Power dissipation associated with surgical operations’ hemodynamics: critical issues and...
12
Journal of Biomechanics 39 (2006) 1583–1594 Power dissipation associated with surgical operations’ hemodynamics: Critical issues and application to the total cavopulmonary connection Mauro Grigioni a, , Giuseppe D’Avenio a , Antonio Amodeo b , Roberto M. Di Donato b a Cardiovascular Bioengineering, Technology and Health Department, Istituto Superiore di Sanita`, Rome, Italy b Department of Cardiac Surgery, Bambino Gesu` Hospital, Rome, Italy Abstract The issue of the correct determination of the mechanical power dissipated by the blood flow in the circulatory system is very important. This parameter is particularly critical when the patient’s circulation has to overcome structural impairments, such as, e.g., in the case of only one functional ventricle. The surgical palliation of such a condition, which is a relatively common form of congenital heart disease, calls for an optimization of the new connection’s hydrodynamics. Starting from the general formulation of the energy dissipation rate in a given control volume, this paper discusses the critical assumptions of the formula usually employed to assess the power dissipation in complex connections, such as the total cavopulmonary connection (TCPC). A new formula is derived, in which the mean elevation of the outlet and inlet sections is shown to be relevant, through the use of the piezometric pressure. Moreover, the flow profile at the boundary of the control volume is also important, since the usual approach implicitly assumes that the flow is perfectly flat: this assumption is doubtful, especially in the venous return (as in the TCPC). In the experimental part of the study, the power dissipation was measured in a physical model of the TCPC, and a large difference was found between the usual method and the proposed one, especially at low regime (85% relative difference, at 1.5 l/min total cardiac output). The proposed approach should be adopted in order to improve the accuracy of the hydrodynamical performance’s assessment of surgical connections (e.g., TCPC) or implantable devices (e.g., valved conduit). r 2006 Elsevier Ltd. All rights reserved. Keywords: Hemodynamics; Total cavopulmonary connection; Power dissipation 1. Introduction The amount of energy lost by the blood as it flows through a given region of the vascular system is a crucial parameter when assessing the quality of implantable devices (e.g., prosthetic heart valves and valved con- duits) and/or surgical techniques. This issue is particu- larly important when Fontan-type interventions are considered, due to the low level of pressure head available in the venous return. Fontan-type procedures are often employed whenever the right heart is affected by congenital diseases. They aim at ensuring a sufficient lung perfusion by shunting partially or totally the right atrium and ventricle (Fontan and Baudet, 1971). In such cases, the pulmonary flow is only driven by the low pressure in the two venae cavae (which carry the venous return). It is thus essential to minimize the energy losses in the connection between the terminal part of the venous system and the pulmonary arteries. The total cavopulmonary connection (TCPC) is a particular implementation of this concept, consisting of the direct anastomosis of the venae cavae to the pulmonary arteries (de Leval et al., 1988). This paper addresses the issue of the rigorous determination of the power lost by the flow across ARTICLE IN PRESS www.elsevier.com/locate/jbiomech www.JBiomech.com 0021-9290/$ - see front matter r 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.jbiomech.2006.04.008 Corresponding author. Department of Technology and Health, Istituto Superiore di Sanita`, Viale Regina Elena 299, 00161 Rome, Italy. Tel.: +39 06 49902855; fax: +39 06 49387079. E-mail address: [email protected] (M. Grigioni).
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Power dissipation associated with surgical operations’ hemodynamics: critical issues and...

ARTICLE IN PRESS
0021-9290/$ - se
doi:10.1016/j.jb
�CorrespondIstituto Superio
Italy. Tel.: +39
E-mail addr
Journal of Biomechanics 39 (2006) 1583–1594
www.elsevier.com/locate/jbiomech
www.JBiomech.com
Power dissipation associated with surgical operations’hemodynamics: Critical issues and application to the total
cavopulmonary connection
Mauro Grigionia,�, Giuseppe D’Avenioa, Antonio Amodeob, Roberto M. Di Donatob
aCardiovascular Bioengineering, Technology and Health Department, Istituto Superiore di Sanita, Rome, ItalybDepartment of Cardiac Surgery, Bambino Gesu Hospital, Rome, Italy
Abstract
The issue of the correct determination of the mechanical power dissipated by the blood flow in the circulatory system is very
important. This parameter is particularly critical when the patient’s circulation has to overcome structural impairments, such as,
e.g., in the case of only one functional ventricle. The surgical palliation of such a condition, which is a relatively common form of
congenital heart disease, calls for an optimization of the new connection’s hydrodynamics. Starting from the general formulation of
the energy dissipation rate in a given control volume, this paper discusses the critical assumptions of the formula usually employed
to assess the power dissipation in complex connections, such as the total cavopulmonary connection (TCPC). A new formula is
derived, in which the mean elevation of the outlet and inlet sections is shown to be relevant, through the use of the piezometric
pressure. Moreover, the flow profile at the boundary of the control volume is also important, since the usual approach implicitly
assumes that the flow is perfectly flat: this assumption is doubtful, especially in the venous return (as in the TCPC). In the
experimental part of the study, the power dissipation was measured in a physical model of the TCPC, and a large difference was
found between the usual method and the proposed one, especially at low regime (85% relative difference, at 1.5 l/min total cardiac
output). The proposed approach should be adopted in order to improve the accuracy of the hydrodynamical performance’s
assessment of surgical connections (e.g., TCPC) or implantable devices (e.g., valved conduit).
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Hemodynamics; Total cavopulmonary connection; Power dissipation
1. Introduction
The amount of energy lost by the blood as it flowsthrough a given region of the vascular system is a crucialparameter when assessing the quality of implantabledevices (e.g., prosthetic heart valves and valved con-duits) and/or surgical techniques. This issue is particu-larly important when Fontan-type interventions areconsidered, due to the low level of pressure headavailable in the venous return. Fontan-type procedures
e front matter r 2006 Elsevier Ltd. All rights reserved.
iomech.2006.04.008
ing author. Department of Technology and Health,
re di Sanita, Viale Regina Elena 299, 00161 Rome,
06 49902855; fax: +39 06 49387079.
ess: [email protected] (M. Grigioni).
are often employed whenever the right heart is affectedby congenital diseases. They aim at ensuring a sufficientlung perfusion by shunting partially or totally the rightatrium and ventricle (Fontan and Baudet, 1971). In suchcases, the pulmonary flow is only driven by the lowpressure in the two venae cavae (which carry the venousreturn). It is thus essential to minimize the energy lossesin the connection between the terminal part of thevenous system and the pulmonary arteries. The totalcavopulmonary connection (TCPC) is a particularimplementation of this concept, consisting of the directanastomosis of the venae cavae to the pulmonaryarteries (de Leval et al., 1988).
This paper addresses the issue of the rigorousdetermination of the power lost by the flow across

ARTICLE IN PRESS
Nomenclature
u velocity vector at a given point and timeu magnitude of uU average value of u over the sectionQ volumetric flow ratem dynamic viscosity of the fluidr density of the fluidg gravitational acceleration (9.8m/s2)p static pressure
h height of the fluid particle above an arbitraryhorizontal plane
rgh elevation pressurep� ¼ pþ rgh piezometric pressureW loss mechanical power dissipated across a con-
nectionW stat contribution of the static pressures to W loss
Wdyn contribution of the dynamic pressures to W loss
n bluntness indexb correction factor
M. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–15941584
a connection with multiple inputs and/or outputs. Thisapproach, as anticipated in Grigioni et al. (2001), will beapplied to the power dissipation across a TCPC, but canobviously be exploited to study also other types ofconnection: an important example is given by themechanical assistance to the circulation, which entailsan alternative route to the natural blood flow, when anoptimization of the overall perfusion conditions is to bepursued by means of the accurate characterization of therelative power losses.
In the calculation of the power dissipation in certainsites of the circulatory system, as will be seen in thefollowing section, it is necessary to use the energyconservation equation, integrated over a given controlvolume. Leaving the details to the following part of thestudy, here we simply point out that the knowledge ofthe local pressure is required. The question arises whichis the correct definition of the pressure to be used.Instead of the measured static pressure p, as will be seenin the following sections, it is necessary to use piezo-metric pressure p� ¼ pþ rgh instead of solely using thestatic pressure p. An elementary example can show thispoint: consider first a cylindrical pipe, placed in ahorizontal position, in which a given flow rate isestablished by means of a certain pressure drop at itsextreme sections. Here the mean quote h is constant ineach section of the pipe, and Dp� ¼ Dp. In laminarconditions, since the mean velocity at the inlet and at theoutlet is the same, no net dynamical pressure contribu-tion exists, and the dissipated power is given by W ¼
Dp�Q ¼ Dp Q ¼ kQ2 (where Q is the volumetric flowrate, Dp ¼ pIN � pOUT, and similarly for Dp�), with k
depending on the viscosity of blood and the length anddiameter of the pipe. If we imagine to incline the pipe ata certain angle, while maintaining the same flow rate,the energy dissipation will be unchanged, since itdepends only (in the laminar regime) on the frictionbetween fluid regions having different velocities: if weapply again the simplified formula W ¼ Dp Q (incor-rectly, because now the relationship Dp�Q ¼ Dp Q is nomore valid, owing to the difference in elevation of thesections), a different result would be provided, since thestatic pressure difference is certainly larger (for an
upward inclination) than in the previous case. It is clear,then, that the potential energy associated with the forceof gravity must be taken into account in the calculationof power dissipation, when the different sections of ahydraulic circuit have a different mean elevation. This issimilar to the consideration of a patient being in ahorizontal or upright position, with a different loadimposed on the heart in the two cases.
Another example can be useful to show the differencebetween exchanged power and dissipated power: if,assuming that the tube is inclined downwards, we takethe limit of W ¼ Dp Q for Q! 0 (this condition may bethought to occur, e.g., when the diameter has a very lowvalue), Dp will tend to the limit Dplim ¼ pin � pout ¼
�rgjDhj, Dh being the difference in height between theinlet and outlet sections. Then, if W ¼ Dp Q isconsidered as a measure of the dissipated power, wecome to the conclusion that in this situation a negativevalue of dissipated power can be found, which isequivalent to state that energy is being accumulatedin the control volume out of dissipation. Evidently,this is inconsistent with physics, so that W ¼ Dp Q
should be correctly assumed to be the power deliveredto the control volume, not the power dissipated in thelatter.
Starting from the energy balance equation for a fluidelement, we will consider the limitations of the usualformula for the power dissipation across circulatorysites. In the present study, we report measurements ofthe power dissipation occurring in an anatomicallyaccurate in vitro model of TCPC, realized with the useof NMR images relative to previously operated childrenat the Pediatric Hospital Bambino Gesu (OPBG) inRome. A study reporting the analysis of the outcome ofsuch operations (Amodeo et al., 1997) concluded thatthe total extracardiac cavopulmonary connection pro-vides good early and midterm results and may reducethe prevalence of late arrhythmias in patients under-going the Fontan operation. The satisfactory hemody-namical performance of this type of extracardiac TCPCwas confirmed by in vitro and numerical studies(Amodeo et al., 2002). With its favourable clinicaloutcome, the extracardiac TCPC realized at the OPBG

ARTICLE IN PRESSM. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–1594 1585
represents a good model to be used in the evaluation ofthe power dissipation relative to the right heart bypass.
In the following, it will be shown that the correctformula for the power dissipated in the circulationrequires some knowledge about the flow profile at theboundary sections of the control volume. This is incontrast to the usual approach, which must then beregarded as a limitative option. The possibility toneglect the gravitational contribution (as in the usualformula) will be discussed, referring to the actual valuesof pressure, flow rates and inlet/outlet ports’ meanelevation.
2. Materials and methods
2.1. Theoretical analysis
The power dissipated in the circulation is an issuewhich is subjected to potential sources of errors,frequently overlooked. It is usually assumed (e.g.,Sharma et al., 1996) that
W loss ¼XmIN
i¼1
piQi �XmOUT
j¼1
pjQj þr2
XmIN
i¼1
U2i Qi �
r2
XmOUT
j¼1
U2j Qj
(1)
or, in compact form, W loss ¼W stat þWdyn, whereW stat ¼
PmIN
i¼1piQi �PmOUT
j¼1 pjQj is the contribution dueto the static pressures, and Wdyn ¼ r=2
PmIN
i¼1U2i Qi �
r=2PmOUT
j¼1 U2j Qj is the contribution due to the dynamical
pressures.In these formulas, Pk;Qk;Uk represent the static
pressure, flow rate and mean velocity in section k,respectively, and mIN (mOUT) is the number of inlet(outlet) ports of the connection.
Eq. (1) is a rather simplified calculation of the powerdissipated across a multiple-input and multiple-outputconnection, such as the TCPC. Actually, a previousinvestigation on the energy loss relative to prosthetic heartvalves (Leefe and Gentle, 1987) proposed a more generalformula, derived from the energy equation for a Lagran-gian fluid element. The integration of the rate of energydissipation (as irrecoverable heat through fluid friction),over a given control volume (bounded by inlet and outletsections as well as by the vascular walls), yields the powerdissipation. The latter can be expressed as follows:
W loss ¼ �
ZIN
ðpþ rghÞu � dA�
ZIN
1
2ru2u � dA
�
ZOUT
ðpþ rghÞu � dA�
ZOUT
1
2ru2u � dA, ð2Þ
where p is the static pressure, r the fluid density, g thegravity acceleration, h the elevation of the fluid particleabove an arbitrary horizontal plane, u the velocity vector,and dA the oriented surface element (dA ¼ dAn, where n is
the outward unit vector normal to the section). In Eq. (2),the first and third term represent the static contribution toW loss, and the second and fourth term represent thedynamical contribution.
The integrals are evaluated on the ensemble of theinflow (IN) or outflow (OUT) sections. In Eq. (2), usehas been made of the steady-flow regime conditions todiscard the time derivative of a volume integraldependent upon the local flow velocity; also the rate ofwork done on the walls by the fluid has been neglected(assuming rigid or perfectly elastic walls). Otherwise, theconstitutive relationship of the wall material shouldhave been taken into proper consideration, which wouldhave refined the analysis, but at a not negligiblemathematical cost.
Eq. (2) was derived in fairly general assumptions, suchas negligible heat transfer between the control volumeand its surroundings, and Newtonian fluid through thecontrol volume. If we make the additional assumptionof the absence of cross-stream velocity components (i.e.,assuming monodimensional flow conditions) at theinflow and outflow sections (this hypothesis is verified,in particular, in the laminar Poiseuillian regime), u �
dA ¼ undA ¼ �udA (with the minus (plus) sign corre-sponding to the inflow (outflow) case), and Eq. (2) canbe cast in a form closer to Eq. (1):
W loss ¼XmIN
i¼1
p�i Qi �XmOUT
j¼1
p�j Qj þr2
ZIN
u3 dA
�r2
ZOUT
u3 dA, ð3Þ
where p� ¼ pþ rgh is the piezometric pressure andmIN; mOUT are the numbers of inflow and outflowsections, respectively. Q ¼
RudA is the volumetric flow
rate at a given section. The analogy to Eq. (1) is evident,the first two terms at the right-hand side of Eq. (3)representing the static contribution and the last two thedynamic contribution to the rate of energy dissipation.
The passage from Eq. (2) to (3) can be assumed to bevalid on the basis of its validity in the important case ofaxisymmetric flows: if we denote with h the spatialaverage value of h in a given section (whose normal issupposed to be perpendicular to the gravity force), thecontribution of the region bounded by the circles ofradius r and r+dr to the integral over that sectionZðpþ rghÞu � dA
is given byR 2pa¼0ðpþ rgðhþ r sin aÞurdrda ¼ 2p pþð
rghÞurdr. Therefore, upon averaging with respect to r,only the mean value of h needs to be considered in theresult, and the integral can be simplified by assumingthat h ¼ constant ¼ h.
Obviously, when the flow profile is skewed, thissimplifying assumption may lose validity; this effect

ARTICLE IN PRESSM. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–15941586
could occur when the boundaries of the control volumeare close to sources of flow disturbances, such asjunctions between vessels or closer to the heart valve.The main objective of the power loss calculationreported here is to evaluate the whole losses due alsoto flow disturbances, selecting appropriate boundariesof the control volume.
As for the kinetic terms with u3, the precise knowledgeof u in each point of the two sections would requiremuch experimental effort (e.g., with laser Doppleranemometry (LDA) or ultrasound echo measurements),so that it is necessary to make some hypothesis about it.SinceZ
Ain=out
u3 dA ¼ Ain=outu3
(the overbar stands for cross-sectional averaging) it isnatural to relate this contribution to the flow rate (Q),which can be expressed in terms of the cross-sectionalaveraging of the flow velocities:
Q ¼ AU
and
U � u ¼1
A
ZA
u dA.
Here there is a subtle point, since generally it cannotbe assumed that the average of the cube of the velocityequals the cube of the average of the velocity, whichwould enable to write simplyZ
Ain=out
u3 dA ¼ Ain=outðuÞ3¼ Ain=out
Q3
Ain=out
� �3¼
Q3
Ain=out
� �2 . ð4Þ
Therefore, a correction factor is required to take intoaccount this difference. We assume axisymmetric flowprofiles, described by the formula
uðrÞ ¼ u0 1�r
R
� �nh i(5)
with n (bluntness index) tending to infinity for acompletely flat profile. In Appendix A, we report thecalculation the ratio between the average of the cube ofthe velocity and the cube of the average of the velocity inthe considered section: this will yield the correctionfactor, denoted as b, to be employed together with theusual measure of the mean flow rate.
Therefore, the terms of the typeRIN u3 dA can be
expressed as
AIN � u3� �
¼ bAIN � uð Þ3 ¼ bAINQ3
IN
AINð Þ3¼ b
Q3IN
AINð Þ2
with b ¼u3
uð Þ3.
Returning again to Eq. (3), the final expression for thetotal power dissipation is the following:
W loss ¼XmIN
i¼1
p�i Qi �XmOUT
j¼1
p�j Qj þr2
ZIN
u3 dA
�r2
ZOUT
u3 dA ¼XmIN
i¼1
p�i Qi �XmOUT
j¼1
p�j Qj þXmIN
i¼1
r
2A2i
biQ3i
�XmOUT
j¼1
r
2A2j
bjQ3j ¼
XmIN
i¼1
p�i Qi �XmOUT
j¼1
p�j Qj þr2
XmIN
i¼1
biU2i Qj
�r2
XmOUT
j¼1
bjU2j Qj, ð6Þ
which, as well as Eq. (1), has the form W loss ¼
W stat þWdyn.There are two differences between this formula and
the one (Eq. (1)) which is usually adopted to calculatethe power dissipation: the first is that the piezometricpressure is used, instead of the static pressure, and thesecond consists in the necessity of multiplying the kineticterms of the type ðr=2ÞU2Q by the ratio b ¼ ðu3= uð Þ3Þ;the latter equals 2, for a Poiseuillian flow, but in all theother cases is such that 1pbo2.
2.2. Experimental assessment
The two approaches to the power loss calculationpreviously described have been experimentally evaluatedreferring to the particular TCPC design realized at theBambino Gesu Pediatric Hospital. In this case, theinflow vessels to the connection are the inferior andsuperior vena cava (IVC and SVC, respectively). Thesevessels are anastomosed to the pulmonary arteries(PAs). The outflows are, then, the right and leftpulmonary artery (RPA and LPA, respectively).
The comparison between the two formulas is notmeant to be a validation of Eq. (6), since the latter isderived from first principles, under reasonable assump-tions, hence an experimental validation is not strictlyrequired; the comparison is made, instead, to show thatthe use of the simpler Eq. (1) leads to sizably differentvalues with respect to those obtained with the proposedmethod.
In the TCPC design considered in this study, theconnection of the IVC to RPA is realized with anextracardiac instead of an intra-atrial tunnel, asproposed in the original formulation of the concept(de Leval et al., 1988; Amodeo et al., 1997). Thesuperiority of the TCPC with respect to the atriopul-monary anastomosis (APA), i.e., the direct connectionof the PAs to the right atrium, was demonstrated invitro (Kim et al., 1995) as well as in vivo (Be’eri et al.,1998), due to the absence of the swirling flow patternswhich characterize the APA.
The discussion is still open about the optimal designparameters which affect a TCPC’s hemodynamical

ARTICLE IN PRESSM. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–1594 1587
performance: offset between venae cavae, angle ofincidence with respect to the arteries, and so on.Actually, the connection with directly opposed venaecavae was seen to be the cause of energy losses (Lardoet al., 1999; Sharma et al., 1996; Amodeo et al., 2002).The use of a prosthetic extracardiac conduit simplifiesthe surgical intervention and gives the surgeons thefreedom to choose between different anastomosesconfigurations.
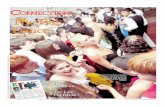
The connection’s model, inserted in a steady-flowloop, was made of blown glass (Grigioni et al., 2000;Amodeo et al., 2002), realized from NMR images ofpediatric patients, previously operated at the BambinoGesu Pediatric Hospital. Fig. 1 shows a scheme of theflow loop. As the control volume for power dissipationcalculation, we chose the region comprised between theinflow and outflow sections placed at 20mm from thecenter of the cross. Then, the height of the SVC (IVC)section was +20 (�20)mm with respect to the meanheight of the two PA sections. The accurate specificationof the extent of the region in which the power loss iscalculated is obviously important in the evaluation ofthe result.
The SVC–IVC flow division was set at 40–60%,corresponding to the physiological unbalance occurringin the circulatory system (Salim et al., 1995). This was
Fig. 1. Schematic of the experimental setup used in the measurements on the
the figure. White arrows denote the flow direction in and out of the TCPC; g
discharge reservoir; black arrows denote the flow from the pump to the VC
repeated for each of the values considered for the totalcardiac output. The connections of pulmonary arteriesto the downstream part of the flow loop were leftunrestricted. For the 40–60% flow partition, equal PAflows were found.
The characteristic dimensions of the TCPC replicawere as follows: caval veins diameter: 11.5mm;pulmonary arteries diameter: 8.6mm; offset betweenthe axes of the venae cavae, at the level of the respectiveanastomosis with the pulmonary artery: 6mm. The IVCformed a 221 angle with the vertical direction, issuingpreferably towards the LPA. For a discussion on theinfluence of geometry on the flow field inside thisimplementation of the TCPC concept, see Amodeo et al.(2002).
The TCPC model was inserted in a steady-flow loop,in which the flow could be controlled in each branch ofthe connection by regulating the pressure of thecorresponding outlet/inlet, with the suitable positioningof the associated reservoir. For the experiments herebydescribed, the flow in the PAs was not controlled;instead, the possibility of regulating the split ofpulmonary flows could be useful for studying the effectof pathologic circulatory conditions, such as, e.g., astenosed PA. As shown in Fig. 1, the reservoirs relativeto each compartment of the connection had an overflow
TCPC. The glassblown model of the latter is shown in the upper part of
ray arrows denote the overflow from the PA and VC reservoirs to the
reservoirs upstream of the TCPC.

ARTICLE IN PRESS
Fig. 2. Pressure measurements [Pa] at the representative sections of the inlet (IVC, SVC) and outlet (LPA, RPA) ports of the TCPC model. Black
(white) bars denote static (piezometric) pressures.
M. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–15941588
connection to the discharge reservoir, in order to keepconstant the level of the free surface of the fluid. In themeasurements, a 35% glycerol–water solution was used,with a kinematic viscosity of 2.44 cSt (value obtained bymeans of measurements with a Cannon–Fenske routineviscometer).
Pressure measurements were performed with a piezo-metric catheter (Millar). Pressures were recorded foreach point of a predefined set of distances from thecenter of the cross, with steps of 10mm, for a total of 30points. The procedure was repeated for each value of theset of total flow rates. In Fig. 2, the difference betweenthe static pressures and the piezometric pressures can beevaluated, at each imposed flow rate.
Flow rate measurements were carried out with a two-channel electromagnetic flowmeter, so that the simulta-neous measurement of the flow rate in the IVC and SVCwas obtained. An alternative arrangement of the set-upenabled us to assess that the total flow rate was equallydistributed in the PAs, when a 40–60% flow partition inthe VCs was imposed.
2.2.1. Application of Eq. (6)
Referring again to Eq. (5) for the flow profile at thecontrol volume boundary sections, we will not make thehypothesis that the flow at each of these sections of ourcontrol volume is Poiseuillian, because these sections arenot sufficiently distant from the junctions. Since the
entrance length, defined as the distance in which the flowprofile changes from a flat to a parabolic shape, is givenby l ¼ 0:06DRe for laminar flow regime (Rouse, 1978),it can be seen that at 2 cm from the center of the TCPC,the flow in the pulmonary arteries is not yet fullyPoiseuillian (x=l51 in Fig. 3), so that we must set n42.
On the other hand, in the venae cavae the fluid hascertainly traveled a sufficient distance to let n ¼ 2 in theequation of the profile. In order to calculate a suitablevalue for n in the pulmonary arteries, we can assumethat the flow is perfectly flat when it enters the artery(n ¼ 1), gradually changing profile as it travels down-stream. At the generic section, at x cm from the entrysection of the pulmonary artery, the bluntness index willbe related to the distance x by the approximatingformula
ð1=nx � 1=nfinalÞ
ð1=ninitial � 1=nfinalÞ¼ 1�
x
l, (7)
which states that nx is a decreasing function of x. It is clearthat, when x ¼ 0, 1=nx ¼ 1=ninitial, or nx ¼ ninitial ¼1;when x ¼ l, instead, 1=nx ¼ 1=nfinal, or nx ¼ nfinal ¼ 2.Eq. (7), moreover, ensures mathematically the continuityof nx with respect to x. Fig. 3 reports the development ofthe flow profile with downstream distance, according toEq. (7).
Using Eq. (7), we calculated the bluntness index foreach pulmonary artery, at every flow rate considered,

ARTICLE IN PRESS
Fig. 3. Flow profiles drawn according to Eq. (7), which accounts for the development of the Poiseuillian profile as the flow travels in a circular pipe,
with a flat entry profile. R is the radius of the pipe, l is the entrance length, defined as l ¼ 0:06DRe. The bluntness index n is shown for each profile.
M. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–1594 1589
once the entrance length was computed as l ¼ 0:06DRe(Rouse, 1978).
3. Results
In Fig. 4 we report the static contribution W static tothe power dissipation according to the two approacheshere considered, given by the first two terms in Eqs. (1)and (6), respectively. The two formulas yield asubstantial difference, due to the effect of the differentmean quote of the vessels the TCPC is composed of.Table 1 summarizes the relative difference between thetwo approaches, for W stat, Wdyn and W loss.
For the evaluation of the difference in the dynamicalcontribution, even though some approximations have tobe made, we proceeded as follows: the flow at theentrance of the PAs was assumed to be perfectly flat,with n ¼ 1. At the section of the measurements (20mmdownstream of the center of the cross), we computed thevalue of n according to Eq. (7). Instead, in the venaecavae the flow profile was assumed to be Poiseuillian,owing to the distance traveled by the fluid upstream ofthe sections in the cavae. Then, the dynamical contribu-tion according to Eq. (3) was plotted in Fig. 5, alongwith its more traditional calculation. The difference inthe two quantities are remarkable, since the values of n
were found to be very high in the pulmonary arteries,from Eq. (6), and bffi 1 as n!1, whereas n ¼ 2 (andb ¼ 2) in the caval veins. It must be underlined,however, that a perfectly flat flow profile at the entranceof the pulmonary artery has been a simplifying
assumption, which should be verified with independentdata. Actually, the flow in the RPA has a predominantSVC contribution (conversely, the flow in the IVC issuespredominantly in the LPA, see also Grigioni et al.,2000), hence the turn made by the flow before the entryin the PA probably renders the skewed profile of theRPA flow, as commonly found in the curved vessels (Heand Ku, 1996; Naruse and Tanishita, 1996). In this case,the value of b could be greater than 1, since a plug flow(associated to b according to Eq. (6)) would not be arepresentative model of the local flow, and the correctvalue of Wdyn should accordingly be calculated bymeans of the last two terms in Eq. (6).
In Fig. 6, finally, the total power loss W loss ¼W stat þ
Wdyn is shown. The power dissipation according to themore accurate approach is larger than W loss, as given byEq. (1).
4. Discussion
The proposed method for the calculation of the powerdissipation relies on the determination of the meanheight and on the knowledge of the correction factor b,for each of the inflow and outflow ports of the controlvolume. In the evaluation of Fig. 6, it must beconsidered that the difference between the dynamicalparts of W loss, according to the two methods, isprobably slightly overestimated, as already said, due tothe hypothesized perfect flatness of the flow profile atthe entrance of the PAs. Nevertheless, it was found thatfor both W static and Wdyn the more general approach to

ARTICLE IN PRESS
Fig. 4. Static contribution (W stat) to the power dissipated in the TCPC, according to the usual Eq (1) and to the proposed method (first two terms in
Eq. (6)). The respective markers are open circles and filled squares.
Table 1
Flow rate (l/
min)
Relative
difference in
Wstat (%)
Relative
difference in
Wdyn (%)
Relative
difference in
Wloss (%)
1.5 55.56 53.11 85.02
2 32.48 53.31 56.90
3 15.22 53.51 36.18
4.167 8.54 53.63 29.58
M. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–15941590
the problem of characterizing the power dissipation insuch hydraulic structures provides higher values thanthe traditional approach. From Fig. 6, it can be seenthat the difference between the values of W loss accordingto the two methods increases for higher values of thecardiac output, so that the proposed method does notlead to a simple rescaling to the power dissipationcalculated with the traditional method. The higherincrease in W loss with the flow rate, according toEq. (6), correlates well with the experience with TCPCpatients, who cannot sustain exercise conditions withoutdifficulty. It is too early, though, to quantify the roleplayed by the enhanced difference, hereby reported, inW loss as the flow rate increases, in the sensation ofdiscomfort experienced by the patient.
The dynamical contributions to the power dissipationin Eqs. (1) and (6), respectively, can be different,depending, in particular, on the local flow field at thecontrol volume’s ends, implicitly taken into account by
the values of b in Eq. (6) . In the simpler Eq. (1), instead,use is being made only of the flow rate and the section’sarea. It can be seen that the two quantities coincide onlyin particular cases: for instance, when the flow profile isperfectly flat. This case is rarely found in the circulatorysystem, particularly in the venous return, so that itshould be advisable to avoid to use Eq. (1), wheneverpossible, and to replace it with Eq. (6).
In the latter formula, the coefficients bi relative to theinlet sections of the TCPC are ’ 2, whereas those of theoutlet sections are equal to 1. Then, the consideration ofthe difference in flow profiles between the VCs and thePAs leads to a higher contribution of the dynamical partthan usuallly assumed. A practical rule for suchconnections, then, could be to impose bIN ¼ 2 andbOUT ¼ 1, in the absence of more detailed informationabout the local flow field.
The case may occur where the knowledge of thequotes hi is not immediate; then, an experimentaldetermination of the terms rghi may be proposed asfollows. In p� ¼ pþ rgh the quote h increases towardsthe upward vertical direction, whereas the pressuresmeasured at zero flow rate increase as decreasing valuesof h are considered. Then, the measured pressures atQi ¼ 0 will be given by pi;0 ¼ pref � rghi, pref being areference pressure. By imposing that the mean quote ofthe ith port is hi ¼ 0 (the quotes are defined with anarbitrary additive constant value), we have thatpref ¼ pi;0, and the terms rghi can be immediatelyderived from the measured pressures at zero flow rate.

ARTICLE IN PRESS
Fig. 5. Dynamical contribution (Wdyn) to the power dissipated in the TCPC, according to the usual Eq (1) and to the proposed method (last two
terms in Eq. (6)). The respective markers are open circles and filled squares.
Fig. 6. Total dissipated power (W loss) in the TCPC, according to the usual Eq. (1) and to the proposed method (Eq. (6)). The respective markers are
open circles and filled squares.
M. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–1594 1591
A correction of the static pressures for the pressure headbias was adopted by de Zelicourt et al. (2005), alsoreferring to an experimental study of the TCPC.
It is to be underlined, though, that this approachyields the value of rghi as a difference between two
measured quantities, so that a direct measurement of thequote hi could be preferable, in terms of accuracy.Actually, the uncertainty associated to the measurementof Dp is twice the uncertainty associated to a singlepressure measurement, then this procedure could be not

ARTICLE IN PRESSM. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–15941592
preferable to the simple use of the values hi in theterms rghi, depending on the characteristics of thepressure measurement system. An issue that can bequantitatively characterized is in which conditions willthe difference in height warrant the required gravitycontribution. Introducing the relative difference in thestatic contribution to the dissipated power:
r ¼ ðW stat; Eq: ð6Þ �W stat; Eq: ð1ÞÞ=W stat; Eq: ð1Þ,
we have that, after some trivial calculations:
r ¼ rg
PmIN
i¼1
hiQi �PmOUT
j¼1
hjQj
PmIN
i¼1
piQi �PmOUT
j¼1
pjQj
.
This value should be compared to an imposedthreshold rmax(e.g., rmax ¼ 5%), above which the grav-itational contribution should not be neglected. It can benoticed how the value of r is very sensitive to the flowrate distribution. For the parameters adopted in theexperimental part of this study, the values of r reportedin Table 1 (second column) confirm that the differencebetween the two approaches is considerable, across theentire range of total cardiac ouput considered, so thatEq. (6) is to be preferred. More generally, the above-written formula enables one to check whether thegravitational contribution should be taken into account.
5. Conclusion
The reassessment of the rate of energy dissipationassociated to the flow through a network of vessels hasshown that the formula usually adopted for the powerloss measurements (Eq. (1)) is inaccurate. This is thecase, in particular, of the TCPC, due to the differentmean elevation of the sections of the vessels theconnection is composed of. A relative difference of85% was found between the power loss provided by thetwo approaches.
The two curves in Fig. 6, drawn according to Eqs. (1)and (6), show that the more general approach does notsimply imply a shift of the level of power dissipation.Actually, the variation in W loss for increasing flow rateis higher than previously assumed. This could beimportant in evaluating the performance of a surgicalconnection such as the TCPC, especially in exerciseconditions.
Due to the importance of the evaluation of dissipa-tions associated to a particular TCPC design, it isadvisable to perform these measurements with a morerigorous approach than that summarized in Eq. (1). Inthis view, Eq. (6) provides the way to account for thedifferent height of the vessels involved in the surgicaldesign and for the type of flow profile in the measure-ment sections. The use of Eq. (6) should be advocated,
since the slight complications in the formula, withrespect to the usual Eq. (1), are justified by sensiblydifferent results, as shown in Table 1 for W loss, as well asfor W stat and Wdyn.
The analysis presented here shows that, even when allsections of the considered connection have the sameheight above a reference plane, there is still a potentialsource of error, due to the fact that the average of thecubed velocity must be evaluated. A correction factor bwas proposed in order to use, with a slight modification,the usual formula for the dynamical contribution to thepower loss.
Appendix A
The ratio between the average of the cube of thevelocity and the cube of the average of the velocity canbe easily calculated in the important case of axisym-metric flows.
For instance, if we consider the Poiseuillian steadyflow (parabolic velocity profile of a fully developedsteady flow)
u ¼ u0 1�r2
R2
� �
in an axially symmetric tube, the average of the velocityis given by
u ¼1
pR2
Z R
0
Z 2p
0
u0 1�r2
R2
� �rdydr ¼
u0
2, (A.1)
whereas the average of V 3 yields
u3 ¼1
pR2
Z R
0
Z 2p
0
u30 1�
r2
R2
� �3
rdydr ¼u30
4(A.2)
and it is evident that ¼ u34 uð Þ3 ¼ u30=8.
More generally, for an axially symmetric flow of theform
u ¼ u0 1�rn
Rn
� �,
where the velocity profile becomes flatter as theexponent n, which could be termed ‘‘bluntness factor’’,increases, which can be useful to simulate the effect ofturbulence or unsteadiness in the flow, or to characterizethe flow downstream of PHVs, at a sufficiently fardistance, i.e., more than two diameters. With straight-forward calculations it can be seen that
u ¼1
pR2
Z R
0
Z 2p
0
u0 1�rn
Rn
� �rdydr ¼
n
nþ 2u0, (A.3)

ARTICLE IN PRESS
Fig. 7. Correction factor b, to be employed in Eq. (6), as a function of the bluntness index n in each section of the control volume.
M. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–1594 1593
u3 ¼1
pR2
Z R
0
Z 2p
0
u30 1�
rn
Rn
� �3
rdydr
¼ 21
2�
3
2þ n�
1
3nþ 2þ
3
ð2nþ 2Þ
� �u30
¼3n3
1þ nð Þ 3nþ 2ð Þ nþ 2ð Þ
� �u30. ðA:4Þ
The correction factor b ¼ u3= uð Þ3, from Eqs. (A.3)and (A.4), is given by
b ¼3 nþ 2ð Þ
2
1þ nð Þ 3nþ 2ð Þ. (A.5)
In Fig. 7 the ratio between u3 and uð Þ3 is plotted as afunction of the exponent n. From Eq. (A.5) it can be
seen that limn!1u3= uð Þ3 ¼ 1, being always u34 uð Þ3, forfinite values of n (see Fig. 7).
References
Amodeo, A., Galletti, L., Marianeschi, S., Picardo, S., Giannico, S., Di
Renzi, P., Marcelletti, C., 1997. Extracardiac Fontan operation for
complex cardiac anomalies: seven years’ experience. Journal of
Thoracic and Cardiovascular Surgery 114 (6), 1020–1030 (discus-
sion 1030-1).
Amodeo, A., Grigioni, M., Oppido, G., Daniele, C., D’Avenio, G.,
Pedrizzetti, G., Ginnico, S., Filippelli, S., Di Donato, R.M., 2002.
The beneficial vortex and best spatial arrangement in total
extracardiac cavopulmonary connection. Journal of Thoracic and
Cardiovascular Surgery 124 (3), 471–478.
Be’eri, E., Maier, S.E., Landzberg, M.J., Chung, T., Geva, T., 1998. In
vivo evaluation of Fontan pathway flow dynamics by multi-
dimensional phase-velocity magnetic resonance imaging. Circula-
tion 98 (25), 2873–2882.
de Leval, M.R., Kilner, P., Gewillig, M., Bull, C., 1988. Total
cavopulmonary connection: a logical alternative to atriopulmonary
connection for complex Fontan operations. Experimental studies
and early clinical experience. Journal of Thoracic and Cardiovas-
cular Surgery 96 (5), 682–695.
de Zelicourt, D.A., Pekkan, K., Wills, L.B.S., Kanter, K., Forbess, J.,
Sharma, S., Fogel, M., Yoganathan, A.P., 2005. In vitro flow
analysis of a patient-specific intraatrial total cavopulmonary
connection. Annals of Thoracic Surgery 79, 2094–2102.
Fontan, F., Baudet, E., 1971. Surgical repair of tricuspid atresia.
Thorax 26, 240–248.
Grigioni, M., Amodeo, A., Daniele, C., D’Avenio, G., Formigari, R.,
Di Donato, R.M., 2000. Particle image velocimetry analysis of the
flow field in the total cavopulmonary connection. Artificial Organs
24 (12), 946–952.
Grigioni, M., Amodeo, A., Daniele, C., D’Avenio, G., Di Donato, R.,
2001. Power dissipation in surgical connections: reassessing its
rigorous calculation. XXVIII ESAO Congress, Gent, 22–25
September 2001. International Journal of Artificial Organs 24 (8),
565.
He, X., Ku, D.N., 1996. Pulsatile flow in the human left coronary
artery bifurcation: average conditions. Journal of Biomechanical
Engineering 118 (1), 74–82.
Kim, Y.H., Walker, P.G., Fontaine, A.A., Panchal, S., Ensley, A.E.,
Oshinski, J., Sharma, S., Ha, B., Lucas, C.L., Yoganathan, A.P.,
1995. Hemodynamics of the Fontan connection: an in-vitro study.
Journal of Biomechanical Engineering 117 (4), 423–428.
Lardo, A.C., Webber, S.A., Friehs, I., del Nido, P.J., Cape, E.G.,
1999. Fluid dynamic comparison of intra-atrial and extracardiac
total cavopulmonary connections. Journal of Thoracic and
Cardiovascular Surgery 117 (4), 697–704.
Leefe, S.E., Gentle, C.R., 1987. Theoretical evaluation of energy loss
methods in the analysis of prosthetic heart valves. Journal of
Biomedical Engineering 9 (2), 121–127.

ARTICLE IN PRESSM. Grigioni et al. / Journal of Biomechanics 39 (2006) 1583–15941594
Naruse, T., Tanishita, K., 1996. Large curvature effect on pulsatile
entrance flow in a curved tube: model experiment simulating blood
flow in an aortic arch. Journal of Biomechanical Engineering 118
(2), 180–186.
Rouse, H., 1978. Elementary Mechanics of Fluids. Dover, New York.
Salim, M.A., DiSessa, T.G., Arheart, K.L., Alpert, B.S., 1995.
Contribution of superior vena caval flow to total cardiac output
in children. A Doppler echocardiographic study. Circulation 92 (7),
1860–1865.
Sharma, S., Goudy, S., Walker, P., Panchal, S., Ensley, A., Kanter, K.,
Tam, V., Fyfe, D., Yoganathan, A., 1996. In vitro flow experiments for
determination of optimal geometry of total cavopulmonary connection
for surgical repair of children with functional single ventricle. Journal of
the American College of Cardiology 27 (5), 1264–1269.