Study of 2708 heroin-related deaths in north-eastern Italy 1985-98 to establish the main causes of...
11
Addiction (2001) 96, 1127–1137 RESEARCH REPORT Study of 2708 heroin-related deaths in north-eastern Italy 1985–98 to establish the main causes of death GIANLUCA QUAGLIO, 1 GIORGIO TALAMINI, 2 ALESSANDRO LECHI, 2 LUCA VENTURINI, 1 FABIO LUGOBONI, 1 GRUPPO INTERSERT DI COLLABORAZIONE SCIENTIFICA (GICS)* & PAOLO MEZZELANI 1 1 Medical Service for Addictive Disorders, Department of Internal Medicine, University of Verona, Italy, 2 Department of Internal Medicine, University of Verona, Italy & *Gruppo Intersert di Collaborazione Scienti ca (GICS) [Group for Co-operation between Public Health Authority Centres for Drug Users], Italy Abstract Aims. To ascertain the causes of deaths among a very large cohort of heroin injecting drug users (IDUs) who, from 1985 to 1998, attended 36 Public Health Authority Centres for Drug Users (PCDUs) in north-eastern Italy. Design. Retrospective analysis of data, obtained from the Annual Register of each Centre and the Municipal Registry Of ce of each local health district. Setting. Thirty-six PCDUs in north-eastern Italy and Medical Service for Addictive Disorders of the University of Verona. Participants. All IDUs who had sought medical care at least once in the PCDUs during the study period. Findings. Of 2708 deaths, overdose was found to be the major cause (37%), followed by AIDS (32.5%) and road accidents (9.4%). The percentage of deaths due to AIDS increased steadily from 2.7% in 1985 to 42.2% in 1996, and then decreased to 16.9% in 1998. Deaths due to overdose remained almost constant. The average age of death per year rose from 26 in the mid eighties to 34 in 1998. The mortality rate among IDUs proved much higher compared to the general population of the same age (13-fold, 95% CI, 11.3–14.6). The proportion of all deaths attributable to regular use of illegal opiates in the 15–34 age group in the general population in 1991 was 16%. HIV prevalence was not a signi cant factor in suicides and deaths by overdose. Conclusions. The mortality rate was 13 times greater than in the general population. To be female and to have dropped out of any kind of treatment proved an important risk factor for overdose. The fall in deaths from AIDS enhances the problem to prevent and treat HCV infection. Decisions in drug projects, in research and in training should be in uenced by the strikingly high percentage of deaths due to drug use. * Members of GICS active in collecting data include: F. Arisi, E. Baggio, V. Balestra, D. Barbiero, G. Bellio, M. Bortolomasi, C. Bossi, R. Bressan, R. Bricolo, D. Cantiero, C. Capra, L. Carraro, F. Celeghin, R. Ceravolo, G. Cicciu ` , P. Civitelli, F. Corso, D. Danieli, D. Dariol, E. Dellantonio, G. Didone `, B. Durano, M. Faccini, S. Ferrari, D. Ferremi, G. Forza, M. Frezza, G. Ghirardello, MA. Giacomin, R. Giusto, F. Guidoboni, E. Levarda, A. Lo Russo, R. Lovaste, G. Mantovani, E. Manzato, M. Mazzo, V. Mecenero, PG. Nardi, A. Padovani, A. Pani, A. Parolin, P. Pili, S. Polli, M. Residori, A. Rovea, R. Sabbion, C. Saccardi, L. Sartori, M. Scaggiante, A. Scandolari, F. Schifano, C. Smacchia, K. Sonnerer, I. Spilimbergo, C. Stimolo, P. Tito, V. Vasi, A. Vendramin, F. Viviani, M. Von Solder, F. Zuin. Correspondence to: Prof. Paolo Mezzelani MD, Medical Service for Addictive Disorders, University of Verona, Policlinico GB Rossi, 37134 Verona, Italy. Tel: 1 1 39 045 8074604; fax: 1 1 39 045 8074269; e-mail: [email protected] Submitted 19th April 2000; initial review completed 23rd June 2000; nal version accepted 8th February 2001. ISSN 0965–2140 print/ISSN 1360–0443 online/01/081127–11 Ó Society for the Study of Addiction to Alcohol and Other Drugs Carfax Publishing, Taylor & Francis Limited DOI: 10.1080/09652140120060725
Transcript of Study of 2708 heroin-related deaths in north-eastern Italy 1985-98 to establish the main causes of...

Addiction (2001) 96, 1127–1137
RESEARCH REPORT
Study of 2708 heroin-related deaths innorth-eastern Italy 1985–98 to establish themain causes of death
GIANLUCA QUAGLIO,1 GIORGIO TALAMINI,2
ALESSANDRO LECHI,2 LUCA VENTURINI,1 FABIO LUGOBONI,1
GRUPPO INTERSERT DI COLLABORAZIONE SCIENTIFICA(GICS)* & PAOLO MEZZELANI1
1Medical Service for Addictive Disorders, Department of Internal Medicine,University of Verona, Italy, 2Department of Internal Medicine, University of Verona,Italy & *Gruppo Intersert di Collaborazione Scienti� ca (GICS) [Group for Co-operationbetween Public Health Authority Centres for Drug Users], Italy
AbstractAims. To ascertain the causes of deaths among a very large cohort of heroin injecting drug users (IDUs)who, from 1985 to 1998, attended 36 Public Health Authority Centres for Drug Users (PCDUs) innorth-eastern Italy. Design. Retrospective analysis of data, obtained from the Annual Register of eachCentre and the Municipal Registry Of� ce of each local health district. Setting. Thirty-six PCDUs innorth-eastern Italy and Medical Service for Addictive Disorders of the University of Verona. Participants.All IDUs who had sought medical care at least once in the PCDUs during the study period. Findings. Of2708 deaths, overdose was found to be the major cause (37%), followed by AIDS (32.5%) and roadaccidents (9.4%). The percentage of deaths due to AIDS increased steadily from 2.7% in 1985 to 42.2%in 1996, and then decreased to 16.9% in 1998. Deaths due to overdose remained almost constant. Theaverage age of death per year rose from 26 in the mid eighties to 34 in 1998. The mortality rate among IDUsproved much higher compared to the general population of the same age (13-fold, 95% CI, 11.3–14.6). Theproportion of all deaths attributable to regular use of illegal opiates in the 15–34 age group in the generalpopulation in 1991 was 16%. HIV prevalence was not a signi� cant factor in suicides and deaths by overdose.Conclusions. The mortality rate was 13 times greater than in the general population. To be female and tohave dropped out of any kind of treatment proved an important risk factor for overdose. The fall in deathsfrom AIDS enhances the problem to prevent and treat HCV infection. Decisions in drug projects, in researchand in training should be in� uenced by the strikingly high percentage of deaths due to drug use.
* Members of GICS active in collecting data include: F. Arisi, E. Baggio, V. Balestra, D. Barbiero, G. Bellio, M.Bortolomasi, C. Bossi, R. Bressan, R. Bricolo, D. Cantiero, C. Capra, L. Carraro, F. Celeghin, R. Ceravolo, G. Cicciu, P.Civitelli, F. Corso, D. Danieli, D. Dariol, E. Dellantonio, G. Didone, B. Durano, M. Faccini, S. Ferrari, D. Ferremi, G.Forza, M. Frezza, G. Ghirardello, MA. Giacomin, R. Giusto, F. Guidoboni, E. Levarda, A. Lo Russo, R. Lovaste, G.Mantovani, E. Manzato, M. Mazzo, V. Mecenero, PG. Nardi, A. Padovani, A. Pani, A. Parolin, P. Pili, S. Polli, M. Residori,A. Rovea, R. Sabbion, C. Saccardi, L. Sartori, M. Scaggiante, A. Scandolari, F. Schifano, C. Smacchia, K. Sonnerer, I.Spilimbergo, C. Stimolo, P. Tito, V. Vasi, A. Vendramin, F. Viviani, M. Von Solder, F. Zuin.
Correspondence to: Prof. Paolo Mezzelani MD, Medical Service for Addictive Disorders, University of Verona,Policlinico GB Rossi, 37134 Verona, Italy. Tel: 1 1 39 045 8074604; fax: 1 1 39 045 8074269; e-mail:[email protected]
Submitted 19th April 2000; initial review completed 23rd June 2000; � nal version accepted 8th February 2001.
ISSN 0965–2140 print/ISSN 1360–0443 online/01/081127–11 Ó Society for the Study of Addiction to Alcohol and Other Drugs
Carfax Publishing, Taylor & Francis Limited
DOI: 10.1080/09652140120060725

1128 Gianluca Quaglio et al.
IntroductionThe mortality rate of injecting drug users (IDUs)is far higher than in the general population of thesame age and sex.1–4 After the appearance of HIV,the AIDS epidemic contributed greatly to a fur-ther increase in mortality among drug users.5–8
Several studies have been carried out on thenumber and causes of deaths of IDUs in order toassess whether the drug problem is becomingmore or less serious.
Unfortunately, most studies of regular illegalopiate use and mortality have been limited9–12
and, as a consequence, many estimates of in-creased mortality due to illegal opiate use areopen to question. Moreover, dif� culties in ob-taining information on the causes of death cou-pled with a lack of accurate information on theappropriate base population, above all the num-ber of drug users, means that the reliability ofthese studies is far from certain.
This research takes into account more thandouble the number of deaths investigated in apreviously published study13 by the authors. Itwas carried out in the Veneto Region and itsneighbouring Region, Trentino-Alto-Adige, with10 Public Health Authority Centres for DrugUsers (PCDUs) included for the � rst time. Datacollection was extended from 1985 to 1998. Weanalysed the causes of death of IDUs attending36 PCDUs.
All PCDUs contributing data were part of aGroup for Co-operation between Public HealthAuthority Centres (known by the Italianacronym GICS) dealing with drug problems.Since 1985, GICS has fostered links between theUniversity of Verona and PCDUs with data in-terchange and mutual scienti� c support.
In Italy, with a population of 58 000 000,there are 569 PCDUs, with a catchment area ofabout 100 000 inhabitants on average. Very dif-ferent numbers of IDUs attend the centres, rang-ing in different regions from less than 100 tomore than 1000 patients. These publicly fundedPCDUs provide counselling, treatment for drugwithdrawal, short-term detoxi� cation with low-dose methadone, methadone maintenance pro-grammes, naltrexone programmes, selection fortherapeutic communities, psychotherapy and soon. Moreover these centres deal with medicalproblems related to addiction such as the assess-ment of liver function, vaccination against HBV,HIV testing, etc.14
North-eastern Italy (Veneto and Trentino-Alto-Adige Regions) is an industrialized areawith an average population density of 170 inhab-itants per square km,15 an unemployment rate of3.95%, very low illiteracy (only among the eld-erly); 4.9% of the population are graduates16 andGDP (in Euro) per inhabitant in 1996 was19 000 (Italian mean GDP 5 15 300 Euro in1996).17 During the years of the study druglegislation was reformed several times, althoughprohibition of all drugs such as heroin, cocaineand cannabinoids remained throughout.
The most noteworthy result of this researchproved to be the dramatic decrease of deaths dueto AIDS and the unchanged death rate due tooverdose, which now represents the principalcause of death; there was a much higher mor-tality rate among IDUs than in the general popu-lation. HIV prevalence was not a signi� cantfactor in the causes of death from overdose andsuicides.
MethodsStudy populationThe study was conducted retrospectively on apopulation of 4 960 000 inhabitants, corre-sponding to 36 PCDUs.
Eligible patients for this study included allIDUs who had sought medical care at least oncein the PCDUs during the study period. All IDUswere white Caucasian opiate users, with the pos-sibility that some were users of other drugs. Thetotal number of IDUs who sought medical carein the 36 PCDUs in the period 1985–98 was33 072. The number of 2708 deaths refers exclu-sively to this number.
To evaluate the relationship between the mor-tality of IDUs and the general population, IDUswho attended PCDUs in 1991, the year of thelast census of the Italian population, were con-sidered, and expected mortality was calculatedon the basis of sex and divided into age groupsstaggered by 5 years.
How mortality data were obtainedThe Annual Register of each Centre and theMunicipal Registry Of� ce of each local healthdistrict were consulted to determine the causesof death. In addition to the information providedon the death certi� cate, more detailed infor-mation from clinical records of the PCDUs and,

Heroin-related deaths in north-eastern Italy 1129
general population in the two Italian Regions(Veneto and Trentino Alto Adige)19,20 involvedin the study. After correction for age and sex onthe basis of the latest census, the observed/ex-pected (O/E) ratio corresponds to the standard-ized mortality ratio (SMR). For the comparisonof observed and expected events,21 tests wereused based on the assumption that the observedcases of death presented a Poisson distribution.Byar’s approximation was used to calculate theSMR con� dence limits21 (p , 0.05 was con-sidered signi� cant). All the information gatheredwas processed with an SPSS (SPSS Inc.,Chicago, IL, USA) statistical program.
ResultsCauses of deathThe causes of 2708 deaths were evaluated(Table 1): 2270 (84%) males and 438 (16%)females. The ratio of males to females was there-fore 5.25:1, re� ecting the ratio of IDUs whoattended the PCDUs in north-eastern Italy (5:1).Overdose was found to be the major cause(37%), followed by AIDS (32.5%), road acci-dents (9.4%); suicide (5.5%), and liver diseases(3.5%); unknown causes accounted for 6.8%,and other causes for 5%.
Among males, the principal cause of death wasoverdose (38.6%), followed by AIDS (31%);whereas in females the principal cause was AIDS(41%) followed by overdose (28.5%). This com-parison between causes of death and gender wassigni� cant ( v 2: p , 0.001). Until 1991 the princi-pal cause of death was overdose, followed byAIDS (Fig. 1); from 1992 to 1996 inclusively,AIDS became the principal cause of death fol-lowed by overdose which again represented theprincipal cause of death from 1997 onwards.
whenever available, hospital charts (in 20% ofcases) or autopsy reports (very rarely carried out)were used. Causes of death were divided intoseven categories: overdose, AIDS, road accident,suicide, liver disease (cirrhosis and hepatocar-cinoma), others (accident, homicide, malignantneoplasm, cerebrovascular disease, heart disease,infectious disease and ill-de� ned conditions) andunknown causes. Unlike previous studies, roadaccidents were considered suf� ciently distinct todeserve a separate category, due to the highnumbers. This enabled an independent evalu-ation to be made without confusion with othercauses of violent death.
In accordance with van Haastrecht et al.,18
drug-related death is de� ned as accidental over-dose in cases of evident recent drug use undercircumstances that do not suggest other causesof death (presence of drug, a syringe or para-phernalia such as a tourniquet, a spoon, lemonor citric acid, cotton wool near the victim) andsuicide when death appears self-in� icted andpremeditated (e.g. accompanied by a suicidenote). A patient with AIDS at the time of deathwas considered an AIDS mortality if othercauses were excluded. In accordance with Galli& Musicco5 the cause of death was consideredunknown if the information available was in-suf� cient to support a causal judgement.
Statistical analysisStatistical analysis was performed by the chi-square test and the ANOVA test to comparedifferences between groups. Bonferroni correc-tion was applied when multiple comparisonswere performed.
The death rate (incidence) was compared forIDUs with the death rate (incidence) of the
Table 1. Causes of death by gender for 2708 IDUs
Cause M (%) F (%) Total (%)
Overdose 876 (38.6) 125 (28.5)† 1001 (36.9)AIDS 702 (30.9) 180 (41.1)† 882 (32.5)Road accident 221 (9.7) 35 (8) 256 (9.4)Suicide 129 (5.7) 22 (5) 151 (5.5)Liver diseases 83 (3.7) 14 (3.2) 97 (3.5)Other causes 106 (4.7) 30 (6.8) 136 (5)Unknown 153 (6.7) 32 (7.3) 185 (6.8)
Total (%) 2270 (84)* 438 (16)* 2708
† 5 Males vs. females p , 0.001; * 5 percentage by row.

1130 Gianluca Quaglio et al.
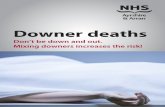
Figure 1. Causes of death for 2078 IDUs and percentages through years 1985–98.
The third cause of death—a constant during the14 years of observation—was road accidents.
The percentage of deaths due to AIDS in-creased steadily from 2.7% in 1985 to 42.2% in1996 (trend test: p , 0.001), then dramaticallydecreased to 16.9% in 1998, while deaths due tooverdose after a steady increase until 1990 sub-sequently remained almost constant. The trendin the causes of deaths over the observation time,from overdose and AIDS, was statisticallysigni� cant (trend test: p , 0.001); no signi� cantchanges were demonstrated for the other causes
of death. Among the category of other causes(Table 2) which accounted for 5%, the order offrequency was as follows: homicide (1.2%), heartdisease (1.2%), cancer (1%), accidents (0.7%),infectious diseases (0.5%), ill-de� ned condition(0.4%) and cerebrovascular diseases (0.1%).
Causes of death in different age groupsThe major causes of death in the different agegroups are listed in Table 3, showing signi� cantdifferences (v 2: p , 0.001). Overdose was re-sponsible for the majority of deaths among the
Table 2. Other causes of death
Cause No. (%)
Accident 18 (0.7)Homicide 32 (1.2)Neoplasm 25 (1)
Lymphatic and haematopoietic tissue 10 (0.4)Other form of neoplasm 15 (0.6)
Cerebrovascular disease 4 (0.1)Heart disease 32 (1.2)
Ischaemic heart disease 10 (0.4)Other forms of heart disease 22 (0.8)
Infectious diseases 15 (0.5)Endocarditis 5 (0.2)Pneumonia 4 (0.1)Septicaemia 4 (0.1)Other forms of infectious diseases 2 (0.1)
Ill-de� ned condition 12 (0.4)
Total 138 5%

Heroin-related deaths in north-eastern Italy 1131
Table 3. Causes of death by age in 2708 IDUs
Road Liver OtherAge Overdose AIDS Suicide accidents diseases causes Unknown Total (%)
15–19 22 0 4 7 2 2 1 38 (1.4)20–24 201 30 33 73 7 14 27 385 (14.2)25–29 330 177 45 83 13 32 65 745 (27.5)30–34 256 378 30 68 42 48 47 869 (32.1)35–39 141 223 27 18 20 20 31 480 (17.7)40–59 51 74 12 7 13 20 14 191 (7.1)
Age groups are staggered by � ve years up to 39, and then in one age group of 20 years.
Table 4. HIV status of 2708 IDUs
Cause of death HIV 1 (%) HIV 2 (%) HIV unknown (%)
Overdose 184 (14.7) 508 (58) 309 (53.5)AIDS 882 (70.3) — —Road accident 39 (3.1) 131 (15) 86 (14.9)Suicide 28 (2.2) 81 (9.2) 42 (7.3)Liver diseases 50 (4) 34 (3.9) 13 (2.2)Other causes 36 (2.9) 62 (7.1) 38 (6.6)Unknown 35 (2.8) 60 (6.8) 90 (15.6)Total (%) 1254 (46.3)* 876 (32.3)* 578 (21.4)*
* 5 Percentage by row.
youngest IDUs (range 15–24 years), followed byroad accidents and suicide. In the 25–29 rangeoverdose was still the principal cause of death,followed by AIDS and road accidents. After theage of 30, AIDS became the primary cause ofdeath, followed by overdose.
HIV statusOf the total number of IDUs observed, 1254(46.3%) were HIV positive (80% male, 20%female), 876 (32.3%) were HIV negative (87%male, 13% female); in 578 (21.4%) cases, theserological status was unknown (Table 4). Pa-tients who died of liver disease had an HIVpositive rate of 51.5%, signi� cantly higher thandeaths in other categories, with the exception ofAIDS ( v 2: p , 0.001). No signi� cant increase ofHIV seropositivity in IDUs who died from over-dose and suicide was found.
Age, period of addiction and years of care in PCDUsThe mean age of death was 31.3 (males 31.3,females 31.2) (Table 5). The patients who diedfrom AIDS and liver diseases (33.5 and 33.4,respectively) were signi� cantly older than thosein all other categories (p , 0.001); IDUs killed inroad accidents or by overdose (respectively, 28.3and 29.9) were considerably younger than inother categories (ANOVA: p , 0.001).
The period of addiction was established in2432 cases (90%) and was not established in 276cases. The mean duration of addiction was 11.7years, similar for both sexes. Patients who diedof AIDS or liver diseases had a much longerhistory of addiction (respectively, 14.3 and 13.9years) than those who died of other causes(ANOVA: p , 0.001); conversely, the period ofaddiction was shorter in IDUs who died throughroad accidents and suicide (respectively, 8.5 and8.2 years) when compared to all other categoriesof deaths (ANOVA: p , 0.001).
The duration of treatment in PCDUs wasknown in 2668 cases (98%) and unknown in 40cases. The mean duration of years of care was6.8 years. IDUs who died of AIDS and liverdiseases had been followed for the longest peri-ods by the centres (respectively, 9 and 8.3 years)(ANOVA: p , 0.001), whereas IDUs who diedin road accidents had undergone shorter periodsof care (4.5 years) followed by IDUs deaths dueto overdose and suicide (respectively, 5.6 and5.7 years) (ANOVA: p , 0.001).
Average age of death per yearThe average age of death per year is shown inFig. 2. The average age rose from 26–27 years inthe mid-1980s to 34.1 years in 1998, asigni� cant difference (ANOVA: p , 0.001).

1132 Gianluca Quaglio et al.
Table 5. Age, years of drug use and years of care in health centres
M (SD) F (SD) Total
OverdoseAge [876 1 125 5 1001] 29.9 (5.8) 30 (6.6)† 29.9 (5.9)Years of drug use [769 1 112 5 881] 10.1 (5,4) 10.5 (5.1)† 10.1 (5.4)Years of care in PCDU [865 1 123 5 988] 5.5 (4.1) 5.8 (4.3)† 5.6 (4.1)
AIDSAge [702 1 180 5 882] 33.5 (4.9) 33.1 (5.4)† 33.4 (5)Years of drug use [652 1 171 5 823] 14.4 (4.3) 13.8 (3.9)† 14.3 (4.2)Years of care in PCDU [693 1 177 5 870] 9 (4.1) 8.8 (4)† 9 (4.1)
Road accidentAge [221 1 35 5 256] 28.7 (5.4) 26.1 (4.7)‡ 28.3 (5.4)Years of drug use [193 1 34 5 227] 8.7 (4.7) 7.2 (4.2)† 8.5 (4.7)Years of care in PCDU [219 1 35 5 254] 4.6 (3.6) 3.8 (3.1)† 4.5 (3.5)
SuicideAge [129 1 22 5 151] 30.5 (7.2) 29 (5.7)† 30.3 (7)Years of drug use [122 1 21 5 143] 9.1 (5.4) 9.7 (4.7)† 9.2 (5.3)Years of care in PCDU [129 1 22 5 151] 5.5 (4.2) 6.6 (3.6)† 5.7 (4.1)
Liver diseasesAge [83 1 14 5 97] 33.4 (5.9) 34.2 (6)† 33.5 (5.9)Years of drug use [77 1 13 5 90] 14 (5.5) 13 (4.3)† 13.9 (5.3)Years of care in PCDU [81 1 13 5 94] 8 (4.8) 10 (3)† 8.3 (4.6)
Other causesAge [106 1 30 5 136] 33.4 (7.3) 31.4 (6.8)† 33 (7.2)Years of drug use [96 1 27 5 123] 12.5 (5.6) 12.1 (5.5)† 12.4 (5.5)Years of care in PCDU [104 1 30 5 134] 6.7 (4.7) 7.9 (5.6)† 7 (4.9)
UnknownAge [153 1 32 5 185] 31.1 (6.1) 30.8 (6.5)† 31 (6.2)Years of drug use [123 1 22 5 145] 11.6 (5.5) 11 (5.7)† 11.5 (5.5)Years of care in PCDU [147 1 30 5 177] 6.7 (4.5) 7.1(4.7)† 6.7 (4.5)
Total patientsAge [2270 1 438 5 2708] 31.3 (6) 31.2 (6.3)† 31.3 (6)Years of drug use [2032 1 400 5 2432] 11.6 (5.5) 11.8 (5)† 11.7 (5.4)Years of care in PCDU [2238 1 430 5 2668] 6.8 (4.4) 7.3 (4.5)‡ 6.8 (4.5)
The number in brackets [males 1 females 5 total] refers to the number of patients taken intoaccount for the variable. † 5 males vs. females p NS; ‡ 5 males vs. females p , 0.05.
Mortality rates of IDUs vs. general populationTable 6 compares the death rate of IDUs and inthe general population on the basis of mortalitydata for 1991, the year of the last census.Columns 2 and 6 indicate the numbers of IDUdeaths observed in 1991 and the numbers ofexpected deaths.
In males the mortality rate of IDUs in thethree age groups covering the range from 25–39was about three times higher than the mortalityrate in the age group from 20–24 and the twoage groups from 40–59; a similar, although lessmarked contrast, was observed in the IDU mor-tality rates among females.
The mortality rate among IDUs attending thecentres was much higher when compared to thegeneral population of the same age (13-fold,95% CI, 11.3–14.6) (Poisson probability:p , 0.001). Taking into account the SMRcon� dence interval among males, mortality forthose aged 20–24 and 40–59 years was similar
and signi� cantly lower than the SMR of thoseaged 25–39 years. For females, SMR did notsigni� cantly differ, due probably to the largecon� dence interval as a result of the scarcity offemales in the IDU population. Comparing gen-ders, male IDUs have an SMR of 8.8 (95% CI,7.7–10.2), signi� cantly lower than females, withan SMR of 21.7 (95% CI, 15.7–29.2).
Finally, in the year of the census, the percent-age of deaths due to drug use in the 15–34 agegroup in the general population (195 deathsamong IDUs/1241 deaths in the general popu-lation, Table 6), was 16%; this broke down as17% in males and 12% in females.
DiscussionCon� rming national2,5 and international stud-ies7,22–24 the SMR among IDUs attending ourcentres was 13 times higher than in the generalpopulation for the same age group. Our mor-tality rate data compared with other studies in

Heroin-related deaths in north-eastern Italy 1133
Figure 2. Distribution of mean age of death from 1985 to 1998.
northern Italy were lower than in Bologna (18-fold) and in Milan (20-fold).3,5
The difference in the SMR calculated in rela-tion to the gender of the IDUs versus the generalpopulation (nine males, 22 females) is not to beattributed to the increase in the mortality rateamong female drug users. In fact, the indirectlystandardized rate of male and female IDUsproves to be similar (2.56 and 2.60, respect-ively). The difference is a consequence of thelower female mortality rate in the general popu-lation (0.12:0.29). These � ndings, con� rmed bya recent study,25 indicate the risk of deaths infemale heroin users and consequently that fe-males require particular targeting by providers ofdrug-treatment services, as Frischer highlights.24
The percentage (16%) of deaths attributableto drug use, in line with another Italian study,26
is striking, considering that in the study area thenumber of IDUs in the same age group is esti-mated at approximately 1% of the population.The continuous increase of deaths among drugusers in the study area, especially after 1988,followed a national trend.27
The important fall in deaths due to AIDS inthe last 2 years of observation was very probablydue to the new antiretroviral therapeutic regi-
mens28 which are provided free for all patients inItaly. A similar trend in all major HIV trans-mission categories and in all demographic groupshas recently been reported in a New York Citystudy.29 The drop in mortality was preceded bya decline in HIV/AIDS case incidence amongdrug users.30 In this regard, prevention and treat-ment of non-AIDS infections, especially hepatitisC virus infection and cancer, will become in-creasingly important in HIV-infected drugusers.31
Why overdose should remain such an import-ant cause of death needs to be explored further.It is to be noted that deaths from overdoseremained constant over the years despite import-ant changes in law and guidelines about access tooral methadone. Methadone dosage restrictionwas lifted in 1993. Therefore, in agreement withother authors,32.33 our data suggest that deathsamong IDUs can only be slightly in� uenced bygovernment policies. Prevention campaignsshould emphasize the danger of overdoses alongwith the danger of AIDS and hepatitis. Drop-outfrom methadone maintenance treatments hasbeen demonstrated as an important risk factorfor overdose.34,35 In our experience, the aboveobservation can be extended to any rehabilitative

1134 Gianluca Quaglio et al.
Table 6. Comparison by means of standardized mortality ratio (SMR) between deaths of IDUs and deaths in the generalpopulation (GP) in 1991 after due correction for age and gender
No. of No. of No. of ExpectedAge deaths No. of deaths in general no. of SMRrange of IDUs IDUs the GP population deaths (O/E) 95% CI p*
Males15–19 4 313 180 182,015 0.31 12.9 3.52–33.03 0.00120–24 21 1983 253 206,961 2.38 8.82 5.46–13.49 0.00125–29 77 3085 253 218,731 3.7 20.81 16.4–26.0 0.00130–34 57 1588 256 190,633 2.06 27.67 21–35.8 0.00135–39 31 575 270 171,824 0.92 33.69 22.9–47.8 0.00140–59 10 284 3351 629,733 1.35 7.41 3.6–13.6 0.00115–59 o 5 200 7796 4563 1,599,897 22.61 8.85 7.7–10.2 0.001
Females15–19 1 90 49 174,281 0.027 37.04 1.1–206.3 0.01320–24 4 428 70 197,072 0.17 23.6 6.4–60.2 0.00125–29 16 609 77 209,005 0.24 66.7 38.1–108.2 0.00130–34 15 333 103 182,043 0.2 75 42–123.7 0.00135–39 6 121 114 166,343 0.08 75 27.5–163.2 0.00140–59 1 72 1566 775,683 0.14 7.14 0.21–39.8 0.07015–59 o 5 43 1653 1979 1,704,427 1.98 21.71 15.7–29.2 0.001
Males 1 females15–59 o 5 243 9451 6542 3,304,374 18.90 12.85 11.3–14.6 0.001
* Poisson two-sided probability; SMR 5 standardized mortality ratio; O/E 5 ratio of observed to expected deaths;CI 5 con� dence interval; IDUs 5 injecting drug users; GP 5 general population. Age groups are staggered by � veyears up to 39, and then in one age group of 20 years.
treatment such as naltrexone programmes, thera-peutic communities as well as psychotherapytreatment on its own. Other important risk fac-tors for overdose are variability in purity of streetheroin rather than increased purity per se, con-current use of other drugs, particularly al-cohol,33,36–38 drug availability, loss of tolerance toheroin39 and, as pointed out above, the youngage and short treatment in PCDUs. Methods topredict and then minimize drop-outs from treat-ment should be re� ned and implemented inorder to effectively reduce risk of death fromoverdose.34 Heroin users need to be educated inthe potentially dangerous practice of concurrentpolydrug abuse, especially the increased vulner-ability of ethanol consumers to the effects ofheroin.36 Campaigns aimed at increasing aware-ness should also emphasize that it is safer toinject heroin in the company of others, and theimportance of calling for an ambulance early inthe event of an overdose. Consideration shouldalso be given to regular analysis of the compo-sition of street heroin,38 to the distribution ofnaloxone,37 preferably provided in a disposablepreloaded syringe,40 and to the fact that the useof illegal heroin and criminal behaviour de-creases when prescribed heroin is available.41 In
addition, it is highly likely that the number ofdeaths by overdose is well underestimated be-cause deaths may be certi� ed as due to naturalcauses in order to avoid autopsy or registrationas an acute drug reaction death, as has beenobserved by many authors.42
The very high proportion of deaths due toroad accidents reported in our previous study13 iscon� rmed, albeit with a slight decrease (from11% to 9.5%). This result, however, is not com-parable with other studies which considered thiscategory as part of the general category of violentdeath by accident or injury.2,11 Suicide ac-counted for only 5.6% of deaths, which is similarto the � ndings of other Italian studies,2,5 butlower than the results of northern-Europeanstudies.43,44
There were a surprisingly small number ofdeaths from liver diseases, although in the studyarea the mean prevalence of HCV positive test-ing is around 70% and the prevalence of HBVpositivity was around 40% in 1985, falling overthe years to around 20% in 1998.45,46 Howeverprevious studies report � gures only slightlyhigher than our data.5,47 Moreover, there is in-creasing evidence that liver disease caused byhepatitis C and D viruses can be more aggressive

Heroin-related deaths in north-eastern Italy 1135
in HIV carriers, leading to more rapid liver fail-ure.48,49
Of deaths from infectious diseases the very lownumber of deaths due to endocarditis is surpris-ing. No case of tuberculosis as cause of deathwas observed, although previous studies haverevealed an increase of tuberculosis amongIDUs.50,51 However, an Italian report hasshowed only a marginally increased risk for TBCamong HIV positive IDUs.52
In relation to the HIV seropositive rate, theonly datum of signi� cance is the higher preva-lence, with the exception of AIDS patients,among those who died of liver diseases,con� rming previous studies.3,18,53 The study didnot reveal a higher rate of HIV seropositivityamong IDUs who died of overdose and suicide.Some previous studies con� rm our data,5,6,18,54
while others do not.1,4,55 In addition, notifyingIDUs of their HIV seropositive status does notappear to lead to a sudden and substantial rise insuicide/overdose deaths.18 Finally, the relativelyhigh number of IDUs with unknown HIV statusis due to the fact that in Italy the test is voluntaryand some patients prefer to be tested in centresother than PCDUs where anonymity may beguaranteed.
The average age of death rose from 26 to 27years in the mid-1980s to 34 years in 1998.Kringsholm56 attributes the steady rise in the ageof death among his cohort of drug users to adecrease in recruitment among the relativelyyoung. This is probably not the case for IDUs inour area, as can be seen from data from theMinistry of Health57 showing a continuous in-crease of IDUs who seek treatment in the PC-DUs. More probably, the increase in age in ourarea depends on the continuous change in thehabits and life-style of IDUs who are more partof society, live in families at home, have a regularjob and are more careful in the concern that theyshow for their everyday state of health thanpreviously.
To our knowledge, this is the largest publishedstudy on opiate-related mortality in Europe. Themost signi� cant result was the dramatic decreaseof deaths due to AIDS, from 1997 onwards, thenumber of deaths due to overdose which repre-sents the principal cause of death and the mor-tality rate among IDUs, which is 13 times higherthan in the general population of the same age.The mean age of death shows a steady increaseover the years. HIV prevalence is not a
signi� cant factor in the causes of suicides anddeaths from overdose.
The practical implications of this study forthose who work in the � eld of addiction are thatmore attention should be paid to female heroinusers, who are particularly at risk of death. Inaddition, the dangers of overdose should bestressed to IDUs as well as the importance of notdropping out of treatment, of whatever kind,because of the increased rate of overdose afterdrop-out. This could be achieved by enhancingcooperation between PCDUs, GPs, the thera-peutic community, prisons and so on. Road acci-dents are a relevant cause of death; drugs forpsychiatric disorders should be administeredwith great care due to the frequent association ofthese drugs with alcohol abuse, a signi� cant con-tributing factor to the causes of road accidents.The fall in deaths from AIDS among IDUsrequires greater efforts to prevent infection byhepatitis C virus in the future and renewed ef-forts to treat infected patients. The strikinglyhigh percentage of deaths due to drug use shouldin� uence decisions in drug projects, research andin training in medical schools.
References1. ZACCARELLI, M., GATTARI, P., REZZA, G., CONTI,
S., SPIZZICHINO, L., VLAHOV, D., IPPOLITO, G.,LELLI, V. & VALENZI, C. (1994) Impact of HIVinfection on non-AIDS mortality among Italianinjecting drug users, AIDS, 8, 345–350.
2. PERUCCI, C. A., DAVOLI, M., RAPITI, E., FORASTI-
ERE, F. & ABENI, D. D. (1991) Mortality of intra-venous drug users in Rome: a cohort study,American Journal of Public Health, 81, 1307–1310.
3. GOEDERT, J. J., PIZZA, G., GRITTI, F. M.,COSTIGLIOLA, P., BOSCHINI, A., BINI, A., LAZZARI,C. & PALARETI, A. (1995) Mortality among drugusers in the AIDS era, International Journal ofEpidemiology, 24, 1204–1210.
4. ESKILD, A., MAGNUS, P., SAMUELSEN, S. O.,SOHLBERG, C. & KITTELSEN, P. (1993) Differ-ences in mortality rates and causes of death be-tween HIV positive and HIV negative intravenousdrug users, International Journal of Epidemiology,22, 315–320.
5. GALLI, M. & MUSICCO, M., FOR THE COMCATSTUDY GROUP (1994) Mortality of intravenousdrug users living in Milan, Italy: role of HIV-1infection, AIDS, 8, 1457–1463.
6. STONEBURNER, R. L., DES JARLAIS, D. C., BEN-
ERZA, D., GORELKIN, L., SOTHERAN, J.L., FRIED-
MAN, S. R., SCHULTZ, S., MARMOR, M., MILDVAN,D. & MASLANSKY, R. (1988) A larger spectrum ofsevere HIV-1-related disease in intravenous drugusers in New York City, Science, 242, 916–919.
7. SELWYN, P. A., HARTEL, D., WASSERMAN, W. &DRUCKER, E. (1989) Impact of the AIDS epi-

1136 Gianluca Quaglio et al.
demic on morbidity and mortality among intra-venous drug users in a New York City metha-done maintenance program, American Journal ofPublic Health, 79, 1358–1362.
8. ORTI, R. M., DOMINGO-SALVANY, A., MUNOZ, A.,MACTARLANE, D., SUELVES, J. M. & ANTO, J. M.(1996) Mortality trends in a cohort of opiateaddicts, Catalonia, Spain, International Journal ofEpidemiology, 25, 545–553.
9. VAILLANT G. E. (1973) A 20-year follow-up ofNew York narcotic addicts, Archives in GeneralPsychiatry, 29, 237–241.
10. THORSEN, K. & HAASTRUP, S. (1975) Follow-upof 97 young non-psychotic male opiate abusers:relationship between achiving abstinence, age,and duration of abuse, Acta Psychiatrica Scandi-navica, 51, 289–296.
11. BARR, H. L., ANTES, D., OTTENBERG, D. J. &ROSEN, A. (1984) Mortality of treated alcoholicsand drug addicts; the bene� ts of abstinence, Jour-nal of Studies on Alcohol, 45, 440–452.
12. BUCKNALL, A. B. V. & ROBERTSON, J. R. (1986)Deaths of heroin users in a general practice popu-lation, Journal of the Royal College of General Prac-titioners, 36,120–122.
13. MEZZELANI, P., QUAGLIO, G. L., VENTURINI, L.,LUGOBONI, F., GICS, FRIEDMAN, S. R. & DES
JARLAIS D. C. (1998) A multicentre study on thecauses of death among Italian injecting drugusers. AIDS has overtaken overdose as the princi-pal cause of death, AIDS Care, 10, 61–67.
14. MEZZELANI, P., VENTURINI, L., TURRINA, G.,LUGOBONI, F. & DES JARLAIS, D. C. (1991) Highcompliance with a hepatitis B virus vaccinationprogram among intravenous drug users, Journalof Infectious Diseases, 163, 923.
15. Popolazione residente per sesso, eta, regioni1999. Istituto Italiano di Statistica (ISTAT),Roma 2000 [Resident population by sex, age, inRegions—Italy 1999, National Institute of Statis-tics, Rome 2000].
16. Indagine trimestrale sulle forze di lavoro 1999,Istituto Italiano di Statistica (ISTAT), Roma2000 [Trimestral report on working class data1999, National Institute of Statistics, Rome2000].
17. Conti economici regionali 1996–1998, IstitutoItaliano di Statistica (ISTAT), Roma 1998 [Re-gional � nancial budget 1996–1998, National In-stitute of Statistics, Rome 1998].
18. VAN HAASTRECHT, H. J. A., MIENTJES, G. H. C.,VAN DEN HOEK, J. A. R. & COUTINHO, R. A.(1994) Death from suicide and overdose amongdrug injectors after disclosure of � rst HIV testresult, AIDS, 8, 1721–1725.
19. Censimento Demogra� co Nazionale 1991; unmodello di analisi per le realta locali (1996) Re-gione Veneto, Dipartimento per la statistica el’informatica [National Population Census 1991;an analysis model for local districts, Veneto Re-gion. Department of Applied Statistics].
20. Tredicesimo censimento della popolazione, 20Ottobre 1991, Istituto Nazionale di Statistica (IS-TAT), Roma 1993 [Thirteenth population cen-
sus, 20 October 1991, National Institute ofStatistics, Roma 1993].
21. BRESLOW, M. & DAY, N. (1986) Rates and RateStandardization. Statistical methods in cancer re-search, pp. 48–79 (Lyon, France, InternationalAgency for Research on Cancer (IARC)).
22. HAASTRUP, S. & JEPSEN, P. W. (1984) Seven-yearfollow-up of 300 young drug abusers, Acta Psy-chiatrica Scandinavica, 70, 503–509.
23. JOE, G. W. & SIMPSON, D. D. (1987) Mortalityrate among opiate addicts in a longitudinal study,American Journal of Public Health, 77, 347–348.
24. FRISHER, M., BLOOR, M., GOLDBERG, D., CLARK,J., GREEN, S. & MCKEGANEY, N. (1993) Mor-tality among injecting drug users: a critical reap-praisal, Journal of Epidemiology and CommunityHealth, 47, 59–63.
25. DAVOLI, M., PERUCCI, C., RAPITI, E., BARBAGLI,A. M., D’IPPOLITI, D., FORASTIERE, F. & ABENI,D. D. (1997) A persistent rise in mortality amonginjection drug users in Rome, 1980 through1992, American Journal of Public Health, 87, 851–853.
26. PERUCCI, C. A., FORASTIERE, F., RAPITI, E.,DAVOLI, M. & ABENI, D. D. (1992) The impact ofintravenous drug use on mortality of young adultsin Rome, Italy, British Journal of Addiction, 81,1247–1249.
27. Relazione annuale della Direzione Centrale per iServizi Antidroga (1998) Ministero dell’Interno,Roma [Annual Report of Head Of� ce of PublicCentres for Drug Users 1998. Home Of� ce,Rome, 1998, 130–132].
28. HOGG, R. S., O’SHAUGHNESSY, M. V., GATARIC,N., YIP, B., CRAIB, K., SCHECHTER, M. T. &MONTANER J. S. (1997) Decline in deaths fromAIDS due to new antiretrovirals, Lancet, 349,1294.
29. CHIASSON, M. A., BERENSON, L., LI, W.,SCHWARTZ, S., SINGH, T., FORLENZA, S., MOJICA,B. A. & HAMBURG, M. A. (1999) Declining HIV/AIDS mortality in New York City, Journal ofAcquired Immune De� ciency Syndromes, 21, 59–64.
30. BAGGIO, E., BOSSI, C., BRESSAN, R., CERAVOLO,R., DURANO, B., GIACOMINI, M.A., LUGOBONI,F., MANZATO, E., ROSSETTO, L., SACCARDI, C. &STIMOLO C. (1995) L’infezione da virusdell’immunode� cienza umana tra i tossicodipen-denti da eroina: studio epidemiologico in 10Servizi per le Tossicodipendenze del Veneto,1985–1992 [HIV infection among heroin drugusers: epidemiological study in 10 Public HealthAuthority Centres for Drug Users in Veneto Re-gion, 1985–1992], Giornale Italiano dell’AIDS, 6,154–156.
31. PRINS, M., SABIN, C. A., LEE, C. A., DEVEREUX,H. & COUTINHO, R. A. (2000) Pre-AIDS mor-tality and its association with HIV disease pro-gression in haemophilic men, injecting drug usersand homosexual men, AIDS, 14, 1829–1837.
32. GHODSE, A. H., SHEEHAN, M., TAYLOR, C. & ED-
WARDS, G. (1985) Deaths of drug addicts in theUnited Kingdom 1967, British Medical Journal,290, 425–428.
33. HULSE, G. K., ENGLISH, D. R., MILNE, E. & HOL-

Heroin-related deaths in north-eastern Italy 1137
MAN C. D. J. (1999) The quanti� cation of mor-tality resulting from the regular use of illicit opi-ates, Addiction, 94, 221–229.
34. DAVOLI, M., PERUCCI, C., FORASTIERE, F.,DOYLE, P., RAPITI, E., ZACCARELLI, M. & ABENI,D. D. (1993) Risk factors for overdose mortality:a case-control study within a cohort of intra-venous drug users, International Journal of Epi-demiology, 22, 273–277.
35. GRONBLADH, L., OHLUND, L. S. & GUNNE, L. M.(1990) Mortality in heroin addiction: impact ofmethadone treatment, Acta Psychiatrica Scandi-navica, 82, 223–227.
36. RUTTENBER, A. J., KALTER, H. D. & SANTINGA, P.(1990) The role of ethanol abuse in the etiologyof heroin-related death, Journal of Forensic Sci-ence, 35, 891–900.
37. ZADOR, D., SUNJIC, S. & DARKE, S. (1996)Heroin-related deaths in New South Wales,1992: toxicological � ndings and circumstances,Medical Journal of Australia, 164, 204–207.
38. DARKE, S., SUNJIC, S., ZADOR, D. & PROLOV, T.(1997) A comparison of blood toxicology ofheroin-related deaths and current heroin users inSidney, Australia, Drug and Alcohol Dependence,47, 45–53.
39. SEAMAN, S. R., BRETTLE, R. P. & GORE, M.(1998) Mortality from overdose among injectingdrug users recently released from prison: data-base linkage study, British Medical Journal, 316,426–428.
40. STRANG, J., DARKE, S., HALL, W., FARRELL, M. &ALI, R. (1996) Heroin overdose: the case fortake-home naloxone, British Medical Journal, 312,1435–1436.
41. BAMMER, G., DOBLER-MIKOLA, A., FLEMING,P.M., STRANG, J. & UCHTENHAGEN, A. (1999)The heroin prescribing debate: integrating sci-ence and politics, Science, 284, 1277–1278.
42. DE LA FUENTE, L., BARRIO, G., VICENTE, J.,BRAVO, M. J. & SANTACREU, J. (1995) The impactof drug-related deaths on mortality among youngadults in Madrid, American Journal of PublicHealth, 85, 102–105.
43. HAASTRUP, S. & JEPSEN, P. W. (1988) Eleven-yearfollow-up of 300 young opioid addicts, Acta Psy-chiatrica Scandinavica, 77, 22–26.
44. FUGELSTAD, A., ANNELL, A., RAJS, J. & AGREN, G.(1997) Mortality and causes and manner of deathamong drug addicts in Stockholm during theperiod 1981–92, Acta Psychiatrica Scandinavica,96, 169–175.
45. LUGOBONI, F., MEZZELANI, P., VENTURINI, L.,FIBBIA, G. C. & DES JARLAIS D. C. (1992) AnHBV vaccination program for street injectingdrug users: implications for testing an HIV vac-cine, VIII International Conference on AIDS, Am-sterdam [abstract PoC 4796].
46. MEZZELANI, P., VENTURINI, L., FIBBIA, G. C.,PERDONA, G. P., LUGOBONI, F., FACCINI, M.,BOSSI, C., SACCARDI, C. & DES JARLAIS D. C.(1992) Parallel decline in both HIV and HBVseroprevalence following AIDS prevention pro-
grams among injecting drug users in North-EastItaly, VIII International Conference on AIDS, Am-sterdam [abstract PoC 4797].
47. SORIANO, V., GARCIA-SAMANIEGO, J., VALENCIA,E., RODRIGUEZ-ROSADO, R., MUNOZ, F. & GON-
ZALEZ-LAHOZ, J. (1999) Impact of chronic liverdisease due to hepatitis viruses as cause of hospi-tal admission and death in HIV-infected drugusers, European Journal of Epidemiology, 15, 1–4.
48. TELFER, P., SABIN, C., DEVEREUX, H., SCOTT, F.& DUSHEIKO, G. (1994) The progression ofHCV-associated liver disease in a cohort ofhaemophilia patients, British Journal of Haema-tology, 87, 555–561.
49. DE POUPLANA, M., SORIANO, V., GARCIA-SA-
MANIEGO, J., ENRIQUEZ, A., MUNOZ, F. & GONZA-
LEZ-LAHOZ, J. (1995) More severe course of Deltahepatitis in HIV-infected patients, GenitourinaryMedicine, 71, 132–133.
50. HAAS, D. W. & DES PREZ, R. M. (1994) Tubercu-losis and acquired immunode� ciency syndrome:a historical perspective on recent developments,American Journal of Medicine, 96, 439–450.
51. BRAUN, M. M., COTE, T. R. & RABKIN, C. S.(1993) Trend in death with tuberculosis duringthe AIDS era, Journal of the American MedicalAssociation, 269, 2865–2868.
52. ANTONUCCI, G., ARMIGNACCO, O. & GIRARDI, E.(1990) Tubercolosi e infezione da HIV: incidenzadella tubercolosi in soggetti con infezione da HIVe prevalenza di sieropositivita per HIV-Ab inpazienti con tubercolosi [Tuberculosis and HIVinfection: incidence of tuberculosis in HIV posi-tive subjects and prevalence of HIV seropositivityin patients with tuberculosis], in: Second ResearchProject on AIDS, 1989, ISTISAN Reports 90/10:133 (Edizioni G. B. Rossi) (Verona, G. B.Rossi).
53. VAN AMEIJDEN, E. J. C., VLAHOV, D., VAN DEN
HOEK, J. A. R., FLYNN, C. & COUTINHO, R. A.(1996) Pre-AIDS mortality and morbidity amonginjection drug users in cohort studies in Amster-dam and Baltimore, XI International Conference onAIDS, Vancouver [abstract ThC220].
54. SOELLNER, R., CASTRUP, U., HECHMANN, W.,TESCHKE, F. & VORWOLD M. (1992) Does anHIV-infection increase the probability of dying bya drug-overdose? VIII International Conference onAIDS, Amsterdam [abstract D402].
55. PRINS, M., AGUADO, I. H., BRETTLE, R. P.,ROBERTSON, J. R., BROERS, B., CARRE, N., GLOD-
BERG, D. J., ZANGERLE, R., COUTINHO, R. A. &VAN DEN HOEK, A. (1997) Pre-AIDS mortalityfrom natural causes associated with HIV diseaseprogression: evidence from the European Sero-convert Study among injecting drug users, AIDS,11, 1747–1756.
56. KRINGSHOLM, B. (1988) Deaths among drug ad-dicts in Denmark in 1968–1986, Forensic ScienceInternational, 38, 139–149.
57. Rilevazione attivita nel settore tossicodipendenze,1997, Dipartimento della Prevenzione, Ministerodella Sanita [National Report on Addictions,1997, Department of Prevention, Ministry ofHealth, Rome 1997].