were not statistically differentfrom the TG to the PG (median absolute change of CRP: -42 and –27 mg/dLrespectively, p=0.63/LDL-C: -31 and –39 mg/dL, p=0.84/triglycerides: -52 and -52mg/dL, p=0.63/HDL-C: +7 and +2 mg/dL, p=0.09).Conclusions: In this trial conducted in subjects with ED and suffering from a re-cent ACS, after 12 weeks of treatment, FMD had significantly increased both inthe group treated with niacin and in the placebo group, but the extent of this risewas not significantly higher in the treatment than in the placebo group. FMD im-provement in both groups may reflect a spontaneous improvement or the effectsof the current recommended therapies. Larger studies maybe using higher niacindoses are required to better address this important topic.
P682 Impact of selective serotonin reuptake inhibitors onarterial stiffness
V. Katsi1, I. Skiadas1, K. Kontoangelos2 , G. Souretis1,D. Tsartsalis1, E. Vergopoulos1, G.N. Papadimitriou2, C. Stefanadis1,I. Kallikazaros1. 1Hippokration General Hospital, Athens, Greece;
2Eginition Hospital of Athens, Athens, Greece
Purpose: In view of the high likelihood that hypertensives will have comorbidanxiety and depression, all hypertensives should be screened for concurrent psy-chiatric illnesses and treatment. The aim of the study was to investigate the re-lationship between the administration of selective serotonin reuptake inhibitors(SSRIs) and arterial stiffness, a hallmark of the cardiovascular aging process.Methods: We studied 210 consecutive untreated stage I-II essential hypertensivesubjects (aged=62±9 years, 110 female, office blood pressure (BP) = 163/91 mmHg). The participants were divided into group A (n=83), those receiving SSRIsand group B (n=127), those without taking any antidepressant therapy. Arterialstiffness was evaluated on the basis of carotid to femoral pulse wave velocity(c-f PWV) by means of a computerized method (Complior SP). Venous bloodsampling was performed for the estimation of routine metabolic profile.Results: The two groups did not differ regarding age, gender, office sys-tolic/diastolic BP as well as serum glucose and triglycerides levels (83±9 vs 84±
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Endothelial function 97
mg/dl and 128±8 vs 119±9 mg/dl, respectively, p=NS in all cases). Group Awas characterized by increased levels of body mass index (32.4±3 vs 29.2±4kg/m2, p=0.015) and elevated cholesterol plasma levels compared to group B(231±32 vs 220±36 mg/dl p<0.05). Group A compared to group B exhibited sig-nificantly increased c-f PWV (8.4±0.3 vs 7.2±0.5 m/sec, p=0.02) and this differ-ence remained significant after adjustment for confounders (p=0.03). In the SSRIstreated- hypertensives, c-f PWV was correlated with age (r=+0.35, p= 0.015) andoffice systolic BP (r=+0.33, p= 0.02), while no significant correlation was demon-strated with cholesterol levels (p=NS).Conclusions: In essential hypertension, the administration of SSRIs exerts anincremental effect on arterial stiffness, accelerating the vascular ageing process.
P683 Favorable effects of omega-3 fatty acids administrationon endothelial function, arterial stiffness and onfibrinolytic process in healthy smokers
M. Zaromitidou1, D. Tousoulis1 , G. Siasos1, A. Verveniotis1,E. Oikonomou1, E. Gialafos1, T. Ntoskas1, A. Plastiras1,
A. Papavassiliou2, C. Stefanadis1. 1Hippokration Hospital, University of Athens,1st Department of Cardiology, Athens, Greece; 2University of Athens MedicalSchool, Department of Biochemistry, Athens, Greece
Purpose: Smoking is associated with endothelial dysfunction and impaired fib-rinolytic status. �-3 fatty acids can modify cardiovascular risk factors. We inves-tigated the effect of �-3 fatty acids on endothelial function, arterial stiffness andfibrinolytic system in healthy smokers.Methods: We studied the effect of a 12 weeks oral treatment with 2gr/day of �-3 fatty acids in 13 healthy smokers (aged 27.5±2.90y) on two occasions (day0: baseline and day 84). The study was carried out on two separate arms, onewith �-3 fatty acids (2 gr/day) and one with placebo according to a randomized,placebo-controlled, double-blind, cross-over design. Measurements were carriedout before (pSm) and immediately after (Sm0) cigarette smoking. Endothelialfunction was evaluated by flow-mediated dilation (FMD) of the brachial artery.Carotid-femoral pulse wave velocity (PWV) was measured as an index of aorticstiffness and augmentation index (AIx) as a measure of arterial wave reflections.Circulating levels of plasminogen activator inhibitor type 1 (PAI-1) were measuredby ELISA.Results: At baseline measurements, compared to pSm, cigarette smokingcaused an increase in AIx (0.64±13.02% vs 5.48±10.05%, p<0.05) and PWV(5.88±0.64 m/sec vs 6.30±0.76 m/sec, p<0.05) as well as a decrease in FMDvalues (7.22±2.54% vs 5.45±2.60%, p<0.05). Treatment with �-3 fatty acidsimproved pSm values of: FMD (7.22±2.54% vs 9.94±5.30%, p<0.05), PWV(5.88±0.64 m/sec vs 5.35±0.86 m/sec, p<0.05) and AIx (.64±13.02% vs -3.82±13.72%, p<0.05) while there was no significant difference with placebo ad-ministration. We also found that, compared with placebo, treatment with �-3 fattyacids, blunted the acute smoking-induced increase in PWV (0.423±0.33 m/secvs 0.013±0.56 m/sec, p<0.05). Finally we found that pSm levels of PAI-1 wereincreased after �-3 fatty acids treatment compared to baseline measurements(23.37±13.39 ng/ml vs 16.28±11.27 ng/ml, p<0.05).Conclusion: Short-term treatment with �-3 fatty acids improves endothelial func-tion and vascular elastic properties of the arterial tree, an effect which is alsoaccompanied by an improvement in the fibrinolytic profile in healthy smokers.
P684 Regulation of proteasomal subunit expression byshear stress
N. Wilck, K. Westphal, S. Meiners, V. Stangl, K. Stangl, G. Baumann,A. Ludwig. Charite - University Medicine Berlin, Campus Mitte, Berlin,Germany
Purpose: Physiological laminar shear stress is atheroprotective and crucial fornormal vessel function. Disturbed nonlaminar flow is known to promote oxidativestress, leading to protein oxidation. Accumulation of dysfunctional proteins is pre-vented by degradation via the ubiquitin-proteasome pathway. Accumulating evi-dence suggests a major role for a proteasomal subtype, the immunoproteasome,in controlling the accumulation of damaged proteins. Therefore, we examined theexpression of proteasomal subunits in response to change in shear stress.Methods and Results: Shear stress experiments were performed with HUVECcultivated on petri dishes using a cone-and-plate system. Endothelial cells wereexposed to static conditions, laminar shear stress of 6.0 dyn/cm2 or turbulentshear stress of 10.0 dyn/cm2 for 24 hours with subsequent analysis of mRNAand protein expression of immunoproteasomal subunits (LMP7, LMP2, MECL-1)by Real Time RT-PCR and Western blotting, respectively. Measurement of intra-cellular ROS formation by DCF fluorescence revealed a significant increase underturbulent conditions. Concomitantly, HUVEC exposed to turbulent shear stressshowed a significant up-regulation of immunoproteasomal subunit mRNA expres-sion as compared to static conditions (LMP2: 2.18±0.21 vs. 1.0±0.27; LMP7:1.86±0.58 vs. 1.0±0.82; MECL-1: 2.56±0.47 vs. 1.0±0.60; mean±SEM). In con-trast, laminar shear stress was characterized by down-regulation of immunopro-teasomal subunit mRNA expression as compared to static conditions (LMP2:0.31±0.18 vs. 1.0±0.07; LMP7: 0.58±0.16 vs. 1.0±0.04; MECL-1: 0.66±0.08vs. 1.0±0.1). Results were confirmed by Western blotting.To substantiate this observation with in vivo data, proteasomal subunit expressionwas analysed in aortae of male Dahl salt-sensitive rats (DSSR). On high-salt diet
(HS), DSSR developed significantly increased systolic blood pressure as com-pared to animals on low-salt diet (LS). DHE fluorescence of frozen vessel sectionsrevealed significant increase of superoxide production in the HS group. mRNA ex-pression of immunoproteasomal subunits LMP2 and MECL-1 were shown to beincreased in the HS group compared to LS animals, whereas expression of con-stitutive proteasomal subunits was not significantly different between HS and LSanimals. Results were confirmed by Western blotting.Conclusion: Expression of immunoproteasomes is increased in endothelial cellsin vitro by turbulent shear stress and in vivo in hypertensive rats. Data suggest arole for immunoproteasomes in degradation of dysfunctional proteins under en-hanced oxidative stress.
P685 Knockout of the peroxisome proliferator coactivator 1enhances vascular oxidative stress and endothelialdysfunction during chronic angiotensin II treatment
E. Schulz, S. Schuhmacher, P. Wenzel, M. Oelze, A. Daiber,T. Muenzel. University Medical Center of the Johannes Gutenberg
University Mainz, Mainz, Germany
Background: Peroxisome proliferator coactivator 1 (PGC-1alpha) is an impor-tant mediator of mitochondrial biogenesis and function. In addition, previouswork showed that the AMP-activated protein kinase (AMPK) protects endothe-lial cells against oxidative stress by preservation of mitochondrial function in aPGC-1alpha dependent manner. Since dysfunctional mitochondria might be in-volved in the pathogenesis of vascular disease, we studied the effects of in vivoPGC-1alpha deletion during chronic angiotensin II (ATII) treatment in vivo.Methods and Results: Deletion of PGC-1alpha had no effect on endothelial func-tion or mitochondrial mass under basal conditions. However, chronic angiotensinII (ATII) infusion at subpressor doses (0.1mg/kg/d) resulted in mild endothelialdysfunction, which was markedly impaired in PGC-1alpha knockout mice. In par-allel, oxidative stress was increased in aortic rings from ATII-treated PGC-1alphaknockout mice while serum antioxidative capacity was decreased. We identi-fied mitochondrial respiratory chain, the NADPH oxidase and xanthine oxidaseas responsible ROS sources during PGC-1alpha deletion. Moreover, expressionstudies using real-time PCR revealed increased mRNA expression of NOX2 andNOX4 in aortas from PGC-1alpha knockout mice.Conclusion: In vivo PGC-1alpha deletion during vascular disease impairs en-dothelial function by augmenting oxidative stress. Mitochondrial dysfunction andassociated ROS production might contribute to this process by activation of sec-ondary ROS sources such as NADPH oxidase and xanthine oxidase.
P686 Endothelial progenitor cells (EPCs), circulatingendothelial cells (CECs) and vascular function in renaltransplant recipients patients
F. Cesari1, C. Fatini1, R. Marcucci1, A.M. Gori1, G. Cioni1,M. Salvadori2, M. Zanazzi2 , E. Bertoni2, G.F. Gensini1, R. Abbate1.
1Department of Medical and Surgical Critical Care, Thrombosis Centre,University of Florence, Florence, Italy; 2Renal Unit, Careggi University Hospital,Florence, Florence, Italy
Introduction: Renal transplant recipients (RTRs) patients are at increased risk ofcardiovascular morbidity and mortality. Endothelial dysfunction contributes to ac-celerated atherosclerosis and few data about the number of endothelial progenitorcells (EPCs) and circulating endothelial cells (CECs) in RTRs are available.Aim: To assess the number of EPCs and CECs in a population of RTRs patientsand to establish a relationship between these cells and endothelial function.Methods: In 87 stable renal transplant recipients (M 61, F 26) with a median ageof 51 (23-73) years, we evaluated EPCs, CECs and endothelial function at leastone year after renal transplantation. Circulating EPCs and CECs were measuredby using flow cytometry. EPCs were defined as CD34+KDR+, CD133+KDR+and CD34+CD133+KDR+, while CECs were defined as CD146+/CD31+/CD45-/CD61-. Endothelial function was assessed by using a finger plethysmograph (En-doPAT; Itamar Medical Ltd,Israel).Results: A significant higher number of CECs was detected in RTRs patientswith a previous history of myocardial infarction [20 (10-47) vs. 7 (0-40) cells/106events p=0.020] and in relation with smoking habit [10 (0-47) vs. 7 (0-30) cells/106events) p=0.04]. As regarding EPCs no differences were detected in relation tocardiovascular risk factors, comorbidities or medications.By dividing our patients populations into tertiles of reactivity hyperaemic index(RHI) [1st <1.70; 2nd 1.71-2.30; 3rd >2.30] a significant trend of increase for allthe three types of EPCs was detected [CD34+/KDR+ 1st 0 (0-20) 2nd 3 (0-17)3rd 7 (0-27) cells/106 events p=0.036; CD133+/KDR+ 1st 0 (0-20) 2nd 3 (0-17)3rd 7 (0-30) cells/106 events p=0.036; CD34+/CD133+/KDR+ 1st 0 (0-17) 2nd 3(0-17) 3rd 7 (0-27) cells/106 events p=0.049].Moreover a significant correlation was observed between RHI and EPCs[CD34+/KDR+ and RHI r=0.21 p=0.04; CD133+/KDR+ and RHI r=0.20 p=0.04].As regarding CECs levels, a trend of decrease, albeit not significant, was de-tected by increasing endothelial function [1st 10 (0-47) 2nd 10 (0-40) 3rd 7 (0-30)cells/106 events]. In relation with marker of renal insufficiency a significant andnegative correlation was observed between parathyroid hormone levels (PTH)levels and EPCs [CD34+/KDR+ and PTH r=-0.40 p=0.005; CD133+/KDR+ andPTH r=-040 p=0.005; CD34+/CD133+/KDR+ and PTH r=-041 p=0.004].
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
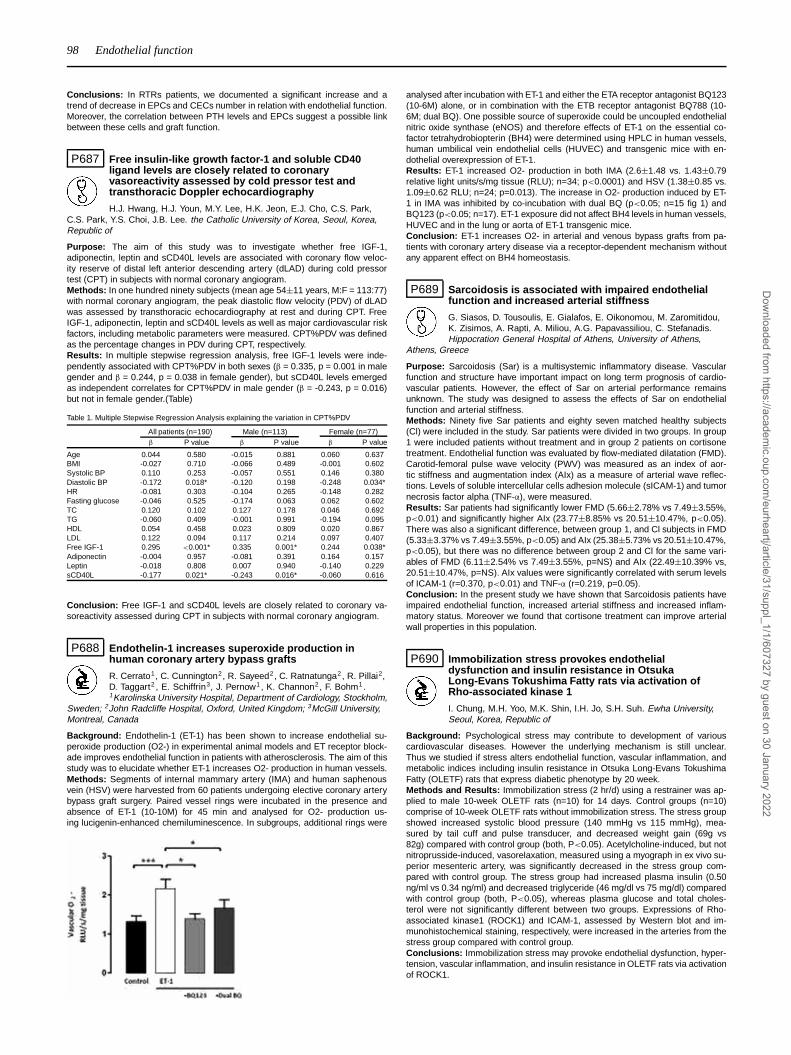
98 Endothelial function
Conclusions: In RTRs patients, we documented a significant increase and atrend of decrease in EPCs and CECs number in relation with endothelial function.Moreover, the correlation between PTH levels and EPCs suggest a possible linkbetween these cells and graft function.
P687 Free insulin-like growth factor-1 and soluble CD40ligand levels are closely related to coronaryvasoreactivity assessed by cold pressor test andtransthoracic Doppler echocardiography
H.J. Hwang, H.J. Youn, M.Y. Lee, H.K. Jeon, E.J. Cho, C.S. Park,C.S. Park, Y.S. Choi, J.B. Lee. the Catholic University of Korea, Seoul, Korea,Republic of
Purpose: The aim of this study was to investigate whether free IGF-1,adiponectin, leptin and sCD40L levels are associated with coronary flow veloc-ity reserve of distal left anterior descending artery (dLAD) during cold pressortest (CPT) in subjects with normal coronary angiogram.Methods: In one hundred ninety subjects (mean age 54±11 years, M:F = 113:77)with normal coronary angiogram, the peak diastolic flow velocity (PDV) of dLADwas assessed by transthoracic echocardiography at rest and during CPT. FreeIGF-1, adiponectin, leptin and sCD40L levels as well as major cardiovascular riskfactors, including metabolic parameters were measured. CPT%PDV was definedas the percentage changes in PDV during CPT, respectively.Results: In multiple stepwise regression analysis, free IGF-1 levels were inde-pendently associated with CPT%PDV in both sexes (β = 0.335, p = 0.001 in malegender and β = 0.244, p = 0.038 in female gender), but sCD40L levels emergedas independent correlates for CPT%PDV in male gender (β = -0.243, p = 0.016)but not in female gender.(Table)
Table 1. Multiple Stepwise Regression Analysis explaining the variation in CPT%PDV
All patients (n=190) Male (n=113) Female (n=77)β P value β P value β P value
Age 0.044 0.580 -0.015 0.881 0.060 0.637BMI -0.027 0.710 -0.066 0.489 -0.001 0.602Systolic BP 0.110 0.253 -0.057 0.551 0.146 0.380Diastolic BP -0.172 0.018* -0.120 0.198 -0.248 0.034*HR -0.081 0.303 -0.104 0.265 -0.148 0.282Fasting glucose -0.046 0.525 -0.174 0.063 0.062 0.602TC 0.120 0.102 0.127 0.178 0.046 0.692TG -0.060 0.409 -0.001 0.991 -0.194 0.095HDL 0.054 0.458 0.023 0.809 0.020 0.867LDL 0.122 0.094 0.117 0.214 0.097 0.407Free IGF-1 0.295 <0.001* 0.335 0.001* 0.244 0.038*Adiponectin -0.004 0.957 -0.081 0.391 0.164 0.157Leptin -0.018 0.808 0.007 0.940 -0.140 0.229sCD40L -0.177 0.021* -0.243 0.016* -0.060 0.616
Conclusion: Free IGF-1 and sCD40L levels are closely related to coronary va-soreactivity assessed during CPT in subjects with normal coronary angiogram.
P688 Endothelin-1 increases superoxide production inhuman coronary artery bypass grafts
R. Cerrato1, C. Cunnington2, R. Sayeed2, C. Ratnatunga2, R. Pillai2,D. Taggart2 , E. Schiffrin3, J. Pernow1, K. Channon2, F. Bohm1.1Karolinska University Hospital, Department of Cardiology, Stockholm,
Sweden; 2John Radcliffe Hospital, Oxford, United Kingdom; 3McGill University,Montreal, Canada
Background: Endothelin-1 (ET-1) has been shown to increase endothelial su-peroxide production (O2-) in experimental animal models and ET receptor block-ade improves endothelial function in patients with atherosclerosis. The aim of thisstudy was to elucidate whether ET-1 increases O2- production in human vessels.Methods: Segments of internal mammary artery (IMA) and human saphenousvein (HSV) were harvested from 60 patients undergoing elective coronary arterybypass graft surgery. Paired vessel rings were incubated in the presence andabsence of ET-1 (10-10M) for 45 min and analysed for O2- production us-ing lucigenin-enhanced chemiluminescence. In subgroups, additional rings were
analysed after incubation with ET-1 and either the ETA receptor antagonist BQ123(10-6M) alone, or in combination with the ETB receptor antagonist BQ788 (10-6M; dual BQ). One possible source of superoxide could be uncoupled endothelialnitric oxide synthase (eNOS) and therefore effects of ET-1 on the essential co-factor tetrahydrobiopterin (BH4) were determined using HPLC in human vessels,human umbilical vein endothelial cells (HUVEC) and transgenic mice with en-dothelial overexpression of ET-1.Results: ET-1 increased O2- production in both IMA (2.6±1.48 vs. 1.43±0.79relative light units/s/mg tissue (RLU); n=34; p<0.0001) and HSV (1.38±0.85 vs.1.09±0.62 RLU; n=24; p=0.013). The increase in O2- production induced by ET-1 in IMA was inhibited by co-incubation with dual BQ (p<0.05; n=15 fig 1) andBQ123 (p<0.05; n=17). ET-1 exposure did not affect BH4 levels in human vessels,HUVEC and in the lung or aorta of ET-1 transgenic mice.Conclusion: ET-1 increases O2- in arterial and venous bypass grafts from pa-tients with coronary artery disease via a receptor-dependent mechanism withoutany apparent effect on BH4 homeostasis.
P689 Sarcoidosis is associated with impaired endothelialfunction and increased arterial stiffness
G. Siasos, D. Tousoulis, E. Gialafos, E. Oikonomou, M. Zaromitidou,K. Zisimos, A. Rapti, A. Miliou, A.G. Papavassiliou, C. Stefanadis.Hippocration General Hospital of Athens, University of Athens,
Athens, Greece
Purpose: Sarcoidosis (Sar) is a multisystemic inflammatory disease. Vascularfunction and structure have important impact on long term prognosis of cardio-vascular patients. However, the effect of Sar on arterial performance remainsunknown. The study was designed to assess the effects of Sar on endothelialfunction and arterial stiffness.Methods: Ninety five Sar patients and eighty seven matched healthy subjects(Cl) were included in the study. Sar patients were divided in two groups. In group1 were included patients without treatment and in group 2 patients on cortisonetreatment. Endothelial function was evaluated by flow-mediated dilatation (FMD).Carotid-femoral pulse wave velocity (PWV) was measured as an index of aor-tic stiffness and augmentation index (AIx) as a measure of arterial wave reflec-tions. Levels of soluble intercellular cells adhesion molecule (sICAM-1) and tumornecrosis factor alpha (TNF-α), were measured.Results: Sar patients had significantly lower FMD (5.66±2.78% vs 7.49±3.55%,p<0.01) and significantly higher AIx (23.77±8.85% vs 20.51±10.47%, p<0.05).There was also a significant difference, between group 1, and Cl subjects in FMD(5.33±3.37% vs 7.49±3.55%, p<0.05) and AIx (25.38±5.73% vs 20.51±10.47%,p<0.05), but there was no difference between group 2 and Cl for the same vari-ables of FMD (6.11±2.54% vs 7.49±3.55%, p=NS) and AIx (22.49±10.39% vs,20.51±10.47%, p=NS). AIx values were significantly correlated with serum levelsof ICAM-1 (r=0.370, p<0.01) and TNF-α (r=0.219, p=0.05).Conclusion: In the present study we have shown that Sarcoidosis patients haveimpaired endothelial function, increased arterial stiffness and increased inflam-matory status. Moreover we found that cortisone treatment can improve arterialwall properties in this population.
P690 Immobilization stress provokes endothelialdysfunction and insulin resistance in OtsukaLong-Evans Tokushima Fatty rats via activation ofRho-associated kinase 1
I. Chung, M.H. Yoo, M.K. Shin, I.H. Jo, S.H. Suh. Ewha University,Seoul, Korea, Republic of
Background: Psychological stress may contribute to development of variouscardiovascular diseases. However the underlying mechanism is still unclear.Thus we studied if stress alters endothelial function, vascular inflammation, andmetabolic indices including insulin resistance in Otsuka Long-Evans TokushimaFatty (OLETF) rats that express diabetic phenotype by 20 week.Methods and Results: Immobilization stress (2 hr/d) using a restrainer was ap-plied to male 10-week OLETF rats (n=10) for 14 days. Control groups (n=10)comprise of 10-week OLETF rats without immobilization stress. The stress groupshowed increased systolic blood pressure (140 mmHg vs 115 mmHg), mea-sured by tail cuff and pulse transducer, and decreased weight gain (69g vs82g) compared with control group (both, P<0.05). Acetylcholine-induced, but notnitroprusside-induced, vasorelaxation, measured using a myograph in ex vivo su-perior mesenteric artery, was significantly decreased in the stress group com-pared with control group. The stress group had increased plasma insulin (0.50ng/ml vs 0.34 ng/ml) and decreased triglyceride (46 mg/dl vs 75 mg/dl) comparedwith control group (both, P<0.05), whereas plasma glucose and total choles-terol were not significantly different between two groups. Expressions of Rho-associated kinase1 (ROCK1) and ICAM-1, assessed by Western blot and im-munohistochemical staining, respectively, were increased in the arteries from thestress group compared with control group.Conclusions: Immobilization stress may provoke endothelial dysfunction, hyper-tension, vascular inflammation, and insulin resistance in OLETF rats via activationof ROCK1.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Endothelial function 99
P691 No clinical complications, but persistent endothelialdysfunction and significantly increased interleukin-18serum levels in a 5-year follow-up of cardiac syndromeX patients
M. Mizia1, K. Mizia-Stec1, M. Mielczarek1, A. Chmiel1, M. Haberka1,J. Janowska2, K. Gieszczyk1, A. Goscinska1, B. Lasota1, Z. Gasior1. 1MedicalUniversity of Silesia, 2nd Department of Cardiology, Katowice, Poland; 2MedicalUniversity of Silesia, Department of Pathophysiology, Katowice, Poland
Background: Cardiac syndrome X (CSX) patients are characterized by endothe-lial dysfunction that seems to be related to metabolic disorders and chronic in-flammation. It is not known yet what is a time-course of endothelial dysfunctionand inflammation and whether it is related to clinical status and treatment of CXSpatients.Aim of the study was to assess clinical data, interleukin-18 (IL-18) serum lev-els and flow-mediated dilatation (FMD) in a 5-year follow-up of CSX patients inrelation to administered therapy.Methods: The study population consisted of thirty CSX patients (M/F=14/16,mean age: 56±10 years) followed-up for five years and 14 healthy individualsas controls (M/F=7/7, mean age: 52±7 years). Our evaluation performed at base-line and after 5 years included clinical status, exercise tolerance test (ETT), high-resolution ultrasound endothelial function parameters (FMD – flow-mediated di-latation, NMD – nitroglycerin-mediated dilatation), transthoracic echocardiogra-phy, and IL-18 serum concentrations (ELISA).Results: CSX patients evaluation after a 5-year period showed similar clinicalsymptoms (CCS), lower positive ETT rate (100 vs 66%, p<0.05), significantlylower LDL-Ch serum levels (123±39 vs 145±39mg/dl; p=0.009), increased LVEF(61±7 vs 58±5%, p=0.037) compared to baseline examination. Twenty eight(93.3%) individuals were hospitalized and eight (26.7%) patients had recurrentcoronary angiography performed within 5 years. Analysis revealed comparableFMD (11.5±9 vs 8.7±5.3%, p=ns), but significantly higher NMD (21.4±13.5 vs15±6.3%, p=0.02) and increased IL-18 serum levels (471±304 vs 243±198pg/dl,p<0.001) obtained after 5-year follow-up compared to the baseline values. In thecontrol group FMD, NMD and IL-18 serum level were as follows: 14.8±5.8%,22.3±6.4%, 272±97pg/dl. There were not significant differences in pharma-cotherapy administered in CSX subjects at the baseline and after 5-year obser-vation. Analysis of CSX patients’ compliance with primary prevention recommen-dations: 21 (70%) patients efficiently achieved goals of the life style recommen-dations and the significant reduction of CCS class, decrease of positive ETT rate,LVMI, and significant increase of LVEF were observed in this subgroup.Conclusions: Five-year observation shows a relatively benign course of CSXwith recurrent symptoms that can be positively modified by non-pharmacologictreatment. Despite pharmacotherapy and compliance with life style recommen-dations, persistent endothelial dysfunction and significant IL-18 serum levels in-crease were found on the control evaluation.
P692 Vitamin D deficiency-induced hypertension isassociated with vascular oxidative stress and alteredgene expression in the heart
J.-F. Argacha1, R. Moreno-Reyes2, D. Egrise2, S. Pochet3 , P. VanDe Borne1, G. Berkenboom1. 1ULB Erasme University Hospital,
Department of Cardiology, Brussels, Belgium; 2ULB Erasme University Hospital,Department of Nuclear Medicine, Brussels, Belgium; 3Free University of Brussels(ULB), Institute of Pharmacy, Lab. of Physiology and Pharmacology, Brussels,Belgium
Aims: Epidemiological studies suggest that Vitamin D deficiency (VDD) is asso-ciated with an increased cardiovascular risk. However, it has not been establishedhow VDD may affect the cardiovascular system. Here, we investigated the effectof VDD on the cardiovascular system in growing male rats fed with a vitamin D-deficient diet.Method and results: We assessed in isolated aorta both superoxide anion andendothelial-dependent relaxations. Microarray technology was used to identifychanges induced by VDD in cardiac gene expression. Compared to control,VDD increases systolic blood pressure (p<0.05) and superoxide anion production(p<0.05) in the aortic wall. However, VDD did not impair endothelial dependentvasorelaxation but tended to slightly improve the maximal relaxation to acetyl-choline from 75±3% to 83±2% (p<0.05). Incubation of aortic rings either with L-NAME alone or L-NAME/catalase did not suppress the enhancement of endothe-lial mediated relaxation observed in vitamin D deficient rats. Only incubation withindomethacin (in the presence of L-NAME) or blockers of calcium-activated potas-sium channels (charybdotoxine plus apamine) abolished the differences betweenthe 2 groups, suggesting a compensatory enhancement via NO- independentpathway. Compared to control, the expression of 53 genes in the heart includingseveral genes involved in the regulation of oxidative stress and the myocardialhypertrophy showed different expression.Conclusions: This experimental study shows that vitamin D deficiency increasesarterial blood pressure, promotes vascular oxidative stress, induces changes incardiac gene expression but does not affect endothelial aorta dependent relax-ation to acetylcholine in the aorta.
P693 Nicorandil, a KATP channel opener, preventspaclitaxel-induced endothelial dysfunction in rats
K. Serizawa1, K. Yogo1, K. Aizawa1, N. Koike1, N. Ishizuka1,H. Ishida2. 1Chugai pharmceutical Co.Ltd, Gotemba Shizuoka, Japan;2Tokai University, Kanagawa, Japan
Background: Despite the excellent anti-restenotic effect of drug-eluting stents,there is a concern of late stent thrombosis due to endothelial dysfunction. Nico-randil (NCR), an anti-anginal drug that induces KATP channel opening and NO-like activity, was reported to have an endothelial protective effect. In this study, weinvestigated the protective effect of NCR on paclitaxel (PTX)-induced endothelialdysfunction in rats.Methods: The % of flow-mediated vasodilation (%FMD) was calculated from achange in diameter of femoral artery after 5 min ligation of iliac artery using ahigh-resolution ultrasound (HRUS) in anesthetized rats. The % of acetylcholine-induced vasodilation (%AchD) and the % of nitroglycerin-induced endothelium-independent vasodilation (%NitD) were calculated from the change of femoralartery after the drug treatments using the HRUS. The %FMD, %AchD and %NitDwere measured, after PTX (5 mg/kg/day) was continuously infused for 7 daysusing an osmotic pump. NCR (15 mg/kg/d), diazoxide (15 mg/kg/d), isosorbidedinitrate (ISDN, 15 mg/kg/d) and tempol (20 mg/kg/d) were orally administratedduring PTX infusion.Results: PTX-treatment significantly reduced both %FMD and %AchD, reduc-tions that were prevented by NCR (Figure). On the other hand, neither PTX norNCR had an effect on %NitD. The reduction of %FMD with PTX was preventedby diazoxide and tempol but not by ISDN (% diazoxide: 18±2, tempol: 18±4,ISDN: 6±1%, n=6-7). PTX increased the mRNA of NADPH oxidase components(p47phox and gp91phox) in the femoral artery, the increase of which was inhibitedby NCR.
Conclusion: These results suggested that PTX-induced endothelial dysfunctionvia an increase in oxidative stress and indicated that NCR prevented PTX-inducedendothelial dysfunction through KATP channel activation.
P694 Effects of the angiotensin II type-1 receptor antagonisttelmisartan on endothelial activation induced byadvanced glycation endproducts
S. Del Turco1, T. Navarra1, G. Basta1, R. De Caterina2. 1Institute ofClinical Physiology of CNR, Pisa, Italy; 2G. D’annunzio, Chieti, Italy
Background: A crosstalk between advanced glycation end products (AGEs),their main receptor (RAGE) and the renin-angiotensin system (RAS) has beenproposed in the pathogenesis of diabetic vascular complications. Telmisartan, anangiotensin II receptor blocker (ARB), has shown a number of pleiotropic effectsin experimental and clinical studies, including anti-inflammatory and antioxidantproperties on the endothelium. We studied the effects of telmisartan on adhesionmolecule expression induced by AGEs or TNF-α in human vein endothelial cells(HUVEC), and the involvement of intracellular reactive oxygen species (ROS).Methods and Results: HUVEC were pretreated with or without losartan ortelmisartan (1, 10 μmol/L) for 30 minutes and stimulated with AGEs (200 μg/mL)or the inflammatory cytokine TNF-α (10 ng/mL) for 18 h to induce vascular ad-hesion molecule-1 (VCAM-1) and intercellular molecule-1 (ICAM-1), and for 10 hto induce E-Selectin expression. Adhesion molecule expression was measuredby surface enzyme immunoassay and intracellular ROS production by the fluo-rescent probe 6-carboxy-2’-7’-dichlorofluoresceine. Telmisartan reduced VCAM-1 expression induced by AGEs (-33%±11% at 10 μmol/L, P<0.001) or TNF-α(-20%±5% at 10 μmol/L, P<0.05), but not of ICAM-1 expression. Telmisartan(10 μmol/L) per se increased E-Selectin expression in a concentration depen-dent manner after TNF-α stimulation (+58%±6% at 10 μmol/L, P<0.001), butprevented its induction by AGEs (-40%±7%, P<0.001). Telmisartan (10 μmol/L)prevented the increase of intracellular ROS after AGEs stimulation (-81%±6%,P<0.05), but not after TNF-α stimulation. Losartan and its active metabolite EXP-3174 used as control, were ineffective in reducing adhesion molecule expressionand ROS production by both AGEs or TNF-α, suggesting a receptor-independenteffect of telmisartan.Conclusions: These results suggest that telmisartan has peculiar regulatorymechanisms on adhesion molecule expression and ROS production induced byeither AGEs or TNF-α. Such anti-inflammatory and antioxidant properties maydisclose a role for this drug in the pro-atherogenic vascular milieu occurring indiabetes.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

100 Endothelial function
P695 Decreased C-type Natriuretic peptide and increasedAsymmetric Dimethylarginine have an additiveunfavourable effect on arterial function and structure
N. Ioakeimidis, C. Vlachopoulos, D. Terentes-Printzios, K. Baou,I. Dima, N. Alexopoulos, A. Samentzas, K. Rokkas, D. Tousoulis,
C. Stefanadis. Hippokration Hospital, University of Athens, 1st Department ofCardiology, Athens, Greece
Purpose: Asymmetric dimethylarginine (ADMA), an endogenous inhibitor of ni-tric oxide (NO) synthase, is a determinant of endothelial dysfunction and C-typenatriuretic peptide (CNP) which is highly expressed in vascular endothelium islikely to exert a strong antiatherogenic activity that might be a key in compensat-ing for deficiencies in NO. In this study, we investigated the combined effect ofhigh ADMA and low CNP levels on arterial function and structure.Methods: ADMA and N-terminal fragment CNP (NT-proCNP) levels were mea-sured 116 consecutive men (mean age 57 years). Aortic stiffness was evaluatedwith carotid-femoral pulse wave velocity (PWV), endothelial function with flow-mediated dilatation of the brachial artery (FMD) and early atherosclerosis withcarotid IMT. The distributions of ADMA and NT-proCNP were split by the median(0.62 μmol/L and 0.23 pmol/L, respectively) and accordingly subjects were strat-ified into those with high and low values.Results: Stepwise regression analysis revealed that ADMA, CNP and the inter-action of ADMA with CNP were independent predictors of FMD, PWV and IMT.The significant interaction between high ADMA and low CNP on arterial struc-ture and function. is additionally reflected by the finding that the subgroup of highADMA/low CNP exhibited the lower FMD and the higher PWV and IMT valuescompared with the subgroups of high ADMA/high CNP, low ADMA/low CNP, andlow ADMA/high CNP after adjustment for age and blood pressure (figure).
NT-proCNP, ADMA and vascular function
Conclusions: Increased ADMA in conjunction with low CNP levels exert an addi-tive detrimental effect on arterial function and structure, accelerating the vascularageing process and promoting atherosclerosis.
P696 Effects of atorvastatin and lisinopril on endothelialdysfunction
M.G. Kaya, T.I. Inanc, N. Kalay, T. Heyit, I. Ozdogru, A. Dogan,M. Duran, A. Kasapkara, O. Gunebakmaz, A. Oguzhan. ErciyesUniversity School of Medicine, Department of Cardiology, Kayseri,
Turkey
Objective: Behcet’s disease is a chronic inflammatory vasculitis. Vascular in-volvement is one of the major complications of Behcet disease, during the courseof the disease. Previous studies showed that ACE inhibitors and statins may im-prove endothelial functions in endothelial dysfunction. The aim of our study is tocompare the effects of atorvastatin and lisinopril to placebo on endothelial dys-function in patients with Behcet’s diseasePatients and methods: We prospectively studied 92 (48 females) Behcet’s pa-tients diagnosed according to the International Study Group criteria. Endothe-lial dysfunction was evaluated by brachial artery flow-mediated dilatation (FMD)method using high-resolution vascular ultrasound device at baseline and afterfor 3 months therapy. Patients were consecutively randomized into three groupsas (atorvastatin (n=31), lisinopril (n=31) and placebo groups (n=30). Patients inatorvastatin group received 20 mg atorvastatin, lisinopril group received 10 mglisinopril per day, and placebo group received placebo per a day for 3 months.Results: The baseline characteristics of patients were similar among threegroups; however, hs-CRP levels were lower in atorvastatin group than placebogroup. A significant improvement in FMD was observed in both atorvastatin(5.0±1.4 vs. 12.8±3.6%, p<0.001) and lisinopril groups (5.0±1.2 vs. 11.4±5.0%,p<0.001). Partial significant enhancement was observed in placebo group(4.8±1.1% vs. 5.7±1.0, p=0.002)., However, it was lower than the cut-off valuefor endothelial dysfunction.Conclusion: These findings suggest that atorvastatin and lisinopril improveendothelial functions in Behcet’s disease patients. However, large studies areneeded to determine the long-term effects of atorvastatin and lisinopril therapy.
P697 Vaccination against influenza A/H1N1 virus adverselyaffects endothelial function in HIV infected patients
P. Xaplanteris1, C. Vlachopoulos1, H. Sambatakou2, I. Mariolis2,D. Terentes-Printzios1, C. Stefanadis1 . 1Hippokration Hospital,University of Athens, 1st Department of Cardiology, Athens, Greece;
2University of Athens Medical School, Hippokration General Hospital, Athens,Greece
Purpose: Vaccines have been shown to induce a transient impairment of en-dothelial function and arterial elastic properties. Newly developed vaccinesagainst the pandemic influenza A/H1N1 virus have been reported to have a safecardiovascular profile; however, their impact on endothelial function and arterialstiffness has not been established.Methods: We recruited 14 HIV infected patients (all male, 3 naïve to antiretroviraltherapy, mean age 35±10 years) with a good functional status (mean CD4 count:719±273). All were free from overt cardiovascular disease. Flow mediated dilata-tion (FMD) of the brachial artery was used as an index of endothelial function;carotid-femoral pulse wave velocity (cfPWV) as a measure of arterial stiffness.Measurements were taken prior to, 8 and 48 hours post vaccination. A singledose of a monovalent, adjuvanted vaccine against influenza A/H1N1 was used.Comparisons were performed by repeated measures ANOVA.Results: Vaccination led to a significant impairment of endothelial function, de-noting a diminished bioavailability of nitric oxide that persisted even after 48h(baseline: 6.5±4.8%, 8h: 2.3±4.9%, 48h: 1.8±4.8%; p=0.05). However, arterialstiffness, as assessed by cfPWV, was not significantly altered (baseline: 7.2±1.2m/sec, 8h: 7.0±1.2 m/sec, 48h:6.8±0.9 m/sec; p=ns).
Flow mediated dilatation
Conclusion: Vaccination against influenza A/H1N1 with a monovalent, adju-vanted vaccine leads to endothelial dysfunction in HIV patients, which lasts forat least 48 hours. Given the increased cardiovascular risk of these patients, thesefindings warrant further research.
P698 The effects of long-term atorvastatin treatment onendothelial function in patients with coronary arterydisease and diabetes mellitus type II
S.H. Chumburidze, T. Shavdatuashvili, G. Shelia. Academician NodarKipshidze National Center of Therapy, Tbilisi, Georgia, Republic of
The aim of this study was to evaluated the effects of long-term atorvastatin treat-ment on endothelial function in patients with coronary artery disease (CAD) anddiabetes mellitus type II.Methods: This was a randomized, double blind, placebo controlled trial with ator-vastatin (Liprimar, Pfizer, USA) (20 mg) administered once daily. 120 patients(aged 40 - 79 years) were randomly assigned to one two treatment group, re-ceiving either atorvastatin (n=60) or placebo (n=60). The flow- mediated dilation(FMD; endothelium dependent) and nitroglycerin-induced dilation (endotheliumindependent) in the brachial artery and the vascular reactivity at the forearm skinwere measured. Background therapy was similar for group. Duration of the studywas 1 year.Results: At the end of the study there were significant and sustained decreasesin plasma level of total (31%), LDL cholesterol (41.6%), triglycerides (25.09%), fib-rinogen (30.12%) and increases in HDL cholesterol level (14.39%) in the atorvas-tatin group compared with the placebo group. At 1 year plasma CRP decreased inthe atorvastatin group compared with baseline (P < 0.05). FMD improved in theatorvastatin-treated subjects when compared with the placebo-treated subjects(atorvastatin, from 3.7±8.5% to 9.8±7.3%; placebo, from 3.9±5.6% to 4.7±4.2%;P= 0.001). No changes were observed in nitroglycerin-induced dilation and themicrocirculation reactivity measurements in either group. The percent changein endothelium-dependent vasodilatation at 1 year correlated with the percentchange in CRP (r = -0.44; P < 0.05), but not with changes in plasma lipids. Ther-apy with atorvastatin was well tolerated.Conclusion: our results suggest that treatment with atorvastatin in patients withcoronary artery disease and type 2 diabetes led to a significant improvementin endothelium-dependent vasodilation, which might be partly related to its anti-inflammatory effect
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Endothelial function 101
P699 Interrelationships of soluble receptor for advancedglycation end products with asymmetricdimethylarginine and arterial stiffness in essentialhypertension: a novel insight into atherosclerosis
K. Dimitriadis, C. Tsioufis, M. Poulakis, L. Lioni, D. Flessas,E. Stefanadi, A. Kasiakogias, D. Tousoulis, C. Stefanadis. First Cardiology Clinic,University of Athens,Hippokration Hospital, Athens, Greece
Purpose: The soluble receptor for advanced glycation end products (sRAGE)participates in the pathogenesis of vascular disease, while arterial stiffening andasymmetric dimethylarginine (ADMA) are related to atherosclerosis progressionand diffuse endothelial dysfunction. In the present study, we investigated the rela-tionships of sRAGE with ADMA and arterial stiffness in essential hypertensives.Methods: Our population consisted of 320 newly diagnosed untreated non-diabetic patients with stage I to II essential hypertension [192 men, mean age=52years, office blood pressure (BP)=145/93 mmHg]. In all participants, arterial stiff-ness was evaluated on the basis of carotid to femoral pulse wave velocity (PWV),by means of a computerized method (Complior SP) and venous blood samplingwas performed to estimate metabolic profile, ADMA and sRAGE levels. The distri-bution of sRAGE was split by the median (1060.1 pg/ml) and accordingly subjectswere stratified into those with high and low values.Results: Patients with low sRAGE (n=164) compared to those with high sRAGEvalues (n=156) had greater body mass index (29.7±4.5 vs 27.1±2.5 kg/m2,p<0.05) and 24-h systolic BP (139±8 vs 131±6 mmHg, p=0.001), while didnot differ regarding metabolic profile (p=NS for all). Moreover, patients with lowsRAGE compared to those with high sRAGE levels exhibited higher ADMA(0.59±0.06 vs 0.51±0.05 μmol/l, p<0.0001) and PWV (9±1.7 vs 7.5±1.2 m/sec,p<0.0001). In the total population, sRAGE was associated with body mass index(r=-0.245, p=0.006), waist to hip ratio (r=-0.462, p<0.0001), 24-h pulse pressure(r=-0.371, p=0.001), ADMA (r=-0.366, p=0.004) and PWV (r=-0.401, p<0.0001).Regarding ADMA, it was related to waist to hip ratio (r=0.324, p=0.004), 24-hsystolic BP (r=0.491, p<0.0001) and PWV (r=0.487, p<0.0001). Multiple regres-sion analysis revealed that body mass index, 24-h systolic BP and ADMA werethe independent predictors of sRAGE (R2=0.44, p<0.0001). Furthermore, analy-sis of covariance showed that ADMA and PWV values were significantly differentbetween groups even after adjustment for confounders (p<0.05).Conclusion: In essential hypertension, attenuated sRAGE levels are associatedwith increased PWV and pronounced endothelial dysfunction. Moreover, the closerelation of sRAGE with arterial stiffening and ADMA, support the potent role ofsRAGE in vascular atherosclerotic disease progression.
P700 Sphingosine 1-phosphate is a bioactive lipid thatconfers high-density lipoprotein with vascularprotection mediated by endothelium-dependentvasodilation
T. Sugiura1, Y. Dohi1, S. Yamashita1, R. Ohkawa2, Y. Yatomi2,G. Kimura1, S. Fujii3. 1Nagoya City University Graduate School
of Medical Scinece, Nagoya, Japan; 2The University of Tokyo, GraduateSchool of Medicine, Tokyo, Japan; 3Nagoya City University Graduate School ofPharmaceutical Sciences, Nagoya, Japan
Introduction: High-density lipoprotein (HDL) exerts atheroprotective effect by re-verse cholesterol transport. HDL is the major carrier in serum of sphingosine 1-phosphate (S1P), a potent bioactive lipid responsible for vascular cell responsesincluding activation of endothelial nitric oxide synthase in endothelial cells andsmooth muscle cells in vitro. Whether HDL-associated S1P favorably regulatesvascular function in patients has not been demonstrated. Accordingly, we testedwhether HDL exerts part of its antiatherogenic effect by S1P in vivo.Methods: Blood was sampled from 20 untreated patients (42 (mean) ± 9(SD) years, male/female=18/2) with low levels of cardiovascular risk factors(blood pressure 135±12/86±10 mmHg) and without any cardiovascular disease.Plasma S1P and dehydro-S1P (DHS1P), another bioactive product of sphingo-sine kinase, levels were measured by HPLC after fluorescent derivatization witho-phthaldialdehyde. At the same time, endothelium-dependent vasodilation, amarker of endothelial function, was measured by flow-mediated dilation (FMD)using ultrasound system, and endothelium-independent vasodilation was mea-sured by glycerol trinitrate-induced dilation (GTD).Results: Plasma S1P level (322±76 nmol/L) was higher than DHS1P level(131±35 nmol/L). S1P levels positively correlated with the level of HDL (58±15mg/dl, r=0.556, p<0.01), and FMD values (3.5±1.6%, r=0.465, p<0.05). S1P lev-els were not correlated with the level of LDL (113±30 mg/dl, r=0.204, p=0.39)or GTD (14.7±3.9%, r=0.418, p=0.67). The level of S1P correlated with hema-tocrit level (46.2±3.6, r=0.540, p<0.05), but not with platelet counts (25.1±4.6,r=0.327, p=0.16). On the other hand as compared with S1P, DHS1P level hadweaker correlations with the level of HDL (r=0.290, p=0.218) and FMD values(r=0.401, p=0.08).Conclusions: Plasma S1P level was closely correlated with the level of HDL, theindex of vascular endothelial function. These results suggest that HDL-associatedS1P is responsible for at least part of the beneficial effects of HDL on vessels.S1P analogues may become a new class of functional HDL mimetic for integratedpatho-biology and cardiovascular therapy. Plasma S1P may be a candidate for anew anti-atherosclerotic biomarker.
P701 Low serum testosterone levels within the referencerange are associated with a decrease of endothelialfunction. Results from the population-based Study ofHealth in Pomerania (SHIP)
K. Empen1, R. Lorbeer2, M. Dorr1, R. Ewert1, H. Volzke2,H. Wallaschofski3, S.B. Felix1. 1Ernst Moritz Arndt University of Greifswald,Department of Internal Medicine B, Greifswald, Germany; 2Ernst Moritz ArndtUniversity of Greifswald, Institute of Community Medicine, Greifswald, Germany;3Ernst Moritz Arndt University of Greifswald, Institute for Clinical Chemistry andLaboratory Medicin, Greifswald, Germany
Purpose: To assess the association between serum testosterone in men and en-dothelial function as measured by flow-mediated dilation (FMD) and nitroglycerin-mediated dilation (NMD) of the brachial artery.Methods: The study population comprised 722 men aged 25 to 85 years from thepopulation-based Study of Health in Pomerania (SHIP). Serum total testosteroneand sexual hormone binding globulin (SHBG) levels were determined by chemilu-minescence immunoassays. Free testosterone levels were calculated accordingto the law of mass action, using measured total testosterone and SHBG levels.FMD and NMD measurements were performed using standardized ultrasoundtechniques. FMD and NMD values below the 20th percentile were considereddecreased.Results: Multivariable logistic regression analyses revealed an association for de-creased FMD with each decrement of total testosterone standard deviation afteradjustment for major potential confounders including waist circumference, smok-ing status, liver, renal disease, and serum low density lipoprotein (LDL) choles-terol (odds ratio 1.28, 95% confidence interval 1.02-1.60; p=0.030). The findingsfor free testosterone were similar: odds ratio 1.33, 95% confidence interval 1.04-1.71; p=0.023. There were no such associations with respect to SHBG in theage-adjusted or in the fully adjusted model. Neither serum total testosterone norfree testosterone nor SHBG were significantly associated with decreased NMD.Conclusion: Lower serum total and free testosterone levels are associated withdecreased FMD. This association might represent a possible link to increasedcardiovascular morbidity and mortality.
P702 Age-related changes in the angiotensin II-inducedvasomotor activity
A. Koller1, Z. Vamos1, P. Cseplo1, P. Toth1, B. Rozsa1, J. Hamar2.1University of Pecs, Medical School, Department of Pathophysiologyand Gerontology, Pecs, Hungary; 2New York Medical College, Dept of
Physiology, Valhalla, United States of America
The primary hormone of the renin-angiotensin-aldosterone system (RAAS) isangiotensin II (Ang II), which is responsible not only for immediate physiologi-cal effects, such as vasoconstriction, but promotes smooth muscle cell growth,hypertrophy, cell migration and events that contribute to normal and pathologictissue function and most importantly to the development of hypertension.Although Ang II-induced vasomotor responses have been extensively investi-gated, less is known regarding the potential aging-induced changes in the mag-nitude of vasomotor responses. We hypothesized that aging induces changes inthe magnitude of vasomotor responses to Ang II.Thus carotid arteries were isolated from newborn (8 days: 8d), young (1 and2 months: 1-, 2m), adult (6-, 9-, 12 months: 6-, 9-, 12m) and old (24 months:24m) rats and placed in a wire myograph and changes in isometric tension weremeasured. Dose response curves to Ang II were obtained in each age group.Peak contractions of vessels from 8d rats to Ang II (1.4±0,2 mN vs.) increased asa function of age, which were similar in magnitude, 2,8±0.7, 4.2±0.9, 5.3±0.5,5,8±0.8, 5.2±0.6 and 5.7±0.4 mN, in vessels from 1-, 2-, 6-, 9-, 12- and 24months rats, respectively). In contrast, the area of under the Ang II contractioncurve from vessels of 8d rats (75±2 cm2), decreased as a function of age (in 1mvessels: 55±1cm2 and in 24m vessels: 45±7 cm2).Compared to the first administration, contractions of vessels to 2nd and 3rdadministrations of Ang II were significantly reduced in vessels from 2 months(3,9±0.4 and 3.7±0.4 mN), 6 months (3.6±1 and 3.4±1 mN, 9 months (1,3±0.5and 1.2±0.4 mN), 12 months (1.8±0,4 and 1.6±0.4 mN) and 24 months(1.05±0.4 and 1.02±0.3 mN) rats, but not in vessels from 1 month (2.4±0.5 and2.3±0.2 mN) and 8 days (1.4±0,2 and 1,5±0,1 mN) rats.In conclusion, these findings suggest that aging has substantial effects on Ang II-induced vasomotor activity. The peak contraction increases, whereas the durationof response decreases with age. Moreover, a substantial tachyphylaxis developswith age. These findings indicate that aging may alter the number and functionof angiotensin II receptors, which can alter not only Ang II-induced vasomotoractivity, but also various signaling mechanisms attached to these receptors, all ofwhich may have clinical significance.
P703 Glucagon-Like Peptide 1 prevents endothelial cellsenescence through the activation of protein kinase A
H.H.W. Sillje, H. Oeseburg, R.A. De Boer, H. Buikema, P. VanDer Harst, W.H. Van Gilst. University medical center Groningen,Groningen, Netherlands
Purpose: Endothelial cell senescence is an important contributor to vascular ag-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

102 Endothelial function / Lipids
ing and is increased under diabetic conditions. In this study we investigated ifthe anti-diabetic hormone, GLP-1, could prevent oxidative stress induced cellularsenescence in endothelial cells.Methods: Vascular senescence was investigated in Zucker Diabetic Fatty (ZDF)rats with or without DPP-4 inhibitor (vildagliptin) treatment. The molecular mech-anisms were investigated using endothelial HUVEC cells in which cellular senes-cence was induced by oxidative stress (H2O2).Results: As compared to lean animals, ZDF rats had a significant 2.0 fold higherlevel of vascular senescence and vildagliptin treatment reduced this to almost nor-mal, lean animal, levels. This effect appeared to be glycemic control independent,since plasma glucose and insulin levels did not change in the treated animals. Invitro studies with HUVEC cells showed that GLP-1 had a direct protective effectand was able to attenuate oxidative stress induced DNA damage and cellularsenescence. The GLP-1 analogue exendin-4 provided similar results, whereasexendin (9-39), a GLP-1 antagonist, abolished this effect. Analysis of the GLP-1-receptor downstream signaling pathways revealed that cAMP/PKA signaling wasboth sufficient and essential for the GLP-1 mediated protective effect. In con-trast to other cell types, the PI3K/Akt kinase survival pathway was not involvedin GLP-1 mediated protection in HUVEC cells. Moreover, nitric oxide generationwas not required for the GLP-1 protective effect; distinguishing it from many otherendothelial protective agents.Conclusions: Here we showed that GLP-1 protects against vascular senescencein a diabetic rat model. In vitro studies with HUVEC cells showed that his effectwas GLP-1 receptor mediated, required PKA activity, but was independent fromthe established Akt and nitric oxide survival pathways.
P704 The effect of nebivolol treatment on endothelial anderectile functions in hypertensive men
B. Ozben Sadic1, U. Kefeli1, A. Cincin1, O. Baykan1, O. Ozgur2,C. Akbal2, Y. Basaran1, O. Yesildag1. 1Marmara University, Facultyof Medicine, Department of Cardiology, Istanbul, Turkey; 2Marmara
University, Faculty of Medicine, Department of Urology, Istanbul, Turkey
Purpose: Impaired nitric oxide (NO) bioactivity is a major pathogenic mechanismin both endothelial and erectile dysfunction. Nebivolol, a third-generation beta-blocker, causes vasodilatation via interaction with the endothelial L-arginine/nitricoxide (NO) pathway. The aim of this study is to evaluate the effects of nebivololon endothelial and erectile functions in hypertensive male patients.Methods: Forty hypertensive male patients (mean age: 53.5±10.1 years) whowere given nebivolol 5mg/day and had complaints of erectile dysfunction wereconsecutively recruited into the study. Endothelial and erectile functions were as-sessed by brachial arterial flow-mediated dilation (FMD) and International Indexof Erectile Functions questionaire, respectively at the baseline, first month andthird month of therapy.Results: The response of blood pressure, heart rate, endothelial and erectilefunctions to nebivolol therapy are presented in Table 1. Both the FMD values anderectile function scores at the third month of therapy were significantly higher thanthe basal values. Nebivolol decreased the number of patients with FMD values <
10% (26 vs 14, p= 0.012) and the number of patients with severe to moderateerectile dysfunction (erectile function scores ≤ 21) (38 vs 26, p<0.001) at the endof the study. There was not any significant correlation between FMD measuresand erectile function scores.
Table 1. The response of blood pressure, heart rate, endothelial and erectile functions to nebivololtherapy
Baseline 1st Month 3rd Month p
Systolic blood pressure (mmHg) 156.5±18.9 143.8±17.7 132.4±13.5 <0.001Diastolic blood pressure (mmHg) 83.1±10.5 80.3±10.9 80.1±9.2 0.061Heart rate (/min) 76±10 72±10 70±8 <0.001Baseline velocity (cm/s) 48.25±13.36 46.75±11.28 46.95±12.62 0.402Baseline diameter (mm) 3.98±0.52 3.88±0.52 3.94±0.55 0.052Post-ischemic flow velocity (cm/s) 106.49±25.23 106.67±28.83 115.83±26.53 0.001FMD absolute (mm) 0.31±0.14 0.38±0.16 0.46±0.16 <0.001FMD percentage (%) 7.98±3.76 9.94±4.44 12.14±4.75 <0.001Erectile function scores 11.2±7.2 13.6±7.3 16.4±8.5 <0.001
Conclusions: Nebivolol improved both the endothelial and erectile dysfunction;thus might be considered in hypertensive male patients with complaints of erectiledysfunction.
LIPIDS
P705 Lipid profile of essential hypertensive patients withminor thalassemia trait
S.-M. Kyvelou1, G. Vyssoulis1, E. Karpanou2, V. Tzamou1,D. Adamopoulos1 , T. Gialernios1, C. Stefanadis1 . 1HippokrationGeneral Hospital, Athens, Greece; 2Onassis Cardiac Surgery Center,
Athens, Greece
Purpose: Minor thalassemia is associated with decreased risk of arterial hyper-tension and myocardial infraction, mainly in men. In the general population, totalcholesterol and LDL levels are lower in patients with minor thalassemia, as is
the blood viscosity. The purpose of the present study was to investigate the lipidprofile of essential hypertensive patients with minor thalassemia in comparison toanemic and non-anemic hypertensives.Methods: The study comprised of 20964 consecutive, essential hypertensive pa-tients who referred to our hypertension clinics for blood pressure control. All studyparticipants were subjected to full clinical and laboratory evaluation. Lipid pro-file was assessed by the measurements of total cholesterol (TC), LDL and HDLcholesterol, triglycerides (TGL) apolipoproteins A and B (ApoA, ApoB, lipoproteina (Lpa) and TC/HDL, ApoB/ApoA, TGL/HDL ratios. Patients under lipid loweringtreatment were excluded from the study. Minor thalassemia trait was assessed bypatients’ medical history and confirmed by laboratory examination.Results: The study population was divided in three groups: group I (n=419,minor thalassemics), group II (n=1665, anemic) and group III (n=18880, non-anemic). Patients in group I presented with significantly lower TC, LDL, TGL,ApoB, ApoB/ApoA ratio, Lpa, TC/HDL ratio and TGL/HDL ratio in comparisonto groups II and III [(193 vs 208 vs 221.5, p<0.001), (122.3 vs 134.4 vs 146.8,p<0.001), (102 vs 122.9 vs 127.5, p<0.001), (105.6 vs 118.1 vs 127.3, p<0.001),(0.72 vs 0.82 vs 0.88, p<0.001), (20.5 vs 23.4 vs 24.3, p=0.003), (4.06 vs 4.49 vs4.75, p<0.001) and (2.28 vs 2.79 vs 2.87, p<0.001) respectively]. In multivariateanalysis, after adjustment for age, gender, BMI, hemoglobin, office BP, smokingstatus, eGFR and glucose the differences in TC, LDL, TGL, ApoB, ApoB/ApoA,HDL, TC/HDL, and TGL/HDL remained significant (R2=0.23, p<0.001).Conclusions: Hypertensive patients with minor thalassemia present with a bet-ter lipid profile in comparison to anemic and non-anemic hypertensives. Thesedifferences are independent and strong and thus it can be hypothized that theprotective effect of the thalassemia trait is mediated through favorable lipid pro-file.
P706 Patients with precocious coronary artery disease showdecreased transfer of free cholesterol toHigh-Density-Lipoprotein (HDL)
F.R.S. Freitas, C.C. Strunz, A.J. Mansur, A.P. Mansur, R.C. Maranhao.Heart Institute (InCor) - University of Sao Paulo Faculty of Medicine
Clinics Hospital, Sao Paulo, Brazil
Purpose: Lipid transfer among lipoprotein classes is mediated by transfer pro-teins such as CETP and PLTP. Formation and metabolism of HDL are largelydependent on lipid transfers to the lipoprotein and are important for HDL role inreverse cholesterol transport and anti-atherogenic functions. Currently, we testedthe hypothesis whether defective lipid transfers to HDL could be related with pre-cocious coronary artery disease (CAD).Methods: Forty-five CAD patients (20 males) were compared with 45 non-CADhealthy controls (20 males), all aged 45-55 yrs. Fasting plasma samples wereincubated for 1 h at 37°C with an artificial donor nanoemulsion labeled with 4radioactive lipids and after chemical precipitation of the nanoemulsion and non-HDL fractions, HDL contained in supernatant was counted for radioactivity andestimation of % transfer from the donor nanoemulsion to HDL.Results: HDL and LDL cholesterol were equal in both groups, but triglycerideswere higher in CAD (157±80mg/dl) than in controls (112±37mg/dl, p<0.002).Transfer of free-cholesterol to HDL was lower in CAD (3.9±1.1%) than in con-trols (7.8±3.5%, p<0.0001). Triglyceride transfer was also lower in CAD (3.8±1.6vs 5.2±1.7%, p<0.0007) but cholesteryl ester transfer was higher (6.4±2.2 vs4.6±1.7%, p<0.0001), whereas phospholipid transfer was equal (17.9±3.6 vs19.2±3.6, NS).Conclusion: Defective free-cholesterol transfer to HDL may alter cholesterol es-terification and reverse cholesterol transport that are major HDL anti-atherogenicfunctions. Alterations in triglyceride and cholesteryl ester transfer to HDL may alsodestabilize the lipoprotein and may contribute to precocious CAD. Those findingsmay serve as disease markers and eventually as therapeutic targets.
P707 Lipids, apolipoproteins and their ratios in relation toarterial stiffness in never-treated hypertensives
D. Terentes-Printzios1, C. Vlachopoulos2, G. Vyssoulis1,N. Alexopoulos1, K. Aznaouridis1, N. Ioakeimidis1, P. Pietri1, I. Dima1,A. Samentzas1, C. Stefanadis1. 1Hippokration Hospital, University of
Athens, 1st Department of Cardiology, Athens, Greece; 2Hippokration GeneralHospital, Athens, Greece
Purpose: Hypertension is associated with increased arterial stiffness. Arterialstiffness, which is a predictor of cardiovascular risk, has been shown to correlatewith lipid profile. However, the effect of alternative measures of lipid profile otherthan low-density lipoprotein (LDL) remains unknown. We assessed the hypothe-sis that arterial stiffness is associated with alternative measures of lipid profile.Method: We enrolled 1225 consecutive essential hypertensives (mean age52.9±11.7 years, 728 males), who did not receive any lipid-lowering treatment.Arterial stiffness was determined with carotid-femoral pulse wave velocity (PWV)using the Complior® device. Levels of total cholesterol, LDL cholesterol, non–high-density lipoprotein (HDL) cholesterol, and apolipoprotein B, as well as ra-tios of total/HDL cholesterol, LDL/HDL cholesterol, and apolipoprotein B/A-I weremeasured in venous blood samples or calculated, accordingly.Results: In multivariable regression analysis, apolipoprotein B/A-I ratio, LDL andtotal/HDL cholesterol ratio exhibited significant positive association with PWV,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Lipids 103
which was independent of age, gender, mean blood pressure, smoking habits,body-mass index, presence of diabetes, triglycerides, C-reactive protein and allthe aforementioned measures of lipid profile (p<0.001, p<0.001 and p<0.05, ad-justed R2 of model=0.402). In further analyses we employed dichotomous out-come variable (PWV ≥75th percentile [9.1 m/s]). Receiver operating character-istic (ROC) curves were generated to evaluate the ability of apolipoprotein B/A-Iratio, LDL and total/HDL cholesterol ratio to discriminate subjects with and withoutsignificant arterial stiffness. The area under the curve (AUC) and 95% CIs of theROC curves for apolipoprotein B/A-I ratio, LDL and total/HDL cholesterol ratio forprediction of significant arterial stiffness (PWV ≥75th percentile [9.1 m/s]) wereAUC=0.64 (95% CI: 0.61-0.67, p<0.001), AUC=0.53 (95% CI: 0.50-0.57, P=0.07)and AUC=0.58 (95% CI: 0.55-0.62, p<0.001). AUC for apolipoprotein B/A-I ratiowas significantly greater than AUCs for LDL (p<0.001) and total/HDL cholesterolratio (p<0.001). AUC for total/HDL cholesterol ratio was significantly greater thanAUC for LDL (p<0.01).Conclusions: Higher apolipoprotein B/A-I and total/HDL ratios are independentpredictors of increased arterial stiffness in never-treated essential hypertensivesand predict increased arterial stiffness better than LDL. These findings strengthenthe clinical usefulness of measurements of lipid profile other than LDL and provideinsights for optimal study design and data interpretation.
P709 Increased plasma levels of non-high-densitylipoprotein (HDL)-bound sphingosine 1-phosphate(S1P) in coronary artery disease are caused byalterations of S1P uptake into HDL
K. Sattler1, P. Keul1, M. Elter-Schulz2, C. Bode3, M. Graeler3,M. Broecker-Preuss4, T. Budde5, R. Erbel6, G. Heusch1, B. Levkau1 . 1Universityof Essen Medical School, Institute of Pathophysiology, Essen, Germany;2University Duisburg-Essen, Institute for Transfusion Medicine, Essen, Germany;3Hannover Medical School, Institute for Immunology, Hannover, Germany;4University Duisburg-Essen, Department of Endocrinology, Essen, Germany;5Alfried Krupp Hospital, Clinic of Internal Medicine and Cardiology, Essen,Germany; 6West German Heart Center Essen, Clinic for Cardiology, Essen,Germany
Purpose: High-density lipoproteins (HDL) are the major carriers of sphingosine1-phosphate (S1P) in plasma, and S1P bound to HDL contributes to some oftheir anti-atherogenic effects. However, the amount of HDL-bound and of non-HDL-bound S1P in plasma is unknown in coronary artery disease (CAD).Methods: HDL were isolated from patients with myocardial infarction (MI, n=83),stable CAD (sCAD, n=95) and controls (n=85), and S1P in HDL and in plasmawas determined by HPLC. The S1P-uptake capacity of HDL isolated from CADpatients and controls as well as of modified isolated HDL and of HDL subfractionswas assessed in vitro.Results: Plasma levels of non-HDL-bound S1P were ∼8-fold higher while thelevels of HDL-bound plasma S1P were ∼1.5-fold lower in MI and sCAD than incontrols. Levels of HDL-bound plasma S1P were dependent on plasma HDL-Clevels. Non-HDL-bound plasma S1P correlated with symptom severity accordingto the Canadian Cardiovascular Score and discriminated MI and sCAD from con-trols in the ROC analysis. Plasma levels of non-HDL-bound S1P were inverselyassociated with the S1P content of isolated HDL in controls, but not in MI or sCAD.In vitro, HDL isolated from controls, but not from CAD patients, acquired exoge-nous S1P proportionally to their initial S1P content. The uptake capacity of HDLfor S1P was reduced by ∼75% by chlorination or oxidation of the lipoprotein, andwas 3.8-fold less for HDL3 than for HDL2.Conclusions: Elevation of plasma levels of non-HDL-bound S1P is a marker forCAD. Lower plasma levels of HDL-bound S1P in CAD may be caused by lowerplasma HDL-C levels, by modifications of HDL components, and by the altereddistribution of HDL subfractions. Elevating plasma HDL-C levels, normalizing thedistribution of HDL subfractions, and preventing HDL modifications may increasethe binding of plasma S1P to HDL in coronary atherosclerosis.
P710 Influence of the Apo E 4 variant in the lipidic profile ofa population with coronary disease
R. Palma Dos Reis1, A.M. Pereira2, A.I. Freitas2, A.C. Sousa2,M.G. Guerra2, S. Freitas2, I. Ornelas2, J.J. Araujo2, A. Brehm3,M.I. Mendonca2 . 1New University of Lisbon, Faculty of Medical
Sciences, Lisbon, Portugal; 2Hospital Funchal, Funchal, Portugal; 3MadeiraUniversity, Funchal, Portugal
The apolipoprotein E4 has been associated with coronary disease (CD), strokeand peripheral arterial disease, possibly due to the allelic gene variation that cod-ifies it (ε2, ε3 and ε4). These polymorphisms regulate alterations in the lipidicmetabolism, platelet aggregation and oxidative stress.Its influence in the plasmatic coronary disease lipid profile is of particular interest.Aim: To investigate the influence of the Apo ε4 allele, that is more associated withatherosclerosis, in the lipidic profile of a population with CD, comparing it with anormal population. Because Apo B and Lp(a) are related with atherosclerosis andfibrinolysis, they were included in the study.Methods: Case-control study that included 848 individuals, of which 458 werecoronary patients admitted consecutively (mean age of 50.6±8.5 years 72%male) and 390 controls without coronary disease (mean age 50.3±12.1 years old
male) selected according not to be significantly different in sex and age, (p=0.647and 0.126, respectively). The genetic study was performed in all subjects, havingonly 188 individuals (98 cases and 90 controls), that is those that presented theε4 allele (ε4/ε4, ε3/ε4, ε2/ε4) been selected for the present study. All the contin-uous variables are presented with the respective averages ± standard deviation(SD), and are compared by the test T Student. The categorical variables werecompared by the Chi square test.Results: The ε4 allele was associated with the highest average found in the pa-tients: Triglycerides: (217.9 in the patients vs. 149.5 in the controls, p=0.06); Lp(a) (45.8 vs. 22.8 p>0,0001) and Apo B (114.9 vs. 107.2, p=0.080). It was asso-ciated with the lowest averages of: Cholesterol HDL (40.0 in the patients vs. 52.0in the controls, p>0.0001); total Cholesterol (200.4 in the patients vs. 222.1 in thecontrols, p=0.019);Conclusion: The ε4 allele of the Apo E polymorphism was associated with thehighest values of triglycerides and lipoprotein (a) as well as with the lowest levelsof HDL Cholesterol, in a significant way. In our coronary population there was noassociation with the high levels of total cholesterol or LDL cholesterol, probablydue to the fact that the patients had been medicated with statins and that thisallelic profile is extremely favourable to the intervention of these drugs, in thereduction of cholesterol levels.
P711 Short-term rosuvastatin therapy decreasesinflammation in metabolic syndrome
Z. Yigit1, A. Kaya1, I. Uzunhasan1, H.E. Ataoglu2, A. Yildiz1,A.A. Ozkan1. 1Istanbul University,Cardiology Institute, Istanbul,Turkey; 2Haseki Training and Research Hospital, Istanbul, Turkey
Aim: Metabolic syndrome is an epidemic with increasing numbers of patientsworldwide. We evaluated the effect of a combination of diet,and short-term rosu-vastatin therapy on inflammatory parameters and ox-LDL, antiox-LDL in metabolicsyndrome.Material and Methods: Data of 100 consecutive (BMI ≥30 kg/m2) patients withmetabolic syndrome who visited outpatient clinic were evaluated. Clinical eval-uation and biochemical work-up (blood glucose,HbA1C, lipids, CRP, fibrinogen,homocystein, ox-LDL and antiox-LDL) was done. Homocystein was quantitatedby immunonephelometry. Systemic oxidative stress was assessed as plasmaconcentrations of ox-LDL and anti Ox-LDL measured using ELISA kit (Marco-dia,Uppsala,Sweden).High sensitive C-reactive protein (hsCRP) by using im-munonephelometry. All patients were given 1x10 mg rosuvastatin and conven-tional light diet for 3 months. Biochemical work up was repeated at the end (Table1).Statistical analysis: Student’s t-test, Mann-Whitney-U test and chi-square testswere used for statistical analysis.p ≤ 0.05 was considered as statistically signifi-cant.Results: Mean age of our patients was 54.00±10.06 years.Their BMI was32,73±3.67 kg/m2.There was a significant decrease in total cholesterol, LDL-C,HbA1C, homocystein and fibrinogen while hsCRP and BMI did not change signif-icantly.OxLDL decreased while antioxLDL increased significantly (p=0.003,0.002)respectively.
Table 1. Biochemical changes induced by short-term rosuvastatin therapy in metabolic syndrome
Initial (n=100) 3rd mo (n=100) p value
Total cholesterol (mg/dl) 213.33±36.97 173,31±41,62 <0.0001HDL cholesterol (mg/dl) 39.60±6.66 47,14±15,30 0.00029LDL kolesterol (mg/dl) 138.31±33.48 99,91±31,35 <0.0001HbA1 C (%) 6.36±1.69 6.0±1,04 0.00041hsCRP 4.55±2.62 4,38±3,83 NSHomocystein 21.30±13.15 16,25±9,91 0.0027Fibrinogen 443.89±107.46 394,34±188,60 0.0001Ox LDL 309.05±1061,88 153,78±695,08 0.0035Antiox LDL 18.61±11.51 39,96±39,98 0,0020
Conclusion: Short term rosuvastatin therapy decreases inflammation by reduc-ing ox-LDL and antiox-LDL in metabolic syndrome.
P712 Cholesterol level of large low-density lipoprotein is adeterminant of carotid intima-media thickness in men
R. Takahashi1 , K. Okumura2, M. Yoshikane1, M. Suzuki1, N. Ikeda1,T. Murohara2 . 1Chunichi Hospital, Nagoya, Japan; 2Nagoya UniversityGraduate School of Medicine, Nagoya, Japan
Background: Precise measurements of cholesterol and triglyceride levels in ma-jor lipoproteins and their subclasses by high-performance liquid chromatography(HPLC) have been established. The aim of this study was to investigate the re-lationship of lipoprotein subclass lipid levels and carotid intima-media thickness(IMT), a surrogate marker of subclinical atherosclerosis.Methods: We studied 116 apparently healthy Japanese men (53±9 years) with-out a history of cardiovascular diseases who were not taking any medication. IMTwas measured by means of high-resolution vascular ultrasound. Plasma choles-terol and triglyceride concentrations in major lipoproteins and their subclasseswere determined by HPLC with gel permeation columns. Malondialdehyde-modified (MDA)-LDL, an oxidized form of LDL, was measured by a sandwichenzyme-linked immunosorbent assay.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

104 Lipids
Results: IMT was significantly correlated with age (r=0.528, p<0.001), smok-ing history (pack-year, r=0.409, p<0.001), hemoglobin A1c (r=0.222, p=0.017),apolipoprotein B (r=0.183, p=0.049), apolipoprotein B/A1 ratio (r=0.192,p=0.039), MDA-LDL (r=0.235, p=0.011), total cholesterol (r=0.196, p=0.035), LDLcholesterol (r=0.218, p=0.019), non-HDL cholesterol (r=0.214, p=0.021), smallVLDL cholesterol (r=0.238, p=0.010), large LDL cholesterol (r=0.240, p=0.001),very small LDL cholesterol (r=0.244, p=0.008), large VLDL triglycerides (r=0.186,p=0.045), medium VLDL triglycerides (r=0.289, p=0.002), small VLDL triglyc-erides (r=0.398, p=0.001), large LDL triglycerides (r=0.208, p=0.025), very smallLDL triglycerides (r=0.191, p=0.040), and estimated glomerular filtration rate(r=-0.293, p=0.001). In stepwise multiple regression analysis, age (β=0.436,F=29.2), smoking history (β=0.225, F=7.7), and large LDL cholesterol (β=0.175,F=5.3) were found to be independent determinants of IMT (adjusted R2=0.347,p<0.001).Conclusion: Cholesterol level of large LDL is an important, independent deter-minant of IMT in men.
P713 Effect of genetic variant in ABCG8 gene in coronaryartery disease and response to atorvastatin therapy
N. Garg, A. Shrivastava, A. Shrivastava, K. Shrivastava, B. Mittal.Sanjay Gandhi PGI, Lucknow, India
Purpose: ATP-binding cassette transporter ABCG8 plays an impor-tant role in excretion of cholesterol from liver. A common genetic polymorphismD19H of ABCG8 may affect cholesterol metabolism and may be causatively re-lated to genetic predisposition of coronary artery disease (CAD) and also to theinterindividual response to atorvastatin therapy. Thus, we aimed to examine therole of ABCG8 D19H polymorphism in susceptibility to CAD and its influence onatorvastatin response.Methods: The study included clinically proven 213 CAD patients and 220 healthycontrols. Genotyping for both the polymorphisms was done by PCR-RFLP andTaqman assay.Results: Our results showed that ABCG8 H allele was conferring significant riskfor CAD in dominant model (p = 0.014; OR = 2.54; 95% CI: 1.2–5.3). This in-creased risk for CAD was more pronounced for males (p = 0.030; OR = 2.69;95% CI: 1.1–6.5). No correlation of ABCG8 genotypes with the risk factors (dia-betes, hypertension and smoking) of CAD was observed. On atorvastatin treat-ment there was a significant decrease in the low density lipoprotein (LDL) level(p=0.021). However, stepwise multiple regression analysis showed that this de-cease in the LDL level on atorvastatin treatment was not associated with ABCG8genetic variant (p=0.845). Observed determinants of variant response to ator-vastatin therapy were pre-treatment LDL (p=0.024) and total cholestrol level(p=0.017).Conclusions: Although the genetic variant 19H of ABCG8 confers risk for CADin north Indian population, it is not associated with the interindividual response toatorvastatin therapy.
P714 Correlations between ldl and hdl subclasses andserum lipoprotein-associated phospholipase a2
D. Rosenbaum1 , R. Bittar2, P. Giral1, B. Hansel1, J.C. Charniot2,E. Bruckert1, X. Girerd1, D. Bonnefont-Rousselot2 . 1Unité deprévention cardiovasculaire - AP-HP - Hospital Pitie-Salpetriere, paris,
France; 2Unité fonctionnelle de biochimie des maladies métaboliques - AP-HP -Hospital Pitie-Salpetriere, Paris, France
Purpose: Lipoprotein-associated phospholipase A2 (Lp-PLA2) is an inflamma-tory biomarker that is secreted in the atherosclerotic plaque. It has been shownthat blood levels of Lp-PLA2 predict future cardiovascular events regarding thepresence of any other traditional cardiovascular (CV) risk factors except LDL-Cholesterol (LDL-C) because Lp-PLA2 is located on its surface. The aim of ourstudy was to assess possible links between Lp-PLA2 and LDL and HDL sub-classes.Methods: Overweighed and obese patients with no history of cardiovascular dis-ease were recruited at our outpatient clinic for CV risk assessment. None shouldbe under any lipid lowering treatment. All patients underwent routine clinical andbiological evaluation, as well as LDL and HDL subclasses determination by elec-trophoresis in a non-denaturing polyacrylamide gradient gel; the diameter of themain LDL peak was calculated. Lp-PLA2 was measured in serum with a Plactest turbidimetric immunoassay. Elevated values (>360 ng/mL) were assayed byELISA.Results: 49 patients were included. Mean body mass index was 31.84kg/m2 (sd:3.45). The Lp-PLA2 ranged from 41 to 407 ng/mL; mean value was 201 ng/mL(sd: 73). Mean values for total cholesterol, LDL-C, HDL-C and apoB were respec-tively 2.31 g/L (sd: 0.38), 1.39 g/L (sd: 0.32), 0.47 g/L (sd: 0.13), and 1.27 g/L(sd: 0.25). 18 patients (37%) had diabetes. Mean LDL size peak was 25.3 nm(sd: 0.94). In univariate analysis, we found a strong linear correlation betweenLp-PLA2, and LDL-C (r=0.42, p<0.028) as well as apoB (r=0.31, p=0.02) and to-tal cholesterol (r=0.44, p=0.001). There was no correlation between percentagesof LDL subclasses (LDL 1,2,3 and 4) or LDL size peak and Lp-PLA2 levels. Inthe opposite, we found no correlation with total HDL-C level but a positive corre-lation with HDL2b percentage (r = 0.29, p= 0.04) and a negative association withHDL3b percentage (r=-0.3, p= 0.03). Mean HDL2b percentage was 11.47% (sd:
7.48). Mean HDL3b percentage was 27.22% (sd: 9.22). Neither ApoA1 (r= 0.061)nor ApoA2 (r=0.059) were correlated with Lp-PLA2 dosages.Conclusion: In our population, LpPLA2 was related with total LDL-C levels with-out any significant relation with the LDL subclasses distribution. By contrast, Lp-PLA2 was not correlated with HDL-C level but with HDL subclasses. Interest-ingly, LpPLA2 was negatively correlated with HDL3b and positively with largeHDL particles (HDL2b). This supports differential properties of HDL subclasses inatherosclerosis and suggests a potential interaction between HDL and LpPLA2.
P715 The effect of rosuvastatin treatment on fastingtriglyceride levels, non fasting triglyceride levels andHsCRP
A. Cakmak, I. Atar, E. Turk, K. Yilmaz, E. Karacaglar, C. Altin,A. Aydinalp, B. Ozin, H. Muderrisoglu. Baskent University, Faculty ofMedicine, Ankara, Turkey
Background: The relationship of hypertriglyceridemia and the risk for coronaryheart disease (CHD) has been an issue of great interest and controversy. Triglyc-erides are usually measured in the fasting state at the lowest triglyceride levelof the day according to the guidelines. Postprandial hypertriglyceridemia, re-flecting an elevated concentration of lipoprotein remnant particles, might changeatherosclerotic lesion content and might show procoagulant, anti-fibrinolytic andpro-inflammatory effects. Recent studies show that statins also have effects inpostprandial lipoprotein metabolism as a beneficial factor for decreasing CHD.We aimed to evaluate effect of rosuvastatin on fasting and non fasting hyper-triglyceridemia and an inflammatory parameter hsCRP.Methods: A total of 49 patients were included in the study. Oral lipid loading wasused in order to measure postprandial triglyceride (PPTG) levels. In the fastingstate and after the lipid rich breakfast (at 4th hour), triglyceride and hsCRP levelswere measured by enzymatic methods at beginning of rosuvastatin therapy andafter the one month 10 mg/day rosuvastatin therapy.Results: Triglyceride levels were significantly increased after fat loading com-pared to baseline levels in patients (P<0.001). There were no significant changesin hsCRP levels at the beginning. After treatment by 10 mg/day rosuvastatin treat-ment during one month both fasting and non fasting triglyceride levels decreasedsignificantly. But no significant change was observed in hsCRP levels (Table 1).
Table 1. Fasting/PPTG & hsCRP levels
Baseline levels After treatment levels at 1st month P value
Fasting TG levels, mg/dl 192±42 SD 154±51 SD <0.001Non fasting TG levels, mg/dl 339±118 SD 259±96 SD <0.001HsCRP levels fasting, mg/L 5,5±5 SD 5,0±4,9 SD 0,306HsCRP levels non fasting, mg/L 6±5,2 SD 4,8±4,7 SD 0,135
Conclusions: Our study demonstrated that rosuvastatin decrease fasting andnon fasting triglyceride levels significantly after oral lipid loading. But hsCRP levelswere not changed.
P716 Effect of increasing doses of rosuvastatin andatorvastatin on apolipoproteins, enzymes involved inlipoprotein metabolism and inflammatory parameters
I. Karalis1, S.C. Bergheanu1 , A. Van Tol2, G.M. Dallinga-Thie3,A.H. Liem4, J.W. Jukema1. 1Leiden University Medical Center,
Department of Cardiology, Leiden, Netherlands; 2Erasmus University MedicalCenter, Department of Celbiology and Genetics, Rotterdam, Netherlands;3Academic Medical Center, Departments of Experimental Vascular Medicine andVascular Medicine, Amsterdam, Netherlands; 4Oosterschelde Hospital, Goes,Netherlands
Purpose: Statins have substantially decreased incidence of cardiovascularevents but the exact pathophysiological mechanism of their beneficial effect is yetunclear. We aimed to examine the effects of up-titrated doses of 2 widely usedstatins (atorvastatin (ATOR) and rosuvastatin (ROSU)) on parameters involved inlipoprotein metabolism, in patients with low high density lipoprotein cholesterolvalues (HDL-C).Methods: 75 male patients, aged 40-80 years, with known cardiovascular dis-ease and low HDL-C (<1.0 mmol/l), were randomized to receive, after an initial6 week dietary run-in phase, either ATOR 20 mg (n=38) or ROSU 10 mg (n=37).The doses were up-titrated (in 6 week intervals) to 80 mg of ATOR or 40 mg ofROSU at 12 weeks. Serum lipoproteins and lipoprotein metabolism parameterswere measured at baseline and at 6 and 18 weeks of follow up.Results: Both statins significantly reduced total cholesterol (TChol) and non-HDL-C values with ROSU being more effective for the doses studied (p<0.05). Nostatistically significant effect on HDL-C was observed for either statin. Apolipopro-teins (apo) B, CI, CIII, AV and E were significantly reduced in both groups(p<0.001), while the ratio of apoAI+AII over apoAI was changed for both statinswith the decrease of apoAI being more prominent in the ATOR group (p=0.01).Cholesterol ester transfer protein (CETP) mass and activity, phospholipid transferprotein (PLTP) activity and platelet activating factor acyl hydrolase (PAFAH) massand activity were all significantly reduced in both treatment groups over the fol-low up period (p<0.001). ATOR displayed a more prominent decrease of PLTPactivity compared to ROSU (p=0.03) while ROSU displayed a more prominent
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
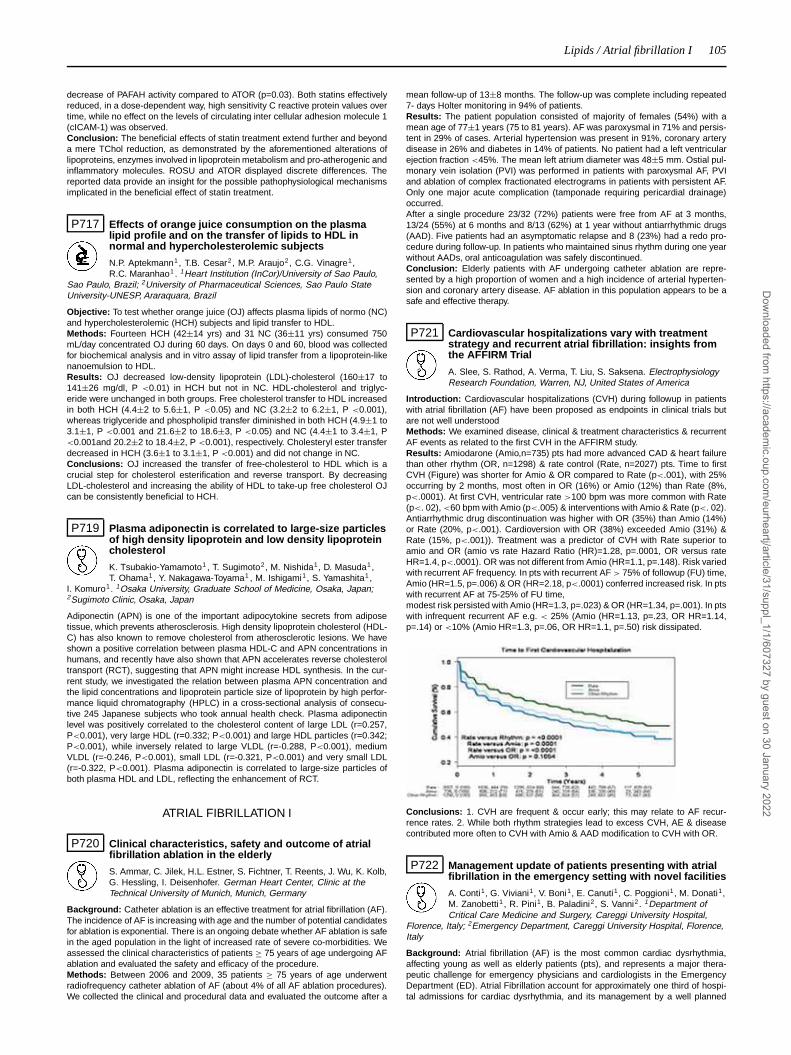
Lipids / Atrial fibrillation I 105
decrease of PAFAH activity compared to ATOR (p=0.03). Both statins effectivelyreduced, in a dose-dependent way, high sensitivity C reactive protein values overtime, while no effect on the levels of circulating inter cellular adhesion molecule 1(cICAM-1) was observed.Conclusion: The beneficial effects of statin treatment extend further and beyonda mere TChol reduction, as demonstrated by the aforementioned alterations oflipoproteins, enzymes involved in lipoprotein metabolism and pro-atherogenic andinflammatory molecules. ROSU and ATOR displayed discrete differences. Thereported data provide an insight for the possible pathophysiological mechanismsimplicated in the beneficial effect of statin treatment.
P717 Effects of orange juice consumption on the plasmalipid profile and on the transfer of lipids to HDL innormal and hypercholesterolemic subjects
N.P. Aptekmann1, T.B. Cesar2, M.P. Araujo2, C.G. Vinagre1,R.C. Maranhao1 . 1Heart Institution (InCor)/University of Sao Paulo,
Sao Paulo, Brazil; 2University of Pharmaceutical Sciences, Sao Paulo StateUniversity-UNESP, Araraquara, Brazil
Objective: To test whether orange juice (OJ) affects plasma lipids of normo (NC)and hypercholesterolemic (HCH) subjects and lipid transfer to HDL.Methods: Fourteen HCH (42±14 yrs) and 31 NC (36±11 yrs) consumed 750mL/day concentrated OJ during 60 days. On days 0 and 60, blood was collectedfor biochemical analysis and in vitro assay of lipid transfer from a lipoprotein-likenanoemulsion to HDL.Results: OJ decreased low-density lipoprotein (LDL)-cholesterol (160±17 to141±26 mg/dl, P <0.01) in HCH but not in NC. HDL-cholesterol and triglyc-eride were unchanged in both groups. Free cholesterol transfer to HDL increasedin both HCH (4.4±2 to 5.6±1, P <0.05) and NC (3.2±2 to 6.2±1, P <0.001),whereas triglyceride and phospholipid transfer diminished in both HCH (4.9±1 to3.1±1, P <0.001 and 21.6±2 to 18.6±3, P <0.05) and NC (4.4±1 to 3.4±1, P<0.001and 20.2±2 to 18.4±2, P <0.001), respectively. Cholesteryl ester transferdecreased in HCH (3.6±1 to 3.1±1, P <0.001) and did not change in NC.Conclusions: OJ increased the transfer of free-cholesterol to HDL which is acrucial step for cholesterol esterification and reverse transport. By decreasingLDL-cholesterol and increasing the ability of HDL to take-up free cholesterol OJcan be consistently beneficial to HCH.
P719 Plasma adiponectin is correlated to large-size particlesof high density lipoprotein and low density lipoproteincholesterol
K. Tsubakio-Yamamoto1 , T. Sugimoto2, M. Nishida1, D. Masuda1,T. Ohama1, Y. Nakagawa-Toyama1 , M. Ishigami1, S. Yamashita1 ,
I. Komuro1. 1Osaka University, Graduate School of Medicine, Osaka, Japan;2Sugimoto Clinic, Osaka, Japan
Adiponectin (APN) is one of the important adipocytokine secrets from adiposetissue, which prevents atherosclerosis. High density lipoprotein cholesterol (HDL-C) has also known to remove cholesterol from atherosclerotic lesions. We haveshown a positive correlation between plasma HDL-C and APN concentrations inhumans, and recently have also shown that APN accelerates reverse cholesteroltransport (RCT), suggesting that APN might increase HDL synthesis. In the cur-rent study, we investigated the relation between plasma APN concentration andthe lipid concentrations and lipoprotein particle size of lipoprotein by high perfor-mance liquid chromatography (HPLC) in a cross-sectional analysis of consecu-tive 245 Japanese subjects who took annual health check. Plasma adiponectinlevel was positively correlated to the cholesterol content of large LDL (r=0.257,P<0.001), very large HDL (r=0.332; P<0.001) and large HDL particles (r=0.342;P<0.001), while inversely related to large VLDL (r=-0.288, P<0.001), mediumVLDL (r=-0.246, P<0.001), small LDL (r=-0.321, P<0.001) and very small LDL(r=-0.322, P<0.001). Plasma adiponectin is correlated to large-size particles ofboth plasma HDL and LDL, reflecting the enhancement of RCT.
ATRIAL FIBRILLATION I
P720 Clinical characteristics, safety and outcome of atrialfibrillation ablation in the elderly
S. Ammar, C. Jilek, H.L. Estner, S. Fichtner, T. Reents, J. Wu, K. Kolb,G. Hessling, I. Deisenhofer. German Heart Center, Clinic at theTechnical University of Munich, Munich, Germany
Background: Catheter ablation is an effective treatment for atrial fibrillation (AF).The incidence of AF is increasing with age and the number of potential candidatesfor ablation is exponential. There is an ongoing debate whether AF ablation is safein the aged population in the light of increased rate of severe co-morbidities. Weassessed the clinical characteristics of patients ≥ 75 years of age undergoing AFablation and evaluated the safety and efficacy of the procedure.Methods: Between 2006 and 2009, 35 patients ≥ 75 years of age underwentradiofrequency catheter ablation of AF (about 4% of all AF ablation procedures).We collected the clinical and procedural data and evaluated the outcome after a
mean follow-up of 13±8 months. The follow-up was complete including repeated7- days Holter monitoring in 94% of patients.Results: The patient population consisted of majority of females (54%) with amean age of 77±1 years (75 to 81 years). AF was paroxysmal in 71% and persis-tent in 29% of cases. Arterial hypertension was present in 91%, coronary arterydisease in 26% and diabetes in 14% of patients. No patient had a left ventricularejection fraction <45%. The mean left atrium diameter was 48±5 mm. Ostial pul-monary vein isolation (PVI) was performed in patients with paroxysmal AF, PVIand ablation of complex fractionated electrograms in patients with persistent AF.Only one major acute complication (tamponade requiring pericardial drainage)occurred.After a single procedure 23/32 (72%) patients were free from AF at 3 months,13/24 (55%) at 6 months and 8/13 (62%) at 1 year without antiarrhythmic drugs(AAD). Five patients had an asymptomatic relapse and 8 (23%) had a redo pro-cedure during follow-up. In patients who maintained sinus rhythm during one yearwithout AADs, oral anticoagulation was safely discontinued.Conclusion: Elderly patients with AF undergoing catheter ablation are repre-sented by a high proportion of women and a high incidence of arterial hyperten-sion and coronary artery disease. AF ablation in this population appears to be asafe and effective therapy.
P721 Cardiovascular hospitalizations vary with treatmentstrategy and recurrent atrial fibrillation: insights fromthe AFFIRM Trial
A. Slee, S. Rathod, A. Verma, T. Liu, S. Saksena. ElectrophysiologyResearch Foundation, Warren, NJ, United States of America
Introduction: Cardiovascular hospitalizations (CVH) during followup in patientswith atrial fibrillation (AF) have been proposed as endpoints in clinical trials butare not well understoodMethods: We examined disease, clinical & treatment characteristics & recurrentAF events as related to the first CVH in the AFFIRM study.Results: Amiodarone (Amio,n=735) pts had more advanced CAD & heart failurethan other rhythm (OR, n=1298) & rate control (Rate, n=2027) pts. Time to firstCVH (Figure) was shorter for Amio & OR compared to Rate (p<.001), with 25%occurring by 2 months, most often in OR (16%) or Amio (12%) than Rate (8%,p<.0001). At first CVH, ventricular rate >100 bpm was more common with Rate(p<. 02), <60 bpm with Amio (p<.005) & interventions with Amio & Rate (p<. 02).Antiarrhythmic drug discontinuation was higher with OR (35%) than Amio (14%)or Rate (20%, p<.001). Cardioversion with OR (38%) exceeded Amio (31%) &Rate (15%, p<.001)). Treatment was a predictor of CVH with Rate superior toamio and OR (amio vs rate Hazard Ratio (HR)=1.28, p=.0001, OR versus rateHR=1.4, p<.0001). OR was not different from Amio (HR=1.1, p=.148). Risk variedwith recurrent AF frequency. In pts with recurrent AF > 75% of followup (FU) time,Amio (HR=1.5, p=.006) & OR (HR=2.18, p<.0001) conferred increased risk. In ptswith recurrent AF at 75-25% of FU time,modest risk persisted with Amio (HR=1.3, p=.023) & OR (HR=1.34, p=.001). In ptswith infrequent recurrent AF e.g. < 25% (Amio (HR=1.13, p=.23, OR HR=1.14,p=.14) or <10% (Amio HR=1.3, p=.06, OR HR=1.1, p=.50) risk dissipated.
Conclusions: 1. CVH are frequent & occur early; this may relate to AF recur-rence rates. 2. While both rhythm strategies lead to excess CVH, AE & diseasecontributed more often to CVH with Amio & AAD modification to CVH with OR.
P722 Management update of patients presenting with atrialfibrillation in the emergency setting with novel facilities
A. Conti1, G. Viviani1, V. Boni1, E. Canuti1, C. Poggioni1, M. Donati1,M. Zanobetti1 , R. Pini1, B. Paladini2, S. Vanni2. 1Department ofCritical Care Medicine and Surgery, Careggi University Hospital,
Florence, Italy; 2Emergency Department, Careggi University Hospital, Florence,Italy
Background: Atrial fibrillation (AF) is the most common cardiac dysrhythmia,affecting young as well as elderly patients (pts), and represents a major thera-peutic challenge for emergency physicians and cardiologists in the EmergencyDepartment (ED). Atrial Fibrillation account for approximately one third of hospi-tal admissions for cardiac dysrhythmia, and its management by a well planned
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

106 Atrial fibrillation I
approach is important in preventing adverse consequences and hospitalizations.In the primary care setting, the availability of novel facilities like an Intensive Ob-servation Unit (IOU) and an Outpatient Clinic for follow-up (OC) could result inimprove global management and reduce admissions. Objective. To prevent andreduce admissions by the management with a IOU and a OC.Methods: We compared three groups of pts presenting to the ED with AF. Pa-tients managed when both the IOU and the OC were unavailable (group A, 2004-2005 years), pts managed when only the IOU was available (group B, 2006-2007y.), and after the final ED reorganization with the OC novel facility (group C, 2008-2009 y.). In pts enrolled, we considered the presence of comorbidities, the AF du-ration (>48 hours or ≤48 hours), and the therapeutic approach (pharmacological:i.v. Flecainide, or Propafenone, or Amiodarone, or DC shock). Logistic regressionanalysis was performed with a stepwise backward model. A two-tailed p value<0.05 was considered significant. Primary endpoint was reduction of admissionrate; secondary endpoint was detection of clinical characteristics predictive ofpoor outcome.Results: Out of 3,324 pts enrolled, group A included 1,087 pts (age 71±13 y.),group B included 970 pts (age 70±13 y.) and group C, 1,267 pts (age 71±12y., n.s. for all comparisons). Admission rate was significantly reduced when theIOU and OC were available (group A, 47%, group B, 38%, and group C, 23%,p<.001). Finally, when the presence of comorbidities (group A, B, and C, 40%,41%, and 24%, respectively; p<.001), AF lasting >48 hours (group A, B, andC, 46%, 43%, and 27%, respectively; p<.001), and group assignment were con-sidered, the presence of comorbidities (HR: 11, 95% CI: 8-13; p<0.001) and AF> 48 hours (HR: 5, 95%CI: 4-6; p<0.001) were independent predictor of pooroutcome. Moreover, the novel ED reorganization was associated with a betteroutcome (HR: 0.78, 95%CI: 0.62-0.98; p=0.035).Conclusions: Present model of management of pts presenting with AF by a novelED organization with a IOU and OC significantly reduces hospital admissions.Comorbidities and AF lasting > 48 hours were independent predictors of higherhospitalizations.
P723 Metabolic syndrome and atrial fibriallation in essentialhypertensive patients
G. Vyssoulis1, E. Karpanou2, D. Adamopoulos1 , S.-M. Kyvelou1,V. Tzamou1, C. Stefanadis1. 1Hippokration General Hospital, Athens,Greece; 2Onassis Cardiac Surgery Center, Athens, Greece
Purpose: Metabolic syndrome (MS) has been recently associated with an in-creased risk for the development of atrial fibrillation (AF) in the general popula-tion. Whether this relation is also apparent in patients with arterial hypertensionremains to be clarified. In the present study we sought to investigate the indepen-dent association of the MS with the AF in a large cohort of hypertensive patients.Methods: The study comprised 15075 consecutive patients with essential hyper-tension (mean age 59±11 years, 51.1% males). All subjects underwent a com-pete clinical and lipid profile assesment as well as a standard 12 lead ECG atdrug free baseline. MS was diagnosted by using 5 different definitions includingthe National Cholesterol Education Program Third Adult Treatment Panel (NCEP-ATPIII) and the GISSI Score.Results: The prevalence of the MS varied from 31.7% to 47.8% according tothe each time definition used. In multivariate logistic regression analysis, MS wasassociated with the presence of AF (odds ratio from 1.68 to 2.13, p<0.001 for all),independenty of the criteria used. All NCEP-ATPIII components were found to beindependently associated with an increased risk for AF. The prevalence of AFincreased progressively with the severity of the metabolic syndrome as assessedby the number of the metabolic syndrome components and the GISSI score.Conclusions: In patients with essential hypertension, the MS is directly and in-dependently related to the AF prevalence pointing to a causal contribution of theMS risk factors to the pathogenesis of the AF.
P724 Baseline apnea/hypopnea index and high-sensitivityC-reactive protein for the risk of recurrence of atrialfibrillation after successful electrical cardioversion
A. Mazza1, M.G. Bendini1, M. Cristofori2, S. Nardi3, M. Leggio4 , R. DeCristofaro1, A. Giordano5, L. Cozzari1, G. Giordano1, R. Cappato6.
1Cardiology Division, Santa Maria della Stella Hospital, Orvieto, Italy;2Epidemiologic and Bio-Statistics Unit, AUSL Terni 4, Terni, Italy; 3CardiologyDivision, Santa Maria Hospital, Terni, Italy; 4Cardiovascular Department, CardiacRehabilitation Operative Unit (S.I.), San Filippo Neri Hospital, Rome, Italy;5Nephrology Unit, Santa Maria della Stella Hospital, Orvieto, Italy; 6Arrhythmiasand Electrophysiology Center, Policlinico San Donato, University of Milan, SanDonato Milanese, Milan, Italy
Purpose: We tested apnea/hypopnea index (AHI), high-sensitivity C-reactive pro-tein (hs-CRP) and clinical/instrumental variables as predictors of atrial fibrillation(AF) recurrence over 1-year follow-up after successful electrical cardioversion.Methods: We enrolled 158 consecutive patients. AHI was assessed with stan-dard overnight polysomnography and hs-CRP with immunonephelometry assaythe day before electrical cardioversion.Results: AF recurrences occurred in 81 patients (51%). Predictors at univariateanalysis were: AHI ≥15 events/h (P= 0.001), hs-CRP >0.30 mg/dl (P= 0.009),AF duration >3 days (P= 0.008), diabetes (P= 0.03) and ongoing antiarrhythmic
therapy at the time of electrical cardioversion (P= 0.03). Survival analysis con-firmed that patients with AHI ≥15 events/h and hs-CRP >0.30 mg/dl had a higherrecurrence rate of AF (log rank P= 0.0006 and P= 0.01, respectively). Predictorsat multivariate analysis were: AHI ≥15 events/h (P= 0.003), hs-CRP >0.30 mg/dl(P= 0.01) and ongoing antiarrhythmic therapy (P= 0.04). A predictive model basedupon the multiple effects of significant variables plus age as a continuous variablestratified the risk of AF recurrence, more than tripled with all dichotomised vari-ables altered with respect to normal variables (85% vs. 27%).
Kaplan-Meier curves
Conclusions: AHI ≥15 events/h and hs-CRP >0.30 mg/dl are the strongest pre-dictors of the predictors chosen of AF recurrence after successful electrical car-dioversion over 1-year follow-up.
P725 Role of left ventricular stiffness in transformation ofprimary paroxysmal atrial fibrillation into permanentform in patients with chronic heart failure
L.G. Tunyan, S.V. Grigoryan. Institute of Cardiology, Yerevan, Armenia
Left ventricular (LV) diastolic dysfunction (DD) causes the higher atrialpressure, increasing the left atrial (LA) volume and may lead to atrial fibrillation(AF).Objective: To assess the role of the LV DD and a higher level of LV stiffness indevelopment of the permanent (Pr) AF in patients (pts) with chronic heart fail-ure (CHF) and with primary diagnosis of paroxysmal AF (PAF) and to prove ahypothesis that pts with PrAF have had higher stiffness of LV.Material and methods: This study included 56 pts (aged 51±14 years, 36 men)with primary diagnosis of PAF <48 h of onset and with clinically stable in NYHA III-IV functional class CHF (dilated cardiomyopathy, LV end-diastolic diameter (EDD)> 60 mm, ejection fraction (EF) < 36%), LA diameter > 44mm, LA maximal vol-ume > 70 ml). All pts received a standard therapy - ACE inhibitors, β-blockers,digoxin and diuretics. The pts passed transthoracal and transesophageal echo-cardiography (echo) after restoration of the sinus rhythm (SR) on the 1st day andat the 180th day. The pts were under observation for 12 months.Results: The analysis of the results showed that PAF transformed into PrAF in 12pts (21.4%, Group A). On the other hand, in 44 pts (78.6%, Group B) SR main-tained till the end of the study period. Retrospective analysis of echo examinationshowed that pts in both groups had similar level of II-IV LV DD. Compared to groupB, the pts in group A had the same LV EDD, LV EF, LA diameter and maximal vol-ume both at the beginning and at the end of the study period (p>0.5). Comparedto group B, the pts in group A on the 1-th and 180-th days had larger minimal LAvolume (1-th day in group A 56.5±8.5ml; 180 day 58.4±9.2.ml; in group B 1-thday 43.3±7.2mm, 180 day was 44.4±5.2.ml p<0.005), increased pulmonary vein(PV) revers atrial flow (RAF) velocity (V) (1-th day in group A was 0.32±0.8m/sec;180 day was 0.35±0.9.m/sec; in group B 1-th day 0.25±0.6m/sec, 180 day was0.26±0.7m/sec; p<0.005), and prolonged PV RAF and transmitral A wave timesdifference (PV RAF-A wave times) (1-th day in group A was 0.32±0.5msec;180 day was 0.33±0.6.msec; 1-th day in group B 0.20±0.4msec, 180 day was0.21±0.6msec; p<0.005).Conclusion: Increased PV RAF V and prolonged PV RAF-A wave times arereliable parameters for LV DD with higher level of LV stiffness. The results showedthat the pts with initial increased RAF V and prolonged PV RAF-A wave times aremore susceptible to the PrAF development. These parameters can be consideredas independent predictors of progression of PrAF in pts with CHF.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
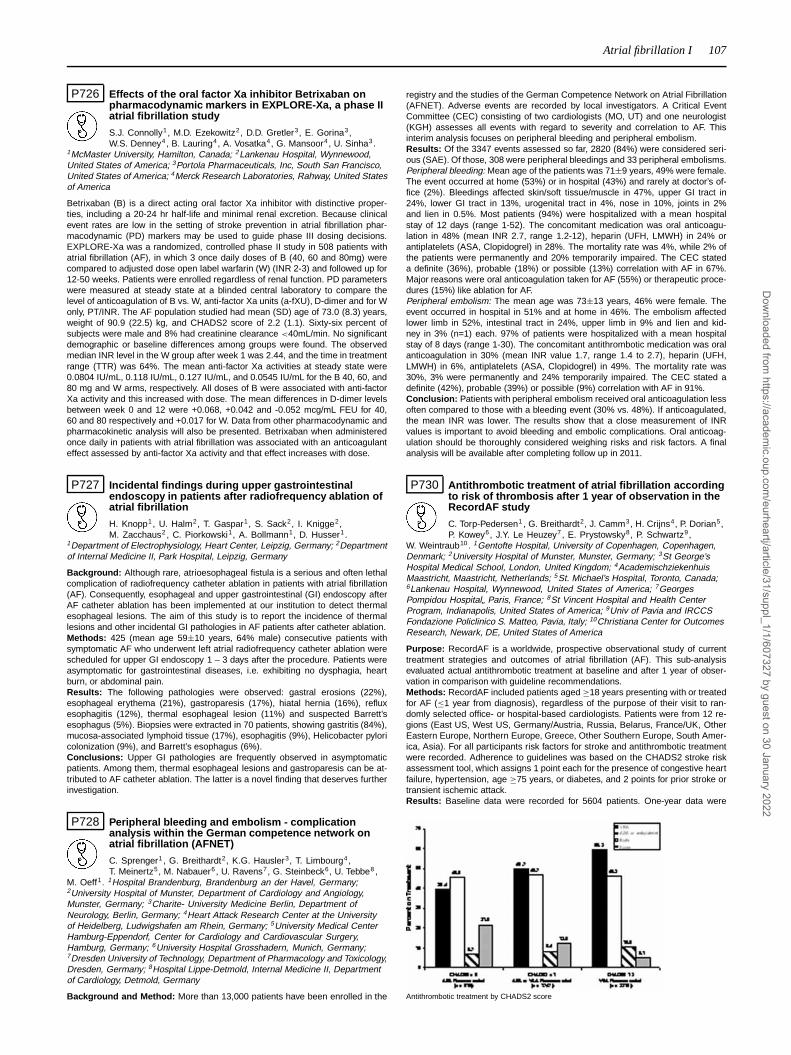
Atrial fibrillation I 107
P726 Effects of the oral factor Xa inhibitor Betrixaban onpharmacodynamic markers in EXPLORE-Xa, a phase IIatrial fibrillation study
S.J. Connolly1, M.D. Ezekowitz2, D.D. Gretler3, E. Gorina3,W.S. Denney4, B. Lauring4, A. Vosatka4, G. Mansoor4 , U. Sinha3.
1McMaster University, Hamilton, Canada; 2Lankenau Hospital, Wynnewood,United States of America; 3Portola Pharmaceuticals, Inc, South San Francisco,United States of America; 4Merck Research Laboratories, Rahway, United Statesof America
Betrixaban (B) is a direct acting oral factor Xa inhibitor with distinctive proper-ties, including a 20-24 hr half-life and minimal renal excretion. Because clinicalevent rates are low in the setting of stroke prevention in atrial fibrillation phar-macodynamic (PD) markers may be used to guide phase III dosing decisions.EXPLORE-Xa was a randomized, controlled phase II study in 508 patients withatrial fibrillation (AF), in which 3 once daily doses of B (40, 60 and 80mg) werecompared to adjusted dose open label warfarin (W) (INR 2-3) and followed up for12-50 weeks. Patients were enrolled regardless of renal function. PD parameterswere measured at steady state at a blinded central laboratory to compare thelevel of anticoagulation of B vs. W, anti-factor Xa units (a-fXU), D-dimer and for Wonly, PT/INR. The AF population studied had mean (SD) age of 73.0 (8.3) years,weight of 90.9 (22.5) kg, and CHADS2 score of 2.2 (1.1). Sixty-six percent ofsubjects were male and 8% had creatinine clearance <40mL/min. No significantdemographic or baseline differences among groups were found. The observedmedian INR level in the W group after week 1 was 2.44, and the time in treatmentrange (TTR) was 64%. The mean anti-factor Xa activities at steady state were0.0804 IU/mL, 0.118 IU/mL, 0.127 IU/mL, and 0.0545 IU/mL for the B 40, 60, and80 mg and W arms, respectively. All doses of B were associated with anti-factorXa activity and this increased with dose. The mean differences in D-dimer levelsbetween week 0 and 12 were +0.068, +0.042 and -0.052 mcg/mL FEU for 40,60 and 80 respectively and +0.017 for W. Data from other pharmacodynamic andpharmacokinetic analysis will also be presented. Betrixaban when administeredonce daily in patients with atrial fibrillation was associated with an anticoagulanteffect assessed by anti-factor Xa activity and that effect increases with dose.
P727 Incidental findings during upper gastrointestinalendoscopy in patients after radiofrequency ablation ofatrial fibrillation
H. Knopp1, U. Halm2, T. Gaspar1, S. Sack2, I. Knigge2,M. Zacchaus2 , C. Piorkowski1, A. Bollmann1, D. Husser1.
1Department of Electrophysiology, Heart Center, Leipzig, Germany; 2Departmentof Internal Medicine II, Park Hospital, Leipzig, Germany
Background: Although rare, atrioesophageal fistula is a serious and often lethalcomplication of radiofrequency catheter ablation in patients with atrial fibrillation(AF). Consequently, esophageal and upper gastrointestinal (GI) endoscopy afterAF catheter ablation has been implemented at our institution to detect thermalesophageal lesions. The aim of this study is to report the incidence of thermallesions and other incidental GI pathologies in AF patients after catheter ablation.Methods: 425 (mean age 59±10 years, 64% male) consecutive patients withsymptomatic AF who underwent left atrial radiofrequency catheter ablation werescheduled for upper GI endoscopy 1 – 3 days after the procedure. Patients wereasymptomatic for gastrointestinal diseases, i.e. exhibiting no dysphagia, heartburn, or abdominal pain.Results: The following pathologies were observed: gastral erosions (22%),esophageal erythema (21%), gastroparesis (17%), hiatal hernia (16%), refluxesophagitis (12%), thermal esophageal lesion (11%) and suspected Barrett’sesophagus (5%). Biopsies were extracted in 70 patients, showing gastritis (84%),mucosa-associated lymphoid tissue (17%), esophagitis (9%), Helicobacter pyloricolonization (9%), and Barrett’s esophagus (6%).Conclusions: Upper GI pathologies are frequently observed in asymptomaticpatients. Among them, thermal esophageal lesions and gastroparesis can be at-tributed to AF catheter ablation. The latter is a novel finding that deserves furtherinvestigation.
P728 Peripheral bleeding and embolism - complicationanalysis within the German competence network onatrial fibrillation (AFNET)
C. Sprenger1 , G. Breithardt2, K.G. Hausler3, T. Limbourg4,T. Meinertz5, M. Nabauer6 , U. Ravens7, G. Steinbeck6, U. Tebbe8 ,
M. Oeff1. 1Hospital Brandenburg, Brandenburg an der Havel, Germany;2University Hospital of Munster, Department of Cardiology and Angiology,Munster, Germany; 3Charite- University Medicine Berlin, Department ofNeurology, Berlin, Germany; 4Heart Attack Research Center at the Universityof Heidelberg, Ludwigshafen am Rhein, Germany; 5University Medical CenterHamburg-Eppendorf, Center for Cardiology and Cardiovascular Surgery,Hamburg, Germany; 6University Hospital Grosshadern, Munich, Germany;7Dresden University of Technology, Department of Pharmacology and Toxicology,Dresden, Germany; 8Hospital Lippe-Detmold, Internal Medicine II, Departmentof Cardiology, Detmold, Germany
Background and Method: More than 13,000 patients have been enrolled in the
registry and the studies of the German Competence Network on Atrial Fibrillation(AFNET). Adverse events are recorded by local investigators. A Critical EventCommittee (CEC) consisting of two cardiologists (MO, UT) and one neurologist(KGH) assesses all events with regard to severity and correlation to AF. Thisinterim analysis focuses on peripheral bleeding and peripheral embolism.Results: Of the 3347 events assessed so far, 2820 (84%) were considered seri-ous (SAE). Of those, 308 were peripheral bleedings and 33 peripheral embolisms.Peripheral bleeding: Mean age of the patients was 71±9 years, 49% were female.The event occurred at home (53%) or in hospital (43%) and rarely at doctor’s of-fice (2%). Bleedings affected skin/soft tissue/muscle in 47%, upper GI tract in24%, lower GI tract in 13%, urogenital tract in 4%, nose in 10%, joints in 2%and lien in 0.5%. Most patients (94%) were hospitalized with a mean hospitalstay of 12 days (range 1-52). The concomitant medication was oral anticoagu-lation in 48% (mean INR 2.7, range 1.2-12), heparin (UFH, LMWH) in 24% orantiplatelets (ASA, Clopidogrel) in 28%. The mortality rate was 4%, while 2% ofthe patients were permanently and 20% temporarily impaired. The CEC stateda definite (36%), probable (18%) or possible (13%) correlation with AF in 67%.Major reasons were oral anticoagulation taken for AF (55%) or therapeutic proce-dures (15%) like ablation for AF.Peripheral embolism: The mean age was 73±13 years, 46% were female. Theevent occurred in hospital in 51% and at home in 46%. The embolism affectedlower limb in 52%, intestinal tract in 24%, upper limb in 9% and lien and kid-ney in 3% (n=1) each. 97% of patients were hospitalized with a mean hospitalstay of 8 days (range 1-30). The concomitant antithrombotic medication was oralanticoagulation in 30% (mean INR value 1.7, range 1.4 to 2.7), heparin (UFH,LMWH) in 6%, antiplatelets (ASA, Clopidogrel) in 49%. The mortality rate was30%, 3% were permanently and 24% temporarily impaired. The CEC stated adefinite (42%), probable (39%) or possible (9%) correlation with AF in 91%.Conclusion: Patients with peripheral embolism received oral anticoagulation lessoften compared to those with a bleeding event (30% vs. 48%). If anticoagulated,the mean INR was lower. The results show that a close measurement of INRvalues is important to avoid bleeding and embolic complications. Oral anticoag-ulation should be thoroughly considered weighing risks and risk factors. A finalanalysis will be available after completing follow up in 2011.
P730 Antithrombotic treatment of atrial fibrillation accordingto risk of thrombosis after 1 year of observation in theRecordAF study
C. Torp-Pedersen1 , G. Breithardt2, J. Camm3, H. Crijns4, P. Dorian5,P. Kowey6, J.Y. Le Heuzey7, E. Prystowsky8, P. Schwartz9,
W. Weintraub10 . 1Gentofte Hospital, University of Copenhagen, Copenhagen,Denmark; 2University Hospital of Munster, Munster, Germany; 3St George’sHospital Medical School, London, United Kingdom; 4AcademischziekenhuisMaastricht, Maastricht, Netherlands; 5St. Michael’s Hospital, Toronto, Canada;6Lankenau Hospital, Wynnewood, United States of America; 7GeorgesPompidou Hospital„ Paris, France; 8St Vincent Hospital and Health CenterProgram, Indianapolis, United States of America; 9Univ of Pavia and IRCCSFondazione Policlinico S. Matteo, Pavia, Italy; 10Christiana Center for OutcomesResearch, Newark, DE, United States of America
Purpose: RecordAF is a worldwide, prospective observational study of currenttreatment strategies and outcomes of atrial fibrillation (AF). This sub-analysisevaluated actual antithrombotic treatment at baseline and after 1 year of obser-vation in comparison with guideline recommendations.Methods: RecordAF included patients aged ≥18 years presenting with or treatedfor AF (≤1 year from diagnosis), regardless of the purpose of their visit to ran-domly selected office- or hospital-based cardiologists. Patients were from 12 re-gions (East US, West US, Germany/Austria, Russia, Belarus, France/UK, OtherEastern Europe, Northern Europe, Greece, Other Southern Europe, South Amer-ica, Asia). For all participants risk factors for stroke and antithrombotic treatmentwere recorded. Adherence to guidelines was based on the CHADS2 stroke riskassessment tool, which assigns 1 point each for the presence of congestive heartfailure, hypertension, age ≥75 years, or diabetes, and 2 points for prior stroke ortransient ischemic attack.Results: Baseline data were recorded for 5604 patients. One-year data were
Antithrombotic treatment by CHADS2 score
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

108 Atrial fibrillation I
available for 4925 patients. The Figure shows percentage of patients receiving vi-tamin K antagonists (VKA) and antiplatelet treatment (>80% aspirin) by CHADS2score.While antithrombotic treatment increased with CHADS2, 39% of patients whoseCHADS2 score was 0 received a VKA, and 35% of patients with CHADS2 ≥2received only antiplatelet therapy.Conclusions: The distribution of antithrombotic treatment after 1 year of observa-tion of patients with AF is surprising in comparison with treatments recommendedby international guidelines. This may reflect a relatively low impact of the guide-lines.
P731 Evaluation of tromboembolic markers, carotid plaqueand intima media thickness in patients with atrialfibrillation (AF) paroxysm more than 48 hours duration
A. Borodai1, O. Sychev1, E. Romanova1, E. Borodai2. 1NationalScientific Center "M.D. Strazhesko Institute of Cardiology, MAS of
Ukraine", Kiev, Ukraine; 2National O.O. Bohomolets Medical University, Kiev,Ukraine
Transesophageal echocardiography is indispensable tool for revealing high riskAF patients before cardioversion. The clinical usefulness of measurement ofcarotid intima media thickness (IMT) and carotid plaque (PL) visualization in thelong term paroxysm AF pts still uncertain.Methods: Transesophageal echocardiography (TEE) and carotid duplex scan-ning were performed in 132 patients (pts) with long term paroxysm AF: mean age59.5 (53.0-67.0) years and mean term of the AF paroxysm 60.0 (25.0-131.0) days.In all patients echo cardiac tromboembolic markers was estimated and it’s interre-lation with common carotid IMT, PL (by NASCET) was evaluated. The associationamong IMT, PL and incidence of previous ischemic cerebrovascular events (CVE)was observed.Pts with severe spontaneous echo contrast (SEC) consist of 33% patients: leftatrial appendage average velocity (LAAV) was 21 (17.9-25.4) cm/s, vs. 36.4(28.28-45.5) cm/s in the group with mild SEC, p<0.0000001. There was straightline correlation between SEC and reduced LAAV, r= -0.6, p<0.000001LAA trombi were founded in the 9% cases: mean LAAV was 19.2 (16.2-24.7) cm/sin that group, vs. 30.7 (24.3-42.9) p<0.000088 in the rest of the patients.Complex atheromas in arch of aorta (AA) and descending aorta more 4 mm, werefounded in 41.6% of the cases. IMT more than 0.09 cm were founded in 37.8%and carotid plaque in 64.2% of the cases.We found correlation between IMT and AA r=0.4, p<0.00002; AA and PL r=0.4,p<0.00002. We found that PL with more than 20% stenosis associated as a ten-dency with presence LAA thrombi OR=3.57, p<0.08 (CI=2.81-4.32). 8 patientshad stroke or transient ischemic attack during their previous or current AF parox-ysm. Interestingly, that IMT more than 0.09 cm associated with previous, CVEChi-square = 7.34, p<0.006 and the same index for SEC 3-4+ was Chi-square= 3.22, p<0.07 in a tendency level. In pts after CVE mean carotid PL stenosiswas 30% (25.0-45.0). We found that low-grade stenosis PL, more than 20% alsoassociated with CVE OR=6.37, p<0.03 (CI=4.29-8.46).Conclusions: There are rapid findings of the markers of trombogenesis andatherosclerosis in long term AF patients group by TEE and carotid duplex scan-ning: LA trombi, low average left atrial appendage velocity, dense echo contrast,complex atheromas in aorta, IMT thickening and carotid PL. This is important thateven low-grade carotid PL may be considered as a strong predictor of CVE in thepts with AF paroxysms. Carotid duplex scanning should be routinely used in AFpts as the tool for evaluation of the cardiovascular risk.
P732 Indexed left atrial volume, C-reactive protein anderythrocyte sedimentation rate as predictors ofrecurrence of non-valvular atrial fibrillation aftersuccessful cardioversion
P. Marchese1, V. Malavasi1, L. Rossi1, G. Delle Donne1,M. Becirovic1, N. Nikolskaya1, A. Colantoni2, A. Luciani2, M.G. Modena1.1University of Modena & Reggio Emilia, Department of Cardiology, Modena,Italy; 2Polyclinic Hospital, Emergency Department, Modena, Italy
Background: The data regarding the relationships between left atrial volume(LAV), inflammation, and atrial fibrillation (AFib) are sparse. Additionally, althoughLAV prognostic role in predicting AFib is wellknown, it has not been prospectivelyevaluated as predictor of recurrence of non-valvular AFib after cardioversion.Methods: We prospectively evaluated 76 consecutive patients (mean age66,1±13.6 years, 65.8% men) who underwent successful cardioversion and withno history of other atrial arrhythmia, stroke, congenital heart disease, valvulardysfunction, surgery, thyroid dysfunction, acute or chronic inflammatory disease,and pacemaker. Baseline clinical and echocardiographic characteristics were ob-tained before cardioversion. The LAV was measured using Simpson’s methodand indexed to BSA. Baseline routine blood samples were obtained in order toevaluate also the inflammatory state. Patients were followed by an ECG after 1st,6th and 12th month and by a Holter ECG performed 3 months aftercardioversion.Results: 39 patients (51.3%) had recurrence of AFib after a median (25th-75thpercentile) follow-up of 165.0 (30.0-270.0) days.Patients with recurrence com-pared to those with no recurrence had larger LAV (36.3±9.9 vs 27.5±8.9 ml/m2,p<0.001), higher level of C-reactive protein (CRP, 0.45±0.49 vs 0.17±0.09 mg/dl,
p=0.04) and erythrocyte sedimentation rate (ESR, 16.2±11.2 vs 10.3±8.8 mm/hr,p=0.04). LA diameter was not associated with recurrence of AFib (RR 1.00,95%CI 0.98-1.23, p=0.09). Each unit increase in indexed LAV was associated with a1.12 fold increased risk of AFib recurrence (RR 1.12, 95% CI 1.04-1.20, p=0.002).When median values were used as cut-off, the association of iLAV >32 ml/m2
with CRP >0,18 mg/dl and/or ERS> 11.0 mm/hr was a associatedwith a 16.2fold increased risk of AFib recurrence (RR 16.2, 95% CI 1.8-42.4, p=0.003).Conclusion: This is the first prospective study to evaluate the relationships be-tween LAV, inflammation, and AFib recurrence after cardioversion. Present workshows, for the first time, that larger indexed LAV before cardioversion, as a moreaccurate measure of LA remodeling than LA diameter, is strongly associated witha higher risk of AFib recurrence. It also shows that inflammation, evaluated bya simple routine blood sample, may provide an adjunctive, easy, and low-costprognostic tool to predict AFib recurrence.
P733 Autonomic dysbalance in nonrheumatic atrialfibrillation
V.B. Barauskiene Vilija, E.M. Egle Martinkute, E.R. Egle Rumbinaite.Kaunas University of Medicine, Kaunas, Lithuania
The autonomic nervous system plays an important role in developmentof atrial fibrillation (AF). One of the most promising markers of autonomic activityis heart rate variability (HRV). Aim of study was to evaluate HRV in patients withnonrheumatic AF. Patients and methods: The study population consisted of 222patients: group I - 75 pts with previous paroxysmal or pesistent nonrheumaticAF without antiarrhythmics drugs; group II - 71 pts with non-AF arrhythmias;group III - 76 healthy controls. HRV was measured by 24-hours Holter moni-toring. Time domain parameters analyzed were average R-R, SDNN, SDANN,SDNNinx, pNN50, and rMSSD. Continuous variables are presented as mean ±standard deviation. Student’s t-test, Pearson Chi-square, and Mann-Whitney testswere applied where appropriate. P-value of <0.05 was considered significant.Results: The results of mean R-R and HRV time domain parameters are pre-sented in table. According to our data HRV was significantly lower in group I ascompared with group II and III (p<0.05): low HRV (rMSSD <30 ms) in groupI (46 pts; 61.3%), group II (21 pts; 29.6%), group III (2pt; 2.6%); medium HRV(30 =< rMSSD < 45 ms) accordingly 27 pts (36.0%), 25 pts (35.2%) and 42 pts(55.2%); high HRV (rMSSD ≥ 45 ms) accordingly 2 pt (2.6%), 25 pts (35.2%),and 32 (42.2%). HRV was significantly higher in group I pts with beta-blockers(27 pts) (p-0.00): rMSSD with beta-blockers 27.44±5.2 ms and no beta-blockers33.2±9.3 ms. Average heart rate was lower in group I when beta-blockers wereused (p<0,05): group I - 59.8±5.7 bpm, group II - 74.4±10.5 bpm, group III –72.7±6.2 bpm.
Time domain variables of study patients
Variable Group I Group II Group III
SDNN (ms) 111.4±47.1 133.0±42.6 134.1±38.0SDANN (ms) 97.0±44.7 112.1±39.5 110.5±36.2SDNNinx (ms) 41.9±18.3 65.8±23.9 68.6±16.5pNN50 (%) 5.3±3.5 11.3±8.9 15.2±8.3rMSSD (ms) 29.5±7.5 45.9±27.9 47.8±13.5
Conclusion: Patients with atrial fibrillation had reduced HRV indicating reducedvagal input in the heart rate regulation. HRV may be used as a prognostic markerfor development of recurrent AF and may be used to optimize treatment. Beta–blockers played a role reducing heart rate in our AF patients and increases HRV.
P734 C-reactive protein, Interleukin-6 and N-terminalpro-Brain Natriuretic Peptide levels followingsuccessful cardioversion of atrial fibrillation: is there arole of biomarkers in arrhythmia recurrence?
D. Chatzopoulos1 , S. Psychari1, M. Katsafados1,A. Charalampopoulos1 , D. Elaiopoulos1, T. Apostolou1, E. Iliodromitis2,D. Kremastinos2. 12nd Department of Cardiology,General Hospital of Nikea,Pireaus, Greece; 2Attikon Hospital, 2nd University Department of Cardiology,Athens, Greece
Purpose: The aim of this study was to investigate possible changes in high sen-sitivity C-reactive protein (hs-CRP), interleukin-6 (IL-6) and N-terminal pro-BrainNatriuretic Peptide (NT pro-BNP), after sinus rhythm restoration and their relationto the recurrence rate.Methods: Eighty patients with first detected episode of AF, that was not self-terminating and was not sustained beyond 2 days, were prospectively studied. Allpatients were medically cardioverted. Echocardiography and measurements ofhs-CRP, IL-6 and NT pro-BNP were performed immediately post- conversion andat 1 month follow-up. All patients were reevaluated 1 month after sinus rhythmrestoration by clinical examination, 12-lead electrocardiogram and 24-hour Holtermonitoring.Results: Recurrence occurred in 30 out of 80 patients and was positively relatedto left atrial volume, (p<0.001). No difference in NT pro-BNP, hs-CRP and IL-6was demonstrated between recurrence and non-reccurence group. DecreasedNTpro-BNP levels were observed in both groups at 1 month (p<0.001, F= 63.4).Left atrial volume was positively related to baseline and 1 month NT pro-BNP
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atrial fibrillation I 109
(p<0.01). Both baseline and 1 month NT pro-BNP levels were lower in the loneAF patients compared with the non-lone group and there was significant drop inthe 1month values (between groups F=9.84, p< 0.001, within groups F=63.46,p< 0.001, interaction F=6.53, p< 0.01).
Biochemical and echocardiographic values
No recurrence Recurrence Total F/χ2 pwithin 1 month 1 month N=80
N=50 N=30
log hs-CRP baseline 1.1±0.8 1.1±0.9 1.1±0.8 0.04 0.8log hs-CRP, 1 month 0.6±0.95 0.7± 0.65±1 0.3 0.6log IL-6 baseline 1.1±0.7 1.4±1 1.2±0.8 1.5 0.2log IL-6, 1 month 1.2±0.7 1.4±1 1.2±0.8 0.3 0.57log NT pro-BNP baseline 5.6±1 5.7±1.1 5.6±1 0.09 0.7log NT pro-BNP, 1 month 4.1±1.1 4.8±1.4 4.4±1.3 4.6 0.03LV ejection fraction, % 58±6 58±6 58±6 0.00 1LA diameter, mm 42±3.5 43±5.5 42.3±4.7 0.8 0.37LA volumeindexed for BSA, mL/m2 27.8±6.5 38.6±5.8 32±8.1 32.8 0.000001
BSA = Body Surface Area, LA = Left atrium, LV = Left Ventricle.
Conclusion: Increased atrial volume was related to AF recurrence, whereas hs-CRP, IL-6 and NT pro-BNP were not reliable biomarkers to anticipate AF relapse.Relation of NTpro-BNP to left atrial volume could indicate a role in the atrial re-modeling process.
P735 The impact of polymorphisms in the promoter regionof tumour necrosis factor-alpha on the vulnerability ofatrial fibrillation in the Chinese Han population
R. Fu1, S. Wu1, J. Qiu2. 1Guangdong Cardiovascular Institute;Guangdong Provincial People’s Hospital, Guangzhou, China, People’s
Republic of; 2Cardiovascular department, Liuhuaqiao Hostpital, Guangzhou,China, People’s Republic of
Aims: The aims of the present study were to investigate the role of TNF-alphaSNPs (mainly -308 position) in the genetic susceptibility to AF in the ChineseHan population and explore the independent risk factors for AF, and thus to helpestablish the relationship between inflammation and AF.Methods: A detailed medical history of each subject was obtained with aquestionnaire. Cardiac morphologic indices were measured with transthoracicechocardiogram. Genotypes were determined by DNA sequencing of target TNF-alpha gene regions. Serum TNF-alpha and CRP levels were detected by Enzyme-Linked ImmunoSorbent Assay (ELISA) and an immunoturbidimetry method, re-spectively.Results: 141 AF patients (90 male, mean age 55.3±10.5 years) and 116 con-trol subjects (62 male, mean age 55.3±8.8years) were enrolled. The two groupsshowed no differences in classic cardiovascular risk factors such as sex, age,history of hyperlipidemia and smoking status. Compared to controls, more AFpatients had hypertension, bradycardia, and mitral regurgitation, and higher val-ues of left atrium diameter (LAd) and left atrium diameter (RAd) were found inthe AF group. They also had significantly higher levels of circulatory TNF-alpha(4.81±2.67 vs 3.61±2.32 pg/ml, p<0.001) and CRP (3.15±4.21 vs 2.01±1.38mg/L, p≤0.003), with the differences remaining statistically significant even afteradjustment for confounding factors.Genotypic analysis showed no significant differences between patients and con-trols in terms of the distribution of TNF-alpha SNP site -857C/T, -806C/T, -782G/A,-646G/A, -575 G/A, -572A/C, -570C/A, -376G/A, -244G/A and -238G/A, while for-308G/A polymorphism, a higher frequency of the rare genotype (-308 GA+AA)was found in the subjects with AF than those without AF (20.6% vs 11.2%). Ahigher OR was seen for individuals with the -308 GA+ AA genotype as opposedto the GG genotype for the risk of AF (OR: 2.052, 95%CI:1.012-4.159, p=0.043).Differences in circulatory TNF-alpha level were not-significant in either the AF orthe control group.After allowance for potential confounders, unconditional logistic analysis revealedthat circulatory TNF-alpha level, rather than -308G/A SNP, was an independentrisk factor for the development of AF (adjusted OR for TNF-alpha level: 1.248;95%CI:1.095-1.423, p = 0.001).Conclusions: An inflammatory state marked by circulating TNF-alpha elevationis present in patients with AF. The TNF-alpha -308G/A polymorphism acts as amodifier rather than risk factor in AF development.
P736 Extracellular matric alterations after sinus rhythmrestoration in patients with persistent atrial fibrillation
E.M. Kallergis, E.G. Manios, E.M. Kanoupakis, H.E. Mavrakis,C.A. Goudis, I.G. Saloustros, C.E. Lathourakis, F.I. Parthenakis,P.E. Vardas. Heraklion University Hospital, Department of Cardiology,
Heraklion, Greece
Purpose: To evaluate the importance of serum markers of collagen turnover inpredicting the outcome of electrical cardioversion (CV) of persistent atrial fibrilla-tion (AF) and to clarify the relationship between AF and fibrosis.Background: Collagen turnover and atrial fibrosis have been implicated in thegeneration and perpetuation of AF.Methods: Serum C-terminal propeptide of collagen type I (CICP) and Cterminal
telopeptide of collagen type I (CITP) were measured in 98 patients with AF beforeand two months after CV.Results: All patients were successfully cardioverted to sinus rhythm (SR) al-though in 23 of them AF recurred. Baseline CICP levels were comparable in pa-tients in sinus rhythm 60 days after CV and in those who experienced a relapse ofAF (82.464±16.65 ng/ml vs. 86.45±10.95 ng/ml, respectively, p=0.18). BaselineCITP levels were significantly higher in patients with AF recurrence compared tothose who remained in SR (0.47±0.15 ng/ml vs. 0.33±0.19 ng/ml, respectively,p=0.001). The restoration and maintenance of SR resulted in a decrease of CICPbut not of CITP levels. In the 75 patients who maintained SR, CICP levels weresignificantly lower at the end of the study as compared to baseline, (61.89±14.18ng/ml vs. 82.464±16.65 ng/ml p<0.001), while there was no difference in plasmaCITP levels, (0.35±0.20 ng/ml vs. 0.33±0.19 ng/ml, respectively, p=0.477).Conclusions: AF can result in alterations in atrial structure and architecture thatmake the atrial myocardium more susceptible to the maintenance of the arrhyth-mia. Sinus rhythm restoration could affect the fibrotic processes that occur orbecome exacerbated during AF course.
P737 Atrial fibrillation and anti-inflammatory medication withNimesulde
S. Grigoryan, K.G. Adamyan, L.G. Hazarapetyan, V.A. Mkrtchyan.Institute of Cardiology, Yerevan, Armenia
Background: Atrial fibrillation (AF) is the most frequent arrhythmiafound in clinical practice. AF is associated with atrial structural changes that mayhave an inflammatory basis. Last year we have suggested a mechanistic link be-tween inflammatory processes and the development of AF. A classical marker ofinflammation, C-reactive protein (CRP) and proinflammation agent Interleukin –6 (IL-6) were found elevated in patients with AF. It is known about inflammationin genesis and perpetuation of AF and possible therapeutic implications for theinhibition of inflammation as an evolving treatment for AF.In this study we aimed to assess the influence of nonsteroid treatment in theprevention of persistent AF by modulating inflammatory pathways.Methods: 76 patients with non-rheumatic persistent AF (mean age 63.6±9.3)where enrolled in this study. After the enrollment the echocardiography examina-tion and 24-hour ambulatory Holter monitoring ECG were registered in each pa-tient. Blood samples were tested on the serum level of high-sensitive C-reactiveprotein (hs-CRP) and plasma level of Interleukin-6 (IL-6). All patients were dividedin two groups. The first group was treated with nonsteroid Nimesulide (N) 200mgdaily, and the second group has been administrated placebo (P) during 4 weeks.Prophylactic drug therapy with Amiodarone (200-300 mg daily dosage) to pre-vent early recurrence of AF was administered to all 76 patients (both placebo andtreatment groups) who were cardioverted into normal sinus rhythm and the pro-phylactic administration of amiodarone was maintained during the entire follow-uptime.Results: The obtained results have shown that the basis data of hs-CRP and ofIL-6 levels in patients with persistent AF were increased ((0.82±0.52 mg/dL and32±21 pg/ml accordingly). After 4 weeks treatment with N these indices weresignificantly reduced ((0.48±0.11 mg/do, p < 0.01 and 22.1±8.9 pg/ml, p<0.05accordingly). The follow-up during 16 weeks has shown that N reduces recurrentAF (primary end-point) from 29% in the placebo group to 8.6% in the N treatmentgroup and permanent AF (expanded end-point) from 19% in the placebo group to4% in the N treatment group.Conclusion: In this study there is the link between inflammation and AF that’swhy nonsteroid, such as N has efficacious in the prevention of AF by modulatinginflammatory pathways.
P738 Efficacy of antiarrhythmic drugs therapy in preventingAF recurrence and long-term cardiovascular prognosisin patients with asymptomatic paroxysmal atrialfibrillation
T. Komatsu, H. Tachibana, Y. Satoh, F. Kunugida, M. Ozawa,M. Nakamura. Division of Cardiology, Department of Internal Medicine, IwateMedical University., Morioka, Japan
Background: The clinical characteristics and cardiovascular prognosis of asymp-tomatic atrial fibrillation (AF) patients have not been elucidated completely.Aim and method: We evaluated the efficacy of antiarrhythmic drug therapy(AAD) and long-term cardiovascular prognosis in patients with asymptomaticparoxysmal AF in comparison to those with symptomatic paroxysmal AF. Thisretrospective study included 334 patients (229 men and 105 women, mean age69±11 years, mean follow-up 60±35 months) who were divided into two groups;patients with symptomatic AF (group I, N=289) and those with asymptomatic AF(group II, N=45) on the basis of subjective symptoms.Results: (1) CHADS2 score was significantly greater in group II (1.63±1.27) thanin Group I (1.14±1.18) (P<0.05). (2) Actuarial rates of patients without AF recur-rence, those with AF recurrence and with electrical/pharmacological cardiover-sion to restore sinus rhythm, and those with conversion to permanent AF despiteAAD after rhythm control therapy were 40%, 41% and 19% respectively in groupI, and 22%, 24% and 54% respectively in group II at the end of follow up period.At 60 months, the percentage of patients with conversion to the permanent formof AF was significantly greater in group II than in group I (P < 0.05, group I versus
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

110 Atrial fibrillation I
group II). (3) Survival rates free from symptomatic thromboembolism at 36, 60 and120 months were 96%, 93% and 88% respectively in group I, and 82%, 76% and71% respectively in group II (P < 0.05, group I versus group II). In patients notundergoing anticoagulant therapy, the annual rate of symptomatic thromboem-bolism was significantly greater in group II (5.3%) than in group I (2.3%) (P <
0.05), while in patients undergoing anticoagulant therapy there was no significantdifference in the annual rate of symptomatic thromboembolism between group I(0.9%) and group II (1.8%).Conclusion: The clinical course of asymptomatic paroxysmal AF is refractory toAAD when compared to symptomatic AF, meaning that anticoagulant therapy isrequired to prevent symptomatic thromboembolism in the asymptomatic paroxys-mal AF group.
P739 Normal left atrial size indicates existence of atrialfibrillation originated from superior vena cava
M. Wada, A. Hirata, H. Nakanishi, K. Kashiwase, S. Hirotani,N. Ogasawara, M. Nishio, T. Nemoto, K. Matsuo, Y. Ueda. OsakaPolice Hospital, Osaka, Japan
Background: Non-pulmonary vein focus of atrial fibrillation (AF) is a major causeof recurrence after catheter ablation of AF. Especially, AF originated from superiorvena cava (SVC) is frequent. It will be important to predict existence of SVC focibefore AF ablation. However, predictors of SVC foci are still unclear.Methods: We evaluated consequent ninety-four patients underwent AF ablationretrospectively. After pulmonary vein isolation, we induced atrial premature con-tractions initiating AF by infusion of isoproterenol (2-5mcg/min) and mapped theirorigins. We also used atrial burst pacing to induce premature contractions in somecases.Results: Age was 61±11years, and 69% were male. 85% were paroxysmalAF, and 15% were persistent AF. Left atrial diameter (LAD) measured by Mmode echocardiography was 42±6mm. SVC foci were seen in 10% of thepatients. The patients with SVC foci had smaller LAD than without SVC foci(36±5mm vs. 42±6mm, p=0.004) and greater left ventricular ejection fraction(71±6% vs. 66±8%, p=0.029). HDL-cholesterol was higher in those with SVCfoci (64±24mg/dl vs. 52±15mg/dl, p=0.033). Multiple logistic regression analysisincluding age, sex, types of AF, hypertension, diabetes mellitus, obesity and LAD(mm) revealed that LAD (mm) was the only predictor of SVC foci (odds ratio 0.81,95% CI 0.67-0.98, p=0.027).Conclusions: Etiology of AF with SVC foci might be different from AF with pul-monary vein foci. We conclude that patients with normal left atrial size should bescreened for SVC foci in AF ablation.
P740 The relationship between the frequency of paroxysmalepisodes of atrial fibrillation and structural remodelingprocess
L.G. Tunyan, S.V. Grigoryan. Institute of Cardiology, Yerevan, Armenia
Objective: To reveal the role of pulsed wave doppler tissue imagingand transesophageal echocardiography in study of the left atrial (LA) functionchanges and evaluate pulmonary venous flow (PVF) in patients (pts) with parox-ysmal atrial fibrillation (PAF), and assess the relationship between the frequencyof symptomatic arrhythmic episodes and echocardiographic data.Methods: The effect of symptomatic arrhythmic episodes on LA and PVF wasstudied in 67 pts with lone PAF (age 49±7 years, 46 men). Pts were divided intotwo groups based on the frequency of the symptomatic AF paroxysms. The firstgroup (n=33) included pts with paroxysms frequency of no more than one timein a three-month period. The pts of the second group (n=34) had more than oneparoxysm during the same three month period. AF paroxysms anamneses in allgroups were 3-9 months. The PVF atrial revers (AR), systolic (S) and diastoliccomponents velocities were measured. As a reference standard the conventionalmeasures of LA function were determined: peak mitral A wave velocity, atrial emp-tying fraction and atrial ejection force. Pulsed wave doppler tissue imaging esti-mated atrial contraction velocity (A’ velocity) of the mitral annulus lateral segment.Results: A’ velocities were significantly higher in pts with frequent PAF (10.5±1.4vs. 7.8±1.3 cm/s; p<0.005). A’ velocity correlated with LA fraction (r=0.53;p<0.005) and LA ejection force (r=0.56; p<0.005). Frequent AF paroxysms corre-lated significantly with LA ejection force (r=0.57; p<0.005), atrial fraction (r=0.61;p<0.005) and A’ velocity (r=0.54; p<0.005). S PVF had an inverse correlation(r=-0.6; p<0.005) with the frequency of PAF episodes (the S PVF was 74±8 cm/svs. 65±6.5 cm/s; p<0.005 among the least and the most frequent episodes ofPAF, respectively). AR PVF had positive correlation (r=0.55, p<0.005) with thefrequency of PAF episodes (the AR PVF was 21±5.5 cm/s vs. 33±4.4 cm/s;p<0.005 among the least and the most frequent episodes of PAF, respectively).There were no significant differences in the other echocardiographic measure-ments or demographic variables.Conclusions: Pulsed wave doppler tissue imaging and transesophageal echo-cardiography provide unique data about global atrial contraction and PVF. Fre-quent arrhythmic episodes significantly diminished S PVF and increased AR PVFand A’ velocities among pts with different frequency of the AF paroxysms. Thissuggests that A’ velocity and PAF components could be used as indicator of grad-ual mechanical remodeling of the atrium, which may favour recurrence and per-petuation of AF.
P741 Smoking is associated with a lower risk ofpostoperative atrial fibrillation
D.O. Arnar1, G.V. Skuladottir2, R. Heidarsdottir2, B. Torfason1,R. Palsson1, V. Edvardsson1, G. Gottskalksson3, O.S. Indridason3.1Landspitali University Hospital and University of Iceland, Reykjavik,
Iceland; 2University of Iceland, Reykjavik, Iceland; 3Landspitali UniversityHospital, Reykjavik, Iceland
Purpose: The adverse effects of smoking on health are well known. Smoking isa major risk factor for the development of heart disease. Population-based stud-ies have shown that both current and former smoking are associated with anincreased risk of atrial fibrillation. However, the results of a recent study suggeststhat smokers may be at lower risk of postoperative atrial fibrillation (POAF) fol-lowing open heart surgery. The aim of this study was to examine the relationshipbetween smoking and POAF in patients undergoing coronary artery bypass graft(CABG) surgery.Methods: This substudy is part of a randomized prospective study on the preven-tion of POAF using omega-3 polyunsaturated fatty acids. Included in this analy-sis were patients undergoing CABG surgery. POAF was defined as an episodelasting more than five minutes, documented by continuous electrocardiographicmonitoring. Wilcoxon-Mann-Whitney and chi-square tests were used to comparethe groups that did and did not develop POAF. multivariable logistic regressionwas used to examine the relationship between smoking and POAF.Results: A total of 125 patients were enrolled with a median age of 66 (range, 45-82) years, 82% were males. POAF occurred in 62 patients (49.6%). The patientsin the POAF group were older (P=0.003). They had a higher maximal serum con-centration of C reactive protein following surgery (P=0.04), and 14.5% of patientsin the POAF group smoked compared to 27% in the non-POAF group (P=0.086).After adjusting for confounding variables, there was a significant relationship be-tween smoking and POAF with an incremental Nagelkerke R2 of 0.067 (P=0.007)and an odds ratio of 0.216 (95%CI 0.070-0.664) for smokers. No interaction wasobserved between smoking and age, BMI, postoperative CRP concentration orlevels of n-3 PUFA in plasma phospholipids, regarding the risk of POAF.Conclusion: The results of this study suggest that smokers are at lower riskof developing POAF following CABG surgery, an effect that is independent ofother major risk factors for this arrhythmia. This association was unexpected andrequires further study. The mechanism behind this is unclear but may possiblybe related to better tolerance to a hyperadrenergic state following major heartsurgery.
P742 Effect of herbal consumption on clinical efficacy ofwarfarin therapy in patients with atrial fibrillation
H.T. Chan1, J. So1, S.W. Li2, C.W. Siu1, C.P. Lau1, H.F. Tse1. 1QueenMary Hospital-The University of Hong Kong, Department of Medicine,Cardiology Division, Hong Kong, China, People’s Republic of; 2Tung
Wah Hospital, Department of Medicine, Hong Kong, China, People’s Republic of
Background: Although it is well known that herbal intake can affect anticoagula-tion effects of warfarin, the long-term impact of herbal intake on anticoagulationcontrol among patients (pts) receiving warfarin is unclear.Objective: We sought to investigate the effect of concomitant herbal intake onanticoagulation control in pts with non-valvular atrial fibrillation (AF) treated withwarfarin.Methods and Results: We studied the effects of common herbs comsumption onthe anticoagulation effect of warfarin as determined by international normalizedratio (INR) in 250 AF pts (69±10 years, 50% male). All pts received warfarin ther-apy for at least 6 months prior enrollment, and their dietary intake, including thetypes and frequency of common herbs were recorded with a standardized ques-tionnaires. Up to 50% of pts reported consumption of foods with herbal ingre-dients, including garlic (80.4%), ginger (74.8%), green tea (50.4%) and papaya(55.2%), but rarely herbal drugs including danshen (1.2%), dong guai (0.8%),fenugreek (1.2%), psyllium seed (0.4%) and ginseng (4%). Furthermore, non-users of herbs (61.1%) had a higher percentage of optimal therapeutic range INRmeasurements (defined by >66.67% time achieved INR level between 2 and 3)as compared with occasional users (> once per month, 28.1%, P=0.022) andfrequent users (> once per week, 37.0%, P=0.045) of herbs (Fig. 1).
Figure 1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
Atrial fibrillation I 111
Conclusion: Pts with AF treated with warfarin had limited knowledge on the po-tential interaction between herbal substances in foods and warfarin, and thosewho consumed common herbs at least once per week was associated subopti-mal anticoagulation control with warfarin.
P743 High incidence of false positive results in detecting leftatrial appendage thrombi in patients with atrialfibrillation
G. Karatasakis, E. Demerouti, A. Dimopoulos, N. Plessas,G. Athanasopoulos, E. Leontiadis. Onassis Cardiac Surgery Center,
Athens, Greece
Anticoagulant therapy is a prerequisite for pts with atrial fibrillation (AF) scheduledfor cardioversion (DC). The presence of left atrial appendage thrombi (LAAT) isconsidered an absolute contraindication for DC. Transesophageal echocardiogra-phy (TEE) is widely used for the exclusion of LAAT despite scarse evidence for itsdiagnostic accuracy in this field. The presence of dense and slow moving spon-taneous echo contrast (SEC) may impede definite diagnosis.The aim of this study is to evaluate the diagnostic value of contrast injection trans-esophageal echocardiography (TEECON) versus plain TEE in ruling out LAAT.We prospectively studied 38 patients (25 males) aged 27-76 years, with AF whowere scheduled for cardioversion. All patients underwent standard transthoracicand TEE study prior to cardioversion. By the end of the TEE study, 0.5 ml of sul-fate hexafluoride solution was injected intravenously in each patient. The analysisof the TEE digitized images was performed by two independent observers off line.By plain TEE there were 7 patients (18.4%) with LAAT, while this finding wasconfirmed by TEECON only in one patient (2.6%,p: 0.029).Pts with LAAT on plain TEE did not differ in left atrial size (58±10 versus 49±9mm p: NS), left ventricular function (EF 52±10 vs 48±11%, p: NS), severity ofSEC and right ventricular systolic pressure (45±17 vs 40±10 mmHg, p:NS) frompatients without the diagnosis of LAAT on plain TEE.Left atrial emptying velocity (LAAV) was lower in patients with LAAT on plain TEE(28±12 vs 45±20, p: 0.038).All patients with negative TEECON underwent successful cardioversion despitepositive plain TEE, with no evidence of thromboembolic events during post-cardioversion follow up.In conclusion, these data confirm our previous observation indicating that theuse of plain TEE for the exclusion of LAAT should be limited only in pts withoutadequate anticoagulant therapy who have higher incidence of LAAT. There is asignificant amount of false positive results of LAAT formation by plain TEE. Theuse of intravenous contrast injection in pts with evidence of LAAT decreases falsepositive results and may prevent us from postponing or deferring cardioversion inpts that may benefit from this procedure.
P744 Determination of the threshold velocity of left atrialappendage blood flow to form intra-atrial thrombus inpatients with atrial fibrillation
A. Watanabe, T. Uejima, S. Watanabe, Y. Tsutsumi, Y. Kataoka, M. Yui,N. Sasaki, T. Tanemura, T. Aizawa, H. Sawada. The Cardiovascular
Institute Hospital, Minato-ku, Japan
Purpose: Atrial fibrillation (Af) is an independent risk factor of thorombo-embolicevents, especially cerebral embolism. Anticoagulation therapy is highly recom-mended to prevent patients from cerebral embolism by stratifying embolic risksusing CHADS2 score. However, several clinical situations such as surgery do notallow us to use anticoagulants during peri-operative period. The purpose of thisstudy was to examine the hypothesis that anticoagulation therapy using warfarincan be safely suspended if the left atrial appendage (LAA) blood flow velocity isenough high. In this study, we determined the threshold velocity of LAA blood flowto form intra-arterial thrombus in the Af patients who do not receive warfarin.Methods: A total number of 1772 non-valvular Af patients with average age of66+11.5 who were examined by transesophageal echocardiography (TEE) wasincluded in this study and (1) the existence of intra-arterial thrombus, (2) left atrialgeometrical and functional parameters determined by TEE, and (3) CHADS2score were evaluated.Results: Of 1772 patients, 1239 patients (69.9%) had persistent Af and remain-ing 533 patients (30.1%) had paroxysmal Af. Seventy six patients (4.3%) hadintra-arterial thrombus and 54 (71.1%) of these patients did not receive warfarin.Maximal LAA blood flow velocity of patients who had thrombus and did not receivewarfarin was 39 cm/sec. Although the existence of thrombus was significantly cor-related with CHADS2 score (p<0.05), 5 patients (6.6% of 76 thrombus-positivepatients) whose CHADS2 score were 0 had thrombus, and their maximal LAAblood flow velocity was 28 cm/sec.Conclusions: In the absence of warfarin, patients whose LAA blood velocity isless than 40 cm/sec have a possibility to form a thrombus in the LAA. Therefore, insuch patients, we suggest that an alternative anticoagulation therapy using short-acting anticoagulant such as heparin is necessary to compensate anticoagulationwhen warfarin is off. Furthermore, we suggest careful observation of LAA andmeasurement of LAA blood flow velocity by TEE even in patients whose CHADS2score is 0.
P745 How Much Amount of Heparin should be used in theAtrial Fibrillation Ablation with therapeuticInternational Normalized Ratio?
T. Hayashi, K. Kumagai, S. Naito, Y. Miki, T. Sakamoto, K. Goto,R. Fukazawa, K. Kaseno, S. Oshima, K. Taniguchi. Gunma Prefectural
Cardiovascular Center, Maebashi, Japan
Background: Warfarin is often discontinued before atrial fibrillation (AF) abla-tion procedures, and intravenous heparin used to ‘bridge’ the patients. However,this ‘bridging therapy’ sometimes increases the thromboembolism risk. This studyaimed to investigate the appropriate heparin dose for AF ablation without stoppingwarfarin.Method: AF ablation was performed in 102 consecutive patients without cessa-tion of warfarin. Intravenous heparin was given every hour to keep the activatedclotting time (ACT) over 300 seconds during the procedure, and additional hep-arin was given according to the pre-procedural prothorombin international normal-ized ratio (PT-INR) after the procedure. The same warfarin dose was continuedthroughout the AF ablation.Results: The average ACT was 321±69 seconds and the injected heparin dosewas 6990±2715U during the procedure. Only one patient had an ischemicstroke as a thromboembolic complication. The patients who had higher pre-procedural PT-INRs, needed significantly lower heparin doses during the proce-dure (R=0.55). The PT-INR increased significantly the day after the procedure(1.78±0.6 to 2.00±0.6, p<0.001). Only one patient had a hematoma as a bleed-ing complication.
Conclusion: AF ablation without cessation of warfarin could be performed safely,and might prevent thromboembolic and bleeding complications. However, the PT-INR should be checked the day after the procedure because the effect of warfarinmay be excessively enhanced by the heparin.
P746 Left atrial thrombus and prognosis afteranticoagulation therapy in patients with atrialfibrillation
S. Fukuda1 , H. Watanabe2, K. Shimada1, S. Jissho1, H. Taguchi1 ,J. Umemura2, M. Yoshiyama3, T. Shiota4, T. Sumiyoshi2,J. Yoshikawa1. 1Osaka Ekisaikai Hospital, Osaka, Japan; 2Sakakibara
Heart Institute, Japan Cardiovascular Research Promotion Society, Tokyo,Japan; 3Osaka City University School of Medicine, Osaka, Japan; 4Cedars-SinaiMedical Center, Los Angeles, United States of America
Background: The anticoagulation therapy reduces the risk of thromboembolicevents by two-thirds in patients with atrial fibrillation (AF), indicating that, in someAF patients, it may not be effective in preventing thromboembolic events.Purpose: To investigate the prevalence of left atrium thrombus (LAT) in patientswith nonvalvular AF after anticoagulation therapy.
Figure 1
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

112 Atrial fibrillation I
Methods: This study consisted of 174 patients with nonvalvular AF who hadtransthoracic (TTE) and transesophageal echocardiographic (TEE) examinationsmore than 3 weeks after anticoagulation therapy. The clinical (age, hyperten-sion, diabetes, congestive heart failure, and the history of cerebral ischemia andCHADS2 index) and TTE characteristics (left ventricular (LV) and LA volumes, LVmass index, LV systolic and diastolic function, and RV pressure) were evaluated.The presence of LAT was estimated by TEE. The international normalized ratio(INR) was assessed before TEE examination.Results: In 174 patients, 17 (10%) patients had LAT after anticoagulation therapy.LAT was observed in 3 (4%) of 74 patients with an INR greater than 2.0. Thepresence of LAT was associated with longer AF duration, greater RV pressure,and higher prevalence of spontaneous echocardiographic contrast. Patients withLAT had worse 1-year outcomes compared with those without LAT (p<0.001).Conclusion: This study demonstrated that TEE found LAT in 10% of patients withnonvalvular AF who had anticoagulation therapy. Importantly, the presence of LATwas associated with worse 1-year outcome in AF patients with anticoagulationtherapy.
P747 CHADS2 score as predictor for the presence of a leftatrial thrombus before pulmonary vein isolation
P. Janse, D.A.M.J. Theuns, Y. Van Belle, T. Szili-Torok, L. Jordaens.Erasmus Medical Center, Thoraxcenter, Department of Cardiology,Rotterdam, Netherlands
Introduction: Before performing a pulmonary vein (PV) ablation, all risk factorsfor thrombo-embolic complication must be reduced to a minimum. Further, it is ad-vised to anti-coagulate before the procedure, irrespective of the CHADS2 score.The presence of a thrombus in the left atrial appendage (LAA) is usually identifiedby a Trans Esophagael Echo (TEE). It would be preferable to identify patients atrisk for having a LAA thrombus to avoid undergoing a TEE.Methods: All 5 variables according to the stroke risk system (CHADS2) were col-lected from a consecutive cohort scheduled for PV isolation in order to determinethe risk level. Sceduled patients were under effective oral anti-coagulation for atleast 4 weeks. The CHADS2 data were paired with echocardiographic data.Results: The cohort consisted of 228 patient (161 males, 67 females) allscheduled for PV ablation from January 2007 until December 2009. In 13 pa-tients (5.7%) a LAA thrombus was discovered. No CHADS2 score exceeded 3.CHADS2 scores of 0, 1, 2, and 3 were detected respectively in 127 patients (4thrombi, 3.1%), 71 patients (6 thrombi, 8.5%), 26 patients (3 thrombi, 11.5%) and4 patients (0 thrombi). No relation between the CHADS2 score and the presenceof thrombi as identified by TEE was found.Conclusion: The risk of a thrombo-embolic events decreases with a lowCHADS2 score. However, a low CHADS2 score was not related to the absenceof thrombi. From this point imaging to identify thrombi before PV ablation is stillmandatory
P748(W) The influence of atrial fibrillation on tricuspidannulus and right ventricular geometry in patientswithout significant tricuspid regurgitation
S.-J. Kim, E.-S. Shin, J.-H. Son, Y.-J. Kim, Y.-R. Ha, H.-K. Kim,S.-G. Lee. Ulsan University Hospital, Ulsan, Korea, Republic of
Background: In patients with severe isolated functional tricuspid regurgitation(TR), annular dilatation secondary to atrial fibrillation is the likely mechanism ofTR. However, the influence of atrial fibrillation on tricuspid annulus and right ven-tricular geometry in patients without significant TR is unknown.Methods: We evaluated 1,008 consecutive patients with atrial fibrillation referedfor echocardiography. We exculded patients with stenotic or regurgitant (morethan grade 2) valvular heart disease, moderate or severe pulmonary hyperten-sion, congenital heart disease, hyperthyroidism, or left ventricular ejection fraction< 50%. Finally, 83 patients participated in the study. Patients were classified intoparoxysmal (Group I, n = 19), persistent (Group II, n = 27), and permanent atrialfibrillation group (Group III, n = 37). We measured right ventricular eccentricity in-dex (RVEI) at parasternal view and right ventricular sphericity index (RVSI), rightventricular fractional area change (RVFAC) and tricuspid annulus (TA) dimensionat apical 4 chamber view.Results: Patients in Group II and III were more older than that in Group I (p= 0.047). Group III had increased left atrial volume index (p < 0.001) and rightatrial volume (p < 0.001) compared with Group I and II. End-diastolic RVSI wasincreased in Group III compared with Group I (p = 0.025). End-systolic TA di-mension were increased in Group III compared with Group I and II (p = 0.018).End-diastolic RVSI (r = 0.58), end-systolic RVSI (r = 0.56) and right atrial volume(r = 0.38) were significantly related to the end-systolic TA dimension in univariateanalysis. However, age, RVFAC, left atrial volume index and systolic pulmonaryartery pressure were not. In multivariate analysis, end-diastolic RVEI (p = 0.038),end-diastolic RVSI (p < 0.001), and right atrial volume (p = 0.008) showed theindependent association with end-systolic TA dimension.Conclusion: Chronic atrial fibrillation in patients without significant isolated func-tional TR may cause tricuspid annuls dilatation, which is associated with end-diastolic RVEI and RVSI, and right atrial volume.
P749 Assessment of global left atrial strain predictsCHADS2 score in atrial fibrillation
S.K. Saha1, P.L. Anderson1, G. Caracciolo2 , A. Kiotsekoglou3,S. Govind4, S. Wilansky2, P. Sengupta2. 1Sundsvall Hospital,Sundsvall, Sweden; 2Mayo Clinic, Scottsdale, United States of
America; 3Saint George’s University, London, United Kingdom; 4Vivus-BMJHeart Center, Bangalore, India
Background: Left atrial volume (LAV) remains elevated in the presence of atrialfibrillation (AF). However, it is unclear whether the dynamic LA function comple-ments assessment of LA volume for risk stratification of subjects with AF as char-acterized on the basis of CHADS2 score. In this project we hypothesized thatglobal LA strain could provide incremental information over LA volume (LAV) forrisk stratification in AF.Subjects and methods: Total 77 subjects of whom 36 had persistent atrial fibril-lation (AF) and 41 had no history of atrial fibrillation (controls) underwent compre-hensive 2-dimensional and Doppler echocardiography with offline assessment ofLA deformation by speckle tracking echocardiography. LA volume was estimatedby area-length method, indexed to body surface area along with longitudinal strain(Global LA S %). Multiple Logistic regression was performed to identify univari-ate and multivariate predictors of AF subjects with CHADS2 score of >2, whileReceiver operated characteristics (ROC) curves were plotted to identify role ofGlobal LA S% and indexed LAV for prediction of CHADS2 score >2.Results: On univariate analysis left ventricular ejection fraction (Odds ratio= 0.89,95% CI 0.84 to 0.96; p < 0.001), ratio of early diastolic flow to mitral annularearly diastolic velocity, E/E’ratio, (OR=1.12, 95% CI = 1,0 to 1,5; p= 0.04) weremost significant predictors. On multivariate regression, Global LA S% was theonly independent predictor of CHADS2 >2 (OR= 0.83, 95% CI = 0.67 to 0.98; p=0.02) and showed higher area under the curve on ROC analysis (Fig) comparedwith LA volume.
ROC analysis for predicting CHADS2 Score
Conclusion: Assessment of LA strain provides incremental information over LAvolume for predicting risk of stroke in AF.
P750 Adding ivabradine to amiodarone better reduces atrialfibrillation recurrence in sinus rhythm patients withdiastolic dysfunction than combination of amiodaroneand bisoprolol
K.G. Adamyan, A.L. Chilingaryan. Institute of Cardiology, Yerevan,Armenia
Left ventricular diastolic dysfunction (DD) represents a common cause of atrialfibrillation (AF) due to overstrained left atrium (LA). We assumed that after AFconversion to sinus rhythm (SR) maximal dose of ivabradine (I) in combinationwith amiodarone (A) might be more effective and safe in sinus rhythm mainte-nance in patients with LV diastolic dysfunction due to impaired relaxation (DD)through better heart rate reduction and thus diastole prolongation than combina-tion of amiodarone and bisoprolol (B) in which B dose increments might be unsafedue to increased risk of AV conduction abnormalities.Methods: 95 pts (31 female) aged 58±4 years with DD and paroxysmal or per-sistent AF after pharmacological or electrical conversion to sinus rhythm wererandomized to two groups in order to receive A 200 mg/day maintenance doseafter loading dose and B titrated to 5 mg/day (n = 45) or combination of I titratedup to 10 mg BID and A 200 mg/day after loading dose (n = 46). DD was definedas E/A < 1.0, DT > 280 ms, IVRT > 80 ms. Transesophageal EchoCG (TEE)were done to measure LA maximal (LAVmax), minimal (LAVmin) and reservoir(LAVr) volumes, LAV at P wave (LAVP), LA passive emptying volume (LAVPE) asLAVmax – LAVP, LA stroke volume (LASV) as (LAVP – LAVmin), LA appendagefilling (LAAFV) and emptying (LAAEV) velocities by investigators unaware of thestudy aim in 1, 90 and 180 days and 1 year follow up.Results: In 1 day all parameters were comparable between groups. In 30 dayLAVPE and LAVP were significantly less in I group (LAVPE: 15.2±4.1 ml vs10.1±2.4 ml, p < 0.05; LAVP 20.3±4.6 ml vs 14.2±2.8 ml, p < 0.05). Other pa-rameters did not reach statistical significance between groups. In 90 day besidesleft atrial better passive emptying properties observed in 30 day, I group patientshad greater LASV, LAAFV and LAAEV and less heart rate (LASV: 7.4±2.1 ml vs4.1±0.9 ml, p < 0.05; LAAFV: 48.6±8.4 m/s vs 31.3±7.5 m/s, p < 0.05; LAAEV:49.2±8.6 m/s vs 32.7±7.7 m/s, p < 0.03; HR: 62±4 vs 71±6). These differencesremained unchanged up to 180 day follow up. During 1 year 11 patients of B and2 patients of I groups had AF recurrence (p < 0.05), more side effects and treat-ment discontinuation (AV node conductance abnormalities, hypotension, fatique)were observed in B (13 pts vs 2 pts, p < 0.03).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atrial fibrillation I 113
Thus combination of I and A compare to B and A is safer and improves LA passiveand active emptying properties and better control sinus rhythm after AF conver-sion in patients with DD AF through heart rate and LA afterload reduction withoutworsening LV relaxation.
P751 Establishment of a new method for clinical evaluationof microcirculation and usage in patients with atrialfibrillation and symptoms of acute coronary syndrome
H. Boenigk, J. Herold, S. Brucks, P.M. Mueller, S. Said, R.C. Braun-Dullaeus. Otto-von-Guericke University of Magdeburg, Departement
of Cardiology, Magdeburg, Germany
Background: Often patients with atrial fibrillation (Afib) present with typical chestpain and mildly elevated parameters of myocardial infarction. Usually, these pa-tients are referred to coronary angiography demonstrating either inconspicuouscoronaries. Additionally, patients discomfort can not be explained by tako-tsubosyndrome, muscle bridging, myocarditis, or vasospasm.Aim of the study: Establishment of a new easy to use, non-invasive techniqueto study microcirculatory changes during Afib, which may explain chest pain andelevation of myocardial necrosis parameters.Methods: Under standard conditions (heating plate, 37 °C) non-invasive, tran-scutaneous examination of finger-perfusion was done with a laser scanner class2 (Perimed, Uppsala, Sweden). After invasive exclusion of coronary heart dis-ease, patients with Afib, chest pain and elevated myocardial infarction parameterswere examined before and 24 hours after effective cardioversion (CV) into sinusrhythm (group A). Age-matched probands in sinus rhythm were used as a control(group B). Additionally, angiological standard-testing to detect relevant micro- ormacroangiopathy was done.Results: Group A: 8 patients (58,25±5,52 years) were examined. During Afib,finger-perfusion was quantified to be 0.55±0.151 (min/max: 0.37-0.77). Twentyfour hours after re-establishment of sinus rhythm, perfusion had increasedto 0.79±0.08 (min/max: 0.64-0.90, p < 0.01). Heart rate had dropped from105±14,11 to 68±7,78 per min (p < 0.01). Group B: 15 probands (57,33±12,64years) were examined and a finger perfusion not significantly different to groupA in sinus rhythm was determined (109±0,14). Heart rate was 67,4±13,3 permin. Ankle brachial index ruled out macroangiopathy in all patients. Photoelectricplethysmography and SpO2 measurements of the extremity/fingers, although ameasure of microangiopathy, did not detect any differences before and after CV.Discussion: Microcirculation is impaired during Afib, which could explain chestpain and upregulation of myocardial markers even in the absence of coronaryheart disease. Re-establishment of sinus rhythm results in a rapid normalization.Whether microcirculation is affected by changes of heart rate or the irregularityof the pulse during Afib needs to be determined. Although this pilot study needsfurther verification and standardization in a larger trial, our data suggest that laserscanning is a very promising tool for determination of microcirculation in humandisease.
P752 Does the CHADS2 score help in assessing risk ofsubsequent mortality after an acute coronarysyndrome?
D. Poci1, M. Hartford2, T. Karlsson2, J. Herlitz2, N. Edvarsson2,K. Caidahl3. 1Orebro University Hospital, Department of Cardiology,Örebro, Sweden; 2Sahlgrenska University Hospital, Gothenburg,
Sweden; 33Department of Molecular Medicine and Surgery, Karolinska Institutet,Stockholm, Sweden
Atrial fibrillation (AF) is associated with an increased morbidity and mortality whenassociated with acute myocardial infarction. We hypothesized that the CHADS2score could be used as a risk assessment tool for mortality in patients with acutecoronary syndromes (ACS), irrespective of the presence or absence of AF.Methods: Consecutive patients with ACS admitted to a coronary care unit be-tween September 1995 and March 2001 were prospectively followed until deathor to the end of follow-up, January 1, 2007. The CHADS2 scores at baseline wereretrospectively calculated from the data collected at admission.Results: Of totally 2335 (66±10 years, 717 women) patients with ACS, 442 hadknown AF, new AF or AF developing during the in-hospital phase. The follow-upperiod was 72±5 months. The mean CHADS2 score was 1.6±1.4 versus 1.0±1.1in patients with and without AF, p<0.0001. The early mortality (<30 days) was13.8% for patients with AF and 5.2% for those without AF (p<0.0001). The all-cause mortality at 10-years showed a strong association with CHADS2 scores inboth groups, although stronger in patients without AF (hazard ratio [HR] per unitincrease in the six-graded CHADS2 score 1.53 [1.42-1.64], p<0.0001 vs 1.28[1.16-1.43], p<0.0001 after adjustment for potential confounders). The all-causemortality at 10-years was 63.6% and 36.3%, respectively, in patients with andwithout AF (p<0.0001).Conclusion: The CHADS2 score was useful in assessing the risk of subsequentshort- and long-term mortality, both in patients with and without AF. A consis-tent use of the CHADS2 score on admission for ACS might help to optimize thetreatment of risk factors, which could, in turn, mitigate subsequent risk of death.
P753 Atrial ischemia and the risk of new onset atrialfibrillation development after myocardial infarction
M. Alasady1, W. Abhayaratna2 , D. Leong1 , K. Robert-Thomson1 ,H. Lim1, D. Chew3, P. Sanders1. 1Cardiovascular Research Centre,Royal Adelaide Hospital, and University of Adelaide, adelaide,
Australia; 2Australian National University, and Department of cardiology at theCanberra Hospital, canberra, Australia; 3Flinders Medical Centre/Department ofCardiology, Adelaide, Australia
Purpose: Myocardial infarction (MI) can be associated with the development ofatrial fibrillation (AF) in up to 20% of the cases and results in significant mor-bidity and mortality. In a prospectively collected clinical cohort, we evaluated thecharacteristics associated with the development of new onset AF.Methods: From a prospectively collected cohort of 3,200 pts with acute MI, 149(4.6%) were identified as having new onset AF within 7 days of MI. After excludingpts with previous AF, severe valvular heart disease, left ventricular hypertrophyor heart failure, using a nested case-control study design, we assessed coronaryanatomy by angiography, and cardiac structure and function by echocardiographyin 42 AF cases and 42 controls (AMI but no AF).Results: The groups were matched for age, gender, LVEF, and cardiovascularrisk factors. AF pts more often had inferior MI (P= 0.002) but less ST segmentelevation MI (P=0.02). Univariate factors associated with AF included increased inleft atrial size (P<0.001), LV filling pressure E/E’ (P<0.001), atrial branch diseaseand left main (LM) disease (P=0.02). In multivariate analysis, lesions in the leftatrial branch of the circumflex artery (P<0.01) and right atrial branches (sinoatrial,right intermediate and atrionodal; p<0.006) were predictors of AF after adjustingfor LM disease, and E/E’. A composite of major cardiovascular outcome (MACE)of death, stroke, bleeding, and heart block were worse in the AF group comparedto controls (P=0.02). In addition, early VF was seen more frequently in the AFgroup (17% vs. 0%; P=0.02)
No AF (n=42) AF (n=42) P-value
Left main disease, n (%) 3 (7.3) 11 (26.6) 0.02Three vessels disease, n (%) 8 (19) 14 (33.3) 0.14Right coronary artery disease, n (%) 9 (21.4) 30 (71.4) 0.009Left circumflex artery disease, n (%) 17 (40.5) 25 (59.5) 0.10Right atrial branches disease, n (%) 8 (19) 28 (66.7) 0.006Left atrial branches disease, n (%) 7 (16.7) 18 (42.9) 0.01
Conclusions: The presence of Atrial ischemia as evident by compromised atrialbranches is an important determinant for the development of AF after MI. Thisfinding was independent of age, gender, pressure load or LV systolic dysfunction.AF was strongly associated with MACE in the 7 days post-MI.
P754 The effects of amiodarone and early cardioversion onpostoperative atrial fibrillation after cardiac surgery
I. Atar, E. Karacaglar, S. Ozbicer, S. Ozcobanoglu, A. Yazici,B. Gultekin, A. Sezgin, H. Muderrisoglu, S. Aslamaci, B. Ozin. BaskentUniversity, Faculty of Medicine, Ankara, Turkey
Background: Previously many strategies have been used to prevent atrial fibril-lation (AF) after cardiac surgery but still there is limited data about postoperativeAF therapy after cardiac surgery. The aim of this study was to evaluate the selec-tive use of amiodarone and early cardioversion postoperatively to restore normalsinus rhythm in patient with postoperative AF after cardiac surgery.Methods: This study was a prospective, randomized, open-controlled trial. A totalof 50 patients [mean age, 68±8 years; 33 men, 17 women] with coronary arterydisease who had new onset AF longer than 30 min after CABG operation werescheduled for the study; 26 patients were randomized to control group and 24 toamiodarone group. The amiodarone group received 300 mg of amiodarone bolusintravenous in 30 min and thereafter received an infusion of 50 mg/hours overa 24-hour period. The control group was received a combination of digoxin andmetoprolol or diltiazem according physician discretion and patients heart rate first24 hours. If NSR was not established within 24 hours, then external electricalcardiversion was performed for two groups.Results: Baseline characteristics were similar between 2 groups. There were sig-nificantly higher NSR at 24th hours in amiodarone group than control group (19patients 79% vs. 13 patients 50%, p=0.042). Cardioversion rate were significantlyhigher in control group than amiodarone group (10 patients 38% vs. 2 patients8%, p=0.019). Normal sinus rhythm at discharge and 1st month were similar be-tween groups. Crossover ratio was significantly higher in control group than amio-darone group (10 patients 38% vs. 2 patients 8%, p=0.019). Complication ratiowas similar in two groups.Conclusions: Our study is the first randomized, prospective controlled study con-ducted to evaluate the effect of amiodarone and early cardioversion on postoper-ative AF after cardiac surgery. Amiodarone therapy seems to effective restoringNSR at 24th hours but not at discharge and 1st month.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

114 Atrial fibrillation I / Atrial fibrillation ablation
P755 Serum resistin level: as a predictor of atrial fibrillationafter coronary artery bypass graft surgery
H. Gungor, M.F. Ayik, B.S. Yildiz, I. Gul, S. Ertugay, S. Nalbantgil,M. Zoghi. Ege University, Faculty of Medicine, Izmir, Turkey
Purpose: Atrial fibrillation (AF) is the most common arrhytmia, withan incidence of 25-40%, after coronary artery bypass grafting (CABG). Previ-ous reports have suggested that AF is associated with an increased incidense ofmortality, stroke, heart failure, renal insufficiency, prolonged hospitalization andincreased social costs. The concept of inflammation as a pathophysiologic deter-minant of AF after CABG is supported by the literature.Resistin is a newly identified adipocyte secreted hormone belonging to a cysteine-rich protein family. It is expressed in white adipose tissues and also has beenfound in several other tissues in human. Recently it was found to be relevant toinflammation-related disease and correlated with serum CRP level. The presentstudy examined relation of preoperative and postoperative early serum resistinlevel, which can play an important role as an inflammatory marker to predict AFafter CABG.Methods: We prospectively analyzed 40 consecutive patients (mean age59,2+10,3 years, 31 male) who were undergoing CABG between September andNovember 2009 at our department. Details of baseline clinical characteristics,preoperative treatment, echocardiographic features, angiographic findings, intra-operative and postoperative findings were recorded. Blood samples were taken toexamine quantities of resistin level the day before surgery and on the 24 th hourin the intensive care unit.Results: The incidence of AF was 25% (n=10, 2,2+1,1. days, 1,2+0,4 episodes).The median age of patients with AF was 68,5+7,1 years compared with 56,1+9,1years for patients with sinus rhythm (SR) (p<0,001). Patients with AF had moreNYHA class II functional capacity (90% vs 50%, p=0,032) compared with SR grup.Preoperative glomerular filtration rate (64,1+23,6 ml/min vs 85,3+26,7 ml/min,p=0,03) and beta-bloker use (40% vs 80%, p=0,04) was significantly lower in AFgrup. Cardiopulmonary bypass time, inotropic medication use, extubation time,intensive care unit following time and postoperative hospitalization time, hospi-tal costs and complication rate were significantly higher in the AF group. Preop-erative resistin level was higher in AF group (10,6+3,3 ng/ml vs 9,1+4,5 ng/ml,p=0,33) but it was not statistically significant. Postoperative resistin level was sig-nificantly higher in AF group (27,4+8,4 ng/ml vs 17,9+9,1 ng/ml, p=0,012) com-pared to SR group.Conclusion: Patients with elevated postoperative resistin level may have high riskfor AF after CABG. This interventions targeting inflammation might help reducingincidence of AF.
P756 Atrial arrhythmias more than 10 years after successfulmaze procedure
T. Kamakura1, H. Okamura1, T. Noda1, K. Satomi1, K. Suyama1,W. Shimizu1, N. Aihara1, S. Kamakura1, J. Kobayashi1, K. Kosakai2.1National Cardiovascular Center, Suita, Osaka, Japan; 2Senri Central
Hospital, Osaka, Japan
Purpose: Sinus rhythm (SR) can be maintained in 50-80% of patients withchronic atrial fibrillation (CAF) in the short to intermediate term after a mazeprocedure (MP) or catheter ablation (CA). However, the percentage of patientswithout AF and the type of atrial arrhythmia in the long term (>10 years) has notbeen reported.Methods: To predict the long-term outcome of CA, postoperative P and F wavemorphology on 12-lead ECG was evaluated in 120 patients (52 males and 68 fe-males; age: 56.6±8.5 years) after successful modified Cox/Kosakai MP for CAF.Successful MP was defined as showing sinus rhythm for at least 1 month af-ter surgery. Mean follow-up time was 13.3±1.8 years. Among the 76 patientswho had maintained normal left ventricular (LV) function (%fractional shortnen-ing (%FS)≥30%) without significant valve failure until final follow-up, 36 patients(Group A) showed preoperative echocardiographic left atrial dimension (LAD)<55mm, and 40 patients (Group B) had LAD ≥55mm. The remaining 44 patients(Group C) showed %FS <30% or valvular regurgitation ≥3/4.Results: Concomitant mitral valve procedures (replacement/plasty) were per-formed in 94%, aortic valve procedures in 35%, and coronary artery bypass graft-ing in 3% of patients. SR, AF and atrial tachycardia (AT) with a cycle length ≥200ms were noted in 33%, 31%, and 36% of patients in Group A, respectively, 35%,45%, and 20% of patients in Group B, respectively, and 28%, 36%, and 36% ofpatients in Group C, respectively, based on the latest ECGs. There was no signifi-cant difference among three groups in the prevalence of arrhythmias (P=0.41). Atlast follow-up, 32% of the patients were free of atrial tachyarrhythmia. AT occurredin 31% of the patients. Only 16% of patients with AT showed positive P waves inV1 and V2 leads. Twenty-one percent of the patients required permanent pace-maker implantation.Conclusions: AT as well as AF frequently occurred after successful modifiedCox/Kosakai MP for CAF. AT of non-pulmonary vein origin and AF developed inabout 60% of patients who had smaller LAD and good LV function for >10 yearsafter successful MP. Atrial arrhythmogenicity may persist even after radical CA forCAF.
P757 Symptoms in atrial fibrillation are related to oxygenuptake at anaerobic threshold
I. Ariansen1, M. Abdelnoor2 , T. Dammen3, E. Edvardsen4, A. Tveit5,K. Gjesdal6. 1Department of Cardiology, Oslo University HospitalUlleval, Oslo, Norway; 2Center for Clinical Research, Oslo University
Hospital Ulleval, Oslo, Norway; 3Department of Psychiatry, Oslo UniversityHospital Ulleval and University of Oslo, Oslo, Norway; 4Department of PulmonaryMedicine, Oslo University Hospital Ulleval, Oslo, Norway; 5Department of InternalMedicine, Asker and Bærum Hospital, Vestre Viken Hospital Trust, Rud, Norway;6Department of Cardiology, Oslo University Hospital Ulleval and University ofOslo, Oslo, Norway
Purpose: Exercise hyperpnea normally occurs after the anaerobic threshold inresponse to increased production of lactic acid. We hypothesized that symptomsand health-related quality of life (HRQoL) scores were associated with exercisecapacity both at the anaerobic threshold and at peak oxygen uptake (VO2 peak)in patients with permanent atrial fibrillation (AF).Methods: 75 year-old patients with permanent AF, recruited from the generalpopulation, underwent maximal treadmill cardiopulmonary exercise testing, mea-suring VO2 peak. The oxygen uptake (VO2) at anaerobic threshold was assessedby the modified V-slope method. The participants filled in the arrhythmia-specificquestionnaire Symptom Checklist Frequency and Severity, where higher scoresdenote more or worse symptoms, in addition to the generic HRQoL questionnaireSF-36 where higher scores represent better HRQoL. SF-36 score results werepooled into a Physical Component Summary score (PCS) and a Mental Compo-nent Summary score (MCS). A similar program was also applied to 75 year-oldsubjects in sinus rhythm.Results: AF patients (n=27) had VO2 peak (mean ± SD) 22.7±5.5 ml/kg/min.VO2 at the anaerobic threshold was 16.6±3.2 ml/kg/min. AF patients had PCSmedian (25th, 75th percentile) 41 (31, 51), MCS 56 (42, 61), Symptom frequencyscore 16 (9, 21) and Symptom Severity score 12 (8, 18). In AF patients Symptomfrequency and Symptom severity scores were strongest related to VO2 at theanaerobic threshold, and PCS score was related to VO2 peak (Table 1). In 70subjects with sinus rhythm PCS score was related both to VO2 peak and VO2 atthe anaerobic threshold.
Table 1. Spearman correlations
Symptom frequency Symptom severity PCS
Atrial fibrillation VO2 at AT - 0.62, p=0.006 - 0.64, p=0.006 0.41, p=0.102VO2 peak - 0.49, p=0.016 - 0.41, p=0.049 0.55, p=0.006
Sinus rhythm VO2 at AT -0.22, p=0.078 -0.24, p=0.064 0.46, p<0.001VO2 peak -0.22, p=0.069 -0.19, p=0.132 0.49, p<0.001
VO2 = oxygen uptake (ml/kg/min). AT = anaerobic threshold. PCS = SF-36 physical componentsummary score.
Conclusion: Symptoms in patients with permanent AF were related to the oxy-gen uptake at the anaerobic threshold, whereas physical HRQoL score was morerelated to maximal exercise capacity.
ATRIAL FIBRILLATION ABLATION
P758 Atrial fibrillation: how far are patients ready to go?
T. Potpara, M. Polovina, M. Petrovic, Z. Vasiljevic, B. Vujisic-Tesic,M. Grujic, M. Ostojic. Institute for Cardiovascular Diseases, ClinicalCenter of Serbia, Belgrade, Serbia
Purpose: to examine atrial fibrillation (AF) patients’ attitude towardsinvasive treatment of AF.Methods: out of 1478 consecutive AF patients referred to our hospital during2007, both for outpatient or in-hospital assessment and treatment, 471 pts wererandomly assigned to complete a set of questions including: "would you acceptany invasive procedure, even if painful and/or risky, if it could cure your AF?"Results: Regardless of tertiary nature of our hospital, these patients were initiallyreferred to our institution immidiately after diagnosis of AF. and we have beenalready following them for 1-6 months (15pts), 1-4 years (35pts), or ≥5 years(421pts). Out of 471 pts, 145 (30.8%) were women, 188 pts (39.9%) had loneAF, 111 pts (23.6%) had paroxysmal, 142 (30.1%) persistent and 218 (46.3%)permanent AF. Asymptomatic AF was documented in 50 pts (10.6%). Mean agewas 62.1±11.7 years, and 130pts (27.7%) were already retired from work. Loweducational level (elementary school) was declared by 56 pts (11.9%), while 130pts (27.7%) reported university or higher education level. Patients answered asfollows: "yes" 224 (47.6%), "no" 125 (26.5%) and "it depends" 122 (25.9%). Mul-tivariate logistic regression analysis identified male gender (OR 2.2, 95%CI 1.4-3.6, p<0.001), persistent AF (OR 2.3, 95%CI 1.2/4.3, p=0.01) and symptoms (OR2.3, 95%CI 1.5-3.5, p<0.001) as predictors of confirmative answer, while high ed-ucation level (OR 1.63, 95%CI 1.1-2.6, p<0.01), retirement from work (OR 1.7,95%CI 1.1-2.7, p<0.05) and asymptomatic AF (OR 2.4, 95%CI 1.4-3.9, p<0.001)were multivariate predictors of negative answer.Conclusions: almost half of AF patients would undoubtedly accept any invasivetreatment of AF. Additional one quarter would probably do so after detailed expla-nation, while only one quarter of AF patients would not consider invasive treat-ment under any condition and these are usually asymptomatic, highly educated
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atrial fibrillation ablation 115
patients who are retired from work. Interestingly, the time from first diagnosed AFhad not significantly influenced the attitude towards invasive treatment of AF.
P759 Adenosine-induced reconnection after pulmonary veinisolation with a novel circular multielectroderadiofrequency ablation catheter
M. Brunelli, S. Raffa, A. Grosse, K. Wauters, J.C. Geller. CentralHospital Bad Berka, Clinic of Cardiology, Division of Electrophysiology,
Bad Berka, Germany
Introduction and Purpose: Pulmonary vein (PV) isolation has been establishedas the goal of treatment in patients (pts) with paroxysmal atrial fibrillation (PAF).However, recurrence rates after catheter ablation remain high and mostly due toPV reconnection. Therefore, additional pharmacological testing has been sug-gested. Aim of the study is to evaluate the effect of adenosine after "apparent"PV isolation in pts with PAF. A low energy phased radiofrequency circular multi-electrode ablation catheter (Pulmonary Vein Ablation Catheter [PVAC], MedtronicAblation Frontiers) was used to achieve electrical disconnection.Methods: The effect of adenosine on left atrial (LA)-PV conduction was prospec-tively evaluated after PV isolation (demonstrated by entry- and exit-block) wasaccomplished. After at least 20 minutes waiting period, repeated boli of 15mg ofadenosine were administered and the response assessed for each vein.Results: In 66 consecutive pts (55% male, mean age 59±11yrs, CHADS2score 1.3±0.9, LVEF 58.1±7.4%, LA diameter 39.6±6.1 mm) PV isolation wasachieved with the PVAC after a mean of 27±7 radiofrequency (RF) pulses(1462±418 seconds). Adenosine revealed residual conduction in 29 out of 264PVs (11%) in 19 pts (28.8%). The right inferior (16.7%) and the left superior(15.1%) showed an higher rate of reconnection compared to the left inferior andright superior (both 6.1%) PV. This response usually preceded any effect on thesinus or AV node. Both transient and permanent reconnection (86% and 14% ofreconnected PVs respectively) were observed. All PVs showing recovery of con-duction were treated with additional PVAC ostial applications (335±259 secondsand 5.9±4.4 RF pulses). In 3 right inferior PVs a cooled-tip catheter was requiredto complete isolation.Conclusions: A considerable number of PVs reconnect on adenosine, there-fore current standards (entry- and exit- block) might not represent a reliable end-point for PV isolation. In our population the left superior and the right inferior PVsshowed the highest percentage of reconnection and this might be explained byinsufficient catheter contact. The outcome of an adenosine-driven PV isolation onlong term success rate needs to be further evaluated.
P760 Small balloon, single freeze, cryo isolation of thepulmonary veins is effective in treating paroxysmalatrial fibrillation, 18 months follow up data
B. Keweloh, S. Siaplaouras, T. Willich, L. Bruch. ukb Berlin, Berlin,Germany
Introduction: Cryo-balloon based pulmonary vein isolation has emerged as asafe and potentially curative therapy for paroxysmal atrial fibrillation (PAF). Sofar two different balloon sizes, one or two transseptal punctures and several longfreezing applications per vein have been used.Hypothesis: We tested the hypothesis that the small 23mm balloon efficientlyoccludes all pulmonary veins in patients with normal atrial sizes and that aftera complete occlusion a single freezing interval efficiently isolates the pulmonaryvein and is sufficient for therapeutic success.Methods: We performed pulmonary vein isolation in 25 consecutive patients withsymptomatic PAF in spite of treatment with β-blockers and with normal atrial sizes.Except in one patient we used exclusively the small 23mm balloon. In 85 from 104treated veins without an early bifurcation a single cryo application per vein wasused. Isolation of the veins was proven by use of a Lasso catheter testing exit- andentrance block. Follow up was done by anamnesis of symptomatic episodes andby 72h ECG at 3, 6, 12 and 18 month, respectively. In 3 patients a second proce-dure was done, two times because of highly symptomatic PAF reoccurances, onetime because of an atrial macroreentry tachycardia.Results: In 25 patients 107 pulmonary veins were treated. We were able to oc-clude 95% of the veins (angiographic prove) and to isolate 98% electrically. 11 of25 patients had few symptomatic reoccurances of atrial fibrillation during the firstweeks after PVI (3 months blanking period). After 3, 6, 12 and 18 months 79, 68,71 and 66% of patients were in SR, respectively.We saw no cases of pulmonary vein stenosis, no fistula to the esophagus, onecase of pericardial effusion and two cases of left atrial flutter. During ablation ofthe right superior pulmonary vein 7 of 25 patients developed acute right phrenicusparesis which was completely regredient in all cases.Conclusion: Small balloon, single freeze cryo balloon ablation is efficient in treat-ing paroxysmal atrial fibrillation. After angiographic complete pulmonary vein oc-clusion a single freezing interval is sufficient to isolate the vein. Isolated rightsuperior veins despite early stopped cryo applications in case of phrenicus pare-sis indicate that much shorter cryo application times than commonly used mightbe sufficient to isolate the veins.
P761 Comparison of 28mm cryoballoon ablation versusradiofrequency catheter ablation of paroxysmal atrialfibrillation
M. Kuhne, Y. Suter, D. Altmann, B. Schaer, S. Osswald, C. Sticherling.University Hospital Basel, Basel, Switzerland
Introduction: Pulmonary vein (PV) isolation (PVI) usually using radiofrequency(RF) energy is the cornerstone of atrial fibrillation (AF) ablation. Cryoballoon ab-lation has emerged as new treatment strategy for patients with AF. The aim ofthis study was to compare procedural data, complications and outcomes aftercatheter ablation of paroxysmal AF using RF versus cryoballoon ablation.Methods: Forty patients (80%male, age of 57±9 years, left ventricular ejectionfraction 57±7%, left atrial size 41±5 mm) with paroxysmal AF referred for PVIwere included. Twenty patients underwent PVI using a single big (28 mm) cry-oballoon (Cryo-PVI) ablation catheter (Arctic Front, Cryocath). In an age- andsex-matched control group of 20 patients, PVI was performed using a 3.5 mm-tip open-irrigation RF ablation catheter (RF-PVI) in conjunction with an elec-troanatomic mapping system. The procedural endpoint was PVI confirmed by acircumferential mapping catheter.Results: There were no differences between the Cryo- and the RF-PVI group atbaseline. Total ablation time was 50±15 min. in the Cryo-PVI group and 45±10min. in the RF-PVI group (p=0.5). Total procedure time was 189±51 min. in theCryo- and 195±37 min. in the RF-PVI group (p=0.6). All PVs were successfullyisolated inthe RF-PVI group. In the Cryo-PVI group, 67/80 PVs (84%) could beisolated with the cryoballoon alone, the remaining 13 PVs (16%) were isolatedusing a conventional catheter. One tamponade requiring drainage occurred in theCryo-PVI group and one groin hematoma resulting in a prolongation of hospital-ization occurred in the RF-PVI group. With a standard postprocedural blankingperiod of three months, 15/20 patients (75%) in the RF-PVI group and 15/20patients (75%) in the Cryo-PVI group were in stable sinus rhythm after a meanfollow-up of 9±4 months.Conclusion: Catheter-based ablation of paroxysmal AF can be performed withsimilar procedure times, complication rates and success rates when compar-ing Cryo-PVI using a single 28mm cryoballoon to RF-PVI. However, randomizedhead-to-head comparisons are needed.
P762 64-MDCT in patients with symptomatic atrial fibrillationprior to pulmonal vein ablation with emphasize toincidental findings
C. Sohns1, S. Sossalla1, D. Vollmann1, L. Luethje1, J. Seegers1 ,M. Dorenkamp1, S. Obenauer2 , M. Zabel1 . 1Cardiology and
Pneumology, Goettingen, Germany; 2Radiology, Goettingen, Germany
Aim: To investigate prevalence of extracardiac findings (ECF) diagnosed by 64-MDCT prior to pulmonary vein (PV) ablation of atrial fibrillation (AF).Methods: 158 patients underwent 64-MDCT to characterize left atrial and PVanatomy prior to AF ablation. Images were evaluated by two reviewer. As well,bone, lung, and soft tissue window settings were used. CT scans with extra-cardiac abnormalities were divided into: Group 1 – clinically significant findings,and Group 2 – clinically non-significant findings.Results: ECF (n=198) were observed in 113/158 (72%) patients. At least onesignificant finding was noted in 49/158 patients (31%). Group 1 abnormalitieswere found in 85/198 findings (43%). Group 2 findings were observed in 113/198findings (72%).
Distribution of clinical significant or potentially significant extra cardiac findings
Clinically significant or potentially significant CT findings Patients [%]
Mediastinal lymph nodes > 10mm 9Moderate or severe degenerative spine disease 6.5Diaphragmatic hernia > 2 cm 5.5Moderate or severe emphysema 4Liver lesion 3.5Air space opacity 2.5Aortic aneurysm > 4 cm 2.5Pleural effusion 4Ground glass attenuation 4Pulmonary nodule > 4 mm 4Pulmonary tumor 1Pericardial effusion 0.5Splenomegaly 0.5Epigastrial lymph nodes 0.5Rib lesion 0.5Total 43
Conclusion: There is a prevalence of prior undiagnosed ECF detected in exami-nation of the PV by MDCT. Clinically significant findings can be expected in ∼40%of patients who undergo cardiac MDCT. Adequately trained personnel is requiredto identify and interpret both cardiac and extra cardiac findings.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

116 Atrial fibrillation ablation
P763 Intermittent atrial tachycardia facilitates atrialfibrillation by a shortening of activation recoveryinterval
J.N. Tenkorang1 , F. Jousset2, P. Ruchat1, J.-M. Vesin2, P. Pascale1,M. Fromer1, S.C. Schaefer1, S.M. Narayan3, E. Pruvot1. 1CentreHospitalier Universitaire Vaudois, Lausanne, Switzerland; 2Signal
Processing Laboratory Swiss Federal Institute of Technology, Lausanne,Switzerland; 3University of California, San Diego, United States of America
Introduction: We recently observed in a chronic ovine model that a shorteningof action potential duration (APD) as assessed by the activation recovery interval(ARI) may be a mechanism whereby pacing-induced atrial tachycardia (PIAT) fa-cilitates atrial fibrillation (AF), mediated by a return to 1:1 atrial capture after theeffective refractory period has been reached. The aim of the present study is toevaluate the effect of long term intermittent burst pacing on ARI before inductionof AF.Methods: We specifically developed a chronic ovine model of PIAT using twopacemakers (PM) each with a right atrial (RA) lead separated by ∼2cm. The 1stPM (Vitatron T70) was used to record a broadband unipolar RA EGM (800 Hz, 0.4Hz high pass filter). The 2nd was used to deliver PIAT during electrophysiologicalprotocols at decremental pacing CL (400 beats, from 400 to 110ms) and longterm intermittent RA burst pacing to promote electrical remodeling (5s of burstfollowed by 2s of sinus rhythm) until onset of sustained AF. ARI was defined asthe time difference between the peak of the atrial repolarization wave and thefirst atrial depolarization. The mean ARIs of paired sequences (before and afterremodeling), each consisting of 20 beats were compared.Results: As shown in the figure, ARIs (n=4 sheep, 46 recordings) decreased postremodeling compared to baseline (86±19 vs 103±12 ms, p<0.05). There was nodifference in atrial structure as assessed by light microscopy between control andremodeled sheep.
Conclusions: Using standard pacemaker technology, atrial ARIs as a surrogateof APDs were successfully measured in vivo during the electrical remodeling pro-cess leading to AF. The facilitation of AF by PIAT mimicking salvos from pul-monary veins is heralded by a significant shortening of ARI.
P764 Superior vena cava isolation using a circularmultielectrode ablation catheter in patients undergoingablation for paroxysmal atrial fibrillation
S. Raffa, A. Grosse, M. Brunelli, K. Wauters, J.C. Geller. CentralHospital Bad Berka, Department of Cardiology, Bad Berka, Germany
Purpose: The potential arrhythmogenic role of the atrial sleeves penetrating thesuperior vena cava (SVC) and the persistent left SVC (PLSVC) has been alreadydocumented. Aim of the study was to report over the feasibility and safety of iso-lating the SVC/PLSVC using a circular multielectrode ablation catheter (PVAC)in patients (pts) undergoing PV isolation and in whom paroxysmal atrial fibrilla-tion (PAF) was triggered by premature atrial complexes (PACs) originating in theSVC/PLSVC.Methods: Pts undergoing ablation for PAF at our institution in the last 10 monthswere included in the analysis. Once PV isolation was achieved using the PVAC,drug challenge using adenosine and isoproterenol was performed. SVC/PLSVCisolation was attempted only in those pts in whom frequent PACs, triggering ornot AF, originated from these veins. Radiofrequency energy was delivered for amaximum of 60 s per application (temperature controlled, 10 Watts, 60°C) onlyfrom those electrodes not demonstrating phrenic nerve capture. Isolation wasproved by entry- and exit-block.Results: During the study period a total of 80 pts (36 female, mean age 61±11yrs) underwent ablation for PAF using the PVAC. In 9 pts (11%) drug-induced(n=6) or spontaneous (n=3) PACs from the SVC (n=9) and the PLSVC (n=1) weredetected (5 female, mean age 60±12 years). All "arrhythmogenic" SVC/PLSVCwere successfully isolated using the PVAC (mean number of applications 4±2,mean energy-application duration 192±115 s). After isolation, repeated drugchallenge did not elicit any other potential AF trigger. No procedure-related com-plications occurred among these pts.Conclusions: 1) SVC/PLSVC-isolation using the PVAC is feasible and safe. 2)In the setting of a PV isolation-procedure, SVC disconnection using the PVACrequires a relatively short additional ablation time. 3) After PV isolation, drugchallenge using adenosine and isoproterenol is able to elicit extra-PV foci in theSVC/PLSVC in a considerable percentage of pts. Elimination of these triggersmight be crucial to improve clinical success.
P765 Incidence of esophageal lesions after pulmonary veinisolation using a remote robotic navigation system
A. Rillig, U. Meyerfeldt, R. Birkemeyer, S. Wiest, B. Sauer, M. Staritz,W. Jung. Schwarzwald-Baar Hospital Villingen-Schwenningen GmbH,Villingen-Schwenningen, Germany
Aims: Esophageal lesions (EL), a potential complication after pulmonary veinisolation (PVI), have been described recently. A new remote robotic navigationsystem (RNS; Hansen medical) provides enhanced catheter stability along withmore effective lesion placement. The aim of this prospective study was to evaluatetemperature monitoring and incidence of EL when using RNS with an irrigated tipradiofrequency (RF) catheter for PVI.Methods: Circumferential PVI using RNS was performed in 73 patients (pts) withparoxysmal (n=46, 63%) and persistent atrial fibrillation. An esophageal temper-ature probe was placed in 58 (79,5%) pts and was integrated in the 3D-map(NavX). Power was limited to 25 watts at the posterior wall, and in the case of anincrease in temperature power was limited to 20 watts. In 42 pts endoscopy wasperformed within 24h after PVI.Results: In 44/58 (75,9%) pts a significant rise in temperature (>39°C) was ob-served. In 6/42 (14,3%) pts an EL was found during endoscopy. In patients withEL the BMI was significantly lower than in pts without EL (24,1±2,0 vs 29,0±5,8,p= 0,047). The BMI of all patients with EL was below 26, whereas all patientswithout EL had a BMI above 26. The EL showed brisk healing after re-endoscopywithin 2 weeks in all pts.Conclusion: In patients undergoing PVI using the RNS, the incidence ofesophageal lesions is 14,3% when using power settings comparable to settingsused in manual ablation. Patients with lower BMI (< 26) are at higher risk foresophageal lesions.
P766 Assessment of cryoballoon ablation lesion formationusing DE-MRI in patients with paroxysmal atrialfibrillation
M. Daccarett1, M. Schmidt2, A. Akoum1, N. Burgon1, T. Haslam1,G. Vergara1, C. Mcgann1, J. Brachmann2, R. Macleod1,
N. Marrouche1. 1University of Utah School of Medicine, Salt Lake City, UnitedStates of America; 2Coburg Clinical Center, Coburg, Germany
Background: Cryoballoon catheter ablation is a promising new alternative fortreatment of paroxysmal atrial fibrillation (AF). As with radiofrequency energy,electrical isolation is achieved by encircling the pulmonary vein’s (PV) antrumwithcryo lesions. Delayed Enhanced MRI (DE-MRI) is a known method use to strat-ify patients prior toablation and delineate the amount of ablation lesion formationpost-procedure. In this study, we aim to evaluate the pre and post procedure le-sion formation characteristics of cryoballoon ablation using DE-MRI.Methods: Patients presenting with paroxysmal AF scheduled to undergo cryobal-loon ablation were prospectively followed. DE-MRI of the left atrium (LA) was per-formed prior to, immediately following, 24 hours and 3 months post-procedure toevaluate lesion behavior. The degree of LA structural remodeling was determinedas a percent of the LA area.Results: A total of 24 patients were included, with a mean age of 59.8±13 yearsold. Electrical isolation of all veins was obtained in 21 (87.5%) of patients whilethe remaining 3 (12.5%) patients had 3 out of the 4PVs isolated. Those patientswith recurrences were found to have a higher amount of fibrosis prior to ablation.
Conclusions: Our multicenter study represents the first prospective cryo-balloonablation lesion visualization study. The results suggest a similar pattern of lesionbehavior compared to radiofrequency ablation. The amount of LA structural re-modeling present prior to ablation was shown to predict recurrence at 6 months.
P767 Evaluating the pulmonary vein anatomy by magneticresonance imaging: an Italian registry
R. De Lucia1, E. Bertaglia2, F. Gaita3, R. Verlato4, M. Paolucci5,M. Del Greco6, C. Pratola7, E. Soldati1, M.G. Bongiorni1. 1SantaChiara Hospital, Cardiovascular Diseases Unit 2, Pisa, Italy; 2Hospital
of Mirano, Mirano, Italy; 3Cardinal Massaia Hospital, Department of Cardiology,Asti, Italy; 4P. Cosma Hospital, Department of Cardiology, Camposampiero, Italy;5Niguarda Ca’ Granda Hospital, Milano, Italy; 6Santa Chiara Hospital in Trento,Department of Cardiology, Trento, Italy; 7University of Ferrara, S. Anna Hospital,Cardiovascular Institute, Ferrara, Italy
Purpose: The aim of this study was to evaluate, by three-dimensional (3D)
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
Atrial fibrillation ablation 117
Magnetic Resonance Imaging (MRI), the prevalence and characterization of pul-monary veins (PVs) anatomical variability (AV) in patients undergoing AF ablation.Method: 3D MRI was performed in 164 patients undergoing PVs isolation fromJanuary 2008 to December 2009 in 7 Italian Centers. MRI data were importedinto electroanatomic mapping workstation (Carto System) and the AV of PVs wasevaluated. For each PV we measured the ostial diameters and circumference,and its neighbouring ridges. The AV analysis and measurements were performedin each Center according to previous standardized definitions and modalities.Results: Typical pattern of 4 PVs with 4 separate ostia was found in 98 patients(pts), 18 pts had an additional PV (APV), 39 pts had a common PV trunk (CPVT)and 9 pts both the anomalies. 100% of CPVT were left-sided and 88.9% of APVwere right-sided. Three different patterns APV were noted: right-sided were 3anterior, 20 middle and 1 posterior, while left-sided were 1 for each pattern.Thesuperior PVs risulted significantly larger when compared with the inferior ones(both p<0.001); the right-sided PVs risulted larger when compared with the corre-sponding left-sided ones (both p=0.05). The average intra-patient variability in PVdiameter was 14.5±5.9mm. The PV ostium was <10 mm in 77 pts and >25 mmin 38 pts. Early branching was found in 67 pts;in 55.2% of these, EB was presentin the right inferior PV. The shortest distance between right-sided PVs risulted sig-nificantly bigger than the same left-sided (7.7±3.9mm vs 5.7±2.5mm,p<0.001).Conclusion: 3D MRI is a pivotal technique for the assessment of PVs AV beforeAF ablation. It allows detection of atypical PVs patterns and of marked intrapatientAV. Information about AV may play a significant role before and during AF ablationprocedures.
P768 Late atrial tachycardia following pulmonary veinsisolation: analysis of discrete sites of successfulablation
F. Zoppo, E. Bertaglia, G. Brandolino, F. Zerbo, A. Lupo, E. Bacchiega.Dept of Cardiology, Mirano, Italy
Introduction: the preventive role of linear lesions added during pul-monary isolation (PVI) to prevent atrial tachycardias (AT) is not yet clear.Objective: to evaluate the mechanism and successful ablation sites of late onsetpost PVI-AT and to understand whether line lesions along the mitral isthmus andleft atrium (LA) roof could have been useful in preventing them.Methods: From March 2002 to August 2008, 366 patients underwent PVI alonefor drug refractory atrial fibrillation (AF). During follow-up, 26 of these patients(7.6%) developed late AT (paroxysmal AT in 13/26; 50%) and were referred forablation. Successful ablation discrete sites were analysed.Results: Twenty-seven ATs were encountered; mean cycle length was (CL) 240m/sec (range 217.5-250). In 3/26 cases, (11%), the mapping failed, while 23/26(88.5%) underwent a successful procedure (cumulative 24 ATs: 3/24 mapped asmitral isthmus-dependent AT, and 1/24 as LA roof dependant). In 15/23 (65.2%)patients, the AT was macroreentrant, and focal in the remaining 8/23 (34.8%). Atthe end of procedure, 22/26 (84.6%) of patients were not inducible. At 23.9±13.4months mean f/u, 23/26 patients (88.4%) remained free of AT, with AAD pre-scribed in 5/26 (19.2%) for AF prevention.Conclusions: in our case series, less than one/fifth of post-PVI ATs were mappedas mitral isthmus or LA roof-dependent circuits. These late onset ATs may besuccessfully ablated once they appear, with good long term outcome, insteadof adopting a preventive extensive ablation stragegy by means of linear lesionsdeploying.
P769 Myocardial injury after catheter ablation of atrialfibrillation: a comparison of cardiac biomarkers afterablation using radiofrequency energy versuscryoenergy
M. Kuhne, Y. Suter, D. Altmann, B. Schaer, S. Osswald, C. Sticherling.University Hospital Basel, Basel, Switzerland
Background: Cardiac biomarkers have been shown to be elevated after radiofre-quency (RF) catheter ablation for atrial fibrillation (AF). Lesion formation and en-ergy application times are different with RF compared to cryoenergy (Cryo). Theaim of this study was to compare the levels of cardiac biomarkers after pulmonaryvein isolation (PVI) of paroxysmal AF using RF versus Cryo and to correlate out-comes.Methods: Forty-two patients (81% male, age of 58±9 years, left ventricular ejec-tion fraction 57±7%, left atrial size 41±5 mm) with paroxysmal AF referred for PVIwere included. Twenty-two consecutive patients underwent PVI using a 28 mmcryoballoon ablation catheter (Arctic Front, Cryocath). In a matched control groupof 20 patients, circumferential antral PVI was performed using a 3.5 mm-tip open-irrigation RF ablation catheter (Thermocool, Biosense Webster) in conjunctionwith an electroanatomic mapping system. The procedural endpoint was PVI con-firmed by a Lasso catheter. Cardiac biomarkers (Troponin T (TrT, normal <0.04mcg/l) and creatine kinase MB (CK-MB, normal <5 mcg/l)) were determined 18hours after completion of the procedure.Results: Baseline characteristics did not differ between the patients treated withRF and Cryo. The mean ablation time was 50±15 min. in the Cryo group and45±10 min. in the RF group (p=0.4). The post-procedure TrT and CK-MB lev-els were elevated in all 42 patients. The mean level of TrT in the RF group was1.25±0.09 mcg/l compared to 0.88±0.14 mcg/l in the Cryo group (p= 0.03). CK-
MB levels did not differ significantly between the groups (33±13 mcg/l in the Cryogroup compared to 15±6 in the RF group, p=0.16). The procedural endpoint ofPVI was reached in all patients. With a postprocedural blanking period of threemonths, 15/20 patients (75%) in the RF group and 17/22 patients (77%) in theCryo group were in stable sinus rhythm after a mean follow-up of 9±4 months(p=ns).Conclusion: Elevations of cardiac biomarkers above cut-off values for myocardialinfarction occur after catheter ablation of paroxysmal AF regardless whether RFor Cryo is used. With similar ablation times, TrT rises were significantly higherafter ablation using RF compared to Cryo. The clinical outcomes between the twogroups were similar.
P770 Monitoring patients with loop recorder postIntervention: classification of AF patterns for informeddecisions. A pilot study
E. Pokushalov, A. Romanov, S. Artemenko, A. Turov, P. Shugaev,D. Losik, V. Shabanov, D. Elesin, S. Panfilov, N. Shirokova. State
Research Institute of Circulation Pathology, Novosibirsk, Russian Federation
Purpose: The significance of such early recurrences (ER) are controversial. Hy-pothesis: If we start typing ER after the first ablation and reveal the patients withmasked and clear focal firing, atrial tachycardia (AT) and atrial flutter (AFI), andperform the second ablation on them, it might improve efficacy rates in the latefollow-up.Methods: One hundred thirty-eight patients with paroxysmal AF underwent cir-cumferential PV isolation. Implantable loop recorder after catheter ablation wereused for typing ER and thereby the ‘real’ success rates. All patients were random-ized in two groups: Typing group (n=71) - all patients if they had ER underwenttyping of ER and patients with masked and clear focal firing, AT and/or AFl un-derwent the second ablation; No typing group (n=68) - patients did not underwentER analysis, blanking period was 3 months.Results: Within the blanking period, 49 (69%) patients of typing group had atleast 1 AF event. 28 (57.2%) of the 49 patients with ER had spontaneous AF initia-tion, 16 (32.6%) had AF initiation by trigger activity and 5 (10.2%) had AF initiationby AT/AFl. 21 patients with AF initiation by trigger/AT/AFl underwent early secondprocedure at a mean of 7±4 weeks after the first procedure. At 6±3 months afterthe final ablation, 39 (54.9%) patients of the typing group and 26 (38.2%) patientsof the no typing group were completely free from AF/AT/AFl in the absence ofantiarrhythmic drugs (log-rang test, p=0.002).
Conclusion: Typing in the early follow up allows us to reveal the categories ofthe patients that need early reablation and thus, to increase the efficacy of theprocedure.
P771 Value of 64-slice multidetector computed tomographyfor coronary angiography prior to pulmonary veinablation
C. Sohns1, S. Kruse1, D. Vollmann1, L. Luethje1 , J. Seegers1 ,M. Dorenkamp1, G. Hasenfuss1, S. Obenauer2 , M. Zabel1 .
1Cardiology and Pneumology, Goettingen, Germany; 2Radiology, Goettingen,Germany
Objective: The aim of our study was to investigate the accuracy of 64-slice mul-tidetector computed tomography (MDCT) for detecting hemodynamically signifi-cant stenoses of the coronary arteries in patients (pts) with symptomatic atrialfibrillation (AF) prior to pulmonary vein ablation (PVA).Methods: In a prospective study, 181 pts (aged 57±11 years) with AF refractoryto antiarrhythmic drug treatment underwent contrast-enhanced 64-MDCT of thechest for identification of PV anatomy and simultaneous assessment of coronaryvessels before PVA. Pretest probability for obstructive CAD was estimated, aswell risk factors and prevalence of angina pectoris (AP) or anginal equivalentswere assessed. Invasive coronary angiography (ICA) was performed as the goldstandard in all pts according to standard techniques. In both ICA and MDCT coro-nary artery stenoses were analyzed using the guidelines of the American HeartAssociation. For each patient and method, 10 vessel segments were identified ona post-processing workstation. Two observer blinded to the results of ICA classi-fied each segment interactively. Significant coronary artery stenosis was definedas luminal narrowing > 50%.Results: Eighty-six patients had ICA and MDCT, 95 patients underwent MDCT
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

118 Atrial fibrillation ablation
alone. ICA revealed significant stenoses in 9% (8/86). Of these one-vessel coro-nary artery disease (CAD) was found in 6/86 pts (7%), and two-vessel CAD in2/86 pts (2%). Overall, 10 total coronary occlusions were found.MDCT detecded CAD in 17/181 of all pts (10%). In this case it revealed one-vessel CAD in 13/181 pts (7%), two-vessel CAD in 3/181 pts (2%), and three-vessel CAD in 1/181 pts (1%). Altogether, prevalence of CAD investigated byMDCT in 181 Patients and 1814 segments was 2%.MDCT investigation lead to a sensitivity of 90% (9/10), specificity of 98%(829/844), PPV of 39% (9/24), and NPV of 100% (829/830) for the detection of> 50% stenoses seen on ICA. All stenoses involving the left anterior descendingcoronary artery (n=5) and the right coronary artery (n=3) were correctly identified.One stenosis in the proximal circumflex artery was correctly detected by MDCT,another one was missed. All pts with a significant stenosis in one or more ves-sels were correctly classified as patients with CAD. Patients with CAD exhibiteddyspnea (n=8) and chest pain (n=6).Conclusion: MDCT coronary angiography is sensitive and highly specific in ptspresenting for PVA. In this patient group a negative scan reliably excludes signif-icant CAD. These data suggest that in pts without AP 64-slice MDCT coronaryangiography can replace ICA prior to PVA for symptomatic AF.
P772 Spatial relationship between left atrial roof or superiorpulmonary veins and bronchi or pulmonary arteries bydual-source computed tomography: implication forpreventing injury of bronchi and pulmona
Y.-G. Li, M. Yang, Y.-H. Li, Q.-S. Wang, S.-B. Lu, L.-W. Yu, J. Sun.Xinhua Hospital of Shanghai Jiao Tong University School of Medicine, Shanghai,China, People’s Republic of
Introduction: The complications due to the ablation procedure are still majorchallenge for the treatment of atrial fibrillation (AF). Dual-source computed to-mography (DSCT) scan has significantly improved temporal resolution of ECG-gated multidetector-row CT, cardiac visualization of AF patients with irregular orhigh heart rate is much more accurate and reliable. Therefore, the objective ofthe present study was to evaluate the spatial relationship between left atrial roofor superior pulmonary veins (PVs) and neighboring structures of AF patients andprovide anatomic guidance for AF ablation to avoid injuring bronchi or pulmonaryarteries (PAs) using DSCT.Methods: DSCT scan was used to depict the left atrium (LA), PVs and nearbystructures including bronchi and PAs in 58 patients with drug-refractory AF (meanage, 64±9 years). The distance between LA roof or superior PVs and bronchi orPAs was measured.Results: The minimal distances from left, middle and right points of LA roofto principal bronchi were 17.0±6.4mm, 23.7±5.1mm and 23.2±7.7mm, respec-tively. LA roof was closer to RPA than LPA in more than 90% patients. Theminimal distances from the left, middle and right points of LA roof to PAs were8.3±5.0mm,5.9±3.1mm and 6.0±2.8mm, respectively. The minimal distancesbetween LSPV and bronchi or left PA (LPA) were 0.32±0.79mm or 0.4±1.0mm,respectively. The minimal distances between RSPV and bronchi or right PA (RPA)were 0.27±0.94mm and 0.0±0.1mm, respectively. Both of the root parts of supe-rior PVs (SPVs) (<6mm from PV ostium) in most patients were in direct contactwith branches of trachea and PAs. The nearest distances between LSPV ostiumto bronchi or PAs were 20.7mm to 31.4mm, and the nearest distances betweenRSPV ostium to bronchi or PAs were 14.8mm to 22.3mm,respectively.Conclusions: DSCT provides important imaging information for determine therelationship between LA, PVs and neighboring structures. Use of preproceduralcardiac CT scan may help avoid ablation-induced injury of bronchi and PAs.
P773 Morphologic analysis of left atrium anatomy bymagnetic resonance angiography in patients with atrialfibrillation undergoing transcatheter ablation
M. Anselmino1, A. Blandino2, S. Beninati1, C. Rovera1, C. Boffano3,S. Miceli2, G. Azzaro2, L. Garberoglio2, F. Cesarani3, F. Gaita1.
1University of Turin, San Giovanni Battista "Molinette" Hospital, Department ofCardiology, Turin, Italy; 2Cardinal Massaia Hospital, Department of Cardiology,Asti, Italy; 3Cardinal Massaia Hospital, Department of Radiology, Asti, Italy
Background: Left atrium (LA) anatomy is of pivotal importance to successfullyaccomplish atrial fibrillation (AF) radiofrequency catheter ablation (RFCA). Aim ofthe study is to describe LA and pulmonary veins (PV) morphology by 3D Mag-netic Resonance Angiography (MRA) in a large cohort of patients undergoing AFablation.Methods: Contrast-enhanced MRA (1.5 Tesla system) was performed in 443patients (352, 79% men; mean age 61±10 years) admitted for RFCA of drug-refractory AF (248, 56% paroxysmal and 195, 44% persistent/long-standing).Maximal, minimal diameters and circumferences (computed at each PVs ostia)were assessed and recorded together with PV branching patterns and LA vol-ume.independently by two experienced radiologists using multiplanar reformattedimages.Results: A typical PV branching pattern, two left and two right, was depicted in178 (40.2%) patients; 149 (33.6%) presented common left trunk (short and long)and 113 (26.2%) at least one accessory PV. Quantitative measurements andcomparisons within the four main PVs are shown in the figure below (RSPV=right
superior pulmonary vein; RIPV=right inferior pulmonary vein; LSPV=left superiorpulmonary vein; LIPV=left inferior pulmonary vein). In general superior PV werelarger than the inferiors and right PV larger than the lefts. AF type did not relate toPV branching pattern (p=0.848) while LA volume resulted superior in patients pre-senting with persistent/long-standing compared to paroxysmal AF (129 vs. 159 mlrespectively, p<0.001).
Conclusions: The present is, to date, the largest experience on left atriumanatomy, assessed by MRA, in patients undergoing RFCA. The evidence that aminority of patients present a "typical" PV branching warrants consideration whenplanning/performing RFCA.
P774 Efficacy and Safety of Epicardial Ablation of CaninePulmonary Veins with Ethanol
M. Ning, J.Z. Dong, C.H. Sang, C.L. Miao, C. Liang, C.S. Ma. BeijingAnzhen Hosp. of the Capital Univ. of Medical Sciences, Beijing Heart,Lung & Blood Vessel, Beijing, China, People’s Republic of
Introduction: Percutaneous endocardial pulmonary vein (PV) isolation using ra-diofrequency (RF) current has become an effective treatment for atrial fibrillation(AF). However, this technique is associated with a significant risk of PV steno-sis, perforation and conduction recurrence. The aim of this study was to identifythe efficacy and safety of epicardial PV ablation with ethanol and explore a newenergy source for catheter ablation of AF.Methods: Twelve mongrel dogs were randomized into ethanol ablation group andcontrol group. In ethanol ablation group (n=6),encircling injection was performedusing an 1ml injector to circumferentially ablate the root of each PV (0.2ml eachsite, 3mm apart) using 95% ethanol. In control group (n=6), saline was injectedinstead of ethanol. PV isolation was confirmed with Lasso immediately after theprocedure and at follow up of 30 days. PV isolation was defined as the absence ofPV potentials at each electrode of the Lasso catheter positioned at the PV side ofthe lesions, as well as complete conduction block into left atrium (LA) during PVpacing. Transthoracic echocardiography indices were collected at baseline and at30 days. Histologic analysis was performed at 30 days.Results: PV electrical isolation with complete bidirectional conduction block wasachieved with ethanol immediately and 30 days, while saline injection caused onlytransient conduction changes between LA and PVs. In ethanol group, histologicanalysis showed transmural lesions at 30 days. And there was no evidence of PVstenosis or thrombus formation. Mean LA diameter was not significantly differentbetween baseline and 30 days (20.5±3.5mm vs. 22±2mm, P<0.05).Conclusions: Epicardial injection of 95% ethanol is a feasible and safe methodto create permanent PV electrical isolation in canine model without stenosis andperforation.
P775 New technical approach for tridimensional oesophagusreconstruction in patients undergoing pulmonary veinisolation
F. Scazzuso, G. Albina, R. Laino, S. Rivera, V. Sammartino, A. Giniger.Cardiovascular Institute of Buenos Aires (ICBA), Buenos Aires,
Argentina
Introduction and Objectives: Previous communications confirmed minimal oe-sophagus movement in patients under general anaesthesia during atrial fibrilla-tion ablation. In order to avoid energy application in direct proximity to the oe-sophagus several strategies were performed.Methods: In this report 24 consecutive patients for circumferential pulmonaryvein isolation were included. We performed a tridimensional reconstruction withnon fluoroscopic system and the fusion with previous multislice tomography. Wedetermine the oesophagus course with a digital analysis of the negative arealimage and their proximity to the pulmonary vein ostia. Sixteen (66%) courseswere central (> 10 mm of ostia), and eight (33%) were lateral (< 10 mm of ostia).Results: Adjustments of the encircling lines were necessary in 8 (33%) patients,approaching the ablations lines to the ostia in one case or diminishing the ra-diofrequency energy in the others. None of them showed lesions after the proce-dure during follow-up of at least three months.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
Atrial fibrillation ablation / Heart failure / Left ventricular dysfunction 119
Oesophagic tridimensional reconstruction
Conclusions: The no fluoroscopic oesophagus reconstruction demonstrates avariable course. In circumferential pulmonary vein isolation, is necessary an indi-vidualized adjustments of ablation lines to diminish risk of oesophagus injury.
P776 Intermediate follow-up of totally thoracoscopicvideo-assisted surgery for pulmonary vein antrumisolation and ganglionated plexi ablation the treatmentof atrial fibrillation
S.P.J. Krul1, A.H.G. Driessen1, G.S.C. Geuzenbroek2 , W.J. VanBoven3, A.C. Linnenbank2 , J.M. De Bakker2, W.M. Jackman4, A.A.M. Wilde1,J.R. De Groot1. 1Academic Medical Center, Department of Cardiology at theUniversity of Amsterdam, Amsterdam, Netherlands; 2Academic Medical Center,Heart Failure Research Center, Dept. of Anatomy, Embryology and Physiology,Amsterdam, Netherlands; 3St Antonius Hospital, Department of Cardiology,Nieuwegein, Netherlands; 4University of Oklahoma Health Sciences Center,Oklahoma City, United States of America
Purpose: Minimal invasive surgical pulmonary vein antrum isolation (PVI) to-gether with ganglionated plexi (GP) ablation is an attractive modality in the treat-ment of atrial fibrillation (AF). We describe our results with totally thoracoscopicvideo-assisted surgical PVI (VATS-PVI) and GP ablation.Methods: Surgery was performed through three ports bilaterally in the intercostalspaces. GPs were localized with high-frequency stimulation (10V, 1000Hz) in-ducing AV-block and subsequently ablated. PVI was performed with a bipolar ra-diofrequency clamp and confirmed with a custom made multi-electrode probe withclosely spaced (1mm) electrode terminals. Additional left atrial ablation lines werecreated and conduction block verified in patients with persistent and permanentAF. The left atrial appendage was stapled and removed. Freedom of AF was as-sessed by ECG’s and 24h Holter monitoring every 3 months or during symptomsof arrhythmia. For 3 months after surgery, investigators were blinded for analysis.Anti-arrhythmic drugs were discontinued after 6 and coumadins after 9 months inpatients with a CHADS2 score of ≤1 in absence of AF recurrence.Results: Seventeen patients (mean age 56±7 yrs, 16 males) underwent VATS-PVI for paroxysmal (n=9), persistent (n=7) or permanent (n=1) AF. Seven of thesepatients had a prior catheter-based PVI (n=4 paroxysmal AF, n=3 persistent AF).After a median follow-up of 274 days (range 97-451 days), 16/17 (94%) patientswere free of AF and symptoms of arrhythmia. One patient with persistent AFhad recurrence of AF. Freedom of AF was confirmed on 5±3 ECG’s and on 2±1Holters in the majority of patients. Ten (59%) patients are off anti-arrhythmic med-ication and 7 (41%) patients are of coumadins. Three patients (18%) had peripro-cedural complications: one pneumothorax requiring ICU admission and two re-quired sternotomy during the procedure because of uncontrolled bleeding. Onepatient (6%) had an asymptomatic pulmonary vein stenosis after six month follow-up on MRI. There were no in-hospital or late deaths.Conclusions: Our present data show that VATS-PVI is a safe and a successfulprocedure with 94% freedom of AF after 3-16 months follow-up. The high suc-cess rate in our centre can be contributed to meticulous confirmation of PVI, GPablation, and additional linear left atrial lesions.
P777 Rate control in atrial fibrillation by cooling: effect oftemperature on negativ dromotropy in perfused rabbithearts
K. Mischke, C. Knackstedt, M. Zink, M. Zarse, M. Lee, A. Napp,O. Rana, E. Saygili, N. Marx, P. Schauerte. University Hospital
Aachen, Medical Faculty RWTH, Aachen, Germany
Introduction: The activity of biological tissue depends on its temperature. Ther-apeutic hypothermia has been used in survivors of cardiopulmonary resuscita-tion, patients with brain trauma and with acute myocardial infarction. Moderatesystemic hypothermia might theoretically be used for rate control in critically illpatients with supraventricular tachycardias instead of or on top of drug therapy.Many drugs with negative dromotropic effects also decrease left ventricular in-otropy and are thus contraindicated in patients with significant heart failure andsupraventricular tachycardias. Investigating the electrophysiologic properties ofisolated Langendorff-perfused rabbit hearts we evaluated the effects of gradualshifts in temperature to determine a temperature-frequency relationship.Methods: In 20 isolated Langendorff-perfused rabbit hearts the temperature ofthe tissue bath was changed between 17 and 42°C. We measured the atrial
and ventricular refractory period (AERP/VERP) and the antegrade and retro-grade Wenckebach period (AWB/RWB). During atrial fibrillation we determinedthe mean ventricular heart rate.Results: With decreasing temperature significant increases of the spontaneoussinus cycle length (SCL), decreases of the mean ventricular heart rate duringatrial fibrillation as well as relevant increases of AERP, VERP, AWB and RWBwere observed (ANOVA p<0.01). An increased ventricular vulnerability was notedat a temperature level of 42°C.
Conclusions: Cardiac hypothermia leads to a significant drop of mean ventricularheart rate during atrial fibrillation. Negative chronotropy and dromotropy inducedby moderate cardiac hypothermia might be a feasible therapeutic approach inpatients with hemodynamically relevant tachyarrhythmias in a CCU/ICU setting.
HEART FAILURE / LEFT VENTRICULAR DYSFUNCTION
P778 Changes in diastolic function with SVR and CABG bycardiac magnetic resonance
G. Ghimire, K. Joshi, P. Hill, S. Boyce, G. Weissman, T. Fuisz.Washington Hospital Center/Medstar Research Institute, Washington,United States of America
Background: CABG with or without surgical ventricular restoration (SVR) im-proves LV systolic parameters but their effect on diastolic parameters is unclear.Cardiac magnetic resonance (CMR) is the gold standard for measuring LV sys-tolic parameters and is an emerging tool useful for evaluation of the LV diastolicprofile.Methods and results: 20 patients who had either CABG + SVR (n=10) or CABGalone (n=10) under-went CMR, pre and post operatively after a mean dura-tion of 32.5 and 4.3 months. LV volumetric quantification was done with man-ual planimetry of the endocardial contours of all contiguous short-axis phases.In the SVR+CABG cohort the sequential EF, LVEDV and LVESV were 41.29%,219.72 mm, 131.09 mm followed by 52.86% (P=0.009), 177.4 mm (p=0.031) and91.41% (p=0.028). In CABG alone cohort, the changes were EF: 49.4% vs. 56.4%(p=0.046), LVEDV: 163.2mm vs. 147.4 mm (p=0.33) and LVES: 112mm vs. 70mm(p=0.162). The LV diastolic parameters obtained are depicted in the table.
Pre-CABG Post-CABG p Pre-CABG Post-CABG p+ SVR + SVR alone alone
Peak filling rate (PFR)ml/sec, mean 351.32 425.94 0.067 286.59 381.04 0.005
Time to peak filling rate (TPFR)msec, mean 190.7 141.5 0.008 153.8 112.9 0.038
Early: atrail filling rate(E/A), mean 1.32 2.35 0.046 0.89 1.494 0.039
Diastolic Volume recovery(DVR) %, mean 57.46 44.55 0.02 67.29 64.59 0.488
Conclusion: Both surgical procedures improved the systolic LVEF and diastolicLV function, and CABG+SVR reduced the LV systolic volumes. SVR did not impairLV diastolic function despite surgical exclusion of a part of the LV.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
120 Heart failure / Left ventricular dysfunction
P779 Diastolic heart failure, device approach
L. Lak1, S.C. Carasso2, Y.F. Feld3, A.S. Sherman1, L.R. Rosen1,A.T. Tubishevitz1 , G.M.B. Meir-Brodnitz1, R.S. Shofti4, S.D. Dubi5,A.E. Elami6. 1CorAssist Cardiovascular, Herzelia, Israel; 2RambamUniversity Hospital, Haifa, Israel; 3Genegrafts, Haifa, Israel;
4Rappaport Faculty of Medicine, Technion, Haifa, Israel; 5Tel Aviv University, TelAviv, Israel; 6Hadassah, Medical Center, Jerusalem, Israel
Introduction: Medical treatment of diastolic heart failure is empirical and disap-pointing. An elastic device designed to enhance left ventricular (LV) filling, gainsenergy during systole and releases it in a recoiling force during diastole. An Extra-ventricular device, attached to the LV epimyocardium, and an Intra-ventricular de-vice, implanted trans-apically was evaluated.Methods: Extra-Ventricular device: In-vivo: Diastolic dysfunction was induced inminipigs by renal wrapping, resulting in hypertension and LV hypertrophy. Studyincluded 5 device implantations and 5 sham procedures as control. Long-termefficacy was evaluated utilizing 2D Echo-strain analysis. Clinical safety study: De-vice was implanted as add-on to Aortic Valve Replacement (AVR) in patients withaortic stenosis (N=7), and compared to a control group (AVR only, N=8). Safetywas evaluated by clinical status, NYHA class, quality of life, adverse event re-porting, BNP. Intra-Ventricular device: The device was implanted in healthy sheepwith up to 6 months follow-up (N=16). Pathological evaluation was performed toevaluate any thrombotic effects.Time of device implantation was measured, acute and chronic bailout performed.Results: Extra-Ventricular device: In the diseased minipigs study, strain analysisrevealed device related global diastolic changes: trends of increased E/S strainrate ratio (1.09±0.2 to 1.29±0.2) compared to a decrease in the control group(1.31±0.3 to 1.08±0.2).Results from 7 patients in the study group (up to 13 months follow-up) and 8patients in control group show similar safety profile. Preliminary indications ofefficacy were observed, with regard to the expected improvement following AVR.Intra-Ventricular device: All animals recuperated after device implantation withoutdecrease in EF. Follow-up for up to 6 months was positive. Pathology evaluationof extra cardiac viscera revealed no evidence of thrombosis or embolism.Implantation time from purse-string to implant positioning confirmation and devicefunctionality verification was less than 10 minutes.Acute bailout post implantation was performed up to 5 times in the same animalwith no sequels to heart performance. Chronic bailout, 2 weeks post implanta-tion was done on beating heart. with no arrhythmias or other heart performancesequels.Conclusion: A passive elastic device, which transfers energy from systole todiastole, is safe and may improve diastolic function with bailout possibility.Internal device percutaneous approach implantation (using dedicated deliverysystem) is in development.
P780 Baroreflex sensitivity impairment mediates cardiacdiastolic dysfunction in rats
I.C. Moraes-Silva1, C.T. Mostarda1, E.D. Moreira1, B. Rodrigues1,A.P. Ferrara1 , E.G. Caldini2, A. Medeiros3, P.C. Brum3, M.C. Irigoyen1.1Heart Institute (InCor), Sao Paulo, Brazil; 2University of Sao Paulo,
Sao Paulo, Brazil; 3School of Physical Education and Sports of University of SaoPaulo, Sao Paulo, Brazil
Purpose: Autonomic dysfunction and reduction of baroreflex sensitivity havebeen associated with higher mortality after myocardial infarction independentlyof cardiac function alterations. However, it is not well understood whether the iso-lated baroreflex impairment influences the cardiac function. In this context, thisstudy evaluated the cardiac morphofunctional changes associated with barore-flex impairment induced by chronic sinoaortic denervation (SAD).Methods: Male Wistar rats were divided into: SAD and control (C) groups. Ratswere catheterized for direct blood pressure measurements and baroreflex sen-sitivity was evaluated by tachycardic and bradycardic responses induced byvasoactive drugs. Cardiac function was directly analyzed by left ventricle (LV)catheterization and cardiac hypertrophy index by the LV weight/body weight ra-tio. LV collagen volume fraction and the expression of regulatory proteins in-volved in intracellular Ca2+ homeostasis (SERCA2a, phospholambam - PLB andNa2+/Ca2+ exchanger - NCX) were also measured.Results: Mean blood pressure was similar between the groups (C=103±2 vs.SAD=105±3 mmHg). Baroreflex sensitivity was sharply reduced in SAD rats(∼80%) in relation to C. Increased LV mass was observed in SAD in compar-ison with C animals (+43%), accompanied by a marked increase in collagenvolume fraction (+175%). Direct LV function evaluation showed enhanced enddiastolic pressure (EDP) and decreased derivative of relaxation (-dP/dt) in theSAD group when compared to C (12±1.5 vs. 5.3±0.2 mmHg and 7422±201 vs.4999±345 mmHg/sec, respectively). SERCA2a expression in the heart was re-duced (-23%), while PLB and NCX expression levels were not changed in SADgroup. However, SAD group presented lower values for both, SERCA2a/NCXand SERCA2a/PLB ratios. Baroreflex sensitivity was correlated with EDP (r2=0.9;p<0.001) and SERCA2a/PLB (r2=0.8; p<0.001). Lastly, SERCA2/PLB was neg-atively correlated with EDP (r2=0.8; p<0.001).Conclusions: The impairment of baroreflex mechanism seems to play a pivotalinfluence in cardiac diastolic dysfunction independently of blood pressure levelsor any other associated cardiovascular risk factor.
P781 Optimizing early diagnostic accuracy in heart failurewith preserved ejection fraction: impact of acousticelectrocardiography
T. Breidthardt1, W.F. Peacock2, A. Maisel3, P. Clopton3, D. Diercks4,B. Hiestand5, M.C. Kontos6, R.M. Nowak7, S. Collins8, C. Mueller1.
1University Hospital Basel, Basel, Switzerland; 2Cleveland Clinic Foundation,Cleveland, United States of America; 3San Diego Veterans Affairs MedicalCenter, San Diego, United States of America; 4University of California-Davis,Sacramento, United States of America; 5Ohio State University, Columbus, UnitedStates of America; 6Virginia Commonwealth University, Richmond, United Statesof America; 7Henry Ford Health System, Detroit, United States of America;8University of Cincinnati, Cincinnati, United States of America
Background: The diagnosis of heart failure with preserved ejection fraction(HFPEF) is dependent on echocardiography and hence time- and resource-consuming. A fast and readily available test would help to identify HFPEF patientsupon their arrival to the emergency department. Our purpose was to determineif analytic processing of the ECG with digitally recorded heart sounds can accu-rately diagnose HFPEF.Methods: Using the HEart failure and Audicor technology for Rapid Diagnosisand Initial Treatment (HEARD-IT) multinational trial database of patients present-ing to the ED with acute heart failure, we evaluated the potential of the acousticcardiographic systolic dysfunction index (SDI) to predict preserved ejection frac-tion. HFPEF was defined as heart failure with a left ventricular ejection fractionexceeding 50%.Results: Overall, 448 patients met all inclusion and no exclusion criteria andreceived a gold standard diagnosis of acute heart failure. 163 of these patientshad echocardiography and admission Audicor SDI results obtained.The area under the SDI-ROC curve (AUC) for the separation of HFPEF from sys-tolic HF was 0.86 (SD: 0.03; 95%CI 0.80-0.92). With an optimal, calculated SDIthreshold of 4.65, sensitivity and specificity were 81% and 82%, with a positiveand negative likelihood ratio of 4.61 and 0.23. The odds ratio for HFPEF was 19.1(95%CI 8.1-45.0). For every unit SDI decrease the likelihood of HFPEF doubles(OD 2.2; 95%CI 1.6-2.8).
Figure 1
Conclusion: Admission SDI measurement by Audicor technology provide a rapidand accurate diagnosis of HFPEF. This will allow future studies to deepen ourunderstanding of acute decompensated HFPEF. Early AHF diagnoses are com-monly erroneous, and the acoustic cardiographic parameters improve early diag-nostic accuracy.
P782 Impaired apical and basal rotation lead to a reductionin twist on exercise in patients with heart failure withnormal ejection fraction (HFNEF)
Y.T. Tan1, F.W.G. Wenzelburger1 , E.S.P. Lee2, G. Heatlie2, F. Leyva1,J.E. Sanderson1 . 1University of Birmingham, Birmingham, United
Kingdom; 2University of North Staffordshire, Stoke-On-Trent, United Kingdom
Background: Many patients presenting with symptoms of heart failure are foundto have normal ejection fraction using standard 2D echocardiography and arelabelled as having Diastolic Heart Failure or HFNEF. It is known that apical rotationis reduced at rest and on exercise in these patients. But there are no data on basalrotation available in this group of patients.Method: 35 Patients (age 73±7years, 25 female) with breathlessness on exer-tion and normal EF (60±6%) underwent cardiopulmonary exercise test to rule outalternative clinical reasons (VO2max 18.4±4.9ml/min/kg). Data were comparedto 26 age-matched control subjects (age 72±7years, 20 female, EF 61±7%)with a normal exercise tolerance (VO2max 29.5±5.2ml/min/kg). All underwent fullDoppler 2D-echocardiography at rest and on supine exercise. Echo images wereanalysed off-line. Rotation was measured by speckle tracking from parasternalshort axis views at mitral valve and apical level. Subsequently LV torsion wascalculated as the difference of rotation at apex and at base in six interpolated
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / Left ventricular dysfunction 121
(three for apical, three for basal rotation) cycles by a specially developed soft-ware.Results: All results are presented in the table. At rest apical but not basal rotationis significantly reduced in patients. On exercise apical and basal rotation are bothsignificantly reduced which leads to a severely impaired torsion in patients. Thiscorrelates with E/e’ on exercise (Pearson Coefficient -.388, p=0.005).
Rotation and Torsion Results
Patients (n=35) Controls (n=26) p-value*
Apical rotation rest (°) 8.7±4.2 12.9±3.6 <0.001Apical rotation exercise (°) 11.4±4.4 16.2±4.1 <0.001Basal rotation rest (°) -8.0±3.0 -7.1±2.7 0.233Basal rotation (°) -7.4±3.3 -9.2±2.6 0.033Torsion rest (°) 16.7±5.3 19.7±3.8 0.016Torsion exercise (°) 18.5±5.2 25.0±5.8 <0.001Diff. Torsion (°) 1.5±6.5 5.4±5.2 0.015
*p-value for unpaired t-Test comparing patients and controls.
Conclusion: Patients with HFNEF show a marked reduction in torsion particu-larly on exercise due to the inability to improve neither apical nor basal rotation.Since this correlates well with E/e’ it might explain in parts the breathlessness onexertion in these patients.
P783 Relationship between LV mass and diastolic function isindependent of NO generation
A.L. Sverdlov1, D.T. Ngo2, A.K. Nightingale1, S. Rajendran1,R.H. Ritchie3, T.H. Marwick4, M.P. Frenneaux5 , J.D. Horowitz1.1University of Adelaide, Queen Elizabeth Hospital, Adelaide, Australia;
2University of South Australia, Adelaide, Australia; 3Baker IDI Heart andDiabetes Institute, Melbourne, Australia; 4University of Queensland, PrincessAlexandra Hospital, Brisbane, Australia; 5University of Aberdeen, Aberdeen,United Kingdom
Introduction: We have recently shown that in an untreated aging populationplasma concentrations of asymmetric dimethylarginine (ADMA) and vascular re-sponsiveness to nitric oxide (NO) are (respectively) direct and indirect correlatesof LV mass. Furthermore, this relationship is partially independent of afterload,implying autocrine/paracrine regulation. NO facilitates relaxation of ventricularmyocardium and therefore represents a potential LVH-independent modulatorof LV diastolic function. Thus, we now sought to evaluate correlations betweenthese findings and 1) myocardial diastolic function; and 2) parameters of collagenturnover.Methods: 74 subjects, aged 67.7±5.8 years, without known cardiovascular dis-ease or treated hypertension were evaluated. LV volumes were calculated fromthe short axis stack of cardiac MRI (Philips Intera 1.5T magnet) and LV mass wasindexed to ht2.7. E/E’ ratio was derived from echocardiographic tissue dopplerimaging. C-terminal telopeptide of collagen I and N-terminal peptide of procolla-gen I were assayed as markers of collagen turnover (and therefore potentially offibrosis). Plasma ADMA concentrations were determined by HPLC. Vascular re-sponsiveness to No donor nitroglycerine was determined via applanation tonom-etry. All putative correlations with LV mass were examined by univariate linearregression analyses and analysis of covariance.Results: None of the subjects had definite LV hypertrophy according to stan-dard clinical definitions. There was a strong relationship between increasing LVmass and E/E’ (R=0.4; p=0.001), which was independent (ANCOVA) of plasmaconcentrations of ADMA and of vascular responsiveness to NO. There was norelationship between LV mass and markers of collagen turnover.Conclusions: Therefore, while NO appears to inhibit the development of LV hy-pertrophy via both local and peripheral actions, it does not significantly modulateLV diastolic (dys)function per unit LV mass.
P784 Different effect of atorvastatin with diastolic andsystolic left ventricular dysfunction in patients withcardiac arrhythmias
E.S. Kozlova, A.S. Popova, F.A. Nemchuk, Y.M. Lopatin. VolgogradState Medical University, Volgograd, Russian Federation
Purpose: To compare the effect of atorvastatin in patients (pts) with heart failure(HF) of ischemic etiology with diastolic and systolic left ventricular dysfunctionand cardiac arrhythmias.Methods: 26-week randomized open trial included 100 pts with ischemic HF(NYHA I-II) and arrhythmias. 60 pts of the cohort had HF with diastolic dysfunc-tion (DHF) and 40 pts had HF with systolic dysfunction (SHF). Every pt was onbasic therapy: amiodarone or sotalol, ACE inhibitor, β-blocker or calcium channelblocker, aspirin and diuretic. Pts with DHF were randomized into two groups –one group of atorvastatin (basic therapy and atorvastatin) and the other groupof control (without statins). Also pts with SHF were randomized into groups ofatorvastatin and control. Data concerning frequency and duration of arrhythmiasand heart rate variability (HRV) from the 24-hour holter monitor ECG and param-eters of echocardiography were recorded and compared at baseline and after sixmonths in every group and between groups.Results: Groups receiving atorvastatin (with DHF and SHF) showed significantlybetter results comparing to corresponding groups of control. Moreover total num-
ber of pts with DHF diminished by 58% (p<0,01) and with SHF – just by 24%(p<0,05). Left atrium dimension in the group of atorvastatin with DHF versusthe group of atorvastatin with SHF decreased by 8,8% vs 5,2%; p<0,05 andleft atrium volume - by 11,2% vs 8,7%; p<0,05. In analysis of HRV we had gotthe increasing in time- and frequency- domain include RMSSD 63,5% vs 44,7%;p<0,05, TP 6,6% vs 4,1%; p<0,05, HF 62% vs 37%; p<0,01 and decreasingLF (-9,5% vs -6,2%; p<0,05) and LF/HF (-28% vs -17,5%; p<0,01). In additionthere was a reduction of the risk of developing recurrent atrial fibrillation (AF)(-69% vs -53%; p<0,05), duration of AF (-88% vs -74%; p<0,05), episodes ofsupraventricular tachycardia (-78% vs -63%; p<0,05), number of supraventricu-lar extrasystoles (-41% vs -32%; p<0,05) and ventricular extrasystoles (-63% vs-55%; p<0,05).Conclusions: Atorvastatin therapy exerts significantly better effect in patientswith left ventricular diastolic dysfunction than with systolic dysfunction in normal-ization of myocardial morphology and improvement of sympatho-vagal balancewhich reduced the risk of developing arrhythmias.
P785 Differences of myocardial systolic deformation andcorrelates of diastolic function in competitive rowersand young hypertensives: a speckle trackingechocardiography study
V. Schiano Lomoriello, A. Santoro, R. Esposito, M. Olibet, R. Raia,M. Galderisi. University Hospital Federico II, Naples, Italy
Purpose: To evaluate differences of myocardial deformation and their relationswith left ventricular (LV) diastolic function in athlete’s and hypertensive heart.Methods: The study population included 19 sedentary controls, 22 top-level row-ers and 18 young newly diagnosed, never treated hypertensive patients, all ofmale gender. Participants underwent Doppler-echo examination including pulsedTissue Doppler of the mitral annulus and off-line Speckle Tracking Echocardio-graphy (STE). The ratio between transmitral early filling peak velocity and TissueDoppler derived early diastolic peak velocity of the mitral annulus (E/Ea ratio)was determined. Peak longitudinal strain was calculated in apical long-axis, 4-chamber and 2-chamber views and values of the 3 views averaged (global lon-gitudinal strain = GLS). Regional circumferential strain and regional radial strainwere calculated at LV base, middle and apical levels and values averaged (globalcircumferential strain = GCS, global radial strain = GRS). LV torsion was deter-mined as the net difference in mean rotation between apical and basal levels.Results: The 3 groups were comparable for age whereas body mass index andblood pressure were higher in hypertensives and heart rate lower in rowers. LVmass index (LVMi) was significantly higher in rowers and in hypertensives than incontrols, without difference in relative wall thickness, ejection fraction and midwallfractional shortening. Left atrial volume index (LAVi) was significantly higher inrowers than in controls and hypertensives. Tissue Doppler derived annular sys-tolic velocity (Sa) (p<0.001) and early diastolic velocity (Ea) (p<0.0001) werelower and E/Ea ratio higher (p<0.0001) in hypertensives. GLS was lower in hyper-tensives (-17.5±2.8%) than in rowers (-22.2±2.7%) and in controls (-21.1±2.0)(p<0.0001). GCS, GRS and torsion were not significantly different among the 3groups. By a multivariate model, after adjusting for age, heart rate, meridionalend-systolic stress, LVMi and LAVi, GLS was an independent contributor of E/Earatio (beta coefficient = -0.39, p<0.0001) in the pooled population (cumulative R2
= 0.42, SE = 1.75, p<0.0001).Conclusions: The heart of young hypertensives is characterized by reducedglobal longitudinal strain whereas circumferential strain and radial strain as wellas torsion are similar to those of the athlete’s heart. The extent of global longitudi-nal systolic function is strongly associated to LV diastolic function, independentlyon afterload changes and degree of LV hypertrophy.
P786 Single ventricle diastolic function and exercisecapacity in patients after Fontan operation
L. Tomkiewicz-Pajak1, J. Kolcz2, M. Pieculewicz1, P. Podolec1,J. Skalski2. 1John Poul II Hospital, Krakow, Poland; 2AmericanChildren’s Hospital, Jagiellonian University Medical College,
Department of Pediatric Ca, Krakow, Poland
Patients who have undergone Fontan operation (FO) may suffer from bothsystolic and diastolic ventricle dysfunction. Recent studies show a prognosticvalue of parameters of cardiopulmonary exercise test (CPX)-peak oxygen up-take (VO2peak), peak VE/VCO2-slope in patients with heart failurein biventricu-lar heart. Using the echocardiography E/E’ ratio, it is possible to determine fillingpressure and consequently to detect ventricle diastolic dysfunction. The aim ofthe study was to evaluate the impact of ventricular diastolic dysfunction on exer-cise capacity in patients after FO.Methods: We investigated twenty eight patients (18F; 10M) after stage FO withventricle of left ventricular morphology aged 17,6±6,1 years in NYHA II-III withEF 43±6%. Pulse-wave Doppler signals from the mitral inflow and tissue Dopplerimaging of the mitral annulus were obtained. All the patients underwent symp-tom limited CPX. We analyzed parameters: mitral annulus systolic velocity (S),early diastolic velocity (E’), E wave peak velocity, E/E’ ratio, exercise time, oxygenuptake at anaerobic threshold (AT), VO2peak and (VE/VCO2).Results: Linear regression analysis revealed a significant positive correlation withE/E’ ratio and patients’ age (r=0,73; p<0,01) and with E/E’ ratio and VE/VCO2-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

122 Heart failure / Left ventricular dysfunction
slope (p=0,93; p<0,01). S velocity showed a positive correlation with VO2peak(r=0,82 p<0,01). There was no correlation between echocardiography Dopplerand CPX parameters.Conclusion: Ventricular diastolic dysfunction reduce exercise capacity in patientsafter Fontan operation. E/E’ ratio increases with age and correlates with ventila-tory inefficiency during exercise, as indicated by the VE/VCO2 slope. Mitral annu-lus systolic velocity correlates with oxygen uptake.
P787 N-Terminal pro brain naturetic peptide correlates withincreased left atrial filling pressures in patients withcarcinoid disease
C.K.L. Wong, D.J. Cuthbertson, G.J. Poston, M.I. Burgess. AintreeUniversity Hospitals, Liverpool, United Kingdom
Introduction: Patients with carcinoid disease have slow growing midgut tumourswhich secrete a serotonin-like vasoactive substance that can cause fibrosis man-ifesting as valvular abnormalities (carcinoid heart disease-CHD). Left ventricularmyocardial effects are not well described in this population but theoretically havethe potential to cause breathlessness by a mechanism related to a progressiverise in left atrial (LA) pressure, a process detectable by echocardiography or neu-rohormonal measurement. We investigated the relationship between echocardio-graphic measurements of LA pressure and N-Terminal pro Brain Naturetic Peptide(NTproBNP) in patients with carcinoid disease.Method: We recruited 58 patients with carcinoid disease and 20 controls. All pa-tients had an echocardiogram, key measurements included LA area, transmitralDoppler assessment of peak early diastolic velocity (E) and peak early diastolictissue velocity of the septal aspect of the mitral annulus (Ea). E/Ea ratio was cal-culated over 3 cardiac cycles. Venous blood was drawn for NTproBNP on thesame day as the echocardiogram.Results: The disease and control groups were age and sex matched (63±11 vs57±14years, p=ns. 51% vs 40% male, p=ns). E/Ea ratio was significantly higherin the carcinoid group (-14.7±7 vs -11.9±3.7, p<0.05). There was no signifi-cant difference in LA area between carcinoid and control groups (14.4±4.6 vs15.4±4.4cm2, p=ns). NTproBNP had a positive correlation to E/Ea ratio (r=0.34,p<0.01) and LA area (r=0.38, p<0.01).
Conclusion: E/Ea is elevated in patients with carcinoid disease indicating eleva-tion of LA pressure in this group. NTproBNP correlates with E/Ea and LA areaand may have a role in the assessment of dyspnea in this patient group.
P788 Associations of persistent diastolic dysfunction aftervalve replacement in aortic stenosis? a study ofhemodynamics and fibrosis
S. Wahi1, R. Leano1, M. Ura1, M. Bansal1, T. Marwick2. 1Universityof Queensland, Princess Alexandra Hospital, Brisbane, Australia;
2Cleveland Clinic Foundation, Cleveland, United States of America
Purpose: Reduction in afterload after aortic valve replacement (AVR) for stenosis(AS) should result in resolution of symptoms and improved functional class. Thereis increasing awareness of the contribution of diastolic dysfunction to ongoingsymptoms after AVR. We sought whether this reflected fibrosis, failure of reverseremodelling of LV hypertrophy or inadequate reduction of AV gradient.Methods: We studied 57 consecutive pts (68±12 years, 24 female) referred forAVR for isolated severe AS. Standard and novel diastolic parameters, early fill-ing (E), late filling (A), deceleration time (DT), early myocardial velocity (E’) andLV torsion were recorded pre – AVR and at 6 months follow - up. LV myocar-dial biopsy to assess myocardial fibrosis was undertaken intra-operatively. Theevolution of diastolic performance was based on change in E’.Results: AVR was associated with improvement of AV area (0.8±0.2 vs 1.5±0.5cm2, p<0.0001), E’ (4.1±1.6 vs 5.1±1.9, p=0.03), and reduction of LVMI (151±39vs 112±28 gm/m2, p<0.0001). Baseline fibrosis was associated with increasedE/E’ (a marker of LV filling pressure) and lower systolic strain (Table). However,change in E’ was associated with change in LVMI (β=0.04, p=0.003), independentof change in gradient and fibrosis.
Table 1
Fibrosis No Fibrosis p value
LVMI (gms/m2) 134±25 150±35 0.25AV mean gradient 51±17 51±14 0.90E/E’ 21.5±10.2 14.9±3.7 0.02Strain -13.9±1.6 -16.3±3.2 0.047
Conclusion: Latent diastolic dysfunction after AVR is associated with failure toregress LV hypertrophy, independent of fibrosis. In the absence of an associationwith change in valve gradient, this may reflect concomitant hypertension.
P789 Segmental diastolic dysfunction of left ventricular wallin patients with 50% coronary artery stenosis
R. Kakihara1, C. Naruse1, H. Hironaka1, T. Tsuzuku2. 1KakiharaClinic, Department of Cardiology, Toyohashi, Japan; 2Kakihara Clinic,Echocardiography Laboratory, Toyohashi, Japan
Purpose: Coronary artery stenosis (CAS) is known to cause segmental diastolicdysfunction of the left ventricular (LV) wall. However, the degree of CAS nec-essary to cause LV diastolic dysfunction is unknown. We utilized strain rate (SR)profile of resting echocardiography to investigate the segmental diastolic dysfunc-tion of patients with various degrees of CAS.Method: Total 126 patients were enrolled in this study. Among them 43 patientshad normal coronary arteries (gr-N). The remaining 83 patients had CAS (gr-S). Three images of apex approach view were analyzed [25% CAS (gr-S1): 24segments (seg.) of 22 patients, 50% CAS (gr-S2): 32 seg. of 20 patients, 75%CAS (gr-S3): 26 seg. of 20 patients, 90%≤ CAS (gr-S4): 21 seg. of 21 patients].There was no statistically significant difference between gr-N and gr-S with regardto age, blood pressure, heart rate and fasting blood glucose level. During thediastolic phase of SR profile, E (1/s: speed of active self-extension of myocardium)and E time (msec: time from the end-systolic time to peak E value time) wereused as variables. Peak E and peak E/E time (acceleration rate of speed of self-extension) were compared. A was not used as a variable, because it expressespassive nonself-extension of myocardium.Results: See the table. By SR profile, diastolic dysfunction of stenotic coronaryartery segments was detectable in patients with 50% CAS.
Segmental diastolic dysfunction and CAS
gr-N gr-S1 gr-S2 gr-S3 gr-S4normal 25% stenosis 50% stenosis 75% stenosis 90%≤ stenosis
Peak E (1/s)values 1.85±0.34 1.75±0.48 1.34±0.5 1.13±1.85 1.03±0.21p < N.S. p<0.05 p<0.001 p<0.001
Peak E/E time (1/s2)values 17.23±10.27 15.22±8.23 10.11±4.57 7.28±2.26 6.67±2.86p < N.S. p<0.01 p<0.001 p<0.001
p<: unpaired t test. By SR profile, segmental diastolic dysfunction was noticed in patients with50% CAS.
Conclusion: Although 50% CAS is not thought to cause myocardial ischemia,segmental diastolic dysfunction in patients with 50% CAS may be an early signof myocardial ischemia. Patients with 50% CAS should undergo further hemody-namic testing to evaluate for diastolic dysfunction.
P790 The potential role of oxidative stress, inflammatory andcoagulation parameters in the development of diastolicdysfunction in patients with hypertension
Z.S. Szelenyi1, G. Szenasi2, M. Kiss3, Z. Prohaszka3, A. Patocs4,I. Karadi3, A. Vereckei3. 1Semmelweis University Cardiology Centre,
Budapest, Hungary; 2EGIS Pharmaceutical Works PLC, Budapest, Hungary;33rd Department of Internal Medicine, Semmelweis University School ofMedicine, Budapest, Hungary; 42nd Department of Medicine, SemmelweisUniversity, School of Medicine, Budapest, Hungary
Purpose: In contrast to systolic heart failure, the incidence of heart failurewith normal ejection fraction (EF) and diastolic dysfunction hasn’t decreased,its pathogenesis is unclear, and efficient therapy is not available. Our aim wasto study the role of oxidative stress, inflammation and hypercoagulability in thepathogenesis of diastolic dysfunction.Methods: Preliminary results from ≥60-year-old 69 patients (6 controls and 63patients with hypertension) with normal EF are presented. All subjects underwentechocardiography with detailed assessment of systolic and diastolic ventricularfunction, online myocardial velocity measurements and offline evaluation of atrialand ventricular myocardial strain and strain rate from recordings by tissue dopplerimaging. Determination of (1) oxidative stress [measurement of total scavengercapacity (TSC) with chemiluminometry and protein carbonylation (PK) with spec-trophotometry], (2) inflammatory [measurement of C-reactive protein (CRP) withultrasensitive immunturbidimetry, interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) levels with ELISA] and (3) coagulation parameters [measurement offibrinogen levels with prothrombin based coagulation test, plasminogen activatorinhibitor-I and von Willebrand factor with ELISA] and (4) chromogranin A (cGA) amarker of overall neuroendocrine activation with RIA was carried out from plasmaor serum samples as well.Results: Echocardiography revealed no diastolic dysfunction in 22/63 (35%) pa-tients with hypertension (HTDD- group), and 41/63 (65%) patients had mild di-astolic dysfunction (HTDD+ group). TSC decreased significantly (p=0.048) inHTDD+ group, but its decrease was non-significant in the HTDD- group comparedwith controls. CRP increased significantly (p=0.026) both in HTDD- and HTDD+groups. PK, cGA, IL-6 and TNF-α levels increased non-significantly in line withthe degree of diastolic dysfunction in patients with hypertension compared with
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / Left ventricular dysfunction 123
controls. No between groups difference was found in the coagulation parameters.TSC showed a significant negative correlation (r= -0.32, p=0.0159) with the meanof the peak left ventricular systolic strain rates and mean atrial contraction strainrate (r=-0.34, p=0.009). The IL-6 (r=0.36, p=0.0178) and TNF-α (r=0.43, p=0.009)levels had significant positive correlation with left atrial volume/body surface val-ues.Conclusions: Oxidative stress and inflammation might have a primary patho-genetic role in the development of diastolic dysfunction, and oxidative stress mayalso result in left ventricular and atrial systolic dysfunction in patients with hyper-tension.
P791 Moderate hypothermia causes increased leftventricular wall stiffness and delayed filling in aporcine model
A. Espinoza1, H. Skulstad2, V. Kerans3, P.S. Halvorsen1, A. Opdahl4 ,J.F. Bugge3, T. Edvardsen2. 1Oslo University Hospital, TheInterventional Centre, Oslo, Norway; 2Oslo University Hospital,
Departement of Cardiology, Oslo, Norway; 3Oslo University Hospital,Departement of Anaesthesia and Intensive Care, Oslo, Norway; 4Johns HopkinsMedical Institutions, Baltimore, United States of America
Introduction: Hypothermia is used for neuroprotection in patients after cardiacarrest. However, hypothermia at 33°C also affects myocardial function. To eluci-date these effects we studied myocardial function during hypothermia in a porcinemodel, with particular focus on diastolic dysfunction.Methods: 8 anesthetized open chest pigs were cooled from baseline (38°C) tohypothermia (33°C). Left ventricle pressure (LVP) was measured with a micro-manometer, and LV dP/dt as well as time constant (τ) of LV relaxation were cal-culated. Diastolic duration was measured from dP/dtmin to following R on ECGand isovolumic relaxation time (IVRt) from dP/dtmin to mitral valve opening. Enddiastolic (EDV) and stroke volumes (SV) were measured by 2D echocardiography.Transmitral flow velocities were obtained by echo/Doppler, and velocity time inte-gral (VTI) of the E and A filling waves calculated as a measure of filling volume.Due to E-A fusion in some animals at 33° C, early diastolic filling was definedas the percentage of VTI occurring before following P on ECG. LV wall stiffness(KLV) was calculated from continuous pressure/m-mode recordings. Measure-ments were obtained at 38° and 33°C.Results: Heart rate decreased during hypothermia, from 91±11 (mean±SD) to79±9 beats per minute (p<0.05, paired t-test). Peak LVP decreased (85±12 to68±11 mmHg, p<0.05), as did LV dP/dtmax (P<0.05). SV and EDV were un-changed. Diastolic duration decreased (311±76 to 281±93 ms, p<0.05) whileIVRt was prolonged at 33° (40±8 to 72±22 ms, p<0.05), resulting in a decreasedfilling time (274±62 to 219±66 s, p<0.05). τ increased from 31±4 to 59±10ms (p<0.05). E was reduced (0.7±0.1 to 0.5±0.2, p<0.05) while A increased(0.5±0.1 to 0.6±0.1, p<0.05), inverting the E/A ratio at 33°C (p<0.05). Duringnormothermia, 67% of the SV entered LV early and E was completed before P inall animals. In contrast, during hypothermia early LV filling was reduced to 33% ofSV, and E not being completed before P on ECG in any animal., KLV increased in-dicating a stiffer LV wall in hypothermia (0.5±0.1 to 0.6±0.1 mm/mmHg, p<0.05).Conclusion: Hypothermia resulted in a substantial decrease in LV diastolic fill-ing time, whereas stroke volume was preserved in our model. We observed amarked reduction in early diastolic filling, consistent with shift from early- to latediastolic filling due to delayed LV relaxation and increased wall stiffness. Our find-ings during hypothermia suggest a compromised LV filling, more dependent onatrial contribution and a slower heart rate.
P792 Metformin is associated with improved diastolicfunction measured by echocardiographic tissueDoppler imaging in diabetes patients
C. Andersson1, P. Soegaard1, S. Hoffmann1, P.R. Hansen1,R. Sorensen1, P. Weeke1 , J.B. Olesen1, L. Kober2, C. Torp-
Pedersen1, G.H. Gislason1. 1Gentofte Hospital - Copenhagen UniversityHospital, Department of Cardiology, Hellerup, Denmark; 2Rigshospitalet,Copenhagen University Hospital, Copenhagen, Denmark
Purpose: Diabetes alters cardiac metabolism, which can lead to impaired di-astolic function and heart failure. Insulin sensitizing agents such as metforminare hypothesized to improve cardiac metabolism and function, but availableclinical studies are sparse. We investigated the influence of different glucose-lowering medications (GLM) on diastolic function measured by trans-thoracic tis-sue Doppler echocardiography in diabetes patients.Methods: Echocardiograms of 242 diabetes patients who underwent coronaryangiography for suspected ischemic heart disease were analyzed. Included pa-tients had a left ventricular ejection fraction (LVEF) ≥20% and were without sig-nificant cardiac rhythm disturbance, bundle branch block or valve disease. Use ofGLM was defined by prescription claims using nationwide registers. Multivariablelinear regression analysis was used to investigate the influence of different GLMon e’.Results: Four groups of GLM were identified: metformin (n=56), sulfonylureas(n=43), insulin (n=61), and combination treatment (n=82, of whom 91% used met-formin). Mean age was 66 (standard deviation [SD] ±10) years, mean LVEF 45(SD ±11) %, similar between the GLM groups (both p >0.05).
Unadjusted mean e’ was 5.3 (SD ±1.6) cm/s for metformin, 4.6 (SD ±1.6) cm/sfor sulfonylureas, 5.3 (SD ±1.8) cm/s for insulin, and 5.4 (SD ±1.7) cm/s for com-bination group, respectively; p for difference between groups=0.04. Adjusted formultiple variables (including treatment duration, coronary pathology, concomitantmedications, comorbidities, LVEF, left ventricular posterior wall thickness, ageand gender), use of metformin remained associated with a relatively higher e’,parameter estimate +0.57 (standard error [SE] ±0.26 cm/s, p=0.03). Use of sul-fonylureas or insulin had no impact on e’ (parameter estimates -0.10 [SE ±0.27]cm/s, p=0.7 and 0.23 [SE ±0.38] cm/s, p=0.5 for sulfonylureas and insulin, re-spectively). The effect of metformin was not altered by concomitant use of sul-fonylureas or insulin (p for interaction =0.7 and 0.5, respectively).There was no significant association between metformin, sulfonylureas or insulinagents and any of S’ and a’, respectively.Conclusions: In patients with diabetes and suspected or confirmed ischemicheart disease, use of metformin is associated with improved diastolic function, ascompared with use of sulfonylureas or insulin.
P793 Comparing outcomes in heart failure patients with orwithout systolic dysfunction: an insolvable question?
F. Saraiva, H. Martins, R. Baptista, P. Mendes, S. Costa, F. Franco,P. Monteiro, L. Goncalves, L.A. Providencia. Coimbra Hospital andMedical School, Coimbra, Portugal
Background: About half of heart failure (HF) patients have a preserved left ven-tricular ejection fraction (LVEF). Their prognosis (versus systolic HF patients) re-mains a subject of great controversy.Objective: To compare the prognosis of HF patients with LVEF> 50% versusLVEF ≤50%.Population and Methods: We studied 384 patients admitted at the same inten-sive care unit, between January 2003 and October 2007. Patients were divided intwo groups: A - patients with LVEF> 50% (n=35) and B - patients with LVEF ≤50%(n=349). LVEF was obtained by echocardiography and determined with the Simp-son method. Groups were studied regarding demographic, clinical and analyticalparameters, HF etiology, prior and post-discharge HF therapy. The combined pri-mary endpoint was cardiovascular death, transplant or re-admission within 180days after discharge; median follow-up was 4.5 years.The survival was expressed with Kaplan-Meyer curves.Results: Mean age was similar, but group A included more female (51.4 vs.32.7%, p=0.001) and less smokers (5.0 vs. 28.8%, p=0.013). Regarding HF etiol-ogy, group A included more cases of restrictive cardiomyopathy (20.6 vs. 1.4%, p<0.001), but less of ischemic (8.8 vs. 34.7%, p=0.001) and dilated cardiomyopa-thy (17.6 vs. 50.7%, p <0.001). The forms of presentation and precipitating factorsof HF were equally prevalent in both groups. Prior to hospitalization, few group Apatients received ACE inhibitors (34.8 vs. 64.2%, p=0.006), beta-blockers (26.1vs. 48.4%, p=0.03), spironolactone (34.8 vs. 54.8% p=0.05) and furosemide (65.2vs. 83.1%, p=0.039). At admission, group A had lower mean hemoglobin levels(p=0.034), but glucose, creatinine, blood pressure and heart rate values revealedno significant differences. Atrial fibrillation was more prevalent in group A (56.3 vs.28.9%, p=0.002). During hospitalization, group A received more often dopamine(44.1 vs. 16.4%, p <0.001), had increased need for dialysis (23.5 vs. 5.2%, p<0.001) and developed more arrhythmias (41.2 vs. 16.4%, p=0.037). Therapy atdischarge was identical in both groups, except for beta-blockers, which were lessprescribed in group A (55.6 vs. 76.2%, p=0.05).No significant differences were found regarding long-term mortality (35.3 vs.24.4%, p=0.148), death or transplantation (47.1 vs. 46.9%, p=0,584) or in theprimary endpoint (64.8 vs. 70.1%, p=0,768).Conclusions: In our population patients with HF and preserved LVEF tended tohave greater mortality and similar morbidity, compared to impaired LVEF patients,thus emphasizing the importance to adequately identify and treat them. Furtherlarge scale studies are warranted on this important subject.
P794 Natriuretic peptide processing in pts with dilatedcardiomyopathy and heart transplant recipients
R. Dierckx, J. Bartunek, L. Delrue, K. Dierickx, M. Goethals,S. Verstreken, M. Vanderheyden. OLV Hospital Aalst, CardiovascularCenter, Aalst, Belgium
Introduction: Corin, a cardiac serine protease converts proBNP (1-108) to itsactive form BNP (1-32). In this study we examined the regulation of corin geneexpression and its relationship to circulating BNP forms in patients (pts) with idio-pathic dilated cardiomyopathy (CCMP) and heart transplant recipients.Methods: Forty five CCMP (EF: 36±3%) and 24 Tx (EF: 75±3%) pts who under-went diagnostic left and right heart catheterization were included in the study. Inall pts blood for proBNP, BNP and Nt-proBNP was sampled at time of diagnosticcatheterization and left ventricular (LV) endomyocardial biopsies were procured.LV mRNA levels of BNP, corin, and ANP were measured by quantitative rt-PCRand normalized for GADPH. The ratio of plasma proBNP/BNP levels was used asan estimate for the degree of unprocessed BNP.Results: As expected CCMP pts had a worse hemodynamic profile and higherplasma proBNP, BNP and Nt-proBNP levels as compared to Tx pts. In CCMPpts myocardial gene expression of BNP (238±37 vs 21±9; p <0.01) and ANP(1606±254 vs 63±26; p < 0.01) was significantly higher whereas that of corin
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
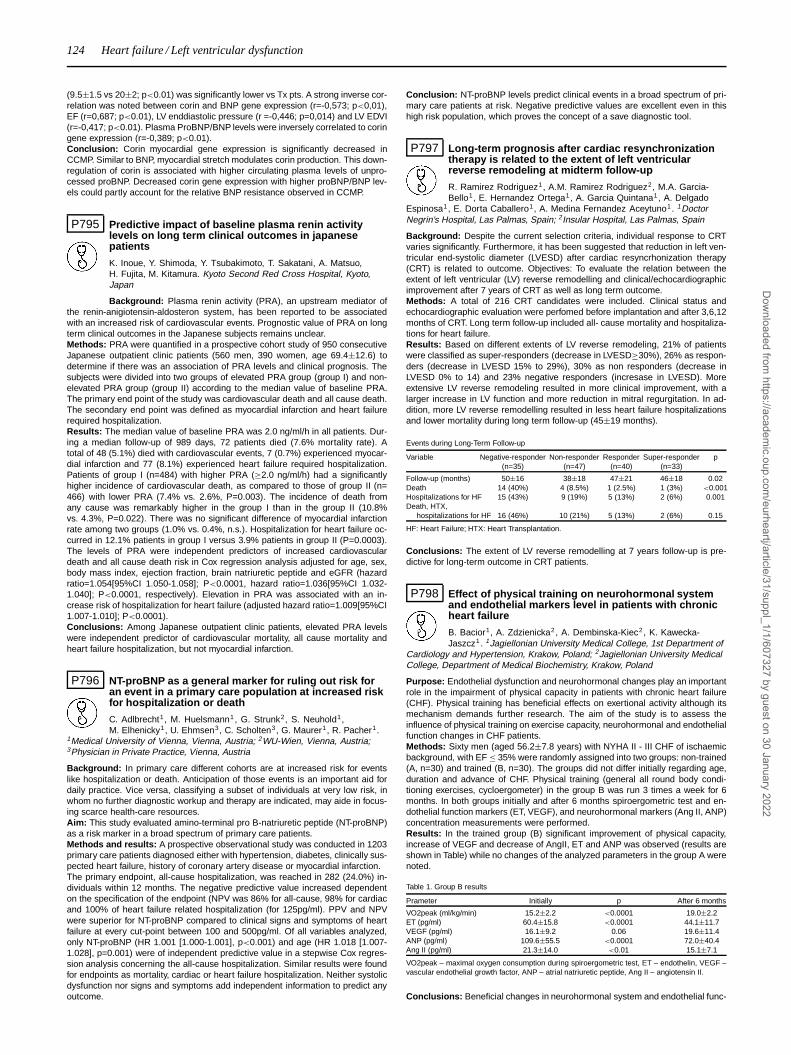
124 Heart failure / Left ventricular dysfunction
(9.5±1.5 vs 20±2; p<0.01) was significantly lower vs Tx pts. A strong inverse cor-relation was noted between corin and BNP gene expression (r=-0,573; p<0,01),EF (r=0,687; p<0.01), LV enddiastolic pressure (r =-0,446; p=0,014) and LV EDVI(r=-0,417; p<0.01). Plasma ProBNP/BNP levels were inversely correlated to coringene expression (r=-0,389; p<0.01).Conclusion: Corin myocardial gene expression is significantly decreased inCCMP. Similar to BNP, myocardial stretch modulates corin production. This down-regulation of corin is associated with higher circulating plasma levels of unpro-cessed proBNP. Decreased corin gene expression with higher proBNP/BNP lev-els could partly account for the relative BNP resistance observed in CCMP.
P795 Predictive impact of baseline plasma renin activitylevels on long term clinical outcomes in japanesepatients
K. Inoue, Y. Shimoda, Y. Tsubakimoto, T. Sakatani, A. Matsuo,H. Fujita, M. Kitamura. Kyoto Second Red Cross Hospital, Kyoto,Japan
Background: Plasma renin activity (PRA), an upstream mediator ofthe renin-anigiotensin-aldosteron system, has been reported to be associatedwith an increased risk of cardiovascular events. Prognostic value of PRA on longterm clinical outcomes in the Japanese subjects remains unclear.Methods: PRA were quantified in a prospective cohort study of 950 consecutiveJapanese outpatient clinic patients (560 men, 390 women, age 69.4±12.6) todetermine if there was an association of PRA levels and clinical prognosis. Thesubjects were divided into two groups of elevated PRA group (group I) and non-elevated PRA group (group II) according to the median value of baseline PRA.The primary end point of the study was cardiovascular death and all cause death.The secondary end point was defined as myocardial infarction and heart failurerequired hospitalization.Results: The median value of baseline PRA was 2.0 ng/ml/h in all patients. Dur-ing a median follow-up of 989 days, 72 patients died (7.6% mortality rate). Atotal of 48 (5.1%) died with cardiovascular events, 7 (0.7%) experienced myocar-dial infarction and 77 (8.1%) experienced heart failure required hospitalization.Patients of group I (n=484) with higher PRA (≥2.0 ng/ml/h) had a significantlyhigher incidence of cardiovascular death, as compared to those of group II (n=466) with lower PRA (7.4% vs. 2.6%, P=0.003). The incidence of death fromany cause was remarkably higher in the group I than in the group II (10.8%vs. 4.3%, P=0.022). There was no significant difference of myocardial infarctionrate among two groups (1.0% vs. 0.4%, n.s.). Hospitalization for heart failure oc-curred in 12.1% patients in group I versus 3.9% patients in group II (P=0.0003).The levels of PRA were independent predictors of increased cardiovasculardeath and all cause death risk in Cox regression analysis adjusted for age, sex,body mass index, ejection fraction, brain natriuretic peptide and eGFR (hazardratio=1.054[95%CI 1.050-1.058]; P<0.0001, hazard ratio=1.036[95%CI 1.032-1.040]; P<0.0001, respectively). Elevation in PRA was associated with an in-crease risk of hospitalization for heart failure (adjusted hazard ratio=1.009[95%CI1.007-1.010]; P<0.0001).Conclusions: Among Japanese outpatient clinic patients, elevated PRA levelswere independent predictor of cardiovascular mortality, all cause mortality andheart failure hospitalization, but not myocardial infarction.
P796 NT-proBNP as a general marker for ruling out risk foran event in a primary care population at increased riskfor hospitalization or death
C. Adlbrecht1, M. Huelsmann1, G. Strunk2, S. Neuhold1,M. Elhenicky1, U. Ehmsen3, C. Scholten3, G. Maurer1, R. Pacher1.
1Medical University of Vienna, Vienna, Austria; 2WU-Wien, Vienna, Austria;3Physician in Private Practice, Vienna, Austria
Background: In primary care different cohorts are at increased risk for eventslike hospitalization or death. Anticipation of those events is an important aid fordaily practice. Vice versa, classifying a subset of individuals at very low risk, inwhom no further diagnostic workup and therapy are indicated, may aide in focus-ing scarce health-care resources.Aim: This study evaluated amino-terminal pro B-natriuretic peptide (NT-proBNP)as a risk marker in a broad spectrum of primary care patients.Methods and results: A prospective observational study was conducted in 1203primary care patients diagnosed either with hypertension, diabetes, clinically sus-pected heart failure, history of coronary artery disease or myocardial infarction.The primary endpoint, all-cause hospitalization, was reached in 282 (24.0%) in-dividuals within 12 months. The negative predictive value increased dependenton the specification of the endpoint (NPV was 86% for all-cause, 98% for cardiacand 100% of heart failure related hospitalization (for 125pg/ml). PPV and NPVwere superior for NT-proBNP compared to clinical signs and symptoms of heartfailure at every cut-point between 100 and 500pg/ml. Of all variables analyzed,only NT-proBNP (HR 1.001 [1.000-1.001], p<0.001) and age (HR 1.018 [1.007-1.028], p=0.001) were of independent predictive value in a stepwise Cox regres-sion analysis concerning the all-cause hospitalization. Similar results were foundfor endpoints as mortality, cardiac or heart failure hospitalization. Neither systolicdysfunction nor signs and symptoms add independent information to predict anyoutcome.
Conclusion: NT-proBNP levels predict clinical events in a broad spectrum of pri-mary care patients at risk. Negative predictive values are excellent even in thishigh risk population, which proves the concept of a save diagnostic tool.
P797 Long-term prognosis after cardiac resynchronizationtherapy is related to the extent of left ventricularreverse remodeling at midterm follow-up
R. Ramirez Rodriguez1, A.M. Ramirez Rodriguez2, M.A. Garcia-Bello1, E. Hernandez Ortega1, A. Garcia Quintana1, A. Delgado
Espinosa1, E. Dorta Caballero1, A. Medina Fernandez Aceytuno1. 1DoctorNegrin’s Hospital, Las Palmas, Spain; 2Insular Hospital, Las Palmas, Spain
Background: Despite the current selection criteria, individual response to CRTvaries significantly. Furthermore, it has been suggested that reduction in left ven-tricular end-systolic diameter (LVESD) after cardiac resyncrhonization therapy(CRT) is related to outcome. Objectives: To evaluate the relation between theextent of left ventricular (LV) reverse remodelling and clinical/echocardiographicimprovement after 7 years of CRT as well as long term outcome.Methods: A total of 216 CRT candidates were included. Clinical status andechocardiographic evaluation were perfomed before implantation and after 3,6,12months of CRT. Long term follow-up included all- cause mortality and hospitaliza-tions for heart failure.Results: Based on different extents of LV reverse remodeling, 21% of patientswere classified as super-responders (decrease in LVESD≥30%), 26% as respon-ders (decrease in LVESD 15% to 29%), 30% as non responders (decrease inLVESD 0% to 14) and 23% negative responders (incresase in LVESD). Moreextensive LV reverse remodeling resulted in more clinical improvement, with alarger increase in LV function and more reduction in mitral regurgitation. In ad-dition, more LV reverse remodelling resulted in less heart failure hospitalizationsand lower mortality during long term follow-up (45±19 months).
Events during Long-Term Follow-up
Variable Negative-responder Non-responder Responder Super-responder p(n=35) (n=47) (n=40) (n=33)
Follow-up (months) 50±16 38±18 47±21 46±18 0.02Death 14 (40%) 4 (8.5%) 1 (2.5%) 1 (3%) <0.001Hospitalizations for HF 15 (43%) 9 (19%) 5 (13%) 2 (6%) 0.001Death, HTX,
hospitalizations for HF 16 (46%) 10 (21%) 5 (13%) 2 (6%) 0.15
HF: Heart Failure; HTX: Heart Transplantation.
Conclusions: The extent of LV reverse remodelling at 7 years follow-up is pre-dictive for long-term outcome in CRT patients.
P798 Effect of physical training on neurohormonal systemand endothelial markers level in patients with chronicheart failure
B. Bacior1, A. Zdzienicka2, A. Dembinska-Kiec2, K. Kawecka-Jaszcz1. 1Jagiellonian University Medical College, 1st Department of
Cardiology and Hypertension, Krakow, Poland; 2Jagiellonian University MedicalCollege, Department of Medical Biochemistry, Krakow, Poland
Purpose: Endothelial dysfunction and neurohormonal changes play an importantrole in the impairment of physical capacity in patients with chronic heart failure(CHF). Physical training has beneficial effects on exertional activity although itsmechanism demands further research. The aim of the study is to assess theinfluence of physical training on exercise capacity, neurohormonal and endothelialfunction changes in CHF patients.Methods: Sixty men (aged 56.2±7.8 years) with NYHA II - III CHF of ischaemicbackground, with EF ≤ 35% were randomly assigned into two groups: non-trained(A, n=30) and trained (B, n=30). The groups did not differ initially regarding age,duration and advance of CHF. Physical training (general all round body condi-tioning exercises, cycloergometer) in the group B was run 3 times a week for 6months. In both groups initially and after 6 months spiroergometric test and en-dothelial function markers (ET, VEGF), and neurohormonal markers (Ang II, ANP)concentration measurements were performed.Results: In the trained group (B) significant improvement of physical capacity,increase of VEGF and decrease of AngII, ET and ANP was observed (results areshown in Table) while no changes of the analyzed parameters in the group A werenoted.
Table 1. Group B results
Prameter Initially p After 6 months
VO2peak (ml/kg/min) 15.2±2.2 <0.0001 19.0±2.2ET (pg/ml) 60.4±15.8 <0.0001 44.1±11.7VEGF (pg/ml) 16.1±9.2 0.06 19.6±11.4ANP (pg/ml) 109.6±55.5 <0.0001 72.0±40.4Ang II (pg/ml) 21.3±14.0 <0.01 15.1±7.1
VO2peak – maximal oxygen consumption during spiroergometric test, ET – endothelin, VEGF –vascular endothelial growth factor, ANP – atrial natriuretic peptide, Ang II – angiotensin II.
Conclusions: Beneficial changes in neurohormonal system and endothelial func-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / Left ventricular dysfunction 125
tion, via blood flow rise and angiogenesis induction in skeletal muscles, play animportant role in the improvement of physical capacity in CHF patients who arephysically trained.
P799 Correlation of ST2 with IL6 and B-type natriureticpeptide in asymptomatic heart failure patients
E. Omer, N. Murphy, M. Ledwidge, I. Dawkins, C. Watson,K. Mcdonald. St Vincent’s University Hospital, Heart Failure Unit,Dublin, Ireland
Background: ST2 is a novel biomarker and a member of the inter-leukin family. It is secreted by monocytes in response to mechanical strain andattenuates inflammatory response and potentially has anti-fibrotic properties. ST2has been shown to be elevated in acute heart failure following myocardial is-chaemia, but its behaviour in chronic heart failure (HF) where inflammation andfibrosis are important characteristics remains poorly studied. In particular the re-lationship between ST2 and B-type natriuretic peptide (BNP), a well establishedmarker of myocardial structural change in heart failure has not been established.Aim: To examine the behaviour of ST2 in a population of patients with stable heartfailure focusing on the relationship between ST2, BNP, inflammatory markers andenzymes involved in collagen turnover.Methods: Patients with stable heart failure had serum analyses of ST2, BNPinflammatory markers (IL6, IL8, MCP) and enzymes involved in collagen turnover(MMP2 and MMP9, TIMP 1, CITP) performed in standard fashion.Results: One hundred and seventy eight patients (60.1% males) with sta-ble heart failure were studied The mean age was 72.8±12.9 and mean LVEFwas 50.5%±14.2%. ST2 was significantly higher in our population (mean12.50±5.92ng/ml) than in published values for patients without HF.Significant correlates of ST2 with plasma BNP levels (P = 0.045), IL6 (P = 0.031)and CITP (p=0.015). In patients with a BNP > 100pg/ml, ST-2 was significantlyelevated (p=0.047).There is no significant correlation between ST2 and MMP-2, MMP-9, TIMP-1,IL-8, MCP-1, TNFa or diastolic parameters on echocardiography.Conclusion: Serum ST2 levels are significantly elevated in stable HF patients.ST2 correlated well with BNP and IL6 for the identification of stable heart failurepatients.Elevated ST2 in stable heart failure patients may be a protective reaction againstinflammation and fibrosis.
P800 Heart rate reduction with ivabradine reduces activationof the renin-angiotensin-aldosterone system in dogswith chronic heart failure
H.N. Sabbah, R.C. Gupta, M. Wang, I. Ilsar, S. Rastogi, M.S. Sabbah,K. Dye, A. Cavanagh. Henry Ford Health System, Detroit, United
States of America
Background: Enhanced activity of the renin-angiotensin-aldosterone system(RAAS) is a hallmark of heart failure (HF). Pharmacologic therapies that down-regulate RAAS activity in HF such as angiotensin-converting enzyme (ACE) in-hibition, angiotensin-receptor blockade and aldosterone (ALDO) blockade, areeffective treatments for chronic HF. We showed that long-term monotherapy withIvabradine (IVA), a novel selective and specific inhibitor of the cardiac pacemakercurrent If, improves LV function and prevent progressive LV remodeling in dogswith moderate HF (LV ejection fraction ∼35%) produced by coronary microem-bolizations. This study examined the effects of IVA on activity of RAAS in dogswith HF.Methods: Studies were performed in plasma and LV tissue obtained from 24 HFdogs randomized to 3 months oral monotherapy with high dose (HD) IVA (30 mgtwice daily, n=8), low dose (LD) IVA (15 mg twice daily, n=8) or to no therapy at all(Placebo control, n=8). Plasma ACE, angiotensin-II (A-II), ALDO, and bradykinin(BRAD) were measured before (PRE) and 3 months after therapy (POST) usingcommercially available RIA kits. The treatment effect � for each neurohormonewas calculated as the difference between PRE and POST therapy. ACE activitywas measured in LV tissue.Results: Heart rate (HR) decreased from PRE to POST therapy by 12±2 bpm inHD-IVA, by 8±2 bpm in LD IVA and by 4±3 bpm in Placebo groups. Comparedto placebo, IVA significantly lowered plasma levels of A-II and ALDO but did notsignificantly affect plasma levels of ACE (Table). HD but not LD IVA significantlyincreased BRAD levels. ACE activity decreased significantly with both HD and LDIVA compared to placebo (Table).
Table of Results (mean ± SEM)
Placebo LD-IVA HD-IVA
�ACE (ng/ml) 0.6±4.3 -8.0±2.9 -9.0±1.3�A-II (pg/ml) 0.4±10.9 -73±23* -132±16*†
�ALDO (pg/ml) 4±164 -1215±430* -1718±308*�BRAD (ng/ml) -1±9 -11±17 54±18*ACE Activity (Fluorescence unit/μg protein/hour) 14.7±2.7 6.4±1.1* 5.2±1.3*
*p<0.05 vs. Placebo; †p<0.05 vs. LD-IVA.
Conclusions: In dogs with moderate HF, long-term HR reduction with IVA re-duces activation of RAAS, which contributes to the beneficial effects of IVA on LV
function and remodeling. This finding supports the use of IVA in the managementof chronic HF.
P801 Evaluation of brain natriuretic peptide (BNP) role asprognostic factor for cardiovascular outcomes inpatients undergoing non-cardiac surgery
V. Talucci, L. Magrini, A. Scarinci, N. Petrucciani, P. Mercantini,A. Mastrantuono, R. Marino, S. Di Somma, V. Ziparo. Sapienza
University of Rome, Sant’Andrea Hospital, Rome, Italy
Purpose: Cardiovascular events in patients undergoing non-cardiac surgery arehigher than other complications; they are associated with high morbidity and mor-tality, and represent the first cause of death. Clinical evaluation itself is not suffi-cient to predict them, especially if patients show heart failure experiencing noneor few symptoms. The chance of having a simple, fast, and not invasive bloodtest such as BNP could be an optimal approach to cardiovascular pre-surgeryrisk stratification. Our aim was to assess the predictive BNP power for adversecardiac events after non-cardiac surgery.Methods: 205 patients admitted in a general surgery department for major, minornon-cardiac surgery have been enrolled (M/F 91/114, mean age 64±15 yrs). Pre-operative data included: patient demographics, vital signs, routine blood samples,plasma BNP before and after surgery (BNP Triage, Biosite), 12-lead ECG, car-diovascular risk evaluation with the Revised Cardiac Risk Index (RCRI) score. Allpatients were reached by phone 90 days after discharge to investigate the onsetof any cardiovascular event.Results: BNP values [median (IQR)] at admission were 28.5 (10.5-90)pg/ml,and at discharge 76.0 (30.2-170.7)pg/ml significantly higher (P<0.0001). Post-discharge cardiac adverse events occurred in 28 patients. Both BNP levels atadmission (118 (46-403)pg/ml) and at discharge (211 (82.3-529)pg/ml) were sig-nificantly higher (p<0.0001) in patients undergoing post-discharge cardiac eventscompared to those without events. BNP at admission was significantly corre-lated to the RCRI index (median 42.0 (16-132)pg/ml for RCRI 2-3, p<0.001).ROC curves for admission and discharge BNP, and cardiac adverse events at 90days have, respectively, an AUC=0.80, p<0.0001, and an AUC=0.76, p<0.0002.Both admission and discharge BNP levels were more accurate in predicting post-discharge cardiac events than RCRI index (ROC curve for RCRI index AUC=0.57,p=not significant). Multivariate analysis showed that BNP median level >29 pg/mlat admission was the only factor independently correlated with cardiovascular ad-verse event (p< 0.001, OR=9,4883).Conclusions: Our data demonstrate the strong power of BNP, in non-cardiacsurgery, in predicting post-discharge adverse cardiac outcomes, higher thanRCRI index, and correlated with anamnestic data of ischemic cardiovascular dis-eases. Pre- and postoperative BNP have a similar predictive power for cardiovas-cular adverse outcomes. Using BNP in a non-cardiac surgery setting is useful toidentify patients at higher risk for cardiovascular events susceptible for a moreaccurate therapeutic control.
P802 Natriuretic peptide receptors A and C: sequencing andcardiac mRNA expression in normal and heart failurepigs
M. Cabiati1, M. Campan1, C. Caselli2, T. Presciimone2, D. Giannessi2,S. Del Ry2. 1High School Sant’Anna, Pisa, Italy; 2CNR Institute of
Clinical Physiology and Gabriele Monasterio Foundation, Pisa, Italy
Purpose: Natriuretic peptide receptors (NPRs) are capable to inhibit cardiac re-modelling in heart failure (HF) targeted by novel pharmacological treatments, buttheir sequencing is still missing in minipig, the elective experimental model of HF.The pig constitutes an animal model largely used in experimental pathology ow-ing of its similarity with human anatomo-physiology but Sus Scrofa genoma is notcompletely sequenced.Aim: To complete the characterization of NPR system in Sus Scrofa, sequenc-ing NPR-A and NPR-C and to evaluate NPRs mRNA expression in experimentalminipig HF models.Methods: to sequence NPR-A and NPR-C gene in Sus Scrofa we exploited thehigh homology between species, in particular between human and pig. For thisreason, the optimal conditions were obtained using human cardiac tissue deriv-ing from left ventricle (LV) of patients undergoing heart transplantation. ANP, BNP,NPR-A and NPR-C mRNA expressions were evaluated using cardiac tissue sam-ples collected from adult male minipigs (weight 35–40 kg) without (control, n=4)and with pacing-induced HF (n=5).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
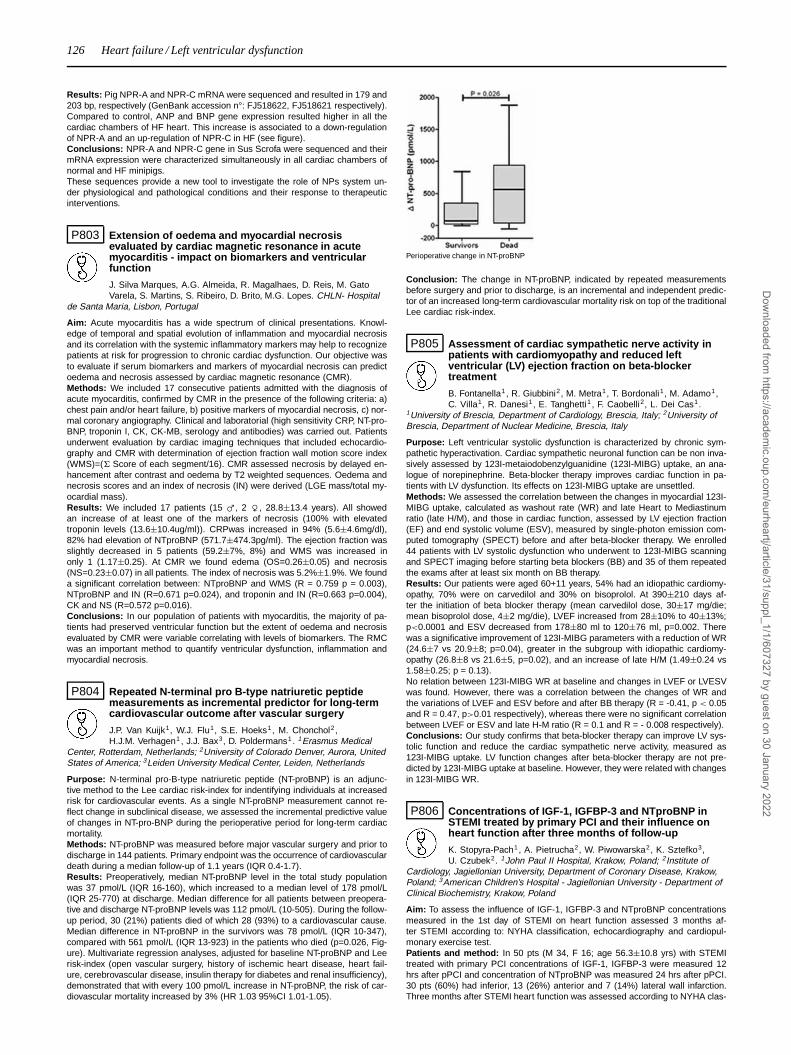
126 Heart failure / Left ventricular dysfunction
Results: Pig NPR-A and NPR-C mRNA were sequenced and resulted in 179 and203 bp, respectively (GenBank accession n°: FJ518622, FJ518621 respectively).Compared to control, ANP and BNP gene expression resulted higher in all thecardiac chambers of HF heart. This increase is associated to a down-regulationof NPR-A and an up-regulation of NPR-C in HF (see figure).Conclusions: NPR-A and NPR-C gene in Sus Scrofa were sequenced and theirmRNA expression were characterized simultaneously in all cardiac chambers ofnormal and HF minipigs.These sequences provide a new tool to investigate the role of NPs system un-der physiological and pathological conditions and their response to therapeuticinterventions.
P803 Extension of oedema and myocardial necrosisevaluated by cardiac magnetic resonance in acutemyocarditis - impact on biomarkers and ventricularfunction
J. Silva Marques, A.G. Almeida, R. Magalhaes, D. Reis, M. GatoVarela, S. Martins, S. Ribeiro, D. Brito, M.G. Lopes. CHLN- Hospital
de Santa Maria, Lisbon, Portugal
Aim: Acute myocarditis has a wide spectrum of clinical presentations. Knowl-edge of temporal and spatial evolution of inflammation and myocardial necrosisand its correlation with the systemic inflammatory markers may help to recognizepatients at risk for progression to chronic cardiac dysfunction. Our objective wasto evaluate if serum biomarkers and markers of myocardial necrosis can predictoedema and necrosis assessed by cardiac magnetic resonance (CMR).Methods: We included 17 consecutive patients admitted with the diagnosis ofacute myocarditis, confirmed by CMR in the presence of the following criteria: a)chest pain and/or heart failure, b) positive markers of myocardial necrosis, c) nor-mal coronary angiography. Clinical and laboratorial (high sensitivity CRP, NT-pro-BNP, troponin I, CK, CK-MB, serology and antibodies) was carried out. Patientsunderwent evaluation by cardiac imaging techniques that included echocardio-graphy and CMR with determination of ejection fraction wall motion score index(WMS)=(� Score of each segment/16). CMR assessed necrosis by delayed en-hancement after contrast and oedema by T2 weighted sequences. Oedema andnecrosis scores and an index of necrosis (IN) were derived (LGE mass/total my-ocardial mass).Results: We included 17 patients (15 m, 2 f, 28.8±13.4 years). All showedan increase of at least one of the markers of necrosis (100% with elevatedtroponin levels (13.6±10.4ug/ml)). CRPwas increased in 94% (5.6±4.6mg/dl),82% had elevation of NTproBNP (571.7±474.3pg/ml). The ejection fraction wasslightly decreased in 5 patients (59.2±7%, 8%) and WMS was increased inonly 1 (1.17±0.25). At CMR we found edema (OS=0.26±0.05) and necrosis(NS=0.23±0.07) in all patients. The index of necrosis was 5.2%±1.9%. We founda significant correlation between: NTproBNP and WMS (R = 0.759 p = 0.003),NTproBNP and IN (R=0.671 p=0.024), and troponin and IN (R=0.663 p=0.004),CK and NS (R=0.572 p=0.016).Conclusions: In our population of patients with myocarditis, the majority of pa-tients had preserved ventricular function but the extent of oedema and necrosisevaluated by CMR were variable correlating with levels of biomarkers. The RMCwas an important method to quantify ventricular dysfunction, inflammation andmyocardial necrosis.
P804 Repeated N-terminal pro B-type natriuretic peptidemeasurements as incremental predictor for long-termcardiovascular outcome after vascular surgery
J.P. Van Kuijk1, W.J. Flu1, S.E. Hoeks1, M. Chonchol2,H.J.M. Verhagen1 , J.J. Bax3, D. Poldermans1. 1Erasmus Medical
Center, Rotterdam, Netherlands; 2University of Colorado Denver, Aurora, UnitedStates of America; 3Leiden University Medical Center, Leiden, Netherlands
Purpose: N-terminal pro-B-type natriuretic peptide (NT-proBNP) is an adjunc-tive method to the Lee cardiac risk-index for indentifying individuals at increasedrisk for cardiovascular events. As a single NT-proBNP measurement cannot re-flect change in subclinical disease, we assessed the incremental predictive valueof changes in NT-pro-BNP during the perioperative period for long-term cardiacmortality.Methods: NT-proBNP was measured before major vascular surgery and prior todischarge in 144 patients. Primary endpoint was the occurrence of cardiovasculardeath during a median follow-up of 1.1 years (IQR 0.4-1.7).Results: Preoperatively, median NT-proBNP level in the total study populationwas 37 pmol/L (IQR 16-160), which increased to a median level of 178 pmol/L(IQR 25-770) at discharge. Median difference for all patients between preopera-tive and discharge NT-proBNP levels was 112 pmol/L (10-505). During the follow-up period, 30 (21%) patients died of which 28 (93%) to a cardiovascular cause.Median difference in NT-proBNP in the survivors was 78 pmol/L (IQR 10-347),compared with 561 pmol/L (IQR 13-923) in the patients who died (p=0.026, Fig-ure). Multivariate regression analyses, adjusted for baseline NT-proBNP and Leerisk-index (open vascular surgery, history of ischemic heart disease, heart fail-ure, cerebrovascular disease, insulin therapy for diabetes and renal insufficiency),demonstrated that with every 100 pmol/L increase in NT-proBNP, the risk of car-diovascular mortality increased by 3% (HR 1.03 95%CI 1.01-1.05).
Perioperative change in NT-proBNP
Conclusion: The change in NT-proBNP, indicated by repeated measurementsbefore surgery and prior to discharge, is an incremental and independent predic-tor of an increased long-term cardiovascular mortality risk on top of the traditionalLee cardiac risk-index.
P805 Assessment of cardiac sympathetic nerve activity inpatients with cardiomyopathy and reduced leftventricular (LV) ejection fraction on beta-blockertreatment
B. Fontanella1 , R. Giubbini2, M. Metra1, T. Bordonali1, M. Adamo1,C. Villa1, R. Danesi1, E. Tanghetti1 , F. Caobelli2, L. Dei Cas1.
1University of Brescia, Department of Cardiology, Brescia, Italy; 2University ofBrescia, Department of Nuclear Medicine, Brescia, Italy
Purpose: Left ventricular systolic dysfunction is characterized by chronic sym-pathetic hyperactivation. Cardiac sympathetic neuronal function can be non inva-sively assessed by 123I-metaiodobenzylguanidine (123I-MIBG) uptake, an ana-logue of norepinephrine. Beta-blocker therapy improves cardiac function in pa-tients with LV dysfunction. Its effects on 123I-MIBG uptake are unsettled.Methods: We assessed the correlation between the changes in myocardial 123I-MIBG uptake, calculated as washout rate (WR) and late Heart to Mediastinumratio (late H/M), and those in cardiac function, assessed by LV ejection fraction(EF) and end systolic volume (ESV), measured by single-photon emission com-puted tomography (SPECT) before and after beta-blocker therapy. We enrolled44 patients with LV systolic dysfunction who underwent to 123I-MIBG scanningand SPECT imaging before starting beta blockers (BB) and 35 of them repeatedthe exams after at least six month on BB therapy.Results: Our patients were aged 60+11 years, 54% had an idiopathic cardiomy-opathy, 70% were on carvedilol and 30% on bisoprolol. At 390±210 days af-ter the initiation of beta blocker therapy (mean carvedilol dose, 30±17 mg/die;mean bisoprolol dose, 4±2 mg/die), LVEF increased from 28±10% to 40±13%;p<0.0001 and ESV decreased from 178±80 ml to 120±76 ml, p=0.002. Therewas a significative improvement of 123I-MIBG parameters with a reduction of WR(24.6±7 vs 20.9±8; p=0.04), greater in the subgroup with idiopathic cardiomy-opathy (26.8±8 vs 21.6±5, p=0.02), and an increase of late H/M (1.49±0.24 vs1.58±0.25; p = 0.13).No relation between 123I-MIBG WR at baseline and changes in LVEF or LVESVwas found. However, there was a correlation between the changes of WR andthe variations of LVEF and ESV before and after BB therapy (R = -0.41, p < 0.05and R = 0.47, p>0.01 respectively), whereas there were no significant correlationbetween LVEF or ESV and late H-M ratio (R = 0.1 and R = - 0.008 respectively).Conclusions: Our study confirms that beta-blocker therapy can improve LV sys-tolic function and reduce the cardiac sympathetic nerve activity, measured as123I-MIBG uptake. LV function changes after beta-blocker therapy are not pre-dicted by 123I-MIBG uptake at baseline. However, they were related with changesin 123I-MIBG WR.
P806 Concentrations of IGF-1, IGFBP-3 and NTproBNP inSTEMI treated by primary PCI and their influence onheart function after three months of follow-up
K. Stopyra-Pach1, A. Pietrucha2, W. Piwowarska2, K. Sztefko3,U. Czubek2. 1John Paul II Hospital, Krakow, Poland; 2Institute of
Cardiology, Jagiellonian University, Department of Coronary Disease, Krakow,Poland; 3American Children’s Hospital - Jagiellonian University - Department ofClinical Biochemistry, Krakow, Poland
Aim: To assess the influence of IGF-1, IGFBP-3 and NTproBNP concentrationsmeasured in the 1st day of STEMI on heart function assessed 3 months af-ter STEMI according to: NYHA classification, echocardiography and cardiopul-monary exercise test.Patients and method: In 50 pts (M 34, F 16; age 56.3±10.8 yrs) with STEMItreated with primary PCI concentrations of IGF-1, IGFBP-3 were measured 12hrs after pPCI and concentration of NTproBNP was measured 24 hrs after pPCI.30 pts (60%) had inferior, 13 (26%) anterior and 7 (14%) lateral wall infarction.Three months after STEMI heart function was assessed according to NYHA clas-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / Left ventricular dysfunction 127
sification, echocardiography and cardiopulmonary exercise test. Heart failure wasobserved in 27 (54%) pts (NYHA I – 11pts, NYHA II- 9pts and NYHA III- 7pts).In echocardiographic examination systolic (EF acc. to Simpson) and diastolic (tis-sue Doppler) heart function and left ventricular mass index (LVMI acc. to Schiller)were assessed. During cardiopulmonary exercise test following parameters wereestablished: VO2peak, AT, VE/VCO2 (in AT), VE/VCO2 peak and METs. Statis-tical analysis was performed using STATISTICA 9.0PL. Multivariate regressionanalysis and correlations were performed, p value <0.05 was treated as statisti-cally significant.Results: The mean concentrations were: IGF-1 176±77 ng/ml; IGFBP-3 4.5±1.3ug/ml; NTproBNP 1428.7±1112.8 pg/ml. The impact of IGF-1 and NTproBNPconcentrations on NYHA class assessed 3months after STEMI was statisticallysignificant (p<0.03 and p<0.02 respectively). The mean values of oxygen con-sumption were as follow: VO2peak 21.3±6 ml/min/kg, AT 13.2±3.1 ml/kg/min,other parameters were: VE/VCO2 13.8±7.4, VE/VCO2peak 39.3±13.8 andMETs 8.43±3.1. Statistically significant correlations were found between IGF-1 and VO2peak (r=0.5; p<0.01) and AT (r=0.36; p<0.05). The mean EF was49.4±6.7%. Mean LVMI was 114±16.2g/m2 . Normal diastolic heart function wasfound in 64% of pts. The concentration of IGF-1 measured in the 1st day of STEMIwas correlated with LVMI determined 3 months after STEMI (r=0.4; p=0.012).Conclusion: 1. Concentration of IGF-1 and NTproBNP measured in 1st day ofSTEMI influence NYHA class in patients treated with primary PCI.2. IGF-1 concentraction during the 1st day of STEMI treated with pPCI correlatespositively with the left ventricular mass index and oxygen consumption in peakexercise and in anaerobic threshold after 3 months follow-up.3. Concentration of IGF-1 and IGFBP-3 in the 1st day of STEMI do not influencethe systolic and diastolic heart function three months after STEMI.
P807 Tumor necrosis factor-a, brain natriuretic peptide andcardiac troponin I in the prediction of 1-year death inpatients with acute decompensated heart failure
M. Zairis, N. Patsourakos, I. Sarris, K. Christodoulopoulos, Z. Katidis,C. Vogiatzidis, K. Katsaros, S. Handanis, J. Panayiotinos, S. Foussas.
Tzanio Hospital, Piraeus, Greece
Purpose: To evaluate a multimarker strategy using circulating levels of tumornecrosis factor alpha (TNF-α), brain natriuretic peptide (BNP) and cardiac tro-ponin I (cTnI) for the prediction of 1-year mortality in patients with acute de-compensated heart failure and preserved (HFPEF) or reduced ejection fraction(HFREF).Methods: A total of 392 and 606 consecutive pts, who were hospitalizedfor acute decompensated HFPEF (LVEF≥50%; mean LVEF:60%) and HFREF(LVEF<50% mean LVEF:35%) respectively, were studied. Biochemical markerswere measured upon admission. The incidence of 1-year death was the prespec-ified primary endpoint.Results: The incidence of the primary endpoint was 19.4% and 21.6% in pts withHFPEF and HFREF, respectively. By separate multivariate Cox analysis in thestudy cohorts, elevated circulating levels of TNF-α (p<0.001and p<0.001 in ptswith HFPEF and HFREF, respectively), BNP (p<0.001and p=0.004 in pts with HF-PEF and HFREF, respectively) and cTnI (p=0.007and p=0.002 in pts with HFPEFand HFREF, respectively) were independently associated with the primary end-point. When the pts were divided according to the number of elevated biomarkers(estimated by ROC analysis) there was a significant gradual increase in the rateof the primary endpoint with increasing of the number of the positive biomarkersin both cohorts (p for trend<0.001 for both cohorts) (Figure).
Conclusions: The present results suggest that serum levels of TNF-α, BNP andcTnI can be used in combination for enhanced early risk stratification in patientswho hospitalized due to either acute decompensated HFPEF or HFREF.
P808 Cardio renal syndrome patients revealed moreneurohormonal and inflammatory activity respect topatients with chronic heart failure
A. Palazzuoli, G. Antonelli, M. Caputo, A. Calabro’, M.S. Campagna,B. Franci, I. Quatrini, A. Santoro, R. Nuti. Department of Internal
Medicine and Metabolic Diseases, Siena, Italy
Purpose: Plasma brain natriuretic peptide (BNP) levels are well established asmarkers of neurohormonal activation in patients with chronic heart failure (CHF).Chronic inflammation, as evidenced by increased levels of pro-inflammatory cy-tokines (such IL-1 and IL-6), is a common feature in patients with chronic re-
nal dysfunction and CHF. Cardio renal syndrome (CRS) is associated with anincreased cardiovascular morbidity and mortality. Therefore Serum NeutrophilGelatinase-Associated Lipocalin (NGAL) is a new marker of tubular damage andrecently associated with poor prognosis in HF patients. Osteoprotegerin (OPG) isa new marker of vascular damage and coronary and systemic calcifications.The aim of this study was to measure inflammatory activation, neurohormonalstatus and vascular damage in patients with CRS (GFR: <50 ml/min) respectto patients with CHF and preserved renal function, analyzing in each group IL6,BNP, NGAL and OPG.Methods: 114 consecutive patients with diagnosis of chronic heart failure (71 withCRS) were enrolled in the study. All laboratory parameters were measured duringhospital admission phase (early 48 hours). Patients with other causes of inflam-matory activation (chronic inflammatory diseases, infective status and neoplasticdiseases), were excluded. We also evaluated eventual correlation between renaldysfunction and all laboratory parameters, and correlation among neurohormonalstatus, inflammatory activation and vascular damage.Results: A significant increase in IL 6, NGAL and BNP plasma levels was foundin CRS patients respect to HF patients without chronic renal dysfunction (IL 6:26±10 ng/ml VS 10±7 ng/ml, p=0,001; NGAL: 152±94 ng/ml VS 61±42 ng/ml,p=0,0002; BNP: 771±50 pg/ml VS 405±80 pg/ml, p=0,01). For OPG, no signifi-cant differences were found between the groups. In the subgroup of patients withCRS (GFR=32,6±13 ml/min) we found a significant correlation between BNP lev-els and GFR (r= -0,27; p=0,02) and between BNP levels and IL 6 levels (r=0,32;p=0,02).Conclusions: in patients with CRS inflammatory and neurohormonal activationare more elevated respect to HF patients. Neurohormonal activity and increasein pro-inflammatory cytokines appear to be related with renal function decrease.These data could explain worsening outcome in patients with HF and renal dys-function.
P809 Serum carbohydrate antigen 125 in patients withsevere aortic stenosis and preserved ejection fraction
C.C. Beladan1, A. Calin1, B.A. Popescu1, M. Rosca1, D. Muraru2,L. Constantin2 , L. Dima2, L. Antohi2, F. Antonini-Canterin3,C. Ginghina1. 1University of Medicine and Pharmacy Carol Davila,
Bucharest, Romania; 2Institute of Cardiovascular Diseases "Prof. Dr. CC Iliescu",Bucharest, Romania; 3Cardiology, ARC, "Santa Maria degli Angeli" Hospital,Pordenone, Italy
Background: Brain natriuretic peptide (BNP) levels are related to symptoms andoutcome in aortic stenosis (AS). Serum levels of carbohydrate antigen CA 125,a tumour marker related to ovarian cancer, have been shown to increase in pa-tients with chronic heart failure (CHF) and to relate with an adverse outcome. Itdemonstrated recently a BNP-like behaviour in patients (pts) with AS and LV dys-function. The significance of CA125 levels in severe AS with preserved EF hasnot been studied yet.Purpose: To assess CA125 levels in pts with severe AS and preserved left ven-tricular ejection fraction (LVEF) and their correlation with clinical symptoms andechocardiographic indices.Methods: CA125 and BNP blood levels were obtained in 35 prospectively en-rolled pts (64±11 years, 24 men) with severe AS (aortic valve area index,AVAi< 0.60 cm2/m2) and preserved LVEF (>50%). Independent evaluation ofheart failure symptoms and a comprehensive echocardiogram were performedin all pts. LV filling pressures were assessed using the E/E’ ratio. Valvulo-arterial impedance (Zva) was calculated based on net mean transvalvular gra-dient (Gmean), systolic arterial pressure, and indexed stroke volume. Skeweddata (CA125 and BNP values) were logarithmically transformed (ln) and used foranalyses.Results: In our population, AVAi was 0.40±0.09 cm2/m2 with a Gmean of 52±19mmHg. Ten pts were in NYHA class I, 19 pts in NYHA II, 6 pts in NYHA III. Me-dian plasma concentrations of BNP and CA125 in the whole population were 173U/ml (interquartile range 75 - 291) and 6 U/ml (interquartile range 4-10), respec-tively. CA125 and BNP levels were significantly correlated to each other (r=0.44,p=0.01) and increased with increasing NYHA functional class, but without reach-ing statistical significance. BNP levels correlated with Gmean (r=0.42, p=0.01),LVEF (r=0.47, p=0.006), indexed left atrial volume (r=0.41, p=0.01) and E/E’ ratio(r=0.48, p=0.009). CA125 levels had a direct relationship with Gmean (r=0.30;p=0.08), indexed left atrial volume (r=0.30; p=0.07), LVEF (r=0.47, p=0.006) andZva (r=0.38; p=0.04).Conclusion: In pts with severe AS and preserved LVEF, BNP levels are signifi-cantly related to AS severity and LV function. In this cohort CA 125, but not BNPserum levels, had a significant relationship with Zva, a proven prognostic markerin AS. The added value of CA 125 serum levels for the optimal decision makingin this setting requires further study.
P810 Prognostic value of pulse wave velocity in patientswith congestive heart failure of ischemic etiology
O.V. Ilyukhin, Y.U.M. Lopatin. State Medical University, Volgograd,Russian Federation
Pulse wave velocity (PWV) is a well known marker of end organ dam-age in patients (pts) with arterial hypertension. Regarding pts with congestive
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
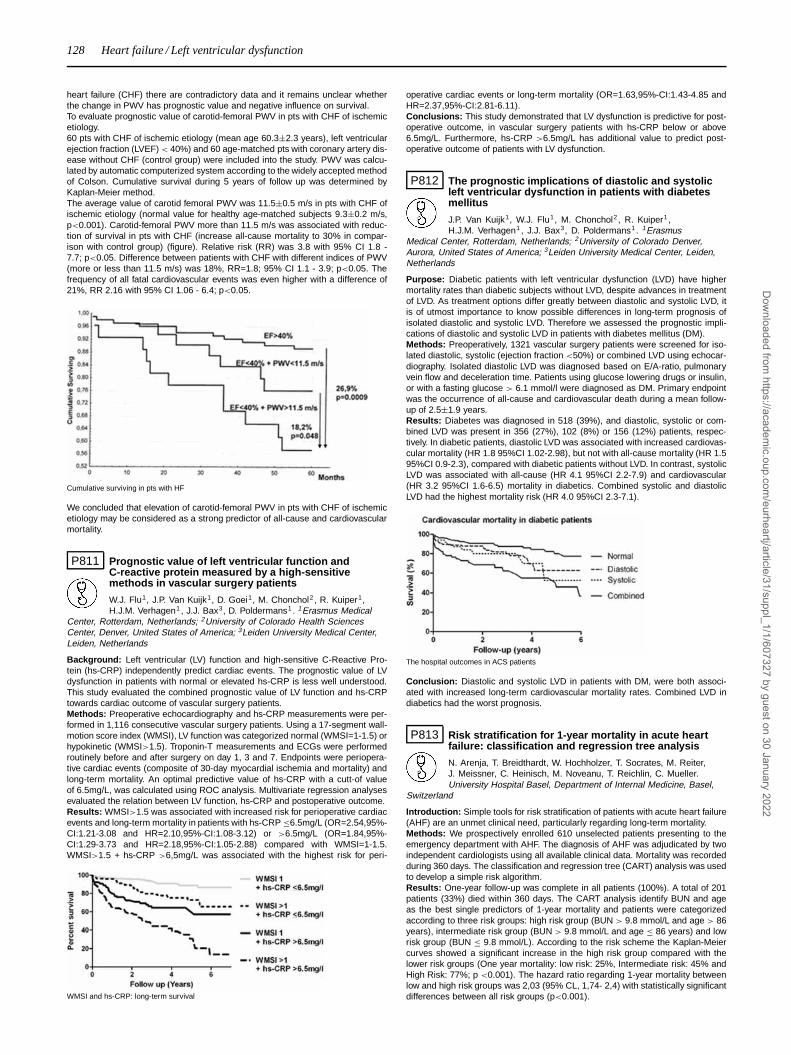
128 Heart failure / Left ventricular dysfunction
heart failure (CHF) there are contradictory data and it remains unclear whetherthe change in PWV has prognostic value and negative influence on survival.To evaluate prognostic value of carotid-femoral PWV in pts with CHF of ischemicetiology.60 pts with CHF of ischemic etiology (mean age 60.3±2.3 years), left ventricularejection fraction (LVEF) < 40%) and 60 age-matched pts with coronary artery dis-ease without CHF (control group) were included into the study. PWV was calcu-lated by automatic computerized system according to the widely accepted methodof Colson. Cumulative survival during 5 years of follow up was determined byKaplan-Meier method.The average value of carotid femoral PWV was 11.5±0.5 m/s in pts with CHF ofischemic etiology (normal value for healthy age-matched subjects 9.3±0.2 m/s,p<0.001). Carotid-femoral PWV more than 11.5 m/s was associated with reduc-tion of survival in pts with CHF (increase all-cause mortality to 30% in compar-ison with control group) (figure). Relative risk (RR) was 3.8 with 95% CI 1.8 -7.7; p<0.05. Difference between patients with CHF with different indices of PWV(more or less than 11.5 m/s) was 18%, RR=1.8; 95% CI 1.1 - 3.9; p<0.05. Thefrequency of all fatal cardiovascular events was even higher with a difference of21%, RR 2.16 with 95% CI 1.06 - 6.4; p<0.05.
Cumulative surviving in pts with HF
We concluded that elevation of carotid-femoral PWV in pts with CHF of ischemicetiology may be considered as a strong predictor of all-cause and cardiovascularmortality.
P811 Prognostic value of left ventricular function andC-reactive protein measured by a high-sensitivemethods in vascular surgery patients
W.J. Flu1, J.P. Van Kuijk1, D. Goei1, M. Chonchol2 , R. Kuiper1,H.J.M. Verhagen1 , J.J. Bax3, D. Poldermans1. 1Erasmus Medical
Center, Rotterdam, Netherlands; 2University of Colorado Health SciencesCenter, Denver, United States of America; 3Leiden University Medical Center,Leiden, Netherlands
Background: Left ventricular (LV) function and high-sensitive C-Reactive Pro-tein (hs-CRP) independently predict cardiac events. The prognostic value of LVdysfunction in patients with normal or elevated hs-CRP is less well understood.This study evaluated the combined prognostic value of LV function and hs-CRPtowards cardiac outcome of vascular surgery patients.Methods: Preoperative echocardiography and hs-CRP measurements were per-formed in 1,116 consecutive vascular surgery patients. Using a 17-segment wall-motion score index (WMSI), LV function was categorized normal (WMSI=1-1.5) orhypokinetic (WMSI>1.5). Troponin-T measurements and ECGs were performedroutinely before and after surgery on day 1, 3 and 7. Endpoints were periopera-tive cardiac events (composite of 30-day myocardial ischemia and mortality) andlong-term mortality. An optimal predictive value of hs-CRP with a cutt-of valueof 6.5mg/L, was calculated using ROC analysis. Multivariate regression analysesevaluated the relation between LV function, hs-CRP and postoperative outcome.Results: WMSI>1.5 was associated with increased risk for perioperative cardiacevents and long-term mortality in patients with hs-CRP ≤6.5mg/L (OR=2.54,95%-CI:1.21-3.08 and HR=2.10,95%-CI:1.08-3.12) or >6.5mg/L (OR=1.84,95%-CI:1.29-3.73 and HR=2.18,95%-CI:1.05-2.88) compared with WMSI=1-1.5.WMSI>1.5 + hs-CRP >6,5mg/L was associated with the highest risk for peri-
WMSI and hs-CRP: long-term survival
operative cardiac events or long-term mortality (OR=1.63,95%-CI:1.43-4.85 andHR=2.37,95%-CI:2.81-6.11).Conclusions: This study demonstrated that LV dysfunction is predictive for post-operative outcome, in vascular surgery patients with hs-CRP below or above6.5mg/L. Furthermore, hs-CRP >6.5mg/L has additional value to predict post-operative outcome of patients with LV dysfunction.
P812 The prognostic implications of diastolic and systolicleft ventricular dysfunction in patients with diabetesmellitus
J.P. Van Kuijk1, W.J. Flu1, M. Chonchol2 , R. Kuiper1,H.J.M. Verhagen1 , J.J. Bax3, D. Poldermans1. 1Erasmus
Medical Center, Rotterdam, Netherlands; 2University of Colorado Denver,Aurora, United States of America; 3Leiden University Medical Center, Leiden,Netherlands
Purpose: Diabetic patients with left ventricular dysfunction (LVD) have highermortality rates than diabetic subjects without LVD, despite advances in treatmentof LVD. As treatment options differ greatly between diastolic and systolic LVD, itis of utmost importance to know possible differences in long-term prognosis ofisolated diastolic and systolic LVD. Therefore we assessed the prognostic impli-cations of diastolic and systolic LVD in patients with diabetes mellitus (DM).Methods: Preoperatively, 1321 vascular surgery patients were screened for iso-lated diastolic, systolic (ejection fraction <50%) or combined LVD using echocar-diography. Isolated diastolic LVD was diagnosed based on E/A-ratio, pulmonaryvein flow and deceleration time. Patients using glucose lowering drugs or insulin,or with a fasting glucose > 6.1 mmol/l were diagnosed as DM. Primary endpointwas the occurrence of all-cause and cardiovascular death during a mean follow-up of 2.5±1.9 years.Results: Diabetes was diagnosed in 518 (39%), and diastolic, systolic or com-bined LVD was present in 356 (27%), 102 (8%) or 156 (12%) patients, respec-tively. In diabetic patients, diastolic LVD was associated with increased cardiovas-cular mortality (HR 1.8 95%CI 1.02-2.98), but not with all-cause mortality (HR 1.595%CI 0.9-2.3), compared with diabetic patients without LVD. In contrast, systolicLVD was associated with all-cause (HR 4.1 95%CI 2.2-7.9) and cardiovascular(HR 3.2 95%CI 1.6-6.5) mortality in diabetics. Combined systolic and diastolicLVD had the highest mortality risk (HR 4.0 95%CI 2.3-7.1).
The hospital outcomes in ACS patients
Conclusion: Diastolic and systolic LVD in patients with DM, were both associ-ated with increased long-term cardiovascular mortality rates. Combined LVD indiabetics had the worst prognosis.
P813 Risk stratification for 1-year mortality in acute heartfailure: classification and regression tree analysis
N. Arenja, T. Breidthardt, W. Hochholzer, T. Socrates, M. Reiter,J. Meissner, C. Heinisch, M. Noveanu, T. Reichlin, C. Mueller.University Hospital Basel, Department of Internal Medicine, Basel,
Switzerland
Introduction: Simple tools for risk stratification of patients with acute heart failure(AHF) are an unmet clinical need, particularly regarding long-term mortality.Methods: We prospectively enrolled 610 unselected patients presenting to theemergency department with AHF. The diagnosis of AHF was adjudicated by twoindependent cardiologists using all available clinical data. Mortality was recordedduring 360 days. The classification and regression tree (CART) analysis was usedto develop a simple risk algorithm.Results: One-year follow-up was complete in all patients (100%). A total of 201patients (33%) died within 360 days. The CART analysis identify BUN and ageas the best single predictors of 1-year mortality and patients were categorizedaccording to three risk groups: high risk group (BUN > 9.8 mmol/L and age > 86years), intermediate risk group (BUN > 9.8 mmol/L and age ≤ 86 years) and lowrisk group (BUN ≤ 9.8 mmol/L). According to the risk scheme the Kaplan-Meiercurves showed a significant increase in the high risk group compared with thelower risk groups (One year mortality: low risk: 25%, Intermediate risk: 45% andHigh Risk: 77%; p <0.001). The hazard ratio regarding 1-year mortality betweenlow and high risk groups was 2,03 (95% CL, 1,74- 2,4) with statistically significantdifferences between all risk groups (p<0.001).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
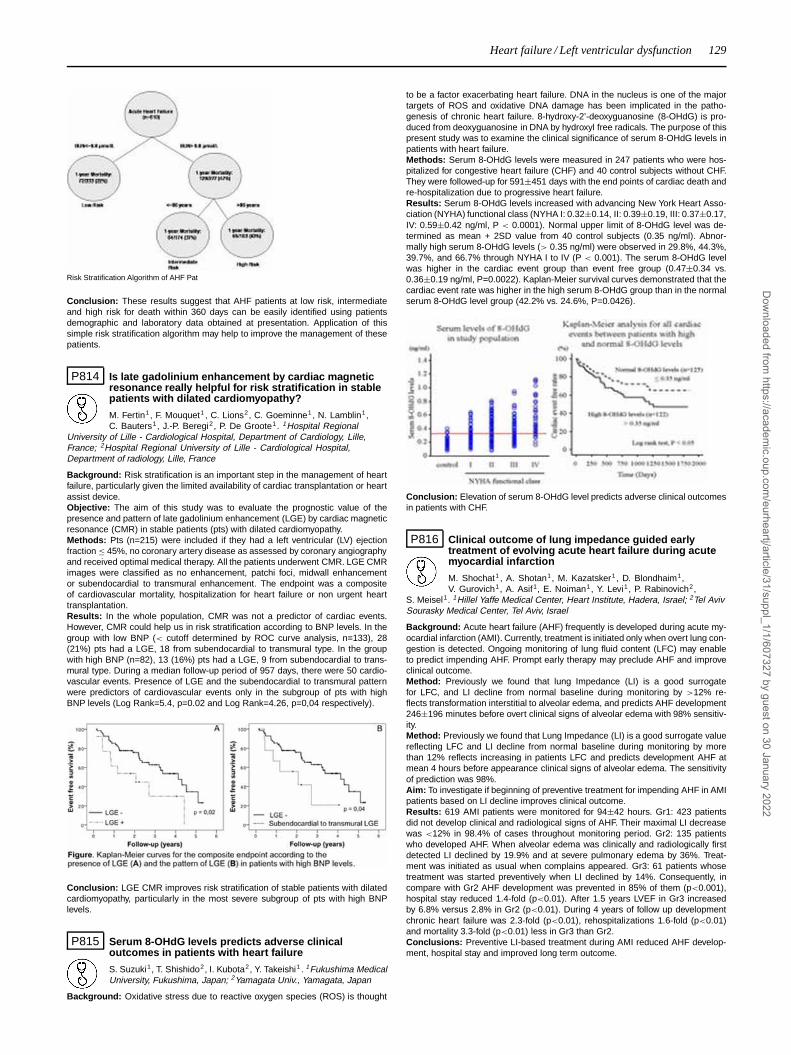
Heart failure / Left ventricular dysfunction 129
Risk Stratification Algorithm of AHF Pat
Conclusion: These results suggest that AHF patients at low risk, intermediateand high risk for death within 360 days can be easily identified using patientsdemographic and laboratory data obtained at presentation. Application of thissimple risk stratification algorithm may help to improve the management of thesepatients.
P814 Is late gadolinium enhancement by cardiac magneticresonance really helpful for risk stratification in stablepatients with dilated cardiomyopathy?
M. Fertin1, F. Mouquet1 , C. Lions2, C. Goeminne1, N. Lamblin1,C. Bauters1, J.-P. Beregi2, P. De Groote1. 1Hospital Regional
University of Lille - Cardiological Hospital, Department of Cardiology, Lille,France; 2Hospital Regional University of Lille - Cardiological Hospital,Department of radiology, Lille, France
Background: Risk stratification is an important step in the management of heartfailure, particularly given the limited availability of cardiac transplantation or heartassist device.Objective: The aim of this study was to evaluate the prognostic value of thepresence and pattern of late gadolinium enhancement (LGE) by cardiac magneticresonance (CMR) in stable patients (pts) with dilated cardiomyopathy.Methods: Pts (n=215) were included if they had a left ventricular (LV) ejectionfraction ≤ 45%, no coronary artery disease as assessed by coronary angiographyand received optimal medical therapy. All the patients underwent CMR. LGE CMRimages were classified as no enhancement, patchi foci, midwall enhancementor subendocardial to transmural enhancement. The endpoint was a compositeof cardiovascular mortality, hospitalization for heart failure or non urgent hearttransplantation.Results: In the whole population, CMR was not a predictor of cardiac events.However, CMR could help us in risk stratification according to BNP levels. In thegroup with low BNP (< cutoff determined by ROC curve analysis, n=133), 28(21%) pts had a LGE, 18 from subendocardial to transmural type. In the groupwith high BNP (n=82), 13 (16%) pts had a LGE, 9 from subendocardial to trans-mural type. During a median follow-up period of 957 days, there were 50 cardio-vascular events. Presence of LGE and the subendocardial to transmural patternwere predictors of cardiovascular events only in the subgroup of pts with highBNP levels (Log Rank=5.4, p=0.02 and Log Rank=4.26, p=0,04 respectively).
Conclusion: LGE CMR improves risk stratification of stable patients with dilatedcardiomyopathy, particularly in the most severe subgroup of pts with high BNPlevels.
P815 Serum 8-OHdG levels predicts adverse clinicaloutcomes in patients with heart failure
S. Suzuki1, T. Shishido2, I. Kubota2, Y. Takeishi1 . 1Fukushima MedicalUniversity, Fukushima, Japan; 2Yamagata Univ., Yamagata, Japan
Background: Oxidative stress due to reactive oxygen species (ROS) is thought
to be a factor exacerbating heart failure. DNA in the nucleus is one of the majortargets of ROS and oxidative DNA damage has been implicated in the patho-genesis of chronic heart failure. 8-hydroxy-2’-deoxyguanosine (8-OHdG) is pro-duced from deoxyguanosine in DNA by hydroxyl free radicals. The purpose of thispresent study was to examine the clinical significance of serum 8-OHdG levels inpatients with heart failure.Methods: Serum 8-OHdG levels were measured in 247 patients who were hos-pitalized for congestive heart failure (CHF) and 40 control subjects without CHF.They were followed-up for 591±451 days with the end points of cardiac death andre-hospitalization due to progressive heart failure.Results: Serum 8-OHdG levels increased with advancing New York Heart Asso-ciation (NYHA) functional class (NYHA I: 0.32±0.14, II: 0.39±0.19, III: 0.37±0.17,IV: 0.59±0.42 ng/ml, P < 0.0001). Normal upper limit of 8-OHdG level was de-termined as mean + 2SD value from 40 control subjects (0.35 ng/ml). Abnor-mally high serum 8-OHdG levels (> 0.35 ng/ml) were observed in 29.8%, 44.3%,39.7%, and 66.7% through NYHA I to IV (P < 0.001). The serum 8-OHdG levelwas higher in the cardiac event group than event free group (0.47±0.34 vs.0.36±0.19 ng/ml, P=0.0022). Kaplan-Meier survival curves demonstrated that thecardiac event rate was higher in the high serum 8-OHdG group than in the normalserum 8-OHdG level group (42.2% vs. 24.6%, P=0.0426).
Conclusion: Elevation of serum 8-OHdG level predicts adverse clinical outcomesin patients with CHF.
P816 Clinical outcome of lung impedance guided earlytreatment of evolving acute heart failure during acutemyocardial infarction
M. Shochat1 , A. Shotan1, M. Kazatsker1, D. Blondhaim1,V. Gurovich1, A. Asif1, E. Noiman1, Y. Levi1, P. Rabinovich2,
S. Meisel1. 1Hillel Yaffe Medical Center, Heart Institute, Hadera, Israel; 2Tel AvivSourasky Medical Center, Tel Aviv, Israel
Background: Acute heart failure (AHF) frequently is developed during acute my-ocardial infarction (AMI). Currently, treatment is initiated only when overt lung con-gestion is detected. Ongoing monitoring of lung fluid content (LFC) may enableto predict impending AHF. Prompt early therapy may preclude AHF and improveclinical outcome.Method: Previously we found that lung Impedance (LI) is a good surrogatefor LFC, and LI decline from normal baseline during monitoring by >12% re-flects transformation interstitial to alveolar edema, and predicts AHF development246±196 minutes before overt clinical signs of alveolar edema with 98% sensitiv-ity.Method: Previously we found that Lung Impedance (LI) is a good surrogate valuereflecting LFC and LI decline from normal baseline during monitoring by morethan 12% reflects increasing in patients LFC and predicts development AHF atmean 4 hours before appearance clinical signs of alveolar edema. The sensitivityof prediction was 98%.Aim: To investigate if beginning of preventive treatment for impending AHF in AMIpatients based on LI decline improves clinical outcome.Results: 619 AMI patients were monitored for 94±42 hours. Gr1: 423 patientsdid not develop clinical and radiological signs of AHF. Their maximal LI decreasewas <12% in 98.4% of cases throughout monitoring period. Gr2: 135 patientswho developed AHF. When alveolar edema was clinically and radiologically firstdetected LI declined by 19.9% and at severe pulmonary edema by 36%. Treat-ment was initiated as usual when complains appeared. Gr3: 61 patients whosetreatment was started preventively when LI declined by 14%. Consequently, incompare with Gr2 AHF development was prevented in 85% of them (p<0.001),hospital stay reduced 1.4-fold (p<0.01). After 1.5 years LVEF in Gr3 increasedby 6.8% versus 2.8% in Gr2 (p<0.01). During 4 years of follow up developmentchronic heart failure was 2.3-fold (p<0.01), rehospitalizations 1.6-fold (p<0.01)and mortality 3.3-fold (p<0.01) less in Gr3 than Gr2.Conclusions: Preventive LI-based treatment during AMI reduced AHF develop-ment, hospital stay and improved long term outcome.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

130 Heart failure / Left ventricular dysfunction
P817 Prognosis of Chagas’ cardiomyopathy versusnon-Chagas’ cardiomyopathy in beta-blockers era:24 month follow-up
G.E. Conceicao-Souza, L.M. Pessoa-De-Melo, J.L. Vieira, V. Batistela,E. Gorobets, L.R. Valim, A.C.P. Barretto, E.A. Bocchi, J.A.F. Ramires.
Heart Institute -InCor, São Paulo, Brazil
Purpose: To compare incidence of an combined endpoint of mortality or hearttransplantation (HT) in patients with systolic heart failure (SHF) due to Chagas’cardiomyopathy (CC) with non-Chagas’ cardiomyopathy (NCC) in a 24-monthfollow-up in the beta-blockers’ era.Methods: Analytical cohort prospective study. Inclusion criteria: left ventricularejection fraction (LVEF) < 45% and onset of symptoms time > 1 month. Pa-tients were allocated in either CC group or NCC group according to results of2 diferent sorologic tests for Trypanosoma cruzi. Exclusion criteria: patients withsevere comorbidities which could affect survival in the next 12 months. Patientswere followed by clinical outpatient evaluation and/or telephone contact after 24months inclusion of the first patient and 8 months after inclusion of the last pa-tient. Sample size was estimated for a power of 90%. P value was consideredstatistically significant if < 0,05. Comparative statistical analysis used Fischer’sexact test for categoric variables; non-paired T-student test for parametric contin-uous variables and Mann-Whitney test for non-parametric continuous variables.Log rank test was used for comparing mortality from Kaplan-Meier curves of bothgroups.Results: From january 2008 to april 2009, 287 patients were included - 140 pa-tients in CC group and 147 patients in NCC group. Medical treatment, clinical andechocardiographic variables were similar in both groups, except for body massindex which was lower in CC group. Use of beta-blockers was not different in G1and G2 (90% vs 95%, respectively). After a 24-month follow-up, transplant-freesurvival was was 70,76% vs 82,15% in G1 and G2 respectively - p=0,0134.Conclusions: Chagasic patients still have a worse prognosis in comparison tonon-chagasic patients, according to transplant-free survival in beta-blockers’ era.
P818 Prognostic role of exercise echocardiography in heartfailure
P. Rubis, L. Drabik, G. Kopec, M. Podolec, M. Olszowska, W. Tracz,P. Podolec. Department of Cardiac and Vascular Disease, John PaulII Hospital, Institute of Cardiology, Krakow, Poland
Aim: We investigated the prognostic role of exercise echocardiography (ex-echo)in systolic HF.Material and Methods: We studied 85 pts, 66 male, mean age of 62.5±11.8 (21-83) years, 35% in NYHA III/IV, LVEF 27.2±9.5% (10-45%). Baseline and ex-echo,with the simultaneous measurement of VO2peak, was performed on semi-supineergometer (20 Watts, 2-min increments). We assessed conventional systolic anddiastolic function parameters (EF, E/A, DT, IVRT), and RVSP. TDI was used forthe assessment peak IVV, IVA, S’, E’, ratio of mitral and tricuspid E to E’ (E/E’).Primary end-point was death and death due to cardio-vascular incident. Duringfollow-up (43±21 months) 21 pts died (group 1).Results: Pts from group 1 were significantly older, had lower exercise capacity,more advanced HF, lower baseline EF, higher baseline RVSP, and more impor-tantly lack of improvement of EF, E/E’, and further increase of RVSP during ex-ercise (Table 1). Among all echocardiographic parameters only peak exercise EF(Wald 6.1; p<0.01), and baseline and peak exercise RVSP (Wald 12.5; P<0.001and Wald 18.7; P<0.001; respectively) were univariate predictors of prognosis onCox-regression and remained independently prognostic when adjusted for ageand sex but were knocked out of the model by NT-proBNP.
Table 1
Variable Group 1 (n=21) Group 2 (n=64) p-value
Age (years) 67.4±10.7 61.3±12.6 0.05VO2 peak (ml/kg/min) 11.9±2.4 15.6±4.7 0.01NT-proBNP (pg/ml) 444.6±146.4 251.3±80.7 0.01Time of exercise (sec) 311.5±107.8 459.5±228.1 0.02EF rest (%) 21.7±7.6 28.3±9.4 0.05EF ex (%) 23.4±7.9 33.2±13.4 0.001RVSP rest (mmHg) 45.4±23.9 25.3±17.3 0.003RVSP ex (mmHg) 56.8±18.6 31.4±21.4 0.001LV-S’ ex (m/s) 4.9±1.8 5.8±2.1 0.05LV-E/E’ ex 21.4±3.1 17.5±5.6 0.01
Conclusions: Lack of augmentation of systolic and diastolic function and in-crease of pulmonary pressure during exercise are more prevalent in HF pts withworse outcome. Ex-echo with the measurement of commonly-used echo param-eters, such as EF and RVSP provides independent, prognostic information in HF.
P819 Prognostic value of the left and right atrial functionalparameters in dilated cardiomyopathy with severechronic heart failure
L.R. Tumasyan, K.G. Adamyan. Institute of Cardiology, Yerevan,Armenia
The aim of study was to assess the significance of the left (LA) and right atrial
(RA) functional parameters in prediction of survival in patients (pts) with dilatedcardiomyopathy (DCM) and severe chronic heart failure (CHF).Methods: 106 pts (age 58.1±0.9) with DCM of ischemic (n=71) or nonischemicorigin and NYHA III-IV functional class CHF in sinus rhythm were prospec-tively studied. LA and RA dimensions, volumes, late diastolic transmitral (Am)and transtricuspid (At) flow velocity (cm/sec), LA (LAKE) and RA kinetic energy(RAKE), LA and RA active emptying fraction (EFakt,%), mitral (MAPSE) and tri-cuspid annulus plane systolic excursion (TAPSE) (mm), LA and RA function index(FI), mitral (MR) and tricuspid regurgitation (TR) were obtained using echocardio-graphy. LAKE and RAKE (kdyn/cm/sec) were calculated using the formula=1/2stroke volume x1.06xAxA, and LA and RA FI =LA (RA) EFx LV (RV) OT –VTI/LA(RA) ESV. MR and TR were quantified as a MR (TR) area/LA (RA) area ratio.Results: During a mean follow-up period of 37±0.7 months 37 (34.5%) pts diedfrom cardiac causes. These pts had more impaired LA and RA functions (p<0.01for all), depicted by LA and RA FI (0.17±0.05 vs. 0.29±0.04 and 0.14±0.02 vs.0.23±0.04), LAKE and RAKE (4.7±0.9 vs. 9.1±1.3 and 4.4±0.8 vs. 8.7±1.2),LA and RA EFakt (12.5±1.1 vs. 18.9±1.9 and 10.1±1.2 vs. 16.8±1.8). MAPSEand TAPSE (5.4±0.7 vs. 9.0±1.1 and 5.1±0.5 vs. 8.6±1.1) and MR and TR(0.41±0.06 vs. 0.2±0.04 and 0.40±0.05 vs. 0.21±0.04) also were markedlyworse (p<0.01) in non-survivors than in survivors. In died pts revealed more se-vere LV and RV diastolic dysfunction with Am and At, respectively, 29.3±3.0 vs.40.2±3.2 and 55.4±6.2 vs. 73.3±7.1, p<0.05. Multivariate stepwise Cox analysisrevealed that independent predictors of cardiac death were LA and RA FI, MAPSEand TAPSE, LAKE and RAKE, LA and RA EFakt, MR and TR. Kaplan-Meier sur-vival curves demonstrated a survival rate of 87% and 84% for pts with LA andRA FI >25 and >20 and 68% and 67% for those with <25 and <20 (p<0.01).Similar probability of survival (p<0.01) was shown in pts with LAKE and RAKE>7.0 (85%) and >6.0 (84%), LA and RA EFakt >15.0 (85%) and >12.5 (83%),MAPSE and TAPSE >7.5 (82%) and >6.5 (86%), MR and TR <0.3 (86% and84%) and in those with LAKE and RAKE <7.0 (62%) and <6.0 (63.5%), LA andRA EFakt <15.0 (67%) and <12.5 (64%), MAPSE and TAPSE <7.5 (64%) and<6.5 (62%) and MR and TR >3.0 (63.5% and 65%).In conclusion, LA and RA functional parameters are the powerful predictors ofsurvival in pts with CHF and could be effectively used in prognostic evaluation ofsuch pts.
P820 In hospital mortality in patients hospitalized for acuteheart failure - AHEAD MAIN Registry
J. Parenica1, J. Spinar1, A. Linhart2, J. Vitovec3, P. Widimsky4,C. Cihalik5, M. Fedorco6 , M. Felsoci1. 1Faculty Hospital, Brno,Czech Republic; 2General Faculty Hospital, Prague, Czech Republic;
3Masaryk University,St. Anne’s Faculty Hospital,1st Department of InternalMedicine-Cardioangiology, Brno, Czech Republic; 4Charles University Prague,3rd Faculty of Med.-Faculty Hospital Kralovske Vinohrady, Cardiocenter, Prague,Czech Republic; 5Bata Regional Hospital Zlin, Department of Cardiology, Zlin,Czech Republic; 6Palacky University, Faculty of Medicine and Dentistry, 1st Deptof Internal Medicine-Cardiology, Olomouc, Czech Republic
Introduction: AHEAD MAIN (Acute HEArt Failure Database) is a prospectiveregistry of patients hospitalized with acute heart failure (AHF) at 7 specializedcardiological departments (available on-line at ahead.registry.cz). Data evaluatedinclude 2742 patients entered in the registry from July 2006 to October 2009.Aim: To divide patients admitted with acute heart failure into groups by clinicalsyndromes (respecting guidelines) and aetiology, to determine in-hospital mortal-ity (IHM).Results: Average age of hospitalized women was 74.9±11.5 yrs, men 68.2±12.3yrs (p<0.001). Median length of hospital stay was 7 days, 2 days for departed pa-tients (N=318) and 8 days for discharged patients (N=2424). The presentation ofclinical syndromes was as follows: (1) minor AHF – 52.2%, (2) pulmonary oedema– 18.3%, (3) cardiogenic shock – 13.5%, (4) hypertensive crisis – 6.2%, (5) highoutput AHF – 5.8%, (6) acute right-ventricle HF – 4.0%. The most frequent etiolo-gies of AHF were ACS (32.6%), chronic IHD (20.6%), valvular defects (11.5%),cardiomyopathies (10.0%), arrhythmias (7.9%), hypertensive crisis (6.5%). TotalIHM was 11.6%, separately for clinical syndromes: (1) – 2.0%, (2) – 7.4%, (3) –61.0%, (4) – 2.4%, (5) – 3.8%, (6) – 16.2%. Using univariant Cox regression, wedetermined mortality-associated risk factors: age >75 yrs (RR = 1.61), BPs <120mmHg (RR = 2.61), BPd <80 mmHg (RR = 2.15), ST elevations (RR = 2.28), LVEF <50% (RR = 1.66), coma (RR = 5.42) and somnolence/sopor (RR = 4.18) atadmission.Conclusion: IHM of patients with acute heart failure is high, depending on clinicalsyndrome manifestation. Predictors of higher mortality are age > 75 yrs, BP <
120/80 ST elevations in acute MI, left ventricle dysfunction and consciousnessfailure at admission
P821 Obesity in heart failure patients: the paradox continuesin the long-term follow-up
E. Zamora, J. Lupon, A. Urrutia, B. Gonzalez, L. Cano, R. Cabanes,G. Bickham, T. Pacual, S. Altimir, C. Diez. Germans Trias I PujolUniversity Hospital, Badalona, Spain
Background: Obesity has paradoxically been associated with improved survivalin heart failure (HF) and we have previously observed that obese patients (P) had
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / Left ventricular dysfunction 131
lower mortality at 2 years than low- and normal-weighed P. It could be speculatedthat with longer follow-up a higher mortality rate of obese P should be expectedafterwards, and then their long-term survival would be similar or even lower thannormal-weighed P.Objective: To analyse the relationship between body mass index (BMI) and long-term mortality in a population with chronic HF.Patients and Method: BMI at first visit and survival status after a minimum of 5years from that visit (5-8.4 years) were available in 504 P (73% men; median age68 years [IQR 58-74]). Aetiology of HF was mainly ischemic heart disease (59%).Median LVEF was 30% [IQR 23-39.7%]. P were divided according to their BMIin 4 groups: low weight (BMI < 20.5 kg/m2), normal weight (BMI 20.5 to <25.5kg/m2), overweight (BMI 25.5 to <30 kg/m2) and obesity (BMI ≥30 kg/m2). Actualmedian follow-up was 68.4 months [IQR 26.5-89.1].Results: mortality at five years differed significantly among BMI groups (p=0.001): low weight 62.5%; normal weight 46.8%; overweight 42.5%; and obe-sity 33.7%. Actuarial survival curves diverged significantly along the eight-yearfollow-up (figure). Obese P had a significant lower mortality than normal-weighedP (HRCox 0.81 [0.69-0.96], p=0.014). After adjustment for age, sex, aetiology,NYHA class, LVEF, hypertension, and diabetes, obesity remained as an indepen-dent predictor of lower mortality.
Survival among BMI groups
Conclusion: Obesity was associated with lower mortality rates during a follow-up of 5-8.4 years. Our results support, even in the long-term assessment, theparadoxical relationship between obesity and outcome in an outpatient populationwith HF.
P822 Comparative and combined prognostic value of redblood cell distribution width and brain natriureticpeptides in acutely decompensated chronic heartfailure patients
L.R. Tumasyan, K.G. Adamyan. Institute of Cardiology, Yerevan,Armenia
The aims of study were to assess the prognostic significance of red blood celldistribution width (RDW) and levels of brain natriuretic peptide (BNP) and N-terminal pro-brain natriuretic peptide (NT-proBNP) in acutely decompensatedchronic heart failure (CHF) patients (pts) and to test whether the combinationof RDW and BNP and NT-pro-BNP better identifies high risk pts.Methods: The predictive value of RDW (%) and its comparison with BNP andNT-proBNP (pg/ml) was performed in 123 pts with acute CHF. Primary endpointwas cardiac death; the secondary endpoint was combined cardiac death or hos-pitalization due to CHF.Results: During mean follow-up of 14±0.5 months from cardiac causes died 41(33.3%) pts. These pts had significantly higher levels (p<0.01) of mean plasmalevels of BNP (942±157 vs. 365±98), NT-pro-BNP (4915±779 vs. 1992±395)and RDW (19.2±1.5 vs. 13.5±1.2) compared with survivors. AUC of ROC were0.89 for BNP, 0.91 for NT-pro-BNP and 0.82 for RWD as predictors of death withan optimised cut off value of 600, 3500 and 15.5 with log rank of 10.7, 10.9 and9.8 (p<0.01), respectively, in Kaplan-Meier analysis. In multivariable Cox’s pro-portional hazards analysis, RDW was a significant independent predictor of 1-year outcome in acute HF [(hazard ratio) HR 1.08 per 1% increase in RDW; 95%CI, 1.03–1.12). Notably, that level of hemoglobin is not independently associatedwith higher mortality when RDW was included in the multivariable model. Accord-ing to levels of BNP, NT-pro-BNP and RDW pts were assigned to 4 groups: group1 (31 pts, level of both markers higher cut off value); group 2 (30 pts, elevatedlevel of peptides and normal value of RDW); group 3 (29 pts, normal level of pep-tides and elevated value of RDW) and group 4 (33 pts, normal values of peptidesand RDW). 1-year survival was 41.9%, 66.7%, 68.9% and 84.8% (p<0.01) andevent-free survival was 23.3%, 36.7%, 34.5% and 54.5%, respectively (p<0.01).In the Cox proportional hazard model elevated levels of both RDW and peptideswere the best predictors of death (HR 13.2 and16.7) and combined endpoint ofcardiac death or hospitalization (HR 11.8 and 14.7).Conclusions: The prognostic value of RDW was highly significant, independentof BNP and NT-pro-BNP levels. Levels of RDW, BNP and NT-pro-BNP were con-sistently associated with risk for cardiac mortality and combined end point ofdeath and hospitalization in acutely decompensated CHF pts. The combined
measurement of BNP, NT-pro-BNP and RDW may improve stratification of ptswith CHF and can help in identification of pts with poor long-term outcome.
P823 Association between hyperuricemia and prognosis injapanese patients with heart failure
K. Masuda, T. Yamashita, N. Enomoto, K. Asada, M. Shoji, T. Otsuka,K. Sagara, H. Sawada, T. Aizawa. The Cardiovascular Institute, Tokyo,Japan
Purpose: Although hyperuricemia is known as one of the risk factors for cardio-vascular events, limited data are available on its association with the prognosisof heart failure (HF) in Japanese. The purpose of this study was to determineassociation between hyperuricemia and prognosis in Japanese patients with HF.Methods: Using a prospective cohort study (Shinken Database 2004-7, n=8917)that comprised all the new patients visiting our hospital, we analyzed the clinicalevents (HF admission, cardiovascular death, and total death) in 2300 patientswith HF (NYHA 1-4) according to the presence of hyperuricemia by using Kaplan-Meier method with log-rank test and Cox proportional hazards model.Results: Out of 2300 HF patients, 1936 were diagnosed as having hyper-uricemia, and 364 were not. Event-free survival rate was significantly lower inpatients with hyperuricemia in any clinical events than those without (figure). Themultivariate Cox proportional hazards model revealed that hyperuricemia was anindependent predictor for HF admission (HR 1.80, P=0.013, 95%CI 1.13-2.87),although it was not in cardiovascular death and total death.
Conclusion: In Japanese HF population, hyperuricemia was significantly associ-ated with worse outcomes as an independent predictor for HF admission.
P824 Reverse epidemiology in different stages of heartfailure
G. Guder1, G. Gelbrich2, B. Pieske3, R. Wachter4 , F. Edelmann4,B. Maisch5, S. Pankuweit5, G. Ertl1, S. Stork1, C.E. Angermann1 .1University of Wurzburg, Department of Internal Medicine I,
Cardiology, Wurzburg, Germany; 2Koordinationszentrum für Klinische StudienLeipzig, Universität Leipzig, Leipzig, Germany; 3Medical University of Graz,Department of Cardiology, Graz, Austria; 4Department of Cardiology andPneumology, University of Goettingen, Goettingen, Germany; 5UniversityHospital Giessen and Marburg, Department of Cardiology, Marburg, Germany
Purpose: Observational studies indicate that in advanced heart failure (HF) ‘clas-sical’ cardiovascular risk factors (RF) as total cholesterol (TC), systolic blood pres-sure (SBP) and body mass index (BMI) are associated with better survival, a phe-nomenon termed ‘reverse epidemiology’. We analyzed associations of these RFwith mood and 1.5-year survival in patients with different HF stages recruited fromthe German Competence Net Heart Failure.Methods: Patients with complete data sets were gleaned from the following sub-projects: HH-BNP-Würzburg; Diast-HF Göttingen; Ikarius Marburg; INH-StudyWürzburg. According to ACC/AHA criteria, the 3,167 patients were allocated tostages A (n=255); B (n=1,339); C1 (New York Heart Association (NYHA) classI+II; n=1,013), C2 (NYHA III, n=488) and D (n=72). Depressive mood was as-sessed using the Patient Health Questionnaire (PHQ).Results: Mean age in stages A, B, C1, C2 and D was64±11/67±8/65±13/67±14/72±13 yrs, and 55/53/33/36/39% of the pa-tients were female. TC and SBP decreased markedly with increasingseverity of HF (TC: 213±41/206±43/196±49/181±56/169±46 mg/dl; SBP:142±19/149±21/134±25/122±22/122±21 mmHg), whereas the associationwith BMI was less pronounced (27.1±4.9/29.5±4.8/28.2±4.8/27.7±5.2/27.0±5.3kg/m2; all P<0.001). The PHQ sum score increased within HF stages A throughD (5.3±4.7/4.9±3.9/6.1±4.6/8.8±5.6/11.7±6.1; P<0.001).Low levels of TC and SBP, but not of BMI, were positively correlated with de-pressed mood. In multivariable Cox regression (adjusted for age, sex, HF stage,ejection fraction) higher levels of TC, SBP and BMI were predictive of better sur-vival (TC per 50 mg/dl: HR 0.69 (95%CI 0.60-0.81), P<0.001; SBP per 10 mmHg:HR 0.91 (95%CI 0.85-0.98), P=0.009 and BMI per 5 kg/m2: HR 0.79 (95%CI 0.67-0.93) P=0.004).Conclusions: Low levels of TC and SBP but not of BMI correlated with depressedmood. Higher levels of TC, BMI and SBP independently predicted better survivalwithin the whole cohort. However, due to low event rates in subgroups A and B, itremains unclear to what extent our results pertain to earlier stages of HF.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
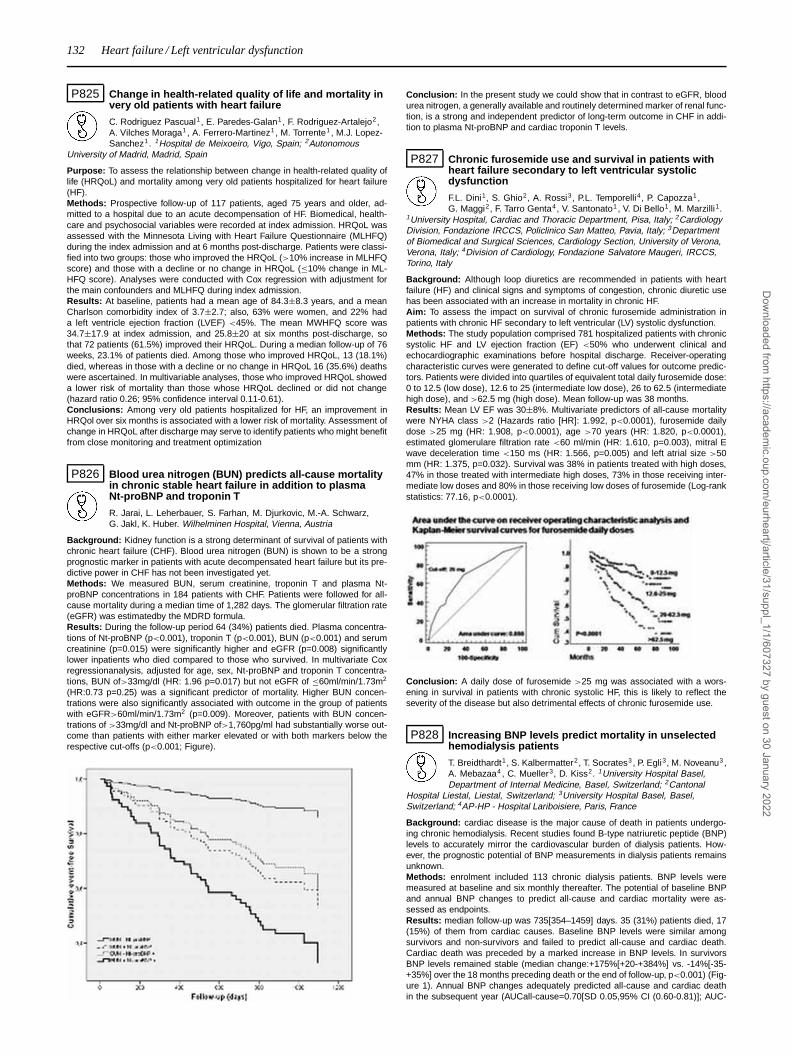
132 Heart failure / Left ventricular dysfunction
P825 Change in health-related quality of life and mortality invery old patients with heart failure
C. Rodriguez Pascual1, E. Paredes-Galan1, F. Rodriguez-Artalejo2,A. Vilches Moraga1, A. Ferrero-Martinez1, M. Torrente1 , M.J. Lopez-Sanchez1. 1Hospital de Meixoeiro, Vigo, Spain; 2Autonomous
University of Madrid, Madrid, Spain
Purpose: To assess the relationship between change in health-related quality oflife (HRQoL) and mortality among very old patients hospitalized for heart failure(HF).Methods: Prospective follow-up of 117 patients, aged 75 years and older, ad-mitted to a hospital due to an acute decompensation of HF. Biomedical, health-care and psychosocial variables were recorded at index admission. HRQoL wasassessed with the Minnesota Living with Heart Failure Questionnaire (MLHFQ)during the index admission and at 6 months post-discharge. Patients were classi-fied into two groups: those who improved the HRQoL (>10% increase in MLHFQscore) and those with a decline or no change in HRQoL (≤10% change in ML-HFQ score). Analyses were conducted with Cox regression with adjustment forthe main confounders and MLHFQ during index admission.Results: At baseline, patients had a mean age of 84.3±8.3 years, and a meanCharlson comorbidity index of 3.7±2.7; also, 63% were women, and 22% hada left ventricle ejection fraction (LVEF) <45%. The mean MWHFQ score was34.7±17.9 at index admission, and 25.8±20 at six months post-discharge, sothat 72 patients (61.5%) improved their HRQoL. During a median follow-up of 76weeks, 23.1% of patients died. Among those who improved HRQoL, 13 (18.1%)died, whereas in those with a decline or no change in HRQoL 16 (35.6%) deathswere ascertained. In multivariable analyses, those who improved HRQoL showeda lower risk of mortality than those whose HRQoL declined or did not change(hazard ratio 0.26; 95% confidence interval 0.11-0.61).Conclusions: Among very old patients hospitalized for HF, an improvement inHRQol over six months is associated with a lower risk of mortality. Assessment ofchange in HRQoL after discharge may serve to identify patients who might benefitfrom close monitoring and treatment optimization
P826 Blood urea nitrogen (BUN) predicts all-cause mortalityin chronic stable heart failure in addition to plasmaNt-proBNP and troponin T
R. Jarai, L. Leherbauer, S. Farhan, M. Djurkovic, M.-A. Schwarz,G. Jakl, K. Huber. Wilhelminen Hospital, Vienna, Austria
Background: Kidney function is a strong determinant of survival of patients withchronic heart failure (CHF). Blood urea nitrogen (BUN) is shown to be a strongprognostic marker in patients with acute decompensated heart failure but its pre-dictive power in CHF has not been investigated yet.Methods: We measured BUN, serum creatinine, troponin T and plasma Nt-proBNP concentrations in 184 patients with CHF. Patients were followed for all-cause mortality during a median time of 1,282 days. The glomerular filtration rate(eGFR) was estimatedby the MDRD formula.Results: During the follow-up period 64 (34%) patients died. Plasma concentra-tions of Nt-proBNP (p<0.001), troponin T (p<0.001), BUN (p<0.001) and serumcreatinine (p=0.015) were significantly higher and eGFR (p=0.008) significantlylower inpatients who died compared to those who survived. In multivariate Coxregressionanalysis, adjusted for age, sex, Nt-proBNP and troponin T concentra-tions, BUN of>33mg/dl (HR: 1.96 p=0.017) but not eGFR of ≤60ml/min/1.73m2
(HR:0.73 p=0.25) was a significant predictor of mortality. Higher BUN concen-trations were also significantly associated with outcome in the group of patientswith eGFR>60ml/min/1.73m2 (p=0.009). Moreover, patients with BUN concen-trations of >33mg/dl and Nt-proBNP of>1,760pg/ml had substantially worse out-come than patients with either marker elevated or with both markers below therespective cut-offs (p<0.001; Figure).
Conclusion: In the present study we could show that in contrast to eGFR, bloodurea nitrogen, a generally available and routinely determined marker of renal func-tion, is a strong and independent predictor of long-term outcome in CHF in addi-tion to plasma Nt-proBNP and cardiac troponin T levels.
P827 Chronic furosemide use and survival in patients withheart failure secondary to left ventricular systolicdysfunction
F.L. Dini1, S. Ghio2, A. Rossi3, P.L. Temporelli4, P. Capozza1,G. Maggi2, F. Tarro Genta4, V. Santonato1, V. Di Bello1, M. Marzilli1.
1University Hospital, Cardiac and Thoracic Department, Pisa, Italy; 2CardiologyDivision, Fondazione IRCCS, Policlinico San Matteo, Pavia, Italy; 3Departmentof Biomedical and Surgical Sciences, Cardiology Section, University of Verona,Verona, Italy; 4Division of Cardiology, Fondazione Salvatore Maugeri, IRCCS,Torino, Italy
Background: Although loop diuretics are recommended in patients with heartfailure (HF) and clinical signs and symptoms of congestion, chronic diuretic usehas been associated with an increase in mortality in chronic HF.Aim: To assess the impact on survival of chronic furosemide administration inpatients with chronic HF secondary to left ventricular (LV) systolic dysfunction.Methods: The study population comprised 781 hospitalized patients with chronicsystolic HF and LV ejection fraction (EF) <50% who underwent clinical andechocardiographic examinations before hospital discharge. Receiver-operatingcharacteristic curves were generated to define cut-off values for outcome predic-tors. Patients were divided into quartiles of equivalent total daily furosemide dose:0 to 12.5 (low dose), 12.6 to 25 (intermediate low dose), 26 to 62.5 (intermediatehigh dose), and >62.5 mg (high dose). Mean follow-up was 38 months.Results: Mean LV EF was 30±8%. Multivariate predictors of all-cause mortalitywere NYHA class >2 (Hazards ratio [HR]: 1.992, p<0.0001), furosemide dailydose >25 mg (HR: 1.908, p<0.0001), age >70 years (HR: 1.820, p<0.0001),estimated glomerulare filtration rate <60 ml/min (HR: 1.610, p=0.003), mitral Ewave deceleration time <150 ms (HR: 1.566, p=0.005) and left atrial size >50mm (HR: 1.375, p=0.032). Survival was 38% in patients treated with high doses,47% in those treated with intermediate high doses, 73% in those receiving inter-mediate low doses and 80% in those receiving low doses of furosemide (Log-rankstatistics: 77.16, p<0.0001).
Conclusion: A daily dose of furosemide >25 mg was associated with a wors-ening in survival in patients with chronic systolic HF, this is likely to reflect theseverity of the disease but also detrimental effects of chronic furosemide use.
P828 Increasing BNP levels predict mortality in unselectedhemodialysis patients
T. Breidthardt1, S. Kalbermatter2, T. Socrates3, P. Egli3, M. Noveanu3,A. Mebazaa4 , C. Mueller3, D. Kiss2. 1University Hospital Basel,Department of Internal Medicine, Basel, Switzerland; 2Cantonal
Hospital Liestal, Liestal, Switzerland; 3University Hospital Basel, Basel,Switzerland; 4AP-HP - Hospital Lariboisiere, Paris, France
Background: cardiac disease is the major cause of death in patients undergo-ing chronic hemodialysis. Recent studies found B-type natriuretic peptide (BNP)levels to accurately mirror the cardiovascular burden of dialysis patients. How-ever, the prognostic potential of BNP measurements in dialysis patients remainsunknown.Methods: enrolment included 113 chronic dialysis patients. BNP levels weremeasured at baseline and six monthly thereafter. The potential of baseline BNPand annual BNP changes to predict all-cause and cardiac mortality were as-sessed as endpoints.Results: median follow-up was 735[354–1459] days. 35 (31%) patients died, 17(15%) of them from cardiac causes. Baseline BNP levels were similar amongsurvivors and non-survivors and failed to predict all-cause and cardiac death.Cardiac death was preceded by a marked increase in BNP levels. In survivorsBNP levels remained stable (median change:+175%[+20-+384%] vs. -14%[-35-+35%] over the 18 months preceding death or the end of follow-up, p<0.001) (Fig-ure 1). Annual BNP changes adequately predicted all-cause and cardiac deathin the subsequent year (AUCall-cause=0.70[SD 0.05,95% CI (0.60-0.81)]; AUC-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / Left ventricular dysfunction / Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) 133
cardiac=0.82[SD0.04,95%CI (0.73-0.90)]. There was no correlation between theBNP increase preceeding cardiac death and changes in body weight (p=0.43).A BNP increase of 40% provided the best cut-off level. Cox-regression analysisconfirmed that annual increases over 40% predicted all-cause (OR 6.77, p=0.015)and cardiac (OR 6.84,p=0.014) mortality within the consequent year.
Figure 1
Conclusions: Annual BNP increases above 40% predicted all-cause and cardiacdeath in the subsequent year. Serially measuring BNP levels may present a noveltool for risk stratification and treatment guidance of ESRD patients on chronicdialysis.
P829 What is the best marker of cardiorenal syndrome inacute heart failure? a prospective hospital cohort study
C. Paulo, J. Mascarenhas, M. Patacho, J. Pimenta, P. Bettencourt.Sao Joao Hospital, Porto, Portugal
Background: Renal impairment is common and related to worse prog-nosis in heart failure (HF). The association between progressive renal and cardiacfailure has been termed cardiorenal syndrome (CRS). The definition of this entityis still unclear and several parameters of renal function (RF) have been exploredas possible markers of CRS. We intended to evaluate the utility of different mark-ers of renal failure in predicting prognosis of acute HF patients.Methods: In a hospital cohort of 241 acute HF patients, we evaluated bloodurea (mg/dL), creatinine (mg/dL) and estimated glomerular filtration rate (eGFR,ml.min-1.m-2, using Modification of Diet in Renal Disease equation) at admissionand discharge and determined variations of these parameters during hospitaliza-tion. Patients were followed up for 6 months, for the occurrence of all-cause deathand hospital readmission. Prognosis was compared between groups using Coxproportional hazards regression.Results: Fifteen patients died during hospitalization; 226 patients were followedup with a median age (interquartile range (IQR)) of 74 (63-81) years; 140 (61.9%)were men; 41 (18%) had new-onset HF, 118 (52%) had coronary heart disease,145 (64%) were hypertensive, 98 (43%) had diabetes mellitus and 154 (69%)were previously treated with furosemide, with a median dose of 80 mg/day. Themedian (IQR) levels of creatinine, urea and eGFR at admission were 1.24 (0.97-1.68), 62 (42-93) and 53 (35-70), respectively, and at discharge were 1.16 (0.96-1.62), 70 (51-98) and 54 (40-69), respectively. The prevalence of 25% increasein urea and of 25% decrease in eGFR was 90 (40%) and 24 (11%), respectively.Higher urea and creatinine levels and lower eGFR both at admission and dis-charge were associated with worse prognosis in univariate analysis. Variations inurea (>25% increase) during hospitalization were associated with better progno-sis. Including all the parameters of RF in a multivariated model, urea at admissionand 25% urea increase remained independent predictors of prognosis (HR 1.12p<0,001, HR 0.57 p=0.028, respectively). Urea at admission (HR 1.12, p<0.001)remained a significant predictor of the outcome after adjusting for other variablesnot related to RF associated to prognosis in univariate analysis.Conclusion: Among several RF parameters, urea at admission was the bestprognostic marker in our sample of acute HF patients, suggesting that a definitionof CRS should take into account the levels of urea.
UPDATE ON COMPUTED TOMOGRAPHY (CT) ANDMAGNETIC RESONANCE IMAGING (MRI)
P830 Evaluability and diagnostic accuracy of a low radiationexposure protocol for prospective ECG-triggeringcoronary multidetector computed tomographyangiography in detection of coronary artery disease
G. Pontone, D. Andreini, E. Bertella, S. Mushtaq, A. Formenti,A.D. Annoni, G. Ballerini, C. Fiorentini, A.L. Bartorelli, M. Pepi. Centrocardiologico Monzino, IRCCS; Cardiovascular Sciences Department, Universityof Milan, Milan, Italy
Purpose: Multidetector computed tomography (MDCT) allows an accurate non-invasive visualization of coronary arteries. However, the radiation exposure is aconcern of issue. Recently, the introduction of prospective ECG-triggering alloweda significant reduction in effective radiation dose (ED). The purpose of our studywas to compare the feasibility (Fe), diagnostic accuracy (Ac) and ED of MDCT
using either a body mass index (BMI)–adapted scanning protocol (MDCT-XTe)or a standard protocol with a tube voltage and current of 120KVp and 650mA,respectively, regardless the patient’s BMI (MDCT-XT). In both cases we utilized aprospective ECG-triggering.Matherials and Methods: We evaluated 170 consecutive patients scheduled forinvasive coronary angiography (ICA) and excluded 14 patients who were not el-igible for MDCT. The remaining 156 patients were randomized to Group 1 (78patients studied using MDCT-XTe) and Group 2 (78 patients studied using MDCT-XT). Eight and eleven patients in Group 1 and 2 were excluded after randomiza-tion for heart rate > 65 bpm, respectively. Datasets were assessed for Fe, signal(SNR) and contrast-to noise ratio (CNR), Ac in detection of coronary stenoses >
50% versus ICA and ED.Blinded results for both modalities were compared using the patient as the pri-mary unit of analysis.Results: There were no significant differences in BMI and HR between groups.The Fe, SNR, CNR, Ac in a segment-based and patient-based model were similarin both groups (97% vs. 97%, 14.5±3.9 vs. 14.2±4.1, 16.0±4.6 vs. 16.5±4.4,95% vs. 94% and 97 vs. 99%, respectively). The ED in Group 1 was 72% lowerthan in Group 2 (2.1±1.2 vs. 7.5±1.8 mSV, respectively; p<001).Conclusions: The use of a BMI–adapted scanning protocol with prospectiveECG-triggering leads to significant reduction in radiation exposure without nega-tive influences on diagnostic performance.
P831 One beat scan with 320-detector computedtomography seems sufficient in clinical practice
T. Imamura, K. Tanabe, S. Kishi, S. Tanimoto, M. Taniwaki, S. Otsuiki,J. Aoki, H. Nakajima, K. Hara. Mitsui Memorial hospital, Tokyo, Japan
Background: Recently, 320-detector row computed tomography (CT)has emerged as the latest generation of CT technology which allows us to ex-amine the entire heart in a single rotation. As a consequence, one beat scan isconsidered to be enough to acquire analyzable images of coronary arteries. How-ever, there have been no clinical studies to investigate whether one beat scan istruly sufficient in clinical setting. Therefore, we have applied 2 beats scan in allcases of 320-detector CT (Toshiba AquilionOne Dynamic Volume CT, Tochigi-ken, Japan) scan, and assessed whether the quality of images derived from halfreconstruction in the first beat (first half recon) was comparable to those in thesecond beat (second half recon), and those derived from segment reconstruction(segment recon) from the 2 beats.Methods: The study population consisted of consecutive 51 patients with sus-pected ischemic heart disease who were scanned by the 320-detector CT fromFebruary 2009 to March 2009. We scanned 2 beats in all patients. The datasetswere reconstructed by the first half recon, the second half recon, and the seg-ment recon, as mentioned above. For analysis of coronary arteries, a previouslydescribed 16-segment American Heart Association model was employed. Theimage quality of all segments was scored into 5 grades, from 1 (poor) to 5 (excel-lent).Result: The patients were 62.4 years old and 38 patients were male (74.5%). TheAgatston score in their coronary arteries averaged as high as 632.0±1501. Themean heart rate (HR) during scanning was 61.1±8.1 bpm. The average imagequality grade of all the segments of the first half recon, second half recon andsegment recon were 3.285±0.95, 3.305±0.864, and 3.292±0.83, respectively.There was no statistical difference among the 3 groups. To note, in the patientswith HR<65, the quality grade of the first half recon was a little higher than thatof segment recon (3.566±0.796 vs 3.466±0.760).Conclusion: One beat scan seems sufficient to visualize coronary artery with the320-detector CT. By utilizing one beat scan, the 320-detector CT has potential tominimize the radiation dose and the amount of contrast together, keeping goodimage quality.
P832 Best calcium score cut-off to predict obstructivecoronary artery disease in cardiac computedtomography
P.J. Sousa, P.A. Goncalves, H. Marques, R. Cale, J. Brito, A. Gaspar,F.P. Machado, J. Roquette. Hospital Luz, Lisbon, Portugal
Purpose: The presence of calcified coronary artery disease is one lim-itation when performing a cardiac Computed Tomography (CT) leading to highernumber of false positive tests and impaired evaluation of more coronary arterysegments. Furthermore, a high Calcium Score (CaSc) value may suggest ob-structive coronary artery disease (CAD) justifying evaluation with a functional orinvasive test, although the best cut-off for this indication has not been establishedyet. The aim of this study is to identify the best CaSc cut-off value to predict thepresence of obstructive CAD and to test variables associated with high coronarycalcification.Methods: From a prospective registry of 1185 consecutive patients that per-formed cardiac CT with a 64 slices dual source scan from February 2007 toNovember 2009, 939 were selected for analysis (patients who performed bothCaSc and CT coronary angiography). CaSc was evaluated as a predictor of ob-structive CAD. Demographic (age, sex) and clinical (hypertension, dyslipidemia,diabetes, smoking habits, obesity) variables were evaluated as predictors of highcalcium score.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

134 Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
Results: Considering patients with coronary calcification (46% of the analyzedgroup), CaSc was a good predictor of obstructive CAD (ROC curve with an AUCof 83%, best cut-off: 297, value used for further analysis).In patients with high CaSc (13%), 75% had obstructive CAD, while only 12% ofpatients with low CaSc had obstructive CAD (p<0.001).Variables associated with high CaSc were: age above 59 years, male gender,obesity and diabetes (table).
Table 1. Variables tested as predictors of high CaSc (≥297)
Variable Calcium score < 297 Calcium score ≥ 297 p
Mean age 57±11 67±9 <0.001Male gender 55% 77% <0.001Body mass index≥30 19% 29% 0.016Diabetes 11% 35% <0.001Hypertension 60% 69% 0.531Dyslipidemia 56% 60% 0.787Smoking habits 28% 30% 0.613
Conclusions: The presence of a CaSc above 297 identifies patients with highprobability of obstructive CAD. This value was observed in 13% of patients and ismore likely to be present in patients with age over 59 years, male gender, obesityor diabetes.
P833 Global evaluation of patients with aortic valve diseaseusing multi-slice computed tomography prior to aorticvalve replacement
J.F. Rodriguez Palomares, C. Llibre Pallares, O. Abdul-JawadAltisent, H. Cuellar Calabria, R. Rios, L. Gutierrez, P. Mahia Casado,
M.T. Gonzalez Alujas, A. Evangelista Masip, D. Garcia-Dorado Garcia. UniversityHospital Vall d’Hebron, Barcelona, Spain
Background: Different imaging techniques are required in patients with aorticvalve disease in order to assess the morphology of the aortic valve, to set theaortic root and ascending aorta diameters, and to rule out the presence of coro-nary artery disease.Purpose: To assess whether multi-slice computed tomography (MSCT) can beused as a unique technique to evaluate patients with a severe aortic valve disease(established by echocardiography) prior to aortic valve replacement.Methods: 81 patients with a severe aortic valvular disease (stenosis or regurgi-tation) were evaluated with a transthoracic echocardiography to measure the tho-racic aorta at different levels: the annulus, sinuses of Valsalva, sinotubular junc-tion and ascending aorta. A coronary angiography was also performed to rule outthe presence of coronary artery disease. The morphology of the aortic valve wasconfirmed by the surgeon at the time of the surgical procedure. All patients under-went a MSCT to evaluate the morphology of the aortic valve, the aortic root andascending aorta diameters and the presence of coronary artery disease. Resultsfrom MSCT and the different imaging modalities were compared.Results: The incidence of coronary artery disease in these patients was 34%.In a per patient analysis, MSCT showed a 96% sensitivity, 94% specificity, 86%positive predictive value and 98% negative predictive value compared to coronaryangiography. According to the surgeon analysis, the aortic valve was tricuspid in60% and bicuspid in 40%. There was a strong and significant agreement betweenMSCT and the surgeon in the morphology of the aortic valve (Kappa= 0.98, p<
0.001). There was also an excellent correlation between echocardiography andMSCT for the assessment of thoracic aorta diameters (intraclass correlation co-efficient): annulus 0.7 (Confidence Interval (CI): 0.5-0.8), sinuses of Valsalva 0.92(CI: 0.86-0.95), sinotubular junction 0.91 (CI: 0.8-0.95), and ascending aorta 0.93(CI: 0.88-0.96).Conclusions: MSCT is an excellent technique for the evaluation of patients witha severe aortic valve disease and can be used as a unique technique for a globalevaluation of these patients before the aortic valve replacement.
P834 Quantitative analysis of contrast-enhanced CTcoronary angiography demonstrates significantreduction in luminal dimensions and changes in plaquecomposition from baseline to 12-month follow-up
S. Rinehart, E. Krivitsky, G. Vazquez, Z. Qian, P. Joshi, A. Kalynych,S. Voros. Piedmont Heart Institute, Atlanta, United States of America
Purpose: Multi-slice computed tomography (MSCT) coronary angiography hasbeen proposed as a tool to evaluate coronary plaque progression. Currently thereis little prospective data available.Methods: 40 patients (mean age 60.8±7.0; 62.5% male) in a prospective studyunderwent 64 or 320-dector row MSCT at baseline and 12 months later. Study le-sions were analyzed using a highly standardized quantitative method. Minimal lu-men diameter (MLD) and area (MLA), % diameter and area stenosis (%DS, %AS)were measured. Calcified, low-density and high-density non-calcified plaque vol-ume and % were determined (CAP [%], LDNCP [%], HDNCP [%]). The vessellumen was first segmented by fitting a model based on attenuation values and ge-ometrical assumptions. Within the vessel wall, non-calcified and calcified plaqueswere characterized in the following manner: LDNCP: -100 to +30 Hounsfield Units(HU); HDNCP: 30-150 HU; CAP≥150 HU. Paired, 2-sided t-test was performed.
Results: CTA plaque parameters are shown in the Figure. On follow-up examina-tion, there was a significant decrease in MLD (1.7±0.7 vs 1.5±0.7; p=0.01), MLA(5.4±2.6 vs 4.4±2.5; p=0.003) and increase in %DS (45.3±18.4 vs 50.4±20.5;p=0.02). While overall plaque volume was similar (227.2 mm3 vs 240.1 mm3;p=0.2), there was a significant increase in the %CAP (25.8±17.5 vs 29.9±18.4;p=0.008) and %LD-NCP (9.1±4.0 vs 11.0±6.4; p=0.04). There was a significantdecrease in %HD-NCP (65.0±16.2 vs 58.9±16.7; p=0.0007).
Figure 1. Plaque Progression on MSCT.
Conclusions: Prospective analysis of coronary plaque progression by MSCTdemonstrates a significant reduction in lumen size from baseline to 1 year. Therewas an approximate 13.7% increase in calcified plaque, 17.3% increase in LD-NCP, and 9.4% decrease in HD-NCP respectively.
P835 Diagnosis and verification of complications ofpermanent pacing with ECG-MSCT - preliminary report
E. Czekajska-Chehab1 , A. Kutarski2, A. Tomaszewski2 ,G. Staskiewicz1, E. Siek1, A. Drop1. 1Medical University of Lublin,Department of Radiology, Lublin, Poland; 2Medical University of
Lublin, Department of Cardiology, Lublin, Poland
Purpose: Complications of permanent pacing related with intravascular and in-tracardiac placement of leads are an important issue, which may be difficult to di-agnose. Transthoracic and transesophageal echocardiography (TTE & TEE) arewidely used, however, both these methods have their limitations. Lead dependentinfective endocarditis is visualized well by TTE, however, vegetations may be lo-cated in precardiac portion of superior vena cava (SVC), or released to pulmonaryarteries. Complications of removal of the leads include remnant vegetations inSVC or pulmonary embolism, which may be well visualized with CT. CT may alsobe particularly useful for visualization of misplaced leads and mechanical injuriesto the cardiac and vascular walls as a result of the implantation or removal of theleads. The aim of the study was to analyze feasibility of ECG-MSCT in diagnosticprocess of intravascular and intracardiac complications of permanent pacing.Method: 4594 ECG-MSCT examinations (2431 males, 2163 females) were ret-rospectively analyzed. Number of patients with permanent pacing and types andfrequency of complications of pacing was analyzed.Results: Permanent pacing was present in 141 patients (3.1% of examinations,75 males and 66 females, mean age: 63.7±13.9 yrs). Complications of perma-nent pacing were found in 73 patients (52% of all patients with pacing; 1,6% of allexams, 42 males and 31 females, mean age: 61.7±16.8 yrs). Forty patients hadprevious echocardiography, which showed 28 cases of thrombosis/vegetations onelectrodes, and 12 cases were referred with suspected postinterventional compli-cations (e.g. removal of infected electrodes).Thrombosis/vegetations were observed in 43 cases (59% of complications), ve-nous narrowing or obstruction in 23 cases (31.5%), pulmonary embolism in 23cases (31.5%). Rare complications were rupture of chordae tendinae (4 cases),intracardiac dislocation of the plastic sheath (3 cases) as well as single casesof piercing of right ventricular wall, fractured tip of permanent lead in pulmonaryartery and hemothorax.Incidentally diagnosed complications accounted for 15 cases (20.5% of compli-cations, 10.6% of exams in patients with pacing, 0.3% of all ECG-MSCTs).Conclusion: ECG-MSCT is a valuable imaging method for diagnosis and verifi-cation of intravascular and cardiac complications of implantation or removal of thepermanent pacing, which allows detailed visualization and documentation of thepatients status, as well as monitoring of the treatment. In the study group, 20% ofcomplications were incidentally diagnosed.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
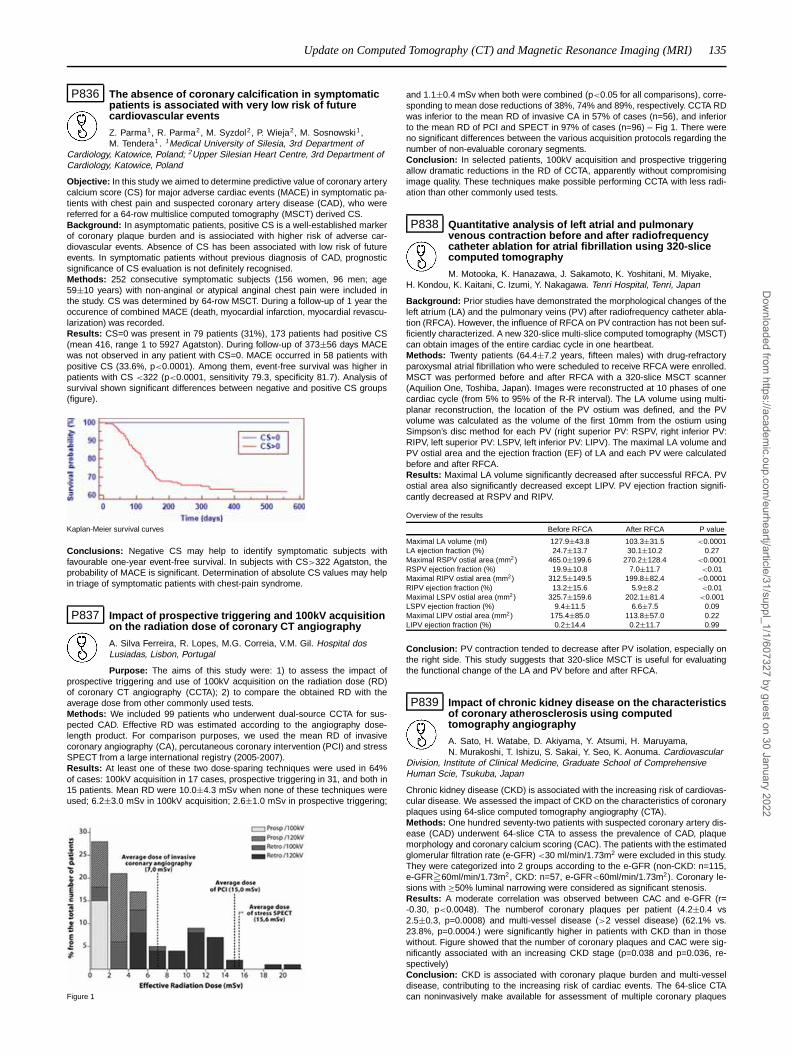
Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) 135
P836 The absence of coronary calcification in symptomaticpatients is associated with very low risk of futurecardiovascular events
Z. Parma1, R. Parma2, M. Syzdol2, P. Wieja2, M. Sosnowski1,M. Tendera1 . 1Medical University of Silesia, 3rd Department of
Cardiology, Katowice, Poland; 2Upper Silesian Heart Centre, 3rd Department ofCardiology, Katowice, Poland
Objective: In this study we aimed to determine predictive value of coronary arterycalcium score (CS) for major adverse cardiac events (MACE) in symptomatic pa-tients with chest pain and suspected coronary artery disease (CAD), who werereferred for a 64-row multislice computed tomography (MSCT) derived CS.Background: In asymptomatic patients, positive CS is a well-established markerof coronary plaque burden and is assiociated with higher risk of adverse car-diovascular events. Absence of CS has been associated with low risk of futureevents. In symptomatic patients without previous diagnosis of CAD, prognosticsignificance of CS evaluation is not definitely recognised.Methods: 252 consecutive symptomatic subjects (156 women, 96 men; age59±10 years) with non-anginal or atypical anginal chest pain were included inthe study. CS was determined by 64-row MSCT. During a follow-up of 1 year theoccurence of combined MACE (death, myocardial infarction, myocardial revascu-larization) was recorded.Results: CS=0 was present in 79 patients (31%), 173 patients had positive CS(mean 416, range 1 to 5927 Agatston). During follow-up of 373±56 days MACEwas not observed in any patient with CS=0. MACE occurred in 58 patients withpositive CS (33.6%, p<0.0001). Among them, event-free survival was higher inpatients with CS <322 (p<0.0001, sensitivity 79.3, specificity 81.7). Analysis ofsurvival shown significant differences between negative and positive CS groups(figure).
Kaplan-Meier survival curves
Conclusions: Negative CS may help to identify symptomatic subjects withfavourable one-year event-free survival. In subjects with CS>322 Agatston, theprobability of MACE is significant. Determination of absolute CS values may helpin triage of symptomatic patients with chest-pain syndrome.
P837 Impact of prospective triggering and 100kV acquisitionon the radiation dose of coronary CT angiography
A. Silva Ferreira, R. Lopes, M.G. Correia, V.M. Gil. Hospital dosLusiadas, Lisbon, Portugal
Purpose: The aims of this study were: 1) to assess the impact ofprospective triggering and use of 100kV acquisition on the radiation dose (RD)of coronary CT angiography (CCTA); 2) to compare the obtained RD with theaverage dose from other commonly used tests.Methods: We included 99 patients who underwent dual-source CCTA for sus-pected CAD. Effective RD was estimated according to the angiography dose-length product. For comparison purposes, we used the mean RD of invasivecoronary angiography (CA), percutaneous coronary intervention (PCI) and stressSPECT from a large international registry (2005-2007).Results: At least one of these two dose-sparing techniques were used in 64%of cases: 100kV acquisition in 17 cases, prospective triggering in 31, and both in15 patients. Mean RD were 10.0±4.3 mSv when none of these techniques wereused; 6.2±3.0 mSv in 100kV acquisition; 2.6±1.0 mSv in prospective triggering;
Figure 1
and 1.1±0.4 mSv when both were combined (p<0.05 for all comparisons), corre-sponding to mean dose reductions of 38%, 74% and 89%, respectively. CCTA RDwas inferior to the mean RD of invasive CA in 57% of cases (n=56), and inferiorto the mean RD of PCI and SPECT in 97% of cases (n=96) – Fig 1. There wereno significant differences between the various acquisition protocols regarding thenumber of non-evaluable coronary segments.Conclusion: In selected patients, 100kV acquisition and prospective triggeringallow dramatic reductions in the RD of CCTA, apparently without compromisingimage quality. These techniques make possible performing CCTA with less radi-ation than other commonly used tests.
P838 Quantitative analysis of left atrial and pulmonaryvenous contraction before and after radiofrequencycatheter ablation for atrial fibrillation using 320-slicecomputed tomography
M. Motooka, K. Hanazawa, J. Sakamoto, K. Yoshitani, M. Miyake,H. Kondou, K. Kaitani, C. Izumi, Y. Nakagawa. Tenri Hospital, Tenri, Japan
Background: Prior studies have demonstrated the morphological changes of theleft atrium (LA) and the pulmonary veins (PV) after radiofrequency catheter abla-tion (RFCA). However, the influence of RFCA on PV contraction has not been suf-ficiently characterized. A new 320-slice multi-slice computed tomography (MSCT)can obtain images of the entire cardiac cycle in one heartbeat.Methods: Twenty patients (64.4±7.2 years, fifteen males) with drug-refractoryparoxysmal atrial fibrillation who were scheduled to receive RFCA were enrolled.MSCT was performed before and after RFCA with a 320-slice MSCT scanner(Aquilion One, Toshiba, Japan). Images were reconstructed at 10 phases of onecardiac cycle (from 5% to 95% of the R-R interval). The LA volume using multi-planar reconstruction, the location of the PV ostium was defined, and the PVvolume was calculated as the volume of the first 10mm from the ostium usingSimpson’s disc method for each PV (right superior PV: RSPV, right inferior PV:RIPV, left superior PV: LSPV, left inferior PV: LIPV). The maximal LA volume andPV ostial area and the ejection fraction (EF) of LA and each PV were calculatedbefore and after RFCA.Results: Maximal LA volume significantly decreased after successful RFCA. PVostial area also significantly decreased except LIPV. PV ejection fraction signifi-cantly decreased at RSPV and RIPV.
Overview of the results
Before RFCA After RFCA P value
Maximal LA volume (ml) 127.9±43.8 103.3±31.5 <0.0001LA ejection fraction (%) 24.7±13.7 30.1±10.2 0.27Maximal RSPV ostial area (mm2) 465.0±199.6 270.2±128.4 <0.0001RSPV ejection fraction (%) 19.9±10.8 7.0±11.7 <0.01Maximal RIPV ostial area (mm2) 312.5±149.5 199.8±82.4 <0.0001RIPV ejection fraction (%) 13.2±15.6 5.9±8.2 <0.01Maximal LSPV ostial area (mm2) 325.7±159.6 202.1±81.4 <0.001LSPV ejection fraction (%) 9.4±11.5 6.6±7.5 0.09Maximal LIPV ostial area (mm2) 175.4±85.0 113.8±57.0 0.22LIPV ejection fraction (%) 0.2±14.4 0.2±11.7 0.99
Conclusion: PV contraction tended to decrease after PV isolation, especially onthe right side. This study suggests that 320-slice MSCT is useful for evaluatingthe functional change of the LA and PV before and after RFCA.
P839 Impact of chronic kidney disease on the characteristicsof coronary atherosclerosis using computedtomography angiography
A. Sato, H. Watabe, D. Akiyama, Y. Atsumi, H. Maruyama,N. Murakoshi, T. Ishizu, S. Sakai, Y. Seo, K. Aonuma. Cardiovascular
Division, Institute of Clinical Medicine, Graduate School of ComprehensiveHuman Scie, Tsukuba, Japan
Chronic kidney disease (CKD) is associated with the increasing risk of cardiovas-cular disease. We assessed the impact of CKD on the characteristics of coronaryplaques using 64-slice computed tomography angiography (CTA).Methods: One hundred seventy-two patients with suspected coronary artery dis-ease (CAD) underwent 64-slice CTA to assess the prevalence of CAD, plaquemorphology and coronary calcium scoring (CAC). The patients with the estimatedglomerular filtration rate (e-GFR) <30 ml/min/1.73m2 were excluded in this study.They were categorized into 2 groups according to the e-GFR (non-CKD: n=115,e-GFR�60ml/min/1.73m2, CKD: n=57, e-GFR<60ml/min/1.73m2). Coronary le-sions with ≥50% luminal narrowing were considered as significant stenosis.Results: A moderate correlation was observed between CAC and e-GFR (r=-0.30, p<0.0048). The numberof coronary plaques per patient (4.2±0.4 vs2.5±0.3, p=0.0008) and multi-vessel disease (>2 vessel disease) (62.1% vs.23.8%, p=0.0004.) were significantly higher in patients with CKD than in thosewithout. Figure showed that the number of coronary plaques and CAC were sig-nificantly associated with an increasing CKD stage (p=0.038 and p=0.036, re-spectively)Conclusion: CKD is associated with coronary plaque burden and multi-vesseldisease, contributing to the increasing risk of cardiac events. The 64-slice CTAcan noninvasively make available for assessment of multiple coronary plaques
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

136 Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
throughout the coronary arteries, which are necessary for intensive treatment toprevent the cardiovascular events.
P840 Diagnostic accuracy of contrast-enhanced 64-rowMSCT-coronary angiography in patients with severecoronary calcification
G. Steinwender1, R. Zweiker1, R. Maier1, K. Preidler2, M. Tillich2,D. Szolar2, N. Watzinger1. 1Medical University of Graz, Department of
Cardiology, Graz, Austria; 2Diagnostikum Graz Süd West, Graz, Austria
Purpose: Our aim was to evaluate the diagnostic accuracy of contrast-enhanced64-MSCT-coronary angiography (MSCT-CA) in patients with severe coronary cal-cification (Agatston-score >400).Methods: One-hundred ten patients with an Agatston-score >400 were includedin this retrospective analysis. Each patient underwent both conventional coronaryangiography and MSCT-CA within a period of 6 months. No patient was excludedfrom the study because of coronary artery bypass grafting or coronary stenting.The results of MSCT-CA were analyzed and compared with those of conventionalcoronary angiography. The diagnostic accuracy for detecting a haemodynamicallysignificant stenosis (defined by a diameter stenosis of ≥50%) was determined forcoronary segments, vessels and patients.Results: The average Agatston-score for the study population was 1368±1105.88% of the patients had at least one significant stenosis on conventional coronaryangiography, defining the gold standard. Artifacts caused by severe coronary cal-cification seem to decrease the diagnostic accuracy of the MSCT-CA. Sensitivityand specifity for detecting a significant stenosis were 54% and 83% for coronarysegments (n=1384), 80% and 70% for coronary vessels (n=440), and 100% and31% for patients (n=110), respectively. The positive and negative predictive val-ues were 52% and 85% for segments, 74% and 77% for vessels, and 92% and100% for patients, respectively. In our patient cohort no significant correlationcould be detected between the degree of coronary calcification and the numberof misclassified coronary segments.
Lesion in RCA (left: MSCT-CA; right: invasive CA)
Conclusions: Performing MSCT-coronary angiography in patients with anAgatston-score >400 should be critically questioned and this decision should bemade on an individual basis.
P841 Correlation of diameter assessment of aortic annulusand bulbus by computed tomography andtrans-esophageal echocardiography prior topercutaneous aortic valve replacement
J. Rixe, J. Wilhelm, A. Rolf, C. Liebetrau, H. Nef, H. Moellmann,D. Erkapic, C.W. Hamm, T. Dill. Kerckhoff Clinic, Department of Cardiology, BadNauheim, Germany
Background: Percutaneous aortic valve replacement is an emerging techniqueapplicable for selected patient collectives not suitable for conventional valvesurgery. However, peri-interventional complications such as severe paravalvularaortic regurgitation are relatively common, so that accurate pre-procedural as-sessment of diameters of the aortic annulus and bulbus is mandatory. Since un-equivocal recommendations concerning applicable imaging modalities are lack-ing, we sought to investigate the correlation between transesophageal echo-cardiography and retrospectively gated Multi-Detector Computed Tomography(MDCT) for the assessment of diameters of the aortic annulus and bulbus prior topercutaneous aortic valve replacement.
Methods: 42 patients (27 male, mean age 81.3±6.4y) underwent retrospectivelygated cardiac CT angiography (Dual Source CT, Siemens Somatom Definition)and transesophageal echocardiography as part of a planning procedure for per-cutaneous aortic valve replacement. The largest diameter of the aortic annulusand aortic bulbus were assessed using both MDCT and echocardiography, forMDCT multiplanar reconstructions at 0.75mm slice thickness were used. Diame-ters were correlated for echocardiography and MDCT.Results: Mean diameter of the aortic annulus and aortic bulbus were26.3±2.5mm and 33.8±3.8mm in MDCT, and they were 26.5±4.3mm and31.7±4.2mm in echocardiography, respectively. In two-sided T-test there were nostatistically significant differences between diameter measurements of the aorticannulus (p=0.88), but assessment of the aortic bulbus by echocardiography leadto significantly smaller diameters as if assessed by MDCT (p=0.039). Amongstpatients with a diameter of the aortic bulbus of ≥ 33.0mm in MDCT (n=18, 43%of all patients) there were 15 with severe aortic calcification under inclusion of theaortic bulbus (35.7% of all patients), potentially leading to a significant overesti-mation of the corresponding diameter.Conclusion: MDCT and transesophageal echocardiography basically show com-parable results for the assessment of pre-procedural diameters of aortic annulusand bulbus. Particularly in patients with severe aortic calcification MDCT yieldssignificantly larger diameters of the aortic bulbus, which may be due to a system-atic overestimation caused by inclusion of calcified areas.
P842 Computed tomography pulmonary angiography: thepowerful prognostic impact of right-to-left ventriculardiameter ratio in acute pulmonary embolism
R. Baptista, I. Santiago, E. Jorge, R. Teixeira, P. Mendes, G. Castro,P. Monteiro, L.A. Providencia. Hospital and Medical School, Coimbra,
Portugal
Introduction: Computed tomography pulmonary angiography (CTA) is useful forthe diagnosis of acute pulmonary embolism (PE) and can give information on thedimensions of several structures related to the pulmonary vasculature. However,current guidelines do not support the use of CTA-derived prognostic indicatorsfor risk assessment in acute PE patients, namely regarding the classification ofpatients in low- or intermediate risk categories.Aims: To assess the prognostic performance of CTA-derived indexes in patientswith acute PE.Methods: A total of 39 consecutive patients admitted in an intensive care unitwith acute PE where studied, regarding clinical, laboratory and radiological data.All patients had a pulmonary CTA on admission in the emergency room as partof the diagnostic algorithm that was reviewed by a single radiologist and the fol-lowing measurements were collected: right-to-left ventricular and pulmonary-to-aorta artery diameter ratio and azygos vein diameter. A mean follow-up of 14.7(9.0-22.3) months was collected, using as endpoint the combined intra-hospitaland follow-up mortality.Results: The study endpoint occurred in 12.8% of patients. Regarding the ra-diological variables, only the right-to-left ventricular diameter ratio (RLVDR) hadpredictive value, being higher in patients who suffered the endpoint (1.6±0.5 vs.1.9±0.4, p = 0.043). Using a cut-off of 1.8, the endpoint incidence was signifi-cantly higher in patients with RLVDR ≥1.8 (33.3 vs 3.7%; OR 13.0, 95% con-fidence interval: 1.3 – 133.6, p < 0.05). Regarding the aforementioned end-point, the area under the receiver operator characteristics curve (c-statistic) was0.779 (95% CI 0.601-0.958) for RLVDR and calibration was good, with a Hosmer-Lemeshow goodness-of-fit p = 0.594, whereas for troponin I the c-statistic was0.655 (95% CI 0.343-0.967). No other radiological index, namely pulmonary-to-aorta artery diameter ratio and azygos vein diameter, had a significant associationwith the endpoint.Conclusions: CTA gives the possibility of determining the diagnosis and assess-ing the prognosis of patients with suspected PE, giving the information needed foracute patient management in a single imagiological procedure. Although furtherstudies are nedded, the simple-to-calculate RLVDR has good discrimination andcalibration for predicting poorer outcomes in patients with acute PE.
P843 Correlation between cardiac troponin T as measuredby two assays and CT-angiographically assessedcoronary artery plaque burden
J. Rixe, A. Rolf, J. Wilhelm, A. Koch, H. Moellmann, H. Nef,C. Liebetrau, D. Erkapic, C.W. Hamm, T. Dill. Kerckhoff Clinic,
Department of Cardiology, Bad Nauheim, Germany
Background: The concept of vulnerable plaque has given new insights intoatherosclerosis, but data on the correlation between coronary plaque burden andserum levels of markers potentially determining plaque instability are rare. SinceMulti Detector-CT (MDCT) is the only non–invasive tool for the detection of coro-nary plaques, we sought to investigate the correlation between coronary plaqueburden assessed by Dual Source-CT (DSCT) and the serum levels of cardiacTroponin T (cTnT) as quantified by two different assays.Methods: 95 patients (69 male, mean age 59±11y) without known CAD under-went DSCT (Siemens Somatom Definition). Before scan, serum levels of cTnTwere determined, using a conventional assay (detection threshold 0.01ng/ml) anda high-sensitive assay (lower limit of detection 1pg/ml). CT data was assessed
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
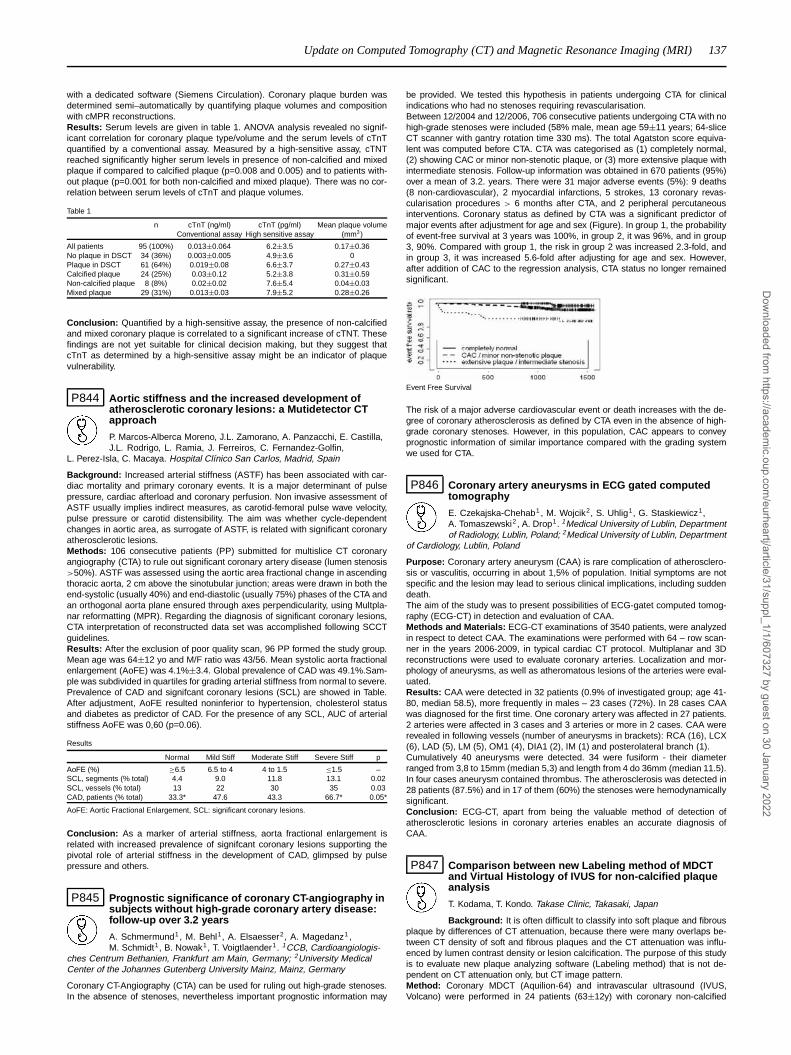
Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) 137
with a dedicated software (Siemens Circulation). Coronary plaque burden wasdetermined semi–automatically by quantifying plaque volumes and compositionwith cMPR reconstructions.Results: Serum levels are given in table 1. ANOVA analysis revealed no signif-icant correlation for coronary plaque type/volume and the serum levels of cTnTquantified by a conventional assay. Measured by a high-sensitive assay, cTNTreached significantly higher serum levels in presence of non-calcified and mixedplaque if compared to calcified plaque (p=0.008 and 0.005) and to patients with-out plaque (p=0.001 for both non-calcified and mixed plaque). There was no cor-relation between serum levels of cTnT and plaque volumes.
Table 1
n cTnT (ng/ml) cTnT (pg/ml) Mean plaque volumeConventional assay High sensitive assay (mm3)
All patients 95 (100%) 0.013±0.064 6.2±3.5 0.17±0.36No plaque in DSCT 34 (36%) 0.003±0.005 4.9±3.6 0Plaque in DSCT 61 (64%) 0.019±0.08 6.6±3.7 0.27±0.43Calcified plaque 24 (25%) 0.03±0.12 5.2±3.8 0.31±0.59Non-calcified plaque 8 (8%) 0.02±0.02 7.6±5.4 0.04±0.03Mixed plaque 29 (31%) 0.013±0.03 7.9±5.2 0.28±0.26
Conclusion: Quantified by a high-sensitive assay, the presence of non-calcifiedand mixed coronary plaque is correlated to a significant increase of cTNT. Thesefindings are not yet suitable for clinical decision making, but they suggest thatcTnT as determined by a high-sensitive assay might be an indicator of plaquevulnerability.
P844 Aortic stiffness and the increased development ofatherosclerotic coronary lesions: a Mutidetector CTapproach
P. Marcos-Alberca Moreno, J.L. Zamorano, A. Panzacchi, E. Castilla,J.L. Rodrigo, L. Ramia, J. Ferreiros, C. Fernandez-Golfin,
L. Perez-Isla, C. Macaya. Hospital Clínico San Carlos, Madrid, Spain
Background: Increased arterial stiffness (ASTF) has been associated with car-diac mortality and primary coronary events. It is a major determinant of pulsepressure, cardiac afterload and coronary perfusion. Non invasive assessment ofASTF usually implies indirect measures, as carotid-femoral pulse wave velocity,pulse pressure or carotid distensibility. The aim was whether cycle-dependentchanges in aortic area, as surrogate of ASTF, is related with significant coronaryatherosclerotic lesions.Methods: 106 consecutive patients (PP) submitted for multislice CT coronaryangiography (CTA) to rule out significant coronary artery disease (lumen stenosis>50%). ASTF was assessed using the aortic area fractional change in ascendingthoracic aorta, 2 cm above the sinotubular junction; areas were drawn in both theend-systolic (usually 40%) and end-diastolic (usually 75%) phases of the CTA andan orthogonal aorta plane ensured through axes perpendicularity, using Multpla-nar reformatting (MPR). Regarding the diagnosis of significant coronary lesions,CTA interpretation of reconstructed data set was accomplished following SCCTguidelines.Results: After the exclusion of poor quality scan, 96 PP formed the study group.Mean age was 64±12 yo and M/F ratio was 43/56. Mean systolic aorta fractionalenlargement (AoFE) was 4.1%±3.4. Global prevalence of CAD was 49.1%.Sam-ple was subdivided in quartiles for grading arterial stiffness from normal to severe.Prevalence of CAD and signifcant coronary lesions (SCL) are showed in Table.After adjustment, AoFE resulted noninferior to hypertension, cholesterol statusand diabetes as predictor of CAD. For the presence of any SCL, AUC of arterialstiffness AoFE was 0,60 (p=0.06).
Results
Normal Mild Stiff Moderate Stiff Severe Stiff p
AoFE (%) ≥6.5 6.5 to 4 4 to 1.5 ≤1.5 –SCL, segments (% total) 4.4 9.0 11.8 13.1 0.02SCL, vessels (% total) 13 22 30 35 0.03CAD, patients (% total) 33.3* 47.6 43.3 66.7* 0.05*
AoFE: Aortic Fractional Enlargement, SCL: significant coronary lesions.
Conclusion: As a marker of arterial stiffness, aorta fractional enlargement isrelated with increased prevalence of signifcant coronary lesions supporting thepivotal role of arterial stiffness in the development of CAD, glimpsed by pulsepressure and others.
P845 Prognostic significance of coronary CT-angiography insubjects without high-grade coronary artery disease:follow-up over 3.2 years
A. Schmermund1, M. Behl1, A. Elsaesser2, A. Magedanz1 ,M. Schmidt1, B. Nowak1, T. Voigtlaender1. 1CCB, Cardioangiologis-
ches Centrum Bethanien, Frankfurt am Main, Germany; 2University MedicalCenter of the Johannes Gutenberg University Mainz, Mainz, Germany
Coronary CT-Angiography (CTA) can be used for ruling out high-grade stenoses.In the absence of stenoses, nevertheless important prognostic information may
be provided. We tested this hypothesis in patients undergoing CTA for clinicalindications who had no stenoses requiring revascularisation.Between 12/2004 and 12/2006, 706 consecutive patients undergoing CTA with nohigh-grade stenoses were included (58% male, mean age 59±11 years; 64-sliceCT scanner with gantry rotation time 330 ms). The total Agatston score equiva-lent was computed before CTA. CTA was categorised as (1) completely normal,(2) showing CAC or minor non-stenotic plaque, or (3) more extensive plaque withintermediate stenosis. Follow-up information was obtained in 670 patients (95%)over a mean of 3.2. years. There were 31 major adverse events (5%): 9 deaths(8 non-cardiovascular), 2 myocardial infarctions, 5 strokes, 13 coronary revas-cularisation procedures > 6 months after CTA, and 2 peripheral percutaneousinterventions. Coronary status as defined by CTA was a significant predictor ofmajor events after adjustment for age and sex (Figure). In group 1, the probabilityof event-free survival at 3 years was 100%, in group 2, it was 96%, and in group3, 90%. Compared with group 1, the risk in group 2 was increased 2.3-fold, andin group 3, it was increased 5.6-fold after adjusting for age and sex. However,after addition of CAC to the regression analysis, CTA status no longer remainedsignificant.
Event Free Survival
The risk of a major adverse cardiovascular event or death increases with the de-gree of coronary atherosclerosis as defined by CTA even in the absence of high-grade coronary stenoses. However, in this population, CAC appears to conveyprognostic information of similar importance compared with the grading systemwe used for CTA.
P846 Coronary artery aneurysms in ECG gated computedtomography
E. Czekajska-Chehab1 , M. Wojcik2, S. Uhlig1, G. Staskiewicz1,A. Tomaszewski2 , A. Drop1. 1Medical University of Lublin, Departmentof Radiology, Lublin, Poland; 2Medical University of Lublin, Department
of Cardiology, Lublin, Poland
Purpose: Coronary artery aneurysm (CAA) is rare complication of atherosclero-sis or vasculitis, occurring in about 1,5% of population. Initial symptoms are notspecific and the lesion may lead to serious clinical implications, including suddendeath.The aim of the study was to present possibilities of ECG-gatet computed tomog-raphy (ECG-CT) in detection and evaluation of CAA.Methods and Materials: ECG-CT examinations of 3540 patients, were analyzedin respect to detect CAA. The examinations were performed with 64 – row scan-ner in the years 2006-2009, in typical cardiac CT protocol. Multiplanar and 3Dreconstructions were used to evaluate coronary arteries. Localization and mor-phology of aneurysms, as well as atheromatous lesions of the arteries were eval-uated.Results: CAA were detected in 32 patients (0.9% of investigated group; age 41-80, median 58.5), more frequently in males – 23 cases (72%). In 28 cases CAAwas diagnosed for the first time. One coronary artery was affected in 27 patients.2 arteries were affected in 3 cases and 3 arteries or more in 2 cases. CAA wererevealed in following vessels (number of aneurysms in brackets): RCA (16), LCX(6), LAD (5), LM (5), OM1 (4), DIA1 (2), IM (1) and posterolateral branch (1).Cumulatively 40 aneurysms were detected. 34 were fusiform - their diameterranged from 3,8 to 15mm (median 5,3) and length from 4 do 36mm (median 11.5).In four cases aneurysm contained thrombus. The atherosclerosis was detected in28 patients (87.5%) and in 17 of them (60%) the stenoses were hemodynamicallysignificant.Conclusion: ECG-CT, apart from being the valuable method of detection ofatherosclerotic lesions in coronary arteries enables an accurate diagnosis ofCAA.
P847 Comparison between new Labeling method of MDCTand Virtual Histology of IVUS for non-calcified plaqueanalysis
T. Kodama, T. Kondo. Takase Clinic, Takasaki, Japan
Background: It is often difficult to classify into soft plaque and fibrousplaque by differences of CT attenuation, because there were many overlaps be-tween CT density of soft and fibrous plaques and the CT attenuation was influ-enced by lumen contrast density or lesion calcification. The purpose of this studyis to evaluate new plaque analyzing software (Labeling method) that is not de-pendent on CT attenuation only, but CT image pattern.Method: Coronary MDCT (Aquilion-64) and intravascular ultrasound (IVUS,Volcano) were performed in 24 patients (63±12y) with coronary non-calcified
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

138 Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
plaques. IVUS image were analyzed by "Virtual Historoly" that was verified bycomparing with histology in many papers. Short axis MDCT images were ana-lyzed by new Labeling software.Result: Outer vessel area (r=0.85,P<0.0001), lumen area (r=0.738, P<0.0001),fibrous plaque (r=0.713,P<0.0001) and soft Plaque (r=0.659, P=0.0005) of CTsignificantly correlated with outer vessel area, lumen area, fibrous plaque andnecrotic core + fibrofatty plaque of IVUS, respectively. Mean CT value of softplaque (54±23 HU) was not significantly lower than that of fibrous plaque (62±12HU).
Conclusion: New plaque analyzing software (Labeling method) correlates withVirtual Histology of IVUS.
P848 MSCT segmental calcium score to predict stenosisseverity in calcified coronary lesions
F. Pugliese1, M.G.M. Hunink2, M. Rengo3, K. Gruszcynska4 ,W.B. Meijboom5, N.R. Mollet4, A.C. Weustink4 , L. Neefjes4,G.P. Krestin4, P.J. De Feyter5 . 1The Essex Cardiothoracic Centre,
Basildon, United Kingdom; 2Erasmus Medical Center, Department ofBioinformatics, Rotterdam, Netherlands; 3Sapienza University of Rome,Department of Radiolgy, Rome, Italy; 4Erasmus Medical Center, Department ofRadiology, Rotterdam, Netherlands; 5Erasmus Medical Center, Department ofCardiology, Rotterdam, Netherlands
Purpose: To develop an algorithm for the prediction of ≥50% coronary stenosesassociated to calcified lesions detected at multi-slice computed tomography coro-nary angiography (MSCT-CA) based on MSCT calcium score (CS) measured persegment and calcification morphology.Methods: Patients (n = 402) with stable or acute chest pain underwent MSCTCS, MSCT-CA and conventional angiography (CAG). One experienced observerunaware of CAG measured CS in individual coronary segments and classifiedcalcification morphology into spotty, wide and diffuse. A derivation dataset and avalidation dataset of equal size were obtained. In the derivation dataset, we de-termined frequency of angiographically proven ≥50% stenoses according to seg-mental CS and morphology, and explored the predictive value of other variables(location within the coronary tree and clinical factors) to derive a multivariableprediction rule. The prediction rule was validated in the validation dataset.Results: In a multivariable model, the OR for stenosis was 1.8-fold greater (p =0.006) in patients with typical chest pain, 2-fold (p = 0.014) greater in patients withacute coronary syndrome, and 2-fold greater (p <0.001) in patients with prior my-ocardial infarction. With distal segments as comparator, each unit of natural logof CS in middle segments corresponded to an OR 1.2-fold (p <0.001) greater;in proximal segments this corresponded to an OR 1.1-fold greater (p = 0.021).Spotty calcifications had an OR for stenosis 2.3-fold (p <0.001) greater than theabsence of calcification, wide calcifications 2.7-fold (p <0.001) greater, and dif-fuse calcifications 4.6-fold (p <0.001) greater. Derivation and validation datasetsrevealed similar results.Conclusion: Focal coronary calcifications may cause false positive diagnoses atMSCT-CA. Combining segmental CS, morphology, lesion location and patient’ssymptoms it is possible to predict the probability of ≥50% stenosis associated toa calcified lesion detected at MSCT-CA. This may help reduce the occurrence offalse positive diagnoses.
P849 Aortic valve annulus pulsatile distention in patientswithout aortic valve disease is asymmetric: analysiswith ECG-gated multislice computed tomography
L.M. De Heer1, K.L. Vincken2, L.A. Van Herwerden1, W.P.T. Mali3,L.W. Bartels2, J. Van Prehn3, R.P.J. Budde3, J. Kluin1. 1University
Medical Center Utrecht, Division Heart and Lungs, Department of CardiothoracicSurgery, Utrecht, Netherlands; 2University Medical Center Utrecht, ImageSciences Institute, Utrecht, Netherlands; 3University Medical Center Utrecht,Department of Radiology, Utrecht, Netherlands
Purpose: A key element of successful transcatheter aortic valve implantation isadequate prosthesis sizing. Cardiac output and aortic compliance result in aorticarea and diameter changes throughout the cardiac cycle. This may result in in-adequate prosthesis sizing. To understand the dynamic changes in stenotic aor-tic valves, the healthy aorta has to be studied first. We assessed the dynamicchanges of the aortic valve annulus using ECG-gated MSCT.
Methods: Fifteen patients with a cardiac MSCT without aortic valve disease wereidentified. 3D datasets were reconstructed at each 10% of the ECG-interval. Perphase a cross-section in-plane with the aortic annulus was reconstructed. Theannulus area was segmented and analysed using in-home developed software(Dynamix, ISI) (figure). Radius changes during the cardiac cycle were measuredover 360 degrees from the center of mass per phase and plotted. The completeannulus shape change in all directions was depicted by an ellipse and describedby radius changes over the major and minor axis. The asymmetry ratio was cal-culated by dividing the major by the minor axis. In addition area change wasdetermined.Results: In all patients distention of the annulus was asymmetric with a ratioof 1.3±0.2. Diameter and area changes were significant in all patients. Meandiameter change was 20±4%. Mean area change was 28±7%.
Aortic segmentation by tresholding
Conclusions: The healthy annulus diameter and area show over 20% changeduring the cardiac cycle and these changes are asymmetrical. Knowledge of dy-namic morphological changes may aid prosthesis sizing and it may have implica-tions for ultimate clinical success.
P850 The significance of enhancement pattern of two-phasecontrast enhanced multidetector computedtomography in reperfused acute myocardial infarction
B.J. Choi, S.J. Tahk, M.H. Yoon, H.S. Lim, S.Y. Choi, J.H. Shin,G.S. Hwang, H.M. Yang, J.S. Park, J.H. Moon. Ajou University School
of Medicine, Suwon, Korea, Republic of
Purpose: The purpose of the present study was to investigate the significance ofeach enhancement pattern of two-phase contrast-enhanced multidetector com-puted tomography (MDCT) in reperfused acute myocardial infarct (AMI) with in-tracoronary physiology studies.Methods: First-onset AMI patients were enrolled. After successful revasculariza-tion, intracoronary physiologic studies were performed with a Doppler wire. Two-Phase Contrast enhanced MDCT was taken within 3 days after revascularization.The patterns of perfusion defects and late enhancement (LE) were classified intothree groups. Group A = absence of early perfusion defect (ED) and absence orpresence of LE without residual perfusion defect (RD), group B = presence of EDand presence of LE without RD, group C = presence of ED and presence of LEwith RD.Results: 53 AMI patients (group A, 9; group B, 20; Group, C; 24) were enrolled.The baseline and hyperemic average peak velocity of the group C were the low-est among 3 groups (24.2±11.5 vs. 20.1±6.9 vs. 13.5±6.9 cm/sec, p=0.037; and48.8±16.7 vs. 37.1±10.8 vs. 25.5±10.8 cm/sec, p=0.018, respectively). Baselineand hyperemic microvascular resistance index of the group C were the great-est among 3 groups (3.16±2.22 vs. 4.03±1.94 vs. 5.86±2.12 mmHg cm-1 sec,p=0.036; and 1.53±1.29 vs. 2.16±1.64 vs. 2.99±1.32 mmHg cm-1 sec, p=0.030,respectively). The baseline and hyperemic diastolic deceleration time of the groupC were the shortest among 3 groups. (669±262 vs. 519±282 vs. 313±152 msec,p=0.021; 751±246 vs. 616±269 vs. 363±104, p=0.033, respectively). However,the 3 groups did not have any significant differences in coronary flow reserve(2.02±0.64 vs. 1.85±0.60 vs. 1.70±0.55, p=0.060).Conclusions: RD in the delayed phase of Two-Phase Contrast enhanced MDCTcorresponded to more severe myocardial necrosis with extensive microvasculardamage than LE. LE might contain greater viable myocardium than RD.
P851 Prevalence and morphology of coronary artery ectasiausing multislice computed tomography coronaryangiography
R. Galal, A. Farrag, A.M.R. El-Faramawy, S. Ghareeb, M.O.H. AliSalem. Kasr Alini -Cairo University -Faculty of medicine -Cardiology
departement, Cairo, Egypt
Aim: To evaluate the prevalence and morphological characteristics of coronaryartery ectasia (CAE) visualized by 64-MSCT coronary angiography and to deter-mine the clinical presentation, the association of CAE with conventional coronaryrisk factors and coexisting coronary artery disease (CAD).Methods: This study included 2600 consecutive patients referred to MSCT coro-nary angiography for a period of 15 months. All patients were subjected to detailedhistory taking, risk factor assessment, ECG-gated CT angiographic studies wereperformed to detect and evaluate the coronary artery disease and morphology.Coronary artery ectasia was defined as an arterial segment with a diameter of at
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
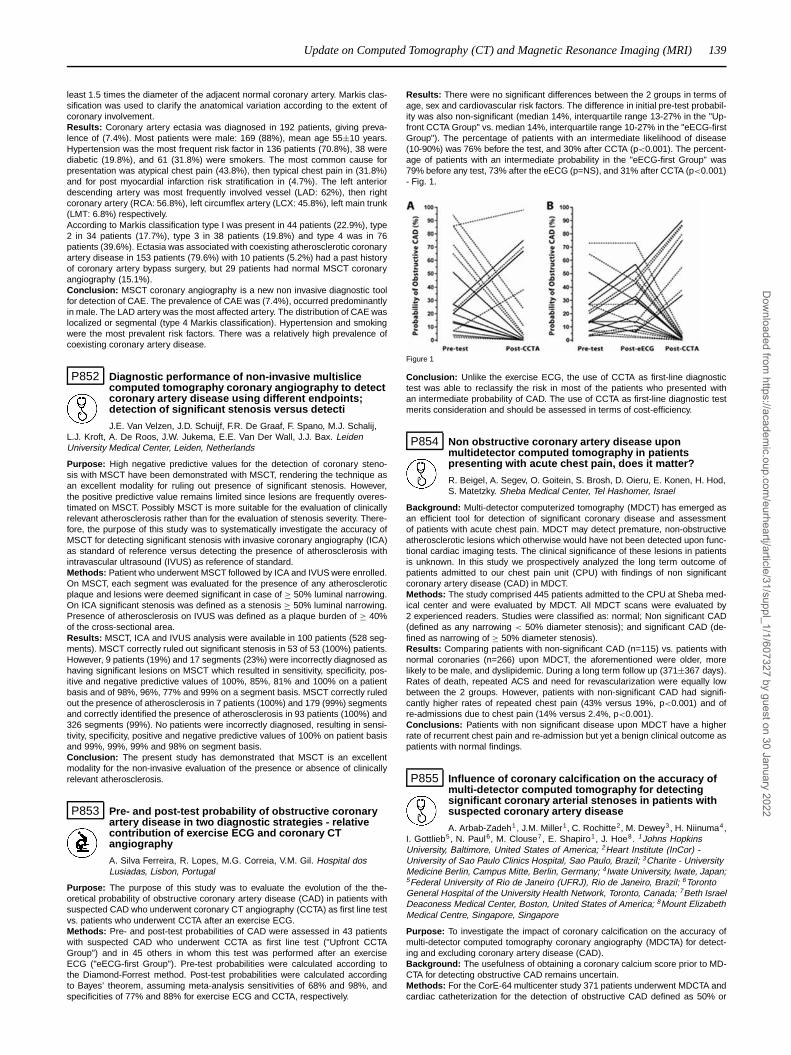
Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) 139
least 1.5 times the diameter of the adjacent normal coronary artery. Markis clas-sification was used to clarify the anatomical variation according to the extent ofcoronary involvement.Results: Coronary artery ectasia was diagnosed in 192 patients, giving preva-lence of (7.4%). Most patients were male: 169 (88%), mean age 55±10 years.Hypertension was the most frequent risk factor in 136 patients (70.8%), 38 werediabetic (19.8%), and 61 (31.8%) were smokers. The most common cause forpresentation was atypical chest pain (43.8%), then typical chest pain in (31.8%)and for post myocardial infarction risk stratification in (4.7%). The left anteriordescending artery was most frequently involved vessel (LAD: 62%), then rightcoronary artery (RCA: 56.8%), left circumflex artery (LCX: 45.8%), left main trunk(LMT: 6.8%) respectively.According to Markis classification type I was present in 44 patients (22.9%), type2 in 34 patients (17.7%), type 3 in 38 patients (19.8%) and type 4 was in 76patients (39.6%). Ectasia was associated with coexisting atherosclerotic coronaryartery disease in 153 patients (79.6%) with 10 patients (5.2%) had a past historyof coronary artery bypass surgery, but 29 patients had normal MSCT coronaryangiography (15.1%).Conclusion: MSCT coronary angiography is a new non invasive diagnostic toolfor detection of CAE. The prevalence of CAE was (7.4%), occurred predominantlyin male. The LAD artery was the most affected artery. The distribution of CAE waslocalized or segmental (type 4 Markis classification). Hypertension and smokingwere the most prevalent risk factors. There was a relatively high prevalence ofcoexisting coronary artery disease.
P852 Diagnostic performance of non-invasive multislicecomputed tomography coronary angiography to detectcoronary artery disease using different endpoints;detection of significant stenosis versus detecti
J.E. Van Velzen, J.D. Schuijf, F.R. De Graaf, F. Spano, M.J. Schalij,L.J. Kroft, A. De Roos, J.W. Jukema, E.E. Van Der Wall, J.J. Bax. LeidenUniversity Medical Center, Leiden, Netherlands
Purpose: High negative predictive values for the detection of coronary steno-sis with MSCT have been demonstrated with MSCT, rendering the technique asan excellent modality for ruling out presence of significant stenosis. However,the positive predictive value remains limited since lesions are frequently overes-timated on MSCT. Possibly MSCT is more suitable for the evaluation of clinicallyrelevant atherosclerosis rather than for the evaluation of stenosis severity. There-fore, the purpose of this study was to systematically investigate the accuracy ofMSCT for detecting significant stenosis with invasive coronary angiography (ICA)as standard of reference versus detecting the presence of atherosclerosis withintravascular ultrasound (IVUS) as reference of standard.Methods: Patient who underwent MSCT followed by ICA and IVUS were enrolled.On MSCT, each segment was evaluated for the presence of any atheroscleroticplaque and lesions were deemed significant in case of ≥ 50% luminal narrowing.On ICA significant stenosis was defined as a stenosis ≥ 50% luminal narrowing.Presence of atherosclerosis on IVUS was defined as a plaque burden of ≥ 40%of the cross-sectional area.Results: MSCT, ICA and IVUS analysis were available in 100 patients (528 seg-ments). MSCT correctly ruled out significant stenosis in 53 of 53 (100%) patients.However, 9 patients (19%) and 17 segments (23%) were incorrectly diagnosed ashaving significant lesions on MSCT which resulted in sensitivity, specificity, pos-itive and negative predictive values of 100%, 85%, 81% and 100% on a patientbasis and of 98%, 96%, 77% and 99% on a segment basis. MSCT correctly ruledout the presence of atherosclerosis in 7 patients (100%) and 179 (99%) segmentsand correctly identified the presence of atherosclerosis in 93 patients (100%) and326 segments (99%). No patients were incorrectly diagnosed, resulting in sensi-tivity, specificity, positive and negative predictive values of 100% on patient basisand 99%, 99%, 99% and 98% on segment basis.Conclusion: The present study has demonstrated that MSCT is an excellentmodality for the non-invasive evaluation of the presence or absence of clinicallyrelevant atherosclerosis.
P853 Pre- and post-test probability of obstructive coronaryartery disease in two diagnostic strategies - relativecontribution of exercise ECG and coronary CTangiography
A. Silva Ferreira, R. Lopes, M.G. Correia, V.M. Gil. Hospital dosLusiadas, Lisbon, Portugal
Purpose: The purpose of this study was to evaluate the evolution of the the-oretical probability of obstructive coronary artery disease (CAD) in patients withsuspected CAD who underwent coronary CT angiography (CCTA) as first line testvs. patients who underwent CCTA after an exercise ECG.Methods: Pre- and post-test probabilities of CAD were assessed in 43 patientswith suspected CAD who underwent CCTA as first line test ("Upfront CCTAGroup") and in 45 others in whom this test was performed after an exerciseECG ("eECG-first Group"). Pre-test probabilities were calculated according tothe Diamond-Forrest method. Post-test probabilities were calculated accordingto Bayes’ theorem, assuming meta-analysis sensitivities of 68% and 98%, andspecificities of 77% and 88% for exercise ECG and CCTA, respectively.
Results: There were no significant differences between the 2 groups in terms ofage, sex and cardiovascular risk factors. The difference in initial pre-test probabil-ity was also non-significant (median 14%, interquartile range 13-27% in the "Up-front CCTA Group" vs. median 14%, interquartile range 10-27% in the "eECG-firstGroup"). The percentage of patients with an intermediate likelihood of disease(10-90%) was 76% before the test, and 30% after CCTA (p<0.001). The percent-age of patients with an intermediate probability in the "eECG-first Group" was79% before any test, 73% after the eECG (p=NS), and 31% after CCTA (p<0.001)- Fig. 1.
Figure 1
Conclusion: Unlike the exercise ECG, the use of CCTA as first-line diagnostictest was able to reclassify the risk in most of the patients who presented withan intermediate probability of CAD. The use of CCTA as first-line diagnostic testmerits consideration and should be assessed in terms of cost-efficiency.
P854 Non obstructive coronary artery disease uponmultidetector computed tomography in patientspresenting with acute chest pain, does it matter?
R. Beigel, A. Segev, O. Goitein, S. Brosh, D. Oieru, E. Konen, H. Hod,S. Matetzky. Sheba Medical Center, Tel Hashomer, Israel
Background: Multi-detector computerized tomography (MDCT) has emerged asan efficient tool for detection of significant coronary disease and assessmentof patients with acute chest pain. MDCT may detect premature, non-obstructiveatherosclerotic lesions which otherwise would have not been detected upon func-tional cardiac imaging tests. The clinical significance of these lesions in patientsis unknown. In this study we prospectively analyzed the long term outcome ofpatients admitted to our chest pain unit (CPU) with findings of non significantcoronary artery disease (CAD) in MDCT.Methods: The study comprised 445 patients admitted to the CPU at Sheba med-ical center and were evaluated by MDCT. All MDCT scans were evaluated by2 experienced readers. Studies were classified as: normal; Non significant CAD(defined as any narrowing < 50% diameter stenosis); and significant CAD (de-fined as narrowing of ≥ 50% diameter stenosis).Results: Comparing patients with non-significant CAD (n=115) vs. patients withnormal coronaries (n=266) upon MDCT, the aforementioned were older, morelikely to be male, and dyslipidemic. During a long term follow up (371±367 days).Rates of death, repeated ACS and need for revascularization were equally lowbetween the 2 groups. However, patients with non-significant CAD had signifi-cantly higher rates of repeated chest pain (43% versus 19%, p<0.001) and ofre-admissions due to chest pain (14% versus 2.4%, p<0.001).Conclusions: Patients with non significant disease upon MDCT have a higherrate of recurrent chest pain and re-admission but yet a benign clinical outcome aspatients with normal findings.
P855 Influence of coronary calcification on the accuracy ofmulti-detector computed tomography for detectingsignificant coronary arterial stenoses in patients withsuspected coronary artery disease
A. Arbab-Zadeh1, J.M. Miller1, C. Rochitte2, M. Dewey3, H. Niinuma4,I. Gottlieb5, N. Paul6, M. Clouse7, E. Shapiro1, J. Hoe8. 1Johns HopkinsUniversity, Baltimore, United States of America; 2Heart Institute (InCor) -University of Sao Paulo Clinics Hospital, Sao Paulo, Brazil; 3Charite - UniversityMedicine Berlin, Campus Mitte, Berlin, Germany; 4Iwate University, Iwate, Japan;5Federal University of Rio de Janeiro (UFRJ), Rio de Janeiro, Brazil; 6TorontoGeneral Hospital of the University Health Network, Toronto, Canada; 7Beth IsraelDeaconess Medical Center, Boston, United States of America; 8Mount ElizabethMedical Centre, Singapore, Singapore
Purpose: To investigate the impact of coronary calcification on the accuracy ofmulti-detector computed tomography coronary angiography (MDCTA) for detect-ing and excluding coronary artery disease (CAD).Background: The usefulness of obtaining a coronary calcium score prior to MD-CTA for detecting obstructive CAD remains uncertain.Methods: For the CorE-64 multicenter study 371 patients underwent MDCTA andcardiac catheterization for the detection of obstructive CAD defined as 50% or
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
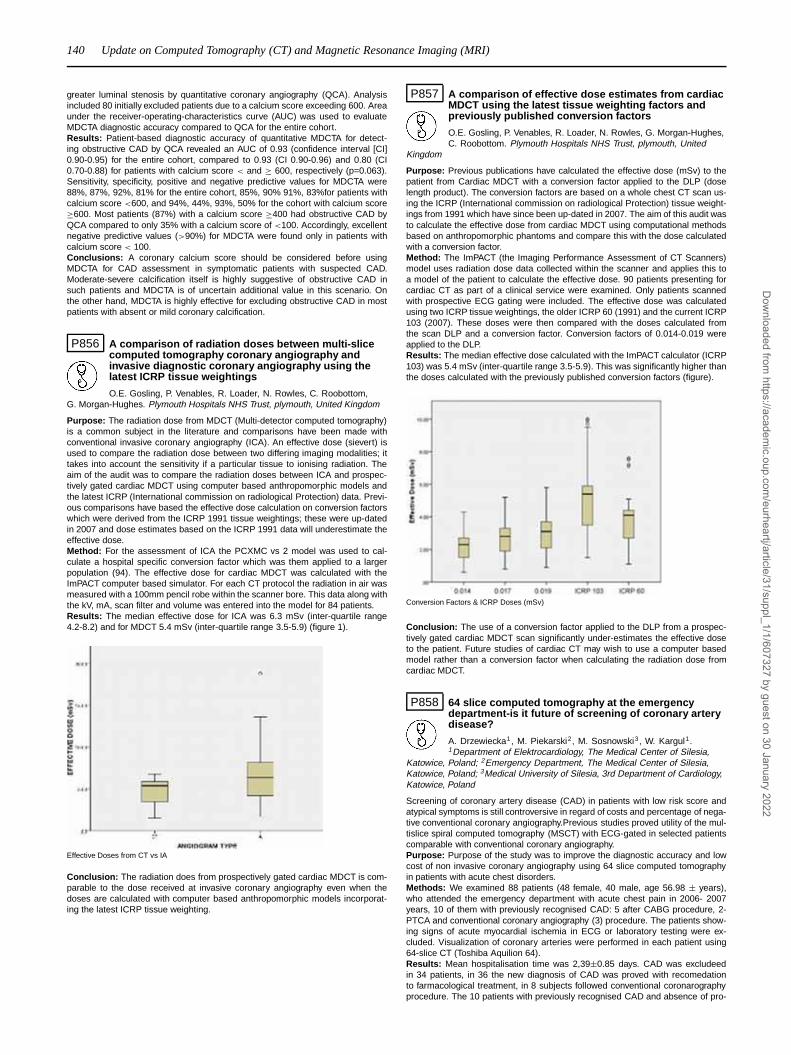
140 Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
greater luminal stenosis by quantitative coronary angiography (QCA). Analysisincluded 80 initially excluded patients due to a calcium score exceeding 600. Areaunder the receiver-operating-characteristics curve (AUC) was used to evaluateMDCTA diagnostic accuracy compared to QCA for the entire cohort.Results: Patient-based diagnostic accuracy of quantitative MDCTA for detect-ing obstructive CAD by QCA revealed an AUC of 0.93 (confidence interval [CI]0.90-0.95) for the entire cohort, compared to 0.93 (CI 0.90-0.96) and 0.80 (CI0.70-0.88) for patients with calcium score < and ≥ 600, respectively (p=0.063).Sensitivity, specificity, positive and negative predictive values for MDCTA were88%, 87%, 92%, 81% for the entire cohort, 85%, 90% 91%, 83%for patients withcalcium score <600, and 94%, 44%, 93%, 50% for the cohort with calcium score≥600. Most patients (87%) with a calcium score ≥400 had obstructive CAD byQCA compared to only 35% with a calcium score of <100. Accordingly, excellentnegative predictive values (>90%) for MDCTA were found only in patients withcalcium score < 100.Conclusions: A coronary calcium score should be considered before usingMDCTA for CAD assessment in symptomatic patients with suspected CAD.Moderate-severe calcification itself is highly suggestive of obstructive CAD insuch patients and MDCTA is of uncertain additional value in this scenario. Onthe other hand, MDCTA is highly effective for excluding obstructive CAD in mostpatients with absent or mild coronary calcification.
P856 A comparison of radiation doses between multi-slicecomputed tomography coronary angiography andinvasive diagnostic coronary angiography using thelatest ICRP tissue weightings
O.E. Gosling, P. Venables, R. Loader, N. Rowles, C. Roobottom,G. Morgan-Hughes. Plymouth Hospitals NHS Trust, plymouth, United Kingdom
Purpose: The radiation dose from MDCT (Multi-detector computed tomography)is a common subject in the literature and comparisons have been made withconventional invasive coronary angiography (ICA). An effective dose (sievert) isused to compare the radiation dose between two differing imaging modalities; ittakes into account the sensitivity if a particular tissue to ionising radiation. Theaim of the audit was to compare the radiation doses between ICA and prospec-tively gated cardiac MDCT using computer based anthropomorphic models andthe latest ICRP (International commission on radiological Protection) data. Previ-ous comparisons have based the effective dose calculation on conversion factorswhich were derived from the ICRP 1991 tissue weightings; these were up-datedin 2007 and dose estimates based on the ICRP 1991 data will underestimate theeffective dose.Method: For the assessment of ICA the PCXMC vs 2 model was used to cal-culate a hospital specific conversion factor which was them applied to a largerpopulation (94). The effective dose for cardiac MDCT was calculated with theImPACT computer based simulator. For each CT protocol the radiation in air wasmeasured with a 100mm pencil robe within the scanner bore. This data along withthe kV, mA, scan filter and volume was entered into the model for 84 patients.Results: The median effective dose for ICA was 6.3 mSv (inter-quartile range4.2-8.2) and for MDCT 5.4 mSv (inter-quartile range 3.5-5.9) (figure 1).
Effective Doses from CT vs IA
Conclusion: The radiation does from prospectively gated cardiac MDCT is com-parable to the dose received at invasive coronary angiography even when thedoses are calculated with computer based anthropomorphic models incorporat-ing the latest ICRP tissue weighting.
P857 A comparison of effective dose estimates from cardiacMDCT using the latest tissue weighting factors andpreviously published conversion factors
O.E. Gosling, P. Venables, R. Loader, N. Rowles, G. Morgan-Hughes,C. Roobottom. Plymouth Hospitals NHS Trust, plymouth, United
Kingdom
Purpose: Previous publications have calculated the effective dose (mSv) to thepatient from Cardiac MDCT with a conversion factor applied to the DLP (doselength product). The conversion factors are based on a whole chest CT scan us-ing the ICRP (International commission on radiological Protection) tissue weight-ings from 1991 which have since been up-dated in 2007. The aim of this audit wasto calculate the effective dose from cardiac MDCT using computational methodsbased on anthropomorphic phantoms and compare this with the dose calculatedwith a conversion factor.Method: The ImPACT (the Imaging Performance Assessment of CT Scanners)model uses radiation dose data collected within the scanner and applies this toa model of the patient to calculate the effective dose. 90 patients presenting forcardiac CT as part of a clinical service were examined. Only patients scannedwith prospective ECG gating were included. The effective dose was calculatedusing two ICRP tissue weightings, the older ICRP 60 (1991) and the current ICRP103 (2007). These doses were then compared with the doses calculated fromthe scan DLP and a conversion factor. Conversion factors of 0.014-0.019 wereapplied to the DLP.Results: The median effective dose calculated with the ImPACT calculator (ICRP103) was 5.4 mSv (inter-quartile range 3.5-5.9). This was significantly higher thanthe doses calculated with the previously published conversion factors (figure).
Conversion Factors & ICRP Doses (mSv)
Conclusion: The use of a conversion factor applied to the DLP from a prospec-tively gated cardiac MDCT scan significantly under-estimates the effective doseto the patient. Future studies of cardiac CT may wish to use a computer basedmodel rather than a conversion factor when calculating the radiation dose fromcardiac MDCT.
P858 64 slice computed tomography at the emergencydepartment-is it future of screening of coronary arterydisease?
A. Drzewiecka1, M. Piekarski2, M. Sosnowski3, W. Kargul1.1Department of Elektrocardiology, The Medical Center of Silesia,
Katowice, Poland; 2Emergency Department, The Medical Center of Silesia,Katowice, Poland; 3Medical University of Silesia, 3rd Department of Cardiology,Katowice, Poland
Screening of coronary artery disease (CAD) in patients with low risk score andatypical symptoms is still controversive in regard of costs and percentage of nega-tive conventional coronary angiography.Previous studies proved utility of the mul-tislice spiral computed tomography (MSCT) with ECG-gated in selected patientscomparable with conventional coronary angiography.Purpose: Purpose of the study was to improve the diagnostic accuracy and lowcost of non invasive coronary angiography using 64 slice computed tomographyin patients with acute chest disorders.Methods: We examined 88 patients (48 female, 40 male, age 56.98 ± years),who attended the emergency department with acute chest pain in 2006- 2007years, 10 of them with previously recognised CAD: 5 after CABG procedure, 2-PTCA and conventional coronary angiography (3) procedure. The patients show-ing signs of acute myocardial ischemia in ECG or laboratory testing were ex-cluded. Visualization of coronary arteries were performed in each patient using64-slice CT (Toshiba Aquilion 64).Results: Mean hospitalisation time was 2,39±0.85 days. CAD was excludeedin 34 patients, in 36 the new diagnosis of CAD was proved with recomedationto farmacological treatment, in 8 subjects followed conventional coronarographyprocedure. The 10 patients with previously recognised CAD and absence of pro-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) 141
gression in coronary arteries avoided next conventional coronary angiographyand prolonged hospitalisation.Conclusions: 1. 64-CT of coronary arteries with its high negative predictive valuesignificanty decrease hospitalisation time of patients with low risk score and atyp-ical symptoms. 2. 64-CT of coronary arteries decrease the diagnostic time and itscost. 3. 64-CT assesment in subjects with recognised CAD allows to avoide nextconventional coronary angiography and its potential adverse event.
P859 Diagnostic accuracy of 64-slice multidetectorcomputed tomography for the evaluation of coronaryartery disease in patients selected for transcatheteraortic valve implantation
G. Pontone, D. Andreini, S. Mushtaq, E. Bertella, A.D. Annoni,M. Muratori, M. Fusari, G. Ballerini, A.L. Bartorelli, M. Pepi. Centro cardiologicoMonzino, IRCCS; Cardiovascular Sciences Department, University of Milan,Milan, Italy
Purpose: transcatheter aortic valve implantation (TAVI) is a new tool for treat-ment of severe aortic stenosis, but for a suitable choice of the surgical tecnique,an accurate assessment of the concomitant coronary artery disease (CAD) ismandatory. Aim of this study is to assess the feasibility (Fe) and accuracy (Ac) ofmultidetetctor computed tomography (MDCT) in the evaluation of CAD in patientsreferred for TAVI, compared with invasive coronary angiography (ICA).Methods and materials: We enrolled 60 patients (22 male, mean age: 80±8years, Logistic Euroscore 20.5±11) who underwent a comprehensive MDCT andICA before TAVI. Regarding to MDCT, the scan parameters were: 64x0.625 mmcollimation, gantry rotation time 350 msec, tube voltage 120 KVp and effectivetube current of 700 mA. All CABG, stented and non-stented segments were in-cluded in our analysis. Two independent and blinded readers classified each graft,stented and non-stented coronary segments as evaluable or not evaluable and forthe presence of significant stenosis, defined as narrowing of the coronary lumenexceeding 50%. Regarding to the coronary arteries, the Fe and Ac was measuredusing a segment-based analysis and a patient-based analysis.Results: the overall Fe of CABG, stented and non-stented segments were 100%,76% and 90%, respectively. The sensitivity (Se), specificity (Sp), negative predic-tive value (NPV), positive predictive value (PPV), and Ac were 100% in CABGand stented-segmented evaluation. In non-stented coronary segments, includingall diagnostic segments, the Se, Sp, NPV, PPV, and Ac were 92%, 96%, 99%,69%, and 95%, respectively. In a patient-based analysis considering as positivethe not-evaluable segments, MDCT demonstrated a Se of 88%, Sp 88%, NPVof 91%, PPV of 85%, and Ac of 88%. In a patient-based analysis including onlypatients with all segments evaluable, the Se, Sp, NPV, PPV, and Ac were 100%,93%, 100%, 92%, and 96%, respectively.Conclusions: the high negative predictive value of MDCT in ruling out concomi-tant CAD may avoid the invasive coronary angiography in negative patients, sug-gesting a promising role of this tecnique in the diagnostic planning of patientsselected for TAVI.
P860 Assessment of coronary arteries in patients with atrialfibrillation by 320-detector computed tomography
T. Imamura, K. Tanabe, S. Kishi, M. Taniwaki, H. Nakajima, K. Ibukuro,J. Aoki, S. Tanimoto, S. Otsuki, K. Hara. Mitsui Memorial hospital,Tokyo, Japan
(Background)Generally, noninvasive coronary angiography by multi-slice com-puted tomography (CT) has been contraindicated to patients with atrial fibrillation(af) because of the difficulty of accurate synchronization of images obtained byseveral beats’ scanning. Because 320-detector row CT can construct analyzableimages from only one beat scan, it is considered to be suitable to analyze coro-nary arteries in af rhythm. However, there have been few clinical data. Thereforewe have applied 320-detector row CT scan to patients with af rhythm and com-pared the image qualities to those with sinus rhythm. (Methods)The study pop-ulation consisted of consecutive 27 patients with af rhythm and 27 patients withsinus rhythm, who were suspected of ischemic heart disease and scanned by the320-detector CT (Toshiba AquilionOne Dynamic Volume CT, Tochigi-ken, Japan)from February 2009 to February 2010. The all datasets were reconstructed byone beat reconstruction. For analysis of coronary arteries, 16-segment Ameri-can Heart Association model was employed. The image quality of all segmentswas scored into 5 grades, from 1 (poor) to 5 (excellent). (Result)Mean Ages ofpatients with af rhythm and sinus rhythm were 68.3 and 62.9 years old, respec-tively. The Agatston calcium score in their coronary arteries averaged as high as369.4±1319 (af rhythm) and 343.4±1028 (sinus rhythm). The mean heart rates(HR) during the scan were 61±25 (af rhythm) and 56±13 (sinus rhythm). Theaverage image quality grade of all the segments of one beat reconstruction were3.505±1.650 (af rhythm), and 3.541±1.280 (sinus rhythm). There was no statis-tical difference between the 2 groups. (Conclusion)One beat scan with the 320-detector CT may allow us to analyze coronary arteries even in the patients withaf rhythm.
P861 The prevalence and severity of coronary artery diseaseamong asymptomatic diabetic patients: thecomparison between coronary computed tomographicangiography and stress testing
T. Kashiyama, Y. Masumura, M. Wada, M. Nishio, Y. Ueda. OsakaPolice Hospital, Osaka, Japan
Background: Myocardial ischemia in diabetic patients is often asymptomatic. Al-though stress testing has been traditionally used for screening, its diagnostic ac-curacy has been varied. Recently, coronary computed tomographic angiography(CCTA) has been demonstrated to be useful for detecting coronary artery disease(CAD). The purpose of this study is to assess the prevalence and severity of silentCAD among asymptomatic diabetic patients using CCTA and stress testing.Methods: A total of 128 asymptomatic patients with type-2 diabetes (33 femalesand 95 males, aged 51 to 82 years, mean 65±7 years) without known nor sus-pected CAD were enrolled in this study. Both CCTA and exercise stress elec-trocardiogram (ECG) testing were performed. If it was difficult to judge the resultof ECG testing, stress Thalium-201 myocardial perfusion imaging was performed.The CCTA studies were classified as having no CAD, nonobstructive (<50% lumi-nal narrowing) CAD, or obstructive CAD. The presence of ischemia was identifiedby exercise-induced ST-segment depression or regional myocardial perfusion ab-normality.Results: CAD was detected in 99 (77%) patients, and ischemia was detected in29 patients (22%). Sixty-seven patients (52%) had obstructive CAD with CCTA,but only 27 patients (40%) among them had ischemia. Patients who were treatedwith cholesterol lowering therapy were more prevalent (62% vs 44%, p=0.03), andcholesterol levels were lower (185±26 vs 198±34 mg/dl, P=0.02) in patients withobstructive CAD, Conventional coronary angiography was performed in 18 of 27patients who had obstructive CAD and ischemia, and whose informed consentwas obtained. Among those 18 patients, 5 underwent percutaneous coronary an-gioplasty and 4 underwent bypass grafting, and 9 were treated by medication.Conclusion: Many diabetic patients have obstructive CAD without symptom norpositive stress test. Patients with dyslipidemia should be treated as high-risk ones,irrespective of their cholesterol levels.
P862 Safety and efficacy of computed tomography inevaluation of coronary artery bypass grafts:comparison with invasive coronary angiography
M. Opolski1, C. Kepka1, J. Pregowski1, M. Kruk1, K.W. Fornalski2 ,Z. Juraszynski1 , A. Witkowski1, W. Ruzyllo1. 1Institute of Cardiology,
Warsaw, Poland; 2A. Soltan Institute for Nuclear Studies, Warsaw, Poland
Background: Computed tomography angiography (CTA) allows noninvasive eval-uation of coronary artery bypass grafts with a high diagnostic accuracy. However,the potential benefit-risk assessment for CTA after coronary artery bypass graft-ing remains unknown. We compared the safety and efficacy profiles between CTAand invasive coronary angiography (ICA) for the assessment of grafts in a singlehigh-volume center.Methods: Sixty one consecutive patients who underwent ICA for bypass graftsevaluation were compared to 60 consecutive patients examined by dual-sourceCT scanner with retrospective ECG gating (0.6 mm collimation, 330 ms gantryrotation time). The effective dose (ED) estimates based on the recommendedconversion factors, contrast volume and examination time were determined.Results: Compared to ICA, CTA studies showed higher ED (18.3±5.7 vs11.0±6.1mSv, p<0.001), less contrast volume (108±10.2 vs 129.4±46mL,p=0.001) and shorter examination time (9.3±6.2 vs 36.1±10.4min, p<0.001).Overall 21% (13 of 61) of patients in the ICA group had at least one graft notvisualized as compared to none in the CTA group (p<0.001). On a per-graft ba-sis, the CTA group had higher incidence of both visualized and interpretable graftscompared to the ICA group (2.3±0.85 vs 1.85±0.95, p=0.007).
Comparison between ICA and CTA Groups
ICA Group CTA Group p value(n=61) (n=60)
Age (yrs) 71.3±8.4 64.1±11.1 <0.001Men 50 (82%) 48 (80%) 0.820BMI (kg/m2) 28.4±3.0 32.1±33.9 0.396No. of grafts 2.2±0.9 2.3±0.8 0.234Contrast volume (mL) 129.4±46.0 108±10.2 0.001Examination time (min) 36.1±10.4 9.3±6.2 <0.001ED (mSv) 11.0±6.1 18.3±5.7 <0.001Pts with any graft not visualized 13 (21%) 0 (0%) <0.001Pts with any graft visualized but not interpretable 3 (5%) 2 (3%) 1.000Pts with all grafts visualized and interpretable 46 (75%) 58 (97%) 0.001
Conclusions: Compared to ICA, CTA provides more efficient method of bypassgraft visualization with shorter examination time and less contrast used, althoughat the expense of higher radiation dose.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

142 Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
P863 Left ventricular function and myocardial fibrosis inisolated left ventricular non-compaction: insights fromcardiac magnetic resonance imaging
G. Nucifora, G. Aquaro, A. Pingitore, P. Masci, M. Lombardi. CNR,Clinical Physiology Institute, Pisa, Italy
Purpose: Cardiac magnetic resonance imaging (MRI) allows accurate assess-ment of left ventricular (LV) function and myocardial fibrosis. However, its potentialclinical value in isolated LV non-compaction (LVNC) has been poorly investigated.Accordingly, the aim of the presence study was twofold. First, to comprehensivelyevaluate the morphological and functional LV features and the prevalence andextent of myocardial fibrosis in patients with isolated LVNC. For this purpose, cineand contrast-enhanced cardiac MRI (1.5 T scanner) were used, respectively. Sec-ond, to investigate the clinical and instrumental correlates of LV systolic function.Methods: The cardiac MRI database of our institution was searched for all pa-tients fulfilling the diagnostic criteria of isolated LVNC (i.e. 1) visual appearance oftwo distinct myocardial layers (a compacted epicardial layer and a non-compactedendocardial layer); 2) marked trabeculation and deep intertrabecular recesseswithin the non-compacted layer; 3) non-compacted to compacted end-diastolicmyocardial ratio >2.3 and 4) absence of other associated congenital or acquiredheart disease). For each patient, cine and contrast-enhanced cardiac MRI im-ages were analyzed to evaluate LV function and the prevalence and extent of lategadolinium enhancement (LGE), a surrogate of myocardial fibrosis.Results: A total of 29 patients (median age 42 years [interquartile range 22-55], 62% male) fulfilled the diagnosis of isolated LVNC. The median number ofLV non-compacted segments per patient was 3 (interquartile range 2-5). MedianLV end-diastolic volume index was 95 ml/m2 (86-122), while median LV ejectionfraction was 50% (36-63). LV dilatation (i.e. increased LV end-diastolic volumeindex) and LV dysfunction (i.e. reduced LV ejection fraction) were observed in 52%and 69% of patients, respectively. LV LGE was observed in 55% of patients, andthe median extent of LGE expressed as percentage of the LV mass (%LV LGE)was 2% (interquartile range 0%-7.5%). No relation was observed between thenumber of LV non-compacted segments and LV systolic function. At multivariateanalysis, only %LV LGE (β = -0.42, p = 0.004) was independently associated withLV systolic function.Conclusions: Myocardial fibrosis is observed in a non-negligible proportion ofpatients with isolated LVNC. Myocardial fibrosis is independently related to LVdysfunction in isolated LVNC, potentially contributing to the vicious circle of pro-gression of heart failure.
P864(W) Congenital heart disease and MRI: our experiencein neonates
G. Puppini1, M. Pilati2, A. Prioli2, D. Cenzi1, P. Biban3,G. Luciani4, C. Vassanelli2, S. Montemezzi1. 1Civil HospitalMaggiore at Borgo Trento, Department of Radiology, Verona,
Italy; 2Civil Hospital Maggiore at Borgo Trento, Department of CardiologyClinical, Verona, Italy; 3Civil Hospital Maggiore at Borgo Trento, Clinical Divisionof Pediatric, Verona, Italy; 4University of Verona, Department of Biomedical andSurgical Sciences, Section of Cardiovasc. Surgery, Verona, Italy
Purpose: Cardiac MRI is an important diagnostic tool for congenital heart dis-ease, as reflected by clear 1 reccomendations by various consensus panels. It isoften use as an alternative to echocardiography or angiography when this imag-ing modalities are unconclusive. Little is known about the clinical utility and safetyof MRI in very young babies. Aim of our study was to analyze the utility and thesafety in a group of neonates studied at our Institution.Methods and Materials: From December 2007 to December 2009 38 childrenunderwent cardiac MRI. All the exams were performed under general anaesthe-sia. The mean age was 3 months, mean weight was 4,6 kg. Indications for thestudies were a better definition of the vascular structures and an anatomical defi-nition before or after surgical correction.Results: During MRI no babies had complications. The mean duration time of theanaesthesia was 65 minutes and 50 minutes of the exams. 16 babies underwentMRI for the study of the aortic arch. 15 of these had an aortic coartation andsurgical correction was performed.9 babies underwent MRI for the study of major aortic-pulmonary collaterals andin all patients excepts 1, MRI images were confirmed by the surgical vision. 8babies were studied after surgical correction for the evaluation of conduits andpulmonary arteries and in 5 babies we performed MRI for a better evaluation ofcardiac anatomy in complex congenital disease.Conclusion: Cardiac MRI can be performed safely with low risk also in veryyoung babies. It provides key informations for their therapeutical mamagement.
P865 MRI based lesion formation comparison betweenradiofrequency and cryoballoon ablation in patientswith of paroxysmal atrial fibrillation
C. Mahnkopf, M. Daccarett, C. Mcgann, T.J. Badger, E. Kholmovski,T. Haslam, N. Burgon, R. Macleod, N. Akoum, N. Marrouche.
University of Utah, Comprehensive Arrhythmia Research and ManagementCenter, Salt Lake City, United States of America
Background: In both cryoballoon and radiofrequency ablation methods for the
treatment of paroxysmal atrial fibrillation (AF), electrical isolation is achieved byencircling the pulmonary vein’s (PV) antrum with lesions. Delayed Enhanced MRI(DE-MRI) is a proven method that can be used to stratify patients pre-ablationand delineate the amount of ablation lesion formation post-ablation. In this study,we aim to compare the pre and post-procedure lesion formation characteristics ofcryoballoon to radiofrequency ablation using DE-MRI.Methods: Patients presenting with paroxysmal AF who qualified for either a cry-oballoon or radiofrequency ablation were prospectively followed. DE-MRI of theleft atrium (LA) was performed prior to, immediately following, 24 hours and 3months post-procedure. The degree of LA fibrosis is reported as a percentage ofthe total LA area.Results: A total of 24 cases and 48 controls were included in the analysis. Elec-trical isolation of all pulmonary veins within the cryo group occurred in 21 (87.5%)patients and 48 (100%) in the radiofrequency group (p=0.03). Those patients withrecurrences were found to have a higher amount of fibrosis prior to ablation. Thelarger the number of veins encircled the greater the odds for a successful ablation(log OR=9.8, p=0.01).Conclusions: Our multicenter case control study represents the first prospectivelesion visualization comparing cryo-balloon vs. radiofrequency ablation. The re-sults suggest a similar pattern of LA structural remodeling caused by cryothermal,when compared to radiofrequency energy. The amount of LA fibrosis present pre-ablation as well as the number of PVs encircled post-ablation independently pre-dicts AF recurrence at 6 months. A study with larger patient population is neededto further detect outcome differences.
P866 Prognostic significance of late gadoliniumenhancement on cardiac magnetic resonance imagesin patients with hypertrophic cardiomyopathycompared with BMIPP and TL SPECT
H. Otsuki1, M. Momose2, T. Nakajima1, Y. Kasai3, A. Takara3 ,C. Kondo2, F. Kimura4, M. Kawana3, K. Kusakabe2, N. Hagiwara1. 1TokyoWomen’s Medical University, Department of Cardiology, Tokyo, Japan; 2TokyoWomen’s Medical University, Department of Diagnostic Imaging and NuclearMedicine, Tokyo, Japan; 3Tokyo Women’s Medical University, Aoyama Hospital,Tokyo, Japan; 4Saitama medical university International medical center,Department of Diagnostic Radiology, Saitama, Japan
Purpose: The purpose of the study is to assess prognostic significance of cardiacMR (CMR) compared to the other imaging and functional parameters in patientswith hypertrophic cardiomyopathy (HCM).Methods: Thirty-eight patients with HCM underwent CMR and BMIPP-TL dualSPECT. BM-TL images were divided into 17 segments, where each segment wasscored 0-4 (0: normal, 4: defect). Total defect score of BM and TL were calcu-lated (BMDS,TLDS). MRI images were also divided into the same segments, andnumber of late gadolinium enhancement segments was calculated (LGE score).LV ejection fraction (EF) and EDV were measured by CMR. Mean follow up pe-riod was 3.1years. All cardiovascular events including cardiac death, heart failure,fatal arrhythmia, and stroke were investigated.Results: Thirteen patients (34%) had cardiovascular events. There was a sig-nificant difference in LGE score between patients with cardiovascular events andthose without (p=0.0013). Kaplan-Meier analysis revealed that LGE score ≥3 hadmuch higher 3-years cardiovascular event rate than LGE score <3 (67% vs. 20%,log rank test: p=0.0017). BMDS also showed a significant difference betweenpatients with cardiovascular event and those without (p=0.03), and there was asignificant difference in Kaplan-Meier analysis (BMDS≥6 vs. BMDS<6, 71% vs.25%, log rank test: p=0.039). TLDS, EF, EDV were not significant predictor of car-diovascular events. Coxhazard multivariate analysis showed LGE score was theonly independent predictor of cardiac events (Wald χ2= 10.3, p=0.0013).
Conclusions: LGE on CMR may be a useful predictor of prognosis in patientswith HCM compared to myocardial perfusion, metabolic and cardiac functionalparameters.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) 143
P867 Arrhythmogenic cardiomyopathy,patterns ofventricular involvement using cardiac magneticresonance
B. Igual Munoz1, E. Zorio Grima1, A. Maceira Gonzalez1, P. LopezLereu1, J. Estornell Erill1, J.V. Monmeneu Menadas1, V. Miro Palau1,A. Quesada Carbona1, A. Lucas1, A. Salvador Sanz2. 1ERESA,
Hospital La Fe, Valencia, Spain; 2Hospital La Fe, Valencia, Spain
Recently, biventricular (ABVC) and left dominant arrhythmogenic cardiomyopathy(LDAC) had been included in the spectrum of arrhythmogenic cardiomyopathy(AC). The aim of the study was to describe, using cardiac magnetic resonance,the patterns of ventricular involvement as well as of late gadolinium enhancement(LGE).Methods: Medical records and databases from 3 hospitals were reviewed in orderto obtain data of patients with AC. Diagnosis of classic ARVC and BVAC wasmade based on Task Force criteria. LDAC was diagnosed if LGE was presentalong with positive family history.Results: 21 consecutive patients were included (38+15yrs, 13 males). Diagnoseswere LDAC in 5 patients (24%), BVAC in 8 (38%) and ARVC in 8 (38%). Right ven-tricular involvement was present in 17 patients (81%). Among them, 10 patients(48%) had ventricular volumes over the upper limit of normality and 7 patients(33%) had mild involvement with wall motion abnormalities and microaneurysms.Also, 10 patients (47%) showed LGE in the right ventricle and 21 patients (100%)in the left ventricle. LGE was more frequent in the inferior and lateral walls (15 pa-tients, 71%) while septum was seldom affected (6 patients, 29%). Usually, LGEwas subepicardial (10 patients, 48%), but in some cases transmural (4 patients,19%) and intramyocardial (2 patients, 10%) LGE were observed. Left ventriclesystolic dysfunction (LVEF<55%, 15patients, 71%) and left ventricular dilatation(LVEDVi>98ml/m2, 24 patients, 19%). Finally, LDAC was the most frequent find-ing in patients referred from the Sudden Cardiac Death Unit (5 patients, 56%),while ARVC was the most frequent abnormality in patients referred from the Ar-rhythmia Unit (5patients, 71%) and BVAC in those referred from the Cardiomy-opathy Unit (3 patients, 60%).Conclusions: LV involvement is the most frequent abnormality found in AC, LGEwas seen in the left ventricle in all the patients studied. LGE was more frequentlysubepicardial and located in the inferior and lateral walls.
P868 Quantification of aortic valve stenosis by a rapidcardiac magnetic resonance protocol: Comparisonwith echocardiography
D.V. Anand, T.R. Burchell, S.A. Mohiddin, L.C. Davies, S.E. Petersen,M.A. Westwood. Barts and The London NHS Trust, London, United
Kingdom
Purpose: Cardiac magnetic resonance (CMR) is an evolving technique for theassessment of aortic valve disease. It can visualise the aortic valve with high res-olution and is independent of acoustic windows. The accuracy of a CMR protocolin which a quick routine assessment of the aortic valve was done, but did not formthe main clinical indication for the study, for quantifying stenotic valve area wasevaluated in comparison to transthoracic echocardiography (TTE).Methods: Out of 2,300 clinical CMR scans done in 2009 (Philips 1.5-T scanner),30 consecutive patients with aortic stenosis who underwent both CMR and TTEwere studied. Our scanning protocol included two long axis cine images of theleft ventricular outflow tract, a velocity encoded flow map piloted perpendicular tothe LVOT views and performed at the level of the sinotubular junction and a cross-sectional cine image across the aortic valve to measure aortic valve area (AVA) byplanimetry. Peak transvalvular gradient was estimated by the modified Bernoulliequation. Estimation of AVA by planimetry was performed in 16 patients. AVA onTTE was estimated from the continuity equation. Correlation between CMR andTTE was tested by regression analysis.Results: Mean age of the patients studied was 64±15 yrs (range 25 – 89 yrs)and 67% were male. 25 patients had calcific aortic stenosis with trileaflet valves.Four patients had bicuspid valves and one patient had supravalvular aortic steno-sis which was correctly identified by CMR. Aortic regurgitation (at least mild) waspresent in 11 patients (37%) and severe in two patients. LV function was signifi-cantly impaired (EF < 35%) in 6 patients (20%). By TTE, mean peak transvalvulargradient was 48 mm Hg (range 19 mm Hg to 130 mm Hg) and mean AVA was 1.2cm2 (range 0.6 cm2 to 1.8 cm2). 8 patients (27%) had severe aortic stenosis. ByCMR, mean peak transvalvular gradient was 38 mm Hg (18 mm Hg to 100 mmHg) and mean AVA by planimetry was 1.4 cm2 (range 0.5 cm2 to 1.8 cm2). Thecorrelation coefficient between peak pressure gradients on CMR and TTE was r= 0.73. The correlation coefficient between AVA estimated by planimetry (CMR)and by continuity equation (TTE) was r = 0.65.Conclusion: A rapid CMR protocol incorporating the routine assessment of theaortic valve by velocity encoded flow mapping and planimetry can be performed inless than 5 minutes and still provides a robust assessment of stenotic aortic valvearea that correlates well with the accepted standard of TTE. The high resolutionof CMR makes it an attractive alternative modality to TTE in the assessment ofaortic valve disease.
P869 Insights into differential regional aortic distensibility inearly chronic kidney disease: a cardiac magneticresonance study
C.D. Chue1, N.C. Edwards1, C.J. Ferro2, C.M. Jones2, J.N. Townend2 ,R.P. Steeds2. 1University of Birmingham, Birmingham, United
Kingdom; 2Queen Elizabeth Hospital, Birmingham, United Kingdom
Background and Objective: The biophysical properties of the aorta vary alongits length with a fall in elastin: collagen ratio proximally to distally. Ageing pref-erentially reduces proximal distensibility. Increased aortic stiffness independentlypredicts adverse cardiovascular outcomes in chronic kidney disease (CKD). Theimpact of CKD on relative contributions of different regions of the aorta to the to-tal "cushioning" effect on left ventricular phasic ejection is unclear. We sought todetermine effects of CKD on regional aortic distensibility using cardiac magneticresonance (CMR) imaging.Methods: 134 patients with stage 2 and 3 non-diabetic CKD were compared to40 non-CKD controls. Aortic distensibility was assessed using CMR (1.5T). As-cending, proximal descending and distal descending aortic distensibility and totalarterial compliance index were calculated using previously validated formulae.Results: Groups were well matched demographically (table). Aortic distensibil-ity increased from ascending to distal descending aorta in both groups. CKDwas associated with significant reductions in aortic distensibility at all three lev-els and reduced total arterial compliance index compared to controls. Regionalheterogeneity in distensibility was preserved as both relative and absolute differ-ences between ascending and distal descending distensibility were similar in bothgroups.
Controls (n=40) CKD (n=134) p value
Age (years) 50.7 53.3 0.15Males 52% 62% 0.26Pulse Pressure (mmHg) 52.2±12.9 55.3±12.7 0.18Ascending Distensibility 4.05±2.1 2.92±1.9 0.002Proximal Descending Distensibility 4.37±1.7 3.39±1.7 0.001Distal Descending Distensibility 5.61±1.8 4.50±2.3 0.005Absolute Asc: Distal Descending Distensibility -1.56 1.6 -1.59 1.6 0.92Relative Asc: Distal Descending Distensibility 0.71±0.3 0.64±0.3 0.15Total Arterial Compliance Index 0.89±0.3 0.75±0.2 0.002
Mean±SD.
Conclusion: Stiffening increases throughout the aorta in patients with earlychronic kidney disease without significant regional differences. This differs fromageing alone, suggesting that processes other than altered elastin: collagen ratiocontribute to increased aortic stiffness.
P870 High field cardiac magnetic resonance diagnosis ofmurine bicuspid aortic valve
D.K. Dawson1, M.A. Jansen1, D.G. Brownstein1, G.D. Merrifield1,S.H. Ralston2, G.A. Gray1, D.E. Newby1, J.J. Mullins1, K.A.A. Fox1.1University of Edinburgh, Centre for Cardiovascular Science,
Edinburgh, United Kingdom; 2University of Edinburgh, Edinburgh, UnitedKingdom
Background: Bicuspid aortic valve (AV) is the commonest congenital abnormal-ity present in the adult population, leading to considerable morbidity, thereforeexperimental models to study potential therapeutic interventions at an early stagewould be of interest.Methods: We studied 17 eNOS-/- mice [10 obtained by disruption of exons 24and 25 (eNOS-/-24,25), 7 by disruption of exon 12 (eNOS-/-12)] and 4 C57Bl/6mice, all at 12 weeks of age (22-28 grams). All mice underwent high field car-diac magnetic resonance (CMR) imaging on a 7T Varian scanner under inhaled1.6% isoflurane anaesthesia with a 39 mm coil, an ECG-gated FLASH sequencewith the following imaging parameters: TR/TE=2.9/1.1 msec, 192x192 matrix,FoV 15x15 mm, yielding superb temporal resolution at 38 frames/cardiac cycle.Mice were euthanized, hearts dissected out, fixed in 10% formalin, embedded inparaffin and 4μm step serial sections were stained with hematoxylin-eosin.Results: High field imaging was feasible with a reproducible protocol and the
Bicuspid (top) and tricuspid (bottom) AV
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

144 Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI)
AV plane was obtained in all cases. 29% of the eNOS-/-12 strain demonstratedbicuspid AV; the eNOS-/-24,25 and C57Bl/6 mice had tricuspid AV. Two indepen-dent blinded readers scored all images (minimum 2 cines/mouse) with excellentlimits of agreement between them (kappa=0.88, p<0.0001) and with histology(kappa=1, p<0.0001 for Reader 1 and kappa=0.88, p<0.0001 for Reader 2). Thefigure shows examples of end-diastolic (a) and end-systolic (b) frames and his-tology (c) of a bicuspid and end-diastolic (d) and end-systolic (e) frames andhistology (f) of a tricuspid AV.Conclusions: High field CMR is well suited for visualisation of murine AV andallows precise in vivo differentiation of bicuspid from tricuspid AV. The presenceof bicuspid AV in the eNOS-/- model is strain specific.
P871 Hemodynamic evaluation of aortic regurgitation aftertranscatheter aortic valve implantation usingcardiovascular magnetic resonance
M. Sherif1, M. Abdel-Wahab1, H.-W. Beurich1, B. Stoecker1,D. Zachow2, V. Geist1, R. Toelg1 , G. Richardt1. 1Segeberger
Clinics, Cardiovascular Center, Bad Segeberg, Germany; 2Segeberger Clinics,Radiology Clinic, Bad Segeberg, Germany
Background: Echocardiography may underestimate the degree of paravalvularaortic regurgitation (AR) after transcatheter aortic valve implantation (TAVI) usingthe Medtronic CoreValve due to inherent limitations of ultrasound imaging in theevaluation of implanted cardiac prostheses.Aim: To evaluate the accuracy and feasibility of cardiovascular magnetic reso-nance (CMR) in quantifying regurgitant volume (RV) and regurgitant fraction (RF)in patients treated with Medtronic CoreValve for severe calcific aortic stenosis,and to compare the results with echocardiography and aortography.Methods & Results: This study included sixteen patients with a mean age of78.7 years (8 women, 8 men) who underwent successful TAVI using MedtronicCoreValve. AR was evaluated by CMR, echocardiography, and aortography. An-giography was performed immediately after valve implantation. CMR and echo-cardiography were performed before hospital discharge. There was a highly sig-nificant correlation between the CMR-derived and the angiographically-estimateddegree of AR (r=0.86, p<0.001). On the other hand, there was only a limitedcorrelation between CMR and echocardiography (r=0.374, p=0.15) as well asangiography and echocardiography (r=0.319, p=0.23) regarding the degree ofAR. The weighted kappa for agreement between echocardiography and angiog-raphy was 0.14, for agreement between echocardiography and CMR 0.20, andfor agreement between angiography and CMR 0.72. Echocardiography underes-timated AR by one degree compared to CMR in 5 patients and 2 degrees in 2patients; in 6 of these, the degree of AR obtained by CMR was similar to angiog-raphy.Conclusion: In patients undergoing TAVI, comparisons between purely quanti-tative measurements of AR by CMR and qualitative assessment by angiographyshowed better correlations than those with echocardiography. This suggests thatechocardiography may underestimate the degree of AR and CMR in these cir-cumstances has a great potential in reliably measuring the severity of AR in aquantitative manner.
P872 Non-invasive evaluation of left atrial appendagemechanical function and risk of LAA thrombogenesisin patients with AtrialFfibrillation (AF) using MRI vsTOE
A.S. Jadidi, M. Lederlin, M. Montaudon, A. Forclaz, S. Miyazaki,I. Nault, N. Sacher, N. Derval, F. Laurent, P. Jais. Hôpital Cardiologique
du Haut-Lévêque, Université Victor Segalen Bordeaux II, Bordeaux, France
Non-invasive evaluation of left atrial appendage (LAA) mechanical function andrisk of LAA thrombogenesis in patients with atrial fibrillation (AF) using MRI vsTOEIntroduction: AF is associatedwith embolic accidents and mortality. The longerthe atria fibrillate, thegreater the electrical/structural remodelling, atrial stunningand likelyhoodof stasis generated thrombi. Transoesophageal echocardiography(TOE) allows toevaluate the LAA mechanical function and risk of LAA throm-boembolisation. Weevaluated LAA mechanical function and thrombogenic risk inAF patients usingnon-invasive MRI.Methods: 45 patientsunderwent 1 day prior to AF ablation both TOE and MRI.TOE evaluated peak LAAemptying velocity (Vep), presence of spontaneous con-trast (SC) or thrombi and biplane LAA shorteningfraction (LAASF). MRI deter-mined LAA max. diastolic and systolic volume,LAA ejection fraction (LAAEF),LAAemptying velocity (Vemax, Vemean). MRI parameters were compared to the4mentioned classical TOE parameters.Results: We found a high correlation between LAAEF mesured at MRI and bothTOEmesured Vep and LAASF (r=0.79 and r=0.91).MRI derived total LAAEF ranged from 0.12 to 0.77. MRI showed an LAA-EFof0.56±0.16, 0.30±0.12 and 0.21±0.07 for patients without SC at TOE,with SCand with LAA thrombus at TOE, respectively.Conclusions: Non-invasive evaluation of the LAA contractile functionusing MRIshows a high correlation to clinically established evaluation of LAAby semi-invasive TOE. MRI allows to evaluate LAA contractile function andthromboem-bolic risk both during AF and SR in patients with AF. Future studiesneed to show
LAA contractiliy and thrombus,MRI vs TOE
the if LAA-contractility as assessed by MRI can guide indicationfor anticoagulationin patients with AF (prior and after AF ablation).
P873 Right ventricular function, assessed by cardiacmagnetic resonance and cardiovascular outcomes inpatients undergoing open heart surgery
L. Lella, G. Bhumireddy, Y. Goldsmith, I. Ahmad, J. Fogel, A. Tortolani,L. Lee, S. Brener, T. Sacchi, J. Heitner. New York Methodist Hopital,
Brooklyn, United States of America
Background: Abnormal right ventricular ejection fraction (RVEF) is known to beassociated with poor outcomes in patients (pts) with severely reduced left ventric-ular ejection fraction (LVEF) undergoing coronary artery bypass grafting (CABG).However, there is scant data evaluating the significance of RVEF independent ofLVEF, in pts undergoing both CABG and valvular surgery.Objective: To determine the significance of abnormal RVEF, independent ofLVEF, in predicting in-hospital and long-term outcomes of pts who undergo open-heart surgery.Methods: We prospectively evaluated 109 consecutive pts referred for pre-operative cardiac magnetic resonance prior to open-heart surgery. RVEF andLVEF were calculated by computer analysis after region of interest curves wereperformed by blinded investigators. Abnormal RVEF and LVEF were considered<35% and <45%, respectively. In-hospital outcomes included length of hospitalstay and duration of mechanical intubation; long-term outcomes included wors-ening congestive heart failure, defined by a decrease in NYHA classification, orre-hospitalization for a cardiac etiology. Follow-up data were obtained via phoneinterview and hospital records. Pts were stratified by the type of surgery: CABG(n=64) or valve surgery (n=45). Analysis of covariance and multivariate logis-tic regression analyses were performed and all analyses were adjusted for age,gender, hypertension, previous myocardial infarction, previous CHF, diabetes andLVEF.Results: The mean age of the sample was 64±19 years and 68 were female.The mean RVEF for pts with reduced systolic function (n=48) compared to ptswith normal RVEF (n=61) was 24% vs 49%, respectively. The mean LVEF for ptswith reduced systolic function (n=54) compared to pts with normal LVEF (n=55)was 28% vs 59%, respectively. The mean follow up was 15±3.5 months. Onmultivariate logistic regression analysis in all surgical pts, an abnormal RVEFhad a greater percentage of re-hospitalization than those with preserved RVEF(31% vs. 13%, OR= 3.05, p=0.02). Abnormal RVEF was a better predictor of re-hospitalization than abnormal LVEF (31% vs. 20%, respectively, OR=3.1, 95% CIof 1.1-9.4, p=0.02). In CABG pts, abnormal RVEF was significantly associatedwith a prolonged hospital stay (mean-17.9 days vs. 12.9 days, p= 0.03). Abnor-mal RVEF was not significantly associated with either in-hospital or long-termoutcomes in the valvular surgery pts.Conclusion: Abnormal RVEF is a stronger predictor for re-hospitalization thanabnormal LVEF in pts who undergo open-heart surgery.
P874 Right ventricular reverse remodelling after pulmonarythrombendarterectomie (PEA) for chronicthrombembolic pulmonary hypertension (CTEPH) bycardiac MRI
A. Rolf1, J. Rixe1, J. Wilhelm1, H. Mollmann1, H.M. Nef1, T. Kramm2,S. Guth2, E. Mayer2 , C. Hamm1, T. Dill1. 1Kerckhoff-Heart-Center,
Bad Nauheim, Germany; 2Kerckhoff-Thorax-Center, Bad Nauheim, Germany
Introduction: About 5% of all patients suffering acute pulmonary embolism willdevelop chronic thrombembolic pulmonary hypertension (CTEPH). This in turncauses continuous detoriation of right ventricular function. Pulmonary thromben-darterectomy (PEA) is a possible cure of this condition with favourable long termprognosis.Cardiac magnetic resonance imaging (cMRI) is an excellent tool for measurementof right ventricular volumes and function.Purpose: This study seeks to measure the changes of right ventricular geom-etry before and after PEA by cMRI and determine its accuracy as compared toinvasive right heart catheter measurements (RHC).Methods: 32 patients (age 67±23) underwent CINE TruFISP MRI (1.5 T,Siemens Sonata) 2 days before and 10±1 days after PEA, volumetric analysis
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Update on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) / YIA Session: Clinical Science 145
was performed on 10 contiguous short axis slices covering the whole right ventri-cle with the Siemens Argus Tool. Ejection Fraction (RVEF), Enddiastolic (RVEDV)-, Endsystolic (RVESV) and stroke (RVSV) volumes as well as right ventricularmass (RVMass) were computed. RVSV and RVEF measurements were corre-lated with pre- and postoperative invasive measurements of cardiac outpout (CO)by PA-catheter.Results: Noninvasive measurements of RVSV and RVEF showed good correla-tion with invasive CO measures (r = 0.6, p = 0.018 for SV and r = 0.66, p = 0.019for EF). RVEF, RVEDV and RVESV improved significantly over time while RVMassremained unchanged (RVEF from 19.6±6.5 to 41.8±10.3 p = 0.0001, RVEDVfrom 187.8±49 to 159.8±62.3 p = 0.03, RVESV from 151.6±42.2 to 94.4±47.4 p= 0.0001, RVMass from 65.8±25.3 to 63.1±19.7 p = 0.67).Conclusion: cMRI measurement showed good accuracy compared with PA-cathmeasurements. It is an excellent tool to document acute changes of RV-functionand volumes before and after PEA. It shows immediate and significant improve-ment of both right ventricular function and volumes as early as ten days postsurgery.
YOUNG INVESTIGATORS AWARDS SESSIONCLINICAL SCIENCE
876 Exercise pulmonary hypertension predicts theoccurrence of symptoms in asymptomatic degenerativemitral regurgitation
J. Magne, K. O’connor, G. Romano, M. Moonen, P. Lancellotti,L.A. Pierard. University of Liege - Sart Tilman, Liege, Belgium
Background: Current ACC/AHA guidelines recommend mitral valve surgery forasymptomatic patients with severe degenerative mitral regurgitation (MR) andpreserved left ventricular systolic function when exercise pulmonary hyperten-sion (PHT) is present. However, the determinants of exercise PHT have not beenevaluated. The aim of this study was to identify the determinants of exercise PHTand the impact on symptom-free survival.Methods and results: Comprehensive resting and exercise transthoracic echo-cardiography were performed in 78 consecutive asymptomatic patients (61±13years, 56% males) with ≥ moderate degenerative MR (effective regurgitant ori-fice [ERO] area =43±20mm2, regurgitant volume [RV] =73±36ml). Resting andexercise PHT were defined as a systolic pulmonary arterial pressure (SPAP)>50mmHg and >60mmHg, respectively. Exercise PHT was more frequent thanresting PHT (48% vs. 15%, p<0.001). In multivariable analysis, exercise EROwas an independent determinant of exercise SPAP (p<0.0001) and exercisePHT (p=0.002). Follow-up collection was complete in 78 (100%) patients witha mean follow-up of 19±14 months (range: 2-56). During follow-up, 40 patients(51%) remained asymptomatic whereas 38 (49%) developed symptoms. In thewhole cohort, symptom-free survival was 71±5%, 54±6% and 40±7% at 1-, 2-and 3-year, respectively. Resting PHT and exercise PHT were associated withmarkedly reduced 2-year symptom-free survival (36±14% vs. 59±7%, p=0.04;35±8% vs. 75±7%, p<0.0001). After adjustment for age and sex, the impactof resting PHT on symptoms was no longer significant. Multivariable Cox pro-portional hazard model identified exercise PHT as an independent predictor ofthe occurrence of symptoms (Hazard-ratio=2.8, 95% confidence interval: 1.4-5.4,p=0.002). Receiver-operating characteristics curves revealed that exercise SPAPwas more accurate than SPAP to predict the occurrence of symptoms duringfollow-up (p=0.032). SPAP> 56mmHg predicted symptoms with good specificity(73%) and sensitivity (82%).Conclusions: Exercise PHT is frequent in patients with asymptomatic degen-erative MR. Exercise MR severity is a strong independent predictor of both ex-ercise SPAP and exercise PHT. Exercise PHT is associated with markedly low2-year symptom-free survival emphasizing the use of exercise stress echocar-diography. An exercise SPAP >56mmHg accurately predicts the occurrence ofsymptoms.
877 Direct comparison of three high-sensitive cardiactroponin assays in the early diagnosis of acutemyocardial infarction -insights from a multicenter study
R. Twerenbold1 , M. Reiter1, T. Reichlin1, J. Meissner1, C. Heinisch1,T. Socrates1, N. Arenja1, T. Breidthardt1, W. Hochholzer2 , C. Mueller1.
1University Hospital Basel, Basel, Switzerland; 2Harvard Medical School,Boston, United States of America
Purpose: High-sensitive troponin (hs-Tn) assays have been shown to signifi-cantly improve the early diagnosis of acute myocardial infarction (AMI). Severalhs-Tn assays that vary considerably in their analytic sensitivity have recently be-come clinically available. Some of these allow the detection of Tn in about 50%of healthy individuals, others are even more sensitive and allow the detection ofTn in up to 90% of healthy individuals. It is unknown, whether this difference inanalytic sensitivity among hs-Tn assays will translate in differences in clinical per-formance.Methods: We conducted a multicenter study to examine the diagnostic accuracyof three hs-Tn assays performed on blood samples obtained in the emergencydepartment from 1087 consecutive patients who presented with symptoms sug-
gestive of acute myocardial infarction. Cardiac troponin levels were determined ina blinded fashion with the use of two hs-Tn assays (Abbott–Architect TnI, SiemensTnI Ultra) that allow the detection of Tn in about 50% of healthy individuals, a hs-Tn assay that allows the detection of Tn in 90% of healthy individuals (Rochehs-TnT) and a conventional Tn assay (Roche TnT). The final diagnosis was adju-dicated by two independent cardiologists.Results: AMI was the adjudicated final diagnosis in 173 (16%) patients. The di-agnostic accuracy for measurements obtained at presentation, as quantified bythe area under the receiver operating characteristic curve (AUC), was similar inall three hs-Tn assays (Architect TnI 0.945; 95% CI 0.929 to 0.957, TnI Ultra0.950; 95% CI 0.935 to 0.962, hs-TnT 0.945; 95% CI 0.929 to 0.957, p=ns forall comparisons among hs-Tn assays) and significantly higher than the conven-tional TnT assay (0.887; 95% CI 0.867 to 0.905, p<0.01 for all comparisons). Inpatients presenting within three hours after the onset of chest pain (n=382, 48patients with AMI), the AUC remained similar among the three hs-Tn assays (Ar-chitect TnI 0.909; 95% CI 0.876 to 0.935, TnI Ultra 0.936; 95% CI 0.907 to 0.959,hs-TnT 0.903; 95% CI 0.868 to 0.930, p=ns for all comparisons among hs-Tn as-says) and significantly lower for the conventional TnT assay (0.750; 95% CI 0.703to 0.792, p<0.001 for all comparisons).Conclusions: The diagnostic performance of hs-Tn assays is excellent, andthese assays can substantially improve the early diagnosis of AMI, particularly inpatients with a recent onset of chest pain. Analytic differences regarding sensitiv-ity in the normal range among hs-Tn assays do not seem to be clinically relevantin the diagnosis of AMI. (ClinicalTrials.gov number, NCT00470587)
878 The effect of erythropoietin as an adjunct to PPCI: arandomised controlled trial
A.J. Ludman1, J.M. Hasleton1, V. Venugopal1 , G. Babu1, J.C. Moon2,V. Muthurangu3 , A. Taylor3 , R. Puranik3, D.M. Yellon1, D.J. Hausenloy1.1University College London, London, United Kingdom; 2The Heart
Hospital, London, United Kingdom; 3Great Ormond Street Hospital for Children,London, United Kingdom
Purpose: Administration of erythropoietin (EPO) at the onset of myocardial reper-fusion reduces myocardial infarct (MI) size by 50% in animal studies. WhetherEPO is beneficial when administered as an adjunct to primary percutaneouscoronary intervention (PPCI) is unknown and is investigated in this randomisedplacebo controlled clinical trial.Methods: 51 STEMI patients presenting for PPCI within 12 hours of chest painwere randomised to receive either intravenous EPO (50,000iu in 10mls) prior toPPCI with a further bolus given 24 hours later, or placebo. Both patient and car-diologist were blinded to the treatment allocation. 24 hour area under the curve(AUC) Troponin-T and CK-MB were measured. Cardiac MR was performed at day2 and 4 months, and were analysed by two blinded observers. The area at riskwas determined by infarct endocardial surface area on CMR and modified BARIand APPROACH jeopardy scores on coronary angiography.Results: Treatment with EPO doubled the incidence of microvascular obstruction(MVO), acutely increased both LV chamber size (indexed LV end diastolic andsystolic volumes: LVEDVi and LVESVi) and index myocardial mass on the initialCMR scan (see table). However, there were no significant differences in MI size(measured by cardiac enzymes or CMR), the myocardial salvage index (MSI)or LV ejection fraction. On repeat CMR at 4 months there were no significantdifferences between the two groups.
Endpoints day 2 post-PPCI
Endpoint Placebo Erythropoietin P value
LV ejection fraction (%) 53 (10) 51 (7) 0.4824 hr AUC Trop-T (μg/l) 101.7 (76.5) 114.6 (78.3) 0.56Infarct mass (g) 25.4 (16.3) 32.8 (15.5) 0.15MSI 0.36 (0.23) 0.29 (0.17) 0.28MVO (% incidence) 47 82 0.02*LVEDVi (ml/m2) 73 (13) 84 (10) 0.003*LVESVi (ml/m2) 34 (11) 41 (9) 0.035*LV mass (indexed, g/m2) 79.4 (11) 89.2 (16) 0.031*
Data are % (SD)or mean (SD).
Conclusions: The administration of EPO as an adjunct to PPCI has detrimentaleffects: it doubled the incidence of MVO; induced acute LV dilatation; and acutelyincreased myocardial mass. This study highlights the importance of using CMRto assess the safety and efficacy of new reperfusion treatment strategies.
879 Cerebral magnetic resonance imaging unmasksmicroembolic cerebral lesions after transcatheter aorticvalve implantation
S. Blazek1, R. Vollmann2, J. Simbrunner2, O. Luha1, R. Hoedl1,G. Stoschitzky1, B. Pieske1, R. Maier1. 1Medical University of
Graz, Department of Cardiology, Graz, Austria; 2Medical University of Graz,Department of Neuroradiology, Graz, Austria
Purpose: Transcatheter aortic valve implantation (TAVI) is an emerging alterna-tive treatment option for patients with symptomatic severe aortic stenosis (AS)and high risk for operative valve replacement. However, stroke can be a catas-trophic complication of TAVI. Stroke has been reported to occur in up to 6.3% of
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

146 YIA Session: Clinical Science / YIA Session: Basic Science
patients undergoing TAVI. This study aimed to assess frequency and extent ofsubclinical microembolic cerebral lesions after TAVI.Patients and methods: In our institution, 46 patients (15 male, 31 female; meanage 81±5 years) with symptomatic severe AS underwent TAVI between July 2008and November 2009. The self-expanding CoreValve prosthesis was implanted viatransfemoral access using the current 18 French delivery catheter system. 37 pa-tients were scheduled for cerebral diffusion-weighted magnetic resonance imag-ing (DW MRI) two days before and up to six days after TAVI. Nine patients werenot eligible due to pacemaker implantation prior to enrolment. 25 patients under-went both pre- and postinterventional DW MRI, while twelve patients could notundergo postinterventional MRI and had to be excluded from analysis (need forpermanent pacemaker implantation, n=2; critical status, n=5; MRI not available,n=5).Results: Thorough physical examination did not reveal any changes in neuro-logical status after TAVI. However, comparison of pre- and postinterventional DWMRI showed that 23 of 25 patients (92%) had newly acquired bright lesions (p<0.001) in accordance with subclinical cerebral embolisation: class I (1-3 newbright lesions), n=9 (36%); class II (4-7 new bright lesions), n= 8 (32%); class III(≥8 new bright lesions or cortical infarction), n=6 (24%). Only in two patients (8%)there was no evidence for any newly acquired bright lesion (class 0).Conclusion: TAVI with the self-expanding CoreValve bioprosthesis is an emerg-ing alternative treatment option for high-risk patients with symptomatic severeAS. Albeit risk of stroke is low, the vast majority of patients show newly acquiredbright lesions in DW MRI compatible with subclinical cerebral embolisation. In thenear future embolic protection devices along with a more detailed assessment ofthe aorta, improved techniques and less traumatic catheters might contribute tominimize cerebral microembolisation and even stroke.
YOUNG INVESTIGATORS AWARDS SESSIONBASIC SCIENCE
881 Genetic deletion of isoforms 1 and 4 of the plasmamembrane calcium pump reveals their differential andimportant roles in cardiac contractility
T.M.A. Mohamed, M. Shaheen, M. Zi, S. Prehar, N. Alatwi, F. Baudoin,R. Abou-Leisa, D. Oceandy, E.J. Cartwright, L. Neyses. University of
Manchester, Manchester, United Kingdom
Recent human genome-wide association studies have linked two members ofa family of calcium pumps, plasma membrane calcium ATPase isoforms 1 and4 (PMCA1 and 4) to clinically important cardiovascular dysfunctions. PMCA1is strongly associated with arterial hypertension, whilst PMCA4 complexed withneuronal nitric oxide synthase (nNOS) has been implicated in the modulation ofQT interval. We have previously shown that cardiac overexpression of PMCA4through its interaction with nNOS modulates the cardiac beta-adrenergic re-sponse (Mohamed et al., JBC, 2009). To understand the role of these genes incardiac physiology we generated and studied mice carrying a genetic deletion ofeither PMCA1 or PMCA4.In vivo basal contractility was enhanced in PMCA4 KO mice (dP/dtmax in8049±628 versus 6604±296 mmHg/s in KO and WT respectively, p<0.05, n=10)with no change in the relaxation rate. Ca2+ transients in cardiomyocytes (CMC)from PMCA4 KO mice showed an increase in amplitude (298.8±24.3nM cal-cium vs 492.2±28.2nM calcium in WT and KO respectively; p<0.05, n=8) with nochange in the rate of Ca2+ decay. This phenotype was imitated by nNOS specificinhibition in WT adult CMC. Although, there is no difference in total nNOS proteinexpression between PMCA4 KO and WT, the nNOS localisation and activity atthe sarcolemmal membrane was decreased by 52% in PMCA4 KO. cGMP levelsin PMCA4 KO mice were markedly decreased suggesting that the phenotype waslikely through nNOS modulation.Since the global deletion of PMCA1 is embryonic lethal, we generated PMCA1cardiomyocyte-specific knockout mice (PMCA1cko) using Cre/LoxP technology.PMCA1cko showed a reduction in the relaxation rate (indicated by an increase inlogistic Tau; 6.9±0.34 versus 5.8±0.29 msec in PMCA1cko and PMCA1flox/floxcontrol respectively; p<0.05, n=11) without any change in cardiac contractil-ity. CMC from PMCA1cko revealed a decreased rate of Ca2+ decay (Tau,0.201±0.009 versus 0.164±0.006 msec in PMCA1cko and PMCA1flox/flox re-spectively; p<0.05, n=16), whilst Ca2+ transient amplitude remained unchanged.The nNOS protein expression, localisation and activity in PMCA1cko mice weresimilar to those in PMCA1flox/flox.In conclusion, using genetically modified mice we have assigned entirely novel,highly differentiated and isoform-specific functions to the cardiac PMCAs. BothPMCA1 and PMCA4 have important roles in cardiac contractility; PMCA4 regu-lates cardiac signalling through modulation of membrane nNOS activity, whilstPMCA1 directly modulates diastolic calcium during excitation-contraction cou-pling.
882 Cardiac raptor deletion impairs adaptive hypertrophy,alters metabolic gene expression and causes heartfailure in mice
P. Shende1, I. Plaisance1, C. Morandi1 , C. Pellieux2, C. Berthonneche3 ,R. Lerch2, M. Hall4, M. Ruegg4, T. Pedrazzini3 , M. Brink1. 1University
Hospital Basel, Department of Biomedicine, Basel, Switzerland; 2UniversityHospital of Geneva, Department of Cardiology, Geneva, Switzerland; 3Universityof Lausanne Medical School, Department of Medicine and CardiovascularAssessment Facility, Lausanne, Switzerland; 4University of Basel, Biozentrum,Basel, Switzerland
Background: Mammalian target of rapamycin (mTOR), a central regulator of cellgrowth, is found in two structurally and functionally distinct multiprotein complexescalled mTOR complex (mTORC)1 and mTORC2. The specific roles of each ofthese branches of mTOR signaling have not been dissected in the adult heart.In the present study, we aimed to bring new insights into the function of cardiacmTORC1-mediated signaling in physiological as well as pathological situations.Methods: We generated mice homozygous for loxP-flanked raptor and positivefor the tamoxifen-inducible Cre recombinase (MerCreMer) under control of the α-myosin heavy chain promoter. The raptor gene encodes an essential componentof mTORC1. Gene ablation was induced at the age of 10-12 weeks, and twoweeks later the raptor cardiac-knockout (raptor-cKO) mice started voluntary cage-wheel exercise or were subjected to transverse aortic constriction (TAC) to inducepressure overload.Results: In sedentary raptor-cKO mice, ejection fractions gradually decreased,resulting in significantly reduced values at 38 days (P < 0.001). Raptor-cKO micestarted to die during the fifth week after the last tamoxifen injection. At that time,the mortality rate was 36% in sedentary (n = 11) and 64% in exercising (n =14) mice. TAC-induced pressure overload resulted in severe cardiac dysfunctionalready at earlier timepoints. Thus, at 7-9 days after surgery, ejection fractionand fractional shortening values were 22.3% vs 43.5% and 10.2% vs 21.5% inraptor-cKO vs wild-type mice, respectively. This was accompanied by significantreductions of ventricular wall and septal thickness as well as an increase in leftventricular internal diameter. Moreover, ventricular weight to tibial length ratioswere increased in wild-type, but not in the raptor-cKO TAC mice. Together, thisshows that raptor-cKO mice rapidly developed dilated cardiomyopathy withoutgoing through a phase of adaptive hypertrophy. Expression of ANP and β-MHCwas induced in all raptor-cKO mice irrespective of the cardiac load conditions.Consistent with reduced mTORC1 activity, phosphorylation of ribosomal S6 ki-nase and 4E-BP1 was blunted, indicating reduced protein synthesis. Moreover,expression of multiple genes involved in the regulation of energy metabolism wasaltered, and followed by a shift from fatty acid to glucose oxidation.Conclusion: Our study suggests that mTORC1 coordinates protein and energymetabolic pathways in the heart. Moreover, we demonstrate that raptor is es-sential for the cardiac adaptation to increased workload and importantly, also fornormal physiological cardiac function.
883 Human beta-3 adrenoreceptor over-expression inhibitsneurohormones-induced cardiac hypertrophy in vitroand in vivo
J. Hammond1, T. Van Assche1, J. Hamelet1, C. Belge1, A. Vanderper2 ,B. Sekkali1, D. Langin3 , P. Herijgers2, C. Dessy1, J.L. Balligand1.
1Université Catholique de Louvain, Brussels, Belgium; 2Katholieke UniversiteitLeuven, Leuven, Belgium; 3Inserm U858, Institut of Molecular Medicine Rangueil(I2MR), Toulouse, France
Background: β3-adrenoreceptors (AR) have been identified in the human heart,where their activation is associated with nitric oxide (NO) synthesis; however, theirrole in cardiac function/remodelling is unclear.Methods: Phenotypical and functional analyses were carried out in wild type(WT) and heterozygote transgenic male mice with cardiac myocyte-specific over-expression of human β3AR (hβ3TG) treated for 10 days with isoproterenol (Iso)or saline by osmotic minipump infusion (30mg/kg/day) or repetitive i-p injection(50mg/kg/day). Some mice were concurrently treated with L-NAME in drinkingwater (2mg/mL). In vitro hypertrophic responses to phenylephrine (PE) and Isowere analyzed in neonatal rat ventricular myocytes (NRVM) infected with a re-combinant adenovirus expressing the human β3AR (AdVhβ3).Results: LV function (DP/dt max (mmHg/sec) at baseline (WT 5894±614vs hβ3TG 8036±1332; p=ns), after acute Iso (WT 9803±119 vs hβ3TG10099±1416; p=ns; n=12-15) and after chronic Iso, was similar between strains.Chronic Iso resulted in cardiac hypertrophy in WT (81.0±3.4mg/TL (Iso) vs.67.1±2.8mg/TL (saline); p<0.05; n=6-11), but not in hβ3TG mice, by morphome-tric (64.7±1.8mg/TL (Iso) vs 65.8±2.6mg/TL (saline; p=ns; n=6-8) or echocar-diographic (Delta LV mass/TL: 0.4±0.14 (Iso) vs 0.10±0.07mg/mm (saline);p=0.078) analyses. L-NAME treatment, at a non-hypertrophic dose, abrogatedthe protection from Iso-induced hypertrophy in hβ3TG mice. Likewise, NRVMsinfected with AdVhβ3 did not show an increase in cell size in response to PEor Iso, (1195±20μm2 (control) vs 1252±19μm2 (PE) vs 1175±21μm2 (Iso);p=ns; n=3 NRVM isolations, 84 cells/condition/isolation), in contrast to NRVMsinfected with control AdVGFP (1247±22μm2 (control) vs 1521±22μm2 (PE) vs1381±21μm2 (Iso): p<0.001). The protection from PE-induced hypertrophy inAdVhβ3 NRVMs was prevented by treatment with L-NAME or KT5823 (a pro-tein kinase G (PKG) inhibitor) (1187±35μm2 (L-NAME alone) vs 1503±48μm2
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

YIA Session: Basic Science / YIA Session: Thrombosis 147
(L-NAME + PE); p<0.001; 1273±33μm2 (KT alone) vs 1439±36μm2 (KT +PE); p<0.05). In acute signalling experiments, increases in PLB and ERK phos-phorylation after Iso and PE stimulation respectively, were similar in AdVGFPand AdVhβ3 NRVMs. VASP Ser239 phosphorylation (PKG target) was higher inAdVhβ3 than AdVGFP NRVMs.Conclusion: Cardiac-specific over-expression of β3ARs inhibits the hypertrophicresponse to chronic AR stimulation in vivo and in vitro, without altering LV func-tion, in part through a NO-dependent mechanism. Cardiac β3ARs may be a ther-apeutic target in the treatment of hypertrophic cardiomyopathies associated withelevated sympathetic tone.
884 Induced pluripotent stem cell-derived cardiomyocytesexhibit limited gene expression variance and surviveafter intramyocardial transplantation
L.W. Van Laake1, L. Qian2, P. Cheng2, Y. Huang2, E.C. Hsiao2,B. Conklin2, D. Srivastava2. 1University Medical Center Utrecht,
Division Heart and Lungs, Utrecht, Netherlands; 2UCSF, Gladstone Institute ofCardiovascular Disease, San Francisco, United States of America
Purpose: To investigate 1) how much variability exists between differentiated lin-eages from independent induced pluripotent stem cell (iPSC) lines and, specif-ically, how similar iPSC-derived cardiomyocytes are to embryonic stem cell-derived cardiomyocytes and 2) if iPSCs could replace ESCs in regenerative ther-apy for myocardial infarction.Methods: In order to facilitate isolation of comparable cardiomyocytes and pro-genitor populations, we generated mouse iPSCs in which expression of Nkx2-5,an early cardiac transcription factor, is marked by transgenic GFP. Differentiationprotocols included embryoid body formation, co-culture with END-2 cells, andselection of the second wave of Flk1-expressing progenitors. GFP+ cells wereselected by FACS and their gene expression was compared to GFP+ cells from2 ESC lines containing the same reporter, using microarrays. Differentiated cellswere injected in the hearts of NOD-SCID mice after coronary artery ligation, andidentified by epifluorescence and immunofluorescence (n=17).Results: The Nkx2-5-GFP iPSCs formed cardiomyocytes in vivo (in chimeric em-bryos and teratomas) and in vitro by several induction protocols. Isolation of theiPSC-derived Nkx2-5-GFP+ cardiac progenitor pool revealed striking similarity ingene expression between independent lines (R=0.99). Only 38 annotated genesout of over 28,000 transcripts were altered greater than 2-fold compared with theESC-derived GFP+ cells. Upon injection in the infarcted mouse heart, unselecteddifferentiated iPSCs formed teratomas but selected Nkx2-5-GFP+ iPSC-derivedcells formed cardiomyocytes only.Conclusions: Our findings suggest that despite the variability of gene expressionin iPSC lines, the variance narrows significantly in specific iPSC-derived cardiacprogenitors, which can be isolated and used for transplantation without generationof unwanted cell types.
YOUNG INVESTIGATORS AWARDS SESSIONTHROMBOSIS
886 Platelet aggregation and association with stentthrombosis and bleeding in clopidogrel-treated patients:initial evidence of a therapeutic window
D. Sibbing1, S.R. Steinhubl2, S. Schulz1, A. Schomig1, A. Kastrati1.1Deutsches Herzzentrum München, München, Germany; 2The
Medicines Company, Zürich, Switzerland
Background: The relationship between P2Y12 receptor inhibition and antithrom-botic efficacy of receptor antagonists is thought to be continuous with increasinglevels of inhibition translating into greater efficacy. However, just as with coumarinderivatives, a threshold effect for both efficacy and bleeding may exist. Here, wesought to evaluate the relationship between the level of platelet inhibition and theincidence of bleeding and stent thrombosis (ST) in clopidogrel-treated patients.Methods: Patients (n=2,533) underwent coronary stenting after 600 mg clopi-dogrel pretreatment. ADP-induced platelet aggregation (in AUC) was assessed
Figure 1
on a Multiplate analyzer prior to PCI. The primary efficacy endpoint was the 30-day incidence of definite or probable ST and the primary safety endpoint was theincidence of in-hospital TIMI major bleeding.Results: Patients were allocated to 3 groups with respect to their level of P2Y12receptor inhibition based on previously established cut-off values for bleeding andST: 975 patients (38%, AUC ≤188)-enhanced responders; 428 patients (17%,AUC ≥468)-low responders; 1130 patients (45%, AUC 189-467)-normal respon-ders. The incidence of bleeding and ST across these cut-off values was signifi-cantly different (Fig. 1). Normal responders were found to be at lower risk of anadverse event (bleeding or ST) compared with the other cohorts (OR=0.40, 95%CI 0.22-0.75; P=0.003) with no difference in ST compared with enhanced re-sponders (P=0.38) and no difference in major bleeding (P=0.78) compared withlow responders.Conclusions: These results are the first to suggest the existence of a therapeuticwindow for P2Y12 inhibition suggesting that above a specific threshold of plateletinhibition higher levels may only increase bleeding and not improve efficacy.
887 Increased short-term risk of thromboembolism afterinterruption of warfarin treatment in patients with atrialfibrillation
J. Raunsoe, M.L. Hansen, C. Torp-Pedersen. Gentofte Hospital -Copenhagen University Hospital, Hellerup, Denmark
Purpose: It is presently unknown whether patients with atrial fibrillation are atincreased short-term risk of thromboembolic adverse events after interruption ofwarfarin treatment. The purpose of this study was to assess the frequency andtiming of thromboembolism after warfarin treatment interruption.Methods: The study was designed as a retrospective, nation-wide cohort studyof 121,005 patients in Denmark hospitalized for atrial fibrillation and subsequentlytreated with warfarin in the period 1997 - 2006. The main outcome measure wasrates of re-hospitalization or death due to thromboembolic events after warfarininterruption. Secondary sensitivity analyses were done to validate the primaryresult.Results: Of 121,005 patients hospitalized with atrial fibrillation, a total of 55,353(45.7%) patients received warfarin treatment. Of these, 36,073 (65.2%) had atleast one episode of treatment interruption and a total of 61,734 episodes wereidentified. Median duration of treatment interruption was 38 days (interquartilerange 14-248). In all, 2110 thromboembolic events occurred during treatment in-terruption with a clustering of events in the initial period. 501, 218, 155, and 142events occurred during 0 to 90, 91 to 180, 181 to 270, and 271 to 360 days aftertreatment interruption, respectively. Correspondingly, the crude incidence rateswere 33.3, 8.1,5.5, and 5.1 events per 100 patient years. In a multivariate analysis, the first 90-day interval was associated with a significantly higher risk of thromboembolism(hazard ratio 2.21; 95% confidence interval 1.71-2.7) versus the interval of 91-180days.Conclusions: In patients with atrial fibrillation, an interruption of warfarin treat-ment is associated with a significantly increased short-term risk of thromboem-bolic events within 90 days of interruption.
888 Effect of upstream clopidogrel treatment in patients withST-elevation myocardial infarction undergoing primaryPCI
S. Koul1, J.G. Smith1, B. Lagerqvist2 , F. Schersten1, S. James2,D. Erlinge1. 1Lund University Hospital, Department of Cardiology, Lund,
Sweden; 2Uppsala University Hospital, Uppsala Clinical Research Center (UCR),Uppsala, Sweden
Purpose: Clopidogrel treatment today constitutes a cornerstone therapy for acutecoronary syndromes. Documentation on the effect of an upstream (prior tothe catheterization laboratory) loading dose (300-600 mg) of clopidogrel in pa-
Figure 1. 30-day mortality in STEMI-patients
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

148 YIA Session: Thrombosis / YIA Session: Population Sciences
tients with ST-Elevation Myocardial Infarction (STEMI) undergoing primary PCI isscarce. This study aimed to investigate the effect of upstream clopidogrel treat-ment in this patient group.Methods: We identified patients presenting with a STEMI and undergoing pri-mary PCI between 2003 and 2008 from the national Swedish Coronary Angiog-raphy and Angioplasty Registry (SCAAR). Patients with previous coronary an-giography/CABG, concomitant warfarin medication and patients not having re-ceived aspirin upstream were excluded. A total of 13 847 patients were identifiedof whom 4034 patients (29%) did not receive upstream clopidogrel treatment.Groups were compared for the outcomes of death, reinfarction and angiograph-ically verified stent thrombosis over 30 days and 1 year using Cox regressionmodels with adjustment for differences in baseline characteristics using propen-sity score methods.Results: The mortality was statistically significant lower in the group with up-stream clopidogrel both at 30 days, hazard ratio 0.76 (95% CI = 0.59-0.98) andat 1 year, hazard ratio 0.77 (95% = 0.63-0.93). No statistically significant effectswere observed on reinfarctions or stent thrombosis. The results remained identi-cal when excluding patients not receiving clopidogrel at hospital discharge.Conclusions: This large observational study suggests a reduction in total mor-tality with upstream clopidogrel treatment in STEMI patients undergoing primaryPCI.
889 Inflammasome formation in the mouse heart duringacute myocardial infarction promotes adverse cardiacremodeling
S. Toldo, B.W. Van Tassell, I.M. Seropian, R. Robati, A. Abbate. VirginiaCommonwealth University, Richmond, United States of America
Background: The ischemic damage to the myocardium during acute myocardialinfarction (AMI) initiates an intense inflammatory response promoting further dys-function and heart failure. Cryopyrin is activated in response to tissue injury andleads to the formation of the inflammasome, a multiprotein complex necessaryfor caspase-1activation and interleukin-1β release. Whether the inflammasomeforms in the myocardium during AMI is unknown.Methods: CD-1 male mice underwent permanent surgical ligation of the left coro-nary artery to simulate AMI. We measured caspase-1 tissue activity after AMIand assessed for the formation of aggregates of the apoptosis speck-like proteincontaining a caspase-recruitment domain (ASC) indicative of the formation of theinflammasome. Finally, we tested whether inhibition of the P2X7 receptor (using apharmacologic inhibitor [PPADS] or small interfering RNA) could prevent cryopy-rin activation thus inhibiting formation of the inflammasome, caspase-1 activation,and adverse cardiac remodeling.Results: Caspase-1 activity was increased as early as 3 hours and up to 14 days,with a peak at 72 hours. ASC aggregates were found at Western blot and im-munohistochemistry 72 hours after AMI. Treatment with a P2X7 pharmacologicinhibitor or targeted small interfering RNA prevented formation of ASC aggre-gates (reduced by 80%, p<0.01), reduced caspase-1 activity (reduced by 50%,p<0.01), and led to a smaller infarct size and a smaller increase in left ventricularend-diastolic and end-systolic diameters.
Conclusions: The inflammasome is formed in the heart during AMI throughP2X7-mediated activation of cryopyrin, and promotes adverse cardiac remod-eling. P2X7, cryopyrin and the inflammasome may represent novel targets forintervention in AMI and heart failure.
YOUNG INVESTIGATORS AWARDS SESSIONPOPULATION SCIENCES
891 Prediction of cardiovascular events by drug inducedchanges in carotid intima media thickness. Ameta-analysis of 41 randomized trials
P. Costanzo, P. Perrone-Filardi, E. Vassallo, S. Paolillo, P. Cesarano,M. Chiariello. University Hospital Federico II, Naples, Italy
Purpose: Carotid Intima-Media Thickness (IMT) increase is associated with araised risk of coronary (CHD) and cerebrovascular (CBV) events. This index isused in several clinical trials as a surrogate end point for cardiovascular out-comes. However, it is undetermined whether favourable changes of IMT reflectprognostic benefits. We assessed whether IMT regression is associated with re-duced incidence of cardiovascular events.
Methods: MEDLINE and the Cochrane Database were searched for articles pub-lished until August 2009. All randomized trials assessing carotid IMT at baselineand at end follow-up and reporting clinical end points were included. Two review-ers independently retrieved, reviewed and extracted data. Discrepancies weresolved by consensus. A weighted random-effect meta-regression analysis wasperformed to test the relationship between mean and max IMT changes and-outcomes. The influence of baseline patients’ characteristics, cardiovascularriskprofile, IMT at baseline, follow up and quality of the trial was alsoexplored. Overallestimates of effect were calculated with a fixed-effects,random effects model orPeto method where appropriate.Results: Forty-one trials enrolling 18307 participants were included. Despite sig-nificant reduction in CHD, CBV events and all cause death induced by activetreatments (for CHD events: Odds Ratio 0.82; 95% Confidence Interval 0.69 to0.96;p=0.02), (for CBV events: OR 0.71; 95% CI 0.51 to 1; p=0.05) and (for allcausedeath: OR 0.71; 95% CI 0.53 to 0.96; p=0.03), there was no significantrelationship between IMT regression and CHD events (Tau 0.91; P=0.37), CBVevents (Tau -0.32; P=0.75), and all cause death (Tau -0.41; P=0.69). In addition,baseline subjects’ characteristics, cardiovascular risk profile, IMT at baseline, fol-low up and quality of the trial did not significantly influence the association be-tween IMT changes and clinical outcomes.Conclusions: Regression or slowed progression of carotid IMT, induced by car-diovascular drug therapies, do not reflect reduction in cardiovascular events. It iswarranted to reconsider the role of carotid IMT as a surrogate end point.
892 The risk of myocardial infarction is similar in rheumatoidarthritis and diabetes - a nationwide cohort study
J. Lindhardsen1 , G.H. Gislason1, O. Ahlehoff1, O.M. Madsen2,P.R. Hansen1. 1Gentofte Hospital - Copenhagen University Hospital,Department of Cardiology, Hellerup, Denmark; 2Gentofte Hospital
- Copenhagen University Hospital, Department of Rheumatology, Hellerup,Denmark
Purpose: To compare the incidence of myocardial infarction (MI) in patients suf-fering from rheumatoid arthritis (RA) or diabetes mellitus (DM) on a nationwidescale.Methods: The study population included the entire Danish population ≥ 10 yearsof age on Jan 1, 1997 (n=4.614.840). Patients developing DM and RA wereidentified by prescription claims, hospitalisations and outpatient visits throughindividual-level-linkage nationwide administrative registers. The population wasfollowed until first MI or Dec 31, 2006. Risk of MI was analysed using Poissonregression models adjusting for date of incidence, cardiovascular treatment, co-morbidity and income.Results: During the study period a total of 10.300 and 132.189 people developedRA and DM, respectively. The overall incidence rate ratio (IRR) of a MI event afterdeveloping RA was inceased to 1.61 ([95% CI] 1.42-1.83), which was comparableto the risk of MI after developing diabetes of 1.70 [1.59-1.83]. After stratifying bygender the risk in RA & DM remained comparable for male patients (RA 1.59[1.33-1.89]; DM 1.58 [1.47-1.70]). The risk for female RA patients was equal toboth RA & DM males, but female DM patients had a slightly higher risk (RA 1.62[1.38-1.91]; DM 1.95 [1.80-2.11]).When further stratifying by age the risk of MI was considerable higher in theyounger patients (table), especially women < 45 years who had an approx. six-fold increase in risk in both RA & DM. While the risk in female RA patients de-creases to a level lower than DM in older age groups, the risk of MI in malesdeveloping RA when > 45 years is the same as in DM.
Risk of myocardial infarction in RA & DM
Age (years) Male Female
RA DM RA DM
<45 0.64 [0.90-4.54]* 4.74 [3.95-5.69] 6.66 [3.4-12.90] 6.13 [4.55-8.26]46-56 2.37 [1.61-3.48] 2.03 [1.80-2.28] 1.92 [1.18-3.11] 2.89 [2.39-3.50]57-67 1.68 [1.23-12.29] 1.54 [1.39-1.72] 1.71 [1.25-2.35] 1.98 [1.72-2.29]>67 1.51 [1.18-1.93] 1.50 [1.35-1.65] 1.28 [1.03-1.59]* 1.58 [1.41-1.77]
Incidence rate ratios by gender & age quartiles (IRR [95% CI]). *p<0.05 compared to correspond-ing DM strata.
Conclusions: RA is an independent risk factor for MI of similar magnitude as DM,and the risk is especially high among younger patients with RA. These resultsunderline the importance of early and aggressive detection and management ofcardiovascular risk factors in patients with RA.
893 Elevated urinary albumin excretion is associated withhigher 10 year cardiovascular risk than predicted by theFramingham risk score and is normalized by treatment
F.P.J. Brouwers, F.W. Asselbergs, J.L. Hillege, R.A. De Boer,R.T. Gansevoort, W.H. Van Gilst. University Medical Center, Groningen,
Netherlands
Background: The PREVEND IT reported a high cardiovascular (CV) eventrate in normotensive and normocholesterolemic subjects with a baseline UAE>50mg/24h. Here, we report on the actual 10-year CV outcome of this popu-lation and compare this with the predicted Framingham Risk Score (FRS). In
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
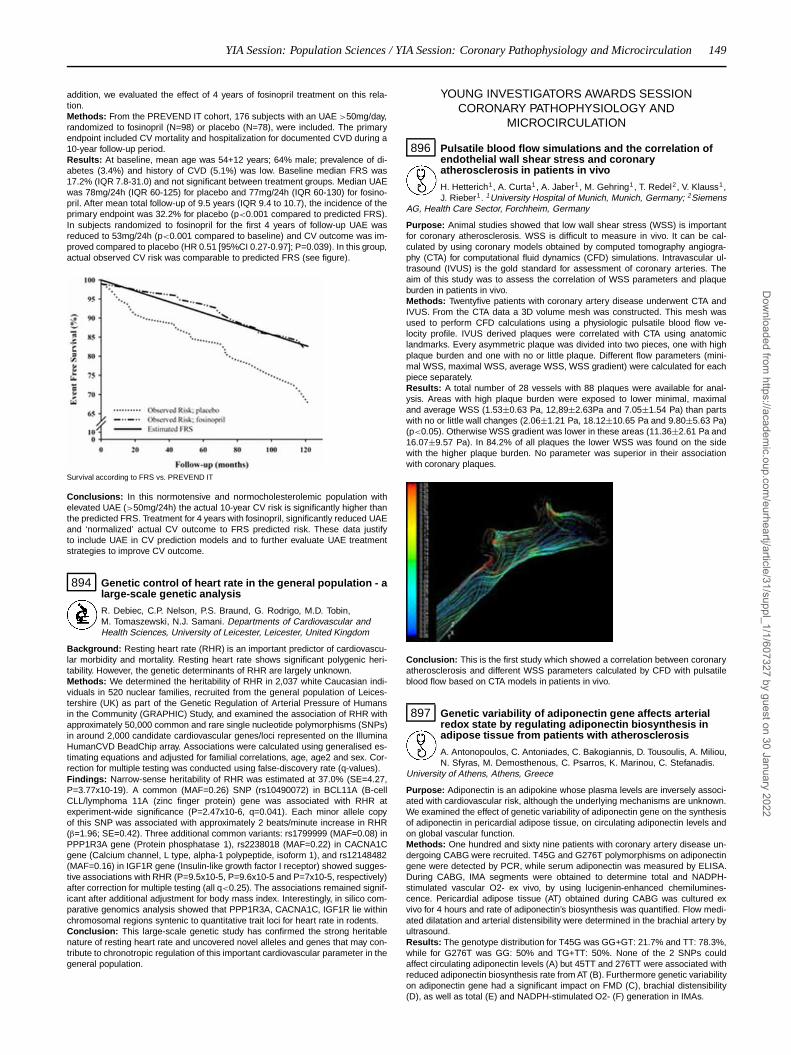
YIA Session: Population Sciences / YIA Session: Coronary Pathophysiology and Microcirculation 149
addition, we evaluated the effect of 4 years of fosinopril treatment on this rela-tion.Methods: From the PREVEND IT cohort, 176 subjects with an UAE >50mg/day,randomized to fosinopril (N=98) or placebo (N=78), were included. The primaryendpoint included CV mortality and hospitalization for documented CVD during a10-year follow-up period.Results: At baseline, mean age was 54+12 years; 64% male; prevalence of di-abetes (3.4%) and history of CVD (5.1%) was low. Baseline median FRS was17.2% (IQR 7.8-31.0) and not significant between treatment groups. Median UAEwas 78mg/24h (IQR 60-125) for placebo and 77mg/24h (IQR 60-130) for fosino-pril. After mean total follow-up of 9.5 years (IQR 9.4 to 10.7), the incidence of theprimary endpoint was 32.2% for placebo (p<0.001 compared to predicted FRS).In subjects randomized to fosinopril for the first 4 years of follow-up UAE wasreduced to 53mg/24h (p<0.001 compared to baseline) and CV outcome was im-proved compared to placebo (HR 0.51 [95%CI 0.27-0.97]; P=0.039). In this group,actual observed CV risk was comparable to predicted FRS (see figure).
Survival according to FRS vs. PREVEND IT
Conclusions: In this normotensive and normocholesterolemic population withelevated UAE (>50mg/24h) the actual 10-year CV risk is significantly higher thanthe predicted FRS. Treatment for 4 years with fosinopril, significantly reduced UAEand ‘normalized’ actual CV outcome to FRS predicted risk. These data justifyto include UAE in CV prediction models and to further evaluate UAE treatmentstrategies to improve CV outcome.
894 Genetic control of heart rate in the general population - alarge-scale genetic analysis
R. Debiec, C.P. Nelson, P.S. Braund, G. Rodrigo, M.D. Tobin,M. Tomaszewski, N.J. Samani. Departments of Cardiovascular andHealth Sciences, University of Leicester, Leicester, United Kingdom
Background: Resting heart rate (RHR) is an important predictor of cardiovascu-lar morbidity and mortality. Resting heart rate shows significant polygenic heri-tability. However, the genetic determinants of RHR are largely unknown.Methods: We determined the heritability of RHR in 2,037 white Caucasian indi-viduals in 520 nuclear families, recruited from the general population of Leices-tershire (UK) as part of the Genetic Regulation of Arterial Pressure of Humansin the Community (GRAPHIC) Study, and examined the association of RHR withapproximately 50,000 common and rare single nucleotide polymorphisms (SNPs)in around 2,000 candidate cardiovascular genes/loci represented on the IlluminaHumanCVD BeadChip array. Associations were calculated using generalised es-timating equations and adjusted for familial correlations, age, age2 and sex. Cor-rection for multiple testing was conducted using false-discovery rate (q-values).Findings: Narrow-sense heritability of RHR was estimated at 37.0% (SE=4.27,P=3.77x10-19). A common (MAF=0.26) SNP (rs10490072) in BCL11A (B-cellCLL/lymphoma 11A (zinc finger protein) gene was associated with RHR atexperiment-wide significance (P=2.47x10-6, q=0.041). Each minor allele copyof this SNP was associated with approximately 2 beats/minute increase in RHR(β=1.96; SE=0.42). Three additional common variants: rs1799999 (MAF=0.08) inPPP1R3A gene (Protein phosphatase 1), rs2238018 (MAF=0.22) in CACNA1Cgene (Calcium channel, L type, alpha-1 polypeptide, isoform 1), and rs12148482(MAF=0.16) in IGF1R gene (Insulin-like growth factor I receptor) showed sugges-tive associations with RHR (P=9.5x10-5, P=9.6x10-5 and P=7x10-5, respectively)after correction for multiple testing (all q<0.25). The associations remained signif-icant after additional adjustment for body mass index. Interestingly, in silico com-parative genomics analysis showed that PPP1R3A, CACNA1C, IGF1R lie withinchromosomal regions syntenic to quantitative trait loci for heart rate in rodents.Conclusion: This large-scale genetic study has confirmed the strong heritablenature of resting heart rate and uncovered novel alleles and genes that may con-tribute to chronotropic regulation of this important cardiovascular parameter in thegeneral population.
YOUNG INVESTIGATORS AWARDS SESSIONCORONARY PATHOPHYSIOLOGY AND
MICROCIRCULATION
896 Pulsatile blood flow simulations and the correlation ofendothelial wall shear stress and coronaryatherosclerosis in patients in vivo
H. Hetterich1, A. Curta1, A. Jaber1 , M. Gehring1, T. Redel2, V. Klauss1,J. Rieber1. 1University Hospital of Munich, Munich, Germany; 2Siemens
AG, Health Care Sector, Forchheim, Germany
Purpose: Animal studies showed that low wall shear stress (WSS) is importantfor coronary atherosclerosis. WSS is difficult to measure in vivo. It can be cal-culated by using coronary models obtained by computed tomography angiogra-phy (CTA) for computational fluid dynamics (CFD) simulations. Intravascular ul-trasound (IVUS) is the gold standard for assessment of coronary arteries. Theaim of this study was to assess the correlation of WSS parameters and plaqueburden in patients in vivo.Methods: Twentyfive patients with coronary artery disease underwent CTA andIVUS. From the CTA data a 3D volume mesh was constructed. This mesh wasused to perform CFD calculations using a physiologic pulsatile blood flow ve-locity profile. IVUS derived plaques were correlated with CTA using anatomiclandmarks. Every asymmetric plaque was divided into two pieces, one with highplaque burden and one with no or little plaque. Different flow parameters (mini-mal WSS, maximal WSS, average WSS, WSS gradient) were calculated for eachpiece separately.Results: A total number of 28 vessels with 88 plaques were available for anal-ysis. Areas with high plaque burden were exposed to lower minimal, maximaland average WSS (1.53±0.63 Pa, 12,89±2.63Pa and 7.05±1.54 Pa) than partswith no or little wall changes (2.06±1.21 Pa, 18.12±10.65 Pa and 9.80±5.63 Pa)(p<0.05). Otherwise WSS gradient was lower in these areas (11.36±2.61 Pa and16.07±9.57 Pa). In 84.2% of all plaques the lower WSS was found on the sidewith the higher plaque burden. No parameter was superior in their associationwith coronary plaques.
Conclusion: This is the first study which showed a correlation between coronaryatherosclerosis and different WSS parameters calculated by CFD with pulsatileblood flow based on CTA models in patients in vivo.
897 Genetic variability of adiponectin gene affects arterialredox state by regulating adiponectin biosynthesis inadipose tissue from patients with atherosclerosis
A. Antonopoulos, C. Antoniades, C. Bakogiannis, D. Tousoulis, A. Miliou,N. Sfyras, M. Demosthenous, C. Psarros, K. Marinou, C. Stefanadis.
University of Athens, Athens, Greece
Purpose: Adiponectin is an adipokine whose plasma levels are inversely associ-ated with cardiovascular risk, although the underlying mechanisms are unknown.We examined the effect of genetic variability of adiponectin gene on the synthesisof adiponectin in pericardial adipose tissue, on circulating adiponectin levels andon global vascular function.Methods: One hundred and sixty nine patients with coronary artery disease un-dergoing CABG were recruited. T45G and G276T polymorphisms on adiponectingene were detected by PCR, while serum adiponectin was measured by ELISA.During CABG, IMA segments were obtained to determine total and NADPH-stimulated vascular O2- ex vivo, by using lucigenin-enhanced chemilumines-cence. Pericardial adipose tissue (AT) obtained during CABG was cultured exvivo for 4 hours and rate of adiponectin’s biosynthesis was quantified. Flow medi-ated dilatation and arterial distensibility were determined in the brachial artery byultrasound.Results: The genotype distribution for T45G was GG+GT: 21.7% and TT: 78.3%,while for G276T was GG: 50% and TG+TT: 50%. None of the 2 SNPs couldaffect circulating adiponectin levels (A) but 45TT and 276TT were associated withreduced adiponectin biosynthesis rate from AT (B). Furthermore genetic variabilityon adiponectin gene had a significant impact on FMD (C), brachial distensibility(D), as well as total (E) and NADPH-stimulated O2- (F) generation in IMAs.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

150 YIA Session: Coronary Pathophysiology and Microcirculation / Atie Immink New Investigator Award in cardiovascular nursing
*p<0.05; **p<0.01; ns: non significant
Conclusions: Even though T45G and G276T polymorphisms on adiponectingene do not alter circulating adiponectin levels, they have a significant effect onadiponectin biosynthesis from pericardial AT and constitute key determinants ofglobal vascular function in coronary patients. These findings provide new insightsin the role of adiponectin in vascular biology.
898 Augmented vascular smooth muscle celldedifferentiation in coronary regions of persistently lowendothelial shear stress co-localize with thin capfibroatheromata in pigs
K.C. Koskinas1, A.B. Baker2, Y.S. Chatzizisis1, A.U. Coskun3,M. Jonas2, M. Papafaklis1, E.R. Edelaman2, P.H. Stone1,
C.L. Feldman1. 1Brigham and Women’s Hospital, Boston, United States ofAmerica; 2Massachusetts Institute of Technology, Cambridge, United States ofAmerica; 3Northeastern University, Boston, United States of America
Purpose: The mechanisms underlying the differential progression of hetero-geneous coronary atherosclerotic plaques are not well understood. Endothelialshear stress (ESS) is a critical determinant of individual plaque formation andprogression. In high-risk, rupture-prone lesions vascular smooth muscle cells(VSMC) undergo phenotypic dedifferentiation characterized by attenuated ex-pression of contractile proteins and adoption of a proliferative phenotype. Weperformed an intravascular ultrasound (IVUS) and histopathology natural historystudy in a porcine model of human-like atherosclerosis and tested the hypoth-esis that low local ESS up-regulates the dedifferentiation of VSMC and therebypromotes the focal formation of high-risk coronary plaques.Methods: Serial IVUS-based geometrically correct 3D reconstruction of all majorcoronary arteries (n=15) was serially performed in vivo at 4, 11, 16, 23 and 36weeks after diabetes induction and initiation of a high-fat diet in five Yorkshire pigs.Each reconstructed artery was divided into 3mm-long segments. We calculatedESS in vivo in all segments at all time points using computational fluid dynamics.Coronary arteries were harvested at final week 36, and 43 segments with signifi-cant plaque by IVUS were identified, cryosectioned and analyzed histopathologi-cally. RNA was isolated and reverse transcribed, and gene expression of the fol-lowing VSMC differentiation markers was assessed by real time RT-PCR in theseplaques: SMC-α-actin, smoothelin, desmin, myocardin, smooth muscle myosinheavy chain (SMMHC), and SMM22a.Results: Local ESS of individual developing plaques changed substantially overtime. At week 36 the analyzed plaques exhibited significant histopathologic het-erogeneity. Thin cap fibroatheromas (TCFAs, n=13 of 43, 30.2%) developed insegments that had been exposed to significantly lower ESS throughout their natu-ral history compared to non-TCFAs (n=30 of 43, 69.8%; p<0.05 at all time points).Gene expression of α-actin, smoothelin, desmin and myocardin was lower in TC-FAs compared to non-TCFAs (p<0.05, p<0.001, p<0.01 and p<0.05, respec-tively), whereas there was no significant difference in the gene expression ofSMMHC and SMM22A. The smoothelin-to- α-actin and desmin-to- α-actin mRNAratio was also lower in TCFAs compared to non-TCFAs (p<0.05).Conclusion: Coronary regions exposed to persistently low ESS throughout theirnatural history exhibit augmented VSMCs dedifferentiation, which may contributeto the formation of high-risk TCFAs.
899 Potential benefit of final-kissing inflation after singlestenting for the treatment of bifurcation lesions: Insightfrom OCT observations
H. Hariki, A. Kozuki, N. Yoshino, N. Miyoshi, H. Kato, H. Kawamori,T. Sawada, T. Shinke, J. Shite, K. Hirata. Kobe University Graduate
School of Medicine, Department of Cardiology, Kobe, Japan
Background: Treatment of coronary bifurcation lesions is complex and challeng-ing even in drug-eluting stent (DES) era. Final-kissing inflation (FKI) after singlestenting to bifurcation lesions may reduce the number of strut hanging over theostium of side branch (jailed struts).Method: 39 true bifurcation lesions treated with single DESs (17 cypher,10 Taxusexpress,12 Taxus liberte) with or without FKI (FKI(+) FKI(-)) were analyzed byoptical coherence tomography (OCT) at 6 and 12 months post implantation. Atbifurcation lesion, % jailed strut (number of jailed strut/total strut) and thrombusattachment were assessed and thickness of neointima on the struts were mea-sured.
Result: % jailed strut was less (25.98±5.94% vs 8.77±6.93%, P<0.01), andthrombus attachment to jailed struts was less frequent (6.7% (1/15) vs. 29.2%(7/24), P<0.05) in FKI(+) than FKI(-) at six months. Neointimal thickness wasprominently increased from 6 months to 12 months on the jailed struts (34±17 to79±26μm, P<0.001) in contrast to slight increase in non-jailed struts (111±122to 120±129μm, P=NS).
Conclusion: FKI reduces the number of jailed strut and the frequency of sub-clinical thrombus at side branch orifice in the setting of single DES stenting tobifurcation coronary lesions, which may have potential long-term benefit.
ATIE IMMINK NEW INVESTIGATOR AWARD INCARDIOVASCULAR NURSING (NIA)
947 Dietary energy density: a mediator of depressivesymptoms and abdominal obesity or independentpredictor of abdominal obesity?
D.A. Grossniklaus1, S.B. Dunbar2, R. Gary2, B.C. Tohill3, J. Frediani4 ,M.K. Higgins2. 1Nurse Consultant, Atl, United States of America;
2Emory University School of Nursing, Atlanta, United States of America;3Consultant, Flagstaff, United States of America; 4Emory University School ofMedicine, Atlanta, United States of America
Purpose: Abdominal obesity (AO), centrally distributed adipose tissue, is a car-diometabolic disease risk (CMDR) factor. In the U.S., AO prevalence has beenincreasing and ≥ 50% of adults have AO; among European adults, similartrends are reported. Depressive symptoms (DSxs) may contribute to AO throughhypothalamic-pituitary-adrenal axis (HTPAA) activation as well as affect contribut-ing dietary patterns such as high energy dense diets. The purpose was to testdietary energy density (kilocalories/gram, [DED]) as a biobehavioral mediator be-tween DSxs and AO.Methods: This prospective, cross-sectional study enrolled overweight adults(n=87); mean age 41.3±10.2 years; 73.6% women; and 50.6% African-American.Variables and measures: Beck Depression Inventory-II (BDI-II) to measure DSxs,weighed 3-day food records analyzed for macronutrients, food group patterns,caloric intake (kilocalories [kcal] and consumed food and beverage weight (grams[g]) to calculate DED. A morning saliva sample was analyzed for cortisol, anindicator of HTPAA activation. Waist circumference (WC), an indicator of AO,was measured. Descriptive statistics and Mann-Whitney U analyzed relationshipsamong variables. Three approaches tested DED as a mediator between DSxsand WC.Results: WC was 103.4±12.7 cm for men and 103.2±14.9 cm for women with73.6% reflecting increased CMDR. BDI-II was 8.67±8.34 with 21.8% reportingDSxs. DED was 0.75±0.22 kcal/g, and those with DSxs consumed less pro-tein (U=438.0; p≤.05) and fewer vegetables (U=448.5; p≤.05) than those withoutDSxs. Mean morning cortisol levels were 0.69±0.45 μg/dl indicating that 81.0%had values within the reference range. Those with WC risk reported greaterDSxs (U=528.5, p≤.05) and higher morning salivary cortisol (U=403.0, p≤.05)than those without WC risk. Sequential regression showed associations betweenDSxs and DED (R2=.391, p≤.05), DSxs and WC (R2=.091, p≤.01), and DEDand WC (R2=.237, p≤.01) showing DED independently predicted WC. Sobel andbootstrap tests were not significant demonstrating DED did not mediate betweenDSxs and WC.Conclusions: DSxs were 3 times higher than the general population, and indi-viduals with DSxs had unfavorable dietary patterns compared to those withoutDSxs. Those with WC risk had greater DSxs and higher morning cortisol com-pared to those without WC risk, and this subtle shift within the reference rangemerits further investigation. Although DED was an independent predictor versusmediator, improving DSxs and modifying DED are important independent targetsof intervention for reducing AO that are amendable to modification.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
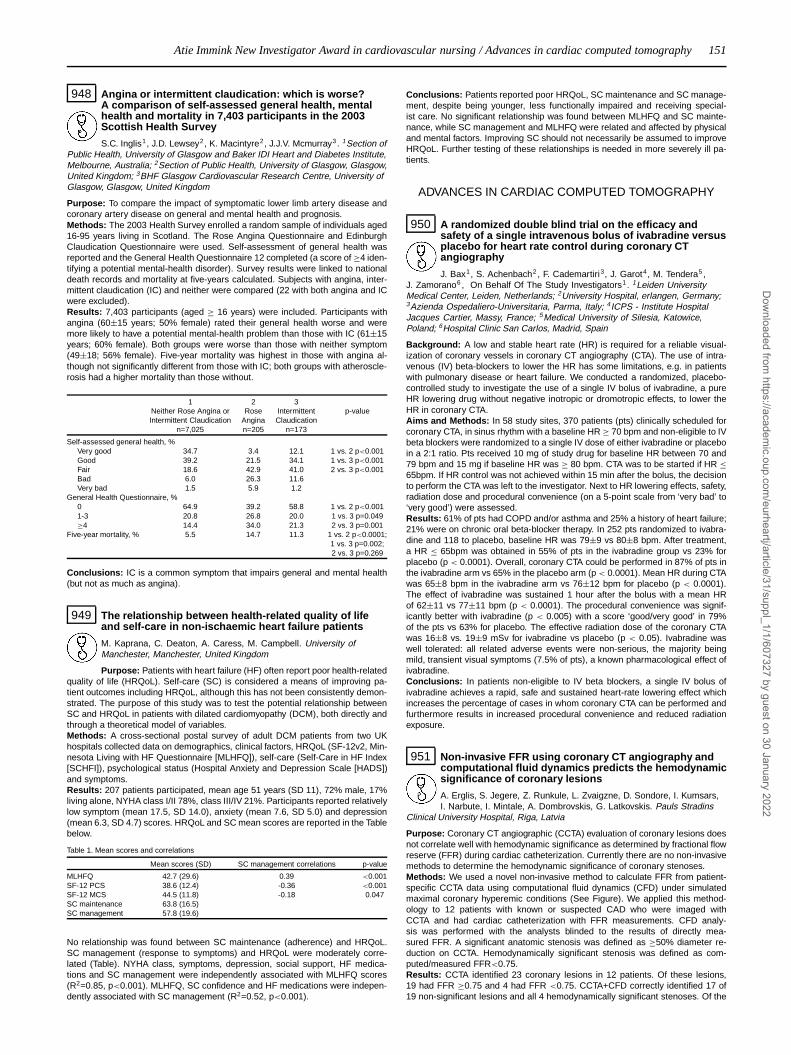
Atie Immink New Investigator Award in cardiovascular nursing / Advances in cardiac computed tomography 151
948 Angina or intermittent claudication: which is worse?A comparison of self-assessed general health, mentalhealth and mortality in 7,403 participants in the 2003Scottish Health Survey
S.C. Inglis1, J.D. Lewsey2, K. Macintyre2, J.J.V. Mcmurray3. 1Section ofPublic Health, University of Glasgow and Baker IDI Heart and Diabetes Institute,Melbourne, Australia; 2Section of Public Health, University of Glasgow, Glasgow,United Kingdom; 3BHF Glasgow Cardiovascular Research Centre, University ofGlasgow, Glasgow, United Kingdom
Purpose: To compare the impact of symptomatic lower limb artery disease andcoronary artery disease on general and mental health and prognosis.Methods: The 2003 Health Survey enrolled a random sample of individuals aged16-95 years living in Scotland. The Rose Angina Questionnaire and EdinburghClaudication Questionnaire were used. Self-assessment of general health wasreported and the General Health Questionnaire 12 completed (a score of ≥4 iden-tifying a potential mental-health disorder). Survey results were linked to nationaldeath records and mortality at five-years calculated. Subjects with angina, inter-mittent claudication (IC) and neither were compared (22 with both angina and ICwere excluded).Results: 7,403 participants (aged ≥ 16 years) were included. Participants withangina (60±15 years; 50% female) rated their general health worse and weremore likely to have a potential mental-health problem than those with IC (61±15years; 60% female). Both groups were worse than those with neither symptom(49±18; 56% female). Five-year mortality was highest in those with angina al-though not significantly different from those with IC; both groups with atheroscle-rosis had a higher mortality than those without.
1 2 3Neither Rose Angina or Rose Intermittent p-valueIntermittent Claudication Angina Claudication
n=7,025 n=205 n=173
Self-assessed general health, %Very good 34.7 3.4 12.1 1 vs. 2 p<0.001Good 39.2 21.5 34.1 1 vs. 3 p<0.001Fair 18.6 42.9 41.0 2 vs. 3 p<0.001Bad 6.0 26.3 11.6Very bad 1.5 5.9 1.2
General Health Questionnaire, %0 64.9 39.2 58.8 1 vs. 2 p<0.0011-3 20.8 26.8 20.0 1 vs. 3 p=0.049≥4 14.4 34.0 21.3 2 vs. 3 p=0.001
Five-year mortality, % 5.5 14.7 11.3 1 vs. 2 p<0.0001;1 vs. 3 p=0.002;2 vs. 3 p=0.269
Conclusions: IC is a common symptom that impairs general and mental health(but not as much as angina).
949 The relationship between health-related quality of lifeand self-care in non-ischaemic heart failure patients
M. Kaprana, C. Deaton, A. Caress, M. Campbell. University ofManchester, Manchester, United Kingdom
Purpose: Patients with heart failure (HF) often report poor health-relatedquality of life (HRQoL). Self-care (SC) is considered a means of improving pa-tient outcomes including HRQoL, although this has not been consistently demon-strated. The purpose of this study was to test the potential relationship betweenSC and HRQoL in patients with dilated cardiomyopathy (DCM), both directly andthrough a theoretical model of variables.Methods: A cross-sectional postal survey of adult DCM patients from two UKhospitals collected data on demographics, clinical factors, HRQoL (SF-12v2, Min-nesota Living with HF Questionnaire [MLHFQ]), self-care (Self-Care in HF Index[SCHFI]), psychological status (Hospital Anxiety and Depression Scale [HADS])and symptoms.Results: 207 patients participated, mean age 51 years (SD 11), 72% male, 17%living alone, NYHA class I/II 78%, class III/IV 21%. Participants reported relativelylow symptom (mean 17.5, SD 14.0), anxiety (mean 7.6, SD 5.0) and depression(mean 6.3, SD 4.7) scores. HRQoL and SC mean scores are reported in the Tablebelow.
Table 1. Mean scores and correlations
Mean scores (SD) SC management correlations p-value
MLHFQ 42.7 (29.6) 0.39 <0.001SF-12 PCS 38.6 (12.4) -0.36 <0.001SF-12 MCS 44.5 (11.8) -0.18 0.047SC maintenance 63.8 (16.5)SC management 57.8 (19.6)
No relationship was found between SC maintenance (adherence) and HRQoL.SC management (response to symptoms) and HRQoL were moderately corre-lated (Table). NYHA class, symptoms, depression, social support, HF medica-tions and SC management were independently associated with MLHFQ scores(R2=0.85, p<0.001). MLHFQ, SC confidence and HF medications were indepen-dently associated with SC management (R2=0.52, p<0.001).
Conclusions: Patients reported poor HRQoL, SC maintenance and SC manage-ment, despite being younger, less functionally impaired and receiving special-ist care. No significant relationship was found between MLHFQ and SC mainte-nance, while SC management and MLHFQ were related and affected by physicaland mental factors. Improving SC should not necessarily be assumed to improveHRQoL. Further testing of these relationships is needed in more severely ill pa-tients.
ADVANCES IN CARDIAC COMPUTED TOMOGRAPHY
950 A randomized double blind trial on the efficacy andsafety of a single intravenous bolus of ivabradine versusplacebo for heart rate control during coronary CTangiography
J. Bax1, S. Achenbach2 , F. Cademartiri3, J. Garot4, M. Tendera5 ,J. Zamorano6 , On Behalf Of The Study Investigators1. 1Leiden UniversityMedical Center, Leiden, Netherlands; 2University Hospital, erlangen, Germany;3Azienda Ospedaliero-Universitaria, Parma, Italy; 4ICPS - Institute HospitalJacques Cartier, Massy, France; 5Medical University of Silesia, Katowice,Poland; 6Hospital Clinic San Carlos, Madrid, Spain
Background: A low and stable heart rate (HR) is required for a reliable visual-ization of coronary vessels in coronary CT angiography (CTA). The use of intra-venous (IV) beta-blockers to lower the HR has some limitations, e.g. in patientswith pulmonary disease or heart failure. We conducted a randomized, placebo-controlled study to investigate the use of a single IV bolus of ivabradine, a pureHR lowering drug without negative inotropic or dromotropic effects, to lower theHR in coronary CTA.Aims and Methods: In 58 study sites, 370 patients (pts) clinically scheduled forcoronary CTA, in sinus rhythm with a baseline HR ≥ 70 bpm and non-eligible to IVbeta blockers were randomized to a single IV dose of either ivabradine or placeboin a 2:1 ratio. Pts received 10 mg of study drug for baseline HR between 70 and79 bpm and 15 mg if baseline HR was ≥ 80 bpm. CTA was to be started if HR ≤65bpm. If HR control was not achieved within 15 min after the bolus, the decisionto perform the CTA was left to the investigator. Next to HR lowering effects, safety,radiation dose and procedural convenience (on a 5-point scale from ‘very bad’ to‘very good’) were assessed.Results: 61% of pts had COPD and/or asthma and 25% a history of heart failure;21% were on chronic oral beta-blocker therapy. In 252 pts randomized to ivabra-dine and 118 to placebo, baseline HR was 79±9 vs 80±8 bpm. After treatment,a HR ≤ 65bpm was obtained in 55% of pts in the ivabradine group vs 23% forplacebo (p < 0.0001). Overall, coronary CTA could be performed in 87% of pts inthe ivabradine arm vs 65% in the placebo arm (p < 0.0001). Mean HR during CTAwas 65±8 bpm in the ivabradine arm vs 76±12 bpm for placebo (p < 0.0001).The effect of ivabradine was sustained 1 hour after the bolus with a mean HRof 62±11 vs 77±11 bpm (p < 0.0001). The procedural convenience was signif-icantly better with ivabradine (p < 0.005) with a score ‘good/very good’ in 79%of the pts vs 63% for placebo. The effective radiation dose of the coronary CTAwas 16±8 vs. 19±9 mSv for ivabradine vs placebo (p < 0.05). Ivabradine waswell tolerated: all related adverse events were non-serious, the majority beingmild, transient visual symptoms (7.5% of pts), a known pharmacological effect ofivabradine.Conclusions: In patients non-eligible to IV beta blockers, a single IV bolus ofivabradine achieves a rapid, safe and sustained heart-rate lowering effect whichincreases the percentage of cases in whom coronary CTA can be performed andfurthermore results in increased procedural convenience and reduced radiationexposure.
951 Non-invasive FFR using coronary CT angiography andcomputational fluid dynamics predicts the hemodynamicsignificance of coronary lesions
A. Erglis, S. Jegere, Z. Runkule, L. Zvaigzne, D. Sondore, I. Kumsars,I. Narbute, I. Mintale, A. Dombrovskis, G. Latkovskis. Pauls Stradins
Clinical University Hospital, Riga, Latvia
Purpose: Coronary CT angiographic (CCTA) evaluation of coronary lesions doesnot correlate well with hemodynamic significance as determined by fractional flowreserve (FFR) during cardiac catheterization. Currently there are no non-invasivemethods to determine the hemodynamic significance of coronary stenoses.Methods: We used a novel non-invasive method to calculate FFR from patient-specific CCTA data using computational fluid dynamics (CFD) under simulatedmaximal coronary hyperemic conditions (See Figure). We applied this method-ology to 12 patients with known or suspected CAD who were imaged withCCTA and had cardiac catheterization with FFR measurements. CFD analy-sis was performed with the analysts blinded to the results of directly mea-sured FFR. A significant anatomic stenosis was defined as ≥50% diameter re-duction on CCTA. Hemodynamically significant stenosis was defined as com-puted/measured FFR<0.75.Results: CCTA identified 23 coronary lesions in 12 patients. Of these lesions,19 had FFR ≥0.75 and 4 had FFR <0.75. CCTA+CFD correctly identified 17 of19 non-significant lesions and all 4 hemodynamically significant stenoses. Of the
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

152 Advances in cardiac computed tomography
two lesions that did not correlate, one had no apparent response to intracoronaryadenosine at the time of FFR and the other had measured FFR of 0.76 and calcu-lated FFR of 0.72. Adding CFD to CCTA increased sensitivity from 75% to 100%,specificity from 58% to 89%, positive predictive value from 27% to 67%, negativepredictive value from 92% to 100% and diagnostic accuracy from 61% to 91%.
Andgiography+FFR versus CCTA+CFD
Conclusions: This is the first demonstration that adding CFD analysis to CCTAcan accurately assess the hemodynamic significance of coronary artery lesions.This provides a new noninvasive method to help select patients who may benefitfrom percutaneous coronary intervention.
952 Adenosine stress perfusion imaging and coronaryangiography using 320 slice cardiac CT- a comparisonwith quantitative coronary angiography and fractionalflow reserve
B. Ko1, J.D. Cameron2, M. Leung1, S.J. Lehman1 , S. Hope1,M. Crossett1, A. Nasis1, P. Antonis1, T. Defrance3, S. Seneviratne1. 1MonashHeart, Melbourne, Australia; 2Monash Cardiovascular Research Centre,Melbourne, Australia; 3Stanford University, Palo Alto, United States of America
Purpose: To determine the accuracy of 320 slice adenosine stress computed to-mography myocardial perfusion imaging (CTP) and coronary angiography (CTA)for detection of significant myocardial ischemia using combined QCA on invasiveangiography (IA) and fractional flow reserve (FFR) as the reference standard.Methods: 42 vessel territories in 14 patients (8 male, 62±8 years) with chestpain were investigated using CTA, CTP and IA. The CT protocol was 1) StressCT: contrast enhanced scan during intravenous adenosine infusion; 2) Delayedscan 10 minutes after stress; 3) Rest CT contrast enhanced scan using prospec-tive triggering. FFR was determined in 26 territories supplied by arteries with≥50% stenosis by visual assessment on IA. Territories were defined as ischemic,if supplied by an artery with FFR ≤0.8, and non ischemic, if supplied by an arterywith QCA <50% or FFR >0.8. Images for CTA and CTP were assessed by con-sensus between two independent blinded observers. QCA on IA was assessedby a single blinded observer.Results: All patients completed the CT protocol (radiation dose 11.42±5mSV).CTP correctly identified 12/15 ischemic territories and 22/27 non ischemic territo-ries. No severe proximal lesion was missed. False negative territories comprisedtwo mid LAD and one distal RCA lesion. CTP yielded a sensitivity of 0.8 (confi-dence interval = 0.5-0.91) and specificity of 0.81 (0.61-0.93) for detection of is-chemia, with positive and negative predictive values of 0.88 (0.68-0.97) and 0.71(0.44-0.88) respectively. The presence of a perfusion defect on CTP or ≥70%stenosis on CTA increased the sensitivity and negative predictive value to 0.87(0.58-0.98) and 0.92 (0.72-0.99) respectively with no significant change in speci-ficity [0.81 (0.61-0.93)]or positive predictive value [0.72 (0.46-0.89)].Conclusions: 320 slice adenosine stress CT accurately identifies stress inducedmyocardial perfusion defects and may be a useful adjunct to CT angiography.Larger studies are needed to further establish the accuracy of myocardial perfu-sion imaging in CT.
953 Detection of coronary artery stenoses in patients withprevious coronary revascularization by 128-slice dualdource computed tomography
T. Pflederer, M. Seltmann, M. Marwan, D. Ropers, W.G. Daniel,S. Achenbach. University of Erlangen-Nuremberg, Department of
Cardiology and Angiology, Erlangen, Germany
Introduction: Coronary CT Angiography (cCTA) allows the detection of coronaryartery stenoses in selected patients. Patients with previous revascularization areusually not considered candidates for cCTA, since imaging may be challenging.The latest Dual-source CT (DSCT) with two detectors that allows simultaneousacquisition of 2x128 slices at 0.28s gantry rotation speed offers unprecedentedtemporal resolution for cCTA. We assessed the accuracy to detect coronary arterystenoses in patients with previous coronary revascularization who were sched-uled for invasive coronary angiography.Methods: 55 patients with previous coronary revascularization (stents, by-pass surgery, or both) were investigated by 128-slice DSCT (Definition FLASH,Siemens Healthcare, Forchheim, Germany, 2x128x0.6 mm collimation, 60-90 mlcontrast agent i.v. at 6 ml/s) prior to conventional coronary angiogram. All patientsreceived 0.8 mg isosorbide dinitrate sublingually and - at heart rates >60 bpm -100mg atenolol orally before the scan. Bypass grafts and native coronary arteries
- including stented segments - as well as each native coronary artery were eval-uated concerning the detection of significant coronary artery stenoses (> 50%diameter reduction) and results were compared to invasive angiography.Results: Mean heart rate was 58±7/min. In the 55 patients, 42 bypass grafts(30 venous and 12 arterial) as well as 78 implanted coronary stents (34 DES, 44BMS) were present (mean stent diameter 3.1±0.4mm). A total of 15 bypass graftstenoses and 16 in-stent stenoses were present. On a per-patient level, DSCTdisplayed a sensitivity and specificity of 92% and 83% to identify patients withbypass lesions or coronary artery stenoses that were not bridged by a bypassgraft (PPV 83% and NPV 92%). Sensitivity, specificity, PPV and NPV of DSCTto identify stenoses with a diameter reduction >50% were 92%, 98%, 92% and98% on a per-segment level, 100%, 96%, 94% and 100% on a per-bypass level,as well as 94%, 90%, 71% and 98% on a per-stent level.Conclusions: Improved image quality of newest DSCT technology as well as anoptimized image acquisition protocol provides high accuracy for the detection ofcoronary artery stenoses in patients with previous coronary revascularization.
954 Prospective randomized trial on radiation doseestimates of CT angiography in patients scanned with asequential scan protocol - impact of different scanalgorithms in the PROTECTION III study
J. Hausleiter1, T. Meyer1, E. Martuscelli2, P. Spagnolo3 , H. Yamamoto4,P. Carrascosa5, T. Anger6, L. Lehmkuhl7 , H. Alkadhi8, A. Achenbach9. 1GermanHeart Center, Clinic at the Technical University of Munich, Munich, Germany;2Tor Vergata Polyclinic, Rome, Italy; 3EMO-GVM Heart Center Columbus,Milan, Italy; 4Nagano Chuo Hospital, Nagano, Japan; 5Diagnóstico Maipú,Buenos Aires, Argentina; 6Hospital Bayreuth, Medical Clinic II - Departmentof Cardiology, Angiology and Pneumology, Bayreuth, Germany; 7University ofLeipzig, Heart Center, Leipzig, Germany; 8University Hospital Zurich, Zurich,Switzerland; 9University of Erlangen-Nuremberg, Department of Cardiology andAngiology, Erlangen, Germany
Background: Concerns have been raised about the radiation exposure duringcoronary CT angiographies (CCTAs). The use of a sequential (SEQ; step-and-shoot) scan protocol effectively lowers CCTA radiation dose compared to conven-tional spiral (SPI) CCTA, but it is unclear, whether image quality is maintained.The prospective, randomized PROTECTION III study is an international, multi-center and multivendortrial investigating the impact of the sequential CCTA protocol on image quality andradiation dose. This subgroup analysis focuses on the efficacy of different scanalgorithms provided by different CT vendors.Methods: 400 patients with suspected coronary artery disease and stable sinusrhythm were randomized to either a sequential or spiral CCTA protocol (200 pts.each). The primary study endpoint was to showthe diagnostic non-inferiority of the sequential scan protocol, which was assessedby a 4-point imagequality grading score (1: nondiagnostic to 4: excellent image quality; predefinednon-inferioritymargin of 0.2 score points). Radiation dose was assessed as secondary endpoint.Results: Mean BMI of all 400 patients was 25.9±3.8kg/m2, mean heart rate54.8±5.8bpm. The overall image quality score did not differ between sequentialand spiral CCTA (SEQ: 3.36±0.59 vs. SPI: 3.37±0.59; P=0.86). The image qual-ity scores for the different vendors were: GE: SEQ: 3.22±0.60 vs. SPI: 3.00±0.66(P=0.047); Philips: SEQ: 3.38±0.60 vs. SPI: 3.57±0.50 (P=0.033); and Siemens:SEQ: 3.47±0.55 vs. SPI: 3.52±0.39 (P=0.56). While the overall radiation dosewas reduced by 69% with SEQ, the lowest radiation dose of 2.9±2.1 mSv wasachieved with the Siemens SEQ algorithm (GE: SEQ: 4.2±2.7 vs SPI: 15.4±6.5mSv; Philips: SEQ: 3.6±0.7 vs SPI: 11.1±3.0 mSv; Siemens: SEQ: 2.9±2.1 vsSPI: 7.3±5.0 mSv; all P<0.001).Conclusions: Compared with spiral CCTA, the overall diagnostic image quality ismaintained with sequential CCTA while radiation dose is reduced by 69%. How-ever, there appear to be small differences in image quality and radiation dose withdifferent CT vendors. Nonetheless, the SEQ scan protocol should be applied in allpatients with stable sinus rhythm to keep radiation exposure as low as reasonablyachievable.
955 Myocardial perfusion assessed through CT coronaryangiography: a comparison with positron emissiontomography
M. Coceani1, R. Favilla2, G. Coppini2, M. Bianchi3, M. Schlueter1,E. Filidei2, A. Mazzarisi2, D. Neglia2, P. Marraccini2. 1Fondazione G.
Monasterio CNR-Regione Toscana, Pisa, Italy; 2Institute of Clinical Physiologyof CNR, Pisa, Italy; 3AOUP Medicina Generale IV, Pisa, Italy
Purpose: CT coronary angiography (CTCA) is a non invasive technique whichallows acquisition of high resolution images of the heart and coronary ves-sels. CTCA may also be used to examine myocardial perfusion. The gold stan-dard technique for the absolute quantification of myocardial blood flow (MBF) ispositron emission tomography (PET). The aim of the present study was to com-pare CTCA with PET in the evaluation of myocardial perfusion.Methods: Twenty five patients (mean age 62±0.7 years, 72% male) underwentboth CTCA and N13-ammonia PET for the evaluation of coronary artery dis-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Advances in cardiac computed tomography / Interventional cardiology, new information from trials and registries 153
ease (CAD). CTCA was performed in normal sinus rhythm with 110 ml of con-trast medium injected at 8 ml/sec. Offline analysis of myocardial perfusion wascarried out according to the following steps: 1) long-axis reformatting and inter-active selection of ventricular VOI 2) extraction of the left ventricular cavity bythresholding and blob growing 3) segmentation of the left ventricle 4) calibra-tion of myocardial enhancement by subtracting the baseline attenuation (esti-mated from standard calcium score scans) 5) generation of 17-segment bull’seye maps depicting the spatial distribution of myocardial contrast enhancement(MCE) expressed in Hounsfield Units, corrected for aortic attenuation. PET imag-ing was performed in basal conditions and after intravenous administration ofdipyridamole; 17-segment polar maps of MBF were then constructed and com-pared with bull’s eye maps obtained through CTCA. Correlations between CTCAMCE and PET MBF were analyzed with Spearman’s rank correlation, under theweak assumption of monotonic dependence.Results: Average values of myocardial blood flow measured by PET were0.55±0.19 ml/min/g (min=0.12, max=1.37) in basal conditions and 1.16±0.49ml/min/g (min=0.20, max=2.81) during pharmacological vasodilatation. AverageMCE at CTCA was 0.14±0.08 (min=0.01, max=0.36). Using Spearman’s analy-sis, a strong association was observed between segmental values of MCE andMBF at rest (rho 0.89, p<10E-15), which became more evident when MCE wascompared with MBF during vasodilatation (rho 0.94, p<10E-15).Conclusions: CTCA allows accurate determination of myocardial perfusion.More specifically, myocardial perfusion assessed through CTCA is more closelylinked to MBF values obtained during vasodilatation induced by dipyridamole.CTCA may, therefore, become a valuable tool not only for the examination ofcoronary anatomy and myocardial contractile function, but also for the evalua-tion of the physiological significance of epicardial stenoses and for the study ofmicrovascular function.
INTERVENTIONAL CARDIOLOGY, NEW INFORMATIONFROM TRIALS AND REGISTRIES
977 Safety and efficacy of a novel metal catheter in chronictotal occlusion lesions. -Corsair First-In-Man (FIM)Registry-
M. Kimura, E. Tsuchikane, O. Katoh, S. Ebisawa, T. Ito, N. Tanaka,N. Kenya, Y. Kinoshita, M. Ehara, T. Suzuki. Toyohashi Heart Center,
Toyohashi, Japan
Background: Successful recanalization of chronic total occlusions (CTO) in na-tive coronary arteries continues to represent the most technically challenging as-pect of percutaneous coronary intervention (PCI). A retrograde approach throughthe collateral channels has recently been proposed and has the potential to im-prove on the success rates of PCI in CTO lesions of the coronary arteries. Theaim of this study was to evaluate the safety and feasibility of a novel metal catheter(CORSAIR) in the retrograde approach for CTO recanalization.Methods: We sought to evaluate the safety and efficacy of this device in retro-grade collateral tracking for CTO lesions. From September 2007 to September2008, CTO recanalization was attempted using CORSAIR in 93 consecutive CTOlesions (>3 months). Clinical outcomes were compared with a matched controlgroup (n=93).Results: Of 93 cases, CTO recanalization was previously attempted in 61 (65%).CTO lesions were most frequently located in the RCA (80%) followed by the LAD(17%), and the LCX (3%). For the retrograde approach with CORSAIR, we usedseptal channels (83%), epicardial channels (15%), and bypass grafts (2%) asan access route. No significant difference was observed in baseline lesion char-acteristics between the 2 groups. The rates of successful channel crossing andaccess into the CTO with CORSAIR were 97% and 91%, respectively. Success-ful recanalization was achieved in 98% of the cases (91% in matched controls,p=0.03) without any major cardiac events or complications such as hematoma orcoronary rupture.Conclusions: In this FIM study, CORSAIR provided a high success rate for PCIvia the retrograde approach for CTO lesions without major complications. Theseresults indicate that this novel device is feasible to use and safe in retrograde ap-proach. Additional clinical trials should be considered to confirm these promisingresults.
978 Experimental and clinical comparison of coronaryluminal dimension between Optical CoherenceTomography (OCT), IntraVascular UltraSound (IVUS) andQuantitative Coronary Angiography (QCA)
K. Hattori, M. Okumura, H. Naruse, S.C. Kan, M. Ishikawa, H. Harigaya,T. Kawai, M. Oota, J. Ishii, Y. Ozaki. Fujita Health University Hospital, Toyoake,Japan
Background: Although OCT has recently entered the clinical arena, the reliabilityof quantitative analysis has not yet been fully established, especially in compari-son with IVUS and QCA measurements.Methods & Results: In experimental phantom series, coronary imaging of 11 in-vitro phantom stenosis (0.5 to 3.0mm diameter) and 90 in-vivo stenosis in 30 pa-tients (pre, post and follow-up) were examined by OCT, IVUS and QCA. In exper-
imental series, minimal luminal diameter (MLD) was compared to true phantomdiameter (PD) using the paired Student’s t-test and linear regression analysis. Inthe clinical series, minimal lumen area (MLA) was compared between OCT, IVUSand QCA, while MLA was calculated from the mathematical equation of MLD byedge-detection QCA (pi x MLD1 x MLD2/4). The mean of the signed differencesbetween the two measurement systems were considered an index of accuracyand the standard deviation of the differences an index of precision. A p-value of<0.05 was considered significant.
Results
Accuracy Precision r p-value
Experimental MLD comparisonQCA vs. Phantom Diam. -0.151mm ±0.116mm 0.999 0.001IVUS vs. Phantom Diam. ... 0.148mm ±0.086mm 0.982 0.001OCT vs. Phantom Diam. 0.108mm ±0.060mm 0.995 0.001
Clinical MLA comparisonOCT vs. IVUS -0.428mm2 ... ±0.965mm2 ... 0.954... 0.001IVUS vs. QCA 2.170mm2 ±2.010mm2 0.770 0.001OCT vs. QCA 1.742mm2 ±2.029mm2 0.775 0.001
Conclusions: In the experimental phantom series, OCT gave the most accuratevalues (i.e. the best accuracy and precision). In the clinical series, calculatedMLA based on the mathematical equation from QCA was significantly smallerthan measured MLA by OCT and IVUS. While MLA by IVUS was significantlygreater than OCT, IVUS might fail to detect true leading edge of coronary lumendue to the limited resolution of ultrasound technology as compared to OCT. Whilein the clinical setting the entire vessel area could occasionally be difficult to traceby current OCT technology as compared to IVUS, OCT could be more reliableto detect the true leading edge of coronary lumen than IVUS as well as than thecalculation from edge-detection QCA.
979 A randomized controlled trial of fractional flow reserveto optimize percutaneous coronary intervention
E. Durand1, M. Gilard2, A. Furber3, P. Coste4, P. Barragan5, J.L. DuboisRande6, P. Dupouy7, S. Rahal1, M. Slama8, A. Lafont1 . 1AP-HP -European Hospital Georges Pompidou, Paris, France; 2University
Hospital of Brest - Hospital Cavale Blanche, Brest, France; 3University Hospitalof Angers, Angers, France; 4University Hospital of Bordeaux - Hospital HautLeveque, Departement of Cardiology, Pessac, France; 5Polyclinic Les Fleurs,Ollioules, France; 6AP-HP - University Hospital Henri Mondor, Department ofCardiology, Creteil, France; 7Clinic Les Fontaines, Melun, France; 8AP-HP -Hospital Antoine-Beclere, Department of Cardiology, Clamart, France
Background: It has been recently demonstrated that measurement of FFR in ad-dition to angiographic guidance results in a significant reduction in major adverseevents in patients with multivessel coronary artery disease before PCI. However,it is unclear whether routine measurement of FFR during PCI improves outcomes.Methods: The FROST 4 study was a French, randomized, multicentre study of571 patients (of 714 planned) with de novo native coronary artery lesions under-going PCI with a bare metal stent (BMS). Patients were randomly assigned toguidance with angiography alone (n=287, angiography-guided PCI group) or byFFR measurements in addition to angiography (n=284, FFR-guided PCI group).Patients assigned to the FFR-guided PCI group during stenting were encouragedto obtain a final FFR > 0.95. The primary end-point was a composite of death,myocardial infarction, and target lesion revascularization (TLR) at 6 months.Results: The primary end point occurred in 21 patients (8.1%) in theangiography-guided PCI group and in 17 (6.6%) in the FFR-guided PCI group (OR0.79, 95 percent confidence interval 0.41 to 1.50, P=0.48). In the FFR-guided PCIgroup, a final FFR > 0.95 was achieved in 77.6%. Furthermore, the primary endpoint was significantly decreased in patients with a final FFR > 0.95 as comparedto those with a final FFR < 0.95 (4.4% vs 13.5%, OR 0.30, 95 percent confidenceinterval 0.10 to 0.87, p=0.048).Conclusions: The results of our study suggest that routine measurement of FFRduring PCI is not significantly associated with clinical benefit. However, a finalFFR > 0.95 is associated with favorable outcome in patients undergoing PCI withBMS (ClinicalTrials.gov number NCT00242892).
980 Clinical outcome after implantation ofzotarolimus-eluting versus sirolimus-eluting stents inpatients with single or multiple lesions. An 18 monthSORT OUT III substudy
H.-H. Tilsted1, M. Maeng2, L.O. Jensen3, A. Kaltoft2, P. Thayssen3 ,J. Ravkilde1, M. Madsen2, H.T. Soerensen2 , L. Thuesen2 , J.F. Lassen2.
1Aalborg Hospital of the Aarhus University Hospital, Center for CardiovascularResearch - Cardiology, Aalborg, Denmark; 2Aarhus University Hospital, Skejby,Department of Cardiology, Aarhus, Denmark; 3Odense University Hospital,Department of Cardiology, Odense, Denmark
Background: The numbers of lesions treated is a predictor for the prognosisafter percutaneous coronary intervention (PCI). We therefore compared clini-cal outcome in patients with single lesions or multiple lesions treated with thesecond-generation zotarolimus-eluting Endeavor stent (ZES) and first-generationsirolimus-eluting Cypher™ stent (SES).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
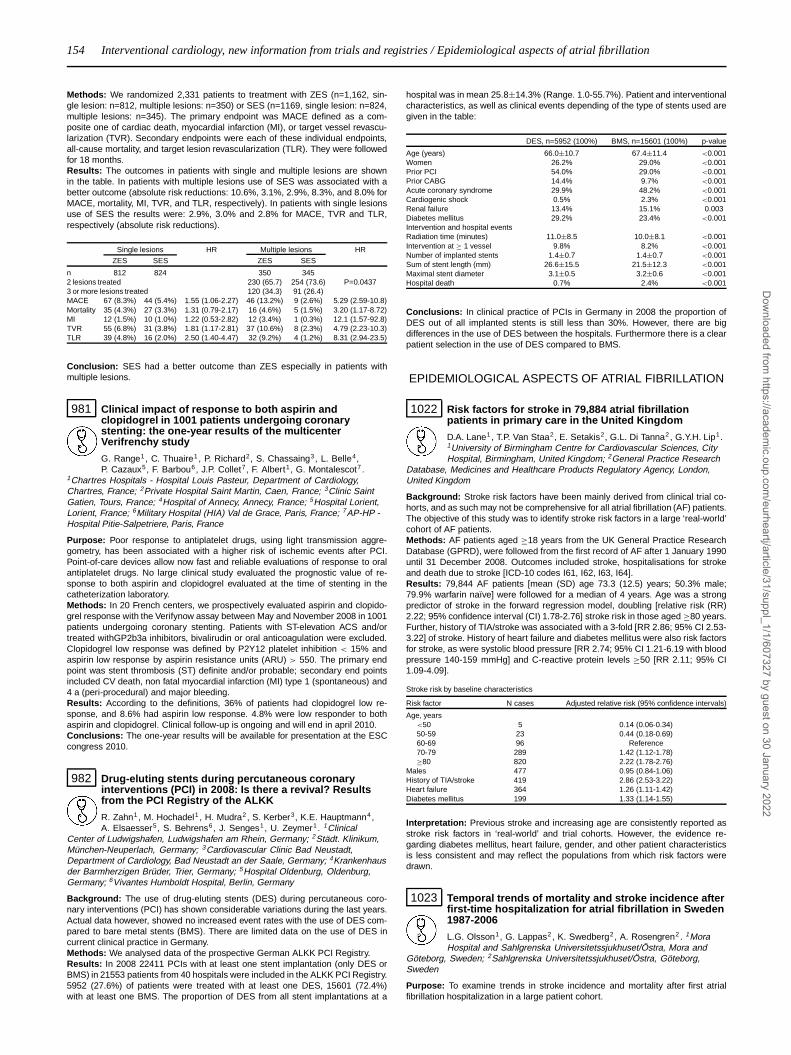
154 Interventional cardiology, new information from trials and registries / Epidemiological aspects of atrial fibrillation
Methods: We randomized 2,331 patients to treatment with ZES (n=1,162, sin-gle lesion: n=812, multiple lesions: n=350) or SES (n=1169, single lesion: n=824,multiple lesions: n=345). The primary endpoint was MACE defined as a com-posite one of cardiac death, myocardial infarction (MI), or target vessel revascu-larization (TVR). Secondary endpoints were each of these individual endpoints,all-cause mortality, and target lesion revascularization (TLR). They were followedfor 18 months.Results: The outcomes in patients with single and multiple lesions are shownin the table. In patients with multiple lesions use of SES was associated with abetter outcome (absolute risk reductions: 10.6%, 3.1%, 2.9%, 8.3%, and 8.0% forMACE, mortality, MI, TVR, and TLR, respectively). In patients with single lesionsuse of SES the results were: 2.9%, 3.0% and 2.8% for MACE, TVR and TLR,respectively (absolute risk reductions).
Single lesions HR Multiple lesions HR
ZES SES ZES SES
n 812 824 350 3452 lesions treated 230 (65.7) 254 (73.6) P=0.04373 or more lesions treated 120 (34.3) 91 (26.4)MACE 67 (8.3%) 44 (5.4%) 1.55 (1.06-2.27) 46 (13.2%) 9 (2.6%) 5.29 (2.59-10.8)Mortality 35 (4.3%) 27 (3.3%) 1.31 (0.79-2.17) 16 (4.6%) 5 (1.5%) 3.20 (1.17-8.72)MI 12 (1.5%) 10 (1.0%) 1.22 (0.53-2.82) 12 (3.4%) 1 (0.3%) 12.1 (1.57-92.8)TVR 55 (6.8%) 31 (3.8%) 1.81 (1.17-2.81) 37 (10.6%) 8 (2.3%) 4.79 (2.23-10.3)TLR 39 (4.8%) 16 (2.0%) 2.50 (1.40-4.47) 32 (9.2%) 4 (1.2%) 8.31 (2.94-23.5)
Conclusion: SES had a better outcome than ZES especially in patients withmultiple lesions.
981 Clinical impact of response to both aspirin andclopidogrel in 1001 patients undergoing coronarystenting: the one-year results of the multicenterVerifrenchy study
G. Range1, C. Thuaire1 , P. Richard2, S. Chassaing3, L. Belle4,P. Cazaux5, F. Barbou6, J.P. Collet7, F. Albert1, G. Montalescot7 .
1Chartres Hospitals - Hospital Louis Pasteur, Department of Cardiology,Chartres, France; 2Private Hospital Saint Martin, Caen, France; 3Clinic SaintGatien, Tours, France; 4Hospital of Annecy, Annecy, France; 5Hospital Lorient,Lorient, France; 6Military Hospital (HIA) Val de Grace, Paris, France; 7AP-HP -Hospital Pitie-Salpetriere, Paris, France
Purpose: Poor response to antiplatelet drugs, using light transmission aggre-gometry, has been associated with a higher risk of ischemic events after PCI.Point-of-care devices allow now fast and reliable evaluations of response to oralantiplatelet drugs. No large clinical study evaluated the prognostic value of re-sponse to both aspirin and clopidogrel evaluated at the time of stenting in thecatheterization laboratory.Methods: In 20 French centers, we prospectively evaluated aspirin and clopido-grel response with the Verifynow assay between May and November 2008 in 1001patients undergoing coronary stenting. Patients with ST-elevation ACS and/ortreated withGP2b3a inhibitors, bivalirudin or oral anticoagulation were excluded.Clopidogrel low response was defined by P2Y12 platelet inhibition < 15% andaspirin low response by aspirin resistance units (ARU) > 550. The primary endpoint was stent thrombosis (ST) definite and/or probable; secondary end pointsincluded CV death, non fatal myocardial infarction (MI) type 1 (spontaneous) and4 a (peri-procedural) and major bleeding.Results: According to the definitions, 36% of patients had clopidogrel low re-sponse, and 8.6% had aspirin low response. 4.8% were low responder to bothaspirin and clopidogrel. Clinical follow-up is ongoing and will end in april 2010.Conclusions: The one-year results will be available for presentation at the ESCcongress 2010.
982 Drug-eluting stents during percutaneous coronaryinterventions (PCI) in 2008: Is there a revival? Resultsfrom the PCI Registry of the ALKK
R. Zahn1, M. Hochadel1 , H. Mudra2, S. Kerber3, K.E. Hauptmann4,A. Elsaesser5, S. Behrens6, J. Senges1, U. Zeymer1. 1Clinical
Center of Ludwigshafen, Ludwigshafen am Rhein, Germany; 2Städt. Klinikum,München-Neuperlach, Germany; 3Cardiovascular Clinic Bad Neustadt,Department of Cardiology, Bad Neustadt an der Saale, Germany; 4Krankenhausder Barmherzigen Brüder, Trier, Germany; 5Hospital Oldenburg, Oldenburg,Germany; 6Vivantes Humboldt Hospital, Berlin, Germany
Background: The use of drug-eluting stents (DES) during percutaneous coro-nary interventions (PCI) has shown considerable variations during the last years.Actual data however, showed no increased event rates with the use of DES com-pared to bare metal stents (BMS). There are limited data on the use of DES incurrent clinical practice in Germany.Methods: We analysed data of the prospective German ALKK PCI Registry.Results: In 2008 22411 PCIs with at least one stent implantation (only DES orBMS) in 21553 patients from 40 hospitals were included in the ALKK PCI Registry.5952 (27.6%) of patients were treated with at least one DES, 15601 (72.4%)with at least one BMS. The proportion of DES from all stent implantations at a
hospital was in mean 25.8±14.3% (Range. 1.0-55.7%). Patient and interventionalcharacteristics, as well as clinical events depending of the type of stents used aregiven in the table:
DES, n=5952 (100%) BMS, n=15601 (100%) p-value
Age (years) 66.0±10.7 67.4±11.4 <0.001Women 26.2% 29.0% <0.001Prior PCI 54.0% 29.0% <0.001Prior CABG 14.4% 9.7% <0.001Acute coronary syndrome 29.9% 48.2% <0.001Cardiogenic shock 0.5% 2.3% <0.001Renal failure 13.4% 15.1% 0.003Diabetes mellitus 29.2% 23.4% <0.001Intervention and hospital eventsRadiation time (minutes) 11.0±8.5 10.0±8.1 <0.001Intervention at ≥ 1 vessel 9.8% 8.2% <0.001Number of implanted stents 1.4±0.7 1.4±0.7 <0.001Sum of stent length (mm) 26.6±15.5 21.5±12.3 <0.001Maximal stent diameter 3.1±0.5 3.2±0.6 <0.001Hospital death 0.7% 2.4% <0.001
Conclusions: In clinical practice of PCIs in Germany in 2008 the proportion ofDES out of all implanted stents is still less than 30%. However, there are bigdifferences in the use of DES between the hospitals. Furthermore there is a clearpatient selection in the use of DES compared to BMS.
EPIDEMIOLOGICAL ASPECTS OF ATRIAL FIBRILLATION
1022 Risk factors for stroke in 79,884 atrial fibrillationpatients in primary care in the United Kingdom
D.A. Lane1, T.P. Van Staa2, E. Setakis2, G.L. Di Tanna2, G.Y.H. Lip1.1University of Birmingham Centre for Cardiovascular Sciences, CityHospital, Birmingham, United Kingdom; 2General Practice Research
Database, Medicines and Healthcare Products Regulatory Agency, London,United Kingdom
Background: Stroke risk factors have been mainly derived from clinical trial co-horts, and as such may not be comprehensive for all atrial fibrillation (AF) patients.The objective of this study was to identify stroke risk factors in a large ‘real-world’cohort of AF patients.Methods: AF patients aged ≥18 years from the UK General Practice ResearchDatabase (GPRD), were followed from the first record of AF after 1 January 1990until 31 December 2008. Outcomes included stroke, hospitalisations for strokeand death due to stroke [ICD-10 codes I61, I62, I63, I64].Results: 79,844 AF patients [mean (SD) age 73.3 (12.5) years; 50.3% male;79.9% warfarin naïve] were followed for a median of 4 years. Age was a strongpredictor of stroke in the forward regression model, doubling [relative risk (RR)2.22; 95% confidence interval (CI) 1.78-2.76] stroke risk in those aged ≥80 years.Further, history of TIA/stroke was associated with a 3-fold [RR 2.86; 95% CI 2.53-3.22] of stroke. History of heart failure and diabetes mellitus were also risk factorsfor stroke, as were systolic blood pressure [RR 2.74; 95% CI 1.21-6.19 with bloodpressure 140-159 mmHg] and C-reactive protein levels ≥50 [RR 2.11; 95% CI1.09-4.09].
Stroke risk by baseline characteristics
Risk factor N cases Adjusted relative risk (95% confidence intervals)
Age, years<50 5 0.14 (0.06-0.34)50-59 23 0.44 (0.18-0.69)60-69 96 Reference70-79 289 1.42 (1.12-1.78)≥80 820 2.22 (1.78-2.76)
Males 477 0.95 (0.84-1.06)History of TIA/stroke 419 2.86 (2.53-3.22)Heart failure 364 1.26 (1.11-1.42)Diabetes mellitus 199 1.33 (1.14-1.55)
Interpretation: Previous stroke and increasing age are consistently reported asstroke risk factors in ‘real-world’ and trial cohorts. However, the evidence re-garding diabetes mellitus, heart failure, gender, and other patient characteristicsis less consistent and may reflect the populations from which risk factors weredrawn.
1023 Temporal trends of mortality and stroke incidence afterfirst-time hospitalization for atrial fibrillation in Sweden1987-2006
L.G. Olsson1, G. Lappas2, K. Swedberg2, A. Rosengren2 . 1MoraHospital and Sahlgrenska Universitetssjukhuset/Östra, Mora and
Göteborg, Sweden; 2Sahlgrenska Universitetssjukhuset/Östra, Göteborg,Sweden
Purpose: To examine trends in stroke incidence and mortality after first atrialfibrillation hospitalization in a large patient cohort.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
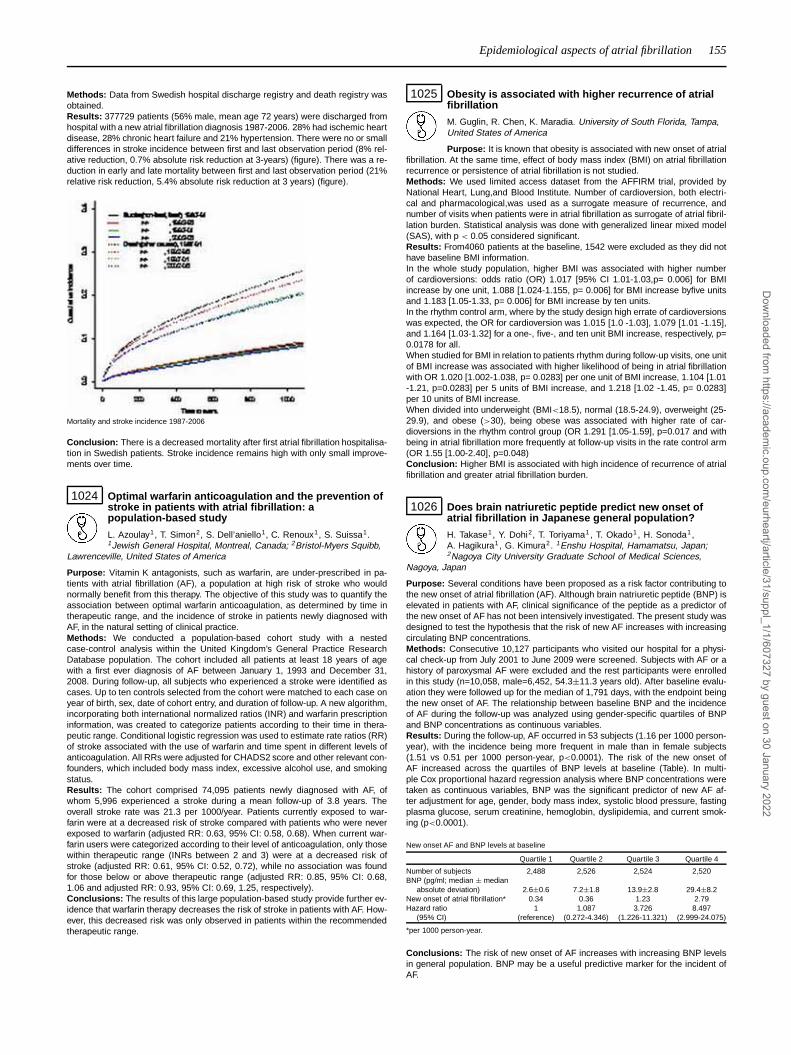
Epidemiological aspects of atrial fibrillation 155
Methods: Data from Swedish hospital discharge registry and death registry wasobtained.Results: 377729 patients (56% male, mean age 72 years) were discharged fromhospital with a new atrial fibrillation diagnosis 1987-2006. 28% had ischemic heartdisease, 28% chronic heart failure and 21% hypertension. There were no or smalldifferences in stroke incidence between first and last observation period (8% rel-ative reduction, 0.7% absolute risk reduction at 3-years) (figure). There was a re-duction in early and late mortality between first and last observation period (21%relative risk reduction, 5.4% absolute risk reduction at 3 years) (figure).
Mortality and stroke incidence 1987-2006
Conclusion: There is a decreased mortality after first atrial fibrillation hospitalisa-tion in Swedish patients. Stroke incidence remains high with only small improve-ments over time.
1024 Optimal warfarin anticoagulation and the prevention ofstroke in patients with atrial fibrillation: apopulation-based study
L. Azoulay1, T. Simon2, S. Dell’aniello1, C. Renoux1, S. Suissa1.1Jewish General Hospital, Montreal, Canada; 2Bristol-Myers Squibb,
Lawrenceville, United States of America
Purpose: Vitamin K antagonists, such as warfarin, are under-prescribed in pa-tients with atrial fibrillation (AF), a population at high risk of stroke who wouldnormally benefit from this therapy. The objective of this study was to quantify theassociation between optimal warfarin anticoagulation, as determined by time intherapeutic range, and the incidence of stroke in patients newly diagnosed withAF, in the natural setting of clinical practice.Methods: We conducted a population-based cohort study with a nestedcase-control analysis within the United Kingdom’s General Practice ResearchDatabase population. The cohort included all patients at least 18 years of agewith a first ever diagnosis of AF between January 1, 1993 and December 31,2008. During follow-up, all subjects who experienced a stroke were identified ascases. Up to ten controls selected from the cohort were matched to each case onyear of birth, sex, date of cohort entry, and duration of follow-up. A new algorithm,incorporating both international normalized ratios (INR) and warfarin prescriptioninformation, was created to categorize patients according to their time in thera-peutic range. Conditional logistic regression was used to estimate rate ratios (RR)of stroke associated with the use of warfarin and time spent in different levels ofanticoagulation. All RRs were adjusted for CHADS2 score and other relevant con-founders, which included body mass index, excessive alcohol use, and smokingstatus.Results: The cohort comprised 74,095 patients newly diagnosed with AF, ofwhom 5,996 experienced a stroke during a mean follow-up of 3.8 years. Theoverall stroke rate was 21.3 per 1000/year. Patients currently exposed to war-farin were at a decreased risk of stroke compared with patients who were neverexposed to warfarin (adjusted RR: 0.63, 95% CI: 0.58, 0.68). When current war-farin users were categorized according to their level of anticoagulation, only thosewithin therapeutic range (INRs between 2 and 3) were at a decreased risk ofstroke (adjusted RR: 0.61, 95% CI: 0.52, 0.72), while no association was foundfor those below or above therapeutic range (adjusted RR: 0.85, 95% CI: 0.68,1.06 and adjusted RR: 0.93, 95% CI: 0.69, 1.25, respectively).Conclusions: The results of this large population-based study provide further ev-idence that warfarin therapy decreases the risk of stroke in patients with AF. How-ever, this decreased risk was only observed in patients within the recommendedtherapeutic range.
1025 Obesity is associated with higher recurrence of atrialfibrillation
M. Guglin, R. Chen, K. Maradia. University of South Florida, Tampa,United States of America
Purpose: It is known that obesity is associated with new onset of atrialfibrillation. At the same time, effect of body mass index (BMI) on atrial fibrillationrecurrence or persistence of atrial fibrillation is not studied.Methods: We used limited access dataset from the AFFIRM trial, provided byNational Heart, Lung,and Blood Institute. Number of cardioversion, both electri-cal and pharmacological,was used as a surrogate measure of recurrence, andnumber of visits when patients were in atrial fibrillation as surrogate of atrial fibril-lation burden. Statistical analysis was done with generalized linear mixed model(SAS), with p < 0.05 considered significant.Results: From4060 patients at the baseline, 1542 were excluded as they did nothave baseline BMI information.In the whole study population, higher BMI was associated with higher numberof cardioversions: odds ratio (OR) 1.017 [95% CI 1.01-1.03,p= 0.006] for BMIincrease by one unit, 1.088 [1.024-1.155, p= 0.006] for BMI increase byfive unitsand 1.183 [1.05-1.33, p= 0.006] for BMI increase by ten units.In the rhythm control arm, where by the study design high errate of cardioversionswas expected, the OR for cardioversion was 1.015 [1.0 -1.03], 1.079 [1.01 -1.15],and 1.164 [1.03-1.32] for a one-, five-, and ten unit BMI increase, respectively, p=0.0178 for all.When studied for BMI in relation to patients rhythm during follow-up visits, one unitof BMI increase was associated with higher likelihood of being in atrial fibrillationwith OR 1.020 [1.002-1.038, p= 0.0283] per one unit of BMI increase, 1.104 [1.01-1.21, p=0.0283] per 5 units of BMI increase, and 1.218 [1.02 -1.45, p= 0.0283]per 10 units of BMI increase.When divided into underweight (BMI<18.5), normal (18.5-24.9), overweight (25-29.9), and obese (>30), being obese was associated with higher rate of car-dioversions in the rhythm control group (OR 1.291 [1.05-1.59], p=0.017 and withbeing in atrial fibrillation more frequently at follow-up visits in the rate control arm(OR 1.55 [1.00-2.40], p=0.048)Conclusion: Higher BMI is associated with high incidence of recurrence of atrialfibrillation and greater atrial fibrillation burden.
1026 Does brain natriuretic peptide predict new onset ofatrial fibrillation in Japanese general population?
H. Takase1, Y. Dohi2, T. Toriyama1, T. Okado1, H. Sonoda1,A. Hagikura1, G. Kimura2. 1Enshu Hospital, Hamamatsu, Japan;2Nagoya City University Graduate School of Medical Sciences,
Nagoya, Japan
Purpose: Several conditions have been proposed as a risk factor contributing tothe new onset of atrial fibrillation (AF). Although brain natriuretic peptide (BNP) iselevated in patients with AF, clinical significance of the peptide as a predictor ofthe new onset of AF has not been intensively investigated. The present study wasdesigned to test the hypothesis that the risk of new AF increases with increasingcirculating BNP concentrations.Methods: Consecutive 10,127 participants who visited our hospital for a physi-cal check-up from July 2001 to June 2009 were screened. Subjects with AF or ahistory of paroxysmal AF were excluded and the rest participants were enrolledin this study (n=10,058, male=6,452, 54.3±11.3 years old). After baseline evalu-ation they were followed up for the median of 1,791 days, with the endpoint beingthe new onset of AF. The relationship between baseline BNP and the incidenceof AF during the follow-up was analyzed using gender-specific quartiles of BNPand BNP concentrations as continuous variables.Results: During the follow-up, AF occurred in 53 subjects (1.16 per 1000 person-year), with the incidence being more frequent in male than in female subjects(1.51 vs 0.51 per 1000 person-year, p<0.0001). The risk of the new onset ofAF increased across the quartiles of BNP levels at baseline (Table). In multi-ple Cox proportional hazard regression analysis where BNP concentrations weretaken as continuous variables, BNP was the significant predictor of new AF af-ter adjustment for age, gender, body mass index, systolic blood pressure, fastingplasma glucose, serum creatinine, hemoglobin, dyslipidemia, and current smok-ing (p<0.0001).
New onset AF and BNP levels at baseline
Quartile 1 Quartile 2 Quartile 3 Quartile 4
Number of subjects 2,488 2,526 2,524 2,520BNP (pg/ml; median ± median
absolute deviation) 2.6±0.6 7.2±1.8 13.9±2.8 29.4±8.2New onset of atrial fibrillation* 0.34 0.36 1.23 2.79Hazard ratio 1 1.087 3.726 8.497
(95% CI) (reference) (0.272-4.346) (1.226-11.321) (2.999-24.075)
*per 1000 person-year.
Conclusions: The risk of new onset of AF increases with increasing BNP levelsin general population. BNP may be a useful predictive marker for the incident ofAF.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

156 Epidemiological aspects of atrial fibrillation / Response to anti-thrombotic treatment
1027 Increased risk of stroke and atrial fibrillation inrheumatoid arthritis - a nationwide cohort study
J. Lindhardsen1, G.H. Gislason1, O. Ahlehoff1, O.R. Madsen2,P.R. Hansen1. 1Gentofte Hospital - Copenhagen University Hospital,Department of Cardiology, Hellerup, Denmark; 2Gentofte Hospital
- Copenhagen University Hospital, Department of Rheumatology, Hellerup,Denmark
Purpose: Rheumatoid arthritis (RA) is increasingly regarded as an independentrisk factor for coronary heart disease. The effect of RA on the risk of stroke isunclear, and the incidence of atrial fibrillation (AFib) in RA patients has not beenestablished in large-scale studies.Methods: The study population included the entire Danish population ≥ 10 yearsof age on Jan. 1, 1997 and was followed until Dec. 31, 2006 or first adverse event,i.e., stroke or AFib. Patients that developed RA in the study period were iden-tified by both claimed prescriptions for disease-modifying antirheumatic drugs(DMARDs) and RA related hospital contacts (admissions and outpatient visits)within the time span of one year through individual-level-linkage nationwide ad-ministrative registers. Adverse events were analysed using multivariate Poissonregression models fitted to age, gender, cardiovascular pharmacotherapy, Charl-sons comorbidity index, and income.Results: A total of 10,300 patients with incident RA were identified, and crude andadjusted incidence rate ratios (IRR [95% CI]) of adverse events were calculatedby comparison with 4,604,540 controls. During follow-up the rates of stroke per1.000 person years were 10.9 in the RA group vs. 4.6 in controls, correspondingto a crude IRR of 2.67 (2.45-2.92). After regression analysis the overall risk ofstroke remained markedly increased in RA patients with IRR 1.32 (1.21-1.45).RA did not change the relative contributions of gender and age to the risk ofstroke, i.e., male gender and high age were similar predictors of stroke in bothRA patients and controls. The rates of AFib in RA patients were also increasedcompared to controls (9.8/1000 vs. 3.7/1000 person years) with a crude IRR of2.67 (2.45-2.92). Indeed, regression analysis showed a 42% increase in risk ofAFib in RA patients compared to the general population (IRR 1.42 [1.30-1.56]).Conclusions: In this nationwide cohort study RA was an independent risk factorfor stroke irrespective of subject gender and age. Furthermore, RA was a signifi-cant risk factor for AFib and this association may contribute to the increased riskof stroke in these patients.
RESPONSE TO ANTI-THROMBOTIC TREATMENT: FROMGENES TO BIOMARKERS TO OUTCOME
1032 Genetic variants besides CYP2C19*2 polymorphism areassociated with major adverse cardiovascular events inhigh risk vascular patients on dual antiplatelet therapy
B. Giusti, C. Saracini, A. Vestrini, A. Magi, R. Marcucci, L. Rossi,A. Cordisco, C. Nanna, G.F. Gensini, R. Abbate. University of Florence,Thrombosis Centre, Dpt of Medical and Surgical Critical Care, Florence, Italy
Persistent platelet reactivity despite antiplatelet treatment confers an increasedrisk of major adverse cardiovascular events (MACE) in patients with acute coro-nary syndrome (ACS) undergoing percutaneous coronary intervention (PCI) withstent implantation. Genetic and non-genetic mechanisms are involved in highon-treatment platelet reactivity. In addition to polymorphisms linked to clopido-grel metabolism, genetic variants in different genes coding for platelet recep-tors and enzymes have been investigated with discordant results. Recently, theCYP2C19*2 polymorphism has been demonstrated a determinant of MACE oc-currence in patients on antiplatelet therapy.In 922 consecutive ACS patients undergoing PCI with stent implantation ondual antiplatelet therapy followed up for 6 months, aim of our study was to as-sess the relation to the risk of MACE of 41 allelic variants in 14 genes codingfor prostaglandin-endoperoxide synthase-1 (PTGS1 or COX1), - 2 (PTGS2 orCOX2), von Willebrand factor (VWF), integrin, alpha 2b (ITGA2B), glycoproteinIb, alpha polypeptide (GP1BA), glycoprotein VI (GP6), selectin P (SELP), integrin,alpha 2 (ITGA2), fibrinogen beta chain (FGB), purinergic receptor P2Y, G-proteincoupled, 12 (P2RY12), ATP-binding cassette, sub-family B (MDR/TAP), member1 (ABCB1), different isoforms of CYP450 (CYP3A4, CYP2C9, and CYP2C19).Genotyping was performed with specific allelic discrimination assays and a realtime PCR detection system.MACE occurred in 54 patients during the follow-up period. Patients with MACEshowed a higher prevalence of carriers of the rs3842788 (Gln41Gln) COX1 poly-morphism and of homozygotes for the rs7969672 VWF polymorphism, and alower prevalence of carriers of the rs5911 ITGA2B polymorphism (18.5% vs 7.9%,p=0.007; 7.4% vs 2.3%; p = 0.022 and 46.3% vs 61.7%, p=0.023, respectively);at the multivariate regression analysis only COX1 polymorphism remained sig-nificantly associated to MACE [OR=3.4 (1.45-8.02), p=0.005]. We confirmed thedata of the independent association of the CYP2C19*2 polymorphism with theoccurrence of MACE [OR adjusted for traditional cardiovascular risk factors 1.6(1.01-2.79, p=0.04)].Our data indicated that, besides the well known CYP2C19*2, other polymor-phisms in genes involved in platelet function play a crucial role in the outcomeof high risk vascular patients.
1033 Impact and interaction of common CYP2C19 geneticvariants on the antiplatelet effects of clopidogrelmaintenance treatment
D. Sibbing1, D. Gebhard1, W. Koch1, S. Braun1, J. Stegherr1,T. Morath1, N. Von Beckerath1 , A. Schomig1, T. Schuster2,
A. Kastrati1. 1Deutsches Herzzentrum München, München, Germany; 2TechnicalUniversity of Munich, Munich, Germany
Background: With the cytochrome P450 (CYP) 2C19*2 allelic variant resultingin loss of enzyme function and the CYP2C19*17 variant that has been linkedto an increased transcriptional activity resulting in extensive metabolization ofCYP2C19 substrates, two common variants in the CYP2C19 gene have beenreported recently. Currently, impact and interaction of both variants on the an-tiplatelet effects of clopidogrel maintenance treatment are unknown. The aim ofthis study was to assess impact and interaction of CYP2C19*2 and *17 on clopi-dogrel responsiveness in patients under clopidogrel maintenance treatment.Methods: Patients (n=968) eligible for this study were under chronic treatmentwith aspirin and clopidogrel (75 mg/d) due to prior coronary stenting. ADP-induced platelet aggregation (PA) was measured on a Multiplate analyzer (inAU*min) and genotypes were determined with a TaqMan assay.Results: PA values were significantly higher in carriers of at least one *2 allele ascompared to homozygous wild-type allele carriers (Fig. 1A). For CYP2C19*17, PAvalues were significantly lower in carriers of at least one *17 allele as compared tohomozygous wild-type allele carriers (Fig. 1B). A gene-dose effect was observedfor both allelic variants with the most pronounced effect of the mutant allele (*2 or*17) in homozygous patients (Fig. 1). Concerning the interaction of both alleleson PA values, a gradual increase of PA values was observed from (+)*17/(-)*2patients, exhibiting the lowest PA values (median 207 AU*min) over (-)*17/(-)*2and (+)*17/(+)*2 to (-)*17/(+)*2 patients, exhibiting the highest values (median309 AU*min) (P<0.001; calculated across groups).
Figure 1
Conclusions: CYP2C19*2 and *17 allele carriage are dominant predictors forthe antiplatelet effect of clopidogrel maintenance treatment.
1034 Impact of inflammatory markers on platelet functionand cardiovascular outcome in patients withsymptomatic coronary artery disease
T. Geisler1, K. Mueller2, S. Aichele2, K. Stellos2, C.S. Zuern2 ,P. Htun2, S. Fateh-Moghadam2 , A.E. May2, M. Flather1, M. Gawaz2.
1Royal Brompton and Harefield NHS Trust, London, United Kingdom; 2UniversityHospital Tübingen, Tübingen, Germany
Aims: There is cumulating evidence of an association between the inflammatorydegree and the incidence of atherothrombotic complications after PCI. The aimof the present analysis was to evaluate the association of inflammatory mark-ers and platelet responses to dual antiplatelet therapy and outcome in patientsundergoing coronary interventions.Methods and Results: In a pilot study, 257 patients with symptomatic coronaryartery disease (CAD) undergoing PCI were consecutively evaluated. Inhibition ofplatelet aggregation (IPA) by clopidogrel and Acetylsalicylic Acid (ASA) was as-sessed using whole blood multiple electrode aggregometry (MEA; Multiplate©).Baseline levels of inflammatory markers IL-6, RANTES, MCP-1 were measuredby Bio-Plex Cytokine assay. CRP was determined by Immunoassay. A signifi-cant association between levels of IL-6, RANTES, CRP and inhibition of ADP and
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Response to anti-thrombotic treatment / Diversity in monocyte and macrophage lineages in atherosclerosis 157
Arachidonic acid (AA)- induced aggregation was observed. In a second step, aretrospective analysis of a cohort of 890 PCI patients was performed to evalu-ate the association of residual platelet aggregation (RPA) under dual antiplatelettherapy, baseline CRP levels and outcome. Baseline CRP correlated with RPA.Patients suffering a subsequent cardiovascular event had a significantly higherlevel of baseline CRP and higher RPA compared to patients without events. Aftermultivariate adjustment baseline CRP was an independent predictor for high RPAand combined major events after PCI.Conclusions: To our knowledge this is the first study linking inflammation,platelet responsiveness to dual antiplatelet therapy and outcome in a largedataset of PCI patients. The results suggest a relevant interaction of these enti-ties and encourage multimodal therapeutic approaches to treat the cardiovascularrisk after PCI.
1035 Leptin levels and clopidogrel non-responsiveness inpatiets undergoing PCI: a dangerous relationship notyet described
L. Gatto, A. Nusca, R. Contuzzi, G. Di Giovanni, E. Ricottini, G. Patti,A. D’ambrosio, G. Di Sciascio. University Campus Bio-Medico of
Rome, Department of Cardiovascular Sciences, Rome, Italy
Purpose: Several studies have demonstrated significant interindividual variabilityin platelet response following clopidogrel treatment. High residual platelet reactiv-ity has been associated to worse outcome in patients undergoing percutaneouscoronary intervention (PCI). Leptin is a 167-amino acid peptide hormone pro-duced by adipose tissue, primarily involved in the regulation of food intake andenergy expenditure. Clinical studies showed that elevated leptin levels representan independent cardiovascular risk factor. Furthermore, leptin receptors are ex-pressed on the platelet surface and this adipocyte hormone may promote ADP-mediated platelet aggregation. The aim of this study was to evaluate the possiblerelationship between leptin levels and clopidogrel response in patients undergo-ing PCI.Methods: We prospectively enrolled 153 patients undergoing PCI at our Insti-tution (100 patients clopidogrel naïve treated with 600 mg loading dose beforethe procedure and 53 patients on 75 mg chronic clopidogrel therapy). In all pa-tients leptin levels were measured before PCI by ELISA and a value > 15 ng/mlwas used to identify hyperleptinemic patients. Platelet aggregation was measuredby VerifyNowP2Y12 assay and expressed such as PRU (P2Y12 Reaction Unit).According to post-treatment PRU value, study population was divided into threeterziles (PRU≤196, N=51; 197>PRU≤267, N=52; PRU>267, N=50). Clopidogrelnon responders were considered patients with post-clopidogrel PRU >240 and/orpatients with a percent decrease in platelet aggregation after treatment comparedto baseline (� aggregation) <30%.Results: Leptin levels were significantly higher in the third terzile (6.56±5.21ng/ml vs 8.46±8.29 ng/ml vs 12.96±18.06 ng/ml; P for trend = 0.022). Clopi-dogrel non-responders showed elevated leptin levels compared to patients clopi-dogrel responders: 11.41±15.71 versus 7.32±6.48 ng/ml, P=0.035 (according topost-treatment PRU >240) and 10.65±14.31 versus 7.03±5.97 ng/ml, P=0.031(according to � aggregation <30%). Leptin levels ≤15 ng/ml were associatedwith lower post-treatment PRU (219.69±81.29 versus 262.63±66.78; P=0.006)and a higher percent decrease in platelet aggregation (25.95±24.35 versus11.42±28.30%; P=0.007).Conclusions: Our results demonstrate, for the first time, a strong relationshipbetween leptin and clopidogrel non-responsiveness. A leptin value > 15 ng/mlidentifies patients with high residual platelet reactivity in whom a more aggressiveantiplatelet therapy may be suggested.
1036 EuroSCORE and 4Ts score could predict thromboticcomplications after cardiac surgery
A.V. Mattioli1, A. Farinetti1, A. Barbieri1, R. Lonardi1, S. Pennella2,G. Ambrosio3. 1University of Modena & Reggio Emilia, Modena,Italy; 2National Institute of Cardiovascular Research, Bologna, Italy;
3University of Perugia, Perugia, Italy
The 4Ts score is a risk assessment tool that classifies patients into low, moderate,and high pretest probability of heparin-induced thrombocytopenia, potentially al-lowing risk-based management. Preliminary observations suggest the 4Ts scoremay rule out HIT in patients with a low score.The European System for Cardiac Operative Risk Evaluation (EuroSCORE) is avalidated score estimating risk in cardiac surgery. Because of its additive nature,the standard EuroSCORE has been found to underestimate risk in certain veryhigh-risk patient groups.Methods: The EuroSCORE and the 4Ts score were evaluated in 600 pts under-going cardiac surgery.Patients were derived from 2 previous studies of HIT. The incidence of HIT wassystematically evaluated using an ELIZA test for detecting antibodies as a refer-ence standard. The follow-up lassessing death and trombotic events lasted 1 yearafter surgery.The 4Ts scoring system produces an integer score between 0 and 8. Scores of0-3, 4-5, and 6-8 are classified as low, moderate, and high pretest probability,respectively, for HIT. The EuroSCORE scoring system produces an integer scorebetween 0 and 8 were score 0-2 identify low risk patients, score 3-5 medium
risk, score 6–24 high risk. We categorized patients according to EuroSCOREand evaluated the 4Ts Score in each categories, then we evaluated the predictiverole of EuroScore and 4Ts with respect to short-teem and long term thrombosis.We reported that pts categorized as high risk from EuroSCORE were more likelyto developed short-term thrombosis (OR 2.1 95%CI 0.9-2.5) whereas pts cat-egorized as high risk from 4Ts score were more likely to developed long termthrombosis (OR 3.5 95%CI 1.6-5.31)In this cohort, a low EuroSCORE was associated with an exceedingly low hard-event rate (0.4% per year) that increased significantly as a function of the 4Tsscore result. The 4Ts score yielded incremental value for the prediction of hardevents (X2 56 to 88, P<0.001) and significantly stratifiedX patients. In patientswith intermediate to high likelihood of cardiac complications as predicted by Eu-roSCORE the 4Ts score significantly increase the prediction of events.Specifically, a 4Ts score of 3 or less appeared to predict a low rate of events and alow rate of serologically confirmed HIT suggesting that patients with a low pretestprobability score may not require a laboratory assessment for HIT and may havetheir heparin continued, on contrary pts with high 4Ts score require a laboratoryconfirmation of antibodies to prevent thrombotic complications
1037 High-on treatment platelet reactivity by different stimuliis a determinant of mortality in acute coronarysyndrome patients: data from ami-florence 2 study
R. Marcucci1, A.M. Gori1, R. Paniccia1, B. Giusti1, D. Balzi2,A. Cordisco1, L. Bagnoli3, R. Santoni4, G.F. Gensini1, R. Abbate1.
1Careggi University Hospital, Florence, Italy; 2Epidemiology Unit, Local Healthunit 10, Florence, Italy; 3Emergency Department, Nuovo San Giovanni di DioHospital, Florence, Italy; 4S.C. Analisi Chimico Cliniche, Nuovo San Giovanni diDio, Florence, Italy
Background: High on treatment platelet reactivity (HPR) by ADP has been as-sociated with an increased risk of stent thrombosis and cardiovascular death inpatients undergoing stent implantation. Scarce data are available on the possiblerole of high on treatment platelet reactivity by other stimuli, such as arachidonicacid (AA).Purpose: We sought to evaluate the role of a high-on treatment platelet reactivityby ADP and/or AA in the occurrence of adverse events at 6-month follow-up ofpatients with acute coronary syndrome (ACS) undergoing PCI.Methods: We have studied patients enrolled in the AMI-Florence 2 study whichis a prospective, observational population-based study designed to evaluate thediagnostic and therapeutic approach to ACS. Platelet function was evaluated byplatelet rich-plasma aggregation (PA) by 10 micromol ADP, 1 mmol/L AA within 24hrs from the hospital admission for an ACS. All patients received 600 mg clopido-grel loading dose followed by 75 mg daily and aspirin 100 mg daily. HPR was de-fined in presence of 10 micromol/L ADP PA ≥70% and/or 1 mmol/L AA PA ≥20%.Results: 333 patients (228 M/105 F) were included in the analysis. All patientsunderwent PCI with stent implantation. 18 deaths were recorded at 6-monthfollow-up. ADP-PA and AA-PA mean values were respectively: 48.3±21.7%(48±21.6% in survivors vs 53.8±23.8% in non survivors) and 16.5±12.9%(16.1±12.6% in survivors vs 23.6±16.6% in non survivors). HPR by ADP and/orAA was detected in 97/333 (29.1%): HPR by ADP was diagnosed in 54/333(16.2%) and HPR by AA in 74/333 (22.2%). At multivariate analysis adjusted forage, sex, cardiovascular risk factors, previous history of cardiovascular or cere-brovascular disease, renal failure, anemia, Killip class, the HPR was an indepen-dent risk factor for 6-month total mortality [HR=2.86, 95%CI 1.07-7.6, p<0.03].Conclusions: We have found that a global HPR is an independent risk factorfor 6-month total mortality. By using different agonists which reflect different path-ways of platelet function, we have demonstrated that ACS patients with a worseprognosis are those with a global hyperactive platelet, independently of the re-sponsiveness to a single antiplatelet drug.
DIVERSITY IN MONOCYTE AND MACROPHAGELINEAGES IN ATHEROSCLEROSIS
1050 TRAF5 deficiency accelerates atherogenesis in mice byincreasing inflammatory cell recruitment and foam cellformation
A. Zirlik1, A. Missiou1, P. Rudolf1, N. Varo2, D. Wolf2, C. Munkel1,P. Libby3, C. Bode1. 1Albert-Ludwig University of Freiburg,
Department of Cardiology and Angiology, Freiburg, Germany; 2University ofNavarra, Pamplona, Spain; 3Brigham and Women’s Hospital, Boston, UnitedStates of America
Rationale: TNF receptor associated factors (TRAFs) are cytoplasmic adaptorproteins for the TNF/IL-1/toll-like receptor superfamily. This family comprisesmultiple important cytokines such as TNFα, CD40L, and IL-1β that promotechronic inflammatory diseases such as atherosclerosis. We recently reportedover-expression of TRAF5 in Murine and human atheromata and demonstrateddependency of classic inflammatory functions on TRAF5 in endothelial cells andmacrophages in vitro.Objective: Here we tested the hypothesis that TRAF5 mediates atherogenesis invivo.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

158 Diversity in monocyte and macrophage lineages in atherosclerosis
Methods and Results: Surprisingly, TRAF5-/-/LDLR-/- mice consuming a highcholesterol diet for 18 weeks developed significantly larger atherosclerotic le-sions compared with TRAF5+/+/LDLR-/- controls. Intimal lesion size increasedby up to 328±11% and 174±15% in sections of the aortic arch and aortic root,respectively (n>13 per group, P<0.01 each). Plaques of TRAF5-deficient animalscontained more lipids and macrophages while smooth muscle cells and collagenremained unchanged. Both deficiency of TRAF5 in endothelial cells and leuko-cytes enhanced adhesion of inflammatory cells to the endothelium in dynamicadhesion assays in vitro and in Murine vessels imaged by intravital microscopy invivo. This coincided with increased expression of the adhesion molecule ICAM-1 on endothelial cells, the integrin VLA-4 on monocytes, and the chemokinesMCP-1 and Kc in blood of TRAF5-deficient mice. Moreover, TRAF5 deficiencypotentiated lipid-uptake and foam cell formation and upregulated the scavengerreceptor CD36 on macrophages. Also, TRAF5-/-/LDLR-/- animals had signifi-cantly reduced regulatory T cell counts. Finally, patients suffering from stable(0.026±0.0016) and acute coronary heart disease (0.023±0.0018) expressedsignificantly lower amounts of TRAF5 mRNA in blood compared with healthy con-trols (0.029±0.0017 TRAF-5/GAPDH mRNA, N=325, P<0.01).Conclusion: We present the novel finding that TRAF 5 deficiency acceleratesatherogenesis in mice, an effect likely mediated by increased inflammatory cellrecruitment to the vessel wall and enhanced foam cell formation.
1051 Metalloproteinases and foam-cell macrophagephenotypes in unstable atherosclerotic plaques
N.P. Jenkins1, J.L. Johnson1 , N. Marx2, G. Pasterkamp3, A. Newby1.1University of Bristol, Bristol, United Kingdom; 2University of Ulm,Faculty of Medicine, Department of Internal Medicine II-Cardiology,
Ulm, Germany; 3University Medical Center Utrecht - Julius Centre for HealthSciences and Primary Care, Utrecht, Netherlands
Introduction: Matrix metalloproteinase (MMP) production from foam cellmacrophages (FCMs) promotes atherosclerotic plaque formation and cap ruptureleading to clinical events. We recently showed diverse patterns of MMP produc-tion in subpopulations of rabbit FCMs. Here we investigate whether FCM pop-ulations expressing different MMPs and tissue inhibitor of MMPs (TIMPs) existin human plaques and associate with histological measures of plaque instability.We also investigate whether lipid-lowering in rabbits or systemic treatment with aPPARγ agonist in humans alters the balance of FCM populations.Methods: Aortic tissue was studied from cholesterol-fed New Zealand White rab-bits, human carotid endarterectomy specimens from the AtheroExpress biobankand human coronary artery specimens from cadaveric donors. Patients (n=12 pergroup) were randomised to receive the PPARγ agonist rosiglitazone or placebofor 4 weeks before carotid endarterectomy.Serial tissue sections were immunostained for CD68 to identify FCMs and forMMPs-2, -12 and -14, TIMP-3, CCR2, COX-2, and CD206 and quantified byblinded analysis.Results: Relationship to plaque vulnerability: A significantly (p<0.05 to 0.001)higher proportion of FCMs in unstable, lipid-rich carotid plaques stained forMMPs-2 (75+9% vs 49+12), -12 (66+6% vs 25+2%) and -14 (59+7% vs 5+2%)and markers of classical activation CCR2 (80+4% vs 28+7%) and COX-2 (72+6%vs 15+4%) than in stable, fibrous plaques. Conversely, a higher percentage ofFCMs in stable plaques stained for TIMP-3 (58+11% vs 19+3) and a marker foralternative activation CD206 (45+11 vs 17+3%) than in unstable plaques. Similardata were obtained in human coronary lesions.Reversal: The percentage of MMP-14 positive plaque FCMs (83+7% and 74±5%)from rabbits fed cholesterol for 8 and 16 weeks declined to 49±4% in rabbitsreturned to a normal diet for the last 8 weeks (n=8 each, p<0.001). PPARγ agonisttreatment did not change FCM expression profiles.Conclusions: Our data implies that MMP-2, -12, -14 positive FCMs may be use-ful to identify vulnerable plaques (e.g. using imaging) and are targets for plaquestabilising therapy. MMP-2,-12. -14 positive FCMs appeared to be classically ac-tivated, whereas TIMP-3 positive FCMs expressed markers of alternative activa-tion. Lipid lowering in rabbits reversed MMP-14 over-expression. Our data withPPARγ agonists are consistent with recent work showing that whereas theseagents predispose monocytes towards alternative activation they do not reverseclassical activation.
1052 Passive immunization with anti-phosphorylcholine IgGantibodies reduces neointimal formation and vascularinflammation in a mouse model for acceleratedatherosclerosis
M.M. Ewing1, M.R. De Vries2, K. Pettersson3, J. Frostegard4 ,D.J. Sexton5, J.W. Jukema1, P.H.A. Quax2. 1Leiden University Medical Center,Department of Cardiology, Leiden, Netherlands; 2Leiden University MedicalCenter, Department of Surgery, Leiden, Netherlands; 3Athera Biotechnologies,Stockholm, Sweden; 4Karolinska Institute, Department of Medicine, Stockholm,Sweden; 5Dyax Corp. 300 Technology Square, Cambridge, MA 02139, UnitedStates of America
Background: Inflammation is important in restenosis and acceleratedatherosclerosis and is elicited by vascular injury and the presence of phospho-rylcholine (PC), the main immunogenic auto-antigen on oxidized LDL (oxLDL)
cholesterol, in the vessel wall during dyslipidemia. Natural anti-PC IgM antibod-ies (abs) prevent foam cell formation, possess anti-inflammatory properties andreduce atherogenesis in mouse models. Unlike IgM, IgG abs can be produced inlarge quantities, allowing clinical application. We compared effects of various IgGand IgM anti-PC abs on oxLDL cholesterol uptake by macrophages and thera-peutic effects of recombinant anti-PC IgG abs in a mouse model for acceleratedatherosclerosis.Methods and Results: We used polyclonal IgM and IgG anti-PC abs purifiedfrom human serum, a recombinant anti-PC IgG construct containing variable re-gions of the murine T15/E06 antibody and the constant region of human IgG1(T15/E06 IgG). Human anti-streptavidin IgG1 (A2) was used as negative control.Effects of these abs on the uptake of oxLDL cholesterol by macrophages wereevaluated in vitro.Macrophages derived from THP-1 by PMA were incubated with 20μg/ml of DiL-labelled, Cu-oxidized LDL cholesterol and abs for 5h. OxLDL cholesterol up-take was measured by FACS. Results showed that the natural IgM abs dose-dependently inhibited oxLDL cholesterol uptake, that the polyclonal IgG abs wereweakly effective and the recombinant anti-PC IgG (T15/E06 IgG) antibody wasineffective.Recombinant anti-PC IgG abs were used to passively immunize ApoE*3Leidentransgenic mice on a Western-type diet twice weekly, using PBS and anti-streptavidin IgG1 (A2) abs as controls. Arterial inflammation was measured asaccumulation of leukocytes and macrophages in the arteries 3d after cuff place-ment and intimal thickening was measured after 14d.Treatment with these abs significantly reduced leukocyte (but not macrophage)adhesion and infiltration in the arterial wall 3d after surgery and reduced intimalthickening by >70% (p=0.000) after 14d. This effect was accompanied by an in-creased relative smooth muscle cell area in the medial layer and reduced relativeleukocyte and macrophage areas in the arterial wall.Conclusions: This study showed therapeutic effectiveness of recombinant anti-PC IgG abs against accelerated atherosclerosis. These effects could not be at-tributed to reduced oxLDL cholesterol uptake by macrophages. Immunization withrecombinant anti-PC IgG has therefore potential as a new treatment against car-diovascular diseases.
1053 Monocyte heterogeneity and cardiovascular riskfactors in coronary artery disease
M. Hristov1, T. Leyendecker2 , C. Schuhmann3, P. VonHundelshausen4 , N. Heussen5, E. Kehmeier2, F. Krotz3,H.-Y. Sohn3, V. Klauss3, C. Weber1 . 1Institute of Molecular
Cardiovascular Research, University Hospital Aachen, RWTH, Aachen,Germany; 2Heinrich-Heine-University, Department of Cardiology, Düsseldorf,Germany; 3LMU Munich, Department of Cardiology, Munich, Germany; 4RWTHAachen University, Department of Cardiology, Aachen, Germany; 5RWTHAachen University, Institute for Medical Statistics, Aachen, Germany
Purpose: Human monocytes in peripheral blood have been divided into func-tional subsets on the basis of their expression of the LPS receptor CD14 and theFc-gamma receptor CD16. CD14++CD16- cells represent the major monocytepopulation, highly express CCR2 and are often described as "classical" mono-cytes. The tissue macrophage-like subset of CD14+CD16+ cells displays higherlevels of the chemokine receptors CX3CR1, CXCR4 and CCR5 but lower expres-sion of CCR2 than CD14++CD16- monocytes. Current data have demonstratedfurther heterogeneity in the CD16+ subset: CD14++CD16+ monocytes differ fromCD14lowCD16+ cells by secretion of TNF-alpha and by expression of VEGFR1and Tie2. The aim of our study was to evaluate possible associations of circulat-ing monocyte subsets with cardiovascular risk and the extent of coronary arterydisease (CAD).Methods and Results: Monocytes were enumerated ex vivo by flow cytom-etry in peripheral venous blood of 80 patients with angiographically docu-mented stable CAD under steady-state conditions without current episodesof ischemia or inflammation; in case of elective catheterization, blood wasdrawn before intervention. Quantitative cell analysis was blinded to patient char-acteristics. CD14lowCD16+ monocytes were reduced (p=0.006), whereas theCD14++CD16- subset was elevated (p=0.001) in high-risk (≥5 risk factors),as compared to low-to-medium risk patients (≤4 risk factors). Univariate sub-analysis revealed a decrease of CD14lowCD16+ monocytes for family predisposi-tion (p=0.003) and smoking (p=0.011), whereas CD14++CD16- monocytes wereincreased in patients with family history for CAD (p=0.024). Multivariate anal-ysis unveiled hypertension as an independent predictor (p=0.039) for reducedCD14lowCD16+ monocytes. Furthermore, the number of risk factors indepen-dently predicted the percentage of CD14++CD16+ monocytes (p=0.042), whileno significant association was observed with the angiographic extent/severity ofCAD or with any medication taken in adherence to high-standard of cardiovascu-lar care (statin, aspirin and ACE-inhibitor).Conclusions: The differential profile of circulating monocyte subsets harbors pre-dictive value for identifying CAD patients at high cardiovascular risk and may openanother option for primary and secondary prevention in individuals with high-riskprofile, family history for CAD, hypertension or in smokers.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Diversity in monocyte and macrophage lineages in atherosclerosis / Important aspects of percutaneous valve therapy 159
1054 Deletion of the S1P receptor S1P3 attenuatesmacrophage-driven inflammation in atheroscleroticlesions of S1P3-/-/ApoE -/- double knockout mice
P. Keul1, S. Lucke1, K. Von Wnuck Lipinski1, M. Graeler2, G. Heusch1,B. Levkau1. 1University of Essen Medical School, Institute of
Pathophysiology, Essen, Germany; 2Hannover Medical School, Hannover,Germany
The causal role of the bioactive sphingolipid sphingosine 1-phosphate (S1P) inatherosclerosis is unknown. We addressed this by examining atherosclerotic le-sion development in mice deficient for the S1P receptor 3 (S1P3-/-/) crossbredon an ApoE -/- background. Atherosclerotic lesion volume in the brachiocephalicartery of S1P3-/-/ApoE -/- double knockout mice fed a normal chow diet for45 weeks was similar to that in ApoE-/- mice. However, the lesions had a dra-matically reduced macrophage content (24% of ApoE-/-) and increased smoothmuscle cell content (174% of ApoE-/-). To search for defects in macrophage re-cruitment in S1P3-deficient mice, we monitored macrophage-driven inflamma-tion in the thioglycolate-induced peritonitis model. In this model, we observed a38% reduction in the numbers of elicited F4/80-positive macrophages in S1P3-deficient mice compared to controls. S1P3-/-macrophages exhibited an alteredcytokine signature with substantially reduced TNFα and MCP-1 mRNA expres-sion levels. S1P concentrations in the peritoneal cavity rapidly increased with amaximum at 48 hours, and elimination of the S1P gradient by application of theS1P analogue FTY720 resulted in an inhibition of macrophage recruitment intothe peritoneal cavity. In Boyden chamber experiments, S1P was chemotactic formacrophages from control but not S1P3-deficient mice. We also observed thatthe S1P-synthesizing enzyme sphingosine kinase 1 was abundantly expressed inmacrophages in atherosclerotic lesions. Finally, atherosclerosis studies in bonemarrow chimeras showed that S1P3-/- in hematopoetic cells is important formacrophage recruitment to atherosclerotic lesions. These data suggest that S1Pacts as a chemoattractant for macrophages via S1P3, and that absence of S1P3alters the cytokine profile of monocyte/macrophages and their recruitment to le-sions of atherosclerosis.
1055 Inflammatory cells are required for endothelialregeneration
C. Endtmann1, B. Haghighat1 , D. Engel2, C. Kurts2, G. Nickenig1,S. Wassmann3, N. Werner1 . 1University of Bonn, Medical Clinic II- Cardiology, Bonn, Germany; 2Institut for molecular medizin und
experimentell immunology, Bonn, Germany; 3McGill University, Montreal,Canada
Background: Circulating endothelial progenitor cells (EPC) contribute to en-dothelial cell (EC) regeneration and are predictors for cardiovascular events. Sys-temic treatment with EPC fosters the repair of damaged endothelium. We haveshown that transfusion of mononuclear cells (MNC) lead to an even more pro-nounced regeneration of the endothelium compared to EPC transfusion poten-tially mediated by paracrine action of inflammatory cells. Here, we determine therole of inflammatory cells in EC regeneration.Methods/Results: Re-endothelialization, neointima formation, and endothelialfunction was determined in wild-type (WT) mice treated with intravenous injec-tions of spleen-derived MNC, CD11b-depleted MNC, CD11b+ cells, or cell-freevehicle after EC denudation. EC regeneration was enhanced and neointima for-mation reduced after transfusion of total MNC and CD11b+ cells but not afterCD11b-depleted cells. In ApoE-/- mice, transfusion of CD11b+ cells and totalMNC but not CD11b-depleted MNCs improved endothelial function. To deter-mine the role of endogenous monocytes on EC repair, mice were treated withclodronate-liposomes (10μl/g bw) to deplete monocytes. Re-endothelializationafter focal EC denudation was significantly diminished in clodronate-treated com-pared to vehicle-treated mice. Next, we selectively depleted CD11b+ monocytesand tissue-residual macrophages using CD11b-DTR transgenic mice. Treat-ment with diphtheria toxin (DT) results in the complete ablation of circulatingmonocytes/tissue-resident macrophages. DT treatment was performed for 10days (15ng/g bw). At day 5 post EC damage, the denuded area was significantlylarger in DT treated compared to vehicle treated mice. Transfusion of Sca1+ cellssignificantly enhanced re-endothelialization in vehicle-treated CD11b-DTR micebut not in DT treated mice. Finally, transfusion of CD11b+ cells in CD11b-DTRmice treated with either vehicle or DT resulted in a comparable enhancement ofre-endothelialization. Interestingly, depletion of CD11c positive dendritic cells inCD11c-DTR mice impaired endothelial dependent vasorelaxation of isolated aor-tic rings in an organ chamber experiment indicating that besides monocytic cells,CD11c dendritic cells contribute to vascular function.Conclusion: Here we demonstrate that circulating CD11b+ monocytes andCD11c+ dendritic cells contribute to EC regeneration. Depletion of inflammatorycells within the acute injury situation is associated with an impaired vascular func-tion/endothelial regeneration.
MODERATED POSTERSIMPORTANT ASPECTS OF PERCUTANEOUS VALVE
THERAPY
P1081 Early benefits of transcatheter aortic valvereplacement on the severity of secondary mitralregurgitation
C. Stoicescu1, M. Vasa-Nicotera2, D. Chin2, D. Vinereanu1,J. Kovac2. 1University of Medicine and Pharmacy Carol Davila,Bucharest, Romania; 2University Hospitals of Leicester, Leicester,
United Kingdom
Background: Few and contradictory data regarding the benefits of transcatheteraortic valve replacement (TAVI) on the severity of secondary mitral regurgitation(MR) are available; thus, data from registries showed that secondary MR is im-proved in >50% of patients receiving TAVI with the CoreValve Medtronic SystemTM. However detailed mechanisms of early improvement after TAVI are not avail-able yet.Methods: 71 patients (81±6 years, 47% male) were studied immediately beforeand after TAVI, and after 30 days. Echocardiography was used to measure leftventricular (LV) dimensions (end-systolic and end-diastolic diameters, and wallthickness) in order to assess LV function (by ejection fraction EF) and LV massindex (LVMI); left atrium (LA) diameter; mitral valve morphology by apical dis-placement of the coaptation point from the plane of the mitral annulus (CPMA),and mitral annulus diameter; and MR severity (by vena contracta, regurgitant vol-ume by PISA, and mitral jet area/LA area). Catheterization was used to measureLV systolic pressure (LVSP) pre- and post- procedure.Results: At 30 days post TAVI, end-systolic diameter decreased from 41±6 to37±4 mm, septal wall thickness from 15.6±1.7 to 14.1±1.2 mm, LVMI from278±70 to 207±51 g/m2 (all p<0.05), while EF increased from 45±11 to 52±10%(p<0.01). Severity of MR decreased: vena contracta from 3.7±0.7 to 2.9±0.6mm, regurgitant volume from 27.1±3.2 to 20.8±2.9 ml, mitral jet area/left atriumarea from 18.1±1.8 to 13.9±1.4% (all p<0.05), however LA diameter did notchange. Decrease of the severity of secondary MR was due to the reduction oftraction forces acting on the mitral valve: CPMA was reduced from 10.2±1.9 to9.1±1.6 mm, p<0.05, while the sphericity index decreased from 1.48±0.13 to1.43±0.10, p=0.07. There were no changes of the mitral annular diameter. TheLVSP decreased from 155.5±26.6 to 130.2±20.8 mmHg (p<0.05). LVSP, CPMA,and sphericity index represented the main independent predictors of MR reduc-tion (R2=0.49; p<0.05).Conclusions: Decrease of LVSP after TAVI is the trigger for reduction of LV wallthickness, ESD, and sphericity index; this leads to an early decrease of the sever-ity of secondary MR, mainly by reducing subvalvar traction acting on the mitralvalve.
P1082 Effectiveness and durability at two years withCoreValve transcatheter aortic valve
G. Schuler1, R. Bonan2, J. Kovac3, P.W. Serruys4, M. Labinaz5,P. Den Heijer6, M. Mullen7, W. Tymchak8, U. Gerckens9. 1Universityof Leipzig, Heart Center, Leipzig, Germany; 2Montreal Heart
Institute, Montreal, Canada; 3University Hospitals of Leicester, GlenfieldHospital, Leicester, United Kingdom; 4Erasmus Medical Center, Thoraxcenter,Rotterdam, Netherlands; 5University of Ottawa Heart Institute, Ottawa, Canada;6Amphia Hospital, Breda, Netherlands; 7Royal Brompton Hospital, London,United Kingdom; 8University of Alberta Hospital, Edmonton, Canada; 9HELIOSHospital, Department of Cardiology, Siegburg, Germany
Purpose: Short-term results from transcatheter aortic valve implantation (TAVI)of the 18-Fr prosthesis in patients with severe aortic stenosis have been reported.We present two-year safety and effectiveness results from a multicenter study.Methods: The 18-Fr study of this TAVI prosthesis evaluated 126 subjects im-planted 2006 to 2008 at 9 centers in Europe and Canada. Subject inclusion re-quirements included ≥ 75 years old, surgical risk with logistic EuroSCORE ≥15%, or 1-2 high-risk co-morbidities. Most subjects were implanted percutaneous(77%), 98% accessed femorally and 2% subclavian.Results: Implanted subjects were 82±6 years old, 57% female, 75% NYHAclass III/IV, logistic EuroSCORE 23±14%. Technical success (functionality withabsence of valve malfunction) at implant was 83%. At two years, follow-up sta-tus was ascertained from 63 subjects, 47 died, 4 withdrew, and 12 were pend-ing evaluation. Two-year safety: Freedom from major adverse cardiovascular andcerebrovascular events was 53.0±4.7%. One paravalvular leak and no valve mi-grations or structural valve deterioration occurred. No emergent cardiac reinter-ventions or non-structural valve dysfunctions occurred after the 30-day visit. Two-
Safety at Two Years Two-Year Effectiveness Baseline Two Years p-valueSurvival at Two Years
All-cause survival 60.0±4.6% Valve orifice area 0.7 cm2 1.8 cm2 p<0.001Cardiac survival 74.2±4.3% Peak trans- 72.5 mmHg 18.0 mmHg p<0.001
valvular gradientFreedom from stroke 83.7±3.8% Mean trans- 46.8 mmHg 8.9 mmHg p<0.001
valvular gradientFreedom from endocarditis 98.6±1.4% LVEF 51.6% 55.0% p=ns
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

160 Important aspects of percutaneous valve therapy
year effectiveness: NYHA improved at least one class in 72% of subjects and 18%had no change (p<0.001, n=61). Aortic valve regurgitation distribution improvedfrom 42% grade 0, 52% grade 1, 6% grade 2, 0 > grade 2 to 61% grade 0, 39%grade 1, 0 > grade 1.Conclusion: The early experience with the 18-Fr TAVI prosthesis in this severeaortic stenosis population is encouraging. Long-term durability and performancewere indicated by sustained improvements in functional class, valve orifice area,and aortic valve regurgitation; the chronic absence of emergent cardiovascularinterventions, non-structural valve dysfunction, and valve migrations; and stablesurvival profiles within expectations for patients presenting with these risk profiles.Subsequent results through four years will be forthcoming.
P1083 In-hospital outcome of aortic regurgitation aftertranscatheter aortic valve implantation: results fromthe prospective multicentre German TAVI registry
M. Abdel-Wahab1, R. Zahn2, M. Sherif1, S. Schneider3,U. Gerckens4, G. Schuler5, H. Sievert6, H. Eggebrecht7 ,
J. Senges3, G. Richardt1. 1Heart and Vascular Center, Segeberger Kliniken,Bad Segeberg, Germany; 2Clinical Center of Ludwigshafen, Department ofCardiology, Ludwigshafen am Rhein, Germany; 3Heart Attack Research Centerat the University of Heidelberg, Ludwigshafen am Rhein, Germany; 4HELIOSHospital, Department of Cardiology, Siegburg, Germany; 5University of Leipzig,Heart Center, Leipzig, Germany; 6CardioVascular Center Frankfurt, SanktKatharinen, Frankfurt am Main, Germany; 7West German Heart Center Essen,Clinic for Cardiology, Essen, Germany
Background: Significant aortic regurgitation (AR) is rare following surgical aorticvalve replacement and is associated with worse outcome. Following transcatheteraortic valve implantation (TAVI), AR is common and is generally believed to bean acceptable and probably transient trade-off, though its effect on outcome isunknown.Methods & Results: We analyzed data from 912 patients with severe aorticstenosis (AS) enrolled in the prospective multicenter German TAVI registry. Meanage was 81.3±7 years, mean aortic valve area 0.7±0.5 cm2 and mean gradient48±17 mmHg. Mean logistic EuroSCORE was 21.4±14.5. Overall, 85% of pa-tients received the CoreValve Revalving system and 15% received the EdwardsSAPIEN valve. The occurrence of AR was evaluated angiographically after devicedeployment and removal of catheter and guidewire. Significant AR was defined asAR ≥2/4 and occurred in 147 patients (16%), while 765 patients (84%) had no ormild AR. Patients with significant AR were more commonly males, had more se-vere AS, were more commonly decompensated and had more severe pulmonaryhypertension at baseline. Aortic annulus diameter was not different between bothgroups, but patients with significant AR had their annulus more commonly es-timated by transoesophageal echocardiography (TEE) than those with no/mildAR (76% vs. 60%, p<0.001), while the latter group had the annulus diametermore commonly determined by computed tomography (40% vs. 24%, p<0.001).In-hospital outcome is shown in the table.
Table 1. In-hospital outcome stratified by the degree of postprocedural AR
Significant (≥2/4) AR No/mild AR p-value OR (95% CI)
Low cardiac output 24 (19.2%) 34 (4.9%) <0.0001 4.59 (2.62-8.06)Respiratory failure 19 (14.4%) 48 (6.6%) <0.01 2.36 (1.34-4.16)Stroke 5 (3.8%) 17 (2.4%) 0.35 1.62 (0.59-4.47)Delirium 20 (15.6%) 35 (5%) <0.0001 3.51 (1.96-6.31)High degree AV block 27 (20.5%) 145 (20.3%) 0.98 1.01 (0.64-1.60)New left bundle branch block 20 (15.2%) 67 (9.4%) <0.05 1.72 (1.01-2.95)In-hospital death 24 (17.9%) 47 (6.5%) <0.0001 3.16 (1.86-5.38)
Conclusion: Significant AR after TAVI is common and is associated with in-creased in-hospital mortality. Long term follow-up is critical to define the impactof AR on clinical outcome. Until these data become available, every effort shouldbe made to prevent and treat this complication.
P1084 Hemodynamic and clinical impact of percutaneousmitral repair using the mitral clip system
J. Hausleiter, J. Pache, P. Barthel, S. Massberg, F. Michalk,H. Lesevic, A. Schoemig. German Heart Center, Clinic at theTechnical University of Munich, Munich, Germany
Background: The catheter-based MitraClip system (Abbott, former Evalve) is anew therapeutic concept to treat patients with significant symptomatic mitral re-gurgitation (MR). Using transesophageal echocardiography (TEE) for procedu-ral guidance, the leaflets of the mitral valve are clipped together to reduce MR,mimicking the surgical "Alfieri stich". The current study evaluates the immediateechocardiographic and hemodynamic outcome after mitral clipping.Methods: 25 consecutive patients (11 female and 14 male patients) with symp-tomatic MR were enrolled. Mitral clipping was attempted in all patients under gen-eral anesthesia. Pre- and post-procedural severity of MR was assessed by TEEand by measurements of the left atrial v-wave and of the change in cardiac outputby thermodilution.Results: 25 patients (mean age: 70.7±8.7 yrs) were enrolled. Degenerative andfunctional MR were present in 19 and 6 patients, respectively. Successful re-
duction of MR by mitral clipping was achieved in 23 of 25 patients; insufficienttransesophageal imaging (1 patient) and an unsuitable anatomy for transseptalpuncture (1 patient) were the reasons for a failed treatment. In the remaining 23patients successful implantations of mitral clips were achieved. Of these, two pa-tients were treated in acute cardiogenic shocks in bail-out situations due to acutemyocardial infarction with rupture of the posterior papillary muscle (1 patient) anddue to acute rupture of the mitral chordae of the posterior leaflet (1 patient). Oneand two clips were placed in 17 and 6 patients, respectively. The grade of MRby TEE improved from 3.1±0.2 to 1.2±0.5 (n=23 patients). The left atrial v-wavewas reduced from 30.1±12.3 mmHg to 16.8±7.8 mmHg (n=16 patients). Con-comitantly, the cardiac output increased from 3.5±1.3 to 5.1±1.7 l/min (n=9 pa-tients). One patient (86 years old) treated in a bail-out situation with acute MI andrupture of the posterior papillary muscle (see above) died 5 days after the pro-cedure; the remaining 22 patients demonstrated without major adverse cardiacevents and with a significant clinical improvement - in general improvement in atleast 1 NYHA class.Conclusions: The minimally invasive catheter-based implantation of clips for sig-nificant MR, which has been shown to be safe and efficacious, represents an al-ternative to surgical mitral reconstructions. However, the long-term durability ofthe promising percutaneous mitral clipping procedure needs to be evaluated andcompared with conventional surgical procedures.
P1085 Transapical aortic valve implantation after previousheart surgery
T. Drews, M. Pasic, S. Buz, A. Unbehaun, S. Dreysse, M. Kukucka,A. Mladenow, R. Hetzer. German Heart Center Berlin, Berlin,Germany
Objective: Transcatheter aortic valve implantation is a new method for treatmentof very high-risk patients with aortic valve stenosis. Especially in patients whohave had previous cardiac surgery the operative risk can be reduced. Never-theless, this new procedure has some potential risks in these patients, due tothe increased danger of endocarditis and in view of potential graft damage afterprevious bypass grafting or prosthesis damage after previous valve replacementcaused by wire manipulation or valve liberation.Methods: Between April 2008 and January 2010, 198 consecutive patients un-derwent transapical aortic valve implantation. Group A consisted of 158 patientswithout previous heart surgery and group B of 40 patients with previous heartoperation (23 coronary artery bypass grafting, 3 aortic valve replacements, 2 mi-tral valve repairs, 1 replacement, and 11 combined operations). Although the ageof patients in group B (75±11) was significantly lower than in group A (80±8)[p=0.003], the preoperative risk score was significantly higher in group B (GroupA: EuroSCORE: 37±18%; STS mortality score: 21±16; Group B: EuroSCORE:53±21%; STS mortality score: 29±18) [p<0.001, p=0.006].Results: The technical success rate was 99% (157/158) in group A and 100%(40/40) in group B. One patient in group A developed after valve liberation a typeA dissection caused by annulus rupture. The postoperative echocardiographicexaminations showed slight central incompetence in 23 patients in group A (15%)and in 2 patients in group B (5%). Minimal paravalvular leakage was seen in 29%of patients in group A and 40% in group B [p=0.034]. The 30-day and 1-yearsurvival was 94% in group A and 92% in group B, and 92% and 85% respectively(not significant).Conclusions: Transcatheter valve implantation can be performed successfullyafter previous heart surgery. Particular care should be taken to achieve optimalvalve positioning and not to damage grafts or prosthetic valves during manipula-tion with guide wires and valve positioning.
P1086 Safety and efficacy comparison between implantedand non-implanted patients in the TITAN trial usingthe CARILLON Mitral Contour System to treatfunctional mitral regurgitation
U.C. Hoppe1, T. Siminiak2, M. Haude3, J. Sadowski4, J. Lipiecki5,J. Fajadet6 , J.C. Wu7, N. Mehta8, D.G. Reuter8. 1Klinikum der universitat zuKoln, Cologne, Germany; 2Poznan University of Medical Sciences, Poznan,Poland; 3Lukas Hospital, Neuss, Germany; 4John Paul II Hospital, Krakow,Poland; 5University Hospital of Clermont-Ferrand - Hospital Gabriel Montpied,Clermont-Ferrand, France; 6Clinic Pasteur of Toulouse, Toulouse, France;7Brigham and Women’s Hospital, Boston, United States of America; 8CardiacDimenions Inc, Kirkland, United States of America
Background: Functional mitral regurgitation (FMR) increases the morbidity andmortality of heart failure patients. The TITAN trial evaluated the safety and efficacyof a coronary sinus based percutaneous mitral annuloplasty device designed totreat FMR.Methods: Inclusion criteria: Dilated ischemic or non-ischemic cardiomyopathy,moderate to severe FMR, LVEF<40%, NYHA Class II-IV, 6 minute walk distance(6MWD) 150-450 meters, and stable heart failure therapy. Permanent implan-tation occurred in patients with a peri-procedural reduction in FMR (n=36). Pa-tients in whom implantation was not achieved served as a non-randomized control(n=17). The primary safety endpoint was the MAEs rate at 1 month. Secondaryendpoints at 1, 6, and 12 months included echo core lab derived quantitativemeasures of FMR (EROA, Vena Contracta, Regurgitant Volume, Jet area/Left
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Important aspects of percutaneous valve therapy / Diagnosis and management of cardiomyopathies 161
atrial area), NYHA Class, 6MWD, and QOL measured by the Kansas City Car-diomyopathy Questionnaire (KCCQ).Results: At baseline, 94% of patients were NYHA III, EF was 28.4%, and LVEDDwas 70mm. The MAE rate at 30-days for all 53 attempted patients was 1.9%.Reductions in 4 quantitative FMR measures ranged from 32-43% at 6 months forimplanted patients. LVESV was reduced from 164±64 (baseline) to 142±52 (6months) (p<0.01). Functional changes are presented in Table 1Final 12 month TITAN data will be presented.
Table 1. Functional Changes
6 mwd (m) NYHA Class KCCQbaseline 6 mo 12 mo baseline 6 mo 12 mo baseline 6 mo 12 mo
Implanted (n=36)302±74 436±208 427±193 3.1±0.2 2.1±0.7 2.1±0.8 43±18 64±23 63±27
p=0.0036 p<0.0001 p=0.00012Non-Implanted (n=17)
338±83 322±105 330±139 2.9±0.2 2.7±0.7 2.4±0.5 40±19 50±22 45±12p=0.915 p=0.135 p=0.655
(mean ± SD, p value by ANOVA).
Conclusion: Percutaneous treatment of FMR was associated with reduction inFMR, reverse remodeling, and a corresponding improvement in functional pa-rameters.
P1087 Failing aortic valve prosthesis treated bypercutaneously implanted CoreValve prosthesis
F. Woitek1, C. Schiefer1, T.H. Walther2, R. Hoellriegel1,N. Mangner1 , S. Moebius-Winkler1, M. Woinke1, F.W. Mohr3,A.H.P. Linke1, G.C. Schuler1. 1University of Leipzig, Heart Center,
Department of Internal Medicine and Cardiology, Leipzig, Germany; 2KerckhoffClinic, Bad Nauheim, Germany; 3University of Leipzig, Heart Center, Departmentof Cardiac Surgery, Leipzig, Germany
Older patients with aortic valve stenosis or regurgitation are commonly treatedby conventional surgical reconstruction or implantation of a bioprosthetic valvewith excellent results. However, a significant number of these valves fail within 15years. At this time, patients are considerably older and their operative mortality forconventional re-operation has increased due to co-morbidities. Retrograde percu-taneous aortic valve replacement (PAVR) with the CoreValve ReValving System- which carries a porcine pericardial bioprosthesis in a self-expandable nitinolframe - represents an alternative to conventional valve surgery. Therefore, it wasaim of the study to elucidate whether PAVR in patients (pts) with a failing aor-tic valve bioprosthesis is safe, feasible and associated with an improvement inhemodynamics.Methods: Pts with symptomatic aortic valve disease, aged ≥ 65 years with a lo-gistic EuroSCORE ≥ 10% were enrolled. Using a retrograde approach, in thosewith a stenotic bioprosthetic valve, valvuloplasty was performed under local anes-thesia followed by CoreValve implantation. In patients with aortic regurgitationof the bioprosthetic valve, CoreValve implantation was performed without priorvalvuloplasty. At 10 and 30 days, respectively, clinical events were recorded anda transthoracic echocardiography was performed to evaluate hemodynamics ofthe new prosthesis at follow-up.Results: A total of 14pts (age 76±6 years) with a Logistic EuroSCORE of 32±6%were treated so far. The duration between conventional AVR and and CoreValveimplantation was 57±43 months, the inner diameter of the bioprosthesis was21.1±1.6mm. Ten patients received the CoreValve for treatment of stenosis of thebioprosthetic valve, whereas four were treated because of regurgitation of the pre-viously implanted bioprosthetic valve. The CoreValve prosthesis was successfullyimplanted in all patients (n=14, 100%). In those with stenosis, the mean gradientdeclined from 48±15mmHg before to 13±7mmHg after CoreValve (p<0.05), inthose with AR the level declined by 2. There was no intraprocedural death, but onepatient died from stroke and one patient from cardiac failure within 24 hours afterCoreValve implantation. There were no further deaths within the 30day follow-up period (30 day mortality: 14%). Only one patient (7%) required a pacemakerimplantation due to AV-Block grade three.Conclusion: These early results suggest that PAVR with the CoreValve ReValv-ing System into a failing aortic bioprosthetic valve is feasible, safe and improveshemodynamics in older patient with higher risk for conventional aortic valve redo-surgery.
P1088 Is redo Percutaneous Mitral balloon Valvuloplasty(PMV) indicated in patients with post-PMV mitralrestenosis?
B. Jerbi, L. Abid, M. Hadrich, I. Trabelsi, M. Hentati, S. Kamoun.HEDI CHAKER HOSPITAL, Sfax, Tunisia
Purposes: The purpose of this study was to assess the immediate and long-termoutcome of repeat percutaneous mitral balloon valvuloplasty (PMV) for post-PMVmitral restenosis.Methods: We report the immediate outcome and long-term clinical follow-up re-sults of 73 patients with symptomatic mitral restenosis after prior PMV,Results: Patients were treated with a repeat PMV at 51, 73±29, 4 months afterthe initial PMV. The mean follow-up period was 58, 85 months with a maximal
follow-up of 10 years. There was a significant increase in the mitral valve area(1,08±0,21 to 1,76±0,32; p<0,001), and decrease in the mean transmitral gradi-ent (15,28±6,84 to 8,67±4,07 mm Hg; p<0.001) and the mean left atrial pressure(25,01±7,33 to 14,75±5,88 mm Hg; p<0,001). Mean pulmonary artery pressuredecreases significantly with redo PMV (47, 5±14, 73 to 34, 38±9, 57; p<0,001).The onset of new mitral regurgitation had occurred in 15 patients and the degreeof mitral regurgitation was increased by one grade in three cases. Successful pro-cedural outcome was achieved in 79, 6% of patients. No patient developed severemitral regurgitation after redo PMV. There were no in-hospital complications.The mean follow-up was 58, 85 months±35, 11. Early symptomatic improvementafter redo PMV of ≥1 NYHA functional class was obtained in 96.7% of the pa-tients. There were no deaths and 10 (13, 69%) patients required mitral valvereplacement (34.21 months after redo PMV) due to recurrent symptoms. Overall,44 patients (60, 27%) were alive without further valvular intervention at follow upafter redo PVM. All of these patients were in NYHA class I or II at follow-up. Theprobability of event-free survival at follow up was 91.2%.By univariate analysis age, history of previous surgical commissurotomy, pre-PMV NYHA functional class, lower echocardiographic score, post-PMV pul-monary artery pressure and atrial fibrillation were identified as univariate pre-dictors of long-term event-free survival in the redo PMV group.Conclusions: Repeat percutaneous mitral valvuloplasty in patients with resteno-sis after a prior percutaneous valvuloplasty is feasible and can be accom-plished with acceptable morbidity and mortality. Immediate procedural successis achieved in most of patients, and the long-term overall survival and event-freesurvival is 91, 2%. In patients with low echo scores and no comorbid diseases,repeat PMV should be the procedure of choice.
MODERATED POSTERSDIAGNOSIS AND MANAGEMENT OF
CARDIOMYOPATHIES
P1089 Mutations in desmosomal genes in heart transplantpatients with idiopathic dilated cardiomyopathy
P. Garcia-Pavia1, P. Syrris2, J. Segovia1, C. Salas3, J. Gonzalez-Mirelis1, M. Gomez-Bueno1, B. Bornstein4, W.J. Mckenna5,L. Alonso-Pulpon1, P.M. Elliott5. 1University Hospital Puerta de
Hierro Majadahonda, Department of Cardiology, Madrid, Spain; 2UniversityCollege London, London, United Kingdom; 3University Hospital "Puerta deHierro Majadahonda", Department of Pathology, Madrid, Spain; 4UniversityHospital "Puerta de Hierro Majadahonda", Department of Biochemistry, Madrid,Spain; 5The Heart Hospital, London, United Kingdom
Background: Idiopathic Dilated cardiomyopathy (DCM) is the most frequentcause of heart transplantation. When systematic screening is applied to relatives,a familial origin of DCM is found in between 20 and 48% of the cases. More than30 different genes have been related with DCM but the number of cases that canbe explained by mutations in the genes described so far is still small. Whethermutations in the desmosomal genes (so far only linked to Arrhythmogenic rightventricular cardiomyopathy, ARVC) could be responsible of a significant numberof cases of end-stage DCM is unknown.Methods: Ninety unrelated patients (mean age 47.9±13.5 years, 80% male)transplanted for DCM underwent mutation screening of the known desmosomalARVC genes (PKP2, DSP, DSC2, DSG2 and JUP). Clinical, familial and anatomo-pathological characteristics were studied. Familial screening was offered to therelatives of patients with sequence variants.Results: Pathogenic mutations were found in 12 patients (13%) (5 patients hadpathogenic mutations in PKP2, 3 in DSP, 3 in DSG2 and 1 in JUP). Eleven addi-tional patients (12%) had genetic variants of uncertain significance (4 in PKP2, 3in DSC2, 2 in DSP, 1 in DSG2, and 1 in JUP). Three patients with pathogenic mu-tations carried also another mutation of unknown significance (2 in DSC2 and 1in DSP). The clinical phenotype of patients with pathogenic mutations in desmo-somal genes was indistinguishable from patients without genetic abnormalities inthese genes. Familial evaluation in 76 relatives from 16 families led to de diagno-sis of 39 carriers with 6 relatives having an overt DCM phenotype.Conclusions: Mutations in desmosomal genes are a frequent cause of DCM inheart transplant patients. The incidence of desmosomal mutations found in ourcohort is higher than those described previously in other genes in DCM. Screen-ing of desmosomal genes should be considered in all idiopathic DCM patients.
P1090 Long-term outcomes in hypertrophic cardiomyopathycaused by mutations in the cardiac troponin T gene
F. Pasquale, P. Syrris, G. Quarta, C. O’ Mahony, M.T. Tome-Esteban,A. Pantazis, J.P. Kaski, W.J. Mckenna, P.M. Elliott. The HeartHospital, London, United Kingdom
Purpose: Hypertrophic cardiomyopathy (HCM) is an autosomal dominant dis-ease caused by mutations in sarcomeric genes. One of the first genotype-phenotype associations to be reported was a high prevalence of sudden cardiacdeath (SCD) in young carriers of troponin T gene mutations (TNNT2m), often inthe presence of mild left ventricular (LV) hypertrophy. Confirmation of this associ-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
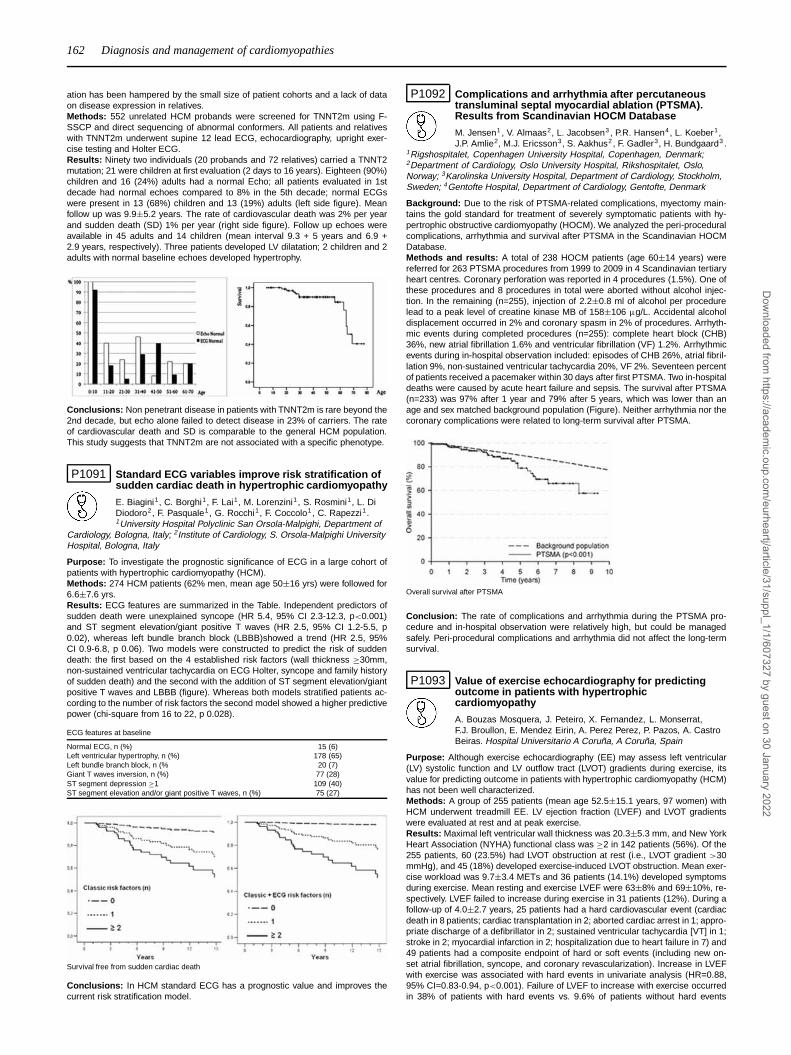
162 Diagnosis and management of cardiomyopathies
ation has been hampered by the small size of patient cohorts and a lack of dataon disease expression in relatives.Methods: 552 unrelated HCM probands were screened for TNNT2m using F-SSCP and direct sequencing of abnormal conformers. All patients and relativeswith TNNT2m underwent supine 12 lead ECG, echocardiography, upright exer-cise testing and Holter ECG.Results: Ninety two individuals (20 probands and 72 relatives) carried a TNNT2mutation; 21 were children at first evaluation (2 days to 16 years). Eighteen (90%)children and 16 (24%) adults had a normal Echo; all patients evaluated in 1stdecade had normal echoes compared to 8% in the 5th decade; normal ECGswere present in 13 (68%) children and 13 (19%) adults (left side figure). Meanfollow up was 9.9±5.2 years. The rate of cardiovascular death was 2% per yearand sudden death (SD) 1% per year (right side figure). Follow up echoes wereavailable in 45 adults and 14 children (mean interval 9.3 + 5 years and 6.9 +2.9 years, respectively). Three patients developed LV dilatation; 2 children and 2adults with normal baseline echoes developed hypertrophy.
Conclusions: Non penetrant disease in patients with TNNT2m is rare beyond the2nd decade, but echo alone failed to detect disease in 23% of carriers. The rateof cardiovascular death and SD is comparable to the general HCM population.This study suggests that TNNT2m are not associated with a specific phenotype.
P1091 Standard ECG variables improve risk stratification ofsudden cardiac death in hypertrophic cardiomyopathy
E. Biagini1, C. Borghi1, F. Lai1, M. Lorenzini1, S. Rosmini1, L. DiDiodoro2, F. Pasquale1, G. Rocchi1, F. Coccolo1, C. Rapezzi1.1University Hospital Polyclinic San Orsola-Malpighi, Department of
Cardiology, Bologna, Italy; 2Institute of Cardiology, S. Orsola-Malpighi UniversityHospital, Bologna, Italy
Purpose: To investigate the prognostic significance of ECG in a large cohort ofpatients with hypertrophic cardiomyopathy (HCM).Methods: 274 HCM patients (62% men, mean age 50±16 yrs) were followed for6.6±7.6 yrs.Results: ECG features are summarized in the Table. Independent predictors ofsudden death were unexplained syncope (HR 5.4, 95% CI 2.3-12.3, p<0.001)and ST segment elevation/giant positive T waves (HR 2.5, 95% CI 1.2-5.5, p0.02), whereas left bundle branch block (LBBB)showed a trend (HR 2.5, 95%CI 0.9-6.8, p 0.06). Two models were constructed to predict the risk of suddendeath: the first based on the 4 established risk factors (wall thickness ≥30mm,non-sustained ventricular tachycardia on ECG Holter, syncope and family historyof sudden death) and the second with the addition of ST segment elevation/giantpositive T waves and LBBB (figure). Whereas both models stratified patients ac-cording to the number of risk factors the second model showed a higher predictivepower (chi-square from 16 to 22, p 0.028).
ECG features at baseline
Normal ECG, n (%) 15 (6)Left ventricular hypertrophy, n (%) 178 (65)Left bundle branch block, n (% 20 (7)Giant T waves inversion, n (%) 77 (28)ST segment depression ≥1 109 (40)ST segment elevation and/or giant positive T waves, n (%) 75 (27)
Survival free from sudden cardiac death
Conclusions: In HCM standard ECG has a prognostic value and improves thecurrent risk stratification model.
P1092 Complications and arrhythmia after percutaneoustransluminal septal myocardial ablation (PTSMA).Results from Scandinavian HOCM Database
M. Jensen1 , V. Almaas2, L. Jacobsen3 , P.R. Hansen4, L. Koeber1,J.P. Amlie2, M.J. Ericsson3, S. Aakhus2, F. Gadler3, H. Bundgaard3 .
1Rigshospitalet, Copenhagen University Hospital, Copenhagen, Denmark;2Department of Cardiology, Oslo University Hospital, Rikshospitalet, Oslo,Norway; 3Karolinska University Hospital, Department of Cardiology, Stockholm,Sweden; 4Gentofte Hospital, Department of Cardiology, Gentofte, Denmark
Background: Due to the risk of PTSMA-related complications, myectomy main-tains the gold standard for treatment of severely symptomatic patients with hy-pertrophic obstructive cardiomyopathy (HOCM). We analyzed the peri-proceduralcomplications, arrhythmia and survival after PTSMA in the Scandinavian HOCMDatabase.Methods and results: A total of 238 HOCM patients (age 60±14 years) werereferred for 263 PTSMA procedures from 1999 to 2009 in 4 Scandinavian tertiaryheart centres. Coronary perforation was reported in 4 procedures (1.5%). One ofthese procedures and 8 procedures in total were aborted without alcohol injec-tion. In the remaining (n=255), injection of 2.2±0.8 ml of alcohol per procedurelead to a peak level of creatine kinase MB of 158±106 μg/L. Accidental alcoholdisplacement occurred in 2% and coronary spasm in 2% of procedures. Arrhyth-mic events during completed procedures (n=255): complete heart block (CHB)36%, new atrial fibrillation 1.6% and ventricular fibrillation (VF) 1.2%. Arrhythmicevents during in-hospital observation included: episodes of CHB 26%, atrial fibril-lation 9%, non-sustained ventricular tachycardia 20%, VF 2%. Seventeen percentof patients received a pacemaker within 30 days after first PTSMA. Two in-hospitaldeaths were caused by acute heart failure and sepsis. The survival after PTSMA(n=233) was 97% after 1 year and 79% after 5 years, which was lower than anage and sex matched background population (Figure). Neither arrhythmia nor thecoronary complications were related to long-term survival after PTSMA.
Overall survival after PTSMA
Conclusion: The rate of complications and arrhythmia during the PTSMA pro-cedure and in-hospital observation were relatively high, but could be managedsafely. Peri-procedural complications and arrhythmia did not affect the long-termsurvival.
P1093 Value of exercise echocardiography for predictingoutcome in patients with hypertrophiccardiomyopathy
A. Bouzas Mosquera, J. Peteiro, X. Fernandez, L. Monserrat,F.J. Broullon, E. Mendez Eirin, A. Perez Perez, P. Pazos, A. CastroBeiras. Hospital Universitario A Coruña, A Coruña, Spain
Purpose: Although exercise echocardiography (EE) may assess left ventricular(LV) systolic function and LV outflow tract (LVOT) gradients during exercise, itsvalue for predicting outcome in patients with hypertrophic cardiomyopathy (HCM)has not been well characterized.Methods: A group of 255 patients (mean age 52.5±15.1 years, 97 women) withHCM underwent treadmill EE. LV ejection fraction (LVEF) and LVOT gradientswere evaluated at rest and at peak exercise.Results: Maximal left ventricular wall thickness was 20.3±5.3 mm, and New YorkHeart Association (NYHA) functional class was ≥2 in 142 patients (56%). Of the255 patients, 60 (23.5%) had LVOT obstruction at rest (i.e., LVOT gradient >30mmHg), and 45 (18%) developed exercise-induced LVOT obstruction. Mean exer-cise workload was 9.7±3.4 METs and 36 patients (14.1%) developed symptomsduring exercise. Mean resting and exercise LVEF were 63±8% and 69±10%, re-spectively. LVEF failed to increase during exercise in 31 patients (12%). During afollow-up of 4.0±2.7 years, 25 patients had a hard cardiovascular event (cardiacdeath in 8 patients; cardiac transplantation in 2; aborted cardiac arrest in 1; appro-priate discharge of a defibrillator in 2; sustained ventricular tachycardia [VT] in 1;stroke in 2; myocardial infarction in 2; hospitalization due to heart failure in 7) and49 patients had a composite endpoint of hard or soft events (including new on-set atrial fibrillation, syncope, and coronary revascularization). Increase in LVEFwith exercise was associated with hard events in univariate analysis (HR=0.88,95% CI=0.83-0.94, p<0.001). Failure of LVEF to increase with exercise occurredin 38% of patients with hard events vs. 9.6% of patients without hard events
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Diagnosis and management of cardiomyopathies / Advances in cardiovascular magnetic resonance 163
(p<0.001). After multivariable adjustment, resting LVEF and METs remained in-dependent predictors of hard events (HR=0.94, 95% CI=0.90-0.98, p=0.008; andHR=0.80, 95% CI=0.70-0.93, p=0.002, respectively), whereas LVEF increase withexercise was marginally associated with hard events (HR=0.93, 95% CI=0.86-1.00, p=0.05), but significantly associated with the combined endpoint of hard orsoft events (HR=0.92, 95% CI=0.87-0.97, p=0.003). Resting or exercise-inducedLVOT obstruction were not significantly associated with either endpoint.Conclusion: Assessment of exercise capacity and LV systolic function during EEmay have a role in risk stratification of patients with HCM.
P1094 Natural history, survival and risk stratification inpre-adolescent hypertrophic cardiomyopathy
J.P. Kaski1, M.T. Tome Esteban2, L. Consuegra3 , J.E. Deanfield1 ,W.J. Mckenna2, P.M. Elliott2. 1University College London, London,United Kingdom; 2The Heart Hospital, London, United Kingdom;
3University Hospital Virgen de la Arrixaca, Department of Cardiology, Murcia,Spain
Background: The natural history of hypertrophic cardiomyopathy (HCM) in adultsis well characterised, and algorithms to identify individuals at high risk of suddendeath have been developed. In contrast, data on the natural history and outcomeof HCM in the paediatric population are limited. This is the first systematic studyto evaluate the natural history and risk of adverse cardiovascular events in youngchildren with HCM.Methods: Ninety-five patients diagnosed with HCM aged ≤13 years underwentresting and ambulatory electrocardiography, echocardiography and cardiopul-monary exercise testing. Follow-up and survival data were collected. Potentialpredictors of adverse cardiovascular events (sudden cardiac death, appropriateICD discharge or cardiac transplantation) were assessed using a univariate Coxregression model and significant variables were analysed in a multivariate Coxregression model.Results: Over a median follow-up time of 6.3 years (IQR 2.6-9.1 years), 13 pa-tients (13.7%) had adverse cardiovascular events, (2.2% per year (95% CI 2.08%- 2.33%)): 7 (7.4%) died suddenly and 1 had appropriate ICD shocks (1.4% peryear [95% CI 1.3-1.5% per year]) and 5 (5.3%) underwent cardiac transplanta-tion. On univariate analysis, 4 significant predictors of adverse cardiovascularevents were identified: NYHA class III/IV; maximal left ventricular wall thickness≥30mm; left atrial z-score ≥+3; and sporadic disease. Sporadic disease (hazardratio (HR) 19.88, 95%CI 1.67-236.70,p=0.018) and NYHA class III/IV (HR 29.97,95%CI 1.89-474.40, p=0.016) were independently predictive of cardiovascularevents. The annual cardiovascular event rate for patients with no risk factors was0.4% (95%CI 0.32% to 0.48%) and 5.84% (95%CI 5.37% to 6.31%) for those with≥2 risk factors. Only sporadic HCM was significantly predictive of sudden deathor appropriate ICD discharges (5.68, 95%CI 1.15-28.17, p=0.03), although max-imal wall thickness ≥30mm and left atrial z-score ≥3 both approached statisticalsignificance (p=0.06 for both).Conclusions: The overall survival rates in this population are higher than previ-ously described, suggesting that most children have a benign prognosis. Childrenwith non-familial disease appear to be at increased risk of sudden death and car-diac transplantation. A subgroup of children at high risk of adverse cardiovascularevents who warrant consideration of prophylactic therapy can be identified usingnon-invasive tests.
P1095 Fulminant myocarditis rescued by mechanicalcirculatory support: outcomes, quality-of-life andincidence of symptoms of post-traumatic stressdisorder, anxiety and depression
M. Mirabel, A. Combes, P. Leprince, J. Chastre. AP-HP - HospitalPitie-Salpetriere, Paris, France
Purpose: Fulminant myocarditis (FM) is a rare but potentially lethal disease af-fecting healthy young patients. Mechanical circulatory support may be required incase of cardiogenic shock non responsive to conventional therapy. Outcomes ofthe disease have been poorly studied.Methods: We analyzed short and long term outcomes of 41 patients admittedfor FM in the intensive care unit (ICU) and treated with mechanical circulatorysupports, such as extracorporeal membrane oxygenator (ECMO) or bi-ventricularassist devices. At follow-up left ventricular ejection fraction (LVEF) was measuredby echocardiography. Health related quality of life (HRQOL) was assessed by theShort Form 36 questionnaire (SF36). Anxiety and depression symptoms, risk forpost-traumatic stress syndrome (PTSD) were assessed by two questionnaires:hospital anxiety and depression scale (HAD) and the impact of event scale (IES).Results: The mean age was 38±12 years. Most patients (85%) had no past med-ical history. Diagnosis was proven by myocardial biopsy in 24 (59%) cases. ECMOwas used in 35 (85%) cases. Multiple organ failure was present in 36 (88%) pa-tients and 13 (31%) patients died in ICU. Mortality was independently associatedwith SAPS II>56 (p=0.01) and troponinIc > 22μg/ml (p=0.03) measured at admis-sion. Complications due to circulatory support were present in 23 (56%) cases.Twenty-three patients (82% of ICU survivors) were followed-up during a meanperiod of 553±347 days. Four patients (10%) received a heart transplant. Amongsurvivors free of heart transplant, mean LVEF was 56±10% at follow-up, and tenpatients (53%) had LVEF≥60%. Using the SF-36, a poorer HRQOL in the phys-
ical domains was identified in patients compared to their sex and age matchedcontrols (aggregate physical component (PCS), p=0.01). Severe symptoms ofanxiety and/or depression according to the HAD score (>10 points) were presentin 3 (13%) and 2 (9%) cases, respectively. High risk for PTSD (IES scoring >30points) was present in 8 (35%) patients.Conclusion: Mechanical circulatory support rescued >65% of otherwise fatalrefractory cardiogenic shock due to fulminant myocarditis. Mortality was signifi-cantly associated with troponinIc level at admission. This widely available markerof myocardial damage may be of great value in identifying at risk patients. Leftventricular systolic function recovered in half of survivors. Need for heart trans-plant was rare. Nevertheless, many patients declared a poor quality of life andwere at risk of PTSD. These findings suggest that medical and psychosocial as-sessment may be beneficial to those individuals.
P1096 A novel risk score for predicting cardiac death inchronic chagas heart disease based on spectralturbulence analysis of the signal-averaged ECG
P.R. Benchimol Barbosa1, B.R. Tura2, E.C. Barbosa3, J. Barbosa-Filho4, B.K. Kantharia5. 1Military Fire Department of Rio de Janeiro,
Rio de Janeiro, Brazil; 2National Institute of Cardiology, Rio De Janeiro, Brazil;3State University of Rio de Janeiro (UERJ), Rio de Janeiro, Brazil; 4Gama FilhoUniversity, Rio de Janeiro, Brazil; 5University of Texas-Health Science Center atHouston, Houston, United States of America
Introduction: Mechanical dysfunction of the heart and arrhytmia are the maincauses of death in chronic Chagas disease (CCD). This study prospectively in-vestigated signal-averaged ECG (SAECG), 24h-ambulatory ECG and echocar-diogram variables in CCD aiming at determining a predictive score for cardiacdeath.Methods: Clinically compensated outpatients with CCD (34 to 74 y.o, 38 males)staged according to Los Andes (Class I: N=28; II: N=48; III: N=24) were en-rolled. Deaths were ascertained by active contact and review of medical records.SAECG was acquired on admission. Spectral turbulence analysis (STA) was car-ried out on XYZ leads after short-time Fourier transform mapping of ventricularactivation, and applying intersegment spectral correlation technique.Results: During a follow-up of (mean±SEM) 95.3±3.1 months, 20 patients died(rate: 26.4±1.4‰/year). In a multivariate Cox proportional-hazard model, nonsus-tained ventricular tachycardia episodes/24h (p=0.006), LVEF<50% (p<0.001),and positive STA (p=0.001) were independent predictors of death (Table inset).A prognostic score was developed by rounding weighted points proportional tobeta coefficient in Cox model (Table inset) to the upper nearest integer. Basedon ROC analysis optimal cut-off value of novel score was set to 5. KM curves ofnovel score for deaths are presented in Figure A (proportional hazard test: rho=-0.5; p=0.06). In 1,000 bootstraps, ROC c-statistic of novel score was superior toboth Rassi score and Ribeiro Score (Figure B).
Figure 1
Conclusions: In chronic Chagas disease, spontaneous nonsustained ventriculartachycardia, LVEF<50% and high SAECG spectral turbulence are independentpredictors of cardiac death. A novel risk score composed by independent predic-tors improves prognostic accuracy in this population.
ADVANCES IN CARDIOVASCULAR MAGNETICRESONANCE
1104 Criteria for the CMR diagnosis of stress induced(Takotsubo) cardiomyopathy: A series of 90 patients inEurope and north America
I. Eitel1, O. Strohm2, H. Abdel-Aty3, M. Gutberlet1, G. Schuler1,M.G. Friedrich2, H. Thiele1. 1University of Leipzig, Heart Center,
Leipzig, Germany; 2University of Calgary Foothills Hospital, Calgary, Canada;3Cardio Center Berlin, Berlin, Germany
Purpose: Stress-induced cardiomyopathy (Takotsubo cardiomyopathy, TTC) isan increasingly recognized acute cardiac syndrome. Cardiovascular magneticresonance (CMR) allows for assessing irreversible injury (late gadolinium en-hancement [LGE]) and myocardial edema and contributes to our understandingand differential diagnosis of this new entity. So far, various CMR criteria have
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

164 Advances in cardiovascular magnetic resonance
been used in rather small populations. We aimed to establish CMR criteria for thediagnosis of TTC and used a comprehensive approach in a large series of TTCpatients recruited by 2 CMR centers in Europe and North America.Methods: Between 2005 and 2010, 90 patients (85 female, age 71±12 years)with acute cardiac symptoms and a left ventricular (LV) dysfunction pattern notexplained by coronary artery disease underwent CMR in a 1.5-T scanner. LV func-tion, T2-weighted triple-inversion-recovery imaging and LGE images after admin-istration of gadolinium-DTPA were evaluated visually. In 37 patients, the recom-mended CMR criteria for acute myocarditis (Lake Louise Criteria) were analyzed.Sixty-one (69%) patients underwent follow-up CMR after three months.Results: In 82 (91%) patients, cine images revealed a typical pattern with api-cal ballooning, in 7 (8%) with midventricular ballooning and in 1 patient (1%) an"inverted", basal pattern with moderate-to-severe reduction of LV ejection frac-tion in all patients (mean 45±9%). A transmural area of high T2 signal in themid and apical regions was visible in 58 (64%) patients matching the distribu-tion of LV dysfunction. In 7 patients (8%) patients, LGE was detected consistentwith focal or patchy myocardial scarring, with a signal intensity lower than thattypically observed in myocardial infarction or myocarditis (<5 standard deviationsabove mean of normal myocardium in all patients). Of 37 TTC patients assessedusing the Lake Louise Criteria, 23 (62%) were positive for acute myocardial in-flammation. Follow-up CMR showed complete normalization of LV function (mean67±6%) and inflammatory parameters in the absence of LGE in all patients.Conclusions: In this largest CMR series to date in TTC patients, the main diag-nostic criteria for TTC are: 1) Typical pattern of mid and apical LV dysfunction;2) Edema in the mid and apical myocardium 3) Absence of LGE >5 standarddeviations; 4) Myocardial inflammation values. Recovery of LV wall motion ab-normalities, inflammatory parameters and LGE at CMR follow-up can be used toconfirm the diagnosis retrospectively. The diagnostic accuracy of these criteriashould be studied.
1105 Patients with persistent microvascular obstructionfollowing acute myocardial infarction remain at highrisk of adverse remodelling despite optimal therapyand may benefit from aldosterone antagonism
R.A.P. Weir1, C.A. Murphy1, C.J. Petrie1, T.N. Martin1, S. Clements1,T. Steedman1, G.S. Wagner2, H.J. Dargie1, J.J.V. Mcmurray1 . 1WesternInfirmary, Glasgow, United Kingdom; 2Duke University Medical Center, Durham,United States of America
Introduction: Microvascular obstruction (MVO) is associated with large acutemyocardial infarction (AMI) and lower left ventricular (LV) ejection fraction, andpredicts greater remodelling, but whether this effect is abolished by contempo-rary anti-remodelling therapies is subject to debate. We examined the influence ofseveral infarct characteristics, including MVO, on LV remodelling in an optimally-treated post-AMI cohort enrolled in a clinical trial investigating the potential anti-remodelling effects of eplerenone, using contrast-enhanced cardiac magnetic res-onance (ceCMR).Methods: 100 patients (mean age 58.9±12 years, 77% male) admitted with AMIin the previous 1-14 days underwent ceCMR at baseline (∼4 days), 12 and 24weeks. The effects on LV remodelling (i.e. change in LV end-systolic volume in-dex [�LVESVI]) of infarct site, transmurality, endocardial extent, and the presenceof early and late MVO were analysed. Tests for interaction between MVO persis-tence and eplerenone therapy were also performed.Results: Mean baseline infarct volume index decreased from 34.0 (21.2) ml/m2
to 20.9 (12.9) ml/m2 at 24 weeks (p<0.001). Infarct site had no influence on re-modelling, but greater baseline infarct transmurality (r=0.47, p<0.001) and endo-cardial extent (r=0.26, p<0.01) were associated with higher �LVESVI. Early MVOwas seen in 69 (69%) of patients and persisted, as late MVO, in 56 (56%). Pa-tients with late MVO underwent significantly greater remodelling than those with-out MVO (�LVESVI +4.1 [13.4] vs. -7.0 [12.7] mL/m2 respectively, p=0.001); thosewith early MVO only displayed an intermediate �LVESVI (-4.9 [13.0] mL/m2).Coronary angiography was undertaken in 85/100 (85%) of the cohort; TIMI 3flow within the infarct-related artery was seen in 42/56 (87.5%) of patients withlate MVO and in 32/44 (86.5%) of those without late MVO (p=ns), thus late MVOwas seen frequently despite optimal coronary blood flow having been restored atangiography. Interestingly, the presence of (late) MVO was associated with signifi-cantly less remodelling in eplerenone- than in placebo-treated patients (�LVESVI0.8 [11.0] ml/m2 vs. 8.1 [15.2] ml/m2 respectively, p<0.001).Conclusions: Late MVO on pre-discharge ceCMR remains an ominous predictorof adverse LV remodelling despite powerful anti-remodelling therapy, and maybe useful in the risk-stratification of survivors of AMI. Eplerenone may attenuateremodelling more powerfully in patients at the highest risk of remodelling, ie. thosewith persistent MVO.
1106 Allopurinol reduces both left ventricular hypertrophyand endothelial dysfunction in cardiorenal patients
M.P. Kao1, D.S. Ang1, S.J. Gandy2, A. Nadir1, C.C. Lang1,A.D. Struthers1. 1University of Dundee, Dundee, United Kingdom;2Ninewells Hospital, Dundee, United Kingdom
Introduction: Oxidative stress (OS) causing left ventricular hypertrophy (LVH)and endothelial dysfunction (ED) is thought to be a major reason why patients
with chronic kidney disease (CKD) suffer more cardiovascular (CV) events thanwould be expected from their conventional risk factors such as BP. One way to re-duce OS is to prevent its formation by using allopurinol to block xanthine oxidase(XO)-induced OS. In this study, we examined if allopurinol really does regress leftventricular (LV) mass and improve ED in CKD patients.Methods: A randomised, double-blind, placebo-controlled, parallel study wasconducted in 67 cardiac patients with chronic kidney disease (CKD) stage 3. Sub-jects received 100mg Allopurinol once a day for the initial 2 weeks, and then in-creased to 300mg Allopurinol once a day for the remaining 9 months, or placebo.Cardiac magnetic resonance (CMR) was performed to measure LV mass index(LVMI). Endothelial function was assessed by flow-mediated dilatation (FMD) ofthe brachial artery, while central arterial stiffness was assessed by pulse waveanalysis (PWA) and pulse wave velocity (PWV).Results: 55 patients completed the study (27 active, 28 placebo). Mean age, es-timated glomerular filtration rate (eGFR) and clinic BP were 72±6 years, 44±10ml/min/1.73m2, and 141/73 (± 16/8) mmHg respectively. LVMI was found toregress in those on allopurinol [� LVMI was -1.4g/m2 (±4.7) in the active groupand +1.3 g/m2 (±4.4) in the placebo group, p = 0.027]. Allopurinol significantlyimproved brachial artery FMD [� FMD was +1.3% (± 3.1%) in the active groupand -0.8% (± 2.9%) in the placebo group (p = 0.020)]. The central augmentationindex (AIx) improved significantly on allopurinol [� AIx was -4.7% (±9.3%) in theactive group and +2.0% (±7.3%) in the placebo group (P=0.005)]. There was alsoa trend towards improvement in PWV in patients on allopurinol [� PWV was -0.4m/sec (±1.1) in the active group and +0.2 m/sec (± 1.3) in the placebo group(P=0.059)]. Allopurinol was well tolerated and renal function remained stable inboth groups throughout the whole study period.Conclusion: This is the first study to demonstrate that allopurinol can regress LVMass. The mechanism by which this is achieved may be mediated via a reductionin oxidative stress and a reduction in afterload, as measured by augmentationindex. As LVH and ED are both important surrogate markers of prognosis, thisstudy should prompt future trials to examine whether allopurinol improves hardclinical end points in cardiorenal patients.
1107 Prognostic value of intramyocardial haemorrhagedetected by cardiac magnetic resonance imaging inacute reperfused ST-elevation myocardial infarction
H. Thiele, K. Kubusch, G. Fuernau, S. De Waha, S. Desch, G. Schuler,I. Eitel. University of Leipzig, Heart Center, Department of Internal
Medicine and Cardiology, Leipzig, Germany
Background: Despite successful reperfusion of the infarcted vessel, recent stud-ies in ST-elevation myocardial infarction (STEMI) patients have frequently shownthe presence of intramyocardial haemorrhage (IMH) in the infarct core. Haem-orrhagic infarction can be accurately detected in vivo by cardiac magnetic reso-nance imaging (CMR) using T2-weighted and T2* imaging because breakdownproducts of haemoglobin are paramagnetic and influence regional magnetic tis-sue properties. Although the relationship of IMH with adverse LV remodelling andinfarct size has been shown in previous trials, the clinical impact and prognosticvalue of IMH remains unknown.Purpose: The purpose of the study was to evaluate the clinical significance ofIMH in a large series of high-risk STEMI patients reperfused by primary PCI.Methods: We analyzed 316 consecutive STEMI patients undergoing primary PCI<12 hours after symptom onset (231 male, mean age 64±12 years). All patientsunderwent CMR within 2-4 days after infarction for assessment of infarct size, mi-crovascular obstruction (MO) and IMH. IMH was detected as areas of hypointensesignal in the core of the high signal intensity region on T2-weighted images. Pa-tients were categorized into 2 groups defined by the presence or absence of IMH.The primary endpoint of the study was the occurrence of major adverse cardio-vascular events (MACE) defined as death, reinfarction and occurrence of newcongestive heart failure within 6 months after the index event.Results: Haemorrhage was present in 143 (45%) patients with acute STEMI.Patients with IMH had significantly larger infarcts, a lower ejection fraction and alarger extent of early as well as late MO (p<0.001, respectively). The extent oflate MO correlated significantly with the extent of haemorrhage in T2-weightedimaging (r=0.59, p<0.001).MACE (13% versus 12%, p=0.96) and mortality (5% versus 4%, p=0.63) rateswere similar between the groups and the presence of IMH was no predictor ofadverse outcomes in uni- and multivariable Cox proportional hazard analysis.Conclusions: Haemorrhage assessed by CMR imaging is a frequent complica-tion in STEMI patients reperfused by primary PCI and is closely related to infarctsize, function, and no-reflow. However, this largest study to date found no prog-nostic significance of IMH regarding hard clinical end-points at 6-month follow-up.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
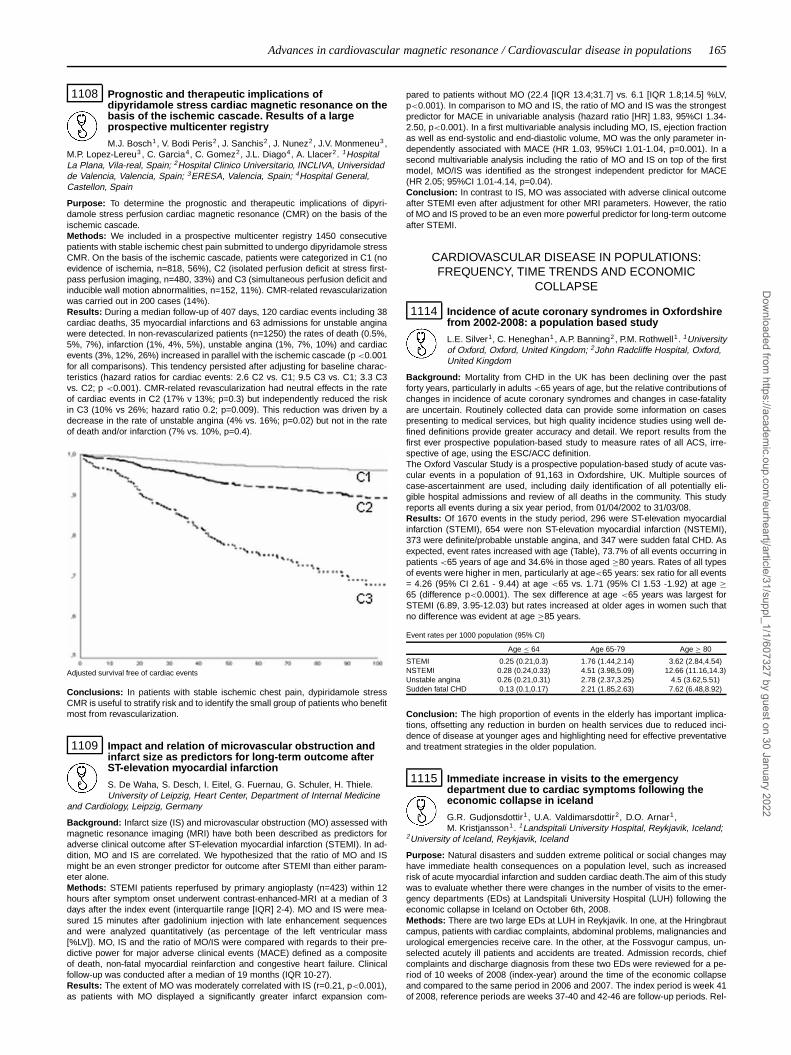
Advances in cardiovascular magnetic resonance / Cardiovascular disease in populations 165
1108 Prognostic and therapeutic implications ofdipyridamole stress cardiac magnetic resonance on thebasis of the ischemic cascade. Results of a largeprospective multicenter registry
M.J. Bosch1, V. Bodi Peris2, J. Sanchis2, J. Nunez2, J.V. Monmeneu3 ,M.P. Lopez-Lereu3 , C. Garcia4, C. Gomez2, J.L. Diago4, A. Llacer2. 1HospitalLa Plana, Vila-real, Spain; 2Hospital Clinico Universitario, INCLIVA, Universidadde Valencia, Valencia, Spain; 3ERESA, Valencia, Spain; 4Hospital General,Castellon, Spain
Purpose: To determine the prognostic and therapeutic implications of dipyri-damole stress perfusion cardiac magnetic resonance (CMR) on the basis of theischemic cascade.Methods: We included in a prospective multicenter registry 1450 consecutivepatients with stable ischemic chest pain submitted to undergo dipyridamole stressCMR. On the basis of the ischemic cascade, patients were categorized in C1 (noevidence of ischemia, n=818, 56%), C2 (isolated perfusion deficit at stress first-pass perfusion imaging, n=480, 33%) and C3 (simultaneous perfusion deficit andinducible wall motion abnormalities, n=152, 11%). CMR-related revascularizationwas carried out in 200 cases (14%).Results: During a median follow-up of 407 days, 120 cardiac events including 38cardiac deaths, 35 myocardial infarctions and 63 admissions for unstable anginawere detected. In non-revascularized patients (n=1250) the rates of death (0.5%,5%, 7%), infarction (1%, 4%, 5%), unstable angina (1%, 7%, 10%) and cardiacevents (3%, 12%, 26%) increased in parallel with the ischemic cascade (p <0.001for all comparisons). This tendency persisted after adjusting for baseline charac-teristics (hazard ratios for cardiac events: 2.6 C2 vs. C1; 9.5 C3 vs. C1; 3.3 C3vs. C2; p <0.001). CMR-related revascularization had neutral effects in the rateof cardiac events in C2 (17% v 13%; p=0.3) but independently reduced the riskin C3 (10% vs 26%; hazard ratio 0.2; p=0.009). This reduction was driven by adecrease in the rate of unstable angina (4% vs. 16%; p=0.02) but not in the rateof death and/or infarction (7% vs. 10%, p=0.4).
Adjusted survival free of cardiac events
Conclusions: In patients with stable ischemic chest pain, dypiridamole stressCMR is useful to stratify risk and to identify the small group of patients who benefitmost from revascularization.
1109 Impact and relation of microvascular obstruction andinfarct size as predictors for long-term outcome afterST-elevation myocardial infarction
S. De Waha, S. Desch, I. Eitel, G. Fuernau, G. Schuler, H. Thiele.University of Leipzig, Heart Center, Department of Internal Medicine
and Cardiology, Leipzig, Germany
Background: Infarct size (IS) and microvascular obstruction (MO) assessed withmagnetic resonance imaging (MRI) have both been described as predictors foradverse clinical outcome after ST-elevation myocardial infarction (STEMI). In ad-dition, MO and IS are correlated. We hypothesized that the ratio of MO and ISmight be an even stronger predictor for outcome after STEMI than either param-eter alone.Methods: STEMI patients reperfused by primary angioplasty (n=423) within 12hours after symptom onset underwent contrast-enhanced-MRI at a median of 3days after the index event (interquartile range [IQR] 2-4). MO and IS were mea-sured 15 minutes after gadolinium injection with late enhancement sequencesand were analyzed quantitatively (as percentage of the left ventricular mass[%LV]). MO, IS and the ratio of MO/IS were compared with regards to their pre-dictive power for major adverse clinical events (MACE) defined as a compositeof death, non-fatal myocardial reinfarction and congestive heart failure. Clinicalfollow-up was conducted after a median of 19 months (IQR 10-27).Results: The extent of MO was moderately correlated with IS (r=0.21, p<0.001),as patients with MO displayed a significantly greater infarct expansion com-
pared to patients without MO (22.4 [IQR 13.4;31.7] vs. 6.1 [IQR 1.8;14.5] %LV,p<0.001). In comparison to MO and IS, the ratio of MO and IS was the strongestpredictor for MACE in univariable analysis (hazard ratio [HR] 1.83, 95%CI 1.34-2.50, p<0.001). In a first multivariable analysis including MO, IS, ejection fractionas well as end-systolic and end-diastolic volume, MO was the only parameter in-dependently associated with MACE (HR 1.03, 95%CI 1.01-1.04, p=0.001). In asecond multivariable analysis including the ratio of MO and IS on top of the firstmodel, MO/IS was identified as the strongest independent predictor for MACE(HR 2.05; 95%CI 1.01-4.14, p=0.04).Conclusion: In contrast to IS, MO was associated with adverse clinical outcomeafter STEMI even after adjustment for other MRI parameters. However, the ratioof MO and IS proved to be an even more powerful predictor for long-term outcomeafter STEMI.
CARDIOVASCULAR DISEASE IN POPULATIONS:FREQUENCY, TIME TRENDS AND ECONOMIC
COLLAPSE
1114 Incidence of acute coronary syndromes in Oxfordshirefrom 2002-2008: a population based study
L.E. Silver1, C. Heneghan1 , A.P. Banning2, P.M. Rothwell1. 1Universityof Oxford, Oxford, United Kingdom; 2John Radcliffe Hospital, Oxford,United Kingdom
Background: Mortality from CHD in the UK has been declining over the pastforty years, particularly in adults <65 years of age, but the relative contributions ofchanges in incidence of acute coronary syndromes and changes in case-fatalityare uncertain. Routinely collected data can provide some information on casespresenting to medical services, but high quality incidence studies using well de-fined definitions provide greater accuracy and detail. We report results from thefirst ever prospective population-based study to measure rates of all ACS, irre-spective of age, using the ESC/ACC definition.The Oxford Vascular Study is a prospective population-based study of acute vas-cular events in a population of 91,163 in Oxfordshire, UK. Multiple sources ofcase-ascertainment are used, including daily identification of all potentially eli-gible hospital admissions and review of all deaths in the community. This studyreports all events during a six year period, from 01/04/2002 to 31/03/08.Results: Of 1670 events in the study period, 296 were ST-elevation myocardialinfarction (STEMI), 654 were non ST-elevation myocardial infarction (NSTEMI),373 were definite/probable unstable angina, and 347 were sudden fatal CHD. Asexpected, event rates increased with age (Table), 73.7% of all events occurring inpatients <65 years of age and 34.6% in those aged ≥80 years. Rates of all typesof events were higher in men, particularly at age<65 years: sex ratio for all events= 4.26 (95% CI 2.61 - 9.44) at age <65 vs. 1.71 (95% CI 1.53 -1.92) at age ≥65 (difference p<0.0001). The sex difference at age <65 years was largest forSTEMI (6.89, 3.95-12.03) but rates increased at older ages in women such thatno difference was evident at age ≥85 years.
Event rates per 1000 population (95% CI)
Age ≤ 64 Age 65-79 Age ≥ 80
STEMI 0.25 (0.21,0.3) 1.76 (1.44,2.14) 3.62 (2.84,4.54)NSTEMI 0.28 (0.24,0.33) 4.51 (3.98,5.09) 12.66 (11.16,14.3)Unstable angina 0.26 (0.21,0.31) 2.78 (2.37,3.25) 4.5 (3.62,5.51)Sudden fatal CHD 0.13 (0.1,0.17) 2.21 (1.85,2.63) 7.62 (6.48,8.92)
Conclusion: The high proportion of events in the elderly has important implica-tions, offsetting any reduction in burden on health services due to reduced inci-dence of disease at younger ages and highlighting need for effective preventativeand treatment strategies in the older population.
1115 Immediate increase in visits to the emergencydepartment due to cardiac symptoms following theeconomic collapse in iceland
G.R. Gudjonsdottir1, U.A. Valdimarsdottir2, D.O. Arnar1,M. Kristjansson1. 1Landspitali University Hospital, Reykjavik, Iceland;
2University of Iceland, Reykjavik, Iceland
Purpose: Natural disasters and sudden extreme political or social changes mayhave immediate health consequences on a population level, such as increasedrisk of acute myocardial infarction and sudden cardiac death.The aim of this studywas to evaluate whether there were changes in the number of visits to the emer-gency departments (EDs) at Landspitali University Hospital (LUH) following theeconomic collapse in Iceland on October 6th, 2008.Methods: There are two large EDs at LUH in Reykjavik. In one, at the Hringbrautcampus, patients with cardiac complaints, abdominal problems, malignancies andurological emergencies receive care. In the other, at the Fossvogur campus, un-selected acutely ill patients and accidents are treated. Admission records, chiefcomplaints and discharge diagnosis from these two EDs were reviewed for a pe-riod of 10 weeks of 2008 (index-year) around the time of the economic collapseand compared to the same period in 2006 and 2007. The index period is week 41of 2008, reference periods are weeks 37-40 and 42-46 are follow-up periods. Rel-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

166 Cardiovascular disease in populations: frequency, time trends and economic collapse
ative risk (RR; cumulative incidence ratios) and 95% confidence intervals (95%CI)of ED visits in weeks 41 through 46 with weekly average number of visits duringweeks 38 through 40 as reference were calculated.Results: Visits to ED at Hringbraut remained at a relatively stable rate during the10 consecutive week periods in 2006 and 2007. In 2008, however, a significantincrease in the number of visits was observed in this ED immediately following thefinancial crisis in week 41. A 26% increase was seen in the number of visits, butthis number decreased again in the coming weeks, returning to similar levels as inprevious years. With the four weeks prior to the economic collapse as reference,the RR for week 41 was 1.26 (95%CI 1.11-1.43); RR 1.41 (95%CI 1.17-1.69)for women and RR 1.15 (95%CI 0.96-1.37) for men. There were more visits dueto suspected cardiac complaints during the first week after the beginning of thefinancial crisis. Moreover, an increase in diagnosis of ischemic heart disease wasobserved among women in the seven days following the economic collapse. Visitsto the ED in Fossvogur were unchanged.Conclusion: The economic collapse in Iceland led to a sudden increased rate ofED visits, especially among patients with suspected cardiac complaints, similar towhat has been described with natural catastrophes. There was interestingly, anincrease in the number of women, but not men, with diagnosis of ischemic heartdisease.
1116 Nation-wide trends for atrial fibrillation in Australia:1998-2008
C.X. Wong, M.T. Sun, D.H. Lau, A.G. Brooks, D.P. Leong, N.J. Shipp,M. Alasady, H.S. Lim, H.S. Abed, P. Sanders. Royal Adelaide Hospital,Cardiovascular Research Centre, Adelaide, Australia
Background: The prevalence of atrial fibrillation (AF) isbelieved to be increasingin developed countries. Despite the substantial public health burden, there is apaucity of epidemiological data on AF in recent years, and very little on AF inAustralia. We thus sought to determine recent nation-wide trends in hospitaliza-tion for AF as a principal diagnosis in Australia from 1998-2008.Methods: We identified all hospitalizations for AF in Australia (population 22 mil-lion) as a principal diagnosis by ICD-10 coding from the Australian Institute ofHealth and Welfare. Population data was obtained from the Australian Bureau ofStatistics.Results: From 1998-2008, a total of 373,197 patients were hospitalized for aprincipal diagnosis of AF. 54.8% of these were for men. Hospitalizations increasedfrom 27,245 to 47,164, or by an average of 6.8% per annum. AF as a percentageof all hospitalizations also increased from 0.48 to 0.60%. Overall, the proportionof individuals hospitalized with AF and aged >75 years rose from 24 to 27% inmen and from 47 to 51% in women during this period. The average length of stayfell for men from 2.8 to 2.7 days and from 4.0 to 3.5 days in women. Despite thisdecrease in length of stay, the increase in AF hospitalisations resulted in a 74 and73% increase in the total number of hospitalization days for AF respectively forboth sexes.
Conclusions: The number of hospitalizations for AF has increased significantin Australia from 1998-2008. This enormous public health burden has importantimplications for health care planning and primary prevention strategies againstthe development of AF.
Abstract 1117 – Table 1. Prevalence and outcomes
1995 (7,170) 1998 (6,827) 2003 (5,513) p-value for trend(adjusted)
AnginaPrevalence, % (unadjusted 95% CI) 3.1 (2.7-3.5) 3.2 (2.8-3.7) 2.3 (1.9-2.7) <0.001All-cause mortality, % (unadjusted 95% CI) 11.4 (7.8-16.4) 5.0 (2.8-8.9) 7.8 (4.1-14.7) 0.1All-cause mortality, MI or stroke, % (unadjusted 95% CI) 17.7 (13.3-23.5) 10.0 (6.7-14.8) 12.3 (7.4-20.0) 0.1
Intermittent ClaudicationPrevalence, % (unadjusted 95% CI) 2.0 (1.7-2.4) 1.7 (1.4-2.0) 1.8 (1.5-2.2) 0.3All-cause mortality, % (unadjusted 95% CI) 7.6 (4.3-13.3) 8.0 (4.2-14.8) 4.1 (1.6-10.6) 0.5All-cause mortality, MI or stroke, % (unadjusted 95% CI) 11.0 (6.9-17.4) 11.5 (6.9-19.0) 5.1 (2.2-11.9) 0.3
1117 Trends in prevalence and 5-year outcomes in subjectsreporting angina and intermittent claudication: ananalysis of three Scottish population health surveysconducted in 1995, 1998 and 2003
S.C. Inglis1, J.D. Lewsey2, K. Macintyre2, J.J.V. Mcmurray3. 1Sectionof Public Health, University of Glasgow and Baker IDI Heart and DiabetesInstitute, Melbourne, Australia; 2Section of Public Health and Health Policy,University of Glasgow, Glasgow, United Kingdom; 3BHF Glasgow CardiovascularResearch Centre, University of Glasgow, Glasgow, United Kingdom
Purpose: We used 3 national health surveys (1995, 1998, 2003) to examinetrends in the prevalence and outcomes related to the 2 major symptomatic man-ifestations of atherosclerosis (angina pectoris and intermittent claudication (IC)).This period saw campaigns to reduce cardiovascular disease, and widespreaduse of antiplatelets, statins and coronary revascularization.Methods: The 3 surveys enrolled random samples of individuals living in Scot-land. The Rose Angina and Edinburgh Claudication Questionnaires were used.Survey records were linked to national hospitalisation and death records and ratesof death and a composite outcome (death, myocardial infarction or stroke) calcu-lated at 5 years. Prevalence and outcome rates (in those aged 18-64 years) wereadjusted for age, sex and socioeconomic status. Subjects with angina, IC and nei-ther condition were compared (42 subjects with both conditions were excluded).Results: 19,510 individuals were included (Table). Prevalence of angina was con-sistently higher than IC and declined across the surveys (p<0.001), contrastingwith that of IC, which did not change (p=0.3). Outcomes were numerically but notstatistically significantly higher in those with angina compared to IC. Outcomesdid not change significantly over time.Conclusion: Angina prevalence in younger individuals in Scotland seems to havedeclined in recent years, while IC prevalence remained stable. Medium-term out-comes did not clearly improve in either group. IC remains a relatively neglected(yet common and dangerous) manifestation of atherosclerosis. Recent changesin practice have neither decreased IC prevalence nor improved its prognosis.
1118 Prevalence study of Keshan disease in China
T. Wang, J. Hou, Q. Li, D. Sun. Institute of Keshan Disease, HarbinMedical University, Harbin, China, People’s Republic of
Background: Keshan disease (KD) is an endemic cardiomyopathywhich is associated with selenium deficiency although the etiology is
not fully known in China. KD is characterized, in pathology, with myocardial de-generation (fresh damage), myocardial necrosis and myocardial fibrosis (old dam-age), and cardiomegaly; and clinically with heart failure and arrhythmia. Commonfindings of abnormal ECG are atrioventricular block, bundle branch block, T-waveand/or ST segment change, Q-T interval prolonged, multi-induced ventricular pre-mature contraction, paroxysmal ventricular or supraventricular tachycardia, atrialfibrillation, atrial flutter, and wave abnormalities. The aim of this study is to findthe national KD prevalence rate and estimated numbers of KD patients in orderto provide evidence for making and adjusting the policy and strategy of and allo-cating health resources in KD prevention and control.Method: Using probability proportional to population size, randomized, multi-stage, and cluster sampling, we surveyed 101,127 people in 178 surveillancesites in 15 provinces. We measured grain selenium levels and surveyed familyincome with pre-designed questionnaires.Results: No case of acute and sub-acute case of KD was found. The crude preva-lence of KD was 2.21% (95% CI: 2.12%, 2.30%) and the standardized nationalprevalence rates of KD, chronic KD and latent KD were 2.12%, 0.46% and 1.65%respectively. Chronic KD patients were mainly in the provinces where KD hadbeen seriously epidemic historically, such as Heilongjiang, Jilin, Sichuan and In-ner Mongolia. The KD prevalence rate was higher in females (2.20%) than inmales (1.98%). KD prevalence rates were higher in older age group in both menand women. The cases younger than 20 years accounted for 13.6%. There wasprobably a small number of KD cases newly occurred. The estimated numbersof national KD and chronic KD patients, with standardized prevalence rates, are1,606,394 and 350,727 (with crude prevalence, 95% CI: 349,300, 410,100) re-spectively. KD prevalence rates were reversely correlated with income. The stan-dardized (age and sex adjusted) prevalence of KD was 2.12%,. We estimated thatthe national numbers of the KD patients were 1.6785 millions (95% CI: 1.6085,1.7473), the chronic KD patients were 379.8 thousands (95% CI: 346.7, 412.8),and the latent KD patients were 1.2381 millions (95% CI: 1.194, 1.3594 millions).Conclusion: KD is still a public health issue of the people of the severe KD en-demic areas. Supplementation of selenium in severe endemic areas and homebased KD patient management should be strengthened.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Cardiovascular disease in populations / Coronary stenting: insights from long term follow up 167
1119 Explaining the decline in coronary heart diseasemortality in Poland between 1991 and 2005
P. Bandosz1, M. O’ Flaherty2, W. Drygas3, J. Koziarek3,B. Wyrzykowski1 , M. Rutkowski1, K. Bennett4, G. Opolski5,T. Zdrojewski1, S. Capewell2. 1Medical University in Gdansk - Dept.
of Hypertension and Diabetology, Gdansk, Poland; 2Department of PublicHealth, University of Liverpool, Liverpool, United Kingdom; 3Department ofEpidemiology, CVD Prevention and Health Promotion, Institute of Cardiology,Warsaw, Poland; 4Trinity Centre for Health Sciences, St James’s Hospital, Dublin,Ireland; 5Medical University of Warsaw, 1st Department of Cardiology, Warsaw,Poland
Purpose: Coronary heart disease (CHD) mortality has declined substantially inPoland over the last two decades. The purpose of this study was to determinewhat proportion of this decline could be associated with changes in CHD riskfactors from 1991-2005.Methods: The validated IMPACT model was used in all calculations. We includeddata describing population size, and CHD mortality and risk factor trends in adultsaged 25-85 years old between 1991 and 2005. Regression coefficients and rel-ative risks from the published literature quantified the relationship between pop-ulation changes for a specific CHD risk factor (i.e., smoking, diabetes, systolicblood pressure, total cholesterol, and obesity) and CHD mortality. The outcomeof interest was the number of deaths prevented or postponed (DPPs) associatedwith changes in each specific CHD risk factor.Results: From 1991-2005, the overall CHD mortality rate in Poland fell from 280to 159 deaths per 100,000 inhabitants, resulting in an estimated 35 176 fewerCHD deaths in 2005. Changes in CHD risk factors produced a total of 12 008CHD deaths (minimum estimate 11 268; maximum estimate 12 798) in Poland.Such reduction accounted for approximately 34% of the total decrease in CHDmortality. The largest contributing risk factor to lower mortality was the substan-tial fall in cholesterol (30%), followed by the increase in physical activity (10%)and reduction in smoking (8%). However, increases in some of risk factors hada negative impact on mortality: diabetes prevalence (-4%), and BMI (-5%) andpopulation systolic blood pressure (-5%), with increasing levels in men aged 45and older, while women and young men showing decreasing trends. Research iscurrently underway to estimate the contribution of treatments to a) the reductionin blood pressure and cholesterol and b) the decrease in case fatality in CHDpatients in Poland.Conclusions: Approximately one third of the large fall in CHD mortality between1991 and 2005 was attributable to reductions in major cardiovascular risk factors.However, adverse trends in blood pressure, obesity and diabetes are worrying.More aggressive food policies may therefore be needed to decrease future CHDdeaths.
CORONARY STENTING: INSIGHTS FROM LONG TERMFOLLOW UP
1132 Long-term bleeding events in patients with prolongeddual antiplatelet therapy after DES implantation
R. Rossini1, G. Musumeci1, C. Lettieri2, N. Lortkipanidze1 ,D. Capodanno3 , N. Cicorella2, T. Nijaradze1, G. Tarantini4 ,A. Gavazzi1, D. Angiolillo5. 1Hospital Riuniti of Bergamo, Bergamo,
Italy; 2Ospedale Carlo Poma, Mantova, Italy; 3Ferrarotto Hospital - Institute forCardiology, Department of Cardiovascular, Catania, Italy; 4Cardiology Division,University of Padova, Padova, Italy; 5University of Florida-Shands Jacksonville,Jacksonville, United States of America
Bleeding has emerged as a predictor of early and late mortality after percuta-neous coronary interventions. However, the prevalence and predictors of long-term bleeding events in patients (pts) on prolonged dual antiplatelet therapy afterdrug-eluting stent (DES) implantation has been poorly explored.Methods: We studied 1358 consecutive pts undergoing DES implantation anddischarged on dual antiplatelet therapy with aspirin and clopidogrel for 1 year.Pts were followed-up for 1 year and the prevalence and predictors of in-hospitaland long-term TIMI major and minor bleeding events were evaluated. The impactof bleeding events on all cause death, major adverse cardiac events (MACE),probable, possible and definite stent thrombosis, and premature discontinuationof antiplatelet therapy were also assessed.Results: The incidence of in-hospital major and minor bleeding was 1.2% and3.7%, respectively. The incidence of cumulative long-term major and minor bleed-ing was 4.2% and 8.2%, respectively. At multivariable analysis, cumulative long-term major bleeding was predicted only by haemoglobin at admission (OR=0.44[0.35-0.55], p<0.001), whereas haemoglobin at discharge (OR=0.62 [0.54-0.72],p<0.001), beta-blockers (OR=0.53 [0.30-0.95], p=0.03), and oral anticoagulantsat discharge (OR=5.59 [2.28-13.70], p<0.001) predicted cumulative long termminor bleeding. The incidence of one-year mortality (23.6% vs 3.8%, p<0.001),MACE (47.3% vs 12.5%, p<0.001), and stent thrombosis (12.7% vs 3.1%,p=0.002) was significantly higher in pts who experienced a major bleeding event.Pts who had a major bleeding event were more likely to prematurely discon-tinue antiplatelet therapy (11.5% vs 63.6%, p<0.001). Minor bleeding was as-sociated with increased rates of MACE (25.2% vs 13%, p=0.001) and prematureantiplatelet therapy discontinuation (44.9% vs 10.9%, p<0.001).
Conclusions: In DES treated pts on dual antiplatelet therapy, long-term majorbleeding is predicted by lower levels of haemoglobin at admission. Pts experi-encing any bleeding event are more likely to discontinue prematurely antiplatelettherapy and have a higher risk of MACE.
1135 Effect of stent length on late outcome afterpercutaneous coronary intervention using thesirolimus-eluting stent: five year results from theprospective multicentre German Cypher stent registry
M. Abdel-Wahab1, C. Hamm2, J. Senges3, R. Zahn4, U. Tebbe5 ,A. Loewe6, T. Pfannebecker7 , B. Levenson6 , G. Richardt1. 1Heart and VascularCenter, Segeberger Kliniken, Bad Segeberg, Germany; 2Kerckhoff Clinic,Department of Cardiology, Bad Nauheim, Germany; 3Heart Attack ResearchCenter at the University of Heidelberg, Ludwigshafen am Rhein, Germany;4Clinical Center of Ludwigshafen, Department of Cardiology, Ludwigshafen amRhein, Germany; 5Hospital Lippe-Detmold, Detmold, Germany; 6KardiologischePraxis, Berlin, Germany; 7Medical Affairs, Cordis Germany, Langenfeld,Germany
Background: Stent length is considered a predictor of target vessel revascular-ization (TVR) after bare-metal coronary stenting. The relationship between stentlength and both efficacy and long term safety after sirolimus-eluting stent (SES)implantation remains controversial.Methods and Results: A total of 8201 patients treated with SES in 51 centers inGermany were entered into the German Cypher Stent Registry. Of these, 5603patients (median age 64 years, 74% males) treated with a single SES consti-tute the population of the current study. We excluded patients treated with morethan one stent to avoid the potential impact of overlapping stents on clinical out-come. A stratified analysis of TVR and major adverse cardiac events (MACE) atsix months and five years, respectively was performed for patients with a stentlength ≤13 mm (1682 patients, 30%), 14-22 mm (2266 patients, 40%) and >22mm (1655 patients, 30%). Patients treated with longer stents had more com-plex baseline and procedural characteristics compared to patients treated withshorter stents (significantly more patients with diabetes mellitus, renal insuffi-ciency, multi-vessel disease and chronic total occlusions in patients in the highesttertile of stent length). However, at 6 months, there was no statistically signifi-cant difference in the rate of TVR between the 3 groups (7.7, 6.8 and 6.9% forthe long, intermediate and short stent groups, respectively, p=0.42). Five yearfollow-up was complete in 80.3% of patients. At long term, the overall MACE rate(a composite of death and myocardial infarction) was numerically higher in thelong stent group compared to the intermediate and short stent groups (22.1, 18.1and 18.3%, respectively; p=0.06). Using multivariate logistic regression analy-sis, the strongest independent predictors of MACE at 5 years were cardiogenicshock (OR 3.94, 95%CI 2.35-6.59), acute coronary syndromes (OR 1.39, 95%CI1.19-1.63), reduced left ventricular ejection fraction (OR 1.7, 95%CI 1.33-2.2), re-nal insufficiency (OR 2.25, 95%CI 1.83-2.77), diabetes mellitus (OR 1.48, 95%CI1.26-1.74), older age (OR 1.32, 95%CI 1.22-1.42), prior myocardial infarction (OR1.62, 95%CI 1.38-1.91) and three vessel disease (OR 1.45, 95%CI 1.23-1.71),but not stent length.Conclusion: Stent length did not impact efficacy and long term safety ofsirolimus-eluting stents in this large "all-comer" patient population. Predictors ofdeath and myocardial infarction at 5 years after SES implantation were predomi-nantly clinical rather than procedural or device-related characteristics. The use oflonger SES when indicated appears safe and effective.
1136 Percutaneous treatment of unprotected left maincoronary stenoses with paclitaxel-eluting stents. 3-yearclinical follow-up of a French prospective multicenterstudy: Friend Registry
D. Carrie1, H. Eltchaninoff2, T. Lefevre3, M. Silvestri4, G. Levy5,P. Brunel6, B. Glatt7, D. Blanchard8, H. Le Breton9, J. Fajadet10. 1Cardiovascularand Metabolic Pole, Rangueil Hospital„ Toulouse, France; 2University Hospital ofRouen - Hospital Charles Nicolle, Rouen, France; 3University Hospital of Poitiers- Hospital of La Miletrie, Poitiers, France; 4Vert Coteau Clinic, Marseille, France;5Millenaire Clinic, Montpellier, France; 6Nouvelles Cliniques Nantaises (NCN),Nantes, France; 7North Cardiologic Center, Saint-Denis, France; 8Clinic SaintGatien, Tours, France; 9University Hospital of Rennes - Hospital Pontchaillou,Department of Cardiology and Vascular Disease, Rennes, France; 10ClinicPasteur of Toulouse, Toulouse, France
Purpose: Percutaneous treatment of unprotected left main coronary artery(ULMCA) disease is progressively gaining acceptance in light of the first resultsfrom drug-eluting stent registries or randomized trial. We thus assessed early andmid-term results of patients treated for ULMCA disease in the FRIEND registry.Methods: After ethical committee approval and informed consent, all consecutivepatients with unprotected left main stenoses treated with Taxus stents were in-cluded in a multicenter prospective study from 23 centers. Major adverse cardiacand cerebro-vascular events (MACCE): death, myocardial infarction, stroke, tar-get lesion revascularisation (TLR), target vessel revascularisation (TVR), acute,sub-acute and late thrombosis were adjudicated at 1and 6 months by an inde-pendent committee. Immediate and 9-month angiographic results were assessedby a central core lab (Corysis, St-Denis, France). For the distal lesion of ULMCA,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

168 Coronary stenting: insights from long term follow up / Basic pathophysiology in heart failure
a strategy of main branch stenting with provisional T-stenting of the side branchfollowed by kissing balloon inflation was strongly recommanded.Results: From December 2005 to July 2006, 151 patients (pts) were included,mean age 68±11 years, 83% male, 41% unstable angina, 3% diabetics, 24% 3-vessel disease.The mean Euroscore was 4.1±2.8. The LM reference diameterwas 3.9±0.5mm. LM lesion was non distal in 34%, and distal in 66% of pts. Inthis group, 72% were located at the bifurcation including LAD, LCX or both ostiaaffected. All patients were successfully treated on the LM (stent length 15.7±5.2mm) and a final kissing balloon inflation was performed in 90%. Apart from the LMstenosis, a total of 1.2±0.8 lesions were treated during the hospitalisation (totalstent length 47±16mm). An intra-aortic balloon pump was used prophylactically in1.3% and glycoprotein IIb-IIIa inhibitors in 10.8%. Transradial approach was usedin 22% of the cases. In-hospital MACCE rate was 4.5% with 2.6% of mortality;at 9-month follow-up (FU), the global rate of event-free survival was 93.5% witha very low angiographic restenosis rate of 3%. Between 9 and 36-month clinicalFU, there were one sudden death, 6 extra-cardiac deaths (total mortality 7%), onerecurrent angina and 1 cardiac failure. Event free survival was 84%.Conclusion: LM PCI using the TAXUS stent is feasible and safe at long-termfollow-up. Stenting deserves to be considered a safe and effective alternative toCABG in institutions performing large numbers of PCIs.
1137 Long-term (more than 15 years) clinical andangiographic outcome after percutaneous coronaryintervention
K. Yamaji1, Y. Soga1, S. Shirai1, K. Ando1, T. Arita1, H. Yokoi1,M. Iwabuchi1, H. Nosaka1, T. Kimura2, M. Nobuyoshi1 . 1KokuraMemorial Hospital, Kitakyushu, Japan; 2Kyoto University Graduate
School of Medicine, Kyoto, Japan
Background: The aim of this single-center study was to evaluate long-term (morethan 15 years) clinical and angiographic outcomes in patients with bare metalstent implantation.Methods: From June 1990 through December 1993, We enrolled a total of 405patients (64±9 years, 79% male) who were discharged alive after successfulPalmaz-shatz stent placement.Results: Results of clinical follow-up: Clinical follow-up information was obtainedin 327 patients (80.7%) at 15 years. The follow-up interval of the 231 survivorswas 13.8±4.2 years (range 1.2-18.8 years, median 15.7 years). The rate ofdeath, myocardial infarction, bypass surgery, and TLR at 15 years was 45.4±2.7,14.2±2.1, 15.3±2.2, and 31.5±2.8%, respectively. The rate of TLR at 14 monthswas 15.4±1.8% and remained on a plateau up to 5 years. Beyond 5 years afterthe stent implantation, TLR occurred steadily at a constant rate of 1.5% per year.Non-TLR occurred at a rate of 2.8% per year after the initial 14 months (Figure).Symptomatic status at the TLR beyond 14 months after the stent implantationwere acute myocardial infarction in 2 patients, class 3 or 4 angina in 14 patients,class 1 or 2 angina in 10 patients, and asymptomatic in 18 patients.
Results of angiographic follow-up: 46 patients underwent complete sequential an-giographic follow-up studies without TLR. Minimum lumen diameter at pre, post,1 year, late studies (4-10 years), and very late studies (more than 10 years) were0.73±0.40, 2.85±0.46, 2.27±0.47, 1.93±0.51 and 1.71±0.70, respectively.Conclusion: Late TLR occurred consistently beyond 5 years after percutaneouscoronary intervention, while significant decrease in MLD was observed from lateto very late follow-up.
BASIC PATHOPHYSIOLOGY IN HEART FAILURE
1138(W) Metformin mediated restoration of mitochondrialintegrity is associated with AMPK activation andimproved cardiac contractility inisoproterenol-induced heart failure
P. Mgandela, R. Brooksbank, T. Maswanganyi, A.J. Woodiwiss,G.N. Norton, S. Makaula. University of the Witwatersrand, Johannesburg, SouthAfrica
Purpose: We investigated whether isoproterenol-induced heart failure (HF) is as-sociated with loss of mitochondrial integrity and whether metformin amelioratesLV dysfunction in non-diabetic failing hearts. Moreover, we investigated the roleof the activation of the cellular energy-sensing enzyme AMPK, in the regulation of
expression of transcription factor genes, the nuclear respiratory factor 1 (NRF-1)and the mitochondrial transcription factor (Tfam), in the control of mitochondrialbiogenesis.Methods: Control rats received no treatment, ISO rats were injected with 0.04mg/kg isoproterenol (ISO) daily for 4 months, METF rats received 300mg/kg met-formin in drinking water and ISO+METF received isoproterenol and metformin.Mitochondrial and myofibrilar changes were assessed using transmission elec-tron microscopy and HF was determined using echocardiography. Changes ingene expression for the AMPK, NRF-1 and Tfam genes were determined usingreal-time PCR.Results: We observed mitochondrial and myofibrilar derangements in ISO-treated rats. However, metformin treatment reversed these ISO-induced deleteri-ous effects. Moreover, echocardiography revealed significant increases in LVEDD(11.9±0.4 mm, p<0.05) and LVESD (4.90±0.40 mm, p<0.05), and a reductionin FSend (41.46±1.68%, p<0.05) compared to controls. ISO+METF treated ratsshowed a significant reduction in LVESD (3.64±0.37 mm, p<0.05 vs ISO) and im-proved FSend (52.10±3.70%, p<0.05 vs ISO). However, moderate changes wereobserved in LVEDD (10.43±0.7 mm, NS vs ISO). Our PCR data showed upregu-lation of the AMPK (3.55±1.22), NRF1 (6.35±3.20) and Tfam (2.89±0.55) genesin ISO-treated rats, compared to controls (1.09±0.47, 2.17±0.78 and 1.00±0.20,respectively). The AMPK gene was upregulated in the METF (4.77±1.33) andISO+METF (5.38±2.29) groups.Conclusion: Metformin mediated restoration of mitochondrial integrity is asso-ciated with improved cardiac contractility in isoproterenol-induced heart failure.There is strong evidence to suggest AMPK activation as a causative factor in theregulation of mitochondrial biogenesis.
1139 Endothelial overexpression of beta-3 adrenergicreceptor in rat, a relevant model of heart failure withpreserved ejection fraction
N. Piriou1, G. Toumaniantz2 , B. Rozec2, M. Erfanian2, S. Erbibou2,S. Menoret3, I. Anegon3, J.N. Trochu1, C. Gauthier2. 1l’Institut du
Thorax, INSERM U915, University Hospital of Nantes -Hôpital G. et R. Laënnec,Nantes, France; 2l’Institut du Thorax, INSERM U915, University Hospital ofNantes, Nantes, France; 3INSERM U643, Nantes, France
Background: Heart failure with preserved ejection fraction (HFPEF) associatesnumerous pathophysiological mechanisms such as diastolic dysfunction, abnor-mal ventricular-arterial interaction, and systolic function abnormalities in myocar-dial deformations. Due to this complexity, developing animal models remains cru-cial to better explore and understand HFPEF mechanisms and to determine po-tential specific therapeutic targets, that still lack in this disease.Methods: We developed a transgenic rat over-expressing the human β3-adrenoceptor (AR) specifically in endothelial cells (Tgβ3). Hemodynamic patternof 12 weeks-old Tgβ3 was compared to age-matched Wistar male rats (wild type).Pressure-volume (PV) loops were performed to assess left ventricle (LV) end-sytolic PV relationship, LV diastolic function, and arterial elastance. Echocardio-graphy was used to assess LV geometry, LV ejection fraction (LVEF), and systolicdeformations through 2D-strain analysis.Results: Tgβ3 had preserved LVEF, but increased LV end-diastolic pressure, al-tered ventricular-arterial coupling, and altered LV systolic deformations (table).
Hemodynamic characterization of Tgβ3 rat
Hemodynamic parameter Wild type Tgβ3(PV: n=7, echo: n=11) (PV: n=7, echo: n=16)
Heart rate (beats/min) 359±15 364±13Mean arterial pressure (mm Hg) 95.08±6.02 114.83±4.50*Arterial elastance (mm Hg/ml) 246.83±32.71 329.33±35.46*LV mass (echo), g 1.49±0.06 1.43±0.06LVEF (echo), % 82.3±2.1 78.7±2.3End systolic pressure at midrange LV volume
(mm Hg), reflecting LV end-sytolic elastance 32.68±3.39 57.22±3.57*LV DP/Dt min (mm Hg/s) -6781±475 -8075±722Time constant of LV isovolumic relaxation, Tau (ms) 8.37±0.40 8.17±0.25LV stiffness constant β 1.71±0.47 2.12±0.58LV end-diastolic pressure (mm Hg) 6.50±1.16 12.67±1.41*Mean of peak LV radial strain (%) 40.56±4.97 23.67±2.83*Global LV circumferential strain (%) -16.39±0.97 -11.34±0.66*
*p<0,05 vs wild type.
Conclusions: Tgβ3 might be a relevant animal model of HFPEF. The link be-tween HFPEF and endothelial overexpression of β3-AR in this model suggests acrucial role of endothelium in HFPEF pathophysiology.
1140 Interleukin-6-deficient mice are resistant todevelopment of cardiomyopathy induced by beta1-adrenergic receptor
L.P. Ma1, G. Premaratne2, E. Bollano2, C. Lindholm3, M. Fu2.1Changhai Hospital, Shanghai, China, People’s Republic of; 2Dept.
of Medicine, Göteborg, Sweden; 3Dept of Rheumatology and Inflammation,Gothenburg, Sweden
IL-6 is known to be an important mediator in immune response and is now sug-gested to be involved in the pathogenesis of autoimmune diseases. However,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
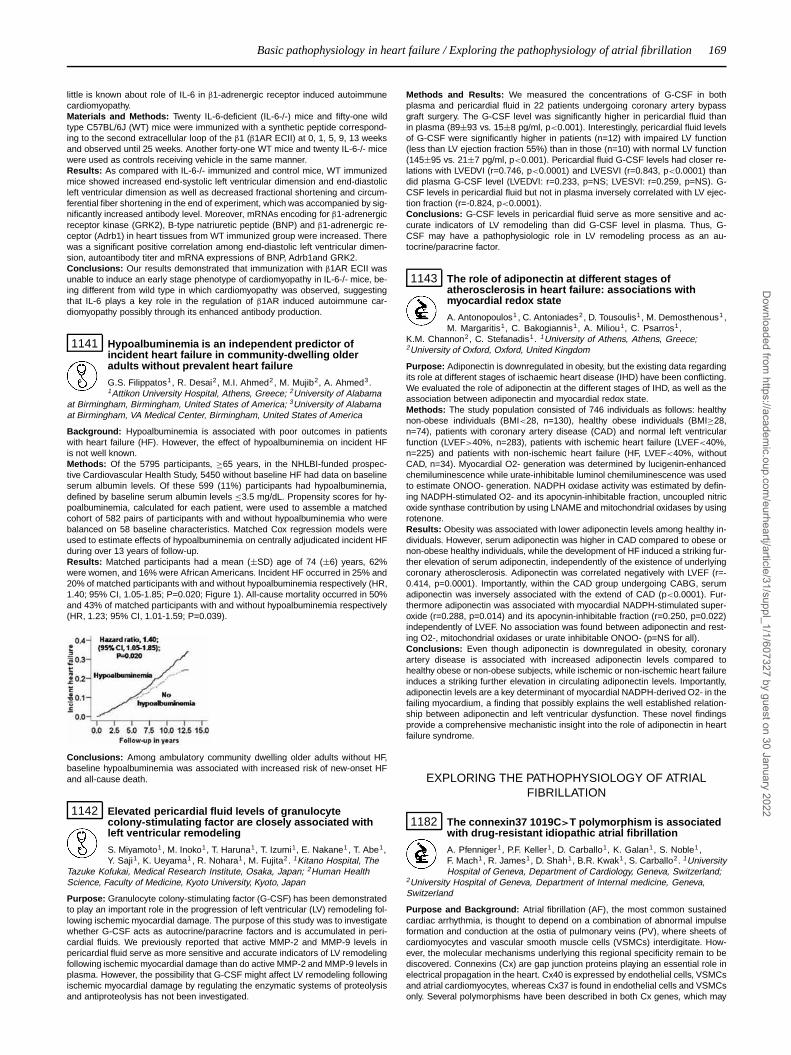
Basic pathophysiology in heart failure / Exploring the pathophysiology of atrial fibrillation 169
little is known about role of IL-6 in β1-adrenergic receptor induced autoimmunecardiomyopathy.Materials and Methods: Twenty IL-6-deficient (IL-6-/-) mice and fifty-one wildtype C57BL/6J (WT) mice were immunized with a synthetic peptide correspond-ing to the second extracellular loop of the β1 (β1AR ECII) at 0, 1, 5, 9, 13 weeksand observed until 25 weeks. Another forty-one WT mice and twenty IL-6-/- micewere used as controls receiving vehicle in the same manner.Results: As compared with IL-6-/- immunized and control mice, WT immunizedmice showed increased end-systolic left ventricular dimension and end-diastolicleft ventricular dimension as well as decreased fractional shortening and circum-ferential fiber shortening in the end of experiment, which was accompanied by sig-nificantly increased antibody level. Moreover, mRNAs encoding for β1-adrenergicreceptor kinase (GRK2), B-type natriuretic peptide (BNP) and β1-adrenergic re-ceptor (Adrb1) in heart tissues from WT immunized group were increased. Therewas a significant positive correlation among end-diastolic left ventricular dimen-sion, autoantibody titer and mRNA expressions of BNP, Adrb1and GRK2.Conclusions: Our results demonstrated that immunization with β1AR ECII wasunable to induce an early stage phenotype of cardiomyopathy in IL-6-/- mice, be-ing different from wild type in which cardiomyopathy was observed, suggestingthat IL-6 plays a key role in the regulation of β1AR induced autoimmune car-diomyopathy possibly through its enhanced antibody production.
1141 Hypoalbuminemia is an independent predictor ofincident heart failure in community-dwelling olderadults without prevalent heart failure
G.S. Filippatos1, R. Desai2, M.I. Ahmed2, M. Mujib2, A. Ahmed3.1Attikon University Hospital, Athens, Greece; 2University of Alabama
at Birmingham, Birmingham, United States of America; 3University of Alabamaat Birmingham, VA Medical Center, Birmingham, United States of America
Background: Hypoalbuminemia is associated with poor outcomes in patientswith heart failure (HF). However, the effect of hypoalbuminemia on incident HFis not well known.Methods: Of the 5795 participants, ≥65 years, in the NHLBI-funded prospec-tive Cardiovascular Health Study, 5450 without baseline HF had data on baselineserum albumin levels. Of these 599 (11%) participants had hypoalbuminemia,defined by baseline serum albumin levels ≤3.5 mg/dL. Propensity scores for hy-poalbuminemia, calculated for each patient, were used to assemble a matchedcohort of 582 pairs of participants with and without hypoalbuminemia who werebalanced on 58 baseline characteristics. Matched Cox regression models wereused to estimate effects of hypoalbuminemia on centrally adjudicated incident HFduring over 13 years of follow-up.Results: Matched participants had a mean (±SD) age of 74 (±6) years, 62%were women, and 16% were African Americans. Incident HF occurred in 25% and20% of matched participants with and without hypoalbuminemia respectively (HR,1.40; 95% CI, 1.05-1.85; P=0.020; Figure 1). All-cause mortality occurred in 50%and 43% of matched participants with and without hypoalbuminemia respectively(HR, 1.23; 95% CI, 1.01-1.59; P=0.039).
Conclusions: Among ambulatory community dwelling older adults without HF,baseline hypoalbuminemia was associated with increased risk of new-onset HFand all-cause death.
1142 Elevated pericardial fluid levels of granulocytecolony-stimulating factor are closely associated withleft ventricular remodeling
S. Miyamoto1, M. Inoko1, T. Haruna1, T. Izumi1, E. Nakane1, T. Abe1,Y. Saji1, K. Ueyama1, R. Nohara1, M. Fujita2. 1Kitano Hospital, The
Tazuke Kofukai, Medical Research Institute, Osaka, Japan; 2Human HealthScience, Faculty of Medicine, Kyoto University, Kyoto, Japan
Purpose: Granulocyte colony-stimulating factor (G-CSF) has been demonstratedto play an important role in the progression of left ventricular (LV) remodeling fol-lowing ischemic myocardial damage. The purpose of this study was to investigatewhether G-CSF acts as autocrine/paracrine factors and is accumulated in peri-cardial fluids. We previously reported that active MMP-2 and MMP-9 levels inpericardial fluid serve as more sensitive and accurate indicators of LV remodelingfollowing ischemic myocardial damage than do active MMP-2 and MMP-9 levels inplasma. However, the possibility that G-CSF might affect LV remodeling followingischemic myocardial damage by regulating the enzymatic systems of proteolysisand antiproteolysis has not been investigated.
Methods and Results: We measured the concentrations of G-CSF in bothplasma and pericardial fluid in 22 patients undergoing coronary artery bypassgraft surgery. The G-CSF level was significantly higher in pericardial fluid thanin plasma (89±93 vs. 15±8 pg/ml, p<0.001). Interestingly, pericardial fluid levelsof G-CSF were significantly higher in patients (n=12) with impaired LV function(less than LV ejection fraction 55%) than in those (n=10) with normal LV function(145±95 vs. 21±7 pg/ml, p<0.001). Pericardial fluid G-CSF levels had closer re-lations with LVEDVI (r=0.746, p<0.0001) and LVESVI (r=0.843, p<0.0001) thandid plasma G-CSF level (LVEDVI: r=0.233, p=NS; LVESVI: r=0.259, p=NS). G-CSF levels in pericardial fluid but not in plasma inversely correlated with LV ejec-tion fraction (r=-0.824, p<0.0001).Conclusions: G-CSF levels in pericardial fluid serve as more sensitive and ac-curate indicators of LV remodeling than did G-CSF level in plasma. Thus, G-CSF may have a pathophysiologic role in LV remodeling process as an au-tocrine/paracrine factor.
1143 The role of adiponectin at different stages ofatherosclerosis in heart failure: associations withmyocardial redox state
A. Antonopoulos1 , C. Antoniades2, D. Tousoulis1 , M. Demosthenous1 ,M. Margaritis1, C. Bakogiannis1, A. Miliou1, C. Psarros1,
K.M. Channon2, C. Stefanadis1. 1University of Athens, Athens, Greece;2University of Oxford, Oxford, United Kingdom
Purpose: Adiponectin is downregulated in obesity, but the existing data regardingits role at different stages of ischaemic heart disease (IHD) have been conflicting.We evaluated the role of adiponectin at the different stages of IHD, as well as theassociation between adiponectin and myocardial redox state.Methods: The study population consisted of 746 individuals as follows: healthynon-obese individuals (BMI<28, n=130), healthy obese individuals (BMI≥28,n=74), patients with coronary artery disease (CAD) and normal left ventricularfunction (LVEF>40%, n=283), patients with ischemic heart failure (LVEF<40%,n=225) and patients with non-ischemic heart failure (HF, LVEF<40%, withoutCAD, n=34). Myocardial O2- generation was determined by lucigenin-enhancedchemiluminescence while urate-inhibitable luminol chemiluminescence was usedto estimate ONOO- generation. NADPH oxidase activity was estimated by defin-ing NADPH-stimulated O2- and its apocynin-inhibitable fraction, uncoupled nitricoxide synthase contribution by using LNAME and mitochondrial oxidases by usingrotenone.Results: Obesity was associated with lower adiponectin levels among healthy in-dividuals. However, serum adiponectin was higher in CAD compared to obese ornon-obese healthy individuals, while the development of HF induced a striking fur-ther elevation of serum adiponectin, independently of the existence of underlyingcoronary atherosclerosis. Adiponectin was correlated negatively with LVEF (r=-0.414, p=0.0001). Importantly, within the CAD group undergoing CABG, serumadiponectin was inversely associated with the extend of CAD (p<0.0001). Fur-thermore adiponectin was associated with myocardial NADPH-stimulated super-oxide (r=0.288, p=0.014) and its apocynin-inhibitable fraction (r=0.250, p=0.022)independently of LVEF. No association was found between adiponectin and rest-ing O2-, mitochondrial oxidases or urate inhibitable ONOO- (p=NS for all).Conclusions: Even though adiponectin is downregulated in obesity, coronaryartery disease is associated with increased adiponectin levels compared tohealthy obese or non-obese subjects, while ischemic or non-ischemic heart failureinduces a striking further elevation in circulating adiponectin levels. Importantly,adiponectin levels are a key determinant of myocardial NADPH-derived O2- in thefailing myocardium, a finding that possibly explains the well established relation-ship between adiponectin and left ventricular dysfunction. These novel findingsprovide a comprehensive mechanistic insight into the role of adiponectin in heartfailure syndrome.
EXPLORING THE PATHOPHYSIOLOGY OF ATRIALFIBRILLATION
1182 The connexin37 1019C>T polymorphism is associatedwith drug-resistant idiopathic atrial fibrillation
A. Pfenniger1, P.F. Keller1, D. Carballo1, K. Galan1, S. Noble1,F. Mach1, R. James1, D. Shah1, B.R. Kwak1, S. Carballo2. 1UniversityHospital of Geneva, Department of Cardiology, Geneva, Switzerland;
2University Hospital of Geneva, Department of Internal medicine, Geneva,Switzerland
Purpose and Background: Atrial fibrillation (AF), the most common sustainedcardiac arrhythmia, is thought to depend on a combination of abnormal impulseformation and conduction at the ostia of pulmonary veins (PV), where sheets ofcardiomyocytes and vascular smooth muscle cells (VSMCs) interdigitate. How-ever, the molecular mechanisms underlying this regional specificity remain to bediscovered. Connexins (Cx) are gap junction proteins playing an essential role inelectrical propagation in the heart. Cx40 is expressed by endothelial cells, VSMCsand atrial cardiomyocytes, whereas Cx37 is found in endothelial cells and VSMCsonly. Several polymorphisms have been described in both Cx genes, which may
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
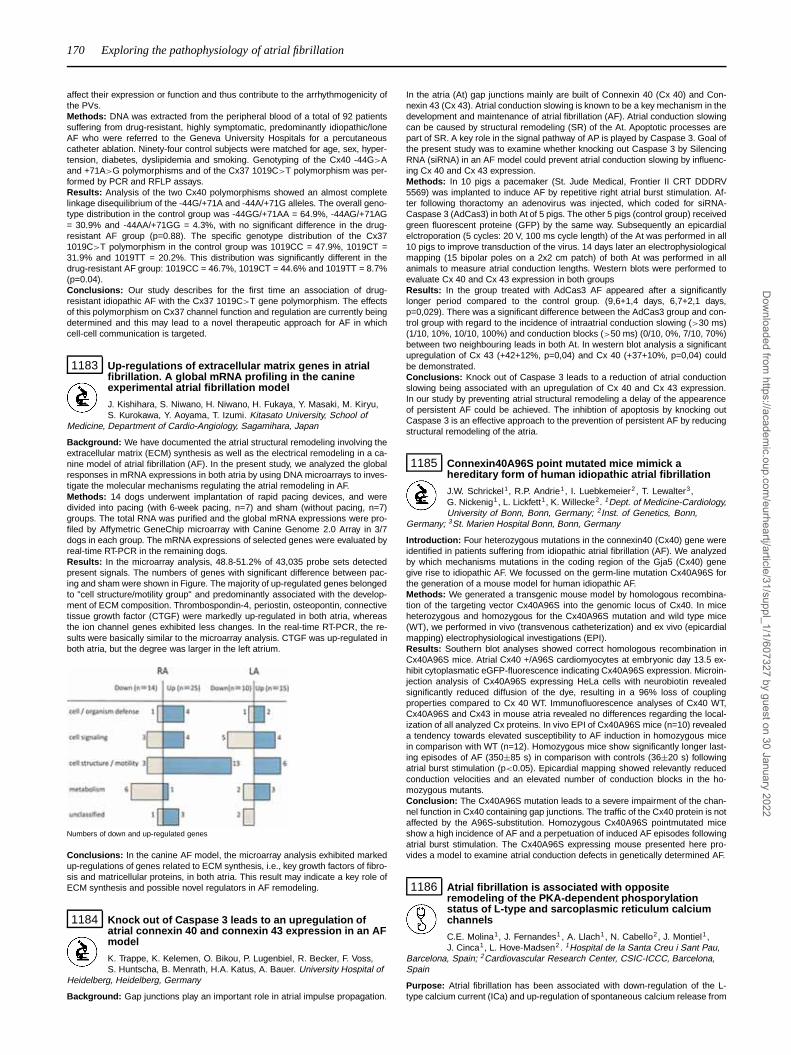
170 Exploring the pathophysiology of atrial fibrillation
affect their expression or function and thus contribute to the arrhythmogenicity ofthe PVs.Methods: DNA was extracted from the peripheral blood of a total of 92 patientssuffering from drug-resistant, highly symptomatic, predominantly idiopathic/loneAF who were referred to the Geneva University Hospitals for a percutaneouscatheter ablation. Ninety-four control subjects were matched for age, sex, hyper-tension, diabetes, dyslipidemia and smoking. Genotyping of the Cx40 -44G>Aand +71A>G polymorphisms and of the Cx37 1019C>T polymorphism was per-formed by PCR and RFLP assays.Results: Analysis of the two Cx40 polymorphisms showed an almost completelinkage disequilibrium of the -44G/+71A and -44A/+71G alleles. The overall geno-type distribution in the control group was -44GG/+71AA = 64.9%, -44AG/+71AG= 30.9% and -44AA/+71GG = 4.3%, with no significant difference in the drug-resistant AF group (p=0.88). The specific genotype distribution of the Cx371019C>T polymorphism in the control group was 1019CC = 47.9%, 1019CT =31.9% and 1019TT = 20.2%. This distribution was significantly different in thedrug-resistant AF group: 1019CC = 46.7%, 1019CT = 44.6% and 1019TT = 8.7%(p=0.04).Conclusions: Our study describes for the first time an association of drug-resistant idiopathic AF with the Cx37 1019C>T gene polymorphism. The effectsof this polymorphism on Cx37 channel function and regulation are currently beingdetermined and this may lead to a novel therapeutic approach for AF in whichcell-cell communication is targeted.
1183 Up-regulations of extracellular matrix genes in atrialfibrillation. A global mRNA profiling in the canineexperimental atrial fibrillation model
J. Kishihara, S. Niwano, H. Niwano, H. Fukaya, Y. Masaki, M. Kiryu,S. Kurokawa, Y. Aoyama, T. Izumi. Kitasato University, School of
Medicine, Department of Cardio-Angiology, Sagamihara, Japan
Background: We have documented the atrial structural remodeling involving theextracellular matrix (ECM) synthesis as well as the electrical remodeling in a ca-nine model of atrial fibrillation (AF). In the present study, we analyzed the globalresponses in mRNA expressions in both atria by using DNA microarrays to inves-tigate the molecular mechanisms regulating the atrial remodeling in AF.Methods: 14 dogs underwent implantation of rapid pacing devices, and weredivided into pacing (with 6-week pacing, n=7) and sham (without pacing, n=7)groups. The total RNA was purified and the global mRNA expressions were pro-filed by Affymetric GeneChip microarray with Canine Genome 2.0 Array in 3/7dogs in each group. The mRNA expressions of selected genes were evaluated byreal-time RT-PCR in the remaining dogs.Results: In the microarray analysis, 48.8-51.2% of 43,035 probe sets detectedpresent signals. The numbers of genes with significant difference between pac-ing and sham were shown in Figure. The majority of up-regulated genes belongedto "cell structure/motility group" and predominantly associated with the develop-ment of ECM composition. Thrombospondin-4, periostin, osteopontin, connectivetissue growth factor (CTGF) were markedly up-regulated in both atria, whereasthe ion channel genes exhibited less changes. In the real-time RT-PCR, the re-sults were basically similar to the microarray analysis. CTGF was up-regulated inboth atria, but the degree was larger in the left atrium.
Numbers of down and up-regulated genes
Conclusions: In the canine AF model, the microarray analysis exhibited markedup-regulations of genes related to ECM synthesis, i.e., key growth factors of fibro-sis and matricellular proteins, in both atria. This result may indicate a key role ofECM synthesis and possible novel regulators in AF remodeling.
1184 Knock out of Caspase 3 leads to an upregulation ofatrial connexin 40 and connexin 43 expression in an AFmodel
K. Trappe, K. Kelemen, O. Bikou, P. Lugenbiel, R. Becker, F. Voss,S. Huntscha, B. Menrath, H.A. Katus, A. Bauer. University Hospital of
Heidelberg, Heidelberg, Germany
Background: Gap junctions play an important role in atrial impulse propagation.
In the atria (At) gap junctions mainly are built of Connexin 40 (Cx 40) and Con-nexin 43 (Cx 43). Atrial conduction slowing is known to be a key mechanism in thedevelopment and maintenance of atrial fibrillation (AF). Atrial conduction slowingcan be caused by structural remodeling (SR) of the At. Apoptotic processes arepart of SR. A key role in the signal pathway of AP is played by Caspase 3. Goal ofthe present study was to examine whether knocking out Caspase 3 by SilencingRNA (siRNA) in an AF model could prevent atrial conduction slowing by influenc-ing Cx 40 and Cx 43 expression.Methods: In 10 pigs a pacemaker (St. Jude Medical, Frontier II CRT DDDRV5569) was implanted to induce AF by repetitive right atrial burst stimulation. Af-ter following thoractomy an adenovirus was injected, which coded for siRNA-Caspase 3 (AdCas3) in both At of 5 pigs. The other 5 pigs (control group) receivedgreen fluorescent proteine (GFP) by the same way. Subsequently an epicardialelctroporation (5 cycles: 20 V, 100 ms cycle length) of the At was performed in all10 pigs to improve transduction of the virus. 14 days later an electrophysiologicalmapping (15 bipolar poles on a 2x2 cm patch) of both At was performed in allanimals to measure atrial conduction lengths. Western blots were performed toevaluate Cx 40 and Cx 43 expression in both groupsResults: In the group treated with AdCas3 AF appeared after a significantlylonger period compared to the control group. (9,6+1,4 days, 6,7+2,1 days,p=0,029). There was a significant difference between the AdCas3 group and con-trol group with regard to the incidence of intraatrial conduction slowing (>30 ms)(1/10, 10%, 10/10, 100%) and conduction blocks (>50 ms) (0/10, 0%, 7/10, 70%)between two neighbouring leads in both At. In western blot analysis a significantupregulation of Cx 43 (+42+12%, p=0,04) and Cx 40 (+37+10%, p=0,04) couldbe demonstrated.Conclusions: Knock out of Caspase 3 leads to a reduction of atrial conductionslowing being associated with an upregulation of Cx 40 and Cx 43 expression.In our study by preventing atrial structural remodeling a delay of the appearenceof persistent AF could be achieved. The inhibtion of apoptosis by knocking outCaspase 3 is an effective approach to the prevention of persistent AF by reducingstructural remodeling of the atria.
1185 Connexin40A96S point mutated mice mimick ahereditary form of human idiopathic atrial fibrillation
J.W. Schrickel1, R.P. Andrie1, I. Luebkemeier2 , T. Lewalter3,G. Nickenig1, L. Lickfett1, K. Willecke2. 1Dept. of Medicine-Cardiology,University of Bonn, Bonn, Germany; 2Inst. of Genetics, Bonn,
Germany; 3St. Marien Hospital Bonn, Bonn, Germany
Introduction: Four heterozygous mutations in the connexin40 (Cx40) gene wereidentified in patients suffering from idiopathic atrial fibrillation (AF). We analyzedby which mechanisms mutations in the coding region of the Gja5 (Cx40) genegive rise to idiopathic AF. We focussed on the germ-line mutation Cx40A96S forthe generation of a mouse model for human idiopathic AF.Methods: We generated a transgenic mouse model by homologous recombina-tion of the targeting vector Cx40A96S into the genomic locus of Cx40. In miceheterozygous and homozygous for the Cx40A96S mutation and wild type mice(WT), we performed in vivo (transvenous catheterization) and ex vivo (epicardialmapping) electrophysiological investigations (EPI).Results: Southern blot analyses showed correct homologous recombination inCx40A96S mice. Atrial Cx40 +/A96S cardiomyocytes at embryonic day 13.5 ex-hibit cytoplasmatic eGFP-fluorescence indicating Cx40A96S expression. Microin-jection analysis of Cx40A96S expressing HeLa cells with neurobiotin revealedsignificantly reduced diffusion of the dye, resulting in a 96% loss of couplingproperties compared to Cx 40 WT. Immunofluorescence analyses of Cx40 WT,Cx40A96S and Cx43 in mouse atria revealed no differences regarding the local-ization of all analyzed Cx proteins. In vivo EPI of Cx40A96S mice (n=10) revealeda tendency towards elevated susceptibility to AF induction in homozygous micein comparison with WT (n=12). Homozygous mice show significantly longer last-ing episodes of AF (350±85 s) in comparison with controls (36±20 s) followingatrial burst stimulation (p<0.05). Epicardial mapping showed relevantly reducedconduction velocities and an elevated number of conduction blocks in the ho-mozygous mutants.Conclusion: The Cx40A96S mutation leads to a severe impairment of the chan-nel function in Cx40 containing gap junctions. The traffic of the Cx40 protein is notaffected by the A96S-substitution. Homozygous Cx40A96S pointmutated miceshow a high incidence of AF and a perpetuation of induced AF episodes followingatrial burst stimulation. The Cx40A96S expressing mouse presented here pro-vides a model to examine atrial conduction defects in genetically determined AF.
1186 Atrial fibrillation is associated with oppositeremodeling of the PKA-dependent phosporylationstatus of L-type and sarcoplasmic reticulum calciumchannels
C.E. Molina1, J. Fernandes1 , A. Llach1, N. Cabello2, J. Montiel1,J. Cinca1, L. Hove-Madsen2 . 1Hospital de la Santa Creu i Sant Pau,
Barcelona, Spain; 2Cardiovascular Research Center, CSIC-ICCC, Barcelona,Spain
Purpose: Atrial fibrillation has been associated with down-regulation of the L-type calcium current (ICa) and up-regulation of spontaneous calcium release from
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Exploring the pathophysiology of atrial fibrillation / Addressing childhood obesity; time to prioritise? 171
the sarcoplasmic reticulum (SR). Opposite changes in the cyclic AMP-dependentphosphorylation status of the L-type calcium channel and the SR calcium releasechannel has been proposed to underlie this remodeling, and the purpose of thisstudy was to determine how this remodeling is affected by equalizing the phos-phorylation status of the two channels.Methods: Human atrial myocytes were isolated from 16 patients with atrial fibril-lation (AF) and 20 patients without the arrhythmia. Cyclic AMP-dependent phos-phorylation was achieved or abolished by exposure of the myocytes to 30 nM iso-proterenol (ISO) or 10 μM H-89 respectively. Perforated patch-clamp techniquewas used to measure ICa and spontaneous Na-Ca exchange currents (INCX)activated by spontaneous calcium release.Results: When exposed to ISO, the down-regulation of ICa and up-regulation ofthe spontaneous INCX frequency in observed at baseline in patients with AF dis-appeared. Consequently, the relative increase in the ICa density was smaller inmyocytes from patients without AF (2.2 fold; 2.8±0.6 to 6.1±0.8 pA/pF, p<0.01)than from patients with AF (4.2 fold; 1.4±0.4 to 5.8±1.3 pA/pF, p<0.001). In con-trast, the relative effect of ISO on the spontaneous INCX frequency was largerin myocytes from patients without AF (4.2 fold; 0.5±0.2 to 2.3±0.6/min, p<0.01)than from patients with AF (2.3 fold; 1.2±0.2 to 2.7±0.6/min, p<0.05). Wheninhibiting Protein Kinase A (PKA)-dependent phosphorylation with H-89, differ-ences in ICa amplitude and spontaneous INCX frequencies between patients withand without AF were also eliminated. As a result, only a minimal inhibitory effectof H-89 on ICa was observed in myocytes from AF patients (from 1.6±0.4 and1.3±0.3pA/pF) while the effect was larger in myocytes from patients without AF(2.5±1.1 and 1.6±0.5pA/pF). Opposite to this, H-89 reduced spontaneous INCXmore strongly in AF myocytes (from 3.3±1.5 to 0.3±0.2/min) than in myocytesfrom patients without AF (from 1.7±0.6/min to 0.3±0.1/min).Conclusions: β-adrenergic stimulation or PKA-inhibition eliminates the differ-ences in ICa amplitude and spontaneous SR calcium release observed amongmyocytes from patients with and without atrial fibrillation, suggesting that atrial fib-rillation leads to opposite changes in the PKA-dependent phosporylation statusof L-type and SR calcium channels.
1187 Lysyl oxidase and connective tissue growth factormediate collagen crosslinking in atrial fibrillation
O. Adam, K. Theobald, D. Lavall, M. Boehm, U. Laufs. SaarlandUniversity Hospital, Department of Internal Medicine III, Cardiology,Homburg, Germany
Introduction: Interstitial fibrosis is a hallmark for the pathogenesis of atrial fibril-lation (AF) and atrial remodeling. Despite its importance is the underlying signaltransduction only partially studied.Methods and Results: Samples of the left atria (LA) from patients with AFshowed a significantly higher collagen content (14.9±2.1% vs. 8.5±1.3%, n=5)and collagen crosslink compared to samples from sinus rhythm (SR) patientsmatched for atrial diameter, left ventricular function and medication. Affymetrix-analysis, RT-PCR and Western Blot analysis revealed that LA of patients withAF are characterised by markedly increased Lysyl Oxidase (LOX; key enzymefor the crosslink of elastin and collagen) mRNA- (206±32%) and protein expres-sion (255±65% vs. SR). This was associated with a 2-fold increased ConnectiveTissue Growth factor (CTGF, profibrotic growth factor) protein expression and a 4-fold higher total protein expression of Rac1 GTPase, an elevated Rac1 membranetranslocation (428±146%), and an increased Rac1 activity (362±98%) comparedto SR patients. Protein expression of Fibronectin was significantly increased in theLA of AF patients. In order to test whether these pro-fibrotic effects were mediatedby Rac1 and CTGF neonatal cardiac fibroblasts were pre-incubated with angio-tensin II (AngII) and the specific inhibitor of Rac1, NSC23766, which completelyprevented the AngII induced upregulation of CTGF (194±34%) expression in fi-broblasts as well as in cardiomyocytes. Treatment of rat neonatal fibroblasts withrecombinant CTGF increased LOX protein expression markedly whereas Rac1expression was unaffected. Transfection of siRNA for CTGF completely inhibitedAngII induced LOX expression. The LOX specific inhibitor BAPN prevented CTGFinduced Fibronectin expression. To further characterize the importance of Rac1in the signalling of fibrosis in vivo, transgenic mice with cardiac overexpression ofRac1 (RacET) were compared to wildtype (WT). LA of RacET mice showed anelevation of CTGF as well as LOX and Fibronectin protein expression. Interstitialcollagen content quantified by sirius red staining and collagen crosslink (colori-metric method) was markedly increased in RacET compared to WT. Importantly,RacET mice developed atrial fibrillation.Conclusion: LA of patients with AF are characterized by upregulation of Rac1 ac-tivity and increased expression of CTGF, LOX, fibronectin and collagen crosslink-ing. In cell culture, Rac1 mediated upregulation of Fibronectin via LOX and CTGF.Inhibition of this signaling pathway may therefore represent a target for the pre-vention of atrial fibrillation.
ADDRESSING CHILDHOOD OBESITY; TIME TOPRIORITISE?
1188 Adipokines are associated with obesity-relatedmetabolic comorbidities and early vascular alterationsin children with obesity
S. Erbs1, E.B. Beck1, R. Hoellriegel1, D. Friebe2, A. Linke1,V. Adams1, C. Walther1, W. Kiess2, G. Schuler1, A. Koerner2.
1University of Leipzig, Heart Center, Leipzig, Germany; 2University HospitalLeipzig, Department of Children and Adolescents, Leipzig, Germany
In adults, adipokines derived from visceral adipose tissue play an essential rolein the regulation of insulin secretion thereby contributing to the development ofdiabetes and finally cardiovascular comorbidities. The impact of adipokines onmetabolic and vascular alterations in childhood obesity is unknown. Therefore, weassessed the impact of serum levels of leptin, nampt and retinol binding protein4 (RBP4) on the extent of metabolic alterations and vascular damage in childrenwith obesity.Methods: In 86 obese (age 12.2±0.3 years, BMI 28.3±0.5) and 70 lean chil-dren (age 12.9±0.4 years, BMI 18.4±0.3) an oral glucose tolerance testingwas performed. Flow-mediated dilation as assessed by reactive hyperemia index(RHI) and carotid artery intima media thickness (cIMT) were obtained. Adipokineserum levels were determined by ELISA. CD34/KDR+ endothelial progenitor cells(EPCs) were quantified by FACS.Results: Already in childhood obesity, serum levels of adipokines are elevated(table, * p<0.05 vs lean). Obesity is associated with insulin resistance (HOMA-IR: 2.6±0.2 vs 1.3±0.1 in lean, p<0.01; peak insulin: 1078±72 pmol/L vs 561±26pmol/L in lean, p<0.01) and impaired insulin sensitivity (Matsuda ISI 5.1±0.3vs 7.3±0.6 in lean, p=0.001) Serum level of nampt correlates with the extent ofobesity (BMI SDS: r=0.35, p<0.0001) as well as insulin sensitivity (Matsuda ISI:r=-0.23, p=0.007). RHI is impaired in obese children (1.30±0.03 vs 1.95±0.08in lean, p<0.01). Also cIMT is altered (0.41±0.01 vs 0.33±0.01 mm in lean,p<0.01). There is an inverse correlation between change in RHI and BMI SDS(r=-0.52, p<0.001), cIMT correlates with BMI SDS (r=0.49, p<0.0001) and HDLcholesterol (r=-0.47, p<0.05). Obese children show a reduced number of EPCs(74±7 vs 97±8 cells/mL blood in lean, p<0.05).
Leptin [ng/mL] Nampt [ng/mL] RBP4 [mg/L]
Obese 29.4±2.1* 3.8±0.3* 32.2±1.2*Lean 6.3±0.8 2.9±0.3 26.4±1.1
Conclusion: Already in childhood obesity, serum levels of adipokines are el-evated and correlate with classical obesity-related comorbidities. These pro-nounced metabolic alterations together with an impaired regenerative capacitymight contribute to generalized vascular damages like endothelial dysfunction andcarotid artery intima media thickening as early stages of atherosclerosis.
1189 Alterations of cerebrovascular flow velocities andregulation in obese children
K. Harada, Y. Harada. Harada Kid’s Clinic, Akita, Japan
Background: Obesity is associated with increased risk for cerebrovas-cular and cardiovascular events, however, there has been little focus on
cerebrovascular function. The purpose of this study is to assess cerebrovascularflow regulation and investigate their relation to cardiovascular risk factors in obesechildren.Methods: Noninvasive ultrasonographic measurements were made in 72 obesechildren (age: 9±2 years, body mass index (BMI): 23±3 kg/m2) and 44 age-matched healthy lean children (BMI: 17±2 kg/m2). Using transcranial colorDoppler sonography, peak systolic (PSV), end-diastolic (EDV), and average peakflow (APV) velocities of middle cerebral artery were measured during spine restand 3 minutes-upright posture. Pulsatile index as a parameter of vascular resis-tance was calculated. Pulsatile index was defined as (PSV-EDV)/APV. Quantita-tive B-mode ultrasound scans were used to measure intima-mediathickness anddiameters of the common carotid artery. Plasma lipid concentrations, indices ofinsulin resistance, and high sensitive C-reactive protein (hs-CRP) were assessedin the obese children.Results: In obese children with BMI≥25 (n = 24),pulsatile index was significantlyhigher compared with controls (1.05±0.12 vs. 0.91±0.13, p < 0.01), becauseAPV and EDV were significantly lower (0.70±0.15 vs. 0.79±0.14 m/sec, p < 0.01and 0.47±0.11 vs. 0.53±0.11 m/sec, p<0.05, respectively), although PSV wasnot significantly different. In obese children with BMI<25 (n = 48), flow velocitiesand pulsatile index were not significantly different compared with controls, how-ever, a significant increase in pulsatile index during upright position was observed(0.87±0.12 vs. 0.93±0.14, p < 0.05). The percent change in pulsatile index dur-ing an upright position correlated significantly with BMI (r =0.53, p < 0.01) andhomeostasis model assessment of insulin resistance (r =0.40, p < 0.05). Bloodpressures, intima-media thickness at carotid artery, hs-CRP, and plasma lipid con-centrations did not correlate with cerebral blood flow velocities.Conclusions: The present study indicates that obesity can adversely affect cere-bral blood flow and resistance in the cerebrovascular bed already in childhood.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

172 Addressing childhood obesity; time to prioritise? / Anti-thrombotic treatment: new drugs and new challenges
Insulin resistance may be a main risk factor for cerebrovascular flow changes.Obesity not only is a risk factor for later cardiovascular disease, but also is asso-ciated with significant impairment of cerebral flow dynamics.
1190 Waist circumference cut offs for German children andadolescents
G.-M. Haas, E. Liepold, P. Schwandt. Arteriosklerose-Praeventions-Institut, Muenchen, Germany
Purpose: Waist circumference as a measure of central adiposity isuseful for the prediction of cardiovascular risk factor clustering. However, there areno generally accepted thresholds for waist circumference predicting risk amongchildren and adolescents. Therefore we calculated cut-off values for 6,888 Ger-man youths aged 6 – 18 years.Subjects and methods: Data were obtained between 2000 and 2008 from 3,250children (1,981 boys) and 3,038 adolescents (1,639 males) participating in thecommunity-based PEP Family Heart Study Nuremberg. Age- and gender- spe-cific percentile curves were constructed for waist circumference using LMS MakerVersion 2.1. The Cut-off-points were calculated from ≥ 3 risk factors out of 7 tra-ditional non-anthropometric risk factors and the sensitivity and specificity valuesof the ROC curves for males and females.Results: 17.5% of boys and 20.9% of girls and 13% of male and 14.6% of femaleadolescents had ≥ 3 risk factors. Among the risk factors hypertriglycridemia hadthe highest values for the area under the curve. The smoothed threshold curveswere quite similar for children and adolescents of both genders. The cut-off rangebetween the 82.5th and 93.5th percentile and the resulting 88th percentile wasnot different between genders though females tended to have a higher waist cir-cumference threshold than males. This 88th percentile threshold is very close tothe 90th percentile proposed by the International Diabetes Federation definingthe main component of the metabolic syndrome in children and adolescents.Conclusions: This cross-sectional study is the first report on gender-and age-specific cut-off values for waist circumference in a large sample of German chil-dren and adolescents and a national contribution to the international definition ofthe pediatric metabolic syndrome.
1191 Early myocardial deformation changes associated toisolated obesity in children: a study based on 3D-Wallmotion tracking analysis
A. Saltijeral1, L. Perez De Isla1, O. Perez1, S. Rueda1, C. Fernandez-Golfin1, C. Almeria1, J. Rementeria2, W. Gorissen2, C. Macaya1 ,
J. Zamorano1 . 1Hospital Clinic San Carlos, Madrid, Spain; 2Toshiba MedicalSystems Europe, Zoetemeer, Netherlands
Background and Aim: Obesity is considered a strong cardiovascular (CV) riskfactor. The association between obesity and CV risk has been difficult to establish,because obesity is strongly associated with other CV risk factors. 3D-Wall motiontracking echocardiography (3D-WMT) provides information regarding myocardialdeformation. Our aim was to assess the presence of early myocardial deformationabnormalities in obese children free from other CV risk factors.Methods: Prospective study in which 30 consecutive non-selected obese chil-dren were enrolled. The control group consisted of 42 healthy volunteer children.Every patient underwent a 2D-echo and a 3D-WMT study.Results: Mean age was 13.90±2.56 and 13.25±2.68 years in the non-obese andobese groups respectively (p=0.30). 43 (59.7%) and 29 (40.3%) patients weremale in the non-obese and obese groups respectively (p=0.66). Main results aredepicted in table below. It is of note the significant modifications in myocardialdeformation in obese children.
Main Results
Non-Obese Obese p
BMI (kg/m2) 19.37±3.02 30.93±6.67 <0.001BSA (m2) 1.47±0.27 1.71±0.27 <0.001PW (cm) 0.78±0.10 0.86±0.11 0.003IVS (cm) 0.79±0.09 0.89±0.12 <0.001Indexed 3D-LVEDV (ml/m2) 44.14±9.71 46.03±9.91 0.42Indexed 3D-LVESV (ml/m2) 14.98±3.66 15.63±3.96 0.48Indexed LAV (ml/m2) 17.27±3.9 18.76±3.30 0.09LV average radial strain (%) 18.47±3.54 28.81±6.93 <0.001LV average circumferential strain (%) -25.14±5.42 -17.44±5.46 <0.001LV average longitudinal strain (%) -20.70±2.70 -15.08±3.39 <0.001LV average twist (deg) 4.64±1.44 5.92±1.39 <0.001LV average torsion (deg/cm) 2.48±0.94 3.03±0.83 0.012
BMI: body mass index; BSA: body surface area; LAV: left atrial volume; 3D-LVEDV: 3D LV enddiastolic volume; 3D-LVESV: 3D LV end systolic volume; IVS: interventricular septum; PW: pos-terior wall; LV: left ventricular.
Conclusions: Isolated obesity in children is accompanied not only by changesin size in the cardiac chambers but also by changes in myocardial deformation.These changes are easily assessed by means of 3D-WMT. This is the first studythat demonstrate these early changes.
1192 Obesity-related vascular functional change starts inearly childhood
K. Harada, Y. Harada. Harada Kid’s Clinic, Akita, Japan
Background: Obesity is associated with structural and functionalchanges in the artery, but there is little information when arterial func-
tional change begins to appear. The purpose of this study is to investigate therelationship between body mass index (BMI) and arterial function from infancy tochildhood.Methods: Echocardiography was performed in 384 healthy children. Subjectswere divided into 3 age groups: infants group, < 1year (0.8±0.3years, n =73);pre-school children group, 4 to 6 years (5±1 years, n = 125);and school childrengroup, 7 to 12 years (9±3 years, n = 186). Cardiac dimensions and relative wallthickness were measured. Stroke volume was calculated using aortic diameterand pulsed Doppler velocity profile. SV was indexed for body surface area (SVI).Effective arterial elastance (Ea) was estimated by end-systolic pressure/SVI andtotal arterial compliance (Ca) by the ratio of pulse pressure/SVI. Quantitative B-mode ultrasound scans were used to measure intima-media thickness and diam-eters of the common carotid artery, and carotid stiffness was calculated.Results: Within each group,left ventricular end-diastolic diameter and relativewall thickness increased significantly with BMI, but intima-media thickness of thecommon carotid artery did not change with BMI. In the infants group, there wereno significant relationships between Ea, Ca, and carotid stiffness and BMI. In thepre-school children group, a weak but significant correlation between Ea and BMIwas found (r = 0.25, p < 0.01), whereas there were no significant relationshipsbetween Ca and carotid stiffness and BMI. In the school children group, Ea andCa increased significantlywith BMI (r =0.27 and 0.34, respectively, p < 0.01). butcarotid stiffness did not change with BMI. The strength of the linear correlationbetween BMI and Ea and the slope of the relation did not differ between thepre-school children group and school children group. There were no significantrelationships between Ea, Ca, and carotid stiffness and left ventricular relativewall thickness.Conclusions: Higher BMI is associated with arterial functional changes in pre-school children and school children, however, remodeling of the common carotidartery is not yet present. Our findings suggest that obesity has a negative effecton vascular function starting already in early childhood.
1193 Obesity as a part of general addiction syndrome inItalian adolescents
F. Denoth, V. Siciliano, P. Iozzo, S. Molinaro. Institute of ClinicalPhysiology of CNR, Pisa, Italy
Purpose: The mounting prevalence of obesity and of drug abuse inthe youth preludes an epidemics in the related cardiovascular complications.Overeating in obese individuals shares similarities with the loss of control andcompulsive behaviour observed in drug-addicted subjects. The aim of this Na-tionwide survey was to investigate the clustering of obesity and addictive attitudesconcerning the abuse of substances with proven cardiovascular side effects, andits relationship with social interactions.Methods: Data were collected by anonymous self-administered questionnaires in40,407 adolescents aged 15-19. Obesity and normal weight were defined as bodymass index (BMI) >90th and 10th≤BMI≤90th percentile, respectively. An addic-tive attitude was defined as use of cocaine, heroin, hallucinogens, stimulants,psychoactive agents ≥10 times and/or cannabis ≥20 times in the last year and/orbinge drinking ≥3 times and/or cigarette smoking ≥11/day in the last month.Results: Obesity was associated with use of cocaine (in females), heroin, hal-lucinogens, binge drinking, cigarette smoking (<0.05 vs normal weight). Whenthe obese category was stratified according to the additional presence vs ab-sence of an addictive attitude, two groups were identified, one without and onewith addictive behaviour. Obesity and substance abuse clustered in a significantproportion of 25% obese adolescents, with a predominance in males (M=29%;F=20%; p<0.01). Addictive-obesity was frequently associated with social or per-sonal maladaptive traits (p<0.01).
Prevalence of social-personal traits
Conclusions: Obesity and food abuse can be part of a general addiction vulner-ability, likely associated with other cardio-toxic substance abuse and social andpersonal maladaptation. An interdisciplinary therapeutic approach is warranted inthe effective prevention.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Anti-thrombotic treatment: new drugs and new challenges 173
ANTI-THROMBOTIC TREATMENT: NEW DRUGS ANDNEW CHALLENGES
1194 Safety and tolerability of YM150 in subjects withnon-valvular atrial fibrillation: a phase II study
A.G.G. Turpie1, G.Y.H. Lip2, K. Minematsu3, S. Goto4, R.W. Renfurm5,K.S.L. Wong6. 1McMaster University, Hamilton, Canada; 2Centre forCardiovascular Sciences, City Hospital, Birmingham, United Kingdom;
3National Cardiovascular Center, Suita, Osaka, Japan; 4Tokai University,Isehara, Japan; 5Astellas Pharma Global Development, Leiderdorp, Netherlands;6Department of Medicine & Therapeutics, Chinese University of Hong Kong,Hong Kong, China, People’s Republic of
Purpose: YM150 is a novel direct inhibitor of activated factor Xa that has demon-strated potential efficacy for prevention of venous thromboembolism in patientsundergoing orthopaedic surgery. This study was designed to evaluate the safetyand tolerability of YM150 in subjects with non-valvular atrial fibrillation (NVAF).Subjects were recruited in the Asia-Pacific region. The primary safety variablewas the incidence of major and clinically relevant non-major (CRNM) bleedingevents.Methods: This study was a prospective, multicentre, double-blind, randomized,parallel-group, dose-finding study evaluating 30, 60, 120 and 240 mg once-dailydoses of YM150, in comparison with open-label warfarin, administered over 12weeks in subjects with NVAF who had a CHADS2 stroke risk stratification score of1–6 (80% of subjects had a score of 1 or 2). Subjects were assessed at Weeks 1,2, 4, 8 and 12 or end of treatment, and at 4 weeks after study drug discontinuation.Results: 448 subjects received 30 (n=90), 60 (n=93), 120 (n=93) or 240 mg(n=78) of YM150, or warfarin (n=94), once daily. Treatment with YM150 240 mgwas terminated early based on the Data and Safety Monitoring Board’s recom-mendation regarding the observed bleeding rate. During the treatment period,the incidences of major and/or CRNM bleeding in the 30, 60, 120 and 240 mgYM150 groups were 2.2, 2.2, 3.2 and 16.7%, respectively, and 2.1% in the war-farin group. There was one major bleed (brainstem haemorrhage), which occurredin the YM150 240 mg group; a subdural haematoma occurred in one warfarin re-cipient during the follow-up period. The incidences of CRNM bleeding in the 30,60, 120 and 240 mg YM150 groups were 2.2, 2.2, 3.2 and 15.4%, respectively,and 2.1% in the warfarin group. The incidence of minor bleeding during the treat-ment period was comparable among the five treatment groups (12.9–16.7%). Theincidence of bleeding appeared to be higher with concomitant aspirin use in boththe YM150 120 and 240 mg groups, but not in the 30 or 60 mg groups. The in-cidence of treatment-emergent adverse events during the treatment period wassimilar in the five treatment groups (56.7–66.7%). There were no thromboembolicstrokes reported during the treatment period.Conclusions: In subjects with NVAF, recruited largely in Asia, 30, 60 and 120 mgdoses of YM150 for 12 weeks were well tolerated. The incidences of major andCRNM bleeding for YM150 doses up to 120 mg were similar to those seen withwarfarin.
1195 Differential effect of ticagrelor versus clopidogrel onthe prevalence of high on-treatment platelet reactivity:results from the ONSET-OFFSET and RESPOND trials
K.P. Bliden1, U.S. Tantry1, M. Antonino1, E. Mahla1, T. Gesheff1,P. Tzevelekos1 , K. Butler2, C. Wei2, P.A. Gurbel3. 1Sinai Center for
Thrombosis Research, Baltimore, United States of America; 2AstraZeneca LP,Wilmington, United States of America; 3Sinai Center of Baltimore, Baltimore,United States of America
Background: High on-treatment platelet reactivity to ADP (HPR), an establishedcardiac risk factor has been strongly linked to adverse event occurrence follow-ing coronary stenting in patients treated with aspirin and clopidogrel (C). Theprevalence of HPR following treatment with ticagrelor (T), a reversible more po-tent oral P2Y12 receptor antagonist developed to overcome the limitations of C isunknown.Methods: The prevalence of HPR was determined in CAD patients treated withT (180mg load, 90mg bid MD [n=102]), and C (600mg load, 75mg qd MD [n=99])with background 75–100mg qd aspirin therapy. HPR was defined by previouslypublished cutpoints associated with post-PCI ischemic risk: >59% 20μM ADP-aggregometry (LTA), >235 PRU-VerifyNow P2Y12 assay (VN), >50% PRI VASP-phosphorylation assay (VASP-P). Proportion differences for T versus C were an-alyzed by Chi-square test for each timepoint. Correlations between assays wereanalyzed by Pearson method.
Prevalence of HPR During Treatment
Ticagrelor Clopidogrel P-value(n=102) (n=99) Ticagrelor vs. Clopidogrel
LTA VN VASP-P LTA VN VASP-P LTA VN VASP-P
HPR (%)Predose 82 97 95 88 96 100 NA NA NA2 hr 2 3 8 49 56 76 <0.0001 <0.0001 <0.00018 hr 0 1 4 28 49 74 <0.0001 <0.0001 <0.000124 hr 0 0 2 30 36 81 <0.0001 <0.0001 <0.0001≥2 weeks 2 0 5 21 35 65 <0.0001 <0.0001 <0.0001
Results: T was associated with significantly lower prevalence of HPR (0-8%)compared with C (21-76%) at all time points post dose (p<0.0001, for all as-says). Correlations (R) between LTA and VN; and LTA and VASP-P were > 0.43,p<0.0001 for both comparisons).Conclusions: Ticagrelor therapy is consistently associated with a very low preva-lence of HPR compared with clopidogrel, as determined by multiple establishedmethods to measure platelet reactivity. The consistent very low prevalence ofHPR provides a mechanism for the clinical benefits of ticagrelor reported inPLATO trial.
1196 Comparison of prasugrel vs. high clopidogrelmaintenance dose to overcome high residual plateletreactivity post stenting
I. Xanthopoulou, G. Dimitropoulos, G. Kasimis, E. Stavrou,A. Panagiotou, G. Tsigkas, P. Davlouros, G. Hahalis, A. Athanassiadou,
D. Alexopoulos. Patras University Hospital, Cardiology Department, Patras,Greece
Background: High residual platelet reactivity as determined with point-of-care(POC) devices is associated with worse clinical outcomes in patients subjectedto PCI. Doubling the maintenance dose (MD) of clopidogrel may reduce plateletreactivity compared to the standard 75 mg/d MD. Prasugrel (10 mg/d) achievesgreater platelet inhibition compared to standard MD of clopidogrel in patients withacute coronary syndromes. We aimed to investigate the relative antiplatelet ef-fects of prasugrel versus double MD of clopidogrel in patients considered resistantto standard clopidogrel treatment post-PCI.Methods: Prospective, single-centre, randomized study, including all consecu-tive patients undergoing PCI with stenting in our centre. Patients were on astandard clopidogrel MD (75 mg/d) for at least 3 days before PCI, or receiveda 600 mg loading dose during PCI in case of no pre-treatment. Platelet reac-tivity was assessed with the Verify-Now POC assay 24 hours post-PCI, or 48hours post-PCI in case of periprocedural administration of IIb-IIIa inhibitors. Us-ing a cut-off value of ≥ 230 Platelet Reactivity Units (PRU) to define clopidogrelnon-responsiveness, non-responders were randomized to either 150 mg/d MD ofclopidogrel (Group-A), or 10mg/d of prasugrel (Group-B), for 30 days. Patientswith contra-indications to prasugrel administration were excluded. Genotyping forthe presence of 681G>A polymorphism in CYP2C19 gene was also performed.Results: Out of 170 patients, 42 (24.7%) were clopidogrel resistant, and 33 ofthem were randomized and completed the 30 days follow-up (14 Group-A and19 group-B). Baseline PRU was 311.9±61.5 and 294.1±48.5 for Group-A andGroup-B respectively (p=0.4). PRU at 30 days was higher in group-A compared togroup-B (210.1±81.9 vs. 150.9±82.9, p=0.05). There was a trend towards morenon-responsive patients in Group-A compared to Group-B (6/14 vs. 3/19, p=0.09).Genotyping for 681G>A variant of CYP2C19 was available in 21 (63.6%) patients(7 patients in Group-A, 14 patients in Group B). Prasugrel administration (Group-B) resulted in higher PRU reduction in patients carrying at least one 681G>Aallele compared to non-carriers (�PRU 248.0±57.4 vs. 120.7±61.3, p=0.01).No such difference was observed in Group-A (�PRU 59.8±44.2 vs. 90.3±24.4,p=0.3).Conclusions: In patients non-responsive to standard clopidogrel treatment onthe basis of PRU assessment post-PCI, prasugrel 10 mg/d may be more effectivecompared to clopidogrel 150 mg/d in further reducing platelet reactivity, especiallyin those carrying at least one 681G>A allele.
1197 Platelet P2Y12 receptor signaling in patients withdiabetes mellitus: an in vitro pharmacodynamic study
M. Ueno, J.L. Ferreiro, K. Dharmashankar, D. Capodanno, R. Alissa,B. Desai, S.D. Tomasello, R.K. Charlton, T.A. Bass, D.J. Angiolillo.University of Florida-Shands Jacksonville, Jacksonville, United States
of America
Purpose: Patients with diabetes mellitus (DM) have reduced pharmacodynamicresponse to the P2Y12 receptor antagonist clopidogrel. The intraplatelet signalingmechanisms leading to poor clopidogrel response in DM patients remain largelyunexplored. The purpose of this study was to investigate if platelets from patientswith DM have altered P2Y12 signaling, which may play a role in their poor re-sponse to clopidogrel.Methods: A total of 58 clopidogrel naïve patients (30 DM and 28 non-DM) withcoronary artery disease on low-dose aspirin therapy were studied. In order toassess the functional status of the P2Y12 signaling pathway, in vitro pharmaco-dynamic experiments using escalating concentrations (1, 3, 10 μM) of the activemetabolite of clopidogrel were performed. The functional activity of the P2Y12 sig-naling pathway was measured by the Platelet Reactivity Index (PRI), determinedby flow cytometric assessment of intraplatelet vasodilator-stimulated phosphopro-tein phosphorylation (VASP-P).Results: There were no differences in baseline PRI between DM (83.9±1.0) andnon-DM (83.5±0.9) patients. Patients with DM had significantly higher PRI withall concentrations of the active metabolite (1μM: 78.9±1.5 vs 72.1±2.8; 3μM:56.3±3.2 vs 46.3±3.9; 10μM: 18.9±2.3 vs 8.8±1.8; p<0.05 for all). The absolutedifferences (�) in PRI before and after in vitro incubation with the three differentconcentrations of the active metabolite were significantly lower in DM comparedwith non-DM patients (Figure).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
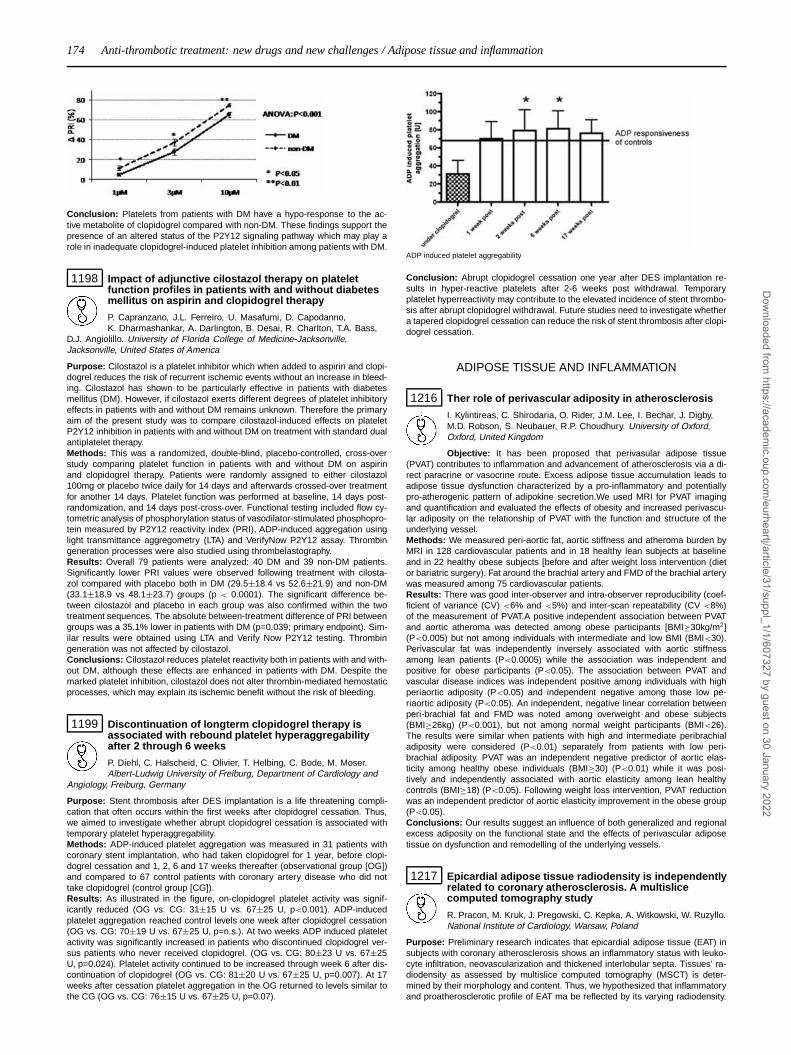
174 Anti-thrombotic treatment: new drugs and new challenges / Adipose tissue and inflammation
Conclusion: Platelets from patients with DM have a hypo-response to the ac-tive metabolite of clopidogrel compared with non-DM. These findings support thepresence of an altered status of the P2Y12 signaling pathway which may play arole in inadequate clopidogrel-induced platelet inhibition among patients with DM.
1198 Impact of adjunctive cilostazol therapy on plateletfunction profiles in patients with and without diabetesmellitus on aspirin and clopidogrel therapy
P. Capranzano, J.L. Ferreiro, U. Masafumi, D. Capodanno,K. Dharmashankar, A. Darlington, B. Desai, R. Charlton, T.A. Bass,
D.J. Angiolillo. University of Florida College of Medicine-Jacksonville,Jacksonville, United States of America
Purpose: Cilostazol is a platelet inhibitor which when added to aspirin and clopi-dogrel reduces the risk of recurrent ischemic events without an increase in bleed-ing. Cilostazol has shown to be particularly effective in patients with diabetesmellitus (DM). However, if cilostazol exerts different degrees of platelet inhibitoryeffects in patients with and without DM remains unknown. Therefore the primaryaim of the present study was to compare cilostazol-induced effects on plateletP2Y12 inhibition in patients with and without DM on treatment with standard dualantiplatelet therapy.Methods: This was a randomized, double-blind, placebo-controlled, cross-overstudy comparing platelet function in patients with and without DM on aspirinand clopidogrel therapy. Patients were randomly assigned to either cilostazol100mg or placebo twice daily for 14 days and afterwards crossed-over treatmentfor another 14 days. Platelet function was performed at baseline, 14 days post-randomization, and 14 days post-cross-over. Functional testing included flow cy-tometric analysis of phosphorylation status of vasodilator-stimulated phosphopro-tein measured by P2Y12 reactivity index (PRI), ADP-induced aggregation usinglight transmittance aggregometry (LTA) and VerifyNow P2Y12 assay. Thrombingeneration processes were also studied using thrombelastography.Results: Overall 79 patients were analyzed: 40 DM and 39 non-DM patients.Significantly lower PRI values were observed following treatment with cilosta-zol compared with placebo both in DM (29.5±18.4 vs 52.6±21.9) and non-DM(33.1±18.9 vs 48.1±23.7) groups (p < 0.0001). The significant difference be-tween cilostazol and placebo in each group was also confirmed within the twotreatment sequences. The absolute between-treatment difference of PRI betweengroups was a 35.1% lower in patients with DM (p=0.039; primary endpoint). Sim-ilar results were obtained using LTA and Verify Now P2Y12 testing. Thrombingeneration was not affected by cilostazol.Conclusions: Cilostazol reduces platelet reactivity both in patients with and with-out DM, although these effects are enhanced in patients with DM. Despite themarked platelet inhibition, cilostazol does not alter thrombin-mediated hemostaticprocesses, which may explain its ischemic benefit without the risk of bleeding.
1199 Discontinuation of longterm clopidogrel therapy isassociated with rebound platelet hyperaggregabilityafter 2 through 6 weeks
P. Diehl, C. Halscheid, C. Olivier, T. Helbing, C. Bode, M. Moser.Albert-Ludwig University of Freiburg, Department of Cardiology and
Angiology, Freiburg, Germany
Purpose: Stent thrombosis after DES implantation is a life threatening compli-cation that often occurs within the first weeks after clopidogrel cessation. Thus,we aimed to investigate whether abrupt clopidogrel cessation is associated withtemporary platelet hyperaggregability.Methods: ADP-induced platelet aggregation was measured in 31 patients withcoronary stent implantation, who had taken clopidogrel for 1 year, before clopi-dogrel cessation and 1, 2, 6 and 17 weeks thereafter (observational group [OG])and compared to 67 control patients with coronary artery disease who did nottake clopidogrel (control group [CG]).Results: As illustrated in the figure, on-clopidogrel platelet activity was signif-icantly reduced (OG vs. CG: 31±15 U vs. 67±25 U, p<0.001). ADP-inducedplatelet aggregation reached control levels one week after clopidogrel cessation(OG vs. CG: 70±19 U vs. 67±25 U, p=n.s.). At two weeks ADP induced plateletactivity was significantly increased in patients who discontinued clopidogrel ver-sus patients who never received clopidogrel. (OG vs. CG: 80±23 U vs. 67±25U, p=0.024). Platelet activity continued to be increased through week 6 after dis-continuation of clopidogrel (OG vs. CG: 81±20 U vs. 67±25 U, p=0.007). At 17weeks after cessation platelet aggregation in the OG returned to levels similar tothe CG (OG vs. CG: 76±15 U vs. 67±25 U, p=0.07).
ADP induced platelet aggregability
Conclusion: Abrupt clopidogrel cessation one year after DES implantation re-sults in hyper-reactive platelets after 2-6 weeks post withdrawal. Temporaryplatelet hyperreactivity may contribute to the elevated incidence of stent thrombo-sis after abrupt clopidogrel withdrawal. Future studies need to investigate whethera tapered clopidogrel cessation can reduce the risk of stent thrombosis after clopi-dogrel cessation.
ADIPOSE TISSUE AND INFLAMMATION
1216 Ther role of perivascular adiposity in atherosclerosis
I. Kylintireas, C. Shirodaria, O. Rider, J.M. Lee, I. Bechar, J. Digby,M.D. Robson, S. Neubauer, R.P. Choudhury. University of Oxford,Oxford, United Kingdom
Objective: It has been proposed that perivasular adipose tissue(PVAT) contributes to inflammation and advancement of atherosclerosis via a di-rect paracrine or vasocrine route. Excess adipose tissue accumulation leads toadipose tissue dysfunction characterized by a pro-inflammatory and potentiallypro-atherogenic pattern of adipokine secretion.We used MRI for PVAT imagingand quantification and evaluated the effects of obesity and increased perivascu-lar adiposity on the relationship of PVAT with the function and structure of theunderlying vessel.Methods: We measured peri-aortic fat, aortic stiffness and atheroma burden byMRI in 128 cardiovascular patients and in 18 healthy lean subjects at baselineand in 22 healthy obese subjects [before and after weight loss intervention (dietor bariatric surgery). Fat around the brachial artery and FMD of the brachial arterywas measured among 75 cardiovascular patients.Results: There was good inter-observer and intra-observer reproducibility (coef-ficient of variance (CV) <6% and <5%) and inter-scan repeatability (CV <8%)of the measurement of PVAT.A positive independent association between PVATand aortic atheroma was detected among obese participants [BMI≥30kg/m2](P<0.005) but not among individuals with intermediate and low BMI (BMI<30).Perivascular fat was independently inversely associated with aortic stiffnessamong lean patients (P<0.0005) while the association was independent andpositive for obese participants (P<0.05). The association between PVAT andvascular disease indices was independent positive among individuals with highperiaortic adiposity (P<0.05) and independent negative among those low pe-riaortic adiposity (P<0.05). An independent, negative linear correlation betweenperi-brachial fat and FMD was noted among overweight and obese subjects(BMI≥26kg) (P<0.001), but not among normal weight participants (BMI<26).The results were similar when patients with high and intermediate peribrachialadiposity were considered (P<0.01) separately from patients with low peri-brachial adiposity. PVAT was an independent negative predictor of aortic elas-ticity among healthy obese individuals (BMI≥30) (P<0.01) while it was posi-tively and independently associated with aortic elasticity among lean healthycontrols (BMI≥18) (P<0.05). Following weight loss intervention, PVAT reductionwas an independent predictor of aortic elasticity improvement in the obese group(P<0.05).Conclusions: Our results suggest an influence of both generalized and regionalexcess adiposity on the functional state and the effects of perivascular adiposetissue on dysfunction and remodelling of the underlying vessels.
1217 Epicardial adipose tissue radiodensity is independentlyrelated to coronary atherosclerosis. A multislicecomputed tomography study
R. Pracon, M. Kruk, J. Pregowski, C. Kepka, A. Witkowski, W. Ruzyllo.National Institute of Cardiology, Warsaw, Poland
Purpose: Preliminary research indicates that epicardial adipose tissue (EAT) insubjects with coronary atherosclerosis shows an inflammatory status with leuko-cyte infiltration, neovascularization and thickened interlobular septa. Tissues’ ra-diodensity as assessed by multislice computed tomography (MSCT) is deter-mined by their morphology and content. Thus, we hypothesized that inflammatoryand proatherosclerotic profile of EAT ma be reflected by its varying radiodensity.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
Adipose tissue and inflammation 175
Our objective was to investigate if EAT radiodensity is associated with coronaryatherosclerosis.Methods: The study included 164 consecutive patients (82 females, mean age58.8±11.1 years) with suspected CAD undergoing MSCT angiography on a 64-slice dual source Siemens scanner. Coronary atherosclerosis was expressed as:1. CAD - defined by the presence of at least one coronary narrowing of ≥ 50%severity; and 2. coronary artery calcium (CAC) determined by Agatston score.Mean EAT radiodensity expressed on the Hounsfield unit (HU) scale was obtainedfrom semi-automatic tracings of the epicardial fat from the cardiac base to apex.Pixels within the range of -30 to -200 HU were assigned to adipose tissue.Results: The mean EAT radiodensity was -81.00±4.64 HU, 36 patients presentedwith CAD, and mean CAC score was 96.0±220.0. Patients with CAD showedhigher EAT radiodensity as compared to patients without CAD (-78.99±4.12 vs.-81.59±4.60 HU, p<0.01). In multivariable model (OR, CI), male gender, EAT ra-diodensity, and age were independently associated with CAD (2.84, 1.06-7.59;1.21, 1.07-1.37; 1.09, 1.04-1.14, respectively). Also, patients in the third tertileof EAT radiodensity showed greater CAC score as compared to patients in thefirst two tertiles (157.7±310.1 vs. 64.8±148.4, p=0.037). EAT radiodensity in-dependently correlated with CAC score in multivariable linear regression model(p<0.001).Conclusions: Increased EAT radiodensity is independently associated with coro-nary atherosclerosis. This may reflect an unfavorable metabolic profile of moreradiodense epicardial fat present in patients with CAD. Whether EAT radiodensityhas the potential to become a diagnostic and prognostic tool in patients with CADremains to be elucidated.
1218 Direct observation of adipose tissue-induced leukocyterecruitment to the artery wall via chemokine signal Apotential link between obesity and atherosclerosis
S. Hagita, M. Osaka, K. Shimokado, M. Yoshida. Tokyo Medical andDental University, Tokyo, Japan
Background: Though inflammation within the adipose tissues thought to play arole in metabolic syndrome, a causative connection between inflamed adiposetissue and atherosclerosis is not fully understood. The present study aimed toexamine the direct effect of adipose tissue on macro vascular inflammation byintravital microscopic analysis of the femoral artery of mouse after perivascularadipose tissue transplantation.Methods and Results: 0.05g of subcutaneous (SQ) or visceral (VIS) adiposetissue harvested from C57BL/6 mice was transplanted to the perivascular area ofthe femoral artery of recipient C57/BL6 mice. A quantitative intravital microscopicanalysis was performed on the artery. The number of adherent leukocyte was in-creased after adipose tissue transplantation in a time-dependent manner (1dayto 7 days). VIS transplantation induced significantly more leukocyte accumula-tion than SQ. Simultaneous flow cytometry showed the expression of CD11b onperipheral neutrophils and monocytes was significantly increased after adiposetissue transplantation with prominent induction with VIS compared to SQ. Induc-tion of oxidative stress in leukocyte was observed after transplantation. Moreover,the expression levels of MCP-1 and MIP-1b were significantly increased in theadipose tissues as well as in the serum of the recipient mice.Conclusion: These data indicate that adipose tissue directly stimulates athero-prone vascular inflammation by inducing leukocyte accumulation. The underlyingmechanisms seem to involve induction of MCP-1 and MIP-1b
1219 Interrelationships between vascular superoxide andadiponectin biosynthesis in perivascular adiposetissue in human atherosclerosis
C. Bakogiannis1 , C. Antoniades2, A.S. Antonopoulos1 ,M. Demosthenous1 , D. Tousoulis1 , A. Miliou1, C. Psarros1,
C. Triantafyllou1, K.M. Channon2 , C. Stefanadis1. 1Hippokration Hospital,University of Athens, Athens, Greece; 2University of Oxford, Oxford, UnitedKingdom
Purpose: Adiponectin (Adipo), an adipokine with anti-atherogenic properties,may serve as a signaling molecule between perivascular adipose tissue (AT) andthe vascular wall.We investigated whether vascular superoxide (O2-) has an impact on Adipo syn-thesis in perivascular AT in human atherosclerosis.Methods: Fifty-one patients undergoing elective CABG were recruited. Seg-ments of saphenous veins (SV) were obtained and vascular O2- production wasmeasured by lucigenin chemiluminescence. The contribution of uncoupled NOSand NADPH-oxidase to vascular O2- generation was quantified by using NOSinhibitor LNAME (100 μM) and NADPH (100 μM). AT speciments (perivascular-surrounding the SV segments obtained, subcutaneous- from the site of incisionand pericardial-) were cultured ex-vivo for 4 hours, and Adipo release was quan-tified in AT culture supernatants.Results: Vascular O2- was positively associated with Adipo release from perivas-cular AT (Fig A) but not from any other AT depots. Similarly, high perivascularAdipo was associated with increased L-NAME inhibitable O2- (Fig. B), indicativeof NOS uncoupling (Fig B). Finally, NADPH-stimulated O2- was not associatedwith Adipo synthesis from perivascular, subcutaneous or pericardial AT (p=NS forall).
Conclusions: Vascular O2- generation is positively associated with adiponectinsynthesis from perivascular (but not from pericardial or subcutaneous) adiposetissue in patients with advanced atherosclerosis. These novel findings introducethe concept of a strong interaction between vascular O2- and adipokines synthe-sis from perivascular adipose tissue in patients with advanced atherosclerosis.
1220 Obesity is related to a higher inflammatory responsivestate of circulating cells after stimulation of toll likereceptor 2 and 4
V.P.W. Scholtes1, D. Versteeg2, E.H.A.M. Elsenberg1, G.T. Rijkers2,P.R. Stella3, P.A. Doevendans3 , D.P.V. De Kleijn1, F.L. Moll4,
G. Pasterkamp1. 1University Medical Center Utrecht, Experimental CardiologyLaboratory, Utrecht, Netherlands; 2St Antonius Hospital, Department of MedicalMicrobiology and Immunology, nieuwegein, Netherlands; 3University MedicalCenter Utrecht, Department of Cardiology, Utrecht, Netherlands; 4UniversityMedical Center Utrecht, Department of Vascular Surgery, Utrecht, Netherlands
Background: Obesity has been recognized as an independent risk factor foratherosclerosis and is associated with increased levels of biomarkers that reflectinflammatory activity. Toll like receptors (TLR’s) are part of the innate immunesystem and can be considered as the first line of defense when the body is chal-lenged by endogenous or exogenous ligands. TLR’s play an important role in theinitiation and progression of atherosclerotic disease. We investigated the associ-ation between obesity and other risk factors for atherosclerosis and whole bloodTLR response in patients with atherosclerotic coronary artery disease.Methods: TLR response was measured in 2 different groups of 2x100 patientswith coronary artery disease. Blood was drawn before Percutaneous CoronaryIntervention (group 1) or before SPECT imaging of the heart (group 2). Wholeblood was stimulated over night with the TLR ligands Pam 3 Cys (TLR2) and LPS(TLR4). TNF- α (group 1) and IL-8 (group 2) were measured in supernatants byELISA. Cd11b expression at baseline was measured by FACS. After exclusionof patients with chronic inflammatory disease or acute myocardial infarction 77(group 1) and 85 (group 2) patients were analyzed.Results: Obese patients (BMI > 25) had significantly higher TNF- α levels afterstimulation of TLR2 compared with non-obese patients (BMI ≤ 25) (median [IQR]:16,8 [7,5 – 49,1] versus 7,5 [1,5 – 19,2], respectively; p = 0.005) and after TLR4 stimulation (362 [192 – 596] versus 219 [175 - 362]; p = 0,049). In addition,obese patients revealed higher levels of IL-8 after stimulation of TLR 4 (3994[2582 – 7647] versus 2851 [2080 – 4085]; p = 0.043). IL-8 levels after stimulationof TLR 2 did not differ. Smoking showed an inverse pattern: Active smokers hadlower TNF-α levels compared with non-smokers after stimulation of TLR 4 (150[69 – 231] versus 340 [184 – 571]; p = 0.013). IL-8 levels after stimulation of TLR2 did not differ. Cd11b expression at baseline significantly correlated with BMI(R = 0,479 p = 0.001). We found no differences in TNF-α levels, IL-8 levels andcd11b expression for the other traditional risk factors.Conclusion: Obesity is associated with an increased whole blood Toll Like Re-ceptor response. TLR’s can be activated by endogenous and exogenous ligandswhich may explain the higher inflammatory status that is observed in obese pa-tients.
1221 Effects of fenofibrate therapy on circulatingadipocytokines in patients with primaryhypertriglyceridemia
K. Koh1, M. Quon2. 1Gachon University, Incheon, Korea, Republic of;2NIH, Diabetes Unit, Bethesda, United States of America
Background: Adipocytokines including adiponectin and leptin mayserve important roles in linking metabolic signals, inflammation, and atherosclero-sis. We investigated effects of fenofibrate therapy on endothelial dysfunction andadipocytokine profiles.Methods: A randomized, single-blind, placebo-controlled, cross-over study wasconducted in 53 patients with primary hypertriglyceridemia. We administeredplacebo or fenofibrate 200 mg daily for 8 weeks.Results: When compared with placebo, fenofibrate therapy decreased non-HDLcholesterol, apolipoprotein B, and triglycerides while increasing HDL-cholesteroland apolipoprotein A-I (all P<0.001) and decreasing total cholesterol (P<0.05).Moreover, fenofibrate therapy substantially improved the percent flow-mediateddilator response to hyperemia by 55±7% (P<0.001), lowered plasma levels of fib-rinogen and TNF-α by 9±2% (P<0.001) and 6±3% (P=0.014), respectively, and
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

176 Adipose tissue and inflammation / Congenital disease of the aorta
lowered hsCRP from 1.10 to 0.90 mg/l (P=0.004). When compared with placebo,fenofibrate therapy increased plasma levels of adiponectin by 17±4% (P=0.001),insulin sensitivity by 4±1% (as assessed by QUICKI, P=0.009), and decreasedplasma levels of leptin and resistin by 4±7% (P=0.022) and 10±3% (P=0.001),respectively. There were correlations between percent changes in QUICKI andpercent changes in adiponectin levels (r= 0.279, P=0.043) or leptin (r= -0.280,P=0.042).Conclusions: Fenofibrate therapy significantly improved percent flow-mediateddilator response to hyperemia, reduced pro-inflammatory biomarkers, and im-proved adipocytokines levels and insulin sensitivity in hypertriglyceridemic pa-tients. Thus, actions of fenofibrate to regulate adipocytokine levels may be linkedto beneficial effects on pro-inflammatory status that simultaneously improve bothendothelial and metabolic function in patients with primary hypertriglyceridemia.
POSTER SESSION 2
CONGENITAL DISEASE OF THE AORTA
P1244 Exercise induced hypertension as a risk factor forsustained hypertension in adult post-coarctectomypatients
P. Luijendijk1, B.J. Bouma1, J.W.J. Vriend2, H.W. Vliegen2,M. Groenink2, B.J.M. Mulder2. 1Academic Medical Center,
Amsterdam, Netherlands; 2Leiden University Medical Center, Leiden,Netherlands
Purpose: Chronic hypertension is an important contributor to late morbidity andmortality in adult post-coarctectomy patients. In healthy subjects, exercise in-duced hypertension is prognostic for the development of sustained hypertension.The prognostic value of exercise induced hypertension in post-coarctectomy pa-tients remains unknown. The aim of the current study was to determine the prog-nostic value of exercise induced hypertension for the development of sustainedhypertension in these patients.Methods: Sixty-seven adult post-coarctectomy patients (58% male; age 31±10years) underwent ambulatory blood pressure measurements, and exercise test-ing in 2001 and after 7±1 years of follow-up. Hypertension was defined as amean daytime systolic RR >140 mmHg and/or a mean diastolic RR >90 mmHg.Exercise induced hypertension was defined as a mean daytime systolic RR <140mmHg, and peak exercise systolic RR ≥200 mmHg.Results: At baseline, 23 (34%) patients were hypertensive, 11 patients (16%)had exercise induced hypertension, and 33 (49%) patients were normoten-sive. At follow-up all 23 hypertensive patients remained hypertensive. Seven pa-tients (64%) with exercise induced hypertension developed chronic hypertension,whereas four exercise-induced hypertensive patients remained exercise-inducedhypertensive. Nine normotensive patients developed exercise induced hyperten-sion, six normotensive patients had developed hypertension, whereas eighteennormotensive patients remained normotensive.Conclusion: Adult post-coarctectomy patients with exercise induced hyperten-sion, have an increased risk to develop sustained hypertension in the future. Ex-ercise testing is useful for early identification of sustained hypertension, which en-ables clinicians to start anti-hypertensive treatment early in the disease in thesepatients who already have a high burden of vascular and myocardial damage.This early treatment might improve the prognosis in adult post-coarctectomy pa-tients.
P1245 Masked hypertension in successfully corrected aorticcoarctation patients: prevalence and impact of on leftventricular geometry and function
G. Di Salvo, B. Castaldi, S. Gala, L. Baldini, F. Del Gaizo,A.F. D’aiello, A. Mormile, G. Pacileo, M.G. Russo, R. Calabro.
Vincenzo Monaldi Hospital, Naples, Italy
Background: The follow-up data subsequent to a successful repair of aorticcoarctation (AoC) show that life expectancy remains reduced. Late arterial hyper-tension, and atherosclerosis are the main determinants of cardiovascular events.Masked hypertension (MH) consists of an elevated daytime ambulatory bloodpressure in the presence of a normal office blood pressure. To the best of ourknowledge, no previous study addressed the impact of MH in children after suc-cessful AoC repair.Aims: 1. To assess the prevalence of MH among AoC patients late (>18 months)after successful repair (isthmus peak gradient <20 mmHg and absence of dias-tolic tail). 2. To evaluate the impact of MH on left ventricular (LV) geometry andfunction.Methods: We studied 80 AoC pts after successful correction and normal bloodpressure, as assessed by office measurement and medical history. All underwent24h-ABPM, standard echo and speckle tracking imaging for the assessment ofLV longitudinal deformation. The 24-ABPM allowed the distinction between realnormotensive (RN) or MH pts (>95°pc for age, sex and height) on the basis ofthe 24h mean systolic and/or diastolic blood pressure.Results: According to 24h-ABPM our sample was divided in Group RN (n=40;mean age 14.62±6.92 yrs, sex 57.5% M, BMI 20.66±3.62, kg/sm) and Group
MH (n=40; mean age 14.23±3.96 yrs, sex 70% M, BMI 22.76±4.44 kg/sm). SeeTable 1.
Table 1
NT MH P
Office SBP 111,28±11,42 114,38±11,98 NSOffice DBP 61,2±8,1 64±7,45 NSHolter 24h SBP 115,35±7,81 133,93±10,24 < 0,0001Holter 24h DBP 64,87±5,41 73,52±11,33 < 0,0001IVSd (mm) 8,33±1,08 8,8±1,01 < 0,05LVMH 2.7 39,91±7,65 43,63±8,55 < 0,05E/A 1,84±0,5 1,61±0,4 < 0,05Mean Long Strain (%) -19,41±2,4 -20,5±3,17 NSBasal Septal Long Strain (s-1) -20,11±5,06 -14,28±8.16 < 0,01
Conclusions: Our study demonstrated for the first time that the prevalence of MHin successfully corrected AoC pts is very high (50%). MH in AoC pts is associatedwith significant changes in LV geometry and function.
P1246 Increased risk for atherosclerosis in adultpost-coarctectomy patients
P. Luijendijk1, E. De Groot1, J.W.J. Vriend2, J. Gort1, B.J. Bouma1,B.J.M. Mulder1. 1Academic Medical Center, Amsterdam,Netherlands; 2Leiden University Medical Center, Leiden,
Netherlands
Purpose: Despite successful surgery of aortic coarctation, cardiovascular mor-tality and morbidity are increased in these patients The increased cardiac risk isthought to be multi-factorial, with atherosclerosis as a major contributor. Carotidintima-media thickness (CIMT) is a validated marker for atherosclerosis. It wasshown in adult post-coarctectomy patients CIMT is increased if compared to un-affected controls. Here, based on longitudinal CIMT data, we describe arterialwall change over time in adult post-coarctectomy patients.Methods: In 55 adult post-coarctectomy patients (33 males, mean age 31.1±9.2years, mean age at surgical repair 8.1±6.7 years) carotid B-mode ultrasoundscans were acquired in 2002 and in 2008. CIMT of pre-coarctic right and leftcarotid conduits were determined. Baseline data were compared with a controlgroup. Also, CIMT progression rates were compared to those described in theliterature.Results: In 2002 CIMT was significantly increased if compared to controls(0.65±0.14 vs 0.49±0.07 mm (p <0.001). During follow up (mean follow up7.11±6.8 years), a significant increase in CIMT (0.65±0.14 mm up to 0.70±0.13mm (p <0.001) e.g. (0.0070±0.015 mm/year) was observed. CIMT progressionover time in patients was somewhat increased if compared to the healthy popula-tion as described in the literature (0.007 vs. 0.005 mm/year). The contribution ofhypertension and/or lipids could not be identified as an independent co-variate tocarotid IMT change (all p >0.3)Conclusion: Carotid IMT in post-coarctectomy patients is increased after surgi-cal repair. In long term follow-up carotid IMT increase is increased in adult post-coarctectomy patients compared to the healthy population. These findings pointtowards an increased risk for atherosclerosis in these patients. Further researchis needed to reveal whether intensive lipid- and blood pressure control in thesepatients normalizes cardiac mortality and morbidity, atherosclerosis progressionand disease risk.
P1247 Impact of antenatal diagnosis on outcomes ofneonates with coarctation of the aorta
S. Di Filippo, D. Abid, R. Henaine, F. Sassolas, C. Ducreux, J. Ninet,A. Bozio. University Hospital of Lyon - Hospital Louis Pradel, Lyon,France
The objective of the study was to review coarctation of the aorta (COAO) inneonates and assess the influence of antenatal diagnosis on prognosis.Material and methods: all patients diagnosed with COAO who underwentsurgery before 2 months of life, from 2004 to 2008, were included.Results: Among 106 neonates (63 males) admitted for diagnosis of COAO at me-dian age 5.5days, 29 (27.3%) had antenatal diagnosis (24 ventricular asymetry,5 aortic arch hypoplasia). The other 81 patients presented with heart failure (23mild, 15 moderate, 19 cardiogenic shock) or no symptom (18 absence of femoralpulse, 6 murmur). PGE was required in 65 (61.3%), mechanical ventilation in 56(52.8%: 77% of patients with PGE). Ventricular septal defect was associated in50 (47%), aortic valve bicuspidia in 53 (50%); mitral valve was normal in 100(94.3%). Antenatal diagnosis was associated with more severe anatomy (LV di-ameter: 15.7 vs 18.2mm, p= 0.004; ascending aorta: 7.2 vs 8.2mm, p= 0.01),less heart failure (p<0.0001), less mechanical ventilation (p= 0.008), higher LVshortening fraction (p= 0.03) and lower pulmonary pressure (p= 0.03). Surgery(Crafoord: 82, Crafoord + banding: 14, Crafoord + VSD patch: 9) was performedat median age 12days (2 to 63days: earlier in antenatal diagnosis cases: 11.5vs 21.5days, p= 0.04), median weight 3kg (1.6 to 5.3), median time from diag-nosis 3days (0 to 59). Postoperative complication occurred in 20 cases (19%),more frequently in case of VSD closure (62.5%). Median CICU stay was 8days(1 to 80), hospital stay 11days (1 to 80), longer in antenatal diagnosis cases:11.5 vs 21.4days, p= 0.02. Aortic restenosis occurred in 6 cases (6%), 45 to
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Congenital disease of the aorta 177
340days postoperative (median 79days), and was associated with postoperativecomplication. Freedom from restenosis at 1month, 2months and 1year was re-spectively 94% and 90%. One patient died before surgery, 3 within 2months aftersurgery. Antenatal diagnosis did not impact on postoperative course, nor survival,nor restenosis.Conclusion: Antenatal diagnosis can detect COAO with most severe anatomy(27.3% of all), allows to anticipate heart failure and LV impairment and leads toearlier surgery, but does not impact on long-term outcome.
P1248 Correlation between magnetic resonance imagingand transthoracic echocardiography in patients withrepaired aortic coarctation
C.N. Lourenco, H. Andrade, N. Antonio, D. Rodrigues, P. Donato,G. Castro, M. Silva, M.J. Ferreira, L. Goncalves, L.A. Providencia.
Coimbra University, Medical School, Coimbra, Portugal
Purpose: The incidence of cardiovascular complications in patients with repairedaortic coarctation warrants a watchful follow-up. Until a few years ago transtho-racic echocardiography (TTE) was the most widely used exam in this setting.Magnetic resonance imaging (MRI) is currently regarded as the reference methodfor aortic morphofunctional evaluation. The aim of our study was to compare TTEand MRI data obtained on the long-term follow-up in a population with repairedaortic coarctation.Methods: Retrospective study including 51 patients with repaired aortic coarc-tation (mean follow-up time was 20±7 years). We compared TTE and MRI dataperformed in 35 patients on average 18 years after the first repair. A reduction inaortic calibre >50% detected by MRI and an ascending/descending aortic gradi-ent detected by TTE >20 mmHg were considered significant.Results: Mean current age was 29±9 y old and at the intervention time was 9±9y old; 61% were male and 87% of the cases were postductal coarctations. Ini-tial repair was made by surgery in 90.2% and by percutaneous intervention in9.8%. MRI evaluation showed normal aortic images in 14.3% of the patients;localized coarctations were detected in 11.4%, hypoplasias in 60% (arch hy-poplasias in 23%), ectasies and persistent left superior vena cava in 5.7%. Nosuggestive dissection images were visualized. Significant reductions of the de-scending aorta calibre were detected in 17% of the cases and mild to moderatereductions in 66%. By TTE, 60% of the cases had ascending/descending aor-tic gradient >20 mmHg. All the patients with significant reduction, and 61% withmild to moderate aortic calibre reduction by MRI, showed ascending/descendingaortic gradient >20 mmHg. However, 28.6% didn’t show a significant gradient byTTE and presented mild to moderate aortic calibre reduction by MRI. There wasconcordance between the exams regarding aortic subvalvular membrane visu-alization (11.4%), aortic regurgitation (31%) and in systolic ventricular functionevaluation.Conclusion: In most cases, there is a concordance between TTE and MRI dataregarding severity of aortic calibre reductions and gradients, aortic valve morpho-functional evaluation and ventricular function. However, MRI allows the detectionof areas with mild to moderate calibre reductions which don’t have significantgradient by TTE, associated vascular anomalies, hypoplasia areas and ectasieshardly observed by TTE, thus becoming an important exam for the evaluation oflate cardiovascular complications in patients with repaired aortic coarctation.
P1249 Does the early surgical correction of aorticcoarctation influence the development ofatherosclerotic changes?
O. Trojnarska1, K. Mizia-Stec2, L. Szczepaniak-Chichel3 ,M. Gabriel4, A. Bartczak1, A. Cieplucha1, J. Chudek5, S. Grajek1,
A. Tykarski3 , Z. Gasior2. 1Poznan University of Medical Sciences, Departmentof Cardiology, Poznan, Poland; 2Silesian Medical University Cardiology Unit,Katowice, Poland; 3Poznan University of Medical Sciences, Department ofHypertension, Poznan, Poland; 4University of Medical Sciences AngiosurgeryUnit, Poznan, Poland; 5Medical University of Silesia, Department ofPathophysiology, Katowice, Poland
Background: Patients after coarctation of the aorta repair (CoAo P) are predis-posed to systemic hypertension (SH) and early atherosclerosis.Aim: to evaluate the following serum markers: nitric oxide (NO; measured as thestable end product of NO, i.e., nitrite/nitrate), assymetric dimethylarginine (ADMA;endogenous competitive inhibitor of NO synthase), high-sensitivity C-reactive pro-tein (hsCRP) and to establish its relation to ultrasound indexes of endothelial func-tion and structural remodeling and to age at operation in CoAo repair patients (P).Patients and methods: 62 CoAo P (37 M, mean age: 34.6±10.3yr) and 20controls (10 M, mean age: 33.6±8.2yr) were analysed. 33 CoAo P were nor-motensive SH(-). The following central: augmentation pressure (AP), augmen-tation index (AI) and peripheral vascular parameters: flow-mediated dilatation(FMD), nitroglycerin-mediated dilatation (NMD), intima-media thickness (IMT),pulse wave velocity (PWV) were measured.Results: ADMA and hsCRP levels were significantly higher, NO lower inthe CoAo P (0.62±0.2umol/l; 2.01±1.7mg/l; 33.0±7.4umol/l) compared to thecontrols (0.46±0.1umol/l, p=0.014; 0.89±0.6mg/l, p=0.001; 37.0±7.1umol/l,p=0.039). ADMA were higher in SH(+) (0.66±0.3umol/l, p=0.001) and SH(-)(0.59±0.24, p=0.014) subgroups compared to controls, significant differences in
NO (31±6.7 umol/l, p=0.025) and hsCRP (2.18±1.9, p=0.02) were found in SH(+)P only.In SH(-) P both peripheral (FMD: 4.75±2.8 vs. 8.5±2.3%, p=0.001); NMD:(11.9±4.8% vs. 19.8±7.2%, p=0.001) and central parameters: AP (7.2±3.9 vs4.3±3.5mmHg; p=0,002), AI (18.7±9.5 vs 12.9±4.1%; p=0,03) was impairedcompared to controls. PWW was increased (6.7±1.1 vs. 5.3±0,7m/s; p=0.003)while IMT was comparable (0,052±0,01 vs. 0,051±0,01 mm; p=0.06).hsCRP correlated with NMD (r=-0.488, p<0.001), IMT (r=0.258, p=0.04), PWV(r=0.337, p=0.007) in all supgroups. ADMA correlated negatively with FMD bothin CoAo P (r=-0.356, p=0.004) and in SH(-) subgroup (=-0.365, p=0.03). Therewere no significant correlations between patient’s age at CoAo repair and anyserum biochemical or arterial ultrasound indexes.Conclusions: CoAo P are characterized by endothelial dysfunction: increasedserum ADMA concentrations as well as impaired FMD. Coexistence of hyperten-sion is associated with decreased NO serum metabolites, increased hsCRP andvascular remodeling. Early operation has no impact on vascular remodeling andearly biochemical atherosclerosis parameters that support the claim that CoAois a systemic vascular disorder which leads to atherosclerosis and progressivevascular damage despite early correction.
P1250 Aortic distensibility and vascular physiology in adultpatients with coarctation of aorta late after repair
A. Moutafi1, C. Delos2, V. Thanopoulos3 , M.A. Gatzoulis4,C.H. Davos1. 1Biomedical Research Foundation, Athens, Greece;2Tzaneio General Hospital, Athens, Greece; 3Agia Sofia Hospital,
Athens, Greece; 4Royal Brompton Hospital, London, United Kingdom
Background: Patients with coarctation of aorta (CoA) present cardiovascularcomplications late after repair such as hypertension, aneurisms and coronaryartery disease which imply a process of chronic vasculopathy. Our prospectivestudy investigated the elastic properties of the aorta and peripheral vessels inadult patients with CoA, late after repair.Methods: We enrolled 19 adult patients (9 male) with repaired CoA (mean age25.3±9.3y, 18.3±8.1 years after repair) and 29 matched healthy controls (14male, mean age 26.1±9.1y). From transthoracic echocardiography (Vivid7, GE,USA) we measured the systolic (ASd) and diastolic diameter (ADd) of the as-cending aorta and we calculated aortic distensibility as [2 x (ASd- ADd)/ADd x(SBP-DBP)] and stiffness index as log [SBP x (ASd - ADd)/(DBP x ADd). We usedarterial applanation tonometry (SphygmoCor 2000, AtCor Medical, Australia) tomeasure the augmentation index (AI%) and the augmented pressure (AP) of thecentral aortic pressure and strain gauge plethysmography (EC6 plethysmograph,DE Hokanson, USA) to measure forearm blood flow (FBF) as an index of en-dothelial function of peripheral arteries.Results: Results are presented in Table 1.
Table 1
CoA Controls p value
Aortic distensibility (dyn-1cm2 10-6 ) 3.09±1.61 4.75±2.64 p=0.02Stiffness index (mmHg) 7.67±12.42 2.61±1.96 p=0.005AP (mmHg) 8.53±5.50 2.33±4.89 p=0.001AIx (%) 26.17±14.98 7.10±13.68 p=0.0007FBF (ml/min/100ml tissue) 13.31±5.10 24.27±13.50 p=0.009
Values in mean±SE.
Conclusions: Adult CoA patients show impaired elastic properties of aorta andperipheral arteries, late after repair, regardless the initial lesion. These resultsmay be due to endothelial dysfunction and suggest a procedure of peripheralvasculopathy which may explain, at least in part, the late complications of repairedCoA.
P1251 Percutaneous dilation of the coarctation of aortathrough balloon angioplasty and/or stent implantation- own experience
M. Szkutnik, J. Bialkowski. Silesian Center for Heart Diseases,Zabrze, Poland
Purpose: Published results of percutaneous dilation of the coarctation of the na-tive aorta (CoA) and recurrent after previous surgical operation (ReCoA) are notfrequent.The aim of this study was to assess results of balloon angioplasty (BAP) and/orstent implantation (SI) in the treatment of such patients (pts).Methods: BAP and/or SI was performed in 203 pts: 110 with native CoA and 93with ReCoA. aged 0,3-57 (median 15) years. In cases of discrete, native CoABAP was performed usually with low pressure balloons whereas in ReCoA - withhigh pressure balloons. According to availability following stents were applied –Palmaz, Cheatham Platinum (CP), covered CP and nitinol self expandable.Results: BAP was performed during 184 procedures and SI in - 63. In case ofnative CoA BAP was efective in 82% pts, whereas SI - in all 45 pts (despite 3stent migrations). In case of ReCoA BAP was effective in 79.2% pts, whereasSI in 72,2% (13/18) pts (stiff lesion). After BAP/SI aortic aneurysm/dissectionoccurred in 1 pt with native CoA and 3 pts with ReCoA – 3 of them were treatedwith covered stent and one surgically. In 53 years old woman with native CoA
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

178 Congenital disease of the aorta
during SI mild stroke occurred and in 6,5 year girl after SI - femoral thrombosis,which required surgical treatment.Conclusions: In majority of the patients with CoA - BAP or SI are an effectivemethods of treatment. The strategy however should be individual.
P1252 Residual hypertension and aortic wall abnormalitiesat mid-term follow-up after native aortic coarctationstenting
J. Bouet, B. Bonello, M. El Tahlawi, V. Fouilloux, T. Cuisset, G. Habib,A. Fraisse. AP-HM - Hospital La Timone, Marseille, France
Purpose: The feasibility of transcatheter primary stenting (TPS) to treat nativeaortic coarctation (Coa) is well-demonstrated as an alternative of surgical repair.However, information on mid-term follow-up remains scarce, especially regardingthe frequency of systemic hypertension and the integrity of the aortic arch. Weretrospectively studied the patient’s outcome after TPS for Coa, paying particularattention to residual hypertension and aortic wall abnormalities, including archobstruction, aneurysm and dissection.Patients and Results: Since 2002, 20 patients (8 female) with Coa were treatedby TPS at a median age and weight of 21 (7 to 52) years and 60 (27 to 94) kg, re-spectively. They were symptomatic in all cases with upper limb hypertension in 16.Twenty stents were successfully implanted and the mean peak systolic pressuregradient dropped from 31 (10 to 60) mmHg to 1,6 (0 to 15) mmHg. One majorcomplication occurred in a patient who experienced bilateral groin hematomas,with hypotension and anemia necessitating transfusion. After a median follow-up of 2,9 (0,12 to 7,8) years, the 20 patients are asymptomatic. Residual up-per limb hypertension is present in 7 cases (35%), including 3 (15%) with mildresidual upper-to-lower limbs gradient (20mmHg). One patient was successfullyredilated for in-stent restenosis. By transthoracic echocardiography (n=20), spiralcomputed tomography (n=4), and magnetic resonance imaging (n=13), there isno aortic aneurysm or dissection.Conclusion: TPS for Coa is successful with minimal morbidity. After mid-termfollow-up, residual hypertension is similar to that observed after surgical repair,whereas aortic wall abnormalities are not encountered. Longer term follow-up ismandatory to confirm this favorable outcome.
P1253 Clinical outcomes in adults following primaryendovascular stenting of aortic coarctation with acovered stent
T. Hamid, B. Clarke, V. Mahadevan. Manchester Royal Infirmary,Manchester, United Kingdom
Introduction: Primary endovascular stenting is a widely recognised treatmentstrategy for treatment of coarctation in adults. The availability of covered stentshas made coarctation stenting more attractive.Objective: To assess early and medium term clinical outcomes and blood pres-sure control in adults with a native aortic coarctation of the aorta undergoingprimary endovascular stenting with a covered stent.Design: Data was collected prospectively from adults with coarctation undergoingstenting using the CP Numed covered stent or the V12 Atrium covered stent overa 3 year period. Patients were assessed with 24 hour ambulatory blood pressuremonitoring (ABP) pre procedure and at 6 weeks and 1 year following endovascu-lar stenting.Results: A total of 24 patients (15 male) underwent primary endovascular stent-ing. The procedure was technically successful in all patients. Mean age was35±15 years. Peak transcatheter aortic gradient across the coarctation fell from29±11 mmHg to 6±5mm Hg (p<0.0001) with stenting. 15 patients were receivinganti-hypertensive medication prior to stenting with 12 receiving 2 or more agents.Blood pressure recordings are given in Table1.At 1 year follow up systolic bloodpressure dropped by 18 mm Hg as compared to pre-procedure (p< 0.05) and13 patients remain on anti-hypertensive medication. One patient had successfulredilatation of his stent 12 months later and there was no mortality. One patienthad a femoral artery false aneurysm post procedure needing repair.
Table 1. Systolic Blood pressure pre-procedure, 6 weeks and 12 months
Pre-stenting 6 weeks 12 months
Rt Arm Systolic BP 155±16 (n=24) 137±23* (n=20) 137±10* (n=21)24 Hrs Average Systolic BP 137±13 (n=17) 127±12* (n=14) 131±10* (n=13)
Conclusion: Primary stenting of aortic coarcation with a covered stent results inexcellent procedural outcomes with significant reduction in clinical and ABP bloodpressures at 6 weeks which is sustained at 1 year. However there is a need forcontinued antihypertensive therapy and long term follow-up is required.
P1254 Vascular remodeling in adults after coarctation repair- impact of descending aorta stenosis and age atsurgery
O. Trojnarska1, L. Szczepaniak-Chichiel2 , K. Mizia-Stec3,A. Bartczak1, S. Grajek1, A. Tukarski2 , Z. Gasior3. 1Poznan
University of Medical Sciences, Department of Cardiology, Poznan, Poland;2University of medical Sciences Hypertension Unit, Poznan, Poland; 3SilesianMedical University Cardiology Unit, Katowice, Poland
Introduction: Patients after successful repair of coarctation of the aorta (CoA)are at risk of hypertension at rest and associated end-organ damage. The aimof the study was to assess arterial stiffness and function in adults after coarcta-tion repair in relation to descending aorta residual coarctation and patient age atoperation.Patients and methods: 85 patients after CoA repair (53 males) aged 34,6±10,3years; median age at operation 0,9±8,2 years. The control group - 30 individuals(18 males) at mean age 33,6±8,2 years. The following central: augmentation(AP) and augmentation index (AI) as well as peripheral vascular parameters flowmediated dilatation (FMD), nitroglicerine-mediated vasodilatation (NMD), intima-media thickness (IMT) and pulse wave velocity (PWV) were measured.Results: 47 CoAo repaired patients were normotensive, and compared to con-trol, they presented higher values of central parameters AP (7,3±4,6 vs 4,4±3,6mmHg; p=0,002) and AI (18, 6±10,4 vs 13,5±4,3% mmHg; p=0,03); as well asthe increased PWV (6,8±1,2 vs 5,4±0,9 m/s; p=0,003), while IMT was compa-rable (0,053±0,01 vs 0,051±0,01mm; p=0,06). The vasodilatation was impairedin the normotensive patients: FMD (4,8±2,8 vs 8,5±2,3%; p=0,00003) and NMD(11,3±4,6 vs 19,8±7,2%; p=0,00001). The comparison of recoarctation (46/54%;gradient across the descending aorta ≥20mmHg) to nonrecoarctation (39/46%)patients did not reveal any significant differences in resting systolic and diastolicpressures, as well as the values of AI and the peripheral vascular parameterers;the value of AP was higher in the recoarctation patients (10,5±6,9 vs 7,5±4,1p= 0,02) and correlated positively with the gradient across the descending aorta(R=0,295, P=0,01). There was no significant linear correlation between age at thetime of surgery and any of peripheral arterial parameters.Conclusions: Residual stenosis in the descending aorta does not affect the arte-rial vasodilatation nor stiffness in patients after CoAo repair. Early operation hasno impact on peripheral vascular remodeling or central pressure which supportsthe claim that coarctation of the aorta is a systemic vascular disorder which leadsto progressive vascular and end-organ damage despite early correction.
P1255 Autonomic nervous system function in adults withcoarctation of the aorta, late after repair
A. Moutafi1, K. Karpouzi1, G. Manis2, C. Delos3, V. Thanopoulos4 ,M.A. Gatzoulis5, C.H. Davos1. 1Biomedical Research Foundation,Athens, Greece; 2University of Ioannina, Ioannina, Greece; 3Tzaneio
General Hospital, Athens, Greece; 4Agia Sofia Hospital, Athens, Greece; 5RoyalBrompton Hospital, London, United Kingdom
Background: There is previous data showing that patients with certain congen-ital heart disease (CHD), such as Tetralogy of Fallot, show impaired autonomicnervous system (ANS) function, late after repair. The aim of this prospective studywas to investigate the ANS function in adult patients with CoA, late after repairby measuring both heart rate variability (HRV) and baroreflex sensitivity (BRS)indices.Methods: Eighteen stable adult patients (9 male) with repaired CoA (mean age25.3±9.6y, 17.8±8.1y after repair) and 27 matched healthy controls (mean age26.1±9.1y) underwent a successive 40-minute ECG and beat-to-beat blood pres-sure recording at rest (TaskForce monitor, CNSystems, Austria). Baroreflex sen-sitivity was computed by the a-index (square root of the ratio between RR intervaland systolic blood pressure (SBP) spectral powers in the low (0.04-0.15Hz, a-LF)and high frequency (0.15-0.4Hz, a-HF) bands and the sequence method (linearregression slope of RR interval vs SBP, BRSseq). Frequency domain (LF and HF)HRV indices and SDNN (standard deviation of all RR intervals), RMSSD (squareroot of the mean squared differences of successive RR intervals) and pNN50 (percent of differences of successive RR intervals >50 ms) were measured.Results: All HRV and BRS indices were not statistically different between CoApatients and healthy controls (Table 1).
Table 1
CoA patients Controls
HRV variables log SDNN 1.90±0.15 1.89±0.22log RMSSD 1.83±0.23 1.81±0.29pNN50 (%) 0.997±0.001 0.997±0.001log LF 2.98±0.46 2.81±0.39log HF 2.99±0.49 2.85±0.49
BRS variables log α-LF 1.19±0.20 1.29±0.21log α-HF 1.40±0.34 1.54±0.25log BRSseq 1.40±0.22 1.33±0.22
Values are mean±SD.
Conclusions: Adult patients late after CoA repair do not present with ANS dys-function. This may be due to the myocardial or haemodynamic stability of thesepatients or other adaptive pathophysiological mechanisms which need further in-vestigation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Congenital disease of the aorta 179
P1256 Dilatative aortopathy in adults with repairedconotruncal defects
T. Rutz, M. Friedrich, A. Wahl, M. Schwerzmann. Bern UniversityHospital, Swiss Cardiovascular Center, Bern, Switzerland
Aim: Dilatative aortopathy is a feature of tetralogy of Fallot (TOF).Structural abnormalities of the medial aorta have been described for otherconotruncal defects like d-transposition of the great arteries (d-TGA). This studyelucidates the aortopathy assessed by cardiac magnetic resonance imaging(CMR) in adults with repaired TOF and d-TGA compared to normal individuals(C).Methods: In 20 individuals of d-TGA, TOF and C aortic diameters were retro-spectively measured by CMR at the levels of aortic sinus (Si), sinotubular junction(STJ), ascending (aA) and descending aorta (dA) at the level of the bifurcation ofthe pulmonary artery (aAP, dAP), diaphragm (D). As a measure of aortic elasticitythe aortic distensibility of aA and dA (aAD, dAD) at the level of the pulmonary bi-furcation was determined from cine images: (maximal cross sectional area (CSA)– minimal CSA)/minimal CSA)/(systolic blood pressure – diastolic blood pres-sure).Results: Age and gender did not differ between groups. Diameters of Si, STJ andaPB were significantly larger in TOF compared to d-TGA and C: Si mm/m2: 21.6vs. 18.2 vs. 17.2, p=.001. STJ mm/m2: 18 vs. 15 vs. 13.7 p=.001. aPB mm/m2:16.8 vs. 15.8 vs. 14.4, p=.008. aAD was significantly reduced in TOF comparedto C and showed a trend to a lower value in d-TGA: aAD 10-3/mmHg: 3.3 vs. 3.6vs. 5.3, p=.014 (figure). dAD showed a trend to a lower value in TOF comparedto d-TGA and C. The diameters of dAP and D did not differ significantly.
Conclusions: The aortopathy in repaired TOF is evident by increased diame-ters and a reduced elasticity of aA. The aortopathy is less evident in d-TGA andprimarily expressed by a reduced elasticity. Nevertheless, aortic dimensions ind-TGA should also be carefully followed, especially with increasing age.
P1257 Surgical aortic management in Marfan syndromecontrasting 20th and 21th century
D. Detaint1, C. Roy2, F. Arnoult3, A. Rezza1, G. Delorme1,M. Gautier1, C. Boileau1, A. Vahanian4, F. Tubach2 , G. Jondeau1 .1Centre de reference syndrome de marfan et apparenté, hopital
Bichat, université Paris VII, APHP, Paris, France; 2URC. Hopital Bichat.Universite Paris 7. AP-HP, Paris, France; 3Explorations fonctionnelles, HopitalBichat, AP-HP, Paris France, Paris, France; 4AP-HP - Hospital Bichat-ClaudeBernard, Department of Cardiology, Paris, France
Background: Major avances have been realised in medical and surgical man-agement in Marfan syndrome (MFS).Methods: We used the data base from the French centre de reference for MFSand related disease to go over the practice and its evolution with time in France.Results: From 1996 to 2009, a total of 3946 patients (2778 adults and 1168children) were seen to our MFS clinic for a suspicion of MFS. Diagnostic of MFSwas based upon international criteria and was confirmed in 1042 (26%). MFSpatients were female in 51%, were 27±16 years at first visit, and were followed4.4±4 years. During this follow-up period, death occurred in 4.3% of patients,related to aortic dissection in 22%, sudden death in 18%, related to surgery in38%, due to other cause in 13% and from unknown cause in 9%.279 (27%) MFS patients underwent cardiac surgery prior their first visit or duringfollow-up.Surgery was performed on the aortic valve in 249 (24%), ascending aorta (AA)in 236 (22%), descending aorta in 54 patients (5,2%), and mitral valve (MV) in58 (5,6%). Aortic root surgery was performed in 17 patients between 1980-1990,92 patients between 1990-2000, and 135 patients between 2000-2010. Compar-isons of surgical techniques between 1990-2000 and 2000-2010 showed that withthe turn of the century, valve sparing surgery became the preferred surgery foraortic root dilatation (82/135, i.e. 59% after year 2000, vs 19/92 i.e. 21% beforeyear 2000). One reason may be that more patients were operated on for aorticdilatation and not dissection after 2000 (77% in the 2000-2010 period vs. 53% inthe 1990-2000 period). When the aortic valve was replaced, a mechanical aorticvalve was used in 95% of the patients, and this percentage remained stable withtime.
Mitral valve repair became the technique of choice over MV replacement in theearly 90ies: 50% between 1980-1990; 65% between 1990-2000; and 75% after2000.Conclusion: the surgical management of French patients with MFS has remark-ably changed over the last 4 decades. The indications of surgery have changedfrom emergency to elective, and contributed to develop aortic valve sparingsurgery, which is since 2000 the favoured technique. This tendency seems tofollow by 10 years MV repair which became predominant in the 90ies.
P1258 Severe deterioration in ascending aorta and aorticarch elastic properties in patients with Marfansyndrome during 11 years follow-up
P. De Witte1, T. Radonic2, K. Laan2, J. Timmermans3, A.J. Scholte4,M.P. Van Den Berg5, A.H. Zwinderman2 , B.J.M. Mulder1,
M. Groenink1. 1Academic Medical Center, Department of Cardiology at theUniversity of Amsterdam, Amsterdam, Netherlands; 2Academic Medical Center,Department of Clinical Epidemiology Biostatistics & Bioinformatics, Amsterdam,Netherlands; 3Radboud University Nijmegen Medical Centre, Departmentof Cardiology, Nijmegen, Netherlands; 4Leiden University Medical Center,Department of Cardiology, Leiden, Netherlands; 5University Medical Center,Department of Cardiology, Groningen, Netherlands
Purpose: In Marfan syndrome aortic elasticity is affected by progressive vesselwall degeneration. Indices of aortic elasticity can be used to assess prognosis inMarfan patients. Aortic elasticity also progressively deteriorates during aging. Weassessed age-related changes in aortic elasticity in 34 individual Marfan patientsin 11 years time and compared these data with data from healthy individuals.Methods: 34 patients (20 male, mean age 30.5) without aortic complications be-yond the aortic root underwent cardiovascular magnetic resonance imaging todetermine aortic diameters and elasticity. Aortic distensibility and diameter weremeasured at 4 levels, e.g. the ascending (level A) and descending (level B) tho-racic aorta, descending aorta at the level of the diaphragm (level C), and theabdominal aorta just above the bifurcation (level D). Flow wave velocity (FWV)was calculated across the entire aorta. After 11 years the protocol was repeated.Blood pressure was recorded during both sessions.Results: Distensibility decreased at all aortic segments, but more in the proximalaorta, compared to the distal aorta (A: 3.3 to 2.4 10-3 mmHg-1, p=0.04. B: 3.8to 2.9 10-3mmHg-1, p=0.055. C: 5.4 to 4.6 10-3 mmHg-1 p=0.07. D: 3.5 to 3.310-3 mmHg-1, p=0.7). Aortic diameters increased in all segments (A: 30.1 to30.6mm, p=0.285. B: 23.1 to 25.1mm, p<0.05. C: 20.1 to 22.8mm, p<0.05. D:18.8 to 20.2mm, p<0.05). FWV in the entire aorta increased from 5.3 to 5.9 m/s(p=0.02), and in the ascending aorta-aortic arch from 4.6 to 6.6 (p<0.001, +0.18m/s per year vs 0.03 to 0.1 m/s per year in healthy individuals).Mean arterialpressure increased from 80 to 90 mmHg (p<0.001).Conclusions: Aortic elasticity in Marfan syndrome decreases significantly aging.This is accompanied by a significant increase in aortic diameter and mean arterialpressure. The decrease in thoracic aortic elasticity beyond the aortic root is muchhigher in Marfan patients compared to healthy individuals.
P1259 Higher plasma levels of TIMP-1 among MarfanSyndrome patients with previous aortic rootreplacement: a marker of improved proteolyticbalance?
A. Lebreiro1, E. Martins1, P. Lorenco1, C. Cruz1, J. Almeida1,M.J. Martins2, P. Bettencourt1, M.J. Maciel1, C. Abreu-Lima2. 1Sao
Joao Hospital, Porto, Portugal; 2University of Porto, Faculty of Medicine, Porto,Portugal
Purpose: Marfan Syndrome (MFS) is a connective tissue disorder that af-fects multiple organ systems. Cardiovascular system is typically involved, mainlythrough aortic dilatation or dissection, the principal cause of death in this popula-tion. Imbalances of the proteolytic cascade involving metalloproteinases (MMPs)and its inhibitors (TIMPs) have been implicated in aortic aneurysm formation andprogression in Marfan Syndrome (MFS) patients. We aimed to investigate the bal-ance between MMPs and TIMPs according to the severity of aortic disease andafter aortic root replacement in a population of MFS patients.Methods: Venous blood samples of 30 MFS patients, all of them fulfillingGhent criteria, were analyzed for MMP-2, MMP-3, MMP-9, TIMP-1, TIMP-2 and α2-macroglobulin. MMP and TIMP levels were measured by enzyme-linked immunosorbent assay and α2-macroglobulin levels were measured by im-munonephelometry. All patients underwent a comprehensive echocardiographicevaluation.Results: In comparison with non operated patients (n=18), those with past his-tory of aortic root replacement (n=12) had higher plasma levels of TIMP-1 [mean(SD) – 134.9 (28.5) vs. 108.2 (21.0) ng/mL; P=.006], and a decreased ratio ofMMP-9/TIMP-1 [median (IQR) – 0.04 (0.03 - 0.09) vs. 0.07 (0.05 - 0.1); P=.03].No significant differences were found between the levels of MMPs, TIMPs, α2-macroglobulin or the ratio MMP/TIMP when comparing patients with and withoutaortic root dilatation.Conclusions: Our results suggest that in aortic root replaced patients, a prote-olytic shift towards a more homeostatic pattern occurs. This better TIMP-1 plasmaprofile may induce a less catabolic molecular milieu in the aortic wall contributing
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

180 Congenital disease of the aorta
to disease stabilization. Our results give insight on mechanisms, beyond hemo-dynamic benefits, for the known prognostic improvement after aortic root replace-ment in Marfan patients, and may open new lines of investigation on the role ofMMPs and TIMPs as biomarkers after aortic surgery in MFS patients.
P1260 Ascending aortic dilation in Turner syndrome: thenatural history
K.H. Mortensen1, B.E. Hjerrild1, K. Stochholm1, N.H. Andersen2,K.E. Sorensen2, E. Lundorf2, A. Hoerlyck2, E.M. Pedersen1,J.S. Christiansen1, C.H. Gravholt1. 1Aarhus University Hospital,
Aarhus Hospital NBG, Aarhus, Denmark; 2Aarhus University Hospital, Skejby,Aarhus, Denmark
Background: Aortic dissection causes excess mortality in Turner syndrome. Therisk of dissection is particularly increased risk in the presence of aortic dila-tion, congenital cardiovascular abnormalities, karyotype 45,X, and elevated bloodpressure. Risk factor identification is, however, inadequate and the natural courseof aortopathy is sparingly investigated.Purpose: To define aortic growth rates along the entire thoracic aorta in Turnersyndrome using magnetic resonance imaging, and to identify the possible predic-tors of aortic growth.Methods: Prospective follow-up study of 102 non-selected patients with Turnersyndrome (recruited from a non-cardiology clinic and examined twice) and 65healthy age-matched females (examined once). The effect parameters were: 3Dnon-contrast, ECG-gated, free-breathing magnetic resonance imaging (thoracicaortic diameter at nine predefined regions), twenty-four-hour ambulatory bloodpressures and echocardiography (aortic valve morphology).Results: The loss to follow-up was: (i) three deaths (two sudden-deaths, onedeath after surgery for severe aortic dilation), (ii) one exclusion (unexpected Stan-ford type A dissection at baseline), and (iii) eight with-drawals of consent (non-health related causes, no cardiovascular events during follow-up). Of the remain-ing, eleven patients were excluded because of unsuccessful magnetic resonanceimaging scans at baseline or follow-up (all declined re-scanning). Eighty patientscompleted the follow-up of 2.4±0.4 years (range 1.4 - 3.5 years). At baseline, thepatients had larger aortas (BSA-indexed) at all regions and the prevalence of aor-tic dilation exceeded 50%. During the follow-up, the aortic caliber increased at thesinuses, sinotubular junction and mid-ascending aorta (all P < 0.02) with growthrates of 0.2 - 0.4 mm/year. All other aortic regions were unchanged (all P > 0.2).In 36 patients (45%) the diameter-increase exceeded the interobserver limits ofagreement (Bland-Altman derived), and in 19 (24%) the increase exceeded twostandard deviations above the mean change in Turner syndrome. Aortic growthrates were not associated with bicuspid aortic valves, aortic coarctation, aorticdilation, karyotype, age and blood pressure.Conclusion: A general aortopathy was evident in unselected TS women with iso-lated ascending aortic enlargement during short-term follow-up. The aortic growthrates were comparable to those seen in other conditions with increased risk ofaortic dissection. Factors believed to confer increased risk of aortic dilatation anddissection did not predict aortic growth.
P1261 Aortic anomalies and dilatation in turner syndrome: acomparison between patients with and withoutbicuspid aortic valves and or coarctation
J.B.W. Elbers, J. Timmermans, J.L.R.M. Smeets. RadboudUniversity Nijmegen Medical Centre, Nijmegen, Netherlands
Purpose: To investigate aortic anomalies and dilatation in patients with TurnerSyndrome (TS).Methods: Study subjects included 99 adult TS patients visiting our multidisci-plinary outpatient clinic. Cardiovascular anomalies were visualized and aortic di-ameters were measured by transthoracic echocardiography and magnetic reso-nance imaging. TS patients were divided into two groups: group A (n=23) withbicuspid aortic valve (BAV) and or aortic coarctation (COA) and group B (n=76)without these anomalies. Aortic diameters were normalized to Body SurfaceArea (BSA) at 6 levels, predicted sinus diameter was calculated and ascend-ing/descending ratios were obtained.Results: In group A, BAV was found in 57%, COA in 14% and BAV plus COAin 29%. Anomalies of aortic arch were present in 30% of group A and in 12%of group B (p=0.04). Ascending aortic diameters/BSA were greater in group A(sinus index p=0,002, ascendens index p<0.001) and ascending/descending ra-tios were greater in group A (p<0.001). Using aorta index >2.1cm/m2 indicativefor dilatation, aortic sinus was dilated in 39% of group A and in 17% of groupB (p=0.03). Using ascending/descending ratio >1.5 indicative for dilation of theascending aorta, 65% of group A and 42% of group B showed dilatation (p=0.01).Conclusion: Bicuspid valve and coarctation are associated with more dilatationof the ascending aorta. In BAV patients without TS, aortic dilatation is progressiveand can lead to aortic dissection. It is unknown if aortic dilatation is equally pro-gressive in TS patients with and without BAV and COA. Therefore cardiovascularfollow up should be obtained.
P1262 Aortic valve disease in patients with congenitalsubaortic stenosis
R. Lopes, P. Lourenco, C. Cruz, M.J. Maciel. Hospital de São João,Porto, Portugal
Background: Aortic valve disease (AVD) frequently coexists withcongenital subaortic stenosis (SAS). This is probably due to a turbulent systolicjet that damage the valve. Aortic regurgitation (AR) is the predominant form ofAVD in SAS, being present in over 50% of patients (pts). AVD progression is un-predictable, even after SAS surgical correction. We aimed to assess predictors ofAVD occurrence and progression in SAS pts.Methods: We retrospectively analysed 51 pts with SAS followed in our congenitalheart disease clinic of a tertiary care hospital, from July 1976 to October 2008.Follow-up (FU) was assessed by reviewing the clinical records. A binary logisticregression was used to assess variables associated with AVD occurrence andAVD progression.Results: Twenty-eight (54.9%) were men, mean age of SAS diagnosis was14.6±14.1 years. Fibrous membrane SAS was present in 46 pts (90.2%). At theinitial evaluation 12 (23.5%) pts presented in NYHA class II, maximal left ven-tricular outflow tract (LVOT) pressure gradient (echocardiogram) was 55.8±28.2mmHg, 23 (46%) pts had left ventricular hypertrophy and all patients had normalleft ventricular function. Aortic regurgitation was present in 23 (45.1%) pts: mildin 18 and moderate in 5. None of our patients had aortic stenosis (AS).In 34 (66.7%) pts SAS was surgically approached. Additional aortic valve surgerywas performed in 6 pts (17.6%): aortic valve replacement (AVR in 3 pts and aorticvalve plasty in 3 pts. The mean time from diagnosis to surgery was 43.6±48.6months.During a mean 212-month FU, 14 pts (27.5%) developed AVD and 10 (19.6%)experienced AVD progression. At the end of FU 37 (72.5%) of our pts had someform of AVD: 34 had AR (mild in 24, moderate in 9 and severe in 1) and 3 anaortic valve prosthesis. In 6 pts mild AS coexisted with AR.Higher LVOT pressure gradient at diagnosis [HR 1.10 (95%CI 1.01-1.20); p =0.04] and higher left ventricular mass (LVm) [HR 1.04 (95%CI 1.01-1.08); p =0.006] were the only independent predictors of AVD occurrence. None of thevariables studied was associated with AVD progression.Conclusions: Aortic valve disease occurrence and progression is very frequentin SAS. No predictors were found for AVD progression. Patients with higher LVOTpressure gradient at diagnosis and higher LVm during FU were more likely to haveAVD. Aortic valve damage by a more turbulent systolic jet at LVOT is the probableexplanation for this AVD susceptibility in SAS.
P1263 Recurrence of congenital subaortic stenosis aftersurgical treatment
R. Lopes, P. Lourenco, C. Cruz, M.J. Maciel. Hospital de São João,Porto, Portugal
Background: Congenital subaortic stenosis (SAS) affects 1-2% ofpatients (pts) with congenital heart disease (CHD). In most of these pts, surgicalcorrection is needed. However, up to one third have SAS recurrence requiring re-intervention. Causes of recurrence are poorly understood. We aimed to assesspredictors of recurrence and reoperation in surgically corrected SAS pts.Methods: We retrospectively analysed 34 pts with surgically corrected SAS fol-lowed in a CHD clinic of a tertiary care hospital, from July 1976 to October 2008.Follow-up (FU) was assessed by reviewing the clinical records.Results: Mean age at diagnosis was 13.3 years and 21 (61.8%) pts were men.Fibrous membrane SAS was present in 31 (91.2%) pts. Association with otherCHD was present in 6 (17.6%) pts. Eight pts (23.5%) presented with NYHA classII. Maximal left ventricular outflow tract (LVOT) pressure gradient was 67.4±27.3mmHg; 17 (46%) pts had left ventricular (LV) hypertrophy and LV function wasnormal in all pts. Mean FU time was 231±80 months.In 25 (73.5%) pts surgical membrane resection was performed along with miec-tomy and in 6 (17.6%) with aortic valve repair. Eight (23.5%) pts had postopera-tive complications: conduction disturbances in 4, mechanical in 3 and medical in1. Eighteen (52.9%) pts had SAS recurrence after surgery and 8 (23.5%) under-went reoperation. Causes for reoperation were: SAS recurrence in 5 pts, aorticregurgitation (AR) in 2 and iatrogenic ventricular septal defect in 1.A shorter time from diagnosis to surgery [HR 0.98 (95%CI 0.96-1.00); p=0.04]was the only independent predictor of SAS recurrence. However, pts operatedat younger age tended to have more SAS recurrence. LVOT pressure gradientat diagnosis was the only independent predictor of reoperation [HR 1.06 (95%CI1.01-1.12); p=0.02]. Moreover, pts with higher post-surgical LVOT pressure gra-dient tended to need more often re-intervention.Conclusion: Congenital SAS recurrence after surgical treatment was frequent;reoperation was needed in about half of those pts. Pts with SAS recurrence wereoperated sooner after diagnosis and at a younger age, suggesting a more severeform of disease. Higher LVOT pressure gradients at diagnosis were associatedwith reoperation, suggesting that a higher turbulent systolic jet may trigger le-sions on the LVOT itself and on the aortic valve. The trend for higher post-surgicalLVOT pressure gradient to be associated with reoperation further supports thishypothesis.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Coronary heart disease: imaging and intervention 181
CORONARY HEART DISEASE: IMAGING ANDINTERVENTION
P1264 Arrhythmias after transcatheter closure of persistentforamen ovale are related to the type of the implanteddevice
M. Pieculewicz, T. Przewlocki, P. Wilkolek, B. Sobien, G. Kopec,L. Tomkiewicz-Pajak, P. Podolec. Jagiellonian University Medical
College - John Paul II Hospital - Department of Cardiac & Vasculare, Krakow,Poland
Transient supraventricular arrhythmias may occur in patients following persistentforamen ovale (PFO) closure. Therefore, the aim of the study was to prospectivelyperform 24-hour ECG monitoring to assess the electrocardiographic effects oftranscatheter closure of PFO depending on the type of implanted devices.Material and methods: 120 consecutive adult subjects (68 F, 52M; mean age:42.3±12.3) were enrolled into the study to undergo PFO closure with an Am-platzer Septal Occluder - ASO (71 pts), and Cardia device (49).Holter monitoring was performed on all patients before, at 1 and 12 months afterthe procedure.Results: The success rate of PFO closure was 94.5% (120 cases from 93 quali-fied in TEE), in 6 cases the PFO tunnels were too small to be forced by a catheter,in one case the PFO device caused an injury of the septum and an ASD Am-platzer device was implanted. During the procedure in 2 (1.7%) cases transientsupraventricular arrhythmia and in 1 (0.8%) case bradycardia to 30 bpm occurred.At 1 month: in 7 (5.8%) pts changes in AV conduction occurred: 1 pt (0.9%) hadcomplete AV dissociation, 6 (5%) pts intermittent first degree AV block; parox-ysmal atrial fibrillation (pAF) occured in 6 (5%) pts, 2 of whom had pAF prior toclosure.A significant increase in the number of SVE premature beats/24h was notedat 1 month after the procedure: 1020.9±431 (27-9600) compared to baselinedata 54.5±43 (0-560) (p<0.0001), at 12 months the SVE number decreased to61.8±51 (4-701) and did not differ significantly from the baseline data.There was no change in the mean number of ventricular arrhythmias/24h afterthe procedure.There was a significant correlation between SVE premature beats/24h at 1 monthafter the procedure and device size (p<0.0001 r =95921).Pts with ASO device had a significantly higher number of SVE ectopy at 1month after PFO closure (1768.9±671) compared to pts with Cardia device(895.9±211), p<0.0001.Conclusions: 1. Transcatheter closure of PFO is associated with a transient in-crease in supraventricular premature beats and a small risk of AV conductionabnormalities and paroxysmal atrial fibrillation in the early follow-up. There is re-gression of periprocedural arrhythmias after 12 months of PFO closure. 2. Tran-scatheter closure of PFO with Cardia device is related to a lower risk of supraven-tricular arrhythmias in the early follow-up. 3. The smaller device is implanted thelower risk of periprocedural arrhythmias is expected.
P1265 Assesment of atrial septal defect size: comparisonbetween 2D-transesophageal echocardiography,3D-transesophageal echocardiography and 64-slicecomputed tomography
D. Garcia Fuertes1, D. Mesa Rubio1, M. Delgado Ortega1, M. RuizOrtiz1, I. Tejero Mateos1, S. Espejo Perez2, R. Ysamat Marfa2, M. Lafuente3,M. Pan Alvarez-Ossorio1, J. Suarez De Lezo Cruz Conde1. 1Department ofCardiology, Reina Sofia University Hospital, Córdoba, Spain; 2Department ofRadiology, Reina Sofia University Hospital, Córdoba, Spain; 3Department ofAnesthesiology, Reina Sofia University Hospital, Córdoba, Spain
Aim: Transcatheter closure of ostium secundum atrial septal defect (ASD) isnowadays the treatment of choice for most patients suffering from this congen-ital defect. Measurement of defect size and selection of device closure sizecan be challenging in some patients considered for percutaneous treatment ofASD. Our aim was to compare 2D-transesophageal echocardiography (TEE),real time three-dimensional transesophageal echocardiography (3D-TEE) and64-slice computed tomography (CT) methods to measure the ASD size beforetranscatheter closure.Methods: From June 1993 to January 2010, 312 patients with ostium secundumASD were percutaneously treated in our hospital. Since January 2009, intrapro-cedural TEE and real time 3D-TEE (iE33, Qlab, Philips), as well as preproceduralCT (General Electric LightSpeed VCT), were perfomed to 21 consecutive patientssubmitted for percutaneous closure of secundum ASD in our center. Maximumand minimum diameters were measured.
Abstract P1265 – Table 1
N=21 N=19 N=19TEE vs 3D-TEE r (p) MD (p) TEE vsCT r (p) MD (p) CT vs 3D-TEE r (p) MD (p)
Maximum Diameter 14.7±9.2 vs 15.3±9.3 0.99 (<0.001) -0.5±0.8 (0.009) 15.3±9.5 vs 17.1±10.6 0.90 (<0.001) -0.7±4.6 (0.11) 17.1±10.6 vs 15.8±9.6 0.92 (<0.001) 1.2±4.0 (0.17)
N=19 N=17 N=19Minimum Diameter 8.3±4.6 vs 8.7±4.7 0.99 (<0.001) -0.3±0.3 (<0.001) 8.8±4.6 vs 12.3±6.2 0.87 (<0.001) -3.5±3.0 (<0.001) 12.3±6.4 vs 9.1±5.0 0.90 (<0.001) 3.2±2.9 (0.17)
TEE: Transesophageal echocardiography; 3D-TEE: real time three dimensional echocardiography; CT: 64-slice computed tomography; r: Pearson’s correlation coefficient; MD: Mean difference.
Results: Twenty one patients were included (female 66%). The mean age was40.8±21.4 years old. All patients successfully underwent percutaneous closure ofASD. An excellent correlation existed between measurements of maximum andminimum ASD diameters obtained by means of TEE, real time 3D-TEE and CT,as shown in table 1. The best correlation was observed between TEE and realtime 3D-TEE. On the other hand, TEE measurements of maximum and minimumdiameters were constantly and significantly lower when compared to those ob-tained with real time 3D-TEE and CT. No significant differences were found when3D-TEE and CT measurements were compared.Conclusion: Although measurements obtained by means of TEE are significantlylower than those obtained with 3D-TEE and CT, all of them are complementarytechniques with an excellent correlation. These findings could be relevant for sizedevice selection.
P1266 Availability and use of different advanced imagingmodalities for congenital heart disease in Europe. Amulticentre survey
E. Valsangiacomo Buechel1 , D. Hoesli1, W.A. Helbing2,L.U.C. Mertens3, J. Simpson4, L. Sieverding5, O. Milanesi6.
1Children’s Hospital Zurich, University Children’s Clinic, Zurich, Switzerland;2Erasmus Medical Center, Sophia Children’s Hospital, Rotterdam, Netherlands;3Hospital for Sick Children, Division of Cardiology, Toronto, Canada; 4Guy’s andSt Thomas’ NHS Trust, London, United Kingdom; 5Eberhard-Karls UniversityTubingen, Children Hospital, Department of Paediatric Cardiology, Tubingen,Germany; 6University of Padua, Department of Paediatrics, Padua, Italy
Background: During the last decade different imaging modalities have been in-troduced for the management of congenital heart disease (CHD). We wanted toassess the availability and use of these techniques in different European tertiaryreferral centres.Methods: A web-based questionnaire was sent to 153 tertiary paediatric cardi-ology centres in 30 European countries. The questionnaire asked for informationon the centre profile, the availability of the different imaging modalities and theprofessional qualifications of the interpreting physicians.Results: The questionnaire was completed by 67 centres in 20 European coun-tries. Each centre had a median of 6 cardiologists (range 2-36), 2 cardiac sur-geons (range 1-6) and performed 250 congenital operations (range 40-850).Regarding the availability of the techniques, all centres had access to cardiaccatheterization and transoesophageal echocardiography (TEE), 86% to 3D echo-cardiography (echo), 81% to tissue Doppler and strain echo, 81% to stress echo.Cardiovascular magnetic resonance (CMR) was available in 92%, computer to-mography (CT) in 88%, and nuclear scintigraphy in 73% of the centres. Cardiaccatheterisation was performed by a paediatric cardiologist alone in 76% and to-gether with an adult cardiologist in 24% of all centres. Adult cardiologists wereperforming stress echo alone in 74% and together with an adult cardiologist in19% of the centres, 3D echo and strain echo alone in 60%, and together withan adult cardiologist in 25%, and TEE alone in 74% and together with an adultcardiologist in 22%. Adult cardiologists performed alone stress echo in 38%, 3Decho and strain echo in 15% and TEE in 2% of the centres. CMR was performedtogether by a cardiologist and a radiologist in 50%, by a radiologist alone in 28%and by a cardiologist alone in 22% of the centres. CT was performed by a radiol-ogist alone in 66% and by a radiologist together with a cardiologist in 33% of thecentres.Conclusions: Most paediatric cardiology centres in Europe have access to themodern advanced imaging techniques. The examinations are often performed inmultidisciplinary teams, with involvement of adult cardiologists for advanced echotechniques and of radiologists for CT and MRI.
P1267 Measurement of cardiac output, intracardiac shuntsand valvular regurgitation using new thermodilutionapparatus
J. Endrys1, J. Stasek1, J. Bis1, J. Dusek1, M. Brtko2, P. Polansky2.1Charles University Prague, Faculty of Medicine in Hradec Kralove,
1st Department of Medicine, Hradec Kralove, Czech Republic; 2CharlesUniversity Prague, Fakulty of Medicine in Hradec Kralove, Department ofCardiosurgery, Hradec Kralove, Czech Republic
Purpose: Commercially available thermodilution apparatus for measurement ofcardiac output (CO) are not able to assess intracardiac shunts (IS). Aim of ourstudy was to develop a method and computer based instrumentation measuringall three basic flow parameters: CO, IS and regurgitation. We were not able tofind any reference about such apparatus in the literature. Apparatus: We havedeveloped a thermo-probe which is 0.035 inch in diameter which can be inserted
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

182 Coronary heart disease: imaging and intervention
through the diagnostic 5F catheter. Thermic signal is fed through the interface intocomputer which measures continuously temperature of the blood, extrapolatesthe curve, calculates flow, displays the curve and all data on screen and produceshard copies, all on line during the procedure.Measurement of L-R shunt: 2 curves are needed. Different algorithm is required inatrial septal defect and in L-R at ventricular and aorto-pulmonary level. Measure-ment in atrial septal defect: the 1 st curve (RA injection - PA sensing) measurespulmonary blood flow (PBF) in l/min. The 2nd curve (LV inj.- AO sens.) measuressystemic blood flow (SBF) in l/min. L-R is calculated as the difference: L-R = PBF- SBF. In ventricular septal defect and patent ductus arteriosus the 1st curve (RAinj. -PA sens.) measures PBF. The 2nd (LV inj. - PA sens.) measures L-R which iscalculated: L-R in l/min=A2/A1 x PBF, where A2 and A1 are areas of the 2nd and1st curve. Measurement of R-L shunt: the 1st curve (LV inj. -AO sens.) measuresSBF. The 2nd one (IVC inj. - AO sens.) measures R-L shunt which is calculatedsimilarly: R-L in l/min = A2/A1 x SBF, where A2 and A1 are areas of the 2nd and1st curve. Sensitivity: 1% of PBF or SBF respectively.Results: Altogether 771 dilution curves were recorded in 116 patients. Using ourapparatus we measured CO simultaneously with commercially available Brauninstrument (BI) in 49 patients (492 curves). Mean value was 5.02 l/min (SD 0.227),while by BI it was 4.98 l/min (SD 0.315), r=0.954. L-R shunt was assessed in 37patients and good correlation was found with oximetry:r =0.936. We measured R-L shunt in 23 patients at rest and during Valsalva ma-neuver. Aortic regurgitation was estimated in 41 patients, mitral in 39 patients andtricuspid in 30 patients. Preciseness of regurgitation measurement is limited byinadequate mixing.Conclusions: The method is fast, precise and safe using cheep indicator. It givesflow parameters in absolute values (l/min), provides unequivocal data and it isapplicable even in infants. Sensitivity of the method in shunts is about 10 timeshigher than oximetry.
P1268 Ventricular interdependence as an important factorfor right and left ventricular systolic function inpatients after repair of tetralogy of Fallot
M. Spiewak, E.K. Biernacka, J. Misko, L.A. Malek, M. Kowalski,J. Petryka, M. Zabicka, B. Milosz, P. Hoffman, W. Ruzyllo. National
Institute of Cardiology, Warsaw, Poland
Purpose: To determine relation between right ventricular (RV) and left ventricular(LV) function in patients after repair of tetralogy of Fallot (TOF).Methods: 82 patients after TOF repair who underwent cardiac magnetic reso-nance (CMR) were studied. The following parameters were measured: LV andRV end-diastolic volume (RVEDV and LVEDV), LV and RV end-systolic volume(RVESV and LVESV), RV and LV ejection fraction (RVEF and LVEF), pulmonaryregurgitation (PR) fraction (PRF) and PR volume (PRV). CMR and echo [peakRV outflow tract (RVOT) gradient] data were analyzed as predictors of RVEF andLVEF.Results: Univariate analysis revealed the following predictors for RVEF: RVEDV(β= -0.09, p<0.0001), LVEDV (β= -0.08, p=0.11), RVESV (β= -0.20, p<0.0001),LVESV (β= -0.29, p=0.0001), LVEF (β=0.81, p<0.0001). On multivariate anal-ysis following variables remained independent predictors for RVEF (RVEDVp<0.0001; RVESV p<0.0001; LVEF p=0.02). On univariate linear regressionanalysis, five factors were associated with LVEF: LVEDV (β= -0.16, p<0.0001),RVEDV (β= -0.06, p=0.0004), RVESV (β= -0.11, p<0.0001), LVESV (β= -0.40,p<0.0001), RVEF (β=0.46, p<0.0001). On multivariate analysis significant vari-ables were: LVEDV (p<0.0001) and LVESV (p<0.0001). Taking into account co-linearity between LVEDV and LVESV separate models were constructed withexclusion of LVEDV or LVESV. In both models RVEF was additional indepen-dent predictor for LVEF (p<0.0001). Comparision between patients with impairedRVEF/LVEF and normal RVEF/LVEF is presented in Table 1.
Table 1
Patients with impaired left and right Patients with normal left and right pventricular systolic function ventricular systolic function
(LVEF <50% and RVEF <35%) (LVEF ≥65% and RVEF ≥50%)(n=7) (n=8)
RVEDV (ml/m2) 192.6±64.0 120.6±30.8 0.01RVESV (ml/m2) 135.0±50.0 53.3±18.5 0.0008RVEF (%) 30.4±4.1 56.6±6.8 <0.0001LVEDV (ml/m2) 106.1±15.9 71.3±8.3 0.0001LVESV (ml/m2) 57.1±9.5 22.5 ± <0.0001LVEF (%) 46.3±2.4 68.4±2.4 <0.0001PRF (%) 22.6±16.7 21.1±16.5 0.87PRV (ml/m2) 15.1±10.6 13.9±12.8 0.84Peak RVOT gradient
(mmHg) 22.0±14.1 19.8±18.1 0.80
Conclusions: RV parameters have a significant impact on LVEF. LV parametershave a significant impact on RVEF.
P1269 New pulmonary vein Doppler echocardiographicindex predicts significant interatrial shunting insecundum atrial septal defect
Y.Y. Lam1, F. Fang2, G.W.K. Yip1, Z.A. Li2, Y. Yang2, C.M. Yu3. 1Div.of Cardiology, Prince of Wales Hospital, Chinese University of Hong
Kong, Hong Kong, China, People’s Republic of; 2Ultrasound Deptartment, BeijingAnZhen Hospital, Capital Medical University, Beijing, China, People’s Republicof; 3Institute of Vascular Medicine, Li Ka Shing Inst. of Health Sciences, ChineseUniversity of Hong kong, Hong Kong, China, People’s Republic of
Background: The relation between pulmonary venous flow (PVF) pattern anddegree of left-to-right interatrial shunting (IAS) in patients with secundum atrialseptal defect (ASD) is not known.Methods: Fifty consecutive ASD patients (14 males, 36±17 yrs) receivedtransthoracic echocardiography (TTE) before and 1 day after transcatheter clo-sure and their results were compared to 40 controls. The ratio of pulmonary-to-systemic flows (Qp/Qs) was assessed by TTE and invasive oximetry.Results: Pre-closure PV systolic (PVs), diastolic (PVd) velocities and velocity-time integral (PV-VTI) increased, time from onset of ECG Q-wave to the peakPV diastolic wave (Q-PVdi) shortened and atrial reversal (Ar) velocity significantlydecreased as compared to normals (Table 1). These findings normalized afterclosure. Patients with large IAS (defined as invasive Qp/Qs≥2) had higher PVs,PVd and PV-VTI, shorter Q-PVDi but lower Ar (all p<0.01) than those with smallIAS. Invasive Qp/Qs ratios correlated with PVs, PVd, PV-VTIi, Q-PVdi and TTE-derived Qp/Qs ratios, ASD sizes and RV end-diastolic dimensions (all p<0.05).Q-PVdi (β=-0.02), PV-VTI (β=0.47) and ASD size (β=0.41) remained independentpredictors of large IAS after multivariate analysis. The corresponding sensitivity,specificity and AUC were 88%, 80% and 0.88 respectively for a PV-VTI of 35cm(p<0.001).
Variables Group 1: Group 1: Group 2: P valuePre-closure Post-closure Controls
(n=50) (n=50) (n=40)Pre- vs. Pre- vs. Post- vs.
post normal normal
PVs velocity, m/s 0.71±0.16 0.55±0.14 0.56±0.14 <0.001 <0.001 NSPVd velocity, m/s 0.52±0.12 0.44±0.12 0.46±0.14 0.002 0.019 NSAr velocity, m/s 0.22±0.11 0.27±0.04 0.27±0.06 0.007 0.011 NSPV VTI, cm 38.3±9.2 30.6±7.6 31.2±10.0 0.001 <0.001 NSQ-PVd, ms 591±118 642±98 641±118 0.022 0.037 NS
Conclusion: ASD patients with significant IAS have distinguishable PVF features.Doppler evaluation of PV-VTI is a new additional tool for assessing the magnitudeof shunting in these patients non-invasively.
P1270 Longitudinal 2D strain is reduced in adults withsystemic right ventricle and is related tosubpulmonary ventricular function and tosymptomatic status
A. Kempny, G.-P. Diller, S.T. Orwat, G. Kaleschke, G. Kerckhoff,R. Schmidt, R. Radke, H. Baumgartner. Adult Congenital and
Valvular Heart Disease Center, University of Muenster, Muenster, Germany
Background: Transposition of the great arteries (TGA) after atrial switch opera-tion and congenitally corrected TGA (ccTGA) are frequently associated with im-paired systemic right ventricular (SRV) function which may be related to morbid-ity and mortality. Echocardiographic assessment of SRV function remains chal-lenging and the interaction between ventricles has not been studied. We investi-gated the value of myocardial deformation indices on speckle-tracking echocar-diography in assessing systemic and subpulmonary ventricular function in ptswith SVR.Methods and Results: 23 pts, 16 with TGA and atrial switch and 7 with ccTGAwere studied (m=16, age 34±11 years). 17 age matched healthy subjects servedas controls. SRV longitudinal 2D- peak systolic strain (2D-LS) was significantly re-duced in pts compared to controls (-13.4±4.4 vs. -20.9±2.6, P<0.0001) and cor-related with NYHA class in TGA pts (r=0.48, P=0.02). In contrast, subpulmonary(LV) 2D-LS was normal in 74% of patients and was not significantly different com-pared to controls (P=0.76). Systemic and subpulmonary 2D-LS correlated in TGApts (r=0.59, P=0.005) suggesting interventricular interaction (see Figure). In addi-tion, patients had evidence of diastolic dysfunction of the systemic (E’ vel. 5.6±2.6
Peak longitudinal 2D strain
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Coronary heart disease: imaging and intervention 183
vs. 8.9±3.1 cm/s pt. vs. ctrl., P=0.0007) and subpulmonary (E’ vel. 5.3±1.8 vs.8.9±3.1 cm/s pt. vs. ctrl., P<0.0001) ventricle.Conclusions: Systemic ventricular global systolic strain is significantly reducedin pts with systemic right ventricle. It is related to the functional state and subpul-monary ventricular function indicating adverse ventriculo-ventricular interaction.Global systolic strain represents an objective and reproducible measure of sys-temic RV function and should be included in outcome studies.
P1271 Transient left ventricular systolic dysfunction posttranscatheter closure of patent ductus arteriosus
K. Hengrussamee, C.H. Burana, P. Porapakkham. Chest DiseaseInstitute, Nonthaburi, Thailand
Background: Amplatzer ductal occluder device (ADOD) is the fa-vorite one using for PDA occlusion. There were some reports in children and fewreports in adults which showed deterioration of the left ventricular systolic functionpost PDA occlusion.Purpose: To assess the immediate, short and intermediate effects of amplatzeroccluder device to the left ventricular remodeling and systolic function in adults.Methods: From october 2008 to december 2009, we studied consecutively theadult patients with PDA who successfully underwent percutaneous transcatheterclosure of PDA with ADOD at Chest Disease Institute. Transthoracic Echocardio-graphy (TTE) was done before and 1 day, 3 months, 6 months and one year afterPDA occlusion. LVEF, LVEDD, LVESD, LVEDV, LVESV were recorded and ana-lyzed. Student paired t test was used to compare between the groups. At p <0.05was considered to be statistificantly significant.Results: There were 61 patients with predominant female (F: M = 5.1:1) andthe mean age of 30.81±10.93 year (range, 16-64 years). TTE revealed the meanLVEF before procedure, 1 day, 3 months, 6 months and 1 year after the procedurewere 60.7±9.2%, 49.2±16.2%, 57.4±13.6%, 58±13.6%, 60.1±13.3% respec-tively. LVEDV and LVEDD before the procedure were 133.8±54.9 ml, 55.7±14.9mm and they decreased significantly to 114.7±47.9 ml, 47.6±13.8 mm at 1 dayand 93.6±31.5 ml and 44.1±9.3 mm at 1 year respectively (p=0.04). LVESV andLVESD before the procedure were 55.8±24.9 ml, 45.2±36.9 mm. and they de-creased significantly to 36.8±18.1 ml and 29.4±7.5 mm at 1 year (p=0.02).Conclusion: Transcatheter closure of PDA in adults using ADOD had influencedon the transient deterioration of left ventricular systolic function in immediate andshort terms. This effect had full recovery within 1 year.
P1272 Detection of coronary complications after coronaryreimplantation surgery: first experience withmultislice computed tomography in children
D. Marini, C. Defilippi, P. Abbruzzese, G. Agnoletti. OspedaleInfantile Regina Margherita, Turin, Italy
Introduction: The main cause of long-term morbidity and mortality after success-ful coronary reimplantation of coronary arteries are complications at the ostialand/or proximal segments. The purpose of this study was to investigate the clini-cal usefulness of multislice computed tomographic angiography in detecting ostialand proximal coronary lesions in children having undergone coronary reimplan-tation surgery for transposition of the great arteries (TGA) and anomalous originof the left coronary artery from the pulmonary artery (ALCAPA).Methods: Twenty-four children (aged 6,4±2,2 years) having had arterial switchoperation for TGA (N=17) and direct reimplantation of the left coronary arteryfor ALCAPA (N=7) underwent systematic selective conventional and multislicecomputed tomographic angiography at a mean follow-up of 6,2±2,3 years fromsurgery. The ability of multislice computed tomography in detecting stenosis andother modifications of the coronary arteries’ course was analyzed by 2 indepen-dent investigators.Results: Multislice computed tomography, as compared with selective conven-tional coronary angiography, permitted the assessment of ostial and proximalcoronary segments in all patients (N=41 coronary arteries). It correctly identified3 (12%) patients with significant coronary lesions (N=1 proximal severe stenosisof the left coronary artery with post stenotic aneurysm, N=1 sub-occlusion andN=1 occlusion of the right coronary artery) whom had been identified by meansof conventional angiography.Conclusions: These results indicate that multislice computed tomographic an-giography is fully accurate in detecting ostial and proximal coronary arterystenoses in paediatric patients having undergone surgical reimplantation of thecoronary arteries. Our results suggest that multislice computed tomography couldbe used as a screening technique for detecting coronary complications in thefollow-up of these patients before having recourse to conventional angiography.
P1273 Application of echocardiography on perventriculardevice closure of ventricular septal defect
H. Tang, Y.U. Kang, H. Song, Q.I. An, K.E. Lin, W.J. Bai. West ChinaHospital, Sichuan University, Chengdu, China, People’s Republic of
Objective: To evaluate the clinical value of echocardiography on per-ventricular device closure of ventricular septal defect (VSD).Methods: From April 2007 to December 2008, 169 patients with VSD were di-
agnosed by transthoracic echocardiography (TTE) and underwent perventriculardevice closure of VSD. They were 81 males and 89 females aged between 6months to 48 years, 68% of which were younger than 7 years old. All patients Un-derwent transesophageal echocardiography (TEE) examination intraoperatively.TTE were used in 3 to 5 days and 3,6,12 months follow-ups.Results: According to the site of VSD shown in preoperative TTE, 169 caseswere classified as 4 subtypes: 27 cases of subarterial, 11 cases of intracristal,121 cases of perimembranous, 10 cases of muscular. Fifteen patients were notsuitable to the device closure based on intraoperative TEE re-evaluation and un-derwent surgical repair of VSD under cardiopulmonary bypass. Perventricular de-vice closure of VSD was successful in 137 case (89.0% of 154 cases). Seventeencases were failed and received surgical repair. Asymmetric occluder was used in96.0% of the subarterial and intracristal VSD (24/25); Symmetric occluder wereused in 88.2% of the perimembranous VSD (90/102). The tricuspid regurgitationin 7 cases decreased or disappeared after the surgery, while the closure causednew mild tricuspid regurgitation in 11 patients and there were 10 cases of mildresidual shunt and 3 cases of mid aortic valve regurgitation by TEE immediateevaluation. Postoperative TTE showed that no displacement of the VSD occluderin any case, residual shunt disappeared in 4 cases, mild-moderate tricuspid re-gurgitation in 1 case and improved left ventricular remodeling in all cases.Conclusion: Perventricular device closure of VSD is a safe and effective treat-ment. Echocardiography plays an important role, including the preoperative diag-nosis and screening, intraoperative real-time monitoring and postoperative short-term and long-term follow-up examination.
P1274 Residual shunt after percutaneous closure of a patentforamen ovale. Results of a 3-year follow-up study
C. Cernigliaro1, G. Cerin1, D. Benea1, B.A. Popa1, A. Popa1,A. Zito1, L. Coppo2, S. Lipari3, E. Novelli4. 1Dpt of Cardiology,Clinica San Gaudenzio, Novara, Italy; 2Clinica Neurologica
A.O.Maggiore, Novara, Italy; 3Dpt of Neuroradiology, Clinica San Gaudenzio,Novara, Italy; 4Dpt of Biostatistics, Clinica San Gaudenzio, Novara, Italy
Purpose: to assess residual shunt, adverse events, migraine disability, up to 7years after a patent foramen ovale (PFO) closure.Methods: between 2002 and 2009, 87 consecutive patients (pts) 48.2±14.7years of age (range, 17-78), 31 males (35.6%), 48 with a history of stroke (55.2%),36 with TIA (41.4%), 3 with ischemic heart disease (3.4%), 53 with refractory mi-graine and aura (60.9%), 19 migraineurs without aura (21.8%) and 15 non mi-graineurs (17.3%), underwent bubble contrast echocardiography to assess thepresence of right-to-left shunt through a PFO. Hypertension was present in 33(37.9%) patients, dyslipidemia in 27 pts (31.0%) and coagulation defects in 3 pts(3.4%). Atrial septal aneurism was present in 36 pts (41.4%). Vascular stroke ter-ritory at MRI was anterior in 24 pts (50%), posterior in 19 pts (39.6%) and in a bor-der zone in 5 pts (10.4%). Migraine severity score (frequency, duration, intensity ofthe attacks and the occurrence of aura) was assessed at baseline and at follow-up. A CARDIA PFO device was successfully implanted under transesophagealechocardiographic monitoring in all patients. Clopidogrel for one month and as-pirin for 1 year was the discharge therapy. Follow-up contrast echocardiographyand transcranial doppler at 6 months and at 1 year, office visits or telephone con-tacts were performed during the observation period (mean 3.3±1.7 years, range:0.5-7.6 years).Results: a 79 years old lady died 6 years after implantation because of heart fail-ure. At 1 year, residual shunt was present in 29 pts (33.3%). Residual shunt cor-related with adverse events: 4 pts had TIAs and 1 surgical closure for intractablemigraine in the residual shunt group vs 1 patient with TIA in the complete clo-sure group (p=0.025). Resolution of migraine occurred in 27 no shunt pts (46.6%)and in 5 pts with shunt (17.2%) (p=0.015). Mean migraine relief was 71.3% inpts with complete PFO closure and 31.9% in pts with residual shunts (p=0.002).Multivariate analysis revealed residual shunt (OR=9.4, 95%CI 0.9-98.2) and aura(OR=11.4, 95%CI 1.5-86.8) as the only independent predictors of adverse eventsafter PFO closure. There were 4 procedure complications (4.6%): esophagealperforation in 1 patient, auricular perforation in 1 patient, inferior NSTEMI in 1 pa-tient and A-V fistula in 1 patient. Minor complications were atrial arrhythmias in 2pts (2.3%).Conclusions: residual shunt after PFO closure is associated with adverse eventsand persistent migraine disability. We believe these findings deserve further test-ing in larger trials.
P1275 Real time three dimensional transesophagealechocardiography in the selection of ventricularoccluder in the device closure of ventricular septaldefect
H. Tang, B. Ren, Y.U. Kang, H. Song, Q.I. An, K.E. Lin. West ChinaHospital, Sichuan University, Chengdu, China, People’s Republic of
Purpose: The application of Real Time Three Dimensional TransesophagealEchocardiography (RT 3D TEE) in the selection of ventricular occluder in thedevice closure of ventricular septal defect (VSD).Methods: 30 cases with echocardiographic evidence for VSD underwent deviceclosure of VSD were included. Patients with pseudomembranous aneurysm andany other cardiac anomaly were excluded. All patients’ weight were above 25 kilo-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

184 Coronary heart disease: imaging and intervention
grams. Philips iE33 echocardiographic system with X7-2t matrix transducer wereused to acquire two dimension (2D) and 3D images. 3D images were acquired byfull volume mode. Philips Advanced Quantification Software QLAB 7.0 was usedin the quantitative analysis of VSD. The area and largest diameter of the VSDwere measured by 3DQA at the end of diastole and systole respectively. The di-ameter calculated by the area of VSD obtained at the end of diastole plus 1-2mmwas used on the selection of VSD occluder intraoperatively.Results: The size of VSD changed during the cardiac cycle, with the largest area(48.3±1.3 mm2) at the end of diastole and the smallest area (38.5±13.6mm2)atthe end of systole. The difference is of statistical significance (P<0.01).The shape of VSD is not regular. The largest diameters obtained by 3DQA(9.7±2.6mm)were larger than diameters obtained by 2D image (8.3±2.0mm).The difference was significant (P<0.01). There were no residual shunt or occluderdisplacement after the surgery.Conclusion: RT 3D TEE can precisely reveal VSD and provide useful informationin the selection of VSD occluder.
P1276 Diagnosis and treatment of patent foramen ovalepatency after percutaneous closure
P. Gerbaudo, C. Bailo, G. Canal, V. Gualtieri, E. Picardi, P. Suriano,D. Castagno, M. Anselmino, F. Gaita, I. Sheiban. University of Turin,S. Giovanni Battista "Molinette" Hospital, Turin, Italy
Purpose: Residual right-to-left shunt (RLS) after patent foramen ovale (PFO) per-cutaneous closure is controversial.Uncertainties remain over preferable methodof assessment (transesophageal echocardiography-TEE or transcranial doppler-TCD) and effectiveness of the implantation of a second closure device.Methods and results: From 1998 to 2008,193 patients underwent transcatheterPFO closure: 88 (46%) patients had suffered a stroke, 75 (39%) a TIA, migrainewith aura was present in 17 (9%),and other neurological events in 13 (6%). Proce-dure was successful in 192 patients (99.5%). Six months follow-up was performedin 155 (81%) patients: 10 (6.4%)underwent TEE, 70 (45%) TCD and 75 (48.4%)both exams. TEE criteria for PFO were based on finding>20 microbubbles in theleft atrium within 3 cardiac cycles after right atrium opacification. TCD was in-dicative of significant RLS if >25 microembolic signals were recorded 5-12 s aftercontrast injection.Complete closure was demonstrate in 100 cases (64.5%), while55 (35.5%) proved residual patency. Patients with residual shunt were youngerthan patients without residual shunt (48.6±13.6 vs 54±12.5, p=0.05), more oftenhad an associated atrial septal aneurysm (47.2% vs 22%, p=0.001) and morefrequently had implanted a device ≥30 mm in diameter (51% vs 27%, p=0.005).Sensitivity and negative predictive value of TCD, assuming TEE as the gold stan-dard, were 100%, specificity was 60.9%, positive predictive value was 30.5% anddiagnostic accuracy was 66.6% (Table). Second closure device implantation wasperformed in 29 patients: in 12 (41%) it was not possible to cross the septumwhile the procedure was successful in 17 (59%) patients. Amongst the latter the6 months TCD follow-up resulted negative for residual RLS in 7 (41%) cases.
ETE Total
Positive Negative
DTC Positive 11 25 36Negative 0 39 39Total 11 64 75
Conclusions: RLS after percutaneous PFO closure is common and easily de-tectable with TCD that is a sensitive test. Second closure device implantation forresidual RLS should be performed in selected cases keeping in mind that it couldbe unfeasible because of the impossibility to successfully cross the interatrial sep-tum.
P1277 Cardiac arrhythmias in ASD patients is related topotassium level but not to ASD size and shunt volume
M. Pieculewicz, T. Przewlocki, P. Wilkolek, L. Tomkiewicz-Pajak,M. Hlawaty, B. Sobien, H. Dziedzic, P. Podolec. JagiellonianUniversity Medical College - John Paul II Hospital - Department of
Cardiac & Vasculare, Krakow, Poland
Hypokalaemia is a common electrolyte abnormality in clinical practice and com-mon cause of arrhythmias. The hight prevelance of arrhytmias is reported in pa-tients with atrial septal defect. We studied the prevalence of hypokalaemia in alarge population of pts with atrial septal defect (ASD) and its relation to arrhyt-mias.Methods: Data on 420 ASD pts (age 42.4±13.0 years, 297 F) who attended ourcentre for the echocardiographic study (TEE) between 2000 and 2009 and hadplasma potassium concentration measured were analysed. Hypokalaemia wasdefined as potassium concentration <3.5. Echocardiographic study and Holtermonitoring was performed on all the pts. A group of 200 healthy volunteers(normal echocardiographic study, normal EKG), (age 42.8±12.1 years, 140 F)),matched for age and gender served as controls. All patients were pharmacologi-cally untreated.Results: The ASD diameter ranged from 6 to 40 mm (26.9±7.8 mm), the shuntvolume (Qp:Qs) ranged from 1.1 to 3.1 mm (1.57±0.9 mm),.Mean potassium concentration in pts with ASD was 3.9±2.4 mEq/L and was sig-
nificantly lower than in the healthy volunteers (4.5±1.9 mEq/L; p<0.0001). Theoverall prevalence of hypokalaemia in ASD group was 25% (n=105) and was sig-nificantly higher than in the healthy volunteers (10%; n= 20, p<0.0001).In Holter monitoring in ASD pts with hypokalaemia there was significantly biggernumber of supraventricular premature beats/24 (p<0.05) as well as number ofepisode of the paroxysmal atrial fibrillation (p<0.001) and supraventricular tachy-cardia (p<0.05) in compare to ASD pts with normal potassium level.There was a significant correlation between number of supraventricular beats/24in Holter and plasma potassium level (p<0,0001 r =90923) as well as numberof episode of the paroxysmal atrial fibrillation in 24-hours monitoring and plasmapotassium level (p<0,0001 r =84525). There was no correlation between numberof supraventricular beats/24 and ASD size and shunt volume.In multivariable analyzes (including 12 clinical and echocardiographic factors)only hipokalaemia was independent risk factors for arrhytmias occurrence (OR4.23 (1.11-4.19), p<0.05).Conclusions: 1. Hypokalaemia affects one in four ASD patients and carries ahigher risk of arrhytmias. 2. The presence of arrhythmias does not depend onASD size and shunt volume but on the potassium level. 3. The screening for hy-pokalaemia is a cheap and simple, but powerful means of risk stratification ofarrhytmias in patients with ASD. Potassium supplementation should be consid-ered in the prevention of arrhythmias in ASD patients who are pharmacologicallyuntreated.
P1278 Assessment of the mitral valve annulus by 3Dechocardiography in children
C. Cardin, B. Arnaudis, S. Hascoet, R. Amadieu, P.E. Seguela,Y. Dulac, B. Leobon, P. Acar. University Hospital of Toulouse -Children’s Hospital, Toulouse, France
Background: Mitral valve repair in children remains a challenge because of thegrowth of the heart. Size of the annulus is crucial in planning optimal surgicaltreatment. Recent advances in real-time 3D echocardiography and 3D computersoftware have made it easier to determine the geometries of non-visualized car-diac structures, such as the mitral valve annulus. However none pediatric studywas reported.Aim: To evaluate the feasibility of 3D echocardiography to measure the size ofthe mitral valve annulus in children.Methods: Eighty pediatric patients (median age 10 years, range 1 day-14 years)with normal cardiac anatomy and function were included. The mean body surfacearea was 1.1 m2 (range from 0.2 to 1.57). 3D transthoracic echocardiographywas performed with the X4-2 or X7-2 matrix probe (ie33, Philips Medical Sys-tems, Andover, MA). The mitral valve volume sweeps were acquired either fromparasternal or apical views. The volumes were analysed with the dedicated anal-ysis softwares (Q Lab 6.0). Surface of the mitral valve annulus was traced andindexed to the body surface area.Results: Feasibility for surface measurements of the mitral valve annulus by 3Dechocardiography was 80% (64/80 patients). Artefacts due to infant mention oc-curred in 10 patients and insufficient resolution in 6 patients. The mean time foracquisition and surface measurement by 3D echocardiography was respectively3 and 2 minutes (total 5 minutes per patient). The surface of the mitral valve an-nulus was related to the age (r=0.3, p<0.001) and the body surface area (r=0.5,p<0.0001). The surface of the mitral valve annulus measured by 3D echocardio-graphy indexed to the body surface aera was 4.94±0.32 cm2/m2. These resultswere comparable to those found in normal adult patient.Conclusion: 3D echocardiography using dedicated software is a feasible and ad-equate method for measurement of the mitral valve annulus in a normal pediatricpopulation. Further studies are needed to validate the accuracy of such methodin patients with congenital mitral regurgitation previously to surgical repair.
P1279 First in vivo experiences with minimally invasivelyimplanted autologous tissue engineered heart valvesbased on sandwich-structured scaffolds andminimally invasively harvested autologous stem cells
D. Schmidt1, C. Mariani2, A. Puolakka2, M. Rissanen2,T. Deichmann3, B. Odermatt4, S.P. Hoerstrup5. 1Department of Cardiology andRegenerative Medicine Program, University Hospital Zurich, Zurich, Switzerland;2Department of Materials Science, Tampere University of Technology, Tampere,Finland; 3Institute for Textile Techniques, RWTH Aachen University, Aachen,Germany; 4Institute of Clinical Pathology, University Hospital Zurich, Zurich,Switzerland; 5Regenerative Medicine Program and Department of SurgicalResearch, University Zurich, Zurich, Switzerland
Purpose: Today’s valve substitutes for minimally invasive implantation are bio-prosthetic suggesting their clinical application primarily in elderly people. A heartvalve tissue engineering concept comprising both the fabrication of the living re-placement from minimally invasively accessible autologous stem cells and a per-cutaneous delivery would overcome these limitations. Here, first experiences withautologous living tissue engineered heart valves based on sandwich-structuredbiodegradable scaffolds and adult stem cells implanted by minimally invasive pro-cedures in an ovine model are presented.Methods: Heart valve scaffolds (n=12) were fabricated from biodegradableP(L,DL)LA-meshes, coated with electrospun nanofibers and integrated in self-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Coronary heart disease: imaging and intervention 185
expanding nitinol stents. Scaffolds were seeded with either autologous stem cells(bone marrow and peripherial blood; n=4) or vascular cells (n=8) and cultured inbioreactors for 6d. Afterwards, constructs (n=6) were implanted as pulmonaryvalve replacements using a minimally invasive approach or analysed directly.In-vivo performance was assed by echocardiography up to 4 weeks. Tissue-analyses comprised histology, biochemistry (extracellular matrix production, cellamount) and tensile tests.Results: Engineered heart valves were successfully minimally invasively im-planted and demonstrated in-vivo functionality. Histology revealed layered neo-tissues including endothelialized surfaces without endogenous inflammatory re-action. The amount of collagen and glycosaminoglycans was higher in stemcell-based than in vascular-based tissues. Cell numbers were comparable in allvalves. Mechanical profiles demonstrated physiological tissue strength but lesselasticity independent of the cell source.Conclusions: These results demonstrate that heart valve tissue engineering us-ing a minimally invasive technique for both adult stem cell harvest and valve im-plantation is feasible. Thus, this new technology may enable minimally invasivetreatment of heart valve diseases also in younger patients.
P1280 Quantitative assessment of pulmonary regurgitationin patients with and without right ventricular tractobstruction
M. Spiewak, L.A. Malek, J. Misko, E.K. Biernacka, J. Petryka,M. Kowalski, B. Milosz, M. Zabicka, P. Hoffman, W. Ruzyllo. National
Institute of Cardiology, Warsaw, Poland
Purpose: There are concerns whether there is a difference in clinical utilityof pulmonary regurgitation (PR) fraction (PRF) and PR volume (PRV) in sub-groups of patients with predominant PR [after exclusion of patients with significantright ventricular outflow tract obstruction (RVOTO)] and individuals with combinedPR+RVOTO. The aim of the study was to compare PRF and PRV in patients withor without RVOTO.Methods: 90 consecutive patients after repair of tetralogy of Fallot (TOF), whounderwent cardiac magnetic resonance (CMR) and echocardiography were stud-ied. Significant RVOTO was defined as peak RVOT gradient ≥30 mmHg.Results: 8 patients were excluded due to poor image quality or incompleteCMR/echo data set. The final analysis comprised 82 patients. A strong corre-lation was seen between PRF and PRV both in patients with and without RVOTO[r=0.93, p<0.0001 and r=0.92, p<0.0001, respectively]. In both subgroups highvariability of PRF was found in subjects with similar degree of PRV [Figure 1;patients with similar values of parameters of PR are marked with circles orsquares (for patients without RVOTO) and with triangles and stars (for patientswith RVOTO)]. There was no difference in PRF between patients with moderateand severe RV dilatation (32±13% vs. 37±12%; p=0.18). On the other hand, sig-nificant difference in PRF was observed between these groups (23±10 ml/m2 vs.31±12 ml/m2, respectively; p=0.02). PRV had better ability than PRF in identifi-cation of severe RV dilatation, both in group with RVOTO [area under the curve(AUC) 0.82 vs. 0.72, p=0.005] and in patients without RVOTO (AUC 0.83 vs. 0.77,p=0.04).
Figure 1
Conclusions: PRV shows better ability than PRF in evaluating influence of PR onRV in patients after TOF repair, both in population with and without concomitantRVOTO.
P1281 Percutaneous balloon mitral valvuloplasty in severemitral stenosis during pregnancy comparing inoueversus multi-track balloons. Comparative studybetween Inoue and multitrack balloon mitralvalvuloplasty in pregnant females with severe mitralstenosis
Y. Sadek, R. Abuallata. National Heart Institute, Cairo, Egypt
Objectives: We sought to compare the maternal and fetal outcomes of patientswith severe mitral stenosis submitted to percutaneous balloon dilation using inoueversus Multi-track balloons during pregnancy.Background: Heart failure in patients with mitral stenosis complicating preg-nancy is a common problem in developing countries. Since 1982, percutaneousdilation of the mitral valve using a balloon catheter has become a therapeutic al-
ternative to open or closed heart surgery. Although the efficacy of percutaneousmitral valve balloon dilation is well established with inoue balloon, its comparisonwith Multi-track balloon during pregnancy is needed.Methods: We compared the clinical and obstetric outcomes in 188 women whowere treated with percutaneous mitral valve balloon dilation Multi-track (groupI, 80 patients) or inoue balloon (group II, 108 patients) for heart failure (NIHAclassII,III,and IV) due to mitral stenosis during pregnancy.Results: In our study, percutaneous balloon dilation of the mitral valve had a suc-cess rate of 99.1% as regard safely completed procedure and a rate of 94.4%for group I and 92.9% for group II as demonstrated by the final mitral valve areaachieved. This improvement was followed by a marked decrease in the mitralvalve gradient, left atrial pressure and pulmonary artery pressure and increase ofmitral valve area by planimetry. Patients in both groups had similar improvementsin symptoms. Patients who underwent percutaneous balloon dilation had no sig-nificant difference fetal complications, with no maternal mortality (2 fetal death ingroup I vs. 1 deaths in group II, p >0.05).Conclusions: Percutaneous balloon mitral valvuloplasty is safe and effective andappears to appropriate using either inoue or Multi-track balloons during preg-nancy.
P1282 Results of radiofrequency ablation of paroxysmaljunctional tachycardias in children and teenagerscompared to an adult population
B. Brembilla-Perrot, P.Y. Zinzius, R. Martins Pedro, S. Jarmouni,L. Muresan, D. Beurrier, J. Schwartz, J.L. Cloez, A. Moulin Zinsch,
F. Marcon. University Hospital of Nancy - Hospital Brabois, Vandoeuvre lesNancy, France
Supraventricular tachycardia (SVT) radiofrequency (RF) ablation is a currentmethod of treatment, but the catheterism-risks and the radiation are factors re-stricting the indications in children and teenagers. The purpose of the study wasto evaluate the clinical and electrophysiological factors of indications of SVT abla-tion in the youth and the results of the procedure compared to an adult population.Methods: Electrophysiological study (EPS) was performed in 1078 patients agedfrom 5 to 97 years, with a normal ECG in sinus rhythm but complaining of SVT;78 of them were children and teenagers aged from 5 to 20 years (16±3). SVTablation was discussed in symptomatic patients or in the case of sport activity.The clinical and electrophysiological factors of the indications of ablation and theresults of ablation were analysed.Results: AP ablation was indicated in 31 children (44%) (group I), for recurrentSVT’s in 28 of them and only sport competition in 3 children; the incidence waslower than in 1000 adults aged from 21 to 97 years where ablation was per-formed in 641 patients (64%) (p <0.0000); ablation was not indicated in 47 chil-dren (group II). Group I patients had the same age as group II (16±3 years).Male gender was as frequent in group I (42%) as II (49%). The mechanism ofSVT differed: AV re-entrant tachycardia (AVRT) through a concealed accessorypathway (AP) was more frequent in group I (13/31) than in group II (8/47) (p<
0.01). Opposite differences were noted in adults: AVRT were less frequent indi-cations of ablations (88/641 (14%) vs 79/359 (22%), p <0.000). Typical or atypicalAV node re-entrant tachycardias (AVNRT) were remaining indications of ablationless frequent in children (18/31 vs 39/47) and more frequent in adults (553/641 vs280/359). Failures or recurrences of SVT after ablation, requiring a second pro-cedure, were more frequent in children and teenagers (8/31; 26%) than in adults(56/641; 9%) (p<0.0001). Complications-related ablation were similar and notedin one group I young population (3%) and 10 adults (1.5%) (NS). Group II chil-dren and teenagers are asymptomatic with antiarrhythmic drugs (n=25) or withouttreatment (n=22). In conclusion, the indications of SVT ablation in the youth arerarer than in adults, because most of them are well with or without drugs. The in-dications are more frequent in SVT related to an AVRT in the youth than in adults.Failures of ablation are more frequent in the youth than in adults, but complica-tions remain rare. It is generally reasonable to wait the adult age for the indicationsof SVT ablations.
P1283 Indications and results of radiofrequency ablation ofaccessory pathway in the young population
B. Brembilla-Perrot, D. Beurrier, P.Y. Zinzius, L. Muresan,J. Schwartz, R. Martins Pedro, S. Jarmouni, C. Oliver-Kazmierczak,C. De Chillou, O. Marcon. University Hospital of Nancy - Hospital
Brabois, Vandoeuvre les Nancy, France
Radiofrequency (RF) ablation of accessory pathway (AP) is widely used, but theindications remain discussed in children and teenagers. The purpose of the studywas to evaluate the clinical and electrophysiological factors of indications of APablation in the youth and the results of the procedure.Methods: Electrophysiological study (EPS) was performed in 139 patients agedfrom 5 to 18 years (13.5±3) with a preexcitation syndrome, for tachycardia (n=51),syncope (n=20), rapid atrial fibrillation (AF) or antidromic tachycardia (ATD) (n=8),or they were asymptomatic (n=60).Results: AP ablation was indicated in 61 children (44%), several years after initialEPS for some of them (group I) and was not indicated in 78 children (group II).Group I was older than group II (15±2 vs 13±4) (p<0.001). Male gender was asfrequent in group I (52%) as in group II (56%); congenital HD tended to be rarer in
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

186 Coronary heart disease: imaging and intervention / Congenital heart disease
group I (6.5%) than in group II (17%) (0.07). Group I was less frequently asymp-tomatic (27%) than group II (73%) (p< 0.001), but symptoms of AVRT or syn-cope did not differ between groups I and II; ablation was performed in all childrenwith spontaneous malignant form. At EPS, group I had a more rapid conductionthrough AP than group II, in control state (207±70 b/min vs 178±51) (< 0.005),but not after isoproterenol (236±74 vs 232±62). AVRT and AF/ATD induction,malignant forms were more frequent in group I (70.5%, 33%, 26%) than in groupII (37.5%, 13%, 6%) (p< 0.001). 5 childrens or teenagers had ablation only for ashort AP refractory period (RP). Failures or reappearances of WPW after abla-tion were frequent (38%), requiring a 2nd procedure in 18 of 23 children and wererelated to the age (15±3 years for the failures vs 17±4; p < 0.05). In 4 AP an-teroseptal locations, ablation was not performed. In group II, one teenager (18 yold) with untreated AVRT died before ablation. Asymptomatic children without ma-lignant form at EPS, are well with disappearance of prexcitation in 2. Symptomaticchildren are well with flecaïnide and beta blockers. In conclusion, indications ofAP ablation in the youth are generally based on recommended data, but there isa high risk of failure or reappearance. If, spontaneous or at EPS malignant formsare absolute indications, it is recommended to indicate ablation in only still symp-tomatic children with antiarrhythmic drugs or for sport competition and to wait theadolescence in other children.
CONGENITAL HEART DISEASE
P1284 Prognostication in adults congenital heart disease:comparative importance and additive value ofexercise parameters
R. Inuzuka, G.P. Diller, F. Borgia, R. Alonso-Gonzalez, E. Tay,M. Silva, K. Dimopoulos, M.A. Gatzoulis. Royal Brompton Hospital,
London, United Kingdom
Purpose: Cardiopulmonary exercise testing (CPET) is used as a prognosticmarker in adults with congenital heart disease (ACHD). We previously reportedthe predictive value of peak VO2, heart rate reserve (HRR) and VE/VCO2 slopein ACHD. We sought to determine how exercise parameters should be used incombination to best predict outcome.Methods: We analysed retrospectively CPET performed on 1375 consecutiveACHD patients between 1999 and 2008. Heart rate reserve was calculated as thedifference between peak and resting heart rates. Cox proportional hazards analy-sis was used to assess the association between exercise variables and mortality.Results: Median age was 31 years and 47% were female. Cyanosis during ex-ercise was present in 19% patients. 84% of patients without cyanosis reachedanaerobic threshold (AT), versus 71% in the cyanotic population. During a me-dian follow-up of 4.8 years, 98 died. On multivariate analysis, HRR was the onlyindependent predictor of death in cyanotic patients (HR 0.83 per 10 bpm increase,CI: 0.72-0.95). In non-cyanotic patients who did not achieve AT, VE/VCO2 slopewas the only independent predictor (HR 1.52 per 10-unit increase, CI:1.13-2.00),whereas in those who achieved AT, HRR and peak VO2 (% of predicted) wereindependent predictors (HR 0.80 per 10 bpm increase, CI: 0.70-0.90 and HR0.75 per 10%, CI: 0.63-0.90, respectively). Patients with both HRR and peak VO2within the lowest quartile (<67 bpm and <58% of predicted, respectively) had theworst survival.
Figure 1. Combination of heart rate reserve (HRR) and peak VO2 in predicting survival.
Conclusions: Prognostication using parameters derived from CPET should beapproached differently according to the type of cardiac defect (cyanotic versusnon) and the achieved exercise level, using a combination of peak VO2, HRR andVE/VCO2 slope.
P1285 Exercise performance and quality of life is moreimpaired in patients with Eisenmenger Syndromethan in those with complex cyanotic congenital heartdisease with pulmonary stenosis
J. Mueller, J. Hess, A. Hager. German Heart Center, Clinic at theTechnical University of Munich, Munich, Germany
Objective: Patients with cyanotic congenital heart disease without correctivesurgery or Fontan palliation survive into adulthood if they have a balanced pul-monary blood flow. This is facilitated by moderate pulmonary stenosis or Eisen-menger syndrome. Both groups show cyanosis, diminished exercise capacity, re-duced ventilatory efficiency and impaired quality of life. This study aimed to com-pare the functional outcome of those two cohorts directly.Patients and methods: In total fifty-eight cyanotic patients with cardiac shunts(28 male, 30 female, aged 14-55 years) were investigated, twenty-three of themwith haemodynamically relevant pulmonary stenosis (PS) and thirty-five of themwith Eisenmenger syndrome (ES). They filled in the health related quality of lifequestionnaire SF-36 and performed a symptom limited cardiopulmonary exercisetest.Results: At exercise, oxygen saturation decreased severely and similarly in bothgroups (PS: 90% to 65% vs. ES: 87% to 64%). Moreover, hemoglobin levelswere comparable in both subgroups. Exercise capacity was markedly reduced,but more diminished in ES (PS: 20.3 (11.9-24.6) ml/min/kg vs. ES: 11.3 (9.7-14.5) ml/min/kg; p<0.001) and ventilatory inefficiency, expressed as VE/VCO2slope, was more enhanced in ES (PS: 45.7 (37.6-52.9) vs. ES: 54.6 (43.4-68.7); p=0.005). Oxygen saturation at rest was correlated to peak VO2 (r=0.436;p=0.001) and VE/VCO2 slope (r=-0.388; p=0.003).Self estimated quality of life was poor in both groups, but worse results in physicaland psychosocial domains in the ES group.Conclusions: Despite similar cyanosis, patients with Eisenmenger syndromeshow less exercise performance, more ventilation-perfusion-mismatch and aworse quality of life compared to complex cyanotic congenital heart disease pa-tients with pulmonary stenosis. Moreover, oxygen saturation at rest seems to pre-dict exercise capacity and ventilatory efficiency in this cohort, but not quality oflife.
P1286 Screening for heart defects in adult patients withdown syndrome is indicated
J.C. Vis1, H.A.C.M. De Bruin-Bon1, B.J. Bouma1, S.A. Huisman2,L. Imschoot3, K. Van Den Brink4, B.J.M. Mulder1. 1AcademicMedical Center, Amsterdam, Netherlands; 2Prinsenstichting,
residential centre for people with intellectual disabilities, Purmerend,Netherlands; 3ASVZ, residential centre for people with intellectual disabilities,Sliedrecht, Netherlands; 4‘s Heeren Loo, residential centre for people withintellectual disabilities, Monster, Netherlands
Purpose: Congenital heart defects (CHD) are common in patients with Downsyndrome. However, adults with Down syndrome who live in residential centreshave not always been screened for CHD in the past. Aim of this study was toinvestigate the prevalence of unknown CHD in adult patients with Down syndromewho live in residential centres and to determine whether cardiac screening shouldbe recommended.Methods: Between January 2007 and November 2009, residential centres na-tionwide were sampled randomly to participate in a two-stage investigation. First,medical files of all patients with Down syndrome were investigated to retrieve doc-umented information on known CHD and then an echocardiogram was performedin those patients with unknown cardiac status.Results: Thirty-one centres with in total 1158 adult patients were included inthe first stage of the study. Overall prevalence of known CHD was 16% (189defects). Echocardiac screening was performed in 138 patients without knownCHD from seven centres. In total, 24 new patients (17%) with a CHD were foundof which six patients needed semi-urgent care. Furthermore, 77% of the screenedpatients had mild to moderate regurgitation in one or more heart valves. Overallprevalence of CHD in Down syndrome patients living in residential centres wouldbe estimated at 33%.Conclusions: Seventeen percent of patients with Down syndrome, living in resi-dential centres had an undiagnosed CHD and valvular regurgitation was presentin the majority of patients. Cardiac screening is recommended in the populationof older Down syndrome patients. New therapeutical options are available for pre-vention of cardiac complications at older age.
P1287 The importance of pulmonary artery pressures andage at repair on late atrial arrhythmia in transcatheterand surgically closed ASD type secundum
A. Van De Bruaene1, M. Delcroix1, A. Pasquet1, J. De Backer2,B. Paelinck3, M. Morissens4, W. Budts1. 1Catholic University of
Leuven, Leuven, Belgium; 2Ghent University, Ghent, Belgium; 3University ofAntwerp, Antwerp, Belgium; 4University Hospital Brugmann, Brussels, Belgium
Aims: Atrial fibrillation and flutter remain an important cause of morbidity in adultswith atrial septal defect (ASD). This study aimed to investigate predictors for late(≥1 month after repair) atrial arrhythmia.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Congenital heart disease 187
Methods: Patients with ASD type secundum, older than 18 years, were selectedthrough the databases of three medical centres in Belgium and were stratifiedinto a surgical and transcatheter treated group. Preprocedural, periproceduraland follow-up data were extracted. Analyzed variables were entered into univari-ate and multivariate Cox regression analysis. Receiver-operating characteristic(ROC) analysis was performed for any independent predictor of late atrial ar-rhythmia.Results: A total of 296 patients (87 men, 209 women) was included. One hun-dred and fourteen patients (median age 25.8 years, range 18.5–79.4 years) un-derwent surgical and 167 (median age 57.4 years, range 18.4–88.1 years) un-derwent transcatheter ASD closure. Only age at repair predicted late atrial ar-rhythmia in surgically treated patients (HR 1.07; 95% CI, 1.02–1.12; P=0.009).However, only mean pulmonary artery pressure (mPAP) independently predictedlate atrial arrhythmia in percutaneously treated patients (HR 1.09; 95% CI, 1.00–1.20; P=0.049). According to ROC analysis, mPAP ≥22.5 mmHg had a sensitivityof 80% and specificity of 81.7% for predicting late atrial arrhythmia (AUC 0.835;95% CI, 0.726–0.944; P<0.0001).Conclusion: Age at repair was the main predictor of late atrial arrhythmia in sur-gically closed ASD patients. However, only mPAP independently predicted lateatrial arrhythmia after transcatheter ASD closure. A mPAP ≥22.5 mmHg pre-dicted late atrial atrial with a sensitivity and specificity of 80% and 81.7% andshould raise increased awareness for atrial arrhythmias and may be used to guidetherapy.
P1288 Long-term prognosis of Kawasaki disease with giantcoronary aneurysms
K. Suda1, M. Iemura1, M. Miura2, S. Ogawa3, M. Ayusawa4,T. Higaki5, Y. Nomura6, M. Matsumura7, T. Matsuishi1. 1KurumeUniversity School of Medicine, Kurume, Japan; 2Kiyose Children’s
Hospital, Kiyose, Japan; 3Nippon Medical School, Tokyo, Japan; 4NihonUniversity, Tokyo, Japan; 5Ehime University, Toon, Japan; 6Kagoshima University,Kagoshima, Japan; 7Tenri Hospital, Tenri, Japan
Background: Still certain number of patients with Kawasaki disease (KD) devel-ops giant coronary aneurysms and coronary stenosis, leading to ischemic heartdisease. The aim of this study was to determine long-term prognosis of KD withgiant aneurysms in large sample volume.Methods: Questionnaires were sent to 6 participating institutions and 170 pa-tients (126 male and 44 female) were identified as the subject of this study whodeveloped giant coronary aneurysms with >8 mm in diameter. From medicalchart, patients’ information concerning demographics such as coronary pathol-ogy (isolated RCA, isolated LCA, and bilateral aneurysm) and medical treat-ment (with warfarin or without warfarin) and catheter and surgical interventionswere collected. Based on these data, we calculated survival rate, cardiac eventfree rate (CEFR), and acute thrombotic event free rate (ATEFR) using Kaplan-Meyer’s analysis. Cardiac events included catheter (PCI) and surgical intervention(CABG) and acute myocardial infarction (AMI). Acute thrombotic events includedAMI and intra coronary thrombolysis (ICT).Results: Subject’s age was 2.9±2.8 years old at the onset of KD and medianobservational period was 13.4 years (range 0-31.2 years). In this period, 11 pa-tients died or underwent cardiac transplantation, giving 96.9, 96.2, and 89.8%of survival rate at 5, 10, and 20 years, respectively. Of 170,78 (45.9%) patientsencountered giving CEFR of 73.5, 63.9, and 39.7% at 5, 10,and 20 years, respec-tively. Concerning coronary pathology, patients with bilateral coronary aneurysmsshowed significantly lower CEFR than those with isolated RCA and LCA lesion(Bilateral vs. LCA and RCA = 65 vs. 80 and 88 at 5 years, 56 vs. 66 and 81% at 10years, 25 vs. 50 and 70% at 20 years, p<0.0001). Patients with warfarin treatment(n=77) showed significantly higher ATEFR than patients without warfarin (n=93)(90 vs. 76% at5 year, 90 vs. 73% at 10 years, 82 vs. 71% at 15 years, p<0.05).Conclusions: Long-term survival of KD with giant coronary aneurysmsis accept-able up to 20 years with various types of catheter and surgical interventions. Pa-tients with bilateral coronary lesion encountered more cardiac events and warfarintreatment can decrease acute coronary thrombosis.
P1289 Cardiac features of Kawasaki disease in France:a single-center esperience
J.C. Lega1, A. Bozio2, F. Sassolas2, C. Ducreux2, S. Di Filippo2.1University Hospital of Lyon- Hospital Lyon Sud, Lyon, France;2University Hospital of Lyon - Hospital Louis Pradel, Lyon, France
Little is known about Kawasaki Disease (KD) features in France. The aims of thisretrospective single-center study were to assess the characteristics of a FrenchKD population over a long period of time, and to describe cardiac lesions.Methods: We retrospectively reviewed the medical records of 417 patients re-ferred to echocardiography for KD suspicion between August 1983 and April2007.Results: 210 patients met criteria for diagnosis of KD, at the age of 2.7±2.5years(median 2). Fever was present in all patients. Time to diagnosis was 7±4.6days(median 6days), time to hospitalization 5.7±4.3days (median 5days). Time to firstechocardiography was 11.4±7.8days (median 9days), shorter in more recent pe-riod. Median time to intravenous immunoglobulin administration was 8 days (1to 39). At initial evaluation, 63.8% were free from cardiac lesions, 23.8% (52
cases) had coronary lesions (aneurisms: 25, dilatation: 27) and 12.4% had "hy-perechogen" coronary arteries. Among 52 cases with abnormal coronary arteries,40 were <5mm in diameter, 9 were 5-8mm, and 3 were >8mm (giant aneurisms):one third localized on one coronary vessel, one third on 2 and one third one all 3coronary arteries. Echographic pericarditis was found in 31 patients, mitral insuffi-ciency in 20 and aortic insufficiency in 2. All patients recovered, except 1 who diedfrom cardiogenic shock due to ruptured chordae. Coronary lesions resolved in 17of 52 cases (32.6%) and persisted in 35 (67.4%, i.e. 16.7% of all patients): 14with aneurisms and 19 with dilatations. No patient developped significant long-term coronary artery stenosis. The incidence of aneurisms was lower over thepast decade (7.2%).Conclusion: In our experience, the occurrence of coronary lesions in KD havelessened over time and long-term cardiac outcome is favourable despite persis-tent coronary lesions.
P1290 Prevalence and spectrum of coronary anomalies inpatients with an isolated congenital left ventricularaneurysm or diverticulum
M.-A.G. Ohlow, J.T. Fuhrmann, B. Lauer. Central Hospital BadBerka, Department of Cardiology, Bad Berka, Germany
Aims: Congenital left ventricular aneurysm (LVA) and diverticulum (LVD) are rarecardiac anomalies and frequently associated with other cardiac anomalies. Wesought to investigate the prevalence and the spectrum of coronary anomalies(CA) in such patients.Methods: We assessed 117 patients with LVA or LVD for the prevalence of coro-nary anomalies and compared the findings to a historical control group (n=1950)without the diagnosis of LV or LVD.Results: 68 of the 117 patients (58.1%) had abnormal CA anatomy. Mean agewas 64 years. 45 (38.5%) were male. Abnormal CA was more prevalent in pa-tients with LVA or LVD compared to control (58.1% versus 5.6%; p<0.001), femalepatients (31% versus 16%; p=0.03), and non-apical location of LVA or LVD (35%versus 65%; p=0.002), whereas age and type (LVA versus LVD) had no influence(41% versus 59%; p=0.4, and 46% versus 54%; p=0.4, respectively). No patientsof our series had a so called "major CA" (ALCA (especially the interarterial type),ARCA, and ALPACA.
Table 1. Prevalence of coronary abnormal
Anomaly LVA/LVD group Control group p117 ptn (%) 1950 ptn (%)
Coronary anomalies (total) 68 (58.1) 110 (5.64) <0.001Split RCA 28 (24) 24 (1.23) <0.001Ectopic RCA (right cusp) 14 (12) 22 (1.13) <0.001Ectopic RCA (left cusp) 1 (0.9) 18 (0.92) 0.9Fistulas 9 (7.7) 17 (0.87) <0.001Absent left main coronary artery 4 (3.4) 13 (0.67) 0.002Circumflex arising from the right cusp 2 (1.8) 13 (0.67) 0.2LCA arising from the right cusp 0 3 (0.15) 0.7Low origination of RCA 3 (2.7) 2 (0.1) <0.001Other anomalies 7 (6) 3 (0.27) <0.001Coronary dominance patternsDominant RCA 97 (82.9) 1641 (89.1) 0.9Dominant LCA 9 (7.7) 164 (8.4) 0.8Codominant arteries 11 (9.4) 48 (2.5) 0.08
Conclusions: This large single center study suggests that the prevalence of ab-normal CA in patients with isolated LVA or LVD is as high as 58.1%. However, thespectrum of the CA is similar to patients without LVA or LVD and we did not findmajor CA with potential lethal consequences.
P1291 Congenital heart defects in live-born children inSardinia (0-365 days): an epidemiologic retrospectivestudy from 2001 to 2007
R. Tumbarello1 , P. Bassareo2, M.C. Tavera1 , P. Neroni1, C. Follese1,S. Montis1, G. Mercuro2. 1G. Brotzu Hospital, Cagliari, Italy;
2University of Cagliari, Cagliari, Italy
Background: Congenital heart disease (CHD) is the most prevalent group of con-genital anomalies. There is considerable variation in the reported epidemiology ofCHD in the world, mainly attributable to methodological differences. Using med-ical records, the current study describes the epidemiology at birth (incidence,treatment modalities and short-term survival) of CHD in a geographically well-defined population of the South of Italy.Methods: We undertook a retrospective review of medical records of all new-borns (0-365 days) who were born in 2001-2007 and were diagnosed, treatedand/or followed-up in Sardinia, a great island in the Italian sea (population:1,680,000; area: 24,090 Km2).Results: In 93,147 births, 1877 newborns with CHD were detected, yielding abirth incidence of 20.2 per 1000, with an increasing trend in the last years. Themost frequently occurring conditions were ventricular septal defects (VSD: 31%),ostium secundum atrial septal defects (29.4%) and persistent ductus arteriosus(13.4%). The severe CHD were 4.7 per 1000. Thirty-nine percent of the childreneither had a cardiosurgical operation or catheter intervention. In this study, 4.4%of the newborns died during the first year of life. The actuarial survival at 6 months
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
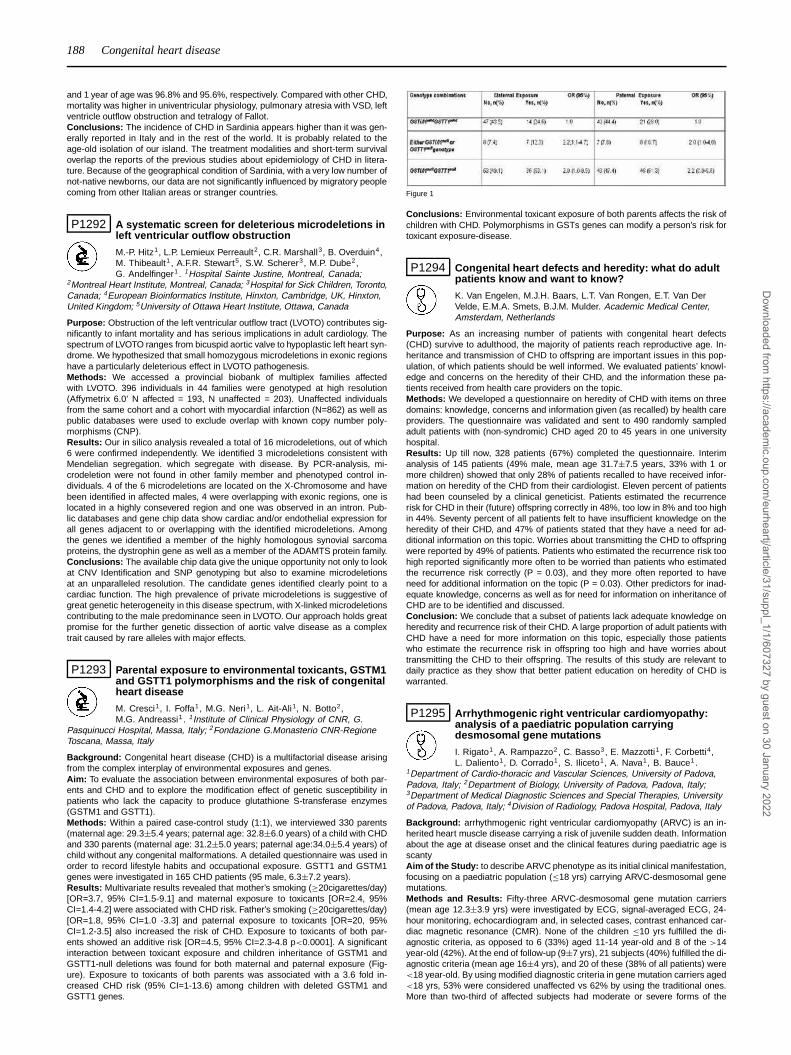
188 Congenital heart disease
and 1 year of age was 96.8% and 95.6%, respectively. Compared with other CHD,mortality was higher in univentricular physiology, pulmonary atresia with VSD, leftventricle outflow obstruction and tetralogy of Fallot.Conclusions: The incidence of CHD in Sardinia appears higher than it was gen-erally reported in Italy and in the rest of the world. It is probably related to theage-old isolation of our island. The treatment modalities and short-term survivaloverlap the reports of the previous studies about epidemiology of CHD in litera-ture. Because of the geographical condition of Sardinia, with a very low number ofnot-native newborns, our data are not significantly influenced by migratory peoplecoming from other Italian areas or stranger countries.
P1292 A systematic screen for deleterious microdeletions inleft ventricular outflow obstruction
M.-P. Hitz1, L.P. Lemieux Perreault2, C.R. Marshall3, B. Overduin4,M. Thibeault1 , A.F.R. Stewart5, S.W. Scherer3, M.P. Dube2,G. Andelfinger1 . 1Hospital Sainte Justine, Montreal, Canada;
2Montreal Heart Institute, Montreal, Canada; 3Hospital for Sick Children, Toronto,Canada; 4European Bioinformatics Institute, Hinxton, Cambridge, UK, Hinxton,United Kingdom; 5University of Ottawa Heart Institute, Ottawa, Canada
Purpose: Obstruction of the left ventricular outflow tract (LVOTO) contributes sig-nificantly to infant mortality and has serious implications in adult cardiology. Thespectrum of LVOTO ranges from bicuspid aortic valve to hypoplastic left heart syn-drome. We hypothesized that small homozygous microdeletions in exonic regionshave a particularly deleterious effect in LVOTO pathogenesis.Methods: We accessed a provincial biobank of multiplex families affectedwith LVOTO. 396 individuals in 44 families were genotyped at high resolution(Affymetrix 6.0’ N affected = 193, N unaffected = 203). Unaffected individualsfrom the same cohort and a cohort with myocardial infarction (N=862) as well aspublic databases were used to exclude overlap with known copy number poly-morphisms (CNP).Results: Our in silico analysis revealed a total of 16 microdeletions, out of which6 were confirmed independently. We identified 3 microdeletions consistent withMendelian segregation. which segregate with disease. By PCR-analysis, mi-crodeletion were not found in other family member and phenotyped control in-dividuals. 4 of the 6 microdeletions are located on the X-Chromosome and havebeen identified in affected males, 4 were overlapping with exonic regions, one islocated in a highly consevered region and one was observed in an intron. Pub-lic databases and gene chip data show cardiac and/or endothelial expression forall genes adjacent to or overlapping with the identified microdeletions. Amongthe genes we identified a member of the highly homologous synovial sarcomaproteins, the dystrophin gene as well as a member of the ADAMTS protein family.Conclusions: The available chip data give the unique opportunity not only to lookat CNV Identification and SNP genotyping but also to examine microdeletionsat an unparalleled resolution. The candidate genes identified clearly point to acardiac function. The high prevalence of private microdeletions is suggestive ofgreat genetic heterogeneity in this disease spectrum, with X-linked microdeletionscontributing to the male predominance seen in LVOTO. Our approach holds greatpromise for the further genetic dissection of aortic valve disease as a complextrait caused by rare alleles with major effects.
P1293 Parental exposure to environmental toxicants, GSTM1and GSTT1 polymorphisms and the risk of congenitalheart disease
M. Cresci1, I. Foffa1, M.G. Neri1, L. Ait-Ali1, N. Botto2,M.G. Andreassi1 . 1Institute of Clinical Physiology of CNR, G.
Pasquinucci Hospital, Massa, Italy; 2Fondazione G.Monasterio CNR-RegioneToscana, Massa, Italy
Background: Congenital heart disease (CHD) is a multifactorial disease arisingfrom the complex interplay of environmental exposures and genes.Aim: To evaluate the association between environmental exposures of both par-ents and CHD and to explore the modification effect of genetic susceptibility inpatients who lack the capacity to produce glutathione S-transferase enzymes(GSTM1 and GSTT1).Methods: Within a paired case-control study (1:1), we interviewed 330 parents(maternal age: 29.3±5.4 years; paternal age: 32.8±6.0 years) of a child with CHDand 330 parents (maternal age: 31.2±5.0 years; paternal age:34.0±5.4 years) ofchild without any congenital malformations. A detailed questionnaire was used inorder to record lifestyle habits and occupational exposure. GSTT1 and GSTM1genes were investigated in 165 CHD patients (95 male, 6.3±7.2 years).Results: Multivariate results revealed that mother’s smoking (≥20cigarettes/day)[OR=3.7, 95% CI=1.5-9.1] and maternal exposure to toxicants [OR=2.4, 95%CI=1.4-4.2] were associated with CHD risk. Father’s smoking (≥20cigarettes/day)[OR=1.8, 95% CI=1.0 -3.3] and paternal exposure to toxicants [OR=20, 95%CI=1.2-3.5] also increased the risk of CHD. Exposure to toxicants of both par-ents showed an additive risk [OR=4.5, 95% CI=2.3-4.8 p<0.0001]. A significantinteraction between toxicant exposure and children inheritance of GSTM1 andGSTT1-null deletions was found for both maternal and paternal exposure (Fig-ure). Exposure to toxicants of both parents was associated with a 3.6 fold in-creased CHD risk (95% CI=1-13.6) among children with deleted GSTM1 andGSTT1 genes.
Figure 1
Conclusions: Environmental toxicant exposure of both parents affects the risk ofchildren with CHD. Polymorphisms in GSTs genes can modify a person’s risk fortoxicant exposure-disease.
P1294 Congenital heart defects and heredity: what do adultpatients know and want to know?
K. Van Engelen, M.J.H. Baars, L.T. Van Rongen, E.T. Van DerVelde, E.M.A. Smets, B.J.M. Mulder. Academic Medical Center,Amsterdam, Netherlands
Purpose: As an increasing number of patients with congenital heart defects(CHD) survive to adulthood, the majority of patients reach reproductive age. In-heritance and transmission of CHD to offspring are important issues in this pop-ulation, of which patients should be well informed. We evaluated patients’ knowl-edge and concerns on the heredity of their CHD, and the information these pa-tients received from health care providers on the topic.Methods: We developed a questionnaire on heredity of CHD with items on threedomains: knowledge, concerns and information given (as recalled) by health careproviders. The questionnaire was validated and sent to 490 randomly sampledadult patients with (non-syndromic) CHD aged 20 to 45 years in one universityhospital.Results: Up till now, 328 patients (67%) completed the questionnaire. Interimanalysis of 145 patients (49% male, mean age 31.7±7.5 years, 33% with 1 ormore children) showed that only 28% of patients recalled to have received infor-mation on heredity of the CHD from their cardiologist. Eleven percent of patientshad been counseled by a clinical geneticist. Patients estimated the recurrencerisk for CHD in their (future) offspring correctly in 48%, too low in 8% and too highin 44%. Seventy percent of all patients felt to have insufficient knowledge on theheredity of their CHD, and 47% of patients stated that they have a need for ad-ditional information on this topic. Worries about transmitting the CHD to offspringwere reported by 49% of patients. Patients who estimated the recurrence risk toohigh reported significantly more often to be worried than patients who estimatedthe recurrence risk correctly (P = 0.03), and they more often reported to haveneed for additional information on the topic (P = 0.03). Other predictors for inad-equate knowledge, concerns as well as for need for information on inheritance ofCHD are to be identified and discussed.Conclusion: We conclude that a subset of patients lack adequate knowledge onheredity and recurrence risk of their CHD. A large proportion of adult patients withCHD have a need for more information on this topic, especially those patientswho estimate the recurrence risk in offspring too high and have worries abouttransmitting the CHD to their offspring. The results of this study are relevant todaily practice as they show that better patient education on heredity of CHD iswarranted.
P1295 Arrhythmogenic right ventricular cardiomyopathy:analysis of a paediatric population carryingdesmosomal gene mutations
I. Rigato1, A. Rampazzo2, C. Basso3, E. Mazzotti1, F. Corbetti4,L. Daliento1, D. Corrado1, S. Iliceto1, A. Nava1, B. Bauce1.
1Department of Cardio-thoracic and Vascular Sciences, University of Padova,Padova, Italy; 2Department of Biology, University of Padova, Padova, Italy;3Department of Medical Diagnostic Sciences and Special Therapies, Universityof Padova, Padova, Italy; 4Division of Radiology, Padova Hospital, Padova, Italy
Background: arrhythmogenic right ventricular cardiomyopathy (ARVC) is an in-herited heart muscle disease carrying a risk of juvenile sudden death. Informationabout the age at disease onset and the clinical features during paediatric age isscantyAim of the Study: to describe ARVC phenotype as its initial clinical manifestation,focusing on a paediatric population (≤18 yrs) carrying ARVC-desmosomal genemutations.Methods and Results: Fifty-three ARVC-desmosomal gene mutation carriers(mean age 12.3±3.9 yrs) were investigated by ECG, signal-averaged ECG, 24-hour monitoring, echocardiogram and, in selected cases, contrast enhanced car-diac magnetic resonance (CMR). None of the children ≤10 yrs fulfilled the di-agnostic criteria, as opposed to 6 (33%) aged 11-14 year-old and 8 of the >14year-old (42%). At the end of follow-up (9±7 yrs), 21 subjects (40%) fulfilled the di-agnostic criteria (mean age 16±4 yrs), and 20 of these (38% of all patients) were<18 year-old. By using modified diagnostic criteria in gene mutation carriers aged<18 yrs, 53% were considered unaffected vs 62% by using the traditional ones.More than two-third of affected subjects had moderate or severe forms of the
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
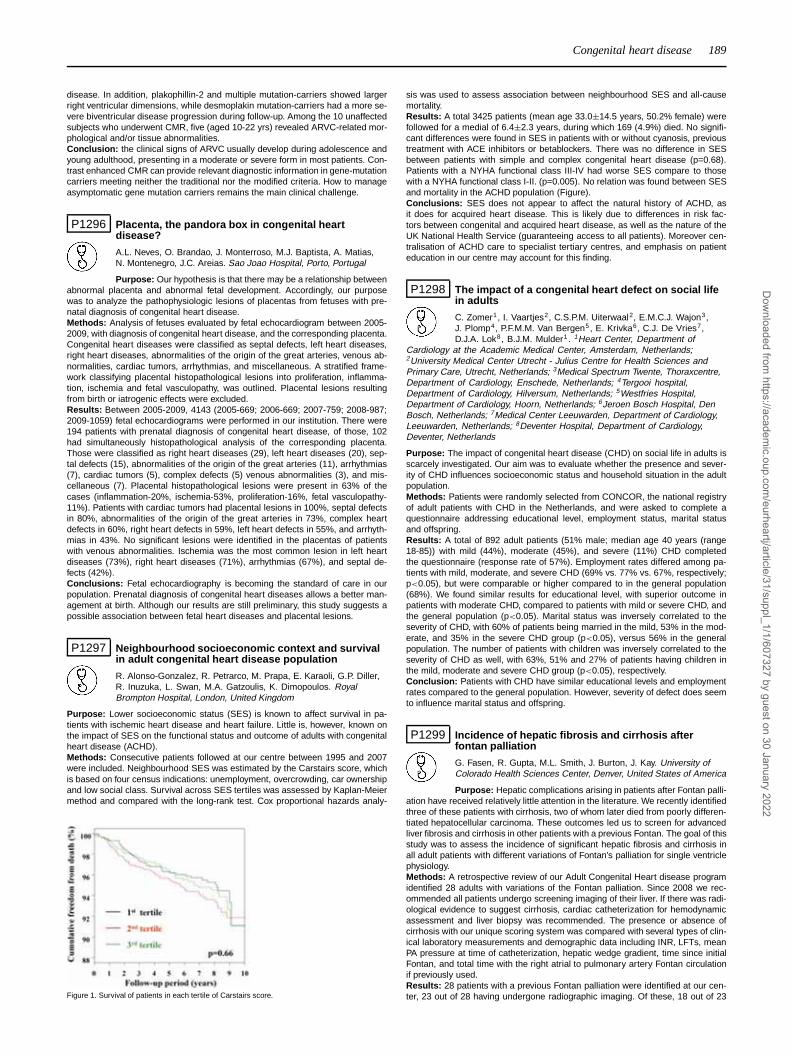
Congenital heart disease 189
disease. In addition, plakophillin-2 and multiple mutation-carriers showed largerright ventricular dimensions, while desmoplakin mutation-carriers had a more se-vere biventricular disease progression during follow-up. Among the 10 unaffectedsubjects who underwent CMR, five (aged 10-22 yrs) revealed ARVC-related mor-phological and/or tissue abnormalities.Conclusion: the clinical signs of ARVC usually develop during adolescence andyoung adulthood, presenting in a moderate or severe form in most patients. Con-trast enhanced CMR can provide relevant diagnostic information in gene-mutationcarriers meeting neither the traditional nor the modified criteria. How to manageasymptomatic gene mutation carriers remains the main clinical challenge.
P1296 Placenta, the pandora box in congenital heartdisease?
A.L. Neves, O. Brandao, J. Monterroso, M.J. Baptista, A. Matias,N. Montenegro, J.C. Areias. Sao Joao Hospital, Porto, Portugal
Purpose: Our hypothesis is that there may be a relationship betweenabnormal placenta and abnormal fetal development. Accordingly, our purposewas to analyze the pathophysiologic lesions of placentas from fetuses with pre-natal diagnosis of congenital heart disease.Methods: Analysis of fetuses evaluated by fetal echocardiogram between 2005-2009, with diagnosis of congenital heart disease, and the corresponding placenta.Congenital heart diseases were classified as septal defects, left heart diseases,right heart diseases, abnormalities of the origin of the great arteries, venous ab-normalities, cardiac tumors, arrhythmias, and miscellaneous. A stratified frame-work classifying placental histopathological lesions into proliferation, inflamma-tion, ischemia and fetal vasculopathy, was outlined. Placental lesions resultingfrom birth or iatrogenic effects were excluded.Results: Between 2005-2009, 4143 (2005-669; 2006-669; 2007-759; 2008-987;2009-1059) fetal echocardiograms were performed in our institution. There were194 patients with prenatal diagnosis of congenital heart disease, of those, 102had simultaneously histopathological analysis of the corresponding placenta.Those were classified as right heart diseases (29), left heart diseases (20), sep-tal defects (15), abnormalities of the origin of the great arteries (11), arrhythmias(7), cardiac tumors (5), complex defects (5) venous abnormalities (3), and mis-cellaneous (7). Placental histopathological lesions were present in 63% of thecases (inflammation-20%, ischemia-53%, proliferation-16%, fetal vasculopathy-11%). Patients with cardiac tumors had placental lesions in 100%, septal defectsin 80%, abnormalities of the origin of the great arteries in 73%, complex heartdefects in 60%, right heart defects in 59%, left heart defects in 55%, and arrhyth-mias in 43%. No significant lesions were identified in the placentas of patientswith venous abnormalities. Ischemia was the most common lesion in left heartdiseases (73%), right heart diseases (71%), arrhythmias (67%), and septal de-fects (42%).Conclusions: Fetal echocardiography is becoming the standard of care in ourpopulation. Prenatal diagnosis of congenital heart diseases allows a better man-agement at birth. Although our results are still preliminary, this study suggests apossible association between fetal heart diseases and placental lesions.
P1297 Neighbourhood socioeconomic context and survivalin adult congenital heart disease population
R. Alonso-Gonzalez, R. Petrarco, M. Prapa, E. Karaoli, G.P. Diller,R. Inuzuka, L. Swan, M.A. Gatzoulis, K. Dimopoulos. RoyalBrompton Hospital, London, United Kingdom
Purpose: Lower socioeconomic status (SES) is known to affect survival in pa-tients with ischemic heart disease and heart failure. Little is, however, known onthe impact of SES on the functional status and outcome of adults with congenitalheart disease (ACHD).Methods: Consecutive patients followed at our centre between 1995 and 2007were included. Neighbourhood SES was estimated by the Carstairs score, whichis based on four census indications: unemployment, overcrowding, car ownershipand low social class. Survival across SES tertiles was assessed by Kaplan-Meiermethod and compared with the long-rank test. Cox proportional hazards analy-
Figure 1. Survival of patients in each tertile of Carstairs score.
sis was used to assess association between neighbourhood SES and all-causemortality.Results: A total 3425 patients (mean age 33.0±14.5 years, 50.2% female) werefollowed for a medial of 6.4±2.3 years, during which 169 (4.9%) died. No signifi-cant differences were found in SES in patients with or without cyanosis, previoustreatment with ACE inhibitors or betablockers. There was no difference in SESbetween patients with simple and complex congenital heart disease (p=0.68).Patients with a NYHA functional class III-IV had worse SES compare to thosewith a NYHA functional class I-II. (p=0.005). No relation was found between SESand mortality in the ACHD population (Figure).Conclusions: SES does not appear to affect the natural history of ACHD, asit does for acquired heart disease. This is likely due to differences in risk fac-tors between congenital and acquired heart disease, as well as the nature of theUK National Health Service (guaranteeing access to all patients). Moreover cen-tralisation of ACHD care to specialist tertiary centres, and emphasis on patienteducation in our centre may account for this finding.
P1298 The impact of a congenital heart defect on social lifein adults
C. Zomer1, I. Vaartjes2, C.S.P.M. Uiterwaal2, E.M.C.J. Wajon3,J. Plomp4, P.F.M.M. Van Bergen5, E. Krivka6, C.J. De Vries7,D.J.A. Lok8, B.J.M. Mulder1. 1Heart Center, Department of
Cardiology at the Academic Medical Center, Amsterdam, Netherlands;2University Medical Center Utrecht - Julius Centre for Health Sciences andPrimary Care, Utrecht, Netherlands; 3Medical Spectrum Twente, Thoraxcentre,Department of Cardiology, Enschede, Netherlands; 4Tergooi hospital,Department of Cardiology, Hilversum, Netherlands; 5Westfries Hospital,Department of Cardiology, Hoorn, Netherlands; 6Jeroen Bosch Hospital, DenBosch, Netherlands; 7Medical Center Leeuwarden, Department of Cardiology,Leeuwarden, Netherlands; 8Deventer Hospital, Department of Cardiology,Deventer, Netherlands
Purpose: The impact of congenital heart disease (CHD) on social life in adults isscarcely investigated. Our aim was to evaluate whether the presence and sever-ity of CHD influences socioeconomic status and household situation in the adultpopulation.Methods: Patients were randomly selected from CONCOR, the national registryof adult patients with CHD in the Netherlands, and were asked to complete aquestionnaire addressing educational level, employment status, marital statusand offspring.Results: A total of 892 adult patients (51% male; median age 40 years (range18-85)) with mild (44%), moderate (45%), and severe (11%) CHD completedthe questionnaire (response rate of 57%). Employment rates differed among pa-tients with mild, moderate, and severe CHD (69% vs. 77% vs. 67%, respectively;p<0.05), but were comparable or higher compared to in the general population(68%). We found similar results for educational level, with superior outcome inpatients with moderate CHD, compared to patients with mild or severe CHD, andthe general population (p<0.05). Marital status was inversely correlated to theseverity of CHD, with 60% of patients being married in the mild, 53% in the mod-erate, and 35% in the severe CHD group (p<0.05), versus 56% in the generalpopulation. The number of patients with children was inversely correlated to theseverity of CHD as well, with 63%, 51% and 27% of patients having children inthe mild, moderate and severe CHD group (p<0.05), respectively.Conclusion: Patients with CHD have similar educational levels and employmentrates compared to the general population. However, severity of defect does seemto influence marital status and offspring.
P1299 Incidence of hepatic fibrosis and cirrhosis afterfontan palliation
G. Fasen, R. Gupta, M.L. Smith, J. Burton, J. Kay. University ofColorado Health Sciences Center, Denver, United States of America
Purpose: Hepatic complications arising in patients after Fontan palli-ation have received relatively little attention in the literature. We recently identifiedthree of these patients with cirrhosis, two of whom later died from poorly differen-tiated hepatocellular carcinoma. These outcomes led us to screen for advancedliver fibrosis and cirrhosis in other patients with a previous Fontan. The goal of thisstudy was to assess the incidence of significant hepatic fibrosis and cirrhosis inall adult patients with different variations of Fontan’s palliation for single ventriclephysiology.Methods: A retrospective review of our Adult Congenital Heart disease programidentified 28 adults with variations of the Fontan palliation. Since 2008 we rec-ommended all patients undergo screening imaging of their liver. If there was radi-ological evidence to suggest cirrhosis, cardiac catheterization for hemodynamicassessment and liver biopsy was recommended. The presence or absence ofcirrhosis with our unique scoring system was compared with several types of clin-ical laboratory measurements and demographic data including INR, LFTs, meanPA pressure at time of catheterization, hepatic wedge gradient, time since initialFontan, and total time with the right atrial to pulmonary artery Fontan circulationif previously used.Results: 28 patients with a previous Fontan palliation were identified at our cen-ter, 23 out of 28 having undergone radiographic imaging. Of these, 18 out of 23
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

190 Congenital heart disease
(78%) demonstrated evidence of liver fibrosis. Of these 18 patients, 10 agreedto undergo cardiac catheterization and liver biopsy. All 10 had either significantbridging fibrosis (n=4) or frank cirrhosis (n=6). None of the clinical laboratory mea-surements or demographic data were significant risk factors for the severity ofhistological changes.Conclusion: Although late arrhythmias, protein losing enteropathy, and embolicevents are well described in this population, few publications have evaluated forhepatic injury as a long term complication. Most of those patients in publishedseries consisted of older atrial pulmonary Fontans with less known about newermodifications. Although larger studies are needed to identify risk factors for cir-rhosis, our study suggests that with a high prevalence of radiological fibrosis, and100% confirmation seen histologically, all adult survivors with Fontan physiologyshould undergo screening. If a malignancy is identified at earlier stages, potentialcures may be obtained without the need for liver transplant.
P1300 Thromboembolic complications in adults withlongstanding Fontan circulation: time course, riskfactors and role of anticoagulation
M. Westhoff-Bleck, O. Tutarel, J. Bleicher, S. Sarikouch, C. Zwadlo,A. Wessel, B. Schieffer, T. Breymann, G.P. Meyer. Hannover Medical
School, Hannover, Germany
Objective: In Fontan circulation thromboembolic complications contribute to sig-nificant morbidity and mortality. In adults time course and impact of anticoagula-tion has not been investigated so far.Method: In 50 adults (age 26.1±5.7years, 17.1±4.5 post Fontan surgery, 38men, NYHA class 1.7±0.6, anticoagulation present in 24 patients) time course,risk factors and impact of anticoagulation on late thromboembolism were ana-lyzed.Results: 12 (24%) patients developed thromboembolic complications. Pa-tients with thromboembolic complications had significantly lower serum Albu-min (41.5±7.8 versus 46.9±6.7 (g/l; p=0.028) and significantly higher degreeof liver fibrosis (APRI score: 0.94±0.52 versus 0.67±0.3; p=0.043). Echocardio-graphically detectable spontaneous echocontrast in the Fontan tunnel was sig-nificantly higher (91.7% versus 42.1%; p=0.003; 95% confidence interval 1.14 -120; p=0.039): Anticoagulation reduced the incidence of thromboembolism sig-nificantly (8.3% versus 39.5%; p=0.002) resulting in significant risk reduction inmultivariate analysis (95% confidence interval 0.005 - 0.055; p=0.013). Actuarialevent free survival rate in patients without anticoagulation was 96%, 89%, 76%,and 57% after 10, 15, 20 and 25 years. This was significantly lower compared toanticoagulated patients (event free survival of 100% up to 15 years and 93% upto 25 years; log-rank p=0.012). The overall incidence of thromboembolic eventswas 5.4/100 patient-years without anticoagulation and 0.6/100 patient-years withanticoagulation respectively. Patients on anticoagulation did not present with sig-nificant bleeding complications.Conclusion: Oral anticoagulation reduces significantly the incidence of throm-boembolic complications occurring with high frequency beyond 13 years postFontan surgery. The presence of spontaneous echocontrast in the Fontan tun-nel can be used for risk stratification.
P1301 Pulmonary restriction in adults with congenital heartdisease relates to complexity of underlying cardiacdefect, previous surgery and outcome
F. Borgia, G.P. Diller, R. Inuzuka, M. Silva, K. Wustmann,R. Alonso-Gonzalez, L. Swan, K. Dimopoulos, M.A. Gatzoulis. Royal
Brompton Hospital, London, United Kingdom
Purpose: Lung function is commonly impaired in adults with congenital heartdisease (ACHD) but its prevalence and relation to cardiac anatomy and prognosisremain unknown.Methods: We retrospectively examined lung function tests performed in our Insti-tution as part of routine clinical assessment between 2000 and 2008. Respiratoryrestriction was classified as mild, moderate or severe according predicted spirom-etry results (respectively, FVC<70, FVC<60 and FVC<50; FEV1/FVC >0.8).Results: A total of 1262 ACHD patients (age 33.8±13.6 years, BMI 23.8±4.6,53.6% male) were included. FVC was 70.2±17.5%, FEV1 72.2±18%, PEF82.3±21%. Moderate or severe lung restriction was present in 28.0% of ACHDpopulation; its prevalence was higher in patients with complex versus simple heartdefects (36% vs 21.4% respectively, p<0.01). Multivariate predictors of moderate
Cox-survival analysis
or severe restrictive lung disease were previous thoracotomy, cardiothoracic ra-tio (from PA chest-X-ray), resting cyanosis and complexity of underlying cardiacdefect. Other univariate predictors (scoliosis, previous sternotomy, lung hypoper-fusion at birth) failed to make it to were not retained in the multivariate model.During a median follow-up was 3.8 years 77 (6.1%) patients died. Moderate-or-severe restrictive lung disease was an independent predictor of death by Cox-survival analysis (HR 2.56, 95%CI 1.64-4.01, p<0.0001, Figure).Conclusions: Restrictive lung disease is highly prevalent in patients with ACHDand predicts outcome. Its severity relates to complexity of cardiac defect, haemo-dynamic status, cyanosis and type of surgery. Pulmonary function tests should beincorporated in the routine, periodic assessment and risk stratification process ofpatients with ACHD.
P1302 Young adults with congenital heart disease show apoor level of information
W. Lesch1, K. Specht1, A. Lux2, M. Frey1, U. Bauer1. 1CompetenceNetwork for Congenital Heart Defects, Berlin, Germany; 2Otto-von-Guericke University of Magdeburg, Institute of Biometry and Medical
Informatics, Magdeburg, Germany
Purpose: More and more patients with congenital heart disease (CoHD) reachadulthood. According to the 2009 Report of the German Advisory Council on theAssessment of Developments in the Health Care System many of these patientsare uninformed about their disease. This can have life threatening consequencesfor their health, if, for example, patients do not take part in follow-up examina-tions or neglect therapeutic measures (Mackie 2009, Somerville 1997). In 2009,1,372 patients with CoHD were surveyed concerning their information behaviourand information needs in order to find out whether they lack knowledge on theirdisease.Methods: In a descriptive cross-sectional study, 1,372 patients enrolled in theNational Registry for Congenital Heart Defects were surveyed using an Internetbased questionnaire. The response rate was 52.3% (174 patients aged 10 – 13years, 147 patients aged 14 – 17 years, 275 patients aged 18 – 30 years).Results: 68.7% of the adult study participants were able to correctly name theirheart defect. On a scale ranging from 1 (not good at all) to 10 (very good), the sur-veyed patients rated their level of information at 7.06. The physician is the mostimportant source of information regarding questions about the CoHD (84.7%),followed by the Internet (52.0%), family and friends (39.3%), books (20.7%), pro-fessional journals (10.5%) and television (9.5%). Only 1.5% of the patients sur-veyed use self-help groups as a source of information. Only 57.5% of the adultpatients with CoHD (ACHD) fully understand the explanations given by their physi-cian. This leads to a considerable lack of information, which is reflected in manyunanswered questions of ACHDs. The issues of greatest interest are exercisecapacity (76.4%), leisure activities/sports/travel (52.4%), health related problems(43.3%), pregnancy/family planning (39.6%) and treatment options (36%). Med-ical issues are covered sufficiently by the treating physicians. However, with re-spect to questions concerning life with the disease, there are statistically signifi-cant discrepancies between the information needs and the information providedby the physicians. Patients are insufficiently informed particularly on matters suchas pregnancy/family planning, insurance, sexuality, anxiety and depression.Conclusions: There is a lack of information in ACHDs regarding their condi-tion. Important issues with respect to living with the disease are not discussedsufficiently by the treating physicians. As they are the most important source ofinformation, there is a need for action in order to prevent health complications.
P1303 Downregulation of bone morphogenetic proteinreceptor type 2 in the pulmonary arteries of the failedFontan patients
H. Ishida1, S. Kogaki1, H. Ichimori1, J. Narita1, T. Ueno1,F. Kayatani2, H. Kishimoto2, M. Nakayama2, Y. Sawa1, K. Ozono1.
1Osaka University, Graduate School of Medicine, Osaka, Japan; 2Osaka MedicalCenter and Research Institute for Maternal and Child Health, Osaka, Japan
Background: The Fontan procedure has been a landmark contribution to thetreatment of congenital heart disease with single ventricle physiology. However,not a few patients suffer from failure of the Fontan circulation due to high pul-monary vascular resistance. Previous studies demonstrated that bone morpho-genetic protein receptor type 2 (BMPR2) dysfunction could lead to pulmonaryendothelial cell apoptosis and vascular smooth muscle cell proliferation, whichresult in pulmonary artery remodeling and elevation of pulmonary vascular re-sistance. The aim of this study is to clarify the possible involvement of BMPR2dysfunction in the the failing Fontan circulation.Subjects and Methods: We examined autopsy lung tissues from the patientsdied of failed Fontan circulation (Group F, n=10), and compared those to age-matched lung tissues from the patients with no cardiovascular disease (GroupN, n=4). We evaluated the histomorphometric alterations and the expression ofBMPR2 in the pulmonary arteries using immunohistochemical analysis and quan-titative real-time PCR.Results: The percent wall thickness of the intra-acinar pulmonary arteries inGroup F was significantly increased as compared to Group N (mean ± stan-dard error, 25.2±4.0% vs. 15.9±2.6%; P < 0.01). The immunostaining of alphasmooth muscle cell actin showed marked proliferation of the vascular smooth
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Congenital heart disease / Management of acute coronary syndromes 191
muscle cells in both intima and media of the distal pulmonary arteries in GroupF. The computational optical density analysis of immunostaining revealed that theexpression level of BMPR2 was significantly decreased in Group F (0.412±0.058vs. 0.580±0.039; P < 0.01), and the quantitative real-time PCR analysis demon-strated that the mRNA expression of BMPR2 was also decreased (1.20±0.33 vs.1.81±0.26, relative to beta-actin expression; P < 0.01).Conclusion: The intra-acinar pulmonary arteries of the patients with failedFontan circulation exhibited significant medial hypertrophy with proliferation ofthe vascular smooth muscle cells. We demonstrated for the first time that theexpression of BMPR2 in the pulmonary arteries of the failed Fontan patients wassignificantly decreased. Downregulation of BMPR2 can deteriorate the Fontancirculation via vascular remodeling with endothelial dysfunction and proliferationof smooth muscle cells. This study supports the hypothesis that the BMP signal-ing may contribute to the pathogenesis in the development of the failing Fontancirculation.
MANAGEMENT OF ACUTE CORONARY SYNDROMES
P1304 Self-referral to the chest pain unit: incidence of acutecoronary syndrome
T. Voigtlaender1, H. Darius2, E. Giannitsis3, G. Miritz4, L.E. Maier5,M. Haude6, T. Muenzel7 , R. Erbel8, G. Heusch9, J. Senges4.1CCB, Cardioangiologisches Centrum Bethanien, Frankfurt
am Main, Germany; 2Vivantes Hospital Neukolln, Department of InternalMedicine-Cardiology, Berlin, Germany; 3Medical Clinic III, University Heidelberg,Heidelberg, Germany; 4Heart Attack Research Center at the University ofHeidelberg, Ludwigshafen am Rhein, Germany; 5Departement for Cardiology,University Heart Centre, Göttingen, Germany; 6Medical Clinic I, Neuss,Germany; 7University Medical Center of the Johannes Gutenberg UniversityMainz, Mainz, Germany; 8West German Heart Center Essen, Clinic forCardiology, Essen, Germany; 9University of Essen Medical School, Institute ofPathophysiology, Essen, Germany
Background: With increasing degree of popularity of chest pain units (CPU) pa-tients refer themselves to the CPU and do not call for emergency services. Up todate, little is known about the characteristics of these patients in comparison topatients referred by emergency services.Patients and methods: From 1st Dec. 2008 until 20th Nov. 2009, the data of2470 patients were prospectively recorded (CPU registry of the German Societyof Cardiology). Self referral (SR) was present in 1012 patients (41%), whereas1458 patients were referred by emergency services (ES). In both groups, the fol-lowing parameter were compared: risk factors, STEMI, NSTEMI, unstable angina,stable angina, PCI, CABG, conservative treatment.Results: SR patients were younger compared to ES patients (66.2 vs. 70.7 years;p<0.0001), in both groups, the percentage of women was comparable (42% vs.42.1%). Hypertension was observed less frequently in the SR than in the ERgroup (p<0.05; OR 0.81; 0.67-0.97), but the other risk factors did not differ. Ahistory of previous coronary artery bypass surgery (CABG) was less prevalent inthe SR group (11.3% vs. 14.3%, p<0.05, OR 0.73; 0.57-0.93), but the incidenceof previous myocardial infarction and PCI did not differ. An acute coronary syn-drome was present in 22.4% of patients with SR and in 39.5% of patients with ER(p<0.0001; OR 0.44 (0.37-0.54). Table. PCI was performed in 31.3% of patientsof SR and in 40.8% of ER (p<0.0001; OR 0.68 (0.57-0.81), CABG in 2 patients ofSR and in 16 patients of ER. The remaining patients were treated conservatively(SR: 67.1% vs. ER: 57.5%, p<0.0001; OR 1.51; 1.26-1.80).
Table 1
SR ER p-Wert OR (95%-KI)
STEMI 1.5% 7.4% 0.0001 0.44 (0.37-0.54)NSTEMI 5.1% 12.7% 0.0001 0.20 (0.11-0.34)unstable AP 15.8% 19.3% 0.05 0.78 (0.62-0.98)stabel AP 8.2% 7.0% 0.3 1.19 (0.86-1.63)
Conclusion: Patients referring themselves present with an acute coronary syn-drome in almost one-quarter of all cases and thus much more frequently thanpreviously thought. Althought STEMI and NSTEMI are more frequent in ER, un-stable angina and stable angina do not differ substantially in self-referred patientsand patients referred by emergency services.
P1305 Speckle tracking-derived circumferential and radialstrain analysis in the evaluation of regional wallmotion in patients with ST-elevation acute myocardialinfarction
C.M. Jorge, N. Cortez-Dias, J. Silva Marques, D. Silva, S. Ribeiro,L. Santos, S. Goncalves, M. Almeida Ribeiro, S. Robalo Martins, M.G. Lopes.Hospital Lisbon North, Hospital Santa Maria, Lisbon, Portugal
Aims: To determine the diagnostic accuracy of circumferential and radial strainparameters as assessed by 2D speckle tracking echo (2DSE) for regionalwall motion (WM) evaluation in patients with ST elevation myocardial infarction(STEMI).
Methods: Consecutive patients (pts) admitted with first-ever STEMI that under-went primary angioplasty (PCI) were studied. Standard Doppler echo and 2DSEstudies were performed within 72 h after PCI. Regional WM was scored by twooperators (normokinesis: 1; hypokinesis: 2; akinesis: 3; dyskinesis: 4) and finalscore was decided by consensus. WM abnormality was defined as WM score≥2. In blinded post-processing, peak systolic circumferential strain (PSCS) andpeak radial strain (PRS) were measured; their distribution was compared accord-ing WM score and ventricular (ANOVA test/Kendall’s Tau b correlation coefficient);and their diagnostic accuracy for detecting WM abnormalities was assessed bythe area under the Receiver Operator Curve (ROC).Results: 69 pts were evaluated (63±14 years; 48 males), with 1-, 2- and 3- ves-sel coronary disease in 62%, 21% and 17%, respectively. The culprit coronaryartery was the anterior descending in 34%, circumflex in 26% and right coronaryartery in 36%. Among the 964 ventricular segments with suitable image quality2DSE analysis, 41% (N=399) had regional WM abnormalities. Both strain param-eters varied with WM score: PSCS was more negative in normokinetic segments(p<0,001), while PRS progressively decreased with WM score (p<0,001). More-over, only in normokinetic and hypokinetic segments PSCS varied with ventricu-lar plan, being more negative in apical segments (p<0,001). Thus, the correlationbetween PSCS and WM score increased from basal (k=0,342) to mid-ventricular(k=0,409) and apical segments (k=0,411) – p<0.001. PSCS had higher diagnos-tic accuracy for detecting WM abnormalities than PRS, ROC: 0.76 and ROC: 0.66respectively. Overall, the PSCS threshold that better identified WM abnormalitieswas >-14.2% (sensibility: 70%; specificity: 70%).Conclusion: Circumferential and radial myocardial deformation parameters al-low quantitative assessment of regional WM. The 2DSE short axis view-derivedparameter that more accurately detected WMA is PSCS.
P1306 Late microvascular obstruction after acute myocardialinfarction: relation with cardiac and inflammatorymarkers
A. Mayr, G. Klug, J. Mair, K. Pedarnig, T. Trieb, O. Pachinger,M. Schocke, W. Jaschke, B. Metzler. Innsbruck Medical University,
Innsbruck, Austria
Background: Cardiac magnetic resonance imaging (CMR) permits accurate as-sessment of microvascular perfusion defects after acute myocardial infarction(AMI). The aim of the present study was to quantify late microvascular obstruction(l-MVO) and to correlate it with cardiac and inflammatory marker concentrations.Methods: CMR was performed in 118 consecutive patients within 8 days af-ter successful interventional reperfused first acute ST-elevation AMI. Infarct vol-umes and l-MVO sizes were calculated from late enhancement (LE) sequencesand functional parameters were determined from short-axis cine MR sequences.Creatine kinase (CK) and cardiac troponin T (cTnT), c-reactive protein (CRP)and fibrinogen as well as lactate dehydrogenase (LD), glutamate-oxalacetat-transaminase (GOT) and glutamate-pyruvate-transaminase (GPT) concentra-tions were determined serially from day 1 to day 4 after symptom onset.Results: L-MVO was detected in 66/118 patients (55.9%) and comprised18.2±10% of infarct size and 4.7±3% of left ventricle myocardial mass. Any sin-gle point-, peak and cumulative release concentration of cTnT (r=0.21 to 0.81,p<0.03), CK (r=0.27 to 0.76, p<0.005), CRP (r=0.39 to 0.51, p<0.003), fibrino-gen (r=0.20 to 0.39, p<0.03) as well as LD (r=0.42 to 0.82, all p<0.0001) andGOT (r=0.28 to 0.77, all p<0.004) significantly correlated with l-MVO size. Re-ceiver operating curve (ROC) analysis indicated a cutoff value of 462 U/l LD tobest identify presence of l-MVO (area under the curve (AUC) 0.916; 95% CI:0.86-0.96; p < 0.0001)).Conclusion: L-MVO sizes significantly correlate with cardiac and inflammatorymarker concentrations as determined early after AMI. LD concentration of > 462U/l could help to identify patients in whom l-MVO is present.
P1307 Cystatin C and structural cardiac compromise inpatients with ST elevation myocardial infarction
D. Silva, N. Cortez-Dias, C. Jorge, C. Calisto, J. Silva Marques,S. Robalo Martins, T. Pessoa, M. Fiuza, A. Nunes Diogo,M.G. Lopes. Hospital Lisbon North, Hospital Santa Maria, Lisbon,
Portugal
Background: Patients with renal dysfunction and acute coronary syndrome havea worse prognosis, not only by the high prevalence of classic risk factors but alsoby the lower use of cardioprotective therapies, increased drug toxicity and abnor-malities of vascular biology (coagulation disorders and endothelial dysfunction).Cystatin C is a surrogate marker of renal dysfunction that has shown to havehigher prognostic value.Aims: To evaluate the correlation of serum cystatin C with the severity of struc-tural cardiac compromise and to assess the association between cystatin Cand coagulation parameters in patients with ST elevation myocardial infarction(STEMI).Methods: In consecutive patients (pts) with STEMI that underwent primary an-gioplasty (PCI), cystatin C and coagulation factors (II, V, VII and VIII) were de-termined in arterial blood samples at the beginning of cardiac catheterization.Echocardiographic study was performed 24 to 72 hours after PCI and the leftventricular (LV) ejection fraction (EF) was measured by the biplane Simpson
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

192 Management of acute coronary syndromes
method. LV systolic dysfunction (SD) was defined as EF ≤40%. The associa-tion between cystatin C levels and EF was determined by Pearson correlation,and the effect of coagulation factors, platelet count, Killip class and systolic bloodpressure at admission in cystatin C levels was assessed by multiple linear regres-sion.Results: 76 pts were evaluated (80% male, 61±13 years), with 1-, 2- and 3-vessels coronary artery disease of in 45%, 40% and 15%, respectively. At admis-sion, Killip class was ≥III in 10% and creatinin was higher than 1.5mg/dL in 75pts. EF was 52±12% (with LVSD in 20%). Cystatin C was significantly higher inpatients with LVSD (1.32±1.65mg/dL vs 0.64±0.27mg/dL, p=0.02), and cystatinC levels were inversely correlated with EF (R2=-0.33, p=0.026). Moreover, in thefinal model, coagulation factors II (R2=-0.33) and VII (R2=0.08) levels were inde-pendently correlated with cystatin C concentration – adjusted R2=0.22; p<0.001.Conclusion: Cystatin C at the time of PCI correlated with the compromise ofcardiac function that had persisted within 72 hours after admission. The higherconcentrations of coagulation factors that tend to be associated with cystatin Clevels may also account for the worse clinical outcome of pts with renal dysfunc-tion.
P1308 Recognition of abnormal glucose metabolism and Itsimpact on treatment in patien with acute myocardialinfarction in Germany: results of the SWEETHEARTregistry
F. Towae1 , T. Bauer1, D. Tschoepe2 , O. Schnell3, E. Standl4,R. Zahn1, A.K. Gitt1. 1Clinical Center of Ludwigshafen, Department ofCardiology, Ludwigshafen am Rhein, Germany; 2Heart and Diabetes CenterNRW, Ruhr-University of Bochum, Bad Oeynhausen, Germany; 3ClinicSchwabing, Munich, Germany; 4Munich Helmholtz Center, Institute for ClinicalDiabetes Research, Munich, Germany
Background: Recent reports from epidemiological studiesdemonstrated a highprevalence of undiagnosed diabetes in patients withcoronary artery disease.These findings led to joint guidelines by the ESC andthe EASD on diabetes, pre-diabetes and cardiovascular disease.Methods: Since 2007, 1,773 consecutive patients withSTEMI or NSTEMI wereenrolled into the MI-registry SWEETHEART to documentpatients’ characteristicsand treatment in clinical practice with specialemphasis on the identification ofabnormal glucose metabolism. In patients withpreviously unknown diabetes, oralglucose tolerance test was performed at day 4after the acute MI. We examinedthe prevalence of abnormal glucose metabolismand its impact on treatment inclinical practice.Results: Out of 1,773 consecutive patients with MI, 919 (52.3%) presented withSTEMI and 837 (47.7%) with NSTEMI. Diabetes was alreadyknown in 33.0% ofpatients. Oral glucose tolerance tests identified another16.1% of patients withmanifest diabetes and 22.4% with impaired fastingglucose or impaired glucosetolerance (pre-diabetes). Only 28.5% of the MIpopulation had no signs of ab-normal glucose tolerance. Medical treatment forsecondary prevention at dis-charge was quite well according to guidelines forantiplatelet therapy, betablock-ers, statins, ACE-inhibitors and ARB for allpatients. Nevertheless, only 61.1% ofpatients with newly diagnosed diabetesdid receive treatment for diabetes at dis-charge, in whom 74.0% only receiveddiet.Conclusion: There was a high prevalence of newly diagnoseddiabetes and pre-diabetes in consecutive patients with myocardial infarction inGermany. Despitenew guidelines by the ESC and the EASD with clearrecommendations for earlyand aggressive therapy of diabetes in patients withcardiovascular disease, 40%of myocardial infarction patients with newlydiagnosed diabetes did not receivediet or an antidiabetic treatment atdischarge.
P1309 The influence of baseline hemoglobin concetration onin-hospital mortality in patients with ST-segmentelevation myocardial infarction treated withpercutaneous coronary intervention
M. Swietlinska, M. Gasior, D. Pres, M. Hawranek, M. Gierlotka,M. Tajstra, A. Lekston, A. Kurek, G. Slonka, L. Polonski. III Chair and Departmentof Cardiology, Silesian Centre for Heart Diseases, Zabrze, Poland
The use of percutaneous coronary intervention (PCI) for treatment of acute my-ocardial infarction significantly improved prognosis of patients. Recently a newprognostic factor is under consideration – the hemoglobin (Hb) level on admis-sion. There are not many evidences that baseline Hb level can affect mortality inpatients with STEMI.Purpose: To assess whether Hb concetration on admission affects in-hospitalmortality in patients with STEMI treated with PCI.Methods: Consecutive patients with STEMI treated with PCI were included in theanalysis. Patients were divided into three groups in dependence on Hb concetra-tion on admission: I group – Hb level ≤ 12g/L, II group - Hb level 12-16 g/L, IIIgroup – Hb level ≥16 g/L. Selected parameters were compared among groups.Results: A total of 3086 patients with STEMI treated with PCI were included inthe analysis. Number of patients in the selected groups was as follows: group I– 245, group II – 2500, group III – 341. Patients with lower Hb level were older,more frequently female, less smokers, had more frequently hypertension, dia-betes and lower left ventricular ejection fraction. The lowest in-hospital mortality
was in patients with Hb 12-16 g/L (4.3%) wheras the highest in patient with Hb ≤12g/L (9.0%) and ≥16 g/L (7.3%) [p=0.0006]. In multivariate analysis comparedwith group II, odds ratios (95% confidence interval) for in-hospital mortality amongthose in groups I and III were 0.99 (0.96-1.04; p=0.99), 2.31 (2.04-5.11; p=0.04),respectively.Conclusion: Higher Hb level on admission in patiets with STEMI treated with PCIis associated with higher in-hospital mortality.
P1310 Distal protection with thrombus aspiration versusthrombus aspiration during primary percutaneouscoronary intervention in patients with acuteST-elevation myocardial infarction
H. Inoue, S. Satoh, E. Mori, K. Takenaka, T. Mori, K. Numaguchi,K. Okamura, N. Tanaka, K. Hiyamuta. National Hospital Organization KyushuMedical Center, Fukuoka, Japan
Purpose: A recent large randomized trial has shown better coronary reperfusionand clinical outcomes by means of thrombus aspiration than conventional primarypercutaneous coronary intervention (PCI) in patients with acute ST-elevation my-ocardial infarction (STEMI), whereas favorable effects of distal protection in pri-mary PCI is still controversial although there exist some beneficial subgroups. Wetested a hypothesis whether distal protection with thrombus aspiration is superiorto simple thrombus aspiration in primary PCI.Methods: Consecutive 107 STEMI patients were enrolled prospectively, andwere assigned to the distal protection group using balloon-occlusion system (DP,n=45) and the thrombus aspiration group (A, n=62) according to anatomical fea-sibility and operator’s decision. We assessed angiographic reperfusion grade, leftventricular function, and clinical outcomes.Results: The onset-to-balloon time was similar between DP and A (5.2±3.5hand 6.5±4.9h). TIMI flow grade was higher in DP than in A (2.8±0.4 and 2.6±0.6,p<0.05). Mortality by 30 days after admission was similar between the two groups(6.7% and 4.8%). In patients who underwent follow-up catheterization after 6months (DP, n=31; A, n=35), (1) there was no significant difference of changesin ejection fraction before and after PCI between the two groups, (2) there wereno significant differences of LVEDVI, LVESVI, or LVEF in the post-PCI state be-tween the two groups (Table). These results were the same in patients with culpritlesions in the left anterior descending artery.
DP A p
TIMI 2.8±0.4 2.6±0.6 <0.05EF change (%) 1.6±9.9 0.3±11.9 nsPost EF (%) 57±13 56±11 nsPost LVEDVI (mL/m2) 67±21 64±17 nsPost LVESVI (mL/m2) 30±18 28±13 ns
Conclusions: Distal protection with thrombus aspiration may be more effectivein the restoration of coronary blood flow than thrombus aspiration alone, but maynot be superior to thrombus aspiration alone in preventing LV remodeling or pre-serving LV function in STEMI patients.
P1311 Early increase in Stromelysin-1 levels is related toinfarct size and predicts long-term LV remodellingfollowing STEMI
S. Orn1, C. Manhenke1 , I.B. Squire2, K. Dickstein3. 1Division ofCardiology, Stavanger University Hospital, Stavanger, Norway;
2University of Leicester, Leicester, United Kingdom; 3University of Bergen,Bergen, Norway
Purpose: Changes in the extracellular cardiac matrix (ECCM) are importantboth in myocardial healing and to the adverse process of left ventricular (LV) re-modelling following acute myocardial infarction (AMI). Recent data suggest thatStromelysin-1 (metalloproteinase-3) may be important for the regulation of ECCMturnover. However, there is limited understanding of the pathophysiological role ofStromelysin-1 following AMI. This study therefore assessed the temporal rela-tionship between Stromelysin-1, infarct size and LV remodelling in ST elevationMI (STEMI).Methods: 42 patients, with first time STEMI, admitted with an occluded singlevessel at time of angiography, successful treated by primary percutanous coro-nary intervention (PCI), were recruited consecutively. Cardiac magnetic reso-nance (CMR) was used to for serial assessment (2 days, 1 week, 2 months and1 year) of infarct size, and LV remodeling. Blood was sampled before PCI and atevery CMR assessment. 25 healthy persons served as reference population.Results: Our major findings were: (1). Prior to PCI, there was a marked elevation(p = 0.001) in plasma levels of Stromelysin-1, reaching maximum 2 days afterPCI, returning towards normal values 1 week after PCI. (2) Stromelysin-1 levelswere closely correlated with CRP levels both prior to PCI (r = 0.44, p = 0.01) and 2days following PCI (r = 0.50, p= 0.001). (3). Stromelysin-1 levels prior to PCI and2 days after PCI were significantly correlated with infarct size and parameters ofLV remodelling 1 year after PCI (table). (4) In multivariable models (correcting forCRP, infarct size and N-BNP at 2 days), Stromelysin-1 (2 days) was an indepen-dent predictor of LV end diastolic volume index (beta = 0.36, p = 0.005), and LVend systolic volume index (beta = 0.29, p = 0.01) at 1 year.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Management of acute coronary syndromes 193
Stromelysin-1 and CMR findings at 1 year
Infarct size LVEF LVEDVi LVESVi(g/m2) (%) (ml/m2) (ml/m2)
Stromelysin-1 r-value p-value r-value p-value r-value p-value r-value p-value
Prior to PCI 0.48 0.005 -0.44 0.01 0.47 0.006 0.51 0.0032 days post PCI 0.37 0.02 -0.36 0.02 0.51 0.0007 0.45 0.0031 week post PCI 0.38 0.01 -0.40 0.01 0.20 0.2 0.30 0.06
Conclusion: Our findings suggest a potential role for Stromelysin-1 both as avery early marker of LV remodelling and as an active participant in the healingand remodelling process following STEMI.
P1312 In-hospital worsening renal function is associatedwith one-year adverse outcome independently frombaseline creatinine levels in patients with myocardialinfarction. The HEROES study
G. Lazaros, D. Tsiachris, A. Patialiakas, A. Karavidas,S. Vogiatzoglou, K. Dimitriadis, C. Tsioufis, C. Vlachopoulos, D. Tousoulis,C. Stefanadis. Hippokration General Hospital, Athens, Greece
Purpose: The association between a history of renal insufficiency and poor out-come in patients with acute myocardial infarction (MI) is well known. However,little information is available about in-hospital worsening of renal function (WRF).Our goal was to determine the prognostic impact of in-hospital WRF in patientswith acute MI.Methods: We studied 522 consecutive patients admitted at our Coronary CareUnit from January 2007 to January 2009 with the diagnosis of acute MI within12 hours of symptoms’ onset and included in our internal MI registry. From bloodsample obtained on admission BNP, white blood count, high sensitivity C-reactiveprotein (CRP), troponin I (TnI), plasma glucose and creatinine (Cr) were deter-mined. Peak TnI and peak Cr levels were also measured throughout hospital-ization. WRF was defined as Cr elevation ≥ 0.3mg/dl. All patients underwentcoronary arteriography and disease extension, LAD involvement, and subsequentrevascularization status (complete or not) were recorded. Ejection fraction wasestimated on admission with 2D echo. The primary endpoint was the compositeof MI, stroke and death during 1-year follow-up period.Results: The incidence of the composite end-point during one-year follow-up was21.9%. Worsening renal function was detected in 96 patients (18.4%). Patientswith WRF compared with those without exhibited significantly higher incidenceof the composite end-point (51.1% vs. 15.2%, p<0.0001), as well as more fre-quently LAD involvement (by 15%, p=0.002) and incomplete revascularization (by17%, p=0.007). Moreover, patients with WRF were older (by 10 years, p<0.001),more frequently females (by 10%, p=0.019), hypertensives (by 15%, p=0.008)and had lower ejection fraction (by 7%, p<0.001), increased glucose (by 33mg/dl, p=0.002), BNP (by 21.5%, p<0.001), CRP (by 26%, p<0.001), white bloodcell count (by 1050 cells/mm3, p=0.041), admission Cr (by 0.3 mg/dl, p<0.001)and TnI levels (by 47%, p=0.002). Multivariate Cox regression analysis revealedthat WRF (HR 2.678 p<0.001), ejection fraction (HR 0.965, p=0.002), BNP (HR1.809, p=0.007), glucose (HR=1.002, p=0.044) and incomplete revascularization(HR=1.579, p=0.048) were the only predictors of the composite end-point.Discussion: WRF reflects a status of exaggerated neurohormonal activation sub-sequent to a greater infarct size and is associated with adverse one-year outcomeindependently from baseline Cr levels. Close monitoring of Cr levels in the acutephase of MI may substantially contribute to long-term risk stratification.
P1313 The ACEF score: a simple but powerful predictor ofshort-term mortality in patients with ST-elevationmyocardial infarction
G.M. Sangiorgi1, L. Bertelli1, G. Biondi Zoccai2 , F. Sgura1,D. Monopoli1, L. Politi1, R. Rossi1, M.G. Modena1. 1University of
Modena & Reggio Emilia, Department of Cardiology, Modena, Italy; 2OspedaleSan Giovanni Battista " Molinette", torino, Italy
Background: several clinical risk scores are available for the risk stratification ofpatients with ST-elevation myocardial infarction (STEMI), such as the CADILLAC,GRACE, PAMI, TIMI, and Zwolle, but all are complex to use and there is uncer-tainty on the best one. The age-creatinine-ejection fraction (ACEF) score, hasbeen recently proven effective and proficient as a risk score in cardiac surgerydespite its user-friendliness. We thus aimed to compare the performance ofthe ACEF score in comparison to the other available risk scores in patient withSTEMI.Methods: subjects with STEMI undergoing primary percutaneous coronary in-tervention at our Institution from 2001 to 2009 were enrolled. The primary end-point was in-hospital all-cause death, whereas long-term all-cause death, long-term cardiac death were appraised as secondary outcomes. ACEF, CADIL-LAC, GRACE, PAMI, TIMI, and Zwolle risk scores were compared with receiver-operating characteristics (ROC) curves with areas under the curve (AUC), andbinary multivariable logistic regression analysis with odds ratios (OR), plus 95%confidence intervals.Results: a total of 746 patients were included, followed for an average of 28months. The best predictors of in-hospital all-cause death were the GRACEscore (AUC=0.78 [0.72-0.85], adjusted OR=1.02 [1.01–1.03], p<0.001) and the
ACEF score (AUC=0.76 [0.69-0.83], adjusted OR=1.64 [1.20-2.24], p=0.002).The GRACE score also proved the best prognostic tool for long-term all-cause death (AUC=0.81 [0.77-0.85], adjusted OR=1.02 [1.01-1.02], p<0.001),together with the CADILLAC score (AUC=0.81 [0.77-0.85], adjusted OR=1,20[1.12-1.29], p<0.001). Finally, the best predictors of long-term all-cause car-diac death were the GRACE score (AUC=0.79 [0.74–0.84], adjusted OR=1.02[1.01–1.03], p<0.001), the CADILLAC score (AUC=0.77 [0.71–0.83], adjustedOR=1.18 [1.10–1.26], p<0.001), and the TIMI score (AUC=0.74 [0.68–0.79], ad-justed OR=0.86 [0.74–0.89], p=0.033).Conclusions: the ACEF score, a risk model limited to only 3 clinical variables,has favorable predictive features compared with more complex risk scores in theprediction of early mortality after STEMI. Conversely, the GRACE score, despiteits greater complexity, provides superior prognostication capability for long-termclinical outlook.
P1314 The increase of pregnancy associated plasmaprotein-A is directly linked to heparin administrationnot only to acute coronary syndrome
P. Hajek1, M. Macek Sr2, A. Lashkevich2 , H. Kluckova2,M. Hladikova1, E. Hansvenclova1, M. Maly1, A. Krebsova3,
J. Veselka1. 1University Hospital Motol, CardioVascular Center, Prague, CzechRepublic; 2University Hospital Motol, Institute of Biology and Medical Genetics,Prague, Czech Republic; 3Charite - Campus Virchow-Klinikum, Department ofCardiology, Berlin, Germany
Purpose: It was recently suggested that serum levels of pregnancy-associatedplasma protein-A (PAPP-A), a potential early marker of acute coronary syndrome(ACS), might be increased by heparin. The aim of our study was to ascertain timecourse of PAPP-A levels in ACS with ST segment elevation (ACS-STE) within first24 hours after the hospital admission and to determine the impact of concomitantclinical conditions, percutaneous coronary intervention (PCI) and heparin admin-istration on PAPP-A levels.Methods: PAPP-A serum levels were studied in 30 ACS-STE patients treated byPCI. Time course of PAPP-A was also evaluated in 10 elective PCI with heparin,in 12 patients with coronary angiography and heparin administration because oftransradial approach and in 5 patients with normal coronary angiogram done bytransfemoral approach without heparin. Samples were examined at admission,immediately after, 1, 2, 4, 6, 12, 24 hours after PCI.Results: Admission PAPP-A levels were higher than 10mIU/L (95th percentile ofnormal levels) in all ACS-STE patients heparinized during transport to the hospitalexcept of the only one patient. Moreover, heparin administration was associatedwith rapid and immense PAPP-A increase not only in ACS–STE patients but alsoin all patients without ACS or even without angiographic signs of atherosclero-sis. Angiography without heparin did not cause any PAPP-A increase. The ef-fect of heparin on PAPP-A increase was directly related to the therapeutic dose,PAPP-A levels significantly correlated with activated clotting time (ACT) (r=0.78;P=0.0001) and inversely to the interval between heparin application and time ofserum sampling. PAPP-A level increase appeared not to be significantly depen-dent on the length of PCI. Rapid increase of PAPP-A after heparin administrationwas followed by rapid decrease within 1-2 hours with return to normal levels <10mIU/L in 80% ACS-STE patients (24/30) within median of 12 hours, comparingto more quicker normalization (P<0.05) in heparinized elective PCI (median 4.3hours) and angiography patients (median 5.4 hours).Conclusions: Our results revealed that PAPP-A increase is directly linked to hep-arin administration. Therefore its diagnostic and prognostic validity in ACS mightbe verified at first after 12 hours after heparin application or if the control ACT levelis in the normal range. The slower return to normal PAPP-A levels in ACS-STEpatients and persistence of PAPP-A increase in some of them might be related toatherosclerotic lesions/plaque instability.
P1315 Factors predicting outcome of primary percutaneouscoronary intervention: role of transradial access
I. Hizoh, G. Szabo, A. Kecskes, G. Kerecsen, N. Kiss, A. Korda,L. Major, R. Markus, R.G. Kiss. State Health Centre, Department ofCardiology, Budapest, Hungary
Background: Transradial (TR) primary percutaneous coronary intervention (PCI)is a procedure with less bleeding and more patient comfort than that via the tra-ditional femoral route. Nevertheless, its effect on mortality is poorly investigated.Methods: Between September 1, 2007, and August 31, 2009, 595 primary percu-taneous coronary interventions have been performed at our department. Sevenpatients were lost for follow up, 588 subjects were further studied for 91-830 days(median: 428.5 days, interquartile range: 236-632.5 days). Transradial procedurewas performed in 80.8% of the cases (475/588), the remaining 113 patients un-derwent transfemoral (TF) primary PCI (19.2%). 8.7% (51/588) of the patientshad cardiogenic shock on admission, 22.6% (133/588) of them were older than75 years, 63.6% (374/588) of the cohort were males. We analyzed 9 variablesplaying a potential role in mortality by backward Cox regression: access site, doorto balloon time, pain to balloon time (total delay to reperfusion), age group (<50,50-75, >75 years), gender, presence of cardiogenic shock, use of intraaortic bal-loon pump, vessel dilated (LAD, D or IM, LCX, RCA, bypass graft, left main stemor multi-vessel), prior CABG operation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

194 Management of acute coronary syndromes
Results: In the entire population for the whole follow up period cardiogenic shock(hazard ratio (HR)=13.7, p<0.0001), age group (HR=2.9, p<0.0001) and accesssite (TF/TR, HR=2.1, p=0.001063) were predictive of mortality, whereas prior by-pass operation had a non-significant protective role (HR=0.15, p=0.06106), theother variables were not included in the model (p>0.1). Similarly, for 30-day mor-tality, shock (HR=21.5, p<0.0001), age group (HR=2.3, p=0.002376), access site(TF/TR, HR=2.2, p=0.009009) were prognostic. Subanalysis of patients survivingbeyond 30 days (n=540) showed that cardiogenic shock still had a reduced butsubstantial prognostic value (HR=5.2, p=0.0006432), risk of age group remainednearly unchanged (HR=2.9, p<0.0001), while role of access site became irrele-vant (p>0.1). In patients who survived beyond 90 days (n=525) age group wasthe only significant factor determining mortality (HR=2.3, p=0.01073), effect ofshock turned out to be negligible (p=0.07307).Conclusions: Our results suggest that access site may be an independent prog-nostic factor of mortality, acting in the first 30 days after primary PCI. The influenceof cardiogenic shock, the strongest predictor of mortality, becomes unimportantbeyond 90 days after the index PCI.
P1316 Safety and long-term clinical benefit of drug-elutingstent in primary percutaneous coronary interventionfor acute thrombotic total occlusion
J.S. Ko1, M.H. Jeong1, Y.K. Ahn1, S.C. Chae2, Y.J. Kim3,D.H. Choi4, I.W. Seung5. 1The heart center of chonnam national
university hospital, Gwangju, Korea, Republic of; 2Gyungbuk Nat’l UniversityHospital, Daegu, Korea, Republic of; 3Yeungnam University Hospital, Daegu,Korea, Republic of; 4Yonsei University, Severance Hospital, Seoul, Korea,Republic of; 5Chungnam National University Hospital, Daejeon, Korea, Republicof
Purpose: Drug eluting stent (DES) has well established benefit in managementof acute coronary syndrome. But concerning clinical setting of acute thromboticocclusion, some debate remained about clinical safety of drug eluting stent com-pared with bare metal stent (BMS). We aimed to verify safety and long term clini-cal outcome of DES for management of acute total occlusion of coronary artery.Methods: We enrolled 3564 patients (male 72.6%, Age 61±12 yr) with acute STelevation myocardial infarction who showed total coronary occlusion in coronaryangiography and underwent primary PCI within 6 hrs from onset of symptom fromKAMIR. We checked baseline clinical characteristics, laboratory findings, and an-giographic data. Incidence of successful PCI, hospital death and the major ad-vance cardiac events (MACE) during 1 year follow up according to stent typewere analyzed.Results: There was no significant difference in baseline characteristics and lab-oratory data between DES and BMS group. The incidence of GpIIbIIIa inhibitorinfusion was lower (9.5% vs. 17.8%, p=0.01) in DES group and stent length waslonger in DES group (26.0±6.12mm vs. 22.1±5.5mm, p<0.001). In echocar-diographic data, LV ejection fraction was lower in DES group (50.4±16.4% vs.53.1±23.6%, p=0.008). Successful PCI was achieved in 97.4% of patients andshowed no significant different between DES and BMS group (97.5% vs. 97.2%,p=0.419). Incidence of in-hospital death was significantly lower in DES group(5.3% vs. 8.5%, p=0.013). In survival analysis, DES was associated of lowerincidence of total MCAE (HR=0.724, p=0.048), but no significant difference inincidence death/myocardial infarction (p=0.690) during one-year follow up.Conclusion: Deployment of drug eluting stent in management acute total occlu-sion of coronary artery was safe and associated with favorable long-term clinicaloutcome
P1317 Difference of prognostic value of thrombolysis inmyocardial infarction flow grade 2 after primarypercutaneous coronary intervention between anteriorand non-anterior ST-elevation myocardial infarction
H. Shibata, S. Yamada, T. Hayashi, Y. Taniguchi, S. Iwata,M. Kumada, T. Takaya, A. Shimane, T. Tagashira, T. Kajiya. HimejiCardiovascular Center, Himeji, Japan
Purpose: Thrombolysis in myocardiar infarction (TIMI) flow grade 2 and 3 afterprimary percutaneous coronary intervention (pPCI) for ST elevation myocardialinfarction (STEMI) has been defined as successful reperfusion. However, whetherTIMI grade 2 is equivalent to TIMI 3 is still controversial especially in anteriorSTEMI.Methods: Between May 2004 and December 2008 we investigated 374 pa-tients with successful pPCI (177 anterior and 197 non-anterior) for STEMI within24 hours from onset. We performed ECG-gated 99m-Technetium-Tetrofosminscintigraphy (TcTF) as an indicator of cardiac function. TcTF were performed 10-14 days after pPCI (acute phase) and repeated at 3 months (chronic phase).Myocardium was divided into 25 segments and segmental score was graded bydegrees according to the relative activity (0: normal, 4: defect). Sum of defectscores (DS) were calculated from SPECT, LV ejection fravtion (EF) and LV end-diastolic volume (LVEDV) were calculated from QGS.Result: Post pPCI TIMI 2 flow were observed in 34 patients (19.2%) in ante-rior STEMI and 33 patients (16.8%) in non-anterior STEMI, respectively. In bothgroup, peak CK and CK-MB did not differ significantly smaller in TIMI2 of anteriorSTEMI. In contrast, these differences were not observed in non-anterior STEMI.
Re-hospitalization due to heart failure during follow-up is more frequent in TIMI2 than TIMI 3 in anteriror STEMI, whereas such difference was also absent innon-anteiror STEMI.
Anterior STEMI Non-Anterior STEMI
TIMI 3 (N=143) TIMI 2 (N=34) p TIMI 3 (N=164) TIMI 2 (N=33 p
peak CK 4222 4679 0.43 3056 2773 0.39peak CK-MB 401 402 0.99 279 251 0.37DS acute 25.4 30.9 0.04 12.2 12.8 0.72EF (%) acute 43.6 38.2 0.01 48.8 51.9 0.17DS chronic 22.4 24.0 0.56 11.6 12.5 0.57EF (%) chronic 51.5 45.7 0.02 56.6 55.8 0.71Rehospitalization
due to heart failure (%) 8.5 20.6 0.04 6.1 9.1 0.54
Conclusion: TIMI flow grade 2 post pPCI predicts poorer cardiac function andclinical outcome only in anterior STEMI.
P1318 Impact of continuous feed-back on thedoor-to-balloon time in patients with ST-segmentelevation myocardial infarction
M.J. Bertrand, L.M. Stevens, S. Champoux, F. Gobeil, A. Kokis,N. Noiseux, J.B. Masson, S. Mansour. Montreal University Hospital
Center, Montreal, Canada
Purpose: Current guidelines for management of patients with ST-elevation my-ocardial infarction (STEMI), recommend a door-to-balloon time (DTB) within 90minutes, although this target is hardly achieved. We aim to determine the impactof a continuous feed-back to referring physician on the DTB in a high volumetertiary center instituted in January 2008.Methods: Consecutive patients with STEMI treated with percutaneous coronaryintervention (PCI) from January 2008 to December 2009, were prospectively an-alyzed. Patients were divided in 4 semesters and data was analysed by ANOVAor Kruskal-Wallis tests as appropriate.Results: Five hundred and fifteen patients with STEMI were included. The meanage was 61±13 years (25% female), 16% of patients had diabetes, 42% ante-rior infarct and the mean left ventricular ejection fraction was 48%±12%. Amongthe four semesters, patients were similar regarding age, gender, co-morbidities,anterior localisation and ejection fraction. Overall median DTB was 97 [80-125]minutes with 42% ≤ 90 minutes. Nevertheless, the median DTB time for eachsemester improved over the study period (104 minutes [83-137] for the firstsemester to 92 minutes [77-108] for the last semester; P < 0.001). This trendwas also observed for PCI performed during the day and night shifts, week-ends and holidays (all p<0.05). The multivariate predictors of long DTB wereearlier semesters (p=0.002), distance (p<0.001), older age (p=0.011), diabetes(p=0.005) and high Killip (p= 0.003).Conclusion: Continuous feed-back to the referring physician was associated withsignificant decrease of the DTB in patients admitted in STEMI. Nevertheless, DTBdo not always meet the recommended standards, other strategies need to bedeveloped especially for high-risk groups.
P1319 Drug-eluting vs. bare-metal stent implantation inST-segment elevation myocardial infarction. Datafrom EUROTRANSFER registry
A. Dziewierz1, Z. Siudak1, T. Rakowski1, W. Zasada1, J.S. Dubiel1,K. Zmudka2 , D. Dudek2. 1Jagiellonian University Medical College,
2nd Department of Cardiology, Krakow, Poland; 2Jagiellonian University MedicalCollege, Department of Interventional Cardiology, Krakow, Poland
Aim: To assess current pattern of drug-eluting stent (DES) implantation and asso-ciated real-life outcomes in patients with ST-segment elevation myocardial infarc-tion (STEMI) transferred for primary percutaneous coronary intervention (PPCI).Methods and results: Data were gathered for 1 650 consecutive STEMI patientstransferred for PPCI from hospital networks in 7 countries in Europe from Novem-ber 2005 to January 2007. We identified 1428 patients with at least one stentimplanted (86.5%). DES were implanted in 382 patients (26.8%) and bare-metalstents (BMS) in 1046 patients (73.2%) of 1428 who received stent. High variabil-ity in DES use in participating centers was observed (range from 0% to 72.1%).In assessed population, DES patients were younger and have higher rate of priorPCI. As shown in the Table, use of DES was associated with significantly lowerrates of ischemic events during follow-up, but observed difference was no longersignificant after adjustment for covariates. These findings were confirmed for both,centers with low (<26.8%) and high (≥26.8%) DES application frequency.
Clinical outcomes
Variable BMS DES P value Adjusted HR (95% CI)
30-day death 4.8% 1.8% 0.014 0.45 (0.20-1.03)30-day death+reinfarction 6.4% 3.4% 0.037 0.59 (0.32-1.11)30-day MACE 7.2% 3.9% 0.026 0.60 (0.34-1.08)1-year death 6.7% 3.1% 0.014 0.56 (0.29-1.07)
Conclusions: Despite positive results of randomized studies comparing DES vs.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Management of acute coronary syndromes 195
BMS in STEMI, a high variability in DES use in such setting is still observed inEurope. In this European prospective registry DES appear to be as safe as BMS,with similar long-term clinical outcomes.
P1320 The development of door-to-balloon time in the last14 years for patients with acute ST-elevationmyocardial infarction treated with primary coronaryintervention: determinants and outcome
F. Towae1, C. Junger2 , H. Mudra3, E. Hauptmann4, T. Voigtlaender5 ,T. Bauer1, U. Zeymer1, J. Senges2, A.K. Gitt1, R. Zahn1. 1Clinical Center ofLudwigshafen, Department of Cardiology, Ludwigshafen am Rhein, Germany;2Heart Attack Research Center at the University of Heidelberg, Ludwigshafen amRhein, Germany; 3Neuperlach Hospital, Department of Cardiology, Pulmonology& Internal Intensive Care, Munich, Germany; 4Hospital of the Merciful Brothers,Department of Cardiology, Trier, Germany; 5CCB, Cardioangiologisches CentrumBethanien, Frankfurt am Main, Germany
Objectives: Aim of the study is to examine the development ofdoor-to-balloontime (DTB) and to evaluate the impact of door-to- balloon timein patients withST-elevation myocardial infarction (STEMI) on hospital and1-year mortality.Methods and Results: From 1994 to 2008, 5078 patients (pts) and known DTB-with acute ST-elevation myocardial infarction were enrolled into the MITRAplu-sand OPTAMI registry in Germany.Our data showed areduction of the door-to-balloon time from 80 minutes to 64minutes in the last14 years (p < 0.001). Over 80% of patients received an angiog-raphy lessthan 2 hours after admission. The main predictors of an increasingdoor-to-balloon time were age over 75 years (p<0.01), a history of priormyocardialinfarction (p<0.001) or coronary bypass graft (p<0.05),diabetes (p<0.05) rightbundle brunch block (p<0.01), blood pressurelower than 100 mmHg (p <0.001)and a prehospital delay time of more than 3 h (p<0.001). In the multivariate re-gression analysis no influence was detectedof door-to-balloon time in hospital or1-year mortality.
Variable ≤60 min >60 min p- Value OR 95% CI
Age [years], median 61.7 63.7 < 0.001Age < 75 years 15.3% 18.6% < 0.01 0.79 0.67-0.93Prior MI 11.1% 17.3% < 0.0001 0.6 0.5-0.72Prior CABG 2.7% 4.5% < 0.05 0.58 0.38-0.89Diabetes 18.3% 21.4% < 0.05 0.82 0.70-0.96Current smoker 43.3% 38.5% < 0.01 1.22 1.05-1.41Hypertension 49.3% 54.9% < 0.001 0.80 0.70-0.90Prehospital delay time
<1 h 15.2% 14.8% 0.69 1.04 0.87-1.231-3 h 50.4% 43.6% < 0.0001 1.31 1.13-1.49>3 h 34.3% 41.6% < 0.0001 0.73 0.65-0.83
Blood pressure < 100 mmHg 12.8% 9.4% < 0.001 1.42 1.16-1.74
Conclusion: In our registries the door-to-balloon time (median)decreased in thelast 14 years and is actually very short in Germany. Weindentified predictors of alonger door-to-balloon time in clinical practice.Given the overall short in-hospitaldelay, the observed door-to-balloon time did not have influence on hospital ansmid term mortality
P1321 Assessing the coverage of a comprehensive STEMIsurvey: prospective recruitment has a potential forselection bias
K.K.M. Koivula1, J.V. Viikila1, J.M. Lilleberg1, M. Syvanne2,V. Salomaa3. 1Helsinki University Central Hospital, Department of
Medicine, Division of Cardiology, Helsinki, Finland; 2Finnish Heart Association,Helsinki, Finland; 3National Institute for Health and Welfare, Helsinki, Finland
Purpose: To assess the coverage of a prospective ST elevation myocardial in-farction (STEMI) survey intended to comprehensively include all cases of STEMI.Methods: In the HUS-STEMI survey we evaluated the results of primary PCI(PPCI) and thrombolysis (lysis) in actively recruited consecutive patients present-ing over a 1-year period at the Hospital District of Helsinki and Uusimaa (HUS) inFinland. Chest pain with ST-elevation or new LBBB and a written informed con-sent were the criteria for inclusion. There were no exclusion criteria. All hospitalsin the HUS district had at least one active investigator. Recruitment time was fromJune 13, 2007 to June 12, 2008. According to local guidelines, low-risk STEMI pa-tients (haemodynamically stable) presenting within 3 hours from chest pain onsetcould be treated with lysis if not contraindicated; the remaining patients were re-ferred for PPCI.In order to estimate the coverage of the study we analysed the first 143 patientsof the HUS-STEMI survey. From hospital databases we searched patients hospi-talised with a STEMI in the same area during the same period but missed for theHUS-STEMI survey. The purpose of the study was to compare the recruited andthe not-recruited patients to evaluate a potential inclusion bias in a survey suchas HUS-STEMI.Results: Fifty-two patients (27% of those eligible) had been missed in the pri-mary recruitment. We found that the omitted STEMI patients were significantlyolder, less actively investigated and treated, and had a worse outcome than therecruited patients (Table).
Comparison of the patient groups
Recruited n Not-recruited n P value
Age (median) 62 143 172 52 0.005Men 69% 98 58% 30 0.159Thrombolysis or PPCI 89% 127 60% 31 <0.001In-hospital mortality 5.6% 8 23% 12 <0.001
PPCI = Primary PCI.
Conclusions: Our results imply that in STEMI studies older patients with a worseoutcome are prone to be omitted despite the specific aim for comprehensive en-rolment. Special measures to avoid selection bias might be necessary in STEMIsurveys
P1322 Influence of prior stroke on the acute therapy andin-hospital events in patients with ST-elevationmyocardial infarction. Results from DHR (GermanMyocardial Infarction Registry)
A.K. Schwarz1, A.K. Gitt1, R. Zahn1, M. Horack2, J. Senges2,U. Zeymer1 . 1Heart Centre Ludwigshafen, Department of Cardiology,Ludwigshafen, Germany; 2Heart Attack Research Center at the University ofHeidelberg, Ludwigshafen am Rhein, Germany
Introduction: Data of treatment and outcome of patients with prior stroke pre-senting with ST elevation myocardial infarction (STEMI) are scarce, since thesepatients are usually excluded from randomized clinical trials. This analysis exam-ines the impact of prior stroke on outcome in clinical practice.Methods: The German Myocardial Infarction Registry is a prospective, multicen-ter registry that enrolled 6714 patients with STEMI. Data were obtained by stan-dardised questionnaires and analysed centrally.Results: In 2007 and 2008 a total of 6714 patients were enrolled of which 5,3%(n=353) had a history of stroke. These patients were older (72,4 vs. 63,0 years;p<0,0001), had significantly more cardiovascular risk factors, (diabetes mellitus,hyperlipidemia, hypertension) and concomitant diseases (renal insufficiency, pe-ripheral arterial disease, previous myocardial infarction, history of percutaneouscoronary intervention (PCI) and coronary artery bypass graft (CABG), and con-gestive heart failure (CHF)). The main differences regarding reperfusion therapy,medical treatment and in-hospital events are displayed in Table 1.
Table 1. Main differences regarding reperfusion therapy, medical treatment, and in-hospital events
Total History of stroke/TIA No history of stroke/TIA p-valuen=6714 n=353 n=6361
Coronary angiography [%] 96,4 89,8 96,8 <0,0001Primary PCI [%] 88,1 79,5 88,5 <0,0001Fibrinolysis [%] 4,1 5,9 4,0 0,08
Aspirin [%] 98,2 95,3 98,4 <0,0001Clopidogrel [%] 94,6 91,1 94,8 <0,01GPIIb/IIIa antagonist [%] 60,8 48,4 61,5 <0,0001
In-hospital mortality [%] 6,8 13,7 6,4 <0,0001Stroke [%] 0,8 3,0 0,6 <0,0001Major bleeding [%] 3,0 5,8 2,8 <0,01
Conclusion: Patients with prior stroke presenting with STEMI significantly lessoften receive reperfusion therapy and had more in-hospital events (death, stroke,major bleeding). The optimal strategy in these patients requires further investiga-tion.
P1323 12-months mortality of STEMI patients treated byprimary PCI with multivessel disease and chronictotal occlusions: analysis from PL-ACS registry
M. Gierlotka1, M. Gasior1, M. Tajstra1, A. Lekston1, P. Buszman2,G. Opolski3, L. Polonski1. 1Medical University of Silesia, Silesian
Center for Heart Diseases, Zabrze, Poland; 2Medical University of Silesia, 3rdDepartment of Cardiology, Katowice, Poland; 3Medical University of Warsaw, 1stDepartment of Cardiology, Warsaw, Poland
Multivessel disease is associated with high mortality after ST-segment elevationmyocardial infarction (STEMI). The purpose of this study was to assess the impactof chronic total occlusions (CTO) found in coronary angiography during primaryPCI for STEMI in patients with 3-vessels disease on 12-months mortality.Methods: All patients with STEMI treated by primary PCI, with 3-vessels dis-eases, who were registered in the prospective Polish Registry of Acute CoronarySyndromes (PL-ACS) from 07.2007 to 11.2008 were included. Patients with priorCABG as well as those with significant stenosis of left main coronary artery wereexcluded. 12-months mortality was obtained from the government database.Results: From 1076 patients, fulfilling inclusion and exclusion criteria, one ormore CTO different than infarct related artery was found in 424 (39.4%). They hadmore often cardiogenic shock on admission and anterior localisation of STEMI (ta-ble). The rates of successful reperfusion of infarct related artery by PCI (TIMI 3)was similar in both groups. In-hospital as well as 12-months mortality was signifi-cantly higher in patients with CTO. After multivariate adjustment for differences inbaseline characteristics presence of CTO remained significantly associated withhigher 12-months mortality (relative risk = 1.48, 95%CI = 1.11-1.96, p=0.0072).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

196 Management of acute coronary syndromes / Focus on stable angina
Table 1
Chronic total occlusion(s) No chronic total occlusion P value
Number of patients, % 424 (39.4%) 652 (60.6%)Age, years (SD) 66.3 (11.1) 66.9 (11.0) 0.42Female sex, % 30.0 35.4 0.062Diabetes, % 25.5 24.2 0.64Killip 4 on admission, % 9.9 4.6 0.0007Anterior infarction, % 44.3 33.7 0.0005Final TIMI flow grade 3 after
PCI of infarct related artery, % 87.7 89.6 0.35In-hospital outcomes– Re-infarction, % 0.9 1.4 0.52– Death, % 13.0 4.9 <0.000112-months mortality, % 29.3 15.8 <0.0001
Conclusion: Chronic total occlusion(s) found in patients with 3-vessels diseaseand STEMI treated by primary PCI are associated with worse 12-months mortal-ity.
FOCUS ON STABLE ANGINA
P1324 Organic nitrates differentially modulate endothelialfunction and circulating angiogenic cells in patientswith symptomatic coronary artery disease
T. Thum1, V. Wiebking1, G. Ertl2, J. Bauersachs2. 1HannoverMedical School, Department of Molecular and Translational
Therapeutic Strategies, Hannover, Germany; 2Julius-Maximilians University,Wurzburg, Germany
Purpose: Symptomatic coronary artery disease (CAD) is usually treated with or-ganic nitrates. Circulating angiogenic cells (CAC) are a cell population participat-ing in angiogenesis and vascular homeostasis in a nitric-oxide (NO)-dependentmanner. We thus investigated the effects of the NO donors isosorbide dinitrate(ISDN) and pentaerythritol tetranitrate (PETN) on numbers and function of CACand endothelial function in patients with symptomatic CAD.Methods and Results: We randomized 36 patients with angiographically provenCAD to treatment with either ISDN (40mg retarded release orally two timesper day; n=18) or PETN (80mg orally two times per day; n=18) for fourteendays (clinical trial number: NCT01030367). Baseline characteristics were simi-lar in both groups. PETN treatment substantially increased numbers of circulat-ing CD34+/KDR+ cells (P=0.02), whereas no effects were observed in patientstreated with ISDN. CAC function assessed by formation of endothelial colonieswas enhanced by 2-fold (P=0.04) in patients treated with PETN. In contrast, nochanges were observed after ISDN treatment. Migratory capacity of CAC was un-changed in both treatment groups. Endothelial function, assessed by peripheralarterial tonometry, remained unchanged during PETN treatment, but was signifi-cantly impaired in patients treated with ISDN.Conclusions: Treatment of symptomatic CAD patients with PETN for fourteendays significantly increased levels of CAC and improved markers for CAC func-tion, whereas ISDN was without effects on CAC and worsened markers of en-dothelial function.
P1325 Benefits of nifedipine GITS in stable coronary arterydisease: further analysis of the "ACTION" database
H.L. Elliott1, P. Meredith2. 1University of Strathclyde, Glasgow,United Kingdom; 2Western Infirmary, Glasgow, United Kingdom
The placebo-controlled ACTION trial examined the effects of Nifedip-ine GITS on clinical outcomes in patients with stable symptomatic coronary arterydisease (CAD). A retrospective further analysis of the database from ACTIONevaluated the potential benefits of nifedipine GITS in combination with other treat-ments.Analyses were performed on an intention-to-treat basis. Treatment groups werecompared by the log-rank test without adjustment for covariates. Hazard ratioswith 95% CI’s were obtained using Cox proportional hazards models with treat-ment allocation as the only covariate.Of 7665 randomised patients 1732 (22.6%) were receiving RAS blockade (ACEinhibitor or ARB) at baseline and 857 were randomised to nifedipine GITS and875 to placebo. Nifedipine significantly reduced a number of endpoints: theseincluded any CV event (-20%; p<0.05), the composite of death, any CV eventand revascularisation (-16%; p<0.05) and coronary angiography (-22%; p<0.01).There were non-significant reductions in the primary composite end-points forefficacy (-14%) and safety (-7%). These benefits were achieved with relativelysmall differences in systolic BP (3.2 mmHg) and diastolic BP (2.3mmHg).Further analyses demonstrated a significant outcome benefit in patients treatedwith nifedipine GITS in the absence of RAS blockade compared to patients re-ceiving RAS blockade and placebo.Since the publication of the HOPE trial there has been a widespread percep-tion that treatment with ACE inhibitor drugs are selectively beneficial in the treat-ment of patients with established CAD and that these benefits are not attributableto BP lowering alone. These retrospective analyses show that in the treatmentof patients with symptomatic CAD additional prognostic benefit can be derived
from the addition of nifedipine GITS even in patients receiving RAS blockade atbaseline. While these findings must be the interpreted cautiously, the treatmentgroups in both analyses were well matched in their demographic features andactive treatments at baseline.
P1326 Gender differences in patients with stable angina:5-year follow-up. Results of the STAR registry
F. Towae1, M. Horack2, T. Bauer1, U. Zeymer1, J. Senges2,R. Zahn1, A.K. Gitt1. 1Clinical Center of Ludwigshafen, Departmentof Cardiology, Ludwigshafen am Rhein, Germany; 2Heart Attack
Research Center at the University of Heidelberg, Ludwigshafen am Rhein,Germany
Background: Registry data of acute coronary syndromes including mid-term andlongterm follow-up have shown gender differences in mortality. However, littledataexist on long term outcome in patients with stable angina and the impactofgender.Methods: Between July 2001 and April2003, 2002 patients with stable anginaCCS I-III and first angiographicdiagnosis of CAD were enrolled in the STAR reg-istry (Stable Angina pectoris Registry). Patient characteristics, medical treatmentand hospital mortality weredocumented at admission, discharge, after 1-year andafter 5-year follow up. Weanalysed gender differences in treatment, presentationand outcome at patientswith stable angina after 5 years follow up.Results: After correcting for differences in baseline characteristics and forinter-ventional and long-term medical treatment using a stepwise logisticregressionanalysis, female gender was associated with a 34% decrease 5year-mortality(OR 0.66; 95% CI 0.51-0.87)
Results
Parameters Female gender (n=600) Male gender (n=1402) p-value
Data at admissionAge (median) 70 65 <0.01Hypertension (%) 79.7 71.3 <0.01Current smoking (%) 15.7 27.8 <0.001Diabetes (%) 31.7 24.2 <0.001
Interventional treatmentPCI (at enrollment) (%) 47.8 45.1 n.s.PCI (1-5 years) 17.3 16.5 n.s.CABG (within 5 years) 24.8 30.6 <0.01
5-years follow upASA (%) 75.7 79.5 n.sBeta-blocker (%) 80.0 75.2 n.s.ACE-Inhibitors (%) 48.9 52.0 n.s.Statins (%) 67.2 66.8 n.s.Death (%) 16.8 18.25 <0.05
Conclusion: Female gender presenting with stable angina were significant 5yearsolder and had more diabetes and less smoking. Considering the differencesin age female gender was associated with a more than one third lower mortalityafter 5years.
P1327 Identification of patients at risk of coronary arterydiease by assessment of digital reactive hyperaemiain an ambulant setting
M. Van Den Heuvel, K. Nieman, O. Sorop, T.W. Galema,P.J. Musters, A.F.L. Schinkel, A.H.J. Danser, W.J. Van Der Giessen.
Erasmus MC, Rotterdam, Netherlands
Purpose: Coronary artery disease (CAD) prediction by risk-scores based on tra-ditional risk-factors lacks specificity in low- to intermediate risk individuals. Coro-nary calcium scoring (CCS) and coronary angiography (CTCA) by multislice com-puted tomography have already proven to be useful in the evaluation of highlysuspected CAD. However, a simple, non-invasive tool that allows reliable iden-tification of low-risk patients in an ambulant setting would be desirable. Sinceperipheral atherosclerosis development correlates with CAD and is more acces-sible for non-invasive examination, we studied this arterial territory with a new testfor the first time outside a research setting.Methods: Digital peripheral arterial tonometry (PAT) was used to measure pulsewave amplitude during reactive hyperaemia and was taken as a measure of pe-ripheral microvascular function in 84 patients referred with stable chest pain com-plaints to our cardiology outpatient department. Of all patients, also CCS andCTCA were determined.Results: Patients with high amounts of coronary plaque or stenosis on CTCAshowed an abnormal PAT-response (P<0.05). However, digital reactive hyper-aemia responses considered to be in the normal range, did not exclude an in-creased CCS, coronary plaque or stenosis.Conclusions: In referred patients with stable chest pain, PAT-response after re-active hyperaemia, CCS, and CTCA may represent independent and separateprocesses in CAD development. By measuring peripheral microvascular functionin an ambulant setting in stead of a research setting, patients with a clear pres-ence of coronary plaque or stenosis cannot be predicted, indicating that this newtest is not able to replace conventional diagnostic procedures.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
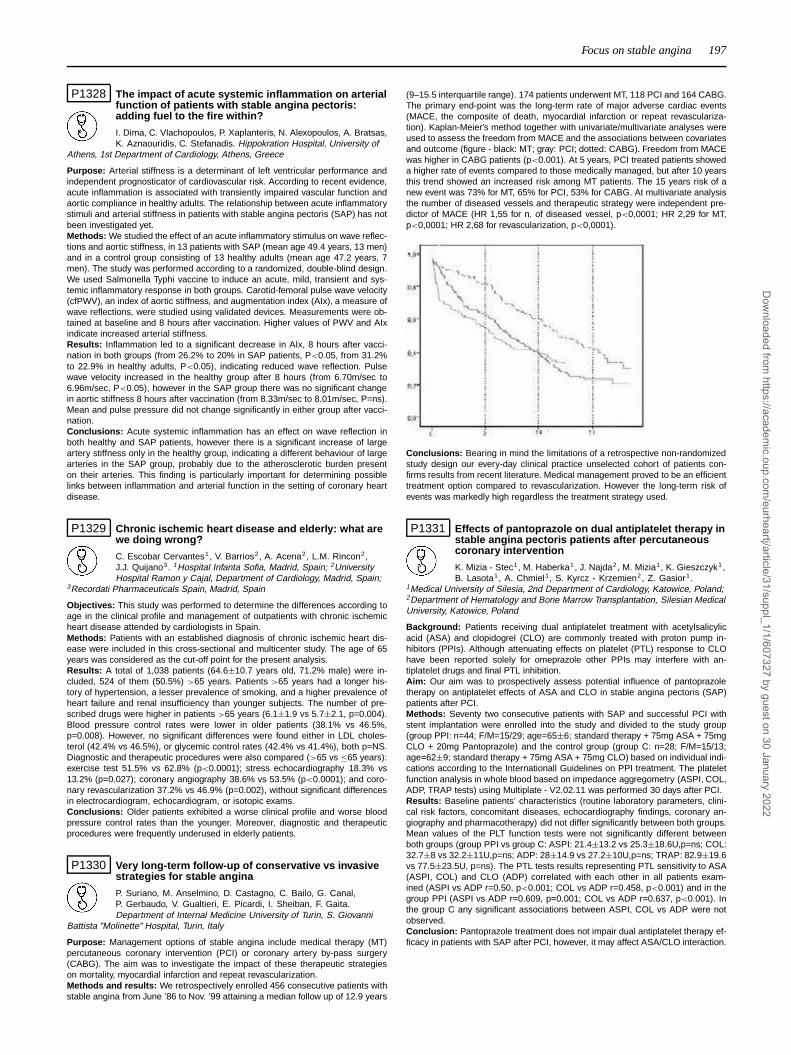
Focus on stable angina 197
P1328 The impact of acute systemic inflammation on arterialfunction of patients with stable angina pectoris:adding fuel to the fire within?
I. Dima, C. Vlachopoulos, P. Xaplanteris, N. Alexopoulos, A. Bratsas,K. Aznaouridis, C. Stefanadis. Hippokration Hospital, University of
Athens, 1st Department of Cardiology, Athens, Greece
Purpose: Arterial stiffness is a determinant of left ventricular performance andindependent prognosticator of cardiovascular risk. According to recent evidence,acute inflammation is associated with transiently impaired vascular function andaortic compliance in healthy adults. The relationship between acute inflammatorystimuli and arterial stiffness in patients with stable angina pectoris (SAP) has notbeen investigated yet.Methods: We studied the effect of an acute inflammatory stimulus on wave reflec-tions and aortic stiffness, in 13 patients with SAP (mean age 49.4 years, 13 men)and in a control group consisting of 13 healthy adults (mean age 47.2 years, 7men). The study was performed according to a randomized, double-blind design.We used Salmonella Typhi vaccine to induce an acute, mild, transient and sys-temic inflammatory response in both groups. Carotid-femoral pulse wave velocity(cfPWV), an index of aortic stiffness, and augmentation index (AIx), a measure ofwave reflections, were studied using validated devices. Measurements were ob-tained at baseline and 8 hours after vaccination. Higher values of PWV and AIxindicate increased arterial stiffness.Results: Inflammation led to a significant decrease in AIx, 8 hours after vacci-nation in both groups (from 26.2% to 20% in SAP patients, P<0.05, from 31.2%to 22.9% in healthy adults, P<0.05), indicating reduced wave reflection. Pulsewave velocity increased in the healthy group after 8 hours (from 6.70m/sec to6.96m/sec, P<0.05), however in the SAP group there was no significant changein aortic stiffness 8 hours after vaccination (from 8.33m/sec to 8.01m/sec, P=ns).Mean and pulse pressure did not change significantly in either group after vacci-nation.Conclusions: Acute systemic inflammation has an effect on wave reflection inboth healthy and SAP patients, however there is a significant increase of largeartery stiffness only in the healthy group, indicating a different behaviour of largearteries in the SAP group, probably due to the atherosclerotic burden presenton their arteries. This finding is particularly important for determining possiblelinks between inflammation and arterial function in the setting of coronary heartdisease.
P1329 Chronic ischemic heart disease and elderly: what arewe doing wrong?
C. Escobar Cervantes1, V. Barrios2, A. Acena2, L.M. Rincon2,J.J. Quijano3. 1Hospital Infanta Sofia, Madrid, Spain; 2UniversityHospital Ramon y Cajal, Department of Cardiology, Madrid, Spain;
3Recordati Pharmaceuticals Spain, Madrid, Spain
Objectives: This study was performed to determine the differences according toage in the clinical profile and management of outpatients with chronic ischemicheart disease attended by cardiologists in Spain.Methods: Patients with an established diagnosis of chronic ischemic heart dis-ease were included in this cross-sectional and multicenter study. The age of 65years was considered as the cut-off point for the present analysis.Results: A total of 1,038 patients (64.6±10.7 years old, 71.2% male) were in-cluded, 524 of them (50.5%) >65 years. Patients >65 years had a longer his-tory of hypertension, a lesser prevalence of smoking, and a higher prevalence ofheart failure and renal insufficiency than younger subjects. The number of pre-scribed drugs were higher in patients >65 years (6.1±1.9 vs 5.7±2.1, p=0.004).Blood pressure control rates were lower in older patients (38.1% vs 46.5%,p=0.008). However, no significant differences were found either in LDL choles-terol (42.4% vs 46.5%), or glycemic control rates (42.4% vs 41.4%), both p=NS.Diagnostic and therapeutic procedures were also compared (>65 vs ≤65 years):exercise test 51.5% vs 62.8% (p<0.0001); stress echocardiography 18.3% vs13.2% (p=0.027); coronary angiography 38.6% vs 53.5% (p<0.0001); and coro-nary revascularization 37.2% vs 46.9% (p=0.002), without significant differencesin electrocardiogram, echocardiogram, or isotopic exams.Conclusions: Older patients exhibited a worse clinical profile and worse bloodpressure control rates than the younger. Moreover, diagnostic and therapeuticprocedures were frequently underused in elderly patients.
P1330 Very long-term follow-up of conservative vs invasivestrategies for stable angina
P. Suriano, M. Anselmino, D. Castagno, C. Bailo, G. Canal,P. Gerbaudo, V. Gualtieri, E. Picardi, I. Sheiban, F. Gaita.Department of Internal Medicine University of Turin, S. Giovanni
Battista "Molinette" Hospital, Turin, Italy
Purpose: Management options of stable angina include medical therapy (MT)percutaneous coronary intervention (PCI) or coronary artery by-pass surgery(CABG). The aim was to investigate the impact of these therapeutic strategieson mortality, myocardial infarction and repeat revascularization.Methods and results: We retrospectively enrolled 456 consecutive patients withstable angina from June ’86 to Nov. ’99 attaining a median follow up of 12.9 years
(9–15.5 interquartile range). 174 patients underwent MT, 118 PCI and 164 CABG.The primary end-point was the long-term rate of major adverse cardiac events(MACE, the composite of death, myocardial infarction or repeat revasculariza-tion). Kaplan-Meier’s method together with univariate/multivariate analyses wereused to assess the freedom from MACE and the associations between covariatesand outcome (figure - black: MT; gray: PCI; dotted: CABG). Freedom from MACEwas higher in CABG patients (p<0.001). At 5 years, PCI treated patients showeda higher rate of events compared to those medically managed, but after 10 yearsthis trend showed an increased risk among MT patients. The 15 years risk of anew event was 73% for MT, 65% for PCI, 53% for CABG. At multivariate analysisthe number of diseased vessels and therapeutic strategy were independent pre-dictor of MACE (HR 1,55 for n. of diseased vessel, p<0,0001; HR 2,29 for MT,p<0,0001; HR 2,68 for revascularization, p<0,0001).
Conclusions: Bearing in mind the limitations of a retrospective non-randomizedstudy design our every-day clinical practice unselected cohort of patients con-firms results from recent literature. Medical management proved to be an efficienttreatment option compared to revascularization. However the long-term risk ofevents was markedly high regardless the treatment strategy used.
P1331 Effects of pantoprazole on dual antiplatelet therapy instable angina pectoris patients after percutaneouscoronary intervention
K. Mizia - Stec1, M. Haberka1, J. Najda2, M. Mizia1, K. Gieszczyk1,B. Lasota1, A. Chmiel1, S. Kyrcz - Krzemien2, Z. Gasior1.
1Medical University of Silesia, 2nd Department of Cardiology, Katowice, Poland;2Department of Hematology and Bone Marrow Transplantation, Silesian MedicalUniversity, Katowice, Poland
Background: Patients receiving dual antiplatelet treatment with acetylsalicylicacid (ASA) and clopidogrel (CLO) are commonly treated with proton pump in-hibitors (PPIs). Although attenuating effects on platelet (PTL) response to CLOhave been reported solely for omeprazole other PPIs may interfere with an-tiplatelet drugs and final PTL inhibition.Aim: Our aim was to prospectively assess potential influence of pantoprazoletherapy on antiplatelet effects of ASA and CLO in stable angina pectoris (SAP)patients after PCI.Methods: Seventy two consecutive patients with SAP and successful PCI withstent implantation were enrolled into the study and divided to the study group(group PPI: n=44; F/M=15/29; age=65±6; standard therapy + 75mg ASA + 75mgCLO + 20mg Pantoprazole) and the control group (group C: n=28; F/M=15/13;age=62±9; standard therapy + 75mg ASA + 75mg CLO) based on individual indi-cations according to the Internationall Guidelines on PPI treatment. The plateletfunction analysis in whole blood based on impedance aggregometry (ASPI, COL,ADP, TRAP tests) using Multiplate - V2.02.11 was performed 30 days after PCI.Results: Baseline patients’ characteristics (routine laboratory parameters, clini-cal risk factors, concomitant diseases, echocardiography findings, coronary an-giography and pharmacotherapy) did not differ significantly between both groups.Mean values of the PLT function tests were not significantly different betweenboth groups (group PPI vs group C: ASPI: 21.4±13.2 vs 25.3±18.6U,p=ns; COL:32.7±8 vs 32.2±11U,p=ns; ADP: 28±14.9 vs 27.2±10U,p=ns; TRAP: 82.9±19.6vs 77.5±23.5U, p=ns). The PTL tests results representing PTL sensitivity to ASA(ASPI, COL) and CLO (ADP) correlated with each other in all patients exam-ined (ASPI vs ADP r=0.50, p<0.001; COL vs ADP r=0.458, p<0.001) and in thegroup PPI (ASPI vs ADP r=0.609, p=0.001; COL vs ADP r=0.637, p<0.001). Inthe group C any significant associations between ASPI, COL vs ADP were notobserved.Conclusion: Pantoprazole treatment does not impair dual antiplatelet therapy ef-ficacy in patients with SAP after PCI, however, it may affect ASA/CLO interaction.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

198 Focus on stable angina
P1332 Cardiac shockwave therapy in patients with end-stagecoronary artery disease and chronic refractory anginapectoris - mid term results
J. Vainer, J. Habets, A. Lousberg, B. Brans, S. Schalla,J. Waltenberger. University Hospital Maastricht, Maastricht,
Netherlands
Despite maximal medical and invasive therapy a substantial number of patientsshows progression to end-stage ischemic coronary artery disease with therapy-refractory angina pectoris. Cardiac shockwave therapy (CSWT) induces a cavita-tion, i.e. rapid formation and collaps of vapor pockets in and outside cells. Thismight stimulate collateral vessel growth in chronic ischemic myocardium leadingto improved regional perfusion and reduced severity of symptoms. This is one ofthe largest studies on CSWT reported so far with a follow-up of 4 months.Methods: 22 pts (18 male, mean age 69±7 years, left ventricular ejection frac-tion 52±13%) with end-stage coronary artery disease and reversible ischemia onmyocardial scintigraphy (SPECT) were included. Nineteen pts had a history ofCABG, 3 pts underwent re-CABG and 7 pts PCI. CSWT was applied to the is-chemic zones (100 impulses/spot, 0.09 mJ/mm2) in an echocardiography-guidedand ECG-triggered fashion. Patients received 3 treatments/week at 0, 1 and 2months, resulting in a total of 9 applications. Per session, 3-6 different spotswere treated. Clinical assessment was performed with exercise test, angina score(CCS class), nitrate use, SPECT at 0, 1 and 4 months after the last treatment ses-sion. Magnetic resonance imaging (MRI) was performed in 8 pts.Results: Following CSWT, the clinical status improved. The use of sublingualnitrates decreased from 10 per week (range 2-25) pre-CSWT to 3 per week (range0-20) at 1 month and to 2 per week (range 0-7) at 4 months post-CSWT (p<0.01).Simultaneously, angina complaints significantly decreased at least by one CCSclass in 18 pts at 1 month and in all but one patient at 4 months after treatment(p<0.01). There was no significant decrease of ischemia burden following CSWTdemonstrated by SPECT. Exercise tolerance did not significantly improve (from7.8±4 to 8.7±4 to 8.5±3 minutes). CSWT was well tolerated without side effectsapart from transient dizziness shortly after the initial treatment session in 4 pts.Creatine kinase did not rise within the first day after treatment. Compared withbaseline, MRI did not show increase in scar tissue volume following CSWT andthere was no change in LV ejection fraction.Conclusions: CSWT resulted in sustained relieve of anginal complaints and de-creased use of nitrates. CSWT was well-tolerated with no relevant side effects.In this relatively small group of patients no significant improvement of exercisetolerance or reduction of ischemia burden could be detected.
P1333 Diagnostic coronary angiography triggers fatalcardiovascular events in patients with chronicmyocardial ischemia due to left main stenosis
T. Sakamoto, M. Tago, K. Nakao. Saiseikai Kumamoto HospitalCardiovascular Center, Kumamoto, Japan
Introduction: Myocardial ischemia due to left main stenosis, or left main dis-ease (LMD) is one of the most serious forms of coronary artery disease, whichneeds revascularization therapy by coronary artery bypass grafting (CABG) orpercutaneous coronary interventions (PCI) as early as possible. We sometimesencounter sudden cardiovascular collapse after diagnostic coronary angiography(CAG) before the treatments even in cases with stable myocardial ischemia withLMD. Appropriate timing for revascularization therapy for stable LMD after diag-nostic CAG is not well elucidated.Methods and Results: To examine whether CAG triggers cardiovascular eventsin cases with chronic myocardial ischemia, consecutive 257 patients with stablemyocardial ischemia who underwent diagnostic CAG at our institute from June2007 to May 2009 were analyzed. All patients were planned to undergo electiveCABG or PCI after diagnostic CAG with significant coronary stenosis. Of thosepatients, 61 cases were diagnosed as having LMD and remaining 196 as non-LMD (NLMD). In the LMD cases, cardiovascular events (myocardial ischemiarequiredemergent CABG or PCI, and cardiovascular death) were observed in11 cases (18%) during queuing periods. Mean event onset duration after CAGwas 4.2 days in those cases. Kaplan-Meier analysis revealed that cardiovascularevents were observed more frequent in LMD as compared with NLMD after CAGeven in stable myocardial ischemia cases (p=0.0033 by logrank). Furthermore,by landmark analysis, cardiovascular events occurred more shortly not after lastischemic symptoms but after diagnostic CAG. This is not the fact in the NLMDcases. That means CAG could be a trigger of cardiovascular events in the LMDbut not in NLMD cases. Multiple regression analysis revealed that existence ofdistal left main lesions was one and only independent predictor of cardiovascularevents after diagnostic CAG (adjusted OR 29.7, p=0.0264).Conclusions: CAG triggers cardiovascular events in patients with chronic andstable myocardial ischemia due to left main disease. Prompt revascularizationtherapy (within 24 hours after CAG) with CABG or PCI is recommended particu-larly in cases with distal left main lesions.
P1334 Outcomes of myocardial bridges in patients withchest pain and normal coronary arteries: Is it really abenign CT finding?
P. Marcos-Alberca Moreno, E. Blanco, E. Castilla, C. Almeria,J. Ferreiros, E. Balbacid, A. Goncalves, J.M. Becerra, C. Macaya,
J.L. Zamorano. Hospital Clínico San Carlos, Madrid, Spain
Background: Myocardial bridge (MB) has traditionally been considered a benignanatomical variant with hardly any clinical relevance.Multidetector Tomography(MDCT) has contributed to an increasing diagnose, so its clinical impact is nowbeing reconsidered.The aim was to know outcomes in patients with non acutechest pain, normal coronary arteries and MB.Methods: Retrospective, single-center observational study of 74 patients (PP)with non acute chest pain and without coronary lesions in MDCT.MB of at leastone coronary segment was diagnosed in 42% of PP.Control group was formedof 43 PP without coronary lesions and without MB.Data included demographiccharacteristics, cardiovascular (CV) risk factors, MB related anatomical features,evolved coronary artery and outcomes: death, myocardial infarction, angina ≥class 2 (CASS), hospitalization, revascularization or antianginal drugs.Results: Mean age was 60±12 yo. and M/F ratio was 30/70. PP with and with-out MB were age and sex matched and there were not differences regarding CVrisk factors.Coronary arteries evolved by MB were middle left anterior descending(LAD) artery (87%) followed by marginal branch of circumflex artery (29%). Out-comes after follow-up (mean 6.4 months, range 1-17) are showed in Table. PPwith normal coronary arteries and at least one MB more frequently had angina(p=0.01) and up to 66% needed antianginal drugs. After adjustment for age, genreand major CV risk factors, MB emerged as an independent predisposing factorfor ongoing angina (OR 6.8 CI 95% 1.5-31.3; p=0.01)
Outcomes (data are %)
Control MB p
Death 0 0 –MI 2.3 3.2 0.46Hospitalization 7 6.4 0.47Angina 7 32 0.01
Conclusion: In PP with non acute chest pain and normal coronary arteries as-sessed by MDCT, regarding the presence of myocardial bridges, outcomes atmidterm showed: 1) scarce serious adverse events; 2) poor quality of life reflectedby ongoing angina and unsatisfactory response to treatment.Further efforts areneeded in order to clarify the physiopathology and optimal clinical addressing ofthis increasing diagnosis.
P1335 Ivabradine improves exercise capacity in patientswith stable angina pectoris receiving maximaltolerated dose of beta-blockers: a subgroup analysisof the ASSOCIATE study
J. Tardif1, P. Ponikowski2, T. Kahan3, On Behalf Of The StudyInvestigators1. 1Montreal Heart Institute, Montreal, Canada; 2Clinical MilitaryHospital, Medical Wroclaw University (2nd Cardiology Department), Wroclaw,Poland; 3Karolinska Institutet, Department of Clinical Sciences, DanderydHospital, Stockholm, Sweden
Ivabradine, a selective If current inhibitor, is a novel agent for angina treatmentdue to its heart rate (HR)-reducing properties. Since the beneficial effect of ivabra-dine in patients already receiving a β-blocker could depend on the β-blocking levelreached in these patients, we analyzed anti-ischemic efficacy of ivabradine in pa-tients already receiving a dose of β-blocker judged as maximal.Method: ASSOCIATE was a double-blind study in 889 patients (84% male) withdocumented CAD and a history of stable angina already treated with atenolol 50mg od and randomized to receive ivabradine (5 mg bid, uptitrated to 7.5 mg bid) orplacebo (n=441 and 434, respectively). Patients underwent treadmill ETT (Bruceprotocol) at baseline and after 4 months at trough of drug activity. Current analysiswas performed in a subgroup of patients in whom atenolol 50 mg od could bejudged as maximal in terms of objective HR, haemodynamic, ECG criteria (restingHR≤ 60 bpm and/or supine systolic BP≤ 100 mmHg and/or mean PR interval ≥200 ms at baseline; n=80 in ivabradine group, n=64 in placebo group).Results: Improvement in all ETT parameters observed with addition of ivabradinein patients in whom dose of atenolol could be judged to be maximal was compa-rable to the improvement observed in whole population of the study (Full analysisset, ivabradine n=441, placebo n=434) (Table).
Ivabradine Placebo P value
Total exercise duration, s Full analysis set 24±65 8±64 <0.001Maximal β-blocker dose 27±63 9±71 0.066
Time to 1-mm ST depression, s Full analysis set 46±93 15±87 <0.001Maximal β-blocker dose 47±85 15±87 0.018
Time to angina onset, s Full analysis set 49±83 23±79 <0.001Maximal β-blocker dose 51±94 18±83 0.013
Time to limiting angina, s Full analysis set 26±66 9±64 <0.001Maximal β-blocker dose 28±63 9±71 0.05
Conclusion: In patients with stable angina receiving doses of β-blockers that
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Focus on stable angina / Focus on antiplatelet treatment 199
could be judged to be maximal, the addition of ivabradine improves exercise ca-pacity equivalent to that observed in patients receiving lower doses of β-blockers.Ivabradine may be valuable addition for patients with remaining ischemia despitehigh doses of β-blockers.
P1336 REALITY: angina treatment in outpatient populationand heart rate monitoring survey in Sweden
A. Hjalmarson. Sahlgrenska University Hospital, Goteborg, Sweden
Background: Reduction of resting heart rate (RHR) has been es-tablished as a strategy to prevent ischemia and angina. In addition,
RHR predicts cardiovascular morbidity and mortality in a very reliable and eas-ily accessible manner. The exact definition of the conditions under which RHR ismeasured appears to be as crucial as the measurement of blood pressure. How-ever, little is known about comparison of RHR measurement by different methodsand under different conditions. The objective of this analysis was to compare themeasurement of HR by different methods and under different conditions in theSwedish REALITY survey.Methods: The REALITY (The cuRrent statE of Angina treatment in outpatientpopuLation and heart rate monIToring surveY) was conducted in Sweden in pa-tients with stable angina attending primary care practice and in four universityhospitals with outpatient departments, which reflects the management of stableangina patients in Sweden. There were no exclusions for age, concurrent illness,or medication. RHR was measured by palpation (for 30 seconds) and by ECG;after 2 or 10 minutes of rest, in the sitting, supine position, and standing positions.Results: 185 patients with stable angina (mean age 71 years; 66% male) wereincluded in this study. 55% had hypertension, 26% diabetes, and 72% had beenhospitalized for acute coronary syndrome. All patients received concomitant stan-dard medication, including statins, aspirin, and angiotensin-converting enzymeinhibitors. 75% of patients were treated with beta-blockers. HR measurement inthe sitting position by pulse counting and HR by ECG recording after 2 min ofsitting at rest provided similar data: 66.7 bpm and 66.8 bpm, respectively. HR inthe supine position was 2 bpm slower (64.7, measured by ECG) than HR in thesitting position, while HR after standing for 2 min was 3 bpm faster (69.7 bpm, byECG) than HR in the sitting position.Conclusion: These data confirm the importance of HR measurement in standardconditions. HR measurement in the sitting position by pulse counting and by ECGrecording after sitting at rest gives reliable and comparable results.
P1337 Severe ST-segment depression on exerciseelectrocardiography test is not always enough topredict the presence of significant coronary arterystenosis
K.S. Cha1, J.H. Kim2, J.H. Lee2, T.H. Park2, M.H. Kim2, Y.D. Kim2.1Pusan National University Hospital, Busan, Korea, Republic of;
2Dong-A Medical Center, Busan, Korea, Republic of
Purpose: Severe ST-segment depression on exercise electrocardiography (ECG)test is regarded as a parameter associated with the presence of multivessel dis-eases and adverse prognosis. However, it may not be always associated with thepresence of significant coronary stenosis. We sought the incidence and predic-tors of the presence of true significant stenosis in patients with severe ST-segmentdepression on exercise ECG test.Methods: The consecutive 139 patients who showed severe (≥ 2.0 mm), hori-zontal or downward sloping, ST-segment depression on exercise ECG test werederived from the 10,694 patients for 6 years. Clinical factors and electrocardio-graphic parameters were compared between the two groups with or without signif-icant coronary stenosis. Multivariate logistic regression analysis was performed.Results: Significant coronary stenosis was present in 82 patients (59%) out of139 patients with severe ST-segment depression on exercise ECG test. Multivari-ate analysis identified clinical and exercise ECG predictors for the presence oftrue significant coronary stenosis which were shown on the table below.
Multivariate analysis Hazard Ratio 95% CI p value
Maximum ST depression during recovery 11.1 2.4∼51.7 0.002Maximum ST depression at stage II 10.3 2.0∼54.1 0.006ST depression in V1∼3, I, and aVL 10.5 1.3∼81.8 0.025Hypertension 4.2 1.3∼13.5 0.007Typical chest pain 4.1 1.3∼14.6 0.023Male gender 3.6 0.9∼14.6 0.068
Conclusions: The incidence of significant coronary stenosis even in patients withsevere (≥ 2.0 mm) ST-segment depression on exercise ECG test was 59% in ourseries of patients. The clinical and ECG predictors for the presence of significantcoronary stenosis were ST-segment depression during recovery and at stage II,ST-segment depression in V1∼3, I, and aVL, hypertension, typical chest pain, andmale gender. Considering the low incidence of significant coronary stenosis evenin patients with severe ST- segment depression on exercise ECG test, our datasupport that second noninvasive stress test may be a reasonable option even inpatients with severe ST-segment depression on exercise ECG test who do nothave clinical and exercise ECG predictors.
P1338 The relation between the SYNTAX score andmyocardial ischemia in multi-vessel coronary arterydisease
C. Shiba, T. Chikamori, H. Tanaka, S. Hida, Y. Igarashi, Y. Ohtaki,Y. Usui, T. Hatano, A. Yamashina. Tokyo Medical University, Tokyo,Japan
Background: Although the SYNTAX Score (SXscore), which is based on thecoronary anatomy such as lesion location and complexity, has recently been de-veloped to delineate technical demand in revascularization procedures due towide variation of disease severity of CAD, no study has evaluated the relation ofSXscore with the extent of inducible ischemia.Methods: Two hundred thirty-one patients with multi-vessel CAD were evaluated.A summed stress score (SSS) and summed difference score (SDS) were calcu-lated, and the SXscore was assessed.Results: In 43 patients with severe SXscore (≥33), where CABG is a betterchoice of revascularization procedure according to the SYNTAX study, the SSS(19.8±11.1 vs 16.8±10.9), SDS (8.9±7.6 vs 8.0±6.0), incidence of transient is-chemic dilation (37 vs 23%) and lung uptake of radiotracers (30 vs 19%) weresimilar to 188 patients with non-severe SXscore (<33). The SSS but not SDScorrelated with SXscore (r=0.208; p=0.001 and r=0.096; p=NS) in all of the pa-tients. By contrast, the SSS and SDS correlated significantly with SXscore in thenon-severe SXscore group (r=0,178; p=0.015 and r=0.163; p=0.026), while nosuch correlation was observed in the severe SXscore group (r=0.272; p=NS andr=0.140; p=NS).Conclusion: The SXscore correlated with myocardial ischemia, but this relationwas limited to modest disease severity of multi-vessel CAD.
P1339 Low incidence of acute heart failure in an adultcontemporary cohort of myopericarditis
R.C. Vidal Perez, E. Abu Assi, J. Elices Teja, P. Cabanas Grandio,R. Agra Bermejo, S. Raposeiras Roubin, J.M. Garcia Acuna, C. PenaGil, A. Varela Roman, J.R. Gonzalez Juanatey. University Clinical
Hospital of Santiago de Compostela, Santiago de Compostela, Spain
Purpose: The clinical manifestations of myopericarditis vary from chest pain tofulminant heart failure. Natural history data come from old series from referral cen-tre populations. The study objective was to assess the incidence of heart failurecomplicating acute myopericarditis diagnosed by using more sensitive markers ofmyocardial necrosis (cardiac Troponin I).Methods: We studied 145 consecutive patients, older than 14 years old, admittedto our Coronary Care Unit between 2000 and 2008. The diagnosis of myocarditisestablished by clinical criteria and evidence of cardiac necrosis markers eleva-tions (Troponin I and CK MB mass). Serial two dimensional echocardiographywas performed in all patients during admission. Coronary angiography was per-formed in 26.9% of patients.Results: Mean age was 28.8±8.5 (16-59) years. There were 93.8% males.46.2% of patients were smokers and 10 had recent used cocaine, previous historyof pericarditis or myopericarditis in 8 patients (5.5%), few patients had risk factorsfor coronary heart disease, mainly dyslipidaemia (8.3%) Evidence of an acute vi-ral infection was present in 64.1%, but witout a seasonal pattern of presentation.23 patients presented fever at admission. Chest pain was present in 86.8% ofpatients. Initial ECG with ST segment elevation (> 1mm) were seen in 71.7% ofpatients, predominantly diffuse elevation pattern. Pericardial effusion was found in18 patients (12.4%), neither with echocardiographic o clinical tamponade findings.On ECG monitoring we found non sustained ventricular tachycardia in 12 patients(8.3%). Serum cardiaca markers: mean CK was 465.7±327.7 ng/mL and CK MBmass was 58.2±47.5 ng/mL, the mean Troponin I peak level was 14.09±10.8ng/mL. Left ventricular wall motion abnormalities were described at admission in28 patients (19.3%) with a complete recovery in all of them at discharge. Meanejection fraction at admission was 60.6±6.3% (range 40-78), of the 17 patients(11.7%) with initial impaired systolic function (Ejection fraction< 55%) ejectionfraction normalized in all of them. Two patients developed transitory heart failureduring admission. Only one patient died in an haematological inmunosuppressioncontext after multiple myopericarditis recurrenceConclusion: Adult contemporary acute myopericarditis have a benign coursewith low incidence of acute heart failure or persistent left ventricle dysfunction.
FOCUS ON ANTIPLATELET TREATMENT
P1340 New antiplatelet regimes for acute coronarysyndrome management: high cost and low costoptions
S. Dawkins, D. Adlam, B. Prendergast. Oxford Heart Centre, JohnRadcliffe Hospital, Oxford, United Kingdom
Background: The UK National Health Service (NHS) spends �150million an-nually on clopidogrel (Plavix, Sanofi) which is the second highest selling drugworldwide. This position will be challenged by new antiplatelet agents, such asprasugrel (Efient, Lilly), ticagrelor (Brilinta, AstraZeneca) and the availability of
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
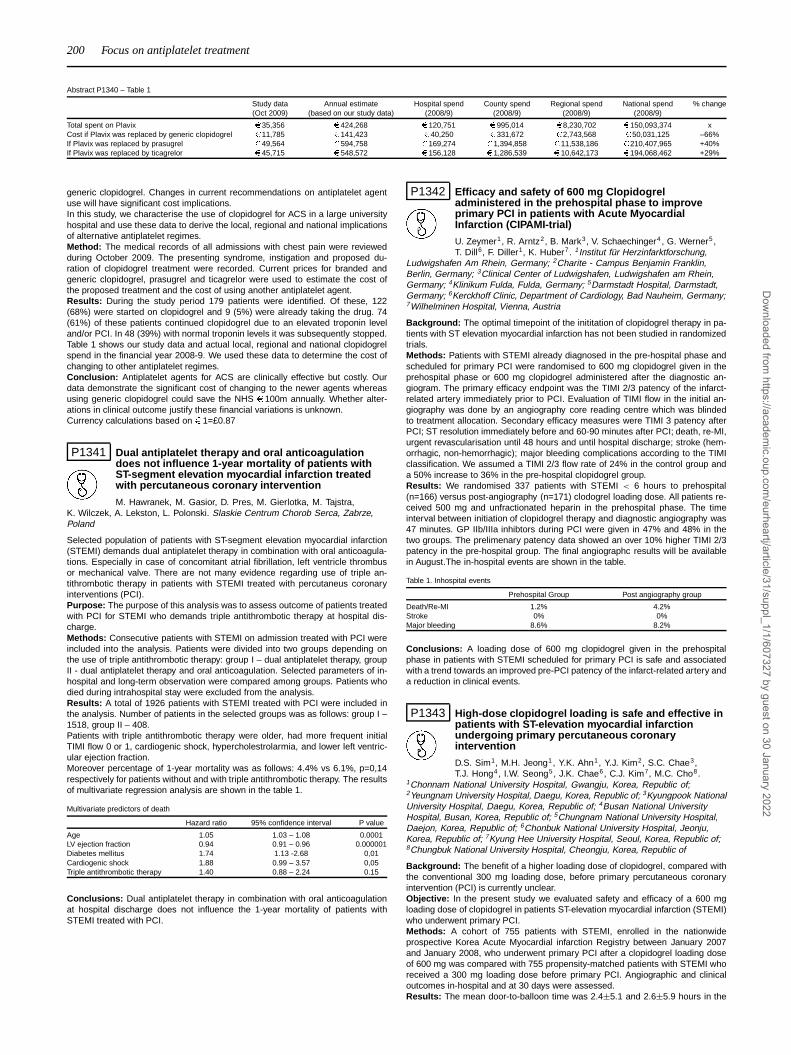
200 Focus on antiplatelet treatment
Abstract P1340 – Table 1
Study data Annual estimate Hospital spend County spend Regional spend National spend % change(Oct 2009) (based on our study data) (2008/9) (2008/9) (2008/9) (2008/9)
Total spent on Plavix � 35,356 � 424,268 � 120,751 � 995,014 � 8,230,702 � 150,093,374 xCost if Plavix was replaced by generic clopidogrel � 11,785 � 141,423 � 40,250 � 331,672 � 2,743,568 � 50,031,125 –66%If Plavix was replaced by prasugrel � 49,564 � 594,758 � 169,274 � 1,394,858 � 11,538,186 � 210,407,965 +40%If Plavix was replaced by ticagrelor � 45,715 � 548,572 � 156,128 � 1,286,539 � 10,642,173 � 194,068,462 +29%
generic clopidogrel. Changes in current recommendations on antiplatelet agentuse will have significant cost implications.In this study, we characterise the use of clopidogrel for ACS in a large universityhospital and use these data to derive the local, regional and national implicationsof alternative antiplatelet regimes.Method: The medical records of all admissions with chest pain were reviewedduring October 2009. The presenting syndrome, instigation and proposed du-ration of clopidogrel treatment were recorded. Current prices for branded andgeneric clopidogrel, prasugrel and ticagrelor were used to estimate the cost ofthe proposed treatment and the cost of using another antiplatelet agent.Results: During the study period 179 patients were identified. Of these, 122(68%) were started on clopidogrel and 9 (5%) were already taking the drug. 74(61%) of these patients continued clopidogrel due to an elevated troponin leveland/or PCI. In 48 (39%) with normal troponin levels it was subsequently stopped.Table 1 shows our study data and actual local, regional and national clopidogrelspend in the financial year 2008-9. We used these data to determine the cost ofchanging to other antiplatelet regimes.Conclusion: Antiplatelet agents for ACS are clinically effective but costly. Ourdata demonstrate the significant cost of changing to the newer agents whereasusing generic clopidogrel could save the NHS �100m annually. Whether alter-ations in clinical outcome justify these financial variations is unknown.Currency calculations based on �1=£0.87
P1341 Dual antiplatelet therapy and oral anticoagulationdoes not influence 1-year mortality of patients withST-segment elevation myocardial infarction treatedwith percutaneous coronary intervention
M. Hawranek, M. Gasior, D. Pres, M. Gierlotka, M. Tajstra,K. Wilczek, A. Lekston, L. Polonski. Slaskie Centrum Chorob Serca, Zabrze,Poland
Selected population of patients with ST-segment elevation myocardial infarction(STEMI) demands dual antiplatelet therapy in combination with oral anticoagula-tions. Especially in case of concomitant atrial fibrillation, left ventricle thrombusor mechanical valve. There are not many evidence regarding use of triple an-tithrombotic therapy in patients with STEMI treated with percutaneus coronaryinterventions (PCI).Purpose: The purpose of this analysis was to assess outcome of patients treatedwith PCI for STEMI who demands triple antithrombotic therapy at hospital dis-charge.Methods: Consecutive patients with STEMI on admission treated with PCI wereincluded into the analysis. Patients were divided into two groups depending onthe use of triple antithrombotic therapy: group I – dual antiplatelet therapy, groupII - dual antiplatelet therapy and oral anticoagulation. Selected parameters of in-hospital and long-term observation were compared among groups. Patients whodied during intrahospital stay were excluded from the analysis.Results: A total of 1926 patients with STEMI treated with PCI were included inthe analysis. Number of patients in the selected groups was as follows: group I –1518, group II – 408.Patients with triple antithrombotic therapy were older, had more frequent initialTIMI flow 0 or 1, cardiogenic shock, hypercholestrolarmia, and lower left ventric-ular ejection fraction.Moreover percentage of 1-year mortality was as follows: 4.4% vs 6.1%, p=0,14respectively for patients without and with triple antithrombotic therapy. The resultsof multivariate regression analysis are shown in the table 1.
Multivariate predictors of death
Hazard ratio 95% confidence interval P value
Age 1.05 1.03 – 1.08 0.0001LV ejection fraction 0.94 0.91 – 0.96 0.000001Diabetes mellitus 1.74 1.13 -2.68 0,01Cardiogenic shock 1.88 0.99 – 3.57 0,05Triple antithrombotic therapy 1.40 0.88 – 2.24 0.15
Conclusions: Dual antiplatelet therapy in combination with oral anticoagulationat hospital discharge does not influence the 1-year mortality of patients withSTEMI treated with PCI.
P1342 Efficacy and safety of 600 mg Clopidogreladministered in the prehospital phase to improveprimary PCI in patients with Acute MyocardialInfarction (CIPAMI-trial)
U. Zeymer1, R. Arntz2, B. Mark3, V. Schaechinger4 , G. Werner5 ,T. Dill6, F. Diller1, K. Huber7. 1Institut für Herzinfarktforschung,
Ludwigshafen Am Rhein, Germany; 2Charite - Campus Benjamin Franklin,Berlin, Germany; 3Clinical Center of Ludwigshafen, Ludwigshafen am Rhein,Germany; 4Klinikum Fulda, Fulda, Germany; 5Darmstadt Hospital, Darmstadt,Germany; 6Kerckhoff Clinic, Department of Cardiology, Bad Nauheim, Germany;7Wilhelminen Hospital, Vienna, Austria
Background: The optimal timepoint of the inititation of clopidogrel therapy in pa-tients with ST elevation myocardial infarction has not been studied in randomizedtrials.Methods: Patients with STEMI already diagnosed in the pre-hospital phase andscheduled for primary PCI were randomised to 600 mg clopidogrel given in theprehospital phase or 600 mg clopidogrel administered after the diagnostic an-giogram. The primary efficacy endpoint was the TIMI 2/3 patency of the infarct-related artery immediately prior to PCI. Evaluation of TIMI flow in the initial an-giography was done by an angiography core reading centre which was blindedto treatment allocation. Secondary efficacy measures were TIMI 3 patency afterPCI; ST resolution immediately before and 60-90 minutes after PCI; death, re-MI,urgent revascularisation until 48 hours and until hospital discharge; stroke (hem-orrhagic, non-hemorrhagic); major bleeding complications according to the TIMIclassification. We assumed a TIMI 2/3 flow rate of 24% in the control group anda 50% increase to 36% in the pre-hospital clopidogrel group.Results: We randomised 337 patients with STEMI < 6 hours to prehospital(n=166) versus post-angiography (n=171) clodogrel loading dose. All patients re-ceived 500 mg and unfractionated heparin in the prehospital phase. The timeinterval between initiation of clopidogrel therapy and diagnostic angiography was47 minutes. GP IIb/IIIa inhibtors during PCI were given in 47% and 48% in thetwo groups. The prelimenary patency data showed an over 10% higher TIMI 2/3patency in the pre-hospital group. The final angiographc results will be availablein August.The in-hospital events are shown in the table.
Table 1. Inhospital events
Prehospital Group Post angiography group
Death/Re-MI 1.2% 4.2%Stroke 0% 0%Major bleeding 8.6% 8.2%
Conclusions: A loading dose of 600 mg clopidogrel given in the prehospitalphase in patients with STEMI scheduled for primary PCI is safe and associatedwith a trend towards an improved pre-PCI patency of the infarct-related artery anda reduction in clinical events.
P1343 High-dose clopidogrel loading is safe and effective inpatients with ST-elevation myocardial infarctionundergoing primary percutaneous coronaryintervention
D.S. Sim1, M.H. Jeong1, Y.K. Ahn1, Y.J. Kim2, S.C. Chae3,T.J. Hong4, I.W. Seong5, J.K. Chae6, C.J. Kim7, M.C. Cho8.
1Chonnam National University Hospital, Gwangju, Korea, Republic of;2Yeungnam University Hospital, Daegu, Korea, Republic of; 3Kyungpook NationalUniversity Hospital, Daegu, Korea, Republic of; 4Busan National UniversityHospital, Busan, Korea, Republic of; 5Chungnam National University Hospital,Daejon, Korea, Republic of; 6Chonbuk National University Hospital, Jeonju,Korea, Republic of; 7Kyung Hee University Hospital, Seoul, Korea, Republic of;8Chungbuk National University Hospital, Cheongju, Korea, Republic of
Background: The benefit of a higher loading dose of clopidogrel, compared withthe conventional 300 mg loading dose, before primary percutaneous coronaryintervention (PCI) is currently unclear.Objective: In the present study we evaluated safety and efficacy of a 600 mgloading dose of clopidogrel in patients ST-elevation myocardial infarction (STEMI)who underwent primary PCI.Methods: A cohort of 755 patients with STEMI, enrolled in the nationwideprospective Korea Acute Myocardial infarction Registry between January 2007and January 2008, who underwent primary PCI after a clopidogrel loading doseof 600 mg was compared with 755 propensity-matched patients with STEMI whoreceived a 300 mg loading dose before primary PCI. Angiographic and clinicaloutcomes in-hospital and at 30 days were assessed.Results: The mean door-to-balloon time was 2.4±5.1 and 2.6±5.9 hours in the
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Focus on antiplatelet treatment 201
600 mg and 300 mg groups, respectively (p=0.388). Initial patency of the infarct-related artery (pre-PCI TIMI grade 2/3) was significantly higher in the 600 mggroup than in the 300 mg group: 54.4% vs. 45.6%, p=0.034). The rate of post-PCI TIMI grade 3 flow was also significantly higher in the 600 mg group indepen-dently of the use of glycoprotein IIb/IIa inhibitor (85.8% vs. 89.3%, p=0.042). Com-pared to the 600mg group, a significantly higher proportion of patients in the 300mg group received bare-metal stents (13.7% vs. 6.1%, p<0.0005) and requiredprolonged anticoagulation during hospitalization (low molecular weight heparin:37.2% vs. 30.9%, 0.009; unfractionated heparin: 70.2% vs. 58.5%, <0.0005). Thelength of hospital stay was significantly longer in the 300 mg group (7.1±6.7 vs.6.2±5.7 days, 0.006). However, the incidence of in-hospital and 30-day ischemicevents (bleeding complications, death, MI, or stent thrombosis) was similar be-tween the two groups.Conclusion: Compared to the conventional 300 mg loading dose, the 600 mgloading dose of clopidogrel before primary PCI improved pre- and post-PCI pa-tency and reduced the need for prolonged anticoagulation and hospital stay with-out increasing the risk of serious bleeding complications.
P1344 Frequency, causes and timing of prematurediscontinuation of double antiplatelet therapy afterdrug eluting stents
I. Lozano Martinez-Luengas, O.C. Garcia, F. Torres, A. Carro,J. Bayon, J. Rondan, P. Avanzas, M. Martin, J.M. De La Hera,
V. Barriales. Hospital Universitario Central de Asturias, Oviedo, Spain
Background: Compliance to double antiplatelet therapy is the most importantfactor to prevent stent thrombosis.Objective: To assess the frequency and causes of premature discontinuation ofdouble antiplatelet therapy in the first year after drug eluting stents.Methods: All the consecutive patients who received at least one drug elutingstent in our center between October 2006 and September 2007 were followedprospectively once every three months during the first year to determine the ad-herence to double antiplatelet therapy and causes of premature discontinuation.Predictors of discontinuation were studied with multivariable analysis.Results: n = 382. Age 67,6±10.2, females 28.5%, diabetes 34.6%. Completefollow-up was achieved in 99%. Fortynine patients (12.8%) discontinued the ther-apy at any moment during the first year. This fact was strongly associated with car-diac mortality and non-fatal stent thrombosis (OR 7.03 IC 95% 2.03-24.7 p=0.002)and all-caused motality and non-fatal stent thrombosis (OR 11.7 IC 95% 3.42-40.48 p<0.000). Eight patients of the 49 who discontinued the DAT died or suf-fered non-fatal stent thrombosis during the follow-up. Importantly, despite all butone discontinued the therapy in the first semester, the moment of the event was inthe second in 5 of the 7 patients. Causes of discontinuation: noncardiac surgery17 patients (34.6%), anticoagulation 7 (14.3%), hemorrhage 7 (14.3%), allergy 5(10.2%), dental procedures 5 (10.2%), endoscopy 4 (8.2%) and poor adherence 4(8.2%). The factors associated with premature discontinuation were male gender,level of hemoglobin and marital status (single or divorced).Conclusions: Premature discontinuation of double antiplatelet therapy in thefirst year after drug eluting stents is relatively common and is associated withmale gender, level of hemoglobin and marital status. Premature discontinuationis strongly associated with stent thrombosis and mortality. The risk of death osrstent thrombosis may persist months after discontinuation of the therapy.
P1345 Clinical impact of short term discontinuation of DualAntiPlatelet Therapy (DAPT) after Drug Eluting Stent(DES) implantation for coronary artery disease
Y. Sakamoto, T. Muramatsu, R. Tsukahara, Y. Ito, H. Ishimori,K. Hirano, M. Nakano, M. Yamawaki, S. Sasaki, M. Araki. saiseikai
yokohama city eastern hospital, Yokohama, Japan
Purpose: After DES implantation for coronary artery diseases when patientsneed surgical operation or suffering bleeding complications, DAPT is often tempo-rally discontinued. However, past studies indicate its strong relationship to stentthrombosis (ST). This study was aimed to investigate the clinical impact of shortterm discontinuation of DAPT after DES implantation in real world.Method: From April 2007 to August 2008, 684 stable angina pectoris patients hadDES implantation during PCI in our hospital and started DAPT with acetylsalicylicacid 100mg and thienopyridine, ticlopidine 200mg or clopidogrel 75mg per day. Af-ter PCI, 57 patients had short term discontinuation (mean period 12.5±9.2 days)of DAPT (DDAPT group) and other 627 patients continued DAPT (CDAPT group)during observational periods of 730 days from procedure (mean period 425±197days). We compared incidence of cardiac events (death, MI, ST, CABG, target le-sion revascularization) of 2 groups, retrospectively. Patients received single APTor discontinued APT by patient’s decision were excluded.Result: Baseline patient characteristics, procedure characteristics of 2 groupswere similar. Comparing incidence of cardiac events in 2 groups, rate of total car-diac events was similar, but death and MI, ST (definite in Academic ResearchConsortium definition) were significantly high in DDAPT group (in picture). More-over, 3 cases of ST in DDAPT group were one case late ST (232 days afterprocedure) and 2 cases very late ST (366 and 450 days after procedure) but 3cases of ST in CDAPT group were all acute or subacute ST which means nocases occurred late or very late ST in CDAPT group.
Picture
Conclusion: Even short term discontinuation of DAPT may contribute to deathand MI, especially late or very late ST.
P1346 24-Hour time dependent aspirin efficacy in patientswith stable coronary artery disease
P. Henry, A. Vermillet, B. Boval, C. Guyetand, T. Petroni,J.G. Dillinger, G. Sideris, C. Bal Dit Sollier, L. Drouet. AP-HP -Hospital Lariboisiere, Paris, France
Background: Aspirin-induced COX-1 acetylation is irreversible and it is assumedthat the platelet thromboxane-A2 aggregation pathway is inhibited for at least 24hafter aspirin ingestion. However, time course of biological efficacy of daily low-dose aspirin has rarely been assessed in patients with coronary artery disease(CAD).Objectives: We aimed to assess the 24-hour biological efficacy of daily low doseaspirin in patients with stable CAD.Patients/Methods: The peak and trough (2h-24h) effect of a chronic treatmentwith once daily dose aspirin (75-250mg/day) were studied in 150 consecutive sta-ble CAD patients. The main outcome measure was light transmission aggregom-etry triggered with 0.5mg/mL arachidonic acid. In the last 47 consecutive patients,time course and platelet function were assessed more precisely.Results: Mean Age was 64±8.9 y.o., 89% were male, 38% were diabetics and32% have been active smokers during past 5 years. Aspirin (no other antithrom-botic treatment) was administered once daily in the morning at a dose ≤100 mg/din 60% of patients and >100 mg/day in 40%. There was 68% of patients treatedwith statin, 17% with insulin and 27% with proton pump inhibitors. On 150 pa-tients, 4.7% were resistant (>20% residual aggregation) 2h after aspirin ingestioncompared to 24.7% 24h after aspirin ingestion (p<0.0001). The more precise as-sessments showed that significant platelet aggregation progressively reappearedwith time after aspirin intake (4% of patients at 2h, 4% at 6h, 11% at 12h, 16% at16h, 19% at 20h and 28% at 24h). Using thromboxane B2 measurement, 2.6%of patients demonstrated elevated TXB2 (>2.45ng/ml) 6h after last aspirin intake.5% after 12h, 8% after 16h, 10.5% after 20h and 24% after 24h. Mean concen-tration of TXB2 was 1.26ng/mL for the patients with aspirin-sensitive platelets asassessed by LTA as compared with 20.17ng/mL for aspirin-insensitive patients24h after last aspîrin intake (p<0.05). Concordant results were observed usingother techniques evaluating arachidonic induced platelet aggregation/activation.No significant differences were found between lower (75-100mg/day) and higher(>100mg/day) dose aspirin. Aspirin resistance at 24h after ingestion was related(univariate) to inflammatory markers (fibrinogen>4g/L, platelet count >270.109/L(median value), HsCRP>8.5 mg/L (median value)), current smoking and dia-betes.Conclusions: Once daily aspirin does not provide stable 24-hour antiplatelet pro-tection in a significant proportion of CAD patients. Biological assessment of as-pirin efficacy should take time since last intake into consideration.
P1347 Clopidogrel loading dose and bleeding outcomes inpatients undergoing urgent coronary bypass surgery
N. Cruden, K. Morch, D.R. Wong, W.P. Klinke, J. Ofiesh, J.D. Hilton.Royal Jubilee Hospital, Victoria, British Columbia, Canada
Purpose: Coronary artery bypass grafting (CABG) performed within5 days of clopidogrel administration is associated with increased bleeding. Theaim of this study was to examine the effect of clopidogrel loading dose on bleedingoutcomes in patients requiring urgent CABG.Methods: Clinical outcomes were examined retrospectively for 196 consecutivepatients undergoing CABG within 5 days of clopidogrel loading between January2003 and June 2009. Major bleeding was defined as a fall in hemoglobin >5g/dL,fatal or intracranial bleeding, or cardiac tamponade.Results: 148 patients received 300mg and 48 patients received ≥600mg clopido-grel loading. Patients were predominantly male (78%) with a mean age of 66±10years. Mean duration from clopidogrel loading to CABG was 3.0±1.5 and 3.0±1.6days for the 300mg and 600mg loading doses respectively. Major bleeding oc-curred in 47% of patients receiving 300mg and 73% of patients receiving ≥600mgclopidogrel loading (p=0.002). Compared to 300mg, patients receiving ≥600mghad greater 24h chest tube output (391±251 vs 536±354 mL, p=0.01), stayedlonger in surgical intensive care (4.3±4.1 vs 5.0±3.1 days,p=0.0001) and trendedtowards greater reoperation for bleeding (4.7% vs 12.5%, p=0.09). Following mul-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

202 Focus on antiplatelet treatment
tivariate analysis, a clopidogrel loading dose ≥600mg (OR 2.8[CI:1.2-6.6]) pre-dicted bleeding.
Clopidogrel loading dose and clinical outcomes in patients undergoing urgent CABG
Outcome 300mg ≥600mg PLoading Dose Loading Dose
(n=148) (n=48)
Major bleeding, n (%) 70 (47%) 35 (73%) 0.002Re-operation for bleeding, n (%) 7 (5%) 6 (12%) 0.09Tamponade, n (%) 4 (3%) 2 (4%) 0.64Mean 24h Chest tube loss, mL 391±251 mL 536±354 mL 0.01Post-operative myocardial infarction, n (%) 8 (5%) 5 (11%) 0.31Post-operative cerebrovascular accident, n (%) 6 (4%) 1 (2%) 0.34Length of stay in surgical intensive care, days 4.3±4.1 5.0±3.1 0.0001In-hospital death, n (%) 7 (5%) 1 (2%) 0.68
Conclusions: Higher clopidogrel loading doses are associated with increasedbleeding when administered within 5 days of CABG. The development of shorter-acting, reversible, oral antiplatelet agents may allow more rapid restoration ofplatelet function and reduce peri-operative bleeding in patients requiring urgentCABG.
P1348 Responsiveness to clopidogrel after percutaneouscoronary intervention can be improved withpolyunsaturated omega-3 fatty acids especially inpatients with CYP 2C19 loss-of-functionpolymorphism
G.P. Gajos1, A. Undas2, P. Rostoff1, J. Nessler1, W. Piwowarska1.1John Paul II Hospital, Department of Coronary Disease, Jagiellonian UniversitySchool of Medicine, Krakow, Poland; 2John Paul II Hospital, Institute ofCardiology, Jagiellonian University School of Medicine, Krakow, Poland
Purpose: To investigate whether omega-3 polyunsaturated fatty acids (PUFA) areable to modify platelet responsiveness to clopidogrel therapy in stable coronaryartery disease patients undergoing percutaneous coronary intervention (PCI), es-pecially in cases of CYP 2C19 loss-of-function polymorphism.Methods: The OMEGA-PCI study was a prospective, single centre, double-blind,placebo-controlled, randomized study.Patients on standard dual antiplatelet therapy (aspirin 75 mg daily and clopidogrel600 mg loading dose followed by 75 mg daily) were randomly assigned to receivethe addition of 1 g of omega-3 ethyl esters (n = 33) or placebo (n = 30) for 1month.Platelet function was measured serially by light transmittance aggregometry (ADPand arachidonic acid were used as agonists) and assessment of the phosphory-lation status of the vasodilator-stimulated phosphoprotein: at baseline, 12 hours,3-5 days and 30 days after randomization. CYP2C19*2 was genotyped at base-line.Results: There were no significant differences among baseline variables, includ-ing genetic polymorphism of CYP2C19.P2Y12 reactivity index was significantly lower after 1 month of treatment withomega-3 PUFA compared with placebo when used on top of dual antiplatelettherapy by 22.2% (p=0.020). Maximal platelet aggregation induced by 5 and 20μmol/L ADP was lower by 13.3% (p=0.026) and 9.8% (p=0.029) respectively after1 month of treatment with omega-3 PUFA as compared with placebo.The beneficial effect of omega-3 PUFA was predominantly demonstrated in carri-ers of CYP 2C19 loss-of-function polymorphism (Fig. 1).
Figure 1
Conclusion: The addition of omega-3 ethyl esters significantly potentiatesplatelet response to clopidogrel after PCI predominantly in patients with CYP2C19 loss-of-function polymorphism.
P1349 Ticagrelor versus clopidogrel in patients with acutecoronary syndromes and diabetes in the PLATOtrial
S. James1, D.J. Angiolillo2, R.C. Becker3, J.H. Cornel4, J. Horrow5,S. Husted6, H. Katus7, J.C. Nicolau8, R.F. Storey9, L. Wallentin1.1Uppsala University Hospital, Uppsala Clinical Research Center
(UCR), Uppsala, Sweden; 2Center for Thrombosis Research, University ofFlorida College of Medicine, Jacksonville, United States of America; 3DukeClinical Research Institute, Durham, United States of America; 4MedischCentrum Alkmaar, Afdeling Cardiologie, Alkmaar, Netherlands; 5Astra ZenecaResearch and Development, Wilmington, Delaware, United States of America;6Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark;7Medizinische Klinik, Universitätsklinikum Heidelberg, Heidelberg, Germany;8Heart Institute, Univeristy of São Paolo Medical School, São Paolo, Brazil;9Department of Cardiovascular Science, University of Sheffield, Sheffield, UnitedKingdom
Purpose: Patients with diabetes mellitus (DM) have poor response to clopidogrel,which contribute to their worse clinical outcomes. In the PLATO trial, ticagrelorreduced the primary composite endpoint of cardiovascular (CV) death, myocardialinfarction (MI) and stroke, but with similar rate of major bleeding. The purpose wasto investigate the effects of ticagrelor vs. clopidogrel in patients with DM and acutecoronary syndrome (ACS).Methods: We investigated outcomes in patients with pre-existing DM (N=4662),including 2573 patients on insulin, and in those without DM (N=13951). Stentedpatients were included in the stent thrombosis analysis.Results: DM was associated with the primary endpoint (HR, 95% CI; 1.66 (1.51-1.82), total mortality HR, 95% CI; 1.84 (1.61-2.10) and major bleeding HR, 95%CI; 1.41 (1.28-1.55). The effects of ticagrelor vs. clopidogrel according to diabeticstatus are summarized.
Table 1
Number Ticagrelor Clopidogrel HR (95% CI) Interaction p
CV death, MI, No DM 13951 8.4 (555) 10.2 (664) 0.83 (0.74-0.93) 0.49or stroke DM 4662 14.1 (309) 16.2 (350) 0.88 (0.76-1.03)
No insulin 2088 11.3 (112) 11.6 (112) 0.99 (0.76-1.28) 0.33Insulin 2573 16.6 (197) 19.8 (237) 0.84 (0.70-1.02)
Total death No DM 13951 3.7 (246) 5.0 (318) 0.77 (0.65-0.91) 0.66DM 4662 7.0 (153) 8.7 (188) 0.82 (0.66-1.01)
No insulin 2088 3.9 (39) 6.3 (62) 0.62 (0.41-0.92) 0.08Insulin 2573 9.7 (114) 10.6 (125) 0.93 (0.72-1.20)
Definite stent No DM 8766 1.3 (53) 1.8 (77) 0.68 (0.48-0.97) 0.89thrombosis DM 2518 1.6 (18) 2.4 (29) 0.65 (0.36-1.17)
No insulin 1085 0.9 (4) 1.6 (9) 0.47 (0.14-1.52) 0.53Insulin 1433 2.1 (14) 2.9 (20) 0.73 (0.37-1.44)
Major bleeding No DM 13798 10.8 (674) 10.0 (624) 1.08 (0.97-1.20) 0.21DM 4621 14.1 (287) 14.8 (305) 0.95 (0.81-1.12)
No insulin 2070 10.5 (93) 9.4 (87) 1.07 (0.80-1.43) 0.39Insulin 2550 17.2 (194) 19.1 (218) 0.91 (0.75-1.11)
Conclusions: Ticagrelor compared with clopidogrel reduces ischaemic end-points and mortality in ACS patients without a significant increase in major bleed-ing with no interaction for diabetes status or insulin treatment.
P1350 Clopidogrel treatment is associated with reduced riskof recurrent myocardial infarction and death inpatients with myocardial infarction revascularised bycoronary artery bypass grafting
R. Sorensen1, S.Z. Abildstrom2, P.R. Hansen1, A. Hvelplund1,C. Andersson1, M.G. Charlot1, J.K. Madsen1, C. Torp-Pedersen1 ,G.H. Gislason1. 1Copenhagen University Hospital Gentofte, Department ofCardiology, Copenhagen, Denmark; 2Copenhagen University Hospital Glostrup,Cardiovascular Research Unit, Copenhagen, Denmark
Purpose: The clinical effect of clopidogrel treatment on recurrent myocardial in-farction (MI) and death among MI patients revascularised by coronary artery by-pass grafting (CABG) is unclear. We examined this question in a nationwide co-hort.Methods: By use of nationwide registers, we identified and followed patients ad-mitted with first-time MI and treated with CABG within 180 days after MI between2002 and 2006. Claimed prescriptions starting at hospital discharge after CABGwere used to determine clopidogrel treatment. Patients were stratified into groupswith or without clopidogrel treatment. Risk of death or recurrent MI was assessedby the Kaplan Meier method and Cox proportional hazard model for all patientsand in a propensity-score matched population.Results: We included 3489 patients with first-time MI that underwent CABG. Ofthese 1064 (30.5%) were treated with clopidogrel after revascularisation. Meanfollow-up was 462 days (±149). Of the 1064 patients treated with clopidogrel,1020 were matched by propensity-score to 1020 patients without clopidogreltreatment. Among all patients treated with clopidogrel 48 (1.4%) died or expe-rienced a new MI whereas these events occurred in 190 (5.5%) of the patientswithout clopidogrel treatment (Log rank p=0.0006). Corresponding figures for thepropensity-matched population were 43 (2.1%) with clopidogrel and 66 (3.2%)without clopidogrel treatment (Log rank p=0.03). Results of the Cox proportionalhazard models are shown in Figure 1.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
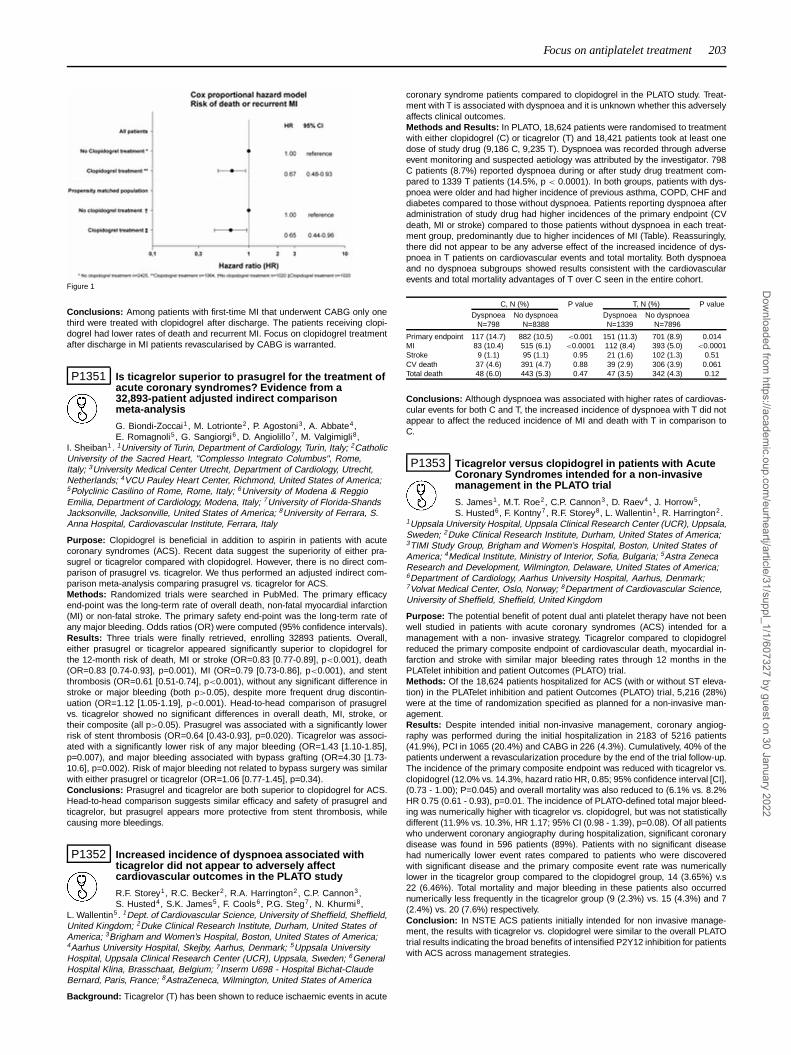
Focus on antiplatelet treatment 203
Figure 1
Conclusions: Among patients with first-time MI that underwent CABG only onethird were treated with clopidogrel after discharge. The patients receiving clopi-dogrel had lower rates of death and recurrent MI. Focus on clopidogrel treatmentafter discharge in MI patients revascularised by CABG is warranted.
P1351 Is ticagrelor superior to prasugrel for the treatment ofacute coronary syndromes? Evidence from a32,893-patient adjusted indirect comparisonmeta-analysis
G. Biondi-Zoccai1, M. Lotrionte2, P. Agostoni3, A. Abbate4,E. Romagnoli5, G. Sangiorgi6, D. Angiolillo7, M. Valgimigli8,
I. Sheiban1. 1University of Turin, Department of Cardiology, Turin, Italy; 2CatholicUniversity of the Sacred Heart, "Complesso Integrato Columbus", Rome,Italy; 3University Medical Center Utrecht, Department of Cardiology, Utrecht,Netherlands; 4VCU Pauley Heart Center, Richmond, United States of America;5Polyclinic Casilino of Rome, Rome, Italy; 6University of Modena & ReggioEmilia, Department of Cardiology, Modena, Italy; 7University of Florida-ShandsJacksonville, Jacksonville, United States of America; 8University of Ferrara, S.Anna Hospital, Cardiovascular Institute, Ferrara, Italy
Purpose: Clopidogrel is beneficial in addition to aspirin in patients with acutecoronary syndromes (ACS). Recent data suggest the superiority of either pra-sugrel or ticagrelor compared with clopidogrel. However, there is no direct com-parison of prasugrel vs. ticagrelor. We thus performed an adjusted indirect com-parison meta-analysis comparing prasugrel vs. ticagrelor for ACS.Methods: Randomized trials were searched in PubMed. The primary efficacyend-point was the long-term rate of overall death, non-fatal myocardial infarction(MI) or non-fatal stroke. The primary safety end-point was the long-term rate ofany major bleeding. Odds ratios (OR) were computed (95% confidence intervals).Results: Three trials were finally retrieved, enrolling 32893 patients. Overall,either prasugrel or ticagrelor appeared significantly superior to clopidogrel forthe 12-month risk of death, MI or stroke (OR=0.83 [0.77-0.89], p<0.001), death(OR=0.83 [0.74-0.93], p=0.001), MI (OR=0.79 [0.73-0.86], p<0.001), and stentthrombosis (OR=0.61 [0.51-0.74], p<0.001), without any significant difference instroke or major bleeding (both p>0.05), despite more frequent drug discontin-uation (OR=1.12 [1.05-1.19], p<0.001). Head-to-head comparison of prasugrelvs. ticagrelor showed no significant differences in overall death, MI, stroke, ortheir composite (all p>0.05). Prasugrel was associated with a significantly lowerrisk of stent thrombosis (OR=0.64 [0.43-0.93], p=0.020). Ticagrelor was associ-ated with a significantly lower risk of any major bleeding (OR=1.43 [1.10-1.85],p=0.007), and major bleeding associated with bypass grafting (OR=4.30 [1.73-10.6], p=0.002). Risk of major bleeding not related to bypass surgery was similarwith either prasugrel or ticagrelor (OR=1.06 [0.77-1.45], p=0.34).Conclusions: Prasugrel and ticagrelor are both superior to clopidogrel for ACS.Head-to-head comparison suggests similar efficacy and safety of prasugrel andticagrelor, but prasugrel appears more protective from stent thrombosis, whilecausing more bleedings.
P1352 Increased incidence of dyspnoea associated withticagrelor did not appear to adversely affectcardiovascular outcomes in the PLATO study
R.F. Storey1, R.C. Becker2, R.A. Harrington2, C.P. Cannon3,S. Husted4, S.K. James5, F. Cools6, P.G. Steg7, N. Khurmi8,
L. Wallentin5. 1Dept. of Cardiovascular Science, University of Sheffield, Sheffield,United Kingdom; 2Duke Clinical Research Institute, Durham, United States ofAmerica; 3Brigham and Women’s Hospital, Boston, United States of America;4Aarhus University Hospital, Skejby, Aarhus, Denmark; 5Uppsala UniversityHospital, Uppsala Clinical Research Center (UCR), Uppsala, Sweden; 6GeneralHospital Klina, Brasschaat, Belgium; 7Inserm U698 - Hospital Bichat-ClaudeBernard, Paris, France; 8AstraZeneca, Wilmington, United States of America
Background: Ticagrelor (T) has been shown to reduce ischaemic events in acute
coronary syndrome patients compared to clopidogrel in the PLATO study. Treat-ment with T is associated with dyspnoea and it is unknown whether this adverselyaffects clinical outcomes.Methods and Results: In PLATO, 18,624 patients were randomised to treatmentwith either clopidogrel (C) or ticagrelor (T) and 18,421 patients took at least onedose of study drug (9,186 C, 9,235 T). Dyspnoea was recorded through adverseevent monitoring and suspected aetiology was attributed by the investigator. 798C patients (8.7%) reported dyspnoea during or after study drug treatment com-pared to 1339 T patients (14.5%, p < 0.0001). In both groups, patients with dys-pnoea were older and had higher incidence of previous asthma, COPD, CHF anddiabetes compared to those without dyspnoea. Patients reporting dyspnoea afteradministration of study drug had higher incidences of the primary endpoint (CVdeath, MI or stroke) compared to those patients without dyspnoea in each treat-ment group, predominantly due to higher incidences of MI (Table). Reassuringly,there did not appear to be any adverse effect of the increased incidence of dys-pnoea in T patients on cardiovascular events and total mortality. Both dyspnoeaand no dyspnoea subgroups showed results consistent with the cardiovascularevents and total mortality advantages of T over C seen in the entire cohort.
C, N (%) P value T, N (%) P value
Dyspnoea No dyspnoea Dyspnoea No dyspnoeaN=798 N=8388 N=1339 N=7896
Primary endpoint 117 (14.7) 882 (10.5) <0.001 151 (11.3) 701 (8.9) 0.014MI 83 (10.4) 515 (6.1) <0.0001 112 (8.4) 393 (5.0) <0.0001Stroke 9 (1.1) 95 (1.1) 0.95 21 (1.6) 102 (1.3) 0.51CV death 37 (4.6) 391 (4.7) 0.88 39 (2.9) 306 (3.9) 0.061Total death 48 (6.0) 443 (5.3) 0.47 47 (3.5) 342 (4.3) 0.12
Conclusions: Although dyspnoea was associated with higher rates of cardiovas-cular events for both C and T, the increased incidence of dyspnoea with T did notappear to affect the reduced incidence of MI and death with T in comparison toC.
P1353 Ticagrelor versus clopidogrel in patients with AcuteCoronary Syndromes intended for a non-invasivemanagement in the PLATO trial
S. James1, M.T. Roe2, C.P. Cannon3, D. Raev4, J. Horrow5,S. Husted6, F. Kontny7, R.F. Storey8, L. Wallentin1, R. Harrington2.
1Uppsala University Hospital, Uppsala Clinical Research Center (UCR), Uppsala,Sweden; 2Duke Clinical Research Institute, Durham, United States of America;3TIMI Study Group, Brigham and Women’s Hospital, Boston, United States ofAmerica; 4Medical Institute, Ministry of Interior, Sofia, Bulgaria; 5Astra ZenecaResearch and Development, Wilmington, Delaware, United States of America;6Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark;7Volvat Medical Center, Oslo, Norway; 8Department of Cardiovascular Science,University of Sheffield, Sheffield, United Kingdom
Purpose: The potential benefit of potent dual anti platelet therapy have not beenwell studied in patients with acute coronary syndromes (ACS) intended for amanagement with a non- invasive strategy. Ticagrelor compared to clopidogrelreduced the primary composite endpoint of cardiovascular death, myocardial in-farction and stroke with similar major bleeding rates through 12 months in thePLATelet inhibition and patient Outcomes (PLATO) trial.Methods: Of the 18,624 patients hospitalized for ACS (with or without ST eleva-tion) in the PLATelet inhibition and patient Outcomes (PLATO) trial, 5,216 (28%)were at the time of randomization specified as planned for a non-invasive man-agement.Results: Despite intended initial non-invasive management, coronary angiog-raphy was performed during the initial hospitalization in 2183 of 5216 patients(41.9%), PCI in 1065 (20.4%) and CABG in 226 (4.3%). Cumulatively, 40% of thepatients underwent a revascularization procedure by the end of the trial follow-up.The incidence of the primary composite endpoint was reduced with ticagrelor vs.clopidogrel (12.0% vs. 14.3%, hazard ratio HR, 0.85; 95% confidence interval [CI],(0.73 - 1.00); P=0.045) and overall mortality was also reduced to (6.1% vs. 8.2%HR 0.75 (0.61 - 0.93), p=0.01. The incidence of PLATO-defined total major bleed-ing was numerically higher with ticagrelor vs. clopidogrel, but was not statisticallydifferent (11.9% vs. 10.3%, HR 1.17; 95% CI (0.98 - 1.39), p=0.08). Of all patientswho underwent coronary angiography during hospitalization, significant coronarydisease was found in 596 patients (89%). Patients with no significant diseasehad numerically lower event rates compared to patients who were discoveredwith significant disease and the primary composite event rate was numericallylower in the ticagrelor group compared to the clopidogrel group, 14 (3.65%) v.s22 (6.46%). Total mortality and major bleeding in these patients also occurrednumerically less frequently in the ticagrelor group (9 (2.3%) vs. 15 (4.3%) and 7(2.4%) vs. 20 (7.6%) respectively.Conclusion: In NSTE ACS patients initially intended for non invasive manage-ment, the results with ticagrelor vs. clopidogrel were similar to the overall PLATOtrial results indicating the broad benefits of intensified P2Y12 inhibition for patientswith ACS across management strategies.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

204 Focus on antiplatelet treatment
P1354 Combination therapy with clopidogrel andlansoprazole, pantoprazole or omeprazole in patientssubmitted to DES implantation
R. Rossini1, G. Musumeci1, D. Capodanno2 , C. Lettieri3,T. Nijaradze1, M. Romano3, N. Lortkipanidze1 , N. Cicorella3,
A. Gavazzi1, D. Angiolillo4. 1Hospital Riuniti of Bergamo, Bergamo, Italy;2Ferrarotto Hospital - Institute for Cardiology, Department of Cardiovascular,Catania, Italy; 3Ospedale Carlo Poma, Mantova, Italy; 4University ofFlorida-Shands Jacksonville, Jacksonville, United States of America
A pharmacodynamic interaction between clopidogrel and proton pump inhibitors(PPI) has been shown, leading to reduced clopidogrel induced platelet inhibitoryeffects. However, data from clinical studies are conflicting. In addition, no studyaddressed the effect of the time of the administration of the two drugs. The aimof the present study is to evaluate the safety of long-term clopidogrel and PPItherapy, administered at least 4 hours apart.Methods: We studied 1201 consecutive patients (pts; age 64±11 yrs; 81% male)undergoing percutaneous coronary drug eluting stent implantation. All pts weretreated with a standard aspirin and clopidogrel treatment regimen for 12 months.The concomitant PPI therapy for the same duration was at the discretion of theclinical cardiologist. PPI therapy included lansoprazole (30 mg/day), pantopra-zole (20 mg/day), or omeprazole (20 mg/day). Clopidogrel and PPI administrationwas at least 4 hours apart. At one year follow-up, major adverse cardiac events(MACE), defined as death, myocardial infarction (MI), acute coronary syndromeleading to hospitalization and non-fatal stroke, were recorded. All cause death,any stent thrombosis (ST) and bleeding (TIMI major and minor) were also as-sessed.Results: Lansoprazole, pantoprazole and omeprazole were administered to 65%,14.2%, and 10.3% of pts, respectively, whereas 10.5% were not prescribed anyPPI therapy. Pantoprazole pts had more often prior MI (22% vs 38% vs 27% vs27%; p<0.001) and multivssel coronary artery disease (55% vs 67% vs 46%vs 55%; p=0.004), whereas previous peptic ulcer was more frequent among ptstreated with omeprazole (13% vs 11% vs 23% vs 10%; p<0.001). The incidenceof 1-year MACE was statistically different among the study groups with pts receiv-ing a combination of clopidogrel and omeprazole experiencing the lowest rate ofevents (10% vs 17% vs 5% vs 11%; p=0.004). Conversely, 1-year rates of allcause death (2.1% vs 3.8% vs 1.7% vs 2.5%; p=0.62) and ST (0.4% vs 0.7% vs1.7% vs 1.7%; p=0.85) did not significantly differ among the 4 groups. Also, thecumulative incidence of major (2.5% vs 3% vs 1.5% vs 1.5%; p=0.50) and minorbleeding (4% vs 4% vs 6% vs 4%; p=0.89) was similar. After statistical adjustmentfor potential confounders, the association of clopidogrel and PPI was no longerassociated with the risk of MACE (OR 1.08, p = 0.85).Conclusions: The association of clopidogrel and PPI, prescribed upon clinicaljudgement and administered at least 4 hours apart, seems to be safe and ef-fective. Lansoprazole, pantoprazole, and omeprazole seem to have comparableclinical safety profiles.
P1355 Exaggerated platelet hypo reactivity increasesbleeding risk as measured by multiplate impedanceaggregometry test after coronary stenting
M. Colic1, B. Calija1, T. Babic1, D. Sarenac1, M. Ljubic1,B. Spasojevic1, A. Grdinic2, V. Bakic-Celic2, M. Dekleva3,
L. Angelkov1. 1Dedinje Cardiovascular Institute, Belgrade, Serbia; 2MedicalCenter Dr Dragisa Misovic-Dedinje, University Clinic for Internal Medicine,Belgrade, Serbia; 3University Clinical Center Zvezdara, Dept. of Cardiology,Belgrade, Serbia
Introduction: Exagerrated platelet hypo reactivity in response to double an-tiplatelet therapy with aspirin and clopidogrel may lead to increased bleeding riskin patients (PTS) after coronary stenting (CS).Purpose: To determine the prognostic value of multiplate impedance aggregome-try tests (adp dependent=ADP and arachidonic acid dependent=ASPI) in relationto minor and major bleeding after coronary stenting procedures.Method: A total of 211 patients (pts) with 307 stents implanted, DES 174 (57%),BMS 133 (43%), recieving standard dual antiplatelet therapy (aspirin 100mg andClopidogrel 75mg/day), was followed for 1 month for the occurence of minor ormajor bleeding. On day 1 after CS in all pts the values of ADP and ASPI testswere determined.Results: Bleeding occured in 11 pts.: 1 major (haemathemesis) and 10 minorbleedings (small haemathomas). The values of ADP and ASPI tests on day 1after CS were significantly lower in pts with bleeding in comparison to pts with-out bleeding: 328.36±110.89 AUC versus 512.69±195.05 AUC, p=0.002 for ADPtest and 160.91±100.66 AUC versus (vs) 282.50±195.73 AUC, p=0.004 for ASPItest. Values of ADP within the lowest quartile, below 347 AUC, were associatedwith higher incidence of bleeding, comparing to the value within other 3 quartiles:6/49 (12%) vs. 5/137 (4%), p=0.04. Values within the lowest quartile for ASPI,below 152 AUC, were associated with higher incidence of bleeding in comparisonto the other 3 quartiles: 7/44 (16%) vs. 4/142 (3%), p=0.004 Group with bleed-ing differed from group without bleeding in higher incidence of female gender6/11 (55%) vs 35/177 (20%), p=0.02, more advanced age 65.64±12.48 yrs. vs59.94±8.78 yrs, p=0.044, lower body weight 73.64±9.53 kg vs 84.47±13.76 kg,p=0.011, frequent previous cerebrovascular accident (CVA) 3/11 (27%) vs 3/177(2%), p<0.001, frequent calcified lesions 2/11 (18%) vs 2/161 (1%), p=0.01. The
above mentioned variables along with the values of ADP and ASPI tests werefound to be independent predictors of bleeding in Cox univariate analysis.Conclusion: Our results suggest that measuring platelet inhibition by multiplateimpedance aggregometry bedside assay, has a prognostic value for bleeding af-ter coronary stenting. Independent predictors of bleeding were: female gender,advanced age, low body weight, previous CVA, calcified lesions and values ofADP and ASPI tests within the lowest quartile.
P1356 Elevated plasma levels of asymmetricdimethylarginine (ADMA) are associated with highresidual platelet reactivity after clopidogrel therapy inpatients undergoing elective PCI
A. Nusca, G. Di Giovanni, L. Gatto, G. Patti, M. Miglionico,R. Contuzzi, A. D’ambrosio, F. Battistoni, G. Dicuonzo, G. Di Sciascio. UniversityCampus Bio-Medico of Rome, Department of Cardiovascular Sciences, Rome,Italy
Aim: Nitric Oxide (NO) suppresses platelet aggregation, leucocyte migration andcellular adhesion to the endothelium. Asymmetric dimethylarginine (ADMA), anendogenous competitive inhibitor of Nitric Oxide Synthase (NOS), is a cause ofendothelial dysfunction and a predictor of occurrence of acute coronary events.Pre-procedural elevated platelet activation represents an important prognosticfactor in patients undergoing percutaneous coronary intervention (PCI). The aimof this study was to evaluate the correlation of ADMA serum levels with residualplatelet reactivity after clopidogrel administration (chronic daily dose of 75 mg orloading dose of 600 mg) in patients (pts) undergoing PCI.Methods and Results: A total of 67 pts were prospectively enrolled and dividedin two groups according to pre-procedural serum ADMA levels measured by highperformance liquid chromatography (35 pts with ADMA ≤ 0.70 mmol/L e 32 ptswith ADMA > 0.70 mmol/L). Platelet inhibition was measured by a "point of care"assay and expressed as P2Y12 reaction units (PRU). The mean serum ADMAconcentration was 0.79±0.20 mmol/L: 0.65±0.07 mmol/L in the first group and0.94±0.17 mmol/L in the second one (p < 0.001). Considering pre-proceduralPRU levels, 37 pts with PRU < 240 showed a significant lower ADMA concen-tration versus 30 pts with PRU > 240 (0.73±0.14 vs 0.83±0.22 mmol/L, p =0.021). In the sub-group receiving 75 mg/die (31 pts),mean pre-procedural PRUlevel was 212±95 in 15 pts with ADMA ≤ 0.70 mmol/L versus 254±76 in 16 ptswith ADMA > 0.70 mmol/L (p=0.176). The rate of clopidogrel-responders (pre-procedural PRU <240) was significantly higher in ADMA ≤ 0.70 mmol/L group(73% vs 37%, p =0.045; 80% vs 31%, p = 0.018), while no differences were ob-served in the 600 mg loading dose sub-group.Conclusions: This is the first study demonstrating the correlation between highserum ADMA levels and residual platelet reactivity after clopidogrel administra-tion. The correlation was stronger in the subgroup receiving 75 mg/die suggest-ing the necessity of a higher clopidogrel maintenance daily-dose or a re-loadingbefore PTCA.
P1357 Impact of staggering clopidogrel and omeprazoleintake on clopidogrel-induced platelet inhibition
J.L. Ferreiro, M. Ueno, D. Capodanno, K. Dharmashankar,A. Darlington, R.K. Charlton, M. Kodali, B. Desai, T.A. Bass,D.J. Angiolillo. University of Florida-Shands Jacksonville,
Jacksonville, United States of America
Purpose: Several studies have reported a drug interaction between clopidogreland omeprazole. Staggering dosing of both drugs has been suggested to mini-mize the risk of interaction due to competitive hepatic metabolism at the level ofthe CYP2C19 enzyme. The aim of this study was to compare clopidogrel-inducedantiplatelet effects when taken concomitantly or staggered from omeprazole ad-ministration.Methods: A total of 20 healthy volunteers were randomized to receive either clopi-dogrel 600-mg loading dose (LD) followed by 75-mg maintenance dose (MD) andomeprazole (40 mg daily) concomitantly (CONC regimen) or staggered by 8-12hours (STAG regimen) for 1 week in a cross-over fashion with a 2-4 week washoutperiod between treatment periods. After another washout period, all randomizedsubjects were treated for 1 week with clopidogrel only (CLOP regimen). Plateletfunction was assessed by flow cytometric analysis of the status of phosphori-lation of the vasodilator-stimulated phosphoprotein (VASP), light transmittanceaggregometry (LTA) following ADP stimulus and VerifyNow P2Y12 system at 3time-points: baseline, 24 hours post LD and 1 week post-MD. The primary end-point was the comparison of P2Y12 reactivity index (PRI) assessed by VASP at 1week between CONC and STAG regimens. Values are expressed as least squaremean [95% confidence interval].Results: No significant difference in PRI was observed between CONC andSTAG regimens after 1 week of treatment (56.1 [49.0-63.2] vs. 61.6 [54.7-68.5];p=NS). However, PRI values were significantly lower in the CLOP regimen (48.8[41.9-55.7]) compared with the CONC (p=0.02) and STAG (p<0.001) regimens.No differences were observed at baseline and 24 hours between regimens. Con-cordant results were obtained by LTA and VerifyNow.Conclusions: Omeprazole use reduces clopidogrel-induced antiplatelet effectsin the maintenance phase of treatment, a phenomenon which is observed irre-spective of regimen (concomitant or staggered) used.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Focus on antiplatelet treatment / Antithrombotics for primary percutaneous coronary intervention 205
P1358 Can we overcome genetic resistance to clopidogrelwith high doses of clopidogrel? The CLOVIS-2 study
J.-P. Collet, J.S.H. Hulot, A.P. Pena, T.C. Chastre, J.S. Sil-vain, G.A. Anzaha, S.G. Gallier, V.G. Gallois, G.C. Cayla,G.M. Montalescot. AP-HP - Hospital Pitie-Salpetriere, Paris, France
Purpose: To compare the pharmacodynamic response of two loading doses (LD)of clopidogrel (300mg vs 900 mg) according to carriage of CYP2C19*2 geneticvariant.Methods: Young patients (aged <45 years) who survived a first MI and all treatedwith 75mg of aspirin and of 75mg of clopidogrel were randomized in this crossoverstudy. Patients were paired according to carriage of CYP2C19*2 variant. Patientsreceived an initial load according to randomization and blood samples were takenat baseline and 6 hours. After loading, clopidogrel 75mg MD dose was continuedand 21 days later patients were crossed over to the alternate LD of clopidogrel.The primary aim was to evaluate the relative change in platelet aggregation be-tween carriers and non carriers of the CYP2C19*2 variant. Platelet aggregationwas expressed as P2Y12 platelet reaction units (PRU) measured with the Veri-fyNow™ P2Y12 (VN-P2Y12) assay.Results: Of 104 randomized patients, 52 were carriers of CYP2C19*2 variant(heterozygous *1/*2, n=45; homozygous *2/*2, n=7). Baseline characteristics be-tween carriers and non carriers of the CYP2C19*2 variant were well-matched.There was a stepwise increase in baseline PRU level between non carriersand carriers with a gene dose-effect among carriers (see table). Carriage of theCYP2C19*2 variant was associated with a reduction of the effect of 300mg load-ing with a gene dose-effect and no detectable effect of 300mg-loading in homozy-gous carriers. 900mg-LD blunted the effect of the CYP2C19*2 variant on plateletinhibition in heterozygous patients, that did not differ from non-carriers of the vari-ant. In contrast, homozygous patients still displayed a reduced effect of 900mgloading.
Non Carriers Carriers P value
*1/*2 (n=45) *2/*2 (n=7)
Baseline PRU level on clopidogrel 76±77 112±61 230±104 <0.001Relative change in PRU 300mg LD -38±36% -25±58% +12±16, 0.02Relative change in PRU 900mg LD -67±68% -63±32% -16±4% 0.008
Conclusion: In stable CAD patients, carriers of CYP2C19*2 variant have lowerlevels of platelet inhibition under a maintenance dose of clopidogrel with a signif-icant gene dose-effect. The gene dose-effect can be overcome by higher dosesof clopidogrel with a drug dose-effect. However clopidogrel resistance remains inhomozygous patients.
P1359 Resistance to antiplatelet therapy in the elderly, a realconcern. Results of the seniors platelet study
J. Silvain, G. Cayla, A. Pena, A. Bellemain-Appaix, F. Beygui,O. Barthelemy, S. Galier, B. Bertin, J.P. Collet, G. Montalescot.Institut de Cardiologie, INSERM CMR937, Pitié-Salpêtrière Hospital
(AP-HP), Université Paris 6, Paris, France
Background: Dual antiplatelet therapy (DAT) effect on platelet inhibition in el-derly patients (>75 y/o) is unknown as they are often excluded from clinical trialsbecause of an increased bleeding risk.Aim: To compare on-treatment platelet reactivity under DAT of elderly vs. youngerpatients (< 75yrs).Methods: The Senior Platelet study included 652 coronary patients treated by amaintenance dose (MD) of aspirin and clopidogrel in whom platelet response wasassessed by Light transmission aggregrometry (LTA) with measure of Maximum(MPA) and Residual Platelet Aggregation (RPA) and VerifyNow with PRU. Ratesof non-responders were established using admitted definitions: >50% RPA with20μM ADP, >235 PRU by VerifyNow P2Y12 assay for clopidogrel response and>20% MPA with AA and >550 ARU by VerifyNow ASA assay for aspirin response.Results: The mean MD of clopidogrel and aspirin were similar between the twogroups. On-clopidogrel platelet reactivity was higher in elderly when comparedto younger patients whatever the test used (figure for PRU). The rate of non-responders with PRU>235 was 37.1% in the 105 elderly patients and 19,01% in
Impact of age on platelet reactivity
the 547 younger patients; p<0,001). Results were even more striking when RPAwas considered with 67.3% of non-responders in elderly vs. 22.8% in youngerpatients; p<0,001. Mean ARU was similar in both groups with 440U in youngerpatients vs. 452U in elderly (p=0.8), but the mean AA induced MPA was 5.5%vs. 10.4% (p=0.01). The rate of non-response was 6.25% and 15% with LTA(p=0.001).Conclusions: Elderly patients have higher levels of on-treatment platelet reactiv-ity for both clopidogrel and aspirin and a two and three fold increase in the rate ofnon-responders to clopidogrel and to aspirin suggesting that elderly patients withCAD or ACS should not be undertreated.
ANTITHROMBOTICS FOR PRIMARY PERCUTANEOUSCORONARY INTERVENTION
P1360 Effects of single high-dose bolus of tirofiban orabciximab during primary angioplasty for acutemyocardial infarction in patients with renal failure
S. Colangelo1 , G. Boccuzzi1, R. Garbo1, P. Noussan2, G. Campo3,M. Valgimigli3. 1Interventional Cardiology, San Giovanni Bosco
Hospital, Turin, Italy; 2Intensive Care Unit, San Giovanni Bosco Hospital, Turin,Italy; 3University of Ferrara, S. Anna Hospital, Cardiovascular Institute, Ferrara,Italy
Introduction: Coronary artery disease is the most important cause of morbidityand mortality in patients with renal failure. We sought to determine the effects oftwo glycoprotein IIb///IIIa inhibitor (tirofiban and abciximab) in patients with renalfailure underwent primary angioplasty for acute myocardial infarction.Methods: 744 patients enrolled in the MULTISTRATEGY trial were stratified byrenal function according with the National Kidney Foundation criteria; both themajor adverse cardiovascular events and mortality were evaluated at 12 monthsin the patients with moderate to end-stage renal disease (class III-IV-V; n=176patients) treated with either tirofiban (group A) or abciximab (group B).Results: Baseline characteristics and angiographic features were comparable inthe two groups as like as bleeding complications (see Table 1), but the need forred blood cells transfusions were significantly higher in the tirofiban group (10.5%vs 2.5%, p= 0.03). Postprocedural TIMI flow grade 3 was not statistically differentin the two groups (87.4% vs 80.2%). Both the overall mortality (11.6% in thetirofiban group vs 8.6% in the abciximab group) and the MACE at 1-year (15.8%vs 14.8%) were not statistically different in the two groups.
Table 1. Baseline characteristics, angiographic features, bleeding complications and outcomes inthe two groups of patients
Characteristics Tirofiban patients Abciximab patients p95 patients 81 patients
Age (yrs) 76±7 75±7 NSDiabetes (%) 24 (25.2%) 12 (14.8%) 0.06LVEF (%) 47±10 46±12 NSMultivessel disease (%) 57 (60%) 50 (61.7%) NSPostprocedural TIMI flow grade 3 83 (87.4%) 65 (80.2%) 0.1TIMI major bleeding (%) 5 (5.3%) 3 (3.7%) NSRBC Transfusions (%) 10 (10.5%) 2 (2.5%) 0.03Death 11 (11.6%) 7 (8,6%) NSMACE 15 (15.6%) 12 (14.8%) NS
Conclusion: The use of tirofiban in patients with moderate to end-stage renalfailure who underwent primary angioplasty seems to be as safe and effective asabciximab. The lack of correlation among the higher rate of RBC transfusions inpatients treated with tirofiban and 1-year mortality should be reassessed duringthe long-term follow-up.
P1361 Use of recombinant factor VII a (NovoSeven) inpatients treated with Fondaparinux ongoing lifethreatening bleeding
F. Schiele, P. Luporsi, N. Meneveau, E. Raccadot, V. Descotes-Genon, R. Chopard, M.F. Seronde, S. Janin. University Hospital
Jean Minjoz, Besancon, France
Rationale: Recombinant factor VIIa (rFVIIa) may be used to reverse the antico-agulant effect of Fondaparinux. We report a single centre experience in 8 patientswith severe bleeding.Methods: Patients pretreated with Fondaparinux, with life-threatening bleedingwere treated with 90μg/kg rFVIIa. Live-threatening bleeding was defined as TIMI3 bleeding or > 5g hemoglobin drop or hemodynamic shock and elevated an-tiXa activity. Endpoints were (1) death, (2) continuation of the bleeding (clinical orcontinued drop of heamoglobin), (3) uncontrolled hemodynamic shock, (4) clinicalarterial or venous thrombosis and (5) peak of thrombin generation.Results: Between June 2008 and November 2009, among 1224 patients treatedwith Fondaparinux, 8 presented with life-threatening bleeding: 3 patients had ve-nous thrombo-embolic disease and 5 acute coronary syndrome (ACS). Patientswith ACS had double (n=2) or triple (n=3) antiplatelet therapy. Bleedings were re-lated to vascular access in 5, gastro-duodenal in 2 and lung in 1. Five patients hadan hemorrhagic shock, mean drop of haemoglobin was 6.1 g/dL. AntiXa activity
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
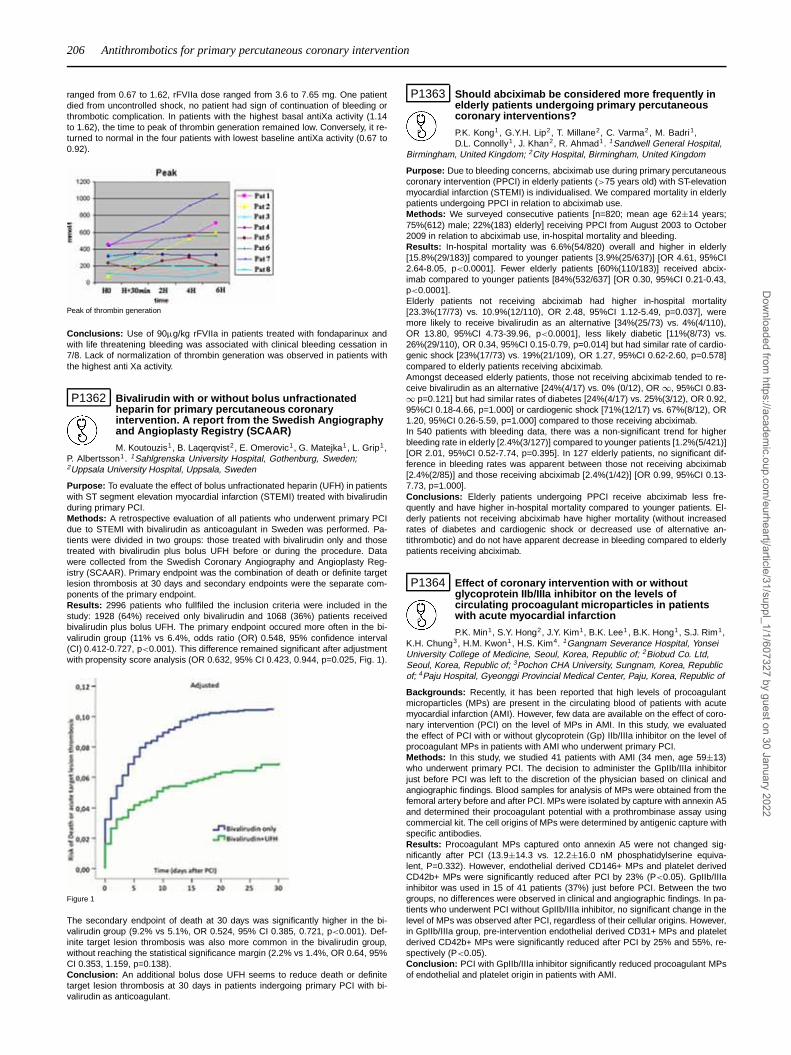
206 Antithrombotics for primary percutaneous coronary intervention
ranged from 0.67 to 1.62, rFVIIa dose ranged from 3.6 to 7.65 mg. One patientdied from uncontrolled shock, no patient had sign of continuation of bleeding orthrombotic complication. In patients with the highest basal antiXa activity (1.14to 1.62), the time to peak of thrombin generation remained low. Conversely, it re-turned to normal in the four patients with lowest baseline antiXa activity (0.67 to0.92).
Peak of thrombin generation
Conclusions: Use of 90μg/kg rFVIIa in patients treated with fondaparinux andwith life threatening bleeding was associated with clinical bleeding cessation in7/8. Lack of normalization of thrombin generation was observed in patients withthe highest anti Xa activity.
P1362 Bivalirudin with or without bolus unfractionatedheparin for primary percutaneous coronaryintervention. A report from the Swedish Angiographyand Angioplasty Registry (SCAAR)
M. Koutouzis1, B. Laqerqvist2 , E. Omerovic1, G. Matejka1, L. Grip1,P. Albertsson1. 1Sahlgrenska University Hospital, Gothenburg, Sweden;2Uppsala University Hospital, Uppsala, Sweden
Purpose: To evaluate the effect of bolus unfractionated heparin (UFH) in patientswith ST segment elevation myocardial infarction (STEMI) treated with bivalirudinduring primary PCI.Methods: A retrospective evaluation of all patients who underwent primary PCIdue to STEMI with bivalirudin as anticoagulant in Sweden was performed. Pa-tients were divided in two groups: those treated with bivalirudin only and thosetreated with bivalirudin plus bolus UFH before or during the procedure. Datawere collected from the Swedish Coronary Angiography and Angioplasty Reg-istry (SCAAR). Primary endpoint was the combination of death or definite targetlesion thrombosis at 30 days and secondary endpoints were the separate com-ponents of the primary endpoint.Results: 2996 patients who fullfiled the inclusion criteria were included in thestudy: 1928 (64%) received only bivalirudin and 1068 (36%) patients receivedbivalirudin plus bolus UFH. The primary endpoint occured more often in the bi-valirudin group (11% vs 6.4%, odds ratio (OR) 0.548, 95% confidence interval(CI) 0.412-0.727, p<0.001). This difference remained significant after adjustmentwith propensity score analysis (OR 0.632, 95% CI 0.423, 0.944, p=0.025, Fig. 1).
Figure 1
The secondary endpoint of death at 30 days was significantly higher in the bi-valirudin group (9.2% vs 5.1%, OR 0.524, 95% CI 0.385, 0.721, p<0.001). Def-inite target lesion thrombosis was also more common in the bivalirudin group,without reaching the statistical significance margin (2.2% vs 1.4%, OR 0.64, 95%CI 0.353, 1.159, p=0.138).Conclusion: An additional bolus dose UFH seems to reduce death or definitetarget lesion thrombosis at 30 days in patients indergoing primary PCI with bi-valirudin as anticoagulant.
P1363 Should abciximab be considered more frequently inelderly patients undergoing primary percutaneouscoronary interventions?
P.K. Kong1, G.Y.H. Lip2, T. Millane2, C. Varma2, M. Badri1,D.L. Connolly1, J. Khan2, R. Ahmad1. 1Sandwell General Hospital,
Birmingham, United Kingdom; 2City Hospital, Birmingham, United Kingdom
Purpose: Due to bleeding concerns, abciximab use during primary percutaneouscoronary intervention (PPCI) in elderly patients (>75 years old) with ST-elevationmyocardial infarction (STEMI) is individualised. We compared mortality in elderlypatients undergoing PPCI in relation to abciximab use.Methods: We surveyed consecutive patients [n=820; mean age 62±14 years;75%(612) male; 22%(183) elderly] receiving PPCI from August 2003 to October2009 in relation to abciximab use, in-hospital mortality and bleeding.Results: In-hospital mortality was 6.6%(54/820) overall and higher in elderly[15.8%(29/183)] compared to younger patients [3.9%(25/637)] [OR 4.61, 95%CI2.64-8.05, p<0.0001]. Fewer elderly patients [60%(110/183)] received abcix-imab compared to younger patients [84%(532/637] [OR 0.30, 95%CI 0.21-0.43,p<0.0001].Elderly patients not receiving abciximab had higher in-hospital mortality[23.3%(17/73) vs. 10.9%(12/110), OR 2.48, 95%CI 1.12-5.49, p=0.037], weremore likely to receive bivalirudin as an alternative [34%(25/73) vs. 4%(4/110),OR 13.80, 95%CI 4.73-39.96, p<0.0001], less likely diabetic [11%(8/73) vs.26%(29/110), OR 0.34, 95%CI 0.15-0.79, p=0.014] but had similar rate of cardio-genic shock [23%(17/73) vs. 19%(21/109), OR 1.27, 95%CI 0.62-2.60, p=0.578]compared to elderly patients receiving abciximab.Amongst deceased elderly patients, those not receiving abciximab tended to re-ceive bivalirudin as an alternative [24%(4/17) vs. 0% (0/12), OR ∞, 95%CI 0.83-∞ p=0.121] but had similar rates of diabetes [24%(4/17) vs. 25%(3/12), OR 0.92,95%CI 0.18-4.66, p=1.000] or cardiogenic shock [71%(12/17) vs. 67%(8/12), OR1.20, 95%CI 0.26-5.59, p=1.000] compared to those receiving abciximab.In 540 patients with bleeding data, there was a non-significant trend for higherbleeding rate in elderly [2.4%(3/127)] compared to younger patients [1.2%(5/421)][OR 2.01, 95%CI 0.52-7.74, p=0.395]. In 127 elderly patients, no significant dif-ference in bleeding rates was apparent between those not receiving abciximab[2.4%(2/85)] and those receiving abciximab [2.4%(1/42)] [OR 0.99, 95%CI 0.13-7.73, p=1.000].Conclusions: Elderly patients undergoing PPCI receive abciximab less fre-quently and have higher in-hospital mortality compared to younger patients. El-derly patients not receiving abciximab have higher mortality (without increasedrates of diabetes and cardiogenic shock or decreased use of alternative an-tithrombotic) and do not have apparent decrease in bleeding compared to elderlypatients receiving abciximab.
P1364 Effect of coronary intervention with or withoutglycoprotein IIb/IIIa inhibitor on the levels ofcirculating procoagulant microparticles in patientswith acute myocardial infarction
P.K. Min1, S.Y. Hong2, J.Y. Kim1, B.K. Lee1, B.K. Hong1, S.J. Rim1,K.H. Chung3, H.M. Kwon1, H.S. Kim4. 1Gangnam Severance Hospital, YonseiUniversity College of Medicine, Seoul, Korea, Republic of; 2Biobud Co. Ltd,Seoul, Korea, Republic of; 3Pochon CHA University, Sungnam, Korea, Republicof; 4Paju Hospital, Gyeonggi Provincial Medical Center, Paju, Korea, Republic of
Backgrounds: Recently, it has been reported that high levels of procoagulantmicroparticles (MPs) are present in the circulating blood of patients with acutemyocardial infarction (AMI). However, few data are available on the effect of coro-nary intervention (PCI) on the level of MPs in AMI. In this study, we evaluatedthe effect of PCI with or without glycoprotein (Gp) IIb/IIIa inhibitor on the level ofprocoagulant MPs in patients with AMI who underwent primary PCI.Methods: In this study, we studied 41 patients with AMI (34 men, age 59±13)who underwent primary PCI. The decision to administer the GpIIb/IIIa inhibitorjust before PCI was left to the discretion of the physician based on clinical andangiographic findings. Blood samples for analysis of MPs were obtained from thefemoral artery before and after PCI. MPs were isolated by capture with annexin A5and determined their procoagulant potential with a prothrombinase assay usingcommercial kit. The cell origins of MPs were determined by antigenic capture withspecific antibodies.Results: Procoagulant MPs captured onto annexin A5 were not changed sig-nificantly after PCI (13.9±14.3 vs. 12.2±16.0 nM phosphatidylserine equiva-lent, P=0.332). However, endothelial derived CD146+ MPs and platelet derivedCD42b+ MPs were significantly reduced after PCI by 23% (P<0.05). GpIIb/IIIainhibitor was used in 15 of 41 patients (37%) just before PCI. Between the twogroups, no differences were observed in clinical and angiographic findings. In pa-tients who underwent PCI without GpIIb/IIIa inhibitor, no significant change in thelevel of MPs was observed after PCI, regardless of their cellular origins. However,in GpIIb/IIIa group, pre-intervention endothelial derived CD31+ MPs and plateletderived CD42b+ MPs were significantly reduced after PCI by 25% and 55%, re-spectively (P<0.05).Conclusion: PCI with GpIIb/IIIa inhibitor significantly reduced procoagulant MPsof endothelial and platelet origin in patients with AMI.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Antithrombotics for primary percutaneous coronary intervention 207
P1365 Heparin or enoxaparin anticoagulation for primary PCI
D. Brieger1, J.P. Collet2, J. Silvain2, A. Landivier2, O. Barthelemy2,F. Beygui2, A. Bellemain-Appaix2, N. Vignolles2, D. Costagliola3,G. Montalescot2 . 1Concord Hospital, Anzac Research Institute,
Sydney, Australia; 2AP-HP - Hospital Pitie-Salpetriere, Department of Cardiology,Paris, France; 3University Pierre & Marie Curie (UPMC), Paris, France
Purpose: The aim of this study was to compare efficacy and safety outcomesamong patients receiving enoxaparin or unfractionated heparin (UFH) while un-dergoing PCI for STEMI (pPCI).Methods: Consecutive eligible patients (580) undergoing pPCI enrolled in theprospective e-PARIS registry were grouped according to whether they receivedUFH or enoxaparin as the sole anticoagulant. Logistic regression modeling andsensitivity analyses were used to evaluate efficacy and safety endpoints forenoxaparin vs UFH.Results: Enoxaparin was administered to 346 patients and UFH to 234. PCI wasperformed through the radial artery in 90%, with 75% use of GPIIb/IIIa antago-nists. Patients receiving enoxaparin were more likely to be therapeutically antico-agulated during the procedure (68% vs 50%, P<0.0001) and were less likely toexperience death or reMI by 30 days (adjusted OR 0.35 95% CI 0.16-0.81). Allcause mortality was also reduced (adjusted OR 0.40 95% CI 0.17-0.99). Otherischemic endpoints were similarly reduced with enoxaparin. In hospital TIMI ma-jor bleeding events were numerically fewer among patients receiving enoxaparin(1.2% vs 2.6%, p=0.2).Conclusions: In patients with STEMI presenting for PCI, enoxaparin was asso-ciated with a reduction in all ischemic complications and no increase in majorbleeding when compared against unfractionated heparin.
P1366 Impact of GPIIb/IIIa inhibitors at the acute stage of MIin diabetics vs non diabetics: data from an age andsex-matched cohort from the FAST-MI registry
J. Ferrieres1, J.Y. Pagny2, A. Dibie3, J.C. Kahn4, M. Zupan5 ,A. Furber6, P. Virot7, E. Ferrari8, T. Simon9, N. Danchin10.
1University Hospital of Toulouse, Department of Epidemiology, Inserm U558,Toulouse, France; 2Clinic Alleray-Labrouste, Paris, France; 3Institut MutualisteMontsouris, Paris, France; 4Hospital Poissy/St Germain en Laye, Department ofCardiology, Poissy, France; 5New Civil Hospital, Cardiovascular Medico-SurgicalActivities, Strasbourg, France; 6University Hospital of Angers, Angers, France;7University Hospital of Limoges - Hospital Dupuytren, Limoges, France;8University Hospital of Nice - Hospital Pasteur, Nice, France; 9AP-HP - HospitalSaint Antoine, Clinical Research Unit (URC) - Est, Paris, France; 10AP-HP -European Hospital Georges Pompidou, Paris, France
Aim: though the Early-ACS trial failed to show a significant reduction in events inpatients with GP IIb/IIIa inhibitors (GPIs), a favorable trend was seen in diabetics.We assessed the impact of GPIs in patients admitted for AMI according to theirdiabetic status.Methods: FAST-MI is a registry conducted in 60% of all French ICUs in 2005.From the 3670 patients included, we built 2 cohorts of 765 diabetic and 765 nondiabetic pts with no previous history of CAD, matched on age and sex. End-points:one-year death or death/MI rates (Kaplan-Meier).Results: Overall, and despite age/sex matching, diabetic pts more often had an-tihypertensive, antiplatelet and lipid lowering medications before the AMI. Earlymanagement was similar for diabetic and non diabetic pts. GPIs were used in 35%of non diabetics (n=271) and 38% of diabetics (n=289) together with clopidogreluse in 95% and 93%, respectively. Overall, 1-year death was 17.4% (diabetics)vs 9.7% (non diabetics), p<0.001, and death/MI was 19.9% vs 11.8% (p<0.001).When stratified by GPI use, death and death/MI were twice as high in diabet-ics vs non diabetics without GPI, whereas the event rates were similar betweendiabetics and non diabetics on GPIs (Figure). Cox x-variate analysis showed thelack of prognostic impact of GPIs in non diabetics (OR for death=0.94 [0.48-1.87];death/MI: 1.29 [0.74-2.26]), but a significant reduction for death (OR=0.53 [0.32-0.88] p=0.013) or death/MI (OR=0.53 [0.34-0.83] p=0.005) in diabetics.
Mortality according to diabetic status
Conclusion: In this real world registry, use of GPIs in diabetic pts was associatedwith improved outcome. One-year event rates in diabetics on GPIs was similar tothat observed in non diabetics.
P1367 Effect of switching to bivalirudin versus adding aGPIIb/IIIa inhibitor in patients with acute myocardialinfarction treated with pre-randomization heparin inthe HORIZONS-AMI trial
G. Dangas1, R. Mehran1, H. White2, A. Caixeta1, A.J. Lansky1,B. Brodie3, B. Witzenbichler4, G. Guagliumi5, D. Dudek6, G.W. Stone1.1Columbia University Medical Center and the Cardiovascular ResearchFoundation, New York, United States of America; 2Auckland City Hospital,Auckland, New Zealand; 3LeBauer Cardiovascular Research Foundation,Greensboro, United States of America; 4Charite - Campus Benjamin Franklin,Berlin, Germany; 5Hospital Riuniti of Bergamo, Bergamo, Italy; 6JagiellonianUniversity, Krakow, Poland
Purpose: The safety and efficacy of switching anticoagulants in the early treat-ment of ST-elevation MI is unknown. In the HORIZONS-AMI randomized trial,bivalirudin monotherapy lowered major bleeding and mortality and had higheracute stent thrombosis but similar overall MACE to heparin plus a GPIIb/IIIa in-hibitor (GPI).Methods: We analyzed the subgroup of HORIZONS-AMI patients (n=2357)treated with heparin before randomization according their subsequent assign-ment to bivalirudin (Switch group, n=1178) or to heparin plus GPI (Control group,n=1179).Results: There were no significant differences in the baseline demographics orprocedural characteristics between the 2 groups, except for higher incidences ofsmoking (65% vs. 61%, p=0.04) and prior CABG (4.2% vs. 2.5%,p=0.03) in theSwitch group. There was lower 2-year cardiac mortality, reinfarction, and bleed-ing in Switch vs. Control. Overall MACE was similar and net adverse event rate(NACE) was lower with Switch. (Table)
2-year Clinical Outcomes
Switch (n=1178) Control (n=1179) p-value
Mortality 4.4% 5.6% 0.15Cardiac death 2.3% 3.8% 0.04MI 4% 7.1% 0.002TVR 13% 12% 0.48Death or MI 7.8% 11.9% 0.001MACE 17.5% 18.6% 0.47Major Bleeding 6% 10% 0.0004TIMI-major bleeding 4% 6.4% 0.007NACE 21.4% 25.3% 0.01Stent Thrombosis* 3.1% 4.3% 0.17
*Academic Research Consortium (ARC) definition.
Conclusions: In patients with acute STEMI who receive early treatment withheparin, switching to bivalirudin for primary angioplasty yields superior ischemicresults and is safer with respect to bleeding complications.
P1368 Early abciximab administration during transfer forprimary percutaneous coronary intervention. Is therea time benefit therapeutic window?
G. Bastos Fernandez, J.E. Carrillo Guevara, E. Paredes Galan,J.A. Baz Alonso, R. Ocaranza Sanchez, A. Ortiz Saez, I. Gomez
Blazquez, J. Sterling Duarte, A. Iniguez Romo. Hospital de Meixoeiro, Vigo,Spain
Purpose: The aim of this observational study was to evaluate benefit of early ab-ciximab administration in ST-elevation myocardial infarction (STEMI) during trans-fer for primary percutaneous coronary intervention (PPCI), compared to late ad-ministration during PPCI.Methods: From January through December 2009, 400 STEMI patients were ad-mitted in a PPCI capable centre, 124 consecutive patients were included. Inclu-sion criteria were STEMI in the first 12 hours with first medical contact at a nonPPCI capable centre. Exclusion criteria were Killip IV class, abciximab contraindi-cation, no 12-lead ECG in the first 60 min. Patients were pretreated with 300mgaspirin and 300mg clopidogrel loading doses plus unfractioned heparin bolus of60 U/kg. Early abciximab administration at the referral non PPCI capable centreor during ambulance transfer was according to the operator choice. One monthclinical follow after discharge was planned. Primary endpoint was initial Throm-bolysis In Myocardial Infarction (TIMI) flow grade. Secondary end points wereST-segment resolution (>50%), left ventricle ejection fraction (LVEF) and mayoradverse cardiac events (death, non fatal myocardial infarction, target lesion revas-cularization, TIMI mayor bleeding) within 30 days.Results: Early abciximab bolus during transfer was administered in 78 (62.9%)with median abciximab administration to reperfusion interval of 58±26 min. Whencomparing early versus late administration baseline characteristics were simi-lar, except for less diabetes mellitus type 2 patients in early abciximab group(29% vs 68%, p =0.04). Median symptom onset to first medical contact interval(136±121 vs 153±116 min, p=0.46), first medical contact to PPCI (110±40.5 vs129±95 min, p=0.12) and symptom onset to reperfusion (246±132 vs 282±138min, p=0.15) were similar. Initial TIMI flow grade was better in the early abciximabgroup (TIMI 0 46.2% vs 71.7%, p=0.006). Only patients in the first quartile of timefrom symptom onset to first medical contact (<90min) had less initial TIMI 0 flowgrade (TIMI 0 26% vs 58%, p=0.01). After first 90 min of symptom onset therewere no differences in early administration of abciximab compared to late admin-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

208 Antithrombotics for primary percutaneous coronary intervention / Predictors of outcome after percutaneous coronary intervention
istration (TIMI 0 58% vs 68%, p=0.4). No immediate ST resolution differenceswere observed (70.6% vs 63.6%, p=0.6). At 30 days there were not differencesin clinical events included bleeding complications.Conclusions: In this study early administration of abciximab in STEMI patientswithin 90 minutes of symptom onset is related with better initial TIMI flow grade.There was no reduction in cardiac events.
P1369 Upstream Abciximab administration in STEMI patientsundergoing timely primary PCI is independentlyassociated with lower in-hospital mortality
G. Crimi1, D. Bartolini1, F. Della Rovere2, S. Bellotti1, A. Gatti2,A. Iannone1 , A. Rolandi2, P. Rubartelli1. 1Ospedale Villa Scassi,
Genoa, Italy; 2Ospedale Galliera, Genoa, Italy
Aims: In patients with STEMI undergoing PCI, upstream Abciximab has beenmainly employed in the attempt to counterbalance the delay related to the proce-dure ("facilitated" PCI). The role of upstream Abciximab in STEMI patients treatedtimely with pPCI is not well defined.Methods: In 1055 consecutive STEMI patients treated with pPCI, 945 receivedAbciximab, which was given just after 1st medical contact (FMC), defined as ei-ther self presentation to the emergency room or contact with the EMS physician.Clopidogrel 300 mg loading dose was given just after the pPCI. Abciximab ad-ministration was defined as upstream when given >20 min before pPCI.Results: pPCI was performed within 120 min from FMC in 80% of patients. Mainbaseline and procedural characteristics and in-hospital results are shown in thetable. Patients treated upstream had a lower prevalence of diabetes and priorMI, but also a longer FMC to balloon time, and presented a lower in-hospitalmortality rate. Multivariate analysis identified the following independent predictorsof mortality (OR, 95% C.I.): age (per year, 1.070, 1.040-1.101), Killip class >1(5.523, 2.679-11.382), FMC-to-balloon time (1.005, 1.001-1.009), and upstreamAbciximab (0.537, 0.289-0.996).
Characteristics and outcome of patients
Upstream (n=694) Periprocedural (n=251) P value
Age (mean± DS) 66.0±12.1 66.4±13.1 nsMale sex (%) 76.8 74.1 nsDiabetes mellitus (%) 20.2 24.3 <.05Previous MI (%) 8.8 14.3 <.05Anterior MI 38.6 37.5 nsKillip Class >1 (%) 5.2 8.0 nsMultivessel disease (%) 40.9 45.0 nsSymptom onset-to-FMC (min, IQR) 93 (50 - 208) 114 (52 - 240) nsFMC-to-balloon (min, IQR) 88 (72 - 110) 75 (50 - 96) <.001TIMI flow 2 or 3 before pPCI (%) 33.1 23.9 <.01In-hospital mortality (%) 4.8 8.4 <.05
Conclusions: In STEMI patients undergoing pPCI with a reasonable delay afterFMC, and not pre-treated with Clopidogrel, upstream Abciximab administration isindependently associated with lower in-hospital mortality.
PREDICTORS OF OUTCOME AFTER PERCUTANEOUSCORONARY INTERVENTION
P1370 Long-term serial angiographic outcomes aftersirolimus-eluting stent implantation: contemporarypractice in real world population
E. Ko, K. Nasu, M. Habara, T. Kurita, Y. Kinoshita, T. Suzuki.Toyohashi Heart Center, Toyohashi, Japan
Aim: Percutaneous coronary intervention (PCI) with drug eluting stent (DES) hassignificantly reduced the rate of repeated target-lesion revascularization. How-ever, the results from a few studies have recently raised concerns regarding ‘latecatch up’ phenomenon of DES. The impact of late restenosis with DES has notbeen uniform across complex subsets and limited data is available examiningpredictors of late restenosis in unselected consecutive population.Method: A total of 3240 lesions were treated with SES from June 2004 to Apr2007 in our institution. Of those, 306 lesions without restenosis at first follow-up (11.2±2.1 months, range: 9.3∼12.4 months) had second follow-up angiogra-phy (29.4±5.2 months, range: 24.2∼49.2 months). We evaluated the extendedterm of angiographic outcomes and predictors of late restenosis among patientstreated with SES beyond 2 years after the index procedure in unselected consec-utive population.Results: Minimal lumen diameter (MLD) at first angiographic follow-up of all le-sions was significantly small compared to that of immediately after procedure(2.72±0.49mm versus 2.83±0.48 mm; p < 0.0001). Also, MLD at second angio-graphic follow-up was significantly smaller than that of first angiographic follow-up (2.57±0.67 mm versus 2.72±0.49 mm; p < 0.0001). Especially, among pa-tients with late restenosis, MLD was significantly decreased from 28.9±0.42 mmat first angiographic follow-up to 2.41±0.33 mm at second angiographic follow-up (p < 0.0001), and LL was significantly increased from 0.48±0.27 mm at firstangiographic follow-up to 1.23±0.49 mm at second angiographic follow-up (p <
0.0001). There were several predictors identified on univariate analysis such as
previous PCI (p = 0.022, OR = 3.938, 95% CI = 1.638-9.464), adjunctive us-age of cutting balloon (p = 0.025, OR = 4.051, 95% CI = 1.195-13.727), post-interventional %DS (p = 0.0007, OR = 0.888, 95% CI = 0.829-0.951), and LL (p< 0.0001, OR = 9.255, 95% CI = 4.022-21.296), MLD (p = 0.018, OR = 0.193,95% CI = 0.069-0.543), %DS (p = 0.0006, OR = 1.070, 95% CI = 1.113) at firstangiographic follow up.Conclusion: Although late regression was observed in BMS era, significant lateprogression beyond 2 years after SES implantation was observed in the presentstudy. Besides, stent under-expansion still remains the important cause of laterestenosis even in DES era. Long term of angiographic follow-up should be rec-ommended to detect ‘late-catch up’ phenomenon especially in patients with sub-optimal stent expansion and moderate progression at first angiographic followup.
P1371 Long-term follow-up after coronary stenting with theSirolimus-eluting stent in clinical practice. Resultsfrom a substudy of the pospective multi-centreGerman cypher stent registry
R. Zahn1, C. Hamm2, G. Sabin3, S. Schneider1 , C. Nienaber4,G. Richardt5, F.J. Neumann6, J. Brachmann7 , J. Senges8. 1Clinical Center ofLudwigshafen, Ludwigshafen am Rhein, Germany; 2Kerckhoff Clinic, Departmentof Cardiology, Bad Nauheim, Germany; 3Elisabeth Hospital, Department ofCardiology & Angiology, Essen, Germany; 4University Hospital Rostock, DptInternal Medicine, Division of Cardiovascular Medicine, Rostock, Germany;5Segeberger Clinics, Cardiovascular Center, Bad Segeberg, Germany;6Heart Centre Bad Krozingen, Bad Krozingen, Germany; 7Coburg ClinicalCenter, Coburg, Germany; 8Heart Attack Research Center at the University ofHeidelberg, Ludwigshafen am Rhein, Germany
Background: In April 2002 the Sirolimus-eluting stent (SES) was introduced forpercutaneaous coronary interventions (PCI). Meanwhile there is accumulatingdata on short and midterm results with this stent. However, long-term follow-up data from unselected patients treated with the SES in clinical practice is stillsparse.Methods: We analysed data from a substudy of the German prospective multi-centre Cypher Registry.Results: Between April 2002 and September 2005 5711 patients treated with atleast one SES from 16 hospitals were included. A follow-up after a Median of 49months (Q1 40, Q3 60 months) was obtained in 5380 patients (94.2%).Mean age of these patients was 65.7 years, with 75.7% male gender. Indica-tion for SES implantation was stable angina in 47.6%, unstable angina in 17.5%,NSTEMI in 10.3% and STEMI in 9.8% of cases. Clinical events until the end offollow-up are given in the table.
Events until the end of follow-up (%)
All death 9.2% (493/5366)Myocardial infarction 6.9% (344/4992)Stroke 2.5% (122/4962)MACCE (death/myocardial infaction/stroke) 16.6% (890/5368)Any revascularization by PCI 31.3% (1568/5017)Any revascularization by CABG 4.9% (241/4966)MACCE orany revasculaization 41.3% (2212/5361)
Multivariate analyses showed clinical characteristics being the main determinatsfor clinical events, whereas interventional characteristics were the major determi-nats for repeat intervntions.Conclusions: Despite many patients treated for acute coronary syndromes, clin-ical event rates after SES implantation during long-term follow-up (median 4.1years) were quite low (MACCE: 16.6%). However, repeat revascularization rateseither by PCI (31.4%) or by CABG (4.9%) were rather high.
P1372 Similar long term outcomes after primary PCI duringoff-hours and regular hours in 1749 acute MI patients
S. De Boer, R.M. Oemrawsingh, M.J. Lenzen, C. Simsek,E. Boersma, P.W.J.C. Serruys, R.T. Van Domburg. Erasmus MedicalCenter, Thoraxcenter, Rotterdam, Netherlands
Purpose: Previous studies have shown contradictory results in outcome in acutemyocardial infarction (AMI) patients who underwent primary percutaneous coro-nary intervention (pPCI) during off-hours versus regular-hours. We aimed to eval-uate the relationship between pPCI timing (off-hours versus regular hours) andmortality in patients with AMI by pPCI.Methods: The study population consisted of 1749 consecutive patients treatedwith pPCI from 2000 to 2005. Descriptive statistics and multivariable survival anal-yses were applied to evaluate the relation between off-hours (Monday- Friday,06.00 PM- 08.00 AM and weekends) versus regular hours and the occurrence ofall-cause death on 30 days and 4 yearsResults: During off-hours 933 patients (56%) were treated and 736 patients(44%) during regular hours. With the exception of age (58.5 vs 60 yrs, p=0.01) nodifferences in baseline characteristics were observed between both groups. Theobserved 30-day mortality was similar in patients treated during regular hours ver-sus patient treated during off-hours (8,6% vs 7,8%, adjusted Hazard Ratio 0.99;
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
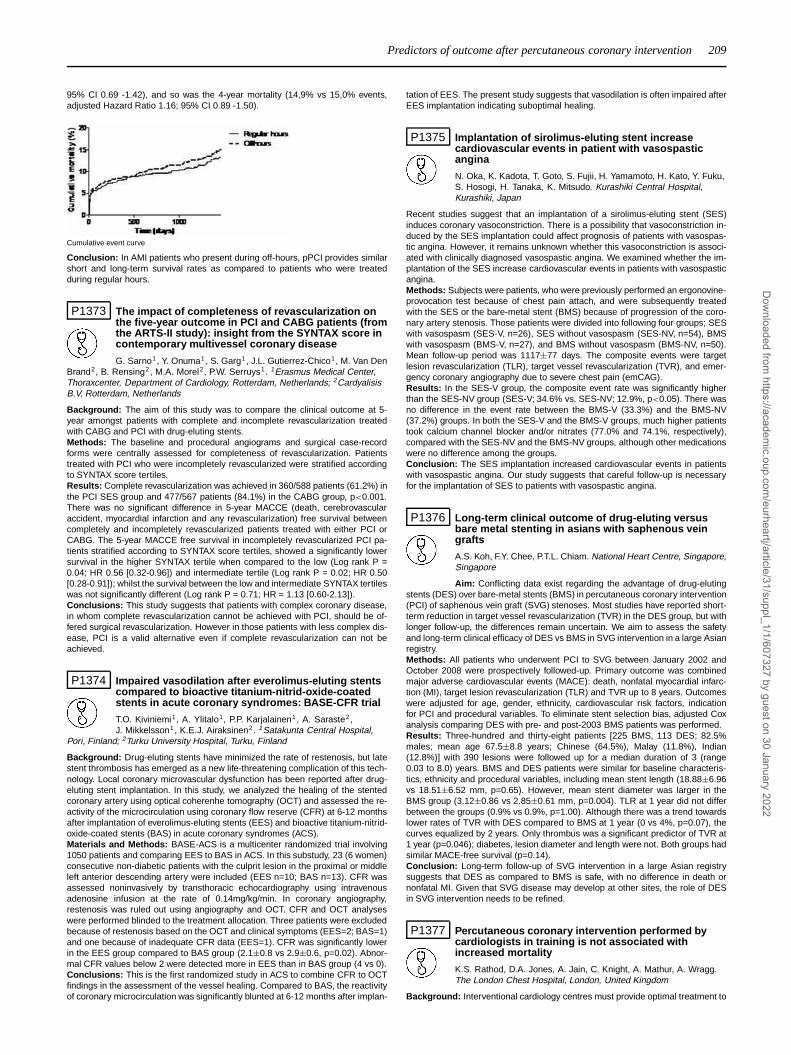
Predictors of outcome after percutaneous coronary intervention 209
95% CI 0.69 -1.42), and so was the 4-year mortality (14,9% vs 15,0% events,adjusted Hazard Ratio 1.16; 95% CI 0.89 -1.50).
Cumulative event curve
Conclusion: In AMI patients who present during off-hours, pPCI provides similarshort and long-term survival rates as compared to patients who were treatedduring regular hours.
P1373 The impact of completeness of revascularization onthe five-year outcome in PCI and CABG patients (fromthe ARTS-II study): insight from the SYNTAX score incontemporary multivessel coronary disease
G. Sarno1, Y. Onuma1, S. Garg1, J.L. Gutierrez-Chico1, M. Van DenBrand2, B. Rensing2, M.A. Morel2, P.W. Serruys1. 1Erasmus Medical Center,Thoraxcenter, Department of Cardiology, Rotterdam, Netherlands; 2CardyalisisB.V, Rotterdam, Netherlands
Background: The aim of this study was to compare the clinical outcome at 5-year amongst patients with complete and incomplete revascularization treatedwith CABG and PCI with drug-eluting stents.Methods: The baseline and procedural angiograms and surgical case-recordforms were centrally assessed for completeness of revascularization. Patientstreated with PCI who were incompletely revascularized were stratified accordingto SYNTAX score tertiles.Results: Complete revascularization was achieved in 360/588 patients (61.2%) inthe PCI SES group and 477/567 patients (84.1%) in the CABG group, p<0.001.There was no significant difference in 5-year MACCE (death, cerebrovascularaccident, myocardial infarction and any revascularization) free survival betweencompletely and incompletely revascularized patients treated with either PCI orCABG. The 5-year MACCE free survival in incompletely revascularized PCI pa-tients stratified according to SYNTAX score tertiles, showed a significantly lowersurvival in the higher SYNTAX tertile when compared to the low (Log rank P =0.04; HR 0.56 [0.32-0.96]) and intermediate tertile (Log rank P = 0.02; HR 0.50[0.28-0.91]); whilst the survival between the low and intermediate SYNTAX tertileswas not significantly different (Log rank P = 0.71; HR = 1.13 [0.60-2.13]).Conclusions: This study suggests that patients with complex coronary disease,in whom complete revascularization cannot be achieved with PCI, should be of-fered surgical revascularization. However in those patients with less complex dis-ease, PCI is a valid alternative even if complete revascularization can not beachieved.
P1374 Impaired vasodilation after everolimus-eluting stentscompared to bioactive titanium-nitrid-oxide-coatedstents in acute coronary syndromes: BASE-CFR trial
T.O. Kiviniemi1, A. Ylitalo1, P.P. Karjalainen1, A. Saraste2 ,J. Mikkelsson1, K.E.J. Airaksinen2. 1Satakunta Central Hospital,
Pori, Finland; 2Turku University Hospital, Turku, Finland
Background: Drug-eluting stents have minimized the rate of restenosis, but latestent thrombosis has emerged as a new life-threatening complication of this tech-nology. Local coronary microvascular dysfunction has been reported after drug-eluting stent implantation. In this study, we analyzed the healing of the stentedcoronary artery using optical coherenhe tomography (OCT) and assessed the re-activity of the microcirculation using coronary flow reserve (CFR) at 6-12 monthsafter implantation of everolimus-eluting stents (EES) and bioactive titanium-nitrid-oxide-coated stents (BAS) in acute coronary syndromes (ACS).Materials and Methods: BASE-ACS is a multicenter randomized trial involving1050 patients and comparing EES to BAS in ACS. In this substudy, 23 (6 women)consecutive non-diabetic patients with the culprit lesion in the proximal or middleleft anterior descending artery were included (EES n=10; BAS n=13). CFR wasassessed noninvasively by transthoracic echocardiography using intravenousadenosine infusion at the rate of 0.14mg/kg/min. In coronary angiography,restenosis was ruled out using angiography and OCT. CFR and OCT analyseswere performed blinded to the treatment allocation. Three patients were excludedbecause of restenosis based on the OCT and clinical symptoms (EES=2; BAS=1)and one because of inadequate CFR data (EES=1). CFR was significantly lowerin the EES group compared to BAS group (2.1±0.8 vs 2.9±0.6, p=0.02). Abnor-mal CFR values below 2 were detected more in EES than in BAS group (4 vs 0).Conclusions: This is the first randomized study in ACS to combine CFR to OCTfindings in the assessment of the vessel healing. Compared to BAS, the reactivityof coronary microcirculation was significantly blunted at 6-12 months after implan-
tation of EES. The present study suggests that vasodilation is often impaired afterEES implantation indicating suboptimal healing.
P1375 Implantation of sirolimus-eluting stent increasecardiovascular events in patient with vasospasticangina
N. Oka, K. Kadota, T. Goto, S. Fujii, H. Yamamoto, H. Kato, Y. Fuku,S. Hosogi, H. Tanaka, K. Mitsudo. Kurashiki Central Hospital,Kurashiki, Japan
Recent studies suggest that an implantation of a sirolimus-eluting stent (SES)induces coronary vasoconstriction. There is a possibility that vasoconstriction in-duced by the SES implantation could affect prognosis of patients with vasospas-tic angina. However, it remains unknown whether this vasoconstriction is associ-ated with clinically diagnosed vasospastic angina. We examined whether the im-plantation of the SES increase cardiovascular events in patients with vasospasticangina.Methods: Subjects were patients, who were previously performed an ergonovine-provocation test because of chest pain attach, and were subsequently treatedwith the SES or the bare-metal stent (BMS) because of progression of the coro-nary artery stenosis. Those patients were divided into following four groups; SESwith vasospasm (SES-V, n=26), SES without vasospasm (SES-NV, n=54), BMSwith vasospasm (BMS-V, n=27), and BMS without vasospasm (BMS-NV, n=50).Mean follow-up period was 1117±77 days. The composite events were targetlesion revascularization (TLR), target vessel revascularization (TVR), and emer-gency coronary angiography due to severe chest pain (emCAG).Results: In the SES-V group, the composite event rate was significantly higherthan the SES-NV group (SES-V; 34.6% vs. SES-NV; 12.9%, p<0.05). There wasno difference in the event rate between the BMS-V (33.3%) and the BMS-NV(37.2%) groups. In both the SES-V and the BMS-V groups, much higher patientstook calcium channel blocker and/or nitrates (77.0% and 74.1%, respectively),compared with the SES-NV and the BMS-NV groups, although other medicationswere no difference among the groups.Conclusion: The SES implantation increased cardiovascular events in patientswith vasospastic angina. Our study suggests that careful follow-up is necessaryfor the implantation of SES to patients with vasospastic angina.
P1376 Long-term clinical outcome of drug-eluting versusbare metal stenting in asians with saphenous veingrafts
A.S. Koh, F.Y. Chee, P.T.L. Chiam. National Heart Centre, Singapore,Singapore
Aim: Conflicting data exist regarding the advantage of drug-elutingstents (DES) over bare-metal stents (BMS) in percutaneous coronary intervention(PCI) of saphenous vein graft (SVG) stenoses. Most studies have reported short-term reduction in target vessel revascularization (TVR) in the DES group, but withlonger follow-up, the differences remain uncertain. We aim to assess the safetyand long-term clinical efficacy of DES vs BMS in SVG intervention in a large Asianregistry.Methods: All patients who underwent PCI to SVG between January 2002 andOctober 2008 were prospectively followed-up. Primary outcome was combinedmajor adverse cardiovascular events (MACE): death, nonfatal myocardial infarc-tion (MI), target lesion revascularization (TLR) and TVR up to 8 years. Outcomeswere adjusted for age, gender, ethnicity, cardiovascular risk factors, indicationfor PCI and procedural variables. To eliminate stent selection bias, adjusted Coxanalysis comparing DES with pre- and post-2003 BMS patients was performed.Results: Three-hundred and thirty-eight patients [225 BMS, 113 DES; 82.5%males; mean age 67.5±8.8 years; Chinese (64.5%), Malay (11.8%), Indian(12.8%)] with 390 lesions were followed up for a median duration of 3 (range0.03 to 8.0) years. BMS and DES patients were similar for baseline characteris-tics, ethnicity and procedural variables, including mean stent length (18.88±6.96vs 18.51±6.52 mm, p=0.65). However, mean stent diameter was larger in theBMS group (3.12±0.86 vs 2.85±0.61 mm, p=0.004). TLR at 1 year did not differbetween the groups (0.9% vs 0.9%, p=1.00). Although there was a trend towardslower rates of TVR with DES compared to BMS at 1 year (0 vs 4%, p=0.07), thecurves equalized by 2 years. Only thrombus was a significant predictor of TVR at1 year (p=0.046); diabetes, lesion diameter and length were not. Both groups hadsimilar MACE-free survival (p=0.14).Conclusion: Long-term follow-up of SVG intervention in a large Asian registrysuggests that DES as compared to BMS is safe, with no difference in death ornonfatal MI. Given that SVG disease may develop at other sites, the role of DESin SVG intervention needs to be refined.
P1377 Percutaneous coronary intervention performed bycardiologists in training is not associated withincreased mortality
K.S. Rathod, D.A. Jones, A. Jain, C. Knight, A. Mathur, A. Wragg.The London Chest Hospital, London, United Kingdom
Background: Interventional cardiology centres must provide optimal treatment to
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
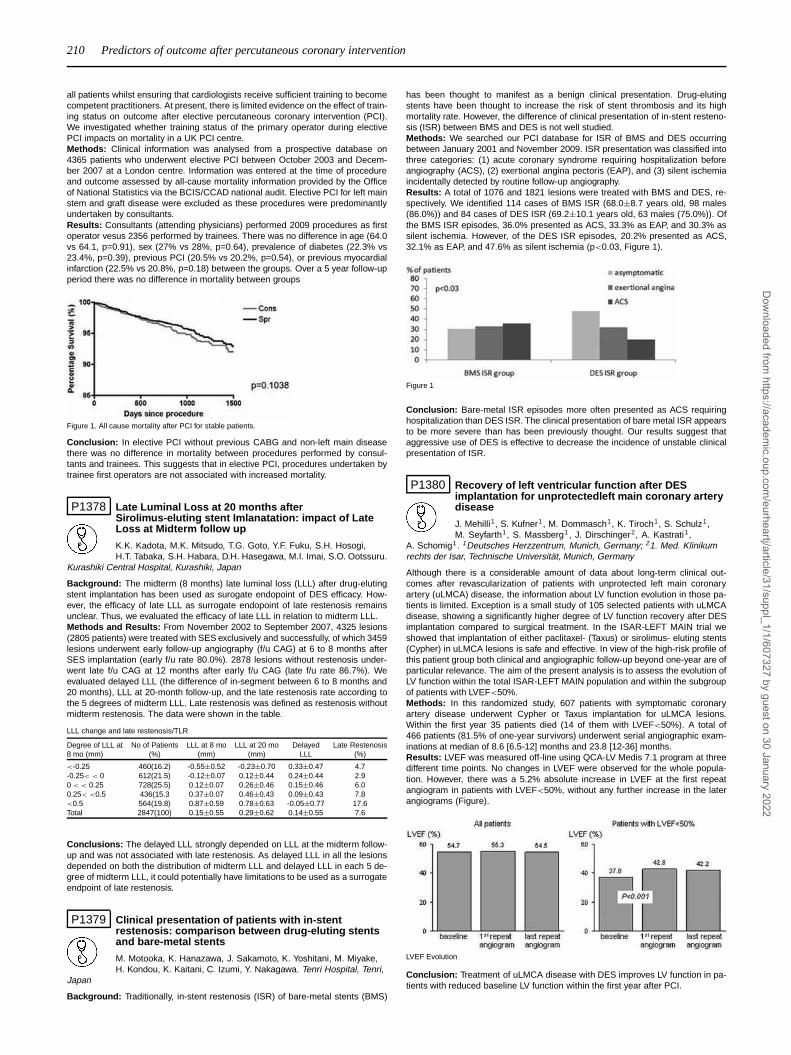
210 Predictors of outcome after percutaneous coronary intervention
all patients whilst ensuring that cardiologists receive sufficient training to becomecompetent practitioners. At present, there is limited evidence on the effect of train-ing status on outcome after elective percutaneous coronary intervention (PCI).We investigated whether training status of the primary operator during electivePCI impacts on mortality in a UK PCI centre.Methods: Clinical information was analysed from a prospective database on4365 patients who underwent elective PCI between October 2003 and Decem-ber 2007 at a London centre. Information was entered at the time of procedureand outcome assessed by all-cause mortality information provided by the Officeof National Statistics via the BCIS/CCAD national audit. Elective PCI for left mainstem and graft disease were excluded as these procedures were predominantlyundertaken by consultants.Results: Consultants (attending physicians) performed 2009 procedures as firstoperator vesus 2356 performed by trainees. There was no difference in age (64.0vs 64.1, p=0.91), sex (27% vs 28%, p=0.64), prevalence of diabetes (22.3% vs23.4%, p=0.39), previous PCI (20.5% vs 20.2%, p=0.54), or previous myocardialinfarction (22.5% vs 20.8%, p=0.18) between the groups. Over a 5 year follow-upperiod there was no difference in mortality between groups
Figure 1. All cause mortality after PCI for stable patients.
Conclusion: In elective PCI without previous CABG and non-left main diseasethere was no difference in mortality between procedures performed by consul-tants and trainees. This suggests that in elective PCI, procedures undertaken bytrainee first operators are not associated with increased mortality.
P1378 Late Luminal Loss at 20 months afterSirolimus-eluting stent Imlanatation: impact of LateLoss at Midterm follow up
K.K. Kadota, M.K. Mitsudo, T.G. Goto, Y.F. Fuku, S.H. Hosogi,H.T. Tabaka, S.H. Habara, D.H. Hasegawa, M.I. Imai, S.O. Ootssuru.
Kurashiki Central Hospital, Kurashiki, Japan
Background: The midterm (8 months) late luminal loss (LLL) after drug-elutingstent implantation has been used as surogate endopoint of DES efficacy. How-ever, the efficacy of late LLL as surrogate endopoint of late restenosis remainsunclear. Thus, we evaluated the efficacy of late LLL in relation to midterm LLL.Methods and Results: From November 2002 to September 2007, 4325 lesions(2805 patients) were treated with SES exclusively and successfully, of which 3459lesions underwent early follow-up angiography (f/u CAG) at 6 to 8 months afterSES implantation (early f/u rate 80.0%). 2878 lesions without restenosis under-went late f/u CAG at 12 months after early f/u CAG (late f/u rate 86.7%). Weevaluated delayed LLL (the difference of in-segment between 6 to 8 months and20 months), LLL at 20-month follow-up, and the late restenosis rate according tothe 5 degrees of midterm LLL. Late restenosis was defined as restenosis withoutmidterm restenosis. The data were shown in the table.
LLL change and late restenosis/TLR
Degree of LLL at No of Patients LLL at 8 mo LLL at 20 mo Delayed Late Restenosis8 mo (mm) (%) (mm) (mm) LLL (%)
<-0.25 460(16.2) -0.55±0.52 -0.23±0.70 0.33±0.47 4.7-0.25< < 0 612(21.5) -0.12±0.07 0.12±0.44 0.24±0.44 2.90 < < 0.25 728(25.5) 0.12±0.07 0.26±0.46 0.15±0.46 6.00.25< <0.5 436(15.3 0.37±0.07 0.46±0.43 0.09±0.43 7.8<0.5 564(19.8) 0.87±0.59 0.78±0.63 -0.05±0.77 17.6Total 2847(100) 0.15±0.55 0.29±0.62 0.14±0.55 7.6
Conclusions: The delayed LLL strongly depended on LLL at the midterm follow-up and was not associated with late restenosis. As delayed LLL in all the lesionsdepended on both the distribution of midterm LLL and delayed LLL in each 5 de-gree of midterm LLL, it could potentially have limitations to be used as a surrogateendpoint of late restenosis.
P1379 Clinical presentation of patients with in-stentrestenosis: comparison between drug-eluting stentsand bare-metal stents
M. Motooka, K. Hanazawa, J. Sakamoto, K. Yoshitani, M. Miyake,H. Kondou, K. Kaitani, C. Izumi, Y. Nakagawa. Tenri Hospital, Tenri,
Japan
Background: Traditionally, in-stent restenosis (ISR) of bare-metal stents (BMS)
has been thought to manifest as a benign clinical presentation. Drug-elutingstents have been thought to increase the risk of stent thrombosis and its highmortality rate. However, the difference of clinical presentation of in-stent resteno-sis (ISR) between BMS and DES is not well studied.Methods: We searched our PCI database for ISR of BMS and DES occurringbetween January 2001 and November 2009. ISR presentation was classified intothree categories: (1) acute coronary syndrome requiring hospitalization beforeangiography (ACS), (2) exertional angina pectoris (EAP), and (3) silent ischemiaincidentally detected by routine follow-up angiography.Results: A total of 1076 and 1821 lesions were treated with BMS and DES, re-spectively. We identified 114 cases of BMS ISR (68.0±8.7 years old, 98 males(86.0%)) and 84 cases of DES ISR (69.2±10.1 years old, 63 males (75.0%)). Ofthe BMS ISR episodes, 36.0% presented as ACS, 33.3% as EAP, and 30.3% assilent ischemia. However, of the DES ISR episodes, 20.2% presented as ACS,32.1% as EAP, and 47.6% as silent ischemia (p<0.03, Figure 1).
Figure 1
Conclusion: Bare-metal ISR episodes more often presented as ACS requiringhospitalization than DES ISR. The clinical presentation of bare metal ISR appearsto be more severe than has been previously thought. Our results suggest thataggressive use of DES is effective to decrease the incidence of unstable clinicalpresentation of ISR.
P1380 Recovery of left ventricular function after DESimplantation for unprotectedleft main coronary arterydisease
J. Mehilli1, S. Kufner1, M. Dommasch1, K. Tiroch1, S. Schulz1,M. Seyfarth1, S. Massberg1, J. Dirschinger2, A. Kastrati1,
A. Schomig1. 1Deutsches Herzzentrum, Munich, Germany; 21. Med. Klinikumrechts der Isar, Technische Universität, Munich, Germany
Although there is a considerable amount of data about long-term clinical out-comes after revascularization of patients with unprotected left main coronaryartery (uLMCA) disease, the information about LV function evolution in those pa-tients is limited. Exception is a small study of 105 selected patients with uLMCAdisease, showing a significantly higher degree of LV function recovery after DESimplantation compared to surgical treatment. In the ISAR-LEFT MAIN trial weshowed that implantation of either paclitaxel- (Taxus) or sirolimus- eluting stents(Cypher) in uLMCA lesions is safe and effective. In view of the high-risk profile ofthis patient group both clinical and angiographic follow-up beyond one-year are ofparticular relevance. The aim of the present analysis is to assess the evolution ofLV function within the total ISAR-LEFT MAIN population and within the subgroupof patients with LVEF<50%.Methods: In this randomized study, 607 patients with symptomatic coronaryartery disease underwent Cypher or Taxus implantation for uLMCA lesions.Within the first year 35 patients died (14 of them with LVEF<50%). A total of466 patients (81.5% of one-year survivors) underwent serial angiographic exam-inations at median of 8.6 [6.5-12] months and 23.8 [12-36] months.Results: LVEF was measured off-line using QCA-LV Medis 7.1 program at threedifferent time points. No changes in LVEF were observed for the whole popula-tion. However, there was a 5.2% absolute increase in LVEF at the first repeatangiogram in patients with LVEF<50%, without any further increase in the laterangiograms (Figure).
LVEF Evolution
Conclusion: Treatment of uLMCA disease with DES improves LV function in pa-tients with reduced baseline LV function within the first year after PCI.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
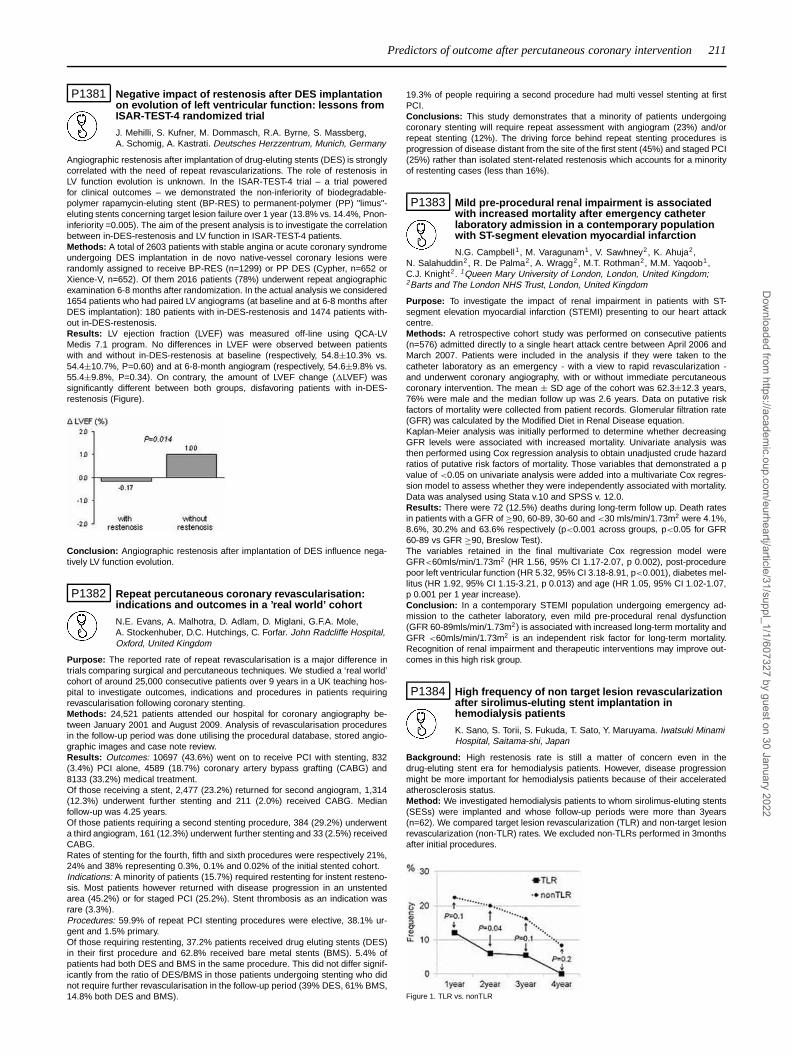
Predictors of outcome after percutaneous coronary intervention 211
P1381 Negative impact of restenosis after DES implantationon evolution of left ventricular function: lessons fromISAR-TEST-4 randomized trial
J. Mehilli, S. Kufner, M. Dommasch, R.A. Byrne, S. Massberg,A. Schomig, A. Kastrati. Deutsches Herzzentrum, Munich, Germany
Angiographic restenosis after implantation of drug-eluting stents (DES) is stronglycorrelated with the need of repeat revascularizations. The role of restenosis inLV function evolution is unknown. In the ISAR-TEST-4 trial – a trial poweredfor clinical outcomes – we demonstrated the non-inferiority of biodegradable-polymer rapamycin-eluting stent (BP-RES) to permanent-polymer (PP) "limus"-eluting stents concerning target lesion failure over 1 year (13.8% vs. 14.4%, Pnon-inferiority =0.005). The aim of the present analysis is to investigate the correlationbetween in-DES-restenosis and LV function in ISAR-TEST-4 patients.Methods: A total of 2603 patients with stable angina or acute coronary syndromeundergoing DES implantation in de novo native-vessel coronary lesions wererandomly assigned to receive BP-RES (n=1299) or PP DES (Cypher, n=652 orXience-V, n=652). Of them 2016 patients (78%) underwent repeat angiographicexamination 6-8 months after randomization. In the actual analysis we considered1654 patients who had paired LV angiograms (at baseline and at 6-8 months afterDES implantation): 180 patients with in-DES-restenosis and 1474 patients with-out in-DES-restenosis.Results: LV ejection fraction (LVEF) was measured off-line using QCA-LVMedis 7.1 program. No differences in LVEF were observed between patientswith and without in-DES-restenosis at baseline (respectively, 54.8±10.3% vs.54.4±10.7%, P=0.60) and at 6-8-month angiogram (respectively, 54.6±9.8% vs.55.4±9.8%, P=0.34). On contrary, the amount of LVEF change (�LVEF) wassignificantly different between both groups, disfavoring patients with in-DES-restenosis (Figure).
Conclusion: Angiographic restenosis after implantation of DES influence nega-tively LV function evolution.
P1382 Repeat percutaneous coronary revascularisation:indications and outcomes in a ’real world’ cohort
N.E. Evans, A. Malhotra, D. Adlam, D. Miglani, G.F.A. Mole,A. Stockenhuber, D.C. Hutchings, C. Forfar. John Radcliffe Hospital,Oxford, United Kingdom
Purpose: The reported rate of repeat revascularisation is a major difference intrials comparing surgical and percutaneous techniques. We studied a ‘real world’cohort of around 25,000 consecutive patients over 9 years in a UK teaching hos-pital to investigate outcomes, indications and procedures in patients requiringrevascularisation following coronary stenting.Methods: 24,521 patients attended our hospital for coronary angiography be-tween January 2001 and August 2009. Analysis of revascularisation proceduresin the follow-up period was done utilising the procedural database, stored angio-graphic images and case note review.Results: Outcomes: 10697 (43.6%) went on to receive PCI with stenting, 832(3.4%) PCI alone, 4589 (18.7%) coronary artery bypass grafting (CABG) and8133 (33.2%) medical treatment.Of those receiving a stent, 2,477 (23.2%) returned for second angiogram, 1,314(12.3%) underwent further stenting and 211 (2.0%) received CABG. Medianfollow-up was 4.25 years.Of those patients requiring a second stenting procedure, 384 (29.2%) underwenta third angiogram, 161 (12.3%) underwent further stenting and 33 (2.5%) receivedCABG.Rates of stenting for the fourth, fifth and sixth procedures were respectively 21%,24% and 38% representing 0.3%, 0.1% and 0.02% of the initial stented cohort.Indications: A minority of patients (15.7%) required restenting for instent resteno-sis. Most patients however returned with disease progression in an unstentedarea (45.2%) or for staged PCI (25.2%). Stent thrombosis as an indication wasrare (3.3%).Procedures: 59.9% of repeat PCI stenting procedures were elective, 38.1% ur-gent and 1.5% primary.Of those requiring restenting, 37.2% patients received drug eluting stents (DES)in their first procedure and 62.8% received bare metal stents (BMS). 5.4% ofpatients had both DES and BMS in the same procedure. This did not differ signif-icantly from the ratio of DES/BMS in those patients undergoing stenting who didnot require further revascularisation in the follow-up period (39% DES, 61% BMS,14.8% both DES and BMS).
19.3% of people requiring a second procedure had multi vessel stenting at firstPCI.Conclusions: This study demonstrates that a minority of patients undergoingcoronary stenting will require repeat assessment with angiogram (23%) and/orrepeat stenting (12%). The driving force behind repeat stenting procedures isprogression of disease distant from the site of the first stent (45%) and staged PCI(25%) rather than isolated stent-related restenosis which accounts for a minorityof restenting cases (less than 16%).
P1383 Mild pre-procedural renal impairment is associatedwith increased mortality after emergency catheterlaboratory admission in a contemporary populationwith ST-segment elevation myocardial infarction
N.G. Campbell1, M. Varagunam1 , V. Sawhney2, K. Ahuja2,N. Salahuddin2, R. De Palma2, A. Wragg2, M.T. Rothman2, M.M. Yaqoob1,C.J. Knight2. 1Queen Mary University of London, London, United Kingdom;2Barts and The London NHS Trust, London, United Kingdom
Purpose: To investigate the impact of renal impairment in patients with ST-segment elevation myocardial infarction (STEMI) presenting to our heart attackcentre.Methods: A retrospective cohort study was performed on consecutive patients(n=576) admitted directly to a single heart attack centre between April 2006 andMarch 2007. Patients were included in the analysis if they were taken to thecatheter laboratory as an emergency - with a view to rapid revascularization -and underwent coronary angiography, with or without immediate percutaneouscoronary intervention. The mean ± SD age of the cohort was 62.3±12.3 years,76% were male and the median follow up was 2.6 years. Data on putative riskfactors of mortality were collected from patient records. Glomerular filtration rate(GFR) was calculated by the Modified Diet in Renal Disease equation.Kaplan-Meier analysis was initially performed to determine whether decreasingGFR levels were associated with increased mortality. Univariate analysis wasthen performed using Cox regression analysis to obtain unadjusted crude hazardratios of putative risk factors of mortality. Those variables that demonstrated a pvalue of <0.05 on univariate analysis were added into a multivariate Cox regres-sion model to assess whether they were independently associated with mortality.Data was analysed using Stata v.10 and SPSS v. 12.0.Results: There were 72 (12.5%) deaths during long-term follow up. Death ratesin patients with a GFR of ≥90, 60-89, 30-60 and <30 mls/min/1.73m2 were 4.1%,8.6%, 30.2% and 63.6% respectively (p<0.001 across groups, p<0.05 for GFR60-89 vs GFR ≥90, Breslow Test).The variables retained in the final multivariate Cox regression model wereGFR<60mls/min/1.73m2 (HR 1.56, 95% CI 1.17-2.07, p 0.002), post-procedurepoor left ventricular function (HR 5.32, 95% CI 3.18-8.91, p<0.001), diabetes mel-litus (HR 1.92, 95% CI 1.15-3.21, p 0.013) and age (HR 1.05, 95% CI 1.02-1.07,p 0.001 per 1 year increase).Conclusion: In a contemporary STEMI population undergoing emergency ad-mission to the catheter laboratory, even mild pre-procedural renal dysfunction(GFR 60-89mls/min/1.73m2) is associated with increased long-term mortality andGFR <60mls/min/1.73m2 is an independent risk factor for long-term mortality.Recognition of renal impairment and therapeutic interventions may improve out-comes in this high risk group.
P1384 High frequency of non target lesion revascularizationafter sirolimus-eluting stent implantation inhemodialysis patients
K. Sano, S. Torii, S. Fukuda, T. Sato, Y. Maruyama. Iwatsuki MinamiHospital, Saitama-shi, Japan
Background: High restenosis rate is still a matter of concern even in thedrug-eluting stent era for hemodialysis patients. However, disease progressionmight be more important for hemodialysis patients because of their acceleratedatherosclerosis status.Method: We investigated hemodialysis patients to whom sirolimus-eluting stents(SESs) were implanted and whose follow-up periods were more than 3years(n=62). We compared target lesion revascularization (TLR) and non-target lesionrevascularization (non-TLR) rates. We excluded non-TLRs performed in 3monthsafter initial procedures.
Figure 1. TLR vs. nonTLR
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

212 Predictors of outcome after percutaneous coronary intervention
Result: Non-TLR was performed more frequently than TLR (35.5% vs. 19.4%,P=0.04). This was especially true in the second year after their initial procedures(figure).Conclusion: Although TLR rate is relatively high even after SES implantation, weshould consider high frequency of non-TLR for dialysis patients as well.
P1385 Longitudinal and sequential follow-up results afterpercutaneous catheter intervention in patients withKawasaki disease
S. Ogawa, R. Fukazawa, M. Kamisago, T. Ohkubo, M. Abe,M. Watanabe, M. Hajikano, N. Suzuki, M. Watanabe, Y. Katsube.
Nippon Medical School, Tokyo, Japan
Objectives: We estimated longitudinal and sequential results after prcuta-neous catheter intervention (PCI) in patients with coronary stenotic sequel afterKawasaki disease using morphological and physiological modalities.¶Subjects: Twenty-four patients (6–28y) with 24 coronary branches who hadtaken PCI before at least 5 years. Percutaneous old balloon angioplasty (POBA)was performed in 20 patients and percutaneous transluminal coronary rotationalablation (PTCRA) was performed in 4 patients. All patients had myocardial is-chemia revealed with stress myocardial scintigraphy before PCI.Methods: We have made sequential follow-up study in these patients more than5 years using the methods of quantitative coronary angiography, intravascularultrasound (IVUS), coronary flow reserve (CFR) by flow wire, myocardial fractionalflow reserve (FFRmyo) by pressure wire, and stress myocardial scintigraphy.Results: Nineteen of 20 patients (95%) performed with POBA showed no signif-icant stenosis after POBA. In these patients myocardial ischemia was improvedand abnormal values of CFR and FFRmyo turned to normal (CFR: 1.2±0.2 to2.1±0.1, FFRmyo 0.64±0.13 to 0.89±0.12). All patients performed POBA withlow inflated pressure (less than 8-10atm) and had no neo-genesis of coronaryaneurysm just inflated portion. Only one patient taking POBA had re-stenosis ofcoronary artery lesion with myocardial ischemia and took PTCRA. Four patientswho had severe calcification just stenotic lesion took PTCRA with drug elutingstent implantation and all of them had lasted good results at least 5 years afterPTCRA. None of them had re-stenosis and myocardial ischemia, and the val-ues of CFR and FFRmyo turned to normal (CFR: 1.3±0.3 to 2.3±0.2, FFRmyo0.61±0.16 to 0.92±0.17). All patients were performed IVUS imaging and showedno thrombosis and re-stenosis.Conclusions: Percutaneous coronary intervention for significant stenotic lesionsafter Kawasaki disease could be effective by appropriated methods at least 5years after PCI.
P1386 Pioglitazone improves endothelial dysfunction aftersirolimus-eluting stent implantation
H. Kitahara, Y. Kobayashi, N. Kuroda, I. Komuro. Chiba UniversityGraduate School of Medicine, Chiba, Japan
Purpose: Previous studies have showed endothelial dysfunction af-ter sirolimus-eluting stent (SES) implantation that may be associated with ad-verse cardiac events during follow-up. Pioglitazone has been reported to improveendothelial function. The present study evaluated the effect of pioglitazone onendothelial function after SES implantation in non-diabetic patients.Methods: The present randomized study included 50 patients undergoing SESimplantation. They were assigned to the pioglitazone (30 mg daily) group (n=25)and the control group (n=25). Endothelial function was estimated at 9-monthfollow-up angiography. Endothelium-dependent vasomotion of coronary segmentfrom the stent edge to 15 mm proximal and distal was assessed with quantitativecoronary angiography, using intracoronary acetylcholine infusion at 10-8 mol/Land 10-7 mol/L. Endothelium-independent vasomotion was assessed after nitrateinfusion (NTG).Results: There was no significant difference in patient, angiographic and pro-cedural characteristics between the 2 groups. There was no restenosis in thepioglitazone group and one in-stent restenosis in the control group. There was nosignificant difference in endothelial function at the proximal edge between the 2groups. However, endothelium-dependent vasoconstriction at the distal edge wasless in the pioglitazone group (Figure).
Figure 1
Conclusions: Pioglitazone improves endothelial dysfunction at the distal edge ofSES in non-diabetic patients.
P1387 Long term results from the first in man application ofbevacizumab eluting stent. Four years follow up
K. Toutouzas1 , A. Synetos1, J. Karampelas1, E. Stefanadi1,E. Tsiamis1, N. Kipshidze2, C. Stefanadis2. 1University of AthensMedical School, 1st Department of Cardiology, Athens, Greece;
2Cardiovascular Research Foundation, New York, United States of America
Purpose: Neovascularization seems to play an important role in the developmentof the vulnerable plaque. Bevacizumab is a monoclonal antibody specific for vas-cular endothelial growth factor, which appears to be the most important mediatorof neovascularisation. In this study we present the long-term results of the safetyand efficacy study of the first-in-man application of bevacizumab–eluting stent.Methods: Patients with acute coronary syndromes and ≥2 angiographically sig-nificant coronary artery stenoses were included in the study. The culprit lesionswere successfully treated. The non-culprit lesions to be included were ≤20 mmin length, producing a significant stenosis (≥50%, in vessels with reference di-ameter ≥2.25mm). Local delivery of bevacizumab was accomplished via Bio-divYsio stents, which bear a phosphorylcholine coating that adsorbs the drugwith a "sponge-like" mechanism. Patients were discharged under aspirin (indefi-nitely) and clopidogrel for 24 months. All patients were scheduled for angiographicfollow-up at 24 months and clinical follow-up at 48 months. Intravascular ultra-sound of the target vessel was performed immediately after the procedure and at24 months.Results: Twenty consecutive patents were included. All stents were successfullydelivered (mean stent length 13.55±4.1 mm) and all patients were dischargedwithout any complication. Acute, subacute or late thrombosis was not observed.Angiographic and intravascular ultrasound follow-up did not reveal any restenosis(50% vessel narrowing) in any target vessel at the angiographic follow-up. Stentmalapposition was not observed in any patient. In-stent late loss was 0.15±0.9mm, and in-lesion late loss was 0.16±0.03 mm. Mean neointimal hyperplasia instented segments as measured with intravascular ultrasound was 0.82±0.29 mm.During a follow-up period of 46.12±3.21 months there were no adverse cardiacevents such as death, myocardial infarction and target vessel revascularization.There was no adverse event between the 2nd and 4th year of clinical follow-upperiod.Conclusions: Bevacizumab-eluting stents seem to be safe for the treatment ofnon-culprit de novo lesions in patients suffering from acute coronary syndromes.The results of the present study provide new insights in the stabilization strategiesof high-risk plaques. These findings warrant further confirmation in larger numberof patients.
P1388 Health economics baseline evaluation of the Germandrug-eluting stent registry (DES.DE)
S.N. Willich1, F. Mueller-Riemenschneider1 , T. Fetsch2, K.H. Kuck3,D. Mcbride1, C.A. Nienaber4 , S. Schneider5, J. Senges5,B. Brueggenjuergen1 . 1Charite University Medical Center, Berlin,
Germany; 2Institute for Clinical Cardiovascular Research, Munich, Germany;3Asklepios Clinic St. Georg, Hamburg, Germany; 4University Hospital Rostock,Rostock, Germany; 5Clinical Center of Ludwigshafen, Department of Cardiology,Ludwigshafen am Rhein, Germany
Background: The efficacy of drug-eluting stents (DES) in patients with coronaryheart disease has been the focus of numerous randomised-controlled trials. Incontrast, data on DES effectiveness in real world settings and cost-effectivenessare limited.Objective: As part of the German DES registry, the health economics evaluationinvestigates effectiveness, economic impact and cost-effectiveness of DES com-pared to bare-metal stents (BMS) and of paclitaxel-eluting stents (PES) comparedto sirolimus-eluting stents (SES). Here, first results regarding study population,baseline findings and in-hospital follow-up are presented.Methods: Patients were recruited between December 2005 and October 2006 in98 centres across Germany. Implantation of PES, SES or BMS was performed atthe discretion of the treating physician. Clinical, economic and quality of life (Qol)data were collected at baseline, 3, 6, 9, and 12 months after index stent implan-tation. Group comparisons (DES vs. BMS and PES vs. SES) were based on chi-square (categorical data) and T-test (continuous data). Two-sided p-values <0.05were considered statistically significant. Cost calculation is based on diagnosis-related group reimbursement to hospitals and average DES surcharges in 2006.Results: In total, 3932 patients (75% male, mean age 65±11 years) were en-rolled into the health-economic evaluation and received DES (3473 patients) orBMS (459 patients). There were few statistically significant differences in clini-cal and procedural characteristics at baseline, but without systematically favour-ing one group. Baseline generic and cardiac-specific Qol was similar betweengroups. Major adverse cardiac and cerebrovascular events occurred in 1.6% and2.2% of DES and BMS patients during in-hospital follow-up (p=0.327), and base-line treatment costs were 4989±1284� and 3607±924� in DES and BMS pa-tients (p<0.001), respectively. No differences were observed in treatment costsof patients receiving PES or SES.Conclusions: This ongoing economic evaluation is one of the largest studies in-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Predictors of outcome after percutaneous coronary intervention / Long term outcome after percutaneous coronary syndrome 213
vestigating the economic impact and the cost-effectiveness of DES in a real-worldsetting. In-hospital treatment costs were considerably higher for DES compared toBMS patients. Longer-term follow up will allow for determining cost-effectivenessand budget impact for the health care system.
P1389 Efficacy, safety and cost-effectiveness of drug-elutingstents over a 4 year time horizon
N. Milic1, B. Parapid2, M.C. Ostojic2, M. Nedeljkovic2, B. Beleslin2,L. Finci3, J. Marinkovic1. 1Institute for Medical Statistics and HealthResearch, School of Medicine University of Belgrade, Belgrade,
Serbia; 2Clinical Center of Serbia, Institute for Cardiovascular Diseases,Belgrade, Serbia; 3Cabinet Médical "Finci", Geneva, Switzerland
Purpose: Drug-eluting stents (DES) reduced the incidence of repeat revascu-larization after stent implantation. 4 year follow up studies showed that DES aresafe in terms of very late stent thrombosis. There is only limited information aboutcost-effectiveness of DES relative to bare metal stents (BMS) with more than 1year follow up data, and no information over a time horizon of 4 years.Methods: We performed an economic evaluation comparing DES to BMS, whereclinical outcome data were obtained from a meta - analysis on randomized con-trolled trials (RCTs) with median follow up of 4 years in patients with symptomaticcoronary artery disease. For stent thrombosis a hierarchical classification of Aca-demic Research Consortium was applied. Costs were drawn as reimbursementrates for diagnosis related groups from the Serbian Health Care Third Party payerperspective, and reported in Euro’s of the financial year 2009. Cost effectivenessoutcomes were expressed as incremental cost- effectiveness ratios (ICER’s) - theincremental cost per quality adjusted life year gained and the incremental cost perrevascularization avoided. All costs and effects were discounted at 5% annually.Results: Of 5261 patients involved in nine double blinded RCTs identified, 2633were randomized to receive DES (Sirolimus or Paclitaxel) and 2628 to BMS.DES resulted in a lower risk of target lesion revascularization (OR=0.37; 95% CI0.32-0.44). Peto’s OR for very late stent thrombosis (definite+probable) was 1.71(95%CI 0.83-3.49). The incremental effects are 0,007 QALYs, while the ICER is>1,000,000 Euro per QALY. Repeat revascularization reduction result in a costdifference of 949 Euro per patient with ICER of 7,908 Euro per revascularizationavoided.Conclusion: DES are safe and effective in reducing target lesion revasculariza-tion in long term follow-up. At current Serbian prices, DES are not cost effectivecompared with conventional stents. Although the technology is clearly effective,general substitution in unselected patients with symptomatic coronary artery dis-ease is not justified.
P1390 Sirolimus-eluting stent does not induce vasospasm atstent edges
T. Morino, Y. Kobayashi, N. Kuroda, I. Komuro. Chiba UniversityGraduate School of Medicine, Department of CardiovascularScience and Medicine, Chiba, Japan
Background: Previous case reports have shown vasospasm at edges ofsirolimus-eluting stent (SES). This study evaluated the incidence of vasospasmat edges of SES compared to bare metal stent (BMS).Methods: Coronary artery vasospasm provocation test was performed in 55 pa-tients at follow-up angiography after coronary stent implantation. Before coronaryangiography, calcium channel blockers and other vasodilators were withheld atleast 3 and 2 days, respectively. Acetylcholine was injected in incremental dosesof 20 and 50 μg for the right coronary artery and 20, 50, and 100 μg for the leftcoronary artery. Coronary vasospasm was defined as total or subtotal occlusionof the epicardial coronary arteries associated with signs of myocardial ischemia,such as chest pain and ischemic ST segment changes. Patients were classifiedinto the SES group (n=29) and the BMS group (n=26).Results: No patients had a history of vasospastic angina. Vasospasm occurred in3 patients (10.3%) with SES and 7 patients (26.9%) with BMS (p=0.16) (proximaledge, 3.4% vs. 0%, p>0.99; distal edge, 6.9% vs. 19%, p=0.24; both, 0% vs.7.7%, p=0.22).Conclusion: SES may not induce vasospasm, although vasospasm may be ob-served in Japanese patients undergoing coronary stenting.
P1391 Drug-eluting stents reduce mortality during the firsttwo years but not beyond. Propensity score analysisof the ACROSS prospective registry
R. Teles, L. Raposo, M. Almeida, P. Goncalves, R. Cale, P. Sousa,J. Brito, J. Baptista, J. Palos, A. Silva. Hospital Santa Cruz,
Carnaxide, Portugal
Background: There is controversy regarding drug-eluting stents (DES) effect onmortality in common practice including off-label indications in patients submittedto percutaneous coronary interventions (PCI). We sought to evaluate the mortalityimpact of DES compared to bare metal stents (BMS).Population and Methods: Single center, prospective, longitudinal registry includ-ing all 4627 consecutive pts submitted to PCI (age 64±11 years, male 74%). Atotal of 3689 DES (79.7%) and 938 BMS (20,3%) procedures were followed by
a median of 529 days (IQ: 422-1012) and death occurred in 334 (7,2%). Demo-graphic, clinical, angiographic and procedural data were considered for multivari-able logistic regression in order to build a predictive model for mortality whichincluded 30 variables (Hosmer and Lemeshow test 0,42; AUC 0,82 95% CI 0,80-83).These model was used to select a total of 1316 pts based on 658 matched casesof DES and BMS. Variables were evenly distributed amongst the two groups ex-cept for non-protected left main (DES 3,2% vs BMS 1,5%, p=0,046). Survivalcurve analysis between groups evidenced that the hazard ratio (HR) was notconstant over time. In the first 630 days the HR favored DES 0,55 (95% CI: 0,36-0,83). However, after these period, there was a tendency for worst DES safety1,92 (95% CI: 0,93-3,94).
Figure 1. Survival curve
Conclusion: In patients undergoing percutaneous coronary intervention drug-eluting stents reduce mortality in the first two years. Beyond this period this effectdisappears and further studies are needed.
LONG TERM OUTCOME AFTER PERCUTANEOUSCORONARY SYNDROME
P1392 ACEF score in the LEADERS trial
J.J. Wykrzykowska1, S. Garg1, T. De Vries2, S. Windecker3,P.W. Serruys1. 1Erasmus Medical Center, Rotterdam, Netherlands;2Cardialysis, Rotterdam, Netherlands; 3Bern University Hospital,Bern, Switzerland
Background: The ACEF score (Age/left ventricular ejection fraction + 1 ifcreatinine> 2.0) has been shown to be an effective predictor of clinical outcomesin patients with multivessel disease undergoing CABG surgery.Objective: We aimed at assessing the predictive value of the ACEF score for ma-jor adverse cardiac events in the "all-comers" patient population of the LEADERStrial, undergoing treatment with percutaneous coronary intervention (using drugeluting stents).Methods: The ACEF score was retrospectively collected in 1,608 of the 1,707 pa-tients enrolled in the LEADERS trial. Post-hoc analysis was performed by strat-ifying clinical outcomes at 1 year follow-up, according to the three ACEF scoretertiles.Results: 1,608 patients were divided into tertiles based on the ACEF score in thefollowing fashion: ACEFlow < 1.0225, 1.0225 < ACEFmid < 1.277 and ACEFhigh> 1.277.At one year follow-up there was a significantly lower number of patients withMACE-free survival in the highest tertile of the ACEF score (ACEFlow=92.1%,ACEFmid=89.5% and ACEFhigh=86.1%; p=0.0218). Cardiac death occurred in0.7% of patients with low ACEF score, 2.2% of patients with intermediate ACEFscore and 4.5% of patients with high ACEF score (HR=2.22; p=0.002). Rate ofmyocardial infarction was significantly higher in patients with high ACEF score(6.7% for ACEFhigh versus 5.2% for ACEFmid and 2.5% for ACEFlow; HR 1.6;p=0.006). Clinically driven TVR also tended to be higher in the ACEFhigh groupbut the difference between the three groups did not reach statistical significance(ACEFlow=5.4%, ACEFmid=6.5% and ACEFhigh=8%; HR=1.22; p=0.16). Therate of composite definite, possible and probable stent thrombosis was also higherin the high ACEF group (ACEFlow=1.2%, ACEFmid=3.5% and ACEFhigh=6.2%;HR 2.04; p<0.001). Patients treated with biolimus and sirolimus stents had equiv-alent event rates across all three ACEF tertiles.Conclusion: ACEF score may be a simple way to stratify risk of events in patientstreated with percutaneous coronary intervention.
P1393 EuroSCORE predicts long-term cardiovascular eventsafter percutaneous coronary intervention in patientswith left main or multivessel coronary artery disease
P.J. Sousa, R.C. Teles, M.S. Almeida, P.A. Goncalves, L. Raposo,R. Cale, J. Brito, J.L. Palos, J. Baptista, J.A. Silva. Hospital de Santa
Cruz - CHLO, Lisbon, Portugal
Purpose: EuroSCORE was created for use in patients undergoing cardiacsurgery. Because it is easy and objective, its application in other settings has
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
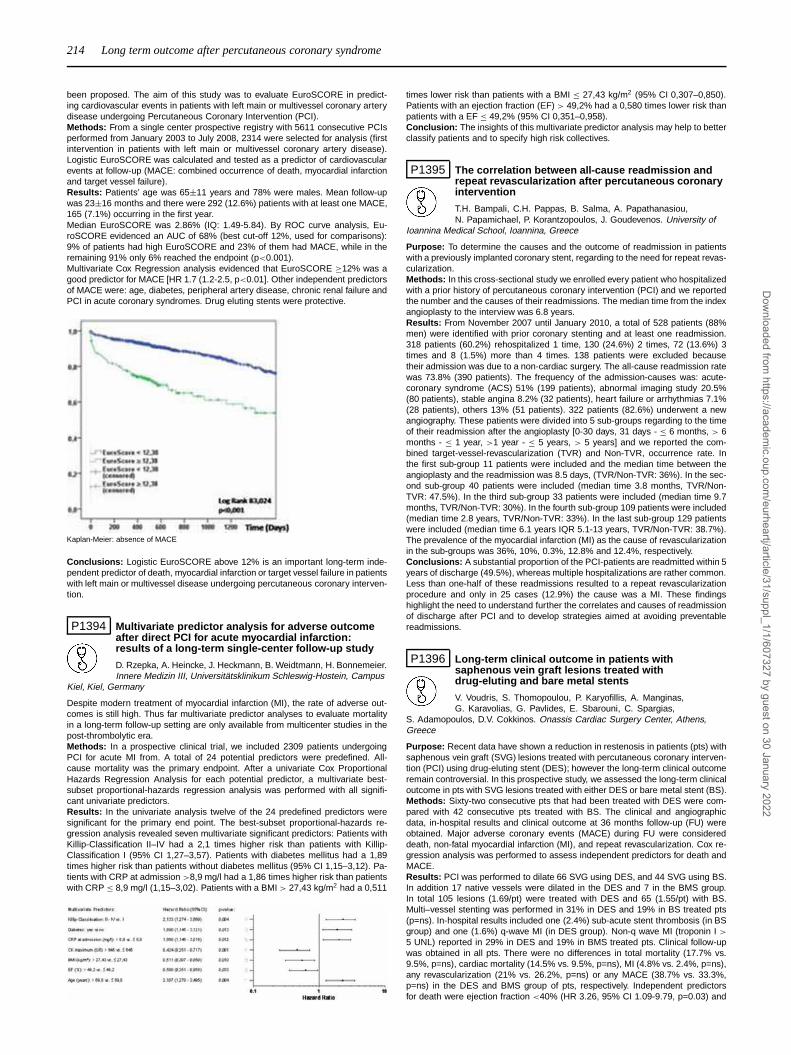
214 Long term outcome after percutaneous coronary syndrome
been proposed. The aim of this study was to evaluate EuroSCORE in predict-ing cardiovascular events in patients with left main or multivessel coronary arterydisease undergoing Percutaneous Coronary Intervention (PCI).Methods: From a single center prospective registry with 5611 consecutive PCIsperformed from January 2003 to July 2008, 2314 were selected for analysis (firstintervention in patients with left main or multivessel coronary artery disease).Logistic EuroSCORE was calculated and tested as a predictor of cardiovascularevents at follow-up (MACE: combined occurrence of death, myocardial infarctionand target vessel failure).Results: Patients’ age was 65±11 years and 78% were males. Mean follow-upwas 23±16 months and there were 292 (12.6%) patients with at least one MACE,165 (7.1%) occurring in the first year.Median EuroSCORE was 2.86% (IQ: 1.49-5.84). By ROC curve analysis, Eu-roSCORE evidenced an AUC of 68% (best cut-off 12%, used for comparisons):9% of patients had high EuroSCORE and 23% of them had MACE, while in theremaining 91% only 6% reached the endpoint (p<0.001).Multivariate Cox Regression analysis evidenced that EuroSCORE ≥12% was agood predictor for MACE [HR 1.7 (1.2-2.5, p<0.01]. Other independent predictorsof MACE were: age, diabetes, peripheral artery disease, chronic renal failure andPCI in acute coronary syndromes. Drug eluting stents were protective.
Kaplan-Meier: absence of MACE
Conclusions: Logistic EuroSCORE above 12% is an important long-term inde-pendent predictor of death, myocardial infarction or target vessel failure in patientswith left main or multivessel disease undergoing percutaneous coronary interven-tion.
P1394 Multivariate predictor analysis for adverse outcomeafter direct PCI for acute myocardial infarction:results of a long-term single-center follow-up study
D. Rzepka, A. Heincke, J. Heckmann, B. Weidtmann, H. Bonnemeier.Innere Medizin III, Universitätsklinikum Schleswig-Hostein, Campus
Kiel, Kiel, Germany
Despite modern treatment of myocardial infarction (MI), the rate of adverse out-comes is still high. Thus far multivariate predictor analyses to evaluate mortalityin a long-term follow-up setting are only available from multicenter studies in thepost-thrombolytic era.Methods: In a prospective clinical trial, we included 2309 patients undergoingPCI for acute MI from. A total of 24 potential predictors were predefined. All-cause mortality was the primary endpoint. After a univariate Cox ProportionalHazards Regression Analysis for each potential predictor, a multivariate best-subset proportional-hazards regression analysis was performed with all signifi-cant univariate predictors.Results: In the univariate analysis twelve of the 24 predefined predictors weresignificant for the primary end point. The best-subset proportional-hazards re-gression analysis revealed seven multivariate significant predictors: Patients withKillip-Classification II–IV had a 2,1 times higher risk than patients with Killip-Classification I (95% CI 1,27–3,57). Patients with diabetes mellitus had a 1,89times higher risk than patients without diabetes mellitus (95% CI 1,15–3,12). Pa-tients with CRP at admission >8,9 mg/l had a 1,86 times higher risk than patientswith CRP ≤ 8,9 mg/l (1,15–3,02). Patients with a BMI > 27,43 kg/m2 had a 0,511
times lower risk than patients with a BMI ≤ 27,43 kg/m2 (95% CI 0,307–0,850).Patients with an ejection fraction (EF) > 49,2% had a 0,580 times lower risk thanpatients with a EF ≤ 49,2% (95% CI 0,351–0,958).Conclusion: The insights of this multivariate predictor analysis may help to betterclassify patients and to specify high risk collectives.
P1395 The correlation between all-cause readmission andrepeat revascularization after percutaneous coronaryintervention
T.H. Bampali, C.H. Pappas, B. Salma, A. Papathanasiou,N. Papamichael, P. Korantzopoulos, J. Goudevenos. University of
Ioannina Medical School, Ioannina, Greece
Purpose: To determine the causes and the outcome of readmission in patientswith a previously implanted coronary stent, regarding to the need for repeat revas-cularization.Methods: In this cross-sectional study we enrolled every patient who hospitalizedwith a prior history of percutaneous coronary intervention (PCI) and we reportedthe number and the causes of their readmissions. The median time from the indexangioplasty to the interview was 6.8 years.Results: From November 2007 until January 2010, a total of 528 patients (88%men) were identified with prior coronary stenting and at least one readmission.318 patients (60.2%) rehospitalized 1 time, 130 (24.6%) 2 times, 72 (13.6%) 3times and 8 (1.5%) more than 4 times. 138 patients were excluded becausetheir admission was due to a non-cardiac surgery. The all-cause readmission ratewas 73.8% (390 patients). The frequency of the admission-causes was: acute-coronary syndrome (ACS) 51% (199 patients), abnormal imaging study 20.5%(80 patients), stable angina 8.2% (32 patients), heart failure or arrhythmias 7.1%(28 patients), others 13% (51 patients). 322 patients (82.6%) underwent a newangiography. These patients were divided into 5 sub-groups regarding to the timeof their readmission after the angioplasty [0-30 days, 31 days - ≤ 6 months, > 6months - ≤ 1 year, >1 year - ≤ 5 years, > 5 years] and we reported the com-bined target-vessel-revascularization (TVR) and Non-TVR, occurrence rate. Inthe first sub-group 11 patients were included and the median time between theangioplasty and the readmission was 8.5 days, (TVR/Non-TVR: 36%). In the sec-ond sub-group 40 patients were included (median time 3.8 months, TVR/Non-TVR: 47.5%). In the third sub-group 33 patients were included (median time 9.7months, TVR/Non-TVR: 30%). In the fourth sub-group 109 patients were included(median time 2.8 years, TVR/Non-TVR: 33%). In the last sub-group 129 patientswere included (median time 6.1 years IQR 5.1-13 years, TVR/Non-TVR: 38.7%).The prevalence of the myocardial infarction (MI) as the cause of revascularizationin the sub-groups was 36%, 10%, 0.3%, 12.8% and 12.4%, respectively.Conclusions: A substantial proportion of the PCI-patients are readmitted within 5years of discharge (49.5%), whereas multiple hospitalizations are rather common.Less than one-half of these readmissions resulted to a repeat revascularizationprocedure and only in 25 cases (12.9%) the cause was a MI. These findingshighlight the need to understand further the correlates and causes of readmissionof discharge after PCI and to develop strategies aimed at avoiding preventablereadmissions.
P1396 Long-term clinical outcome in patients withsaphenous vein graft lesions treated withdrug-eluting and bare metal stents
V. Voudris, S. Thomopoulou, P. Karyofillis, A. Manginas,G. Karavolias, G. Pavlides, E. Sbarouni, C. Spargias,
S. Adamopoulos, D.V. Cokkinos. Onassis Cardiac Surgery Center, Athens,Greece
Purpose: Recent data have shown a reduction in restenosis in patients (pts) withsaphenous vein graft (SVG) lesions treated with percutaneous coronary interven-tion (PCI) using drug-eluting stent (DES); however the long-term clinical outcomeremain controversial. In this prospective study, we assessed the long-term clinicaloutcome in pts with SVG lesions treated with either DES or bare metal stent (BS).Methods: Sixty-two consecutive pts that had been treated with DES were com-pared with 42 consecutive pts treated with BS. The clinical and angiographicdata, in-hospital results and clinical outcome at 36 months follow-up (FU) wereobtained. Major adverse coronary events (MACE) during FU were considereddeath, non-fatal myocardial infarction (MI), and repeat revascularization. Cox re-gression analysis was performed to assess independent predictors for death andMACE.Results: PCI was performed to dilate 66 SVG using DES, and 44 SVG using BS.In addition 17 native vessels were dilated in the DES and 7 in the BMS group.In total 105 lesions (1.69/pt) were treated with DES and 65 (1.55/pt) with BS.Multi–vessel stenting was performed in 31% in DES and 19% in BS treated pts(p=ns). In-hospital results included one (2.4%) sub-acute stent thrombosis (in BSgroup) and one (1.6%) q-wave MI (in DES group). Non-q wave MI (troponin I >
5 UNL) reported in 29% in DES and 19% in BMS treated pts. Clinical follow-upwas obtained in all pts. There were no differences in total mortality (17.7% vs.9.5%, p=ns), cardiac mortality (14.5% vs. 9.5%, p=ns), MI (4.8% vs. 2.4%, p=ns),any revascularization (21% vs. 26.2%, p=ns) or any MACE (38.7% vs. 33.3%,p=ns) in the DES and BMS group of pts, respectively. Independent predictorsfor death were ejection fraction <40% (HR 3.26, 95% CI 1.09-9.79, p=0.03) and
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
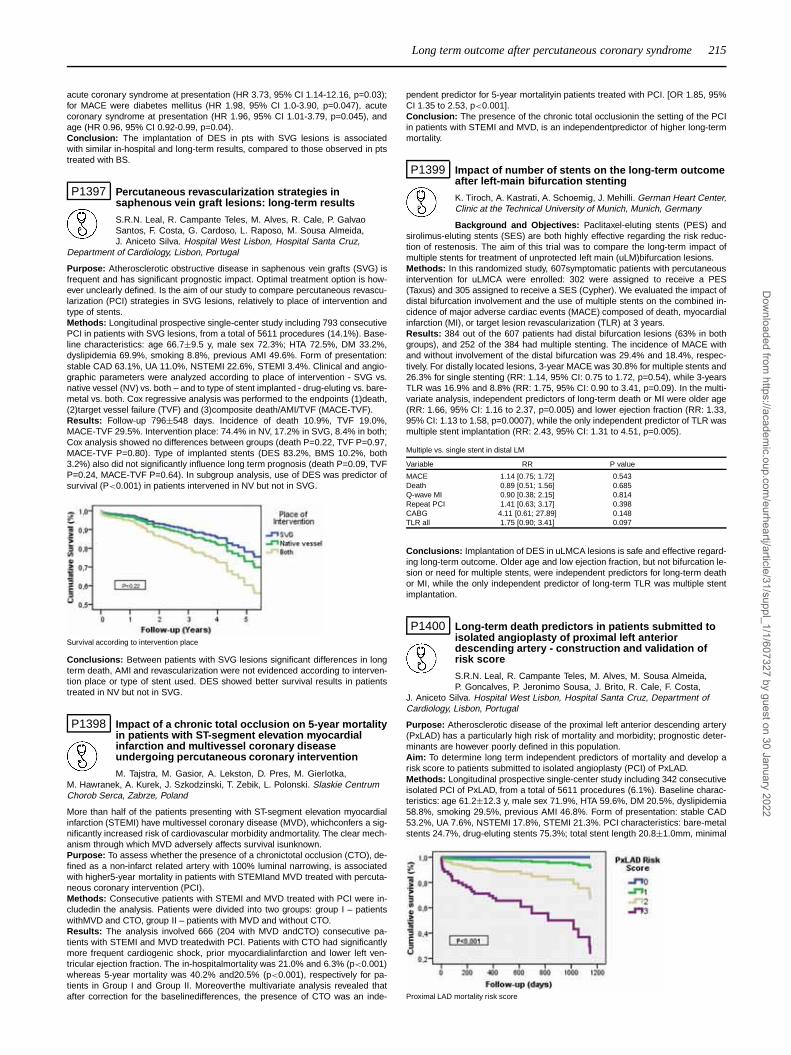
Long term outcome after percutaneous coronary syndrome 215
acute coronary syndrome at presentation (HR 3.73, 95% CI 1.14-12.16, p=0.03);for MACE were diabetes mellitus (HR 1.98, 95% CI 1.0-3.90, p=0.047), acutecoronary syndrome at presentation (HR 1.96, 95% CI 1.01-3.79, p=0.045), andage (HR 0.96, 95% CI 0.92-0.99, p=0.04).Conclusion: The implantation of DES in pts with SVG lesions is associatedwith similar in-hospital and long-term results, compared to those observed in ptstreated with BS.
P1397 Percutaneous revascularization strategies insaphenous vein graft lesions: long-term results
S.R.N. Leal, R. Campante Teles, M. Alves, R. Cale, P. GalvaoSantos, F. Costa, G. Cardoso, L. Raposo, M. Sousa Almeida,J. Aniceto Silva. Hospital West Lisbon, Hospital Santa Cruz,
Department of Cardiology, Lisbon, Portugal
Purpose: Atherosclerotic obstructive disease in saphenous vein grafts (SVG) isfrequent and has significant prognostic impact. Optimal treatment option is how-ever unclearly defined. Is the aim of our study to compare percutaneous revascu-larization (PCI) strategies in SVG lesions, relatively to place of intervention andtype of stents.Methods: Longitudinal prospective single-center study including 793 consecutivePCI in patients with SVG lesions, from a total of 5611 procedures (14.1%). Base-line characteristics: age 66.7±9.5 y, male sex 72.3%; HTA 72.5%, DM 33.2%,dyslipidemia 69.9%, smoking 8.8%, previous AMI 49.6%. Form of presentation:stable CAD 63.1%, UA 11.0%, NSTEMI 22.6%, STEMI 3.4%. Clinical and angio-graphic parameters were analyzed according to place of intervention - SVG vs.native vessel (NV) vs. both – and to type of stent implanted - drug-eluting vs. bare-metal vs. both. Cox regressive analysis was performed to the endpoints (1)death,(2)target vessel failure (TVF) and (3)composite death/AMI/TVF (MACE-TVF).Results: Follow-up 796±548 days. Incidence of death 10.9%, TVF 19.0%,MACE-TVF 29.5%. Intervention place: 74.4% in NV, 17.2% in SVG, 8.4% in both;Cox analysis showed no differences between groups (death P=0.22, TVF P=0.97,MACE-TVF P=0.80). Type of implanted stents (DES 83.2%, BMS 10.2%, both3.2%) also did not significantly influence long term prognosis (death P=0.09, TVFP=0.24, MACE-TVF P=0.64). In subgroup analysis, use of DES was predictor ofsurvival (P<0.001) in patients intervened in NV but not in SVG.
Survival according to intervention place
Conclusions: Between patients with SVG lesions significant differences in longterm death, AMI and revascularization were not evidenced according to interven-tion place or type of stent used. DES showed better survival results in patientstreated in NV but not in SVG.
P1398 Impact of a chronic total occlusion on 5-year mortalityin patients with ST-segment elevation myocardialinfarction and multivessel coronary diseaseundergoing percutaneous coronary intervention
M. Tajstra, M. Gasior, A. Lekston, D. Pres, M. Gierlotka,M. Hawranek, A. Kurek, J. Szkodzinski, T. Zebik, L. Polonski. Slaskie CentrumChorob Serca, Zabrze, Poland
More than half of the patients presenting with ST-segment elevation myocardialinfarction (STEMI) have multivessel coronary disease (MVD), whichconfers a sig-nificantly increased risk of cardiovascular morbidity andmortality. The clear mech-anism through which MVD adversely affects survival isunknown.Purpose: To assess whether the presence of a chronictotal occlusion (CTO), de-fined as a non-infarct related artery with 100% luminal narrowing, is associatedwith higher5-year mortality in patients with STEMIand MVD treated with percuta-neous coronary intervention (PCI).Methods: Consecutive patients with STEMI and MVD treated with PCI were in-cludedin the analysis. Patients were divided into two groups: group I – patientswithMVD and CTO, group II – patients with MVD and without CTO.Results: The analysis involved 666 (204 with MVD andCTO) consecutive pa-tients with STEMI and MVD treatedwith PCI. Patients with CTO had significantlymore frequent cardiogenic shock, prior myocardialinfarction and lower left ven-tricular ejection fraction. The in-hospitalmortality was 21.0% and 6.3% (p<0.001)whereas 5-year mortality was 40.2% and20.5% (p<0.001), respectively for pa-tients in Group I and Group II. Moreoverthe multivariate analysis revealed thatafter correction for the baselinedifferences, the presence of CTO was an inde-
pendent predictor for 5-year mortalityin patients treated with PCI. [OR 1.85, 95%CI 1.35 to 2.53, p<0.001].Conclusion: The presence of the chronic total occlusionin the setting of the PCIin patients with STEMI and MVD, is an independentpredictor of higher long-termmortality.
P1399 Impact of number of stents on the long-term outcomeafter left-main bifurcation stenting
K. Tiroch, A. Kastrati, A. Schoemig, J. Mehilli. German Heart Center,Clinic at the Technical University of Munich, Munich, Germany
Background and Objectives: Paclitaxel-eluting stents (PES) andsirolimus-eluting stents (SES) are both highly effective regarding the risk reduc-tion of restenosis. The aim of this trial was to compare the long-term impact ofmultiple stents for treatment of unprotected left main (uLM)bifurcation lesions.Methods: In this randomized study, 607symptomatic patients with percutaneousintervention for uLMCA were enrolled: 302 were assigned to receive a PES(Taxus) and 305 assigned to receive a SES (Cypher). We evaluated the impact ofdistal bifurcation involvement and the use of multiple stents on the combined in-cidence of major adverse cardiac events (MACE) composed of death, myocardialinfarction (MI), or target lesion revascularization (TLR) at 3 years.Results: 384 out of the 607 patients had distal bifurcation lesions (63% in bothgroups), and 252 of the 384 had multiple stenting. The incidence of MACE withand without involvement of the distal bifurcation was 29.4% and 18.4%, respec-tively. For distally located lesions, 3-year MACE was 30.8% for multiple stents and26.3% for single stenting (RR: 1.14, 95% CI: 0.75 to 1.72, p=0.54), while 3-yearsTLR was 16.9% and 8.8% (RR: 1.75, 95% CI: 0.90 to 3.41, p=0.09). In the multi-variate analysis, independent predictors of long-term death or MI were older age(RR: 1.66, 95% CI: 1.16 to 2.37, p=0.005) and lower ejection fraction (RR: 1.33,95% CI: 1.13 to 1.58, p=0.0007), while the only independent predictor of TLR wasmultiple stent implantation (RR: 2.43, 95% CI: 1.31 to 4.51, p=0.005).
Multiple vs. single stent in distal LM
Variable RR P value
MACE 1.14 [0.75; 1.72] 0.543Death 0.89 [0.51; 1.56] 0.685Q-wave MI 0.90 [0.38; 2.15] 0.814Repeat PCI 1.41 [0.63; 3.17] 0.398CABG 4.11 [0.61; 27.89] 0.148TLR all 1.75 [0.90; 3.41] 0.097
Conclusions: Implantation of DES in uLMCA lesions is safe and effective regard-ing long-term outcome. Older age and low ejection fraction, but not bifurcation le-sion or need for multiple stents, were independent predictors for long-term deathor MI, while the only independent predictor of long-term TLR was multiple stentimplantation.
P1400 Long-term death predictors in patients submitted toisolated angioplasty of proximal left anteriordescending artery - construction and validation ofrisk score
S.R.N. Leal, R. Campante Teles, M. Alves, M. Sousa Almeida,P. Goncalves, P. Jeronimo Sousa, J. Brito, R. Cale, F. Costa,
J. Aniceto Silva. Hospital West Lisbon, Hospital Santa Cruz, Department ofCardiology, Lisbon, Portugal
Purpose: Atherosclerotic disease of the proximal left anterior descending artery(PxLAD) has a particularly high risk of mortality and morbidity; prognostic deter-minants are however poorly defined in this population.Aim: To determine long term independent predictors of mortality and develop arisk score to patients submitted to isolated angioplasty (PCI) of PxLAD.Methods: Longitudinal prospective single-center study including 342 consecutiveisolated PCI of PxLAD, from a total of 5611 procedures (6.1%). Baseline charac-teristics: age 61.2±12.3 y, male sex 71.9%, HTA 59.6%, DM 20.5%, dyslipidemia58.8%, smoking 29.5%, previous AMI 46.8%. Form of presentation: stable CAD53.2%, UA 7.6%, NSTEMI 17.8%, STEMI 21.3%. PCI characteristics: bare-metalstents 24.7%, drug-eluting stents 75.3%; total stent length 20.8±1.0mm, minimal
Proximal LAD mortality risk score
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

216 Long term outcome after percutaneous coronary syndrome
stent caliber 3.1±0.4mm. Clinical and imagiological parameters were analyzedby multivariate Cox regression to determine the independent predictors of longterm mortality and to develop and validate a multifactorial additive mortality riskscore to this population (PxLAD Score).Results: Follow-up 723±485d, incidence of death 8.6%. Independent predictorsof long term mortality: ACS presentation (P=0.03), left ventricular ejection frac-tion <50% (P=0.017), extracardiac vascular disease (P=0.027) and minimal stentdiameter <3.0mm (P=0.012). These predictors were used to construct PxLADScore, ranging from 0 to 4 according to the number present in each patient(0=14.9% pts, 1=52.9% pts, 2=27.5% pts, 3=4.7% pts, 4=0% pts). Cox anal-ysis showed significant mortality differences between PxLAD Score subgroups(P<0.001).Conclusions: The application of the developed PxLAD mortality risk score mayconstitute a useful clinical tool to the correct stratification of this high risk popula-tion.
P1401 Proximal left anterior descendent coronary arteryST-elevation myocardial infarction. Additionalangiographic findings and outcome
K. Arinell1, J. Josefsson1, A. Magnuson2 , O. Frobert1 . 1OrebroUniversity Hospital, Department of Cardiology, Orebro, Sweden;
2Orebro University Hospital, Departments of Statistics and Epidemiology,Orebro, Sweden
Background: Acute proximal occlusion of the left anterior descendent coronaryartery (LAD) is a critical medical condition often leading to heart failure and death.Objective: Our objective was to investigate how additional angiographic findingsmight influence prognosis.Methods: In a single center setting by using consecutive data from the Swedishangiography and angioplasty registry (SCAAR) we identified all patients withacute myocardial infarction (AMI) related to the proximal LAD referred for primarycoronary angioplasty. Clinical and angiographic data were collected from January2004 through December 2008.Results: In the study period, 359 patients (mean age 67.9±12.3 years, 106women) were identified as having proximal LAD-related culprit lesion. Follow-upwas up to 5.5 years. Having both a small conus branch and an occluded firstseptal perforator was associated with increased risk of death after adjustment forage, diabetes mellitus and prior AMI (hazard ratio 4.5 (1.1 - 18), P=0.033). Multi-vessel coronary artery disease and occlusion of the first septal perforator branchand having a small conus branch was also associated with increased risk of death(hazard ratio 5.2 (1.3 - 20), P=0.018).Conclusion: In patients with STEMI because of a proximal LAD lesion treatedby primary PCI, the combination of a small conus branch and an occluded firstseptal perforator branch is associated with a poorer outcome. Additional presenceof multivessel coronary artery disease further aggravate outcome.
P1402 Isolated PCI to the proximal LAD: long term follow upof DES vs BMS
D. Jones, K. Rathod, A. Prinja, A. Swanpillai, A. Jain, C. Knight,A. Mathur, A. Wragg. Barts and The London NHS Trust, London,United Kingdom
Background: There are limited studies with long term follow up comparing in-sertion of bare metal (BMS) vs drug-eluting stent (DES) in isolated proximal leftanterior descending artery (pLAD) lesions in patients with stable angina. We stud-ied the long term outcome of these 2 groups of patients.Methods: 827 consecutive patients with angina underwent elective PCI for signif-icant isolated proximal LAD lesions at a teaching centre between October 2003and December 2008. The primary end point used was major adverse cardiacevents (MACE), defined as death, myocardial infarction (MI), stroke and targetvessel revascularization (TVR).Results: There were 335 patients who underwent PCI with BMS and 492 ptswith DES. The mean follow-up period was 1039±470 days for the BMS group
Abstract P1401 – Table 1
Follow up data
LAD occlusion Small conus Occluded Occluded S1 Multivessel Multivessel disease Mulitivessel disease Occluded S1, small conus branch,only branch S1 AND disease AND AND AND
small conus branch small conus branch occluded S1 multivessel disease
n 77 49 31 32 60 56 32 22Death 3 (4%) 2 (4%) 5 (16%) 6 (19%) 9 (15%) 10 (18%) 8 (25%) 9 (41%)Unadjusted HR (95% Cl) reference 0.9 (0.1–5.6) 3.9 (0.9 -16) 5.1 (1.3 - 20) 4.0 (1.1 - 15) 4.6 (1.3 – 17) 6.3 (1.6 – 24) 11 (2.9 – 40)p value p=0.940 p=0.064 p=0.021 p=0. 037 p=0.020 p=0.007 p<0.001Adjusted by age, HR (95% Cl) reference 0.9 (0.1 – 5.4) 3.7 (0.9 – 16) 4.4 (1.1 – 18) 3.0 (0.8 – 11) 3.5 (0.9 – 13) 3.8 (0.9 – 15) 7.1 (1.9 – 27)p value p=0.906) p=0.072 p=0.035 p=0.098 p=0.058 p=0.052) p=0.004)Adjusted by age and diabetes
mellitus, HR (95%Cl) reference 1.0 (0.2-6.1) 4.2 (0.9 – 18) 4.5 (1.1-18) 3.1 (0.8-12) 3.7 (1.0-14) 4.1 (1.0-16) 6.4 (1.7-25)p value p=0.995 p=0.053 p=0.034 p=0.090 p=0.049 p=0.042 p=0.007Adjusted by age, DM and prior
AMIHR (95% Cl) reference 1.0 (0.1 – 5.9) 4.0 (0.9-17) 4.5 (1.1 – 18) 3.1 (0.8 –11) 3.4 (0.9 – 13) 3.8 (0.9-15) 5.2 (1.3-20)p value p=0.968 p=0.061 p=0.033 p=0.094 p=0.056 p=0.056 p=0.018
Values are numbers or percentage. Hazard ratios (HR) from Cox regression supplemented with 95% confidence intervals (CI) and p-values. Both unadjusted and adjusted models are presented. Ageare categorised in four categories: <60-69, 70-79 and 80 years or more.
and 920±369 days for the DES group. Baseline characteristics were the sameother than diabetes, which was more common in the DES treated group (21% v15%). Per lesion there was a large number of stents used in the DES group (1.57vs 1.27, p <0.0001), with a longer average length (20.43 vs 16.8, p<0.0001),there was no difference in stent width. There was a significant difference in MACEbetween the two groups in favour of DES (9% BMS v 3% DES group [P<0.001]at 1 year; 14% BMS v 8% DES group [P<0.001] at 4 year). MACE was driven byin-stent restenosis in both groups and the difference between both groups wasdue to increased TVR in the BMS group (figure 1). There was no difference indeath, MI or stroke.
Figure 1. K-M Curve comparing DES vs BMS
Conclusions: As expected DES resulted in a lower MACE than BMS due to adecreased need for repeat revascularisation, this is more impressive consideringa higher risk group (longer lesion length, diabetes). This adds evidence that overthe medium term DES are superior to BMS with regard to repeat revascularisa-tion.
P1403 Long term clinical outcomes of final kissing balloonangioplasty after a simple strategy of stenting themain vessel only in coronary bifurcation lesions
S.E. Lee1, J.Y. Rhew1, Y. Moon2, J.P. Park1, J.H. Lim1, S.H. John1,J.H. Kim3. 1Jeonju Presbyterian Medical Center, Jeonju, Korea,
Republic of; 2gospel medicine clinic, jeonju, Korea, Republic of; 3ChonnamNational University Hospital, The Heart Center, Gwangju, Korea, Republic of
Objectives: In the treatment of coronary bifurcation lesions with drug-elutingstent (DES), we sought to the angiographic and clinical outcomes of final kiss-ing balloon angioplasty (KBA) after stenting main vessel only.Methods: Between January 2004 and December 2006, a total of 364 patientswho underwent drug-eluting stent implantation only the main vessel for a coronarybifurcation lesions were grouped according to perform final KBA: Group I: no finalKBA (n=264, 173 men); Group II: final KBA (n=100, 75 men). We carried out postKBA only if the thrombolysis in myocardial infarction (TIMI) flow of side branchwas reduced grade 0 or 1, or when the ostium of side branch become obstructedover 90% after stenting only the main vessel. We evaluated the major adversecardiac events (MACE; death, non-fatal myocardial infarction, and target vesselrevascularization) at three-year follow-up.Results: Final TIMI flow of the side branch was significantly decreased in thegroup I (p=0.007). The fluoroscopic time and amount of contrast media weresignificantly less in the group I during coronary bifurcation intervention. Therewere no significant differences in the incidences of cardiac death (1.1% vs. 0%,p=0.380), MI (1.9% vs. 1%, p=1.000), TLR (5.3% vs. 8%, p=0.332), TVR (7.6%vs. 9%, p=0.667), and total MACE (9.8% vs. 10%, p=0.552) between two groups.Conclusion: Unless the TIMI flow was reduced grade 0, 1, or become obstructedover 90% of side branch after stenting only the main vessel in the bifurcationlesions, final KBA does not reduce the clinical outcomes compared to no finalKBA during a three-year clinical follow-up.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
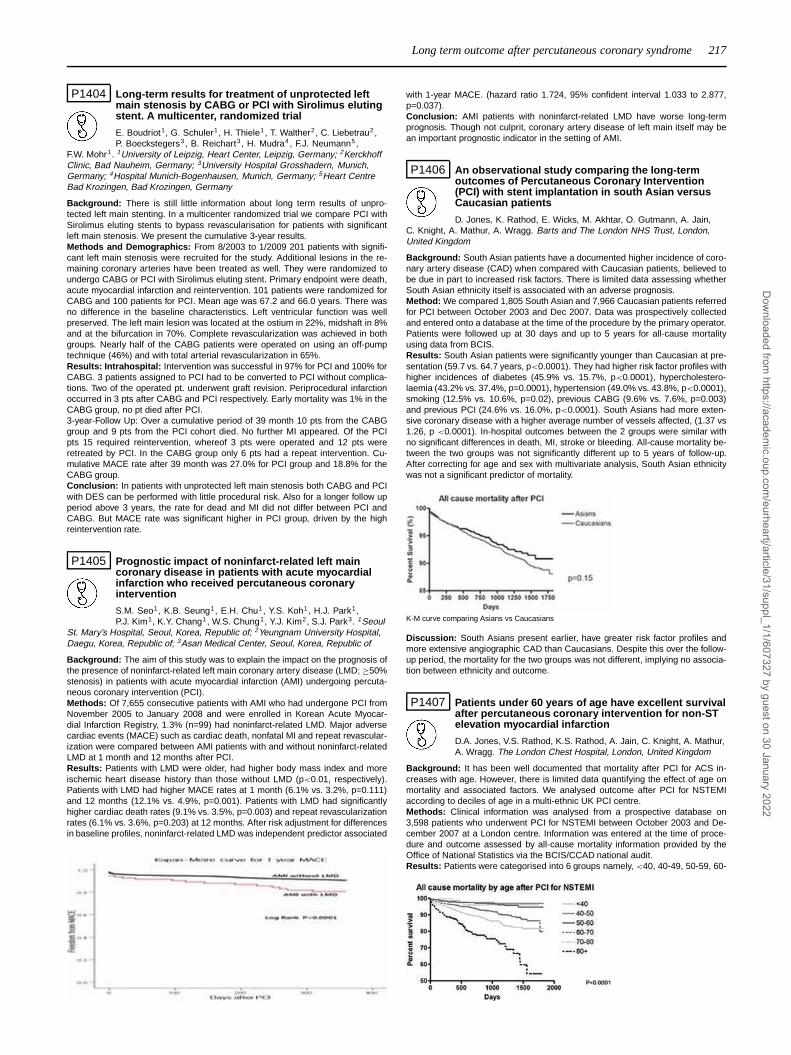
Long term outcome after percutaneous coronary syndrome 217
P1404 Long-term results for treatment of unprotected leftmain stenosis by CABG or PCI with Sirolimus elutingstent. A multicenter, randomized trial
E. Boudriot1, G. Schuler1, H. Thiele1, T. Walther2, C. Liebetrau2,P. Boeckstegers3 , B. Reichart3, H. Mudra4, F.J. Neumann5,
F.W. Mohr1. 1University of Leipzig, Heart Center, Leipzig, Germany; 2KerckhoffClinic, Bad Nauheim, Germany; 3University Hospital Grosshadern, Munich,Germany; 4Hospital Munich-Bogenhausen, Munich, Germany; 5Heart CentreBad Krozingen, Bad Krozingen, Germany
Background: There is still little information about long term results of unpro-tected left main stenting. In a multicenter randomized trial we compare PCI withSirolimus eluting stents to bypass revascularisation for patients with significantleft main stenosis. We present the cumulative 3-year results.Methods and Demographics: From 8/2003 to 1/2009 201 patients with signifi-cant left main stenosis were recruited for the study. Additional lesions in the re-maining coronary arteries have been treated as well. They were randomized toundergo CABG or PCI with Sirolimus eluting stent. Primary endpoint were death,acute myocardial infarction and reintervention. 101 patients were randomized forCABG and 100 patients for PCI. Mean age was 67.2 and 66.0 years. There wasno difference in the baseline characteristics. Left ventricular function was wellpreserved. The left main lesion was located at the ostium in 22%, midshaft in 8%and at the bifurcation in 70%. Complete revascularization was achieved in bothgroups. Nearly half of the CABG patients were operated on using an off-pumptechnique (46%) and with total arterial revascularization in 65%.Results: Intrahospital: Intervention was successful in 97% for PCI and 100% forCABG. 3 patients assigned to PCI had to be converted to PCI without complica-tions. Two of the operated pt. underwent graft revision. Periprocedural infarctionoccurred in 3 pts after CABG and PCI respectively. Early mortality was 1% in theCABG group, no pt died after PCI.3-year-Follow Up: Over a cumulative period of 39 month 10 pts from the CABGgroup and 9 pts from the PCI cohort died. No further MI appeared. Of the PCIpts 15 required reintervention, whereof 3 pts were operated and 12 pts wereretreated by PCI. In the CABG group only 6 pts had a repeat intervention. Cu-mulative MACE rate after 39 month was 27.0% for PCI group and 18.8% for theCABG group.Conclusion: In patients with unprotected left main stenosis both CABG and PCIwith DES can be performed with little procedural risk. Also for a longer follow upperiod above 3 years, the rate for dead and MI did not differ between PCI andCABG. But MACE rate was significant higher in PCI group, driven by the highreintervention rate.
P1405 Prognostic impact of noninfarct-related left maincoronary disease in patients with acute myocardialinfarction who received percutaneous coronaryintervention
S.M. Seo1, K.B. Seung1, E.H. Chu1, Y.S. Koh1, H.J. Park1,P.J. Kim1, K.Y. Chang1, W.S. Chung1, Y.J. Kim2, S.J. Park3. 1Seoul
St. Mary’s Hospital, Seoul, Korea, Republic of; 2Yeungnam University Hospital,Daegu, Korea, Republic of; 3Asan Medical Center, Seoul, Korea, Republic of
Background: The aim of this study was to explain the impact on the prognosis ofthe presence of noninfarct-related left main coronary artery disease (LMD; ≥50%stenosis) in patients with acute myocardial infarction (AMI) undergoing percuta-neous coronary intervention (PCI).Methods: Of 7,655 consecutive patients with AMI who had undergone PCI fromNovember 2005 to January 2008 and were enrolled in Korean Acute Myocar-dial Infarction Registry, 1.3% (n=99) had noninfarct-related LMD. Major adversecardiac events (MACE) such as cardiac death, nonfatal MI and repeat revascular-ization were compared between AMI patients with and without noninfarct-relatedLMD at 1 month and 12 months after PCI.Results: Patients with LMD were older, had higher body mass index and moreischemic heart disease history than those without LMD (p<0.01, respectively).Patients with LMD had higher MACE rates at 1 month (6.1% vs. 3.2%, p=0.111)and 12 months (12.1% vs. 4.9%, p=0.001). Patients with LMD had significantlyhigher cardiac death rates (9.1% vs. 3.5%, p=0.003) and repeat revascularizationrates (6.1% vs. 3.6%, p=0.203) at 12 months. After risk adjustment for differencesin baseline profiles, noninfarct-related LMD was independent predictor associated
with 1-year MACE. (hazard ratio 1.724, 95% confident interval 1.033 to 2.877,p=0.037).Conclusion: AMI patients with noninfarct-related LMD have worse long-termprognosis. Though not culprit, coronary artery disease of left main itself may bean important prognostic indicator in the setting of AMI.
P1406 An observational study comparing the long-termoutcomes of Percutaneous Coronary Intervention(PCI) with stent implantation in south Asian versusCaucasian patients
D. Jones, K. Rathod, E. Wicks, M. Akhtar, O. Gutmann, A. Jain,C. Knight, A. Mathur, A. Wragg. Barts and The London NHS Trust, London,United Kingdom
Background: South Asian patients have a documented higher incidence of coro-nary artery disease (CAD) when compared with Caucasian patients, believed tobe due in part to increased risk factors. There is limited data assessing whetherSouth Asian ethnicity itself is associated with an adverse prognosis.Method: We compared 1,805 South Asian and 7,966 Caucasian patients referredfor PCI between October 2003 and Dec 2007. Data was prospectively collectedand entered onto a database at the time of the procedure by the primary operator.Patients were followed up at 30 days and up to 5 years for all-cause mortalityusing data from BCIS.Results: South Asian patients were significantly younger than Caucasian at pre-sentation (59.7 vs. 64.7 years, p<0.0001). They had higher risk factor profiles withhigher incidences of diabetes (45.9% vs. 15.7%, p<0.0001), hypercholestero-laemia (43.2% vs. 37.4%, p=0.0001), hypertension (49.0% vs. 43.8%, p<0.0001),smoking (12.5% vs. 10.6%, p=0.02), previous CABG (9.6% vs. 7.6%, p=0.003)and previous PCI (24.6% vs. 16.0%, p<0.0001). South Asians had more exten-sive coronary disease with a higher average number of vessels affected, (1.37 vs1.26, p <0.0001). In-hospital outcomes between the 2 groups were similar withno significant differences in death, MI, stroke or bleeding. All-cause mortality be-tween the two groups was not significantly different up to 5 years of follow-up.After correcting for age and sex with multivariate analysis, South Asian ethnicitywas not a significant predictor of mortality.
K-M curve comparing Asians vs Caucasians
Discussion: South Asians present earlier, have greater risk factor profiles andmore extensive angiographic CAD than Caucasians. Despite this over the follow-up period, the mortality for the two groups was not different, implying no associa-tion between ethnicity and outcome.
P1407 Patients under 60 years of age have excellent survivalafter percutaneous coronary intervention for non-STelevation myocardial infarction
D.A. Jones, V.S. Rathod, K.S. Rathod, A. Jain, C. Knight, A. Mathur,A. Wragg. The London Chest Hospital, London, United Kingdom
Background: It has been well documented that mortality after PCI for ACS in-creases with age. However, there is limited data quantifying the effect of age onmortality and associated factors. We analysed outcome after PCI for NSTEMIaccording to deciles of age in a multi-ethnic UK PCI centre.Methods: Clinical information was analysed from a prospective database on3,598 patients who underwent PCI for NSTEMI between October 2003 and De-cember 2007 at a London centre. Information was entered at the time of proce-dure and outcome assessed by all-cause mortality information provided by theOffice of National Statistics via the BCIS/CCAD national audit.Results: Patients were categorised into 6 groups namely, <40, 40-49, 50-59, 60-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
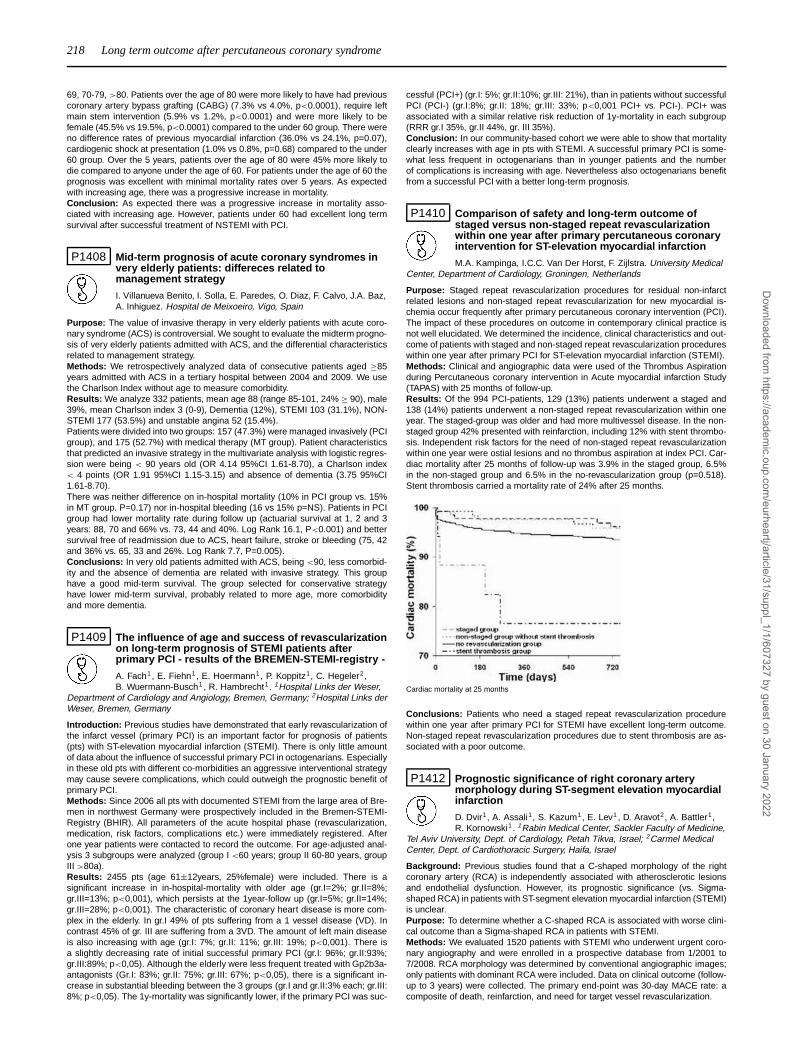
218 Long term outcome after percutaneous coronary syndrome
69, 70-79, >80. Patients over the age of 80 were more likely to have had previouscoronary artery bypass grafting (CABG) (7.3% vs 4.0%, p<0.0001), require leftmain stem intervention (5.9% vs 1.2%, p<0.0001) and were more likely to befemale (45.5% vs 19.5%, p<0.0001) compared to the under 60 group. There wereno difference rates of previous myocardial infarction (36.0% vs 24.1%, p=0.07),cardiogenic shock at presentation (1.0% vs 0.8%, p=0.68) compared to the under60 group. Over the 5 years, patients over the age of 80 were 45% more likely todie compared to anyone under the age of 60. For patients under the age of 60 theprognosis was excellent with minimal mortality rates over 5 years. As expectedwith increasing age, there was a progressive increase in mortality.Conclusion: As expected there was a progressive increase in mortality asso-ciated with increasing age. However, patients under 60 had excellent long termsurvival after successful treatment of NSTEMI with PCI.
P1408 Mid-term prognosis of acute coronary syndromes invery elderly patients: differeces related tomanagement strategy
I. Villanueva Benito, I. Solla, E. Paredes, O. Diaz, F. Calvo, J.A. Baz,A. Inhiguez. Hospital de Meixoeiro, Vigo, Spain
Purpose: The value of invasive therapy in very elderly patients with acute coro-nary syndrome (ACS) is controversial. We sought to evaluate the midterm progno-sis of very elderly patients admitted with ACS, and the differential characteristicsrelated to management strategy.Methods: We retrospectively analyzed data of consecutive patients aged ≥85years admitted with ACS in a tertiary hospital between 2004 and 2009. We usethe Charlson Index without age to measure comorbidity.Results: We analyze 332 patients, mean age 88 (range 85-101, 24% ≥ 90), male39%, mean Charlson index 3 (0-9), Dementia (12%), STEMI 103 (31.1%), NON-STEMI 177 (53.5%) and unstable angina 52 (15.4%).Patients were divided into two groups: 157 (47.3%) were managed invasively (PCIgroup), and 175 (52.7%) with medical therapy (MT group). Patient characteristicsthat predicted an invasive strategy in the multivariate analysis with logistic regres-sion were being < 90 years old (OR 4.14 95%CI 1.61-8.70), a Charlson index< 4 points (OR 1.91 95%CI 1.15-3.15) and absence of dementia (3.75 95%CI1.61-8.70).There was neither difference on in-hospital mortality (10% in PCI group vs. 15%in MT group. P=0.17) nor in-hospital bleeding (16 vs 15% p=NS). Patients in PCIgroup had lower mortality rate during follow up (actuarial survival at 1, 2 and 3years: 88, 70 and 66% vs. 73, 44 and 40%. Log Rank 16.1, P<0.001) and bettersurvival free of readmission due to ACS, heart failure, stroke or bleeding (75, 42and 36% vs. 65, 33 and 26%. Log Rank 7.7, P=0.005).Conclusions: In very old patients admitted with ACS, being <90, less comorbid-ity and the absence of dementia are related with invasive strategy. This grouphave a good mid-term survival. The group selected for conservative strategyhave lower mid-term survival, probably related to more age, more comorbidityand more dementia.
P1409 The influence of age and success of revascularizationon long-term prognosis of STEMI patients afterprimary PCI - results of the BREMEN-STEMI-registry -
A. Fach1, E. Fiehn1, E. Hoermann1, P. Koppitz1, C. Hegeler2,B. Wuermann-Busch1 , R. Hambrecht1 . 1Hospital Links der Weser,
Department of Cardiology and Angiology, Bremen, Germany; 2Hospital Links derWeser, Bremen, Germany
Introduction: Previous studies have demonstrated that early revascularization ofthe infarct vessel (primary PCI) is an important factor for prognosis of patients(pts) with ST-elevation myocardial infarction (STEMI). There is only little amountof data about the influence of successful primary PCI in octogenarians. Especiallyin these old pts with different co-morbidities an aggressive interventional strategymay cause severe complications, which could outweigh the prognostic benefit ofprimary PCI.Methods: Since 2006 all pts with documented STEMI from the large area of Bre-men in northwest Germany were prospectively included in the Bremen-STEMI-Registry (BHIR). All parameters of the acute hospital phase (revascularization,medication, risk factors, complications etc.) were immediately registered. Afterone year patients were contacted to record the outcome. For age-adjusted anal-ysis 3 subgroups were analyzed (group I <60 years; group II 60-80 years, groupIII >80a).Results: 2455 pts (age 61±12years, 25%female) were included. There is asignificant increase in in-hospital-mortality with older age (gr.I=2%; gr.II=8%;gr.III=13%; p<0,001), which persists at the 1year-follow up (gr.I=5%; gr.II=14%;gr.III=28%; p<0,001). The characteristic of coronary heart disease is more com-plex in the elderly. In gr.I 49% of pts suffering from a 1 vessel disease (VD). Incontrast 45% of gr. III are suffering from a 3VD. The amount of left main diseaseis also increasing with age (gr.I: 7%; gr.II: 11%; gr.III: 19%; p<0,001). There isa slightly decreasing rate of initial successful primary PCI (gr.I: 96%; gr.II:93%;gr.III:89%; p<0,05). Although the elderly were less frequent treated with Gp2b3a-antagonists (Gr.I: 83%; gr.II: 75%; gr.III: 67%; p<0,05), there is a significant in-crease in substantial bleeding between the 3 groups (gr.I and gr.II:3% each; gr.III:8%; p<0,05). The 1y-mortality was significantly lower, if the primary PCI was suc-
cessful (PCI+) (gr.I: 5%; gr.II:10%; gr.III: 21%), than in patients without successfulPCI (PCI-) (gr.I:8%; gr.II: 18%; gr.III: 33%; p<0,001 PCI+ vs. PCI-). PCI+ wasassociated with a similar relative risk reduction of 1y-mortality in each subgroup(RRR gr.I 35%, gr.II 44%, gr. III 35%).Conclusion: In our community-based cohort we were able to show that mortalityclearly increases with age in pts with STEMI. A successful primary PCI is some-what less frequent in octogenarians than in younger patients and the numberof complications is increasing with age. Nevertheless also octogenarians benefitfrom a successful PCI with a better long-term prognosis.
P1410 Comparison of safety and long-term outcome ofstaged versus non-staged repeat revascularizationwithin one year after primary percutaneous coronaryintervention for ST-elevation myocardial infarction
M.A. Kampinga, I.C.C. Van Der Horst, F. Zijlstra. University MedicalCenter, Department of Cardiology, Groningen, Netherlands
Purpose: Staged repeat revascularization procedures for residual non-infarctrelated lesions and non-staged repeat revascularization for new myocardial is-chemia occur frequently after primary percutaneous coronary intervention (PCI).The impact of these procedures on outcome in contemporary clinical practice isnot well elucidated. We determined the incidence, clinical characteristics and out-come of patients with staged and non-staged repeat revascularization procedureswithin one year after primary PCI for ST-elevation myocardial infarction (STEMI).Methods: Clinical and angiographic data were used of the Thrombus Aspirationduring Percutaneous coronary intervention in Acute myocardial infarction Study(TAPAS) with 25 months of follow-up.Results: Of the 994 PCI-patients, 129 (13%) patients underwent a staged and138 (14%) patients underwent a non-staged repeat revascularization within oneyear. The staged-group was older and had more multivessel disease. In the non-staged group 42% presented with reinfarction, including 12% with stent thrombo-sis. Independent risk factors for the need of non-staged repeat revascularizationwithin one year were ostial lesions and no thrombus aspiration at index PCI. Car-diac mortality after 25 months of follow-up was 3.9% in the staged group, 6.5%in the non-staged group and 6.5% in the no-revascularization group (p=0.518).Stent thrombosis carried a mortality rate of 24% after 25 months.
Cardiac mortality at 25 months
Conclusions: Patients who need a staged repeat revascularization procedurewithin one year after primary PCI for STEMI have excellent long-term outcome.Non-staged repeat revascularization procedures due to stent thrombosis are as-sociated with a poor outcome.
P1412 Prognostic significance of right coronary arterymorphology during ST-segment elevation myocardialinfarction
D. Dvir1, A. Assali1, S. Kazum1, E. Lev1, D. Aravot2, A. Battler1,R. Kornowski1. 1Rabin Medical Center, Sackler Faculty of Medicine,
Tel Aviv University, Dept. of Cardiology, Petah Tikva, Israel; 2Carmel MedicalCenter, Dept. of Cardiothoracic Surgery, Haifa, Israel
Background: Previous studies found that a C-shaped morphology of the rightcoronary artery (RCA) is independently associated with atherosclerotic lesionsand endothelial dysfunction. However, its prognostic significance (vs. Sigma-shaped RCA) in patients with ST-segment elevation myocardial infarction (STEMI)is unclear.Purpose: To determine whether a C-shaped RCA is associated with worse clini-cal outcome than a Sigma-shaped RCA in patients with STEMI.Methods: We evaluated 1520 patients with STEMI who underwent urgent coro-nary angiography and were enrolled in a prospective database from 1/2001 to7/2008. RCA morphology was determined by conventional angiographic images;only patients with dominant RCA were included. Data on clinical outcome (follow-up to 3 years) were collected. The primary end-point was 30-day MACE rate: acomposite of death, reinfarction, and need for target vessel revascularization.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Long term outcome after percutaneous coronary syndrome / Antithrombotic therapy after percutaneous coronary intervention 219
Results: Among patients with left coronary system-related STEMI, those with C-shaped RCA had significantly worse outcome than those with Sigma-shaped RCA(30 days: death- 8.2% vs. 2.9%, p=0.037; MACE- 22.6% vs. 12.6%, p= 0.004).These differences were independent of existing RCA stenosis (p=0.007) and weresustained to end of follow-up (Figure). Among patients with RCA-related STEMI,there was no association between RCA morphology (C vs. Sigma) and outcome(30 days: death- 5.9% vs. 4.4%, p=0.69; MACE- 9.8% vs. 8.9%, p=0.85).
Figure 1
Conclusions: STEMI patients with a culprit in the left coronary system haveworse clinical outcome in the presence of a C-shaped RCA than a Sigma-shaped.Evaluating RCA morphology in patients with left STEMI may improve risk strat-ification. The underlying pathophysiological mechanism warrants further evalua-tion.
P1413 Results in long term outcome of patients withmultiple vessel disease treated with drug eluting,baremetal stents and coronary bypass surgery: insightsfrom five years follow up of ERACI III study
A. Rodriguez1, M. Hlatky2, L. Grinfeld3, J. Mieres1, M.A. Rodriguez-Granillo1, D. Berrocal3, D. Boothroyd2, C. Fernandez-Pereira1 , I.P. Palacios4,W. Oneill4. 1Sanatorium Otamendi, Buenos Aires, Argentina; 2StanfordUniversity Medical Center, Division of Cardiovascular Medicine, Stanford, UnitedStates of America; 3Italian Hospital, Buenos Aires, Argentina; 4Harvard MedicalSchool, Massachusetts General Hospital, Boston, United States of America
Background: One year follow up (FU) of this study, EuroIntervention Journal2006, showed significantly better outcome with drug eluting stents (DES) com-pared to bare metal stents (BMS) or coronary artery bypass surgery (CABG).Methods: The ERACI III was a comparison among previous randomized data inpatients with multiple vessel disease (MVD) treated with BMS and CABG (ERACIII) with a prospective MVD cohort of patients treated with DES. 675 patients wereincluded. 5years FU was required by study design to ascertain the primary endpoint of major adverse cardiovascular events (MACCE) defined as death (D) my-ocardial infarction (MI) stroke (S)and target vessel revascularization (TVR). D andD+MI+stroke are secondary end points.DES were compared with BMS and CABG using multivariable Cox model in theentire population and a propensity matched subset.Results: 5 years FU are shown on Table.DES compared to BMS had highermortality in the overall group (odds ratio (OR) 0.490 confidence limits (CL)0.236-1.019 p=0.056) and after propensity matched (OR 0.280CL672 p=0.004).DEScompared to BMS had higher incidence of D+MI+S in overall (OR 0.506 CL0.276-0.927 p=0.028) and after matching (OR 0.291 CL0.134-0.633 p=0.002).MACCE was similar in overall (OR1.062 CL 0.669-1.686 p=0.80) and matched(OR0.739 CL0.418-1.306 p=0.298)groups.DES and CABG showed no differ-ences in D,D+MI+S or MACCE (p=0.42,0.80 and 0.30 respectively). Only 17.7%of DES patients were taking clopidogrel at 5 years FU.
Table 1. 5 years Follow Up
BMS (225) DES (225) CABG (225)
Death 7.1% 13.8% 11.6%Non cardiac death 1.8% 6.7% 2.3%MI 2.7% 9.8% 6.2%TVR 28.4% 18.7% 7.6%MACCE 34.6% 33.8% 24.5%
Conclusions: In ERACI III,when compared to BMS,patients with MVD treatedwith DES are at higher risk of D and D+MI+S; differences remained after propen-sity matched.
ANTITHROMBOTIC THERAPY AFTER PERCUTANEOUSCORONARY INTERVENTION
P1414 Does clinical profile predict doublenon-responsiveness to aspirin and clopidogrel?
A. Moynagh1 , P. Jariwala1, T. Hovasse1, M.C. Morice1, Y. Louvard1,T. Unterseeh2, H. Benamer1, B. Chevalier1, T. Lefevre3. 1InstitutHospitalier Jacques Cartier - ICPS, Massy, France; 2Hôpital Privé
Claude Galien, ICPS, Quincy, France; 3ICPS - Institute Hospital Jacques Cartier,Massy, France
Purpose: Double antiplatelet treatment is the gold standard after percutaneouscoronary angioplasty (PCI). However, variability of platelet response to aspirinand plavix remains problematic.Methods: 500 consecutive patients were enrolled in a prospective dedicateddatabase after PCI.All patients had Plavix testing using VASP and aspirin testing using PFA 100.All patients were pretreated with a loading dose of 600mg clopidogrel and hada daily maintenance dose of 75mg, or 150mg if their weight was greater than80kg and aspirin 160mg/day. VASP >50% and PFA 100 <170 sec. were definedas clopidogrel and aspirin resistance. We compared patients who were doublenon-responders with double responders.Results: 246 patients (49.2%) were responders to both aspirin and clopidogrel,while 58 (11.6%) were double non-responders.Results of univariate analysis comparing both groups are shown in the table.By multivariate analysis, male gender (p=0.06), previous myocardial infarction(p=0.06), hypertension (p=0.03) and weight<75kg (p=0.02) were more likely tobe double responders.
Double responders Double non-responders P value
Male (%) 77.6 86.2 0.15Age (yrs) 67.3±10.6 63.8±11.5 0.06Weight (kg) 77.7±15.3 79.2±14.6 0.48BMI 25.4±7.2 27.2±5.4 0.04Smoking (%) 36.2 35.5 0.81Dyslipidaemia (%) 61.8 61.4 0.96Diabetes (%) 4.7 6.1 0.22Hypertension (%) 64.6 50.1 0.06Family history (%) 7.3 3.5 0.20Past PCI (%) 35.8 33.3 0.73Past CABG (%) 3.7 3.5 0.96Past MI (%) 10.1 19.2 0.11Weight <75kg (%) 46.8 31.0 0.02
Conclusion: Combined aspirin and clopidogrel non-responsiveness is found inalmost 12% of patients. The main predictor of double non responsiveness isweight>75kg. Influence of double non responsiveness on clinical outcome willbe available at the time of the meeting.
P1415 An international examination of the variations in themanagement pathway of ACS patients undergoingPCI: Results from the Antiplatlet TreatmentObservational Registry (APTOR)
A. Mohacsi1 , G. Pavlides2, G. Berkenboom3, K. Norrbacka4,J. Goedicke5, M.-A. Paget6, M.E. Tomlin7, A. Bakhai8. 1Gottsegen Institute ofHungarian Cardiology, Budapest, Hungary; 2Onassis Cardiac Surgery Center,Athens, Greece; 3ULB Erasme University Hospital, Brussels, Belgium; 4Eli Lillyand Company, Helsinki, Finland; 5Eli Lilly and Company, Hamburg, Germany;6Eli Lilly and Company, Paris, France; 7Eli Lilly and Company, Indianapolis,United States of America; 8Barnet General Hospital, London, United Kingdom
Purpose: To assess the management pathway of ACS patients undergoing PCI.Methods: Prospective, observational registry of 14 countries grouped into 9 clus-ters, each with ∼500 ACS patients undergoing PCI, capturing practice patternsfrom 2007-2009.Results: Median age ranged from 59-66 yrs, and the % of patients with STEMIranged from 33-61%. Wide variations were observed with access site; prevalenceof bare metal (BMS) and drug-eluting stents (DES); time from index ACS event tohospital admission, time from ACS to clopidogrel loading dose, time to PCI; andnumber of ambulance transfers (Table 1, see p 220).Conclusions: The management pathway for ACS patients undergoing PCI variessignificantly by geography. These registry data suggest an ongoing need to pro-mote best practices locally and internationally and suggest there is some scopefor harmonization of practices and some opportunity for improvement of out-comes.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

220 Antithrombotic therapy after percutaneous coronary intervention
Abstract P1415 – Table 1
Spain UK France Czech Republic Germany Greece Nordic Countries Austria-Hungary Belgium-Netherlands(N=538) (N=504) (N=483) (N=507) (N=500) (N=558) (N=496) (N=496) (N=484)
UA/NSTEMI (%) 67 65 53 43 53 63 56 39 40Age (median, IQR) 65 (55, 74) 63 (53, 70) 61 (54, 72) 63 (57, 73) 66 (54, 74) 64 (55, 73) 66 (58, 74) 62 (54, 70) 63 (56, 75)BMS only (%) 24 29 53 74 62 10 59 50 59DES only (%) 57 46 29 22 35 87 35 45 37Radial access site (%)* – – – 23 4 2 45 24 21% patients Time (0 days) from qualifying ACS to hospital
admission 69 88 81 70 81 79 82 85 90Time (0 days) from qualifying ACS to first loading dose 53 65 67 70 77 78 72 78 80% with ≥2 ambulance transfers 30 8 31 17 5 1 24 11 35% Time (≤3 days) from ACS qualifying event to PCI 63 31 81 80 91 76 74 90 79STEMI (%) 33 35 47 57 47 37 44 61 60Age (median, IQR) 59 (51, 68) 60 (53, 68) 58 (50, 69) 61 (53, 67) 61 (52, 70) 56 (49, 66) 62 (55, 70) 61 (53, 70) 61 (53, 71)BMS only (%) 32 52 75 90 76 35 69 78 72DES only (%) 49 33 13 8 22 60 29 20 27Radial access site (%)* – – – 14 0 2 25 25 12% patients with time (0 days) from qualifying ACS to hospital
admission 86 87 86 93 91 86 92 93 94% patients with time (0 days) from qualifying ACS to first loading
dose 73 74 85 94 91 89 93 93 95% with ≥2 ambulance transfers 15 15 27 12 2 4 34 12 21% patients with time (≤1 day) from ACS qualifying event to PCI 71 51 80 97 97 67 94 97 94
*PCI access site was not collected in APTOR I (Spain, France, and UK).
P1416 Impact of oral anticoagulation on cardiovascularevents after Drug-eluting stent implantation inpatients with atrial fibrillation. Results of the DES.deRegistry
U. Zeymer1, R. Zahn2, P. Bramlage3, M. Hochadel1 ,J. Senges1, K. Kuck4, C. Nienaber5, U. Tebbe6 . 1Institut für
Herzinfarktforschung, Ludwigshafen Am Rhein, Germany; 2Clinical Center ofLudwigshafen, Ludwigshafen am Rhein, Germany; 3Dresden University ofTechnology, Department of Pharmacology and Toxicology, Dresden, Germany;4Asklepios Clinic St. Georg, Hamburg, Germany; 5University Hospital Rostock,Department of Cardiology, Rostock, Germany; 6Hospital Lippe-Detmold, InternalMedicine II, Department of Cardiology, Detmold, Germany
Background: The optimal antithrombotic therapy in patients with atrial fibrillation(AFib) and drug-eluting stent is still a matter of debate. There are no randomizedclinical trials available comparing different regimens. Therefore we sought to in-vestigate the impact of oral anticoagulation on outcome in patients with AFib afterDES.Methods: The first phase of the German DES.de registry included 5782 patientswith DES implantation. Follow-up and data processing were performed centrallyin the IHF Ludwigshafen. For this analysis patients with AFib were divided intotwo groups according to their medication at discharge: patients with and withoutoral anticoagulation (OAC).Results: 532 (9%) patients had AFib. Baseline characteristics and cardiovascularevents occuring during the 12-month follow-up are listed in the table.
With OAC (n=137) Without OAC (n=395) p-value
Age 71.2 yrs 71.6% 0.4Prior stroke 8.8% 8.3% 0.8Diabetes 42.3% 42.0% 0.7Clopidogrel 98% 99% 0.4Death 12.0% 11.0% 0.8Stroke 3.5% 2.7% 0.7MACCE 18.4% 16.3% 0.7Stent thrombosis 7.2% 9.1% 0.5Bleeding 5.6% 4.2% 0.4
Conclusions: In clinical practice in Germany only 25% of the patients with AFibare treated with OAC after DES. Overall cardiovascular event rate in patients withAFib is high, without any differences between patients with and without OAC. Theoptimal antithrombotic regimen in these patients still needs to be defined.
P1417 Uninterrupted oral anticoagulation and short termdual antiplatelet therapy duration after coronarystenting to improve long term prognosis of warfarinpatients: a prospective registry
P.F. Lesault1, A. Veugeois1 , A. Amara1, S. Champagne1, B. Gellen1,G. Mouillet1, A. Belarbi1, K. Boughalem1, J.L. Dubois-Rande2, E. Teiger1.1AP-HP - University Hospital Henri Mondor, Interventional Cardiology Unit,Department of Physiology, Creteil, France; 2AP-HP - University Hospital HenriMondor, Department of Cardiology, Creteil, France
Introduction: After coronary angioplasty (PCI),Patients with indication for longterm oral anticoagulation (AC) are exposed to high bleeding risk and worse longterm prognosis compared to overall population admitted in the cathlab unit. Re-cent retrospective studies or registries suggest that uninterrupt AC during PCI,radial access and short time duration of dual antiplatelet therapy in associationwith oral anticoagulation after PCI, can limit outcomes events in this high riskpopulation. The aim of this monocentric prospective registry is to evaluate prog-
nosis after PCI in anticoagulated patients using a systematic strategy with radialaccess, AC during angioplasty and follow up and a minimal duration of dual an-tiplatelet therapy.Methods: All patients with indication for long term AC who underwent PCI forstable angina or non STEMI were registred between July 2007 and January 2010.Radial access, uninterrupt oral anticoagulation with INR value <2.5 the day of PCIand minimal dual antiplatelet therapy duration (i.e. 1 month for Bare Metal Stentand 2 to 6 months for Drug ElutingStent -DES-) were recommended for eachpatient. Clinical events were recorded at 1, 6 months and 1 year after PCI.Results: 100 patients with AC (mean age 73±11years, male gender 81%)underwent PCI during 31 months. Indication for oral anticoagulation was atrial fib-rillation in 69% of cases with CHADS score ≥ 2 in 74% of them. Angioplasty wasperformed with radial access in 82% of cases and 97% had BMS implantationwith final TIMI III in all patients. The mean INR value the day of PCI was 2.13±0.7.Bleeding in the arterial access site occurred in 1 case, after radial access for onepatient with low molecular weight heparin overdose. During follow up (281±60days) AC was sustained for 92% of patients and dual antiplatelet therapy wasprescribed during 113±45days. The rate of Major Adverse Cardiovascular Eventwas 13%, with 3% of stent thrombosis and 4% of cardiac death. Total bleedingoccurred in 14% of cases with 6% major bleeding and no stroke were recorded.Conclusion: Uninterrupt oral anticoagulation, radial access and short term dualantiplatelet therapy after stenting offer a protective strategy for warfarin patientswith a low rate of access site bleeding, a low rate of major bleeding and no strokeduring folllow up. Nevertheless, prognosis remains poor in this high risk popula-tion.
P1418 Optimal versus "over-optimal" duration of dualantiplatelet therapy after coronary stent implantation.Primum non nocere
T.H. Bampali, C.H. Pappas, B. Salma, A. Papathanasiou,P. Korantzopoulos, S. Pappas, J. Goudevenos. University of Ioannina
Medical School, Ioannina, Greece
Purpose: The current recommendations state that the patients with previouslyimplanted coronary stent should be treated with dual antiplatelet therapy (as-pirin 100 mg plus clopidogrel 75mg for one month after Bare-Metal-Stent (BMS)and one year after Drug-Eluting-Stent (DES) implantation, followed by aspirin forlifetime. Our purpose was to evaluate the compliance of patients/doctors in NWGreece with the above.Methods: In this cross-sectional study, we enrolled every patient who proceededfor hospitalization in our department and had undergone coronary stent implan-tation.Results: From November 2007 until January 2010, 526 patients (88% men) wereidentified with history of prior coronary stenting. 60% of them (316 patients) hadbeen treated with BMS, 27.2% (143 patients) with DES and 12.8% with bothtypes. The median time from the angioplasty to the interview was 6.6 years (IQR1-15 years). 420 patients had received long-time dual antiplatelet therapy for amedian time of 3.2 years and only 39 patients had been treated according tothe recommendations. 6 cases of premature discontinuation were reported. Inthe sub-group of the BMS-treated patients only 25 (7.9%) had received dual an-tiplatelet therapy for 1 month, whereas the rest for longer period (median 2.9years). Respectively, in the DES-treated subgroup only 14 patients had receiveddual therapy for 1 year, whereas the majority (90.2%) for a median time of 3.4years. In this category of the "over-complianced" patients 76 bleedings occurred(44 in the BMS subgroup). The severity of the bleedings was major (3), inter-mediate (12), low risk (61), according to the GUSTO stratification). Furthermore,we reported 125 cases of acute coronary syndromes (ACS) (71 in the BMS sub-group). Respectively in the category of the "complianced" patients 6 bleedings (1intermediate, 5 of low risk) and 18 ACSs occurred.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Antithrombotic therapy after percutaneous coronary intervention 221
Conclusions: Despite of the recommendations for the optimum duration of thedual antiplatelet treatment after angioplasty, 79.8% of the patients in our studycontinued to receive them, and this was correlated with a 2-fold increase of thebleeding risk (19.2% vs 9.2%, p <0.02). No significant difference in the occur-rence of the ACSs (31.7% vs 27.6%, p>0.7) was shown. These findings highlightthe need to take under option the possible increase of the side effects of thelong-term prescribed clopidogrel, especially in off-label treatment.
P1419 Hyper-responsiveness to clopidogrel in the real world
A. Moynagh, P. Jariwala, T. Hovasse, T. Lefevre, M.C. Morice,Y. Louvard, T. Unterseeh, H. Benamer, B. Chevalier. InstitutHospitalier Jacques Cartier - ICPS, Massy, France
Purpose: Clopidogrel in association with aspirin have proven effi-cacy in the prevention of stent thrombosis. Low responsiveness is a well knownproblem associated with a higher risk of stent thrombosis. On the opposite, hy-per responsiveness has not been studied carefully. We sought to describe theclopidogrel hyper responsiveness using the VASP test in a population of patientsundergoing percutaneous coronary intervention (PCI).Methods: 630 consecutive patients were prospectively included in a dedicateddatabase after PCI. VASP test was performed in all cases. All patients were pre-treated with a loading dose of 600mg clopidogrel and had a daily maintenancedose of 75mg, or 150mg if their weight was >80kg. Hyper-responsiveness toClopidogrel was defined as a VASP ≤ 10%.Results: Clopidogrel hyper-responsiveness was found in 7.3% of patients. Byunivariate analysis no predictors of hypre responsiveness were found (table).
Variable VASP ≤ 10% VASP > 10% p
Male 31 (67.4%) 445 (76.2%) 0.26Age (yrs) 66.7±11.9 66.8±10.9 0.94Weight 74.4±14.8 78.6±14.7 0.06BMI 26.2±4.3 26.5±6.3 0.76Weight >80kg 21 (45.7%) 258 (44.2%) 0.85Weight <45kg 1 (2.3%) 16 (3.2%) 1Smoking 18 (39.1%) 223 (38.2%) 0.88Dyslipidaemia 28 (60.9%) 361 (61.8%) 0.87Diabetes 11 (23.9%) 151 (25.8%) 0.86Hypertension 26 (56.5%) 367 (62.8%) 0.4Family history 6 (13.0%) 43 (7.4%) 0.28Past PCI 11 (23.9%) 194 (33.2%) 0.16Past CABG 3 (6.5%) 26 (4.5%) 0.59Past MI 8 (17.4%) 66 (11.3%) 0.31
Conclusion: Clopidogrel hyper-responsiveness is observed in less than 10% ofthe population. No predictors were identified. Due to the bleeding risk and theuse of longer durations of treatment, it is important to identify these patients andadapt clopidogrel dose accordingly. The inflmuence on long term outcome will bepresented at the meeting.
P1420 Safety and efficacy of reloading doses of clopidogreland aspirin before elective PCI to optimizeperiprocedural outcome in elderly
A. Ntalianis, C. Trana, O. Muller, F. Mangiacapra, A. Peace,M. Hamilos, T. Cuisset, M. Conte, J. Bartunek, W. Wijns. OLV
Hospital Aalst, Cardiovascular Center, Aalst, Belgium
Purpose: Age relates to prognosis in patients undergoing elective percutaneouscoronary intervention (PCI). Whether age affects residual platelet reactivity (RPR)and periprocedural myocardial infarction (MI) after oral administration of highreloading doses of clopidogrel and aspirin is unknown.Methods: In this open-label multicenter registry, 144 elderly (≥75 years) and 411non-elderly (<75 years) consecutive patients, on maintenance daily doses of 75mg of clopidogrel and 100 mg of aspirin, scheduled for elective PCI were prospec-tively included. All patients received high reloading doses of clopidogrel (600 mg)and aspirin (500 mg) 12-24 hours before PCI. Blood was collected before and 24hours after PCI to determine: a) RPR using the point-of-care assay VerifyKnowand b) Troponin T, as a marker of MI. MI was defined as an increase in troponingreater than 3×99th percentile of the upper reference limit.Results: Elderly patients had higher RPR, as expressed by higher P2Y12 units(236±92 vs 208±87 in non-elderly, p=0.001). There was a trend for higher aspirinreaction units in elderly (459±77 vs 446±65 in non-elderly, p=0.13). By multivari-
Predictors of PRU and ARU
Beta SE p 95% CI
Multivariate analysis: predictors of PRUAge 2.1 0.5 <0.001 1.2–3.1BMI 2.5 1.1 0.02 0.4–4.5DM 25.6 10.4 0.015 5.1–46
Multivariate analysis: predictors of ARUAge 0.9 0.4 0.012 0.2–1.6Previous PCI/CABG/MI -22.2 7.1 0.002 (-36.2)–(-8.2)
BMI: body mass index, DM: diabetes mellitus, PCI: percutaneous coronary intervention, CABG:coronary artery bypass grafting, AMI: acute myocardial infarction, SE: standard error, CI: confi-dence interval.
able analysis, age was an independent predictor of PRU and ARU (table). Agewas not an independent predictor of MI [Odds ratio (OR): 1.02; 95% Confidenceinterval (CI): 0.99-1.06, p=0.2)] nor of myonecrosis [OR: 1.02; 95% CI: 0.99-1.06,p=0.2)]. None of the patients presented TIMI major bleeding.Conclusions: Reloading doses of clopidogrel and aspirin in elderly before elec-tive PCI are safe but do not optimize residual platelet reactivity. Periproceduralmyocardial infarction rates though, are similar with that in younger patients.
P1421 Clopidogrel discontinuation and long-term outcomeafter percutaneous coronary intervention
R.M. Oemrawsingh, R.T. Van Domburg, J. Onuma, J.W.I. Van Nierop,P.P.T. De Jaegere, E. Boersma, P.W.J.C. Serruys. Erasmus MedicalCenter, Thoraxcenter, Department of Cardiology, Rotterdam,
Netherlands
Purpose: Recent data suggest that the duration of clopidogrel treatment may in-fluence clinical outcome after PCI, particularly in the case of drug eluting stent(DES) use. Our objective was to evaluate early and long-term outcome bothduring and after discontinuation of 3 clopidogrel treatment regimes (3 months,6 months and 12 months post-PCI).Methods: The RESEARCH/TSEARCH Registry, a prospective observational co-hort PCI study conducted between January 2000 and December 2005, included6200 consecutive patients. Detailed patient information was collected on an-tiplatelet therapy. Endpoints were all cause mortality and stent thrombosis (ST).Results: Median duration of clopidogrel treatment was 4.7 months (interquartilerange 2.6 to 6.1 months). Mean follow-up after clopidogrel discontinuation was3.9 years (range 0 to 9 years). Clopidogrel discontinuation after 6 months (groupII) was associated with lower mortality (adjusted HR 0.83; 95%CI 0.68-0.98) ascompared to clopidogrel discontinuation after 3 months (group I). Clopidogrel dis-continuation after 12 months (group III) was also related with lower mortality ascompared to group I (HR 0.50; 95%CI 0.24-1.00). Cumulative Kaplan-Meier mor-tality rates at 1-, 3- and 5 years were 4%, 9% and 14% in group I, 3%, 7% and11% in group II, and 1%, 4% and 9% in group III, respectively (logrank p<0.01).ST occurred in 179 patients of whom 123 patients after DES. No association be-tween clopidogrel treatment duration and occurrence or time-distribution of stentthrombosis was found.Conclusion: Extended use of clopidogrel after PCI may be associated with a re-duced risk of mortality. However, large randomized clinical trials are the preferreddesign for proper determination of the appropriate duration of post-PCI clopido-grel administration.
P1422 A comparison of paclitaxel vs. bare metal stentthrombosis in patients with STEMI using clopidogrelwith proton pump inhibitors after postfibrinolysisangioplasty. A GRACIA-3 substudy
P.L. Sanchez Fernandez1 , F. Gimeno2, P. Ancillo3, J.J. Sanz4,J.H. Alonso Briales5, F. Bosa6, I. Santos7, J. Sanchis8, J.A. San Roman2,F. Fernandez Aviles1. 1University General Hospital Gregorio Maranon, Madrid,Spain; 2University Hospital of Vallodolid, ICICOR, Valladolid, Spain; 3HospitalGeneral de Segovia, Segovia, Spain; 4Hospital Río Hortega, Valladolid, Spain;5University Hospital Virgen de la Victoria, Malaga, Spain; 6University Hospitalof Canarias, Tenerife, Spain; 7University Hospital of Salamanca, Salamanca,Spain; 8University Hospital Clinic, Valencia, Spain
Purpose: Recent reports suggest there may be an increase in late stent throm-bosis in paclitaxel eluting-stent (PES) treated patients. Furthermore, there areconcerns about the reduced efficacy of clopidogrel when used concurrently withproton pump inhibitors (PPIs). We studied the potential for one-year increasedrisk of stent thrombosis in the GRACIA-3 study.Method: The GRACIA-3 study (n=436) evaluated in a randomised manner theefficacy of the PES in STEMI patients treated with postfibrinolysis angioplasty.The main analysis showed that compared with bare-metal stents (BMS), PESresulted in reduced late loss but did not reduce in-segment binary restenosis at 1-year angiographic follow-up. At the end of the study 77.4% and 77.0% (P=0.773)in the PES and BMS groups were on aspirin and clopidogrel. Similarly, 74.7%and 78.1% (P=0.619) of patients in the PES and BMS groups were on PPIs.We report here the rates of stent thrombosis in patients with PES vs. BMS. Wefollowed the Academic Research Consortium (ARC) criteria for classifying stent-related thrombosis.Results: Overall stent thrombosis was comparable for PES and BMS at 12months (1.8% [4/217] PES vs. 2.3% [5/216] BMS; P=0.751). The rates of defi-nite and probable stent thrombosis were also similar for both the PES and BMSgroups; 0.9% (2/217) vs 1.4% (3/216), P=0.685 for definite stent thrombosis and0.9% (2/217) vs. 0.9% (2/216), P=1.000 for probable stent thrombosis. No differ-ences were observed in patients with or without clopidogrel and PPIs.Conclusions: PES showed similar one-year-safety profile to BMS in STEMI pa-tients undergoing postfibrinolysis angioplasty with clopidogrel plus PPIs.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

222 Antithrombotic therapy after percutaneous coronary intervention
P1423 Identification of patients at risk for prematurediscontinuation of oral antiplatelet therapy afterelective percutaneous coronary intervention
G. Cayla1, J.P. Collet2, J.C. Macia3, J. Sivain2, L. Schmutz1,B. Ledermann1 , R. Gervasoni3, L. Cornillet3, F. Leclercq3,
P. Messner-Pellenc1. 1CHU Caremeau, Nimes, France; 2AP-HP - Hospital Pitie-Salpetriere, Paris, France; 3University Hospital of Montpellier, Montpellier, France
Background: Premature discontinuation of antiplatelet therapy is a major risk fac-tor of stent thrombosis after drug-eluting stent placement leading to an increasedrisk of death.Objectives: We sought to determine by a simple questionnaire the prevalence ofpatients at risk for premature discontinuation of oral antiplatelet therapy in electivepercutaneous coronary intervention (PCI).Methods: Patients scheduled for elective PCI underwent a routine interview (RI)and a specific questionnaire (SQ) by two independent physicians the day beforethe intervention. The SQ was designed to identify bleeding disorders, suspectedcancer, planned invasive procedures and self evaluation of compliance. The finaldecision of drug eluting stent (DES) implantation was made by a third indepen-dent physician who performed the planned PCI and who had full access to thepatient record.Results: At least one contraindication to DES implantation was found in one thirdof the study population (82/302, 27%) after the RI. All these patients were alsoidentified by the SQ. At total of 31 additional patients were identified by the SQ asnon eligible for DES implantation. Active bleeding (n=14) and scheduled biopsies(n=4) were the two main contraindications to DES implantation isolated by theSQ. Patients characteristics and angiographic findings identified 59.9% patients(n=181/302) eligible for a DES implantation. Finally the physician performing thePCI excluded 66.3% of the patients (n=79/302) who could receive a DES andimplanted a bare metal stent (BMS) instead. This decision was based on thefindings of the dedicated questionnaire on top of the interview in 30 patients (38%)and in 49 patients (62%) for other reasons.Conclusions: In elective PCI, a simple questionnaire used before DES implan-tation can improve identification of patients at high risk for premature discontinu-ation of antiplatelet therapy.
P1424 Impact of the duration of dual antiplatelet therapy oncardiovascular events after drug-eluting stentimplantation. Results of the DES.de registry
U. Zeymer1, R. Zahn2, M. Hochadel1 , S. Silber3, J. Senges1,K. Kuck4, C. Nienaber5. 1Institut für Herzinfarktforschung,
Ludwigshafen Am Rhein, Germany; 2Clinical Center of Ludwigshafen,Ludwigshafen am Rhein, Germany; 3HKL Dr Mueller Klinik, Munich, Germany;4Asklepios Clinic St. Georg, Hamburg, Germany; 5University Hospital Rostock,Department of Cardiology, Rostock, Germany
Background: The optimal duration of dual antiplatelet therapy (DAT) is still amatter of deate. Recent studies have shown an increase in cardiovascular eventswith early determination of clopidogrel. Therefore we sought to investigate theimpact of duration of DAT on outcome in patients after DES.Methods: The first phase of the German DES.de registry included 5782 patientswith DES implantation. Follow-up and data processing were performed centrally inthe IHF Ludwigshafen. Patients were devided into four groups related the durationof dual antiplatelet therapy. 874 Patients (15%) with unknown duration of dualantiplatelet therapy were excluded from the analysis.Results: The majority of patients (55%) were treated for > 6 months with dual an-tiplatelet therapy. The cardiovascular events occuring during the 12-month follow-up are listed in the table.
Table 1. Clinical events
Duration of dual antiplatelets <3 months 3-6 months 6-9 months 9-12 monthsn=697 (12%) n=1013 (18%) n=923 (16%) n=2275 (39%)
Death 6.7% 2.5% 1.3% 0%MACCE 12.3% 4.9% 4.6% 5.9%Stent thrombosis 5.6% 2.1% 1.3% 2.1%Bleeding 3.6% 2.6% 3.0% 2.2%TVR 9.6% 7.4% 8.1% 16. 1%
Conclusions: In clinical practice in Germany more than half of the patients aretreated with DAT for more than 6 months after DES implantation. Longer DATis associated with a decreased rate of MACCE without an increase in bleedingcomplications.
P1425 Background, incidence, and predictors of antiplatelettherapy discontinuation during the first year afterdrug eluting stent implantation (ACDC study)
I. Ferreira Gonzalez1, A. Ribera1, J.R. Marsal1, B. Garcia DelBlanco1, G. Marti1, P. Cascant1, M. Sabate2, V. Matin2, D. Garcia
Dorado1, G. Permanyer Miralda1. 1University Hospital Vall d’Hebron, Barcelona,Spain; 2University of Barcelona, Hospital Clínic, Barcelona, Spain
Purpose: To assess the incidence, background and predictors of antiplatelet ther-
apy discontinuation (ATD) during the first year after drug eluting stent (DES) im-plantation.Methods: Prospective study with 3, 6, 9, and 12 months follow up. All patientsreceiving at least one DES between January and April 2008 in 29 hospitals wererecruited. Main outcome measures: One year rate of ATD, reasons for ATD (i.e.bleeding event or medical invasive procedure, medical decision not associatedwith bleeding event or invasive procedure, patient initiative), and individual-leveland hospital-level predictors of ATD assessed bymultinomial-multilevel regressionanalysis.Results: 234 (14.4%) interrupted at least one AT, predominantly clopidogrel(n=182; 11.8%). In 123 patients (7.6%) the ATD was permanent, and temporal in111 (6.8%) (median 7 days; interquartile range 5-10 days). Bleeding event or in-vasive procedure led to ATD in 109 patients (although a major episode occurred inonly 56), and it was predicted by renal impairment (OR 2.81;95% CI 1.48 – 5.34),prior major haemorrhage (OR 3.77; 95% CI 1.41 – 10.03), and peripheral arte-rial disease (OR 1.78; 95% CI 1.01 – 3.15). Medical decision not associated withbleeding event or invasive procedure led to ATD in 70 patients; it was predictedby long term antiocoagulant therapy (OR 3.88; 95% CI 1.26 – 11.98), undergoingthe procedure in a private hospital (OR 13.3; 95% CI 1.69 – 105), and not re-ceiving instructions about medication (OR 2.8; 95% CI 1.23 – 6.36). 39 patientsinterrupted ATD on their own initiative, mainly immigrants (OR 3.78; 95% CI 1.2 –11.98), and psychotropic drugs consumers (OR 2.58; 1.3 – 5.12).Conclusions: ATD is not exceptional during the first year after DES implantation,and it can occur in different scenarios. In most instances ATD is based on patientdecision or medical decision not associated with major bleeding events or majorsurgical procedures. Predictors of ATD depend on the specific scenario consid-ered, both individual-level andhospital-level variables being important to explainit.
P1426 Percutaneous coronary intervention and diabetesmellitus. An indication for long-term dual antiplatelettreatment?
T.H. Bampali, C.H. Pappas, B. Salma, A. Papathanasiou,N. Papamichael, P. Korantzopoulos, J. Goudevenos. University of
Ioannina Medical School, Ioannina, Greece
Purpose: According to ex-vivo platelet function tests, the morbidity of diabetesmellitus (DM) increases platelet aggregability, due to micro inflammation andendothelial dysfunction, and several data from trials indicate the treatment withclopidogrel. Moreover, in the specific population of the coronary stent implantedpatients the dual antiplatelet (DAP) treatment, (aspirin plus clopidogrel) is cru-cial, although the optimal duration of this therapy, is not well established. Thus,we sought to evaluate the relative value of the long- term DAP treatment in thispopulation.Methods: In this cross-sectional study, we enrolled every patient with prior coro-nary stenting and comorbidity of DM, who proceeded for hospitalization in ourdepartment. The main outcome was the combined (atherothrombotic/bleeding)complication rate.Results: From January 2008 until January 2010, 486 patients were identified withhistory of coronary stenting. 157 of them (32%) had also DM (age 65.35±8.71,men 81%, 53% (83 patients) had been treated with Bare-Metal-Stent, 34% (53)with Drug-Eluting-Stent and 13% (21) with both types). 129 pateints were receiv-ing DAP treatment for a median time of 3.1 years. We divided them into 3 sub-groups regarding to the duration of the DAP treatment (≤ 1 year, >1 - ≤ 5 years,>5 years) and we reported the occurrence of an acute coronary syndrome (ACS)or a bleeding event. In the first subgroup (55 patients, mean time 6.4 months) 18cases of ACS (32.7%) and 6 bleedings (10.1%) were reported. In the second sub-group (46 patients, mean time 2.9 years) we reported 22 ACSs (47.8%) and 11bleedings (23.9%). In the last subgroup (28 patients, mean 7.1 years) 11 patients(39.3%) suffered an ACS and 9 (32.1%) a bleeding event.Conclusions: Despite our initial hypothesis, that in patients with prior implantedcoronary stent and DM, the adherence to long-term DAP treatment would be po-tentially effective, more than 12 months treatment was associated with a 2.7-foldincrease of the bleeding risk (10.1% vs. 27%, p<0.01) and a 1.3-fold increase inthe occurrence of the ACSs (32.7% vs. 44.6%, p<0.05). These data indicate thatthe effectiveness of the clopidogrel may be diminished in this specific category ofpatients.
P1427 Stent thrombosis: incidence, predictors andoutcomes in a population of the real world
F. Moscoso Costa, L. Raposo, R. Teles, P. Sousa, R. Cale, M. Alves,M. Almeida, A. Silva. Hospital West Lisbon, Hospital Santa Cruz,Department of Cardiology, Lisbon, Portugal
Background: Stent thrombosis (ST) is an adverse event of percutaneous coro-nary intervention (PCI) associated with adverse clinical outcomes.Objective: Evaluate incidence, timing, predictors and implications on long termmortality of ST in a real world population with coronary artery disease submittedto PCI.Methods: We studied a population of 5661 patients (pts) submitted to PCI be-tween January 2003 and June 2008; 294 (5,2%) were excluded because of un-available follow up (FUP). Average age was 64 (±11) years, 7% males, 28%
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Antithrombotic therapy after percutaneous coronary intervention 223
diabetic and 85% had an ejection fraction (EF)>50%. In 41% an acute coronarysyndrome (ACS) was the indication for PCI and with ≥1 DES was implanted in69,4%. ST was identified using the Academic Research Consortium definition(ARC). We determined the absolute incidence of ST according to the year of PCIand used a Cox regression model to establish the predictors of ST (total anddefinitive) and their impact on total mortality (M).Results: Median FUP was 17 months (IQR: 14;35), we identified 189 cases of ST(absolute incidence 3,6%): 108 (57,1%) definite ST, 6 probable ST and 75 possi-ble ST. The proportion of definite ST was higher in early cases [<30days] (86% vs50,3%; p=0,0002). The absolute incidence of ST increased between 2003-2006and decreased beyond that period, especially due to definite ST (p=0,001 for thetendency). Total mortality was lower in patients treated with ≥1 DES (6,1% vs11,1%) and no association was noted between DES use and the occurrence oflate/very late ST (1,5% vs 1,6%). Clinical predictors of definite ST were PCI inthe setting of an ACS (HR 2,3 CI 95% 1,4-3,6), EF<50% (HR 2,2 CI95% 1,4-3,6)and the presence of peripheral vascular disease (HR 2,1 CI 95% 1,2-3,7). Thediameter of the smallest implanted stent was the main angiographical predictor ofST and was inversely related to the cumulative risk of ST (HR 0,99 CI95% 0,98-0,99; p<0,012 for each step-up from 2,25 to 5,0 mm stents). Total mortality inpatients with ST was 48,1% (3,3% in first 30 days after ST) and the median timeuntil death was 447 days. ST (any) was a powerful predictor of death (adjustedHR 4,72 CI95% 3,5-6,2; p<0,0001); however definite ST did not have the sameimpact on survival (adjusted HR 0,9 CI95% 0,5-1,6; p=NS). The risk profile ofpatients with probable/possible ST was significantly worst than those with definiteST.Conclusion: ST appears to be decreasing in this population and we could notdemonstrate any correlation between its cumulative risk and the use of DES. Thewide definition of ARC may overestimate the real clinical impact of ST.
P1428 Differences in coronary intravascular ultrasoundfindings in early, late, and very late stent thrombosisafter sirolimus-eluting stent implantation
M. Kimura, S. Ebisawa, Y. Ko, T. Kurita, T. Ito, M. Habara, N. Tanaka,K. Nasu, Y. Kinoshita, T. Suzuki. Toyohashi Heart Center, Toyohashi,
Japan
Background: Stent thrombosis (ST) after sirolimus-eluting stent (SES) implan-tation is a fatal complication. However, the pathophysiology has not been fullyevaluated. The aim of this study was to evaluate acute and long-term intravascu-lar ultrasound (IVUS) findings in pts with ST.Method: Of 3,902 pts (4,171 lesions) treated with SES between May 2004 andApril 2009, serial quantitative IVUS analysis was performed at the minimum lu-men site before and after SES implantation and after ST in 25 pts (0.64%) withARC definite ST.Results: Early ST (n=12), late ST (n=7) and very late ST (n=6) occurred me-dian 10 (IQR 2.5-14), 85 (IQR 35-260), and 675 (IQR 461-1020) days after SESimplantation, respectively. There was no significant difference in baseline demo-graphic features or baseline IVUS findings among the 3 groups. When post-SES implantation cross-sectional area (CSA; mm2) was compared among the3 groups, pts with very late ST had a higher rate of change in vessel CSA com-pared with those with early and late ST (P=0.0071), although the rates of changein lumen and stent CSA among the 3 groups were similar. (Figure) Of 6 pts withvery late ST, late acquired incomplete stent apposition (ISA) was observed in 4pts, and 3 of these 4 pts discontinued dual antiplatelet therapy in the month priorto experiencing ST.Conclusions: After SES implantation, late ISA caused by positive remodeling iscommon in pts with very late ST. If late ISA is observed at follow-up angiography,continuation of dual antiplatelet therapy may be warranted.
P1429 Effect of common cyclooxygenase-2 genepolymorphisms on the long-term outcome aftersuccessful single-vessel percutaneous coronaryintervention: a pilot study
P. Rostoff1, W. Szczeklik2, J. Nessler1, M. Sanak2, W. Piwowarska1,A. Szczeklik2. 1Jagiellonian University Medical College, Institute of Cardiology,Dept. of Coronary Disease, Krakow, Poland; 2Jagiellonian University MedicalCollege, Department of Medicine, Krakow, Poland
There is evidence that G-765C polymorphism (rs20417) of cyclooxygenase-2(COX-2) gene can affect the risk of myocardial infarction and stroke. Little isknown about the role of COX-2 T8473C (rs5275) polymorphism in atherogen-esis and plaque instability. No study has been performed so far to determine theeffect of common COX-2 polymorphisms on the long-term outcome after PCI.The aim of this study was to evaluate the influence of two common COX-2gene polymorphisms on the risk of death, cardiac death, myocardial infarction(MI), stroke, restenosis, and need for hospitalization after single-vessel PCI at 36months of follow-up.Methods: 119 consecutive Caucasians (92 M, aged 39-86 yrs, mean age62.4±10.7 yrs), were enrolled based on the following inclusion criteria: (a) sta-ble CAD (67 pts) or acute NSTEMI (52 pts) treated with single-vessel PCI; (b) nocontraindications to aspirin or clopidogrel. All patients received standard medicaltherapy.
Results: In the stable CAD group, the prevalence of MI was significantly higherin homozygotes -765C-765C, as compared to –765G-765G (100.0% vs 4.4%;p=0.002). No significant differences were found in the occurrence of death, car-diac death, stroke, restenosis, and need for hospitalization among genotypesof G-765C and T8473C polymorphisms in stable CAD. No significant associa-tion was apparent between the COX-2 polymorphisms and study end-points inNSTEMI pts.
Conclusions: 1. The COX-2 G-765C polymorphism is associated with an in-creased risk for myocardial infarction after single-vessel PCI in stable CAD pts inlong-term follow-up. 2. There is no significant association of G-765C and T8473Cpolymorphisms with all-cause mortality, cardiac mortality, risk of stroke, resteno-sis and need for hospitalization after PCI both in pts with stable CAD and NSTEMI.
P1430 The effect of long-term dual antiplatelet treatment onclinical outcome of diabetic patients treated withsirolimus-eluting stents
P. Karyofillis, C. Doulaptsis, S. Thomopoulou, D. Cokkinos,V. Voudris. Onassis Cardiac Surgery Center, Athens, Greece
Purpose: Despite encouraging short-term results with drug-eluting stents in di-abetes mellitus (DM) patients (pts) with coronary artery disease, the long-termsafety is unknown, because of late-onset stent thrombosis (LST). We investi-gated the influence of long-term dual antiplatelet treatment (APLT) with aspirinand clopidogrel on clinical outcome in DM pts treated with sirolimus-eluting stent(SES).Methods: We assessed 267 consecutive DM pts (male 83%, mean age 64±9years, range 37-86) that had been treated with SES and received dual APLTtreatment for 12 months. Long-term (5 years) clinical follow-up (FU), obtainedin 264/267 (99%) of them; 119 (45%) pts were on single APLT (SAPLT) and145 (55%) on dual APLT (DAPLT). Adverse events on clinical FU was consid-ered death (D), myocardial infarction (MI), cerebrovascular accident (CVA), andhard end-points (HEDP) was considered D, MI and CVA. LST was defined as an-giographic documentation of stent occlusion associated with an acute ischemicevent, unexplained sudden D or MI not clearly attributable to another coronarylesion > 12 months post-procedure.Results: There was no difference in gender, age, risk factors profile, history MI,previous CABG, unstable angina on presentation, extent and location of coronaryartery disease, and systolic left ventricular function, between two pts groups. Thetotal stent length was 25.7±14.1 mm in SAPLT vs. 26.4±14.5 mm in DAPLT andcomplete revascularization was obtained in 41% and 53% (p=0.07), respectively.Clinical FU at 5 years showed total mortality 8.4% vs. 11.7%, cardiac D 3.4% vs.7.6%, MI 2.5% vs. 2.8%, CVA 2.5% vs. 3.4%, and HEDP 9.2% vs. 15.9% betweenpts in SAPLT and DAPLT, respectively (p:ns). The incidence of LST was 1.7%in SAPLT (mean time 34±28 months) and 6.9% in DAPLT (mean time 33±20months), (p=0.07). In a multivariate model predictors for LST was ejection frac-tion (HR 0.08, 95% CI 0.02-0.30, p<0.001), acute coronary syndrome (HR 0.22,95% CI 0.06-0.85, p=0.03), and DAPLT (HR 0.17, 95% CI 0.03-0.87, p=0.03); forcardiac D/MI was ejection fraction (HR 0.22, 95% CI 0.08-0.57, p<0.002), andage (HR 1.06, 95% CI 1.01-1.13, p=0.04). Non-cardiac operation required 22%of pts in SAPLT and 15% in DAPLT (p:ns); 85% in both groups discontinued APLTbefore operation and there was one LST (in DAPLT group).Conclusion: Long-term DAPLT (5 years) in DM pts treated with SES implantationis not associated with better clinical outcome or lower risk of LST.
P1431 Intracoronary or intravenous abciximabadministration in patients with ST-segment elevationmyocardial infarction undergoing percutaneouscoronary intervention? An hypothesis generatingmeta-analysis
F. Piscione, R. Piccolo, S. Cassese, G. Galasso, R. De Rosa,T. Niglio, M. Chiariello. University of Naples Federico II, Dpt of Clinical Medicine,Cardiovascular & Immunological Science, Naples, Italy
Purpose: Although abciximab remains a mainstay in the treatment of acute St-segment elevation myocardial infarction (STEMI), recently intracoronary admin-istration has been proposed as an alternative strategy to standard intravenousbolus. Therefore, we performed a meta-analysis of randomized trials to assess
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

224 Antithrombotic therapy after percutaneous coronary intervention
angiographic and electrocardiographic outcomes associated with intracoronaryabciximab bolus application as compared with intravenous bolus.Methods: We undertook a literature search using Medline, EMBASE, theCochrane Central Register of Controlled Trials, scientific session abstracts andrelevant websites, until January 2010. The following searching words were used:randomized, myocardial infarction, intracoronary, intravenous, abciximab, Reo-Pro, primary angioplasty, reperfusion. Main outcomes were: ST-segment reso-lution, myocardial blush grade 2/3, post-procedural Thrombolysis in MyocardialInfarction (TIMI) flow grade 3.Results: Three trials were included, involving 249 STEMI patients (124 random-ized to intracoronary abciximab and 125 to intravenous abciximab). Intracoronarybolus administration significantly improved ST-segment resolution (79.5 versus67.2% respectively, p=0.03) and myocardial blush grade 2/3 (92.9 versus 77.0%respectively, p=0.003). In addition, no difference was found in terms of post-procedural TIMI flow grade 3 between groups (87.9 versus 82.4% respectively,p=0.26).Conclusions: In STEMI patients treated with percutaneous coronary interven-tion, intracoronary bolus administration of abciximab is associated with a sig-nificant improvement in angiographic and electrocardiographic outcome. Largerrandomized trials are warranted to evaluate whether these findings translate intoimproved clinical outcome.
P1432 Prevalence and clinical profile of aspirin resistance inpatients undergoing percutaneous coronaryintervention
P.V. Jariwala1, T. Lefevre2, T. Hovasse1, M.C. Morice1, Y. Louvard1,T. Unterseeh3, H. Benamer1 , B. Chevalier1, O. Tavolaro3 , P. Garot3.
1Institut Hospitalier Jacques Cartier - ICPS, Massy, France; 2ICPS - InstituteHospital Jacques Cartier, Massy, France; 3Hôpital Privé Claude Galien, ICPS,Quincy, France
Introduction: Aspirin resistance remains a controversial issue. Beside Thienopy-ridine resistance, it may play an important role in stent thrombosis after coronarystenting. Platelet Function Analysis (PFA-100) is now available for the assess-ment of platelet function in the cathlab and may be an important tool to decreasethe risk of stent thrombosis.Methods: Platelet function was studied in 2270 consecutive patients (Femalegender 30.4%, age 66.4±11.2 years, acute coronary syndrome 26.4%, diabetes28.2%, BMI 27.8±4.5) undergoing percutaneous coronary interventions (PCI)in our institution. Only patients with acute myocardial infarction were excluded.All patients were taking aspirin before PCI (160 mg/day). Using PFA-100 (DadeBehring), the epinephrine closure time was studied during PCI. Aspirin resistancewas defined as an epinephrine closure time < 170 s. In case of aspirin resistancethe dose of 160 mg of aspirin was given BID. Predictors of aspirin resistance werestudied by univariate analysis using Fisher’s exact test.Results: Aspirin resistance was found in 23% of cases. The average value of PFAin patients with aspirin resistance was 117.83±30.54s. By univariate analysis,Male gender (P=0.003), weight > 85 kg (P=0.005), smoking habit (P=0.004), dia-betes (P=0.001), family history of coronary artery disease (P=0.044), past historyof myocardial infarction (P=0.0001) and past history of CABG (P=0.024) were as-sociated with increased resistance. While hypertension (P=0.80), dyslipidaemia(P=0.21) and past history of PCI (P=0.08) were not associated with aspirin resis-tance.Conclusions: Aspirin resistance as assessed by PFA-100 is frequent. Althoughthe potential mechanisms of aspirin resistance still remain uncertain, we foundthat platelet responsiveness to aspirin is reduced in patients with diabetes, pasthistory of myocardial infarction, smoking habits, male gender and overweight(weight >85kg). The impact of these results on long term outcome will be pre-sented at the meeting.
P1433 Recurrence and prognosis of first generation drugeluting stent thrombosis after successful treatment
J.-Y. Moon1, J.-H. Sung1, I.-J. Kim1, S.-W. Lim1, D.-H. Cha1,M.-H. Jeong2. 1CHA Bundang Medical Center, CHA University,Sungnam, Korea, Republic of; 2Chonnam National University
Hospital, The Heart Center, Gwangju, Korea, Republic of
Background: The purpose of the present analysis was to determine the recur-rence rate and the long term clinical outcomes of patients who survived from DESthrombosis.Methods: The 2,663 consecutive patients who performed successful implanta-tion of the first generation DES (TAXUS and/or Cypher® stent) between May.2003 and Dec. 2007 were investigated. From this registry, 31 patients (incidence:1.16%) were treated with definite ST. The long-term clinical outcomes were retro-spectively investigated for all of the 31 patients.Results: In-hospital mortality of definite stent thrombosis (ST) was 9.7%. Duringthe median follow up duration of 34.9 months, Cardiac death was occurred in4 patients (14.3%) and recurrent ST was in 4 patients (14.3%). Target lesionrevascularization (including the emergent PCI for recurrent ST) was needed in7 patients (25%). Totally, MACE was occurred in 9 of 28 patients (32.1%). Thestenting in proximal left anterior descending artery (hazard ratio 3.89, 95% CI1.022 to 14.784, p=0.046) was the only significant risk factor for predicting the
primary endpoint. Even though successful revascularization was undergone, in-hospital mortality in patients with ST remains high (9.7%).Conclusions: The recurrence rate of ST was 14.3% and showed higher mortalityrates. In real world clinical practice, ST continues to be a serious complication ofcontemporary DES use and even though successful revascularization of occludedstent, the long-term outcomes including recurrent ST were not good.
P1434 The dynamics of blood lymphocyte subpopulationsafter coronary stenting with rapamycin eluting stents
E. Pylaeva1, A. Potekhina2, V. Sokolov2, S. Provatorov2,V.P. Masenko2, N. Kukhtina2, T.L. Krasnikova2, E. Noeva2,T. Arefieva2. 1State University, Moscow, Russian Federation;
2Russian Cardiology Research and Production Center, Moscow, RussianFederation
Purpose: Coronary stenting with rapamycin-eluting stents (RES) is effective forCAD treatment as it was shown to reduce significantly the rate of restenosis.Recent data have proved the immumodulating properties of rapamycin in vitrohowever the systemic effects of RES implantation were not investigated. The aimof this study was to evaluate the parameters of cell immunity in patients afterintracoronary RES implantation.Methods: We assigned 62 patients underwent coronary angiography (CA), 42patients with stable angina and angiographically proved coronary stenosis weretreated with RES. Blood samples were obtained before, 24, 48 hours, 7 days,1, 3 months and 6 after angiography/stenting. The main lymphocyte subpop-ulations (T-, B-, NK-) were assayed with Simultest IMK-Lymphocyte Kit, acti-vated and regulatory T-cells were identified as CD4+CD25lowCD127high andCD4+CD25highCD127low, respectively. Blood concentration of sCD25 (solublealpha-subunit of IL2 receptor) was studied in both groups at all time points bychemiluminiscent method.Results: No changes in whole leucocytes, relative levels of lymphocytes, mainsubpopulations of CD3+ lymphocytes and activated CD4+CD25+lowCD127highT-cells, were observed at all time points. Tregs were significantly increased inpatients who received RES one month after PCI (7.52±1.58% of CD3+CD4+lymphocytes) vs initial levels (5.89±1.59%, p< 0.001). sCD25 concentration wasalso increased 1 month after RES implantation (554.6±36.7 vs. 625.6±39.5 U/ml,p<0.001) but not after CA (529,2±31,5 vs. 530,5±40,0 U/ml). Treg level did notchange in patients after CA (5.92±1.90 vs. 5.78±1.80). The level of B-cells wasreduced in 7 days and a month after PCI with RES implantation (0.21±0.12vs. 0.14±0.10 and 0.13±0.07 x103/μl, p<0.05) but not after CA (0.26±0.12 vs.0.24±0.09 and 0.24±0.08).Conclusion: The data reveals that regulatory T-cells and sCD25 rise markedlyone month after RES implantation. At the same time the level of circulating B-cellswas reduced. We speculate that even small doses of rapamycin have a systemicimmunomodulating effect, more research is needed to find out if these changesaffect the prognosis after coronary stenting with RES. Tregs play an important rolein regulating immune response. Rapamycin in vitro inhibits T-effectors’ prolifera-tion while selectively increasing the number of Tregs.Tregs localise in atheroscle-rotic plaques and are thought to impair vessel wall remodeling. We speculate thatthe inhibitory effect of rapamycin on neointima growth is depended in part on itsinfluence on Tregs expansion.
P1435 Intracoronary electrocardiogram ST segment shiftduring fractional flow reserve measurement: a PCIcost saving strategy
V. Balian1, C. Marcassa2, G. Cecchin1, R. Michi1, M. Crenna1,E. Petrucci1, M. Onofri1. 1Circolo Hospital of Busto Arsizio, Busto
Arsizio, Italy; 2Salvatore Maugeri Foundation, IRCCS, Division of CardiologyRehabilitation, Veruno, Italy
Purpose: Fractional Flow Reserve (FFR) is an index of the physiological sig-nificance of a coronary stenosis. Unipolar intracoronary (IC) electrocardiogram(ECG) recording from angioplasty guidewire is more sensitive than standard ECGin detecting regional myocardial ischemia. To assess if IC ST recording duringmaximal pharmacologic vasodilation could be used as an indirect estimation ofFFR results.Methods: We recorded IC ECGs in 55 clinically stable patients undergoing FFRevaluation of an intermediate coronary stenosis during intravenous adenosineinfusion and correlated the IC ECG findings with FFR results. During adenosineinfusion, IC ST shift (elevation or depression) was considered significant if ≥ 1mm compared to the corresponding baseline value.Results: During adenosine infusion, a significant IC ST segment shift was docu-mented in 28 patients (51%; ST segment elevation in 21 patients and ST depres-sion in 7 other patients). FFR values were ≤ 0.80 in 33 patients (60%) and > 0.80in 22 (40%); IC ST segment shift was documented in 25 out of 33 patients withFFR ≤ 0.80 (60%) and in 3 out of 22 patients with FFR > 0.80 (p<0.0001).Sensitivity of IC ST segment shift during adenosine infusion for predicting a patho-logical FFR value was 76%, specificity 86%, the positive and negative predic-tive accuracies were 89% and 70%, respectively; the overall accuracy was 80%.Owing to these data, it can be suggested that in presence of IC ECG shift dur-ing adenosine infusion, an additional FFR evaluation with pressurewire could beunecessary (predictive positive accuracy 89% of IC data), and PCI can be per-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Antithrombotic therapy after percutaneous coronary intervention / Has the recession made US more cost-effective? 225
formed. In presence of a negative IC ECG result, patients should be evaluatedwith FFR and PCI performed in the presence of a FFR ≤ 0.80.Conclusions: Intracoronary ST segment shift evaluation during adenosine infu-sion may result in a significant cost saving strategy, able in reducing pressurewireutilization.
HAS THE RECESSION MADE US MORECOST-EFFECTIVE?
P1436 The cost-effectiveness of rosuvastatin 20 mg for theprevention of cardiovascular morbidity and mortality -a swedish economic evaluation of the JUPITER trial
R.L. Ohsfeldt1, A.G. Olsson2, M.M. Jensen3, S.K. Gandhi4,T. Paulsson5. 1Department of Health Policy and Management,
College Station, United States of America; 2Faculty of Health Sciences,Linköping University, Linköping, Sweden; 3AstraZeneca, Lund, Sweden;4AstraZeneca, Wilmington, United States of America; 5AstraZeneca, Södertälje,Sweden
Objectives: This study estimates long-term outcomes, health-care costs, andcost-effectiveness of rosuvastatin 20 mg therapy (versus placebo) in the primaryprevention of major cardiovascular disease (CVD).Methods: Based on data from the JUPITER (Justification for the Use of statinsin Primary prevention: an Intervention Trial Evaluating Rosuvastatin) trial long-term CVD event outcomes with rosuvastatin versus no active treatment were es-timated. Using a decision-analytic model, CVD event rates were combined withepidemiological and unit cost data specific for the Swedish setting. Initial andsubsequent CVD events and death were estimated over 10 years, 20 years, andlifetime of patients. CVD event rates observed in the JUPITER trial were appliedin the rosuvastatin and placebo groups, respectively. The observed relative riskreduction of rosuvastatin versus placebo was extrapolated beyond trial duration.Following an initial CVD event, probabilities of subsequent CVD events and deathwere estimated based upon the assumption that patients initially treated with ro-suvastatin 20 mg continued on the same therapy, while placebo patients wereinitiated on available statins as observed in clinical practice. Incremental effec-tiveness was measured as life-years gained (LYG) or quality-adjusted life-years(QALYs) gained. The incremental cost-effectiveness ratio was computed by divid-ing the incremental costs with the incremental QALYs for the rosuvastatin treat-ment arm. Long term costs and effects were also estimated for a subpopulation ofthe JUPITER trial with an elevated baseline risk (Framingham risk score ≥ 10%).Results: Treating 100,000 patients with rosuvastatin 20 mg avoided an estimated11,038 events over the lifetime (5,812 non-fatal MIs, 2,297 non-fatal strokes, and3,765 CVD deaths). This translated into an estimated gain of 28,029 years infull health (QALYs) and 28,972 total life years (LYG) versus placebo. Over 20-year and 10-year timeframes, corresponding QALY gains were 19,907 and 7,227,respectively. Estimated incremental cost-effectiveness ratio (cost per QALY) wasSEK 12,712 (lifetime), SEK 29,587 (20-year horizon), and SEK 192,892 (10-yearhorizon). In patients with an elevated baseline risk, the incremental cost per QALYgained was SEK 1,051 for the lifetime and SEK 134,930 for the 10-year horizon,respectively.Conclusions: Results indicate that rosuvastatin 20 mg treatment is a cost-effective treatment option in patients comparable to the JUPITER trial popula-tion in Sweden. The cost-effectiveness of rosuvastatin is further improved in thesub-population with higher baseline CVD event risk.
P1437 Cost-effectiveness of ferric carboxymaltose inpatients with chronic heart failure: an analysis fromthe FAIR-HF trial
P.R. Blank1, M. Schwenkglenks2, T.D. Szucs2. 1University of Zurich,Institute of Social and Preventive Medicine, Zurich, Switzerland;
2European Center of Pharmaceutical Medicine (ECPM), Basel, Switzerland
Purpose: Chronic heart failure (CHF) is a common and severe medical condi-tion frequently associated with anaemia and iron deficiency. Several studies haveshown clinical and quality of life benefits of anaemia treatment in CHF patients.CHF symptoms, functional capacity and quality of life can be enhanced by replet-ing iron stores and improving iron bioavailability. Ferric carboxymaltose (FCM) isa dextran-free, intravenous (i.v.) iron preparation that allows the administration ofa single dose of up to 1000 mg iron in 15 minutes. This study evaluated the costeffectiveness of iron repletion using i.v. FCM in CHF patients with and withoutanaemia, from a third party payer perspective in Switzerland.Methods: Using data from a randomized, double-blind, controlled clinical study(FAIR-HF, n=459), per-patient costs and clinical effectiveness of i.v. FCM were es-timated. Economic assessment was based on published Swiss costs associatedwith New York Heart Association (NYHA) functional classes. Effectiveness wasassessed as the number of quality-adjusted life years (QALYs) gained, derivedfrom the European Quality of life-5 Dimensions (EQ-5D) Visual Analogue Scalescores. The incremental cost-effectiveness ratio (ICER) of i.v. FCM was deter-mined compared to placebo. The time horizon of this within-trial analysis was 24weeks.Results: In the FAIR-HF trial, NYHA functional classes were significantly im-
proved in the FCM group compared with placebo (p<0.001). Estimated per-patient costs during 24 weeks (excluding i.v. iron) were �2,461 and �2,541 fori.v. FCM and placebo, respectively. Based on the reimbursed price for FCM inSwitzerland (�22.5 per 100 mg iron) and the mean iron dosage of the clinicalstudy (1850 mg iron) plus administration costs, a net investment of �389 (opti-mized dosing regimen per SmPC) to �480 (per FAIR-HF regimen) per patientwould be required. FCM resulted in improved quality of life (increased EQ-5Dscores), translating into a gain of 0.0254 QALYs over the 24 week study period.Depending on the FCM dosing regimen, the ICER of i.v. FCM ranged between�15,331 and �18,917 per QALY gained for the SmPC and the FAIR-HF dosingregimen, respectively, compared to the placebo group.Conclusion: From the Swiss payers’ perspective, managing iron deficiency withand without anaemia in CHF patients using i.v. FCM can be considered cost-effective. Improved symptoms and better quality of life contribute to the economicbenefits seen with FCM.
P1438 Cost effectiveness of Implantable CardioverterDefibrillator (ICD) therapy in clinical practice
J. Groarke, N. Orfali, P. Nolan, A. Heerey, S. Kasim, J. Crowley,K. Daly, P. Nash. University College Hospital Galway, Galway, Ireland
Purpose: Widening evidence based indications for ICD implantationhave cost implications. Published cost analyses are dated, industry driven andclinical trial based. Cost effectiveness of ICDs in the real world and by patientsubgroup requires review.Methods: A cost analysis of 67 ICD patients was performed in an Irish universityteaching hospital. Comparisons were drawn with cost effectiveness data frompivotal ICD clinical trials.Results: The male:female ratio among the 67 patients was 7.4:1. The medianage of patients was 60 years [SD=12 years; range: 21-78 years]. The medianfollow-up was 1.6 years [range: 0.4 to 2.7 years]. The median implantation time inthe catherterisation laboratory was 90 minutes. The median length of stay (LOS)at time of implantation was 2 days [SD=1.9 days; range: 1-12 days]. 6 patients(9%) had an ICD-related readmission.17 episodes were terminated in 7 patients by shock delivery and 9 episodes in4 patients by anti-tachy pacing (ATP). 1 patient received both therapies. Thus,it is assumed that 10 lives were saved [18 Quality Adjusted Life Years (QALYs)gained] during the follow up period.Total device costs, staff and bed costs at implantation (+5% for any additionalcosts) were �1,164,674. Thus, the cost of ICD implantation per patient was�17,383. When the costs of 329 device checks, 8 ICD-related readmissions and5 repeat procedures for these patients over the follow up period were added, thetotal cost was � 1,190,083.For this cohort, it cost �119,008/life saved; � 45,772/appropriate device therapy;and �66,115/QALY over the median follow-up period of 1.6 years.The cost per life saved at 1 year for those with ischaemic LV dysfunction (pa-tients similar to patients in the MADIT and MUSTT trials) was �126,029 and�209,437 for those with non-ischaemic left ventricular (LV) dysfunction. The costper QALY gained for patients resembling MADIT and MUSTT populations was�49,701 while the cost per QALY for patients resembling SCD-HeFT populations(patients with ischaemic and non-ischaemic LV dysfunction) was �57,200.Conclusions: Relative to the cost of dialysis (�39,000–� 78,000/QALY), ICDtherapy in the above various subgroups is cost effective. Cost effectiveness variesby subgroup. The cost/QALY in the MADIT/MUSTT-like patients and SCD-HeFT-like patients was 2.5 times and 2 times higher respectively than costs quoted intrials. Higher costs are likely due to inflation, sample size, independence fromindustry and a shorter median follow-up (19 versus 39-45 months).ICD costliness mandates delivery to populations for whom they confer provenbenefits.
P1439 Cost-effectiveness of an early invasive versusconservative strategy in ST-elevation myocardialinfarction treated with thrombolysis
E. Bohmer1, I.S. Kristiansen2, H. Arnesen3, S. Halvorsen4.1Department of Medicine, Innlandet Hospital Trust, Lillehammer,
Norway; 2University of Oslo, Institute of Health Management and HealthEconomics, Oslo, Norway; 3Center for Clinical Heart Research, Department ofCardiology, Ulleval University Hospital, Oslo, Norway; 4Department of Cardiology,Oslo University Hospital, Ulleval, Oslo, Norway
Purpose: The health benefits and optimal timing of invasive treatment afterthrombolysis is not established. In the NORwegian study on DIstrict treatment ofST-Elevation Myocardial Infarction (NORDISTEMI), a strategy with early transferfor percutaneous coronary intervention (PCI) after thrombolysis was comparedto a conservative, ischemia-guided strategy in patients living in areas with longtransfer distances to an invasive centre. The clinical outcomes of the study havebeen published recently, showing a reduction in the composite of death, reinfarc-tion and stroke with the early invasive strategy. The aim of this substudy wasto explore the health-related quality of life (HRQoL) and cost consequences ofreplacing conservative treatment with early angioplasty.Methods: Patients with STEMI of < 6 h duration and >90 min transfer delays toPCI were treated with thromolysis and randomised to either early invasive (n=134)
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

226 Has the recession made US more cost-effective?
or conservative (n= 132) strategy. The HRQoL (Sintonen 15D) and use of healthresources were assessed at baseline, 1, 3, 7 and 12 months follow-up. Data onin-patient care, out-patient care, transportations, pharmaceuticals and work ab-senteeism were collected. The costs of in-patient care were based on a detailedhospital accounting system. Other costs were based on fee schedules and mar-ket prices. Costs were analysed in a societal perspective and on the basis ofintention-to-treat analysis. Bootstrapping with 1000 replications was used to testfor differences.Results: In total, 266 patients were randomised. Complete data on costs andHRQoL was available in 259 patients. The unadjusted mean differences in thenumber of quality adjusted life years (QALYs) as well as total costs after 12months are shown in the table. When adjusting for the difference in baselineHRQoL, the mean difference in QALYs was reduced to 0.008 (95%CI= -0.027,0.043).
Early invasive Conservative Mean difference (95% CI)
Quality of life,baseline values 0.913 0.902 0.011 (-0,011,0.033)QALYS 0.885 0.870 0.016 (-0.023,0.055)Total costs (� ) 19047 17861 1185 (-1683,4167)
Conclusion: There was no significant difference in health related quality of life orcosts between early invasive and conservative strategy in STEMI patients treatedwith thrombolysis.
P1440 The health and economic impact of switching fromatorvastatin to generic simvastatin in the Netherlands
D. Liew1, W.J. Meerding2, S. Ong3, K. Webb3 . 1The Universityof Melbourne, Department of Medicine, St Vincent’s Hospital,Melbourne, Australia; 2Pfizer bv, Capelle a/d IJssel, Netherlands;
3Pfizer Ltd, Surrey, United Kingdom
Purpose: Since January 2009, Dutch clinicians have been required to justify theprescription of branded statins using an authorization form. This has led to signifi-cant switching of patients from atorvastatin to generic simvastatin. However, datafrom the first three months of 2009 indicated that 34% of this switching occurredat less than equipotent doses. We sought to assess the potential impact of this.Methods: A Markov micro-simulation model was populated with 1046 Dutchpatients drawn from the PHARMO Institute database who were free of cardio-vascular disease (CVD) and being prescribed atorvastatin in December 2008.Risks of initial CVD were estimated from a calibrated Framingham risk equation.Follow-up occurred for 20 years or until age 100. Decision analysis estimated themarginal effects of switching all patients to generic simvastatin. Dose-specific,lipid-modifying effects of the two statins and CVD costs were sourced from pub-lished data. Annual discount rates of 4% and 1.5% were applied to costs andhealth effects, respectively, as per Dutch recommendations.Results: Of the 1046 subjects on atorvastatin, 207 (19.8%) were predicted todevelop CVD over 20 years. In the switched-to-simvastatin group, the predictednumber was 229 (21.9%), equating to a ‘number needed to harm’ of 48. Althoughswitching led to a net cost saving of �549 (discounted) per subject, each alsolost 0.015 life-years (discounted) and 0.029 QALYs (discounted). These equatedto ICERs of �36,653 and �18,716 per life-year and QALY gained, respec-tively (atorvastatin vs simvastatin). Sensitivity analyses, which included a 20%decrease in the percentage of switches to less potent simvastatin doses, indi-cated the results to be robust. Furthermore, the analysis is likely to have under-estimated the true effects of non-equivalent switching as it was limited to theprimary prevention of CVD, where absolute risks are lower than in the secondarypreventive setting.Conclusions: In the Netherlands, patients are being switched from atorvastatinto generic simvastatin at non-equipotent doses, which may increase CVD risk.Maintaining patients on atorvastatin is sound from a health economic perspective.[Disclaimer: the views expressed in this abstract are only those of the authors,and not necessarily those of the PHARMO Institute.]
P1441 Longterm cost-effectiveness analysis of atelemedicine programme for patients with chronicheart failure
H. Janssen. Institute of Health Economy, Bremen, Germany
Purpose: Telemedicine support services are now well establishedand both their educational role as well as its outcomes improving po-
tential are already recognised in international guidelines. There exists, however,still scepticism and reservation towards the long-term effects of telemedicine.The purpose of our study was therefore to compare the long-term effects of atelemedicine programme versus conventional care on relevant outcome mea-sures.Methods: A longterm study with a controlled trial design was conducted, com-paring patients with additional telemedicine support (n=220) versus patients withconventional treatment (n=220). Patients were randomly selected from patientclusters (previously matched by age class, gender and time in service) of a healthcare insurance. Cardiologically relevant aetiology has been controlled for. Thetime period under investigation was 2003-2009. The main outcome measureshave been the all-cause mortality rate, the hospitalisation rate, duration and costs
(cardiac and all-cause hospitalizations), costs of medication (cardiac and all-cause costs), number and costs of emergencies, as well as the total costs. Theresults have been validated by a comparison of the intervention group (n=220)with a threefold control group (n=660).Results: Our analyses showed a clear reduction in the overall average costs perpatient per year, a reduction of the mortality rate, as well as a reduction of bothhospitalisation rate and duration (both cardiac and all-cause hospitalizations) dueto the intervention. Beside this, our analyses revealed a lower number of emer-gencies and myocardial infarcts after service start in favour of the interventiongroup. The relative risk reduction was 43% in hospitalisation and 57% in mor-tality. The overall savings per patient per year due to the telemedicine supportamounted nearly 70%. Interventional effects in the out-patient sector (use of med-ications and number of visits at specialist or general practitioner) have not beenfound. Subgroup analyses revealed higher effects for older patients. All tenden-cies could have been validated from the threefold control group.Conclusions: All in all the telemedicine support can be regarded as more effi-cient and effective compared to the conventional treatment. Future studies shouldfurther investigate, which patients benefit most from the intervention and whichimpact on the patients quality of life and behaviour exists, so that telemedicineprograms can be tailored more target-specific
P1442 Cost-effectiveness of thrombus aspiration comparedto conventional PCI in acute myocardial infarction: 1year follow-up of the TAPAS-trial
M.A. Kampinga1, Y.L. Gu1, P. Pechlivanoglou2, M.J. Postma2,B.J.G.L. De Smet1, A.F.M. Van Den Heuvel1, E.S. Tan1, F. Zijlstra1.
1University Medical Center, Department of Cardiology, Groningen, Netherlands;2University of Groningen, Department of PharmacoEpidemiology, Groningen,Netherlands
Purpose: Improved 1-year clinical outcome with thrombus aspiration before stentimplantation compared to conventional percutaneous coronary intervention (PCI)was demonstrated in the Thrombus Aspiration during Percutaneous coronary in-tervention in Acute myocardial infarction Study (TAPAS). No previous study hasevaluated the cost-effectiveness of thrombus aspiration. We analyzed the cost-effectiveness up to 1 year of thrombus aspiration compared to conventional PCIin ST-segment elevation myocardial infarction (STEMI) patients.Methods: Medical resource utilization in our hospital, unit costs and clinical out-come up to 1 year were tracked for all 1071 patients enrolled in TAPAS. Effec-tiveness was calculated using estimated life expectancy after myocardial infarc-tion based on the Framingham Heart Study and literature data. Incremental cost-effectiveness ratio was calculated. Uncertainty surrounding the cost-effectivenessratio was determined by bootstrapping.Results: Cardiac death or non-fatal reinfarction after 1 year occurred in 5.6% ofthe thrombus aspiration-group and 9.9% of the conventional PCI-group (logrankp=0.008). Mean costs per patient within 1 year in the thrombus aspiration-groupwas 9 674 euro compared to 9 333 euro in the conventional PCI-group. The incre-mental cost-effectiveness ratio for thrombus aspiration was 7 964 euro per cardiacdeath or non-fatal reinfarction avoided and 2548 euro per life year gained. Cost-effectiveness ratio below 20.000 euro per life year gained was found in 91% ofthe bootstrap replications.
Bootstrap of cost-effectiveness
Conclusions: In the TAPAS trial, thrombus aspiration reduces cardiac deathsand non-fatal myocardial infarctions, while increasing 1-year costs only modestly.Therefore, thrombus aspiration is long-term cost-effective compared to conven-tional PCI in STEMI patients.
P1443 Advantages and restrictions of telemonitoring inchronic heart failure - experiences and results fromthe integrated care concept Telemedicine for the heart
T.M. Helms1, J. Pelleter1, A. Kroettinger1, K. Budych1, E. Thoden1,S. Sohn2, A. Mueller3. 1German Foundation for the Chronically
Ill (GFCI), Fuerth, Germany; 2Chair of Business Administration, Public HealthManagement, FAU Erlangen-Nuremberg, Nuremberg, Germany; 3HospitalChemnitz, Chemnitz, Germany
Cardiovascular diseases such as chronic heart failure (CHF) have evolved into a
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Has the recession made US more cost-effective? 227
major challenge for the healthcare sector. CHF is characterized by a considerablereduction in the patients’ quality of life as well as a poor long term prognosis, atthe same time being linked to an above average frequency of costly hospital ad-missions. Nevertheless, CHF is statistically under-diagnosed and under-treatedwith the patients themselves suffering from a lack of knowledge about the condi-tion and its treatment.To compensate for these deficiencies, the Techniker Krankenkasse (TK) and theGFCI developed the program "Telemedicine for the heart" which aims at reachingthree essential goals. First, at improving the patients’ knowledge about their dis-ease. Second, at decreasing the number of emergencies and hospital admissionsby optimized medical outpatient treatment. And third, at minimizing mortality. Toevaluate the program’s performance the TK conducted a patient survey. In addi-tion a health economic study involving more than 1.000 patients was conductedto validate the assumed cost-effectiveness, reduction of hospital admissions andmortality.The survey depicted high satisfaction scores with regard to both the program’sconcept and the positive impact on the patients’ ability to deal with their CHF.96.0% of the patients stated that they felt better informed about their CHF. 92.8%agreed that due to the program they could take a more active part when planningtheir treatment with their physician.The evaluation proved that the program’s focus on improving the quality of medicaltreatment led to a considerable modification of drug therapy. Regarding mortalityand hospital admissions, the patients participating in the program showed con-siderably better results than those of the control group. The number of hospitaladmissions per patient and year was reduced by 21.5% while mortality was de-creased by 35.1%. As an additional benefit, these results could be achieved with-out additional spending, average yearly treatment costs of patients participatingin the program being by 2.633,40 � (25,0%) smaller as those of their respectivematches.It became clear that the program is capable of achieving the predicted results –improved quality of life, improved medical treatment and reduced costs. The focuson patient-empowerment and close cooperation between all players involved inpatient-care seems well suited for the support of patients with CHF who are willingto accept a certain amount of responsibility for their own health. Patient educationimproved understanding, active involvement in their treatment and compliance.
P1444 Canadian cost-effectiveness analysis of dronedaronein patients with atrial fibrillation based on theATHENA trial
J. Berg1, L. Sauriol2, P. Lindgren1. 1i3 Innovus, Stockholm, Sweden;2sanofi-aventis, Quebec, Canada
Purpose: The ATHENA trial randomized 4,628 patients with atrial fibrillation (AF)or atrial flutter (AFL), aged ≥70 years with risk factors or ≥75 years without riskfactors, to receive 400 mg dronedarone or placebo on top of standard therapy. Pa-tients on dronedarone showed a 24% reduction in cardiovascular hospitalizationsor all-cause mortality over a mean follow-up of 22 months (p<0.0001). The ob-jective of the present study was to assess the cost-effectiveness of dronedaronein ATHENA from a Canadian health-care payer perspective.Methods: Patient-level data from ATHENA was used. Data on medical resourceuse (cardiovascular hospitalizations, hospitalizations due to treatment-related ad-verse events, outpatient examinations and procedures, study drug and concomi-tant medications) were aggregated for all randomized patients during the entiretrial period and multiplied with standard Canadian unit costs (2008 prices). Effec-tiveness was measured using the number of cardiovascular hospitalizations anddeaths from any cause, projected survival and projected quality-adjusted survival(QALYs) using life tables adjusted for AF mortality and data on determinants ofutility in AF. A yearly discount rate of 5% was applied to both costs and effects.Uncertainty was assessed using bootstrapping (1000 replications).Results: The total medical and medication cost in the dronedarone arm wasCan$7,200, out of which the cost of the study drug was Can$1,897. This canbe compared to a cost of Can$6537 in the placebo arm, indicating that part ofthe treatment cost is offset by savings from fewer hospitalizations. On average,patients on dronedarone had 0.18 fewer events. Including extrapolated survival,patients on dronedarone gained 0.13 life-years, corresponding to 0.09 QALYs.The cost per event avoided was Can$3,669 and the cost per QALY Can$7,470.The results were sensitive to the cost of cardiac arrhythmia.Conclusions: Dronedarone on top of standard therapy appears to be a cost-effective treatment strategy for AF/AFL patients in the ATHENA study.
P1445 The COACH program is cost-effective for thesecondary prevention of coronary heart disease
D. Liew1, M. Vale1, J. Kingston2, M. Jelinek3, A.M. Tonkin4 ,J.D. Best1. 1The University of Melbourne, Department of Medicine,St Vincent’s Hospital, Melbourne, Australia; 2The COACH Program,
Melbourne, Australia; 3St Vincent’s Hospital, Melbourne, Australia; 4MonashUniversity, Department of Epidemiology & Preventive Medicine, Melbourne,Australia
Purpose: The COACH (Coaching On Achieving Cardiovascular Health) Programis a 6-month, telephone-delivered disease management program that coachespatients to achieve risk factor targets and maintain compliance with evidence-
based treatment. Its efficacy in the secondary prevention of coronary heart dis-ease (CHD) has been shown in two randomized controlled trials, and follow-updata indicated sustained benefits up to 18 months after coaching. We soughtto determine the cost-effectiveness of The COACH Program from an Australianhealthcare perspective.Methods: A Markov micro-simulation model of recurrent CHD was populated with1400 Australian patients who had enrolled in The COACH Program at public andprivate hospitals between 2007 and 2009. For each subject individually, his/herrisk of non-fatal myocardial infarction (MI) or coronary death was estimated from aFramingham risk equation, with calibration against local data. Follow-up was sim-ulated for 5 years. Decision analysis compared the health and cost consequencesof The COACH Program versus no coaching. Reflecting the key randomized trial,The COACH Program was assumed to reduce serum total cholesterol and sys-tolic blood pressure by 7.4% (p<0.0001) and 3.3% (p=0.001), respectively. Con-servatively, no impact on other risk factors was assumed. Costs were estimatedfrom published sources. A 5% annual discount rate was applied to costs andyears of life lived.Results: Of the 1400 subjects in the no coaching group, 167 (12.0%) were pre-dicted to suffer non-fatal MI or coronary death over 5 years. In The COACHProgram Group, the predicted number was 158 (11.3%), equating to a numberneeded to treat of 151. Over the 5-year period, The COACH Program was esti-mated to have saved 0.007 life years (discounted) per person, at a net cost ofAUD$215 (discounted). These equated to an incremental cost effectiveness ratioof AUD$28,679 per life-year gained. Sensitivity analyses, which included the un-certainty limits of coaching efficacy and costs, indicated the results to be robust.Sub-analyses by insurance status revealed no differences between public andprivate patients.Conclusion: The COACH Program represents a cost-effective means of prevent-ing recurrent disease and death among patients post CHD. Its cost-effectivenessis at least as good as, and in many cases better than, currently-recommendedsecondary preventive strategies. Further appeal of The COACH Program lies inits safety, high-level of acceptance and broad applicability, including to those un-able to access cardiac rehabilitation programs.
P1446 Cost-utility analysis of 10-years cardiovascularprevention program in Russian primary care
A. Kontsevaya1, A. Kalinina1, A. Deev1, R. Rajan2. 1NationalResearch Center for Preventive Medicine, Moscow, RussianFederation; 2Peoples Friendship University of Russia (RPFU),
Moscow, Russian Federation
Purpose: To evaluate the economic efficiency of 10-years cardiovascular preven-tion program in primary care of Russian Federation.Methods: In 1977-1990 in Moscow a large prevention project was realized. Theproject was realized in two primary care areas of Moscow and included men withbaseline age 40-59. One primary care area was intervention area where cardio-vascular prevention program was realized during the 5 years. Other area wascontrol, where no additional interventions were conducted. Participants of inter-vention (n=3488) and control primary care areas (n=3168) had the similar age,education and cardiovascular morbidity. The cardiovascular prevention programincluded physician’s consultations for patients with hypertension and ischemicheart disease (8.0 in year), individual preventive counseling for participants withhypercholesterolemia overweight and obesity and sedentary lifestyle and grouppreventive counseling for the smoking patients. All cardiovascular endpoints (car-diovascular death, nonfatal myocardial infarction and non fatal stroke) were regis-tered during the 5 years of intervention and 5 years after the intervention (totallyduring 10 years). The decreasing of cardiovascular and total mortality in inter-vention group compared with control group was demonstrated early. In this studywe calculated the gain of life years saved (LYS) and quality adjusted life years(QALY) in intervention group compared with control group (on 1000 participants)during the 5 years on the intervention and during 10 years of total follow up pe-riod. Also we calculate the total cost of the program including the first screening,intervention costs and follow-up costs in the prices of 2008 years. The cost utilityanalysis was conducted with calculation of cost per gained QALY during 5 yearsand during 10 year.Results: The number of gained LYS in the intervention group was 45.7 on 1000participants in 5 years and 139.4 – in 10 years. The number of QALY was 46.2and 132.7 on 1000 participants in 5 and 10 years accordingly. The total costswere 174 124$ on 1000 participant in 5 years and 237 928$ in 10 years. Cost perQALY gained was 3769$ during the 5 years and 1793$ during the 5 years. Thegross domestic product on capita in 2008 was 11 806$.Conclusion: Cardiovascular prevention program for men aged 40-59 is highlycost-effective.
P1447 Economic benefit of copeptin for rapid rule out ofacute myocardial infarction
R. Twerenbold1 , T. Reichlin1, M. Reiter1, J. Meissner1, C. Heinisch1,T. Socrates1, N. Arenja1, M. Noveanu1, K. Winkler2, C. Mueller1.1University Hospital Basel, Basel, Switzerland; 2Hospital Del Mar,
Barcelona, Spain
Purpose: The purpose of this multicenter study was to examine the economic
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

228 Has the recession made US more cost-effective?
benefit of copeptin for rapid rule out of acute myocardial infarction (AMI). In twoindependent previous studies the combination of cardiac troponin T (cTnT) andcopeptin resulted in a very high negative predictive value for AMI already at pre-sentation.Methods: In 1251 consecutive chest pain patients presenting to the emergencydepartment (ED), we measured levels of copeptin at presentation. The final diag-nosis was adjudicated by two independent cardiologists. Treatment costs in theED were determined for each patient both for the current guideline-based algo-rithm and a new, investigational algorithm using copeptin. In the investigationalalgorithm, AMI was ruled out in patients who had undetectable levels of cTnT(<0.01ug/l) and Copeptin level <14pmol/l at presentation.Results: AMI was the adjudicated diagnosis in 199 patients (16%). The investi-gational algorithm allowed to rule out AMI in 712 patients (57%) and enabled dis-charge after 90 minutes in patients without and after 225 minutes in patients withsuspected pulmonary embolism or aortic dissection, respectively. Median time todecision could be reduced from 350 minutes (Interquartile range [IQR], 205 to 480minutes) to 90 minutes (IQR, 90 to 266 minutes) (p<0.001). The mean treatmentcost was 1’283.70 $ per patient using the current guideline-based algorithm. Theadditional use of copeptin resulted in a 30% reduction of the total treatment cost(mean, 386 $; 95% confidence interval, 362-410 $) (p<0.001).
Cumulative frequency distribution curve
Conclusions: In consecutive chest pain patients, the additional use of copeptinseems to reduce total treatment costs in the ED by 30%. (ClinicalTrials.gov num-ber, NCT00470587)
P1448 Inverse correlation between socioeconomic statusand risk of cardiovascular death
K. Kozakiewicz1, A. Michalewska-Wludarczyk1, B. Korzeniowska1,G. Broda2, A. Pajak3, T. Zdrojewski4, M. Tendera1 . 1MedicalUniversity of Silesia, 3rd Department of Cardiology, Katowice,
Poland; 2Cardinal Stefan Wyszynski University, Department of Psychology,Warsaw, Poland; 3CMUJ - Institute of Public Health, Institute of ClinicalEpidemiology and Population Studies, Krakow, Poland; 4Medical University ofGdansk, Gdansk, Poland
Socioeconomic status (SES) is one of the factors of cardiovascular diseases de-velopment. In highly industrialized countries a decline in death from CVD hasbeen found in subjects with high SES.Aim: Assessment of SCORE-based CV death risk in the study population and itscorrelation with education and income.Methods: Study population consisted of randomly screened inhabitants of South-ern Poland. Depending on the population size, 3 categories of communities weredefined, with <8000, 8000-40000 and >40000 inhabitants. 18 communities wererandomly sampled (6 per category) and 100 males and 100 females aged from20 to 74 years were invited to participate. Out of 3600 subjects, 2287 (63,5%)took part in the study. In each subject questionnaire data (age, sex, smokinghabits, socioeconomic factors), anthropometric data, blood pressure measure-ments as well as blood glucose and lipids were obtained. Education level and netmonthly income per person were further analyzed after categorization: incom-plete secondary, secondary and higher (education) and income. After exclusionof those with a diagnosed cardiovascular disease, in the remaining 1821 subjects(816m,1005f) the risk of CVD death according to SCORE algorithm (for higherrisk countries) was calculated.Results: Results are presented in the table.
Education Income(subjects with high CV risk – in %) (subjects with high CV risk – in %)
Incomplete Secondary Higher P value Low Intermediate High P valuesecondary
Whole group 41,5 24,3 21,6 <0,0001 29,7 31,7 40,7 0,0001Male 49,7 37,6 34,4 0,0006 43,7 42,4 49,2 0,17Female 33,3 15,3 13,4 <0,00001 18,4 23,3 32,2 0,0006
Conclusion: Higher education is associated with lower calculated risk of cardio-
vascular death both in men and women. For income an inverse association wasobserved.
P1449 How to truly price an ICD: daily cost or up-front cost?
M. Biffi, M. Ziacchi, M. Bertini, B. Gardini, A. Mazzotti, V. Mantovani,E. Cervi, I. Diemberger, C. Martignani, G. Boriani. Institute ofCardiology, Bologna, Italy
Purpose: We firstly reported that ICD longevity is significantly dif-ferent among manufacturers. Health care systems are sensitive to ICD up-frontcost, but this may prove an unreliable indicator for the device-purchasing process,being not related to longevity. We calculated the daily cost of ICDs from differentmanufacturers based on their actual longevity as measured at device replace-ment, to understand whether the daily cost or the up-front cost should be used asa guide to price devices.Methods: Longevity of single chamber (SC), double chamber (DC), and biven-tricular (BiV) ICDs from Medtronic (MDT), Guidant (GDT) and St. Jude Medical(SJM) was measured in all the patients implanted in years 2000, 2001, 2002 whoreached device replacement within December 31st 2009. The cost of each ICD(device + lead/s) was divided for its own longevity. Data are expressed as median(25th-75th percentile).Results: 123/153 patients implanted in the above-mentioned period survived untilICD replacement. 107/153 patients (70%) were alive at a median 8.3 years (7.5-9.4) follow up. Longevity of SC devices was 86 (80-101), 53 (45-63), and 56 (50-60) respectively for MDT, GDT, SJM (p<0.001), whereas it was 84 (79-86), 51(45-55), and 41 (37-56) months respectively for MDT, GDT, and SJM DC devices(p< 0.001).CRT-Ds were respectively replaced after 81 (67-89) (MDT), 44 (43-45)(GDT), and 44 (43-45) (SJM) months (p<0.05). MDT devices had a significantlylower daily cost compared to other manufacturers (table, p<0.001)A 9-years ICD longevity would have saved 67% of ICD replacements within thefollow up period.
Cost per service life of 123 ICDs
ICD cost/day (� ) Single Chamber (n=63) Double chamber (n=50) CRT-D (n=10) P
Medtronic (n=23) 4.8 (4.6-5.7) 6.9 (6.8-7.7) 8.5 (8.3-10.3) 0.004*Guidant (n=43) 6.8 (6.2-9.2) 12.6 (11.8-13.3) 15.4 (15.1-15.8) <0.001*St Jude M (n=57) 6.9 (6.2-7.6) 13.4 (10.3-16.1) 14.6 (14.1-14.9) <0.001*P <0.001* 0.001* 0.10*
*Kruskal-Wallis.
Conclusions: Based on the improved survival of ICD carriers, ICD treatmentshould be priced based on ICD longevity and daily cost rather than on up-frontcost. Independent observations in the real-life scenario are needed to properlyvalue newer technologies against actual benchmark.
P1450 A cost-effectiveness assessment of theSirolimus-Eluting Stent in diabetic and non-diabeticpatients versus Bare Metal Stents (BMS): Analysis ofthe French cohort EVASTENT
G. Barone-Rochette1 , C. Combescure2, P. Motreff3, A. Foote4,J.L. Quesada4, C. Castelli2, G. Vanzetto1, J.P. Daures2, N. Danchin5 ,J. Machecourt1 . 1Cardiology department, Grenoble University Hospital,Grenoble, France; 2Division of Biostatistics, University Hospital of Nîmes,Nîmes, France; 3Cardiology department, Clermont-Ferrand University Hospital,Clermont-Ferrand, France; 4INSERM Clinical Research Center, GrenobleUniversity Hospital, Grenoble, France; 5Hôpital Européen Georges Pompidou,Paris, France
Objectives: To assess the cost-effectiveness of the Sirolimus-Eluting Stent (SES)in diabetic and in non-diabetic patients after 3-years follow-up versus Bare MetalStents (BMS).Background: Concerns persist about the long-term safety results in multiple ves-sel disease diabetic patients and the cost-effectiveness of the SES remains un-certain.Methods: Patients undergoing revascularization exclusively with SES (1731)were included in the EVASTENT matched-cohort registry; for each diabetic pa-tient (db+) included, stratified as single (SVD) or multiple (MVD) vessel disease,a non-diabetic patient (db-) was subsequently included. The Direct hospital costsfor hospitalization, PCI (Percutaneous coronary intervention), BMS, SES, CABG(Coronary Artery Bypass Graft), as well as costs for drugs were measured forthe SES arm. Trajectories for costs and clinical outcomes were derived from aMarkov model and Monte Carlo simulations, with 3 month intervals over a 3-yeartime horizon. The parameters in the SES arm were derived from EVASTENTdata, whereas transition probabilities in the BMS arm were derived from the SESarm according to previous randomized studies: RR of TLR = 0.30 with SES/BMSduring the first year, then RR=1 after one year, with no difference for the 3-yeardeath. Sensitivity analyses according to the price premium and RR of TLR havebeen performed. SES were considered cost effective if <10,000 � /TLR avoided.Results: The all-cause mortality rate was 6.9%, 2.8 times higher in db+ thandb- patients, and cardiovascular mortality rate was higher (p≤0.001) in db+ MVD(8.4%) than in db+ SVD, db-MVD and db-SVD (5.5, 2.9 and 1.4% respectively).Definite, definite or probable, or any Academic Research Consortium (ARC) def-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Has the recession made US more cost-effective? / Looking beyond the heart: psychosocial factors in heart disease 229
inition of stent thrombosis occurred respectively in 1.9%, 2.5% and 3.5%, signif-icantly more often in db+ MVD (3.9%, 4.8% and 6.1%), with a 0.55%/year rateof very late stent thrombosis (any ARC definition). Target lesion revasculariza-tion was needed in 7.1% of patients, and any revascularization in 16.4%. Com-pared to BMS the SES was cost-effective only in db+ MVD (7494 � per avoidedrevascularization vs. >10,000 � in other groups, and 70,466 � per QALYs vs.>100,000� ). Sensitivity analyses demonstrated dominance of SES in such pa-tients if the price premium between SES and BMS is 400 � .Conclusion: SES is cost effective in diabetic multiple disease patients, patientswho experience more stent thrombosis.
LOOKING BEYOND THE HEART: PSYCHOSOCIALFACTORS IN HEART DISEASE
P1451 Follow up of adults with congenitally malformedhearts with focus on computer-based education andpsychosocial support improves knowledge, resultsfrom a randomised intervention study
H. Ronning, N.E. Nielsen, E. Swahn, A. Stromberg. LinkopingUniversity, Department of Medical and Health Sciences, Linkoping, Sweden
Purpose: Adults with congenitally malformed hearts have previously been foundto have a poor level of knowledge about various aspects of their congenital car-diac malformation and there is a lack of educational materials. Therefore, we con-ducted a clinical randomised trial to test whether a nurse-led intervention consist-ing of computer-based education, an individualised care-plan and psychosocialsupport would increase knowledge.Method: Adults with congenitally malformed hearts as ventricular septal defect,atrial septal defect, coarctation of the aortae, aortic valve stenosis (uncomplicatedheart malformations) and tetralogy of Fallot, complete transposition of the greatarteries, congenitally corrected transposition of the great arteries, single ventricle,Ebstein anomaly and Eisenmenger syndrome (complicated heart malformations)were randomised to either experimental or control group. The experimental groupreceived education and psychosocial support by a nurse, computer-based edu-cation and an individualised care-plan was made in addition to usual care. Thecontrol group received usual care consisting of traditional follow-up visits to aphysician.Results: The participants (n=114) had a mean age 34 years (rang 18-74) and56 were women. Twenty-six had complicated heart malformations in the experi-mental group (n=55) and 31 in the control group (n=59). Results after 3-monthsshowed that the experimental group had a significantly better general knowl-edge about their congenital cardiac malformation compared to the control group(P<0.001). Out of 114 participants, 75 were recommended prevention of endo-carditis at baseline. The knowledge about prevention of endocarditis was signif-icantly increased in the experimental group (n= 37) but remained unchanged inthe control group (P<0.001).Conclusion: Our results indicate that a more extensive follow-up focusing onindividualised and interactive education and care-planning in combination withpsychosocial support significantly increased the participants’ general knowledgeabout their congenital cardiac malformation and prevention of endocarditis. Dataregarding the effects of the intervention on quality of life, anxiety, depression andperceived control will be further analysed. Results from 1-year data will be avail-able late autumn 2010.
P1452 Symptoms of anxiety and depression and the role ofsocial support in patients with chest pain
G. Mourad1, G. Rondahl1 , T. Jaarsma1, A. Stromberg2. 1Linkopinguniversity, Department of Social and Welfare Studies, Norrkoping,Sweden; 2Linkoping University, Department of Medical and Health
Sciences, Linkoping, Sweden
Background and aim: Being admitted to a coronary care unit due to chest painis stressful. Limited data is available on anxiety and depression in chest painpatients during the acute phase. Social support may act as a buffer to the psy-chological impact of an acute cardiac event. Therefore, the aim of this study wasto describe the prevalence of symptoms of anxiety and depression and their re-lationship to social support in patients admitted to a coronary care unit (CCU) foracute chest pain.Methods: The study had a descriptive, cross sectional design based on datacollected by standardised questionnaires. Data was collected consecutively at auniversity hospital in central Sweden between October 2006 and October 2007.Eligible for the study were patients younger than 75 years, hospitalized due tochest pain at the CCU, who spoke and read Swedish and were in a general stateof health to participate in the study. Patients were asked to answer three dif-ferent questionnaires: State-Trait Anxiety Inventory (STAI), Hospital Anxiety andDepression Scale (HADS) and Medical Outcome Study-Social Support Survey(MOS-SSS) within 24 hours after being admitted to CCU.Results: A total of 337 patients were included in the study (mean age 60.5 years,73% men, 73% married). Only two patients were free from symptoms of anxietyand depression, while 7% of the patients had clinically significant levels of bothanxiety and depression. A total 71% had a clinically significant or severe level
of anxiety and 22% were at a borderline level for anxiety. A total of 14% hada clinically significant level of depression and 67% were at a borderline level ofdepression. Regression analysis showed that social support was independentlyrelated to anxiety and depression.Conclusion: Patients admitted to CCU experience extreme levels of psycholog-ical distress in the acute phase and social support seems to play an importantrole. Assessment of anxiety and depression as well as interventions includingsupport and information should be considered in the CCU setting in order to im-prove mental well-being of patients with chest pain.
P1454 Coronary artery bypass graft patients experienceunmet physical and psychosocial symptoms duringtheir early rehabilitation. Results from theintervention group in a randomized controlled trial
I. Lie1, E.H. Bunch2, N.A.A. Smeby1, H. Arnesen1, G. Hamilton1.1Oslo University Hospital, Ulleval, Oslo, Norway; 2University of Oslo, Oslo,Norway
Background: Patients‘ experiences after CABG reveal unmet physical, psycho-logical and educational needs after surgery. Foremost are symptoms of anxi-ety and depression that significantly predict increased morbidity and mortality.A structured information and psychological supportive psycho-educative methodto perform health education and teaching coping skills are warranted.Purpose: To implement an individualized intervention that explores the CABGpatients‘ symptoms, and promotes symptom management in the early rehabilita-tion.Method: A randomized controlled trial recruited 101 patients (n = 101) to a home-based intervention at 2 and 4 weeks after surgery. The psycho-educative inter-vention consisted of an intervention protocol with 7 predefined themes knownto be important. The narrative interviews were analyzed using thematic contentanalysis before sub-themes were quantified to give a background on how oftenspecific experiences were addressed in the interviews.Results: A total of 93 patients completed the intervention. Patients‘ experi-ences revealed 16 sub themes related to the 7 predefined themes. 1. Phys-ical theme: postoperative pain (84% at 2 weeks/66% at 4 weeks), assess-ment of surgical site (55%/53%), numb feeling at chest surgery site (23%/22%),physical activity/exercise (almost 100%) and issues with compression stocking(7%/13%). 2. Prescribed discharge medication theme: uncertainty about medica-tions (15%/12%). 3. Anxiety and/or depression themes: living alone (12%/5%),changed sleep pattern (11%/9%), irritability "short fuse" (15%/7%), postopera-tive complications (16%/13%), security of grafts after CABG (10%/15%), return towork (13%/3%) and driving a car (7%/15%). 5. Sexuality theme: impotence (erec-tile dysfunction) (20% at 4 weeks). 7. Open themes: discharge phase (15% at 2weeks) and missing link to hospital (6%/28%).Conclusion: This study indicates the need to extend hospitals‘ discharge care forCABG patients to the first month after surgery for specific symptoms to enhancethe patients‘ symptom management.
P1455 Family partnership and education interventions toreduce dietary sodium by patients with heart failurediffer by family functioning
S.B. Dunbar1, P.C. Clark2, A.L. Smith3, C.M. Reilly1, R.A. Gary1,F. Mccarty4, N. Kaslow5. 1Emory University School of Nursing,
Atlanta, United States of America; 2Georgia State University School of Nursing,Atlanta, United States of America; 3Emory University School of Medicine,Division of Cardiology, Atlanta, United States of America; 4Georgia StateUniversity School of Public Health, Atlanta, United States of America; 5EmoryUniversity School of Medicine, Atlanta, United States of America
Purpose: Lowering dietary sodium by persons with heart failure (HF) is difficultand often occurs within the home and family context. We examined whether familyfunctioning influenced response to interventions aimed at reducing dietary sodiumby NYHA Class II and III patients.Method: HF patients and a family member (FM) (n=117 dyads) were randomizedto receive structured patient and family education (PFE), PFE plus family partner-ship intervention (FPI) or usual care (UC). PFE included education on selectionand preparation of low sodium foods and label reading. FPI added family supportcommunication and empathy using autonomy support concepts. Family function-ing (FF) was measured using the Family Assessment Device (FAD), and dyadswere identified as high or low FF based on standard scores. Depressive symp-toms were measured by Beck Depression Inventory II (BDI-II). Dietary sodiumintake was measured by 24 hour urinary sodium (Urine NA) and a three-day foodrecord analyzed with a nutrient software program (Diet NA) at baseline (BL), 4and 8 months (M). Analyses included descriptive statistics, as well as ANOVAbased pairwise contrasts by group and time adjusted for age, gender, body massindex, NYHA class, BDI-II, and diuretic equivalents, stratified by FF.Results: HF subjects were 64% male, 58% African American, age 56±10 years;LVEF 26.9 + 13%. FMs were 81% female, age 52 +13 years, and 53% spouses.At BL, groups did not differ on demographic, clinical, FAD scores or Diet or UrineNA variables. At 4 M, FPI group had decreased mean Urine NA from BL (3754 +1854 to 3001 + 2011, p=.02) which also differed from UC (4071 + 1884; p=.056).At 8 M, PFE differed from UC on mean Urine NA (3018 + 2087 vs. 4165 + 1848,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

230 Looking beyond the heart: psychosocial factors in heart disease
p=.04). For high FF, there were no differences between intervention groups onNA over time. For low FF group, FPI and PFE had lower mean Urine NA thanUC (p<.05) at 4 M, and FPI remained lower than UC at 8 months (p<.05). WithinPFE, low FF did not change, yet within FPI low FF reduced Urine NA at 4 m(p=.005) and 8 month (p=.04) from BL.Conclusion: Both FPI and PFE reduced dietary sodium compared to UC, how-ever FPI and support achieved a decrease in dietary sodium initially while struc-tured PFE showed slower sustained decrease over time. Intervention responsesvaried based on high and low FF, with FPI having a greater effect for those withlow FF. Further research is warranted to determine if tailoring patient and familyeducation the family context yields better dietary sodium adherence. Efforts tooptimize family-focused interventions into heart failure clinical care are indicated.
P1456 Psychometric properties of the swedish version ofthe Control Attitudes Scale (CAS) for patients withcardiac disease and their partners
K. Arestedt1, S.Å. Susanna Agren2, I.F. Inger Flemme3, D.M. BedbraMoser4, A.S. Anna Stromberg2. 1Linnaeus University, School
of Health and Caring Sciences, Kalmar, Sweden; 2Linkoping University,Department of Medical and Health Sciences, Linkoping, Sweden; 3HalmstadUniversity, School of Social and Health Sciences, Halmstad, Sweden; 4Universityof Kentucky, College of Nursing, Lexington, United States of America
Purpose: Perceived control is considered to be a robust predictor of well-beingthat is instrumental for effective self-care in cardiac patients. The 4-item ControlAttitudes Scale was developed to measure the level of control perceived by in-dividuals with cardiac disease. As the scale previously not have been extensivetested, the aim was to evaluate the psychometric properties of the patient andfamily version of the Control Attitudes Scale in a Swedish sample of internal car-dioventer defibrillator (ICD) recipients, heart failure patients and their partners.Methods: A pooled sample (n=391) of ICD recipients, heart failure patients andpartners were used. Descriptive statistics, exploratory factor analysis, ordinal re-gression modeling and Cronbach’s alpha were used to evaluate data quality, di-mensionality, absence of differential item functioning for age and sex, and internalconsistency reliability.Results: The findings revealed that the CAS is a multidimensional scale. In ad-dition to the total scale, two subscales can be calculated, the control and help-lessness subscales. The internal consistency was satisfactory for all scales (α=0.74-0.85) except the family version total scale (α=0.62). No differential itemfunctioning for age and sex was detected, which implies that the scale can beused to make invariant comparisons between groups of different age and sex.Conclusions: The psychometric properties, together with the simple and shortformat of the CAS, make it to a useful tool for measuring perceived control amongpatients with cardiac diseases and their family members.
P1457 Association between depressive symptoms andC-reactive protein levels in general population
J. Piwonski1, T. Zdrojewski2, A. Piwonska1, W. Drygas3, P. Kurjata1,J. Gluszek4, K. Kozakiewicz5, A. Pajak6. 1National Institute ofCardiology, Warsaw, Poland; 2Medical University, Gdansk, Poland;
3Medical University, Lodz, Poland; 4Poznan University of Medical Sciences,Poznan, Poland; 5Medical University of Silesia, Katowice, Poland; 6JagiellonianUniversity, Krakow, Poland
Purpose: There is an increasing evidence of independent relation of psychoso-cial risk factors to cardiovascular diseases (CVD) risk. It could be via inflammatoryprocess. Some epidemiological studies confirmed the relationship between de-pression and inflammatory markers, but some did not. We try to assess the rela-tion between one of the inflammatory markers: high-sensitivity C-reactive protein(hsCRP) and depressive symptoms (DS).Methods: The representative sample of 6392 men and 7153 women, aged 20-74, were examined in 2003-2005, in the frame of the National Multicenter HealthSurvey (WOBASZ Study). DS were assessed using Beck’s Depression Inven-tory (BDI; DS ≥ 10pts). Questionnaire, physical examination and laboratory datawere obtained. Persons with hsCRP > 10 mg/l were excluded from the analyses.Because of non-normal distribution of the hsCRP we use the logarithmic transfor-mation for hsCRP data.Results: Out of screened persons 24,1% men and 34.3% women had DS. Per-sons with DS were significantly older, had more CVD risk factor and higher levelsof hsCRP than those without DS (geometric means: men - 1,62 mg/dl ± 2,29 vs1,27 mg/dl ± 2,44, p < 0,0001; women - 1,61±2,43 mg/l vs 1,31±2,44 mg/l, p <
0,0001). HsCRP > 3 mg/l were significantly more often found in persons with DSthan without DS (men: 23,0% vs 16,8%, p < 0,0001; women 25,8% vs 17,5%,p < 0,0001). In the univariate logistic regression performed in 3 age-group (<40 year old, 40-59 year old, ≥ 60 year old) we found a significant relationshipbetween hsCRP and DS only in the 40-59 age-group, both in men (OR for DS= 1.22, p=0.0072) and in women (OR for DS = 1.18, p=0.0114). In the multiplelogistic regression, after adjustment for the additional risk factors, the significantrelationship between hsCRP and DS maintained only in men (OR for DS = 1.15,p < 0.05).Conclusions: There is a very high prevalence of depressive symptoms in Polishpopulation, especially in women. Persons with depressive symptoms had higher
levels of hsCRP. The level of hsCRP occurred significantly associated with de-pressive symptoms only in middle-aged persons, especially in men.
P1458 Depression among cardiology patients: findings fromcollaborative cardiology and psychiatry "heart andmind clinic"
M.I. Vidovich, G. Bhardwaj, R. Manev, S. Schmid, H. Manev.University of Illinois at Chicago, Chicago, United States of America
Background: 12 million people in the US suffer from coronary heart diseasewhich is the single most common cause of death among adults. Comorbid depres-sion increases the risk of adverse cardiac events in patients with heart diseasehowever routine screening for depression is infrequently performed in outpatientcardiology settings.Objective: By routinely screening cardiology patients for depression, we soughtto determine the prevalence of depressive symptoms and to correlate depressivesymptoms with guideline-recommended quality measures in an outpatient cardi-ology clinic.Methods and Results: 154 patients who presented to University CardiologyClinic between August 2008 and May 2009 were screened for depression usingPatient Health Questionnaire-9 (PHQ-9) and cardiology care followed guideline-based recommendations (median blood pressure 137/73 mmHg, median LDLcholesterol 84 mg/dL). Prevalence of depression, (PHQ-9 score ≥ 10), was 26%.Patients who screened positive for depression were more likely to be youngerthan 50 years (p=0.047). The scores on the somatic component of PHQ-9 (items3, 4, 5) were consistently higher (mean 3.04) than the scores on the cognitivecomponent (mean 1.66; items 2, 6, 7, 9) (p<0.001). No significant associationwas found between PHQ-9 scores and gender, blood pressure, cholesterol levelsand underlying cardiovascular disease.
PHQ-9 Frequency per Age Group
Conclusions: Findings suggest a higher prevalence of self-reported symptomsof depression in patients presenting for cardiology evaluation as compared togeneral population and support current American Heart Association guidelines forroutine depression screening in outpatient cardiology clinics. Certain subgroupsof cardiology patients may be at higher risk for depressive symptoms.
P1459 Frequency of negative psychosocial risk factors inpolish obese persons. Results of National MulticenterHealth Survey (WOBASZ)
J. Piwonski1, A. Piwonska1, W. Drygas2, T. Zdrojewski3,J. Gluszek4, A. Pajak5, K. Kozakiewicz6. 1National Institute of
Cardiology, Warsaw, Poland; 2Medical University, Lodz, Poland; 3MedicalUniversity of Gdansk, Gdansk, Poland; 4Poznan University of Medical Sciences,Poznan, Poland; 5Jagiellonian University, Krakow, Poland; 6Medical University ofSilesia, Katowice, Poland
Purpose: During last years depressive symptoms and low social support levelhave become a still growing problem in many worldwide populations. Negativepsychosocial risk factors such as depression or lack of social support can beboth risk factors of obesity due to their effect on person’s behaviour as well asthey can be a result of being obese because of the lack of acceptance of obesepersons by family or population. We want to evaluate the frequency of depressivesymptoms (DS) and low social support level (SSL) in obese persons comparedto the rest of population.Methods: The polish population sample - 6392 men and 7153 women, aged 20-74, examined in 2003-2005 in the frame of National Multicenter Health Survey(WOBASZ). Study procedure covered questionnaire, physical examination andlaboratory tests. DS were assessed by Beck Depression Scale (≥ 10 pt) and SSLusing Berkman and Syme questionnaire.Results: 1313 men - M (21%) and 1612 women - W (22%) were obese. Obesepersons were older and independently of age had higher levels of risk factors.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Looking beyond the heart: psychosocial factors in heart disease 231
Both men and women with obesity compared to persons without obesity signifi-cantly more often had DS (M – 29% vs 22%, p< 0.0001; W – 46% vs 30%, p<
0.0001). Lack or low SSL were observed in 58% of obese M and in 79% obeseW (compared respectively to 64% M and 68% W without obesity). The significantassociation between obesity and DS and low SSL, both in men and women, wasobserved. In obese, compared to not obese men, the chance of getting DS (in-dependently of age) was higher by 14% (OR=1.14, p<0.05), and in women evenby 40% (OR=1.40, p<0.0001). In obese man the chance of getting low SSL waslower by 29% (OR=0.71, p=0.0014), but in women increased by 19% (OR=1.19,p<0.05) compared to not obese persons.Conclusions: In obese persons, both men and women, depressive symptomswere observed more often than in persons without obesity, but low social supportwas observed more often only in obese women.
P1460 Premature atherosclerosis in patients withdepression and coronary risk factors
C. Pizzi1, S. Mancini2, F. Fontana1 , G.M. Costa1. 1University ofBologna, Bologna, Italy; 2University of Modena & Reggio Emilia,Modena, Italy
Purpose: The aim of this study was the association of the intima-media thicken-ing (IMT) as expression of preclinical atherosclerosis, in depressed patients withcoronary risk factors but free to coronary artery disease.Methods: We studied 391 asymptomatic subjects, with a cluster of risk factors,and we evaluated the depression mood. Depression was evaluated at baselineusing the Beck Depression Inventory. IMT of the common carotid artery was de-termined by B-mode ultrasound imaging. Traditional risk factors for atheroscle-rosis and disease-related factors were recorded. Markers of inflammation (C-reactive protein, CRP; interleukin 6, IL-6) and heart rate variability (time domaincomponents: SDNN, SDANN, RMSSD, pNN50%) were determined.Results: A total of 90 (23.0%) subjects showed a depressive symptomatology.Of these, 48 were mildly, 27 moderately, and 15 severely depressed. AverageIMT was increased in depressed patients (0.87±0.35 mm) at risk for CHD butfree from disease compared to controls (0.77±0.019 mm; p<0.001). Heart ratevariability was reduced in depressed patients. Levels of SDNN (108±35 ms) andSDANN (93±20 ms) were decreased in depressed patients as compared to non-depressed patients (113±22 ms and 103±14 ms p:<0.001). Whereas, RMSSD,pNN50% did not differ between both groups. Patients with depression mood hadhigher CRP (2.00±1.00 mg/dL) and IL-6 (2.00±0.40 pg/ml) than patients with nondepression moods (CRP: 0.79±0.34 mg/dL; IL-61.14±0.65 pg/ml; p<0.001). Inmultivariate analysis, depression was positively correlated with C-reactive protein,IL-6 and inversely associated with levels of SDANN and IMT.Conclusions: The IMT is higher in depressed patients, indicating that atheroscle-rosis is accelerated in this sub-group of patients. This is mainly due to disease-related risk factors, as inflammation and imbalance of autonomic nervous system.
P1461 Anxiety is related to increased carotid intima-mediathickness in patients with first acute myocardialinfarction
A. Stefanatou1, I. Oikonomidis1, N. Kouris2, I. Lekakis1 ,D. Kremastinos1, M. Nana1. 1Attikon Hospital, 2nd University
Department of Cardiology, Athens, Greece; 2Thriassio General Hospital, Athens,Greece
Purpose: Emotional disorders have been associated with mechanisms that pro-mote atherosclerosis, but most of the research has been focused on depression.The potential impact of anxiety on the progress of atherosclerosis has not beenfully investigated. We examined the association of anxiety and depression withcarotid intima media thickness in CAD patients during their hospitalisation foracute myocardial infarction (MI).Methods: A cohort of 74 consecutive patients (age:59±10, range: 30 to 75 years)with a first episode of myocardial infarction (MI) (64% STEMI and 36% NonSTEMI) were included. Sixty non CAD patients also admitted in the cardiologydepartment for other reasons served as controls. Mean intima-media thickness(IMT) in common carotids and carotid bulbs using ultrasound imaging was mea-sured at study entry. All patients completed the Hospital Anxiety and DepressionScale (HADS) in the first 3 days of admission and the corresponding anxiety anddepression scores were calculated. Patients were interviewed according to thestructured clinical interview of the DSM-IV masked to the self-reports of symp-toms.Results: Patients with MI had higher incidence of anxiety and depression thannon CAD patients (67% vs 46% for anxiety and 74% vs 47% for depressionp<0.05) Patients with MI and pre-infarction angina had a higher incidence of anx-iety (75% vs. 25% P<0.01) compared to those without. There were no differencein atherosclerotic risk factors medication and socioeconomic status, location ofMI and STEMI between patients with [n=49 (67%)] and without anxiety. Howeverpatients with anxiety had increased IMT compared to those without (0.1±0.01 vs.0.08±0.01 cm p<0.05). The anxiety score as assessed by HADS was related withIMT (r=0.40 p<0.01). After adjustment for atherosclerotic risk factors, (hyperlipi-demia,diabetes,smoking, hypertension) socioeconomic status and medication,)anxiety was independently associated with increased IMT values (b regressioncoefficient =0.37 p<0.05).
Conclusion: The present study suggests that increased anxiety is an indepen-dent determinant of IMT, an established surrogate marker of atherosclerosis, inpatients with acute myocardial infarction. This finding might imply links of thepathophysiology of emotional disorders to CAD and vascular structure. Treatinganxiety disorder might also have cardiac prognostic implications.
P1462 Selective serotonin reuptake inhibitors in patientswith depression and coronary heart disease: ameta-analysis
C. Pizzi1, A.W.S. Rutjes2, G.M. Costa1, F. Fontana1 , A. Mezzetti2,L. Manzoli2. 1University of Bologna, Bologna, Italy; 2G. D’Annunzio
University, Chieti, Italy
Purpose: The occurrence of depression in patients with coronary heart disease(CHD) substantially increases the likelihood of a poorer cardiovascular prognosis.Although antidepressants are generally effective in reducing depression, their usein CHD patients is controversial. We carried out a meta-analysis to evaluate thehealth effects of SSRI versus placebo or no antidepressants in patients with CHDand depression.Methods: Randomized controlled trials (RCTs) were searched in MEDLINE, EM-BASE, PsycINFO, the Cochrane Controlled Clinical Trial Register and other trialregistries, and references of relevant articles. The primary outcomes were read-mission for CHD and all-cause mortality; the secondary outcome was the severityof depression symptoms.Results: Seven articles on six trials involving 2461 participants were included.One study incorrectly randomized participants, and another one was a re-analysisof RCT data. Both were excluded from the main analysis; however sensitivitymeta-analyses were performed including these trials in order to consider all of theavailable information. When only properly randomized trials were considered (pa-tients n.=734), SSRIs patients showed no significant improvement in mortality orCHD readmission rates, as compared to controls. Two of the three RCTs showedRRs that were reduced, but not significant (p=0.24). Conversely, when all stud-ies were considered, patients assuming SSRI showed a significantly lower rateof CHD readmissions during the follow-up as compared with controls (RR=0.63;95% CI: 0.46-0.86). Similarly, when all studies that assessed all-cause mortalitywere combined, a significantly lower risk of death (RR=0.56; 95% CI: 0.35-0.88)was observed for SSRI patients, but this association was no longer significantwhen the two studies with incorrect randomization were excluded (p=0.26). Fourstudies compared the remission rate for depression in patients assuming SSRIsversus controls. No relevant differences emerged excluding the trial with incorrectrandomization: compared with control, the assumption of SSRI determined a 35%increase in the rate of remissions during the follow-up (95% CI: 15%-60%), andsuch a difference was highly significant (p<0.001).Conclusion: In patients with CHD and depression, SSRI medication reduce de-pression symptoms and may improve CHD prognosis. However, the evidence isscarce and future adequately powered trials are urgently needed.
P1463 Prospective association of depressive symptomswith coronary heart disease and stroke incommunity-dwelling elderly. The 3C Study
R. Pequignot1 , C. Tzourio2, J.F. Dartigues3, K. Ritchie4,P. Ducimetiere5, J.P. Empana1. 1INSERM U970, Paris
Cardiovascular Research Center, Paris V University, Paris, Paris, France;2INSERM U708, Paris, Paris, France; 3INSERM, U897, Bordeaux, France;4Inserm U888, University Montpellier 1, Montpellier, France; 5Paris SudUniversity, Paris, France
Purpose: To assess prospectively the association of depressive symptoms withincident coronary heart disease (CHD) and stroke in community-dwelling elderlyparticipating to the 3C Study.Methods: Depressive symptoms at baseline were defined as a CESD score ≥16in 7358 subjects who were free of prevalent CHD, stroke or dementia. CHD andstroke events occurring during 6 years of follow up were validated by two indepen-dent expert committees. Hazard ratios (HRs) were estimated by Cox proportionalhazard regressions.Results: The mean age was 73.8 years (range: 65 – 100) and 37% were male. Atbaseline, 22.9% had depressive symptoms and 6.7% used antidepressant. Aftera median follow up of 55 months, 601 subjects died, 273 had a first CHD eventincluding 57 fatal and 137 had a first stroke including 25 fatal. After adjustmentfor age, gender, study centre, living alone, education level, smoking status, alco-hol consumption, hypertension, diabetes mellitus, total cholesterol, MMSE score,antidepressant use and IADL impairment, association with depressive symptomsexisted for total mortality (HR=1.22, 95%CI: 1.01 – 1.48), fatal CHD (HR=1.90,95%CI: 1.05 – 3.44) and fatal stroke (HR=2.44, 95%CI: 1.01 – 5.87), but not fornon-fatal events. The multivariate-adjusted HR of depressive symptoms for thecombined end point of fatal CHD and stroke was 2.05 (95%CI: 1.26 – 3.35). Inthis latter model, antidepressant use (HR=2.09, 95%CI: 1.11 – 3.94) and IADLimpairment (HR=3.37, 95%CI: 1.93 – 5.86) were additional strong predictors.Conclusion: In community-dwelling elderly, depressive symptoms are indepen-dent predictors of fatal but not non-fatal CHD and stroke. This may have relevanceto the inability to cope with an acute event, the severity of the event or the aggres-siveness of hospital care more than to the development of the disease.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

232 Looking beyond the heart: psychosocial factors in heart disease
P1464 National survey of australian cardiologists beliefs andpractice regarding screening, diagnosis andmanagement of depression in cardiac patients
A.G.O. Stewart1, A. Driscol2, D.L. Hare3. 1Austin Hospital,Melbourne, Australia; 2Monash University, Melbourne, Australia;
3University of Melbourne, Melbourne, Australia
Over one third of cardiac patients are depressed. It is unclear whether depressionis thought important by cardiologists.Purpose: (1) Examine cardiologists’ beliefs and practice in relation to depressionscreening, diagnosis, treatment and referral Method: A national survey of all Aus-tralian cardiology members of the Cardiac Society of Australia & New Zealand(CSANZ) was conducted with a single page questionnaire.Results: Sixty percent of members responded (511 of 822 eligible). The major-ity screened for depression "sometimes", 49.8%, and 32.4%, "often" or "always".While 96.8% reported using no standard screening tool, 71.3% reported theywould use a short screening questionnaire if available. For responsibility of de-pression identification, General Practitioners (GPs) were highest ranked, followedby cardiologists and cardiac rehabilitation. For treatment of depression, GPs wereranked highest, followed closely by psychiatrists, then cardiologists and psychol-ogists. Most referred patients "sometimes" (40%) to GPs, psychiatrists and psy-chologists, and 56% of all surveyed "very much" wanted feedback on patientprogress. Most reported never treating depression with antidepressant medica-tion (40%), and the strongest predictor treatment was confidence in treating de-pression (r=0.616, p<0.0001), followed by, nomination of cardiologists for treat-ment (0.387, p<0.0001), belief in antidepressant efficacy (r=0.358, p<0.0001),and depression having an etiological role in CVD (r=0.158, p<0.0001). Most be-lieved depression was only "slightly" related to CVD development (41.2%), but"moderately" related to cardiac events and death, 53% and 49% respectively.Conclusions: Australian cardiologists are interested in depression but don’t usediagnostic screening tools. These results will assist the development of clinicalpathways.
P1465 Depression: a threat for both the heart failure patientand the family caregiver
G.-A. Dan1, A. Dan2, A. Buzea1, C. Stanescu1, D. Gologanu2 ,C. Adam2. 1University of Medicine and Pharmacy Carol Davila,Bucharest, Romania; 2Colentina University Hospital, Bucharest,
Romania
Depressive symptoms (DS) are encountered in one third of patients (pt) with heartfailure (HF) and the outcome consequences of DS in HF pt are well-known. Lessis known about the impact on family caregivers of the DS in HF pt.The purpose of our study was to demonstrate the differences in the quality of lifeof family caregivers of HF pt with or without DS as demonstrated by the difficulty ofcaregiving, time spent for caregiving and perception of the caregiving burden. Inour prospective transversal study we included 94 HF pt in stable condition, livingat home (mean age 65±11 yrs), recruited from a hospital database. The meanNYHA class was 3.1 and the mean ejection fraction was 29.6%. The presence ofDS in HF patients was measured by Beck Depression Inventory (BDI) with a cut-off point of ≥ 14 defining the presence of DS. The caregiver’s interview was doneby two independent observers in two different days. The time spent for caregivingand the perception of difficulty of caregiving were measured with the 15 itemsOberst Caregiving Burden Scale (OCBS) and the perception of the caregivingburden was evaluated with Zarit Burden Interview (ZBI) considering a score ≥ 17as indicating a perception of severe burden. In 85% of pt the caregiver was thespouse. A BDI score ≥ 14 was noticed in 36% of HF pt. There were no significantdifferences in the therapy in HF pt with or without DS. Caregivers of HF pt withDS demonstrated higher scores for the caregiving time spent and significantly(p=0.05) higher scores evaluating the difficulty of caregiving. 67% of caregiversin HF pt with DS demonstrated a ZBI score ≥ 17 vs. 23% in caregivers of HFpt without DS. (p=0.03). The mean ZBI score of caregivers in HF pt with DSwas significantly higher than in caregivers of pt without DS. Re-hospitalizationswere more frequent in pt in whom caregivers demonstrated a severe caregivingburden.Conclusions: DS in HF pt have an important impact on time spent for caregiving,difficulty of caregiving and caregiving burden. Further guidelines should focus onpertinent tools able to reduce both the DS in HF pt and the perception of highcaregiving burden.
P1466 Fear and negative affectivity significantly predictfuture cardiovascular events among patients withangiographically proven stable coronary arterydisease
V. Kiene1, V. Drexel1, A. Vonbank1, P. Langer1 , P. Rein2, C. Saely1,H. Drexel1. 1VIVIT Institute, Feldkirch, Austria; 2Private University,
Triesen, Liechtenstein
Purpose: Psychological patient characteristics in various clinical settings are im-portant predictors of outcome. We aimed at investigating the impact of fear andof negative affectivity on future cardiovascular events in patients with stable coro-nary artery disease (CAD).
Methods: We recorded cardiovascular events in 408 patients with angiographi-cally proven stable CAD over a mean follow-up period of 5.3±1.3 years. Negativeaffectivity and fear were recorded by validated standardized questionnaires.Results: Pathological fear scores at baseline were diagnosed in 8.8% and neg-ative affectivity in 39.8% of our patients. During the follow-up period, vascularevents occurred in 30.6% (n = 125) of the patients. High scores of fear (standard-ized adjusted hazard ratio (HR) = 1.33 [1.11-1.59]; p = 0.002) and of negativeaffectivity (HR = 1.26 [1.06-1.50]; p = 0.009) strongly and significantly predictedfuture vascular events.Conclusion: Fear and negative affectivity predict vascular events in patients withstable CAD. Therapeutic interventions targeted at these traits apart over andabove improving the patients’ quality of life may improve their cardiovascular out-come.
P1467 Influence of type d personality on the evolution overtime of quality of life, anxiety and depression
H. Miljoen1, K. Siebens1, C. Vrints1, J. Denollet2. 1University ofAntwerp Hospital (Edegem), Department of Cardiology, Antwerp,Belgium; 2Tilburg University, CoRPS Center of Research on
Psychology in Somatic diseases, Tilburg, Netherlands
Purpose: Patient-centered outcomes are becoming more and more important.The present study set out to evaluate the effect of the presence of Type D per-sonality on the evolution over time of health related quality of life, anxiety anddepression.Methods: 260 patients admitted to a chest pain unit of a university hospital withsymptoms suggestive of an acute coronary syndrome were included in a pre-post intervention trial to evaluate the implementation of a critical pathway. Theywere asked to fill in the following questionnaires during admission and at 1 and6 months: DS14, HADS A and D, EQ-5D and a visual analog scale to evaluatequality of life and anxiety. The results were then analyzed using multivariate anal-ysis for the influence of the baseline value, intervention group, presence of typeD, diagnosis type (cardiac vs. non-cardiac), age, sex and presence of heart failureon the outcome after six months.Results: Type D personality was present in 29% of patients. The table showsthe results of the multivariate analysis. In all cases baseline value was the mostimportant predictor. When this value was left out of the equation, the presenceof Type D personality has a deleterious effect on all the outcome measures. In-creasing age is important for quality of life and depression, female sex increasesthe score of HADS A, and the presence of heart failure decreases the EuroQOLscore and increases HADS A.
Outcome Variable Baseline Intervention Type D Diagnosis Age Sex Heart R2group Failure
EuroQOL 0.667*** – -0.099*** – -0.003** – -0.172* 0.348VAS QOL 0.552*** – -7.434*** – -0.364*** – – 0.342HADS A 0.454*** – 2.634*** – – -1.177* 2.910* 0.135VAS Anxiety 0.386*** – 1.415*** – – – – 0.277HADS D 0.631*** – 2.085*** – 0.080*** – – 0.361
Values reported are the B-coefficients. The R2 reported is that of the model without the baselinevalue. The stars indicate the level of significance: *p<0.05, **p<0.01, ***p<0.001.
Conclusions: the presence of Type D personality has a deleterious effect onquality of life, anxiety and depression six months after admission. This finding isimportant for possible future attempts to influence these outcome measures. Asage, sex and the presence of heart failure cannot be modified, efforts should bedirected to the modification of personality traits like Type D.
P1468 Development of type-d-personality in coronarypatients: a longitudinal study
V. Kiene1, V. Drexel1, P. Rein2, A. Vonbank1 , P. Langer1 ,C.H. Saely1, H. Drexel1. 1VIVIT Institute, Feldkirch, Austria; 2PrivateUniversity, Triesen, Liechtenstein
Purpose: Recently, the association between Type-D-personality, a combination ofnegative affectivity and social inhibition with cardiovascular events has attractedgreat interest. No longitudinal data are available on the development of Type-D-personality in patients with established coronary artery disease (CAD).Methods: Over a follow-up period of 6 years we investigated the developmentof Type-D-personality in 129 patients with angiographically proven stable CAD bymeans of a validated standardised questionnaire (DS-14).Results: The initial prevalence of Type-D-Personality was 24.8% in our cohort ofcoronary patients; during the follow-up of 6 years it increased to 40.3% (p for trend= 0.003). The prevalence rates of the two components of Type-D-Personality, so-cial inhibition and negative affectivity initially were 37.2% and 40.3%, respectively.Whereas the prevalence of social inhibition increased to 72.9% over 6 years(p <0.001), the prevalence of negative affectivity did not change substantially(45.7% after 6 years, p = 0.324).Conclusion: The prevalence of Type-D-personality in patients with stable CADincreases significantly over time, due to an increase in social inhibition. Giventhe important role of Type-D-personality for the prognosis for these patients, earlypreventive psychological interventions in coronary patients appear necessary.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Looking beyond the heart: psychosocial factors in heart disease / What affect quality of life and clinical outcomes 233
P1469 Sub-acute and acute stress could act as trigger foratrial fibrillation
A.V. Mattioli1, A. Farinetti1, S. Pennella2, S. Bonatti1, E. Giuliani1.1University of Modena & Reggio Emilia, Modena, Italy; 2NationalInstitute of Cardiovascular Research, Bologna, Italy
Background: Symptoms of depression and anxiety and major depression andanxiety disorders have been reviewed extensively as potential risk factors forcoronary artery disease, on contrary few studies evaluated the role of acute stressand anxiety on the development of atrial fibrillation (AF). The present study aimsto evaluate psychosocial factors and anxiety in patients (pts) with AF.Methods: Study population included 400 pts (200 men and 200 women, meanage 54±10.9 years) with first diagnosed AF. Pts with underline cardiac diseasewere excluded from the study. Of the total population, 171 pts (42.75%) spon-taneously recovered SR within 48 hours, the remaining were cardioverted usingdrugs or DC shock. All pts underwent the Recent Life Change Questionnaire,a test developed to evaluate sub-acute and acute psychological stress (stressrange 0-150). Pts were followed for 12 weeks to assess recurrences of AF.Result: Pts were divided in quintiles according to the Recent Life Change Ques-tionnaire. The median value of questionnaire was 33 with a range from 0 to 150,25° percentile was 22 and 75° percentile was 98. Of the 171 pts who sponta-neously recovered sinus rhythm, 129 were included in higher quintiles (3-4-5)and 42 in lower quintiles. We referred to first quintile as 1 and O.R. for sponta-neous cardioversion was 4.9 (95% CI 1.4-6) in the higher quintile. Recurrencesof AF were more frequent in patients in lower quintile (O.R. 2.1 95%CI 1.1-3.0)Conclusion: Stress influenced AF. Pts developing AF after an acute stress aremore likely to have a spontaneous recover of sinus rhythm. On contrary, recur-rences were more frequent in pts that developed the arrhythmia independentlyfrom an acute stress. This feature suggests a role of acute stress as a trigger ofAF and support the hypothesis that AF in healthy pts had a better prognosis interm of spontaneous cardioversion.
WHAT AFFECT QUALITY OF LIFE AND CLINICALOUTCOMES
P1470 Intravenous ferric carboxymaltose improves qualityof life in patients with chronic heart failure and irondeficiency regardless the presence of anaemia: ananalysis from the FAIR-HF study
J. Comin-Colet1, M. Lainscak2, K. Dickstein3, G. Filippatos4,P. Johnson5, T.F. Luscher6 , C. Mori5, R. Willenheimer7, P. Ponikowski8,S.D. Anker9. 1Heart Failure Program, Department of Cardiology, Hospital delMar, Barcelona, Spain; 2University Clinic of Respiratory and Allergic DiseasesGolnik, Division of Cardiology, Golnik, Slovenia; 3Stavanger University Hospitaland University of Bergen, Stavanger and Bergen, Norway; 4Athens UniversityHospital Attikon, Athens, Greece; 5Vifor Pharma, Glattbrugg, Switzerland;6University Hospital Zurich, Department of Internal Medicine, Division ofCardiology, Zurich, Switzerland; 7Health Heart Group and Lund University,Malmo, Sweden; 8Military Hospital, Medical University, Department of HeartDiseases, Wroclaw, Poland; 9Charite - Campus Virchow-Klinikum, Departmentof Cardiology, Division of Applied Cachexia Research, Berlin, Germany
Background: Patients with chronic heart failure (CHF) show impaired health-related quality of life (HRQoL), and iron deficiency may contribute to this.Aims and methods: We evaluated the effect of iron repletion using intravenousferric carboxymaltose (FCM) on HRQoL of iron-deficient CHF patients. The FAIR-HF trial randomized 459 CHF patients with impaired left ventricular ejection frac-tion and iron deficiency to FCM or placebo (2:1). HRQoL was assessed usingthe Kansas City Cardiomyopathy Questionnaire (KCCQ) and the generic EQ-5Dquestionnaire (Visual Analogue Scale [VAS]) at baseline and after 4, 12, and 24weeks of therapy. In both, higher scores indicate better HRQoL.Results: Baseline HRQoL directly correlated with serum ferritin and percenttransferrin saturation (r=0.11–0.18, p<0.05 for all) and FCM significantly improvedHRQoL measures at all time points (see table). This effect was observed regard-
QoL at baseline and changes with therapy
Baseline % Change from baseline(mean±SD) week 4 week 12 week 24
Placebo FCM Placebo FCM Placebo FCM Placebo FCM
EQ-5D VAS 54.1±15.2 54.3±17.1 1.5 11.0‡ 4.4 14.5‡ 6.3 16.8‡
KCCQ-OS 52.5±17.2 52.4±19.6 6.7 17.9‡ 8.8 23.3‡ 11.8 24.4‡
KCCQ-CS 55.4±17.4 55.5±20.0 5.6 18.7‡ 6.0 22.9‡ 7.0 21.6‡
KCCQ-TS 58.9±18.5 58.9±20.9 4.6 15.8‡ 5.6 19.7‡ 7.1 19.3‡
KCCQ Domain ScoresPhysical limitation 51.9±19.9 52.1±22.6 4.4 15.7‡ 6.4 20.1‡ 8.7 20.5†
Symptom stability 52.5±14.7 53.7±17.0 3.0 23.6‡ 3.2 26.4‡ 8.6 24.6‡
Symptom frequency 57.7±20.9 58.6±22.5 7.1 17.2‡ 5.5 20.5‡ 8.0 19.6‡
Symptom Burden 60.2±17.8 59.3±21.0 3.5 18.2‡ 5.5 22.4‡ 5.5 21.1‡
Self-efficacy 63.5±25.7 63.6±24.3 9.0 10.8 6.8 14.0† 9.4 15.2QoL 48.0±21.3 47.4±22.1 7.5 18.3† 9.4 28.0‡ 14.1 31.2‡
Social limitation 50.9±23.3 51.3±25.7 8.0 20.0† 14.1 23.6 * 16.7 25.5
*P<0.05; †P<0.01; ‡P<0.001 all vs placebo.OS: overall score; CS: clinical summary; TS: totalsymptom.
less of anaemia status (p-values for interaction: 0.93 [VAS] and 0.66 [KCCQ over-all score]).Conclusions: Intravenous FCM resulted in significant improvements in HRQoLduring 24 weeks of therapy. The positive effects were seen after 4 weeks of treat-ment and were independent of anaemia status.
P1471 Changes in patients’ behaviour and impact on qualityof life with the use of telemedicine (Motiva-Philips) inan heart failure unit: the CARME study (CAtalanRemote Management Evaluation)
B. Gonzalez1, M. Domingo1, J. Lupon1, R. Lopez1, A. Ramos1,E. Crespo1, A. Urrutia1, L. Cano1, C. Diez1, J. Valenzuela2. 1Germans TriasI Pujol University Hospital, Badalona, Spain; 2Philips Health Care, Barcelona,Spain
Background: Telemedicine can be useful in the management of patients withheart failure (HF) and can help nurses in their educative intervention and it canalso collaborate in improving the perception of Quality of Life (QOL) of HF pa-tients.Objective: To evaluate the changes in the patients’ behaviour obtained after aprogram of Remote Patient Management (RPM) in patients already managed ina HF Unit, and also to assess the impact of such program in the perception ontheir QOL.Methods: Patients were randomized in 2 groups: A) Motiva system without mea-surement devices (educative videos, messages, charts, questionnaires); and B)Motiva system + telemonitoring of blood pressure, pulse rate and weight. P inNYHA class I, those unable to cope with home monitoring in opinion of HF nurse,not having a TV or telephone, nor participating in another trial were excluded.Results: 97 patients were initially included in the study. 22 out of them voluntar-ily discontinued, 5 patients withdrew consent for last evaluation and 3 patientsdied during the study (1 after early de-installation). Then, 68 P (71% men; meanage 65.8±10.9 years; 85% in NYHA class II and 15% in class III) completedthe evaluation period (1 year) and the study questionnaires. Positive changes inpatients’ behaviour were mostly observed although no effect on nutritional and ex-ercise data recording was obtained (figure). The perception of QOL significantlyimproved both with EuroQOL (p<0.001) and MLWHFQ (p=0.005) when paireddata were analyzed (Wilcoxon test).
Changes in patients’ behaviour
Conclusion: Although the number of patients who discontinued RPM was farfrom negligible, positive changes in several aspects of patients’ behaviour wereobserved with the use of RPM, together with the improvement in the perceptionof their QOL.
P1472 Better clinical outcomes of participants in clinicalresearch: Trial effect of an observational study inpatients with non ST elevation acute coronarysyndrome (NSTE-ACS)
G.N. Viswanathan1, J. Jardine2, M. Bhardwaj3, P. Adams4,S. Marshall1, A. Zaman5. 1Institute of cellular medicine, Newcastle University,Newcastle upon Tyne, United Kingdom; 2Newcastle University, Newcastle uponTyne, United Kingdom; 3Cesagen, Cardiff University, Cardiff, United Kingdom;4Newcastle upon Tyne Hospitals NHS foundation trust, Newcastle upon Tyne,United Kingdom; 5The Cardiothoracic Centre, Freeman Hospital, Newcastleupon Tyne, United Kingdom
Participants in randomized clinical trials have favourable outcomes than non-participants (trial effect). There is paucity of data on trial effect in observationalstudies and acute medical illness.Methods: We prospectively screened 458 patients admitted with Non-ST Ele-vation – Acute Coronary Syndrome (NSTE-ACS) and eligible patients were re-quested to take part in an observational study, which compares the efficacy ofdual antiplatelet therapy in patients with and without type 2 diabetes mellitus. Allpatients were treated as per ESC/AHA guidelines. 66 patients who volunteered(attendees) were compared to 30 who, for personal reasons, withdrew from thestudy (refusers). No study specific interventions were performed and there wereno alterations to further treatment.Results: Baseline cardio vascular risk profile, secondary prevention therapy andsocial deprivation indices were similar but there were more males in the ‘atten-dees’ group (77.3% v 60.0%, p<0.05). All cause re-admission was significantlylower in ‘attendees’ group. (21.2% v 63.3%, p <0.05, OR 0.06). This group had
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
234 What affect quality of life and clinical outcomes
lower re- admissions due to a cardiac cause (6.1% v 53.3%, p<0.05, OR 0.06)and mortality (1.5% v 16.7%, p<0.05, OR 0.08).There were no evidence of treat-ment effect, protocol effect, Hawthorne effect, care effect or placebo effect. Betterself motivation, acceptance of illness and adherence to medical advice were thelikely factors. Psycho-social factors such as altruism, belief in common good andhope may have influenced the outcomes of the attendees.
Conclusion: Clinical study participants had significantly better outcomes and ob-servational studies should routinely present this data to ascertain their general-isability.Large scale studies should explore this phenomenan which may improveclinical outcomes.
P1473 Optimising education for heart failure patients with aself-care manual
M. Boyde1, C. Turner2 , D.R. Thompson3 , S. Stewart4. 1Universityof Queensland, Princess Alexandra Hospital, Brisbane, Australia;2University of Queensland, Brisbane, Australia; 3University of
Leicester, Leicester, United Kingdom; 4Baker IDI Heart and Diabetes Institute,Melbourne, Australia
Purpose: Heart failure management has routinely incorporated patient educationto promote self-care activities which assist patients to maintain their own health.Health care professionals need disease specific patient centered education re-sources to optimise education for this cohort of chronically ill patients.Method: A self-care manual was developed following investigation of the learn-ing style and the learning needs of heart failure patients. A Heart Failure LearningStyle and Needs Inventory was completed by 55 heart failure patients: mean age64.25 years ±13.21; 69% were males; 44% NYHA Class II, 44% NYHA Class III.From this group a purposive sample of 12 patients representing each of the learn-ing styles participated in semi-structured interviews to identify their preferencesfor information delivery.Results: With regard to learning style 64% preferred multimodal educational re-sources, with read/write being identified as the strongest single style (18%). Pa-tients preferred to read, record and refer back to written information establishingthe need for a comprehensive written manual as the platform for an educationalstrategy. Patients ranked their key learning needs firstly as signs and symptomsand secondly the significance of their disease and whether it can be cured. Riskfactors and medications were ranked third and fourth respectively. Four themesemerged: 1) knowledge quest (L-loading); 2) barriers to learning (L-inhibitors);3) facilitators for learning (L-agonists); and 4) meeting educational needs (L-titration). Integral to these themes was the participant’s relationship with healthcare professionals. The ‘GO-Getting on with heart failure manual’ was developedbased on this quantitative and qualitative data and provides a patient-centeredapproach divided into sections which address the patients identified learningneeds.Conclusion: This study has developed a unique self-care manual for patientsthat is now being evaluated in the ‘Guided Heart Failure study’, a randomisedcontrolled trial.
P1474 Sleep disordered breathing in community dwellingelderly-associations to cardiovascular disease,impaired systolic function and mortality. A six yearfollow-up
P. Johansson1 , M. Ulander2, U. Alehagen1, E. Svanborg2,U. Dahlstrom1, A. Brostrom2. 1Department of Cardiology,University
Hospital of Linköping, Linköping, Sweden; 2Department of ClinicalNeurophysiology, Linköping University Hospital, Linköping, Sweden., Linköping,Sweden
Study Objectives: To investigate whether sleep disordered breathing (SDB) isa factor that affects mortality in elderly people, with special focus on those witha cardiovascular disease (CVD) and/or signs of impaired cardiac function. Set-ting: Community. Participants: 331 elderly aged between 71-87 years. Measure-ments: SDB was recorded by whole night polygraphic recordings in the subjectshomes. Presence of CVD and impaired systolic function were established by clin-
ical and echocardiographic examinations, as well as by N-terminal fragment ofproBNP (NT-proBNP). Those with ischemic heart disease (IHD) and TIA/strokewere amalgamated into one group labelled CVD. Mortality data were collectedafter six years.Results: In the total population no significant associations between mortality anddifferent degrees of SDB were found. In those with CVD oxygen desaturationindex (ODI)≥10 was associated to mortality. The hazard ratio of 6.1 (CI 95% 1.9-19.9, p=0.002) remained statistically significant after adjustments for age, gender,smoking, BMI, diabetes, LVEF<50% and plasma values of NT-proBNP.Conclusion: SDB in community dwelling elderly has no overall association tomortality irrespective degree of SDB. However hypoxia events (i.e., ODI≥10) wasa predictor for mortality in the group who had CVD in combination with an im-paired systolic function as measured by the plasma marker of ipmpaired systolicfunction (NT-proBNP).
P1475 Sleeping patterns in patients with ICD
S. Kikkenborg Berg1, M. Higgins2, S. Dunbar2. 1Rigshospitalet,Copenhagen University Hospital, Copenhagen, Denmark; 2EmoryUniversity School of Nursing, Atlanta, United States of America
Purpose: Sleep disorders contribute to the development of chroniccardiovascular conditions, and contribute increased morbidity and mortality in car-diac patients. The purpose of this study was to describe sleep patterns and as-sociated psychological and physical factors in patients during the first 6 monthsafter ICD implantation.Methods: Data were from a longitudinal study of ICD patients (n=235) in whichthe Pittsburgh Sleep Quality Index (PSQI) and The Epworth Sleepiness Scale(ESS) were used to measure sleep quality and daytime sleepiness. Variables andmeasures were anxiety (State-Trait Anxiety Inventory, STAI), depressive symp-toms (Beck Depression Inventory II, BDI-II), functional status (Duke Activity Sta-tus Inventory, DASI), pain (Brief Pain Inventory, BPI).Results: Participants were 75% men, mean age 58.5 years, 33.8% NYHA IIIand IV, mean LVEF 26.3%. Fifty percent had a history of SCD. 13 patients (6.8%)received ICD shock within 6 months. There was a change in PSQI score over time(p<.0001) with 57-77% having scores >5 indicating poor sleep quality (Table).Mean PSQI scores were higher for those with lower DASI CO-efficient –0.056(SE=0.01), higher BPI severity 0.08 (SE=0.02), and higher BDI-II 0.13 (SE=0.03)scores at BL. Approximately 40% had ESS scores of 10 or more which decreasedover time. ESS score was predicted by lower baseline DASI, NYHA III or IV andhigher BDI-II scores at baseline.
PSQI and ESS score results
BL (n=235) 1 month (n=212) 3 month (n=194) 6 month (n=190)
PSQIRange 1-19 2-20 0-21 1-18Mean ± SD 7.8±4.2 8.5±4 6.8±4.3 7±4.3% score > 5 77.2% 75% 52.6% 57.4%ESSRange 0-24 0-24 0-22 0-22Mean ±SD 8.2±5.2 8.1±5 7.9±4.5 7.6±4.9% score >10 40.4% 36.8% 29.5% 32.6%
Change in PSQI and ESS score over time p<0.001.
Conclusions: More than half the patients with ICD experience poor sleep qualityduring the first 6 month, and 1/3 experience daytime sleepiness. Low sleep qualityis associated with low physical function, depression and pain. Daytime sleepinessis associated with low physical function, depression and NYHA III and IV.
P1476 A prospective, randomized trial of kinetic therapy inpatients with cardiogenic shock
G. Simonis, K. Steiding, K. Schaefer, T. Rauwolf, R.H. Strasser.Dresden University of Technology, Dresden, Germany
Background: Kinetic therapy (KT) has been shown to reduce com-plications and to shorten hospital stay in trauma patients. Data in non-surgicalpatients is inconclusive. Retrospective data suggest a beneficial effect of KT inpatients with cardiogenic shock (CS) requiring ventilator therapy. KT, however,has not been tested prospectively in those patients.Methods: A prospective, randomized, open-label trial was performed to compareKT using oscillating beds (Triadyne, KCI) with standard care (SC). Patients withcardiogenic shock requiring ventilator therapy for more than 24 h were included.End points were the occurrence of hospital-acquired pneumonia and of pressureulcers during the hospital stay and 1-year all-cause mortality.Measurements and main results: 45 patients were randomized to KT, and 44patients to SC. All patients required at least one inotropic agent and one va-sopressor for circulatory assistance. The groups were comparable in age, bodymass index, use of balloon counterpulsation, and APACHE-II-score (33 vs 34)and SOFA-score (11 vs. 11) at inclusion. Hospital-acquired pneumonia occurredin 10 patients in KT and 28 pts in SC (p<0.001); pressure ulcers were reduced by80% (p<0.001). Hospital mortality tended to be lower in KT, and 1-year all-causemortality was 40% in KT and 61% in SC.Conclusion: The use of KT shortens hospital stay and reduces rates of pneumo-nia and pressure ulcers as compared to SC. Moreover, in this study, patients with
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
What affect quality of life and clinical outcomes 235
KT had a better outcome. The study suggests that KT should be used in patientswith cardiogenic shock requiring ventilator therapy for a prolonged time.
P1477 Nurse-led early triage of chest pain patients: anobservational study to evaluate a servicedevelopment aimed at improving the management ofpatients with non-ST-elevation acute coronarysyndromes
L. O’neill1, C.C. Lang2. 1University of Brighton, Brighton, UnitedKingdom; 2NHS Tayside, Dundee, United Kingdom
Background: Patients presenting with non-ST-elevation acute coronary syn-dromes (NSTE-ACS) are at risk of early death. This may be reduced by promptassessment and therapeutic intervention.Objectives: (i)To evaluate if nurse-led chest pain triage can improve time to as-sessment and the management of ACS patients. (ii)To re-evaluate if any benefitsare sustained several years later when established as routine care.Methods: NET-1 study – Initial data on 79 consecutive chest pain patients ad-mitted before the introduction of chest pain triage and on 103 patients admittedin the 1st 6 months of the service, was re-examined. The primary outcome mea-sure was time to 12-lead ECG. NET-2 study - Data was gathered on 92 patientsadmitted to the current CCU triage service and on 22 patients admitted to acuteadmissions, who were denied access to CCU triage. End-points were comparedbetween all groups and differences analysed by the CHI squared test for categor-ical variables and the Mann Whitney-U test to compare median times.Results: NET-1 - Nurse-led early triage resulted in statistically significant im-provements in the number of chest pain patients who had their 12-lead ECGperformed within 10mins of admission (94% vs 32%, p<0.001) and the numberof high risk NSTE-ACS patients receiving Clopidogrel (72% vs 42%, p<0.05) andbeing managed in CCU (82% vs 34%, p<0.001). Completion of NET-2 and com-parison of current triage with NET-1 non-triage (baseline control) demonstratedthat these measurable benefits were sustained with p-values of p<0.001 forcomparative ECG times, Clopidogrel prescribing and whether managed in CCU.There were no significant differences in outcomes between NET-2 triage andNET-1 triage demonstrating that current triage is as effective as it was when theservice was introduced. Comparison of the current triage group with the currentnon-triage group (of relatively smaller sample number) revealed that there wereno significant differences between the number of high risk NSTE-ACS patientsprescribed Clopidogrel or referred for angiography however patients in triage re-ceived these drugs more promptly and the difference in median time was signifi-cant (1hr 37m vs 9hr 50m, p<0.05).Conclusions: The current study demonstrated the positive impact of nurse-ledearly triage on the management of patients with non ST-elevation ACS and thatinitial benefits seen when the service was first introduced have been sustained.
P1478 Nursing role in clinical pathways to improve care topost operative patients after bypass surgery. A 10years experience
M. Wit, A. Schaap, C. Burgersdijk, V.A. Umans. Medical CenterAlkmaar, Alkmaar, Netherlands
Background: Critical pathways attempt to increase efficiency by organizing thecare delivery process into individual analysable steps. However, full advantagemay only be reached if the process is governed by a ‘process care taker’.Currently, new opportunities are emerging for nurses to become involved assovereign health care specialists and may become an intermediate between pa-tient and clinical team. We evaluate a critical pathway with a nurse-practitioner inthe ongoing consecutive experience in critical practice.Methods: The introduction of a critical pathway into the hospital information sys-tem allows continuous surveillance of clinical outcome as well as variance in-dicators. Primary goals were improved guideline-adherence and reduced walk-through times in the 1336 consecutive pathway versus 235 consecutive controlpts.
Results: The pathway was launched in 01-2000. Since then, 1671 all-comer,post-operative pts have been treated using this integrated critical pathway. Duringthe 10 yrs period, 1436 patients were treated by the nurse practitioner (NP) and235 by residents (C). A total of 1671 patients were transferred from the surgery tothe teaching hospital at a mean of 5.5 and 6.3 days after the operation (NP vs C,
respectively). Typically these patients were men (79%) with a mean age of 67±11years. The NP pts were discharged significantly sooner than those C pts (4.5 vs 6days;p<0.001). The 30-day mortality rate was comparable in both groups: 0.4%.
P1479 Outcomes from the first year of a nurse-led preadmission clinic for elective PCI patients
A. Pottle, J. Breen, C. Hayes, T. Joseph, S. King. CardiologyDepartment, Harefield, United Kingdom
Purpose: In the UK, most patients being admitted to hospital forelective procedures/operations, attend a pre-admission clinic. In January 2009a nurse-led pre admission clinic was established for patients admitted for electivePCI or angio ? proceed.Method: Patients were asked to attend the clinic initially if they were under thecare of one of the institutions cardiologists. The clinic is run weekly on a Tuesdayafternoon and is nurse and pharmacist led. Two nurses are present in the cliniceach week, the Consultant nurse and a nurse specialist. A maximum of 10 pa-tients are booked into the clinic. A 3-month pilot study was carried out and theclinic was then extended to all elective PCI patients.Patients attend the clinic 1-2 weeks prior to the planned date of admission. Detailsof symptoms, medical history and clinical examination are recorded in the inte-grated care pathway. The procedure is explained and any additional informationgiven. The pharmacist reviews the medication and prescribes Clopidogrel to start1 week before admission, to those patients not already taking dual anti-platelettherapy. Baseline vital signs are recorded. Routine blood tests are taken includingrenal function and patients are screened for MRSA. Results of these investiga-tions are checked following the clinic and action taken as necessary. Patientswere asked to complete a satisfaction survey during the pilot study.Results: 267 patients were reviewed in the clinic in the first year. The followingresults are from the 66 patients seen during the 3-month pilot study. 1 patient wasfound to be MRSA positive and therefore had his admission delayed. 3 patientswere found to have impaired renal function which had not been known. They wereadmitted earlier than planned for pre-hydration and acetyl-cysteine. 4 patientswere not sure what procedure they were being admitted for and 1 patient wasundecided as to whether to have the PCI. Attendance at the clinic allowed timefor explanation and discussion of the pros and cons to facilitate informed consent.12 patients had a variety of problems related to medication which were addressedin the clinic and a total of 43 patients were issued with a prescription. 54 surveyswere returned (82%). 83% of patients were ‘very satisfied’ with all aspects of theclinicConclusion: Attendance at a pre-admission clinic facilitates a smooth admis-sion to hospital. Patients appear to be better informed if they have attended theclinic. Important co-morbidites can be treated prior to admission thereby reduc-ing patient risk. The pre-admission clinic can be successfully run by nurses andpharmacists.
P1480 Does telephone follow-up after discharge for acutemyocardial infarction affect patient experience withhospital care?
T.A. Hanssen1, J.E. Nordrehaug2, K. Oterhals2, B. Rokne3.1Division of Cardiothoracic and Respiratory Medicine, Tromsoe,
Norway; 2Haukeland University Hospital, Bergen, Norway; 3University of Bergen,Bergen, Norway
Background: Patient experience assessments are increasingly used to describehealth care from the patient’s point of view and evaluate outcome of health care.In a context where existing follow-up services were poorly developed, we havepreviously demonstrated that a telephone follow-up intervention after dischargefrom hospital, showed positive effects after 6 months on the primary endpoint,the physical dimension of health related quality of life. No long term effects onphysical or mental health related quality of life were found.Purpose: To assess whether the telephone follow-up intervention improved pa-tient’s experience of quality of hospital care and analyse what factors are associ-ated with satisfaction/dissatisfaction with hospital care.Method: Out of 413 screened patients with a diagnosis of acute myocardial in-farction, 288 patients consented to participate, and were randomized to an in-tervention or a control group. The intervention group received weekly telephonefollow-up by a nurse the first four weeks after discharge, thereafter in week 6,8, 12 and 24, in addition to the standard post discharge follow-up of the controlgroup. Endpoint data in this study was collected through mailed questionnairessix weeks after discharge using the Patient Experiences Questionnaire and aquestionnaire assessing perception of received information.Results: There were no significant differences between the intervention- and con-trol group on the ten summated rating scales in the Patient Experiences Ques-tionnaire. Patients in the intervention group to a smaller extent experienced thatthere were need to improve information and follow-up after discharge, comparedto the control group. Further, they experienced lack of information after dischargeto a significant smaller extent. Factors associated with satisfaction/dissatisfactionwith hospital care are to be presented and discussed.Conclusion: The telephone follow-up intervention did not affect the patient’s ex-perience of hospital health care. However, the telephone follow-up contributedpositively to satisfaction with follow-up and reduced the information needs experi-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

236 What affect quality of life and clinical outcomes / Culture and society: how do they affect heart disease and treatment
enced after discharge. Predictors of satisfaction/dissatisfaction with hospital careare identified.
P1481 Anxiety and quality of life in teenagers withparoxysmal tachycardia
A. Maryniak1, A. Bielawska1, K. Bieganowska1, M. Miszczak-Knecht1, L. Szumowski2, F. Walczak2. 1Children’s Memorial HealthInstitute, Warsaw, Poland; 2Institute of Cardiology, Warsaw, Poland
From the stress theory, the attacks of tachycardia are a particularly difficult sit-uation, characterized among other by a high unpredictability in terms of time (itcan be expected that a further attack will take place, but without knowing when)and the low ability of control – the patient has a limited effect of the course ofthe attack. The aim of the study was to assess the emotional functioning, espe-cially anxiety, and quality of life in teenagers with paroxysmal supraventricular oratrio-ventricular tachycardia.Methods: 129 patients (71 F, 58 M), aged 11-18, among them 74 with WPW Syn-drome, qualified for ablation due to paroxysmal atrial or atrio-ventricular tachycar-dia, were examined psychologically. A detailed interview concerning the symp-toms of arrhythmia and every-day functioning was performed. Utilizing State-TraitAnxiety Inventory the level of anxiety was tested in two aspects - as its currentstate and as a trait, i.e. general tendency to respond with anxiety to perceivedthreats in the environment. To assess QoL applied Cantrill Ladder – tests on ascale of 0 to 10 assessing their current satisfaction with life as well as the bestand worst levels in the last year.Results: In the analyzed group boys showed a significantly higher level of stateanxiety than girls (t=-2.11; p=0.03). A difference between the sex was also notedin results of QoL assessment – the worst level was decidedly lower assessed byboys (z=2.04; p=0.04). Patients often declared that the appearance of arrhythmiawas their worst period. A significant negative correlation was ascertained betweenthe anxiety and the age of the appearance of the first symptoms (p=0.005).Conclusions: the occurrence of AVNRT or AVRT attacks, particularly appearingin early childhood, can affect emotional development, expressed in a constantlyhigher level of anxiety as a trait. The biggest threat of improper development isamong boys, who emotionally have worse toleration of arrhythmia than girls.
P1482 Can lifestyle and risk factors explain differences inmortality and cardiovascular incidence in men inFrance and Northern Ireland? Evidence from thePrime study
J.W.G. Yarnell1, C.C. Patterson1, J. Woodside1 , D.R. Arveiler2,P. Amouyel3, J. Ferrieres4, A. Bingham5, P. Ducimetiere5. 1Queen’s University,Belfast, United Kingdom; 2MONICA-Strasbourg, Strasbourg, France; 3MONICA-Lille, Lille, France; 4MONICA-Toulouse, Toulouse, France; 5INSERM U780,Paris, France
Purpose: We examine the contributions of health behaviours and biological riskfactors to the differences in all- cause mortality and cardiovascular incidence be-tween France and Northern Ireland.Methods: 10,593 men aged 50-59 years were examined in 1991–94 in centresin Northern Ireland and France. Men were screened for evidence of coronaryheart disease (CHD) and prior stroke, and followed annually for 10 years by ques-tionnaire for incident cases of CHD and stroke. Deaths and cardiovascular (CV)events (coronary deaths, myocardial infarction and stroke) were documented byclinical records and were reviewed by a medical committee. Health behaviours(lifestyle) included lifetime smoking habit (pack years), inhalation, alcohol con-sumption, physical activity and fruit and vegetable consumption.Biological riskfactors included lipids and fibrinogen, measured in the same central laboratoriesfor all men, blood pressure, diabetes and body mass index. Statistical analysiswas performed using Cox Proportional Hazards. Bootstrapping was used to ob-tain 95%CIs for the explained percentages.Results: At 10 years of follow-up there were 510 deaths from any cause and409 fatal and non fatal CV events in men without evidence of CV disease atbaseline. All-cause mortality was 49% higher and CV incidence 92% higher inNorthern Ireland. Adjustment for biological risk factors attenuated the differencein all-cause mortality by 7% and in CV incidence by 24%. Separate adjustment forlifestyle explained 31% of the difference in all-cause mortality and 39% of that inCV incidence. Combining risk factors and lifestyle explained 34% of the differencein all-cause mortality and 56% of that in CV incidence.Conclusion: Health behaviours and biological risk factors "explain" about half ofthe difference in cardiovascular incidence and a third of the difference in all-causemortality, but health behaviours make the greater contribution.
Abstract P1482 – Table 1. Risk of death or cardiovascular event at 10 years follow-up in Northern Ireland compared to France - hazard ratios (95% CI)
Outcome Age Age and lifestyle Age and risk factors Age and both Explained by lifestyle Explained by risk factors Explained by both
All deaths 1.49 (1.24,1.79) 1.32 (1.07,1.63) 1.45 (1.19,1.77) 1.30 (1.05,1.62) 31% (5%,85%) 6% (-13%,37%) 34% (5%,93%)CV events 1.92 (1.57,2.35) 1.49 (1.19,1.87) 1.64 (1.33,2.03) 1.34 (1.05,1.69) 39% (21%,63%) 24% (12%,42%) 56% (33%,89%)
Explained percentages (95% CIs) calculated on logarithmic hazard ratio scale.
P1483 Organisation of care for swedish patients with animplantable cardioverter defibrillator, a nationalsurvey
K. Bolse1, I. Johansson2 , A. Stromberg2. 1School of Socialand Health Sciences, Halmstad University, Halmstad, Sweden;2Linkoping University Hospital, Linkoping, Sweden
Background: ICD implantations have developed rapidly in recent years and isnow an established arrhythmia treatment. The expanding indication for ICD im-plantation demands new competencies and resources in the ICD team members.Objectives: To describe the clinical aspects of Implantable Cardioverter Defibril-lators (ICD) care in Sweden with focus on organisation, the role and education ofnurses, patient information and education, and areas in need of improvement.Methods: Participants were recruited among physicians and nurses in all of thehospitals implanting ICDs (N=16). Data was collected by a questionnaire. Thequestionnaire was constructed based on a systematic literature review and thenguided by an expert group with clinical and research expertise within the ICDarea. The format was inspired by existing questionnaires on heart failure care.The questionnaire comprised of 23 questions, including both multiple choicequestions and open questions. Additionally, all written educational materials pro-vided to patients pre- and post-ICD implant were collected from all 16 hospitals.Deductive content analysis using Sarvimäki and Stenbock-Hult’s five holistic di-mensions was employed to ascertain how information was provided in brochuresand information materials.Results: This study revealed variations in the organisation and follow-up of ICDpatients between the different centres in Sweden. Half of the hospitals (n=8)had nurse-based outpatient clinics and several others planned to introduce them.Three hospitals carried out distance follow-ups by means of tele-monitoring. Thenurses had received specific ICD education from ICD companies and/or variousuniversity courses. In all hospitals, ICD patients received verbal and written infor-mation both before and after implantation. The biophysical dimension dominatedin the information material while the emotional, intellectual, and socio-cultural di-mensions were scarcely described, and the spiritual- existential was not referredto at all. The majority of the ICD teams were in favour of the development ofresearch and quality assurance by means of check lists, guidelines and the ICD-registry.Conclusion: Holistic care of ICD patients can be achieved by means of a multi-disciplinary ICD team and more patient-centred educational strategies. In Swe-den, the organisation of ICD care and follow-up is developing towards more nurse-based clinics. The content of the written educational materials need to be moreholistic, rather than mainly focusing on the biophysical and technical aspects ofliving with an ICD.
CULTURE AND SOCIETY: HOW DO THEY AFFECTHEART DISEASE AND TREATMENT
P1484 Standing at the crossroads between new and oldforms of heart disease in urban black Africans:the Heart of Soweto cohort study
S. Stewart1, M.J. Carrington1, A. Becker2, S. Pretorius2,P. Methusi2, K. Sliwa3. 1Baker IDI Heart and Diabetes Institute,
Melbourne, Australia; 2Soweto Cardiovascular Research Unit, Johannesburg,South Africa; 3(1)Hatter Institute for Cardiovascular Research, Groote SchuurHospital, University of Cape Town, Cape Town, South Africa
Background: The Heart of Soweto Study is tracking the contemporary burdenimposed by well established ("old") versus emerging ("new") forms of heart dis-ease (HD) in an urban African community in epidemiologic transition.Methods: Chris Hani Baragwanath Hospital in Soweto, South Africa, provideshealth care to >1 million mainly black Africans. We systematically captured datafrom all de novo cases (n = 5328) attending the hospital’s Cardiology Unit during2006-2008.Results: There were 3168 female (aged 52±18 years) versus 2160 male (aged53±17 years) cases, with black African women predominating (n = 2859, 54%).Three distinct clinical groups were identified (pre-specified criteria): 1) 999cases (19% of all cases) with a single diagnosis (mostly hypertension [HT]),2) 1862 cases (35%) of new, non-communicable HD (1146 and 581 cases ofhypertensive heart failure [HF] and coronary artery disease, respectively) and 3)2092 cases (39%) of older forms of HD in Africa. The latter comprised 724 withprimary valve disease and 502 idiopathic dilated cardiomyopathies in addition toa large component of underlying HT (n= 611, 29%). Cases were often complex,with a mean of 1.9±0.9 diagnoses; those with the least education present-ing with the most diagnoses (p = 0.045). Presentation with old forms of HDwas highest in those aged 20 - 49 years (rising from 19 to 60 cases/100,000 popu-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Culture and society: how do they affect heart disease and treatment 237
lation p.a.), but infrequent in the same age group for new forms of HD (peak of343 cases/100,000 in > 60 years age group). On an adjusted basis, those witholder forms of HD were younger (mean age 47±18 vs. 59±14 years: adjusted OR0.98, 95% 0.97-0.99, p<0.0001), more likely to be black African (93% vs. 79%:OR 3.76, 95% 2.23-6.63, p<0.001) and originate from Soweto (55% vs. 51%:OR 1.37, 95% 1.00-1.89, p=0.049). Alternatively, the presence of a family history,hyperlipidaemia, hypertension and obesity increased the risk of presenting withnewer forms of HD. Secondary valve dysfunction (advanced pathology) in thosewith older forms of HD was independently associated with being male (22% vs.16%, OR 1.38, 95% CI 1.04-1.83, p=0.027), little or no education (23% vs. 15%,OR 1.40, 95% CI 1.08-1.81, p=0.012), a history of smoking (23% vs. 14%, OR1.66, 95% CI 1.26-2.19, p<0.0001) and a greater body mass index (26.1±6.5 vs.26.7±6.1 kg/m2, OR 1.02, 95% CI 1.00-1.04, p=0.038).Summary: These data suggest that urban regions in sub-Saharan Africa stand atthe cross-roads between more traditional and newer forms of HD. Dynamic socio-economic and lifestyle factors appear to be modulating the type and severity ofunderlying HD.
P1485 Socioeconomic deprivation is associated with ahigher risk of all forms of cardiovascular disease over25 years: a cohort study of over 15,000 men andwomen
P.S. Jhund1, J.D. Lewsey2, C.L. Hart2, K. Macintyre2,J.J.V. Mcmurray1. 1University of Glasgow, BHF Glasgow
Cardiovascular Research Centre, Glasgow, United Kingdom; 2University ofGlasgow, Department of Public Health and Health Policy, Glasgow, UnitedKingdom
Purpose: To examine the association between socioeconomic deprivation (SED)and cardiovascular disease (CVD) after adjustment for major CVD risk factors.Methods: We analysed a cohort study of 15,378 men and women, age 45-64,surveyed between 1972-76 in Renfrew and Paisley, Scotland. Those with nohistory of coronary heart disease (CHD) (angina, myocardial infarction (MI), is-chaemia on ECG) at screening were followed up through register linkage for hos-pitalisation for 25 years. We calculated hazards ratios (HR) for a first dischargewith, MI, any CHD, stroke, heart failure (HF) or any cardiovascular disease (CVD)using Cox regression. Analyses were adjusted for age, sex, cholesterol, smoking,systolic blood pressure, and history of diabetes. The strength of association be-tween SED and MI and SED with stroke was compared using a competing riskanalysis. SED was defined by the Carstairs deprivation index and by social class.Results: 12795 men and women with no history of CHD could be assigned aCarstairs index and 12480 a social class. SED was associated with a higher risk ofeach form of CVD using both measures of SED (Table). The association betweenSED and MI was similar to that of SED and stroke (P=0.23 for comparison ofassociation using Carstairs and P=0.04 using social class).
Adjusted hazard of CVD according to SED
Number with event HR (Most vs least deprived) 95% CI P
Carstairs IndexCVD 4529 1.39 1.21-1.58 <0.001CHD 1761 1.61 1.28-2.02 <0.001MI 1314 1.48 1.14-1.92 0.003Stroke 1238 1.78 1.36-2.33 <0.001HF 661 1.49 1.06-2.09 0.022
Social ClassCVD 4433 1.40 1.17-1.68 <0.001CHD 1735 1.43 1.07-1.90 0.015MI 1299 1.44 1.03-2.01 0.032Stroke 1212 1.50 1.07-2.09 0.017HF 649 1.78 1.12-2.18 0.014
Conclusions: SED is associated with all forms of CVD over 25 years of followup. No difference in the association with stroke and MI was observed.
P1486 Socioeconomic and environmental factors are themain determinants of regional differences incardiovascular mortality in Poland ecological analysis
G. Broda, W. Piotrowski, P. Kurjata, M. Polakowska, E. Sygnowska,A. Waskiewicz, A. Piwonska, J. Piwonski. National Institute of
Cardiology, Department of CVD Epidemiology & Prevention & Health Promotion,Warsaw, Poland
Background: Cardiovascular disease (CVD) are the leading cause of death in all16 administrative provinces in Poland. CVD mortality rates and prevalence of CVDrisk factors vary considerably by province however data from National Surveyshowed that the mortality rates are not clearly corresponded with the prevalenceof CVD risk factors in particular provinces. It suggests that other factors can playimportant role in the differences in CVD mortality within country.Aim: To assess the extent to which classical CVD risk factors and wide rangeof socioeconomic, medical care and environmental determinants are related towithin country differences in CVD mortality.Methods: The main outcome measures were age-standardized CVD mortalityrates (ICD-10: codes I.00-I.99) in each of 16 provinces for men and women ages
20-74. Also for each province 90 indicators, were collected in 9 categories fromseveral sources: prevalence of risk factors, medical care, economy, education,welfare state, environmental pollution, demography, living conditions, health sta-tus.The analysis was based on univariate correlation and discrimination model andmultivariate stepwise regression models. Partial and multivariate coefficient ofdetermination was calculated with determinants significant in univariate models.Results: In men about 73% of the within country variance in CVD mortality weresignificantly explained by the differences between provinces in the level of airpollution, urbanization, employment rate, monthly income and expenditure on en-vironmental protection. For women: 42% of those differences were explained bydifferences in expenditure on environmental protection. Differences in the preva-lence of classical CVD risk factors explained only 5-15% between province differ-ences in CVD mortality.Conclusion: The results promote a deeper understanding and awareness of so-cioeconomic health determinants including living and environmental conditions,which should contribute to the development of a multisectoral health policy toimprove population health.
P1487 Radiological (un)awareness in cardiologists, and howto improve it: the SUIT-Heart (Stop Useless ImagingTesting in Heart Disease) Project
G. Kraft1, C. Carpeggiani2, D. Caramella3, M. Lazzeri2, C. Traino4,E. Picano5. 1Istituto di Informatica e Telematica, CNR, Pisa, Italy;
2Institute of Clinical Physiology of CNR, Pisa, Italy; 3University of Pisa, RadiologyDept., Pisa, Italy; 4Health Physics of AOUP, Pisa, Pisa, Italy; 5Institute of ClinicalPhysiology - Istituto Toscano Tumori, Pisa, Italy
Background: International Atomic Energy Agency launched in September 2009the "3 A’s campaign": Audit, Appropriateness and Awareness for radiological jus-tification, which is an effective tool for cancer prevention. Cardiologists prescribethe majority of radiological testing, but their awareness of doses and risks ofcardio-radiological exams is low.Aim: To assess radiological awareness of cardiologists before and after 1-dayintensive radioprotection primer course as a part of the SUIT-Heart (Stop UselessImaging Testing in Heart Disease) project.Methods: A 1-day 6-hours primer of radioprotection for a closed number (<35) ofcardiologists (providing 8 education credits of Italian Health Ministry) was held 9times over 3 years for a total of 294 physicians. For each attendee, a radiologicalawareness score was obtained before and after the course, with a 10 multiple-choice (4 answers) survey on radioprotection basics (doses of common examina-tions in multiples of chest x-rays; associated cancer risk, etc.). Each answer wasscored from 1 ("severe mistake") to 4 ("right").Results: The radiological awareness score of the 294 attendees improved from31±3 (before) to 37±2 (after training, p<.001 vs pre). At baseline, 47 physicians(15.9%) thought that radiation risk is independent from age and gender (whereasit is 4-fold higher in children <1 year and 38% higher in females), 196 (66.6%) thatstochastic cancer risk is absent and 65 (22.1%) that radiation risk disappears overtime (whereas it is cumulative over the lifetime): see figure.
Conclusions: Awareness of radiological doses and risks, albeit essential for risk-benefit assessment of radiological testing, is poor among cardiologists, but candramatically improve with a limited teaching effort through targeted training.
P1488 Effects of Ramadan on renal function and frequencyof contrast induced nephropathy in patientsundergoing coronary angiography
F.A. Choudry, L.A. Mcgill, S.P. Page, M. Ozcor, A. Archbold,M.T. Rothman, C. Knight, S.A. Mohiddin. The London Chest
Hospital, London, United Kingdom
Purpose: The requirement for coronary angiography in subjects of Bangladeshiorigin is due to their high rate of vascular disease and associated risk factors in-cluding diabetes. Dehydration can result in renal failure and predisposes to con-trast induced nephropathy (CIN) in susceptible subjects. We sought to determinewhether fasting during Ramadan contributes to renal dysfunction or CIN in pa-tients undergoing coronary angiography.Methods: The study cohort comprised all patients of Bangladeshi origin whounderwent coronary angiography at the London Chest Hospital, East London,during the months of Ramadan in 2005-2008 (n=109). A control group consistedof Bangladeshi patients who underwent coronary angiography in the 2 monthspreceding Ramadan in the same three years (n=164). Patients established on
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

238 Culture and society: how do they affect heart disease and treatment
dialysis were excluded. Renal function was assessed by serum creatinine con-centration ([Cr]) and estimated glomerular filtration rate (eGFR). Comparisonsof pre-procedure renal function and changes following angiography were madebetween Ramadan and non Ramadan. Contrast induced nephropathy was de-fined as a decrease in serum [Cr] of >25%, and patients on dialysis were ex-cluded.Results: The characteristics of patients in the two groups were similar for age(58±12 years in Ramadan vs. 57±13 years for control months), gender (17% vs.26%), type of admission (elective in 59% vs. 64%, p=ns). There were no differ-ences between groups for pre-procedure serum [Cr] (109±87 vs. 109±134μmol/l;p=ns), eGFR (75±23 vs. 79±23 ml/kg/m2; p=ns) and in the proportion of patientsadmitted with an eGFR<60 mls/min; 16 vs. 14%; p=ns). For unplanned urgentand emergency admissions, pre-procedure renal function tended to be worse dur-ing Ramadan (serum [Cr] 129±124 vs. 104±108 μmol/l, p=ns; and eGFR 71±26vs. 78±21 mls/kg/m2, p=ns). Ninety patients (45 in each group) had renal functionassessed following angiography at (mean 1.9±2 days). In these patients, therewas no significant change from baseline in mean serum [Cr] or eGFR in either ofthe groups and CIN occurred in similar proportions (4/45 vs. 5/45; p=ns). Whenonly those patients with a pre-procedure eGFR<60 were considered, no signifi-cant differences between admission and post angiography renal parameters wereobserved, although CIN developed in 15% (14% vs. 15%; p=ns).Conclusion: These data suggest that fasting during Ramadan does not have aclinically important effect on renal function or renal function after administration ofcontrast agents. While recommended for patients with pre-existing renal dysfunc-tion, prehydration during Ramadan is not supported by these data.
P1489 ICD reutilization: Can referral centers provide devicesfor donation to developing world countries?
T. Baman1, L. Gakenheimer1 , J. Romero1, P. Sovitch1,J.N. Kirkpatrick2, P. Meier1, S. Kai1, J. Azizi1, H. Oral1, K.A. Eagle1.1University of Michigan Hospital, Ann Arbor, United States of
America; 2University of Pennsylvania, Philadelphia, United States of America
Purpose: In light of increasing healthcare disparities between industrialized anddeveloping nations, reuse of electrophysiological devices is a safe, efficacious,and ethical way to address the medical needs for the poor in need of device ther-apy. ICD’s are indicated in some cases of Chagas cardiomyopathy (South Amer-ica) and sudden unexplained death syndrome (Southeast Asia) and can also bereused as pacemakers for those with symptomatic bradycardia. The purpose ofthis study is to determine whether referral centers can provide devices for reuse.Methods: We conducted a retrospective chart review of all patients with an ex-tracted Medtronic or Boston Scientific/Guidant ICD from January 2007 to Jan-uary 2010 at a single tertiary referral center. Key clinical parameters of deviceswere collected along with patient demographic and clinical data. Devices wereconsidered a possible resource for developing world nations if battery longevitywas ≥ 24 months (Medtronic) or >50% battery life was remaining (Boston Scien-tific/Guidant).Results: 328 ICDs were extracted during this time period. Of this group, 118devices were ICDs with cardiac resynchronization therapies (CRT-D). Overall,193/328 (59%) devices were explanted due to elective replacement interval (ERI).Acceptable battery longevity was estimated in 99/328 (30%) of all devices rou-tinely explanted. Controlling for age of patient and duration of device implan-tation, ICDs explanted prior to upgrade to a CRT-D device (n=29; HR 57.9, CI13.9-240.5, p<0.01) and devices removed during heart transplantation (n=30;HR 4.98, CI 1.38-17.95, p=0.01) remained independent predictors of adequatebattery life for possible reuse in multivariate anlaysis. Device removal secondaryto infection (n=35, p=0.21) was not a predictor of adequate battery life.Conclusions: >50% of ICDs explanted for reasons other than ERI have an ad-equate battery life and should be considered for reutilization in the developingworld. Specifically, devices explanted prior to CRT-D upgrade or heart transplan-tation can be a possible resource for ICD reutilization programs to underservednations.
P1490 Level of adherence to the Mediterranean diet inrelation to lifestyle characteristics among Greekadolescents. Data from the 3L Study
D. Tsiachris, C. Tsioufis, A. Mazaraki, I. Andrikou, M. Selima,T. Psaltopoulou, D. Tousoulis, D. Panagiotakos, C. Stefanadis. First
Cardiology Clinic, University of Athens,Hippokration Hospital, Athens, Greece
Purpose: Observational studies have exhibited an association between televi-sion viewing and adolescent adiposity. The Mediterranean diet (MD), has beenpostulated as having a protective role against cardiovascular diseases. Our aimwas to evaluate the relationship between television viewing, dietary habits andanthropometric characteristics among Greek adolescents.Methods: During 2009, 496 schoolchildren (304 boys and 192 girls), aged 12-17years participated in the Lyceum Leontio ALbuminuria Study (3L study). Height,weight, waist and hip circumference were measured and the body mass index(BMI) was calculated. For each child a questionnaire was completed that was de-veloped to retrieve information on dietary habits (through a semi-quantitative FoodFrequency Questionnaire), lifestyle and socio-economic characteristics. Adher-ence to the MD was assessed by the KIDMED score. Based on television viewing
≥2 hours, adolescents were classified as those with increased and those withdecreased television viewing.Results: Among Greek adolescents 294 (59.3%) reported increased televisionviewing. Only 6.0% of the sample was classified as high adherers of MD (KIDMEDscore>7), whereas 52.1% had an average KIDMED score (4-7) and 41.9% hada poor KIDMED score (<4). Adolescents with increased television viewing spentless time for studying (2.8 vs. 3.2 hours, p<0.001) compared to those with de-creased television viewing, while there was no difference regarding gender, bodymass index, waist circumference and waist to hip ratio. Moreover, adolescentswith increased television viewing exhibited significantly lower KIDMED score(3.7±2.1 vs. 4.6±2.1, p<0.001) as well as a higher prevalence of poor adherenceto MD (47.9 vs. 33.1, p=0.001). In these lines, adolescents with increased televi-sion viewing compared to those with decreased television viewing reported morefrequently eating from canteen (53.1% vs. 41%, p=0.01) and smoking amongfamily members (68.3% vs. 58.2%, p=0.028) as well as owned a mobile phoneat a greater percentage (89.2% vs. 79.8%, p=0.016). Hours of television viewingwas negatively correlated with KIDMED score (r=-0.189, p<0.001) and hours ofstudying (r=-0.192, p<0.001).Conclusions: Greek adolescents with increased television viewing are charac-terized by an extremely poor adherence to MD. Taking into account that unhealthyeating habits have been related to adverse cardiovascular outcomes, school- orcommunity-based programmes should be conducted promoting healthy dietaryand lifestyle behaviors.
P1491 Pediatric cardiac surgery: is the girl child neglected?
S. Ramakrishnan, R. Khera, S. Jain, A. Saxena, K. Suparna,R. Juneja, B. Bhargava, S.S. Kothari, V.K. Bahl. All India Institute ofMedical Sciences (AIIMS), New Delhi, India
Background: Several socio-economic factors govern the complianceto surgical treatment in patients with congenital heart disease (CHD). These fac-tors have not been studied systematically.Methodology: Parents or guardians of patients (aged 1 day to 12 years) be-ing recommended a surgical procedure for a CHD were interviewed using apredesigned validated proforma. Those who had not opted for surgery beyond3 months of recommendation were considered to have significantly delayedsurgery. A qualitative thematic analysis was done among 20 patients with sig-nificant delay.Results: Of the total 405 patients studied (median age - 2 years), 271 were maleand 134 were female. Definite repair of ventricular septal defect and tetrologyof Fallot were the common surgeries advised. Only 15% of male patients hadsignificantly delayed surgery, as opposed to 46% of female patients (p < 0.0001).There is a significant correlation between percentage delay and socio-economicclass (p < 0.0001), cost of surgery (p < 0.0001) and the number of siblings of theindex case (p < 0.001). For each socio-economic class except the upper class,the percentage of female patients with delay is 2 to 5 times that of male patients(p < 0.0001 for each). Qualitative analysis suggested that economical, logisticaland lack of social support were the major thematic reasons for a delayed surgery.Conclusion: Female sex emerges as an important factor governing the delay inopting for surgery and the difference between sexes persist even within individualsocio-economic classes.
P1492 Adverse cardiovascular risk profile in adisadvantaged minority community consistent withthe thrifty phenotype hypothesis. Findings from theAll-Ireland Traveller Health Study
C.M. Mcgorrian, S. Abdalla, L. Daly, P. Fitzpatrick, C. Kelly,R.G. Moore, R. Niccarthaigh, B. Quirke, J. Turner, C.C. Kelleher. UniversityCollege Dublin, School of Public Health, Physiotherapy & Population Science,Dublin, Ireland
Purpose: The thrifty phenotype hypothesis suggests that individuals who surviveadverse developmental circumstances may be predisposed to cardiovascular dis-eases (CVD) in adult life. The Traveller community is an indigenous minority groupin Ireland with higher premature and infant mortality than the general Irish pop-ulation. The All Ireland Traveller Health Study (AITHS) is a census survey of thehealth status of the estimated 10,000 Irish Traveller families. This analysis exam-ines both the frequency of typical cardiovascular risk factors in Travellers, and theassociation between measures of social capital and typical CVD risk factors withCVD.Methods: All Traveller families on the island of Ireland were located and invitedto participate in the census, with an overall 80% response rate. A 20% randomsubsample completed a detailed Adult Health survey (n=2003). Data were col-lected by trained peer researchers using a novel oral-visual computer assistedpersonal interview instrument, to overcome literacy issues. CVD was defined asdoctor diagnosis of heart attack, angina or stroke in the preceding 12 months.Typical CVD risk factors (measured by respondent self-report) and measures ofsocial capital such as trust and social support were examined in simple adjustedand multivariable logistic regression models, with CVD as the dependent variable.Results: Overall self-report of CVD was 5.6%, higher than in the general Irishpopulation. Prevalence of CVD increased with age (p<0.001) and these respon-dents had a high prevalence of risk factors such as tobacco use (57.3%)and di-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
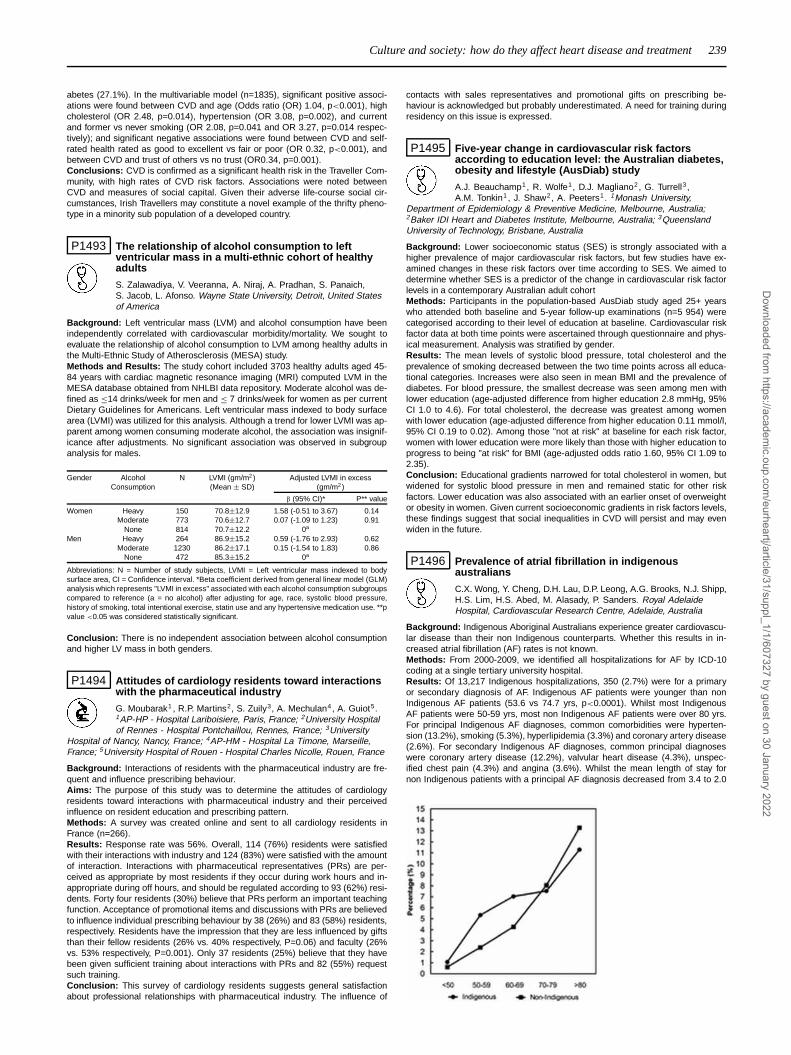
Culture and society: how do they affect heart disease and treatment 239
abetes (27.1%). In the multivariable model (n=1835), significant positive associ-ations were found between CVD and age (Odds ratio (OR) 1.04, p<0.001), highcholesterol (OR 2.48, p=0.014), hypertension (OR 3.08, p=0.002), and currentand former vs never smoking (OR 2.08, p=0.041 and OR 3.27, p=0.014 respec-tively); and significant negative associations were found between CVD and self-rated health rated as good to excellent vs fair or poor (OR 0.32, p<0.001), andbetween CVD and trust of others vs no trust (OR0.34, p=0.001).Conclusions: CVD is confirmed as a significant health risk in the Traveller Com-munity, with high rates of CVD risk factors. Associations were noted betweenCVD and measures of social capital. Given their adverse life-course social cir-cumstances, Irish Travellers may constitute a novel example of the thrifty pheno-type in a minority sub population of a developed country.
P1493 The relationship of alcohol consumption to leftventricular mass in a multi-ethnic cohort of healthyadults
S. Zalawadiya, V. Veeranna, A. Niraj, A. Pradhan, S. Panaich,S. Jacob, L. Afonso. Wayne State University, Detroit, United Statesof America
Background: Left ventricular mass (LVM) and alcohol consumption have beenindependently correlated with cardiovascular morbidity/mortality. We sought toevaluate the relationship of alcohol consumption to LVM among healthy adults inthe Multi-Ethnic Study of Atherosclerosis (MESA) study.Methods and Results: The study cohort included 3703 healthy adults aged 45-84 years with cardiac magnetic resonance imaging (MRI) computed LVM in theMESA database obtained from NHLBI data repository. Moderate alcohol was de-fined as ≤14 drinks/week for men and ≤ 7 drinks/week for women as per currentDietary Guidelines for Americans. Left ventricular mass indexed to body surfacearea (LVMI) was utilized for this analysis. Although a trend for lower LVMI was ap-parent among women consuming moderate alcohol, the association was insignif-icance after adjustments. No significant association was observed in subgroupanalysis for males.
Gender Alcohol N LVMI (gm/m2) Adjusted LVMI in excessConsumption (Mean ± SD) (gm/m2)
β (95% CI)* P** value
Women Heavy 150 70.8±12.9 1.58 (-0.51 to 3.67) 0.14Moderate 773 70.6±12.7 0.07 (-1.09 to 1.23) 0.91
None 814 70.7±12.2 0a
Men Heavy 264 86.9±15.2 0.59 (-1.76 to 2.93) 0.62Moderate 1230 86.2±17.1 0.15 (-1.54 to 1.83) 0.86
None 472 85.3±15.2 0a
Abbreviations: N = Number of study subjects, LVMI = Left ventricular mass indexed to bodysurface area, CI = Confidence interval. *Beta coefficient derived from general linear model (GLM)analysis which represents "LVMI in excess" associated with each alcohol consumption subgroupscompared to reference (a = no alcohol) after adjusting for age, race, systolic blood pressure,history of smoking, total intentional exercise, statin use and any hypertensive medication use. **pvalue <0.05 was considered statistically significant.
Conclusion: There is no independent association between alcohol consumptionand higher LV mass in both genders.
P1494 Attitudes of cardiology residents toward interactionswith the pharmaceutical industry
G. Moubarak1 , R.P. Martins2, S. Zuily3, A. Mechulan4, A. Guiot5.1AP-HP - Hospital Lariboisiere, Paris, France; 2University Hospitalof Rennes - Hospital Pontchaillou, Rennes, France; 3University
Hospital of Nancy, Nancy, France; 4AP-HM - Hospital La Timone, Marseille,France; 5University Hospital of Rouen - Hospital Charles Nicolle, Rouen, France
Background: Interactions of residents with the pharmaceutical industry are fre-quent and influence prescribing behaviour.Aims: The purpose of this study was to determine the attitudes of cardiologyresidents toward interactions with pharmaceutical industry and their perceivedinfluence on resident education and prescribing pattern.Methods: A survey was created online and sent to all cardiology residents inFrance (n=266).Results: Response rate was 56%. Overall, 114 (76%) residents were satisfiedwith their interactions with industry and 124 (83%) were satisfied with the amountof interaction. Interactions with pharmaceutical representatives (PRs) are per-ceived as appropriate by most residents if they occur during work hours and in-appropriate during off hours, and should be regulated according to 93 (62%) resi-dents. Forty four residents (30%) believe that PRs perform an important teachingfunction. Acceptance of promotional items and discussions with PRs are believedto influence individual prescribing behaviour by 38 (26%) and 83 (58%) residents,respectively. Residents have the impression that they are less influenced by giftsthan their fellow residents (26% vs. 40% respectively, P=0.06) and faculty (26%vs. 53% respectively, P=0.001). Only 37 residents (25%) believe that they havebeen given sufficient training about interactions with PRs and 82 (55%) requestsuch training.Conclusion: This survey of cardiology residents suggests general satisfactionabout professional relationships with pharmaceutical industry. The influence of
contacts with sales representatives and promotional gifts on prescribing be-haviour is acknowledged but probably underestimated. A need for training duringresidency on this issue is expressed.
P1495 Five-year change in cardiovascular risk factorsaccording to education level: the Australian diabetes,obesity and lifestyle (AusDiab) study
A.J. Beauchamp1, R. Wolfe1, D.J. Magliano2, G. Turrell3,A.M. Tonkin1 , J. Shaw2, A. Peeters1. 1Monash University,
Department of Epidemiology & Preventive Medicine, Melbourne, Australia;2Baker IDI Heart and Diabetes Institute, Melbourne, Australia; 3QueenslandUniversity of Technology, Brisbane, Australia
Background: Lower socioeconomic status (SES) is strongly associated with ahigher prevalence of major cardiovascular risk factors, but few studies have ex-amined changes in these risk factors over time according to SES. We aimed todetermine whether SES is a predictor of the change in cardiovascular risk factorlevels in a contemporary Australian adult cohortMethods: Participants in the population-based AusDiab study aged 25+ yearswho attended both baseline and 5-year follow-up examinations (n=5 954) werecategorised according to their level of education at baseline. Cardiovascular riskfactor data at both time points were ascertained through questionnaire and phys-ical measurement. Analysis was stratified by gender.Results: The mean levels of systolic blood pressure, total cholesterol and theprevalence of smoking decreased between the two time points across all educa-tional categories. Increases were also seen in mean BMI and the prevalence ofdiabetes. For blood pressure, the smallest decrease was seen among men withlower education (age-adjusted difference from higher education 2.8 mmHg, 95%CI 1.0 to 4.6). For total cholesterol, the decrease was greatest among womenwith lower education (age-adjusted difference from higher education 0.11 mmol/l,95% CI 0.19 to 0.02). Among those "not at risk" at baseline for each risk factor,women with lower education were more likely than those with higher education toprogress to being "at risk" for BMI (age-adjusted odds ratio 1.60, 95% CI 1.09 to2.35).Conclusion: Educational gradients narrowed for total cholesterol in women, butwidened for systolic blood pressure in men and remained static for other riskfactors. Lower education was also associated with an earlier onset of overweightor obesity in women. Given current socioeconomic gradients in risk factors levels,these findings suggest that social inequalities in CVD will persist and may evenwiden in the future.
P1496 Prevalence of atrial fibrillation in indigenousaustralians
C.X. Wong, Y. Cheng, D.H. Lau, D.P. Leong, A.G. Brooks, N.J. Shipp,H.S. Lim, H.S. Abed, M. Alasady, P. Sanders. Royal AdelaideHospital, Cardiovascular Research Centre, Adelaide, Australia
Background: Indigenous Aboriginal Australians experience greater cardiovascu-lar disease than their non Indigenous counterparts. Whether this results in in-creased atrial fibrillation (AF) rates is not known.Methods: From 2000-2009, we identified all hospitalizations for AF by ICD-10coding at a single tertiary university hospital.Results: Of 13,217 Indigenous hospitalizations, 350 (2.7%) were for a primaryor secondary diagnosis of AF. Indigenous AF patients were younger than nonIndigenous AF patients (53.6 vs 74.7 yrs, p<0.0001). Whilst most IndigenousAF patients were 50-59 yrs, most non Indigenous AF patients were over 80 yrs.For principal Indigenous AF diagnoses, common comorbidities were hyperten-sion (13.2%), smoking (5.3%), hyperlipidemia (3.3%) and coronary artery disease(2.6%). For secondary Indigenous AF diagnoses, common principal diagnoseswere coronary artery disease (12.2%), valvular heart disease (4.3%), unspec-ified chest pain (4.3%) and angina (3.6%). Whilst the mean length of stay fornon Indigenous patients with a principal AF diagnosis decreased from 3.4 to 2.0
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

240 Culture and society: how do they affect heart disease and treatment
days, the mean length of stay in Indigenous patients remained at approximately3 days. Furthermore, principal Indigenous AF diagnoses as a percentage of allIndigenous AF hospitalizations increased from 7.1 to 24.1%.Conclusions: Indigenous Australians have significantly greater rates of AF atan earlier age than their non Indigenous counterparts. Furthermore, this datasuggests that the AF accounts for an increasing number of their hospitalizations.The burden of AF in this racial subgroup is substantial and likely to contribute totheir early morbidity and mortality.
P1497 Augmentation index and marriage in men: it is arelationship you cannot disparage
A. Siama, C. Vlachopoulos, G. Vyssoulis, P. Pietri, D. Terentes-Printzios, P. Xaplanteris, A. Samentzas, N. Ioakeimidis, K. Baou,C. Stefanadis. Hippokration General Hospital, Athens, Greece
Purpose: Hypertension is associated with increased arterial stiffness and wavereflections, which are predictors of cardiovascular risk. However, the relationshipbetween marital status and arterial function in never-treated hypertensives hasnot been investigated. We assessed the hypothesis that marital status is associ-ated with arterial stiffness and wave reflections in never-treated hypertensives.Method: We enrolled 639 essential hypertensives (mean age 52.9±11.7 years).Arterial stiffness was determined with carotid-femoral pulse wave velocity (PWV)using the Complior® device and aortic augmentation index (AIx), an index of wavereflections, was measured using the Sphygmocor® device. Subjects were classi-fied as singles (83 males [SM], 51 females [SF]), if they were never married,divorced or widowed, and as married (256 males [MM], 249 females [MF]).Results: AIx was higher in females than males (34.1 vs 23.4%, p<0.001). Amongthe 4 groups SM had the lowest AIx, which was significantly lower than the aug-mentation index of MM, SF and MF (15.8 vs 28.4, 33.1 and 34.2%, respectively, allp<0.001). (Figure) The abovementioned differences remained significant even af-ter adjustment for possible confounders, such as age, mean blood pressure, bodymass index, blood glucose, low-density lipoprotein, smoking status, presence ofdiabetes, heart rate and C-reactive protein (all p<0.001). There were no signif-icant differences among MM, SF and MF. There were no significant differencesamong the 4 groups in PWV.
AIx and marital status im men and women
Conclusions: In never-treated hypertensives SM have lower augmentation indexthan MM. However, never-treated hypertensives SF and MF are found to havesimilar levels of AIx. This finding provides further insights on the role of socioeco-nomic factors on arterial stiffness and cardiovascular risk.
P1498 Will the habits and customs of the native americansof Chubut (Patagonia Argentina) influence thepresence of cardiovascular risk factors?
R. Ingaramo, D. Williams, A. Daroca, M. Del Popolo, F. Suarez,G. Guevara, S. Zambianchi, M.I. Carletti, L. Carrizo. Hypertension
Center and Cardiovascular Diseases, Trelew, Argentina
The native south americans of Chubut (NA), Patagonia Argentina, Mapuches andTehuelches races, whom live in relatively isolated communities, retain certain an-cestral customs. One is mostly food based on lamb meat.Purpose: to assess the prevalence of cardiovascular risk factors and their possi-ble impact on arterial and cardiac structure in relation to their eating habits.Methods: 285 subjects, 181 NA and 106 zonal residents (ZR), answered to aquestionnaire on habits and socio-economic condition. Fasting blood sampleswere obtained, in order to measure cholesterol (CHOL), triglycerides (TGL) andglucose (GL). Their body mass index (BMI), abdominal circumference (AB), sys-tolic (SBP) and diastolic blood presure (DBP), were obtained. The subjects under-went an echocardiogram (ECHO) to assess the left ventricular mass index (LVMI),a carotid ultrasound to assess the intima-media thickness (IMT) and presenceof plaques (CP) and to an ophtalmoscopic examination (OF). Student’s t-test,chi-square test and a multivariate model of logistic regresion were used for thestatistical analysis. A p value < 0,05 was considered statistically significant.Results: The mean age in the NA was slightly, nonsignificant, higher (47,1±19,4vs. 44,6±17,6; p = 0,288) The diet was different in both groups (p = 0,037), char-acterizing the NA by the increased consumption of meat only. The percentage of
alcohol (12% in the NA and 6% for ZR, p = 0,123) and smokers (27% for NA and24% in the ZR, (p = 0,615) were higher in the NA, although not significant. Hy-pertension (HT) were more common in the NA (25% vs. 17% for ZR, p = 0,152)but the difference was not significant. The prevalence of obesity (p = 0,163) wassimilar in both populations. The average values of SBP, DBP, BMI and AB, weresignificantly higher (p = 0,009, p = 0,043, p = 0,002, p = 0,013 respectively) in theNA, while values of CHOL were lower (p = 0,025) and no differences in the valuesof TGL (p = 0,8263) and GL (p = 0,5954) were obtained. The distribution of CPwas similar in both populations (24% in the NA and 19% for ZR, p = 0,382) whilethe values of IMT did not differ significantly (p = 0,416) LVMI values was higher inthe NA (94,9±28,2 vs. 86,8±28,5 p = 0,026). We found no differences in the OF(p = 0,094)Conclusions: The NA consume more lamb meat, and have the BP, BMI andAB, higher than ZR. However, the results did not show a clear difference in theprevalence of risk factors and in cardiovascular compromise to them in relation toone of its customs
P1499 Gender disparity in coronary revascularisationmanagement in Europe: a report from the Euro HeartSurvey
H.T. Jorstad1, M.J. Lenzen2, W.J. Scholte Op Reimer1, S.E. Hoeks2,W. Wijns3, J.G. Tijssen1, R.J.G. Peters1. 1Academic Medical Center,Amsterdam, Netherlands; 2Erasmus Medical Center, Department
of Cardiology, Rotterdam, Netherlands; 3OLV Hospital Aalst, Department ofCardiology, Aalst, Belgium
Purpose: To evaluate gender differences in revascularisation choices in the Eu-roHeart survey on coronary revascularisaton.Methods: We analysed gender differences in the decision to perform coronaryartery bypass grafting (CABG) versus percutaneous coronary intervention (PCI)or no revascularisation in patients with angiographically documented coronaryartery disease (≥50% stenosis) without prior revascularisation procedures in theEuro Heart survey.Results: Women were less likely than men to be treated with CABG (26.7 vs21.7%, p<0.001) and more likely to be treated with PCI (59.8 vs 55,6%, p<0.001)in a population of 3939 revascularisation naive patients (2959 men, 980 women).In patients younger than 60 years, the proportion of revascularisation proceduresin men and women was 20.4% vs. 22.0% (ns) for CABG and 64.6 vs. 66.1% (ns)for PCI. In patients older than 60 years, these proportions were 31.6% vs. 21.6%for CABG (p<0.001) and 48.6% vs. 57.8% for PCI (p<0.001) for men and womenrespectively (Figure 1). These differences remained significant after adjusting forco-morbidities and patient characteristics.
Choice of treatment
Conclusion: Women above 60 years were significantly less likely to be treatedwith CABG and more likely to be treated with PCI than men above 60 years,indicating an age-dependent gender disparity in revascularisation choices.
P1500 Preventive effect of cocoa on impaired flow-mediateddilation in working night shifts
W. Kim1, E.K. Cho2, C.S. Park2, S.H. Park2, H.H. Park2,W.Y. Kang2, S.H. Hwang2, S.J. Ha1, W. Kim2. 1Kyung HeeUniversity Hospital, Seoul, Korea, Republic of; 2Gwangju Veterans
Hospital, Gwangju, Korea, Republic of
Background: Previous our study suggests that three sequential night shifts de-teriorated endothelial function through decreased production of NO. Flavanolshave been suggested to mediate the favorable effects on cardiovascular health.The aim of this study is to examine the effect of flavanol-rich cocoa on endothelialfunction and oxidative stress in healthy medical personnel with three sequentialnight shifts.Method: This Prospective, open-label, case-control study was designed for fortyyoung healthy nurses divided into two groups. The cocoa group (n=20, 28.5±4.5years) received dark chocholate 48g/day (containing 813mg polyphenols) for 3days and control group (n=20, 27.4±3.2 years) did not received chocholate. Weexamined Flow-Mediated Dilatation (FMD), hs-CRP, oxidative markers (Nitric ox-ide and malondialdehyde) before and after three-night shift.Results: Baseline characteristics were not different between the two groups.FMD was significantly decreased after continuous 3-night shift in both two groups
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Culture and society: how do they affect heart disease and treatment / Hypertension: from bench to bedside 241
(p<0.001). FMD change which means deterioration of vascular endothelial func-tion was lower in cocoa group than control group (5.83% vs 3.14%, p=0.041).Result of inflammatory marker (hs-CRP), oxidative markers (NOx and malondi-aldehyde) will be presented.Conclusion: This study indicated that 3-night shift aggravated endothelial func-tion. However, consumption of small amount of polyphenol-rich dark chocolatemay improve the endothelial function.
P1501 Heart rate variability and human immudeficiencyvirus treatment
P. Lotufo1 , M. Eira2, E.L. Dorea1, E.M. Eduardo3, J.G. Mill3,I.M. Bensenor1 . 1University of Sao Paulo, Hospital Universitario,Sao Paulo, Brazil; 2Instituto de Infectologia Emilio Ribas, Sao Paulo,
Brazil; 3Federal University Espirito Santo, Vitoria, Brazil
Several epidemiological studies have been describing that patients with infec-tion due to human immunodeficiency virus (HIV) and under treatment with highlyactive antiretroviral treatment (HAART) have alterations in the functioning of theautonomic nervous system related to heart rate frequency and to postural hy-potension. Our aim is to compare heart rate variability among patients with HIVinfection (under and without HAART) to patients without HIV infection, but at ahigher risk of cardiovascular diseases, as people with diabetes type 2.Methods: we recruited consecutively from an outpatient clinic 29 patients un-der HAART for at least one year, 28 people with HIV without HAART (naïve),44 patients with diabetes type 2. We recruited as control group from a worksitehealth program, 30 apparently healthy volunteers. We used a digital electrocar-diograph at a sampling ratio of 250 Hz. Wincardio (4.4a) software was used togenerate automatically the R-R interval series from a selected EGG lead. Exposi-tions evaluated were sociodemographic characteristics, HIV-related information,anthropometrics, and heart rate variability. Median (interquartile interval) of heartrate variability time and frequency indices of the four groups was compared usinga Kruskall-Wallis test.Results: for both sexes, no age differences among the four groups were verified.The overall mean age (± standard deviation) was 42.9 years (± 7.9) for men and42.3 (± 7.2) for women. HIV infected patients using HAART and naïve patientswere leaner compared to diabetics (P<0.01). Diabetics presented higher valuesof waist measurement compared to the other groups (P<0.001) Systolic bloodpressure, and pulse pressure averages were similar among these groups. No dif-ference was found among groups for time domain index. However, HIV-infectedHAART, naïve and diabetic patients presented a significant (P<0.04) lower me-dian values of the "Low Frequency/High Frequency area" when they were com-pared to controls: HAART, 1.1 (o.3-1.7); naïve, 0.8 (0.6-2.3); diabetics, 0.9 (0.3-1.4) and controls, 2.3 (0.8-3.3). No difference was found in time and frequencydomain indices according to gender. Comparing the percentages of time and fre-quency domain indices below, within and above with the interquartile interval ofcontrols, showed a decreased heart rate variability in HIV-infected and diabeticpatientsConclusion: decrease in heart rate variability detected in HIV-infected patientsis similar to that also observed in diabetics, and the treatment of HIV-infectedpatients with antiretroviral agents did not improve the autonomic variations amongthese patients.
HYPERTENSION: FROM BENCH TO BEDSIDE
P1502 Periodontal disease severity and urinary albuminexcretion in hypertensive patients: a cross-talkbetween teeth and kidneys beyond systemicinflammation
C. Thomopoulos, C. Tsioufis, N. Soldatos, A. Kasiakogias,I. Andrikou, E. Stefanadi, S. Sideris, G. Giamarelos, C. Stefanadis.
First Cardiology Clinic, Univ. of Athens, Hippokration Hospital, Athens, Greece
Objectives: Focal (i.e. periodontal disease) and systemic low-grade inflammationmay contribute to the initiation and perpetuation of widespread vascular damage.We aimed to address whether periodontal disease indices (PDIs) are associatedwith urinary albumin to creatinine ratio (UACR) in conditions of high and low sys-temic inflammation, as evaluated by the levels of high sensitivity C reactive protein(hsCRP), in untreated middle aged hypertensive patients.Methods: We studied 242 – aged 51±9 years – hypertensive patients (24-h sys-tolic/diastolic blood pressure [BP] 132±10/83±8mmHg) with diverse severity ofperiodontal disease evaluated by 3 PDIs (i.e. mean clinical loss of attachment,maximum probe depth and gingival bleeding index). Patients underwent BP mea-surements, echocardiography, and periodontal examination, while from fastingblood samples we assessed metabolic profile, and hsCRP. Finally, UACR wascalculated from 2 nonconsecutive overnight spot urine samples.Results: With respect to the median of hsCRP and UACR (1.67 mg/Land 10mg/g) the total population was divided into 4 groups: patients withlow-UACR/low-hsCRP (n=65), low-UACR/high-hsCRP (n=63), high-UACR/low-hsCRP (n=51) and high-UACR/high-hsCRP (n=63). There was difference in allPDIs between the 4 groups, and those with high UACR had significantly higher24-h systolic BP with respect to those with low UACR. All 3 PDIs, hsCRP and the
interaction of each single PDI with hsCRP were determinants of UACR. AmongPDIs, mean clinical loss of attachment was the stronger determinant of the highUACR/high hsCRP pattern.Conclusion: In untreated middle aged hypertensive patients, PDI and hsCRPhave a synergistic effect on UACR levels. These findings suggest that focal in-flammatory sources, such as deteriorated periodontal tissue, could contribute tothe incremental UARC beyond systemic inflammatory load in the setting of es-sential hypertension, suggesting a direct cross-talk between teeth and kidneys.
P1503 Decreased levels of soluble receptor for advancedglycation end-products are accompanied bypronounced arterial stiffening, albuminuria andattenuated glomerular filtration rate in hypertension
K. Dimitriadis, C. Tsioufis, A. Kasiakogias, A. Miliou, S. Sideris,H. Sotiropoulos, I. Kallikazaros, C. Stefanadis. First Cardiology Clinic, Universityof Athens,Hippokration Hospital, Athens, Greece
Purpose: Emerging evidence implicates the soluble receptor for advanced glyca-tion end-products (sRAGE) in the development of vascular disease, while arterialstiffening, urinary albumin excretion and impaired renal function are associatedwith atherosclerosis progression. In the present study, we investigated the inter-relationships of sRAGE with urinary albumin excretion, expressed as the albuminto creatinine ratio (ACR), estimated glomerular filtration rate (eGFR) and arterialstiffness in essential hypertensives.Methods: Our population consisted of 320 newly diagnosed untreated non-diabetic patients with stage I to II essential hypertension [192 men, mean age=52years, office blood pressure (BP)=145/93 mmHg]. In all participants, ACR val-ues were determined as the mean of two non-consecutive morning spot urinesamples and aortic stiffness was evaluated on the basis of carotid to femoralpulse wave velocity (PWV), by means of a computerized method (Complior SP).Moreover, eGFR was assessed using the Modification of Diet in Renal Diseaseequation and venous blood sampling was performed for estimation of sRAGEconcentrations. The distribution of sRAGE was split by the median (1060.1 pg/ml)and accordingly subjects were stratified into those with high and low values.Results: Patients with low sRAGE (n=164) compared to those with high sRAGEvalues (n=156) had greater body mass index (29.7±4.5 vs 27.1±2.5 kg/m2,p<0.05) and 24-h systolic BP (139±8 vs 131±6 mmHg, p=0.001), while didnot differ regarding metabolic profile (p=NS for all). Moreover, patients withlow sRAGE compared to those with high sRAGE levels exhibited higher ACR(50.56±14.3 vs 20.75±15.5 mg/g, p=0.011) and PWV (9±1.7 vs 7.5±1.2 m/sec,p<0.0001), whereas had lower eGFR (65.9±7.2 vs 92.6±9.1 ml/min/1.73m2,p<0.05), independently of confounders. In the total population, sRAGE was as-sociated with body mass index (r=-0.245, p=0.006), waist to hip ratio (r=-0.462,p<0.0001), 24-h pulse pressure (r=-0.371, p=0.001), ACR (r=-0.274, p=0.019),eGFR (r=0.236, p=0.03) and PWV (r=-0.401, p<0.0001). Multiple regressionanalysis revealed that body mass index, 24-h systolic BP, ACR and PWV werethe independent predictors of sRAGE (R2=0.57, p<0.0001).Conclusions: In essential hypertension, decreased sRAGE levels are associatedwith increased PWV, pronounced albuminuria and impairment of renal function.Moreover, the close relation of sRAGE with arterial stiffening, ACR and eGFR,supports the potent role of sRAGE in renal and vascular atherosclerotic diseaseprogression.
P1504 Increased Circulating CD31+/Annexin V+ ApoptoticMicroparticles and Decreased Circulating EndothelialProgenitor Cells Levels in Hypertensive Patients withMicroalbuminuria
P.H. Huang, S.S. Huang, J.W. Chen, S.J. Lin. Taipei VeteransGeneral Hospital, Taipei, Taiwan
Objective: Microalbuminuria is associated with an increased risk for all-causeand cardiovascular mortality, but the pathophysiologic mechanism remains un-clear. We tested the hypothesis that enhanced endothelial apoptotic microparti-cles and decreased endothelial progenitor cells (EPCs) levels might contribute tothe pathophysiology of micro- or macroalbuminuria in cardiovascular disease.Methods: Flow cytometry was used to assess endothelial cell apoptosis andcirculating EPC levels by quantification of circulating CD31+/Annexin V+ apop-totic microparticles and EPC markers (defined as KDR+CD133+, CD34+CD133+,CD34+KDR+) in peripheral blood.Results: Totally, 125 subjects with hypertension were enrolled in the study, inwhich 80 patients (64%) with normoalbuminuria (albumin excretion rate [AER] of< 20 μg/min, overnight urine samples), 35 patients (28%) with microalbuminuria(an AER of 20 to 200 μg/min), and 10 patients (8%) with macroalbuminuria (anAER > 200 μg/min). Among the 3 groups, patients with micro- or macroalbu-minuria had significantly increased CD31+/Annexin V+ apoptotic microparticles(1.8±2.2 vs 3.0±4.3 vs 5.2±6.2%, p=0.044), and decreased circulating EPCnumbers (p<0.05). By multivariate analysis, CD31+/Annexin V+ apoptotic mi-croparticles level was an independent predictor of urinary albumin excretion ratein hypertensive patients (p<0.001). Microparticles isolated from hypertensive pa-tients with micro- or macroalbuminuria attenuated EPCs proliferation, migration,and increased H2O2 production, cellular senescence and apoptosis in compari-son with those from hypertensive patients with normoalbuminuria.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

242 Hypertension: from bench to bedside
Conclusion: These findings suggest that hypertensive patients with micro- ormacroalbuminuria have increased endothelial apoptotic microparticles and de-creased circulating EPC levels, which may contribute to atherosclerotic dis-ease progression and enhanced cardiovascular risk in hypertensive patients withnephropathy.
P1505 Low testosterone and increased fibrinogen levelshave an additive detrimental effect on vascularfunction and structure in essential hypertensivepatients with erectile dysfunction
N. Ioakeimidis, C. Vlachopoulos, N. Alexopoulos, I. Dima,D. Terentes-Printzios, A. Siama, A. Samentzas, P. Pietri, E. Christoforatou,C. Stefanadis. Hippokration Hospital, University of Athens, 1st Department ofCardiology, Athens, Greece
Purpose: In this study, we investigated the combined effect of increased fibrino-gen and low androgen level on vascular function and structure in essential hyper-tensive subjects.Methods: A total of 127 untreated patients with stage I-II essential hypertensionunderwent B-mode ultrasonographic measurements of the carotid intima mediathickness (IMT) and pharmacologically stimulated peak systolic velocity (PSV) ofcavernous arteries evaluation. The distributions of fibrinogen and testosteronewere split by the median (290 mg/dL and 4.06 ng/mL, respectively) and accord-ingly subjects were stratified into those with high and low values.Results: Patients with high compared with those with low fibrinogen levels ex-hibited greater IMT and lower PSV values (by 0.13 mm, P < 0.001 and 5 cm/s,P<0.05, respectively), whereas patients with low compared with those with hightestosterone levels had higher IMT and lower PSV values (by 0.08 mm, P < 0.01and 4.5 cm/s, P<0.05). Stepwise regression analysis revealed that age, systolicBP, fibrinogen and testosterone were independent predictors of IMT and PSV.Interestingly, a significant interaction between high fibrinogen and low testos-terone on PSV and IMT is reflected by the finding that the subgroup of highfibrinogen/low testosterone exhibited the higher IMT and the lower PSV valuescompared with the subgroups of high fibrinogen/high testosterone, low fibrino-gen/low testosterone, and low fibrinogen/high testosterone (overall P < 0.001and P<0.01, respectively).
↓Testo and ↑ fibrinogen in ED hypert pts
Conclusions: In essential hypertension, pronounced low-grade inflammation inconjunction with low androgen level exerts an additive detrimental effect on pe-ripheral vascular function and structure, accelerating the atherosclerotic process.
P1506 Early cardiac gene transcript levels in peripheralblood mononuclear cells of patients with essentialhypertension associate with left ventricular massindex
J.E. Kontaraki1, M.E. Marketou2, E.A. Zacharis2, F.I. Parthenakis2,P.E. Vardas2. 1Univ. of Crete, Faculty of Medicine, Molecular
Cardiology Lab, Heraklion, Greece; 2Heraklion University Hospital, Departmentof Cardiology, Heraklion, Greece
Purpose: Cardiomyocyte hypertrophy is one of the many structural alterationsin hypertensive heart disease. Cardiac hypertrophy is associated with an alteredgene expression profile. We evaluated gene transcript levels of the early cardiacmarker genes Nkx2.5, GATA4 and myocardin that are part of the "fetal gene pro-gramme" and participate in the hypertrophic growth of the adult heart, in periph-eral blood mononuclear cells of patients with essential hypertension in relation toechocardiography findings, defining left ventricular geometry.Methods: Echocardiography and blood sampling were obtained in 48 untreatedparticipants with essential hypertension (25 men, 23 women, mean age 65±6.9years). Peripheral blood mononuclear cells were isolated and gene transcript lev-els were determined by quantitative real time reverse transcription PCR.Results: Transcript levels of Nkx2.5 (r=0.512, p<0.001), GATA4 (r=0.415,p=0.003) and myocardin (r=0.339, p=0.020), showed significant positive corre-lations with left ventricular mass index.Conclusions: Our study for the first time provides data that demonstrate a cor-relation between early cardiac gene transcript levels in peripheral blood cells andleft ventricular mass index in patients with essential hypertension. This indicates
that there is a possible induction of the hypertrophic response network in hyper-tensive heart disease, and genes participating in the hypertrophic response mightbe important markers of left ventricular hypertrophy development in hypertensivepatients.
P1507 Prevalence of asymptomatic coronary artery diseasein essential hypertensive middle-aged men witherectile dysfunction. A prospective angiographicstudy
D. Terentes-Printzios, C. Vlachopoulos, N. Ioakeimidis, A. Aggelis,A. Samentzas, A. Siama, P. Xaplanteris, A. Bratsas, K. Rokkas,
C. Stefanadis. Hippokration Hospital, University of Athens, 1st Department ofCardiology, Athens, Greece
Purpose: Hypertension is the most common comorbidity in patients with erectiledysfunction (ED). ED may be considered a clinical manifestation of a generalizedvascular disease affecting also the penile arteries. The aim of this prospectivestudy was to evaluate angiographically the incidence of asymptomatic coronaryartery disease (CAD) in hypertensive middle-aged men with ED of vascular origin.Methods: 138 consecutive asymptomatic non-diabetic treated hypertensive(Grade I-II) men (40-60 y/o) with ED were comprehensively evaluated using med-ical history and examination, exercise treadmill test and stress echocardiogra-phy. Patients who had positive one or both of the two non-invasive procedureswere referred for coronary arteriography in order to document CAD and evalu-ate the severity of the disease. The penile vasculature was assessed using colorDoppler ultrasonography. Lower Doppler velocities indicate severe penile vascu-lar disease.Results: Coronary arteriography performed in 21 patients with non-invasive evi-dence for myocardial ischemia demonstrated that three patients had three-vesseldisease, six patients had two-vessel disease, nine patients had single-vessel dis-ease and three patients had coronary artery ectasias. Men with angiographicallydocumented CAD compared to men without CAD, had a higher prevalence ofGrade II hypertension, lower testosterone levels (3.6 vs 4.5 ng/ml), longer dura-tion of ED (33±21 vs 25±20 months, P<0.05), a greater impairment of erectilefunction as estimated by ultrasonographic measurements of penile peak systolicvelocity (28.5±5 vs 33.2±7 cm/s, P<0.01) and a higher prevalence of severepenile arterial insufficiency (SAI) (34 vs 19%, P<0.01). In multivariable logisticregression analysis SAI [odds ratio (OR) 4.8, 95% confidence interval (CI) 1.4-18.5, P<0.01], time interval between clinical onset of ED and angiographicallydocumented CAD [OR 2.2, 95% CI 1.1-6.3, P<0.01], presence of Grade II hy-pertension [OR 3.3, 95% CI 1.2–11.8, P<0.01] and low androgen levels (< 4.0ng/ml) [OR 1.8, 95% CI 1.0–4.6, P=0.03] remained independent predictors for thepresence of CAD.Conclusions: A considerable proportion (18/138 or 13%) of hypertensive middle-aged men with ED has angiographically documented silent CAD. These ap-proaches to diagnosis and evaluation of severity of ED could become a powerfulclinical tool to help with early detection of CAD and enhance overall vascularhealth prevention in men with hypertension.
P1508 Longitudinal evaluation of blood pressure values andtarget organ damage in subjects with high normalblood pressure in a general population in NorthernItaly
A. Paini, M.L. Muiesan, M. Salvetti, C. Agabiti Rosei, C. Aggiusti,D. Stassaldi, F. Bertacchini, F. Beschi, M. Castellano, E. Agabiti
Rosei. University of Brescia, Department of Internal Medicine, Brescia, Italy
Background: Subjects with high-normal (HN) blood pressure (BP) may be atincreased risk of progression to hypertension (HT) and of cardiovascular events,in comparison with normotensives (NT). Aim of our study was to evaluate theprogression to hypertension and the development of target organ damage in ageneral population in Northern Italy.Methods: In 585 subjects (age 50±8 years, 46% males) a baseline visit and labo-ratory examinations were performed. Subjects were divided into 3 groups accord-ing to systolic (SBP) and diastolic blood pressure (DBP) values: NT (SBP/DBP <
130/85 mmHg); HN (SBP/DBP >130/85 and < 140/90 mmHg) and HT (SBP/DBP> 140/90 mmHg). In 478 subjects a follow up (FU) visit, laboratory examinations,measurement of carotid femoral pulse wave velocity (PWV) and carotid intimamedia thickness (IMT) were performed after 8.7±2.3 years.Results: at baseline 30% of patients were NT, 25% were HN and 45% were HT.Among patients classified as HN at baseline, 71% developed hypertension atFU, 18% had HN BP, 11% were NT. Among subjects classified as NT at base-line, 34% developed hypertension at FU, 23% were classified as HN and 43%were NT. Mean BP values at FU were 129±13/82±7 in NT, 139±13/87±6 in HN,146±15/89±8 mmHg in HT, respectively (ANOVA p<0.001). At FU in HN and inHT, as compared with NT, a significant increase of PWV (11.2±2.1 and 12.4±3.3vs 10.1±1.9 m/sec, ANOVA p<0.01) and of common carotid IMT (1.00±0.19 and1.09±0.27 vs 0.93±0.15 mm, ANOVA p<0.01) was observed.Conclusions: In a general population in Northern Italy a large proportion of sub-jects with high normal BP developed hypertension and vascular target organ dam-age during a 9 years follow up.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Hypertension: from bench to bedside 243
P1509 Distinct prognostic value of different definitions ofchronic kidney disease for cardiovascular events inhypertension. A Greek 6-year follow-up study
D. Tsiachris, C. Tsioufis, L. Raftopoulos, V. Antonakis, D. Flessas,M. Poulakis, S. Lalos, A. Moulakakis, I. Kallikazaros, C. Stefanadis.
First Cardiology Clinic, University of Athens,Hippokration Hospital, Athens,Greece
Purpose: We assessed the comparative prognostic role of chronic kidney dis-ease (CKD) for major CV events defined according to glomerular filtration rate(GFR) or creatinine clearance (CrCl) in a prospective observational study inGreek hypertensives.Methods: We followed-up 1652 hypertensives (mean age 54.3 years, 696 males,office BP=147/93 mmHg) free of CV disease for a mean period of 6 years. Fivemajor risk factors [age>65, gender, current smoking, diabetes mellitus (DM) anddyslipidemia (LDL>160mg/dl)] were evaluated at baseline along with the pres-ence of CKD defined either according to MDRD-estimated GFR between 15 and59 ml/min/1.73m2 or based on estimated CrCl between 15 and 59 ml/min (by us-ing Cockroft-Gault formula). End-points of interest were the incidence of coronaryartery disease (CAD), stroke, all cause mortality and their composite.Results: The prevalence of CKD according to Cockroft-Gault formula was lowerthan the one based on estimated GFR (8.8% vs. 13.3%). At the end of followup, CAD was the most prevalent (5.2%), followed by stroke (5%) and total mor-tality (3.1%). In univariate Cox regression analysis, age>65 (HR 2.53, p<0.001),male gender (HR 1.97, p=0.004), DM (HR 4.01, p<0.001) and the presence ofCKD, based either on GFR (HR 1.91, p=0.039) or CrCl estimation (HR 2.67,p=0.003) were correlated with the incidence of CAD. In multivariate analysis,CKD based only on estimated CrCl (adjHR 2.34, p=0.018) along with age>65,male gender and DM remained independents prognosticator of CAD. In addi-tion, age>65 (HR 5.98, p<0.001) and CKD based either on estimated CrCl (HR3.56, p<0.001 and or estimated GFR (HR 1.91, p=0.048) were associated withthe incidence of stroke. In multivariate analysis, only CrCl-estimated CKD (adjHR2.17, p=0.029) and age>65 was a predictor of stroke. Finally, age>65 (HR 4.65,p<0.001), male gender (HR 1.34, p=0.041), DM (HR 2.00, p=0.001) and CKDbased either on estimated CrCl (HR 3.42, p<0.001) or estimated GFR (HR 1.96,p=0.001) were correlated with the composite end-point. In multivariate analysis,apart from age and sex, CKD based on estimated CrCl (adjHR 2.31, p<0.001)and on GFR (adjHR 1.55, p=0.045) were independent predictors of the compositeend-point.Conclusions: In hypertensive subjects free of CV disease, CKD estimated ac-cording to CrCl formula, although less prevalent than estimation based on GFR,contains enhanced predictive significance for major CV events.
P1510 Rennin-angiotensin-aldosterone systempolymorphisms in resistant hypertension andadverse cardiovascular events: GENHART-RIO Study
P.R. Benchimol Barbosa1, P.C. Silva1, I. Cordovil2, J. Barbosa-Filho2. 1Gama Filho University, Rio de Janeiro, Brazil; 2National
Institute of Cardiology, Rio De Janeiro, Brazil
Introduction: Renin-angiotensin-aldosterone system (RAAS) polymorphisms in-fluence 24h arterial pressure fluctuation. Resistant systemic arterial hypertension(RSAH) has an increased risk of end organ damage and unfavorable prognosis.The aim of this study was to prospectively investigate, in subjects with RSAH ina tropical South American city: 1) Adverse cardiovascular events defined as fataland non-fatal stroke or acute myocardial infarction (AMI); and 2) the associationof RAAS polymorphisms and adverse cardiovascular events in this population.Methods: Between 2001 and 2006, 212 subjects in investigation for RSAH atthe hypertension unit were admitted. All subjects received standard drug ther-apy, aiming at achieving <140/90mmHg and were re-evaluated up to four weekslater, including 24h ambulatory arterial pressure monitoring. Subjects with sec-ondary causes of RSAH were excluded. Ninety three subjects (age 57±10 y.o, 61women, and hypertension duration time 16.5±8.1 years) underwent genotypingto RAAS polymorphisms: renin (G1051A), angiotensinogen (M235T), ACE (I/D),angiotensin II type 1 receptor (A1166C), aldosterone synthase (C344T) and min-eralcorticoid receptor (G3514C). In this group, 66.7% had RSAH and 33.3% hadpseudo-RSAH. During regular follow-up, a composite of fatal and nonfatal strokeand/or AMI were assessed. The analysis of risk for composite outcome was car-ried out in a Cox proportional hazard model, for age, gender, hypertension time,RSAH and RAAS polymorphisms. Alpha error revel was <0.05.Results: During a median follow-up of 4.7 years, 28 subjects had compositeendpoint (respectively, mean 1.2 years of follow-up). No significant differencesaccording to age, gender and hypertension duration time were found. Compos-ite endpoint was observed in 56.8% of RSAH and 30.4% of pseudo-SRAH (RRof RSAH: 1.5 95%CI [1.0-2.3]; p=0.04). Hardy-Weinberg equilibrium was con-firmed in all RAAS polymorphism analyzed. Renin polymorphisms in homozygo-sis was associated with increased incidence of composite endpoint (GG =71.4%vs AA=27.3%; RR = 2.3 95%CI [1.0-5.4]; p=0.02). In univariate Cox proportionalhazard model, only renin G allele in homozygosis achieved significance (GG vs.AA: Hazard ratio 1.9; 95%CI [1.0-3.7]; p=0.04).Conclusion: RSAH determines increased cardiovascular risk for a compositeof fatal and nonfatal stroke and AMI. Renin G allele in homozygosis shows anincreased hazard for composite endpoint, in a selected tropical population.
P1511 Toll-like receptor 4 selectively activates MCP-1 toinduce cardiac hypertrophy and dysfunction inangiotensin II-induced hypertension
S. Matsuda1, S. Umemoto2, H. Yoshino1, T. Nakashima1, S. Ito3,H. Aoki4, K. Yoshimura5, T. Murata6 , M. Matsuzaki5. 1Department
of Medicine and Clinical Science, Yamaguchi University Graduate School ofMedicine, Ube, Japan; 2Pharmaceutical Clinical Research Center,YamaguchiUniversity Hospital, Ube, Japan; 3Shimonoseki Saiseikai General Hospital,Shimonoseki, Japan; 4Cardiovascular Research Institute Kurume University,Kurume, Japan; 5Yamaguchi University Graduate School of Medicine,Department of Molecular Cardiovascular Biology, Ube, Japan; 6YamaguchiUniversity, Science Research Center, Ube, Japan
Purpose: Angiotensin II (ATII) plays an important role in the development of car-diac hypertrophy and subsequent heart failure through the production of reactiveoxygen species (ROS) in the heart. Furthermore, it is reported that ATII stimu-lates the expression of monocyte chemoattractant protein-1 (MCP-1) depend onthe level of ROS. Toll-like receptor 4 (TLR4) is reported to be involved in cardio-vascular events and we have previously shown that TLR4 upregulates superoxidecontent in the heart in ATII-induced hypertension. However, it remains unknownwhether TLR4 is involved in the upregulation of MCP-1 and cardiac function byATII stimulation. We investigated the effects of TLR4 on oxidative stress and theexpression of MCP-1 in the heart, and cardiac function in ATII-induced hyperten-sion in vivo.Methods: TLR4 deficient mice (Tlr4lps-d) and wild-type (WT) mice were random-ized into ATII, NE or sub-depressor dose ATII type 1 receptor blocker irbesartan(IRB) with ATII treatment groups for 2 weeks. Cardiac hypertrophy and cardiacfunction were estimated based on transthoracic echocardiography. We measuredNAD(P)H oxidase activity by a luminescence assay and evaluated the superoxide(. O2-) content in the heart. We evaluated the expression of SAPK/JNK, Erk, Akt,p38 and MCP-1 with immunoblots.Results: ATII and NE similarly and significantly increased systolic blood pressurein all the drug treated groups throughout the experiments (p<0.05). In WT mice,ATII significantly induced cardiac hypertrophy and cardiac dysfunction, whereasthe Tlr4lps-d mice showed little effects of ATII on these indices. In WT mice,IRB treatment significantly rescued the cardiac hypertrophy and dysfunction com-pared with those in the ATII-treatment alone. ATII treated WT mice showed a 5-fold increase in NAD(P)H oxidase activity and •O2- content in the heart comparedwith the control mice, whereas IRB significantly reduced the NAD(P)H oxidaseactivity and •O2- content compared with those in the ATII-treatment alone. More-over, ATII significantly increased the expression of MCP-1 compared with those inthe control mice, and the treatment of sub-depressor dose IRB suppressed MCP-1 expression in the heart to the same level as that in the control mice. In contrast,ATII did not show any significant effect on the expression of SAPK/JNK, Erk, Aktand p38 in the heart of both WT and Tlr4lps-d mice. NE showed little effects onany indices in the WT and Tlr4lps-d mice.Conclusions: TLR4 may selectively activate MCP-1 through the increase in ox-idative stress and induce cardiac hypertrophy and dysfunction in ATII-inducedhypertension.
P1512 Genetic polymorphism on type 2 receptor ofangiotensin II, increases cardiovascular risk inhypertensive patients by modifying inflammatorymechanisms
N. Koumallos, D. Tousoulis, C. Antoniades, A. Miliou,A. Antonopoulos, D. Mentzikof, K. Marinou, C. Bakogiannis,
E. Kallikazarou, C. Stefanadis. University of Athens, Athens, Greece
Purpose: Evidence suggests that there is a balance between angiotensin II ef-fects on proatherogenic constitutive type 1, and antiatherogenic inducible type 2(AT2R) receptors. The AT2R gene is located on chromosome X, and the biologicaleffect of a newly described polymorphism (A1675G) in this gene is unclear. Weexamined the impact of A1675G polymorphism on AT2R, on the risk for coronaryatherosclerosis, and its effect on the expression of proatherogenic inflammatorymolecules.Methods: The study population consisted of 437 males: 155 with coronary arterydisease (111 with hypertension) and 282 healthy age-matched controls (121 withhypertension). The presence of A1675G polymorphism on AT2R gene (locatedin chromosome X) was determined by PCR. Serum levels of C-reactive pro-tein, fibrinogen, interleukin-6 (IL-6) and soluble vascular cell adhesion molecule-1(sVCAM-1) were measured in all the participants.Results: The frequency of the A allele was similar among healthy individuals(41.8% 118/282) and CAD patients (47.7%, 74/155, p=NS). However the pres-ence of the A allele was more frequent in hypertensives with CAD (55%, 59/107)than in hypertensives without CAD (35.8%, 43/120, p<0.01). Importantly, the Aallele was associated with increased risk for CAD among hypertensive individuals(OR: 2.201[95%CI: 1.291-3.752], p=0.004), an effect which was not seen amongnormotensive subjects (p=NS). Importantly, the presence of the A allele was alsoassociated with significantly higher levels of CRP (mean[25th-95th percentile]:A:3.52[1.98-6.08] vs G:1.18[0.66-1.71] mg/ml, p=0.0001), fibrinogen (A:407[347-513] vs G:369[320-416] mg/dl, p=0.001), IL-6 (A:1.55[3.63-5.40] vs G:0.99[0.51-2.46] pg/ml, p=0.002), and sVCAM-1 (A:702[648-925] vs G:621[476-799] ng/ml,p=0.03).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

244 Hypertension: from bench to bedside
Conclusions: Genetic polymorphism A1675G on AT2R affects systemic inflam-matory mechanisms, since the presence of the A allele is associated with higherlevels of CRP, fibrinogen, IL-6 and sVCAM-1. In addition, the A allele is associatedwith elevated cardiovascular risk among hypertensive individuals.
P1513 Pre-existing type 2 diabetes and history of coronaryheart disease on cardiovascular risk in high-riskhypertensive patients: a subanalysis of the CASE-Jtrial
S. Yasuno1, K. Ueshima1, K. Oba1, T. Ogihara2, T. Saruta3,K. Nakao4. 1EBM Research Center, Kyoto University Graduate
School of Medicin, Kyoto, Japan; 2Osaka General Medical Center, Osaka,Japan; 3Keio University School of Medicine, Tokyo, Japan; 4Kyoto University,Graduate School of Medicine, Department of Medicine and Clinical Science,Kyoto, Japan
Objective: Several studies have reported that pre-existing diabetes mellitus hasthe same impact on the incidence of cardiovascular (CV) events as a history of CVdisease or myocardial infarction. However, there is little evidence regarding thisissue in high-risk Japanese hypertensive patients. Thus, we examined the impactof pre-existing type 2 diabetes and a history of coronary heart disease (CHD)on the incidence of CV events in high-risk Japanese hypertensive patients, as asubanalysis of the CASE-J (Candesartan Antihypertensive Survival Evaluation inJapan) trial.Methods: The CASE-J trial compared the effects of the angiotensin II receptorblocker candesartan and the calcium channel blocker amlodipine on the incidenceof CV events in high-risk Japanese hypertensive patients. There were 4,703 high-risk hypertensive patients (mean age: 63.8 years) to be analyzed in the trial. Wedivided them into four groups according to baseline characteristics as follows,non-diabetics without a history of CHD (n=2292), non-diabetics with a history ofCHD (n=393), diabetics without a history of CHD (n=1815), and diabetics witha history of CHD (n=203). We used the multivariate Cox regression analysis toestimate the hazard ratio (HR) and corresponding 95% confidential interval (CI)with adjustment for baseline characteristics as standard covariates and subse-quent systolic and diastolic blood pressure (BP) during the trial as time-varyingcovariates. HR of non-diabetics without a history of CHD for CV events was setto a reference value of 1.0.Results: BP was strictly controlled to the level as low as less than 140/80 mmHgin all groups. Of 4,703 patients, 268 (5.7%) patients experienced CV events fora rate of 17.7 per 1000 person-years during 3.2±0.9 years of follow-up. Diabet-ics with a history of CHD most frequently experienced CV events among fourgroups (adjusted HR: 5.25; 95%CI: 3.52-8.13; P<0.001). Both non-diabetics witha history of CHD and diabetics without a history of CHD also more frequentlyexperienced CV events compared to non-diabetics without a history of CHD (ad-justed HR: 2.66; 95%CI: 1.68-4.19; P<0.001, adjusted HR: 2.40; 95%CI: 1.79-3.22; P<0.001, respectively). However, there was no significant difference in therisk of CV events between non-diabetics with a history of CHD and diabetics with-out a history of CHD (P=0.648).Conclusion: Pre-existing type 2 diabetes was associated with the risk of CVevents as strongly as a history of CHD was in high-risk Japanese hypertensivepatients.
P1514 From a stiff aorta to a hypertrophied ventricle: arterialstiffness is a better predictor of echocardiagraphicleft ventricular hypertrophy than wave reflections andpulse pressure in hypertensives
P. Xaplanteris, C. Vlachopoulos, G. Vyssoulis, I. Dima, D. Terentes-Printzios, A. Siama, C. Stefanadis. Hippokration Hospital, University of Athens,1st Department of Cardiology, Athens, Greece
Purpose: Echocardiographic assessment of left ventricular mass index (LVMI)has been implemented into clinical practice for detecting subclinical organ dam-age in hypertension. Brachial and aortic pulse pressure, as well as aortic stiffnessand wave reflections have been proposed as useful measures for risk stratifica-tion. We sought to evaluate the ability of these indices to predict left ventricularhypertrophy in a cohort of newly diagnosed hypertensives.Methods: We enrolled 1200 subjects with a new diagnosis of hypertension forwhich they had never received treatment. Left ventricular mass index (LVMI) wascalculated by echocardiography. Hypertrophy was defined as LVMI ≥ 125 g/m2 formen and ≥ 110 g/m2 for women, according to guidelines. Carotid-femoral pulsewave velocity (cfPWV), an index of aortic stiffness, was measured using a vali-dated device. Aortic pressures and augmentation index (AIx), an index of wavereflections, were measured by applanation tonometry. Receiver operating char-acteristic (ROC) curves and the area under each curve (AUC) were calculated foreach variable.Results: Aortic stiffness had the higher predictive value for left ventricular hy-pertrophy; cfPWV exhibited the larger AUC:0.73 (95% CI:0.70-0.76, p<0.001).AIx had the smaller AUC:0.654 (95% CI:0.624-0.685, p<0.001) among studiedvariables. AUCs for aortic and brachial PP were 0.704 (95% CI:0.674-0.734,p<0.001) and 0.676 (95% CI:0.646-0.707, p<0.001) respectively.Conclusion: cfPWV can accurately predict left ventricular hypertrophy in nevertreated hypertensives; moreover, it is a better predictor than AIx, brachial or aor-
ROC curves for PWV, AIx, pulse pressures
tic pulse pressure. These findings underscore the importance of aortic stiffnessevaluation as an adjunct for assessing target organ damage.
P1515 Early stages of hypertension are characterized by adeficiency of the cardioprotetive hormone BNP
A. Cataliotti, F. Macharet, P.M. Mckie, R.J. Rodeheffer, L.S. Malatino,K.R. Bailey, J.C. Burnett. Mayo Clinic, Rochester, MN, United Statesof America
The objective of the current study was toassess the relationship between hyper-tension (HTN) and 3 distinct circulatingforms of B-type Natriuretic Peptide (BNP),including mature active BNP1-32determined by Shionogi and by Biosite, non-active NT-proBNP1-76 by Roche, and, for the first time, the precursor proBNP1-108 by BioRad. We also evaluated their relationship with cardiac hypertrophyand renal function. BNP forms were measured in 2,036 randomly selected adultsfrom Olmsted County, MN (age>45). There were 571 normotensives, 755 withpre-HTN, 492 with stage 1HTN, and 218 with stage 2 HTN. All forms of BNP in-creased with age, were lowerin male as compared with female and were inverselyrelated with BMI. Averagelevels of all BNP forms were higher in subjects with leftventricular hypertrophy (LVH) and increased with the severity of HTN and withreduced renalfunction. However, in a multivariate model adjusted for age, gen-der, BMI, LVH,and renal function (Table 1), BNP1-32 (both assays) was lower inearly stages of HTN (pre-HTN and stage 1 HTN) and elevated in stage 2 HTN(by Biosite) as compared to normotensives. Similarly, NT-proBNP1-76 was lowerin the pre-HTN andhigher in stage 2 HTN as compare with the normotensives.More importantly,proBNP1-108 was lower in stage 1 HTN and did not increase instage 2 HTN. The lack of elevation of the precursor proBNP1-108 demonstratesimpaired BNPproduction in HTN.
Table 1. BNP forms in 2,036 subjects
Variable proBNP1-108 p BNP1-32 p BNP1-32 p NT-proBNP p(BioRad) (Shionogi) (Biosite) (Roche)
Normotensive(n=571) reference na reference na reference na reference na
Pre-Hypertensive(n=755) -38.9 0.174 -70.5 0.016 -56.8 0.034 -65.2 0.011
HypertensionStage 1 (n=492) -66.7 0.038 -90.6 0.006 -73.2 0.015 -27.4 0.343Stage 2 (n=218) 1.2 0.978 30.2 0.493 77.7 0.052 77.2 0.045
These results obtained from a large, well characterized community sample con-firm and extend our previous observation made in a smallgroup of hypertensivesubjects and support the hypothesis a deficiency state ofthe cardiorenal protec-tive natriuretic peptide system may play a role in the development of HTN.
P1516 The powerful additive predictive value of nighttimehemodynamics and aortic stiffness on thedevelopment of microalbuminuria in hypertension:a 6-year follow-up study
E. Andrikou, C. Tsioufis, C. Thomopoulos, I. Andrikou, A. Mazaraki,V. Tzamou, L. Lioni, I. Kallikazaros, C. Stefanadis. First Cardiology Clinic,University of Athens,Hippokration Hospital, Athens, Greece
Objective: To assess whether aortic stiffening as defined by carotid-femoral pulsewave velocity (PWV) has either additive or synergistic effect with ambulatory BPload in new-onset microalbuminuria during follow-up.Methods: We prospectively studied 163 white hypertensive non-diabetic patients(52±10 years, 98 men, 59 smokers, body mass index=28.8±5.4kg/m2) in a 6-year period. All patients underwent 24-hour ambulatory monitoring, and PWVmeasurement with Complior SP, whereas metabolic profile, estimated creatinineclearance (eGFR) and echocardiographic measurements were also performedat both baseline and last outpatient clinic visit (follow-up: 4.5±0.89 years). Mi-croalbuminuria was defined as ACR between either 20 or 30 (men and womenrespectively) and 300mg. All subjects were under optimal antihypertensive ther-apy complemented by supplementary vasoactive drugs where appropriate andthe spectrum of drugs implemented within the last 6-month period before lastvisit consisted of: renin-angiotensin system inhibitors RAASI (49%), diuretics
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Hypertension: from bench to bedside 245
(25%), calcium-channel blockers (20%), beta-blockers (13%), statins (16%) andantiplatelet agents (18%).Results: Baseline nighttime systolic and diastolic BP were 121±13 and73±9mmHg, while the incidence of microalbuminuria was 13.5% (n=22). Be-tween baseline and last follow-up visit it was accomplished a decrease in BMIby 1.9±4.1kgr/m2, while PWV was increased by 1.83±1.37m/s (7.9±1.5 vs.9.6±1.5m/s). During follow-up, 24h systolic and diastolic BP were decreased by12.7±9.1 and 8.2±6.2mmHg (130±12 vs. 122±12 and 80±9 vs. 75±8mmHg)respectively. In Cox regression models after adjustment for confounders, it wasfound that independent predictors (HR [95% CI]) of microalbuminuria were: base-line nighttime systolic BP, 1.034 [1.001-1.068], p=0.046, baseline PWV, 1.317[1.048-1.654], p=0.018, and the interaction term of nighttime systolic BP x base-line PWV, 1.003 [1.001-1.004], p<0.001.Conclusion: Baseline nighttime systolic BP and PWV have an additive effect onthe incidence of microalbuminuria suggesting that integrated stiffening measuresmay predict kidney damage in the early course of hypertension.
P1517 Treatment of hypertension in acute ischemic stroke
K. Fouad1 , S. Said2. 1Ain Shams University Hospital, Departmentof Cardiology, Cairo, Egypt; 2Alexandria University, Department ofNeurology, alexandria, Egypt
Introduction: There has been substantial controversy regardingtreatment of blood pressure in the management of acute ischemic stroke. Non-Uniformity of study design and reporting makes it difficult to draw conclusionsfrom previous data. When to treat hypertension in the acute setting is one of theunsettled questions yet.Aim of the study: To study stroke outcome in relation to treatment of hyperten-sion in the management of acute ischemic stroke and its impact on the cardio-vascular system.Patients and methods: This was a prospective study in which all admitted pa-tients for acute ischemic stroke within 24 hours throughout the year 2006 wereincluded. The severity of the stroke was based on the National Institutes of HealthStroke Scale (NIHSS). The 2005 AHA/ASA guidelines in the management ofacute ischemic stroke were followed. We also followed the same guidelines inthe treatment of hypertension in adults with acute ischemic stroke in the first 24hours. However, patients who continued to have hypertension grade II&III afterthe first 24 hours were also treated.Results: A total of 356 patients were initially included and managed in the acutephase. Only 241 completed the study and attended the clinics for their follow upassessment at 3 months. The majority were males (76%), preexisting hyperten-sion was found in 68.9% and most of the patients had hypertension on admission(87.5%). In 223 patients (92.53%) no antihypertensive medication was given inthe 1st 24 hours. In 134 patients (55.6%) the blood pressure continued to beon the hypertensive side after the first 24 hours and they received antihyperten-sive medications. The 223 patients (92.53%) who did not receive antihyperten-sive treatment achieved 57.1%, 78.09% and 73.87% of the total reduction in SBP,DBP and MBP respectively at the end of the 1st 24 hours. All cardiac compli-cations (ten patients, 4.15%) were reported in the first 24 hours only. The meanNIHSS score on admission was 22.98±10.38, while the mean score at the 3rdmonth was 9.4±6.5. The differences were highly significant (p< 0.0001). Whenthe stepwise regression analysis was used, only the increase in stroke severity atthe onset (p<0.0001), followed by the decrease in SBP at the 3rd day (p< 0.001)and lastly the increase in SBP on admission (p< 0.05) were predictive for poorstroke outcome.Conclusion: Introducing antihypertensive medications after the first 24 hours ofacute ischemic stroke in patients who continued to have hypertension grade II&IIIhas no negative impact on stroke outcome and limits the cardiovascular compli-cations
P1518 Pulse pressure is a predictor of vascular endothelialfunction in middle-aged subjects with no apparentheart disease
R. Beigel1, D. Dvir2, Y. Arbel3, A. Shechter1, M.S. Feinberg1,M. Shechter1. 1Chaim Sheba Medical Center, Tel Hashomer, Israel;
2Rabin Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Dept. ofCardiology, Petah Tikva, Israel; 3Sorasky Medical Center, Tel Aviv, Israel
Objective: To investigate whether pulse pressure (PP) is associated with en-dothelial function in subjects with no apparent heart disease.Background: Elevated PP is increasingly being recognized as a cardiovascularrisk factor.Methods: We prospectively assessed brachial flow-mediated dilation (FMD) in525 middle-aged, consecutive subjects with no apparent heart disease [320(61%) men, mean age 52±11 years, mean body mass index 26±4 kg/m2]. Fol-lowing an overnight fast and discontinuation of all medications for ≥ 12 hours, per-cent improvement in FMD (%FMD) and endothelium-independent, nitroglycerin-mediated vasodilation (%NTG) were assessed using high resolution linear arrayultrasound.Results: Linear regression analysis revealed a significant inverse associationbetween %FMD and PP (r=-0.65, p<0.01), systolic blood pressure (r=-0.52,p<0.01) and age (r=-0.21, p<0.05). Multivariate analysis showed that PP was
the strongest independent predictor of %FMD. We therefore divided subjects intotwo groups: those with ≤ (n=290) and > (n=235) a median PP of 50 mmHg. Age,gender, body mass index, concomitant medications, lipids, resting heart rate, ho-mocysteine, C-reactive protein and fasting blood glucose were comparable in bothgroups. %FMD but not %NTG was significantly greater in patients with PP ≤ com-pared with > 50mmHg (14.9±5.0% vs. 10.8±5.0%, p<0.001 and 16.1±4.8% vs.14.8±4.9%, p=0.38, respectively) [Figure; subjects with PP ≤ (closed bars) and> (open bars) the median PP of 50 mmHg].
Conclusion: PP is inversely associated with brachial FMD in middle-aged sub-jects with no apparent heart disease, suggesting a potential mechanism wherebyelevated PP contributes to cardiovascular disease. Long-term follow-up is war-ranted to elucidate the incidence of coronary artery disease in both study groups.
P1519 Increased perioperative complications after majorvascular surgery in patients with a hypertensive orhypotensive exercise blood pressure response
I.I. De Liefde, G. Welten, J. Klein, R.T. Van Domburg,H.J.M. Verhagen, R.J. Stolker, D. Poldermans. Erasmus Medical
Center, Rotterdam, Netherlands
Background: Recent studies have shown that a pre-operative hypertensive orhypotensive blood pressure response at treadmill exercise test in patients withknown or suspected peripheral arterial disease (PAD) is associated with a two foldincreased risk of cardiovascular events and mortality. However, the complicationrisk in these patients after major vascular surgery is still unknown.Methods: Between 1993 and 2006, 665 consecutive PAD patients underwentelective major vascular surgery (carotid endarterectomy, abdominal aorta repairor lower extremity revascularization surgery) in the Erasmus MC. Complications(post-operative infection, myocardial infarction, angina pectoris, cardiac arrhyth-mia, heart failure, cerebrovascular accident or spinal cord ischemia, dialyses, am-putation, thrombectomy, re-operation and death) within one month after majorvascular surgery were collected using medical records and computerised hospi-tal databases. Postoperative myocardial infarction, angina pectoris, heart failure,new cardiac arrhythmia’s and 30-day cardiac mortality together were classified ascardiac complications.Results: Mean age was 64 years with 75% males. The complication rate rangedfrom 1% for angina pectoris till 15% for postoperative infections. The 30 day mor-tality was 3%.Patients with a hypertensive blood pressure response (n=66) demonstrated ahigher risk of thrombectomy (HR 2.80 95%CI (1.24 - 6.33)) compared to patientswith a normal blood pressure response. No differences were observed for 30-daymortality risk or postoperative cardiac complications.Patients with a hypotensive blood pressure response (n=18) showed an increasedrisk of postoperative myocardial infarction (HR 3.69 95% CI (1.08 - 12.64)), car-diac complications (HR 2.90 95% CI (1.02-8.19).Conclusion: Patients with an abnormal blood pressure response have an in-creased risk of cardiovascular complications after elective major vascular surgery.Addition prospective research is needed to confirm these results and to investi-gate the underlying mechanisms and therapy.
P1520 Exaggerated exercise blood pressure response isassociated with increased levels of C-reactiveprotein, osteoprotegerin and urinary albuminexcretion in essential hypertensive subjects
K. Dimitriadis, C. Tsioufis, D. Syrseloudis, M. Selima, E. Stefanadi,A. Agelis, A. Miliou, I. Kallikazaros, C. Stefanadis. First Cardiology Clinic,University of Athens,Hippokration Hospital, Athens, Greece
Purpose: The data regarding the association of a hypertensive response to exer-cise (HRE) with cardiovascular risk are controversial, while low-grade inflamma-tory processes, osteoprotegerin (OPG) and urinary albumin excretion are linkedto atherosclerosis progression and unfavourable outcome. In this study we exam-ined the correlations between HRE, high-sensitivity C-reactive protein (hs-CRP),OPG and urinary albumin excretion, expressed as the albumin to creatinine ratio(ACR), in essential hypertensives.Methods: 240 newly diagnosed untreated non-diabetics with stage I to II es-sential hypertension [155 men, mean age=51 years, office blood pressure(BP)=150/96 mmHg] with a negative treadmill exercise test (Bruce protocol) weredivided into those with HRE (n=70) (peak exercise systolic BP ≥210mmHg in menand ≥190 mmHg in women) and to those without HRE (n=170). Moreover, in allsubjects ACR values were determined as the mean of two non-consecutive morn-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

246 Hypertension: from bench to bedside / Atherosclerosis
ing spot urine samples and venous blood samples were drawn for estimation ofmetabolic profile, hs-CRP and OPG levels according to established techniques.Results: Patients with HRE compared to those without HRE were older (54±8vs 49±5 years, p<0.05), had greater 24-h systolic BP (143±9 vs 131±8 mmHg,p<0.05), while did not differ regarding metabolic profile, left ventricular mass in-dex and relative wall thickness (p=NS for all). Furthermore, patients with HREas compared to those without HRE exhibited higher levels of ACR (72.9±17 vs14.1±2.8 mg/g, p<0.0001), hs-CRP (5.3±1.1 vs 2.3±0.9 mg/l, p<0.0001) andOPG (5.4±0.1 vs 4.1±0.5 pmol/l, p<0.05). In the total population, peak exercisesystolic BP was related to 24-h systolic BP (r=0.249, p<0.05), hs-CRP (r=0.429,p<0.0001), OPG (r=0.214, p<0.05) and ACR (r=0.422, p<0.0001), while hs-CRPwas associated with ACR (r=0.644, p<0.0001). By analysis of covariance it wasrevealed that ACR, OPG and hs-CRP values remained significantly different be-tween groups after adjustment for confounders (p<0.05).Conclusions: In the setting of essential hypertension, an HRE is associated withheightened hs-CRP, OPG and ACR levels, reflecting diffuse vascular dysfunction.These findings suggest that HRE may be a useful tool in identifying hypertensivesubjects with adverse proatherosclerotic profile.
P1521 Exercise capacity as strong predictor of progressionfrom pre-hypertension to hypertension inAfrican-American Men
A. Pittaras1, C. Faselis2, M. Doumas2, A.J. Manolis3,L. Korshak2, L. Poulimenos3, I. Zacharopoulou3 , A. Mazarakis3 ,
V. Papademetriou2, P.F. Kokkinos2. 1Mediton Medical Center, Athens, Greece;2VA & Georgetown University Medical Centers, Washington Dc, United States ofAmerica; 3Asclepion Voulas Hospital, Athens, Greece
Background: Predictors of the progression from pre-hypertension to hyperten-sion (HTN) have not been adequately defined, especially in African-Americans.Since fitness is associated with cardiovascular health, we assessed the asso-ciation between fitness and the rate of progression to HTN in pre-hypertensiveAfrican-American men.Methods: From March of 1985 to June 2007, we identified 1,081 pre-hyper-tensive African-American men (mean age: 54±12) who underwent an exerciseevaluation to rule out ischemia. All had normal exercise response, were not re-ceiving cardiac or antihypertensive medications and had resting blood pressurewithin the established pre-hypertension criteria. We established four fitness cat-egories based on the age and MET level achieved. Individuals who achieved apeak MET level within the lowest 20th percentile of their respective age group(mean: 5.2 MET) comprised the Lowest-Fit category (n=210). Those with a METlevel between the 21st and 50th percentile (mean: 7.1 MET) comprised the Low-Fit category (n=359). Subjects with a MET level between 51st and 85th percentile(mean: 8.8 MET) comprised the Moderate-Fit category (n=352) and those witha MET level above the 85th percentile (mean 10.1 MET), comprised the High-Fitcategory (n=160).Results: The overall rate of progression from pre-hypertension to HTN within thefollow-up period of 8.2±5.8 years was 33.3% and the yearly rate was 4.1%. Thehighest rate (41.4%) was observed in the Lowest-Fit category, followed by 39.3%,28.4% and 20% for the Low, Moderate, and High-Fit categories respectively. CoxProportional hazard analysis (adjusted for age, BMI, smoking, resting BP, and di-abetes) revealed a 10% lower risk for developing HTN for every 1-MET increasein exercise capacity. When compared to the High-Fit category, the risk for hyper-tension was 66% higher (hazard ratio= 1.66; CI 1.1-2.4) in the Low-Fit and 82%higher (hazard ratio=1.82; CI: 1.1-2.7) in the Lowest-Fit category individuals.Conclusions: Exercise capacity is inversely related to the risk for developingHTN. The risk was 10% lower for each 1-MET increase in exercise capacity. Therelative risk for developing HTN in the two lowest fit categories was approximately60% to 80% higher when compared to the High-Fit.
P1522 Arterial stiffness a marker or a mediator ofparoxysmal atrial fibrillation in essentialhypertension?
I. Skiadas1, C. Tsioufis1, P. Sarafis2, I. Vagena1, S. Veioglanis1,D. Papoutsis1, C. Stefanadis1 , I. Kallikazaros1. 1HippokrationGeneral Hospital, Athens, Greece; 2Attikon University Hospital,
Athens, Greece
Purpose: The structural and functional characteristics of the vasculature plays animportant role in the pathopysiology of hypertension and its complications. More-over, the sequels of essential hypertension on rhythm disturbances is currentlyunder vigorous investigation as an unexplored topic. Thus, the present study wasconducted to investigate the contribution of the elasticity status of the great ves-sels to the genesis of atrial fibrillation in hypertensives.Methods: We studied 46 consecutive essential hypertensive subjects (aged 64years, 22 men, office blood pressure (BP) 144/86mmHg) with a history of parox-ysmal atrial fibrillation and no other evident comorbidity and 49 consecutive es-sential hypertensives without any evidence of PAF, matched for age, sex and BP.All included subjects were on sinus rhythm and underwent a complete conven-tional and tissue doppler imaging (TDI) echocardiographic study. Left Ventricular(LV) diastolic function was estimated by TDI, averaging the diastolic mitral annularvelocities measurements. Aortic stiffness was evaluated, on the basis of carotid
–femoral pulse wave velocity (PWV) measurements by means of a computerizedmethod (Complior SP).Results: Hypertensives with PAF compared to those without PAF had increasedbody mass index (28.1 vs 26.9kg/m2, p<0.05), were smokers in a higher percent-age (45 vs 31%, p<0.05), had a longer duration of hypertension (5 vs 2 years,p< 0.05), showed significantly increased relative wall thickness (0.46 vs 0.44,p<0.05), left atrial volume indexed for body surface area (LAV index) (23.7±7vs 19.7±3 ml/m2 p<0.05) and lower Em (7.5±1.6 vs 8.4±1.4cm, p<0.05) andEm/Am values (0.8±0.1 vs 0.9±0.4 p<0.05). Hypertensive subjects with PAFcompared to those without PAF had increased PWV (9.65 vs 8.44 m/sec, p<0.05)and it was positively correlated with age (r=0.54, p<0.001), office systolic BP(r=0.35, p<0.05), relative wall thickness (r=0.32, p<0.005) and LA volume index(r=0.29, p<0.05).A PWV cut-off value of 8m/sec classified hypertensive patientsin the two groups with sensitivity of 66% and specificity of 72%.Conclusions: Hypertensive subjects with PAF have significantly stiffer aorta andaltered cardiac geometry. A PWV cut-off value of 8.0 m/sec yielded a specificityof 72%. Although the underlying pathophysiological mechanisms are largely un-determined, this association could at least partially explain the increased vulner-ability of such patients for development of PAF.
P1523 Comparative role of different definitions of leftventricular hypertrophy as predictors ofcardiovascular events in hypertension: a Greek 6-yearfollow-up study
D. Tsiachris, C. Tsioufis, K. Dimitriadis, C. Thomopoulos,D. Syrseloudis, S. Lalos, I. Kallikazaros, C. Stefanadis. First
Cardiology Clinic, University of Athens,Hippokration Hospital, Athens, Greece
Purpose: We assessed the comparative prognostic role of two different defini-tions of left ventricular hypertrophy (LVH) for major cardiovascular (CV) events ina prospective observational study in Greek hypertensives.Methods: We followed-up 1652 hypertensives (mean age 54.3 years, 696 males,office BP=147/93 mmHg) free of CV disease for a mean period of 6 years.Five major risk factors [age >65, gender, current smoking, diabetes mellitus(DM) and dyslipidemia (LDL>160mg/dl)] were evaluated at baseline along withechocardiographically-detected LVH (defined either as LV mass indexed for bodysurface area (BSA) ≥125 g/m2 for men and ≥110 g/m2 for women according tocurrent guidelines or defined as LV mass indexed for height2.7 ≥49 g/m2.7 for menand ≥45 g/m2.7 for women). End-points of interest were the incidence of coronaryartery disease (CAD), stroke, all cause mortality and their composite.Results: The prevalence of LVH, based on indexation for height2.7, was higherthan the one by using indexation for BSA (60.5% vs. 35.6%). At the end of followup, CAD was the most prevalent (5.2%), followed by stroke (5%) and total mortal-ity (3.1%). In univariate Cox regression analysis, age>65 (HR 2.53, p<0.001),male gender (HR 1.97, p=0.004), DM (HR 4.01, p<0.001) and the presenceof LVH, indexed either for height2.7 (HR 2.50, p=0.007) or for BSA (HR 1.76,p=0.048) were correlated with the incidence of CAD. In multivariate analysis, LVHindexed only for height2.7 (adjHR 2.40, p=0.012) along with age>65, male gen-der and DM remained independents prognosticator of CAD. Age>65 (HR 5.98,p<0.001) in addition to LVH indexed either for height2.7 (HR 3.06, p=0.002 andadjHR 2.34, p=0.025, respectively) or BSA (HR 2.31, p=0.003 and adjHR 1.86,p=0.033 respectively) were independently associated with the incidence of stroke.Finally, age>65 (HR 4.65, p<0.001), male gender (HR 1.34, p=0.041), DM (HR2.00, p=0.001) and LVH indexed both for height2.7 (HR 2.74, p=<0.001) andfor BSA (HR 1.75, p=0.001) were correlated with the incidence of the compos-ite end-point. In multivariate analysis, apart from age and sex, LVH indexed bothfor height2.7 (adjHR 2.74, p=<0.001) and for BSA (adjHR 1.75, p=0.001) wereindependent predictors of the composite end-point.Conclusions: In hypertensives free of CV disease, LVH is an independent prog-nosticator of stroke and the composite end-point irrespectively from its definition.Normalization of LV mass for height2.7, estimates more accurately the prevalenceof LVH in overweight subjects and enhances the predictive value of LVH regardingthe incidence of CAD.
ATHEROSCLEROSIS
P1524 Role of surgical repair in coronary intimal thickeningformation in patients with congenital cardiovasculardefects
R.A. Guerri-Guttenberg1, E. De Mateo2, D.R. Grana1, I. Marco2,J. Milei1. 1Institute of Cardiological Research UBA-CONICET,
Buenos Aires, Argentina; 2Pathology Division, Ricardo Gutiérrez Children’sHospital, Buenos Aires, Argentina
Purpose: Patients with specific congenital heart disease (CHD) have a high-riskfor accelerated atherosclerosis. Some surgeries for CHD involve manipulation ofcoronary arteries, a setting were coronary ostial stenosis may develop leading toincreased risk of associated atherosclerosis. The aim of this study is to assessthe presence of intimal thickenings in autopsies of CHD patients with (Group 1)and without (Group2) surgical repair, in order to appraise the role of surgery indeveloping intimal thickenings in a high-risk group for accelerated atherosclerosis.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atherosclerosis 247
Method: The coronary tree of 67 patients (age range; 3 months-14 years) whodied of congenital heart disease was analyzed. This group of patients had thefollowing structural pathologies of the heart either isolated or combined; ASD(n=28), Tetralogy of Fallot (n=21), Ductus (n=19), VSD (n=10), Troncus arterio-sus (n=5), coarctation of the aorta (n=3), DORV (n=3), CTGA (n=3), Pulmonarystenosis (n=2), Pulmonary atresia (n=2), Coronary artery anomalies (n=2), Eb-stein anomaly (n=2), TAPVR (n=1), Bicuspid aortic valve (n=1) and Single ventri-cle (n=1). A total of 804 samples of coronary arteries of a thickness of 2mm wereanalyzed by serial sectioning.Results: Coronary intimal thickenings were more frequent in Group 1 (see Ta-ble 1). The most frequently affected vessel was the right coronary artery (RCA)in Group 1, and the left anterior descending coronary artery (LAD) in Group 2.Lesions ranged from focal to diffuse intimal hyperplasia with infiltration of smoothmuscle cells and internal elastic membrane rupture.
Table 1. Intimal thickenings in CHD
Groups Coronary Intimal Thickenings
Total RCA LAD PDA LCX
G 1. CHD with surgical repair(n=16) 87.5% (14) i 56.3% (9) ii 43.8% (7) iii 12.5% (2) iv 6.3% (1) v
G 2. CHD without surgery (n=51) 45.1% (23) i 15.7% (8) ii 17.6% (9) iii 17.6% (9) iv 9.8% (5) v
Fisher exact test: i - p=0.0035, ii - p=0.0025, iii - p=0.04, iv - ns, v - ns.
Conclusion: Surgical repair of congenital heart disease increases the presenceof intimal thickenings. Extracorporeal circulation may be involved in the patho-physiology of these findings. Intimal thickenings in the presence of risk factorssuch as sedentary lifestyle resulting from limitations in the ability to perform phys-ical activity could explain the accelerated atherosclerosis in these set of patients.Intimal thickenings could regress, stabilize or progress to overt atheroscleroticlesions.
P1525 The influence of the transcriptional regulation factorHIF (hypoxia inducible factor) on the progression ofatherosclerotic plaques in vivo
C. Pfluecke1, M. Christoph1, K. Hesse1, D. Poitz1, K. Ibrahim1,R.C. Braun-Dullaeus2, R.H. Strasser1, A. Schmeisser2. 1Dresden
University of Technology, Heart Center, Dept. of Cardiology and Intensive Care,Dresden, ; 2Otto-von-Guericke University of Magdeburg, Magdeburg, Germany
Background: The development of atherosclerosis has been well characterizedmorphologically. Which role hypoxia plays in the genesis of atherosclerosis hasnot been well elucidated. It has been postulated that the transcription factor hy-poxia inducible factor (HIF) contribute to the regulation of the genetic expressionprofile in these processes. HIF also has been suggested to promote the formationof microvessels (angiogenesis) within the atherosclerotic plaque by inducing highlevels of endothelial growth factors and their receptors (VEGF and VEGF-R)Hypothesis: The transcriptional regulation factor HIF has a fundamental influ-ence on the plaque progression by regulation of local proliferation, chronic in-flammation and neointimal angiogenesis in vivo.Methods: As an in vivo model of atherosclerosis, an endothelial denudation offemoral arteries in Apolipoprotein E knock-out-mice was performed. At specifictime intervals femoral arteries after treatment were examined as to atheroscle-rotic plaque progression using HE staining. Moreover, to examine the influence ofHIF on the atherosclerotic plaque progression, we performed a systemic or localtransfection of the femoral arteries with a viral vector which encodes a dominantnegative mutant of HIF. After the denudation the viruses were injected either sys-temically into the tail vein of the mouse, or were applied locally around the femoralartery. The transfection efficiency was checked with a viral LacZ encoding vectorand subsequent histological quantification.Results: Seven days after denudation of the femoral artery early phases of anatherosclerotic plaque could be observed. Over 4 weeks a continuous plaque pro-gression up to subtotal stenosis of the denudated vessel was obvious. After localtransfection, a stable expression of LacZ and thus an effective suppression of HIFin about 80 percent of the cells of the vessel wall could be reached in a period of1-4 weeks. The systemic administration of viral vectors, however was inefficient.In mice with an efficient local suppression of HIF, a dramatically reduced plaqueprogression and a decrease of the late lumen loss could be demonstrated.Conclusion: The local suppression of the oxygen-dependent transcription factorHIF via adenoviral transfection is able to reduce the plaque progression. Thesedata document that HIF has a relevant impact in the development of atheroscle-rosis in vivo. The new paradigm that hypoxia and HIF play a central role in thegenesis of atherosclerosis may open new routes for the understanding and inhi-bition of the progression of atherosclerosis.
P1526 Insulin resistance and oxidative stress precedeinflammation during the development of themetabolic syndrome and atherosclerosis in obesemice
B. Geeraert, M. Hulsmans, P. Holvoet. Catholic University of Leuven,Department of Cardiovascular Diseases, Leuven, Belgium
Purpose: Obesity-associated inflammation and oxidative stress are regarded as
key disease processes related to insulin resistance (IR) and atherosclerosis. How-ever, it remains to be determined if infiltration of inflammatory cells causes or re-sults from the development of IR and oxidative stress. Furthermore, we want todetermine the sequence of underlying molecular events in adipose and vasculartissues, and their associations with the development of the metabolic syndrome(MetS) and atherosclerosis.Methods: We studied mice with combined leptin and LDL-receptor deficiency(double knockout or DKO) at 6, 12, and 24 weeks. At 24 weeks, these mice fea-ture all MetS components except low HDL cholesterol. Since an important rolefor PPARs was suggested, we evaluated the effect of rosiglitazone and fenofi-brate treatment. We compared blood variables and size and composition of thevisceral adipocytes and atherosclerotic plaques of the DKO mice with those inlean C57BL6 mice of the same age and determined gene expressions.Results: Obesity-associated downregulation of Ppar expressions in the adiposetissue of DKO mice occurred from the age of 6 weeks on. This was associ-ated with impaired adipogenesis, hypertriglyceridemia, IR and systemic oxida-tive stress, which all deteriorated with further weight gain during aging. Theplasma adiponectin concentration decreased with increasing weight. Macrophageinfiltration started at 12 weeks, but only reached a maximum at 24 weeks.These results were confirmed on the RNA level. Simultaneous changes wereobserved in the aorta. The decrease in gene expression of Ppars and markergenes related to insulin signalling (Insr, Irs1, Irs2), glucose transport (Glut4), lipidmetabolism (Lpl, Fabp4) and oxidative defence (Sods, Cat) preceded the infiltra-tion of macrophages and atherogenesis. Furthermore, adiponectin was not onlyinversely related to weight and IR, but also to markers of macrophages and oxida-tive defence in the adipose tissue and the vascular wall. Rosiglitazone, more thanfenofibrate, improved adipogenesis, thereby upregulating adiponectin, increasinginsulin sensitivity and decreasing oxidative stress, inflammation and atheroscle-rosis.Conclusions: Our observations indicate that IR and oxidative stress developearly in obese mice, rendering them susceptible to macrophage-driven inflam-mation and atherogenesis. Common molecular pathways were identified in adi-pose and vascular tissues, most of which are under transcriptional control ofPPARgamma. Furthermore, our data support the importance of adiponectin assignalling molecule between the adipose tissue and vascular wall.
P1527 Tissue factor dependent thrombin generation during1 year-follow-up in acute coronary syndromes
S. Fedi1, A. Rogolino2, R. Marcucci1, A. Fabbri1 , A. Cordisco1,C. Giglioli3, S. Valente3, R. Abbate1, G.F. Gensini1, A.M. Gori2.1University of Florence, Department of Critical Care Medicine,
Florence, Italy; 2Careggi University Hospital - Thrombosis Centre, Department ofHeart and Vessels, Florence, Italy; 3Department of Heart and Vessels, AziendaOspedaliero-Universitaria Careggi, Florence, Italy
Background: The acute coronary syndrome (ACS) is a clinical state induced bythe thrombosis consequent to the rupture of an unstable atherosclerotic plaque.After the occurrence of the acute cardiovascular event a hypercoagulable statehas been documented, but no definite data about the durability of blood clottingactivation are available. Recently it has been available a global assay sensitive toprothrombotic factors and to activated protein C dysfunction.Purpose: Our aim was to evaluate the balance between anticoagulant and pro-coagulant factors, by using a tissue factor dependent thrombin generation assay,during a follow-up of 1, 6 and 12 months after an acute voronary event in 115 (87males and 28 females) patients with ACS undergoing PCI with stent implantation.Methods: Tissue factor dependent thrombin generation analysis was performedin patients on dual antiplatelet treatment at the time of the acute coronary event(TØ), and after 1 (T1), 6 (T2) and 12 (T3) months. Tissue factor dependent throm-bin generation values were defined on the basis of mean minus 2SD of the resultsobtained in control population (n=150) and was set at 77.31% protac-induced co-agulation inhibition (PICI).Results: Baseline values (TØ) of PICI (%) were significantly lower in ACS patientthan in control subjects [78.84 (40.82-94.11) vs 87.48 (72.50-97.65), p <0.0001].PICI % values significantly increased during the 12 month follow-up (p<0.0001).At T1 (1 month after the acute event) PICI % values were slightly but not signif-icantly higher than those observed at TØ [80.62 (51.00-91.02) vs 78.84 (40.82-94.11)]. After 6 and 12 months of follow-up a marked increased with respect tobaseline values was observed [T2: 82.42 (53.96-91.39) PICI%, T3: 83.32 (67.07-91.77) PICI%, p<0.0001 vs TØ]. At TØ altered PICI values (defined as PICI %values < 77.31) were found in 46.1% (53/115) of ACS patients. Similar figure wasfound at T1: altered PICI % values were present in 41.7% (48/115) of patients.Abnormal PICI values significantly (p<0.01) decreased to 25.2% (29/115) at T2and 21.7% (25/115) at T3.Conclusions: This is the first study which evaluated the variation in the coagula-tion cascade balance during 1 year-follow-up in ACS patients undergone PCI. Wedocumented that a marked unbalance of coagulation cascade persists 1 monthafter the acute coronary event. In spite of the progressive decrease in tissue fac-tor dependent thrombin generation values during the follow-up, in these patients,a hypercoagulable state is yet present 6 and 12 months after the vascular events.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
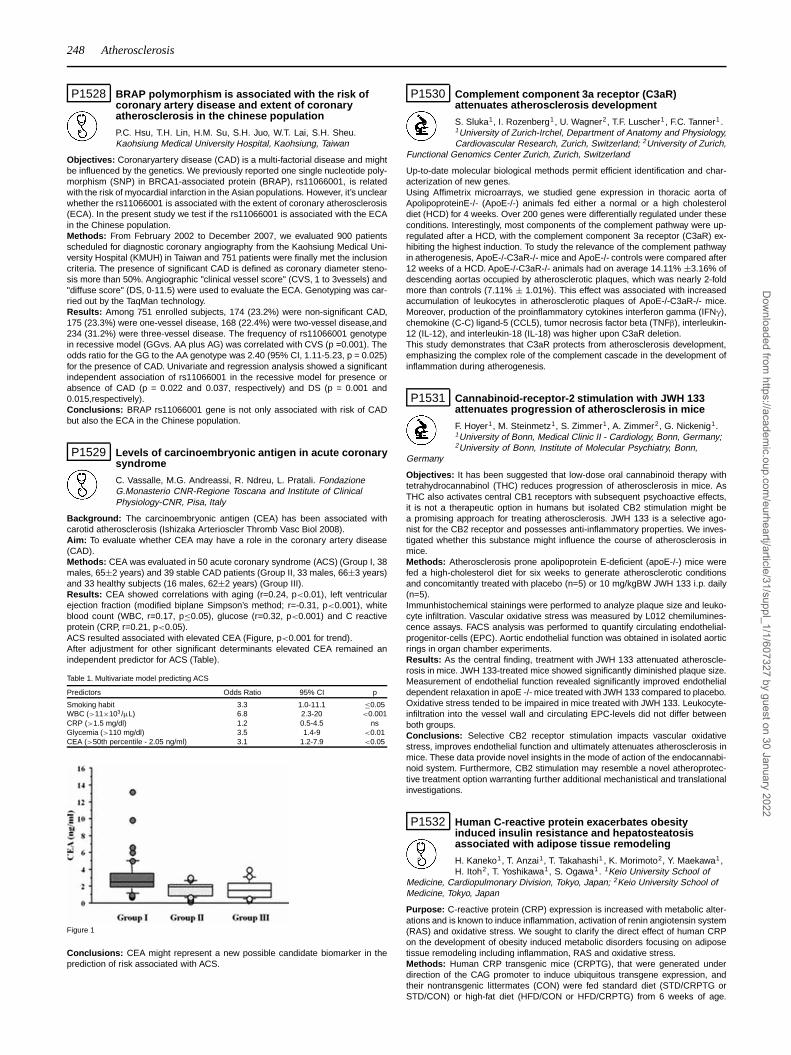
248 Atherosclerosis
P1528 BRAP polymorphism is associated with the risk ofcoronary artery disease and extent of coronaryatherosclerosis in the chinese population
P.C. Hsu, T.H. Lin, H.M. Su, S.H. Juo, W.T. Lai, S.H. Sheu.Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
Objectives: Coronaryartery disease (CAD) is a multi-factorial disease and mightbe influenced by the genetics. We previously reported one single nucleotide poly-morphism (SNP) in BRCA1-associated protein (BRAP), rs11066001, is relatedwith the risk of myocardial infarction in the Asian populations. However, it’s unclearwhether the rs11066001 is associated with the extent of coronary atherosclerosis(ECA). In the present study we test if the rs11066001 is associated with the ECAin the Chinese population.Methods: From February 2002 to December 2007, we evaluated 900 patientsscheduled for diagnostic coronary angiography from the Kaohsiung Medical Uni-versity Hospital (KMUH) in Taiwan and 751 patients were finally met the inclusioncriteria. The presence of significant CAD is defined as coronary diameter steno-sis more than 50%. Angiographic "clinical vessel score" (CVS, 1 to 3vessels) and"diffuse score" (DS, 0-11.5) were used to evaluate the ECA. Genotyping was car-ried out by the TaqMan technology.Results: Among 751 enrolled subjects, 174 (23.2%) were non-significant CAD,175 (23.3%) were one-vessel disease, 168 (22.4%) were two-vessel disease,and234 (31.2%) were three-vessel disease. The frequency of rs11066001 genotypein recessive model (GGvs. AA plus AG) was correlated with CVS (p =0.001). Theodds ratio for the GG to the AA genotype was 2.40 (95% CI, 1.11-5.23, p = 0.025)for the presence of CAD. Univariate and regression analysis showed a significantindependent association of rs11066001 in the recessive model for presence orabsence of CAD (p = 0.022 and 0.037, respectively) and DS (p = 0.001 and0.015,respectively).Conclusions: BRAP rs11066001 gene is not only associated with risk of CADbut also the ECA in the Chinese population.
P1529 Levels of carcinoembryonic antigen in acute coronarysyndrome
C. Vassalle, M.G. Andreassi, R. Ndreu, L. Pratali. FondazioneG.Monasterio CNR-Regione Toscana and Institute of ClinicalPhysiology-CNR, Pisa, Italy
Background: The carcinoembryonic antigen (CEA) has been associated withcarotid atherosclerosis (Ishizaka Arterioscler Thromb Vasc Biol 2008).Aim: To evaluate whether CEA may have a role in the coronary artery disease(CAD).Methods: CEA was evaluated in 50 acute coronary syndrome (ACS) (Group I, 38males, 65±2 years) and 39 stable CAD patients (Group II, 33 males, 66±3 years)and 33 healthy subjects (16 males, 62±2 years) (Group III).Results: CEA showed correlations with aging (r=0.24, p<0.01), left ventricularejection fraction (modified biplane Simpson’s method; r=-0.31, p<0.001), whiteblood count (WBC, r=0.17, p≤0.05), glucose (r=0.32, p<0.001) and C reactiveprotein (CRP, r=0.21, p<0.05).ACS resulted associated with elevated CEA (Figure, p<0.001 for trend).After adjustment for other significant determinants elevated CEA remained anindependent predictor for ACS (Table).
Table 1. Multivariate model predicting ACS
Predictors Odds Ratio 95% CI p
Smoking habit 3.3 1.0-11.1 ≤0.05WBC (>11×103 /μL) 6.8 2.3-20 <0.001CRP (>1.5 mg/dl) 1.2 0.5-4.5 nsGlycemia (>110 mg/dl) 3.5 1.4-9 <0.01CEA (>50th percentile - 2.05 ng/ml) 3.1 1.2-7.9 <0.05
Figure 1
Conclusions: CEA might represent a new possible candidate biomarker in theprediction of risk associated with ACS.
P1530 Complement component 3a receptor (C3aR)attenuates atherosclerosis development
S. Sluka1, I. Rozenberg1, U. Wagner2, T.F. Luscher1 , F.C. Tanner1 .1University of Zurich-Irchel, Department of Anatomy and Physiology,Cardiovascular Research, Zurich, Switzerland; 2University of Zurich,
Functional Genomics Center Zurich, Zurich, Switzerland
Up-to-date molecular biological methods permit efficient identification and char-acterization of new genes.Using Affimetrix microarrays, we studied gene expression in thoracic aorta ofApolipoproteinE-/- (ApoE-/-) animals fed either a normal or a high cholesteroldiet (HCD) for 4 weeks. Over 200 genes were differentially regulated under theseconditions. Interestingly, most components of the complement pathway were up-regulated after a HCD, with the complement component 3a receptor (C3aR) ex-hibiting the highest induction. To study the relevance of the complement pathwayin atherogenesis, ApoE-/-C3aR-/- mice and ApoE-/- controls were compared after12 weeks of a HCD. ApoE-/-C3aR-/- animals had on average 14.11% ±3.16% ofdescending aortas occupied by atherosclerotic plaques, which was nearly 2-foldmore than controls (7.11% ± 1.01%). This effect was associated with increasedaccumulation of leukocytes in atherosclerotic plaques of ApoE-/-C3aR-/- mice.Moreover, production of the proinflammatory cytokines interferon gamma (IFNγ),chemokine (C-C) ligand-5 (CCL5), tumor necrosis factor beta (TNFβ), interleukin-12 (IL-12), and interleukin-18 (IL-18) was higher upon C3aR deletion.This study demonstrates that C3aR protects from atherosclerosis development,emphasizing the complex role of the complement cascade in the development ofinflammation during atherogenesis.
P1531 Cannabinoid-receptor-2 stimulation with JWH 133attenuates progression of atherosclerosis in mice
F. Hoyer1, M. Steinmetz1, S. Zimmer1, A. Zimmer2, G. Nickenig1.1University of Bonn, Medical Clinic II - Cardiology, Bonn, Germany;2University of Bonn, Institute of Molecular Psychiatry, Bonn,
Germany
Objectives: It has been suggested that low-dose oral cannabinoid therapy withtetrahydrocannabinol (THC) reduces progression of atherosclerosis in mice. AsTHC also activates central CB1 receptors with subsequent psychoactive effects,it is not a therapeutic option in humans but isolated CB2 stimulation might bea promising approach for treating atherosclerosis. JWH 133 is a selective ago-nist for the CB2 receptor and possesses anti-inflammatory properties. We inves-tigated whether this substance might influence the course of atherosclerosis inmice.Methods: Atherosclerosis prone apolipoprotein E-deficient (apoE-/-) mice werefed a high-cholesterol diet for six weeks to generate atherosclerotic conditionsand concomitantly treated with placebo (n=5) or 10 mg/kgBW JWH 133 i.p. daily(n=5).Immunhistochemical stainings were performed to analyze plaque size and leuko-cyte infiltration. Vascular oxidative stress was measured by L012 chemilumines-cence assays. FACS analysis was performed to quantify circulating endothelial-progenitor-cells (EPC). Aortic endothelial function was obtained in isolated aorticrings in organ chamber experiments.Results: As the central finding, treatment with JWH 133 attenuated atheroscle-rosis in mice. JWH 133-treated mice showed significantly diminished plaque size.Measurement of endothelial function revealed significantly improved endothelialdependent relaxation in apoE -/- mice treated with JWH 133 compared to placebo.Oxidative stress tended to be impaired in mice treated with JWH 133. Leukocyte-infiltration into the vessel wall and circulating EPC-levels did not differ betweenboth groups.Conclusions: Selective CB2 receptor stimulation impacts vascular oxidativestress, improves endothelial function and ultimately attenuates atherosclerosis inmice. These data provide novel insights in the mode of action of the endocannabi-noid system. Furthermore, CB2 stimulation may resemble a novel atheroprotec-tive treatment option warranting further additional mechanistical and translationalinvestigations.
P1532 Human C-reactive protein exacerbates obesityinduced insulin resistance and hepatosteatosisassociated with adipose tissue remodeling
H. Kaneko1, T. Anzai1, T. Takahashi1 , K. Morimoto2, Y. Maekawa1,H. Itoh2, T. Yoshikawa1, S. Ogawa1. 1Keio University School of
Medicine, Cardiopulmonary Division, Tokyo, Japan; 2Keio University School ofMedicine, Tokyo, Japan
Purpose: C-reactive protein (CRP) expression is increased with metabolic alter-ations and is known to induce inflammation, activation of renin angiotensin system(RAS) and oxidative stress. We sought to clarify the direct effect of human CRPon the development of obesity induced metabolic disorders focusing on adiposetissue remodeling including inflammation, RAS and oxidative stress.Methods: Human CRP transgenic mice (CRPTG), that were generated underdirection of the CAG promoter to induce ubiquitous transgene expression, andtheir nontransgenic littermates (CON) were fed standard diet (STD/CRPTG orSTD/CON) or high-fat diet (HFD/CON or HFD/CRPTG) from 6 weeks of age.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atherosclerosis 249
After 12 weeks, oral glucose tolerance tests (OGTT) and intraperitoneal insulintolerance tests (IPITT) were performed and epididymal adipose tissue (EAT) andliver were excised.Results: High-fat diet feeding resulted in increased body, liver and EAT weightcompared with standard diet both in CON and CRPTG. OGTT and IPITT showedthat glucose tolerance and insulin sensitivity were tended to be deteriorated inSTD/CRPTG compared with STD/CON. Moreover, those were significantly dete-riorated in HFD/CRPTG and HFD/CON. Histological analysis of liver showed thathepatocellular ballooning, oil-drops and perisinusoidal fibrosis were prominent inHFD/CRPTG compared with HFD/CON. Hepatic triglyceride content (303.0±43.6vs. 133.0±72.8 mg/g, p< 0.01) were higher in HFD/CRPTG than HFD/CON. EATweight and mean adipocyte area were comparable between HFD/CRPTG andHFD/CON. The number of Infiltrating Mac-3 positive macrophages and CD3 pos-itive T lymphocytes in EAT were higher in HFD/CRPTG than HFD/CON. EATmRNA expression of Emr-1 and intereferon-γ in HFD/CRPTG was upregulatedthan that in HFD/CON. Serum adiponectin levels (11.1±2.7 vs. 16.9±0.9 μg/mL,p< 0.01) in HFD/CRPTG were lower than those in HFD/CON. Expression of an-giotensinogen (p< 0.01) and angiotensin II type 1A receptor (p< 0.05) mRNAin EAT was upregulated in HFD/CRPTG than HFD/CON. EAT mRNA expres-sion of glutathione peroxidase (GPX)1 and GPX3 was lower in HFD/CRPTG thanHFD/CON (both p< 0.05). Immunohistochemistry of EAT showed 8-Hydroxy-2’-deoxyguanosine was increased in CRPTG compared with CON.Conclusions: Human-CRP overexpression facilitated the development of insulinresistance and hepatosteatosis under high-fat diet in association with provokinginflammation, RAS activation, adiponectin downregulation, and enhanced oxida-tive stress in adipose tissue. Increased CRP and metabolic alterations may syn-ergistically accelerate adipose tissue remodeling and insulin resistance.
P1533 PTX3 is involved in the pathogenesis of unstableplaque associated with intraplaque hemorrhage
K. Hatakeyama1, Y. Matsuura1, T. Imamura1, T. Tsuruda1,K. Nishihira1, Y. Shibata2, T. Kodama3, Y. Asada1. 1Univ ofMiyazaki, Miyazaki city, Japan; 2Miyazaki Association Hospital,
Miyazaki city, Japan; 3Tokyo Univ, Tokyo, Japan
Background: Pentraxin 3 (PTX3), which has C-terminal sequence homology withC-reactive protein, is a multifunctional protein acting as an important componentof innate immunity and inflammation. Recently, plasma PTX3 levels were de-scribed to be increased in acute myocardial infarction (AMI) and unstable anginapectoris (UAP). However, the role of PTX3 in atheromatous plaque to its instabilityremains unknown.Methods: First, immunohistochemistry for PTX3 was performed using 121 coro-nary specimens (AHA classification type II-III, IV, Vc, Va and VI, n = 17, 17, 16,20 and 51, respectively) obtained from 37 autopsy cases. Immunopositive area ofPTX3 was quantified and compared its abundance among lesion types. Next, weimmunohistochemically examined the relationship between abundance of PTX3in plaque and clinical presentation using 44 coronary culprit plaques obtainedby directional coronary atherectomy (DCA) from patients with 22 acute coronarysyndromes (18 UAP, 4 AMI) and 22 stable angina pectoris (SAP). DCA speci-mens were stained with antibodies against PTX3, CD68 (macrophage), CD163(Hemoglobin scavenger receptor; M2 macrophage), smooth muscle cell actin,CD3 (T lymphocytes) and adipophilin (lipid store marker). Lastly, coronary thrombiobtained from 105 AMI patients who had undergone thrombus removal using as-piration catheter were assessed for PTX3 immunoreactivity.Results: In autopsy cases, PTX3 accumulation significantly differed only betweentype VI and other lesion types (type VI vs all other lesion types, p<0.01), andabundant PTX3 was present especially at site of intraplaque hemorrhage. In DCAcases, quantitative analysis exhibited that PTX3 was more intense in patients withACS than those with SAP (p<0.001). Among histological components, PTX3 wascorrelated with CD68, CD163, iron (an indicator of intraplaque hemorrhag) andadipophilin. In coronary thrombi, many macrophages in atheromatous componentwere immunopositive for PTX3.Conclusions: PTX3 is involved in pathogenesis of unstable plaque associatedwith intraplaque hemorrhage.
P1534 Uncovering the role of circulating soluble receptor foradvanced glycation end products in hypertension:relationships with albuminuria
C. Tsioufis, K. Dimitriadis, A. Agelis, M. Poulakis, M. Selima,A. Kasiakogias, A. Miliou, K. Toutouzas, C. Stefanadis. First
Cardiology Clinic, University of Athens,Hippokration Hospital, Athens, Greece
Purpose: The soluble receptor for advanced glycation end-products (sRAGE)participates in the development and acceleration of atherosclerosis, while albu-minuria is an established marker of target organ damage. We investigated therelationships of urinary albumin excretion, expressed as the albumin to creatinineratio (ACR), with sRAGE in essential hypertensives.Methods: Our population consisted of 320 newly diagnosed untreated non-diabetic patients with stage I to II essential hypertension [192 men, mean age=52years, office blood pressure (BP)=145/93 mmHg]. According to the ACR valuesdetermined as the mean of two non-consecutive morning spot urine samples, thestudy population was divided into microalbuminurics (n=64) (mean ACR=30-300
mg/g) and normoalbuminurics (n=256) (mean ACR<30 mg/g). Moreover, in allpatients venous blood sampling was performed for estimation of lipid profile andsRAGE concentrations.Results: Microalbuminurics compared to normoalbuminurics were older (55±6vs 49±4 years, p<0.05), had higher 24-h systolic BP (140±11 vs 131±8 mmHg,p=0.001), while did not differ regarding sex, smoking status and metabolic profile(p=NS for all). Moreover, microalbuminurics compared to normoalbuminurics ex-hibited lower levels of sRAGE (1015±451 vs 1505±932 pg/ml, p=0.003). In thetotal population, ACR was positively related to age (r=0.344, p=0.004), body massindex (r=0.217, p<0.005) and 24-h systolic BP (r=0.415, p<0.0001), whereas itwas negatively correlated with sRAGE (r=-0.274, p=0.019). Regarding sRAGE,it was associated with body mass index (r=-0.245, p=0.006), waist to hip ratio(r=-0.462, p<0.0001) and 24-h pulse pressure (r=-0.371, p=0.001). Multiple re-gression analysis revealed that age, 24-h systolic BP and sRAGE were the in-dependent predictors of ACR (R2=0.48, p<0.0001). Furthermore, analysis of co-variance showed that sRAGE values were significantly different between groupseven after adjustment for confounding factors (p<0.05).Conclusion: In essential hypertension, microalbuminuria is accompanied by at-tenuated levels of sRAGE, reflecting pronounced vascular dysfunction. Moreover,the close association of sRAGE with ACR, suggests active involvement of sRAGEin atherosclerotic target organ damage progression in non-diabetic essential hy-pertensives.
P1535 Notch signaling enhances BMP-2-induced osteogenicconversion and mineralization of vascular smoothmuscle cells
T. Shimizu, T. Tanaka, T. Iso, M. Kurabayashi. Gunma UniversitySchool of Medicine, Gunma, Japan
Background: Vascular calcification is closely correlated with cardiovascular mor-bidity and mortality. Bone morphogenetic protein-2 (BMP-2) is considered as amaster regulator of its formation. However, it is widely accepted that BMP-2 perse is not sufficient to execute the entire process of its development, and a spe-cial mechanism that support BMP-2-initiated vascular calcification has been ex-pected. Here we demonstrate that Notch signaling supports to amplify BMP-2-induced osteogenic differentiation of vascular smooth muscle cells (SMCs).Methods and Results: Despite an established role of BMP-2 in in vivo vascu-lar calcification, alkaline phosphatase (ALP) activity, a marker of osteogenic dif-ferentiation, was not apparently induced in BMP-2-treated human aortic SMCs(HASMCs). Immunohistochemistry of human atherosclerotic specimens revealedcolocalized expression of BMP-2 and Notch1, a receptor of Notch signaling, sug-gesting a possible correlation between Notch signaling and osteogenic processinduced by BMP-2. Interestingly, overexpression of Notch1 intracellular domain(N1-ICD) drastically upregulated ALP activity as well as mineralization in BMP-2-treated HASMCs and C3H10T1/2 cells. RT-PCR analysis and Western blot-ting revealed that the Msx2 gene, a key modulator of vascular calcification aswell as osteogenesis, was synergistically induced by N1-ICD overexpression andBMP-2 treatment. Conversely, a specific silencing of Msx2 using siRNA stronglydiminished the osteogenic phenotype. Sequencial analysis of Msx2 promoter re-vealed a putative binding site of RBP-Jk, a transcription factor crucial for Notchsignaling. Furthermore, it is located at the very proximity of Smad binding ele-ment (SBE), suggesting a crosstalk between Notch and BMP-2 signaling at tran-scriptional level. In fact, reporter gene assay confirmed that the putative RBP-Jkbinding site, as well SBE, were essential for the drastic Msx2 gene activation.Correspondingly, cells deficient of RBP-Jk did not show such an enhanced Msx2gene transcription and ALP activity.Conclusion: We showed in vitro results that Notch signaling markedly potentiateBMP-2-induced osteogenic conversion of HASMCs, in a manner dependent onMsx2. Furthermore, these results suggest a novel role of Notch signaling to assistBMP2-triggered process of vascular calcification.
P1536 Dietary alpha-linolenic acid (ALA) diminishesatherogenesis and restricts T cell-driven inflammation
S. Winnik1, C.M. Matter1, C. Lohmann1 , E.K. Richter2, N. Schaefer3 ,W.-L. Song4, F. Leiber2 , G.A. Fitzgerald4, T.F. Luescher1 , J.H. Beer5.1University Hospital Zurich, Department of Internal Medicine,
Division of Cardiology, Zurich, Switzerland; 2Federal Institute of TechnologyZurich - Department of Agricultural and Food Science, Zurich, Switzerland;3University of Zurich - Zurich Center of Integrative Human Physiology, Zurich,Switzerland; 4University of Pennsylvania - Institute for Translational Medicine andTherapeutics, Philadelphia, United States of America; 5Cantonal Hospital Baden- Department of Medicine, Baden, Switzerland
Background and Aims: Epidemiological studies report an inverse associa-tion between plant-derived dietary alpha-linolenic acid (ALA) and cardiovascularevents. However, little is known about the mechanism of this protection. Here, weassessed the cellular and molecular mechanisms of dietary ALA (flaxseed) onplaque formation using a mouse model of atherosclerosis.Methods and Results: 8-week-old male apolipoprotein E knockout (ApoE-/-)mice were fed a 0.21 g% cholesterol diet for 16 weeks containing either a highALA (7.3 g%; n=10) or low ALA proportion (0.03 g%; n=10). Bioavailability, chainelongation, and fatty acid metabolism were measured by gas chromatography
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

250 Atherosclerosis
of tissue lysates and urine. Plaques were assessed using immunohistochem-istry. T cell proliferation was investigated in primary murine CD3-positive lympho-cytes. T cell differentiation and activation was assessed by expression analysesof interferon gamma, interleukin-4, and tumor necrosis factor alpha (TNFα) usingquantitative PCR and ELISA. Dietary ALA increased aortic tissue levels of ALAas well as of the n-3 long chain fatty acids (LC n-3 FA) eicosapentaenoic acid,docosapentaenoic acid, and docosahexaenoic acid. The high ALA diet reducedplaque area by 50% and decreased plaque T cell content as well as expressionof vascular cell adhesion molecule-1 and TNFα. Both dietary ALA and direct ALAexposure restricted T cell proliferation, differentiation, and inflammatory activity.Dietary ALA shifted prostaglandin and isoprostane formation towards 3-seriescompounds, potentially contributing to the atheroprotective effects of ALA.Conclusions: Dietary ALA diminishes experimental atherogenesis and restrictsT cell-driven inflammation. Therefore, plant-derived ALA may provide a valuablealternative to marine LC n-3 FA. Prospective clinical studies are necessary toprove the clinical relevance of this principle.
P1537 Asymmetric dimetihylarginine, Vascular CellAdhesion Molecule-1 and subclinical atherosclerosis
E.E. Babes, M.I. Popescu, V.V. Babes, A. Ardelean, M. Rus,C. Bustea. Faculty of Medicine, Oradea, Romania
Background: Asymmetric dimethylarginine (ADMA) is a novel riskfactor for atherosclerosis that impair endothelial function by interfering with en-dothelial nitric oxide synthesis. Vascular cell adhesion molecule-1 (VCAM-1) isexpressed on the surface of endothelial cells in early atherosclerosis.The aim of the study was to investigate in young asymptomatic subjects the re-lationship between plasma ADMA and soluble VCAM with surrogate markers ofsubclinical atherosclerosis (SA): endothelial dysfunction evaluated with brachialflow mediated dilation (FMD) and carotid intima-media thickness (CIMT) and withcardiovascular risk factors.Methods: Study was performed on 68 (52 men) asymptomatic young healthyadults with cardiovascular risk factors aged between 20-40 years. Conventionalcardiovascular risk factors, plasma ADMA and VCAM, FMD and CIMT were de-termined in all subjects.Results: Mean values for ADMA were 0,69±0,19 ymol/l. Plasma ADMA levelscorrelated directly with age (r=0,53, p=0,0001), glicemia (r=0,29, p=0,04), LDL-cholesterol (r=0,34, p=0,01), systolic-blood pressure (r=0,28, p=0,04), diastolic-blood pressure (r=0,35, p=0,01) and also strongly correlated with CIMT (r=0,78,p<0,0001) and VCAM (r=0,8, p<0,0001) and inversely with FMD (r= - 0,76, p<
0,0001). In multiple regression analysis ADMA remained correlated with FMD(p=0,002, r= - 0,76), VCAM (p=0,035, r=0,8) and IMT (p=0,04, r= 0,78) (R2=0,74).Mean values for VCAM were 536,72±77,93 ng/ml. Plasma levels of VCAM cor-related directly with age (r=0,43, p=0,0017), glicemia (r=0,39, p=0,004), systolic-blood pressure (r=0,31, p=0,02), diastolic-blood pressure (r=0,31, p=0,02) andalso strongly correlated with CIMT (r=0,75, p<0,0001) and inversely with FMD(r= - 0,75, p<0,0001). In multiple regression analysis VCAM remained correlatedwith ADMA (p= 0,038, r= 0,8); FMD (p=0,04,r= - 0,76) and CIMT (p=0,04,r=0,75)(R2=0,69).Conclusions: Plasma ADMA and VCAM were positively correlated one withthe other. Both markers are correlated with surrogate markers of subclinicalatherosclerosis (FMD and CIMT) in young asymptomatic adults. Both markersare probably valuable markers for subclinical atherosclerosis detection and canserve as basis for early and intensive secondary prevention.
P1538 Cyanate selectively disrupts anti-atherogenicactivities of high-density lipoprotein in humanatherosclerotic lesions
M. Holzer, M. Gauster, C. Wadsack, G. Marsche. Medical Universityof Graz, Graz, Austria
Rationale: Carbamylation of proteins through the reactive species cyanate hasbeen demonstrated to predict an increased cardiovascular risk, but the under-lying mechanisms remain unclear. Cyanate is formed at sites of inflammationby the myeloperoxidase (MPO)-H2O2-thiocyanate system of activated phago-cytes. Since MPO is a component of high-density lipoproteins (HDL) in humanatherosclerotic intima, cyanate may selectively target HDL in the vessel wall.Objective: To test the hypothesis that cyanate affects atheroprotective propertiesof HDL.Methods and Results: We observed that the carbamyllysine content of lesionderived HDL was about 5-fold increased compared to circulating plasma HDL andabout 7-fold compared with atherosclerotic tissue. Immunohistochemical analysisof atheroma sections revealed marked co-localization of carbamyllysine, apoA-I and macrophages expressing the HDL receptor scavenger receptor class B,type 1 (SR-BI). HDL exposed to cyanate that produced a carbamyllysine con-tent observed in lesion derived HDL induced (i) cholesterol accumulation inmacrophages by a pathway requiring SR-BI and (ii) significantly reduced the ac-tivity of the main HDL-located anti-inflammatory enzyme paraoxonase.Conclusion: The present results provide strong evidence that carbamylation ofHDL is a pathophysiological relevant mechanism resulting in loss of atheropro-tective functions.
P1539 The impact of a single nucleotide polymorphism ofthe palladin gene on cardiovascular outcome amongpatients with prevalent atherosclerosis
M. Hoke1, M. Schillinger1, R. Koppensteiner1 , E. Minar1,W. Mlekusch1, O. Wagner2 , O. Schlager1, P. Dick1, M. Exner2,
C. Mannhalter2 . 1Medical University Vienna, Department of Internal MedicineII,Division of Angiology, Vienna, Austria; 2Medical University Vienna,Departmentof Medical and Chemical Laboratory Diagnostics, Vienna, Austria
Purpose: A single nucleotide polymorphism (SNP) in the palladin gene (PALLD,rs7439293) has recently been reported to be associated with coronary heart dis-ease (CHD) in two case-control studies as well as in a large population-basedcohort (Atherosclerosis Risk in Communities study, ARIC). Its clinical relevance,however, has not been evaluated prospectively. We investigated whether the riskallele (A) of PALLD rs7439293 (G>A) is associated with the occurrence of futuremajor cardiovascular events (MACE) in a cohort of patients with prevalent carotidatherosclerosis.Methods: 1283 patients with neurologically asymptomatic carotid atherosclerosiswere included in the study and followed for a median of 3.5 years (interquartilerange 3 to 4 years). We analyzed whether the risk allele is associated with pro-gression of carotid atherosclerosis after a 6 to 9 months period as measured byduplex Doppler sonography. Patients were then followed for the occurrence of afirst MACE, a composite of myocardial infarction, stroke, coronary revascularisa-tion and death.Results: After a median of 7.5 months (interquartile range 6 to 9 months) pro-gression of carotid stenosis was observed in 103 (8.1%) patients. Cardiovascularevents occurred in 337 (30%) patients after a median follow up of 3.5 years (in-terquartile range 3 to 4 years). The risk allele of PALLD was neither associatedwith progressive carotid atherosclerosis (p=0.21) nor with MACE (p=0.58). Ad-justed hazard ratios for a first MACE in heterozygous and homozygous carrierswere 0.83 (95% CI 0.58 to 1.18) and 0.94 (95% CI 0.65 to 1.35) compared towild-type, respectively.Conclusion: The A-allele of PALLD rs7439293 was not associated with progres-sive carotid atherosclerosis as measured by duplex Doppler sonography nor didit represent a risk factor for adverse cardiovascular outcome among patients withprevalent carotid atherosclerosis.
P1540 Association between Syntax Score, soluble CD40ligand and matrix metalloproteinase-3 in patients withstable coronary artery disease
M. Griva1, R. Naplava1, C. Cihalik1, O. Hlinomaz2. 1Department ofCardiology, Bata Regional Hospital, Zlin, Czech Republic; 2Masaryk
University, Faculty Hospital Brno, Department of Internal Cardiology Medicine,Brno, Czech Republic
Objective: The Syntax Score is an angiographic tool grading the complexity ofcoronary artery disease (CAD). Since atherosclerosis is an inflammatory disease,circulating factors related to inflammation such as proinflammatory cytokine solu-ble CD40 ligand (sCD40L) may be predictors of CAD. Matrix metalloproteinases(MMPs) play an important role in the pathogenesis of vascular diseases, such asatherosclerosis, plaque rupture and aneurysms but the mechanisms are not yetfully understood. The aim of this study was to evaluate the association betweensCD40L, MMP-3 and Syntax Score.Methods: Serum levels of sCD40L and MMP-3 were measured in 128 patientswith stable coronary artery disease (69% diabetics), then coronary angiographyand Syntax Score assessment followed.Results: Plasma level of MMP-3 was significantly higher in 2 type diabetes mel-litus patients 37.0 (13.7; 82.5) compared with non-diabetic patients 25.8 (11.9;82.8), p = 0.044. MMP-3 was also significantly higher in men 42.1 (15.7; 85.2)compared with women 21.9 (11.3; 44.8), p<0.001. According to Spearman’s cor-relations analysis – the Syntax Score correlated with MMP-3 levels in the en-tire patient group (0.358) as well as in diabetic (0.378) and non-diabetic (0.335)subgroups. There was no significant correlation between sCD40L and SyntaxScore in the entire group (0.159) nor any subgroup (diabetics 0.138, non-diabetics0.156)Conclusion: Our results suggest that in patients with stable coronary artery dis-ease MMP-3 level correlates with extensity of coronary artery impairment regard-less of diabetes mellitus presence. Association between sCD40L and grade ofCAD was not found.
P1541 Endothelial dysfunction, atherosclerosis andinflammation
A. Petrosyan. Yerevan State Medical University after M. Heratsi,Yerevan, Armenia
Cardiovascular diseases (CVD) remains a major cause of morbidityand mortality in developed societies. Early diagnosis and prevention of endothelialdysfunction (ED) as the 1st sign of atherosclerosis is important. Among classicalFraming CVD risk factors during last decades critical role have been consideredto inflammation.Purpose of our study was to find out role of inflammation in development of EDamong patients suffering from Familial Mediterranean Fever (FMF), which is a
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atherosclerosis 251
chronic auto inflammatory disease prevalent among Eastern Mediterranean pop-ulations, mainly Armenians, Sephardic Jews, Arabs.Methods: We involved in our study 74 middle age, male FMF patients, anddivided them in three groups. 22 patient regularly receiving anti-inflammatorycolchicinotherapy, 30 patients with irregular treatment and 22 patients with FMFcomplication amyloidosis. In control group we involved same age and gender30 healthy males. We studied endothelium dependent vasodilatation (EDVD) ofbrachial artery (BA), C-reactive protein (CRP) level as a marker of inflammationand lipid profile.Results: We revealed that ED is more expressed and CRP level is higher amongpatients with amyloidoses EDVD,% 6,77±0,198, CRP 9,87±0,17 (p<0.05), thenamong those who were receiving irregular anti-inflammatory treatment EDVD,%7,357±0,16, CRP 8,66±0,18 (p<0.05), then among FMF patients with regulartreatment EDVD,% 9,086±0,138, CRP 5,59±0.13 (p<0.05). In all groups lipidslevel was in normal range. As well as we revealed positive correlation betweenactivity of inflammation and ED and negative correlation between ED, inflamma-tion and lipid profile. Our data are presented in table below.
EDVD of BA and CRP among FMF patients
Control FMF patients with regular FMF patients with FMF patients withgroup colchicinotherapy irregular colchicinotherapy amyloidosis(n=30) (n=22) (n=30) (n=22)
EDVD,% 13,15±0,156 9,086±0,138 7,357±0,16 6,77±0,198CRP mg/l 3,4±0,11 5,59±0.13 8,66±0,18 9,87±0,17
Conclusions: 1) Inflammation has it’s own etholopatological role in developmentof ED. 2)Among patients with chronic inflammatory diseases anti-inflammatorytreatment may prevent development and progression of ED and atherosclerosis.3) In early preclinical stages CVD may be diagnosed by evaluating of endothelialfunction by determination of EDVD, % of BA. 4) CRP level may have a diagnosticand prognostic meaning for ED, atherosclerosis and CVD among patients withchronic inflammatory diseases.
P1542 Real-time observation of leukocyte recruitment tomouse femoral artery after wire injury
M. Osaka, S. Hagita, M. Yoshida. Tokyo Medical and DentalUniversity, Tokyo, Japan
Purpose: Wire injury of an artery has been recognized as a standardmodel of vascular inflammation and atherosclerosis. However, the mechanism ofleukocytes recruitment has not been studied in this model. Here, we documentedthe recruitment of leukocytes to murine femoral artery after wire injury.Methods: Transluminal mechanical injury was generated by inserting a wire(0.015 inch diameter) to the femoral artery of C57BL/6J mice (male, 7w-13w).Mice, anesthetized and ventilated after tracheotomy, were protected from hy-pothermia by a warming lamp. Body temperature (36.0-36.9 °C) and blood pH(pH7.4) did not significantly change during the experiment. Interaction betweenRhodamine-6G labeled leukocytes and injured femoral artery was monitored us-ing an epifluorescent microscope. Captured images were then evaluated usinga computer-assisted image analysis program. To identify adhesion moleculesresponsible for the initial and later phases of leukocyte recruitment, antibodiesagainst anti-P-selectin or anti-GP1b-alpa were injected after wire injury.Results: In the absence of injury, virtually no leukocyte adhesion was observed(2.20±2.63/10-2 mm2 vessel surface, n=10). In contrast, the number of adherentleukocytes was increased at 4 hours (36.3±6.96, P <0.005 vs. 0 h, n=10) and24 hours (19.5±2.84, P <0.005 vs. 0h, n=10) after injury. The number of leuko-cyte adhesion was reduced when we examined 72 hours after injury (3.5±0.82, P<0.005 vs. 24h, n=10). Interestingly, we identified another peak of leukocyte ad-hesion at 7 days after injury (22.8±3.64, P< 0.005 vs. 72 h, n=11). It was shownthat the treatment of anti-P-selectin or anti-GP1b-alpa significantly decreased thecellular adhesion to the vessel wall.Conclusion: In conclusion, we have established a novel experimental systemto directly observe leukocyte recruitment to injured femoral artery. Our systemrevealed previously undetected unique profile of leukocytes recruitment duringvascular injury. In addition, it was suggested that the role of platelets are importantto the leukocyte accumulation in the wire injury model.
P1543 Differences in responsiveness of circulatingmonocytes are related to differences in expression ofthe predictive local atherosclerotic plaque markerosteopontin
V.P.W. Scholtes1, J.P. De Vries2, G.T. Rijkers3, D.P.V. De Kleijn1,F.L. Moll4, G. Pasterkamp1. 1University Medical Center Utrecht,
Experimental Cardiology Laboratory, Utrecht, Netherlands; 2St AntoniusHospital, Department of Vascular Surgery, Nieuwegein, Netherlands; 3StAntonius Hospital, Department of Medical Microbiology and Immunology,nieuwegein, Netherlands; 4University Medical Center Utrecht, Department ofVascular Surgery, Utrecht, Netherlands
Background: Recently, we described that local atherosclerotic plaque markersin single plaques may hide strong predictive value for secondary cardiovascularcomplications in all vascular territories. Although these plaque markers may re-
veal a predictive value for events, clinical utility is limited. We hypothesized thatcirculating monocyte activation is associated with expression of plaque markersthat have found to be predictive for events. We conducted a prospective study in-vestigating the relation of the predictive local plaque marker osteopontin and theactivation state of the circulating monocyte.Methods: 41 patients scheduled for carotid artery endarterectomy participitatedin this study. Blood was drawn after anaesthesia and whole blood was stimulatedfor 30 minutes with LPS (Toll like receptor 4 ligand) and Pam 3 Cys (Toll Likereceptor 2 ligand). Cd11b expression on circulating monocytes was measured byFACS. After dissection, atherosclerotic plaques wereimmediately frozen in liquidnitrogen. Plaque osteopontin (OPN) levels were determined by ELISA.Results: Patients were divided into 3 equal groups based on their OPN plaquelevels; LOW < 4.6 ng/ml (n=14), MEDIUM: 4.7 - 6.6 ng/ml (n=14) and HIGH:> 7.3 ng/ml (n=13). Patients with higher plaque OPN levels had higher Cd11bexpression at baseline: (median and IQR) LOW: 9.7 [7.7–13.0], MEDIUM: 11.5[8.7–18.2], HIGH: 11.6 [5.7–20.4]. Cd11b expression following stimulation of LPSincreased to higher levels in patients with higher plaque OPN levels: LOW: 24.9[21.3–31.5], MEDIUM: 25.0 [20.8–35.1], HIGH: 31.8 [23.6–45.5]. The same asso-ciation was observed after stimulation of P3C: LOW: 19.2 [15.2–25.8], MEDIUM:20.4 [17.5–28.8] and HIGH: 23.7 [18.9–38.0]. When patients were compared us-ing a visually selected cut-off point, differences were more striking. Patients witha plaque OPN level of > 10 ng/ml (high n=8) had compared with patients with aplaque OPN level of < 10.0 ng/ml (low n=33) higher Cd11b expression at base-line: low: 10.0 [7.9–14.0] and high: 20.0 [9.5–23.4](p = 0.067). Cd11b levels werealso higher after stimulation of LPS: low: 20.0 [17.5–22.8] and high: 28.7 [21.7–38.9](p = 0.000). Similar results were obtained after stimulation with P3C.Conclusion: This is the first study demonstrating that activated circulating cellshide markers that are associated with local plaque phenotype. A higher level ofthe local predictive marker osteopontin was related with higher levels of Cd11bexpression on the circulating monocyte at baseline and after stimulation.
P1544 Effect of aleglitazar, a balanced dualPPARalpha/gamma agonist, on pro-inflammatorybiomarkers of atherothrombotic vascular disease andHDL functionality in non-human primates withmetabolic syndrome
A. Corsini1, S. Raab2, X. Zhang3, J. Wang3, R. Xiao3, P. Huang4,E. Sebokova2. 1University of Milan, Laboratory of Cellular Pharmacology ofAtherosclerosis, Milan, Italy; 2F. Hoffmann-La Roche AG, Basel, Switzerland;3Peking University, Primate Research Center, Beijing, China, People’s Republicof; 4Massachusetts General Hospital, Boston, United States of America
Introduction: Vascular endothelial dysfunction is a prominent feature of theearly stages of atherogenesis. A number of pro-inflammatory stimuli can acti-vate endothelial cells, resulting in increased expression of adhesion moleculesand chemoattractants. Several findings support a cardioprotective role for HDL inpreventing development of endothelial dysfunction in humans. Aim: To investigatethe effect of the novel dual peroxisome proliferator-activated receptor (PPAR) al-pha/gamma agonist aleglitazar on circulating levels of pro-inflammatory markersof atherothrombotic vascular disease and the anti-inflammatory properties of HDLisolated from non-human primates with metabolic syndrome.Methods: Nine obese rhesus monkeys with metabolic syndrome received vehi-cle for 2 weeks, followed by a 6-week aleglitazar 0.03 mg/kg/day treatment period.Effects on circulating markers were evaluated by measuring levels of fibrinogen(coagulant biomarker), P-selectin and E-selectin (surrogate markers for plateletand endothelial cell activation), IL-8 (marker of chronic inflammatory disorders),and hsCRP (marker for cardiovascular risk assessment) using Hitachi and ELISAassays. Anti-inflammatory properties of isolated HDL were studied following ad-dition of human recombinant TNFα in human umbilical vein endothelial cells (HU-VEC) incubated in the presence or absence of HDL. Cell surface expression ofVCAM-1 and ICAM-1 were analyzed using flow cytometry. Expression of eNOSwas analyzed in cell lysates.Results: Plasma analysis of circulating markers after 6 weeks’ treatment withaleglitazar demonstrated reductions in fibrinogen (34%), P-selectin (60%), E-selectin (7%), IL-8 (80%), and hsCRP (37%). Flow cytometry analysis showedthat treatment of HUVEC with HDL isolated from monkeys treated with aleglitazarreduced cell surface expression of adhesion molecules VCAM-1 (-36.2% ± 36.3)and ICAM-1 (-26.2% ± 13.5). Conversely, the expression of eNOS, the major con-stitutive enzyme involved in NO production in endothelial cells, was significantlyincreased by HDL by 40%.Conclusions: Taken together, decreased levels of circulating pro-inflammatorymarkers and improved HDL functionality, as demonstrated by anti-inflammatoryproperties of HDL in HUVEC, may represent an important mechanism in theatheroprotective effect of aleglitazar.
P1545 In vivo caspase inhibition augments vascular repairby progenitor cells and decreases atherosclerosis inapolipoprotein E deficient mice
W.S. Speidl, R. Hutter, V. Fuster, J.J. Badimon. Mount Sinai Schoolof Medicine, New York, United States of America
Background: Bone marrow progenitor cells (BMPCs) play a role in vascular re-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

252 Atherosclerosis
pair and may thereby counteract atherosclerotic lesion progression. These BM-PCs are exposed to pro-apoptotic ox-LDL particles in lipid-rich plaques that couldresult in insufficient vascular repair. To test this hypothesis we evaluated the ef-fect of caspase-inhibition on c-kit progenitor cells and atherosclerotic lesions in amouse model of atherosclerosis in vivo.Methods and Results: In vitro, oxLDL induced apoptosis in Lin-c-kit+ BMPCs.Likewise, Apo-E -/- mice on atherogenic diet showed an increased apoptosis rateof circulating c-kit cells as compared to normolipidemic controls. 48 hours afterinjection of Lin-c-kit+ BMPCs from GFP-transgene mice in Apo-E -/- mice onlyapoptotic remnants were detectable within the atherosclerotic plaques of aorticroots. However, after ex vivo pretreatment with a caspase inhibitor GFP+Lin-c-kit+BMPCs were found within the plaques and showed signs of vascular repair. Dailytreatment of Apo-E -/- mice with caspase inhibitor or control-peptide for threeweeks resulted in a significant lower apoptosis rate of c-kit+ BMPCs in the circu-lation and within the aortic plaques. The treatment significantly decreased aorticplaque size and inflammatory cell content and increased staining for smooth mus-cle cells.Conclusions: BMPC viability may be of key importance for adequate vascu-lar repair and attenuation of atherosclerosis progression. Therefore, reducingBMPC apoptosis by caspase-inhibitors could become a powerful tool to bettertreat atherosclerosis progression.
P1546 Effects of frequently prescribed statins onatherosclerotic plaque composition: cross-sectionalanalysis of 1117 carotid plaques
G.W. Van Lammeren1, F.L. Moll2, B.A.N. Verhoeven3 , D.P.V. DeKleijn1, J.P.P.M. De Vries3, G. Pasterkamp1. 1University Medical
Center Utrecht, Experimental Cardiology Laboratory, Utrecht, Netherlands;2University Medical Center Utrecht, Department of Vascular Surgery, Utrecht,Netherlands; 3St Antonius Hospital, Department of Vascular Surgery,Nieuwegein, Netherlands
Background: The hypothesized pleiotrophic effect of statins remains an ongoingsubject of discussion. We present cross-sectional data concerning atheroscleroticplaque composition and inflammatory status of a large cohort of patients whounderwent carotid endarterectomy in relation to pre-operative statin use.Methods: Between 2002 and 2009, 1117 consecutive patients undergoingcarotid endarterectomy were enrolled, including individuals without statin use(n=297), pravastatin use (n=94), simvastatin use (n=392) and atorvastatin use(n=334). Atherosclerotic plaques were quantitatively examined for the presence ofmacrophages, smooth muscle cells (SMC) and the amount of vessels and semi-quantitatively examined for calcifications, collagen, intraplaque hemorrhage andfat (lipid core > 40% of the plaque area). Expressions of a total of 27 cytokines,chemokines and proteases were assessed in a subgroup of 535 randomly se-lected patients. After adjusting for cardiovascular risk factors and baseline dif-ferences through multivariable analyses, odds ratios (OR) with 95% confidenceinterval were calculated.Results: Atorvastatin use was independently associated with higher meanamount of macrophages 1.26 (±0.083) versus 0.87 (±0.077) in no statin use OR1.82 [1.3-2.5]. Pravastatin and simvastatin were associated with reduced pres-ence of large lipid cores: 25.5% (24/94) and 29.1% (114/392) respectively, versus37.4% (111/297) for no statin use, OR 0.55 [0.32-0.93] and 0.64 [0.46-0.90] re-spectively. A similar trend was observed for atorvastatin 29.6% (99/334) OR 0.71[0.51-1.0]. A decreased amount of intraplaque hemorrhage was seen in plaquesfrom patients under simvastatin use 77.7% (188/242) as compared to no statinuse 89.4% (186/208) OR 0.47 [0.27-0.82].No differences were observed in plaque concentrations of pro- or anti-inflammatory cytokines, chemokines or proteases amongst the different groups.Conclusions: Simvastatin use was associated with less intraplaque hemor-rhages and together with pravastatin associated with fewer large lipid pools. Thiscan be considered as the presence of a more stable plaque phenotype under theuse of these statins and therefore a beneficial effect might be present. Atorvas-tatin was associated with an increased amount of macrophages in the plaque, butthis inflammatory status could not be confirmed at protein level.
P1547 Endothelial regeneration in Apolipoprotein E-deficientmice is disturbed by altered progenitor cellmobilization from the bone marrow
M. Steinmetz, E. Lucanus, C. Peseke, K. Paul, S. Zimmer,G. Nickenig, N. Werner. Rheinische Friedrich-Wilhelms-Universitaet,
Bonn, Germany
Introduction: Bone-marrow derived progenitor cells are reduced in patients withatherosclerotic disease potentially due to a direct negative impact of cardiovas-cular risk factors and increased consumption of circulating endothelial progenitorcells (EPC) within atherosclerotic lesions. To date, the impact of atherosclerosison bone marrow (BM) residual progenitor cells has not been deciphered. Here wehypothesize that atherosclerotic ApoE-/- mice display an additional mobilizationdefect on the BM level.Methods and results: ApoE-/- mice (age 6 months, C57bl6 background) withhigh-cholesterol diet were compared to age-matched littermates without diet, andwildtype mice (C57bl6). Stromal derived factor-1α (SDF-1α) essentially partici-
pates in mobilization of progenitor cells from the BM into peripheral blood. Theconcentration of plasmatic SDF-1α was highest in cholesterol treated ApoE-/-mice suggesting a strong mobilizing stimulus in severely atherosclerotic mice.SDF-1α concentrations within the BM supernatant were comparable in all groups.Despite a strong mobilization stimulus, circulating sca1/flk1 positive EPC and exvivo cultivated early and late EPC were significantly reduced in ApoE-/- mice oncholesterol diet. In order to determine the underlying reasons for the reducedlevels of circulating EPC in ApoE-/- mice despite strong mobilization signals, wedetermined the rate of progenitor cell apoptosis in BM-residual sca1/flk1 positiveEPC. EPC apoptosis within the BM did not differ between evaluated groups. Next,we determined EPC proliferation rates within the BM which showed a slightly in-creased proliferation rate in ApoE-/- mice on cholesterol diet. To test the bonemarrow capacity for EPC mobilization, mice were treated with granulocyte colonystimulating factor (G-CSF;0.05μg/g body weight). EPC levels were significantlyincreased in ApoE-/-mice with or without diet. No changes within the BM residuallevels of sca1/flk1 positive EPC were observed.Conclusion: Atherosclerosis not only affects peripheral progenitor cell functionbut also the bone marrow microenvironment. Accelerated turnover of endothe-lial regenerating cells in atherosclerotic lesions of ApoE-/- mice is associatedwith insufficient mobilization of progenitor cells from bone marrow to peripheralblood despite strong mobilization signals. The net results are low levels of bonemarrow-derived, circulating, early, and late EPC which can be reconstituted byG-CSF mobilization indicating a potential therapeutic pathway in patients withatherosclerotic disease.
P1548 Apelin/APJ and adiponectin/T-cadherin expression inhuman aortic arterial wall and periaortic adiposetissue in correlation with atherosclerosis
C. Kostopoulos, S. Spiroglou, J. Varakis, H. Papadaki. University ofPatras, Patras, Greece
Purpose: Adipokines have been implicated in vascular physiology and pathol-ogy, including cardiovascular disease. We investigated the expression of apelin,adiponectin and their receptors APJ and T-cadherin in human aortic arterial walland periaortic fat as well as their correlation with aortic atherosclerosis.Methods: Paraffin embedded samples of human aortas (n=40) including periad-ventitial fat were evaluated for apelin, adiponectin, APJ and T-cadherin expressionusing immunohistochemistry. AHA classification was used for atherosclerosis as-sessment. SPSS for Windows was used for statistical analysis.Results: Apelin was expressed by periadventitial fat and vascular smooth mus-cle cells (VSMCs) in 40/40 samples and endothelia in 38/40 samples, whileadiponectin was expressed by periadventitial fat in 37/40 samples. APJ and T-cadherin were detected in VSMCs (40/40 and 40/40 samples, respectively) andendothelia (29/40 and 34/40, respectively). Apelin expression in periaortic fat andaortic VSMCs was positively correlated with APJ in VSMCs (r=0.517, p=0.001and r=0.319, p=0.045, respectively). Periadventitial fat adiponectin expres-sion was positively correlated with endothelial T-cadherin expression (r=0.345,p=0.029). Atherosclerosis was detected in 34/40 aortas. Aortic atherosclerosiswas negatively correlated with VSMC apelin (r=-0.450, p=0.004), periaortic fatadiponectin (r=-0.701, p<0.001), VSMC T-cadherin (r=-0.404, p=0.010) and en-dothelial T-cadherin (r=-0.419, p=0.007) expression.Conclusion: Apelin/APJ and adiponectin/T-cadherin expression pattern in aorticwall and periaortic fat in correlation with atherosclerosis suggests a putative roleof these adipokines in the atherosclerotic process.
P1549 Cytokine-induced expression of VCAM-1, ICAM-1,E-selectin and monocyte adhesion on HUVECs arenot associated with gender
K. Kunert, M. Lorenz, G. Baumann, K. Stangl, V. Stangl. Charite -University Medicine Berlin, Campus Mitte, Department of Cardiology
and Angiology, Berlin, Germany
Background: Gender differences in the expression of atherosclerotic markerscorrelate with the incidence and severity of cardiovascular diseases (CVD). Nev-ertheless, the mechanisms responsible for these differences are not well under-stood. Oxidative stress contributes to the expression of adhesion molecules at thevascular endothelium, which is a precondition for migration of inflammatory cellsinto the vessel wall and thus an early event in atherogenesis. Gender related dif-ferences in the expression of adhesion molecules might contribute to differencesin the incidence and severity of CVD in men and women.Purpose: Aim of the study was to determine whether the expression of intercellu-lar adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1),endothelial leukocyte adhesion molecule-1 (E-selectin) and monocyte adhesionon human umbilical vein cells (HUVECs) are influenced by gender. Therefore weisolated HUVECs from 40 different human umbilical veins (20 male/20 female)and developed three different assays.Methods: Cell culture. HUVECs were isolated by collagenase digestion of humanumbilical veins by standard techniques and cultured in EC medium. THP-1 cellswere cultured in RPMI 1640 medium. ELISA. HUVECs were treated for 4-16h withTNF-α (5ng/ml) or IL-1β (8ng/ml) and the expression of VCAM-1, ICAM-1 and E-selectin was measured. Adhesion assay. THP-1 cells were flourescence-labeled.For static adhesion assays HUVECs were treated with TNF-α for 4h before ad-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atherosclerosis 253
dition of labeled THP-1 cells. Adherent monocytes were measured in a fluores-cence plate reader. Model of Oxidative Stress. Cells were flourescence-labeledwith Dichlorodihydrofluorescein (DCF). For induction of oxidative stress HUVECswere incubated with 50/100 μM H2O2. The fluorescence intensity was propor-tional to the reactive oxygen species levels within the cell cytosol and could beread on a fluorescence plate reader.Results: Although there were indications that HUVECs from female individualsshowed higher baseline values compared to male and lower values after stimu-lation with H2O2 or TNF-α/IL-1β we could not find any significant differences be-tween male and female HUVECs concerning the expression of VCAM-1, ICAM-1,E-selectin, oxidative stress levels and monocyte adhesion.Conclusion: In the present study gender had no impact on the expression ofVCAM-1, ICAM-1, E-selectin and on monocyte adhesion on HUVECs. Althoughseveral reports suggest that oxidative stress affects male and female vascularbeds differently we could not find any significant differences between male andfemale HUVECs in our cell assays.
P1551 Glucagon-like peptide-1 (1-37) inhibitschemokine-induced migration of human CD4-positivelymphocytes
M. Burgmaier1, D. Walcher2, P. Heinz2, M. Ostertag2, A. Hausauer2 ,H. Bach2, R. Durst2, V. Hombach2, N. Marx1. 1University HospitalAachen, RWTH, Internal Medicine I, Cardiology, Pulmonology &
Vascular Medicine, Aachen, Germany; 2University of Ulm, Faculty of Medicine,Department of Internal Medicine II-Cardiology, Ulm, Germany
Objective: The present study examined the effect of GLP-1(1-37) on chemokine-induced CD4-positive lymphocyte migration as one of the early and critical stepsin atherogenesis.Methods and Results: Stimulation of isolated human CD4-positive lympho-cytes with SDF-1 led to a 3.4±1.7 fold (p<0.01; n=9) increase in cell migration.Pretreatment of cells with GLP-1(1-37) reduced this effect in a concentration-dependent manner to a maximal 1.1±0.7 fold induction at 1 nmol/L GLP-1(1-37)(p<0.01 compared to SDF-1-treated cells, n=9). Similar effects were seen whenRANTES was used as a chemokine to induce cell migration. GLP-1(1-37)’s effecton CD4-positive lymphocyte migration was mediated through an early inhibitionof chemokine-induced PI-3 kinase activity. Downstream, GLP-1(1-37) inhibitedSDF-induced phosphorylation of MLC and cofilin and limited f-actin formation aswell as ICAM3 translocation. However, exendin-4, a GLP-1 receptor agonist, didnot inhibit SDF-induced migration of human CD4-positive lymphocytes despite anexpression of the GLP-1 receptor in these cells.Conclusion: Thus, GLP-1(1-37) inhibits chemokine-induced CD4-positive cellmigration by inhibition of the PI3-kinase pathway, which is at least partially in-dependent of the known GLP-1 receptor. The effect seen provides a potentialnovel mechanism of how GLP-1(1-37) may modulate vascular disease.
P1552 Accelerated early atherosclerosis in mice deficient inL-selectin
S. Sluka1, I. Rozenberg1 , E.E. Eriksson2, P. Mocharla1,A. Hallenberg3, P. Rotzius3, J. Boren4, L. Borsig5, T.F. Luscher1 ,F.C. Tanner1 . 1University of Zurich-Irchel, Department of Anatomy
and Physiology, Cardiovascular Research, Zurich, Switzerland; 2KarolinskaUniversity Hospital, Department of Molecular Medicine & Surgery, Stockholm,Sweden; 3Karolinska Institute, Stockholm, Sweden; 4Sahlgrenska UniversityHospital, Wallenberg Laboratory for Cardiovascular Research, Gothenburg,Sweden; 5University of Zurich, Zurich, Switzerland
Members of the selectin family of adhesion molecules are important mediators ofleukocyte extravasation.To investigate the importance of L-selectin (L-sel) in atherogenesis, we crossed L-sel-/- animals with mice lacking Apolipoprotein E (ApoE-/-). We analyzed double-knockout ApoE/L-sel (ApoE-/- L-sel-/-) mice and the corresponding ApoE-/- con-trols both without and with a high cholesterol diet (HCD).After 6 weeks of HCD ApoE-/- L-sel-/- mice developed on average 2.46% ± 0.54%aortic lesions, which is two-fold higher than ApoE-/- controls (1.28% ± 0.24%).A similar effect was observed in 6 month old ApoE-/- L-sel-/- animals fed a nor-mal diet. In contrast, after 12 weeks of HCD, there was no difference in atheromaformation between the two groups of animals. Leukocyte rolling in atheroscle-rotic aorta was similar in ApoE-/- and ApoE-/- L-sel-/- animals. In line with this,atherosclerotic plaques did not exhibit any alterations in cellular composition uponL-sel deletion. Mice lacking L-sel exhibited reduced size and cellularity of periph-eral lymph nodes, increased size of spleen, and increased number of blood lym-phocytes both after 6 weeks and after 12 weeks of HCD.These results indicate that L-sel is a negative regulator of early, but not advancedatherosclerosis. This effect is neither associated with leukocyte capture nor ab-normal leukocyte distribution.
P1553 A low SCORE risk and calcium score, interrelationand the value for coronary atherosclerosis riskstratification
R. Avram1, F. Parv1, G. Miclaus2, T. Ciocarlie1, M. Tudoran1 ,L. Branzan1, M. Balint1. 1County Hospital, Timisoara, Romania;
2Neuromed Imagistic Centre, Timisoara, Romania
Purpose: A low "SCORE" risk cannot exclude a coronary artery disease, evenin the presence of atypical clinical symptomalogy. We evaluated the coronaryarteries using multislice computed tomography and the calcium score, in patientsof both gender, with low risk and atypical thoracic pain.Methods: We selected a group of 54 women and 54 men, with a SCORE riskscore <5% and identical anamnesis, clinical and laboratory data, with atypicalsymptoms for angina, a normal ECG and a negative or inconclusive stress test, inwhich we performed coronary angiography using 64 multislice Siemens SomatronSensation computed tomography. Calcium score was calculated using Agatsonformula on reconstructed 3 and 0.6 mm sections.Results: Calcium score was 155±238.64 (0-697) in women vs. 373.125±344.43(0-1056) in men with p=0.047, a 0 calcium score was more frequent in womenp=0.049 and score over 100 in 43% women and 74% men. Plaque calcificationwas present in 8 (14%) women and 24 (44%) men (p=0.01), plaque without calci-fication in 24 (43%) women and 16 (29%) men (p=0.40), mixed in 8 (14%) womenand 10 (19%) men (p=0.72). The number of the affected coronary segments was2.42±2.06 in women and 3.5±2.42 in men (p=0.20). Regarding stenosis sever-ity, severe stenosis > 75% was present in 4 women and 24 men (p=0.0001), 0occlusions in women and 6 in men. Under 75% lesions were present in 93% ofwomen and 56% of men. We found moderate stenosis in 16 (33%) women and18 (33%) men (p=0.77), mild stenosis in 40 (74%) in women and 46 (85%) in men(p=0.32), very mild stenosis in 46 (85%) women and 38 (70%) men (p=0.35%).Conclusions: In the presence of atypical thoracic pain, a low "SCORE" risk anda negative stress test do not exclude coronary atherosclerosis,. A calcium scoreover 100 identifies the patients with coronary risk, especially men, women havingless significant stenosis and plaque calcification.
P1554 Low plasma adiponectin is associated withobstructive coronary disease in asymptomaticpatients with diabetes
R. Djaberi, J.D. Schuijf, C.J. Roos, A. Van Der Laarse, A.M. Pereira,J.W. Smit, J.A. Romijn, E.E. Van Der Wall, J.J. Bax, J.W. Jukema.
Leiden University Medical Center, Leiden, Netherlands
Purpose: In patients with type 2 diabetes (DM2), the mechanisms of coronaryartery disease (CAD) as well as the most effective approach for early identificationof this disease remain unclear. We examined the relation between the plasmaadiponectin and the presence of obstructive CAD in asymptomatic patients withDM2.Methods: Prospectively, 97 asymptomatic patients with DM2 were included(mean age 53, male 49%). Multi-slice computed tomography (MSCT) coronaryangiography was performed to determine the presence of obstructive CAD (≥50%luminal narrowing).Plasma adiponectin was assessed using radio-immunoassay. Adiponectin levelswere compared in patients with and without obstructive CAD.Thereafter, univariate analysis of risk factors was performed to identify the po-tential predictors of obstructive CAD. Risk factors with p≤0.05 were included in amultivariate logistic regression model to determine the independent predictors.Results: Obstructive CAD was revealed in 27 patients (28%). Median plasmaadiponectin was significantly lower in patients with obstructive CAD (3.9 mcg/ml(2.9-6.2)) as compared to those without CAD (8.3 mcg/ml (4.6-12.8)) (P<0.001).Importantly, multivariate analysis revealed low plasma adiponectin to be an inde-pendent predictor of obstructive CAD (Hazard Ratio 0.79 (0.68-0.92), P=0.002).A plasma adiponectin cut-off value of <4.50 mcg/ml yielded a sensitivity and aspecificity of respectively 80% and 71% for predicting the presence of obstructiveCAD on MSCT.Conclusions: The current study suggests that in asymptomatic patients withDM2, lower levels of plasma adiponectin are associated with the presence ofobstructive CAD.
P1555 Association of intimal thickening with thin capfibroatheroma in culprit lesions of patients with acutecoronary syndromes
A. Karanasos, K. Toutouzas, M. Riga, E. Tsiamis, A. Synetos,J. Karampelas, E. Stefanadi, C. Tsioufis, D. Tousoulis, C. Stefanadis.
Hippokration Hospital, University of Athens, Athens, Greece
Background: Intimal thickening is implicated in the pathogenesis of the earlystages of atheromatosis. The introduction of optical coherence tomography(OCT), a high resolution imaging method, has enabled precise measurementsof intimal thickness of non-atheromatic coronary segments. Yet, the significanceof such measurements has not been investigated so far. We aimed to investigatein patients with acute coronary syndromes (ACS) the association of intimal thick-ness in proximal non-atheromatic segments of the culprit lesions (CLs) with thincap fibroatheroma (TCFA) and rupture of the CL.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

254 Atherosclerosis
Methods: Thirty four consecutive patients with ACS that underwent cardiaccatheterization within 24 hours from symptom onset were enrolled. Optical co-herence tomography study was then performed in all CLs. Images from proximalnon-atheromatic segments and from the culprit lesion were stored and analysedoffline. Maximum intimal thickness was measured at proximal sites where thevessel wall had a three-layered appearance in the OCT image, without eccentricthickening (as defined by a ratio of maximum intimal thickness/minimum intimalthickness>3). Presence of culprit lesion plaque rupture was recorded and fibrouscap thickness (FCT) was measured at the thinnest part of the plaque of culpritlesions. TCFA was defined as a plaque with cap thickness ≤ 65μm.Results: Images were successfully acquired from all 34 CLs and correspond-ing proximal non-atheromatic segments. Mean intimal thickness of proximal seg-ments in all patients was 266±89 μm. Twenty four patients (70.4%) had at leastone TCFA at the CL. Mean intimal thickness of the proximal segments in patientswith TCFA was greater than that of patients without TCFA (293±84 μm versus201±65 μm, p<0.01). Sixty five percent of the plaques (n=22) were ruptured. Nosignificant difference was found in the intimal thickness of proximal segments be-tween patients with or without plaque rupture (270±97 μm versus 259±76 μm,p=NS).Conclusions: Proximal segments of plaques containing TCFA are associatedwith increased intimal thickness in patients with ACS. However, in the same pa-tients increased intimal thickness of proximal segments is not associated withruptured plaques. Our findings suggest that atherosclerotic changes of the vesselwall are associated with culprit plaque morphology in acute coronary syndromes.
P1556 Coronary flow velocity assessment on left anteriorcoronary artery as a marker of atherosclerosis:reliability and accuracy of transthoracicechocardiographic study compared to Doppler flowwire
F. Rigo1, F.R. Tona2, A. Cati1, E. Grolla1, A. Djordjevic-Dikic3,C. Sarais2, T. Milorad Tesic3 , S. Iliceto2. 1dell’Angelo Hospital Departmentof Cardiology, Mestre-Venice,Italy, Italy; 2University of Padua cardiologyDepartment, Padova, Italy; 3University of Belgrade, School of Medicine, CCS,Institute for Cardiovascular Diseases, Belgrade, Serbia
Background: Doppler flow wire investigation (DFW) is the reference tool to getfunctional information about the flow limiting effect of a coronary stenosis. Tran-thoracic echocardiograpic selective mapping of Doppler velocities (DFVm) hasbeen proposed as a tool enables to offer information about left anterior coronary(LAD) disease, but so far its diagnostic value has not been tested yet.Aim: To compare the reliability and the relative diagnostic value of DFVm restvelocities in the 3 main segments of LAD coronary artery (Proximal=I- Middle=II,distal=III) with coronary angiography (CA),CFR and FFR assessed invasively.Methods: In 2009 we enrolled 17 chest pain patients (12 men, 70%), mean age68±9 years by using TTE-Doppler mapping of LAD, employing a dedicated vas-cular Doppler software of analysis. Each of them underwent dipyridamole (up to0.84 mg/kg over 6’) stress echo one day before CA. A higher flow velocity inmid-distal LAD was considered due to coronary stenosis, and we considered asabnormal a CFR value <2.0. All pts underwent CA considering as significant astenosis ≥50%. We performed Doppler flow wire analysis to highlight pressuregradient, segmental coronary flow velocities, CFR and FFR on LAD.Results: Significant LAD coronary artery disease was found in 10 (59%) patients.As summarized in the table, we found similar values of flow velocity between TTEand DFW on LAD: LAD I (r=0.711, p=0.004) LAD II (r=0.654, p=0.004) and LADIII (r=0.520, p= 0.03).
CA stenosis % DFW cm/s TTE cm/s r p
LAD I 33±7 69±36 59±24 0.711 0.004LAD II 41±7 83±36 75±44 0,654 0.004LAD III 8±3 73±33 67±26 0,521 0,003CFR 2,1±0,7 2,0±0,6 0,98 0,001FFR 0,8±0,1
Conclusions: DFVm of LAD showed good values in terms of reliability and diag-nostic accuracy as well as a good overlap with those values obtained by DFW.Therefore, the finding of a significant difference between proximal to distal rest ve-locity on LAD can be considered a reliable marker of LAD coronary narrowing andmay become an option for simple non-invasive screening of patients suspectedof having CAD, before performing CFR or any invasive procedure.
P1557 Sphingomyelin content of erythrocyte membranes isincreased and in linear association with membranesloading with cholesterol in acute coronary syndromepatients
K.E. Mitrousi1, D.N. Tziakas1, G.K. Chalikias1, D.A. Stakos1,I. Tentes1, A. Thomaidi1, P. Kikas1, A. Lantzouraki1 , H. Boudoulas2,S.K. Konstantinidis1. 1Democritus University of Thrace, Alexandroupolis,Greece; 2Biomedical Research Foundation, Athens, Greece
Purpose: Histopathological studies have suggested that cholesterol transportedby erythrocytes and deposited into the necrotic core of atheromatous plaques,
contributes to lipid core growth and thus to plaque instability. Previous studieshave reported that total cholesterol content of erythrocyte membranes (TCEM)is significantly higher in patients with acute coronary syndromes (ACS), com-pared to chronic stable angina (CSA) patients. Sphingolipids and especially sph-ingomyelin (SM) are particularly important for cellular membrane physiology. SMhas a molecular attraction for cholesterol and it is postulated that "traps" choles-terol within a particular membrane site preventing its normal cellular movementand metabolism. The precise mechanisms, however, by which erythrocyte mem-branes are loaded with cholesterol are still unknown. With the present studysought to assess whether SM content of erythrocyte membranes (SMEM) is as-sociated with TCEM.Methods: We prospectively assessed 72 patients of whom 21 had CSA (12men,age 61±12 years), 39 ACS (36 men, age 62±11years) and 12 with normalcoronary arteries (NCA) (9 men, age 51±18years). Total cholesterol and sphin-gomyelin content in erythrocyte membranes (TCEM and SMEM) were measuredusing an enzymatic assay, while protein content was measured by the Bradfordmethod.Results: TCEM content was higher in ACS patients (118±27.2 ug/mg) comparedto CSA patients (102.3±15.6 ug/mg, p=0.011) and NCA controls (100.8±8.3ug/mg, p=0.021). No difference was found between CSA and NCA study group(p=0.847). Similarly, SMEM was higher in ACS subgroup (156.8 ug/mg) com-pared to CSA (127.7 ug/mg, p=0.028) and NCA (108.5 ug/mg, p=0.003) sub-group. SMEM levels were similar between CSA and NCA study participants(p=0.271). There was a positive linear association between TCEM and SMEMlevels (r=0.476, p<0.001). In a multivariable linear regression model includingpossible cofounders (i.e. statins) of erythrocyte membrane’s cholesterol loading(R=0.608), SMEM remained independently and positively associated with TCEM(b=0.444, p=0.001). No association between TCEM or SMEM with plasma lipidlevels were observed.Conclusions: The present study showed that SMEM levels in parallel with TCEMare also significantly higher in ACS patients compared to CSA patients. Further-more, a positive and independent linear association between TCEM and SMEMlevels was observed suggesting a pathophysiological role for SM in regulating theexchange of cholesterol between erythrocytes and plasma. Further studies areneeded to elucidate the complex biology of erythrocyte membrane cholesterolefflux.
P1558 Bone mass density and severity of atheroscleroticcoronary disease in unstable and stable patients
A. Macchi, I. Franzoni, I. Rosa, F. Buzzetti, L. Ferri, M.C. Pedrigi,I. Villa, M. Sirtori, A. Rubinacci, A. Margonato. San RaffaeleHospital, Milan, Italy
Purpose: Cardiovascular disease and osteoporosis have a major impact on mor-bidity and mortality. These two pathologies share several risk factors such as age,smoking, obesity and physical inactivity. Recently, there has been growing evi-dence linking low bone mass density (BMD) with coronary artery disease (CAD).Arterial tissue calcification derives from an organized process similar to thosein bone mineralization. Moreover calcified plaques express several bone matrixproteins. ST-elevation myocardial infarction (STEMI) usually occurs because ofnon-critical plaques rupture while stable angina (SA) often subtend diffuse coro-nary atherosclerosis. In the present study, we investigate the relationship betweenBMD and severity of atherosclerotic coronary disease in unstable and stable pa-tients (pts).Methods: We enrolled two groups of male pts: in the first group 28 pts with SA(63,6±10,03 years) and in the second 24 pts with STEMI (64,9±11,5 years).We excluded pts with previous myocardial infarction, neoplastic, renal, hepatic,bone metabolic disease and pts already submitted to revascularization proce-dures. BMD was measured by vertebral and femoral computerized bone miner-alometry. BMD results were classified according to World Health Organizationcriteria. Coronary angiography was performed in all pts. The severity of CADwas estimated using the Syntax Score (low risk=22; intermediate risk=23-32; highrisk≥33).Results: We observed an high prevalence of low BMD in our study groups thatwas 35,6% in pts with SA and 28% in pts with STEMI. According to Syntax Scorewe estimated 18 pts at low, 7 pts at intermediate and 3 pts at high risk in SAand 18 pts at low, 4 pts at intermediate and nobody at high risk in STEMI. More-over we counted 15 pts with normal BMD; 9 pts with osteopenia and 1 pts withosteoporosis in SA and 16 pts with normal BMD, 8 pts with osteopenia and no-body with osteoporosis in STEMI. We observed a significant inverse correlationbetween BMD and Syntax Score in SA (p=0,017), while there was no statisticalcorrelation between these two variables in STEMI (p=0,82). A multivariate analy-sis confirmed this difference in the two groups considering the levels of BMD andSyntax Score (p=0,018).Conclusions: Low BMD is a very frequent condition in pts with CAD. In stable pts,BMD levels are inversely correlated with the severity of atherosclerotic coronarydisease probably because of elevate percentage of calcified plaques. On the con-trary, we couldn’t observe this relationship in pts with STEMI that is characterizedby a mostly thrombotic component.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atherosclerosis 255
P1559 Usefulness of an abnormal aortic/penile index topredict the presence of coronary artery disease inerectile dysfunction patients
N. Ioakeimidis, C. Vlachopoulos, K. Rokkas, D. Terentes-Printzios,A. Aggelis, N. Alexopoulos, A. Samentzas, C. Aggeli, C. Stefanadis.
Hippokration Hospital, University of Athens, 1st Department of Cardiology,Athens, Greece
Purpose: It has been reported that there is a strict correlation between erectiledysfunction (ED) and coronary artery disease (CAD), but the importance of anindex to predict CAD in ED patients needs to be addressed. We investigated anaccurate arterial function parameter linking ED with CAD.Methods: Carotid-femoral pulse wave velocity (PWV) as an index of aortic stiff-ness and pharmacologically stimulated peak systolic velocity (PSV) of cavernousarteries were used to assess vascular function in two groups of ED patients withsimilar age and risk factor profile: 57 men with angiographically documented CADand 124 men without CAD. Lower PSV values indicate impaired penile arterialfunction and vice versa. Aortic/penile index (API) was developed to describe theseverity of extracoronary vascular dysfunction with the formula: API=PWV/PSV.Results: Subjects were divided into tertiles based on the level of API. Therewas a linear relation of API with prevalence of CAD (left plot). API was also sig-nificantly correlated with the extent of coronary atherosclerosis as assessed bymodified Gensini’s score (r=0.43, P<0.001, middle plot). ROC curve analysis forthe prediction of the presence of CAD showed that the area under the curve(AUC) for API was significantly greater than AUC for PWV (difference betweenAUCs 12.2%, P<0.05, right plot).
API and extent of CAD
Conclusion: API allows an accurate interpretation for the association betweenED and CAD and predicts the presence of CAD, with high values of both sensitiv-ity and specificity.
P1560 Alpha-Defensin: a risk factor for atherosclerosis butnot for plaque rupture
R.A. Abu Fanne1, B. Shmuel1, A. Finkelstein1, I. Herz1, U. Chorin1,Y. Arbel1, A. Halkin1, S. Heyman2, G. Keren1, A.A. Higazi3. 1telaviv suorasky medical center, tel aviv, Israel; 2Hadassah-Hebrew
University Medical Center, Jerusalem, Israel; 3university of pennsylvania,philadelphia, United States of America
Background: Increased neutrophil activation is known to be associated withatherosclerosis severity and acute coronary syndrome. Neutrophil peptides de-fensins are essential elements of the innate immunity and are present inatherosclerotic plaques in humans. They are negatively involved in lipoproteinmetabolism and fibrinolysis, enhance endothelial dysfunction, activate plateletaggregation/adhesion and are a potential regulator of neovascularization. In aprevious pilot study (53 patients) we found that deposition of alpha-defensin inthe skin is a strong independent predictor of coronary artery disease (CAD) inmen.Purpose: We sought to investigate the relationship between neutrophil activationand atherosclerosis/thrombosis via measuring alpha-defensin levels.Methods: Defensin was Immunohistochemically quantified in skin biopsies takenfrom 338 consecutive patients (age 55±12) immediately prior to coronary an-giography. The patients‘ diagnosis, established biomarkers for CAD and acceptedclinical risk factors were obtained concurrently; including questionnaire for infec-tious/inflammatory status.Results: In the meantime we increased the number of patients in our series andare now presenting data obtained from 338 patients.Our new data support our previous results showing that defensin is a risk fac-tor for the development of CAD; furthermore, the new data strengthen our initialconclusion that deposition of alpha-defensin in the skin is a strong independentpredictor of CAD in men. The correlation found between alpha-defensin in skinand the severity of CAD was highly significant, with a Pearson chi-square testof p<0.0001. Multiple regression analysis showed that skin alpha-defensin is anindependent predictor for CAD severity (p=0.005).We found no correlation between the amount of defensin in the skin and the de-velopment of acute myocardial infarction (AcMI). We even found a trend towardsan inverse relationship between defensin and AcMI, suggesting that defensin is arisk factor for the development of the atherosclerotic lesion, but may increase itsstability.Conclusions: The new data confirm our previous results showing a significantcorrelation between defensin and atherosclerosis in men and support the ab-sence of such a correlation in women.Taken together our data support the role of inflammation in general and specifi-
cally that of a defensin in the development of the atherosclerotic plaque. Amongother players in the inflammatory milieu traditionally linked with plaque rup-ture/destabilization, alpha defensins seem to divert the pendulum toward stabi-lization of the atherosclerotic lesions.
P1561 Lymphocyte subset characterization in patients withearly onset coronary heart disease
N.D. Brunetti, C. D’antuono, M. Rana, G. D’arienzo, L. De Gennaro,M. Di Biase. University of Foggia, Foggia, Italy
Aim: To investigate lymphocyte activation in young non-diabetic pa-tients with coronary heart disease (CHD).Methods: Twenty-five consecutive young (<55 yrs) out-patients with coronaryheart disease (CHD) (acute myocardial infarction in the previous 3 months)and stable clinical conditions (>1 month) underwent venous blood sampling inorder to determinate CD3+ (T lymphocytes), CD19+ (B lymphocytes), CD4+(Helper/Inducer lymphocytes) and CD8+ (Suppressor/Cytotoxic lymphocytes)populations. Patients with diabetes, heart failure symptoms, recent revasculariza-tion (<30 days) were excluded. Twenty-five patients matched for age, gender andrisk factors were enrolled as controls. All patients with CHD previously underwentcoronary angiography.Results: CHD patients showed lower CD3+ levels (70.96%±4.72% vs74.12%±4.93%, p<0.05) and CD8+ (37.80%±7.15% vs 46.36%±5.22%,p<0.001) but higher CD4+ (37.32%±7.99% vs 31.64%±4.72%, p<0.01) andCD4/CD8 ratio (1.06±0.43 vs 0.69±0.13, p<0.001). Difference in CD19+ levelswas not statistically significant. Subjects with an impaired (≤55%) left ventricu-lar ejection fraction were characterized by lower levels of CD8+ (33.23%±7.04%vs 43.76%±7.40%, p<0.05) and higher levels of CD4+ (38.31%±8.23% vs32.73%±6.08%, p<0.05) and CD4/CD8 ratio (1.06±0.38 vs 0.79±0.34, p<0.05).CD8+ levels inversely related to severity of coronary atherosclerosis (r -0.37,p<0.01).Conclusions: Subjects with early presentation of CHD are characterized by analtered CD4/CD8 ratio and lower CD3+ levels.
P1562 PON2 S311C polymorphism and risk factors areindependently associated with atherothromboticevents
J. Campolo1, L. Cozzi1, R. Caruso1, R. De Maria1, M. Parolini1,M.C. Patrosso2, A. Marocchi2, S. Penco2, O. Parodi1. 1CNR ClinicalPhysiology Institute - Niguarda Ca’ Granda Hospital, Milan, Italy;
2Laboratory of Medical Genetics, Niguarda Ca’ Granda Hospital, Milan, Italy
Purpose: Several authors link oxidative stress to cardiovascular events, whichare usually triggered by arterial thrombosis. Polymorphisms in genes encodingenzymes involved in oxidant stress modulation provide a potentially powerful ap-proach to study disease susceptibility and paraoxonase genes represent goodcandidates. Aim of our study is to investigate the possible association amongPONs polymorphisms, clinical and metabolic factors with atherothrombotic eventsin an Italian population.Methods: We evaluated in 108 subjects, with or without atherosclerotic risk fac-tors, the presence of PON1 L55M, PON1 Q192R and PON2 S311C genetic vari-ants, as well as lipid profile, the concentration of aminothiols (blood reduced glu-tathione, plasma total glutathione, homocysteine, cysteine, cysteinylglycine), andmalondialdehyde as marker of lipid peroxidation. Clinical, biochemical and ge-netic variables were correlated with a history of atherothrombosis.Results: Previous atherothrombotic events were found in 45 patients (43%) whilePON2 311C allele was present in 31 subjects (29%). By multiple logistic regres-sion analysis, hypertension (OR=5.538; 95% CI 2.202 to 13.902, P<0.001), HDLcholesterol concentration (OR=0.947; 95% CI 0.910 to 0.985, P=0.007) and thepresence of C allele in PON2 gene (OR=3.595; 95% CI 1.247 to 10.361, P=0.018)were independently associated with atherothrombotic events.Conclusions: Our study sheds light on the role of PON2 as possible cofactorin determining the risk of events together with the well-known risk markers HDLcholesterol and hypertension.Study partially supported by a grant from FP7-ICT-2007 project (grant agreement224297, ARTreat)
P1563 Atherosclerosis subclinical in adolescents: itsrelationship with metabolic syndrome
E. Silva, L. Chacin, J. Villasmil, G. Bemudez, M. Bracho,A. Gonzalez, C. Esis. Instituto Regional de Investigacion y Estudiosde Enfermedades Cardiovasculares, Universidad del Zul, Maracaibo,
Venezuela
Objective: To determine the predictive value of the metabolic syndrome (MetS)for subclinical atherosclerosis in adolescents.Methods: This study included 163 adolescents, males (n=71) and females(n=92), age - mean = 14 years (SD=2). Demographic (age, gender), anthropomet-ric data [weight, height, body mass index, waist circumference (WC)] and bloodpressure (BP) were recorded. It was determined serum glucose, HDL-cholesteroland triglycerides. The MetS was defined by definitions of the National Cholesterol
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

256 Atherosclerosis
Education Program, Adult Treatment Panel III modified for adolescents. Subclini-cal atherosclerosis (SA) was assessed by carotid intima-media thickness (c-IMT)on B-mode ultrasonography, and adolescents with c-IMT abnormal for their ageand gender were considered with SA. The logistic regression was applied to esti-mate the model for the prediction of the probability (P) of SA. The factors includedin this model were determined by correlation analysis and chi square test.Results: The prevalence of SA was 30.1% (n=49) in all subjects, and it was39.4% (n=28) for males and 22.8% (n=21) for females (p<0.01). There were sta-tistically significant associations between SA with: male gender (p=0.02), MetS(p=0.001), WC (p=0.001), systolic BP (p=0.01), weight (p=0.003) and height(p=0.03). The logistic regression analysis evidenced significant effects of theMetS (odds ratio=4.785; 95% CI=1.835-12.477; p=0.001) on the probability ofthe presence of SA [P(SA) = 0.59], excluding the rest of the factors that showedassociations with SA (Cox and Snell R2 = 0.063; Nagelkerde R2 = 0.089).Conclusions: This study evidence high prevalence of SA in adolescents. TheMetS has an important predictive value of the presence of SA in adolescents,and therefore for cardiovascular risk. These results suggest the importance ofscreening and intervention in early life stages.
P1564 RANKL/OPG serum concentration ratio as a newbiomarker for coronary artery calcification
A.H. Mohammadpour1 , M. Ramezani1, S. Nazemi2,H. Falsoleiman3, J. Shamsara4, S. Ghadirzadeh4. 1PharmaceuticalResearch Center & School of Pharmacy, Mashad University of
Medical Science, Mashad, Iran (Islamic Republic of); 2Razavi Hospital, Mashad,Iran (Islamic Republic of); 3Ghaem Hospital, Mashad University of MedicalScience, Mashad, Iran (Islamic Republic of); 4School of Pharmacy, MashadUniversity of Medical Science, Mashad, Iran (Islamic Republic of)
Purpose: The numerous studies have attempted to use serum level of osteo-protegrin (OPG) or receptor activator of nuclear factor-κB ligand (RANKL) as apredictor of atherosclerosis and coronary artery calcification (CAC) but conflict-ing results have been obtained. In our view, inhibitory effect of OPG on RANKLis the main cause of these disconformities. Therefore the aim of this study isconcomitant determination of both serum level of RANKL/OPG and calculation ofRANKL:OPG ratio as a biomarker for CAC.Method: 50 patients with coronary artery disease (CAD) who fulfilled inclusionand exclusion criteria entered in this pilot study. These patients underwent CTAngiography and coronary artery calcium score in LMCA, LAD, RCA, CX andtotal CAC were determined in these patients. Also serum concentration of RANKLand OPG were determined by ELISA method at this time. Correlation betweenCAC and serum level of OPG, RANKL and RANKL:OPG ratio were determinedstatistically.Results: There was positive significant correlation between total CAC andRANKL:OPG ratio (P=0.01 and pearson correlation=0.519) and this correlationwas significant only with LAD calcium score (p=0.01 and pearson correlation=0.545).There was no significant correlation between serum level of RANKL andtotal CAC but the results indicated negative significant correlation between serumlevel of OPG and total CAC (p=0.03 and pearson correlation = -0.468).Conclusion: The serum level RANKL:OPG ratio could be a biomarker for CACbut larger studies is needed.
P1565 Correlations of different parameters of carotid intimamedia thickness with complexity of coronary arterydisease
S.K. Chua1, N.H. M1, T.K. Ong1, A. Rapaee2, A.Y.Y. Fong1,B.C. Chang1, K.L. Yew1, Y.L. Cham1, N.Z. Khiew1, K.H. Sim1.
1Sarawak General Hospital, Kuching, Malaysia; 2University Malaysia Sarawak(UNIMAS), Kuching, Malaysia
Background and Purpose: Although widely accepted as a screening tool forcoronary artery disease (CAD), carotid intima media thickness (CIMT) has shownat best only a moderate correlation with CAD severity. Possible reasons includethe variability of atherosclerosis development in different vascular beds, uncer-tainties about the best site to measure CIMT and no standard method of quanti-fying CIMT.ObjectiveTo evaluate how different measurements of CIMT correlate with the Syntax scorein CAD patients.Methods: 96 patients who underwent coronary angiography from October 2009to January 2010 were recruited. Common carotid artery (CCA) Ultrasound B-mode scanning was performed with a L11-3 linear array transducer on the PhillipsiE33 Echocardiography System. Three measurements were made on each sideof the neck - (a) mid CIMT over 10 mm at mid CCA level, (b) maximum CIMT atany point along the entire length of the CCA, and (c) diameter of CCA to calculatemidCIMT index and maxCIMT index. The Syntax Score was calculated based onthe coronary angiogram. Statistical analysis was done with the SPSS 13 softwareusing Spearman’s 1 tailed correlation test.Results: The mean age of our study population was 56.4±11.1 years. Thefollowing CIMT measurements were obtained - Left midCIMT 0.62±0.17mm,Left midCIMT index 0.85±0.22, Left maxCIMT 0.70±0.38mm, Left maxCIMT in-dex 0.94±0.51, Right midCIMT 0.63±0.20mm, Right midCIMT index 0.85±0.24,
Right maxCIMT 0.76±0.43mm, Right maxCIMT index 0.99±0.54. Mean Syntaxscore was 18.4±11.3 with mininum of 1 and maximum of 61.5. Statistical anal-ysis showed significant correlations between the Syntax Score and maxCIMT(Left maxCIMT p=0.025, Right maxCIMT p=0.04) as well as maxCIMT index (LeftmaxCIMT index p=0.012, Right maxCIMT index p=0.001). The meanCIMT andmeanCIMT index did not correlate with the Syntax Score.Conclusions: The maxCIMT may predict complexity of CAD. However, due tovariation in CCA diameter, it might be better to use maxCIMT index rather thanmaxCIMT. Larger studies are needed to validate the results of this study.
P1566 The effect of high dose pitavastatin on intima-mediathickness and distensibility of the carotid artery inasymptomatic patients with progressiveatherosclerosis
Y.S. Lee, K.S. Kim, M.J. Sung, J.B. Lee, J.K. Ryu, J.Y. Choi,S.G. Chang. Catholic University of Daegu, Daegu, Korea, Republic
of
Purpose: The various statin might contribute to a reduction of atheroscleroticburden. The aim of this study was to investigate the effect of high dose pitavas-tatin on structure and function of the carotid artery in asymptomatic patients withprogressive atherosclerosis.Methods: We enrolled 33 patients with progressive atherosclerosis (maximumintima media thickness (IMT) > 0.7 mm). They were treated pitavastatin 4mgfor 6 months. We evaluated the maximal and mean IMT and distensibility of thecarotid artery using by B mode ultrasound. Also, we measured C-reactive protein(CRP), apoprotein B/A1, and lipid profile at baseline, and 6 months later.Results: The lipid profile and apoprotein B/A1 were significantly decreased at 6months later. However, CRP was slightly decreased, but not significant (p=0.210).The maximal and mean carotid IMT were significantly decreased at 6 monthslater (0.965±0.142 vs. 0.882±0.154, 0.691±0.132 vs. 0.648±0.129, respectively)(p<0.001). In addition, the carotid distensibility at 6 months was significantly im-proved compared to it at baseline (2.80±1.12 vs. 1.75±0.78 mmHg-1 x103, re-spectively) (p<0.001). These changes were not correlated to lipid change.
Conclusions: High dose pitavastatin might improve the carotid IMT and disten-sibility.
P1567 Pitavastatin LDL-C target attainment in elderly andCHD risk populations in a Phase 3 programme
N. Hounslow. Kowa Research Europe Ltd, Wokingham, UnitedKingdom
In previously reported studies, approximately 58% and 77% of pa-tients with primary hypercholesterolaemia or combined dyslipidaemia reachedEAS treatment targets with pitavastatin (PIT) 2 mg or 4 mg once daily: thesedoses were non-inferior to both simvastatin (SIM, 20 mg or 40 mg) and atorvas-tatin (ATO, 10 mg or 20 mg) therapy.In higher risk patients, a 12-week, double-blind, parallel group study in 942 elderlypatients (≥65 years) demonstrated non-inferiority of PIT 1, 2 and 4 mg to pravas-tatin (PRA) 10, 20 and 40 mg for LDL-C reduction, and EAS target attainment wassignificantly greater following PIT than PRA (p<0.001, all comparisons). Target at-tainment increased from 55.9-88.1% across the doses of PIT vs. 37.9-65.7% withPRA; similar trends were seen with NCEP criteria.In a 60-week, open-label extension to this study (n=545), target attainment wasmaintained in elderly patients: 91.0% and 98.7% of the PIT 2 mg group achievedEAS and NCEP targets. Patients who failed to meet targets on PIT 2 mg (n=90)benefitted from up-titration to PIT 4 mg, with 79.2% and 70.1% meeting EAS andNCEP targets, respectively, at Week 60.In a separate 12-week study (n=355), patients with at least two additional riskfactors for CHD were randomised to PIT 2 mg or SIM 20 mg and then force-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Atherosclerosis / Invasive electrophysiological studies 257
titrated to PIT 4 mg or SIM 40 mg; 87.1% and 81.4% of PIT and SIM patientsattained EAS targets, respectively. In a 44-week extension phase (n=178), SIM40 mg patients not achieving targets in the core study were up-titrated to SIM 80mg. After 44 weeks, attainment of EAS targets fell from 94.9% to 84.2% with PIT4 mg, compared with 92.7% to 73.7% with SIM 40/80 mg.In conclusion, PIT 2 mg and 4 mg was associated with a higher proportion ofEAS target attainment than PRA 20 mg and 40 mg (p<0.001, all comparisons) inelderly patients. In patients at high risk of CHD, up-titration from SIM 40 mg to 80mg produced little benefit for target attainment vs. sustained treatment with PIT 4mg.
P1568 Vascular morphopathological particularities ofsubclinical atherosclerosis in elderly
R. Avram, F. Parv, A. Dema, T. Ciocarlie, M. Balint, L. Branzan,M. Tudoran, I. Avram. County Hospital, Timisoara, Romania
Purpose: Subclinical atherosclerosis in elderly is not well under-stood. Our objective is to identify morphological, histochemical and immunohisto-chemical particularities of subclinical atherosclerosis in elderly.Methods: We have selected 40 patients (20 males, 20 females), over 70 yearsold, deceased from causes other than vascular disease with no history of cardiacdisease. We have studied vascular lesions in the aorta, carotid, coronary and re-nal arteries, in segments from 1 to 5 cm, focusing on morphological aspects, mus-cle and collagen fibers, calcium deposits, lipid deposits, T and B lymphocytes, thepresents of inflammatory cells in plaque with calculation of the Redgrave score,plaque neovascularization and estrogen receptors. Morphological (Hematoxylinand Eosin, Tricrom Masson, Van Gieson), histochemical (Scharlach R, Verhoeff,Giemsa) and immunohistochemical techniques (anti-actin monoclonal antibodies,anti-muscle, anti-CD45, anti-CD45-RO, anti-CD68, anti-ER (estrogen receptors)and anti-CD34) were used in our study.Results: 70% of the dominant lesions on the carotid arteries were type 3, 4 and 5.Renal artery lesions were moderate, mostly type 1-4. As to the coronary arteries,type 5 lesions represented 80% of the coronary injuries while 60% of the pa-tients had stenosis over 50%. 10% of the plaques were calcified, inflammation ofthe adventitia (Type T CD3+ lymphocytes) was situated in the fibrous layer and,together with neovascularization (CD34), in the plaque shoulder. Aortic lesionswere 10% of type 6, 60% showed calcification and 20% were positive for inflam-mation. The study showed that carotid, renal, aortic, and coronary lesions foundin women were less extensive compared to men, however this finding was statis-tically insignificant (p=0,52, p=0,89, p=0,75, p=0,52). Also renal artery injuries inwomen were more advanced (p=0,04) and aortic calcifications were more severein women (80% vs. 40% in men) with less inflammation.Conclusion: Subclinical atherosclerosis is common to the entire vascular bed inelderly, predominantly as aortic calcifications and with the least extent in renal ar-teries. Neovascularization and inflammation most likely suggest plaque instability.As to differences between sexes, less inflammation was present in women, withmore extensive calcifications of the aorta and more frequent renal artery lesionsversus men.
INVASIVE ELECTROPHYSIOLOGICAL STUDIES
P1569 Prognostic stratification of the subjects with Brugadaelectrocardiogram: the role of programmed electricalstimulation with 2 and 3 extrastimuli
N. Cerrato1, C. Giustetto1, A. Mazzanti1, E. Marras2, G. Allocca2,M. Bortnik3, P. Dalmasso4, R. Riccardi5, P. Delise2, F. Gaita1.
1Cardinal Massaia Hospital, Department of Cardiology, Asti, Italy; 2ConeglianoHospital, Department of Cardiology, Conegliano, Italy; 3Maggiore Della CaritaHospital, Department of Cardiology II, Novara, Italy; 4Medical Statistics,University of Torino, Torino, Italy; 5E. Agnelli Hospital, Department of Cardiology,Pinerolo, Italy
Purpose: Brugada syndrome is an arrhythmogenic disease characterized by anincreased risk of sudden cardiac death (SCD). Until now, an implantable car-dioverter defibrillator (ICD) is the only proven therapy. Therefore, it is mandatoryto identify the subjects at high risk of SCD. The aim of the study was to evalu-ate the prognostic value of clinical and genetic variables (gender, family history,ECG features, symptoms, SCN5A mutation) and the role of programmed electri-cal stimulation (PES) in the risk stratification of the subjects with a Brugada ECG,comparing the predictive value of 2 different stimulation protocols, with 2 and 3extrastimuli.Methods: 286 patients with spontaneous or drug-induced type 1 Brugada ECGwere enrolled in 2 regions of Italy. PES was performed in 77% of them: 94 pa-tients underwent a protocol with up to 2 extrastimuli until refractoriness, while 127patients were studied up to the third extrastimulus. In both cases extrastimuli weredelivered from two ventricular sites.Results: Population features at diagnosis: mean age 44±14 years; 49% sponta-neous type 1 ECG; 64% asymptomatic individuals, 34% with history of syncope,2% with aborted sudden death. Ventricular fibrillation (VF) was induced in 39%of patients studied with up to 2 extrastimuli and in 40% of those studied with upto 3 extrastimuli. During a follow-up of 38±28 months the incidence of arrhyth-
mic events was 1.6% per year (3%-year in symptomatic patients vs 0.6%-year inasymptomatic ones). Induction of VF at PES (p=0.001), syncope (p=0.019) andspontaneous type 1 ECG (p=0.03) were predictors of arrhythmic events at follow-up. None of the patients with syncope and negative PES had events during follow-up. At PES, both protocols revealed high negative predictive value and sensitivity,with higher positive predictive value and specificity in the protocol with up to 2extrastimuli [2 extrastimuli: sensitivity 100% (CI=59.0-100); NPV 100% (CI=93.7-100); PPV 19% (CI=8-35.2); specificity 66% (CI=54.5-75.4); 3 extrastimuli: sensi-tivity 100% (CI=29.2-100); NPV 100% (CI=95.3-100); PPV 5.9% (CI=1.23-16.2);specificity 61% (CI=51.2-69.9)].Conclusions: PES, history of syncope and spontaneous type 1 ECG were theonly predictors of arrhythmic events. PES resulted to be useful especially for riskstratification of patients with syncope of unknown origin (no events at follow-up inthose with negative PES), while the best approach to asymptomatic subjects hasstill to be established (low PPV of PES). PES with up to 3 extrastimuli comparedwith PES with a maximum of 2 extrastimuli did not show a greater accuracy inpredicting outcome.
P1570 Circumferential pulmonary vein isolation with pointby point ablation using a high density mesh mappercatheter versus the one-shot ablation technique withthe high density mesh ablator
A. Meissner, G.P. Plehn, T.B. Butz, H.Y. Yeni, M.B. Van Bracht,P.M. Maagh, M.C. Christ, H.J.T. Trappe. University Hospital Bochum, Herne,Germany
Purpose: The purpose of this prospective study was to evaluate fluoroscopy- andprocedural times of circumferential pulmonary vein (PV) isolation using the highdensity mesh ablator (HDMA), a novel single, expandable electrode catheter forboth mapping and radiofrequency (RF) delivery at the left atrium/PV junctions incomparison to irrigated point to point ablation around an only mapping catheter,the high density mesh mapper (HDMM).Methods: The HDMA study group consists of 26 patients (pts) with highly symp-tomatic paroxysmal AF (14, 53.8%) and persistent AF (12, 46.2%). Segmental PVisolation via the HDMA was performed using a customized pulsed RF energy de-livery program (target temperature 55-60 degrees, power 70-100 Watt, 600-900seconds RF application time/PV).The HDMA study group consists of 72 pts with highly symptomatic, drug refrac-tory AF, 47 (65.2%) with PAF, 12 (16.7%) with persistent and 13 (18.1%) withpermanent AF. Segmental PV isolation was performed by circumferential abla-tion around the HDMA on the atrial side of the PV by irrigated RF application.All pts were investigated during conventional fluoroscopy in biplane technique, anadditional navigation system was not in use.Results: In the HDMA study group all 104 PV in 26 pts could successfully beablated by the HDMA. Segmental PV isolation was achieved with a mean of3.25±1.4 circumferential RF applications for a mean of 603±185 sec. Entranceconduction block was obtained in >94% of all PV. Mean total procedure and flu-oroscopy time was 159±32 min and 33.5±8.6 min respectively. In the HDMMstudy group overall 288 PV in 72 pts had to be examined. 284 PV (98.6%) couldbe analysed by this approach. In 93% the primary end point of an entrance blockand in 81% the secondary end point of an exit block was achieved. Mean total pro-cedure and fluoroscopy time was 235±41 min and 62.5±14.7 min respectively.Hence, point by point ablation around the HDMM by irrigated ablation requiredboth significant longer procedural and fluoroscopy times compared to the newHDMA technique with the one-shot ablation technique (p<0.01). Severe compli-cations did not occur in both study groups.Conclusions: Comparing circumferential PV isolation using a conventional ap-proach with point by point irrigated ablation around the diagnostic only HDMMcatheter versus the mapping and ablating HDMA catheter in a single unit bothyields to good primary success rates. The HDMA simplifies the complex proce-dure of AF ablation, favorably impacting procedure and fluoroscopy times.
P1571 Intra- and postprocedural lesion visualization ininterventional electrophysiology using MRI: earlydelineation of isthmus ablation lesions in patientswith typical atrial flutter
P. Nordbeck1, W.R. Bauer1, F. Fidler2, M. Warmuth3, K.H. Hiller2,M. Nahrendorf4, P.M. Jakob3, G. Ertl1, O. Ritter1. 1Internal Medicine I, Universityof Würzburg, Würzburg, Germany; 2Research Center Magnetic ResonanceBavaria, Würzburg, Germany; 3Experimental Physics V, University of Würzburg,Würzburg, Germany; 4Harvard Medical School, Center for Molecular ImagingResearch, Boston, United States of America
Background: Imaging of myocardial ablation lesions during electrophysiology(EP) procedures would allow superior guidance of interventions and immediateidentification of potential complications. The aim of the current study was to es-tablish MRI-based imaging techniques feasible for intraprocedural lesion visual-ization in interventional EP.Methods: Interventional EP was performed under MR guidance in an animalmodel, using a custom setup including MR-conditional catheters. Various pulsesequences were explored for intraprocedural lesion visualization after RF abla-tion. The developed contrast agent-enhanced and non-enhanced visualization
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

258 Invasive electrophysiological studies
techniques were then used to investigate lesion formation in patients immediatelyafter ablation of atrial flutter.Results: The animal studies in 9 mini pigs showed that Gadolinium-DTPA-enhanced T1 weighted and non-enhanced T2 weighted pulse sequences are sim-ilarly feasible for lesion visualization immediately after RF ablation. Comparisonof MRI-derived lesion size with autopsy revealed good agreement. Non-contrastagent-enhanced techniques were suitable for repetitive lesion visualization duringEP interventions, thus allowing for intraprocedural monitoring of ablation success.After extensive testing in animal models, we used contrast enhanced T1 and non-enhanced T2 weighted MRI to image therapeutic lesions in 24 patients with typicalright atrial flutter several minutes to hours after cavo-tricuspid isthmus ablation.Therapeutic lesions could be visualized in all patients successfully using contrastenhanced and also non-enhanced MRI. Complete isthmus block was associatedwith a continuous ablation lesion along the cavo-tricuspid isthmus.Conclusion: MRI allows for precise lesion visualization in EP interventions justminutes after RF ablation. Non-enhanced T2 weighted MRI is particularly feasi-ble for intraprocedural delineation of lesion formation as lesions are detectableonly minutes after RF delivery and imaging is unrestrictedly repeatable duringinterventions.
P1572 Diagnostic and prognostic value of theelectrophysiological study in patients withnon-documented palpitations
E. Valles, V. Bazan, F. Suarez, L. Portillo, D. Cian, J. Marti. HospitalDel Mar, Barcelona, Spain
Introduction: Documentation of the arrhythmia helps predicting the tachycar-dia mechanism in patients presenting with palpitations, thus guiding the man-agement. Documentation of the arrhythmia is not always feasible, generally dueto self-termination. In these situations the diagnostic value of electrophysiologicstudy (EPS) is of concern. Otherwise we do not know the long-term prognosis ofpatients with undocumented palpitations.Methods: One hundred and seventy two patients (132 women) with normal basalECG and undocumented palpitations suggesting supraventricular tachycardia un-derwent EPS.Results: Symptoms were long in duration (>5minutes) in 56%. Sudden termina-tion was present in 65%. Neck palpitations were reported in 36%. Only 86 pa-tients (50%) had electrophysiologic abnormalities (induced atrioventricular nodalreentrant tachycardia (AVNRT) in 43, orthodromic reentrant tachycardia (ORT)in 9, and atrial tachycardia/fibrillation (AT/AF) in 34. Long duration episodes(p<0.001), sudden termination (p<0.001) and neck palpitations (p=0.01) wereclinical predictors of arrhythmia induction in the bivariate analysis and werealso linked to induction of AVNRT (p<0.001). Patients were followed for 53±36months. All the patients with AVNRT or ORT underwent effective ablation andremained symptom-free at follow up. Among patients with negative EPS results,92% remained symptom-free compared to 32% in the group with AT/AF induced(p<0.001). Kaplan-Myers analysis showed recurrence among those patients withdiminished left ventricle ejection fraction (LVEF), <50 years (p<0.0001), or AT/AF(p<0.0001). Age >50 years and diminished LVEF were independent predictorsfor recurrences in the multivariate analysis.Conclusions: Only 50% of patients with undocumented palpitations have an ab-normal EPS. Certain clinical characteristics are helpful in predicting tachycardiainducibility and can help selecting patients for study. Most of the patients with neg-ative EPS results remain symptom-free at long-term follow up. AT/AF induction,age>50 years and diminished LVEF are predictors for recurrences.
P1573 Endocardial voltage mapping for diagnosis ofarrhythmogenic right ventricular dysplasia: remotemagnetic navigation maps are more accurate thanmanual maps
D.G. Latcu, P. Ricard, I. Popescu, M. Arnoult, T. Hugues, N. Saoudi.The Princess Grace Hospital Centre, Monaco, Monaco
Purpose: Electroanatomic endocardial mapping in arrhythmogenic right ventric-ular dysplasia (ARVD) using the CARTO system has shown to be useful in iden-tifying low voltage areas (LVA) as a marker of fatty infiltration. However, using theconventional manual technique, poor tissue-electrode contact may result in falsepositive LVA. For instance areas such as the paratricuspid inferior region may bedifficult to reach using the conventional femoral approach with single curve steer-able catheter. Additionally, distortions in the right ventricle (RV) silhouette maybe expected because of excessive catheter pressure on the RV wall. We postu-lated that magnetic navigation (MN) may produce more accurate maps as it mayovercome these limitations.Methods: Twenty patients (pts; 15 males, 42±16 y) with suspected ARVD wereprospectively included. All had sustained or non-sustained ventricular arrhyth-mias, but complete work-up according to current guidelines was unable to con-firm ARVD. During a single procedure, 2 RV voltage maps were sequentially per-formed: the first one manually and the second one remotely with a MN system(Stereotaxis). For both maps a 4 mm non-irrigated tip catheter was used. Carewas taken to map the RV as completely as possible with each technique with atleast 100 evenly distributed acquired points. LVA was defined as bipolar voltage<1.5 mV at at least 3 adjacent points.
Results: Both maps were successfully performed in all pts. A comparable numberof points were acquired with each technique (133±51 points for the conventionalmap vs. 129±38 points for the MN map, p=0.92), MN mapping time being slightlylonger (39±11 min vs. 50±15 min, p=0.01). Magnetic maps yielded higher RVvolumes (135±59 ml vs. 182±73 ml, p=0.0004) and a higher RV surface (189±55cm2 vs. 214±64 cm2, p=0.003). Almost systematically, basal inferior RV areas(underneath the tricuspid valve) were incompletely mapped with the stiff manualcatheters, as seen after comparing to the MN maps. LVA were found in 14 pts withthe conventional technique and in 7 pts with MN (p=0.21), with LVA surface beingsignificantly smaller for the magnetic maps (13.53±13.06 cm2 vs. 6.46±10.99cm2, p=0.009, for conventional and MN maps, respectively).Conclusions: Using the same number of mapping points, magnetic maps resultin higher RV volume and surface and smaller low voltage areas than manual ones.These data suggest that MN voltage maps are more accurate and may result inless false positive ARVD diagnosis.
P1574 The effect of different mapping modalities on theassessment of pulmonary vein disconnection
M. Gwechenberger, B. Richter, C. Adlbrecht, J. Sipoetz,H. Goessinger. Medical University of Vienna, Vienna, Austria
Purpose: Pulmonary vein (PV) isolation (PVI) is a corner stone inthe ablation of atrial fibrillation. The study aim was to evaluate whether the as-sessment of PV is dependant on the applied mapping modality.Methods: A total of 37 patients aged 60.1±11.27 undergoing PVI were included.After the delivery of 18 energy application/patient to all 4 PVs with a novel mul-tielectrode catheter (PVAC) the presence or absence of PV potentials was as-sessed using three different mapping modalities: a PVAC, a quadripolar ablationcatheter (Navistar Thermocool) and a conventional circular catheter (Lasso).Results: Of 148 analysed PVs, 61 (41.2%) were found to be not isolated with thePVAC. In contrast, with the LASSO catheter 68 (45.9%) were detected to be nonisolated, while the Navistar yielded the lowest rate with 37 (25%). The correlationbetween PVAC and LASSO was 0.660 (p<0.001); between Lasso and Navistar0.595 (p<0.001) and between PVAC and Navistar 0.499 (p<0.001). These find-ings were independent from the PV localisation.Conclusion: The assessment of PVI is dependent on the applied mappingmodality. Therefore the kind of mapping has to be taken into account, when abla-tion results are compared.
P1575 Intraoperative VV-delay does not predict response tocardiac resynchronization therapy
M. Mutschelknauss1 , D. Altmann1, M. Kuehne1, B. Schaer1,S. Osswald1, P. Ammann2, C. Sticherling1. 1University HospitalBasel, Department of Cardiology, Basel, Switzerland; 2Cantonal
Hospital St. Gallen, St. Gallen, Switzerland
Purpose: Approximately 30% of patients treated with cardiac resynchronizationtherapy (CRT) are non-responders. To date, no hemodynamic, clinical or echocar-diographic predictors of failure to response to CRT could be identified. We soughtto study whether the intraoperatively measured width of the electrical interventric-ular delay (VV delay) between the right ventricular (RV) and the left ventricular(LV) electrogram predicts narrowing of the resulting QRS complex and responseto CRT.Methods: 48 pts (36 m, median age 63 y, IQR 59-71 y) were implanted with CRT.The underlying cardiac condition was coronary heart disease (ICMP) in 33% andnon-ischemic cardiomyopathy (NICMP) in 67%. LVEF was severely depressed(median 20%, IQR 15-25%) at baseline. Median NYHA class was III and the me-dian intrinsic QRS width 160 ms (IQR 140-168 ms). 10/48 pts (21%) suffered fromatrial fibrillation. VV-Delay (ms) was measured intraoperatively from the electricaldelay of the local EGM between the tip of the RV lead and the LV lead duringintrinsic conduction. Operators were encouraged to place the LV lead at the po-sition with the longest VV-delay. For better comparisons within our population aratio (VV/QRS) between intraoperative VV-delay (ms) and intrinsic QRS duration(ms) was calculated. Response to CT was defined as improvement of at least oneNYHA class.Results: 25 pts (52%) improved significantly after CRT implantation. In 15/25 ptsmedian NYHA functional class improved one class while 10/25 pts showed clinicalimprovement of more than one NYHA class. However, 23 pts remained clinicalnon-responders. Median LVEF increased significantly after CRT (20% vs 31%,p<0.0001). However, for 22 pts no echocardiographic follow-up was available.Responders (QRS pre 160 ms, IQR 134-165; delta QRS pre/post 26 ms, IQR14-40 ms) as well as non-responders (QRS 166 ms, IQR 140-175; delta QRSpre/post 33 ms, IQR 11-63) showed a significant narrowing of median QRS dura-tion (p=0.13 for comparison between both groups). Mean VV/QRS ratio showedno significant correlation to clinical response (p=0.71), narrowing of QRS complex(p>0.1 for both groups) or the underlying cardiac disease (p=0.73 for comparisonbetween ICMP and NICMP).Conclusions: Measurement of intraoperative VV delay and calculation of a ratiobetween intrinsic QRS duration and intraoperative VV delay did neither predictnarrowing of the resulting QRS width nor response to CRT.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Invasive electrophysiological studies / Non invasive studies 259
P1576 In vivo characterization of murine cardiacelectrophysiology in aging
P. Francia1 , A. Ricotta1, C. Balla1, A. Uccellini1, S. Carosio2,L. Barberi2, G. Dobrowolny2, A. Musaro’2, F. Cosentino1, M. Volpe1.1Sapienza University of Rome, Sant’Andrea Hospital, 2nd Faculty of
Medicine, Rome, Italy; 2Sapienza University of Rome, Department of Histologyand Medical Embryology, Rome, Italy
Background: Cardiac brady- and tachyarrhythmias increase with age in bothheart-diseased patients and healthy individuals. Major advances in gene targetingtechnology made available mutant mice protected against age-related cardiovas-cular disease. Although maturational physiology of the atrio-ventricular (AV) nodehas been described in mice, it is unknown whether aging may affect sino-atrial(SA) and AV conduction as well as propensity for tachyarrhythmias in the mouse.This information would help to establish a murine model suitable for studying age-related cardiac arrhythmias.Methods: Nine 6 month-old male SV129 WT (young) and six 24 month-old maleSV129 WT mice (old) were studied. All mice underwent baseline ECG and com-plete EP study after IP injection of 33 mg/kg pentobarbital. An octopolar catheter(1.1 F, EPR-800, Millar Instruments) was used for recording cardiac electrogramsand pacing. The catheter was inserted through the right jugular vein and the tipadvanced into the right ventricle. Standard ECG time intervals (RR, P, PR, QRS,and QTc) were determined for each mouse. A complete transvenous in vivo EPstudy was performed to assess (1) SA node function (corrected sinus nodere-covery time, SNRTc), (2) AV conduction (decremental atrial pacing to the pointof Wenckebach block and programmed premature atrial extrastimuli to determinethe AV node effective refractory period, AVNRP), and (3) arrhythmia induction byprogrammed atrial and ventricular stimulation.Results: Baseline heart rate was comparable in young and old mice (479±32 vs448±70 bpm). Old mice had significantly longer P wave (15.9±1 vs 12.7±3 ms;p= 0.01) and QRS (18.8±4 vs 14.2±3; p= 0.02) duration as compared to younganimals. Old mice displayed longer A-H interval (40.5±7 vs 27.8±5 ms; p= 0.03)and similar H-V interval (15.5±5 vs 13.9±2 ms). The mean SNRTc was compa-rable among young and old mice (46±11 vs 52±19 ms, respectively), whereasWenckebach block cycle and AVNRP were higher in old vs young mice (100±10vs 80±5 ms; p<0.01 and 75±18 vs 52±10 ms; p= 0.05, respectively). Inducibleruns of atrial tachycardia were elicited in two old mice, while none of the younganimals was inducible.Conclusions: These data suggest that WT mice develop age-dependent slowingof intra-atrial and intra-ventricular conduction as well as AV node dysfunction andpropensity for atrial tachyarrhythmias. Characterization of murine electrophysiol-ogy in physiological aging may provide insights into the mechanisms linking agingand arrhythmias and is crucial to study cardiac electrophysiology in geneticallymodified long-living animals.
P1577 Can we accept an atrioventricular nodal echo beatafter cryoablation of atrio-ventricular nodal re-entranttachycardia?
B. Godin, A. Savoure, F. Anselme. University Hospital of Rouen -Hospital Charles Nicolle, Rouen, France
Purpose: Cryoablation has been introduced to reduce the risk of atrio-ventricular(AV) block in patients treated for atrio-ventricular nodal re-entrant tachycardia(AVNRT). If persistent AV nodal jump and single nodal echo beat are acceptedafter radiofrequency ablation, the predictive value of residual slow pathway con-duction after cryoablation is not known.Methods: Between October 2007 and September 2009, 27 patients (pts) un-derwent cryoablation of AVNRT, in our center using a 6 mm-tip CRYO catheterablation. Acute success was defined by non-inducibility of AVNRT during isopro-terenol infusion. We evaluated the recurrence rate of AVNRT at 4 months afterablation according to whether the slow pathway conduction was abolished or not.Results: Typical AVNRT was induced at the beginning of the EP study. Thecryoablation was anatomically guided. Following cryoablation, complete slowpathway disappearance, a jump without nodal echo beat, a jump with one echobeat, more than one echo beat but less than three, were recorded in respec-tively 4, 4,16 and 3 pts. In all cases, at the end of the procedure, AVNRT wasno longer inducible at baseline and under isoproterenol infusion. In none of thepts, AV nodal conduction impairment was documented at the end of the study.No PR prolongation was recorded on surface ECG the day after the procedure.Mean fluoroscopy time (7.7±6.6 min; p=0.8), mean procedure time (104±29 min;p=0.9) or mean number of cryoablations (5.7±5; p=0.3) were not significantly dif-ferent within groups. Anti-arrhythmic drugs were stopped 3 days before the proce-dure and not reintroduced at discharge. After 4 months, two of the three pts withmore than one echo beat had recurrence of AVNRT, but none of the other 23 pts.Three of the 16 pts for whom a single echo beat was tolerated experienced shortepisodes of palpitations which could not be documented as AVNRT recurrences.Conclusions: In this series, all of the recurrences occurred when more than oneecho beat was recorded after the end of procedure. Persistence of a jump withone echo beat appeared an acceptable endpoint for AVNRT cryoablation.
P1578 The high density mesh ablator technology is highlyeffective in curing from paroxysmal atrial fibrillation.A novel mesh electrode catheter for both mappingand radiofrequency delivery in a single uni
A. Meissner, G.P. Plehn, H.Y. Yeni, T.B. Butz, M.C. Christ,P.M. Maagh, M.V.B. Van Bracht, H.J.T. Trappe. University Hospital Bochum,Herne, Germany
Purpose: Interventional therapy of atrial fibrillation (AF) still is a complex proce-dure often associated with long examination- and fluoroscopy times. The use ofmapping catheters in addition to the ablation catheter requires multiple transsep-tal sheets for left atrial access.The purpose of this prospective study was to evaluate feasibility and safety ofpulmonary vein (PV) isolation using the High Density Mesh Ablator (HDMA), anovel single, expandable electrode catheter for both mapping and radiofrequency(RF) delivery at the left atrium/PV junctions.Methods: 40 patients with highly symptomatic paroxysmal AF (27, 57.5%) andpersistent AF (17, 42.5%) were studied. Segmental PV isolation via the HDMAwas performed using a customized pulsed RF energy delivery program (targettemperature 55-60 degrees, power 70-100 Watt, 600-1000 seconds RF applica-tion time/PV).Results: All 158 PV in 40 patients could be ablated by the HDMA. SegmentalPV isolation was achieved with a mean of 3.75±1.5 RF applications for a meanof 715±197 sec. Entrance conduction block was obtained in 92.7% of all PV.Mean total procedure and fluoroscopy time was 152±34 min and 28.7±9.7 minrespectively. None of the patients experienced severe acute complications. After3 month no PV stenosis was observed, 78% and 41% of the patients with PAFand persistent AF respectively were completely free of AF.Conclusions: In this first study of PV isolation using the HDMA, our findings sug-gest that this method is safe and yields good primary success rates. Anatomicalorientation and signal quality were good, allowing for excellent electrophysiologi-cal control. The HDMA simplifies the complex procedure of AF ablation, favorablyimpacting procedure and fluoroscopy times.
NON INVASIVE STUDIES
P1579 Assessment of Baroreflex sensitivity by bivariatephase-rectified signal averaging and prediction ofmortality after myocardial infarction
A. Bauer1, P. Barthel2, A. Mueller2, J. Kanters3, M. Malik4,G. Schmidt2. 1Eberhard-Karls University Tubingen, Internal
Medicine III, Department of Cardiology, Tubingen, Germany; 2I. MedizinischeKlinik, Klinikum Rechts der Isar, Technische Universität München, Munich,Germany; 3Laboratory of Experimental Cardiology, Dept. of BiomedicalSciences, University of Copenhagen, Copenhagen, Denmark; 4Division ofCardiac and Vascular Sciences, St George’s University of London, London,United Kingdom
Background: Baroreflex sensitivity (BRS) provides important prognostic informa-tion in various cardiac diseases. However, traditional methods for assessment ofspontanous BRS are limited by non-stationarities and noise. We developed thetechnique of bivariate phase-rectified signal averaging (biPRSA) and propose anovel method for assessment of spontaneous baroreflex sensitivity.Methods: The Autonomic Regulation Trial (ART study) prospectively enrolled 941consecutive survivors of acute MI presenting with sinus rhythm and aged ≤80years. All patients underwent a 30-minute recording of ECG and arterial bloodpressure (BP, Finapress) within the second week after MI. Baroreflex sensitivitywas assessed by biPRSA (BRS-PRSA) and compared with two standard meth-ods of BRS assessment, i.e. the sequence method (BRS-SEQ) and the transferfunction method (BRS-TF). Primary endpoint was total mortality within five years.Predictive power of different methods was compared by using the area under thereceiver operator characteristics curve (AUC).
Risk stratification by BRS-PRSA
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

260 Non invasive studies
Results: During follow-up, 72 patients died. BRS-PRSA was highly significantlyassociated with the primary endpoint (p<0.0001). AUC of BRS-PRSA was sig-nificantly larger (71.5±3.2) than AUC of BRS-SEQ (62.4±4.9) and BRS-TF(62.3±3.9) (p<0.0001 for both). Multivariately, predictive value of BRS-PRSA wasindependent from LVEF ≤30%, history of previous MI, age>65 years and pres-ence of diabetes mellitus.Conclusion: BRS-PRSA is a strong and independent predictor of mortality aftermyocardial infarction which yields significant advantages over standard methodsof BRS assessment.
P1581 Arrhythmogenic right ventricular cardiomyopathylong-term single centre experience: ECG,echocardiographic and MR predictors of adverseoutcome
A. Blandino1, C. Gallo2, C. Giustetto1, M. Anselmino2, M. Leuzzi1,R. Bonamini2, S. Miceli1, M. Morello2, F. Gaita2. 1Cardinal Massaia
Hospital, Department of Cardiology, Asti, Italy; 2University of Turin, San GiovanniBattista "Molinette" Hospital, Department of Cardiology, Turin, Italy
Background: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is an in-herited heart-muscle disease that primarily affects the right ventricle (RV). Pur-pose of this study is to describe ECG, echocardiographic and magnetic reso-nance (MR) parameters related to ARVC long-term prognosis.Methods and results: 67 patients (49, 73% men; mean age 48±15 years; 11,16% familiar cases) with an ARVC diagnosis, Task Force Criteria 1994, withmean follow-up of 14.5±11 years. During this period 11 (16%) patients died (3sudden cardiac deaths, 3 heart failures, 5 non-cardiac causes). Sustained ven-tricular tachycardia (SVT) was experienced by 43 (64%) patients, syncope by32 (48%); 23 (35%) patients were implanted with an ICD, 8 (12%) had abortedsudden deaths (aSD), 17 (25%) heart failures (HF), 1 (1,5%) heart transplant, 8(12%) strokes and 16 (24%) atrial fibrillation. Baseline and end of the study ECGparameters were recorded at a mean distance of 7.7±5.4 years. Registered pa-rameters changing overtime were: left anterior fascicular block (LAFB) (11% vs.20%, p=0.04), QRS duration in lead 1 (0.10 vs 0.11 ms respectively, p=0.005), Swave upstroke in leads 1-3 > 55ms (61% vs 68%, p=0.02), epsilon wave (32%vs 52%, p=0.004), r wave voltage reduction in the leads 4-6 (9.7 vs 6.9 in lead4, p=0.001; 10.3 vs 8.4 in lead 5, p=0.002; 8.7 vs 7.5 mV in lead 6 respectively,p=0.019), and T wave inversion in leads 2-5 (61% vs 63,6% in lead 2, p=0.02;52% vs 63,6% in lead 3, p=0.03; 33% vs 45% in lead 4, p=0.03; 22% vs 32% inlead 5, p=0.003). Based on the end of study ECG, r wave reduction in leads 4-6predicted long-term incidence of stroke (p=0.02 in lead 4, p=0.02 in lead 5, p=0.03in lead 6), syncope (p=0.025) and HF (p=0.024) while LAFB and inverted T wavein lead 4 related with aSD incidence (p=0.04 and p=0.04 respectively). Epsilonwave did not relate with any clinical events recorded. Based on echocardiogra-phy (n=66, 98%) right ventricular outflow dilatation predicted long-term incidenceof HF (p=0.02) and increased left ventricular diameter with aSD (p=0.001) andstroke (p=0.002). MR imaging (n=60, 89%) related left ventricular involvement ofthe disease and segmental dyskinesia with stroke (p=0.014) and HF (p=0.028).Conclusion: During a long term follow-up, patients with ARVC show high in-cidence of adverse outcomes, not only SVT, but also death, heart failure andstrokes. In addition to more complex echocardiographic and MR parameters, thesimpler ECG features, marks of disease progression as r wave voltage reductionin left precordial leads and progressive T wave inversion in lead 4, relate with aworse outcome.
P1582 Correlation between ventricular pacing andventricular arrhythmias occurrence in single anddouble chamber ICDs: preliminary results from theFIRST registry
O. Piot1, B. Degand2, M. Lopez3, P. Sbragia4, A. Da Costa5,A. Rousseau6, L. Padeletti7. 1Centre Cardiologique du Nord, St
Denis, France; 2CHU La Milétrie, Poitiers, France; 3Hôpital St Joseph & St Luc,Lyon, France; 4CHU Nord Marseille, Marseille, France; 5Université Jean MonnetSt Etienne, St Etienne, France; 6Sorin CRM SAS, Clamart, France; 7OspedaleCareggi Florence, Florence, Italy
Aims: The FIRST study is an international registry on Implantable CardioverterDefibrillator (ICD) patients (pts) designed to assess pts’ outcome and clinicalpractice over a 2 years follow up (FU). This analysis assessed the relationshipbetween Ventricular pacing (Vp) and V arrhythmias occurrence over a 3 months(M) FU according to ICD double (DR) or single (VR) chamber model.Methods: 42 european centres contributed data from 239 pts implanted fromNovember, 2007 to 2009 with an ICD. At 3M (72.9±22 days) FU, VT/VF episodeswere ascertained from device memories as sustained treated V Tachycardia (VT)and Fibrillation (VF). Pts implanted with DR (including a specific algorithm to avoidunnecessary Vp) or VR ICDs were then classified in G1 or G2 whether or not theypresented with VT/VF episode and the distribution of Vp (1st quartile Q1, median,3rd quartile Q3) was analyzed.Results: Data were available for 111 pts at 3M (65.3±11.8 yrs, 84% male, LVEF34±12%, NYHA 15% Class I, 70% Class II, 15% Class III, 56 VR/55 DR) im-planted for primary (41%) and secondary (59%) prevention. Mean %Vp was sig-nificantly higher in DR (13.9±28.0%) versus VR (3.99±18.3% – p=0.006) im-
planted pts. 8 (14.5%) DR and 2 (3.6%) VR implanted pts were classified in G1(p=0.05). %Vp distribution significantly differed between groups in VR implantedpts (0, 0.004, 0.03 in G1 and 0.5, 8.9, 17.3 in G2) (p=0.05), while no significantdifference was observed in DR implanted pts (0, 0.03, 14.3 in G1 and 0.09, 1.8,6.2 in G2).
Conclusions: In the era of DR ICD featuring specific algorithm to avoid unnec-essary Vp, significantly higher %Vp and VT/VF incidence were observed in DRversus VR implanted pts. However, VT/VF incidence was correlated to %Vp onlyin VR implanted pts. No impact of %Vp was observed in DR implanted pts.
P1583 Pulse pressure variation predicts mortality after acutemyocardial infarction
G. Schmidt1, P. Barthel1, A. Muller1, S. Schneider1, M. Malik2.1Technische Universität München, Munich, Germany; 2St George’sHospital Medical School, London, United Kingdom
Background: Increased pulse pressure (PP) is associated with increased riskof cardiovascular events but little is known about its beat-to-beat variation. Theaim of this study was to assess PP variation and its association with mortality inpost-infarction patients.Methods: 938 consecutive post-infarction patients in sinus rhythm aged ≤80years were prospectively included. Non-invasive 30-min recordings of arterialpressure (Portapres) were obtained 7±2 days after index infarction. PP varia-tion was quantified by PP standard deviation (PPSD), and PP phase rectifica-tion (PPPR) assessed by modified phase-rectified signal averaging. Figure showsPPPR examples. Follow-up period was 5 years. Primary endpoint was total mor-tality.
Results: During follow-up, 61 patients (6.5%) died. Mortality was moderately cor-related with PPSD (p<0.05) strongly correlated with PPPR (p<0.0001) but notcorrelated with the mean values of PP. High values of PPSD and PPPR indicatedincreased mortality risk. In the multivariable Cox regression adjusted for knownrisk predictors (age, history of a previous infarction, diabetes mellitus, LVEF, meanheart rate, heart rate turbulence and deceleration capacity), PPPR was signifi-cantly associated with mortality (p=0.001).Conclusions: Increased beat-to-beat pulse pressure variation is a strong andindependent predictor of mortality after myocardial infarction.
P1584 Malignant arrhythmias in patients witharrhythmogenic right ventricular cardiomyopathy arerelated to right ventricular mechanical dispersion
S.I. Sarvari1, K.H. Haugaa1, O.G. Anfinsen1, T.P. Lerent2,O.A. Smiseth1, J.P. Amlie1, T. Edvardsen1. 1Oslo University
Hospital, Rikshospitalet, Department of Cardiology, Oslo, Norway; 2OsloUniversity Hospital, Rikshospitalet, Department of medical genetics, Oslo,Norway
Background: Life-threatening ventricular arrhythmias are frequent in arrhythmo-genic right ventricular cardiomyopathy (ARVC). Electrical dispersion is a wellknown trigger of arrhythmias in these patients and may result in mechanical dis-persion (heterogeneous contraction) which can be assessed by strain echocar-diography. We hypothesised that mechanical dispersion by myocardial strain canpredict risk for ventricular arrhythmia in patients with ARVC.Methods: We included 59 patients with ARVC diagnosis based on clinical cri-teria (n=36) or genetic mutation criteria (n=23). Ventricular arrhythmia was doc-umented in 36 (61%) patients. ARVC related mutations were confirmed in 43
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Non invasive studies 261
(73%) patients, (37 PKP2, 5 DSP and 1 RYR2). Mutation was not found in 16(27%) patients. Strain was assessed by speckle tracking echocardiography. Con-traction duration (CD) was measured as time from onset R on ECG to maximumright ventricular (RV) shortening by strain. Standard deviation (SD) of CD wascalculated as a parameter of mechanical dispersion, in a 6 RV segment model.Results: Patients with arrhythmias had decreased RV function by strain (-19±7%) compared to those without (-24±5%, p<0.05). RV mechanical disper-sion in patients with arrhythmias was substantially increased compared to thosewithout (53±25ms vs 33±20ms, p<0.05). Fig. shows increased mechanical dis-persion in an ARVC patient with arrhythmias.
Mechanical dispersion in ARVC patients
Conclusion: RV mechanical dispersion assessed by strain was increased andRV strain was decreased in ARVC patients with arrhythmias. These novel markersmay become important tools in risk stratification of ARVC patients.
P1585 Clinical characteristics and referral patterns of theBrugada population in a UK tertiary cardiac centre
L.M. Nunn, J. Bhar-Amato, M.D. Lowe, P.M. Elliott, W.J. Mckenna,P.D. Lambiase. The Heart Hospital, University College Hospital &Institute of Cardiovascular Sciences, UCL, London, United Kingdom
Purpose: To audit the Brugada patient population seen in a tertiary cardiac centrein the UK.Methods: Retrospective analysis of specialist arrhythmia and Sudden ArrhythmicDeath (SADS) clinic referrals.Results: 95 patients were diagnosed with Brugada syndrome. Mean follow-up1.9 yrs. 15% of those genetically tested had pathological SCN5A mutation. Table1 presents the demographics and clinical characteristics of each group of Bru-gada patients based upon referral route. 6 patients had Type 1 ECG changes inhigh leads only during drug provocation (standard leads negative). 28 patientsreceived an ICD. 1 received an appropriate shock for VF (cardiac arrest survivor)and there were no inappropriate shocks. A further 2 patients had non-sustainedVT (both received implant for a positive VT stimulation study in asymptomatictype 1 patients.) 14% complication rate: 1 system extraction for infection, 2 pa-tients underwent lead revision for lead fracture and noise respectively and 1 pa-tient RV lead perforation. Those positive for a pathological SCN5A mutation hadsignificantly longer PR interval than those testing negative (p=0.005).
Table 1. Demographics and clinical characteristics of Brugada patients grouped by referralmethod
Cardiac 1st degree Incidental Assessment Family Familyarrest relatives of ECG of cardiac screening screening
survivors SADS victims finding symptoms of survivors
Total no. 7 39 13 12 20 4% male 71 20 77 75 25 75Mean age yrs 50 44 56 43 41 46Spontaneous type 1
ECG % 28 0 23 50 0 0Spontaneous type 2
ECG % 0 0 30 0 5 25Ajmaline type 1
response % 83 59 64 100 63 75Ajmaline type 2
response % 17 38 36 0 16 25Ajmaline type 1 on high
lead recording % 0 3 0 0 21 0Infero-lateral early
repolarisation % 29 24 8 20 41 25
Conclusions: 1. There is a high incidence of type 1 ECG (spontaneous or drugprovocation) in those assessed for cardiac symptoms & Low incidence of spon-taneous type 1 ECG in family screening (of SADS relatives, survivors or knownBrugada cases). 2. A significant proportion had infero-lateral J point elevation. 3.Despite 1 ICD patient receiving appropriate therapy, there was a significant ICDmorbidity.
P1586 The artery of the left atrial lateral ridge detected bymultidetector computed tomography: a potentialcause of atrial fibrillation recurrence after pulmonaryvein catheter isolation
G. Pizarro1, D. Sanchez-Quintana2, M. Murillo2, E. Gonzalez-Caballero1, B. Fuertes1 , S. Bayona1, V. Martinez1, J.A. Cabrera1. 1HospitalQuiron-Madrid. Universidad Europea de Madrid, Madrid, Spain; 2University ofExtremadura, Department of Anatomy and Cell Biology, Badajoz, Spain
Purpose: Recovery of the left atrium-pulmonary vein conduction is the majorcause of atrial fibrillation (AF) recurrence after catheter ablation. As previouslyreported by anatomical studies, the lateral ridge (LR) is located between the leftatrial appendage (LAA) and the left superior pulmonary vein (LSPV). Occasion-ally, there is an artery following the course of the LR, which can be a cause ofunablated gaps due to flow-mediated convective tissue cooling.Methods: A prospectively acquired 64-Slice Computed Tomography Angiographywas performed in 60 consecutive patients (mean age 57±6 years, 43 males).We analyzed the presence and anatomical characteristics of the LR artery. Itsrelationship with the sinoatrial node (SAN) artery was also evaluated.Results: The LR artery was identified in 20 cases (33%). This vessel was abranch of the circunflex artery in all cases, 8 from the proximal segment and12 from the distal segment. The presence of this vessel was not related to thecoronary dominance (91% right dominant) nor the presence of atherosclerosis(58%). The minimal distance between the LR artery and the LSPV endocardiumwas 1.33 mm (Range: 0.6 to 5.3) (Figure). Among patients in whom a LR arterywas identified, the SAN artery was a branch of the LR artery in 65% (S-shapedartery), whereas it arose from another branch of the left circunflex in 15% andfrom the right coronary artery in 20%.
Left atrium lateral ridge artery
Conclusions: The lateral ridge artery detected by Multi-Slice Computed Tomog-raphy has not been previously analized. It could be a common cause of AF recur-rence after catheter ablation due to a flow-mediated cooling effect.
P1587 Sinus-node modulation with ivabradine in patientswith inappropriate sinus tachycardia
J. Borbola, P. Abraham. Gottsegen György Hungarian Institute ofCardiology, Budapest, Hungary
Purpose: Inappropriate sinus-node tachycardia (IST) is a rare dis-ease defined as increased heart rate at rest and/or inadequate response to phys-ical or emotional stress. The aim of this study was to investigate the If-channelblocker ivabradine in IST.Methods: In the last years, 15 patients (13 women, 2 men; age: 19-57 (30±3)years) with IST were treated with ivabradine due to palpitations. Patients hadno structural heart disease (LVEF: 66±2%), TSH values were within normal lim-its, but resting heart rates were repeatedly high: 105±3/min. Standard 24-hoursHolter monitorings and excercise tests were performed.Results: Holter recordings (expressed as minimal-maximal and average heartrate/min) without medication showed high heart rate values: 58±2 -171±4 -96±2/min. The bicycle ergometry showed an average exercise capacity of 106±6W (heart rate: control (C):114±7/min, top (T):174±8/min). The ivabradine de-creased the heart rate significantly and dose-dependently compared to controlvalues: ivabradine 5 mg b.i.d.: 50±2 -131±5 -76±2/min (p<0.001), ivabradine7.5 mg b.i.d.: 50±2 -128±9 -71±3/min (p<0.001). Ivabradine improved the ex-ercise capacity of IST patients: ivabradine 5 mg b.i.d.: 112±6 W (ns) heart rate:C: 87±5/min (p<0.005), T:142±6 (p<0.001), ivabradine 7.5mg b.i.d.: 138±7 W(p<0.001) heart rate: C: 72±2/min (p<0.001), T: 134±12/min (p<0.03) and de-creased the heart rate frequencies. The ivabradine treatment was well tolerated,there was no sinus bradicardiac episode.Conclusions: Based on our clinical experiences, IST can be treated with thesinoatrial node modulator drug ivabradine successfully and safely. Ivabradine sig-nificantly decreased, improved the heart rate ferquency spectrum not only duringHolter monitoring, but also during exercise test. The disadvantage of the ivabra-dine is the lack of approval for IST therapy. The ivabradine treatment might beconsidered as an alternetive to the invasive transcatheter radiofrquency modifi-cation of the sinus-node with the inherent risk of pacemaker implantation.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
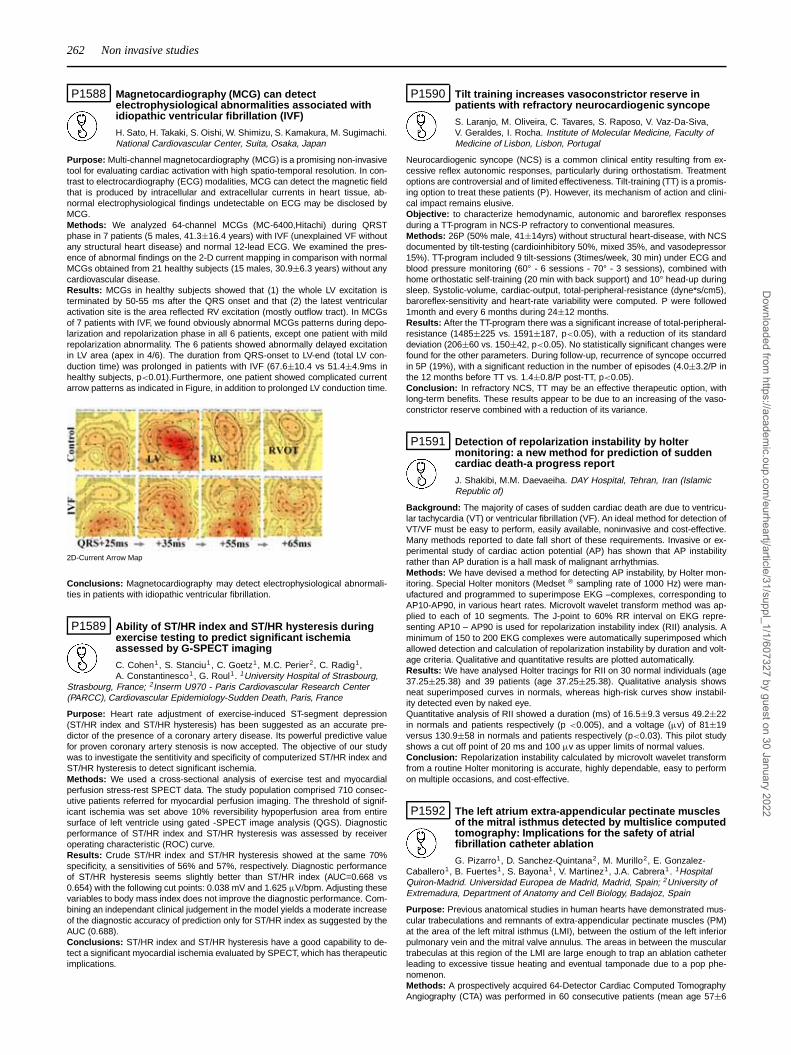
262 Non invasive studies
P1588 Magnetocardiography (MCG) can detectelectrophysiological abnormalities associated withidiopathic ventricular fibrillation (IVF)
H. Sato, H. Takaki, S. Oishi, W. Shimizu, S. Kamakura, M. Sugimachi.National Cardiovascular Center, Suita, Osaka, Japan
Purpose: Multi-channel magnetocardiography (MCG) is a promising non-invasivetool for evaluating cardiac activation with high spatio-temporal resolution. In con-trast to electrocardiography (ECG) modalities, MCG can detect the magnetic fieldthat is produced by intracellular and extracellular currents in heart tissue, ab-normal electrophysiological findings undetectable on ECG may be disclosed byMCG.Methods: We analyzed 64-channel MCGs (MC-6400,Hitachi) during QRSTphase in 7 patients (5 males, 41.3±16.4 years) with IVF (unexplained VF withoutany structural heart disease) and normal 12-lead ECG. We examined the pres-ence of abnormal findings on the 2-D current mapping in comparison with normalMCGs obtained from 21 healthy subjects (15 males, 30.9±6.3 years) without anycardiovascular disease.Results: MCGs in healthy subjects showed that (1) the whole LV excitation isterminated by 50-55 ms after the QRS onset and that (2) the latest ventricularactivation site is the area reflected RV excitation (mostly outflow tract). In MCGsof 7 patients with IVF, we found obviously abnormal MCGs patterns during depo-larization and repolarization phase in all 6 patients, except one patient with mildrepolarization abnormality. The 6 patients showed abnormally delayed excitationin LV area (apex in 4/6). The duration from QRS-onset to LV-end (total LV con-duction time) was prolonged in patients with IVF (67.6±10.4 vs 51.4±4.9ms inhealthy subjects, p<0.01).Furthermore, one patient showed complicated currentarrow patterns as indicated in Figure, in addition to prolonged LV conduction time.
2D-Current Arrow Map
Conclusions: Magnetocardiography may detect electrophysiological abnormali-ties in patients with idiopathic ventricular fibrillation.
P1589 Ability of ST/HR index and ST/HR hysteresis duringexercise testing to predict significant ischemiaassessed by G-SPECT imaging
C. Cohen1, S. Stanciu1, C. Goetz1, M.C. Perier2, C. Radig1,A. Constantinesco1, G. Roul1. 1University Hospital of Strasbourg,
Strasbourg, France; 2Inserm U970 - Paris Cardiovascular Research Center(PARCC), Cardiovascular Epidemiology-Sudden Death, Paris, France
Purpose: Heart rate adjustment of exercise-induced ST-segment depression(ST/HR index and ST/HR hysteresis) has been suggested as an accurate pre-dictor of the presence of a coronary artery disease. Its powerful predictive valuefor proven coronary artery stenosis is now accepted. The objective of our studywas to investigate the sentitivity and specificity of computerized ST/HR index andST/HR hysteresis to detect significant ischemia.Methods: We used a cross-sectional analysis of exercise test and myocardialperfusion stress-rest SPECT data. The study population comprised 710 consec-utive patients referred for myocardial perfusion imaging. The threshold of signif-icant ischemia was set above 10% reversibility hypoperfusion area from entiresurface of left ventricle using gated -SPECT image analysis (QGS). Diagnosticperformance of ST/HR index and ST/HR hysteresis was assessed by receiveroperating characteristic (ROC) curve.Results: Crude ST/HR index and ST/HR hysteresis showed at the same 70%specificity, a sensitivities of 56% and 57%, respectively. Diagnostic performanceof ST/HR hysteresis seems slightly better than ST/HR index (AUC=0.668 vs0.654) with the following cut points: 0.038 mV and 1.625 μV/bpm. Adjusting thesevariables to body mass index does not improve the diagnostic performance. Com-bining an independant clinical judgement in the model yields a moderate increaseof the diagnostic accuracy of prediction only for ST/HR index as suggested by theAUC (0.688).Conclusions: ST/HR index and ST/HR hysteresis have a good capability to de-tect a significant myocardial ischemia evaluated by SPECT, which has therapeuticimplications.
P1590 Tilt training increases vasoconstrictor reserve inpatients with refractory neurocardiogenic syncope
S. Laranjo, M. Oliveira, C. Tavares, S. Raposo, V. Vaz-Da-Siva,V. Geraldes, I. Rocha. Institute of Molecular Medicine, Faculty ofMedicine of Lisbon, Lisbon, Portugal
Neurocardiogenic syncope (NCS) is a common clinical entity resulting from ex-cessive reflex autonomic responses, particularly during orthostatism. Treatmentoptions are controversial and of limited effectiveness. Tilt-training (TT) is a promis-ing option to treat these patients (P). However, its mechanism of action and clini-cal impact remains elusive.Objective: to characterize hemodynamic, autonomic and baroreflex responsesduring a TT-program in NCS-P refractory to conventional measures.Methods: 26P (50% male, 41±14yrs) without structural heart-disease, with NCSdocumented by tilt-testing (cardioinhibitory 50%, mixed 35%, and vasodepressor15%). TT-program included 9 tilt-sessions (3times/week, 30 min) under ECG andblood pressure monitoring (60° - 6 sessions - 70° - 3 sessions), combined withhome orthostatic self-training (20 min with back support) and 10° head-up duringsleep. Systolic-volume, cardiac-output, total-peripheral-resistance (dyne*s/cm5),baroreflex-sensitivity and heart-rate variability were computed. P were followed1month and every 6 months during 24±12 months.Results: After the TT-program there was a significant increase of total-peripheral-resistance (1485±225 vs. 1591±187, p<0.05), with a reduction of its standarddeviation (206±60 vs. 150±42, p<0.05). No statistically significant changes werefound for the other parameters. During follow-up, recurrence of syncope occurredin 5P (19%), with a significant reduction in the number of episodes (4.0±3.2/P inthe 12 months before TT vs. 1.4±0.8/P post-TT, p<0.05).Conclusion: In refractory NCS, TT may be an effective therapeutic option, withlong-term benefits. These results appear to be due to an increasing of the vaso-constrictor reserve combined with a reduction of its variance.
P1591 Detection of repolarization instability by holtermonitoring: a new method for prediction of suddencardiac death-a progress report
J. Shakibi, M.M. Daevaeiha. DAY Hospital, Tehran, Iran (IslamicRepublic of)
Background: The majority of cases of sudden cardiac death are due to ventricu-lar tachycardia (VT) or ventricular fibrillation (VF). An ideal method for detection ofVT/VF must be easy to perform, easily available, noninvasive and cost-effective.Many methods reported to date fall short of these requirements. Invasive or ex-perimental study of cardiac action potential (AP) has shown that AP instabilityrather than AP duration is a hall mask of malignant arrhythmias.Methods: We have devised a method for detecting AP instability, by Holter mon-itoring. Special Holter monitors (Medset ® sampling rate of 1000 Hz) were man-ufactured and programmed to superimpose EKG –complexes, corresponding toAP10-AP90, in various heart rates. Microvolt wavelet transform method was ap-plied to each of 10 segments. The J-point to 60% RR interval on EKG repre-senting AP10 – AP90 is used for repolarization instability index (RII) analysis. Aminimum of 150 to 200 EKG complexes were automatically superimposed whichallowed detection and calculation of repolarization instability by duration and volt-age criteria. Qualitative and quantitative results are plotted automatically.Results: We have analysed Holter tracings for RII on 30 normal individuals (age37.25±25.38) and 39 patients (age 37.25±25.38). Qualitative analysis showsneat superimposed curves in normals, whereas high-risk curves show instabil-ity detected even by naked eye.Quantitative analysis of RII showed a duration (ms) of 16.5±9.3 versus 49.2±22in normals and patients respectively (p <0.005), and a voltage (μv) of 81±19versus 130.9±58 in normals and patients respectively (p<0.03). This pilot studyshows a cut off point of 20 ms and 100 μv as upper limits of normal values.Conclusion: Repolarization instability calculated by microvolt wavelet transformfrom a routine Holter monitoring is accurate, highly dependable, easy to performon multiple occasions, and cost-effective.
P1592 The left atrium extra-appendicular pectinate musclesof the mitral isthmus detected by multislice computedtomography: Implications for the safety of atrialfibrillation catheter ablation
G. Pizarro1, D. Sanchez-Quintana2, M. Murillo2, E. Gonzalez-Caballero1, B. Fuertes1 , S. Bayona1, V. Martinez1, J.A. Cabrera1. 1HospitalQuiron-Madrid. Universidad Europea de Madrid, Madrid, Spain; 2University ofExtremadura, Department of Anatomy and Cell Biology, Badajoz, Spain
Purpose: Previous anatomical studies in human hearts have demonstrated mus-cular trabeculations and remnants of extra-appendicular pectinate muscles (PM)at the area of the left mitral isthmus (LMI), between the ostium of the left inferiorpulmonary vein and the mitral valve annulus. The areas in between the musculartrabeculas at this region of the LMI are large enough to trap an ablation catheterleading to excessive tissue heating and eventual tamponade due to a pop phe-nomenon.Methods: A prospectively acquired 64-Detector Cardiac Computed TomographyAngiography (CTA) was performed in 60 consecutive patients (mean age 57±6
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Non invasive studies 263
years, 43 males). We analyzed the presence and anatomical characteristics ofthe extra-appendicular PM along the LMI.Results: In 20 cases (33%), the anterior ostial margin of the left atrial appendage(LAA) did not present as a clear-cut border and muscular trabeculations werefound extending inferiorly from the LAA to the vestibule of the mitral valve. Theywere all located at the posterior LA wall, extending to the mitral valve (Figure).The average distance between the PM and the ostium of the LAA was 11,9 mm(Range 3,9 to 31 mm). The regions in between the extra-appendicular PM werefound to have a thinner wall, compared to the rest of the LA posterior wall.
Extra-appendicular pectinate muscles
Conclusions: The detection of extra-appendicular posterior pectinate musclesby Multidetector CTA has not been previously reported. This information could berelevant to perform the procedures of atrial fibrillation ablation more safely.
P1593 Multiresolution wavelet analysis of heart ratevariability predicts total mortality in heart failurepatients
P. Arsenos1, K. Gatzoulis1, G. Manis2, P. Dilaveris1,E. Kartsagoulis3, K. Masoura1 , L. Raftopoulos1, D. Tsiachris1,G. Lazaros1, C. Stefanadis1 . 1First Department of Cardiology,
Medical School, National & Kapodistrian University of Athens, Athens, Greece;2Department of Computer Science,University of Ioannina, Ioannina, Greece;3Cardiology Department, Thriasio General Hospital, Elefsina, Greece
Purpose: To evaluate the scale dependent wavelet-coefficient standard deviation[σwav (m)] of Multiresolution wavelet analysis (MWA) in comparison to the con-ventional non invasive Electrophysiological indices as Total Mortality (TM) predic-tors in Heart Failure (HF) patients (pts).Methods: MWA method decomposes the ECG signal into several scales. Thestandard deviation of each one of those scales was computed. "Haar" waveletand 8th scale was used for MWA. We screened 172 HF pts (age: 65.6±13.4,male: 84%, Left Ventricular Ejection Fraction (LVEF): 31.9±10.1, NYHA: 2.3±0.5,CAD: 83%, DCMP: 17%) under optimum treatment with ECG, SAECG, ECHOand 24 hours HOLTER. After 15.0±13.4 months of follow up, 29 deaths occurred(Sudden Cardiac: 11, Pump Failure: 12, Non Cardiac: 6). Statistical analysis wasperformed with Log rank test. The correlation of the non invasive markers withTM was analyzed through survival analysis method utilizing Kaplan Meier curvesadjusted for possible confounders under building of appropriate Cox statisticalmodels.Results: In univariate analysis σwav was a statistically significant predictor of TM(Logrank p=0.001). Furthermore, after Cox regression analysis adjusted for gen-der, age, LVEF, fQRS from SAECG, ventricular premature beats (VPBs/24 hours),NSVT episodes/24 hours, QTc, SDNN from heart rate variability analysis (HRV),σwav remained the most significant and independent predictor of TM [HR:0.990,(p=0.004, 95%CI:0.984-0.997)].Conclusions: MWA may predict TM in HF patients significantly and in-dependently of gender, age, LVEF, SAECG fQRS, VPBs/24hours, NSVTepisodes/24hours, QTc and SDNN from HRV analysis. A cut off point of σwav<
233ms (50% percentile) presented sensitivity of 75%, specificity of 55%, positivepredictive value: 26% and negative predictive value:92% for predicting TM in thispreliminary HF patients sample.
P1594 Influence of different atrial lead positions oninteratrial and atrioventricular conduction andpercentage of ventricular stimulation in populationwith SSS treated by atrioventricular pacing
P. Skoczynski, A. Slawuta, J. Gajek, A. Mysiak. Wroclaw MedicalUniversity, Department of Cardiology, Wroclaw, Poland
Background: Many patients with sick sinus syndrome (SSS) suffer from intera-trial and atrioventricular conduction disorder, what often leads to atrial fibrillation.Atrial lead localization may be very important in this population. Implantation ofatrial lead in right atrium appendage is the reason of longer time of interatrial andatrioventricular conduction even in patients without prior interatrial and atrioven-tricular conduction disorder. Such a situation may be the cause of higher per-centage of ventricular stimulation and its hemodynamic consequence which mayprognose atrial fibrillation development, especially in population with preservedventriculoatrial conduction.Purpose: The aim of this study was to assess influence of atrial pacing site on in-
teratrial and atrioventricular conduction and percentage of ventricular stimulationin population with SSS without prior atrioventricular conduction disorder treatedby atrioventricular pacing.Methods: The study group consisted of 66 patients (40 F, 26 M) aged 69,6±16,7years. Patients were divided in two groups: group 1 (n=36) with right atrium ap-pendage stimulation, group 2 (n= 30) with Bachman area stimulation. Differencesin atrioventricular conduction in sinus heart rate and AAI 60 and 90/min pacingwere assessed. Also width of P wave at sinus rate and during atrial pacing as wellas percentage of ventricular stimulation were compared.Results: The differences between atrioventricular conduction time during sinusrate and atrial pacing at 60 and 90/min were significantly bigger in patients withthe right atrium appendage stimulation (35±16,5 vs 3±6,7 ms p<0.005 and60±30,5 vs 22±11,4 ms p<0,005).P wave duration in atrial stimulation was longer (141,7±24,6 vs 113±14,9 msp<0,005) and percentage of ventricular stimulation was grater (0,17±0,1 vs0,04±0,03) in group 1.Conclusions: 1.The localization of the artial lead in Bachman area causes lessinteratrial conduction disorder than in right atrium appendage.2. Right atrium appendage pacing in SSS leads to more pronounced atrioven-tricular conduction disorder and the rise of the percentage of ventricular pacin inDDD mode.
P1595 Effects of cardiac resynchronization therapy onmyocardial contractile reserve during exercise
C. Valzania1, F. Gadler2, G. Boriani1, M.J. Eriksson3. 1UniversityHospital Polyclinic San Orsola-Malpighi, Department of Cardiology,Bologna, Italy; 2Karolinska University Hospital, Department of
Cardiology, Stockholm, Sweden; 3Karolinska University Hospital, Department ofClinical Physiology, Stockholm, Sweden
Background: Myocardial Contractile Reserve (MCR) is a marker of myocardialviability. To date, the impact of Cardiac Resynchronization Therapy (CRT) onMCR during exercise has been little studied.Aim: To investigate the effects of CRT on global and regional MCR by exerciseechocardiography.Methods: Twenty-seven CRT responders (81% men, 63±9 yr, 56% ischemic)were assessed by echocardiography during rest and supine bicycle exercise. Im-ages were acquired during spontaneous rhythm ("off") and active CRT ("on").Global MCR was expressed as the change (�) in left ventricular ejection fraction(LVEF) and aortic velocity-time integral (VTI) from rest to exercise. Regional MCRwas expressed as the rest-to-exercise change in peak systolic tissue velocity (Sm)of the basal and mid interventricular septum and lateral wall.Results: LVEF and aortic VTI increased during "on" at rest and during exercise,and the improvement in global MCR during exercise was higher during "on" than"off" (� LVEF 6±6 vs. 3±3%, p=0.009; � aortic VTI 2.9±2.1 vs. 1.9±1.8 cm,p=0.036). Septum Sm increased during "on" at rest (p=0.01), and it was stillhigher during exercise (p≤0.01 vs. "off"), although the change from rest to ex-ercise was similar during "on" and "off". Lateral wall Sm did not change at restduring "on", but basal lateral wall MCR during exercise was higher at "on" than"off" (p=0.036). Ischemic and non ischemic patients showed a similar increasein LVEF during exercise. Regional MCR of the basal septum was higher during"on" in non ischemic than in ischemic patients (� basal septum Sm 1.0±0.7 vs.0.5±0.5 cm/s, p = 0.05).Conclusion: Chronic response to CRT is characterized by a pacing-dependentincrease in global MCR during exercise. The changes in regional MCR of the sep-tum and the lateral wall tend to have different patterns. These factors may help tounderstand the determinants of improved exercise tolerance in CRT responders.
P1596 The value of beat-to-beat variability of repolarisationand T-wave alternans as markers for arrhythmogenicremodeling early after myocardial infarction in a pigmodel
V. Flore1, P. Claus2, G. Antoons1, K. Sipido1, R. Willems1.1Catholic University of Leuven, Department of Cardiology, Leuven, Belgium;2Catholic University of Leuven, Dept Cardiovascular Dis., Division Imaging &Cardiovascular Dynamics, Leuven, Belgium
Introduction: The temporal variability of repolarisation is an interesting conceptin the non-invasive risk stratification for sudden cardiac death (SCD). T-wave alter-nans (TWA) has been subject of exhaustive research but lacks sufficient supportfor clinical application. Beat-to-beat variability of repolarisation (BVR) is a newparameter quantifying repolarisation variability and is also linked with arrhythmia.We investigated TWA and BVR in a pig model of myocardial infarction.Methods: In 9 (MI) pigs the mid-LAD coronary artery was balloon-occluded for 1h. We studied 6 (SHAM) pigs as control. TWA was tested with the spectral methodduring right atrial pacing before and 21 days after myocardial infarction. A cardiacmagnetic resonance (CMR) scan was made on day 21. BVR was quantified asshort-term variability (STV) of 60 consecutive QT and RR intervals obtained bymanual measurement on 1kHz Holter ECG recordings.Results: CMR showed a transmural ischemic myocardial infarction with an infarctsize of 21.1±4.4% and a decreased LVEF (36.8±7.8%). At the clinical thresholdfor TWA testing (110/min), in none of the pigs TWA was positive. At higher pacing
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

264 Non invasive studies
rates a physiological increase in TWA was seen in both MI and SHAM pigs (55 vs50%, p = 0.79).In the MI group, before and during acute ischemia there was a significant increasein STV QT at intrinsic rhythm (2.44±0.43 vs. 3.55±0.41 msec., p<0.001). Onday 21 STV QT had increased even more (5.80±1.2 msec.). Before instrumen-tation, there was no difference in STV QT between both groups (2.44±0.43 vs.2.42±0.52 msec. p=0.95). On day 21 STV QT in the MI was significantly higherthan in the SHAM (5.80±1.2 msec. vs. 2.14±0.54 msec. p=0.002).A clinical VT induction protocol was positive in 2 of 9 MI pigs and in none of the6 SHAM pigs. When plotting the individual results for STV QT at intrinsic rhythmand paced rates, we see that STV in MI pigs is clearly distinct from the SHAMpigs with almost no overlap. The STV values of the inducible pigs are amongstthe highest of the MI group.Conclusions: In the early phase after an acute myocardial infarction with mod-erate infarct size, BVR measured on ECG tracings is a consistent phenomenon,whereas TWA is not. The prognostic meaning of BVR remains unknown but ourdata might indicate usefulness for predicting arrhythmia in the early post-infarctperiod, during which the risk of sudden cardiac death is known to be the highest.
P1597 Heart rate turbulence indices identify risk of mortalityafter acute myocardial infarction
B. Sredniawa, A. Musialik-Lydka, J. Kowalczyk, A. Sliwinska,A. Wozniak, S. Cebula, A. Sedkowska, A. Krawczynska, Z. Kalarus.Department of Cardiology, Medical University of Silesia, Silesian
Center for Heart Diseases, Zabrze, Poland
Heart rate turbulence (HRT), closely related to baroreflex sensitivity, is a newfactor in the identifying patients being at high risk of sudden cardiac death (SCD).The aim of the study was to assess the relation between the type of HRT in-dices and mortality in 2 years follow-up in patients after optimally treated acutemyocardial infarction (MI).Methods: Study group consisted of 270 pts (94F, 176M, mean age 60±11 years)with acute MI. All patients were treated invasively just after admission. In 223pts STEMI and in 47 NSTEMI was present. During 2 years follow-up 16 (6%)pts died due to any cause. In all pts in 5th (mean) day of MI 24 hours Holtermonitoring was performed. After arrhythmia analyze, following HRT parametersusing HRTView program were calculated: turbulence onset – TO [%] and turbu-lence slope [ms/RR interval]. Values of TO≥0% and TS≤2.5 ms/RR interval wereassumed as correlated with increased risk of SCD and therefore as abnormal.Results: In the group of pts who died during 2 years follow-up significantly greaterpercentages of pts with abnormal TO (81.3 vs 26.8%; p<0.001) and TS (62.5 vs22.4%; p<0.001) were present, as well as both abnormal HRT parameters werenoted (43.8 vs 11.8%; p<0.001). Significantly lower percentage of pts with both(TO and TS) parameters survived 2 years follow-up than patients with at least one(TO or TS) normal parameter (22% vs 94%; p<0.005) respectively.
Conclusions: The presence of both abnormal HRT parameters early after op-timally treated acute MI indicate on high risk of mortality in long-term follow-up.Patients with at least one normal HRT index are characterized by favorable out-come after MI.
P1598 The diagnostic value of adenosine test in sick sinussyndrome is affected by a history of syncope orpresyncope
N. Fragakis1 , A. Antoniadis2, P. Kyriakoy1, V. Skeberis1,G. Katsaris2, P. Geleris1. 1Hippokration Hospital, 2nd Propedeutic
Department, Cardiology Unit, Thessaloniki, Greece; 2General Hospital G.Papanikolaou, 2nd Department of Cardiology, Thessaloniki, Greece
Purpose: We sought to investigate the diagnostic value of adenosine test inthe identification of sick sinus syndrome (SSS) in relation to a history of syn-cope/presyncope.Methods: We investigated 28 patients with SSS and history of syncope/presyn-cope (group A) and 10 with SSS without history of syncope/presyncope (groupB). Controls for group A were 7 subjects with syncope of unknown origin while
for group B 15 subjects who underwent electrophysiological testing for other in-dications. Corrected sinus node recovery time after intravenous adenosine (0.15mg/kg) was determined and values >525msec were considered abnormal.Results: Adenosine test showed high specificity for SSS diagnosis in bothgroups, with intermediate negative predictive values. The test sensitivity was no-tably higher in group A as well as its positive predictive value (Table 1).
Table 1. Diagnostic indices of adenosine test in the identification of SSS in patients with (GroupA) vs without (Group B) history of syncope/presyncope
Group A Group B
Sensitivity 79% 30%Specificity 100% 87%Positive Predictive Value 100% 60%Negative Predictive Value 54% 65%
Conclusion: A positive adenosine test is highly specific for SSS, irrespectiveof syncope/presyncope. However, ruling out SSS by means of a negative resultwould be much more accurate in the presence of syncope/presyncope.
P1599 A novel magnetocardiographic approach forestimating the whole ventricular activation with useof 3-directional measurements
S. Kawakami, H. Takaki, S. Oishi, H. Sato, W. Shimizu, S. Kamakura,M. Sugimachi. National Cardiovascular Center, Suita, Osaka, Japan
Background: Multichannel magnetocardiography (MCG) is a potentially usefulnoninvasive tool for evaluating cardiac activation with high spatio-temporal reso-lution. However, 2-D mapping obtained by a standard method over anterior chestalone may not provide sufficient information to estimate the whole heart activation(especially in the posterior site of heart), because magnetic fields rapidly decaywith distance.Methods: Using a MCG system (Hitachi) with 64-channel magnetic sensors, werepeated 3 measurements (1-ms sampling) with sensors placed close to anterior,posterior, and left lateral chest wall (in the supine, prone, and lateral decubituspositions, respectively) in 25 healthy volunteers. We averaged MCG signals (>20beats) with simultaneously digitized ECG, which was used to synchronize 2-Dcurrent arrow QRS maps for each measurement.Results: During the ventricular activation in all subjects, we found 3 distinct car-diac currents. Left lateral mapping was particularly useful for the recognition. Af-ter early rightward anterior-directed currents (corresponding to "septal activation",Max at 17±4 ms after QRS onset), we could observe two different currents virtu-ally simultaneously arising from separate sites; anterior downward- and posteriorupward-propagating currents (appearing at 27±4, and 26±4 ms, respectively). LVactivation was promptly completed at 51±5 ms, followed by RV activation (totalQRS duration = 89±6 ms).
Representative Maps (Anterior & Lateral)
Conclusions: We, for the first time to our knowledge, noninvasively visualized thetwo separate electrical propagations in the left ventricle arising from left anteriorand posterior fascicles. This MCG approach allows accurate estimation of thewhole ventricular activation with high spatio-temporal resolution, possibly servingto identify arrhythmogenic substrates.
P1600 Detection of the Ca2+ overload in patients presentingwith delayed aftedepolarization using cardiacmagnetic field mapping at rest
V.M. Sosnytskyy1, L.A. Stadnyuk2, T.V. Sosnytska2. 1NationalScientific Center "M.D. Strazhesko Institute of Cardiology, MAS
of Ukraine", Kiev, Ukraine; 2P.L. Shupik Medical Academy for PostgraduateEducation, Kiev, Ukraine
Purpose: Human ventricular cells studies have shown that the Na+/Ca2+ ex-change current (INa/Ca) contribute to the transient inward current (Iti). Iti is re-sponsible for the proarrhythmic delayed afterdepolarizations (DADs). AlthoughDADs are generally accepted to be Ca2+-dependent, the relationship betweensarcoplasmic reticulum Ca2+ release and DAD amplitude has not been mea-sured, partly because the underlying Ca2+ -activated currents are hard to con-trol. The overall objective of the present study was to demonstrate the efficacy ofmagnetocardiography (MCG) in the diagnosis of the Ca2+ overload in an area ofthe heart in patients presenting with DADs.Methods: Standard clinical examination (e.g. Tissue Doppler echocardiograms,
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Non invasive studies / Electrocardiography 265
12-channel ECG, 24-h Holter monitoring) and MCG were performed in 24 patients(age 27±1.9) affected by DADs and 22 (age 25±2.5) healthy controls. MCG wasrecorded by means of 4x3–channel MCG system in an unshielded setting. Cur-rent density vector (CDV) maps were plotted by the magnetic moments methodof the "inverse problem solution". MCG based indices, namely direction of thelargest CDV, its deviation and shift, current density total sum and maximum valueof current density vectors during Tpeak-Tend and electric diastole intervals wereperformed utilizing an automated MCG analysis program.Results: Two MCG based indices showed a significant difference between DADspatients and the control group. Although Tpeak-Tend interval was shortened inpatients presenting with DADs they had additional current density peak duringelectric diastole interval. We localized and visualized the current source distribu-tion corresponding to the Ca2+ -activated currents successfully. If such currentreaches threshold, it induces the onset of a focal extrasystole. We also foundeffect of verapamil, the prototype calcium-channel blocker, on these indices inDADs patients.Conclusion: We conclude MCG is a promising procedure for a non-invasive test-ing as well as screening method as for localization of an area of the heart withthe Ca2+ overload which provides a substrate that favors electrical abnormalitiesand might initiate a focal extrasystole.
P1601 P wave dispersion and atrial electromechanical delayin patients with prehypertension
N. Ermis, N. Acikgoz, E. Yasar, H. Tasolar, H. Atas, H. Pekdemir,J. Yagmur, M. Cansel, R. Ozdemir. Inönü University, Turgut ÖzalMedical Center, Malatya, Turkey
Purpose: Prolonged P wave dispersion (PWD) and intra/inter-atrial electrome-chanical delay estimated by tissue Doppler imaging (TDI) is related to develop-ment of atrial fibrillation. In our study, we aimed to evaluate intra-atrial and inter-atrail conduction times in patients with prehypertension by PWD and TDI.Methods: 46 prehypertensive patients (56.5±12.3 years) and normotensive con-trols (55.8±11.7 years) recruited to the study. The difference between the maxi-mum (Pmax) and minimum P wave durations was calculated and defined as PWD.Using TDI, atrial electromechanical coupling (PA) was measured from the lateralmitral annulus (lateral PA), septal mitral annulus (septum PA), and right ventriculartricuspid annulus (tricuspid PA).Results: Maximum P wave duration (Pmax) and PWD were prolonged accordingto the controls (p<0.001, p<0.001). Atrial electro mechanic coupling intervalsmeasured at lateral (lateral PA) and septal mitral annulus (septal PA) were delayedin prehypertensive group compared to the controls (p <0.001, p=0.0021). Bothof inter-atrial (lateral PA – tricuspid PA) and intra-atrial (septal PA – tricuspid PA)conduction times were delayed in prehypertensive group according to the controls(p<0.001, p=0.008).
Table 1. Electrocardiographic and echocardiographic findings of patients with prehypertensionand controls
Prehypertensive patientsn (46) Controls n (39) p value
Heart rate (beat per minute) 78.6±11.3 80.1±12.7 NSPmax (ms) 110.1±13.8 91.4±7.7 <0.001Pmin (ms) 54.4±10.7 55.1±5.3 NSPWD (ms) 55.7±11.1 36.8±5.7 <0.001Left atrium diameter (mm) 35.4±4.7 34.3±4.9 NSLateral PA (ms) 76.5±10.1 65.4±10.4 < 0.001Septal PA (ms) 59.0±6.4 53.5±7.5 0.02Tricuspid PA (ms) 49.8±7.6 48.1±6.4 NSLateral PA – Tricuspid PA (ms) 25.8±9.3 17.0±9.5 < 0.001Septal PA – Tricuspid PA (ms) 9.2±3.7 6.7±3.0 0.008
NS: nonsense.
Conclusion: Atrial conduction interval delay and PWD are prolonged in prehy-pertensives compared to healthy persons. This situation indicates that the risk ofdeveloping of atrial fibrillation is increased in patients with prehypertension.
P1602 T-wave alternans testing in pacemaker patients:comparison of pacing modes and long-termprognostic relevance
M. Dorenkamp1, C. Breitwieser2, A.J. Morguet3 , S. Behrens4,M. Zabel1. 1Universitaetsmedizin Goettingen, Heart Center,
Cardiology, Goettingen, Germany; 2HELIOS Hospital Berlin-Buch, Berlin,Germany; 3Charite - University Medicine, Campus Benjamin Franklin,Department of Cardiology and Pulmonology, Berlin, Germany; 4VivantesHumboldt Hospital, Berlin, Germany
Aims: Microvolt T-wave alternans (MTWA) is an effective tool for identifying pa-tients who are at risk for sudden cardiac death. Since MTWA is heart rate de-pendent, testing requires controlled increase of heart rate which can be achievedby either physical exercise or by pacemaker stimulation.We aimed to determinethe effects of different pacing modes on test results and long-term prognosticrelevance of MTWA in patients with prior DDD (dual-chamber) pacemaker im-plantation.Methods and results: Sixty-three patients (mean age 68±13 years) with struc-tural heart disease and implanted DDD pacemaker were enrolled. Left ventric-
ular (LV) function was normal or moderately impaired (mean LV ejection frac-tion 61±13%). All patients underwent sequential MTWA testing during atrial andventricular pacing, respectively. During atrial pacing, 21% of MTWA tests werepositive, 50% negative, and 29% indeterminate. When using ventricular pacing,18% of tests were positive, 41% negative, and 41% indeterminate. When posi-tive and indeterminate tests were grouped as non-negative, the concordance be-tween atrial and ventricular pacing was 70%. After a mean follow-up of 8.1±2.8years, 26 (41%) patients had died. Better survival was predicted by the absenceof MTWA during atrial pacing (p = 0.0324) but not during ventricular pacing (p =0.82).Conclusion: In patients with permanent pacemakers, there is a low concordanceof MTWA test results among different pacing protocols. During long-term follow-up, only MTWA during atrial pacing is of prognostic relevance and should there-fore remain one of the standards of MTWA measurements.
ELECTROCARDIOGRAPHY
P1603 Value of the surface electrocardiogram in detectingright ventricular dilatation in the presence of leftbundle branch block
R.J. Van Bommel1, N. Ajmone Marsan1, V. Delgado1, M.J. Schalij1,J.J. Bax1, H.J. Wellens2. 1Leiden University Medical Center,
Leiden, Netherlands; 2Cardiovascular Research Institute Maastricht (CARIM),Maastricht, Netherlands
Background: Approximately 20% of patients with heart failure have a left bundlebranch block (LBBB) on the surface ECG. In this group of patients, the possibil-ity of detecting right ventricular (RV) dilatation using a standard ECG can be ofclinical relevance, since RV enlargement is an important prognostic marker. Con-sequently, aim of this study was to test the diagnostic accuracy for several ECGcriteria in determining significant RV dilatation in patients with heart failure andLBBB.Methods: Standard 12-lead ECGs were obtained in 173 heart failure patientswith known LBBB. From the ECG, 3 criteria for RV dilatation were defined; pres-ence of terminal positivity in lead aVR (late R wave in lead aVR), low voltage(<0.6 mV) in all extremity leads and an R/S ratio ≤1 in lead V5 (Figure). Addi-tionally, all patients underwent comprehensive echocardiographic evaluation, in-cluding assessment of RV dimensions. Measurements were performed blindedto ECG results. Significant RV dilatation was defined in 2 ways: RV base-to-apexlength ≥86 mm, and RV diastolic area ≥33 cm2.Results: Eighty-six patients (50%) had a late R wave in lead aVR, 36 patients(21%) had low voltage in the extremity leads and 67 patients (39%) had an R/Sratio ≤1 in lead V5. An RV base-to-apex length ≥86 mm was present in 67 pa-tients (39%), while 62 patients (36%) had an RV diastolic area ≥33 cm2. Anycombination of 2-3 positive criteria predicted an RV base-to-apex length ≥86 mmwith a positive predictive value (PPV) of 89% and a negative predictive value(NPV) of 88%. Similarly, an RV diastolic area ≥33 cm2 could be predicted with aPPV of 80% and a NPV of 88%.
Example of the 3 different ECG criteria
Conclusions: Combining 2-3 distinct ECG criteria allows for accurate detectionof RV dilatation in heart failure patients with a LBBB.
P1604 Prediction of sudden death in diabetic post-infarctionpatients
A. Bauer1, P. Barthel2, A. Mueller2, M. Malik3, G. Schmidt2.1Eberhard-Karls University Tubingen, Internal Medicine III,Department of Cardiology, Tubingen, Germany; 2I. Medizinische
Klinik, Klinikum Rechts der Isar, Technische Universität München, Munich,Germany; 3Division of Cardiac and Vascular Sciences, St George’s University ofLondon, London, United Kingdom
Background: Prevalence of sudden death is twice as high in diabetic as in non-diabetic post-infarction patients. The present study therefore aimed to identify
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
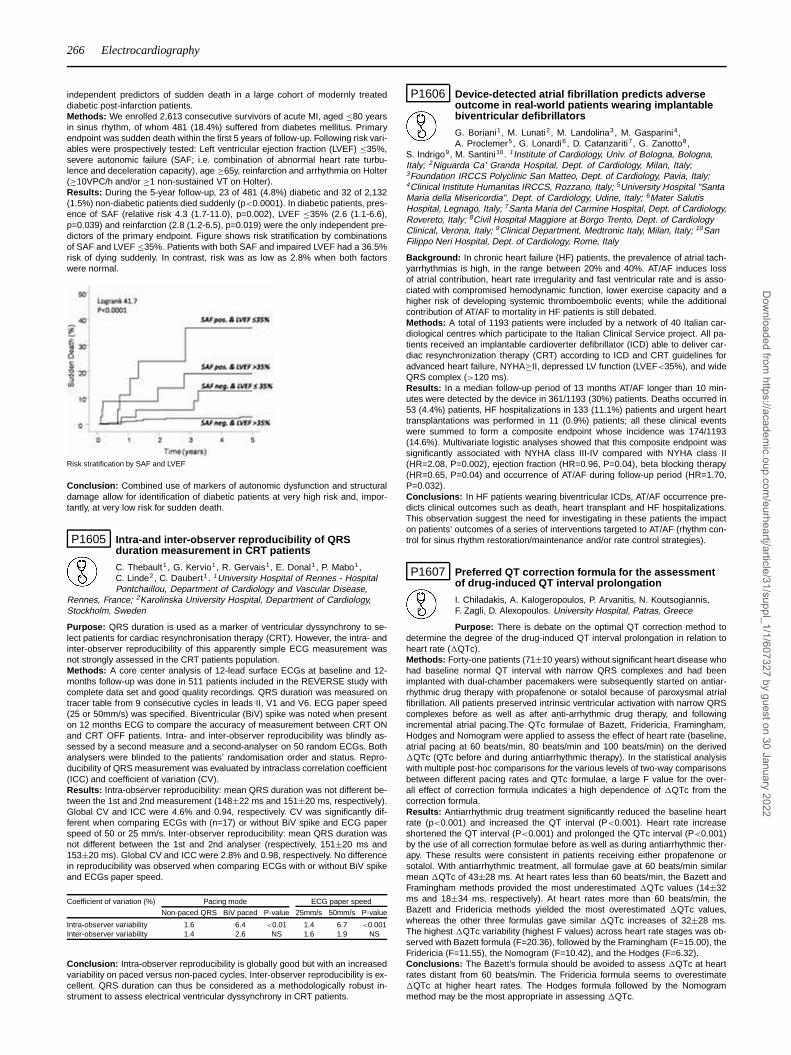
266 Electrocardiography
independent predictors of sudden death in a large cohort of modernly treateddiabetic post-infarction patients.Methods: We enrolled 2,613 consecutive survivors of acute MI, aged ≤80 yearsin sinus rhythm, of whom 481 (18.4%) suffered from diabetes mellitus. Primaryendpoint was sudden death within the first 5 years of follow-up. Following risk vari-ables were prospectively tested: Left ventricular ejection fraction (LVEF) ≤35%,severe autonomic failure (SAF; i.e. combination of abnormal heart rate turbu-lence and deceleration capacity), age ≥65y, reinfarction and arrhythmia on Holter(≥10VPC/h and/or ≥1 non-sustained VT on Holter).Results: During the 5-year follow-up, 23 of 481 (4.8%) diabetic and 32 of 2,132(1.5%) non-diabetic patients died suddenly (p<0.0001). In diabetic patients, pres-ence of SAF (relative risk 4.3 (1.7-11.0), p=0.002), LVEF ≤35% (2.6 (1.1-6.6),p=0.039) and reinfarction (2.8 (1.2-6.5), p=0.019) were the only independent pre-dictors of the primary endpoint. Figure shows risk stratification by combinationsof SAF and LVEF ≤35%. Patients with both SAF and impaired LVEF had a 36.5%risk of dying suddenly. In contrast, risk was as low as 2.8% when both factorswere normal.
Risk stratification by SAF and LVEF
Conclusion: Combined use of markers of autonomic dysfunction and structuraldamage allow for identification of diabetic patients at very high risk and, impor-tantly, at very low risk for sudden death.
P1605 Intra-and inter-observer reproducibility of QRSduration measurement in CRT patients
C. Thebault1 , G. Kervio1, R. Gervais1, E. Donal1, P. Mabo1,C. Linde2, C. Daubert1. 1University Hospital of Rennes - HospitalPontchaillou, Department of Cardiology and Vascular Disease,
Rennes, France; 2Karolinska University Hospital, Department of Cardiology,Stockholm, Sweden
Purpose: QRS duration is used as a marker of ventricular dyssynchrony to se-lect patients for cardiac resynchronisation therapy (CRT). However, the intra- andinter-observer reproducibility of this apparently simple ECG measurement wasnot strongly assessed in the CRT patients population.Methods: A core center analysis of 12-lead surface ECGs at baseline and 12-months follow-up was done in 511 patients included in the REVERSE study withcomplete data set and good quality recordings. QRS duration was measured ontracer table from 9 consecutive cycles in leads II, V1 and V6. ECG paper speed(25 or 50mm/s) was specified. Biventricular (BiV) spike was noted when presenton 12 months ECG to compare the accuracy of measurement between CRT ONand CRT OFF patients. Intra- and inter-observer reproducibility was blindly as-sessed by a second measure and a second-analyser on 50 random ECGs. Bothanalysers were blinded to the patients’ randomisation order and status. Repro-ducibility of QRS measurement was evaluated by intraclass correlation coefficient(ICC) and coefficient of variation (CV).Results: Intra-observer reproducibility: mean QRS duration was not different be-tween the 1st and 2nd measurement (148±22 ms and 151±20 ms, respectively).Global CV and ICC were 4.6% and 0.94, respectively. CV was significantly dif-ferent when comparing ECGs with (n=17) or without BiV spike and ECG paperspeed of 50 or 25 mm/s. Inter-observer reproducibility: mean QRS duration wasnot different between the 1st and 2nd analyser (respectively, 151±20 ms and153±20 ms). Global CV and ICC were 2.8% and 0.98, respectively. No differencein reproducibility was observed when comparing ECGs with or without BiV spikeand ECGs paper speed.
Coefficient of variation (%) Pacing mode ECG paper speed
Non-paced QRS BiV paced P-value 25mm/s 50mm/s P-value
Intra-observer variability 1.6 6.4 <0.01 1.4 6.7 <0.001Inter-observer variability 1.4 2.6 NS 1.6 1.9 NS
Conclusion: Intra-observer reproducibility is globally good but with an increasedvariability on paced versus non-paced cycles. Inter-observer reproducibility is ex-cellent. QRS duration can thus be considered as a methodologically robust in-strument to assess electrical ventricular dyssynchrony in CRT patients.
P1606 Device-detected atrial fibrillation predicts adverseoutcome in real-world patients wearing implantablebiventricular defibrillators
G. Boriani1, M. Lunati2, M. Landolina3, M. Gasparini4,A. Proclemer5, G. Lonardi6 , D. Catanzariti7, G. Zanotto8,
S. Indrigo9, M. Santini10. 1Institute of Cardiology, Univ. of Bologna, Bologna,Italy; 2Niguarda Ca’ Granda Hospital, Dept. of Cardiology, Milan, Italy;3Foundation IRCCS Polyclinic San Matteo, Dept. of Cardiology, Pavia, Italy;4Clinical Institute Humanitas IRCCS, Rozzano, Italy; 5University Hospital "SantaMaria della Misericordia", Dept. of Cardiology, Udine, Italy; 6Mater SalutisHospital, Legnago, Italy; 7Santa Maria del Carmine Hospital, Dept. of Cardiology,Rovereto, Italy; 8Civil Hospital Maggiore at Borgo Trento, Dept. of CardiologyClinical, Verona, Italy; 9Clinical Department, Medtronic Italy, Milan, Italy; 10SanFilippo Neri Hospital, Dept. of Cardiology, Rome, Italy
Background: In chronic heart failure (HF) patients, the prevalence of atrial tach-yarrhythmias is high, in the range between 20% and 40%. AT/AF induces lossof atrial contribution, heart rate irregularity and fast ventricular rate and is asso-ciated with compromised hemodynamic function, lower exercise capacity and ahigher risk of developing systemic thromboembolic events; while the additionalcontribution of AT/AF to mortality in HF patients is still debated.Methods: A total of 1193 patients were included by a network of 40 Italian car-diological centres which participate to the Italian Clinical Service project. All pa-tients received an implantable cardioverter defibrillator (ICD) able to deliver car-diac resynchronization therapy (CRT) according to ICD and CRT guidelines foradvanced heart failure, NYHA≥II, depressed LV function (LVEF<35%), and wideQRS complex (>120 ms).Results: In a median follow-up period of 13 months AT/AF longer than 10 min-utes were detected by the device in 361/1193 (30%) patients. Deaths occurred in53 (4.4%) patients, HF hospitalizations in 133 (11.1%) patients and urgent hearttransplantations was performed in 11 (0.9%) patients; all these clinical eventswere summed to form a composite endpoint whose incidence was 174/1193(14.6%). Multivariate logistic analyses showed that this composite endpoint wassignificantly associated with NYHA class III-IV compared with NYHA class II(HR=2.08, P=0.002), ejection fraction (HR=0.96, P=0.04), beta blocking therapy(HR=0.65, P=0.04) and occurrence of AT/AF during follow-up period (HR=1.70,P=0.032).Conclusions: In HF patients wearing biventricular ICDs, AT/AF occurrence pre-dicts clinical outcomes such as death, heart transplant and HF hospitalizations.This observation suggest the need for investigating in these patients the impacton patients’ outcomes of a series of interventions targeted to AT/AF (rhythm con-trol for sinus rhythm restoration/maintenance and/or rate control strategies).
P1607 Preferred QT correction formula for the assessmentof drug-induced QT interval prolongation
I. Chiladakis, A. Kalogeropoulos, P. Arvanitis, N. Koutsogiannis,F. Zagli, D. Alexopoulos. University Hospital, Patras, Greece
Purpose: There is debate on the optimal QT correction method todetermine the degree of the drug-induced QT interval prolongation in relation toheart rate (�QTc).Methods: Forty-one patients (71±10 years) without significant heart disease whohad baseline normal QT interval with narrow QRS complexes and had beenimplanted with dual-chamber pacemakers were subsequently started on antiar-rhythmic drug therapy with propafenone or sotalol because of paroxysmal atrialfibrillation. All patients preserved intrinsic ventricular activation with narrow QRScomplexes before as well as after anti-arrhythmic drug therapy, and followingincremental atrial pacing.The QTc formulae of Bazett, Fridericia, Framingham,Hodges and Nomogram were applied to assess the effect of heart rate (baseline,atrial pacing at 60 beats/min, 80 beats/min and 100 beats/min) on the derived�QTc (QTc before and during antiarrhythmic therapy). In the statistical analysiswith multiple post-hoc comparisons for the various levels of two-way comparisonsbetween different pacing rates and QTc formulae, a large F value for the over-all effect of correction formula indicates a high dependence of �QTc from thecorrection formula.Results: Antiarrhythmic drug treatment significantly reduced the baseline heartrate (p<0.001) and increased the QT interval (P<0.001). Heart rate increaseshortened the QT interval (P<0.001) and prolonged the QTc interval (P<0.001)by the use of all correction formulae before as well as during antiarrhythmic ther-apy. These results were consistent in patients receiving either propafenone orsotalol. With antiarrhythmic treatment, all formulae gave at 60 beats/min similarmean �QTc of 43±28 ms. At heart rates less than 60 beats/min, the Bazett andFramingham methods provided the most underestimated �QTc values (14±32ms and 18±34 ms, respectively). At heart rates more than 60 beats/min, theBazett and Fridericia methods yielded the most overestimated �QTc values,whereas the other three formulas gave similar �QTc increases of 32±28 ms.The highest �QTc variability (highest F values) across heart rate stages was ob-served with Bazett formula (F=20.36), followed by the Framingham (F=15.00), theFridericia (F=11.55), the Nomogram (F=10.42), and the Hodges (F=6.32).Conclusions: The Bazett’s formula should be avoided to assess �QTc at heartrates distant from 60 beats/min. The Fridericia formula seems to overestimate�QTc at higher heart rates. The Hodges formula followed by the Nomogrammethod may be the most appropriate in assessing �QTc.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Electrocardiography 267
P1608 The normal ECG in advanced age: findings on 11,805geriatric electrocardiograms
D. Nicolis, G. Morani, G. Pesarini, E. Raytcheva, C. Vassanelli.Civil Hospital Maggiore at Borgo Trento, Department of CardiologyClinical, Verona, Italy
Purpose: The old are a growing component of the industrialized nations. Despitethat, even if ECG is one of the most frequently performed examination, no large-scale analysis of normal geriatric electrocardiogram exists to date.Methods: This was a retrospective study: we collected data from baseline ECGsfor a overall number of 11.805 geriatric single individuals (age over 65 years). TheECGs were performed in our cardiology division from 01/01/2006 to 31/12/2009and were interpreted by cardiologists as normal ECGs. We examined the meanvalues and correlations with sex and age of heart rate, PR, QRS, QTc-Bazettduration and axis.Results: Age range from 65 to 101 years. The mean age was 73,86±6,67 yrs.Women were 57,5% of the population. Mean values of QRS (91,2±10 msec Vs84,9±9 msec p < 0.001) and PR (165,5±22,8 msec Vs 160,6±22 msec p <
0.001) where significatively lower in women than in men, instead HR (72,1±10,4bpm Vs 73,8±10,1 bpm p < 0.001) and QTc (428,5±21,6 msec Vs 434,4±20,9msec p < 0.001) were significatively higher. Mild but significant correlations werenoted between age and QRS duration (r = -0.148, p < 0.001) and between ageand QTc duration (r = 0.139, p < 0.001).Conclusion: We observed sex-related variations in electrocardiogram values ofnormal geriatric ECG. The most surprising finding is a mild but progressive nar-rowing of QRS with advancing age. Also a lengthening of QTc with age is noted.PR tract and heart rate remain, substantially, stable with age. The significance ofthese variation in geriatric ECGs are uncertain. Duration of QRS may be simplyan epiphenomenon of aging and due to progressive muscular atrophy but oth-erwise we can speculate that a narrower QRS might identify a population withmore probability of successful aging. Finally, our findings should be considered indefining normal reference values of electrocardiogram in elderly.
P1609 An alternative criterion for Brugada syndromediagnosis
L. Ferreira Santos1, E. Correia1, B. Rodrigues1, L. Nunes1,A. Costa1, C. Henriques2, A. Matos2, J. Machado3, S. Castedo3,J. Oliveira Santos1. 1Hospital São Teotónio, Viseu, Portugal; 2School
of Technology of Viseu - Polytechnic Institute, Viseu, Portugal; 3IPATIMUP,Oporto, Portugal
Purpose: For Brugada syndrome (BS) diagnosis only coved-type ECG patternwith more than 2 mm ST-segment elevation (type 1) in at least two right precordialleads is defined as diagnostic.Methods: We studied 75 members of a family with BS including 30 carriers (CA+)of a specific mutation of SCN5A gene. We compared the number of diagnosticECGs by conventional criterion (CC) against the number of diagnostics with aproposed alternative criterion (AC): type 1 ECG in at least one right precordiallead. Right precordial leads V1 and V2 were placed in 4th intercostal space (IS)and then in 2nd IS.Results: From the 75 elements, 4 were excluded because they had a definitivepacemaker, resulting 28 CA+ (11 men) and 43 non-carriers (NC) (22 men). TheCC (with V1 and V2 placed in the 4th IS) made 6 diagnosis (without false posi-tives) in spontaneous ECG and 3 more diagnosis after the drug challenge (DC)(plus 2 false positives): sensitivity (SE) = 32.1% and specificity (SP) = 95.3%. TheAC made 12 diagnosis (without false positives) and 6 more after DC (with 3 falsepositives): SE = 64.3% and SP = 93%. The AC led to a significant increase in SE(p=0.002), without a significant decrease in SP (p=0.5). The CC (with V1 and V2placed in the 2nd IS) made 11 diagnosis (and additionally 2 false positives), andafter DC 4 more diagnosis (without false positives): SE = 53.8% and SE = 95.3%.With AC were made 14 diagnosis (with the same 2 false positives) and the same4 after DC (with one 1 false positive): SE = 64.3% and SP = 93%. However, nei-ther the increase in SE nor the decrease in SP achieved with AC were statisticallysignificant (p = 0.125, p = 0.5, respectively). Finally there are no significant differ-ences in SE and SP between the CC with leads V1 and V2 in the 2nd IS and theAC with leads V1 and V2 in the 4th IS (p = 0.25, p = 0.5, respectively).Conclusions: In this family, with leads V1 and V2 in the 4th IS the AC is moreeffective in BS diagnosis than the CC. AC with the right precordial leads in the4th IS showed the same diagnostic effectiveness that CC with leads V1 and V2 inthe 2nd IS, with an obvious advantage: this maneuver is rarely performed in dailyclinical practice which contributes to the underdiagnosis of SB. We suggest thatthe AC should be considered to be tested in more patients leading to a possiblereview of the current diagnostic criteria.
P1610 Patent accessory pathways close to the conductionsystem of the heart: electrocardiographic recognitionand ablation results
A. Cortell Fuster1, R. Ruiz Granell1, S. Morell Cabedo2, A. FerreroDe Loma-Osorio1, A. Martinez Brotons1, M.T. Izquierdo De
Francisco1 , E. Dominguez Mafe1, R. Garcia Civera1. 1University HospitalClinic, Cardiology Department, Valencia, Spain; 2University General Hospital ofValencia, Valencia, Spain
Purpose: Proximity to conduction system can complicate the ablation ofparahisian superior paraseptal and midseptal accessory pathways (AP). Our ob-jective was to search for a characteristic electrocardiographic (ECG) pattern ofparahisian location among superior paraseptal (SPS) and midseptal (MS) AP andto review the results of their ablation procedures.Methods: We retrospectively reviewed the ECG records and the ablation data of364 consecutive patients with preexcitation referred to our laboratory for ablation,excluding patients with previous procedures.Results: A total of 382 AP were found in 364 patients; 34 (8.9%) were SPS (20parahisian) and 35 (9.2%) were MS (4 parahisian, p<0.001). A QS pattern inV1 was present in 93% of parahisian SPS-AP (area under the ROC curve 0.7;sensitivity 93%; specificity 48%) and a QS pattern in V1 and V2 in 29% (area un-der the ROC curve 0.64; sensitivity 29%; specificity 100%). No distinctive patternwas found for parahisian MS-AP. Ablation was attempted in 66 AP; complicativepermanent AV block developed in 2 (both MS), risk of AV block led to suspendablation in 5 (3 MS) and ablation failed in 2 (both MS).Conclusions: QS pattern in V1 is a sensitive criteria to detect parahisian SPS-APbeing QS in V1 and V2 a more especific criteria. Parahisian MS-AP are infrequentand difficult to predict by the ECG. Complications during ablation presented ex-clusively in MS-AP.
P1611 Evaluation of the specificity of morphologicalelectrocardiographic criteria for the differentialdiagnosis of wide QRS complex tachycardia inpatients with Tetrallogy of Fallot
E. Diaz Caraballo, R. Peinado, R. Cozar, J.M. Oliver, L. Pena,A. Gonzalez, J.L. Merino, A. Perez, S. Moreno, I. Valverde. University HospitalLa Paz, Madrid, Spain
Purpose: Many patients (P) with repaired Tetralogy of Fallot (RTOF) developatrial or ventricular tachycardias by adulthood. Althoughseveral ECG criteria havebeen described for the differential diagnosis oftachycardias with a wide QRS com-plex, their applicability in patients with RTOFis unknown. This study was aimed atanalysing the specificity of previouslydescribed criteria in these P.Methods: The ECGs during sinus rhythm of 82 P withRTOF ramdomly selectedfrom the database of the Adult Congenital Heart DiseaseUnit were analysed bytwo independent observers. Fifty-six of them (age 34±9years), had a QRS widthduring sinus rhythm greater than 0,12 seconds and wereincluded in this study.Predominant R wave in V1 was observed in 42 P (rightbundle branch block –RBBB- configuration) and predominant S wave in V1 in 14 (left bundle branchblock –LBBB- configuration). We analyzed the specificity ofthe QRS morphologi-cal criteria previously described in ECGs during sinusrhythm.Results: Only two of 12 analyzed criteria had specificity greater than 0.90 amongour P:a concordant pattern in all precordial leads (0.98) and the absence of anRScomplex in all precordial leads (0.98). QRS duration >140 and an R to Sin-terval >100 ms in one precordial lead had a specificity of 0.25 and 0.7respec-tively. Specific morphological criteria in the presence of a RBBBconfiguration hadfairly high specificity: a monophasic (R), biphasic (qR, QR,Rs or RS) or tripha-sic (Rsr’or Rr’) QRS complex in V1 (0.88), aright superior axis (0.88), a QS, QR,or R QRS pattern in V6 (0.86) or a leftsuperior axis (-30 to -90°; 0.74). Mor-phological criteria in the presence of aleft bundle branch block (LBBB) morphol-ogy had lower specificity: >60 msfrom QRS onset to S nadir (0.79), a notcheddownstroke S wave (0,71), any Q inV6 (0.5), or an R >30 ms in lead V1 or V2(0.36).Conclusions: These findings suggest an acceptable applicability of QRS mor-phologicalcriteria in P RTOF and wide QRS tachycardia with RBBB configurationbut a limitedusefulness in P with wide QRS tachycardia and LBBB morphology.
P1612 QRS changes in ECG leads with ST-segment elevationdifferentiate epicardial and transmural myocardialinjury
R.F. Wiegerinck, C. Galvez-Monton, E. Jorge, R. Martinez, E. Ricart,J. Cinca. Hospital de Sant Pau, Barcelona, Spain
Purpose: QRS duration and R wave amplitude are increased in acute transmuralischemic injury due to depressed intramyocardial activation. Theoretically, whenmyocardial injury is confined to the epicardium, the intramyocardial activation willnot be affected and thus no QRS changes will occur. We assessed whether anal-ysis of the QRS complex can differentiate epicardial from transmural myocardialinjury.Methods: The effects of local or diffuse epicardial injury induced respectively bytopical or intrapericardial exposure to potassium solutions were compared withtransmural injury induced by acute left anterior descending coronary artery occlu-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

268 Electrocardiography
sion in 17 pigs. The effects were measured in local electrograms from transmuralneedles inserted in the left ventricular free wall or in the peripheral 12-lead ECG.Results: Local epicardial application of 50 mM potassium (7 pigs) inducedST segment elevation in epicardial local electrograms (from 0.2±0.06 mV to0.5±0.09 mV; p<0.05) but not underneath in midmyocardial local electrograms(from 0.1±0.07 mV to -0.1±0.09 mV). Intrapericardial injection of potassium (10pigs) induced ST segment elevation on average in 9/12 ECG-leads. Acute leftanterior descending coronary artery occlusion induced ST segment elevation as-sociated with increased QRS duration (69±1.2 ms to 89±3.6 ms; p<0.001) andincreased R wave amplitude (0.1±0.01 mV to 0.7±0.09 mV; p<0.001), but thisassociation did not occur after exposure to potassium. In addition, local midmy-ocardial activation times were not affected by epicardial application of potassium(from 182±5.9 ms to 183±5.8 ms), but increased significantly during acute leftanterior descending corornary artery occlusion (246±20.9 ms; p<0.01).Conclusion: Transmural but not epicardial myocardial injury is associated withQRS prolongation and increased R wave amplitude in leads with ST segmentelevation. This differential QRS pattern is due to a delayed local activation intransmural but not in epicardial injury.
P1613 Specificity of the provocative test in the Brugadasyndrome: the fall of a myth?
L. Ferreira Santos1, R. Faria1, D. Moreira1, L. Nunes1, A. Costa1,J. Machado2, S. Castedo2, C. Henriques3, A. Matos3, J. OliveiraSantos1. 1Hospital São Teotónio, Viseu, Portugal; 2IPATIMUP,
Oporto, Portugal; 3School of Technology of Viseu - Polytechnic Institute, Viseu,Portugal
Purpose: Pharmacological provocative test to unmask concealed forms of Bru-gada syndrome (BS) is performed under the assumption that the number of falsepositives (patients developing a type 1 ECG without being affected by the disease)is extremely low but the real specificity of sodium channel blockage to identify af-fected elements is uncertain.Methods: 22 adults from a genotyped family with BS (including 13 carriers (CA+)of a specific SCN5A mutation) with non diagnostic spontaneous ECG underwentpharmacological provocative test with flecainide or ajmaline. Structural heart dis-ease was excluded in all patients.Results: 22 family members (36.36±12.3 years old; 9 men); 13 CA+ (4 men).Three patients had history of syncope. After provocative test, 66.7% of non carri-ers (NC) and 23.1% of CA+ kept the same ECG pattern but this difference was notstatistically significant (p=0.08). ECG changes in CA+ included intraventricularconduction disturbances (15.4%), Brugada suggestive (type 2 and type 3 repolar-ization) (38.5%) and Brugada diagnosis (23.1%). ECG changes in NC includedBrugada suggestive (11.1%) and Brugada diagnosis (22.2%). With leads V1 andV2 in the 4th intercostal space (IS) the provocative test was positive in 5 patients(3 CA+) with sensitivity (SE) of 23.1%, specificity (SP) of 77.8%, positive predic-tive value (PPV) of 60% and negative predictive value (NPV) of 41.2%. With leadsV1 and V2 in the 2nd IS the test was positive in 9 patients (7 CA+) increasing theSE to 53.8%, PPV to 77.8%, VPN to 53.8%, without changes of SP. The higherSE with the alternative lead position was not statistically significant (p=0.063).Conclusion: As long as every single patient developing a type 1 ECG is definedas affected by BS, it will be impossible to find a false positive, thus perpetuatingthe perception that the pharmacological test is 100% accurate. In this family thespecificity of provocative test is 77.8% and two NC would be misdiagnosed asBrugada patients if genetic tests weren’t available. At present, no data derivedfrom systematic studies support or disprove the concept that sodium channelblockers provide an accurate diagnosis of the syndrome. More studies in geno-typed families are necessary to accurately establish the specificity of provocativetest in BS.
P1614 Use of novel HRV-parameters for risk stratification inpatients with dilated cardiomyopathy
T. Demming, B. Weidtmann, N. Frey, H. Bonnemeier. Innere MedizinIII, Universitätsklinikum Schleswig-Hostein, Campus Kiel, Kiel,Germany
Novel Holter-derived HRV-Parameters such as Deceleration Capacity (DC) andApproximate Entropy (AppEn) have gained recent interest and prove to give valu-able prognostic information in various populations of patients. Their use for riskstratification in patients with Dilated Cardiomyopathy which certainly have a highrisk for major arrhythmic events and sudden cardiac death has not yet been ex-amined.Methods and Results: Holter-ECG recordings of 228 Patients treated in theyears from 2000 until 2006 for Dilated Cardiomyopathy in the Hospital of theUniversity of Lübeck, were retrospectively analysed and used to obtain param-eters of Heart Rate Variability. A total of 59 Patients died during the follow up ofnot less than 40 month. AppEn and DC of patients which died during follow upwhere significantly lower than of the surviving patients (DC survivors 4.55±0.3msvs. DC non survivors 3.01±0.91ms; AppEn survivors 0.85±0.05 vs. AppEn nonsurvivors 1.15±0.11) (Figure 1).Conclusion: Patients with Dilated Cardiomyopathy have not yet been examinedfor new parameters of HRV. This study presents that DC and AppEn are signifi-cantly lower in patients which died within the time of follow up than in the surviv-
Figure 1
ing cohort. A use of these parameters for risk stratification in patients with DilatedCardiomyopathy seems therefore possible and may be capable to give additionalinformation to the classical prognostic risk predictors such as left ventricular ejec-tion fraction.
P1615 Usefulness of t wave amplitude in lead avr forpredicting cardiac events in patients with st elevatedmyocardial infarction
M. Musialowska, J. Forys, J.D. Kasprzak. Second Chair andDepartment of Cardiology Medical University of Lodz, Lodz, Poland
Background: Since there are some independent informations about prognos-tic value of T wave amplitude in lead aVR as a powerful prognostic marker forestimating risk of CV death in males we investigated the association betweenupward pointing T waves in patients with ST elevated myocardial infarction whounderwent pPCI.Methods: Retrospective cohort was performed at Second Chair and Departmentof Cardiology, Lodz, Poland, which included 602 patients with ST elevated my-ocardial infarction treated with pPCI, who were hospitalized between years 2001-2002. Analysis of 12-lead resting ECGs was performed of all subjects at the ad-mission and the last day of hospitalization and it was excluding patients with atrialfibrillation, WPW, QRS duration > 120 ms, and paced rhythms. Average follow-upwas 8 years during which time there were 84 CV deaths.Results: While ST segment measurements in aVR were univariately predictiveof CV death, T wave amplitude superseded them in multivariate survival analysis.In addition, T wave amplitude in aVR outperformed repolarization measurementsin all other leads as well as other ECG criteria (Q waves, LVH) for predictingCV mortality. As T wave amplitude became less negative in aVR, there was aprogressive increase in relative risk (RR). When the T waves in aVR had a positivedeflection (i.e., upward pointing) the RR for CV death was 4.0
Baseline characteristic and mortality
Characteristic Total Negative T waves Positive T waves P valuepopulation in aVR in aVR
N=602 N=488 N=114
Age (yrs) 57,4±17,0 54,9±16,8 62,3±12,3 <0,001HR 74,2±15,8 72±13,8 75,3±15,6 <0,001T wave amp in lead I (microvolts) 146±10 172±101 -40±106 <0,001Left ventricular hypertrophy (LVH) 30 (5%) 19 (4%) 24 (21%) <0,001Cardiovascular death 84 (10,3%) 22 (4,5%) 62 (54%) <0,001
Conclusions: T wave amplitude in lead aVR is a powerful prognostic marker forestimating risk of CV death in patients with STEMI. Upward pointing T waves (asimple visual criterion) was prevalent (10.3% of a clinical population) and wasassociated with an annual CV mortality of 3.4% and a risk of four times.
P1616 Predicting factors of infrahisian conductionabnormality in Myotonic Dystrophy
B. Brembilla-Perrot1, J.D. Luporsi1, S. Louis2, P. Kaminsky3.1University Hospital of Nancy - Hospital Brabois, Vandoeuvre lesNancy, France; 2Neurology, Nancy, France; 3Internal Medicine,
Orphan diseases; CHU of Brabois, Vandoeuvre Les Nancy, France
Patients with type I myotonic dystrophy (MD) are at high of conduction distur-bances. The exact methods for their detection are discussed. The purpose ofstudy was to evaluate the factors implicated in the prediction of infrahisian blockin patients with MD.Methods: Our population comprised 52 patients, 30 men, 21 women aged from17 to 69 years (mean 47±14) with confirmed type I MD consecutively recruitedfor an electrophysiological study (EPS); they were asymptomatic, except 3. ECG,left ventricular ejection fraction (LVEF), Holter monitoring with evaluation of heart
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Electrocardiography 269
rate variability (HRV) by measurement of standard deviation of the mean RR in-tervals (SDNN) during the 24 hour period and signal-averaged ECG (SAECG)with the measurement of QRS duration, low amplitude signal duration (LAS) androot mean square voltage of the last 40 ms of QRS (RMS 40), were obtained andthe results compared to those of EPS. Multivariate analysis of several parameters(age, abnormal conduction at ECG, SDNN, QRS duration, data of SAECG, con-duction abnormality at Holter monitoring, LVEF) used a linear logistic regressionmodel.Results: Infrahisian conduction abnormality was noted in 20 patients (38%),never in 9 patients with normal ECG, in 1 of 9 (11%) with first degree AV block(AVB), in 6 of 10 (60%) with left hemiblock (LH), in 6 of 8 (75%) with bundle branchblock (BBB), 3 of 6 (50%) with the association first degree AVB and LH, and 4 of7 (57%) with first degree AVB and BBB. Patients with infrahisian block exhibiteda higher QRS duration than the others (137.8±32.2 ms vs 112.8±19.8 ms; p <
0.02). However, neither age (50.4±9.0 years vs 49.4±11.2; p= 0.8), nor LVEF(56.9±14.0% vs 54.0±16.5%; p=0.9), nor SDNN (130±57 ms vs 132±50 ms;p=0.8), nor RMS40 (13.2±9.4 μv vs 20.2±14.4 μv; p=0.06) nor LAS (48.0±28.7ms vs 33.9±14.4 ms; p=0.13) significantly differed between the patients with orwithout infrahisian block. Abnormal conduction noted at ECG was significantlysensitive to predict infrahisian block (relative risk RR 5.82), as well as QRS du-ration higher than 130 ms (RR 2.45). Multivariate analysis indicated that onlyabnormal conduction at ECG (first d AVB associated with LH or BBB or isolatedBBB) was an independent predictor for infrahisian block.Conclusions: In patients with MD, the only independent predictor of infrahisianconduction abnormality is the presence of conduction disturbance at ECG, a lefthemiblock or a bundle branch block, mainly when they were associated with a firstdegree AVB. Infrahisian conduction was always normal in patients with normalECG, whatever the age of the patient.
P1617 Abnormal electrocardiographic findings are commonin cirrhotic patients undergoing liver transplantationand predict post-transplant morbidity and mortality
A. Josefsson1, M. Fu1, E. Bjornsson2, M. Olausson3,E. Kalaitzakis1. 1Sahlgrenska University Hospital, Department
of Internal Medicine, Gothenburg, Sweden; 2Landspitali University Hospital,Department of Internal Medicine, Reykjavik, Iceland; 3Sahlgrenska UniversityHospital, Transplantation Center, Gothenburg, Sweden
Background: Cardiac complications are common during and after liver trans-plantation in patients with cirrhosis. However, data on electrocardiographic (ECG)findings of cirrhotics undergoing pre-transplant evaluation and their impact ontransplantation outcome are scarce. We aimed to assess the prevalence of ECGabnormalities in patients with cirrhosis at pre-transplant evaluation and their prog-nostic impact post-transplantation.Methods: A retrospective study was performed on consecutive cirrhotics under-going liver transplantation in a single institutiton (1999-2007). Available ECGs,clinical and biochemical data at pretransplant evaluation were analyzed. ECGswere analyzed using the Minnesota coding system. The corrected QT time inter-val (QTc) was calculated (Bazett formula). Patients were followed up for a meanof 4 years. Adverse events and mortality were analyzed during the immediatepost-transplant inpatient period (early events) and from discharge from hospitalpost-transplant until last follow-up (late events).Results: A total of 186 out of 243 cirrhotics who underwent transplantation hadan available baseline ECG (mean age 52yr, 29% F, 38% with alcoholic liver dis-ease (ALD), 29% had Hepatitis C, mean Model of end-stage liver disease (MELD)score 16,2). In all 137/186 (74%) had an abnormal ECG. Common abnormalitieswere prolonged QTc (25%), QRS transition zone to the left of lead V3 (23%), ab-normal QRS axis deviation (21%), Q wave (12%) and pathologic T-wave (10%).In logistic regression analysis prolonged QTc time was independently related toage (Odds Ratio (OR) 1.06, 95% confidence interval (CI) 1.02-1.1), ALD (OR3.35, 95% CI 1.61-7) and beta-blockers (OR 0.41, 95%CI 0.19-0.85); Q wave toolder age (OR 1.09, 95% CI 1.03 – 1.16); both QRS axis deviation (OR 4.13,95% CI 1.652-10.3) and abnormal T wave (OR 3.33, 95% CI 1.05-10.62) wererelated to arterial hypertension. Prolonged QTc time was associated with earlycardiac complications (60% vs 26%, p<0.01), suspect early heart failure as as-sessed by the Boston criteria (63% vs 20%, p<0.01), prolonged stay in the in-tensive care unit post-transplant (8.6 vs 4.7 days, p<0.01) and increased overallmortality (Kaplan-Meier analysis, log-rank test p<0.01). Q-wave was related to in-creased late cardiac events (Kaplan-Meier analysis, log-rank test (KM), p<0.01)and overall mortality (KM p<0.05).Conclusions: Abnormal ECG findings are common in cirrhotic patients under-going pre-transplantation evaluation. They are related to ALD, history of arterialhypertension, older age and predict post-transplant cardiac events and mortality.
P1618 Prognostic role of ST segment changes in lead aVR inpatients with inferior ST segment elevationmyocardial infarction
P. Kukla1, L. Bryniarski2, D. Dudek3, K. Kawecka-Jaszcz2 .1Specialist Hospital, Gorlice, Poland; 2I Dept. of Cardiology and
Hypertension, Cracow, Poland; 3II Dept. of Cardiology, Cracow, Poland
Background: Inferior myocardial infarction with ST segment elevation is consid-
ered a low risk STEMI but 30- 40% patients with inferior STEMI present complica-tions during in-hospital stay. The latest results suggest that ST segment elevationin lead aVR, so far mostly ignored, is associated with a worse prognosis. The aimof the study was to determine whether or not the ST segment changes in leadaVR could predict prognosis in inferior STEMI.Material and methods: The data of 320 consecutive patients with inferior STEMIwere analyzed, 206 men and 114 women (65,6±11,1 years). The patients weredivided into 2 groups: group A – treated with primary angioplasty (pPCI) - 134patients and group B – treated not invasively - 186 patients. There were no differ-ences between the group A and B taking to consider age, typical risk factors orejection fraction.Results: ST segment changes in lead aVR were observed in 135 (42.2%) pa-tients, ST elevation in 47 (14.7%), ST depression in 88 (27.5%) patients. In pa-tients with ST segment elevation, ST depression and without ST changes themortality rate was: 27.7%, 16.5% and 1.0%, p<0.001, respectively. In the pPCIgroup, in patients with ST segment elevation, ST depression and without STchanges the mortality rate was: 15.4%, 21.0% and 1.2% (p<0.001). In patientstreated with fibrynolysis in the groups with ST segment elevation, ST depressionand without ST changes in lead aVR, the mortality was: 33.3%, 12.9% and 0%,p=0.006 respectively. In patients without the reperfusion therapy, in the groupswith ST segment elevation, ST depression and without ST changes in lead aVR,the mortality was: 32.0%, 12.5% and 2.0%, p=0.001 respectively. In the multivari-ate analysis the predictors of ST segment elevation in lead aVR were: sex (fe-male), diabetes, hypertension, lower ejection fraction (EF%), cardiogenic shockon admission.Conclusion: ST segment changes in lead aVR in inferior STEMI are frequentand present in 42% of the patients. The presence of ST segment changes (STelevation and ST depression) in lead aVR is associated with a poor prognosisand it is independent of the type of the treatment strategy. Patients with inferiorSTEMI with ST segment changes in lead aVR should be considered as a highrisk group.
P1619 Left atrial enlargement evaluated by the 12-leadelectrocardiogram is a predictor of mild diastolicdysfunction in outpatients with hypertension
A.T. Yamada1, D.T. Carvalho1, N.G. Vieira Filho2, W.N. Ribeiro2,A.J. Mansur1 . 1Heart Institute (InCor) University of Sao Paulo
Medical School, Sao Paulo, Brazil; 2Hospital Municipal Dr. Fernando MauroPires da Rocha, Sao Paulo, Brazil
The objective of this study was to evaluate the accuracy of the rest 12-lead elec-trocardiogram (ECG) in the diagnosis of left atrial enlargement compared to theechocardiography and its association with mild diastolic dysfunction.From January of 2007 to March of 2009 all outpatients in sinus rhythm submittedto the elective ECG and echocardiography referred by physicians of health basicunits were invited to participate of this study. Patients with moderate and importantdiastolic dysfunction, pericardial diseases, valvular heart disease and patientswith left ventricular systolic dysfunction were excluded. The diastolic function wasestimated by the Doppler indices of left ventricular diastolic filling velocities in theechocardiography and an expert cardiologist evaluated the ECG.Were evaluated 394 patients, 177 (45%) patients with mild diastolic dysfunctionwith a mean age of 64 + 8 years, 95 (54%) women and 217 (55%) patients withoutdiastolic dysfunction with a mean age of 60 + 12 years, 116 (53%) women wasconsidered the control group.Were found 96 (24.3%) patients with left atrial enlargement and 228 (73.6%) with-out atrial enlargement in the ECG. Evaluating patients with left atrial enlargementin the ECG, 61 (63.5%) had mild diastolic dysfunction and 35 (36.5%) had normalpattern of A and E waves and E/A ratio (OR: 2.73; IC: 1.72 – 4.33).Were found in the echocardiography 98 patients with left atrial enlargement, 53(54%) of them had diastolic dysfunction and 45 (46%) patients had normal E/Aratio (OR: 1.63; CI: 1.03 – 2.57). The ECG had a sensibility of 49% and specificityof 84% to identify left atrial enlargement compared to the echocardiography.Conclusion: The presence of left atrial enlargement in the ECG had better corre-lation with mild left ventricular diastolic dysfunction when compared with left atrialenlargement in the echocardiography.
P1620 Electrocardiographic patterns of atrial fibrillation inV1 and inferior leads as predictors for successfulelectric cardioversion
J. Benezet-Mazuecos, L. Duarte, J.M. Rubio, P. Sanchez-Borque,E. Macia, S. Del Castillo, A. Pastor, J. Farre. Foundation Jimenez
Diaz, Madrid, Spain
Introduction: Fibrillatory waves in atrial fibrillation (AF) vary considerably be-tween patients, and their characteristics may be related with the clinical charac-teristics of the patient and other structural or mechanical properties of the atria.The different ECG patterns of AF at the moment of electrical cardioversion (ECV)may predict the probability of conversion to sinus rhythm.Methods: We have analyzed the morphology of the fibrillatory waves in lead V1and inferior leads of 100 consecutive patients (64±12 year; 57% male) submittedto ECV for AF. In 54% was a first episode of AF. We excluded those patients withsevere valvular heart disease, mechanical prosthesis and severely dilated atria
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

270 Electrocardiography / Ventricular arrythmias
(AP diameter >55 mm). We have also studied the amplitude and duration of theP wave after successful ECV.Results: We have identified four different ECG patterns of AF: Type I (organizedfibrillatory waves visible in V1 and II, III or aVF) 40%, Type II (organized activityonly in V1) 39%, Type III (organized activity only in II, III or aVF) 4%, Type IV(without any organized activity) 17%. Successful ECV was achieved in 85% ofpatients. The successful rate for each patter was: Type I (98%); Type II (87%);Type III (100%) and type IV (47%; p<0.001). There were no significant differ-ences between groups in atrial dimension, mitral regurgitation or age. Type IVpattern was significantly associated with a lower amplitude of the P wave in V1(0.93±0.32 mm) compared to the other patterns (1.44±0.58 mm; p<0.05), butwithout differences in the P wave duration (96±13 vs. 96±18 ms; p=NS).
Organized and disorganized patterns
Conclusions: In AF, different ECG patterns of the fibrillatory wave may be recog-nized. Organized patterns in V1 and/or the inferior leads at the moment of ECVpredict a higher probability of conversion to sinus rhythm.
VENTRICULAR ARRYTHMIAS
P1621 Mortality and ventricular tachyarrhythmia occurrencein implantable cardioverter defibrillator recipientswith left ventricular dysfunction: are secondaryprevention recipients at higher risk?
S. Rose1, A.M. Gillis2, D.V. Exner2, K. Kavanagh2, G. Veenhuyzen2 ,R.S. Sheldon2, H.J. Duff2, F.R. Quinn2, M.R. Cassidy2, L.B. Mitchell2. 1AlbertaHealth Services, Calgary, Canada; 2Libin Cardiovascular Institute of Alberta,Calgary, Canada
Purpose: The implantable cardioverter defibrillator (ICD) has become an ac-cepted therapy for prevention of sudden death in high risk populations. At present,there is limited data about the predictors of survival and ventricular tachyarrhyth-mia (VT/VF) occurrence after implantation. The objective of this analysis was todetermine if survival and occurrence of VT/VF is different in patients with primaryvs secondary prevention ICD recipients with coronary artery disease (CAD).Methods: We prospectively followed 599 patients with left ventricular systolic dys-function secondary to CAD for a median of 3 years (IQR = 2.0 – 5.5) following ICDimplantation. Predictors of overall survival were examined using a proportionalhazards model where the time to VT/VF occurrence, VT storm and appropriateshocks were modeled as time dependent covariates. Results are presented ashazard ratios (HR) with 95% confidence intervals (CI). In a separate model, pre-dictors of VT/VF recurrence were examined using a competing risk model whereprior death was the competing risk and the risk ratio is expressed as the subhazard ratio (SHR).Results: There was no evidence of a difference in survival between patients withprimary vs. secondary prevention (HR = 0.90, 95% CI 0.66 – 1.22, p = 0.478).In the multivariate model predicting survival, VT storm (HR = 3.4, 95% CI 2.1 –5.4, p < 0.001) and appropriate shocks (HR = 1.9, 95% CI 1.3 – 2.7, p < 0.001)were the most significant predictors of death after controlling for age, NYHA class,LVEF, drug use (ACE/ARB (p = 0.004), Class I/III antiarrythmic (p = 0.008) andstatins (p =<0.001) and year of implant (p = 0.032). Patients with a CRT ICD wereat the highest risk compared to patients with a VVI (HR for VVI compared to CRT= 0.47, 95% CI 0.26 – 0.83, p = 0.009). In the competing risks model, patients withsecondary prevention had a higher risk of VT/VF (SHR = 2.0, 95% CI 1.6 – 2.6, p< 0.001) after controlling for age and drug use. Beta-blockers were protective ofrecurrent VT (SHR = 0.64, 95% CI 0.49 – 0.84), as were class I/III antiarrythmicdrugs (SHR = 0.83, 95% CI 0.74 – 0.92, p 0.001). Patients with revascularizationwere less likely to experience VT/VF providing they did not have atrial fibrillation(interaction p = 0.045).Conclusions: Survival is similar in patients receiving ICDs for primary ver-sus secondary prevention, whereas patients with secondary prevention are ata higher risk of VT/VF recurrence. VT storm and appropriate shock therapies arestrongly predictive of mortality.
P1622 Epicardial catheter ablation of left ventriculartachycardias: the anatomic risk of inducing leftphrenic nerve injury
M. Murillo1, D. Sanchez-Quintana1 , G. Pizarro2, E. Gonzalez2,B. Fuertes2 , S. Bayona2, V. Climent1, J.A. Cabrera2. 1University
of Extremadura, Department of Anatomy and Cell Biology, Badajoz, Spain;2Hospital Quiron-Madrid. Universidad Europea de Madrid, Madrid, Spain
Purpose: Epicardial catheter ablation is an increasingly important technique inthe treatment of left ventricular tachycardia. The left phrenic nerve (LPN) is astructure especially at risk when procedures are carried out at the vicinity of thehigh left ventricular wall (HLVW). Detailed information of the anatomic relationsbetween the LPN and the HLVW may be useful to perform the ablation proceduresmore safely.Methods: Twenty-two human cadavers (14 m, 8 f; 64±9 years old) without ob-vious signs of thoracic pathology or prior surgery were carefully dissected. Weexamined by gross inspection and histological sections the course of the LPN inrelation with the epicardial aspect of the HLVW.Results: The LPN, a branch of the left cervical plexus runs dorsal along the leftbrachiocephalic vein. It continues closely applied over the aortic arch, pulmonarytrunk and descends in front of the root of the left lung embedded in betweenthe fibrous pericardium to course between the mediastinal pleura and the lateralsurface of the left ventricle. The course of the LPN along the border of the leftventricle was variable. In 4 specimens (18%), the nerve took an anterior courseand was related to the anterior interventricular groove, high part of the right ven-tricular outflow tract and anterior part of the HLVW (distance LPN to HLVW was3.5±0.5 mm; range 2.5-5.5 mm). In 13 specimens (59%) the nerve descendedlateral to the HLVW (distance LPN to HLVW was 2.3±0.5 mm; range 1.5-5 mm).In 5 specimens (23%) with an inferior course the distance between the LPN andthe HLVW was 2.0±0.5 mm (range 1.5-4.5 mm).
Left Phrenic Nerve and Ventricular Wall
Conclusions: The left phrenic nerve can be extremely close to the high left ven-tricular wall. This structure can be potentially damaged during epicardial ablationof left ventricular tachycardia.
P1623 Association of statin therapy with incidence ofventricular arrhythmia in patients with acute coronarysyndrome
S. Apiyasawat1, T. Ngarmukos1 , C. Sriratanasathavorn2,P. Kasemsuwan3, P. Sritara1. 1Faculty of Medicine Ramathibodi
Hospital of Mahidol University, Bangkok, Thailand; 2Her Majesty’s CardiacCenter, Siriraj Hospital, Bangkok, Thailand; 3BMA Medical College & VajiraHospital, Bangkok, Thailand
Purpose: Besides lowering cholesterol, statin stabilizes atherosclerotic plaqueand potentially reduces ventricular arrhythmia. We tested the hypothesis that priorstatin therapy was associated with lower incidence of in-hospital ventricular ar-rhythmia and cardiac death in patients with acute coronary syndrome.Methods: The study populations were 2009 patients (mean age 64, 67.5% male)enrolled in Thai Registry of Acute Coronary syndrome (TRACS), a prospective,multicenter, nation-wide, observational study of patients with acute coronary syn-drome. Patients were categorized into statin user and non-user according to theirreports of use before the initial presentation. Primary composite endpoint wasin-hospital ventricular arrhythmia and cardiac death. Age and sex-adjusted oddsratios (ORs) and 95% confidence interval (CI) for primary composite endpointwere calculated.Results: During the mean hospital stay of 7 days, a total of 96 patients (4.8%)died; 82 (4.1%) were due to cardiac cause. The primary composite endpoint wasreached in 209 patients (10.4%). Compared to statin non-users, the users hadhigher incidence of prior MI or coronary intervention (42% vs 8.2%), heart fail-ure (62.1% vs. 20.6%), dyslipidemia (30.3% vs. 5.8%), hypertension (36.5% vs.11.2%), and diabetes (31.7% vs. 20.3%) (P<0.0001 for all). Statin users wereless likely to develop ventricular arrhythmia (5.5% vs. 9%; OR=0.59; 95% CI,0.39-0.91; P=0.02) and to reach primary composite endpoint (7.4% vs. 11.5%;OR= 0.59; 95% CI, 0.41-0.85; P=0.005). The odds of primary composite end-point were lower among patients with history of ischemic stroke (OR=0.31; 95%CI, 0.10-0.93; P=0.04), heart failure (OR=0.31, 95% CI 0.14-0.69, P=0.004), andchronic renal failure (OR=0.37; 95% CI, 0.15-0.93; P=0.03).Conclusions: Use of statin may reduce the incidence of ventricular arrhythmiaand cardiac death during acute coronary syndrome especially in patients withhistory of ischemic stroke, heart failure, and chronic renal failure.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Ventricular arrythmias / Heart failure / LV dysfunction 271
P1624 Incidence and clinical significance of ventriculararrhythmias occurring during cardiopulmonaryexercise testing
A. Stuto, E. Cosentino, A. Ambu, G. Bottaro, F. Raineri, C. Sgroi,A. Lo Giudice, B. Armaro, L. Vitale, G. Basile. STAR FOR LIFE
Cardiac Rehabilitation Centre, Siracusa, Italy
Purpose: the aims of this study were to assess the incidence and clinical signifi-cance of ventricular arrhythmias (VA) occurring during cardiopulmonary exercisetesting (CPET) in subjects with and without evidence of heart diseases (HD).Methods: this study concerns 1913 males who performed a CPET from January2007 to January 2009. Based on evidence of HD the subjects were divided in twogroups: 1500/1913 (78.4%), mean age 61.9±11.5 years, with HD (group A) and413/1913 (21.6%), mean age 45.6±14.9 years, without evidence of HD (group B).During CPET were measured the ventilatory equivalent for the CO2 (VE/VCO2)and the end-expiratory tension of the CO2 (PETCO2) at anaerobic threshold (AT)and the oxygen uptake at the peak of exercise, and recorded the occurrence ofVA. The subjects with VA occurrence were followed for 24,03±7,07 months andthe end points were the occurrence of acute coronary syndrome (ACS), heartfailure (HF) and sudden cardiac death (SCD).Results: from the analysis of the data: 1) ectopic ventricular beats (EVB) oc-curred in 421/1500 (28,06%) in group A and 99/413 (23,97%) in group B, 2) nonsustained ventricular tachycardia (NSVT) occurred in 3/413 (0,73%) in group B,only during the exercise, and in 24/1500 (1,6%) in group A, respectively in 10/24(41,6%) during exercise, in 9/24 (37,5%) during recovery and in 5/24 (20,8%)during exercise and recovery from exercise, 3) sustained ventricular tachycardia(SVT) occurred during exercise only in one patient in group A that underwentICD implantation, because a resuscitated cardiac arrest, after six months fromCPET. The follow-up was uneventful in all cases of EVB occurrence and in allcases of NSVT occurrence during exercise, but 4/9 (44,4%) of NSVT occurrenceduring recovery with VE/VCO >32 and PETCO2<36 at AT developed clinical ev-idence of heart failure during the follow-up, and 3/5 (60%) of NSVT occurrenceduring exercise and recovery developed clinical evidence of ACS, whereas 1/5(20%) underwent ICD implantation, because a resuscitated cardiac arrest after 8months of follow-up.Conclusions: the follow-up was uneventful in all cases of EVB occurrence, butone with VT and twenty percent of NSVT occurrence during exercise and recoveryunderwent ICD implantation because of a resuscitated cardiac arrest, about fortyfive percent of patients with NSVT occurrence during recovery developed clinicalevidence of heart failure, and sixty percent of patients with NSVT occurrenceduring exercise and recovery developed clinical evidence of ACS.
P1625 Predictors of electrical storm and its recurrences inpatients with implantable cardioverter-defibrillators
F. Streitner, J. Kuschyk, E. Mahl, C. Dietrich, N. Schoene,C. Veltmann, R. Schimpf, C. Wolpert, M. Borggrefe. Univ. HospitalMannheim, Medical Faculty, Medical Clinic I, Mannheim, Germany
Background: Electrical storms (ES) are associated with a high mortality earlyafter the event. The present study sought to determine prevalence and predic-tors of an ES and its recurrence in patients with cardioverter-defibrillators (ICDs)implanted for primary or secondary prevention.Methods: Single center study analyzing data of consecutive patients who re-ceived an ICD between 1998 and 2008.Results: 955 patients (mean age 66.9±12.8 years; mean left ventricular ejectionfraction (LVEF) 35.7±15.6%) were followed for 54.2±35.5 months (4313 patientyears). 800 of 955 patients (83.8%) received an ICD for primary prevention. In274 of 955 patients (28.7%), 2871 ventricular tachyarrhythmia episodes were ob-served during follow-up. An ES occurred in 63 patients (6.6%). Overall, 153 ESepisodes were seen. 32 of 63 patients with ES (50.8%) experienced more thanone ES episode. 26 of 32 patients (81.2%) with ES recurrences experienced thesecond ES episode within one year. Multivariable Cox regression analysis iden-tified only age >65 years to be predictive for the occurrence of the initial ESevent (OR 2.6; 95%-CI 1.282-5.419; p=0.008) as well as for ES recurrences (OR3.5; 95%-CI 1.207-10.176; p=0.021). LVEF ≤30% (OR 2.2; 95%-CI 1.021-4.856;p=0.044) was identified to be an independent predictor only for ES recurrences.Patients with angiotensin-converting enzyme (ACE) inhibitor therapy after the ini-tial ES event were less likely to experience an ES recurrence (OR 0.39; 95%-CI0.187-0.817; p=0.013).Conclusions: ES occurs in 6.6% of ICD-recipients. The risk for ES recurrenceswithin the first year is high (50.8%). Only age >65 years is predictive for an initialES event and for ES recurrences. LVEF ≤30% and a lack of ACE-inhibitor therapyare independent predictors for ES recurrences.
P1626 Efficacy of pharmacological treatment and geneticanalysis in early diagnosed patients affected by longQT syndrome with impaired A-V conduction
B. Sarubbi1, G. Frisso2, E. Romeo1, E. Evangelista2, A. Cordella2,G. Santarpia1, M.G. Russo1, F. Salvatore2, R. Calabro’1. 1Vincenzo
Monaldi Hospital, Naples, Italy; 2CEINGE-Biotecnologie Avanzate, Naples, Italy
Purpose: The coexistence of QT prolongation, torsade de pointes ventricular
tachycardia (TdPVT) and impaired atrio-ventricular (AV) conduction is a rare ma-lignant variant of the long QT syndrome (LQTS) in infants potentially leading tosudden death. We examined the clinical presentation, genetic background andoutcome of 9 medically treated infants with LQTS and impaired AV conductionreferred to a single centre.Methods: Nine infants referred within the first three weeks of life for occasionallong QTc evaluated with standard ECG and/or 24-hour ECG before and afterantiarrhythmic drugs were studied.Results: 24-hour ECG revealed TdPVT episodes in 5 patients and non-sustainedVT episodes in one. Four patients with TdPVT had 2:1 AV block, the fifth aWenckebach-type AV block. Two others had 2:1 AV block with non-sustained VTor without arrhythmias. Two others had episodes of impaired left bundle branchconduction without arrhythmias. All patients underwent propranolol treatment (1-6mg/kg/day per os) alone or associated with mexiletine (1-6mg/kg/day per os),which resolved life-threatening VT and AV conduction impairments. During follow-up, one patient, aged 3 months, with TdPVT and 2:1 AV block died from untreat-able cardiac arrest; one (aged 13 months) was lost to follow-up. At a medianfollow-up of 84 months (12 to 113 months), seven patients are alive, undergoingtreatment, without arrhythmias or conduction arrhythmias. DNA mutations wereidentified in KCNH2 (n = 2), SCN5A (n = 2) and KCNQ1 (n = 1) genes.Conclusion: Conduction abnormalities associated with LQTS represent"pseudo" impairment of AV conduction resulting from sinus intervals shorter thanrefractoriness of the conduction system. Beta-blockers alone or combined withmexiletine can benefit impaired AV conduction associated with LQTS. Screeningfor SCN5A, KCNQ1, KCNH2, KCNE1 and KCNE2 genes does not identify thisparticular subset of high-risk patients, which suggests that factors other than theprimary mutation affect probability of manifesting symptoms of LQTS, as occursfor the common variant in NOS1AP gene.
HEART FAILURE / LV DYSFUNCTION
P1627 Risk stratification in chronic ischemic heart disease:Is scar a better predictor of adverse outcome then LVejection fraction?
R. Shakur, C. Yu, C. Bucciarelli-Ducci, I. Roussin, M. Dweck,R. O’hanlon, C. Parsai, S. Rizvi, D.J. Pennell, S.K. Prasad. Royal
Brompton Hospital, Cardiovascular Magnetic Resonance Unit, London, UnitedKingdom
Introduction: Risk stratification in chronic coronary artery disease is challeng-ing. Whilst conventional risk stratification is based on LVEF, it has a relatively lowpositive predictive value with a reasonable negative predictive value for guidingdelivery of expensive device therapy. An important mechanism for arrhythmia andheart-failure is the presence of significant amounts of scar tissue. Recent ad-vances in cardiovascular magnetic resonance have enabled the in-vivo detectionof scar tissue in high resolution. In this study we assessed the comparative valueof both parameters in predicting outcome in patients with chronic stable coronaryartery disease.Methods: 151 consecutive chronic ischaemic heart disease patients underwent aCMR scan (age, 72.0±9.8years) between 2002-2007 (Siemens 1.5T scanner). Allpatients had a previous history of myocardial infarction >6months and underwentcine MRI to measure LV function, volume and mass. A late contrast-enhancedstudy was also performed to assess the amount of scar. Patients were divided intogroups according to LVEF (<35%, >35%). LVEF was calculated from a 3D stackof short-axis slices, using the modified Simpson’s method. Infarct size was de-termined by a blinded observer using semi-automated software, Medis (Leiden).A primary composite endpoint of major adverse cardiovascular events (MACE)including all-cause mortality, unplanned cardiovascular hospitalisation, and majorarrhythmia was used.Results: Across both subgroups of LVEF, the amount of scar tissue was highlypredictive of adverse outcomes (p=0.001) in both patients with severe and mod-erate levels of LV dysfunction.Conclusion: Both LVEF and scar tissue are important predictors of MACE inpatients with chronic stable ischaemic heart disease. The amount of scar tissueremains an important predictor of adverse events in patients with both severe andmoderate levels of functional impairment.
P1628 May men and women have different predictors forcardiac mortality in chronic heart failure?
G. Kozdag, M. Yaymaci, G. Ertas, U. Bildirici, T. Kilic, G. Kahraman,D. Ural. Kocaeli University, Faculty of Medicine, Department ofCardiology, Kocaeli, Turkey
Background and Aim: Understanding the influence of gender differencies onpredictors for cardiac mortality in chronic heart failure may allow for longer lifetimeand better life style. This study described the gender differences in chronic heartfailure (HF) patients on cardiac mortality.Methods: Consecutive patients (373 men vs. 207 women) from 2003 and 2009were recruited from a single HF unit. Mean follow-up was 39±14 months.Results: Mean age was 63±13 years; left ventricular ejection fraction (LVEF)26±9%. Women had lower mean LVEF than male (25±9% vs 27±10%, p=0.016),
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

272 Heart failure / LV dysfunction
and similar New York Heart Association (NYHA) functional class and BNP levelswith men. By the end of the study, both genders had similar cardiovascular mor-tality (35% men vs 38% women, p=NS). Age, NYHA functional class, BNP lev-els, uric acid levels, ejection fraction and cardiac dimensions were predictors ofmortality in men with chronic heart failure. Age, NYHA functional class, hs-CRPlevels, uric acid levels, triglyceride levels were predictors of mortality in womenwith chronic heart failure. In multivariate analysis, age was the strongest pre-dictor of mortality in men (95% CI 1.04-1.09, p<0.001), and women (95% CI1.02-1.08, p=0.004) with chronic HF. If we removed the age from multivariateanalysis NYHA class (95% CI 2.41-7.98, p<0.001) and uric acid levels (95% CI1.07-1.31, p=0.001) were important predictors for men. For women, NYHA class(95% CI 2.41-13.12, p<0.001) and hs-CRP levels (95% CI 1.16-1.29, p=0.005)were important predictors for cardiac mortality after the age was removed fromthe analysis.Conclusions: In a contemporary tertiary referral heart failure clinic, predictors ofcardiac mortality were similar between the genders.
P1629 Cardiac Troponin T as a predictor of long timesurvival after cardiac resynchronization therapy
M. Aarones1, L. Gullestad1, S. Aakhus2, T. Ueland3, R. Skaardal2,R. Wergeland4, H. Aass5, H.J. Smith6, P. Aukrust7, E. Kongsgaard2.1Oslo University Hospital, Dept. of Cardiology and University of
Oslo, Oslo, Norway; 2Oslo University Hospital, Department of Cardiology, Oslo,Norway; 3Oslo University Hospital, Section of Endocrinology, Oslo, Norway;4Oslo University Hospital, Dep. of Medical Boichemistry, Oslo, Norway; 5VestfoldHospital, Tonsberg, Norway; 6University of Oslo and Oslo University Hospital,Dep. of Radiology, Oslo, Norway; 7University of Oslo and Oslo UniversityHospital, Section for Clinical Immunology and Infectious Dis, Oslo, Norway
Aims: Predicting response to cardiac resynchronization therapy (CRT) is chal-lenging. High sensitive cardiac Troponin T (hsTnT) might predict response to CRTand identify patients at a high risk of experiencing severe cardiovascular events.We investigated whether baseline levels of hsTnT were associated with responseto CRT and with severe cardiovascular events after long term follow-up.Methods: 81 consecutive patients were included according to the current guide-lines for cardiac resynchronization therapy. Biochemical, functional, and clinicalparameters were assessed at baseline and at 3, 6 and 12 months follow up(FU), and mortality/cardiac transplantation after 46±6 months FU was investi-gated. Cardiac magnetic resonance imaging (MRI) and echocardiography wereused to assess left ventricular function including viability and remodeling.Results: 75 patients completed 12 months FU and after a follow-up of 46±6months a total of 15 patients died, 13 of these from cardiovascular causes and 7underwent heart transplantation. Baseline hsTnT < 15ng/L predicted response toCRT and was associated with a more favourable outcome with regard to severecardiovascular events. Multivariate analysis found that presence of transmuralscar tissue/fibrosis on MRI, use of statins and relatively lower ejection fractionon echocardiography were independently associated with higher concentrationsof hsTnT at baseline. There was a strong correlation between hsTnT and NT-proBNPConclusions: HsTnT levels were elevated in the majority of HF patients that werescheduled for CRT. HsTnT levels predicted response to CRT as well long timesurvival. CRT is associated with a significant reduction in hsTnT concentration.
P1630 Prognostic value of cancer antigen 125 (ca 125) inmild to moderate heart failure patients
E. Vizzardi, N. Pezzali, A. D’ Aloia, G. Faden, M. Metra, L. Dei Cas.Sec. of Cardiovasc. Diseases, Department of Experimental andApplied Med., University and Hospital, Brescia, Italy
Purpose: Plasma levels of tumoral carbohydrate 125 antigen marker (CA 125)have been found elevated among patients (pts) with heart failure (HF). They relateto clinical condition and to diastolic and systolic left ventricular (LV) parameters,as previously observed. Also, CA125 is independently related to mortality amongacute and advanced HF pts. We evaluated the prognostic value of CA125 in apopulation of pts with mild to moderate HF.Methods: Serum levels of CA 125 were obtained in 102 pts with mild to moder-ate HF due to idiopathic (48%) or ischemic (52%) dilated cardiomyopathy (age64±10.6 years, left ventricular ejection fraction (LVEF), 34.36±8.54%, NYHAclass 2±0.3) under optimized medical therapy according to the guidelines (95%ACE inhibitors-ARBs, 86% beta-blockers). All the pts underwent a complete clini-cal examination and transthoracic echocardiography. Events occurring in a mean1380.4±487.5 days follow-up were recorded.Results: During the follow-up, 16 (15.68%) cardiovascular deaths and 23(22.54%) cardiovascular deaths+hospitalizations occurred. 15 (14.7%) ptsshowed CA125 levels >30U/ml (established cut-off value). Considering cardiacdeath, comparison between Kaplan Meyer survival curves by the logrank testshowed that pts with CA125 levels higher than the cut-off value had a worse sur-vival vs the others (p<0.0001, HR 0.01722 among pts with CA125 levels lowerthan the cut-off value, 95% CI 0.003173-0.09344). This was also observed whenconsidering cardiovascular death+hospitalizations as the end-point (p=0.0003,HR 0.07248 among the pts with CA125 lower than the cut-off value, 95% CI0.01723-0.3049). Moreover, pts with CA125 levels ≥ 75% percentile showed a
worse survival vs the other quartiles groups, with a higher incidence of cardiacdeaths as well as cardiovascular death+hospitalizations (p<0.0001).Conclusions: In mild-to-moderate HF pts under optimized therapy, higher plasmaCA 125 levels are an effective prognostic marker in forecasting cardiovascularevents and hospitalization and may contribute to a better risk stratification.
P1631 Prevalence of myocardial fibrosis in thalassemiamajor assessed by late gadolinium enhancementcardiovascular magnetic resonance
P. Kirk, J.-P. Carpenter, M.A. Tanner, D.J. Pennell. Royal BromptonHospital, London, United Kingdom
Purpose: In transfusion dependent thalassemia major (TM), heart failure dueto cardiac siderosis remains a dominant cause of mortality but can be reversedwith intensive chelation therapy. The role of myocardial fibrosis in the genesisof cardiac failure is unclear. Late gadolinium enhancement (LGE) cardiovascularmagnetic resonance (CMR) detects replacement fibrosis in a wide range of car-diomyopathies and is linked to the development of heart failure and arrhythmias.CMR also measures storage cardiac iron using T2*, a non-invasive, highly repro-ducible technique. We used LGE and cardiac T2* to investigate the incidence ofmacroscopic fibrosis and its correlation with myocardial iron and cardiac functionin TM patients.Methods: 45 TM patients (19 male, mean age 27.1±9.6 years) were scannedat 1.5T (Siemens Sonata, Erlangen, Germany). A single breath-hold, multi-echosequence with 8 echo times (2.6–16.7ms) was used to acquire a single mid-ventricular short axis slice for T2* measurement. Left ventricular volumes andejection fraction (LVEF) were measured from a set of long axis and contigu-ous short axis cines. LGE images were acquired 10 minutes after intravenousgadolinium-DTPA (0.1mmol/kg). Data analysis was performed by two experi-enced independent readers using CMRtools (CVIS, London UK).Results: Fibrosis was detected in only one patient, whose T2* was 20.1ms andLVEF 57%. There were 5 patients with a history of heart failure with recovery, 3patients with current LV dysfunction undergoing treatment, and 18 patients withmyocardial iron loading (T2*<20ms) at the time of scan, but none of these pa-tients had fibrosis. 27 patients had no significant iron loading (T2*>20ms), 15had mild/moderate loading (T2* 10-20ms) and 3 had severe myocardial iron load-ing (T2*<10). There was no difference in LVEF between patients with T2*>20msand those with T2* between 10-20ms (LVEF 68.3±8.3% vs 64.1±6.2%; P=0.34)but in comparison to patients with T2*>20ms, those with T2*<10ms had a signif-icantly reduced LVEF (68.3±8.3% vs 54.7±3.5%; P <0.01).Conclusions: This study demonstrates that macroscopic cardiac fibrosis is un-common in TM over a broad range of iron loading. No fibrosis was detected inpatients with current or prior heart failure, or in patients with cardiac iron loadingwithout heart failure. Our results show no relation between cardiac iron levels andfibrosis, and no relation between fibrosis and heart failure in TM patients. It istherefore unlikely that macroscopic fibrosis plays a major role in the pathophysi-ology of this reversible cardiac dysfunction.
P1632 Potential pathophysiological role of chronic Fcγ-IIreceptor stimulation in DCM
L.R. Herda, C. Mueller, L.G. Eckerle, Y. Reinke, S.B. Felix, A. Staudt.Ernst Moritz Arndt University of Greifswald, Department of InternalMedicine B, Greifswald, Germany
Introduction: Cardiotropic autoantibodies, which have been described in dilatedcardiomyopathy (DCM), can induce signals into the cell via two mechanisms: oneis mediated by binding to the respective antigen via the Fab-part, the other viabinding to Fcγ receptors. This study aimed to evaluate the role of Fcγ receptor IIin mediating reduced myocardial contractility in dilated cardiomyopathy.Methods: 10 male Lewis rats each, age 4-6 weeks, were immunized by sub-cutaneous injection of an Fcγ receptor II peptide or vehicle and followed up byechocardiography. Isolated cardiomyocytes were cultured with goat IgG and Fcγ
receptor II antibodies. Western blotting was performed to assess the phospho-rylation status of Akt. Cellular contractility was measured in cardiomyocytes byfield-stimulation using a video-imaging edge detector system.Results: Animals developing an Fcγ receptor II-antibody showed progressive leftventricular dilatation (LVEDD: 0.36±0.01cm to 0.41±0.01cm; p<0.05) and re-duced myocardial contractility (LVEF: 77.8±2.4% to 52.9±3.5%; p<0.001). An-tibody level was negatively associated with left ventricular function (r=-0.596;p<0.001). Contractility analyses of isolated cardiomyocytes showed negative in-otropy after incubation with anti-Fcγ receptor II antibodies, while goat IgG didnot influence contractility in comparison to medium control (-18.1±4.5% vs. -2.6-±2,7%; p<0.05). Phosphorylation of Akt was markedly reduced after addition ofanti-Fcγ receptor II antibodies in isolated cardiomyocytes compared to controland goat IgG.Conclusions: Immunization against the Fcγ receptor II led to left ventricular di-latation and dysfunction. Activation of this receptor might therefore be involved inantibody-mediated DCM. Negative inotropy in this model might be mediated byreduced activation of Akt.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / LV dysfunction 273
P1633 Diabetes mellitus worsens cardiac remodeling inaged spontaneously hypertensive rats
K. Okoshi1, C.M. Rosa1, N.P. Xavier1, A.A.H. Fernandes2 ,D.H.S. Campos1, M.D.M. Cezar1, P.F. Martinez1, A.H.R. Takamoto1 ,A.C. Cicogna1, M.P. Okoshi1. 1UNESP - Sao Paulo State University
- Botucatu Medical School, Botucatu, Brazil; 2UNESP - Botucatu BiosciencesInstitute, Botucatu, Brazil
Purpose: The association of diabetes mellitus (DM) and systemic arterial hy-pertension induces greater structural and functional cardiac damage than eithercondition alone. However, few studies have examined this association, especiallyin aged rats.Therefore, this study aimed to analyze the influence of DM on left ventricular andatrial remodeling in senescent hypertensive rats (SHR).Methods: Thirty 18 month old male SHR’s were divided into two groups: con-trol (CTL, n=15) and diabetic (DM, n=15). DM was induced by streptozotocin (40mg/kg, i.p.). Nine weeks after DM induction, the animals underwent echocardio-graphy and myocardial functional study of left ventricular (LV) isolated papillarymuscle. LV myocardial alpha and beta-myosin heavy chain isoforms (alpha-MyHCand beta-MyHC), sarcoplasmic reticulum Ca++ ATPase (SERCA), and atrial na-triuretic peptide (ANP) gene expression was assessed by real time RT-PCR. Ox-idative stress was determined by measuring serum levels of lipid hydroperox-ide (LPO), superoxide dismutase (SOD), and glutathione peroxidase (GPx). Datawere analyzed by Student’s t test (p<0.05).Results: DM group showed increased LV (CTL, 24.6±3.18; DM, 30.6±5.34mm/kg; p<0.05) and left atrial (CTL, 21.5±3.72; DM, 26.3±5.82 mm/kg; p<0.05)diameters normalized to body weight, and LV relative wall thickness reduction(CTL, 0.44±0.07; DM, 0.40±0.05; p<0.05). Indexes of in vivo LV systolic func-tion (fractional shortening: CTL, 48.6±7.9; DM, 40.0±8.6%; p<0.05; posteriorwall shortening velocity: CTL, 31.8±6.70; DM, 26.4±5.93 mm/s; p<0.05) and invitro myocardial contractile function (developed tension: CTL, 5.38±2.76; DM,3.56±1.82 g/mm2; p<0.05; positive derivative of tension: CTL, 43.2±22.5; DM,25.7±15.4 g/mm2/s; p<0.05; time to peak of developed tension: CTL, 236±30;DM, 264±24 ms; p<0.05) were impaired in the DM group. DM did not cause al-terations in diastolic function. ANP expression was higher in DM (p=0.009). Alphaand beta-MyHC, and SERCA expression did not differ between groups. LPO lev-els (CTL: 8.80±0.84; DM: 11.1±1.04 nmol/ml; p<0.05) were increased and SOD(CTL: 687±84; DM: 396±50 U/g protein; p<0.05) and GPx (CTL: 20.7±2.0; DM:17.6±1.95 nmol/ml; p<0.05) decreased in the DM group.Conclusions: Diabetes mellitus causes dilation of the left cardiac chambers andimpairs LV myocardial and ventricular function in aged spontaneously hyperten-sive rats. These alterations are associated with increased oxidative stress andhigher ANP gene expression.
P1634 Growth-differentiation factor-15, a novel biomarker ofseverity disease in hypertrophic cardiomyopathy
D. Hernandez-Romero1 , E. Jover1, J.A. Vilchez1, A. Garcia-Honrubia2, B. Bonacasa1, G. De La Morena1, V. Climent2,P. Martinez1, M. Valdes1, F. Marin1. 1Hospital Universitario Virgen
de la Arrixaca, Murcia, Murcia, Spain; 2General University Hospital of Alicante,Alicante, Spain
Hypertrophic cardiomyopathy (HCM) is characterised by inappropriate hypertro-phy, small-vessel coronary artery disease, myocyte disarray and increased inter-stitial fibrosis. Growth-differentiation factor-15 (GDF-15) is a new marker of riskand prognosis in acute coronary syndrome and it has recently been proposed toregulate myocite hypertrophy. However there is no evidence of studies performedin HCM patients and their functional status. We hypothesised that GDF-15 couldbe raised in HCM patients with severe disease evolution.Methods: We included a very selected population in a case-control study con-sisted of 56 stable HCM patients from two monographic HCM outpatient clinics,and age- and sex-matched healthy controls (exclusion criteria diabetes, hyperten-sion, hemodynamic unstability and atrial fibrillation). Secondly, in order to evaluatewhether GDF-15 levels were associated with parameters of severity of the dis-ease, we performed a study including up to 140 consecutive HCM patients, 71%males aged 47±15 years. All patients fulfilled conventional criteria for HCM. Acomplete history and clinical examination was performed, including 12-lead elec-trocardiogram, echocardiography, 24 hours ECG-Holter monitoring, and symptomlimited treadmill exercise test. MET values (metabolic equivalent units) were cal-culated. A cardiac MRI was performed with late myocardial-enhanced study withGadolinium. We determined two established biomarkers of cardiac remodelling:matrix metalloproteinase-2 (MMP-2) and NT-proBNP. Plasma GDF-15 levels wereassayed by commercial ELISA.Results: We found no differences in GDF-15 plasma levels between patientsand controls (p:0.386) in the case-control study. For the HCM population associa-tion study, we found that GDF-15 level correlated with age (r:0.47, p<0.001) andexercise capacity (r:-0.48, p<0.001). In addition, GDF-15 was found raised in pa-tients with severe functional class, atrial fibrillation and female gender (p:0.002,p:0.016, and p: 0.028; respectively, Mann-Whitney U test). GDF-15 levels pos-itively correlated with MMP-2, and NT-proBNP (r:0.41, p:0.008; r:0.29, p:0.039;respectively). We did not find any significant association with non sustained ven-tricular tachycardia, abnormal blood pressure response, presence of obstructionor late Gadolinum enhancement.
Conclusions: We show, for the firt time, that GDF-15 is a potential biomarker ofdisease severity in patients with HCM, as it shows high levels in patients present-ing worse exercise capacity and functional class. Levels of GDF-15 are associ-ated with different biomarkers related to cardiac remodeling of the disease.
P1635 Functional correlates of increased NT-proBNP andTroponin I in cardiac AL amyloidosis
F. Musca1, F. Salinaro1, G. Palladini1, I. Fracchioni1 , G. Palladini2,R. Albertini3, R. Moratti3, C. Rapezzi4 , G. Merlini2, S. Perlini1.1Clinica Medica II, Fondaz IRCCS S.Matteo, University of Pavia,
Pavia, Italy; 2Center for Amyloidosis, Biotechnology Laboratories IRCCS SanMatteo, Pavia, Italy; 3University of Pavia, Department of Biochemistry "A.Castellani", Pavia, Italy; 4University Hospital Polyclinic San Orsola-Malpighi,Department of Cardiology, Bologna, Italy
Background: Increased concentrations of both NT-proBNP and Troponin I (TnI)characterize high-risk patients with cardiac AL amyloidosis and a dismal progno-sis. Little is known on the functional correlates of the increase of these biomark-ers.Methods: To evaluate the relationships between NT-proBNP and TnI serum con-centrations and indices of both systolic and diastolic function in cardiac AL amyloi-dosis, a complete echocardiographic evaluation was performed in 221 consecu-tive newly diagnosed patients with cardiac AL amyloidosis, referred to our centerbetween 2006 and 2009. Patients in whom cardiac involvement was excludedserved as controls (n=81). Diastolic function was characterized in terms of: trans-mitral Doppler early (E)and atrial (A) velocities, E deceleration time, pulmonaryvenous flow velocity, early Tissue Doppler (TDI) peak velocity (E’) and E/E’ ratio.Systolic function was evaluated as: left ventricular (LV) ejection fraction (EF), lon-gitudinalmitral annulus septum excursion (MAPSE), isovolumic (IVVm) and sys-tolic (Sm) TDI peak velocity. Serum NT-proBNP and TnI were concomitantly as-sessed. Patients with significant valve disease, previous myocardial infarction,atrial fibrillation, or chronic obstructive lung disease were excluded.Results: When compared with AL patients without myocardial involvement, car-diac AL was characterized by increased wall thickness (p<0.001) and reducedend-diastolic LV volumes (p<0.001). Global systolic function, as assessed by LVejection fraction, was preserved. In cardiac AL patients, highly significant univari-ate correlations were found between NT-proBNP concentrations and indices ofboth diastolic and systolic dysfunction. In contrast, TnI concentrations did onlycorrelate with MAPSE, IVVm, and Sm, i.e. with indices of depressed regionalsystolic function, whereas no correlation was found with markers of diastolic(dys)function. At multivariate regression analysis, the main NT-proBNP determi-nant was the diastolic index E/E’ ratio, whereas MAPSE and TDI systolic peakvelocity resulted as TnI determinants. Patients with increased TnI concentrationsshowed the highest extent of regional systolic dysfunction.Conclusions: In cardiac AL amyloidosis, higher TnI concentrations (characteriz-ing a subset of patients with a worse prognosis) are related to a more profoundextent of myocardial systolic dysfunction.
P1636 Left ventricular sphericity as an early indicator ofdecompensated hypertrophy in experimental aortaregurgitation
M.G. Roscani, B.F. Polegato, A.P.M. Lousada, S.E. Tanni,M.F. Minicucci, P.S. Azevedo, M.B. Bruno, E.P. Jamas,
L.S. Matsubara, B.B. Matsubara. Sao Paulo State University, Botucatu MedicalSchool, Department of Internal Medicine, Botucatu, Brazil
Purpose: Increased left ventricular (LV) diastolic diameter (DD) has been usedas a marker for surgical replacement of insufficient aortic valve. However, this en-largement may occur after irreversible damage of myocardium. The aim of thisstudy was to evaluate in vivo temporal changes of the heart and how this is asso-ciated with LV function.Methods: Male Wistar rats (BW: 250g) underwent surgical procedure (anesthe-sia: ketamine-50mg/kg plus xylazine-1mg/kg) for inducing acute aorta regurgi-tation (AR group, n= 23) or sham operation (SH group, n= 12). Transthoracicechocardiograms were performed at 1, 4, 8 and 16 weeks after procedure.Anatomic variables were: LVDD, LV sphericity index (SI), normalized left atriumarea (LAA) and LV relative wall thickness (RWT) and functional index was LV frac-tional shortening (FS). Statistical analyses used GEE model (General EstimativeEquation, STATA 10.0) or repeated measures ANOVA (p<0.05).Results: There were interactions between time and AR for increasing LVDD(p<0.001), LAA (p=0.0011) and SI (p<0.001), and for decreasing RWT (p=0.002)and FS (p<0.001). Compared to week 1, the increased SI at week 4 (0.72±0.09vs. 0.65±0.64; p<0.001) preceded the LVDD enlargement (9.0±1.3mm vs.7.6±0.63mm; p<0.05) and LAA increasing (1.56±0.32 vs. 1.45±0.20; p<0.05)observed at week 8 and RWT decreasing observed at week 16 (0.175±0.044 vs.0.20±.025; p=0.003). There was an interaction between time and SI for reducingFS (p<0.001). LV systolic dysfunction was detected at week 8 and preceded LAAenlargement at week 16. This suggested increased LV diastolic pressure and itwas coincident with the decreased RWT indicating LV dilation.Conclusion: Left ventricular spherical geometry in aorta regurgitation is an earlysign of decompensated hypertrophy, preceding systolic and diastolic LV dysfunc-tion.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

274 Heart failure / LV dysfunction
P1637 Micro RNAs could play key roles in progression of leftventricular diastolic dysfunction involved inmyocardial fibrosis in patients with heart failure
H. Izawa1, Y. Kato2, H. Yokoi1, W. Fujiwara1, C. Xian Wu3,Y. Mizoguchi1 , S. Morimoto2, T. Murohara3, Y. Ozaki2, M. Nomura1.
1Fujita Health University, Banbuntanehotokukai Hospital, Nagoya, Japan; 2FujitaHealth University, Toyoake, Japan; 3Nagoya University Graduate School ofMedicine, Nagoya, Japan
Purpose: Left ventricular (LV) diastolic dysfunction induces diastolic heart fail-ure. However, the molecular mechanisms that underlie LV diastolic dysfunctionremain incompletely understood. MicroRNAs (miRNAs) are recently discovered,posttranscriptional regulators of gene expression. We hypothesized that miRNAsmight play key roles in the pathogenesis of LV diastolic dysfunction.Methods: We measured the following parameters obtained by conventional andtissue Doppler echocardiography in 8 patients with idiopathic dilated cardiomy-opathy (5 male and 3 female): peak early (E) and late (A) diastolic velocity of themitral inflow, E/A ratio, peak early myocardial diastolic velocity (E’), and E/E’ ratio.We also performed genome-wide miRNA expression profiling in each endomy-ocardial biopsy specimens obtained from these 8 patients.Results: Four patients had increased E/E’ ratio (> 15; mean ± SD, 20.2±5.5) in-dicating elevated LV diastolic filling pressure (Group I) and 4 had normal E/E’ ratio(<15; 8.9±0.9) (Group II). LV ejection fraction did not differ between groups I andII (34±7 vs. 28±9%, respectively). Collagen volume fraction in biopsy samples ingroup I were increased compared with those in group II (4.4±0.9 vs. 2.3±0.3%,respectively). Out of 650 miRNAs measured, 7 were differentially expressed ingroup I compared with group II (p < 0.01). The expressions of 6 miRNAs weresignificantly (p < 0.01) reduced and the expressions of 1 miRNA was significantly(p < 0.01) increased in group I compared with group II.Conclusion: We demonstrated that specific miRNAs could play keyl roles in thepathogenesis of LV diastolic dysfunction in patients with idiopathic dilated car-diomyopathy. These findings call attention to the potential of miRNAs to provideetiologic insights as well as therapeutic targets for progression of diastolic dys-function in patients with chronic heart failure.
P1638 Low HDL cholesterol and newly diagnosed type IIdiabetes or insulin resistance are major determinantsof impaired myocardial blood flow in dilatedcardiomyopathy
D. Neglia1, D. Rovai2, C. Vecoli3, G. Rossi2, F. Bigazzi2, P. Iozzo2,S. Pardini2, D. Giannessi2, A. L’abbate3, T. Sampietro1. 1Fondazione G.Monasterio CNR - Regione Toscana, Pisa, Italy; 2CNR institute of ClinicalPhysiology, Pisa, Italy; 3Scuola Superiore Sant’Anna, Pisa, Italy
Purpose: In patients with dilated cardiomyopathy (DCM), absolute myocardialblood flow (MBF) at rest and during stress is frequently impaired likely due tocoronary endothelial/microvascular dysfunction. We tested the hypothesis thatDCM and impaired MBF are related with cardiovascular risk factors and with anincreased 10- year risk of Coronary Heart Disease (CHD risk).Methods: Eighty-three consecutive patients (61 males, aged 60±10 yrs) withsystolic left ventricular dysfunction (ejection fraction [EF] 38±10%) and angio-graphically normal coronary arteries were studied. The diagnosis of DCM wasposed in patients with a LVEF <45% associated with a LV end-diastolic diame-ter >60mm at 2D-echocardiography. Absolute MBF was measured by positronemission tomography, using 13N-Ammonia as flow tracer, both at rest and duringdipyridamole infusion (0.56 mg/kg I.V. over 4 min). MBF was considered abnormalif <0.65 ml/min/g at rest, and <1.36 ml/min/g after dipyridamole. Cardiovascularrisk factors (age, sex, family history of CHD, newly diagnosed type II diabetes mel-litus or insulin resistance [NIDD/IR], arterial hypertension, hypercholesterolemia,low HDL cholesterol, smoking habit and obesity) were entered in a logistic modelto derive the independent determinants of DCM and impaired MBF. Individual10-year CHD risk was estimated from Framingham CHD risk score.Results: DCM was diagnosed in 44/83 patients (53%). An abnormal MBF waspresent in 28/44 (64%) DCM patients and in 16/39 (41%) non DCM patients(P<0.05). Age, NIDD/IR and low HDL cholesterol (<40 mg/dl) were independentpredictors of DCM; the hazard ratio was 1.07 (95% confidence interval [CI] 1.00-1.13; P<0.05) for age, 3.47 (95% CI 1.21-9.97; P<0.05) for NIDD/IR and 3.73(95% CI 1.32-10.54; P<0.01) for low HDL cholesterol. NIDD/IR and low HDLcholesterol were also independent predictors of abnormal MBF, with hazard ra-tios of 3.20 (95% CI 1.17-8.75; P<0.05) and 3.36 (95% CI 1.28-8.81, P<0.01),respectively. LV function was not an independent predictor of abnormal MBF. The10-year CHD risk was higher (18±11%) in patients with DCM and abnormal MBFthan in the others (11±7%, P<0.05).Conclusion: DCM and impaired myocardial blood flow are related with low HDLcholesterol levels, presence of newly diagnosed type II diabetes or insulin resis-tance and increased 10-year CHD risk. These results suggest possible commonpathogenetic pathways between DCM and CHD.
P1639 The relationship between CA 125 levels and rightventricular function in patients with chronicobstructive pulmonary disease
O. Uz, D. Tas, E. Kardesoglu, G. Acar, M. Aparci, Z. Isilak,B.Y. Cingozbay, B.S. Cebeci. GATA Haydarpasa Training Hospital,
Istanbul, Turkey
Objective: A few studies have shown that elevated CA 125 levels are associatedwith chronic obstructive pulmonary disease (COPD) However, there are no dataconcerning the associaton between serum CA 125 levels and right ventricularfunction in COPD patients. Aim of this study was to evaluate the role of serumCA 125 in patients with COPD and its possible relationship with right ventricularechocardiography parameters.Methods: Fifty-two patients with COPD (38 males/14 females, mean age68,9±5,7 years) were studied. The control group consisted of 30 age-gendermatched healthy volunteers (23 males/7 females, mean age 64,2±6,3 years).Coventional echocardiographyic parameters, tissue doppler imaging (TDI) andserum CA 125 level measurement was performed in all subjects.Results: Serum CA 125 levels were significantly higher in COPD patients thanin controls (26,7±22,5 vs. 7,3±1,4 pg/mL, P<0.05). Pulmonary artery pressure(PAP) (P=0.0001), right ventricular enddiastolic volume (RVEDV) (P=0.0001),and right ventricle (RV) myocardial performance index (MPI) (P=0.0001) val-ues were higher in COPD patients. There was a powerful correlation betweenserum CA 125 levels and PAP values (r=0.70, P<0.0001). Additionally, the serumCA 125 levels correlated with RVEDV (r=0.49, P<0.0001), and RV MPI (r=0.34,P<0.0001).Conclusion: This study shows that there is a significant correlation between rightheart haemodynamic parameters and levels of CA 125 in the serum of patientswith COPD. It that appears CA 125 levels may be useful in evaluating right ven-tricular function in these patients.
P1640 The clinical significance of combined determinationon cardiac troponin T and myocardial zymogram inearly diagnosis of myocardium injury in patients withacute mountain sickness
Q. Zhou, Y. Luo, P. Guo. Department of High Altitude Disease, ThirdMilitary Medical University, Chongqing, China, People’s Republic of
Background: Acute mountain sickness (AMS) is one of main threats to humanhealth in people who rapidly advance towards high altitude. Of the 3,184 cases ofacute mountain disease that we examined, we found that 70% of patients sufferedfrom abnormal heart dysfunction. However, due to a lack of effective test method,the rate of early diagnosis of myocardial injury in patients with acute mountainsickness is not high.Objective: To make an early diagnosis of myocardial injury in patients with acutemountain disease, cardiac troponin T (cTnT) and CK-MB were measured in 29patients with high altitude pulmonary edema (HAPE) at 3,658 meters, and thenthe value of testing for both cTnT and CK-MB for the early diagnosis of myocardialinjury in AMS was determined.Methods: Of 29 male patients with HAPE, 8 had mild HAPE, 15 had moderateHAPE, and 6 had severe HAPE. With the permission of the patients, blood sam-ples (3 ml) were obtained from the cubital veins were obtained. One-step incuba-tion ELISA Kits (Boehringer Mannheim Corporation, Germany) for the detection ofcTnT were used to determine the levels of cTnT in the serum. Serum Ck-MB wasdetermined by rate assay kits provided by Shanghai Changzheng Medical Sci-ence CO., Ltd. in China. Then, the patients were given routine treatment and weregiven nitric oxide (NO) to inhale, and the serum cTnT and CK-MB were deter-mined at the same time that ECG and B-mode echocardiography were performed.Results: Contents of serum cTnT and CK-MB in HAPE patients with abnormalcardiac function are abnormally high, and these abnormal changes are markedlyearlier than those observed in ECG or B-mode echocardiography examinations.There were significant increases of serum cTnT (0.215±0.123 μg/L) and CK-MB (25.01±5.83μ/L).Both of them recovered to the normal range after resolutionof HAPE: cTnT (0.054±0.0513μg/L) and CK-MB (16.3±4.243μ/L). There was apronounced difference between before and after treatment levels of cTnT and CK-MB (P < 0.01).The data indicates that determination of both cTnT and CK-MB isvaluable in the early diagnosis of high altitude-induced myocardial injury and thatwe can use these serum markers to obtain an early diagnosis of this condition inpatients with high-altitude exposure.Conclusions: Serum cTnT is a highly sensitive and special biochemical markerfor myocardial injury. Combined determination of cTnT and CK-MB can increasethe early diagnosis rate of high altitude myocardial injury, minimizing the rate ofmisdiagnosis and improving the rate of early diagnosis.
P1641 Determinants of ventilator inefficiency in heart failurewith normal left ventricular ejection fraction: role ofchanges in wedge pressure during exercise
M.T. Maeder1, N.M. Htun2, D.M. Kaye1. 1Baker IDI Heart andDiabetes Institute, Melbourne, Australia; 2The Alfred Hospital,
Melbourne, Australia
Purpose: Patients with heart failure (HF) due to reduced left ventricular fraction
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / LV dysfunction 275
(LVEF; HFREF) are well characterized by abnormalities of haemodynamics andby indices of the ventilatory response to exercise including the peak oxygen con-sumption (pVO2) and the slope of the relationship between minute ventilation andcarbon dioxide production (VE/VCO2 slope). Recently several of these parame-ters have been documented in patients with HF and a normal LVEF (HFNEF)although their pathophysiological significance in this group remains uncertain. Inorder to better understand the mechanisms contributing to exercise limitation inHFNEF, we aimed to compare the VE/VCO2 slope between patients with HFREF,HFNEF, and healthy controls, and to assess the association between exercisehaemodynamics and the VE/VCO2 slope in patients with normal LVEF.Methods: We studied 36 patients with advanced HFREF, 10 patients with HFNEF,and 8 asymptomatic controls (LVEF 24±8, 68±5, 64±8%; pVO2 12.7±3.7,15.1±4.9, 26.5±12.5 ml/kg/min) undergoing cardiopulmonary exercise testingand right heart catheterisation. Patients with normal LVEF (ie, the control andHFNEF groups) underwent exercise right heart catheterisation with arterial bloodgas analysis.Results: The VE/VCO2 slope in the HFREF, HFNEF, and control groups was42±11, 34±5, and 28±3 respectively (p=0.001). When looking at parametersavailable at rest, lower mean arterial pressure (p=0.037) was the only parame-ter significantly associated with higher VE/VCO2 slope in the HFREF group. Inpatients with normal LVEF, only higher age (p=0.02) was independently asso-ciated with higher VE/VCO2 slope. If exercise haemodynamics were analysed,lower peak exercise partial pressure of arterial carbon dioxide (PaCO2; p=0.046),higher increase in pulmonary capillary wedge pressure per work rate per kilo-gram body weight (dPCWP/WR; p=0.003), lower left ventricular end-diastolicdiameter (p=0.036), and lower peak exercise tidal volume (p=0.017) were as-sociated with higher VE/VCO2 slope. In the multivariable analysis, lower peakexercise PaCO2 (β=-0.41; p=0.036) and higher dPCWP/WR (β=0.60; p=0.005)were independently associated with higher VE/VCO2 slope (r2 of the total model0.61).Conclusions: In patients with HFNEF, the VE/VCO2 slope is intermediate be-tween asymptomatic controls and HFREF patients. In subjects with normal LVEF,high dPCWP/WR is closely related to the VE/VCO2 slope, indicating that theVE/VCO2 slope may assist in the diagnosis of HFNEF and may be a useful follow-up parameter in those with an established diagnosis of HFNEF.
P1642 Multiple coronary artery spasm can induce transientheart failure: we called this state as vasospastic heartfailure
H. Kohno, S. Sueda, T. Sakaue, T. Matsunaka, H. Habara. EhimePrefectural Niihama Hospital, Hongo, Japan
Background: There have been no reports concerning the correlation betweentransient heart failure (HF) and coronary artery spasm (CAS). We examined thefrequency of provoked spasm in patients with HF after controlling state beforedischarge, retrospectively.Methods & Results: From Jan 2000 and Dec 2007, 201 patients with HF werehospitalized at our institution. We could perform coronary arteriography andspasm provocation tests in 37 (22 men, 67±11 years, LVEF < 45% or BNP >
100 pg/dl on admission) out of 201 patients with HF before discharge, consistedof 9 DCM, 4 HHD, 3 valvular heart diseases, and 21 other disease. Atrial fibrilla-tion was observed in 13 patients (35%). After controlling HF and 24 hour cessa-tion of vasoactive drugs, pharmacological selective spasm provocation tests wereperformed. Positive spasm was defined as > 90% luminal narrowing. CAS wasobserved in 12 patients (32%), including 11 positive acetylcholine tests and onepositive ergonovine test. Multiple spasm was recognized in 10 (83%) out of 12patients (2 vessels spasm: 5 pts, 3 vessels spasm: 5 pts). Though ejection frac-tion on admission was not different between the two groups (42±18 vs. 43±11%,ns), LVEDVI (74±31 vs. 82±34, p<0.01), LVESVI (42±29 vs. 46±23, p<0.01),LVSVI (32±12 vs. 38±19, p<0.01), and LVEDP (10±6 vs. 14±7, p<0.01) be-fore discharge (11 days) was significantly smaller in patients with positive spasmthan that in those with negative spasm. There was no difference concerning clin-ical backgrounds, acute phase therapy, and initial medications between the twogroups. Only one patient was coronary spastic angina before admission.Conclusions: CAS, especially multiple spasm may cause transient HF in a smallpart of unknown origin HF in Japan. It is necessary to investigate CAS accuratelyin patients with HF.
P1643 Clinical and prognostic significance of plasmaviscosity in heart failure
P. Rubis, K.M. Goode, H. Loh, D. Cullington, J. Zhang, A. Yassin,Y. Al-Najjar, A.L. Clark, J.G.F. Cleland. University of Hull, KingstonUpon Hull, United Kingdom
Background and Aims: We investigated determinants of plasma viscosity (PV)and its prognostic significance in a broad spectrum of patients referred with heartfailure (HF).Material and Methods: Patients referred with suspected heart failure to a spe-cialist clinic serving a local community between 2004-2009 were enrolled. Aftertreatment optimisation, patients had symptoms quantified, were examined, hadan ECG and echo and blood taken for haematology, including PV, biochemistryand NT-proBNP and, when able, a corridor walk test.
Results: Of 1625 patients, mean age was 71±11years, 63% were men, 30%were in NYHA III/IV and 45% had LVEF<45%. Median PV was 1.69 (IQR: 1.62-1.78). Compared to those in the lowest quartile, patients in the highest quartileof PV had shorter 6-minute walk test distance, lower eGFR and higher total pro-tein, hsCRP, NT-proBNP, white cell count and platelets, were on higher dose ofloop diuretics, and had lower LVEF but had similar haematocrit. Significant cor-relations were observed between PV and total protein (r=0.5; p<0.001), CRP(r=0.28; p<0.001), NT-proBNP (r=0.37; p<0.001), and total daily dose of loopdiuretics (r=0.2; p<0.001). PV was a univariate predictor of prognosis on Cox-regression (Wald=35, p<0.001) and remained independently prognostic whenadjusted for age and sex (PV, Wald=36, p<0.001); but was knocked out of themodel by NT-proBNP and LVEF.
Characteristics by Quartile of PV
Variable Q1 Q2 Q3 Q4 ANOVAp-value
Distance walked [m] 390 (262-450) 334 (180-410) 345 (224-405) 300 (120-390) =0.001Furosemide or
Equiv [mg/d] 0 (0-40) 20 (0-40) 40 (0-40) 40 (20-80) <0.001GFR [ml/min/1.73m2] 66 (53-80) 68 (54-82) 62 (50-77) 56 (41-75) <0.001WCC [×109/l] 6.25 (5.3-7.5) 6.6 (5.6-7.9) 7.1 (6-8.3) 7.7 (6.4-9) <0.001Platelets [×109 /l] 200 (167-241) 225 (188-258) 229 (197-268) 247 (205-304) <0.001NT-proBNP [pg/ml] 551 (169-1951) 553 (152-2029) 537 (151-1400) 1365 (357-3061) 0.036CRP [mg/l] 1.7 (0.8-3.8) 2.6 (1.2-5.6) 3.8 (1.6-7.4) 7.1 (3.6-15) <0.001EF [%] 47 (36-58) 49 (36-59) 50 (37-60) 44 (32-57) <0.001
Conclusions: Higher PV is related to more advanced HF, use of higher dosesof diuretic and inflammatory markers. PV may be a readily accessible prognosticmarker in patients with HF when more sophisticated tests are not available. Fur-ther studies are required to determine if PV can serve as a therapeutic target inHF.
P1644 Subclinical myocardial dysfunction in patients withFriedreich ataxia and normal left ventricular ejectionfraction
C. Dedobbeleer1 , M. Pandolfo2, P. Unger1. 1ULB Erasme UniversityHospital, Department of Cardiology, Brussels, Belgium; 2ULB
Erasme University Hospital, Department of Neurology, Brussels, Belgium
Purpose: Iron deposits, diffuse fibrosis and focal necrosis are found in Friedre-ich’s cardiomyopathy. We hypothesized that subclinical left ventricular (LV) dys-function might occur in patients with Friedreich ataxia who present with normalLV ejection fraction (LVEF).Methods: Twelve patients with Friedreich ataxia (mean age: 36±18 years) andtwelve age-matched healthy controls (mean age: 36±17 years) were submitted tostandard echocardiography. Short axis basal and apical views were analyzed us-ing speckle tracking software. LV twist was defined as the net difference betweenthe apical rotation and basal rotation. The degree of LV untwisting was calculatedas the percentage of systolic twist: (twist max-twist(t)/twist max x100).Results: The two groups did not differ in terms of LVEF (65±4% and 65±6% inpatients and controls, respectively), LV mass index (93±23 g/m2 vs 86±18 g/m2),and in systolic mitral annular velocities (7.6±1.3 cm/s in patients and 8.3±1.2cm/s in controls, p=NS). The LV filling parameters did not differ between the 2groups (Table). However, early diastolic mitral annular velocity (Ea) was lowerand the ratio of early transmitral flow velocity to Ea was higher in Friedreich ataxiapatients. Peak LV twist was significantly reduced in patients as compared to con-trols, unlike early diastolic LV untwisting (at 5%, 10% and 15% of diastole) whichwas not significantly different.
Friedreich Control p value
E wave (cm/s) 73±10 73±10 NSE/A 1.7±0.7 1.95±0.7 NSEa (cm/s) 9.3±1.9 12.1±3.4 0.02E/Ea 8.6±2.1 6.6±1.9 0.03Peak LV twist (°) 9.2±3.4 12.1±2.4 0.02
Conclusions: In patients with Friedreich ataxia and normal LVEF and mass, thedetection of a reduction in LV twist and an alteration in mitral annular diastolicvelocities suggests the presence of subtle myocardial dysfunction. Evaluation ofthese parameters may prove useful as an outcome measure for the assessmentand follow-up of new therapies in the early stages of the disease.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

276 Heart failure / LV dysfunction
P1645 Systolic dysfunction index (SDI) determined byacoustic electrocardiography improves diagnosticaccuracy in elderly patients with acutedecompensated heart failure
M. Noveanu1, F. Peacock2, A. Maisel3, P. Clopton3, D. Diercks4,B. Hiestand5, M.C. Kontos6, R. Nowak7, S.P. Collins8, C. Mueller1. 1UniversityHospital Basel, Basel, Switzerland; 2Cleveland Clinic Foundation, Cleveland,United States of America; 3Veterans Affairs San Diego Health Care System, SanDiego, United States of America; 4University of California Davis, Davis, UnitedStates of America; 5Ohio State University, Ohio, United States of America;6Virginia Commonwealth University, Richmond, United States of America;7Henry Ford Health System, Detroit, United States of America; 8University ofCincinnati, Cincinnati, United States of America
Background: Diagnosis of acute decompensated heart failure (ADHF) in elderlypatients presenting with dyspnea to the emergency department (ED) is challeng-ing due to multiple co-morbidities and decreased accuracy of natriurtetic pep-tides. Rapidly and easy determined parameters including systolic dysfunction in-dex (SDI) derived from acoustic electrocardiography and analytic processing ofthe ECG may be of early diagnostic value. SDI is a product of the acoustic S3strength, the electrocardiogram QRS duration and QR interval, and the % of theelectromechanical activation time.Methods: Using the HEart failure and Audicor technology for Rapid Diagnosisand Initial Treatment (HEARD-IT) multinational trial database (n=1076), we eval-uated the diagnostic property of SDI in consecutive patients > 70 years of agepresenting with acute dyspnoea to the ED. Treating ED physicians blinded to theacoustic electrocardiography results, estimated ADHF probability from 0 to 100%on a visual analog scale (VAS) after initial history and physical examination. Thepotential of SDI to improve early ADHF diagnosis before arrival of laboratory re-sults or additional diagnostic was evaluated.Results: 377 patients (median [IQR] age 78 [74-83] years, 53% male) with acous-tic electrocardiography results were included in this analysis. ADHF was finallydiagnosed in 197 patients (52%). After initial history and physical examination,ED physicians remained uncertain about the underlying disorder in 225 patients(59%) of all cases (VAS for ADHF between 20 and 80%). In these patients, finalgold standard diagnosis resulted in 46% true positive ADHF diagnoses and 26%true negative ADHF exclusions. Consideration of a calculated SDI cutoff of 4.55during initial evaluation increased true negative HF exclusions by 10%. The areaunder the combined (primary ED evaluation and SDI) ROC curve for the diag-nosis of ADHF was 0.88 (95%CI 0.84-0.91) compared to an AUC of 0.82 for theprimary ED diagnosis alone (95%CI 0.78-0.87) (p=0.013).Conclusion: In patients > 70 years presenting with dyspnoea to the ED, SDIdetermined by acoustic electrocardiography improved early diagnostic accuracyfor ADHF.
P1646 Diabetes is a predictor of effort tolerance andventilatory efficiency in patients with moderatesystolic dysfunction on beta-blocker therapy
L.E. Pastormerlo1, M. Emdin2, A. Giannoni1, R. Poletti2,M. Fontana2 , C. Prontera2, C. Passino1. 1Scuola Superiore
Sant’Anna, Pisa, Italy; 2Gabriele Monasterio Foundation, Pisa, Italy
Background: Cardiopulmonary exercise test (CPT), through evaluation of func-tional capacity and ventilatory efficiency, is an important clinical tool to assessdisease severity with established prognostic value in heart failure patients. Type 2diabetes mellitus (DM) has been independently associated with lower peak oxy-gen consumption (VO2) and higher slope of ventilation to carbon dioxide produc-tion ratio (VE/VCO2) in HF patients without beta-blockers therapy.Purpose: We aimed to confirm the association of DM to lower VO2 and higherVE/VCO2 in a population with high percentage (70%) of beta-blockers users; fur-thermore, to evaluate the relationships between diabetes and CPT variables insubsets of patients with different degree of systolic dysfunction.Methods: We prospectively studied 310 patients with CHF (mean age of 61±13(mean ±SD), left ventricular ejection fraction (EF) 32±9%) on optimal treatment.98 of them (30%) had DM. All patients underwent CPT, clinical assessment,Doppler echocardiography and neurhormonal evaluation. For subgroup analysisa LVEF cut-point of 30% was considered.Results: Diabetic patients showed lower VO2 at peak exercise and at anaerobicthreshold (10.6±3.4 vs 13.1±5.4, p<0.01 and 8.2±2.3 vs. 9.5±3.6 ml/kg/min,p=0.012 respectively) and higher VE/VCO2 slope (41±10.5 vs. 37±10, p< 0.01),than their non diabetic counterparts. When patients were divided according todegree of left ventricular dysfunction, these findings were confirmed only in thegroup of patients with a LVEF > 30% (VO2: 10.8±3.3 vs. 13.7±5.4 ml/kg/min,p<0.01; VO2 AT: 8±2.3 vs. 10±4 ml/kg/min, p<0.01; VE/VCO2 slope: 40.4±10.8vs. 35.4±9.6 p<0.01, diabetic vs non diabetic patients). Moreover, at multivariateanalysis, only in this group, after correction for age, NYHA class, and neurohor-monal activation, DM resulted an independent predictor of VO2 and VE/VCO2slope (beta coefficients: -0.33 IC: -2.8 to 0.13, p=0.013 and 0.12 CI 0.04 to 4.5,p=0.03 respectively).Conclusion: DM negatively affects exercise tolerance and ventilatory efficiencyin HF patients treated with beta-blockers. This statement is particularly clear in pa-tients with moderate systolic dysfunction, also after correction for neurohormonalactivation and other variables, such as age and NYHA class. These findings sug-
gest the presence of DM-driven pathophysiological mechanisms (e.g. lung andperipheral microcirculatory alterations, impaired skeletal muscle metabolism, de-fects in muscular oxygen utilization), acting at early stages of the disease.
P1647 Relationship between serum testosterone and clinicalcharacteristics in men with heart failure
D. Ahmed, J. Zhang, A. Yassin, A. Crundall, N. Sherwi, L. Buga,J.P. Hobkirk, K.M. Goode, A.L. Clark, J.G.F. Cleland. University ofHull, Kingston Upon Hull, United Kingdom
Background:- Testosterone (T) deficiency may be common in men with heartfailure (HF) either due to ageing, concomitant disease and treatment or severityof HF.Aim:- To describe the clinical characteristics according to serum T concentrationof men with HF and to identify factors that may explain T deficiency.Methods:- Patients diagnosed with HF at a single specialist service were en-rolled. After treatment optimisation, patients had symptoms quantified, were ex-amined, had an ECG and echo and blood was taken for haemoglobin (Hb), bio-chemistry, NT-proBNP and T.Results:- Of 695 men enrolled in 2008/2009, mean age was 71±11years, 250(36%) were in NYHA class III/IV, mean LVEF 42±12% and median NT-proBNPwas 837pg/ml. On univariate analysis, low serum T was associated with greaterage, higher body mass index (BMI), lower Hb, higher urea, lower eGFR and higherlogNT-proBNP. On multi-variable analysis, age, BMI, Hb, urea and absence ofspironolactone treatment were associated with low T. In the lowest quintile of T,32 (23%) were taking T lowering treatment for prostatic disease. Further analysesexcluding patients on T lowering therapy and on survival will be presented.
Table 1
Q1 Q2 Q3 Q4 Q5
Serum T 6.2 (4.0-7.4) 9.4 (8.8-10.0) 12 (12-13) 15 (14-16) 21 (19-24)Age 75 (68-81) 73 (66-81) 71 (63-79) 71 (64-78) 69 (61-76)BMI 30 (27-36) 30 (26-33) 29 (26-32) 28 (25-31) 26 (23-31)AF 43 (31%) 38 (27%) 25 (18%) 31 (22%) 35 (25%)LVSD 70 (50%) 81 (59%) 73 (53%) 69 (50%) 76 (55%)NT-proBNP (pg/ml) 1040 1090 736 744 693
(346-1962) (430-2190) (266-1763) (262-1729) (271-1539)Haemoglobin 13.1 13.5 13.8 13.8 14.2
(11.7-14.3) (12.2-14.7) (12.6-14.6) (12.8-14.8) (13.1-14.9)Serum Urea 7.6 (5.7-11.0) 7.7 (5.9-10.1) 6.7 (5.4-9.0) 6.9 (4.8-9.6) 5.8 (4.5-8.0)eGFR 59 (43-77) 60 (45-80) 63 (47-77) 62 (48-78) 70 (56-81)Spironolactone 40 (29%) 48 (35%) 38 (27%) 51 (37%) 48 (34%)
Data are median and IQR or proportions by quintiles of testosterone.
Conclusions:- Low serum T is common in patients with HF and may be dueto therapy for prostatic disease. Low T is associated with adverse prognostic fea-tures including greater age, worse renal function, lower Hb and higher NT-proBNPbut also with some that are not, such as BMI. Whether T replacement therapyshould be considered for treating HF will be addressed by randomised trials
P1648 Metabolomics and heart failure: a new and promisingscientific approach
M. Deidda1, C. Cadeddu1, L. Barberini1, F. Torri1, C. Fattuoni2 ,E. Cadoni2, M. Lussu3, F. Murgia3, L. Atzori3, G. Mercuro1.1University of Cagliari, Dept. of Cardiovascular and Neurological
Sciences, Monserrato, Italy; 2University of Cagliari, Dept. of Chemical Sciences,Monserrato, Italy; 3University of Cagliari, Dept. of Toxicology, Monserrato, Italy
Purpose: Heart failure (HF) is characterized by a series of maladaptive metabolicchanges, which have recently been proposed as a new therapeutic target for
Figure 1. Discrimination between high BNP (>200 pg/ml; A) low BNP (<100 pg/ml; B) patientsand healthy controls (C).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / LV dysfunction 277
HF. Metabolomics (MBS) enables the parallel assessment of a broad range ofmetabolites.Methods: A proton nuclear magnetic resonance (1H NMR)-based MBS analysiswas performed on blood samples of 3 groups of individuals: HF patients withBNP >200 pg/ml BNP (n=6; A); HF patients with BNP <100 pg/ml (n=7; B) andage- and sex-matched healthy controls (n=6; C). Specimens were analyzed witha 1H-NMR 400MHz spectrometer. A supervised PLS-DA Projection on LatentStructures Discriminant Analysis was applied to realize a descriptive model ofHF, also on a still limited database of 1H-NMR spectra. BNP plasma concentrationwas measured using a non-competitive immunofluorimetric test.Results: The application of Pattern-recognition methods to 1H-NMR spectra wasable to identify 3 metabolic clusters related to A, B and C groups, respectively(Figure 1). The discrimination of the latent structures were related to a metabolicfingerprint depending on a limited set of metabolites: Acetone, Glucose, Glyc-erol, 3-Hydroxybutyric acid, Ornithine, Proline, Asparagine, Creatine, Creatinine,Valine, Aspartic acid and Phenylalanin.Conclusions: Our preliminary data show that MBS is a sensitive method, whichcan be effectively used in investigations on HF pathophysiology and therapy.This new tool may improve our knowledge of 1. perturbed metabolic pathwaysin HF, 2. their correlation with impaired myocardial function, 3. clinical monitor-ing in HF patients, 4. identification and management of innovative therapeuticapproaches.
P1649 Heterogeneous pattern of mechanical dyssynchronyin patients with systolic heart failure revealed byadvanced echocardiographic technologies
Q. Zhang1, R.J. Van Bommel2, J.Y.S. Chan3, V. Delgado2,Y.J. Liang1, M.J. Schalij2, J.J. Bax2, F. Fang3, G.W.K. Yip3,
C.M. Yu4. 1Department of Cardiology, West China Hospital, Sichuan University,Chengdu, China, People’s Republic of; 2Department of Cardiology, LeidenUniversity Medical Centre, Leiden, Netherlands; 3Division of Cardiology, Princeof Wales Hospital, The Chinese University of Hong Kong, Hong Kong, China,People’s Republic of; 4Li Ka Shing Institute of Health Sciences, The ChineseUniversity of Hong Kong, Hong Kong, China, People’s Republic of
Purpose: With the development of advanced and quantitative echocardiographicimaging tools, systolic dyssynchrony as a common mechanical phenomenon inpatients with advanced heart failure, could further be investigated for differentcomponents according to the directions of left ventricular (LV) motions.Methods: The current study examined the occurrence of longitudinal and/or ra-dial dyssynchrony and the pattern of latest contraction in 448 heart failure patients(65±12yrs, 75%) with ejection fraction≤35% from the 2 cardiac centers, by usingtissue Doppler imaging (TDI) and 2D speckle tracking imaging.Results: Longitudinal dyssynchrony was identified in 263 (59%) patients whileradial dyssynchrony in 186 (42%). There were 125 (28%) patients who had bothlongitudinal and radial dyssynchrony, 138 (31%) had only longitudinal, 61 (13%)had only radial, and 124 (28%) had neither form of dyssynchrony. By using TDI,the single most delayed segment in septum, lateral, anterior, inferior, anterosep-tum, posterior and multi-segmental delay occurred in 12%, 27%, 12%, 19%, 7%,13% and 10% patients. Whereas, the figures were 10%, 8%, 5%, 10%, 12%,14% and 41% by using 2D speckle tracking. When compared between patientswith wide (≥120ms, n=241) and narrow (<120ms, n=207) QRS complexes, thewide QRS group had a more prolonged dyssynchrony indices by TDI (39.2±16.0vs. 36.0±17.8ms) and 2D speckle tracking (150±122 vs. 118±104ms) methods(both p<0.05). The prevalence of both longitudinal (63% vs. 53%) and radial(54% vs. 36%) dyssynchrony were significantly higher in wide QRS patients (bothp<0.05). However, the distribution of the most delayed segment revealed by ei-ther method was not different between the 2 groups.Conclusion: The assessment of systolic dyssynchrony by advanced echocardio-graphic techniques indicates the heterogeneous pattern and complex nature ofmechanical dyssynchrony in heart failure, which would provide complementaryinformation to QRS duration.
P1650 Clinical significance of clinical scenarios in acuteheart failure syndromes: A report from ATTENDregistry
N. Sato1, K. Kajimoto2, R. Munakata1 , K. Asai1, Y. Minami3,M. Mizuno3, D. Yumino3, K. Tanaka1 , K. Mizuno1, T. Takano1 .1Nippon Medical School, Tokyo, Japan; 2Sensoji Hospital, Tokyo,
Japan; 3Tokyo Women’s Medical University, Tokyo, Japan
Clinical scenarios (CS) has been suggested for urgent management of acuteheart failure syndromes (AHFS) (Crit Care Med 2008), based on AHFS experts’opinions. Therefore, clinical significance of CS has not been demonstrated in real-world AHFS.Goal/Methods: Our goal was to clarify their usefulness. Clinical profiles werecompared between CS1 (SBP>140mmHg), CS2 (100≤SBP≤140mmHg), andCS3 (SBP<100mmHg) in 1856 AHFS patients enrolled in ATTEND registry, themulticenter prospective observational cohort study of AHFS in Japan.Results (see Table 1): The present study demonstrated specific characteristicsof each CS, i.e., a higher proportion of CS1 patients presented with hypertensiveheart disease and preserved left ventricular ejection fraction (>40%), lower B-
type natriuretic peptide, and better in-hospital mortality. In contrast, CS3 patientswere younger and clinically severer.
Table 1. Clinical differences between CSs
Variables Total CS1 CS2 CS3 P-value(n=1856) (n=966) (n=747) (n=143)
Age (yr) 73.1±13.8 73.3±13.1 74.1±13.8 66.5±17.2 <0.001Underlying diseases
Ischemic 592 (31.9%) 325 (33.6%) 225 (30.1%) 42 (29.4%) <0.001Hypertensive 341 (18.4%) 266 (27.5%) 71 (9.5%) 4 (2.8%)Cardiomyopathy 243 (13.1%) 78 (8.1%) 129 (17.3%) 36 (25.2%)
Medical historyPrior hospitalization
for heart failure 699 (37.7%) 300 (31.1%) 313 (41.9%) 86 (60.1%) <0.001Hypertension 1275 (68.7%) 796 (82.4%) 429 (57.4%) 50 (35.0%) <0.001
Clinical profile at admissionEjection fraction�40% 1052 (56.7%) 518 (53.6%) 441 (59.0%) 93 (65.0%) 0.01
Systolic bloodpressure (mmHg) 146.0±37.5 174.2±28.2 120.6±11.0 87.8±8.6 <0.001
B-type natriureticpeptide (pg/ml)* 740 [374-1250] 726 [365-1249] 745 [379-1226] 902 [446-1452] 0.111
Blood urea nitrogen(mg/dl) 27.6±23.6 25.4±19.8 29.0±27.4 34.4±23.8 <0.001
Estimated GFR(mL/min/1.73m2 ) 49.9±29.0 50.0±24.3 51.1±34.9 43.4±22.8 0.016
In-hospital mortalityTotal death 145 (7.8%) 31 (3.2%) 83 (11.1%) 31 (21.7%) <0.001Cardiovascular death 104 (5.6%) 17 (1.8%) 60 (8.0%) 27 (18.9%) <0.001
Plus minus value: mean ± sd; *median [interquartile range].
Conclusion: the present study revealed that CS was useful for clinical assess-ment at urgent stage of AHFS.
P1651 Characterisation of interventricular and intra-leftventricular dyssynchrony in new-onset idiopathicdilated cardiomyopathy, and their response to therapy
D. Leong1, N. Shipp1, P. Molaee1, A. Penhall2, R. Perry2,M. Shirazi2, A. Chakrabarty2 , C.G. Depasquale2 , P. Sanders1,
J.B. Selvanayagam2. 1University of Adelaide, Adelaide, Australia; 2FlindersMedical Centre, Adelaide, Australia
Background: Although interventricular and intra-left ventricular (LV) dyssyn-chrony have been used as criteria for cardiac resynchronisation therapy for treat-ment of severe systolic heart failure (HF), the prevalence and prognostic signifi-cance of dyssynchrony at presentation of new onset HF are unknown. We there-fore sought to assess dyssynchrony at baseline and followup among patients withnewly diagnosed idiopathic dilated cardiomyopathy (IDC). We hypothesised thatdegree of dyssynchrony at diagnosis would be associated with the extent of im-provement in systolic LV function.Methods: Fifty-nine patients were prospectively studied a median of 9 days(IQR 6-15 days) and 6 months (IQR 5-7 months) following presentation withIDC, and compared with 19 healthy volunteers. In patients, significant coronaryartery disease was excluded by angiography. All subjects underwent standard-ised transthoracic echocardiography. LV volumes weremeasured by Simpson’smethod. Interventricular dyssynchrony was assessed by interventricular mechan-ical delay (IVMD): the difference in time from QRS onset to onset of systolic flowin the right and left ventricular outflow tracts, as measured by pulse-wave Dopplerimaging. Intra-LV dyssynchrony was evaluated by septal-posterior wall motion de-lay (SPWMD) as measured by colour M-mode imaging in the parasternal shortaxis view and tissue Doppler dyssynchrony index (TD DI): the standard deviationof time-to-peak systolic tissue velocity values from 12 myocardial segments in the3 apical views.Subjects also underwent 6-minute walk test and cardiopulmonaryexercise testing for the measurement of VO2 PEAK.Results: IDC patients exhibited significantly greater dyssynchrony than con-trols: IVMD 33±22 v 17±12ms, p=0.02; SPWMD 85±59 v 42±30ms, p=0.02;TD DI 41±14 v 26±16ms, p=0.001. IVMD (r=0.55, p=0.005), SPWMD (r=0.48,p=0.03) and TD DI (r=0.48, p=0.01) correlatedwith QRS duration. At follow-up, IDC patients displayed significant increase in LV ejection fraction (29±8 v41±12%,p<0.001) and 6-minute-walk distance (419±97 v 466±88m,p=0.04).IVMD (33±22 v 43±37ms,p=0.6), SPWMD (85±59 v.83±55ms,p=0.9) and TDDI (41±14 v 38±21ms,p=0.1) did not change at follow-up. Dyssynchrony indiceswere not associated with degree of improvement in LV volume or ejection fraction,nor were they predictive of functional improvement.Conclusions: Patients with newly diagnosed IDC exhibit marked dyssynchronyearly in the disease course that does not improve despite optimal medical ther-apy and significant increase in LV systolic function.Degree of dyssynchrony atpresentation does not predict response to medical therapy.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
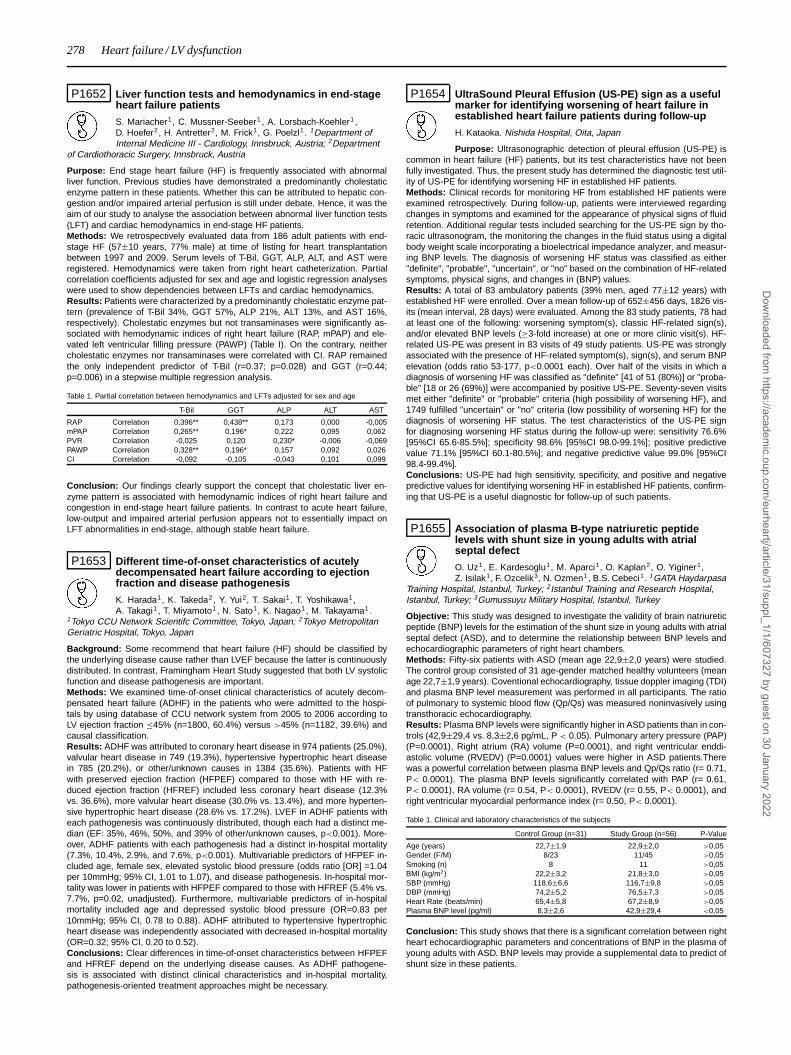
278 Heart failure / LV dysfunction
P1652 Liver function tests and hemodynamics in end-stageheart failure patients
S. Mariacher1, C. Mussner-Seeber1 , A. Lorsbach-Koehler1 ,D. Hoefer2, H. Antretter2, M. Frick1, G. Poelzl1. 1Department ofInternal Medicine III - Cardiology, Innsbruck, Austria; 2Department
of Cardiothoracic Surgery, Innsbruck, Austria
Purpose: End stage heart failure (HF) is frequently associated with abnormalliver function. Previous studies have demonstrated a predominantly cholestaticenzyme pattern in these patients. Whether this can be attributed to hepatic con-gestion and/or impaired arterial perfusion is still under debate. Hence, it was theaim of our study to analyse the association between abnormal liver function tests(LFT) and cardiac hemodynamics in end-stage HF patients.Methods: We retrospectively evaluated data from 186 adult patients with end-stage HF (57±10 years, 77% male) at time of listing for heart transplantationbetween 1997 and 2009. Serum levels of T-Bil, GGT, ALP, ALT, and AST wereregistered. Hemodynamics were taken from right heart catheterization. Partialcorrelation coefficients adjusted for sex and age and logistic regression analyseswere used to show dependencies between LFTs and cardiac hemodynamics.Results: Patients were characterized by a predominantly cholestatic enzyme pat-tern (prevalence of T-Bil 34%, GGT 57%, ALP 21%, ALT 13%, and AST 16%,respectively). Cholestatic enzymes but not transaminases were significantly as-sociated with hemodynamic indices of right heart failure (RAP, mPAP) and ele-vated left ventricular filling pressure (PAWP) (Table I). On the contrary, neithercholestatic enzymes nor transaminases were correlated with CI. RAP remainedthe only independent predictor of T-Bil (r=0.37; p=0.028) and GGT (r=0.44;p=0.006) in a stepwise multiple regression analysis.
Table 1. Partial correlation between hemodynamics and LFTs adjusted for sex and age
T-Bil GGT ALP ALT AST
RAP Correlation 0,396** 0,438** 0,173 0,000 -0,005mPAP Correlation 0,265** 0,196* 0,222 0,095 0,062PVR Correlation -0,025 0,120 0,230* -0,006 -0,069PAWP Correlation 0,328** 0,196* 0,157 0,092 0,026CI Correlation -0,092 -0,105 -0,043 0,101 0,099
Conclusion: Our findings clearly support the concept that cholestatic liver en-zyme pattern is associated with hemodynamic indices of right heart failure andcongestion in end-stage heart failure patients. In contrast to acute heart failure,low-output and impaired arterial perfusion appears not to essentially impact onLFT abnormalities in end-stage, although stable heart failure.
P1653 Different time-of-onset characteristics of acutelydecompensated heart failure according to ejectionfraction and disease pathogenesis
K. Harada1, K. Takeda2, Y. Yui2, T. Sakai1, T. Yoshikawa1,A. Takagi1 , T. Miyamoto1, N. Sato1, K. Nagao1, M. Takayama1 .
1Tokyo CCU Network Scientifc Committee, Tokyo, Japan; 2Tokyo MetropolitanGeriatric Hospital, Tokyo, Japan
Background: Some recommend that heart failure (HF) should be classified bythe underlying disease cause rather than LVEF because the latter is continuouslydistributed. In contrast, Framingham Heart Study suggested that both LV systolicfunction and disease pathogenesis are important.Methods: We examined time-of-onset clinical characteristics of acutely decom-pensated heart failure (ADHF) in the patients who were admitted to the hospi-tals by using database of CCU network system from 2005 to 2006 according toLV ejection fraction ≤45% (n=1800, 60.4%) versus >45% (n=1182, 39.6%) andcausal classification.Results: ADHF was attributed to coronary heart disease in 974 patients (25.0%),valvular heart disease in 749 (19.3%), hypertensive hypertrophic heart diseasein 785 (20.2%), or other/unknown causes in 1384 (35.6%). Patients with HFwith preserved ejection fraction (HFPEF) compared to those with HF with re-duced ejection fraction (HFREF) included less coronary heart disease (12.3%vs. 36.6%), more valvular heart disease (30.0% vs. 13.4%), and more hyperten-sive hypertrophic heart disease (28.6% vs. 17.2%). LVEF in ADHF patients witheach pathogenesis was continuously distributed, though each had a distinct me-dian (EF: 35%, 46%, 50%, and 39% of other/unknown causes, p<0.001). More-over, ADHF patients with each pathogenesis had a distinct in-hospital mortality(7.3%, 10.4%, 2.9%, and 7.6%, p<0.001). Multivariable predictors of HFPEF in-cluded age, female sex, elevated systolic blood pressure (odds ratio [OR] =1.04per 10mmHg; 95% CI, 1.01 to 1.07), and disease pathogenesis. In-hospital mor-tality was lower in patients with HFPEF compared to those with HFREF (5.4% vs.7.7%, p=0.02, unadjusted). Furthermore, multivariable predictors of in-hospitalmortality included age and depressed systolic blood pressure (OR=0.83 per10mmHg; 95% CI, 0.78 to 0.88). ADHF attributed to hypertensive hypertrophicheart disease was independently associated with decreased in-hospital mortality(OR=0.32; 95% CI, 0.20 to 0.52).Conclusions: Clear differences in time-of-onset characteristics between HFPEFand HFREF depend on the underlying disease causes. As ADHF pathogene-sis is associated with distinct clinical characteristics and in-hospital mortality,pathogenesis-oriented treatment approaches might be necessary.
P1654 UltraSound Pleural Effusion (US-PE) sign as a usefulmarker for identifying worsening of heart failure inestablished heart failure patients during follow-up
H. Kataoka. Nishida Hospital, Oita, Japan
Purpose: Ultrasonographic detection of pleural effusion (US-PE) iscommon in heart failure (HF) patients, but its test characteristics have not beenfully investigated. Thus, the present study has determined the diagnostic test util-ity of US-PE for identifying worsening HF in established HF patients.Methods: Clinical records for monitoring HF from established HF patients wereexamined retrospectively. During follow-up, patients were interviewed regardingchanges in symptoms and examined for the appearance of physical signs of fluidretention. Additional regular tests included searching for the US-PE sign by tho-racic ultrasonogram, the monitoring the changes in the fluid status using a digitalbody weight scale incorporating a bioelectrical impedance analyzer, and measur-ing BNP levels. The diagnosis of worsening HF status was classified as either"definite", "probable", "uncertain", or "no" based on the combination of HF-relatedsymptoms, physical signs, and changes in (BNP) values.Results: A total of 83 ambulatory patients (39% men, aged 77±12 years) withestablished HF were enrolled. Over a mean follow-up of 652±456 days, 1826 vis-its (mean interval, 28 days) were evaluated. Among the 83 study patients, 78 hadat least one of the following: worsening symptom(s), classic HF-related sign(s),and/or elevated BNP levels (≥3-fold increase) at one or more clinic visit(s). HF-related US-PE was present in 83 visits of 49 study patients. US-PE was stronglyassociated with the presence of HF-related symptom(s), sign(s), and serum BNPelevation (odds ratio 53-177, p<0.0001 each). Over half of the visits in which adiagnosis of worsening HF was classified as "definite" [41 of 51 (80%)] or "proba-ble" [18 or 26 (69%)] were accompanied by positive US-PE. Seventy-seven visitsmet either "definite" or "probable" criteria (high possibility of worsening HF), and1749 fulfilled "uncertain" or "no" criteria (low possibility of worsening HF) for thediagnosis of worsening HF status. The test characteristics of the US-PE signfor diagnosing worsening HF status during the follow-up were: sensitivity 76.6%[95%CI 65.6-85.5%]; specificity 98.6% [95%CI 98.0-99.1%]; positive predictivevalue 71.1% [95%CI 60.1-80.5%]; and negative predictive value 99.0% [95%CI98.4-99.4%].Conclusions: US-PE had high sensitivity, specificity, and positive and negativepredictive values for identifying worsening HF in established HF patients, confirm-ing that US-PE is a useful diagnostic for follow-up of such patients.
P1655 Association of plasma B-type natriuretic peptidelevels with shunt size in young adults with atrialseptal defect
O. Uz1, E. Kardesoglu1, M. Aparci1, O. Kaplan2, O. Yiginer1,Z. Isilak1, F. Ozcelik3, N. Ozmen1, B.S. Cebeci1. 1GATA Haydarpasa
Training Hospital, Istanbul, Turkey; 2Istanbul Training and Research Hospital,Istanbul, Turkey; 3Gumussuyu Military Hospital, Istanbul, Turkey
Objective: This study was designed to investigate the validity of brain natriureticpeptide (BNP) levels for the estimation of the shunt size in young adults with atrialseptal defect (ASD), and to determine the relationship between BNP levels andechocardiographic parameters of right heart chambers.Methods: Fifty-six patients with ASD (mean age 22,9±2,0 years) were studied.The control group consisted of 31 age-gender matched healthy volunteers (meanage 22,7±1,9 years). Coventional echocardiography, tissue doppler imaging (TDI)and plasma BNP level measurement was performed in all participants. The ratioof pulmonary to systemic blood flow (Qp/Qs) was measured noninvasively usingtransthoracic echocardiography.Results: Plasma BNP levels were significantly higher in ASD patients than in con-trols (42,9±29,4 vs. 8,3±2,6 pg/mL, P < 0.05). Pulmonary artery pressure (PAP)(P=0.0001), Right atrium (RA) volume (P=0.0001), and right ventricular enddi-astolic volume (RVEDV) (P=0.0001) values were higher in ASD patients.Therewas a powerful correlation between plasma BNP levels and Qp/Qs ratio (r= 0.71,P< 0.0001). The plasma BNP levels significantly correlated with PAP (r= 0.61,P< 0.0001), RA volume (r= 0.54, P< 0.0001), RVEDV (r= 0.55, P< 0.0001), andright ventricular myocardial performance index (r= 0.50, P< 0.0001).
Table 1. Clinical and laboratory characteristics of the subjects
Control Group (n=31) Study Group (n=56) P-Value
Age (years) 22,7±1,9 22,9±2,0 >0,05Gender (F/M) 8/23 11/45 >0,05Smoking (n) 8 11 >0,05BMI (kg/m2) 22,2±3,2 21,8±3,0 >0,05SBP (mmHg) 118,6±6,6 116,7±9,8 >0,05DBP (mmHg) 74,2±5,2 76,5±7,3 >0,05Heart Rate (beats/min) 65,4±5,8 67,2±8,9 >0,05Plasma BNP level (pg/ml) 8,3±2,6 42,9±29,4 <0,05
Conclusion: This study shows that there is a significant correlation between rightheart echocardiographic parameters and concentrations of BNP in the plasma ofyoung adults with ASD. BNP levels may provide a supplemental data to predict ofshunt size in these patients.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / LV dysfunction 279
P1656 Prognostic values of left ventricular ejection fractionat starting of hemodialysis therapy on cardiovascularand all-cause mortality in patients with end-stagerenal disease
H. Ishii1, T. Toriyama2, Y. Kumada2, T. Aoyama2, H. Takahashi2 ,M. Tanaka2 , Y. Kawamura2, T. Amano1, T. Matsubara3, T. Murohara1. 1NagoyaUniversity Graduate School of Medicine, Department of Cardiology, Nagoya,Japan; 2Nagoya Kyoritsu Hospital, Nagoya, Japan; 3Aichi Gakuin University,School of Dentistry, Nagoya, Japan
Purpose: Left ventricular (LV) dysfunction directly affects cardiac failure, partic-ularly, LV systolic dysfunction is strongly associated with a survival in end-stagerenal disease (ESRD) patients. The aim of the present study is to clarify prognos-tic value of reduced LV ejection fraction (LVEF) for mortality in patients with ESRDfrom the beginning of hemodialysis (HD) therapy.Methods: 1,254 consecutive ESRD patients who electively started HD therapywere screened by echocardiography within 1 month after induction of HD ther-apy. They were divided into 5 groups according to LVEF levels with decreasingof 0.1 each and were followed-up for up to 7 years. Survival comparisons wereexamined with the Kaplan-Meier method and compared using the log-rank test.Results: Of 1,254 patients, LVEF levels ≥ 0.6, 0.5-0.6, 0.4-0.5, 0.3-0.4, and <0.3were seen in 842 (67.1%), 247 (19.7%), 107 (8.5%), 41 (3.3%), and 17 (1.4%) pa-tients, respectively. On Kaplan-Meier analysis, 7-year event free rates from cardio-vascular death were 84.2%, 83.7%, 73.6%, 59.4% and 30.9% in order of groupswith decreasing LVEF of 0.1 each (p<0.0001), respectively. For all-cause death,7-year survival were 69.2%, 61.7%, 57.1%, 45.9% and 23.1% in the same orderof groups (p<0.0001), respectively. Even after adjustment for other risk factors,decreasing LVEF was a strong independent predictor for cardiovascular deathand all-cause death.Conclusions: Reduced LVEF at starting HD therapy could stratify risk of cardio-vascular and all-cause mortality in ESRD patients. The screening by echocar-diography at starting HD therapy might be recommended to predict prognosis inpatients with ESRD.
P1657 Circulating timp1 and beta2microglobulin asbiomarkers of cardio-renal remodelling in heartfailure and in the athlete’s heart
A. Vianello, P. Pietrini, G. Santoro, L. Caponi. Gabriele MonasterioFoundation, Pisa, Italy
Background: Tissue inhibitor of matrix metalloproteinase 1 (TIMP1) is now rec-ognized as a biomarker of ongoing adverse LV remodelling in heart failure pa-tients. Circulating beta2microglobulin (beta2M), the beta chain of HLA class Imolecule, represents a biomarker of decreased glomerular filtration rate, of in-flammation and high tissue turnover. Its role in heart remodelling has been inves-tigated only in dialysis-related amyloidosis.Aims: To evaluate the relationships between plasma profile of TIMP1 and beta2Min heart failure (HF) and in the athlete’s heart (AH).Methods: We investigated plasmatic levels of TIMP1 and beta2M in 25 subjectswith stable HF, in 42 veteran marathoners with AH, 48 hours after training, andin 25 sedentary controls. TIMP1 levels were assayed with ELISA; beta2M withAxSym, Abbott. All subjects with acute or chronic inflammatory disease, neoplas-tic disease, renal or hepatic failure were excluded.Results: TIMP1 and beta2M showed a strong positive correlation between themboth in HF (r=0.6, p<0.005) and in the AH (r=0.5, p=0.001), but not in controls.Circulating levels of TIMP1 and beta2M were much higher in patients with stableHF (TIMP1: 322.1±31.2 ng/ml vs 230.8±9.5 ng/ml in the athlete, p<0.01 and228.3±11.3 ng/ml in controls, p<0.005; beta2M: 2539.7±294.3 vs 1147.3±37.6in the athlete, p<0.001 and 1215.2±45.1 in controls, p<0.001) and correlate alsowith NTpro-BNP and creatinine.Conclusions: The strong correlation between TIMP1 and beta2M in HF and AHand the correlation of both with proBNP and creatinine in HF suggest their clinicalapplication in following the development of pathological cardio-renal remodelling.
P1658 Diagnostic utility of serum intact parathyroidhormone in predicting impaired cardiachemodynamics combined with brain natriureticpeptide in patients with heart failure
T. Sugimoto1, K. Dohi2, H. Nakajima1, K. Ichikawa1, S. Nakamori1,M. Tanabe1 , K. Onishi1, M. Miyahara1, M. Nakamura1, M. Ito1. 1Mie UniversityGraduate School of Medicine, Department of Cardiology, Tsu, Japan; 2MieUniversity Graduate School of Medicine, Department of Molecular & LaboratoryMedicine, Tsu, Japan
Purpose: This study sought to evaluate diagnostic utility of serum intact parathy-roid hormone (intact PTH) in predicting impaired cardiac hemodynamics com-bined with brain natriuretic peptide (BNP) in patients with heart failure.Methods: We prospectively studied 21 non-ischemic heart failure patients. Pa-tients with stage 4 or 5 chronic kidney disease were excluded. Blood sampling forintact PTH and BNP were performed simultaneously with invasive measurementsof pulmonary capillary wedge pressure (PCWP) and cardiac index (CI).Results: Both intact PTH (51±32 pg/ml, median 38 pg/ml) and BNP (539±643
pg/ml, median 282 pg/ml) were significantly correlated with mean PCWP (intactPTH: r = 0.71, BNP: r = 0.78, p< 0.05, respectively, shown in Figure) and CI (intactPTH: r = -0.48, BNP: r = -0.58, p< 0.05, respectively). When divided patients into3 groups according to median levels of intact PTH and BNP (Group 1; n = 5: intactPTH< 38 pg/ml and BNP< 282 pg/ml, Group 2; n = 9: intact PTH≥ 38 pg/ml andBNP< 282 pg/ml, or intact PTH< 38 pg/ml and BNP≥ 282 pg/ml, Group 3; n= 7: intact PTH≥ 38 pg/ml and BNP≥ 282 pg/ml), Group 1 had normal cardiachemodynamic parameter (mean PCWP: 11±5 mmHg, CI: 3.1±0.4 L/min/m2).In contrast, these two parameters were significantly impaired in Group 3 (meanPCWP: 25±11* mmHg, CI: 1.9±0.3* L/min/m2, *p <0.05 vs. Group 1).
Conclusion: Intact PTH had high diagnostic utility in predicting impaired cardiachemodynamics combined with BNP in patients with heart failure.
P1659 Urinary 8-Hydroxy-2’-Deoxyguanosine as a newoxidative stress biomarker in patients with chronicheart failure
T. Susa, S. Kogayashi, T. Tanaka, S. Okuda, M. Doi, Y. Wada,J. Yamada, T. Ueyama, M. Yano, M. Matsuzaki. Yamaguchi
University Graduate School of Medicine, Department of Medicine and ClinicalScience, Ube, Japan
Background: The oxidative stress is known to play a crucial role in thepathogenesis of heart failure. We investigated whether urinary 8-hydroxy-2’-deoxyguanosine (8-OHdG), a product of oxidative DNA damage, is a clinicallyuseful biomarker for evaluating the severity of chronic heart failure (CHF) as wellas the response to the treatment with beta blocker in patients with CHF.Methods and results: In our preliminary study, the level of serum 8-OHdG(ng/ml), a marker of oxidative DNA damage, was higher in coronary sinus (CS)than in artery (A) in CHF (n=30), while it was not in normal subjects (N:n=10)(CHF: 0.55±0.43 in CS; 0.28±0.15 in A; N: 0.17±0.07 in CS; 0.16±0.06 in A), in-dicating that reactive oxygen species is produced in failing cardiac tissue. There-fore, we measured the urinary 8-OHdG and other biomarkers: e.g. plasma brainnatriuretic peptide (BNP), urinary 8-isoprostane, high sensitive (hs) CRP, IL-6,TNF-alpha, in 30 control subjects (no prior clinical history of HF or LV dysfunction,age and gender-matched) and 140 patients with CHF (mean age: 57±16 years;male: 52%; LVEF: 34±13%). Then, we examined the relationship between uri-nary 8-OHdG and LVEF, PCWP or BNP. The urinary 8-OHdG level indeed corre-lated with the NYHA class (r=0.62, p<0.001), LVEF (r=0.43, p<0.001) and PCWP(r=0.54, p<0.001), while other biomarkers of oxidative stress and inflammationsuch as the urinary 8-isoprostane, serum IL-6, serum TNFα and hs CRP did not.Furthermore, we investigated whether urinary 8-OHdG was useful in evaluatingthe effectiveness of beta blocker therapy (mean follow-up periods: 12 months) inthirty patients with CHF, who had no medication of beta blocker before the follow-up. The responder was defined as a clinical improvement of either more than 10%in LVEF or more than 1 class of NYHA functional classification before and afteraddition of beta blocker. In responder patients (n=17), urinary 8-OHdG was signif-icantly decreased (urinary 8-OHdG;ng/mg•creatinine: before treatment;15.3±6.1vs. after treatment;9.9±3.3, P<0.01) in parallel with an improvement of NYHAclass, LVEF, LV end-diastolic diameter and BNP levels after treatment of betablocker. On the other hand, in non-responder patients (n=13), it did not.Conclusions: In heart failure, the urinary 8-OHdG seems to reflect the level ofoxidative stress especially produced in failing cardiac tissue, and it correlates wellwith various parameters upon symptomatic or functional severity of CHF as wellas evaluates the effectiveness of beta blocker therapy in patients with CHF.
P1660 Circadian body temperature variability correspondsto significant decline in left ventricular functionduring decompensated heart failure incardiomyopathic hamsters
A. Ahmed1, S. Gondi1, C. Cox1, M. Zheng1, A. Mohammed1,I. Stupin1, A. Brewer1, S.W. Casscells2, J.M. Wilson3. 1Texas Heart Institute,Houston, United States of America; 2University of Texas HSC at Houston,Houston, United States of America; 3Baylor College of Medicine, Houston,United States of America
Background: We have previously established that a declining amplitude of bodytemperature circadian rhythm (BTCR) predicts decompensation or death in car-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
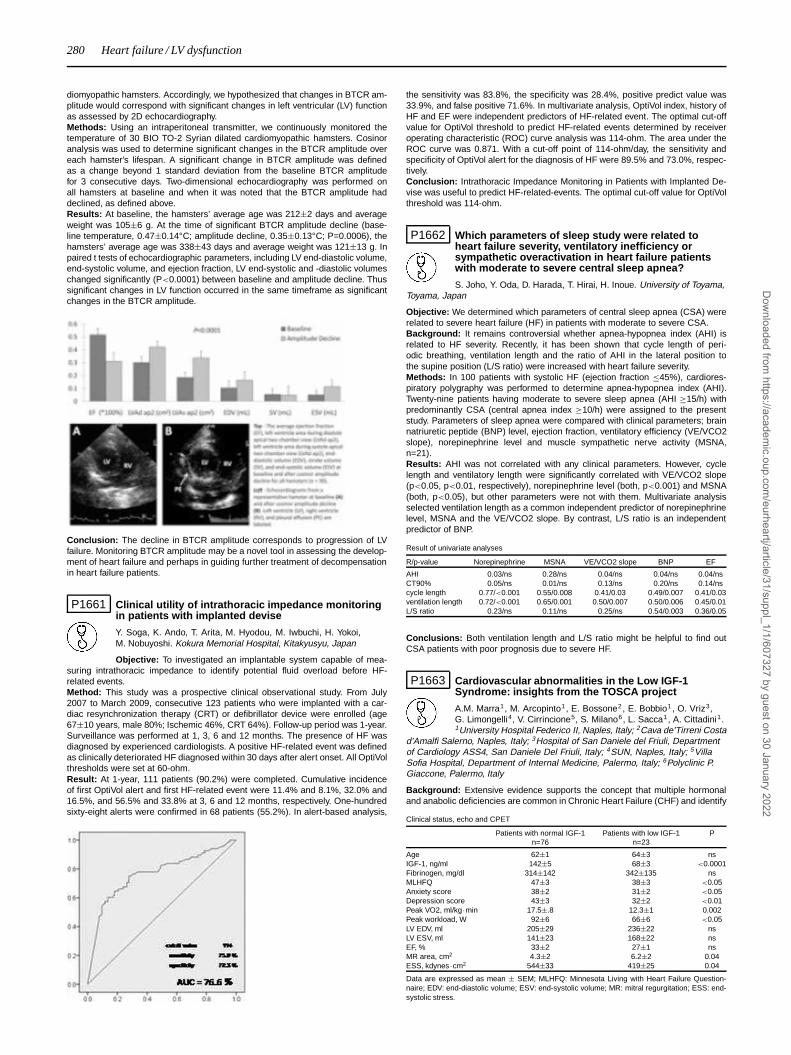
280 Heart failure / LV dysfunction
diomyopathic hamsters. Accordingly, we hypothesized that changes in BTCR am-plitude would correspond with significant changes in left ventricular (LV) functionas assessed by 2D echocardiography.Methods: Using an intraperitoneal transmitter, we continuously monitored thetemperature of 30 BIO TO-2 Syrian dilated cardiomyopathic hamsters. Cosinoranalysis was used to determine significant changes in the BTCR amplitude overeach hamster’s lifespan. A significant change in BTCR amplitude was definedas a change beyond 1 standard deviation from the baseline BTCR amplitudefor 3 consecutive days. Two-dimensional echocardiography was performed onall hamsters at baseline and when it was noted that the BTCR amplitude haddeclined, as defined above.Results: At baseline, the hamsters’ average age was 212±2 days and averageweight was 105±6 g. At the time of significant BTCR amplitude decline (base-line temperature, 0.47±0.14°C; amplitude decline, 0.35±0.13°C; P=0.0006), thehamsters’ average age was 338±43 days and average weight was 121±13 g. Inpaired t tests of echocardiographic parameters, including LV end-diastolic volume,end-systolic volume, and ejection fraction, LV end-systolic and -diastolic volumeschanged significantly (P<0.0001) between baseline and amplitude decline. Thussignificant changes in LV function occurred in the same timeframe as significantchanges in the BTCR amplitude.
Conclusion: The decline in BTCR amplitude corresponds to progression of LVfailure. Monitoring BTCR amplitude may be a novel tool in assessing the develop-ment of heart failure and perhaps in guiding further treatment of decompensationin heart failure patients.
P1661 Clinical utility of intrathoracic impedance monitoringin patients with implanted devise
Y. Soga, K. Ando, T. Arita, M. Hyodou, M. Iwbuchi, H. Yokoi,M. Nobuyoshi. Kokura Memorial Hospital, Kitakyusyu, Japan
Objective: To investigated an implantable system capable of mea-suring intrathoracic impedance to identify potential fluid overload before HF-related events.Method: This study was a prospective clinical observational study. From July2007 to March 2009, consecutive 123 patients who were implanted with a car-diac resynchronization therapy (CRT) or defibrillator device were enrolled (age67±10 years, male 80%; Ischemic 46%, CRT 64%). Follow-up period was 1-year.Surveillance was performed at 1, 3, 6 and 12 months. The presence of HF wasdiagnosed by experienced cardiologists. A positive HF-related event was definedas clinically deteriorated HF diagnosed within 30 days after alert onset. All OptiVolthresholds were set at 60-ohm.Result: At 1-year, 111 patients (90.2%) were completed. Cumulative incidenceof first OptiVol alert and first HF-related event were 11.4% and 8.1%, 32.0% and16.5%, and 56.5% and 33.8% at 3, 6 and 12 months, respectively. One-hundredsixty-eight alerts were confirmed in 68 patients (55.2%). In alert-based analysis,
the sensitivity was 83.8%, the specificity was 28.4%, positive predict value was33.9%, and false positive 71.6%. In multivariate analysis, OptiVol index, history ofHF and EF were independent predictors of HF-related event. The optimal cut-offvalue for OptiVol threshold to predict HF-related events determined by receiveroperating characteristic (ROC) curve analysis was 114-ohm. The area under theROC curve was 0.871. With a cut-off point of 114-ohm/day, the sensitivity andspecificity of OptiVol alert for the diagnosis of HF were 89.5% and 73.0%, respec-tively.Conclusion: Intrathoracic Impedance Monitoring in Patients with Implanted De-vise was useful to predict HF-related-events. The optimal cut-off value for OptiVolthreshold was 114-ohm.
P1662 Which parameters of sleep study were related toheart failure severity, ventilatory inefficiency orsympathetic overactivation in heart failure patientswith moderate to severe central sleep apnea?
S. Joho, Y. Oda, D. Harada, T. Hirai, H. Inoue. University of Toyama,Toyama, Japan
Objective: We determined which parameters of central sleep apnea (CSA) wererelated to severe heart failure (HF) in patients with moderate to severe CSA.Background: It remains controversial whether apnea-hypopnea index (AHI) isrelated to HF severity. Recently, it has been shown that cycle length of peri-odic breathing, ventilation length and the ratio of AHI in the lateral position tothe supine position (L/S ratio) were increased with heart failure severity.Methods: In 100 patients with systolic HF (ejection fraction ≤45%), cardiores-piratory polygraphy was performed to determine apnea-hypopnea index (AHI).Twenty-nine patients having moderate to severe sleep apnea (AHI ≥15/h) withpredominantly CSA (central apnea index ≥10/h) were assigned to the presentstudy. Parameters of sleep apnea were compared with clinical parameters; brainnatriuretic peptide (BNP) level, ejection fraction, ventilatory efficiency (VE/VCO2slope), norepinephrine level and muscle sympathetic nerve activity (MSNA,n=21).Results: AHI was not correlated with any clinical parameters. However, cyclelength and ventilatory length were significantly correlated with VE/VCO2 slope(p<0.05, p<0.01, respectively), norepinephrine level (both, p<0.001) and MSNA(both, p<0.05), but other parameters were not with them. Multivariate analysisselected ventilation length as a common independent predictor of norepinephrinelevel, MSNA and the VE/VCO2 slope. By contrast, L/S ratio is an independentpredictor of BNP.
Result of univariate analyses
R/p-value Norepinephrine MSNA VE/VCO2 slope BNP EF
AHI 0.03/ns 0.28/ns 0.04/ns 0.04/ns 0.04/nsCT90% 0.05/ns 0.01/ns 0.13/ns 0.20/ns 0.14/nscycle length 0.77/<0.001 0.55/0.008 0.41/0.03 0.49/0.007 0.41/0.03ventilation length 0.72/<0.001 0.65/0.001 0.50/0.007 0.50/0.006 0.45/0.01L/S ratio 0.23/ns 0.11/ns 0.25/ns 0.54/0.003 0.36/0.05
Conclusions: Both ventilation length and L/S ratio might be helpful to find outCSA patients with poor prognosis due to severe HF.
P1663 Cardiovascular abnormalities in the Low IGF-1Syndrome: insights from the TOSCA project
A.M. Marra1, M. Arcopinto1, E. Bossone2, E. Bobbio1 , O. Vriz3,G. Limongelli4, V. Cirrincione5, S. Milano6, L. Sacca1, A. Cittadini1.1University Hospital Federico II, Naples, Italy; 2Cava de’Tirreni Costa
d’Amalfi Salerno, Naples, Italy; 3Hospital of San Daniele del Friuli, Departmentof Cardiology ASS4, San Daniele Del Friuli, Italy; 4SUN, Naples, Italy; 5VillaSofia Hospital, Department of Internal Medicine, Palermo, Italy; 6Polyclinic P.Giaccone, Palermo, Italy
Background: Extensive evidence supports the concept that multiple hormonaland anabolic deficiencies are common in Chronic Heart Failure (CHF) and identify
Clinical status, echo and CPET
Patients with normal IGF-1 Patients with low IGF-1 Pn=76 n=23
Age 62±1 64±3 nsIGF-1, ng/ml 142±5 68±3 <0.0001Fibrinogen, mg/dl 314±142 342±135 nsMLHFQ 47±3 38±3 <0.05Anxiety score 38±2 31±2 <0.05Depression score 43±3 32±2 <0.01Peak VO2, ml/kg ·min 17.5±.8 12.3±1 0.002Peak workload, W 92±6 66±6 <0.05LV EDV, ml 205±29 236±22 nsLV ESV, ml 141±23 168±22 nsEF, % 33±2 27±1 nsMR area, cm2 4.3±2 6.2±2 0.04ESS, kdynes ·cm2 544±33 419±25 0.04
Data are expressed as mean ± SEM; MLHFQ: Minnesota Living with Heart Failure Question-naire; EDV: end-diastolic volume; ESV: end-systolic volume; MR: mitral regurgitation; ESS: end-systolic stress.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / LV dysfunction 281
subgroups of patients with higher mortality. Chief among these is the reducedactivity of the GH/IGF-1 axis.Patients and Methods: Ninety-nine patients with CHF, selected from a largercohort participating in a multicenter trial, were divided according to their IGF-1levels. Low IGF-1 syndrome was defined in CHF patients with IGF-1 levels belowthe 25th percentile of an age and sex-matched population.Results: Results are shown in the table below. Patients with low IGF-1 levels dis-played higher depression and anxiety scores, reduced indexes of quality of life aswell as of cardiopulmonary performance compared with CHF patients with normalIGF-1 levels. Moreover, LV volumes tended to be higher in low IGF-1 patients withsignificantly higher wall stress and larger mitral regurgitation jets.Conclusion: low IGF-1 syndrome defines a subgroup of CHF patients character-ized by worse clinical status, cardiopulmonary performance, and LV dynamics.
P1664 Lack of gadolinium late enhancement in noncompaction myocardium
D. Perez De Arenaza, M. Falconi, M. Pietrani, L. Distefano, G. Maid,C. Belziti, N. Vulcano, J. Krauss, R. Garcia Monaco, A. Cagide.Italian Hospital of Buenos Aires, Buenos Aires, Argentina
Purpose: Isolated ventricular non-compaction (IVNC) is an idiopathic form of car-diomyopathy. Little is known about the pathogenesis of this cardiomyopathy. Manycardiomyopathies have late enhancement with gadolinium in cardiovascular ma-gentic resonance (CMR) scans that suggests the presence of fibrosis, necrosisor infiltration of the myocardium. The aim of this study was to assess if late en-hancement gadolinium CMR technique identify potential pathogenic mechanismsof IVNC.Methods: Patients with suspected IVNC by Doppler echocardiography were re-ferred to a CMR scan to confirm diagnosis. CMR scans were performed in 1.5Tesla scanners (Vision or Avanto, Siemens). Morphology was assessed by T1,T2 and Haste sequences, ventricular function and volumes by cines sequences,and late enhancement gadolinium by inversion recovery sequences. Diagnosisof non-compaction was confirmed by a ratio of non compacted/compacted my-ocardium > 2.3 in the left ventricle at end-diastole. A 17-segment model wasused for location of non-compacted myocardium.Results: We studied 45 patients that had criteria for non-compaction by Dopplerechocardiography and CMR. The mean age was 38±18 years, 63% were male,the mean left ventricle ejection fraction was 47±17%, left ventricle end-diastolicvolume was 215±89 ml and left ventricle end-systolic volume was 123±88 ml.The mean non-compacted/compacted ratio was 2.98±0.78. The most frequentlyinvolved segments were mid inferolateral (16%), mid anterolateral (16%), api-cal lateral (21%), apical anterior (10%), and apex (10%). None of the segmentwith non-compacted myocardium had late enhancement after gadolinium injec-tion. Only seven patients have intramyocardium gadolinium late enhancement inremote areas from the non-compacted myocardium. Patients with late enhance-ment in remote areas had lower ejection fraction (32% vs 49%, p=0.015) andlarger left ventricle end-systolic volume (113 vs 186ml, p=0.042) compared withpatients without enhancementConclusions: The lack of late enhancement in areas of noncompation suggeststhat necrosis, fibrosis or infiltration may not play a role in the pathogenesis ofthis idiopathic form of cardiomyopathy (IVNC). The late enhancement of remoteareas from the non-compacted myocardium may indicate a more advance dilatedcardiomyopathy and greater left ventricular systolic disfunction.
P1665 Inflammation results in increased levels of NT-proBNPand an increased NT-proBNP/BNP ratio
J. Jensen1 , L.P. Ma2, M. Fu3, O. Hammarsten1. 1SahlgrenskaUniversity Hospital, Department of Clinical Chemistry, Gothenburg,Sweden; 2Changhai Hospital, Shanghai, China, People’s Republic
of; 3Dept. of Medicine, Göteborg, Sweden
Objectives: The purpose of this study was to search for conditions that affect therelation between BNP and NT-proBNP.Background: Plasma BNP and NT-proBNP are often regarded as interchange-able parameters to assess severity and prognosis in patients with heart failure(HF). The level of NT-proBNP, measured in ng/L, is expected to be 9.7 timeshigher compared to BNP. Kidney failure is a known factor that result in dispro-portionate increases of NT-proBNP. Kidney function is therefore considered whenNT-proBNP is used to assess HF.Methods: To look for other factors that affect BNP and NT-proBNP levels differ-ently we examined the NT-proBNP/BNP ratio, 26 other lab parameters and clinicalfactors in 218 patients from the HF ward.Results: As expected, we found a strong correlation between kidney functionand levels of BNP, NT-proBNP and the NT-proBNP/BNP ratio. In addition, wealso found a significant correlation between the NT-proBNP/BNP ratio and in-flammation as measured by orosomucoid (r=0.525, p<0,0001), CRP (r= 0.333,p<0,0001), Haptoglobulin (r= 0.201, p=0,02) and Alfa1-antitrypsin (r= 0.223,p=0,01). The reverse correlation was found to transferring (r= -0.323, p<0,0001),albumin (r= -0.251, p=0,003) and S-Fe (r= -0.205, p=0,02) parameters known todecrease in response to long-standing inflammation. By comparing the levels ofBNP and NT-proBNP among patients with the same level of HF we found that in-flammation resulted in increased levels of NT-proBNP but no significant increase
of BNP. Inflammation affected the NT-proBNP/BNP ratio to the same extent aslow kidney function.Conclusions: NT-proBNP should be evaluated together with inflammation toavoid overestimation of HF.
P1666 Cheyne-Stokes respiration in patients with chronicheart failure: central CO2-receptor sensitivity isdependent of left ventricular filling pressures
O. Oldenburg, C. Piper, T. Bitter, D. Horstkotte. Department ofCardiology, Heart and Diabetes Centre North Rhine-Westphalia,
Ruhr University Bochum, Bad Oeynhausen, Germany
Purpose: Cheyne-Stokes respiration (CSR) in chronic heart failure (CHF) is ofmajor prognostic impact, however its pathophysiology is not fully understood.Besides other contributing factors, sensitivity of central chemoreceptors to CO2seems to be involved. This chemosensitivity is supposed to be influenced by sym-pathetic drive and filling pressures. Aim of the present study was to analyse therole of left-ventricular filling pressures on hyperoxic-hypercapnic ventilatory re-sponse (HCVR) in CHF (NYHA ≥ II, LV-EF ≤ 45%) patients.Methods and Results: HCVR was measured according to Read’s rebreathingmethod (93% O2, 7% CO2) in 48 consecutive patients with CHF (44 male, age64.3±11.9 years, LV-EF 32.2±7.3%, NT-proBNP 3511±4256pg/ml) and noctur-nal CSR (apnoea-hypopnoea-index ≥ 5/h) within 24h after simultaneous rightand left heart catheterisation. Cardiac index was 2.17±0.6 l/min/m2, LVEDP20.1±8.6mmHg, RVEDP 8.6±4.7mmHg, PAPmean 28.6±12.1mmHg, PCWP-mean 19.0±9.7mmHg and HCVR 4.08±3.9l/min/mmHg. Significant correlation(Spearman) was found between HCVR and PCWP (r=0.5; p=0.004), PAP (r=0.5;p=0.004) and LVEDP (r=0.4; p<0.05). In this cohort, no significant correlation wasdocumented for RVEDP and HCVR (r=0.3; p=0.133).Conclusions: In patients with symptomatic CHF due to left ventricular dysfunc-tion, elevated left ventricular filling pressures are associated with increased cen-tral CO2-receptor sensitivity. This augmented sensitivity might at least in part ex-plain hyperventilation and respiratory instability in CHF patients with CSR.
P1667 Left ventricular function assessed by global strain inHodgkin’s lymphoma long-term survivors afteradjuvent anthracycline chemotherapy– a two-dimensional speckle tracking echocardiographicstudy
H.R. Tsai1, O. Gjesdal1, T. Wethal1, K.H. Haugaa1, A. Fossa2,S.D. Fossa3, T. Edvardsen1. 1University of Oslo, Faculty Division RikshospitaletUniversity Hospital, Department of Cardiology, Oslo, Norway; 2Cancer Clinic,The Norwegian Radium Hospital, Oslo, Norway; 3University of Oslo,FacultyDivision Norwegian Radium Hospital,Department of Clinical Cancer Research,Oslo, Norway
Purpose: Anthracycline therapy is associated with cardiovascular morbidity andmortality. There are, however, limited studies for long-term follow up of myocar-dial function in adult Hodgkin’s lymphoma survivors receiving adjuvant anthra-cycline. Two-dimensional speckle tracking echocardiography (2D-STE) is an ac-curate angle-independent modality for quantification of regional and global leftventricular (LV) function. The aim of the present study was to investigate the long-term impact of adjuvant anthracycline therapy on left ventricular systolic function.Method: Echocardiography was performed in 47 Hodgkin’s lymphoma survivors22±2 years following successful mediastinal radiotherapy with (n=27) or without(n=20) adjuvant anthracycline treatment, and in 20 healthy controls. LV functionwas assessed by left ventricular ejection fraction (LVEF) and global longitudinalstrain, calculated as the average of peak systolic strain by 2D-STE in a 16 seg-ments LV model.Results: Both patient groups received similar dosage of radiation (41±3Gyvs. 41±1Gy, ns). Patients with adjuvant anthracycline treatment received a to-tal dose of 313±92 mg/m2. Global longitudinal strain was reduced in patientsreceiving combined anthracycline and mediastinal radiation therapy comparedto those receiving radiotherapy alone (-16.1±1.9% vs. -17.5±1.7%, p<0.05),and both groups had reduced strain compared to healthy controls (-20.4±1.7%,both p<0.05). LVEF did not separate between the patient groups (55±8% vs.56±6%, ns), but patients had reduced function compared to controls (62±5%,both p<0.05).Conclusions: Myocardial function was reduced in Hodgkin’s lymphoma survivorstwo decades after successful treatment, indicating irreversible myocardial im-pairment. Patients receiving adjuvant anthracycline chemotherapy had additionalnegative long-tem effect on left ventricular systolic function. Global longitudinalstrain is an excellent tool for assessment of LV dysfunction following anthracy-cline therapy.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

282 Heart failure / LV dysfunction
P1668 Consistent cardiac symptoms in chronic disease -does the autonomic dysfunction play a pivotal role?A comparison of chronic heart failure and pancreaticcancer
T. Kung1, C. Misgeld1, C. Heinz1, Y. Mori1, T. Szabo1, W. Doehner1 ,S.D. Anker1, M. Rauchhaus2 , S. Von Haehling1. 1Charite - Campus Virchow-Klinikum, Department of Cardiology, Division of Applied Cachexia Research,Berlin, Germany; 2University Hospital Rostock, Department of Cardiology,Rostock, Germany
Background: Patients with chronic heart failure (CHF) and pancreatic cancer(PCA) frequently present with similar clinical symptoms: Dyspnea and fatigue.Neuroendocrine activation plays a significant role in the pathophysiology of CHFand cancer fatigue syndrome (CFS) by decoupling of physiological pathways andisolation of constituent organs. We hypothesized that symptoms of CHF and CFSfollow similar pathways and assessed exercise capacity and heart rate variability(HRV), a measure of autonomic function in patients with CHF and PCA and inhealthy controls.Methods: We assessed 29 patients with CHF (age: 62±10 years, mean±SD, 28male, body-mass-index (BMI): 28.1±4.0 kg/m2, hemoglobin (Hb): 13.2±1.3 g/dl,left ventricular ejection fraction (LVEF): 35.4±8.6%, NYHA class 2.2±0.5), 96patients with PCA (58.9±9 years, 60 male, BMI: 23.1±3.7 kg/m2, Hb: 11.3±1.5g/dl) and 74 healthy controls (CON, 59.7±1.3 y, 40 male, BMI: 26.2±0.5 kg/m2,Hb: 13.9±0.2 g/dl) in exercise capacity, cardiac function and heart rate variabilityin patients and controls. In a subgroup of 42 PCA patients and 22 CON TNF-α,Interleukin-6 and TNF-Receptor1/2 (TNF-R1/2) were analysed.Results: Patients with CHF and PCA displayed significantly impaired autonomicfunction as compared to CON when measured as time domain analysis bythe standard deviation of normal RR intervals (SDNN, CHF: 116.9±29.8, PCA:100.3±30.8, CON: 142±36.9 ms, all p<0.05) and SDNN index (CHF: 46.1±15.0,PCA 35.3±13.6, CON 54.3±16.7, p<0.05). Both SDNN and SDNN index weresignificantly lower in PCA than in CHF (both p<0.05). Other parameters of au-tonomic function were likewise reduced in CHF and PCA compared to controls:Very Low Frequency (CHF: 2018±2297, PCA: 971±699, CON: 2268±1274 ms2,p=ns vs. CHF, p<0.05 vs. PCA), Low Frequency (CHF: 421±361, PCA: 275±265,CON: 742±430 ms2, all p<0.05) and High Frequency (CHF: 210±271, PCA:81.6±86.8, CON: 196±207 ms2, all p<0.05). There was no difference in LVEFbetween PCA and CON (61.2±8.4 vs. 62.1±6.1). Patients with CHF and PCA dis-played impaired exercise capacity compared to CON (peak VO2 CHF: 17.4±4.6,PCA 21.1±5.8 mL/min/kg, CON 27.2±7.9 mL/min/kg, all p<0.02). In PCA pro-inflammatory markers were elevated compared to CON (IL-6: 5.2±0.8 pg/mLvs. 1.8±0.2 pg/mL, TNF-R1: 1828±132 pg/mL vs. 1245±69 pg/mL, TNF-R2:2811±143 pg/mL vs. 2018±120pg/mL) (all p<0.05).Conclusions: Autonomic dysfunction, reduced exercise capacity and elevatedpro-inflammatory markers are present in patients with CHF as well as in thosewith PCA. The involved mechanisms and the clinical implications require furtherelucidation.
P1669 Late gadolinium enhancement is related to increasedleft ventricular wall stress and mass in patients withnon-ischemic cardiomyopathy
P. Alter, H. Rupp, M.B. Rominger, F. Stoll, P. Adams, B. Maisch.Philipps University of Marburg, Marburg, Germany
Introduction: Late gadolinium enhancement (LGE) as assessed by cardiac mag-netic resonance (CMR) imaging is suspected to be related to various myocardialinjuries. LGE was associated with a poor prognosis and increased myocardial col-lagen content in dilated cardiomyopathy. A reduced cardiac function is frequentlylinked with left ventricular (LV) dilatation and is the strongest worse prognosticindicator in heart failure. In parallel, the indication of cardioverter-defibrillators forprimary prevention largely depends on LV function and dilatation. Since dilatationis frequently associated with an increased wall stress, LGE could be expected tooccur involving an increased capillary leakage due to stretch and impaired con-trast agent redistribution. We therefore hypothesized that LGE is associated withLV wall stress.Methods: A total of 300 patients with suspected cardiomyopathy were examined.CMR imaging was used to assess LV volume, mass, wall stress, and LGE.Results: Increased LV enddiastolic wall stress (>4 kPa) was found in 112 pa-tients (37%), increased endsystolic wall stress (>18 kPa) in 121 patients (40%).Presence of LGE was observed in 93 patients (31%). Enddiastolic (94±43 vs.79±42 ml/m2, P=0.006) and endsystolic LV volume (62±44 vs. 44±37 ml/m2,P<0.001) and LV mass (95±34 vs. 78±31 g/m2, P<0.001) was increased in pa-tients exhibiting LGE. In particular, LV enddiastolic and endsystolic wall stress wasincreased (4.5±2.8 kPa vs. 3.6±3.0 kPa, P=0.025; 19.6±9.1 kPa vs. 17.5±8.2kPa, P=0.045). LGE was observed more frequently than expected from randomoccurrence in patients with increased enddiastolic (39% vs. 26%, P=0.02) andendsystolic wall stress (41% vs. 24%, P=0.002). Both normal enddiastolic andendsystolic wall stress had a high negative predictive value for the absence ofLGE (75% and 76%).Conclusions: In the present study, occurrence of LGE was associated with in-creased LV wall stress and mass in patients with non-ischemic cardiomyopathy.It is suggested that increased ventricular wall stress enhances the capillary leak-age and thus favours contrast medium emission from the vasculature into the
interstitial space. Also, redistribution into the vasculature can be impaired. Basedon the present findings, increased ventricular wall stress appears to be a pre-viously unrecognized major determinant of LGE. It is proposed to consider wallstress-associated LGE as potential prognostic determinant regarding progressionof heart failure, occurrence of sudden cardiac death, and its usefulness as riskstratification for prophylactic treatment with an implanted cardioverter-defibrillator.
P1670 Do women with acute heart failure differ from men?
J.S. Spinar1, J.P. Parenica1, J.V. Vitovec1, P.V. Widimsky2,A.L. Linhart2, R.M. Miklik1, L.S. Spinarova1, J.S. Spac1,L.D. Dusek1, D.T. Tomcikova1. 1University hospital, Brno, CzechRepublic; 2University Hospital, Prague, Czech Republic
The AHEAD (Acute HEArt failure Database) programme consists of the AHEADMAIN, AHEAD CORE and AHEAD NETWORK studies. The AHEAD MAIN studyincludes 2 742 patients – 1 137 (41.5%) female and 1 605 (58.5%) male hospi-talised with acute heart failure in 7 university hospitals – all with 24 hour cath labservice – in 3 cities. The registry started in July 2006 and continued till November2009.57.5% of the patients had de novo acute heart failure, 42.5% had decompensa-tion of chronic heart failure. Women had more frequently de novo heart failure(61.2%) than men (54.9%) (p=0.001). The mean age was 70.9 years (most of thepatients – 32.6%, were in age 70-79 years); mean BMI was 28.0 kg/m2. Femaleswere older 74.9 vs 68.2 years (p<0.001), males had higher BMI. History of hyper-tension was present in 70.1% and diabetes in 40.9%. Females had significantlyhigher systolic blood pressure (140.5 vs. 134.1 mmHg, p<0.001). No differencein diastolic blood pressure between genders was present. The mean ejectionfraction was 38.1%, women had statistically higher ejection fraction (42.8% vs.34.8%, p<0.001). Women had lower creatinine (118.3 vs. 134.9 umol/l, p<0.001),lower hemoglobin (125.2 vs. 134.9 g/l, p<0.001), lower uric acid (394.6 vs. 435.1umol/l, p<0.001). BNP at admission was similar for both sexes (1020.4 vs. 1152.7pg/ml, p = ns).The duration of hospitalisation was 7.0 days for both females and males. Thehospital mortality was 11.7% for females and 11.5% for males (p = ns).Summary: women hospitalised for acute heart failure were significantly older, hadslightly more frequent de novo heart failure, more elevated systolic blood pres-sure and more frequently preserved ejection fraction than men. Females havemore frequently anaemia and less frequently renal insufficiency. The in-hospitalmortality is similar, but when adjusted to age, the prognosis of female patients isclearly better.
P1671 Myocardial longitudinal deformation in thalassemicpatients. An Echocardiographic 2D-Speckle trackingstudy
L. Sirugo, V. Bottari, S. Licciardi, I.P. Monte. University of Catania,Catania, Italy
The patients with thalassemia major (TM) show complications due to chroniceffectsof anaemia but especially to excess iron transfusion, believed to bemainly responsible for the morbidity and mortality and cardiac complications ofTM.Unfortunately, heart disease becomes clinically evident only when ventricularfunction is impaired or when symptomatic arrhythmias appear; after the expres-sion of clinical signs, evolution can be very rapid up to refractory heart failure.Purpose: The aim of our study was to identify early abnormalities of cardiacfunction, through the analysis of longitudinal deformation by global strain (GS)of the left ventricle (LV) and left atrium (LA), using 2D speckle tracking, and thepossible changes following therapy.Methods: We examined the echo parameters of 63 subjects with TM divided into2 groups:TM1: 58 asymptomatic pts age 28,3 +7,2, BSA 1,56 + 0,2) without clinical signsof cardiac dysfunction.TM2: 5 pts (age 33 + 10, BSA 1,50 + 0,25), with heart failure symptoms and LVEF<53%.We have comparedtherefore the echo parameters with those of 16 normal sub-jects (N) matched for age and BSA.Results: TM1and TM2, compared to N, showed increased dimension and vol-ume of LV, RV, LA,RA, E/E’ and LV performance index (TEI), decreased systolicmyocardial velocity (S’) and strain (LV-GS andLA-GS). Subsequently 14 TM1 ptswhohad LAVI>30 ml, E/E ’>10, TEI>0.40 were treated with low dose ACEin-hibitor and all patients TM2 begins therapy with ACE inhibitor, digitalis and beta-blockers.At 6 months follow up in the subgroup TM1 reduces LAVi, improves LA-GS (from12,5 to 18,11% p>0.001), while the other parameters remain the same function.The TM2 is reduced LV size and volume, improved EF, while the lack of normal-ization of LV-GS and LA-GS.Conclusions: The decrease of LA and LV volume after therapy is probably re-lated to overload reduced, whereas the persistent abnormal longitudinal deforma-tion may be related to fatal myocardial damage.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Heart failure / LV dysfunction 283
P1672 Utility of radiological score for verification of evolvingheart failure in the course of acute myocardialinfarction
M. Shochat1, A. Shotan1, M. Kazatsker1, D. Blondheim1,V. Gurovich1, A. Asif1, E. Noiman1, Y. Levi1, P. Rabinovich2,
S. Meisel1. 1Hillel Yaffe Medical Center, Heart Institute, Hadera, Israel; 2Tel AvivSourasky Medical Center, Tel Aviv, Israel
Background: Near twenty percents of patients sustaining acute myocardial in-farction (AMI) develop acute heart failure (AHF) as a result of increased lung fluidcontent (LFC). There is no method to monitor LFC. Lung impedance (LI) thatdecreases with increasing LFC may be indicator of LFC, but needs verification.For this we designed radiological score (RS) based on numerical summation lungedema signs.Aim: To evaluate, in AMI patients developing AHF, the RS by comparison withthe clinical stage (CS) of AHF. We assessed RS and LI correlation, in attempt tovalidate the pathophysiological significance of LI measurement.Method: Patients admitted for AMI and without signs of lung edema were mon-itored by LI device. Absence of lung rales was interpreted as no or interstitiallung edema (CS0). Detection lung rales signified alveolar edema graded as mild(CS1), moderate (CS2), severe (CS3) according to their level.Results: 476 of 622 patients did not develop overt AHF (CS0) during 96 hrsmonitoring. Their RS was 1.4±1.3 and LI decreased from initial by 6.3±6.1%(p<0.001). 146 patients developed overt AHF. At CS1RS was 5.1±0.9 (p<0.001)and LI decreased by 21.6±5.2% (p<0.001). At CS2 and 3, RS were 6.9±1.1 and9.8±0.5 (p<0.001). LI decreased by 29.5±8.2% and 37.4±7.2%, respectively(p<0.001). An RS of 0-2 characterized patients with no edema, 3-4 with inter-stitial edema on chest radiograph, a 5-6 mild edema, and 7-8 and 9-10 signifiedmoderate and severe alveolar edema (Table). AHF CS correlated with RS (r=0.6,p<0.001) and with LI (r=-0.6, p<0.001). RS correlated with LI (r=-0.85, p<0.001).Changes in RS and LI strikingly preceded the detection of lung rales.Conclusions: RS was shown to be a simple and reliable method to assess LFCin patients developing AHF and correlated with the degree of lung congestion.
P1673 Association between QRS duration and increased LVend systolic volume and early LV dysfunction inpatients at high cardiovascular risk in theONTARGET/TRANSCEND cardiac MRI sub-study
R.A.H. Stewart1, A. Young1, B. Cowan1, M. Plijmert1, C. Anderson2,T. Koon3, G. Jennings4 . 1The University of Auckland, Auckland, New Zealand;2George Institute for International Health, Sydney, Australia; 3McMasterUniversity, Hamilton, Canada; 4Baker IDI Heart and Diabetes Institute,Melbourne, Australia
Background: Longer QRS duration on ECG has been associated with increasedcardiovascular mortality but the reasons are uncertain. This study evaluated asso-ciations between increased QRS duration without bundle branch block (≤120ms)and left ventricular (LV) mass, LV end systolic (ESV) and end diastolic volume(EDV), and LV ejection fraction (EF), in 273 patients with increased cardiovascu-lar risk who participated in the ONTARGET and TRANSCEND cardiac magneticresonance imaging (MRI) sub-studies.Methods: Cross-sectional analyses of ECG and cardiac MRI parameters at base-line and 2 year follow-up were performed. ECG measures were performed by asingle trained recorder using standard methods. QRS duration was determinedby computer in most cases. Mean (±SD) cardiac MRI measurements adjustedby height to power of 2.7 are presented for each 10ms band increase in QRSduration.Results: See Table. LV EDV and ESV both increased as the QRS duration length-ened. LV mass also increased with QRS duration but not LV mass/EDV. On aver-age, patients with a QRS duration >110ms had a lower EF. Results were similarfor analysis of 2 year follow-up data.
Cardiac MRI measurements by QRS duration
QRS duration, ms <90 90-99 100-109 110-120 p-value
Number of subjects 109 81 56 27LV mass, g/m2 34.7 (6.8) 36.9 (7.7) 37.3 (7.5) 39.9 (7.3) 0.017EDV, ml/m2 34.2 (7.2) 37.2 (7.0) 36.2 (8.0) 40.6 (9.4) 0.072ESV, ml/m2 12.8 (5.1) 15.4 (5.3) 14.7 (6.4) 20.3 (9.6) 0.0016Ejection fraction, % 63 (8) 59 (9) 61 (10) 52 (13) 0.0003LV mass/EDV 1.03 (0.18) 1.01 (0.19) 1.05 (0.21) 1.01 (0.22) 0.46
Conclusion: Longer QRS duration on the ECG is arisk marker for early LV dys-function. This may explain the association between increased QRS duration andhigher cardiovascular mortality
P1674 Occult endocardial thrombosis in idiopathic leftventricular dysfunction
A. Frustaci, P. Severino, E. Canali, C. Centurion, M. Mancone,F. Fedele, C. Chimenti. Sapienza University of Rome, Rome, Italy
Purpose: Left ventricular (LV) dysfunction is a recognized causeof cardiac thrombo-embolism. However because of limitations of imaging tech-
niques, the real prevalence of LV thrombosis is unknown as uncertain is its rela-tionship with the underlying myocardial disease.Methods: Endocardial thrombus apposition was retrospectively checked in LV en-domyocardial biopsies (4-6 each patient) of 2525 patients (218 without anticoag-ulation) undergoing LV biopsy because of idiopathic LV dysfunction. No echocar-diographic evidence of LV thrombosis was relieved in all before invasive study.Endocardial thrombosis was correlated with patients’ age, sex, LV end diastolicdiameter, LV ejection fraction, duration of LV dysfunction and the histological sub-strate.Results: At histology, an organizing/organized LV endocardial thrombus was de-tected in 14 of 2307 (0.6%, 8 F, 6 M, mean age 47±16) patients on anticoagulationand 17 of 218 (7.7%, 10 F, 7 M, mean age 48±13) patients without (Figure 1). Inboth groups thrombosis strongly correlated (p 0.013; OR: 6.835; IC95%: 1.511-10.929) with the presence of endomyocardial inflammation (CD45RO >14/2mmassociated with focal myocyte necrosis in 11 of 14 pts of group 1 and in 15 of 17of group 2) but not with severity and duration of cardiac disease. LV thrombosiswas associated in pts with inflammation to endocardial PAI-1 expression.
Figure 1
Conclusions: Occult endocardial thrombosis can be histologically detected in upto 7.7% of patients with idiopathic LV dysfunction and no anticoagulation, 13 foldhigher than patient cohort on anticoagulation. It strongly correlates with endocar-dial inflammation and activation of inflammatory cytokines.
P1675 Myocardial fibrosis predicts appropriate devicetherapy in patients with implantable cardioverterdefibrillators for primary prevention of suddencardiac death
L. Iles, H. Pfluger, L. Lefkovits, M.J. Butler, P.M. Kistler, D.M. Kaye,A.J. Taylor. The Alfred Hospital, Melbourne, Australia
Purpose: Patients with heart failure are at risk of sudden cardiac death (SCD).Current guidelines recommend internal cardioverter-defibrillator (ICD) devices fora subgroup based on impaired left ventricular function. A significant proportionof devices never discharge, hence a more accurate method for targeting thoseat risk is desirable. We evaluated the association between regional myocardialfibrosis and ventricular arrhythmia in patients with cardiomyopathy.Methods: We prospectively enrolled 103 patients meeting criteria for ICD implan-tation for primary prevention of SCD. Cardiac magnetic resonance imaging (CMR)was performed prior to device implantation. Regional fibrosis was identified withlate gadolinium enhancement (LGE).Results: Median follow-up was 573 days (interquartile range 379-863 days). LGEidentified regional fibrosis in 31/61 (51%) patients with non-ischemic cardiomy-opathy (NICM) and in all 42 patients with ischemic cardiomyopathy (ICM). Therewas a 29% (9/31) discharge rate in the NICM group with LGE compared to a 14%(6/42) discharge rate in the ICM group (p=NS). There were no ICD discharges inthe NICM group without LGE, which was significantly lower than the rate observedin both the ICM patients (p=0.04) and the NICM patients with LGE (p<0.01). Leftventricular ejection fraction was similar in those with and without device therapy(24±12% vs 26±8%, p=NS) and those with or without LGE (25±9% vs 26±9%,p=NS).Conclusions: Patients with advanced cardiomyopathy and myocardial fibrosisdemonstrated by LGE on CMR have a high likelihood of appropriate ICD ther-apy. Correspondingly, absence of LGE may indicate a lower risk for malignantventricular arrhythmias.
P1676 Growth differentiation factor 15, a marker for earlydetection of heart failure
F.F. Wang, W. Gao. Peking University Third Hospital, Beijing, China,People’s Republic of
Purpose: The reliability of clinical diagnosis for early stage heart fail-ure is poor.Growth differentiation factor 15 (GDF-15) is a member of transforminggrowth factor β (TGF-β) cytokine superfamilies. In animal models, GDF-15 was
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

284 Heart failure / LV dysfunction / Non Imaging
elevated in heart in response to ischemia- reperfusion injury and pressure over-load,manifesting a cardioprotective effect.This population-based study examinedvalue of plasma GDF-15 for detection of early stage heart failure patients andassessing its relationship with collagen turnover.Methods: 174 patients were selected from the Department of Cardiology of Hos-pital from July 2007 and September 2008. They were classified according toACC/AHA guidelines for the chronic heart failure. The group A and B were as-sumed as the early stage of heart failure. Diagnostic accuracies of GDF-15 andNT-proBNP were assessed by ROC curve analysis.Results: 1.The plasma concentration of GDF-15 had positive relationship withthe stages of heart failure (group A: 697.5±324.3 ng/L, group B: 978.9±278.5ng/L, group C: 1302.3±324.4 ng/L, r=0.554,P<0.001) and they were all sig-nificantly higher compared with the Cont group (482.2±170.7 ng/L, P<0.01).2.GDF-15 was associated with NYHA heart function classification. (class I, II,III: 796.0±363.6ng/L,1059.3±357.7 ng/L and 1329.5±318.3ng/L,P < 0.001). 3.There was positive correlation between the GDF-15 and the NT-proBNP at groupC (r=0.392,P=0.016). 4. Left ventricular ejection fraction (LVEF) and left ventricu-lar mass index (LVMI) were independent predictors of GDF-15 value. 5. In distin-guishing the patients with or without cardiac structural disease, areas under thecurves were 0.809 (95% confidence interval, 0.735-0.804) for GDF-15 and 0.818(0.690-0.947) for NT-proBNP (P<0.000). Cutoff values with a largest Youden In-dex (sensitivity + specificity - 1) for cardiac structural disease were 843.6ng/L forGDF-15 and 204.2pg/ml for NT-proBNP. 6. The biomarkers of collagen turnover(ICTP, PINP, PIIINP) were all elevated in group OMI-HF compared with the con-trol group (3.31±1.05 vs. 2.22±1.02 μg/L,23.35±7.20 vs. 17.33±5.94μg/L and13.90±9.23 vs. 6.93±6.04 μg/L, P<0.05). GDF-15 were positively correlated withICTP and PIIINP (r=0.300, 0.259, P<0.05) and had negative relationship withLVEF (r=-0.238, r=-0.282,P=0.011).Conclusions: The levels of plasma GDF-15 were positively correlated with thestages of heart failure. GDF-15 has value for detecting cardiac structural disease.Plasma GDF-15 was associated with the indicators of type I collagen degradationand type III collagen turnover.
P1677 Metalloproteinase-9 serum levels and restrictivediastolic filling pattern as major predictors ofoutcome in patients with ischemic cardiomyopathy
F.L. Dini1, P. Fontanive2, P. Capozza1, A. Pieroni2, M.G. DelleDonne1, P. Caravelli1, E. Orsini1, M. Marzilli1. 1University Hospital,
Cardiac and Thoracic Department, Pisa, Italy; 2Santa Chiara Hospital,Cardiology Unit 2, Pisa, Italy
Objective: Assessment of matrix metalloproteinase-9 (MMP-9) serum levels andDoppler markers of increased left ventricular (LV) filling pressure may be added toprognostic stratification of patients with LV ischemic cardiomyopathy. Therefore,we aimed at investigating the value of serum MMP-9 and restrictive diastolic filling(RDF) in patients with ischemic cardiomyopathy.Methods: Eighty-eight consecutive patients with LV dysfunction (LV ejectionfraction <45%) due to post-infarction LV remodeling were enrolled. A completeM-mode and two-dimensional Doppler-echocardiographic examination was per-formed. Patients were defined as having RDF if they had a mitral E wave decelera-tion time <150 msec. Serum MMP-9 and plasma N-terminal protype-B natriureticpeptide levels were assessed at the time of the index echocardiogram. End pointswere clinical events including all-cause morality mortality or heart failure-relatedhospital admissions. Follow-up period was 30±18 months.Results: On univariate analysis, a number of measurements predicted clinicalevents including: NYHA class >2, MMP-9 >149 ng/ml, RDF, LV ejection frac-tion <30% and N-terminal protype-B natriuretic peptide >1965 pg/ml. However,on multivariate analysis the only independent variables of clinical events wereserum MMP-9 (OR=3.79, p=0.002), NYHA class (OR=3.03, p=0.020), and RDF(OR=2.39, p=0.019). The addition of RDF and MMP-9 to conventional clinical andechocardiographic variables significantly improved the chi-square for the predic-tion of the outcome (from 32.9 to 45.5). Kaplan-Meier survival curves of patientscategorized according to MMP-9 levels and RDF are illustrated.
Conclusion: This study shows the value of serum MMP-9 levels and RDF to riskstratify patients with LV systolic dysfunction due to ischemic cardiomyopathy.
P1678 The role of pulmonary hypertension in thedevelopment of heart failure after acute myocardialinfarction
D. Aronson, D. Mutlak, H. Hammerman, Y. Agmon. Rambam HealthCare Campus, Haifa, Israel
Background: Elevated pulmonary artery systolic pressure (PASP)often accompanies systolic or diastolic left ventricular (LV) dysfunction. In patients(pts) with acute myocardial infarction (AMI), the acute reduction in LV systolic anddiastolic function may lead to an abrupt elevation in PASP. We sought to define theprevalence, severity, and clinical significance of elevated PASP in pts with AMI.Methods: We studie704 pts with AMI. LV systolic and diastolic function and PASPwere assessed by echocardiography. Pts with moderate or severe mitral regurgi-tation were excluded. The primary endpoint of the study was readmission for thetreatment of HF. The relationship between PASP categories and new-onset HFwas examined using Cox regression, adjusting for age, gender, hypertension, di-abetes, Killip class on admission, coronary revascularization, creatinine, LV ejec-tion fraction, and presence of restrictive filling pattern. The primary endpoint wasreadmission for heart failure (HF).Results: Normal (<35 mmHG), mildly elevated (35-49 mmHG) and moderately-severely elevated (≥50 mmHG) PASP was present in 414 (59%), 227 (32%) and63 (9%) pts, respectively. During a mean follow-up of 16 months, readmission forHF occured in 17 (4%), 35 (15%), and 20 (32%) of the respective PASP groups(Figure). In a multivariable Cox regression, compared with patients with normalPASP, the adjusted hazard ratio for HF was 2.3 (95% CI 1.2-4.3) in patients withmildly elevated PASP and 3.1 (95% CI 1.5-6.4) in pts with moderately-severelyelevated PASP.
Conclusions: Elevated PASP is highly prevalent in patient after AMI. There is agraded independent association between the severity of PASP and developmentof HF in pts after AMI. The predictive value of PASP is independent of both systolicand diastolic LV dysfunction.
NON IMAGING
P1679 Investigation on the effect of the wall thickness inrupture risk estimation of AAA by a probabilistic finiteelement approach
S. Celi1, F. Di Puccio2, P. Forte2, M. Mariani3, S. Berti3. 1Instituteof Clinical Physiology of CNR, G. Pasquinucci Hospital, Massa,
Italy; 2University of Pisa, Department of Mechanical, Nuclear and ProductionEngineering, Pisa, Italy; 3Gabriele Monasterio Foundation, Massa, Italy
Purpose: In clinical practice the commonly used predictors for AAA rupture riskare the maximum transverse diameter (Dmax) and its expansion rate; however,they are only general rules and not reliable indicators since also small aneurysmcan rupture. From a biomechanical perspective, both morphology and materialproperties play an important role and the rupture event occurs when the mechan-ical wall stress exceeds the tensile strength of the tissue.The aim of this study is to investigate the effect of morphological parameters(eccentricity, maximum transverse diameter, length and wall thickness reductionin the bulge) on the rupture risk estimation.Methods: CT images from our patient database were analysed and the maingeometrical features of abdominal aortic diseases were identified by means ofa specific routine developed in Matlab. Sensitivity analyses were performed byusing a probabilistic Finite Element approach to investigate the stress field at thepeak systolic pressure. Due to the difficulties to evaluate the wall thickness in-vivo,experimental thickness measurements on 13 specimens were employed.Results: Results of the sensitivity analysis show that the mean value of the maxi-mum stress is 0.29 MPa (sd 0.13 MPa). The peak stress, under the assumption of
Figure 1. Maximum von Mises wall stress (MPa).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
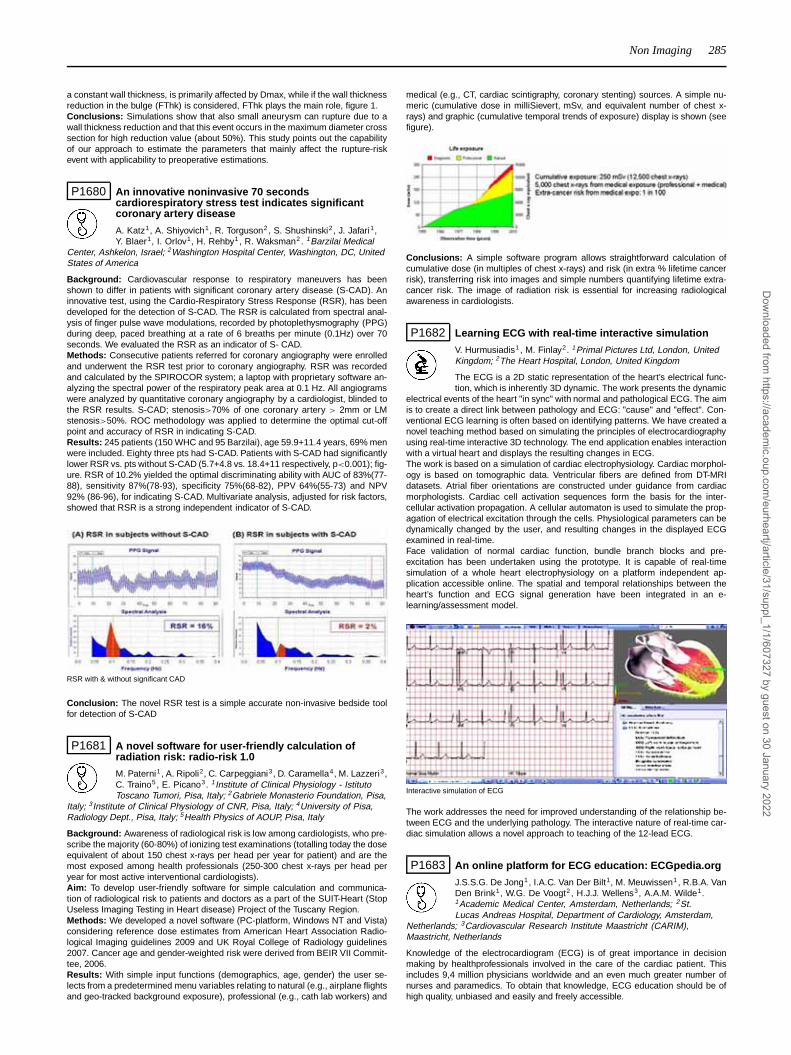
Non Imaging 285
a constant wall thickness, is primarily affected by Dmax, while if the wall thicknessreduction in the bulge (FThk) is considered, FThk plays the main role, figure 1.Conclusions: Simulations show that also small aneurysm can rupture due to awall thickness reduction and that this event occurs in the maximum diameter crosssection for high reduction value (about 50%). This study points out the capabilityof our approach to estimate the parameters that mainly affect the rupture-riskevent with applicability to preoperative estimations.
P1680 An innovative noninvasive 70 secondscardiorespiratory stress test indicates significantcoronary artery disease
A. Katz1, A. Shiyovich1, R. Torguson2 , S. Shushinski2, J. Jafari1,Y. Blaer1, I. Orlov1, H. Rehby1, R. Waksman2. 1Barzilai Medical
Center, Ashkelon, Israel; 2Washington Hospital Center, Washington, DC, UnitedStates of America
Background: Cardiovascular response to respiratory maneuvers has beenshown to differ in patients with significant coronary artery disease (S-CAD). Aninnovative test, using the Cardio-Respiratory Stress Response (RSR), has beendeveloped for the detection of S-CAD. The RSR is calculated from spectral anal-ysis of finger pulse wave modulations, recorded by photoplethysmography (PPG)during deep, paced breathing at a rate of 6 breaths per minute (0.1Hz) over 70seconds. We evaluated the RSR as an indicator of S- CAD.Methods: Consecutive patients referred for coronary angiography were enrolledand underwent the RSR test prior to coronary angiography. RSR was recordedand calculated by the SPIROCOR system; a laptop with proprietary software an-alyzing the spectral power of the respiratory peak area at 0.1 Hz. All angiogramswere analyzed by quantitative coronary angiography by a cardiologist, blinded tothe RSR results. S-CAD; stenosis>70% of one coronary artery > 2mm or LMstenosis>50%. ROC methodology was applied to determine the optimal cut-offpoint and accuracy of RSR in indicating S-CAD.Results: 245 patients (150 WHC and 95 Barzilai), age 59.9+11.4 years, 69% menwere included. Eighty three pts had S-CAD. Patients with S-CAD had significantlylower RSR vs. pts without S-CAD (5.7+4.8 vs. 18.4+11 respectively, p<0.001); fig-ure. RSR of 10.2% yielded the optimal discriminating ability with AUC of 83%(77-88), sensitivity 87%(78-93), specificity 75%(68-82), PPV 64%(55-73) and NPV92% (86-96), for indicating S-CAD. Multivariate analysis, adjusted for risk factors,showed that RSR is a strong independent indicator of S-CAD.
RSR with & without significant CAD
Conclusion: The novel RSR test is a simple accurate non-invasive bedside toolfor detection of S-CAD
P1681 A novel software for user-friendly calculation ofradiation risk: radio-risk 1.0
M. Paterni1, A. Ripoli2, C. Carpeggiani3, D. Caramella4, M. Lazzeri3,C. Traino5, E. Picano3. 1Institute of Clinical Physiology - IstitutoToscano Tumori, Pisa, Italy; 2Gabriele Monasterio Foundation, Pisa,
Italy; 3Institute of Clinical Physiology of CNR, Pisa, Italy; 4University of Pisa,Radiology Dept., Pisa, Italy; 5Health Physics of AOUP, Pisa, Italy
Background: Awareness of radiological risk is low among cardiologists, who pre-scribe the majority (60-80%) of ionizing test examinations (totalling today the doseequivalent of about 150 chest x-rays per head per year for patient) and are themost exposed among health professionals (250-300 chest x-rays per head peryear for most active interventional cardiologists).Aim: To develop user-friendly software for simple calculation and communica-tion of radiological risk to patients and doctors as a part of the SUIT-Heart (StopUseless Imaging Testing in Heart disease) Project of the Tuscany Region.Methods: We developed a novel software (PC-platform, Windows NT and Vista)considering reference dose estimates from American Heart Association Radio-logical Imaging guidelines 2009 and UK Royal College of Radiology guidelines2007. Cancer age and gender-weighted risk were derived from BEIR VII Commit-tee, 2006.Results: With simple input functions (demographics, age, gender) the user se-lects from a predetermined menu variables relating to natural (e.g., airplane flightsand geo-tracked background exposure), professional (e.g., cath lab workers) and
medical (e.g., CT, cardiac scintigraphy, coronary stenting) sources. A simple nu-meric (cumulative dose in milliSievert, mSv, and equivalent number of chest x-rays) and graphic (cumulative temporal trends of exposure) display is shown (seefigure).
Conclusions: A simple software program allows straightforward calculation ofcumulative dose (in multiples of chest x-rays) and risk (in extra % lifetime cancerrisk), transferring risk into images and simple numbers quantifying lifetime extra-cancer risk. The image of radiation risk is essential for increasing radiologicalawareness in cardiologists.
P1682 Learning ECG with real-time interactive simulation
V. Hurmusiadis1 , M. Finlay2. 1Primal Pictures Ltd, London, UnitedKingdom; 2The Heart Hospital, London, United Kingdom
The ECG is a 2D static representation of the heart’s electrical func-tion, which is inherently 3D dynamic. The work presents the dynamic
electrical events of the heart "in sync" with normal and pathological ECG. The aimis to create a direct link between pathology and ECG: "cause" and "effect". Con-ventional ECG learning is often based on identifying patterns. We have created anovel teaching method based on simulating the principles of electrocardiographyusing real-time interactive 3D technology. The end application enables interactionwith a virtual heart and displays the resulting changes in ECG.The work is based on a simulation of cardiac electrophysiology. Cardiac morphol-ogy is based on tomographic data. Ventricular fibers are defined from DT-MRIdatasets. Atrial fiber orientations are constructed under guidance from cardiacmorphologists. Cardiac cell activation sequences form the basis for the inter-cellular activation propagation. A cellular automaton is used to simulate the prop-agation of electrical excitation through the cells. Physiological parameters can bedynamically changed by the user, and resulting changes in the displayed ECGexamined in real-time.Face validation of normal cardiac function, bundle branch blocks and pre-excitation has been undertaken using the prototype. It is capable of real-timesimulation of a whole heart electrophysiology on a platform independent ap-plication accessible online. The spatial and temporal relationships between theheart’s function and ECG signal generation have been integrated in an e-learning/assessment model.
Interactive simulation of ECG
The work addresses the need for improved understanding of the relationship be-tween ECG and the underlying pathology. The interactive nature of real-time car-diac simulation allows a novel approach to teaching of the 12-lead ECG.
P1683 An online platform for ECG education: ECGpedia.org
J.S.S.G. De Jong1, I.A.C. Van Der Bilt1, M. Meuwissen1, R.B.A. VanDen Brink1, W.G. De Voogt2 , H.J.J. Wellens3, A.A.M. Wilde1.1Academic Medical Center, Amsterdam, Netherlands; 2St.Lucas Andreas Hospital, Department of Cardiology, Amsterdam,
Netherlands; 3Cardiovascular Research Institute Maastricht (CARIM),Maastricht, Netherlands
Knowledge of the electrocardiogram (ECG) is of great importance in decisionmaking by healthprofessionals involved in the care of the cardiac patient. Thisincludes 9,4 million physicians worldwide and an even much greater number ofnurses and paramedics. To obtain that knowledge, ECG education should be ofhigh quality, unbiased and easily and freely accessible.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
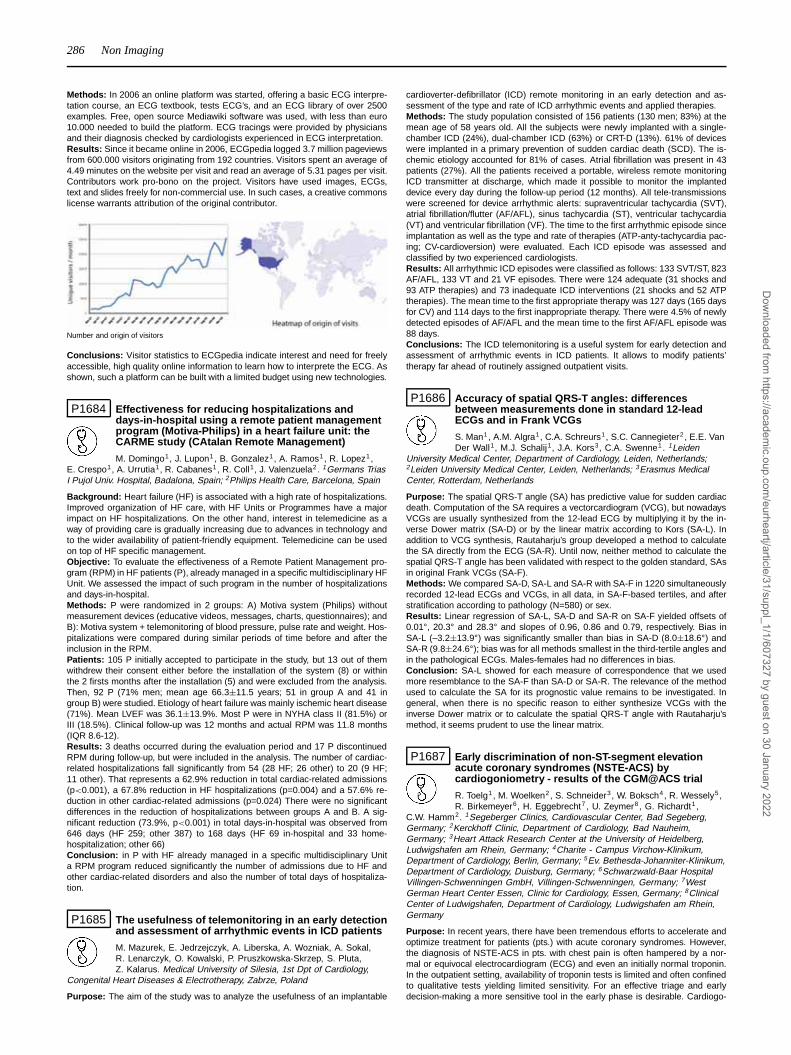
286 Non Imaging
Methods: In 2006 an online platform was started, offering a basic ECG interpre-tation course, an ECG textbook, tests ECG’s, and an ECG library of over 2500examples. Free, open source Mediawiki software was used, with less than euro10.000 needed to build the platform. ECG tracings were provided by physiciansand their diagnosis checked by cardiologists experienced in ECG interpretation.Results: Since it became online in 2006, ECGpedia logged 3.7 million pageviewsfrom 600.000 visitors originating from 192 countries. Visitors spent an average of4.49 minutes on the website per visit and read an average of 5.31 pages per visit.Contributors work pro-bono on the project. Visitors have used images, ECGs,text and slides freely for non-commercial use. In such cases, a creative commonslicense warrants attribution of the original contributor.
Number and origin of visitors
Conclusions: Visitor statistics to ECGpedia indicate interest and need for freelyaccessible, high quality online information to learn how to interprete the ECG. Asshown, such a platform can be built with a limited budget using new technologies.
P1684 Effectiveness for reducing hospitalizations anddays-in-hospital using a remote patient managementprogram (Motiva-Philips) in a heart failure unit: theCARME study (CAtalan Remote Management)
M. Domingo1, J. Lupon1, B. Gonzalez1, A. Ramos1, R. Lopez1,E. Crespo1, A. Urrutia1, R. Cabanes1, R. Coll1, J. Valenzuela2 . 1Germans TriasI Pujol Univ. Hospital, Badalona, Spain; 2Philips Health Care, Barcelona, Spain
Background: Heart failure (HF) is associated with a high rate of hospitalizations.Improved organization of HF care, with HF Units or Programmes have a majorimpact on HF hospitalizations. On the other hand, interest in telemedicine as away of providing care is gradually increasing due to advances in technology andto the wider availability of patient-friendly equipment. Telemedicine can be usedon top of HF specific management.Objective: To evaluate the effectiveness of a Remote Patient Management pro-gram (RPM) in HF patients (P), already managed in a specific multidisciplinary HFUnit. We assessed the impact of such program in the number of hospitalizationsand days-in-hospital.Methods: P were randomized in 2 groups: A) Motiva system (Philips) withoutmeasurement devices (educative videos, messages, charts, questionnaires); andB): Motiva system + telemonitoring of blood pressure, pulse rate and weight. Hos-pitalizations were compared during similar periods of time before and after theinclusion in the RPM.Patients: 105 P initially accepted to participate in the study, but 13 out of themwithdrew their consent either before the installation of the system (8) or withinthe 2 firsts months after the installation (5) and were excluded from the analysis.Then, 92 P (71% men; mean age 66.3±11.5 years; 51 in group A and 41 ingroup B) were studied. Etiology of heart failure was mainly ischemic heart disease(71%). Mean LVEF was 36.1±13.9%. Most P were in NYHA class II (81.5%) orIII (18.5%). Clinical follow-up was 12 months and actual RPM was 11.8 months(IQR 8.6-12).Results: 3 deaths occurred during the evaluation period and 17 P discontinuedRPM during follow-up, but were included in the analysis. The number of cardiac-related hospitalizations fall significantly from 54 (28 HF; 26 other) to 20 (9 HF;11 other). That represents a 62.9% reduction in total cardiac-related admissions(p<0.001), a 67.8% reduction in HF hospitalizations (p=0.004) and a 57.6% re-duction in other cardiac-related admissions (p=0.024) There were no significantdifferences in the reduction of hospitalizations between groups A and B. A sig-nificant reduction (73.9%, p<0.001) in total days-in-hospital was observed from646 days (HF 259; other 387) to 168 days (HF 69 in-hospital and 33 home-hospitalization; other 66)Conclusion: in P with HF already managed in a specific multidisciplinary Unita RPM program reduced significantly the number of admissions due to HF andother cardiac-related disorders and also the number of total days of hospitaliza-tion.
P1685 The usefulness of telemonitoring in an early detectionand assessment of arrhythmic events in ICD patients
M. Mazurek, E. Jedrzejczyk, A. Liberska, A. Wozniak, A. Sokal,R. Lenarczyk, O. Kowalski, P. Pruszkowska-Skrzep, S. Pluta,Z. Kalarus. Medical University of Silesia, 1st Dpt of Cardiology,
Congenital Heart Diseases & Electrotherapy, Zabrze, Poland
Purpose: The aim of the study was to analyze the usefulness of an implantable
cardioverter-defibrillator (ICD) remote monitoring in an early detection and as-sessment of the type and rate of ICD arrhythmic events and applied therapies.Methods: The study population consisted of 156 patients (130 men; 83%) at themean age of 58 years old. All the subjects were newly implanted with a single-chamber ICD (24%), dual-chamber ICD (63%) or CRT-D (13%). 61% of deviceswere implanted in a primary prevention of sudden cardiac death (SCD). The is-chemic etiology accounted for 81% of cases. Atrial fibrillation was present in 43patients (27%). All the patients received a portable, wireless remote monitoringICD transmitter at discharge, which made it possible to monitor the implanteddevice every day during the follow-up period (12 months). All tele-transmissionswere screened for device arrhythmic alerts: supraventricular tachycardia (SVT),atrial fibrillation/flutter (AF/AFL), sinus tachycardia (ST), ventricular tachycardia(VT) and ventricular fibrillation (VF). The time to the first arrhythmic episode sinceimplantation as well as the type and rate of therapies (ATP-anty-tachycardia pac-ing; CV-cardioversion) were evaluated. Each ICD episode was assessed andclassified by two experienced cardiologists.Results: All arrhythmic ICD episodes were classified as follows: 133 SVT/ST, 823AF/AFL, 133 VT and 21 VF episodes. There were 124 adequate (31 shocks and93 ATP therapies) and 73 inadequate ICD interventions (21 shocks and 52 ATPtherapies). The mean time to the first appropriate therapy was 127 days (165 daysfor CV) and 114 days to the first inappropriate therapy. There were 4.5% of newlydetected episodes of AF/AFL and the mean time to the first AF/AFL episode was88 days.Conclusions: The ICD telemonitoring is a useful system for early detection andassessment of arrhythmic events in ICD patients. It allows to modify patients’therapy far ahead of routinely assigned outpatient visits.
P1686 Accuracy of spatial QRS-T angles: differencesbetween measurements done in standard 12-leadECGs and in Frank VCGs
S. Man1, A.M. Algra1, C.A. Schreurs1, S.C. Cannegieter2 , E.E. VanDer Wall1, M.J. Schalij1, J.A. Kors3, C.A. Swenne1. 1Leiden
University Medical Center, Department of Cardiology, Leiden, Netherlands;2Leiden University Medical Center, Leiden, Netherlands; 3Erasmus MedicalCenter, Rotterdam, Netherlands
Purpose: The spatial QRS-T angle (SA) has predictive value for sudden cardiacdeath. Computation of the SA requires a vectorcardiogram (VCG), but nowadaysVCGs are usually synthesized from the 12-lead ECG by multiplying it by the in-verse Dower matrix (SA-D) or by the linear matrix according to Kors (SA-L). Inaddition to VCG synthesis, Rautaharju’s group developed a method to calculatethe SA directly from the ECG (SA-R). Until now, neither method to calculate thespatial QRS-T angle has been validated with respect to the golden standard, SAsin original Frank VCGs (SA-F).Methods: We compared SA-D, SA-L and SA-R with SA-F in 1220 simultaneouslyrecorded 12-lead ECGs and VCGs, in all data, in SA-F-based tertiles, and afterstratification according to pathology (N=580) or sex.Results: Linear regression of SA-L, SA-D and SA-R on SA-F yielded offsets of0.01°, 20.3° and 28.3° and slopes of 0.96, 0.86 and 0.79, respectively. Bias inSA-L (–3.2±13.9°) was significantly smaller than bias in SA-D (8.0±18.6°) andSA-R (9.8±24.6°); bias was for all methods smallest in the third-tertile angles andin the pathological ECGs. Males-females had no differences in bias.Conclusion: SA-L showed for each measure of correspondence that we usedmore resemblance to the SA-F than SA-D or SA-R. The relevance of the methodused to calculate the SA for its prognostic value remains to be investigated. Ingeneral, when there is no specific reason to either synthesize VCGs with theinverse Dower matrix or to calculate the spatial QRS-T angle with Rautaharju’smethod, it seems prudent to use the linear matrix.
P1687 Early discrimination of non-ST-segment elevationacute coronary syndromes (NSTE-ACS) bycardiogoniometry - results of the CGM@ACS trial
R. Toelg1 , M. Woelken2, S. Schneider3, W. Boksch4, R. Wessely5 ,R. Birkemeyer6, H. Eggebrecht7 , U. Zeymer8 , G. Richardt1,
C.W. Hamm2. 1Segeberger Clinics, Cardiovascular Center, Bad Segeberg,Germany; 2Kerckhoff Clinic, Department of Cardiology, Bad Nauheim,Germany; 3Heart Attack Research Center at the University of Heidelberg,Ludwigshafen am Rhein, Germany; 4Charite - Campus Virchow-Klinikum,Department of Cardiology, Berlin, Germany; 5Ev. Bethesda-Johanniter-Klinikum,Department of Cardiology, Duisburg, Germany; 6Schwarzwald-Baar HospitalVillingen-Schwenningen GmbH, Villingen-Schwenningen, Germany; 7WestGerman Heart Center Essen, Clinic for Cardiology, Essen, Germany; 8ClinicalCenter of Ludwigshafen, Department of Cardiology, Ludwigshafen am Rhein,Germany
Purpose: In recent years, there have been tremendous efforts to accelerate andoptimize treatment for patients (pts.) with acute coronary syndromes. However,the diagnosis of NSTE-ACS in pts. with chest pain is often hampered by a nor-mal or equivocal electrocardiogram (ECG) and even an initially normal troponin.In the outpatient setting, availability of troponin tests is limited and often confinedto qualitative tests yielding limited sensitivity. For an effective triage and earlydecision-making a more sensitive tool in the early phase is desirable. Cardiogo-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Non Imaging / Imaging 287
niometry (CGM) is a novel electrodiagnostic method utilizing computer-assisted3-dimensional information of cardiac potentials. It is performed at rest, simple touse and fast to apply. We sought to investigate the potential of CGM for the earlyidentification of NSTE-ACS upon arrival in a chest-pain unit.Methods: In the prospective German CGM@ACS observational trial, a total of200 pts. with acute chest pain or dyspnea undergoing coronary angiography willbe included. The results of CGM at admission will be correlated with the ultimateclinical diagnosis after coronary angiography (NSTE-ACS vs. no NSTE-ACS). Wepresent an interim analysis of 180 pts. so far included into the trial.Results: Mean age of the patients was 67 years with 32% being females, 25%were diabetics, 31% were smokers, 10% had renal insufficiency and 84% hadarterial hypertension. Pts. presenting with NSTE-ACS (n=133) or no NSTE-ACS(n=47) had previous myocardial infarction in 24.4% vs. 12.8% (n.s.), had previ-ous revascularization in 54.2% vs. 29.8% (n.s.), had an angiographic significantcoronary artery disease in 84.2% vs. 28.9% (p<0.0001), were treated with PCIin 53.4% vs. 8.5% (p<0.0001), had a positive troponin at admission in 30.0%vs. 10.9% (p<0.05) and a pathologic CGM at admission in 68.4% vs. 51.1%(p<0.05). In discriminating between NSTE-ACS and no NSTE-ACS Troponin atadmission revealed 30.0% sensitivity, 89.1% specificity, 88.6% positive predic-tive value and 31.1% negative predictive value. Respectively, CGM at admissionshowed 68.4% sensitivity, 48.9% specificity, 79.1% positive predictive value and35.4% negative predictive value.Conclusion: These preliminary results indicate that CGM has a high potentialfor detecting patients with NSTE-ACS probably at an earlier stage compared totroponin. Since CGM measures ischemic myocardium, specificity is somewhatlower in this setting, as a remarkable number of patients without NSTE-ACS haveestablished coronary artery disease.
P1688 QRS-T morphology measured from exerciseelectrocardiogram as a predictor of cardiac death
T. Kentta1, M. Karsikas1, M.J. Junttila1, J.S. Perkiomaki1,T. Seppanen1 , T. Nieminen2, T. Lehtimaki2, J. Viik2, M. Kahonen2,H.V. Huikuri1. 1University of Oulu, Oulu, Finland; 2University of
Tampere, Tampere, Finland
Purpose: Total cosine R-to-T (TCRT) measured from standard 12-lead ECG re-flects the spatial relationship between depolarization and repolarization wave-fronts. Reduced TCRT value indicates an increased risk of mortality. We testedthe hypothesis that measurement of TCRT or QRS/T angle from exercise ECGgives even more powerful prognostic information.Methods: The prognostic significance of the rate-dependence of TCRT andQRS/T angle were assessed from standard exercise ECG recordings in 1297patients (age 56±13 years [mean±SD], 67% males) undergoing a clinically indi-cated bicycle stress-test.Results: During an average follow-up of 45±12 months, 74 patients died (5.7%);34 (2.6%) were cardiac deaths and 24 (1.9%) were sudden cardiac deaths. TCRTand QRS/T angle had a correlation with the RR intervals in the total cohort, but theindividual responses were variable, e.g. median correlation coefficient betweenTCRT and RR intervals (TCRT-RR) was 0.89 with an inter-quartile range of 0.55- 0.98. After adjustments with age, β-blockers, body mass index, coronary heartdisease, diabetes, left ventricular ejection fraction, maximum heart rate, metabolicequivalent, previous infarction, sex and smoking, reduced TCRT-RR value duringthe recovery phase of exercise ECG was a stronger predictor of cardiac death(adjusted HR 3.6; 95%CI: 1.8-7.2; p=0.001) than TCRT measured from baseline12-lead ECG (adjusted HR 1.8; 95% CI: 1.2-2.9; p=0.01). Poor TCRT-RR corre-lation coefficient both during the exercise and recovery was specifically related toa high risk of sudden cardiac death (adjusted HR 7.1; 95%CI; 2.5-20.3; p<0.001;Figure 1).
Kaplan-Meier curve for SCD
Conclusions: Loss of rate-dependence of depolarization and repolarizationwavefronts is a strong predictor of cardiac death, especially of sudden cardiacdeath.
P1689 What is the reproducibility of non-linear measures ofheart rate variability analysis carried out on shortECG recordings?
J. Sacha1, J. Sobon2, S. Barabach1, G. Bilinski2, W. Pluta1.1Department of Cardiology, Regional Medical Center, Opole,
Poland; 2Faculty of Physical Education and Physiotherapy, Opole University ofTechnology, Opole, Poland
It is not clear if non-linear heart rate variability (HRV) methods can be employedto analyse short ECG recordings – in particular little is known about the repro-ducibility of such measurements.Purpose: To explore the reproducibility of non-linear and linear HRV measurescalculated from short ECG recordings.Methods: 792 ECG recordings were performed among 18 healthy persons (ina sitting position twice daily over 30 days) – 706 recordings (512 RR intervalseach) were suitable for the analysis (39.2 recordings/person on average). Coeffi-cients of variation (CV) were calculated for each patient for the following parame-ters: Temporal analysis: mean RR interval (mRR), standard deviation (SD) of RR(SDRR), mean heart rate (mHR), SDHR, RMSSD, pNN50%; Geometric methods:TINN, RR triangular index (Tri index); SPECTRAL ANALYSIS: total power (TP),VLF, LF, HF, LF/HF, nLF, nHF; Nonlinear methods: approximate entropy (ApEn);sample entropy (SampEn); correlation dimension (Corr Dim); Detrended Fluctua-tion Analysis: Alfa 1, Alfa 2; Poincare Plot: SD1, SD2; Recurrence Plot Analysis:mean line length (MLine L), max line length (MxLine L), recurrence rate (REC),determinism (DET), Shannon entropy (SchanEn).Results: Figure exhibits CV’s of all parameters ordered from the highest to lowestupper quartile (Friedman test, p<0.00001) – significant difference between neigh-boring CV’s are marked with signs. Majority of non-linear measures revealed highreproducibility (low CV’s) – excellent reproducibility was seen for DET, SchanEnand ApEn.
Coefficients of variation HRV parameters
Conclusions: Non-linear HRV measures calculated from short ECG recordingspresent high reproducibility in healthy persons in steady conditions – thus theyseem to be useful for monitoring sick people. Further studies are needed to testthis approach in selected patients groups.
IMAGING
P1690 Endocardial acceleration versus ultrasound-derivedtime intervals in recipients of cardiacresynchronization therapy systems
E. Donal1, L. Giorgis2, S. Cazeau3, C. Leclercq1, L. Senhadji4,A. Amblard2, G. Jauvert5, M. Burban6, A. Hernandez4 , P. Mabo1.
1CHU Rennes, Rennes, France; 2Sorin CRM SAS, Clamart, France; 3St JosephHospital, Paris, France; 4INSERM U642 Rennes, Rennes, France; 5INPARYSClinical Research Group, St Cloud, France; 6Nouvelles Cliniques Nantaises,Nantes, France
Background: Optimization of cardiac resynchronization therapy (CRT) requiresthe gathering of cardiac functional information. An accurate timing of the phasesof the cardiac cycle is key in the optimization process.Methods and Results: We compared Doppler echocardiography to an auto-mated system, based on the recording of sonR (formerly endocardial accelera-tion) in the detection of mitral and aortic valves closure and measurements of du-ration of systole and diastole. We prospectively studied, under various conditionsof cardiac stimulation, 75 recipients of CRT systems (69% men), whose meanage was 72±9.2 years, left ventricular ejection fraction 35±11%, baseline QRSduration 154±29 ms, and New York Heart Association functional class 3.0±0.7.We simultaneously recorded a) sonR, detected by a non-invasive piezoelectricmicro-accelerometer sensor clipped onto an electrode located in the parasternalregion, b) electrocardiogram, and c) Doppler audio signals, using a multichanneldata acquisition and analysis system. The correlation between timing of mitraland aortic valves closure by sonR versus Doppler signals was examined by lin-ear regression analysis. Correlation coefficients and average absolute error werecalculated. A concordance in the timing of the mitral (r = 0.86, error = 9.7 ms) andaortic (r = 0.93, error = 9.7ms) valves closure was observed between the 2 meth-ods in 94% of patients. Similarly, sonR and the Doppler-derived measurements of
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022
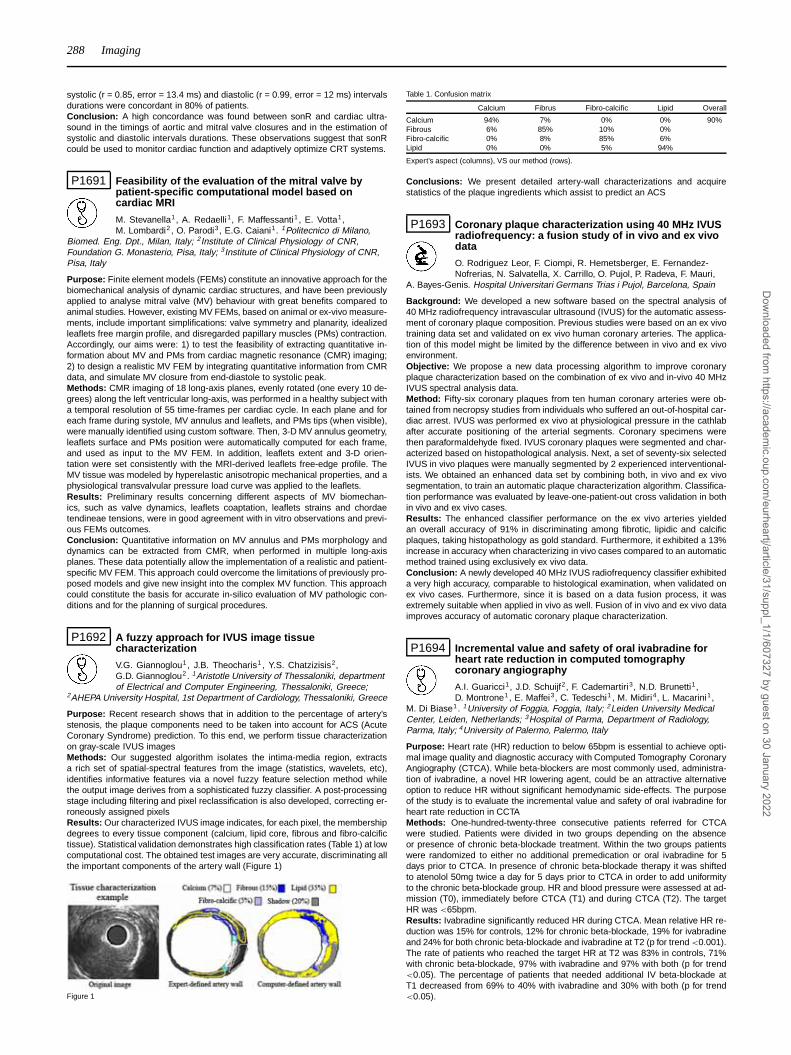
288 Imaging
systolic (r = 0.85, error = 13.4 ms) and diastolic (r = 0.99, error = 12 ms) intervalsdurations were concordant in 80% of patients.Conclusion: A high concordance was found between sonR and cardiac ultra-sound in the timings of aortic and mitral valve closures and in the estimation ofsystolic and diastolic intervals durations. These observations suggest that sonRcould be used to monitor cardiac function and adaptively optimize CRT systems.
P1691 Feasibility of the evaluation of the mitral valve bypatient-specific computational model based oncardiac MRI
M. Stevanella1, A. Redaelli1, F. Maffessanti1 , E. Votta1,M. Lombardi2 , O. Parodi3, E.G. Caiani1. 1Politecnico di Milano,
Biomed. Eng. Dpt., Milan, Italy; 2Institute of Clinical Physiology of CNR,Foundation G. Monasterio, Pisa, Italy; 3Institute of Clinical Physiology of CNR,Pisa, Italy
Purpose: Finite element models (FEMs) constitute an innovative approach for thebiomechanical analysis of dynamic cardiac structures, and have been previouslyapplied to analyse mitral valve (MV) behaviour with great benefits compared toanimal studies. However, existing MV FEMs, based on animal or ex-vivo measure-ments, include important simplifications: valve symmetry and planarity, idealizedleaflets free margin profile, and disregarded papillary muscles (PMs) contraction.Accordingly, our aims were: 1) to test the feasibility of extracting quantitative in-formation about MV and PMs from cardiac magnetic resonance (CMR) imaging;2) to design a realistic MV FEM by integrating quantitative information from CMRdata, and simulate MV closure from end-diastole to systolic peak.Methods: CMR imaging of 18 long-axis planes, evenly rotated (one every 10 de-grees) along the left ventricular long-axis, was performed in a healthy subject witha temporal resolution of 55 time-frames per cardiac cycle. In each plane and foreach frame during systole, MV annulus and leaflets, and PMs tips (when visible),were manually identified using custom software. Then, 3-D MV annulus geometry,leaflets surface and PMs position were automatically computed for each frame,and used as input to the MV FEM. In addition, leaflets extent and 3-D orien-tation were set consistently with the MRI-derived leaflets free-edge profile. TheMV tissue was modeled by hyperelastic anisotropic mechanical properties, and aphysiological transvalvular pressure load curve was applied to the leaflets.Results: Preliminary results concerning different aspects of MV biomechan-ics, such as valve dynamics, leaflets coaptation, leaflets strains and chordaetendineae tensions, were in good agreement with in vitro observations and previ-ous FEMs outcomes.Conclusion: Quantitative information on MV annulus and PMs morphology anddynamics can be extracted from CMR, when performed in multiple long-axisplanes. These data potentially allow the implementation of a realistic and patient-specific MV FEM. This approach could overcome the limitations of previously pro-posed models and give new insight into the complex MV function. This approachcould constitute the basis for accurate in-silico evaluation of MV pathologic con-ditions and for the planning of surgical procedures.
P1692 A fuzzy approach for IVUS image tissuecharacterization
V.G. Giannoglou1, J.B. Theocharis1 , Y.S. Chatzizisis2,G.D. Giannoglou2. 1Aristotle University of Thessaloniki, departmentof Electrical and Computer Engineering, Thessaloniki, Greece;
2AHEPA University Hospital, 1st Department of Cardiology, Thessaloniki, Greece
Purpose: Recent research shows that in addition to the percentage of artery’sstenosis, the plaque components need to be taken into account for ACS (AcuteCoronary Syndrome) prediction. To this end, we perform tissue characterizationon gray-scale IVUS imagesMethods: Our suggested algorithm isolates the intima-media region, extractsa rich set of spatial-spectral features from the image (statistics, wavelets, etc),identifies informative features via a novel fuzzy feature selection method whilethe output image derives from a sophisticated fuzzy classifier. A post-processingstage including filtering and pixel reclassification is also developed, correcting er-roneously assigned pixelsResults: Our characterized IVUS image indicates, for each pixel, the membershipdegrees to every tissue component (calcium, lipid core, fibrous and fibro-calcifictissue). Statistical validation demonstrates high classification rates (Table 1) at lowcomputational cost. The obtained test images are very accurate, discriminating allthe important components of the artery wall (Figure 1)
Figure 1
Table 1. Confusion matrix
Calcium Fibrus Fibro-calcific Lipid Overall
Calcium 94% 7% 0% 0% 90%Fibrous 6% 85% 10% 0%Fibro-calcific 0% 8% 85% 6%Lipid 0% 0% 5% 94%
Expert’s aspect (columns), VS our method (rows).
Conclusions: We present detailed artery-wall characterizations and acquirestatistics of the plaque ingredients which assist to predict an ACS
P1693 Coronary plaque characterization using 40 MHz IVUSradiofrequency: a fusion study of in vivo and ex vivodata
O. Rodriguez Leor, F. Ciompi, R. Hemetsberger, E. Fernandez-Nofrerias, N. Salvatella, X. Carrillo, O. Pujol, P. Radeva, F. Mauri,
A. Bayes-Genis. Hospital Universitari Germans Trias i Pujol, Barcelona, Spain
Background: We developed a new software based on the spectral analysis of40 MHz radiofrequency intravascular ultrasound (IVUS) for the automatic assess-ment of coronary plaque composition. Previous studies were based on an ex vivotraining data set and validated on ex vivo human coronary arteries. The applica-tion of this model might be limited by the difference between in vivo and ex vivoenvironment.Objective: We propose a new data processing algorithm to improve coronaryplaque characterization based on the combination of ex vivo and in-vivo 40 MHzIVUS spectral analysis data.Method: Fifty-six coronary plaques from ten human coronary arteries were ob-tained from necropsy studies from individuals who suffered an out-of-hospital car-diac arrest. IVUS was performed ex vivo at physiological pressure in the cathlabafter accurate positioning of the arterial segments. Coronary specimens werethen paraformaldehyde fixed. IVUS coronary plaques were segmented and char-acterized based on histopathological analysis. Next, a set of seventy-six selectedIVUS in vivo plaques were manually segmented by 2 experienced interventional-ists. We obtained an enhanced data set by combining both, in vivo and ex vivosegmentation, to train an automatic plaque characterization algorithm. Classifica-tion performance was evaluated by leave-one-patient-out cross validation in bothin vivo and ex vivo cases.Results: The enhanced classifier performance on the ex vivo arteries yieldedan overall accuracy of 91% in discriminating among fibrotic, lipidic and calcificplaques, taking histopathology as gold standard. Furthermore, it exhibited a 13%increase in accuracy when characterizing in vivo cases compared to an automaticmethod trained using exclusively ex vivo data.Conclusion: A newly developed 40 MHz IVUS radiofrequency classifier exhibiteda very high accuracy, comparable to histological examination, when validated onex vivo cases. Furthermore, since it is based on a data fusion process, it wasextremely suitable when applied in vivo as well. Fusion of in vivo and ex vivo dataimproves accuracy of automatic coronary plaque characterization.
P1694 Incremental value and safety of oral ivabradine forheart rate reduction in computed tomographycoronary angiography
A.I. Guaricci1, J.D. Schuijf2, F. Cademartiri3, N.D. Brunetti1,D. Montrone1, E. Maffei3, C. Tedeschi1 , M. Midiri4, L. Macarini1,
M. Di Biase1. 1University of Foggia, Foggia, Italy; 2Leiden University MedicalCenter, Leiden, Netherlands; 3Hospital of Parma, Department of Radiology,Parma, Italy; 4University of Palermo, Palermo, Italy
Purpose: Heart rate (HR) reduction to below 65bpm is essential to achieve opti-mal image quality and diagnostic accuracy with Computed Tomography CoronaryAngiography (CTCA). While beta-blockers are most commonly used, administra-tion of ivabradine, a novel HR lowering agent, could be an attractive alternativeoption to reduce HR without significant hemodynamic side-effects. The purposeof the study is to evaluate the incremental value and safety of oral ivabradine forheart rate reduction in CCTAMethods: One-hundred-twenty-three consecutive patients referred for CTCAwere studied. Patients were divided in two groups depending on the absenceor presence of chronic beta-blockade treatment. Within the two groups patientswere randomized to either no additional premedication or oral ivabradine for 5days prior to CTCA. In presence of chronic beta-blockade therapy it was shiftedto atenolol 50mg twice a day for 5 days prior to CTCA in order to add uniformityto the chronic beta-blockade group. HR and blood pressure were assessed at ad-mission (T0), immediately before CTCA (T1) and during CTCA (T2). The targetHR was <65bpm.Results: Ivabradine significantly reduced HR during CTCA. Mean relative HR re-duction was 15% for controls, 12% for chronic beta-blockade, 19% for ivabradineand 24% for both chronic beta-blockade and ivabradine at T2 (p for trend <0.001).The rate of patients who reached the target HR at T2 was 83% in controls, 71%with chronic beta-blockade, 97% with ivabradine and 97% with both (p for trend<0.05). The percentage of patients that needed additional IV beta-blockade atT1 decreased from 69% to 40% with ivabradine and 30% with both (p for trend<0.05).
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Imaging 289
Conclusions: Ivabradine is safe and effective in increasing the rate of patientsat target HR and in reducing the need for additional IV beta-blockade in patientsreferred for CTCA.
P1695 The comparison of dual-source computedtomography, coronary angiography and intravascularultrasound in the evaluation of restenosis after theleft main coronary artery stenting
D. Zemanek1 , P. Bradacova2, T. Adla2, J. Veselka1. 1CharlesUniversity Prague, 1st Faculty of Medicine, University Hospital Motol, Prague,Czech Republic; 2University Hospital Motol, Prague, Czech Republic
Purpose: Percutaneous coronary intervention (PCI) of the left main coronaryartery (LMCA) is a challenging topic in recent cardiology. Restenosis of LMCAafter previous stenting is potentially associated with fatal myocardial infarction.Therefore, it was widely accepted to repeatedly perform coronary angiography(CAG). The aim of this study was to determine whether CAG and dual-sourcecomputed tomography (DSCT) are accurate methods in the evaluation of theLMCA after PCI with stent implantation.Methods: Thirty-two consecutive patients (56% males, 68±13 years) wereprospectively enrolled for follow-up CAG, intravascular ultrasound (IVUS) andDSCT examinations after LMCA stenting (4 and 9 moths follow up in patient withdrug-eluting stents, 3 and 6 moths with bare-metal stents, respectively). Resteno-sis was defined by CAG as > 50% of luminal diameter loss, by DSCT and IVUS asa minimal luminal area (MLA) < 6mm2. IVUS was considered the gold standard.Results: Thirty-nine complete examinations were performed. There were no sig-nificant complications during all the examinations. We found 2, 8 and 1 significantrestenosis according to CAG, MSCT and IVUS, respectively. Positive predictivevalues according to CAG and DSCT were 50% and 12, 5%, by contrast to 100%negative predictive values for both methods. The correlation coefficient betweenMSCT and IVUS for MLA was 0.44 (graph).
Conclusion: These results suggest that all used methods are safe. Positive pre-dictive value of CAG and mainly DSCT seems to be limited, in opposite to nega-tive predictive value. Thus, DSCT is a useful, non-invasive method in the evalu-ation of the post-PCI restenosis of LMCA. However, finding of restenosis of anysignificance should be re-evaluated by CAG and eventually by IVUS.
P1696 Manual thrombectomy reduces infarct size andimproves left ventricular function in patients withacute ST-elevation myocardial infarction undergoingprimary percutaneous coronary intervention
D.S. Sim, Y. Ahn, Y.H. Kim, S. Choi, H.J. Seon, J.H. Kim, M.H. Jeong,J.G. Cho, J.C. Park, J.C. Kang. Chonnam National University Hospital, Gwangju,Korea, Republic of
Purpose: The role of manual thrombectomy during primary percutaneous coro-nary intervention (PCI) remains open for further exploration. We sought to assesswhether manual thrombectomy could reduce infarct size and improve left ven-tricular (LV) function in patients with acute myocardial infarction (MI) undergoingprimary PCI.Methods: Between April 2009 and November 2009, 45 consecutive patients pre-senting with stable (Killip≤II) first acute ST-elevation MI within <12 hours after thesymptom onset who had TIMI flow grade≤1 in the culprit artery were enrolled inthis study. The patients underwent primary PCI after a 600-mg loading dose ofclopidogrel with the use of thrombectomy or glycoprotein IIb/IIIa inhibitor (GPI) atthe discretion of the operator. All patients underwent delayed enhanced MDCTimmediately after PCI without injection of an additional contrast media to assessinfarct size, determined as the total volume of myocardium showing delayed en-hancement. The primary endpoint was infarct size reduction at 2 months betweenpatients who received thrombectomy (group I, N=13) and who did not (group II,N=32).Results: Baseline clinical characteristics and angiographic findings were similarbetween the two groups. There were no differences between group I and II in theuse of GPI (46.2 vs. 53.1%, p=0.672) and drug-eluting stents (61.5 vs. 65.6%,p=0.795); the presence of anterior MI (53.8 vs. 50.0%, p=0.815); and the rateof post-PCI TIMI 3 (92.3 vs. 84.4%, p=0.656). Markers of myocardial reperfu-sion (ST-resolution rate, myocardial blush grade, and corrected TIMI frame count)were not different between the groups. Group I had, however, more reduced in-farct size (13.7 vs. 27.7 ml, p=0.006) and more preserved LV ejection fraction(LVEF) after PCI (61.2 vs. 54.1%, p=0.032). In multiple linear regression analysis,
significant determinants of infarct size were the presence of anterior MI (B=23.7,95% CI=9.603∼37.972, p=0.002) and the use of thrombectomy (B=-18.84, 95%CI=-33.088∼-4.583, p=0.012). GPI use, total volume of contrast media, and timebetween the last contrast injection and CT scan were not associated with in-farct size. At 2 months, in-hospital and clinical outcome were similar betweenthe groups. Still, group I showed improved LVEF (61.6 vs. 52.8%, p=0.048) andtendency toward reduced infarct size (13.2 vs. 25.7 ml, p=0.061).Conclusion: Manual thrombectomy, independent of GPI use, reduced infarct sizeand improved LV function in patients with acute ST-elevation MI undergoing pri-mary PCI after a 600-mg clopidogrel loading.
P1697 Usefulness of 64-detector computed tomographicangiography for left main coronary artery stentevaluation
G. Roura I Ferrer, J.A. Gomez-Hospital, F. Fernandez-Alarza,E. Carreno, M. De Albert, J. Gomez-Lara, J. Maristany, L.M. Teruel,
E. Esplugas, A. Cequier. University Hospital of Bellvitge, Barcelona, Spain
Background and Objective: Percutaneous Coronary Intervention (PCI) of LeftMain Coronary Artery (LMCA) disease is currently an alternative to CoronaryArtery Bypass Graft (CABG) in some patients. Multislice Computed Tomography(MSCT) is a novel technique for the non invasive study of coronary arteries anduseful for evaluating large stents, such as those placed in the LMCA. The role ofthis diagnostic approach is not yet defined. The objective of this study is to eval-uate the accuracy of MSCT in assessing stent patency compared with coronaryangiography plus 3D intravascular Ultrasound (3D-IVUS)Methods: Patients with LMCA disease treated with stent were consecutively in-cluded. Chronic renal failure, atrial fibrillation or history of contrast allergic reactionwere exclusion criteria. All demographic and clinical data were registered. Duringfollow up, a MSCT, a coronary angiography and an IVUS study were performed.In MSCT study we analysed binary angiographic restenosis rate (>50% obstruc-tion), Minimal Lumen Diameter (MLD), Mean Stent Diameter (MSD), Minimal Lu-men Area (MLA), Mean Stent Area (MSA) and Maximum Hyperplasia by twoindependent observers. IVUS images were analyzed using three-dimensional in-tracoronary ultrasound software. Binary angiographic restenosis rate, MLD, MSD,MLA, MSA, In-Stent Neointimal hyperplasia volume, Maximal neointimal hyper-plasia (mm), Vessel volume, Stent volume and Lumen volume were registered byan investigator blinded to the MSCT result.Results: 41 patients were analyzed with a median follow-up time of 315 days.The binary restenosis rate of the LMCA stent by MSCT was 13.9% and the bi-nary restenosis rate by IVUS was 11.1% (p >0.05) with no false negative casesand one false positive case. Sensibility was 100% and especificity was 96.9%with a Kappa index of 0.873. If we analysed the binary restenosis rate of theLMCA stent plus side branch ostium we found a restenosis rate of 16.7%. MSCTdiagnostic accuracy of 89.9%. When we have compared diameters and areasan underestimation tendency of in-stent diameter and area was found: MLD byMSCT 2.74mm vs MLD by IVUS 3,5mm p=0.07 and MLA by MSCT 5,6mm2 vsMLA by IVUS 7.47mm p=0.001, even though, intraclass correlation index were0.801 for diameter comparison and 0.809 for area comparison. Correlation be-tween two independent MSCT observers was 0.842.Conclusions: MSCT appears as useful technique to rule out stent restenosis inLMCA with an excellent diagnostic accuracy. Although MSCT quantitative mea-sures are underestimated due to the metallic artefact, exists a good correlationbetween MSCT and 3D-IVUS quantitave measures.
P1698 Comparative study of carotid artery intima-mediathickness and coronary artery disease as evaluatedby CT angiography correlated to plasma inflammatorymarkers
A.I. Guaricci1, N.D. Brunetti1, M. De Luca1, R. Ieva1,F. Cademartiri2, E. Maffei2, C. Tedeschi1 , L. Macarini1, M. Midiri3, M. DiBiase1. 1University of Foggia, Foggia, Italy; 2Hospital of Parma, Department ofRadiology, Parma, Italy; 3University of Palermo, Palermo, Italy
Purpose: Coronary artery disease (CAD) is associated with both mean maximumcarotid artery intima-media thickness (CIMT) and plasma inflammatory markers.Catheter-based angiography is the gold standard in the detection of CAD. Weevaluated the correlation between common carotid artery intima-media thickness,as evaluated by b-mode ultrasound, and serum levels of inflammatory markerswith the presence, severity and extent of CAD, as evaluated by computed tomog-raphy coronary angiography (CCTA).Methods: One-hundred-two consecutive patients with known or suspected CADreferred for CTCA were studied (mean age 60±10,1 ys). All patients underwentclinical evaluation, ecg, laboratory tests, b-mode ultrasound CIMT and CCTA.Results: CIMT >0,9 mm was correlated with significant CAD, severity of stenosis,number of vessels with critical stenosis and the number of segments with criticalstenosis (p<0.001, r 0.52, r 0.52, r 0.45, r 0.42 respectively). IL 6 was significantlyhigher in patients with significant CAD (p<0.05). The IL 6 levels were associatedwith the number of vessels with critical stenosis (p for trend<0.05) and with thenumber of the segment with critical stenosis (p<0.01, r 0.28)Conclusions: Mean maximum carotid artery IMT and IL 6 values are significantlycorrelated with presence, severity and extent of CAD as evaluated by CCTA.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

290 Imaging
There is a weak correlation between other plasma inflammatory markers (IL 1b,IL 2R, IL8, IL10, TNFα, BNP, hs PCR, CA 125, alpha 1 glycoprotein, alpha 1antitrypsin) and CAD.
P1699 Head to head comparison of multislice coronarytomography and conventional coronary angiogram inthe setting of systematic screening of coronaryvasculopathy after orthotopic heart transplantation
O. Barthelemy, S. Varnous, D. Toledano, F. Fernandez, E. Berman,C. Le Feuvre, I. Gandjbakhch, J.P. Metzger, A. Pavie, P. Cluzel. AP-HP - HospitalPitie-Salpetriere, Paris, France
Aim: to determine if conventional invasive coronary angiogram (CA) can be re-placed by multislice coronary tomography (MSCT) (64- and 256-row) for the sys-tematic screening of coronary vasculopathy of heart transplant patients.Methods: Electrocardiogram-gated contrast-enhanced MSCT (Philipps, Bril-liance, 64-row for the first 25 patients and 256-row for last 11 patients) was per-formed 24 hours before annual CA. MSCT parameters, adapted to the patient’sweight, include 120 kV, 800mAs, 0.625 mm slice thickness, 0.42s/0.27s rotationtime.Primary endpoint was the negative predictive value of CT for the detection ofsignificant (stenosis>50%) coronary artery disease (CAD). Secondary endpointwas the comparison of X-Ray (mSv) and iodine contrast agent (ml) exposure. Thestudy obtained the approval of ethical committee and all patients sign an informedconsent. We expect to include 100 patients and present the preliminary results.Results: Thirty six patients were prospectively included. Mean age was 53±14years. Transplantation occurred 5±5 years before inclusion. Of the 612 angio-graphic coronary segments, 577 (94.3%) were evaluable by MSCT. Analyse bysegments shows a good concordance of 98.6% between the two techniques.Only 4 patients (11.1%) had significant CAD on CA. Only one of them had a cor-rect coronary assessment on MSCT. The negative predictive value was 91% bypatient analysis and 99% by segment analysis.The total amount of iodine injected was higher 127±39 ml vs 58±31 ml, as theeffective dose 19±11 mS vs 6±5 mSv with MSCT.Conclusions: New generation of multidetector MSCT (64 or 256-row) have agood negative predictive value for the systematic screening of significant (>50%)coronary vasculopathy of heart transplant patients. MSCT can represent an al-ternative to invasive coronary angiogram in patient without significant stenosis.However, safety concerns (contrast agent, radiation) remain in the setting of an-nual coronary assessment.
P1700 Feasibility and diagnostic accuracy of ultra-low dosemultidetector computed tomography coronaryangiography in the evaluation of coronary arterybypass grafts
D. Andreini, G. Pontone, S. Mushtaq, A. Annoni, A. Formenti,E. Bertella, S. Cortinovis, G. Ballerini, M. Pepi. University of Milan, FoundationMonzino (IRCCS), Center Cardiology, Dpt of Cardiology, Milan, Italy
Aim of the study was to compare the diagnostic performance and effective doseof a BMI-adapted scanning protocol with prospective ECG-triggering (MDCT-XTe)versus MDCT with prospective ECG-triggering using the standard scanning pro-tocol (MDCT-XT) versus MDCT with conventional retrospective ECG triggering(MDCT-Helical), compared to traditional ICA, in the assessment of patency ofgrafts.Materials and methods: One hundred and nineteen patients were randomizedto Group 1 based on BMI-adapted scanning protocol with prospective ECG-triggering (MDCT-Xte, 40 patients), group 2 with prospective ECG-triggering(MDCT-XT, 39 patients) and group 3 (MDCT-Helical, 40 patients) with retrospec-tive ECG-triggering, followed by ICA. MDCT data were acquired using a 64-sliceCT.Results: MDCT was able to assess the patency of all CABG in both groups. Over-all, after comparison with ICA, MDCT was able to correctly detect the occlusionor significant stenosis of CABG in all the groups, with the exception of one caseof group 3. In group 3, in segment-based analysis, sensitivity, specificity, posi-tive predictive value, negative predictive value and accuracy were 100%, 98.4%,96.7%, 100% e 98.9%, respectively. In group 1 and 2 the diagnostic accuracywas 100%. Effective radiation dose was 3.5±1.4 mSv in group 1 vs 7.4±2.6 mSvin group 2 vs 27.8±9.4 mSv.Our results indicated that MDCT-XTe has a diagnostic performance in the evalu-ation of CABG similar to MDCT-XT and MDCT-Helical, with a further significantreduction of radiation exposure.
P1701 Impact of coronary calcium on neointimal formationfollowing sirolimus-eluting stent implantation
S. Kishi, K. Tanabe, S. Yachi, T. Imamura, Y. Nakajima, M. Taniwaki,S. Tanimoto, J. Aoki, Y. Nakajima, K. Hara. Mitsui Memorial Hospital,Tokyo, Japan
Background: Sirolimus-Eluting stents (SES) have dramatically reduced in-stentrestenosis, however, there is a concern that the drug elution from the stent might
be hampered by calcium in coronary vessel wall. Recently, multidetector spiralcomputed tomography (MDCT) has emerged as non-invasive modality which al-lows us to assess coronary stenosis as well as coronary calcium. Therefore, weinvestigated the relationship between the Agatston calcium score of target lesionand in-stent late luminal loss.Methods: The study population consisted of consecutive 71 patients who werediagnosed as having coronary artery disease by 64-slice MDCT (SOMATOM Sen-sation Cardiac 64, Siemens) and 320-slice MDCT (AquilionOne, Toshiba), andsubsequently underwent percutaneous coronary intervention (PCI) with SES be-tween February 2005 and January 2009. The Agatston calcium scores in thetarget lesions were analyzed by a physician blinded to clinical outcomes. Thepatients underwent follow-up angiograms at 8-months. The in-stent late lumenloss was determined by quantitative coronary angiography (QCA) with automatededge-detection system (CMS, Medis Medical Imaging Systems BV).Results: The patients were 67±8 years old and 37 (71%) were male. 30 (58%)were diabetic and 4 (8%) were on hemodialysis. The patients had 69 de novocoronary target lesions. Coronary calcium in the lesion was present in 61 (88%)patients. The calcium score of the target lesion averaged 214.7±372.5. The8-month follow-up angiogram revealed that in-stent late lumen loss averaged0.47±0.58mm. there was a week positive correlation between the calcium scoreand the in-stent late lumen loss at 8-month (R=0.469, P<0.001).Conclusion: Coronary calcium might be one of the key components which de-flate the effect of drug-eluting stents to prevent neointimal formation.
P1702 Left atrial appendage and left atrial volumes inpatients with normal sinus rhythm and recurrent atrialfibrillation by 64-slice computed tomography
K. Steffen1, K. Bernd1, S. Newman1, I. Usherenko1, L. Wetzel2,T. Rosamond1. 1Mid-America Cardiology Associates, Inc. University
of Kansas Medical Center, Kansas City, United States of America; 2University ofKansas Medical Center, Kansas City, United States of America
Purpose: The aim of the study was to define normal left atrial (LA) and left atrialappendage (LAA) volumes, corrected for body mass index (BMI) in patients withno history of atrial fibrillation (AF), compared to patients with recurrent atrial fibril-lation referred for 64-slice cardiac computed tomography (CTA) prior to pulmonaryvein isolation.Methods: We identified 300 consecutive patients, 245 in normal sinus rhythm(gender: male 150, female 95; age: 58+14; BMI: 29+5; EF: 64%+10) and 55 withrecurrent AF (gender: male 43, female 12; age: 61+11; BMI: 29+5; EF: 61%+8)who underwent CTA. LA and LAA volumes were measured by 3D volume render-ing techniques using General Electric’s AW Workstations. Pulmonary veins wereexcluded from volume determination.Results: LAA and LA volumes and volume indices were significantly higher inpatients with atrial fibrillation than those in sinus rhythm (Table 1). The normalLAA volume in patients with normal sinus rhythm was 7.15mls + 2.8 vs. 8.47mls +3.56 in patients with recurrent atrial fibrillation (P=0.003). The normal LA volumewas 77.5 mls for patients in normal sinus rhythm vs. 95.4 mls for AF patients(P=<0.0001).
Table 1. Left atrial appendage and left atrial volumes by computerized tomography
Normal Sinus Atrial Fibrillation P Value
LA Volume (ml) all 77.47 + 23.81 95.40 + 27.77 <0.0001LA Volume (ml) male 81.87 + 23.72 96.21 + 29.06 <0.001LA Volume (ml) female 70.53 + 22.37 92.53 + 23.45 <0.001LA Volume Index all (LA volume/BMI) 2.70 + 0.94 3.34 + 0.96 <0.0001LA Volume Index male (LA volume/BMI) 2.84 + 0.95 3.39 + 1.00 <0.001LA volume Index female (LA volume/BMI) 2.50 + 0.88 3.14 + 0.81 0.02LAA Volume (ml) all 7.15 + 2.80 8.47 + 3.56 0.003LAA Volume (ml) male 7.50 + 2.96 8.62 + 3.90 0.04LAA Volume (ml) female 6.62 + 2.96 7.95 + 1.93 0.08LAA Volume Index all (LAA volume/BMI) 0.25 + 0.11 0.29 + 0.12 0.02LA/LAA 11.86 + 4.61 12.2 + 4.20 0.53
Conclusion: Normal values for LAA and LA volume are established and cor-rected for BMI using 64-slice CTA. Increased LAA and LA volumes and indicesare associated with refractory atrial fibrillation in both males and females.
P1703 Aortic annulus measurement in patients referred fortranscatheter aortic valve implantation: comparisonbetween multi-detector computed tomography andtransoesophageal echocardiography
S. Sen, S.S. Kaneria, B. Ariff, G.W. Mikhail, I. Malik, J. Mayet,J.E. Davies, C.F. Juli, N. Sutaria. Imperial College Healthcare NHS Trust,London, United Kingdom
Background: Transcatheter aortic valve implantation (TAVI) offers an alternativetreatment for patients with severe aortic stenosis who are unsuitable for conven-tional surgery. Accurate assessment of aortic annular size is critical for patientselection, valve sizing and successful implantation. Transoesophageal echocar-diography (TOE) is the current standard for annular assessment, but is not with-out risk and only assesses the annulus in the sagittal dimension. If cardiac gatedmultidetector computed tomography (MDCT) with multi-planar reconstruction can
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Imaging 291
provide equivalent data it could provide an alternative to TOE; combining the as-sessment of the aortic valve with that of the peripheral vasculature in a singlenon-invasive study. We examined the differences in aortic annular measurementsusing MDCT and TOE in patients referred for TAVI.Methods: 52 consecutive patients referred for TAVI were studied (28 female, me-dian age 82, range 61-94). Contrast enhanced MDCT was performed using acardiac gated 64-slice scanner (Brilliance 64-slice, Philips Medical Systems). Im-age reconstruction of the aortic annulus was obtained in the sagittal plane andcoronal plane using the Philips workstation (Version 2.1, Phillips Medical Sys-tems). Multiplane 2 dimensional TOE was performed under conscious sedationusing a Philips IE33 ultrasound scanner (Philips Medical Systems). Aortic annu-lar dimension was assessed in the 120-140 degree long-axis view in mid systoleusing a zoomed view of the aortic root and measuring the diameter at the leafletinsertion points. Data were analysed using Wilcoxon signed rank test. Analyseswere performed using Instat software (version 3.1, Graphpad).Results: TOE mean aortic annulus diameter was 22.7 mm ± 2.3 mm. MDCTmean aortic annulus diameter was 23.1±3.0 mm (sagittal view) and 24.8±2.8mm (coronal view). There was no significant difference between TOE and sagittalMDCT measurements (mean difference 0.4 mm 95% CI -0.04, 0.93, p=0.07).Coronal MDCT measurements were significantly larger than TOE measurements(mean difference 2.1 mm, 95% CI 1.56, 2.68, p < 0.0001) reflecting the ellipticalshape of the aortic annulus.Conclusion: Cardiac gated MDCT can provide an alternative to TOE for the as-sessment of aortic annular size. The ability of MDCT to combine aortic valve andperipheral vascular assessment in a single study makes it an attractive investiga-tion for screening patients referred for TAVI.
P1704 Less downstream test utilization of front-linediagnostic evaluation by coronary computedtomography as compared toexercise-electrocardiography
L.N. Lene Nielsen1, J.M. John Markenvard2, J.M.J. Jesper MollerJensen1, H.M. Hans Mickley3, B.L. Norgaard1. 1Department
Cardiology, Vejle Hospital, Vejle, Denmark; 2Department Internal Medicine,Fredericia Hospital, Fredericia, Denmark; 3Odense University Hospital,Department of Cardiology, Odense, Denmark
Purpose: Despite a suboptimal diagnostic accuracy exercise-electrocardiogaphy(Ex-ECG) is widely used as the primary diagnostic method in patients suspectedof angina. Numerous studies have documented a high diagnostic accuracy ofCTA in patients with stable angina, however, there is no universal agreement onthe mainstream use of CTA. The clinical benefit of CTA has been questioned be-cause CTA as compared to conventional functional tests identify more patientswith atherosclerosis, hence add the risk of introducing more downstream diag-nostic test utilization (DTU) and consequently increase costs. The purpose of thisstudy was to investigate the influence of a frontline diagnostic strategy using Ex-ECG versus CTA on the DTU in a "real world" cardiology practice.Methods: In two adjacent community hospitals using either Ex-test (group A, n=247) or CTA (Dual Source technique, group B, n =251) as the front-line diagnos-tic tool in patients suspected of angina, cohorts of consecutive patients were ret-rospectively identified (Jan. 2007 – Febr. 2008). During a follow-up of 12 monthsDTU (coronary angiography, CA; myocardial scintigraphy, MPS) was registered.Results: There was no differences between study cohorts in demographic char-acteristics or pretest risk of significant coronary artery disease. Mean (± SD) agewas 56 (11) years, 52% were men, and 69% of the total study cohort was atintermediate pretest risk of significant disease. DTU was more frequent appliedin group A as compared to group B patients, 32% versus 21% (P =0.003). CAwas the most frequent mode of DTU in both groups, 70% of the total number ofadditional tests in group A versus 85% in group B (P =0.19). Subsequent MPSwas more frequent applied (28% versus 19%, P = 0.03), whereas CA tended tobe more frequent applied (23% versus 18%, P =0.16) in group A as compared togroup B patients. The prevalence of significant disease at subsequent CA (steno-sis >50%) was lower in group A as compared to group B, 34%% versus 65%%(P =0.02).Conclusions: A frontline diagnostic strategy using Ex-ECG in comparison to aCTA based strategy in patients suspected of angina is associated to a more fre-quent use of additional downstream diagnostic test utilization. CTA seems moreaccurate in detecting significant coronary artery disease than Ex-ECG. Futurerandomized trials are needed in order of defining the most cost-effectively diag-nostic use of CTA relative to conventional ischemia testing.
P1705 Assessment of coronary atherosclerosis related tovulnerable plaque using multislice computedtomography in uncomplicated hypertensive patientswith left ventricular hypertrophy
K. Harada, A. Saito, Y. Yokoyama, T. Okumura, N. Kageyama,T. Yamamoto, H. Fujinaga. Tokushima Prefectural Central Hospital, Tokushima,Japan
Background: Left ventricular hypertrophy (LVH) has been identified as one ofthe risk factors for sudden cardiac death. However, it is unexpectedly unknownthe characteristics of coronary artery disease (CAD) in hypertensive patients with
LVH. The purpose of this study was to evaluate the presence and the severity ofcoronary atherosclerosis using multislice computed tomography (MSCT) in un-complicated hypertensive patients with LVH.Methods: MSCT was performed in 665 consecutive patients. Coronary arterycalcium (CAC) scores were calculated according to Agatston’s method. To eval-uate coronary plaque and coronary artery stenosis accurately, the object waslimited to the patients with coronary calcium score < 400. Of these patients, 75patients who had uncomplicated hypertension were included. They were dividedinto patients with LVH (n=35) and without LVH (n=45), according to echocardio-graphic recordings of LV mass index (LVH: LV mass index >111 g/m2 in menand >106 g/m2 in women). In this study, high-risk patients threatened by acutecoronary syndrome was defined as the patients who had lipid-rich plaques (<50Hounsfield Unit) with positive remodeling (remodeling index >1.05) and/or signif-icant coronary artery stenosis (>50% luminal narrowing).Results: Patients with LVH was significantly older compared with patients withoutLVH (71±10 vs. 66±10 years, p<0.05). There were no significant differences inCAC score (54 vs. 32, p=0.15) and the presence of significant coronary arterystenosis (9% vs. 7%, p =0.10). Patients with LVH group had more presence ofnoncalcified plaques (69% vs. 38%, p<0.01), number of noncalcified plaques (1.7vs. 0.8, p<0.01), presence of lipid-rich plaques with positive remodeling (43%vs. 13%, p < 0.01) and frequency of high-risk patients (43% vs. 18%, p<0.05)than without LVH. On multivariate analysis, male gender (OR=3.4, p<0.05), coro-nary calcification (CAC score ≥100, OR=4.2, p<0.05) and LVH (OR=3.2, p<0.05)were independent predictors of high-risk patients.Conclusions: With the use of MSCT, the present study shows that LVH relatesto the presence of noncalcified plaques with vulnerable characteristics that maycause sudden cardiac death.
P1706 Low-dose coronary CT angiography in three hundredpatients: utilization of a novel high-pitch spiral,sequential, and conventional spiral scan modes in alarge, consecutive cohort
K.T. Ho, C. Panknin, K.C. Chua. Tan Tock Seng Hospital, Singapore,Singapore
Purpose: There are currently 3 scan modes available for CTA. These include thespiral, prospectively ECG-triggered axial sequential acquisition ("step and shoot"mode), and prospectively ECG-triggered high-pitch spiral acquisition ("FLASH")modes. We decided to: 1) describe our experience with 300 consecutive patientsundergoing coronary CTA. These were all-comers and reflect a real-world ex-perience for coronary CTA imaging. 2) explore the extent to which the FLASH,Adaptive Sequence, and Spiral studies could be used in routine practice.Methods: The first 300 consecutive patients undergoing coronary CTA at our fa-cility using the new dual-source CT (Definition FLASH, Siemens Healthcare) aredescribed. The indications included evaluation of chest pain, post-coronary an-gioplasty/stenting and post-bypass surgery. They encompassed the spectrum oflow-to-intermediate likelihood of CAD to those with established CAD. All patientsreceived betablockers prior to the study. Those with heart rate< 65bpm under-went FLASH scanning and those with heart rate >65bpm underwent scanningwith sequential or spiral modes. The tube current voltage was set at 80kV for pa-tients < 55kg, 100kV for those between 55kg to 100kg, and 120kV for >100kg.In patients <100kg, the tube current was 320mAs/rotation, and 400mAs/rotation> 100kg. Pitch was 3.4 in patients undergoing FLASH scanning.Results: In the population of 300, 67% were males,mean age 55±12 years, BMI25.4±4.3 kg/m2. 30% underwent CTA for evaluation of cardiac risk, 50% of thepatients were previously known to have CAD, with 60% having undergone pre-vious PCI and/or CABG. 94% of 300 patients successfully underwent FLASHexamination, 6% Adaptive Sequence & none spiral scanning. The mean heartrate at time of scan was 53±7 bpm (FLASH) and 67±7 (Adaptive Sequence).98% of all patients were administered betablockers. 18%, 70% and 12% wereimaged with a tube-voltage of 80kV, 100kVand 120kV respectively. The radiationdose of patients imaged with FLASH and Adaptive Sequence was 0.9±0.5mSvand 2.7±1.3 mSv respectively. 30% of all patients with scanned with 80kV, andthe radiation dose in this group was 0.32±0.9mSv.Diagnostic quality was attainedin 95% of all coronary segments using the17-segment ACC model, with 2% and3% of non-diagnostic segments due to motion artefacts and blooming artefactsrespectively.Conclusions: 1) 94% of 300 consecutive patients had successful CTAs per-formed with the FLASH mode, with mean radiation dose of 0.9±0.5mSv.2) Only6% required scanning with Adaptive Sequence, with mean dose of 2.7±01.3mSv.
P1707 Prospective ECG-triggered high pitch spiral CTcoronary angiography provides high image quality ata substantially reduced effective radiation dose
D.V. Anand, R. Shakur, M.A. Westwood, S.E. Petersen, A. Mathur,L.C. Davies. Barts and The London NHS Trust, London, United
Kingdom
Purpose: CT coronary angiography (CTCA) is an evolving technique for the di-agnosis of coronary artery disease (CAD). A new scan mode for CTCA utilising adual source CT scanner has been recently described. This mode (FLASH spiralCTCA) uses a higher pitch and faster table speed thus enabling image acquisition
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

292 Imaging
within a single cardiac cycle. We compared the image quality and radiation doseof FLASH spiral with retrospective spiral CTCA in patients with suspected CAD.Methods: 40 consecutive patients (mean age: 55±11 yrs; 60% male) underwentCTCA on a dual source CT scanner using either the FLASH (n = 20) or the ret-rospective spiral mode (n = 20). FLASH CTCA was performed with 2 x 128 x 0.6mm collimation, 0.28 sec rotation time, a pitch of 3.2, 100 kV tube voltage andcurrent of 320 mA s. Scans were triggered at 60% of the R-R interval and com-pleted within one cardiac cycle. Retrospective spiral CTCA was performed usinga tube voltage of 100 -120 kV according to body weight. Metoprolol was adminis-tered to lower heart rate < 70 bpm. Image quality (IQ) was graded subjectively ona 4-point scale (1-excellent with no artefacts to 4-uninterpretable) and objectivelyby measuring the signal to noise ratio (SNR) in the left main stem artery. Effectivedose (ED) was estimated from the dose-length product, using a conversion factorof 0.014.Results: 52% of patients were hypertensive, 8% were diabetic and 50% hadhyperlipidaemia. 7 patients (18%) had atrial fibrillation. 60% had coronary cal-cification (Median calcium score: 6 Agatston units [IQR: 0-237 AU]). CTCA wasnormal in 19 patients (47%). 21 (53%) patients had CAD (non-obstructive: 8; ob-structive: 13). IQ of FLASH CTCA was comparable to that of retrospective spiralCTCA i.e. IQ scores of 1, 2 and 3 were seen in 80%, 15% and 5% of subjectsundergoing FLASH and 75%, 20% and 5% of subjects undergoing retrospectivespiral CTCA respectively (χ2 = 0.8; p = NS). SNR was not significantly differ-ent between FLASH and retrospective spiral modes (mean SNR: 27.2[9.3] HUfor FLASH and 25.3[16.3] HU for retrospective; p = NS). In contrast, the FLASHmode had a 10-fold lesser ED (1.14±0.43 mSv) when compared to the retrospec-tive mode (11.92±6.5 mSv); p <0.0001. The FLASH mode was associated withan ED below 1 mSv in 60% of patients (n = 12).Conclusion: In non-obese patients with a stable heart rate, FLASH spiral CTCAhas comparable image quality with that of retrospective spiral CTCA and providesa 10-fold reduction in the ED. The ability to provide high image quality at a verylow ED makes this mode extremely promising, especially in younger patients.
P1708 Very low-dose coronary artery calcium score usinghigh-pitch spiral acquisition mode: comparisonbetween standard 120 kV versus 100 kV tube voltageprotocols
M. Marwan, M. Seltmann, T. Pflederer, D. Ropers, W.G. Daniel,S. Achenbach. University of Erlangen-Nuremberg (Friedrich-Alexander-University), Erlangen, Germany
Aim: We prospectively compared 120 kV and 100kV tube voltage in low-doseacquisition protocols for coronary artery calcium scoring (CACS) protocols usinghigh pitch spiral acquisition mode.Methods: 60 consecutive patients referred for CACS were subjected to a stan-dard 120 kV followed by a 100 kV scan both using high-pitch spiral acquisitionmode. Tube current for both protocols was set at 80 mAs. All patients were insinus rhythm with a heart rate ≤ 60/min and a body weight < 100 kg. CT wasperformed using Dual Source CT with 0.28s gantry rotation, 2x128 slices, a pitchof 3.4, triggered at 60% of the R-R interval. Using a medium sharp reconstruc-tion kernel (Siemens B35f), cross-sectional images were reconstructed with 3.0mm slice thickness and 1.5 mm increment. For both scans a threshold of 130Hounsfield units (HU) was adopted for calcium detection.Results: The mean Agatston score for 120 kV scans vs. 100 kV scans was273±236 vs. 317±295 (p = 0.003). Mean DLP was 26±7 cm*cGy for 120 kVscaning protocol vs. 15±4 cm*cGy for 100 kV protocol, corresponding to averageeffective doses of 0.4 and 0.2 mSv (p < 0.0001). In spite of excellent correla-tion (r=0.99, p< 0.0001), Bland-Altman analysis revealed a significant systematicoverestimation of the Agatston score using lower dose 100 kV tube voltage (meandifference 44±75).Conclusion: High-pitch spiral acquisition allows coronary calcium scoring witheffective doses below 0.5 mSv. 100 kV tube voltage further reduces dose as com-pared to the standard of 120 kV. However, it leads to significant overestimation ofthe Agatston Score when the standard threshold of 120 kV is used. When using100 kV for calcium scoring, the quanitifcation threshold needs to be adjusted.
P1709 Diagnostic accuracy of 64-slice multidetectorcomputed tomography for the evaluation of aorticroot in patients selected for transcatheter aortic valveimplantation
G. Pontone, D. Andreini, E. Bertella, S. Mushtaq, A.D. Annoni,G. Tamborini, M. Fusari, G. Ballerini, A.L. Bartorelli, M. Pepi. University of Milan,Foundation Monzino (IRCCS), Center Cardiology, Dpt of Cardiology, Milan, Italy
Purpose: Transcatheter aortic valve implantation (TAVI) is a new tool for treat-ment of severe aortic stenosis, but for a suitable choice of the valve prosthesisan accurate assessment of the aortic root anatomy (AoA) is mandatory. Aim ofthis study is to assess the feasibility and accuracy of multidetetctor computedtomography (MDCT) in the evaluation of AoA compared with transthoracic echo-cardiography (TTE).Methods and materials: We enrolled 60 patients (22 male, mean age: 80±8years, Logistic Euroscore 20.5±11) who underwent a comprehensive TTE andMDCT before TAVI. Measurements of the AoA with TTE (AoATTE) were per-
formed in systole in a parasternal long-axis view on the left ventricular outflowtract at the point of insertion of the right aortic and non-coronary aortic cusp. Re-garding to MDCT, the scan parameters were: 64x0.625 mm collimation, gantry ro-tation time 350 msec, tube voltage 120 KVp and effective tube current of 700 mA.Aortic Annulus (AoAMDCT) was defined as a virtual ring formed by joining basalattachments of aortic leaflets. For each AoAMDCT, the maximum (Max-AoA-DMDCT), the minimum (Min-AoA-DMDCT) diameter, the area (AoA-AMDCT) inan orthogonal plane on the center line of the aorta and the lumen morphologyindex of AAoMDCT (LMI) defined as Max-AoA-DMDCT/Min-AoA-DMDCT ratiowere measured in systole and diastole, respectively. The Spearman’s correlationand Bland-Altman analysis were performed to compare MDCT versus echocar-diography. LMI and AAo-AMDCT/Prosthesis mismatch were included in a mul-tivariate logistic regression with a backward selection of independent variables,with a significant level of p<0.05.Results: Max-AoA-DMDCT, Min-AoA-DMDCT, AoA-AMDCT were 25.1±2.8 mm,21.2±2.2 mm, 410±81.5 mm2 respectively. No differences were detected be-tween systole and diastole. There was a good agreement between MDCT andechocardiography, as assessed with Pearson’s correlation (r: 0.86) and Bland-Altman plot analysis particularly between Min-AAo-DMDCT and AAoTTE regard-less the cardiac phase (mean difference: 0.3±1.7 mm and 0.2±2.3 mm in systoleand diastole, respectively). Occurrence of paraortic leakage was related to higherLMI and AoA-AMDCT/prosthesis discongruence.Conclusions: The aortic annulus area could be the best parameter in choosingthe size of the prosthesis to reduce the incidence of paraprosthetic regurgitation,but also to avoid excessive oversizing prosthetic that could alter the function andduration of device. The high reproducibility and accuracy of MDCT in the definitionof A-Ao suggesting a promising role in the diagnostic planning of patients selectedfor TAVI.
P1710 Atrial fibrillation ablation: long term follow up inpatients studied with 64 slice cardiac computedtomographic angiography (CTA)
K. Steffen1, I. Usherenko1, S. Newman1, M. Feldkamp1, L. Wetzel2,T. Rosamond1. 1Mid-America Cardiology Associates, Inc. University
of Kansas Medical Center, Kansas City, United States of America; 2University ofKansas Hospital, Kansas City, United States of America
Purpose: We sought to define the long term outcome of patients treated for atrialfibrillation (AFIB) with pulmonary venous isolation (PVI) to define clinical and CTAcharacteristics that predict recurrence.Methods: Patients were identified with AFIB by review of our CTA laboratory’sexperience for all patients referred prior to PVI. Clinical outcomes were analyzedbased upon follow up review of our electronic medical record system.Findings: From a total of 1961 CTA’s performed we retrospectively identified 769CTA studies in patients referred for PVI of AFIB: 543 male (70.6%), mean age61±10years, BMI=30.8±6, CTA EF =60±12%, and calcium score mean=536.Mean time to follow up was 429±289 (range 35-1345) days. For the entire group:659 (85.7%) were in normal sinus rhythm at the time of follow up. Atrial fibrillationwas present in 110 (14.3%). Subgroup oneway ANOVA indicated no significantdifference between those with and without sinus rhythm at time of follow up interms of age, gender, BMI, CTA EF, calcium score, LV end diastolic volume, LVwall thickness, HDL or LDL levels. Contingency analysis indicated no differenceacross pt groups for history of smoking, hypertension, diabetes, or prior historyof hyperlipidemia. However, the combined volume of the left atrium and left atrialappendage (LAV) was significantly larger in patients with recurrent AFIB thanthose in normal sinus at follow up: 126±13mls vs. 99±31mls prob>F= 0.0089.Left atrial appendage volume alone (LAA) was also larger in patient with recurrentafib: 10.7±2.9 mls vs. 8±3.4 mls, prob >F=0.0254. Non-vascular complications ofPVI were infrequent: diaphragm paralysis: 7pts, radiation dermatitis: 3pts, patchburn: 1pt. Vascular access complications were also infrequent: pseudoaneurysmor AV fistulae: 10pts, hematoma: 8 pts. Mild-moderate pulmonary venous (PV)narrowing (i.e., less than 70%) was noted on follow up CTA in 19 cases but wassevere in only 7 pts, 3 requiring PV stenting. In pts with PV narrowing only 4 werein AFIB at the time of follow-up.Conclusion: PVI for AFIB has a high rate of long term success when defined sim-ply as normal sinus rhythm at the time of follow up regardless of many commonlymeasured clinical and CTA characteristics and has a low rate of procedural com-plications. Significant PV stenosis was infrequent. However recurrent AFIB ptshad a significantly larger LAV and LAA volumes prior to PVI. Mild pulmonary ve-nous narrowing post PVI may partially reflect resolution of venous engorgementafter successful establishment of normal sinus rhythm.
P1711 High-pitch Dual-source CT allows triple-rule-out witha high accuracy and a low radiation dose in real livepatients: first experience in nonselected symptomaticpatients
H. Schuchlenz1, W. Weihs1, D. Botegal1, P. Kullnig2. 1LKH GrazWest, Graz, Austria; 2DiagnostikZentrum, Graz, Austria
Objectives/Background: In patients with heart rates <60/min, multislice coro-nary computed tomography is associated with a high diagnostic accuracy for theexclusion and assessment of coronary artery stenoses. However radiaton expo-
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Imaging 293
sure, especially in triple rule out scans are a cause of concern. The objective ofthis prospective evaluation was to test the diagnostic accuracy and efficiency of anew high-pitch dual-source computed tomography in non-selected symptomaticpatients for the diagnosis of significant coronary stenosis, pulmonary embolismor aortic dissection.Methods: We evaluated 72 consecutive chest pain patients from our emergencydepartment/cardiac outpatient clinic with a low to intermediate likelihood of coro-nary disease including patients with a previous stentimplantation, patients withheart rates > 60/min or with atrial fibrillation. CT was performed using a dual-source CT system with 2 x 128 x 0.6 mm collimation, 0.28 s rotation time andtemporal resolution of 75ms. Invasive coronary angiography (ICA) was performedin patients with significant stenosis (> 50%) on CTCA.Results: In 70 patients (98%) imaging was successful with diagnostic image qual-ity for a triple-rule-out evaluation. Of 1008 coronary artery segments, 28 (3%)were uninterpretable in 3 patients. In 39 patients (56%) CTA could exclude a sig-nificant coronary artery stenosis but diagnosed pulmonary embolism in 2 pts. ICAwas performed in 31 Patients (54%) and analysed 434 coronary artery segments.ICA served as golden standard. In a vessel-based analysis, sensitivity, specificity,positive predictive value, and negative predictive values of CTA were 97%, 98%,93%, and 99%, respectively. The effective radiation dose was 3.5±2 mSv.Conclusion: In real live symptomatic non selcted patients, high-pitch spiral coro-nary CTA provides excellent image quality to diagnose significant coronary arterystenosis at a consistent low radiation dose.
P1712 Image quality and radiation exposure of low-doseprotocols for coronary CT angiography: comparisonof prospectively triggered axial scanning andhigh-pitch spiral CT
M. Seltmann1, S. Achenbach1 , T. Goroll1, M. Marwan1,T. Pflederer1, D. Ropers1 , M. Lell2, K. Anders2, M. Uder2, W.G. Daniel1.1University of Erlangen-Nuremberg, Department of Cardiology and Angiology,Erlangen, Germany; 2University of Erlangen-Nuremberg, Radiological Institute,Erlangen, Germany
Introduction: We conducted a prospective, randomized comparison of two low-dose data acquisition protocols for coronary CT angiography (CTA). Using dualsource CT (DSCT), image quality and the rate of fully evaluable data sets werecompared for prospectively ECG gated axial acquisition ("step-and-shoot") versushigh-pitch spiral acquisition ("Flash Mode").Methods: 100 consecutive patients in whom coronary CTA was scheduled forsuspected coronary artery disease, with sinus rhythm and a rate ≤60 bpm afterpre-treatment with beta blockers and a body weight < 100 kg were randomizedto prospectively ECG gated axial acquisition ("step-and-shoot") versus high-pitchspiral acquisition ("Flash Mode"). Coronary CTA was performed using dual sourceCT, with 0.28 s rotation time, 2x128x0.6 mm collimation. 100 kV and 320 mAs.For high-pitch spiral CT ("Flash Mode") a pitch of 3.4 was used and acquisition,prospectively triggered at 60% of the cardiac cycle, was completed in approxi-mately 250 ms. Prospectively ECG-triggered axial scans ("step-and-shoot") wereacquired at 70% of the R-R interval. Temporal resolution was 75 ms per imagefor both modes. 60 ml contrast agent was injected with a rate of 6 ml/s. For all 18coronary segments, image quality was rated by blinded observers on a 4 pointscale (1= no artefact to 4 = unevaluable).Results: Mean age was 57±13 years, mean weight 75±13 kg and heart rate55±5 bpm (p = n.s. between the two groups). Mean dose length product (DLP)was 93±7 cm*cGy for axial acquisition vs. 57±4 cm*cGy for high-pitch spiral CT,corresponding to estimated effective doses of 1.3 und 0.8 mSv (p < 0.001). Inprospectively triggered axial scans, an image quality score of "1" was found in694/798 segments (88%), "2" in 86 segments (11%), "3" in 14 segments (2%)and "4" in 4 segments (0.5%). For high-pitch spiral CT, image quality was "1"in 706/770 segments (91%), "2" in 46 segments (6%), "3" in 15 segments (2%)and "4" in 3 segments (0.4%). The number of incompletely evaluable patient datasets (at least 1 segment with a score of "4") was not significantly different betweenthe two groups. Mean image quality score per patient was 1.2±0.2 for axial and1.1±0.1 for high-pitch spiral acquisition (p = n.s.).Summary: Both prospectively ECG triggered axial acquisition ("step-and-shoot")and the newly developed high pitch spiral acquisition ("Flash Mode") permit coro-nary CTA with a low rate of unevaluable coronary segments in selected patients.Image quality is high and not significantly different between the two scan proto-cols. Radiation dose is lower for high-pitch spiral acquisition.
P1713 Cardiac computed tomography with and withoutECG-triggering: accuracy regarding thrombusdetection in the left atrial appendage prior to atrialfibrillation ablation
C. Jilek, S. Fichtner, T.S. Meyer, E. Hendrich, T. Reents, H.L. Estner,C. Kolb, J. Hausleiter, G. Hessling, I. Deisenhofer. German Heart Center, Clinicat the Technical University of Munich, Munich, Germany
Purpose: Catheter ablation has become an established treatment for patientswith atrial fibrillation (AF). Pre-procedural cardiac computed tomography (cCT)has a high negative predictive value in detecting thrombus in the left atrial ap-pendage (LAA).
Objective: Comparison between ECG-triggered and non-ECG-triggered cCTwith regard to accuracy in excluding LAA thrombus.Methods: Analysis of consecutive patients who underwent a contrast-enhancedcCT and transesophageal echocardiography (TEE) prior to AF ablation. The ab-sence of a thrombus in cCT was judged according to the LAA filling with contrastmedium. The ratio of Hounsfield-units measured in the LAA and left atrium (HU-ratio) was used as quality marker for LAA filling. Presence of LAA thrombus wasassumed when a clear LAA filling defect was present. The number of patientswith unclear LAA filling was compared between the two groups.Results: 564 patients were included: 263 patients (mean age 61±9.2 yrs, 68%male, mean BMI 25.8±6.3 kg/m2) received an ECG-triggered cCT whereas 301patients (mean age 60±10.2 yrs, 70% male, mean BMI 27.2±6.4 kg/m2; p=0.43)received a non-ECG-triggered cCT.The quality of LAA contrast filling did not differ between the two groups: the meanHU-ratio was 0.78±0.31 in the ECG-triggered group vs 0.68±0.38 (p=0.18). Inthe ECG-triggered group, 8.8% of cCT showed an unclear LAA filling versus11.7% in the non-ECG-triggered group (p=0.58) resulting in a specificity of 91.2%(CI 87-94) vs 88.3% (CI 84-91).The 3 thrombi detected in TEE were all adequately detected in the cCT regardlessof the ECG triggering.Conclusion: ECG-triggering does not have a significant influence on the ade-quate assessment of the LAA in patients prior to AF ablation.
P1714 A pulsatile in-vitro model to establishmultidetector-row computed tomography imagingcharacteristics of mechanical prosthetic valves
P. Symersky1, R.P.J. Budde2, M. Prokop2, B.A.J.M. De Mol3. 1IsalaClinics, Zwolle, Netherlands; 2University Medical Center Utrecht,
Department of Radiology, Utrecht, Netherlands; 3Academic Medical Center,Amsterdam, Netherlands
Purpose: Multidetector-row CT (MDCT) is a promising imaging technique forevaluation of mechanical prosthetic heart valves (PHV). However, image qual-ity and artifacts vary between valves types and no in-vitro studies havebeen un-dertaken to explore these differences to date. We constructed a pulsatile in-vitromodel to study the MDCT imaging characteristics of common PHV.Methods: Björk-Shiley (BS), St Jude (SJ), Medtronic Hall (MH), Carbomedics(CM), and ON-X (ON-X) valves were inserted in a custom-made in-vitro pulsatilemodel and scanned five times each using a 64-detector row scanner. Image qual-ity regarding visualization of leaflets, prosthetic detail and periprosthetic detail aswell as presence of artifacts was scored on a four-point scale by two observers.Results: Image quality for the BS valve was scored poor to moderate for all cri-teria and wasworse than all other PHV. Leaflet visualization was excellent for allotherPHV. Visualization of prosthetic detail was good for MH and SJ, and excel-lent for CM and ON-X. Visualization of periprosthetic detail was good for MH, SJand CM, and excellent for ON-X. Artifacts were moderate for MH and SJ, minorfor CM and minimal for ON-X. All differences were significant (p<0.001).
MDCT images of prosthetic valves
Conclusions: The pulsatile in-vitro model is an effective tool to detect differencesin MDCT imaging characteristics of PHV. Image quality is determined by prosthe-sis components and, to a lesser degree, by prosthesis design. Modern carbon-titanium PHV yield good to excellent image quality on MDCT.
P1715 Trends in radiation dose of coronary CT angiography
J. Hausleiter, B. Bischoff, T. Meyer, B. Gramer, F. Hein,M. Hadamitzky, E. Hendrich, A. Will, S. Martinoff, A. Schoemig.German Heart Center, Clinic at the Technical University of Munich,
Munich, Germany
Background: Coronary CT angiography (CCTA) is a frequently used diagnosticmethod, but the associated radiation exposure still raises concerns. Improved CT
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

294 Imaging
technology has lead to numerous dose-saving strategies. The latest and verypromising technique for dose reduction is high-pitch, single heart beat CCTA with2nd generation dual-source CT (DSCT) systems.Objective: To determine trends in radiation dose with improving CT technologyin a single centre analysis.Methods: In 4374 consecutive patients, radiation dose of CCTA was analysed bydetermination of median estimated radiation dose of every single month. FromOctober 2004 to September 2006, a 64-slice single-source CT system was used.Between October 2006 and March 2009, patients were examined with a 1st gen-eration dual-source CT. Since April 2009, 2nd generation dual-source CT systemis in use. Dose-saving strategies were used whenever possible. Radiation doseestimates were derived from the dose length product (DLP) and a conversioncoefficient for the chest (0.014 mSv mGy-1 cm-1).Results: During the single-source 64-CT period, 1771 patients were examinedwith a median radiation dose of 8.6 mSv [7.3; 12.9]. Dose-saving strategies suchas a sequential scan technique and aggressive ECG-dependent tube currentmodulation allowed for a median radiation dose of only 4.9 mSv [2.6; 9.2] in 1704patients examined with the 1st generation dual-source CT system. With introduc-tion of single heart beat CCTA, a further reduction of radiation dose to a medianof 1.9 mSv [1.0; 2.9] was achieved in 899 patients using a 2nd generation dual-source CT system (see figure).
CCTA radiation dose 2004 - 2009
Conclusions: The current analysis demonstrates that significant reduction of ra-diation dose can be achieved when using modern CT systems and applying dose-saving strategies whenever possible.
P1716 Non-tagged magnetic resonance longitudinal andvolumetric diastolic strain rate for the evaluation ofleft ventricular filling pressures
B.P. Paelinck1, P. Van Herck1, H.J. Lamb2, J.M. Bosmans1,P.M. Parizel1, C.J. Vrints1. 1Antwerp University Hospital, Edegem,
Belgium; 2Leiden University Medical Center, Leiden, Netherlands
Purpose: Transmitral flow is unreliable for the estimation of left ventricular (LV)filling pressures in hypertrophy and normal systolic function. Global diastolic strainrate (SR) during peak filling provides a relatively load independent measurementof global myocardial performance. We aimed to determine the feasibility of non-tagged cardiovascular magnetic resonance (CMR) assessed global diastolic SRand its potential implications for the estimation of filling pressure, in comparisonwith invasive measurement.Methods: Sixteen patients with hypertensive heart disease (LV mass index:111±18 g/m2), absence of valvular regurgitation and with normal systolic func-tion (LV ejection fraction: 67±7%) referred for cardiac catheterization were stud-ied. Measurement of mitral flow (early peak filling velocity E and late peak fillingvelocity A) was performed by phase-contrast CMR. Global longitudinal SR dur-ing early peak filling was measured using long-axis cine CMR images. Globalvolumetric diastolic SR during early peak filling was measured using long-axisand using short-axis cine CMR images. These data were compared with meanpulmonary capillary wedge pressure (PCWP).Results: Mitral flow E/A had no significant correlation with mean PCWP. Longi-tudinal diastolic SR (r=0.65, p<0.01), long-axis volumetric diastolic SR (r=0.51,p<0.05) and short-axis volumetric diastolic SR (r= 0.60, p<0.05) related to inva-sively measured mean PCWP.Longitudinal volumetric diastolic SR and long-axis volumetric diastolic SR hadsimilar sensitivity (respectively 87.5% and 75%), specificity (respectively 62.5%and 87.5%) and area under the curve (respectively 0.80 and 0.80, p<0.05) forthe prediction of elevated mean PCWP.Conclusions: In patients with LV hypertrophy and normal systolic function, non-tagged CMR assessed longitudinal and volumetric diastolic SR provided similarpredictors of elevated LV filling pressure.
P1717 Quantitative assessment of aortic regurgitation bycardiac magnetic resonance is dependent on the siteof flow assessment in the ascending aorta
M. Desai, R. Gabriel, R. Renapurkar, M. Bolen, D. Verhaert,P. Schoenhagen, S. Flamm, B. Griffin. Cleveland Clinic Foundation,
Cleveland, United States of America
Background: Similar to transthoracic echocardiography (TTE), cardiac magneticresonance (CMR) can also assess the severity of aortic regurgitation (AR) byquantifying regurgitant fraction (RF) in ascending aorta (AA) using phase contrast(PC) measurements. We sought to a) assess whether the RF cutoff for moderate-severe AR by CMR is different at different aortic levels b) and the potential factorsresulting in these differences.Methods: In 107 consecutive patients (mean age 48 years, 72% male, 39% bi-cuspid aortic valve, mean mid AA dimension 3.9 cm) undergoing CMR and TTEevaluation, PC flow RF measurement was performed at 3 levels in the AA (sino-tubular junction or STJ, mid and distal) on a 1.5 Tesla scanner. AR was classifiedusing multiple TTE criteria as 0-4+.Results: AR severity by TTE was graded as: 0 in 43%, 1+ in 17%, 2+ in 16%, 3+in 12% and 4+ in 12% patients. The mean RF was significantly lower (p < 0.001)in the mid (11.7±13.3%) and distal (9.4±12.6%) AA vs. STJ (13±13.3%). The RFcutoff which best differentiates ≥ 3+ and < 3 + AR on TTE is >15% (sens 96%,spec 89%) at STJ, >12% (sens 100%, spec 93%) at mid and >12% (sens 100%,spec 93%) at distal AA. Potential predictors of differences in RF measurementsat STJ and distal AA, on logistic regression analysis, are listed in Table 1.
Table 1
Univariate Multivariate
Beta Statistic P value Beta Statistic P value
Age (years) +0.03 0.26Sex (male) +1.39 0.20BSA +2.91 0.13Systolic BP –0.004 0.87Trileaflet vs. nontrileaflet aortic valve –2.62 0.007 –2.62 0.009Sinotubular junction maximum dimension +1.49 0.02 +0.82 0.34Distal aortic maximum dimension +1.59 0.048 +1.24 0.32Hypertension +0.67 0.50Beta-blocker +0.16 0.87Angiotensin converting enzyme-inhibitor +1.34 0.18
Conclusion: The grading of AR by CMR differs based on the level of flow as-sessment in AA. Abnormal aortic valve morphology appears to be a significantcontributor to this difference.
P1718 Comparison of myocardial deformation analysis bystrain-encoded cardiac magnetic resonance imagingwith speckle-tracking echocardiography - quantitativeanalysis of left ventricular function
E. Altiok1, M. Neizel2, S. Tiemann1, V. Krass2, M. Becker1,E. Grabskaya1 , R. Koos1, N. Marx1, R. Hoffmann1. 1University Hospital Aachen,RWTH, Internal Medicine I, Cardiology, Pulmonology & Vascular Medicine,Aachen, Germany; 2Heinrich-Heine University of Dusseldorf, Department ofCardiology, Dusseldorf, Germany
Background: Quantitative analysis of segmental myocardial function for differentmyocardial layers has become possible using strain-encoded cardiac magneticresonance imaging (SENC) as well as speckle tracking echocardiography. Wesought to evaluate and compare both methods for detailed analysis of myocardialfunction.Methods: In 20 patients (mean age 60.7±12.5 years) SENC using a 1.5-T MRIand 2D speckle tracking echocardiography (Echo) was performed. Quantitativelayer specific analysis of segmental left ventricular function was performed todetermine circumferential peak systolic strain values by SENC and by Echo ofan endocardial layer (Endo) and an epicardial myocardial layer (Epi). Analysisincluded 169 segments. In addition, segmental function was defined as normoki-netic, hypokinetic or akinetic by visual analysis of MRI cine sequences.Results: Endo as well as Epi strain defined by SENC or Echo differ significantlybetween different function states (table 1). Endo strain by SENC correlated toEndo strain by Echo (R=0.43; p<0.001). Correlation of Epi strain between themethods was less (R=0.14; p=0.063). Endo strain by echo was larger than Endostrain by SENC (bias=6.8; -18.6 to 32.3). Epi strain defined by the two methodswas less different (bias between Echo and SENC= 0.0; -19.2 to 19.3). There wasa trend for better distinction of hypokinesia/akinesia from normokinesia defined byvisual analysis of MRI using Endo strain by echo than Endo strain by SENC (AUCROC: 0.873 vs 0.802, p=0.105). Distinction of hypkinesia/akinesia from normoki-nesia was more accurate using Epi strain by echo than by SENC (AUC ROC:0.820 vs 0.680, p= 0.014).
Table 1. Circumferential peak systolic strain values in %
Wall Motion by MRI cine sequences SENC Endo Echo Endo SENC Epi Echo Epi
Normokinesia (n=113) -20.4±4.5 -30.9±13.4 -16.0±4.8 -18.0±9.1Hypokinesia (n=45) -14.0±5.9 -14.5±7.1 -12.3±5.2 -9.3±4.7Akinesia (n=11) -15.4±6.1 -10.5±9.4 -13.7±4.9 -5.9±5.8
p≤0.001 p≤0.001 p≤0.001 p≤0.001
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

Imaging 295
Conclusion: Quantitative analysis of segmental function by SENC and 2D Echoallows accurate distinction of different function states. However, strain values forthe two imaging modalities are on different levels. Strain by SENC tends to belower than by Echo. There is significant correlation of strain by SENC and 2DEcho for endocardial function, but not for epicardial function.
P1720 Left ventricular scarring and aortic stiffness arebetter predictors of mortality than ejection fraction,sphericity and volumes in severe ischemiccardiomyopathy: A cardiac magnetic resonance study
A. Lewis, Z. Popovic, D. Kwon, C. Halley, P. Schoenhagen, S. Flamm,B. Griffin, R. Starling, M. Desai. Cleveland Clinic Foundation, Cleveland, UnitedStates of America
Background: Left ventricular (LV) ejection fraction, sphericity & volumes predictoutcomes in ischemic cardiomyopathy (ICM). Myocardial scarring & aortic stiff-ness also predict outcomes. We assessed the incremental impact of aortic stiff-ness & myocardial scarring over volumetric indices on survival in ICM.Methods: ICM patients (n = 279, 77% men, 66±11 years, LV ejection fractionof 22% ± 11 & > 70% disease in ≥1 coronary artery) were studied. Cardiacmagnetic resonance (CMR) was used for evaluation of LV volumes & scar. LVsphericity was measured on end-diastolic 4-chamber cine view as D1 (apical) +D2(mid) + D3(basal)/3L(length of LV). LV scar was measured >2SD above viablemyocardium as % of total LV. Pulse wave velocity (PWV, m/s), a measure of aorticstiffness, was recorded on velocity-encoded CMR as �x/�t (�x = aortic pathlength between ascending & descending aorta, and �t = time between arrival offoot of PW between 2 points). Cardiac transplantation (CTx) & all-cause mortalitywere recorded.Results: Over 3.7±1.7 years, there were 80 events (75 deaths & 5 CTx). Resultsof Cox survival analysis are shown in Table 1.
Table 1
Univariable Forward StepwiseAnalysis Multivariable Analysis
Hazard ratio (CI) p-value Hazard ratio (CI) p-value
Age 1.04 (1.01-1.06) 0.001 1.04 (1.02-1.07) 0.001Female Gender 2.06 (1.29-3.28) 0.002 1.87 (1.17-3.01) 0.02Statins 0.72 (0.46-1.12) 0.14Beta-blockers 0.74 (0.47-1.16) 0.2Angiotensin converting enzyme-
inhibitors 0.75 (0.48-1.18) 0.2Post-CMR coronary bypass
grafting 0.63 (0.40-0.99) 0.04Post-CMR mitral valve repair/
replacement 1.12 (0.66-1.89) 0.2Post-CMR defibrillator or
cardiac resynchronization 0.78 (0.46-1.30) 0.2LV ejection fraction 0.99 (0.96-1.01) 0.3LV end-systolic volume index 1.003 (0.99-1.007) 0.3Indexed (D1+D2+D3)/3L (cm/m2) 1.20 (1.06-1.44) 0.006Mean scar % on CMR 1.01 (1.001-1.02) 0.03 1.02 (1.006-1.03) 0.001Pulse wave velocity on CMR 1.02 (1.007-1.04) 0.003 1.02 (1.002-1.034) 0.01
Conclusions: In severe ICM patients, aortic stiffness and scar are better predic-tors of outcomes than volumetric indices.
P1721 Non-invasive quantification of myocardial fibrosis indiabetic cardiomyopathy: T1 mapping or integratedbackscatter?
C. Jellis1, J. Wright2, J. Sacre1, D. Kennedy3, B. Haluska1,C. Jenkins1, J. Martin1, T. Marwick1. 1University of Queensland,
Brisbane, Australia; 2Hearts 1st, Greenslopes Private Hospital, Brisbane,Australia; 3Queensland X-ray, Greenslopes Private Hospital, Brisbane, Australia
Purpose: Interstitial fibrosis is believed to be one of several contributors to di-abetic cardiomyopathy (DCM), manifesting as myocardial dysfunction in the ab-sence of ischemic heart disease in subjects with type 2 diabetes (T2DM). Myocar-dial ultrasound reflectivity is proportionate to fibrosis, but use of the pericardiumas a frame of reference (calibrated integrated backscatter, cIB) may be limitedby signal saturation. Recently, diffuse fibrosis has been shown to be inverselyproportionate to T1 time on post-contrast T1 mapping using cardiac magneticresonance imaging. We sought to compare the association of cIB and T1 timewith DCM.Methods: Demographic, anthropometric, hemodynamic and biochemical datawere measured in 107 apparently healthy, asymptomatic subjects with T2DM (65men, 60±9 years). LV dysfunction (LVD) was sought on resting echo (early di-astolic tissue velocity [Em] < 1SD from mean for age). Ischemia was excludedby exercise echo. Standard 2D and color TDI measures (tissue velocity, strainand strain rate) were acquired in apical long axis views. Calibrated integratedbackscatter (cIB) was calculated from a parasternal long axis view. Tonometricaortic pulse wave velocity (APWV) was used to determine arterial stiffness. T1mapping was performed in those with LVD and matched controls.Results: LVD was identified in 23 subjects (28%) who also demonstrated sig-nificantly poorer diabetic control (HbA1c 8.2±2.0 vs 7.3±1.4 mmol/L) but no re-
lationship with cIB. T1 mapping was performed in 26 subjects (17 men, 60±10years) comprising 20 with LVD and 6 controls. Em was independently associatedwith age (β=-0.76 p<0.001), body mass index [BMI] (β=-0.65, p<0.001), strain(β=0.51, p=0.003) and post-contrast T1 time (β=0.36, p=0.04) [model R Square =0.63] but not cIB. Post-contrast T1 time was independently associated with insulinresistance (HOMA-IR β=-0.63, p=0.016) [model R Square = 0.38] but not withcIB, APWV, BMI or low density lipoprotein (LDL). The only independent correlateof cIB was APWV (β=0.59, p=0.009) [model R Square = 0.39] and not HOMA-IR,BMI or LDL.Conclusions: Quantitative tissue characterisation of fibrosis (T1 time) was in-dependently associated with subclinical DCM, in addition to systolic dysfunction(strain), age and BMI. The association of T1 mapping with insulin resistance con-trasts with the link between cIB and arterial stiffness, suggesting potential differ-ences between fibrosis in DCM and hypertension.
P1722 Imaging monocytes with iron oxide nanoparticlestargeted towards the monocyte integrin MAC-1 doesnot result in improved atherosclerotic plaquedetection by in vivo MRI
C. Von Zur Muhlen1, A. Fink2, J. Salaklang2, D. Von Elverfeldt1,D. Paul1, I. Neudorfer3, V. Berti3, C. Bode3, K. Peter4. 1Albert-Ludwig Universityof Freiburg, Freiburg, Germany; 2School Federal Polytechnic of Lausanne,Lausanne, Switzerland; 3Albert-Ludwig University of Freiburg, Department ofCardiology and Angiology, Freiburg, Germany; 4Baker IDI Heart and DiabetesInstitute, Melbourne, Australia
Introduction: Imaging of macrophages with superparamagnetic iron oxide par-ticles (SPIO) has been performed to improve detection of atherosclerotic plaqueinflammation in human and mouse studies by molecular magnetic resonanceimaging (MRI). Since affinity of the monocyte/macrophage integrin MAC-1(CD11b/CD18) is upregulated in inflammation, we generated a contrast agenttargeting CD11b (CD11b-SPIOs) for improved macrophage detection in plaques.Methods: CD11b-SPIOs and non-targeted SPIOs (control-SPIOs) were incu-bated in vitro with human monocytes/macrophages, and SPIO-typical MRI sig-nal extinction was quantified. The aortic arch and vessel branches of ApoE-/–Knockout mice on a western-type diet were imaged before and 48h after con-trast agent injection of either CD11b-SPIOs or control-SPIOs, using a 9.4 TeslaMRI-scanner with a coronal multi slice FLASH-sequence (isotropic resolution of104 μm). The SPIO-induced signal was quantified, as well as the macrophage-content by anti-CD68 immunhistochemistry and the iron-content by Prussian-bluestaining.Results: Intracellular iron-content was significantly higher in mono-cytes/macrophages incubated with CD11b-SPIO than with control-SPIO in vitro(p<0.05). SPIO-induced signal extinction in in vivo-MRI was similar in CD11b-SPIO and control-SPIO-injected animals, with a non-significant trend towards animproved uptake of CD11b-SPIOs in the subclavian artery and subsections ofthe aortic arch. These data correlated well with the results obtained by histology.Conclusion: Although in vitro MRI-data indicate an increased uptake of targetedCD11b-SPIOs in monocytes/macrophages, in vivo mouse data do not allow im-proved atherosclerotic plaque detection compared to non-targeted SPIOs. There-fore, CD11b-targeted MRI contrast labelling of monocytes/macrophages does notseem to be a successful strategy in stable atherosclerotic plaques. However, theimpressive correlation between MRI and histology data encourages further de-velopment of inflammation- and plaque-specific contrast agents for vulnerableplaque imaging.
P1723 Mid-wall fibrosis is an independent predictor ofmortality in patients with aortic stenosis
M. Dweck1, S. Joshi1, T. Murigu1, F. Alpendurado1 , A. Gulati1,W. Banja1, R. Mohiaddin1, D. Newby2, D. Pennel1, S. Prasad1.1Royal Brompton Hospital, Cardiovascular Magnetic Resonance
Unit, London, United Kingdom; 2University of Edinburgh, Centre forCardiovascular Science, Edinburgh, United Kingdom
Introduction: Predicting adverse outcomes in patients with aortic stenosis (AS) ischallenging. An important mechanism is fibrosis. Using late gadolinium enhance-ment (LGE) we assessed the prognostic significance of mid-wall vs myocardialinfarction patterns of fibrosis in patients with AS.Methods: Consecutive patients (n=143) with moderate or severe AS underwentCMR with LGE and were followed up for an average of 2.0 years.
Baseline data
No LGE Mid-Wall LGE Infarct pattern of LGE P value(NG) (MG) (IG)
Number of Patients 49 54 40 –Mean Age (SD) 64 (15.5) 70 (11) 70 (13) 0.031Male Sex % 52 70 80 0.018Documented CAD % 37 42 100 0.0001Mean AVA mm2 (SD) 1.04 (0.37) 1.00 (0.31) 0.91 (0.26) 0.111EF (SD) 69 (13) 58 (21) 44 (18) 0.001LV mass index (SD) g/m2 98 (33) 118 (34) 100 (23) 0.001Mortality rate (deaths
per 1000 patient years) 15.7 146.4 123.2 –
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022

296 Imaging
Results: Despite similar severities of AS and concomitant coronary artery dis-ease, patients with mid-wall LGE (MG) had a 7-fold increase in mortality com-pared to patients with no LGE (NG). This compares with a 5-fold increase inpatients with an infarct pattern of LGE (IG). Multivariate analysis showed thatmid-wall LGE (p=0.049) and ejection fraction (p=0.019) were the only two inde-pendent predictors of mortality.
Kaplan Meier curve
Conclusion: Mid-wall fibrosis is a powerful predictor of survival in AS.
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/suppl_1/1/607327 by guest on 30 January 2022