
Smoking and All-cause Mortality in Older Adults
11
Smoking and All-cause Mortality in Older Adults Results From the CHANCES Consortium Aysel Müezzinler, PhD, 1,2 Ute Mons, PhD, 1 Carolin Gellert, PhD, 1 Ben Schöttker, PhD, 1 Eugène Jansen, PhD, 3 Frank Kee, MD, 4 Mark G. O’Doherty, PhD, 4 Kari Kuulasmaa, PhD, 5 Neal D. Freedman, PhD, MPH, 6 Christian C. Abnet, PhD, MPH, 6 Alicja Wolk, DMSc, 7 Niclas Håkansson, PhD, 7 Nicola Orsini, PhD, 7 Tom Wilsgaard, PhD, 8 Bas Bueno-de-Mesquita, MD, PhD, MPH, 3,9,10,11 Yvonne T. van der Schouw, PhD, 12 Petra H.M. Peeters, MD, PhD, 12 Lisette C.P.G.M. de Groot, PhD, 13 Annette Peters, PhD, 14 Philippos Orfanos, PhD, 15,16 Allan Linneberg, PhD, 17,18,19 Charlotta Pisinger, PhD, MPH, 17 Abdonas Tamosiunas, MD, PhD, 20 Migle Baceviciene, PhD, 20 Dalia Luksiene, PhD, 20 Gailute Bernotiene, PhD, 20 Pekka Jousilahti, MD, PhD, 5 Ulrika Petterson-Kymmer, MD, PhD, 21,22 Jan Håkan Jansson, MD, PhD, 21 Stefan Söderberg, MD, PhD, 21 Sture Eriksson, MD, PhD, 23 Nicole Jankovic, MSc, 13 María-José Sánchez, MD, PhD, 24,25 Giovanni Veronesi, PhD, 26 Susana Sans, MD, PhD, 27 Wojciech Drygas, MD, PhD, 28 Antonia Trichopoulou, MD, PhD, 15,16 Paolo Boffetta, MD, MPH, 15,29 Hermann Brenner, MD, MPH 1 Introduction: Smoking is known to be a major cause of death among middle-aged adults, but evidence on its impact and the benefits of smoking cessation among older adults has remained limited. Therefore, we aimed to estimate the influence of smoking and smoking cessation on all- cause mortality in people aged Z60 years. Methods: Relative mortality and mortality rate advancement periods (RAPs) were estimated by Cox proportional hazards models for the population-based prospective cohort studies from Europe and the U.S. (CHANCES [Consortium on Health and Ageing: Network of Cohorts in Europe and the U.S.]), and subsequently pooled by individual participant meta-analysis. Statistical analyses were performed from June 2013 to March 2014. From the 1 Division of Clinical Epidemiology and Aging Research, German Cancer Research Center (DKFZ), Heidelberg, Germany; 2 Network Aging Research, University of Heidelberg, Heidelberg, Germany; 3 National Insti- tute for Public Health and the Environment, Bilthoven, the Netherlands; 4 UKCRC Centre of Excellence for Public Health, Queen’s University Belfast, Belfast, Northern Ireland; 5 National Institute for Health and Welfare, Helsinki, Finland; 6 Division of Cancer Epidemiology and Genetics, National Cancer Institute, Bethesda, Maryland; 7 Institute of Environmental Medicine, Karolinska Institutet, Stockholm, Sweden; 8 Department of Community Medicine, UiT the Arctic University of Norway, Tromsø, Norway; 9 Depart- ment of Gastroenterology and Hepatology, University Medical Center Utrecht, Utrecht, the Netherlands; 10 Department of Epidemiology and Biostatistics, School of Public Health, Imperial College London, London, United Kingdom; 11 Department of Social and Preventive Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia; 12 Department of Epidemiology, Julius Center, University Medical Center Utrecht, Utrecht, the Netherlands; 13 Division of Human Nutrition, Wageningen University, Wageningen, the Netherlands; 14 Institute of Epidemiology II, Helmholtz Zentrum München, Neuherberg, Germany; 15 Hellenic Health Foundation, Athens, Greece; 16 Department of Hygiene, Epidemiology and Medical Statistics, University of Athens Medical School, Athens, Greece; 17 Research Centre for Prevention and Health, Glostrup University Hospi- tal, Glostrup, Denmark; 18 Department of Clinical Experimental Research, Glostrup University Hospital, Glostrup, Denmark; 19 Faculty of Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark; 20 Laboratory of Population Studies, Institute of Cardiology of Medical Academy, Lithuanian University of Health Sciences, Kaunas, Lithuania; 21 Department of Public Health and Clinical Medicine, Medicine, Skellefteå Research Unit, Cardiology, Umeå University, Umeå, Sweden; 22 Depart- ment of Pharmacology and Clinical Neurosciences, Umeå University, Umeå, Sweden; 23 Department of Community Medicine and Rehabilitation, Geriatric Medicine, Umeå University, Umeå, Sweden; 24 Escuela Andaluza de Salud Pública, Instituto de Investigación Biosanitaria de Granada (Granada.ibs), Granada, Spain; 25 CIBER de Epidemiología y Salud Pública, Barcelona, Spain; 26 Department of Clinical and Experimental Medicine, Research Center in Epidemiology and Preventive Medicine, University of Insubria, Varese, Italy; 27 Institute of Health Studies, Barcelona, Spain; 28 Department of Epidemiology, Cardiovascular Disease Prevention and Health Promotion, Institute of Cardiology, Warsaw, Poland; and the 29 Tisch Cancer Institute and Institute for Translational Epidemiology, Mount Sinai School of Medicine, New York, New York Address correspondence to: Ute Mons, PhD, Division of Clinical Epide- miology and Aging Research, German Cancer Research Center (DKFZ), Im Neuenheimer Feld 581, 69120 Heidelberg, Germany. E-mail: [email protected]. 0749-3797/$36.00 http://dx.doi.org/10.1016/j.amepre.2015.04.004 & 2015 American Journal of Preventive Medicine Published by Elsevier Inc. Am J Prev Med 2015;](]):]]]–]]] 1
Transcript of Smoking and All-cause Mortality in Older Adults

From the 1DCancer ReseResearch, Utute for Pub4UKCRC CeBelfast, NorHelsinki, FinCancer InstiKarolinskaMedicine, Ument of GaUtrecht, UtBiostatistics,United Kingof Medicine,of EpidemiUtrecht, theUniversity, WHelmholtz ZFoundation,Medical Sta17Research Ctal, Glostrup
& 2015 Am
Smoking and All-cause Mortality inOlder Adults
Results From the CHANCES ConsortiumAysel Müezzinler, PhD,1,2 Ute Mons, PhD,1 Carolin Gellert, PhD,1 Ben Schöttker, PhD,1
Eugène Jansen, PhD,3 Frank Kee, MD,4 Mark G. O’Doherty, PhD,4 Kari Kuulasmaa, PhD,5
Neal D. Freedman, PhD, MPH,6 Christian C. Abnet, PhD, MPH,6 Alicja Wolk, DMSc,7
Niclas Håkansson, PhD,7 Nicola Orsini, PhD,7 Tom Wilsgaard, PhD,8
Bas Bueno-de-Mesquita, MD, PhD, MPH,3,9,10,11 Yvonne T. van der Schouw, PhD,12
Petra H.M. Peeters, MD, PhD,12 Lisette C.P.G.M. de Groot, PhD,13 Annette Peters, PhD,14
Philippos Orfanos, PhD,15,16 Allan Linneberg, PhD,17,18,19 Charlotta Pisinger, PhD, MPH,17
Abdonas Tamosiunas, MD, PhD,20 Migle Baceviciene, PhD,20 Dalia Luksiene, PhD,20
Gailute Bernotiene, PhD,20 Pekka Jousilahti, MD, PhD,5 Ulrika Petterson-Kymmer, MD, PhD,21,22
Jan Håkan Jansson, MD, PhD,21 Stefan Söderberg, MD, PhD,21 Sture Eriksson, MD, PhD,23
Nicole Jankovic, MSc,13 María-José Sánchez, MD, PhD,24,25 Giovanni Veronesi, PhD,26
Susana Sans, MD, PhD,27 Wojciech Drygas, MD, PhD,28 Antonia Trichopoulou, MD, PhD,15,16
Paolo Boffetta, MD, MPH,15,29 Hermann Brenner, MD, MPH1
ivarnivlicntthlatutIniTstrecSdoUoloN
enAtise, D
e
Introduction: Smoking is known to be a major cause of death among middle-aged adults, butevidence on its impact and the benefits of smoking cessation among older adults has remainedlimited. Therefore, we aimed to estimate the influence of smoking and smoking cessation on all-cause mortality in people aged Z60 years.
Methods: Relative mortality and mortality rate advancement periods (RAPs) were estimated byCox proportional hazards models for the population-based prospective cohort studies from Europeand the U.S. (CHANCES [Consortium on Health and Ageing: Network of Cohorts in Europe andthe U.S.]), and subsequently pooled by individual participant meta-analysis. Statistical analyses wereperformed from June 2013 to March 2014.
ision of Clinical Epidemiology and Aging Research, Germanch Center (DKFZ), Heidelberg, Germany; 2Network Agingersity of Heidelberg, Heidelberg, Germany; 3National Insti-Health and the Environment, Bilthoven, the Netherlands;
re of Excellence for Public Health, Queen’s University Belfast,ern Ireland; 5National Institute for Health and Welfare,nd; 6Division of Cancer Epidemiology and Genetics, Nationale, Bethesda, Maryland; 7Institute of Environmental Medicine,stitutet, Stockholm, Sweden; 8Department of Communitythe Arctic University of Norway, Tromsø, Norway; 9Depart-roenterology and Hepatology, University Medical Centerht, the Netherlands; 10Department of Epidemiology andchool of Public Health, Imperial College London, London,m; 11Department of Social and Preventive Medicine, Facultyniversity of Malaya, Kuala Lumpur, Malaysia; 12Departmentgy, Julius Center, University Medical Center Utrecht,etherlands; 13Division of Human Nutrition, Wageningenageningen, the Netherlands; 14Institute of Epidemiology II,trum München, Neuherberg, Germany; 15Hellenic Healththens, Greece; 16Department of Hygiene, Epidemiology andtics, University of Athens Medical School, Athens, Greece;ntre for Prevention and Health, Glostrup University Hospi-enmark; 18Department of Clinical Experimental Research,
Glostrup University Hospital, Glostrup, Denmark; 19Faculty of Health andMedical Sciences, University of Copenhagen, Copenhagen, Denmark;20Laboratory of Population Studies, Institute of Cardiology of MedicalAcademy, Lithuanian University of Health Sciences, Kaunas, Lithuania;21Department of Public Health and Clinical Medicine, Medicine, SkellefteåResearch Unit, Cardiology, Umeå University, Umeå, Sweden; 22Depart-ment of Pharmacology and Clinical Neurosciences, Umeå University,Umeå, Sweden; 23Department of Community Medicine and Rehabilitation,Geriatric Medicine, Umeå University, Umeå, Sweden; 24Escuela Andaluzade Salud Pública, Instituto de Investigación Biosanitaria de Granada(Granada.ibs), Granada, Spain; 25CIBER de Epidemiología y Salud Pública,Barcelona, Spain; 26Department of Clinical and Experimental Medicine,Research Center in Epidemiology and Preventive Medicine, University ofInsubria, Varese, Italy; 27Institute of Health Studies, Barcelona, Spain;28Department of Epidemiology, Cardiovascular Disease Prevention andHealth Promotion, Institute of Cardiology, Warsaw, Poland; and the29Tisch Cancer Institute and Institute for Translational Epidemiology,Mount Sinai School of Medicine, New York, New York
Address correspondence to: Ute Mons, PhD, Division of Clinical Epide-miology and Aging Research, German Cancer Research Center (DKFZ), ImNeuenheimer Feld 581, 69120 Heidelberg, Germany. E-mail: [email protected].
0749-3797/$36.00http://dx.doi.org/10.1016/j.amepre.2015.04.004
rican Journal of Preventive Medicine � Published by Elsevier Inc. Am J Prev Med 2015;](]):]]]–]]] 1

Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]]2
Results: A total of 489,056 participants aged Z60 years at baseline from 22 population-basedcohort studies were included. Overall, 99,298 deaths were recorded. Current smokers had 2-fold andformer smokers had 1.3-fold increased mortality compared with never smokers. These increases inmortality translated to RAPs of 6.4 (95% CI¼4.8, 7.9) and 2.4 (95% CI¼1.5, 3.4) years, respectively.A clear positive dose�response relationship was observed between number of currently smokedcigarettes and mortality. For former smokers, excess mortality and RAPs decreased with time sincecessation, with RAPs of 3.9 (95% CI¼3.0, 4.7), 2.7 (95% CI¼1.8, 3.6), and 0.7 (95% CI¼0.2, 1.1) forthose who had quit o10, 10 to 19, and Z20 years ago, respectively.
Conclusions: Smoking remains as a strong risk factor for premature mortality in older individualsand cessation remains beneficial even at advanced ages. Efforts to support smoking abstinence at allages should be a public health priority.(Am J Prev Med 2015;](]):]]]–]]]) & 2015 American Journal of Preventive Medicine
Introduction
Tobacco smoking is a strong risk factor for multi-ple chronic diseases, including cancer1,2 andcardiovascular diseases,3–5 and, consequently,
for all-cause mortality.6 Although the harmful effects oftobacco smoking among middle-aged adults have beenwell established,7,8 evidence on the consequences ofsmoking at older age has only recently received specificattention.5,9,10 The impact of smoking on older individ-uals is of considerable public health interest, given theincreasing numbers of older people in both developedand developing countries, which will increase healthcarecosts.11 Even though smoking is less common in olderthan in younger people,12,13 smoking in older adults isone of the most important factors leading to general lossof function, mobility, and independence.14,15 On theother hand, smoking is a modifiable risk factor andsmoking cessation is highly and rapidly beneficial even atthe oldest ages (Z80 years).10
Although recent research has assessed the impact ofsmoking and smoking cessation on health-related out-comes at older ages,9,10 summative evidence from large-scale prospective studies from different parts of the worldremains sparse. The present study addresses this questionin the Consortium on Health and Ageing: Network ofCohorts in Europe and the U.S. (CHANCES), whichincludes a large number of cohorts from all over Europeand the U.S. Apart from traditional measures of relativemortality, the impact of smoking and smoking cessationamong older adults was quantified by mortality rateadvancement periods (RAPs).16 RAPs quantify the agedifference by which a risk factor advances diseaseincidence or mortality among exposed compared withunexposed individuals. They could be particularly effec-tive at communicating the associated risks of cigarettesmoking and the benefits of cessation.9
MethodsStudy Design and Study Population
This investigation was based on 489,066 participants, aged Z60years, from 22 population-based cohorts of the CHANCESconsortium (www.chancesfp7.eu/).17 The overall recruitment ofdifferent studies took place between 1979 and 2005 and their meanfollow-up time was between approximately 8 and 13 years for moststudies. Detailed cohort descriptions are provided in the Appendix(available online).
All variables used for the project were created by each cohortaccording to the pre-agreed harmonization rules of the CHANCESconsortium. All CHANCES cohort studies have been conducted inaccordance with the Declaration of Helsinki.
Measures
Smoking status, amount of smoking, and age at smoking cessationwere assessed via self-administered questionnaires at baseline. Thenumber of currently smoked cigarettes was not available in theMultinational Monitoring of Trends and Determinants in Car-diovascular Diseases (MONICA) Risk, Genetics, Archiving andMonograph (MORGAM) North Sweden cohort and the Survey inEurope on Nutrition and the Elderly; a Concerted Action(SENECA) cohort. In the NIH-AARP (previously known asAmerican Association of Retired Persons Diet and Health Study)cohort, time since smoking cessation was collected only incategories (cessation last year, 1�4 years ago, 5�9 years ago,Z10 years ago) that could not be fully harmonized with theinformation from the other cohorts. Therefore, these results arereported separately. All cohorts, except the Survey of Health,Ageing and Retirement in Europe (SHARE), obtained the exactdate of death from an official death register or death certificate. InSHARE, the date of death was obtained from an “end of lifeinterview” with household members. Covariates comprised impor-tant sociodemographic variables, potential confounders, and well-known risk factors for mortality (age, sex, education, BMI, alcoholconsumption, physical activity, history of diabetes, total choles-terol, and systolic blood pressure). A detailed overview of avail-ability of different variables across the cohorts is provided inAppendix Table 1 (available online).
www.ajpmonline.org

Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]] 3
Statistical Analysis
Statistical analysis was carried out from June 2013 to March 2014.Analyses were performed separately for each cohort using uniformanalysis scripts. Cox proportional hazards regression was used toestimate hazard ratios (HRs) and 95% CIs for the associations ofsmoking with all-cause mortality. Time of follow-up was used asthe underlying time variable. The following covariates wereadjusted for in the main model: age (continuous), sex, BMI,education (r9 years, 10�11 years, and Z12 years), alcoholconsumption (abstainer, low intake, medium intake, and highintake, which were defined as follows: men, 0.1�39.9 g/week,40�59.9 g/week, and Z60 g/week; women, 0.1�19.9 g/week,20�39.9 g/week, andZ40 g/week, respectively18), physical activity(inactive and active, which were defined as follows: 0 hours ofvigorous physical activity/week and >0 hours of vigorous physicalactivity/week). All analyses were carried out on the whole sample,separately for women and men and in two age groups (60�69years and Z70 years).RAPs and 95% CIs were calculated from the results of the
multivariable regression models.16 Briefly, RAPs are calculated asratio of the regression coefficients of the smoking-relatedexposure variable and age (more details in the Appendix,available online). The MORGAM Kaunas cohort includedparticipants with a very narrow age range, which did not allowfor reliable estimates of regression coefficients for age. Therefore,RAPs were not calculated for this cohort. Following the estima-tion of HRs and RAPs in single studies, individual participantmeta-analyses were performed to calculate summary HRs andRAPs across the cohorts.19
All analyses were conducted with SAS software, version 9.2, andstatistical tests were two-sided using a 5% significance level. TheComprehensive Meta-Analysis software, version 2.0, was used tocarry out all meta-analyses. In a conservative approach, therandom effects estimates were taken as “main results” to allowfor variation of true effects across studies.20 Random effectsestimates were derived using the DerSimonian-Laird method.21,22
Heterogeneity was assessed by I2-statistics and Q-statistics.
ResultsAge and sex distributions of the 489,056 individualsincluded from 22 cohorts are shown in Table 1. The totalstudy population was composed of 44% (n¼213,941)women and 56% (n¼275,115) men. Eighty-six percent(n¼422,676) of participants were aged 60 to 69 years and14% (n¼66,390) were aged Z70 years at baseline.Overall, there were 55,728 (11%) current, 221,727(45%) former, and 182,389 (37%) never smokers atbaseline examination (Appendix Figures 1 and 2, avail-able online, show distributions of smoking status andsmoking intensity across cohorts). The total number ofdeaths was 99,298.Sensitivity analyses for meta-analyses, excluding those
studies lacking adjustments for physical activity, alcoholconsumption, or both, did not yield considerably differ-ent estimates. Therefore, we report in each case thesummary meta-analyses estimates including all cohorts.
] 2015
Further sensitivity analyses included history of diabetes,blood pressure, and total cholesterol level as additionalcovariates. However, these inclusions did not materiallyaffect any of the results and are therefore not reportedseparately.The association of smoking status with all-cause
mortality is shown in Figure 1. HRs and RAPs forcurrent and former smokers compared to never smokersare shown separately for each cohort (Figure 1A and 1B,respectively). Meta-analyses indicated that current smok-ers had a 2-fold and former smokers had a 1.3-foldincreased mortality compared with never smokers. Thesummary estimates from the meta-analyses of RAPs were6.4 and 2.4 years for current and former smokers,respectively. Owing to a much stronger association ofsmoking with mortality in the NIH-AARP cohort, thelargest cohort in the consortium, the fixed effects modelsgiving a large weight to this cohort would yield consid-erably higher estimates (current smokers, HR=2.73, 95%CI=2.67, 2.78, po0.001, RAP=8.70, 95% CI=8.44, 8.96,po0.001; former smokers, HR=1.58, 95% CI=1.56, 1.60,po0.001, RAP=4.22, 95% CI=4.05, 4.39, po0.001). Sex-specific summary estimates were similar in men andwomen (Appendix Table 2, available online). Those aged60�69 years at baseline had larger relative excess risksthan those aged Z70 years (Appendix Table 3, availableonline).Figure 2 shows the association of the average number
of cigarettes smoked per day by current smokers withall-cause mortality. The total number of deaths in thisanalysis was 44,935. A clear dose�response relation-ship was observed. Summary estimates of individualHRs were 1.83, 2.35, and 2.54 for smoking 1�10cigarettes/day, 11�19 cigarettes/day, and Z20 ciga-rettes/day, respectively. The meta-analyses of RAPssuggested that those who smoked 1�10 cigarettes/dayhad mortality advancement by 5.2 years, whereas thosewho smoked 11�19 and Z20 cigarettes/day had anoverall 7.3 and 8.2 years advancement in mortality ratesrespectively, compared with never smokers. Similardose�response relationships were observed in sex-and age-specific analyses (Appendix Tables 2 and 3,available online).Meta-analyses according to year since smoking cessa-
tion were carried out separately for the NIH-AARPcohort and the other cohorts, given practical incompa-tibilities of the categories used. HRs and RAPs for formersmokers according to time since smoking cessation withreference to never smokers (excluding the NIH-AARPcohort) are presented in Figure 3. The total number ofdeaths from 20 cohorts was 19,685. A clear reduction ofexcess mortality with time since cessation was observed,with summary HRs of 1.53, 1.35, and 1.08 and summary

Table 1. Description of Cohorts
Cohorts NDeaths,
n
Meanfollow-uptime, y
Agedistribution, n (%)
Sexdistribution (%)
60�69 y 60�69 y Male Female
ELSA (England) 10,816 2,246 9.8 5,065 (47) 5,751 (53) 6,044 (56) 4,772 (44)
EPIC Greece 9,863 1,970 10.0 7,056 (72) 2,807 (28) 5,942 (60) 3,921 (40)
EPIC Netherlands 6,896 960 12.6 6,891 (99.9) 5 (0.1) 6,579 (95) 317 (5)
EPIC Spain 5,185 629 13.2 5,185 (100) 0 2,946 (57) 2,239 (43)
EPIC Sweden 3,364 490 13.3 3,324 (99) 40 (1) 1,780 (53) 1,584 (47)
ESTHER (Germany) 6,545 896 10.8 4,981 (76) 1,564 (24) 3,566 (54) 2,979 (46)
MORGAMKORA-Augsburg(Germany)
4,494 1,601 13.8 3,372 (75) 1,122 (25) 2,174 (48) 2,320 (52)
MORGAM Brianza(Italy)
713 235 15.4 713 (100) 0 338 (47) 375 (53)
MORGAMCatalonia (Spain)
740 81 8.5 740 (100) 0 299 (40) 441 (60)
MORGAM FINRISK(Finland)
6,106 2,067 12.9 5,257 (86) 849 (14) 3,007 (49) 3,099 (51)
MORGAM Glostrup(Denmark)
2,970 752 14.8 1,973 (66) 997 (34) 1,468 (49) 1,502 (51)
MORGAM Kaunas(Lithuania)
647 149 10.0 647 (100) 0 334 (52) 313 (48)
MORGAM NorthernSweden
906 111 7.8 763 (84) 143 (16) 438 (48) 468 (52)
MORGAM SHIP(Germany)
1,442 378 9.0 793 (56) 619 (44) 648 (46) 794 (54)
MORGAM Warsaw(Poland)
829 229 9.7 829 (100) 0 425 (51) 404 (49)
NHANES III(USA)
6,596 3,631 9.9 2,608 (40) 3,988 (60) 3,479 (53) 3,117 (47)
NIH-AARP(USA)
366,919 77,895 11.4 345,580 (94) 21,339 (6) 143,567 (39) 223,352 (61)
SENECA(Europe)
2,584 822 8.6 8 (0.3) 2,576 (99.7) 1,303 (50) 1,281 (50)
SHARE (Europe) 40,004 444 2.0 20,310 (51) 19,734 (49) 21,667 (54) 18,337 (46)
SMC (Sweden) 4,699 96 4.8 3,120 (66) 1,579 (34) 4,699 (100) 0
Tromsø(Norway)
5,851 3,056 11.9 3,099 (53) 2,752 (47) 3,238 (55) 2,613 (45)
Zutphen(The Netherlands)
887 560 9.6 362 (41) 525 (59) 0 887 (100)
Sum 489,056 99,298 422,676 (86.4) 66,390 (13.6) 213,941 (43.7) 275,115 (56.3)
ELSA, English Longitudinal Study of Ageing; EPIC, European Prospective Investigation into Cancer and Nutrition; ESTHER, Early Recognition andOptimised Treatment of Chronic Diseases in the Older Population; MORGAM, Multinational Monitoring of Trends and Determinants inCardiovascular Diseases (MONICA) Risk, Genetics, Archiving and Monograph; NHANES, National Health and Nutrition Examination Survey; NIH-AARP, previously known as American Association of Retired Persons Diet and Health Study; SENECA, Survey in Europe on Nutrition and the Elderly;a Concerted Action; SHARE, Survey of Health, Ageing and Retirement in Europe; SMC, Swedish Mammography Cohort.
Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]]4
www.ajpmonline.org

Figure 1. Meta-Analysis of Association Between All-CauseMortality and Smoking Status. (A). All-causemortality (HRs and RAPs) in cur-rent smokers in reference to never smokers. (B) All-cause mortality (HRs and RAPs) in former smokers in reference to never smokers.*Random effects model.**Fixed effects model.ELSA, English Longitudinal Study of Ageing; EPIC, European Prospective Investigation into Cancer and Nutrition; ESTHER, Early Recognition and OptimisedTreatment of Chronic Diseases in the Older Population; HR, hazard ratio; MORGAM, Multinational Monitoring of Trends and Determinants in CardiovascularDiseases (MONICA) Risk, Genetics, Archiving and Monograph; NHANES, National Health and Nutrition Examination Survey; NIH-AARP, previously known asAmerican Association of Retired Persons Diet and Health Study; RAP, rate advancement period; SENECA, Survey in Europe on Nutrition and the Elderly; aConcerted Action; SHARE, Survey of Health, Ageing and Retirement in Europe; SMC, Swedish Mammography Cohort.
Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]] 5
RAPs of 3.8, 2.8, and 0.7 years for o10 years, 10�19years, andZ20 years after cessation, respectively. Never-theless, excess mortality Z20 years after smoking cessa-tion remained statistically significant (po0.001).In the NIH-AARP cohort, the overall number of
deaths was 74,716. A clear reduction of excess mortalitywith time since cessation was likewise observed, but HRsand RAPs for former smokers compared with neversmokers were again higher than those from other studies.HRs were 2.43 (95% CI¼2.38, 2.49) and 1.41 (95%CI¼1.38, 1.44) and RAPs were 8.6 (95% CI¼8.3, 8.9)
] 2015
and 3.3 (95% CI¼3.1, 3.5) for those who quit o10 andZ10 years ago, respectively.
DiscussionThis is the first study to provide relative risk estimatesand RAPs (and their summary estimates from meta-analyses) of all-cause mortality for current and formersmoking in a large number of cohorts of older adultsfrom different countries. The CHANCES consortium,which includes countries with different cultures and at

Figure 2. Meta-Analysis of Association Between All-Cause Mortality and Number of Currently Smoked Cigarettes. (A) All-causemortality (HRs and RAPs) in current smokers smoking 1�10 cigarettes daily in reference to never smokers. (B) All-causemortality (HRs and RAPs) in current smokers smoking 11�19 cigarettes daily in reference to never smokers. (C) All-causemortality (HRs and RAPs) in current smokers smoking Z20 cigarettes daily in reference to never smokers.*Random effects model.**Fixed effects model.ELSA, English Longitudinal Study of Ageing; EPIC, European Prospective Investigation into Cancer and Nutrition; ESTHER, Early Recognition andOptimised Treatment of Chronic Diseases in the Older Population; HR, hazard ratio; MORGAM, Multinational Monitoring of Trends and Determinants inCardiovascular Diseases (MONICA) Risk, Genetics, Archiving and Monograph; NHANES, National Health and Nutrition Examination Survey; NIH-AARP,previously known as American Association of Retired Persons Diet and Health Study; RAP, rate advancement period; SENECA, Survey in Europe onNutrition and the Elderly; a Concerted Action; SHARE, Survey of Health, Ageing and Retirement in Europe; SMC, Swedish Mammography Cohort.
Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]]6
www.ajpmonline.org
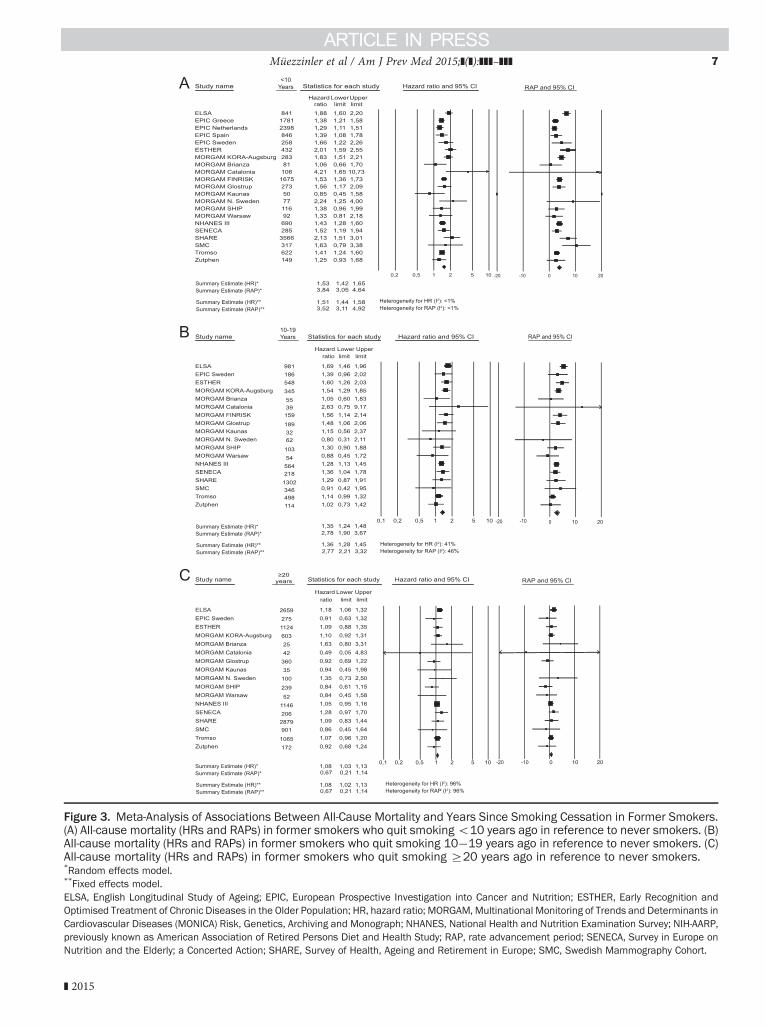
Figure 3. Meta-Analysis of Associations Between All-Cause Mortality and Years Since Smoking Cessation in Former Smokers.(A) All-cause mortality (HRs and RAPs) in former smokers who quit smokingo10 years ago in reference to never smokers. (B)All-cause mortality (HRs and RAPs) in former smokers who quit smoking 10�19 years ago in reference to never smokers. (C)All-cause mortality (HRs and RAPs) in former smokers who quit smoking Z20 years ago in reference to never smokers.*Random effects model.**Fixed effects model.ELSA, English Longitudinal Study of Ageing; EPIC, European Prospective Investigation into Cancer and Nutrition; ESTHER, Early Recognition andOptimised Treatment of Chronic Diseases in the Older Population; HR, hazard ratio; MORGAM, Multinational Monitoring of Trends and Determinants inCardiovascular Diseases (MONICA) Risk, Genetics, Archiving and Monograph; NHANES, National Health and Nutrition Examination Survey; NIH-AARP,previously known as American Association of Retired Persons Diet and Health Study; RAP, rate advancement period; SENECA, Survey in Europe onNutrition and the Elderly; a Concerted Action; SHARE, Survey of Health, Ageing and Retirement in Europe; SMC, Swedish Mammography Cohort.
Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]] 7
] 2015

Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]]8
different stages of the smoking epidemic,23 provides anexcellent opportunity to investigate these associations inalmost 500,000 older adults from the U.S. and Europe.Notwithstanding their heterogeneous cultural and polit-ical backgrounds, the results are remarkably consistentacross the included cohort studies. Furthermore, theseresults accord with those of a meta-analysis of previouslyreported studies10 and, with the inclusion of olderparticipants, strongly expand the so far very limitedevidence on RAPs reported from single studiesonly.5,9,24,25
Summarizing results from 22 cohorts, we observe anincrease of total mortality by >100% and by more thanone-third for current and former smokers, respectively,compared with never smokers. These increases in mor-tality translate to 6.7 and 2.6 years of mortality advance-ment in current and former smokers, respectively. Aclear dose�response relationship between currentlysmoked cigarettes and mortality is consistently observedacross the cohorts. Relative mortality of former smokersdecreases with time since smoking cessation. Never-theless, some (albeit very modest) excess mortality is stillobserved in former smokers who had quitZ20 years ago.Sex-specific meta-analyses yield similar results for menand women. In age-group�specific analyses, smoking-related relative mortality decreases with increasing age,but smoking remains a strong risk factor even after age70 years. The point estimates are in agreement with thosefrom previous studies on smoking and mortality amongolder adults, which have been based on a much smallernumber of cohorts and a smaller number of partici-pants.3,9,10 However, the large sample size enablesestimation of the associations with a much greaterprecision.Tobacco use continues to be a leading global cause of
preventable death, and the smoking epidemic continuesworldwide. Although evaluation of the impact of smok-ing and smoking cessation among older adults in differ-ent populations is challenging because of methodologicissues, such as possible differentially attenuated relativerisks as the force of general mortality increases in theelderly and the attendant “depletion of susceptibles,”26,27
it has been previously shown that the hazardous effects ofsmoking and benefits of cessation persist even in olderages.9,10 These results are remarkably consistent withthose obtained among middle-aged adults.6,28,29 Thepatterns strongly suggest that smoking remains a keyrisk factor after age 60 years, with an absolute toll ofmortality likely to be even much larger than at youngerages. Efforts to reduce smoking and promote smokingcessation even at older age are likely to bear a majorpublic health impact. Considering the current demo-graphic processes of population aging, a substantial
increase in the burden of smoking-related morbidityand mortality is expected, unless a reduction in smokingprevalence is achieved. Efforts to curb the smokingepidemic at all ages are therefore needed. In this respect,effective risk communication is crucial. RAPs can beparticularly helpful for risk communication to the gen-eral public and in clinical settings. The message thatRAPs convey is direct, simple, and strong. Explaining to a60-year-old heavy smoker that he or she has the samerisk of dying within the next few years as a 68-year-oldnever smoker is a rather clear statement that might helpto increase motivation to quit smoking. An advantage ofRAPs over other related measures, such as years of lifelost, is that they can be directly estimated from theavailable cohort data, without having to rely on externalinformation (e.g., from population life tables).The fixed effects model shows that the heterogeneity in
the results across studies is mostly introduced by thelarge NIH-AARP cohort, which yields higher estimatesfor the hazards of smoking than most other cohorts.These relatively high effect estimates could be a result ofdifferences in the study design or in characteristics of thestudy participants. Unlike any other included cohort,NIH-AARP exclusively used a single mailed question-naire for baseline data collection. The response rate to the3.5 million questionnaires sent was 17.6%.30 It is plau-sible that health-conscious and highly motivated peoplemight be over-represented among the respondents,which might have led to under-representation of smokerson one hand, but also to higher validity of reportedsmoking habits. Higher validity of self-reported smoking,on the other hand, might explain the higher (and possiblyless biased) hazard estimates in this cohort. BecauseNIH-AARP had almost as much weight in the fixedeffects meta-analysis as all other studies combined owingto its large sample size, excluding this study from thefixed effects model in sensitivity analyses led to attenu-ated estimates, approaching the estimates of the randomeffects model (details not shown). Excluding it from therandom effects model left estimates mostly unchanged.In order to account for the heterogeneity in the riskestimates between the studies, we used a conservativestatistical approach and considered the summary esti-mates from the random effects models of meta-analysesas the main results.
LimitationsThis study has specific strengths and limitations. Onlysmoking information collected at baseline was availablefor this analysis. Therefore, it is possible that someformer smokers resumed smoking afterward, leading tounderestimation of benefits related to smoking cessation.
www.ajpmonline.org

Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]] 9
Similarly, it is quite likely that some current smokers quitsmoking during the follow-up time, which would haveled to underestimation of hazards related to continuingsmoking. Moreover, some of the former smokers mighthave quit smoking because of ill health; hence, they couldhave had higher baseline mortality than those whocontinued smoking (sick-quitter bias).31 Additionally,all smoking data were self-reported without validationby biological markers such as cotinine. Therefore, mis-classification and recall bias are possible, particularlybecause of under-reporting of smoking. Taking theselimitations together, the true associations of smoking andsmoking cessation with mortality are therefore probablystronger than observed in our study. Although theassociations are consistent across studies, are biologicallyplausible, show clear dose�response patterns, and persistafter controlling for relevant confounders, the possibilityof residual confounding by less-than-perfect measure-ment of covariates or by unmeasured confounderscannot be excluded. Strengths include the large samplesize covering a wide range of countries, as well as detailedassessment of smoking histories and relevant confound-ers. Although there was also some heterogeneity in datacollection across studies, this was minimized by majorefforts of data harmonization, which is not commonlypossible in meta-analyses of published data.
ConclusionsIn this large consortium of cohort studies of older adults,strong associations of smoking status, smoking intensity,and time since smoking cessation with all-cause mortal-ity were found. Owing to the increase in mortality withage, the impact of smoking is even larger on an absolutescale. Excess mortality decreased with time since smok-ing cessation. In summary, our results provide strongevidence for the detrimental effects of smoking also atolder age, and emphasize the need for, and considerablepotential of, prevention efforts that support smokingabstinence at all ages. Communicating the risks associ-ated with continued smoking and benefits of cessationeven at older ages should remain a top public healthpriority.
Aysel Müezzinler, MSc, Ute Mons, PhD, and Carolin Gellert,PhD made equal contributions to the preparation of themanuscript.Data used throughout the present study are derived from the
Consortium on Health and Ageing: Network of Cohorts inEurope and the U.S. (CHANCES) project. The project iscoordinated by the Hellenic Health Foundation, Greece. Theresearch leading to this publication has received funding fromthe European Union Seventh Framework Programme (FP7/
] 2015
2007-2013) under grant agreement no. HEALTH-F3-2010-242244. The data of the English Longitudinal Study of Ageing(ELSA) cohort were made available through the United King-dom Data Archive (UKDA). ELSA was developed by a team ofresearchers based at the NatCen Social Research, UniversityCollege London and the Institute for Fiscal Studies. The datawere collected by NatCen Social Research. Funding is providedby the National Institute of Aging in the U.S., and a consortiumof UK government departments coordinated by the Office forNational Statistics. The developers and funders of ELSA andthe Archive do not bear any responsibility for the analyses orinterpretations presented here. The European ProspectiveInvestigation into Cancer and Nutrition (EPIC) NetherlandsStudy was funded by the following institutions: Dutch Ministryof Public Health, Welfare and Sports (VWS), NetherlandsCancer Registry (NKR), LK Research Funds, Dutch PreventionFunds, Dutch Zorg Onderzoek Nederland (ZON), WorldCancer Research Fund (WCRF), and Statistics Netherlands.EPIC Greece was funded by the Hellenic Health Foundation.EPIC Spain was supported by Health Research Fund (FIS) ofthe Spanish Ministry of Health RTICC ‘Red Temática deInvestigación Cooperativa en Cáncer (grant numbers, Rd06/0020/0091 and Rd12/0036/0018), Regional Governments ofAndalucía, Asturias, Basque Country, Murcia (project 6236)and Navarra, and Instituto de Salud Carlos III, Redes deInvestigacion Cooperativa (RD06/0020). EPIC Sweden wasfunded by the Swedish Cancer Society, the Swedish ScientificCouncil and the Regional Government of Skåne. The Epide-miological Study on the Chances of Prevention, Early Recog-nition and Optimised Treatment of Chronic Diseases in theOlder Population (ESTHER) study was funded by the Baden-Württemberg state Ministry of Science, Research and Arts(Stuttgart, Germany), the Federal Ministry of Education andResearch (Berlin, Germany), and the Federal Ministry ofFamily Affairs, Senior Citizens, Women and Youth (Berlin,Germany). Support for the National Institutes of Health-AARP(NIH-AARP) Diet and Health Study was provided by theIntramural Research Program of the National Cancer Institute(NCI), NIH. The National Health and Nutrition ExaminationSurvey (NHANES) is conducted by the National Center forHealth Statistics (NCHS), CDC. The findings and conclusionsin this paper are those of the authors and not necessarily thoseof the agency. In addition to the FP7 funding for CHANCES(HEALTH-F3-2010-242244), the MONICA (MultinationalMonitoring of Trends and Determinants in CardiovascularDiseases) Risk, Genetics, Archiving and Monograph (MOR-GAM) Project has received funding during the work fromEuropean Union FP 7 projects ENGAGE (HEALTH-F4-2007-201413) and BiomarCaRE (278913). This has supportedcentral coordination, workshops, and part of the activities ofThe MORGAM Data Centre, at THL in Helsinki, Finland.MORGAM Participating Centres are funded by regional andnational governments, research councils, charities, and other

Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]]10
local sources. The Survey in Europe on Nutrition and theElderly; a Concerted Action (SENECA) is a Concerted Actionwithin the EURONUT program of the European Union. TheSurvey of Health, Ageing and Retirement in Europe (SHARE)data collection has been primarily funded by the EuropeanCommission through the 5th Framework Programme (projectQLK6-CT-2001-00360 in the thematic programme Quality ofLife), through the 6th Framework Programme (projectsSHARE-I3, RII-CT-2006-062193, COMPARE, CIT5-CT-2005-028857, and SHARELIFE, CIT4-CT-2006-028812) andthrough the 7th Framework Programme (SHARE-PREP, no.211909, SHARE-LEAP, no. 227822, and SHARE M4, no.261982). Additional funding from the U.S. National Instituteon Aging (U01 AG09740-13S2, P01 AG005842, P01 AG08291,P30 AG12815, R21 AG025169, Y1-AG-4553-01, IAG BSR06-11, and OGHA 04-064) and the German Ministry of Educationand Research, as well as from various national sources isgratefully acknowledged (see www.share-project.org for a fulllist of funding institutions). The Swedish MammographyCohort (SMC) received funding by the Swedish ResearchCouncil and Strategic Funds from Karolinska Institutet.Tromsø was funded by UiT The Arctic University of Norway,the National Screening Service, and the Research Council ofNorway. Zutphen Elderly Study was funded by the NetherlandsPrevention Foundation. The work of Aysel Müezzinler wassupported by a scholarship from the Klaus Tschira Foundation.
The study sponsors did not have any role in the study design,analysis, or interpretation of data, in writing of the report, or inthe decision to submit the article for publication.
We acknowledge contributions to this manuscript (i.e., datacollection, assistance in data analysis, and manuscript revision)from the following members of the CHANCES group: AnoukGeelen (Division of Human Nutrition, Wageningen Univer-sity, Wageningen, the Netherlands), Jukka Kontto (Depart-ment of Chronic Disease Prevention, National Institute forHealth and Welfare (THL), Helsinki, Finland), Daan Kromhout(Division of Human Nutrition, Wageningen University, Wage-ningen, the Netherlands), Max Leenders (Institute for RiskAssessment Sciences (IRAS), Utrecht University, The Nether-lands), Roberto Lorbeer (Institute for Community Medicine,SHIP/Clinical-Epidemiological Research Unit, UniversityMedicine Greifswald, Greifswald, Germany), Ellisiv B. Mathie-sen (Department of Clinical Medicine, UiT The Arctic Uni-versity of Norway, Tromsø, Norway), Inger Njølstad(Department of Community Medicine, UiT the Arctic Uni-versity of Norway, Tromsø, Norway), Barbara Schaan (MunichCenter for the Economics of Aging (MEA), Munich,Germany), Andrea Schneider (Institute of Epidemiology II,Helmholtz Zentrum München, Neuherberg, Germany),Galatios Siganos (Department of Community Medicine, UiTThe Arctic University of Norway, Tromsø, Norway), Marti-nette Streppel (Division of Human Nutrition, WageningenUniversity, Wageningen, the Netherlands), Eveline Waterham
(Division of Human Nutrition, Wageningen University, Wage-ningen, the Netherlands), Patrik Wennberg (Department ofPublic Health and Clinical Medicine, UiT the Arctic Universityof Norway, Tromsø, Norway).
References1. Peto R, Darby S, Deo H, Silcocks P, Whitley E, Doll R. Smoking,
smoking cessation, and lung cancer in the UK since 1950: combinationof national statistics with two case-control studies. BMJ. 2000;321(7257):323–329. http://dx.doi.org/10.1136/bmj.321.7257.323.
2. Doll R, Peto R, Boreham J, Sutherland I. Mortality from cancer inrelation to smoking: 50 years observations on British doctors. Br JCancer. 2005;92(3):426–429. http://dx.doi.org/10.1038/sj.bjc.6602359.
3. Pencina MJ, D'Agostino RB, Larson MG, Massaro JM, Vasan RS.Predicting the 30-year risk of cardiovascular disease the FraminghamHeart Study. Circulation. 2009;119(24):3078–3084. http://dx.doi.org/10.1161/CIRCULATIONAHA.108.816694.
4. Ferrie J, Singh-Manoux A, Kivimaeki M, et al. Cardiorespiratory riskfactors as predictors of 40-year mortality in women and men. Heart.2009;95(15):1250–1257. http://dx.doi.org/10.1136/hrt.2008.164251.
5. Gellert C, Schöttker B, Müller H, Holleczek B, Brenner H. Impact ofsmoking and quitting on cardiovascular outcomes and risk advance-ment periods among older adults. Eur J Epidemiol. 2013;28(8):649–658. http://dx.doi.org/10.1007/s10654-013-9776-0.
6. Thun MJ, Carter BD, Feskanich D, et al. Fifty-year trend in smoking-related mortality in the United States. N Engl J Med. 2013;368(4):351–364. http://dx.doi.org/10.1056/NEJMsa1211127.
7. Menotti A, Kromhout D, Blackburn H, Jacobs D, Lanti M. Forty-yearmortality from cardiovascular diseases and all causes of death in the USRailroad cohort of the Seven Countries Study. Eur J Epidemiol. 2004;19(15):417–424.
8. Puddu PE, Menotti A, Tolonen H, Nedeljkovic S, Kafatos AG.Determinants of 40-year all-cause mortality in the European coh-orts of the Seven Countries Study. Eur J Epidemiol. 2011;26(8):595–608. http://dx.doi.org/10.1007/s10654-011-9600-7.
9. Gellert C, Schöttker B, Holleczek B, Stegmaier C, Müller H, Brenner H.Using rate advancement periods for communicating the bene-fits of quitting smoking to older smokers. Tob Control. 2013;22(4):227–230. http://dx.doi.org/10.1136/tobaccocontrol-2012-050572.
10. Gellert C, Schoettker B, Brenner H. Smoking and all-cause mortality inolder people systematic review and meta-analysis. Arch Intern Med.2012;172(11):837–844. http://dx.doi.org/10.1001/archinternmed.2012.1397.
11. Megyesiovà S, Hajduovà Z. Demographic challenges across the Euro-pean Union member states. Workplace Health Saf. 2012;60(7):321–326. http://dx.doi.org/10.3928/21650799-20120625-05.
12. Cancer Research UK. Tobacco statistics. www.cancerresearchuk.org/cancer-info/cancerstats/causes/tobacco-statistics/. Accessed May 19, 2015.
13. Lugo A, La Vecchia C, Boccia S, Murisic B, Gallus S. Patterns ofsmoking prevalence among the elderly in Europe. Int J Environ ResPublic Health. 2013;10(9):4418–4431. http://dx.doi.org/10.3390/ijerph10094418.
14. Kleykamp BA, Heishman SJ. The older smoker. JAMA. 2011;306(8):876–877. http://dx.doi.org/10.1001/jama.2011.1221.
15. Granados JA. Health at advanced age: social inequality and otherfactors potentially impacting longevity in nine high-income countries.Maturitas. 2013;74(2):137–147. http://dx.doi.org/10.1016/j.maturitas.2012.11.013.
16. Brenner H, Gefeller O, Greenland S. Risk and rate advancementperiods as measures of exposure impact on the occurrence of chronicdiseases. Epidemiology. 1993;4(3):229–236. http://dx.doi.org/10.1097/00001648-199305000-00006.
www.ajpmonline.org

Müezzinler et al / Am J Prev Med 2015;](]):]]]–]]] 11
17. Boffetta P, Bobak B, Borsch-Supan A, et al. The Consortium on Healthand Ageing: Network of Cohorts in Europe and the United States(CHANCES) project—design, population and data harmonization of alarge-scale, international study. Eur J Epidemiol. 2014;29(12):929–936. http://dx.doi.org/10.1007/s10654-014-9977-1.
18. Ezzati M, Lopez AD, Rodgers A, Murray CJL. Alcohol use. In: WorldHealth Organisation. Comparative Quantification of Health Risks:Global and Regional Burden of Disease Attributable to Selected MajorRisk Factors. Geneva, Switzerland: WHO; 2004.
19. Riley RD, Lambert PC, Abo-Zaid G. Meta-analysis of individual part-icipant data: rationale, conduct, and reporting. Br Med J. 2010;340:c221.
20. Normand SL. Meta-analysis: formulating, evaluating, combining, andreporting. Stat Med. 1999;18(3):321�359. http://dx.doi.org/10.1002/(SICI)1097-0258(19990215)18:3o321::AID-SIM2843.0.CO;2-P.
21. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control ClinTrials. 1986;7(3):177–188. http://dx.doi.org/10.1016/0197-2456(86)90046-2.
22. Lipsey MW,Wilson DB. Practical Meta-Analysis. Thousand Oaks, CA:Sage, 2001.
23. ThunM, Peto R, Boreham J, Lopez AD. Stages of the cigarette epidemicon entering its second century. Tob Control. 2012;21(2):96–101. http://dx.doi.org/10.1136/tobaccocontrol-2011-050294.
24. Liese AD, Hense HW, Brenner H, Löwel H, Keil U. Assessing the impactof classical risk factors on myocardial infarction by rate advancementperiods. Am J Epidemiol. 2000;152(9):884–888. http://dx.doi.org/10.1093/aje/152.9.884.
25. Keil U, Liese AD, Hense HW, et al. Classical risk factors and theirimpact on incident non-fatal and fatal myocardial infarction and all-cause mortality in southern Germany. Results from the MONICAAugsburg cohort study 1984-1992. Monitoring trends and determi-nants in cardiovascular diseases. Eur Heart J. 1998;19(8):1197–1207. http://dx.doi.org/10.1053/euhj.1998.1089.
] 2015
26. Morida Y, Abenhaim L. Evidence of the depletion of susceptibles effectin non-experimental pharmacoepidemiologic research. J Clin Epide-miol. 2004;57(1):111.
27. Tournier M, Moride Y, Lesk M, Ducruet T, Rochon S. The depletion ofsusceptibles effect in the assessment of burden-of-illness: the exampleof age-related macular degeneration in the community-dwellingelderly population of Quebec. Can J Clin Pharmacol. 2008;15(1):e22–e35.
28. Pirie K, Peto R, Reeves GK, Green J, Beral V, Million Women StudyCollaborators. The 21st century hazards of smoking and benefits ofsmoking: a prospective study of one million women in the UK.Lancet. 2013;381(9861):133–141. http://dx.doi.org/10.1016/S0140-6736(12)61720-6.
29. Jha P, Ramasundarahetitige C, Landsman V, et al. 21st Century hazardof smoking and benefits of cessation in the United States.N Engl J Med.2013;368(4):341–350. http://dx.doi.org/10.1056/NEJMsa1211128.
30. Schatzkin A, Subar AF, Thompson FE, et al. Design and serendipity inestablishing a large cohort with wide dietary intake distributions: theNational Institutes of Health�American Association of RetiredPersons Diet and Health Study. Am J Epidemiol. 2001;154(12):119–125. http://dx.doi.org/10.1093/aje/154.12.1119.
31. He Y, Jiang B, Li LS, et al. Changes in smoking behavior and subsequentmortality risk during a 35-year follow-up of a cohort in Xi'an, China.Am J Epidemiol. 2014;179(9):1060–1070. http://dx.doi.org/10.1093/aje/kwu011.
Appendix
Supplementary data
Supplementary data associated with this article can be found at,http://dx.doi.org/10.1016/j.amepre.2015.04.004.




















