Strategic costs and preferences revelation in the allocation of resources for health care
19
Strategic costs and preferences revelation in the allocation of resources for medical treatments Laura Levaggi * and Rosella Levaggi † June 2005 Abstract This article examines the resource allocation process in the internal market for health care and argues that the observed allocation is the re- sult of the maximisation procedure of different agents, whose behaviour might not be fully detected by the system and whose preferences might not even enter the decision tree. Internal markets for health care foresee a separation between the purchaser and the provider which generates asym- metry of information. In this paper we analyse the strategic behaviour of the provider which, by misrepresenting its cost and reservation utility, might shift the allocation of resources away from the purchaser’s objec- tives. Although we do not wish to deny the fundamental importance of equity and efficiency considerations which have been the traditional focus of the literature on the allocation of resources, this paper shows that the organisation of production is not a neutral instrument and more research should be devoted to studying these effects. JEL Classification: I11, I18 Keywords: Internal market, asymmetry of information, devoted worker * Department of Mathematics, University of Genova, Via Dodecaneso 35 - 16146 Genova (Italy). E-mail: [email protected]. † Department of Economics, University of Brescia, Via S. Faustino, 74b, 25122 Brescia (Italy). E-mail: [email protected]. 1
Transcript of Strategic costs and preferences revelation in the allocation of resources for health care

Strategic costs and preferences revelation
in the allocation of resources
for medical treatments
Laura Levaggi∗ and Rosella Levaggi†
June 2005
Abstract
This article examines the resource allocation process in the internal
market for health care and argues that the observed allocation is the re-
sult of the maximisation procedure of different agents, whose behaviour
might not be fully detected by the system and whose preferences might
not even enter the decision tree. Internal markets for health care foresee a
separation between the purchaser and the provider which generates asym-
metry of information. In this paper we analyse the strategic behaviour
of the provider which, by misrepresenting its cost and reservation utility,
might shift the allocation of resources away from the purchaser’s objec-
tives. Although we do not wish to deny the fundamental importance of
equity and efficiency considerations which have been the traditional focus
of the literature on the allocation of resources, this paper shows that the
organisation of production is not a neutral instrument and more research
should be devoted to studying these effects.
JEL Classification: I11, I18
Keywords: Internal market, asymmetry of information, devoted worker
∗Department of Mathematics, University of Genova, Via Dodecaneso 35 - 16146 Genova(Italy). E-mail: [email protected].
†Department of Economics, University of Brescia, Via S. Faustino, 74b, 25122 Brescia(Italy). E-mail: [email protected].
1

1 Introduction
The definition of the criteria used to allocate resources in the context of anyhealth care system is one of the fundamental steps in its architecture. Thisprocess in fact translates the general objective of providing an acceptable levelof health care to those in need into a set of rules to allocate resources and into anorganisational design that regulates the relationship among the different actors.This process is not straightforward because each agent has his own competingobjectives, information is asymmetric and the institutional setting might itselfinfluence the outcome.
The literature on resources allocationhas studied the rules that should beused to maximise the welfare of the population treated, taking for granted thatthe decision-maker has full control of the whole process. However, this might notbe the case especially in the presence of an internal market for health care.Theinternal market for health care is in fact only virtually competitive both on theoutput and the input side. As regards the output, i.e. health care, the demandcannot drive the price to be equal to the marginal cost of production because thepatient does not usually pay for the care he receives. Providers often competefor patients through quality [7, 10, 9] but the cost for health care is still mainlydetermined by a bargaining between the purchaser and the provider, usuallycharacterised by information asymmetry on costs and unverifiable quality [1].
Furthermore, input factors are seldom paid on their marginal productivitygiven the barriers to entry in the market and the fact that the medical staff mightpursue more complex objectives than a straight maximisation of the differencebetween reward and effort [14, 13, 3, 5].
The observed allocation of resources will then be the result of the maximisa-tion procedure of different agents, whose behaviour might not be fully detectedby the system. The focus of the analysis presented in this paper is on the effectsthat the organisation of health care might have on the process of allocating re-sources. This article shows how costs and utility can be misrepresented to alterthe perception of the true health possibility frontier and ultimately to shift theallocation of resources away from the purchaser’s objectives.
This consideration has important policy implications: the contract itselfis not a neutral instrument in determining the allocation of resources. Thisimplies that restricting the analysis to the maximands of the purchasers’ utilityfunctions and to priority setting might be misleading. The analysis should infact be extended to study the interactions between contract rules and resourcesallocation.
The article will be organised as follows: in the first part we present the mainactive participants in the resources allocation process and describe how theirbehaviour is going to determine the final outcome. In section two we model theallocation of resources implicit in the literature to show that this is just one ofthe possible equilibria; in section three we show how the provider can influenceresources allocation by misrepresenting its cost and utility function; section fourpresents a numerical simulation and finally section five concludes the paper.
2

2 The allocation process in the internal market
In a public health care system, the allocation process is the end result of theinteractive behaviour of different players with competing objectives. Hospitalcare accounts for about 50% of total health care and in this respect it representsby far and large the most important type of expenditure. Public health caresystems often envisage the provision of hospital care through some form of quasimarkets, where public agencies act as the sole purchasers on behalf of consumersin their area of jurisdiction. In this way a more competitive environment iscreated in which costs are minimized and quality enhanced.
Median voter/General public
Collectivedecisionmaker
P
U
R
C
H
A
S
E
R
P
R
O
V
I
D
E
R
MedicalStaff
Management
Pressure Groupslobbies
Industry
Figure 1: The actors in the allocation process
In health care there is an important dichotomy between individual and totaldemand for health care. While the first is the result of an agency relationshipbetween the patient and his doctor, the second process which determines theallocation of resources among competing treatments is delegated to a collectivebody usually defined as the purchaser. Our analysis focuses on the relationshipbetween the purchaser and the provider, but in order to understand the mech-anisms leading to preferences and budget formation, it is important to describethe entire allocation process.
3

The left side of figure one represents total demand formation which meanssetting the budget for health care and its allocation to hospital care and thento competing treatments.
The budget is usually set by a collective decision-maker that acts either inthe best interest of the whole community (a benevolent planner as in [8]) andmaximises a social welfare function or a re-election oriented body in which caseit will maximise the utility of the median voter [6].
The shape of the preferences can be altered by the action of patient pressuregroups whose objective is to maximise the health gain of a specific group. Inthis battle they can receive financial support from industries and information ontreatments and their effectiveness from medical pressure groups. To simplify theanalysis, it will be assumed that the purchaser is a perfect agent of the collectivedecision-maker so that its preferences are equal to those of the general public(median voter). The behaviour of the purchaser can then be represented bythe maximisation of a function of the health gains of each patient’s group andwhose shape has long been debated in the theoretical literature [16, 17, 12].
The supply side of the internal market is represented by the hospital, theprovider, whose behaviour depends on the combined effect of the maximisationof the objectives of the management and the medical staff.
The hospital managers have a series of objectives ranging from output max-imisation to surplus/slack maximisation. In this model they are merely playingthe role of contracting with the purchaser and of getting their medical staff to dothe work they have contracted for. Doctors are assumed to be devoted workers,i.e. they take care of their work and of what they produce [3, 4, 5].
This assumption can be justified on several grounds: in the agency relation-ship with his patient, the doctor is a benevolent agent that truly believes thatbetter health outcomes for patients can be reached through some types of treat-ment. Alternatively, we might assume that the medical staff are motivated byselfish interests and might be biased towards the implementation of new tech-nologies whose adoption might quicken their career and enhance their personalreputation.
The extra effort deriving from the devoted aspect of the medical staff cannotbe observed or verified by the other actors. This means that physicians are notpaid for their unverifiable effort, but they can use this variable strategically tochange the outcome of the resources allocation process.
Industries are of course interested in playing a role in resources allocationbecause this process determines their profits. Pharmaceutical industries try topromote the care of patients for which drugs are more important than othermedical/surgical procedures; the producers of new technologies try to inducephysicians to opt for an early adoption despite the higher costs 1. In doing this,they can help out and finance pressure groups campaigning for increased budgetsto their target patients or can subsidise the cost of the hospital in specific sectorsby using discounts and rebates on meeting specific volume requirements or by
1See [11]
4

added value clauses in the contract.2 In our model we focus on the supply sideof health care and show how it can actively influence the resource allocationprocess.
3 The model
Internal markets have been created for publicly provided health care in an at-tempt to enhance competition among providers. The idea is that by establish-ing public agencies to act as the sole purchasers on behalf of consumers in theirarea of jurisdiction, the asymmetry of information can be moderated and a morecompetitive environment created in which costs will be minimized and qualityenhanced3. In this paper, given the focus on resources allocation we take thepayment scheme as a given and assume that the contract provides for a PPSscheme. The literature has pointed out the problems relating to this scheme asregards cost and quality matters [1, 9], but in order to concentrate on asymme-try of information on cost and effort verifiability, in the model presented herewe abstract from any risk-sharing considerations, i.e. we assume that the costof treating a patient does not depend on the state of nature (the severity of thepatient).
The environmentTo describe the allocation process, we assume that society can be divided intos groups of individuals with different health needs, each of them having size ni.Their health needs are assessed outside the model and no party in the allocationprocess can influence the size ni of the reference population. Health improve-ments depend on the effectiveness of the treatment received; each treatment isappropriate and allows the receiver to get a health gain equal to hi, indepen-dently of any specific characteristics of the patient4. The total health gain foreach group will then be equal to:
(H1 −H0)xi = hixi (1)
where H1 and H0 is the health status before and after the treatment, xi is thenumber of treatments for group ni (with xi < ni) and hi is the health gain. Thecost incurred by the hospital to produce health care can be written as:
Cj = kj − ej − βj(xj) (2)
where kj is a fixed cost, ej is the effort of the medical staff and βj(xj) is afunction that captures reduction in costs due to several factors such as special
2By added value we mean the supply of goods and services, free of charge, that should beused in combination with the product sold, for example the appliance that is necessary to usebotulin.
3The theoretical literature casts some doubts on the effectiveness of internal markets inpromoting competition. [10, 9, 2] especially when a prospective payment system is used.
4An alternative way of interpreting this assumption is to assume that hi is the expectedhealth gain from treatment that depends on some characteristics of the patient that cannotbe predicted by any of the actors in the allocation process.
5

contracts with the supplier of drugs and medical devices which provides quantitydiscounts. This element is assumed to be private information to the hospitalmanagement. For each treatment j, the cost of taking care of a patient of typei is equal to kj − βj(xj), but it can be lowered through the effort ei whichproduces a disutility linear in the patients treated, but increasing in the effort.We assume that
f(e, x) = nf(e) nfe(e) > 0; nfee(e) > 0; (3)
Given that utility is linear in the number of patients, the purchaser can set thecontract for each single treatment and it can then replicate it for all the patientsthat will be treated.
The providerBelow we identify the objectives pursued by the provider with the utility func-tion of the medical staff. The provider participates in the production processonly if the reward received, net of the production cost, produces a positive util-ity. It is interesting to note that the medical staff are devoted workers, i.e.they receive utility from the outcome of their effort. For this reason, the utilityfunction of the provider for each treatment offered can be written as:
U(pj + αjej − Cj − f(ej)) (4)
where pi is the reimbursement scheduled. The devoted quality of the effortof the medical staff is private information to the hospital, i.e. αj cannot beobserved by the purchaser. The literature often assumes that the utility of thedevoted worker depends on the outcome of his effort; in this analysis we havepreferred to assume that the physician receives utility directly from the efforthe makes. This assumption relies on the observation that the medical staff careabout his patients and receives an further reward from their effort if the patientgets well. We think that this formulation is the most suitable to capture theidea that the physician care about the outcome of their work5
pj + αjej − Cj − f(ej) (5)
The purchaser
In the internal market for health care, the purchaser acts as the agent of thecitizens and buys services on their behalf.
The purchaser’s behaviour can then be represented by the maximisation ofa function defined over the health gains of each patient’s group. The literaturehas long discussed the shape of this function, the rationality of having differentweights on different people, and the arguments of the utility function, i.e. if oneshould consider health gains for each group or perhaps health after treatment.
5The formulation of the cost function in eq (2) can in any case be interpreted in terms ofdevoted worker in a more traditional way. βj(xj) can in fact be interpreted as a lower costthat derives from the devoted characteristic of the medical staff.
6

Given that in this article the main focus is on the factors other than the pref-erences of the provider that might drive the allocation process, we assume thatthe provider maximises a well-behaved, concave and twice differentiable utilityfunction:
V (xjhj) (6)
subject to the fixed budget constraint B that the central decision-maker hasassigned to the purchaser. This function can be separated into the differentarguments or not, depending on the objectives of the purchaser.
3.1 The resources allocation process: the traditional frame-
work
A benchmark model reproducing the traditional framework to resources alloca-tion will now be presented. The medical staff are assumed to have no preferencesover the case mix, i.e. their utility function is maximised over the reward theyreceive and the disutility of their effort. The timing of the model can be repre-sented as follows:
P observes utility of H P sets the contract H accepts
The purchaser observes the utility of the provider and sets the contract accord-ingly; given its predominant position, it can act as a Stackelberg leader. Withthis information, it will then maximise its utility over competing treatments.Togive a picture of the problem we can reduce the number of competing treatmentsto two so that the optimal allocation problem can be written as:
Maxej ,xi,pj V (x1h1;x2h2)
s.t.
Cj = kj − ej j = 1, 2
pj − Cj − fj(ej) ≥ 0 j = 1, 2
2∑
j=1
pixi = B
The F.O.C for the problem can be written as:
f ′j(ej) = 1 j = 1, 2
pj = Cj + f(ej) j = 1, 2∂V∂x1
∂V∂x2
h1
h2
=p1
p2
2∑
j=1
pixi = B
7

Therefore, the effort e∗j is determined by the first equation f ′j(ej) = 1 whichpermits definition of the price p∗j = kj − e∗j + fj(e
∗
j ). Finally, the last twoequations determine the allocation process followed by the purchaser and canbe written as:
x∗1 = d1(B, p∗1, p∗
2, h1, h2) (7)
x∗2 = d2(B, p∗1, p∗
2, h1, h2)
The set of equations (7) represents the optimal number of people that are goingto be treated for each treatment given the preferences of the provider and theprices for both treatments. They can however be interpreted as the functionalrepresentation of the purchaser’s decision-making procecss. The first derivativeswith respect to the parameters of the demand function can be interpreted asthe purchaser’s reaction function to a change in the environment. The problemcan be represented in a diagram as follows: The Edgeworth box in Figure 2
x2
x1
U1
U2
U2=0
U1=0
*2x
*1x
Figure 2: Edgeworth box for purchaser and provider
allows us to represent the purchaser and the provider’s objective at the sametime. Let’s examine the problem from the purchaser’s point of view. Its utilityfunction is increasing NE and it is represented by the indifference curve HH.In maximising its utility it has to comply with its budget constraint BB whoseslope and position is determined by the behaviour of the provider. The latterreceives utility from both treatments, but being a follower in this game canonly impose on the purchaser a reservation utility which has been assumed tobe separate (it must apply to both simultaneously) for both services produced.The reservation utility is represented in the diagram by the lines U1 = 0 and
8

U2 = 0. These lines define the prices (hence their ratio) and allow us to drawthe budget constraint for the purchaser which can then maximise its utility bychoosing the point where the indifference curve is tangent to the budget line.
3.2 The true allocation framework: devoted physicians
If the purchaser could truly observe the utility and the cost faced by the provider,the allocation process just presented would reflect the preferences of the former.This is the reason why the literature on the allocation of resources has focusedon the purchaser’s objective and huge effort has been devoted by the normativeliterature to finding an optimal trade-off between efficiency (defined in terms ofhealth produced or restored by the treatment offered) and an equity (defined interms of access to health care). From a positive point of view, some authors havelong observed that the final allocation of resources depends on several elements,some of which might be even more important than equity and efficiency and themost recent literature seems to advocate the use of a more integrated approachto resources allocation [15].
So far, however, very few authors have modelled this problem, especiallythe effects on the allocation of resources of the providers’ objectives. In ourapproach we have identified the provider with the medical staff. We assume thatthey are devoted workers, i.e. they take pride in their work and receive a positiveutility from what they produce. The additional effort deriving from motivationcannot be verified, but it has important consequences on the production of thatspecific good and on the incentive structure of the employment contract [3, 4, 5].Given the above assumption, the utility function of the hospital for each unitof treatment j will be written as:
pj + αjej − Cj − f(ej) (8)
If the provider reveals his devoted worker characteristic, the reservation pricefor producing the two treatments will be reduced and if the physician has pref-erences over treatments (α1 6= α2) the price ratio will change, i.e. being devotedhas a price and income substitution effect on the allocation of resources. Thefinal effect depends on the intensity of the devoted characteristic αj and onthe shape of the functional form for the provider as will be shown in this sec-tion. The information on the exact value of αj is private information to thepurchaser which will then reveal to the purchaser the level that maximises itsutility function. The timing of the problem can be written as:
H reveals reservation utility P sets the contract H accepts
Given that the provider has full information, the problem can be solved bybackward induction, i.e. the medical staff sets α∗
j so as to maximise its totalutility. Since the objective relation f ′j(ej) = 1 + α∗
j has to be satisfied, setting
9

α∗
j is equivalent to setting the effort ej , which naturally affects both the pricep∗j and the demanded bundle. Obviously it must be α∗
j ∈ [0, αj ] for any j and
correspondingly we will get ej ∈ [emj , eMj ] with f ′j(emj ) = 1 and f ′j(e
Mj ) = 1+α∗
j .With this in mind, we study the following optimization problem in the effort:
Maxe1,e2∈E
2∑
j=1
x∗j (p∗
j + αjej − Cj − f(ej))
s.t
Cj = kj − ej j = 1, 2
p∗j = kj − (1 + α∗
j )ej + f(ej) j = 1, 2
f(ej) = 1 + α∗
j j = 1, 2
x∗1 = d1(B, p∗1, p∗
2, h1, h2)
x∗2 = d2(B, p∗1, p∗
2, h1, h2),
where E is the set {(e1, e2) : ei ∈ [emj , eMj ]}. Let’s call U(e1, e2) the objectivefunction. Then
U(e1, e2) = x∗1(1 + α1 − f ′1(e1))e1 + x∗2(1 + α2 − f ′2(e2))e2
=: x∗1g1(e1) + x∗2g2(e2).
Since U(em1 , em2 ) > 0 while U(eM1 , eM2 ) = 0, a sufficient condition for the medicalstaff to have interest in (partially) revealing the devoted quality of their workis the existence of a feasible direction v = (v1, v2) in which U is increasing, i.e.
(
∇U · v)
ej=emj> 0, for some v1, v2 ≥ 0. (9)
Of course this expression depends on various factors, such as the shape of thedemand function and the disutility of the effort, but essentially it is satisfiedwhen the parameters αj are not too small. The economic interpretation behindthis condition is quite straightforward. If the medical staff do not reveal theirbeing devoted, they receive a total positive utility which is equal to x∗jαje
mj .
If they partially declare their utility in treating patients, they will receive thefollowing utility xj(αj−α∗
j )ej . The term in brackets is clearly decreasing in α∗
j ,but the other two increase because of the revelation of the devoted characteristic:the effort through f ′j(ej) = 1 + α∗
j and the quantity xj because of an incomeeffect (produced by the reduction in the price) and a price effect (the price ratiomight change as a result of an asymmetric declaration of α∗
j ).Once this necessary condition is checked, we can look for a maximum in
the interior of E by writing down the F.O.C. of the problem. We obtain thefollowing system of equations:
∂d1
∂p∗1
dp∗1de1
g1(e1) + x∗1dg1
de1
+∂d2
∂p∗1
dp∗1de1
g2(e2) = 0
∂d2
∂p∗2
dp∗2de2
g2(e2) + x∗2dg2
de2
+∂d1
∂p∗2
dp∗2de2
g1(e1) = 0.
(10)
10

The equations above can be rewritten in terms of elasticities. Let εi(dj) be theelasticity of the demand of good j with respect to the i-th price, ε(p∗j ) and ε(gj)be the elasticities with respect to the effort ej of p∗j and gj respectively. Thensystem (10) becomes
x∗1 g1
(
ε1(d1) +ε(g1)
ε(p∗1)
)
+ x∗2 g2 ε1(d2) = 0
x∗2 g2
(
ε2(d2) +ε(g2)
ε(p∗2)
)
+ x∗1 g1 ε2(d1) = 0.
(11)
Moreover, recalling the following elasticity identities
εj(dj) = −1− εj(di)p∗i x
∗
i
p∗jx∗
j
, i, j = 1, 2 i 6= j
The optimal solution can be derived by solving the following system for ej .
x∗1 g1
(
ε(g1)
ε(p∗1)− 1
)
+∂d2
∂p∗1
[g2p∗
1 − g1p∗
2] = 0
x∗2 g2
(
ε(g2)
ε(p∗2)− 1
)
+∂d1
∂p∗2
[g1p∗
2 − g2p∗
1] = 0.
(12)
This result shows that the devoted characteristic of the physician has a veryimportant impact on the allocation of resources that goes completely undetectedby the system. The first interesting result is that if the medical staff are devoted,the purchaser will never be able to pay a reward simply equal to their reservationutility. As in any model with private information, also in this case the agentcommands a rent deriving from the variable he can privately observe.
The final effect of the allocation of the budget among competing treat ments(Bi) depends on the relative preferences of the physician for the two treatmentsand on the shape of the utility function of the provider. This relationship hasa power effect: the more the two treatments are substitutes in terms of healthgain, the more budget can be shifted by the provider.
The effect on the revelation of α∗
j is not clear-cut since in general there aredifferent incentives working in several directions. In general it can be shownthat the value for α∗
j depends on:
• how devoted the medical staff are, which is measured by αj ;
• the relative degree of the devoted aspect implied by their work whichdepends on α1/α2;
• the utility function of the provider, namely whether it is separable in thetreatments;
• the initial price ratio p∗1/p∗
2 which determines the budget share.
11

The first effect is quite straightforward and does not need any further ex-planation. The relationship between αj and α∗
j is monotonically increasing andwhile its shape might depend on the utility function of the provider, its firstderivative is always positive. The type of utility function might influence theactual level of α∗
j because in this case there are two different forces at work.If the utility is separable, the only incentive to revealing the devoted aspectderives from the motivation to increase access to health care; if the function isnot separable the provider influences the allocation process.
If the function is not separable, the provider should also take account of theratio α1/α2 because an increase in one of the two parameters can cause, throughthe reduction in the budget, a decrease in the total utility enjoyed by treatingpatients affected by the other condition.
For a better understanding of the problem, let’s analyse two cases in detail.For the first, assume that the utility function is separable in the two goodsand the cross price elasticities are equal to zero. Here the maximisation can becarried out separately in each treatment. In this case condition (9) becomes
(
∂U
∂ej
)
ej=emj
> 0, j = 1, 2, (13)
which is satisfied if
αj >[ dj f
′′
j (ej) ]ej=emj[
−∂dj∂p∗j
f ′′j (ej) + dj]
ej=emj
. (14)
Whenever this is true, an optimal couple (e1, e2) exists for the given optimizationproblem, which from (12) is a solution of
ε(gj) = ε(p∗j ), j = 1, 2. (15)
From (3) both gj and p∗j are concave, therefore this solution is unique. Theoptimal revealed qualities α∗
1, α∗
2 are then obtained by inverting the relationα∗
j + 1 = f ′j(ej).Another interesting case is when the devoted quality of the staff work can
be applied to just one treatment, say the first, while α2 = 0. Then g2 = 0 andU depends on e1. Again (9) is written as above and from (11) the optimumsatisfies
ε1(d1) +ε(g1)
ε(p∗1)= 0. (16)
A simple calculation of the derivative of the elasticities ratio ε(g1)/ε(p∗
1) showsthat this function is increasing in α∗
1. Suppose that the elasticity ε1(d1) isgreater than −1, as for example when V is a CES utility function. Then, otherparameters being equal, the optimal α∗
1 will be less than the optimum for theseparable case, which verifies (15).
If the own price elasticity is less than -1, we can then conclude that if theutility of the purchaser is separable in x1 and x2, the provider has a greater
12

incentive in revealing its being devoted. This result, which might seem counter-intuitive at first sight, depends on two factors: a moderate own price effect andan income effect which increases the production of x2, but not the utility of theprovider.
3.3 The true allocation framework: quantity discounts
In this section we consider another form of information asymmetry that mightarise from contracts that the industry offers to the hospital in order to createloyalty in the use of its product.
Some of these are legal practices while others, which in general go under thename of added value, are illegal in some countries, especially in the context ofpublic health care systems. If implemented, they reduce the cost of productionof the treatment both directly (through a quantity discount) and indirectly (theindustry supplies for free some sort of medical device that has to be used eitherfor increasing the effectiveness of the product supplied or to improve its generaluse).
We consider here quantity discounts on the use of specific devices (drugs orother medical appliances), either proportional to the quantity used or dependentthemselves on the volume of purchases. This process is somehow different fromthe one presented in the previous section, but it still has very important policyimplications.
The timing of the game can be written as follows:
Ind sets price H reveals res. utility P sets contract H accepts for technology
and the problem can be written as:
Maxβ1,β2
2∑
j=1
x∗j (p∗
j − Cj − f(ej))
s.t.
p∗j = kj − βj + fj(ej)− ej
Cj = kj − β(x∗j )− ej
x∗1p∗
1 + x∗2p∗
2 = B
f ′j(ej) = 1
x∗1 = d1(B, p∗1, p∗
2, h1, h2)
x∗2 = d2(B, p∗1, p∗
2, h1, h2).
The above problem can be solved as a free maximum problem. For the F.O.C.
13

we get the following system of equations
∂d∗i∂pi
[(Ci + fi(ei))− x∗i β′
i(x∗
i )] +∂d∗j∂pi
[(Cj + fj(ej))− x∗j β′
j(x∗
j )] = 0
for i, j = 1, 2, i 6= j. Since the matrix
∂d1
∂p1
∂d2
∂p1
∂d1
∂p2
∂d2
∂p2
is non-singular, the F.O.C. are satisfied if and only if
Ci + fi(ei)− x∗i β′
i(x∗
i ) = 0, i = 1, 2. (17)
Since Ci is a unitary cost, the variable part can be better written as β(xi) =hi(xi)/xi, where hi(xi) is the total quantity discount. Note also that ei doesnot depend on βi and that for βi = 0 we have p∗i (0) = ki + fi(ei) − ei. Then(17) can be written as
p∗i (0) = h′i(x∗
i ), i = 1, 2.
In this context, it is interesting to study the problem with reference to thetype of discount offered. If the rate of the price reduction is independent ofthe number of treatments offered and ultimately of the quantity of the specificdevice bought, h′(xj) is constant and in this case there is no incentive for theprovider to reveal that it is receiving the discount. This result is independentof the shape of the purchaser utility function.
4 Numerical simulations
The results presented in the previous section show that the presence of devotedstaff has a dramatic impact on the resources allocation process. Given thatseveral incentives are working in different directions, to show their separateeffect we now present some numerical simulations.
The utility of the purchaser is represented by the following CES utility:
V = ((h1x1)ρ + (h2x2)
ρ)1
ρ
which presents a different degree of substitution between the two goods accord-ing to the value of ρ ∈ (−∞, 1]. The demand functions are then given by
x1 =B
p1
(p1h2)r
(p1h2)r + (p2h1)rx2 =
B
p2
(p2h1)r
(p1h2)r + (p2h1)r
with r = ρ1−ρ
.
14
As regards the provider, we will assume that the disutilty of the effort canbe written as:
fj(ej) =1
2e2
j ,
therefore p∗j = kj −1
2e2j , ej = 1 + α∗
j , emj = 1 and eM1 = 1 + α1. In order to
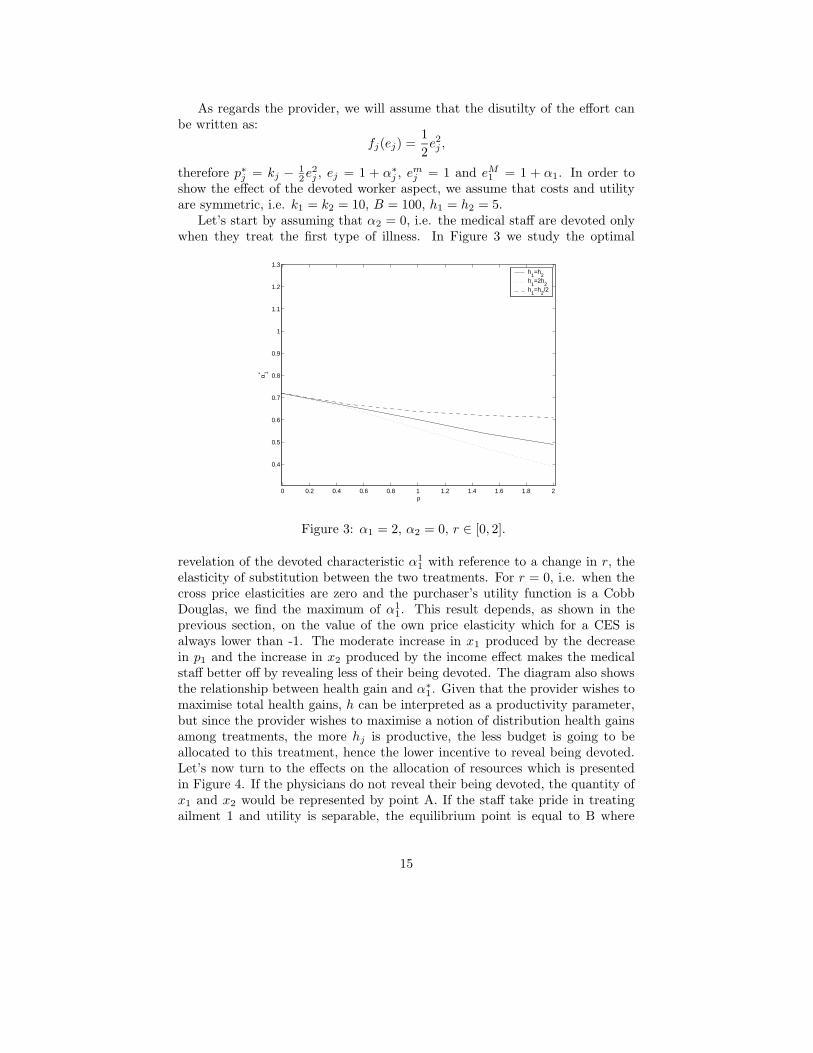
show the effect of the devoted worker aspect, we assume that costs and utilityare symmetric, i.e. k1 = k2 = 10, B = 100, h1 = h2 = 5.
Let’s start by assuming that α2 = 0, i.e. the medical staff are devoted onlywhen they treat the first type of illness. In Figure 3 we study the optimal
0 0.2 0.4 0.6 0.8 1 1.2 1.4 1.6 1.8 2
0.4
0.5
0.6
0.7
0.8
0.9
1
1.1
1.2
1.3
ρ
α 1*
h1=h
2h
1=2h
2h
1=h
2/2
Figure 3: α1 = 2, α2 = 0, r ∈ [0, 2].
revelation of the devoted characteristic α11 with reference to a change in r, the
elasticity of substitution between the two treatments. For r = 0, i.e. when thecross price elasticities are zero and the purchaser’s utility function is a CobbDouglas, we find the maximum of α1
1. This result depends, as shown in theprevious section, on the value of the own price elasticity which for a CES isalways lower than -1. The moderate increase in x1 produced by the decreasein p1 and the increase in x2 produced by the income effect makes the medicalstaff better off by revealing less of their being devoted. The diagram also showsthe relationship between health gain and α∗
1. Given that the provider wishes tomaximise total health gains, h can be interpreted as a productivity parameter,but since the provider wishes to maximise a notion of distribution health gainsamong treatments, the more hj is productive, the less budget is going to beallocated to this treatment, hence the lower incentive to reveal being devoted.Let’s now turn to the effects on the allocation of resources which is presentedin Figure 4. If the physicians do not reveal their being devoted, the quantity ofx1 and x2 would be represented by point A. If the staff take pride in treatingailment 1 and utility is separable, the equilibrium point is equal to B where
15

A
B
Figure 4: α1 = 2, α2 = 0, r ∈ [0, 2].
all the beneficial effect is used to increase the production of x1. However, ifthe function is not separable, the price effect permits an increase also in theproduction of x2, so that there is a spillover effect between the two treatments.
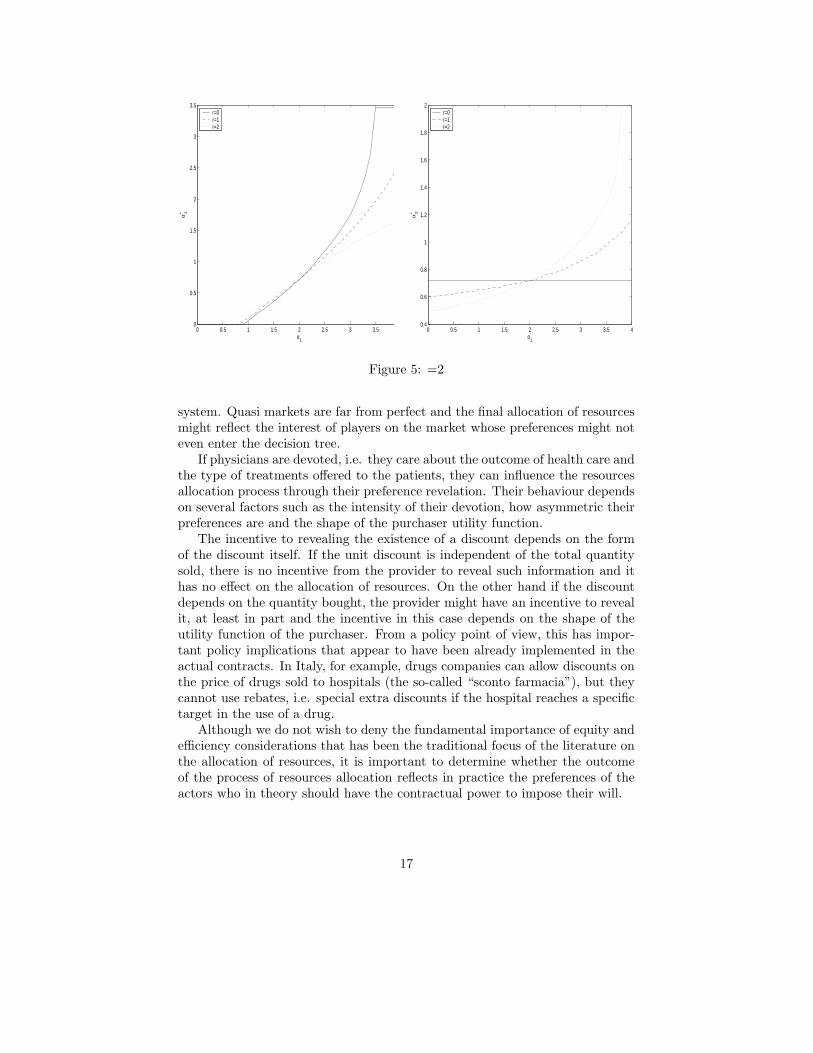
Let’s now examine the case where the staff are devoted for both treatments.In this case, studying the different relationships is even more complicated andthere are several numerical simulations that it would be interesting to present.We have chosen the one we think is most significant for our analysis. In Figure5 we show the relationship between α∗
1 and α∗
2 when α2 is set to 2 and α1
can vary between 0 and 4. The relationship between the two values is now
clear. The provider is clearly trying to declare anα∗
1
α∗2
as close as possible to 1
to reduce the cross-price effect. The lines, drawn for different levels of r, allcross at α1 = 2, i.e. where the devoted characteristic would be symmetric. Thisis an interesting result per se: if the provider is indifferent between the twotreatments, the revelation of the level of utility that it derives from treatingpatients is independent of the purchaser’s utility.
The effect of h is similar to the one presented in Figure 3 and k has the sameeffect as h, as one might expect.
When the staff are devoted in both treatments, the final effect on the al-location of resources is rather more difficult to predict given that in this caseseveral factors play a determinant role.
5 Conclusions
This article examines the resource allocation process in health care provision andargues that the observed allocation of resources is the result of the maximisationprocedure of different agents, whose behaviour might not be fully detected by the
16
0 0.5 1 1.5 2 2.5 3 3.5 40
0.5
1
1.5
2
2.5
3
3.5
α1
α1*
r=0r=1r=2
0 0.5 1 1.5 2 2.5 3 3.5 40.4
0.6
0.8
1
1.2
1.4
1.6
1.8
2
α1
α2*
r=0r=1r=2
Figure 5: =2
system. Quasi markets are far from perfect and the final allocation of resourcesmight reflect the interest of players on the market whose preferences might noteven enter the decision tree.
If physicians are devoted, i.e. they care about the outcome of health care andthe type of treatments offered to the patients, they can influence the resourcesallocation process through their preference revelation. Their behaviour dependson several factors such as the intensity of their devotion, how asymmetric theirpreferences are and the shape of the purchaser utility function.
The incentive to revealing the existence of a discount depends on the formof the discount itself. If the unit discount is independent of the total quantitysold, there is no incentive from the provider to reveal such information and ithas no effect on the allocation of resources. On the other hand if the discountdepends on the quantity bought, the provider might have an incentive to revealit, at least in part and the incentive in this case depends on the shape of theutility function of the purchaser. From a policy point of view, this has impor-tant policy implications that appear to have been already implemented in theactual contracts. In Italy, for example, drugs companies can allow discounts onthe price of drugs sold to hospitals (the so-called “sconto farmacia”), but theycannot use rebates, i.e. special extra discounts if the hospital reaches a specifictarget in the use of a drug.
Although we do not wish to deny the fundamental importance of equity andefficiency considerations that has been the traditional focus of the literature onthe allocation of resources, it is important to determine whether the outcomeof the process of resources allocation reflects in practice the preferences of theactors who in theory should have the contractual power to impose their will.
17

Aknowledgements
Financial support from PRIN n. 2003130120 004 and the MIUR cofinancedproject “Control, optimization and stability of non-linear systems: geometricaland analytical methods” is gratefully acknowledged.
References
[1] M. Chalkley and J. Malcomson, “Cost sharing in health service provi-sion: an empirical assessment of cost saving,” Journal of Health Economics,vol. 84, pp. 219–249, 2002.
[2] A. Enthoven, “Introducing market forces into health care: a taleof two countries,” presented at the Proc. of the 4th EuropeanConference on Health Economics, Paris, July 2002. [Online]. Available:http://perso.wanadoo.fr/ces/Pages/english/PLS3.pdf
[3] P. Francois, “Public service motivation as an argument for governmentprovision,” Journal of Public Economics, vol. 78, pp. 275–299, 2000.
[4] ——, “Not-for-profit provision of public services,” Economic Journal, vol.113, pp. C53–C61, 2003.
[5] A. Glazer, “Motivating devoted workers,” International Journal of Indus-
trial Economics, vol. 22, pp. 427–440, 2004.
[6] M. Gouveia, “Majority rule and the public provision of a private good,”Public Choice, vol. 1, pp. 1–24, 1997.
[7] H. Gravelle, “Capitation contracts: Access and quality,” Journal of Health
Economics, vol. 18, no. 3, pp. 315–340, 1999.
[8] J. Laffont and J.Tirole, A Theory of Incentives in Procurement and Regu-
lation. Cambridge, MA: The MIT Press, 1993.
[9] R. Levaggi. (2004) Hospital health care: Cost reimbursement and qualitycontrol in a spatial model with asymmetry of information. SSRN WorkingPaper. [Online]. Available: http://ssrn.com/abstract=538822
[10] ——. (2004) Internal markets for hospital care: cost and quality controlin a spatial competition model. SSRN Working Paper. [Online]. Available:http://ssrn.com/abstract=539362
[11] R. Levaggi and M. M. (2004) Investment in hospital care technology underdifferent purchasing rules: A real option approach. FEEM Working Papern. 75.04. [Online]. Available: http://ssrn.com/abstract=536002
[12] J. Macinko and B. Starfield, “Annotated bibiliography on equity in health,”International Journal on Equity in Health, vol. I, pp. 1–20, 2002. [Online].Available: http://www.equityhealthj.com/content/pdf/1475-9276-1-1.pdf
18

[13] T. McGuire, Physician Agency. Elsevier Science, 2000, vol. 1, ch. 9, pp.461–536.
[14] A. Scott, The Economics of General Practice. Amsterdam: Elsevier Sci-ence, 2000, vol. 1B, ch. 22, pp. 1175–1200.
[15] L. Terry, “An integrated approach to resource allocation,” Health-care
Analysis, vol. 17, no. 2, pp. 171–80, 2004.
[16] A. Wagstaff, “Qalys and the equity-efficiency trade off,” Journal of Health
Economics, vol. 10, pp. 21–41, 1991.
[17] A. Williams and P. Kind, “The present state of play abouti qualys,” inMeasures of the quality of life, A. Hopkins, Ed. London: Royal College ofPhysicians, 1992, pp. 21–34.
19