SITUATIONAL ASSESSMENT ON THE HEALTH OF CAMBODIAN IRREGULAR MIGRANTS, IOM 2011
101
THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT S S I I T T U U A A T T I I O O N N A A L L A A S S S S E E S S S S M M E E N N T T O O N N T T H H E E H H E E A A L L T T H H O O F F C C A A M M B B O O D D I I A A N N I I R R R R E E G G U U L L A A R R M M I I G G R R A A N N T T S S A A J J o o i i n n t t A A s s s s e e s s s s m m e e n n t t b b y y t t h h e e I I n n t t e e r r n n a a t t i i o o n n a a l l O O r r g g a a n n i i z z a a t t i i o o n n f f o o r r M M i i g g r r a a t t i i o o n n i i n n C C o o l l l l a a b b o o r r a a t t i i o o n n w w i i t t h h t t h h e e D D e e p p a a r r t t m m e e n n t t o o f f C C o o m m m m u u n n i i c c a a b b l l e e D D i i s s e e a a s s e e C C o o n n t t r r o o l l , , M M i i n n i i s s t t r r y y o o f f H H e e a a l l t t h h C C a a m m b b o o d d i i a a 2 2 0 0 1 1 1 1
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of SITUATIONAL ASSESSMENT ON THE HEALTH OF CAMBODIAN IRREGULAR MIGRANTS, IOM 2011

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT
SSSIIITTTUUUAAATTTIIIOOONNNAAALLL AAASSSSSSEEESSSSSSMMMEEENNNTTT OOONNN TTTHHHEEE HHHEEEAAALLLTTTHHH OOOFFF CCCAAAMMMBBBOOODDDIIIAAANNN IIIRRRRRREEEGGGUUULLLAAARRR MMMIIIGGGRRRAAANNNTTTSSS
AAA JJJoooiiinnnttt AAAsssssseeessssssmmmeeennnttt bbbyyy ttthhheee IIInnnttteeerrrnnnaaatttiiiooonnnaaalll OOOrrrgggaaannniiizzzaaatttiiiooonnn fffooorrr MMMiiigggrrraaatttiiiooonnn
iiinnn CCCooollllllaaabbbooorrraaatttiiiooonnn wwwiiittthhh ttthhheee DDDeeepppaaarrrtttmmmeeennnttt ooofff CCCooommmmmmuuunnniiicccaaabbbllleee DDDiiissseeeaaassseee CCCooonnntttrrrooolll,,,
MMMiiinnniiissstttrrryyy ooofff HHHeeeaaalllttthhh
CCCaaammmbbbooodddiiiaaa 222000111111

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT
IOM Cambodia would like to acknowledge the support of the IOM 1035 facility and the collaborative partnership with the Migration Health focal point, Dr Sok Touch from the Department of Communicable Disease Control within the Ministry of Health in making this report possible.
This report is written by Brett Dickson, Dr. Mark Kavenagh and Erin Flynn. The opinions expressed in this publication are those of the authors and do not necessarily reflect the views of IOM.
Contact: International Organization for Migration (IOM)
Mission in Cambodia
No. 31, Street 71, Khan Chamkarmon,
Phnom Penh, Cambodia
Telephone: +855 (0) 23 216 532
Fax: +855 23 216 423
Email: [email protected]
© 2011 International Organization for Migration and Ministry of Health

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT
SITUATIONAL ASSESSMENT ON SITUATIONAL ASSESSMENT ON THE HEALTH OF CAMBODIAN THE HEALTH OF CAMBODIAN
IRREGULAR MIGRANTSIRREGULAR MIGRANTS
A Joint Assessment by A Joint Assessment by
tthe Internatihe International Organization for Migrationonal Organization for Migration
in Collaboration within Collaboration with
the Department of Communicable Dthe Department of Communicable D isease isease ControlControl ,, Ministry of HealthMinistry of Health
Cambodia 2011Cambodia 2011

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 1
ACKNOWLEDGEMENTS This publication presents migrant health and socio-‐economic data collected in 2011 through a collaborative process of field research and inter-‐agency dialogue on the Health of Migrants, involving many colleagues from national and provincial health and non-‐health authorities and local NGOs who actively participated in each stage of this situational assessment.
This publication would not have been possible without their committed collaboration and substantial contributions. Therefore IOM Cambodia would like to express its sincere gratitude and appreciation to the following:
• Dr Sok Touch and his deputy Dr Teng Srey, the assigned Migration Health focal point and research assistant from MOH CDC for their commitment to promoting migrant health resolution and continuing regional Migrant Health dialogue at country level at national and provincial consultations.
• Dr. Keo Sopheaktra, Director of BMC PHD and Dr. Vorn Vinnara, Deputy Director of Svay Rieng PHD for their coordination and management of the staff to work with IOM to conduct interviews and data collection.
• Mr. Choam Phoip from the Poipet International Border Immigration Unit for coordinating between the Data Collection Team and the migrants for interviews and data collection.
• The Data Collection Team: Dr. Sin Eap, Mr. Keo Samnang, Mr. On Chanry and Mr. Ta Hear from BMC PHD, Dr. Oum Saron, Dr. Leuk Sambath, Mr. Ke Samuth and Ms. Phok Usaphea from SVR PHD, Mr. Heung Kleung, Mr. Kang Savuth, Mr. Chan Chhom, Mr. Hem Saphorn and Mr. Toch Sopheap from SVR DSVY, Mr. Leu Chandara from the BMC Anti-‐human Trafficking and Juvenile Protection Unit, Ms. Run Sarom from SEADO, Mr. Sim Samnang from Poipet Transit Centre for their field work of interviewing and data collection.
• All key personnel from International organizations and NGOs (UNAIDS, ILO, UNDP, WHO, UNICEF, UNIAP, SEADO, WORLD VISION, TPO, CCPCR, CHC) who contributed invaluable inputs at national and provincial consultations.
• The IOM Project Team; Mr Brett Dickson for coordinating the overall research process; Mr. Phiev Khay and Mr. Nuth Sam Ol for training the Data Collection Team on interviewing skills and data collection, coordinating the data collection process; Mr. Soy Thol for managing the data collection logistics.
• All returned migrants who participated in the interviews and provided valuable information on their migration patterns, personal experiences, health problems and access to health services.
• IOM 1035 facility and IOM colleagues at Headquarters for supporting this Situational Assessment financially.
• Dr Jaime Calderon and Dr Poonam Dhavan, our regional and Global IOM Migration Health colleagues, for their timely reviews and technical inputs into the final report.
• The Globalroom Consulting, Dr Mark Kavenagh and Erin Flynn for their professional services providing statistical analysis and drafting of the report.
Ms. Iuliana Stefan Chief of Mission
International Organization for Migration, IOM Cambodia

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 2
THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 3
FOREWORD
The joint situational assessment into the health of Cambodian irregular migrants in two border
provinces was conducted under the collaboration of the Ministry of Health, respective Provincial
Health Departments (PHD) in Cambodia and the International Organization for Migration (IOM) with
the objective of gaining an in-‐depth understanding of the health issues faced by returned
Cambodian irregular migrant groups and the general population in two border provinces of Banteay
Meanchey and Svay Rieng.
This report aims to inform future Migrant Health programming for the Ministry of Health and IOM to
build on a future collaborative partnership in realizing high-‐level Health policies regarding the health
of migrants such as the World Health Assembly’s resolution on the “Health of Migrants.”
The situational assessment has managed to establish baseline data on certain inter-‐related socio-‐
economic factors that lead to irregular migration in the border areas, including documentation of
the health risks irregular migrants are exposed to while abroad and their access to health services
upon return. The findings and recommendations from this report will ultimately lead to a better
understanding of migrant health concerns, including barriers to accessing health services and
provide relevant Government Ministries, partner organizations and other stakeholders, baseline
data that will inform future appropriate interventions and key recommendations for policy
development.
Dr Sok Touch
Director Department of Communicable Disease Control
Ministry of Health

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 4
LIST OF ACRONYMS
AIDS Acquired Immunodeficiency Syndrome
CARAM Coordination of Action Research on AIDS and Mobility
DOTS Directly Observed Treatment Short-‐Course
DSVY Department of Social Affairs, Veterans and Youth Rehabilitation
GMS Greater Mekong Sub-‐region
Hep C Hepatitis C
HIV Human Immunodeficiency Virus
IOM International Organization for Migration
MoH Ministry of Health
MoU Memorandum of Understanding
NCDD National Committee for Decentralization and De-‐concentration
NGO Non-‐Government Organization
PHD Provincial Health Department
PMCT Prevention of Mother to Child Transmission
STI Sexually Transmitted Infection
TB Tuberculosis
VCCT Voluntary and Confidential Counselling and Testing

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 5
LIST OF TABLES Table 1: The sample of migrants and non-‐migrants ............................................................................ 19
Table 2: Marital status of respondents ................................................................................................ 25
Table 3: Marital status of respondents ................................................................................................ 26
Table 4: Types of loans ........................................................................................................................ 35
Table 5: Types of violence experienced ............................................................................................... 44
Table 6: Illnesses experienced by migrants ......................................................................................... 47
Table 7: Future plans of migrants ........................................................................................................ 54
Table 8: Most common health problems reported by healthcare workers ......................................... 60
Table 9: Challenges of providing healthcare to cross-‐border migrants ............................................... 62
LIST OF FIGURES Figure 1: Migrant status by province ................................................................................................... 23
Figure 2: Gender of respondents ......................................................................................................... 24
Figure 3: Gender of respondents by province ..................................................................................... 24
Figure 4: Age of respondents ............................................................................................................... 25
Figure 5: Years of schooling ................................................................................................................. 26
Figure 6: Living situation in Cambodia ................................................................................................. 27
Figure 7: Housing materials of owned homes ..................................................................................... 28
Figure 8: Land ownership .................................................................................................................... 29
Figure 9: Income while in Cambodia by migrant status ....................................................................... 30
Figure 10: Income while in Cambodia by province .............................................................................. 30
Figure 11: Monthly income by migrant status and sex ........................................................................ 31
Figure 12: Monthly income by province .............................................................................................. 31
Figure 13: Migrant monthly income by source .................................................................................... 33
Figure 14: Non-‐migrant monthly income by source ............................................................................ 33
Figure 15: Financial position of families .............................................................................................. 34
Figure 16: Reason for loan by migrant status ...................................................................................... 35
Figure 17: Specific uses of loaned money ............................................................................................ 36
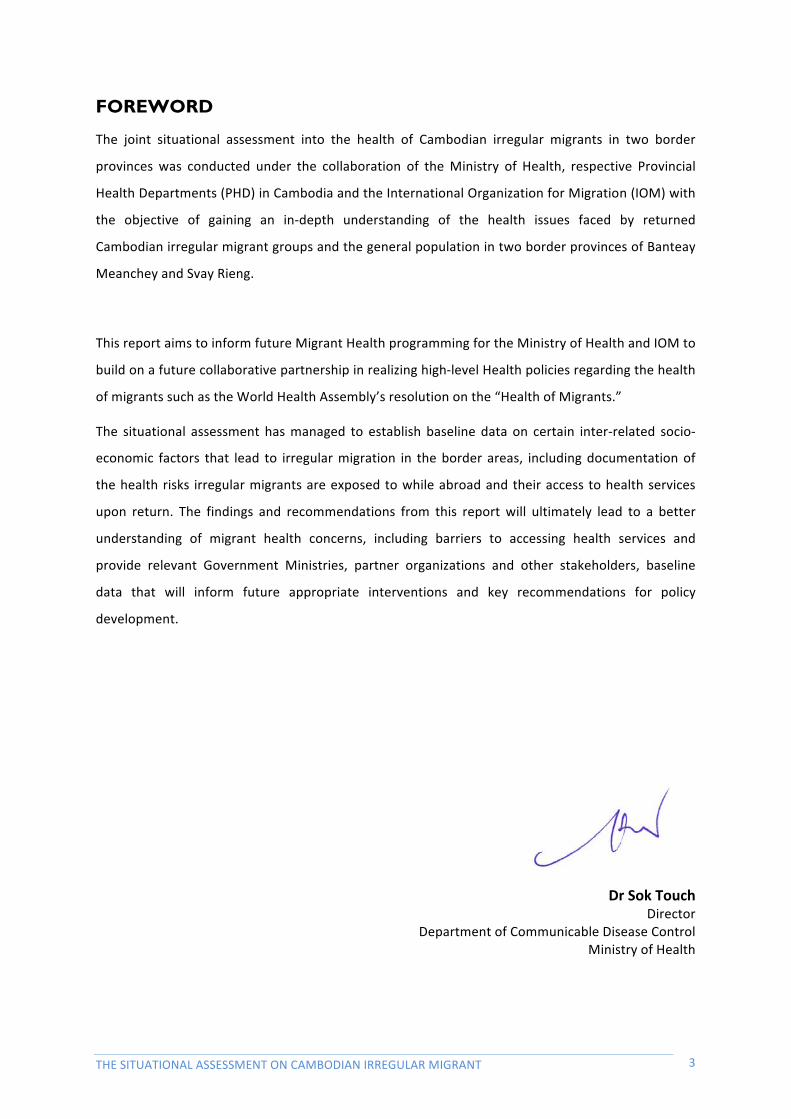
Figure 18: Debt for health care ............................................................................................................ 37
Figure 19: Strategy to pay back debt ................................................................................................... 37
Figure 20: Reason for migrating .......................................................................................................... 38
Figure 21: Migration documentation .................................................................................................. 39
Figure 22: Frequency of migration ...................................................................................................... 39
Figure 23: Type of work during last migration ..................................................................................... 40
Figure 24: Type of work ....................................................................................................................... 41

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 6
Figure 25: Experienced health risks ..................................................................................................... 42
Figure 26: Health risks at work ............................................................................................................ 42
Figure 27: Migrants held in detention ................................................................................................. 43
Figure 28: Healthcare provider in Cambodia ....................................................................................... 45
Figure 29: Reason for selecting public/private healthcare providers .................................................. 45
Figure 30: Causes of illness .................................................................................................................. 46
Figure 31: Symptoms while abroad ..................................................................................................... 48
Figure 32: Knowledge of common health problems between Migrant and Non-‐migrants and according to gender .................................................................................................................... 49
Figure 33: Knowledge of HIV prevention ............................................................................................. 49
Figure 34: Knowledge of TB transmission ............................................................................................ 50
Figure 35: First source of health information ...................................................................................... 52
Figure 36: Obstacles to seeking health information ............................................................................ 52
Figure 37: Health testing in the past 12 months ................................................................................. 53
Figure 38: Awareness of HIV and TB healthcare services .................................................................... 53
Figure 39: Who would you talk to if you had HIV, STIs or TB .............................................................. 54
Figure 40: Age of healthcare workers .................................................................................................. 55
Figure 41: Position of healthcare workers ........................................................................................... 56
Figure 42: Highest year of schooling .................................................................................................... 56
Figure 43. Training received by healthcare staff ................................................................................. 57
Figure 44: Last time workers received training ................................................................................... 57
Figure 45. Types of training needed .................................................................................................... 58
Figure 46: Supplies not available to health workers ............................................................................ 58
Figure 47: Inadequate supplies for health workers ............................................................................. 59
Figure 48: Adequate supplies for health workers ................................................................................ 59
Figure 49: Perceived main cause of illnesses ....................................................................................... 60
Figure 50: Services offered to HIV or TB patients by health workers .................................................. 61
Figure 51: First place migrants seek health care ................................................................................. 61
Figure 52: Perceived reason irregular migrants selected health services ........................................... 62
Figure 53: Most effective source of health information to reach migrants ........................................ 62

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 7
TABLE OF CONTENTS Executive Summary .................................................................................................................. 9 Chapter I: Introduction .......................................................................................................... 12
The Study ...................................................................................................................... 12 Study Objectives ......................................................................................................................... 12 Overall Assessment Questions .................................................................................................... 13 Definitions of Irregular Migrants ................................................................................................. 13 Report Structure ......................................................................................................................... 13 Cambodia’s Cross-‐Border Provinces ........................................................................................... 13 Cross-‐border Migration Trends: Regular vs. Irregular ................................................................. 14 Irregular Migration to Thailand and Malaysia ............................................................................. 15 Irregular Migration to Viet Nam ................................................................................................. 16 Health Problems Faced by Migrants ........................................................................................... 16
Chapter II: Methodology ........................................................................................................ 19 Sample ........................................................................................................................................ 19 Instruments ................................................................................................................................. 20 Data Analysis ............................................................................................................................... 22 Limitations .................................................................................................................................. 22
Chapter III: Findings ............................................................................................................... 23 Migrants and Non-Migrants ....................................................................................... 23
Demographics ............................................................................................................................. 23 Housing and Land Ownership ..................................................................................................... 27 Employment, Income and Financial Status ................................................................................. 29 Migration and Mobility ............................................................................................................... 38 Conditions Abroad ...................................................................................................................... 40 Health of Migrants ...................................................................................................................... 41 Health Seeking Behaviour ........................................................................................................... 44 Experience of Illness .................................................................................................................... 46 Health Knowledge ....................................................................................................................... 48 Future Plans for Migration .......................................................................................................... 54
Health Staff ................................................................................................................... 55 Demographics ............................................................................................................................. 55 Healthcare setting and resources ............................................................................................... 58 Healthcare workers experience with irregular migrants ............................................................ 61
Chapter IV: Discussion on Findings ...................................................................................... 64 Chapter V: Conclusion & Recommendations ...................................................................... 67 Bibliography ............................................................................................................................. 69 Annex A: Source Villages for Migrants and Non-migrants ................................................ 70 Annex B: English Versions of Questionnaire ....................................................................... 71 Annexe C: Letter of Approval from the National Ethic Committee for Health Research, Ministry of Health (MoH) ....................................................................................................... 95

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 8
Picture 1: Data Collection Team in Kompong Ro District, Svay Rieng

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 9
Executive Summary
The Situational Assessment of the Health of Cambodian Irregular Migrants was conducted in early 2011. In the initial stages of the project IOM worked closely with partners from the Ministry of Health (MoH) and the Provincial Health Department (PHD) to identify migrants and coordinate with border authorities in Banteay Meanchey and Svay Rieng provinces. Data collection focused on the mobility of irregular migrants and health outcomes. A control group of non-‐migrants from source communities in Banteay Meanchey and Svay Rieng were also interviewed for a comparison. The Situational Assessment was designed as an operational and policy oriented study aiming to provide an in-‐depth understanding of the health issues faced by Cambodian irregular migrants.
Methodological Design
Two structured questionnaires (migrants and non-‐migrants) were developed in collaboration with MoH and PHD partners. The questionnaires were complementary, allowing for comparisons to be made between the two groups. An additional questionnaire was also developed for government and community health workers to gain greater understanding of service delivery for returned Cambodian migrants.
In Svay Rieng migrants were selected for interviews using case files from the Department of Social Affairs, Veterans and Youth Rehabilitation for migrants that had returned to Cambodia in the last twelve months. Cases were randomly selected. In Banteay Meanchey, primary interviews with returned migrants were conducted at the Poipet Immigration Centre. Respondents were randomly chosen from scheduled daily deportations and list of those returned.
For the non-‐migrant sample, villages were selected close to the borders. Households were selected using a sampling interval calculated by dividing the number of households in each village by the desired village sample.
Provincial and district health staff and social workers, including NGO staff that provided healthcare and health education to irregular migrants, conducted the data collection. Prior to data collection interviewers were trained by IOM on how to carry out interviews using the questionnaires.
The Sample
The demographic data of the sample is described in detail on page 22 of this report. The sample included 220 adult migrants and 218 adult non-‐migrants, with proportions of males and females roughly equal between the two groups. The most common age range of respondents was between 20 to 29 years of age.
A Snapshot of Irregular Migrants
Socio-‐economic status of migrants was generally lower than non-‐migrants. The average monthly income of migrants (USD 73.45) was significantly lower than non-‐migrants (USD 92.42). Nearly half of the migrants had only completed between one and three years of primary education.
Home ownership and ownership of agricultural land were significantly lower among migrants compared to non-‐migrants. Migrants were also more likely to have lost or sold agricultural land and acquired household debt. Debts were often taken out to pay for basic needs or to pay off other debts.
The majority of migrants reported migrating three to four times per year. Begging and construction work were the two most commonly reported types of work while recently working abroad. Of the 220 migrants in the sample only five possessed a Cambodian passport and one had obtained a visa. The largest proportion of the respondents had never applied for a Cambodian passport, as they believed that it was not required to work in either Viet Nam or Thailand. As a result of being

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 10
undocumented 184 migrants were arrested and deported. Of those who were arrested only 16.36 per cent were not held in detention.
Risk Factors
Migrants reported being exposed to more health risks while abroad than their counterparts in Cambodia. Both groups reported dangerous working conditions as the biggest risk factor. Alarmingly, twice the number of migrants compared to non-‐migrants reported risk of abuse and limited access to healthcare.
As described above a large number of the migrants were held in detention while abroad. The length of time spent in detention ranged from one month up to six months. While in detention half reported being treated ‘not so well’, more men described this than women.
Fewer than 30 per cent of migrants also reported experiencing abuse, most often verbal abuse; however a larger proportion of those who were abused experienced physically abuse.
Living conditions while working abroad were poor. 34.55 per cent of the sample reported living on the street, which women were four times more likely than men to be living on the street.
Health Concerns
A larger proportion (85.45%) of the migrant sample reported experiencing illness while working abroad. Environmental, social, economic and lifestyle factors were all reported to have contributed to the illnesses experienced by migrants. Lifestyle factors were not reported as a cause of illness by any of the non-‐migrants.
Knowledge of some common health problems was significantly lower among migrants. Knowledge of HIV transmission and prevention was slightly lower among women (71%) compared to men (81%). Practice of safe sex was low for both men and women. 87.61 per cent of those that responded stated that they did not use a condom during their last sexual encounter, a significantly higher proportion were women.
Knowledge of Tuberculosis (TB) transmission and prevention was slightly higher among non-‐migrants compared to migrants.
A predictably large proportion of both migrants and non-‐migrants reported needing health testing of some description. Knowledge about where to go for testing in Cambodia was good, however only 33.33 per cent of the total sample had had health testing in the past 12 months. Fear of arrest and cost were obstacles for those migrants who did not have health testing done while working abroad.
Summary
The cross-‐border migration of Cambodians to Thailand and Viet Nam is likely to continue increasing. While there are potential economic and livelihood benefits there are also related costs. Poor living conditions, limited access to healthcare and exploitation as a result of no documentation greatly increase their vulnerability and risk of illness.
It will be important for stakeholders – government and civil society -‐ to use this new evidence to identify and fill gaps in health service delivery in these border areas where there is a high incidence of irregular migration and mobility. It will be crucial that future policy development focuses on the potential benefits of cross-‐border migration, while at the same time, addressing ways to reduce risks and improve the health of irregular migrants and border populations.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 11
Picture 2: Map of Targeted study sites marked in red in the two border provinces-‐ Banteay Meanchey and Svay Rieng Provinces

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 12
Chapter I: Introduction
THE STUDY
The overall objective of the Situational Assessment is to gain an in-‐depth understanding of the health issues faced by Cambodian irregular migrants and source communities in cross-‐border areas. The study sampled migrants returned across the Thai border in Banteay Meanchey province and migrants returned across the Vietnam border at Svay Rieng province. The migrants are compared with control groups from source communities in Banteay Meanchey and Svay Rieng provinces. Due to the high number of people who cross the border in Poipet, control villages were selected from Nimit commune, which is 15km from the border along the highway in the same district (O’Chrov). Control villages in Svay Rieng province were selected nearby migrant villages within the same districts.
In order to improve health outcomes in Cambodian border communities, including for irregular migrants, it will be important to identify and fill gaps in health service delivery in these border areas where there is a high incidence of cross border migration and mobility. This report describes data, which will inform improvements to health, particularly outlining health-‐seeking behaviour of migrants and source communities.
The Situational Assessment is broadly designed as an operational and policy-‐oriented study looking at the health perceptions of both returning migrants and their source communities in Banteay Meanchey and Svay Rieng provinces. In addition, equal importance is given to data that may help identify and fill gaps in health service delivery with a focus on the capacity building of health care workers and village health support groups to respond to migrant health challenges in cross-‐border areas.
The Situational Assessment provides important data for IOM and project stakeholders, which can be used to inform specific project interventions and provide the Ministry of Health (MoH) and other relevant stakeholders with overall migrant health policy guidance to improve the health of irregular Cambodian migrants and health service delivery. The Situational Assessment aims to contribute to overall research and analysis on the health of migrants in the Greater Mekong Sub-‐region by sampling deported and repatriated Cambodian irregular migrants and representatives from source communities in Banteay Meanchey and Svay Rieng provinces.
Study Objectives The objectives of the Situational Assessment in two border provinces of Cambodia are as follows:
1. Assess and document the socio-‐economic and migration patterns of returned migrants and source communities in the two target border provinces;
2. Assess and document the current health status and access to health services of returned migrants and the source communities, including their health seeking behaviour;
3. Promote better understanding of migrant health concerns, including barriers to accessing health services among the health workforce, relevant Government Ministries, partner organizations and other stakeholders;
4. Develop and prioritize follow up interventions and key recommendations for policy development.
The Situational Assessment and subsequent findings within this report will be disseminated and presented to multiple stakeholders at national and provincial levels resulting in a better understanding of the patterns of migration, health issues, availability and access to health care services, and potential health interventions. Furthermore, the Situational Assessment report will provide information on the existing migration patterns and health of migrants that will be

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 13
disseminated and available to the MoH and provincial health authorities for future evidence-‐based migration health programming and policy development.
The Situational Assessment report will help to inform the current collaborative IOM and MoH Migrant Health project promoting better understanding of migrant health concerns, including barriers to accessing health services among the health workforce, relevant Government Ministries, partner organizations and other stakeholders. The findings and subsequent discussions will lead to the development of piloted, evidence-‐based interventions, such as migrant health training for health workers and technical assistance to provide health screenings to returned migrants.
Overall Assessment Questions • What are the factors or circumstances that lead to irregular migration and impacts on the
health of irregular migrants in the two targeted border provinces?
• How do irregular migrants perceive their own health risks and health problems? How do they seek health care while abroad compare to in Cambodia?
• Do irregular migrants have specific health needs not being met by current public health services? Are there health disparities between irregular migrants and source communities? What are the specific health disparities and how can they be addressed?
Definitions of Irregular Migrants The 2008 census defines a migrant as “a person who has moved to the place of enumeration from another village (or another country) which was the person’s last previous residence. In Cambodia 26.52 per cent of the total population is classified as migrants. It is 57.93 per cent in the urban areas and 18.90 in the rural areas. Around half of all migrants are male (50.46%) and half female (49.54%)” (NIS, 2009).
Defined by the International Organization for Migration (IOM, 2011), an irregular migrant worker is a person who: “Owing to unauthorized entry, breach of a condition of entry, or the expiry of his or her visa, lacks legal status in a transit or host country”.
Report Structure This report is laid out under four chapters: Introduction, Methodology, Findings and Conclusion. The findings section is divided into five sub-‐topics: Demographics, Socio-‐economic factors, Migration and mobility, Health and Future migration. The demographics section describes the characteristics of the sample including migrant status, age and gender. Socio-‐economic factors include housing, land ownership, employment and income, illustrating the differences between migrants and non-‐migrants. Migration and mobility looks at practices of irregular migrants in the study, specifically documentation, frequency of migration and risks associated with working abroad. The health section of the report identifies the differences between migrants and non-‐migrants in terms of health status, health seeking behaviour and health knowledge. Future migration explores the plans of the migrants in the study.
The conclusion of the report highlights the identified immediate health needs of Cambodian irregular migrants. Recommendations for future programming to improve health outcomes of irregular migrants and border populations are addressed. Supporting this report is a policy paper, to be used as an advocacy tool to increase awareness about the needs of irregular migrants and mobilize funds that address their needs.
Cambodia’s Cross-‐Border Provinces The border town of Poipet within Banteay Meanchey province is a main route of cross-‐border migration between Cambodia and Thailand. In 2006 Thailand was one of the three main destinations for Cambodian migrant workers. In October 2005 there were 182,007 Cambodians registered with

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 14
the Ministry of Interior in Thailand. While the number of undocumented Cambodians currently in Thailand is not known, it is estimated that there may be as many as documented migrants (Maltoni, 2006).
Migration from Svay Rieng province is often the result of poor agricultural conditions, particularly in the past few years as water shortages have been common. Cambodians often migrate, both within Cambodia, and across the border to nearby Viet Nam. The unique shape of Svay Rieng province means that almost every district in the province shares a border with Viet Nam. Svay Rieng is dissected by National Road 1, which continues directly to Ho Chi Minh City in Viet Nam.
Cross-‐border Migration Trends: Regular vs. Irregular Migration in Cambodia is mostly internal and intra-‐provincial (Maltoni, 2006), but in recent years, cross-‐border migration has been increasing, particularly along the Cambodian-‐Thai and Cambodian-‐Viet Nam borders that are described as porous. The two border provinces of Banteay Meanchey and Svay Rieng are used by a number of different cross-‐border migrant groups, defined largely on different movements and legal status (Maltoni 2008; Sciortino & Punpuing, 2009). Cross-‐border migrant groups can be classified into two categories; 1) short-‐term, short range depicted by daily cross-‐border work and long-‐term, 2) long-‐range characterized by the migration to central, eastern and southern provinces of Thailand and Ho Chi Minh City in Viet Nam (Maltoni, 2006).
Cross-‐border migration can also be defined by the legal nature of crossings and the type of documentation required for each individual cross-‐border migrant. In most short-‐term cross-‐border migration, day migrants with local national identity cards obtain a border pass. These passes are based on provincial cross-‐border agreements that allow locals registered in the border province, to commute daily into Thailand and Viet Nam to work in trade or agricultural work, and return in the evenings. Border passes are the main document in cross border areas. Passports are rarely used. It has been reported that often it is difficult to assess if those crossing are regular day migrants under the provincial agreements or long-‐term migrants entering on short-‐term border passes who eventually overstay and continue, as irregular migrants, deeper into Thailand or Viet Nam. (Sciortino & Punpuing 2009; PATH, 2010).
Cross-‐border migration relies on social networks on both sides of the borders, often with the help of friends, relatives or facilitators in the places of origin and destination. Most migrants choosing irregular channels to migrate long-‐term to Thailand are using facilitators or brokers linking them with Thai employers (Maltoni, 2006). These networks are also described as "chain migration" when one family member successfully migrates to another country and makes the necessary contacts to facilitate the migration of other family members (PATH, 2010). Often it is successful first migrations that lead others to follow. The stay could vary from three months to more than 10 years (Chan, 2009; Kavenagh & Buller, 2010).
Push & Pull Factors to Migration
Reasons to migrate, either internally or cross-‐border, are based on sets of “push and pull factors.” In Cambodia, the push factors driving internal migration are also driving international cross-‐border migration, such as lack of employment opportunities for a growing workforce; landlessness; financial debt to pay for health care; or responses to natural calamities, such as drought or floods (Maltoni, 2008; IOM, 2008; Biddulph, 2004; Phiev, 2004). Equally, the pull factors that spur international migration are forces such as a growing industrial demand for low skilled migrant labour and relatively higher wages compared to Cambodian labour work. Most cross-‐border migration from Cambodia is to Thailand, due to proximity, high economic growth and similar job markets (IOM, 2008). According to Chan, push factors to migrate are not only a lack of jobs and income in the country or place of origin, but in some situations a result of fraudulent money saving schemes that have left people financially in–debt, who now see migration as the last resort to overcome their dire situation (Chan, 2009).

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 15
Push and pull factors to migrate, internally or cross-‐border, are often interconnected and related to peoples’ inability to cope with overwhelming socio-‐economic issues, including inability to afford basic health care. Often agricultural land is sold to pay for unexpected health treatment for a family member. According to Biddulph (2004), in Cambodia one of the main causes of landlessness is financial debt from out-‐of-‐pocket expenses for health care. Another example of a push factor is low yields of annual crops that result in accumulative debt to ensure food security.
Migration therefore becomes a short-‐term coping strategy to overcome these health and socio-‐economic problems. Others would say a long-‐term strategy as cross-‐border migration increases (Sciortino & Punpuing, (2009).
Irregular Migration to Thailand and Malaysia In the Greater Mekong sub-‐region (GMS), Thailand is the largest destination country for an estimated one to two million, mainly low-‐skilled, migrant workers with families from Cambodia, Laos and Myanmar. The majority of migrant workers looking to work long term out of Cambodia choose to migrate via irregular channels that increase vulnerabilities to exploitation and forms of human trafficking, making it harder for Governments to protect, and ensure access to health care (IOM, 2008). The majority of migrants choose to migrate through irregular channels due to factors of high cost and long processing time associated with legal channels compared to irregular migration options (Maltoni, 2006; IOM 2008; Sciortino & Punpuing, 2009).
It is estimated that irregular migrants in Thailand could be two or four times higher than the 932,255 who have documented status (Thailand Ministry of Labour, 2011). The World Bank (2005) has estimated that 90 per cent of migrants in Thailand are irregular. Others estimate there to be one million undocumented migrants working in Thailand, mostly Burmese, but also, large numbers of Cambodians and Laotians (Hall, 2010).
It is reported that some Cambodian migrants in Thailand and Malaysia enter legally but become irregular by over-‐staying their work visas. Cambodian regular migrants in Malaysia are mostly female working as domestic workers sent through the private recruitment agencies under the Ministry of Labour. Under the bilateral Memorandum of Understanding (MOU) agreements since 2006 the Ministry of Labour has sent 4,771 migrant workers and 6,114 to Thailand (Chan, 2009). Not being a country bordering Cambodia, most Cambodians enter Malaysia legally but CARAM, an NGO working on migration issues, reports that many overstay their visas. This results when migrants change employers, which is not permitted by the Malaysian Immigration Act. Thus, when undocumented, they are more vulnerable and subject to deportation (IOM, 2008).
Deportation from Thailand and Malaysia
According to Sciortino and Punpuing (2009), many who failed to re-‐register or obtain a work permit remain in Thailand due to demand for low-‐skilled work. Many are subsequently deported for being unregistered or in breach of registration rules. There are anecdotal reports from NGOs and Immigration officials that many return to Thailand immediately after deportation or after a brief respite in villages in the border areas. The growing groups of deportees being expelled via Thai border check-‐points with the surrounding countries are largely vulnerable migrant population from Myanmar, Cambodia and Laos who have limited social protection and health care.
The main border checkpoint for deported Cambodian migrants is the Poipet and Aranyaprathet International border between Sa Kaeo province on the Thailand side and Banteay Meanchey province on the Cambodia side.
The reception of deported migrants on the Cambodian side is under the authority of the Border Immigration Police under the Ministry of Interior. According to the Chief of the Anti-‐trafficking Unit under the Ministry of Interior in Banteay Meanchey province, the number of deported irregular migrants from Thailand to Poipet International border rose from 91,268 in 2009 to a staggering

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 16
98,083 in 2010 (Chief of Poipet Immigration Centre, personal communication, January 25th 2011) Cambodian migrants are deported from centres in Thailand on average 150 to 200 per day according to immigration police and senior border officials.
In Poipet, the majority of those irregular migrants being deported originally have come from the inner provinces of Cambodia. Many are currently living in Poipet and have become totally reliant on irregular migration to all parts of Thailand to make a living. The total population of Poipet City is 92,143 people, of which 1,400 families stay on a temporary basis to participate in cross-‐border migration (NCDD, 2009).
Irregular Migration to Viet Nam Svay Rieng province borders Viet Nam and is considered a high migration area for Cambodia. Irregular migration to Viet Nam from Svay Rieng province is both long term and short term (Kavenagh & Buller, 2010; Phiev, 2004). Daily migrants travel across the border for daily work in agriculture and other low skilled manual labour. With support from IOM, the Department of Social Affairs, Veterans and Youth Rehabilitation has supported and collected data on a number of migrants deported from Ho Chi Minh City and other cross-‐border provinces for begging (Social Development Research & Consultancy, SRDC, 2002).
Migration trends and the number of returned irregular migrants are much different in Svay Rieng province compared to other cross-‐border migration trends in Banteay Meanchey province. While the push factors are similar the pull factors of demand for low-‐skilled labour are generally concentrated in the cross-‐border areas and are largely seasonal. Those long-‐range irregular migrants are predominately begging in Ho Chi Minh City or participating in informal activities. The majority of those irregular migrants being deported from Viet Nam are from impoverished districts along the border in Svay Rieng, rather than internal provinces. Between 2007 and 2008, the total number of returned irregular migrants from Viet Nam to Svay Rieng province reached 2,869, with a significant 67 per cent of them being children aged 12-‐17 years and 60 per cent female1.
Deportation from Viet Nam
Based on the data from Svay Rieng Department of Social Affairs, the majority of irregular migrants come from Kompong Ro and Chantrea districts near the border. The population of the two districts combined is 92,898 people (The National Committee for Sub-‐ National Democratic Development (NCDD, 2009); of which approximately 369 families have irregular migrant family members based on the deportation statistics from the Department of Social Affairs in Svay Rieng. These irregular migrant families are mostly poor farmers or hired agriculture labourers with limited or no agricultural land that migrate seasonally to supplement their scarce daily subsistence activities with begging in Ho Chi Minh City and in other border provinces of South Viet Nam.
Health Problems Faced by Migrants One critical concern is the health of migrants at all points of the migration process, from origin, transit, destination and return. Migrants, who migrate through irregular channels without legal documentation, often find themselves more vulnerable and at risk of exploitation by employers or traffickers, that impacts on their overall physical health and psychological well-‐being.
Migrants in Thailand and Malaysia are reportedly subject to physical abuse, harassment, excessive working hours, poor living conditions, lack of food, confinement (detention), no health care or limited access, and work related accidents that impact on the overall health and well-‐being of migrants (Maltoni, 2006; PATH, 2010).
Migrants are generally concentrated in jobs deemed dirty, dangerous and degrading that have a considerable impact on their health. Low skilled migrants are often expected to do dangerous work 1Data is from statistics kept by the Department of Social Affairs Svay Rieng 2007-‐2009

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 17
that locals refuse to do, such as spraying harmful chemicals or working under sub-‐standard conditions that increase certain health and occupational risks. Apart from the working conditions, migrants predominately live in crowded, unhygienic and poor sanitary conditions in low-‐socio-‐economic areas that increase their susceptibility to infections and communicable diseases in confined living spaces.
In their study to find out health and mortality differences among Myanmar, Laos and Cambodian migrants residing in Thailand, Nucharee and Punpuing (2009), highlighted that the work and living conditions of irregular migrants intensify certain vulnerability to health problems and mortality. Data from annual epidemiological reports during 1998 to 2006 and vital registration statistics during 2004 to 2008 showed that major causes of sickness among these migrants were acute diarrhoea, malaria and pyrexia of unknown origin. Cambodian migrants had surprisingly high fatality rates for pneumonia, tuberculosis, hepatitis, malaria, meningitis and tetanus when compared with migrants from Myanmar, Laos and local Thai people. Results from the vital registration revealed that majority of Cambodian migrants died from infectious diseases and accidents (Nucharee and Punpuing, 2009).
Other prevalence studies among 818 fishermen (582 Thai, 137 Burmese, 99 Cambodian) found HIV prevalence rates among migrant workers were significantly high at 15.5 per cent. For Cambodians it was 20 per cent HIV prevalence attributed to visiting sex workers (40%) (PATH, 2010).
Health Risks Faced by Migrants
Migrant groups often find themselves exposed to a range of health risks, as many lack the knowledge and skills to stay healthy and often have low perception of their health vulnerabilities, which in turn affects their health seeking behaviour (Phiev, 2009). While migration in itself is not a risk factor to health, the circumstances surrounding the migration process can increase their vulnerability and exposure to certain diseases or infections.
The lengthy detention and conditions in detention centres abroad are considerable risk factors. According to consultations with Immigration and Social Affairs Officials in Cambodia, the length of detention varies from one to two months in Thailand and from two to three months in Viet Nam. In 2010, 20 per cent of the 98,083 deported from Thailand had spent more than one month in detention and were confined to cells crowded with up to 30 people that potentially increases certain health risks to tuberculosis and other airborne infections. It was reported that access to health care and general exercise was restricted (Dickson, 2010).
Health Seeking and Access to Health Services in Destination and Origin
Irregular migrants are potentially more at risk of infection and illness, largely due to frequent mobility, poor socio-‐economic conditions and limited access to health services due to illegal status, which pose considerable challenges to ensuring the health of migrants and source communities.
In Thailand, only registered migrants have access to health care under the universal coverage policy including coverage under migrant health schemes such as, the Compulsory Migrant Health Insurance Scheme that aims to provide migrant workers and their families with access to essential health care services. Membership under such schemes is in compliance with migrant registration and involves annual fees paid by the migrant, or can be paid by the employer.
It is much more difficult for undocumented migrants to access the same health services largely due to their undocumented legal status. For undocumented migrants health care options are limited to hospital exemptions and out of pocket payments. Many do not even attempt access due to fear of arrest if presented at public health facilities. Most in emergencies pay upfront fees for treatment at hospitals or apply for hospital exemption. Many delay to seek health services until conditions are serious. Most migrants resort to self-‐medication and treatment such as traditional coining and

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 18
buying medicines over the counter at pharmacies. (IOM & WHO 2009, Health Care Financing for Migrants: A case study from Thailand; PATH, 2010)
Frequent cross-‐border mobility may also lead migrants to forget or run out of their daily medicine leaving them vulnerable to opportunistic infections and more serious conditions with limited access to health services in the destination. Treatment defaults among mobile TB and HIV patients also contribute to problems with multi-‐drug resistance.
In light of the World Health Assembly Resolution on the Health of Migrants (WHA, 2008) that calls on member states such as Cambodia to promote the health of migrants and migrant sensitive health services, there is a need to analyse the major challenges to health associated with migration.
In light of the secretariat reports on the progress of the resolution WHA 61.17 there is a particular concern for migrants in an irregular situation and the associated health risks and lack of access to health services. This Situational Assessment intends to document the trends of Cambodian irregular migrant groups in border areas; identify and fill gaps in service delivery to meet irregular migrant health needs; disaggregate health information by gender, age and origin and by socioeconomic and migratory status; encourage health and migration knowledge production; documenting and disseminating data on irregular migrants' health needs in countries of origin or return, transit and destination.
Data on distinct national groups such as irregular migrants compared to non-‐migrant households will pave the way for recognizing public health issues associated with voluntary or forced migration and work toward addressing their repercussions for health service delivery systems. Additionally, specific migrant health data presents a model in how to reduce health disparities among different demographic population groups.
Picture 3: Returned Irregular Migrants receiving HIV awareness education from NGO worker from SEADO at the Poipet Immigration Centre

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 19
Chapter II: Methodology
Sample A total of 438 adult migrants and non-‐migrants were interviewed by Government and NGO interviewers recruited by IOM, as part of the Situational Assessment. 220 irregular migrants were interviewed in villages in Banteay Meanchey and Svay Rieng provinces. A control group of 218 non-‐migrants from source communities in the same two provinces were also interviewed in order to conduct comparisons.
The study sites were identified during multi-‐stakeholder consultations in the two operational districts near the international border crossings in Poipet, O’Chrov District in Banteay Meanchey province and Kampong Ro and Chantrea districts, Svay Rieng Province. These two major border crossings receive deported and repatriated Cambodian irregular migrants from Thailand and Viet Nam, including those who have been trafficked. Table 1 below summarizes the sample.
Table 1: The sample of migrants and non-‐migrants
Migrants Non-‐Migrants Svay Rieng (Kampong Ro & Chantrea Districts) 102 99 Banteay Meanchey (Poipet & Nimit Communes, O’Chrov District)
118 119
Total 220 218
Migrants
The selection of migrants for interview varied according to the different situation of migrants in each target border province.
a) Svay Rieng Province
In Svay Rieng province, interviews with returned irregular migrants were carried out in source villages within two border districts. Migrants were identified based on repatriation records of irregular migrants managed by the Department of Social Affairs in coordination with government departments and border authorities.
A list of irregular migrants returned in 2009 and 2010 was generated and acted as the target population sample frame. In order to ensure the same probability of being selected for interview, the research team used a simple randomization method assigning every irregular migrant on the sample frame list, a number on a small piece of paper, folded and placed in a hat. Once all irregular migrants had an assigned number and were placed in the hat. Each research team member took it in turns selecting one piece of paper at random from the hat and recorded the number, marking the correlating name. The list of 100 names was then matched with the corresponding case file that included name and brief family history, a photo, and location of village.
The remaining 37 irregular migrants that were not selected were used as a substitute list in case people were absent or had returned to Viet Nam.
b) Banteay Meanchey Province
In Banteay Meanchey province, interviews were conducted with returned irregular migrants at the Poipet Immigration Centre in collaboration with border police and centre staff.
The research team conducted the migrant interviews in the immigration centre during the reception of deported Cambodians. The research team coordinated with immigration police and NGOs to randomly select participants from the groups of arrivals at the centre using a sampling interval

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 20
calculated by dividing the number of returnees by the desired number of interviews. For example 50 migrants per truck; the team divided the number of 12 interviewers by 50, which gave the interval of four. Using the interval the research team counted every fourth migrant, which was selected for interview. Due to the stressful circumstances of deportation and presence of police, those selected were given the chance not to participate and volunteers were asked to participate.
Irregular migrants who had been previously deported were also interviewed in nearby villages within Poipet commune when there was no scheduled deportation. Local NGOs and village leaders were consulted to develop a list of migrant households with family members that had been recently deported. From the list using a simple random selection used in Svay Rieng, irregular migrants were selected for interview. (see Annex A for the full list of villages).
Non-‐migrants
Non-‐migrants were selected from villages close to the border in Nimit commune. These villages were geographically within the same district of O’Chrov and close to Poipet commune and were socio-‐economically similar. In Svay Rieng province non-‐migrants were drawn from villages in Chantrea and Kampong Ro districts (see Annex A for the list of villages).
Within the identified villages, houses were selected using a sampling interval calculated by dividing the number of households in the village by the desired village sample. The research team selected houses by counting the interval along the road from each proceeding interview. To avoid bias the first house was always randomly chosen. This systematic random sampling technique allowed the number of interviews to be proportionally spread out across the village and the sample to be relatively representative of the entire village population.
Health Staff
Health service delivery was assessed through interviews with 100 health care workers and community health volunteers – including peer educators from two health centres and referral hospitals in O’Chrov and Chipou Operational Districts. Community-‐based health workers and peer educators were selected from the same target villages from which migrants were drawn.
Instruments IOM and project partners from the MoH and PHD jointly developed the questionnaires adapted from previous IOM questionnaires on migration, influenza and other communicable disease studies targeting migrants. Two structured questionnaires (migrant and non-‐migrant) were developed, composed of mostly closed questions, with single and multiple-‐choice answers. The migrant and non-‐migrant questionnaires were complementary, allowing for comparisons to be made between data from the two groups. A limited number of qualitative questions were included with probes to solicit more in-‐depth answers. For government and community health workers, a separate questionnaire was developed using similar questions (see Annex B). The questionnaires were separated into seven sections that collected data on the following areas:
1. General demographics
2. Socio-‐economic background
3. Migration and mobility
4. Health risks
5. Health issues and health seeking behavior
6. Health knowledge and awareness
7. Sources of health information

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 21
Data Collection Due to potential ethical concerns and the sensitivity of the research, substantial care was taken in managing data collection. Provincial and district health and social workers, including NGO staff who regularly provide health care and health education, case management and family support to returned irregular migrants were identified by IOM as the best interviewers to conduct data collection. These individuals were respected authority figures with a good understanding of the migrant issues having first-‐hand experience working with migrants and border communities.
The interviewers were trained by IOM staff on how to carry out interviews using the migrant and non-‐migrant questionnaires. The training focused on interviewing skills, with particular emphasis on techniques such as staying neutral and avoiding the use of leading questions, as well as probing and re-‐phrasing questions to ensure clarity without changing the meaning of the question. IOM field staff supported the interviewers to pre-‐test the questionnaires with some irregular migrants in the target sites.
The National Ethics Committee for Health Research, under the Ministry of Health formally approved the Situational Assessment and research protocol followed by interviewers. Interviews were conducted in Khmer using a bilingual version of the questionnaire so IOM and MoH staff – both international and local – could monitor the entire interview process to ensure questions were not missed or interviewers were not leading interviewees. The research teams introduced themselves to participants and provided an explanation of the study (see Annex B). Participants volunteered their participation verbally and had a chance to ask any questions about the study before commencing the interview. Individual interviews lasted approximately one hour.
Two MoH and IOM staff, as well as an international research consultant checked each questionnaire for errors. At the end of each day, informal debriefing sessions were held with the interviewers to evaluate progress and provide insight into the data collection process.
Picture 4: Returned Irregular migrants during interviews with a Government Social worker from Provincial Social Affairs Department in Svay Rieng Province

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 22
Data Analysis Once all data collection activities were complete, three IOM staff entered data and conducted preliminary analysis in collaboration with the project research assistant from the MoH. Following the data entry, IOM ran a series of technical meetings in collaboration with the MoH and Provincial Health Department focal points. Preliminary findings in the data were identified for further exploration. Finally, detailed quantitative data analysis was conducted using the STATA statistics programme.
Limitations While every effort was made to ensure that the sample of both migrants and non-‐migrants were representative of the relevant populations, the nature of irregular migration creates some research challenges.
Sampling irregular migrants is incredibly difficult. The clandestine nature of irregular migration means that the authorities only come into contact with migrants when they are deported or return so ‘finding’ the population can be difficult. The experiences of IOM and stakeholders working in migration – including from civil society and government – were used to carefully design the sampling for this research. Participants were drawn both at the point of return -‐ in immigration centres at the border, and from official lists of returnees identified from repatriation records to maximize representativeness of the migrant population.
The Situational Assessment also took great care to ensure that the impact of migration on entire communities was captured. Both migrants and non-‐migrants were interviewed in target locations.
IOM is also well aware that the migration experience can differ remarkably in different locations and the research responded to this by sampling in two provinces where the migration story is known to vary. While migrants leaving from Banteay Meanchey province technically came from source communities in the province – in many cases, individuals internally move to the province from elsewhere in Cambodia first. This migration situation differs in Svay Rieng province where the majority of migrants originate from within the province. In order to account for this, comparisons were made during analysis to explore this difference and where significant, data that indicated population factors had an influence is reported throughout the report.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 23
Chapter III: Findings
MIGRANTS AND NON-MIGRANTS
Demographics The final sample (n=438) consisted of 50.23 per cent migrants and 49.77 per cent non-‐migrants. This section introduces the demographics and the socio-‐economic characteristics of both migrants and non-‐migrants sampled. Specifically, comparisons will be made by gender, age, marital status, education level, living situation and income. The findings are based on two sets of comparisons: migrants and non-‐migrants in two border provinces.
Migrant Status
Figure 1 describes the sample by migrant status and location. The number of migrants and non-‐migrants in the two provincial locations were roughly equal2. This allows for simple comparisons of actual characteristics between migrants and non-‐migrants
Figure 1: Migrant status by province
Gender
Figure 2 below shows that overall the proportions of males and females were roughly equal between the migrant and non-‐migrant groups3. This allows for simple comparisons between the groups based on gender.
2 Non significant Chi-‐square (χ2=0.04, df=1, p=0.842) 3 Non significant Chi square analysis (χ2=0.22, df=1, p=0.638)
50.75% 49.25% 49.79% 50.21%
Svay Rieng Banteay Meanchey
Migrant Non Migrant Graphs by Place of Interview: Province?
n=438 Migrant Status by Province

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 24
34.55%
65.45%
36.70%
63.30%
Migrant Non Migrant
Male Female
Graphs by Migrant status
n=438Gender of respondents
Figure 2: Gender of respondents
However, it should be noted that there were differences between the proportions of males and females within the locations, seen in Figure 3. In Svay Rieng province a higher proportion of the migrants were women (80.39% of Svay Rieng migrants) than in Banteay Meanchey (52.54%). This difference was significant4 and as the research is based on a carefully constructed random sample, this finding suggests that in Svay Rieng province, migrants are more likely to be women than men. Given the lack of information of gender composition of irregular migrants5, this new evidence is something that should be explored.
19.61%
80.39%
40.40%
59.60%
Migrant Non Migrant
Male Female
Graphs by Migrant status
(n=201)Gender of respondents: Svay Rieng
47.46%52.54%
33.61%
66.39%
Migrant Non Migrant
Male Female
Graphs by Migrant status
(n=237)Gender of respondents: Banteay Meanchey
Figure 3: Gender of respondents by province
4This difference was statistically significant (χ2=10.38, df=1,p=0.001) 5 IOM (2006). Review of Labour Migration Dynamics in Cambodia. IOM: Phnom Penh.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 25
Age
Figure 4 indicates that migrants were almost all aged between 20 and 49 years. The most common age category was 20 – 29 years. Within this category, respondents were almost twice more likely to be migrants than non-‐migrants. In Banteay Meanchey Province, migrants were most likely to be in the 20-‐29 years category. In Svay Rieng province, migrants were most likely to be in the 40-‐49 years category.
74
28
1917
26
40
32
6
18
4
14
4
57
25 25
45
21
33
1
10
2
020
4060
18-19 20-29 30-39 40-49 50-59 60-69 18-19 20-29 30-39 40-49 50-59 60-69
Sv ay Rieng Banteay Meanchey
Migrants Non-migrants
coun
t of c
ases
.
(n=438)Age of respondent
Figure 4: Age of respondents
Marital Status
Table 2 illustrates that the largest proportion of the total sample were married. However a smaller proportion of migrants (69.55%) were married compared to non-‐migrants (84.86%) thus migrants were statistically more likely to be single than non-‐migrants6.
Table 2: Marital status of respondents
Migrant Non-‐Migrant Single/never married 45 20.45% 17 7.8% Married 153 69.55% 185 84.86% Separated/divorced/widowed 22 10.00% 16 7.34%
6This difference was statistically significant (χ2=16.61, df=2, p=0.00)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 26
Number of Dependents
Table 3 shows that overall 63 per cent of respondents had between three and six dependents. There was no significant difference between non-‐migrants and migrants for the number of dependents7.
Table 3: Marital status of respondents
Dependents % of migrants & non-‐migrants No dependents 04.34% One or two 13.47% Three or four 30.37% Five or six 33.56% Seven or eight 11.64% Nine or ten 04.34% More than ten 02.28% Total 100%
Level of Education
Figure 5 illustrates that over one fifth (23.52%) of the total sample had never attended school.
109
56
22
46
16
33
4
148
13
5 81
5548
020
4060
8010
0
coun
t of c
ases
1-3 grades 6 grades 7-8 grades 9 grades 10-11 grades 12 grades Uni None
(n=438)Years of schooling
Mig Non
Figure 5: Years of schooling
The overall education levels among migrants in the two border provinces are low compared to non-‐migrant groups. Nearly half, (i.e., 49.55%) of the migrants only completed between one and three years of primary education. Migrant levels of education between the two provinces were similar. Respondents that had completed primary or secondary education were more likely to be non-‐migrants than migrants. In the sample, limited formal education was clearly related to migration. This may be due to the fact that often, young people drop out of education to pursue migrant work. In turn, lower levels of complete formal education may also exclude migrants from local job markets, perpetuating their need to migrate for employment.
7Chi square (χ2=7.23, df=6, p=0.30)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 27
Housing and Land Ownership Living Situation
Figure 6 shows results regarding the living situations of respondents. A greater proportion of non-‐migrants (90.83%) reported that they owned both their house and plot or their house without plot, when compared to migrants (79.55%)8.
050
100
150
200
coun
t of c
ases
Own house/plot Own house Rent house Rent room With relative Homeless
(n=438)Living situation in Cambodia
Migrants Non-Migrants
16.82%
4.13%
62.73%
86.70%
6.82%
12.27%8.72%
0.91%
Figure 6: Living situation in Cambodia
When analysing the two border provinces, a larger proportion of Svay Rieng respondents (92.04%) owned their own house than those from Banteay Meanchey (79.33%). 6.82 per cent of migrants reported renting a house while no non-‐migrants rented. All those that reported renting a house or a room were from Banteay Meanchey province. Migrants (12.27%) were only slightly more likely than non-‐migrants (8.72%) to live with relatives or friends. Two migrants, both from Banteay Meanchey reported to be living in temporary structures.
These findings may be an indication of differences between the two cross-‐border locations. A large number of Banteay Meanchey residents have relocated from elsewhere in Cambodia before going on to Thailand. Of the 118 migrants from the Banteay Meanchey sample, 22 were originally from other provinces in Cambodia, which highlights the internal migration particularly from provincial to cross-‐border areas in the past 10 to 15 years since reopening of the Poipet border. These people are more likely to be living in insecure housing reflecting the transient nature of cross-‐border populations in Poipet. In contrast cross-‐border migration for Cambodians is very much localized in Svay Rieng, only one migrant was not born and raised in Svay Rieng province.
8This difference was statistically significant (χ2=56.41, df=2, p=0.000)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 28
Housing Materials
Figure 7 shows that among the respondents that owned their house (n=373), there were significant differences9 between migrants and non-‐migrants in the housing materials, which their houses were constructed from.
050
100
150
coun
t of c
ases
Good Adequate Poor
(n=373)Housing materials
Migrants Non-Migrants
6.86%
14.71%
37.71%
56.86%
55.43%
25.49%
Figure 7: Housing materials of owned homes
More than half (55.43%) of the migrants reported housing materials categorized as ‘poor’ compared to 25.49 per cent of non-‐migrants (the ‘poor’ category included palm leaves or plastic sheeting). On the other hand, more than half of the non-‐migrants (56.86%) reported ‘adequate’ housing (permanent structures using hard wood and corrugated metal sheeting), compared to 37.71 per cent of migrants. Twice as many non-‐migrant respondents who owned their houses reported that their houses were of ‘good’ quality (two-‐storey structures with tiled roofs and bricked downstairs living spaces).
Land Ownership
As shown in Figure 8 below, there was a significant difference between the ownership of agricultural land among migrants and non-‐migrants.10 The majority of non-‐migrants (72.48%) reported ownership of agricultural land used for cultivating rice or small crops, compared with only 39.55 per cent of migrants. More than half of the migrants (58.18%) had no agricultural land. A very small proportion of the total sample rented agricultural land (n=15). These findings indicate that a lack of agricultural land is probably a strong push factor for migration amongst the sample.
9This difference was statistically significant (χ2=33.75, df=2, p=0.000) 10(This difference was statistically significant (χ2=56.41, df=2, p=0.000)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 29
050
100
150
coun
t of c
ases
Owned Rented No
(n=438)Ownership of agricultural land
Migrants Non-Migrants
39.55%
72.48%
4.59%2.27%
22.94%
58.18%
Figure 8: Land ownership
As with the home ownership statistics cited above, when comparing the two provinces, a larger proportion of people in Svay Rieng province (70.65% of Svay Rieng respondents) owned land than of people in Banteay Meanchey province (43.46% of Banteay Meanchey respondents).
More than 90 per cent of Cambodians are subsistence farmers; ownership of agricultural land therefore provides stability for many families. Often in a time of crisis, families are forced to sell their land. Although interconnected with many other factors, landlessness is a contributing cause pushing people to migrate for work. In the sample, there was a significant difference between the number of migrants compared with non-‐migrants that had sold or lost agricultural land in the past.11 Twice the proportion of migrants (35%) had sold or lost agricultural land in the past compared to non-‐migrants (16.51%), suggesting that migrants are more financially vulnerable to losing land than non-‐migrants. Of those respondents who had sold land, 66.23 per cent reported they sold land to pay for basic needs including food, health care and shelter. 18.18 per cent needed money to pay back the debt incurred to pay for the same basic needs. The other 10.39 per cent indicated that authority figures, other family members, or powerful people had taken their land. These findings support theories that those faced with a financial crisis and unable to support basic needs (for example unable to buy food, healthcare, education and shelter) are likely to sell their agricultural land, and as a result are pushed to migrate in order to generate income.
Employment, Income and Financial Status Sources of Income in Cambodia
Highlighted in Figure 9 and Figure 10 agriculture was the most commonly reported source of income for both migrants and non-‐migrants. However, smaller proportions of migrants (57%) compared to non-‐migrants (79%) derived their income from agricultural work.12 When making statistical comparisons by province respondents from Svay Rieng were more likely to get income from agriculture than those in Banteay Meanchey.13
11(χ2=19.55, df=1, p=0.000) 12 This was statistically significant (χ2=24.65, df=1, p=0.000) 13 This was statistically significant (χ2=77.70, df=1, p=0.000)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 30
020
4060
80
perc
enta
ge
Migrant Non Migrant
(n=438)Sources of income while in Cambodia: Migrant Status
Agriculture FactoryFishing Small businessConstruction Domestic workMoto taxi/cart CasinoGovernment UnemployedOther
Figure 9: Income while in Cambodia by migrant status
020
4060
80
perc
enta
ge
Svay Rieng Banteay Meanchey
(n=438)Sources of income while in Cambodia: Province
Agriculture FactoryFishing Small businessConstruction Domestic workMoto taxi/cart CasinoGovernment UnemployedOther
Figure 10: Income while in Cambodia by province
The second most frequently reported income source was small business; once more a smaller proportion of migrant (21%) compared to non-‐migrants (33%) reported this as an income source.14 When comparing the two provinces, respondents from Banteay Meanchey more frequently reported small business as a source of income than those in Svay Rieng.15 Migrants (11%) were slightly more likely to get income from construction than non-‐migrants (7%) though this was not statistically significant.
The survey included sex work and begging as possible categories however no one in the sample reported these as a source of income. A total of 23 respondents reported being unemployed.
14 This was statistically significant (χ2=6.98, df=1, p=0.000) 15 This was statistically significant (χ2=15.39, df=1, p=0.000)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 31
Frequency of Work
There were significant differences between the reliability of income throughout the year for non-‐migrants and migrants for work they did in Cambodia.16Half of the (50.25%) employed migrants (n=197) reported that their source of income was irregular, compared to 39.45 per cent of non-‐migrants. Work during the dry season was the second most frequently reported source of income for migrants, 51 per cent of the total. More than double the number of non-‐migrants (n=51) reported income during the wet season than migrants (n=17). A small proportion of both the migrant (6.09%) and the non-‐migrant (8.72%) groups reported having income all year round.
Average Income
Figure 11 illustrates the average monthly income of respondents. There was a significant difference in the average monthly income between migrants (USD 73.45) and non-‐migrants (USD 92.42).17Figure 12 illustrates the income bands compared by province. There was also a significant difference18 in the reported mean income of respondents from Banteay Meanchey (USD 98.67)
010
2030
40
perc
enta
ge
Migrant Non MigrantMale Female Male Female
* 23 Missing values among unemployed migrants
(n=415*)Monthy income: Migrant Status
Under $50 $50-100$100-200 $200-300None
Figure 11: Monthly income by migrant status and sex
89
81
207
63
70
6718
050
100
150
200
Svay Rieng Banteay Meanchey
* 23 Missing values among unemployed migrants
(n=415*)Monthy income: Province
Under $50 $50-100$100-200 $200-300None
Figure 12: Monthly income by province
16 This was statistically significant (χ2=19.69, df=4, p=0.001) 17 This was confirmed by a significant independent sample t-‐test (t=-‐2.5414, df=413, p=0.0114, two-‐tailed) 18This was confirmed by a significant independent sample t-‐test (t=-‐4.3682, df=413, p=0.000, two-‐tailed)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 32
Picture 5: An irregular migrant being interviewed by a Government Social Worker at the Poipet Immigration Centre

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 33
Stability of Income
Highlighted in Figure 13 and Figure 14, some interesting patterns can be seen in the relationship between stability of work and income. For example income from ‘irregular’ work, for both the migrant and non-‐migrant, was most likely to be less than USD 50 per month. These patterns were similar for migrants and non-‐migrants. However, as noted already, migrants are likely to earn less and have less stable work thus being more affected by these patterns.
36
2 1
19
25
6
1
9
53 3
7 6
2
44
33
19
3
010
2030
40
num
ber r
epor
ted
All year Dry season Wet season Daily Irregular
*23 missing values
(n=197*)Monthly income by stability of source: Migrants
Under $50 $50-100$100-200 Over $200
Figure 13: Migrant monthly income by source
4
10
3 2
14
21
11
4
18
14 14
5
1
8
2 1
37
22 21
6
010
2030
40
num
ber r
epor
ted
All year Dry season Wet season Daily Irregular
(n=218)Monthly income by stability of source: Non-Migrants
Under $50 $50-100$100-200 Over $200
Figure 14: Non-‐migrant monthly income by source

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 34
Perceived Financial Position
Figure 15 illustrates that a larger proportion of migrants than non-‐migrants reported that they did not have enough money to pay for their family’s basic needs.
050
100
150
200
coun
t of c
ases
Not enough Enough food Enough food/health Pay for most Cover all
(n=438)Financial position of families
Migrants Non-Migrants
84.09%
57.80%
10.91%
22.94%
3.64%6.42%
0.91%
10.55%
0.45% 2.29%
Figure 15: Financial position of families
More than double the number of non-‐migrants compared to migrants reported having ‘enough money for food’. A significantly larger 28 non-‐migrants reported having sufficient money to ‘pay for most’ and ‘cover all’, in contrast to just three migrants.
The mean income of those respondents that reported that they did not have enough money was USD 76.96, which is USD 3.51 higher than the mean monthly income of migrants (USD 73.45) and USD 15.46 lower than the mean monthly income of non-‐migrants (USD 9 2.42). The mean monthly income of those respondents that reported having enough money for food was USD 87.94. Therefore, it is likely, that migrants whose families rely solely on their income will not have enough money to meet their basic needs for food and health care, putting them at great risk of ill health and pushing them further into the poverty trap.
Household Debt
Of the total sample, 68.49 per cent reported having outstanding household loans or debts. Migrants (77.73%) were significantly more likely19 to have household debt than non-‐migrants (59.17%). In line with prior research, these findings indicate that household debt is a major factor pushing Cambodian people to migrate for work.
Of the 300 respondents that reported having loans, just under half (49.33%) reported having one loan, split almost evenly between migrants and non-‐migrants. 28 per cent reported having two loans and 13.33 per cent reported having three. There was no significant difference between migrants and non-‐migrants in these categories. There was a significant difference between respondents that
19 This was statistically significant (χ2=17.46, df=1, p=0.000)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 35
reported having four or more loans, 14.62 per cent of migrants compared to 2.33 per cent of non-‐migrants.20
The mean amount of money owed was significantly higher for non-‐migrants (USD 748.05) than for migrants (USD 472.65).21 This finding aligns with the knowledge that those people earning more money are more likely to have larger debts.
Almost the same proportions of migrants and non-‐migrants owed their money to informal moneylenders and banks/microfinance agents. However, migrants (68.13%) were more likely to have loans with their neighbours than non-‐migrants.22 Table 4 below documents the number of respondents by the type of loan they reported.
Table 4: Types of loans
Lender % of migrants % of non-‐migrants Parents/relatives 21.05% 19.38% Friends 9.94% 7.75% Neighbours 36.26% 22.48% Informal money lender 29.82% 29.46% Bank/microfinance 34.50% 39.53% NGO 0.00% 1.55% Private clinic 1.75% 0.00% Other 0.00% 4.65%
* Respondents could owe in more than one category if they had numerous loans
Reason for Debt
Figure 16 illustrates the reasons that migrants and non-‐migrants had loans.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=300)Reason for loans: Migrant Status
Basic needs HealthEducation Livelihood inputsBuy/rent land CeremoniesPay loan/debt Migration
Figure 16: Reason for loan by migrant status
20 This was statistically significant (χ2=14.988, df=3, p=0.002) 21 This was confirmed by a significant independent sample t-‐test (t=-‐2.6373, df=298, p=0.0088, two-‐tailed) 22 This was statistically significant (χ2=6.60, df=1, p=0.01)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 36
Although loans were common amongst migrants and non-‐migrants, there were important differences in the reasons these loans were taken out. Crucially, migrants (54.39%) were twice more likely to take out loans for basic needs than non-‐migrants (24.03%). This Cambodian data is in line with previous research indicating that household debt as a major push factor leading to migration.
Seen in
Figure 17 below, migrants were twelve times more likely (9.36%) than non-‐migrants (0.78%) to take out loans to pay off other debts. The graphs also show that non-‐migrants (13.95%) were twice more likely than migrants (5.85%) to take out loans for education. Similarly, non-‐migrants (66.22%) were 1.5 times more likely to take loans for livelihood, such as agriculture, than migrants (44.11%).
Figure 17: Specific uses of loaned money
The high number of migrants in debt largely indicates money lending is common among migrant households. The capacity of migrant households to save money is low indicated by the use of these loans to pay for basic needs. Non-‐migrants however are taking out larger loans, corresponding to their larger incomes, and investing into livelihoods such as agriculture and small businesses that have the potential to increase their income and probability of repaying original loans. This distinguishes the different coping strategies and levels of socio-‐economic status among migrants and non-‐migrants.
Figure 18 below indicates that migrants (49.12%) were still more likely than non-‐migrants (38.76%) to take out loans for healthcare. However, this difference was not statistically significant.23
23 This was not statistically significant (χ2=3.19, df=1, p=0.074)
57.89%
42.11%31.78%
68.22%
Migrant Non Migrant
No Yes
Graphs by Migrant status
n=300Debt: Livelihood
94.15%
5.85%
86.05%
13.95%
Migrant Non Migrant
No Yes
Graphs by Migrant status
n=300Debt: Education
90.64%
9.36%
99.22%
0.78%
Migrant Non Migrant
No Yes
Graphs by Migrant status
n=300Debt: Pay off loans
45.61%54.39%
75.97%
24.03%
Migrant Non Migrant
No Yes
Graphs by Migrant status
n=300Debt: Basic needs
THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 37
50.88%49.12%
61.24%
38.76%
Migrant Non Migrant
No Yes
Graphs by Migrant status
n=300Debt: Healthcare
Figure 18: Debt for health care
Strategy to Pay Back Debt
Figure 19 shows that of the 300 respondents who had loans, 90 per cent of migrants and 97 per cent of non-‐migrants reported that they would work and save to pay their loans.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=300)Strategy to pay back loan
Work and save Send family member to workMigrate to work Sell landAnother loan Other
Figure 19: Strategy to pay back debt
Unsurprisingly, more migrants (31%) compared to non-‐migrants (2%) reported that they would migrate for work to pay their loans. A small proportion of both groups reported that they would send family to work to as a strategy to pay back the money they owed.
It appears that migrants find themselves in more vicious cycles of debt than non-‐migrants. Taking out loans for basic needs, owing money to several moneylenders and using one loan to pay off another. Non-‐migrants tend to loan larger sums of money, investing into land or businesses, that have the potential to make money, and are therefore more likely pay off the original loan.
These findings indicate that migrants have a lower socio-‐economic status than non-‐migrants. Confirming push factors described earlier, including household debt, which lead to a reliance on irregular migration as the means to repay accumulative debt and interest.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 38
Migration and Mobility Reason for Migrating
Illustrated in Figure 20, the primary reasons to migrate differ significantly between migrants from the two provinces. Migrants in Banteay Meanchey (69.84%) are twice more likely than those from Svay Rieng (30.16%) to migrate for a ‘better job/income’.24 This may be closely linked the greater demand for low skilled migrant labour work in Thailand compare to Viet Nam. Migrants from Svay Rieng (62.64%) were more likely to migrate to pay off family debt than those in Banteay Meanchey (37.36%)25. Lack of jobs at home was equally reported as a reason for migrating by both Svay Rieng and Banteay Meanchey migrants.
020
4060
80pe
rcen
t
Svay Rieng Banteay Meanchey
(n=220)Reasons for migrating
Better job/income More jobs at destLack of jobs at home Pay off family debtLoss of land Earn for familyEarn for business With family
Figure 20: Reason for migrating
Migration Documentation
Figure 21 shows that of the 220 migrants in the sample, only five (2.27%) possessed a Cambodian passport and one (0.45%) had a visa for the country that they migrated to but had overstayed the time stipulated. Only eleven (5%) migrants had border passes, and it is likely that these migrants crossed the border daily for work. The other 204 (92.73%) migrants were undocumented, illegally crossing the border into either Viet Nam or Thailand for work. Of all migrants only 17.73 per cent had Cambodian National ID cards. Of those migrants who did not have a passport (n=216) only six had ever tried to apply for one. The largest proportion reported they did not need a passport as the reason for never applying. This data is not surprising given access to non-‐formal migration routes and the financial position of most migrants explained previously. The passport application process is costly compared to Neighbouring countries26 and time consuming, which results in many migrants taking a short cut through irregular channels (Chan, S (2009).
24 This was statistically significant (χ2=31.14, df=1, p=0.000) 25 This was statistically significant (χ2=16.53, df=1, p=0.000) 26 According to a cost benefit study passports in Cambodia can range from 139 USD up to 224 USD depending on time in which passport is needed. In comparison Cambodian passports are significantly more expensive when comparing with Viet Nam (12 USD) and Thailand (30USD). Chan, S (2009).

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 39
020
4060
80pe
rcen
t
(n=220)Documentation while migrating
Passport VisaBorder pass ID cardNothing
Figure 21: Migration documentation
Frequency of Migration
Highlighted in Figure 22, of the 220 migrants interviewed, the majority from both provinces reported migrating three or four times per year. Double the number of migrants in Banteay Meanchey crossed the border once per year than from Svay Rieng. A small proportion of the total migrant sample (10.45%) migrated weekly, fortnightly or monthly. For eight respondents this was their first international migration.
Figure 22: Frequency of migration
4 5 6 8
66
56
4 1
9 13 13
27
8
0
20
40
60
80
number of cases
Week/fortnightly Monthly 3 or 4 per year 5 or 6 per year Twice a year Once a year Other
(n=220) Frequency of migration
Svay Rieng Banteay Meanchey

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 40
Conditions Abroad Types of Migrant Work
As illustrated in Figure 23, the largest proportion of the migrant sample (35.45%) reported begging as the main type of work for their most recent cross-‐border migration. Interestingly, as documented above, no one in the same group reported begging as their main source of income while in Cambodia. The next most frequently reported work was ‘construction’ (21.82%) followed by ‘street vendor’ (this includes selling lottery tickets and flowers and is sometimes a euphemism for begging). Smaller numbers of migrants reported small business, factory, agriculture, domestic work, hospitality and fishing as their main source of income. When comparing sources of income while in Cambodia, to the reported type of work during most recent migration, a much smaller proportion relied on agricultural work while in Viet Nam and Thailand.
5% 7%1%
17%
22%3%
35%
2%8%
Agriculture FactoryFishing Street vendorConstruction Domestic workBegging Hospital itySmall business/service
(n = 220)Main type of work
Figure 23: Type of work during last migration
Figure 24 breaks down the type of work by province and some differences were evident. Those who earn their income from begging in Vietnam were mostly from Svay Rieng, where there are fewer formal work opportunities and less demand for low-‐skilled migrants. In comparison, Thailand provides good opportunity for migrant manual labour in the construction sector. Small business, such as food shops, mechanics and factories also absorb migrants for low skilled work.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 41
Figure 24: Type of work
Living Conditions While Abroad
Of the migrant sample, a small percentage (34.08%) reported renting accommodation. This was sharing a rented house with others, renting a room with family, sharing a room with between a few and more than 8 people. 34.55 per cent of the sample reported living on the streets. Those living on the streets were four times more likely to be women (n=61) than men (n=15). 30.91 per cent reported that they lived in their workplace, of which 39 are men and 29 are women.
Time Spent Abroad
The largest proportion of migrants spent less than six months working abroad during their most recent migration. However, 90.97 per cent of women reported working abroad for less than six months compared to 72.37 per cent of men. Of those who went away for more than a year they were more often men27. When comparing by province, migrants from Banteay Meanchey were more likely than those from Svay Rieng to spend one or more years working abroad28. This is further evidence that migrants to Viet Nam from Svay Rieng province were more likely to be migrating as a short term, seasonal coping strategy.
Health of Migrants Health Risks
When comparing the perceived health risks, highlighted in Figure 25, migrants experienced greater physical and emotional risks while working abroad (72%) compared to their non-‐migrant counterparts in Cambodia (48%). This difference was significant.29
27This difference was statistically significant (χ2=15.87, df=3, p=0.001) 28This difference was statistically significant (χ2=15.97, df=3, p=0.001) 29 This was statistically significant (χ2=26.57, df=1, p=0.000)
1
10 15
3
34
3 1
47
2 5
64
14
4
17
0
20
40
60
number of cases
Agriculture Factory Fishing Street vendor Construction Domestic work Begging Hospitality Business
(n=220) Main type of migrant work
Svay Rieng Banteay Meanchey

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 42
020
4060
80pe
rcen
t
(n=438)Experienced a health risk
Non-migrants Migrants
Figure 25: Experienced health risks
Figure 26 shows, that when respondents were asked to specify their perceived health risks, the largest proportions of both migrants and non-‐migrants reported dangerous working conditions. Alarmingly, twice the number of migrants compared to non-‐migrants reported risk of physical/emotional abuse30 and limited access to healthcare.31Additionally, only migrants reported risk of being detained in crowded conditions32 and being forced to do something against their will, such as use harmful chemicals and work without safety gear.33. This evidence clearly highlights that migrants are exposed to greater health risks while working abroad.
Figure 26: Health risks at work
When comparing the health risks while working as migrants, there were no significant differences between males and females. For migrants in Thailand, it was reported that the lack of occupational health and safety protocols and equipment in factories and on construction sites, place migrants at risk of exposure to harmful chemicals or serious accidents when working on machinery or on scaffolding. It should be noted that no respondent, migrant or non-‐migrant, reported lifestyle choice or risk taking behaviour as health risks while working.
30 This was statistically significant (χ2=8.83, df=1, p=0.003) 31 This was statistically significant (χ2=14.31, df=1, p=0.000) 32 This was statistically significant (χ2=50.93, df=1, p=0.000) 33 This was statistically significant (χ2=66.24, df=1, p=0.000)
35
72
46 52
58
15
80
0
22
0 0
20
40
60
80
Migrant Non Migrant
(n=438) Health Risks while working
Physical/emotional abuse Dangerous work conditions Detained in crowded conditions Limited health access Forced to do something
num
ber o
f res
pond
ents

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 43
Experience of Detention and Abuse while Abroad
Of the total number of migrants, 83.64 per cent were arrested by authorities and returned to Cambodia. Of those migrants that returned to Cambodia on their own (16.36%) -‐ twice the proportion were from Banteay Meanchey (though many had previous detention histories). Figure 27 captures the number of migrants held in detention in each province by sex.
2 2
95
2
10
38
7
1 0
10
17
35
19
1
14
45
1 1 1
010
2030
4050
num
ber r
epor
ted
Male FemaleSvay Rieng Banteay Meanchey Svay Rieng Banteay Meanchey
(n=220)Migrants held in detention
Not held <1 month1-2 months 3-4 months5-6 months
Figure 27: Migrants held in detention
Amongst those who were arrested (n=184), the length of time spent in detention ranged from one month up to six months. Just under half were held in detention for more than one month (44.56%), with a slightly greater proportion of women compared to men. Disturbingly, 14.13 per cent of migrants were held in detention for three to four months, with nearly twice the proportion of women than men. A total of 4 migrants were detained for five to six months.
When comparing by province a significantly higher proportion of migrants from Svay Rieng were held in detention for more than one month (69.61%) compared to a majority of migrants from Banteay Meanchey being held for under one month (70.34%).34 The reason for this is likely due to the vast difference between the number of migrants hosted by Thailand and Vietnam, and the quota of detainees set for the Vietnamese authorities to initiate deportation35. Time in detention is often prolonged, and authorities wait until fifty to sixty detainees are held before initiating deportation.
When looking at treatment while in detention just over half reported being treated ‘not so well’. A greater number of migrants from Svay Rieng (46.67%) reported being treated ‘well’ compared to Banteay Meanchey (25.53%). Migrants who reported being treated ‘badly’ and ‘not so well’ were significantly more likely to be from Banteay Meanchey than Svay Rieng.36 From the reports, women were twice more likely to report being treated ‘well’ than men.37
Generally speaking, those that spend longer periods of time in detention are at higher risk of communicable diseases such as tuberculosis, especially if they are kept in crowded conditions with no access to healthcare. The questionnaire did not include specific questions about the conditions of detention, however, previous consultation with deported migrants at Poipet Immigration highlight 34This difference was statistically significant (χ2=87.99, df=4, p=0.000) 35 The quota is usually 50-‐70 detainees in the centre for their to be a scheduled deportation 36This difference was statistically significant (χ2=10.03, df=2, p=0.007) 37This difference was statistically significant (χ2=8.01, df=2, p=0.018)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 44
overcrowding in Thai detention centres to the point where deportees are unable to lay down to sleep in their cells due to the larger number of people. Other deportees have also indicated that detained migrants have limited access to outside areas for exercise.38
While working abroad, 29.09 per cent of migrants reported that they had been abused, 32 respondents from each province. In similar findings to those above, men (35.53%) were more likely than women (25.69%) to have experienced abuse while working abroad. One respondent confirmed they had been abused sexually or touched inappropriately. Five respondents indicated others had physically tortured them. It should be noted that these statistics maybe an underestimate as some respondents would not have felt comfortable discussing their experiences of abuse.
Table 5: Types of violence experienced
Total Male Female
Physical 23 12 11
Verbal 48 17 31
Sexual 1 0 1
Torture 4 1 3
Other 2 1 1 * some respondents reported multiple types of violence
More than half (n=36) of those who experienced abuse reported being abused by ‘centre staff’, twice as many were from Svay Rieng than Banteay Meanchey. Others commonly reported include abuse by police (5 in Svay Rieng and 7 in Banteay Meanchey), and employers (13 only in Banteay Meanchey).
Drug Use
Of the entire sample only two people reported injecting drugs. Both were migrants. One stated that they had shared needles. Responses were rather limited given the level of criminalization surround such practices particularly currently in Cambodia. There is no specific data to support that migrants are more exposed to this phenomenon.
Health Seeking Behaviour The following section looks at the health seeking behaviour of migrants and non-‐migrants, including migrants’ health seeking behaviour while working abroad.
Health Providers in Cambodia
Figure 28 highlights that for the entire sample, the majority of respondents reported that while in Cambodia the public health centre would be the first place they would go when they are sick. The second most commonly reported place was a private clinic and thirdly the pharmacy. The trend was the same when broken down by migrants and non-‐migrants. Only four migrants reported traditional medicine/healer as the first place they would go for healthcare.
38Group Interview at Immigration Centre, July 20th 2011

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 45
18%
27%
1%
53%
1%0%
Pharmacy Private cl inicNGO clinic Health centreTraditional healer Other
(n = 438)First place to seek healthcare in Cambodia
Figure 28: Healthcare provider in Cambodia
More than 70 per cent of the total sample sought medical care within the last six months. 7.31 per cent had never sought medical care. There was no significant difference between the last time medical treatment was sought for migrants and non-‐migrants. Of those that sought healthcare, there was however, a significant difference between the healthcare provider for migrants and non-‐migrants. A greater proportion of migrants (67.68%) sought medical care last from the public health service compared to non-‐migrants (57.49%).39 Only 2.72 per cent of the total sample sought care from NGO clinics. Gender was not a significant factor in the type of health services accessed; on the other hand location did have an effect. When looking at the entire sample, a significantly greater number of respondents overall from Svay Rieng sought medical treatment from the public health services than those from Banteay Meanchey. This however was not significant when only comparing migrants from the two provinces.
Reasons for Using Private or Public Healthcare
As seen in Figure 29, there was little variation between migrants and non-‐migrants reasons for accessing either public or private health services. A larger proportion of those who used the public health system reported reasonable cost, location, trusting staff, quality of care and medicine supply as reasons for their choice. When comparing only by choice of service there was a significantly greater proportion of respondents that used public health services, compared to those that selected private services, who stated reasonable cost as a motivating factor.
020
4060
80pe
rcen
t
Migrant Non MigrantPrivate Public Private Public
* 33 Missing values for those not sought/cant remember last health seeking/sought from NGO service
(n=394*)Reason for chosing public/private services
Reasonable cost LocationTrust staff Quality of careMedicine supply No other choiceFree Convenient hours
Figure 29: Reason for selecting public/private healthcare providers
39This difference was statistically significant (χ2=6.68, df=2, p=0.035)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 46
Experience of Illness Of the migrant sample a total of 85.45 per cent (n=188) reported illness while working abroad. The following section looks at the causes and types of illness reported by migrants and non-‐migrants.
Causes of Illness
Figure 30 illustrates that double the number of migrants compared to non-‐migrants felt that environmental factors, such as occupational hazards and poor living conditions, contributed to their ill health.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Causes of illness
Environmental factors Social factorsEconomic factors Lifestyle factorsDon't know Other
Figure 30: Causes of illness
Almost an equal number in each group reported economic factors as a cause of ill health (60 migrant and 65 non-‐migrants). Social factors, such as personal risk taking, physical and emotional abuse and fear of being arrested when accessing healthcare were higher for migrants. Lifestyle factors including substance abuse, unprotected sex, drugs and poor nutrition was reported by 51 migrants as causes of sickness, while none of the non-‐migrants reported this as a problem.
Picture 6: Government Doctors interpreting a chest X-‐ray of a returned migrant at Chipou Referral Hospital in Svay Rieng Province
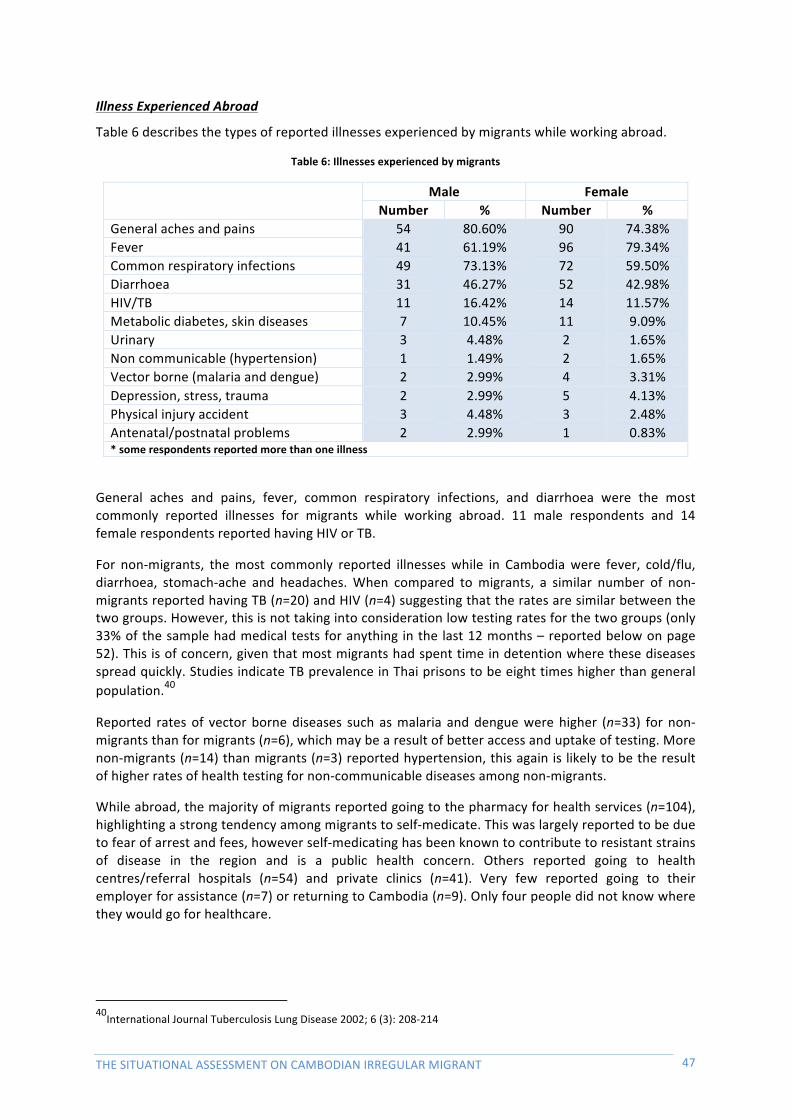
THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 47
Illness Experienced Abroad
Table 6 describes the types of reported illnesses experienced by migrants while working abroad.
Table 6: Illnesses experienced by migrants
Male Female Number % Number %
General aches and pains 54 80.60% 90 74.38% Fever 41 61.19% 96 79.34% Common respiratory infections 49 73.13% 72 59.50% Diarrhoea 31 46.27% 52 42.98% HIV/TB 11 16.42% 14 11.57% Metabolic diabetes, skin diseases 7 10.45% 11 9.09% Urinary 3 4.48% 2 1.65% Non communicable (hypertension) 1 1.49% 2 1.65% Vector borne (malaria and dengue) 2 2.99% 4 3.31% Depression, stress, trauma 2 2.99% 5 4.13% Physical injury accident 3 4.48% 3 2.48% Antenatal/postnatal problems 2 2.99% 1 0.83% * some respondents reported more than one illness
General aches and pains, fever, common respiratory infections, and diarrhoea were the most commonly reported illnesses for migrants while working abroad. 11 male respondents and 14 female respondents reported having HIV or TB.
For non-‐migrants, the most commonly reported illnesses while in Cambodia were fever, cold/flu, diarrhoea, stomach-‐ache and headaches. When compared to migrants, a similar number of non-‐migrants reported having TB (n=20) and HIV (n=4) suggesting that the rates are similar between the two groups. However, this is not taking into consideration low testing rates for the two groups (only 33% of the sample had medical tests for anything in the last 12 months – reported below on page 52). This is of concern, given that most migrants had spent time in detention where these diseases spread quickly. Studies indicate TB prevalence in Thai prisons to be eight times higher than general population.40
Reported rates of vector borne diseases such as malaria and dengue were higher (n=33) for non-‐migrants than for migrants (n=6), which may be a result of better access and uptake of testing. More non-‐migrants (n=14) than migrants (n=3) reported hypertension, this again is likely to be the result of higher rates of health testing for non-‐communicable diseases among non-‐migrants.
While abroad, the majority of migrants reported going to the pharmacy for health services (n=104), highlighting a strong tendency among migrants to self-‐medicate. This was largely reported to be due to fear of arrest and fees, however self-‐medicating has been known to contribute to resistant strains of disease in the region and is a public health concern. Others reported going to health centres/referral hospitals (n=54) and private clinics (n=41). Very few reported going to their employer for assistance (n=7) or returning to Cambodia (n=9). Only four people did not know where they would go for healthcare.
40International Journal Tuberculosis Lung Disease 2002; 6 (3): 208-‐214

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 48
Symptoms while Abroad
Highlighted in Figure 31, while abroad the most commonly reported symptoms were on-‐going fatigue (more frequently reported by women), severe headaches (more frequently reported by men) and fever. 45 per cent of men reported experiencing chest pain while abroad compared to 34 per cent of women. A large number of migrants reported specific symptoms that are clinical indications for TB; 28 per cent of males compared to 18 per cent females reported experiencing a cough for more than two weeks and 18 per cent of males and 13 per cent of females reported blood in their sputum. Eight per cent of women and three per cent of men reported herpes symptoms and another seven per cent of men and 13 per cent of women reported genital discharge, and indication of an STI.
020
4060
80pe
rcen
t
Male Female
(n=438)Reported symptoms while abroad
Cough +2 weeks
Cough blood
Severe headache
Nausea/cramps/vomitingChest pain
Weight loss
Ongoing fatigue
Fever
Skin disease
Herpes
Difficulty swallowingMental health
Severe diarrhea
Vision loss
Genital discharge
Other
Figure 31: Symptoms while abroad
Health Knowledge Knowledge of common health problems
When looking at knowledge of common health problems, illustrated in Figure 32, there was a significant difference between migrants and non-‐migrants. Migrants are less likely to have knowledge about malaria/dengue41 and typhoid.42 Similarly, migrants are less likely to have knowledge about TB.43 Among the 24 per cent of migrants that knew about STIs and Hepatitis C there was significantly higher knowledge among men than women44.
41This difference was statistically significant (χ2=6.17, df=1, p=0.013) 42This difference was statistically significant (χ2=13.88, df=1, p=0.000) 43This difference was statistically significant (χ2=5.02, df=1, p=0.025) 44This difference was statistically significant STIs (χ2=11.18, df=1, p=0.001). Hepatitis C (χ2=8.30, df=1, p=0.004)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 49
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Knowledge of common health problems: Overall
HIV/AIDS STIsInfluenza TyphoidDiarrhea/Cholera TBMalaria/Dengue Dep/Stress/TraumaHep C OtherDon't know
020
4060
80pe
rcen
t
Male Female
(n=438)Knowledge of common health problems: Migrants
HIV/AIDS STIsInfluenza TyphoidDiarrhea/Cholera TBMalaria/Dengue Dep/Stress/TraumaHep C OtherDon't know
Figure 32: Knowledge of common health problems between Migrant and Non-‐migrants and according to gender
Of the entire sample 72.15 per cent believed that they had close contact with a person with one of the illnesses/diseases described in figure 33. These people were most likely to be a family member, relative or neighbours.
Knowledge of HIV/AIDS
Figure 33 shows the ways respondents reported that HIV/AIDS could be avoided. 71 per cent of migrants and 81 per cent of non-‐migrants stated condoms were a way of preventing HIV transmission. Interestingly, staying faithful to one’s partner is a less popular choice as a way to avoid getting infected with HIV among migrants compared to non-‐migrants.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Knowledge of how to avoid HIV/AIDS
Abstain from sex Use condoms
Stay faithful to one partner Limit sexual partners
Avoid sex with prostitutes Avoid sex with those have many partners
Avoid homosexual sex Avoid sex with IDUs
Avoid blood transfusions Avoid shared needles
Don't know Other
Figure 33: Knowledge of HIV prevention
Looking within the migrant population, women had significantly lower levels of knowledge about preventing the transmission of HIV considering that 16.67 per cent said they did not know how to prevent it.45 Women also had extensively lower knowledge about preventing HIV through condom
45This difference was statistically significant (χ2=5.82, df=1, p=0.016)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 50
use46. These findings are similar to those of the 2005 Demographic Health Survey, where it was reported that men have higher knowledge of HIV prevention than women47.
Knowledge of HIV transmission and condom use as the best preventative measure is high, but practice is low. 87.61 per cent of those that responded (n=438) said that their partner had not used a condom during their last sexual encounter. A significantly higher proportion that responded no, were women.48 Of the non-‐married respondents (n=60) 83.33 per cent did not use a condom, again a higher proportion were women.49 Of those that were married (n=338) 87.87 per cent reported that they did not use a condom, a higher proportion were also women.50 Lower condom use among women corresponds with women’s knowledge of preventing transmission as described above. This data suggests that migrants are at high risk of being infected with HIV or an STI during their migration. For migrants that are single they also place future partners at risk and for those that are married it is likely they place their partners at risk when they return.
Knowledge of Tuberculosis
Figure 34 shows that knowledge about TB transmission was slightly higher among non-‐migrants. 90 per cent of non-‐migrants and 82 per cent of migrants knew that TB was airborne. 77 per cent of non-‐migrants compared to 62 per cent of migrants also stated sharing food and utensils as a transmission route for TB.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Knowledge of how TB spreads
Shaking hands AirborneSharing food/utensils Touching public i temsDon't know Other
Figure 34: Knowledge of TB transmission
A slightly lower proportion of non-‐migrants and migrants reported wearing a mask when near TB patients than those that reported it was airborne. This may be because wearing a mask is not a realistic option for everyone. However, 53 per cent of non-‐migrants and 44 per cent of migrants reported TB patients covering their coughs as another prevention method. 58 per cent of non-‐migrants and 39 per cent of migrants also reported avoiding sharing utensils with TB patients as a prevention technique. It was not asked whether respondents could identify symptoms of TB.
46This difference was statistically significant (χ2=6.41, df=1, p=0.011) 47 RGOC (2005) Cambodian Demographic and Health Survey, Ministry of Planning: Phnom Penh. 48This difference was statistically significant (χ2=17.58, df=1, p=0.000) 49This difference was statistically significant (χ2=3.30, df=1, p=0.069) 50This difference was statistically significant (χ2=12.51, df=1, p=0.000)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 51
Picture 7: IOM Project Vehicle at Poipet border

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 52
Sources of Health Information
Figure 35 shows that over half of the migrants and non-‐migrants reported the radio as their first source of health information. The second most frequently reported source for both groups was health workers, and thirdly television.
57.73%14.55%
11.36%
6.36%
60.09%12.84%
12.39%
5.05%
Migrant Non Migrant
Radio Health workersTV Family/friends/othersNewspapers/magazines Don't knowPrinted materials BillboardsLocal authorities OtherTeachers
Graphs by Migrant status
(n=438)First source of information
Figure 35: First source of health information
Figure 36 below shows that the largest proportion of both migrants and non-‐migrants reported no obstacles in obtaining health information. The most frequently reported obstacle for both migrants and non-‐migrants was lack of transport. Twice the number of migrants reported being afraid of health staff and as an obstacles, more women reported being afraid than men. Cost and no information available was also a reported among migrants as a barrier more frequently than non-‐migrants.
020
4060
80pe
rcen
t
Male Female
(n=438)Obstacles to seeking health information
Cost Technical languageDistance Afraid of health staffFear losing job Lack transportNo information available No obstaclesNo time Other
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Obstacles to seeking health information
Cost Technical languageDistance Afraid of health staffFear losing job Lack transportNo information available No obstaclesNo time Other
Figure 36: Obstacles to seeking health information
Voluntary Health Testing
Predictably a large, and similar, proportion of migrants (92.27%) and non-‐migrants (92.66%) reported that they required health testing of some description. 97.72 per cent stated they knew where to go for health testing in Cambodia – with more than 95 per cent of both migrants and non-‐migrants reported that they would go to either a public health centre or referral hospital for testing. Despite good knowledge of testing locations and a self-‐identified need, in the past twelve months only 33.33 per cent of the total sample had voluntarily gone to a health facility for health testing of any kind. Of those that had health testing a significantly larger proportion were migrants51. Looking 51This difference was statistically significant (χ2=10.09, df=1, p=0.001)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 53
at data for previous questions, it is likely that fear of arrest and cost were obstacles for those migrants who did not have health testing done while abroad. A slightly higher number of migrants (89.88%) had health testing done at public health centres and referral hospitals than non-‐migrants (71.93%). Double the proportion of non-‐migrants (24.56%) compared to migrants attended private clinics for health testing.
Figure 37describes the types of health tests voluntary taken by migrants and non-‐migrants in the past twelve months. A greater proportion of migrants reported being voluntary tested for TB, HIV and Hepatitis C than non-‐migrants.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Tests in past 12 months
Sputum smear (TB) HIVHepatitis C STINone
Figure 37: Health testing in the past 12 months
Figure 38 shows that migrants and non-‐migrants reported similar levels of awareness about HIV and TB services. However, 25 per cent of migrants had no awareness of HIV or TB services. For those who were aware of specific HIV and TB services the largest proportion were aware of free medicine being available for HIV and TB patients, followed by food support and free testing and diagnosis at Voluntary Confidential Counseling and Testing (VCCT) facilities. Very few respondents were aware of directly observed treatment short-‐course for TB patients and HIV networks.
020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Awareness of HIV and TB services
Free diagnosis Free medicineHIV+ networks Food for HIV/TB patientsDirectly observed treatments (DOTS) Don't know
Figure 38: Awareness of HIV and TB healthcare services

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 54
Illustrated in Figure 39, migrants are less likely than non-‐migrants to talk to their spouse about TB, HIV and STIs. The most frequently reported person for both groups was doctor/medical worker. Amongst both migrants and non-‐migrants, around 30 people reported they would speak to their parents or other family members.
0.87
0.54
0.30 0.31
0.15
0.00 0.01
0.87
0.77
0.33 0.34
0.11
0.00 0.00020
4060
80pe
rcen
t
Migrant Non Migrant
(n=438)Person to talk to if had TB/HIV/STI
Doctor/medical worker SpouseParent Other family memberClose friend No oneOther
Figure 39: Who would you talk to if you had HIV, STIs or TB
The majority of both migrants (82.27%) and non-‐migrants (86.70%) reported that they would seek treatment as soon as they realized that they might have TB, HIV or STI symptoms. Only a small number of migrants (2.73%) reported that they would not go to the doctor. Other respondents reported that they would go to the doctor when self-‐treatment did not work (4.11%), when symptoms lasted longer than three to four weeks (3.88%) or when they could no longer work (5.48%). There was not a significant difference between migrants and non-‐migrants in these categories.
When asked about their immediate health needs at the time of interviewing, 52.05 per cent of the total samples report that they required a health check and treatment. The second largest proportion, 29.91 per cent, reported that they had no immediate health needs. There was no significant difference between the immediate needs of migrants and non-‐migrants.
Future Plans for Migration Of the migrants 40.91 per cent stated that they would continue to migrate abroad for work. There was no significant difference between Svay Rieng and Banteay Meanchey. Of those that reported they would migrate again for work (n=90) 31.11 per cent stated earning money to pay off debt as the main reason and 21.22 per cent reported future migration due to lack of family income. 16.67 per cent reported lack of job prospects in Cambodia and 15.56 per cent stated earning money to support their family as reasons why they would continue to migrate.
Table 7 describes where migrants reported they would go now they are back in Cambodia.
Table 7: Future plans of migrants
Where Number % Return to home province 122 55.45% Return to current place of residence 66 30.00% Migrate back to Thailand or Viet Nam 24 10.91% Migrate within Cambodia to another province 3 1.36% Stay on the border are and look for work 2 0.91% Other 3 1.36%

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 55
Of the migrants that stated they would not continue to migrate for work (n= 130) more than half (56.92%) reported fear of arrest and detention as the motive. The second largest proportion (6.92%) reported difficulty in finding work abroad as the reason. Only 2.31 per cent reported health problems as a deterrent.
Picture 8: Garment Workers returning Home from work at local factories on the border in Svay Rieng Province
HEALTH STAFF
Demographics To gain better understanding about the healthcare service delivery available in Cambodia to returned irregular migrants 105 government health workers and village health volunteers were interviewed. Of those who were interview 60 per cent were males and 40 per cent were females.
Figure 40 illustrates that the most common age of healthcare workers in the sample was 40 – 49 years. The next most prevalent age was 30 -‐39 years.
1%13%
27%
39%
18%
2%
18-19 years 20-29 years30-39 years 40-49 years50-59 years 60-66 years
(n = 105)Age of health workers
Figure 40: Age of healthcare workers

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 56
Position and training
Described in Figure 41, nurses made up just under half of the sample (46%), as did village health volunteers (40%). A small proportion of the sample was midwives and doctors.
4%
46%
7%
40%
4%
Doctor NurseMidwife Village Health Support WorkerOther
(n = 105)Positions of health workers
Figure 41: Position of healthcare workers
Illustrated in Figure 42, the largest proportion of medical staff had completed 7 to 8 grades of schooling (34.29%). With another 20.95 per cent having completed upper secondary school. It is not clear whether anyone in the sample completed university level education; this may be a result of how the question was formulated.
12%
10%
34%11%
11%
21%
1-5 grades 6 grades7-8 grades 9 grades10-11 grades 12 grades
(n = 105)Highest year of school
Figure 42: Highest year of schooling
Figure 43 illustrates the type of training that healthcare staff had received. All but 2 staff had received training of some description. The most common type of training was basic counselling for HIV/AIDS and TB drugs, followed by dissemination of health information and referring and counselling and testing for Prevention of Mother to Child Transmission (PMCT).

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 57
020
4060
80pe
rcen
t(n=105)
Training received by staff
VCCT Counselling and testing for PMTCT
Pre-service counselling and testing training Diagnostic counselling and testing (DCT)
Basic counselling for HIV/AIDS or TB drugs Management of patients on ARV or TB drugs
Management of oportunistic infections Home based care for HIV/AIDS patients
Direct observation treatment (DOTS) Community DOTS
Disseminating health information and referring ARV or TB program management
Other
Figure 43. Training received by healthcare staff
Figure 44 highlights that most healthcare workers had received training within the last 6 months (68%).
21%
27%
20%
7%
8%
14%2%2%
Less than 1 month 1-3 months3-6 months 6-9 months9-12 months More than 1 yearDon't remember Never
(n = 105)Last time you received training?
Figure 44: Last time workers received training
Figure 45 shows the future training needs of the healthcare workers. The most commonly reported training requirements was in the area of basic counselling for HIV/TB, dissemination of health information, VCCT training and Community DOTS.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 58
020
4060
80pe
rcen
t
(n=105)Further training needed
VCCT Training Counselling/testing for PMTCT
Pre-service counselling and testing training Diagnostic counselling and testing
Basic counselling for HIV/TB Management of patients on ARV/TB drugs
Management of opportunistic infections Home based care for HIV
DOTS CDOTS
Dissemination of health info ARV/TB program management
Other
Figure 45. Types of training needed
Healthcare setting and resources Graphs in this section depict responses from facility based health care workers (n=63), which exclude village health support group workers. Illustrated in Figure 46, few health workers indicated that essential supplies were not available to them.
0
3
2
3 3
4
3
01
23
4
num
ber
(n=63)Supplies not available
Gloves Gowns
Disposable sharps container Bleach solution
Soap Running water
Essential medicines
Figure 46: Supplies not available to health workers
Seen in Figure 47, over 50 per cent of healthcare workers stated that essential medicine was in short supply. Gloves, bleach solution, soap and running water were also reported to be inadequate in almost a quarter or more of cases.
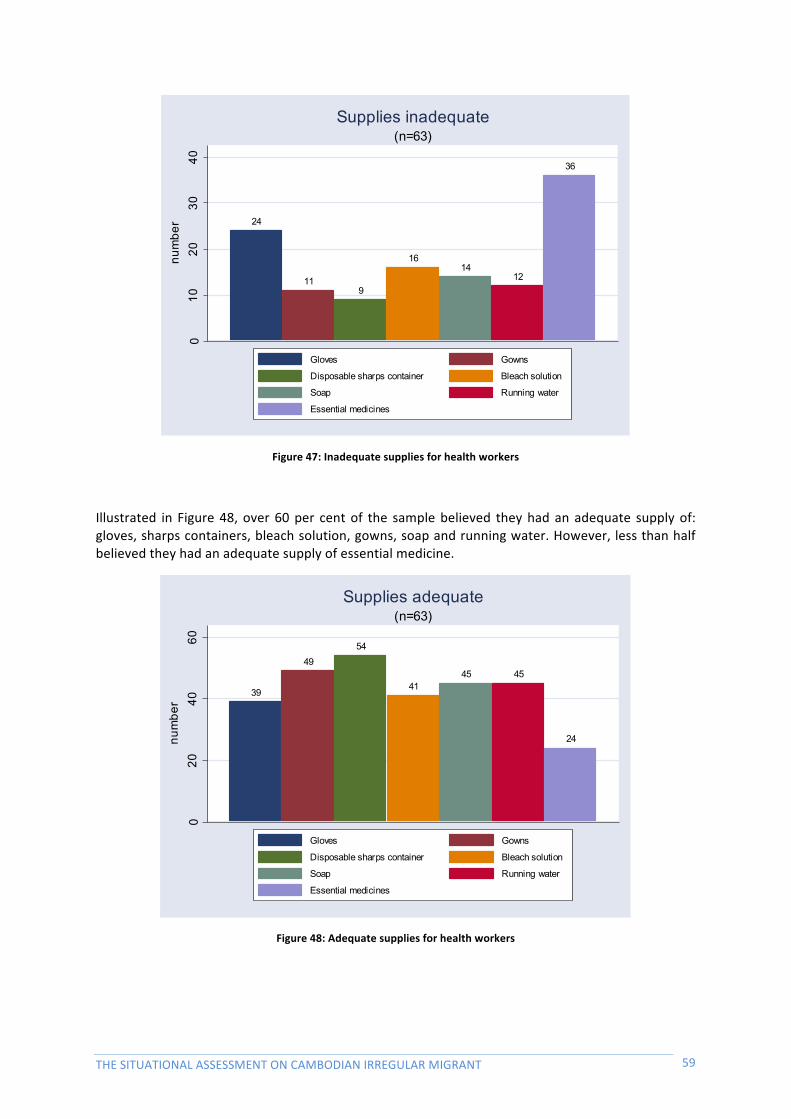
THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 59
24
119
1614
12
36
010
2030
40nu
mbe
r
(n=63)Supplies inadequate
Gloves Gowns
Disposable sharps container Bleach solution
Soap Running water
Essential medicines
Figure 47: Inadequate supplies for health workers
Illustrated in Figure 48, over 60 per cent of the sample believed they had an adequate supply of: gloves, sharps containers, bleach solution, gowns, soap and running water. However, less than half believed they had an adequate supply of essential medicine.
39
4954
4145 45
24
020
4060
num
ber
(n=63)Supplies adequate
Gloves Gowns
Disposable sharps container Bleach solution
Soap Running water
Essential medicines
Figure 48: Adequate supplies for health workers

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 60
Common Health Problems
Table 8 describes the most common health problems reported by healthcare workers.
Table 8: Most common health problems reported by healthcare workers
Problem Number TB 88 Respiratory 41 HIV/AIDS 38 STIs 29 Diarrhoea 23 Fever 22 Cold/flu 19 Antenatal 18 High blood pressure 17 Typhoid 14 Malaria 10 Other physical 10 Depression 9 Road accident 9 Other 8 Dengue 7 Diabetes 5 Postnatal 4 Skin disorders 3 Urinary 3 Headache 2 Eye/Ear 1 Stomach ache 1
Illustrated in Figure 49, healthcare workers viewed the most common cause of illness as living conditions, lack of income, poor nutrition and personal risk taking.
020
4060
80pe
rcen
t
(n=105)Perceived causes of most common illnesses
Unsafe employment Living/housing conditions
Personal risk taking Physical/emotional abuse
Lack income Lack access to higher paid work
Substance abuse Risky behaviour
Poor nutrition Don't know
Other Climate change
Figure 49: Perceived main cause of illnesses

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 61
Figure 50 shows the types of service offered to HIV and TB patients by the healthcare workers. The most commonly reported services were free medicine and food for TB and HIV patients. Free diagnosis was also offered by over 70 per cent of the healthcare workers.
020
4060
80pe
rcen
t(n=105)
Services offered to HIV or TB patients
Free diagnosis Free medicine
HIV+ networks Food for TB/HIV patients
DOTS Don't know
Other
Figure 50: Services offered to HIV or TB patients by health workers
Healthcare workers reported 24-‐hour service (n=21), adequate medicines (n=16) and staff commitment (n=12) as the main strengths of the public health care system. Areas that were most commonly reported as needing improvement were limited capacity of health facility (n=61) and poor quality of care (n=19).
Healthcare workers experience with irregular migrants Of the healthcare worker sample 83.81 per cent stated that they had come across Cambodians who had migrated across the border during their work and 16.19 per cent of healthcare workers had not.
Figure 51 shows that the majority of healthcare workers believed that the first place irregular migrants sought healthcare in Cambodia was at public health facilities (Health centres 76 per cent and Referral hospitals 3 per cent). A smaller proportion believed that some sought healthcare at private clinics (10%) and pharmacies (10%).
10%
10%
3%
76%
1%
Pharmacy Private cl inicReferral hospital Health centreOther
(n = 105)First place to seek healthcare
Figure 51: First place migrants seek health care

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 62
Demonstrated in Figure 52, most healthcare workers felt that irregular migrants selected health services based on reasonable cost (62%). Other common reasons were trust in health personnel (45%), location of service (40%) and quality of care (49%).
0.62
0.400.45
0.49
0.26
0.060.10
0.00
0.24
020
4060
80pe
rcen
t(n=105)
Reason for chosing health services
Reasonable cost Location of services
Trust health personnel Quality of care
Regular supply of medicine No other choice
Free service Convenient working hours
Other
Figure 52: Perceived reason irregular migrants selected health services
The three most commonly reported special health needs of migrants reported by healthcare workers were health screening/treatment (62.85%), health education (10.47%) and pregnancy checks (9.52%).
Table 9 shows the five more commonly reported challenges by healthcare workers to providing care to cross-‐border migrants
Table 9: Challenges of providing healthcare to cross-‐border migrants
Challenge Number Frequent movement 23 Migrants do not want to participate 13 Lack of care takers 12 Poverty 12 Difficult to take care and provide counselling to them 10
Shown in Figure 53, 60 per cent of healthcare workers believed that radio was the most effective form of media to reach migrant populations with health information. The second largest proportion believed that television (23%) was also an effective source.
60%23%
1%6%
10%
Radio TVBillboards Printed materialHealth workers
(n = 105)Most effective source of information
Figure 53: Most effective source of health information to reach migrants

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 63
Picture 9: Data collection Team (from left to right: Dr Leuk Sambath, Mr. Ta Hear, Mr. Orn Chanry, Mr Keo Samnang, Mr Hem Saporn, MrHeung Kleung, Ms. Ron Sarom, Mr Toch Sopheap, Mr Nuth Sam Ol, Dr Ke Samut, Mr Phiev Khay) in
Nimit commune, Banteay Meanchey Province

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 64
Chapter IV: Discussion on Findings
Differences in Cross-‐border Migration Trends and Irregular Migrant Groups
The demographics of age highlight the different migrant trends in Svay Rieng and Banteay Meanchey, the two border provinces with the highest population mobility in Cambodia. Migrants going to Thailand appear to be a much younger mobile migrant group compared to other migrants going to Viet Nam who appear to be more middle-‐aged and predominantly married women. The migration from Svay Rieng to Viet Nam is mostly women due to the nature of begging activities in Viet Nam being more profitable if led by females and their small children.
Overall, most migrants spend less than six months abroad. Women are more likely to stay less than six months compared to men, while men are more likely to migrate longer-‐term. For Svay Rieng, cross border migration appears to be more of a short-‐term coping strategy on seasonal basis to pay back household debt and overcome health and socio-‐economic problems. For Banteay Meanchey, cross-‐border migration is more of a long-‐term strategy to Thailand where there is a greater demand for low skilled migrant labour for people in search of a better job and income.
The majority of irregular migrants returned are undocumented. Many irregular migrants lack the most basic form of identification, such as Cambodian National Identification Cards. This finding highlights the particular trend that most long-‐distance cross-‐border migration is via informal channels that appear to be cheaper and less bureaucratic compared to regular legal channels. This finding also highlights a lack of information on the legal process to migrate among this migrant group.
Living situations abroad are mostly rental accommodation or living at workplace. A third of migrants reported living on the streets and those living on the street were four times more likely to be women.
In regards to education, non-‐migrants were more likely to have completed their primary and secondary education compared to migrants. The lack of both primary and secondary certificates among migrants greatly reduces chances in a competitive job market for skilled labour, it also potentially increases the likeliness of them considering opportunities to join low skilled migrant labour abroad. Lower educational levels are also strong social determinants regarding accessing health information and healthcare.
Types of work abroad contrasted from types of work while in Cambodia. Abroad, the largest proportions of migrants were begging, followed by construction and street vendors. While in Cambodia, majority were involved in agriculture and no one reported begging while in the country.
Again the type of work differs between the two provinces. Most of the migrants from Svay Rieng province are women going for begging in Viet Nam, while in Thailand migrants are mostly involved in construction work. This is consistent with the demand for low skilled migrant labour in Thailand compared to Viet Nam.
Socio-‐Economic Push factors leading to Migration
The findings strongly support and reaffirm that certain socio-‐economic push factors that are known social determinants of the health of migrants52 are driving cross-‐border migration, such as lack of employment opportunities at home for a growing workforce; landlessness; accumulative household debt to pay for health care. Equally, the pull factors were highlighted such as better jobs and income in the destination, as low skilled migrant labour.
From the findings, three major push factors for migration appear strongly, namely:
1) Lack of agricultural land tenure creates a sense of instability, insecure employment, absence of income and subsistence.
52 Davies, Dr Anita, Basten, A & Frattini, C (2009). Migration: A Social Determinant of the Health of Migrants, IOM Geneva.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 65
A strong push factor for migration, the findings support the notion that certain push and pull factors to migrate, internally or cross-‐border, are often interconnected and related to peoples’ ability to cope with overwhelming socio-‐economic issues, including ability to afford basic needs: shelter, food and health care. Migrants were twice as likely to have lost or sold agricultural land compared to non-‐migrants. Their land was sold reportedly to pay back outstanding debt, pay for basic needs, including health care and treatment.
2) Household debt for basic needs, including health care and treatment
Significantly, migrants were found more likely to have household debt as reported in previous studies and publications. Migrants were more likely to have four or more loans at one time, indicating a continuous cycle of debt. These findings support the assumptions that household debt is another major factor pushing Cambodian people to migrate for work.
The high number of migrants in debt indicates money lending is common among migrant households. Capacity to save or invest the loans is low indicated by the use of loans to pay for basic needs. Migrants were more likely to take out loans for healthcare. Migrants were more likely to use migration as a strategy to pay back debt.
3) Lack of secure employment and regular income.
Migrants appear to have less consistent work and regular income throughout the year compared to non-‐migrants. Migrants have much lower average income, particularly in Banteay Meanchey province. This highlights poor economic factors leading to migration. This finding also reflects migrants’ limited ability to pay for and access healthcare.
The Overall Health of Irregular Migrants
Migrants are more likely to be exposed to certain health risks, such as dangerous working conditions while abroad. The health risks abroad were mostly associated with lack of occupational health and safety in the workplace.
Periods of detention pose one of the major risks to migrant health. Migrants in Vietnam spend longer periods in detention compared to migrants in Thailand. Conditions in detention centres are a considerable factor when analysing the health risks. Generally speaking those that spend longer periods of time in detention are at higher risk of airborne infectious diseases such as tuberculosis, especially if they are kept in crowded conditions with no access to healthcare.
Causes of illness are much more diverse among migrants suggesting the circumstances of irregular migration contribute to increased health risks and illness. Migrants indicated more social and lifestyle factors compared to non-‐migrants. Migrants were more exposed to physical and emotional abuse, detention, substance abuse, unprotected sex and poor nutrition. A third of migrants experienced either physical or verbal abuse while abroad. Migrant men were more likely exposed to these health risks than women.
Health seeking behaviour in Cambodia between migrants and non-‐migrants is generally the same. The first most commonplace migrants would seek health care is from a public health centre, the second most common place would be a private clinic and third, a pharmacy. Health workers interviewed indicated and confirmed this health seeking behaviour trend exists among migrants.
Most migrants and non-‐migrants chose the public health system reportedly for the reasonable cost, location, trusting staff, quality of care and medicine supply. The choice between public over private was largely determined by the cost of health care. Migrant health seeking abroad greatly differs from at home. There was a strong tendency to self-‐medicate while abroad largely due to fear of arrest if intercepted by Thai authorities as irregular migrants.
General aches and pains, fever, common respiratory infections, and diarrhoea were the most commonly reported illnesses for migrants while working abroad. For non-‐migrants the most commonly reported illnesses while in Cambodia were fever, cold or flu, diarrhoea, stomachache and headaches. Both migrants and non-‐migrants reported similar health problems regarding tuberculosis

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 66
and HIV although a larger number of migrants reported clinical symptoms of TB that raises concern when considering risk factors associated with long periods in detention centres with crowded conditions.
For health care workers the most common health problems differed from the migrants and non-‐migrants, tuberculosis and respiratory disease were the most common health problems they treated followed by HIV and STIs as the top most common health problems in the border areas.
Migrant women had significantly lower levels of knowledge about preventing the transmission of HIV compared to men. Single migrant women were much less likely to have used a condom in their last sexual encounter. This data suggests that migrants, particular women, are at high risk of being infected with HIV or an STI before, during and upon returned from their migration. For migrants that are single there is potential future risk of infection to partners and for those that are married it is likely their partners face the same risk of infection if un-‐checked upon return.
The first most frequent reported source of health information for both migrant and non-‐migrant was the “radio” and second most frequently reported source was “health workers”, and third the “television”.
Both migrants and non-‐migrants are equally concerned about their health and require a health test. In the past twelve months, only a small proportion has been tested. Migrants show to be tested for TB, HIV and Hepatitis C more than non-‐migrants possibly visiting health services upon return due to having no access to such health testing abroad. Health workers highlighted three most commonly reported special health needs of migrants were health screening and treatment, health education and pregnancy checks.
In light of the World Health Assembly resolution of the health of migrants and the strong recommendations from the Dialogue on the Health of Asian Labour Migrants held in Bangkok in July 2010, IOM together with WHO have begun to strengthen key partnerships with the Ministry of Health and the National TB Programme managed by the National Centre for Tuberculosis and Leprosy Control (CENAT), to actively screening for TB among returning irregular migrant workers and guaranteeing adequate management of migrant TB cases detected.
Although national and provincial consultations have been held, continued encouragement and support to relevant government ministries to review existing policies, laws and practices related to labour migration and health, is crucial in achieving an overall coherence among policies that may affect migrants’ health and their ability to access services. This is most evident in light of the recent Cambodian Prime Minister’s ban on recruiting and sending labour migrants a decision based on continued reports of abuse and violation of rights of recruitment agencies in Cambodia and abroad. Without the encouragement and support of international agencies and NGOS in reviewing certain policies and mechanisms to protect potential and returned migrants, abusive practices and vulnerabilities to exploitation will continue to profoundly impact on the physical and psychological well being of migrants. Through this field research, IOM has worked with the department of communicable disease control under the MoH and identified a focal entity for migration health and continues to work with other concerned ministries tasked to initiate inter-‐ministerial and cross-‐sectoral dialogue. This has been proven to be difficult at the national level compared to provincial levels. Certain inter-‐ministerial collaboration between health and immigration departments at major border points engaged in these active TB screenings are forging a model of future inter-‐ministerial collaborations that have the potential to strengthen mechanisms for health education and delivery of health services upon return, including safe migration and reintegration information, covering all major points of the migration process.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 67
Chapter V: Conclusion & Recommendations
Cambodian cross-‐border migration to Thailand and Viet Nam is likely to continue increasing and while cross-‐border migration can provide improved economic and livelihood opportunities there are also risks. Irregular migrants are a high-‐risk population for communicable diseases such as TB, STIs and HIV. Poor living conditions, limited access to healthcare, and exploitation as a result of having no formal documentation greatly increase migrants’ vulnerability. However, it is unlikely that any of these factors will be a deterrent for cross-‐border migration for those in the poverty trap and mitigating these risks is important. Below are key conclusions from the Situational Assessment.
Vulnerability of undocumented migrants
Under the law, undocumented migrants do not receive any form of protection in receiving countries. The fear of deportation and detention leaves irregular migrants vulnerable to harassment and exploitation. As cross-‐border migration from Cambodia increases, it will be important to address migrant needs for support and also work towards documented migration as a realistic alternative for these populations. Following the MOU on Cooperation in the Employment of Workers signed between Cambodia and Thailand to reduce illegal and unsafe migration it will be important to continue to support the government in promoting legalization and protection regarding all migrants.
Time spent in detention high risk factor to TB
When irregular migrants are arrested it is likely they will spend time in detention before being repatriated to Cambodia. Detention conditions are often overcrowded, unhygienic and violent, and places migrants at great risk of communicable disease, such as Tuberculosis. Without active TB case detection and screening of returnees, these diseases may spread amongst border communities in higher rates.
Poor HIV prevention practice
While knowledge of HIV prevention is good among migrants, condom use during sexual encounters is low. This is of great concern, especially when considering the higher HIV rates in Thailand. A greater understanding of the decision-‐making processes and barriers regarding condom use and other prevention practices among irregular migrants, coupled with interventions to improve practices will best prevent transmission of HIV and STIs in this group.
Frequency of cross-‐border migration
Frequency of migration may provide an opportunity to link returned irregular migrants to health services, including testing at the border immigration centres receiving returned migrants. Given the strong desire of irregular migrants to get health testing, it is likely, if barriers are reduced, that more irregular migrants will access healthcare on their return. Creating supportive environments will be the key.
Recommendations
In light of the study findings, and in the background of the WHA resolution and the framework for migration health [Madrid 2010 report], the following recommendations are proposed –
(I) Monitoring migrant health
1. Promote and support voluntary HIV, TB and STI testing of returning migrants through Government health services in the two border provinces and guarantee adequate management and treatment of potential diseases or infections.
2. Integrate data collection on health of returned migrants in Cambodia within existing national and local surveillance and public health systems.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 68
3. Ensure that feedback from returning migrants is included in pre-‐departure orientation and awareness-‐raising activities with the active participation from migrants themselves.
(II) Migrant-‐sensitive health systems
1. Continue to support existing and potential focal points for migration health within concerned ministries tasked to initiate inter-‐ministerial and cross-‐sectoral dialogue.
2. Promote better understanding of migrant health concerns, including barriers to accessing health services encountered by migrants throughout the migration cycle, among the health workforce, embassies, partner organizations and other stakeholders.
(III) Policy and Legal frameworks
1. Strongly encourage and support relevant government ministries to review existing policies, laws and practices related to labour migration and health, aiming at an overall coherence among policies that may affect migrants’ health and their ability to access services.
2. Present and analyse Migrant Health data through the Health Secretariat and
3. Develop and provide a basic package of safe migration information on legal rights, health and services to better prepare, protect and inform migrants before they migrate.
(IV) Partnerships
1. Further develop inter-‐ministerial collaboration, including UN partners and NGOs, to strengthen mechanisms of health education and delivery of country-‐ and occupation-‐specific information, covering major health risks, prior to overseas travel for employment.
2. Collaborate and coordinate with Government authorities and civil society organizations in the two border provinces on issues related to protection of the rights of all migrant workers and their families, with special attention to health issues.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 69
Bibliography
Biddulph, (2004), IOM Situation Report on Migration in South East Asia, 2008, Return of Cambodians from Viet Nam.
Chan, S (2009). Costs & Benefits of Cross-‐Country Labour Migration in the GMS: A Cambodian Case Study. Cambodian Development Research Institute, CDRI.
Dickson, B. (2010). A Situational Assessment of Cambodian Families and Children in Svay Rieng Province going for begging in Viet Nam. IOM: Phnom Penh, Cambodia.
Davies, Dr Anita, Basten, A & Frattini, C (2009). Migration: A Social Determinant of the Health of Migrants. IOM Geneva.
International Organization for Migration, (2011). Key Migration Terms. Retrieved 12/09/2011 from www.iom.int.
International Organization for Migration, (2008). Regional Thematic Working Group on International Migration including Human Trafficking, 2008. Situation Report on International Migration in East and South-‐East Asia. IOM: Regional Office for Southeast Asia
Kavenagh, M. & Buller, K. (2010). The Landscape of Migration in four districts of Svay Rieng Province. Child Fund: Phnom Penh, Cambodia.
Maltoni, B. (2007). Migration in Cambodia: Internal Vs. External Flows: 8th ARPMN Conference on “Migration, Development and Poverty Reduction”, in Fuzhou (China), 25-‐29 May 2007. IOM: Phnom Penh, Cambodia.
Maltoni, B. (2006). Review of Labour Migration Dynamics in Cambodia. IOM: Phnom Penh, Cambodia.
National Committee for sub-‐National Democratic Development NCDD, (2009). Chantrea, Kompong Ro & Bavet District Data Books 2009, Svay Rieng Province. NCDD: Phnom Penh, Cambodia.
National Committee for sub-‐National Democratic Development NCDD, (2009). O’Chrov Poipet District Data Books 2009, Banteay Meanchey Province. NCDD: Phnom Penh, Cambodia.
National Institute of Statistics (2009). General Population Census of Cambodia 2008. National Institute of Statistics, Ministry of Planning: Phnom Penh, Cambodia.
PATH. (2010). Catalyzing healthier labor migration. Working on health and development in source communities in Cambodia and destinations in Thailand. PATH: Phnom Penh, Cambodia.
Phiev, K. (2004). Needs Assessment and Situational Analysis of Migration and Trafficking from Svay Rieng Province, Cambodia to Vietnam for Begging: The Long-‐Term Recovery and Re-‐integration Assistance to Trafficked Women and Children Project. U.S. Department of State, Bureau of Population, Refugees and Migration.
Phiev, K (2009). Situation Assessment for Preparedness for Pandemic and Other Emergencies among Migrants and Host Communities in Svay Rieng. IOM: Phnom Penh, Cambodia.
Sciortino, R & Punpuing, S (2009). International Migration in Thailand. IOM: Thailand.
Srivirojana, N. and Punpuing, S. (2009). Health and Mortality differential among Myanmar, Laos and Cambodia Migrants in Thailand.
Social Development Research & Consultancy (SRDC), (2002). A Study on the Situation of Cambodian Victims of Trafficking in Vietnam and Returned Victims of Trafficking from Vietnam to Cambodia: IOM Return and Reintegration of Trafficked and Other Vulnerable Women and Children Between Selected Countries in the Mekong Region. AusAID and IOM: Ho Chi Minh City, Vietnam.
Thailand Ministry of Labour (2011). Statistics on Migrant Workers. Royal Government of Thailand, Office of Foreign Workers Administration, Department of Employment, Ministry of Labour: Thailand.
World Health Organization, (2010). Health of migrants: the way forward -‐ report of a global consultation. WHO: Madrid, Spain.
61st World Health Assembly. (2008) Health of Migrants, Secretary Report 2008.

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 70
Annex A: Source Villages for Migrants and Non-migrants
Migrants
Province Village Number Percentage
Svay Rieng Kbal Thnol 34 15.45%
Svay Rieng Bon 11 5.00%
Svay Rieng Chantrea 3 1.36%
Svay Rieng Taeng Mao 20 9.09%
Svay Rieng Tuol Ompil 10 4.55%
Svay Rieng Trapang Run 4 1.82%
Svay Rieng Tuol Spean 7 3.18%
Svay Rieng Thom 5 2.27%
Svay Rieng Prasab Leak 5 2.27%
Svay Rieng Koul Laveang 3 1.36%
Banteay Meanchey Procheathom 26 11.82%
Banteay Meanchey Kbal Spean 30 13.64%
Banteay Meanchey Palelai 57 25.91%
Banteay Meanchey Oreusey 5 2.27%
Total 220 100%
Non-‐migrants
Province Village Number Percentage
Svay Rieng Thnal Kaeng 13 5.96%
Svay Rieng Traok 17 7.80%
Svay Rieng Trapang Run 15 6.88%
Svay Rieng Po Maam 20 9.17%
Svay Rieng Prey Robeus 19 8.27%
Svay Rieng Trapeang Deakraom 15 6.88%
Banteay Meanchey Dong Aranh 27 12.39%
Banteay Meanchey Kon Domrey 25 11.47%
Banteay Meanchey Nimit Muoy 20 9.17%
Banteay Meanchey Sorya 47 21.56%
Total 218 100%

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 71
Annex B: English Versions of Questionnaire
1. Migrant Questionnaire
Hello. My name is ……………………………… and I work for …….. We are conducting a survey on health issues. I would like to ask you a few questions on your migration experience and the circumstances that led to possible health problems you may have encountered. There are no risks or direct benefits to you from participating in the survey but your participation will contribute to improving health services for migrant in health facilities and develop other health and social services for migrants.
You would need about ……minutes to answer these questions. Please be assured that the information will be confidential and will not be shown to other persons and you may choose to stop your participation at any time or refrain from answering any questions. However, we hope that you will participate in this survey and answers the questions openly and honestly because your opinions are very important to us. If you have questions of your own please feel free to ask.
Would you like to participate in the interview now? ( Yes No)
Interview Date ____/___/20______
DD MM YYYY
Name of Interviewer
Place of Interview Village: __________________ ;
Commune: ____________________ ;
District ______________________ ;
Province ________________________
Sex of Respondent Male (1) Female (2)
Starting Time: ______________________ End Time: _________________________
Checked by supervisor: __________________ Signature: ______________________
Date: ____/____/20____ Time: __________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 72
1. General Demographic
1.1 How old are you? [………..] Years
1.2 What is your current Marital Status? (Tick answer)
Single/Never Married (1) Separated (2) Widowed (3) Married (4) Divorced (5) Refuse to answer (6)
1.3 How many family members do you support financially? (Children, Parents, Siblings, Grandparents, Wives etc.)
________Family members (dependents)
1.4 Have you ever attended school?
Yes (1) No (2) (If No, go to Q1.6)
1.5 What is your highest grade of education complete? (need to probe if Old or New grading system) (Tick Box)
OLD Grading System (1) NEW Grading System (2) [………….] Grades completed (To be circled by supervisor)
1. Some primary (1-‐3 grades) 2. Completed Primary School (6 grades) 3. Some lower Secondary (7-‐8 grades) 4. Completed Lower Secondary School (9 grades) 5. Some Upper Secondary (10-‐11 Grades) 6. Completed Upper Secondary School (12 grades) 7. University any level 8. Technical / Vocational
1.6 Where is your permanent address?
Village: __________________ Commune/Sangkat: ____________________
District/City: ______________________ Province: ________________________
1.7 Where are you living now?
Village: __________________ Commune/Sangkat: ____________________
District/City: ______________________ Province: ________________________
1.8 How long have you been living in your current place?
_________Years (1) _________ Months (2) _________Weeks (3)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 73
2. Socio-‐economic Background
2.1 What is your living situation like in Cambodia? (Tick one answer)
Own house & plot (1) Own house but not plot(2) Rent a house(3) Rent a room(4) Live with relative/friend(5) Live in a house of someone without paying rent(6) Live in the work place (7) Lived on the streets (8) Homeless living under temporary structure(9) Other__________________________(99)
2.2 What is the housing material like? (Tick one answer)
Good (tiles/brick/concrete)(1) Adequate (wood/corrugated iron)(2) Poor(thatch/palm leaves/plastic sheet)(3)
2.3 Do you currently have agricultural land? (Rice, Chamcar etc.)
Yes (1)-‐> Owned (a) or Rented (b)? __________________ No (2)
2.4 Have you sold or lost agricultural land in the past?
Yes (1) -‐> what was reason for this decision/loss? __________________________ (a) No (2)
2.5 What are your main sources of income while in Cambodia? (Tick more than 1)
Agriculture(1) Factory(2) Fishing(3) Seller/small business(4) Construction(5) Domestic work(6) Begging(7) Sex work(8) Moto taxi/cart puller(9) Unemployed(10) Other(99) ______________________________________________________________
2.6 How regular are these sources of income throughout the year?
All year round (1) Dry Season (2) Wet Season (3) Day to day basis (4) Irregular (5)
2.7 On average how much can you earn from these income sources per day? month? year?
………………….. Riel(1) ………………..Baht(2) ………...……..Dong(3) ……………..USD(4)
2.8 Which of the following better describes the financial position of your family?
(Tick one answer) We do not have enough money(1) We have enough money for food(2) We have enough money for food and healthcare(3) We can pay for most food, health & education needs(4) We can cover all family needs and extra things we need(5)
2.9 Does your household have any outstanding loans or debts to repay?
Yes (1) No (2) (If No, go to 3.1)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 74
2.10 How many moneylenders do you owe these loans/debts too?
Number of Debtors: _________ Who? (a)-‐> Parents/Relatives (1) Friends (2) Neighbours (3) Informal Money Lenders (4) Banks/ Microfinance Firms/Credit (5) NGO (6) Other (99) ___________________________________________
2.11 What are these loans/debts for? (Tick more than one)
Basic needs (Food, Shelter) (1) Healthcare/treatment (2) Children’s Education (3) Livelihood inputs (agriculture e.g.) (4) Buy back/or rent land (5) Family Ceremonies (Weddings, Funerals e.g.) (6) Pay off other Loan/debt repayments (7) Migration (Travel costs) (8) Other(99) ________________________________________________________________
2.12 What is the total amount of these loans/debts?
………………….. Riel(1) ………………..Baht(2) ………...……..Dong(3) ……………..USD(4)
2.13 What are you expecting to do to settle the loans/debts?
Will try to work and save money (1) Will send family members to work (2) Will migrate myself to look for work (3) Sell my land (4) Take out another loan (5) Other (99) _______________________________________________________________
3. Migration & Mobility
3.1 Which best describes your experiences of migrating? (Choose more than one)
Short distance/day migration across the border (1) Long distance/seasonal migration across the border (2) Internal migration within Cambodia (3) Undocumented (without passport, visa, border pass) (4) Documented (with passport, visa, border pass) (5) Other (99) _______________________________________________________________
3.2 Why did you decide to migrate away from your home?
Search for better jobs/incomes (1) More jobs at destination (2) Lack of jobs at home (3) Pay off family debt (4) Loss of land (5) Earn money for family (education, food, health care) (6) Earn money for making business (7) Problems at home (8) Forced to go ….who? (9) ___________________________________________________ Went voluntarily to accompany other family members/friends (10) Other (99) _______________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 75
3.3 Throughout the year, how often would you migrate across the border?
Daily or most days (1) Once a week or every two weeks (2) Once a month (3) Three or four times per year (4) Dry season (5) Wet season (6) Other (99)________________________________________________________________
3.4 For the most recent migration, where did you spend most of your time?
Name of place ____________ Vill:______ Comm: ______ Dist:______ Prov: _____ Count: ____
3.5 What documentation did you have while migrating/ and working abroad?
Passport (1) Visa (Destination) (2) Border pass/laissez-‐passer (3) Cambodian ID card (4) Nothing (5) Other (99) _____________________
3.6 Have you ever applied for a Cambodian passport?
Yes (1) (Go to 3.8) No (2)
3.7 If you have never applied for a Cambodian passport, why not?
Have no money(1) Waste of money(2) Takes too long to do(3) Too expensive(4) Do not know where to apply(5) Do not need it(6) Other (99) ________________________________________________________________
3.8 For the most recent migration, what was the main type of work you did?
Agriculture(1) Factory(2) Fishing(3) Seller/small business(4) Construction(5) Domestic work(6) Begging(7) Sex work(8) Moto taxi/cart puller(9) Unemployed(10) Other(99) _________________________________________________________________
4. Health Risks
4.1 While working abroad, did you ever experience any health risks that impacted on your physical health and emotional well-‐being?
Yes (1) No (2) (If No, go to 4.3)
4.2 What were the specific risks to your health?
Experiencing physical & emotional abuse (1) Dangerous types of employment/working conditions (2) Being detained and locked up in crowded conditions (3) Lifestyle choices/risk taking behaviour (4) Limited access to health services (5) Being forced or having no choice (6) Other (99) _________________________________________________________________
4.3 What was your living arrangement abroad?
Own house and plot(1) Own house but not plot (2) Shared rented house with others (3) Rented a room to live (with family)(4) Shared room with up to 4 persons (5)
Shared room with 5 to 8 persons (6) Shared room with more than 8 people (7) Lived in the working place (8) Lived on the streets (9) Other (99) __________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 76
4.4 For the recent migration, how long were you working abroad?
Less than Six Months (1) One Year (2) Two or more years (3) Other (99) _________________________________________________________________
4.5 Did you have adequate food while abroad?
3 meals a day (1) 2 meals a day (2) 1 meal a day (3) No, food was inadequate (4)
4.6 How did you come to be returned to Cambodia?
Arrested by police, placed in a shelter then returned (1) Came back on my own (2) Came back with person I came with (3) Other, (specify) (99) __________________________________________________________
4.7 If you were arrested, how long were you in detention before being deported or repatriated?
[..........] Years (1) [..........] Months (2) [..........] Weeks (3) [..........] Days (4)
4.8 How were you treated during detention?
Badly (1) Not so well (2) Well (3) Very well (4)
4.9 Did you experience any abuse while abroad?
Yes (1) No (2) (If No, go to 5.1)
4.10 If so, what kind of abuse?
Hit (1) Verbal (2) Touched sexually/or inappropriately (3) Tortured (4) Other (99) _____________________________________________
4.11 From whom did you receive abuse?
________________________________________________________________________________ ________________________________________________________________________________
5. Health Issues & Health Seeking Behaviour
5.1 Did you have any health problems while aboard?
Yes (1) No (2) (If No, go to 5.4)
5.2 What were the health problems you had?
(Tick all mentioned, probe on highlighted) Stomach ache (1) Back pain (2) Head ache (3) Ear/Eye pain (4) Fever (5) Diarrhea (6) Cold/Flu (7) Respiratory problem (8) Tuberculosis (cough with blood) more than 21 days (9) Diabetes (10) Disease: urinary system (11) High blood pressure (12) Typhoid fever (13) Dengue fever (14) Skin disorder (15) Malaria (16) HIV (or AIDS) and Opportunity Infections (17) STI symptoms (genital discharges, ulcers etc.) (18) Depression, Stress, Trauma (19) Other physical injury (20) Antenatal issues (22) Postnatal issues (23) Road accident (24) Other (99) _______________________
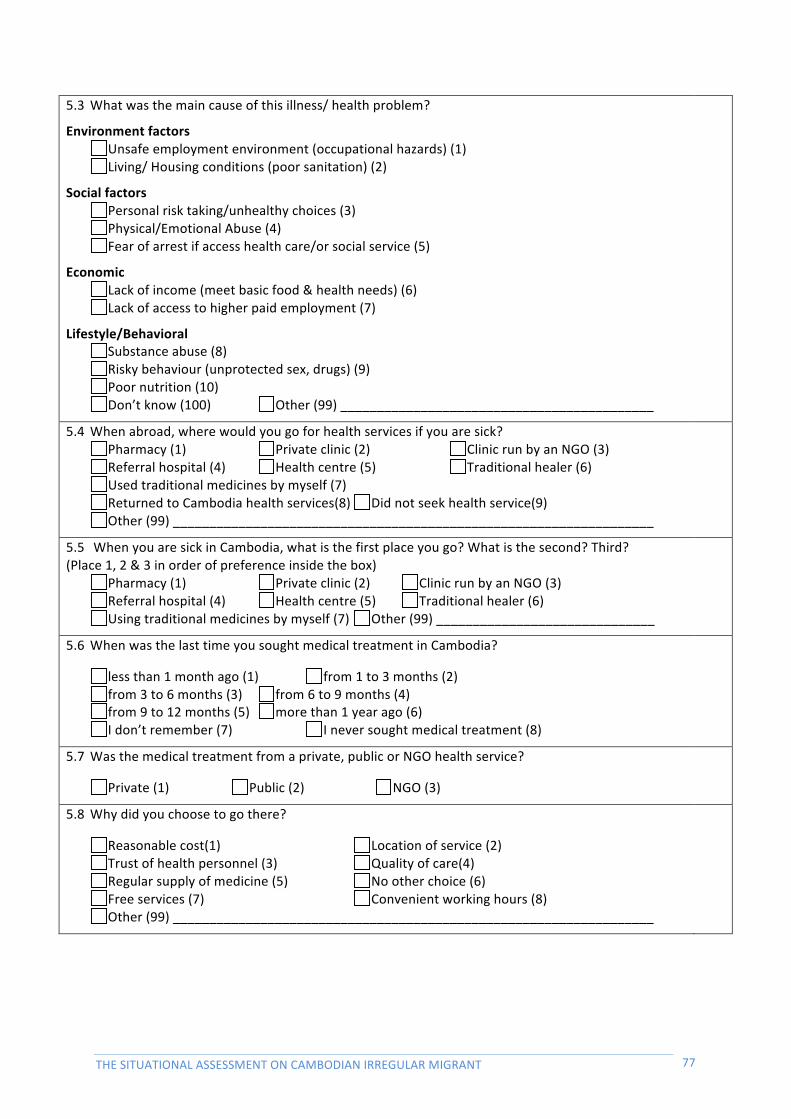
THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 77
5.3 What was the main cause of this illness/ health problem?
Environment factors Unsafe employment environment (occupational hazards) (1) Living/ Housing conditions (poor sanitation) (2)
Social factors Personal risk taking/unhealthy choices (3) Physical/Emotional Abuse (4) Fear of arrest if access health care/or social service (5)
Economic Lack of income (meet basic food & health needs) (6) Lack of access to higher paid employment (7)
Lifestyle/Behavioral Substance abuse (8) Risky behaviour (unprotected sex, drugs) (9) Poor nutrition (10) Don’t know (100) Other (99) ___________________________________________
5.4 When abroad, where would you go for health services if you are sick? Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Used traditional medicines by myself (7) Returned to Cambodia health services(8) Did not seek health service(9) Other (99) __________________________________________________________________
5.5 When you are sick in Cambodia, what is the first place you go? What is the second? Third? (Place 1, 2 & 3 in order of preference inside the box)
Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Using traditional medicines by myself (7) Other (99) ______________________________
5.6 When was the last time you sought medical treatment in Cambodia?
less than 1 month ago (1) from 1 to 3 months (2) from 3 to 6 months (3) from 6 to 9 months (4) from 9 to 12 months (5) more than 1 year ago (6) I don’t remember (7) I never sought medical treatment (8)
5.7 Was the medical treatment from a private, public or NGO health service?
Private (1) Public (2) NGO (3)
5.8 Why did you choose to go there?
Reasonable cost(1) Location of service (2) Trust of health personnel (3) Quality of care(4) Regular supply of medicine (5) No other choice (6) Free services (7) Convenient working hours (8) Other (99) __________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 78
6. Health Knowledge & Awareness
6.1 What are the most common diseases you have heard?
(Tick those mentioned-‐ Don’t Read out) HIV/AIDS (1) Sexually Transmitted Infections (2) Influenza (3) Typhoid (4) Diarrhea/Cholera (5) Tuberculosis (6) Malaria/Dengue Fever (7) Depression/Stress/Trauma (8) Hepatitis C (9) Other (99) _____________________________
6.2 Did you have any close contact with a person with one of these diseases/illnesses?
Yes (1)-‐> Who? _______________________________________ No (2)
6.3 Have you ever had any of the following symptoms while abroad?
(Read list out for interviewee to choose) Cough longer than 2 weeks (1) Coughing up blood (2) Severe headache & neck stiffness (3) Nausea, abdominal cramps, & vomiting (4) Chest pain (5) Weight loss (6) Ongoing fatigue (7) Frequent fevers and sweats (8) Skin diseases (9) Mouth, genital, or anal sores (herpes) (10) Seizures and lack of coordination (11) Difficult or painful swallowing (12) Mental symptoms such as confusion and forgetfulness (13) Severe and persistent diarrhea (14) Vision loss (15) Genital discharges, rashes, pain, ulcers in/around genitals etc. (16) Other (99) _________________________________ Do not remember (100)
6.4 Have you ever injected drugs before?
Yes (1)-‐>Did you share a needle with another person? Yes (a) No (b) No (2)
6.5 What can someone do to avoid getting HIV?
(Can tick more than one) Abstain from sex (1) Use condoms (2) Limit sex to one partner/Stay faithful to one partner (3) Limit number of sexual partners (4) Avoid sex with prostitutes (5) Avoid sex with persons who have many partners (6) Avoid sex with homosexuals (7) Avoid sex with persons who inject drugs intravenously (8) Avoid blood transfusions (9) Avoid injections with shared needles (10) Don’t know (100) Other (99) __________________________________________________________________
6.6 Did you or your partner use a condom in your last sexual encounter?
Yes (1) No (2)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 79
6.7 How does TB spread from one person to another?
(Please tick all that are mentioned.) Through shaking hand (1) Through the air when a person with TB coughs or sneezes (2) Sharing utensils and food from the same plate (3) Through touching items in public places (doorknobs, handles in transportation, etc.) (4) Do not know (100) Other (99) _________________________________________________________________
6.8 What can someone do to avoid getting TB?
(Can tick more than one) Wear mast when near a TB patient (1) Avoid sharing utensils with a TB patient (2) TB patients cover their coughs (3) Wash hands regularly (4) Avoid close contacts with TB patients (5) Do not know (100) Other (99) _________________________________________________________________
6.9 Are you worried about your health?
Yes (1) No (2)
6.10 Do you think need to be tested?
Yes (1) No (2)
6.11 Do you know where to get tested in Cambodia?
Yes (1) -‐>Where? _____________________________ No (2)
6.12 Did you have any of the following tests in the past 12 months? (Origin or Destination) (Read list out for interviewee to choose)
Sputum smear (TB) (1) HIV test (2) Hepatitis C test (3) STI test (4) I didn’t get tested (100)
6.13 If so, where did you get the test done?
(Please tick one) Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Other (99) _________________________________________________________________
6.14 What services are you aware that are offered to HIV or TB patients in Cambodia?
(Tick all that are mentioned.) Free diagnosis (TB, HIV & STI) in all provinces/districts of Cambodia (VCCT Clinics) (1) Free medicine for HIV/TB patients (2) HIV + networks (3) Food for TB/HIV patients (4) Directly observed therapy DOTS (5) Do not know (100) Other (99) _________________________________________________________________
6.15 What would be your reaction if you were found to have TB, HIV or a STI?
(Tick all that are mentioned.) Fear (1) Surprise (2) Shame (3) Embarrassment (4) Sadness or hopelessness (5) Other (99) _________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 80
6.16 Who would you talk to about your illness if you had TB, HIV or a STI?
(Tick all that are mentioned.) Doctor or other medical worker (1) Spouse (2) Parent (3) Other family member (4) Close friend (5) No one (6) Other (99) ______________________
6.17 Where would you go if you thought you had symptoms of TB, HIV or a STI?
(Tick all that apply.) Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Using traditional medicines by myself (7) Not seeking any health service(8) Other (99) ________________
6.18 If you had symptoms of TB, HIV or STI when would you seek professional medical care at a private or public clinic?
(Please Tick one.) When treatment on my own does not work (1) When symptoms that look like TB, HIV signs last for 3–4 weeks (2) As soon as I realize that my symptoms might be related to TB, HIV or STI (3) When I could no longer work or became very ill (4) I would not go to the doctor (5) Other (99) _________________________________________________________________
7. Awareness and Source of Health Information
7.1 What are the obstacles you encounter if you want information about communicable diseases or other illnesses from health facilities?
(Please tick where applicable) Cost (having to pay) (1) Language (technical terms, lack of literacy) (2) Distance (specify)_________KM (3) I am afraid of receptionist (4) I am afraid of the nurse (5) I am afraid of the doctor (6) I am afraid of the laboratory technician (7) Fear of losing my job if I find out I have the infection (8) Lack of transport (9) No health information is available(10) I have no obstacles (11) Other (99) _________________________________________________________________
7.2 What are the sources of information that you think can most effectively reach people like you with information on Communicable diseases or other illnesses?
(Please tick the three most effective sources.) Newspapers and magazines (1) Radio (2) TV (3) Billboards (4) Brochures, posters and other printed materials (5) Health workers (6) Family, friends, neighbours and colleagues (7) Religious leaders (8) Teachers (9) Other (99) _________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 81
7.3 Where will you go now you are back in Cambodia?
Return to home province (1) Return to current place of residence (2) Migrate back to Thailand or Viet Nam (3) Migrate within Cambodia to another province (4) Stay in the border area and look for work (5) Other (99) _________________________________________________________________
7.4 Will you continue to migrate abroad for work?
Yes (1) No (2)
Why? Why not? ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________
7.5 What are your immediate health needs? ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 82
2. Non-‐ Migrant Questionnaire
Hello. My name is ……………………………… and I work for …….. We are conducting a survey on health issues. I would like to ask you a few questions on your life experience and the circumstances that led to possible health problems you may have encountered. The information you give will be used only by my team and will be very important for us to improve and develop other health and social services for migrants and communities.
You would need about ……minutes to answer these questions. Your participation in this survey is voluntary and you have the right not to answer any personal questions or to stop your participation at any time during the discussion. If you choose not to answer some questions, it will not affect your rights or opportunities to access any health or social service in the future. However, we hope that you will participate in this survey and answers the questions openly and honestly because your opinions are very important to us.
If you agree to participate in the interview, everything you tell us will be confidential. This means that the information is private between us. I will not note down your name. You do not have to answer any question you are not comfortable answering, and if you have questions of your own please feel free to ask.
Would you like to participate in the interview now? ( Yes No)
Screening questions: 1. Have you ever migrated across the border? (No-‐>Start) 2. If Yes, What type of migration? SHORT DISTANCE/ DAY MIGRATION ACROSS THE BORDER (Start Interview) (1) LONG DISTANCE/ SEASONAL MIGRATION ACROSS THE BORDER (refer to Migrant survey) (2)
Interview Date ____/___/20___
DD MM YYYY
Name of Interviewer
Place of Interview Village: __________________ ;
Commune: ____________________ ;
District ______________________ ;
Province ________________________
Sex of Respondent Male (1) Female (2)
Starting Time: ______________________ End Time: _________________________
Checked by supervisor: __________________ Signature: ______________________
Date: ____/____/20___ Time: __________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 83
1. General Demographic
1.9 How old are you? [………..] Years
1.10 What is your current Marital Status? (Tick answer)
Single/Never Married (1) Separated (2) Widowed (3) Married (4) Divorced (5) Refuse to answer (6)
1.11 How many family members do you support financially? (Children, Parents, Siblings, Grandparents, Wives etc.)
________Family members (dependents)
1.12 Have you ever attended school?
Yes (1) No (2) (If No, go to Q1.6)
1.13 What is your highest grade of education complete? (need to probe if Old or New grading system) (Tick Box)
OLD Grading System (1) NEW Grading System (2) [………….] Grades completed (To be circled by supervisor)
1. Some Primary (1-‐3 grades) 2. Completed Primary School (6 grades) 3. Some Lower Secondary (7-‐8 grades) 4. Completed Lower Secondary School (9 grades) 5. Some Upper Secondary (10-‐11 Grades) 6. Completed Upper Secondary School (12 grades) 7. University any Level 8. Technical/Vocational
1.14 Where is your permanent address?
Village: __________________ Commune/Sangkat: ____________________
District/City: ______________________ Province: ________________________
1.15 Where are you living now?
Village: __________________ Commune/Sangkat: ____________________
District/City: ______________________ Province: ________________________
1.16 How long have you been living in your current place?
_________Years (1) _________ Months (2) _________Weeks (3)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 84
2. Socio-‐economic Background
2.14 What is your living situation like? (Tick one answer)
Own house & plot (1) Own house but not plot(2) Rent a house(3) Rent a room(4) Live with relative/friend(5) Live in a house of someone without paying rent(6) Live in the work place (7) Lived on the streets (8) Homeless living under temporary structure(9) Other (99) _________________________________________________________________
2.15 What is the housing material like? (Tick one answer)
Good (tiles/brick/concrete)(1) Adequate (wood/corrugated iron)(2) Poor(thatch/palm leaves/plastic sheet)(3)
2.16 Do you currently have agricultural land? (Rice, Chamcar etc.)
Yes (1)-‐> Owned (a) or Rented (b)? __________________ No (2)
2.17 Have you sold or lost agricultural land in the past?
Yes (1) -‐> what was reason for this decision/loss? __________________________ (a) No (2)
2.18 What are your main sources of income? (Tick more than one)
Agriculture(1) Factory(2) Fishing(3) Seller/small business(4) Construction(5) Domestic work(6) Begging(7) Sex work(8) Moto taxi/cart puller(9) Unemployed(10) Other(99) ___________________________________________________________________
2.19 How regular are these sources of income throughout the year?
All year round (1) Dry Season (2) Wet Season (3) Day to day basis (4) Irregular (5)
2.20 On average how much can you earn from these income sources per day? month? year?
………………….. Riel(1) ………………..Baht(2) ………...……..Dong(3) ……………..USD(4)
2.21 Which of the following better describes the financial position of your family?
(Tick one answer) We do not have enough money(1) We have enough money for food(2) We have enough money for food and healthcare(3) We can pay for most food, health & education needs(4) We can cover all family needs and extra things we need(5)
2.22 Does your household have any outstanding loans or debts to repay?
Yes (1) No (2) (If No, go to 2.14)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 85
2.23 How many moneylenders do you owe these loans/debts too?
Number of Debtors: _________ Who? (a)-‐> Parents/Relatives (1) Friends (2) Neighbours (3) Informal Money Lenders (4) Banks/ Microfinance Firms/Credit (5) NGO (6) Other (99) ______________________________
2.24 What are these loans/debts for? (Tick more than one)
Basic needs (Food, Shelter) (1) Healthcare/treatment (2) Children’s Education (3) Livelihood inputs (agriculture e.g.) (4) Buy back/or rent land (5) Family Ceremonies (Weddings, Funerals e.g.) (6) Pay off other Loan/debt repayments (7) Migration (Travel costs) (8) Other(99) _____________________
2.25 What is the total amount of these loans/debts?
………………….. Riel(1) ………………..Baht(2) ………...……..Dong(3) ……………..USD(4)
2.26 What are you expecting to do to settle the loans/debts?
Will try to work and save money (1) Will send family members to work (2) Will migrate myself to look for work (3) Sell my land (4) Take out another loan (5) Other (99) _______________________
2.27 Why don’t you migrate to Viet Nam/Thailand?
______________________________________________________________________________
2.28 Have you ever applied for a Cambodian passport?
Yes (1) (Go to 3.8) No (2)
2.29 If you have never applied for a Cambodian passport, why not?
Have no money(1) Waste of money(2) Takes too long to do(3) Too expensive(4) Do not know where to apply(5) Do not need it(6) Other (99) ___________________________________________________________________
7. Health Risks
7.1 While working/doing business here, have you ever experienced any health risks that impacted on your physical health and emotional well-‐being?
Yes (1) No (2) (If No, go to 3.3)
7.2 What were the specific risks to your health?
Experiencing physical & emotional abuse (1) Dangerous types of employment/working conditions (2) Being detained and locked up in crowded conditions (3) Lifestyle choices/risk taking behaviour (4) Limited access to health services (5) Being forced or having no choice (6) Other (99) __________________________________________________________________
7.3 Did you have adequate food in this area?
3 meals a day (1) 2 meals a day (2) 1 meal a day (3) No, food was inadequate (4)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 86
8. Health Issues & Health Seeking Behaviour
8.1 Did you ever have any health problems living here?
Yes (1) No (2) (If No, go to 4.4)
8.2 What were the health problems you had?
(Tick all mentioned, probe on highlighted) Stomach ache (1) Back pain (2) Head ache (3) Ear/Eye pain (4) Fever (5) Diarrhea (6) Cold/Flu (7) Respiratory problem (8) Tuberculosis (cough with blood) more than 21 days (9) Diabetes (10) Disease: urinary system (11) High blood pressure (12) Typhoid fever (13) Dengue fever (14) Skin disorder (15) Malaria (16) HIV (or AIDS) and Opportunity Infections (17) STI symptoms (genital discharges, ulcers etc.) (18) Depression, Stress, Trauma (19) Other physical injury (20) Antenatal issues (22) Postnatal issues (23) Road accident (24) Other (99) __________________________
8.3 What was the main cause of this illness/ health problem?
Environment factors Unsafe employment environment (occupational hazards) (1) Living/Housing conditions (poor sanitation) (2)
Social factors Personal risk taking/unhealthy choices (3) Physical/Emotional Abuse (4)
Economic Lack of income (meet basic food & health needs) (6) Lack of access to higher paid employment (7)
Lifestyle/Behavioral Substance abuse (8) Risky behaviour (unprotected sex, drugs) (9) Poor nutrition (10) Don’t know (100) Other (99) _____________________
8.4 When you are sick, what is the first place you go? What is the second? Third?
(Place 1, 2 & 3 in order of preference inside the box) Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Using traditional medicines by myself (7) Other (99) ________________________
8.5 When was the last time you sought medical treatment?
less than 1 month ago (1) from 1 to 3 months (2) from 3 to 6 months (3) from 6 to 9 months (4) from 9 to 12 months (5) more than 1 year ago (6) I don’t remember (7) I never sought medical treatment (8)
8.6 Was the medical treatment from a private, public or NGO health service?
Private (1) Public (2) NGO (3)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 87
8.7 Why did you choose to go there?
Reasonable cost(1) Location of service (2) Trust of health personnel (3) Quality of care(4) Regular supply of medicine (5) No other choice (6) Free services (7) Convenient working hours (8) Other (99) _________________________________________________________________
9. Health Knowledge & Awareness
9.1 What are the most common diseases you have heard? (Tick those mentioned-‐ Don’t Read out)
HIV/AIDS (1) Sexually Transmitted Infections (2) Influenza (3) Typhoid (4) Diarrhea/Cholera (5) Tuberculosis (6) Malaria/Dengue Fever (7) Depression/Stress/Trauma (8) Hepatitis C (9) Other (99) _____________________________
9.2 Did you have any close contact with a person with one of these diseases/illnesses? Yes (1)-‐> Who? _______________________________________ No (2)
9.3 Have you ever injected drugs before? Yes (1)-‐>Did you share a needle with another person? Yes (a) No (b) No (2)
9.4 What can someone do to avoid getting HIV? (Can tick more than one)
Abstain from sex (1) Use condoms (2) Limit sex to one partner/Stay faithful to one partner (3) Limit number of sexual partners(4) Avoid sex with prostitutes (5) Avoid sex with persons who have many partners (6) Avoid sex with homosexuals (7) Avoid sex with persons who inject drugs intravenously(8) Avoid blood transfusions (9) Avoid injections with shared needles (10) Don’t know (100) Other (99) ____________________________________
9.5 Did you or your partner use a condom in your last sexual encounter? Yes (1) No (2)
9.6 How does TB spread from one person to another? (Please tick all that are mentioned.)
Through shaking hand (1) Through the air when a person with TB coughs or sneezes (2) Sharing utensils and food from the same plate (3) Through touching items in public places (doorknobs, handles in transportation, etc.) (4) Do not know (100) Other (99) ____________________________________
9.7 What can someone do to avoid getting TB?
(Can tick more than one) Wear mast when near a TB patient (1) Avoid sharing utensils with a TB patient (2) TB patients cover their coughs Wash hands regularly Avoid close contacts with TB patients Do not know (100) Other (99) __________________________________________________________________
9.8 Are you worried about your health?
Yes (1) No (2)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 88
9.9 Do you think need to be tested?
Yes (1) No (2)
9.10 Do you know where to get tested in Cambodia?
Yes (1) -‐>Where? _____________________________ No (2)
9.11 Did you have any of the following tests in the past 12 months? (Read list out for interviewee to choose)
Sputum smear (TB) (1) HIV test (2) Hepatitis C test (3) STI test (4) I didn’t get tested (100)
9.12 If so, where did you get the test done?
(Please tick one) Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Other (99) _________________________________________________________________
9.13 What services are you aware that are offered to HIV or TB patients in Cambodia?
(Tick all that are mentioned.) Free diagnosis (TB, HIV & STI) in all provinces/districts of Cambodia (VCCT Clinics) (1) Free medicine for HIV/TB patients (2) HIV + networks (3) Food for TB/HIV patients (4) Directly observed therapy DOTS (5) Do not know (100) Other (99) _______________________
9.14 What would be your reaction if you were found to have TB, HIV or a STI?
(Tick all that are mentioned.) Fear (1) Surprise (2) Shame (3) Embarrassment (4) Sadness or hopelessness (5) Other (99) __________________________________________________________________
9.15 Who would you talk to about your illness if you had TB, HIV or a STI?
(Tick all that are mentioned.) Doctor or other medical worker (1) Spouse (2) Parent (3) Other family member (4) Close friend (5) No one (6) Other (99) ________________________
9.16 Where would you go if you thought you had symptoms of TB, HIV or a STI?
(Tick all that apply.) Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Using traditional medicines by myself (7) Not seeking any health service(8) Other (99) _________________
9.17 If you had symptoms of TB, HIV or STI when would you seek professional medical care at a private or public clinic?
(Please Tick one.) When treatment on my own does not work (1) When symptoms that look like TB, HIV signs last for 3–4 weeks (2) As soon as I realize that my symptoms might be related to TB, HIV or STI (3) When I could no longer work or became very ill (4) I would not go to the doctor (5) Other (99) ___________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 89
6. Awareness and Source of Health Information
6.1. What are the obstacles you encounter if you want information about communicable diseases or other illnesses from health facilities?
(Please tick where applicable) Cost (having to pay) (1) Language (technical terms, lack of literacy) (2) Distance (specify)_________KM (3) I am afraid of receptionist (4) I am afraid of the nurse (5) I am afraid of the doctor (6) I am afraid of the laboratory technician (7) Fear of losing my job if I find out I have the infection (8) Lack of transport (9) No health information is available(10) I have no obstacles (11) Other (99) ________________________
6.2. What are the sources of information that you think can most effectively reach people like you with information on Communicable diseases or other illnesses?
(Please tick the three most effective sources.) Newspapers and magazines (1) Radio (2) TV (3) Billboards (4) Brochures, posters and other printed materials (5) Health workers (6) Family, friends, neighbours and colleagues (7) Religious leaders (8) Teachers (9) Other (99) _____________________________________________
6.3. What are your immediate health needs? ____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 90
3. Health Care Worker Questionnaire
Hello. My name is ……………………………… and I work for …….. We are conducting a survey on health issues. I would like to ask you a few questions on your experience as a health care worker and your management of health problems in the community. The information you give will be used only by my team and will be very important for us to improve health and social services for migrants and communities.
You would need about ……minutes to answer these questions. Please be assured that the information will be confidential and will not be shown to other persons and you may choose to stop your participation at any time or refrain from answering any questions. However, we hope that you will participate in this survey and answers the questions openly and honestly because your opinions are very important to us. If you have questions of your own please feel free to ask.
Would you like to participate in the interview now? ( Yes No)
Interview Date ____/___/20___
DD MM YYYY
Name of Interviewer
Place of Interview Village: __________________ ;
Commune: ____________________ ;
District ______________________ ;
Province ________________________
Sex of Respondent Male (1) Female (2)
Starting Time: ______________________ End Time: _________________________
Checked by supervisor: __________________ Signature: ______________________
Date: ____/____/20___ Time: __________________________
2. General
1.17 How old are you? [……] years of age
1.18 What is your position at this health facility/or within this village?
Medical Doctor (1) Nurse (2) Mid-‐wife (3) Administrator (4) Village Health Support Worker (5) Peer Educator (6) Other (99) ___________________________________________________________________
1.19 What is your highest grade of education complete? (need to probe if Old or New grading system)
OLD Grading System (1) NEW Grading System (2) […….] Grades completed
1.20 How long have you been in this position?
[……… ] Years [……… ] Months

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 91
1.21 Would you say the supply of (gloves….read each item in list) is adequate, inadequate, or not available in this Health Center or Hospital?
Not Available
Inadequate supply
Adequate
1. Gloves 2. Gowns 3. Disposal container for sharps 4. Bleach solution (disinfectant) 5. Soap 6. Running water 7. Essential medicines
3 Health Problems & Health Seeking Behaviour
3.1 What are the most common health problems you deal with on a day-‐to-‐day basis?
(Tick all mentioned, probe on highlighted) Stomach ache (1) Back pain (2) Head ache (3) Ear/Eye pain (4) Fever (5) Diarrhea (6) Cold/Flu (7) Respiratory problem (8) Tuberculosis (cough with blood) more than 21 days (9) Diabetes (10) Disease: urinary system (11) High blood pressure (12) Typhoid fever (13) Dengue fever (14) Skin disorder (15) Malaria (16) HIV (or AIDS) and Opportunity Infections (17) STI symptoms (genital discharges, ulcers etc.) (18) Depression, Stress, Trauma (19) Other physical injury (20) Antenatal issues (22) Postnatal issues (23) Road accident (24) Other (99) ____________
3.2 What are the priority health problems that take up most of your time?
(Tick all mentioned, probe on highlighted) Stomach ache (1) Back pain (2) Head ache (3) Ear/Eye pain (4) Fever (5) Diarrhea (6) Cold/Flu (7) Respiratory problem (8) Tuberculosis (cough with blood) more than 21 days (9) Diabetes (10) Disease: urinary system (11) High blood pressure (12) Typhoid fever (13) Dengue fever (14) Skin disorder (15) Malaria (16) HIV (or AIDS) and Opportunity Infections (17) STI symptoms (genital discharges, ulcers etc.) (18) Depression, Stress, Trauma (19) Other physical injury (20) Antenatal issues (22) Postnatal issues (23) Road accident (24) Other (99) _______________
3.3 What are the main causes of these illness/ health problems?
Environment factors Unsafe employment environment (occupational hazards) (1) Living/ Housing conditions (poor sanitation) (2)
Social factors Personal risk taking/unhealthy choices (3) Physical/Emotional Abuse (4)
Economic Lack of income (meet basic food & health needs) (5) Lack of access to higher paid employment (6)
Lifestyle/Behavioral Substance abuse (7) Risky behaviour (unprotected sex, drugs) (8) Poor nutrition (9) Don’t know (100) Other (99) _________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 92
3.4 What is the first place a person goes when they are sick? What is the second? Third?
(Place 1, 2 & 3 in order of preference inside the box) Pharmacy (1) Private clinic (2) Clinic run by an NGO (3) Referral hospital (4) Health centre (5) Traditional healer (6) Using traditional medicines by myself (7) Other (99) _______________________
3.5 Why do they choose first to go there?
Reasonable cost(1) Location of service (2) Trust of health personnel (3) Quality of care(4) Regular supply of medicine (5) No other choice (6) Free services (7) Convenient working hours (8) Other (99) __________________________________________________________________
4 Health of Migrants (Think about Khmer people who leave their homes to migrate across the border to Viet
Nam and Thailand to find work and are arrested and deported back to Cambodia.)
4.1 Have you ever come across Khmers who migrate across the border during your work as a health care provider?
Yes (1) No (2)
4.2 What important or special health needs do you feel that they have?
______________________________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________________
4.3 What are the challenges in providing healthcare or health information to cross-‐border migrants?
______________________________________________________________________________________________________________________________________________________________________________ _______________________________________________________________________________________
5 Training
5.1 Have you ever received any training? Yes (1) No (2)
5.2 What kind of training did you receive?
Yes(1) No (2) 1. VCT training 2. Counselling and testing for PMTCT 3. Pre-‐service counselling and testing training 4. Diagnostic counselling and testing (DCT) 5. Basic counselling for HIV/AIDS or TB patients 6. Management of patients on ARV or TB drugs 7. Management of opportunistic infections 8. Home based care for HIV/AIDS patients 9. Direct Observation Treatment (DOTS) 10. Community Direct Observation Treatment (CDOTS) 11. Disseminating Health Information and making referrals 12. ARV or TB program management 13. Other: _______________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 93
5.3 When was the last time you received technical trainings to improve or upgrade your skills as a health care worker? less than 1 month ago (1) from 1 to 3 months (2) from 3 to 6 months (3) from 6 to 9 months (4) from 9 to 12 months (5) more than 1 year ago (6) I don’t remember (7) I never received any training (8)
5.1 Would you say you are highly confident, moderately confident or you have low confidence in….(Read each item and circle appropriate response)
Not
Apply(1)
Mod
era
te (2
)
Confide
nt (3
)
Highly
Confide
nt (4
)
1. Recommending HIV, TB or STI testing to a patient? 2. Counselling a patient who has accepted to test for HIV, TB or
STI before testing?
3. Counselling a patient whose HIV, TB or STI test is positive? 4. Counselling a patient whose HIV, TB or STI test is negative? 5. Couple counselling?
5.2 Would you say you are highly competent, moderately competent, or have low competence in…(Read each item in list and circle one response)
Not
Apply(1)
Mod
erate
(2)
Confiden
t (3)
Highly
Confiden
t (4)
1. Clinical assessment of patients with communicable diseases or other health issues
2. Assessing patient readiness for taking medicine (e.g. antiretroviral therapy (ART)
3. Management of opportunistic infections (OIs) or side effects 4. Adherence counselling for patients on ARV or TB treatment 5. Monitoring patients on Anti-‐retroviral therapy or C-‐DOTS 6. Home based care for HIV/AIDS patients 7. Nutritional support for HIV/AIDS and TB patients 8. Psycho-‐social support for HIV/AIDS and TB patients 9. Providing health information and making referrals of patients
5.3 What services do you offer to HIV or TB patients as a health care worker? (Tick all that are mentioned.) Free diagnosis (TB, HIV & STI) in all provinces/districts of Cambodia (VCCT Clinics) (1) Free medicine for HIV/TB patients (2) HIV + networks (3) Food for TB/HIV patients (4) Directly observed therapy DOTS (5) Do not know (100) Other (99) ________________________________
5.4 What further training do you think you need to improve your skill and quality of work as health care worker?
VCT training Counselling and testing for PMCT Pre-‐service counselling and testing training Diagnostic counselling and testing (DCT) Basic counselling for HIV/AIDS or TB patients Management of patients on ARV or TB drugs Management of opportunistic infections Home based care for HIV/AIDS patients Direct Observation Treatment (DOTS) Community Direct Observation Treatment (CDOTS) Disseminating Health Information and making referrals ARV or TB program management Other _______________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 94
5. Awareness and Source of Health Information
5.1 What are the obstacles people encounter if they want information about communicable diseases or other illness from health facilities?
(Please tick where applicable) Cost (having to pay) (1) Language (technical terms, lack of literacy) (2) Distance (specify)_________KM (3) They are afraid of receptionist (4) They are afraid of the nurse (5) They are afraid of the doctor (6) They are afraid of the laboratory technician (7) Fear of losing their job if they find out they have the infection (8) Lack of transport (9) No health information is available(10) They have no obstacles (11) Other (99) ___________________________
5.2 What are the sources of information that you think can most effectively reach migrants on Communicable diseases or other illnesses?
(Please tick the three most effective sources.) Newspapers and magazines (1) Radio (2) TV (3) Billboards (4) Brochures, posters and other printed materials (5) Health workers (6) Family, friends, neighbours and colleagues (7) Religious leaders (8)
Teachers (9) Other (99) _____________________________________________
5.3 What are the weaknesses of the local public health system? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
5.4 What are the strengths of the local public health system? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 95
Annexe C: Letter of Approval from the National Ethic Committee for Health Research, Ministry of Health (MoH)

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 96

THE SITUATIONAL ASSESSMENT ON CAMBODIAN IRREGULAR MIGRANT 97