![100019.ppt [\254\333\256e\274\322\246\241]](https://static.fdokumen.com/doc/165x107/631ce499b8a98572c10d1be1/100019ppt-254333256e274322246241.jpg)
Spinal Tuberculosis: Clinicoradiological Findings in 274 Patients
10
Clinical Infectious Diseases Spinal Tuberculosis in HIV-Prevalent Setting • CID 2018:67 (1 July) • 89 Spinal Tuberculosis: Clinicoradiological Findings in 274 Patients Suzaan Marais, 1,2 Izanne Roos, 1,2 Ayesha Mitha, 3 Sepelong J. Mabusha, 4 Vinod Patel, 1,2 and Ahmed I. Bhigjee 1,2 1 Department of Neurology, Inkosi Albert Luthuli Central Hospital, 2 Department of Neurology, University of KwaZulu-Natal, 3 Department of Radiology, Inkosi Albert Luthuli Central Hospital; and 4 Department of Orthopedics, King Dinuzulu Hospital, Durban, South Africa Background. Mycobacterium tuberculosis is a major cause of myelopathy and radiculopathy in settings with a high prevalence of tuberculosis/human immunodeficiency virus (HIV) coinfection. However, a paucity of publications exists on the spectrum of neurological and magnetic resonance (MR) imaging findings of spinal tuberculosis in these populations. Methods. We conducted a retrospective study of adults with spinal tuberculosis at a referral center in South Africa for patients with spinal disease without bony involvement seen at plain film radiography. We report the clinical, laboratory and spinal MR imag- ing findings, compare HIV-infected and HIV-uninfected patients, and correlate clinical and cerebrospinal fluid findings with those of MR imaging. Results. Of 274 patients, 209 (76%) were HIV infected and 49 (18%) were HIV uninfected. Radiculomyelitis occurred in 77% (n = 210), and spondylitis in 39% (n = 106). Subdural abscess (n = 42) and intramedullary tuberculoma (n = 33) were common. In 24% of HIV-infected and 14% of HIV-uninfected patients, spinal disease manifested as a paradoxical tuberculosis reaction, fre- quently following tuberculous meningitis. e triad of neurological deficit, fever, and back pain was similar in patients with spondy- litis (24%), epi/subdural abscess without bony disease (14%), meningoradiculitis (17%), and isolated myelitis (17%). Conclusions. Radiculomyelitis is a common manifestation of spinal tuberculosis in settings with high tuberculosis/HIV preva- lence, oſten presenting as a paradoxical reaction. We describe a high frequency of rarely reported spinal tuberculosis manifestations, suggesting that these are more common than implied by the literature. Keywords. radiculomyelitis; spondylitis; HIV; meningoradiculitis. Central nervous system (CNS) tuberculosis includes involve- ment of the brain, such as tuberculous meningitis (TBM), tuber- culoma/abscess, and cerebritis, and, less commonly, the spinal cord, including radiculomyelitis [1], vertebral tuberculosis with neurological compromise [2], and primary epidural abscess [3]. Several studies have reported tuberculosis as a major cause of myelopathy and or radiculopathy in settings with a high prev- alence of human immunodeficiency virus (HIV)/tuberculosis coinfection [4–6], accounting for 68% of HIV-infected patients (84 of 123) with myelopathy or cauda equina syndrome in whom an etiological cause was confirmed [4]. However, there is a paucity of literature on the clinical presentations and the spec- trum of magnetic resonance (MR) imaging findings of spinal tuberculosis in HIV-infected patients [4, 6–15]. Furthermore, there are only a few studies comparing these findings to those in HIV-uninfected patients [2, 8, 12]. Here we report the clinical, investigative, and MR imaging findings in adults with spinal tuberculosis in a setting with a high tuberculosis/HIV burden. We compare HIV-infected and HIV-uninfected patients and correlate clinical and cerebrospinal fluid (CSF) findings with those of spinal MR imaging. METHODS We conducted a retrospective study at Inkosi Albert Luthuli Central Hospital (IALCH), a public-sector referral facility in KwaZulu-Natal, South Africa. The hospital is the main referral center for patients with spinal disease without plain film radio- graphic evidence of bony involvement; those with bony disease are preferentially referred to the orthopedic spinal unit at King Dinuzulu Hospital (KDH). Hence, the study was biased toward nonbony spinal disease. We screened clinical records of all adults (aged ≥18 years) assessed with a diagnosis of tuberculosis involv- ing the CNS and/or vertebral column from June 2003 through December 2015 at IALCH. Patients were identified based on International Classification of Diseases, 10th Revision, codes from the hospital’s electronic record system (Supplementary Data). We included patients who presented with new-onset mye- lopathy or radiculopathy and underwent MR imaging of the spine. Clinical data were extracted from hospital records. All MR images were reported by a neuroradiologist and reviewed by a neurologist. Results of tuberculosis and CSF investigations MAJOR ARTICLE © The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: [email protected]. DOI: 10.1093/cid/ciy020 Received 9 November 2017; editorial decision 24 December 2017; accepted 10 January 2018; published online January 11, 2018. Correspondence: S. Marais, Department of Neurology, Level 3 D Block, Inkosi Albert Luthuli Central Hospital, 800 Vusi Mzimela Rd, Cato Manor 4091, Durban, South Africa (marais. [email protected]). Clinical Infectious Diseases ® 2018;67(1):89–98 Downloaded from https://academic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Spinal Tuberculosis: Clinicoradiological Findings in 274 Patients
Clinical Infectious Diseases
Spinal Tuberculosis in HIV-Prevalent Setting
Spinal Tuberculosis in HIV-Prevalent Setting • CID 2018:67 (1 July) • 89
Spinal Tuberculosis: Clinicoradiological Findings in 274 PatientsSuzaan Marais,1,2 Izanne Roos,1,2 Ayesha Mitha,3 Sepelong J. Mabusha,4 Vinod Patel,1,2 and Ahmed I. Bhigjee1,2
1Department of Neurology, Inkosi Albert Luthuli Central Hospital, 2Department of Neurology, University of KwaZulu-Natal, 3Department of Radiology, Inkosi Albert Luthuli Central Hospital; and 4Department of Orthopedics, King Dinuzulu Hospital, Durban, South Africa
Background. Mycobacterium tuberculosis is a major cause of myelopathy and radiculopathy in settings with a high prevalence of tuberculosis/human immunodeficiency virus (HIV) coinfection. However, a paucity of publications exists on the spectrum of neurological and magnetic resonance (MR) imaging findings of spinal tuberculosis in these populations.
Methods. We conducted a retrospective study of adults with spinal tuberculosis at a referral center in South Africa for patients with spinal disease without bony involvement seen at plain film radiography. We report the clinical, laboratory and spinal MR imag-ing findings, compare HIV-infected and HIV-uninfected patients, and correlate clinical and cerebrospinal fluid findings with those of MR imaging.
Results. Of 274 patients, 209 (76%) were HIV infected and 49 (18%) were HIV uninfected. Radiculomyelitis occurred in 77% (n = 210), and spondylitis in 39% (n = 106). Subdural abscess (n = 42) and intramedullary tuberculoma (n = 33) were common. In 24% of HIV-infected and 14% of HIV-uninfected patients, spinal disease manifested as a paradoxical tuberculosis reaction, fre-quently following tuberculous meningitis. The triad of neurological deficit, fever, and back pain was similar in patients with spondy-litis (24%), epi/subdural abscess without bony disease (14%), meningoradiculitis (17%), and isolated myelitis (17%).
Conclusions. Radiculomyelitis is a common manifestation of spinal tuberculosis in settings with high tuberculosis/HIV preva-lence, often presenting as a paradoxical reaction. We describe a high frequency of rarely reported spinal tuberculosis manifestations, suggesting that these are more common than implied by the literature.
Keywords. radiculomyelitis; spondylitis; HIV; meningoradiculitis.
Central nervous system (CNS) tuberculosis includes involve-ment of the brain, such as tuberculous meningitis (TBM), tuber-culoma/abscess, and cerebritis, and, less commonly, the spinal cord, including radiculomyelitis [1], vertebral tuberculosis with neurological compromise [2], and primary epidural abscess [3]. Several studies have reported tuberculosis as a major cause of myelopathy and or radiculopathy in settings with a high prev-alence of human immunodeficiency virus (HIV)/tuberculosis coinfection [4–6], accounting for 68% of HIV-infected patients (84 of 123) with myelopathy or cauda equina syndrome in whom an etiological cause was confirmed [4]. However, there is a paucity of literature on the clinical presentations and the spec-trum of magnetic resonance (MR) imaging findings of spinal tuberculosis in HIV-infected patients [4, 6–15]. Furthermore, there are only a few studies comparing these findings to those in HIV-uninfected patients [2, 8, 12]. Here we report the clinical, investigative, and MR imaging findings in adults with spinal
tuberculosis in a setting with a high tuberculosis/HIV burden. We compare HIV-infected and HIV-uninfected patients and correlate clinical and cerebrospinal fluid (CSF) findings with those of spinal MR imaging.
METHODS
We conducted a retrospective study at Inkosi Albert Luthuli Central Hospital (IALCH), a public-sector referral facility in KwaZulu-Natal, South Africa. The hospital is the main referral center for patients with spinal disease without plain film radio-graphic evidence of bony involvement; those with bony disease are preferentially referred to the orthopedic spinal unit at King Dinuzulu Hospital (KDH). Hence, the study was biased toward nonbony spinal disease. We screened clinical records of all adults (aged ≥18 years) assessed with a diagnosis of tuberculosis involv-ing the CNS and/or vertebral column from June 2003 through December 2015 at IALCH. Patients were identified based on International Classification of Diseases, 10th Revision, codes from the hospital’s electronic record system (Supplementary Data).
We included patients who presented with new-onset mye-lopathy or radiculopathy and underwent MR imaging of the spine. Clinical data were extracted from hospital records. All MR images were reported by a neuroradiologist and reviewed by a neurologist. Results of tuberculosis and CSF investigations
M A J O R A R T I C L E
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: [email protected]: 10.1093/cid/ciy020
Received 9 November 2017; editorial decision 24 December 2017; accepted 10 January 2018; published online January 11, 2018.
Correspondence: S. Marais, Department of Neurology, Level 3 D Block, Inkosi Albert Luthuli Central Hospital, 800 Vusi Mzimela Rd, Cato Manor 4091, Durban, South Africa ([email protected]).
Clinical Infectious Diseases® 2018;67(1):89–98
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022

90 • CID 2018:67 (1 July) • Marais et al
Marais et al
performed elsewhere and outcome (alive 9 months after admis-sion) were obtained from the National Health Laboratories Service database. After diagnosis, patients with tuberculosis spondylitis were referred to KDH. We perused records at KDH for management and outcome (neurological disability) in these patients. The Biomedical Research Ethics Committee (BREC) of the University of KwaZulu-Natal approved the study (BREC class approval number BCA325/15).
Patients received tuberculosis treatment according to national tuberculosis guidelines for ≥9 months [16] and were prescribed prednisone at variable doses (starting dose, 40 mg/d to 1.5 mg/kg/d) for 4–6 weeks. Since South Africa’s national antiretroviral therapy (ART) program was implemented in 2004, all patients with neurological tuberculosis were eligible to start triple ther-apy. Tuberculosis treatment and ART were provided by and monitored at primary tuberculosis/HIV care facilities and dis-trict-level hospitals.
MR imaging was performed with a 1.5- or 3.0-T imager (Siemens Magnetom Aera 1.5 T TIM DOT System and Siemens Magnetom Skyra 3 T TIM DOT System). Sagittal and axial T1-weighted (T1W) and T2-weighted (T2W) imaging were routinely performed. Gadolinium-enhanced T1W imaging was performed in most patients.
DEFINITIONS
Clinical Definitions
Definite spinal tuberculosis was defined by positive results of microscopy, culture, histology, or Xpert MTB/RIF assay of any CNS sample. Probable spinal tuberculosis was defined as any of the following: (1) clinical or radiological improvement in neurological symptoms/signs after tuberculosis treatment initiation; (2) concomitant TBM [17]; (3) spondylitis with the presence of extra-CNS tuberculosis (ie, Mycobacterium tuber-culosis identified from an extra-CNS source or suggestive radi-ological features, eg, chest radiography) or with the patient alive at 9-month follow-up; (4) radiculomyelitis without spon-dylitis with features of extra-CNS tuberculosis plus exclusion of other causes by CSF examination for fungi, bacteria, viruses, cancer, and syphilis and appropriate blood tests. Patients were excluded if any of the following criteria were met: (1) undoc-umented spinal neurological findings; (2) neurological signs explained by findings of brain MR imaging; or (3) additional CNS infection, or noninfectious disease, identified or empir-ically treated.
Radiological Definitions
Spondylitis with or without diskitis was defined by any of the following: (1) abnormal vertebral signal (with or without abnormal disk signal) on T2W (hyperintense) and T1W (hypo/isointense) images, with contrast enhancement if gadolinium was administered; (2) end-plate destruction; or (3) vertebral height loss/collapse, with or without disk destruction.
Myelitis was defined by a cord appearing hyperintense on T2W images and hypo- or isointense on T1W images, with or without cord expansion, along with (1) no cord compression (ie, subdural/epidural abscess or spondylitis) or (2) in case of cord compression, intramedullary enhancement. Meningoradiculitis was defined by any of the following: (1) spinal subarachnoid space loculations/obliteration; (2) nerve root thickening, nod-ularity, or clumping; or (3) spinal meningeal, root or subdural enhancement; radiculomyelitis was defined as meningoradicu-litis and or myelitis. Subdural abscess was defined as a collection appearing iso/hypointense to the spinal cord on T1W images and of mixed signal intensity on T2W images with rim enhance-ment; this includes areas of T1 hypointensity (breakdown) within hypertrophic meninges and lesions in the subdural space that meet criteria for “liquefied tuberculoma” (defined below for intramedullary tuberculoma). (Note that “subdural tuber-culoma” and “subdural abscess” are used interchangeably in the literature and may also be referred to as “subdural/intradural tuberculous granuloma” or “subdural/intradural “tuberculous empyema” [18].)
Intramedullary tuberculoma was defined as a well-circum-scribed intramedullary lesion appearing (1) hypointense on T1W and hyperintense on T2W images with homogeneous enhancement (solid, noncaseating); (2) isointense to hypoin-tense on both T1W and T2W images with rim enhancement (caseating); or (3) hypointense on T1W images and hyperin-tense on T2W images with rim enhancement (liquefied). Syrinx was defined as an intramedullary lesion appearing isointense to CSF on T1W and T2W images without enhancement.
Statistical Analysis
Statistical analysis was performed using GraphPad Prism soft-ware, version 6. Continuous variables are presented as medians and interquartile ranges (IQRs), and categorical variables as percentages. Categorical and continuous variables were com-pared between groups using Fisher exact and Mann-Whitney U tests, respectively. Differences were considered statistically significant at P < .05.
RESULTS
Baseline Characteristics
During the study period, 343 adults with spinal tuberculo-sis were assessed and underwent MR imaging of the spine. Figure 1 shows the reasons for study exclusion or inclusion. Of 274 included patients, the majority (73%) either had a diag-nosis of definite neurological tuberculosis (n = 52) or showed clinical and or radiological improvement after tuberculosis treatment was initiated (n = 147). The baseline and outcome findings in the whole study group and in HIV-infected (n = 209; 76%) and HIV-uninfected (n = 49; 18%) patients are pre-sented in Table 1. The median CD4 cell count for HIV-infected patients was 175/μL (IQR, 100–292/μL). Of these patients, 53%
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022

Spinal Tuberculosis in HIV-Prevalent Setting • CID 2018:67 (1 July) • 91
Spinal Tuberculosis in HIV-Prevalent Setting
were receiving ART at presentation, for a median duration of 204 days (IQR. 40–593 days). Twenty-five patients were known to start ART a median of 20 days (IQR, 13–52 days) after starting tuberculosis treatment. HIV-uninfected patients presented more often with noncommunicable diseases (28% vs 8%; P <.001), including diabetes mellitus, that was present in 10% (Table 1). In 71 patients (26%), spinal symptoms developed during tuberculosis treatment; these included 62 HIV-infected and 8 HIV-uninfected patients and 1 with unknown HIV status; TBM was the initial disease presentation in 51, with improve-ment before presentation in 48. Reasons for deterioration in HIV-uninfected patients included paradoxical reaction (n = 7) [19], manifesting a median of 27 days (IQR, 12–43) after initia-tion of tuberculosis treatment, and progressive deterioration of CNS tuberculosis (n = 1). Among HIV-infected patients, 16 of 62 had paradoxical tuber-culosis-immune reconstitution inflammatory syndrome (IRIS) [20, 21], occurring a median of 23 days (IQR, 12–40 days) after ART initiation. Among HIV-infected patients, 27 had para-doxical reactions unrelated to ART initiation, including 18 not receiving ART and 9 who were well established with ART before tuberculosis treatment; these events occurred a median of 31 days (IQR, 13–68 days) after tuberculosis treatment was ini-tiated. In addition, 7 of 62 HIV-infected patients had paradoxi-cal worsening after initiation of tuberculosis treatment and were receiving ART, but the date of ART initiation was unknown; 1 of 62 had progressive multidrug-resistant tuberculosis, and in
11 of 62 no specific cause could be identified owing to incom-plete data (eg, incomplete data on compliance with treatment and ART). Although HIV-infected patients presented with some form of paradoxical reaction more frequently than HIV-uninfected patients (24% vs 14%), this difference did not reach statistical significance (P = .18).
Clinical Findings
Limb weakness was present in 269 patients (98%) and most fre-quently involved lower limbs only (n = 213). The clinical pres-entation did not differ significantly between HIV-infected and uninfected patients (Table 1), but concomitant TBM was more common in HIV-coinfected patients (48% vs 29%; P = .02).
MR Imaging Findings
All patients underwent MR imaging of the whole spine except 1 who underwent imaging of the thoracolumbar spine only. Gadolinium-enhanced imaging was performed in 207 patients (76%). Spinal MR findings in the study group and by HIV status are presented in Table 2. Radiculomyelitis was present in 210 patients (77%; Figure 2A and 2B) and spon-dylitis in 106 (39%). Of 163 patients (59%) who had radic-ulomyelitis without spondylitis, 24 had features of myelitis only. Seventy patients with radiculomyelitis had no asso-ciated TBM or spondylitis. Three patients without spon-dylitis had an epidural abscess (Figure 2C). Of those who underwent gadolinium-enhanced imaging, 42 (20%) had a
Figure 1. Flow diagram of patients with neurological tuberculosis who had spinal symptoms/signs and underwent magnetic resonance (MR) imaging of the spine. The “dual pathology” category included patients with bacterial infection (n = 5), cytomegalovirus radiculopathy (n = 8), neurosyphilis (n = 4), toxoplasmosis encephalitis (n = 4), varicella zoster virus myelitis (n = 3), vitamin B12 deficiency myeloneuropathy (n = 3), neurocysticercosis (n = 2), herpes simplex virus myelitis (n = 2), human T-lymphotropic virus myelitis (n = 2), cryptococcal meningitis (n = 2), and other conditions (n = 4). The 24 patients with insufficient information were all lost to follow-up and included 3 with bony tuberculosis with no extra–central nervous system (CNS) tuberculosis and 21 with radiculomyelitis and (1) features of extra-CNS tuberculosis but without sufficient exclusion of other causes (n = 8), (2) no features of extra-CNS tuberculosis (n = 10), or (3) no features of extra-CNS tuberculosis and without sufficient exclusion of other causes (n = 3). Patients with definite spinal tuberculosis had a positive CNS sample for any of the following: acid-fast bacilli seen with microscopy, Mycobacterium tuberculosis cultured, M. tuberculosis identified by a commercial nucleic acid amplification test, or histological features consistent with tuberculosis. Most patients with probable spinal tuberculosis fulfilled >1 diagnostic criterion. Abbreviations: MRI, magnetic resonance imaging; TBM, tuberculous meningitis.
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022
92 • CID 2018:67 (1 July) • Marais et al
Marais et al
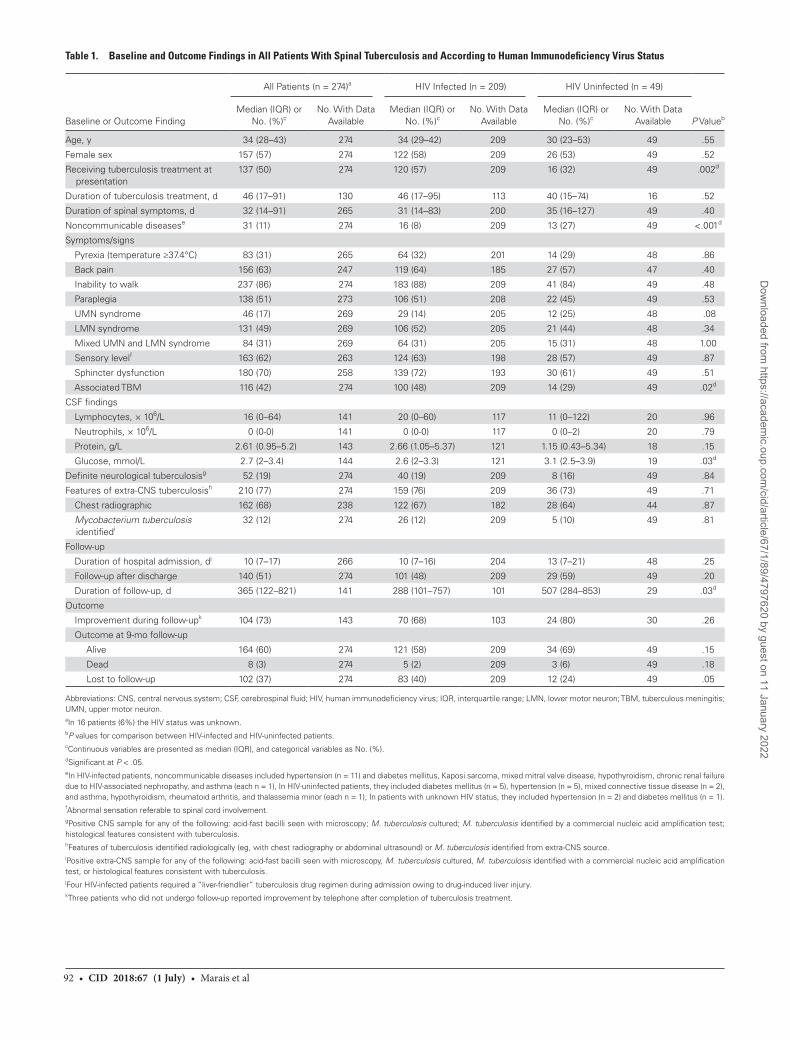
Table 1. Baseline and Outcome Findings in All Patients With Spinal Tuberculosis and According to Human Immunodeficiency Virus Status
Baseline or Outcome Finding
All Patients (n = 274)a HIV Infected (n = 209) HIV Uninfected (n = 49)
P ValuebMedian (IQR) or
No. (%)cNo. With Data
Available Median (IQR) or
No. (%)cNo. With Data
Available Median (IQR) or
No. (%)cNo. With Data
Available
Age, y 34 (28–43) 274 34 (29–42) 209 30 (23–53) 49 .55
Female sex 157 (57) 274 122 (58) 209 26 (53) 49 .52
Receiving tuberculosis treatment at presentation
137 (50) 274 120 (57) 209 16 (32) 49 .002d
Duration of tuberculosis treatment, d 46 (17–91) 130 46 (17–95) 113 40 (15–74) 16 .52
Duration of spinal symptoms, d 32 (14–91) 265 31 (14–83) 200 35 (16–127) 49 .40
Noncommunicable diseasese 31 (11) 274 16 (8) 209 13 (27) 49 <.001d
Symptoms/signs
Pyrexia (temperature ≥37.4°C) 83 (31) 265 64 (32) 201 14 (29) 48 .86
Back pain 156 (63) 247 119 (64) 185 27 (57) 47 .40
Inability to walk 237 (86) 274 183 (88) 209 41 (84) 49 .48
Paraplegia 138 (51) 273 106 (51) 208 22 (45) 49 .53
UMN syndrome 46 (17) 269 29 (14) 205 12 (25) 48 .08
LMN syndrome 131 (49) 269 106 (52) 205 21 (44) 48 .34
Mixed UMN and LMN syndrome 84 (31) 269 64 (31) 205 15 (31) 48 1.00
Sensory levelf 163 (62) 263 124 (63) 198 28 (57) 49 .87
Sphincter dysfunction 180 (70) 258 139 (72) 193 30 (61) 49 .51
Associated TBM 116 (42) 274 100 (48) 209 14 (29) 49 .02d
CSF findings
Lymphocytes, × 106/L 16 (0–64) 141 20 (0–60) 117 11 (0–122) 20 .96
Neutrophils, × 106/L 0 (0-0) 141 0 (0-0) 117 0 (0–2) 20 .79
Protein, g/L 2.61 (0.95–5.2) 143 2.66 (1.05–5.37) 121 1.15 (0.43–5.34) 18 .15
Glucose, mmol/L 2.7 (2–3.4) 144 2.6 (2–3.3) 121 3.1 (2.5–3.9) 19 .03d
Definite neurological tuberculosisg 52 (19) 274 40 (19) 209 8 (16) 49 .84
Features of extra-CNS tuberculosish 210 (77) 274 159 (76) 209 36 (73) 49 .71
Chest radiographic 162 (68) 238 122 (67) 182 28 (64) 44 .87
Mycobacterium tuberculosis identifiedi
32 (12) 274 26 (12) 209 5 (10) 49 .81
Follow-up
Duration of hospital admission, dj 10 (7–17) 266 10 (7–16) 204 13 (7–21) 48 .25
Follow-up after discharge 140 (51) 274 101 (48) 209 29 (59) 49 .20
Duration of follow-up, d 365 (122–821) 141 288 (101–757) 101 507 (284–853) 29 .03d
Outcome
Improvement during follow-upk 104 (73) 143 70 (68) 103 24 (80) 30 .26
Outcome at 9-mo follow-up
Alive 164 (60) 274 121 (58) 209 34 (69) 49 .15
Dead 8 (3) 274 5 (2) 209 3 (6) 49 .18
Lost to follow-up 102 (37) 274 83 (40) 209 12 (24) 49 .05
Abbreviations: CNS, central nervous system; CSF, cerebrospinal fluid; HIV, human immunodeficiency virus; IQR, interquartile range; LMN, lower motor neuron; TBM, tuberculous meningitis; UMN, upper motor neuron.aIn 16 patients (6%) the HIV status was unknown. bP values for comparison between HIV-infected and HIV-uninfected patients.cContinuous variables are presented as median (IQR), and categorical variables as No. (%).dSignificant at P < .05.eIn HIV-infected patients, noncommunicable diseases included hypertension (n = 11) and diabetes mellitus, Kaposi sarcoma, mixed mitral valve disease, hypothyroidism, chronic renal failure due to HIV-associated nephropathy, and asthma (each n = 1), In HIV-uninfected patients, they included diabetes mellitus (n = 5), hypertension (n = 5), mixed connective tissue disease (n = 2), and asthma, hypothyroidism, rheumatoid arthritis, and thalassemia minor (each n = 1); In patients with unknown HIV status, they included hypertension (n = 2) and diabetes mellitus (n = 1).fAbnormal sensation referable to spinal cord involvement.gPositive CNS sample for any of the following: acid-fast bacilli seen with microscopy; M. tuberculosis cultured; M. tuberculosis identified by a commercial nucleic acid amplification test; histological features consistent with tuberculosis.hFeatures of tuberculosis identified radiologically (eg, with chest radiography or abdominal ultrasound) or M. tuberculosis identified from extra-CNS source.iPositive extra-CNS sample for any of the following: acid-fast bacilli seen with microscopy, M. tuberculosis cultured, M. tuberculosis identified with a commercial nucleic acid amplification test, or histological features consistent with tuberculosis.jFour HIV-infected patients required a “liver-friendlier” tuberculosis drug regimen during admission owing to drug-induced liver injury.kThree patients who did not undergo follow-up reported improvement by telephone after completion of tuberculosis treatment.
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022
Spinal Tuberculosis in HIV-Prevalent Setting • CID 2018:67 (1 July) • 93
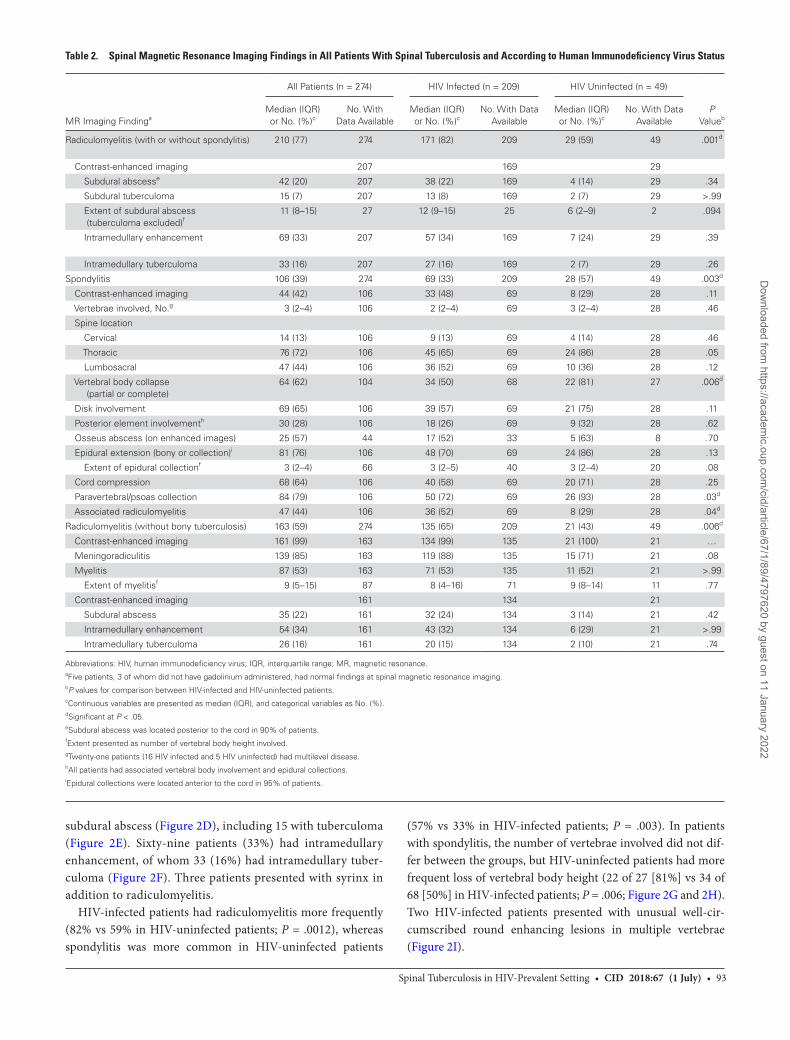
Spinal Tuberculosis in HIV-Prevalent Settingsubdural abscess (Figure 2D), including 15 with tuberculoma (Figure 2E). Sixty-nine patients (33%) had intramedullary enhancement, of whom 33 (16%) had intramedullary tuber-culoma (Figure 2F). Three patients presented with syrinx in addition to radiculomyelitis.
HIV-infected patients had radiculomyelitis more frequently (82% vs 59% in HIV-uninfected patients; P = .0012), whereas spondylitis was more common in HIV-uninfected patients
(57% vs 33% in HIV-infected patients; P = .003). In patients with spondylitis, the number of vertebrae involved did not dif-fer between the groups, but HIV-uninfected patients had more frequent loss of vertebral body height (22 of 27 [81%] vs 34 of 68 [50%] in HIV-infected patients; P = .006; Figure 2G and 2H). Two HIV-infected patients presented with unusual well-cir-cumscribed round enhancing lesions in multiple vertebrae (Figure 2I).
Table 2. Spinal Magnetic Resonance Imaging Findings in All Patients With Spinal Tuberculosis and According to Human Immunodeficiency Virus Status
MR Imaging Findinga
All Patients (n = 274) HIV Infected (n = 209) HIV Uninfected (n = 49)
P Valueb
Median (IQR) or No. (%)c
No. With Data Available
Median (IQR) or No. (%)c
No. With Data Available
Median (IQR) or No. (%)c
No. With Data Available
Radiculomyelitis (with or without spondylitis) 210 (77) 274 171 (82) 209 29 (59) 49 .001d
Contrast-enhanced imaging 207 169 29
Subdural abscesse 42 (20) 207 38 (22) 169 4 (14) 29 .34
Subdural tuberculoma 15 (7) 207 13 (8) 169 2 (7) 29 >.99
Extent of subdural abscess (tuberculoma excluded)f
11 (8–15) 27 12 (9–15) 25 6 (2–9) 2 .094
Intramedullary enhancement 69 (33) 207 57 (34) 169 7 (24) 29 .39
Intramedullary tuberculoma 33 (16) 207 27 (16) 169 2 (7) 29 .26
Spondylitis 106 (39) 274 69 (33) 209 28 (57) 49 .003d
Contrast-enhanced imaging 44 (42) 106 33 (48) 69 8 (29) 28 .11
Vertebrae involved, No.g 3 (2–4) 106 2 (2–4) 69 3 (2–4) 28 .46
Spine location
Cervical 14 (13) 106 9 (13) 69 4 (14) 28 .46
Thoracic 76 (72) 106 45 (65) 69 24 (86) 28 .05
Lumbosacral 47 (44) 106 36 (52) 69 10 (36) 28 .12
Vertebral body collapse (partial or complete)
64 (62) 104 34 (50) 68 22 (81) 27 .006d
Disk involvement 69 (65) 106 39 (57) 69 21 (75) 28 .11
Posterior element involvementh 30 (28) 106 18 (26) 69 9 (32) 28 .62
Osseus abscess (on enhanced images) 25 (57) 44 17 (52) 33 5 (63) 8 .70
Epidural extension (bony or collection)i 81 (76) 106 48 (70) 69 24 (86) 28 .13
Extent of epidural collectionf 3 (2–4) 66 3 (2–5) 40 3 (2–4) 20 .08
Cord compression 68 (64) 106 40 (58) 69 20 (71) 28 .25
Paravertebral/psoas collection 84 (79) 106 50 (72) 69 26 (93) 28 .03d
Associated radiculomyelitis 47 (44) 106 36 (52) 69 8 (29) 28 .04d
Radiculomyelitis (without bony tuberculosis) 163 (59) 274 135 (65) 209 21 (43) 49 .006d
Contrast-enhanced imaging 161 (99) 163 134 (99) 135 21 (100) 21 …
Meningoradiculitis 139 (85) 163 119 (88) 135 15 (71) 21 .08
Myelitis 87 (53) 163 71 (53) 135 11 (52) 21 >.99
Extent of myelitisf 9 (5–15) 87 8 (4–16) 71 9 (8–14) 11 .77
Contrast-enhanced imaging 161 134 21
Subdural abscess 35 (22) 161 32 (24) 134 3 (14) 21 .42
Intramedullary enhancement 54 (34) 161 43 (32) 134 6 (29) 21 >.99
Intramedullary tuberculoma 26 (16) 161 20 (15) 134 2 (10) 21 .74
Abbreviations: HIV, human immunodeficiency virus; IQR, interquartile range; MR, magnetic resonance. aFive patients, 3 of whom did not have gadolinium administered, had normal findings at spinal magnetic resonance imaging. bP values for comparison between HIV-infected and HIV-uninfected patients.cContinuous variables are presented as median (IQR), and categorical variables as No. (%).dSignificant at P < .05.eSubdural abscess was located posterior to the cord in 90% of patients.fExtent presented as number of vertebral body height involved.gTwenty-one patients (16 HIV infected and 5 HIV uninfected) had multilevel disease.hAll patients had associated vertebral body involvement and epidural collections.iEpidural collections were located anterior to the cord in 95% of patients.
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022
94 • CID 2018:67 (1 July) • Marais et al
Marais et al
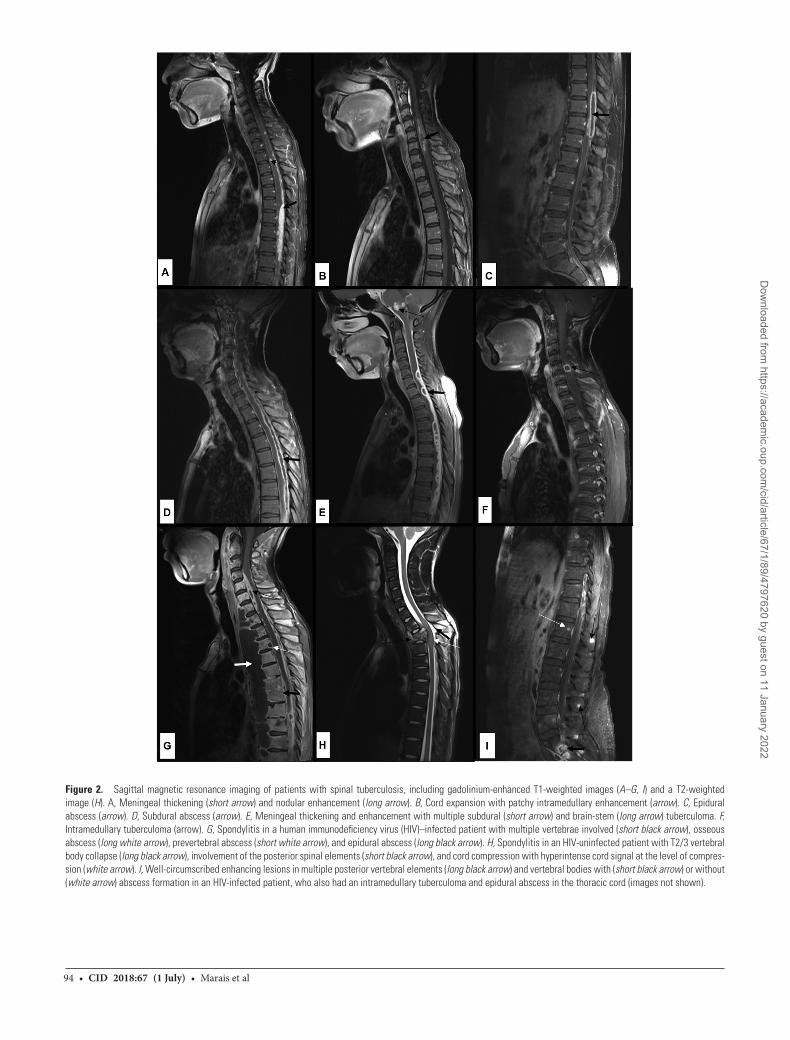
Figure 2. Sagittal magnetic resonance imaging of patients with spinal tuberculosis, including gadolinium-enhanced T1-weighted images (A–G, I) and a T2-weighted image (H). A, Meningeal thickening (short arrow) and nodular enhancement (long arrow). B, Cord expansion with patchy intramedullary enhancement (arrow). C, Epidural abscess (arrow). D, Subdural abscess (arrow). E, Meningeal thickening and enhancement with multiple subdural (short arrow) and brain-stem (long arrow) tuberculoma. F, Intramedullary tuberculoma (arrow). G, Spondylitis in a human immunodeficiency virus (HIV)–infected patient with multiple vertebrae involved (short black arrow), osseous abscess (long white arrow), prevertebral abscess (short white arrow), and epidural abscess (long black arrow). H, Spondylitis in an HIV-uninfected patient with T2/3 vertebral body collapse (long black arrow), involvement of the posterior spinal elements (short black arrow), and cord compression with hyperintense cord signal at the level of compres-sion (white arrow). I, Well-circumscribed enhancing lesions in multiple posterior vertebral elements (long black arrow) and vertebral bodies with (short black arrow) or without (white arrow) abscess formation in an HIV-infected patient, who also had an intramedullary tuberculoma and epidural abscess in the thoracic cord (images not shown).
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022
Spinal Tuberculosis in HIV-Prevalent Setting • CID 2018:67 (1 July) • 95
Spinal Tuberculosis in HIV-Prevalent Setting
Brain imaging was performed in 96 patients (MR imaging in 62 and computed tomography in 34); contrast material was administered in 88%. Features of TBM seen in 76 patients (79%) included meningeal enhancement (n = 50), tuberculoma (n = 33), hydrocephalus (n = 27), and infarcts (n = 20).
Correlation Between Clinical and MR Imaging Findings
Supplementary Table S1 shows the clinical findings in patients with spondylitis (n = 106) compared with those in patients with-out bony disease (n = 168); patients with spondylitis were older (median age [IQR], 38 [30–50] vs 31 [27–38], years; P < .001) and had a longer symptom duration (47 [22–107] vs 28 [13–78] days; P = .004). The triad of neurological deficits, fever, and back pain, were seen in similar proportions of patients with spon-dylitis (24%), subdural/epidural abscess without bony disease (14%), meningoradiculitis (17%), and isolated myelitis (17%).
In 205 patients with cord involvement at MR imaging, 39 (19%) presented with an upper motor neuron (UMN) syn-drome, 93 (45%) with a lower motor neuron (LMN) syndrome and 69 (34%) with mixed UMN and LMN signs. Spinal symp-tom duration varied according to these clinical presentations; patients with a pure UMN syndrome had the longest duration (median [IQR], 91 [33–171] days), those with mixed signs had
an intermediate duration (35 [16–91] days), and those with an LMN syndrome had the shortest duration (23 [12–50] days) (P < .001 for UMN vs mixed and P = .03 for mixed vs LMN signs).
Correlation Between CSF and MR Imaging Findings
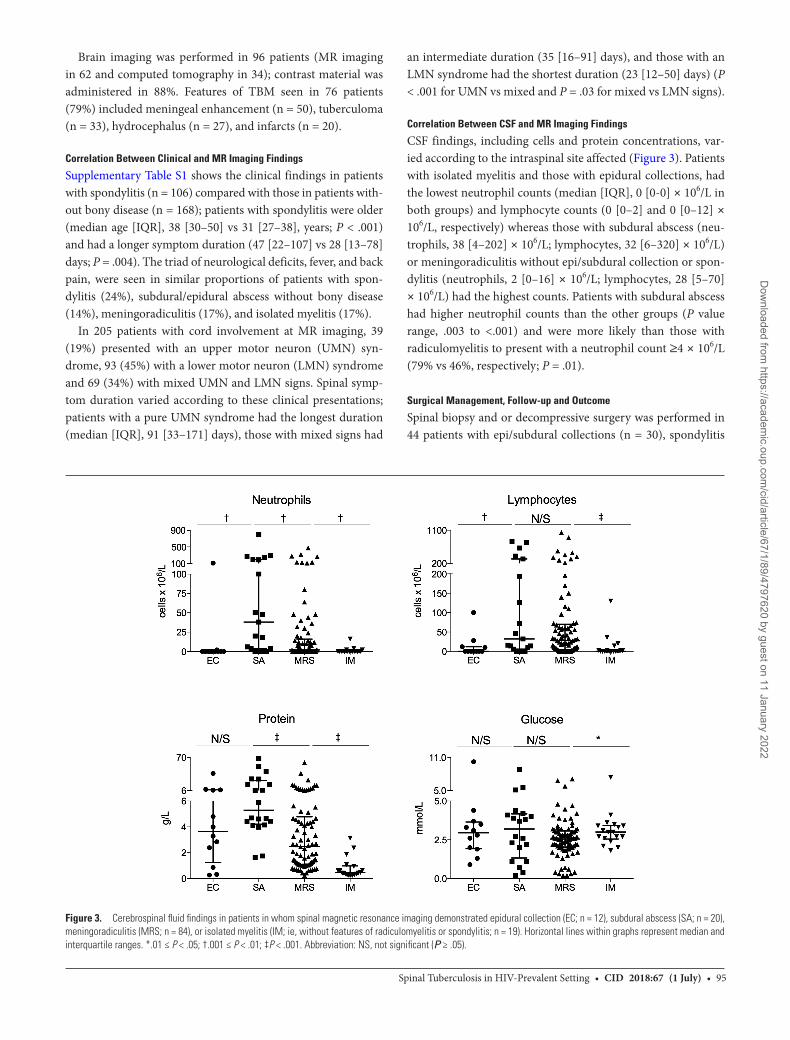
CSF findings, including cells and protein concentrations, var-ied according to the intraspinal site affected (Figure 3). Patients with isolated myelitis and those with epidural collections, had the lowest neutrophil counts (median [IQR], 0 [0-0] × 106/L in both groups) and lymphocyte counts (0 [0–2] and 0 [0–12] × 106/L, respectively) whereas those with subdural abscess (neu-trophils, 38 [4–202] × 106/L; lymphocytes, 32 [6–320] × 106/L) or meningoradiculitis without epi/subdural collection or spon-dylitis (neutrophils, 2 [0–16] × 106/L; lymphocytes, 28 [5–70] × 106/L) had the highest counts. Patients with subdural abscess had higher neutrophil counts than the other groups (P value range, .003 to <.001) and were more likely than those with radiculomyelitis to present with a neutrophil count ≥4 × 106/L (79% vs 46%, respectively; P = .01).
Surgical Management, Follow-up and Outcome
Spinal biopsy and or decompressive surgery was performed in 44 patients with epi/subdural collections (n = 30), spondylitis
Figure 3. Cerebrospinal fluid findings in patients in whom spinal magnetic resonance imaging demonstrated epidural collection (EC; n = 12), subdural abscess (SA; n = 20), meningoradiculitis (MRS; n = 84), or isolated myelitis (IM; ie, without features of radiculomyelitis or spondylitis; n = 19). Horizontal lines within graphs represent median and interquartile ranges. *.01 ≤ P < .05; †.001 ≤ P < .01; ‡P < .001. Abbreviation: NS, not significant (P ≥ .05).
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022

96 • CID 2018:67 (1 July) • Marais et al
Marais et al
(n = 13), or intramedullary lesions (n = 1). In addition to 57 patients who initially presented with a paradoxical reaction, 6 patients experienced paradoxical CNS worsening after study entry; 3 patients showed clinical deterioration, including an HIV-infected patient with a recurrence of spinal tuberculo-sis-IRIS symptoms 5 months after presentation secondary to a new subdural tuberculoma and 2 HIV-uninfected patients with recurrent spinal abscess (2.5 months after tuberculosis treat-ment initiation) and new subdural tuberculoma (8 months after tuberculosis treatment initiation), respectively. Asymptomatic radiological deterioration was seen on follow-up images in the other 3 patients, including worsening myelitis (n = 1) and increased size of tuberculoma (n = 1) in HIV-infected patients not receiving ART, and new intracranial tuberculoma in an HIV-uninfected patient. Of patients who were followed up for 9 months, 38 of 87 (44%) were able to walk at end of follow-up. Similar proportions of HIV-infected and HIV-uninfected patients showed improvement.
MR imaging of the spine was repeated in 50 patients at a median follow-up of 12 months (IQR, 6–26 months). Improvement was seen in 35 of 50 patients; findings were unchanged in 8, and 7 showed deterioration with new syrinx formation (n = 3), new enhancing lesions (n = 5; due to para-doxical reaction in 3 and to poor compliance with tuberculosis treatment in 2), and cord atrophy (n = 1).
DISCUSSION
This is, to our knowledge, the largest series of patients with spinal tuberculosis thus far published. Radiculomyelitis, which was present in 77% of patients, is commonly reported as a com-plication of (1) TBM, through downward disease extension, or (2) tuberculosis spondylitis, through epidural disease progres-sion [10, 22]. Primary nonbony spinal tuberculosis is the third scenario that occurs, owing to hematological dissemination to the diseased area [3, 22]. In our study, a third of patients with radiculomyelitis presented with primary intraspinal tuberculo-sis, emphasizing the importance of considering the diagnosis in patients with spinal symptoms without the more common fea-tures of neurological tuberculosis (ie, meningitis or spondylitis). Subdural abscess/tuberculoma [7, 10, 11, 18, 23–25], epidural abscess (without spondylitis) [3, 26–28], and intramedullary tuberculoma [7, 10, 27, 29–34] are rarely reported in the litera-ture; only case reports and small case series exist. A review of all cases of spinal complications of TBM reported 147 cases, which included subdural tuberculoma (n = 36), intramedullary tuber-culoma (n = 13) and abscess (n = 13) [35]. We report 42 cases of subdural abscess (including 15 tuberculoma), 33 of intramedul-lary tuberculoma, and 3 of epidural abscess without spondylitis.
Noncommunicable comorbid conditions were common in HIV-uninfected patients (28% vs 8% in HIV-infected patients), and probably contributed to tuberculosis susceptibility. In par-ticular, diabetes, a known risk factor for active tuberculosis,
was present in 10% of HIV-uninfected patients [36]. Spinal tuberculosis was associated with significant morbidity. At pres-entation 86% were unable to walk, which probably reflects a combination of factors, such as delayed treatment initiation and extensive CNS involvement. However, the full magnitude of the long-term clinical consequences of spinal tuberculosis could not be assessed, considering the limited proportion of patients who were followed up for the duration of tuberculo-sis treatment (32%) and the sizable proportion of patients for whom mortality data were unavailable (37%). The gap in the lit-erature regarding long-term outcome in spinal tuberculosis (in particular radiculomyelitis) therefore remains, which should be addressed in future studies.
Even though IALCH is not the primary referral center for patients with bony involvement, spondylitis was a frequent finding, especially in HIV-uninfected patients. There is a predi-lection of tuberculosis for the anterior vertebral body. Posterior element involvement is rare, especially in isolation [37]. In our study, a high proportion of patients with bony disease had posterior element involvement (28%), all in association with vertebral body disease. These findings are similar to those in a small study that detected extension of vertebral body tubercu-losis into the posterior vertebral arch in 53% of patients (10 of 19) with spinal tuberculosis demonstrated by MR imaging [38]. Similar to a previous report [8], vertebral destruction was more common in HIV-uninfected than in HIV-infected patients with spondylitis. It has been suggested that the reduced bony destruction associated with HIV occurs because of an impaired type IV hypersensitivity reaction and consequently reduced granulation formation [8]. In a study of patients with spinal tuberculosis lesions, the granulomatous architecture and mac-rophage activation seen at biopsy were similar in HIV-infected (n = 9) and HIV-uninfected (n = 13) patients [39], so the reason for our observation remains unclear.
Paradoxical clinical and or radiological deterioration after effective tuberculosis treatment initiation, referred to as “par-adoxical reaction”, is common in both HIV-infected and HIV-uninfected patients with CNS tuberculosis [19, 40]. HIV-infected patients are particularly vulnerable to paradoxical tuberculosis-IRIS, which occurs after ART is started during tuberculosis treatment; in 1 study, neurological tuberculo-sis-IRIS developed in almost half of patients with TBM who started ART 2 weeks after tuberculosis treatment [21]. In our study, paradoxical reaction occurred mostly after TBM and accounted for a significant proportion of spinal tuberculosis cases. Although a minority of paradoxical reactions in HIV-infected patients (16 of 50) occurred after ART initiation, only 25 patients were known to start ART during tuberculosis treat-ment; furthermore, the time of ART initiation was unknown for 7 HIV-infected patients who presented with paradoxical reaction. There is no diagnostic test for paradoxical reaction or tuberculosis-IRIS and it is therefore vital to consider and
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022

Spinal Tuberculosis in HIV-Prevalent Setting • CID 2018:67 (1 July) • 97
Spinal Tuberculosis in HIV-Prevalent Setting
exclude other causes for deterioration, such as poor adherence to tuberculosis treatment or ART, drug reactions or toxic effect, other infections, and tuberculosis drug resistance [20].
The triad of fever, back pain, and neurological symptoms, which is suggestive of epidural abscess [41], occurred at similar frequencies in patients with spondylitis, epi/subdural abscess, radiculomyelitis, or isolated myelitis, emphasizing its limita-tion in predicting the presence of epi/subdural abscess in spinal tuberculosis. However, increased CSF neutrophil counts may suggest the presence of subdural abscess in patients with sus-pected spinal tuberculosis. Patients with isolated tuberculosis myelitis frequently had minimal features of CSF inflammation; a diagnosis of spinal tuberculosis should therefore not be dis-missed in patients with such findings.
Limitations of our study include its retrospective nature and therefore the limited information on long-term patient outcome. Complications that occurred after presentation, such as para-doxical reaction/IRIS and drug-induced hepatitis, were probably diagnosed and managed at referring hospitals and were rarely doc-umented during follow-up; these complications probably contrib-uted to the significant loss to follow-up. Patients with tuberculosis spondylitis evident at plain film radiography are usually referred elsewhere, and the contribution of spondylitis to spinal tuber-culosis (regardless of HIV status) was probably underestimated. A relatively small proportion of patients were HIV-uninfected, and differences according to HIV status could have been missed. A minority of patients had definite neurological tuberculosis that could be explained by the large proportion of patients (50%) already receiving tuberculosis treatment at presentation. However, the majority of patients with probable neurological tuberculosis showed neurological improvement with tuberculosis treatment in the absence of other disease-specific therapies, and the remaining cases were included according to stringent criteria.
In conclusion, we describe a high frequency of previously rarely reported manifestations of spinal tuberculosis, suggest-ing that they are more common than what the literature implies. These findings will contribute to the clinical knowledge of spi-nal tuberculosis in setting with a high prevalence of tuberculo-sis/HIV coinfection.
Supplementary DataSupplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the authors to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the authors, so questions or comments should be addressed to the corresponding author.
NotePotential conflicts of interest. All authors: No reported conflicts.
All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the con-tent of the manuscript have been disclosed.
References1. Patkar D, Narang J, Yanamandala R, Lawande M, Shah GV. Central nervous sys-
tem tuberculosis: pathophysiology and imaging findings. Neuroimaging Clin N Am 2012; 22:677–705.
2. Dunn R, van der Horst A, Lippross S. Tuberculosis of the spine—prospective neurological and patient reported outcome study. Clin Neurol Neurosurg 2015; 133:96–101.
3. Arora S, Kumar R. Tubercular spinal epidural abscess involving the dorsal-lum-bar-sacral region without osseous involvement. J Infect Dev Ctries 2011; 5:544–9.
4. Candy S, Chang G, Andronikou S. Acute myelopathy or cauda equina syndrome in HIV-positive adults in a tuberculosis endemic setting: MRI, clinical, and pathologic findings. Am J Neuroradiol 2014; 35:1634–41.
5. Modi G, Ranchhod J, Hari K, Mochan A, Modi M. Non-traumatic myelopathy at the Chris Hani Baragwanath Hospital, South Africa—the influence of HIV. QJM 2011; 104:697–703.
6. Bhigjee AI, Madurai S, Bill PL, et al. Spectrum of myelopathies in HIV seroposi-tive South African patients. Neurology 2001; 57:348–51.
7. Alessi G, Lemmerling M, Nathoo N. Combined spinal subdural tuberculous empyema and intramedullary tuberculoma in an HIV-positive patient. Eur Radiol 2003; 13:1899–901.
8. Anley CM, Brandt AD, Dunn R. Magnetic resonance imaging findings in spinal tuberculosis: comparison of HIV positive and negative patients. Indian J Orthop 2012; 46:186–90.
9. Cormican L, Hammal R, Messenger J, Milburn HJ. Current difficulties in the diag-nosis and management of spinal tuberculosis. Postgrad Med J 2006; 82:46–51.
10. Gupta R, Garg RK, Jain A, Malhotra HS, Verma R, Sharma PK. Spinal cord and spinal nerve root involvement (myeloradiculopathy) in tuberculous meningitis. Medicine (Baltimore) 2015; 94:e404.
11. Hernández-Albújar S, Arribas JR, Royo A, González-García JJ, Peña JM, Vázquez JJ. Tuberculous radiculomyelitis complicating tuberculous meningitis: case report and review. Clin Infect Dis 2000; 30:915–21.
12. Leibert E, Schluger NW, Bonk S, Rom WN. Spinal tuberculosis in patients with human immunodeficiency virus infection: clinical presentation, therapy and out-come. Tuber Lung Dis 1996; 77:329–34.
13. Woolsey RM, Chambers TJ, Chung HD, McGarry JD. Mycobacterial meningo-myelitis associated with human immunodeficiency virus infection. Arch Neurol 1988; 45:691–3.
14. Metta H, Corti M, Redini L, Yampolsky C, Schtirbu R. Spinal epidural abscess due to Mycobacterium tuberculosis in a patient with AIDS: case report and review of the literature. Braz J Infect Dis 2006; 10:146–8.
15. Bono CM. Spectrum of spine infections in patients with HIV: a case report and review of the literature. Clin Orthop Relat Res 2006; 444:83–91.
16. Antimycobacterials. In: Gibbon CJ, Blockman M, eds. South African medicines formulary. 8th ed. Cape Town, South Africa: Division of Clinical Pharmacology, Faculty of Health Sciences, University of Cape Town, 2008:301–2.
17. Marais S, Thwaites G, Schoeman JF, et al. Tuberculous meningitis: a uniform case definition for use in clinical research. Lancet Infect Dis 2010; 10:803–12.
18. Roca B. Intradural extramedullary tuberculoma of the spinal cord: a review of reported cases. J Infect 2005; 50:425–31.
19. Garg RK, Malhotra HS, Kumar N. Paradoxical reaction in HIV negative tubercu-lous meningitis. J Neurol Sci 2014; 340:26–36.
20. Meintjes G, Lawn SD, Scano F, et al. International Network for the Study of HIV-associated IRIS. Tuberculosis-associated immune reconstitution inflammatory syndrome: case definitions for use in resource-limited settings. Lancet Infect Dis 2008; 8:516–23.
21. Marais S, Meintjes G, Pepper DJ, et al. Frequency, severity, and prediction of tuberculous meningitis immune reconstitution inflammatory syndrome. Clin Infect Dis 2013; 56:450–60.
22. Bernaerts A, Vanhoenacker FM, Parizel PM, et al. Tuberculosis of the cen-tral nervous system: overview of neuroradiological findings. Eur Radiol 2003; 13:1876–90.
23. Luo L, Pino J. An intradural extramedullary tuberculoma of the spinal cord in a non-HIV-infected patient: case report and review of the literature. Lung 2006; 184:187–93.
24. Ozates M, Ozkan U, Kemaloglu S, Hosoglu S, Sari I. Spinal subdural tuberculous abscess. Spinal Cord 2000; 38:56–8.
25. Sandler AL, Thompson D, Goodrich JT, et al. Infections of the spinal subdural space in children: a series of 11 contemporary cases and review of all published reports. A multinational collaborative effort. Childs Nerv Syst 2013; 29:105–17.
26. Mantzoros CS, Brown PD, Dembry L. Extraosseous epidural tuberculoma: case report and review. Clin Infect Dis 1993; 17:1032–6.
27. Wasay M, Arif H, Khealani B, Ahsan H. Neuroimaging of tuberculous mye-litis: analysis of ten cases and review of literature. J Neuroimaging 2006; 16:197–205.
28. Zhang Q, Koga H. Tubercular spinal epidural abscess of the lumbosacral region without osseous involvement: comparison of spinal MRI and pathological find-ings of the resected tissue. Intern Med 2016; 55:695–8.
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022

98 • CID 2018:67 (1 July) • Marais et al
Marais et al
29. Garg RK, Sharma R, Kar AM, et al. Neurological complications of miliary tuber-culosis. Clin Neurol Neurosurg 2010; 112:188–92.
30. Chitre PS, Tullu MS, Sawant HV, Ghildiyal RG. Co-occurrence of intracerebral tuber-culoma with lumbar intramedullary tuberculoma. J Child Neurol 2009; 24:606–9.
31. Kemaloğlu S, Gür A, Nas K, Cevik R, Büyükbayram H, Saraç AJ. Intramedullary tuberculoma of the conus medullaris: case report and review of the literature. Spinal Cord 2001; 39:498–501.
32. Li H, Liu W, You C. Central nervous system tuberculoma. J Clin Neurosci 2012; 19:691–5.
33. Sharma MC, Arora R, Deol PS, Mahapatra AK, Sinha AK, Sarkar C. Intramedullary tuberculoma of the spinal cord: a series of 10 cases. Clin Neurol Neurosurg 2002; 104:279–84.
34. Varghese P, Abdul Jalal MJ, Kandathil JC, Mathew IL. Spinal intramedullary tuberculosis. Surg J (N Y) 2017; 3:e53–7.
35. Garg RK, Malhotra HS, Gupta R. Spinal cord involvement in tuberculous menin-gitis. Spinal Cord 2015; 53:649–57.
36. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med 2008; 5:e152.
37. Currie S, Galea-Soler S, Barron D, Chandramohan M, Groves C. MRI character-istics of tuberculous spondylitis. Clin Radiol 2011; 66:778–87.
38. Le Page L, Feydy A, Rillardon L, et al. Spinal tuberculosis: a longitudinal study with clinical, laboratory, and imaging outcomes. Semin Arthritis Rheum 2006; 36:124–9.
39. Danaviah S, Sacks JA, Kumar KP, et al. Immunohistological characterization of spinal TB granulomas from HIV-negative and -positive patients. Tuberculosis (Edinb) 2013; 93:432–41.
40. Singh AK, Malhotra HS, Garg RK, et al. Paradoxical reaction in tuberculous men-ingitis: presentation, predictors and impact on prognosis. BMC Infect Dis 2016; 16:306.
41. Patel AR, Alton TB, Bransford RJ, Lee MJ, Bellabarba CB, Chapman JR. Spinal epidural abscesses: risk factors, medical versus surgical management, a retrospec-tive review of 128 cases. Spine J 2014; 14:326–30.
Dow
nloaded from https://academ
ic.oup.com/cid/article/67/1/89/4797620 by guest on 11 January 2022

![HKIFM CPD MVAC.ppt [\254\333\256e\274\322\246\241]](https://static.fdokumen.com/doc/165x107/63175591c72bc2f2dd056c30/hkifm-cpd-mvacppt-254333256e274322246241.jpg)




![100040.ppt [\254\333\256e\274\322\246\241]](https://static.fdokumen.com/doc/165x107/633baafca215b3a22b0d61d3/100040ppt-254333256e274322246241.jpg)











![Betty_Eng.ppt [\254\333\256e\274\322\246\241]](https://static.fdokumen.com/doc/165x107/6320bdd6aaa3e1b19f07a319/bettyengppt-254333256e274322246241.jpg)

