
Subject NGO's Topic - Inter Aide
45
HMF Annual Report 2008 Inter Aide Comment Keywords Author(s) Eamon Kelly, Kumar Shailabh, Dr. Abhijeet Sale, Dr Amit, Vrushali Vengurlekar, Shital Bhosale, Dr. Deepali Kulkarni, Inter aide/Swabhimaan/Uplift India Created 05/1/2009 Status: Version Final Last Edited March 19 th , 2009 Editing Time HMF Annual Report – 2008 Subject Uplift Health NGO’s Annapurna Parivar Vikas Sandhan (APVS) and Parvati Swajamrojgar (PSW) Topic Annual Report Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road, Sadhu Vaswani Circle, Pune-411001 Page 1 of 45
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Subject NGO's Topic - Inter Aide
HMF Annual Report 2008 Inter Aide
Comment
Keywords
Author(s) Eamon Kelly, Kumar Shailabh, Dr. Abhijeet Sale, Dr Amit, Vrushali Vengurlekar, Shital Bhosale, Dr.
Deepali Kulkarni, Inter aide/Swabhimaan/Uplift India
Created 05/1/2009 Status:
Version Final Last Edited March 19th, 2009 Editing Time
HMF Annual Report – 2008
Subject Uplift Health NGO’s Annapurna Parivar Vikas Sandhan (APVS) and Parvati Swajamrojgar (PSW)
Topic Annual Report
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 1 of 45
HMF Annual Report 2008 Inter Aide
1 Introduction to Uplift Health.......................................................................................................................................3
1.1 Background .........................................................................................................................................................3 1.2 Idea behind HMF ................................................................................................................................................3 1.3 Mutual Insurance Key Features...........................................................................................................................3 1.4 Health Mutual Fund Product ...............................................................................................................................4 1.5 Mutuals Main Achievements...............................................................................................................................4 1.6 Remaining Challenges.........................................................................................................................................4 1.7 Development Plans..............................................................................................................................................5 1.8 UpLift Partners....................................................................................................................................................5 1.9 Operations organization ......................................................................................................................................5
2 Executive Summary ....................................................................................................................................................6 2.1 Members covered ................................................................................................................................................6 2.2 Services & protection provided...........................................................................................................................6 2.3 Implementing NGO’s..........................................................................................................................................8 2.4 Technical support (ie Uplift) ...............................................................................................................................9
3 Members coverage ....................................................................................................................................................10 3.1 Policies & renewals...........................................................................................................................................10 3.2 Member details..................................................................................................................................................11
4 Services & protection provided.................................................................................................................................13 4.1 Health Services..................................................................................................................................................13 4.2 Protection provided ...........................................................................................................................................18 4.3 Claims analysis..................................................................................................................................................19 4.4 Plan for 2009 .....................................................................................................................................................26
5 Implementing NGO’s - Parvati .................................................................................................................................27 5.1 Main indicators..................................................................................................................................................27 Services review .................................................................................................................................................27 5.2 27 5.3 Performance according to the business plan......................................................................................................28 5.4 Other matters .....................................................................................................................................................28
6 Implementing NGO’s – APVS Pune.........................................................................................................................30 6.1 Main indicators..................................................................................................................................................30 6.2 Services review .................................................................................................................................................30 6.3 Performance according to the business plan......................................................................................................31
7 Implementing NGO’s – APVS Mumbai ...................................................................................................................33 7.1 Main indicators..................................................................................................................................................33 7.2 Services review .................................................................................................................................................33 7.3 Performance according to the business plan......................................................................................................34
8 Technical support (Uplift & Swabhimaan) ...............................................................................................................35 8.1 Summary of 2008..............................................................................................................................................35 8.2 Health services ..................................................................................................................................................35 8.3 Front office........................................................................................................................................................36 8.4 Back office ........................................................................................................................................................41 8.5 Risk Management..............................................................................................................................................42 8.6 MIS....................................................................................................................................................................44
APVS : Annapurna Parivar Vikas Sandhan BPI: Business Process In-sourcing CM: Collector-Motivator (Loan Programme) FDP : Family Development Programme. FSF : Family Security Funds (Life Insurance) HCP: Health Care Providers HMF : Health Mutual Funds ICU : Intensive Care Unit IGP : Income Generating Programme (Microfinance) IPD : In-patient Department LIC : Life Insurance Corporation of India MIU : Micro-insurance units OOPE : Out of Pocket Expenses OPD : Out-patient Department PCM : Partner committee Meeting PSW : Parvati Swajamrojgar SE : Service executives (Field staff in charge of HMF operations)
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 2 of 45

HMF Annual Report 2008 Inter Aide
1 Introduction to Uplift Health
1.1 Background Community Based Health Mutual Funds were initiated by Uplift India Association in response to the health care access need of women members of self help groups in the slums of Pune in 2003. The concept is based on health funds managed through mutual contributions and a network of health care services that provide quality treatment at concessional rates. An elaborate system of referrals and guidance towards the network services with a 24X7 helpline has been created to assist the members in accessing services. To aid members for their daily health needs a network of general practitioners has been recently created. In Pune the project is being implemented by Annapurna Parivar Vikas Samvardhan and Parvati Swayam Rojgar. The project was expanded to rural areas of Osmanabad and Solapur through Swayam Sikshan Prayog in 2006. The mutual product was designed through the responses of member’s capacity to pay and the claim settlement is done by communities themselves. There is an in house developed software that takes care of database management and daily operations.
1.2 Idea behind HMF During illness, and especially at time of hospitalizations the problems of the poor are:
Financial distress of the family: hospital expenses and loss of daily wages, which is a double burden.
Lack of health understanding and health consciousness
Poor access to adequate healthcare facilities Hence there is a need for a service which gives an entry point to access quality health care at most affordable prices. Health mutual funds allow people to share the risk through saving a small amount on the basis of ‘One for all, all for one’ so that in times of health crises a lump sum amount can be made available to meet the hospitalization expenditure, smoothening the financial shock when facing such events. While the system is similar to the insurance industry, here the risks are not “transferred” to an insurer, but shared under the community’s responsibility.
1.3 Mutual Insurance Key Features Fund is created and governed by communities;
fund money is kept in community’s name. Claims are settled in democratic and transparent
way by communities themselves Referral and guidance services provided through
localized branches and field workers. Preventive and promotive health measures,
member education is a key component of the programme
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 3 of 45

HMF Annual Report 2008 Inter Aide
1.4 Health Mutual Fund Product
1.5 Mutuals Main Achievements • Outreach has improved to 60000 lives
• Has been able to achieve 60% sustainability
• Has been able to bargain concessions with health care providers from 10-50%;
• In-house database management system provides effective management of information.
• Its a people governed model where health and access to quality health care at reasonable rates, is the prime concern
• With its focus on specific demand based health check up camps and OPD network services reduce the frequency of hospitalisation
• Has been able to save lakhs of rupees through referral and guidance services to members
1.6 Remaining Challenges The mutual model has still to address the following main challenges:
• Reduce operations cost to reach a 100% sustainability level of the project
• To reduce the out of pocket expenditure (which has risen due to rise in health care costs) through public financing as increasing premium is not an option.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 4 of 45

HMF Annual Report 2008 Inter Aide
• To promote a redistribution system with public money to cater to the lowest segment of the population
• Establish governing structures to have people’s ownership and management
• To increase renewal ratio from to 70% by end of 2009
1.7 Development Plans • Increase membership to reach 100,000 by 2009 end
• Reengineer processes to prepare for replicability and up scaling
• Automated MIS for increased efficiency
• New business partners for Upscaling
1.8 UpLift Partners UpLift has developed since 2003, relationship and partnership with various famous organisations who support in their manner the objective of building access to quality health care for the poor:
• Inter Aide: A French NGO, catalyst at the origin of UpLift, implements development programmes for the urban poor in the domains of productive microfinance, family development, early childhood and health mutual funds.
• MACIF: the biggest French insurance mutual recently associated with Inter Aide to provide technical support.
• GTZ: Support on liasoning with govt schemes etc.
• ILO: identified and documented Uplift’s best practices.
• Tieto : A Finland IT Development company, having a development centre in Pune allocates 1man – year for the development requirements of SysLift the UpLift’s MIS.
• Extensia: An Indian IT company providing technical support for development of Impact software
1.9 Operations organization
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 5 of 45

HMF Annual Report 2008 Inter Aide
2 Executive Summary The document sets out a review of the Health Mutual Funds (HMF) operations for the period Jan 2008- Dec 2008 for 2 implementing NGOs running Community based health insurance in Pune and in Mumbai as well as detail the technical services & tools delivered by Swabhimaan and Uplift support teams.
We set out the achievements of 2008, as follows:
Members covered
Health & Protection Services provided
Developments in implementing NGO’s
Developments in Technical support
2.1 Members covered The graph below summarises the numbers of policies starting and the renewal ratio in the last 3 years
Numbers & Renewal ratio
42%
54%59%
0
10,000
20,000
30,000
40,000
50,000
60,000
2006 2007 20080%
10%
20%
30%
40%
50%
60%
Policies Starting Ongoing Members Renewal Ratio
Comments as follows:
There was a substantial increase in member numbers in 2007 (40%). In 2008 there was an even greater increase in numbers starting due to significant growth in APVS Pune and also the initiation of HMF in Mumbai (in mid 2008). Numbers starting for PSW have been relatively stable the last 3 years.
There has also been a steady increase in aggregate renewal ratio from 2006 to 2008, due to both compulsory enrolment of HMF alongside IGP for Annapurna and also increased services and education of members regarding services. HMF is voluntary for PSW but the renewal ratio is only slightly below that of Annapurna.
Family size has been relatively stable in the order of 3.7 members for each policy. There is some variation by NGO due to differences in verification documents used and in the enrolment procedure.
2.2 Services & protection provided Key developments in the year include:
Launch of the New member product in mid 2008
o This provided increased coverage for members (from 3 to 5 categories, with a maximum increased
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 6 of 45

HMF Annual Report 2008 Inter Aide
from Rs5,000 Rs15,000) with an increased contribution from Rs60 to Rs100 per member.
o To ensure certain poorer members are not at a disadvantage, we provided a subsidy of Rs40 for members at SLL3 or lower (thus effectively keeping the contribution unchanged) for PSW
o Policy restricted to network hospitals only (except in case of emergencies)
o Pre-existing covered from 3rd renewal (previous product had full exclusion of pre-existing)
OPD coupons; we introduced the OPD coupons for members which are collected from OPD providers to provide detailed analysis of OPD usage by members
The Health Care provider (HCP) network has grown from 100 at start of the year to 150 by December 2008. There have been few deletions from the network and a number of new public HCP providers have been tied up and use concessional rates. We have also seen in increased use of referral letters by members to the HCP.
Mumbai project: We launched HMF in Mumbai with Annapurna as a compulsory rider on IGP. HMF policies started in June 2008. The product contribution, terms and cover are the same as the Pune product. The Health Services are still at an early stage with a basic HCP network set up, health talks and health camps and some initial referrals.
Staff product: we launched a product for staff of implementing NGO’s (including Swabhimaan and Uplift) from 1st May 2008, with premium of Rs300 per member and maximum cover of Rs30,000. Claims experience has been quite benign to date
An in-house study was completed in 2008, which analysed the impact of HMF services on IGP members and concluded that the HMF programme may improve the economic stability and hence the long term socio economic conditions of the insured families. Being an insured member in addition of being a borrower made a difference in terms of:
o Improved access to health care and health coverage
o Increased economic stability in the family for insured members
o Greater awareness on the importance of health
o Positive impact on saving behaviour
o Improvement in the health status of the family
Results for the year
Health Services:
The graph below summarises the health services (excluding claims) & savings for 2007 & 2008
Services & Savings
12,964
20,973
14,631
30,557
50% 49%
0
5,000
10,000
15,000
20,000
25,000
30,000
2007 20080%
10%
20%
30%
40%
50%
60%
Members Services Total Saving R'00 Services Ratio
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 7 of 45

HMF Annual Report 2008 Inter Aide
Comments as follows:
Numbers of members receiving services has grown substantially in 2008. This largely reflects the increased member numbers and consistent growth in services to match this growth (via a stable services ratio in the order of 50%)
However the savings have grown substantially reflecting a maturing program with a fuller range of services available to members (including an enlarged HCP network). The average saving per member (excluding claims) has increased from 113 to 143 – a 29% increase. When compared to the premium of Rs100, this in effect is a strong positive return for the policy holder.
However, there is potential for further growth and coverage of members – refer to health services section for further details.
Claims:
The graph below summarises the claim numbers and frequency since 2004
78169
247
434
604
1 .6%
1.4%1.3%
1.7%
1 .4%
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
1.8%
0
100
200
300
400
500
600
2004 2005 2006 2007 2008
C la im N um b ersC laim s
C laim F req uency (per m em ber)
Comments as follows:
Claim numbers have grown largely in line as the program has grown.
The claim frequency steadily decreased until 2006 and then increased in 2007 (largely due to poor experience for PSW). The total frequency has reduced in 2008, primarily due to low frequency for APVS outweighing a continued high frequency for PSW.
Further details are provided in the main body of the report
2.3 Implementing NGO’s Results for the year
As noted above there has been a marked increase in policies for APVS-Pune in 2008 (from 3600 to 9600) whereas PSW has reduced slightly from 3516 to 3456. The renewal ratio for APVS-Pune has also increased this year compared to 2007 (from 53% to 61%) and is also higher than PSW which is largely unchanged from 2007 (ie 56%)
Number of ongoing members for APVS Pune has more than doubled to be just over 36,000 while for PSW member numbers have reduced slightly (to 13235).
Key developments
HR issues:
o there continued to be a high turnover of field staff (SE’s) with worse turnover for APVS. This had some impact on renewals and services. APVS Pune has appointed an additional co-ordinator (now 2
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 8 of 45

HMF Annual Report 2008 Inter Aide
across 8 branches) plus an assistant Manager (from 1 December). This is in line with increased workload with increasing enrolments plus some organisational changes at Annapurna. Annapurna plan to hire 2 new SE’s in 2009 to handle the increased workload.
o PSW hired a co-ordinator during the year but the person was not suited to the work and so maintained a Manager (the previous co-ordinator) managing the 7 SE’s. PSW plan to hire a new CO in 2009 and split the HMF manager role across IGP & HMF.
Governance for each NGO:
o PSW has implemented separate accounts for claims and admin costs, plus enforced compulsory attendance of a PCM at claims meetings and co-signature on claims cheque. PCM’s are also empowered to provide referrals for members to the HCP network
o APVS has increase the numbers of PCM members from 7 (1 per branch) to 25 (based on number of members)
Other changes:
o Annapurna has moved to new Headquarters at Warje and the previous HO has become a branch and community meeting hall.
2.4 Technical support (ie Uplift) Uplift continued to provide the technical support to the implementing NGO’s throughout 2008 with the same services including developments listed below.
Back office: 2008 was the first full year of BPI provided by Uplift. This handled a number of developments including the new member product, the introduction of the staff product, OPD coupons, inclusion of Mumbai HMF, changes to Nidhi cards and a significantly increased workload (enrolments, claims etc).
Front office: front office support continued with assistance on the new product (and staff product), development and new tools, continual training (field staff & members), audits of front office function in the field and governance changes for Uplift.
Health Services: 2008 saw the appointment of a new network doctor for Pune (from January), regular services review, guidance centre, referrals, assistance to field staff and development and maintenance of the HCP
MIS: continual upgradation of Syslift including for the new product and the staff product and various developments in reporting.
Governance: Uplift implemented a new governance model including, project review meetings, operational committee, executive committee and representative committee. These all cover various issues (some independent) with continual feedback (between committee) and development.
Members on Uplift representative committee
Risk management: Uplift continued to provide technical support via reporting and claims analysis and reserve management and monitoring.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 9 of 45

HMF Annual Report 2008 Inter Aide
3 Members coverage As noted earlier, HMF is distributed via IGP for the implementing NGO’s. It is compulsory for IGP with Annapurna and voluntary with Parvati (with 85% take-up). As such the numbers of new HMF policies issued are directly linked to the number of IGP loans in that period. This requires a close co-operation between the IGP and HMF teams and an alignment of process where possible. The growth in numbers of HMF policies are therefore a reflection of the success of IGP for the NGO’s and the demand for IGP with those NGO’s by members in the community plus the experience of current and previous HMF members.
The compulsory nature of the distribution has the following effects;
• Is an effective and efficient distribution of HMF (and thus lower costs)
• Reduces the selection risk of members taking out HMF (who may be aware of poorer health status)
• HMF member profile is representative of the profile of members taking out a loan (and thus the capacity to service a loan)
3.1 Policies & renewals The graph below summarises the numbers of policies starting and renewal ratio since inception in 2003
1%
34%
42%
54%59%
70%
0%
10%
20%
30%
40%
50%
60%
70%
80%
0
5,000
10,000
15,000
20,000
25,000
2003 2004 2005 2006 2007 2008 2009
No of policies starting & Renewal ratio
APVS-Mumbai APVS-PunePSW Renewal ratio
Comments as follows:
There has been a steady increase in the total numbers starting each year up to 2007. In 2008 there was a substantial increase in numbers starting due to significant growth in APVS Pune and also the initiation of HMF in Mumbai in mid 2008.
Numbers starting for PSW have been relatively stable the last 4 years at between 3000 to 3500 per annum
There has also been a steady increase in aggregate renewal ratio from 2005 to 2008, due to both compulsory enrolment of HMF alongside IGP for Annapurna and also increased services and education of members regarding services.
For 2009 we are targeting a renewal ratio of 70% and a growth of just over 50% in policies and members. This is due to continued growth in Mumbai (plus 2 new branches), very strong targets per CM for APVS, and a revised IGP product for PSW.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 10 of 45
HMF Annual Report 2008 Inter Aide
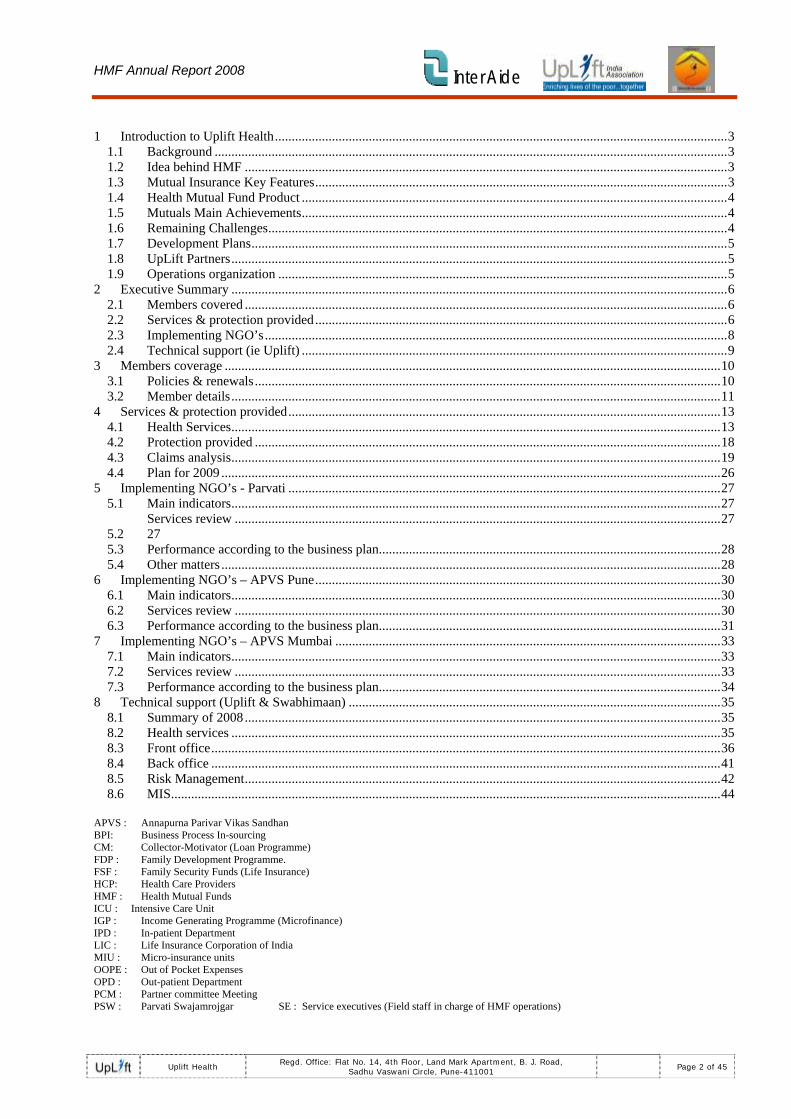
3.2 Member details Member Numbers:
The graph below summarises the numbers of members covered since inception (at each year end)
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
2003 2004 2005 2006 2007 2008 2009
No of ongoing members (at Dec end)
APVS-Mumbai APVS-Pune PSW
Comments as follows:
As illustrated in the previous graph we see steady growth from 2004 to 2007 and then a marked increase in 2008, due primarily to significant growth for APVS Pune and the initiation of HMF program in Mumbai.
We also note the stabilisation of PSW numbers since 2006 at just under 14,000 ongoing members (with a slight reduction in 2008).
For 2009 we are projecting an increase of 57% in ongoing members from 56,000 to 88,000. This is based on just under 40% growth for PSW & APVS-Pune and very significant growth in Mumbai (tripling of ongoing members) as we move into post 12 months operations with renewals plus the opening of 2 new branches.
Member Profile:
The graph below summarises the proportions of IGP borrowers across various Standard of living assessment levels. Field workers use a poverty assessment tool to assess poverty level of each IGP borrower based on answers to a number of qualitative and quantitative questions.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 11 of 45

HMF Annual Report 2008 Inter Aide
0%5%
10%15%20%25%30%35%40%45%50%
SLL 1 SL L 2 SL L 3 SL L 4 SL L 5 SLL 6 SL L 7
SLL proportions for IGP in 2008
PSW APVS Pune
Comments as follows:
This data relates to IGP borrowers but is broadly indicative of HMF members given the very strong link between distribution of HMF with IGP. This is based on survey data for 2008 which for PSW is just under 80% of borrowers. For APVS Pune the data is for 7 months of the year and surveyed at 15% of the total borrowers for that period. There is significant variation in the proportions from month to month and some subjective nature to the quality of the results. Therefore, these proportions should be considered as broad indicators of SLL across the IGP borrowers.
SLL3 is generally considered to be close to the poverty line. SLL4 and above indicate increasing levels of economic and social standing (and thus further away from poverty level).
The data indicates that PSW have a greater proportion of borrowers at the lower SLL level (3&4) and APVS have a greater proportion at the higher SLL level. This is consistent with anecdotal evidence from field staff and member interaction. This will also be related to the slum areas that the NGO’s operate and the borrowing capacity of the IGP people.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 12 of 45

HMF Annual Report 2008 Inter Aide
4 Services & protection provided In this section we discuss the health services available to members, the financial protection available under the HMF scheme, claims experience in 2008 and the key points in the plan for 2009.
4.1 Health Services Key services:
Maintaining members health is a major concern for the Health mutual fund. Therefore, we have a number of ways whereby members can avail services from the network in order to keep healthy.
1. going to OPD doctors 2. specialty clinics 3. hospitals for consulting and admissions 4. investigatory centres 5. medicine and medical equipment 6. health camps 7. NGOs
Usage of services
The table below summarises services since inception
All Dec-04 Dec-05 Dec-06 Dec-07 Dec-08
Ongoing Members (at June) 4,855 12,027 19,005 25,728 43,234
Health Camp - number 21 0 0 79 70Health Camp - members 1,554 0 0 4,112 3,876
Health Camp - Savings 0 0 377,930 795,911Health Talk - number 0 0 94 337
Health Talk - members 0 0 1,316 4,718OPD 0 0 2,112 4,302
OPD - savings 0 0 37,358 85,715Network Doctor 0 0 1,500 2,336
Members receiving service 1,554 0 0 9,040 15,232
Referrals 145 750 943 2,684 6,210Positive referrals 43 417 728 1,952 4,877Referral savings 9,570 219,985 577,051 1,047,836 2,174,070Call Centre 0 0 1,972 864Total services 1,597 417 728 12,964 20,973Total savings 9,570 219,985 577,051 1,463,124 3,055,696
Notes re the data as follows:
Health camps began in 2004 but very limited data is available for camps prior to 2007
Health talks began in 2007
OPD joined the network in 2006 but monitoring and regular data collection began in 2007
Call Centre: prior to 2007 all such calls were handled by the network doctor. Formal monitoring and regular data collection began in 2007.
The graph below summarises the health services since program inception, at each year end (please note that data prior to 2007 is incomplete)
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 13 of 45

HMF Annual Report 2008 Inter Aide
0
5,000
10,000
15,000
20,000
Dec‐04 Dec‐05 Dec‐06 Dec‐07 Dec‐08
Health services (member numbers)
Call centre Positive Referrals
OPD & Network doctor Health prevention
The graph below summarises the savings from health services since program inception, at each year end (please note that data prior to 2007 is incomplete)
0
500000
1000000
1500000
2000000
2500000
3000000
Dec‐04 Dec‐05 Dec‐06 Dec‐07 Dec‐08
Health services (savings)
Positive Referrals OPD & Network doctor
Health prevention
Comments as follows:
Numbers of members receiving services (and associated savings) has grown substantially in recent years including further significant growth in 2008. This reflects a maturing program with a fuller range of services available to members and growing member numbers. However, there is potential for further growth and coverage of members – refer to plan for 2009 for further details.
The number of members attending health camps has reduced slightly but the total saving has doubled. This is largely due to an increased number of eye camps which have a typical saving of Rs7500 per cataract operation.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 14 of 45
HMF Annual Report 2008 Inter Aide
There was also an extensive 2 week health camp in December at Bharti Hospital with free OPD and IPD
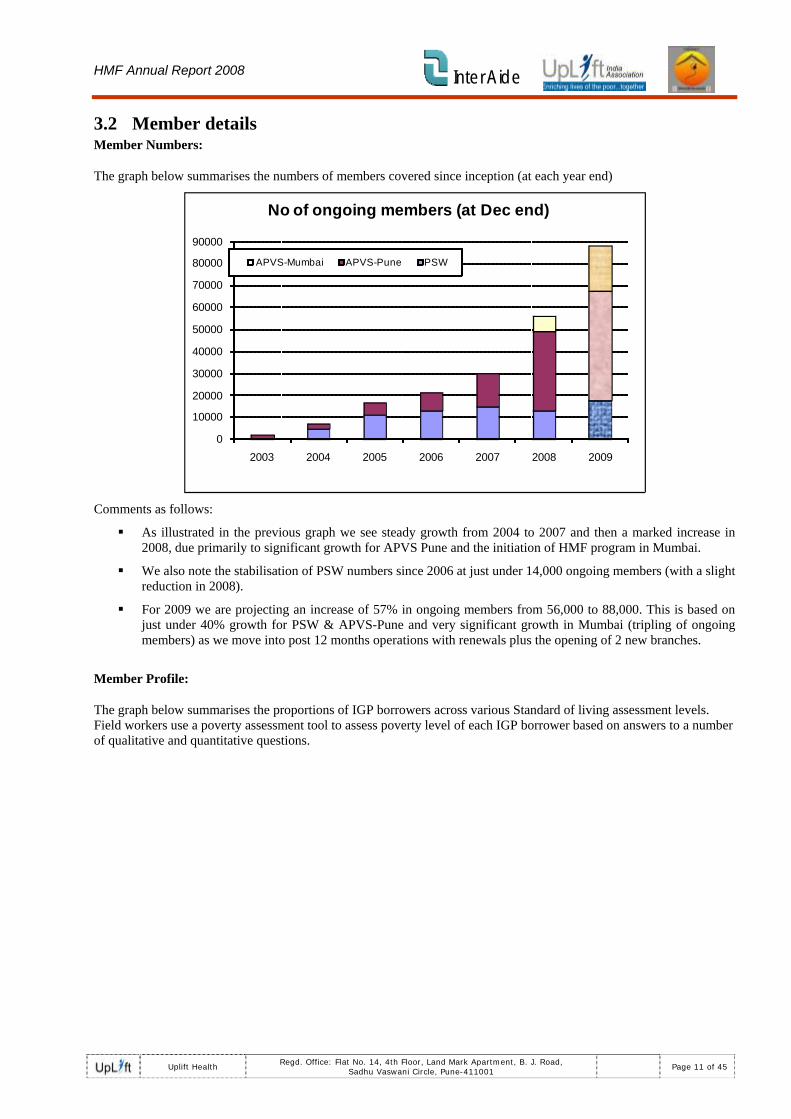
Network range:
The graph below summarises the members of the HCP at the end of 2008.
UPLIFT NETWORK HCP-150
30
15
2926
8
13
188 111
PUBLICTRUSTPRIVATEGPSP.CLINICINVEST.CENTREPHARMACYNGOOPTICIANORTHO REHAB CENTRECANCER CENTRE
At the end of 2007, there were 100 HCP in the Uplift network. By the end of 2008,the network has reached 150 (+50 new tie ups as compared to 2007). There were 54 new HCP added, as mentioned below and 4HCP de-panelled.
Additions in 2008 include;
4 Public Hospitals &12 Clinics
6 Trust Clinics
8 multi-specialities hospitals
2 Speciality doctor.
9 General Practitioners.
3 Laboratories
9 medical stores
1 NGO
Out of the 150 health care providers available in the network, 58 are hospitals. But the range of facilities available in those 58 hospitals is wide. In fact, there are 12 different combinations of facilities ranging from full fledged facilities like OPD, IPD, ICU (Intensive Care Unit), Investigation centers, radiology, medical shop and operational theatres to simple OPD/IPD facilities.
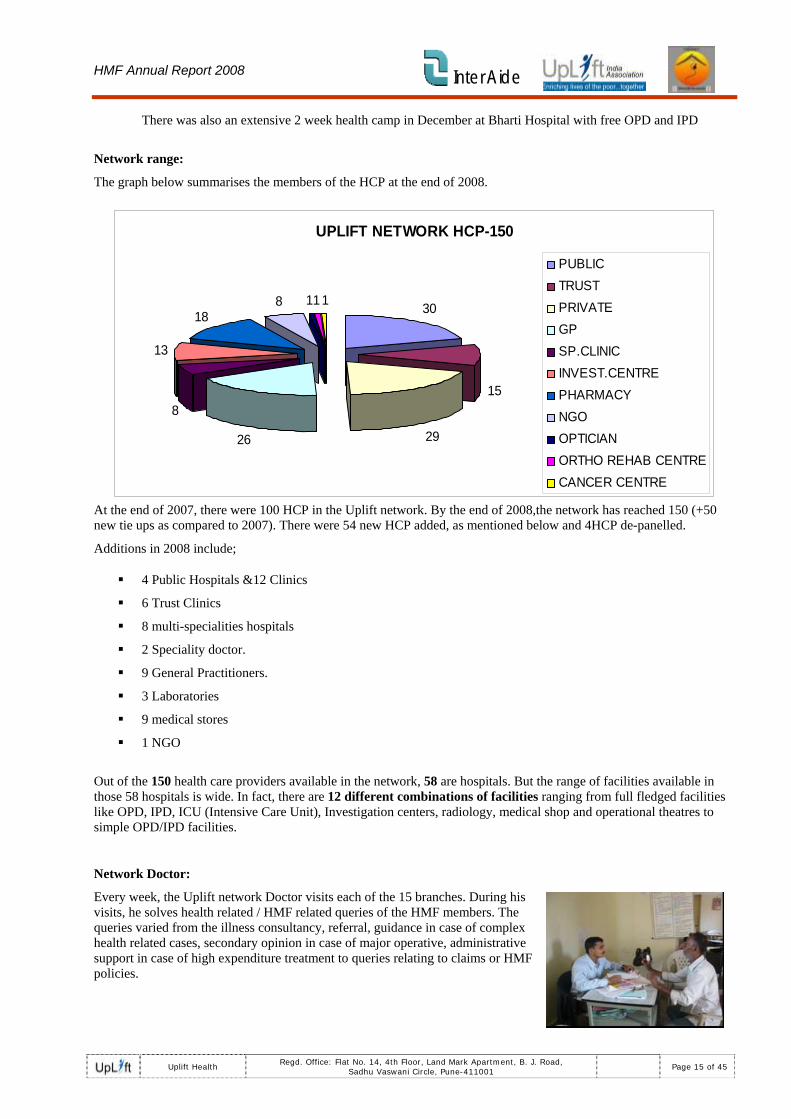
Network Doctor:
Every week, the Uplift network Doctor visits each of the 15 branches. During his visits, he solves health related / HMF related queries of the HMF members. The queries varied from the illness consultancy, referral, guidance in case of complex health related cases, secondary opinion in case of major operative, administrative support in case of high expenditure treatment to queries relating to claims or HMF policies.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 15 of 45

HMF Annual Report 2008 Inter Aide
Though the aggregate number of HMF members visiting the network doctor is over 2,300, the frequency of members visiting the network doctor showed a slight downward trend since June 2007 as the General Practitioner (OPD) setup is complete in most of the branches. The OPD are available as per HMF members timing and give concessions on medical treatment, i.e. primary care, ranging from 25% to 50%.
OPD
The year 2006 saw the initiation of the setup of OPD in Uplift Health Care Provider network. By the end of 2007 there were 12 OPD per NGO (total of 24). We now have 26 OPD in the network.
The main aim of the OPD setup was to provide the HMF members with medical facility such as primary screening and quality treatment at concessional rate in their vicinity through qualified Health Care Professionals. This also reduces the need for members to attend the network doctor clinics and is consistent with our approach of working with current health care providers rather than creating an alternative system.
Main highlights of the General Practitioners:
1. More visibility of the organization at ground level
• Frequency of visiting General Practitioners per member is 3-4 times more than going to a specialist doctor and 10-15 times more than getting admitted in a hospital, which results in an increased use of network facility. This also meets the primary care needs for members.
• Members use Nidhi Cards (identity cards); therefore there is no need to go to the Branch office to get referral. By using Nidhi Card for this service, members associate themselves with the organization and also realize that through the organization they can receive this medical facility at concessional rates.
2. Easy accessibility and less medical expenses: therefore there is an increased usage of the facility i.e. people don’t push their luck but go to the General Practitioners in time to avail the medical facility.
3. Cheaper treatments than in hospitals e.g. Concealed lacerated wound which needs suturing under local anesthesia is 40% less in OPD than at the hospital.
Referral System
The referral system acts in 2 ways:
1. Referral letter: mostly for specialist consulting, admissions, planned operative procedure, investigations and medicines. Also used at the time of emergency admissions since this letter is kept as a record in the hospitals and used at the time of yearly audit.
2. Telephone helpline and Identity card: in case of emergency admissions, emergency operatives or accidental cases the patient avails the treatment in network hospital on showing the Nidhi card (identity card) or through telephone helpline but has to submit the referral letter to the said HCP within 24hrs after admission.
Service executives are responsible for the follow-up of the referrals and guidance. They should check whether the reference has been used, and, whenever required, should inquire about members health status especially if they undergo long treatments. References follow-up is included in the service executive incentive scheme.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 16 of 45

HMF Annual Report 2008 Inter Aide
9%16%
44%
10%
4% 8%9%
Referral Usage 2008
PUBLIC TRUST PRIVATEGP SP.CLINIC INVEST.CENTREPHARMACY
Comments as follows:
• About 70% of the total referrals given were for different hospitals. The main reason behind this is that the hospitals cater to a variety of health needs, be it general consulting, specialized consulting, investigations, operatives, admissions, etc. Even though 70% of the referrals were given to the hospitals only 15%-18% of them were converted into admissions. Those referrals are largely to specialist doctors working in those hospitals and the rest of referrals are primarily for OPD and/or investigations
• 8% referrals were given to investigatory centres (radiological centres + laboratories) as these give more concessions of approx. 50%-60% compared to the 10%-30% concessions given for investigations in network hospitals.
• 4% referrals were given to speciality clinics like eye clinic E.g. Takewade eye clinic.
• 10% referrals were given to general practitioners (where the member actually has to use Nidhi Card). This helps make the members more familiar with the network general practioners. This is done to build the members’ trust in the general practitioners and in the organization.
• 9% referrals were given to medicine shops
Telephone helpline (call centre):
The 24X7 helpline was started in the year 2006 taking into consideration the needs of the HMF members. In the year 2007 the centralization of the telephone helpline took place (October 2007) and the helpline was called UPLIFT Arogyanidhi Phone Sewa.
Most of the calls today are received by the Network doctor and we have been encouraging the members to use confidently the new helpline; for this we have started issuing visiting cards of UPLIFT Arogyanidhi Phone Sewa to the HMF members and printing the helpline number on the nidhi cards of new and renew members.
Every time they are in contact with the members, the SEs also tell them to make more use of the helpline.
Members use the telephone helpline in the following cases:
• Health related problems
• Health Care Provider related problems
• Regarding administrative support
• Regarding Health Mutual Fund policy queries
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 17 of 45

HMF Annual Report 2008 Inter Aide
• Complaints from the members
• Complaints from the HCPs
• Information from the HCPs
• Emergency admissions
• Telephonic referrals during off days or in case the member is living far from the branch office and is not able to take the referral letter.
CALL CENTRE 24X7
2332
53
37 40 3626
53 53
32
50
82
11
2637
29 3328 28 32
22 2633
42
0102030405060708090
JAN
FEB
MARCHAPRIL
MAYJU
NEJU
LYAUG
SEPTOCT
NOVDEC
APVSPSW
The number of phone calls has been relatively stable since March with some variation by month and an increase at the year end. This is an average of 72 calls per month which is below target and also below the average for 2007 (which was in the order of 150pm).
The possible reasons for this are as follows.
• The S.E. is the main person giving reference to the HMF members as per their health needs taking their financial status into consideration.
• There is increased awareness of the Network HCPs due to increased use of nidhi card and HCP information given during the community directors’ training and community meeting.
• Increase awareness of the Network HCPs due to increased frequency of health camps carried out by the Network HCPs.
Due to the above factors the telephone helpline is now increasingly used in case of emergency admissions only.
4.2 Protection provided The health protection is the insurance component of the HMF product. As noted in the 2007 report there was an extensive process to review the product in light of increased medical costs and high out of pocket expenses for members (further detail on options considered and process followed is provided in the 2007 annual report)
In 2008 we launched a new version of the member product with some key changes as detailed below:
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 18 of 45

HMF Annual Report 2008 Inter Aide
Comparison of new product and old product (after May2008)
Old product New Product
Premium Rs60 Rs100Claims/Expense split 36/24 60/40Hospitals reimbursement
Public 100% 100%Network Low Cost 80% 80%
Network Private 80% 80%Non-network Private 40% Nil
Pre-existings Fully excluded Covered after 3rd renewal
Key Exclusions
9 key types including Chronic illness, self harm,
war, etc
HIV added to exclusions
Wage Loss Rs50 pday (max 15 days) Removed
CategoriesDay Care 1000 2500
General 2500 5000Semi-Special 7500
Special 5000 10000Super Special 15000
Comments as follows:
Key elements of change are the increase in the number of categories from 3 to 5, with a substantial increase in the maximum benefit for each category, and
Coverage of pre-existing diseases after the 3rd renewal
Removal of wage loss cover
No payment for non-network private hospital claims – to keep total costs down and also given the extensive and substantial network that now exists.
Increase in total premium from Rs60 to Rs100 (and for claims component from Rs36 to Rs60)
4.3 Claims analysis We discuss in this section the claims experience for the past number of years, with particular focus on experience in 2008.
4.3.1 Claim Numbers
The table below summarises claim numbers for the past 3 years from 2006 to 2008
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 19 of 45

HMF Annual Report 2008 Inter Aide
Claim frequencyNGO: All APVS ‐ Pune PSW APVS‐MumTotal 2006 2007 2008 2006 2007 2008 2006 2007 2008 2008Members 19005 25728 43239 6689 11696 25691 12316 14032 14061 3488Claims Incurred 247 434 623 92 156 243 155 278 330 50Claim frequency 1.3% 1.7% 1.4% 1.4% 1.3% 0.9% 1.3% 2.0% 2.3% 1.4%
Settled Unpaid(Rejected) 40 60 50 18 29 24 22 31 24 2Settled Paid(Disbursd) 207 320 491 66 108 171 141 212 296 24Check 247 380 541 84 137 195 163 243 320 26%Rejected 16% 16% 9% 21% 21% 12% 13% 13% 8% 8%
The graph below summarises claim numbers & frequency since 2004 for all NGO’s combined
78169
247
434
604
1.6%
1.4%1.3%
1.7%
1.4%
0.0%
0.2%
0.4%
0.6%
0.8%
1.0%
1.2%
1.4%
1.6%
1.8%
0
100
200
300
400
500
600
2004 2005 2006 2007 2008
Claim NumbersClaims
Claim Frequency (per member)
Comments as follows:
There was an increase in frequency in 2007 which was largely driven by PSW experience. The frequency has reduced in 2008 to be similar to levels prior to 2007. However this is due to low frequency for APVS outweighing a higher frequency for PSW.
Possible reasons for higher frequency for PSW are
o A higher proportion of renewals and thus greater awareness for members of Health services and the claims process.
o Lower turnover of SE for PSW and thus more consistency of information flow and relation with members (and senior/experienced SE’s)
o Greater geographical spread for APVS which may reduce the interaction between the SE and member
The proportion of claims rejected has reduced in 2008, for both NGO’s. In particular there has been a significant reduction for APVS. The reduction in rejection ratio may be due to improved awareness of product rules at the branch level (via training and also with increased numbers of claims and thus experience of dealing with claims)
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 20 of 45

HMF Annual Report 2008 Inter Aide
4.3.2 Comparative claim analysis Claims by Category
The table below shows the proportional split of claims by category (for the old product)
Proportional Split (claim numbers)
Claim Category 2006 2007 2008 Grand Total
On Day Discharge 0% 7% 10% 7%General 66% 59% 56% 59%Special 34% 34% 33% 34%Grand Total 100% 100% 100% 100%
Comments as follows: On Day discharge (ODD) was added at end of 2006.
There has been an increase in proportion at ODD for 2008 (largely due to PSW), with a corresponding reduction in proportion of general category claims.
There has been no significant change in the proportion in special category
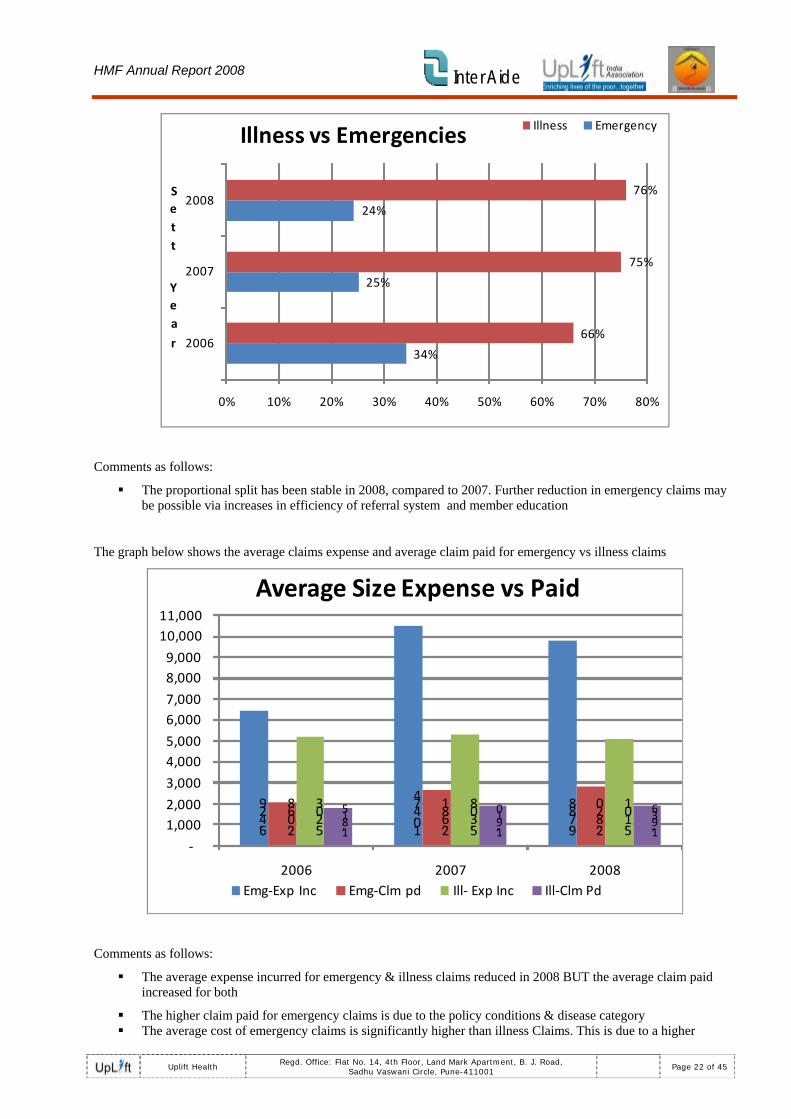
Illness Vs Emergency
The claims are divided into 2 categories depending upon the condition of the patient at the time of admission:
Illness: deterioration of the patient condition wherein there is no immediate threat to the life and / or no partial or total disability in any sense. All diseases not requiring ICU treatment, operative procedures that can be planned, accidental cases wherein treatment was not taken on the day of accident are all included in the illness category.
Emergency: deterioration of the patient condition wherein there is immediate threat to the life and / or partial or total disability in any sense. All diseases requiring ICU treatment, emergency operative procedures and accidental cases requiring prompt treatment and /or taken treatment on the same day are included in the emergency category.
The graph below shows the proportional split of claims between emergency and illness types of claims (based on numbers)
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 21 of 45
HMF Annual Report 2008 Inter Aide
34%
25%
24%
66%
75%
76%
0% 10% 20% 30% 40% 50% 60% 70% 80%
2006
2007
2008Sett
Yea
r
Illness vs Emergencies Illness Emergency
Comments as follows:
The proportional split has been stable in 2008, compared to 2007. Further reduction in emergency claims may be possible via increases in efficiency of referral system and member education
The graph below shows the average claims expense and average claim paid for emergency vs illness claims
6,429
10,474
9,788
2,068
2,681
2,820
5,203
5,308
5,101
1,815
1,910
1,936
‐
1,000 2,000
3,000
4,000 5,000
6,000 7,000
8,000 9,000
10,000 11,000
2006 2007 2008
Average Size Expense vs Paid
Emg‐Exp Inc Emg‐Clm pd Ill‐ Exp Inc Ill‐Clm Pd
Comments as follows:
The average expense incurred for emergency & illness claims reduced in 2008 BUT the average claim paid increased for both
The higher claim paid for emergency claims is due to the policy conditions & disease category The average cost of emergency claims is significantly higher than illness Claims. This is due to a higher
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 22 of 45

HMF Annual Report 2008 Inter Aide
percentage of Emergency Claims in Private Hospitals rather than in network or Low Cost Hospitals (especially for PSW)
Emergency Claims include High Cost Claims such as Head Injuries and Multiple Fractures resulting from Road Traffic Accidents and also Cardio Respiratory problems
Emergency Claims represent over 30% of the Claims Costs Paid. Claims Cost Paid is a lower percentage due to sub limits in the policy impacting very large claims. The maximum payable is 15000 RPs (under the New product) but some claims are above 60000 RPs expenses incurred. In 2009, Uplift plans to introduce a Solidarity Fund which would make additional payments in the case of some very large cases where the Out of Pocket Expenses are very high.
Claims by Hospital Type
The graph below shows the proportional split of claims between hospital type
13%
10%
13%
44%
40%
44%
43%
50%
44%
0% 10% 20% 30% 40% 50% 60%
2006
2007
2008
Frequancy ‐ Hospital type
Private Network Low Cost Network
Comments as follows:
The use of private hospital has reduced (in 2008) with concurrent increase in use of Network & Low cost hospital.
In 2009 we expect further reductions in proportion using private hospital with the new product rules and improvements in the referral system (with greater member awareness). Ideally the proportion of private hospitals is the same as the proportion of emergency claims and all planned treatment is via the network.
The graph below shows the average claims expense per Hospital type
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 23 of 45

HMF Annual Report 2008 Inter Aide
2,028
3,253
2,8095,
250
6,050
5,356 7,
094
7,787
8,044
5,621
6,635
6,208
‐
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
2006 2007 2008
Average Expense incurred per Hospital type
Low Cost Network Network Private All
The graph below details average claim paid per Hospital type
1253 16
69181121
68 2380
2246
1826 20
202167
1901 21
28
2157
0
500
1000
1500
2000
2500
2006 2007 2008
Average claim paid per Hospital type
Low Cost Network Network Private All
Comments as follows:
Average expense varies significantly between hospital, but claim paid broadly similar across hospital.
The average %Paid for low cost/network/private is 64%, 42% and 27%.
4.3.3 Out of pocket expenses The table below details the out of pocket expenses and % paid for claims
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 24 of 45

HMF Annual Report 2008 Inter Aide
Total %OOPE Sett Year
2006 2007 2008APVS-Pune 66% 62% 54%PSW 66% 71% 72%All 66% 68% 65%
Average %Paid (across each claim)Sett Year
2006 2007 2008 TotalAPVS-Pune 58% 52% 59% 57%PSW 50% 47% 46% 47%All 53% 49% 51% 51%
Comments as follows:
The out of pocket expenses (“OOPE”) is based on total expenses vs total claims paid for all claims combined. The % paid is the actual % paid for each claim, then averaged across all claims. The % paid is a more consistent view of how much money each claimant receives.
We note that the % Paid is generally higher for APVS vs PSW. This is largely due to PSW claims experience, refer to notes below in section 4.3.4.
4.3.4 New product experience As noted earlier we launched a new product in 2008 with additional categories, increased coverage and an increased premium.
While experience to date is very limited we note below a number of key items of experience.
Details for new vs old product (claims settled in 2008)
Old New TotalNumber Settled 406 54 460Amount Paid 813355 178840 992195Expenses Incurred 2482487 377886 2860373Average of % Paid 50% 57% 51%OOPE % 67% 53% 65%
Average expense incurred 6115 6998 6218Average Claim paid 2003 3312 2157
Product Type
Details for new vs old product (claims settled in 2008)
Average of % PaidProduct Type APVS PSW Grand TotalNew Product ‐ 100RPS 65% 48% 57%Old Product ‐ 60 RPS 58% 45% 50%Grand Total 59% 46% 51%
NGO
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 25 of 45

HMF Annual Report 2008 Inter Aide
Comments as follows:
The OOPE is lower for the new product and the % Paid is higher. This is consistent with the intention of the new product to reduce out of pocket expenses for members with the higher claim category limits and higher premium.
We note significantly different experience for PSW vs APVS, with APVS having higher % paid on old and on new product. For the APVS claims settled to date, the % paid has risen to 65% compared to 58% on Old product.
The lower proportion of %paid for PSW is likely due to
o continuation of old policy rules and use of private hospitals which reduces % paid and also reduces funds available for other members
o The expense incurred for private claims is much higher than the relevant category limit thus reducing the possible % paid if people use private hospital.
o Number of ongoing members is lower and thus the funds available is lower and
o PSW has a higher claims frequency
4.4 Plan for 2009 Given the increasing numbers of members it is essential that the Health Services continually develop to match member growth. The key plans for Health services & protection for 2009 are as follows:
• Improve core services (Health talks, health camps, OPD, referrals, health guidance, call centre) • Systemisation of data – review format, recording, quality & reporting of data collected on services
• HCP management: review & renewal of MOU’s, review rate list, development & growth as HMF numbers grow (location & volume)
• Investigate the possible provision of additional services
• Detailed review of product benefits and pricing including the impact of the new product on out of pocket expenses and the adequacy of the revised premium (in particular for Mumbai)
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 26 of 45

HMF Annual Report 2008 Inter Aide
5 Implementing NGO’s - Parvati
5.1 Main indicators The table below summarises the main indicators for PSW since inception;
PSW Dec-03 Dec-04 Dec-05 Dec-06 Dec-07 Dec-08
New Policies 59 1398 2556 1826 1757 14Renewal Policies 4 408 1352 1759 1980Renewal Ratio 7% 29% 46% 55% 56%Ongoing Policies 58 1402 3184 3470 3797 3456Ongoing Members 256 4854 11456 13176 14887 13235Services Ratio 3% 4% 60% 68%
76
Comments as follows:
Total ongoing members reduced by 11% in 2008 compared to end of 2007. This is due to reduced numbers of policies starting and a slightly lower average family size per policy.
Total policies starting reduced by 9% over the year with new policies reducing by 16% and renewals increasing by 13%.
Renewal ratio stabilised in 2008 at 56% (though below target of 70%). This is largely a reflection of the renewal ratio for IGP as HMF is directly related to IGP numbers.
Services ratio has increased from 60% in 2007 to 67% in 2008 (more details below)
5.2 Services review Indicator Planned Actual Difference
No of Health Check-up Camps 52 33 -19
No of Health camp beneficiaries 3900 1973 1927
Health Talks 168 162 -6
No of health talk beneficiaries 3060 2249 811
No of Referrals 3707 1685 2022
Percentage of referral follow-up 80% 79% -1%
No of telephonic guidance @ 20 calls average/day
319
No of members using OPD services 1901 2468 +567
Money saved thanks to services(references
601915 Rs
Comments as follows:
The number of health camps is below target due to SE turnover in some branches plus the availability of Hospitals (& NGO’s) being less than expected. Number of members attending health camps is just under 60 while target was 75. This can very across the year and by branch due to timing, location and camp type.
Number of health talks was close to expected but beneficiaries lower than target due to lower average
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 27 of 45

HMF Annual Report 2008 Inter Aide
attendance.
Number of referrals lower than expected but target may have been too ambitious and also actual enrolments were substantially lower than expected thus reducing the number of possible referrals. The positive referral follow up proportion is very close to expected.
Number of members using OPD significantly higher than expected which illustrates the stabilisation of the OPD network and member familiarity and comfort in using the OPD in the network.
5.3 Performance according to the business plan.
Indicator Planned till Dec 2008
Actual
HMF New Members 7353 5580
Renew members 9582 7655
Ongoing Members 21843 13235
Renewal ratio 70% 56%
Number of Claims 371 327
Paid Indemnities 450181 Rs
12 months Indemnities / earned contribution Ratio
80% 77 %
12 months claim frequency Ratio
0.17% 0.20 %
FSF
New and renew Members 4171 2453
Ongoing Members 4220 2453
No of claims 25 15
Paid Indemnities 25000 13000 Rs
12 months Indemnities / earned contribution Ratio
60% 26%
12 months claim frequency ratio 0.06% 0.05%
Comments as folows:
the main reasons for lower policy & member numbers (as advised by PSW) are as follows:
o Increased competition for IGP by new entrants in Pune
o Shortfall in IGP capital available for lending
o Temporary cessation of new loans in 2 branches for almost 6 months due to low PAR
o Anecdotal impact of higher HMF premium on affordability for members (though we attempt to offset this via a subsidy for SLL3 families)
o SE turnover and IGP staff turnover (and lack of IGP program manager throughout 2008 at PSW)
5.4 Other matters
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 28 of 45

HMF Annual Report 2008 Inter Aide
A. Subsidy to SLL3 level families. During the survey for the launch of the new 100Rs product ,strong feedback was received from the community ,that for some families ,who were very poor (SSL3 and below families according to Uplift U Impact) , this product would be unaffordable-though they preferred the higher coverage in the new product.
Subsequently it was decided by PSW and it’s supporting agency InterAide, that such families should not be excluded from the benefits of the new proposed product, because of their less paying capacity. Therefore it was decided that those families who came under the SLL3 or below category would pay the earlier contribution of Rs 60 per person/year and the remaining 40 Rs would be subsidized by InterAide grants to PSW. The first month of enrolment of SLL3 families showed an unexpected rise with 73 families .The analysis of the enrolment and Impact form showed that though the families
belonged to family level 3 (according to the poverty assessment tool) , the per capita income was high enough to afford the premium. Thus the criteria for subsidizing the family on only the level was not sufficient and so the second criteria of families having per capita income below Rs 1200 was added from May onwards. The enrolments were consistent until October but again showed a rise in November and December. This time along with the checking of forms a detail discussion was carried out with the field team to understand any gaps in the current system.
1. The SE’s were not getting the Impact forms when they go for verification of the families
2. There was no compulsory impact form filling for non IGP cases.
3. The CM’s were calculating the SLL level only according to per capita income and not on the seven indicators.
4. Some SE’s had complete misunderstanding about the concept of per capita income.
5. The SE’s were not filling Impact forms for renewed cases that were referred to subsidy. They were renewed for subsidy if the SE’s felt that they were very poor and should get a subsidy.
The system was redesigned to overcome the above gaps along with the HMF manager and the field team. A training was given to the SE’s again on how to fill the Impact forms. We will be continually monitoring this and also reviewing the appropriateness of the subsidy in 2009. B. Non-IGP enrolments Typically enrolments are alongside IGP but PSW also enrol non-IGP members. PSW began enrolling non-IGP policies in 2007 and continued with this in 2008. Service executives arrange orientation meetings from non-IGP families in the community. Else, Family development project’s field workers get an incentive for their HMF enrolments. For 2007 274 non-IGP policies and 991 members were enrolled. In 2008 this increased to 320 non-IGP policies and 1092 members.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 29 of 45

HMF Annual Report 2008 Inter Aide
6 Implementing NGO’s – APVS Pune
6.1 Main indicators The table below summarises the main indicators for APVS Pune since inception;
APVS Pune Dec-03 Dec-04 Dec-05 Dec-06 Dec-07 Dec-08
New Policies 515 665 1130 1612 2477 7416Renewal Policies 2 290 471 1,107 2,189Renewal Ratio 0% 43% 33% 53% 61%Ongoing Policies 515 667 1482 2195 3865 9605Ongoing Members 2047 2552 5192 8185 15207 36174Services Ratio 5% 3% 39% 45%
Comments as follows:
Total ongoing members reduced by a factor of 1.4 in 2008 compared to end of 2007. This is due to significant growth in numbers of policies starting, in particular in the later part of 2008.
Total policies starting increased by a factor of 1.5 over the year with new policies increasing by a factor of 2.0 and renewals doubling
Renewal ratio increased in 2008 to 61% (though below target of 70%). This is largely a reflection of the renewal ratio for IGP as HMF is directly related to IGP numbers.
Services ratio has increased from 39% in 2007 to 45% in 2008 (more details below)
6.2 Services review
Indicator Planned Actual No of Health Check-up Camps 48 39 No of Health camp beneficiaries 3085 2180 Health Talks 192 175 No of health talk benefeciaries 2880 2469 No of Referrals 3085 4525 Percentage of referral follow-up 80% 78% No of telephonic guidance @ 20 calls average/day 1543 517 No of members using OPD services 3085 1834 Money saved thanks to services(references , camps,opd
2,108,176 Rs
Comments as follows:
The number of health camps is below target due to SE turnover in some branches plus the availability of Hospitals (& NGO’s) being less than expected. Number of members attending health camps is 56 while target was 65. This can very across the year and by branch due to timing, location and camp type.
Number of health talks was lower than expected due to SE turnover in some branches
Number of referrals is much higher than expected due to some very strong performance by some SE’s in a number of branches. The positive referral follow up proportion is very close to expected.
Numbers of calls to call centre is well below expected- we discuss this in more detail in the services section (Section 3)
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 30 of 45

HMF Annual Report 2008 Inter Aide
Number of members using OPD significantly higher than expected which illustrates the stabilisation of the OPD network and member familiarity and comfort in using the OPD in the network.
6.3 Performance according to the business plan.
Indicator Planned till Dec 2008
Actual
HMF New Members 33744 26772
Renew members 6812 9402
Ongoing Members 40556 36174
Renewal ratio 70% 61 %
Number of Claims 617 224
Paid Indemnities 443792
12 months Indemnities / earned contribution Ratio
80% 52%
12 months claim frequency Ratio
0.14% 0.08%
FSF
New and renew Members 11206 10887
Ongoing Members 11206 10887
No of claims 92 61
Paid Indemnities 93000 Rs 57000 Rs
12 months Indemnities / earned contribution Ratio
60% 39%
12 months claim frequency ratio 0.06% 0.07%
Comments as follows:
the main reasons for lower than target policy & member numbers is largely due to lower than expected performance in the first half of 2008
o Increased competition for IGP by new entrants in Pune
o Poor performance of IGP staff unable to meet targets
o Target had planned opening of a new branch in 2008 which did not happen
o SE turnover and IGP staff turnover
Renewal ratio is lower than target but an improvement on 2007, this is largely linked to the renewal of IGP loans
Number of claims are below target due to members being below target and a much lower than expected claim frequency. It is not clear if this is due to the health status of APVS members and/or understanding of the HMF program. There has been a focus in the latter half of 2008 to ensure member understanding of claims entitlements and this has coincided with an increased claims ratio for those months.
Renewals in APVS
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 31 of 45

HMF Annual Report 2008 Inter Aide
After a not so encouraging experience in voluntary enrolment of HMF Annapurna started with compulsory enrolment of HMF with loans. As long as the member was an APVS loanee he/she was re-enrolled in HMF too. The SE was supposed to visit each member for renewals.
With the increase in new loans and reloans in 2008 APVS decided to opt for automatic renewal system whereby the member got his policy automatically renewed if he was supposed to get the next loan from APVS. From now onwards members who were defaulters or who did not wish to go for a second loan were not eligible for HMF re-enrolment.
It was observed that the automatic renewal system has it’s own limitations
The members who disqualified for second loans were not renewed due to the new system. The policies of such members lapsed. These members after qualifying for the loans again joined as new policies. Though they were actually renewed due to the break in the policies they appeared as new policies.
Some members showed dissatisfaction if their loans were cancelled due to some reasons after the renewal of their policies.
Renewal ratio is heavily dependent upon IGP activity i.e the month with high number of defaulter cases or write off cases automatically lowered the renewal ratio. Therefore while computing performance indicators renewal ratios won’t have the same significance as before.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 32 of 45

HMF Annual Report 2008 Inter Aide
7 Implementing NGO’s – APVS Mumbai Annapurna commenced operations in 2008 with enrolment in May 2008 and the first HMF policy starting in June 2008.
7.1 Main indicators The table below summarises the main indicators for APVS Mumbai:
APVS Mumbai Dec-08
New Policies 2,004Renewal Policies "n/aRenewal Ratio "n/aOngoing Policies 2,004Ongoing Members 6,964Services Ratio 20%
Comments as follows:
At the end of 2008 total ongoing policies are just over 2,000 and ongoing members almost 7,000
7.2 Services review
Indicator Planned Achieved
No of Health Check-up Camps 28
No of Health camp beneficiaries 1400
Health Talks 56 51
No of health talk beneficiaries 1120 1308
No of Referrals 160 168
Percentage of referral follow-up 80% 68 %
Money saved thanks to services(references
With the Health care providers network still taking root for APVS Mumbai the new HMF team started to provide the members with some set of important health services like
Health talks : The SE’s were trained to take health talks in the community the result of which total 51 health talks were taken with total attendance of 1308 members.
Some Doctors from the newly associated HCP network also showed their initiative by conducting health talks for the community.
Referrals: 168 referrals were given by the SE’s against the target of 160.all the referrals were given to the Public hospitals.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 33 of 45

HMF Annual Report 2008 Inter Aide
7.3 Performance according to the business plan.
Indicator Planned till Dec
2008 Actual
HMF
New Members 6041 6964
Ongoing Members 6041 6964
Number of Claims 32 49
Paid Indemnities 22111 Rs
Indemnities / earned contribution Ratio
80% 41%
claim frequency 0.14% 0.20 %
FSF
New Members 1729 2738
Ongoing Members 2738
No of claims 5
Paid Indemnities 5000
Indemnities / earned contribution Ratio
60% 26%
Claim frequency ratio 0.06% 0.04 %
Comments as follows:
Member numbers are 15% above target due to very strong IGP activity in the later part of 2008.
The claim numbers and frequency is higher than expected but at such an early stage is difficult to say if this is a major cause for concern. However the claims ratio is well below expected due to lower than expected average claim size and strong usage of the public health system in Mumbai
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 34 of 45

HMF Annual Report 2008 Inter Aide
8 Technical support (Uplift & Swabhimaan) Uplift provides the technical support to the implementing NGO’s of the HMF program with the assistance of Inter Aide (via the program manager who managed the Uplift operations in 2008).
In doing so Uplift receives a network support charge from the implementing NGO’s (Rs20 per member) to cover expenses. There is additional financial support provided to Uplift by Inter Aide.
Swabhimaan is a partner NGO providing technical support to the implementing NGO’s for other programs and works with Uplift in knowledge, resource (and actual office) sharing.
8.1 Summary of 2008 The year 2008 saw Uplift Health develop its portfolio as well as its governance model. The impact on health care access through referrals saw an increased growth as also the increase in the amount saved that amounted to more than 3 million rupees.
The revision of product saw tripling the coverage along with doubling of the contribution. The new product also saw the launch of the OPD coupon system to make the project more tangible and increase the usage of OPD services. The project saw an up scaling to Mumbai with back office operations being held from the Pune office itself.
The monthly federation meeting gave way to the new governance structure where by the management was realigned at two levels and three committees. The first committee is the Representatives committee where the community representatives are brought at Uplift level and secondly the Executive committee comprising of the MDs. A third committee to represent front line management (Operations committee) has also been instituted to discuss the operational issues.
The year also saw Uplift representing its model idea to the Pune Municipal Corporation as well as to the Family welfare department (GOM) in association with GTZ. Uplift also pursued the up scaling agenda with BUCCS. With up scaling and resource mobilization becoming as the next step in operations Uplift teamed up with UNITUS and GV to co draft a grant proposal for the ILO Micro Insurance Innovation Fund which did not meet the desired results. However, the ILO did produce a very informative short film about Uplift during 2008 and have proposed to perform a case study on the Uplift model in 2009.
Uplift strategy to promote people led social security systems played a critical role in setting up the CLASS as a national level initiative and also joined the prestigious ICMIF as a full member.
Uplift this year was called as a resource person in the ASIA MICROFINANCE SUMMIT held at Bali, the GTZ-USAID national workshop on health micro insurance in New Delhi and by CARE in Tamil Nadu. The Uplift model was presented to the UK institute of actuaries (London) in September. Uplift was also represented at the 3rd international micro-insurance conference held in November in Columbia.
Towards the year end a strategy document was prepared and validated by the Board which outlined the need for changes in the model so that it became replicable and democratic. These needs have been identified and the ensuing year will bring new changes at Uplift.
8.2 Health services 1. Network Services:
Network facilities are developed and maintained by the Uplift Association team. This is primarily led by the Network Doctor and the BPI manager (previously the network doctor) with assistance from the rest of the team.
Their targets are:
• Providing quality health services to HMF members at reasonable rates (average of 30% discount)
• Increasing the level of Primary level of treatment.
• Raising health awareness among HMF members.
• Increasing members’ confidence in the scheme.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 35 of 45

HMF Annual Report 2008 Inter Aide
• Increasing members’ participation in the scheme. 2. Means of operation:
• Develop & maintain a network of health care providers as per the needs of HMF members
• Provision of quality health care at concessional rates through the Health Care Providers (HCPs).
• Proper functioning and monitoring of referral system.
• Proper monitoring of the network OPDs.
• Maintain good relations with HCPs.
• Arrangement of health camps.
• Arrangement of health talks.
• Increased access to the National Health Programmes.
• Early scanning of diseases, more emphasis of referrals on primary treatment than secondary and tertiary level.
• Helping the members to get administrative support in case of very high cost treatment procedures.
• Helping the members to take proper decision during the health crises.
3. HCP status as on December 2008
In 2006, there were 69 HCPs part of our network. In 2007, the network reached 100 and now at December 2008 the network has reached 150 providers.
There were 54 new HCPS added, as mentioned below and 4 HCPs depanelled.
Public and trust hospitals represent 25% of the network and thus supply health care at a very minimal rate. 75% of health care providers of our network are private ventures.
Uplift is also developing a health care network for Mumbai and with the assistance of Dr Swapna Jambhekar identified almost 30 health care providers for this network. Uplift has also recently hired a doctor to fill the position of Network doctor for Mumbai.
Additions
New healthcare providers have entered in the network in order to cater the needs of the 2 new branches (Upper Indiara Nagar and Hadapsar) at primary as well as specialty level and, also to cope with the members’ growth.
Deletions
The de-panelments happened because of lapses in the MOU signed or refusal of HCPS to continue with Uplift’s schedule of rates.
4. Plan for 2009
Given the increasing numbers of members it is essential that the Health Services continually develop to match member growth. The key plans for Health services for 2009 are as follows:
• Improve core services (Health talks, health camps, OPD, referrals, health guidance, call centre) • Systemisation of data – review format, recording, quality & reporting of data collected on services
• HCP management: review & renewal of MOU’s, review rate list, development & growth as HMF numbers grow (location & volume)
• Investigate the possible provision of additional services
8.3 Front office
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 36 of 45

HMF Annual Report 2008 Inter Aide
Uplift provides support to the Front office functions of the implementing NGO’s as follows:
• Product review & development
• Monitoring, evaluation & reporting
• New project development
• Tools development
• Capacity building & HR development
• Governance & Administration
1. Product review and development
A. HMF product
Study on claims and OOPES
Claim analysis in 2007 had highlighted the following trends • Percentage of OOPES increased to 68%. High level of out-of-pocket expenses, particularly for larger claims • The average claim size increased from over Rs 5000 in 2006 to under Rs 7000 in 2007 Maximum coverage
was not sufficient to cover the increased size. Health care cost from 2003 to 2006 rose by 20 % thereby significantly increasing medical expenses while the caps did not.
• The claim frequency had increased markedly between 2006 and 2007.
New product proposed
Taking into consideration the above trends a new product was proposed. The proposed contribution was Rs 100 in which 4 options were given for the maximum reimbursement. The final option chosen was one with maximum coverage of Rs15000, with coverage for pre-existing diseases from the 3rd continuous year of membership and all other services as before.
New service features in the new product (OPD coupon)
With the aim of improving access to OPD services in the network and creating value for money, a new feature of providing the members with 3 OPD coupons each along with the new product was introduced in 2008.These OPD coupons were designated as discount coupons valid for the policy period ,keeping in mind the variation in the concessions provided by different Health care providers on OPD basis. Further these coupons were intended to be collected back every month from the HCP’s .The intention was to clearly account for the frequency of OPD service usage as well as record how many times a member availed this service and saved money. The Coupons (For members ) and the coupon boxes(For OPD doctors) were designed. The Service executives were trained on the new system .The OPD doctors in the slums were given instruction on the new process.
NGO No of coupons used for OPD (Till
Nov 08) PSW 228 APVS Pune 44
. (Printing cost of the coupon/member =84 paisa)-.
B. FSF product revision.
The following changes were made in the FSF product • One spouse and two elder children (staying in the same house) to be covered. No age limit for children .
• No exclusions only death has to be certified for processing the claim
• Claim should be paid within 8 days of the death.
• Death Pass as the minimum document required for claim settlement .
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 37 of 45

HMF Annual Report 2008 Inter Aide
2. Monitoring evaluation and reporting
• Monitoring & Evaluation system
The monitoring of the branches continued with monthly branch audits in 2008 also. NGO Number of branch audits -2008 APVS Pune 21 APVS Mumbai 10 (From May 08-Dec 08) PSW 17
The evaluation of per month front office activities was done in the monthly project review meetings with the Managing directors of each NGO. 12 project review meetings were conducted with each NGO.
• Reports
a) ‘The activity report’ was revised according to the new product
b) The ‘HMF Branch monitoring report’ revised according to the needs of the Coordinators.
c) ‘Annual branch audit summary’ sheet prepared which highlighted the proportion of issues each branch had (the lesser issues the better the branch is) and helped to compare the performance as compared to the last audit.
3. New project development
A. APVS Mumbai
Annapurna Parivar which has it sister concerns in Mumbai for the last two decades planned to upscale the Pune HMF model to it’s Mumbai operations along with it’s fast track IGP model. HMF operations started in May 08 in the following four branches
1. Chembur
2. Mankhurd
3. Kalwa
4. Shivdi
HR for new operations A five day induction and training was conducted by Uplift and APVS Pune staff for the newly appointed HMF team in Mumbai . B. Staff HMF
The member organization of Uplift Health decided to replicate the community based health mutual model for their staff members so as to follow the ‘preach and practice’ paradigm as well as to further the spirit of solidarity and provide social protection cover as part of good practices of employment. The member organizations decided to pool this fund at Uplift and all their staff would be contributing to this fund known as ‘Staff Health Mutual Fund’. The Member organization would contribute 75 Rs per employee and his/her nuclear family up to 4 members.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 38 of 45
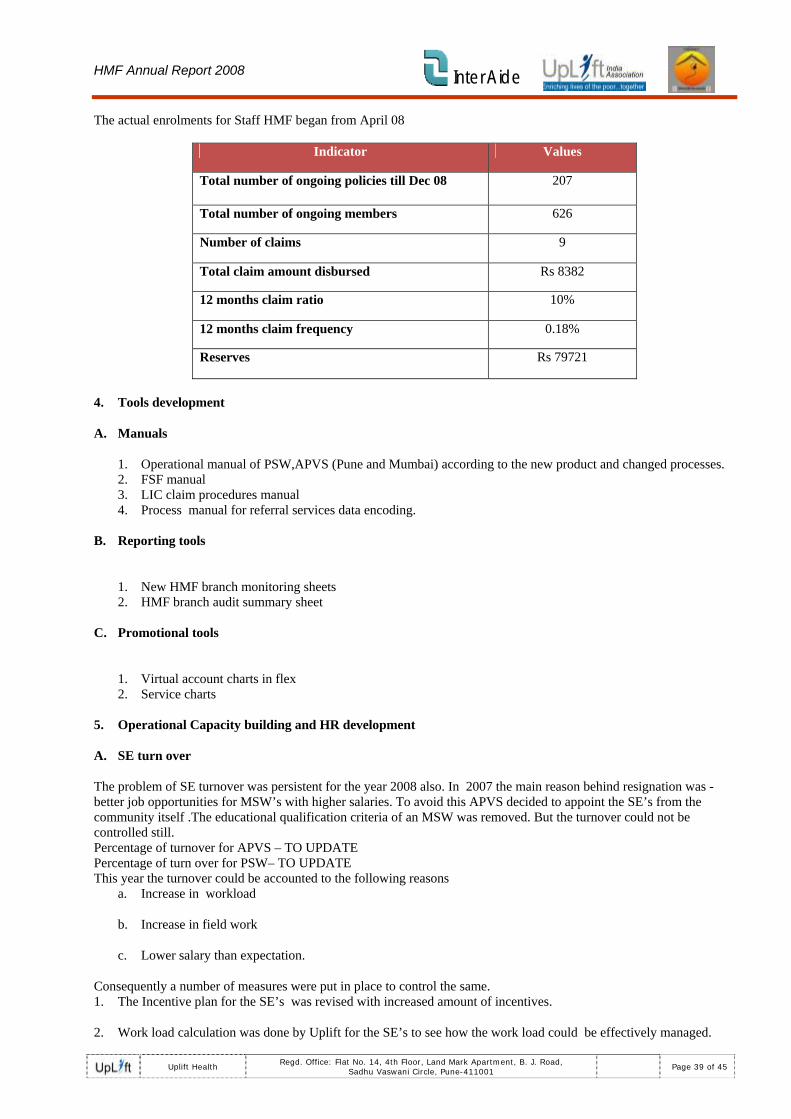
HMF Annual Report 2008 Inter Aide
The actual enrolments for Staff HMF began from April 08
Indicator Values
Total number of ongoing policies till Dec 08 207
Total number of ongoing members 626
Number of claims 9
Total claim amount disbursed Rs 8382
12 months claim ratio 10%
12 months claim frequency 0.18%
Reserves Rs 79721
4. Tools development
A. Manuals
1. Operational manual of PSW,APVS (Pune and Mumbai) according to the new product and changed processes. 2. FSF manual 3. LIC claim procedures manual 4. Process manual for referral services data encoding.
B. Reporting tools
1. New HMF branch monitoring sheets 2. HMF branch audit summary sheet
C. Promotional tools
1. Virtual account charts in flex 2. Service charts
5. Operational Capacity building and HR development
A. SE turn over
The problem of SE turnover was persistent for the year 2008 also. In 2007 the main reason behind resignation was - better job opportunities for MSW’s with higher salaries. To avoid this APVS decided to appoint the SE’s from the community itself .The educational qualification criteria of an MSW was removed. But the turnover could not be controlled still. Percentage of turnover for APVS – TO UPDATE Percentage of turn over for PSW– TO UPDATE This year the turnover could be accounted to the following reasons
a. Increase in workload
b. Increase in field work
c. Lower salary than expectation.
Consequently a number of measures were put in place to control the same. 1. The Incentive plan for the SE’s was revised with increased amount of incentives.
2. Work load calculation was done by Uplift for the SE’s to see how the work load could be effectively managed.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 39 of 45

HMF Annual Report 2008 Inter Aide
B. SE training
The intense monitoring and evaluation helped to figure out what training should be given to the field staff to minimize the error percentage and standardize each process. Accordingly the training modules were designed. The main feature of 2008 training was the effective participation of the Service executives in the trainings as trainers. This helped the junior SE’s to understand the nitty-gritty’s of the field process.
The following topics were taken for the training.
Month Topic Jan 1. Referral services
March 2. Exposure visit to SEWA
April 3. Concept of CBHMF and the product details
May 4. Communication skills during visit to member. Health talk-Cancer
June 5. Claim and referral services
July 6. Review of Operational manual
Aug 7. Training on how to conduct effective orientation .Health talk on antenatal care
Sep 8. Attitude test and required soft skills .Health talk on Home remedies
Oct 9. Attitude test and required soft skills-Part 2 .Health talk on Dengue.
Nov 10. Tech report and VAC filling. Health talk on Malaria and typhoid Dec 11. Enrolment form filling, MIS issues and health talks- Eye care and
Immunization.
Other trainings conducted by Swabhimaan
Type of training NGO Number of days/hours Month Junior SE’s training PSW- 2 days Jan 08 APVS 4 days March 08 and July 08 New project implementation
APVS Mumbai 5 days April 08
Staff training PSW 4 hours 24th March APVS 4 hours Revised HMF operations SSP 3 days 9-11 Jan Internal trainings APVS Pune and Mumbai
Smart Shrimati game 4 hours 1st September and
SE work load 4 hours 29th September
6. Governance
Uplift in 2008 not only focused to increase the involvement and ownership of the community members in HMF fund but also their participation in HMF services. The representatives were trained accordingly on the following
A. Referral services
One member from each branch was provided with referral letter pad and the list of Health care providers to give
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 40 of 45

HMF Annual Report 2008 Inter Aide
referral letters to the needy members incase the SE or the network doctor is not available. B. Claim service
Their involvement in the claim meetings in regards of taking decisions considerably increased. They even helped the other members in gathering the essential documents for claims.
C. Enrolment
In PSW motivation was also given to them to increase the enrolments in HMF as a result of which the PCM’s were trying to get new members in the fund.
7. 2009 Plan
Given the increasing numbers of members and the workload in the field it is essential that the front office support is continually developing to support field operations. The key plans for Front office support for 2009 are as follows:
• Proactive management of activities (health services, enrolments, renewals etc)
• Referral follow up and review of OPD coupons (usage etc)
• Standardisation of key process in the field (via audit, review etc)
• Increased member interaction and development of member information tools
• Research & development into process and promotion tools
• Continual training of field staff
8.4 Back office 1. Key function
In mid 2007 Uplift centralised the back office processes of the implementing NGO’s.
The BPI service includes the following;
• Encoding of HMF policies
• Encoding of FSF policies
• Production of Nidhi cards
• Production of OPD coupons (from June 2008)
• Encoding of staff HMF policies
• Validation and encoding of Claims
2. 2008 key achievements
2008 was the first full year of operation of the BPI function at Uplift. This was a crucial year as it involved
• the stabilisation of process for BPI
• handling introduction of new product (revised enrolment form, claims form etc)
• set up for handling of Staff HMF policies (encoding, Nidhi card, claims)
• production of OPD coupons (introduced in June 2008)
• handling increased workload for growth in APVS Pune (in late 2008)
• handling workload for APVS Mumbai (launched in May 2008)
• adaptation to changes in IGP & HMF process for the implementing NGO’s
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 41 of 45

HMF Annual Report 2008 Inter Aide
• development & implementation of quality & process controls for encoding (eg via time targets & quality standards)
• adaptation to changes in community structure for the implementing NGO’s
• updated Nidhi cards (format & preparation process)
• developments in claims process (primarily related to new product);
o revised claim guidelines for the new product (for validation)
o revised claims form
o revised claims categories
o revised claims recording process
3. Workload
The graph below summarises the workload volumes for BPI in the last 18 months (since centralisation in July 2007)
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
Sep‐07 Dec‐07 Mar‐08 Jun‐08 Sep‐08 Dec‐08
HMF enrolments FSF enrolments Nidhi Cards Claims
Comments as follows:
• there has been a regular growth in workload quarter on quarter with a significant increase in the last 2 quarters of 2008.
• There was also additional workload from June 2008 with the production of OPD coupons (3 per member) 4. 2009 plan
Given the increased volume and level of workload for BPI it is essential that the process are as efficient as possible to handle current workload and future increases in workload. As such the key plans for BPI for 2009 are as follows:
• Continual quality improvement for NGO’s
• Detailed review of BPI process (including Research & development)
• Standardisation of claims validation, review of claims categories and updation of related documentation
• Input of BPI into health services delivery (including the call centre)
• Revision of infrastructure needs and preparation for upscaling
8.5 Risk Management
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 42 of 45

HMF Annual Report 2008 Inter Aide
1. Current status
Risk management has been developed to be as practical as possible and implementable at a field level. Therefore Uplift has developed basic tools to assist the implementing NGO’s for risk management.
The key tools are;
• Monthly technical report which details key statistics such as claims ratio, reserves, claims frequency etc. These are monitored monthly and reviewed and discussed at NGO and branch level
• Claims decision tool – a simplified tool to assist co-ordinators in recording claims and determining maximum amount payable and relate to earned premium
• Reserves utilisation sheet – which allows the use of reserves when the earned premium is insufficient to cover claims in a particular month
• Sharing of reserves and/or earned premium by branches for each NGO when paying claims
• Member involvement in claim decision via claims meeting – this ensures member understanding of funds available and encourages risk management at the community level, to ensure claims paid when necessary and encourage healthy behaviour by members
2. Reserve level
The graph below summarises the total reserves since program inception (at each year end)
Reserves Rs'000 (at Dec end)
0
500
1000
1500
2000
2500
3000
3500
2003 2004 2005 2006 2007 20080
10
20
30
40
50
60PSW APVS-PuneAPVS-M umbai Ave per member
Comments as follows:
The reserves have grown steadily since inception of the program up to 2007.
There has been a marked increase in 2008 due to the introduction of the program in Mumbai plus significant growth in APVS-Pune (with relatively low claims ratio). This is at December year end and overstates the true position due to some claims yet to be settled and substantial unearned premium.
These reserves may be used for a solidarity fund due to be set up in early 2009.
3. Plan for 2009
Given the increasing member numbers and claim numbers there are a number of key developments in risk management planned for 2009, as follows:
• Setting up of solidarity fund
• Investigate and/or set up of reinsurance arrangements
• Quarterly claims analysis
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 43 of 45

HMF Annual Report 2008 Inter Aide
• Detailed product & pricing review on new product (both staff and member)
• Review of risk management tools & training for Uplift and field staff
• Development of a Risk management scorecard
8.6 MIS 1. Introduction
The key MIS used for HMF is the Syslift software developed with the assistance of Tieto. This is the key software and is a very important tool used for Data Processing, Back office Management, Monitoring & Evaluation of Field Processes and Services, Decision Making & Product Designing
The Uplift MIS team manage and provide the following key services to the operations;
• Syslift development
• Uimpact development
• BPI support
• Implement new projects for Syslift
• Development of new tools
• Capacity building
2. Key achievements in 2008
Syslift developments:
• Amendments to partner window, claims window, policy window and product definition window
• Development of a database switch
• Design & Implement crystal reports for OPD coupons, OR report for SLL3 & below, encoder reporting
• Patch development & testing: in 2008 total 14 versions of the Syslift were released by Tieto and the same were continuously tested at Uplift. Ver_3.30 is the latest patch release and is under testing.
• Major updates and new versions released on field & at BPI
o a key version was meant for the solution of two major errors on the databases named as Overflow and Index out of Bounds error
o Ver_3.22.07 was updated in Nov-08, mainly to solve Run Time error on Syslift.
o Installation in the Uplift BPI for APVS Mumbai.
o In May 2008, the fresh Syslift (ver 3.22) installation was done for Annapurna Parivar Vikas Samvardhan Head Office, Dadar - Mumbai. The training of Syslift installation and troubleshooting was provided to MIS executive of Annapurna Parivar Vikas Samvardhan, Mumbai.
o In May 2008, the Syslift software was installed in the BPI for Uplift Staff Health Mutual Fund.
o In Sept 2008, fresh installation of Syslift 3.22 was done for PSW head office when the the HMF (Syslift) server was shifted.
Uimpact developments:
• Uimpact is the software used for recording and analysis of poverty impact assessment tool
• In Feb 2008, Uplift started working with Extentia (A Pune based IT Company) for UImpact software developments. Extentia first reviewed the entire source code for UImpact and resolved the previous bugs.
• UImpact version 3.24 was released by Extentia in Apr 2008, the main feature of UImpact 3.24 is dynamic
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 44 of 45

HMF Annual Report 2008 Inter Aide
reports, analysis reports, action reports and action encoding/configuration facility etc.
• From May to Sept 2008, Extentia developed 8 to10 SQL views to get the data of common IGP+HMF members for impact study 2008. The same were continuously tested. Out of these views; two views are currently used for the monthly analysis. These views are consisting of the detail information of the surveys with the indicators values like Food, Health, Housing, Education, Documentation, Economic Activity, Financial Links etc.
• Enhancement in the actions configuration facility is developed and tested.
• In Oct 2008, AND/OR facility in the dynamic report made workable and it’s under testing
• In Dec 2008, developments/enhancements of the reports is done and it’s under testing.
• Fresh UImpact installation was done for APVS Mumbai in the BPI for encoding in Jan 2008.
Other developments:
• Syslift quality checking & monitoring
• Regular & ongoing BPI support
• Incorporation of new projects in syslift (APVS Mumbai)
• Incorporation of staff product (including staff premium calculation tool)
• Updation for new member product
• Capacity bulding through training for BPI team and NGO staff
3. Plan for 2009
There are a number of key developments in MIS planned for 2009, as follows:
• Review reporting and standardisation to reduce manual workload and avoid duplication
• Add New Users + Increase for existing users from current Functionalities from Syslift
• Replacement of Excel reporting where possible
• Additional encoding functionality for services & claims data
• Tools development for improved reporting
• Develop & implement a testing protocol in a standard process for syslift patches
• Continual Syslift developments
o TblPremiumStat Implementation.
o Policy Condition Storage & Printing Facility.
o Formula Designer Window for Indemnity Calculation.
o Benefit Providers Module Development.
o Database Consolidations.
o To develop the facility in Syslift to Import the Data (for partners / policies / contributions).
o Non- Monitory Benefits Module Development.
• UImpact developments
o Efficient Statistical and analytical Reports development/enhancement.
o Actions encoding followed by actions report.
o Web based development.
Uplift Health Regd. Office: Flat No. 14, 4th Floor, Land Mark Apartment, B. J. Road,
Sadhu Vaswani Circle, Pune-411001 Page 45 of 45




















