Somatostatin, Somatostatin Analogs and Somatostatin Receptor Dynamics in the Biology of Cancer...
17
Send Orders of Reprints at [email protected] Current Molecular Medicine 2012, 12, 1-17 1 1566-5240/12 $58.00+.00 © 2012 Bentham Science Publishers Somatostatin, Somatostatin Analogs and Somatostatin Receptor Dynamics in The Biology of Cancer Progression Massimiliano Ruscica 1 , Marica Arvigo 2 , Liliana Steffani 1 , Diego Ferone 2 and Paolo Magni *,1 1 Dipartimento di Scienze Farmacologiche e Biomolecolari, Università degli Studi di Milano, Milan, Italy 2 Department of Internal Medicine and Center of Excellence for Biomedical Research, University of Genova, Italy Abstract: The pharmacological effects (i.e., inhibition of endocrine secretion and cell proliferation) mediated by the hormone somatostatin (SRIF) are derived from its universal high-affinity binding to five different G protein- coupled receptors (GPCRs), named sst1-5. However, SRIF has a half-life of less than 3 min, whereas the available mono- and bi-specific SRIF preferential analogs show prolonged half-life and increased potency. These compounds may control tumor development, cell proliferation and metastatization by direct actions, including cell division arrest in G0/G1 phase (i.e., induction of cyclin-dependent kinase inhibitor p27 kip1 or p21 Cip1 ), induction of apoptosis (i.e., induction of p53 and Bax) and suppression of cell invasion. Along with these direct actions on the biology of cancer progression, in vivo SRIF analogs may also regulate tumor growth through indirect actions, by suppressing the secretion of growth-promoting hormones and growth factors and angiogenesis. Interestingly, when ssts are co-expressed, they may interact forming homo- or heterodimers, also with other GPCRs such as type 2 dopamine receptor and the -opioid receptor 1, altering their original pharmacological and functional properties. Dimers can be not only constitutive, but perhaps also ligand- promoted: hence, compounds with high affinity for different ssts isoforms may be used to achieve effects elicited by specific dimers. Future developments in the knowledge of ssts dynamics upon SRIF and SRIF analogs binding in neoplastic tissues may allow the full elucidation of the pathophysiological role of this system and the exploitation of the therapeutic potential of its modulation. Keywords: Angiogenesis in cancer, cancer cell proliferation, metastatization, somatostatin, somatostatin analogs in cancer, somatostatin receptors in cancer. INTRODUCTION It has been over three decades since the first isolation and structural elucidation of somatostatin [1], as the hypothalamic factor responsible for the suppression of growth hormone (GH/somatotropin) secretion; hence the abbreviation SRIF (somatotropin- releasing inhibiting factor). Since then, compelling evidence has implicated SRIF in the inhibition of the growth and development of various normal and tumor cells. The medical applications of SRIF and its chemically designed analogs have expanded, along with an increasing knowledge of the pharmacological effects of these compounds [2]. Among them, octreotide and lanreotide are currently used in the clinical practice to treat patients with acromegaly or symptoms of carcinoid syndrome due to metastatic neuroendocrine tumors (NETs) [3]. Conversely, somewhat confusing in vivo and in vitro data exist on SRIF effects on solid tumors (for review, see [3]). Some of the major approaches for treatment of metastatic cancer, such as conventional chemotherapy, show relevant limitations, partly due to non-specificity that *Address correspondence to this author at the Dipartimento di Scienze Farmacologiche e Biomolecolari, Università degli Studi di Milano, via G. Balzaretti, 9, 20133 Milan, Italy; Tel: ++39-02- 5031.8229; Fax: ++39-02-5031.8204; E-mail: [email protected] results in toxic side effects and drug resistance. Thus, considerable interest has been placed on "biological" receptor-targeted cancer therapy, since certain receptors were found to be expressed in high concentrations in cancer cells. Specifically, SRIF receptors (ssts) are highly expressed in different tumor cells and primary tumor tissues, including NETs at different sites (lung, gastrointestinal, pancreatic, pituitary, thyroid medullary cancer, prostate and others) [4-6] and non-NETs (breast, lung, colorectal, prostate, ovary and others) [7-10]. The effects of treatment with the clinically-available SRIF analogs octreotide and lanreotide, which mainly target the sst2 receptor isoform, have thus been evaluated in clinical studies on solid tumors, unfortunately substantially failed [3]. Probably such results derived from (a) the lack of characterization of ssts in solid tumors, which may not be routinely performed in clinical studies [3] and (b) the complex biological dynamics of ssts, which includes the cyclic process of signaling, desensitization, internalization, resensitization, and recycling to the plasma membrane. For these reasons, the present review discusses the role of the SRIF system in the context of the biology of cancer progression, focusing on sst dynamics in terms of trafficking, receptor- receptor interaction, dimerization and indirect effects (i.e., angiogenesis and cell invasion) of SRIF on cell growth.
Transcript of Somatostatin, Somatostatin Analogs and Somatostatin Receptor Dynamics in the Biology of Cancer...

Send Orders of Reprints at [email protected]
Current Molecular Medicine 2012, 12, 1-17 1
1566-5240/12 $58.00+.00 © 2012 Bentham Science Publishers
Somatostatin, Somatostatin Analogs and Somatostatin Receptor Dynamics in The Biology of Cancer Progression
Massimiliano Ruscica1, Marica Arvigo2, Liliana Steffani1, Diego Ferone2 and Paolo Magni*,1
1Dipartimento di Scienze Farmacologiche e Biomolecolari, Università degli Studi di Milano, Milan, Italy
2Department of Internal Medicine and Center of Excellence for Biomedical Research, University of Genova,
Italy
Abstract: The pharmacological effects (i.e., inhibition of endocrine secretion and cell proliferation) mediated by
the hormone somatostatin (SRIF) are derived from its universal high-affinity binding to five different G protein-
coupled receptors (GPCRs), named sst1-5. However, SRIF has a half-life of less than 3 min, whereas the
available mono- and bi-specific SRIF preferential analogs show prolonged half-life and increased potency.
These compounds may control tumor development, cell proliferation and metastatization by direct actions,
including cell division arrest in G0/G1 phase (i.e., induction of cyclin-dependent kinase inhibitor p27kip1
or
p21Cip1
), induction of apoptosis (i.e., induction of p53 and Bax) and suppression of cell invasion. Along with
these direct actions on the biology of cancer progression, in vivo SRIF analogs may also regulate tumor growth
through indirect actions, by suppressing the secretion of growth-promoting hormones and growth factors and
angiogenesis. Interestingly, when ssts are co-expressed, they may interact forming homo- or heterodimers,
also with other GPCRs such as type 2 dopamine receptor and the -opioid receptor 1, altering their original
pharmacological and functional properties. Dimers can be not only constitutive, but perhaps also ligand-
promoted: hence, compounds with high affinity for different ssts isoforms may be used to achieve effects
elicited by specific dimers. Future developments in the knowledge of ssts dynamics upon SRIF and SRIF
analogs binding in neoplastic tissues may allow the full elucidation of the pathophysiological role of this system
and the exploitation of the therapeutic potential of its modulation.
Keywords: Angiogenesis in cancer, cancer cell proliferation, metastatization, somatostatin, somatostatin analogs in cancer, somatostatin receptors in cancer.
INTRODUCTION
It has been over three decades since the first isolation and structural elucidation of somatostatin [1], as the hypothalamic factor responsible for the suppression of growth hormone (GH/somatotropin) secretion; hence the abbreviation SRIF (somatotropin-releasing inhibiting factor). Since then, compelling evidence has implicated SRIF in the inhibition of the growth and development of various normal and tumor cells. The medical applications of SRIF and its chemically designed analogs have expanded, along with an increasing knowledge of the pharmacological effects of these compounds [2]. Among them, octreotide and lanreotide are currently used in the clinical practice to treat patients with acromegaly or symptoms of carcinoid syndrome due to metastatic neuroendocrine tumors (NETs) [3]. Conversely, somewhat confusing in vivo and in vitro data exist on SRIF effects on solid tumors (for review, see [3]). Some of the major approaches for treatment of metastatic cancer, such as conventional chemotherapy, show relevant limitations, partly due to non-specificity that
*Address correspondence to this author at the Dipartimento di Scienze Farmacologiche e Biomolecolari, Università degli Studi di
Milano, via G. Balzaretti, 9, 20133 Milan, Italy; Tel: ++39-02-5031.8229; Fax: ++39-02-5031.8204; E-mail: [email protected]
results in toxic side effects and drug resistance. Thus, considerable interest has been placed on "biological" receptor-targeted cancer therapy, since certain receptors were found to be expressed in high concentrations in cancer cells. Specifically, SRIF receptors (ssts) are highly expressed in different tumor cells and primary tumor tissues, including NETs at different sites (lung, gastrointestinal, pancreatic, pituitary, thyroid medullary cancer, prostate and others) [4-6] and non-NETs (breast, lung, colorectal, prostate, ovary and others) [7-10]. The effects of treatment with the clinically-available SRIF analogs octreotide and lanreotide, which mainly target the sst2 receptor isoform, have thus been evaluated in clinical studies on solid tumors, unfortunately substantially failed [3]. Probably such results derived from (a) the lack of characterization of ssts in solid tumors, which may not be routinely performed in clinical studies [3] and (b) the complex biological dynamics of ssts, which includes the cyclic process of signaling, desensitization, internalization, resensitization, and recycling to the plasma membrane. For these reasons, the present review discusses the role of the SRIF system in the context of the biology of cancer progression, focusing on sst dynamics in terms of trafficking, receptor-receptor interaction, dimerization and indirect effects (i.e., angiogenesis and cell invasion) of SRIF on cell growth.
massimilianoruscica
Barra
massimilianoruscica
Barra
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Font monospazio
massimilianoruscica
Font monospazio
massimilianoruscica
Font monospazio

2 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
SOMATOSTATIN
SRIF peptide, originally identified by Krulich [11], was first isolated from ovine hypothalamic fragments [1], and subsequently in porcine hypothalamus, as well as in pigeon and anglerfish pancreas [12]. It is a cyclic tetradecapeptide ((H-Ala
1-Gly
2-cyclic[Cys
3-Lys
4-Asn
5-
Phe6-Phe
7-Trp
8-Lys
9-Thr
10-Phe
11-Thr
12-Ser
13 Cys
14]-
OH) containing a disulfide bond linking the cysteine residues at position 3 and 14 (cys
3-cys
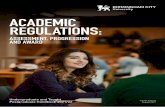
14) (Fig. 1A).
SRIF was classified as a hypothalamic neurohormone which potently inhibits GH secretion and it is produced throughout the central and peripheral nervous systems. In the periphery, the endocrine pancreas and the gut are the main sources of SRIF, but SRIF-producing cells are also present in the thyroid, adrenals, submandibular glands, kidneys, prostate, and placenta
[13-16]. Furthermore, SRIF immunoreactive cells are present in the retina and in endocrine areas where the activity of somatostatinergic neurons is regulated by the light (i.e., the pineal gland) (reviewed in [17]). SRIF mainly inhibits the secretion of multiple pituitary, pancreatic, and gastrointestinal (GI) hormones, like thyroid stimulating hormone, insulin, glucagon [18], as well as locomotor activity and cognitive functions [19]. Moreover, this hormone also appears to mediate antiproliferative effects by cell cycle arrest or apoptosis induction in cancer [20-24] (see section “Somatostatin and somatostatin analogs in cancer cell proliferation”).
The human SRIF gene is located on chromosome 3q28 and it codes for a pro-hormone which undergoes tissue specific processing to produce either the tetradecapeptide SRIF-14 or the octacosapeptide
Fig. (1). (A) structure of cyclic tetradecapeptide SRIF-14 which contains the peculiar tetrapeptide-active pharmacophore (Phe7-
Trp8-Lys
9-Thr
10) and a disulfide bond linking the cys
3-cys
14; (B) structure of some cyclooctapeptide synthetic SRIF analogs
(octreotide, vapreotide, lanreotide and TT-232) with some substitutions into the active pharmacophore; (C) structure of
pasireotide (SOM-230). Dec, diaminoethylcarbamoyl; HyPro, hydroxyproline; Phg, phenylglicine; Tyr(Bzl), (4-O-benzyl)-L-
tyrosine.

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 3
SRIF-28 isoforms. SRIF-28 was isolated from porcine intestine [25] and pig and ovine hypothalamus [12, 26] and represents a congener of SRIF-14 extended at the N-terminus by 14 amino acids (aa) residues (Ser-Ala-Asn-Ser-Asn-Pro-Ala-Met-Ala-Pro-Arg-Glu-Arg-Lys-(SRIF-14)). In mammals both SRIF isoforms originate from a 116 aa prepro-SRIF precursor (12.7-kDa) which is synthetized in the anterior hypothalamic periventricular nuclei and contains a 24 aa signal sequence (cleavage at gly
-1-ala
+1 junction). Hence, the
prepro-SRIF is translated into a 92 aa residues pro-hormone, 10.3-kDa pro-SRIF, which undergoes, from the N-terminus (first aa) to the C-terminus (92
nd aa),
both monobasic (Arg64
) and dibasic (Arg77
-Lys78
) cleavages. These latter events release the two bioactive peptides SRIF-28 and SRIF-14 (reviewed in [27]). Production of SRIF-14 and -28 is quantitatively variable from tissue to tissue as well as in different cell types [28].
EXPRESSION OF SOMATOSTATIN RECEPTORS IN CANCER
The biological effects of SRIF are mediated by specific plasma membrane receptors that have been identified in normal and neoplastic tissues by binding studies and receptor autoradiography techniques (reviewed in [29]). Human ssts, named sst1-5, are encoded by different intronless (except for sst2) genes located at chromosomes 14q13, 17q24, 22q13.1, 20p11.2 and 16p13.3, respectively. However, introns have been found in the 5’-untraslated regions of SSTR2, SSTR3 and SSTR5 genes (reviewed in [30]).
The presence of a cryptic splice site (i.e., lacking a typical exon-intron structure) at the 3’ end of the coding region of SSTR2 gene gives rise to two membrane proteins with 7 trans-membrane domain (TMDs) which differ only in the length of the cytoplasmic tail, a long variant of 369 aa (sst2A) and a shorter one of 346 aa (sst2B) [31, 32]. The other sst proteins, which belong to the so-called ‘‘superfamily’’ of GPCRs, consist of 391- (sst1), 418- (sst3), 388- (sst4) and 363-aa (sst5), respectively [33-36].
These receptors are classified as GPCR subtypes within the GPCRDB database [37-39], which divides the GPCRs into six classes (Class A: Rhodopsin-like, with over 80% of all GPCRs in humans; Class B: Secretin-like; Class C: Metabotropic glutamate receptors; Class D: Pheromone receptors; Class E: cyclic adenosine monophosphate (cAMP) receptors; and the much smaller Class F: Frizzled/smoothened family) [40]. Specifically, ssts are categorized in class A if they rapidly dissociate from -arrestin during internalization or in class B if they remain associated with -arrestin. These differences translate into a quicker recycling to the plasma membrane for the GPCRs class A than the class B one [41]. Moreover, GPCRs may exist as either homo- or heterodimers and dimerization could have an important role in ligand binding, signaling, receptor desensitization, and receptor trafficking [42].
All sst isoforms possess a highly conserved sequence motif, YANSCANPI/VLY, in the seventh transmembrane region, which serves as a signature sequence for this receptor family [43]. Duran-Prado [44] and Cordoba-Chacon [45] have also found the existence of novel spliced functional variants of sst5 in humans, rodents and porcine due to non-canonical splicing events which cannot follow the GT-AG rule [45] and give rise to different truncated sst5 receptor variants with five or four TMDs in humans (hsst5TMD5 and hsst5TMD4, respectively). Human sst5TMD4 variant expression is very uncommon in normal tissues, is present at low levels in lung, kidney, liver, brain and is abundant in several types of pituitary tumors. Interestingly, this evidence could have clinical implications in justifying the octreotide non-responder GH-secreting tumors. A study conducted on 25 somatotropinomas highlighted that expression of hsst5TMD4 variant worsens the ability of octreotide to reduce GH levels in vivo and is partially negatively correlated with inhibition of GH secretion by a monospecific sst5 BIM-23268 in vitro, using dispersed pituitary tumor cells [46]. Moreover, the presence of the hsst5TMD4 variant in sporadic ductal invasive breast cancer and human breast adenocarcinoma MCF-7 cells was associated with enhanced malignant behaviour, promoting invasion and proliferation ability [47].
The novel spliced functional sst5 variants have also been identified in other species like mice which display four, two and one TMDs (msst5TMD4, msst5TMD2 and msst5TMD1, respectively); rat with one TMD (rsst5TMD1); and porcine with six and three TMDs (psst5TMD6 and psst5TMD3) [48].
The association of sst and cancer has also been investigated in different retrospective studies that compared the SSTRs gene variants in prostate [49], breast [50] and pancreatic [51] cancers, as well as in acromegaly [52]. While SSTR2 gene polymorphisms were significant but weakly associated with breast cancer risk, and no association between SSTR1-5 gene polymorphisms and prostate cancer (PCa) risk were identified, in pancreatic tumors the SSTR5 P109S variant allele was associated with 1.62-fold increase risk. Interestingly, in a cohort of 48 patients with acromegaly and 96 control subjects, 19 single nucleotide polymorphisms (SNPs) were identified in the SSTR5 gene locus and among them rs34037914, rs169068 and rs642249 SNPs were significantly associated with the presence of acromegaly.
Ssts are highly and variably expressed in various primary tumor tissues, including NETs (GI, pancreatic, pituitary, medullary cancers, prostate, pancreatic) and non-NETs (breast, lung, colorectal, ovarian, cervical cancers). In general, many tumor cells, along with blood vessels of peritumoral veins, most frequently express sst2 at a high concentration, some also express sst1, sst3 and sst5, whereas fewer express sst4 (reviewed in [53]).
The gene expression of a single SSTR isoform in cancer may represent a useful marker in predicting a
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

4 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
better survival [54, 55]. Moreover, a high SSTR5/SSTR2 gene expression ratio has been associated to a positive outcome to long-term treatment with SRIF analogs in patients affected by TSHoma [56, 57].
SOMATOSTATIN ANALOGS
The unique pharmacological effects mediated by SRIF are derived from its universal high-affinity binding to all sst subtypes (sst1-sst5). However, SRIF has a very short in vivo half-life of less than 3 min, limiting its therapeutic utility in humans [58]. This shortcoming led chemists (a) to reduce the size, (b) to prolong the biological half-life, and (c) to enhance the specificity [59]. Moreover, a combinatorial chemistry approach has also been implemented for the identification of nonpeptide agonists selective for each sst subtype, i.e., L-363,377 which shows high affinity for sst2 and L-817,818 with high affinity for sst5 [60].
After elucidating the 3-dimensional structure, the enzymatic degradation pattern (which includes at least five sites [61]) and the minimal chain length for biological activity of the natural hormone, the synthesis of a large number of analogs was started already before 1974 [62]. Since 1976, numerous (> 450) modified analogs with prolonged half-life and increased potency have been developed [63] and few of them are widely used in the treatment of acromegaly [64]. SRIF-14 native molecule possesses a peculiar tetrapeptide-active pharmacophore (Phe
7-Trp
8-Lys
9-Thr
10) (Fig. 1A),
which was kept into the first octapeptide synthetized, octreotide (Sandostatin - octapeptide SMS 201-995) [65, 66]. Its short chain, along with one disulfide bridge and the terminal Thr-COOH group reduced to an alcohol function, allowed octreotide a half-life of 90-120 min when administrated subcutaneously, and a pharmacodinamic action lasting up to 8-12 hours [67]. Interestingly, cyclooctapeptide synthetic analogs, such as lanreotide (Somatuline - BIM 23014, Fig. 1B) and vapreotide (RC-160, Fig. 1B), and the hexapeptide MK-678, had some substitutions into the active pharmacophore including D-Trp, which contributes to the prolonged half-life of the these molecules (Fig. 1B). All of these molecules, as well as octreotide, bind with high affinity to sst2 and to sst5 subtypes and sst3 with moderate affinity and show little or no affinity for sst1 and sst4 receptors [68]. At present, among SRIF analogs, octreotide, octreotide long-acting-release (LAR), lanreotide-sustained-release and lanreotide autogel are approved for clinical use [69].
SRIF agonists differ from SRIF in their affinities for the different sst subtypes. This feature is an important aspect to be evaluated since each of the sst subtypes is involved in multiple physiological and biological functions and is expressed in multiple tissues throughout the body [70]. Thus, targeting a single receptor is unlikely to achieve either functional or therapeutic specificity [71]. This concept has led to the development of new compounds, the so called bi-specific molecules (i.e., sst1/sst2 BIM-23704; sst2/sst5 BIM-23244) [72]. Specifically, BIM-23244 shows
approximately 2-fold greater affinity at sst2 and approximately 20-fold greater affinity at sst5 than octreotide and lanreotide which have high affinity for sst2 and moderate for sst5. However, there was a need to develop new analogs with multi-receptor binding profile (i.e., SOM230, KE108 and BIM-23A779) to be potentially effective not only in patients with acromegaly or carcinoid tumors who respond to octreotide, but also in patients unresponsive or refractory to octreotide, as well as in other diseases associated with ssts expression other than sst2, then increasing tumor responsiveness [73]. Pasireotide (SOM230) binds with high affinity to SRIF receptor subtypes sst1, sst2, sst3 and sst5, displays a 30- to 40-fold higher affinity for sst1 and sst5 than octreotide or lanreotide and shows a serum 23-h half-life in SOM230-treated animals [74].
The development of SOM230 (Fig. 1C) is currently rather advanced, since the results of a phase III study for Cushing’s disease have been released [75] and the drug is now under registration for this disease [76]. The results of a phase III study for acromegaly have been recently announced [77] and a phase III study for NETs is presently ongoing [76].
KE108 (a SRIF analog with a reduced-size and stabilized structure, Tyr0–(cyclo-D-Dab–Arg–Phe–Phe–D-Trp–Lys–Thr–Phe)) (Fig. 1B) is an extremely potent molecule that acts as an agonist at all five sst subtypes, but in vivo characterizations regarding its stability, metabolism, biodistribution and toxicology will represent further necessary steps before clinical applications [78]. Moreover, there are only few data about the pan-inhibitor BIM-23A779 (binding affinity for sst1, sst2, sst3, sst5, respectively: 2.5, 0.3, 0.6, 0.6 nmol/l) and they are considered not encouraging [79, 80].
The discovery that some SRIF and dopamine (DA) receptor subtypes are able to form heterodimers (i.e., sst5/D2R [81]) represented an interesting possibility in terms of physiological theory and drug development [82]. A series of chimeric compounds that incorporate structural elements of both SRIF and DA into a single molecule have been synthesized [71], based on the evidence that, in acromegaly, the combination of SRIF and DA agonists therapy (octreotide and bromocriptine, respectively) achieves a greater suppression of GH secretion than treatment with either agent alone [83, 84]. The dihybrid sst2/D2R BIM-23A387, compared to sst2- and D2R-monospecific compounds, showed an enhanced potency in suppressing GH and prolactin (PRL) secretion from human pituitary somatotroph adenoma cells in vitro [85]. However, the evidence that the improved GH-suppressive effect was interpreted as a rescue of response acting through the highly expressed SSTR5 in tumors expressing low levels of SSTR2 [86] led to synthesize molecules which display activity at the sst5 subtype, in addition to sst2/D2R. Some of these chimeric compounds are BIM-23A760 (IC50, nM of 0.03 for sst2, 15 for D2R and 42 for sst5), BIM-23A761 (IC50, nM of 0.06 for sst2, 27 for D2R and
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 5
3.7 for sst5) and BIM-23A765 (IC50, nM of 0.2 for sst2, 7 for D2R and 9 for sst5).
Besides the above described bi-specific or chimeric compounds, there are also some mono-specific sst subtype analogs (BIM-23745 and BIM-23926, sst1-selective; BIM-23197 and BIM-23120, sst2-selective; BIM-23268 and BIM-23206 sst5-selective) which resulted effective in mediating both antisecretive and antiproliferative features in experimental in vitro models [24, 46, 87-93].
So far we have reviewed compounds able to bind with high affinity to sst1, sst2, and sst5 subtypes. Concerning the sst3 subtype, BIM-23056 is classified both as a sst3 agonist with a relative selectivity which would appear to be species-dependent, and an antagonist blocking sst5 signaling [68]. The ODN-8 analog binds selectively to sst3 subtype, but it works as an antagonist [94]. New SRIF analogs with replacement of the tryptophan residue (Trp8) by one of the two enantiomers of 3-(3'-quinolyl)-alanine (Qla8) and binding sst1 and sst3 have been synthetized [95].
SSTR4 is expressed in human cerebellum, frontal cortex and hippocampus [96]. Within the past decade, revolving around this evidence, various high affinity sst4 peptides and non-peptide mimetics have been synthesized and shown to produce potent pharmacological activity [97].
TT-232, a heptapeptide sst4/sst1 receptor agonist and J-2156, a high affinity sst4 receptor-selective peptidomimetic agonist have been demonstrated to be potent anti-inflammatory and anti-nociceptive agents [98, 99]. Moreover, TT-232 also displayed direct antitumor effects, likely mediated by sst1 binding [99].
Interestingly, the hepta-back-bone cyclic peptide PTR-3173 (Somatoprim), which binds with high affinity to sst2, sst4 and sst5 subtypes, shows no inhibitory effect on glucagon and insulin secretion [100], but it is able to strongly suppress GH and PRL in human pituitary secreting cell culture [101].
Taking into consideration all the above reported data, we can conclude that increasing knowledge about sst subtypes expression and function in malignant diseases indicates a need for new analogs that can be incorporated into the therapeutic arsenal.
SOMATOSTATIN ANALOG ACTIVATION AFFECTS SOMATOSTATIN RECEPTOR MEMBRANE TRAFFICKING
GPCRs are synthesized and processed in the endoplasmic reticulum (ER) and post-translational modifications such as glycosylation and ubiquitination, oligomerization with other receptor molecules, association with accessory chaperone proteins and folding, take place in this compartment and are necessary for export. Subsequent trafficking through the ER and Golgi intermediate compartment (ERGIC) and Golgi apparatus also facilitates maturation and correct targeting to the cell surface (see review by [102]). Thus, the internalization of plasma membrane
receptors in response to drugs, hormones, and post-translational modifications are a well recognized phenomenon [103] which prevents cells from undergoing excessive receptor stimulation or periods of prolonged inactivity [104]. SRIF receptors differently internalize after agonist binding and, specifically, sst2, sst3 and sst5 are internalized to a higher extent than sst1 or sst4 [105].
In 2001, Liu [106] showed for the first time that human sst1 undergoes rapid, agonist-stimulated phosphorylation and that receptor phosphorylation correlates with homologous desensitization but not with receptor internalization. Hence, receptor uncoupling rather than receptor endocytosis seems responsible for sst1 desensitization and suggests that receptor phosphorylation is involved in the desensitization process. Conversely, using improved methods to quantify internalization of sst1, Roosterman [107] found that SRIF-14 stimulation induced a fast dynamic process of endocytosis, recycling, and reendocytosis of both the rsst1 receptor and the ligand, in rats. Therefore, the reported species-specific (human [106] vs rat [107]) trafficking of sst1 is to be ascribed to the differences in the methodology used.
SRIF-14 was not routed to lysosomal degradation, but it was continuously internalized and released as intact and biological active peptide. Hence, in contrast with data on human sst1 [106], where SRIF-14 did not or only slowly promoted its uptake during chronic stimulation, SRIF-14 continuously accumulated in the cells and such accumulation is accomplished by mobilization of intracellularly present receptors and by endocytosed receptors that recycled to the plasma membrane [107].
After internalization, ssts are either resensitized and recycled to plasma membrane or transferred into the lysosomal compartment and subjected to proteolytic degradation.
Among all subtypes, the agonist-mediated trafficking of both sst2 splicing variants are the most described [105]. Octreotide and lanreotide are used as first medical choice of NETs (i.e., acromegaly and gastro-enteropancreatic NETs) in controlling hormonal overproduction as well as in Cushing’s disease, characterized by adrenocorticotroph hormone (ACTH) hypersecretion. However, after one year of treatment, about 1/3 of patients treated with octreotide shows an escape of response. Octreotide response in these patients depends on the presence of sst2. Within this context, agonist binding to sst2 has been found to diminish the expression of this receptor [108], rapidly desensitized and internalized after agonist-mediated phosphorylation [105]. Upon ligand binding, sst2 is rapidly and powerfully internalized from cell membrane to the cytoplasm, specifically into endosome-like cellular structures (in vivo animal tumor models) [109] and to a small extent in lysosomes (human NETs) [110]. Moreover, exposure to different concentrations of ligand is associated with a different sst2 pattern of internalization, since NET samples from patients receiving a high dose of octreotide showed
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

6 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
predominantly internalized sst2, and patients with a low dose of octreotide had a variable ratio of internalized vs membranous sst2, whereas untreated patients had exclusively membrane sst2 [110]. The internalization process includes receptor phosphorylation, which involves sites located in the third intracellular loop and in the C terminal tail, subsequent recruitment of -arrestins ( -arrestin-1 and -2) to the receptor forming a stable complex, which is internalized into the endocytotic vesicles [111]. Sst2 desensitization and escape from octreotide therapy remain important events which are repeatedly debated and the understanding of ssts ability to undergo agonist-induced desensitization and internalization may provide important clues for the clinical use of SRIF analogs. In this context, experiments conducted on HEK-293 cells, stably expressing the human ssts, demonstrated that SOM230 was less potent than octreotide in inducing signaling and internalization of the sst2 receptor. Whereas octreotide-activated sst2 receptors co-internalized with -arrestin-2 into the same endocytic vesicles, SOM230-mediated sst2 activation led to the formation of unstable complexes, dissociated at or near the plasma membrane. Sst2 receptors recycled faster to the plasma membrane in SOM230- than in octreotide-treated cells. The accelerated recycling of SOM230-activated receptors may counteract homologous desensitization in sst2-expressing cells, hence, resulting in longer lasting functional responses of cells to SOM230 [112]. Similar data were obtained in AR42J-tumor bearing rat where intra-venous administration of 0.21 mg/animal of SOM230 failed to trigger sst2 internalization, differently from octreotide which, after 1 hour treatment, elicited a massive and rapid internalization of sst2 [109]. This body of evidence could explain the reasons why preclinical studies have shown that the inhibitory effects of SOM230 on GH and IGF-I secretion are more potent and have a longer duration than those of octreotide, and in animal models tachyphylaxis during long-term therapy with SOM230 may not occur [73].
Sst3, which shows high affinity for SRIF-14, internalizes after agonist stimulation through a pathway involving adaptor protein complex 2 (AP2) and clathrin and is regulated by -arrestin [113]. Sst3 trafficking requires functional Rabs and specifically it traffics through Rab4 and Rab21 early endosomes, and through Rab11 recycling endosomes [114]. However, basal cycling of sst3 has been detected and it regulates the level of surface sst3 which is available to mediate the responsiveness of cells to agonist [113]. Regarding sst4, scanty and conflicting data are present in the literature, also due to the lack of selective agonists. Some studies on human embryonic kidney HEK cells or on transfected rat insulinoma cells, expressing rsst4, did not demonstrate SRIF-driven receptor internalization, whereas CHO-K1 expressing hsst4 underwent internalization after [
125I]-LTT SRIF-28 [115]
and [125
I]-[Tyr11
]-SRIF [116] binding. However, the rate of endocytosis is very low and mediated by clathrin-coated pit formation with subsequent rapid recycling of ligand to the extracellular media [116].
In contrast to sst2 and sst3, the cellular distribution characteristics of sst5 are unusual. Experiments conducted on COS-7 cells, exogenously expressing rsst5, showed that sst5-SRIF complexes are internalized via the endocytic pathway, but functional sst5 are highly maintained at the cell surface [117]. Conversely, in HEK-sst5 cells the balance between depletion of the intracellular sst5 pool and sst5 internalization in the presence of SRIF resulted in a net internalization. Hence, the ability of sst5 analogs to facilitate the formation of a stable receptor-arrestin complex determines their effectiveness for stimulating endocytosis [111]. Indeed, sst5 internalization seems to depend on clathrin-coated pits formation [118], as incubation with endocytosis polyamine oxidase or in hypertonic sucrose entirely blocked sst5 internalization [119]. Interestingly, SRIF-28 induces the recruitment of
-arrestin-2, but not -arrestin-1, to the plasma membrane where it colocalized with sst5 and after prolonged agonist exposure, sst5 internalized in endocytotic vescicles, whereas arrestin redistributed in the cytoplasm [120]. Hukovic showed that the cytoplasmic terminal (C-tail) of hsst5 serves as multifunctional purpose in mediating effector coupling, agonist-dependent desensitization, and internalization, hypothesizing that receptor coupling to adenylyl cyclase is dependent on the length of the C-tail, whereas desensitization and internalization require specific structural domains [121]. Conversely, by using a series of C-terminal tail-truncated forms of sst5, Peverelli clearly demonstrated that a short or absent C-terminal tail did not reduce, but enhanced the internalization process. The agonist-receptor activation promotes a sequential phosphorylation of residues, first on the C-terminal tail and then within the third cytoplasmatic loop, thus allowing these two domains to dissociate and arrestin to bind to the activated third loop [120]. Interestingly, a study conducted on CHO-K1 cells stably expressing the hsst5 possessing the C-tail of hsst1 (R5CR1 chimera) and hsst1 possessing the C-tail of hsst5 (R1CR5 chimera) revealed that the replacement of sst5 C-tail with the sst1 one completely abolished the agonist mediated internalization. This evidence suggests the presence of a negative internalization signal in the hsst1 C-tail sufficient to block the internalization of hsst5 [122].
HOMO- AND HETERODIMERIZATION OF SOMATOSTATIN RECEPTORS ARE AFFECTED BY SOMATOSTATIN ANALOGS
When co-expressed in the cell membrane, ssts may interact forming homo- and heterodimers also with other GPCRs (Fig. 2), thus altering their original pharmacological and functional profiles [123, 124]. The dimer formation can be not only constitutive, but also ligand-promoted; hence, compounds with high affinity for the different receptor subtypes can be used to achieve effects elicited by specific dimers [86]. A series of studies, carried out on transfected cell lines, have shown that dimers can consist of two identical sst subtypes (homodimers) or two different subtypes (heterodimers), with a range of possible combinations
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 7
depending on the specific subtype and, probably, on the specific sst-expressing population [125].
Human sst1 naturally occurs as a monomer and its status is agonist-binding independent [81, 126]. This evidence was further confirmed by photobleaching fluorescence resonance energy transfer (pbFRET) and fluorescence correlation spectroscopy, which revealed that hsst1 did not form homodimers either in the absence or in the presence of ligand and that hsst5 robustly dimerizes upon agonist exposure [127]. When both receptors were co-expressed in the same cell, two populations of dimers were present, hsst5 homodimers and hsst1/hsst5 heterodimers [127]. By using CHO-K1 cells stably expressing the hsst5 possessing the C-tail of sst1 (R5CR1 chimera) and the hsst1 possessing the C-tail of sst5 (R1CR5 chimera), Grant [122] showed that only a ligand-driven hsst5 and R1CR5 homodimer formation exists, indicating that the C-tail of sst1 is responsible for its inability to homodimerize. However, the co-expression of both hsst1 and hsst5 at the cell surface resulted either in greater signaling efficiency (i.e., inhibition of forskolin-induced cAMP production) or in a different pattern of receptor trafficking [122]. In fact, hsst1 internalized only as a heterodimer, but not when expressed alone on the cell membrane, suggesting that co-expression of this receptor with hsst5 or possibly
another subtype is crucial to determine its agonist-dependent regulatory responses [81, 126].
When co-expressed in HEK-293 cells, rsst2A and rsst3 form heterodimers resulting in a new receptor with enhanced sst2A-like and diminished sst3-like activity. This heterodimer involves noncovalent hydrophobic interactions of the receptor proteins, not requiring C-tail involvement [128]. Specifically, the functional inactivation of sst3 by heterodimerization with sst2A modifies sst3 internalization, which is drastically impaired, whereas sst2A endocytosis remains unchanged [128]. However, when expressed alone, rsst2A and rsst3 exist as constitutive homodimers [128]. Regarding hsst3, pbFRET and immunoprecipitation analysis clearly demonstrated that this isoform exists as a preformed homodimer in basal conditions. After binding of SRIF-14 or sst3 agonist L-796778, hsst3 underwent internalization as monomer [129] as described above for rsst3 [128].
Hence, heterodimerization of ssts is a specific process that is restricted to some but not all receptor subtype combinations. The human sst2/sst5 heterodimerization is mediated by the selective stimulation of sst2 and not of both receptors. Dimerization occurs after sst2-selective agonist L-779,975 treatment, but not after L-817,818 sst5 agonist. Conversely, activation of sst5 with the native
Fig. (2). (A) constitutive presence of hssts on plasma membrane as monomers or homodimers; (B) constitutive or ligand-driven
h- and rssts heterodimerization on plasma membrane; (C) hssts heterodimerization with μ-opioid (MOR1) receptor or dopamine
receptor subtype 2 (D2R).
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

8 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
ligand SRIF-14 resulted in an increased sst5 homodimers stabilization [130]. These data are in line with previous evidence, which showed that the ligand-driven murine sst2/sst5 dimer reduced sst2 internalization, increased receptor recycling, and decreased its desensitization [131]. However, it is important to highlight that hsst2 exists preferentially as membrane-bound homodimers under basal conditions and dissociates into monomers upon ligand-binding [132]. Subsequently, hsst2 monomers themselves undergo internalization via clathrin-coated vesicles and interact with -arrestin [111, 133]. Some interspecies differences in the internalization/trafficking dynamics of sst2, possibly related to differences in the aa sequence, have been reported [128, 132, 134]. In particular, psst2 is present in the plasma membrane as dimer under unstimulated conditions, dissociates upon ligand binding and rapidly reassociates [134], whereas hsst2 does not reassociate [132].
On the wave of these data, it is interesting to note that G-proteins themselves can regulate the homo- and heterodimerization of hsst2 and hsst5. Treatment with pertussis toxin (PTX) resulted in a disruption of G i/hsst2 coupling leading to a dissociation of hsst2 dimers. This event is similar to what happened after a specific sst2 agonist (L-799,976)-binding [135]. Furthermore, both treatment with PTX and L-799,996 similarly increased the association of human heterodimers sst2/sst5 as monitored by pbFRET and co-immunoprecipitation experiments [135]. Conversely, PTX did not influence either hsst5 basal monomeric status, nor the stabilization of sst5 homodimers following from SRIF-14 stimulation [135].
This body of evidence is referred to cell systems (CHO-K1 or HEK-293) transfected with specific ssts subtype, depending on the experimental needs. In this context, we showed that human androgen dependent PCa LNCaP cells constitutively express sst1/sst2 and sst2/sst5 dimers, which were further stabilized by treatment with BIM-23704 (sst1/sst2 agonist) and BIM-23244 (sst2/sst5 agonist), respectively [24].
According to what has been described so far, there is a great diversity (increasing, decreasing or no changes) between sst subtypes in response to agonist-induced dimerization. As previously described for hsst5, also for hsst4 homodimerization formation, the C-tail aa sequences play a crucial role. Deletion of 74 aa residues resulted in the complete loss of hsst4 preformed dimers [136]. Interestingly, the same authors demonstrated that hsst4, when co-expressed with hsst5 and activated by a specific agonist (i.e., L-803087), forms heterodimers. These hsst4/hsst5 heterodimers internalized upon activation of sst4 alone, whereas hsst5 stimulation led to a greater accumulation of hsst4/hsst5 at the cell membrane, indicating that hsst4 retains the heteromeric complex. Conversely, when hsst4 is co-expressed with hsst1, only an agonist-driven hsst4/hsst4 homodimerization is possible [136].
However, in this scenario it should not be forgotten that ssts can also heterodimerize with other G-protein-
coupled receptors, such as D2R [93] and the -opioid receptor (MOR1) [137]. The co-expression of ssts and D2R in endocrine [57] and pituitary [138, 139] tumors has been extensively reviewed. Specifically, hD2R has been shown to heterodimerize preferentially with either hsst2 [125] or hsst5 [81]. However, almost all of in vitro studies have been carried out in transfected cell models [81, 140] and most of them did not evaluate receptor interaction [141]. Conversely, in two in vitro non-endocrine tumors constitutively expressing ssts and D2R, Arvigo [93] clearly demonstrated the ability of ssts and D2R to interact, even in the absence of ligands, whereas treatment with a SRIF/DA chimeric compound (BIM-23A760) significantly increased the sst5/D2R and sst2/D2R complexes. The combination of the above-mentioned molecular data with those from clinical reports suggesting enhanced efficacy of combined SRIF and DA analog treatment (i.e., suppression of GH hypersecretion) represents the rationale for generating chimeric molecules combining structural features of both compound classes (reviewed in [142]).
MOR1 and sst2A, which share 38% sequence homology, are highly co-localized in the locus coeruleus and can functionally interact in pain-processing pathways [143]. Since extensive cross-talk between opioid- and somatostatin-mediated analgesic response have been demonstrated [144], the sst2A/MOR1 heterodimer [137] could have functional relevance in vivo, in part explaining the attenuation of opioid withdrawal syndrome in patients treated with octreotide [145].
SOMATOSTATIN AND SOMATOSTATIN ANALOGS IN CANCER CELL PROLIFERATION
As previously reported in the “Somatostatin” section, along with the mainly inhibitory effects on endocrine/exocrine secretions exerted by SRIF, this hormone also appears to mediate antiproliferative effects by cell cycle arrest or apoptosis induction. SRIF analogs can control tumor development and progression/metastatization by at least two separate mechanisms: direct actions, mediated by the ssts expressed at the tumor cell membrane [146], and indirect actions which involve the inhibitory effect on secretory products such as GH and IGF-I [147]. Specifically, the direct antiproliferative actions include inhibition of the mitogenic signaling of growth factor receptor kinases [106], arrest of cell division (reviewed in [148]), suppression of cell invasion and induction of apoptosis (programmed cell death) [146]. SRIF can control cell growth arrest by recruiting several signal transduction pathways, which include activation of tyrosine kinases (Janus kinase (JAK), c-src) and tyrosine phosphatases (src homology 2-containing tyrosine phosphatase 1 (SHP1), src homology 2-containing tyrosine phosphatase 2 (SHP2), protein tyrosine phosphatase eta (PTPeta)), activation/ inhibition of nitric oxide synthase/cyclic guanosine monophosphate (cGMP)-dependent protein kinase, Ras/extracellular signal-regulated kinase (ERK)
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 9
pathway and inhibition of phosphoinositide 3-kinase (PI3-K)/Akt pathway, which in turn lead to induction of the cyclin-dependent kinase inhibitor p27
kip1 or p21
Cip1
[24], induction of the tumor suppressor Zac1 [149] and cell cycle arrest [146].
SRIF seems to fit well in counteracting the main mechanisms underlying the ability of cancer to be malignant as defined by the list of “essential hallmarks” of cancer, reviewed by Hanahan [150].
SRIF-driven antineoplastic and antiproliferative activities are generally attributed mainly to activation of sst2, followed by sst1 and sst5, which are the most frequently expressed subtypes in tumors. A minority of tumors expresses SSTR3 and SSTR4 (reviewed in [3]). Hence, the tissue expression patterns of ssts, the binding profile of agonists and the ssts effector coupling confer functional and therapeutic specificity to ligand activity [2]. The sst-mediated effect on tumor cell proliferation has been considered to include several mechanisms, related to both specific receptor and cell subtype. Different ssts (sst1, sst2, sst4 and sst5) have been implicated in vitro in G0/G1 cell cycle blockade, whereas the apoptotic effect seems to be mediated through sst2 and sst3.
A direct inhibitory effect of SRIF or analogs on cell growth has been demonstrated in various cancer cell lines which express endogenous SRIF receptors. In Chinese hamster ovary-DG-44 cells stably expressing sst2, the SRIF analog RC-160-mediated cell proliferation inhibition and p27
Kip1 induction involve a
marked and transient ERK2 activation. This mechanism for ERK2 activation results from PI3-K and both SHP-1 and SHP-2 activation, which triggers both Ras and Rap1 small GTPases and B-Raf mitogen-activated protein (MAPK) activation [151]. The same modular mechanism of signal transduction of ssts, involving both tyrosine kinases and phosphatases was identified also for sst1, which mediates antiproliferative effects through the sequential activation of JAK2, SHP-2, c-src and PTPeta [152]. In human pituitary cells, as well as in GH3 cell line, sst-mediated growth inhibition is associated with downregulation of pERK [153] and upregulation of p27 [154]. A similar pattern of signaling activation, associated to growth inhibition, was described in C6 rat glioma cells, both in vivo (xenografted in nude mice) [155] and in vitro, where sst1, -2 and -5 agonists (BIM-23745, BIM-23120 and BIM-23206 respectively) inhibited ERK1/2 phosphorylation through PTPeta-activation [156]. Different levels of cooperativity among the ssts were identified in C6 cells, since the cumulative activation of sst1, -2 and -5 receptors was required to mimic SRIF-mediated effects and the combined activation of sst1 and -2 showed only a partial synergism, whereas sst2 and -5 activation resulted in effects similar to sst5 activation [156]. Upregulation of the cyclin-dependent kinase inhibitors p27, along with that of p21 and inhibition of cyclin E, were found associated with the antiproliferative effects of some SRIF agonists in LNCaP cells [24]. Zatelli et al. [157] demonstrated that SRIF, by activating Src homology-2-containing protein,
inhibits cell proliferation of the human medullary thyroid carcinoma cell line, TT, which expresses all ssts. Moreover, sst2 selective agonist BIM-23120 inhibits TT cell proliferation and DNA synthesis, by a transient accumulation of TT cells in G2/M phase [158].
SRIF can exhibit antiproliferative properties also by upregulating proapoptotic genes like p53, death receptors, and BAX, and downregulating anti-apoptotic bcl-2 [159]. A pro-apoptotic effect is achieved by regulation of the two main signalling pathways, the cell-extrinsic pathway (triggered by death receptors) and the cell-intrinsic pathway (also called the mitochondrial pathway) [23, 146]. The receptor subtypes primarily involved in SRIF-induced apoptosis are sst3 and sst2, via a mechanism involving intracellular acidification, activation of endonucleases and induction of p53 and Bax and via a p53-independent mechanism, when sst2 is involved [160]. Consistent with this data, Gruszka [161] found that treatment with octreotide and bromocriptine, alone or in combination, causes a significant increase in Bax expression in the rat prolactinoma cells. These findings indicate that anti-tumoral actions of bromocriptine and to some extent the action of octreotide in experimental rat prolactinoma is connected with the induction of apoptosis and is associated with increased Bax expression. Moreover, octreotide has been reported to induce apoptosis in human somatotroph tumors by involving the putative antiapoptotic gene Seladin-1 [162], and to increase the enzymatic activity of caspase 3 [22]. Conversely, lanreotide was not able to change the G0/G1 cell cycle profile, but promoted radiation-induced apoptosis in rat GH3 cells [159].
With regards to hsst3-mediated antiproliferative effects, it is important to highlight how these events are uniquely triggered by apoptosis [163]. Interestingly, this latter process is mediated by aa residues present in the sst3 C-tail [129]. Treatment with SRIF-14 and L-796778 (sst3 agonist) inhibited HEK-293 cell growth only in cells transfected with hsst3, whereas deletions of some aa in the C-tail altered the physiological response of cells to agonist [129].
Since the mechanism by which SRIF analogs exert antiproliferative activity depends on the tumor cell type and the receptor subtype to which it binds, a SRIF analog like SOM230 that targets multiple sst receptor subtypes may have a further potent antiproliferative effect. This hypothesis was supported by in vitro studies on primary cultures of human corticotroph tumors expressing multiple ssts in which SOM230 significantly suppressed cell proliferation and ACTH secretion, supporting the hypothesis that SOM230 may have a role in the medical therapy of corticotroph tumors [164]. Lattuada [165] proved that SOM230 performed a more potent inhibitory effect on human lymphocyte proliferation than octreotide and this different growth inhibitory behaviour could be an apoptotic phenomenon mediated by sst2A, in the case of octreotide, and by sst3 or by sst2/sst3 heterodimerization when SOM230 is used.
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

10 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
Previous data were confirmed in in vivo studies in mice bearing GH- and PRL-secreting pituitary tumors, where the effect of SOM230 was significantly stronger than that of octreotide, resulting in tumor shrinkage, whereas octreotide only significantly slowed down the progression of the tumor without inducing regression [166].
Conversely, there was no statistical difference between SOM230 and octreotide in the control of cell growth of 18 human skin malignant melanoma cell lines, even though the employed concentration of octreotide was 50- 1000-fold higher than that of SOM230 [167].
SOMATOSTATIN AND SOMATOSTATIN ANALOGS IN CANCER-ASSOCIATED ANGIOGENESIS
Angiogenesis consists in the development of new blood vessels from previously formed venules followed by transformation of endothelial cells from a quiescent phenotype into a proliferating phenotype [168]. These sprouted capillaries develop in a direct manner towards a chemoattractant [169]. Angiogenesis is a fundamental process occurring during embryonic development and in a few normal physiological processes such as growth, reproductive cycle, fertility and wound healing. In pathological events, angiogenesis is involved in retinopathies, psoriasis and tumor growth [170]. Folkman originally postulated the importance of angiogenesis for tumor growth and metastasis more than 30 years ago [168]; nowadays tumor angiogenesis represents a chronic unregulated angiogenetic state which falls into the general category of pathological angiogenesis [171]. A considerable body of evidence has documented that tumor growth and metastasis require persistent new blood vessels growth as well as inducers of angiogenesis including vascular endothelial growth factor (VEGF), basic fibroblast growth factor, transforming growth factor , proliferin, platelet-derived growth factor (PDGF), interleukin-8 and hepatocyte growth factor.
Being the inhibition of angiogenesis a primary target for antineoplastic therapy, SRIF and SRIF analogs may be endogenous agents that maintain endothelial cells in quiescence and thus regulate angiogenesis [172]. The expression of sst subtypes in endothelial cells are tissue specific [91, 173] and SRIF seems to act through the direct inhibition of endothelial cell proliferation and indirectly through the inhibition of production of angiogenic factors such as VEGF or the inhibition of the migration of monocytes [174]. By using the human placental vein angiogenesis model (HPVAM) and the rabbit cornea or the chicken chorioallantoic membrane (CAM) models, Woltering [172] demonstrated that RC-160, octreotide and lanreotide were potent inhibitors of angiogenesis via G-protein, cAMP and calcium signal transduction involvement. Interestingly, in Kaposi’s sarcoma (KS), a highly angiogenic lesion, which represents a prototype of tumor angiogenesis, SRIF inhibited growth and cell invasion of a reconstituted basement membrane (Matrigel) of human endothelial-like immortalized cells EAhy926 stimulated with KS cell
products [175]. SRIF showed a multiple anti-angiogenetic activity inhibiting endothelial cells both directly and indirectly through monocyte inhibition, which results to be one of the major mediator of angiogenesis [176]. In addition, monocyte migration has been shown to be promoted by VEGF [177], which stimulates proliferation and migration of endothelial cells both in physiogical and pathological angiogenesis. Hence, VEGF downregulation could be an indirect pathway of chemotaxis inhibition by SRIF analogs. Interestingly, Gulec [178] demonstrated that the anti-angiogenic properties of SRIF and SRIF analogs are a potentially significant anti-cancer tool, even for ssts-negative tumors. In fact, the tumoricidal effects of 111-In-JIC 2DL (a sst2-preferring SRIF analog) were seen only in sst2 positive IMR-32 cells (human neuroblastoma), whereas the angiogenic response was inhibited in both IMR-32 and SSTR2 negative MDA MB-231 (human breast) cells independent of the sst2 status of tumor cells [178]. To support this latter evidence, Florio [179] clearly demonstrated that in KS models, the antiangiogenetic effects driven by SRIF require the activation of SSTR3, which, in turn, transduces a signal resulting in the inhibition of endothelial nitric oxide synthase and ERK1/2, two key pathways of angiogenesis.
Nevertheless, the in vitro use of sst1 agonists (BIM-23926 and BIM-23745) has determined significant inhibition of human endothelial cell proliferation, migration, and sprouting in an extracellular matrix as well as of VEGF expression, suggesting a possible therapeutic role of these selective peptides on various proliferative and chronic diseases involving angiogenesis. Hence, SRIF could counteract the “angiogenic switch” that occurs when the concentration or actions of pro-angiogenic agents exceed those of anti-angiogenic agents [180]. Moreover, in anti-angiogenic therapy, which requires a continuous treatment, since most anti-angiogenic drugs are ‘angiostatic’ rather than cytotoxic, SRIF should be used as an adjuvant anti-angiogenic treatment, administrated after or during conventional therapy (surgical, radiological and chemical) [175].
SOMATOSTATIN AND SOMATOSTATIN ANA-LOGS IN CANCER CELL MATRIX INVASION AND METASTATIZATION
The subsequent steps of cancer progression, following angiogenesis, involve proteolytic degradation of the basement membrane (BM) and surrounding extracellular matrix (ECM) through involvement of matrix metalloproteinases (MMP) and urokinase, endothelial cell proliferation, endothelial cell migration and tube formation, and structural reorganization leading to the tumor cell metastatization. Metastasis development is one of the major causes of mortality in cancer and it is a process composed by multiple steps [181].
SRIF is a potent anti-migratory and anti-invasive agent for various tumor cells including pancreatic cancer, neuroblastoma and glioma cells [146].
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Matita
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 11
Moreover, since SRIF receptor subtypes are highly expressed in peritumoral/intratumoral veins, but not in arteries; indeed they represent promising drug delivery enhancers in cytotoxic cancer treatment. The camptothecin (CPT)-SRIF conjugate exhibited anti-invasive and anti-angiogenic properties as evidenced by a series of in vitro experiments, including cell adhesion, migration, invasion and capillary-like tube formation of PC3 (human androgen-independent PCa cells) and HUVEC cells, respectively, and in vivo bFGF-induced angiogenesis in C57B1/6N female mice. Moreover, CPT-SRIF reduced, in PC3 cells, the secretion of MMP-2 and -9, which are highly expressed in more aggressive tumor cells and are associated with angiogenesis and metastasis [182]. Specifically, MMPs are utilized by the primary tumor to facilitate invasion into the surrounding stroma and by metastatic tumor cells to intravasate into and extravasate out of the vasculature, and to degrade extracellular matrix and stroma as it migrates to establish metastatic foci [180].
Along with the SRIF-conjugate compounds, the expression of SSTR2 was reported to be crucial in pancreatic cancer. Loss of SSTR2 expression confers a growth advantage in these tumors, but when re-expressed in pancreatic cancer cell line BXPC-3, led to the inhibition of migration and invasion through the downregulation of MMP-2, thus resulting in a less aggressive phenotype [29, 183].
Along with its action on MMP-2 and -9 expression and secretion, SRIF potently inhibits the invasive effect of PDGF, which is a mitogen mostly for cells of mesenchymal origin, able to induce chemotaxis and actin reorganization and to prevent cells from dying by apoptosis. In this context, SRIF-mediated PDGF inhibition resulted a potent anti-migratory and anti-invasive agent for neuroblastoma, with a potential use to limit the spread of tumor cells, i.e., the metastatic process [184]. Moreover, SRIF was able to inhibit PDGF-stimulated motility of two human tumoral cell lines U87-MG and T98G glioma cells. In addition, the hormone strongly reduced the motility induced by PDGF, but also the hyperactive basal motility detected in U87-MG cells in the absence of extracellular stimuli. It is of particular interest the ability of SRIF to block glioma cell migration even without an added stimulus; gliomas locally invade the surrounding normal brain tissue and form multifocal lesions that are almost impossible to control [185]. Moreover, SRIF and its analogs inhibit PDGF-induced cell proliferation and motility, and VEGF and MMP-2 gene expression in human endometrial cells, suggesting their possible role in the treatment of endometriosis [186].
SRIF also induces cell growth inhibition through restoration of functional gap junctions by rescuing the expression of connexins. Restoration of cell density inhibition of human pancreatic cancer BxPC-3 cells by sst2 activation is actually due to overexpression of endogenous connexins 26 and 43 and consequent formation of functional gap junctions [187].
FUTURE DIRECTIONS
According to the evidence reported in the present review, most specific patterns of sst activation seem to be associated to important and peculiar antitumoral actions, with potential relevance for the therapy of some solid tumors expressing these receptor isoforms. In addition, dimerization studies confirm that the activity of ssts and DA receptors could be peculiar to specific cell types in which they are expressed. Therefore, not only the receptor profiles, but also the cell types, as well as the dimerization, are responsible for the final effect of a given ligand. The inhibitory effects of SOM230 on ACTH, GH and IGF-I secretion in humans and animal models are more potent and have a longer duration than those of octreotide, with only minor tachyphylaxis [73]. Such differences may derive from different ssts internalization and trafficking patterns by the two analogs [112]. Moreover, upregulation of certain GPCRs in many tumor cells has led to the development of novel, safe, and efficacious receptor-targeted drugs [188]. Since peptides are the endogenous ligands of many of these tumor-associated GPCRs, they offer an exciting paradigm for drug design and development [53]. Nowadays, adopting Paul Ehrlich’s concept of the “magic bullet” [189], regulatory peptides can be considered ideal agents for diagnostic and therapeutic applications. Since peptide receptors are often expressed in many primary tumors, they can be targeted specifically by the peptide or different labelled analogs [190]. Hence, peptides as potential therapeutics or drug-delivering vehicles, possess a number of attractive characteristics such as rapid circulatory clearance and good tumor tissue-penetrating ability. Nevertheless, the identification and validation of effective and physiologically relevant tumor cell models are critical components for the successful design and development of novel therapeutic interventions. Thus, it should be kept in mind that, due to the large tissue distribution of ssts and their different-coupled intracellular pathways, it is important to deliver selective drugs to avoid producing untoward effects.
ABBREVIATIONS
aa = Amino acids
AP = Adaptor protein complex
BM = Basement membrane
CPT = Camptothecin
CAM = Chorioallantoic membrane
cAMP = Cyclic adenosine monophosphate
cGMP = Cyclic guanosine monophosphate
C-tail = Cytoplasmic terminal
DR = Dopamine receptor
DA = Dopamine
ER = Endoplasmic reticulum
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

12 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
ECM = Extracellular matrix
ERK = Extracellular signal-regulated kinase
GPCR = G protein-coupled receptors
GH = Growth hormone
HPVAM = Human placental vein angiogenesis model
IGF = Insulin-like growth factor
i.v. = Intra-venous
JAK = Janus kinase
KS = Kaposi’s sarcoma
MMPs = Metalloproteinases
MAPK = Mitogen-activated protein
NET = Neuroendocrine tumor
PTX = Pertussis toxin
PI3-K = Phosphoinositide 3-kinase
pERK = Phosphorylated extracellular signal- regulated kinase
pbFRET = Photobleaching fluorescence resonance energy transfer
PDGF = Platelet-derived growth factor
PRL = Prolactin
PCa = Prostate cancer
PTP = Protein tyrosine phosphatase
SSTR = Somatostatin receptor subtype (gene)
sst = Somatostatin receptor subtype (protein)
SRIF = Somatotropin-releasing inhibiting factor
SHP-1 = Src homology 2-containing tyrosine phosphatase 1
SHP-2 = Src homology 2-containing tyrosine phosphatase 2
TMD = Trans-membrane domain
VEGF = Vascular endothelial growth factor
MOR1 = -opioid receptor
CONFLICT OF INTEREST
There is no conflict of interest to disclose.
ACKNOWLEDGEMENT
Declared none.
REFERENCES
[1] Brazeau P, Vale W, Burgus R, et al. Hypothalamic polypeptide that inhibits the secretion of immunoreactive
pituitary growth hormone. Science 1973; 179: 77-9. [2] Zatelli MC. Antiproliferative effects of somatostatin analogs in
endocrine tumours. F1000 Med Rep 2009; 1: 40.
[3] Hasskarl J, Kaufmann M, Schmid HA. Somatostatin receptors in non-neuroendocrine malignancies: the potential role of somatostatin analogs in solid tumors. Future Oncol
2011; 7: 895-913.
[4] Righi L, Volante M, Tavaglione V, et al. Somatostatin
receptor tissue distribution in lung neuroendocrine tumours: a clinicopathologic and immunohistochemical study of 218 'clinically aggressive' cases. Ann Oncol 2010; 21: 548-55.
[5] Ioannou M, Papagelopoulos PJ, Papanastassiou I, Iakovidou I, Kottakis S, Demertzis N. Detection of somatostatin receptors in human osteosarcoma. World J Surg Oncol 2008;
6: 99. [6] Klagge A, Krause K, Schierle K, Steinert F, Dralle H, Fuhrer
D. Somatostatin receptor subtype expression in human
thyroid tumours. Horm Metab Res 2010; 42: 237-40. [7] Schaer JC, Waser B, Mengod G, Reubi JC. Somatostatin
receptor subtypes sst1, sst2, sst3 and sst5 expression in
human pituitary, gastroentero-pancreatic and mammary tumors: comparison of mRNA analysis with receptor autoradiography. Int J Cancer 1997; 70: 530-7.
[8] Volante M, Rosas R, Allia E, et al. Somatostatin, cortistatin and their receptors in tumours. Mol Cell Endocrinol 2008; 286: 219-29.
[9] Fujita T, Yamaji Y, Sato M, Murao K, Takahara J. Gene expression of somatostatin receptor subtypes, SSTR1 and SSTR2, in human lung cancer cell lines. Life Sci 1994; 55:
1797-806. [10] Reubi JC, Waser B, Liu Q, Laissue JA, Schonbrunn A.
Subcellular distribution of somatostatin sst2A receptors in
human tumors of the nervous and neuroendocrine systems: membranous versus intracellular location. J Clin Endocrinol Metab 2000; 85: 3882-91.
[11] Krulich L, Dhariwal AP, McCann SM. Stimulatory and
inhibitory effects of purified hypothalamic extracts on growth hormone release from rat pituitary in vitro. Endocrinology 1968; 83: 783-90.
[12] Esch F, Bohlen P, Ling N, Benoit R, Brazeau P, Guillemin R. Primary structure of ovine hypothalamic somatostatin-28 and somatostatin-25. Proc Natl Acad Sci USA 1980; 77: 6827-31.
[13] Polak JM, Pearse AG, Grimelius L, Bloom SR. Growth-hormone release-inhibiting hormone in gastrointestinal and pancreatic D cells. Lancet 1975; 1: 1220-2.
[14] Alumets J, Sundler F, Hakanson R. Distribution, ontogeny and ultrastructure of somatostatin immunoreactive cells in the pancreas and gut. Cell Tissue Res 1977; 185: 465-79.
[15] Reichlin S. Somatostatin. N Engl J Med 1983; 309: 1495-501.
[16] Reichlin S. Somatostatin (second of two parts). N Engl J Med
1983; 309: 1556-63. [17] Helboe L, Moller M. Localization of somatostatin receptors at
the light and electron microscopial level by using antibodies
raised against fusion proteins. Prog Histochem Cytochem 2000; 35: 3-64.
[18] Lewin MJ. The somatostatin receptor in the GI tract. Annu
Rev Physiol 1992; 54: 455-68. [19] Epelbaum J, Dournaud P, Fodor M, Viollet C. The
neurobiology of somatostatin. Crit Rev Neurobiol 1994; 8: 25-
44. [20] Danila DC, Haidar JN, Zhang X, Katznelson L, Culler MD,
Klibanski A. Somatostatin receptor-specific analogs: effects
on cell proliferation and growth hormone secretion in human somatotroph tumors. J Clin Endocrinol Metab 2001; 86: 2976-81.
[21] Ferone D, Pivonello R, Van Hagen PM, et al. Quantitative and functional expression of somatostatin receptor subtypes in human thymocytes. Am J Physiol Endocrinol Metab 2002;
283: E1056-66. [22] Ferrante E, Pellegrini C, Bondioni S, et al. Octreotide
promotes apoptosis in human somatotroph tumor cells by
activating somatostatin receptor type 2. Endocr Relat Cancer 2006; 13: 955-62.
[23] Florio T. Molecular mechanisms of the antiproliferative
activity of somatostatin receptors (SSTRs) in neuroendocrine tumors. Front Biosci 2008; 13: 822-40.
[24] Ruscica M, Arvigo M, Gatto F, et al. Regulation of prostate
cancer cell proliferation by somatostatin receptor activation. Mol Cell Endocrinol 2010; 315: 254-62.
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 13
[25] Pradayrol L, Jornvall H, Mutt V, Ribet A. N-terminally
extended somatostatin: the primary structure of somatostatin-28. FEBS Lett 1980; 109: 55-8.
[26] Schally AV, Huang WY, Chang RC, et al. Isolation and
structure of pro-somatostatin: a putative somatostatin precursor from pig hypothalamus. Proc Natl Acad Sci USA 1980; 77: 4489-93.
[27] Barnett P. Somatostatin and somatostatin receptor physiology. Endocrine 2003; 20: 255-64.
[28] Brakch N, Lazar N, Panchal M, et al. The somatostatin-28(1-
12)-NPAMAP sequence: an essential helical-promoting motif governing prosomatostatin processing at mono- and dibasic sites. Biochemistry 2002; 41: 1630-9.
[29] Benali N, Ferjoux G, Puente E, Buscail L, Susini C. Somatostatin receptors. Digestion 2000; 62 Suppl 1: 27-32.
[30] Patel YC. Somatostatin and its receptor family. Front
Neuroendocrinol 1999; 20: 157-98. [31] Baumeister H, Meyerhof W. Gene regulation of somatostatin
receptors in rats. J Physiol Paris 2000; 94: 167-77.
[32] Olias G, Viollet C, Kusserow H, Epelbaum J, Meyerhof W. Regulation and function of somatostatin receptors. J Neurochem 2004; 89: 1057-91.
[33] Yamada Y, Post SR, Wang K, Tager HS, Bell GI, Seino S. Cloning and functional characterization of a family of human and mouse somatostatin receptors expressed in brain,
gastrointestinal tract, and kidney. Proc Natl Acad Sci USA 1992; 89: 251-5.
[34] Corness JD, Demchyshyn LL, Seeman P, et al. A human somatostatin receptor (SSTR3), located on chromosome 22,
displays preferential affinity for somatostatin-14 like peptides. FEBS Lett 1993; 321: 279-84.
[35] Rohrer L, Raulf F, Bruns C, Buettner R, Hofstaedter F,
Schule R. Cloning and characterization of a fourth human somatostatin receptor. Proc Natl Acad Sci USA 1993; 90: 4196-200.
[36] Panetta R, Greenwood MT, Warszynska A, et al. Molecular cloning, functional characterization, and chromosomal localization of a human somatostatin receptor (somatostatin
receptor type 5) with preferential affinity for somatostatin-28. Mol Pharmacol 1994; 45: 417-27.
[37] Horn F, Weare J, Beukers MW, et al. GPCRDB: an
information system for G protein-coupled receptors. Nucleic Acids Res 1998; 26: 275-9.
[38] Horn F, Bettler E, Oliveira L, Campagne F, Cohen FE, Vriend
G. GPCRDB information system for G protein-coupled receptors. Nucleic Acids Res 2003; 31: 294-7.
[39] Vroling B, Sanders M, Baakman C, et al. GPCRDB:
information system for G protein-coupled receptors. Nucleic Acids Res 2011; 39: D309-19.
[40] Davies MN, Secker A, Halling-Brown M, et al. GPCRTree:
online hierarchical classification of GPCR function. BMC Res Notes 2008; 1: 67.
[41] Reiter E, Ahn S, Shukla AK, Lefkowitz RJ. Molecular
Mechanism of b-Arrestin-Biased Agonism at Seven-Transmembrane Receptors. Annu Rev Pharmacol Toxicol 2012; 52: 179-97.
[42] Agnati LF, Ferre S, Lluis C, Franco R, Fuxe K. Molecular mechanisms and therapeutical implications of intramembrane receptor/receptor interactions among
heptahelical receptors with examples from the striatopallidal GABA neurons. Pharmacol Rev 2003; 55: 509-50.
[43] Kreienkamp HJ, Soltau M, Richter D, Bockers T. Interaction
of G-protein-coupled receptors with synaptic scaffolding proteins. Biochem Soc Trans 2002; 30: 464-8.
[44] Duran-Prado M, Gahete MD, Martinez-Fuentes AJ, et al.
Identification and characterization of two novel truncated but functional isoforms of the somatostatin receptor subtype 5 differentially present in pituitary tumors. J Clin Endocrinol
Metab 2009; 94: 2634-43. [45] Cordoba-Chacon J, Gahete MD, Duran-Prado M, et al.
Identification and characterization of new functional truncated
variants of somatostatin receptor subtype 5 in rodents. Cell Mol Life Sci 2010; 67: 1147-63.
[46] Duran-Prado M, Saveanu A, Luque RM, et al. A potential
inhibitory role for the new truncated variant of somatostatin
receptor 5, sst5TMD4, in pituitary adenomas poorly
responsive to somatostatin analogs. J Clin Endocrinol Metab 2010; 95: 2497-502.
[47] Duran-Prado M, Gahete MD, Hergueta-Redondo M, et al.
The new truncated somatostatin receptor variant sst5TMD4 is associated to poor prognosis in breast cancer and increases malignancy in MCF-7 cells. Oncogene 2012; 31:
2049-61. [48] Cordoba-Chacon J, Gahete MD, Duran-Prado M, Luque RM,
Castano JP. Truncated somatostatin receptors as new
players in somatostatin-cortistatin pathophysiology. Ann N Y Acad Sci 2011; 1220: 6-15.
[49] Johansson M, McKay JD, Wiklund F, et al. Genetic variation
in the SST gene and its receptors in relation to circulating levels of insulin-like growth factor-I, IGFBP3, and prostate cancer risk. Cancer Epidemiol Biomarkers Prev 2009; 18:
1644-50. [50] Canzian F, McKay JD, Cleveland RJ, et al. Genetic variation
in the growth hormone synthesis pathway in relation to
circulating insulin-like growth factor-I, insulin-like growth factor binding protein-3, and breast cancer risk: results from the European prospective investigation into cancer and
nutrition study. Cancer Epidemiol Biomarkers Prev 2005; 14: 2316-25.
[51] Li D, Tanaka M, Brunicardi FC, Fisher WE, Gibbs RA,
Gingras MC. Association between somatostatin receptor 5 gene polymorphisms and pancreatic cancer risk and survival. Cancer 2011; 117: 2863-72.
[52] Ciganoka D, Balcere I, Kapa I, et al. Identification of
somatostatin receptor type 5 gene polymorphisms associated with acromegaly. Eur J Endocrinol 2011; 165: 517-25.
[53] Sun LC, Coy DH. Somatostatin receptor-targeted anti-cancer therapy. Curr Drug Deliv 2011; 8: 2-10.
[54] Sestini R, Orlando C, Peri A, et al. Quantitation of
somatostatin receptor type 2 gene expression in neuroblastoma cell lines and primary tumors using competitive reverse transcription-polymerase chain reaction.
Clin Cancer Res 1996; 2: 1757-65. [55] Slaby O, Sachlova M, Bednarikova M, et al. Gene expression
of somatostatin receptor 4 predicts clinical outcome of
patients with metastatic neuroendocrine tumors treated with somatostatin analogs. Cancer Biother Radiopharm 2010; 25: 237-43.
[56] Gatto F, Barbieri F, Castelletti L, et al. In vivo and in vitro response to octreotide LAR in a TSH-secreting adenoma: characterization of somatostatin receptor expression and role
of subtype 5. Pituitary 2011; 14: 141-7. [57] Gatto F, Barbieri F, Gatti M, et al. Balance between
somatostatin and D2 receptor expression drives TSH-
secreting adenoma response to somatostatin analogues and dopastatins. Clin Endocrinol (Oxf) 2012; 76: 407-14.
[58] Lewis I, Albert R, Kneuer R, et al. Medicinal chemistry of
somatostatin analogs leading to the DTPA and DOTA conjugates of the multi-receptor-ligand SOM230. J Endocrinol Invest 2005; 28: 15-20.
[59] Marbach P, Bauer W, Briner U, Dopfner W, Petcher T, Pless J. Structure-function relationships of somatostatin analogs. Horm Res 1988; 29: 54-8.
[60] Rohrer SP, Birzin ET, Mosley RT, et al. Rapid identification of subtype-selective agonists of the somatostatin receptor through combinatorial chemistry. Science 1998; 282: 737-40.
[61] Marks N, Stern F. Inactivation of somatostatin (GH-RIH) and its an analogs by crude and partially purified rat brain extracts. FEBS Lett 1975; 55: 220-4.
[62] Pless J. The history of somatostatin analogs. J Endocrinol Invest 2005; 28: 1-4.
[63] Pawlikowski M, Melen-Mucha G. Somatostatin analogs -
from new molecules to new applications. Curr Opin Pharmacol 2004; 4: 608-13.
[64] Melmed S. Medical progress: Acromegaly. N Engl J Med
2006; 355: 2558-73. [65] Veber DF, Freidlinger RM, Perlow DS, et al. A potent cyclic
hexapeptide analogue of somatostatin. Nature 1981; 292:
55-8.
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

14 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
[66] Bauer W, Briner U, Doepfner W, et al. SMS 201-995: a very
potent and selective octapeptide analogue of somatostatin with prolonged action. Life Sci 1982; 31: 1133-40.
[67] Anthony L, Freda PU. From somatostatin to octreotide LAR:
evolution of a somatostatin analogue. Curr Med Res Opin 2009; 25: 2989-99.
[68] Hannon JP, Nunn C, Stolz B, et al. Drug design at peptide
receptors: somatostatin receptor ligands. J Mol Neurosci 2002; 18: 15-27.
[69] De Martino MC, Hofland LJ, Lamberts SW. Somatostatin and
somatostatin receptors: from basic concepts to clinical applications. Prog Brain Res 2010; 182: 255-80.
[70] Reubi JC, Schaer JC, Markwalder R, Waser B, Horisberger
U, Laissue J. Distribution of somatostatin receptors in normal and neoplastic human tissues: recent advances and potential relevance. Yale J Biol Med 1997; 70: 471-9.
[71] Culler MD. Evolving concepts in the quest for advanced therapeutic analogues of somatostatin. Dig Liver Dis 2004; 36 Suppl 1: S17-25.
[72] Jaquet P, Saveanu A, Gunz G, et al. Human somatostatin receptor subtypes in acromegaly: distinct patterns of messenger ribonucleic acid expression and hormone
suppression identify different tumoral phenotypes. J Clin Endocrinol Metab 2000; 85: 781-92.
[73] Schmid HA. Pasireotide (SOM230): development,
mechanism of action and potential applications. Mol Cell Endocrinol 2008; 286: 69-74.
[74] Bruns C, Lewis I, Briner U, Meno-Tetang G, Weckbecker G. SOM230: a novel somatostatin peptidomimetic with broad
somatotropin release inhibiting factor (SRIF) receptor binding and a unique antisecretory profile. Eur J Endocrinol 2002; 146: 707-16.
[75] Colao A, Petersenn S, Newell-Price J, et al. A 12-month phase 3 study of pasireotide in Cushing's disease. N Engl J Med 2012; 366: 914-24.
[76] Oncology TPoN. A Pipeline that Spans All Phases. Available at: http://www.novartisoncology.com/research-innovation/pipeline.jsp. [accessed 2012].
[77] Colao A, Bronstein M, Freda PU, et al. Pasireotide LAR is significantly more effective than octreotide LAR at inducing biochemical control in patients with acromegaly: results of a
12-month randomized, double-blind, multicenter, Phase III study. 2012 Joint 15th International Congress of Endocrinology and 14th European Congress of
Endocrinology; 7 May 2012; Florence: BioScientifica; 2012. [78] Reubi JC, Eisenwiener KP, Rink H, Waser B, Macke HR. A
new peptidic somatostatin agonist with high affinity to all five
somatostatin receptors. Eur J Pharmacol 2002; 456: 45-9. [79] Jaquet P, Gunz G, Saveanu A, et al. BIM-23A760, a chimeric
molecule directed towards somatostatin and dopamine
receptors, vs universal somatostatin receptors ligands in GH-secreting pituitary adenomas partial responders to octreotide. J Endocrinol Invest 2005; 28: 21-7.
[80] Saveanu A, Gunz G, Guillen S, Dufour H, Culler MD, Jaquet P. Somatostatin and dopamine-somatostatin multiple ligands directed towards somatostatin and dopamine receptors in
pituitary adenomas. Neuroendocrinology 2006; 83: 258-63. [81] Rocheville M, Lange DC, Kumar U, Patel SC, Patel RC,
Patel YC. Receptors for dopamine and somatostatin:
formation of hetero-oligomers with enhanced functional activity. Science 2000; 288: 154-7.
[82] Prinster SC, Hague C, Hall RA. Heterodimerization of g
protein-coupled receptors: specificity and functional significance. Pharmacol Rev 2005; 57: 289-98.
[83] Flogstad AK, Halse J, Grass P, et al. A comparison of
octreotide, bromocriptine, or a combination of both drugs in acromegaly. J Clin Endocrinol Metab 1994; 79: 461-5.
[84] Li JK, Chow CC, Yeung VT, et al. Treatment of Chinese
acromegaly with a combination of bromocriptine and octreotide. Aust N Z J Med 2000; 30: 457-61.
[85] Saveanu A, Lavaque E, Gunz G, et al. Demonstration of
enhanced potency of a chimeric somatostatin-dopamine molecule, BIM-23A387, in suppressing growth hormone and prolactin secretion from human pituitary somatotroph
adenoma cells. J Clin Endocrinol Metab 2002; 87: 5545-52.
[86] Saveanu A, Gunz G, Dufour H, et al. Bim-23244, a
somatostatin receptor subtype 2- and 5-selective analog with enhanced efficacy in suppressing growth hormone (GH) from octreotide-resistant human GH-secreting adenomas. J Clin
Endocrinol Metab 2001; 86: 140-5. [87] Zatelli MC, Piccin D, Tagliati F, et al. Somatostatin receptor
subtype 1 selective activation in human growth hormone
(GH)- and prolactin (PRL)-secreting pituitary adenomas: effects on cell viability, GH, and PRL secretion. J Clin Endocrinol Metab 2003; 88: 2797-802.
[88] Ludvigsen E, Stridsberg M, Taylor JE, Culler MD, Oberg K, Janson ET. Subtype selective interactions of somatostatin and somatostatin analogs with sst1, sst2, and sst5 in BON-1
cells. Med Oncol 2004; 21: 285-95. [89] Zatelli MC, Piccin D, Bottoni A, et al. Evidence for differential
effects of selective somatostatin receptor subtype agonists
on alpha-subunit and chromogranin a secretion and on cell viability in human nonfunctioning pituitary adenomas in vitro. J Clin Endocrinol Metab 2004; 89: 5181-8.
[90] Zatelli MC, Maffei P, Piccin D, et al. Somatostatin analogs in vitro effects in a growth hormone-releasing hormone-secreting bronchial carcinoid. J Clin Endocrinol Metab 2005;
90: 2104-9. [91] Bocci G, Culler MD, Fioravanti A, et al. In vitro antiangiogenic
activity of selective somatostatin subtype-1 receptor
agonists. Eur J Clin Invest 2007; 37: 700-8. [92] Ludvigsen E, Stridsberg M, Taylor JE, et al. Regulation of
insulin and glucagon secretion from rat pancreatic islets in vitro by somatostatin analogues. Regul Pept 2007; 138: 1-9.
[93] Arvigo M, Gatto F, Ruscica M, et al. Somatostatin and dopamine receptor interaction in prostate and lung cancer cell lines. J Endocrinol 2010; 207: 309-17.
[94] Reubi JC, Schaer JC, Wenger S, et al. SST3-selective potent peptidic somatostatin receptor antagonists. Proc Natl Acad Sci USA 2000; 97: 13973-8.
[95] Ramon R, Martin-Gago P, Verdaguer X, et al. SSTR1- and SSTR3-Selective Somatostatin Analogues. Chembiochem 2011; 12: 625-32.
[96] Kumar U. Expression of somatostatin receptor subtypes (SSTR1-5) in Alzheimer's disease brain: an immunohistochemical analysis. Neuroscience 2005; 134:
525-38. [97] Crider AM, Witt KA. Somatostatin sst4 ligands: chemistry and
pharmacology. Mini Rev Med Chem 2007; 7: 213-20.
[98] Elekes K, Helyes Z, Kereskai L, et al. Inhibitory effects of synthetic somatostatin receptor subtype 4 agonists on acute and chronic airway inflammation and hyperactivity in the
mouse. Eur J Pharmacol 2008; 578: 313-22. [99] Kuriyama I, Miyazaki A, Tsuda Y, et al. Inhibitory effect of
somatostatin Peptide analogues on DNA polymerase activity
and human cancer cell proliferation. Anticancer Res 2010; 30: 4841-9.
[100] Afargan M, Janson ET, Gelerman G, et al. Novel long-acting
somatostatin analog with endocrine selectivity: potent suppression of growth hormone but not of insulin. Endocrinology 2001; 142: 477-86.
[101] Shimon I, Rubinek T, Hadani M, Alhadef N. PTR-3173 (somatoprim), a novel somatostatin analog with affinity for somatostatin receptors 2, 4 and 5 is a potent inhibitor of
human GH secretion. J Endocrinol Invest 2004; 27: 721-7. [102] Jean-Alphonse F, Hanyaloglu AC. Regulation of GPCR
signal networks via membrane trafficking. Mol Cell
Endocrinol 2011; 331: 205-14. [103] Salahpour A, Barak LS. Visualizing receptor endocytosis and
trafficking. Methods Mol Biol 2011; 756: 311-23.
[104] van Koppen CJ, Jakobs KH. Arrestin-independent internalization of G protein-coupled receptors. Mol Pharmacol 2004; 66: 365-7.
[105] Jacobs S, Schulz S. Intracellular trafficking of somatostatin receptors. Mol Cell Endocrinol 2008; 286: 58-62.
[106] Liu Q, Schonbrunn A. Agonist-induced phosphorylation of
somatostatin receptor subtype 1 (sst1). Relationship to desensitization and internalization. J Biol Chem 2001; 276: 3709-17.
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 15
[107] Roosterman D, Kreuzer OJ, Brune N, et al. Agonist-induced
endocytosis of rat somatostatin receptor 1. Endocrinology 2007; 148: 1050-8.
[108] Plockinger U, Albrecht S, Mawrin C, et al. Selective loss of
somatostatin receptor 2 in octreotide-resistant growth hormone-secreting adenomas. J Clin Endocrinol Metab 2008; 93: 1203-10.
[109] Waser B, Tamma ML, Cescato R, Maecke HR, Reubi JC. Highly efficient in vivo agonist-induced internalization of sst2 receptors in somatostatin target tissues. J Nucl Med 2009;
50: 936-41. [110] Reubi JC, Waser B, Cescato R, Gloor B, Stettler C, Christ E.
Internalized somatostatin receptor subtype 2 in
neuroendocrine tumors of octreotide-treated patients. J Clin Endocrinol Metab 2010; 95: 2343-50.
[111] Cescato R, Schulz S, Waser B, et al. Internalization of sst2,
sst3, and sst5 receptors: effects of somatostatin agonists and antagonists. J Nucl Med 2006; 47: 502-11.
[112] Lesche S, Lehmann D, Nagel F, Schmid HA, Schulz S.
Differential effects of octreotide and pasireotide on somatostatin receptor internalization and trafficking in vitro. J Clin Endocrinol Metab 2009; 94: 654-61.
[113] Kreuzer OJ, Krisch B, Dery O, Bunnett NW, Meyerhof W. Agonist-mediated endocytosis of rat somatostatin receptor subtype 3 involves beta-arrestin and clathrin coated vesicles.
J Neuroendocrinol 2001; 13: 279-87. [114] Tower-Gilchrist C, Lee E, Sztul E. Endosomal trafficking of
the G protein-coupled receptor somatostatin receptor 3. Biochem Biophys Res Commun 2011; 413: 555-60.
[115] Smalley KS, Feniuk W, Humphrey PP. Differential agonist activity of somatostatin and L-362855 at human recombinant sst4 receptors. Br J Pharmacol 1998; 125: 833-41.
[116] Smalley KS, Koenig JA, Feniuk W, Humphrey PP. Ligand internalization and recycling by human recombinant somatostatin type 4 (h sst(4)) receptors expressed in CHO-
K1 cells. Br J Pharmacol 2001; 132: 1102-10. [117] Stroh T, Jackson AC, Dal Farra C, Schonbrunn A, Vincent
JP, Beaudet A. Receptor-mediated internalization of
somatostatin in rat cortical and hippocampal neurons. Synapse 2000; 38: 177-86.
[118] Hukovic N, Panetta R, Kumar U, Patel YC. Agonist-
dependent regulation of cloned human somatostatin receptor types 1-5 (hSSTR1-5): subtype selective internalization or upregulation. Endocrinology 1996; 137: 4046-9.
[119] Koenig JA, Edwardson JM, Humphrey PP. Somatostatin receptors in Neuro2A neuroblastoma cells: ligand internalization. Br J Pharmacol 1997; 120: 52-9.
[120] Peverelli E, Mantovani G, Calebiro D, et al. The third intracellular loop of the human somatostatin receptor 5 is crucial for arrestin binding and receptor internalization after
somatostatin stimulation. Mol Endocrinol 2008; 22: 676-88. [121] Hukovic N, Panetta R, Kumar U, Rocheville M, Patel YC. The
cytoplasmic tail of the human somatostatin receptor type 5 is
crucial for interaction with adenylyl cyclase and in mediating desensitization and internalization. J Biol Chem 1998; 273: 21416-22.
[122] Grant M, Patel RC, Kumar U. The role of subtype-specific ligand binding and the C-tail domain in dimer formation of human somatostatin receptors. J Biol Chem 2004; 279:
38636-43. [123] Duran-Prado M, Malagon MM, Gracia-Navarro F, Castano
JP. Dimerization of G protein-coupled receptors: new
avenues for somatostatin receptor signalling, control and functioning. Mol Cell Endocrinol 2008; 286: 63-8.
[124] Csaba Z, Peineau S, Dournaud P. Molecular mechanisms of
somatostatin receptor trafficking. J Mol Endocrinol 2012; 48: R1-12.
[125] Baragli A, Alturaihi H, Watt HL, Abdallah A, Kumar U.
Heterooligomerization of human dopamine receptor 2 and somatostatin receptor 2 Co-immunoprecipitation and fluorescence resonance energy transfer analysis. Cell Signal
2007; 19: 2304-16. [126] Rocheville M, Lange DC, Kumar U, Sasi R, Patel RC, Patel
YC. Subtypes of the somatostatin receptor assemble as
functional homo- and heterodimers. J Biol Chem 2000; 275:
7862-9. [127] Patel RC, Kumar U, Lamb DC, et al. Ligand binding to
somatostatin receptors induces receptor-specific oligomer
formation in live cells. Proc Natl Acad Sci USA 2002; 99: 3294-9.
[128] Pfeiffer M, Koch T, Schroder H, et al. Homo- and
heterodimerization of somatostatin receptor subtypes. Inactivation of sst(3) receptor function by heterodimerization with sst(2A). J Biol Chem 2001; 276: 14027-36.
[129] War SA, Somvanshi RK, Kumar U. Somatostatin receptor-3 mediated intracellular signaling and apoptosis is regulated by its cytoplasmic terminal. Biochim Biophys Acta 2011; 1813:
390-402. [130] Grant M, Alturaihi H, Jaquet P, Collier B, Kumar U. Cell
growth inhibition and functioning of human somatostatin
receptor type 2 are modulated by receptor heterodimerization. Mol Endocrinol 2008; 22: 2278-92.
[131] Sharif N, Gendron L, Wowchuk J, et al. Coexpression of
somatostatin receptor subtype 5 affects internalization and trafficking of somatostatin receptor subtype 2. Endocrinology 2007; 148: 2095-105.
[132] Grant M, Collier B, Kumar U. Agonist-dependent dissociation of human somatostatin receptor 2 dimers: a role in receptor trafficking. J Biol Chem 2004; 279: 36179-83.
[133] Tulipano G, Stumm R, Pfeiffer M, Kreienkamp HJ, Hollt V, Schulz S. Differential beta-arrestin trafficking and endosomal sorting of somatostatin receptor subtypes. J Biol Chem 2004; 279: 21374-82.
[134] Duran-Prado M, Bucharles C, Gonzalez BJ, et al. Porcine somatostatin receptor 2 displays typical pharmacological sst2 features but unique dynamics of homodimerization and
internalization. Endocrinology 2007; 148: 411-21. [135] Grant M, Kumar U. The role of G-proteins in the dimerisation
of human somatostatin receptor types 2 and 5. Regul Pept
2010; 159: 3-8. [136] Somvanshi RK, Billova S, Kharmate G, Rajput PS, Kumar U.
C-tail mediated modulation of somatostatin receptor type-4
homo- and heterodimerizations and signaling. Cell Signal 2009; 21: 1396-414.
[137] Pfeiffer M, Koch T, Schroder H, Laugsch M, Hollt V, Schulz
S. Heterodimerization of somatostatin and opioid receptors cross-modulates phosphorylation, internalization, and desensitization. J Biol Chem 2002; 277: 19762-72.
[138] Ferone D, Gatto F, Arvigo M, et al. The clinical-molecular interface of somatostatin, dopamine and their receptors in pituitary pathophysiology. J Mol Endocrinol 2009; 42: 361-70.
[139] Hofland LJ, Feelders RA, de Herder WW, Lamberts SW. Pituitary tumours: the sst/D2 receptors as molecular targets. Mol Cell Endocrinol 2010; 326: 89-98.
[140] Ren SG, Kim S, Taylor J, et al. Suppression of rat and human growth hormone and prolactin secretion by a novel somatostatin/dopaminergic chimeric ligand. J Clin Endocrinol
Metab 2003; 88: 5414-21. [141] Kidd M, Drozdov I, Joseph R, Pfragner R, Culler M, Modlin I.
Differential cytotoxicity of novel somatostatin and dopamine
chimeric compounds on bronchopulmonary and small intestinal neuroendocrine tumor cell lines. Cancer 2008; 113: 690-700.
[142] Culler MD. Somatostatin-dopamine chimeras: a novel approach to treatment of neuroendocrine tumors. Horm Metab Res 2011; 43: 854-7.
[143] Schulz S, Schreff M, Schmidt H, Handel M, Przewlocki R, Hollt V. Immunocytochemical localization of somatostatin receptor sst2A in the rat spinal cord and dorsal root ganglia.
Eur J Neurosci 1998; 10: 3700-8. [144] Bereiter DA. Morphine and somatostatin analogue reduce c-
fos expression in trigeminal subnucleus caudalis produced
by corneal stimulation in the rat. Neuroscience 1997; 77: 863-74.
[145] Bell JR, Young MR, Masterman SC, Morris A, Mattick RP,
Bammer G. A pilot study of naltrexone-accelerated detoxification in opioid dependence. Med J Aust 1999; 171: 26-30.
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

16 Current Molecular Medicine, 2012, Vol. 12, No. 10 Ruscica et al.
[146] Pyronnet S, Bousquet C, Najib S, Azar R, Laklai H, Susini C.
Antitumor effects of somatostatin. Mol Cell Endocrinol 2008; 286: 230-7.
[147] Susini C, Buscail L. Rationale for the use of somatostatin
analogs as antitumor agents. Ann Oncol 2006; 17: 1733-42. [148] Steffani L, Passafaro L, Ferone D, Magni P, Ruscica M.
Somatostatin (SS), SS receptors and SS analog treatment in
tumorigenesis. Atlas of Genetics and Cytogenetics in Oncology and Haematology 2011; [http://AtlasGeneticsOncology.org/Deep/SomatostatinID2009
4.html]. [149] Theodoropoulou M, Zhang J, Laupheimer S, et al.
Octreotide, a somatostatin analogue, mediates its
antiproliferative action in pituitary tumor cells by altering phosphatidylinositol 3-kinase signaling and inducing Zac1 expression. Cancer Res 2006; 66: 1576-82.
[150] Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell 2011; 144: 646-74.
[151] Lahlou H, Saint-Laurent N, Esteve JP, et al. sst2
Somatostatin receptor inhibits cell proliferation through Ras-, Rap1-, and B-Raf-dependent ERK2 activation. J Biol Chem 2003; 278: 39356-71.
[152] Arena S, Pattarozzi A, Massa A, et al. An intracellular multi-effector complex mediates somatostatin receptor 1 activation of phospho-tyrosine phosphatase eta. Mol Endocrinol 2007;
21: 229-46. [153] Hubina E, Ruscica M, Nanzer AM, et al. Novel molecular
aspects of pituitary adenomas. J Endocrinol Invest 2005; 28: 87-92.
[154] Hubina E, Nanzer AM, Hanson MR, et al. Somatostatin analogues stimulate p27 expression and inhibit the MAP kinase pathway in pituitary tumours. Eur J Endocrinol 2006;
155: 371-9. [155] Barbieri F, Pattarozzi A, Gatti M, et al. Differential efficacy of
SSTR1, -2, and -5 agonists in the inhibition of C6 glioma
growth in nude mice. Am J Physiol Endocrinol Metab 2009; 297: E1078-88.
[156] Barbieri F, Pattarozzi A, Gatti M, et al. Somatostatin
receptors 1, 2, and 5 cooperate in the somatostatin inhibition of C6 glioma cell proliferation in vitro via a phosphotyrosine phosphatase-eta-dependent inhibition of extracellularly
regulated kinase-1/2. Endocrinology 2008; 149: 4736-46. [157] Zatelli MC, Tagliati F, Taylor JE, Piccin D, Culler MD, degli
Uberti EC. Somatostatin, but not somatostatin receptor
subtypes 2 and 5 selective agonists, inhibits calcitonin secretion and gene expression in the human medullary thyroid carcinoma cell line, TT. Horm Metab Res 2002; 34:
229-33. [158] Zatelli MC, Piccin D, Tagliati F, et al. Selective activation of
somatostatin receptor subtypes differentially modulates
secretion and viability in human medullary thyroid carcinoma primary cultures: potential clinical perspectives. J Clin Endocrinol Metab 2006; 91: 2218-24.
[159] Ning S, Knox SJ, Harsh GR, Culler MD, Katznelson L. Lanreotide promotes apoptosis and is not radioprotective in GH3 cells. Endocr Relat Cancer 2009; 16: 1045-55.
[160] Ferjoux G, Bousquet C, Cordelier P, et al. Signal transduction of somatostatin receptors negatively controlling cell proliferation. J Physiol Paris 2000; 94: 205-10.
[161] Gruszka A, Kunert-Radek J, Pawlikowski M. The effect of octreotide and bromocriptine on expression of a pro-apoptotic Bax protein in rat prolactinoma. Folia Histochem
Cytobiol 2004; 42: 35-9. [162] Luciani P, Gelmini S, Ferrante E, et al. Expression of the
antiapoptotic gene seladin-1 and octreotide-induced
apoptosis in growth hormone-secreting and nonfunctioning pituitary adenomas. J Clin Endocrinol Metab 2005; 90: 6156-61.
[163] Sharma K, Patel YC, Srikant CB. Subtype-selective induction of wild-type p53 and apoptosis, but not cell cycle arrest, by human somatostatin receptor 3. Mol Endocrinol 1996; 10:
1688-96. [164] Batista DL, Zhang X, Gejman R, et al. The effects of
SOM230 on cell proliferation and adrenocorticotropin
secretion in human corticotroph pituitary adenomas. J Clin
Endocrinol Metab 2006; 91: 4482-8. [165] Lattuada D, Casnici C, Crotta K, et al. Inhibitory effect of
pasireotide and octreotide on lymphocyte activation. J
Neuroimmunol 2007; 182: 153-9. [166] Fedele M, De Martino I, Pivonello R, et al. SOM230, a new
somatostatin analogue, is highly effective in the therapy of
growth hormone/prolactin-secreting pituitary adenomas. Clin Cancer Res 2007; 13: 2738-44.
[167] Martinez-Alonso M, Llecha N, Mayorga ME, et al. Expression
of somatostatin receptors in human melanoma cell lines: effect of two different somatostatin analogues, octreotide and SOM230, on cell proliferation. J Int Med Res 2009; 37: 1813-
22. [168] Folkman J. Angiogenesis in cancer, vascular, rheumatoid
and other disease. Nat Med 1995; 1: 27-31.
[169] Hanahan D, Folkman J. Patterns and emerging mechanisms of the angiogenic switch during tumorigenesis. Cell 1996; 86: 353-64.
[170] Lyons J, 3rd, Anthony CT, Woltering EA. The role of angiogenesis in neuroendocrine tumors. Endocrinol Metab Clin North Am 2010; 39: 839-52.
[171] Dvorak HF, Weaver VM, Tlsty TD, Bergers G. Tumor microenvironment and progression. J Surg Oncol 2011; 103: 468-74.
[172] Woltering EA, Watson JC, Alperin-Lea RC, et al. Somatostatin analogs: angiogenesis inhibitors with novel mechanisms of action. Invest New Drugs 1997; 15: 77-86.
[173] Ribatti D, Conconi MT, Nussdorfer GG. Nonclassic
endogenous novel [corrected] regulators of angiogenesis. Pharmacol Rev 2007; 59: 185-205.
[174] Garcia de la Torre N, Wass JA, Turner HE. Antiangiogenic
effects of somatostatin analogues. Clin Endocrinol (Oxf) 2002; 57: 425-41.
[175] Albini A, Florio T, Giunciuglio D, et al. Somatostatin controls
Kaposi's sarcoma tumor growth through inhibition of angiogenesis. FASEB J 1999; 13: 647-55.
[176] Polverini PJ. Role of the macrophage in angiogenesis-
dependent diseases. EXS 1997; 79: 11-28. [177] Clauss M, Gerlach M, Gerlach H, et al. Vascular permeability
factor: a tumor-derived polypeptide that induces endothelial
cell and monocyte procoagulant activity, and promotes monocyte migration. J Exp Med 1990; 172: 1535-45.
[178] Gulec SA, Drouant GJ, Fuselier J, et al. Antitumor and
antiangiogenic effects of somatostatin receptor-targeted in situ radiation with (111)In-DTPA-JIC 2DL. J Surg Res 2001; 97: 131-7.
[179] Florio T, Morini M, Villa V, et al. Somatostatin inhibits tumor angiogenesis and growth via somatostatin receptor-3-mediated regulation of endothelial nitric oxide synthase and
mitogen-activated protein kinase activities. Endocrinology 2003; 144: 1574-84.
[180] Harper J, Moses MA. Molecular regulation of tumor
angiogenesis: mechanisms and therapeutic implications. EXS 2006; (96): 223-68.
[181] Terranova VP, Hic S, Diflorio RM, Lyall RM. Tumor cell
metastasis. Crit Rev Oncol Hematol 1986; 5: 87-114. [182] Sun LC, Luo J, Mackey LV, Fuselier JA, Coy DH. A
conjugate of camptothecin and a somatostatin analog
against prostate cancer cell invasion via a possible signaling pathway involving PI3K/Akt, alphaVbeta3/alphaVbeta5 and MMP-2/-9. Cancer Lett 2007; 246: 157-66.
[183] Feng Y, Huang T, Gao J, Chang Q, Qin R. Inhibition of metastatic progression of SSTR2 gene transfection mediated by adenovirus in human pancreatic carcinoma cells. J
Huazhong Univ Sci Technolog Med Sci 2006; 26: 68-71. [184] Pola S, Cattaneo MG, Vicentini LM. Anti-migratory and anti-
invasive effect of somatostatin in human neuroblastoma
cells: involvement of Rac and MAP kinase activity. J Biol Chem 2003; 278: 40601-6.
[185] Cattaneo MG, Gentilini D, Vicentini LM. Deregulated human
glioma cell motility: inhibitory effect of somatostatin. Mol Cell Endocrinol 2006; 256: 34-9.
[186] Annunziata M, Luque RM, Duran-Prado M, et al.
Somatostatin and somatostatin analogues reduce PDGF-
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea

Somatostatin Analogs in Cancer Progression Current Molecular Medicine, 2012, Vol. 12, No. 10 17
induced endometrial cell proliferation and motility. Hum
Reprod 2012; 27: 2117-29. [187] Lahlou H, Fanjul M, Pradayrol L, Susini C, Pyronnet S.
Restoration of functional gap junctions through internal
ribosome entry site-dependent synthesis of endogenous connexins in density-inhibited cancer cells. Mol Cell Biol 2005; 25: 4034-45.
[188] Schally AV, Nagy A. Cancer chemotherapy based on
targeting of cytotoxic peptide conjugates to their receptors on tumors. Eur J Endocrinol 1999; 141: 1-14.
[189] Strebhardt K, Ullrich A. Paul Ehrlich's magic bullet concept:
100 years of progress. Nat Rev Cancer 2008; 8: 473-80. [190] Ruscica M, Dozio E, Motta M, Magni P. Role of neuropeptide
Y and its receptors in the progression of endocrine-related
cancer. Peptides 2007; 28: 426-34.
Received: May 30, 2012 Revised: September 13, 2012 Accepted: September 19, 2012
massimilianoruscica
Font monospazio
2013, 13(4):555-71
massimilianoruscica
Linea




















