
Self-management of oral anticoagulation in the elderly: Rationale, design, baselines and oral...
7
Regular Article Self-management of oral anticoagulation in elderly patients – Effects on treatment-related Quality of Life Andrea Siebenhofer a, ⁎, Lars G. Hemkens b , Ivo Rakovac c , Stephan Spat c , Ulrike Didjurgeit d and for the SPOG 60+ Study Group a Institute for General Practice, Goethe University, Frankfurt am Main, Germany b Institute for Quality and Efficiency in Health Care (IQWiG), Cologne, Germany c HEALTH - Institute for Biomedicine and Health Sciences, JOANNEUM RESEARCH Forschungsgesellschaft mbH, Graz, Austria d DIeM - Institute for Evidence-based Medicine GmbH, Cologne, Germany abstract article info Article history: Received 9 March 2012 Received in revised form 29 May 2012 Accepted 13 June 2012 Available online xxxx Background – rationale for study: In elderly patients, long-term self-management of oral anticoagulation has been shown to reduce the number of major thromboembolic and bleeding complications and improve the quality of oral anticoagulation (OAC) control compared to routine care for a mean follow-up period of three years. This article presents the results of the predefined secondary endpoint treatment-related quality of life (QoL). Methods and Results: The effect of self-management on five aspects of QoL was evaluated in comparison with routine care. A validated questionnaire specifically designed for patients receiving OAC was used. The evaluation was possible for 141 patients, comprising 90% of surviving patients on OAC. At baseline, all patients had high scores for the following QoL-aspects: general treatment satisfaction, self- efficacy, daily hassles and strained social network. A high proportion of patients in both groups explicitly reported high distress, indicating that general psychological distress seems to be of particular concern in this population. After about 3 years of follow-up, patients performing self-management showed a significantly great- er improvement in general treatment satisfaction than controls (median score increase [25th percentile, 75th percentile]: 0.9 [0.0, 1.6] vs. 0.0 [−0.2, 0.6], p=0.002; scale 1–6). Changes in general psychological distress, self-efficacy, daily hassles and strained social network were not significant. Conclusion: Treatment related quality of life in elderly patients performing self-management of OAC was similar as for patients in routine care setting, with a tendency of higher general treatment satisfaction, after three years of follow up. © 2012 Elsevier Ltd. All rights reserved. Introduction In elderly patients, oral anticoagulation therapy seem to benefit most from oral anticoagulation therapy [1–3]. However, physicians seem to be reluctant in prescribing OAC particularly in elderly indi- viduals for various reasons [4–8]. A major barrier seems to be the physicians’ concern that OAC may lead to a hemorrhage [4–7]. In pa- tients over 70 years of age, the risk of such an event is twice as high as in younger patients [9]. In a recent observational study for this age group, the risk of major bleeding events was 3-times higher during the 90 days following the initiation of OAC and 2.75 times higher in patients ≥80 years of age, than in younger patients [10]. Self-management can help to reduce the risk of severe anticoagulation- related complications [11–15], but conclusive evidence demonstrating the beneficial effects of OAC self-management in elderly patients is scarce. The meta-analysis published by Heneghan in 2011 demonstrat- ed that even in the very elderly self-management showed no significant adverse effects of the intervention for all outcomes [14]. We know of only one such randomized single center study, and that showed a signif- icant reduction in the number of thromboembolic complications in pa- tients with a mean age of 64 to 67 over an average follow-up of one year [16]. Another trial indicated that self-testing in elderly patients may ef- fectively reduce excessive bleeding rates [17]. Against this background, the SPOG 60+ (structured teaching and self-management program for patients who are over 60 years of age and receiving OAC) trial aimed to compare self-management with routine care in elderly patients receiving long-term anticoagulation treatment by using thromboembolic and hemorrhagic complications as the combined primary outcome. Predefined secondary and tertiary outcomes were frequency and duration of hospitalization, mortality, Thrombosis Research xxx (2012) xxx–xxx ⁎ Corresponding author at: Institute for General Practice, Goethe University, Theodor-Stern-Kai 7, 60590 Frankfurt am Main, Germany. Tel.: + 49 69 6301 7296; fax: +49 69 6301 6428. E-mail address: [email protected] (A. Siebenhofer). TR-04790; No of Pages 7 0049-3848/$ – see front matter © 2012 Elsevier Ltd. All rights reserved. doi:10.1016/j.thromres.2012.06.012 Contents lists available at SciVerse ScienceDirect Thrombosis Research journal homepage: www.elsevier.com/locate/thromres Please cite this article as: Siebenhofer A, et al, Self-management of oral anticoagulation in elderly patients – Effects on treatment-related Quality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Self-management of oral anticoagulation in the elderly: Rationale, design, baselines and oral...
Thrombosis Research xxx (2012) xxx–xxx
TR-04790; No of Pages 7
Contents lists available at SciVerse ScienceDirect
Thrombosis Research
j ourna l homepage: www.e lsev ie r .com/ locate / thromres
Regular Article
Self-management of oral anticoagulation in elderly patients – Effects ontreatment-related Quality of Life
Andrea Siebenhofer a,⁎, Lars G. Hemkens b, Ivo Rakovac c, Stephan Spat c, Ulrike Didjurgeit d
and for the SPOG 60+ Study Groupa Institute for General Practice, Goethe University, Frankfurt am Main, Germanyb Institute for Quality and Efficiency in Health Care (IQWiG), Cologne, Germanyc HEALTH - Institute for Biomedicine and Health Sciences, JOANNEUM RESEARCH Forschungsgesellschaft mbH, Graz, Austriad DIeM - Institute for Evidence-based Medicine GmbH, Cologne, Germany
⁎ Corresponding author at: Institute for GeneralTheodor-Stern-Kai 7, 60590 Frankfurt am Main, Germfax: +49 69 6301 6428.
E-mail address: [email protected]
0049-3848/$ – see front matter © 2012 Elsevier Ltd. Alldoi:10.1016/j.thromres.2012.06.012
Please cite this article as: Siebenhofer A, eQuality of Life, Thromb Res (2012), doi:10.
a b s t r a c t
a r t i c l e i n f oArticle history:
Received 9 March 2012Received in revised form 29 May 2012Accepted 13 June 2012Available online xxxxBackground – rationale for study: In elderly patients, long-term self-management of oral anticoagulation hasbeen shown to reduce the number of major thromboembolic and bleeding complications and improve thequality of oral anticoagulation (OAC) control compared to routine care for a mean follow-up period ofthree years. This article presents the results of the predefined secondary endpoint treatment-related qualityof life (QoL).Methods and Results: The effect of self-management on five aspects of QoL was evaluated in comparison with
routine care. A validated questionnaire specifically designed for patients receiving OACwas used. The evaluationwas possible for 141 patients, comprising 90% of surviving patients on OAC.At baseline, all patients had high scores for the following QoL-aspects: general treatment satisfaction, self-efficacy, daily hassles and strained social network. A high proportion of patients in both groups explicitlyreported high distress, indicating that general psychological distress seems to be of particular concern in thispopulation. After about 3 years of follow-up, patients performing self-management showed a significantly great-er improvement in general treatment satisfaction than controls (median score increase [25th percentile, 75thpercentile]: 0.9 [0.0, 1.6] vs. 0.0 [−0.2, 0.6], p=0.002; scale 1–6). Changes in general psychological distress,self-efficacy, daily hassles and strained social network were not significant.Conclusion: Treatment related quality of life in elderly patients performing self-management of OAC was similaras for patients in routine care setting, with a tendency of higher general treatment satisfaction, after three yearsof follow up.© 2012 Elsevier Ltd. All rights reserved.
Introduction
In elderly patients, oral anticoagulation therapy seem to benefitmost from oral anticoagulation therapy [1–3]. However, physiciansseem to be reluctant in prescribing OAC particularly in elderly indi-viduals for various reasons [4–8]. A major barrier seems to be thephysicians’ concern that OAC may lead to a hemorrhage [4–7]. In pa-tients over 70 years of age, the risk of such an event is twice as high asin younger patients [9]. In a recent observational study for this agegroup, the risk of major bleeding events was 3-times higher duringthe 90 days following the initiation of OAC and 2.75 times higher inpatients ≥80 years of age, than in younger patients [10].
Practice, Goethe University,any. Tel.: +49 69 6301 7296;
frankfurt.de (A. Siebenhofer).
rights reserved.
t al, Self-management of ora1016/j.thromres.2012.06.012
Self-management canhelp to reduce the riskof severeanticoagulation-related complications [11–15], but conclusive evidence demonstratingthe beneficial effects of OAC self-management in elderly patients isscarce. The meta-analysis published by Heneghan in 2011 demonstrat-ed that even in the very elderly self-management showed no significantadverse effects of the intervention for all outcomes [14]. We know ofonly one such randomized single center study, and that showed a signif-icant reduction in the number of thromboembolic complications in pa-tientswith amean age of 64 to 67 over an average follow-up of one year[16]. Another trial indicated that self-testing in elderly patients may ef-fectively reduce excessive bleeding rates [17].
Against this background, the SPOG 60+ (structured teaching andself-management program for patients who are over 60 years of ageand receiving OAC) trial aimed to compare self-management withroutine care in elderly patients receiving long-term anticoagulationtreatment by using thromboembolic and hemorrhagic complicationsas the combined primary outcome. Predefined secondary and tertiaryoutcomes were frequency and duration of hospitalization, mortality,
l anticoagulation in elderly patients – Effects on treatment-related

2 A. Siebenhofer et al. / Thrombosis Research xxx (2012) xxx–xxx
recurrence of stroke, quality of oral anticoagulation, and cost-effectiveness evaluations as well as treatment-related quality of life.The main results of the SPOG 60+ trial have already been published[18]. In summary, over a mean follow-up of up to three years, self-management in elderly patients showed statistically significant bene-fits compared to routine care. The combined risk of thromboembolicevents requiring hospitalization and of all major bleeding complica-tionswas halved (HR: 0.50; 95% CI: 0.25 to 1.00; p=0.049). Sensitivityanalyses focusing solely on patients who successfully received their al-located intervention reinforced the reported benefits (HR 0.27; 95%CI:0.13 to 0.71; p=0.006). OAC control was significantly better in theself-management group (SMG) than in the routine care group (RCG).
Quality of life (QoL) in patients performing self-management of OAChas been compared with routine care in several randomized controlledtrials [19–25], aswell as in ameta-analysis [11].While some trials foundimprovements in some aspects of QoL, others failed to find significantdifferences [20,21,23,26]. The majority of these studies were short-term trials involving relatively young patients.
In the following we show the results of the predefined secondaryoutcome “treatment-related quality of life” of the SPOG 60+ study inan elderly population over a mean follow-up of three years.
Patients and Methods
Design Overview
The rationale and design of the SPOG 60+ trial have been pres-ented in detail elsewhere [27]. In brief, patients aged 60 or overwho were undergoing long-term anticoagulation therapy with ei-ther phenprocoumon or acenocoumarol were included. Patientswho had previously participated in a self-management OAC programor who had severe cognitive impairment or a terminal illness wereexcluded. Patients were informed by their physician of their individ-ually defined INR therapeutic target ranges. Consenting patients wereallocated to self-management or routine care via central telephone ran-domization using a concealed, computer generated and block-sized,center-stratified randomization scheme. The study centers were in Co-logne, Vienna, and Graz.
In Brief, patients in both groups were asked to attend trainingcourses (details in [27]). RCG patients received basic theoretical infor-mation on OAC (potential risk of thromboembolism and bleeding, po-tential problems in special situations such as exercise, travel and dietchanges) during a single session. SMG patients underwent the SPOG60+ training course (structured teaching and self-management pro-gram for patients of more than 60 years of age receiving OAC). Trainedanticoagulation nurses instructed patients in four consecutive weeklysessions with the aim of providing themwith a theoretical understand-ing of oral anticoagulation and empowering them to practice OACman-agement. All patients gave their written informed consent and the trialprotocol was approved by all local ethics committees and performed inaccordance with the Declaration of Helsinki.
Outcomes and Follow-up
The trial started in March 2002 and ended in February 2007, twoyears after the final patient was randomized. Follow-up visits werescheduled at baseline and at 6-month intervals. Patients were clini-cally examined and questioned about minor or major bleeding orthromboembolic events, any illnesses in the meantime, changes inlong-term medications, and hospitalizations. Patients who withdrewfrom the study were either invited to visit once last time at studyend or the attending physicians were contacted by telephone to ob-tain complete data for the primary endpoint, as well as death andhospitalization rates.
Treatment-related quality of life (QoL) was assessed at baselineand during a final visit by means of a structured questionnaire. The
Please cite this article as: Siebenhofer A, et al, Self-management of oraQuality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
results of the questionnaire were recorded by personnel blinded tothe treatment arm.
The structured questionnaire used for the evaluation of quality of lifein patients receiving oral anticoagulation was developed by our work-ing groupwith the help of members of German and Austrian patient or-ganisations. It has been validated and used in several randomizedcontrolled trials [19,22,24]. The questionnaire comprises 32 items spe-cially designed for patients receiving oral anticoagulation and coversfive socio-psychological treatment-related topics: general treatmentsatisfaction, self-efficacy, strained social network, daily hassles, and generalpsychological distress.
The study patients estimated the impact of every item on theirself-perceived treatment-related quality of life on a graded scaleranging from not noticeable [1], barely noticeable [2], somewhat no-ticeable [3], moderately noticeable [4], quite noticeable [5] extremelynoticeable [6]. By dividing the total score by the number of includeditems, an overall score ranging from a minimum of 1 to a maximumof 6 was calculated for every topic.
General treatment satisfaction refers to general aspects pertaining toindividual treatment-associated satisfaction. Self-efficacy reflects apatient's belief in being able to take care of him or herself. High scoreson these items represent a high treatment-related QoL. Social networkfactors are, for example, important when a patient has problemsaccepting the inconveniences associated with oral anticoagulation:this is particularly true for the elderly. Possible negative effects arecaptured by the item strained social network. Daily hassles refer tominor stressful events that can frequently have a negative impacton quality of life. Low scores on the item daily hassles and on theitem general psychological distress indicate high treatment-relatedQoL.
Statistical Analysis
Data were analysed in accordance with participants' randomizedtreatment (intention to treat), with the randomization date being thestarting point for the follow-up. For continuous variables, differenceswere assessed by means of the Wilcoxon test, unpaired for inter-group and paired for intra-group comparisons. Categorical data werecompared using χ2 tests. The significance level was set at α=0.05. Ifnot otherwise stated data are presented as themedian [25th percentile,75th percentile]. Treatment-related QoL was a secondary outcome ofthe SPOG-60+trial andwas not part of the power calculation. Statisticalanalyses were performed using version 2.4.1 of the R package for statis-tical computing [28]. Further details concerning the statistical analyseshave already been reported [27].
Results
Overall, 43% of eligible patients invited to participate at the studycentres were randomized.
Fig. 1 shows the numbers of patients that were randomized andfollowed up on by the time the study closed. Of the 99 patients ran-domized to the SMG, 89 successfully completed training. In the RCG94 of 96 randomized patients attended the training session. Reasonsfor not receiving the allocated intervention are described in the trialprofile in Fig. 1. Twenty-six of the 195 randomized patients died dur-ing follow-up and 12 discontinued OAC treatment. Of the 157 pa-tients on OAC who survived, 141 (90%) provided complete qualityof life data and were included in the main analysis of the effect ofOAC self-management on treatment-related quality of life (QoL).The characteristics of and results for the total study population arepresented in a previous publication [27].
Table 1 shows the characteristics of both groups. At baseline, therewere no significant differences in terms of age, gender, intended INRranges, co-morbidities, previous thromboembolic and hemorrhagiccomplications or other long-term medications. The patients’ diaries
l anticoagulation in elderly patients – Effects on treatment-related
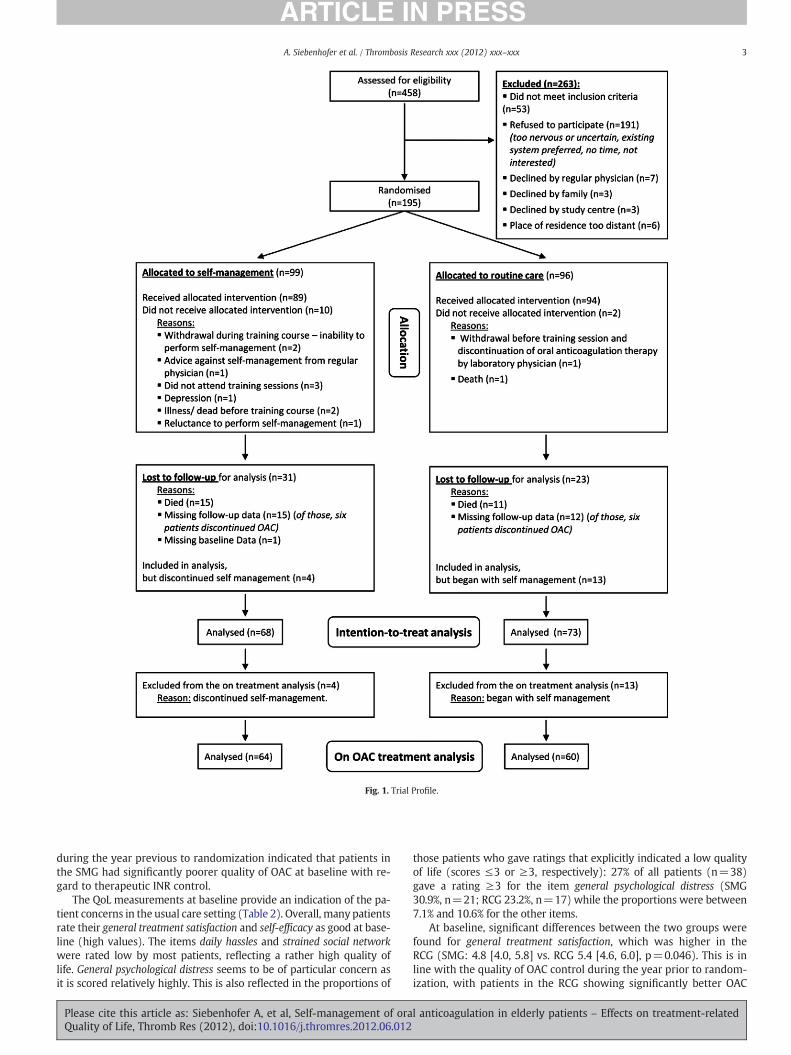
Fig. 1. Trial Profile.
3A. Siebenhofer et al. / Thrombosis Research xxx (2012) xxx–xxx
during the year previous to randomization indicated that patients inthe SMG had significantly poorer quality of OAC at baseline with re-gard to therapeutic INR control.
The QoL measurements at baseline provide an indication of the pa-tient concerns in the usual care setting (Table 2). Overall, many patientsrate their general treatment satisfaction and self-efficacy as good at base-line (high values). The items daily hassles and strained social networkwere rated low by most patients, reflecting a rather high quality oflife. General psychological distress seems to be of particular concern asit is scored relatively highly. This is also reflected in the proportions of
Please cite this article as: Siebenhofer A, et al, Self-management of oraQuality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
those patients who gave ratings that explicitly indicated a low qualityof life (scores ≤3 or ≥3, respectively): 27% of all patients (n=38)gave a rating ≥3 for the item general psychological distress (SMG30.9%, n=21; RCG 23.2%, n=17) while the proportions were between7.1% and 10.6% for the other items.
At baseline, significant differences between the two groups werefound for general treatment satisfaction, which was higher in theRCG (SMG: 4.8 [4.0, 5.8] vs. RCG 5.4 [4.6, 6.0], p=0.046). This is inline with the quality of OAC control during the year prior to random-ization, with patients in the RCG showing significantly better OAC
l anticoagulation in elderly patients – Effects on treatment-related

Table 1Patients' baseline characteristics.
Variable Self-managementgroup
Routine Caregroup
p-value
Patients, n 68 73Mean age±SD, years 69.7±6.5 69.4±6.6 0.836Females 43% (29) 36% (26) 0.392Indication for oralanticoagulation treatment
0.085
Atrial fibrillation 54% (37) 33% (24)Venous thromboembolism 16% (11) 26% (19)Mechanical heart prothesis 18% (12) 18% (13)Pulmonary embolism 4% (3) 11% (8)Other 7% (5) 12% (9)
Intended INR target range 0.0872-3 84% (57) 79% (58)2.5-3.5 16% (11) 14% (10)Other 0% (0) 7% (5)
Duration of oral anticoagulationtreatment, years
5.6±6.7 6.4±7.4 0.770
Oral anticoagulation medication 0.922Phenprocoumon 90% (60) 89% (65)Acenocoumarol 10% (7) 11% (8)
Co-morbiditiesCardiovascular disease other thanatrial fibrillation or mechanicheart valve replacement
75% (51) 82% (60) 0.297
Hypertension 44% (30) 45% (33) 0.897Diabetes mellitus 22% (15) 21% (15) 0.827Pulmonary disease 9% (6) 10% (7) 0.875Disease of the gastrointestinaltract
15% (10) 10% (7) 0.351
Cancer 6% (4) 7% (5) 0.814Previous complications
Thromboembolic 41% (28) 45% (33) 0.629Severe hemorrhagic 4% (3) 7% (5) 0.532
Other long-term medicationsAntihypertensive agents (incl.diuretics)
79% (54) 79% (58) 0.995
Cardiac therapy 49% (33) 41% (30) 0.375Lipid modifying agents 28% (19) 41% (30) 0.101Anti-ulcer agents 13% (9) 12% (9) 0.872Anti-diabetic agents 13% (9) 16% (12) 0.593Psychotropic drugs 15% (10) 10% (7) 0.351
Anti-inflammatory and anti-analgetic agents
10% (7) 11% (8) 0.898
Hospitalization within previous12 months
60% (41) 58% (42) 0.739
Data are mean±SD or % (n).
4 A. Siebenhofer et al. / Thrombosis Research xxx (2012) xxx–xxx
control at baseline with regard to therapeutic INR [18,27]. This alsoapplies to the 141 patients included in the QoL analysis (data notshown).
Mean follow-up was (mean±standard deviation) 3.1±1.0 and3.1±0.9 years in the SMG and RCG, respectively. Cronbach α values
Table 2Quality of life at baseline and end of follow-up.
Baseline(n=68)
SMG RCG
GeneralTreatment Satisfaction
4.8[4.0, 5.8]
5.4[4.6, 6.0]
Self-efficacy 5.0[4.3, 5.8]
5.0[3.8, 5.8]
Generalpsychological distress
2.14[1.57, 3.29]
2.00[1.57, 2.86]
Daily hassles 1.86[1.29, 2.43]
1.71[1.29, 2.14]
Strainedsocial network
1.40[1.00, 2.38]
1.38[1.00, 2.13]
Data are median [25th percentile, 75th percentile]. P values, obtained by Wilcoxon test, derespectively. SMG: Self-management Group. RCG: Routine Care Group.
Please cite this article as: Siebenhofer A, et al, Self-management of oraQuality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
varied between 0.68 and 0.88 (baseline) and 0.52 and 0.75 (follow-up) depending on the item.
During follow-up all investigated aspects of treatment-related QoLimproved in both groups (Table 2). The score differences betweenbaseline and follow-up are shown in the form of a boxplot in Fig. 2.The most pronounced improvement was found in general treatment sat-isfaction after participation in the self-management program (medianscore increase SMG: 0.9 [0.0, 1.6] vs. RCG: 0.0 [−0.2, 0.6], p=0.002). Ad-ditionally, patients performing self-management showed improvementsin their median scores for the items general psychological distress (SMG:−0.14 [−0.57, 0.29] vs. RCG:−0.43 [−0.86, 0.0], p=0.092) and strainedsocial network (SMG: −0.13 [−0.63, 0.00] vs. RCG: 0.00 [−0.50, 0.38],p=0.073), but these differences were not significant. No differenceswere found in daily hassles (SMG: −0.15 [−0.71, 0.13] vs. RCG: −0.14[−0.57, 0.29], p=0.49) and self-efficacy (SMG: 0.38 [0.0, 1.25] vs. RCG:0.50[0.0, 1.25], p=0.8).
Patient populations in both groups who gave ratings indicating anexplicitly low quality of life (≤3 or ≥3, respectively) seemed to benefitfrom participation in the trial: after participation no patient in eithergroup gave such ratings for general treatment satisfaction, and only2.9% of patients gave such ratings for self-efficacy in the SMG. Likewisean improvementwas observed in both groups for strained social network(SMG: 2.9%; RCG 6.8%) and daily hassles (SMG: 2.9%; RCG 4.1%). The rel-atively higher proportion of patients who gave low ratings for generalpsychological distress at baseline decreased substantially in both groups(SMG: 11.8%; RCG 16.4%). However, for this item, particular improve-ment was shown by patients in the self-management group (SMG:−19.1% vs.RCG: −6.8%, p=0.169).
Subgroup analyses of different routine care settings, i.e. general prac-tice (n=32) or hospital-based anticoagulation clinic (n=41) were con-sistent with the main analysis: The most pronounced improvement wasfound in general treatment satisfaction independent of whether self-management is compared to routine care in a general practice setting(SMG: 0.90 [0.0, 1.60] vs. GP-RCG: 0.0 [0.0, 0.60], p=0.048) or to routinecare in an anticoagulation clinic (SMG: 0.90 [0.0, 1.60] vs. Clinic-RCG: 0.0[−0.6, 0.6], p=0.002). An interaction test for the different settings wasperformed for all five items but no significant difference was revealed.
Analysis of the patient population that completed the entire trialon their allocated treatment, i.e. after exclusion of those patients thatcrossed over treatment (in OAC treatment analysis) showed no sub-stantial changes in the main results. Likewise, an analysis of patientsin the group that (at least for their last treatment) had crossed overtreatments confirmed the main results.
Discussion
To our knowledge, this is the first multi-center randomized con-trolled trial that has assessed the efficacy of self-management of oral
Follow-Up(n=73)
p-value SMG RCG p-value
0.046 6.00[5.55, 6.0[
5.80 [5.00, 6.0] 0.10
0.65 5.75[5.25, 6.0]
5.50[5.0, 6.0]
0.042
0.31 1.71[1.39, 2.32]
1.71[1.29, 2.43]
0.82
0.19 1.40[1.13, 1.78]
1.50[1.13, 1.75]
0.99
0.84 1.13[1.00, 1.75]
1.38[1.00, 2.13]
0.054
note statistical significance for between group comparisons at baseline and follow up,
l anticoagulation in elderly patients – Effects on treatment-related
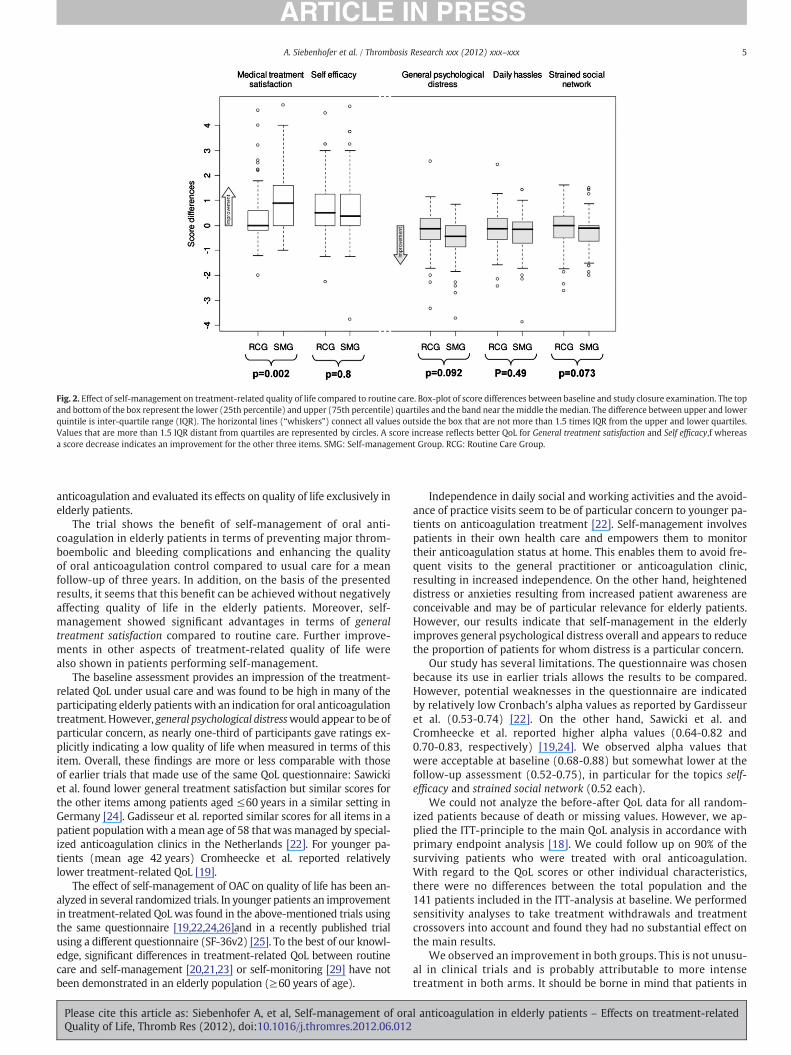
Fig. 2. Effect of self-management on treatment-related quality of life compared to routine care. Box-plot of score differences between baseline and study closure examination. The topand bottom of the box represent the lower (25th percentile) and upper (75th percentile) quartiles and the band near themiddle themedian. The difference between upper and lowerquintile is inter-quartile range (IQR). The horizontal lines (“whiskers”) connect all values outside the box that are not more than 1.5 times IQR from the upper and lower quartiles.Values that are more than 1.5 IQR distant from quartiles are represented by circles. A score increase reflects better QoL for General treatment satisfaction and Self efficacy,f whereasa score decrease indicates an improvement for the other three items. SMG: Self-management Group. RCG: Routine Care Group.
5A. Siebenhofer et al. / Thrombosis Research xxx (2012) xxx–xxx
anticoagulation and evaluated its effects on quality of life exclusively inelderly patients.
The trial shows the benefit of self-management of oral anti-coagulation in elderly patients in terms of preventing major throm-boembolic and bleeding complications and enhancing the qualityof oral anticoagulation control compared to usual care for a meanfollow-up of three years. In addition, on the basis of the presentedresults, it seems that this benefit can be achieved without negativelyaffecting quality of life in the elderly patients. Moreover, self-management showed significant advantages in terms of generaltreatment satisfaction compared to routine care. Further improve-ments in other aspects of treatment-related quality of life werealso shown in patients performing self-management.
The baseline assessment provides an impression of the treatment-related QoL under usual care and was found to be high in many of theparticipating elderly patients with an indication for oral anticoagulationtreatment. However, general psychological distresswould appear to be ofparticular concern, as nearly one-third of participants gave ratings ex-plicitly indicating a low quality of life when measured in terms of thisitem. Overall, these findings are more or less comparable with thoseof earlier trials that made use of the same QoL questionnaire: Sawickiet al. found lower general treatment satisfaction but similar scores forthe other items among patients aged ≤60 years in a similar setting inGermany [24]. Gadisseur et al. reported similar scores for all items in apatient population with a mean age of 58 that wasmanaged by special-ized anticoagulation clinics in the Netherlands [22]. For younger pa-tients (mean age 42 years) Cromheecke et al. reported relativelylower treatment-related QoL [19].
The effect of self-management of OAC on quality of life has been an-alyzed in several randomized trials. In younger patients an improvementin treatment-related QoL was found in the above-mentioned trials usingthe same questionnaire [19,22,24,26]and in a recently published trialusing a different questionnaire (SF-36v2) [25]. To the best of our knowl-edge, significant differences in treatment-related QoL between routinecare and self-management [20,21,23] or self-monitoring [29] have notbeen demonstrated in an elderly population (≥60 years of age).
Please cite this article as: Siebenhofer A, et al, Self-management of oraQuality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
Independence in daily social and working activities and the avoid-ance of practice visits seem to be of particular concern to younger pa-tients on anticoagulation treatment [22]. Self-management involvespatients in their own health care and empowers them to monitortheir anticoagulation status at home. This enables them to avoid fre-quent visits to the general practitioner or anticoagulation clinic,resulting in increased independence. On the other hand, heighteneddistress or anxieties resulting from increased patient awareness areconceivable and may be of particular relevance for elderly patients.However, our results indicate that self-management in the elderlyimproves general psychological distress overall and appears to reducethe proportion of patients for whom distress is a particular concern.
Our study has several limitations. The questionnaire was chosenbecause its use in earlier trials allows the results to be compared.However, potential weaknesses in the questionnaire are indicatedby relatively low Cronbach's alpha values as reported by Gardisseuret al. (0.53-0.74) [22]. On the other hand, Sawicki et al. andCromheecke et al. reported higher alpha values (0.64-0.82 and0.70-0.83, respectively) [19,24]. We observed alpha values thatwere acceptable at baseline (0.68-0.88) but somewhat lower at thefollow-up assessment (0.52-0.75), in particular for the topics self-efficacy and strained social network (0.52 each).
We could not analyze the before-after QoL data for all random-ized patients because of death or missing values. However, we ap-plied the ITT-principle to the main QoL analysis in accordance withprimary endpoint analysis [18]. We could follow up on 90% of thesurviving patients who were treated with oral anticoagulation.With regard to the QoL scores or other individual characteristics,there were no differences between the total population and the141 patients included in the ITT-analysis at baseline. We performedsensitivity analyses to take treatment withdrawals and treatmentcrossovers into account and found they had no substantial effect onthe main results.
We observed an improvement in both groups. This is not unusu-al in clinical trials and is probably attributable to more intensetreatment in both arms. It should be borne in mind that patients in
l anticoagulation in elderly patients – Effects on treatment-related

6 A. Siebenhofer et al. / Thrombosis Research xxx (2012) xxx–xxx
the RCG participated in only a single training session at which theywere provided with basic theoretical information on oral anti-coagulation. Regression-to-the-mean and Hawthorne effects may alsobe of relevance in this context and should be taken into account wheninterpreting any conclusions drawn from before-after-comparisonswithin the treatment groups.
It should be noted that treatment-related QoLwas not included in thesample size calculation and we evaluated it as a predefined secondaryendpoint without adjusting for multiple testing. Furthermore, we shouldpoint out that scores for treatment satisfaction at baseline were lower inthe self-management group than in the routine care group. However,any effect thismay have hadwasmore than offset by amore pronouncedincrease in the self-management group at follow-up. In this context onecould argue that there was more potential for optimization in the SMGand that a ceiling effect had occurred.We cannot rule out this explanationand would therefore like to emphasize that these results are descriptiveand should be carefully interpreted as such. Nevertheless, it is worthy ofemphasis that self-management of OAC increased treatment satisfactionin most of the elderly patients and that about 80% of the patients in theSMG returned the highest possible score for treatment satisfaction ontheir final visit.
Therefore, although we found self-management to be statistically su-perior in some aspects of quality of life, these results should be interpretedwith caution andneed confirmation in further studies. Themajor strengthof our trial lies in the explicit focus on elderly patients, the randomizedcontrolled multicenter study design and the long follow-up period of ap-proximately three years. In terms of the quality of oral anticoagulation,the prevention of major thromboembolic complications, and bleedingcomplications, we have already shown that for elderly patients the self-management of oral anticoagulation therapy is superior to routine caremanaged by specialised anticoagulation clinics or general practitioners.In this paper, we have demonstrated that in addition to this, self-management of OAC therapy can significantly improve treatment satis-faction and has a positive effect on treatment-related quality of life.
Role of Funding Source
The sponsor of the study, Roche Diagnostics, played no role in thestudy design, in data collection and analysis, data interpretation, orin the writing of the report. The corresponding author had full accessto all the data in the study and had final responsibility for the deci-sion to submit this work for publication.
Conflict of interest statement
The DIeM - Institute for Evidence-based Medicine, Cologne, Ger-many received scientific grants from Roche Diagnostics, Germany,for the study conducted by Sawicki et al. on a structured teachingand self-management program for patients receiving oral anti-coagulation [24] and for the present study on the evaluation of self-management of oral anticoagulation in the elderly. Lars G. Hemkenswas employed at DIeM until February 2009. For this study the MedicalUniversities of Graz and Vienna received financial support fromRocheDi-agnostics, Germany, for patient supervision in the trial. Ulrike Didjurgeitparticipated in the development of the SPOG program, and receives copy-right fees from the publisher of educational materials. There are no fur-ther conflicts of interests to be declared.
Acknowledgement
We should like to thank Margit Seimel, Ute Sternenberg,Elisabeth Waclawiczek and Brigitte Krinninger, who together withthe principal investigators were responsible for the training andpractical and administrative follow-up of the patients, Peter T.Sawicki for protocol development in year 2001 and critical revisionfor intellectual content, Karl Horvath, Klaus Jeitler, Caroline
Please cite this article as: Siebenhofer A, et al, Self-management of oraQuality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
Kleespies and Andreas Waltering for evaluation of endpoints, andPhillip Elliot for proof reading the manuscript.
References
[1] Aguilar MI, Hart R. Oral anticoagulants for preventing stroke in patients withnon-valvular atrial fibrillation and no previous history of stroke or transient is-chemic attacks. Cochrane Database Syst Rev 2005(3):CD001927.
[2] Ansell J, Hirsh J, Poller L, BusseyH, JacobsonA, Hylek E. The pharmacology andmanage-ment of the vitamin K antagonists: the Seventh ACCP Conference on Antithromboticand Thrombolytic Therapy. Chest 2004;126(3 Suppl.):204S–33S.
[3] Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of anti-thrombotic therapy in atrial fibrillation. Analysis of pooled data from five ran-domized controlled trials. Arch Intern Med 1994;154(13):1449–57.
[4] Bungard TJ, Ghali WA, Teo KK, McAlister FA, Tsuyuki RT. Why do patients withatrial fibrillation not receive warfarin? Arch Intern Med 2000;160(1):41–6.
[5] Choudhry NK, Anderson GM, Laupacis A, Ross-Degnan D, Normand SL, SoumeraiSB. Impact of adverse events on prescribing warfarin in patients with atrial fibril-lation: matched pair analysis. BMJ 2006;332(7534):141–5.
[6] Cohen N, Almoznino-Sarafian D, Alon I, Gorelik O, Koopfer M, Chachashvily S,et al. Warfarin for stroke prevention still underused in atrial fibrillation: patternsof omission. Stroke 2000;31(6):1217–22.
[7] Gage BF, Boechler M, Doggette AL, Fortune G, Flaker GC, Rich MW, et al. Adverseoutcomes and predictors of underuse of antithrombotic therapy in medicare ben-eficiaries with chronic atrial fibrillation. Stroke 2000;31(4):822–7.
[8] Hylek EM, D'Antonio J, Evans-Molina C, Shea C, Henault LE, Regan S. Translatingthe results of randomized trials into clinical practice: The challenge of warfarincandidacy among hospitalized elderly patients with atrial fibrillation. Stroke2006;37(4):1075–80.
[9] Palareti G, Leali N, Coccheri S, Poggi M, Manotti C, D'Angelo A, et al. Bleeding com-plications of oral anticoagulant treatment: An inception-cohort, prospective col-laborative study (ISCOAT). Italian Study on Complications of Oral AnticoagulantTherapy. Lancet 1996;348(9025):423–8.
[10] Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage andtolerability of warfarin in the first year of therapy among elderly patients withatrial fibrillation. Circulation 2007;115(21):2689–96.
[11] Bloomfield HE, Krause A, Greer N, Taylor BC, MacDonald R, Rutks I, et al.Meta-analysis: Effect of patient self-testing and self-management oflong-term anticoagulation on major clinical outcomes. Ann Intern Med2011;154(7):472–82.
[12] Christensen TD, Johnsen SP, Hjortdal VE, Hasenkam JM. Self-management of oralanticoagulant therapy: A systematic review and meta-analysis. Int J Cardiol2007;118(1):54–61.
[13] Heneghan C, Alonso-Coello P, Garcia-Alamino JM, Perera R, Meats E, Glasziou P.Self-monitoring of oral anticoagulation: A systematic review and meta-analysis.Lancet 2006;367(9508):404–11.
[14] Heneghan C,Ward A, Perera R, Bankhead C, Fuller A, Stevens R, et al. Self-monitoringof oral anticoagulation: Systematic review and meta-analysis of individual patientdata. Lancet 2012;379(9813):322–34.
[15] Wells PS, Brown A, Jaffey J, McGahan L, Poon MC, Cimon K. Safety and effective-ness of point-of-care monitoring devices in patients on oral anticoagulant thera-py: A meta-analysis. Open Med 2007;1(3):e131–46.
[16] Menendez-Jandula B, Souto JC, Oliver A, Montserrat I, Quintana M, Gich I, et al.Comparing self-management of oral anticoagulant therapy with clinic manage-ment: A randomized trial. Ann Intern Med 2005;142(1):1–10.
[17] Beyth RJ, Quinn L, Landefeld CS. A multicomponent intervention to prevent majorbleeding complications in older patients receiving warfarin. A randomized, con-trolled trial. Ann Intern Med 2000;133(9):687–95.
[18] Siebenhofer A, Rakovac I, Kleespies C, Piso B, Didjurgeit U. Self-management oforal anticoagulation reduces major outcomes in the elderly. A randomized con-trolled trial. Thromb Haemost 2008;100(6):1089–98.
[19] Cromheecke ME, Levi M, Colly LP, de Mol BJ, Prins MH, Hutten BA, et al. Oral anti-coagulation self-management and management by a specialist anticoagulation clinic:a randomised cross-over comparison. Lancet 2000;356(9224):97–102.
[20] Fitzmaurice DA, Murray ET, Gee KM, Allan TF, Hobbs FD. A randomised controlledtrial of patient self management of oral anticoagulation treatment compared withprimary care management. J Clin Pathol 2002;55(11):845–9.
[21] Fitzmaurice DA, Murray ET, McCahon D, Holder R, Raftery JP, Hussain S, et al. Selfmanagement of oral anticoagulation: randomised trial. BMJ 2005;331(7524):1057.
[22] Gadisseur AP, Kaptein AA, Breukink-Engbers WG, van der Meer FJ, Rosendaal FR.Patient self-management of oral anticoagulant care vs. management by special-ized anticoagulation clinics: positive effects on quality of life. J Thromb Haemost2004;2(4):584–91.
[23] Jowett S, Bryan S, Murray E, McCahon D, Raftery J, Hobbs FD, et al. Patientself-management of anticoagulation therapy: a trial-based cost-effectivenessanalysis. Br J Haematol 2006;134(6):632–9.
[24] Sawicki PT. A structured teaching and self-management program for patientsreceiving oral anticoagulation: a randomized controlled trial. Working Groupfor the Study of Patient Self-Management of Oral Anticoagulation. JAMA1999;281(2):145–50.
[25] Soliman Hamad MA, van Eekelen E, van Agt T, van Straten AH. Self-managementprogram improves anticoagulation control and quality of life: a prospective ran-domized study. Eur J Cardiothorac Surg 2009;35(2):265–9.
l anticoagulation in elderly patients – Effects on treatment-related

7A. Siebenhofer et al. / Thrombosis Research xxx (2012) xxx–xxx
[26] McCahon D, Murray ET, Murray K, Holder RL, Fitzmaurice DA. Doesself-management of oral anticoagulation therapy improve quality of life andanxiety? Fam Pract 2011;28(2):134–40.
[27] Siebenhofer A, Rakovac I, Kleespies C, Piso B, Didjurgeit U. Self-management of oralanticoagulation in the elderly: rationale, design, baselines and oral anticoagulation con-trol after one year of follow-up. A randomized controlled trial. Thromb Haemost2007;97(3):408–16.
Please cite this article as: Siebenhofer A, et al, Self-management of oraQuality of Life, Thromb Res (2012), doi:10.1016/j.thromres.2012.06.012
[28] R Development Core Team. R: A Language and Environment for Statistical Com-puting. www r-project org Available from:www.R-project.org2006.
[29] Khan TI, Kamali F, Kesteven P, Avery P, Wynne H. The value of education andself-monitoring in the management of warfarin therapy in older patients with un-stable control of anticoagulation. Br J Haematol 2004;126(4):557–64.
l anticoagulation in elderly patients – Effects on treatment-related




















