Subgenual prefrontal cortex of child and adolescent bipolar patients: a morphometric magnetic...
7
Subgenual prefrontal cortex of child and adolescent bipolar patients: a morphometric magnetic resonance imaging study Marsal Sanches a,b,c , Roberto B. Sassi d , David Axelson e , Mark Nicoletti a,b , Paolo Brambilla f , John P. Hatch a , Matcheri S. Keshavan e , Neal D. Ryan e , Boris Birmaher e , Jair C. Soares a,b, * a Division of Mood and Anxiety Disorders, Department of Psychiatry, The University of Texas Health Science Center at San Antonio, San Antonio, TX, USA b South Texas Veterans Health Care System, Audie L. Murphy Division, San Antonio, TX, USA c Department of Psychiatry, Federal University of Sao Paulo, Sao Paulo, Brazil d Department of Psychiatry, University of Sao Paulo School of Medicine, Sao Paulo, Brazil e Department of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh Medical Center, Pittsburgh, PA, USA f Department of Pathology and Experimental and Clinical Medicine, Section of Psychiatry, University of Udine, Udine, Italy Received 18 March 2004; received in revised form 26 November 2004; accepted 27 November 2004 Abstract The subgenual prefrontal cortex (SGPFC) plays an important role in emotional processing. We carried out a magnetic resonance imaging (MRI) study comparing the volume of the SGPFC in child and adolescent bipolar patients and healthy controls. The sample consisted of 15 children and adolescents who met DSM-IV criteria for bipolar disorder (mean ageFS.D.=15.5F3.5 years) and 21 healthy adolescents (mean ageFS.D.=16.9F3.8 years). MR images were obtained with a 1.5 T GE Signa Imaging System with Signa 5.4.3 software. SGPFC volumes were measured with the semi-automated software MedX (Sensor Systems, Sterling, VA, USA). ANCOVAwas performed to compare SGPFC volumes between groups, using age, gender and intra-cranial volume (ICV) as covariates. The volumes (meanFS.D.) of the right and left SGPFC for bipolar patients were 291.27F88.70 mm 3 and 284.86F83.98 mm 3 , respectively. For healthy controls, the right and left SGPFC volumes were 284.95F73.33 mm 3 and 307.55F73.67 mm 3 , respectively. There were no statistically significant differences between groups regarding right or left SGPFC volumes. We found no evidence of volumetric abnormalities in the SGPFC of bipolar children and adolescents. D 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Neuroimaging; Prefrontal cortex; Bipolar disorder; Adolescents 0925-4927/$ - see front matter D 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.pscychresns.2004.11.004 * Corresponding author. Division of Mood and Anxiety Disorders, Department of Psychiatry, The University of Texas Health Science Center at San Antonio, 7703 Floyd Curl Drive, San Antonio, TX 78229, USA. Tel.: +1 210 5675492; fax: +1 210 5673759. E-mail address: [email protected] (J.C. Soares). Psychiatry Research: Neuroimaging 138 (2005) 43 – 49 www.elsevier.com/locate/psychresns
-
Upload
childrenslearninginstitute -
Category
Documents
-
view
0 -
download
0
Transcript of Subgenual prefrontal cortex of child and adolescent bipolar patients: a morphometric magnetic...
www.elsevier.com/locate/psychresns
Psychiatry Research: Neuroim
Subgenual prefrontal cortex of child and adolescent bipolar
patients: a morphometric magnetic resonance imaging study
Marsal Sanchesa,b,c, Roberto B. Sassid, David Axelsone, Mark Nicolettia,b,
Paolo Brambillaf, John P. Hatcha, Matcheri S. Keshavane, Neal D. Ryane,
Boris Birmahere, Jair C. Soaresa,b,*
aDivision of Mood and Anxiety Disorders, Department of Psychiatry, The University of Texas Health Science Center at San Antonio,
San Antonio, TX, USAbSouth Texas Veterans Health Care System, Audie L. Murphy Division, San Antonio, TX, USA
cDepartment of Psychiatry, Federal University of Sao Paulo, Sao Paulo, BrazildDepartment of Psychiatry, University of Sao Paulo School of Medicine, Sao Paulo, Brazil
eDepartment of Psychiatry, Western Psychiatric Institute and Clinic, University of Pittsburgh Medical Center, Pittsburgh, PA, USAfDepartment of Pathology and Experimental and Clinical Medicine, Section of Psychiatry, University of Udine, Udine, Italy
Received 18 March 2004; received in revised form 26 November 2004; accepted 27 November 2004
Abstract
The subgenual prefrontal cortex (SGPFC) plays an important role in emotional processing. We carried out a magnetic
resonance imaging (MRI) study comparing the volume of the SGPFC in child and adolescent bipolar patients and healthy
controls. The sample consisted of 15 children and adolescents who met DSM-IV criteria for bipolar disorder (mean
ageFS.D.=15.5F3.5 years) and 21 healthy adolescents (mean ageFS.D.=16.9F3.8 years). MR images were obtained with a
1.5 T GE Signa Imaging System with Signa 5.4.3 software. SGPFC volumes were measured with the semi-automated software
MedX (Sensor Systems, Sterling, VA, USA). ANCOVA was performed to compare SGPFC volumes between groups, using
age, gender and intra-cranial volume (ICV) as covariates. The volumes (meanFS.D.) of the right and left SGPFC for bipolar
patients were 291.27F88.70 mm3 and 284.86F83.98 mm3, respectively. For healthy controls, the right and left SGPFC
volumes were 284.95F73.33 mm3 and 307.55F73.67 mm3, respectively. There were no statistically significant differences
between groups regarding right or left SGPFC volumes. We found no evidence of volumetric abnormalities in the SGPFC of
bipolar children and adolescents.
D 2004 Elsevier Ireland Ltd. All rights reserved.
Keywords: Neuroimaging; Prefrontal cortex; Bipolar disorder; Adolescents
0925-4927/$ - s
doi:10.1016/j.ps
* Correspon
Center at San A
E-mail addr
aging 138 (2005) 43–49
ee front matter D 2004 Elsevier Ireland Ltd. All rights reserved.
cychresns.2004.11.004
ding author. Division of Mood and Anxiety Disorders, Department of Psychiatry, The University of Texas Health Science
ntonio, 7703 Floyd Curl Drive, San Antonio, TX 78229, USA. Tel.: +1 210 5675492; fax: +1 210 5673759.
ess: [email protected] (J.C. Soares).
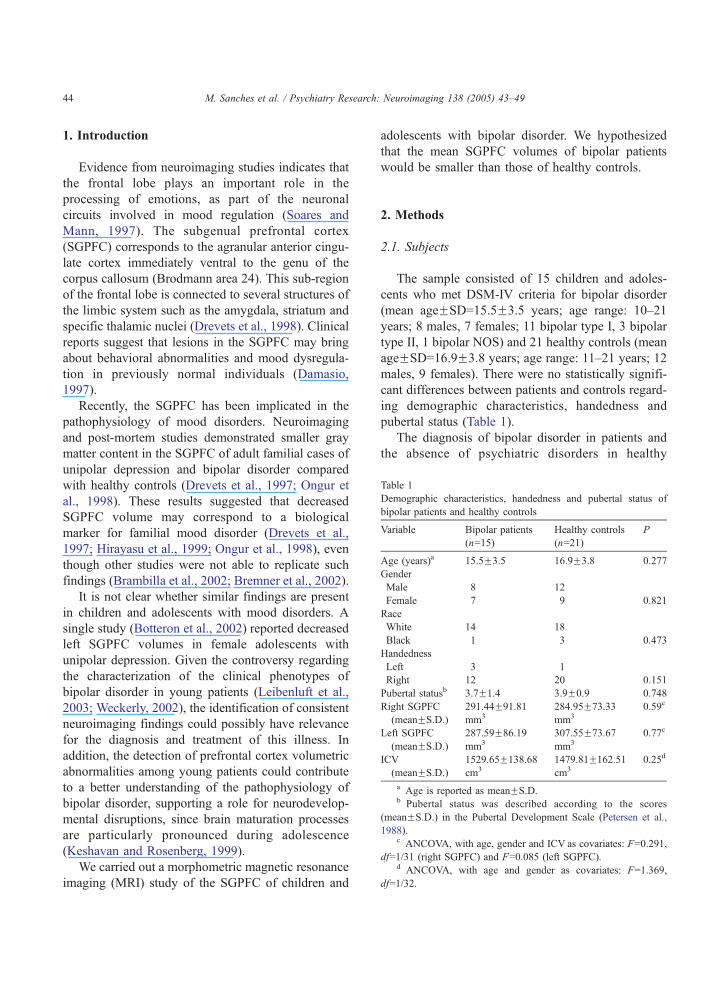
Table 1
Demographic characteristics, handedness and pubertal status of
bipolar patients and healthy controls
Variable Bipolar patients
(n=15)
Healthy controls
(n=21)
P
Age (years)a 15.5F3.5 16.9F3.8 0.277
Gender
Male 8 12
Female 7 9 0.821
Race
White 14 18
Black 1 3 0.473
Handedness
Left 3 1
Right 12 20 0.151
Pubertal statusb 3.7F1.4 3.9F0.9 0.748
Right SGPFC
(meanFS.D.)
291.44F91.81
mm3
284.95F73.33
mm3
0.59c
Left SGPFC
(meanFS.D.)
287.59F86.19
mm3
307.55F73.67
mm3
0.77c
ICV
(meanFS.D.)
1529.65F138.68
cm3
1479.81F162.51
cm3
0.25d
a Age is reported as meanFS.D.b Pubertal status was described according to the scores
(meanFS.D.) in the Pubertal Development Scale (Petersen et al.,
1988).c ANCOVA, with age, gender and ICV as covariates: F=0.291,
df=1/31 (right SGPFC) and F=0.085 (left SGPFC).d ANCOVA, with age and gender as covariates: F=1.369,
df=1/32.
M. Sanches et al. / Psychiatry Research: Neuroimaging 138 (2005) 43–4944
1. Introduction
Evidence from neuroimaging studies indicates that
the frontal lobe plays an important role in the
processing of emotions, as part of the neuronal
circuits involved in mood regulation (Soares and
Mann, 1997). The subgenual prefrontal cortex
(SGPFC) corresponds to the agranular anterior cingu-
late cortex immediately ventral to the genu of the
corpus callosum (Brodmann area 24). This sub-region
of the frontal lobe is connected to several structures of
the limbic system such as the amygdala, striatum and
specific thalamic nuclei (Drevets et al., 1998). Clinical
reports suggest that lesions in the SGPFC may bring
about behavioral abnormalities and mood dysregula-
tion in previously normal individuals (Damasio,
1997).
Recently, the SGPFC has been implicated in the
pathophysiology of mood disorders. Neuroimaging
and post-mortem studies demonstrated smaller gray
matter content in the SGPFC of adult familial cases of
unipolar depression and bipolar disorder compared
with healthy controls (Drevets et al., 1997; Ongur et
al., 1998). These results suggested that decreased
SGPFC volume may correspond to a biological
marker for familial mood disorder (Drevets et al.,
1997; Hirayasu et al., 1999; Ongur et al., 1998), even
though other studies were not able to replicate such
findings (Brambilla et al., 2002; Bremner et al., 2002).
It is not clear whether similar findings are present
in children and adolescents with mood disorders. A
single study (Botteron et al., 2002) reported decreased
left SGPFC volumes in female adolescents with
unipolar depression. Given the controversy regarding
the characterization of the clinical phenotypes of
bipolar disorder in young patients (Leibenluft et al.,
2003; Weckerly, 2002), the identification of consistent
neuroimaging findings could possibly have relevance
for the diagnosis and treatment of this illness. In
addition, the detection of prefrontal cortex volumetric
abnormalities among young patients could contribute
to a better understanding of the pathophysiology of
bipolar disorder, supporting a role for neurodevelop-
mental disruptions, since brain maturation processes
are particularly pronounced during adolescence
(Keshavan and Rosenberg, 1999).
We carried out a morphometric magnetic resonance
imaging (MRI) study of the SGPFC of children and
adolescents with bipolar disorder. We hypothesized
that the mean SGPFC volumes of bipolar patients
would be smaller than those of healthy controls.
2. Methods
2.1. Subjects
The sample consisted of 15 children and adoles-
cents who met DSM-IV criteria for bipolar disorder
(mean ageFSD=15.5F3.5 years; age range: 10–21
years; 8 males, 7 females; 11 bipolar type I, 3 bipolar
type II, 1 bipolar NOS) and 21 healthy controls (mean
ageFSD=16.9F3.8 years; age range: 11–21 years; 12
males, 9 females). There were no statistically signifi-
cant differences between patients and controls regard-
ing demographic characteristics, handedness and
pubertal status (Table 1).
The diagnosis of bipolar disorder in patients and
the absence of psychiatric disorders in healthy

M. Sanches et al. / Psychiatry Research: Neuroimaging 138 (2005) 43–49 45
controls was established through the Schedule for
Affective Disorders and Schizophrenia for School-
Age Children—Present and Lifetime Version (Kauf-
man et al., 1997); the Structured Clinical Interview for
DSM-IV (Spitzer et al., 1994) was used instead
subjects were 18 or older. Trained postdoctoral
fellows and study coordinators administered the
diagnostic instruments to the subjects and their
parents, and the results were reviewed by a senior
study psychiatrist. The information obtained was
supplemented by review of the patients’ medical
charts.
Exclusion criteria included mental retardation,
previous head trauma with loss of consciousness for
more than 1 h, and report of substance abuse during
the 6 months that preceded the interview.
Among the bipolar patients, 13 were euthymic
(Hamilton Depression Rating Scale score b8 and
Young Mania Rating Scale score b6) and 2 were
mildly depressed (Hamilton Depression Rating Scale
scores between 8 and 13). All reported a familial
history of mood disorders, defined as having a first-
degree relative who ever received a diagnosis of
unipolar or bipolar disorder. Thirteen patients were
receiving mood-stabilizing treatment for bipolar dis-
order (six on lithium, three on valproate and four on
lithium plus valproate). The doses of lithium ranged
from 675 to 1350 mg/day, and the blood levels from
0.4 to1.26 mEq/l. The doses of valproate ranged from
500 to 2000 mg/day, and the blood levels ranged from
10 to 150 Ag/ml. Ten patients reported previous use of
antipsychotic drugs.
The mean duration of the disease was 3.8 (S.D.=2.4,
median 4.5) years. Comorbid mental disorders were
found in seven patients and consisted of attention-
deficit/hypeactivity disorder (five subjects), opposi-
tional defiant disorder (one subject) and conduct
disorder (one subject). This study was approved by
the University of Pittsburgh Institutional Review
Board, and informed consent was obtained from all
subjects and their parents or legal representatives.
2.2. MRI procedure
MR images were obtained with a 1.5 T GE Signa
Imaging System running the program Signa 5.4.3
(General Electric Medical Systems, Milwaukee, WI)
at the University of Pittsburgh. Images were acquired
using 3D-gradient echo imaging (Spoiled Gradient
Recalled Acquisition) in the coronal plane (TR=25
ms, TE=5 ms, nutation angle=408, FOV=24 cm, slice
thickness=1.5 mm, NEX=1, matrix size=256�192). A
sagittal scout series was first obtained to verify the
position of the subject and to locate a midline sagittal
slice. A T1-weighted sagittal scout image was
obtained for graphic prescription of the coronal
images. To screen for neuroradiological abnormalities,
T2 and proton density images were obtained in the
axial plane. The 3D SPGR images were realigned to
the AC-PC line before volumetric measurements of
the SGPFC were performed.
2.3. SGPFC measurement
SGPFC measurements were obtained using the
semi-automated software MedX version 3.2 (Sensor
System, Sterling, VA). Manual tracing was performed
by a trained evaluator (intra-class correlation coef-
ficient r=0.92 for the right SGPFC and r=0.94 for the
left SGPFC), according to methods proposed by
Drevets et al. (1997). Likewise, intra-cranial volumes
(ICV) were obtained by another trained evaluator
(ICC=0.98) using the semi-automated software Scion
Image Beta-4.0.2 for Windows (Scion, Frederick,
MD, USA). The evaluators were blind to subjectsTdiagnosis and identity.
2.4. Anatomical landmarks
2.4.1. SGPFC
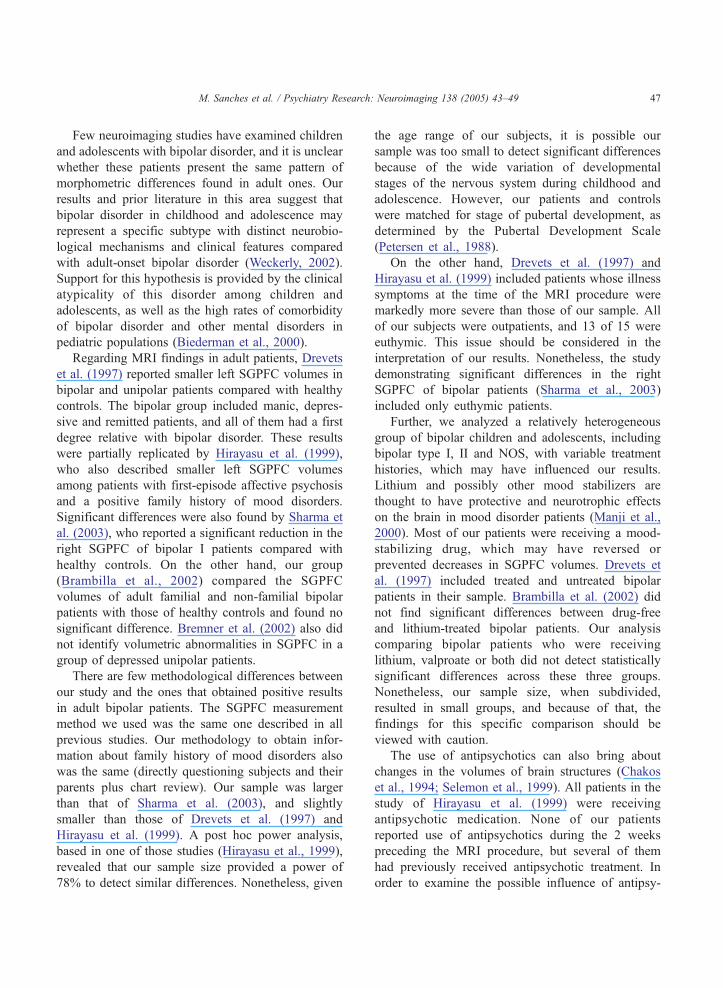
The gray matter of the gyrus immediately below
the corpus callosum was traced in the coronal plane,
after realigning the images along the anterior–poste-
rior commissure line (Fig. 1). Tracing started at the
most rostral slice where the corpus callosum could be
seen and continued to the slice anterior to the one
where the internal capsule no longer divided the
striatum. The tracing procedure was exactly as
previously reported (Brambilla et al., 2002).
2.4.2. ICV
The outer border of the brain was traced in the
coronal plane from the most anterior to the most
posterior slice that contained brain matter. Total
cerebral gray and white matter, cerebro-spinal fluid,
dura matter and sinuses were included in the tracing.
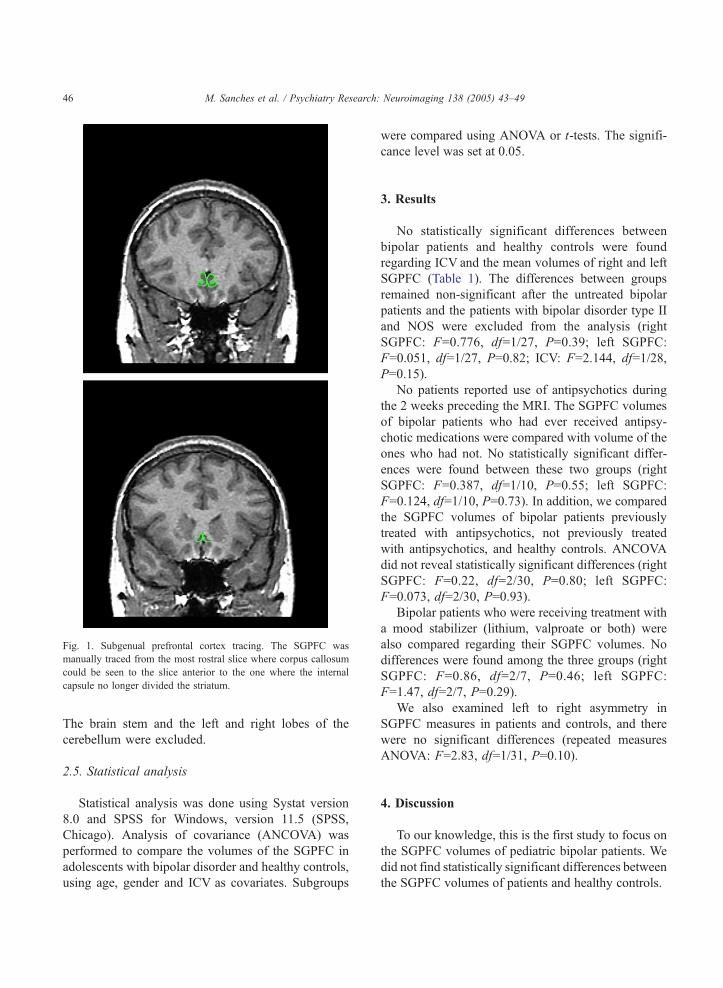
Fig. 1. Subgenual prefrontal cortex tracing. The SGPFC was
manually traced from the most rostral slice where corpus callosum
could be seen to the slice anterior to the one where the internal
capsule no longer divided the striatum.
M. Sanches et al. / Psychiatry Research: Neuroimaging 138 (2005) 43–4946
The brain stem and the left and right lobes of the
cerebellum were excluded.
2.5. Statistical analysis
Statistical analysis was done using Systat version
8.0 and SPSS for Windows, version 11.5 (SPSS,
Chicago). Analysis of covariance (ANCOVA) was
performed to compare the volumes of the SGPFC in
adolescents with bipolar disorder and healthy controls,
using age, gender and ICV as covariates. Subgroups
were compared using ANOVA or t-tests. The signifi-
cance level was set at 0.05.
3. Results
No statistically significant differences between
bipolar patients and healthy controls were found
regarding ICV and the mean volumes of right and left
SGPFC (Table 1). The differences between groups
remained non-significant after the untreated bipolar
patients and the patients with bipolar disorder type II
and NOS were excluded from the analysis (right
SGPFC: F=0.776, df=1/27, P=0.39; left SGPFC:
F=0.051, df=1/27, P=0.82; ICV: F=2.144, df=1/28,
P=0.15).
No patients reported use of antipsychotics during
the 2 weeks preceding the MRI. The SGPFC volumes
of bipolar patients who had ever received antipsy-
chotic medications were compared with volume of the
ones who had not. No statistically significant differ-
ences were found between these two groups (right
SGPFC: F=0.387, df=1/10, P=0.55; left SGPFC:
F=0.124, df=1/10, P=0.73). In addition, we compared
the SGPFC volumes of bipolar patients previously
treated with antipsychotics, not previously treated
with antipsychotics, and healthy controls. ANCOVA
did not reveal statistically significant differences (right
SGPFC: F=0.22, df=2/30, P=0.80; left SGPFC:
F=0.073, df=2/30, P=0.93).
Bipolar patients who were receiving treatment with
a mood stabilizer (lithium, valproate or both) were
also compared regarding their SGPFC volumes. No
differences were found among the three groups (right
SGPFC: F=0.86, df=2/7, P=0.46; left SGPFC:
F=1.47, df=2/7, P=0.29).
We also examined left to right asymmetry in
SGPFC measures in patients and controls, and there
were no significant differences (repeated measures
ANOVA: F=2.83, df=1/31, P=0.10).
4. Discussion
To our knowledge, this is the first study to focus on
the SGPFC volumes of pediatric bipolar patients. We
did not find statistically significant differences between
the SGPFC volumes of patients and healthy controls.
M. Sanches et al. / Psychiatry Research: Neuroimaging 138 (2005) 43–49 47
Few neuroimaging studies have examined children
and adolescents with bipolar disorder, and it is unclear
whether these patients present the same pattern of
morphometric differences found in adult ones. Our
results and prior literature in this area suggest that
bipolar disorder in childhood and adolescence may
represent a specific subtype with distinct neurobio-
logical mechanisms and clinical features compared
with adult-onset bipolar disorder (Weckerly, 2002).
Support for this hypothesis is provided by the clinical
atypicality of this disorder among children and
adolescents, as well as the high rates of comorbidity
of bipolar disorder and other mental disorders in
pediatric populations (Biederman et al., 2000).
Regarding MRI findings in adult patients, Drevets
et al. (1997) reported smaller left SGPFC volumes in
bipolar and unipolar patients compared with healthy
controls. The bipolar group included manic, depres-
sive and remitted patients, and all of them had a first
degree relative with bipolar disorder. These results
were partially replicated by Hirayasu et al. (1999),
who also described smaller left SGPFC volumes
among patients with first-episode affective psychosis
and a positive family history of mood disorders.
Significant differences were also found by Sharma et
al. (2003), who reported a significant reduction in the
right SGPFC of bipolar I patients compared with
healthy controls. On the other hand, our group
(Brambilla et al., 2002) compared the SGPFC
volumes of adult familial and non-familial bipolar
patients with those of healthy controls and found no
significant difference. Bremner et al. (2002) also did
not identify volumetric abnormalities in SGPFC in a
group of depressed unipolar patients.
There are few methodological differences between
our study and the ones that obtained positive results
in adult bipolar patients. The SGPFC measurement
method we used was the same one described in all
previous studies. Our methodology to obtain infor-
mation about family history of mood disorders also
was the same (directly questioning subjects and their
parents plus chart review). Our sample was larger
than that of Sharma et al. (2003), and slightly
smaller than those of Drevets et al. (1997) and
Hirayasu et al. (1999). A post hoc power analysis,
based in one of those studies (Hirayasu et al., 1999),
revealed that our sample size provided a power of
78% to detect similar differences. Nonetheless, given
the age range of our subjects, it is possible our
sample was too small to detect significant differences
because of the wide variation of developmental
stages of the nervous system during childhood and
adolescence. However, our patients and controls
were matched for stage of pubertal development, as
determined by the Pubertal Development Scale
(Petersen et al., 1988).
On the other hand, Drevets et al. (1997) and
Hirayasu et al. (1999) included patients whose illness
symptoms at the time of the MRI procedure were
markedly more severe than those of our sample. All
of our subjects were outpatients, and 13 of 15 were
euthymic. This issue should be considered in the
interpretation of our results. Nonetheless, the study
demonstrating significant differences in the right
SGPFC of bipolar patients (Sharma et al., 2003)
included only euthymic patients.
Further, we analyzed a relatively heterogeneous
group of bipolar children and adolescents, including
bipolar type I, II and NOS, with variable treatment
histories, which may have influenced our results.
Lithium and possibly other mood stabilizers are
thought to have protective and neurotrophic effects
on the brain in mood disorder patients (Manji et al.,
2000). Most of our patients were receiving a mood-
stabilizing drug, which may have reversed or
prevented decreases in SGPFC volumes. Drevets et
al. (1997) included treated and untreated bipolar
patients in their sample. Brambilla et al. (2002) did
not find significant differences between drug-free
and lithium-treated bipolar patients. Our analysis
comparing bipolar patients who were receiving
lithium, valproate or both did not detect statistically
significant differences across these three groups.
Nonetheless, our sample size, when subdivided,
resulted in small groups, and because of that, the
findings for this specific comparison should be
viewed with caution.
The use of antipsychotics can also bring about
changes in the volumes of brain structures (Chakos
et al., 1994; Selemon et al., 1999). All patients in the
study of Hirayasu et al. (1999) were receiving
antipsychotic medication. None of our patients
reported use of antipsychotics during the 2 weeks
preceding the MRI procedure, but several of them
had previously received antipsychotic treatment. In
order to examine the possible influence of antipsy-
M. Sanches et al. / Psychiatry Research: Neuroimaging 138 (2005) 43–4948
chotic use on our findings, we compared bipolar
patients with and without previous antipsychotic
therapy. We found neither statistically significant
differences between treated and untreated groups of
bipolar patients, nor between patients and healthy
controls.
Because childhood and adolescence are important
transitional phases regarding maturation of the
nervous system (Bartzokis et al., 2001; Giedd et
al., 1999), studies involving young psychiatric
patients may provide valuable information about
the role of neurodevelopmental processes in the
pathophysiology of mental disorders, as well as
about the timing of some brain abnormalities found
in adults (Friedman et al., 1999; Keshavan and
Rosenberg, 1999). This may be especially important
when frontal lobe abnormalities are considered, since
this brain region seems to show particularly impor-
tant changes between adolescence and early adult-
hood (Sowell et al., 1999). Even though Botteron et
al. (2002) described the same finding of decreased
left SGPFC volume among adolescents and middle-
aged women with unipolar depression, no similar
studies were carried out among bipolar patients.
Therefore, an alternative explanation to our negative
findings is that SGPFC abnormalities in bipolar
disorder may be observed late in the course of the
illness and cannot be found in its earliest phases.
Nonetheless, findings by Brambilla et al. (2002)
suggest that such abnormalities are only present in
severely ill patient samples.
In conclusion, the results of our study suggest no
abnormalities in the SGPFC of children and adoles-
cents with bipolar disorder. Future studies should
examine untreated patients and involve longitudinal
designs to compare the volumes of the SGPFC before
and after psychotropic treatment and across various
phases of the illness.
Acknowledgments
This work was partly supported by grants MH
01736, MH 55123, MH 30915 and MH 59929 from
the National Institute of Mental Health, NARSAD, the
Krus Endowed Chair in Psychiatry (The University of
Texas Health Science Center at San Antonio) and
CAPES Foundation (Brazil).
References
Bartzokis, G., Beckson, M., Lu, P.H., Nuechterlein, K.H., Edwards,
N., Mintz, J., 2001. Age-related changes in frontal and temporal
lobe volumes in men: a magnetic resonance imaging study.
Archives of General Psychiatry 58, 461–465.
Biederman, J., Mick, E., Faraone, S.V., Spencer, T., Wilens, T.E.,
Wozniak, J., 2000. Pediatric mania: a developmental subtype of
bipolar disorder? Biological Psychiatry 48, 458–466.
Botteron, K.N., Raichle, M.E., Drevets, W.C., Heath, A.C., Todd,
R.D., 2002. Volumetric reduction in left subgenual prefrontal
cortex in early onset depression. Biological Psychiatry 51,
342–344.
Brambilla, P., Nicoletti, M.A., Harenski, K., Sassi, R.B., Mallinger,
A.G., Frank, E., Kupfer, D.J., Keshavan, M.S., Soares, J.C.,
2002. Anatomical MRI study of subgenual prefrontal cortex in
bipolar and unipolar subjects. Neuropsychopharmacology 27,
792–799.
Bremner, J.D., Vythilingam, M., Vermetten, E., Nazeer, A., Adil, J.,
Khan, S., Staib, L.H., Charney, D.S., 2002. Reduced volume of
orbitofrontal cortex in major depression. Biological Psychiatry
51 (4), 273–279.
Chakos, M.H., Lieberman, J.A., Bilder, R.M., Borenstein, M.,
Lerner, G., Bogerts, B., Wu, H., Kinon, B., Ashtari, M., 1994.
Increase in caudate nuclei volumes of first-episode schizo-
phrenic patients taking antipsychotic drugs. American Journal of
Psychiatry 151, 1430–1436.
Damasio, A.R., 1997. Neuropsychology. Towards a neuropathology
of emotion and mood. Nature 386, 769–770.
Drevets, W.C., Price, J.L., Simpson Jr., J.R., Todd, R.D., Reich, T.,
Vannier, M., Raichle, M.E., 1997. Subgenual prefrontal cortex
abnormalities in mood disorders. Nature 386, 824–827.
Drevets, W.C., Ongur, D., Price, J.L., 1998. Neuroimaging
abnormalities in the subgenual prefrontal cortex: implications
for the pathophysiology of familial mood disorders. Molecular
Psychiatry 3 (220–226), 190–221.
Friedman, L., Findling, R.L., Kenny, J.T., Swales, T.P., Stuve, T.A.,
Jesberger, J.A., Lewin, J.S., Schulz, S.C., 1999. An MRI study
of adolescent patients with either schizophrenia or bipolar
disorder as compared to healthy control subjects. Biological
Psychiatry 46, 78–88.
Giedd, J.N., Blumenthal, J., Jeffries, N.O., Castellanos, F.X.,
Liu, H., Zijdenbos, A., Paus, T., Evans, A.C., Rapoport,
J.L., 1999. Brain development during childhood and ado-
lescence: a longitudinal MRI study. Nature Neuroscience 2,
861–863.
Hirayasu, Y., Shenton, M.E., Salisbury, D.F., Kwon, J.S., Wible,
C.G., Fischer, I.A., Yurgelun-Todd, D., Zarate, C., Kikinis, R.,
Jolesz, F.A., McCarley, R.W., 1999. Subgenual cingulate cortex
volume in first-episode psychosis. American Journal of Psy-
chiatry 156, 1091–1093.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P.,
Williamson, D., Ryan, N., 1997. Schedule for Affective
Disorders and Schizophrenia for School-age Children—present
and lifetime version (K-SADS-PL): initial reliability and
validity data. Journal of the American Academy of Child and
Adolescent Psychiatry 36, 980–988.
M. Sanches et al. / Psychiatry Research: Neuroimaging 138 (2005) 43–49 49
Keshavan, M.S., Rosenberg, D.R., 1999. New trends in devel-
opmental neuroimaging in psychiatry. Progress in Neuro-
Psychopharmacology & Biological Psychiatry 23, 557–560.
Leibenluft, E., Charney, D.S., Towbin, K.E., Bhangoo, R.K., Pine,
D.S., 2003. Defining clinical phenotypes of juvenile mania.
American Journal of Psychiatry 160, 430–437.
Manji, H.K., Moore, G.J., Chen, G., 2000. Clinical and preclinical
evidence for the neurotrophic effects of mood stabilizers:
implications for the pathophysiology and treatment of manic-
depressive illness. Biological Psychiatry 48, 740–754.
Ongur, D., Drevets, W.C., Price, J.L., 1998. Glial reduction in the
subgenual prefrontal cortex in mood disorders. Proceedings of
the National Academy of Science of the United States of
America 95, 13290–13295.
Petersen, A.C., Crockett, L., Richards, M., Boxer, A., 1988. A self-
report measure of pubertal status: reliability, validity, and initial
norms. Journal of Youth and Adolescence 17, 117–133.
Selemon, L.D., Lidow, M.S., Goldman-Rakic, P.S., 1999. Increased
volume and glial density in primate prefrontal cortex associated
with chronic antipsychotic drug exposure. Biological Psychiatry
46, 161–172.
Sharma, V., Menon, R., Carr, T.J., Densmore, M., Mazmanian, D.,
Williamson, P.C., 2003. An MRI study of subgenual prefrontal
cortex in patients with familial and non-familial bipolar I
disorder. Journal of Affective Disorders 77 (2), 167–171.
Soares, J.C., Mann, J.J., 1997. The anatomy of mood disorders—
review of structural neuroimaging studies. Biological Psychiatry
41, 86–106.
Sowell, E.R., Thompson, P.M., Holmes, C.J., Jernigan, T.L., Toga,
A.W., 1999. In vivo evidence for post-adolescent brain
maturation in frontal and striatal regions. Nature Neuroscience
2 (10), 859–861.
Spitzer, R.L., Williams, J.B.W., Gibbon, M., Williams, J.B.W.,
1994. Structured Clinical Interview for DSM-IV (SCID-IV).
American Psychiatric Press, Washington, DC.
Weckerly, J., 2002. Pediatric bipolar mood disorder. Journal of
Developmental and Behavioural Pediatrics 23, 42–56.