Sex and relationship education for 13–16 year olds: evidence from England
17
This article was downloaded by: [Durham University Library] On: 15 August 2013, At: 13:00 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Sex Education: Sexuality, Society and Learning Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/csed20 Sex and relationship education for 13–16 year olds: evidence from England Vicki Strange a , Simon Forrest b , Ann Oakley a , Judith Stephenson c & the RIPPLE Study Team a University of London, UK b The Sex Education Forum, UK c University College London Medical School, UK Published online: 23 Jan 2007. To cite this article: Vicki Strange , Simon Forrest , Ann Oakley , Judith Stephenson & the RIPPLE Study Team (2006) Sex and relationship education for 13–16 year olds: evidence from England, Sex Education: Sexuality, Society and Learning, 6:1, 31-46 To link to this article: http://dx.doi.org/10.1080/14681810500508964 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms & Conditions of access and use can be found at http://www.tandfonline.com/page/terms- and-conditions
Transcript of Sex and relationship education for 13–16 year olds: evidence from England
This article was downloaded by: [Durham University Library]On: 15 August 2013, At: 13:00Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Sex Education: Sexuality, Society andLearningPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/csed20
Sex and relationship education for13–16 year olds: evidence from EnglandVicki Strange a , Simon Forrest b , Ann Oakley a , JudithStephenson c & the RIPPLE Study Teama University of London, UKb The Sex Education Forum, UKc University College London Medical School, UKPublished online: 23 Jan 2007.
To cite this article: Vicki Strange , Simon Forrest , Ann Oakley , Judith Stephenson & the RIPPLEStudy Team (2006) Sex and relationship education for 13–16 year olds: evidence from England, SexEducation: Sexuality, Society and Learning, 6:1, 31-46
To link to this article: http://dx.doi.org/10.1080/14681810500508964
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoeveror howsoever caused arising directly or indirectly in connection with, in relation to orarising out of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Sex and relationship education for 13–
16 year olds: evidence from England
Vicki Strange*a, Simon Forrestb, Ann Oakleya, JudithStephensonc and the RIPPLE Study Team1
aUniversity of London, UK; bThe Sex Education Forum, UK; cUniversity College London
Medical School, UK
This article examines the quantity and content of sex and relationship education (SRE) delivered to
students in Years 9–11 (aged 13–16 years) in 12 coeducational state secondary schools in England
during 1997–2000. Teachers reported the delivery of an average of seven (range 0–12) sessions of
SRE across the three years, with no SRE delivered in up to five schools in each year. Most teachers
reported having covered contraception, sexually transmitted diseases and relationships at least once.
Topics such as homosexuality and the negotiation of relationships and sexual encounters were rarely
covered. Data collected from students provided a slightly different picture. At least one-half of
students in all schools reported having received some SRE during Year 9 and at least 85% reported
receiving some SRE during Years 10 and/or 11. Teachers identified various factors that limited the
quality of the SRE delivered. The article discusses some of the challenges that arose when attempting
to reconcile data gathered from students and teachers.
Introduction
In recent years, UK government policy has focused on the need to improve sex and
relationship education (SRE) in schools (Department for Education and Employment
[DfEE], 2000; Department of Health, 2002). This is part of wider concerns to reduce
rates of teenage pregnancies and the number of young people contracting sexually
transmitted infections (Social Exclusion Unit, 1999; Department of Health, 2001). In
order to evaluate these efforts to improve sex education and to make decisions about
the future provision of SRE, it is important to have a clear idea about provision in
schools, prior to the introduction of such policy and guidance, and the salient issues
for those involved in the organization and delivery of this.
Research focusing on SRE in schools has indicated that often little time is
allocated for the delivery of SRE, it is delivered too late for many students and tends
to have an overly biological focus. SRE has been criticized for failing to address
*Corresponding author. Social Science Research Unit (SSRU), Institute of Education, University
of London, 18 Woburn Square, London WC1H ONS, UK. Email: [email protected]
Sex Education
Vol. 6, No. 1, February 2006, pp. 31–46
ISSN 1468-1811 (print)/ISSN 1472-0825 (online)/06/010031-16
# 2006 Taylor & Francis
DOI: 10.1080/14681810500508964
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013

affective issues around emotions and relationships, attitudes or skills development
(Allen, 1987; Holland et al., 1998; Measor et al., 2000). Studies examining the
organization and delivery of school-based SRE have identified factors influential in
determining the quality of SRE provision, such as a lack of time available for
planning and delivery; teachers’ confidence and commitment, embarrassment and
lack of training; and difficulties with implementing and monitoring a cross-curricular
approach (Scott & Thomson, 1992; Lawrence et al., 2000).
While much of this research provides important insights into ways in which SRE
might be improved, it is limited with regards to its ability to provide definite
information about either the amount or content of SRE received by students in
schools. For example, few studies have attempted to establish how much time has
been allocated for the delivery of SRE or which aspects of SRE are being addressed.
The report by the Office for Standards in Education (Ofsted), based on a survey of
SRE in 1000 schools and 20 local education authorities, inspections by Her
Majesty’s Inspectors of 140 schools and analysis of Ofsted inspections carried out
during 2000/02, is a good example of this (Ofsted, 2002). The report provides no
detail about the content of SRE being delivered in schools nor about how much time
in the formal curriculum of schools is allocated to this. Rather, it focuses on the
quality of the teaching observed in schools and on recommendations for topic areas
(e.g. sexuality, HIV/AIDS and parenthood) considered to require more attention.
Few studies have attempted to collect information in systematic ways from
representative samples of schools or students. One exception is a survey of SRE
provision carried out by Lawrence et al. (2000); however, generalization from these
findings is limited, as demographic information about the schools is not provided. It
is also difficult to draw conclusions about the total amount of SRE received by
students throughout their school careers. For example, Lawrence et al. (2000) report
estimates of intended provision, rather than figures for SRE actually delivered, and
assess provision only at one point in time across different year groups.
This paper aims to fill a research gap concerning what is known about SRE
provision in English schools. Data gathered from both teachers and students are
drawn on to establish the amount and content of SRE delivered to two cohorts of
students during Years 9–11 (aged 13–16 years) in 12 coeducational state secondary
schools in England over the period 1997–2000. We also examine teachers’ views
about the factors that need to be addressed for SRE to be delivered successfully. By
focusing on the period immediately prior to the most recent government guidance
on sex and relationship education (DfEE, 2000) we hope to provide data against
which future studies can compare more current information about sex education,
thus allowing some assessment of the possible impact of such guidance. We also
discuss some of the challenges that arose in our attempts to combine data from
teachers and students in order to establish what SRE was actually delivered in the
study schools. Combining data gathered by different methods and from different
sources is commonly referred to as ‘triangulation’ and is considered by some as an
appropriate approach for establishing the validity/credibility of findings (Patton,
1980). A second contribution of the paper is to these methodological debates.
32 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013

Methods
In 1997, approximately 350 mixed-sex state schools in central and southern England
were contacted by letter and invited to take part in a randomized controlled trial of
peer-led sex education—the Randomised Intervention of Pupil Peer-led Sex
Education (RIPPLE) Study. Forty-nine schools expressed an interest in taking part
in the study and, following visits by members of the research team to discuss the
study in more detail, 29 schools were randomly allocated either to receive peer-led
sex education or to continue with their usual sex education curriculum. Schools
chose not to take part in the study for a variety of reasons, some unrelated to the
delivery of sex education. A few schools were only interested in taking part in the
study if they could implement peer-led sex education. Others were excluded by
the research team because they were too far from the study base in London. Full
details of the RIPPLE study, including the process by which schools were recruited
to the study and the methods employed, can be found elsewhere (Stephenson et al.,
2003). This paper reports on the data collected in the 12 schools randomized to the
control group in which the usual sex education curriculum was implemented.
Between 1997 and 2000 in-depth interviews were carried out in all the RIPPLE
Study schools with the teachers who were responsible for coordinating, and in some
cases delivering, SRE. Some teachers were interviewed more than once. The
interviews were semi-structured and consisted mainly of open questions that aimed
to establish the following: what SRE had been delivered to two cohorts of students in
Years 9–11; what external agencies had contributed to the programme; what the
main issues were in organizing and delivering it; and whether any of the teachers
delivering SRE had received any training. In order to standardize the information
collected from the schools, teachers were also asked to complete, with the
researcher, a table indicating whether particular topics had been covered in the
SRE programme, and in which years. Teachers were also asked to indicate the extent
to which they were satisfied with a number of factors thought to influence the
organization and delivery of SRE. These topics and factors were based on very
similar questions asked in a recent survey of school sex education by Lawrence et al.
(2000). All the interviews were transcribed. Information from these was extracted
and combined with other study data.
Two cohorts of students, in all schools, were asked to complete questionnaires in
Year 9 (aged 13/14 years), Year 10 (aged 14/15 years) and Year 11 (aged 15/16
years). Students completed the questionnaires under the supervision of researchers
and/or teachers, and were asked to work alone. The questionnaires comprised about
50 items including demographics, sexual knowledge, attitudes, cognitions and
behaviour and attitudes to school and the future. One section, the data from which
are reported here, covered students’ experiences of SRE. Frequencies were
calculated using the Statistical Package for the Social Sciences. This paper presents
data from questionnaires completed by students attending the schools in Years 10
and 11. Data from those students who joined the schools after the autumn term of
Year 9 were excluded as these students may not have been enrolled in the study
schools when the SRE was delivered. Data referring to SRE covered during Year 9
Sex and relationship education for 13–16 year olds 33
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
are taken from the questionnaires completed by students in Year 10, and data
referring to SRE covered in Years 10 and 11 are taken from questionnaires
completed in Year 11, unless otherwise stated.
Results
A comparison of the RIPPLE Study control schools with other maintained
secondary schools in the same four Government office regions in 19972 indicates
that in relation to key demographic criteria these schools are a fairly representative
sample. The study schools had slightly fewer students with statements of special
educational needs (1.8% versus 2.3%) and the academic attainment of students, as
indicated by the average GCSE3 points score, was very slightly lower (36.1 versus
37.8). The proportion of students who were eligible for free schools meals was very
similar (13.7% versus 13.0%) and levels of absenteeism (authorized and
unauthorized) were also very similar (8.6% versus 8.8% of half-days).
Interviews were carried out with 17 teachers and one school nurse in the 12
control schools. Eight of the teachers were personal social and health education
(PSHE) coordinators and three of these also held other positions as a head of year,
head of science and deputy head of the school, respectively. Seven of the teachers
were year heads with responsibility for coordinating the SRE provision for their year.
One teacher was a religious education (RE) teacher and another was a science
teacher.
A total of 3331 students (86% of those enrolled in the schools since Year 9)
completed questionnaires in Year 10 (1622 in cohort 1 and 1709 in cohort 2) and
2920 (80% of those enrolled in the schools since Year 9) did so in Year 11 (1433 in
cohort 1 and 1487 in cohort 2). The sample in each year comprised approximately
50% girls and 50% boys.
What SRE was provided and by whom?
Data from teachers
In eight of the 12 schools, most of the SRE was delivered by form tutors. In one of
these schools, the form tutors chose the area of PSHE that they would like to teach,
and consequently most of the form groups received SRE from the same teacher. In
another school, SRE had previously been delivered by form tutors, but in recent
years had not been delivered at all because form tutors were not confident and/or
comfortable with teaching the subject. In two schools, most of the SRE was
delivered by one or two dedicated teachers with form tutors covering classes where
necessary. In one school the SRE was delivered on three days during the school year.
On these days the timetable was collapsed and most of the SRE was delivered by the
school nurse and outside agencies. Teachers in two other schools reported that the
school nurse contributed to the SRE programme, and in one of these almost all
the SRE was delivered by her. In another two schools, teachers reported that school
nurses used to contribute to the SRE programme, but that more recently these
34 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013

services had been cut and they were no longer able to commit time to the
programme. In three of the 12 schools, teachers reported that some of the SRE had
been delivered by external speakers or organizations other than the school nurse.
These included sessions delivered by a representative from a company promoting
sanitary products and a drama company that worked with students in Year 9, a
session with a nurse from a family-planning clinic aiming to promote local services
and abstinence from sexual intercourse, and discussion-based sessions delivered by
volunteers from a local church youth group. In most schools the SRE delivered in
PSHE time was supplemented by that covered as part of the national curriculum in
science. This covered fertilization, physical and emotional changes in adolescence
(puberty), the menstrual cycle, the effects of sex hormones and development of the
foetus (www.nc.uk.net). In at least one school, PSHE was also supplemented by
work carried out in RE, which included discussion about abortion. No teachers
indicated any awareness of topics related to SRE having being covered in other
subject areas.
How much time was allocated to SRE?
Data from teachers
Table 1 summarizes data from teachers about the amount of SRE delivered to each
cohort of students in each school in Years 9–11. As all the interviews were completed
before the end of the school year 2000/01, data about the SRE provided to students
in the second cohort during Year 11 were not obtained. In order to provide some
idea of the total probable amount of SRE delivered across the three years, we have
assumed that the SRE delivered in this year was the same as for those students in the
first cohort (these data are shown in italics in the table). Table 1 does not include any
SRE that was stated as having been delivered in science or RE as part of the national
curriculum.
Over the three years, teachers reported that students in the first cohort received
between 0 and 12 sessions of SRE with an average between six and seven sessions.
Students in the second cohort received between three and 12 sessions with an
average between seven and eight sessions.4 The number of sessions delivered in each
year ranged from zero to six in Year 9, zero to seven in Year 10 and zero to five in
Year 11. Teachers reported that no SRE was delivered to students in Year 9 in four
schools, to students in Year 10 in four schools and to students in Year 11 in five
schools. In one school, teachers reported that students in the first cohort received no
SRE in Years 9, 10 or 11. Data were missing for at least two of the three years for
students in two schools—one for students in the first cohort and one for students in
the second cohort.
Data from students
Table 1 also presents data from students (see emboldened characters). Between 49%
and 99% of students in the first cohort and 65% and 99% of students in the second
Sex and relationship education for 13–16 year olds 35
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
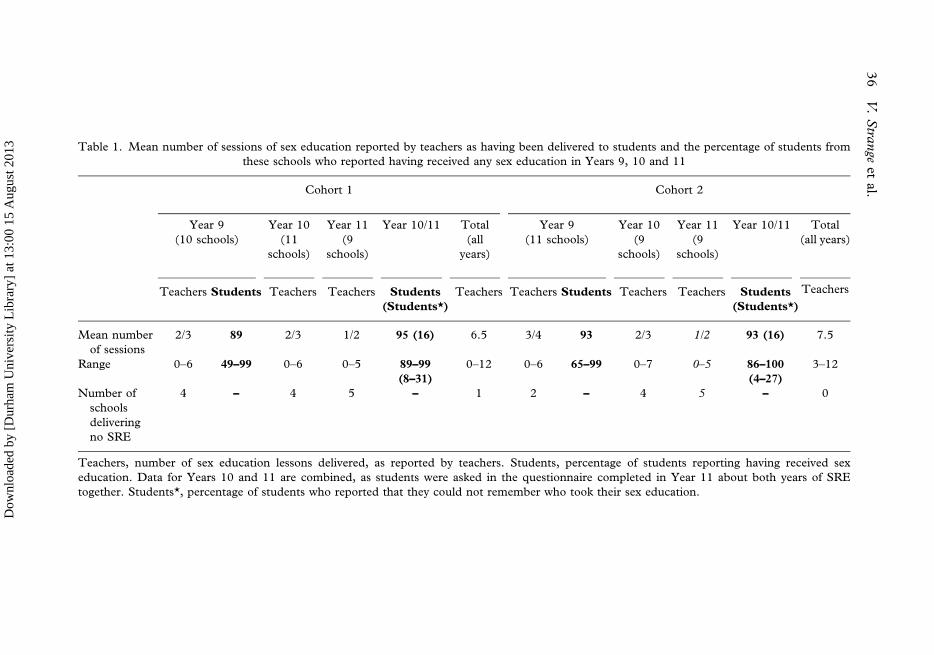
Table 1. Mean number of sessions of sex education reported by teachers as having been delivered to students and the percentage of students from
these schools who reported having received any sex education in Years 9, 10 and 11
Cohort 1 Cohort 2
Year 9
(10 schools)
Year 10
(11
schools)
Year 11
(9
schools)
Year 10/11 Total
(all
years)
Year 9
(11 schools)
Year 10
(9
schools)
Year 11
(9
schools)
Year 10/11 Total
(all years)
Teachers Students Teachers Teachers Students
(Students*)
Teachers Teachers Students Teachers Teachers Students
(Students*)
Teachers
Mean number
of sessions
2/3 89 2/3 1/2 95 (16) 6.5 3/4 93 2/3 1/2 93 (16) 7.5
Range 0–6 49–99 0–6 0–5 89–99
(8–31)
0–12 0–6 65–99 0–7 0–5 86–100
(4–27)
3–12
Number of
schools
delivering
no SRE
4 – 4 5 – 1 2 – 4 5 – 0
Teachers, number of sex education lessons delivered, as reported by teachers. Students, percentage of students reporting having received sex
education. Data for Years 10 and 11 are combined, as students were asked in the questionnaire completed in Year 11 about both years of SRE
together. Students*, percentage of students who reported that they could not remember who took their sex education.
36
V.
Stra
nge
etal.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013

cohort reported receiving SRE in Year 9. Between 89% and 99% of students in the
first cohort and 86% and 100% of students in the second cohort reported receiving
SRE in Years 10 or 11. Of those who reported having received some SRE, between 4%
and 31% said they could not remember who took the sessions.
Comparison of data from teachers and students
In order to obtain as complete a picture as possible of the provision of SRE, we asked
for data from both teachers and students. We found a number of discrepancies
between these two sources of information. While teachers in some schools reported
that SRE was not delivered to students during PSHE in some years, at least one-half
of the students in all schools in each of the three years reported having received some
SRE. For example, teachers in four schools reported that no SRE was delivered to
students in the first cohort in Year 9; but between 49% and 96% of students in these
same four schools said they had received some SRE.
What topics/activities were covered and when?
Data from teachers
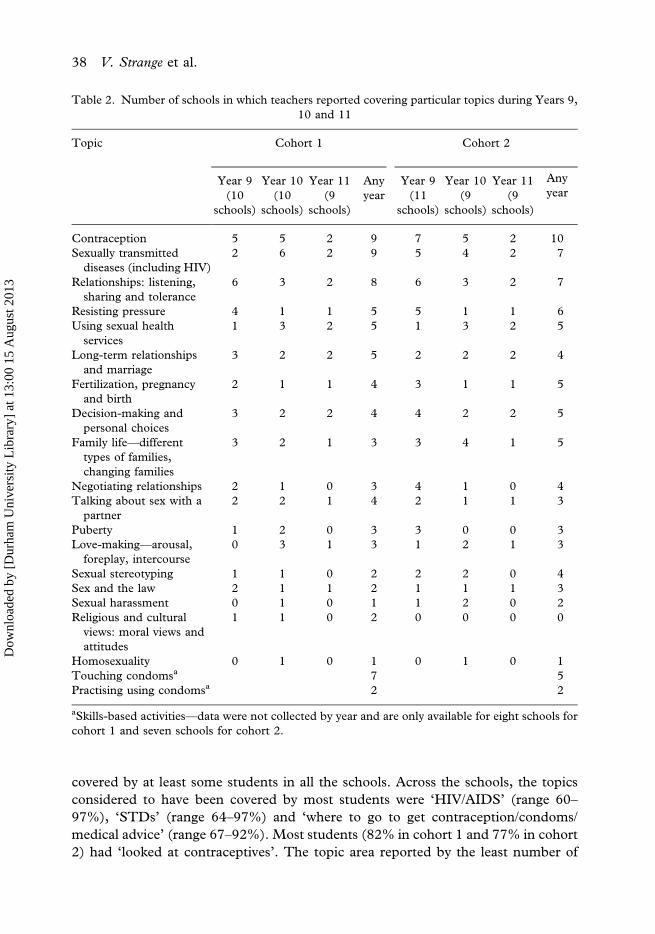
Table 2 presents teacher reporting of the coverage of SRE topics in each year. The
topics most commonly reported by teachers as having being covered at all were
‘contraception’ (nine schools in cohort 1 and 10 in cohort 2) and ‘sexually
transmitted diseases’ (nine in cohort 1 and seven in cohort 2). The next most
frequently covered were ‘relationships’ (eight in cohort 1 and seven in cohort 2),
resisting pressure (five in cohort 1 and five in cohort 2) and ‘using sexual health
services’ (five in cohort 1 and five in cohort 2). Some topics were reported as having
been covered by very few teachers. These included ‘homosexuality’ (which was
reported as being covered in just one school in each cohort), religious and cultural
views (two schools in cohort 1 and no schools in cohort 2) and ‘sexual harassment’
(one school for the first cohort and two schools for the second). ‘Talking about sex
with a partner’ was also reported as being covered in just four schools in the first
cohort and three in the second cohort. Three schools in the first cohort and four in
the second reported having covered how to ‘negotiate relationships’.
Teachers were also asked whether students in their schools were provided with the
opportunity to touch and practise using condoms in the classroom. In seven schools
in cohort 1 and five schools in cohort 2, teachers reported that some students would
have had the opportunity to touch condoms. Teachers from two schools in each
cohort reported that, in some classes, the teacher would have demonstrated how to
use a condom and some students may have practised using a condom themselves.
Data from students
Table 3 presents comparable data from students on the coverage of particular topics
within SRE. All topics and skill-based activities were considered to have been
Sex and relationship education for 13–16 year olds 37
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
covered by at least some students in all the schools. Across the schools, the topics
considered to have been covered by most students were ‘HIV/AIDS’ (range 60–
97%), ‘STDs’ (range 64–97%) and ‘where to go to get contraception/condoms/
medical advice’ (range 67–92%). Most students (82% in cohort 1 and 77% in cohort
2) had ‘looked at contraceptives’. The topic area reported by the least number of
Table 2. Number of schools in which teachers reported covering particular topics during Years 9,
10 and 11
Topic Cohort 1 Cohort 2
Year 9
(10
schools)
Year 10
(10
schools)
Year 11
(9
schools)
Any
year
Year 9
(11
schools)
Year 10
(9
schools)
Year 11
(9
schools)
Any
year
Contraception 5 5 2 9 7 5 2 10
Sexually transmitted
diseases (including HIV)
2 6 2 9 5 4 2 7
Relationships: listening,
sharing and tolerance
6 3 2 8 6 3 2 7
Resisting pressure 4 1 1 5 5 1 1 6
Using sexual health
services
1 3 2 5 1 3 2 5
Long-term relationships
and marriage
3 2 2 5 2 2 2 4
Fertilization, pregnancy
and birth
2 1 1 4 3 1 1 5
Decision-making and
personal choices
3 2 2 4 4 2 2 5
Family life—different
types of families,
changing families
3 2 1 3 3 4 1 5
Negotiating relationships 2 1 0 3 4 1 0 4
Talking about sex with a
partner
2 2 1 4 2 1 1 3
Puberty 1 2 0 3 3 0 0 3
Love-making—arousal,
foreplay, intercourse
0 3 1 3 1 2 1 3
Sexual stereotyping 1 1 0 2 2 2 0 4
Sex and the law 2 1 1 2 1 1 1 3
Sexual harassment 0 1 0 1 1 2 0 2
Religious and cultural
views: moral views and
attitudes
1 1 0 2 0 0 0 0
Homosexuality 0 1 0 1 0 1 0 1
Touching condomsa 7 5
Practising using condomsa 2 2
aSkills-based activities—data were not collected by year and are only available for eight schools for
cohort 1 and seven schools for cohort 2.
38 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
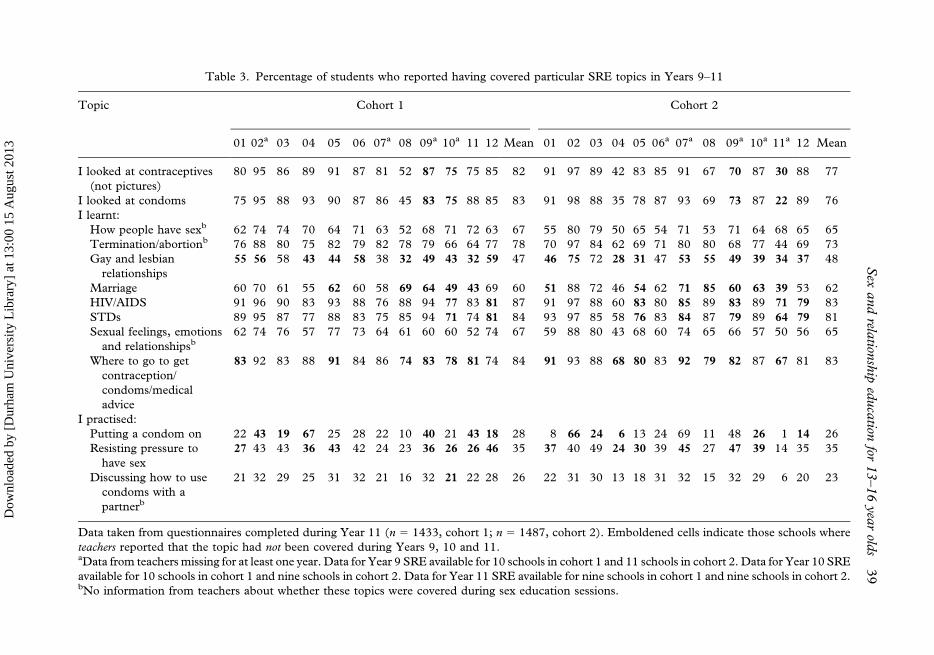
Table 3. Percentage of students who reported having covered particular SRE topics in Years 9–11
Topic Cohort 1 Cohort 2
01 02a 03 04 05 06 07a 08 09a 10a 11 12 Mean 01 02 03 04 05 06a 07a 08 09a 10a 11a 12 Mean
I looked at contraceptives
(not pictures)
80 95 86 89 91 87 81 52 87 75 75 85 82 91 97 89 42 83 85 91 67 70 87 30 88 77
I looked at condoms 75 95 88 93 90 87 86 45 83 75 88 85 83 91 98 88 35 78 87 93 69 73 87 22 89 76
I learnt:
How people have sexb 62 74 74 70 64 71 63 52 68 71 72 63 67 55 80 79 50 65 54 71 53 71 64 68 65 65
Termination/abortionb 76 88 80 75 82 79 82 78 79 66 64 77 78 70 97 84 62 69 71 80 80 68 77 44 69 73
Gay and lesbian
relationships
55 56 58 43 44 58 38 32 49 43 32 59 47 46 75 72 28 31 47 53 55 49 39 34 37 48
Marriage 60 70 61 55 62 60 58 69 64 49 43 69 60 51 88 72 46 54 62 71 85 60 63 39 53 62
HIV/AIDS 91 96 90 83 93 88 76 88 94 77 83 81 87 91 97 88 60 83 80 85 89 83 89 71 79 83
STDs 89 95 87 77 88 83 75 85 94 71 74 81 84 93 97 85 58 76 83 84 87 79 89 64 79 81
Sexual feelings, emotions
and relationshipsb62 74 76 57 77 73 64 61 60 60 52 74 67 59 88 80 43 68 60 74 65 66 57 50 56 65
Where to go to get
contraception/
condoms/medical
advice
83 92 83 88 91 84 86 74 83 78 81 74 84 91 93 88 68 80 83 92 79 82 87 67 81 83
I practised:
Putting a condom on 22 43 19 67 25 28 22 10 40 21 43 18 28 8 66 24 6 13 24 69 11 48 26 1 14 26
Resisting pressure to
have sex
27 43 43 36 43 42 24 23 36 26 26 46 35 37 40 49 24 30 39 45 27 47 39 14 35 35
Discussing how to use
condoms with a
partnerb
21 32 29 25 31 32 21 16 32 21 22 28 26 22 31 30 13 18 31 32 15 32 29 6 20 23
Data taken from questionnaires completed during Year 11 (n 5 1433, cohort 1; n 5 1487, cohort 2). Emboldened cells indicate those schools where
teachers reported that the topic had not been covered during Years 9, 10 and 11.aData from teachers missing for at least one year. Data for Year 9 SRE available for 10 schools in cohort 1 and 11 schools in cohort 2. Data for Year 10 SRE
available for 10 schools in cohort 1 and nine schools in cohort 2. Data for Year 11 SRE available for nine schools in cohort 1 and nine schools in cohort 2.bNo information from teachers about whether these topics were covered during sex education sessions.
Sex
and
relation
ship
educa
tionfor
13–16
yea
rold
s39
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
students as having been covered was ‘gay and lesbian relationships’ (range 31–75%).
Fewer students reported having covered skills-based activities; 26% of students in
cohort 1 and 23% in cohort 2 said they had practised discussing how to use condoms
with a partner; 28% in cohort 1 and 26% in cohort 2 reported having practised
putting a condom on; and 35% in each cohort said they had practised how to resist
pressure to have sex.
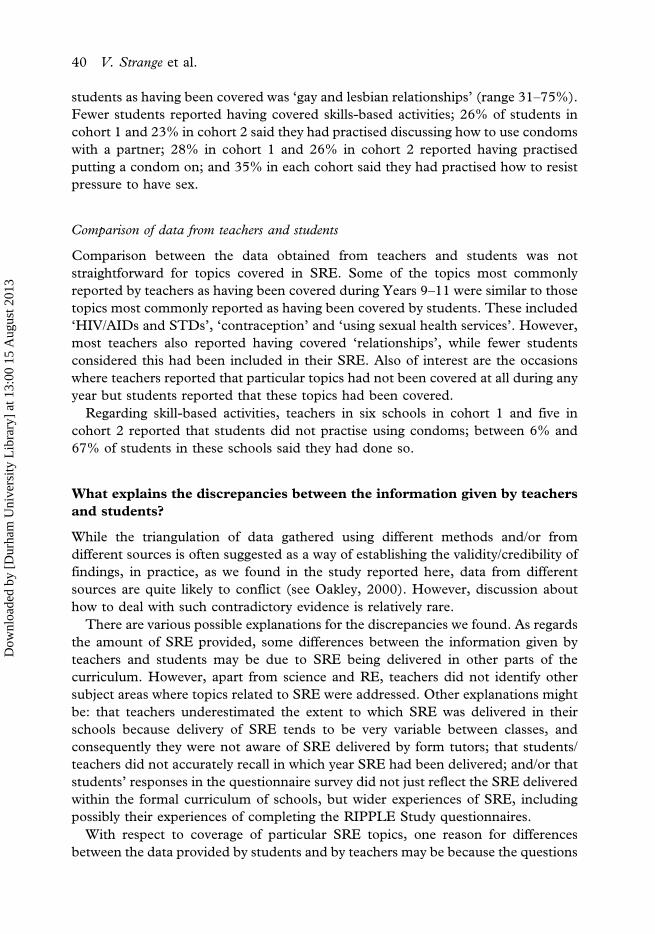
Comparison of data from teachers and students
Comparison between the data obtained from teachers and students was not
straightforward for topics covered in SRE. Some of the topics most commonly
reported by teachers as having been covered during Years 9–11 were similar to those
topics most commonly reported as having been covered by students. These included
‘HIV/AIDs and STDs’, ‘contraception’ and ‘using sexual health services’. However,
most teachers also reported having covered ‘relationships’, while fewer students
considered this had been included in their SRE. Also of interest are the occasions
where teachers reported that particular topics had not been covered at all during any
year but students reported that these topics had been covered.
Regarding skill-based activities, teachers in six schools in cohort 1 and five in
cohort 2 reported that students did not practise using condoms; between 6% and
67% of students in these schools said they had done so.
What explains the discrepancies between the information given by teachers
and students?
While the triangulation of data gathered using different methods and/or from
different sources is often suggested as a way of establishing the validity/credibility of
findings, in practice, as we found in the study reported here, data from different
sources are quite likely to conflict (see Oakley, 2000). However, discussion about
how to deal with such contradictory evidence is relatively rare.
There are various possible explanations for the discrepancies we found. As regards
the amount of SRE provided, some differences between the information given by
teachers and students may be due to SRE being delivered in other parts of the
curriculum. However, apart from science and RE, teachers did not identify other
subject areas where topics related to SRE were addressed. Other explanations might
be: that teachers underestimated the extent to which SRE was delivered in their
schools because delivery of SRE tends to be very variable between classes, and
consequently they were not aware of SRE delivered by form tutors; that students/
teachers did not accurately recall in which year SRE had been delivered; and/or that
students’ responses in the questionnaire survey did not just reflect the SRE delivered
within the formal curriculum of schools, but wider experiences of SRE, including
possibly their experiences of completing the RIPPLE Study questionnaires.
With respect to coverage of particular SRE topics, one reason for differences
between the data provided by students and by teachers may be because the questions
40 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013

asked of the two groups were not exactly the same. For example, whereas teachers
were asked whether ‘using sexual services’ had been covered during SRE, students
were asked whether they had ‘learnt where to go to get contraception/condoms/
medical advice’. In addition, data were missing from teachers from four schools in
cohort 1 and five schools in cohort 2 for at least one year. In some schools these
missing data reflected teachers’ (particularly year heads’) limited knowledge of the
SRE provision delivered to year groups other than their own. In other schools,
the interviews were carried out with teachers who had joined the school and/or taken
over the responsibility for the SRE programme when the RIPPLE study was already
underway, and they may therefore not have been aware of the SRE provided before
this date. Often teachers who may have known more about the SRE had either left
the school or researchers were not able to make contact and organize an interview. In
some cases it is possible that students had covered particular topics in another
subject lesson. For example, the teacher in school 12 reported that sexually
transmitted diseases/HIV was not covered in any year during PSHE; however,
around 80% of students reported having covered this topic (most probably in
science). For other topics, the differences between the reports of the students and
the teachers are more difficult to explain. For example, just one teacher reported that
‘homosexuality’ was covered as part of the SRE programme, while between 31% and
75% of students in all schools reported having covered gay and lesbian relationships.
In this case it is less obvious in which other part of the curriculum this topic might
have been addressed.
Some possible explanations for differences between students and teachers in
reporting skills-based activities are that teachers may sometimes have been unaware
that other teachers were carrying out SRE lessons where students were encouraged to
practise using condoms, and/or that students interpreted this question to include
occasions on which they may have watched others/teachers demonstrating condom use.
What issues influenced the organization and delivery of SRE?
Throughout the interviews, teachers talked about the factors that they felt influenced
the organization and delivery of SRE. The issues most often mentioned were
differences in confidence and enthusiasm, management support, timetable space
and training.
Variability in teachers’ confidence and enthusiasm for delivering SRE
This was highlighted by teachers in seven of the 12 schools. Many teachers
commented that the SRE was ‘patchy’ and that the quality and quantity of SRE
delivered to the different form or class groups was highly dependent on the
enthusiasm and confidence of the staff delivering it. All these teachers indicated that
they thought that the quality of SRE would be improved if delivered by a core team
of staff who were interested in delivering SRE as distinct from form tutors, some of
whom felt uncomfortable providing SRE and/or did not value it.
Sex and relationship education for 13–16 year olds 41
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
Support from the senior management team
All the teachers interviewed thought that this was important and that support for
SRE from the senior management team (SMT) was essential in order for space to be
allocated in the timetable for SRE and so that the importance of PSHE was
promoted within the staff team. In four schools, teachers identified the lack of
support from the SMT as a problem for the implementation of the SRE in their
school. In three schools, teachers reported that whole year groups had failed to
receive SRE because of a lack of clarity regarding who was responsible for the
coordination of the programme. In one school, the teacher interviewed explained
how a recent Ofsted report highlighting the lack of timetabled provision had assisted
her with negotiating more support from the SMT to promote SRE. Some teachers
felt that the SRE was more likely to be implemented successfully if responsibility for
the coordination of SRE was taken by a member of the SMT.
Space on the timetable
Many teachers said they would like more time to deliver SRE. In two schools,
teachers reported that there was no time allocated to the delivery of SRE. Some
teachers expressed concerns that the time available for SRE was likely to decrease as
more subjects (e.g. citizenship) are incorporated into the PSHE framework and as
the pressure increases for schools to invest time in improving examination grades in
curriculum subjects.
Training and INSET time
About one-half the teachers interviewed specifically identified the lack of training for
teachers and the lack of INSET time to develop and coordinate the SRE programme
as factors influencing the implementing of SRE. Teachers in five of the 12 schools
reported that they had received some training or support from an external agency
related to the delivery of SRE since 1997. This included sessions coordinated by the
local education authority (three teachers) and a two-day course held at a local
hospital for teachers and health professionals that covered information about
contraception and sexually transmitted infections and classroom-based activities
such as condom demonstrations (one teacher). A teacher in one school had received
advice about the content of the SRE programme from someone in the local health
promotion team. Teachers in five schools said that either INSET or some other time
had been allocated to support staff around issues relating to PSHE. Just two of the
teachers interviewed (in the same school) reported that they had received training in
the delivery of sex education during their initial teacher training.
Discussion
This paper has examined the quantity and content of SRE delivered to students in
Years 9, 10 and 11 in 12 mixed-sex state schools in England between 1997 and 2000
42 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
using evidence from a national study of sex education. Comparison of these schools
with others in central and southern England suggests this to be a broadly
representative sample.
The amount of SRE reported by teachers to have been delivered to students
during Years 9–11 was very variable between schools and across the three years and
the two cohorts. Teachers in one school reported that students received no SRE. In
contrast, teachers in other schools reported that students received as many as 11 or
12 sessions. On average, teachers reported the delivery of around six to seven
sessions of SRE across the three years. Data collected from students provide a
slightly different picture. At least one-half of students in all schools reported having
received some SRE during Year 9 and at least 90% reported receiving SRE during
Year 10 and/or Year 11.
Teachers in most schools reported having covered ‘contraception’, ‘sexually
transmitted diseases’ and ‘relationships’ at least once during the three years. This
was heartening, as these topics are listed in government guidance (DfEE, 2000) as
topics that should be addressed as part of the SRE programme in secondary schools.
However, other topics such as ‘homosexuality’ and the negotiation of relationships
and sexual encounters, including dealing with sexual harassment, were rarely
covered. Again, the data from students on topics covered provided a slightly
different picture. At least 10% of students in all schools reported having covered
each of the SRE topics. Some of the topics (e.g. HIV/AIDS and contraception) most
commonly identified by students as having been addressed were the same as those
identified by most teachers. But others topics (e.g. relationships) that were
commonly reported by teachers as having been covered during SRE were reported
by fewer students. While teachers in just two schools reported that students in some
classes might have been given the opportunity to practise using condoms, some
students in all schools said they had practised these skills during SRE.
These findings echo those from other research and suggest that, while many
schools may have successfully given students factual information, most were not
providing them with opportunities to develop skills that may enable them to use
condoms and negotiate sexual situations with partners (Buston et al., 2002). The
development of such skills has been highlighted as important in government
guidance (DfEE, 2000) and is supported by research examining the factors
predicting young people’s sexual behaviour (Abraham & Sheeran, 1994).
In the RIPPLE Study, from which the data reported in this paper are taken, we
collected information on the same issues from multiple sources, including, with
respect to SRE provision, both teachers and students. However, attempting to
combine these data to yield a complete picture of the amount and content of SRE
currently provided in the study schools was a problematic enterprise. We have
suggested a number of reasons why the ‘facts’ as reported by teachers and students
might be different, and why a simple approach to the triangulation of data is unable
to solve this problem. While contradictions in data gathered from different sources
may present researchers with difficulties in terms of establishing ‘what actually
happens’, such contradictions may ultimately result in more rigorous analyses, as
Sex and relationship education for 13–16 year olds 43
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013

researchers are motivated, in order to understand the findings, more fully to
interrogate both the data themselves and the methods by which these were collected.
The teachers interviewed in this study were, almost without exception, extremely
committed and enthusiastic about SRE. However, they identified a number of
factors that have also been highlighted in previous research examining SRE both in
England and other parts of the United Kingdom (Buston et al., 2001, 2002) that
limited the quality of SRE delivered to students. The four most commonly discussed
were: the variability in teachers’ confidence and enthusiasm for delivering SRE, a
lack of support from the senior management team, competition for space on
crowded timetables, and a lack of training and INSET time.
These findings suggest a number of ways in which the quality of SRE in schools
might be improved. Lawrence et al. (2000) have recommended that SRE should
become a statutory part of the national curriculum. They argue that statutory status
would raise the profile of SRE in schools and increase its recognition by those in
senior management positions. This in turn would increase the likelihood that
adequate space on the timetable would be allocated to the delivery of SRE, and that
those taking responsibility for coordinating SRE would be seen to hold a valuable
role within the school and be given time to design, develop and review programmes.
With school timetables becoming ever more crowded and teachers and students
already under pressure to meet increasing numbers of academic targets, the
likelihood of schools being able successfully to implement comprehensive SRE
programmes may be highly dependent on policy-makers resolving some difficult
questions regarding which other aspects of the school curriculum should be
compromised.
Clearly with such limited time available to deliver SRE it is not possible for most
schools to address all the topics suggested by government guidance (DfEE, 2000).
Suggested topics include relationships, the responsibilities of parenthood, self-
esteem, contraception, safe sex, how to access local services, resisting pressure, peer
pressure, sex and the law, arguments for delaying sexual activity and human
sexuality and prejudice. Schools require clear guidelines about which core topics
they should cover and how these can realistically be addressed in the time available.
Such guidance should focus particularly on how teachers should address skill
development and how they can enable students to examine their personal attitudes
towards, for example, gender and sexuality.
Finally, the findings of this study indicate that the quality of SRE is greatly
dependent on the confidence and enthusiasm of the classroom teachers responsible
for its delivery. Both teachers and young people (see also Forrest et al., 2002) say
that the characteristics and values of both the teachers coordinating the programme
and of individual classroom teachers have an important influence on the quality of
SRE provided in schools. While it is important that all teachers have a basic
awareness of issues related to SRE, it might be preferable for most sex education to
be delivered by teams of SRE specialists—a recommendation outlined in the most
recent Ofsted report on SRE (Ofsted, 2002). Our findings also suggest that a greater
emphasis should be given to the training of teachers coordinating and delivering
44 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
SRE. Activities such as condom demonstrations and role-plays may be particularly
difficult for teachers who lack confidence about delivering SRE and/or do not have
the skills or experience to facilitate such activities (Buston et al., 2002). A recent
report outlining progress with regards to the implementation of the government’s
teenage pregnancy strategy describes further developments to ensure the effective
delivery of SRE and indicates that some of these issues are being addressed
(Department of Health, 2004). For example, a specialist PSHE certification
programme for teachers (which includes SRE as a component) has been
implemented, with over 600 teachers from 44 education authorities participating
during 2003/04. A similar programme for community nurses is currently being
piloted and evaluated. In addition, new standards for initial teacher training have
been developed to ensure that trainee teachers are familiar with the PSHE
framework, and a ‘best practice toolkit on PSHE’ has been commissioned and were
circulated to initial teacher training providers by autumn 2004. In exploring the
possible impacts of such initiatives, future research should aim to compare data
about SRE provision, such as those provided in this paper, with similar data
describing the quantity, quality and content of subsequent SRE provision in schools.
Acknowledgements
The authors would like to thank the schools and all the young people attending them
for their support of the project. The study is funded by the Medical Research Council.
Notes
1. The RIPPLE team includes the authors and Prof. Anne Johnson, Helen Monteiro
(Department of Sexually Transmitted Diseases, University College London Medical
School) and Angela Flux (State of Flux). It previously included Susan Charleston, Gayle
Johnson and Sarah Hambidge.
2. The Government office regions were East Midlands, West Midlands, Eastern and South East.
All figures are for 1997 except the GCSE points score, which is for students taking GCSE
examinations in June 1999 (DfEE, 1998, 2000).
3. General Certificate of Secondary Education—examinations usually taken at age 16, at the end
of Year 11.
4. This assumes that the sex education delivered in Year 11 to the second cohort of students was
the same as that delivered to those in the first cohort.
References
Abraham, C. & Sheeran, P. (1994) Modelling and modifying young heterosexuals’ HIV
preventative behaviour: a review of theories, findings and educational implications, Patient
Education and Counselling, 23, 173–186.
Allen, I. (1987) Education in sex and personal relationships (London, Policy Studies Institute).
Buston, K., Wight, D. & Scott, S. (2001) Difficulty and diversity: the context and practice of sex
education, British Journal of Sociology of Education, 22(3), 353–367.
Buston, K., Wight, D., Hart, G. & Scott, S. (2002) Implementation of a teacher-delivered sex
education programme: obstacles and facilitating factors, Health Education Research, 17(1),
101–114.
Sex and relationship education for 13–16 year olds 45
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013
Department for Education and Employment (2000) Sex and relationship guidance (Nottingham,
DfEE).
Department for Education and Skills (1998) Secondary school performance tables – Ref. PER98SEC.
Available online at: http://www.dfes.gov.uk/rsgateway.
Department for Education and Skills (2000) Secondary school performance tables – Ref. PER00/SEC.
Available online at: http://www.dfes.gov.uk/rsgateway.
Department of Health (2001) The national strategy for sexual health and HIV (London, HMSO).
Department of Health (2002) Government response to the first annual report of the independent advisory
group on teenage pregnancy (London, HMSO).
Department of Health (2004) Teenage pregnancy strategy progress report March. Available online at:
www.info.doh.gove.uk/tpu/tpu.nsf (accessed July 2004).
Forrest, S., Strange, V., Oakley, A.the RIPPLE Study Team (2002) A comparison of students’
evaluations of a peer-delivered sex education programme and teacher-led provision, Sex
Education, 2(3), 195–214.
Holland, J., Ramazanoglu, C., Sharpe, S. & Thomson, R. (1998) The male in the head—young
people, heterosexuality and power (London, The Tufnell Press).
Lawrence, J., Kanabus, A. & Regis, D. (2000) A survey of sex education provision in secondary schools
(Horsham, AVERT).
Measor, L., Tiffin, C. & Miller, K. (2000) Young people’s views on sex education: attitudes and
behaviour (London, RoutledgeFalmer).
Office for Standards in Education (2002) Sex and relationship education in Schools (London,
Ofsted).
Oakley, A. (2000) Experiments in knowing (Cambridge, Polity Press).
Patton, M. Q. (1980) Qualitative evaluation methods (Beverly Hills, CA, Sage Publications).
Social Exclusion Unit (1999) Report on teenage pregnancy (London, HMSO).
Scott, L. & Thomson, R. (1992) School sex education: more a patchwork than a pattern, Health
Education Journal, 51, 132–134.
Stephenson, J. M., Oakley, A., Johnson, A. M., Forrest, S., Strange, V., Charleston, S., Black, S.,
Copas, A., Petruckevitch, A. & Babiker, A. (2003) A school-based randomised controlled
trial of peer-led sex education in England, Controlled Clinical Trials, 24, 643–657.
46 V. Strange et al.
Dow
nloa
ded
by [
Dur
ham
Uni
vers
ity L
ibra
ry]
at 1
3:00
15
Aug
ust 2
013