Sickle Cell Disease: International collaboration and global issues
31
Sickle Cell Disease International collaboration and global issues Jacques Elion, MD, PhD National Reference Centers for Sickle Cell Disease Department of Medical Genetics Robert Debré University Hospital, 75019 Paris, France Inserm UMR 665 National Institute for Blood Transfusion, 75015 Paris Guadeloupe University Hospital, 97139 Les Abymes (French West Indies) Institut national de la santé et de la recherche médicale La Havana 20-24 May 2013
-
Upload
univ-paris-diderot -
Category
Documents
-
view
0 -
download
0
Transcript of Sickle Cell Disease: International collaboration and global issues

Sickle Cell DiseaseInternational collaboration and global issues
Jacques Elion, MD, PhD National Reference Centers for Sickle Cell Disease
Department of Medical Genetics Robert Debré University Hospital, 75019 Paris, France
Inserm UMR 665National Institute for Blood Transfusion, 75015 ParisGuadeloupe University Hospital, 97139 Les Abymes (French West Indies)
Institut national de la santé et de la recherche médicale
La Havana20-24 May 2013
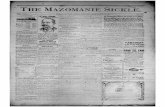
Map is from Piel FB et al: Nature Communications, Nov 2010
Independent origins of SCD in Africa and India

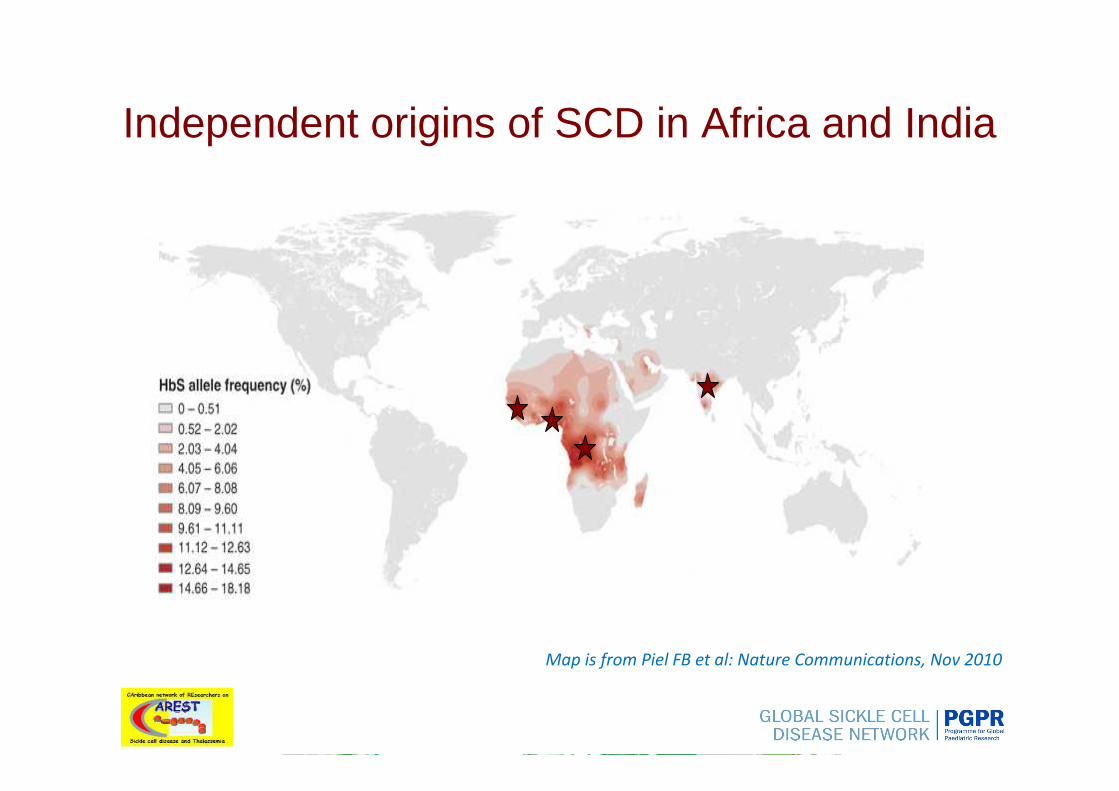
Spread by the slave trade
Royaume Uni Pays-Bas
Espagne
Portugal
Belgique
AllemagneFrance
Italie
Grèce
Irlande
Luxembourg
Danemark
Norvège
Suède
Finlande
ββββS
…or modern economical migrations
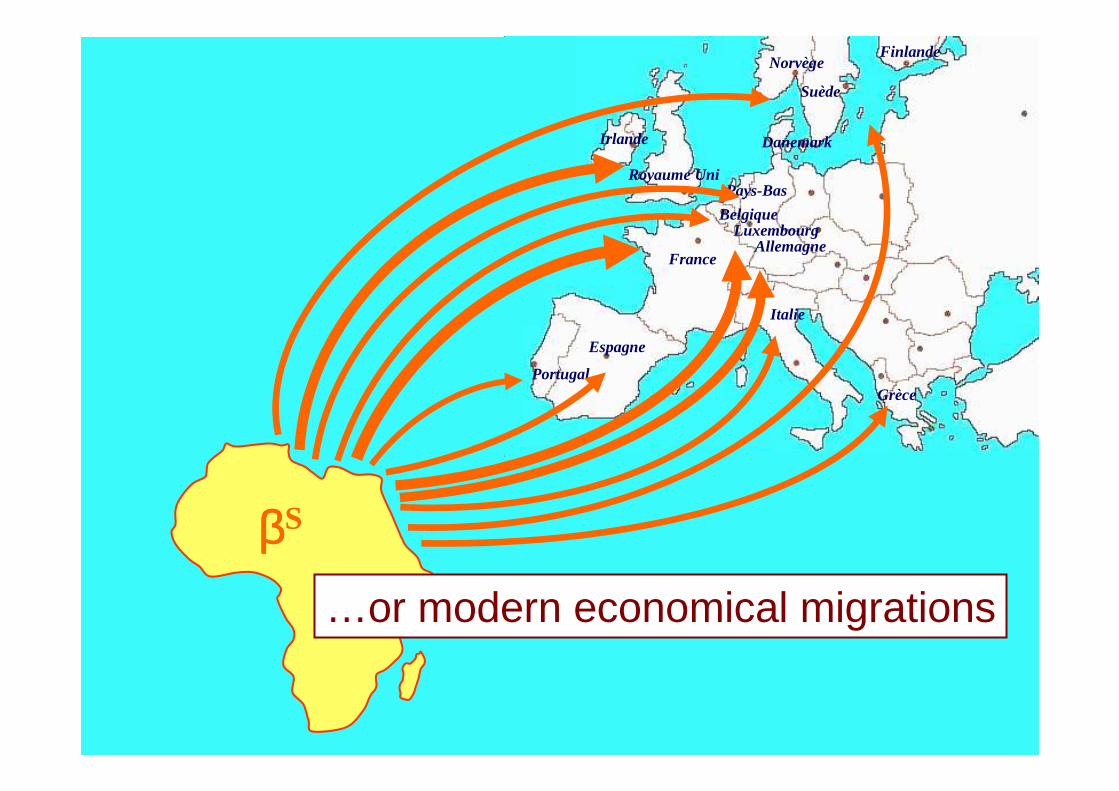
It is estimated that in excess of 300 000 children are born each year with a severe inherited disorder of hemoglobin and that approximately 80% of these births occur in low- or middle-income countries.
Major hemoglobin disorder No. of annual births
β thalassaemia major 22 989HbE β thalassaemia 19 128HbH disease 9 568Hb Bart hydrops (α°) 5 183SS disease 217 331S β thalassaemia 11 074SC disease 54 736
Sickle cell anaemia is by far the commonest and data suggests that close to 180 000 babies are born each year in sub-Saharan Africa with this condition
The burden of the haemoglobinopathies
Weatherall DJ. Blood. 2010
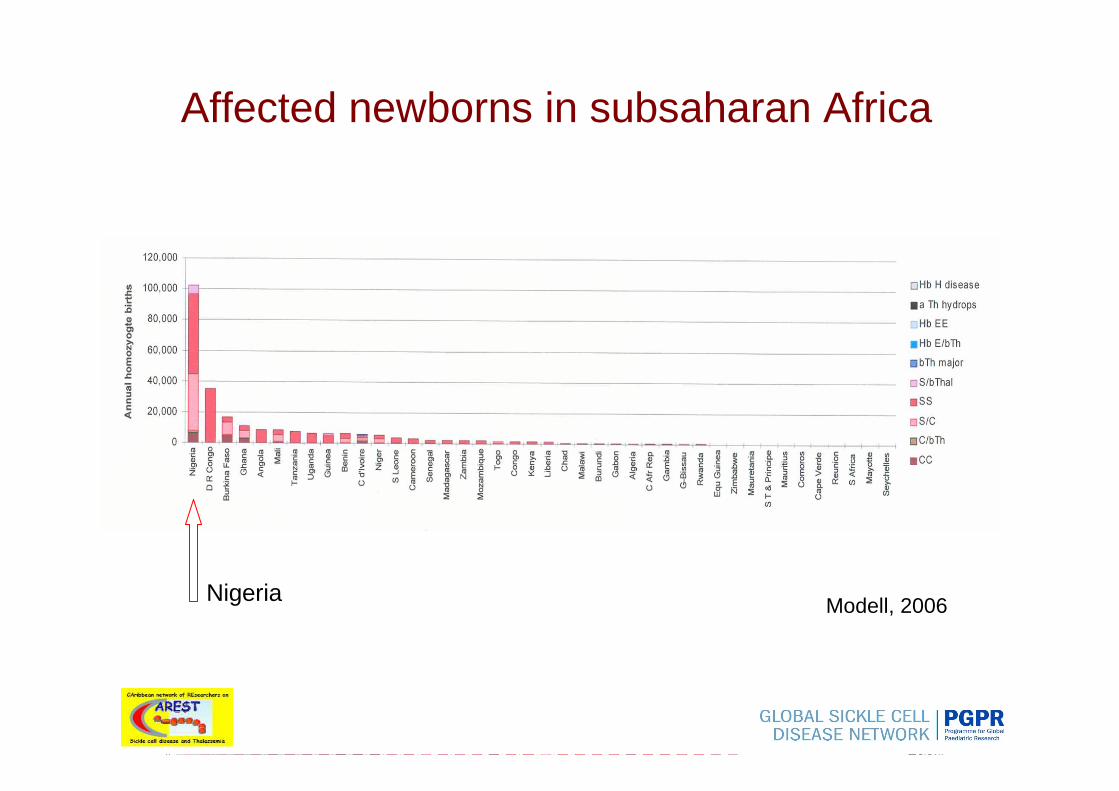
Affected newborns in subsaharan Africa
Modell, 2006Nigeria
(0-18%)(0-18%
(0-1%)
(0-2%)
(0-12%)
(0-35%)
(0-31%)
(0-33%)
(0-34%)
(0-23%)
(0-20%)
(0-31%)
(0-30%)
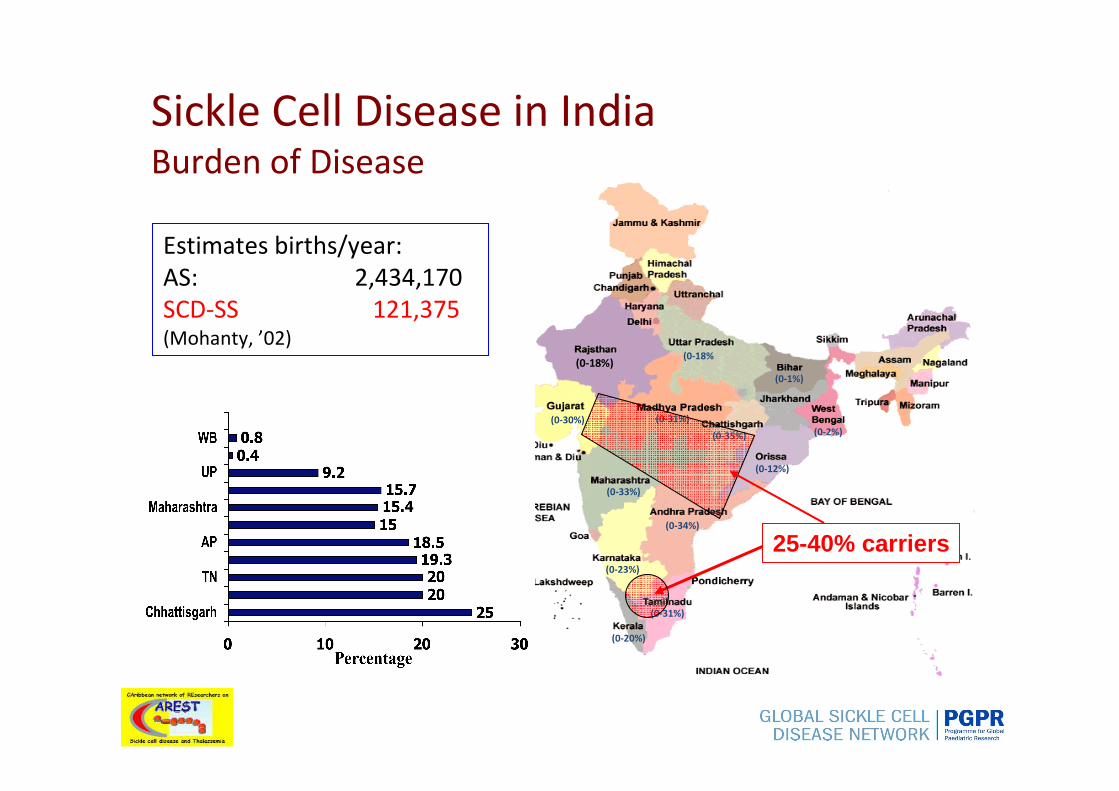
Sickle Cell Disease in IndiaBurden of Disease
Estimates births/year:
AS: 2,434,170
SCD-SS 121,375(Mohanty, ’02)
25-40% carriers

• African Union: Assembly decision/AU/ Dec. 81 July 2005
• UNESCO General Assembly September 2005
• WHO resolutions: WHA59.20 and EB 118 May 2006• UN General Assembly resolution: A/63/237
December 2008
• WHO-AFRO resolution: AFR/RC60/8 August 2010Sickle-cell disease: a strategy for the WHO African Region
SCD is recognized as a global public health issue
Still many issues remain unanswered
- based mainly on studies that were carried out before 1980 (in Africa)- obtained from a very limited number of centers in each of the countries - even in many richer countries, data of this kind are scarce
Epidemiological data must be interpreted with extreme caution
Thus, there is an urgent need of sound epidemiological data to estimate the health burden that will be encountered, particularly by the poorer countries as the haemoglobin disorders become even more frequent in the future.
unresolved issue 1
Weatherall DJ. Blood. 2010

- improved nutrition- better control of infectious disease
…childhood mortality rates are decreasing
Under these circumstances, the prevalence of genetic disorders like haemoglobinopathies tends to increase
The epidemiologic transition
Because of:
Furthermore, in many cases this affects countries with the highest rate of increase of their population.
But census data are uncertain
unresolved issue 2
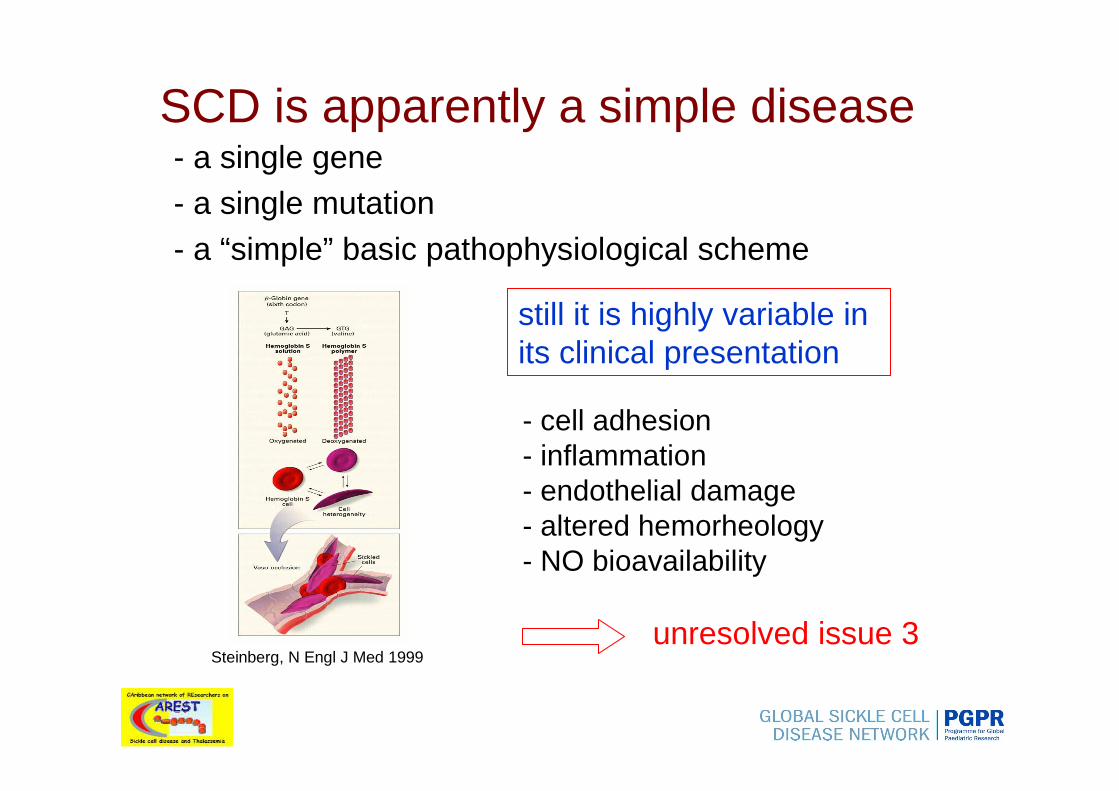
SCD is apparently a simple disease- a single gene - a single mutation- a “simple” basic pathophysiological scheme
still it is highly variable in its clinical presentation
unresolved issue 3
- cell adhesion- inflammation- endothelial damage- altered hemorheology- NO bioavailability
Steinberg, N Engl J Med 1999

What is the problem?
- basic research has been done in the North, mostlyin the USA
- all the tools are there (pharmalogical labs, facilities for GWAS studies…)
but- we lack epidemiological data
- we know almost nothing about the natural history ofSCD in its natural environment
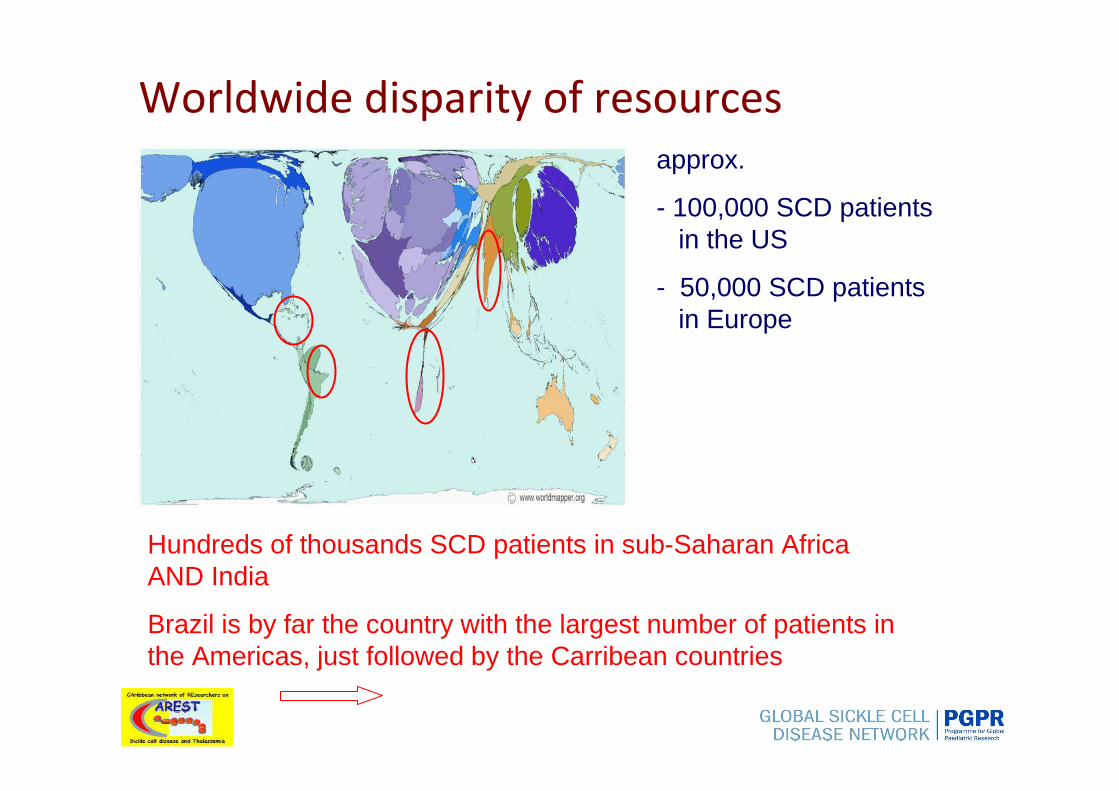
Worldwide disparity of resources
Hundreds of thousands SCD patients in sub-Saharan Africa AND India
Brazil is by far the country with the largest number of patients in the Americas, just followed by the Carribean countries
approx.
- 100,000 SCD patients in the US
- 50,000 SCD patients in Europe

Worldwide disparity of resources
Hundreds of thousands SCD patients in sub-Saharan Africa AND India
Brazil is by far the country with the largest number of patients in the Americas, just followed by the Carribean countries
approx.
- 100,000 SCD patients in the US
- 50,000 SCD patients in Europe
Global issue → clear necessity of coordinated efforts
- South-South sustainable collaboration- North-South equitable & sustainable collaboration- triangular partnerships
regional and international (global) networks

International collaboration is crucial
It is clear that research, training of doctors and health workers and education can be the driving force to improve clinical care globally
to the mutual benefit of both low- or middle-income countries and high-income countries and for the good of the patients.

Examples of fruitful collaborative networks- France – French-speaking African countries- UK - Tanzania- Portugal – Angola- Holland – Curaçao - USA – Ghana- Brazil – Ghana, Senegal, Benin, Angola
International collaboration
Within this frame, regional networks and international coordination are pivotal to promote:
- research- training and education- patients follow-up and management

Definition of the phenotype is crucial. Given the level of complexity of SCD it is is difficult to achieve an agreed classification of the different degrees of severity.
It is vital to attempt to produce a workable description of severity as a prelude to the potential international collaborations and to normalise clinical and biological data collection.
Comparative cohort studies are badlyneeded
Results of projects such as the Jamaican Cohort Study or the USA Cooperative Study of Sickle Cell Disease are clear indications that such initiatives should be pursued in a comparative manner.
Weatherall et al. Blood. 2005

The Central AfricanSCD network
- Cameroon Angola- DRC Ouganda- Congo Zambia- CAR Kenya- Gabon Burundi- Tanzania Ruanda- South Sudan
REDAC
Africa (1)
Examples of successful regional networks
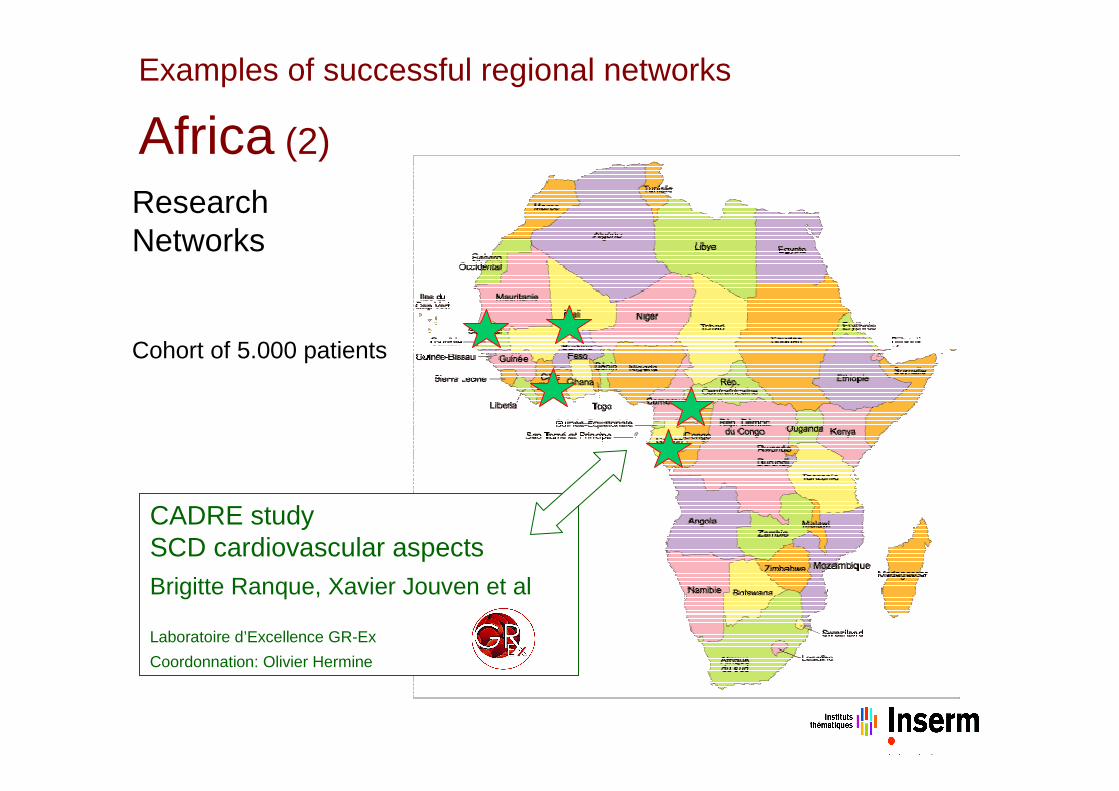
CADRE studySCD cardiovascular aspectsBrigitte Ranque, Xavier Jouven et al
Laboratoire d’Excellence GR-Ex
Coordonnation: Olivier Hermine
ResearchNetworks
Cohort of 5.000 patients
Examples of successful regional networks
Africa (2)
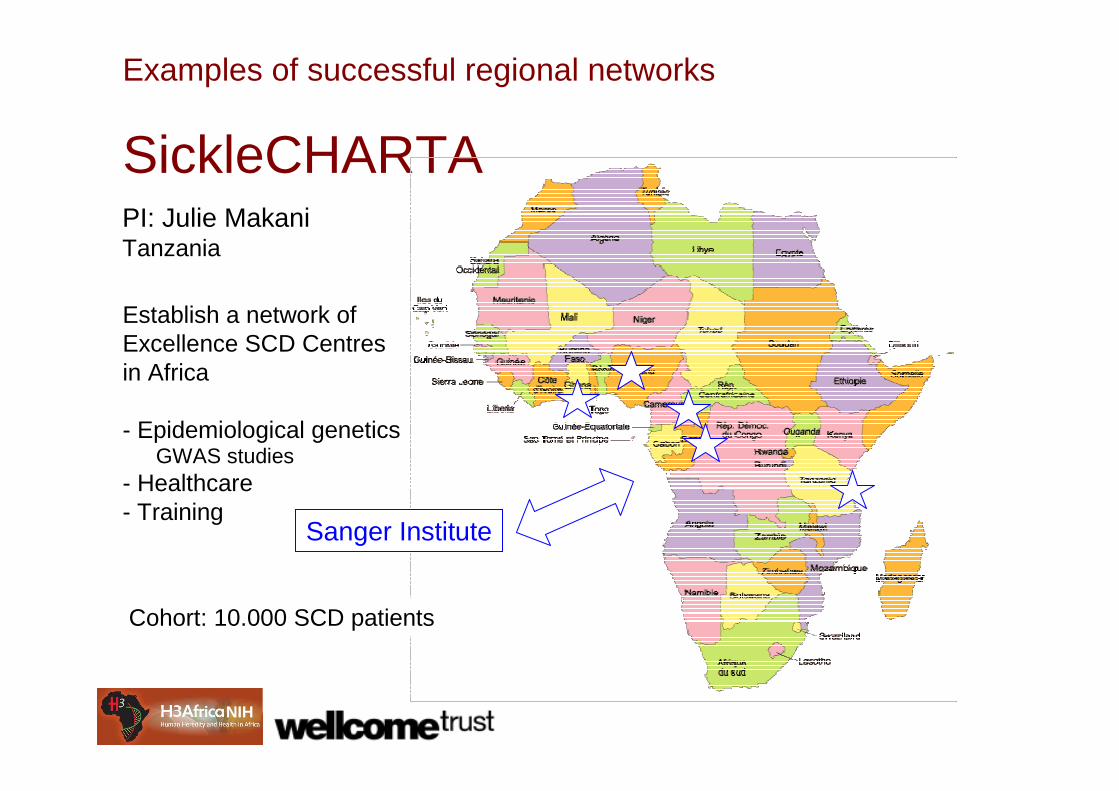
SickleCHARTA
NIH
Sanger Institute
PI: Julie MakaniTanzania
Establish a network of Excellence SCD Centres in Africa
- Epidemiological geneticsGWAS studies
- Healthcare- Training
Cohort: 10.000 SCD patients
Examples of successful regional networks

CAribbean network of REsearchers on
Sickle cell disease and Thalassemia
Caribbean Network
11 Caribbean countries
- Newborn screening- Follow-up- Education- Research
Relationship between Acute Chest Syndrome and the sympatho-vagal balance in adults with hemoglobin SS disease; a case control study Knight-Madden JM,
Connes P, Bowers A, Nebor D, Hardy-
Dessources MD, Romana M, Reid H,
Pichon AP, Barthélémy JC, Cumming VB,
Elion J, Reid M. 2012, sous presse.
President : MD Hardy-Dessources
Examples of successful regional networks
The Global SCD Network
• Mission
– Furthering research and advancing clinical care globally
• Goals
– Facilitate North-South, South-South and triangular partnerships
• Research
• Training
• Education
• Clinical programs
Medical Director: Isaac OdameSickKids Hospital, Toronto
International Advisory Board:
Jacques Elion, Chairman

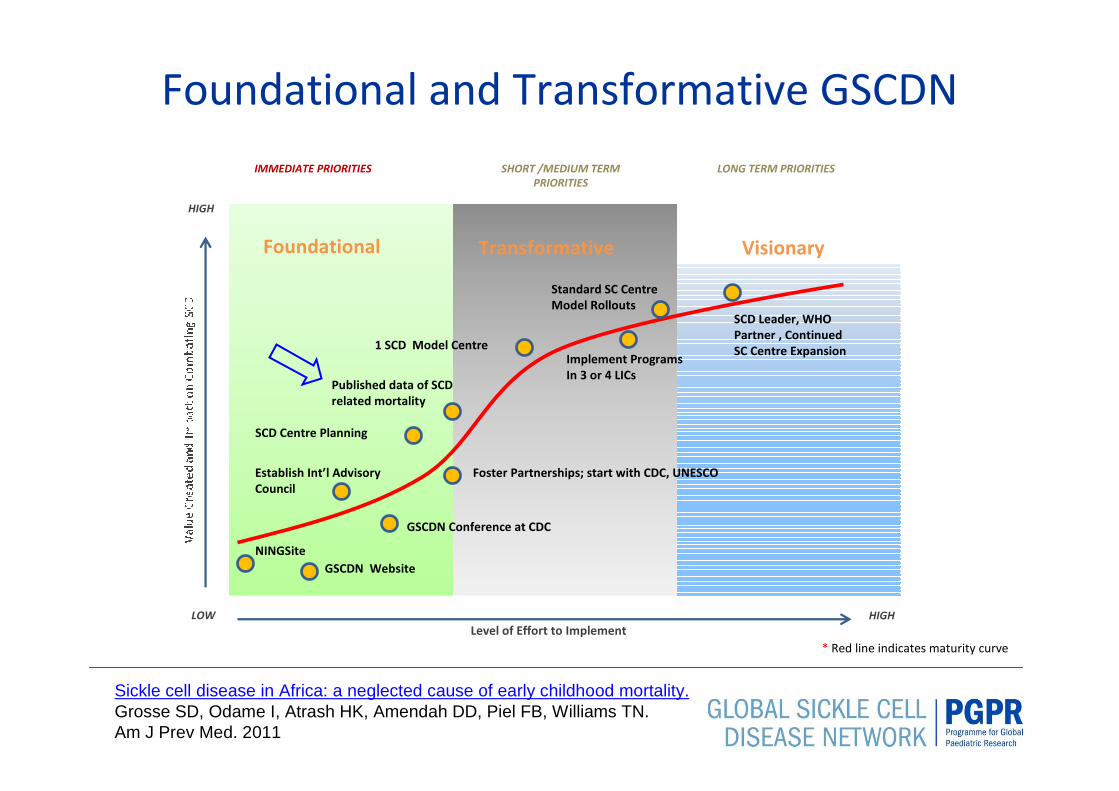
Foundational and Transformative GSCDN
NINGSite
GSCDN Website
Foundational Transformative Visionary
Establish Int’l Advisory
Council
HIGH
HIGH
LOW
Level of Effort to Implement
IMMEDIATE PRIORITIES SHORT /MEDIUM TERM
PRIORITIES
LONG TERM PRIORITIES
* Red line indicates maturity curve
GSCDN Conference at CDC
Published data of SCD
related mortality
Foster Partnerships; start with CDC, UNESCO
SCD Centre Planning
1 SCD Model CentreImplement Programs
In 3 or 4 LICs
Standard SC Centre
Model RolloutsSCD Leader, WHO
Partner , Continued
SC Centre Expansion

www.globalsicklecelldisease.org
GSCDN Website

http://www.globalsicklecelldisease.org/
Interactive Treatment Centres Map
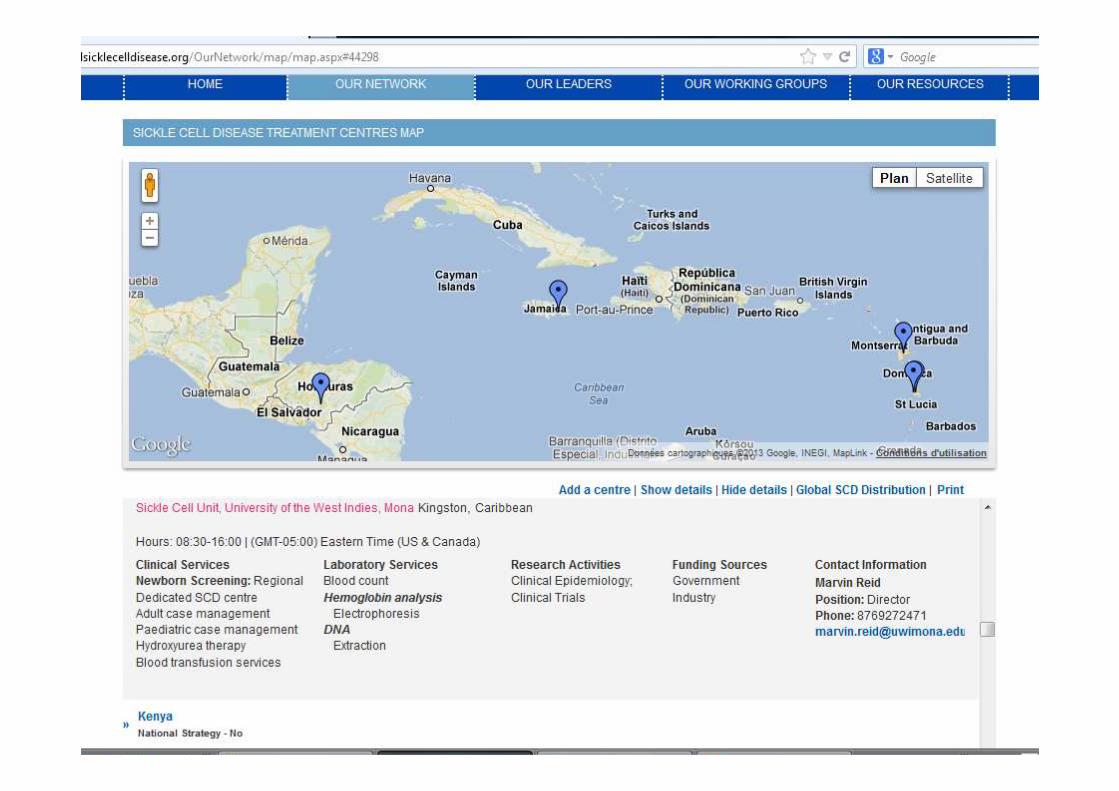

http://globalscd.ning.com
GSCDN ‘Ning’ Online Community
Foundational and Transformative GSCDN
NINGSite
GSCDN Website
Foundational Transformative Visionary
Establish Int’l Advisory
Council
HIGH
HIGH
LOW
Level of Effort to Implement
IMMEDIATE PRIORITIES SHORT /MEDIUM TERM
PRIORITIES
LONG TERM PRIORITIES
* Red line indicates maturity curve
GSCDN Conference at CDC
Published data of SCD
related mortality
Foster Partnerships; start with CDC, UNESCO
SCD Centre Planning
1 SCD Model CentreImplement Programs
In 3 or 4 LICs
Standard SC Centre
Model RolloutsSCD Leader, WHO
Partner , Continued
SC Centre Expansion
Sickle cell disease in Africa: a neglected cause of early childhood mortality.Grosse SD, Odame I, Atrash HK, Amendah DD, Piel FB, Williams TN.Am J Prev Med. 2011
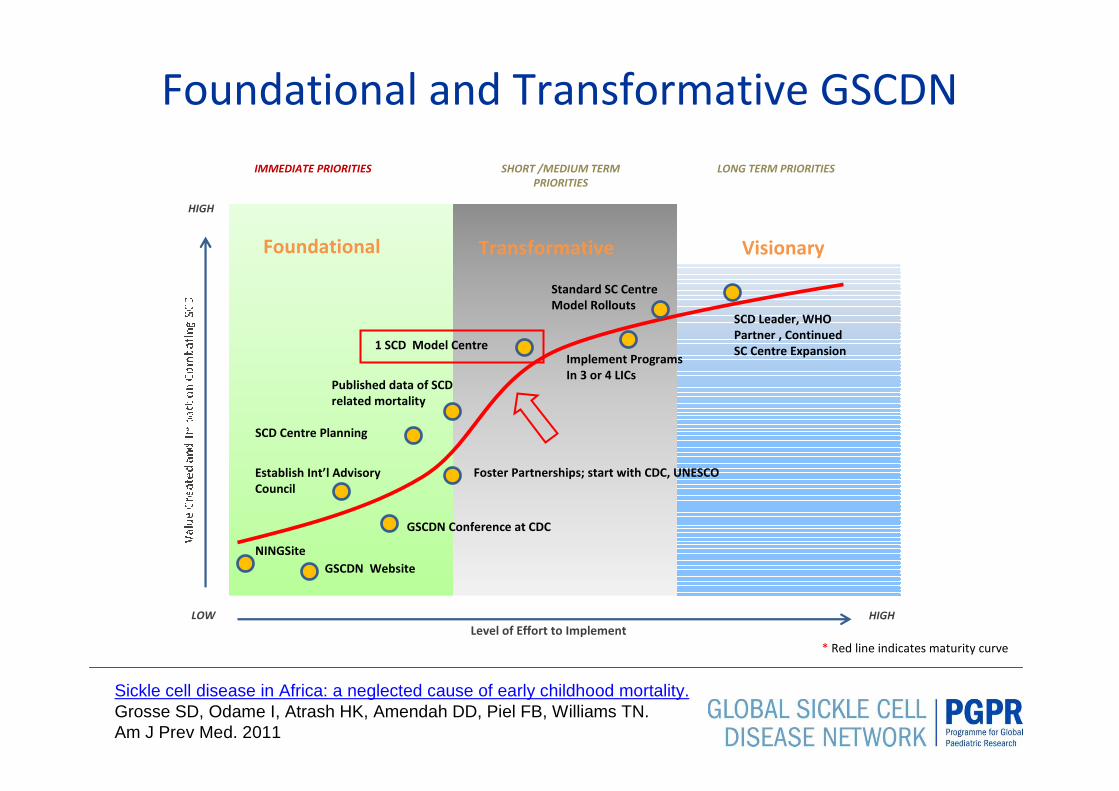
Foundational and Transformative GSCDN
NINGSite
GSCDN Website
Foundational Transformative Visionary
Establish Int’l Advisory
Council
HIGH
HIGH
LOW
Level of Effort to Implement
IMMEDIATE PRIORITIES SHORT /MEDIUM TERM
PRIORITIES
LONG TERM PRIORITIES
* Red line indicates maturity curve
GSCDN Conference at CDC
Published data of SCD
related mortality
Foster Partnerships; start with CDC, UNESCO
SCD Centre Planning
1 SCD Model CentreImplement Programs
In 3 or 4 LICs
Standard SC Centre
Model RolloutsSCD Leader, WHO
Partner , Continued
SC Centre Expansion
Sickle cell disease in Africa: a neglected cause of early childhood mortality.Grosse SD, Odame I, Atrash HK, Amendah DD, Piel FB, Williams TN.Am J Prev Med. 2011

The importance of local management in reinforcing the whole
GSCDN and the regional SCD Networks
CAREST
REDAC
GLOBAL SICKLE CELL
DISEASENETWORK

Juntos mas fuertes
Together we will be stronger
Ensemble nous serons plus forts
Ansanm nou ké pli fô
Organize / Join SCD Networks!