
STAR: A Transformative Learning Framework for Nurse Educators
18
http://jtd.sagepub.com/ Education Journal of Transformative http://jtd.sagepub.com/content/9/1/42 The online version of this article can be found at: DOI: 10.1177/1541344611426010 2012 2011 9: 42 originally published online 5 January Journal of Transformative Education Margaret McAllister STAR : A Transformative Learning Framework for Nurse Educators Published by: http://www.sagepublications.com can be found at: Journal of Transformative Education Additional services and information for http://jtd.sagepub.com/cgi/alerts Email Alerts: http://jtd.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://jtd.sagepub.com/content/9/1/42.refs.html Citations: What is This? - Jan 5, 2012 OnlineFirst Version of Record - Mar 23, 2012 Version of Record >> at Univ of the Sunshine Coast on July 16, 2012 jtd.sagepub.com Downloaded from
Transcript of STAR: A Transformative Learning Framework for Nurse Educators
http://jtd.sagepub.com/Education
Journal of Transformative
http://jtd.sagepub.com/content/9/1/42The online version of this article can be found at:
DOI: 10.1177/1541344611426010
2012 2011 9: 42 originally published online 5 JanuaryJournal of Transformative Education
Margaret McAllisterSTAR : A Transformative Learning Framework for Nurse Educators
Published by:
http://www.sagepublications.com
can be found at:Journal of Transformative EducationAdditional services and information for
http://jtd.sagepub.com/cgi/alertsEmail Alerts:
http://jtd.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://jtd.sagepub.com/content/9/1/42.refs.htmlCitations:
What is This?
- Jan 5, 2012OnlineFirst Version of Record
- Mar 23, 2012Version of Record >>
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
STAR: A TransformativeLearning Frameworkfor Nurse Educators
Margaret McAllister1
AbstractContemporary nursing education in Australia needs to respond to the imperatives
facing clinical practice (A* that nurses be work-ready, resilient, multi-skilled, good
team communicators, compassionate and responsive to the diverse needs of clients
and families. Transformative learning principles combined with effective, action-
based learning experiences can provide a focused pedagogical basis for cultivating
and achieving these graduate outcomes. In this paper, a novel framework is pre-
sented that provides a structure to support educators and curriculum development.
The STAR framework, which stands for Sensitivity, Taking action and reflection,
is easily remembered and embodies key aspects of transformative learning.
Keywordscritical reflection, transformative education, transformative learning
Introduction
Australia, like the rest of the world, has been experiencing a severe shortage of
registered nurses for over three decades (Australian Institute of Health and Welfare
[AIHW], 2010). While this is a multifaceted problem, there has been recent
1 School of Health & Sport Sciences, University of the Sunshine Coast, Maroochydore DC, Queensland,
Australia
Corresponding Author:
Margaret McAllister, School of Health & Sport Sciences, University of the Sunshine Coast, Locked Bag 4,
Maroochydore DC, Queensland 4558, Australia
Email: [email protected]
Journal of Transformative Education9(1) 42-58
ª The Author(s) 2011Reprints and permission:
sagepub.com/journalsPermissions.navDOI: 10.1177/1541344611426010
http://jted.sagepub.com
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
acknowledgment that the crisis has deepened to include a shortage of nurse educators
(Benner, Sutphen, Leonard, & Day, 2009). Many are reaching retirement age and the
numbers of qualified educators replacing them are inadequate (Sayers & DiGiacomo,
2010). There has tended to be an overreliance on part-time educators, usually clinical
experts, who have had little preparation for an education role (Halcombe, Andrews,
Peters, Salamonson, & Jackson, 2009).
At the same time as developments within health care and the consumer movement
have added complexity to the nursing role, the challenges for nurse educators have
also increased.
There is a regulatory- and industry-driven imperative to equip nursing graduates
with specialized techniques needed in a highly complex technological health care
environment; and also interpersonal effectiveness so that they can work in and lead
teams, problem-solve ethical dilemmas, and communicate respectfully with clients
and families (Morison, Johnstone, & Stevenson, 2010).
There is also awareness that nursing education needs to play a more active role in
resolving the widening health inequities, particularly within vulnerable populations
such as those who are ageing, who have mental health problems, or who are living
with enduring and multiple health conditions (De Chesnay, 2007). Furthermore, edu-
cators are teaching to a more diverse student body and larger class sizes because of the
widened access to university education (Potempa, Redman, & Landstrom, 2009).
Thus, nursing educators need to alter the curriculum to prepare graduates for this
more complex health environment and yet not overwhelm students with content
knowledge and swiftly engage, captivate, and inspire nursing students to commit
themselves to a challenging and changing health career. For all of these reasons, the
principles of transformative learning resonate soundly for nurse educators.
Originally coined by Mezirow (2000), transformative learning can be defined as
the process by which we call into question our taken-for-granted frames of reference,
or habits of mind, to make them more inclusive, open, and reflective so that they may
generate beliefs to guide action (Taylor, 2009). In nursing education, these habits of
mind may include technorationalist discourse, teaching as transmission, and learning
to understand. Transformative learning theory helps to problematize such habits of
mind and stimulates awareness of other ways of knowing.
Over time, transformative learning theory has been developed and applied by
many educationalists, with different implications for instructional design and facil-
itation (Brookfield, 2000; Cranton, 2006; Dirkx, 2001). This article will primarily be
working from the perspective that Mezirow elaborates, particularly in relation to his
notion of critical reflection.
The Learning and Teaching Context
At the University of the Sunshine Coast in Queensland, Australia, a 3-year under-
graduate nursing program produces approximately 200 entry-to-practice nursing
graduates annually. Over 40% of these students are mature-aged and others are
McAllister 43
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

recent high school leavers. Approximately 90% are female. This program, like most
others offered across the country, relies on input from a range of nurse educators.
Some are experienced, educationally qualified academics, but the majority are
clinical experts who lack educational preparation and who also tend to lack an
explicit pedagogy to drive their practice (McAllister, Mosel Williams, Gamble,
Malko-Nyhan, & Jones, 2011). It was within this context that a teacher-oriented tool
encapsulating transformative learning principles, and termed the sensitizing, taking
action, and promoting reflection (STAR) framework, was developed. The frame-
work’s aim is to provide a useful tool for developing curriculum experiences that inte-
grate the principles of transformative learning.
It was developed because the theory of transformative learning, while arguably
well fitting for nursing and health programs, is unfamiliar to many educators
working within health, and important concepts may be difficult to remember. When
educators have difficulty with new concepts, they tend to revert to that which is
familiar, such as the ‘‘chalk-and-talk’’ method, didactic lectures, and the like (Iron-
side, 2004). Therefore, the STAR framework aims to be a simple, easily memorized
framework that assists educators to apply the principles of transformative learning.
It brought together a number of concepts discussed in transformative learning and
relevant to empowered action in nursing and health care.
Transformative Learning for Nursing Students
A meta-review of educational research articles found transformative learning to be
the most researched and discussed topic in the field of adult education (Taylor,
2007). Despite wide variations in approaches, this theoretical perspective on adult
learning usually emphasizes a process of (a) awakening or sensitizing students to
issues of social justice and impressing upon them their role in making a difference;
(b) engaging students with innovative, action-based, powerful learning modes that
develop critical, creative, and constructive cognitive skills; and (c) reflection to
make meaning of the learning experience and to revise and replace unhelpful habits
of mind (Cranton, 2006).
The value of transformative learning for nursing students lies in its ability to
awaken them to issues of injustice that lead to and sustain health inequities and to pro-
mote in them critical thinking and questioning of previously held assumptions,
beliefs, values, and perspectives, so that they may be part of systemic change. Exam-
ples include exploring the health and well-being of vulnerable populations, people
who experience marginalization, and those who are not well served by the health ser-
vices. Transformative learning experiences fit well with the pursuits of nurses because
both entail applied humanism; the use of liberal educational strategies such as narra-
tive, poetry, metaphors, film, and literature can evoke imagination, empathy, and care
(O’Sullivan & Morrell, 2002). These qualities are vital for the contemporary nurse.
The concept of taking action, as it is explained by Mezirow (2000), also
offers important insights for health and nursing educators. Nursing is inherently
44 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
action-based. Indeed, the noun and title itself draw on the verbs ‘‘to nurse’’ and ‘‘to
be nursed.’’ Without a theoretical lens to help identify when, and what kind of,
action is needed in client care, students may be tempted to ‘‘nurse’’ a client, regard-
less of need and without attention to the facilitation of empowered action.
According to Mezirow (2000), it is not all action that precipitates transformative
learning, only that action that evokes disorienting dilemmas among the learners.
Establishing an environment of reflective discourse is therefore vital to the educa-
tor–student relationship in nursing so that the students are encouraged to reflect
on what actions, if any, are needed and who should be the change agent. A simple
example is the student working with a new mother who is tentative about bathing
her baby. It could be that the mother simply requires from the nurse supportive
words. Alternatively, it may be that hidden within this situation is a deeper dilemma
that reflective dialogue may help to uncover—that health workers who take control
may be encouraging dependence and miss opportunities to foster parental self-
efficacy. By encouraging hesitation, contemplation, and questioning the very idea
of action in nursing, learners may be able to move beyond understanding toward the
achievement of new insights that facilitate empowered action—be that within them-
selves, colleagues, clients, or communities.
In Mezirow’s (2000) view, individuals and groups experience disorienting dilem-
mas that can become a trigger for deep learning. Thus, it is not the objective for edu-
cators to protect students from these dilemmas but rather to assist them to reflect on
them and arrive at new understandings to better equip them for future practice and
for the advancement of the profession. For example, one dilemma frequently expe-
rienced by students is that nursing was once the main profession that laid claim to the
central place of care (Watson, 1979), but there are now many professions who incor-
porate caring theory into their practice (Gilligan, 1982; Noddings, 2003). Students
often experience a disconcerting threat to a once firm social role. Experiencing this
dilemma for the first time may challenge students’ identity within the health care
team (Bandali, Parker, Mummery, & Preece, 2008), but it may also lead to new
insights about shared care and collaboration and the importance of continuing to
develop nursing’s role.
Another dilemma students may experience once they have mastered the suite of
technical procedures needed for health care monitoring and treatment is to notice
that technical rationalism has its value but also its limitations (Dirkx, 2001),
especially when procedures are not sufficient to help clients and families accept and
integrate their health problem into their lives (Smythe, 2003). Simply administering
an insulin injection into a newly diagnosed adolescent diabetic who feels anger or
distress about having the disease illustrates this insufficiency. Thus, challenges for
educators are many and include efforts to develop and enact positive professional
identity, interprofessional respect, and competent technical abilities as well as
psychosocial capabilities.
Rather than it be the case that technical know-how is unnecessary, it is more help-
ful to see that technical and communicative knowledge are useful. Thus, educators
McAllister 45
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
can assist students to notice, discuss, and work through dialectical tensions and
the need for both—and thinking, rather than binary thinking (Nelson, Palonsky, &
Carlson, 2007).
Transformative learning also sees that the crowded curriculum is not an inevita-
ble or insurmountable problem but rather a challenge that is powerfully reframed by
considering threshold concepts. As Meyer and Land (2006) explained, there is a ten-
dency among educators to stuff their curriculum with content, and this is an issue
often discussed in the nursing education literature (Diekelmann, 2004; Ironside,
2004). Meyer and Land argue that this additive approach, closely connected to trans-
mission models of learning, ultimately burdens both the educator with the task of
transmitting vast amounts of knowledge bulk and the students with the imperative
to absorb and then reproduce it. By examining threshold concepts in the curriculum,
nurse educators are provided with a strong rationale for including learning
challenges on topics that are particularly troubling or debated in nursing, and where
unlearning, interruption or reenvisioning is required.
The STAR Framework
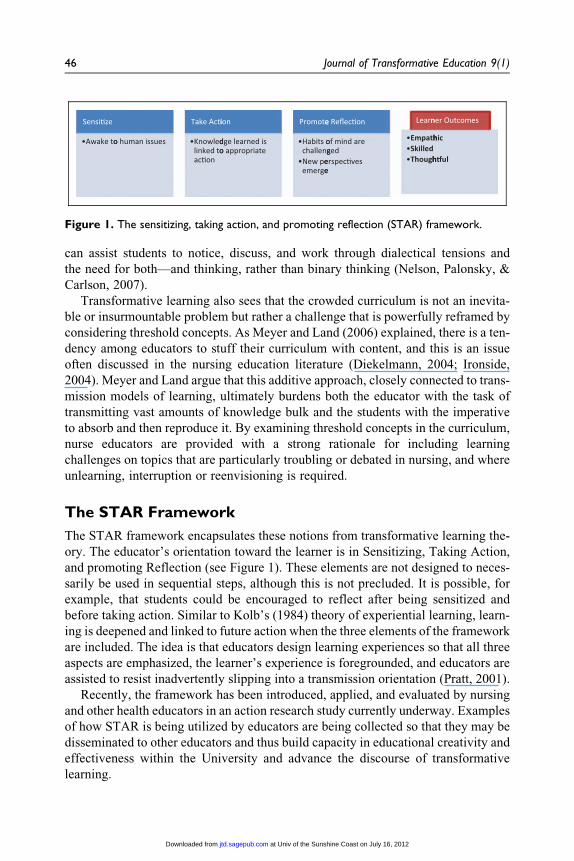
The STAR framework encapsulates these notions from transformative learning the-
ory. The educator’s orientation toward the learner is in Sensitizing, Taking Action,
and promoting Reflection (see Figure 1). These elements are not designed to neces-
sarily be used in sequential steps, although this is not precluded. It is possible, for
example, that students could be encouraged to reflect after being sensitized and
before taking action. Similar to Kolb’s (1984) theory of experiential learning, learn-
ing is deepened and linked to future action when the three elements of the framework
are included. The idea is that educators design learning experiences so that all three
aspects are emphasized, the learner’s experience is foregrounded, and educators are
assisted to resist inadvertently slipping into a transmission orientation (Pratt, 2001).
Recently, the framework has been introduced, applied, and evaluated by nursing
and other health educators in an action research study currently underway. Examples
of how STAR is being utilized by educators are being collected so that they may be
disseminated to other educators and thus build capacity in educational creativity and
effectiveness within the University and advance the discourse of transformative
learning.
Sensi�ze
•Awake too human issues
Take Acti
•Knowledlinked toac�on
ion
dge learned is o appropriate
Promote
•Habits ochalleng
•New peemerge
e Reflec�on
of mind are ged
erspec�ves e
Learn
•Empath•Skilled•Though
ner Outcomes
hic
h�ul
Figure 1. The sensitizing, taking action, and promoting reflection (STAR) framework.
46 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
Sensitizing
The first principle of the STAR framework is the value in sensitizing students to
issues of social import. Unfortunately, many students of nursing are not aware of
important historical, political, and social issues that have shaped and continue
to influence health care, patient participation, and their own professional practice
(Nelson & Gordon, 2004). This leads to fragile self-identity and self-confidence
(Madsen, McAllister, Godden, Greenhill, & Reed, 2009). Frequently, students do
not understand why they are studying particular concepts and are instead eager to
go out to the clinical world to practice (Gallagher, 2004). They are also not suffi-
ciently sensitized to the impact that health inequalities are having on peoples’ lives
and as a result have not been galvanized into committed action (Daiski, 2004;
Farmer, 2004; Reutter, Sword, Stewart, & Rideout, 2004). As a result, there has been
a disappointing lack of progress by nurses in effecting health system change
(Lynam, 2009; Vonfrolio, 2006).
According to the principles of transformative learning, it is these health inequi-
ties, as well as nursing’s lack of progress in addressing them, that ought to become
threshold concepts and be explored in depth. Cousin (2010) explains that educators
have an important role in identifying threshold concepts in disciplines and also in
listening to students’ misunderstandings about these, providing a holding environ-
ment for the toleration of confusion, and expecting that it may involve a number
of takes for such a concept to be learned by students. The STAR framework, with
its appreciation for needing to sensitize learners about issues that they may have
become inured to, or ignorant about, is a succinct explanation of why and how
threshold concepts are necessary to explore within a curriculum.
Nursing students can be made aware of these and other issues and hopefully be
inspired to contribute to change. They also need to appreciate that much of what
nurses do and learn to do operates at an unconscious or tacit level. This awareness
can, in itself, be liberating because it helps them see how the dominant paradigm in
health care—medical science—sets the agenda, creates hegemony, and co-opts
many nurses into unwittingly supporting practices that are ultimately self-
defeating and that constrain change. Freire (1972) and other critical theorists would
term this conscientization.
An engaging way to apply the transformative aim of awakening students to issues
of importance in nursing is the idea of ‘‘sensitizing’’ students to patients’ health care
experiences and nurses’ parts in either exacerbating or ameliorating distress.
The key to sensitization is to engage learners’ senses in listening, observing, feeling,
and touching through using powerful media such as first-person testimonials, film,
music, poetry, and novels (Infinito, 2003). The aim for nursing students is to
appreciate the (a) significance of a learning issue on peoples’ lives and (b) to expe-
rience a disorienting dilemma that challenge habits of mind that tend to be routinely
taken by nurses and by students that would have ordinarily been used to understand
the situation. In this way, the objective is transformation.
McAllister 47
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

Consider this example: The issue of nursing the person experiencing schizophrenia
is raised. Students may be asked to draw upon and reveal their feelings, concerns, and
aspirations about this work. Frequently, this elicits discussion around fear, stigma,
feeling out of one’s depth or concern about exacerbating symptoms in clients. Next,
a 2-min video advertisement, located through YouTube and part of the ‘‘Time to
change’’ U.K. media campaign to end discrimination can be played. One production
is entitled ‘‘Schizophrenic man terrifies kids at party’’—a headline familiar to students,
often used by journalists, and which subtly yet insidiously reinforces the notion that
people with mental illness are terrifying and unsafe. Yet the video goes on to dismantle
this habit of mind, by showing a gentleman entertaining children at a party by ‘‘scaring’’
them with balloons and a game of hide-and-seek (http://www.time-to-change.org.uk/).
Playing the video sensitizes students on the issue of stigma, creates some levity in the
classroom and a freedom to speak about other fears and uncertainties.
In other words, auditory, visual, kinesthetic, or immersion experiences can
sensitize students in novel and powerful ways to significant health and social issues
such as marginalization of minority groups, sexism, the poverty cycle, inertia, fear,
loneliness, disability, and the journey of living with a chronic illness. As Dirkx
(1997) has explained, learning can be transformative when we open our minds to
feeling rather than logically interpreting—what he has termed soulful learning. The
STAR framework, with its emphasis on sensitizing reminds educators of the impor-
tance of taking the time to nurture this soulful learning, and develop in students, not
just dispassionate logic, but an engaged empathic stance, for both will be important
in their work as nurses.
The process of sensitization assists students to make meaning of the learning and
to see its relevance to the nurse’s role and to life. In this way, students can be awa-
kened to issues of social and health inequities and they can be assisted to identify
their role in making a positive difference in professional practice.
Taking Action
Taking action is the second principle in the STAR framework. This relates to the idea
that there is value in educators making space within the learning experience for stu-
dents to take action or put into practice newly learned knowledge or skills. Without
this space, students may simply learn for understanding, achieving accumulation of
knowledge, and this may do little to effect social change. In a transformative class-
room in nursing the aim is to produce clinicians who are committed to take action—
be this in the stance that they take with clients, or with their colleagues, in actions
that they choose not to take, or in new behaviors. Several educational theorists
(Hooks, 1994; Freire, 1972; Brookfield, 2000) have powerfully argued that theoriz-
ing and reflecting can also be radical actions because they lead to social change.
Thus, students in nursing who are assisted to theorize and reflect are also in a sense
taking relevant and radical action that can ultimately change the health care world.
48 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
Similarly, when actions are not linked to knowledge in nursing, they are downright
dangerous. For example, proceeding to take routine blood pressure measurements
when the client has a more important need for pain relief can be harmful, and requires
the nurse to think first, before acting.
In order for new educators in nursing to remember this notion and convey this to
students, STAR emphasizes the importance of ‘‘taking action,’’ but stresses that
action needs to be linked to knowledge and theory and students need time to discuss
and invent new ways of taking action around an issue.
Unfortunately, however, literature and local experiences indicate that nursing edu-
cation continues to emphasize a one-way flow of knowledge, usually emanating from
the active educator (Ironside, 2004), and this leads to at least two deficiencies.
Declarative knowledge, modeled by the all-knowing educator, becomes favored by
students over knowing how and why, which are understandings revealed in context and
in action; and students get very little time to develop praxis, or the practice of ideas.
A simple medical example, illustrating the problem resulting from an imbalance
between knowing that and knowing why, is that teaching nursing students to under-
stand oxygen is pointless if students do not know how, why, and when to safely
administer it. Knowing that oxygen is a gas is not sufficient. Knowing when it is
indicated, and how to give it for different conditions are crucial. For students to
come to appreciate this knowledge linked to action, they need time and space within
the learning experience.
Other situations when knowledge might exist, but not be put into action include
knowing about anatomy and physiology, yet failing to interpret signs of pathology
using clinical reasoning (Tanner, 2006); knowing the value of active listening but
failing to utilize it during client distress (Bowles, Mackintosh, & Torn, 2001); know-
ing that professional behavior entails demonstrating respect yet failing to show this
in multidisciplinary teams (Zwarenstein & Reeves, 2006), and knowing self-care is
an important healthy practice yet failing to utilize it themselves (Jackson, Firtko, &
Edenborough, 2007). Unfortunately, opportunities for students to convert knowl-
edge into action are not always a priority for time-pressured nurse educators. How-
ever, if educators appreciate the need to make space for STAR elements within
lectures, then theory would be discussed in the context for how it will be later linked
to nursing actions.
A powerful strategy to assist students to enact the practice of ideas, or praxis, is to
have them use the think-aloud technique (Offredy, 2002), whenever they are practi-
cing a nursing technique. This can be powerfully modeled by educators explaining
what they are doing as they are doing it and can be emulated, critiqued, revised, and
reconstructed by students during laboratory sessions or clinical placements.
Another strategy that may prompt students to challenge habits of mind and put
into action alternatives is to encourage conscientious objection. For example, after
learning about a health inequity, students could be requested to write a letter to a
political organization explaining why they no longer intend to support an irrational
or damaging policy, highlighting the shift in thinking they have undergone. In this
McAllister 49
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

action, students are revealing the aspects of their thinking that have been trans-
formed and also implementing political action while drawing on research-based
information. In this way, students have been encouraged to notice that inequities
do not need to be accepted and have shown that it is their role to seek to drive sys-
temic change and achieve better health outcomes for all. Such strategies that encour-
age students to take action and put knowledge into use are likely to be far more
engaging than simply listening and absorbing and may trigger the achievement of
transformational objectives.
Reflective Learning
In achieving empowered nursing practice, thinking is bound to action (Freire, 1972).
This is praxis. Therefore, for students to be able to ‘‘Take Action,’’ they need to be
putting into place deep thinking. This comes about through reflective learning. Thus,
the ‘‘TA’’ and the ‘‘R’’ in the STAR framework are inextricably linked. Indeed, the
‘‘R’’ can also be linked to the sensitization phase, for if students are to make sense of
affective learning experiences they need to be reflecting.
However, not all reflection is, or leads to, transformative learning. For example,
students may be asked to recall what happened during a simulation learning experi-
ence and recollect actions, verbal exchanges, and outcomes. But this may not result
in a transformed perspective. On the other hand, activities that provoke meaning
making in students by acting as disorienting dilemmas, and are followed through
with dialogue that produces new ideas, and the possibility for new practices, can
be transformative. This is the critical reflection Mezirow (2000) has discussed.
Critical reflection refers to questioning the integrity of deeply held assumptions
and beliefs that are based on prior experience. Critical reflection may not come natu-
rally to all students (Freshwater, 2002). Indeed for it to be well executed, it may need
to be learned and practiced repeatedly like any new thinking skill. Learning how to
reflect can lead to a transformation in perspective, particularly if students learn to
distinguish reflection that is based on content, processes, and premises (Mezirow,
2000). In content reflection, one reflects on what we perceive or think about the
problem. In process reflection, one reflects on how we problem solve and the stra-
tegies we use. In premise-based reflection, one has an awareness of why we perceive
in this way, and the problem itself is questioned. For example, we may ask, Why is
this problem even important? or Why do you think we created this simulation learn-
ing experience to include paramedics and nurses responding to this home-based
emergency? Why not nurses alone, why not in the hospital emergency department?
Such questions cannot produce certainty in answers and may act as a disorienting
dilemma—to carry on learning in single-disciplinary ways may build up nursing
knowledge but not collaboration skills. Answers from students are likely to be ten-
tative and to yield insights on the benefits of students learning with other health/
emergency workers, and how and why this might work to produce social changes.
50 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

According to the literature and my experience, in nursing education, there is a
tendency for reflection to be delimited to content reflection (Ironside, 2004). Educa-
tors, particularly those who lack confidence, preparation, or explicit pedagogy, may
lack the repertoire of questioning strategies to facilitate critical reflection. Therefore,
dialogue among educators about how to cultivate deeper levels of reflection in nur-
sing students is important. Educators need to claim the space for collegial dialogue
because it is likely to enrich the learning experience for nursing students and propel
reflection into deeper layers.
The STAR framework explains that reflection ought to form part of every learn-
ing experience. Reflection activities are those that challenge students’ habits of
mind, invite a rethink on existing nursing practices, or provide thinking tools that
empower students to be able to resist oppressive work practices and resist becoming
dominating agents themselves in the future. Examples for when and how they can be
used are discussed next.
During After-Action Reviews
In military culture, the mission is not over until the after-action review (AAR)
process is complete because soldiers know that errors cost lives, and uncorrected errors
will cost more lives. AAR is a structured review for analyzing what happened, why it
happened, and how it can be done better. AARs are more commonly termed debriefing
sessions in nursing and routinely follow simulation or clinical learning experiences.
By attributing a new name to what has become a taken-for-granted practice in nur-
sing education, raises the possibility of deconstructing the notion of the ‘‘debrief.’’
Debriefing connotes the removal of something from students, rather than an active
meaning-making process that students and educators engage in. AARs can encour-
age students to transfer the learning acquired to other contexts (Dreifuerst, 2009).
For example, a common learning activity is for students to learn suctioning skills
on a manikin. Following the experience, students may be prompted to reflect on
what they think and feel about doing the suctioning therapy. They may be able to
recall modes of administering suction; and they may have felt clumsy, uncertain,
or afraid of hurting the patient. After reflecting on the self, they may now feel more
able to reflect on how the patient might have felt, what other experiences of having
your basic bodily drives (to breathe, to move, to urinate, etc.) controlled by another.
With prompting, they may reflect that uncertain feelings are generated whenever
they are reminded of being a novice or by being with a seriously ill patient, or by
not having a colleague to provide support. These premise reflections, which can
be difficult to elicit, could be prompted by asking learners: Why do you find yourself
becoming clumsier when there is a lack of support?
In this way, students are assisted to appreciate the limits of their own abilities and to
understand the connection between feelings and actions. These insights can be lifelong
learnings for students. Too often, novices fail to realistically appraise their own abil-
ities, and dangerous mistakes, mistakes that may remain uncorrected, can occur.
McAllister 51
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

A more abstract strategy, known as synectics exercises (Joyce & Weil, 2009), that
can be useful in prompting critical reflection after actions is to provide students with a
metaphorical image, such as a tour guide or a lighthouse keeper, and assist them
through careful questioning to reflect on what happened, could have happened, or
what might happen differently in the future in the clinical situation. Students can be
challenged to find similarities and differences between a nurse’s actions in assisting
a client’s journey of recovery (or illness adaptation) and the actions of a good tour
guide or lighthouse keeper (McAllister, 1995). The power of the use of metaphor is
in making the familiar strange, and the strange familiar and thus in prompting novel
associations between ideas and developing in students constructive thinking abilities.
Throughout the Student’s Journey
Activities that prompt learners to write, either online or in reflective journals, can also
be useful (Boyer, Maher, & Kirkman, 2006). Indeed, the written format potentially
strengthens the reflective experience by creating an actual object of what were previ-
ously ideas of the mind. Writing requires learners to externalize their reflective expe-
rience. Writing also provides a means for sharing with others and helps to consolidate
one’s beliefs. However, journals require caution as they are quite difficult to assess
(Cranton, 2006, p. 147), and one needs to clarify the difference between reflective
learning and mere personal reflections (Bradbury-Jones, Sambrook, & Irvine, 2008).
Learning to be critically reflective is a mature cognitive skill (Merriam, 2004).
Thus, to assist students to understand the difference between personal reflections and
learning, it may be helpful to provide frameworks for students so that they reflect on
nursing issues using a particular lens.
For example, students can be encouraged to analyze their own practice using a
framework such as Tanner’s (2006) clinical reasoning model. Frameworks such as this
may be beneficial because they provide the structure needed to move students beyond
their usual habit of mind and to use a new lens to broaden perspective. Tanner’s frame-
work consists of four consecutive phases in thinking critically about effective clinical
care: noticing, interpreting, responding, and reflecting. Tanner explains that the frame-
work embodies ‘‘thinking-in-action’’ and ‘‘thinking-on-action.’’ She views the frame-
work as a means to promote learning by guiding students to break down the components
of clinical judgment. In this way, thoughts and actions, which would otherwise be impli-
cit, hidden, and not open to review, critique, or revision, are made explicit.
This process of converting the implicit to the explicit is potentially transformative
because disorienting dilemmas may be revealed that prompt a new way of thinking
about the world. For example, students may begin to appreciate that they are noticing
signs (outward manifestation of illness) but not symptoms (the patient’s personal
experiences of illness). They may then appreciate that discussion with clients is nec-
essary to be able to achieve sound clinical reasoning.
Learners are first asked to ‘‘think out loud’’ the cues that they have noticed in
the environment. For example, ‘‘the patient looks pale, her respiratory rate has
52 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
increased, and she has had no medications for 3 hours.’’ The cues can then be sorted
to make an interpretation, such as, ‘‘I think this patient is in pain.’’ The student can
then be encouraged to respond by taking action, such as to discuss with the patient
preferred comfort and pain-relief measures. Finally, students can be reminded to
reflect on the expected effects, and then proceed to take further action; for example,
to evaluate the patient’s response within a specific time period, and to seek further
assistance from the team should the pain not be relieved.
Many other theoretical frameworks can similarly be provided to prompt students’
critical thinking and clinical reasoning. Examples include the CARE framework that
assists nurses to recognize the treatment paradigm and to move beyond it to promote
patient empowerment (McAllister & Walsh, 2003); Kotter’s (1990) change frame-
work that differentiates qualities needed as a leader or a manager; and Kanel’s
(2007) applied behavior change framework, which provides a simple method for
showing clinicians how to first attend to a person’s problem, then to break down
goals into manageable tasks, and finally to facilitate coping during crisis. Each
framework can trigger transformation, if they are used to challenge previous habits
of mind and assist students to appreciate new perspectives on an issue.
Throughout All Educator–Student Dialogical Encounters
The transformative learning literature asserts the importance of creating the possibility
for meaningful dialogue with students (Taylor, 2009). Ideas are generated, shared,
tested, and changed during meaningful dialogue (Hooks, 1994). However, educators
need to be reminded that dialogue is not necessarily debate, and nor is it simply discus-
sion. Dialogue is trustful communication, in which two-way self-disclosure is sup-
ported. Self-knowledge may also be enhanced through gentle challenging, with
mutual consent and on the understanding that suggestions will be validated.
Gentle challenging, also called interruption, is an important part of the transfor-
mative educator’s role (McAllister, Tower, & Walker, 2007). Educators have a
responsibility to take learners to the edge of their knowledge and then to prompt
them to learn something new. In this way, deeply held assumptions and beliefs based
on prior experience are challenged, and critical reflection is achieved. Reaching the
space at the edge of one’s knowledge can be uncomfortable—nobody likes to be in a
position of not knowing something—so educators need to be aware, supportive,
respectful, and encouraging. Challenges can be put to students, such as, Has this
practice always been done like this? What’s the history behind it? Would it always
be the right thing to do? What would be the limits around this practice? Then, stu-
dents need to be given voice. Here, it is important for educators to self-reflect and
consider: Is my voice really needed? Can I make more space for students to speak?
Students also need affirmation that being wrong sometimes is normal, that to occa-
sionally not know something is acceptable, and that changing your mind about what
you believe is permissible. Importantly, students need to understand the expectations
McAllister 53
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

that are placed on nurses. They then have every opportunity to live up to those
expectations and to learn how to meet established professional standards.
When Critiquing Performance of Self or Other
Dialectical critique is another strategy to promote reflection that produces new per-
spectives. Dialectics is a term coined by Hegel (Nicholson, 1950), a German philo-
sopher and was originally used to explain the reality of tensions in all things
coexisting. For example, all people have feminine as well as masculine traits, but
to recognize this, one needs to engage in conscious analysis, such as to ask, ‘‘In what
way am I feminine? In what way am I not feminine? In what way am I masculine? In
what way am I not masculine?’’ These sets of opposing questions offer a way to see
both sides of an issue, to examine the thesis and antithesis. Students are thus aided to
see new complexity in issues. Simple examples to use after a learning experience are
to ask, In what ways was that a successful/helpful intervention? In what ways was it
not? In what ways is this patient making good progress, and where are his obstacles?
What were my strengths in that intervention? Where have I room for further
improvement? Deliberately looking for the antithesis is one way of revealing hidden
or unconscious aspects of the self and others (Dirkx, 2001) and may yield a deeper
understanding and appreciation for complexity.
When Leaving the Clinical Field
Commonly in nursing, memorable experiences occur for students during clinical
placement. It is here where students encounter real people experiencing real-life
crises and where nursing work is undertaken in the context of dynamic, busy health
care settings. These experiences have transformative potential when meaning is
made about and with them. Questions posed by the educator to encourage not just
a retelling, but an interpretation of the significance of the events help to achieve
transformative learning. Asking students to share what, how, and why events hap-
pened may be good discussion triggers. But questions that prompt premise reflec-
tions or affective knowing can deepen the learning. Students could be asked to
paint the experience, write a haiku, or choose a symbol that illustrates the lessons
about the nursing role they will take with them from that experience. Then students
can be asked to explain their choices. Importantly, students do not have to directly
experience these events to learn from them. Even by discussing events with each
other during end of day groups, students may share in the experience of transforma-
tion, drawing lessons, and enduring meaning from those events.
Conclusion
The STAR framework summarizes complex concepts such as multiple ways of
knowing, threshold concepts, praxis, and critical reflection. It may be a useful guide
54 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

in prompting educators to apply transformative learning theory. It also may become
a useful tool for curriculum development, helping to influence decisions about
which topics to select within a crowded curriculum, and in what experiences stu-
dents may require longer periods to practice newly learned concepts and skills.
Faculty and industry-based nurses can have meaningful discussions to renew nursing
programs by considering the issues around which students are not sufficiently sen-
sitized, or that nurses seek to avoid discussing, developing, or rethinking (threshold
concepts). They can then go on to consider how learning in academic and clinical
fields can be oriented toward accepting that these concepts may require unlearning,
holding, reiteration and repeated practice. Together they may consider strategies to
develop reflection at critical junctures throughout the nursing program. This may be
a more valuable discussion than to consider only what procedural skills should be
taught and therefore risk overloading an already crowded curriculum (Tanner,
Gubrud-Howes, & Shores, 2008).
Alternative pedagogies such as transformative learning are much needed because
health care systems all over the world are in crisis, a major cause of which is the
continuing nursing shortage. There may be many reasons for the nursing shortage,
but an important remedy is the production of new graduates who are informed and
committed agents of change. The simple STAR framework, which summarizes the
transformative learning philosophy, may be a useful tool to remind educators to cre-
ate powerful, transformative learning experiences and to incorporate them into their
everyday teaching practices. Such experiences should aim to sensitize, engage, and
radicalize students to commit to changed actions in future practice. The experiences
should include active student participation and opportunities to observe, ponder, cri-
tique, and reflect, in order that nursing practices are not simply accepted and blindly
followed. Capabilities beyond treatment, monitoring, or those related to psychomo-
tor tasks should be cultivated in students at every opportunity. These capabilities
include team work, leadership, delegation, communication, and problem-solving
skills, all of which align well with the principles of transformative learning: shifts
in perspective and knowledge linked with action.
Acknowledgments
The author acknowledges Julie Hanson for assistance with the literature review, and Dr. Leigh
Findlay for editorial assistance with an early version of the manuscript.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship,
and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship,
and/or publication of this article: The Office of the Vice Chancellor, University of the
Sunshine Coast, provided funding for this project.
McAllister 55
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from
References
Australian Institute of Health and Welfare. (2010). Nursing and midwifery labour force 2008.
Bulletin no.81. Canberra, ACT: Author. Retrieved March 4, 2011, from http://www.aihw.
gov.au/publications/index.cfm/title/12017
Bandali, K., Parker, K., Mummery, M., & Preece, M. (2008). Skills integration in a simulated
and interprofessional environment: An innovative undergraduate applied health curricu-
lum. Journal of Interprofessional Care, 22, 179-189.
Benner, P., Sutphen, M., Leonard, V., & Day, L. (2009). Educating nurses: A call for radical
transformation. San Francisco, CA: Jossey-Bass.
Bowles, N., Mackintosh, C., & Torn, A. (2001). Nurses’ communication skills: An evaluation
of the impact of solution-focused communication training. Journal of Advanced Nursing,
36, 347-354.
Boyer, N., Maher, P., & Kirkman, S. (2006). Transformative learning in online settings: The
use of self-direction, metacognition and collaborative learning. Journal of Transformative
Education, 4, 335-361.
Bradbury-Jones, C., Sambrook, S., & Irvine, F. (2008). Power and empowerment in nursing: a
fourth theoretical approach. Journal of Advanced Nursing, 62, 258-266.
Brookfield, S. (2000). The power of critical theory. San Francisco, CA: Jossey-Bass.
Cousin, G. (2010). Neither teacher-centred nor student-centred: threshold concepts and
research partnerships. Journal of Learning Development in Higher Education, 2, 1-10.
Cranton, P. (2006). Understanding and promoting transformative learning (2nd ed.). San
Francisco, CA: Jossey-Bass.
Daiski, I. (2004). Changing nurses’ dis-empowering relationship patterns. Journal of
Advanced Nursing, 48, 43-50.
De Chesnay, M. (2007). Caring for the vulnerable (2nd ed.). New York, NY: Jones & Bartlet.
Diekelmann, N. (2004). Covering content and the additive curriculum: How can I use my time
with students to best help them learn what they need to know? Journal of Nursing Educa-
tion, 43, 341-344.
Dirkx, J. (1997). Nurturing soul in adult learning. In P. Cranton (Ed.), Transformative learn-
ing in action: insights from practice (pp. 79-88). San Francisco, CA: Jossey-Bass.
Dirkx, J. (2001). Images, transformative learning and the work of soul. Adult Learning, 12,
15-16.
Dreifuerst, K. (2009). The essentials of debriefing in simulation learning: A concept analysis.
Nursing Education Perspectives, 30, 109-114.
Farmer, P. (2004). An anthropology of structural violence. Current Anthropology, 45, 305-326.
Freire, P. (1972). Pedagogy of the oppressed. Harmondsworth, England: Penguin.
Freshwater, D. (2002). Therapeutic nursing: Improving patient care through self-awareness
and reflection. London, England: SAGE.
Gallagher, (2004). How the metaphor of a gap between theory and practice has influenced
nursing education. Nurse Education Today, 24, 263-268.
Gilligan, C. (1982). In a different voice: Psychological theory and women’s development.
Cambridge, MA: Harvard University Press.
56 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

Halcombe, E., Andrews, S., Peters, K., Salamonson, Y., & Jackson, D. (2009). Casualisation
of the teaching workforce: Implications for nursing education. Nurse Education Today, 30,
528-532.
Hooks, B. (1994). Teaching to transgress: Education as the practice of freedom. New York,
NY: Routledge Kegan Paul.
Infinito, J. (2003). Jane Elliot meets foucault: The formation of ethical identities in the class-
room. Journal of Moral Education, 32, 67-76.
Ironside, P. (2004). Covering content and teaching thinking: Deconstructing the additive
curriculum. Journal of Nursing Education, 43, 5-12.
Jackson, D., Firtko, A., & Edenborough, M. (2007). Personal resilience as a strategy for sur-
viving and thriving in the face of workplace adversity: A literature review. Journal of
Advanced Nursing, 60, 1-9.
Joyce, B., & Weil, M. (2009). Synectics: The art of enhancing creative thought. In B. Joyce &
M. Weil (Eds.), Models of teaching (pp. 213-246). Boston: Allyn & Bacon.
Kanel, K. (2007). A guide to crisis intervention (3rd ed.). Fullerton: California State University.
Kolb, D. A. (1984). Experiential learning: Experience in the source of learning and develop-
ment. Englewood cliffs, New Jersey, NJ: Prentice-Hall.
Kotter, J. (1990). A force for change: How leadership differs from management. New York,
NY: Simon & Schuster.
Lynam, M. J. (2009). Reflecting on issues of enacting a critical pedagogy in nursing. Journal
of Transformative Education, 7, 44-64.
Madsen, W., McAllister, M., Godden, J., Greenhill, J., & Reed, R. (2009). Nursing’s orphans:
How the system of nursing education in Australia is undermining professional identity.
Contemporary Nurse, 32, 9-18.
McAllister, M. (1995). The nurse as tour guide: A metaphor for debriefing nursing students.
Issues in Mental Health Nursing, 16, 395-405.
McAllister, M., Mosel Williams, L., Gamble, T., Malko-Nyhan, K., & Jones, C. (2011). Steps
towards empowerment: An examination of the needs of Australian nurse educators work-
ing in training colleges, health services and universities. Contemporary Nurse Journal
Special Issue: Advances in Contemporary Nurse Education, 38(1-2), 6-17.
McAllister, M., Tower, M., & Walker, R. (2007). Gentle interruptions: Transformative
approaches to clinical teaching. Journal of Nursing Education, 46, 304-313.
McAllister, M., & Walsh, K. (2003). C. A. R. E: A framework for mental health practice.
Journal of Psychiatric and Mental Health Nursing, 10, 39-48.
Merriam, S. (2004). The role of cognitive development in Mezirow’s transformational learn-
ing theory. Adult Education Quarterly, 55, 60-68.
Meyer, J., & Land, R. (2006). Overcoming barriers to student understanding: Threshold con-
cepts and troublesome knowledge. New York, NY: Routledge Kegan Paul.
Mezirow, J. (2000). Learning as transformation. San Francisco, CA: Jossey-Bass.
Morison, S., Johnstone, J., & Stevenson, J. (2010). Preparing students for interprofessional prac-
tice: Exploring the intra-personal dimension. Journal of Interprofessional Care, 24, 412-421.
Nelson, J., Palonsky, S., & Carlson, K. (2007). Critical issues in education: Dialogues and
dialectics. New York, NY: McGraw-Hill.
McAllister 57
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from

Nelson, S., & Gordon, S. (2004). The rhetoric of rupture: nursing as a practice with a history?
Nursing Outlook, 52, 255-261.
Nicholson, J. A. (1950). Philosophy of religion (p. 108). New York, NY: Ronald Press.
Noddings, N. (2003). Caring: A feminine approach to ethics and moral education (2nd ed.).
Berkeley: University of California Press.
Offredy, M. (2002). Decision-making in primary care: Outcomes from a study using patient
scenarios. Journal of Advanced, 40, 532-541.
O’Sullivan, E., & Morrell, A. (2002). Expanding the boundaries of transformative learning:
Essays on theory and praxis (p. 18). New York, NY: Palgrave Press.
Potempa, K., Redman, R., & Landstrom, G. (2009). Human resources in nursing education:
A worldwide crisis. Collegian, 16, 19-23.
Pratt, D. (2001). Good teaching: One size fits all? In J. Ross-Gordon (Ed.), An up-date on
teaching theory. San Francisco, CA: Jossey-Bass.
Reutter, L., Sword, W., Meagher-Stewart, D., & Rideout, E. (2004). Nursing students’ beliefs
about poverty and health. Journal of Advanced Nursing, 48, 299-309.
Sayers, J. M., & DiGiacomo, M. (2010). The nurse educator role in Australian hospitals:
Implications for health policy. Collegian, 17, 77-84.
Smythe, E. (2003). Uncovering the meaning of ‘‘being safe’’ in practice. Contemporary
Nurse, 14, 195-204.
Tanner, C. (2006). Thinking like a nurse: A research-based model of clinical judgment in nur-
sing. Journal of Nursing Education, 45, 204-211.
Tanner, C., Gubrud-Howe, P., & Shores, L. (2008). The oregon consortium for nursing education:
A response to the nursing shortage. Policy, Politics & Nursing Practice, 9, 203-209.
Taylor, E. (2007). An update of transformative learning theory: A critical review of the
empirical research (1999–2005). International Journal of Life Long Learning, 26, 173-191.
Taylor, E. (2009). Fostering transformative learning. In J. Mezirow & E. TaylorAssociates.
(Eds.), Transformative learning in practice. Insights from community, workplace, and
higher education (pp. 3-17). San Francisco, CA: Jossey-Bass.
Vonfrolio, L. (2006). It’s time to roar. RN, 69, 16.
Watson, J. (1979). Nursing. The philosophy and science of caring. Boston, MA: Little, Brown.
Zwarenstein, M., & Reeves, S. (2006). Knowledge translation and interprofessional colla-
boration: Where the rubber of evidence-based care hits the road of teamwork. Journal
of Continuing Education in the Health Professions, 26, 46-54.
Bio
Margaret McAllister is professor of Nursing at the University of the Sunshine Coast. She is
the program leader of the Master of Mental Health Nursing, and is a credentialed mental
health nurse with higher degrees in Arts and Education. Her research areas include solution
focused therapy, resilience, self-injury, the history and future of nursing and enhancing the
quality of education through transformative learning and inter-professional learning.
58 Journal of Transformative Education 9(1)
at Univ of the Sunshine Coast on July 16, 2012jtd.sagepub.comDownloaded from




















