student's self-study guidelines for practice activities
252
Іgnatenko G.А., Taktashov G.S., Bragina R.Sh., Sherbakov K.S., Pola M.K., Kontovskyy Y.A. STUDENT’S SELF-STUDY GUIDELINES FOR PRACTICE ACTIVITIES 0BPropedeutics of the Internal Medicine For Third Year Students Of International Medical Faculty Module 2. SYMPTOMES AND SYNDROME OF INTERNAL DISEASE Donetsk 2009 cardiology.dsmu.edu.ua
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of student's self-study guidelines for practice activities

Іgnatenko G.А., Taktashov G.S., Bragina R.Sh., Sherbakov K.S.,
Pola M.K., Kontovskyy Y.A.
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
0BPropedeutics of the Internal Medicine
For Third Year Students Of International Medical Faculty
Module 2. SYMPTOMES AND SYNDROME OF INTERNAL DISEASE
Donetsk 2009
1
cardi
ology
.dsmu.e
du.ua

УДК 616-07(075.8) ББК 54.1я7 S90 Іgnatenko G.А., Taktashov G.S., Bragina R.Sh., Sherbakov K.S., Pola M.K., Kontovskyy Y.A., Guidelines for practice activities on propedeutics of internal medicine for third year students of international medical faculty. The Main Methods of Examination of Patient on Internal Diseases Course Guidelines for practice activities. The Main Methods of Examination of Patient on Internal Diseases Course -Donetsk: the Donetsk national Gorky’s medical university 2009 Методические указания по пропедевтике внутренней медицины для студентов 3 курса международного медицинского факультета. – Донецк: Донецкий национальный медицинский университет им. М.Горького, 2009. – 252 с. In the guideline to practical training of propedeutic of internal medicine for the third year students of international faculty the ones are represented according to a method and dedicate to research and diagnostic of organs and systems with factors of anatomico-physiological data. The method is prepared with the modern requirements of high school and directed on increase of studies efficiency for students of higher medical institutes. Reviewers: Putincev V.G. – professor doctor of medicine, head of department of hospital therapy of the Lugansk state medical university; Kolomiec V.І. – professor doctor of medicine, head of department of faculty therapy of the Lugansk state medical university; Linevskiy U.V. – professor doctor of medicine of the department of internal disease №2 DonSMU. Puzik A.A. – Dr., PhD, head of foreing language department of the Donetsk national medical university.
36BIt is ratified on the conference DonSMU UMK Committee 30.10.08 №7
© Іgnatenko G.А., Taktashov G.S., Bragina R.Sh., Sherbakov K.S., Pola M.K., Kontovskiy Y.A.
2
cardi
ology
.dsmu.e
du.ua

UCONTENTS 1BFOREWORD………………………………………………………………….……..5 Subject 1. Examination of the blood. Clinical study of the blood. Clinical estimation of blood investigation. Main syndromes and symptomes in anaemia……....………..…..……6 Subject 2. The main hematologic syndromes. Haemorrhagic syndrome. Main syndromes in leukemia. …………………………………..………………………...23 Subject 3. Syndrome of heart failure: main clinical and instrumental investigation. Syndrome of acute and chronic vascular insufficiency.………………....……..........38 Subject 4. Mitral heart valve disease: main syndromes and symptomes according to clinical and instrumental investigation. Tricuspid heart valve disease.……..............49 Subject 5. Aortic heart valve disease: main syndromes and symptomes according to clinical and instrumental investigation.………………..……………………….........65 Subject 6. The main syndromes and symptomes in the arterial hypertention and arterial hypotention. Hypertensic crisis. …………………..………………………...83 Subject 7. Syndrome of the myocardial affection. Syndrome heart rhythm disorders. Syndrome hydropericardium. The main syndromes and symptomes in angina pectoris and myocardial infarction. Acute coronary syndrome.……………………………...99 Subject 8. Instrumental diagnostics and laboratory investigation of the respiratory system. Examination of the respiratory function. Investigation of sputum and pleural fluid…………………………………..……………..……………………………....114 Subject 9. Syndrome of acute and chronic respiratory failure. Disorders of ventilatory capacity of the lungs. Types and stages of the respiratory failure. Restrictive and obstructive respiratory failure.…. ……………..…………………..127 Subject 10. Syndrome of air and fluid in the pleural cavity. Bronchial obstructive syndrome. Syndrome of increased airiness of the lungs. Pickwickian syndrome. Syndrome of pulmonary cavity. Syndrome of pulmonary consolidation.……….....138 Subject 11. Syndrome of pulmonary hypertention. Syndrome of cor pulmonale. Respiratory distress syndrome. Syndrome of extra-respiratory failure.…………....153 Subject12. Instrumental diagnostics and laboratory investigation of digestive system. Examination of the secretory and acid-forming functions of the stomach, duodenal contents. Coprological studies. Technique and indications to gastroscopy and colonoscopy. X-ray of stomach.…………………………………………….....166 Subject13. Syndrome of abdominal pain. Dyspeptic syndrome. Malabsorption syndrome. Irritable colon syndrome. ……………..……………………..…………178 Subject 14. Instrumental diagnostics and laboratory investigation of diseases of hepatobiliary system. Jaundice syndrome. Cholestatic syndrome. Hereditary hyperbilirubinemia syndrome. Hepatomegaly syndrome. Hepatolienal syndrome..…. ………………………………..……………………..……………………..……….190 Subject 15. Syndrome of portal hypertension. Hepatorenal syndrome. Syndrome of acute and chronic hepatic failure. Syndrome of hepatarhia……………..…………200 Subject 16. Instrumental diagnostics and laboratory investigation of kidneys and urinary system. Main syndromes and symptomes of diseases of urinary system.
3
Disuric syndrome. Urinary syndrome. Hematuric syndrome. Arterial blood pressure syndrome.Syndrome of renal colic..……………………………… ………...……..215
cardi
ology
.dsmu.e
du.ua

4
Subject 17. Nefritic syndrome. Nefrotic syndrome. Tubulo-interstitial syndrome..……………………………………………………………………....….224 Subject 18. Syndrome of acute and chronic renal failure. Uremic coma and chlorohydropenic coma. ……………..……………………..…………………..….236 Question Checklist for Final Test……………..……………………..………...…245 Practical Skill Checklist……………..……………………..……………………..247 Literature……………..……………………..……………………..……………...249
cardi
ology
.dsmu.e
du.ua

5
Module 2 Symptomes and Syndromes of Internal Diseases Key objectives of the module: 1. To master practical skills and analyse the data of main laboratory and instrumental methods of examination 2. To master practical skills and detemine main syndromes and syndromes of pathology. Topic 6 Module. Blood disorders, musculoskeletal disordes, endocrine disease, interpretation data of laboratory investigation. Topic 7 Module. Main syndromes and symptomes of cardiovascular diseases. Topic 8 Module. Main syndromes and symptomes of respiratory diseases, interpretation data of instrumental diagnostics and laboratory investigation. Topic 9 Module. Main syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation. Topic 6 Module. Blood disorders, musculoskeletal disordes, endocrine disease, interpretation data of laboratory investigation. Specific Goals: - To learn how to enquire and examine patients with pathologies blood system, musculoskeletal system, endocrine system. - To identify the main syndromes of pathology of the blood system, musculoskeletal system, endocrine system. - To interpret the received data of laboratory investigation for recognition of pathology of blood system and endocrine system - To choose appropriate methods of investigation for certain blood,endocrine, musculoskeletal diseases.
cardi
ology
.dsmu.e
du.ua

Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptomes and Syndromes of the Internal Diseases
Topic 6 Module Blood disorders, musculoskeletal disordes,
endocrine disease, interpretation data of laboratory investigation.
Practice Examination of the blood. Clinical study of the blood. Clinical estimation of blood investigation. Main syndromes and symptomes in anaemia
Course 3
Faculty International Medical Faculty
Donetsk 2009
6
cardi
ology
.dsmu.e
du.ua

7
UImportance of the Subject U: Ability to interpret a clinical blood analysis and reveal clinical signs of blood system disorders is necessary for the doctor of any speciality because changes in peripheral blood are both specific for haematological pathology and for disorders of other organs and systems.
UKey ObjectiveU: To be able to estimate the blood analysis, make inquiries about haematological pathology, carry out phisical examination of patients with blood disorders and reveal the main syndromes, symptomes and laboratory criterions of anaemia.
USpecific Goals:
1. To estimate clinical blood analysis 2. To learn how to enquire patients with haematological pathologies about their most
disturbing complaints 3. To develop skills in carrying out the inspection and palpation of lymph nodes,
inspection, palpation and percussion of the bones 4. To develop skills in revealing the main syndromes and symptomes in anaemia.
Level of Knowledge and Skills before the Practice:
1. To have knowledge of the links of the haemopoiesis (Described in the Histology course)
2. To distinguish the cellular elements of blood on their morphological properties (Described in the Histology course) 3. To carry out clinical analysis of the blood – blood taking, preparation of smears (for microscopic examination), cell count, ESR determination (Described in the Physiology course) 4. To have knowledge of anatomical details and projection of the lymph nodes and spleen (Described in the Human Anatomy course) Questions for Self-Assessment of the Pre-Practice Knowledge Q1. Patient with hypochromic anemia has splitting hair and loss of hair, increased nail brittling and taste alteration. What is the mechanism of the development of these symptoms? A. Decreased production of parathyrin B. Decreased production of thyroid hormones C. Deficiency of vitamin ВR12 D. Deficiency of vitamin А E. Deficiency of iron-containing enzymes Q2. Punctata hemorrhage was found out in the patient after application of a tourniquet. With disfunction of what blood cells is it connected? A. Eosinophiles B. Lymphocytes C. Monocytes
cardi
ology
.dsmu.e
du.ua

8
D. Neutrophiles E. Platelets Q3. In the blood smear, stained according to Romanovsky-Giemsa method, there are 20% big (20 mcm in diametre), rounded cells with pale-basophilic cytoplasm and bean-shaped nucleus. How is this condition characterised clinically? A. Neutrophilosis B. Leukopenia C. Monocytosis D. Lymphocytosis E. Reticulocytosis Q4. Blood sampling for bulk analysis is recommended to be performed on an empty stomack and in the morning. What changes in blood composition can occur if to perform blood sampling after food intake? A. Reduced contents of erythrocytes B. Increased contents of erythrocytes C. Increased contents of leukocytes D. Increased plasma proteins E. Reduced contents of thrombocytes Q5. Which of the following are the last precursors of red blood cells? A. Platelets B. Normocytes C. Monocytes D. Reticulocytes E. Erythroblasts Answer Keys: E, E, C, C, D
The following printed materials can be of help to improve your pre-practice knowledge and skills: 1. Test book of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 2. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 3. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy
UContents of Practice
UTopics of Theory:
1. Clinical study of the blood. Clinical estimation of blood investigation. 2. Classification of the anaemia. 3. The main clinical and laboratory features of anaemia. 4. The iron deficiency anaemia: reasons, clinical features, syndromes,
investigations, laboratory signs. 5. The vitamin B12 and folate deficiency anaemia: reasons, clinical features,
syndromes, investigations, laboratory signs. 6. Congenital and acquired haemolyic anaemia: reasons, clinical features,
syndromes, investigations, laboratory signs.
cardi
ology
.dsmu.e
du.ua

Practical skills: UStudents should be able to demonstrate mastery of the following pratical skills To estimate clinical blood analysis 1. To enquire patients with haematological pathologies about their most disturbing
complaints 2. To carry out the inspection and palpation of lymph nodes, inspection, palpation
and percussion of the bones, spleen 3. To reveal the main laboratory criterions, clinical syndromes and symptomes of the
anaemia
Required Glossary to Practice
Term Definition
Anemia
is pathological condition characterized by decreased number of erythrocytes and the blood haemoglobin level is below the normal range in blood unit volume for the patient’s age, sex.
Hydraemia
is abnormally watery blood, due to dilution of blood in renal ,cardiac and other oedema without absolute reduction of erythrocytes (relative erythrocytopenia).
Erythrocytosis (polycythemia)
increased number of erythrocytes in the cirulating blood. The increase may or may not be associated with an elevation in the total quantity of RBC in the body.
Relative polycythemia
The concentration of the RBC becomes greater than normal (but total red cell mass is normal)in the circulating blood. This occurs as a result of loss blood plasma. (dehadration -low fluid intake,diarrhoea,vomiting, sweating)
Absolute polycythemia (erythrocytosis)
There is an increase in the total red cell mass.
Primary polycythemia (erythramia, polycythemia vera, primary proliferative polycythemia, Vakeza disease)
It is one of the chronic myelopolyferative disorders.It is characterized by increased production of all cell, however the disease is generally dominated by an elevated RBC, haemoglobin concentration.
Colour index
Haemoglobin content (haemoglobin saturation) of each erythrocyte, it compare with normal saturation= 1
Colour index = U 3 * Hb U RBC(first three figures).
Normochromia colour index - 0,85-1,05 (normochromic anemia)
9
cardi
ology
.dsmu.e
du.ua

Hyperchromia
colour index more than 1,05 – the volume of erythrocyte is higher than normal. It occurs in hyperchromic anemia - vitamin B-12 deficiency anemia.
Microcytosis (microtic red cells)
decrease in diameter of RBC less than < 7 μm, it occurs in iron deficiency anemia
Macrocytosis (macrocytic red cells)
increase in diameter of RBC more >9 to 11μm it develops in vitamin B12 folate deficiency anaemia; haemopoietic dysfunction of the liver liver disease,
Anisocytosis Exessive variation in the size of RBC. It occurs in different anaemias.
Poikilocytosis
The changes in the shape of RBC in severe anaemia. Specificpoikilocytosis- micropherocytic haemolytic anaemia (microcytic, spherocytic shape). .
Polychromasia
Presence in peripheral blood the polychromatophilic, immature erythrocytes which have different colour because they are stained acid and alkaline stains.
Normoblasts Immature nuclear (still containing nuclei) red cells. They delivered into the blood from bone marrow in its erythropoietic hypofunction.
Reticulocyt Immature red cells; last precursor of red cells. They have reticular formation.
Pernicious anemia Anemia caused by a deficiency of vitamin B12; commonly caused by absence of intrinsic factor in the stomach.
10
cardi
ology
.dsmu.e
du.ua

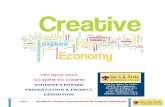
Flow chart 1
USyndrome of Anaemia
Anaemia
11
Clinical Signs
UComplaints:U weakness, dizziness, fainting, fast fatigue, dyspnoea, ear noise, palpitation, decreased appetite.
UInspection:U pallor of skin and mucous membrane, trophic changes of skin and mucous membrane
UPhysical examination:U dyspnoea, tachicardia, functional systolic murmurs over heart and vessels, cervical venous hum.
Wax-like pailness
Pailness with lemon like tinge, smooth and glossy tongue.
Pailness with golden yellow tinge
Pica, dyspeptic complaints, dysphagia.
Burning sensation of the tongue, skin paraesthesia, changed gait, deranged sleep, irritability.
Increased body temperature Increase in spleen and liveer
Laboratory investigation
UBlood analysis Haemoglobin and RBC are reduced, anisocytosis, poikilocytosis, increased ESR.
UOther investigations
Hypochromia, microcytosis, frequently thrombocytoleucopenias, eosinopenia
Hyperchromia, macro- and megalocytosis, Jolly boddies, Cabot rings, neutropenia, eosinopenia, relative lymphocytosis, thrombocytopenia.
Normochromia, microspherocytosis, sicle cells.
Decrease in plasma iron
Insignificant increase in unconjugated bilirubin
Increase in unconjugated bilirubin in the blood, increase in stercobilin , decrease in osmotic resistance of RBC .
Absence of reticulotes, thrombocytopenia., relative monocytosis and lymphocytosis .
UBone marrow study: Hypocellular and acellular marrow.
Based on the cause of aneamia
UPosthaemorrhagic Acute and chronic
UDue to inadequate production of red cells
UHaemolytic
Iron deficiency ВR12R and folate deficiency Hypoplastic and aplastic
metaplastic
cardi
ology
.dsmu.e
du.ua

USuggested Reading List URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Functional investigation of the blood 5. Methodical guideline for students 6. Flow charts for Practice 7. Website of department: www.cardiology.dsmu.edu.ua
UAdditional Reading
1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
UClinical Study of the Blood
Includes: UQuantitativeU and
UQualitative Determination:
12
↓ ↓
Cell count Leucocyte formula: cellular changes of the size, shape (morphology of the cells)
- erythrocyte count - level of haemoglobin - reticulocyte count - platelet count - leucocyte count
URed Blood study
- Red blood cells (erythrocytes) - Haemoglobin - Colour index - Hemotocrit - Reticulocyte count The main function of “Red” blood is taking part in gas exchange.
cardi
ology
.dsmu.e
du.ua

Haemoglobin There are three main methods for determining UHaemoglobinU.
1)colorimetric (widely used in practical medficine-Sali’s method) 2)Gasometric 3)Determination by the iron contained in the haemoglobin molecule.
The most accurate technique –cyanmethaemoglobin method. *concentration of haemoglobin in healthy people varies from :
120-260 g/l in women 130-170 g/l in men
Neutrophils are classified into: 1) juvenile (metamylocytes) neutrophils (0%)- in peripheral blood 2) stab (band) neutrophils 2-7% 3) segmented neutrophils (50-70%) - mature neutrophils Granules of neutrophilic leucocytes are small, stained brown-voilet colour. Segmented neutrophils have nuclei which consist of 2 to 5 segments of various size and shape connected by thready bridges The main function of the neutrophils is phagocytining. PLATELETS (Thrombocytes) are derived from marrow megakaryocytes; normal life span is about 7-10days; blue or puple non-nucleated discs, with granular centre. Their normal number is 180,0 – 320* 10P
9P/l per microlitre.per 1L (180,000-320,000
per 1 ML) of blood . The main function of platelets is formation of mechanical plug during the haemostatic response to vascular injury.
- adhesion - aggregation - platelet release reaction (vasoconstriction – tromboxane
A2, heparin neutralizing factor, fibrinogen, serotonin). IF the number of thrombocytes decreases significantly – thrombocytopenia a tendency to haemorrhages develops. Critical figure at which haemorrhage occurs is believed to 30-50*10 /L. 9
THROMBOCYTOPENIA - immune (idiopathic) thombocytopenic purpura - Vergolf’s disease (antiplatelet antibodies) due to virus and bacterial infections (including HIV infections), drugs (aspirin, indomethacin, penicillins, heparin) -marrow aplasia (idiopathic,drugs) (apalastic condition) -marrow infilterations (leucaemia, myeloma). -SLE,Vasculatis, DIC (dissminated intravascular coagulation) -uraemia -sepsis -hypersplenism (portal hpertension, lymphomas, myeloproliferative disorders). -B12, folate deficiency anaemia
13
cardi
ology
.dsmu.e
du.ua

THROBOCYTOSIS Increase in risk of clots. Occurs after haemorrhages, operations. - polycythemia - splenectomy - malignant tumours
NEUTROPENIA
It is a kind of leucopenia (decrease in neutrophils). Due to disturbed or inhibted leukopoiesis. It is observed in action of various toxic substances 1)The poisoning with benzelen, arsenic, sulphonamides. 2) ionising radiation 3) some drugs (sulpha drugs,aspirinamidobutrin, lutostic. Actions some infections 4) typhoid fever, brucellosis, virus infections- influenza, measles,German measles, chicken pox, infectious hepatitis. Sometimes leukopenia is manifested in the form of agranulocytes which is characterized by strong decrease or even absence of neutrophils and other granulocytes in blood,when the number of granulocytes is below 0,75*10 9 /L or total number of leukocytes is below 1*10 9 /L.
NEUTROPHILIA: 1) bacterial infections, pyogenic processes 2) different in toxications (uraemia, diabetes, acidosis, lead poisoning, digitalis, mercury) 3) necrosis, damage of the tissues - myocardial infaction, burn, operations. 4) malignancies (carcionomas, sarcomas). 5) systemic diseases of the connective tissue
ACCELERATION OF ESR Develops due to changes ratio between proteins in blood (globulins, albumin, fibrinogen) and increased content of high dispersed protiens (globulins,fibrinogen) these protiens absorbed on negative changed RBC and thus promote their agglutination and sedimentation- infections and inflammatory processes 1) bacterial infections (non - viral infections) 2) tbs 3) immune connective tissue diseases. 4) miocardial infarction 5) malignant tumours 6) liver diseases 7) multiple myeloma 8) amilodosis 9) nephrotic syndrome
14
cardi
ology
.dsmu.e
du.ua

15
10) anaemia – decreased number RBC accelarates ERS due to agglutination arises more easier 11) pregnancy, vaccination
DECREASE IN ESR 1) polycythemia vera- Vakeza’s disease. 2) typhoid fever. 3) viral infections 4) obstructive jaundice with significant cholemia. UANAEMIA U- is pathological condition characterized by decreased number of red blood cells and blood haemoglobin level is below the normal range in blood unit volume for the patient’s age, sex. CLASSIFICATION: Based on the cause of anaemia. There are three main groups. 1) DUE TO BLOOD LOSS-Postthaemorrhagic anaemia. a) Acute posthaemorrhagic anaemia- acute blood loss (trauma, postpartum bleeding)-large volume over short period. b) Chronic posthaemorrhagic anaemia- chronic blood loss small volume over long period.it may considered as iron deficiency anaemia.(bleeding peptic ulcer, haemorrhoids, excessive mentraual loss, look worms). 2) DUE TO INADEQUATE PRODUCTION OF RED CELLS:(disordered haemopoiesis). a) Iron deficiency anaemia due to iron deficiency- -increased demand- physiological –pregnancy,lactation,adolescent growth,mesuration. -iron loss due to bleeding- hook worm infestation,menorrhagic postpartum haemorrhage,peptic ulcer,piles, neoplastic diseases,erosion from in flammatory drugs. -malabsorption- inflammatory bowel disease a tropic gastritis. -in adequate diet- postgastectomy. b) Vitamin B12, folate deficiency anaemia.due to vitamin B12 and folate deficiency - malabsorption syndrome, postgastrectomy, atropic gastritis (lack of intrinsic factor), gastric cancer, entritis, intestineotomy, helminthic infestation, inadequate nutrition (alcoholics, purevegetarians), hepatitis, liver cancer, cirrhosis. c) Influence of toxic factors - chronic inflammatory and infective disease, renal failure, hepatic failure d) Marrow failure - hypoplastic, aplastic anaemia (condition) - endogenous or exogenous toxicosis (inhibition of the bone marrow), radiation; drugs (cytotoxic drugs, antibacterial drugs, tranquillizers, antirheumatic drugs), chemicals (benzene,arsenic, mecury), viral and bacterial infections (viral hepatitis, mononucleosis, HIV, parvovirus; tbs). e) Metaplastic anaemia due to marrow invasion - red bone marrow is replaced by other tissue (leukaemias, multiple mieloma, fibrosis, metastasis).
cardi
ology
.dsmu.e
du.ua

16
3) DUE TO EXESSIVE DESTRUCTION OF RED CELLS (HAEMOLYTIC ANAEMIAS) 1) UCongenital genetic defectsU a) Red cell membrane defects - spherocytosis- Microspherocytosis anaemia Minkovskiy – Shoffar’s anaemia (hereditary spherocytosis) - Elliptocytosis b) Haemogloblin defects: sickle cell anaemia- results from an abnormal haemoglobin known as Hb –S or sickle cell Hb. The molecular lesion in Hbs is the subsituation of valine for glutamic acid at the beta chain. Thalasimia- reduction or absence synthesis of one of globulin chains – alpha or beta thalassaemia it depends on which chains are affected. c) Enzyme defects – G6PD (glulose 6- phosphate dehydrgenase) deficiency, pyruvate kinase deficiency. 2) UAcquired U- influence of extra-erythrocytic factors: - Infections (malaria, sepsis, influenza) - Haemolytic disease of new borns. - Bruns - Mushroom poisoning - Incompatible blood transfusion - Drugs (asprin, sulphamides, nitrofrurtion, L-Dopa) - Autoimmune process- antibodies against RBC. - Proxysmal cold haemoglobinuria - attack of acute haemolysis on exposure to cold.
Normal blood values Haemoglobin (males) – 130 -170g ⁄ l Haemoglobin (females)- 120-160g ⁄ l Red blood cells (m)- 4·10P
12P/l -5,5·10P
12P/l
Red blood cells ( f )- 3,5· 10P
12P/l -5,0·10P
12P/l
Colour index - 0,85- 1,05 Diameter of RBC -7-9µm Haematocrit (m) – 40-55% Haematocrit (f) – 35-42% Reticulocytes – 0, 2 -1,2% (2-12‰) White blood cells (m)- 4,5 ·10P
9P/l -8,0 ·10P
9P/l
White blood cells ( f )- 3,5 ·10P
9P/l -7,0 ·10P
9P/l
Average white blood cell count - 4 ·10P
9P/l - 9 ·10P
9P/l
Eosinophils -0,5 – 3% Basophiles -0-1% Stab neutrophils -2-7% Segmented neutrophils- 50-70% Lymphocytes – 20- 35% Monocytes – 5-10% Myelocytes - 0%
cardi
ology
.dsmu.e
du.ua

17
Metamyelocytes - 0% Platelets – 190 ·10P
9P/l - 320·10P
9P/l
ESR(m) – 3-12mm/l ESR(f) – 5- 20mm/l Osmotic resistance of red blood cells (osmotic fragitity test ) Minimal – 0,42 -0,46%NaCL Maximum – 0,30 -0,36%NaCL
cardi
ology
.dsmu.e
du.ua

UHaemopoiesis
Pluripotent stem cell
18
UErythropoesis ↓ Erythroblast ↓ Pronormocyte ↓ Basofile normocyte ↓ Polychromatofile normocyte with nucleus ↓ Oxyfile normocyte ↓ Reticulocyte ↓ RBC (life span 120days) UMyelopoiesis ↓ Myeloblast ↓ Promyelocyte ↓ Myelocyte ↓ Metamyelocyte (juvenile) ↓ Stab neutrophils ______ appear in peripheral blood
UThrombopoiesis ↓ Megacaryoblast ↓ Promegacaryoblast ↓ Megacaryocyte ↓ Platelet (tb) - life span 7-10days ULymphopoiesis ↓ Lymphoblast ↓ Prolymphocyte T-cell
↓ Segmented neutrophils (basophils, eosinophils, neutrophils) UMonopoiesis ↓ Monoblast ↓ Promonocyte ↓ Monocyte ↓ Macrophage (in tissue)
↓ Lymphocyte B-cell ↓ Plasma cells
cardi
ology
.dsmu.e
du.ua

19
Revision Questions
Q1. Choose the parameter which is not included into the clinical study of the blood: A. platelet count B. reticulocyte count C. level of haemoglobin D. haematocrit E. leucocyte formula Q2. Macrocytosis is characteristic for: A. iron deficiency anaemia B. relative erythrocytosis C. vitamin B12 anaemia D. aplastic anaemia E. any anaemia Q3. Choose normal leukocyte count for women in the clinical investigation of the blood : A. 2,5·10P
9P/l
B. 3,0·10P
9P/l
C. 3,3·10P
9P/l
D. 7,0·10P
9P /l
E. 11,0·10P
9P/l
Q4. The reason of haemolytic anemia may be: A. enteritis B. helminthic infestation C. congenital defects of red blood cells D. metastasises in the bone marrow E. all listed variants Q5. Anisocytosis is characteristic for: A. iron deficiency anaemia B. vitamin B12 anaemia C. R Raplastic anaemia D. any anaemia E. relative erythrocytosis Q6. Choose the normal level of hemoglobin for men in the clinical investigation of the blood : A. 100 g/l B. 110 g/l C. 150 g/l D. 180 g/l E. 200 g/l Q7. High ESR is typical for: A. multiple myeloma B. influenza C. cardiac failure D. polycythaemia vera
cardi
ology
.dsmu.e
du.ua

20
E. all listed variants Q8. Define the color index, if level of hemoglobin is 138 g/l and red blood cell count is 4,4·10P
12P/l :
A. 0,74 B. 0,87 C. 0,94 D. 1,0 E. 1,2 Q9. Macrocytosis is characteristic for: A. iron deficiency anaemia B. aplastic anaemia C. folate deficiency anaemia D. severe anaemia E. relative erythrocytosis Q10. Choose the normal level of hemoglobin for men in the clinical investigation of the blood : A. 100 g/l B. 110 g/l C. 120 g/l D. 170 g/l E. without correct previous variants of answers
Answer Keys: Q1D, Q2C, Q3D, Q4C, Q5D, Q6C, Q7A, Q8C, Q9C, Q10D.
2BSUMMARY OF PROCEDURES
The practice lesson shall begin in the study room, with the homework assignment checked and students’ testing carried out.
Then students with teacter discuss signs of blood investigations for diagnostics of different pathology and their diagnostic value. Teacher gives students blood analyses for revelation the changes in these analyses and discuss disorders which may cause these changes. Then the symptoms and sings characteristic of anaemic syndrome, the methods of it’s determination (clinical, laboratory), mechanisms of anaemia development and it’s type are discussed. After that students examine patients independently, divided into groups for 2-3 men. At the end of the practice teacher makes short general conclusion concerning obtained findings and students do final tests.
Final Tests Q1. Define character of the anemia if in the peripheral blood: red blood cell count is 2,8· 10P
12P/l, hemoglobin is 64 g/l, reticulocyte count is 4 %:
A. hypochomic аregenerative B. hypochomic regenerative C. normochomic hyporegenerative D. normochomic regenerative E. hyperchomic аregenerative
cardi
ology
.dsmu.e
du.ua

21
Q2. Microcytosis is characteristic for: A. iron deficiency anaemia B. relative erythrocytosis C. vitamin B12 anaemia D. severe anaemia E. any anaemia Q3. Decreased level of the haematocrit is occurred in: A. increased quantity of red blood cells in the peripheral blood B. increased quantity of white blood cells in the peripheral blood C. increased quantity of platelets in the peripheral blood D. hypovolemia (decreased plasma volume) E. massive hemorrhage Q4. High ESR is typical for: A. multiple myeloma B. myocardium infarction C. nephrotic syndrome D. tuberculosis E. all listed variants Q5. Poikilocytosis is characteristic for: A. iron deficiency anaemia B. vitamin B12 anaemia C. aplastic anaemia D. severe anaemia E. relative erythrocytosis Q6. Increased level of the haematocrit is occurred in: A. increased quantity of red blood cells in the peripheral blood B. increased quantity of white blood cells in the peripheral blood C. increased quantity of platelets in the peripheral blood D. hypervolemia (increased plasma volume) E. haemolysis of red blood cells Q7. Choose the normal reticulocyte count in the clinical investigation of the blood : A. 0,1% B. 0,5% C. 3% D. 5% E. 10% Q8. The term "microcytosis" means: A. presence of red blood cells with various shape in blood B. presence of white blood cells with small sizes in blood C. presence of red blood cells with small sizes in blood D. presence of red blood cells with various diameter in blood E. presence of red blood cells with high haemoglobin content in blood Q9. The reason of vitamin B12 deficiency anemia may be: A. mushroom poisoning B. burns
cardi
ology
.dsmu.e
du.ua

22
C. helminthic infestation D. without correct previous variants of answers E. all listed variants Q10. The reason of the acquired haemolytic anemia may be: A. enteritis B. helminthic infestation C. metastasises in the bone marrow D. malaria E. all listed variants
cardi
ology
.dsmu.e
du.ua

The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptomes and Syndromes of the Internal Diseases
Topic 6 Module Blood disorders, musculoskeletal disordes,
endocrine disease, interpretation data of laboratory investigation.
Practice The main hematologic syndromes. Haemorrhagic syndrome. Main syndromes in leukemia.
Course 3
Faculty International Medical Faculty
Donetsk 2009
23
cardi
ology
.dsmu.e
du.ua

24
UImportance of the Subject U: Early diagnostics of blood disorders is necessary at the adequate estimation of basic clinical symptoms and syndromes. It provides, at first, the choice of method of treatment and prevention worsening of pathological process before making final diagnosis and secondly choice of methods of examination as much as possible quickly provides confirmation of final diagnosis UKey Objective:U Students should be able to reveal features and signs of syndromes of blood pathology (haemorrhagic syndrome, disseminated intravascular clotting syndrome, syndrome of enlarged lymph nodes, syndrome of leukemia) using enquiry, inspection, palpation and laboratory diagnostics for confirmation of these syndromes
USpecific Goals: 1. To develop skills in revealing haemorrhagic syndrome according to equiry, main clinical signs and laboratory criterions 2. To develop skills in revealing disseminated intravascular clotting syndrome
according to equiry, main clinical signs and laboratory criterions 3. To develop skills in revealing the syndrome of enlarged lymph nodes according to
equiry, main clinical signs and laboratory criterions 4. To develop skills in revealing the syndrome of leukemia according to equiry,
main clinical signs and laboratory criterions
Level of Knowledge and Skills before the Practice: 1. To have knowledge of the mechanism of haemostasis, coagulation cascade (Described in the Physiology course) 2. To have knowledge of anatomical details and projection of the lymph nodes and spleen (Described in the Human Anatomy course) 3. To distinguish the cellular elements of blood on their morphological properties (Described in the Histology course) 4. To carry out clinical analysis of the blood – blood taking, preparation of smears (for microscopic examination), cell count, ESR determination (Described in the Physiology course)
Questions for Self-Assessment of the Pre-Practice Knowledge Q1 A patient's blood was analyzed and the decreased erythrocyte’s sedimentation rate (ESR) was discovered. What disease from the listed below is accompanied with decreased ESR? A. Myocardial infarction B. Hepatitis C. Splenomegaly D. Polycytemia E. Vitamin B deficiency Q2. A patient with tissue trauma was taken a blood sample for the determination of blood clotting parameters. Specify the right sequence of extrinsic pathway activation. A. III – VIII: TF – Xa
cardi
ology
.dsmu.e
du.ua

25
B. III – VIIa – Xa C. III – IV – Xa D. IV – VIII: TF – Xa E. IV – VIIa – Xa Q3. A couple came for medical genetic counseling. The man has hemophilia, the woman is healthy and there were no cases of hemophilia in her family. What is the risk of having a sick child in this family? A. 25% B. 0 C. 100% D. 75% E. 50% Q4. During physical examination incresed size of spleen was revealed in patient with leukemia. Choose normal length of spleen A. 1-3 cm B. 5-7 cm C. 22-25 cm D. 18-20 cm E. 11-13 cm. Q5. During physical examination incresed size of spleen was revealed in patient with leukemia. Name normal projection of transversal size of spleen A. Between V and VII ribs B. Between VII and VIII ribs C. Between IX and XI ribs D. Below XII rib E. Level of navel Answer Keys: D, B, B, E, C. The following printed materials can be of help to improve your pre-practice knowledge and skills: 1. Test book of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 2. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 3. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy
UContents of Practice UTopics of Theory: The main coagulation components, coagulation cascade 1. Haemorrhagic syndrome in thrombocytopenia, coagulopathy, hemorrhagic
vasculatis. 2. Laboratory investigations of haemorrhagic syndrome, coagulation tests 3. Reasons, pathogenesis, laboratory signs of disseminated intravascular clotting 4. Main clinical symptomes and laboratory signs in leukemia
cardi
ology
.dsmu.e
du.ua

Practical skills: UStudents should be able to demonstrate mastery of the following pratical skills 1. To reveal haemorrhagic syndrome according to equiry, main clinical signs and
laboratory criterions 2. To reveal disseminated intravascular clotting syndrome according to equiry, main
clinical signs and laboratory criterions 3. To reveal the syndrome of enlarged lymph nodes according to equiry, main
clinical signs and laboratory criterions 4. To reveal the syndrome of leukemia according to equiry, main clinical signs and
laboratory criterions Required Glossary to Practice
Term Definition
Myeloplastic syndrome (panmyelophtisis)
Is a large group of conditions of various aetiology and pathogenesis whose main clinical syndroms are determined by the inhibition of blood formation in the bone marrow
Hypoplastic and aplastic condition
Incomplete or complete inhibition of bone marrow
Panmyelophthisis In which the regeneration function of bone marrow is inhibited in all directions
Haemorrhagic syndrome
There are hemorrhagic diseases in which bleeding disorders are main leading symptomes (bleeding into skin, mucous membranes, muscles, joints, bleeding from wounds, easy bruising) in haemophilia, thrombocytopenic purpura
Immune idiopathic thrombocytopenic purpura (Werlhof’s disease)
Increased destruction of platelets due to production anti-thrombocytic antibodies which fix on surface of platelets and damage them
Haemophilia Is X – linked recessive genetic disorders of coagulation. It results from reduction of coagulation factors (haemophilia A - VIII factor, haemophilia B - IX factor, haemophilia C - X factor)
Leukaemia Is characterized by a failure of cell maturation (differentiation), proliferation of immature cells which fill up the bone marrow so replacement (metaplasia) of these pathological cells for normal cells of the haemopoietic organs develops
Hiatus leucaemicus
Is typical for acute leukaemia. Presence blasts, mature forms in leucocyte formule in peripheral blood and absence intermediate forms
26
cardi
ology
.dsmu.e
du.ua

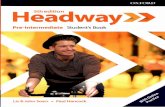
Flow chart 1
Enlargement of Lymph Nodes
Local Generalized
Local infections
Systemic connective tissue disease
27
1- size 2- presence or absence of tenderness 3- consistensy 4- mobility 5- fusing with skin 6- fusing between each other 7- changes of skin over lymph nodes
Tumours Immune process
Granuloma Features
1 2 3 4 5 6
Tumours tous process
Hereditarity process
Lymphoproliferative syndrome
7
cardi
ology
.dsmu.e
du.ua

28
Flow chart 2
Reasons Of Enlargement Of The Lymph Nodes
Enlarged lymph nodes
Common reasons of enlargement of lymph nodes
Cervical lymph nodes
Tonsillitis Pharyngitis Scarlatina (scarlet fever) Diptheria Lymphangioma Tumour of thyroid gland
Submandibular lymph nodes
Caries Gingivitis Tumour of larynx Carcinoma of lips
Supraclavicular lymph nodes
Tumour of mammary gland Tumour of stomach (Virchow's metastasis)
Subclavicular lymph nodes
Tumour of thyroid gland Tumour of the lung
Axillary lymph nodes
Furunculosis Paronychia Pararitium (felon,whitlow) Tumour of mammary gland Tumour of lung
Inguinal lymph nodes
Paronychia, paraitium Blister foot Syphilis Gonorrhea Bartholinitis
General enlargement of lymph nodes
Tbs Sarcoidosis Syphilis Mononucleosis Lymphoid leukaemia Lymphogranulomatosis Lymphosarcoma Systemic connective tissue diseases HIV
cardi
ology
.dsmu.e
du.ua

Flow chart 3
Leukaemia
The main clinical syndrome
Myeloproliferative Lymphoproliferative syndrome syndrome
Enlargement of lymph nodes
Splenomegaly
Splenomegaly Hepatomegaly
29
Pain in the bones Skin damages
Added syndromes
Prolifera Haemorra Immunode ficiency
Hematolo gic
Anaemic
tive gic
Sings
Proliferation of immature cells
Failure of cell maturation
(differentiation)
Replacement (metaplasia) of
the bone marrow
Development of pathological
foci ( leukaemic infiltrations)
cardi
ology
.dsmu.e
du.ua

30
USuggested Reading List URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Functional Investigation of the Blood 5. Methodical guideline for students 6. Flow charts for Practice 7. Website of department: www.cardiology.dsmu.edu.ua
UAdditional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
UHAEMORRHAGIC SYNDROME There haemorrhagic diseases in which bleeding disorders are the main leading symptoms. In some diseases the haemorragic syndrome is secondary one (liver diseases; leukemia, aplastic, hypoplastic anaemias). Clinic: 1) Bleeding into skin - purpura, petechia, echymoses 2) Bleeding into mucous membranes-epistaxis, haemorrhagic bullae in oral mucosa; genitourinary, gastrointestinal bleeding 3) Bleeding into viscera, muscles, joints 4) Easy brusing 5) Prolonged bleeding from wounds 6) Intracranial haemorrhage
UCoagulation Tests 1. Whole blood clotting time (blood coagulation time time - Lee and White method). Venous blood specimen is placed in a test tube and kept at 37deg.CP
oP. In the norm
blood coagulation is 5-10 minutes. *Less than 5min. – Hypercoagulation. *More than 10min. – Hypocoagulation (deficiency of factors- haemophilia A, B; administration of heparin). *Vasopathy, Thrombocytopenia- N. 2. Bleeding time (By Duke’s method) - finger tip in punctured by blood lancet to depth 3mm then touch to skin with special paper every 15sec, until all bleeding ceases. Normal time is 2-4min. It estimates adherence and fusing (aggregation) features of Tb.
cardi
ology
.dsmu.e
du.ua

31
*Increase in time- in thrombocytopenia, thrombopathy, N- in haemophilia. 3. Retraction of blood clot (clot retraction): Also depends on number and activity of Tb, retrozyne which realizes by Tbs and causes retraction. Norm- 0,3 – 0,5 : *decrease in the thrombocytopenia,thrombocytopathy. 4. Platelet count (decrease in thrombocytopenia, leukaemia, hypoplastic conditions). 5. Activated partial thromboplastin time (APTT). 6. Thrombin time. 7. Prothrombin time. 8. Prothrombin index:- prothrombin time of donor’s plasma / prothrombin time of the patient’s plasma= N- 80-10% 9. Fibrinogen level 10. Fibrin degradation products.(FDPs). 11. INR ( International Normalized Ratio) 12. Capillary permeability tests (capillary resistance tests): a) Konchalovosky-Rumpel-Leede sign (tourniquet test –Hess test):- A tourniguet is applied to the forearm and changes occuring in the skin are assessed. If petechiae appear on the skin below the tourniquet, the test is positive. b) Cupping glass test. c) Pinch test. d) Mallet symptom- ecckymosis develops on the skin after tapping percussion mallet. * These tests estimate vascular component and they are positive in vessel wall abnormilities – vasopathy sometimes in thrombocytopenia, thrombocytopathy.
UImmune (Idiopathic) Thrombocytopenic Purpura (ITP) (Werlhof’s disease) Anti-thrombocytic antibodies of IgG type are produced and fixed on surface of TB to damage them. Reasons: Viral and bacterial infections, drugs, vaccination. Clinic: Multiple haemorrhages into skin- petechiae, echymoses (large spots), purpura and mucous membrane. - Prolonged bleeding from superficial cuts. - Bleeding immediately after sugery, trauma. Local pressure effective. History of drug intake especially non-steroidal anti –inflammatory drugs (like Aspirin), viral infections Investigation: - Decrease in Tbs. - Prolonged bleeding time. -Clot retraction is decreased. -Blood coagulation time- N - May be positive capillary resistance tests.
UHaemophilia Haemophilia is X-linked recessive genetic disorder of coagulation. It results from reduction of (VIIIP
th Pcoagulation factor – Haemophilia A, IXP
thP- B, X th
P -C). P
cardi
ology
.dsmu.e
du.ua

32
Clinic: - Bleeding into viscera, muscles - Into joints (haemarthroses); bleeding wounds - Bleeding starts several hours after surgery or trauma (delayed bleeding) - Local pressure ineffective - East bruising - Life- long history, family history Investigation: - Bleeding time, prothrombin time and platelet count are normal - Clot retraction is normal - Blood coagulation time is proglonged (more than 10 min) - Negative capillary resistance tests. - Prolonged time of plasma recalciffication factor.(norm is 60-70sec) - Activated partial thromboplastin time (APTT) is typically prolonged. - Deficiency of specific coagulation factor (VIII ,IX ,X).
ULeukaemia
Leukaemia is characteized by a faliure of the maturation (diffrentiation), proliferation of immature cells which fill up the bone marrow; replacement (metaplasia) of these pathological cells for normal cells of the haemopoietic organs and development of pathological foci (leukaemic infilterations) in other organs. 1) Acute - lymphoid (lymphoblastic) - myeloid (myelogenous) 2) Chronic – lymphoid (lymphocytic) - myeloid (myelocytic) *It should be remembered that differentiation between chronic and acute leucosis first of all depends on the cytomorphological sign (the degree of cell mature) not on the clinical course of the disease.( its morphological diagnosis) - Myeloproliferative syndrome - Lymphoproliferative syndrome - Added symptoms: Anaemia- anaemic syndrome. Granulocytopenia- infections at various sites (oral, pharyngeal ulcers, pneumonias, fever, septicaemia) Thrombocytopenia – Haemorrhagic syndrome Expanding cell mass in bone marrow (bone pains, sternal tendeness) Leukaemic infilteration of tissues. ULeukaemias can have the following three variants - Leukaemic form- with considerable increase in the quantity of pathological cells in the periphiral blood - Subleukaemic form – with moderate increase in their number. - Aleukaemic form – Normal or decreased number of leucocytes.
cardi
ology
.dsmu.e
du.ua
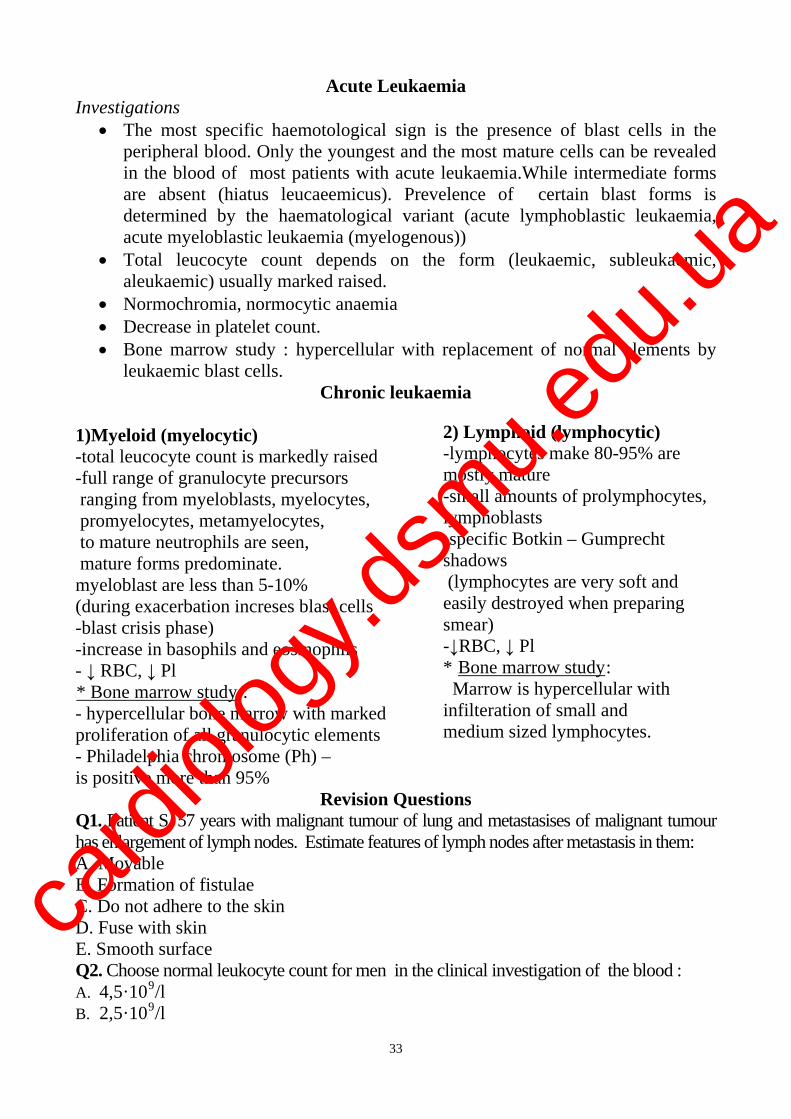
Acute Leukaemia Investigations
The most specific haemotological sign is the presence of blast cells in the peripheral blood. Only the youngest and the most mature cells can be revealed in the blood of most patients with acute leukaemia.While intermediate forms are absent (hiatus leucaeemicus). Prevelence of certain blast forms is determined by the haematological variant (acute lymphoblastic leukaemia, acute myeloblastic leukaemia (myelogenous))
Total leucocyte count depends on the form (leukaemic, subleukaemic, aleukaemic) usually marked raised.
Normochromia, normocytic anaemia Decrease in platelet count. Bone marrow study : hypercellular with replacement of normal elements by
leukaemic blast cells. Chronic leukaemia
2) Lymphoid (lymphocytic) 1)Myeloid (myelocytic) -lymphocytes make 80-95% are mostly mature
-total leucocyte count is markedly raised -full range of granulocyte precursors
-small amounts of prolymphocytes, lymphoblasts
ranging from myeloblasts, myelocytes, promyelocytes, metamyelocytes,
-specific Botkin – Gumprecht shadows
to mature neutrophils are seen, mature forms predominate.
(lymphocytes are very soft and easily destroyed when preparing smear)
myeloblast are less than 5-10% (during exacerbation increses blast cells -blast crisis phase)
-↓RBC, ↓ Pl -increase in basophils and eosinophils * UBone marrow study
33
- ↓ RBC, ↓ Pl U: Marrow is hypercellular with infilteration of small and
U* Bone marrow studyU : - hypercellular bone marrow with marked
medium sized lymphocytes. proliferation of all granulocytic elements - Philadelphia chromosome (Ph) –
is positive more than 95% Revision Questions
Q1. Patient S. 57 years with malignant tumour of lung and metastasises of malignant tumour has enlargement of lymph nodes. Estimate features of lymph nodes after metastasis in them: A. Movable B. Formation of fistulae C. Do not adhere to the skin D. Fuse with skin E. Smooth surface Q2. Choose normal leukocyte count for men in the clinical investigation of the blood : A. 4,5·10P
9P/l
B. 2,5·10P
9P/l
cardi
ology
.dsmu.e
du.ua

34
C. 3,5·10P
9P/l
D. 3,9·10P
9P /l
E. 11,0·10P
9P/l
Q3. Choose the parameter which is not included into the clinical study of the blood: A. platelet count B. reticulocyte count C. level of haemoglobin D. leucocyte formula E. prothrombin index Q4. Choose normal quantity of the myelocytes in the clinical investigation of the blood for women: A. 0,5-1 % B. 1-3% C. 3-5 % D. 5-7% E. they must be absent Q5. Patient A. 60 years has enlargement of cervical lymph node. Estimate features of lymph nodes which are characteristic for lymphadenitis: A. Usual colour above damaged lymph node B. Firm consistency C. Fuse with each other D. Painless E. Elastic consistency Q6. What lymph nodes may be palpated in the norm: A. submandibular lymph nodes B. axillary lymph nodes C. inguinal lymph nodes D. all listed groups of lymph nodes E. without correct previous variants of answers Q7. Patient D. 56 years with lymphogranulomatosis has enlargement of lymph nodes. Estimate features of lymph nodes which are characteristic for lymphogranulomatosis: A. Painful B. Do not fuse with each other C. Fuse with skin D. Elastic consistency E. Firm consistency Q8. Patient E. 64 years has general enlargement of lymph nodes. Which diseases do cause general enlargement of lymph nodes? A. Pharyngitis B. Diphtheria C. Lymphogranulomatosis D. Lymphadenitis E. Tonsillitis Q9. Choose normal platelet count in the clinical investigation of the blood : A. 150·10P
9P/l
cardi
ology
.dsmu.e
du.ua

35
B. 170·10P
9P/l
C. 300·10P
9P/l
D. 340·10P
9P /l
E. 400·10P
9P/l
Q10. Thrombocytosis is characteristic for: A. leukemia B. polycythaemia vera C. systemic lupus erythematos D. influenza E. all listed variants Answer Keys: Q1D, Q2A, Q3E, Q4E, Q5E, Q6D, Q7E, Q8C, Q9C, Q10B.
3BSUMMARY OF PROCEDURES Practice begins in the classroom from the testing. Then the symptoms and
sings characteristic of haemorrhagic syndrom, leukaemia the methods of their determination (clinical, laboratory and instrumental), mechanisms of development of haemorrhagic syndrom and it’s type discuses. After that students examine patients independently, divided into groups for 2-3 men. This part of the practice should fulfilled in the ward. Then students examine patients independently, divided into groups for 2-3 men.
At the end of the practice teacher makes short general conclusion concerning obtained findings and students do final tests.
Final Tests
Q1. Expressed hepatosplenomegaly is characteristic for: A. anemic syndrome B. hemorrhagic syndrome C. myeloproliferative syndrome D. lymphoproliferative syndrome E. all listed syndromes Q2. Immunodeficiency is characteristic for: A. anemic syndrome B. hemorrhagic syndrome C. total myeloaplastic syndrome D. all listed variants E. without correct previous variants of answers Q3. Patient M. 55 years has enlargement of axillary lymph node. Estimate features which are characteristic for lymphadenitis of axillary node: A. Usual colour above damaged lymph node B. Fuse with each other C. Firm consistency D. Painless E. Hyperemic colour above damaged lymph node Q4. Anaemia is characteristic for: A. myeloproliferative syndrome
cardi
ology
.dsmu.e
du.ua

36
B. hemorrhagic syndrome C. syndrome of the enlarged lymph nodes D. without correct previous variants E. all listed variants Q5. The thrombocytopenia is characteristic for: A. malignant tumours B. polycythaemia vera C. radioactive irradiation D. splenectomy E. all listed variants Q6.Considerable enlargement of the lymph nodes is characteristic for: A. anemic syndrome B. hemorrhagic syndrome C. lymphoproliferative syndrome D. all listed variants E. without correct previous variants of answers Q7. Patient V. 56 years with malignant tumour of intestines and metastasises of malignant tumour has enlargement of lymph nodes. Estimate features of lymph nodes after metastasis in them: A. Smooth surface B. Rough surface C. Formation of fistulae D. Elastic consistency E. Do not adhere to the skin Q8. The thrombocytopenia is characteristic for: A. posthemorragic syndrome B. splenectomy C. hypersplenism D. polycythaemia vera E. all listed variants Q9. Patient E. 64 years has general enlargement of lymph nodes.Which diseases do cause general enlargement of lymph nodes? A. Lymphosarcoma B. Diphtheria C. Tonsillitis D. Lymphadenitis E. Pharyngitis Q10. Patient W. 54 years has general enlargement of lymph nodes.Which diseases do cause general enlargement of lymph nodes? A. Tonsillitis B. Pharyngitis C. Lymphadenitis D. Gingivitis E. Leukemia
cardi
ology
.dsmu.e
du.ua

37
Topic 7 Module. Main syndromes and symptomes of cardiovascular diseases. Specific Goals: - To estimate data of the enquering, physical examination, instrumental diagnostics of patient with cardiovascular pathology. - Make primary conclusion of disorders of cardiovascular system - To interpret the received data of the examination for recognition of clinical syndromes of the cardiovascular system - To know new classifications of cardiovascular diseases
cardi
ology
.dsmu.e
du.ua

The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module № 2 The symptoms and syndromes at diseases of internal
Topic 7 Module Basic symptoms and syndromes at diseases of cardio-vascular system
Practice Syndrome of heart failure: basic clinical and instrumental methods of investigation. Acute and chronic circulatory collapse.
Course 3
Faculty International Medical Faculty
Donetsk 2009
38
cardi
ology
.dsmu.e
du.ua

39
UImportance of the SubjectU: Early diagnostics of circulatory collapse signs permits optimization of the future diagnostic walkback process and timely beginning of patients’ treatment what can improve their prognosis. UKey Objective:U to determine leading syndromes and symptoms in clinic of internal diseases, to analyze results of basic laboratory and instrumental methods of examination. USpecific Goals:U
1. To determine heart failure and basic pathogenetic ways of its development. 2. To classify heart failure (stages of heart failure, hemodynamic type, functional classes of patients). 3. To characterize basic clinic signs of heart failure. 4. To interpret data of instrumental methods of examination which confirm its presence. 5. To differ circulatory collapse and its basic kinds. 6. To have an idea of syncopal state, mechanism of its origin and basic clinical signs. Level of Knowledge and Skills before the Practice: 1. To assess basic physiological characteristics of cardiovascular system, mechanisms of haemodynamics regulation. “Physiology” 2. To know anatomic features of separate parts of cardiovascular system. “Anatomy” Questions for Self-Assessment of the Pre-Practice Knowledge Task 1: Systolic (stroke) volume of ventricles is: A. 45-50 mL B. 50-60 mL C. 65-70 mL D. 80-90 mL E. 100-105 mL Task 2: What anatomic structure finishes greater systemic circulation? А. Aorta В. Pulmonary artery С. Left atrium D. Left ventricle Е. Right ventricle Task 3: Musculation of ventricles has: A. One layer of muscles (longitudinal) B. Two layers of muscles (longitudinal and circular). C. Three layers of muscles (two longitudinal and circular). D. Four layers of muscles (two longitudinal, oblique and circular) E. Two layers of muscles (oblique and circular)
cardi
ology
.dsmu.e
du.ua

40
Task 4: Name three- valvate valves of heart А. all valves of heart В. aortal and pulmonary when breathlessness С. right and left atrioventricular D. semilunar and right atrioventricular Е. semilunar and left atrioventricular Task 5: Frank-Starling law provides: A. decrease of stroke volume when increasing of venous inflow. B. increase of stroke volume when increasing of venous inflow C. decrease of stroke volume when decreasing of venous inflow D. increase of stroke volume when decreasing of venous inflow E. increase of stroke volume when increasing of heart beat rate Answer Keys. Task 1: С. Task 2: Е. Task 3: С. Task 4: D. Task 5: В. UContents of Practice
UTopics of Theory:
1. Definition of heart failure and basic pathogenetic ways of its development 2. Modern classification of heart failure (stages of heart failure, hemodynamic type, functional classes of patients). 3. Basic clinic signs of heart failure and data of instrumental methods of examination that confirm its presence. 4. Circulatory collapse and its basic kinds: syncope, collapse, shock. 5. Definition of syncopal state, mechanism of its origin and basic clinical signs.
Practical skills:
1. Conduction of patient's questioning and determination of complaints typical for patients with circulatory insufficiency. 2. Conduction of objective examination and selection of circulatory insufficiency and heart failure signs. 3. Interpretation of data of instrumental methods of examination of patients with heart and circulatory insufficiency (ECG, echocardiography, radiography)
cardi
ology
.dsmu.e
du.ua

41
Required Glossary to Practice
Term Definition
Cyanosis A bluish-purple discoloration of skin and
mucous membranes usually resulting from a deficiency of oxygen in the blood
Ascites Accumulation of serous fluid in the peritoneal cavity
Orthopnea It is shortness of breath (HTUdyspneaUTH) which occurs when lying flat, causing the person to have to sleep (take a rest) propped up in bed or sitting in a chair. Mainly develops due to pulmonary congestion which results in pulmonary edema as a result of left-sided (left ventricular) heart failure
ESR The erythrocyte sedimentation rate (ESR), also called a sedimentation rate, is the rate at which HTUred blood cellsUTH precipitate in a period of 1 hour. It is a common HTUhematologyUTH test which is a non-specific measure of HTUinflammationUTH. To perform the test, anticoagulated HTUbloodUTH is placed in an upright tube, known as a Westergren tube, and the rate at which the HTUred blood cellsUTH fall is measured and reported in mm/h
Kitaev Reflex Narrowing of lungs arterioles in reply to increase in pressure in the left atrium and pulmonary veins.
For mastering of contents of practice get acquainted with flow charts.
cardi
ology
.dsmu.e
du.ua

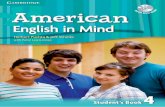
Flow chart: 1
Diagnostics of circulatory insufficiency
Questioning
42
UComplaints: U breathlessness, attacks of breathlessness, properties of sputum, feeling of heart beat intermittency, pain in the right hypochondrium, thirst, edema, diuresis
UMedical history, life history: Beginning of disease, circulatory insufficiency, course.
Objective examination
UInspection:U UPercussionU: UAuscultationU: UPalpation of Uabdomen: Cyanosis, Heart borders, Gallop rhythm Enlargement position in comparative heart murmurs of liver, bed, RR, percussion of arrhythmia, spleen; cervical veins, lungs moist rales ascites Additional investigations
U Blood:U UUrineU: USputumU: UECGU: Radiography of chest: Leukocyte Relative Leukocytes, Disturbances Increase of heart, formula, density protein, erythrocytes, of rhythm, configuration, erythro- erythrocytes, cells of heart conduction, cytosis, cylinder disease local and hydrothorax ESR, diffuse protein miocardial fractions changes
cardi
ology
.dsmu.e
du.ua

43
URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture. 5. Methodical guideline for students 6. Flow charts for practice: 7. Website of department: www.cardiology.dsmu.edu.ua
UAdditional Reading
1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Algorithm of heart failure determination
Step 1 Determination of heart failure course Acute Chronic Step 2 Determination of heart failure type Left ventricular Right ventricular Total Step 3 Determination of heart failure stage
I IIA IIB III
Situational tasks.
Task 1. 65 year old patient A. has been admitted to the clinic with diagnosis of acute transmural myocardial infarction of left ventricle. General state of patient is very severe: sluggishness, pale and grey cyanosis of face, skin is moist and cold, tongue is dry Pulse rate is 130 per minute, ABP is 70/0 mm of mercury. Pressor drugs are not effective. Urinary bladder is free. Respiration rate is 28 per minute. Edema is absent. Does this patient has circulatory insufficiency signs? Which one?
cardi
ology
.dsmu.e
du.ua

44
Task 2 Patient is ill with rheumatism and mitral stenosis. He complains of breathlessness during fast walk, dry cough, palpitation, weakness, podedema appearing in the evening and disappearing in the morning. There is moderate lips’ cyanosis, acrocyanosis, sponginess of shins. Pulse rate is 105 per minute, it is rhythmical. Breathing is vesicular, in the lower parts of lungs there are moist rales. Abdomen is soft, the liver goes beyond ribs on 3sm and it is painful. Diuresis is 900 mL. Determine grade of circulatory insufficiency. Task 3 67 year old patient L. About a year ago have had myocardial infarction. He got up in the night because of breathlessness that was rapidly increasing. Orthopnea, remote moist rales, respiration rate is 40 per minute. There is pale-grey cyanosis of face, cold sweat. Pulse rate is 140 per minute, it regular, arterial blood pressure is 110/70mm of mercury. Cough is with pink colored sputum. In the lungs there is clear pulmonary sound and dullness on percussion in the lower parts. Breathing is vesicular and diminished. There are a lot of medium and coarse moist rales. Heart borders are extended to the left on 1sm. There is accentuation of the II sound on the pulmonary artery. Liver is not enlarged, edema are absent. What are the symptoms of cardiovascular insufficiency of that patient? What is the most probable cause of the heart failure?
Revision Questions
Task 1 Patient E. has been treated of rheumatic heart disease over 15 years. He complains of inspiratory dyspnea during minimal physical activity. During auscultation of the heart it was revealed that the Ist sound was sharply depressed on the cardiac apex and there is rough pansystolic murmur of the descending configuration that is conducted to the left axillary region. This patient is sick with: A. Acute left ventricular insufficiency B. Acute right ventricular insufficiency C. Chronic left ventricular insufficiency D. Chronic right ventricular insufficiency E. Acute circulatory insufficiency Task 2 Patient has expressed heart failure. During inspection tachypnea, rapid small pulse, tachycardia, protodiastolic gallop rhythm on the apex, edema of lower extremities were revealed. Sigh of right ventricular insufficiency is: A. Tachypnea B. Rapid small pulse C. Tachycardia D. Protodiastolic gallop rhythm E. Edema of lower extremities. Task 3 25 year old patient G. suffers from essential hypertension. During the last 3 months he has been marking inspiratory dyspnea and palpitation at the usual moderate
cardi
ology
.dsmu.e
du.ua

45
physical activity. Mentioned complaints do not disturb him at rest. During examination: there is normal vesicular breathing in the lungs. Left border of cardiac dullness is displaced on 1sm to the left from midclavicular line. Heart activity is rhythmical. Heart rate is 76bpm. On the heart apex the Ist sound is lauder than the IInd one, there is accentuation of the IInd sound on aorta. ABP 170/100mm of mercury, Liver is near the edge of the costal margin. Edema is absent. This patient has: A. Chronic heart failure of the 1grade. B. Chronic heart failure of the 2A grade. C. Chronic heart failure of the 2B grade D. Chronic heart failure of the 3 grade. E. Chronic heart failure is absent. Task 4 Patient is in the clinic with severe heart failure. He complains of expressed dyspnea at rest. In case of severe heart involvement during dyspnea patient as a rule is in the forced attitude: A. Lying on the left side; B. Lying on the right side; C. Lying on the back; D. Lying on the abdomen; E. Sitting. Task 5 Patient is in the special care ward because of myocardial infarction. Suddenly patient’s state worsened. Pulmonary edema was diagnosed by the doctor on duty. At pulmonary edema dyspnea is usually combined with: A. cough; B. hyperemia of face; C. decrease of hemithorax; D. rapid formation of cardiac hump; E. rapid augmenting of emphysema of lungs. Task 6 Patient has been suffering from arterial hypertension during a long time. Her state has worsened 2 weeks ago when dyspnea and weakness increased. Currently there is dyspnea at rest increasing at the minor physical activity, conversation. During heart auscultation protodiastolic gallop rhythm was heard. If gallop rhythm appears on he ground of severe arterial hypertension it can be auscultated the best on: A. Aorta; B. Pulmonary artery; C. Heart apex; D. Near xiphoid process; E. On the 5P
thP point.
Task 7 Right ventricular heart failure developed of patient suffering from the pulmonary valve artery stenosis for a long time. What symptom is the most typical for right ventricular heart failure?
cardi
ology
.dsmu.e
du.ua

46
A. dyspnea B. cough C. hemoptysis D. ascites E. asthmatic fits Task 8 Patient with acute right ventricular insufficiency was admitted to the intensive care department. What from the listed below diseases could become possible cause of acute right ventricular insufficiency? A. Pulmonary embolism B. Chronic bronchitis C. Mitral stenosis D. Pulmonaryvalvular insufficiency E. Myocardial infarction of the left ventricle Task 9 36 year old woman gave birth about an hour ago. Postpartum hemorrhage was about 1L. Ear noise, blackout and short time loss of consciousness appeared. Acute circulatory insufficiency was diagnosed. What from the listed below is typical for collapse? A. paleness of skin B. deep noisy breathing C. increased systolic pressure D. slowing of pulse E. diffuse cyanosis
SUMMARY OF PROCEDURES The practice lesson shall begin in the study room, with the homework
assignment checked and students’ testing carried out. After that instructor gives instruction about peculiarities of patients’ examination with heart failure. Then in the wards under control of instructor students collect data of complaints and case history, conduct all the necessary examinations (inspection, borders of heart and lungs, auscultation of heart and lungs, respiration rate, heart rate, ABP, arterial pulse, palpation of liver, spleen etc). After that diagnostic significance of the found symptoms is discussed. Students determine presence of acute and chronic heart failure, grade of chronic circulatory insufficiency, syndromes of acute circulatory collapse. In the studying room instructor gives data of additional examinations (ECG, echocardiography, X-ray examination etc.) Than test control of the topic is conducted by tests of A format, students’ mistakes are discussed. Study shall be summed up and students’ works to be assessed.
Final Tests
Q1. The IP
PClass of the patients with heart failure according to classification of New
York Heart Association characterised by the following:
cardi
ology
.dsmu.e
du.ua

47
A. no limitation of physical activity, no symptoms with ordinary exertion B. slight acrocyanosis at rest, swelling of the ankles at evening C. marked limitation of physical activity, less than ordinary activity causes appearance of dyspnoea, palpitation, fatigue, and weakness D. slight limitation of physical activity, ordinary activity causes appearance of dyspnoea, palpitation, fatigue, and weakness E. dyspnoea at rest, attacks of cardiac asthma, anasarca, cardiac cachexia Q2. Expressed right-sided (right-ventricular) heart failure is characterized by A. arterial hypertension B. ascites C. cardiac asthma D. cough with a pink foamy sputum E. rales in lights Q3. Choose the disease resulting in acute heart failure: A. vascular dystonia B. mitral stenosis C. mitral regurgitation D. myocardial infarction E. aortic stenosis Q4. Choose the disease resulting in left ventricular (left-sided) heart failure: A. constrictive (adhesive) pericarditis B. polycytaemia rubra vera C. stenosis of the renal artery D. primary pulmonary hypertension E. attack of bronchial asthma Q5. Choose the clinical feature characteristic of a chronic cor pulmonale: A. pallor of the skin B. hyperemia C. pulsation of jugular veins D. pulsation of carotid arteries E. dilatation of the heart to the left and downwards Q6. Choose the disease resulting in difficulty of the blood discharging from the left ventricle: A. essential hypertension B. secondary arterial hypertension in patient with a chronic glomerulonephritis C. secondary arterial hypertension in patient with the renal artery stenosis, i.e. renovascular hypertension D. secondary arterial hypertension in patient with coarctation of the aorta E. all listed above Q7. Choose the disease which is characterized by heart failure due to primary affection of coronary arteries:
cardi
ology
.dsmu.e
du.ua

48
A. ischemic heart disease B. hypertrophic cardiomyopathy C. toxic affection of myocardium D. atrial septal defect E. mitral stenosis Q8. Severe left ventricular heart failure is characterized by: A. dry rhonchi during inspiration B. dry rhonchi during expiration C. dry rhonchi during both inspiration and expiration D. moist rales in combination with a crepitation E. pericardial friction rub Q9. The left-ventricular (systolic) dysfunction should be diagnosed at: A. presence of crepitation B. X-ray findings of pulmonary venous congestion C. swelling of the ankles D. left ventricle ejection fraction less than 45-40% (by ECHOCG) E. liver enlargement Q10. For evaluation of severity of heart failure clinical manifestations according to the classification of New York Heart Association the following criteria are used: A. intensity (character) of the peripheral edema B. liver enlargement C. level of activity which provokes the appearance of dyspnoea, palpitation, fatigue, and weakness D. presence of ascites E. all listed above
cardi
ology
.dsmu.e
du.ua

The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of Internal Medicine
Module 2 4BSymptoms and syndromes at diseases of internal organs
Topic-based Module 1 Subject
Mitral valvular diseases: main symptoms and syndromes based on clinical instrumental methods of investigation. Tricuspid valvular diseases.
Year 3
Faculty Faculty of Medicine for International Students
Donetsk 2009
49
cardi
ology
.dsmu.e
du.ua

50
Importance of the Subject : the ability to apply objective methods and to properly interpret investigation results at mitral and tricuspid valvular diseases helps to suspect pathology of the valvular apparatus, prescribe timely effective treatment, avoid complications.
Key Goal: to develop skills in determining syndromes of mitral and tricuspid valves damage by means of objective methods (interview, examination, percussion, palpation, auscultation) and laboratory instrumental methods( results of serum test, ECG, echocardiograph, phonocardiogram, X-ray examination of the thorax organs). Specific Goals:
1. To interview a patient, to state the main complaints of a patient with the valvular apparatus disorder, i.e. mitral and tricuspid valvuar diseases (dyspnea, apnoe, palpitation, heart intermittence, dizziness, loss of consciousness fits, hemoptysis, heartache), anamnestic data, their pathogenic significance. 2. To perform an objective investigation: examination (stating a patient’s position in bed, examining mucous membranes, skin, cardiac region and peripheral vessels), investigation of heartbeat, arterial and venous pulses, BP; percussion of the heart and lungs (heart borders, hydrothorax), auscultation of the heart and lungs (heart sounds, cardiac murmurs, respiratory murmurs), palpation of the stomach (enlarged liver, spleen), diagnostic estimation of the results obtained. 3. To estimate peculiarities of changes in biochemical results of blood serum(general protein albumin, proteinogram, CRP, rheumatoid factor, titer antistreptolysine O, diphenylamine, sialic acids, general bilirubin and its fractions, aloninamino transferase, AST , cholesterol) and instrumental methods of investigation (ECG, phonocardiogram, echocardiograph, X-ray examination of the thorax organs). Diagnostic significance. 4. To determine syndromes of mitral and tricuspid valves damage, pathogenic mechanisms of development of different cardiac regions overload, disorders of intracardiac and systemic haemodynamics. Goals of Prerequisite Knowledge and Skills Level: 1. To estimate the main hydrodynamic mechanisms of heart murmur formation at liquid passage in tubes (Department of Biophysics) 2. To distinguish the main characteristics of the heart cycle – systole and diastole, their phases (Department of Physiology) 3. To possess knowledge of the structure of heart cavities and valvular apparatus, points of the valves projection on the thoracic cage (Department of Normal Anatomy)
Questions for Self-Assessment of Prerequisite Knowledge and Skills: (with answer keys after the last test question)
Q 1: What is a phase of asynchronous tension? A. a period of ventricle contraction with valves closed
cardi
ology
.dsmu.e
du.ua

51
B. a period of ventricle contraction with valves open C. ventricle muscle tension without shortening of muscle fiber length D. ventricle muscle tension with shortening of muscle fiber length E. combined phases of asynchronous and isometric contraction Q 2: Which level does the left ventricle pressure reach in a healthy person during the period of blood expulsion? А. 120-130 mm of mercury column В. 100-105 mm of mercury column С. 90-80 mm of mercury column D. 60-70 mm of mercury column Е. 30-40 mm of mercury column Q 3: Give the definition of heart murmur. A. a sound caused by acceleration or retardation of blood flow B. a sound caused by vibration of the valvular apparatus C. a sound with vibration frequency < 300 Hz D. a sound with vibration frequency > 300 Hz E. a sound caused by vibration of the cardiac muscle Q4: Where is the left atrioventricular valve situated? А. in the aorta В. in the pulmonary artery С. in the pulmonary veins D. between the left atrium and left ventricle Е. between the right atrium and right ventricle Q 5: Give the definition of Reynolds number. A. a ratio of blood viscosity to vessel radius B. a ratio of blood flow velocity and vessel radius to blood viscosity C. a ratio of vessel radius and blood viscosity to blood flow velocity D. a ratio of blood viscosity to blood flow velocity E. a ratio of blood viscosity to blood flow velocity and vessel radius Answer Keys: Q1. – C; Q2. – A; Q3. – D; Q4. –D; Q5. – B;
PRACTICE OVERVIEW After you have made sure that you have the prerequisite knowledge and skills, you can proceed to the “PRACTICE OVERVIEW” section below.
Theory Topics Addressed by the Practice Activities 1. Occurrence and frequency of mitral and tricuspid valves damage. 2. Main causes and mechanisms of development of mitral and tricuspid valvular
diseases (stenosis and insufficiency). 3. Haemodynamic changes at mitral and tricuspid valvular diseases. Importance of
Kitaev’s reflex.
cardi
ology
.dsmu.e
du.ua

52
4. Main complaints, data of examination, palpation of the precordial region and percussion at mitral and tricuspid valvular diseases.
5. Auscultation picture of mitral stenosis and mitral insufficiency. 6. Auscultation picture of tricuspid stenosis and tricuspid insufficiency. 7. ECG and phonocardiogram signs of mitral and tricuspid valvular diseases. 8. X-ray signs of mitral and tricuspid valvular diseases. 9. Changes in laboratory results depending on etiologic factor and expressed cardiac
failure. 10. The concept of mitral valve prolapse.
Practical skills:
1. Collecting complaints and anamnesis of patients with mitral and tricuspid valvular diseases.
2. Examining a patient. Palpating the precordial region. 3. Determining heart borders. 4. Carrying out heart auscultation. 5. Interpreting and estimating results of ECG, phonocardiogram, echocardiograph,
X-ray examination of the thorax organs of patients with mitral and tricuspid valvular diseases.
6. Estimating laboratory investigation results. 7. Identifying a clinical syndrome.
cardi
ology
.dsmu.e
du.ua

53
Required Glossary to Practice
Term Definition Kitaev’s reflex A reflex narrowing of arterioles in the lungs
due to irritation of baroreceptors at increased pressure in the left atrium and pulmonary veins (accompanied by increased pressure in the left atrium).
Mitral valve prolapse A dysfunction of the mitral valve at which one or both cusps are turned out into the left atrium cavity during ventricular systole resulting in inverse blood flow from the left ventricle into the left atrium.
Vinogradov’s sign Pulsation of jugular veins with synchronic throwing back of the head – a sign of a
tricuspid valvular disease.
Popov-Saveliev’s sign Different pulse on hands at mitral stenosis. Rivero-Corvallo’s sign Increased systolic murmur at inspiration at
tricuspid valve insufficiency. Frank-Starling law Increased power of left ventricle contraction at
its blood overflow. Angiocardiography A method of X-ray examination allowing
obtaining pictures of some heart cavities or great vessels.
Siderophagus A cell of yellow and brown color (due to hemosiderin’s presence) found in sputum at mitral valvular diseases.
Phonocardiography Graphic registration of sound vibrations arising in the heart and great vessels due to their activity.
To master the material on the subject study the following flow charts:
cardi
ology
.dsmu.e
du.ua

Flow chart 1
54
cardi
ology
.dsmu.e
du.ua

Flow chart 2
55
cardi
ology
.dsmu.e
du.ua

USuggested Reading List URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Mitral valve disease 5. Methodical guideline for students 6. Flow charts 1, 2. 7. Website of department, e-mail: www.cardiology.dsmu.edu.ua
UAdditional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 4. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
UGuide Sequence of ActionsU.
Algorithm of actions at auscultation of patients with mitral and tricuspid valvular diseases:
Carrying out auscultation in the
points of listening to the valves
56
Estimating sound characteristics and presence of additional
sounds
Giving characteristics of the sounds
Determining direction of sound conduct
Mitral valve Tricuspid valve
Region of apical beat STEP 1 Near xiphoid process
STEP 2
STEP 3
STEP 4 cardi
ology
.dsmu.e
du.ua

57
Additional methods of investigation in diagnosis of mitral stenosis. 1. ECG reveals hypertrophy of the left atrium (P wave is dilated more than 0.12s and two-humped) and of the right ventricle (axis deviation to the right, dislocation of the transitional zone to the left, increased range of wave R in the right chest leads). Atrial fibrillation is possible. 2. Phonocardiography reveals a great range of sound I in the region of cardiac apex (2-3 times as much as the norm); lengthening of Q-I interval to 0.08-0.12s (N-0.04-0.06s); splitting and accent of sound II above the pulmonary artery; appearance of opening snap (sound) of mitral valve 0.04-0.10s after sound II; decreasing diastolic murmur and increasing presysolic one, fused with sound I. 3. Echocardiograph reveals thickening of mitral valve, their abnormal fusion along commissures limiting their opening in diastole. The method allows measuring degree of left atrium dilatation and area of mitral ring, intra-atrial thrombus visualization is possible. 4. X-ray examination of the thorax organs reveals increased left atrium (mitral configuration of the heart – flatness of waist of heart). Congestion signs in the pulmonary circulation are revealed through interstitial edema of the lungs, presence of Kerli’s lines (edema of interlobular septa). At the development of pulmonary hypertension enlargement of the right ventricle and dilatation of pulmonary arteries are observed. In oblique lie with esophagus opacification the shadow of the latter is slanted backwards along the minor radius arch.
Additional methods of investigation in diagnosis of mitral insufficiency. 1. ECG reveals increased left atrium (P wave is dilated more than 0.12s and two-humped) and hypertrophy of the right ventricle (axis deviation to the left, dislocation of the transitional zone to the right, increased range of wave R in left chest leads V5 -V6, lengthening of the period of intrinsic deflection in V5 -V6 more than0.05s ). 2. Echocardiograph reveals the following: increased left atrium, myocardium hypertrophy and dilatation of the left ventricle cavity; reflux of blood stream from the left ventricle into the left atrium. 3. Phonocardiography reveals the following: decrease or complete disappearance of sound I on the apex; increase in the range of sound II and its splitting above the pulmonary artery; decreasing or ribbon protosysolic murmur is sometimes pansystolic. 4. X-ray examination of the thorax organs reveals increased left atrium and left ventricle, flatness of cardiac arc. In oblique lie with esophagus opacification the shadow of the latter is slanted along the major radius arch. Increased right ventricle is revealed at late stages. Signs of pulmonary hypertension and congestion are moderately expressed. Additional methods of investigation in diagnosis of tricuspid stenosis. 1. ECG reveals hypertrophy of the right atrium (high-amplitude, usually more than 2.5 mm, sharp-tipped, non-broadened P waves).
cardi
ology
.dsmu.e
du.ua

58
2. Echocardiograph reveals structural changes of tricuspid valves and degree of narrowing of the right atrioventricular opening, considerable enlargement of the right atrium. 3. Phonocardiography reveals the following: high-amplitude high-frequency tricuspid component of sound I; sound(snap) of tricuspid valve opening(0.10-0.12s after sound II ); diastolic low-frequency murmur of spindle shape, not fused with sound I; lengthening of interval Q-I. All phonocardiographic signs are best revealed at inspiration in intercostal space V along the left border of the breastbone on the right side. 4. X-ray examination of the thorax organs reveals absence of venous congestion signs in the lungs, considerable enlargement of the right atrium, flatness of cardiac diaphragmal angle. Additional methods of investigation in diagnosis of tricuspid insufficiency. 1. ECG reveals hypertrophy of the right atrium (high-amplitude, usually more than 2.5 mm, sharp-tipped, non-broadened P waves) and hypertrophy of the right ventricle(axis deviation to the right, dislocation of the transitional zone to the left, increased range of wave R in right chest leads V1 –V2 more than 7mm, increased period of intrinsic deflection in V1 more than 0.03s, shift of interval ST downwards and appearance of negative asymmetrical T wave in leads III, VF, V1 –V2 ). 2. Echocardiograph reveals paradoxical movement of the interventricular septum, systolic flow of regurgitation into the right atrium. Enlargement of the right atrium and right ventricle is observed. 3. X-ray examination of the thorax organs reveals enlarged right regions of the heart. Signs of pulmonary congestion are not pronounced. 4. Phonocardiography registers decreased amplitude of sound I, decreased protosystolic murmur above the xiphoid process of the breastbone. Right ventricular sound III may be observed. Additional methods of investigation in diagnosis of mitral valve prolapse. 1. At primary mitral valve prolapse ECG of people of asthenic build reveals axis deviation to the right. Different rhythm disorders are frequently registered (supraventricular and ventricular extrasystolе, paroxysmal tachycardia, bradyarrhythmia and atrioventricular conduct disorders). Presence of early repolarization syndrome is possible. However, more often there are no changes in ECG. 2. Echocardiograph reveals thickening of mitral valves; deflection of one or both septa more than 4mm with respect to the surface of mitral ring into the left atrium cavity during left ventricle systole; at mitral regurgitation – increased left atrium, later – left ventricle. 3. Phonocardiography reveals systolic snap and systolic murmur in the area of heart apex and along the left breastbone border. 4. X-ray examination of the thorax organs reveals “suspended”, “elongated” heart. Pulmonary pattern is not changed.
cardi
ology
.dsmu.e
du.ua

59
Situational test questions.
Q1. 38-year-old patient S. has been admitted to hospital with complaints of dyspnea increasing on little exertion, pain in the right hypochondrium, gradually increasing edema of the legs. The objective examination is significant for acrocyanosis with icteric tint, pulsation and dilatation of jugular veins; heart percussion reveals considerable cardiomegaly to the right, heart auscultation shows increased sound I, opening snap of tricuspid valve and middiastolic murmur increasing at inspiration along the left breastbone border, sound II over thee pulmonary trunk is weakened, the liver is 3 cm enlarged, of dense elastic consistency, feet and shin edema. What syndrome can be suspected? Explain the change in auscultation picture from the point of view of hemodynamic disorders. Work out a plan of examination. Q 2. 59-year-old patient D. complains of general weakness, dyspnea on exertion accompanied by sweating; the patient also suffers from fits of irregular, accelerated palpitation. Objectively: apical beat in 5,6P
thP intercostal space, 1.5 сm outwards to the
left midclavicular line, diffuse, high, resistant. Boundary of the heart relative dullness: right – 1 cm outwards from the right breastbone edge, upper – III rib, left –2 cm outwards from the left midclavicular line. The heart auscultation is significant for weakened sound I on the apex, accompanied by intensive murmur conducted to point 0, as well as along the left breastbone edge. Accent and splitting of sound II above the pulmonary artery are observed. What pathological syndrome is the most probable one? What is accent of sound II above the pulmonary artery conditioned by? What ECG changes can be revealed in the patient? Q 3. 68-year-old patient B. complains of dyspnea and palpitation on exertion, dry cough, sleepless nights because of suffocation fits, episodic hemoptysis. He has cyanotic blush on the cheeks. The apical beat in V intercostal space is 0.59 inches inwards from the left midclavicular line. Boundary of the heart relative dullness: right – 1 cm outwards from the right breastbone edge, upper – II rib, left –1 cm inwards from the left midclavicular line. The heart auscultation is significant for increased sound I on the apex, a short interval after sound II is followed by an additional sound. After a short pause following sound II the additional sound is accompanied by murmur increasing before sound I. Accent and splitting of sound II above the pulmonary artery are observed. Determine the phase of cardiac cycle when the murmur occurs. What is increased sound I on the apex conditioned by? What disease is this clinical picture typical of?
cardi
ology
.dsmu.e
du.ua

60
Tests for self-training purposes Q 1 On physical examination signs of Facies mitralis were found in a patient with rheumatoid damage of mitral valve. Which of the options offered corresponds to Facies mitralis? A. cyanotic blush on cheeks B. skin hyperemia, shining eyes, excited expression of the face C. widening of palpebral fissures, increased shining of eyes, exophthalmus D. falling back eyes, pointed nose, pale skin, cold sweat E. expressionless, pale face of light icteric tint Q 2 Expressed dyspnea, weakened sound I and intensive protosystolic murmur on the heart apex with conduct to the left appeared in a patient as a result of postnecrotic tear of papillary muscles of the left ventricle. Which additional symptom can be revealed on the patient’s examination? A. cyanosis B. carotid artery pulsation C. jugular vein pulsation A. negative heart push B. narrowing and widening of pupils simultaneously with pulse (Landolfi’s symptom) Q 3 Weakened sound I and systolic murmur arising simultaneously with sound I and having decreasing character are auscultated on the heart apex. Choose the disease characterized by the following auscultation picture. A. mitral insufficiency B. mitral stenosis C. aortic insufficiency D. aortic stenosis E. ventricular septal defect Q 4 Echocardiograph of a patient suffering from rheumatism reveals mitral stenosis. Which hemodynamic disorder is characteristic of this disease? A. increased preload on the left ventricle B. increased afterload on the left ventricle C. increased preload on the right ventricle D. increased afterload on the right ventricle E. simultaneously increased preload and afterload on the left ventricle Q 5 Which are the peculiarities of heart beat at a sharp widening of the right ventricle, for example, in a patient with diastolic “ cat’s purr”? A. it is shifted only to the left, high, about 3 сm in diameter B. it is shifted only to the left, not high, about 2 сm in diameter C. it is shifted to the left and downwards, high, about 3 сm in diameter D. it is shifted to the left and downwards, low, about 1 сm in diameter
cardi
ology
.dsmu.e
du.ua

61
E. it is not shifted, low, diffuse, about 3 сm in diameter Q 6 A patient has expressed cyanosis of the skin, the right border is 2.5 cm to the right from the right breastbone edge, weakening of sound I at xiphoid process base, protosystolic murmur occupies a greater part of systole and is increased at inspiration. Choose the most typical complaint.
A. increased stomach due to ascites, edema of the lower extremities B. hemoptysis C. dyspnea at rest D. fits of suffocation at night forcing the patient to sit down E. cough with pink foamy sputum during dyspnea Q 7 A patient’s echocardiograph reveals expressed tricuspid valve insufficiency. What can the patient’s examination reveal? A. negative venous pulse B. positive venous pulse C. carotid artery pulsation D. Musse’s symptom E. narrowing and widening of pupils simultaneously with pulse (Landolfi’s symptom) Q 8 Increased preload on the right ventricle in a patient with relative tricuspid insufficiency leads to the following: A. decreased power of myocardium contraction of the right ventricle B. does not change power of myocardium contraction of the right ventricle C. decreased systole duration of the right ventricle D. does not change myocardium systole duration of the right ventricle E. increased power of myocardium contraction of the right ventricle Q 9 A patient’s objective examination is significant for the right heart border being 1.5 сm to the right from the right breastbone edge, weakening of sound I at xiphoid process base, protosystolic murmur occupying a greater part of systole, positive Rivero-Korvalio’s test. Choose the clinical findings typical of this disease. A. moist rales in the lungs B. transudate accumulation in the left pleural cavity C. inspiratory dyspnea D. liver enlargement E. cough with pink foamy sputum Q 10 Examination of a patient with infectious endocarditis reveals the heart right border 1.5 сm to the right from the right breastbone edge, weakening of sound I at xiphoid process base, protosystolic murmur occupying a greater part of systole, positive Rivero-Korvalio’s test. Which disease could lead to such clinical picture? A. tricuspid insufficiency B. tricuspid stenosis
cardi
ology
.dsmu.e
du.ua

62
C. thrombosis of the pulmonary artery small branches D. chronic pulmonary heart E. mitral stenosis Answer Keys: Q1. – A, Q2. – A; Q3. – A; Q4. –D; Q5. – B; Q6. – A; Q7 – B; Q8 – E; Q9 – D; Q10 – A.
SUMMARY OF PROCEDURES
The practice lesson shall begin in a classroom, with the homework assignment checked and students’ testing carried out. Then the instructor considers diagnostic peculiarities of mitral, tricuspid valvular diseases and mitral valve prolapse. Another part of the practice shall be conducted in the Therapeutic Department. During it the instructor demonstrates patients carrying out all stages of the objective examination step by step. After that, using data of additional investigations in the patient’s case history, the main clinical syndrome is determined. Later students pass over to examining patients themselves. The practice shall continue in a classroom where students are supposed to do test questions on the subject material and the results of the practice are summed up.
Final test questions Q 1 Echocardiograph of a patient with Marfan's disease reveals moderate mitral valve insufficiency. Which auscultation melody is characteristic of this disease? A. systolic murmur starting with a short (0.03 s) interval after sound I B. systolic murmur starting with a big (>0.1 s) interval after sound I C. systolic murmur starting simultaneously with sound I D. diastolic murmur starting with a short (0.03 s) interval after sound II E. diastolic murmur starting with a big (>0.1 s) interval after sound II Q 2 Rheumatic heart disease is identified in a patient. Objective examination is significant for shifted left and upper boundary outwards, weakened sound I on the apex and short protosystolic murmur. Which position is the best for such murmur auscultation? A. vertical position at inspiration B. vertical position at expiration C. horizontal position at inspiration D. horizontal position at expiration E. vertical position with bending forward at inspiration Q 3 According to examination data, a patient has eccentric hypertrophy of the left ventricle as a result of increased preload on the left ventricle. Choose the disease characterized by such hemodynamic disorder: A. mitral insufficiency B. pulmonary valve stenosis C. interatrial septum defect
cardi
ology
.dsmu.e
du.ua

63
D. aortic stenosis E. mitral stenosis Q 4 Presence of expressed inspiratory dyspnea, shifted apical beat (outwards from the midclavicular line in 6P
thP intercostal space), eccentric hypertrophy of the left ventricle
in a patient are conditioned by diastolic overflow of the left ventricle. Point out the cause of the left ventricle overload. A. mitral stenosis B. tricuspid stenosis C. aortic stenosis D. mitral insufficiency E. pulmonary stenosis Q 5 A patient with rheumatism has weakened sound I and protosystolic murmur on the apex with conduct to the left. Which hemodynamic disorder is characteristic of this disease? A. increased preload on the left ventricle B. increased afterload on the left ventricle C. increased preload on the right ventricle D. increased preload on the left atrium E. simultaneously increased preload and afterload on the right ventricle Q 6 A patient has expressed cyanosis of the skin, the right border is 2.5 cm to the right from the right breastbone edge, weakening of sound I at xiphoid process base, protosystolic murmur occupies a greater part of systole and is increased at inspiration. Choose the most typical complaint: A. increased stomach due to ascites, edema of the lower extremities B. hemoptysis C. dyspnea at rest D. fits of suffocation at night forcing the patient to sit down E. cough with pink foamy sputum during dyspnea Q 7 A patient has cyanotic skin with icteric tint, swollen jugular veins. Weakening of sound I and murmur are auscultated at xiphoid process base. Positive Sherba’s test. ECG reveals high-amplitude wave Р, wave R> 7 mm in V1-V2. Point out the character and possible direction of the murmur conduct. A. systolic murmur is conducted into II intercostal space to the left from breastbone B. systolic murmur is conducted along the right breastbone edge C. systolic murmur is conducted into the left axillary region D. diastolic murmur is conducted along the right breastbone edge E. diastolic murmur is conducted to the heart apex Q 8 A patient has cyanosis of the skin, positive venous pulse. Weakening of sound I and murmur are auscultated at xiphoid process base. Which is the result of Sherba’s test in the patient?
cardi
ology
.dsmu.e
du.ua

64
A. increased systolic murmur B. decreased systolic murmur C. increased diastolic murmur D. decreased diastolic murmur E. systolic murmur intensity does not change Q 9 A patient has expressed inspiratory dyspnea, cyanotic blush on the cheeks, moist rales in the lungs, liver enlargement, shin and feet edema. Boundary of heart dullness is shifted to the right, left, upwards. “Quail’s rhythm” is auscultated on the apex. Echocardiograph reveals relative tricuspid insufficiency. Which is the cause of relative tricuspid insufficiency in the patient? A. rheumatic damage of tricuspid valve B. prolonged arterial hypertension C. expressed hydropericardium D. aortic disease in decompensation stage E. expressed mitral stenosis Q 10 Loud and flapping sound I, opening snap of tricuspid valve, presystolic and middiastolic murmur are auscultated in the region of xiphoid process. How will the heart melody change during Rivero-Korvalio’s test? A. weakened intensity of middiastolic murmur B. disappearance of presystolic murmur C. appearance of protodiastolic murmur D. increased volume of “quail’s rhythm” E. decreased volume of “quail’s rhythm”
cardi
ology
.dsmu.e
du.ua
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of Internal Medicine
Module 2 5BSymptoms and syndromes at diseases of internal organs
Topic-based Module 1 Subject
Aortal valvular diseases: main symptoms and syndromes based on clinical instrumental methods of investigation. Congenital heart disease.
Year 3
Faculty Faculty of Medicine for International Students
Donetsk 2009
65
cardi
ology
.dsmu.e
du.ua

66
Importance of the Subject: concord of traditional objective and modern instrumental methods of investigation of acquired (aortal) and congenital (septal heart defects, pulmonary artery narrowing, aorta dextraposition) diseases allows to timely diagnose the valvular apparatus damage and administer well-timed treatment. Key Goal: to develop skills in determining syndromes of aortal valve damage and congenital heart diseases (septal heart defects, pulmonary artery narrowing, aorta dextraposition )by means of objective methods (interview, examination, percussion, palpation, auscultation) and laboratory instrumental methods( results of serum test, ECG, echocardiograph, phonocardiogram, X-ray examination of the thorax organs). Specific Goals:
1. To interview a patient, to state the main complaints of a patient with the valvular apparatus disorder, i.e. aortal valvuar diseases and congenital heart diseases (dyspnea, apnoe, palpitation, heart intermittence, dizziness, loss of consciousness fits, hemoptysis, heartache), anamnestic data, their pathogenic significance. 2. To perform an objective investigation: examination (stating a patient’s position in bed, examining mucous membranes, skin, cardiac region and peripheral vessels), investigation of heartbeat, arterial and venous pulses, BP; percussion of the heart and lungs (heart borders, hydrothorax), auscultation of the heart and lungs (heart sounds, cardiac murmurs, respiratory murmurs), palpation of the stomach (enlarged liver, spleen), diagnostic estimation of the results obtained. 3. To estimate peculiarities of changes in biochemical results of blood serum(general protein albumin, proteinogram, CRP, rheumatoid factor, titer antistreptolysine O, diphenylamine, sialic acids, general bilirubin and its fractions, aloninamino transferase, AST , cholesterol) and instrumental methods of investigation (ECG, phonocardiogram, echocardiograph, X-ray examination of the thorax organs). Diagnostic significance. 4. To determine syndromes of acquired disease of aortal valve and congenital heart diseases (septal heart defects, pulmonary artery narrowing, aorta dextraposition), pathogenic mechanisms of development of different cardiac regions overload, disorders of intracardiac and systemic haemodynamics. Goals of Prerequisite Knowledge and Skills Level: 1. To estimate the main hydrodynamic mechanisms of heart murmur formation at liquid passage in tubes (Department of Biophysics) 2. To distinguish the main characteristics of the heart cycle – systole and diastole, their phases (Department of Physiology) 3. To possess knowledge of the structure of heart cavities and valvular apparatus, points of the valves projection on the thoracic cage (Department of Normal Anatomy) 4. To possess knowledge of hemodynamics within normal limits and its disorders at aortal and congenital diseases. (Department of Pathological Physiology)
cardi
ology
.dsmu.e
du.ua

67
Questions for Self-Assessment of Prerequisite Knowledge and Skills: (with answer keys after the last test question)
Q 1: 38-year-old patient K. complains of sudden weakness, pain in the right hypochondrium, increased stomach, edema of the legs, slight dyspnea. Objective examination results: acrocyanosis with icteric tint, swollen jugular veins, right ventricle and liver pulsation, heart boundary shift to the right. Which increased anatomic formation of the heart is heart boundary shift to the right conditioned by? А. right atrium В. right ventricle С. right atrium and ventricle D. left atrium Е. left ventricle Q 2: Point out the correct position of aortal valve: А. between the left atrium and aorta and transmits blood in the direction of atrium В. between the left atrium and aorta and transmits blood in the direction of aorta С. between the right ventricle and aorta and transmits blood in the direction of aorta D. between the left ventricle and aorta and transmits blood in the direction of
ventricle Е. between the left ventricle and aorta and transmits blood in the direction of aorta Q 3: Left ventricle pumps blood: A. arterial blood into the pulmonary artery B. venous blood into the pulmonary artery C. arterial blood into the aorta D. venous blood into the upper cava E. venous blood into the lower cava Q 4: Hemodynamic changes at inspiration: A. decreased right ventricle filling, increased pulmonary circuit blood inflow,
decreased left ventricle filling B. increased right ventricle filling, increased pulmonary circuit blood inflow,
increased left ventricle filling C. decreased right ventricle filling, decreased pulmonary circuit blood inflow,
decreased left ventricle filling D. increased right ventricle filling, increased pulmonary circuit blood inflow,
decreased left ventricle filling E. increased right ventricle filling, decreased pulmonary circuit blood inflow,
increased left ventricle filling Q 5: At increased final diastolic volume (FDV) power of heart contractions: A. grows at increased FDV up to 180 ml, then decreases B. decreases at increased FDV up to 180 ml, then grows C. grows at increased FDV irrespective of its definite rate
cardi
ology
.dsmu.e
du.ua
68
D. decreases at increased FDV irrespective of its definite rate E. FDV changes do not influence power of heart contractions Answer Keys: Q1. – B; Q2. – E; Q3. – C; Q4. –D; Q5. – A;
PRACTICE OVERVIEW After you have made sure that you have the prerequisite knowledge and skills,
you can proceed to the “PRACTICE OVERVIEW” section below.
Theory Topics Addressed by the Practice Activities 1. Prevalence and frequency of aortal valve damage. 2. Prevalence and frequency of septal defects (interatrial and interventricular septal defects), pulmonary artery narrowing, aorta dextraposition. 3. Main causes and mechanisms of development of aortal diseases (stenosis and insufficiency) and congenital heart diseases. 4. Hemodynamic changes at aortal and congenital diseases (interatrial and interventricular septal defects, pulmonary artery narrowing, aorta dextraposition). 5. Main complaints, data of examination, palpation of the precordial region and percussion at aortal and congenital heart diseases. 6. Auscultation picture of aortal stenosis and aortal insufficiency. 7. Auscultation picture at interatrial and interventricular septal defects, pulmonary artery narrowing, aorta dextraposition. 5. ECG and phonocardiogram signs of aortal and congenital heart diseases. 6. X-ray signs of aortal and congenital heart diseases. 7. Changes in laboratory results depending on etiologic factor and expressed cardiac failure.
Practical skills:
1. Collecting complaints and anamnesis of patients with aortal and congenital heart diseases. 2. Examining a patient. Palpating the precordial region. 3. Determining heart borders. 4. Carrying out heart auscultation. 5. Interpreting and estimating results of ECG, phonocardiogram, echocardiograph, X-ray examination of the thorax organs of patients with aortal valvular diseases. 6. Estimating laboratory investigation results. 7. Identifying a clinical syndrome.
cardi
ology
.dsmu.e
du.ua

69
Required Glossary to Practice
Term Definition Heart disease A persistent congenital or acquired
pathological change of heart structure causing its dysfunction.
Dilatation of heart Dilatation of heart chambers which can be a compensatory mechanism (tonogenic dilatation of heart) and a decompensation sign (myogenic dilatation).
Capillary pulse Visible arteriole pulsation at nail bed compression, rubbing forehead skin and pressing red border with glass slide.
Phonocardiography Graphic registration of sound vibrations arising in the heart and great vessels due to their activity.
Valsav’s maneuver Decreased murmurs at stenosis of aorta and pulmonary artery after a straining effort with closed glottis.
Durasie’s sign Double (systolic diastolic) murmur on the femoral artery at aortal valvular insufficiency.
Korrigan’s pulse Fast, high and bouncing pulse at aortal semilunar valves insufficiency.
Tolochinov-Roger A congenital heart disease – a nonclosure of interventricular septum
Tetrology of Fallot A congenital heart disease characterized by a tetrad of signs: a high ventricular septal defect, right-sided position (dextraposition) of aorta, right ventricle hypertrophy and pulmonary artery stenosis.
To master the material on the subject study the following flow charts:
cardi
ology
.dsmu.e
du.ua

Flow chart 1
70
cardi
ology
.dsmu.e
du.ua

71
Flow chart 2
cardi
ology
.dsmu.e
du.ua

72
Flow chart 3
cardi
ology
.dsmu.e
du.ua

73
Table 1
cardi
ology
.dsmu.e
du.ua

74
USuggested Reading List URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Aortic valve disease 5. Methodical guideline for students 6. Flow charts 1, 2, 3, 4. 7. Website of department, e-mail: www.cardiology.dsmu.edu.ua
UAdditional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
UGuide Sequence of ActionsU.
Algorithm of actions at auscultation of patients with aortal valvular diseases:
Carrying out auscultation in the
points of listening to the heart
Estimating volume and quality of sounds
Giving characteristics of the sounds
STEP 1 Aortal stenosis Aortal insufficiency
Determining direction of sound conduct
STEP 2
STEP 3
STEP 4
II intercostal space to the right from
breastbone
II intercostal space to the right from breastbone,
V point
Carotid arteries, jugular fossa,
interscapular space
Botkin-Erb’s point (if the epicenter is above
aorta)
cardi
ology
.dsmu.e
du.ua

75
Additional methods of investigation in diagnosis of aortal stenosis. 1. ECG reveals hypertrophy of the left atrium (axis deviation to the left,
increased range of wave R in left chest leads V5 -V6; deep waves SV1, SV2; a sum of range of waves SV1 + RV5 ( Sokolov-Layon’s index) > 35mm; dislocation of the transitional zone to the left, increased duration of internal deviation in leads V5, V6 > 0,05s; signs of systolic overload of the left ventricle.
2. Echocardiograph reveals thickening and decreased range of aortal valve opening; hypertrophy and/or dilatation of the left ventricle; increased linear velocity of blood flow in aorta; increased gradient of systolic pressure between the left ventricle and aorta.
3. Phonocardiography reveals a decreased range of sound I in the region of cardiac apex and of sound II in II intercostal space to the right from breastbone. Systolic murmur starts with small range vibrations some time after sound I, then its range grows, reaches its peak, more often in the middle of systole, later it decreases and fades without reaching sound II (diamond shape).
4. X-ray examination of the thorax organs reveals aortic configuration of heart, poststenotic dilatation of ascending region of aorta. At the development of left ventricular cardiac insufficiency there appear signs of pulmonary venous congestion.
Additional methods of investigation in diagnosis of aortal insufficiency.
1. ECG reveals hypertrophy of the left ventricle myocardium (axis deviation to the left, increased range of wave R in the left chest leads V5 -V6; deep waves SV1, SV2; a sum of range of waves SV1 + RV5 ( Sokolov-Layon’s index) > 35mm; dislocation of the transitional zone to the left, increased duration of internal deviation in leads V5, V6 > 0,05s; signs of diastolic and later systolic overload of the left ventricle.
2. Echocardiograph reveals structure changes of aortal valve septa and a degree of expressed aortal regurgitation. Thickening of walls and increase of the left ventricle cavity in size. Diastolic fremitus of the mitral valve frontal septum (this sign is conditioned by reverse turbulent blood flow from aorta into the left ventricle, which causes Flint’s murmur).
3. Phonocardiography reveals decreased range of sound I on the apex. Sometimes a high-amplitude sound of aortal distention in systole is registered. Protodiastolic decreasing murmur in Botkin-Erb’s point or II intercostal space on the right is determined. Sometimes Flint’s diastolic murmur (relative mitral stenosis) and systolic murmur (relative aortal stenosis) can be determined.
4. X-ray examination of the thorax organs reveals increased left ventricle, increased pulsation, waist of heart is distinctly expressed.
cardi
ology
.dsmu.e
du.ua

76
Situational test questions. Q 1. 37-year-old patient L. complains of compressing pains behind the breastbone irradiating into the left arm, pulsation in the region of neck vessels, arms, dizziness, loss of consciousness, palpitation. Objectively: “carotid shudder”, Landolfi’s symptom, apical beat in VI-VII intercostal space 1.5 сm outwards from the left midclavicular line, diffuse, high, resistant. Boundary of the heart relative dullness: right – 1 cm outwards from the right breastbone edge, upper – III rib, left –2 cm outwards from the left midclavicular line. The heart auscultation is significant for weakened sound I on the apex, weakened sound II above the aorta, accompanied by soft, heaving murmur which decreases by the end of a big pause; the murmur is best auscultated in Botkin-Erb’s point. BP is 160/40 mm of mercury column. Estimate the objective data. What syndrome is the most probable one? Q 2 40-year-old patient A. complains of loss of consciousness fits caused by exertion, burning pain behind the breastbone, irradiating into the left arm, arising on exertion and sometimes – at rest. Apical beat in VI intercostal space is 2 сm outwards from the left midclavicular line, diffuse, high, resistant. Boundary of the heart relative dullness: right – 1 cm outwards from the right breastbone edge, upper – III rib, left –1.5 cm outwards from the left midclavicular line. The heart auscultation is significant for weakened sound I on the apex, weakened sound II above the aorta. Rough systolic murmur, reaching its peak in II intercostal space and conducted on carotid and subclavian arteries is heard above all auscultation points. What are the pains behind the breastbone conditioned by? What disease is the given auscultation picture characteristic of? Administer investigation scheme. Q 3 20-year-old patient B. has been admitted to hospital with complaints of dyspnea at rest and insignificant physical exercise, dizziness, general weakness, increased tiredness, periodic heartache. The objective examination is significant for the following: skin paleness, crimson colour of the cheeks, nose tip, fingers, “watch glass” and “drumstick” syndromes, cardiac hump, apical beat is not determined, systolic fremitus is palpated in ІІ intercostal space on the left. At percussion the heart is dilated to the right. Auscultation reveals rough systolic murmur in IІ intercostal space to the left from the breastbone, conducted on the neighbouring arteries and into the interscapular space on the left at II intercostal space level, sound ІІ above the pulmonary trunk is weakened, the pulse is rapid, of weak filling and tension, BP is decreased, physical development lagging attracts attention. What syndrome can be suspected? Describe hemodynamic disorders. What investigations can substantiate the diagnosis?
cardi
ology
.dsmu.e
du.ua

77
Tests for self-training purposes Q1 A patient’s examination revealed skin paleness, apical beat shifted to the left and downwards, diffuse, high, resistant. In II intercostal space midsystolic murmur is auscultated. ECG results: heart electrical axis shifted to the left; Rv5-Rv6>Rv4; Rv5+Sv1>35mm; segment ST shifted downwards and negative asymmetric wave Т in leads I and V5-6. Which region hypertrophy is present in the patient? A. left atrium B. right ventricle C. left ventricle D. left ventricle and right atrium simultaneously E. both ventricles Q 2 A patient’s auscultation reveals weakened sound I on the apex and weakened sound II above the aorta, midsystolic murmur above the aorta conducted on the neck vessels and into interscapular space. Which hemodynamic disorder arises at the given disease? A. left ventricle volume overload B. left atrium volume overload C. left ventricle pressure overload D. left atrium pressure overload E. left ventricle and right atrium pressure overload Q 3 A doctor revealed skin paleness, apical beat shifted to the left and downwards, diffuse, high, resistant. Auscultation results: weakened sound I on the apex and weakened sound II above the aorta, midsystolic murmur above the aorta, conducted on the neck vessels and into interscapular space. Choose the most typical cause of the disease formation. A. Marfan’s disease B. aortic aneurysm C. Bechterew’s disease D. infective endocarditis E. traumatic rupture of aortal valve septum Q 4 Left ventricle concentric hypertrophy arose in a patient as a result of rheumatic heart disease. Choose the pathology characterized by such increase in left ventricle afterload. A. aortal insufficiency B. aortal stenosis C. aneurismal dilatation of aortal descending region D. mitral stenosis E. mitral insufficiency
cardi
ology
.dsmu.e
du.ua

78
Q 5 A patient complains of frequent fits of dizziness and loss of consciousness. Apical beat is shifted to the left and downwards, diffuse, high, resistant. Echocardiograph reveals signs of aorta narrowing. The patient’s complaints are conditioned by the following: A. brain tissue increased need in oxygen and metabolic substrates at their normal
supply B. worsening of cerebral circulation due to problematic blood expulsion from the
right ventricle into Tr. pulmonalis C. worsening of cerebral circulation due to problematic blood expulsion from the
left ventricle into the aorta D. worsening of cerebral circulation due to problematic venous outflow from the
brain E. considerable decrease in circulating blood volume, erythrocyte and hemoglobin
content Q 6 Cardiac region examination reveals epigastric pulsation, moderate dilatation on the right border, systolic murmurs of different quality in ІІ - ІІІ and ІІІ- ІV intercostal spaces at the left breastbone edge. Echocardiograph shows aorta dextraposition. Choose the corresponding heart disease: A. coarctation of aorta B. narrowing of pulmonary artery C. atrial septal defect D. ventricular septal defect E. Fallot’s tetrad Q 7 A patient with congenital heart disease is remarkable for a well developed muscular system of the shoulder girdle and hypertrophy of the lower extremities musculature. Apical beat is increased, diffuse, shifted to the left. Arterial pressure is 250/150 mm of mercury column. Which is the patient’s arterial hypertension conditioned by? A. excess rennin elimination into blood B. excess catecholamine elimination into blood C. excess cortisol and adrenocorticotropic hormone elimination into blood D. hypovolemia of arterial canal of the upper extremities, body and head E. hypovolemia of arterial canal of pelvic organs and lower extremities Q 8 Examination of a patient with Fallot’s tetrad reveals: inspiratory dyspnea, iron blue cyanosis of the skin, swollen jugular veins, edema of the lower extremities, enlarged liver. Which is the patient’s liver enlargement conditioned by? A. hepatitis B. polycythemia C. portal hypertension D. blood congestion in the pulmonary circuit
cardi
ology
.dsmu.e
du.ua

79
E. blood congestion in the systemic circuit Q9 A patient’s examination revealed expressed skin paleness, apical beat is shifted to the left and downwards, diffuse, high, resistant; systolic “cat’s purr” is determined. Auscultation of the heart in II intercostal space to the right from the breastbone reveals: A. systolic murmur starting with a small(about 0.03 s) interval after sound I B. systolic murmur starting with a big(more than 0.1 s) interval after sound I C. systolic murmur starting simultaneously with sound I D. diastolic murmur starting with a small(about 0.03 s) interval after sound II E. diastolic murmur starting with a big(more than 0.1 s) interval after sound II Q 10 In a patient with heart disease apical beat is shifted to the left and downwards, diffuse, high, resistant. The patient’s echocardiograph shows signs of aortal stenosis. Choose the variant of murmur melody in II intercostal space to the right from the breastbone: A. systolic murmur starting with a small(about 0.03 s) interval after sound I B. systolic murmur starting with a big(more than 0.1 s) interval after sound I C. systolic murmur starting simultaneously with sound I D. diastolic murmur starting with a small(about 0.03 s) interval after sound II E. diastolic murmur starting with a big(more than 0.1 s) interval after sound II Answer Keys: Q1. – C, Q2. – C; Q3. – D; Q4. –B; Q5. – C; Q6. – E; Q7 – A;Q8 – E; Q9 – A; Q10 – A.
SUMMARY OF PROCEDURES
The practice lesson shall begin in a classroom, with the homework assignment checked and students’ testing carried out.
Then the instructor considers diagnostic peculiarities of aortal valvular and congenital heart diseases.
Another part of the practice shall be conducted in the Therapeutic Department. During it the instructor demonstrates patients carrying out all stages of the objective examination step by step. After that, using data of additional investigations in the patient’s case history, the main clinical syndrome is determined.
Later students pass over to examining patients themselves. The practice shall continue in a classroom where students are supposed to do test questions on the subject material and the results of the practice are summed up.
cardi
ology
.dsmu.e
du.ua

80
Final test questions Q 1 A patient has skin paleness, apical beat is shifted to the left and downwards, diffuse, high, resistant. Auscultation results: weakened sound I on the apex and weakened sound II above the aorta, midsystolic murmur above the aorta, conducted on the neck vessels and into interscapular space. Choose the most typical complaint for this patient. A. jugular pulse B. sensation of fever and flush C. heavy weight and swelling sensation in the right hypochondrium D. increased stomach E. short-term losses of consciousness Q 2 A patient has skin paleness, apical beat is shifted to the left and downwards, diffuse, high, resistant. Auscultation results: weakened sound I on the apex and weakened sound II above the aorta, midsystolic murmur above the aorta, conducted on the neck vessels and into interscapular space. Choose the most typical complaint for this patient. A. dizziness (especially on exertion) B. jugular pulse C. diffuse cyanosis D. heavy weight sensation in the right hypochondrium due to hepatomegaly E. increased stomach due to ascites Q 3 A patient complains of frequent fits of dizziness and loss of consciousness. Apical beat is shifted to the left and downwards, diffuse, high, resistant. Systolic “cat’s purr” is determined. Which could be found on the patient’s examination?
A. skin paleness B. diffuse cyanosis C. jugular pulse D. considerable enlargement and pulsation of liver E. negative cardiac beat Q 4 A patient with atherosclerotic damage of aortal valve complains of frequent fits of dizziness and loss of consciousness, inspiratory dyspnea. Echocardiograph shows signs of aortal stenosis, left ventricle dilatation. Apical beat in the patient at transition from tonogenic to myogenic dilatation of heart becomes as follows: A. more resistant and diffuse B. less resistant and diffuse C. less resistant and more diffuse D. less diffuse and more resistant E. disappears
cardi
ology
.dsmu.e
du.ua

81
Q 5 A patient has weakness, fits of dizziness and loss of consciousness, infective endocarditis in past history. Auscultation results: weakened sound I on the apex and weakened sound II above the aorta, midsystolic murmur above the aorta, conducted on the neck vessels and into interscapular space. Apical beat: A. is shifted to the left and becomes diffuse, resistant B. is shifted to the left, but remains local and nonresistant C. is shifted to the left and downwards, becoming diffuse and resistant D. is shifted to the left and downwards, but remains local and nonresistant E. is shifted to the left and upwards, becoming diffuse and resistant Q 6 Choose the pathology at which a patient’s echocardiograph shows eccentric hypertrophy of the right ventricle: A. a combination of ventricular septal defects and pulmonary artery insufficiency B. a combination of pulmonary artery stenosis and tricuspid stenosis C. a combination of ventricular septal defects and pulmonary artery stenosis D. a combination of mitral stenosis and coarctation of aorta E. a combination of mitral and aortal valves insufficiency Q 7 A patient has expressed skin paleness; temporary cyanosis appears on exertion. Auscultation results are as follows: right auricular presystolic gallop, rough midsystolic murmur in II intercostal space on the left, accompanied by thorax fremitus. Choose the most typical variant of congenital heart disease. A. pulmonary artery stenosis B. coarctation of aorta C. atrial septal defect D. Fallot’s tetrad E. ventricular septal defect Q 8 ECG of a patient with a long-term hemodynamic disorder against the background of atrial septal defect reveals apart from high-amplitude wave Р and wave R >7mm one of the following A. left bundle-branch block B. right bundle-branch block C. sinoauricular block D. АВ block І degree E. АВ block ІІ degree Q 9 A patient has weakness, fits of dizziness and loss of consciousness, infective endocarditis in past history. Apical beat is shifted to the left and downwards, diffuse, high, resistant. Echocardiograph shows signs of aortal stenosis. Auscultation picture characteristic of this patient is: A. weakened sound I , protosystolic decreasing murmur, with its peak on the apex,
conducted into point 0
cardi
ology
.dsmu.e
du.ua

82
B. weakening of sound I on the apex and sound II above the aortal valve, protodiastolic soft “heaving” decreasing murmur, with its peak in point V, practically not conducted
C. increased sound I on the apex(flapping sound I ), protosystolic decreasing murmur, with its peak on the apex, conducted into point 0
D. increased sound I on the apex(flapping sound I ), opening sound of mitral valve, midsystolic murmur with presystolic enhancement
E. weakening of sound I on the apex and sound II above the aortal valve, midsystolic rhomboid murmur, with its peak in II intercostal space at the right breastbone edge, conducted on the neck vessels
Q 10 A patient’s auscultation reveals rough systolic murmur in II intercostal space on the right. Which position is this murmur best auscultated in? A. in a horizontal position B. in a vertical position C. in a position lying on the stomach D. in a sitting position E. in any of the positions mentioned above
cardi
ology
.dsmu.e
du.ua

83
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve»
meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 6BThe symptoms and syndromes at diseases of internal
Topic 7 Module Basic symptoms and syndromes at diseases of cardio-vascular system
Practice 7BBasic symptoms and syndromes at arterial hypertension and hypotension (hypertensive and hypotensive syndromes). Hypertensic crisis
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

84
UImportance of the Subject U: Arterial hypertension is one of the most serious medical problems. It is conditioned by its wide popularity, high risk of severe injuries of vitally important organs what leads to loss of quality of life and high mortality. Arterial hypertension is considered to be the leading risk factor of coronary heart disease, stroke, chronic heart failure, renal failure and atherosclerotic affection of peripheral arteries.
UKey Objective: UTo be able to diagnose arterial hypertension and hypotension syndromes, symptomatic character of hypertension, stage and degree of essential hypertension.
USpecific Goals:U
1. To mark out arterial hypertension syndrome on the basis of complaints, anamnesis and physical examination. 2. To measure arterial pressure (on hands and legs) and assess detected changes in conditions of pathology. 3. To interpret electrocardiographic changes of patients with essential hypertension and symptomatic hypertensions. 4. To draw a plan of additional examinations of patients with arterial hypertension syndrome and interpret their results. 5. To be able to distinguish essential hypertension from symptomatic one. 6. To know and be able to diagnose complications of essential hypertension.
Level of Knowledge and Skills before the Practice:
1. To interpret physiological parameters of arterial blood pressure (department of physiology). 2. To measure arterial blood pressure of healthy people (department of physiology). 3. To assess changes of waves and intervals in norm (department of physiology) and pathology (department of pathologic physiology). 4. To determine necessary extent of examinations and chain of laboratory and instrumental methods of examination, assess results (department of pathologic physiology). 5. To interpret various causes of arterial hypertension syndrome development (department of pathologic physiology). 6. To know causes and basic mechanisms of development of essential hypertension’s complications (department of pathologic physiology and anatomical pathology).
Questions for Self-Assessment of the Pre-Practice Knowledge
Q 1:
A 50-year old patient P. was admitted to the hospital with complaints of headache, sensation of heaviness in the head. During his inspection the following
cardi
ology
.dsmu.e
du.ua

85
abnormalities have been discovered: displacement of left border of relative cardiac dullness to the left on 2sm, apex beat is amplified, “metallic inflection”, accentuation of the 2nd sound on aorta. ABP is 190/140 mm of mercury. ECG: deviation of electric axis to the left, QRS>0,09”, RV6+SV1=45mm, elevation of ST segment, negative wave T in V5, V6, I, II, avL leads, RV6>RV5. Displacement of left border of relative cardiac dullness testifies about: A. Left ventricular hypertrophy. B. Right ventricular hypertrophy. C. Biventricular hypertrophy. D. Left atrial and ventricular hypertrophy. E. Right atrial and ventricular hypertrophy. Q 2: A 42-year old patient B. has been suffering from essential hypertension during 8 years. He applied for help with complaints of headache, dizziness, single vomiting. Patient is excited, ABP is 180/95 mm of mercury, and pulse is 120bpm. Hypertensic crisis was suspected. What kind of examination is necessary to be fulfilled for patient in case of emergency? A. Aortography B. ECG C. Ultrasonography of kidneys D. Clinical urine analysis E. Roentgenography of thorax organs Q 3: A 56-year old patient S. suffers from arterial hypertension. Which of the following methods permits arterial blood pressure measuring of this patient? A. Korotkoff’s apparatus B. Bodyplethysmography C. Thermometry D. Pneumonography E. Examination of fundus of eye Q 4: A 58-year old patient S. suffers from essential hypertension. Heart rate is 70bpm; ABP is 210/140 mm of mercury. Right border of relative cardiac dullness is on 1sm to the left from the edge of breast bone, upper border – is the 2nd rib, left – is on 1,5sm outside midclavicular line. Cardiac sounds are of usual volume. There is accentuation of the 2nd sound on aorta. What objective sign shows the presence of left ventricular hypertrophy? A. Extension of left border of relative cardiac dullness B. Extension of upper border of relative cardiac dullness C. Magnitude of arterial blood pressure D. Heart rate E. Presence of accentuation of the 2nd sound on aorta
cardi
ology
.dsmu.e
du.ua

86
Q 5: A 44-year old patient L. complains of headache and dizziness. He has been suffering from essential hypertension since 20 years old. ABP is 220/120mm mercury. Borders of relative cardiac dullness are: right – right edge of breast bone, upper – the 3rd rib, left – on 3sm to the left from midclavicular line. Heart activity is rhythmical, 1 sound is depressed on the cardiac apex, and systolic murmur is conducted to the left and increases on the left side. Heart rate is 75bpm. Which heart trouble’s sound is heard? A. Murmur of secondary mitral regurgitation B. Murmur of mitral stenosis C. Murmur of pulmonic regurgitation D. Murmur of aortic stenosis E. Murmur of tricuspid stenosis Q 6: Patient S., 30 years old receives beta-blocker on account of increased arterial blood pressure. Pulse rate is 55bpm. On ECG there is sinus bradycardia. Point out ECG-sign of sinus bradycardia: A. Increase of RR interval B. Decrease of RR interval C. Increase of T wave D. Expansion of P wave E. Shortening of QT interval Answer Keys. Q 1: A, Q 2: B, Q 3: A, Q 4: A, Q 5: A, Q 6: A. Information for securing of initial level of knowledge can be found in following literature:
UContents of Practice
UTopics of Theory:
1. Factors and causes of arterial hypertension syndrome development. 2. Classification of essential hypertension 3. Basic complaints of patient with arterial hypertension, data of objective examination: palpation of precardiac region, characteristics of apex beat, percussion and auscultation of borders of relative cardiac dullness. 4. Changes on ECG of patients with arterial hypertension syndrome. 5. Diagnostics of hypertensive crisis Practical skills: UStudents should be able to demonstrate mastery of the following practical skills 1. Palpation of precardiac region and assessment of apex beat characteristics of patients with arterial hypertension syndrome. 2. Determination of heart absolute and relative cardiac dullness.
cardi
ology
.dsmu.e
du.ua

87
3. Auscultation of heart and vessels of patients with essential hypertension 4. Measurement of blood pressure
Required Glossary to Practice
Term Definition
Hypertensive syndrome
Stable rise of arterial blood pressure more than 140/90 mm of mercury
Hypotensive syndrome Stable fall of arterial blood pressure
Hypertensic crisis Rapid and significant rise of arterial blood pressure with signs of target organs lesions (brain, heart, organ of vision)
For mastering of contents of practice get acquainted with flow charts.
cardi
ology
.dsmu.e
du.ua

88
Flow chart 1.
Assessment of complaints, data of anamnesis and objective examination
Provisional diagnosis
Additional methods of examination
Laboratory: Instrumental: Roentgenological: Common blood and urine analysis
ECG Roentgenography of thorax Examination of fundus of eye
Glucose, cholesterol, electrolytes, creatinine, hormones
Monitoring of ECG and blood pressure
Computer tomography of kidneys and suprarenal glands Echocardiogram, stress-
echocardiogram Aortography US of suprarenal glands, kidneys, US of kidneys’vessels
Excretory urography
Exception or confirmation of symptomatic character of hypertension
Assessment of possibility of development and prophylaxis of complications: Miocardial infarction, stroke, nephrosclerosis, chronic renal insufficiency, aortic aneurysm dissection, retinopathy, pulmonary edema, nasal hemorrhage, arrhythmia, acute heart failure.
cardi
ology
.dsmu.e
du.ua

89
URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture. 5. Methodical guideline for students 6. Flow charts for Practice 7. Website of department: www.cardiology.dsmu.edu.ua UAdditional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 4. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
cardi
ology
.dsmu.e
du.ua

90
Sequence of physician’s actions in case of patient’s syndrome
of arterial hypertension.
To assess general condition of patient
Step 1
Examination, measurement of arterial blood pressure and pulse rate
Presence of
crisis
Absence of crisis
To make urgent examinations – ECG, fundus of eye, urine analysis
Step 2
To assess severity of patient’s state and type of crisis
Scheduled
examination
Complicated crisis
Non-complicated
Step 3
Transportation of patient to the special
care ward
Unassisted relocation of the
patient to the department
Step 5
Em
ergency
Adm
ission of the patient to the
therapeutic/cardiologic departm
ent
Step 4
Out-patient
treatment
cardi
ology
.dsmu.e
du.ua

91
cardi
ology
.dsmu.e
du.ua

92
Technique of arterial blood pressure measurement 1P
stP Stage. In the studying room students get acquainted with components of
apparatus for arterial blood pressure measurement. Origin of vascular sounds that are heard during measurement of ABP by Korotkoff’s method is discussed. Students give diagnostic interpretation of results received during ABP measurement. 2P
ndP Stage. Patient is notified about prohibition of smoking, tonics drinking and
eating during 30-60 minutes before measurement of ABP. Patient should stay in calm sitting position during 5 minutes. 3P
rdP Stage. Measurements are run on both hands. Cuff is closely located on hand on
3sm higher than the bend of elbow. Air injection is made on 30 mm of mercury higher than supposed level of blood pressure. Vascular sounds appearing in arteries during ABP measurement are to be determined. Their origin should be explained. Diagnostic interpretation of results received during ABP measurement has to be given. 4P
thP Stage. Air from cuff should be released with speed 3-5mm of mercury per
second. 5P
thP Stage. Duplicate measurement should be made in 1-2 minutes after cuff
emptying. Situational Question. Q 1. 56 year old patient R. complains of headache. He has been ill for some years and never appealed for medical aid. During objective examination: left border of relative cardiac dullness is displaced on 2,5sm to the left from midclavicular line. Heart activity is rhythmical; there is accentuation of the 2nd sound on aorta. ABP is 195/100 mm of mercury. On ECG there is depression of ST segment in I, avL, leads V5-6, RV5>RV4. QRS=0,09sec. What was the cause of left heart border displacement in this case? A. Left ventricular hypertrophy B. Right ventricular hypertrophy C. Left atrial hypertrophy D. Right atrial hypertrophy E. Right ventricular dilatation Q 2. 28-year old patient L. came to consult a doctor for the first time with complaints of palpitation, headache, and pains in lumbar region on both sides. She considers herself sick for half a year. There is vesicular respiration in lungs. Borders of relative cardiac dullness are displaced to the left on 1sm. Heart activity is rhythmical, sounds are sonorous, heart rate is 98bpm, ABP is 165/95mm of mercury. Right lobe of liver is on 1,5sm lower than the edge of costal margin, edemata are absent. On the ECG there are: electrical axis of heart is deviated to the left (angle alpha – 50), depression of ST segment on 0,5 mm in I, avL, V5-V6,
cardi
ology
.dsmu.e
du.ua

93
SV2+RV5=35mm. What primary laboratory examination is necessary for determination of renal cause of hypertension? A. Roentgenography of thorax organs B. Sonography of the liver C. Common urine analysis D. Investigation of bilirubin of the blood E. Determination of glucose in the urine Q 3. 68 year old patient K. has been suffering from essential hypertension during 15 years. Some years ago he had ischemic stroke. On the ECG there are: heart rate is 52bpm, left ventricular hypertrophy. Indicate stage of essential hypertension. A. Essential hypertension of the 1 stage B. Essential hypertension of the 2 stage C. Essential hypertension of the 3 stage D. Essential hypertension of the 4 stage E. Essential hypertension of the 0 stage
Revision Questions Q 1. 65 year old patient K. complains of morning headache, periodic dizziness, breathlessness during physical activity. He has been ill for some years and never appealed for medical aid. During objective examination: rales are not heard in the lungs. Left border of relative cardiac dullness is displaced on 2,5sm to the left from midclavicular line. Heart activity is rhythmical; the Ist sound is depressed on the cardiac apex, there is accentuation of the 2nd sound on aorta, ABP is 185/110mm of mercury. Abdomen is smooth and painless. Edemata are absent. On the ECG there are RV5-6>RV4, QRS=0,09sec. Point out the guiding syndrome. A. Total heart failure B. Arterial hypertension C. Right ventricular heart failure D. Pulmonary hypertension E. Left ventricular heart failure Q 2. 60 year old patient M. complains of headache, periodic dizziness, breathlessness during physical activity. He has never been examined and knew nothing about his own disease. Patient’s case record is absent. During objective examination it was revealed that there are moist congestive rales on both sides of the lungs. Heart activity is rhythmical; the Ist sound is depressed on the cardiac apex, there is accentuation of the 2nd sound on aorta, ABP is 200/130mm of mercury. On the ECG there is depression of ST segment in I, avL, V5-V6 up to 0,5mm, RV5>RV4<RV6, QRS=0,10sec. What do these changes of ECG indicate? A. Small-focal myocardial infarction B. Q-myocardial infarction C. Left ventricular hypertrophy
cardi
ology
.dsmu.e
du.ua

94
D. Right ventricular hypertrophy E. Left bundle-branch block Q 3. 34-year old patient complains of periodic headache. She has been sick with chronic pyelonephritis and nephrogenous hypertension from childhood. Borders of relative cardiac dullness are displaced to the left on 2sm. Heart activity is rhythmical, sounds are sonorous, heart rate is 66bpm, ABP is 190/120mm of mercury. On the ECG there are: electrical axis of heart is deviated to the left (angle alpha= -45), depression of ST segment on 0,5 mm in I, avL, V5-V6, SV2+RV5=45mm. What do these changes of ECG indicate? A. Biventricular hypertrophy B. Right ventricular hypertrophy C. Left ventricular hypertrophy D. Myocardial infarction E. Syndrome of early ventricular repolarization Q 4. 56 year old patient B. has been admitted to the hospital on account of arterial hypertension diagnosed for the first time. ABP is 210/100 mm of mercury. In anamnesis there are: urolithiasis, Quincke's edema, bronchial asthma, constipations, and diabetes mellitus. There are signs of left ventricular hypertrophy on the ECG. What disease could result in arterial hypertension syndrome’s development in this case? A. Urolithiasis B. Quincke's edema C. Bronchial asthma D. Constipations E. Diabetes mellitus Q 5. 23 year old patient G. complains of paroxysmal appearance of headache, tremor, fear, and increase of blood pressure up to 170/100 mm of mercury during palpitation. According to the data of sonography there is enlargement of left adrenal gland up to 3×3sm. In urine analysis: specific gravity is 1022, protein is absent, leukocytes – 1-2, and erythrocytes are absent. Point out the cause of crisis increase of blood pressure. A. Pheochromocytoma B. Polycystic kidneys C. Essential hypertension D. Chronic pyelonephritis E. Chronic glomerulonephritis Q 6. 42 year old patient during 8 years has been suffering from essential hypertension. Today after emotional stress he is irritable, feels dry mouth. During objective examination tremor of hands, hyperemia of face, skin is moistened, and polyuria were revealed. Patient is consciousness. ABP is 210/100mm of mercury. Heart rate
cardi
ology
.dsmu.e
du.ua

95
is 110bpm. Movement and sensory disorders are absent. Blood glucose is 4,5mmol/l. What kind of complication has developed? A. Hypertensic crisis B. Hypoglycemia C. Ischemic stroke D. Hemorrhagic stroke E. Diabetic coma Keys To Answers. Q 1 : B; Q 2 : C; Q 3 : C; Q 4 : A; Q 5 : A; Q 6 : A.
SUMMARY OF PROCEDURES The practice lesson shall begin in the study room, with the homework assignment checked and students’ testing carried out. Then the instructor will demonstrate technique of arterial blood measurement by auscultatory Korotkoff’s method to the students. During demonstration typical for arterial blood pressure measurement mistakes shall be marked. Another part of the practice shall be conducted in the hospital wards. The instructor will demonstrate technique and features of taking the case history, complaints, and physical skills of examination of patients with arterial hypertension to the students. The instructor also will demonstrate chain and technique of arterial blood pressure measurement of patients suffering from arterial hypertension. Then technique of arterial blood pressure measurement of patients suffering from arterial hypertension and hypotension shall be practiced by each of the students individually. For that purpose students shall be divided in groups of two-three people. Sphygmomanometer Riva-Rocci shall be used. According to the topic of the study students shall examine patients: questioning, inspection, physical examination, acquaintance and interpretation of additional methods of examination. Then probable causes of arterial hypertension syndrome development shall be discussed together with instructor. Practice shall be continued in the study room where students will be supposed to solve control Qs on the topic of the study. Study shall be summed up. Final Tests Q 1. 34 year old patient B. suffers from chronic glomerulonephritis. ABP is 180/95mm of mercury. Amount of protein in the urine analysis is 0,56g/l. Edematic syndrome and impairment of nitrogen-excretory function of kidneys were revealed. What kind of symptomatic hypertension the patient is sick with? A. Renoparenchymal hypertension B. Essential hypertension C. Vasorenal hypertension D. Pheochromocytoma E. Primary aldosteronism (Conn's syndrome)
cardi
ology
.dsmu.e
du.ua

96
Q 2. 49-year old patient K. complains of intensive headache. In lungs there is vesicular respiration, rales are absent. Left border of relative cardiac dullness is displaced on 2sm to the left from midclavicular line. Heart activity is rhythmical; the Ist sound is depressed on the cardiac apex, there is accentuation of the 2nd sound on aorta, ABP is 210/180mm of mercury. Edemata are absent. On the ECG there is depression of ST segment in I, avL, V5-6, RV5-6>RV4, QRS=0,09sec. Point out guiding syndrome. A. Total heart failure B. Arterial hypertension C. Left ventricular heart failure D. Syndrome of bronchial obstruction E. Hepatic failure Q 3. 58-year old patient M. complains of headache. In lungs there is vesicular respiration. Left border of relative cardiac dullness is displaced on 2sm to the left from midclavicular line. Heart activity is rhythmical, there is accentuation of the 2nd sound on aorta, ABP is 220/180mm of mercury. On the ECG there is depression of ST segment in I, avL, V5-6, RV5>RV4, QRS=0,10sec. What do these changes of ECG indicate? A. Atrioventricular heart block B. Myocardial infarction C. Left ventricular hypertrophy D. Right ventricular hypertrophy E. Left bundle-branch block Q 4. 56-year old patient P. complains of headache. During objective examination it was revealed that left border of relative cardiac dullness is displaced on 2,5sm to the left from midclavicular line. Heart activity is rhythmical, there is accentuation of the 2nd sound on aorta, ABP is 195/100mm of mercury. On the ECG there is depression of ST segment in I, avL, V5-6, RV5>RV4, QRS=0,09sec. What was the cause of left heart border displacement? A. Left ventricular hypertrophy B. Right ventricular hypertrophy C. Left atrial hypertrophy D. Right atrial hypertrophy E. Right ventricular dilatation Q 5. 68-year old patient O. came to consult a doctor with complaints of intensive pain in the heart region appeared about one hour ago for the first time. She has been suffering from essential hypertension during more than 20 years. Heart activity is rhythmical, sounds are sonorous, heart rate is 100bpm, and ABP is 200/100mm of mercury. Edemata are absent. On the ECG there are: electrical axis of heart is deviated to the left (angle alpha= -50), PQ interval is 0,18sec, depression of ST
cardi
ology
.dsmu.e
du.ua

97
segment on 10 mm in I lead, avL, V5-V6, deep negative T wave up to 10mm of depth, SV2+RV5=35mm. What complication of essential hypertension has developed? A. Mesenteric ischemia B. Myocardial infarction C. Brain infarction D. Heart rhythm disturbance E. Atrioventricular heart block of the 3 grade Q 6. 49-year old patient N. came to consult a doctor with complaints of periodic headache. Borders of relative cardiac dullness are displaced on 2sm to the left. Heart activity is rhythmical, sounds are sonorous, heart rate is 66bpm, and ABP is 190/120mm of mercury. On the ECG there are: electrical axis of heart is deviated to the left (angle alpha= -45), depression of ST segment on 0,5 mm in I lead, avL, V5-V6, SV2+RV5=35mm. What do these changes of ECG indicate? A. Biventricular hypertrophy B. Interventricular septum hypertrophy C. Left ventricular hypertrophy D. Myocardial infarction E. Extrasystole Q 7. 76 year old patient B. has been admitted to the hospital on account of arterial hypertension diagnosed for the first time. ABP is 210/100 mm of mercury. During 10 years he has been suffering from urolithiasis, chronic bronchitis, persistent hepatitis, adenoma of prostate gland. Pancreatic diabetes was diagnosed a year ago. On the ECG there are signs of left ventricular hypertrophy. Indicate the most probable cause of arterial hypertension syndrome development. A. Urolithiasis B. Adenoma of prostate gland. C. Chronic persistent hepatitis D. Chronic bronchitis E. Pancreatic diabetes Q 8 33 year old patient H. has been admitted to the cardiological department of the hospital on account of increased ABP up to 170/100mm of mercury. Heart activity is rhythmical; heart rate is 80bpm. On the ECG there are signs of left ventricular hypertrophy. What kind of primary routine examination should be made to the patient with the purpose of exception of hypertension’s renal origin? A. Roentgenography of stomach B. To examine urine analysis C. Sonography of the spleen D. Sonography of the liver E. To examine common blood analysis
cardi
ology
.dsmu.e
du.ua

98
Q 9. 23 year old patient G. complains of paroxysmal headache, tremor, fear, and increase of blood pressure up to 170/100 mm of mercury during palpitation. According to the data of sonography there is enlargement in projection of left adrenal gland up to 1×3sm. In urine analysis: specific gravity is 1022, protein is absent, leukocytes – 1-2, and erythrocytes are absent. Point out the cause of crisis increase of blood pressure. A. Pheochromocytoma B. Cancer of kidney C. Essential hypertension D. Chronic pyelonephritis E. Chronic glomerulonephritis Q 10. 56 year old patient G. complains of paroxysmal appearance of headache, tremor, fear, and increase of blood pressure up to 200/120 mm of mercury during palpitation. According to the data of computer-aided tomography there is tumor-like mass in projection of left adrenal gland up to 5×2sm. Pheochromocytoma was diagnosed. What is the cause of paroxysmal increase of arterial blood pressure? A. Low concentration of potassium in the blood B. High concentration of catecholamines in the blood C. High concentration of cortisol in the blood D. Increased of cardiac output of left ventricle E. High concentration of aldosterone in the blood
cardi
ology
.dsmu.e
du.ua

99
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 1 8BThe Main Methods of Examination of Patient on Internal Diseases Course
Topic 2 Module 9BSyndrome of myocardial affection. Syndrome of cardiac rhythm disturbance. Hydropericardium syndrome. Basic symptoms and syndromes of stenocardia and myocardial infarction. Acute coronary syndrome.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

100
UImportance of the Subject.U A heart disease is one of the most urgent social and medical problems of practical health protection. It’s explained not only by considerable morbidity and mortality but also by objective complexity in diagnostic and treatment of such patients. Modern diagnostic of heart affection allows optimization of medical aid and improvement of prognosis of such patients.
UKey ObjectiveU: To be able to diagnose syndromes of myocardial and pericardial affection, cardiac rhythm disturbances, of stenocardia and myocardial infarction. USpecific Goals:
1. To characterize general clinical manifestations of myocardial affection and classify them according to etiological principle. 2. To characterize hemodynamic disorders and clinical manifestations of hydropericardium syndrome. To distinguish causes of its development and variants of classical clinical course. 3. To determine disorders of automatism, conduction, excitability of heart and differentiate their clinical manifestations. 4. To determine basic symptoms and syndromes of stenocardia. 5. To characterize basic symptoms and syndromes of myocardial infarction.
Level of Knowledge and Skills before the Practice:
1. To assess basic anatomic parameters of cardiovascular system. “Anatomy” 2. To assess basic physiological characteristics of human’s cardiovascular system. “Physiology” 3. Mental and ethical interrelations in the society. “Philosophy”
Questions for Self-Assessment of the Pre-Practice Knowledge
Q 1. Determine quantity of valves of the human being.
A. 2 B. 3 C. 4 D. 5 E. 6 Q 2. Determine quantity of myocardium layers of the left ventricle.
A. 1 B. 2 C. 3 D. 4 E. 5 Q 3. The centre of the first order automatism of the heart is: A. Synoatrial [S-A] node B. Atrioventricular [A-V] node
cardi
ology
.dsmu.e
du.ua

101
C. Interatrial bundle of Bachman D. Right bundle-branch E. Left posterior hemiblock Q 4.What is the minute volume of bloodflow of the right ventricle in norm? A. 1,5 L/min B. 2,5 L/min C. 3,0 L/min D. 3,5 L/min E. 5,0 L/min Q 5.What is transmembrane resting potential of cardiac hystiocyte? A. 30mV B. 50mV C. 65mV D. 90mV E. 105mV Answer Keys 1 - С; 2 - С; 3 - А; 4 - Е; 5 - D. Contents of Practice
Topics of Theory:
1. To have a clear idea of clinical manifestations of cardiac affection. 2. To know hemodynamic disorders and clinical manifestations of hydropericardium 3. To know disorder of automatism, conductance, excitability of heart. 4. To know basic symptoms and syndromes of stenocardia and myocardial infarction.
Practical skills:
UStudents should be able to demonstrate mastery of the following practical skills
1. Diagnostics of clinical manifestations of myocardial affection. 2. Skills of hydropericardium symptoms’ diagnostics. 3. Verification of cardiac rhythm disturbances by clinical and instrument methods. 4. Skills of diagnostics of basic symptoms and syndromes of stenocardia and myocardial infarction.
cardi
ology
.dsmu.e
du.ua

102
Required Glossary to Practice
Term Definition
Automatism Ability of organs and single tissues to rhythmic activity regardless of connection with external exciter.
Asystolia Complete termination of activity of one or every heart parts in the absence of bioelectrical activity.
Veloergometry Method of functional heart examination with use of graduated physical weight bearing on bicycle ergometer.
Ischemia Abatement of blood supply of body region, organ or tissue as result of constriction or occlusion of the appropriate artery.
Megalocardia Increase of heart’s sizes and mass
Cardiac tamponade
Compression of heart as a result of rapid accumulation of large quantity of fluid in the pericardial cavity with the increase of pressure in it.
For mastering of the theme content get acquainted with flow charts.
cardi
ology
.dsmu.e
du.ua

103
Flow chart 1.
Clinical manifestations of heart arrhythmia
Palpitation Intermission of heart activity
Syncopes Retrosternal pain
Heart failure
General clinical manifestations of myocardial affection.
Pains in the heart area
Tachycardia or bradycardia
Extrasystole Thromboembolism
Breathlessness Dullness of heart sounds
Blockades Ciliary arrhythmia
Hydropericardium (signs of cardiac tamponade)
Haemodynamics ECG Echocardiography
- Impediment of filling of cardiac chambers with blood; increase of intrapericardial pressure. - Decrease of cardiac output - Appearance of breathlessness - Increase of central venous - Presence of paradoxical pulse - Decrease of ABP - Short time impairment of consciousness
Decrease of voltage of waves Inversion of T wave Upward dislocation of ST segment
Free space between movable epicardium and immobile pericardium
cardi
ology
.dsmu.e
du.ua

104
USuggested Reading List
URequired Reading
1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990
2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986
3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004
4. Lecture.
5. Methodical guideline for students
6. Flow charts for practice: Clinical manifestations of heart arrhythmia. General clinical manifestations of myocardial affection. Hydropericardium (signs of cardiac tamponade).
7. Website of department: www.cardiology.dsmu.edu.ua
UAdditional Reading
1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 4. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Algorithm of ECG sequencing of patient with rhythm disturbances.
Step 1 Determination of cardiac beat’s regularity. Step 2 Determination of heart rate. Step 3 Determination of electrical axis of heart. Step 4 Analysis of P waves, QRS complex, PQ interval, ST segment, T
wave. Step 5 Determination of excitation source. Step 6 Assessment of conduction function. Step 7 ECG conclusion.
Assessment of conduction function
1. Measurement of P wave length (determination of atrial conduction) 2. Measurement of PQ interval length (determination of atrial, ventriculoatrial [V-A], and His’ system conduction). 3. Measurement of QRS complex length (determination of ventricular conduction) 4. Determination of internal deviation interval in V1 V6R.
cardi
ology
.dsmu.e
du.ua

105
Situational Questions.
Q 1.
Patient complains of dyspnea at rest, dull retrosternal pain, palpitation. During objective examination it was revealed: patient is sitting in the bed bending forward, cyanosis of lips is present. Respiration rate is 28 per minute; pulse rate is 115 per minute, it almost disappears during deep breath. ABP is 100/65mm of mercury. Cervical veins are swelled. There is legs’ edema. Apex beat can not be determined. Borders of absolute cardiac dullness are: the right one is on 2,5sm to the right from the right edge of breast bone, the upper border is the 3 rib, and the left one is on the anterior axillary line. Sounds are dull. Abdomen is soft. The liver goes beyond ribs on 2sm. What pathology is in question?
Q 2.
Patient was admitted to the hospital with complaints of compressive retrosternal pain, spreading to the left arm and neck. Duration of pain is more than 30 minutes, it doesn’t stop by nitroglycerine. During objective examination it was revealed: skin is pale and moist, there is acrocyanosis. Pulse rate is 96bpm, it is arythmic. ABP is 110/70mm of mercury. Borders of cardiac dullness are not displaced. Sounds are dull. There is moderate systolic murmur on the cardiac apex. Lungs are without peculiarities. Assess pain syndrome.
Q 3.
Patient was admitted to the hospital with suspicion on myocardial infarction. During objective examination it was revealed: skin is pale and moist. Pulse rate is 46 per minute, pulse is rhythmical. ABP is 110/70mm of mercury. Borders of relative cardiac dullness were displaced to the left on 1sm. Heart activity is rhythmical, occasionally there is considerably intensified the 1 sound. This phenomenon has been described by N.D.Strazhesko as “cannon sound”. Determine pathology when described sound can be found.
Revision Questions
Q 1.
Patient points out on intermittency in heart’s work, low grade fever during the evening. It is known that in the childhood he suffered from rheumatism. During auscultation gallop rhythm is determined. On the ECG there is sinus rhythm. Heart rate is 90bpm. P – 0.08sec, PQ – 0.23sec, QRS – 0.09sec. T wave is low-negative. Determine complication of the disease.
A. Sinoatrial block B. I grade A-V block C. II grade A-V block D. III grade A-V block E. Right bundle-branch block
cardi
ology
.dsmu.e
du.ua

106
Q 2.
Patient was admitted to the hospital with complaints of palpitation attacks following by retrosternal pain, spastic polyuria. He stops the attack by breath-holding and straining effort. During attack on the ECG there is: rhythm is regular, heart rate is 220bpm. P waves are negative, QRS – 0.09sec. T waves are smoothed. Determine rhythm disorder.
A. Sinus tachycardia B. Supraventricular paroxysmal tachycardia C. Ventricular paroxysmal tachycardia D. Atrial flutter, regular shape E. Ventricular flutter Q 3.
Patient was admitted to the hospital with complaints of compressing retrosternal pain spreading to the left arm and neck. Duration of pain is more than 30 minutes, it doesn’t stop by nitroglycerine. During objective examination it was revealed: skin is pale and moist, there is acrocyanosis. Pulse rate is 96bpm, it is arythmic. ABP is 110/70mm of mercury. Borders of cardiac dullness are displaced to the left on 1sm. Sounds are dull. There is moderate systolic murmur on the cardiac apex. Lungs are without peculiarities. In blood analysis: leukocytes – 9,7g/l. Myocardial infarction was suspected. This disease can be complicated by:
A. Atrial extrasystole B. Ventricular premature beats C. Ciliary arrhythmia D. Everything listed above E. Rhythm disturbances are not typical Q 4.
Patient was admitted to the hospital with suspicion of myocardial infarction. During objective examination it was revealed: skin is pale and moist. Pulse rate is 130bpm, it is arythmic. ABP is 105/70mm of mercury. Sounds are dull. In blood analysis: Enzymes: AST – 1.56mmol/hl, ALT – 0.44mmol/hl. ECG: there are f waves instead of P waves, QSRV3-6R. There is elevation of ST segment in V3-6, depression of ST in III, aVF. What is the patient’s pathology?
A. Small-focal non-Q wave myocardial infarction, sinus tachycardia B. Small-focal non-Q wave myocardial infarction, paroxysmal tachycardia C. Large-focal myocardial Q-wave infarction, paroxysmal tachycardia D. Large-focal myocardial Q-wave infarction, atrial flutter E. Large-focal myocardial Q-wave infarction, atrial fibrillation Q 5.
During auscultation of the heart abatement of the Ist sound and low-frequency sound appeared after 0.14sec after the IInd sound was determined. Determine pathology corresponding to the auscultation data.
cardi
ology
.dsmu.e
du.ua

107
A. Mitral stenosis B. Tricuspid stenosis C. Focal myocarditis D. Diffuse myocarditis E. Fibrinous pericarditis (pericarditis sicca) Q 6.
Patient complains of inspiratory dyspnea at rest. He fell ill after supercooling. During objective examination it was revealed: patient is sitting in the bed bowing down, cyanosis of lips is present. Respiration rate is 33 per minute; pulse rate is 120 per minute. ABP is 105/70mm of mercury. Cervical veins are swelled. There is legs’ edema. Apex beat is not determined. Borders of absolute cardiac dullness are: the right one is on 2,5sm to the right from the right edge of breast bone, the upper border is the 3 rib, and the left one is on the anterior axillary line. Sounds are dull. Abdomen is soft. The liver goes beyond ribs on 2sm. What pathology is in question?
A. Acute myocarditis B. Dilated cardiomyopathy C. Fibrinous pericarditis (pericarditis sicca) D. Exudative pericarditis E. Aterosclerotic cardiosclerosis Q 7.
Patient complains of compressing retrosternal pain spreading to the left arm and shoulder-blade. Pain arises during physical activity and can be stopped by nitroglycerine during 1 minute. During objective examination it was revealed that evident edema is absent. Pulse rate is 72bpm, it is rhythmic. ABP is 135/90mm of mercury. Borders of cardiac dullness are displaced to the left on 1,5sm. Sounds are dull. Lungs are without peculiarities. On the ECG: rhythm is regular; heart rate is 72bpm, electrical axis of heart is normal. P – 0,09s; PQ – 0,15s; QRS – 0,09s. There is transient (during one hour) inversion of T wave in chest leads. What is the patient’s pathology?
A. Intercostal neuralgia B. Small-focal non-Q wave myocardial infarction C. Large-focal myocardial Q-wave infarction D. Instable angina E. Exertional angina Q 8.
Patient was admitted to the hospital with complains of compressing retrosternal pain spreading to the both arms and back, inspiratory dyspnea, nausea. He fell ill about 1 hour ago. During objective examination: skin is pale and moist. Pulse rate is 130bpm, it is arythmic. ABP is 105/70mm of mercury. In blood analysis: leukocytes – 14,2G/l. Enzymes: AST – 1,12mmol/hl, ALT – 0,42mmol/hl. ECG:QRIIIR, aVF 0,04s. There is elevation of ST segment in III, aVF; depression of
cardi
ology
.dsmu.e
du.ua

108
ST in chest leads. Presence of such Q waves indicates presence of:
A. Myocardial necrosis B. Myocardial ischemia C. Ischemic injury D. Left ventricular hypertrophy E. Metabolic disorders Q 9.
Patient is ill with non-rheumatic myocarditis. He complains of walking dyspnea, irregular heart work, increase of body temperature up to 37,8ºC. During auscultation of the heart gallop rhythm was revealed. In blood analysis: erythrocytes – 4,35T/l; Hb – 135g/l; color index of blood – 0,93; leukocytes – 11,3G/l; eosinophils - 0%, stab neutrophils 8%, segmental leukocytes – 62%, lymphocytes – 22%, monocytes – 8%, ESR – 26mm/h. Assess blood analysis:
A. Anemia B. Neutrophilous right shift C. ESR decrease D. Lymphopenia E. Neutrophilous left shift Q 10.
Patient complains of rest dyspnea with inspiration’s difficulty, feeling of heaviness in precardiac area, palpitation, pain in right hypochondrium. Disease began 3 weeks ago after overcooling when body temperature increased and listed above complaints appeared. During objective examination there is cyanosis of lips, respiration rate is 30 per minute, pulse rate 110bpm. ABP is 105/70mm of mercury. Apex beat can’t be determined. Borders of absolute cardiac dullness are: the right one is on 3sm to the right from the right edge of breast bone, the upper border is the 3 rib, and the left one is on 3sm to the left from midclavicular line. Sounds are dull. Abdomen is soft. The liver goes beyond ribs on 4sm. What pathology is in question?
A. Exudative pericarditis B. Fibrinous pericarditis (pericarditis sicca) C. Acute myocarditis D. Dilated cardiomyopathy E. Aterosclerotic cardiosclerosis Standards of answers
1 – B; 2 – B; 3 – D; 4 – E; 5 – D; 6 – D; 7 – E; 8 – A; 9 – E; 10 – A.
cardi
ology
.dsmu.e
du.ua

109
SUMMARY OF PROCEDURES
The practice lesson shall be conducted in the study room and therapeutic department. After short introduction (topicality of the heart injuries’ studying in modern conditions) tests of initial level are carried out, students’ mistakes are analyzed and discussed.
Independent work of students shall be conducted in therapeutic department. Under control of the instructor students shall examine patients with different pathology of cardiovascular system. Another part of the practice shall be conducted in the study room, received data shall be discussed and mistakes shall be analyzed. Instructor shall give results of laboratory and instrumental examination. On the basis of anamnesis, objective examination, additional methods of examination symptoms of the disease shall be determined, united into syndromes and leading syndrome shall be chosen. Stage of heart failure shall be determined.
Test control and its results shall be carried out at the end of the study. Sum up shall be made by instructor.
Final tests
Q 1. During interpretation of ECG results of patient suspected of myocarditis it was revealed that rhythm is sinus, non-regular, there is atrial and ventricular premature beats; heart rate is110bpm; electrical axis of heart is not deviated; P – 0,10s, PQ – 0,24, QRS – 0,12S and in leads VR1R and VR2R it has shape rSRP
1P; there is also inversion
of T wave in right chest leads (VR1R – VR2R). Determine ECG changes typical for myocarditis. A. Disorders of processes of ventricular repolarization B. Extrasystole C. Right bundle-branch block D. Atrioventricular heart block E. Any of the listed above signs Q 2. Patient complains of pains in the heart area without strict connection with physical activity, weakness, increase of body temperature up to 37,5ºC. Borders of relative cardiac dullness are: right is on 1sm to the right from the right edge of breast bone, upper – the 3P
rdP rib; left – midclavicular line. Heart sounds are of usual volume, on
the left side near breast bone there is systolic and diastolic murmurs increasing when bending forward. Heart beat rate is 96bpm. ABP is 110/75mm of mercury. Abdomen is soft and painless. What pathology may be suspected? A. Congenital heart disease (CHD): atrial septal defect B. CHD: ventricular septal defect C. CHD: patent ductus arteriosus D. Aortal multivalvular disease E. Fibrinous pericarditis (pericarditis sicca) Q 3.
cardi
ology
.dsmu.e
du.ua

110
Patient complains of compressive retrosternal pain spreading to the left arm and shoulder. Pain arises while walking therefore he should stop every 100m, and dyspnea while going upstairs. During objective examination: visible edema is absent. Pulse rate is 70bpm and it’s rhythmical. ABP is 140/90mm of mercury. Borders of relative cardiac dullness are displaced to the left on 1,5sm. On the heart apex sounds are dull; there is accentuation of the II sound on aorta. Lungs are without peculiarities. Abdomen is soft. Liver and spleen can’t be palpated. On the ECG: rhythm is regular, 70bpm, electrical axis of heart is deviated to the left. There is also horizontal depression (up to 2mm) of ST segment in VR3-5R. What is the patient’s pathology? A. Intercostal neuralgia B. Exertional angina C. Instable angina D. Small-focal non-Q wave myocardial infarction E. Large-focal myocardial Q-wave infarction Q 4. Patient was admitted to the hospital with complaints of asphyxia, severe retrosternal pin spreading to the back. During objective examination it was revealed that skin is pale and moist. Pulse rate is 116bpm and it’s rhythmical. ABP is 11/65mm of mercury. Borders of relative cardiac dullness are displaced to the left on 1,5sm. Sounds are dull. There is the 3P
rdP sound in the protodiastole.
Respiration in lungs is vesicular. Abdomen is soft and painless. In blood analysis: erythrocytes – 5,1G/l; Hb – 148g/l; leukocytes – 13,6G/l. Enzymes: AST – 1,22mmol/hl, ALT – 0,48mmol/hl. ECG: QRv2-5R 0,04s. There is elevation of ST segment in VR2-5R; depression of ST in III, aVF. What is the patient’s disease? A. Instable angina B. Exertional angina C. Intercostal neuralgia D. Large-focal myocardial Q-wave infarction E. Small-focal non-Q wave myocardial infarction Q 5. Resorption-necrotic syndrome is one of the basic signs of acute period of myocardial infarction. Determine its signs: A. Increase of body temperature B. Leukocytosis C. Increase of ESR D. Increase of aspartate aminotransferase (AST) level E. Any of the listed above Q 6. Patient is ill with non-rheumatic myocarditis. During examination it was found that apex beat is located in the 5P
thP intercostal space on 2sm to the outside from
midclavicular line, and it’s diffuse and non-resistant. Borders of relative cardiac dullness are: right is on 1,5sm to the right from the right edge of breast bone, upper – the 2P
ndP intercostal space; left –on 1,5sm outside midclavicular line. Determine
cardi
ology
.dsmu.e
du.ua

111
configuration of heart. A. Normal B. Mitral C. Aortic D. Trapezoid E. Shape of “sitting duck” Q 7. Patient complains of rest dyspnea, dull retrosternal pain, palpitation. About week ago he had a sore throat. During examination: patient is sitting in the bed bending forward. There is cyanosis of his lips. Respiration rate is 28 per minute. Pulse rate is 115bpm. Cervical veins are swelled; there is also edema of legs. apex beat can’t be determined. Borders of relative cardiac dullness are: right is on 2,5sm to the right from the right edge of breast bone, upper – the 3P
rdP rib; left – anterior axillary
line. Sounds are dull. Abdomen is soft; The liver goes beyond ribs on 2sm. What pathology can be accompanied by paradoxical pulse? A. Myocarditis B. Dilated cardiomyopathy C. Fibrinous pericarditis (pericarditis sicca) D. Mitral stenosis E. Exudative pericarditis Q 8. Patient was admitted to the hospital with complaints of attacks of palpitation that are accompanied by retrosternal pain in the heart and spastic polyuria. She stops the attacks by breath-holding and straining efforts. On the ECG in the moment of attack: rhythm is regular, heart rate is 220bpm. P waves are negative, QRS – 0,09s. T waves are smoothed. Determine rhythm disorder. A. Sinus tachycardia B. Supraventricular paroxysmal tachycardia C. Ventricular paroxysmal tachycardia D. Atrial flutter, regular shape E. Ventricular flutter Q 9. Patient was admitted with complaints of asphyxia, severe retrosternal pin spreading to the back. He fell ill about 2 hours ago. Myocardial infarction was suspected. On the ECG there is complete left bundle-branch block what complicates verification of the disease. Assistance in diagnostics is possible in case of biochemical markers of cardiac hystiocytes’ death use. Determine such marker (-s) from the suggested list: A. Aspartate aminotransferase (AST) B. Creatine phosphokinase MB fraction C. Lactate dehydrogenase-1 (LDG-1) D. Troponin T E. Any of the listed above
cardi
ology
.dsmu.e
du.ua

112
Q 10. Patient was admitted to the hospital with suspicious myocardial infarction. During objective examination it was found that skin is pale and moist. Pulse rate is 46bpm, regular. ABP is 110/70mm of mercury. Borders of relative cardiac dullness are displaced to the left on 1,0sm. Heart activity is rhythmical. There is periodic significantly intensive 1P
stP sound on the apex of heart. This phenomenon was
described by N.D. Strazhesko as “cannon sound”. Determine pathology when this sound can be heard. A. Right bundle-branch block B. Left bundle-branch block C. Atrioventricular heart block of the 1P
st Pdegree
D. Atrioventricular heart block of the 2P
ndP degree
E. Atrioventricular heart block of the 3P
rdP degree
cardi
ology
.dsmu.e
du.ua

113
Topic 8 Module. Main syndromes and symptomes of respiratory diseases, interpretation data of instrumental diagnostics and laboratory investigation. Specific Goals: - To estimate data of the enquering, physical examination, instrumental diagnostics of patient with respiratory pathology - Make primary conclusion of disorders of respiratory system - To interpret the received data of the examination for recognition of clinical syndromes of the respiratory system - To know new classifications of respiratory diseases
cardi
ology
.dsmu.e
du.ua

114
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptomes and Syndromes of the Internal Diseases
Topic 8 Module Main syndromes and symptomes of
respiratory diseases, interpretation of instrumental diagnostics and laboratory investigation data
Practice Instrumental diagnostics and laboratory investigation of the respiratory system. Examination of the respiratory function. Investigation of sputum and pleural fluid.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

115
UImportance of the Subject U: Instrumental diagnostics and laboratory investigation of the respiratory system are widely used at medical practice. They allow to quickly identify abnormal changes in respiratory organs, diagnose disease and confirm diagnosis together with physical examination. UKey ObjectiveU: To master knowledge and skills in identifying necessary laboratory and instrumental investigations for certain syndrome of respiratory disorders and analyzing laboratory and instrumental investigations in respiratory pathology. USpecific Goals: 1. To be able to demonstrate mastery of analyzing respiratory functions in spirometry and estimate diagnostic value of the discovered changes in a patient. 2. To reveal changes and interpret findings of investigation of sputum. 3. To reveal changes and interpret findings of investigation of pleural fluid, be able to demonstrate mastery of making distinction of transsudate and exudate. 4. To explain the mechanism of occurence of changes in laboratory and instrumental investigations for certain respiratory pathology.
Level of Knowledge and Skills before the Practice:
1. To identify main parameters in the act of breathing (i.e. its frequency, depth, mode and rhythm) and factors which constitute them in normal and abnormal conditions (Described in the Physiology course)
2. To have knowledge of a histological structure of alveoli, bronchi, bronchioles and pleural layers (Described in the Histology course.)
3. To identify main parameters in the act of breathing, features of ventilatory capacity of the lungs and gas exchange (Described in the Physiology course.)
4. To have knowledge of the structure and features of different parts of respiratory system (Described in the Human Anatomy course.)
Questions for Self-Assessment of the Pre-Practice Knowledge
Q1. Air clarification from dust and microorganisms in lung alveoli is conducted by: A. respiratory epithelial cells (alveolocyte of 1 type) B. large epithelial cells (alveolocyte of 2 type) C. brush epithelial cells (alveolocyte of 3 type) D. alveolar macrophages E. secretor cells of bronchiole Q2. Quiet exhalation after inhalation in norm happens due to: A. Constriction of bronchial tubes and alveolus. B. Constriction of expiratory mussels. C. Constriction of diaphragm. D. Constriction of prelum abdominale mussels
cardi
ology
.dsmu.e
du.ua

116
E. Relaxation of inspiratory mussels. Q3. Deep inhalation after exhalation in norm happens due to: B. Constriction of bronchial tubes and alveolus C. Constriction of expiratory mussels D. Constriction of diaphragm E. Relaxation of expiratory mussels F. Relaxation of inspiratory mussels Q4. Chouse anatomical formations, which not provide the ventilation, but considerable influent on intensity of gas exchange: A. Alveoli and their capillaries B. Alveoli and visceral pleura C. Alveoli and parietal pleura D. Alveoli and bronchial tubes (8-16 generation) E. Alveoli and middle bronchus (4-8 generation), pleura
Q5. A 44-year-old woman was admitted to the therapeutic department because of right-side pleuritis. The examination confirmed the presence of liquid in the pleural cavity. What sinus of the pleura will have the biggest accumulation of the serosity A. Right mediastinodiaphragmatic B. Right costodiaphragmatic C. Right costomediastinal D. Left mediastinodiaphragmatic E. Left costomediastinal
Answer Keys: D, E, C, A, B
The following printed materials can be of help to improve your pre-practice knowledge and skills: 1. Test book of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 2. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 3. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy UContents of Practice UTopics of Theory: 1. Spirometry, body pletyzmograph, the main respiratory parametres, estimation finding of these investigations 2. Investigation of sputum, types of sputum (macroscopic, micriscopic and bacteriological investigations of sputum), interpreting the findings, diagnostic value of changes 3. Investigation of pleural fluid, diagnostic value of changes in pleural fluid, difference between transsudate and exudate, character of exudate 4. Mechanism of occurence of changes in laboratory and instrumental investigations for certain respiratory pathology Practical skills: UStudents should be able to demonstrate mastery of the following pratical skills
cardi
ology
.dsmu.e
du.ua

117
1. To be able to demonstrate mastery of analyzing respiratory functions in spirometry and estimate diagnostic value of the discovered changes in a patient. 2. To reveal changes and interpret findings of investigation of sputum 3. To reveal changes and interpret findings of investigation of pleural fluid, be able to demonstrate mastery of making distinction of transsudate and exudates
Required Glossary to Practice
Term Definition Respiratory Volume (RV)
volume of air which correspond to normal inhalation and exhalation N-300-900 ml
Vital Capacity (VC) volume of air which correspond to maximal deep inhalation and exhalation ( RV + ERV+ IRV ) N- 3700 ml ± 15%
Expiratory Reserve Volume ( ERV)
volume of air which is possible to exhale after normal exhalation N-1500-2000ml
Inspiratory Reserve Volume (IRV )
volume of air which is possible to inhale after normal inhalation N-1500-2000ml
Residual Volume (RV ) volume of air which stays in lung after maximal deep exhalation N-1000-1500 ml
Total Lung Capacity ( TLC)
(VC + RV ) N- 5000 - 6000 ml
Forced Vital Capacity (FVC)
volume of air which correspond to maximal quick exhalation N- 85%VC
Forced Expiratory Volume in 1 sec (FEV1)
volume of air which correspond to maximal quick exhalation during first second
Maximal voluntary ventilation (MVV)
maximal volume of air which pass through lung in 1 minute under forced breathing- respiratory depth (l) · respiratory rate N -80-200 l/min
Low voluntary ventilation (LVV)
maximal volume of air which passes through lung in 1 minute under normal breathing N- 5000 ml
cardi
ology
.dsmu.e
du.ua

118
Index Tiffeneau
FEV1 /VC
Transsudate
is noninflammatory fluid, ultrafiltrative of plasma, resulting from increased hydrostatic pressure or decreased serum oncotic pressure.This is essentially an effusion with normal pleura (right heart failure, nephrotic syndrome, liver cirrhosis)
Exudate
is inflammatory fluid, rich in proteins. This results from increased capillary permeability. This is essentially an effusion with diseased pleura (pleurisy)
Curschmann spirals casts of bronchial lumen, mucous white curled threads (Ubronchial asthmaU, pneumonia, tumor of lung)
Charcot-Leyden crystals
crystals of destroyed eosinophils – (Ubronchial asthmaU, chronic bronchitis)
Dittrich's plugs – corpuscular from elastic fibers, bacteriae and fats, greenish-yellow colour with stinking odour in lung (abscess, bronchiectasis, pulmonary gangrene)
cardi
ology
.dsmu.e
du.ua

119
Macroscopic investiga tion of sputum
Colour
Character
Consistence
Visible Elements
Microscopic investiga tion of sputum
Blood cells Elastic fibres
Tumour cells Alveolar macrophages
Chacot-Leyden crystals
Bacteriae
Curschmann spirals
Fungi
Epithelium cells Hemosiderin crystals
Dittrich’s plugs Clots of fibrin
Bacterio logical investiga tion of sputum
Bacterioscopic investigation
Investigation of Sputum
Inoculation of medium
cardi
ology
.dsmu.e
du.ua

120
USuggested Reading List URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Functional investigation of the lungs. Main syndromes and symptomes of respiratory diseases. 5. Methodical guideline for students 6. Flow charts for Practice 7. Website of department: www.cardiology.dsmu.edu.ua UAdditional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Macroscopic investigation of sputum
Character
Consistence and colour Diseases Mucous viscous, colorless acute bronchitis, after attack of
bronchial asthma Serous liquid, foamy pulmonary oedema Mucopurulent
viscous, yellowish chronic bronchitis, tracheitis bronchopneumonia-lobular pneumonia, bronchiectasis
Purulent semi-fluid, yellow-greenish
lung abscess, pleural empyema which communicates with bronchus
Bloody liquid, reddish, red tbs, cancer of lung, bronchiectasis, actinomycosis
Mucobloody viscous, blood streaks lung infarction, mitral valve disease, bronchiectasis, bronchogenic cancer
Bloody-purulent
semi-fluid, grey- brown lung abscess, pulmonary gangrene
Rusty viscous, brown- yellow lobar pneumonia
cardi
ology
.dsmu.e
du.ua

121
- Consistence depends on present of mucous, epithelium, formed elements - Quantity Small quantity- bronchitis, tracheitis in their onset first 2-3 days Moderate quantity - bronchitis, tracheitis in 2 -3 days Large quantity (0,5-2 litres) – bronchiectasis, lung abscess (after its rupture), tuberculous cavity Chronic inflammatory process (abscess, bronchoectasis, tuberculous cavity ) – sputum divided into three layers:
1) upper – Mucopurulent 2) middle – Serous 3) lower – Purulent
-Odour putrefactive, stinking odour in prolonged purulent infections, putrefactive destruction, anaerobic infection (abscess, bronchoectasis, tbs, pulmonary gangrene, cancer of lung) Microscopic investigation of sputum :
- stratified epithelium – epithelium of oral cavity, nasopharynx - columnar ciliated epithelium - bronchitis, tracheitis, bronchial asthma - clots of fibrin - fibrinous bronchitis - Curschmann spirals – mucous white curled threads -Ubronchial asthmaU,
pneumonia, tumor of lung - Charcot-Leyden crystals – destroyed eosinophils - Ubronchial asthmaU, chronic bronchitis. - Dittrich's plugs – corpuscular from elastic fibers, bacteriae and fats – greenish-yellow colour with stinking odour in lung - abscess, bronchiectasis, pulmonary gangrene
- compact lenticular greenish –yellow formations consisting of calcified elastic fibres,
cholesterol crystals and soaps containing tuberculosis mycobacteria - tbs - granules of lime - granules of actinomycetes – fungus infection (after antibiotic treatment) - necrotizing parts of lung - pulmonary gangrene
- hemosiderin crystals- destroyed haemoglobin in hemorrhages - elastic fibre – destruction of lung tissue (tbs, abscess of lung, tumor of lung.) - eosinophils - bronchial asthma. - neutrophils – purulent infections. - alveolar macrophages ( siderophages)- cells of heart valve disease
(macrophages with hemosiderin) – mitral heart valve disease - dust cells ( macrophage with coal particles ) - atypical cells - neoplastic cells – pulmonary cancer - erythrocytes - lung infarction, bronchiectasis, cancer, tbs, pulmonary oedema - bacteriae
cardi
ology
.dsmu.e
du.ua

122
Microscopy of stained preparations 1. Romanovsky-Giemsa staining – common use 2. Ziehl-Neelsen staining – tbs 3. Gram staining – tbs 4. Leishmann staining - atypical cells
Pleural fluid
Character of pleural fluid Sign
Transsudate Exudate transparency transparent, opalescent turbidity (cloudy) colour pale-yellow pale-yellow, golden-yellow,
yellow, grey, greenish, reddish, brown, pink, milk - like
consistence fluid may be thick smell without may be with stinking odour relative density <1,015 >1,015 quantity of protein <3% ( 5-25g/l) >3% (> 30g/l) albumin >60% <60% fibrinogen absence present Rivalta's test negative positive Lucaerini test negative positive cellular sediment (WBC, RBC)
minimal(WBC< 15 ) significant(WBC >15 )
Sterility
sterile with bacteriaе
Rivalta's test - a cylinder is filled with water acidified with a few drops of acetic acid; 1 or 2 drops of the punctate are added; as effusion sinks to the bottom it leaves a cloudy trace (like cigarette smoke), while in case of transudate the reaction is negative. Lucaerini test - 2 ml of hydrogen peroxide (3 per cent solution) are placed on a watch glass (against a black background) and a drop of the punctate is added: opalescence appears in case of the positive reaction. Both reactions are used to detect the presence of seromucin in the effusion. This is a mucopolysaccharide complex which is absent from transudates. Character of Exudate - serous, serofibrinous in exudative pleurisy associated with tbs, connective
tissue diseases, cancer (increase in lymphocytes) - purulent - exudative purulent pleurisy ( increase in neutrophils) - putrefactive- with stinking odour in prolonged purulent infections, putrefactive destruction, anaerobic infection( increase in neutrophils)
cardi
ology
.dsmu.e
du.ua

123
- hemorrhagic – trauma of pleura, tumours, tbs, hemorrhagic syndrome ( a lot of red blood cells) - chylous – turbidity, lacteal, with fat drops due to congestion of lymph(pressing
by enlanged lymph nodes, tumour) or destruction of the thoracic lymph duct by tumour or trauma. It is determined by test opacity disappears after addition of ether)
- chylous- like- turbidity, milk – like colour, pleural fluid by fatty degeneration of cells contained in ample quantity. Opacity does not disappear after ether.
- cholesteric - yellowish, thick, cholesterol crystals, destroyed cells in prolonged encysted pleurisy
Colour – pale-yellow, golden-yellow, yellow, grey, greenish, reddish, brown, pink, and milky
Microscopic investigation of pleural fluid Cells – erythrocytes, neutrophil, eosinophil, lymphocytes, monocyte, macrophage, Atypical neoplastic cells, bacteriae, Mesothelium cells - pleural mesothelioma, cancer, tbs (often pleural fluid is
hemorrhagic). Transsudate - small quantity erythrocytes, leucocytes, mesothelium cells Bacteriological investigation - inoculation of medium
Revision Questions
Q1. The pleural fluid is exudate if: A. colour is milk like B. colour is pale yellow C. relative density 1010 D. relative density 1012 E. relative density 1014 Q2. Presence of elastic fibers in sputum is typical for: A. acute bronchitis B. pneumonia C. bronchial asthma D. pulmonary tuberculosis E. chronic bronchitis Q3. The pleural fluid is exudate if it has : A. reddish colour B. pale yellow colour C. relative density 1010 D. relative density 1009 E. relative density 1014 Q4. The pleural fluid is transudate if: A. Rivalta`s test is positive B. Rivalta`s test is negative C. relative density 1020 D. relative density 1022 E. protein content is 35g/l
cardi
ology
.dsmu.e
du.ua

124
Q5. The pleural fluid is transudate if it has : A. relative density 1012 B. redish colour C. milk like colour D. yellow- green colour E. relative density 1017 Q6. Presense of Charcot - Leyden crystals in the sputum is typical for: A. tyberculosis of the lung B. pneumonia C. abscess of the lungs D. eosinophilic pneumonia E. exudative pleurisy Q7.What colour is typical for chylous exudate: A. milk- like colour (lacteal) B. red color (hemorrhagic) C. yellow color (purulent) D. brown E. grey Q8. Presence of blood in the sputum is typical for: A. bronchial asthma B. chronic bronchitis C. exadative pleurisy D. cavernous tuberculosis E. pneumothorax Q9. The pleural fluid is exudate if: A. colour is pale yellow B. milk like colour C. relative density 1010 D. relative density 1012 E. relative density 1014 Q10. Choose the pathology which is characterized by presence of mucobloody sputum: A. pneumothorax B. bronchial asthma C. mitral valve disease D. exudative pleurisy E. chronic bronchitis Answer Keys: Q1A, Q2D, Q3A, Q4B, Q5A, Q6D, Q7A, Q8D, Q9B, Q10C.
10BSUMMARY OF PROCEDURES The practice lesson shall begin in the study room, with the homework assignment checked and students’ testing carried out. Then students with teacter discuss signs of instrumental, laboratory investigations for diagnostics of respiratory pathology and their diagnostic value. Teacher gives
cardi
ology
.dsmu.e
du.ua

125
students analyses of sputum, pleural fluid, data of spirometry for revelation the changes in these analyses and discuss respiratory disorders which may cause these changes. Then students are invited to the room for spirometry and body pletyzmograph where the instructor will demonstrate to the students technique of spirometry and discuss revealed data..
At the end of the practice teacher makes short general conclusion concerning obtained findings and students do final tests.
Final Tests Q1. Presence of Charcot –Leyden crystals in sputum is typical for: A. pulmonary oedema B. acute bronchitis C. pneumonia D. bronchial asthma E. pulmonary tuberculosis Q2. Choose disease which is characterised by expectoration plenty of sputum: A. acute pneumonia and multiple bronchiectasis; B. bronchial asthma and chronic lung abscess; C. tubercular cavity and exudative pleurisy; D. chronic lung abscess and multiple bronchiectasis; E. bronchial asthma and pulmonary embolism. Q3. Which substance does help to distinguish chylous exudate from chylous-like exudate (opacity disappears after its addition)? A. hydrogen peroxide B. sulphuric acid C. acetic acid D. hydrosulphuric acid E. ether Q4. Choose typical reason of accumulation of transsudate in pleural cavity: A. left heart failure B. nephrotic syndrome C. acute bronchitis D. attack of bronchial asthma E. exudative pleurisy Q5. Choose the pathology which is characterized by presence of purulent sputum: A. bronchial asthma B. pulmonary oedema C. exudative pleurisy D. lung abscess E. pneumothorax Q6. Choose characteristic reason of the presence of bloody--purulent sputum A. chronic bronchitis B. bronchial asthma C. lung abscess
cardi
ology
.dsmu.e
du.ua

126
D. exudative pleurisy E. pneumothorax Q7. Presense of oesinophils in the sputum is typical for: A. pulmonary oedema which associated with mitral stenosis B. acute bronchitis C. pulmonary cancer D. bronchial asthma E. bronchiectasis Q8. The pleural fluid is transudate if protein level is : A. 18 g / l B. 22 g / l C. 25 g / l D. 1-3 answers are correct E. 1-3 answers are wrong Q9. Name chronic inflammatory process which characterized by division of sputum into 3 layers: A. pneumonia B. bronchial asthma C. exudative pleurisy; D. chronic lung abscess E. pulmonary embolism Q10. What does microcopic investigation of sputum include: A. colour of sputum B. inoculation of medium C. presence of atypical cells D. character of sputum E. odour of sputum
cardi
ology
.dsmu.e
du.ua

127
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptomes and Syndromes of the Internal Diseases
Topic 8 Module Main syndromes and symptomes of
respiratory diseases, interpretation of instrumental diagnostics and laboratory investigation data
Practice Syndrome of acute and chronic respiratory failure. Abnormal ventilatory capacity of the lungs. Types and stages of the respiratory failure. Restrictive and obstructive respiratory failure
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

128
UImportance of the Subject U: Respiratory failure is the most frequent syndrome which is caused by affection of the respiratory system. Respiratory failure is complication of acute and chronic respiratory diseases. Syndrome of respiratory failure often is accompanied with other syndromes of affection of the respiratory system (syndrome of bronchial obstruction, fluid or air in the pleural cavity). Determining the clinical signs of this syndrome allows to quickly define necessary future investigations (laboratory and instrumental) for examination of the patient . UKey ObjectiveU: To master knowledge and skills in determining clinical sings of respiratory failure, cases of acute and chronic respiratory failure, dividing the respiratory failure into restrictive and obstructive types using clinical signs and pathophysiological mechanisms, identifying laboratory and instrumental investigations of respiratory failure.
USpecific Goals: 1. To determine and distinguish signs of respiratory failure. 2. To determine features of acute and chronic respiratory failure. 3. To be able to define type (restrictive and obstructive) and stage of respiratory failure using clinical laboratory and instrumental signs.
Level of Knowledge and Skills before the Practice: 1. To have knowledge of the structure and features of different parts of respiratory system (Described in the Human Anatomy course.) 2. To identify main parameters in the act of breathing, features of ventilatory capacity of the lungs and gas exchange (Described in the Physiology course.)
34BQuestions for Self-Assessment of the Pre-Practice Knowledge Q1. Patient H., 27 years, complains of attacks of breathlessness (dyspnoea). They arise at night-time. During attacks expiration becomes difficult. Auscultation of the lungs: markedly prolonged expiration accompanied by high-pitched rhonchi.What anatomic formation of the respiratory system hinders in this case to ventilation of lungs? A. Trachea B. Large and mean bronchi (2-8 generation) C. Small bronchi and bronchioles D. Alveoli E. Pleura Q2. Quiet exhalation after inhalation in norm is provided: A. By contraction of shallow bronchi and alveoli. B. By contraction of expiratory muscles. C. By contraction of diaphragm. D. By contraction of muscles of the anterior abdominal wall. E. By relaxation of inspiratory muscles.
cardi
ology
.dsmu.e
du.ua

129
Q3. Deep exhalation after inhalation in norm is provided: A. By contraction of shallow bronchi and alveoli. B. By contraction of expiratory muscles. C. By contraction of diaphragm. D. By relaxation of expiratory muscles. E. By relaxation of inspiratory muscles. Q4. Choose the caliber of bronchi in which rate of movement of air is the least: A. Trachea. B. Large bronchi (2-5 generation). P. Mean bronchi (5-8 generation). D. Shallow bronchi and bronchioles (8-16 generation). E. Respiratory bronchioles (20-23 generations). Q5. Choose anatomic formation providing the gases exchange in the lungs: A. Trachea. B. Large and mean bronchi (2-8 generation). C. Shallow bronchi and bronchioles. D. Alveoli. E. Pleura. Answer Keys: C, E, B, E, D. The following printed materials can be of help to improve your pre-practice knowledge and skills: 1. Test book of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 2. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 3. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy UContents of Practice UTopics of Theory: 1. Pulmonary ventilation and mechanisms of gases exchange in the lungs, pathophysiological mechanisms of respiratory failure 2. Collecting of complaints and anamnesis, physical methods of examination of the patients with respiratory diseases. 3. Clinical sings of respiratory failure 4. Cases of acute and chronic respiratory failure 5. Restrictive and obstructive types of respiratory failure 6. Laboratory and instrumental investigations of the patients with respiratory diseases. Practical skills: UStudents should be able to demonstrate mastery of the following pratical skills 1. To determine and distinguish signs of respiratory failure. 2. To determine features of acute and chronic respiratory failure 3. To be able to perform physical examination of the patients with respiratory diseases
cardi
ology
.dsmu.e
du.ua

130
4. To be able to define type (restrictive and obstructive) and stage of respiratory failure using clinical laboratory and instrumental signs.
Required Glossary to Practice
Term Definition
Ventilation-perfusion coupling
Mechanisms which maintain the correct proportion between alveolar airflow and pulmonary capillary blood flow.
Diffusion
The movement of materials from a region of higher concentration to lower concentration as a result of their kinetic energy. Pulmonary diffusion of gases develops when carbon dioxide and oxygen pass through alveolar capillary membrane (oxygen is supplied from the alveoli to the blood and carbon dioxide is diffused from blood to the alveolar air.
Partial pressure (PaCO2, PaO2)
The pressure exerted by an individual gas in a mixture of gases; it is directly proportional to the percentage of the gas in the total gas mixture
Respiratory failure is the condition with abnormal gas composition of the blood, or abnormality, which is compensated for by intensive work of the external respiratory apparatus and higher load on the heart. Respiratory failure is present when PaCO2 in excess of 45 mmHg and PaO2 less than 60 mmHg
Obstructive type of respiratory failure
is characterized by difficult passage of air thourgh the bronchi (narrowing of airways), ventilatory defect
Restrictive type of respiratory failure
Occurs in limited ability of the lungs to expand and collapse and during decrease in respiratory surface
Mixed type of respiratory failure
Happens with domination of one type of respiratory failure in long –standing diseases
cardi
ology
.dsmu.e
du.ua

131
Flow chart 1
Clinical sings:
Complaints – expiratory, inspiratory or mixed dyspnoea in physical exertion or at rest, palpitation, fatigue
Inspection – central cyanosis, barrel-shape like chest, clubbing of fingers, nails in form of watch glass (in chronic hypoxia)
Other Signs of Physical Examination – increase in respiratory rate, decrease in movements of lower border of lungs, at late stage signs of right heart failure
Examination of blood gases - PaCOR2R N<40 mmHg, if more – hypercapnic changes - PaOR2R N 90-100 mmHg, if less – hypoxemic changes
Laboratory diagnostic:
Clinical examination of blood - increase in Hb, erythrocytes, decrease in ESR
Instrumental diagnostic: - Examination of the external respiration:VC, ERV, IRV, FEV1 and other
cardi
ology
.dsmu.e
du.ua

132
USuggested Reading List URequired Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Functional Investigation of the Lungs 5. Methodical guideline for students 6. Flow charts for Practice 7. Website of department: www.cardiology.dsmu.edu.ua UAdditional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Respiratory failure is the condition with abnormal gas composition of the blood, or abnormality, which is compensated for by intense work of the external respiratory apparatus and higher load on the heart. Types of respiratory failure:
Obstructive Restrictive Mixed Diseases bronchial
asthma, foreign body, tumor of the bronchus.
pneumosclerosis, kyphoscoliosis, hydrothorax, pneumothorax, costal or muscle affection, ankylosing spondylitis, pleural adhesions
chronic obstructive pulmonary disease (COPD) with pneumosclerosis, emphysema of lungs
Dyspnoea expiratory inspiratory Cyanosis central central Cough productive absent Rales present, arising
at forced exspiration
missing
Spirography decrease in FEV1
decrease in VC
Shape of chest
barrel-like shape
without changes
cardi
ology
.dsmu.e
du.ua

133
Clinical course: Acute – attack of bronchial asthma, spontaneous pneumothorax, obstructive atelectasis, pulmonary embolism, pulmonary oedema, acute respiratory distress syndrome, trauma, stroke, sometimes in botulism, lobar pneumonia Chronic –
chronic pulmonary disease, pulmonectomy. kyphoscoliosis, ankylosing spondylitis, myasthenia, dermatomyositis, Pickwickian syndrome.
Pathogenetic mechanisms:
Pulmonary failure obstructive restrictive mixed
(combined)diffuse pulmonary changes
Stages of respiratory failure
1 stage - dyspnoe and tachycardia become evident only at moderate or significant physical load . Arterial blood gas levels are normal.
2 stage - dyspnoe develops during light exercise and at rest cyanosis only during physical load. Hypertrophy of right ventricle. Changes in blood gas level.
3 stage – cardiopulmonary failure. Dyspnoe and cyanosis at rest as manifestation of arterial hypoxaemia. Pneumofibrosis. Significant changes in functional pulmonary tests, gas level. Dilation of right ventricle, right heart failure
cardi
ology
.dsmu.e
du.ua

134
Revision Questions
Q1. Patient K., 38 years old, complains of a breathlessness with difficulty on inspiration which occurs during insignificant exertion and at rest, fever - 38,5-39°C, weakness, fatigue, heaviness in the right part of the chest for 2 week. Physical examination: from the level of the lower angle of the right scapula percussion note is dull, in this site the breath sounds are absent. The type of respiratory failure in this is case: A. obstructive respiratory failure associated with obstructive bronchitis B. respiratory failure with the obstruction of respiratory tracts. C. restrictive respiratory failure associated with syndrome of hydrothorax D. restrictive respiratory failure associated with syndrome of pneumothorax E. none listed above Q2. Choose the disease which is characteristic of hypoxaemic respiratory failure: A. hereditary muscular dystrophy B. polymyositis C. myxedema D. pneumonia E. myasthenia Q3. Patient T., 57 years old suffers from chronic bronchitis for 8 years. He complains of prolonged dyspnoea, palpitation during going upstairs at 5th floor. What degree of respiratory failure characterised by the following: A. respiratory failure I stage B. respiratory failure II stage C. respiratory failure III stage D. heart failure I stage E. cardiopulmonary failure Q4. Choose diseases with dyspnoea which is caused by affection of the lung tissue A. pleural adhesions B. bronchiectasis C. tumours of bronchi D. tuberculosis of the lungs E. pneumothorax Q5. Patient T., 57 years old suffers from chronic bronchitis for a long time. Physical examination: oedema of inferiot limbs, enlargement of liver, ascites, dyspnoe at rest. What degree of respiratory failure characterised by the following: A. respiratory failure I stage B. respiratory failure II stage C. respiratory failure III stage D. heart failure I stage E. heart failure II stage Q6. Choose the disease which is not characteristic of hypercapnic respiratory failure: A. hereditary muscular dystrophy B. polymyositis
cardi
ology
.dsmu.e
du.ua
135
C. pneumofibrosis D. myxedema E. myasthenia Q7. Patient H., 56 years old, complains of a breathlessness with difficulty on inspiration which occurs during insignificant exertion and at rest, fever - 38,5-39°C, weakness, fatigue, heaviness in the right part of the chest for 2 week. Physical examination: from the level of the lower angle of the right scapula percussion note is dull, in this site the breath sounds are absent. The type of respiratory failure in this is case: A. restrictive respiratory failure B. obstructive respiratory failure C. mixed respiratory failure D. none listed above Q8. The division of types of respiratory failure( acute, chronic) according to classification is based on: A. features of dyspnoea B. features of cough C. data of anamnesis D. severity of cyanosis E. swollen of cervical veins Q9. Patient T., 67 years old, complains of a breathlessness with difficulty on inspiration which occurs during insignificant exertion and at rest, fever - 38,5-39°C, weakness, fatigue, heaviness in the right part of the chest for 2 week. Physical examination: from the level of the lower angle of the right scapula percussion note is dull, in this site the breath sounds are absent. The most informing parameter of the spirometry in this case is : A. forced expiratory volume in 1 sec (FEV1). B. inspiratory reserve volume (IRV). C. forced expiratory vital capacity (FEVC). D. residual volume (RV). E. expiratory reserve volume (ERV). Q10. Compression of the lungs which accompanied with dyspnoea arises in: A. hydrothorax B. hemothorax C. chylothorax D. 1-3 answers are wrong E. 1-3 answers are right
Answer Keys: Q1C, Q2D, Q3A, Q4D, Q5C, Q6C, Q7A, Q8C, Q9 B, Q10E.
11BSUMMARY OF PROCEDURES Practice begins in the classroom from the testing. Then the symptoms and
sings characteristic of respiratory failure, the methods of it’s determination (clinical, laboratory and instrumental), mechanisms of respiratory failure development and it’s type discuses. After that students examine patients
cardi
ology
.dsmu.e
du.ua

136
independently, divided into groups for 2-3 men. This part of the practice should fulfilled in the ward. Then students examine patients independently, divided into groups for 2-3 men.
At the end of the practice teacher makes short general conclusion concerning obtained findings and students do final tests. Final Tests Q1. The cause of obstructive type of respiratory failure is: A. pneumosclerosis; B. hydrothorax; C. fibrosis of the lungs; D. pleural adhesions (commissures); E. tumour of bronchus. Q2. Patient T., 45 years old, was admitted to a hospital. Phisical examination: position of body is forced (sits, leaning against hands), moderate cyanosis of lips and face, distention of the neck veins. The supraclavicular fossae are protrude over the clavicles, expansion of thorax, tension of muscles of neck are present. Percussion of the lungs: percussion note is hyperresonant (bandbox sound). Auscultation of the lungs: decreased vesicular breath sounds with prolonged expiration accompanied by high-pitched rhonchi. The most informing parameter of the spirometry in this case is : A. forced expiratory volume in 1 sec (FEV1). B. inspiratory reserve volume (IRV). C. forced inspiratory vital capacity (FIVC). D. respiratory (tidal) volume (TO). E. expiratory reserve volume (ERV). Q3. Disorders of pulmonary compliance which accompanied with dyspnoea arises in: A. dilatation of the bronchi B. constriction of the bronchi C. acute bronchitis D. pneumonia E. pleural adhesions Q4. Choose the reasons of the acute respiratory failure: A. pulmonary emphysema B. pneumoconiosis C. kyphoscoliosis D. spontaneous pneumothorax E. chronic obstructive bronchitis Q5. Patient G., 27 years old, complains of sudden severe dyspnoea after physical exertion. Physical examination:cyanosis, swollen cervical veins, respiratory rate- 32 respirations per minute, from the level of the lower angle of the scapula percussion note is hyperresonant, in this site the breath sounds are absent. The cause of respiratory failure in this is case: A. chronic obstructive bronchitis which causes chronic obstructive respiratory failure. B. acute respiratory failure with the obstruction of respiratory tracts.
cardi
ology
.dsmu.e
du.ua

137
C. syndrome of pneumothorax which causes acute restrictive respiratory failure. D. syndrome of hydrothorax which causes acute restrictive respiratory failure. E. none listed above Q6. Choose types of dyspnoea and cyanosis which is characteristic for restrictive respiratory failure: A. inspiratory dyspnoea B. expiratory dyspnoea C. mixed dyspnoea D. cyanosis is absent E. local cyanosis Q7. Constriction of the bronchi which accompanied with dyspnoea arises in: A. pneumonia B. tumour of the trachea C. affection of the trachea D. bronchiectasis E. bronchitis, bronchiolitis Q8. Choose the reasons of the restrictive respiratory failure: A. foreign body B. massive pleural adhesions C. obstructive bronchitis D. bronchial asthma E. tumour of the bronchus Q9. The most accurate parameter for assessment of degree ( stages) of respiratory failure is : A. complaints B. anamnesis C. auscultation D. blood gas level (CO2 saturation, O2 saturation) E. spirometry Q10. Respiratory failure II degree characterized by: A. dyspnoea during moderate physical activity B. changes in respiratory depth and rhythm C. severe duffuse cyanosis D. cardiac rhythm disorders (tachycardia at rest) E. dyspnoea during significant physical activity
cardi
ology
.dsmu.e
du.ua

138
Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptomes and Syndromes of the Internal Diseases
Topic 8 Module Main syndromes and symptomes of respiratory
diseases, interpretation of instrumental diagnostics and laboratory investigation data
Practice Syndrome of air and fluid in the pleural cavity. Bronchial obstructive syndrome. Syndrome of increased airiness of the lungs. Pickwickian syndrome. Syndrome of pulmonary cavity. Syndrome of pulmonary consolidation.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua
139
UImportance of the SubjectU: Early diagnostics of respiratory pathology is most effective at the adequate estimation of basic clinical symptoms and syndromes. It provides, at first, the choice of method of treatment and prevention worsening of pathological process before making final diagnosis and secondly choice of methods of examination as much as possible quickly provides confirmation of final diagnosis. UKey ObjectiveU: Students should be able to reveal features and signs of syndromes of respiratory pathology (syndrome of air and fluid in the pleural cavity, bronchial obstructive syndrome, syndrome of increased airiness of the lungs, Pickwickian syndrome, syndrome of pulmonary cavity, syndrome of pulmonary consolidation) according to ispection and palpation of the chest, percussion and auscultation of the lungs; be able to select and use the methods of laboratory and instrumental diagnostics for confirmation of these syndromes. USpecific Goals: 1. To learn how to enquire patients with pathologies in respiratory organs about their most disturbing complaints and estimate findings. 2. To develop skills in carrying out the inspection and palpation of the chest, percussion and auscultation of the lungs and in identifying the pathologies discovered. 3. To be able to demonstrate mastery at analyzing of clinical, instrumental, laboratory investigations for confirmation of the certain syndrome. Level of Knowledge and Skills Before the Practice: 1. To have knowledge of the structure of the lungs and their location within the human body (Described in the Human Anatomy course) 2. To have knowledge of a location of the identification points and topographic lines within the chest, as well as of a projection of parts of the lungs onto the chest (Described in the Human Anatomy course) 3. To identify main parameters in the act of breathing (i.e. its frequency, depth, mode and rhythm) and factors which constitute them in normal and abnormal conditions. (Described in the Physiology course.) 4. To identify main features of ventilatory capacity of the lungs and gas exchange (Described in the Physiology course.) 5. To have knowledge of a histological structure of alveoli, bronchi, bronchioles and pleural layer (Described in the Histology course.) Questions for Self-Assessment of the Pre-Practice Knowledge Q1. X-ray examination discovered lungs emphysema in the patient. What is the reason of short breath development in this case? A. Decreased lungs elasticity B. Decreasing of alveoli receptors sensitivity C. Increased lungs elasticity
cardi
ology
.dsmu.e
du.ua

140
D. Inhibition of respiratory center E. Excitation of respiratory center Q2. A patient who had been suffering for many years from bronchial asthma died from asphyxia. The histological examination of his lungs revealed the following: much mucus with eosinophiles contents in the lumen of bronchioles and small bronci, sclerosis of interalveolar septa, dilation of alveolar lumen. Which of the mechanisms of allergy development is it? A. Immunocomplex B. Cytolysis, caused by lymphocytes C. Cytotoxic D. Reagin E. Granulomatosis Q3. The patient complains of dry cough. What is location of cough receptors? А. In alveoli В. In acinus С. On forward wall of pharynx D. In pleura Е. In auricle Q4. A patient because of pathological process has thickened alveolar membrane. What will be reduced directly as a result this? A. Oxygen capacity of blood B. Alveolar lung ventilation C. Alveolar diffusion D. Reserve expiratiory capacity E. Minute respiratory capacity Q5. The patient has productive cough. What normal quantity of mucus is formed in tracheobronchial tract a day? А. 20-30 ml В. 30-50 ml С. 50-90 ml D. 100-300 ml Е. 350-500 ml Answer Keys: A, D, D, C, C.
The following printed materials can be of help to improve your pre-practice knowledge and skills:
1. Test book of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 2. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 3. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy
cardi
ology
.dsmu.e
du.ua

141
UContents of Practice
UTopics of Theory:
1. General rules, method of questioning of patient; typical complaints for certain syndrome of respiratory pathology 2. Physical examination (inspection and palpation of the chest, percussion and auscultation of the lungs, vocal fremitus and vocal resonance) in identifying the syndromes of respiratory pathology.
3. Laboratory, instrumental diagnostics syndromes of respiratory pathology. 4. Diagnostic value of findings. After mastering of the questions listed above, familiarize with flow charts and tables for this subject
Practical skills:
Students should be able to demonstrate mastery of the following pratical skills
1. To enquire patients with pathologies in respiratory organs about their most disturbing complaints and estimate findings.
2. To carrying out the inspection of the chest, percussion and auscultation of the lungs and in identifying the syndrome of respiratory pathology discovered.
3. To be able to demonstrate mastery of the analyzing of clinical, instrumental, laboratory investigations for confirmation of the certain syndrome.
cardi
ology
.dsmu.e
du.ua

142
Required Glossary to Practice
Term Definition
Syndrome of consolidation of pulmonary tissue
The syndrome of focal consolidation of lung tissue is caused by filling of the alveoli with the inflammatory fluid and fibrin (pneumonia - inflammatory consolidation), blood (lung infarction), growing connective tissue in the lung (pneumosclerosis) or developing tumour, atelectasis (noninflammatory consolidation) .
Syndrome of lobar pneumonia
Pneumococcal pneumonia with inflammatory consolidation (infiltration) of whole lobe associated with pleural affection (dry pleuritis). It has 3 stages. 1 stage- acute hyperaemia of the lung tissue, exudation. Alvelar wall are impregnated by exudate, impaired –hyperresonant note is revealed during percussion, auscultation-decreased vesicular breath sounds, crepitation indux 2 stage- red and grey hepatization of lung tissue, lung tissue is airless by consolidation, dull note is revealed during percussion, auscultation-bronchial breath sounds,consonating moist rales, pleural rub. 3 stage-resolution stage, impaired-hyperresonant note is found out during percussion. decreased vesicular breath sounds, crepitation redux
Syndrome of atelectasis Decrease or absence of airness of pulmonary region caused by obstruction of bronchial lumen by tumour, foreing body (incomplete or complete obstructive atelectasis) or compression of lung tissue from the outside by pleural effusion, air (compressive atelectasis)
Syndrome of pneumothorax
a state in which air accumulation is present in the pleural cavity and which occurs spontaneously as a result of disease of the lung (in subpleural tuberculosis cavern or abscess), puncture of the chest wall or injury of the chest.
Syndrome of pulmonary abscess
is a purulent melting of the lung tissue with formation cavity which filled with pus circum-scribed by an inflammatory swelling
cardi
ology
.dsmu.e
du.ua

143
Syndrome of bronchiectasis
This disorder is characterized by abnormal destruction and local dilitation of bronchi. Bronchiectatic conditions are divided into primary (congenital, which are very rare) and secondary (secondary to various diseases of the bronchi, lungs)
Syndrome of emphysema of the Lungs
Lung emphysema is characterized by increased airiness of the lungs due to abnormal enlargement and overdistention of the alveolar air spaces accompanied by destructive changes of the alveolar walls.
Syndrome of accumulation of pleural fluid
occurs in hydrothorax (accumulation of non-inflammatory effusion, i.e. transudate, for example in cardiac failure), or in pleurisy with effusion (inflammation of the pleura).
Pickwickian syndrome Represents patients with morbid gross obesity who have chronic sleep-induced central hypoventilation and develop daytime somnolence. Many of these patients also have obstructive sleep apnoea. These patients have hypoxaemia, hypercapnia, polycythaemia,pulmonary hypertention and rigth-sided heart failure.
cardi
ology
.dsmu.e
du.ua

144
Syndromes of pathology of lungs and pleura
Increased airiness Pulmonary inflammatory
infiltration of the lungs
Compression by air in pleural cavity
Bronchial asthma
Pulmonary emphysema
Tuberculous infiltration
Pneumonia
Obstructive atelectasis (complete, incomplete)
Compressive atelectasis
Obstruction by tumour
Obstruction by foreing body
Compression by fluid in pleural cavity
Fluid in pleural cavity
Air in pleural cavity
Hydrothorax Exudative pleurisy
Pneumothorax Haemothorax. Chylothorax
Pulmonary cavity
Abscess Bronchiecta sis
Dry cyst of lung
Echinococ cus cyst of lung
Tuberculous cavern
cardi
ology
.dsmu.e
du.ua

145
Table № 1
*Topographic percussion of the lungs (upper level of lung apices, their width (Kroenig’s area), lower border of the lungs, range of movement of the lower pulmonary borders (diaphragmatic movement)
Syndromes of pulmonary pathology
Static inspec tion
Dynamic inspection
Topog raphic percus sion of the lungs*
Com parative percus sion of the lungs
Main breath sounds
Added breath sounds
Vocal fremitus, vocal resonance
Increased airiness of the lungs (emphysema)
Bronchial spasm Pulmonary cavity (in upper lobe, it communicates with bronchus)
Air in a pleural cavity (Pneumothorax)
Fluid in a pleural cavity (Hydrothorax)
Exudative pleurisy in initial and resolution stage
Exudative pleurisy in middle stage
Air and fluid in a pleural cavity (Hydropneumothorax)
Obstructive atelectasis (incomplete)
Obstructive atelectasis (complete)- collapse
Compressive atelectasis
Inflammatory pulmonary consolidation (lobar pneumonia1-3 stages)
cardi
ology
.dsmu.e
du.ua

146
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Lecture: Functional Investigation of the Lungs 5. Methodical guideline for students 6. Flow charts for Practice 7. Website of department: www.cardiology.dsmu.edu.ua
Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Syndrome of pulmonary cavities
- Abscess - Bronchiectasis
- Kartagener's syndrome – situs viscerus inversus, sinusitis, bronchiectasis. - Williamsa-Kempebla – congenital bronchoectasis due to hypoplasia of
bronchial cartilages. - Tuberculous cavern - Cystic lung hypoplasia - Dry cyst - Echinococcus cyst - Lung infarction
Pulmonary cavity with communication with bronchus Inspection - visual changes are absent; percussion- hyperresonant or impaired- hyperresonant (it depends on size of cavity, presence of inflammatory capsule which surroundes it, presence fluid in it); auscultation- bronchial amphoric breath sounds, moist consonating rales, vocal fremitus and vocal resonance are increased Bronchiectasis - this is a condition characterized by local dilatation of the bronchi. Bronchiectatic conditions are divided into primary (congenital, which are very rare) and secondary (complication of various diseases of the bronchi, lungs and pleura). Bronchiectases develop in bronchitis only when the inflammatory process extends onto the muscular layer of the bronchial wall or onto all its layers.
The main symptom is cough with expectoration of seromucopurulent (three layers) or purulent sputum (sometimes foul-smelling). The daily amount of expectorated sputum varies from 50 to 500 ml and more. Blood streaks may be seen. Cough is paroxysmal in character and occurs mainly in the morning.
cardi
ology
.dsmu.e
du.ua
147
Haemoptysis, dyspnoea, excess sweating, weakness, headache, dyspepsia, deranged sleep and appetite, and wasting can also be observed.
The body temperature rises, leucocytosis develops, and ESR increases. General inspection of the patient reveals acrocyanosis (at later stages of the disease) and oedematous face; in some cases the terminal phalanges of the fingers become clubbed (Hippocratic fingers), and the nails resemble the watch glass. Bronchial obstructive syndrom Complaints – dyspnoea with difficulties in exhalation, dyspnoea with
intensification at night and in cold weather, cough,wheezes Inspection – protrusion of intercostals space, supra- and infraclavicular fossea. Palpation – deacreased vocal fremitus. Percussion – hyperresonant( bandbox note), elevation of upper level of pulmonary
(apices), lowering of lower borders. Decrease in movement of both sides of the chest
Auscultation – harsh, vesicular breath sound with prolonged expiration, wheezes, rhonchi which increase during forced expiration
Syndrome of increased airiness of the lungs – emphysema – vicarious- (pulmonectomy, pneumothorax, hydrothorax, so another lung works more severe) - primary - secondary (complication of chronic obstructive pulmonary diseases) - limited - diffuse Inspection – barrel like chest, protrusion of intercostals space, supra- and
infraclavicular fossea. Palpation – deacreased vocal fremitus. Percussion – hyperresonant( bandbox note), elevation of upper level of pulmonary
(apices), lowering of lower borders. Decrease in movement of both sides of the chest
Auscultation – deacreased vesicular breath sound Stages of emphysema:
1. Decreased range of movement of lower pulmonary borders – less than 4 cm, decrease in absolute dullness of heart
2. Decreased range of movement of lower pulmonary borders – less than 2cm, lowering of lower border on 1 rib, wide intercostal spaces
3. Absence range of movement of lower pulmonary borders , lowering of lower border on 2 ribs, participation of accessory muscles, swollen cervical veins, enlargement of liver
Pickwickian syndrome hereditary predisposition obesity→ high level of diaphragm→ alveolar hypoventilation
cardi
ology
.dsmu.e
du.ua

148
pathologically somnolence or hypersomnia (excessive sleepiness) – during conversation or taking a meal, sleep apnoea, dyspnoea, cyanosis, polycythemia, high level of Hb, cor pulmonale ( signs of right heart failule)
Syndromes of pneumothorax
- Traumatical pneumothorax ( blunt trauma of the chest, fracture of ribs, penetrating wound of the chest by knife, bullet)
- Iatrogenic pneumothorax ( after resuscitation -external cardiac massage, unsuccessful puncture of pleural cavity) - Spontaneous pneumothorax – neonatal – primary (unknown reasons)
– secondary (COPD, BA, pneumonia, infarction, tumor, endometriosis, tbs, X- Ray examination with contrast, cystic fibrosis, eosinophilic granuloma, Marfan's syndrome, pregnancy)
- Tension pneumothorax (when air can’t go out from pleural cavity and new portions come in it again) – it gives dullish note during percussion
Syndrome of atelectasis Obstructive atelectasis - complete (collapse) - indrawing of the intercostals spaces, lagging of affected side, dull note, absence of breath sounds, vocal fremitus and vocal resonance are absent - incomplete – normal or small indrawing of the intercostals spaces, impaired-hyperresonant note, decreased vesicular breath sounds, vocal fremitus and vocal resonance are decreased Compressive atelectasis (compression of lung tissue by tumour, hydrothorax, pneumothorax) Cause of complicated pulmonary compliance which accompanied with dyspnoea:
- pneumosclerosis - pleural adhesion
Revision Questions
Q1. A 66 –year old patient A, the miner, was admitted to a hospital with complaints of severe dyspnoea at rest and small physical activity. In inspection the syndrome of increased pulmonary airness has been found. Determine the following main symptoms which characterize the syndrome of the increased pulmonary airness. In static inspection the following shape of the chest is determined: A. Normosthenic B. Asthenic C. Hypersthenic
cardi
ology
.dsmu.e
du.ua

149
D. Emphysematous (barrel-chest) E. Paralytic Q2.What auscultatory data can be defined in patients with syndrome of large pulmonary cavity (more than 6-7 cm): A. impaired (dullish) percussion note B. hyperresonant percussion note C. dull percussion note D. dullish- hyperresonant (impaired-tympanitic) percussion note E. resonant percussion note Q3. Patient R., 25 years old, has sudden onset of breathlessness with difficulty on inspiration after physical exertion. Physical examination: respiratory rate- 34 respirations per minute, cyanosis, swollen cervical veins, from the level of the lower angle of the left scapula percussion note is hyperresonant, in this site the breath sounds are absent . In dynamic inspection the following shape of the chest is determined: A. Equal participation of the two sides of the chest in the respiration act B. Lagging of the right side of the chest during respiration C. Lagging of the left side of the chest during respiration D. Lagging of the both sides of the chest during respiration E. None of above listed Q4.The syndrome of cavity in the lung is observed at: A. pneumothorax B. lungs emphysema C. hydrothorax D. tubercular cavern E. bronchial asthma Q5. Narrowing of bronchi resulting in rising of dyspnoea, occurs at: A. pneumonia B. tumour of trachea C. bronchocarcinoma D. affection of diaphragm E. bronchiectasis Q6. Choose the reason resulting in obstructive atelectasis of lung: A. diminishing of the bronchial lumen (from within) B. hydrothorax C. growing up of connective tissure D. pneumothorax E. hydropneumothorax Q7. Patient N., 67 years old, complains of a breathlessness which occurs during insignificant exertion and at rest, fever - 38,5-39°C, weakness, fatigue, heaviness in the right part of the chest for 2 week. Physical examination: from the level of the lower angle of the right scapula percussion note is dull, vocal fremittis and vocal resonance are not determined. Determine the following main symptoms which characterize the syndrome of accumulation of fluid in the pleural cavity. Auscultation of the lungs on affected side determines in this case:
cardi
ology
.dsmu.e
du.ua

150
A. Bronchial breath sounds over root region and over other regions breath sounds are absent B. Vesicular breath sounds С. Diminished vesicular breath sounds D. Increased vesicular breath sounds E. Breath sounds are absent Q8. Choose pathological syndrome of the lungs and pleura which is characterized by decreased vocal resonance (fremitus) (but it is not absent): A. syndrome of the inflammatory pulmonary consolidation B. syndrome of incomplete atelectasis of the lung C. syndrome of complete atelectasis of the lung (pulmonary collapse) D. syndrome of massive accumulation of air in the pleural cavity E. syndrome of massive accumulation of fluid in the pleural cavity Q9. Choose the syndrome of pathology of lungs and pleura which is characterized by decreased bronchophony (but it is not absent): A. syndrome of massive accumulation of air and fluid in the pleural cavity B. syndrome of inflammatory consolidation of pulmonary tissue C. syndrome of massive accumulation of air in the pleural cavity D. syndrome of massive accumulation of fluid in the pleural cavity E. syndrome of accumulation of small amount of liquid in the pleural cavity Q10. Choose the disease which is the reason of formation of cavity in the lung: A. hydrothorax B. pleural empyema C. hydrothorax D. dry cyst of lung E. focal tuberculosis
Answer Keys: Q1D, Q2B, Q3C, Q4D, Q5C, Q6A, Q7E, Q8B, Q9E, Q10D.
12BSUMMARY OF PROCEDURES
The given practice shall begin in the study room with the homework assignment checked and students’ testing carried out. Then students with teacter discuss signs of phisical examination, instrumental, laboratory investigations for diagnostics of certain syndrome of respiratory pathology and their diagnostic value. Then students examine patients with different respiratory pathology, divided into groups for 2-3 men. Diagnostic value of the revealed changes of breath sounds in examined patients shall be discussed outside of the ward.
At the end of the practice teacher makes short general conclusion concerning obtained findings and students do final tests.
Final Tests
Q1. Which percussion data can be defined in patients with syndrome of the increased airiness of the lungs? A. dullish- hyperresonant( dullish-tympanitic) note B. dullish note C. elevation of the lower borders of the lungs with restricted range of the their
cardi
ology
.dsmu.e
du.ua

151
movement D. lowering of the lower borders of the lungs with restricted range of the their
movement E. lower borders of the lungs and range of their movement without changes Q2. Choose the signs which can be determined in patients with syndrome of air in the pleural cavity (tension pneumothorax) during percussion: A. impaired (dullish) percussion note B. hyperresonant (tympanitic)percussion note C. dull percussion note D. dullish-hyperresonant percussion note E. resonant percussion note Q3. Choose the signs which can be determined in patients with syndrome of the pulmonary cavity during inspection: A. enlargement of the affected side of the chest during breathing B. enlargement of the healthy side of the chest during breathing C. emphysematous (barrel-like) chest D. levelling or protrusion of the supraclavicular fossae E. changes are absent Q4. Which percussion data can be defined in patients with syndrome of the increased airiness of the lungs? A. dullish- hyperresonant( dullish-tympanitic) note B. dullish note C. hyperresonant (bandbox) note D. elevation of the lower borders of the lungs with restricted range of the their
movement E. lower borders of the lungs and range of their movement without changes Q5. Which percussion data can be defined in patients with syndrome of the inflammatory pulmonary consolidation (lobar pneumonia, I or III stages) ? A. dullish- hyperresonant( dullish-tympanitic) note B. dullish note C. hyperresonant (bandbox) note D. dull percussion note E. resonant percussion note Q6. Choose the signs which can be determined in patients with syndrome of small pulmonary cavity ( less than 2-3 cm) during percussion: A. impaired (dullish) percussion note B. hyperresonant (bandbox)percussion note C. dull percussion note D. dullish-hyperresonant percussion note E. resonant percussion note Q7. Choose the signs which can be determined in patients with syndrome of moderate accumulation of of fluid in the pleural cavity during percussion: A. impaired (dullish) percussion note B. hyperresonant (bandbox)percussion note
cardi
ology
.dsmu.e
du.ua

152
C. dull percussion note D. dullish-hyperresonant percussion note E. resonant percussion note Q8. Which auscultatory data can be defined in patients with syndrome of the inflammatory pulmonary consolidation (lobar pneumonia, I or III stages)? A. diminished vesicular breath sounds B. increased vesicular breath sounds C. bronchial breathing D. rhonchi E. non - consonating moist rales Q9. Choose possible reasons of the compressive pulmonary consolidation: A. decrease in intrinsic lumen of bronchus B. hydropneumothorax C. pneumosclerosis D. foreign body in bronchus E. pressing of bronchus from the outside Q10. Choose the signs which can be determined in patients with Pickwikian syndrome: A. paralytic chest B. pronounced supraclavicular fossae C. funnel chest D. oedema of inferior limbs E. wide and assimetrical intercostals spaces
cardi
ology
.dsmu.e
du.ua

153
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
_ ”_ ____”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptomes and Syndromes of the Internal Diseases
Topic 8 Module Main syndromes and symptomes of respiratory
diseases, interpretation of instrumental diagnostics and laboratory investigation data
Practice Syndrome of pulmonary hypertention. Syndrome of cor pulmonale. Respiratory distress syndrome. Syndrome of extra-respiratory failure.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

154
Importance of the Subject: Syndrome of pulmonary hypertention and syndrome of cor pulmonale.are important, serious complication of respiratory and heart pathology. Respiratory distress syndrome and extra-respiratory failure need quick diagnostics and treatment. Determining the clinical signs of these syndromes allows to define necessary future investigations (laboratory and instrumental) for examination and treatment of the patient. Key Objective Students should be able to determine features and signs of syndrome of pulmonary hypertention,. syndrome of cor pulmonale, respiratory distress syndrome, syndrome of extra-respiratory failure according to physical examination; be able to select and use the methods of laboratory and instrumental diagnostics for confirmation of these syndromes. Specific Goals: 1. To enquire patients with pathologies in respiratory organs about their most disturbing complaints and estimate findings. 2. To develop skills in identifying the syndrome of pulmonary hypertention and cor pulmonale according to physical examination, instrumental and laboratory investigations, to know reasons of these syndromes 3. To develop skills in identifying the respiratory distress syndrome and syndrome of extra-respiratory failure. according to physical examination, instrumental and laboratory investigations, to know reasons of these syndromes 4. To be able to demonstrate mastery at analyzing of clinical, instrumental, laboratory investigations for confirmation of the certain syndrome. Level of Knowledge and Skills Before the Practice: 1. To have knowledge of a histological structure of alveoli, bronchi, bronchioles and pleural layer (Described in the Histology course.) 2. To have knowledge of the structure of the lungs and their location within the human body (Described in the Human Anatomy course) 3. To identify main parameters in the act of breathing (i.e. its frequency, depth, mode and rhythm) and factors which constitute them in normal and abnormal conditions. (Described in the Physiology course.) 4. To identify main features of ventilatory capacity of the lungs and gas exchange (Described in the Physiology course.) Questions for Self-Assessment of the Pre-Practice Knowledge Q1. Gaseous exchange in the lungs occurs in: A. Trachea B. Primary and lobar bronchi C. Segmental bronchi and bronchioles D. Alveoli E. Pleura
cardi
ology
.dsmu.e
du.ua

155
Q2. Patient V. 40 years old admitted in therapeutics department with diagnosis: Right-sided pleurisy. Evaluation of the patient acknowledged presence of the fluid in pleural cavity. In what pleural sinus will be greatest quantity of serous fluid? A. Right costophrenic B. Right costomediastinal C. Left mediastenodiaphragmatic D. Left costomediastinal E. Right mediastenodiaphragmatic Q3. Upon examination under the microscope of the specimen of airways surface epithelium with a lot of cellula ciliata and goblet cells is determined What basic function of these cells? A. Incretory B. Air cooling C. Air clarification D. Air heating E. Gas exchange Q4. Surfactant is synthesized by: A. respiratory epithelial cells (alveolocyte of 1 type) B. large epithelial cells (alveolocyte of 2 type) C. brush epithelial cells (alveolocyte of 3 type) D. alveolar macrophages E. secretor cells of bronchiole Q5. Lung of premature infant is presented on electronic photomicrography of biopsy material. Collapse of the alveolar wall caused by the deficiency of surfactant was revealed. Disfunction of what cells of the alveolar wall caused it? A. Fibroblasts B. Alveolar macrophages C. Secretory cells D. Alveocytes type II E. Alveocytes type I Answer Keys: Q1D, Q2A, Q3C, Q4B, Q5D.
The following printed materials can be of help to improve your pre-practice knowledge and skills:
1. Test book of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 2. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 3. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy
cardi
ology
.dsmu.e
du.ua

156
Contents of Practice
Topics of Theory:
1. Pulmonary hypertension; primary and secondary pulmonary hypertension, acute and chronic pulmonary hypertension, its reasons, complaints, data of physical examination, instrumental and laboratory investigations 2. Cor pulmonale, reasons, types, complaints, data of physical examination, instrumental and laboratory investigations 3. Respiratory distress syndrome, reasons, mechanism of occurence, clinical signs, instrumental and laboratory investigations 4. Extra-respiratory failure, reasons, mechanism of occurence, clinical signs
Practical Skills:
Students should be able to demonstrate mastery of the following pratical skills
1. To enquire patients with pathologies in respiratory organs about their most disturbing complaints and estimate findings.
2. To determine the syndrome of pulmonary hypertention according to physical examination, instrumental and laboratory investigations
3. To reveal the syndrome of cor pulmonale according to physical examination, instrumental and laboratory investigations
4. To determine the respiratory distress syndrome and syndrome of extra-respiratory failure. according to physical examination, instrumental and laboratory investigations 5. To demonstrate mastery of analyzing of clinical, instrumental, laboratory investigations for confirmation of the certain syndrome.
cardi
ology
.dsmu.e
du.ua

157
Required Glossary to Practice
Term Definition
Pulmonary hypertention is defined as a pulmonary artery systolic pressure greater than 30 mmHg
Euler-Liliestrand reflex
This reflex mechanism in response to insufficient lung ventilation and alveolar hypoxia (hypertension in the vessels of the lesser circulation in diffuse affections of the lungs) is an important adaptation means limition of blood supply to in-sufficiently ventilated alveoli and increase in blood supply to parts of the lungs which ventilated more.
Graham Steel murmur This is soft, blowing , early diastolic murmur which begins immediately after loud P2 over pulmonary artery. The murmur results from relative pulmonary regurgitation due to rigth ventricle dilation and pulmonary valve ring dilation caused by pulmonary hypertention
Extra-pulmonary failure This is respiratory failure caused by extra-pulmonary reasons
Cor pulmonale Hypertrophy or dilation of right ventricle due to pulmonary hypertention which caused by bronchopulmonary diseases, defects of pulmonary vessels, chest wall
Acute respiratory distress syndrome
(ARDS)
Non-cardiogenic pulmonary oedema. This serious condition characterized by damage of alveolar epithelium and pulmonary capillary endothelium. Alveolar spaces are filled by oedema fluid and it causes acute respiratory failure.
cardi
ology
.dsmu.e
du.ua

158
Flow chart № 1
Pulmonary hypertension
Primary hypertension Secondary hypertension
Aer’s disease- primary affection of pulmonary arteries
chronic pulmonary diseases
mitral valvular diseases
kyphoscoliosis
septal heart defects
acute respiratory distress syndrome
attack of bronchial asthma
Chronic pulmonary hypertension
left heart failure
thrombosis of the pulmonary artery
Acute pulmonary hypertension
cardi
ology
.dsmu.e
du.ua

159
Acute respiratory distress syndrome (ARDS)
Pathogenesis – influence of membrane damage substance There are remedies, drugs, uraemic substance, aspiration of gastric contents, trauma of thorax, sepsis, affection of central nervous system, inhalation of smoke or hot air, acute pancreatitis This leads to:
- quick accumulation of fluid in lung tissue - increase of permeability of alveolar-capillary membrane - disorder of lung compliance - disturbance in gas exchange
Symptoms: – acute onset in dyspnoea – cyanosis – disseminated intravascular clotting (DIC), – low blood pressure, tachycardia – interstitial oedema of lungs which passes to alveolar oedema (harsh
breathing, moist rales, crepitation) – sings of heart failure – blood gas abnormalies
Cor pulmonary Reasons: Bronchopulmonary reasons (chronic obstructive bronchitis, bronchial asthma, emphysema, pneumofibrosis,bronchiectasis) Vascular reasons (affection of vessels in lesser circulation)-pulmonary thrombosis, vasculatis, compression of pulmonary artery Thoracodiaphragmatic reasons (chest wall abnormalities) –gross obesity-Pickwickian syndrome, kyphoscoliosis, ankylosing spondylitis (Bechterev’s disease), disorders of neuromuscular transmission Complaints:
- dyspnoea - palpitation - constricting pain in heart region - fast fatigue - oedema - dizziness - heavy feeling in the rigth hypochondrium
Clinical sings: Inspection, palpation
- central cyanosis - dilatation and pulsation of jugular veins, positive venous pulse - pulsation in epigastric region, absolute dullness of heart (dilation of rigth
ventricle), may be pulmonary artery pulsation - peripheral oedema, ascites, hydrothorax, hydropericardium - hepatomegaly
cardi
ology
.dsmu.e
du.ua

160
Percussion- - increaserd vascular bundle due to pulmonary artery enlargement - displacement of heart dullness right
Auscultation - accent of second sound over lung artery, its splitting - Graham Steel murmur - positive Rivella-Korvalo sign - positive Shcherba sign
ECG - signs of right ventricular hypertropy - P-pulmonale - rigth bundle branch block
X- ray - increase in right ventricle - increase in second arch of pulmonary artery - distension of vessels in lesser circulation
Extra-pulmonary failure
central disturbance of breathing (failure of respiratory drive) – stroke, trauma, neuroinfection, respiratory depressant drugs
disturbance of neuromuscular transmission poliomyelitis, tetanus, polyradiculoneuritis, botulism, trauma, polymyositis, myasthenia gravis
thoraco-diaphragmatic disturbance – trauma, kyphoscoliosis, ankylosing spondylitis (Bechterev’s disease), gross obesity – Pickwickian syndrome.
Suggested Reading List
Required Reading
1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990
2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986
3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004
4. Lecture: Examination of the respiratory system: Functional investigation of the lungs. Main syndromes and symptomes of respiratory diseases.
5. Methodical guideline for students
6. Flow charts for Practice
7. Website of department: www.cardiology.dsmu.edu.ua
cardi
ology
.dsmu.e
du.ua

161
Additional Reading
1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Revision Questions
Q1. During physical examination of patient with chronic obstructive bronchitis doctor heard murmur over pulmonary artery. Choose the characteristic murmur in patients with cor pulmonale which can be detected over pulmonary artery: A. mesosystolic murmur B. presystolic murmur C. early diastolic murmur D. late diastolic murmur E. mesodiastolic murmur Q2. During physical examination of patient with chronic obstrucrive bronchitis doctor revealed systolic murmur over xiphoid process. Choose the most characteristic feature of systole murmur in patients with cor pulmonale which can be detected at the base of xiphoid process: A. intensive «scraping» murmur which increases during expiration B. soft systolic murmur which does not depend on respiratory phase C. soft systolic murmur which increases during inspiration D. soft systolic murmur which increases during expiration E. intensive «scraping» murmur which does not depend on respiratory phase Q3. A 73 –year old patient A. was admitted to a hospital with complaints of dyspnoea at rest and small physical activity. In inspection the syndrome of increased pulmonary airness has been found. Choose the method of instrumental investigation, which is most informative for diagnostics of chronic cor pulmonale: A. bronchoscopy B. ECHO C. phonocardiography D. spirography E. pneumotachography Q4. Doctor heard murmur over pulmonary artery in patient with chronic obstructive pulmonary disease during physical examination. Choose the name of early diastolic murmur in patients with cor pulmonale which can be detected over pulmonary artery: A. Graham Steell murmur B. Cumb’s murmur C. Flint’s murmur D. Rivello-Corvalo sign E. Obraztsov`s click
cardi
ology
.dsmu.e
du.ua

162
Q5. ECG recording was peformed for patient with cor pulmonale. Choose the ECG sign which is characteristic of chronic cor pulmonale: A. left electrical axis deviation B. Rs,R,qR in V1,V2 C. normal position of electrical axis D. high R waves in V5-6 E. pathological Q wave in V5-6 Q6. During physical examination the patient doctor determined clinical features of cor pulmonale. Choose the clinical feature characteristic of a chronic cor pulmonale: A. displasment of apex beat to the left and down B. hypertermia C. displacement of cardiac dullness to the right D. pulsation of carotid arteries E. enlargment of spleen Q7. There is swelling (enlargement) of liver in case of the markedly expressed chronic increased airiness of the lungs. It caused: A. by shifting back of the liver and neck veins by extended (hyperairiness) lungs; B. by dilatation of right ventricle as a result of hypertension in the system of
pulmonary artery; C. by the often developing thrombosis of vena cava inferior; D. by the thrombosis of small branches of pulmonary artery; E. by the considerable consolidations of the bronchial walls Q8. Some diseases have complication as a pulmonary hypertension. Secondary pulmonary hypertension is caused by: A. renal diseases B. septal heart disease C. tricuspid valvular diseases D. coartation of aorta E. essential hypertention Q9. Choose the state which results in rising of pulmonary hypertension: A. pulmonary thromboembolism B. essential hypertension C. tricuspid regurgitation D. tricuspid stenosis E. portal vein thrombosis Q10. Choose the extrapulmonary reasons of respiratory failure due to disorders of neuromuscular transmission A. gross obesity B. spontaneous pneumothorax C. ankylosing spondylatis D. tetanus E. inhibition of respiratory center (drive) Answers Keys: Q1C, Q2C, Q3B, Q4A, Q5B, Q6C, Q7B, Q8B, Q9A, Q10D.
cardi
ology
.dsmu.e
du.ua

163
SUMMARY OF PROCEDURES The given practice shall begin in the study room with the homework assignment checked and students’ testing carried out. Then students with teacter discuss signs of phisical examination, instrumental, laboratory investigations for diagnostics of syndrome of pulmonary hypertention, syndrome of cor pulmonale, respiratory distress syndrome, syndrome of extra-respiratory failure, their diagnostic value. Then students examine patients with different respiratory pathology, divided into groups for 2-3 men. Diagnostic value of the revealed changes in examined patients shall be discussed in the study room.
At the end of the practice teacher makes short general conclusion concerning obtained findings and students do final tests.
Final Tests
Q1. Choose the reason of cor pulmonale: A. essential hypertension B. tricuspid heart valve disease C. aortic heart valve disease D. respiratory distress syndrome E. endocrine diseases Q2. Choose the clinical feature characteristic of a chronic cor pulmonale: A. displasment of apex beat to the left and down B. hypertermia C. pulsation of carotid arteries D. enlargment of liver E. dilatation of heart to the left and downwards Q3. Choose the clinical feature characteristic of a chronic cor pulmonale: A. pulsation of carotid arteries B. pallor of the skin C. hyperemia D. dilatation of heart to the left and downwards E. oedema of inferior limbs Q4. Reason of acute pulmonary hypertension is: A. chronic pulmonary diseases B. attack of bronchial asthma C. mitral valvular diseases D. essential hypertension E. kyphoscoliosis Q5. Choose the method of instrumental investigation which has the most diagnostic value in case of chronic cor pulmonale: A. phonocardiography; B. bronchoscopy; C. spirography; D. electrocardiography; E. measurement of the blood pressure.
cardi
ology
.dsmu.e
du.ua

164
Q6. Compression of the lungs which accompanied with dyspnoea arises in: A. pneumothorax B. pleural adhesions C. pneumosclerosis D. pneumoconiosis E. pulmonary emphysema Q7. Choose the extrapulmonary reasons of respiratory failure due to thoracodiaphragmatic disorders A. polymyositis B. myasthenia gravis C. ankylosing spondylitis D. myositis E. laryngeal obstruction Q8. Choose the extrapulmonary reasons of respiratory failure due to central hypoventilation A. spontaneous pneumothorax B. pleural effusion C. disturbance of neuromuscular transmission of nervous impulse D. gross obesity E. inhibition of respiratory center (drive) Q9. Reason of acute pulmonary hypertension is: A. chronic pulmonary diseases B. acute left heart failure C. mitral valvular diseases D. essential hypertension E. kyphoscoliosis Q9. Sign of pulmonary hypertension which reveals during auscultation: B. Loud S1 and its splitting over second left intercostal space C. Loud S2 and its splitting over second left intercostal space D. Loud S1 and its splitting over second right intercostal space E. Loud S2 and its splitting over second right intercostal space F. Loud S1 and its splitting over heart apex Q10. The main laboratory signs of respiratory distress syndrome are characterized by: A. blood gas abnormalies B. changes in troponin level C. changes in glucose level D. changes in cholesterol E. decreased level of red blood cells
cardi
ology
.dsmu.e
du.ua

165
Topic 9 Module. Main syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation. Specific Goals: - To estimate data of the enquering, physical examination, instrumental diagnostics of patient with diseases of digestive system and urinary system - Make primary conclusion of disorders of digestive system and urinary system - To interpret the received data of the examination for recognition of clinical syndromes of the alimentary system diseases and urinary system diseases. - To know new classifications of alimentary system diseases and urinary system diseases
cardi
ology
.dsmu.e
du.ua

166
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 13BThe Main Methods of Examination of Patient on Internal Diseases Course
Topic 9 Module
14BMain syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice
Instrumental diagnostics and laboratory investigation of digestive system. Examination of the secretory and acid-forming functions of the stomach, duodenal contents. Coprological studies. Technique and indications to gastroscopy and colonoscopy. X-ray of stomach.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

167
Importance of the Subject: Instrumental diagnostics and laboratory investigation of digestive system one of the most important parts of examination of digestive system, that can defined or confirm pathology. Examination of the secretory and acid-forming functions of the stomach, duodenal contents, coprological studies, technique and indications to gastroscopy and colonoscopy, X-ray of stomach are the main variants of examination of digestive system. Key Objective: To know main variants of instrumental diagnostics and laboratory investigation of digestive system. To know indication and contraindication for them and can assess results. Specific Goals: 1. To have knowledge about examination of the secretory and acid-forming functions of the stomach, indication and contraindication, can assess results. 2. To have knowledge about examination of the duodenal contents, indication and contraindication, can assess results. 3. To have knowledge about coprological studies, indication and contraindication, can assess results. 4. To have knowledge about gastroscopy and colonoscopy, indication and contraindication, can assess results. 5. To have knowledge about X-ray of stomach, indication and contraindication, can assess results.
Level of Knowledge and Skills before the Practice: 1. To know anatomy of digestive symptoms. 2. To know physiology of digestive symptoms.
Questions for Self-Assessment of the Pre-Practice Knowledge 1. Which type of cells in stomach mucous membrane do you know? A. Mucous cells B. Parietal (oxyntic) cells C. Chief (zymogenic) cells D. Enteroendocrine (APUD) cells E. All listed above 2. Which hormones are controlled the movement and the flow of chemicals into the stomach? A. Gastrin B. Cholecystokinin (CCK) C. Secretin D. Gastric inhibitory peptide E. All listed above 3. How many anatomical parts in duodenum? A. 1. B. 2.
cardi
ology
.dsmu.e
du.ua

168
C. 3. D. 4. E. 5. 4. On what anatomical part major duodenal papilla present? A. Superior B. Descending C. Inferior (horizontal) D. Ascending E. None of them 5. What enter into the bile content? A. Cholesterol B. Phospholipids (mainly Lecithin) C. Bile pigments (bilirubin diglucoronoide) D. Bile salts (sodium glycocholate & sodium taurocholate) and bicarbonate ions E. All listed above Key answers: E, E, D, B, E
Contents of Practice
Topics of Theory:
1. Examination of the secretory and acid-forming functions of the stomach 2. Examination of the duodenal contents. 3. Examination of the coprological studies. 4. Technique and indications to gastroscopy and colonoscopy. 5. X-ray of stomach. Practical skills:
Students should be able to demonstrate mastery of the following practical skills
1. To have knowledge about examination of the secretory and acid-forming functions of the stomach, indication and contraindication, can assess results. 2. To have knowledge about examination of the duodenal contents, indication and contraindication, can assess results. 3. To have knowledge about coprological studies, indication and contraindication, can assess results. 4. To have knowledge about gastroscopy and colonoscopy, indication and contraindication, can assess results. 5. To have knowledge about X-ray of stomach, indication and contraindication, can assess results.
cardi
ology
.dsmu.e
du.ua

169
Required Glossary to Practice
Term Definition
Gastric juice is a strong HacidicH liquid, HpHH 1 to 3 in humans, which is close to being colourless. The hormone HgastrinH is released into the bloodstream when HpeptidesH are detected in the stomach. This causes gastric glands in the lining of the HstomachH to secrete gastric juice. Its main components are digestive enzymes HpepsinH and HrenninH, Hhydrochloric acidH, and HmucusH.
Nasogastric tube or Ryle's Tube is a thin rubber tube used for nasogastric feeding of a patient who can not take food by his mouth because of some disease. It is also used for emptying stomach in case of poisoning or Intestinal Obstruction or Intestinal Perforation. It is made up of soft PVC and usually available 5 french gauge size to 20 french gauge size. A Ryle's Tube is inserted through the nose of the patient via Pharynx it is pushed in esophagus. There are 2-3 holes at the lateral side of the lower end of the tubes, lower end is closed. This tube is lined with radio-opaque lining so that it can be seen in a X Ray film.
HBariumH sulfate is a white crystalline solid with the chemical formula BaSO4. It is poorly HsolubleH in HwaterH and other traditional solvents. Barium sulfate is frequently used clinically as a HradiocontrastH agent for HX-rayH HimagingH and other diagnostic procedures. It is most often used in imaging of the HGI tractH during what is colloquially known as a 'HBarium mealH'.
cardi
ology
.dsmu.e
du.ua

170
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006 After the above-mentioned topics have been studied, turn to get familiar with relevant Flow charts for practice given in the Appendices Normal gastric secretion
Index of secretion
Units
On empty stomach
Basal secretion
Submaximal stimulation (histamine)
Maximal stimulation (pentagastrin)
Volume of juice ml less than 50 50-80 100-140 180-220 Total acidity titrating
units 10-20 40-60 80-100 100-120
Free hydrochloric acid
titrating units
0-10 20-40 65-85 90-110
Hydrochloric acid discharge
mmol - 0-5 6-16 16-24
cardi
ology
.dsmu.e
du.ua

171
Investigation of ВАO (Basal Acid Output) 15% irritation of cells and SAO (Submaximal Acid Output) 45% and
MAO (Maximal Acid Output) 90% (mmol/l)
ВАО SАО
male female male female
Norm 0-5,0 0-4,0 6,1-16,0 5,1-13,0
Moderate hypoacidity 5,1-10,0 4,1-7,0 16,1-26,0 13,1-20,0
Expressed hypoacidity >10,0 >7,0 >26,0 >20,0
Moderate hyposecretion
3,0-6,0 3,0-5,0
Expressed hyposecretion
<3,0 <3,0
Free hydrochloric acid = amount of NaOH (ml) that was spent at 1P
stP stage of
titration * 20 (titrating units) Total acidity = amount of NaOH (ml) that was spent for the entire titration (from red colour to red) * 20 (titrating units) Bound hydrochloric acid = Total acidity – NaOH was spent for the titration with alizarin * 20 Hydrochloric acid discharge - amount of hydrochloric acid excreted by stomach during hour Hydrochloric acid discharge (mg) = 0,0365 * V * C, Σ four portions during hour Hydrochloric acid discharge (mmol) = V * C/1000 V– volume of portion (1,2,3,4 portions) C – acidity in these portions
cardi
ology
.dsmu.e
du.ua

172
Acidity is expressed in millilitres of NaOH which are spent to neutralize 100 ml of the juice. It has become usual now to express acidity in milligrams of HC1 or milli-equivalents (MEq). Two drops of a 0.5 per cent alcoholic solution of dimethylamidoazobenzene and two drops of a 1 per cent alcoholic solution of phenolphthalein (phenol red is now very popular) are added to a 5- or 10-ml aliquot.
1) Dimethylamidoazobenzene turns red in the presence of free HC1. Alkali is buretted, drop by drop, to the gastric juice until it turns pinky orange to indicate the point of equivalence. The amount of the alkali spent is determined and titration is continued.
2) The liquid first turns yellow and then red again: all acid has been neutralized and phenolphthalein turns red. The new spent volume of alkali is measured again. The number of millilitres of the alkali that were spent at the first stage of titration are multiplied by 20 to give the amount of free hydrochloric acid. The amount of alkali spent for the entire titration should also be multiplied by 20 to determine total acidity. This is the sum of all acids contained in the stomach, e.g. free and bound hydrochloric acid, organic acids, and acid phosphates. Bound acid is non-dissociated hydrochloric acid of protein hydrochloride molecules of gastric juice. Normal gastric juice contains proteins (pepsin, gastromucoprotein). The protein content increases in gastritis, bleeding ulcer, or degradation of a tumour; the amount of bound hydrochloric acid increases accordingly.
3) Bound acid is determined indirectly by titrating a small (5 ml) portion of the juice in the presence of alizarin sodium sulphonate which is yellow in the presence of any free acid. When acid is neutralized, the solution turns violet. Bound HCl is determined by subtracting the number of millilitres of alkali spent for titration with alizarin from total acidity and multiplying the difference by the factor of 20. Indices of acidity that were considered to be normal for decades have now been revised.
Thus the normal content of hydrochloric acid in the fasting stomach of a healthy subject was considered to be maximum 10-20 titrating units (t.u.), or the acid might be absent at all. Normal acidity after taking a test meal was 20-40 titrating units for free HCl and 40-60 for total acidity. Findings of many investigators who observed a great number of healthy people show that "normal" acidity is found in only 50 per cent of them, while in others acidity is either below or above this "normal" level and is their constitutional feature. Total acidity below 20 t.u. should therefore be considered hypo-acidity and over 100 t.u. hyperacidity.
cardi
ology
.dsmu.e
du.ua

173
Normal duodenal content
Portions
Index А ( 1 ) В ( П ) С (Ш)
• Colour Golden- yellow Dark brown (olive- coloured)
Golden- yellow
• Transparency transparent transparent transparent • Reaction subalkaline alkaline alkaline • Epithelium 5-10 in
microscope’s vision field
1-3 in microscope’s vision field
1-3 in microscope’s vision field
• White blood cells
2-4 in microscope’s vision field
5-10 in microscope’s vision field
5-10 in microscope’s vision field
• Cholesterol crystals
Absent 1-3 in microscope’s vision field
Absent
• Bilirubinate calcium crystals
Absent 1-3 in microscope’s vision field
Absent
• Bilirubin 255,0-770,0
-310,0 mcmol/l
• Bile id
~115,0 g/l 7,0-14,0 g/l
• Cholesterol ~4,0 g/l 0,8-2,1 g/l • Protein~ ~4,5 g/l 1,4-2,7 g/l
cardi
ology
.dsmu.e
du.ua

174
Normal coprological investigation
Index Characteristic
• Reaction => Neutral or subalkaline
• Muscle fibres => Single digestible fibres
(without transverse striated pattern) • Connective tissue => Absent
• Neutral fat =» Small amount
• Fatty acids => Small amount
• Soaps => Small amount
• Digestible vegetable cellulose => Single cells
• Not digestible
vegetable cellulose
=> Different amount
• Starch =» Absent
• Mucus => Absent
• Epithelium => Absent
• White Blood Cells => Single cells
Revision Questions
Q1 Which contrast substance is used for the X-ray studies of intestine? A 100 g of barium sulphate in an equal quantity of water B 100 g of magnesium hydroxide C Physiologic solution D Iodine solution E Ammonium fluoroborate solution Q2 Which portions of large intestine could be examined with rectosigmoidoscopy? A Only rectum B Rectum and the lower portion of the sigmoid colon C Rectum, sigmoid colon and descendence colon D Rectum, sigmoid colon, descendence and transverses colon E Rectum, sigmoid colon, descendence, transverses and ascendence colon Q3 Which is characteristic of faces in case of rectal bleeding? A Brown color B White color C Blood streaks in faces
cardi
ology
.dsmu.e
du.ua
175
D Black color E Yellow color Q4 The pathological component of stools, such as bloodstained mucus, is characteristic of: A Gastritis B Oesophagitis C Dysentery and ulcerative colitis D Pancreatitis E All listed above Q5 Increased starch content of the faeces (amylorrhoea) is usually associated with diseases of: A Oesophagus B Small intestine C Large intestine D Stomach E Any listed above Q6 Which solution is used for determination of acidity of gastric juice by titrating? A Ammonium hydroxide B Magnesium hydroxide C Sodium hydroxide solution D Barium hydroxide E Physiological (salt) solution Q7 What could be finded with gastroscopy? A Polyp B Ulcer C Tumor D Mucosa E All listed above Q8 Find normal duodenal content for portion A A Golden-yellow, clear and transparent with absence of cholesterol crystal which delivered the first B Dark-yellow, brown or olive with presents of small amount of cholesterol crystal C Golden-yellow, clear and transparent with absence of cholesterol crystal which delivered the last D Golden-yellow, cloudy and not transparent which delivered the first E Golden-yellow, clear and transparent with presents of 60-80 white blood cells in microscope’s vision field which delivered the first Q9 What portion of duodenal content corresponded hepatic bile? A A B B C C D D E E
cardi
ology
.dsmu.e
du.ua

176
Q10 Chouse contraindications for gastroscopy A Burn of oesophagus B Esophageal stricture C Aortic aneurysm D Grave condition E All listed above Key answers: A, B, C, C, B, C, E, A, C, E
SUMMARY OF PROCEDURES The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out. Than have brief discussion about instrumental diagnostics and laboratory investigation of digestive system. Then begin individual working with results of examination of the secretory and acid-forming functions of the stomach, duodenal contents, coprological studies, technique and indications to gastroscopy and colonoscopy, X-ray of stomach. After in an educational room diagnostic values of results are discussed. At end of lesion the final tests are dispense to the students.
Final tests
Q1 Which colour of faces is characteristic of stomach bleeding? A Brown B White C Red D Black E Yellow Q2 Unaltered blood is seen on the surface of stools in case of: A Gastritis B Oesophagitis C Dysentery and ulcerative colitis D Pancreatitis E Haemorrhoidal bleeding Q3 What is steatorrhoea? A Presents of starch in stools B A condition in which the stools are abnormally fatty C Presents of vegetable cellular tissue in stools D Presents of muscular fibres in stools in great amount E Large accumulations of leucocytes in stools Q4 What is creatorrhoea? A Presents of starch in stools B A condition in which the stools are abnormally fatty C Presents of vegetable cellular tissue in stools D Presents of muscular fibres in stools in great amount E Large accumulations of leucocytes in stools
cardi
ology
.dsmu.e
du.ua

177
Q5 What could be assessed with X-ray examination of the stomach? A Evacuatory function B Ulcer C Tumor D Shape E All listed above Q6 How many portions received during examination of duodenal content? A One B Two C Three D Four E Five Q7 Find normal duodenal content for portion B A Golden-yellow, clear and transparent with absence of cholesterol crystal which delivered the first B Dark-yellow, brown or olive with presents of small amount of cholesterol crystal C Golden-yellow, clear and transparent with absence of cholesterol crystal which delivered the last D Golden-yellow, cloudy and not transparent which delivered the first E Dark-yellow, cloudy and not transparent with presents of small amount of cholesterol crystal Q8 What portion of duodenal content corresponded evacuation of the gall bladder? A A B B C C D D E E Q9 What is Total acidity A Total acidity minus NaOH was spent for the titration with alizarin * 20 B Amount of NaOH (ml) that was spent for the entire titration (from red colour to red) * 20 C Amount of NaOH (ml) that was spent at 1P
stP stage of titration * 20
D Amount of hydrochloric acid excreted by stomach during hour E All listed above Q10 Hydrochloric acid discharge A Total acidity minus NaOH was spent for the titration with alizarin * 20 B Amount of NaOH (ml) that was spent for the entire titration (from red colour to red) * 20 C Amount of NaOH (ml) that was spent at 1P
stP stage of titration * 20
D Amount of hydrochloric acid excreted by stomach during hour E All listed above
cardi
ology
.dsmu.e
du.ua

178
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 15BThe Main Methods of Examination of Patient on Internal Diseases Course
Topic 9 Module
16BMain syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice
Syndrome of abdominal pain. Dyspeptic syndrome. Malabsorption syndrome. Irritable colon syndrome.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

179
Importance of the Subject: Syndrome of abdominal pain is the most widespread syndrome above all other abdominal ones. Most of pains are not bring any jeopardy and relieve independently without treatment, but some pains may be important signs of dangerous pathology. Dyspeptic syndrome is not less widespread than abdominal pain syndrome and has different clinical features that are why the importance of knowing of this pathology is actual. Malabsorption syndrome and irritable colon syndrome met in clinical practice and proper treatment prevent development of complication. Key Objective: To be able to reveal signs of abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. Distinguish complications of these syndromes. To know the methods of laboratory and instrumental diagnostics of these pathology. Specific Goals: 1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. 2. Assess data of additional laboratory and instrumental examination (biochemical, X-ray examination, colonoscopy) at abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. 3. To be able to diagnose these pathology.
Level of Knowledge and Skills before the Practice: 1. To know anatomy of digestive symptoms. 2. To know physiology of digestive symptoms.
Questions for Self-Assessment of the Pre-Practice Knowledge 1. What is normal pH in colon? A. varies between 2.0 and 3.0 (acidic) B. varies between 5.0 and 6.5(slightly acidic). C. varies between 5.5 and 7 (slightly acidic to neutral). D. varies between 7.0 and 9.0 (alkaline) E. Any 2. Which pancreatic enzymes do you know? A. Trypsin and Chymotrypsin, is a peptidases that breaks down peptides in the small intestine. B. Steapsin, degrades triglycerides into fatty acids and glycerol. C. Carboxypeptidase, splits peptide fragments into individual amino acids. It is a protease. D. Pancreatic amylase that, besides starch, glycogen and cellulose, degrades most other carbohydrates. Cholecystokinin (CCK) E. All listed above
cardi
ology
.dsmu.e
du.ua

180
3. What is the length of small intestine? A. 1 to 2 meters. B. 3 to 5 meters. C. 6 to 7 meters. D. 10 to 15 meters. E. 50to 60 meters. 4. What is the length of large intestine? A. 0.5 meters. B. 1.5 meters. C. 3 meters. D. 5 meters. E. 12 meters. 5. What are in the gut going from inside the lumen radially outwards? A. mucosa, submucosa, muscularis externa, serosa B. submucosa, muscularis externa, serosa, mucosa C. muscularis externa, serosa, mucosa, submucosa D. serosa, mucosa, submucosa, muscularis externa E. serosa, subserosa, muscularis externa, mucosa Key answers: C, E, C, B, A
Contents of Practice
Topics of Theory:
1. Classification of abdominal pain syndrome. 2. Enquiring of patient with abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. 3. Objective examination – inspection, palpation, percussion of patient with these pathology. 4. Laboratory and instrumental diagnostic of abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. Practical skills:
Students should be able to demonstrate mastery of the following practical skills
1. To demonstrate correct enquiring of patient and perform objective examination (inspection, palpation, percussion, auscultation) of patients with abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. 2. Assess laboratory analysis and information given with instrumental examination at patients with abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome. 3. Suggest possible development of complications at abdominal pain, dyspeptic, malabsorption and irritable colon syndromes. 4. Be able to put correct diagnose at (abdominal pain syndrome, dyspeptic syndrome, malabsorption syndrome, irritable colon syndrome).
cardi
ology
.dsmu.e
du.ua

181
Required Glossary to Practice
Term Definition
Villi are vaginations of the mucosa and increase the overall surface area of the intestine
Goblet cells are glandular simple columnar epithelial cells whose sole function is to secrete mucus. They use both HapocrineH and HmerocrineH methods for secretion.
embolism occurs when an object (the embolus, plural emboli) migrates from one part of the HbodyH (through HcirculationH) and causes a blockage (HocclusionH) of a Hblood vesselH in another part of the body.
amyloidosis refers to a variety of conditions in which HamyloidH HproteinsH are abnormally deposited in HorgansH and/or HtissuesH, causing disease.
Crohn's disease
is a HdiseaseH of the Hdigestive systemH which may affect any part of the Hgastrointestinal tractH from HmouthH to HanusH. The main gastrointestinal symptoms are Habdominal painH, HdiarrheaH (which may be visibly bloody), HvomitingH, or Hweight lossH. Crohn's disease can also cause complications outside of the gastrointestinal tract such as Hskin rashesH, HarthritisH, and Hinflammation of the eyeH.
sprue Coeliac disease, also spelled celiac disease, is an HautoimmuneH disorder of the Hsmall intestineH that occurs in Hgenetically predisposedH people of all ages from middle infancy. Symptoms include chronic HdiarrhoeaH, Hfailure to thriveH (in children), and HfatigueH, but these may be absent and symptoms in all other organ systems have been described. It is estimated to affect about 1% of all HIndo-EuropeanH populations, but is thought to be significantly underdiagnosed. Coeliac disease is caused by a reaction to HgliadinH, a HglutenH protein found in HwheatH (and similar proteins of the HtribeH HTriticeaeH which includes other HcultivarsH such as HbarleyH and HryeH). Upon exposure to gliadin, the enzyme Htissue transglutaminaseH modifies the protein, and the Himmune systemH cross-reacts with the bowel tissue, causing an Hinflammatory reactionH. That leads to flattening of the lining of the small intestine (called villous atrophy).
Protein losing enteropathy
refers to any condition of the Hgastrointestinal tractH that results in a net loss of HproteinH from the body.
Steatorrhea is the presence of excess fat in HfecesH. Stools may also float due to excess gas, have an oily appearance and be foul smelling. An oily anal leakage or some level of Hfecal incontinenceH may occur. There is increased HfatH excretion, which can be measured by determining the fecal fat level. While definitions have not been standardised, fat excretion in feces in excess of 0.3 (g/kg)/day is considered indicative of steatorrhea.
cardi
ology
.dsmu.e
du.ua

182
Suggested Reading List
Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006 After the above-mentioned topics have been studied, turn to get familiar with relevant Flow charts for practice given in the Appendices
cardi
ology
.dsmu.e
du.ua

183
Abdomen pain
Type Mechanism Clinical feature Causes Spastic Spasm of
smooth muscles of hollow organs, ducts
Acute, intensive, paroxysmal (attack-like), sudden onset (certain time of onset and end), with typical radiation. May be with vomiting without reliving and local muscle tension of abdomen wall.
Renal, intestinal, stomach, biliary colic (colic pain), pancreas tracts
Disten-sional
Distension of wall of hollow organs and ligaments tension
Dull, mild, not intensive, diffuse, persistent, without certain location and typical radiation.
Meteorism, hyposecretory syndrome
Peritoneal «acute abdomen»
Inflammation of parietal peritoneum and its irritation after perforation of hollow organs
They are started gradually or sharply (in perforation-attack of stabling pain), constant, progressive, its intensity rapidly increases to become very severe. They are accompanied by vomiting, limitation of abdominal respiration, abdomen muscle tension-board like (muscular defense), absent or decreased intestinal peristaltic sounds, reduction or absence of liver dullness ( after perforation) positive Blumberg's sign. Symptoms of general intoxication- pallor, cold sweat, weak and rapid pulse, low blood pressure, facies Hippocratica
Peritonitis due to appendicitis, cholecystitis; perforation of duodenal or gastric ulcer.
Vascular (vassal)
Acute blood supply disturbance (angina abdominis)
Acute, duffuse, sudden onset, constant, intensity, severe pain.
mesenteric ischemia(atherosclerosis of mesenteric arteries), mesenteric embolism, mesenteric spasm.
cardi
ology
.dsmu.e
du.ua

184
Malabsorption Syndrome This symptom complex is due to upset absorption in the small intestine. The syndrome often develops in combination with the syndrome of inadequate digestion. Primary and secondary malabsorption syndromes are distinguished. Primary malabsorption is probably explained by congenital disorders in the fine structure of the intestinal mucosa and genetically determined intestinal enzymopathy. The onset of the secondary malabsorptioan syndrome is due to acquired structural changes in the intestinal mucosa evoked by: 1. Inadequate digestion
- chronic pancreatitis - obstructive [mechanical, surgical] jaundice
2. Small intestine disorders - intentional resection - gluten enteropathy - infiltration by – amyloidosis, Crohn's disease - chronic enteritis - dysbacteriosis - sprue - intestinal lipodystrophy
3. Impairment lymph circulation - lymphomas in abdominal cavity
- tuberculosis of mesenteric lymph nodes - exudative [protein-losing] enteropathy
The upset intestinal digestion and accelerated passage of chyme through the intestine are decisive in acute and subacute diseases. In chronic conditions the decisive factors are dystrophy and atrophic fibrous changes in the mucosa of the small intestine, shortening and levelling of the villi and crypts, significant reduc-tion of the microvilli number, fibrous tissue formation in the intestinal wall with impairment of blood and lymph circulation, and disordered parietal digestion. All these changes limit absorption of the products of hydrolysis of: in the intestinal wall - proteins, fats, and carbohydrates, - minerals, Fe, Ca - vitamins B and K Clinical picture. Course. Gradual lose of weigh, symptoms of metabolic disorders of all types (protein, fat, vitamin, water-salt), dystrophic changes in the internal organs with their subsequent dysfunction, and also constant steatorrhoea, creatorrhoea, and amylorrhoea are characteristic. Hypoproteinaemia develops (mostly at the expense of reduction of the serum albumin level); hypocholesterolaemia, hypocalcaemia – fractures, cramps, bone pains, and
cardi
ology
.dsmu.e
du.ua

185
moderate hypoglycaemia occur. Hypoproteinaemic oedema develops in the presence of hypoproteinaemia below 40-50 g/1. The characteristic symptoms of polyhypovitaminosis are osteoporosis, anaemia (hypochromic anaemia in predominant malabsorption of iron, and hyperchromic anaemia in upset absorption of vitamin B12), trophic changes in the skin, nails, mucous membrane – stomatitis, glossitis, gingival and nasal hemorrhage, progressive atrophy of the muscles, signs of polyglandular insufficiency, weakness, and (in severe cases) acidosis and cachexia. Laboratory examinations determine hypoproteinaemia, hypocholesterolaemia, hypoglycaemia, and other disorders due to malabsorption. Coprologic studies reveal increased content of undigested food in the faeces and also increased excretion of the products of enzymic decomposition of food, steatorrhoea, creatorrhoea, and amylorrhoea . Enterobiopsy reveals atrophic changes in the mucosa of the proximal parts of the small intestine. Since the walls of the small intestine absorb great amounts of various substances, different methods are used to study their absorption. These are tests with carotine, folic acid, galactose, D-xylose absorption test, etc. Caseine, albumin, oleic acid, methionine, glycine, vitamin Bi2, folic acid, and other substances labelled with radioactive isotopes have recently beed used. The method is based on the determination of concentration of labelled substances and the time of their appearance in the blood, their excretion with the urine or faeces, and assessment of residual radioactivity of faecal masses that is indicative of the amount of unabsorbed substances. Determination of the absorbed nutrients is based on the study of the chemical composition of food and stools during a certain period of time.
Irritable colon [irritable bowel] syndrome Upset colon function:
- diarrhea - constipation
Causes: - after colon infection - continuous improper feeding - lead-poisoning (saturnism) - antibiotic receiving
Clinic features: - pain in abdomen - diarrhea in morning - vegetative disbalance - meteorism - depression, hysteria - cardialgia - palpitation - weakness - dizziness
cardi
ology
.dsmu.e
du.ua
186
Revision Questions
Q1 Percussion of the abdomen in patient with distension pains is characterized by the following: A It can not be performed because of intensive abdominal pain and tension of abdominal wall; B Reveals the dull percussion sound; C Reveals the horizontal level of dull percussion sound (at the level of navel) in vertical position of the patient; D Hyperresonant (tympanitic) percussion sound over the whole abdominal wall E Any of previous variants. Q2 Peritoneal pain in abdomen region is typical for: A Renal colic; B Meteorism; C Mesenteric thrombosis; D Inflammations of parietal peritoneum at appendicitis; E Intestinal colic. Q3 Distensional pains in the abdomen region can be caused by: A Inflammation of the parietal peritoneum B Distension of hollow organs wall C Strong contraction of smooth muscles of intestines D Strong contraction of smooth muscles of channels (biliary, pancreas, urinary tracts) E Blood supply disturbance Q4 Malabsorption manifests: A By obesity; B By intensive abdominal pain; C By permanent constipations; D By heartburn; E By loss of weight and weakness. Q5 Choose the reason of malabsorption which is caused by pathology of small intestine: A Hypersecretion of parietal cells B Chronic pancreatitis C Obstruction of bile ducts D Enterectomy E Anyone Q6 Choose the reason resulting in the irritable bowel syndrome: A Chronic intestinal bleedings B Esophageal obstruction C Intestinal infection in anamnesis D Chronic diseases bile ducts E Application of antacids Q7 Intensive pain occurs in case of: A Biliary colic
cardi
ology
.dsmu.e
du.ua

187
B Flatulence C Enlargement of the liver D Distention of stomach wall Q8 Any of previous variants of answers Shchetkin-Blumberg sign is characteristic of: A Biliary colic B Hyposecretory syndrome C Flatulence D Perforations of peptic duodenal ulcer E Renal colic Q9 Chouse characteristic of distensional pains in abdomen region: A Not intensive long and monotonous; B Intensive and constantly increasing; C Intensive and wavy; D Intensive with signs of peritoneum irritations; E Any listed variants of pains. Q10 Choose reason of irritable colon: A After colon infection B Inadequate [inappropriate] feeding C Lead-poisoning (saturnism) D Antibiotic intaking E Anyone Key answers: D, D, B, E, D, C, A, D, A, E
SUMMARY OF PROCEDURES The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out. Than have brief discussion about instrumental diagnostics and laboratory investigation of digestive system. Then begin individual working with results of examination of the secretory and acid-forming functions of the stomach, duodenal contents, coprological studies, technique and indications to gastroscopy and colonoscopy, X-ray of stomach. After in an educational room diagnostic values of results are discussed. At end of lesion the final tests are dispense to the students.
Final tests Q1 Severe pain arises at: A Meteorism B Peritonitis C Hyposecretory symptoms D Stretching of a wall of a stomach E All listed variants Q2 Choose characteristics of spastic pains in abdominal area: A Intensive and progressively arising;
cardi
ology
.dsmu.e
du.ua

188
B Intensive and wavy; C Not intensive, long; D Intensive with signs of peritoneal irritations; E All listed variants. Q3 Distension abdominal pain is characteristic of: A Thrombosis of mesenteric vessels B Intestine colic C Renal colic D Biliary colic E Flatulence Q4 Vascular pain in abdomen region is typical for: A Meteorism B Renal colic C Thrombosis of the mesenterial vessels D Calculous cholecystitis E Intestinal colic Q5 Choose the reason of malabsorption which is caused by pathology of small intestine: A Tuberculosis of mesenteric lymph nodes B Crohn’s disease C Chronic pancreatitis D Obstruction of bile ducts E Anyone Q6 Spastic abdominal pain occurs in case of affection of the: A Parietal peritoneum B Intestine C Hepatic parenchyma D Renal parenchyma Q7 Pancreatic parenchyma Shchetkin-Blumberg sign, as a rule, combines with: A Peritoneal pain; B Spastic pain; C Distensive pain; D Vascular pain; E Any types of pain. Q8 Vascular abdominal pain is caused by: A Tension of the walls of the hollow organs; B Strong constriction of smooth muscles of intestine; C Strong constriction of smooth muscles of ducts (biliary, pancreatic or urinary tracts); D Inflammation of parietal peritoneum; E Disordes of the blood circulation. Q9 Choose reason of secondary malabsorbtion: A Chronic pancreatitis
cardi
ology
.dsmu.e
du.ua
189
B Obstructive [mechanical, surgical] jaundice C Intention resection D Exudative [protein-losing] enteropathy E Anyone Q10 Choose possible laboratory sign of malabsorbtion: A Steatorrhoea, creatorrhoea, and amylorrhoea B Hypoproteinaemia C Polyhypovitaminosis D Hypochromic or hyperchromic anaemia E All listed above
cardi
ology
.dsmu.e
du.ua

190
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 17BThe Main Methods of Examination of Patient on Internal Diseases Course
Topic 9 Module 18BMain syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice
Instrumental diagnostics and laboratory investigation of diseases of hepatobiliary system. Jaundice syndrome. Cholestatic syndrome. Hereditary hyperbilirubinemia syndrome. Hepatomegaly syndrome. Hepatolienal syndrome.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

191
Importance of the Subject: Affection of hepatobiliary system (viral hepatitis, stones in gal bladder, cholangitis and other) is one of the most frequent affection of digestive system. They are lead to the temporary lose of ability to work and some times to invalidism and even death. Key Objective: To be able to reveal symptoms of affection of hepatobiliary system. To be able to determine character of jaundice, cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome by clinical signs and pathophysiological mechanisms. To be able to distinguish them by clinical and laboratory data, instrumental examination. Specific Goals: 1. Enquiring of patient. Objective examination (inspection, palpation, percussion, auscultation). Finding the most characteristic signs of hepatobiliary system affection (cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome). 2. Assess data of additional laboratory and instrumental examination (biochemical, sonography, cholecystography). 3. Assess data of duodenal intubation. 4. Determine peculiarities of pain syndrome at hepatic colic. 5. To be able to diagnose next syndromes, such as cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome.
Level of Knowledge and Skills before the Practice: 1. To know anatomy of liver and bile ducts 2. To know bile production and bile components.
Questions for Self-Assessment of the Pre-Practice Knowledge 1. What is Sphincter Oddi? A. Present in the common bile duct in the Hampulla of VaterH. B. Present in the left hepatic duct C. Present in the cystic duct D. Present in the right hepatic duct E. Present in the Hpancreatic duct 2. What is cystic duct? A. Start from gall bladder. B. Start from liver C. Gather left and right hepatic ducts D. Start from pancreas E. None of them 3. What is common bile duct? A. Start from gall bladder. B. Start from liver C. Gather left and right hepatic ducts
cardi
ology
.dsmu.e
du.ua

192
D. Start from pancreas E. Gather common hepatic duct and cystic duct 4. What is common hepatic duct? A. Start from gall bladder. B. Start from liver C. Gather left and right hepatic ducts D. Start from pancreas E. Gather common hepatic duct and cystic duct 5. How many lobes in liver? A. 1 B. 2 C. 3 D. 4 E. 5 Key answers: A, A, E, C, D
Contents of Practice
Topics of Theory:
1. Anatomy of hepatobiliary system 2. Particularies of bile secretion 3. Enquiring of patients with hepatobiliary system affection (cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome). 4. Objective examination – inspection, palpation, percussion, auscultation. 5. Laboratory and instrumental diagnostic of cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome. Practical skills:
Students should be able to demonstrate mastery of the following practical skills
1. To demonstrate correct enquiring of patient and perform objective examination (inspection, palpation, percussion, auscultation) of patients with hepatobiliary system affection (cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome). 2. Assess laboratory analysis and information given with instrumental examination at patients with cholestasis, hereditary hyperbilirubinemia, hepatomegaly and hepatolienal syndrome. 3. Suggest possible development of complications at liver diseases. 4. Be able to put correct diagnose at (hepatobiliary system affection (cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome).
cardi
ology
.dsmu.e
du.ua

193
Required Glossary to Practice
Term Definition
AST Aspartate HtransaminaseH (AST) also called serum glutamic oxaloacetic transaminase (SGOT) or aspartate aminotransferase (ASAT/AAT) is similar to Halanine transaminaseH (ALT) in that it is another enzyme associated with liver HparenchymalH cells. Normal range is 0,1-0,6 mmol/l.
ALT Alanine transaminase or ALT is a HtransaminaseH HenzymeH. It is also called serum glutamic pyruvic transaminase (SGPT) or alanine aminotransferase (ALAT). ALT is found in HserumH and in various bodily tissues, but is most commonly associated with the HliverH; Normal range is 0,1-0,4 mmol/l.
GGT gamma-glutamyltransferase is an HenzymeH that HcatalyzesH the Hchemical reactionH, belongs to the family of HtransferasesH. Normal range is 0,6-3,9 mmol/l.
Gilbert's syndrome
Gilbert's syndrome, often shortened to the acronym GS, is the most common HhereditaryH cause of increased HbilirubinH, and is found in up to 5% of the population (though some Gastroenterologists maintain that it is closer to 10%). The main symptom is otherwise harmless HjaundiceH which does not require treatment, caused by elevated levels of unconjugated bilirubin in the bloodstream (HhyperbilirubinemiaH).
Crigler-Najjar syndrome
Crigler-Najjar Syndrome or CNS is a rare disorder affecting the HmetabolismH of HbilirubinH, a chemical formed from the breakdown of HbloodH. The disorder results in an HinheritedH form of non-HhemolyticH HjaundiceH, often leading to Hbrain damage in infants. H
Dubin-Johnson syndrome
Dubin-Johnson syndrome is an Hautosomal recessiveH disorder which causes an increase of conjugated HbilirubinH without elevation of HliverH HenzymesH (HALTH, HASTH). Thiscondition is associated with a defect in the ability of hepatocytes to secrete conjugated HbilirubinH into the bile. It is usually diagnosed in early infancy.
Rotor's syndrome Rotor syndrome is a rare, relatively benign Hautosomal recessiveH HbilirubinH disorder of unknown origin.
cardi
ology
.dsmu.e
du.ua

194
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice
Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
Hereditary hyperbilirubinemia
Gilbert's syndrome
Crigler-Najjar syndrome
Dubin-Johnson syndrome
Rotor's syndrome
Glucuronil-transferase deficiency and other
Expressed glucuronil-transferase deficiency
Disturbance of excretion bilirubin in bile
Disturbance of excretion bilirubin in bile
↑↑ unconjugated bilirubin
↑↑↑ unconjugated bilirubin
↑ unconjugated bilirubin
↑ unconjugated bilirubin
N conjugated bilirubin
↑ conjugated bilirubin
↑↑↑ conjugated bilirubin
↑↑↑ conjugated bilirubin
absent urobilin in urine
absent urobilin in urine
↑ urobilin in urine ↑ urobilin in urine
Syndrome of cholestasis Disorders of bile outflow (from intrahepatic and extrahepatic biliary tracts) Causes: intrahepatic –viral hepatitis, biliary cirrhosis, tumour of liver, sarcoidosis . extrahepatic biliary tracts – obstruction of common bile duct (obstructive jaundice), sclerosing cholangitis Clinical signs: - Jaundice - Scratch (itcing) of skin (due to cholemia)
cardi
ology
.dsmu.e
du.ua

195
- Xanthomas, xanthelasmas - Dark urine - Stool pale like putty or clay - Night blindness (hen blindness- our term) Laboratory investigation: Increase in - Conjugated bilirubin - Cholesterol - Alkaline phosphatase - Gamma –glutamyl transpeptidase (GGTP) - Absent of urobilin of urine and stercobilin of stool Syndrome of hepatomegaly 1.Venous congetion in the liver ( right heart failure, constrictive pericarditis, tricuspid heart valvular diseases, obstruction of hepatic veins – Budd -Chiari disease) 2. nonparasitic infections 3. viral hepatitis( A,B,C, D, E) 4. cirrhosis ( B, C, D) 5. leptospirosis 6. tbs, brucellosis, syphilis 7. actinomycosis 8. parasitic infections (amebiasis, echinococcosis, schistosomiasis) 9. obstruction of the biliary tracts (gall stones in the common bile duct, tumours, stricture of common bile duct, enlarged lymph nodes, sclerosing cholangitis) 10. hepatomegaly without connection with infection ( tumours metastasis, hepatitis, cirrosis due to alcohol, drugs, toxic substances , autoimmune disease, polycystic liver, sarcoidosis, lymphogranulomatous ) Infective
o Glandular fever (Infectious mononucleosis) This is caused by the Epstein-Barr virus (EBV).
o Hepatitis (Although not all hepatitis viruses cause hepatomegaly) o Liver abscess o Malaria o Amoeba infections o Hydatid cyst o Leptospirosis o Actinomycosis
Neoplastic o Hemangiomas o Hepatocellular carcinoma o Myeloma o Leukaemia
cardi
ology
.dsmu.e
du.ua

196
o Lymphoma Cirrhotic
o Portal o Biliary o Cardiac o Haemochromatosis
Metabolic o Fatty infiltration o Amyloidosis o Gaucher's disease
Drugs and Toxins o Alcoholism o Poisoning o Drugs
Congenital o Hemolytic anemia o Riedel's lobe o Polycystic disease
Others o Hunter syndrome o Zellweger's syndrome o Carnitine palmitoyltransferase I deficiency o Carnitine palmitoyltransferase II deficiency o Carnitine-acylcarnitine translocase deficiency
Revision Questions
Q1. A hepatomegaly with focal changes in the liver is characteristic of: A. Liver carcinoma B. Liver cirrhosis C. Liver amyloidosis D. Liver hemochromatosis E. Chronic hepatitis Q2. Choose the reason of the hepatomegaly caused by venous congestion in the liver: A. Tricuspid valve diseases B. Mitral valve diseases C. Aortic valve diseases D. Myocardial infarction E. Left ventricular hart failure Q3. Choose the reason of hepatomegaly doesn’t caused by infection: A. Viral hepatitis B. Drugs or toxic affection of the liver C. Amebiasis
cardi
ology
.dsmu.e
du.ua

197
D. Echinococcosis E. Tuberculosis Q4. Choose reason of the hepatomegaly caused by the obstruction of bile ducts: A. Stone in a gall-bladder B. Gilbert′s syndrome C. Stone in intrahepatic bile ducts D. Budd-Chiari syndrome E. Chronic cholecystitis Q5. A hepatomegaly with the diffuse affection of liver is characteristic of: A. Single liver cyst B. Polycystic liver disease C. Cancer of liver D. Angioma of liver E. Chronic hepatitis Q6. Choose the laboratory sign of cholestasis: A. Increased content of AST B. Increased content of ALT C. Increased content of alkaline phosphatase D. Increased content of lactate dehydrogenase E. Increased content of stercobilin in an excrement Q7. Choose the clinical signs of cholestasis: A. Scratch (itcing) of skin B. Macrohaematuria C. Acute severe increasing of arterial blood pressure D. Fever E. Expressed edema of face and feet Q8. Choose the cause of hepatomegaly which caused by parasitogenic infections: A. Tuberculosis B. Actinomycosis C. Syphilis D. Echinococcosis E. All listed above Q9. Excretion of urine of “color of beer” is characteristic of: A. Hepatocellular (parenchymatous) jaundice only B. Cholestatic (obstructive) jaundice only C. Hemolytic jaundice only D. Hepatocellular (parenchymatous) and cholestatic (obstructive) jaundices E. Hemolytic and cholestatic (obstructive) jaundices Q10. The skin itch is characteristic of: A. Parenchymatous jaundice only B. Cholestatic (obstructive) jaundice only C. Haemolytic jaundice only
cardi
ology
.dsmu.e
du.ua

198
D. Parenchymatou and cholestatic (obstructive) jaundices E. Parenchymatou and haemolytic jaundicees Key answers: A, A, B, C, E, C, A, E, D, B
SUMMARY OF PROCEDURES
The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out. Than have brief discussion about objective and subjective syndromes of hepatobiliary system affection (cholestasis, hereditary hyperbilirubinemia, hepatomegaly or hepatolienal syndrome). Consideration about clinical, laboratory and instrumental importance without patient and on the example of concrete patient. After teacher demonstrate methodic of percussion of liver and spleen, their palpation. Next is showed palpation of the kidneys in upstanding and lying positions. Under the control of the teacher students perform all methodic. Then begin individual working with the patient under the control of the teacher and discussion of the revealed symptoms. After in an educational room diagnostic value of available symptoms is discussed. At end of lesion the final tests are dispense to the students.
Final tests
Choose the reasons of hepatomegaly which is caused by parasitogenic infections: A. Syphilis B. Amebiasis C. Actinomycosis D. Brucellosis E. All listed above Choose the clinical signs of cholestasis: A. Dark stool B. Light or colourless urine C. Pallor of the skin D. Cyanosis of the skin E. Xanthelasmaes Choose the reason of hepatomegaly caused by parasitogenic infections: A. Amebiasis B. Brucellosis C. Echinococcosis D. Schistosomiasis E. Any of the represented answers Choose the reason of hepatomegaly caused by the obstruction of bile ductus: A. Stones in the gallbladder; B. Stone in the cystic duct; C. Stone in the common bile duct; D. Budd-Chiari syndrome;
cardi
ology
.dsmu.e
du.ua

199
E. Sclerosis and obliteration of gallbladder. Choose the reason of the hepatomegaly caused by venous congestion in the liver: A. Right-sided (right-ventricular) heart failure B. Mitral valvular disease C. Aortic valvular disease D. Pericarditis with effusion E. Myocardial infarction Choose the laboratory signs of cholestasis: A. Increase of total bilirubin level due to conjugated fraction; B. Increase of total bilirubin level due to unconjugated fraction; C. Increase of total bilirubin level due to due to both conjugated and unconjugated fractions; D. The level of total bilirubin does not rise; E. Decrease the level of cholesterol in the blood serum. Choose the clinical signs of cholestasis: A. Skin itching B. Dark stool Colourless urine C. Pallor of skin D. Cyanosis Absence of urobilin in urine is characteristic of: A. Hepatocellular (parenchymatous) jaundice only B. Cholestatic (obstructive) jaundice only C. Haemolytic jaundice only D. Haemolytic and cholestatic (obstructive) jaundices E. Hepatocellular (parenchymatous) and haemolytic jaundices Hepatomegaly with the focal changes in the liver is characteristic of: A. Liver cirrhosis B. Haemochromatosis of liver C. Polycystic liver disease D. Amyloidosis of liver E. Chronic hepatitis Hepatosplenomegaly is characteristic of: A. Hepatic cancer; B. Diskinesia of bile duct; C. Polycytaemia rubra vera; D. Chronic posthemorrhagic anaemia; E. Polycystic liver disease.
cardi
ology
.dsmu.e
du.ua

200
Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 19BThe Main Methods of Examination of Patient on Internal Diseases Course
Topic 9 Module
20BMain syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice
Syndrome of portal hypertension. Hepatorenal syndrome. Syndrome of acute and chronic hepatic failure. Syndrome of hepatargia.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

201
Importance of the Subject: These syndromes are frequent signs or complications of acute and chronic liver diseases. In most cases one patient have even several hepatic syndromes, which aggravate disease. Key Objective: To be able to reveal syndromes of portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome on basis of clinical, laboratory and instrumental signs. Specific Goals: 1. Enquiring of patient. Objective examination (inspection, palpation, percussion, auscultation). Finding the most characteristic signs of portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome. 2. Assess data of additional laboratory and instrumental examination (biochemical, sonography). 3. To be able to diagnose next syndromes, such as portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome. Level of Knowledge and Skills before the Practice: 1. To know anatomy of liver and system of vena porta 2. To know functions of liver. Questions for Self-Assessment of the Pre-Practice Knowledge 1. What liver do? A. HGluconeogenesisH (the synthesis of HglucoseH from certain Hamino acidsH, HlactateH or HglycerolH) B. HGlycogenolysisH (the breakdown of HglycogenH into HglucoseH) (muscle tissues can also do this) C. HGlycogenesisH (the formation of glycogen from glucose) D. The breakdown of HinsulinH and other Hhormones E. All listed above 2. What liver do? A. The liver is responsible for the mainstay of protein HmetabolismH. B. HCholesterolH synthesis C. HLipogenesisH, the production of HtriglyceridesH (fats). D. The liver produces Hcoagulation factorsH HIH (fibrinogen), HIIH (prothrombin), HVH, HVIIH, HIXH, HXH and HXIH, as well as Hprotein CH, Hprotein SH and HantithrombinH. E. All listed above 3. What liver do? A. The liver breaks down HhaemoglobinH, creating HmetabolitesH that are added to HbileH as pigment (HbilirubinH and HbiliverdinH). B. The liver breaks down HtoxicH substances and most medicinal products in a process called Hdrug metabolismH. C. The liver converts HammoniaH to HureaH.
cardi
ology
.dsmu.e
du.ua

202
D. The liver stores a multitude of substances, including glucose (in the form of HglycogenH), Hvitamin B12H, HironH, and HcopperH. E. All listed above 4. What portal anastomosis do you know? A. haemorrhoidal venous plexus B. oesophagogastric plexus C. paraumbilical veins D. none of them E. All listed above 5. What is normal weight of a liver? A. 0,5 kilo B. 1,5 kilo C. 2,5 kilo D. 5 kilo E. 8,0 kilo Key answers: E, E, E, E, B
Contents of Practice
Topics of Theory:
1. Classification of chronic hepatitis 2. Ethnology of liver affection 3. Enquiring of patients with hepatic pathology. 4. Objective examination – inspection, palpation, percussion, auscultation. 5. Laboratory and instrumental diagnostic of portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome. Practical skills:
Students should be able to demonstrate mastery of the following practical skills
1. To demonstrate correct enquiring of patient and perform objective examination (inspection, palpation, percussion, auscultation) of patients with portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome. 2. Assess laboratory analysis and information given with instrumental examination at patients with portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome. 3. Suggest possible development of complications at liver diseases. 4. Be able to put correct diagnose at (portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndrome.).
cardi
ology
.dsmu.e
du.ua

203
Required Glossary to Practice
Term Definition
Child-Paquet classification Classification of patient with cirrhosis for assessment of prognosis
Cirrhosis is a consequence of chronic HliverH HdiseaseH characterized by replacement of liver HtissueH by fibrous HscarH tissue as well as regenerative HnodulesH (lumps that occur as a result of a process in which damaged tissue is regenerated), leading to progressive loss of liver function.
Cholestasis is a condition where HbileH cannot flow from the HliverH to the HduodenumH.
Portal hypertension is HhypertensionH (high blood pressure) in the Hportal veinH and its branches. It is often defined as a portal pressure gradient (the difference in pressure between the portal vein and the hepatic veins) of 5 mm Hg or greater.
Splenomegaly is an enlargement of the HspleenH, Hypersplenism is characterized by anaemia, leucopenia and
thrombocytopenia and splenomegaly HBsAg is the surface HantigenH of the HHepatitisH-B-Virus
(HHBVH).
cardi
ology
.dsmu.e
du.ua

204
cardi
ology
.dsmu.e
du.ua

205
cardi
ology
.dsmu.e
du.ua

206
cardi
ology
.dsmu.e
du.ua

207
cardi
ology
.dsmu.e
du.ua

208
cardi
ology
.dsmu.e
du.ua

209
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice
Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
After the above-mentioned topics have been studied, turn to get familiar with relevant Flow charts for practice given in the Appendices
Portal hypertension Portal hypertension is characterized by a stable increase in the blood pressure in the portal vein. Portal hypertension develops due to obstructed blood outflow from the portal vein:
1) syprahepatic - as a result of its compression from the outside (by a tumour, enlarged lymph nodes of the porta hepatis in cancer metastases, vein cava inferior thrombosis, constrictive pericarditis, right ventricle failure, tricuspid heart diseases etc.)
2) hepatic - or by obliteration of part of its intrahepatic branching in chronic affections of the liver parenchyma (in cirrhosis or other liver diseases)
3) infrahepatic - or due to thrombosis of the portal vein or its branches. Growth and subsequent cicatrization of connective tissue at the site of degraded hepatic cells of a cirrhotic liver cause stenosis or complete obliteration of part of hepatic sinusoids and intrahepatic vessels. An obstacle is thus created to the blood flow which increases portal pressure and interferes with blood outflow from the abdominal viscera. In these conditions, transudation of fluids from the vessels into the abdominal cavity is intensified to account for the development of ascites. Decreased oncotic pressure of plasma is an important factor in the development of ascites associated with liver cirrhosis. The pressure decreases because of upset synthesis of albumins in the liver. Sodium and water retention is also important. It
cardi
ology
.dsmu.e
du.ua

210
occurs due to hypersecretion of aldosterone by the adrenal glands (secondary aldosteronism) and its inadequate inactivation in the liver. The time of the onset of ascites depends on the degree of development of collateral circulation, i.e. on portocaval anastomoses. For a long time the disturbed portal circulation can be compensated for by delivery of blood into the superior and inferior venae cavae from the portal vein via normally existing anastomoses. But in portal hypertension these anastomoses become highly developed. There exist three groups of natural portocaval anastomoses: 1) in the zone of haemorrhoidal venous plexus; these are anastomoses between the inferior mesenteric vein (the portal vein system) and haemorrhoidal veins emptying into the inferior vena cava; haemorrhoidal nodes develop in portal hypertension which rupture to cause rectal haemorrhage; 2) anastomoses in the zone of the oesophagogastric plexus: this is a collateral leading through the left gastric vein, the oesophageal plexus, and hemiazygos vein into the superior vena cava. In pronounced portal hypertension, marked varicose nodes are formed in the lower portion of oesophagus whose injury (e.g. by hard food) is responsible for possible haemorrhage in the form of haematemesis (blood vomiting), which is the most serious complication of diseases attended by portal hypertension and which is a frequent cause of death; 3) anastomoses in the system of paraumbilical veins communicating with the veins of the abdominal wall and the diaphragm, carrying blood to the superior and inferior venae cavae. In portal hypertension, varicose veins radiate from the umbilicus to give a peculiar pattern known as the caput medusae. Auscultation of vein collaterals – phonendoscope put above navel – listen continuous murmur not connected with cardiac cycle. The degree of increase in the pressure in the portal vein system can be determined by a special needle and a water pressure gauge. The pressure is measured in the spleen (splenometry) or in varicose veins of the oesophagus. In the latter case the needle is introduced through the oesophagoscope. It is believed that pressure in the spleen is the same as in the portal vein trunk. Normally it is 70—150 mm H2O, while in portal hypertension it rises to 400—600 mm H2O. Contrast techniques are used to reveal obstruction of the portal vein: these are splenoportography and in rare cases transumbilical portohepatography. The spleen may be somewhat enlarged (splenomegaly) in venous congestion associated with portal hypertension. Treatment. In order to remove portal hypertension, whose first danger are oesophagogastric and haemorrhoidal haemorrhages, the patients are operated on for placing anastomoses between the portal vein system and the inferior vena cava.
cardi
ology
.dsmu.e
du.ua

211
Revision Questions
Q1. Hepatorenal syndrome characterized by: A. Increased level of creatinine in the blood serum B. Decreased level of creatinine in the blood serum C. Decreased level of urea in a blood serum D. Massive (gross, nephrotic) proteinuria (more than 3,5 g/l) E. Glucosuria Q2. Hepatorenal syndrome is characterized by: A. Low creatinine content in the blood serum B. Low urea content in the blood serum C. Moderate proteinuria (less than 3,5 g/24 hrs) D. Massive (gross, nephritic) proteinuria (more than 3,5 g/24 hrs) E. Glucosuria Q3. Hepato-cellular failure is characterized by: A. Progressive jaundice without the skin itch B. Enlargement of liver C. Progressive jaundice with expressed skin itch D. Spastic pains beneath right hypochondrium (biliary colic) E. Diminishing of jaundice and strengthening of skin itch Q4. Choose the cause resulting in intrahepatic portal hypertension: A. Vena cava thrombosis B. Occlusion of portal vein C. Portal vein thrombosis D. Exsudate pericarditis E. Diseases of the liver Q5. The thrombosis of portal vein results in rising of the following variants of portal hypertension: A. Intrahepatic only B. Extrahepatic pre-sinusoidal only C. Extrahepatic post-sinusoidal only D. Intrahepatic and extrahepatic pre-sinusoidal E. Extrahepatic pre-sinusoidal and post-sinusoidal Q6. Patient with cirrhosis of liver starved from hemorrhoidal bleeding and dilatation of rectal veins. Chouse more correct explanation of this. A. The normal phenomenon. B. Porto-caval anastomosis (shunt for blood in vein cava superiors) C. Cava-caval anastomosis. D. Anevrismatic expansion of a vein. E. Porto-caval anastomosis (shunt for blood in vein cava inferior). Q7. Choose type of breathing at hepatic coma A. Cheyne-Stokes breathing B. Kussmaul's breathing C. Biot's breathing D. Grokko
cardi
ology
.dsmu.e
du.ua

212
E. Normal breathing Q8. What is hepatorenal syndrome? A. Liver failure in patients with chronic kidney disease B. Renal failure in patients with chronic heart disease C. Renal affection without renal failure in patients with chronic liver disease D. Renal failure in patients with chronic liver disease E. Chronic liver failure Q9. What is the main reason for hemorrhagic syndrome in case of liver failure? A. Decrease in detoxication function of liver B. Poor production of coagulation factor in liver C. Increase in direct bilirubin D. High ALT level in blood E. Enlargement of liver Q10. Patient has liver cirrhosis. What may be the reason for black color of stool? A. Oesophageal bleeding B. Hemorrhoidal bleeding C. Obstruction of common bile duct D. Anemia E. High level of conjugated bilirubin in blood Key answers: A, C, C, C, D, E, C, D, B, A
SUMMARY OF PROCEDURES The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out.
Than have brief discussion about objective and subjective syndromes of portal hypertension, hepatorenal syndrome, acute and chronic hepatic failure, hepatodepression syndromes. Consideration about clinical, laboratory and instrumental importance without patient and on the example of concrete patient.
Then begin individual working with the patients under the control of the teacher and discussion of the revealed symptoms. After in an educational room diagnostic value of available symptoms is discussed.
At end of lesion the final tests are dispense to the students.
Final tests Q1. Exudative pericarditis results in rising of the fallowing variants of portal hypertension: A. Intrahepatic only B. Extrahepatic pre-sinusoidal only C. Extrahepatic post-sinusoidal only D. Extrahepatic pre-sinusoidal and post-sinusoidal
cardi
ology
.dsmu.e
du.ua

213
E. Intrahepatic and extrahepatic post-sinusoidal Q2. Hepatocellular failure is characterized by: A. Bitter taste in to the mouth B. Spastic pain in abdomen C. Enlargement of the liver D. Specific (sweetish) smell of mouth E. Heartburn Q3. Choose the cause resulting in extrahepatic pre-sinusoidal (subhepatic) portal hypertension: A. Thrombosis of vena cava inferior; B. Occlusion of intrahepatic veins; C. Tricuspid heart diseases; D. Thrombosis of portal vein; E. Pericardial effusion. Q4. Patient with cirrhosis of liver has dilatation of lower part of oesophageal veins. Chouse more correct explanation of this. A. The normal phenomenon. B. Porto-caval anastomosis (shunt for blood in vein cava superiors) C. Cava-caval anastomosis. D. Anevrismatic expansion of a vein. E. Porto-caval anastomosis (shunt for blood in vein cava inferior). Q5. Chouse possible reasons for acute hepatic coma A. Acute viral hepatitis B, C B. Arsenic poisoning C. Mushroom poisoning D. Drugs poisoning E. All listed above Q6. Chouse sings of hepatorenal syndrome A. Oliguria or anuria B. High creatine level C. Increase in potassium level in blood D. Progressive portal hypertention and hepatic failure E. All of them Q7. What is Caput Medusae? A. Dilatation of veins and arteries on head B. Number of prominent collateral vessels radiating from the umbilicus C. Dilatation of veins and arteries on eye ground D. Protruding belly due to ascitis E. None of them Q8. What is the reason of hepatorenal syndrome? A. Cirrhosis B. Acute viral hepatitis C. Operation on liver and bile tracts D. All of them
cardi
ology
.dsmu.e
du.ua

214
E. None of them Q9. Portal thrombosis leads to the following variants of portal hypertension: A. Intrahepatic only B. Extrahepatic pre-sinusoidal only C. Extrahepatic post-sinusoidal only D. Intrahepatic and extrahepatic pre-sinusoidal E. Extrahepatic post-sinusoidal and extrahepatic pre-sinusoidal Q10. Portal hypertension is characterized by: A. Ascites B. Shins varices C. Cyanosis D. Pulsation of liver E. Pulsation of jugular veins
cardi
ology
.dsmu.e
du.ua

215
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptoms and Syndromes of the Internal Diseases
Topic 9 Module Main syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice
Instrumental diagnostics and laboratory investigation of kidneys and urinary system. Main syndromes and symptomes of diseases of urinary system. Disuric syndrome. Urinary syndrome. Hematuric syndrome. Arterial blood pressure syndrome. Syndrome of renal colic.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

216
Importance of the Subject: Basis of clinical knowledge about kidney diseases is covered with the main syndromes, such as disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic, etc. For proper diagnosis these syndromes is important to know instrumental diagnostics and laboratory investigation of kidneys and urinary system. Key Objective: To be able to reveal syndromes, such as disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. To know the methods of instrumental diagnostics and laboratory investigation of kidneys and urinary system. Specific Goals: 1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. 2. Assessment data of additional laboratory and instrumental examination at disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. 3. To be able to diagnose disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic.
Level of Knowledge and Skills before the Practice:
1. To know anatomy of kidney and urinary tract 2. To know physiology of kidney.
Questions for Self-Assessment of the Pre-Practice Knowledge
Q1. What is normal volume of urine? A. 10-100 ml B. 100-500 ml C. 800-1500 ml D. 2000-5000 ml E. 8000-15000 ml Q2. What is normal colour of urine? A. red B. amber yellow C. blue D. orange E. any Q3. What is normal pH reaction of urine? A. varies between 2.0 and 3.0 (acidic) B. varies between 5.5 and 6.5(slightly acidic). C. varies between 7.0 and 8.0 (slightly acidic to neutral). D. varies between 8.0 and 10.0 (alkaline) E. Any
cardi
ology
.dsmu.e
du.ua

217
Q4. What is normal specific gravity (concentration) of urine? A. 21B100-400 B. 22B800-960 C. 23B1001-1040 D. 24B1051-1089 E. 25B2000-250 Q5. What should not be present in urine normally? A. Bacterias B. Glucose C. Urobilin D. Ketone bodies E. All listed above Key answers: C, B, B, C, E
Contents of Practice
Topics of Theory:
1. Etiology and pathogenesis of disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. 2. Clinical features and laboratory changes at disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. 3. Instrumental diagnostics and laboratory investigation of kidneys and urinary system Practical skills:
Students should be able to demonstrate mastery of the following practical skills
1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. 2. Assess data of additional laboratory and instrumental examination (biochemical, sonography, X-ray examination) at disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. 3. To be able to diagnose disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic.
cardi
ology
.dsmu.e
du.ua

218
Required Glossary to Practice
Term Definition
Isosthenuria refers to the excretion of urine, the Hspecific gravityH (concentration) of which is neither greater (more concentrated) nor less (more dilute) than that of protein-free HplasmaH. This is the hallmark of such disease states as chronic and acute Hrenal failureH in which the HkidneysH lack the ability to concentrate or dilute the HurineH and so the initial filtrate of the blood remains unchanged despite the need to conserve or excrete water based on the body's hydration status.
ischuria also known as Urinary retention is a lack of ability to HurinateH. It is a common complication of Hbenign prostatic hypertrophyH (also known as benign prostatic hyperplasia or BPH), although HanticholinergicsH may also play a role, and requires a HcatheterH or HProstatic stentH.
Bence Jones protein is a monoclonal HglobulinH HproteinH found in the HbloodH or HurineH. Finding this protein in the context of end-organ manifestations such as Hmalignant bone marrow cancerH, Hrenal failureH, Hlytic bone diseaseH, or HanemiaH, or large numbers of Hplasma cellsH in the Hbone marrowH of patients can be diagnostic of Hmultiple myelomaH, in which it is present in 2/3 of cases.
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice
Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania
cardi
ology
.dsmu.e
du.ua

219
2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006 After the above-mentioned topics have been studied, turn to get familiar with relevant Flow charts for practice given in the Appendices Examination: - ultrasonography - angiography - excretory (descending, intravenous) urography - scintigraphy – function accordingly accumulation - renography – excretory function - biopsy Amount of urine – 800-1500 ml (2000ml) Colour and aspect – amber yellow and clear Transparency – transparent pH (Reaction) – 5,5 – 6,5 (subacid) Specific gravity – 1001-1040, normally – 1015 – 1025 1030 Epithelium – 1-3 in microscope`s vision field (high power field) Leucocytes – 2-5 in microscope`s vision field, Addis-Kakovsky test - <2000000/day, Nechiporenko's method <2000/ml Erythrocytes – 0-2 unaltered in microscope`s vision field, Addis-Kakovsky test - <1000000/day, Nechiporenko's method <1000/ml Casts – 0, Addis-Kakovsky test - <20000/day, Nechiporenko's method - hyaline casts- 0-1 on 4 microscope`s chambers Bacteria - <50000 - 100000/ml Protein – 0 (0,033 g/ml), < 0,05 g/day, «pronounced proteinuria» >3,5 g a day Glucose – 0 Acetone – 0 Ketone bodies – 0 Urobilin – 0 Bilirubin – 0 Clearance of creatinine – 100-130 (80-120) Tubular reabsorption – 98,5-99% Chemical constituents: a-Nitrogenous constituents : urea, uric acid, creatinine, urinary pigments (urochromogen, uroerythrin, urobilinogen). b-Non-nitrogenous compound: HCO3, K, Nacl, Ca, SO4. Glucose & ketones are absent.
cardi
ology
.dsmu.e
du.ua

220
Revision Questions
Q1. A 34 –year old patient G., was admitted to a hospital with complaints of acute pain in lumbar region and red colour urine after this pain. Laboratory investigation of urine confirmed the presence of hematuria. How is hematuria explained in renal diseases? A. inflammation of renal pelvis B. inflammation of urinary bladder C. trauma of a mucous membrane renal pelvis by stone D. inflammation of urethra E. inflammation of ureter Q2. Choose complaints, which are most typical for patients with acute pyelonephritis A. the expressed oedema on the face and legs B. gross hematuria C. lumbar pain D. considerable increase in blood pressure E. excessive thirst Q3. At examination of patients with renal disease can be detected next typical sign A. changes of distal phalanx of fingers by type of clubbing fingers B. oedema of the face and on the legs C. ascites which caused by portal hypertension D. oedema only on the legs E. skin cyanosis Q4. The urinary syndrome is characterized by A. hematuria, combined with oedema and arterial hypertension B. pronounced proteinuria, combined with oedema C. asymptomatic hematuria D. hematuria, combined with expressed oedema E. proteinuria, combined with oedema and arterial hypertension Q5. Doctor ordered the clinical examination of morning portion of urine. What is possible to estimate by clinical examination of morning portion of urine? A. fluctuations of specific gravity of urine B. crystals of uric acid C. daily loss of protein D. daily glucosuria E. nycturia Q6. The analysis of urine according to Nechiporenko's method allows to define: A. fluctuations of specific gravity of urine; B. daily diuresis; C. quantity of red blood cells in microscope`s vision field; D. quantity of red blood cells in the certain volume of urine; E. quantity of white blood cells and casts in microscope`s vision field.
cardi
ology
.dsmu.e
du.ua

221
Q7. Choose variant of the answer, which corresponds to the term «pronounced proteinuria» A. 0,1 g a day B. 0,55 g a day C. 1,35 g a day D. 3,25 g a day E. 7,5 g a day Q8. Choose the diseases resulting in «postrenal proteinuria» A. renal amyloidosis B. glomerulonephritis C. urethritis D. massive hemolysis E. diabetic nephrosclerosis Q9. A 45 –year old patient K., with pyelonephritis has following data of urine analasis by Nechiporenko's method: RBC- 1,5 x 10P
6P/l, WBC- 4,5 x 10P
6P/l, casts
100 x 10P
6P/l. Choose amount of leukocytes analyzed with Nechiporenko's
method which corresponds to norm A. 1,5 x 10P
6P/l
B. 4,5 x 10P
6P/l
C. 6,0 x 10P
6P/l
D. 9,5 x 10P
6P/l
E. 20,5 x 10P
6P/l
Q10. At examination patients with renal diseases it is possible to reveal typical sign A. oedema only on the legs B. ascitis, caused by a portal hypertension C. pallor skin D. skin cyanosis E. changes distal phalanx of fingers by type of clubbing fingers Key answers: C, C, B, C, B, D, E, C, A, C
SUMMARY OF PROCEDURES
The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out. Than have brief discussion about objective and subjective signs of disuric, urinary, hematuric, arterial blood pressure, syndrome of renal colic. Consideration about clinical, laboratory and instrumental importance without patient and on the example of concrete patient. Then begin individual working with the patients under the control of the teacher and discussion of the revealed symptoms. After in an educational room diagnostic value of available symptoms is discussed. At end of lesion the final tests are dispense to the students.
cardi
ology
.dsmu.e
du.ua

222
Final tests Q1. Hematuria can be explained in renal diseases by A. inflammation of renal pelvis B. glomerulonephritis C. inflammation of urinary bladder D. inflammation of urethra E. inflammation of ureter Q2. A 34 –year old patient N. suffers from pyelonephritis associated with urolithiasis for 3 years. Choose complaints, which are most typical for patients with urolithiasis A. the expressed oedema on the face and legs B. considerable increase in body temperature C. attack-like pain in lumbar area D. considerable increase in blood pressure E. expressed thirst Q3. A 56 –year old patient K., was admitted to a hospital with complaints of massive oedemas associated with renal pathology. How is occurrence of oedema explained in renal diseases? A. the high content renin in blood B. the high content of angiotensin in blood C. the high content of sodium and water in blood due to increase in level of aldosterone D. the low content renin in blood E. the low content of angiotensin in blood Q4. Clinical analysis of morning urine it is possible to define A. fluctuations of specific gravity of urine B. proteinuria for the day C. amount of erythrocytes or leukocytes in microscope`s vision field D. glucosuria for the day E. nycturia Q5. Choose variant of the answer, which corresponds to the term «pronounced proteinuria» A. 3,7 g a day B. 4,55 g a day C. 6,35 g a day D. 9,25 g a day E. all listed variants Q6. Choose the diseases resulting to «postrenal proteinuria» A. glomerulonephritis B. renal amyloidosis C. massive hemolysis D. cystitis E. diabetic nephrosclerosis
cardi
ology
.dsmu.e
du.ua

223
Q7. Choose amount of leukocytes which corresponds to norm according to Nechiporenko's method A. 0,5 x 10P
6P/l
B. 6,5 x 10P
6P/l
C. 7,0 x 10P
6P/l
D. 9,9 x 10P
6P/l
E. 11,5 x 10P
6P/l
Q8. The pain in lumbar region (or abdomen) is the most typical for: A. pronounced proteinuria B. inflammation of renal pelvis C. gross hematuria D. moderate proteinuria E. microhematuria Q9. Doctor ordered the method for estimation of filtrative function of kidneys for patient with renal failure. The filtrative function of kidneys can be revealed with the help of A. Nechiporenko's method B. Zimnitsky's test C. Clearance test D. X-ray examination of kidneys E. nephrosonography Q10. Occurrence of expressed leucocyturia is typical for A. trauma of a mucous membrane of pelvis by stone B. inflammation of glomerulus C. renal infarction D. inflammation of pelvis E. trauma of mucous membrane of ureter
cardi
ology
.dsmu.e
du.ua

224
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY GUIDELINES FOR
PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptoms and Syndromes of the Internal Diseases
Topic 9 Module
Main syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice Nephritic syndrome. Nephrotic syndrome. Tubulo-interstitial syndrome.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

225
Importance of the Subject: nephrotic, nephritic and tubulo-interstitial syndromes are the most widespread variants of kidney pathology allover the world. Frequently they are met at glomerulonephritis, diabetic affection of kidney, vasculitis, systemic diseases etc.
Nowadays the peculiarities of glomerulonephritis and pyelonephritis are latent and occult course of disease that prevents timely indication of correct treatment. Key Objective: To be able to reveal nephrotic, nephritic and tubulo-interstitial syndromes on basis of clinical, laboratory and instrumental signs at different diseases of kidney and urinary tracts. Specific Goals: 1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of nephrotic, nephritic and tubulo-interstitial syndromes. 2. Assess data of additional laboratory and instrumental examination (biochemical, sonography, X-ray examination) at primary and secondary kidney diseases. 3. To be able to diagnose nephrotic, nephritic and tubulo-interstitial syndromes.
Level of Knowledge and Skills before the Practice:
1. To know anatomy of kidney and urinary tract 2. To know functions of kidney. 3. To know kinds of urine analysis and variants of instrumental examination of kidney
Questions for Self-Assessment of the Pre-Practice Knowledge
Q1. The electronic microphoto of kidney fragment has exposed afferent glomerular arteriole, which has giant cells under its endothelium, containing secretory granules. Name the type of these cells: A. Smoothmuscular B. 26BInterstitial C. Juxtavascular D. Juxtaglomerular E. Mesangial Q2. A 16 year-old patient got numerous traumas in automobile accident. Now the patient is haning a shock. АP - 80/60 mm Hg. daily urine volume 60-80 ml. What pathogenic mechanism leads to kidneys function violation? A. Increased vasopressin blood concentration B. Increased osmotic pressure in glomerular capillaries C. Increased pressure in Bowman’s capsule D. Trauma of the urinary bladder E. Decreased hydrostatic pressure in glomerular capillaries
cardi
ology
.dsmu.e
du.ua

226
Q3. An autopsy has revealed that kidneys are enlarged, surface is large-granular because of multiple cavities with smooth wall, which are filled with clear fluid. What kidney disease did the patient have? A. 27BInfarction B. Glomerulonephritis C. Polycystic kidney D. Pyelonephritis E. Necrotic nephrosis Q4. Periodic renal colics attacks are observed in a woman with primery hyperparathyroidizm. Ultrasonic examination revealed small stones in the kidneys. What is the most plausible reason of the stones's formation? A. 28BHyperphosphatemia B. Hypercalcemia C. Hypercholesterinemia D. Hyperuricemia E. Hyperkalemia Q5. For a long time a 49-year-old woman had suffered from glomerulonephritis which caused death. The autopsy revealed that the size of her kidneys was 7х3х2,5 sm, weight 65,0 g, they were dense and small-grained. Microscopically: fibrinogenous inflammation of serous and mucous capsules, dystrophic changes of parenchymatous organs, brain edema. What complication can cause such changes of serous capsules and inner organs? A. Sepsis B. DIC-syndrome C. Anemia D. Uraemia E. Thrombopenia Key answers: D, E, C, B, D
Contents of Practice
Topics of Theory:
1. Etiology and pathogenesis of nephrotic, nephritic and tubulo-interstitial syndromes. 2. Clinical features and laboratory changes at nephrotic, nephritic and tubulo-interstitial syndromes. 3. Diagnosing of nephrotic, nephritic and tubulo-interstitial syndromes. 4. Complications of nephrotic, nephritic and tubulo-interstitial syndromes. Practical skills:
Students should be able to demonstrate mastery of the following practical skills
1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of nephrotic, nephritic and tubulo-interstitial syndromes.
cardi
ology
.dsmu.e
du.ua

227
2. Assess data of additional laboratory and instrumental examination (biochemical, sonography, X-ray examination) at primary and secondary kidney diseases. 3. To be able to diagnose nephrotic, nephritic and tubulo-interstitial syndromes.
Required Glossary to Practice
Term Definition
Nephrotic syndrome is a nonspecific disorder in which the HkidneysH are damaged, to leak large amounts of HproteinH (at least 3.5 grams per day per 1.73m2 body surface area) from the HbloodH into the HurineH.
Nephritic syndrome is a collection of signs (known as a HsyndromeH) associated with disorders affecting the HkidneysH, more specifically HglomerularH disorders.
Interstitial nephritis (Tubulo-interstitial syndrome)
is a form of nephritis affecting the interstitium of the kidneys surrounding the tubules. Common causes include infection (pyelonephritis), or reaction to medication (such as an analgesic or antibiotics).
Glomerulonephritis also known as glomerular nephritis, abbreviated GN, is a HrenalH disease characterized by HinflammationH of the HglomeruliH, or small blood vessels in the kidneys.H[1]H It may present with isolated HhematuriaH and/or HproteinuriaH (blood resp. protein in the HurineH); or as a Hnephrotic syndromeH, a Hnephritic syndromeH, acute Hrenal failureH, or chronic renal failure. They are categorised into several different pathological patterns, which are broadly grouped into non-proliferative or proliferative types. Diagnosing the pattern of GN is important because the outcome and treatment differs in different types. Primary causes are one which are intrinsic to the kidney, whilst secondary causes are associated with certain infections (bacterial, viral or parasitic pathogens), drugs, systemic disorders (HSLEH, vasculitis) or HcancersH.
Pyelonephritis is an ascending Hurinary tract infectionH that has reached the pyelum (HpelvisH) of the HkidneyH (nephros in HGreekH). If the infection is severe, the term "urosepsis" is used interchangeably (HsepsisH being a Hsystemic inflammatory response syndromeH due to infection). It requires HantibioticsH as therapy, and treatment of any underlying causes to prevent recurrence. It is a form of HnephritisH. It can also be called pyelitis.
cardi
ology
.dsmu.e
du.ua

228
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006 After the above-mentioned topics have been studied, turn to get familiar with relevant Flow charts for practice given in the Appendices Interstitial nephritis (Tubulo-interstitial syndrome) - is a form of nephritis affecting the interstitium of the kidneys surrounding the tubules. Common causes include infection (pyelonephritis), or reaction to medication (such as an analgesic or antibiotics). Etiological [causative] agent affects tubules and in tissue appears complexes (foreign substance, during reabsorption, affect basal membrane of tubules and, with appearing destroyed proteins, compose complex) with antigenic properties. Reflective spasm of vessels and their inflammatory end exudative constriction lead to deterioration of kidney blood circulation. In severe case acute renal failure developed. When the proximal tube is injured sodium, potassium, bicarbonate, uric acid, and phosphate intake may be reduced or changed, resulting in - low bicarbonate, known as metabolic acidosis, - low potassium, low uric acid known as hypouricemia, and - low phosphate known as hypophosphatemia. - protein, proteinuria Damage to the distal tubule may cause loss of urine concentrating ability and polyuria.
– glucosuria – hyposthenuria – increase in quantity of bicarbonates in urine - Electrolyte disbalance
cardi
ology
.dsmu.e
du.ua

229
Treatment – antisensitizer, glucocorticoid Nephrotic syndrome
- proteinuria (more than 3,5 g/l) - oedema - pronounced - hypoproteinemia – hypoalbuminemia – white nails - leuconychia - hypergamma globulinemia - disproteinemia - hyperlipemia – due to metabolic disfunction at uremia - hypocalcemia – tetany - rise in serum coagulation factors
Nephritic syndrome - proteinuria - mild - oedema - erythrocyturia - hypertension - pallor
Polycystic renal disease - can be diagnosed by nephrosonography or X-ray examination of kidneys - high probability of inheritance of illness - increase in both kidneys
Post-infectious GN Post-infectious glomerulonephritis occurs after Streptococcal infection - usually of the skin, after a latency of 10-14 days. Approximately 1-2% of patients with poststreptococcal glomerulonephritis progress to CRF and ESRD. This condition is essentially defined as an inflammation of the kidneys. Light microscopy shows diffuse hypercellularity due to proliferation of endothelial and mesangial cells, inflammatory infiltrate with neutrophils and with monocytes. The Bowman space is reduced (compressed), in severe cases might see cresent formation. However, biopsy is seldom done because the disease usually regresses. Patients present with a nephritic syndrome. Diagnosis is suggested by positive streptococcal titers in the blood (ASOT). Treatment is supportive, and the disease resolves (as a rule) in 2 weeks. Rapidly progressive glomerulonephritis or crescentic glomerulonephritis: Approximately 90% of patients progress to ESRD (end-stage renal disease) within weeks or months. Mesangiocapillary glomerulonephritis or Membranoproliferative glomerulonephritis: Approximately 40% of patients with membranoproliferative glomerulonephritis progress to CRF and ESRD in 10 years. 35BThis is primary, or secondary to SLE, viral hepatitis, hypocomplementemia. One sees 'hypercellular and hyperlobular' glomeruli due to proliferation of both cells and the matrix within the mesangium. Presents usually with as a nephrotic syndrome but can be nephritic, with inevitable progression to ESRF. Additionally two further causes present as solely RPGN.
cardi
ology
.dsmu.e
du.ua

230
One is Goodpasture's syndrome, an autoimmune disease whereby antibodies are directed against antigens found in the kidney and lungs. As well as kidney failure, patient has hemoptysis (cough up blood). Wegener's granulomatosis is a form of vasculitis that affects the lungs, kidneys and other organs. Membranous nephropathy: Approximately 20-30% of patients with membranous nephropathy progress to chronic renal failure (CRF) and ESRD in 10 years. A third of people continue having the disease, 1/3 remit, 1/3 progress to end-stage kidney failure. It is usually idiopathic, but may be associated with cancers (lung, bowel), infection (hepatitis, malaria), drugs (penicillamine), SLE. Minimal change GN This form of GN causes 80% of nephrotic syndrome in children, but only 20% in adults. As the name indicates, there are no changes visible on simple light microscopy, but on electron microscopy there is fusion of podocytes (supportive cells in the glomerulus). Immunohistochemistry staining is negative. Treatment consists of supportive care for the massive fluid accumulation in the patients body (= oedema) and as well as steroids to halt the disease process (eg Prednisone 1 mg/ kg). Over 90% of children respond well to steroids, being essentially cured after 3 months of treatment. Adults have a lower response rate (80%). Failure to respond to steroids ('steroid resistant') or return of the disease when steroids are stopped ('steroid dependent') may require cytotoxic therapy (eg cyclosporin) which is associated with many side-effects. Focal segmental glomerulosclerosis FSGS. Approximately 80% of patients progress to ESRD in 10 years. Patients with the collapsing variant, which is termed malignant focal segmental glomerulosclerosis, have a more rapid progression. This form may be idiopathic or related to HIV infection. IgA disease (Berger's nephropathy) - mesangioproliferative This is the most common type of glomerulonephritis in adults world-wide. It usually presents as macroscopic haematuria (visibly bloody urine). It occasionally presents as a nephrotic syndrome. It often affects young males within days (24-48hrs) after an upper respiratory tract or gastrointestinal infection. Microscopic examination of biopsy specimens shows increased number of mesangial cells with increased matrix (the 'cement' which holds everything together). Immuno-staining is positive for immunoglobulin A deposits within the matrix. Prognosis is variable, 20% progress to ESRF. Steroids and immunosuppression are not effective treatments for this disease; ACE inhibitors are the mainstay of treatment. Henoch-Schonlein purpura (HSP) This is a systemic variant of IgA nephropathy which causes vasculitis of small vessels of which GN is a feature. IgA nephropathy: Approximately 10% of patients with IgA nephropathy progress to CRF and ESRD in 10 years. Lupus nephritis: Overall, approximately 20% of patients with lupus nephritis progress to CRF and ESRD in 10 years; however, patients with certain histologic variants (eg, class IV) may have a more rapid decline.
cardi
ology
.dsmu.e
du.ua

231
cardi
ology
.dsmu.e
du.ua

232
Revision Questions
Q1. The nephrotic syndrome is characterized by A. low proteinuria (0,3 – 1,0 g/l) B. moderate proteinuria (1,0 – 3,5 g/l) C. increase in total protein of plasma due to globulin D. increase in total protein of plasma due to albumin E. decrease in total protein of plasma Q2. Choose instrumental methods of examination which allow to confirm nephrotic syndrome A. plan radiography of kidneys B. excretory pyelography C. nephrosonography D. computed tomography E. none of them Q3. Choose signs of tubulo-interstitial syndrome A. oliguria B. anuria C. glucosemia D. glucosuria E. arterial hypotension Q4. Nephrotic syndrome is characterize by A. disproteinaemia due to decrease in globulin B. hyperproteinaemia C. disproteinaemia due to increase in albumin D. disproteinaemia due to decrease in albumin E. hypoproteinaemia without disproteinaemia Q5. Choose the sign, which is obligatory for nephritic syndrome A. hematuria B. acute renal failure C. acute left ventricular failure D. nausea E. spasmes Q6. Choose the sign, which is obligatory for nephritic syndrome A. proteinuria B. nausea C. spasmes D. acute renal failure E. renal eclampsia Q7. Choose sings that are characterize tubulo-interstitial syndrome A. oliguria B. anuria C. hyposthenuria D. glucosemia E. arterial hypotension
cardi
ology
.dsmu.e
du.ua

233
Q8. Electrolyte disbalance in the tubulo-interstitial a syndrome is characterized with A. decrease in quantity of bicarbonates in urine B. increase in concentration of calcium in plasma of blood C. decrease in concentration potassium in plasma of blood D. decrease in nitrogen metabolic product in blood E. increase in quantity of bicarbonates in urine Q9. The nephrotic syndrome is characterized by: A. low proteinuria (0,3 – 1,0 g/l) B. moderate proteinuria (1,0 – 3,5 g/l) C. pronounced proteinuria (more than 3,5 g/l) D. increase in the total protein of plasma due to globulin E. increase in the total protein of plasma due to albumin Q10. Choose sign, which is not related to nephrotic syndrome: A. hypoproteinemia B. disproteinemia C. isohyposthenuria D. hyperlipemia E. proteinuria (more than 3,5 g/l) Key answers: E, E, D, D, A, A, C, E, C, C
SUMMARY OF PROCEDURES
The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out. Than have brief discussion about objective and subjective signs of nephrotic, nephritic and tubulo-interstitial syndromes. Consideration about clinical, laboratory and instrumental importance without patient and on the example of concrete patient. Then begin individual working with the patients under the control of the teacher and discussion of the revealed symptoms. After in an educational room diagnostic value of available symptoms is discussed. At end of lesion the final tests are dispense to the students.
Final tests
Q1. Choose biochemical method of examination which allows to confirm nephrotic syndrome: A. increase in the total protein of blood plasma B. increase in plasma of blood C. increase in triglycerides of blood plasma D. increase in creatinine of blood plasma E. increase in blood urea Q2. Clinical expression of nephrotic syndrome is A. oedema B. skin cyanosis
cardi
ology
.dsmu.e
du.ua

234
C. hyperemia of skin D. rising of the body temperature E. positive Pasternatsky's symptom Q3. Nephrogenic diabetes insipidus is based on: A. poisonous action of high concentration antidiuretic hormone on tubular apparatus of kidneys B. poisonous action of high concentration antidiuretic hormone on glomerular apparatus of kidneys C. dysfunction glomerular apparatus of kidneys due to low concentration in blood of antidiuretic hormone D. resistency of tubular cell of kidneys to normal concentration antidiuretic hormone E. dysfunction of tubular apparatus of kidneys due to low concentration in blood antidiuretic hormone Q4. Choose variant of the answer, which corresponds to the term «pro-nounced proteinuria»: A. 1,37 g a day B. 1,55 g a day C. 2,35 g a day D. 3,25 g a day E. none of them Q5. Examination of patient with renal damage in gout can reveal: A. the high concentration of blood urea B. nephrotic syndrome C. disproteinemia D. the high concentration of uric acid in blood E. renal glucosuria Q6. Clinical expression of nephrotic syndrome is A. skin cyanosis B. positive Pasternatsky's symptom C. elevation of the body temperature D. all listed variants E. none of the listed variants Q7. Choose laboratory method of examination which allows to confirm nephrotic syndrome: A. Rehberg test B. Zimnitsky's test C. the clinical analysis of blood D. lipid level of blood plasma E. creatinine level of blood plasma Q8. Choose the sign which is obligatory for nephritic syndrome: A. pyuria B. nycturia C. small amount of urine or anuria
cardi
ology
.dsmu.e
du.ua

235
D. disproteinemia E. hypoproteinemia Q9. Choose sign, which is not related to nephrotic syndrome A. proteinuria (more than 3,5 g/l) B. hypoproteinaemia C. disproteinaemia D. leucocyturia E. lyperlipemia Q10. Nephrotic syndrome is characterized by A. disproteinaemia due to decrease in globulin B. disproteinaemia due to increase in albumin C. hypoproteinaemia without disproteinaemia D. disproteinaemia due to increase in globulin E. hyperproteinaemia
cardi
ology
.dsmu.e
du.ua

236
The Health Ministry Of Ukraine Donetsk National Medical University
«Approve» meeting of propedeutics of internal medicine department #2 Head of department
Associate Member of AMSc of Ukraine, Professor G. A. Ignatenko
”______”___________________2009
STUDENT’S SELF-STUDY
GUIDELINES FOR PRACTICE ACTIVITIES
Subject Propedeutics of the Internal Medicine
Module 2 Symptoms and Syndromes of the Internal Diseases
Topic 9 Module Main syndromes and symptomes of diseases of digestive system and urinary system, interpretation data of instrumental diagnostics and laboratory investigation.
Practice Syndrome of acute and chronic renal failure. Uremic coma and chlorohydropenic coma.
Course 3
Faculty International Medical Faculty
Donetsk 2009
cardi
ology
.dsmu.e
du.ua

237
Importance of the Subject: acute renal failure may arise in different ages because of different reasons, such as shock, trauma, glomerulonephritis, occlusion of ureter. Some cases are needed in using of kidney machine. Chronic renal failure developed when presents of functional nephrons near 10%. The main causes are chronic glomerulonephritis, interstitial nephritis, diabetes mellitus. Key Objective: To be able to reveal signs of acute and chronic renal failure, uremic coma and chlorohydropenic coma. Distinguish complications of acute and chronic renal failure. To know the methods of laboratory and instrumental diagnostics of syndromes acute and chronic renal failure. Specific Goals: 1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of acute and chronic renal failure, uremic coma and chlorohydropenic coma. 2. Assess data of additional laboratory and instrumental examination (biochemical, sonography, X-ray examination) at acute and chronic renal failure, uremic and chlorohydropenic comas. 3. To be able to diagnose acute and chronic renal failure, uremic and chlorohydropenic comas.
Level of Knowledge and Skills before the Practice: 1. To know anatomy of kidney and urinary tract 2. To know physiology of kidney. 3. To know kinds of urine analysis and variants of instrumental examination of kidney
Questions for Self-Assessment of the Pre-Practice Knowledge Q1. What is the level of kidney according vertebra? A. IX-XII thorax B. X-XII thorax C. XI thorax – I lumbar D. XII thorax – II lumbar E. XII thorax – III lumbar Q2. What is interrelation between right and left kidney? A. Left lower on 1-1,5 cm B. Left lower on 2-4 cm C. Right lower on 1-1,5 cm D. Right lower on 2-4 cm E. Level is equal Q3. What projection of pelvis of the kidney on X-ray according to vertebra? A. XII thorax B. I-II lumbar
cardi
ology
.dsmu.e
du.ua

238
C. II-III lumbar D. III-IV lumbar E. V lumbar Q4. What is averaged amount of initial urine? A. 29B1 liter B. 30B5 liter C. 31B10 liter D. 32B100 liter E. 33B1000 liter Q5. Choose correct sequence of nephron? A. Glomerulus and Bowman's capsule, proximal tubule, loop of Henle, distal convoluted tubule B. Glomerulus and Bowman's capsule, loop of Henle, distal convoluted tubule, proximal tubule C. Loop of Henle, glomerulus and Bowman's capsule, proximal tubule distal, distal convoluted tubule D. Loop of Henle, glomerulus and Bowman's capsule, distal convoluted tubule, proximal tubule E. Glomerulus and Bowman's capsule, loop of Henle, proximal tubule distal, distal convoluted tubule Key answers: E, C, B, D, A Contents of Practice Topics of Theory: 1. Etiology and pathogenesis of acute and chronic renal failure, uremic and chlorohydropenic comas. 2. Clinical features and laboratory changes at acute and chronic renal failure, uremic and chlorohydropenic comas. 3. Diagnosing of acute and chronic renal failure, uremic and chlorohydropenic comas. 4. Complications of acute and chronic renal failure, uremic and chlorohydropenic comas. Practical skills: Students should be able to demonstrate mastery of the following practical skills 1. Enquiring of patient. Objective examination (inspection, palpation). Finding the most characteristic signs of acute and chronic renal failure, uremic coma and chlorohydropenic coma. 2. Assess data of additional laboratory and instrumental examination (biochemical, sonography, X-ray examination) at acute and chronic renal failure, uremic and chlorohydropenic comas. 3. To be able to diagnose acute and chronic renal failure, uremic and chlorohydropenic comas.
cardi
ology
.dsmu.e
du.ua

239
Required Glossary to Practice
Term Definition
Acute renal failure (ARF)
also known as acute kidney failure or acute kidney injury, is a rapid loss of Hrenal functionH due to damage to the HkidneysH, resulting in retention of nitrogenous (HureaH and HcreatinineH) and non-nitrogenous waste products that are normally excreted by the kidney. Depending on the severity and duration of the renal dysfunction, this accumulation is accompanied by metabolic disturbances, such as Hmetabolic acidosisH (acidification of the blood) and HhyperkalaemiaH (elevated potassium levels), changes in body Hfluid balanceH, and effects on many other organ systems. It can be characterised by HoliguriaH or HanuriaH (decrease or cessation of urine production), although nonoliguric ARF may occur. It is a serious disease and treated as a Hmedical emergencyH.
Chronic kidney disease (CKD)
also known as chronic renal disease, is a progressive loss of Hrenal functionH over a period of months or years through five stages. Each stage is a progression through an abnormally low and deteriorating HglomerularH filtration rate, which is usually determined indirectly by the HcreatinineH level in Hblood serumH.
Uremia is a term used to loosely describe the illness accompanying Hkidney failureH (also called renal failure). In kidney failure, HureaH and other waste products, which are normally excreted into the urine, are retained in the blood. Early symptoms include anorexia and lethargy, and late symptoms can include decreased mental acuity and coma. It is usually diagnosed in Hkidney dialysisH patients when the Hglomerular filtration rateH, a measure of kidney function, is below 50% of normal.
HAzotemiaH is another word that refers to high levels of urea, but is used primarily when the abnormality can be measured chemically but is not yet so severe as to produce symptoms. Uremia can also result in Hfibrinous pericarditisH. There are many dysfunctions caused by uremia affecting many systems of the body, such as blood (lower levels of erythropoietin), sex (lower levels of testosterone/estrogen) and bones (osteoporosis and metastatic calcifications).
cardi
ology
.dsmu.e
du.ua

240
Suggested Reading List Required Reading 1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination. Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. A system of case recording and clinical examination of patients on propaedeutic of internal diseases. 4. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 5. Methodical guideline for students 6. Website of department: www.cardiology.dsmu.edu.ua 7. Flow charts for Practice Additional Reading 1. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 2. History and Physical Examination. Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 3. Davidson’s Medicine, Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006
After the above-mentioned topics have been studied, turn to get familiar with relevant Flow charts for practice given in the Appendices
Acute renal failure Causes Prerenal – shock, occlusion of artery Renal – acute or malignant glomerulonephritis, Goodpasture's syndrome (primary pulmonary hemosiderosis with glomerulonephritis), hemolytic-uremic syndrome, trauma, necrosis Postrenal – occlusion of ureter Stages 1. initial - adverse effect of etiological agent 2. oligoanuric 3. polyuric 4. recovery Changes - uremia (azotemia), water-electrolytic disbalance, acidic- basic disbalance
Chronic renal failure
Causes: chronic glomerulonephritis, interstitial nephritis, diabetes mellitus, congenital abnormality, secondary glomerulonephritis, primary nephrosclerosis, occlusion, multiple [plasma cell] myeloma, drugs.
cardi
ology
.dsmu.e
du.ua

241
Changes: - creatine increasing - urea increasing - uric acid increasing - potassium increasing - magnesium increasing - phosphorus increasing - calcium decreasing - anemia - leukocytosis - thrombocytopenia
Clinical features: thirst, polyuria, nicturia, arterial hypertension Uremia signs:
- itch - convulsions - mussels weakness - Kussmaul's respiration - Pericarditis - fibrinous pleurisy - hypersomnia; excessive sleepiness, drowsiness - hiccup - haemorrhage - pain in bones - nausea - vomiting - diarrhea - anemia
Revision Questions
Q1. Choose the reason resulting in development renal form of acute renal failure A. acute retention of urine (prostate gland adenoma) B. radiographic contrast medium C. retention of urine (cancer of urinary bladder) D. shock E. primary water-electrolytic disbalance Q2. For polyuric stage of acute renal failure is typical A. high specific gravity of urine B. normal specific gravity of urine C. increase in contents of urea and creatinine in blood D. increase in hematuria E. low specific gravity of urine Q3. Laboratory sign of expressed chronic renal failure is A. hypersthenuria B. polyuria
cardi
ology
.dsmu.e
du.ua

242
C. pyuria D. anemia E. pronounced proteinuria Q4. Changes of respiratory system in terminal chronic renal failure A. lung emphysema B. lobar pneumonia C. fibrinous pleurisy D. multiple abscesses E. pneumothorax Q5. Changes of gastrointestinal tract in severe chronic renal failure are A. bitterness in a mouth B. heartburn C. diarrhea D. early pains E. late "hungry" pains Q6. Choose the reason resulting in development of postrenal form of acute renal failure: A. acute cardiac failure B. ureteric obstruction by stones C. glomerulonephritis D. pyelonephritis E. poisoning with salts of heavy metals Q7. Chronic renal failure can be revealed with the help of: A. Zimnitsky's test B. determination of proteinuria for the day C. two-glass test D. Nechiporenko's method E. Sonography of kidneys Q8. Choose a parameter, which is necessary for definition creatinine clearance test A. concentration of creatinine in urine B. volume of intaking liquid for last day C. specific gravity of urine D. fluctuations of specific gravity of urine E. concentration of urea in blood plasma Q9. Choose the laboratory examination which allows to reveal renal failure A. Nechiporenko's method B. the clinical urine analysis C. level of creatinine in the blood D. level of haematuria E. daily proteinuria Q10. Chronic renal failure arises in A. decrease in glomerular function of one kidney B. decrease in tubular function of one kidney C. decrease in glomerular and tubular functions of one of kidneys
cardi
ology
.dsmu.e
du.ua

243
D. decrease in glomerular and tubular functions of both kidneys E. all listed variants Key answers: B, E, D, C, C, B, A, A, C, D
SUMMARY OF PROCEDURES
The practice lesson shall be begun in the study room. Checking of the homework, the test control is carried out.
Than have brief discussion about objective and subjective signs of acute and chronic renal failure, uremic and chlorohydropenic comas. Consideration about clinical, laboratory and instrumental importance without patient and on the example of concrete patient.
Then begin individual working with the patients under the control of the teacher and discussion of the revealed symptoms. After in an educational room diagnostic value of available symptoms is discussed.
At end of lesion the final tests are dispense to the students.
Final tests
Q1. Laboratory signs of expressed chronic renal failure A. hyposthenuria B. isohyposthenuria C. polyuria D. pyuria E. pronounced proteinuria Q2. Third stage of acute renal failure is characterized by: A. anasarca B. high specific gravity of urine C. anuria D. polyuria E. oliguria Q3. Choose the reason resulting in development of renal form of acute renal failure A. primary water-electrolytic disbalance B. antibiotics C. acute retention of urine (at prostate gland adenoma) D. retention of urine (cancer of urinary bladder) E. shock Q4. Choose correct sequence of stages occurrence acute renal failure A. oliguric (anuric) → polyuric → shock → recovery B. oliguric (anuric) → shock → polyuric → recovery C. shock → oliguric (anuric) → polyuric → recovery D. shock → polyuric → oliguric (anuric) → recovery E. polyuric → oliguric (anuric) → shock → recovery
cardi
ology
.dsmu.e
du.ua

244
Q5. What is typical urinary sediment in oliguric (anuric) stage of acute renal failure? A. only proteins B. only casts C. only leukocytes D. only erythrocytes E. all listed variants Q6. Third stage of acute renal failure reveals: A. oliguria B. anuria C. low specific gravity of urine D. high specific gravity of urine E. anasarca Q7. Choose the reason resulting in development postrenal form of acute renal failure: A. shock B. acute retention of urine (in prostate gland adenoma) C. primary water-electrolytic disbalance D. glomerulonephritis E. poisoning with salts of heavy metals Q8. Second stage of acute renal failure is characterized by A. polyuria B. anuria C. pyuria D. increases in specific gravity of urine E. anasarca Q9. Urinary sediment in oliguric (anuric) stage of acute renal failure reveals A. only epithelium B. only leukocytes C. only proteins D. only casts E. all listed variants 10. Choose reasons of occurrence of hypochloric coma: A. severe vomitting B. profused diarrhea C. paracentesis D. all above listed E. none above listed
cardi
ology
.dsmu.e
du.ua

245
Question Checklist for Final Test Module 2: Symptomes and Syndromes of Internal Diseases
1. Syndrome of pulmonary consolidation: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
2. Syndrome of increased airiness of the lungs: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
3. Syndrome of accumulation of fluid in a pleural cavity: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
4. Syndrome of accumulation of air in a pleural cavity: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
5. Syndrome of bronchial spasm : ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
6. Syndrome of pain in the heart region: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
7. Syndrome of heart failure: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
8. Syndrome of left heart failure: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
9. Syndrome of right heart failure: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
10. Syndrome of circulatory failure: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
11. Syndromes of the arterial hypertension: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics
12. Dyspeptic syndrome : ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
13. Syndrome of dysphagia : ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
14. Syndrome of portal hypertention: ethiology, pathogenesis,clinical and laboratory investigation, instrumental diagnostics.
15. Hepatorenal syndrome. 16. Syndrome of acute and chronic hepatic failure. Syndrome of hepatarhia. 17. Types of biliary dyskinesia: the main clinical and laboratory signs. 18. Syndrome of jaundice : ethiology, pathogenesis,clinical and laboratory
investigation, instrumental diagnostics. 19. Cholestatic syndrome. 20. Syndrome of hereditary hyperbilirubinemia. 21. Hepatomegaly syndrome. 22. Hepatolienal syndrome. 23. Syndrome of pain in abdomen region. 24. Dyspeptic syndrome. 25.Malabsorption syndrome. 26.Irritable colon syndrome. 27.Syndrome of gastrointestinal hemorrhage: ethiology, pathogenesis,clinical and
cardi
ology
.dsmu.e
du.ua

246
laboratory investigation, instrumental diagnostics. 28. Disuric syndrome. 29. Hematuric syndrome. 30. Tubulo-interstitial syndrome. 31. Nefritic syndrome. Nefrotic syndrome: ethiology, pathogenesis,clinical and
laboratory investigation, instrumental diagnostics. 32. Urinary syndrome: ethiology, pathogenesis,clinical and laboratory
investigation, instrumental diagnostics. 33. Syndrome of acute renal failurу: ethiology, pathogenesis,clinical and laboratory
investigation, instrumental diagnostics. 34. Syndrome of chronic renal failure: ethiology, ,clinical and laboratory
investigation, instrumental diagnostics. 35. Uremic and chlorohydropenic comas. 36. Anaemic syndrome: ethiology, pathogenesis,clinical and laboratory
investigation, instrumental diagnostics. 37. Hyperplastic syndrome in blood system disorders: ethiology, pathogenesis,
clinical and laboratory investigation, instrumental diagnostics. 38. Haemorrhagic syndrome: classification, pathogenesis, clinical and laboratory
investigation. 39. Syndrome of hyperthyroidism: main reasons, clinical signs,clinical and
laboratory investigation. 40. Syndrome of hypohyroidism: main reasons, clinical signs,clinical and
laboratory investigation. 41. Diseases of the mitral valve: main clinical signs, diagnostics.
42. Diseases of the aortic valve: main clinical signs,The main clinical signs and diagnostics of angina pectoris.
43. Acute coronary syndrome.Main clinical signs and diagnostics of myocardial infarction.
44. Syndromes of the arterial hypertension: , clinical signs,diagnostics. 45. Secondary hypertention: clinical and laboratory investigation, instrumental
diagnostics. 46. Articular syndrome (inflammatory and degenerative affections of joints).
Muscular syndrome. 47. Anaemia: classification, the main syndromes. 48. Iron deficiency anaemia: reasons, pathogenesis, clinical features, laboratory signs. 49. Vitamin B12 and folate deficiency anaemia: reasons, pathogenesis, clinical
features, laboratory signs. 50. Haemolyic anaemia: classification, the main features, laboratory signs. 51. Chronic leukemia: main symptomes, blood characteristic. 52. Hemophilia: classification, the main clinical signs, laboratory sings. 53. Thrombocytopenic purpura: the main clinical signs, laboratory sings. 54. Hemorrhagic vasculitis: the main clinical signs, laboratory sings. 55. Diabetes mellitus: classification, the main clinical syndromes, laboratory signs.
cardi
ology
.dsmu.e
du.ua

247
Practical Skill Checklist for Final Test Module 2: Symptomes and Syndromes of Internal Diseases
1. To carry out a physical examination of patient with mitral heart valve disease. To determine the main symptomes and syndromes.
2. To carry out a physical examination of patient with aortic heart valve disease. To determine the main symptomes and syndromes.
3. To carry out a physical examination of patient with arterial hypertention. To determine the main symptomes and syndromes.
4. To carry out an enquiry on the possible presence of ischemic heart disease (stable angina pectoris), to detail a pain syndrome and determine patient|`s functional class.
5. To cary out general inspection and physical examination of patient with acute coronary syndrome (myocardial infarction). To determine .
6. To estimate ECG of patient with myocardial infarction and determine character and location of myocardilal affection.
7. To carry out a physical examination of patient with heart failure. To determine the main symptomes, syndromes and functional class.
8. To carry out an enquiry and inspection of patient with obstructive pulmonary disease, to determine the main symptomes and syndromes, using spirometry to make conclusion about stage of disease.
9. To carry out a palpation, percussion of the chest and auscultation of the lungs of patient with obstructive pulmonary disease, to determine the main symptomes and syndromes.
10. To carry out an enquiry and physical examination of patient with syndrome of pulmonary consolidation (pneumonia). To determine the main symptomes and syndromes.
11. To carry out an enquiry and physical examination of patient with pleuritis. To determine the character of pleural fluid, main symptomes and syndromes of pleuritis.
12. To carry out an inspection and palpation of abdomen of patient with digestive pathology. To determine the main symptomes and syndromes.
13. To analyse the data of gastric content. Estimate secretory and acid-forming functions of the stomach.To carry out an enquiry, inspection and palpation abdomen of patient`s with biliary duct pathology .To determine the main symptomes and syndromes. Estimate the main symptomes of gall-bladder pathology. To determine the main syndromes.
14. Estimate duodenal content in patient with biliary duct pathology. To determine the main syndromes and location of affection .
15. To carry out an enquiry and inspection of patient with liver disease (hepatitis, cirrhosis). To determine the main symptomes and syndromes.
16. To carry out an physical examination of patient with hepatitis (or liver cirrhosis). To determine the main syndromes according to biochemical blood and urine analysis.
17. To carry out an physical examination of patient with kidney disease. To determine the main syndromes.
cardi
ology
.dsmu.e
du.ua

248
18. To analyse the data of urine analysis of patient with kidney disease, Zimnitsky’s test, Nechiporenko’s test. To draw a conclusion about kidney pathology.
19. To carry out an physical examination of patient with anemia. To determine the main syndromes and symptomes according to blood analysis and determine type of anemia.
20. To analyse the blood analysis of patient with leukemia. To determine the main laboratory symptomes and type of chronical leukemia.
21. To carry out an enquiry and general inspection of patient with diabetes mellitus. 22. To examine properties of pulse on arteries of upper annd lower limbs. To
determine the main syndromes and symptomes.
cardi
ology
.dsmu.e
du.ua

249
LITERATURE
1. Internal Diseases, an Introductory Course. Edited by V.Vasilenko and Grebenev, Mir Publishers, Moscow, 1990 2. Clinical Examination, Edited by Jonh Macleod, Jonh Munro, Churchill Livingsone, 1986 3. Medicine, Edited by K. George Mathew, Praveen Aggarwal, Elsevier, 2004 4. Davidson’s Medicine, Edited by Nicholas A. Boon, Nicki R. Colledge, Davidson, 2006 5. Textbook of Physical Diagnosis. History and Examination / Mark H. Swartz 2002, W. B. Saunders Company Pennsylvania 6. History and Physical Examination . Current Clinical Strategies, Edited Paul P. Chan, Peter, J. Winkle, 2005 7. Manual for the Case Record. D., Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 8. Manual for General Inspection of the Patient. Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 9. Manual for the Respiratory System. Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 10. Manual for the Cardiovascular System. Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 11. Manual for the Electrocardiography. Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 12. Manual for the Urinary System. Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 13. Manual for the Gastrointestinal System. Edited by Ignatenko G.A., Department of Propaedeutic Therapy and Clinical Cardiology, Donetsk, 2007 14. Testbook of Medical Physiology / Arthur C. Guyton, John I. Hall 2001, W. B. Saunders company Pennsylvania 2001 15. Gray's Anatomy. Edited by T. Pickering Pick, F.R.C.S., 1995 16. M. Prives, N. Lysenkov, V. Bushovich; Human Anatomy
cardi
ology
.dsmu.e
du.ua

250
cardi
ology
.dsmu.e
du.ua

251
cardi
ology
.dsmu.e
du.ua

252
Здано 29.08.2009 р. Підписано до друку 16.10.2009 р. Формат 145х215 (60х90/16). Друк офсетний. Папір офсетсупер. Ум. др. л. 19,09. Замовлення № 161008. Тираж 100 примірників. Друкарня Донецького національного медичного університету ім. М. Горького. Україна, 83003, м. Донецьк, пр. Ілліча, 16.
Тел.: (062) 385-95-22
cardi
ology
.dsmu.e
du.ua