
Type-1 pericytes participate in fibrous tissue deposition in aged skeletal muscle
Upload
independentCategory
view
1download
0
British Journal ofOphthalmology, 1981, 65, 737-749
Structural basis of contraction in vitreal fibrousmembranesI. GRIERSON AND A. H. S. RAHI
From the Department of Pathology, Institute of Ophthalmology, 17/25 Cayton Street, London ECIV 9AT
SUMMARY A combined ultrastructural and immunofluorescent study was conducted on experi-mentally induced fibrous membranes in the vitreous of adult rabbits. Autochthonous tissuecultured fibroblasts were injected into the mid-vitreous ofone eye of each of25 rabbits. The animalswere monitored routinely with an ophthalmoscope and slit-lamp and were killed at various timeperiods between 5 minutes and 6 months. Appropriate tissue was taken for light microscopy,transmission electron microscopy, scanning electron microscopy, and indirect immuno-fluorescence. With this model we were able to show that the contractile elements in fibrousmembranes are probably modified fibroblasts called myofibroblasts which are most abundant 3 to 6weeks after injection. This is the time when retinal detachment usually occurs. It is our impressionthat, as traction membranes develop, there is not so much an increase in the contractile elements ofthe constituent cells as a rearrangement of the existing cytoplasmic microfilaments into compacthighly organised bundles called stress cables. The behaviour and ultrastructural characteristics ofintravitreal fibroblasts compare with the action of fibroblasts in the healing of wounds.
Experimental vitreal fibrous membranes have beenproduced in the rabbit eye by the injection of autoch-thonous (autologous) cultured skin fibroblasts intothe centre of the vitreous cavity. 1-3 These membranesare contractile and can produce traction detach-ments of the retina. Indeed in their preliminary studyGrierson and Forrester3 found that of the 7 animalswhich were followed up for at least 4 weeks 5developed detachments. More extensive investiga-tions have been conducted by Algvere and Kock' and-Sugita et al.2 in whose experimental series detachmentdeveloped in 50% and 55% of the injected eyesrespectively.
It would seem, then, that the rabbit model is auseful means of studying the basic mechanismsinvolved in the process of membrane contraction andsubsequent retinal detachment. The experimentalfibrous membranes produced in the rabbit appear tohave a similar biological behaviour to those found inhuman pathological specimens. Nonvascular fibrousmembranes develop in association with the vascularproliferations which characterise diabetic retin-opathy, and undoubtedly they contribute to the pro-gressive visual disability.4 Retinal detachment is acommon late complication following trauma to theposterior globe of the eye, and the detachments occur
Correspondence to Dr 1. Grierson.
when sheets of scar tissue form within the vitrealcavity."8 Further serious visual complications canensue in eyes with rhegmatogenous retinal detach-ment due to the action of vitreal fibrous tissue inexacerbating the initial detachment.9
Clearly with a better understanding of the nature ofmembrane contraction and the precise pathogeneticevents which take place during the formation offibrous membranes decisions regarding the best timefor surgical intervention will have a less empiricalbasis. Also the possibility of pharmacological inhi-bition of membrane development or contraction willbe brought a step nearer.
In the present investigation ultrastructural and im-munofluorescent techniques were used to study thedevelopment of scar tissue in the rabbit vitreous andto study the basis of contraction in the developingmembranes. Comparisons were made between fibro-blast activity in wound healing of the skin andmembrane formnation in the vitreous.
Material and methods
EXPERIMENTAL PROCEDURESSkin biopsies were taken from the backs of 25 albinorabbits which weighed between 1-5 and 3-0 kg. Thehair in the area to be biopsied was closely croppedand then cleaned with 70% alcohol. Local anaesthesia
737
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

1. Grierson and A. H. S. Rahi
was induced by the intradermal injection of lignocainehydrochloride, and thereafter a segment of skin wasremoved and sliced into 3 or 4 blocks which wereapproximately 1 mm wide. The blocks were thenintroduced into Falcon flasks and fixed into positionwith a double layer of chick plasma clot.'0 Theseflasks were kept in an incubator at 37-38°C, fed twiceevery week with tissue culture medium," and main-tained in an environment of 5% CO2 and air. Afterapproximately 2 weeks in primary culture a mono-layer of fibroblasts had formed and the clot had splitand disintegrated. The fibroblasts were subculturedfor a further 2 to 3 weeks until there was a sufficientcrop of cells for for intravitreal injection. To harvestthe cells the monolayer was dissociated with a solutionof 0-25% trypsin in phosphate-buffered saline orscraped off with a rubber 'policeman' and thencollected in a sterile syringe. The cells were finallywashed 3 or 4 times in isotonic phosphate-bufferedsaline prior to being centrifuged at 1000 rpm for 6minutes.The cells were resuspended in phosphate-buffered
salt solution, cell frequency was checked with ahaemocytometer, and 0-2 ml of fluid containing400000 to 1000000 fibroblasts was taken up into asyringe. A second sample of cells was vitally stainedwith trypan blue, and the frequency of dead anddamaged cells in the fibroblast population waschecked.At this time the appropriate rabbit was anaes-
thetised with intravenous sodium pentobarbitone(30 mg per kg body weight) and one eye softened bythe withdrawal of 0-2 ml of aqueous humour (seeForrester and Grierson'2). Subsequently the 0 2 ml ofsuspended fibroblasts were injected into the centralvitreous cavity via the pars plana. The wholeprocedure was carried out under ophthalmoscopiccontrol. Routine examination included ophthalmo-scopic and slit-lamp observation of the experimentaleyes for the duration of the study. In this way aphotographic record of the key changes during thedevelopment of the vitreal membranes and the sub-sequent retinal detachment (if it took place) wasavailable for each animal.
HISTOLOGICAL PROCEDURES
The animals were killed with an intravenous overdoseof sodium pentobarbitone 5 min, 2 h, 4 h, 1 day, 2days, 3 days, 6 days, 2 weeks, 3 weeks, 6 weeks, 10weeks, 3 months, and 6 months after the intravitrealinjection of fibroblasts. The eyes were opened in theappropriate plane depending on the position of thefibroblasts or the developing membranes and fixed in3% glutaraldehyde solution in cacodylate buffer.After macroscopic photography and a minimum of 4hours in primary fixative samples of retina, opticnerve, vitreous, lens, ciliary body, and limbus weredissected out for post-fixation in 1% osmium tet-roxide. Thereafter the segments were dehydrated in
Fig. 1 Indirect immunofluorescent staining with sera rich in 'smooth-muscle' antibody. (a) A frozen section from normalskin with positive staining in the epidermis (arrows) but not in the dermis. (b) A frozen section from a 14-day scar: there isstrongfluorescence in the dermis (arrows) corresponding to the presence ofactivatedfibroblasts. (x 80).
738
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

Structural basis of contraction in vitreal fibrous membranes
Fig. 2 An electron micrograph which shows part ofafibroblastfrom a 14-day scar. There is a thick bundle of6 to 7 nmdiameter microfilaments within the cytoplasm (arrows). (Uranyl acetate/lead citrate stained section; x 30 000).
ascending grades of ethanol. Some tissue segmentswere dried in a critical point drier (Polaron), mountedon standard stubs, coated with gold in a sputter coater(Polaron), and studied in a Cambridge S4-10 scanningelectron microscope. However, after dehydration inethanol most of the tissue was cleared in propyleneoxide and embedded in Araldite. Sections were cuton an LKB Ultrotome III or a Huxley microtome andviewed in a JEOL IOOC electron microscope.Some of the established monolayers of skin fibro-
blasts not needed for intravitreal injection were fixedand processed for electron microscopy in the mannerdescribed above. Other monolayers were fixed in10% formol basic-salt solution and stained withperiodic acid Schiff and haematoxylin.Segments of the scar tissue which formed at the
sites of the skin biopsies were taken from 3 days to 5weeks following the initial wound. These were either
processed conventionally for wax histology or fortransmission electron microscopy.
IMMUNOFLUORESCENT STUDIESFor this part of the investigation monolayers ofcultured fibroblasts, early fibroblast aggregates fromthe vitreous, and mature membranes of various ageswere washed in isotonic saline and fixed in acetone.When normal skin, skin scar tissue, and whole globeswere required for examination, they were first frozenand then sectioned on a cryostat.Blood from patients with chronic uveitis or intra-
ocular melanoma which had high titres (that is, 1/160or better) of antibodies to smooth muscle proteins,particularly actin 13-1 served as the source of anti-serum to localised contractile cytoplasmic proteins.Reactivity and specificities were assessed by detailedexamination of various tissues from a rat-for
739
V.
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

I. Grierson and A. H. S. Rahi
Fig. 3 Indirect immunofluorescentstaining with sera rich in'smooth-muscle' antibody ofafibroblast at the growing edgeofa culture. (x 816).
Fig. 4 Phase-contrast micrograph from a squashpreparation of vitreous which was removed 4 hours after theintravitreal injection offibroblasts. The cells are rounded andform clusters. Dead cells appear pigmented because ofuptake oftrypan blue. (x 570).
example, skeletal muscle, liver, kidney, stomach wall,and salivary gland-which had been frozen, sectionedand treated with the sera. 6 After treatment with thesera the appropriate sections and tissues wereexposed to fluorescein-labelled antihuman immuno-globulins. 3 14 The specimens were studied and photo-graphed in a Zeiss epifluorescent microscopeequipped with an FITC interference filter.
Results
WOUND HEALING IN THE SKINThe fibroblasts of normal skin are scattered through-out the papillary and reticular dermis. When we
examined these cells under the electron microscope
they were seen to have ovoid nuclei with a prominentheterochromatin pattern, and their cytoplasm con-tained a few small mitochondria and poorly developedrough endoplasmic reticulum. The cytoskeletalframework of the fibroblasts consisted of a fewscattered microtubules, intermediate filaments(10-12 nm in diameter), and contractile micro-filaments 6-7 nm in diameter). Correspondingly,indirect immunofluorescent staining for 'smoothmuscle' antigens in normal skin was positive in thecase of vascular endothelium and epidermal keratin-ocytes, but was only faintly positive in the dermalconnective tissue where the inactive fibroblasts(fibrocytes) were located (Fig. la).During the process ofwound healing the number of
fibroblasts increased after the initial inflammatoryepisode (from day 4 onwards). From 10 to 21 daysbands of elongated spindle shaped cells wereprominent. Under the electron microscope thespindle shaped fibroblasts had the characteristics ofactively synthesising cells, being rich in both mito-chondria and rough endoplasmic reticulum. Some ofthe fibroblasts had distinctive bundles of micro-filaments (Fig. 2) and these cells became progressivelymore abundant over the 10- to 21-day time period.
Consistent with this finding strongly fluorescentcells were observed in the scar tissue followingtreatment with 'anti-smooth muscle' sera Fig. lb).Cells ofthis type have been called 'myofibroblasts"7-20and by 4 to 5 weeks myofibroblasts were still presentbut were less prominent than at earlier periods.
FIBROBLASTS IN CULTUREWhen the fibroblasts from the skin explants began togrow in culture they were found to have 'smoothmuscle' antigens in their cytoplasm (Fig. 3). Cyto-plasmic fluorescence was particularly prominent inthose cells at the growing edge of the culture. Wellestablished primary cultures and subcultures con-sisted of a compact mass of spindle-shaped cells, andby 3 to 4 weeks there were usually sufficient cells forintravitreal injection.
CULTURED FIBROBLASTS INJECTED INTO THEVITREOUSImmediately after their injection into the vitreous thefibroblasts rounded up and formed clusters. Theseclusters persisted for at least 4 hours. After they werestained with trypan blue it was found that between 10and 15% of the cells in the initial injections weredead. After 4 hours in the vitreous the incidence ofdead cells had increased (20 to 40%) (Fig. 4). Theintact viable cells could be seen by electronmicroscopy to contain large numbers of lysosomalinclusions. Their cytoskeleton consisted of a fewmicrotubules and 10 to 12 nm intermediate filaments.
740
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

Structural basis of contraction in vitreal fibrous membranes
Fig. 5 Indirect immunofluorescentstaining ofaggregates ofroundedfibroblasts 4 hours after intravitreal injection. (a) Inthis example scattered cells on the surface ofthe bolus arehighly fluorescent, whereas others deeper in the bolus showlittle evidence ofstaining (arrows). (b) Another aggregatewhere a larger proportion ofthefibroblasts are stronglyfluorescent. (x 110).
Those microfilaments (6-7 nm) which make up thecontractile system were rare and only sporadicallydistributed within the cell cytoplasm. Immuno-fluorescent studies of the intravitreal bolus 1 hourafter injection showed that the bulk of the cellpopulation were only weakly positive. However, by 4hours some of the fibroblasts at the periphery of theaggregate had a distinct and diffuse cytoplasmicfluorescence (Fig. 5).One day after injection into the vitreous the cells
had begun to form elongated strands. By this stagemost of the cells were intensely fluorescent, but thepattern was always of the diffuse form (Fig. 6).Electron microscopy showed that 6-7 nm micro-filaments were common and were spread throughoutthe cell cytoplasm.Between the 3rd and the 6th days the cells migrated
towards the vitreous base, and the optic nerve headand sheets of cells occupied a retrolental position.During this period the cells progressively lost their
Fig. 6a, b The strands which form I day after intravitrealinjection are highlyfluorescent after treatment withanti-'smooth muscle'sera. (x 175).
rounded form and they adopted a more characteristicfibroblastic shape (Figs. 7 and 8). The cells hadobvious 'ruffles' (Fig. 7) and filopodia (Fig. 8), both ofwhich are features indicating cellular mobility. Onday 3 microfilaments were abundant but were alwaysdiffusely spread throughout the cell cytoplasm (Fig.9), whereas on day 6 we began to find cells in whichthe 6-7 nm microfilaments were aggregated into loosebundles (Fig. 10). Usually by the 3rd day the vitreousface was detached, and variable numbers of inflam-matory cells were present. The inflammatory responsebecame apparent on either the 1st or 2nd day andconsisted almost entirely of neutrophils. By the 6thday few neutrophils remained, and there was a pre-dominance of lymphocytes. The lymphocytes per-sisted up to the 3rd week after injection.At day 6 the fibroblasts had formed sheets through-
out the vitreous (Fig. 11a). By now some of the cellsappeared to be producing thin branching extracellularmicrofibrils (Fig. 12) and were distinguished by thepresence of a well-developed Golgi system, manymitochondria, and abundant rough endoplasmic
741
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

I. Grierson and A. H. S. Rahi
Fig. 7 A squash preparation ofvitreal material 3 days afterintravitreal injection. Thefibroblasts have 'ruffles' which are acharacteristic feature oftheirlocomotion and some cells arespindle-shaped. (Phase contrast;x 325).
reticulum. From 6 days onwards immunofluorescentstaining of the newly formed membranes gave onlyweakly positive results. Indeed by 2 weeks thefluorescence was so poor it was difficult to distinguishthe cells.
Particularly well established membranes werefound between 3 and 6 weeks, by which time retinaldetachment had occurred in most eyes (Fig. Ilb).Sheet-like membranes occupying an equatorial orretrolental position were common as were columnaror stalk membranes some extending between the lensand the optic nerve head. The membranes werehypercellular and the collagen within them wascomposed of predominantly 10 to 20 nm diameterfibrils which, with our staining technique, had noobvious periodicity. At the 3-week stage the fibro-blasts were elongated spindle-shaped cells in closecontact with each other (Fig. 13). The highly
orientated bands of cells had formed gap junctions atpoints of cell-to-cell contact (Fig. 14). Mitochondria,Golgi vesicles, and rough endoplasmic reticulum wereno longer profuse within the majority of cells.Compact bands of microfilaments were a frequentfinding and these aggregates were located in the cyto-plasm immediately beneath the plasma membrane(Fig. 15). Similar bands of closely associated micro-filaments have been observed in a variety of cells invitro and have been called 'stress-cables' (seediscussion). Occasionally the 'stress-cables' extendedinto thin cytoplasmic processes to constitute micro-tendons (Fig. 15) that either joined neighbouringcells or were embedded in the extracellular matrix.Some of the cells in the membranes had heavilyindented nuclei (Fig. 13), but otherwise the nucleiwere unremarkable.
Immunofluorescent staining showed fine fluor-
Fig. 8 An electron micrograph ofafibroblast 6 days after intravitrealinjection. The cell has numerousfilopodia and a more characteristicfibroblastic shape. (Uranylacetate/lead citrate staining;x 3950).
742
:8.
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from
Structural basis of contraction in vitreal fibrous membranes
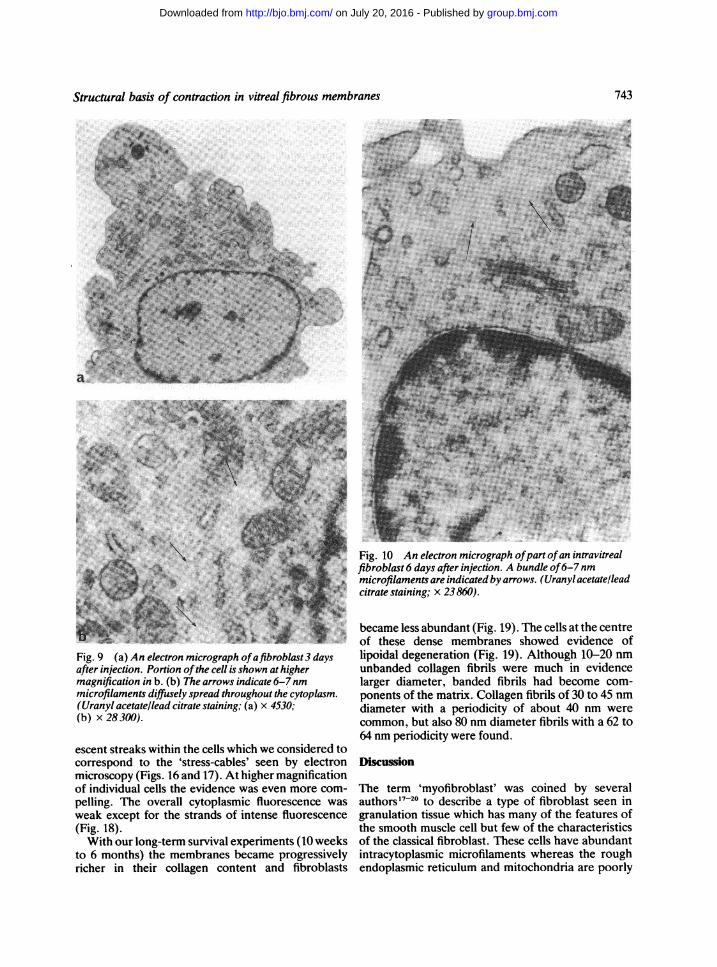
'LeC~~~~~~~~~~~~JFig. 10 An electron micrograph ofpart ofan intravitrealfibroblast 6 days after injection. A bundle of6-7nmmicrofilaments are indicated by arrows. (Uranyl acetate/leadcitrate staining; x 23860).
Fig. 9 (a) An electron micrograph ofafibroblast3 daysafter injection. Portion ofthe cell is shown at highermagnification in b. (b) The arrows indicate 6-7nmmicrofilaments diffusely spread throughout the cytoplasm.(Uranyl acetate/lead citrate staining; (a) x 4530;(b) x 28 300).
escent streaks within the cells which we considered tocorrespond to the 'stress-cables' seen by electronmicroscopy (Figs. 16 and 17). At higher magnificationof individual cells the evidence was even more com-
pelling. The overall cytoplasmic fluorescence wasweak except for the strands of intense fluorescence(Fig. 18).With our long-term survival experiments (10 weeks
to 6 months) the membranes became progressivelyricher in their collagen content and fibroblasts
became less abundant (Fig. 19). The cells at the centreof these dense membranes showed evidence oflipoidal degeneration (Fig. 19). Although 10-20 nmunbanded collagen fibrils were much in evidencelarger diameter, banded fibrils had become com-ponents of the matrix. Collagen fibrils of 30 to 45 nmdiameter with a periodicity of about 40 nm werecommon, but also 80 nm diameter fibrils with a 62 to64 nm periodicity were found.
Discussion
The term 'myofibroblast' was coined by severalauthors'720 to describe a type of fibroblast seen ingranulation tissue which has many of the features ofthe smooth muscle cell but few of the characteristicsof the classical fibroblast. These cells have abundantintracytoplasmic microfilaments whereas the roughendoplasmic reticulum and mitochondria are poorly
743
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

7. Grierson and A. H. S. Rahi
Fig. II (a) A macrophotograph showing membranoussheets throughout the vitreous 6 days after injection. (b) Amacrophotograph ofan eye enucleated 6 weeks afterintravitreal injection offibroblasts. Retinal detachment isevident.
developed. '820 Their similarity to smooth muscle cellshas been confirmed on the basis ofimmunofluorescentstaining which showed the presence of actomyosin-like materials within the fibroblasts.2" Also detailedtests of granulation tissue in vitro7 18 has shown con-traction with drugs which stimulate smooth muscleand relaxation with relaxant drugs. Subsequentlymyofibroblasts have been identified in woundhealing,22 in the normal rat testicular capsule23 inrat duodenal villi24 and many other sites includ-ing the fibrous membranes which develop in thevitreous.23The identification of myofibroblasts in experi-
mental fibrous vitreal membranes has been basedentirely on ultrastructural observations,23 whereas inthe present investigation attempts have been made(a) to determine whether vitreal fibroblasts contain'smooth muscle' elements as indicated by indirectimmunofluorescence; (b) to correlate the patterns ofcytoplasmic fluorescence with the fine structure of thefibroblasts; and (c) to compare the behaviour andultrastructural characteristics with the fibroblastsinvolved in wound healing of the skin and fibroblastsin tissue culture.
It was evident that the fibroblasts in the vitreouswent through several stages during which their mor-phology and presumably also their activities wereradically different. Table 1 is an attempt to summarisethe main characteristics of the fibroblasts at thevarious time intervals. Herschel et al.2 and Gabbianiet al. 8 have found that there is an intensely positivereaction in the cytoplasm of the myofibroblast withanti-smooth muscle serum, whereas normal fibro-blasts are negative. Equally they were able to showthat fibroblasts in tissue culture could adopt a myo-
Table I Summary table showing the main characteristics of intravitreal autochthonousfibroblasts at various time periods
Time period Activities Membrane General Morphological Immunofluorescence Immunofluorescence Generalappearance characteristics pattem comments
0-I days Quiescence Bolus of cells Rounded Large nuclear to Weak Diffuse Inflammatorycytoplasmic ratio response after I day
2-4 days Motility Strands of cells Intermediate Decreased nuclear to Strong Diffuse Detached vitreousform cytoplasmic ratio, cells face
have microvilli6 days to Synthesis Membrane Typical Large quantities of Moderate to weak Reticular Liquefied vitreous2 wks sheets fibroblastic r.e.r., many
form mitochondria, welldeveloped golgi
3 wks to Contraction Retrolental, Thin elongated Aggregates of Moderate Stress cables Retinal detachment10 wks equatorial, stalk spindle shape microfilaments within has taken place
membranes the cellsSome nuclei are crenatedgap junctions haveformed
10 wks to Remodelling and " Elongated Large accumulations of " Mixed Neovascularisation,6 mths maturation (fixed irregular lipid within some cells epiretinal glial
scar) proliferation mayhave taken place
744
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

Structural basis of contraction in vitreal fibrous membranes
fibroblast form.25 Indeed it is well known thatcultured fibroblasts contain contractile proteinswithin their cytoplasm,26 and immunofluorescencestudies on our cultured cells confirmed this finding.
After injection into the vitreous, however, the cellscontained few contractile microfilaments, andstaining with sera rich in 'smooth muscle' antibodiesgave only weakly positive results. It was an extremelyinteresting finding that in the vitreous the mostintense reaction was not with the so-called myo-fibroblasts but at the earlier presynthesis motile stagewhen a strongly positive diffuse cytoplasmic stainingreaction was observed. In this particular model ourimmunofluorescent and ultrastructural studies in-dicate that, as traction membranes develop, there isnot so much an overall increase in the contractileelements of the constituent cells as a rearrangementof the microfilaments into compact highly organisedbundles orientated parallel to the long axis of the cell.The characteristics of the myofibroblasts in thevitreous are (a) they are not rich in rough endo-plasmic reticulum and mitochondria; (b) they areelongated spindle shaped cells; (c) they form compact
Table 2 A comparison of the main features ofskin andvitreal myofibroblasts. The characteristics ofskinmyofibroblasts are based on our own observations and thefindings ofRyan et al., '9 Montandon et al.,20 Gorgas andBock, 23 and Gabbiani et al.2
Featutres Skin Vitrealmvofihroblasts mYofibroblasts
I Microfilaments (dispersed throughout + + + + +the cvtoplasm)
2. Microfilaments (forming stress cables) + + + . . ±3. Dense bodies ± . . +4. Microtendons + + + ± . .
5. Indented nuclei 4- + + + +4-6. Gap junctions + + + + + +7. Desmosomes (Maculae adhaerentes) + ++ 4+8. Hemidesmosomes + +
Kev: +--+ + =Abundant: + + =common: + =rare.
sheets; (d) gap junctions link adjacent cells; (e) somecells have highly invaginated nuclei; (f) microtendonsare frequently evident; and (g) the contractilefilaments are arranged into thick bundles of 6 to 7 nmmicrofilaments.
Myofibroblasts elsewhere in the body have the
Fig. 12 An electron micrograph showingpartofan intravitrealfibroblast6 days after injection. Thin branching extracellularmicrofibrils (arrows) are seen to be in intimate association with the plasma membrane. (Uranvl acetate/lead citrate sectionstaining; x 60 000).
745
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

1. Grierson and A. H. S. Rahi
S:.-;.:....................
< :F+. . . ................................;:.....: .
.."XW..Fig. 13 Electron micrographs ofmembranes at 3 weeks. (a) Themembrane is hypercellularconsisting ofconnectingspindle-shaped cells. Attachments abetween cells are by thin elongatedprocesses. (b) A similar membraneto that in a. The nuclei (n) havemany infoldings. (Uranyl acetateand lead citrate staining; x 4230).
:.4
bX
.~~~~~ ~ ~ ~ ~~~ ~ ~~~~~~~~~~~~~~~~.. ..
io
Fig. 14 An electron micrograph showing a gap junction(arrow) at a point of cell-to-cell contact. From a membranewhich hasformed 6 weeks after the injection offibroblastsinto the vitreous. (Uranyl acetate/lead citrate staining;x 27500).
features we have described but in addition 'densebodies,"9 maculae adhaerentes, and hemidesmo-somes20 have been noted. We have seen all 3 in ourcells, but they were not particularly prominent andcertainly were too rare to be considered as dis-tinguishing features of the vitreal myofibroblasts. InTable 2 the main features of skin and vitreal myo-fibroblasts are compared.To have an effective contractile membrane which
will produce retinal detachment several criteria mustbe satisfied. The membrane must have a stablescaffold on which to develop, it will require firmattachment to the retina, there have to be contractileelements capable of co-ordinated action, and, finally,the contractile elements (myofibroblasts) must befirmly adherent to the scaffold.As yet we know little about the adhesion of the
746
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

Structural basis of contraction in vitreal fibrous membranes
Fig. 15 Higherpower electron micrographs ofareas shownin Fig. 13b. (a) A stress-cable ofcompact microfilaments isindicated by arrows. (b) A stress-cable (large arrows) and amicrotendon (small arrows) can be seen. (Uranylacetate/lead citrate staining; x 8700).
myofibroblasts to their collagen scaffold. Hemi-desmosomes usually have a prominent role in cell toextracellular matrix associations but unlike other
tissues where myofibroblasts abound202223 we wereunable to find significant numbers of attachmentzones. Our evidence that the fibroblasts are the con-tractile elements is indirect but compelling. The fibro-blasts are organised into sheets and have linking gapjunctions. Gap junctions are thought to be couplingdevices and serve as low resistance pathways by whichions and metabolites can pass between cells.27 Thusthe fibroblasts have the necessary attachments forco-ordinated action. Bundles of microfilamentsusually considered to be rich in actin are presentwithin the fibroblasts, and by immunofluorescencethese bundles have been shown to selectively bindsera rich in anti-'smooth muscle' antibodies. Thus,having the necessary contractile apparatus, the in-dentation of the cell nuclei is an indication that con-traction may have taken place.28 The nuclei of smoothmuscle cells,29 vascular endothelia,8 and heartmuscle cells30 show a similar pattern of deep in-foldings and multiple indentations during contraction.Obviously it is important to undertake a pharmaco-logical study of the effects on the fibrous membranesofdrugs which can produce relaxation and contractionof smooth muscle.
It should not be considered that the fibroblast isunique in its ability to adopt a different arrangementof its contractile proteins in response to externalstimuli. Many cells can do this both in vivo andvitro,'3 1426 although perhaps not in quite such aspectacular manner. During locomotion the micro-filaments of the mobile cell are dispersed throughoutthe cytoplasm and appear to be arranged in a hap-hazard manner. On the other hand the so-calledstress-fibres or organised bundles of microfilaments
Fig. 16 Indirect immunofluorescent staining with sera rich Fig. 17 Indirect immunofluorescent staining with sera richin anti-'smooth muscle' antibodies ofa sheet membrane 3 in anti-'smooth muscle' antibodies ofa membrane 6 weeksweeks after the injection offibroblasts into the vitreous. after the injection offibroblasts into the vitreous.Streaks ofpositive staining corresponding to 'stress-cables' Stress-cables can be seen (x 275).can be identified (x 200).
747
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

I. Grierson and A. H. S. Rahi
i -...oo s ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.:..... ....
*S.._r .cu
* ~ it,.S r _ ? -
a , '_ ~ * . e .. - ' _ *i
At.- , - .S ~~~~A
$ F
Fig. 19 Light micrographs of toluidine blue stained
semithin sections through parts ofmembranes 3 months after
the injection offibroblasts. (a) There is a well developed
extracellular matrix in the long-term membranes. (b) In
addition the cells in the 'middle of these membranes show
evidence of lipoidal degeneration (arrows). (x 350).
Fig. 18 A cell at the periphery ofa 6-week intravitrealmembrane treated with sera rich in anti-'smooth muscle'antibodies. The overall cytoplasmic fluorescence is poorexceptfor a distinctive strand offluorescence which probablycorresponds to the 'stress-cables' seen in the electronmicrographs. (x 1000).
are associated with cells which are anchored firmly toa substrate.26"" Whether the prominent actin-richmicrofilamentous bundles in the cytoplasm of myo-fibroblasts merely bind the cells to the collagenousscaffold or are the contractile system responsible forretinal detachment remains to be established.
It has been proposed that collagen formation is thebasis of the contraction of fibrous membranes,'32 butnormal collagen does not contract and as we3 andothers2 have shown the basis of membrane retractionis cellular rather than extracellular. However,maturation of the extracellular matrix from the thinunbanded microfibrils which initially were the solecomponents of the scaffold to the complex of un-banded and banded collagen microfibrils (seen at 10
weeks) may be the locking mechanism whereby thecontracted membrane develops into a fixed scar. Theprocesses involved have been studied in woundhealing of the skin33 but they remain an importantarea for future research in vitreal fibrosis.We acknowledge with thanks the advice and comments of Mr D.McLeod, Moorfields Eye Hospital, and Professor A. Garner,Department of Pathology. Institute of Ophthalmology, London. Wealso thank Miss E. Robins, Mr R. C. Howes. Mr S. Ahmed. and MissL. Millar for their technical assistance. The secretarial help was
provided by Miss L. S. Hart.
References
1 Algvere P, Kock E. Experimental fibroplasia in the rabbitvitreous. Retinal detachment induced by autologous fibroblasts.Albrecht von Graefes Arch Klin Ophthalmol 1976; 199: 215-22.
2 Sugita G, Tano Y, Machemer R, Abrams G, Claflin AJ,Fiorentino G. Intravitreal autotransplantation of fibroblasts. AmJ Ophthalmol 1980; 89:121-30.
3 Grierson 1, Forrester JV. Vitreous haemorrhage and vitrealmembranes. Trans Ophthalmol Soc UK 1980; 100: 40-50.
4 Constable IJ, Pathology of vitreous membranes and the effect ofhaemorrhage and new vessels on the vitreous. Trans OphthalmolSoc UK 1975; 95: 382-6.
748
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

Structural basis of contraction inz vitreal fibrous membranes
5 Faulborn J, Topping TM. Proliferation in the vitreous cavity afterperforating injuries: a histopathologic study. Albrecht von
Graefes Arch Klin Ophthalmol 1978; 205:'157-66.6 Winthrop SR, Cleary PE, Minckler DS, Ryan SJ. Penetrating eye
injuries: a histopathological review. Br J Ophthalmol 1980; 64:809-17.
7 Machemer R. Aaberg TM. Vitrectomv. 2nd ed. New York. SanFrancisco, London: Grune and Stratton, 1979.
8 Coles WH, Haik GM. Vitrectomy intraocular trauma. Itsrationale and its indications and limitations. Arch Ophthalmol1972: 87: 621-8.
9 Machemer R. Massive periretinal proliferation. A logicalapproach to therapy. Trans Am Ophthalmol Soc 1977; 75:556-86.
10 Tripathi B. Retinal vascular complex of rabbit and its response tohyperoxia in tissue culture. PhD Thesis, London University.1971.
t t Grierson I. Robins E, Howes RC. Preliminary observations on
human trabecular meshwork cells in vitro. Albrecht von GraefesArch Klin Ophthalmol 1980; 212: 173-86.
12 Forrester JV. Grierson 1. The cellular response to blood in thevitreous, an ultrastructural study. J Pathol 1979; 129: 43-52.
13 Rahi A, Grierson 1. Ashton N. Contractile proteins in oculartissues: role in health and disease. Trans Ophthalmol Soc UK1980; 100:155-61.
14 Rahi A, Ashton N. Contractile proteins in retinal endotheliumand other non-muscle tissues of the eye. Br J Ophthalmol 1978;62: 627-43.
15 Grierson 1. Rahi AHS. Microfilaments in the cells of the humantrabecular meshwork. Br J Ophthalmol 1979: 63: 3-8.
16 Trenchev P. Holborow EJ. The specificitv of anti-actin serum.
lmmunology 1976; 31: 509-17.17 Majno G, Gabbiani G. Hirschel BJ, Ryan GB, Statkov PR.
Contraction of granulation tissue in vitro: similaritv to smoothmuscle. Science 1971;173: 548-9.
18 Gabbiani G, Herschel BJ, Ryan GB, Statkov PR, Majno G.Granulation tissue as a contractile organ. A study of structure andfunction. J Exp Med 1972; 135: 719-34.
19 Ryan GB, Cliff WJ, Gabbiani G, et al. Myofibroblasts in humangranulation tissue. Human Pathol 1974; 5: 55-67.
20 Montandon D, Gabbiani G. Ryan GB, Majno G. The contractilefibroblast. Its relevance in plastic surgery. Plast Reconstr Surg1973; 52: 286-92.
21 Herschel BJ, Gabbiani G, Ryan GB, Majno G. Fibroblasts ofgranulation tissue: immunofluorescent staining witb anti-smoothmuscle serum. Proc Soc Exp Biol Med 1971; 138: 466-9.
22 Squier CA, Kremenak CR. Myofibroblasts in healing palatalwounds of the beagle dog. J Anat 1980; 130: 585-94.
23 Gorgas K, B6ck P. Myofibroblasts in the rat testicular capsule.Cell Tissue Res 1974; 154: 533-41.
24 Guldner FH, Wolff JR, Keyserlingk DG. Fibroblasts as a part ofthe contractile system in duodenal villi of rat. Z ZellforschMikrosk Anat 1972: 135: 349-53.
25 Gabbiani G, Majno G, Rvan GB. The fibroblast as a contractilecell. The mvofibroblast. In: Pikkarainen J, Kulonen K, eds.Biology of the Fibroblast. New York: Academic Press, 1973:139-54.
26 Lazarides E. Immunofluorescence studies on the structure ofactin filaments in tissue culture cells J Histochem Cvtochem 1975:23: 507-28.
27 Gilula NB, Reeves OR, Steinbach A. Metabolic coupling and cellcontacts. Nature 1972; 235: 262-5.
28 Majno G. Shea SM, Leventhal M. Endothelial contractioninduced by histamine-type mediators. An electron microscopicstudy. J Cell Biol 1969; 42: 647-72.
29 Lane BP. Alterations in the cytologic detail of intestinal smoothmuscle in various stages of contraction. J Cell Biol 1965; 27:199-213.
30 Bloom S, Cancilla PA. Conformational changes in myocardialnuclei of rats. Circ Res 1969; 24: 189-96.
31 Pollack R, Rifkin D. Actin-containing cables within anchoragedependent rat embryo cells are dissociated by plasma and trypsin.Cell 1975; 6: 495-506.
32 Havener WH. Massive vitreous retraction. Ophthalmic Surg1973; 4: 22-67.
33 Rudolph R, Guber S. Suzuki M. Woodward M. The life cycle ofthe myofibroblast. Surg Gvnecol Obstet 1977; 145: 389-94.
749
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from

vitreal fibrous membranes.Structural basis of contraction in
I Grierson and A H Rahi
doi: 10.1136/bjo.65.11.7371981 65: 737-749 Br J Ophthalmol
http://bjo.bmj.com/content/65/11/737Updated information and services can be found at:
These include:
serviceEmail alerting
Sign up in the box at the top right corner of the online article. Receive free email alerts when new articles cite this article.
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 20, 2016 - Published by http://bjo.bmj.com/Downloaded from
Copyright © 2022 FDOKUMEN




















