Sex and the ‘recently single’: perceptions of sexuality and HIV risk among mature women and...
18
This article was downloaded by:[Grant, Kathryn] On: 22 June 2008 Access Details: [subscription number 794168475] Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Culture, Health & Sexuality An International Journal for Research, Intervention and Care Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713693164 Sex and the 'recently single': perceptions of sexuality and HIV risk among mature women and primary care physicians Kathryn Grant a ; Kathleen Ragsdale b a Department of Sociology and Anthropology, University of North Florida, USA b Department of Sociology, Anthropology and Social Work, Mississippi State University, USA Online Publication Date: 01 June 2008 To cite this Article: Grant, Kathryn and Ragsdale, Kathleen (2008) 'Sex and the 'recently single': perceptions of sexuality and HIV risk among mature women and primary care physicians', Culture, Health & Sexuality, 10:5, 495 — 511 To link to this article: DOI: 10.1080/13691050801948094 URL: http://dx.doi.org/10.1080/13691050801948094 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Sex and the ‘recently single’: perceptions of sexuality and HIV risk among mature women and...
This article was downloaded by:[Grant, Kathryn]On: 22 June 2008Access Details: [subscription number 794168475]Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Culture, Health & SexualityAn International Journal for Research,Intervention and CarePublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713693164
Sex and the 'recently single': perceptions of sexualityand HIV risk among mature women and primary carephysiciansKathryn Grant a; Kathleen Ragsdale ba Department of Sociology and Anthropology, University of North Florida, USAb Department of Sociology, Anthropology and Social Work, Mississippi StateUniversity, USA
Online Publication Date: 01 June 2008
To cite this Article: Grant, Kathryn and Ragsdale, Kathleen (2008) 'Sex and the 'recently single': perceptions ofsexuality and HIV risk among mature women and primary care physicians', Culture, Health & Sexuality, 10:5, 495 —511
To link to this article: DOI: 10.1080/13691050801948094URL: http://dx.doi.org/10.1080/13691050801948094
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article maybe used for research, teaching and private study purposes. Any substantial or systematic reproduction,re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expresslyforbidden.
The publisher does not give any warranty express or implied or make any representation that the contents will becomplete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should beindependently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings,demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with orarising out of the use of this material.

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
Sex and the ‘recently single’: perceptions of sexuality andHIV risk among mature women and primary care
physicians
KATHRYN GRANT1 & KATHLEEN RAGSDALE2
1Department of Sociology and Anthropology, University of North Florida, USA, and 2Department of
Sociology, Anthropology and Social Work, Mississippi State University, USA
AbstractPrimary care physicians may mistakenly conclude that sexual issues are unimportant to divorced orwidowed mature women, based on age and gender biases. Although research suggests that manysingle mature women are sexually active, physicians are often reluctant to discuss sexual matters withthem. Structured and open-ended interviews explored perceptions regarding mature women’ssexuality and HIV-related risk for patient-physician communication among 44 ‘recently single’mature women aged 45–68 and 31 primary care physicians. Age and ethnic group comparisons withthe mature women suggest that younger and African-American women reported higher HIV and STIrisk perception than older and White women. Many mature women (64%) believed that they were at-risk for HIV and STIs, whereas physicians considered younger patients most at-risk and that riskdeclined with patients’ advancing age and with female status. Mature women and physicians haddifferent expectations regarding initiation of clinical sexual health discussions, with 44% of themature women placing the onus of responsibility on the patient, whereas 74% of physicians believed itwas the role of both doctors and patients to bring up these topics. The findings are instructive toprimary care physicians and healthcare policy makers, indicating that sexual health issues are relevantto mature women’s continued health and well-being.
ResumeLes medecins en soins primaires peuvent considerer a tort, en se basant sur leurs perceptions de l’ageet du genre, que les questions de sexualite n’ont pas d’importance pour les femmes divorcees ou pourles veuves d’age mur. Bien que la recherche suggere que beaucoup de femmes seules et d’age mursont sexuellement actives, les medecins sont souvent reticents a l’idee d’aborder ces questions avecelles. Des entretiens structures et ouverts ont permis d’explorer les perceptions sur la sexualite desfemmes d’age mur et les risques lies au VIH, dans le cadre de la communication entre patients etmedecins, chez 44 femmes d’age mur, « seules depuis peu » et agees de 45 a 68 ans, et chez 31medecins en soins primaires. Concernant les 44 femmes d’age mur, les comparaisons par tranchesd’age et par groupes ethniques suggerent que les taux de perceptions des risques lies au VIH et auxIST sont plus eleves chez les femmes les plus jeunes et chez les Afro-Americaines que chez les femmesles plus agees et les femmes de race blanche. Beaucoup de femmes d’age mur (64 %) considerentqu’elles sont exposees au VIH et aux IST; alors que les medecins croient que seules les plus jeunespatientes sont les plus exposees et que ces risques diminuent en fonction de l’age et du statut desfemmes. Concernant l’initiation des discussions sur la sante sexuelle, les femmes d’age mur expriment
Correspondence: Kathryn Grant, Department of Sociology and Anthropology, University of North Florida, 1 UNF Drive,
Jacksonville, 32224, USA. Email: [email protected]
Culture, Health & Sexuality, June 2008; 10(5): 495–511
ISSN 1369-1058 print/ISSN 1464-5351 online # 2008 Taylor & Francis
DOI: 10.1080/13691050801948094

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
des attentes differentes de celles des medecins, 44 % d’entre elles considerant qu’il revient auxpatientes d’initier ces discussions, et 74 % des medecins considerant qu’il est du role aussi bien desmedecins que des patientes d’aborder ces questions. Les resultats sont instructifs pour les medecinsen soins primaires et les responsables des politiques des soins: ils indiquent que les questions de santesexuelle sont tout a fait pertinentes dans le domaine du maintien de la sante et le bien-etre des femmesd’age mur.
ResumenLos medicos de atencion primaria pueden llegar a la conclusion erronea de que los problemas sexualesno son importantes para mujeres maduras divorciadas o viudas basandose en prejuicios de edad ygenero. Aunque los estudios indican que muchas mujeres maduras solteras son sexualmente activas,con frecuencia los medicos son reacios a hablar con ellas sobre temas sexuales. Mediante entrevistasestructuradas y abiertas a 44 mujeres maduras solteras con edades comprendidas entre los 45 y 68 anosy 31 medicos de atencion primaria, se analizo que percepciones tenıan de la sexualidad de mujeresmaduras y el riesgo de infeccion del virus del sida y cual era la relacion comunicativa medico-paciente.Las comparaciones realizadas en funcion de la edad y el grupo etnico entre las mujeres maduras indicanque las mujeres mas jovenes y de origen afroamericano eran mas conscientes del riesgo de contagio delVIH y de infecciones de transmision sexual que las mujeres mas mayores y de raza blanca. Muchasmujeres maduras (64%) creıan que corrıan riesgos de contagiarse del virus del sida y de infecciones detransmision sexual mientras que los medicos pensaban que las pacientes mas jovenes corrıan masriesgos y que este riesgo disminuıa si los pacientes era mas mayores y mujeres. Las mujeres maduras ylos medicos tenıan expectativas diferentes en cuanto al inicio de charlas sobre salud sexual: el 44% de lasmujeres maduras pensaban que era responsabilidad del paciente, mientras que el 74% de medicoscreıan que eran los medicos y las pacientes quienes debıan ocuparse de hablar de estos temas. Estosresultados son instructivos para los medicos de atencion primaria y los responsables de la polıticasanitaria porque indican que las mujeres maduras tambien tienen problemas de salud sexual y que sonimportantes para su salud y el continuo bienestar.
Keywords: HIV/AIDS, risk perception, patient communication, older women, STIs
Introduction
Interest in exploring the dynamics of provider-patient communication about sexuality
issues has taken on new significance in the wake of the HIV epidemic. This interest is
apparent in patient-service provider communication studies that address sensitive topics
and behaviours, including those that may be difficult to articulate, embarrassing or
stigmatising among populations that vary by gender, age, ethnicity and sexual orientation
(Makadon and Silin 1995, Kerr et al. 1996, Haas and Coe 1997, Skiest and Keiser 1997,
Epstein et al. 1998, Coates 1999, Wilson and Kaplan 2000, Rich 2001, Roter et al. 2002,
Nusbaum et al. 2002, Lindau et al. 2006, Smith et al. 2007). Such studies have explored
physicians’ communication behaviours with patients in terms of sexual function and
sexual health (such as HIV prevention) within the clinical setting; physician and patient
attitudes towards discussing sexual health issues within clinical contexts; and the impact
of physician or patient characteristics (i.e. age, gender, ethnicity). However, many of
these studies on HIV prevention and/or sexual communication within clinical contexts
have not delineated all findings by age, gender or ethnicity and most have primarily
focused on young populations historically at higher risk for HIV (Makadon and Silin
1995, Kerr et al. 1996, Haas and Coe 1997, Epstein et al. 1998, Coates 1999, Nusbaum et
al. 2002).
Indeed, what often comes to mind when the dating scene and HIV/STI risk are
mentioned are people in their 20s and 30s. Yet many mature women and men remain
496 K. Grant and K. Ragsdale
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
sexually active well into their later years, practicing a full range of sexual behaviours
(Stall and Catania 1994, American Association of Retired Persons (AARP) 1999, 2003,
Winningham et al. 2004, Lindau et al. 2006, Smith et al. 2007). As baby boomers age,
research on mature sexuality is expected to take on more social and clinical importance
(Yates et al. 1999). Despite this projected trend within the USA, cultural emphasis on
sexuality in youth, and the implication that older persons should not be concerned
about sexuality (or the potential health risks associated with some sexual behaviour),
does not prepare older persons or their healthcare providers for clinical communication
about sexual issues. This paper presents data from research that focused on mature
women’s concepts of sexuality and their notions about HIV and STI risks, comparing
those concepts with those of primary care physicians in an urban north Florida
community.
Background
Within the USA, healthcare providers would seem an ideal source of HIV prevention
information, since adults average almost three visits a year to a physician and physicians are
believed to be highly credible sources of health information (Makadon and Silin 1995,
Haas and Coe 1997). Indeed, most patients surveyed indicate that they would like to talk
with physicians about sexual health concerns, including HIV and AIDS (Makadon and
Silin 1995, Nusbaum et al. 2002, Smith et al. 2007). However, this resource often goes
untapped due, in part, to physicians’ perceptions of what constitutes appropriate medical
care, their discomfort with discussing sensitive issues, such as sexuality and intravenous
drug use, limited conceptions about who is at risk for HIV and time and resource
constraints (Strombeck and Levy 1998). Additionally, some physicians’ ageist attitudes
towards mature adults preclude the notion that older women and men can be at risk for
HIV infection (Strombeck and Levy 1998). Yet, the continuing rise of HIV cases among
populations not traditionally considered at high risk of infection indicates that physicians
may be interacting ‘with HIV-positive patients and other patients who are at risk for
infection that may not fall into the ‘‘traditional’’ high-risk categories’ (Haas and Coe 1997,
p. 403).
Although reported cases of HIV and AIDS decreased among children and persons aged
25–34 years between 1998 and 2002, they increased among persons aged 45 and older
(CDC 2002). In 2003, 9% of all people living with HIV/AIDS in the USA were aged 55
and older (CDC 2003). In Florida, the site of the present study, persons aged 50 and over
account for 15% of AIDS cases and 11% of the HIV (not AIDS) cases; non-Hispanic
Blacks account for 52% of all seniors (age 50 and over) diagnosed with AIDS, as compared
with 32% of non-Hispanic Whites and 16% of Hispanics (Florida Department of Health
2004). African-American women in all age groups have been severely affected by HIV and
AIDS in Florida, representing 69% of all AIDS cases and 66% of all HIV cases in women
(Florida Department of Health 2006a).
The primary mode of transmission for all adult women is through heterosexual contact,
accounting for 86% of HIV cases in Florida (Florida Department of Health 2006b).
Despite growing concern about female-to-female HIV transmission (CDC 2006),
heterosexual transmission continues to be the area of greatest concern for women aged
50 and older, particularly among those re-entering the dating scene after divorce or
widowhood (Rich 2001, Florida Department of Health 2004). Furthermore, HIV risk
perceptions, rates of testing and consistent condom use are relatively low among mature
Culture, Health and Sexuality 497

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
persons (Mack and Bland 1999, Theall et al. 2003, Zablotsky and Kennedy 2003,
Paranjape et al. 2006).
Given that HIV transmission is increasing among older people, research on mature
sexuality should address how sociocultural factors mediate and moderate effective
patient-physician communication regarding HIV- and STI-related risk. This research
was designed to address the following questions: Do physicians hold age- and/or gender-
based assumptions about discussing sexuality and/or HIV and STI-related topics with
mid-life and older women? Do physicians feel their education prepared them to address
HIV and STI-related topics with their mature women patients? Are physicians’ concepts
about sexuality and aging different from women’s own sexuality and aging concepts? Are
there differences in women’s perceptions about discussing sexuality issues in clinical
contexts based on age, marital/partner status and ethnicity? Are there differences in
women’s HIV and STI risk perceptions based on age, marital/partner status and
ethnicity?
Methods
Qualitative and quantitative data were collected from a sample of 44 recently divorced,
widowed or separated mature women (referenced here as ‘recently single’ due to their
marital status and recent participation in a displaced homemaker programme) and a sample
of 31 primary care physicians, in the same north Florida community. Recently single
participants completed a demographic survey and in-depth interview. Physician partici-
pants completed a demographic/practice characteristics survey and some also completed an
in-depth interview. The details of each method are described below.
Recently single participants
The 44 recently single women aged 45–68 years were recruited through a state-
sponsored displaced homemaker programme between October 2002 and June 2004.
Interviews with programme staff indicated that most of the women attending the
programme had been single for six months to a year, though this information was not
systematically collected. The female investigator conducted the interviews with
participants in their homes, places of work or at the community college campus where
the displaced homemaker programme was conducted. The investigator attended sessions of
each three-week programme that occurred during the recruitment period. Eligible
participants met the following inclusion criteria: they were > 45 years of age and divorced,
widowed, separated or had ended a long-term heterosexual consensual union (women who
had lived with a man in a long-term consensual union for periods ranging from about 5–15
years, but had never married). Eligible women who did not complete the interview on the
spot were interviewed later at a pre-arranged time and place of their choosing. The
Institutional Review Board of the University of Florida approved the consent procedures
for this project, which included informing participants of the sexuality theme of the
research and their right to refuse to answer any question or to terminate the interview at any
time. Participants were also assured that no individual identifiers would be associated with
their interview responses in data reports. Respondents were compensated for their
participation with a US$20 gift certificate.
498 K. Grant and K. Ragsdale

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
Physician participants
The majority of the physicians recruited into the study were resident or attending
physicians at a university-based family practice clinic that serves an urban, low-income,
largely African-American neighbourhood. Their female patient population is made up of
all age groups and is approximately 70% African-American and 30% White. Between June
2003 and June 2004, 28 physicians were recruited through a family practice residency
programme, and three physicians were from other primary care departments in the same
university-based hospital. The inclusion criteria for physicians were: a patient base that
included women aged 45 and older; and training in a primary care speciality (i.e. family
medicine, general medicine, internal medicine, obstetrics/gynaecology, etc.). All 31
physicians completed the survey and 18 also participated in one-on-one interviews. The
approved consent procedures were largely the same as those for the recently single
women, except for clarification regarding level of participation (survey only or both survey
and interview) and compensation based on level of participation (survey only participants
received a US$10 gift certificate and survey/interview participants received a US$20 gift
certificate).
Recently single participant survey
The structured survey for the recently single women elicited information in the following
areas: sociodemographic data on age, ethnicity, marital status, number of children, number
in current household, level of education, years lived in the area, health status, most recent
doctor visits and type of doctor visited. For purposes of analysis, the following variables
were recoded as follows: ethnicity was dichotomised as White or African-American; ages
were grouped as 45–55 versus 56-or-above; ‘divorced’ and ‘ended consensual union’ were
combined into one variable.
Physician participant survey
The structured survey for the physicians elicited information in the following areas: age;
status as a resident or attending physician; recentness of medical training; type of practice;
demographic profile of physicians’ patient population (percentages based on age, gender
and ethnicity); perceptions of medical education and HIV/STI prevention preparedness;
perceptions of patients’ HIV knowledge; sexual health risk for their patients aged 45 and
older; and opinions about patient and physician responsibility regarding discussing sexual
health issues.
A five-point Likert scale format was used for the following questions: (1) ‘How well
informed are the majority of your adult patients (aged 45 and older) about HIV and other
STIs?’ (ranging from ‘well informed’ to ‘not at all informed’); and (2) ‘Do you feel that
your medical education adequately prepared you for addressing current sexuality issues
(including STIs and HIV) with a wide range of patients?’ (ranging from ‘strongly agree’ to
‘strongly disagree’). The following multiple-choice question was used: ‘Do you think it is
primarily the patient’s or the physician’s responsibility to bring up sex life issues in a clinical
encounter?’ Responses codes were ‘doctor’s’, ‘patient’s’ or ‘both’.
The initial survey included a question about the percentage of adult patients that
physicians considered at-risk. Early interviews with physicians suggested that they deemed
men to be at higher risk than women, which prompted a revision to the survey to assess
Culture, Health and Sexuality 499

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
this difference. Therefore three of the physicians were not asked this question in the
survey or interview format. The revised version of the survey asked physicians (n518) to
rate their patients’ HIV and STI risk with: ‘Generally, what percentage of your adult
patients do you consider at-risk for HIV or other STIs?’ (males …%, females …%). A
further revision of the survey was given to eight of the physicians, which asked them to
address the differences in risk by age groups. Additional data on age/gender risk
perceptions was gleaned from interviews.
Recently single participant interview
All interviews were audio taped with the participants’ permission. Interviews required
between 30 and 60 minutes to complete. Some qualitative interview data was coded for
quantitative analysis using responses from the following questions related to HIV and
AIDS knowledge and risk: (1) ‘Tell me a little bit about what you know about HIV and
AIDS’; (2) ‘Do you think that you are at-risk for HIV or other STIs?’ (responses coded
as ‘yes’, ‘no’ or ‘don’t know’, even though responses often included qualification for
why they gave the responses they gave); and (3) ‘Do you think that other recently single
women your age and older think that they are at-risk for HIV or other STIs?’ (responses
coded as ‘yes’, ‘yes, most’, ‘no’, ‘no, not most’, ‘don’t know’). All responses to closed-
ended questions listed above and were followed by probes, such as, ‘Why do you think
that you are (or are not) at risk?’ To determine how these women felt about physicians
talking to their older patients about sexual health issues, participants were asked: (1)
‘Do you think that doctors should assume their mature patients are sexually active?’
(responses coded as ‘yes’ or ‘no, don’t assume, ask’); (2) ‘Do you think doctors ought
to address the topic sexually transmitted infections with their mature patients?’
(responses coded as ‘yes’ or ‘no’); and (3) ‘Do you think that it is the patient’s or the
doctor’s responsibility to bring up sex life issues?’ (responses coded as ‘doctor’s’,
‘patient’s’ or ‘both’). Probes followed the questions above to assess the reasons for their
answers.
Physician participant interview
The physician participant interviews were used to elicit information about physicians’ age-,
gender-, marital status- and ethnicity-based perceptions regarding mature sexuality. The
interview schedule included the following questions and probes related to HIV-risk
perceptions and discussing sexual health issues with mature patients: (1) ‘Do you think
physicians should assume that all of their mature patients are sexually active?’ (responses
coded as ‘yes’ or ‘no, don’t assume, ask’); (2) ‘When do you think sexuality issues should be
addressed between physician and patient?’; and (3) ‘What percentage of your patients do
you consider at-risk for HIV or other STIs?’ Follow-up probes included, ‘Why this
number?’ and ‘Does their age/ethnicity/sex/sexual orientation influence risk status?’ Data
collected from these qualitative questions were not quantified for statistical analysis.
Data analyses
SPSS 12.0 (Chicago, Il) was used for analysis of quantitative data. Standard inferential
tests were used to assess significance within groups and between-groups using two-by-two
500 K. Grant and K. Ragsdale
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
comparison tables for Fisher’s Exact Test with two-sided significance (p-values only). Only
findings from those tests that yielded significance are reported. Percentages of comparisons
with multiple variables are given without further statistical analysis because of sample size
limitations on Pearson Chi-Square statistics. NUD*IST qualitative software was used
primarily as an organizing tool to sort the interview data for coding of relevant themes.
Themes were identified by the primary researcher and supported with the assistance of her
dissertation committee. Comments on a given theme were supported by a minimum of a
fifth of participants for each sample (physicians or ‘recently’ single women) mentioning a
topic to be considered a theme for analysis. Qualitative data presented here maintains the
confidentiality of the respondents and serves to support and clarify the statistical data and
percentage data.
Results
Recently single participants
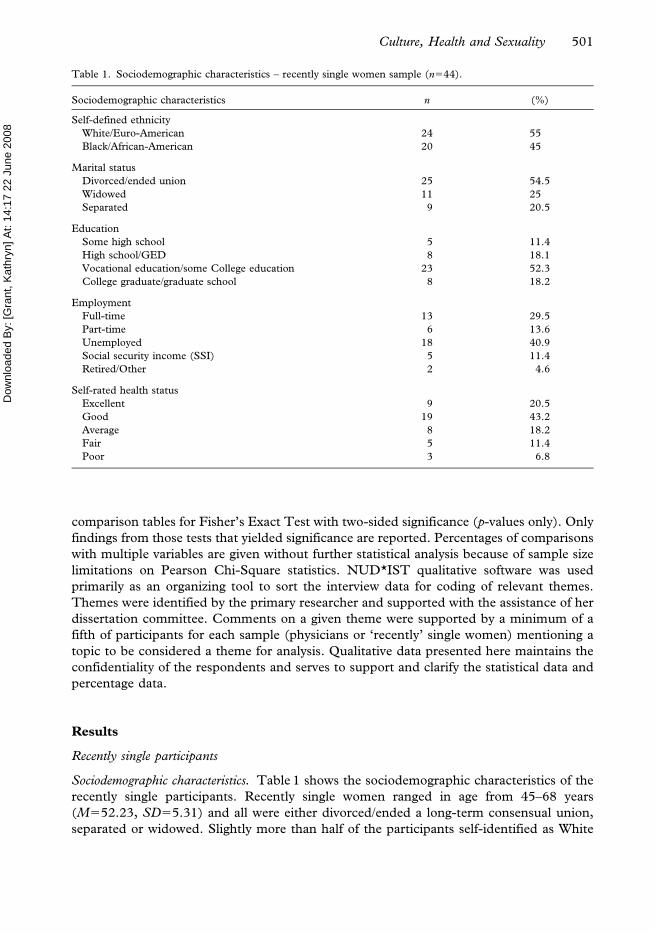
Sociodemographic characteristics. Table 1 shows the sociodemographic characteristics of the
recently single participants. Recently single women ranged in age from 45–68 years
(M552.23, SD55.31) and all were either divorced/ended a long-term consensual union,
separated or widowed. Slightly more than half of the participants self-identified as White
Table 1. Sociodemographic characteristics – recently single women sample (n544).
Sociodemographic characteristics n (%)
Self-defined ethnicity
White/Euro-American 24 55
Black/African-American 20 45
Marital status
Divorced/ended union 25 54.5
Widowed 11 25
Separated 9 20.5
Education
Some high school 5 11.4
High school/GED 8 18.1
Vocational education/some College education 23 52.3
College graduate/graduate school 8 18.2
Employment
Full-time 13 29.5
Part-time 6 13.6
Unemployed 18 40.9
Social security income (SSI) 5 11.4
Retired/Other 2 4.6
Self-rated health status
Excellent 9 20.5
Good 19 43.2
Average 8 18.2
Fair 5 11.4
Poor 3 6.8
Culture, Health and Sexuality 501
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
(including one Middle-Eastern woman who self-identified as ‘other’) and 45% identified
as African-American. More than half had vocational training or some college education
and about a fifth were college graduates or had advanced degrees. Nine percent of
African-American women had not completed high school compared to 2% of White
women, but African-American women were more likely to have some college or
vocational training (60%) than were white women (43.5%). Almost two-thirds rated their
health as ‘good’ or ‘excellent’, just under a fifth rated their health as average and the
remaining fifth reported their health was ‘fair’ or ‘poor’. A slight majority was
unemployed or on Supplemental Security Income (a Federal income programme
funded by general tax revenues for people who are aged, disabled or unable to generate
sufficient income for food and shelter) and 43% were working either part- or full-time.
Since the primary purpose of the displaced homemaker programme is to assist women
with gaining employment after marital disruption, the low employment rate is not
surprising.
Twenty-three percent (n510) of the participants were in new sexual relationships with
steady partners, 15.9% (n57) were in new sexual relationships with non-steady partners,
6.8% (n53) had recently ended a dating/sexual relationship within the past two weeks to a
month, 36.4% (n516) were single and were not actively pursuing a new sexual
relationship, but would consider dating the ‘right person’ and 15.9% (n57) expressed no
interest in finding a new sexual partner or dating. These categories were gleaned from
interview data to best reflect the variety of responses to a question (and probes) regarding
current partner status.
Dating and HIV/STI risk among recently single participants. Sixty-four percent said that
they considered themselves to be ‘at risk’ for HIV and other STIs. Partner status was
important in determining their risk perception, with 82.4% of those with partners
declaring that they believed they were at risk, as compared to 51.9% of those without a
current partner. Women between 45 and 55 years of age (70.6%, n524) were more likely
to report that they were ‘at risk’ than women 56 years of age or above (40%, n54) and
African-American women were slightly more likely to think that they were at risk (70%,
n514) than White women (58.3%, n514), but these difference were not statistically
significant.
Explanations of HIV/STI risk perceptions. In the interviews, some of the women cited
infidelity by husbands and lovers for their risk perception and some mentioned the
uncertainty of knowing a partner’s status:
‘… even if you’re in a monogamous relationship, just because you are doesn’t mean that …your
partner isn’t, you know, going someplace.’ (divorced woman with steady partner in her
mid-50s)
Other reasons focused on the newness of safer sex practices:
‘Well, I have never had sex with a condom – never had to … That’s going to be a whole new
experience for me when that comes to pass. Asking, you know, ‘let’s use protection,’ [or] ‘do you
have any?’ Or going to a store and buying some condoms to keep in my nightstand – totally
something that I have never done and never expected to do.’ (separated woman in her mid-50s
without a current partner)
502 K. Grant and K. Ragsdale
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
Some of the women without a current sexual partner who felt that they were at-risk for HIV
and STIs explained that they did not intend to remain single and that they were cognizant
of the risks involved with sexual relationships:
‘Yes, I will be [at-risk], ‘cause I’m planning on getting back into the game.’ (separated woman in
her mid-50s)
Some participants without partners who did not consider themselves at risk explained that
they were not sexually active and had no interest in finding a partner:
‘No ma’am, because it’s like I told you, I’m scared and I don’t want to be bothered. And um, I
don’t like, what do you call it, protection [condoms]? I don’t care for that.’ (divorced woman in her
late 50s)
Tested for HIV. Forty-one percent (n518) of recently single women spontaneously
volunteered during interviews that they had been previously tested for HIV; 59% (n510)
of women with partners or in dating relationships had been tested, as compared to 29.6%
(n58) of women without partners. Though not statistically significant, women between the
ages of 45 and 55 (47.1%, n516) and African-American participants (55%, n511) were
more likely than participants over 55 years of age (20%, n52) and White participants
(29.1%, n57) to report that they had been previously tested for HIV. HIV testing was
motivated by fear of exposure and inconsistency in using condoms, although in some cases
it was also related to having personal knowledge of someone with HIV or who had died of
AIDS. The following quote summarized several of the issues raised in the interviews about
dating, safer sex practice and reasons for HIV testing:
‘So many people like me are divorced and we date and we’re not always careful. We don’t like
condoms. We hardly ever use them … We take chances, thinking that, well, it doesn’t happen in
my age group or in my class, but it does. But when you have a steady boyfriend, you don’t think of
yourself, and you don’t know what he’s doing on the days he’s not seeing you, and I don’t trust
men anymore, so I figure they’re going to be out doing something … I know myself, and I’ve lied to
men before about other men, so if I’ll do it, then I’m sure they’ll do it ‘cause I’m not that different
… But I’ve had myself tested.’ (divorced woman in her early 60s)
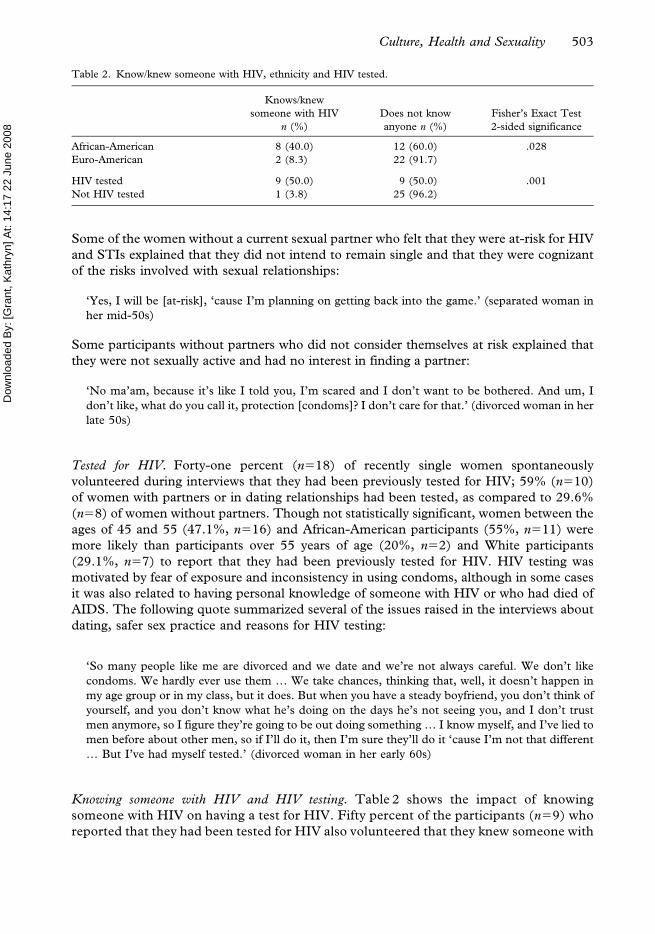
Knowing someone with HIV and HIV testing. Table 2 shows the impact of knowing
someone with HIV on having a test for HIV. Fifty percent of the participants (n59) who
reported that they had been tested for HIV also volunteered that they knew someone with
Table 2. Know/knew someone with HIV, ethnicity and HIV tested.
Knows/knew
someone with HIV
n (%)
Does not know
anyone n (%)
Fisher’s Exact Test
2-sided significance
African-American 8 (40.0) 12 (60.0) .028
Euro-American 2 (8.3) 22 (91.7)
HIV tested 9 (50.0) 9 (50.0) .001
Not HIV tested 1 (3.8) 25 (96.2)
Culture, Health and Sexuality 503
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
the disease or who had died of AIDS, whereas only one of the participants that knew
someone with the disease had not been tested. On the other hand, the majority of those
who did not mention being tested (96.2%) did not know anyone with HIV (p5.001).
Knowing someone with HIV was significantly related to ethnicity with 40% of African-
American participants as compared to 8.3% of White participants knowing someone who
has or had HIV (p5.028).
Perceptions of HIV risk for self and other recently single women. In response to the question,
‘Do you think that other recently single women your age and older think that they are at
risk for HIV?’, 57.5% (n523) said ‘yes’ or ‘yes, most’ as compared to 42.5% (n517) who
said ‘no’ or ‘no, not most’. Respondents often qualified their ideas about the perceptions
of others by saying that they think that they know of the risk, but do not consistently take
steps to protect themselves and that emotional and socioeconomic issues also come into
play:
‘Probably in the back of their minds [they know of the risk], but they really don’t … think that it
can happen to them. They don’t want to face reality, ‘cause they want to live for the moment.’
(divorced woman in her early 50s)
‘I think we’re a lot more cognizant than any of us would have been 10 years ago. Maybe not as
vigilant as we probably should be.’ (separated woman in her mid-40s)
‘Yes, I think we’re more at risk than some of these young people because we’re more settled …
Then especially when you’re unemployed, lost a loved one and depression, low self-esteem,
sometimes you can just fall into a lurch where you just don’t think sometimes.’ (widow in her mid-
40s)
Physician participants
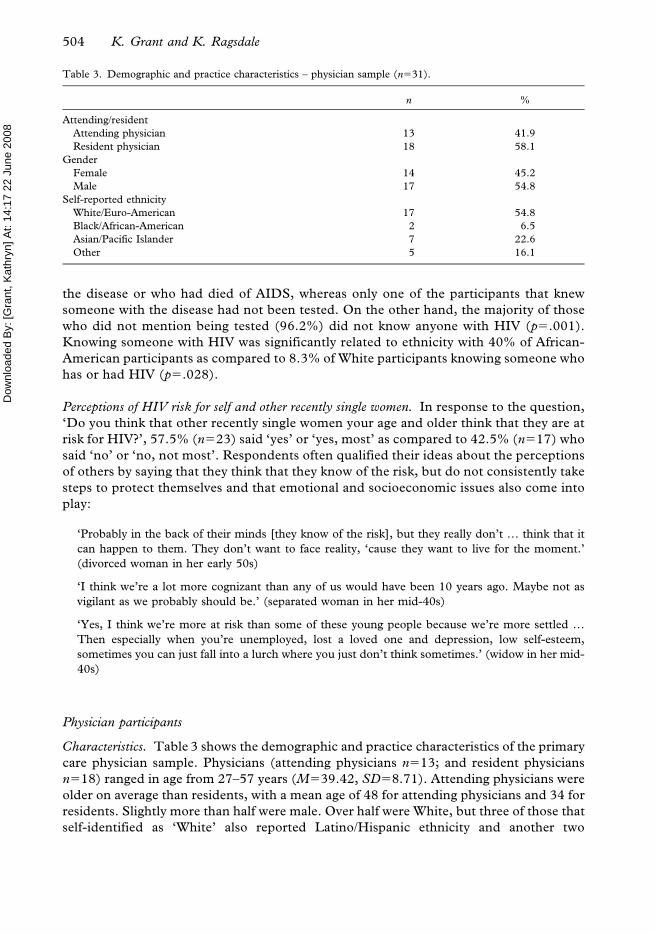
Characteristics. Table 3 shows the demographic and practice characteristics of the primary
care physician sample. Physicians (attending physicians n513; and resident physicians
n518) ranged in age from 27–57 years (M539.42, SD58.71). Attending physicians were
older on average than residents, with a mean age of 48 for attending physicians and 34 for
residents. Slightly more than half were male. Over half were White, but three of those that
self-identified as ‘White’ also reported Latino/Hispanic ethnicity and another two
Table 3. Demographic and practice characteristics – physician sample (n531).
n %
Attending/resident
Attending physician 13 41.9
Resident physician 18 58.1
Gender
Female 14 45.2
Male 17 54.8
Self-reported ethnicity
White/Euro-American 17 54.8
Black/African-American 2 6.5
Asian/Pacific Islander 7 22.6
Other 5 16.1
504 K. Grant and K. Ragsdale

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
identified with a Latin American nationality without selecting the ‘White’ identity as well.
Almost one quarter identified themselves as Asian/Pacific Islander, two identified with a
middle-eastern nationality, two identified as African-American and one identified as ‘West
Indian’.
Physicians’ perceptions of HIV risk for their patients. All of the physicians surveyed and
interviewed work in an area serving mostly a lower income population that is largely
African-American. Forty-three percent of the physicians (n513) considered the majority of
their patients aged 45 years or older ‘partially informed’ about HIV and STIs, while 36.7%
(n511) considered these patients ‘poorly informed’, 10% (n53) considered them
‘moderately informed’ and 10% (n53) considered them ‘well informed’. There were no
significant differences by gender or attending/residency status on this topic. Despite
physicians’ sense that many of their mature patients lacked adequate knowledge about HIV
risks, few physicians considered them at significant risk for HIV and STIs.
Interview and survey follow-up questions suggested that physicians’ perception of
HIV and STI risk generally declined with patients’ increasing age, female status and
intact marriage. Eight physicians completed a revised version of the survey that asked
them to give percentages of patients they considered at risk by gender and age group.
Averages from percent rankings showed that these physicians considered 29.38% of
their male patients aged 45–64 years at risk, as compared to 24.38% of their female
patients in the same age group, and 18.13% of their male patients aged 65 and older at
risk, as compared to 15.63% of their female patients in the same age group. Although
mature women and men were considered to be at a similar risk for HIV and STIs for
these age groups, risk for men was slightly higher. When asked which patient sub-
population they considered most at risk, several physicians mentioned either sex
workers and their clients, or drug users, whereas others referred to patients with
‘multiple sex partners’ or those they believed were not in a ‘committed monogamous
relationship’. Only one physician mentioned her population of gay male patients. As
indicated in the percentages above and interview comments about mature men with
multiple partners, visiting sex workers, etc., physicians were slightly more likely to
consider their mature male patients to be at greater HIV risk than mature female
patients.
Age and marital factors in risk perceptions for patients. Although physicians acknowledged that
most of their patients have some degree of risk for HIV and STIs, several felt that younger
patients and single patients were more at-risk:
‘It’s like, you’re young, you’re healthy you’re out there … so for me it’s probably more age and
general physical abilities … although I had a patient who was in her 80’s in a wheelchair with a
chronic Foley catheter who was still having intercourse and I just wasn’t frankly thinking that that
was in her life, but it was.’ (attending physician in mid-40s)
A few physicians also raised the topic of ethnicity when discussing their patients’ risk for
HIV and STIs. A resident physician in his early 30s voiced the opinion that the largely poor,
African American community that these physicians serve in their clinic might affect their
views about who is at risk.
Medical education and HIV prevention readiness. On a Likert-scale survey question regarding
how physicians felt about their medical training and HIV prevention, most (58%, n518)
Culture, Health and Sexuality 505

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
attending and resident physicians reported that their medical training had prepared them
well to address HIV and STIs with a variety of patients. However, attending physicians
were more likely to ‘disagree’ (38.5%, n55) with the statement that their ‘training had
prepared them well’ than were resident physicians (11.1%, n52). Thirty-three percent
(n56) of the resident physicians selected ‘neutral’ in response to this question compared to
none of the attending physicians.
Responsibility of physicians or patients to raise sexuality topics. Physicians (74.1%, n520) were
much more likely to consider ‘both’ patients and physicians responsible for raising sexual
health issues compared to 27.9% (n512) of the recently single women. About one quarter
(25.9%, n57) of both the physicians and the women (27.9%, n512) placed the onus on the
physician, whereas 44.2% of the women believed that the patient was responsible,
compared to none of the physicians. Qualitative analysis of the interview data showed that
many of the women who said it was the responsibility of the patient to raise sexual health
topics also commented that physicians needed to ‘open the door’ to make patients feel it
was ‘OK’ to talk about it. Even though all of the physicians felt that either physicians alone
or both physicians and patients were responsible for raising sexual health topics, their
comments revealed that some actually place more responsibility on the patient: ‘I think the
patient will bring it up if there’s an issue’; or ‘The physician can’t be expected to just dig for
everything’; or ‘They [patients] have a responsibility, particularly if they have questions or
concerns … to bring it to the physician’s attention and not expect us to be a magician’.
In response to probes following questions about sexual health communication, several
physicians commented that it was ‘usually’ or ‘always’ appropriate to discuss sexual health
risk issues with their patients. However, some physicians also acknowledged that they
seldom raise the topic with their mature patients, citing time constraints, concerns about
offending mature patients or a belief that patients will raise the topic if it is something they
want to discuss. Generally, they talk to those they think are at risk, which tends to be
younger, unmarried patients and those they believe might engage in some high-risk
behaviours. These perspectives and practices point to their perceptions about who is
sexually active and potentially at risk for HIV and STIs.
Assuming mature patients are sexually active. Among the 18 physicians who participated in
the interview, 83.3% (n515) believed that doctors should assume that their mature
patients are sexually active, compared to 51.2% (n522) of the recently single women
(p5.023) (see Table 4). Although physicians overwhelmingly agreed that they should
assume mature patients are sexually active, a few acknowledged that they had on occasion
made the wrong assumption and stereotyped mature patients as sexually inactive:
‘I tend to assume, too often, that they are not sexually active. I think this is kind of a stereotype that
goes on in my mind.’ (attending physician in early 50s)
Table 4. Women and physicians assuming older patients are sexually active.
Yes, assume
n (%)
No, or don’t assume,
ask n (%)
Fisher’s Exact Test
2-sided significance
Recently single women 22 (51.2) 21 (48.8) .023
Physicians 15 (83.3) 3 (16.7)
506 K. Grant and K. Ragsdale

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
‘I think we should assume it because … we’ve had older patients with HIV that people just
assumed weren’t sexually active. And you know, I had a patient with syphilis and I just assumed
that she wasn’t sexually active.’ (attending physician in mid-40s)
Although half of the recently single women did not want physicians to assume mature
patients were sexually active, many said that physicians should ask their patients about it to
be sure:
‘No, because like I said, in assuming, you don’t really know … It’s better to be sure than assume,
because with assumptions sometimes you miss out on something that’s important.’ (divorced
woman in her mid-40s)
‘I don’t think a doctor should make that assumption. But I think they could bring [it] up.’ (widow
in her early 50s)
Some of the women who thought physicians should assume their patients are sexually
active expressed the sentiment that ‘it’s better to be safe than sorry’ and that ‘appearances
can be deceiving’ when is comes to sexual activity:
‘We’re all human … Yes, they should assume that they’re sexually active. They may not be, but if
they’re not right now they probably will be later’ (widow in her late 40s with a new partner)
In addition, 88.6% (n539) of the recently single women thought that physicians should
discuss HIV/STIs issues with their mature patients.
Discussion
The sexual health risks of mature women have generally been ignored in both medical
literature and practice. That HIV and other STI risks are not confined to younger, male or
other identified groups remains poorly recognized among healthcare professionals and
the general public. The present study collected qualitative and quantitative data from
mature women and primary care physicians regarding clinical communication about
sexual health and HIV and STI-related risks. Findings suggest that physicians bring
societal age and gender biases to their perceptions regarding which patients are sexually
active (and therefore possibly at risk for heterosexual HIV and STI transmission) that
influence their communication about sexual health issues with mature female patients.
Mature women and physicians also differ in their perceptions of responsibility to initiate
sexual health communication within the clinical encounter, which may play an important
role during the process of physician/patient communication about this particular health
risk.
Previous research showed a low perception of risk among mature women (Binson et al.
1997). More recent research suggests that more mature women believe they are at-risk for
HIV than earlier cohorts (Zablotsky and Kennedy 2003) and that mature African-
American women are more likely than White women to report making behavioural changes
to reduce their risk of exposure (Lindau et al. 2006). The present analysis suggests that
personal HIV risk perception was high among the recently single women included in this
sample. The higher-than-expected risk perception was linked to dating status, with those in
new relationships expressing the most concern over HIV and STI-related risk. Several
factors may have influenced risk perception among this sample of women: (1) the particular
‘relationship’ circumstances of the women interviewed for this project, in that this study
Culture, Health and Sexuality 507
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
focused specifically on recently single women, who might be more likely to have
experienced partner infidelity than women in previous studies; (2) the newness of condom
use and/or inconsistency in safer sex practices; (3) changes that have occurred in the
demographics in the spread of the disease since some of the earlier studies were conducted
in the early 1990s; and (4) having personal knowledge of someone with HIV or who has
died of AIDS.
Younger women and African-American women reported higher HIV and STI risk
perception than older women and those who were White. This may be due to the fact that
HIV is more prevalent among African-Americans (Florida Department of Health 2006a,
CDC 2007); that several African-American women in the study reported personal
knowledge of a friend or family member who was living with HIV or had died of AIDS; and
that several had been tested for HIV. Consistent with previous research, younger women
and African-American women were the most likely to reveal that they had been tested
(Mack and Bland 1999, Florida Department of Health 2003, Theall et al. 2003). Although
perception of being at sexual risk may have motivated some women to have an HIV test,
their narrative comments suggest that risk perception may not be motivating the
participants to engage in safer sex practices. Specific data on condom use was not
collected, but the interview data suggests that condom use may be low or inconsistent
among this sample of mature women, which corresponds with previous research (Binson et
al. 1997, Zaboltsky 1998; Mack and Bland 1999, Yates et al. 1999, AARP 2003, Theall et
al. 2003, Zaboltsky and Kennedy 2003, Lindau et al. 2006).
Several respondents reported that age influenced women’s knowledge of sexual health
risk and safer sex behaviour and, therefore, doctors should address sexual health risks with
their mature patients. In contrast, although physicians also considered age an important
factor in patient knowledge of HIV and risk for HIV, they tended to perceive that married
patients and older patients were generally not at risk for HIV and STIs and, therefore,
many physicians were reluctant to discuss sexual risk due to concerns about offending
mature patients. Such misperceptions among physicians have been reported previously
(Makadon and Silin 1995, Kerr et al. 1996, Haas and Coe 1997, Skiest and Keiser 1997,
Epstein et al. 1998). Despite the apparent disinclination to discuss sexual health issues
with certain patients, most physicians thought that they were adequately prepared for such
discussions. Resident physicians were less likely to feel that their medical education failed
to prepare them for clinical communication about sexual health issues and HIV and STI
risks, though the pattern was not as strong as that reported by Haas and Coe (1997), who
found that 78% of more recently trained physicians felt that they were better prepared by
their medical education to address HIV- and AIDS-related topics than physicians trained
earlier.
Most of the recently single women believed that physicians should discuss HIV and STI
issues with their older patients, but close to half of the women participants placed the
responsibility of raising sexual health topics on patients, whereas a majority of physicians
believed that both parties were responsible. However, the recently single participants also
thought that physicians had a responsibility to create a favourable atmosphere for sexual
discussions within the clinical setting.
This study has several limitations. First, it was conducted among a small purposive sample of
recently single women and a small convenience sample of physicians. Although non-
representative sampling is regularly used in qualitative studies (Bernard 1995, Handwerker
2001), care is needed when generalizing results to other recently single women and other
primary care physicians. Given that the recently single participants were seeking guidance
508 K. Grant and K. Ragsdale

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
through a state sponsored programme, these findings may not be representative of other
recently single women who do not choose to participate in such programmes. Second, data on
the length of time between divorce, widowhood or separation and participation in the
programme was not systematically collected either by the programme staff or the project
researcher, which may be an important factor in explaining differences between participants.
Third, multiple domains of HIV risk perception may limit the utility of comparing findings
across studies (see Theall et al. 2003). Fourth, the sociodemographic characteristics of the
recently single participants were somewhat different from the patients of the physician
participants. The physicians treat a largely low-income, African American population of all
ages, whereas the recently single women participants were all aged 45 and over and came from
a range of socioeconomic backgrounds.
The present study adds to the scant literature on mature women’s HIV and STI risk
perceptions and some of the factors that affect it. The focus on a sample of divorced,
separated and widowed mature women provided unique information about an under-
studied segment of the population in HIV and STI prevention studies. These findings
suggest that factors such as the age, gender and ethnicity of patients are important factors in
physician perceptions about sexuality and sexual health risks. Physician perceptions about
marital/partner status are also important factors in physicians’ HIV risk perceptions for
their patients and all of these factors influence the discussion of sexual issues in clinical
contexts. Physicians’ preconceptions of ‘at risk’ populations appear to limit their
perceptions, such that they may miss important primary prevention opportunities among
populations not traditionally conceived as vulnerable to HIV and STIs. This study suggests
that physicians may need to revisit their perceptions regarding mature sexuality in order to
better address HIV risks among mature women patients. The findings are instructive to
primary care physicians, healthcare delivery programmes and policy makers that sexual
health issues are not only important to mature women, but also extremely relevant to
mature women’s continued health and well-being.
Acknowledgements
This paper is based upon research supported by the National Science Foundation under
Grant No. 0241675 and a Woodrow Wilson/Johnson and Johnson Dissertation Grant in
Women’s Health. We are grateful to Celia B. Fisher for insightful perspectives and
commentary during the development of this manuscript and to Kathryn Grant’s
dissertation committee (James P. Stansbury, Leslie Sue Lieberman, Sharleen Simpson
and Barbara Zsembik) for invaluable assistance with funding proposals and critical analysis.
We would also like to thank the recently single women and the physicians who participated
in this study. The participants’ generosity in sharing their time and perspectives made this
research possible.
References
American Association of Retired Persons (AARP) (1999) Sexuality study ‘AARP/Modern Maturity’. Available
from: http://www.aarp.org/research/reference/publicopinions/aresearch-import-726.html, full report: http://
assets.aarp.org/rgcenter/health/mmsexsurvey.pdf [Accessed 26 January 2008].
AARP (2003) Lifestyles, dating and romance: a study of midlife singles (Washington DC: AARP).
Bernard, R. H. (1995) Research methods in anthropology: qualitative and quantitative approaches (Walnut Creek, CA:
AltaMira).
Culture, Health and Sexuality 509
Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
Binson, D., Pollack, L. and Catania, J. (1997) AIDS-related risk behaviours and safer sex practices of women in
midlife and older in the United States: 1990–1992. Health Care for Women International, 18, 343–354.
Centers for Disease Control and Prevention (CDC) (2007) Fact Sheet: HIV/AIDS among African Americans.
Available from: http://www.cdc.gov/hiv/topics/aa/resources/factsheets/aa.htm [Accessed 4 October 2007].
CDC (2006) HIV/AIDS among women who have sex with women. Available from: http://www.cdc.gov/hiv/topics/
women/resources/factsheets/wsw.htm [Accessed 4 October 2007].
CDC (2003) HIV/AIDS surveillance report, 2003. Volume 15 (Atlanta, GA: CDC).
CDC (2002) HIV/AIDS surveillance report 2002. Volume 14 (Atlanta, GA: CDC).
Coates, T. J. (1999) HIV prevention in clinical practice. AIDS Clinical Care, 11(1), 1–4.
Epstein, R. M., et al., (1998) Awkward moments in patient-physician communication about HIV risk. Annals of
Internal Medicine, 128, 435–442.
Florida Department of Health (FDOH) (2006a) HIV/AIDS among blacks: 2006 fact sheet. FDOH, Bureau of HIV/
AIDS. Available from: http://www.doh.state.fl.us/Disease_ctrl/aids/updates/facts/2006_Black_Fact_Sheet.pdf
[Accessed 28 September 2007].
FDOH (2006b) HIV/AIDS among women: 2006 fact sheet. FDOH, Bureau of HIV/AIDS. Avail-
able from: http://www.doh.state.fl.us/Disease_ctrl/aids/updates/facts/2006WomenFactsheet.pdf [Accessed
28 September 2007].
FDOH(2004) HIV/AIDS among persons age 50+ in Florida, 2004. FDOH, Bureau of HIV/AIDS. Available from:
http://www.doh.state.fl.us/disease_ctrl/aids/updates/facts/BW04_50.pdf [Accessed 30 June 2005].
FDOH (2003) Florida behavioural risk factor data. Available from: http://www.floridacharts.com/charts/brfss.aspx
[Accessed 7 May 2004].
Haas, D. M. and Coe, R. M. (1997) Do physicians discuss HIV and AIDS with patients? A survey of physician
practices. Journal of Community Health, 22(6), 401–416.
Handwerker, W. P. (2001) Quick ethnography. Walnut Creek, CA: Altamira.
Kerr, S. H., et al., (1996) Primary care physicians and their HIV prevention practices. AIDS Patient Care, 10(4),
222–235.
Lindau, S. T., et al., (2006) Older women’s attitudes and communication about sex and HIV: a community-based
study. Journal of Women’s Health, 15(6), 747–753.
Mack, K. A. and Bland, S. D. (1999) HIV testing behaviours and attitudes regarding HIV/AIDS of adults aged
50–64. Gerontologist, 39(6), 687–694.
Makadon, H. J. and Silin, J. G. (1995) Prevention of HIV infection in primary care: current practices, future
possibilities. Annals of Internal Medicine, 123(9), 715–719.
Nusbaum, M. R. H., Gamble, G. R. and Pathman, D. E. (2002) Seeking medical help for sexual concerns:
frequency, barriers and missed opportunities. Journal of Family Practice, 51(8), 706–710.
Paranjape, A., et al., (2006) Effect of relationship factors on safer sex decisions in older inner-city women. Journal
of Women’s Health, 15(1), 90–97.
Rich, E. R. (2001) Negotiation of HIV preventive behaviours in divorced and separated women re-entering the
sexual arena. Journal of the Association of Nurses in AIDS Care, 12(4), 25–35.
Roter, D. L., Hall, J. A. and Aoki, Y. (2002) Physician gender effects in medical communication. Journal of the
American Medical Association, 288(6), 756–764.
Skiest, D. J. and Keiser, P. P. (1997) Human immunodeficiency virus infection in patients older years: a survey of
primary care physicians’ beliefs, practices and knowledge. Archives of Family Medicine, 6, 289–294.
Smith, L. J., et al. (2007) Sex after seventy: a pilot study of sexual function in older persons. Journal of Sexual
Medicine, 4, 1247–1253.
Stall, R. and Catania, J. (1994) AIDS risk behaviours among late middle-aged and elderly Americans. Archives of
Internal Medicine, 154, 57–63.
Strombeck, R. and Levy, J. (1998) Educational strategies and interventions targeting adults age 50 and older for
HIV/AIDS prevention. Research on Aging, 20(6), 912–936.
Theall, K. P., et al., (2003) Perceived susceptibility to HIV among women: differences according to age. Research
on Aging, 25(4), 405–432.
Wilson, I. B. and Kaplan, S. (2000) Physician-patient communication in HIV disease: the importance of patient,
physician and visit characteristics. Journal of Acquired Immune Deficiency Syndromes, 25(5), 417–425.
Winningham, A., et al., (2004) The changing age of HIV: sexual risk among older African American women living
in rural communities. Preventive Medicine, 39, 809–814.
Yates, M. E., et al., (1999) The importance of AIDS-related knowledge for mid-life and older women. AIDS
Education and Prevention, 11(3), 224–231.
Zaboltsky, D. L. (1998) Overlooked, ignored and forgotten: older women at risk for HIV infection and AIDS.
Research on Aging, 20(6), 760–775.
510 K. Grant and K. Ragsdale

Dow
nloa
ded
By:
[Gra
nt, K
athr
yn] A
t: 14
:17
22 J
une
2008
Zablotsky, D. L. and Kennedy, M. (2003) Risk factors and HIV transmission to midlife and older women:
knowledge, options and the initiation of safer sexual practices. Journal of Acquired Immune Deficiency
Syndromes, 33, S122–S130.
Culture, Health and Sexuality 511