
Social Variables Predict Gains in Cognitive Scores across the Preschool Years in Children with Birth...
9
Social Variables Predict Gains in Cognitive Scores across the Preschool Years in Children with Birth Weights 500 to 1250 Grams Brett J. Manley, MB BS 1,2,3 , Robin S. Roberts, MSc 4 , Lex W. Doyle, MD 1,3,5,6 , Barbara Schmidt, MD 4,7 , Peter J. Anderson, PhD 3,6 , Keith J. Barrington, MB ChB 8 , Birgitta B € ohm, PhD 9 , Agneta Golan, MD 10 , Aleid G. van Wassenaer-Leemhuis, PhD 11 , and Peter G. Davis, MD 1,2,3 , on behalf of the Caffeine for Apnea of Prematurity (CAP) Trial Investigators* Objective To determine the extent that social variables influence cognitive development of very low birth weight (VLBW) infants across the preschool years. Study design Participants were VLBW (500-1250 g) children enrolled in the Caffeine for Apnea of Prematurity ran- domized trial between 1999 and 2004. We investigated the relationships between 4 potential social advantages: higher maternal education, higher paternal education, caregiver employment, and 2 biologic parents in the same home—and gain in cognitive scores. Cognitive assessments were performed at the corrected ages of 18 months (Mental Development Index score on the Bayley Scales of Infant Development II) and 5 years (Full Scale IQ on the Wechsler Preschool and Primary Scale of Intelligence III). Cognitive gain was computed by subtracting each individual 18-month Mental Development Index score from the corresponding Full Scale IQ at 5 years. Results Data were available for 1347 children. Mean (SD) cognitive scores were 90.8 (15.7) at 18 months and 98.9 (14.5) at 5 years. Multivariable regression showed that higher maternal education, higher paternal education, and caregiver employment had independent and additive effects of similar size on cognitive gain (P < .001); the mean cognitive gain between 18 months and 5 years increased by 3.6 points in the presence of each of these ad- vantages. When all 3 were present, cognitive scores improved on average by 10.9 points compared with children without any of these advantages. Conclusion In VLBW children, a count of 3 social advantages strongly predicts gains in cognitive scores across the preschool years. (J Pediatr 2015;-:---). See editorial, p and related article, p P reterm birth is a leading cause of infant morbidity and mortality in indus- trialized countries. 1 Infants who are born very preterm (<32 weeks) or with very low birth weight (VLBW, <1500 g) are at greater risk of poor neurobehavioral outcomes. 2,3 The Caffeine for Apnea of Prematurity (CAP) trial is a large, international, randomized controlled trial of the safety and efficacy of neonatal caffeine therapy in children with birth weights of 500-1250 g. 4,5 The pri- mary outcome was a composite of death, cerebral palsy, cognitive delay, deafness, or blindness at a corrected age of 18 months. Caffeine reduced the rates of this composite outcome and 2 of its components, cerebral palsy and cognitive delay. These treatment benefits were attenuated at a corrected age of 5 years, although secondary motor outcomes were still improved in children who had been as- signed randomly to neonatal caffeine therapy. 6 The frequency of cognitive scores less than 2 SDs below the mean in the CAP trial cohort was lower and the mean cognitive scores were greater at 5 years than at 18 months. 6 These cognitive scores were measured with different instruments From the 1 Department of Obstetrics and Gynecology, The University of Melbourne; 2 Neonatal Services and Newborn Research Centre, The Royal Women’s Hospital; 3 Murdoch Childrens Research Institute, Melbourne, Australia; 4 Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Ontario, Canada; 5 Research Office, The Royal Women’s Hospital; 6 Department of Pediatrics, The University of Melbourne, Melbourne, Australia; 7 Division of Neonatology, Children’s Hospital of Philadelphia and Department of Pediatrics, University of Pennsylvania, Philadelphia, PA; 8 McGill University, Montreal, Quebec, Canada; 9 Department of Women’s and Children’s Health, Karolinska Institutet, Stockholm, Sweden; 10 Soroka Medical Center, Beer Sheva, Israel; and 11 Department of Neonatology, Emma Children’s Hospital AMC, Amsterdam, The Netherlands *List of investigators of the Caffeine for Apnea of Prematurity (CAP) Trial is available at www.jpeds.com (Appendix). Funded by the Canadian Institutes of Health Research (MCT 13288) and the National Health and Medical Research Council (Australia; 108706). B.S., L.D., and K.B. received travel and related expenses for attending scientific meetings from Chiesi Pharmaceuticals. B.S. received a speakers’ honorarium from the Nemours Foundation. The other authors declare no conflicts of interest. Registered with ClinicalTrials.gov: NCT00182312. 0022-3476/$ - see front matter. Copyright ª 2015 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.jpeds.2014.12.016 Bayley-III Bayley Scales of Infant and Toddler Development, 3rd Edition BSID-II Bayley Scales of Infant Development II CAP Caffeine for Apnea of Prematurity FSIQ Full Scale IQ MDI Mental Development Index VLBW Very low birth weight WPPSI-III Wechsler Preschool and Primary Scale of Intelligence III 1
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Social Variables Predict Gains in Cognitive Scores across the Preschool Years in Children with Birth...

Social Variables Predict Gains in Cognitive Scores across the PreschoolYears in Children with Birth Weights 500 to 1250 Grams
Brett J. Manley, MB BS1,2,3, Robin S. Roberts, MSc4, Lex W. Doyle, MD1,3,5,6, Barbara Schmidt, MD4,7,
Peter J. Anderson, PhD3,6, Keith J. Barrington, MB ChB8, Birgitta B€ohm, PhD9, Agneta Golan, MD10,
Aleid G. van Wassenaer-Leemhuis, PhD11, and Peter G. Davis, MD1,2,3, on behalf of the
Caffeine for Apnea of Prematurity (CAP) Trial Investigators*
Objective To determine the extent that social variables influence cognitive development of very low birth weight(VLBW) infants across the preschool years.Study design Participants were VLBW (500-1250 g) children enrolled in the Caffeine for Apnea of Prematurity ran-domized trial between 1999 and 2004. We investigated the relationships between 4 potential social advantages:higher maternal education, higher paternal education, caregiver employment, and 2 biologic parents in the samehome—and gain in cognitive scores. Cognitive assessments were performed at the corrected ages of 18 months(Mental Development Index score on the Bayley Scales of Infant Development II) and 5 years (Full Scale IQ onthe Wechsler Preschool and Primary Scale of Intelligence III). Cognitive gain was computed by subtracting eachindividual 18-month Mental Development Index score from the corresponding Full Scale IQ at 5 years.Results Data were available for 1347 children. Mean (SD) cognitive scores were 90.8 (15.7) at 18 months and 98.9(14.5) at 5 years. Multivariable regression showed that higher maternal education, higher paternal education, andcaregiver employment had independent and additive effects of similar size on cognitive gain (P < .001); themean cognitive gain between 18 months and 5 years increased by 3.6 points in the presence of each of these ad-vantages. When all 3 were present, cognitive scores improved on average by 10.9 points compared with childrenwithout any of these advantages.Conclusion In VLBW children, a count of 3 social advantages strongly predicts gains in cognitive scores acrossthe preschool years. (J Pediatr 2015;-:---).
See editorial, p ��� andrelated article, p ���
reterm birth is a leading cause of infant morbidity andmortality in indus-
From the 1Department of Obstetrics and Gynecology,The University of Melbourne; 2Neonatal Services andNewborn Research Centre, The Royal Women’sHospital; 3Murdoch Childrens Research Institute,Melbourne, Australia; 4Department of ClinicalEpidemiology and Biostatistics, McMaster University,Hamilton, Ontario, Canada; 5Research Office, The RoyalWomen’s Hospital; 6Department of Pediatrics, TheUniversity of Melbourne, Melbourne, Australia; 7Divisionof Neonatology, Children’s Hospital of Philadelphia andDepartment of Pediatrics, University of Pennsylvania,Philadelphia, PA; 8McGill University, Montreal, Quebec,Canada; 9Department of Women’s and Children’sHealth, Karolinska Institutet, Stockholm, Sweden;10Soroka Medical Center, Beer Sheva, Israel; and11Department of Neonatology, EmmaChildren’s HospitalAMC, Amsterdam, The Netherlands
*List of investigators of the Caffeine for Apnea ofPrematurity (CAP) Trial is available at www.jpeds.com(Appendix).
P trialized countries.1 Infants who are born very preterm (<32 weeks) orwith very low birth weight (VLBW, <1500 g) are at greater risk of poor
neurobehavioral outcomes.2,3 The Caffeine for Apnea of Prematurity (CAP) trialis a large, international, randomized controlled trial of the safety and efficacy ofneonatal caffeine therapy in children with birth weights of 500-1250 g.4,5 The pri-mary outcome was a composite of death, cerebral palsy, cognitive delay, deafness,or blindness at a corrected age of 18 months. Caffeine reduced the rates of thiscomposite outcome and 2 of its components, cerebral palsy and cognitive delay.These treatment benefits were attenuated at a corrected age of 5 years, althoughsecondary motor outcomes were still improved in children who had been as-signed randomly to neonatal caffeine therapy.6
The frequency of cognitive scores less than 2 SDs below the mean in the CAPtrial cohort was lower and the mean cognitive scores were greater at 5 years thanat 18 months.6 These cognitive scores were measured with different instruments
Funded by the Canadian Institutes of Health Research(MCT 13288) and the National Health and MedicalResearch Council (Australia; 108706). B.S., L.D., andK.B. received travel and related expenses for attendingscientific meetings from Chiesi Pharmaceuticals. B.S.received a speakers’ honorarium from the NemoursFoundation. The other authors declare no conflicts ofinterest.
Registered with ClinicalTrials.gov: NCT00182312.
0022-3476/$ - see front matter. Copyright ª 2015 Elsevier Inc.
All rights reserved.
http://dx.doi.org/10.1016/j.jpeds.2014.12.016
Bayley-III Bayley Scales of Infant and Toddler Development, 3rd Edition
BSID-II Bayley Scales of Infant Development II
CAP Caffeine for Apnea of Prematurity
FSIQ Full Scale IQ
MDI Mental Development Index
VLBW Very low birth weight
WPPSI-III Wechsler Preschool and Primary Scale of Intelligence III
1

THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
but both are age-standardized to have a mean of 100 and SDof 15. However, not all children experienced the same degreeof cognitive improvement. The relationship between cogni-tive gain at 5 years and Mental Development Index (MDI)scores at 18 months was linear but with a downward slopesuch that the greatest gains were seen in those who performedthe worst at 18 months.6 This observation may be partly dueto the statistical phenomenon of “regression to the mean”: bychance those who scored low at 18months would be expectedto score higher at 5 years, and vice versa. However, other fac-tors may have influenced the magnitude of the observedchanges in cognitive scores over time.
As a child grows, the environment plays a progressivelylarger role in cognitive development compared with the child’sgenetic make-up and early health problems. In the generalpopulation, social variables are positively associated with gen-eral intelligence7-9 and with more specific cognitive domainssuch as language and executive function.10-12 In relation tomore distal social-environmental factors, parenting practicesthat provide for a stimulating home environment are associ-ated with improved cognitive development.13
Social disadvantage is also a risk factor for poorer develop-mental outcomes in preterm infants.14 Yet, the extent towhich social variables affect the rate of change in cognitivedevelopment over the preschool years in preterm childrenhas not been adequately described. Social variables thathave been associated with cognitive development includematernal education, paternal education, and family in-come.8,15-17 We undertook this study to examine the effectof social variables on cognitive gains and losses across thepreschool years in this international cohort of VLBW infants.
Methods
Infants with birth weights of 500-1250 g were enrolled in theCAP trial between October 11, 1999, and October 22, 2004,and followed to a corrected age of 18 months.4,5 All but 4of the original 35 study centers performed further follow-up to a corrected age of 5 years. These 31 academic hospitalswere located in Canada, Australia, Europe, and Israel and hadenrolled 1932 (96.3%) of the 2006 CAP trial participants.6
We have previously demonstrated the importance of correct-ing for prematurity at follow-up testing to avoid bias incognitive test scores.18,19
The research ethics boards of the 31 study centersapproved the original and the 5-year follow-up protocols.Written informed consents were obtained from a parent orguardian of each study participant at entry into the trialand before the 5-year follow-up assessments.
TheMDI score on the Bayley Scales of Infant DevelopmentII (BSID-II) was our measure of cognitive development at18 months.20 Children who were too cognitively impairedto be tested were assigned an “imputed” score of 49, because50 is the lowest MDI score on the BSID-II.
The Full Scale IQ (FSIQ) on the Wechsler Preschool andPrimary Scale of Intelligence III (WPPSI-III) was themeasureof general cognitive ability at age 5 years.21 Children who
2
were too cognitively impaired to be tested were assigned an“imputed” score of 39, because 40 is the lowest FSIQ onthe WPPSI-III. A total of 44 children were tested with otherstandardized intelligence tests because a national version ofthe WPPSI-III was not available or because it was no longerappropriate for the age of the child at the time of the assess-ment.Demographic data collection at both follow-up visits
included the following information for maternal andpaternal caregivers: their level of education, current employ-ment status, relationship to the child, and whether both par-ents lived in the same home.
Statistical AnalysesLinear regression was used to investigate the relationships be-tween prespecified social variables and the change in stan-dardized cognitive scores between ages 18 months and5 years. Because the cognitive scores of most—althoughnot all—children improved during this period, we refer tothis difference as “cognitive gain,” defined as the WPPSI-IIIFSIQ minus the BSID-II MDI score. We excluded childrenwho were not tested with the BSID-II at 18 months or withthe WPPSI-III at 5 years and those who had imputed cogni-tive scores at either age. The 4 prespecified social advantagevariables were: (1) higher maternal education (ie, started orcompleted college or university); (2) higher paternal educa-tion (ie, started or completed college or university); (3)parental employment (at least 1 employed or self-employedcaregiver at both 18 months and 5 years); and (4) 2 biologicparents in the same home at 18 months and 5 years.These social advantage variables were categorized as “pre-
sent” (coded as 1) or “absent” (coded as 0). A small numberof missing values (<1%) also were included as “absent.”Because the dependent variable “cognitive gain” decreasedwith increasing values of the 18-month MDI, this score wasincluded as an explanatory variable in all models.The separate effect of each social advantage variable on
cognitive gain was estimated by fitting a series of regressionmodels (Models 1 to 4 in Table I) that contained the 18-month MDI score and an indicator variable for thepresence or absence of the respective social advantage. Thismodel incorporates a common linear trend of cognitivegain with MDI score but allows the position of the trendline to vary depending on the presence or absence of thesocial advantage being considered. An interaction term (theproduct of the social advantage variable and the MDIscore) was included in a secondary analysis to explore thepossibility that the social advantage variables may affect theslope of the relationship between cognitive gain at 5 yearsand MDI score at 18 months. The fitted regressioncoefficient associated with each social variable estimatedthe mean difference in cognitive gain between childrenwith, as opposed to without, the social advantage.Statistical significance was derived from the ratio of thiscoefficient and its SE.The presence or absence of the 4 social advantages may be
correlated and thus their effects, analyzed separately, may
Manley et al

Table I. Regression models
Model number Regression model
Fitted model Interaction P value
Coefficient (SE)* P value MDI slope† Nonadditivityz
1 Higher maternal education 6.0 (0.68) <.00118-month MDI �0.56 (0.021) <.001 .38
2 Higher paternal education 5.9 (0.67) <.00118-month MDI �0.56 (0.021) <.001 .34
3 Employed or self-employed caregiver 5.6 (1.0) <.00118-month MDI �0.56 (0.021) <.001 .33
4 Two biologic parents 3.0 (0.79) <.00118-month MDI �0.55 (0.022) <.001 .61
5 Combined-effects of social advantagesHigher maternal education 3.9 (0.76) <.001 .70Higher paternal education 3.5 (0.77) <.001Employed or self-employed caregiver 2.7 (1.1) .01Two biologic parents 0.90 (0.83) .2818-month MDI �0.58 (0.021) <.001 .75
6 Final combined-effects modelHigher maternal education 3.9 (0.76) <.001 .82Higher paternal education 3.6 (0.76) <.001Employed or self-employed caregiver 3.2 (1.0) .00218-month MDI �0.58 (0.021) <.001 .49
7 Social advantage count modelSocial advantage count 3.6 (0.33) <.00118-month MDI �0.58 (0.021) <.001 .34
*The model coefficient is the estimated difference in mean cognitive gain per unit change in the explanatory variable. For a social advantage, the coefficient equals the mean difference in cognitivegain due to the presence of the social advantage. For the 18-month MDI, the coefficient equals the difference in mean cognitive gain per 1-point increase in MDI.†Test of the influence of the presence of each social advantage on the slope of cognitive gain with MDI (ie, nonparallelism).zGlobal test of the pair-wise interactions between the individual social advantages (ie, nonadditivity).
- 2015 ORIGINAL ARTICLES
overlap. To eliminate this potential overlap, the combined ef-fect of these variables was estimated using a multivariableregression model containing the MDI score and each of the4 separate social advantage variables (Model 5 in Table I).Nonsignificant social variables were eliminated by using abackwards elimination process to obtain what is called theFinal combined-effects model (Model 6 in Table I).Secondary analyses explored the possibility of nonadditivesocial advantage effects in this reduced model (ie, that thecombined effect of 2 social advantages being present wasdifferent from the sum of their individual effects afterallowance for intercorrelation) and the effects of socialadvantages on the linear trend with the MDI score.Additional interaction terms evaluated the effects of sex,geographic region (Canada, Australia, Europe, and Israel),and of the randomized allocation to neonatal caffeinetherapy or placebo. Finally, we constructed a “Socialadvantage count” model (Model 7 in Table I) using thenumber of social advantages present and containing theMDI score as an additional explanatory variable. All Pvalues were 2-sided and considered significant if P < .05.SAS version 9.2 (SAS Institute Inc, Cary, North Carolina)was used for all statistical analyses and regression modelswere fitted with PROC REG (SAS Institute Inc).
Results
Study Population and Cognitive Outcomes at18 Months and 5 YearsThe number of children who were included in the analysisand the reasons for exclusion of others are shown inFigure 1 (available at www.jpeds.com). The characteristics
Social Variables Predict Gains in Cognitive Scores across the Pres500 to 1250 Grams
of the 1347 children and their families in this analysiscohort are shown in Table II. The mean (SD) MDI score at18 months was 90.8 (15.7) and FSIQ at 5 years was 98.9(14.5).
Effects of Social Advantages on Cognitive Gainbetween 18 Months and 5 YearsFor ease of data display, the children were divided into sub-groups according to the respective quartiles of their MDIscores at age 18 months. The plots in Figure 2 illustrate therelationships between the mean cognitive gains at age5 years and the mean MDI scores in the 4 quartiles at age18 months in children with and without each of thehypothesized social advantages. All plots in Figure 2 showa similar pattern: a general downward linear trend suchthat children with lower MDI at 18 months experiencedlarger cognitive gains at 5 years and, superimposed on thistrend, an approximately constant mean increase incognitive gain associated with the presence of each socialadvantage. The net effect of these influences is a pair ofapproximately parallel and approximately linearrelationships between cognitive gain at 5 years and MDIscores at 18 months, with the vertical displacementrepresenting the effect of the social advantage.Table I summarizes the regression analyses. The presence
of each individual social advantage was associated with asignificantly larger mean cognitive gain (Models 1-4). Forexample, Model 1 shows that the presence of the socialadvantage of “Higher maternal education” was associatedwith an increased mean cognitive gain at 5 years of 6.0points compared with not having the social advantage.Mean cognitive gain at 5 years trends downwards with a
chool Years in Children with Birth Weights 3

Table II. Characteristics of the children and theirfamilies*
CharacteristicsStudy group(n = 1347)
ChildrenBirth weight, mean (SD), g 971 (180)Gestational age, mean (SD), wk 27.4 (1.8)Female sex, no. (%) 675 (50.1)Birth weight <10th percentile for gestational
age,† no. (%)203 (15.1)
Exposure to antenatal corticosteroids, no. (%) 1199 (89.0)Singleton birth, no. (%) 950 (70.5)Neonatal morbidities, no. (%)
Bronchopulmonary dysplasiaz 552 (41.0)Brain injuryx 135 (10.3)Severe retinopathy of prematurity{ 64 (4.8)Any neonatal morbidity 612 (46.9)
Cognitive outcomesMDI score at 18 mo, mean (SD) 90.8 (15.7)WPPSI-III FSIQ at 5 y, mean (SD) 98.9 (14.5)
Families, no. (%)Maternal college or university education at 5 y 759 (56.3)Paternal college or university education at 5 y 665 (49.4)Employed or self-employed caregiver at 18 mo
and at 5 y1175 (87.2)
Two biologic parents as caregivers at 18 moand at 5 y
1157 (85.9)
*These data are for the 1347 children with adequate cognitive scores at 18 months and at5 years.†The 10th percentile for gestational age in a normal population was as reported by Krameret al.22
zThe need for supplemental oxygen at a postmenstrual age of 36 weeks.xEchodense intraprenchymal lesions, periventricular leukomalacia, or ventriculomegaly with orwithout intraventricular hemorrhage diagnosed on cranial ultrasound.{Unilateral or bilateral stage 4 or 5 retinopathy or received cryotherapy or laser therapy to atleast one eye.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
decrease of 0.56 for each 1 point increase in the 18-monthMDI. None of the social advantages influenced the slope ofthe relationship between cognitive gain and MDI score.The smallest P value for an interaction in these 4 analyseswas .33, confirming the visual impression in Figure 2 thatthe linear relationships separating children with andwithout each of the 4 social advantages are parallel over theentire range of MDI scores at 18 months. Thus each socialadvantage is associated with a fixed independent positiveeffect superimposed on the general downward trend ofcognitive gain with 18-month MDI.
Examination of the combined effects of the 4 socialadvantage variables showed that higher maternal andpaternal education both remained strongly associatedwith cognitive gain (Model 5). Caregiver employment orself-employment was associated with a significant butweaker effect than parental education, and having 2 bio-logic parents in the same home at ages 18 months and5 years did not contribute significantly to this multivari-able regression model. As in the individual models, theslope of the relationship between cognitive gain andMDI score was not influenced by the 4 social advantages(P = .75), and the combined effect of the social advantageswas purely additive (nonadditivity P = .70). After thebackwards elimination process the Final combined-effectsmodel retained higher maternal and paternal educationand having an employed or self-employed caregiver as
4
strongly significant explanatory variables of cognitivegain at 5 years (Model 6). Note that estimated effect sizesof these 3 social advantages are now somewhat smallerthan in Models 1-3 as a result of eliminating the overlapdue to intercorrelation.Exploratory analyses of possible interactions with sex,
geographic region, and neonatal caffeine treatment did notimprove the fit of the Final combined-effects model, withthe exception of female sex. It was associated with an addi-tional small cognitive gain of 1.6 points, independent of thepresence or absence of the social advantages. The slope ofthe relationship between mean cognitive gain and meanMDI did not vary with the presence or absence of each socialadvantage (P= .49). This finding suggests that the presence ofsocial advantages was associated with greater cognitive gainsat 5 years, but without altering the trend for cognitive gains tobe smallest in the children with the greatest MDI scores at18 months. Moreover, there was no evidence that the com-bined effect of the 3 social advantage variables was anythingother than additive (P = .82).This prognostic independence, together with the observa-
tion that the cognitive gain associated with each of the 3 so-cial advantages was of similar size, implies that a simple countof the number of social advantages that are present would fitthe observed data well. This “Social advantage count” model(Model 7) explained only 0.02% less of the variation than theFinal combined-effects model and suggested that the meancognitive gain between 18 months and 5 years increased by3.6 points (P < .001) for each social advantage that was pre-sent. The fit of the Social advantage count model is shown inFigure 3. When higher maternal education, higher paternaleducation, and caregiver employment or self-employmentwere all present, cognitive scores improved on average by10.9 points compared with the scores of the childrenwithout any of these 3 social advantages. Adjusting for thepresence of 3 prognostically important neonatalmorbidities (bronchopulmonary dysplasia, brain injury,and severe retinopathy of prematurity)23 did not affect thestrength of the relationship between cognitive gain andsocial advantage count (data not shown). In a regressionmodel, 3.1% of the variance in 18-month MDI wasexplained by the social advantage count, and at 5 years, itexplained 10.1% of the variance in FSIQ.
Discussion
Previous research has demonstrated that social advantagesare associated with better cognitive outcomes in VLBW chil-dren.15,24 However, this study examined the impact of mul-tiple social advantages on the change in cognitive scoresover time in these children. In this large longitudinal studywe demonstrated that children with 3 social advantageshad, on average, an increment in cognitive scores betweenages 18 months and 5 years that was more than two-thirdsof a SD greater than children without any of the advantages,a clinically important difference. Thus, the trajectory ofcognitive development for VLBW children from socially
Manley et al
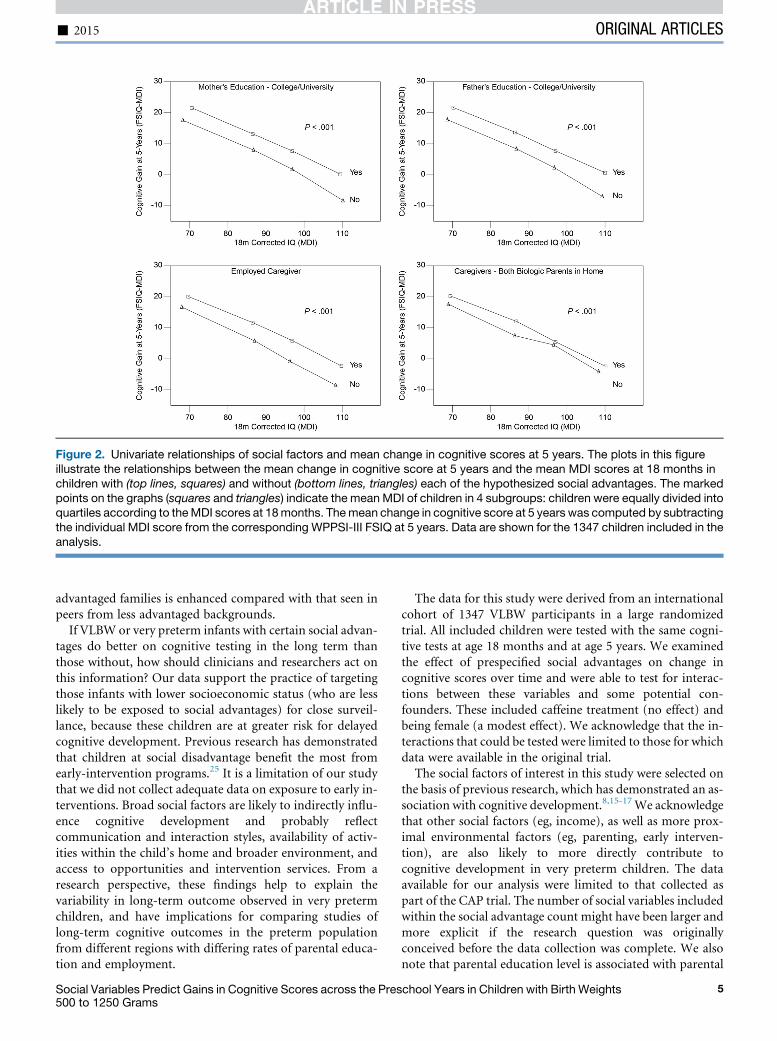
Figure 2. Univariate relationships of social factors and mean change in cognitive scores at 5 years. The plots in this figureillustrate the relationships between the mean change in cognitive score at 5 years and the mean MDI scores at 18 months inchildren with (top lines, squares) and without (bottom lines, triangles) each of the hypothesized social advantages. The markedpoints on the graphs (squares and triangles) indicate the mean MDI of children in 4 subgroups: children were equally divided intoquartiles according to theMDI scores at 18months. Themean change in cognitive score at 5 years was computed by subtractingthe individual MDI score from the corresponding WPPSI-III FSIQ at 5 years. Data are shown for the 1347 children included in theanalysis.
- 2015 ORIGINAL ARTICLES
advantaged families is enhanced compared with that seen inpeers from less advantaged backgrounds.
If VLBW or very preterm infants with certain social advan-tages do better on cognitive testing in the long term thanthose without, how should clinicians and researchers act onthis information? Our data support the practice of targetingthose infants with lower socioeconomic status (who are lesslikely to be exposed to social advantages) for close surveil-lance, because these children are at greater risk for delayedcognitive development. Previous research has demonstratedthat children at social disadvantage benefit the most fromearly-intervention programs.25 It is a limitation of our studythat we did not collect adequate data on exposure to early in-terventions. Broad social factors are likely to indirectly influ-ence cognitive development and probably reflectcommunication and interaction styles, availability of activ-ities within the child’s home and broader environment, andaccess to opportunities and intervention services. From aresearch perspective, these findings help to explain thevariability in long-term outcome observed in very pretermchildren, and have implications for comparing studies oflong-term cognitive outcomes in the preterm populationfrom different regions with differing rates of parental educa-tion and employment.
Social Variables Predict Gains in Cognitive Scores across the Pres500 to 1250 Grams
The data for this study were derived from an internationalcohort of 1347 VLBW participants in a large randomizedtrial. All included children were tested with the same cogni-tive tests at age 18 months and at age 5 years. We examinedthe effect of prespecified social advantages on change incognitive scores over time and were able to test for interac-tions between these variables and some potential con-founders. These included caffeine treatment (no effect) andbeing female (a modest effect). We acknowledge that the in-teractions that could be tested were limited to those for whichdata were available in the original trial.The social factors of interest in this study were selected on
the basis of previous research, which has demonstrated an as-sociation with cognitive development.8,15-17We acknowledgethat other social factors (eg, income), as well as more prox-imal environmental factors (eg, parenting, early interven-tion), are also likely to more directly contribute tocognitive development in very preterm children. The dataavailable for our analysis were limited to that collected aspart of the CAP trial. The number of social variables includedwithin the social advantage count might have been larger andmore explicit if the research question was originallyconceived before the data collection was complete. We alsonote that parental education level is associated with parental
chool Years in Children with Birth Weights 5
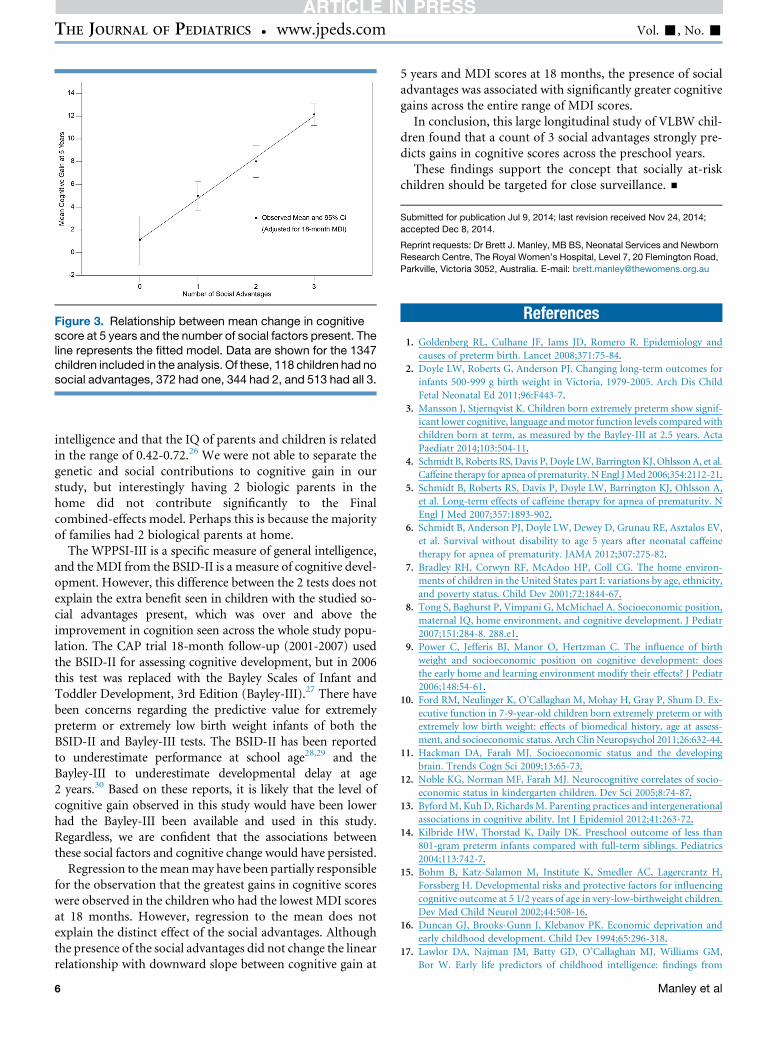
Figure 3. Relationship between mean change in cognitivescore at 5 years and the number of social factors present. Theline represents the fitted model. Data are shown for the 1347children included in the analysis. Of these, 118 children had nosocial advantages, 372 had one, 344 had 2, and 513 had all 3.
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
intelligence and that the IQ of parents and children is relatedin the range of 0.42-0.72.26 We were not able to separate thegenetic and social contributions to cognitive gain in ourstudy, but interestingly having 2 biologic parents in thehome did not contribute significantly to the Finalcombined-effects model. Perhaps this is because the majorityof families had 2 biological parents at home.
The WPPSI-III is a specific measure of general intelligence,and theMDI from the BSID-II is a measure of cognitive devel-opment. However, this difference between the 2 tests does notexplain the extra benefit seen in children with the studied so-cial advantages present, which was over and above theimprovement in cognition seen across the whole study popu-lation. The CAP trial 18-month follow-up (2001-2007) usedthe BSID-II for assessing cognitive development, but in 2006this test was replaced with the Bayley Scales of Infant andToddler Development, 3rd Edition (Bayley-III).27 There havebeen concerns regarding the predictive value for extremelypreterm or extremely low birth weight infants of both theBSID-II and Bayley-III tests. The BSID-II has been reportedto underestimate performance at school age28,29 and theBayley-III to underestimate developmental delay at age2 years.30 Based on these reports, it is likely that the level ofcognitive gain observed in this study would have been lowerhad the Bayley-III been available and used in this study.Regardless, we are confident that the associations betweenthese social factors and cognitive change would have persisted.
Regression to themeanmay have been partially responsiblefor the observation that the greatest gains in cognitive scoreswere observed in the children who had the lowest MDI scoresat 18 months. However, regression to the mean does notexplain the distinct effect of the social advantages. Althoughthe presence of the social advantages did not change the linearrelationship with downward slope between cognitive gain at
6
5 years and MDI scores at 18 months, the presence of socialadvantages was associated with significantly greater cognitivegains across the entire range of MDI scores.In conclusion, this large longitudinal study of VLBW chil-
dren found that a count of 3 social advantages strongly pre-dicts gains in cognitive scores across the preschool years.These findings support the concept that socially at-risk
children should be targeted for close surveillance. n
Submitted for publication Jul 9, 2014; last revision received Nov 24, 2014;
accepted Dec 8, 2014.
Reprint requests: Dr Brett J. Manley, MB BS, Neonatal Services and Newborn
Research Centre, The Royal Women’s Hospital, Level 7, 20 Flemington Road,
Parkville, Victoria 3052, Australia. E-mail: [email protected]
References
1. Goldenberg RL, Culhane JF, Iams JD, Romero R. Epidemiology and
causes of preterm birth. Lancet 2008;371:75-84.
2. Doyle LW, Roberts G, Anderson PJ. Changing long-term outcomes for
infants 500-999 g birth weight in Victoria, 1979-2005. Arch Dis Child
Fetal Neonatal Ed 2011;96:F443-7.
3. Mansson J, Stjernqvist K. Children born extremely preterm show signif-
icant lower cognitive, language andmotor function levels compared with
children born at term, as measured by the Bayley-III at 2.5 years. Acta
Paediatr 2014;103:504-11.
4. Schmidt B, Roberts RS, Davis P, Doyle LW, BarringtonKJ,OhlssonA, et al.
Caffeine therapy for apnea of prematurity. N Engl JMed 2006;354:2112-21.
5. Schmidt B, Roberts RS, Davis P, Doyle LW, Barrington KJ, Ohlsson A,
et al. Long-term effects of caffeine therapy for apnea of prematurity. N
Engl J Med 2007;357:1893-902.
6. Schmidt B, Anderson PJ, Doyle LW, Dewey D, Grunau RE, Asztalos EV,
et al. Survival without disability to age 5 years after neonatal caffeine
therapy for apnea of prematurity. JAMA 2012;307:275-82.
7. Bradley RH, Corwyn RF, McAdoo HP, Coll CG. The home environ-
ments of children in the United States part I: variations by age, ethnicity,
and poverty status. Child Dev 2001;72:1844-67.
8. Tong S, Baghurst P, Vimpani G, McMichael A. Socioeconomic position,
maternal IQ, home environment, and cognitive development. J Pediatr
2007;151:284-8. 288.e1.
9. Power C, Jefferis BJ, Manor O, Hertzman C. The influence of birth
weight and socioeconomic position on cognitive development: does
the early home and learning environment modify their effects? J Pediatr
2006;148:54-61.
10. Ford RM, Neulinger K, O’Callaghan M, Mohay H, Gray P, Shum D. Ex-
ecutive function in 7-9-year-old children born extremely preterm or with
extremely low birth weight: effects of biomedical history, age at assess-
ment, and socioeconomic status. Arch Clin Neuropsychol 2011;26:632-44.
11. Hackman DA, Farah MJ. Socioeconomic status and the developing
brain. Trends Cogn Sci 2009;13:65-73.
12. Noble KG, Norman MF, Farah MJ. Neurocognitive correlates of socio-
economic status in kindergarten children. Dev Sci 2005;8:74-87.
13. ByfordM, KuhD, RichardsM. Parenting practices and intergenerational
associations in cognitive ability. Int J Epidemiol 2012;41:263-72.
14. Kilbride HW, Thorstad K, Daily DK. Preschool outcome of less than
801-gram preterm infants compared with full-term siblings. Pediatrics
2004;113:742-7.
15. Bohm B, Katz-Salamon M, Institute K, Smedler AC, Lagercrantz H,
Forssberg H. Developmental risks and protective factors for influencing
cognitive outcome at 5 1/2 years of age in very-low-birthweight children.
Dev Med Child Neurol 2002;44:508-16.
16. Duncan GJ, Brooks-Gunn J, Klebanov PK. Economic deprivation and
early childhood development. Child Dev 1994;65:296-318.
17. Lawlor DA, Najman JM, Batty GD, O’Callaghan MJ, Williams GM,
Bor W. Early life predictors of childhood intelligence: findings from
Manley et al

- 2015 ORIGINAL ARTICLES
the Mater-University study of pregnancy and its outcomes. Paediatr
Perinat Epidemiol 2006;20:148-62.
18. Rickards AL, Kitchen WH, Doyle LW, Kelly EA. Correction of develop-
mental and intelligence test scores for premature birth. Aust Paediatr J
1989;25:127-9.
19. Wilson-Ching M, Pascoe L, Doyle LW, Anderson PJ. Effects of correct-
ing for prematurity on cognitive test scores in childhood. J Paediatr
Child Health 2014;50:182-8.
20. Bayley N. Manual for the Bayley Scales of Infant Development. 2nd ed.
San Antonio (TX): Psychological Corporation; 1993.
21. Wechsler Preschool and Primary Scale of Intelligence. 3rd ed. Toronto,
Canada: Psychological Corporation; 2002.
22. Kramer MS, Platt RW, Wen SW, Joseph KS, Allen A, Abrahamowicz M,
et al. A new and improved population-based Canadian reference for
birth weight for gestational age. Pediatrics 2001;108:E35.
23. Schmidt B, Asztalos EV, Roberts RS, Robertson CM, Sauve RS,
Whitfield MF. Impact of bronchopulmonary dysplasia, brain injury,
and severe retinopathy on the outcome of extremely low-birth-weight
infants at 18 months: results from the trial of indomethacin prophylaxis
in preterms. JAMA 2003;289:1124-9.
24. Potharst ES, Houtzager BA, van Sonderen L, Tamminga P, Kok JH,
Last BF, et al. Prediction of cognitive abilities at the age of 5 years
Social Variables Predict Gains in Cognitive Scores across the Pres500 to 1250 Grams
using developmental follow-up assessments at the age of 2 and 3
years in very preterm children. Dev Med Child Neurol 2012;54:
240-6.
25. Koldewijn K, van Wassenaer A, Wolf MJ, Meijssen D, Houtzager B,
Beelen A, et al. A neurobehavioral intervention and assessment program
in very low birth weight infants: outcome at 24 months. J Pediatr 2010;
156:359-65.
26. Bowles S, Gintis H. The inheritance of inequality. J Econ Perspect 2002;
16:3-30.
27. Bayley N. Bayley Scales of Infant and Toddler Development. 3rd ed. San
Antonio (TX): Psychological Corporation; 2006.
28. Hack M, Taylor HG, Drotar D, Schluchter M, Cartar L, Wilson-
Costello D, et al. Poor predictive validity of the Bayley Scales of Infant
Development for cognitive function of extremely low birth weight chil-
dren at school age. Pediatrics 2005;116:333-41.
29. Roberts G, Anderson PJ, Doyle LW. The stability of the diagnosis of
developmental disability between ages 2 and 8 in a geographic
cohort of very preterm children born in 1997. Arch Dis Child
2010;95:786-90.
30. Anderson PJ, De Luca CR, Hutchinson E, Roberts G, Doyle LW. Under-
estimation of developmental delay by the new Bayley-III Scale. Arch Pe-
diatr Adolesc Med 2010;164:352-6.
chool Years in Children with Birth Weights 7

Appendix
Additional members of the CAP Trial include:McMaster University Medical Center, Hamilton, ON,
Canada: Barbara Schmidt, MD, MSc, Judy D’Ilario, RN,Janice Cairnie, RN, Joanne Dix, RN, BScN, MSN, BethAnne Adams, PhD, Erin Warriner, PhD, CPsych, Mee-HaiMarie Kim, MD, MSc; Royal Women’s Hospital, Mel-bourne, Australia: Peter Anderson, PhD, Peter Davis, MD,Lex Doyle, MD, Brenda Argus, RN, Catherine Callanan,RN, RM, Noni Davis, MBBS, Julianne Duff, B Med Sci,MB, BS, Marion McDonald, RN; Sunnybrook Health Sci-ences Center, Toronto, Canada: Elizabeth Asztalos, MD,MSc, Denise Hohn, BScOT, OTReg (Ont), Maralyn Lacy,BSc, RN; Women’s and Children’s Hospital, Adelaide,Australia: Ross Haslam, MBBS, Christopher Barnett,MBBS, FCCMG, Louise Goodchild, RN, Rosslyn MarieLontis, RN, RM, NICC, Dip of Nursing (CommunityHealth), BN; Mercy Hospital for Women, Melbourne,Australia: Simon Fraser, MBBS, MPPM, Julie Keng,MHlthSc, Kerryn Saunders, MBBS, Gillian Opie, MBBS,IBCLC, Elaine Kelly, MA, MAPsS, LACST, MAASH,CPSP, Heather Woods, RN, RM, Emma Marchant, RN,Anne-Marie Turner, MBBS, Noni Davis, MBBS, EmmaMa-grath, MBBS, MHth&MedLaw, AmandaWilliamson, MPsy;Centre Hospitalier Universitaire de Quebec, Quebec City,Canada: Aida Bairam, MD, PhD, Sylvie B�elanger, MD, An-nie Fraser, MPs; Ottawa Hospital, Ottawa, ON, Canada:Marc Blayney, MB BCh, Brigitte Lemyre, MD, Jane Frank,RN; Children’s & Women’s Health Centre of BC, Vancou-ver, BC, Canada: Alfonso Solimano, MD, Anne Synnes,MDCM, MHSC, Ruth E. Grunau, PhD, Philippa Hubber-Richard, RN, BScN, BSc, Marilyn Rogers, BSR, PT, MargotMackay, BScO.T, Julianne Petrie-Thomas, PhD, ArsalanButt, MSc; Academic Medical Center, Amsterdam, TheNetherlands: Aleid van Wassenaer, MD, PhD, Debbie Nuy-temans, CRC, Bregje Houtzager, PhD, Loekie van Sonderen,MD; Meir General Hospital, Kfar-Saba, Israel: Rivka Regev,MD, Netter Itzchack, MA, Shmuel Arnon, MD, Adiba Cha-laf, RN; Mount Sinai Hospital, Toronto, Canada: ArneOhlsson, MSc, Karel O’Brien, MB BCh BAO, MSc, Anne-Marie Hamilton, PT, MSc, May Lee Chan, BA; RoyalUniversity Hospital, Saskatoon, SK, Canada: KoravangattuSankaran, MD, FCCM, Pat Proctor, RN; Soroka UniversityMedical Center, Beer Sheva, Israel: Agneta Golan, MD,Esther Goldsch-Lerman, PhD; The Canberra Hospital, Can-berra, Australia: Graham Reynolds, MB BS, DCH MHP,MHEd, Barbara Dromgool, MN, Sandra Meskell, RN, Va-nessa Parr, MN, Catherine Maher, RN, Margaret Broom,BN RN RM, Zsuzsoka Kecskes, Dr Med, PhD, Cathy Ring-land, RN; Foothills Hospital and Alberta Children’s Hospi-tal, Calgary, AB, Canada: Douglas McMillan, MD, ElizabethSpellen, RN, BN, Bed, Reginald S. Sauve, MD, MPH, Heath-er Christianson, BA, Deborah Anseeuw-Deeks, BN, DianneCreighton, PhD, RPsych, Jennifer Heath, MD; St. Boniface,Winnipeg, MB, Canada: Ruben Alvaro, MD, Aaron Chiu,
MD, Ceceile Porter, RNBN CEI, NICU, Gloria Turner,RN, Diane Moddemann, MD, Med, Naomi Granke, RN,CCRP, Karen Penner, PhD (candidate), MSc, BMROT,Jane Bow, PhD, CPsych; University Hospital Maastricht,Maastricht, The Netherlands: Antonius Mulder, MD,PhD, Renske Wassenberg, PhD, Markus van der Hoeven,MD, PhD; Kingston General Hospital, Kingston, ON, Can-ada: Maxine Clarke, MBBS, DCH, Judy Parfitt, RN, BA, Ke-vin Parker, BA, MDiv, MA, PhD; Windsor RegionalHospital, Windsor, ON, Canada: Chukwuma Nwaesei,MD, MPH, Heather Ryan, RN, BSc, BScN, Cory Saunders,PhD, CPsych; Ludwig Maximilian University, Munich, Ger-many: Andreas Schulze, MD, Inga Wermuth, MD, AnneHilgendorff, MD, PhD, Andreas W. Flemmer, MD, PhD;Astrid Lindgren Children’s Hospital, Stockholm, Sweden:Eric Herlenius, MD, PhD, Lena Legnevall, RN, BSc, HugoLagercrantz, MD, PhD; Victoria General Hospital, Victoria,BC, Canada: Derek Matthew, MD (retired), Wendy Amos(retired), Suresh Tulsiani, MD, Cherrie Tan-Dy, MD, Mari-lyn Turner (retired), Constance Phelan, RN (retired); Ka-plan Medical Center, Rehovot, Israel: Eric S. Shinwell,MD, Michael Levine, RN, MPHA, Ada Juster-Reicher,MD; Royal Victoria Hospital, Montreal, QC, Canada: MayKhairy, MD, CM, Patricia Grier, BScN, Julie Vachon,PhD, Larissa Perepolkin, BA, Keith J Barrington, MB,ChB; James Cook University Hospital, Middlesbrough,United Kingdom: Sunil Kumar Sinha, MD, Win Tin, MD,Susan Fritz, SRN, RSCN; University of Sherbrooke, Sher-brooke, QC, Canada: Herve Walti, MD, Diane Royer, RN;Royal Maternity Hospital Belfast, Northern Ireland, UnitedKingdom: Henry Halliday, MD, DCH D(Obst)RCOG, Da-vid Millar, MB, MRCP, Clifford Mayes, MD, ChristopherMcCusker, MSc, PhD, CPsycho, Olivia McLaughlin, BSc;Basel Children’s Hospital, Basel, Switzerland: Hubert Fah-nenstich, MD, Bettina Tillmann, MD, Peter Weber, MD;Royal Victoria Infirmary, Newcastle upon Tyne, UnitedKingdom: Unni Wariyar, BSc, MBBS, DCH, DCCH, MD,Nicholas Embleton, MD, Ravi Swamy, MD, MRCPCH;University Hospital Zurich, Zurich, Switzerland: Hans U.Bucher, MD, Jean-Claude. Fauchere, MD, Vera Dietz,MD; Northern Neonatal Initiatives, Middlesbrough, UnitedKingdom: Chidambara Harikumar, MD, MRCP, DM(Neo), DCH RCPCH, Win Tin, MD, Susan Fritz, SRN,RSCN.Steering Committee for 5-Year Follow-Up: Barbara
Schmidt (Chair), MD, MSc (McMaster University, Hamil-ton, Ontario, Canada, and University of Pennsylvania, Phil-adelphia, Pennsylvania), Peter J. Anderson, PhD (Universityof Melbourne, Melbourne, Victoria, Australia), Elizabeth V.Asztalos, MD, MSc (University of Toronto, Toronto, On-tario, Canada), Keith J. Barrington, MB, ChB (Universityof Montreal, Montreal, Quebec, Canada), Peter G. Davis,MD (University of Melbourne, Melbourne, Victoria,Australia), Deborah Dewey, PhD (University of Calgary, Cal-gary, Alberta, Canada), Lex W. Doyle, MD (University ofMelbourne, Melbourne, Victoria, Australia), Ruth E. Gru-nau, PhD (University of British Columbia, Vancouver,
THE JOURNAL OF PEDIATRICS � www.jpeds.com Vol. -, No. -
7.e1 Manley et al

British Columbia, Canada), Diane Moddemann, MD, MEd(University of Manitoba, Winnipeg, Manitoba, Canada),Arne Ohlsson, MSc (University of Toronto, Toronto, On-tario, Canada), Robin S. Roberts, MSc (McMaster Univer-sity, Hamilton, Ontario, Canada), Alfonso Solimano, MD(University of British Columbia, Vancouver, BritishColumbia, Canada), Win Tin, MD (The James Cook Univer-sity Hospital, Middlesbrough, UK).
External Safety Monitoring Committee: Michael Gent(Chair), BSc, MSc, DSc (McMaster University, Hamilton,Ontario, Canada), William Fraser, MD, MSc (University of
Montreal, Montreal, Quebec, Canada), Edmund Hey, DPhil(deceased), Max Perlman, MB, BS (Hospital for Sick Chil-dren, Toronto, Ontario, Canada), Kevin Thorpe, BMath,MMath (McMaster University, Hamilton, Ontario, Can-ada).Consultant Pharmacist: Shari Gray, BScPhm, RPh
(McMaster University, Hamilton, Ontario, Canada).Coordinating and Methods Center, McMaster University,
Hamilton, Ontario, Canada:Robin S. Roberts, MSc, Carole Chambers, Lorrie Costan-
tini, BA, Wendy Yacura, Erin McGean, Lori Scapinello.
2006 Infants were randomized in the CAP Trial
191 Excluded 74 Enrolled in centers that did not
participate in 5-year follow-up 117 Did not survive to 5 years
1815 Children were eligible for assessments at 18 months and 5 years
396 Did not have quantitative cognitive data at 18 months and/or 5 years 28 Had imputed cognitive scores
at 18 months and/or 5 years 44 Were not tested with the WPPSI-III at 5 years
1347 Children were included in this analysis
Figure 1. Study flow.
- 2015 ORIGINAL ARTICLES
Social Variables Predict Gains in Cognitive Scores across the Preschool Years in Children with Birth Weights500 to 1250 Grams
7.e2




















