To be seated ‘with great courtesy and veneration’: Contextual aspects of the Taíno Duho

lable at ScienceDirect
Heart & Lung 43 (2014) 105e111
Contents lists avai
Heart & Lung
journal homepage: www.heartandlung.org
Seated and semi-recumbent positioning of the ventilated intensivecare patient e Effect on gas exchange, respiratory mechanics andhemodynamics
Peter Thomas, BPhty (Hons), PhD, FACP a,*, Jennifer Paratz, MPhty, PhD, FACP b,Jeffrey Lipman, MBBCh, DA (SA), FFA (SA), FFA (CritCare), FCICMb,c
aDepartment of Physiotherapy, Royal Brisbane and Women’s Hospital, Brisbane, AustraliabBurns Trauma and Critical Care Research Centre, University of Queensland, Brisbane, AustraliacDepartment of Intensive Care Medicine, Royal Brisbane and Women’s Hospital, Brisbane, Australia
a r t i c l e i n f o
Article history:Received 2 April 2013Received in revised form25 November 2013Accepted 26 November 2013
Keywords:Intensive careRespiratory mechanicsPostureSemi-recumbentWeaning
Abbreviations: Aea gradient, alveolar gas to arterference; ALI, acute lung injury; APACHE, acute physevaluation II score; BMI, body mass index; Cdyn, dyclosing volume; FiO2, fraction of inspired oxygen; FRCHR, heart rate; MABP, mean arterial blood pressure;linear mixed model main effect analysis for positionP � T, linear mixed model analysis for position and timpressure of carbon dioxide in arterial blood; PaO2, parterial blood; PIPaw, peak inspiratory airway pressurshallow breathing index; SaO2, arterial hemoglobisepsis-related organ failure assessment; SpO2, pulse oliner mixed model main effect analysis for time; T0, tistarting position; T5, time of measurement, 5 min pomeasurement, 30 min post intervention; VE, minute vConflicts of interest: All authors have none to decla* Corresponding author. Tel.: þ61 (0)7 3646 7288;
E-mail address: [email protected]
0147-9563/$ e see front matter Crown Copyright � 2http://dx.doi.org/10.1016/j.hrtlng.2013.11.011
a b s t r a c t
Objectives: To compare the effect of semi-recumbent and sitting positions on gas exchange, respiratorymechanics and hemodynamics in patients weaning from mechanical ventilation.Background: Upright positions are encouraged during rehabilitation of the critically ill but there effectshave not been well described.Methods: A prospective, randomized, cross-over trial was conducted. Subjects were passively mobilizedfrom supine into a seated position (out of bed) and from supine to a semi-recumbent position (>45�
backrest elevation in bed). Arterial blood gas (PaO2/FiO2, PaO2, SaO2, PaCO2 and Aea gradient), respi-ratory mechanics (VE, VT, RR, Cdyn, RR/VT) and hemodynamic measurements (HR, MABP) were collected insupine and at 5 min and 30 min after re-positioning.Results: Thirty-four intubated and ventilated subjects were enrolled. The angle of backrest inclination insitting (67 � 5�) was greater than gained with semi-recumbent positioning (50 � 5�, p < 0.001). Therewere no clinically important changes in arterial blood gas, respiratory mechanic or hemodynamic valuesdue to either position.Conclusions: Neither position resulted in significant changes in respiratory and hemodynamic parame-ters. Both positions can be applied safely in patients being weaned from ventilation.
Crown Copyright � 2014 Published by Elsevier Inc. All rights reserved.
ial blood oxygen tension dif-iological and chronic healthnamic lung compliance; CV,, functional residual capacity;MLI, Murray lung injury; P,(sitting or semi-recumbent);e interaction; PaCO2, partialartial pressure of oxygen ine; RR, respiratory rate; RR/VT,n oxygen saturation; SOFA,ximeter oxygen saturation; T,me of measurement, baselinest intervention; T30, time ofentilation; VT, tidal volume.re.fax: þ61 (0)7 3646 1665.(P. Thomas).
014 Published by Elsevier Inc. All
Introduction
The practice of early mobilization of the intensive care patient isconsidered to be safe1,2 and appears to positively influence inten-sive care outcomes. For example, a focus on early mobilization canimprove the functional ability of patients during the intensivecare period3,4 and at hospital discharge.1 Additionally, it may in-crease ventilator-free days1 and reduce intensive care and hospitallength of stay.5 As part of these early mobilization strategies, thepositioning of patients upright in bed or out of bed is encouraged inorder to overcome possible respiratory and/or cardiovascularcomplications of immobility.1 Positioning patients semi-recumbentup to 60� is usually well tolerated hemodynamically, with minimalimpact on cardiac output6,7 and 45� semi-recumbent positioninghas been shown to significantly reduce the incidence of ventilator-associated pneumonia.8 Outside of the intensive care unit, researchinvolving subjects fromboth normal and diseased populations haveshown significant improvement in pulmonary function associatedwith movement from a supine to an erect semi-recumbent (in bed)
rights reserved.

P. Thomas et al. / Heart & Lung 43 (2014) 105e111106
or seated position (out of bed).9e14 These benefits include increasesin functional residual capacity (FRC),10e12 lung compliance14,15 andadoption of large tidal volume-low respiratory rate patterns ofbreathing.14 In some people, the changes in lung volume and me-chanics on moving from a supine to seated position may result inimprovement in the partial pressure of oxygen in arterial blood(PaO2) and other indices of gas exchange.10,11
Knowledge of the influence of position on gas exchange and/orrespiratory mechanics is important during weaning from mechan-ical ventilation. If adoption of a seated or semi-recumbent positionresults in improved gas exchange, lung compliance and/or tidalvolume and a reduction in respiratory rate and work of breathing,their utilizationmay prevent respiratorymuscle fatigue and shortenthe weaning process. Additionally, there could be advantages inmoving a patient out of bed and into a seated position. Investigationin normal subjects suggests that positioning a patient into a seatedposture may result in greater improvements in FRC than are gainedwith a semi-recumbent position.13 Maintaining a patient in a semi-recumbent position can be challenging in clinical practice16e18 andif patients slide out of a semi-recumbent position into a slumpedposition it may further reduce lung volume.13
Several studies have examined the effect of a semi-recumbentor seated position on gas exchange and/or respiratory mechanicsin specific intensive care populations including patients withacute lung injury,19e22 abdominal distension23 and post-operativeabdominal surgery.24,25 However, only two studies have recruitedpatients specifically during the stages of weaning frommechanicalventilation.26,27 These two studies report no significant deleteriouseffects of sitting or semi-recumbent positions. However, respira-tory effort may be higher in sitting26; and sitting may result insmaller improvements in inspiratory muscle strength.27 Neitherstudy has reported the effect on arterial blood gas measurements.Changes in compliance may account for increased respiratoryeffort,26 and have previously been hypothesized to impact onchanges in oxygenation indices.20,22
The aim of this study was to compare the effects of sitting out ofbed and semi-recumbent positioning in bed when applied inventilated (>48 h) intensive care patients. The null hypothesis wasthat a change in position from supine to either a seated or semi-recumbent position would not affect gas exchange, respiratorymechanics, or hemodynamic values.
Methods
A prospective, randomized, cross-over trial design was usedwith concealed allocation to the first position examined.
Ethical approval for this study was gained from the relevantinstitutional human research ethics committee. Written informedconsent to participation was gained from participants and/ortheir authorized legal guardian. Participants were recruited from
Table 1Study inclusion and exclusion criteria.
Inclusion criteria
Age >18 yearsIntubated and receiving mechanical ventilation (>48 h)Suitable candidates to mobilize into either the seated or semi-recumbent position.To ascertain this, clinical characteristics had to include:PaO2 >60 mm HgFiO2 <0.6PIPaw <40 cm H2OStable hemodynamic parametersHR 60e130 beats/minMABP 70e120 mm Hg
Arrhythmias (if present) stable and not compromising blood pressure
the intensive care unit of a tertiary-referral, university-affiliated,metropolitan centre. Patients receiving mechanical ventilation formore than 48 h were screened and consent for participation soughtif there were no absolute contraindications to sitting and theircardiovascular and respiratory parameters were stable according tothe criteria outlined in Table 1.
As there was limited published data investigating the effect ofupright positioning on arterial blood gas measurements and res-piratory mechanics in patients weaning from mechanical ventila-tion, an interim analysis was conducted after enrollment of 20patients and was used to estimate the standard deviation for paireddifferences in PaO2/FiO2 and VE from supine to sitting and semi-recumbent positioning. A sample size estimate of 34 patients wascalculated to detect moderate effect sizes and clinically significantchanges in PaO2/FiO2 (difference ¼ 20, s ¼ 35, a ¼ 0.05,power ¼ 0.9) and VE (sample estimate ¼ 27, difference ¼ 1 L/min,s ¼ 1.55 L/min, a ¼ 0.05, power ¼ 0.9) in a repeated measuresdesign.28
Admission diagnosis, demographic information, sepsis-related organ failure assessment (SOFA) scores29 and Murraylung injury (MLI) scores30 were calculated from data collected onthe day of the study. Automated calculations for acute physio-logical and chronic health evaluation II (APACHE) scores31 wereobtained from the intensive care unit’s clinical informationsystem.
Ventilator settings and respiratory mechanics (respiratory rate(RR), tidal volume (VT), minute ventilation (VE), peak inspiratoryairway pressure (PIPaw), dynamic lung compliance (Cdyn) wererecorded via electronic transfer of data from the serial port of theventilator (Mallinckrodt Puritan Bennet 7200� or 840� ventilator),which were calibrated according to manufacturer’s recommenda-tions. A shallow breathing index was also calculated as RR/VT.Ventilator measurement of pressure, volume and flow are consid-ered to be accurate and have low variability.32,33 However, at eachdata collection point, 5-min periods of respiratory mechanic mea-surements were collected and averaged to reduce any breath-to-breath variability of measurements.34,35
Variations in gas exchange were monitored through arterialblood gas sampling (ABL 700 Series machines e Radiometer,Copenhagen, Denmark) and analysis of the ratio of PaO2 to FiO2(PaO2/FiO2), PaO2, the partial pressure of carbon dioxide in arterialblood (PaCO2), arterial hemoglobin oxygen saturation (SaO2), andalveolar gas to arterial blood oxygen tension difference (Aeagradient).
Heart rate (HR), MABP and SpO2 were recorded from the patientmonitoring system (Philips Intellivue). For MABP measurements,arterial blood pressures were manually checked for accuracy/cali-bration against sphygmomanometer readings prior to data collec-tion and the arterial line transducer placement was re-zeroed priorto each recording.
Exclusion criteria
Signs of new or sustained sepsis on the day of enrollmentHemoglobin <70 g/LPlatelets <30 � 109/L
Vasopressor or neuromuscular blockade medicationsNitric oxidePulmonary barotrauma (e.g. flail chest, untreated pneumothorax)Burn injuriesDialysisContraindications to upright positioning (e.g. unstable spinal column fracturesor spinal cord injury)Intracranial pressure monitoring

Table 2Baseline characteristics of the patients.
Characteristic Value Range
Age (years) 65.5 � 14.4 18e87Female e N (%) 13 (38%)Body mass index (kg/m2) 28.6 � 6.9 18.7e50.8APACHE IIa 23.2 � 6.7 10e37Primary diagnosis e NGastrointestinal (post-operative) 9Gastrointestinal (non-surgical) 2Multi-trauma (post-operative) 2Cardiovascular (post-operative) 3Respiratory 7Neurological (post-operative) 1Neurological (non-surgical) 3Cardiovascular 4Metabolic/renal (non-surgical) 1Diabetic ketoacidosis 1Drug overdose 1
Glasgow coma score e medianEye 4 3e4Motor 6 1e6Verbal 3 1e5Total 13 5e15
SOFA scoreb
Respiratory 2.29 � 0.58 1e3Coagulation 0.24 � 0.65 0e3Liver 0.44 � 0.82 0e3Cardiovascular 0.44 � 0.56 0e3Central nervous system 0.85 � 0.89 0e4Renal 0.59 � 1.0 0e4Total SOFA score 4.85 � 2.0 1e9
MLI scoreb 1.25 � 0.6 0e2.7Days prior to enrollment of:Hospital admission 16.4 � 9.3 5e36ICU admission 12.8 � 8.7 3e36Mechanical ventilation 12.5 � 8.5 3e36
Tracheostomy e N (%) 21 (62%)Ventilator mode e NSIMV (volume controlled) 6Pressure support ventilation 28
FiO2 0.35 � 0.06 0.25e0.5Pressure support (cm H20) 11.5 � 2.8 8e20PEEP (cm H20) 5.7 � 1.44 5e10Hemoglobin (g/L) 90.2 � 13.7 70e14124-h fluid balance (L) �0.20 � 1.5 �3.4e2.1
a APACHE II scores were collated from admission data.b SOFA scores and MLI scores were calculated from data collected on the day of
the study.
P. Thomas et al. / Heart & Lung 43 (2014) 105e111 107
A goniometer/protractor was used to measure the angle ofbackrest inclination achieved36 and a tape measure was used todetermine the static maintenance of the two upright positions overthe study period. The reference points measured were the distancebetween a patient’s popliteal crease and the bed end (semi-recum-bent positioning) or the chair base (sitting). All goniometer and tapemeasure recordings were taken by the primary investigator.
The study period began with a minimum of 2 h during whichventilator settings were left unchanged, other interventions limitedand a 30minperiod in the supine position immediately prior to datacollection. The dose of sedative medications was not altered duringthe study period. To attain the semi-recumbent position, the pa-tient’s bed was simply adjusted from a horizontal position to havingthe head of bed elevated. The seated position was achieved bytransferring the patient out of bed (via sliding board) into aHausted� chair (APC series, HaustedMedina, Ohio). Neither positionrequired the patient to actively assist or contribute to the transferand/or change in position. Both the Hausted� chair and beds usedwere able to have their backrest adjusted through a 0e80� range.With either position, a minimum of 45� backrest elevation wastargeted,with higher elevations usedwhen reported comfortable bythe patient. This reflected clinical practice. Patients were main-tained in either position for 30 min, at which point, data collectionfinished. Patients were later returned supine, with a minimum of30 min supine before the alternate position was studied.
For each position, data was collected at three time pointsincluding the baseline supine position (T0), then 5 min postimplementation of the semi-recumbent or sitting position (T5)and/or at 30 min post implementation (T30). Arterial blood gassamples were taken at T0 and T30 only. Respiratory mechanics, HR,BP and SpO2 measurements were collected at T0, T5 and T30.Goniometer and tapemeasure recordings were taken at T5 and T30.
During the data collection periods, the position was ceased ifintolerance to either position was noted. This was defined by: a>10% increase in fraction of inspired oxygen (FiO2) required tomaintain pulse oximeter oxygen saturation (SpO2) >90% or thepartial pressure of oxygen in arterial blood (PaO2) >60 mm Hg; thealteration of heart rate by �30 beats/min; the onset of a newarrhythmia or ischemic electrocardiograph changes or a reductionin blood pressure due to arrhythmia; or change in mean arterialblood pressure (MABP) by �30 mm Hg). Additionally, occurrencesof any adverse events (e.g. accidental extubation, removal ofindwelling catheters) were recorded. If any intolerance or adverseevent occurred, medical staff were notified immediately andappropriate action taken.
An intention-to-treat analysis was used for this study. Contin-uous variables were assessed for normality of distribution, trans-formed as appropriate and analyzed using a linear mixed model(within subject main effects: position (sitting or semi-recumbent)(P) and time (T) and their interaction (P � T); subjects wererandom effects). Incorporated into this model was assessment foran order effect, and analysis of covariates, which included a sub-jects’ age, body mass index (BMI), extent of lung pathology(determined from the chest radiograph rating of the MLI score),degree of hypoxemia (determined from the respiratory systemrating of the SOFA score) and 24-h fluid balance for the day of thestudy. Paired sample t-tests were used to compare the angle ofinclination and displacement out of position measured betweenthe two positions. Results are expressed as mean � standard de-viation and a significance level of <0.05 was used.
Results
Thirty-four patients were enrolled in the study. Diagno-stic and demographic information is presented in Table 2.
Recruitment of patients during the weaning period from me-chanical ventilation is reflected by the majority of patientsbeing ventilated on pressure support ventilation (Table 2), andonly eight (24%) of patients receiving sedative or opioid in-fusions (two patients received Propofol, six patients receivedFentanyl).
At the time of enrollment, nine patients (26%) had previously satout of bed on days prior to recruitment to the study. The random-ization procedure resulted in three of these patients being examinedfirst in the semi-recumbent position and six in the seated position.The median time between assessment of the semi-recumbent andseated positions was 2.5 h (inter-quartile range ¼ 1e3.5 h). Threepatients completed only one part of the protocol, resulting in 33assessments in the seated position and 32 in the semi-recumbentposition. Reasons for non-completion of the entire protocol wereelective extubation prior to completion (N ¼ 2) and the onset ofhemodynamic instability requiring commencement of inotropes(N ¼ 1), which occurred more than 3 h after the first intervention.Review by the investigators and attending medical staff determinedthat there was no direct temporal or causal relationship with thisdeterioration and the study protocol. No patients required cessation
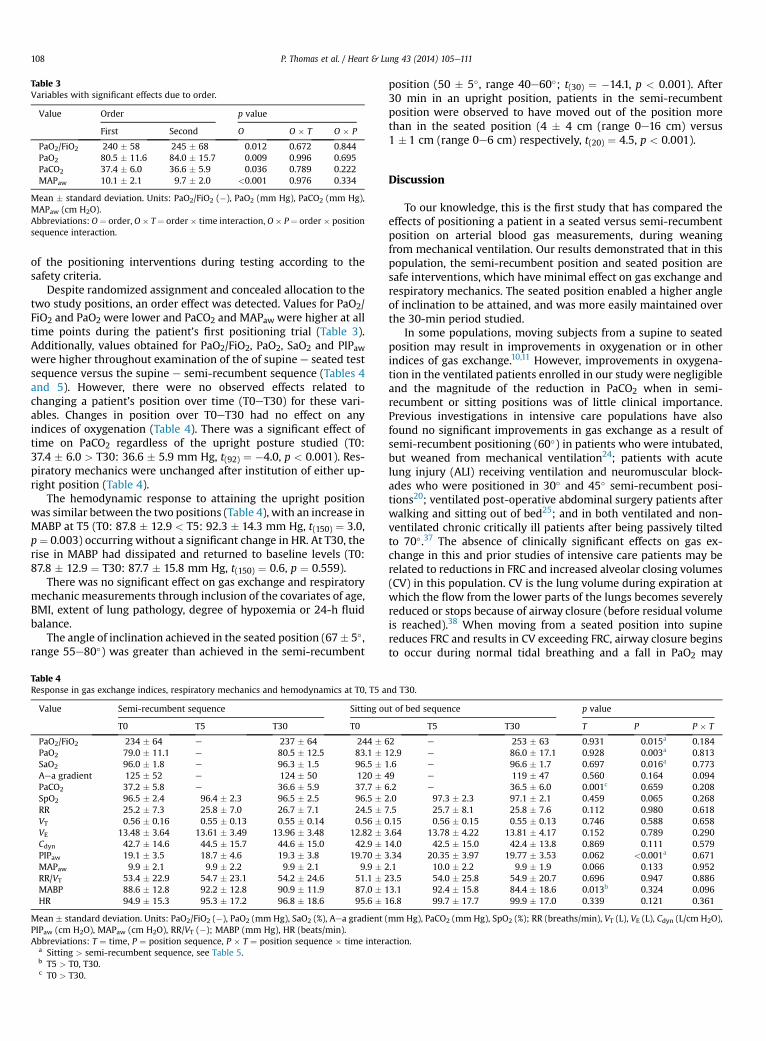
Table 3Variables with significant effects due to order.
Value Order p value
First Second O O � T O � P
PaO2/FiO2 240 � 58 245 � 68 0.012 0.672 0.844PaO2 80.5 � 11.6 84.0 � 15.7 0.009 0.996 0.695PaCO2 37.4 � 6.0 36.6 � 5.9 0.036 0.789 0.222MAPaw 10.1 � 2.1 9.7 � 2.0 <0.001 0.976 0.334
Mean � standard deviation. Units: PaO2/FiO2 (�), PaO2 (mm Hg), PaCO2 (mm Hg),MAPaw (cm H2O).Abbreviations: O¼ order, O� T¼ order� time interaction, O� P¼ order � positionsequence interaction.
P. Thomas et al. / Heart & Lung 43 (2014) 105e111108
of the positioning interventions during testing according to thesafety criteria.
Despite randomized assignment and concealed allocation to thetwo study positions, an order effect was detected. Values for PaO2/FiO2 and PaO2 were lower and PaCO2 and MAPaw were higher at alltime points during the patient’s first positioning trial (Table 3).Additionally, values obtained for PaO2/FiO2, PaO2, SaO2 and PIPawwere higher throughout examination of the of supine e seated testsequence versus the supine e semi-recumbent sequence (Tables 4and 5). However, there were no observed effects related tochanging a patient’s position over time (T0eT30) for these vari-ables. Changes in position over T0eT30 had no effect on anyindices of oxygenation (Table 4). There was a significant effect oftime on PaCO2 regardless of the upright posture studied (T0:37.4 � 6.0 > T30: 36.6 � 5.9 mm Hg, t(92) ¼ �4.0, p < 0.001). Res-piratory mechanics were unchanged after institution of either up-right position (Table 4).
The hemodynamic response to attaining the upright positionwas similar between the two positions (Table 4), with an increase inMABP at T5 (T0: 87.8 � 12.9 < T5: 92.3 � 14.3 mm Hg, t(150) ¼ 3.0,p¼ 0.003) occurring without a significant change in HR. At T30, therise in MABP had dissipated and returned to baseline levels (T0:87.8 � 12.9 ¼ T30: 87.7 � 15.8 mm Hg, t(150) ¼ 0.6, p ¼ 0.559).
There was no significant effect on gas exchange and respiratorymechanic measurements through inclusion of the covariates of age,BMI, extent of lung pathology, degree of hypoxemia or 24-h fluidbalance.
The angle of inclination achieved in the seated position (67� 5�,range 55e80�) was greater than achieved in the semi-recumbent
Table 4Response in gas exchange indices, respiratory mechanics and hemodynamics at T0, T5 a
Value Semi-recumbent sequence Sitting ou
T0 T5 T30 T0
PaO2/FiO2 234 � 64 e 237 � 64 244 �PaO2 79.0 � 11.1 e 80.5 � 12.5 83.1 �SaO2 96.0 � 1.8 e 96.3 � 1.5 96.5 �Aea gradient 125 � 52 e 124 � 50 120 �PaCO2 37.2 � 5.8 e 36.6 � 5.9 37.7 �SpO2 96.5 � 2.4 96.4 � 2.3 96.5 � 2.5 96.5 �RR 25.2 � 7.3 25.8 � 7.0 26.7 � 7.1 24.5 �VT 0.56 � 0.16 0.55 � 0.13 0.55 � 0.14 0.56 �VE 13.48 � 3.64 13.61 � 3.49 13.96 � 3.48 12.82 �Cdyn 42.7 � 14.6 44.5 � 15.7 44.6 � 15.0 42.9 �PIPaw 19.1 � 3.5 18.7 � 4.6 19.3 � 3.8 19.70 �MAPaw 9.9 � 2.1 9.9 � 2.2 9.9 � 2.1 9.9 �RR/VT 53.4 � 22.9 54.7 � 23.1 54.2 � 24.6 51.1 �MABP 88.6 � 12.8 92.2 � 12.8 90.9 � 11.9 87.0 �HR 94.9 � 15.3 95.3 � 17.2 96.8 � 18.6 95.6 �
Mean � standard deviation. Units: PaO2/FiO2 (�), PaO2 (mm Hg), SaO2 (%), Aea gradientPIPaw (cm H2O), MAPaw (cm H2O), RR/VT (�); MABP (mm Hg), HR (beats/min).Abbreviations: T ¼ time, P ¼ position sequence, P � T ¼ position sequence � time inter
a Sitting > semi-recumbent sequence, see Table 5.b T5 > T0, T30.c T0 > T30.
position (50 � 5�, range 40e60�; t(30) ¼ �14.1, p < 0.001). After30 min in an upright position, patients in the semi-recumbentposition were observed to have moved out of the position morethan in the seated position (4 � 4 cm (range 0e16 cm) versus1 � 1 cm (range 0e6 cm) respectively, t(20) ¼ 4.5, p < 0.001).
Discussion
To our knowledge, this is the first study that has compared theeffects of positioning a patient in a seated versus semi-recumbentposition on arterial blood gas measurements, during weaningfrom mechanical ventilation. Our results demonstrated that in thispopulation, the semi-recumbent position and seated position aresafe interventions, which have minimal effect on gas exchange andrespiratory mechanics. The seated position enabled a higher angleof inclination to be attained, and was more easily maintained overthe 30-min period studied.
In some populations, moving subjects from a supine to seatedposition may result in improvements in oxygenation or in otherindices of gas exchange.10,11 However, improvements in oxygena-tion in the ventilated patients enrolled in our study were negligibleand the magnitude of the reduction in PaCO2 when in semi-recumbent or sitting positions was of little clinical importance.Previous investigations in intensive care populations have alsofound no significant improvements in gas exchange as a result ofsemi-recumbent positioning (60�) in patients who were intubated,but weaned from mechanical ventilation24; patients with acutelung injury (ALI) receiving ventilation and neuromuscular block-ades who were positioned in 30� and 45� semi-recumbent posi-tions20; ventilated post-operative abdominal surgery patients afterwalking and sitting out of bed25; and in both ventilated and non-ventilated chronic critically ill patients after being passively tiltedto 70�.37 The absence of clinically significant effects on gas ex-change in this and prior studies of intensive care patients may berelated to reductions in FRC and increased alveolar closing volumes(CV) in this population. CV is the lung volume during expiration atwhich the flow from the lower parts of the lungs becomes severelyreduced or stops because of airway closure (before residual volumeis reached).38 When moving from a seated position into supinereduces FRC and results in CV exceeding FRC, airway closure beginsto occur during normal tidal breathing and a fall in PaO2 may
nd T30.
t of bed sequence p value
T5 T30 T P P � T
62 e 253 � 63 0.931 0.015a 0.18412.9 e 86.0 � 17.1 0.928 0.003a 0.8131.6 e 96.6 � 1.7 0.697 0.016a 0.77349 e 119 � 47 0.560 0.164 0.0946.2 e 36.5 � 6.0 0.001c 0.659 0.2082.0 97.3 � 2.3 97.1 � 2.1 0.459 0.065 0.2687.5 25.7 � 8.1 25.8 � 7.6 0.112 0.980 0.6180.15 0.56 � 0.15 0.55 � 0.13 0.746 0.588 0.6583.64 13.78 � 4.22 13.81 � 4.17 0.152 0.789 0.29014.0 42.5 � 15.0 42.4 � 13.8 0.869 0.111 0.5793.34 20.35 � 3.97 19.77 � 3.53 0.062 <0.001a 0.6712.1 10.0 � 2.2 9.9 � 1.9 0.066 0.133 0.95223.5 54.0 � 25.8 54.9 � 20.7 0.696 0.947 0.88613.1 92.4 � 15.8 84.4 � 18.6 0.013b 0.324 0.09616.8 99.7 � 17.7 99.9 � 17.0 0.339 0.121 0.361
(mm Hg), PaCO2 (mm Hg), SpO2 (%); RR (breaths/min), VT (L), VE (L), Cdyn (L/cm H2O),
action.

Table 5Variables with significant effects due to position sequence.
Value Supine e semi-recumbent Supine e seated p value
PaO2/FiO2 236 � 64 249 � 62 0.018PaO2 79.8 � 11.8 84.6 � 15.1 0.003SaO2 96.1 � 1.7 96.6 � 1.6 0.015PIPaw 19.0 � 4.0 20.0 � 3.6 0.007
Mean � standard deviation. Units: PaO2/FiO2 (�), PaO2 (mm Hg), SaO2 (%), PIPaw(cm H2O).
P. Thomas et al. / Heart & Lung 43 (2014) 105e111 109
arise.10,39 However, when FRC volume is significantly reduced, orCV significantly increased so that CV exceeds (FRC þ VT) in both theseated and supine position, significant airway closure is present inboth positions. Subsequently, changes in regional alveolar ventila-tion may be small and diminish any potential for upright posi-tioning to induce a change in oxygenation.10,39 Factors that areknown to decrease the elastic recoil of the lung and subsequentlyincrease CV include advancing age, smoking, respiratory diseaseand/or obesity.10,11,39 Alternatively, FRC may be reduced by thepresence of: respiratory failure40,41; mechanical ventilation, anes-thesia and paralysis42,43; ALI44; major chest X-ray abnormalities45;a low FEV1/FVC ratio11; and abdominal surgery.46 Many of theseconditions were features of the subjects in this study and the widerintensive care population.
The decision to mobilize a patient out of bed who is weaningfrom mechanical ventilation can be delayed due to concerns of theeffort involved by the patient and the impact this may have onrespiratory system function. In this study, the change to eitherupright position resulted in no significant effect on RR, VT, VE, or RR/VT. Deye et al26 also found no change in these variables after 15 minof supine, semi-recumbent positioning and a seated position in bed.As seated positions produce negligible changes in RR, VT, VE, or RR/VT, they could be utilized during the weaning of patients frommechanical ventilation in order to promote arousal, function andinteraction of patients with their environment. However, Deyeet al26 also measured work of breathing and respiratory effort andfound them to be slightly lower with semi-recumbent positioning.Subsequently, they concluded that the semi-recumbent position isuseful in difficult to wean patients in order to unload (rest) therespiratory muscles. While this unloading may be important whenrecovery is required, the benefits of early mobilization in the crit-ically ill have been gained by mobilizing patients out of bed andincrementally loading (training) the respiratory system. Thesebenefits have also been demonstrated in patients who are slow towean.5,47,48 Therefore, the utilization of seated positioning couldinstead be viewed as an important component of early rehabilita-tion strategies in order to slightly increase respiratory effort and/orprovide a stable and more optimal position for rehabilitation ex-ercises. When periods of sitting are well tolerated, progression maythen occur to standing or tilt table rehabilitation, which are moredemanding and generate increases in VT and/or VE.25,37
A reduction in compliance with the use of upright positioningwas not observed in this study. Variations in compliance have beenobserved in ventilated patients with ALI when positioned fromsupine to a 30� or 45� semi-recumbent position20 but not withseated positions in bed.19 Differences in the level of sedation and/or use of neuromuscular blocking agents may account for the dif-ferences observed. In heavily sedated and/or paralyzed patientscompliance is decreased because spontaneous diaphragmaticcontractions are reduced and diaphragmatic excursion is reliant onthe positive pressure ventilation to overcome resistance from theabdominal compartment.
We encountered no adverse events during the application of thesemi-recumbent or seated position in patients who met our studycriteria and only a small increase inMABPwas evident immediately
after positioning in to the upright position. Prior investigations alsoappear to support the safety specifically of sitting and/or semi-recumbent positioning,20,22 with no adverse event reported and/or no requirement for additional sedation, neuromuscular blockadeor vasoactive drugs.20 Bourdin et al49 reported the frequent use ofsitting out of bed in 20 patients receiving mechanical ventilation,and concluded it to be safe with minimal changes in HR or MABP.Other studies have assessed hemodynamic changes with semi-recumbent positioning in patients who are hemodynamically sta-ble, ventilated and/or receiving vasoactive drugs with resultsindicating that altering position from supine to a semi-recumbentposition up to 60� is generally well tolerated, with minimalchange to cardiac output.6,7
Moving a patient in to a semi-recumbent position is easier andinvolves less staff compared to sitting a patient out of bed. However,discomfort may contribute to the ability to sustain the semi-recumbent position and several authors have outlined the diffi-culties of implementing and/or maintaining the semi-recumbentposition in clinical practice.16e18 While we did not record thelevel of comfort experienced by patients in either position, webelieve comfort was the main factor that limited achievement ofhigher backrest elevations with semi-recumbent positioning.Additionally, the results of this study suggest that an advantage ofseated positions is the ability to achieve a greater angle of incli-nation and to remain stable in the position. This may have signifi-cant implications for patient safety and comfort and considerationsin pressure area management with the use of upright positioning.
Erect postures enhance the mechanics of the thoracic cage andincrease the caudal excursion of the diaphragm.50 As patients slideout of the semi-recumbent position, they assume a slumpedposture. As the degree of kyphosis increases, lung volumes andchest wall mechanics may be adversely affected. For example, innormal subjects, a slumped semi-recumbent position significantlyreduces FRC13 and a slumped sitting position has been shown todecrease VE and VT.50 Therefore, it is possible, that with a longerduration of semi-recumbent positioning, adverse effects of pul-monary function may have become evident in this population.
The results of this study support clinicians to implement earlymobilization strategies, in that the adoption of seated positions outof bed can be commenced with the knowledge that short applica-tions of 30 min are generally not detrimental to a patient’s respi-ratory or cardiovascular status. Additionally, clinicians should notexpect improvements in oxygenation indices to routinely occurwhen utilizing upright positions in patients that are weaningfrom mechanical ventilation. While a potential benefit of passivelymoving patients out of bed into specialized chairs is that patientsmay not slide out of the upright position, clinicians should be awareof the risk that static positioning also poses to skin integrity andtherefore the duration of seated upright positioningmay need to belimited and/or guided by a patient’s skin tolerance.
A limitation of this study was the short period of data collection.Thirty minutes in the upright position was chosen for the conve-nience and ability to complete data collection for both positions inclose proximity, in an environment where various interventionsand investigations compete for time. Similar and/or shorter timeperiods have been used in prior research in this population anddetected significant changes in respiratory function.13,20,24,25 Themedian time between the position sequences was 2.5 h and anorder effect was observed. While the magnitude of these changeswere small and would not be clinically significant, it may indicatethat small improvements in respiratory function occur through therepeated utilization of these position changes. A longer time periodfor data collection and the effect of repeated applications of uprightposition may have been able to detect significant changes in res-piratory function. Variation in respiratory responses to upper limb

P. Thomas et al. / Heart & Lung 43 (2014) 105e111110
exercise has been found when ventilated patients are comparedwith non-ventilated patients.14 As patients were still supported onmechanical ventilation, if any detrimental effect of either positionarose, the impact of the change on respiratory function may havebeen lessened.51 Therefore, replication of this study in patients whohave been recently extubated, are undergoing a slow weaningprocess or are undergoing spontaneous breathing trials may yielddiffering results.
In addition to investigating the effect of utilizing upright posi-tions over longer time periods and/or during different phases ofventilator support, more specific measures of a patients lung vol-ume, work of breathing and fatigue are required in future studies todirect prescription of seated positions under varying circum-stances. For example, if the success or duration of a T-piece trial ina difficult to wean patient was known to be affected by semi-recumbent or seated positions, then positions that benefit lungvolumes or work of breathing or reduce fatigue could be utilizedduring the trial. Positions that may provide an additional challengeto the respiratory system e.g. by increasing work of breathing maybe utilized at different times to a T-piece trial, to prevent over-loading the respiratory system of the slow to wean patient. Furtherinvestigation into the variety of real and/or perceived barriers tomobilizing patients out of bed is also warranted52 including patientfactors (e.g. comfort, arousal, dyspnea) and environmental factors(e.g. equipment, sedation practices). By increasing our under-standing of the impact of positioning practices throughout variousstages of critical illness, clinicians will be able to refine earlyrehabilitation strategies that include the appropriate timing andapplication of upright positioning.
Acknowledgments
Warren Stanton, School of Health and Rehabilitation Sciences,University of Queensland, Brisbane.
Ross Darnell, Statistician, School of Health and RehabilitationSciences, University of Queensland, Brisbane.
Financial support for this project was gained from the AustralianPhysiotherapy Association, Dorothy Hopkins Award for clinicalresearch.
References
1. Schweickert WD, Pohlman MC, Pohlman AS, et al. Early physical and occupa-tional therapy in mechanically ventilated, critically ill patients: a randomisedcontrolled trial. Lancet. 2009;373(9678):1874e1882.
2. Bailey P, Thomsen GE, Spuhler VJ, et al. Early activity is feasible and safe inrespiratory failure patients. Crit Care Med. 2007;35(1):139e145.
3. Nava S. Rehabilitation of patients admitted to a respiratory intensive care unit.Arch Phys Med Rehabil. 1998;79(7):849e854.
4. Thomsen GE, Snow GL, Rodriguez L, Hopkins RO. Patients with respiratoryfailure increase ambulation after transfer to an intensive care unit where earlyactivity is a priority. Crit Care Med. 2008;36(4):1119e1124.
5. Morris PE, Goad A, Thompson C, et al. Early intensive care unit mobility therapyin the treatment of acute respiratory failure. Crit Care Med. 2008;36(8):2238e2243.
6. Lambert CW, Cason CL. Backrest elevation and pulmonary artery pressures:research analysis. Dimens Crit Care Nurs. 1990;9(6):327e335.
7. Doering L. The effect of positioning on hemodynamics and gas exchange in thecritically ill: a review. Am J Crit Care. 1993;2(3):208e216.
8. Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M. Supine bodyposition as a risk factor for nosocomial pneumonia in mechanically ventilatedpatients: a randomised trial. Lancet. 1999;354(9193):1851e1858.
9. Behrakis PK, Baydur A, Jaeger MJ, Milic-Emili J. Lung mechanics in sitting andhorizontal body positions. Chest. 1983;83(4):643e646.
10. Craig DB, Wahba WM, Don HF, Couture JG, Becklake MR. “Closing volume” andits relationship to gas exchange in seated and supine positions. J Appl Physiol.1971;31(5):717e721.
11. Hardie JA, Morkve O, Ellingsen I. Effect of body position on arterial oxygentension in the elderly. Respiration. 2002;69(2):123e128.
12. Ibanez J, Raurich JM. Normal values of functional residual capacity in the sittingand supine positions. Intensive Care Med. 1982;8(4):173e177.
13. Jenkins SC, Soutar SA, Moxham J. The effects of posture on lung volumes innormal subjects and in patients pre- and post- coronary artery surgery. Phys-iotherapy. 1988;74(10):492e496.
14. Vitacca M, Clini E, Spassini W, Scaglia L, Negrini P, Quadri A. Does the supineposition worsen respiratory function in elderly subjects? Gerontology.1996;42(1):46e53.
15. Lorino AM, Atlan G, Lorino H, Zanditenas D, Harf A. Influence of posture onmechanical parameters derived from respiratory impedance. Eur Respir J.1992;5(9):1118e1122.
16. Cook DJ, Meade MO, Hand LE, McMullin JP. Toward understanding evidenceuptake: semirecumbency for pneumonia prevention. Crit Care Med.2002;30(7):1472e1477.
17. Grap M, Munro C, Bryant S, Ashtiani B. Predictors of backrest elevation incritical care. Intensive Crit Care Nurs. 2003;19(2):68e74.
18. van Nieuwenhoven C, Vandenbroucke-Grauls C, van Tiel F, et al. Feasibility andeffects of the semirecumbent position to prevent ventilator-associated pneu-monia: a randomized study. Crit Care Med. 2006;34(2):396e402.
19. Dellamonica J, Lerolle N, Sargentini C, et al. Effect of different seated positionson lung volume and oxygenation in acute respiratory distress syndrome.Intensive Care Med. 2013;39(6):1121e1127.
20. Bittner E, Chendrasekhar A, Pillai S, Timberlake GA. Changes in oxygenationand compliance as related to body position in acute lung injury. Am Surg.1996;62(12):1038e1041.
21. Hoste EAJ, Roosens CDVK, Bracke S, et al. Acute effects of upright position ongas exchange in patients with acute respiratory distress syndrome. J IntensiveCare Med. 2005;20(1):43e49.
22. Richard JC, Maggiore SM, Mancebo J, Lemaire F, Jonson B, Brochard L. Effects ofvertical positioning on gas exchange and lung volumes in acute respiratorydistress syndrome. Intensive Care Med. 2006;32(10):1623e1626.
23. Burns S, Egloff M, Ryan B, Carpenter R, Burns J. Effect of body position onspontaneous respiratory rate and tidal volume in patients with obesity,abdominal distention and ascites. Am J Crit Care. 1994;3(2):102e106.
24. Bonnet F, Bourgain JL, Matamis D, Tesseire B, Viars P. The influence of positionon ventilation-perfusion distribution after abdominal surgery. Acta Anaes-thesiol Scand. 1988;32(7):585e589.
25. Zafiropoulos B, Alison JA, McCarren B. Physiological responses to the earlymobilisation of the intubated, ventilated abdominal surgery patient. Aust JPhysiother. 2004;50(2):95e100.
26. Deye N, Lellouche F, Maggiore SM, et al. The semi-seated position slightly re-duces the effort to breathe during difficult weaning. Intensive Care Med.2013;39(1):85e92.
27. Chang MY, Chang LY, Huang YC, Lin KM, Cheng CH. Chair-sitting exerciseintervention does not improve respiratory muscle function in mecha-nically ventilated intensive care unit patients. Respir Care. 2011;56(10):1533e1538.
28. Dupont WD, Plummer WD. Power and sample size calculations: a review andcomputer program. Control Clin Trials. 1990;11:116e128.
29. Vincent JL, Moreno R, Takala J, et al. The SOFA (sepsis-related organ failureassessment) score to describe organ dysfunction/failure. Intensive Care Med.1996;22(7):707e710.
30. Murray JF, Matthay MA, Luce JM, Flick MR. An expanded definition ofthe adult respiratory distress syndrome. Am Rev Respir Dis. 1988;138(3):720e723.
31. Knauss WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity ofdisease classification system. Crit Care Med. 1985;13:818e829.
32. Banner MJ, Blanch PB, Kirby RR. Imposed work of breathing and methods oftriggering a demand-flow, continuous positive pressure system. Crit Care Med.1993;21(2):183e190.
33. Gammage GW, Banner MJ, Blanch PB, Kirby RR. Ventilator displayed tidalvolume e what you see may not be what you get [abstract]. Crit Care Med.1988;16:454.
34. Petrini MF, Evans J, Wall MA, Norman JR. Variability, reproducibility and data-collection time of pulmonary bedside monitoring. Biomed Instrum Technol.1998;32:273e281.
35. Tobin MJ. Respiratory monitoring in the intensive care unit. Am Rev Respir Dis.1988;138:1625e1642.
36. Hummel R, Grap M, Sessler C, Munro C, Corley M. Continuous measurement ofbackrest elevation in critical care: a research strategy. Crit Care Med.2000;28(7):2621e2625.
37. Chang AT, Boots RJ, Hodges PW, Thomas PJ, Paratz JD. Standing with theassistance of a tilt table improves minute ventilation in chronic critically illpatients. Arch Phys Med Rehabil. 2004;85(12):1972e1976.
38. Stedman TL. Stedman’s Medical Dictionary. Philadelphia: Lippincott Williamsand Wilkins; 2000.
39. Leblanc P, Ruff F, Milic-Emili J. Effects of age and body position on “airwayclosure” in man. J Appl Physiol. 1970;28(4):448e451.
40. Katz JA, Ozanne GM, Zinn SE, Fairley HB. Time course and mechanisms of lung-volume increase with PEEP in acute pulmonary failure. Anesthesiology.1981;54(1):9e16.
41. Ramachandran PR, Fairley HB. Changes in functional residual capacity duringrespiratory failure. Can Anaesth Soc J. 1970;17(4):359e369.
42. Hedenstierna G, Strandberg A, Brismar B, Lundquist H, Tokics L. What causesthe lowered FRC during anaesthesia? Clin Physiol. 1985;5:S133eS141.
43. Wahba RW. Perioperative functional residual capacity. Can J Anaesth.1991;38(3):384e400.
P. Thomas et al. / Heart & Lung 43 (2014) 105e111 111
44. Rylander C, Hogman M, Perchiazzi G, Magnusson A, Hedenstierna G. Functionalresidual capacity and respiratory mechanics as indicators of aeration andcollapse in experimental lung injury. Anesth Analg. 2004;98(3):782e789.
45. Wiren JE, Lindell SE, Hellekant C. Pre- and postoperative lung function in sittingand supine position related to postoperative chest X-ray abnormalities andarterial hypoxaemia. Clin Physiol. 1983;3(3):257e266.
46. Meyers JR, Lembeck L, O’Kane H, Baue AE. Changes in functional residual ca-pacity of the lung after operation. Arch Surg. 1975;110(5):576e583.
47. Burtin C, Clerckx B, Robbeets C, et al. Early exercise in critically ill patients en-hances short-term functional recovery. Crit Care Med. 2009;37(9):2499e2505.
48. Clini EM, Crisafulli E, Antoni FD, et al. Functional recovery following physicaltraining in tracheotomized and chronically ventilated patients. Respir Care.2011;56(3):306e313.
49. Bourdin G, Barbier J, Burle JF, et al. The feasibility of early physical activity inintensive care unit patients: a prospective observational one-center study.Respir Care. 2010;55(4):400e407.
50. Landers M, Barker G, Wallentine S, McWhorter W, Peel C. A comparison oftidal volume, breathing frequency, and minute ventilation between twositting postures in healthy adults. Physiother Theory Pract. 2003;19:109e119.
51. El-Khatib MF, Jamaleddine GW, Khoury AR, Obeid MY. Effect of continuouspositive airway pressure on the rapid shallow breathing index in patientsfollowing cardiac surgery. Chest. 2002;121(2):475e479.
52. Mendez-Tellez PA, Dinglas VD, Colantuoni E, et al. Factors associated withtiming of initiation of physical therapy in patients with acute lung injury. J CritCare. 2013;28(6):980e984.
Copyright © 2022 FDOKUMEN