Cartografía digital.Conjunto de operaciones con - Geoportal IGM

Rheumatol Int (2008) 28:851–857
DOI 10.1007/s00296-008-0535-6ORIGINAL ARTICLE
Serum IgG activity against cyclic citrullinated peptide in patients evaluated for rheumatoid factor correlates with the IgM isotype
M. G. Zavala-Cerna · A. Nava · E. García-Castañeda · J. Durán-González · M. J. Arias-Merino · M. Salazar-Páramo
Received: 18 August 2007 / Accepted: 14 January 2008 / Published online: 6 February 2008© Springer-Verlag 2008
Abstract The purpose of this study was to evaluate thefrequency of seric antibodies against cyclic citrullinatedpeptide (a-CCP) in patients tested for rheumatoid factor(RF) reactivity, and to analyze the correlation between theirtiters. We obtained serum from 112 consecutive patients(85 female), aged 47.2 § 13.4 years and from 46 clinicallyhealthy subjects (CHS). Patients where stratiWed into foursubgroups: rheumatoid arthritis (RA), probable RA (PRA),spondylarthropathies and other diagnosis. The a-CCP anti-
bodies were determined by enzyme linked immunoassay(ELISA), RF by nephelometric test (IgM) and ELISA (IgGand IgM). Analysis of variance (ANOVA) showed statisti-cally that a-CCP antibodies diVers among RA versus CHSand other diagnosis; PRA versus CHS and other diagnosis.A signiWcant Rho value of 0.84 (P < 0.05, Spearman’s cor-relation) was identiWed between a-CCP antibodies and RFin PRA subgroup. When a correlation of a-CCP antibodieswith RF (both isotypes) was done, the higher correlationwas observed against IgM RF. The data suggests diVerentpathways and times for each antibody generation.
Keywords Rheumatoid arthritis · Anti-cyclic citrullinated peptide antibodies · Rheumatoid factor
Introduction
A broad range of autoantibodies has been detected in rheu-matoid arthritis (RA) patients. The best known is the rheu-matoid factor (RF), which is often negative or present atlow titer in early disease stages. Other autoantibodiesdescribed in RA patients include antinuclear antibodies(ANA), anti RA33, anti-Sa, and anti-perinuclear factor(APF) antibodies among others but they lack speciWcity [1].
Currently, the most speciWc autoantibody system for RAinvolves antibodies against cyclic citrullinated peptide (a-CCP), directed to citrulline residues as Wrst described bySchellekens et al. [2]. These antibodies are detected usingcyclic citrullinated proteins as substrate in an immuneenzymatic assay, binds antigenic determinants containingcitrulline, which are generated post-translationally by theaction of peptidylarginine deaminases (PAD) [3]; suchdeterminants have been found in several proteins, includingWllagrin, Wbrin, vimentin [4, 5] and �-enolase [6].
M. G. Zavala-Cerna · A. Nava · E. García-CastañedaUnidad de Investigación Médica en Epidemiología Clínica, UMAE, HE, CMNO, IMSS, Guadalajara, Jalisco, México
M. G. Zavala-CernaDoctorado Ciencias Biomédicas, CUCS, Universidad de Guadalajara, Guadalajara, Jalisco, México
A. NavaDirección de Investigación, Ciencias de la Salud, Universidad Autónoma de Guadalajara, Guadalajara, Jalisco, México
J. Durán-GonzálezPrograma de Doctorado en Genética, CUCS, Universidad de Guadalajara, Guadalajara, Jalisco, México
M. J. Arias-MerinoLaboratorio Clínico, UMAE, HE, CMNO, IMSS, Guadalajara, Jalisco, México
M. Salazar-Páramo (&)División de Investigación, UMAE, Hospital de Especialidades, CMNO, IMSS, Belisario Domínguez 1000, PB. S.L. Col. Independencia, 44320 Guadalajara, Jalisco, Méxicoe-mail: [email protected]; [email protected]
M. Salazar-PáramoDepartamento de Fisiología, CUCS, Universidad de Guadalajara, Guadalajara, Jalisco, México
123

852 Rheumatol Int (2008) 28:851–857
DiVerent studies have described the sensitivity and spec-iWcity of the a-CCP antibodies in patients with RA, whichis 68 and >97%, respectively [7, 8]; appearing early in thecourse of the disease, sometimes years before the symp-toms come evident [9], and being able to diVerentiatebetween RA from other undiVerentiated polyarthritis [10].
Recent evidence suggests that RF and a-CCP are twoseparate autoantibody systems: (1) the a-CCP antibodiesare associated with the shared epitope more than RF does;(2) extra-articular manifestations are related more speciW-cally to the RF and not to a-CCP antibodies [11]; and (3)anti-CCP antibodies appear very early, even before theonset of symptoms [9, 12].
Despite the overlap between RF and a-CCP antibodies inRA patients, none or little has been made with respect toother diseases and the presence of these two autoantibodies,when polyarthritis is the initial form of presentation. There-fore, more information regarding the role of these autoanti-bodies in the diagnosis evaluation of rheumatic and non-rheumatic diseases is needed. The purpose of this study wasto evaluate the frequency of seric a-CCP antibodies in con-secutive patients who were evaluated for RF test, and toanalyze the correlation between their titers.
Methods
Patients and samples
Serum samples were collected from each of 112 consecutivepatients and sent to the Clinical Immunology Laboratory forRF (IgM isotype) testing upon physician request and fulWll-ing other inclusion criteria: established or suspected diagno-sis of reference and age >18 years. Exclusion criteria wereinsuYcient serum sample volume after RF determinationand incomplete clinical data. All the clinical informationwas obtained from laboratory database, and compared withmedical records. As a comparison group, consecutive sam-ples from clinically healthy subjects (CHS) were included.
Sample storage
All samples were obtained, identiWed and stored at ¡20°Cuntil tested for antibodies.
The protocol was reviewed and accepted by an institu-tional research and ethics committee, and the additionaltests performed did not have implications in the treatmentor medical attention for patients.
Detection of a-CCP antibodies
The a-CCP antibodies (IgG) were measured using a com-mercially available second generation enzyme-linked
immunosorbent assay (ELISA-II), according to the manu-facturer instructions (EUROIMMUN, UK®). BrieXy, testsamples, calibrator and controls are incubated in the respec-tive wells, containing the citrullinated peptide. IgG antibod-ies will bind and non-bound material is removed bywashing. Next, peroxidase conjugated anti-human IgG isadded to each well. After incubation with substrate solu-tion, the reaction is stopped and optical densities were mea-sured with spectrophotometer at a wave length of 405/620 nm. Results were expressed in relative units per millili-ter RU/ml, considering positive when the result was¸5 RU/ml. The cut-oV point was obtained with themean § 2 SD of the control group.
RF (IgM) determination
The RF was measured on IU/ml, and assessed using stan-dard nephelometric assay according to the manufacturer’sspeciWcations (Dade Behring, DE). A positive result wasdeWned as a level of >20 UI/ml.
RF (IgG and IgM) by ELISA
Two RF subtypes were determined by a commerciallyavailable ELISA assay, according to the manufacturerinstructions (EUROIMMUN, UK®). Results wereexpressed in optical densities, it was considered positivewhen the result was >0.30 OD for RF IgG and >1.63 ODfor RF IgM.
Statistical analysis
Mean and standard deviation were included for descriptivepurpose; inferential phase was supported by analysis of var-iance (ANOVA) and Student’s t test, Kruskal–Wallis fornon-parametric data. SigniWcance level was established atP < 0.05.
Results
Demographics and clinical
From the 112 patients, the mean age of the whole group ofpatients was 47 § 13.4 years (range 20–80); 85 (76%) werefemale gender (Table 1). Patients were stratiWed into foursubgroups according to reference diagnosis: (1) RA n = 45;(2) probable RA (PRA; patients who have not fulWlledACR criteria for RA classiWcation) n = 16; (3) spond-ylarthropathies (SpA) n = 12; and (4) patients with sys-temic rheumatic disorders (systemic lupus erythematosus,Sjögren’s syndrome, Wbromyalgia) and other diagnosis(systemic diseases from endocrinological origin, infectious
123
Rheumatol Int (2008) 28:851–857 853
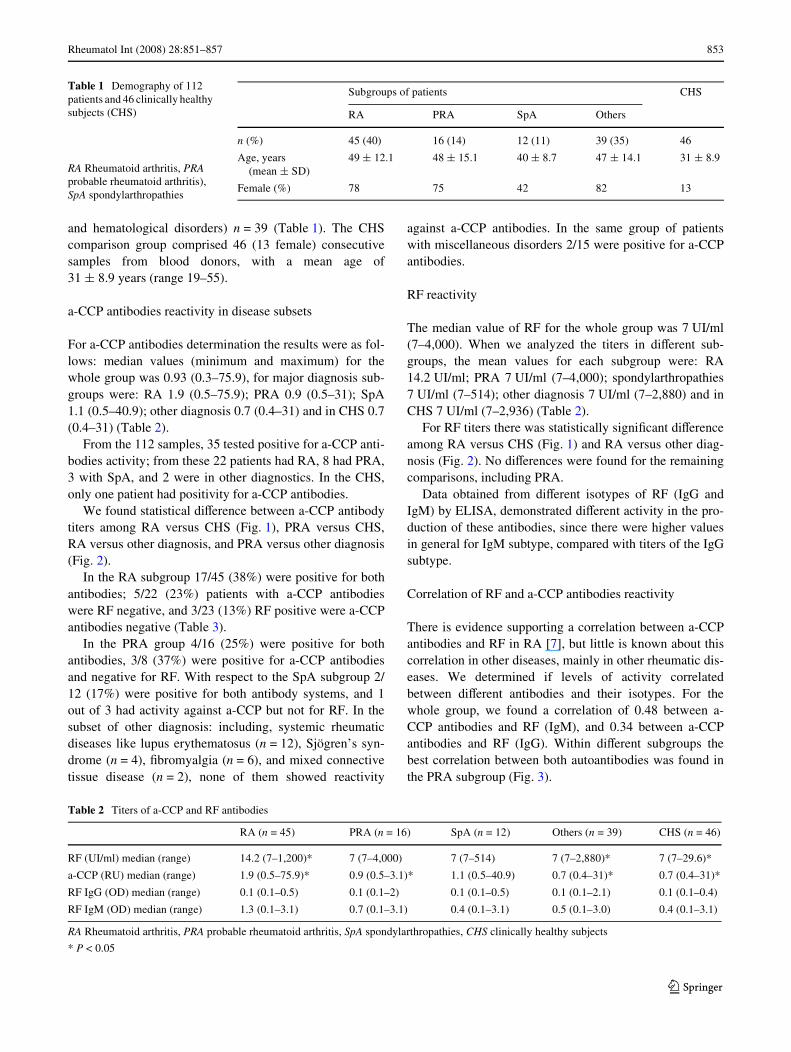
and hematological disorders) n = 39 (Table 1). The CHScomparison group comprised 46 (13 female) consecutivesamples from blood donors, with a mean age of31 § 8.9 years (range 19–55).
a-CCP antibodies reactivity in disease subsets
For a-CCP antibodies determination the results were as fol-lows: median values (minimum and maximum) for thewhole group was 0.93 (0.3–75.9), for major diagnosis sub-groups were: RA 1.9 (0.5–75.9); PRA 0.9 (0.5–31); SpA1.1 (0.5–40.9); other diagnosis 0.7 (0.4–31) and in CHS 0.7(0.4–31) (Table 2).
From the 112 samples, 35 tested positive for a-CCP anti-bodies activity; from these 22 patients had RA, 8 had PRA,3 with SpA, and 2 were in other diagnostics. In the CHS,only one patient had positivity for a-CCP antibodies.
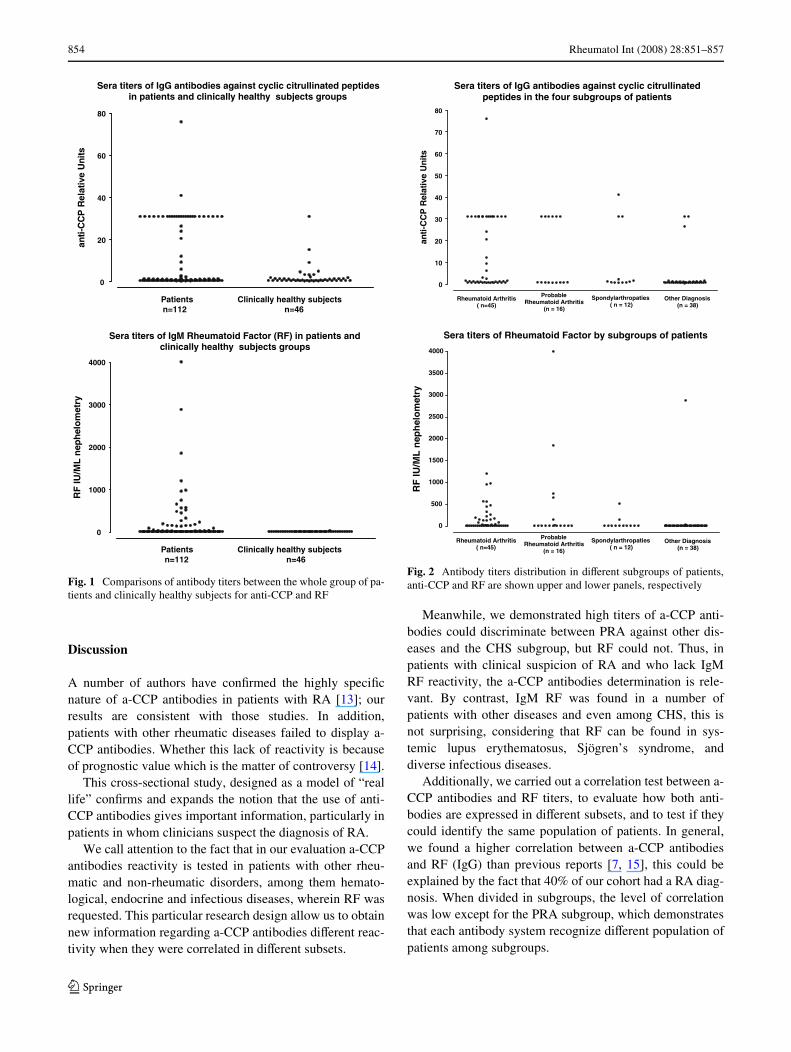
We found statistical diVerence between a-CCP antibodytiters among RA versus CHS (Fig. 1), PRA versus CHS,RA versus other diagnosis, and PRA versus other diagnosis(Fig. 2).
In the RA subgroup 17/45 (38%) were positive for bothantibodies; 5/22 (23%) patients with a-CCP antibodieswere RF negative, and 3/23 (13%) RF positive were a-CCPantibodies negative (Table 3).
In the PRA group 4/16 (25%) were positive for bothantibodies, 3/8 (37%) were positive for a-CCP antibodiesand negative for RF. With respect to the SpA subgroup 2/12 (17%) were positive for both antibody systems, and 1out of 3 had activity against a-CCP but not for RF. In thesubset of other diagnosis: including, systemic rheumaticdiseases like lupus erythematosus (n = 12), Sjögren’s syn-drome (n = 4), Wbromyalgia (n = 6), and mixed connectivetissue disease (n = 2), none of them showed reactivity
against a-CCP antibodies. In the same group of patientswith miscellaneous disorders 2/15 were positive for a-CCPantibodies.
RF reactivity
The median value of RF for the whole group was 7 UI/ml(7–4,000). When we analyzed the titers in diVerent sub-groups, the mean values for each subgroup were: RA14.2 UI/ml; PRA 7 UI/ml (7–4,000); spondylarthropathies7 UI/ml (7–514); other diagnosis 7 UI/ml (7–2,880) and inCHS 7 UI/ml (7–2,936) (Table 2).
For RF titers there was statistically signiWcant diVerenceamong RA versus CHS (Fig. 1) and RA versus other diag-nosis (Fig. 2). No diVerences were found for the remainingcomparisons, including PRA.
Data obtained from diVerent isotypes of RF (IgG andIgM) by ELISA, demonstrated diVerent activity in the pro-duction of these antibodies, since there were higher valuesin general for IgM subtype, compared with titers of the IgGsubtype.
Correlation of RF and a-CCP antibodies reactivity
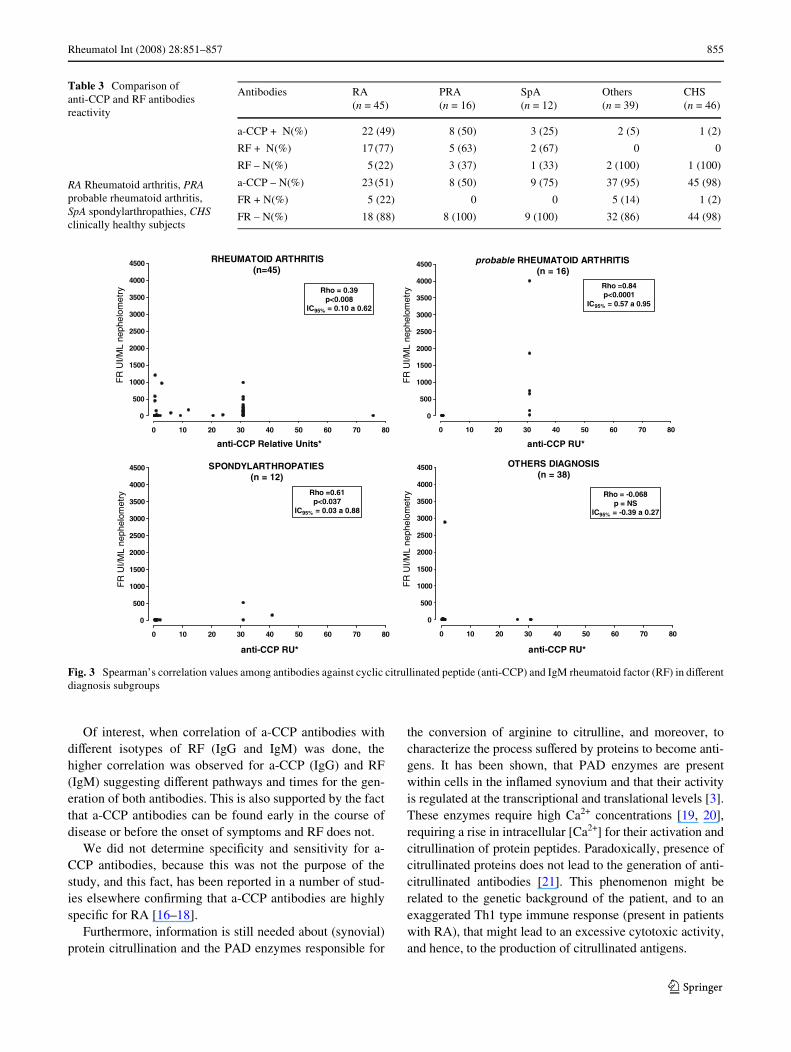
There is evidence supporting a correlation between a-CCPantibodies and RF in RA [7], but little is known about thiscorrelation in other diseases, mainly in other rheumatic dis-eases. We determined if levels of activity correlatedbetween diVerent antibodies and their isotypes. For thewhole group, we found a correlation of 0.48 between a-CCP antibodies and RF (IgM), and 0.34 between a-CCPantibodies and RF (IgG). Within diVerent subgroups thebest correlation between both autoantibodies was found inthe PRA subgroup (Fig. 3).
Table 1 Demography of 112 patients and 46 clinically healthy subjects (CHS)
Subgroups of patients CHS
RA PRA SpA Others
n (%) 45 (40) 16 (14) 12 (11) 39 (35) 46
Age, years (mean § SD)
49 § 12.1 48 § 15.1 40 § 8.7 47 § 14.1 31 § 8.9
Female (%) 78 75 42 82 13
RA Rheumatoid arthritis, PRA probable rheumatoid arthritis), SpA spondylarthropathies
Table 2 Titers of a-CCP and RF antibodies
RA Rheumatoid arthritis, PRA probable rheumatoid arthritis, SpA spondylarthropathies, CHS clinically healthy subjects
* P < 0.05
RA (n = 45) PRA (n = 16) SpA (n = 12) Others (n = 39) CHS (n = 46)
RF (UI/ml) median (range) 14.2 (7–1,200)* 7 (7–4,000) 7 (7–514) 7 (7–2,880)* 7 (7–29.6)*
a-CCP (RU) median (range) 1.9 (0.5–75.9)* 0.9 (0.5–3.1)* 1.1 (0.5–40.9) 0.7 (0.4–31)* 0.7 (0.4–31)*
RF IgG (OD) median (range) 0.1 (0.1–0.5) 0.1 (0.1–2) 0.1 (0.1–0.5) 0.1 (0.1–2.1) 0.1 (0.1–0.4)
RF IgM (OD) median (range) 1.3 (0.1–3.1) 0.7 (0.1–3.1) 0.4 (0.1–3.1) 0.5 (0.1–3.0) 0.4 (0.1–3.1)
123
854 Rheumatol Int (2008) 28:851–857
Discussion
A number of authors have conWrmed the highly speciWcnature of a-CCP antibodies in patients with RA [13]; ourresults are consistent with those studies. In addition,patients with other rheumatic diseases failed to display a-CCP antibodies. Whether this lack of reactivity is becauseof prognostic value which is the matter of controversy [14].
This cross-sectional study, designed as a model of “reallife” conWrms and expands the notion that the use of anti-CCP antibodies gives important information, particularly inpatients in whom clinicians suspect the diagnosis of RA.
We call attention to the fact that in our evaluation a-CCPantibodies reactivity is tested in patients with other rheu-matic and non-rheumatic disorders, among them hemato-logical, endocrine and infectious diseases, wherein RF wasrequested. This particular research design allow us to obtainnew information regarding a-CCP antibodies diVerent reac-tivity when they were correlated in diVerent subsets.
Meanwhile, we demonstrated high titers of a-CCP anti-bodies could discriminate between PRA against other dis-eases and the CHS subgroup, but RF could not. Thus, inpatients with clinical suspicion of RA and who lack IgMRF reactivity, the a-CCP antibodies determination is rele-vant. By contrast, IgM RF was found in a number ofpatients with other diseases and even among CHS, this isnot surprising, considering that RF can be found in sys-temic lupus erythematosus, Sjögren’s syndrome, anddiverse infectious diseases.
Additionally, we carried out a correlation test between a-CCP antibodies and RF titers, to evaluate how both anti-bodies are expressed in diVerent subsets, and to test if theycould identify the same population of patients. In general,we found a higher correlation between a-CCP antibodiesand RF (IgG) than previous reports [7, 15], this could beexplained by the fact that 40% of our cohort had a RA diag-nosis. When divided in subgroups, the level of correlationwas low except for the PRA subgroup, which demonstratesthat each antibody system recognize diVerent population ofpatients among subgroups.
Fig. 1 Comparisons of antibody titers between the whole group of pa-tients and clinically healthy subjects for anti-CCP and RF
Sera titers of IgG antibodies against cyclic citrullinated peptidesin patients and clinically healthy subjects groups
0
20
40
60
80
Patients Clinically healthy subjects n=112 n=46
stinU evitale
R P
CC-itna
Sera titers of IgM Rheumatoid Factor (RF) in patients andclinically healthy subjects groups
0
1000
2000
3000
4000
Patients Clinically healthy subjects n=112 n=46
yrtem
oleh
pen
LM/
UI F
R
Fig. 2 Antibody titers distribution in diVerent subgroups of patients,anti-CCP and RF are shown upper and lower panels, respectively
Sera titers of IgG antibodies against cyclic citrullinatedpeptides in the four subgroups of patients
0
10
20
30
40
50
60
70
80
Rheumatoid Arthritis( n=45)
ProbableRheumatoid Arthritis
(n = 16)
Spondylarthropaties( n = 12)
Other Diagnosis(n = 38)
stin
U evitaleR
PC
C-itna
Sera titers of Rheumatoid Factor by subgroups of patients
0
500
1000
1500
2000
2500
3000
3500
4000
Rheumatoid Arthritis( n=45)
ProbableRheumatoid Arthritis
(n = 16)
Spondylarthropaties( n = 12)
Other Diagnosis(n = 38)
yrtem
oleh
pen
LM/
UI F
R
123
Rheumatol Int (2008) 28:851–857 855
Of interest, when correlation of a-CCP antibodies withdiVerent isotypes of RF (IgG and IgM) was done, thehigher correlation was observed for a-CCP (IgG) and RF(IgM) suggesting diVerent pathways and times for the gen-eration of both antibodies. This is also supported by the factthat a-CCP antibodies can be found early in the course ofdisease or before the onset of symptoms and RF does not.
We did not determine speciWcity and sensitivity for a-CCP antibodies, because this was not the purpose of thestudy, and this fact, has been reported in a number of stud-ies elsewhere conWrming that a-CCP antibodies are highlyspeciWc for RA [16–18].
Furthermore, information is still needed about (synovial)protein citrullination and the PAD enzymes responsible for
the conversion of arginine to citrulline, and moreover, tocharacterize the process suVered by proteins to become anti-gens. It has been shown, that PAD enzymes are presentwithin cells in the inXamed synovium and that their activityis regulated at the transcriptional and translational levels [3].These enzymes require high Ca2+ concentrations [19, 20],requiring a rise in intracellular [Ca2+] for their activation andcitrullination of protein peptides. Paradoxically, presence ofcitrullinated proteins does not lead to the generation of anti-citrullinated antibodies [21]. This phenomenon might berelated to the genetic background of the patient, and to anexaggerated Th1 type immune response (present in patientswith RA), that might lead to an excessive cytotoxic activity,and hence, to the production of citrullinated antigens.
Table 3 Comparison of anti-CCP and RF antibodies reactivity
Antibodies RA (n = 45)
PRA (n = 16)
SpA (n = 12)
Others (n = 39)
CHS (n = 46)
a-CCP + N(%) 22 (49) 8 (50) 3 (25) 2 (5) 1 (2)
RF + N(%) 17 (77) 5 (63) 2 (67) 0 0
RF – N(%) 5 (22) 3 (37) 1 (33) 2 (100) 1 (100)
a-CCP – N(%) 23 (51) 8 (50) 9 (75) 37 (95) 45 (98)
FR + N(%) 5 (22) 0 0 5 (14) 1 (2)
FR – N(%) 18 (88) 8 (100) 9 (100) 32 (86) 44 (98)
RA Rheumatoid arthritis, PRA probable rheumatoid arthritis, SpA spondylarthropathies, CHS clinically healthy subjects
Fig. 3 Spearman’s correlation values among antibodies against cyclic citrullinated peptide (anti-CCP) and IgM rheumatoid factor (RF) in diVerentdiagnosis subgroups
elbaborp SITIRHTRA DIOTAMUEHR )61 = n(
0 01 02 03 04 05 06 07 08
0
005
0001
0051
0002
0052
0003
0053
0004
0054
48.0= ohR1000.0<p
CI %59 59.0 a 75.0 =
*UR PCC-itna
FR
UI/M
L ne
phel
omet
ry
SEITAPORHTRALYDNOPS)21 = n(
0 01 02 03 04 05 06 07 08
0
005
0001
0051
0002
0052
0003
0053
0004
0054
16.0= ohR730.0<p
CI %59 88.0 a 30.0 =
*UR PCC-itna
FR
UI/M
L ne
phel
omet
ry
SISONGAID SREHTO)83 = n(
0 01 02 03 04 05 06 07 08
0
005
0001
0051
0002
0052
0003
0053
0004
0054
860.0- = ohRSN = p
CI %59 72.0 a 93.0- =
*UR PCC-itna
FR
UI/M
L ne
phel
omet
ry
SITIRHTRA DIOTAMUEHR )54=n(
0 01 02 03 04 05 06 07 08
0
005
0001
0051
0002
0052
0003
0053
0004
0054
93.0 = ohR800.0<p
CI %59 26.0 a 01.0 =
*stinU evitaleR PCC-itna
FR
UI/M
L ne
phel
omet
ry
123

856 Rheumatol Int (2008) 28:851–857
There is evidence supporting the fact of antibody pro-duction within the inXamed joint and that the proportion ofIgG found is higher when compared with serum [22].
For plasma cells to secrete antibodies there must be acti-vation via CD4+ T cells. It has been shown that the conver-sion of arginine to citrulline in the peptide interacting withthe shared epitope (HLA-DRB1) signiWcantly increasedCD4+ T cells activation [23], but this activation is not suY-cient for intramolecular epitope restriction in antibody pro-duction, there must be additional mechanisms of B celltolerance such as deletion, receptor editing, or inactivation,occurring during exposure to self antigens, combined withother factors like genetic background or environmental fac-tors; altogether inducing this imbalance towards a Th1 typeimmune response.
There are still many questions unresolved about the linkbetween the etiology of the disease and the generation ofspeciWc autoantibodies. However, in order to establish a-CCP antibodies as diagnostic markers, more standardizedand comparative assays must be introduced. In our cohort,a-CCP antibodies were more frequent among RA patients,than we observed with RF. The absence of a-CCP antibod-ies in systemic rheumatic diseases other than RA and in thegroup of miscellaneous disorders increases its utility in theclinical setting (“real life”) in order to discriminate diVeren-tial diagnosis. Nevertheless, taking into account the closestfrequency from both antibodies and the fact that they prob-ably recognize diVerent populations of patients, we suggestthe request and the use of these antibodies when RA is sus-pected.
Acknowledgments This study was Wnancially supported by FOFOIfrom Instituto Mexicano del Seguro Social (registry number 2005/1/I/118).
References
1. van Boekel MA, Vossenaar ER, van den Hoogen FH, van Ven-rooij WJ (2002) Autoantibody systems in rheumatoid arthritis:speciWcity, sensitivity and diagnostic value. Arthritis Res Ther4:87–93
2. Schellekens GA, Visser H, de Jong BA, van den Hoogen FH, Haz-es JM, Breedveld FC, van Venrooij WJ (2000) The diagnosticproperties of rheumatoid arthritis antibodies recognizing a cycliccitrullinated peptide. Arthritis Rheum 43:155–163
3. Vossenaar ER, Zendman AJ, van Venrooij WJ, Pruijn GJ (2003)PAD, a growing family of citrullinating enzymes: genes, featuresand involvement in disease. Bioessays 25:1106–1118
4. Suzuki A, Yamada R, Ohtake-Yamanaka M, Okazaki Y, SawadaT, Yamamoto K (2005) Anti-citrullinated collagen type I antibodyis a target of autoimmunity in rheumatoid arthritis. Biochem Bio-phys Res Commun 333:418–426
5. Chapuy-Regaud S, Nogueira L, Clavel C, Sebbag M, Vincent C,Serre G (2005) IgG subclass distribution of the rheumatoid arthri-tis-speciWc autoantibodies to citrullinated Wbrin. Clin Exp Immu-nol 139:542–550
6. Kinloch A, Tatzer V, Wait R, Peston D, Lundberg K, Donatien P,Moyes D, Taylor PC, Venables PJ (2005) IdentiWcation of citrulli-nated alpha-enolase as a candidate autoantigen in rheumatoidarthritis. Arthritis Res Ther 7:R1421–R1429
7. Lee DM, Schur PH (2003) Clinical utility of the anti-CCP assay inpatients with rheumatic diseases. Ann Rheum Dis 62:870–874
8. Vallbracht I, Rieber J, Oppermann M, Forger F, Siebert U, HelmkeK (2004) Diagnostic and clinical value of anti-cyclic citrullinatedpeptide antibodies compared with rheumatoid factor isotypes inrheumatoid arthritis. Ann Rheum Dis 63:1079–1084
9. Nielen MM, van Schaardenburg D, Reesink HW, van de Stadt RJ,van der Horst-Bruinsma IE, de Koning MH, Habibuw MR, Van-denbroucke JP, Dijkmans BA (2004) SpeciWc autoantibodies pre-cede the symptoms of rheumatoid arthritis: a study of serialmeasurements in blood donors. Arthritis Rheum 50:380–386
10. Nell VP, Machold KP, Stamm TA, Eberl G, Heinzl H, UVmann M,Smolen JS, Steiner G (2005) Autoantibody proWling as early diag-nostic and prognostic tool for rheumatoid arthritis. Ann RheumDis 64:1731–1736
11. De Rycke L, Verhelst X, Kruithof E, Van den Bosch F, HoVmanIE, Veys EM, De Keyser F (2005) Rheumatoid factor, but not anti-cyclic citrullinated peptide antibodies, is modulated by inXiximabtreatment in rheumatoid arthritis. Ann Rheum Dis 64:299–302
12. van Gaalen FA, Linn-Rasker SP, van Venrooij WJ, de Jong BA,Breedveld FC, Verweij CL, Toes RE, Huizinga TW (2004) Auto-antibodies to cyclic citrullinated peptides predict progression torheumatoid arthritis in patients with undiVerentiated arthritis: aprospective cohort study. Arthritis Rheum 50:709–715
13. Nishimura K, Sugiyama D, Kogata Y, Tsuji G, Nakazawa T, Kaw-ano S, Saigo K, Morinobu A, Koshiba M, Kuntz KM, Kamae I,Kumagai S (2007) Meta-analysis: diagnostic accuracy of anti-cy-clic citrullinated peptide antibody and rheumatoid factor for rheu-matoid arthritis. Ann Intern Med 146:797–808
14. Visser H, le Cessie S, Vos K, Breedveld FC, Hazes JM (2002)How to diagnose rheumatoid arthritis early: a prediction model forpersistent (erosive) arthritis. Arthritis Rheum 46:357–365
15. Hill JA, Al-Bishri J, Gladman DD, Cairns E, Bell DA (2006)Serum autoantibodies that bind citrullinated Wbrinogen are fre-quently found in patients with rheumatoid arthritis. J Rheumatol33:2115–2119
16. Sauerland U, Becker H, Seidel M, Schotte H, Willeke P, SchoratA, Schluter B, Domschke W, Gaubitz M (2005) Clinical utility ofthe anti-CCP assay: experiences with 700 patients. Ann N Y AcadSci 1050:314–318
17. Jansen AL, van der Horst-Bruinsma I, van Schaardenburg D, vande Stadt RJ, de Koning MH, Dijkmans BA (2002) Rheumatoidfactor and antibodies to cyclic citrullinated Peptide diVerentiaterheumatoid arthritis from undiVerentiated polyarthritis in patientswith early arthritis. J Rheumatol 29:2074–2076
18. Matsui T, Shimada K, Ozawa N, Hayakawa H, Hagiwara F, Na-kayama H, Sugii S, Ozawa Y, Tohma S (2006) Diagnostic utilityof anti-cyclic citrullinated peptide antibodies for very early rheu-matoid arthritis. J Rheumatol 33:2390–2397
19. Vossenaar ER, van Venrooij WJ (2004) Citrullinated proteins:sparks that may ignite the Wre in rheumatoid arthritis. Arthritis ResTher 6:107–111
20. Curis E, Nicolis I, Moinard C, Osowska S, Zerrouk N, Benazeth S,Cynober L (2005) Almost all about citrulline in mammals. AminoAcids 29:177–205
21. Vossenaar ER, Smeets TJ, Kraan MC, Raats JM, van VenrooijWJ, Tak PP (2004) The presence of citrullinated proteins is notspeciWc for rheumatoid synovial tissue. Arthritis Rheum50:3485–3494
22. Masson-Bessiere C, Sebbag M, Durieux JJ, Nogueira L, Vincent C,Girbal-Neuhauser E, Durroux R, Cantagrel A, Serre G (2000) In therheumatoid pannus, anti-Wlaggrin autoantibodies are produced by
123
Rheumatol Int (2008) 28:851–857 857
local plasma cells and constitute a higher proportion of IgG than insynovial Xuid and serum. Clin Exp Immunol 119:544–552
23. Hill JA, Southwood S, Sette A, Jevnikar AM, Bell DA, Cairns E(2003) Cutting edge: the conversion of arginine to citrulline allows
for a high-aYnity peptide interaction with the rheumatoid arthritis-associated HLA-DRB1*0401 MHC class II molecule. J Immunol171:538–541
123
Copyright © 2022 FDOKUMEN