Scoping Exercise on Fallers’ Clinics Report to the National Co-ordinating Centre for NHS Service...
214
Scoping Exercise on Fallers’ Clinics Report to the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO) March 2007 prepared by Sarah Lamb*† Simon Gates* Joanne Fisher* Matthew Cooke* Yvonne Carter* Christopher McCabe‡ *Warwick Medical School, University of Warwick, Coventry †Kadoorie Critical Care Research Centre, University of Oxford, Oxford ‡Leeds Institute of Health Sciences, University of Leeds, Leeds Address for correspondence Professor Sarah Lamb Warwick Medical School, The University of Warwick, Coventry CV4 7AL, UK E-mail: [email protected] Telephone: 024 7657 4658
Transcript of Scoping Exercise on Fallers’ Clinics Report to the National Co-ordinating Centre for NHS Service...

Scoping Exercise on Fallers’ Clinics
Report to the National Co-ordinating Centre for NHS Service Delivery and Organisation R & D (NCCSDO)
March 2007
prepared by
Sarah Lamb*†
Simon Gates*
Joanne Fisher*
Matthew Cooke*
Yvonne Carter*
Christopher McCabe‡
*Warwick Medical School, University of Warwick, Coventry
†Kadoorie Critical Care Research Centre, University of Oxford, Oxford
‡Leeds Institute of Health Sciences, University of Leeds, Leeds
Address for correspondence
Professor Sarah Lamb
Warwick Medical School, The University of Warwick, Coventry CV4
7AL, UK
E-mail: [email protected]
Telephone: 024 7657 4658

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 2
Contents
Glossary 5
Acknowledgements 5
Executive Summary 6
The Report 9
Section 1 Introduction 9 1.1 Background 9
1.2 Aims and objectives 10
1.3 A definition of a fallers’ clinic 10
1.4 Overview of methods 10
Section 2 National survey of fallers’ clinics and services 12 2.1 Introduction 12
2.2 Methods 12
2.2.1 Methodology 12
2.2.2 Sampling 12
2.2.3 Data capture 13
2.2.4 Analysis 15
2.2.5 Ethical approval 16
2.3 Results 16
2.3.1 Sample 16
2.3.2 Site of the clinic 17
2.3.3 Aims of the service 18
2.3.4 Referral to the service 19
2.3.5 Eligibility criteria 20
2.3.6 Age 21
2.3.7 Attendances 22
2.3.8 Staffing 22
2.3.9 Assessment 23
2.3.10 Interventions 26
2.3.11 Post-intervention follow-up 31
2.3.12 Cost of services and economic data available 31
2.4 Summary 31
Section 3 Estimates of the effectiveness of fallers’ clinics 33 3.1 Introduction 33
3.2 Eligibility criteria 33
3.2.1 Types of studies 33
3.2.2 Population 33
3.2.3 Types of intervention 34
3.2.4 Outcomes 34
3.3 Search strategy for eligible studies 35
3.3.1 Cochrane review 35
3.3.2 Update of the Cochrane review’s searches to 2003–2006 35

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 3
3.3.3 Specific search for studies of falls clinics 35
3.4 Review methods 35
3.5 Included and excluded studies 36
3.6 Methodological quality of included studies 37
3.6.1 Randomisation 38
3.6.2 Blinding 38
3.6.3 Losses and exclusions 38
3.6.4 Follow-up 38
3.6.5 Recording of falls outcomes 39
3.6.6 Cluster-randomised trials 39
3.7 Results 39
3.7.1 Falls 39
3.7.2 Recurrent falls 40
3.7.3 Fall-related injury 40
3.7.4 Hospitalisation 40
3.7.5 GP attendance 40
3.7.6 Emergency department attendance 40
3.7.7 Death 41
3.7.8 Move to institutional care 41
3.7.9 Health-related quality of life and physical activity 41
3.7.10 Sensitivity analysis for inclusion of cluster-randomised trials 41
3.8 Discussion 41
Section 4 Systematic review of screening instruments to predict fallers among community-living older people 84 4.1 Introduction 84
4.2 Methods 84
4.2.1 Eligibility 84
4.2.2 Search strategy 85
4.2.3 Data extraction 86
4.2.4 Quality assessment of included studies 86
4.3 Statistical analysis 86
4.4 Results 86
4.4.1 Searches 86
4.4.2 Characteristics of studies 87
4.4.3 Methodological quality 88
4.4.4 Measurement performance 88
4.5 Discussion 91
4.5.1 Design, reporting and methodological quality of existing studies 92
4.5.2 Searching for relevant studies 93
Section 5 Cost-effectiveness systematic review 115 5.1 Introduction 115
5.2 Methods 115
5.2.1 Selection criteria 116
5.2.2 Search strategy 116
5.3 Results 117
5.4 Discussion 118

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 4
Section 6 Feasibility of constructing a cost-effectiveness model of multi-factorial interventions for falls prevention 119 6.1 Background 119
6.2 Structure and parameter specification for a cost-effectiveness model 119
6.3 Evidence on parameters in cost-effectiveness models 121
6.3.1 Patient identification and eligibility 121
6.3.2 Effectiveness 121
6.3.3 Resource utilisation 122
6.4 Discussion 122
6.5 Conclusion 124
References 125
Appendices 156
Appendix 1 Summary economic data 156
Appendix 2 Search strategies for systematic review of effectiveness of faller’s clinics 175
Appendix 3 Quality-assessment tool for systematic review of effectiveness in fallers’ clinics 180
Appendix 4 Studies excluded from the systematic review of effectiveness of fallers’ clinics 182
Appendix 5 Search strategies for the systematic review of screening instruments 184
Appendix 6 Quality-assessment tool for the systematic review of screening instruments 192
Appendix 7 Studies excluded from the systematic review of screening instruments 194
Appendix 8 Search strategy for systematic review of cost-effectiveness of fallers’ clinics 198
Appendix 9 Quality-assessment tool used for the systematic review of economic studies 200
Appendix 10 Studies excluded from the economic systematic review 204

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 5
Glossary
CI confidence interval
FPP falls-prevention programme
FRAT Fall Risk Assessment Tool
ICC intracluster correlation coefficient
MMSE Mini Mental State Examination
NICE National Institute for Health and Clinical Excellence
NPV negative predictive value
p.a. per annum
PPA physiological profile assessment
PPV positive predictive value
ProFANE Prevention of Falls Network Europe
RCT randomised controlled trial
ROC receiver operating characteristics
RR relative risk
SD standard deviation
SWWT test Stops Walking When Talking test
TUG test Timed Up and Go test
Acknowledgements
This research was supported with a project grant from the NHS
Service Delivery and Organisation R&D Programme (SDO/139/2006).
The authors would like to thank the following members of the National
Co-ordinating Centre for NHS Service Delivery and Organisation R&D
Steering Committee – Damian O’Boyle, Emma Hawkridge, Stuart
Anderson and Donna Cox – for constructive comments during the
project.
The authors would also like to thank Rachel Potter, Tarla Patel and
Heather Cooke for their assistance with data collection, Rachel
Lancaster for advising on the development of the search strategy for
the cost-effectiveness systematic review, Christopher McCarthy for his
assistance with data extraction for the systematic review of the
effectiveness of fallers’ clinics and Christelle Evaert for her assistance
in the preparation of this report.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 6
Executive Summary
The National Service Framework for Older People has stated the need
for fall-prevention programmes. An appraisal of fallers’ clinics
launched by the National Institute for Health and Clinical Excellence
(NICE) was suspended because of a lack of information regarding
existing services and typology. This project aimed to determine the
feasibility of conducting economic modelling to appraise fallers’ clinics.
To achieve this a national survey of services and reviews of the
evidence of effectiveness of various models of fallers’ clinics and
screening tools were undertaken.
We have defined a fallers' clinic as ‘a facility based in either primary or
secondary health care that administers services to individuals with the
purpose of preventing falls and involves qualified health professionals
in the delivery of some or all of the assessment and intervention.’ The
national survey was conducted by contacting all falls services in the
UK by telephone or e-mail. Interviews were undertaken using a
standardised template previously developed by the Prevention of Falls
Network Europe (ProFANE) group, establishing the approach of the
clinic, its geographical base and characteristics, the assessments
undertaken and the interventions used. A total of 298 services were
identified and 231 (78%) agreed to participate. Most services were
urban (61.5%) with an equal split between community- and acute-
sector bases. Only 2% of services were based in emergency
departments. Referral was mostly from health professionals (63%),
although some had open referral systems and 3% required referral
from a doctor. Most (92%) used specified criteria for referral, with
most using falls/near falls/fear of falls (74%) and/or specified
screening tools (61%). The most common tool was the Falls Risk
Assessment Tool (FRAT). The median number of attendances was 180
per annum and most clinics were staffed by a multi-disciplinary team
(92%) although composition was highly variable. Ninety-nine per cent
undertook a multi-factorial assessment but the components varied
considerably. The majority (91%) undertook gait and balance
assessment and many undertook environment (76%), medication
(72%) and cardiovascular (69%) assessments. The most commonly
used interventions were information provision (94%), exercise (81%)
and medication review (66%). Post-intervention follow-up was
undertaken by 51% of services. The total cost of services provided in
the UK is estimated to be approximately £32 million per annum.
A systematic review of randomised studies of effectiveness of fallers’
clinics was undertaken. The search strategy included Cochrane reviews
(including repeating their search strategies) and searches of the
MEDLINE and EMBASE databases. All articles were reviewed by two
authors. A total of 202 studies were reviewed of which 18 were studies
of eligible interventions. The quality of some of the studies since the

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 7
last Cochrane review is poor. The evidence to support multi-factorial
fall-prevention interventions is inconclusive; with a range of
conclusions from no advantage to a 20% reduction in falls. The overall
estimate of risk reduction for further falls is 0.9 (95% confidence
interval 0.8–1.0). There were no clear advantages of location, of
selecting high-risk populations or from inclusion of a doctor in the
multi-disciplinary team. There is no clear effect on subsequent fall-
related injury, health-related quality of life or health care usage.
The systematic review of screening instruments focused on
prospective studies of community-dwelling people. A range of
electronic databases were searched (MEDLINE, EMBASE, PsycINFO,
CINAHL and Social Science Citation Index Expanded). This was
supplemented by hand searching of journals. Assessment was by two
independent reviews, using recognised quality-assessment tools.
Twenty-three articles were determined to be suitable for inclusion,
which included data on 28 different screening tools. Many studies were
excluded because they failed to report the data necessary for
evaluating test performance. The tests assessed by most studies were
the Tinetti mobility test, the Stops Walking When Talking test (SWWT
test) and the Timed Up and Go test (TUG test). There was, however,
variation in cut-off points to determine a positive test, the way tests
were utilised and the definitions of outcomes. It was therefore not
possible to combine results from different studies. The Tinetti mobility
test had an overall positive predictive value (PPV) of 0.31–0.68 and a
negative predictive value (NPV) of 0.67–0.88, with a reduced PPV if
only the balance element was used. The SWWT test in an unselected
population has a high PPV (83%) and NPV (76%), although sensitivity
was low (48%).The TUG test had variable cut-offs and hence studies
could not be combined. There is insufficient evidence to reliably
determine the quality and effectiveness of the screening tests.
A third systematic review was undertaken to study the cost-
effectiveness of fallers’ clinics in the UK. An extensive search strategy
was developed from that used by NICE and searched MEDLINE,
CINAHL, EMBASE, NHS EED, OHE HEED, the National Research
Register and bibliographic review. Data extraction and appraisal used
the Drummond and Jefferson framework. No suitable studies were
found on cost-effectiveness of UK fallers’ clinics although one study is
due to report in 2007. International studies were found but cannot be
used to inform UK cost-effectiveness.
The limitation of the information available means that the
effectiveness of various models cannot be confidently assessed and
economic modelling cannot be recommended. Present service
provision is highly variable in its format and activity. Hence it is not
possible to construct a cost-effectiveness model representative of
present falls-prevention activity in the NHS. To establish cost-benefit
outcomes we need reliable data, which are not available. Present
policy recommendations are not based on high-quality evidence. More
primary research on the predictive performance of screening tools, the

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 8
effectiveness of interventions and the cost-effectiveness of falls
prevention programmes are required. In the absence of such research,
we cannot be confident that falls-prevention programmes are an
efficient use of limited NHS resources.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 9
The Report
Section 1 Introduction
1.1 Background
The National Service Framework for Older People (Department of
Health, 2001) requires that the NHS establish fall-prevention
programmes. Little operational guidance was provided until publication
of the National Institute for Health and Clinical Excellence (NICE)
clinical practice guideline for the assessment and prevention of falls in
older people in 2004 (National Institute for Clinical Excellence, 2004).
This guidance is summarised below.
Case/risk identification should be undertaken by screening older
people for the occurrence of falls in the past year. Among those
reporting a fall, or considered to be at risk of falling, further
observations of balance and gait should be undertaken and ability to
benefit from strength and balance interventions should be considered.
Multi-factorial assessment should be undertaken and may include
assessments of falls history, gait/balance/mobility, muscle weakness,
osteoporosis risk, perceived functional ability and fear relating to
falling, visual impairment, cognitive impairments and neurological
examination, urinary incontinence, home hazards, cardiovascular
examination and medication review. Individualised multi-factorial
interventions should be considered; they may include strength and
balance training, home-hazard assessment and intervention, vision
assessment and referral, and medication review with
modification/withdrawal.
Practitioners who are involved in developing falls-prevention
programmes (FPPs) should ensure that such programmes are flexible
enough to accommodate participants’ different needs and preferences
and should promote the social value of such programmes.
Specialist falls services may vary among providers in the detail of
configuration, staffing and leadership. The most cost-effective
configuration is not yet established. Specialist falls services should,
however, be operationally linked to both bone health (osteoporosis)
services and cardiac pacing services.
An appraisal of fallers’ clinics was launched in 2004 by NICE but was
subsequently suspended because of lack of information regarding
existing services and their typology. The general perception before
this project was commissioned was that services have evolved
disparately in terms of selection criteria, screening procedures and
localities, and with variation in the treatment modalities offered.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 10
1.2 Aims and objectives
The objective of this project was to determine the feasibility of
conducting economic modelling as part of an appraisal of UK fallers’
clinics, utilising either published or unpublished sources of data.
This objective was broken down in to series of aims.
1 To identify current models of fallers’ clinics (and hence the
pathway that should be modelled) by conducting a national
survey of existing services.
2 To review the published evidence of effectiveness of various
models of fallers’ clinics, and undertake evidence synthesis to
identify factors that are likely to determine the success of fallers’
clinics, estimate parameters for economic models and identify
areas where information is lacking.
3 To formulate a framework for economic modelling of fallers’ clinics
and to determine from (1) and (2) the feasibility of conducting
economic modelling with current information.
1.3 A definition of a fallers’ clinic
There is no definition of the term fallers’ clinic in the literature. In the
initial phases of the project we developed a broad definition of a
fallers’ clinic: ‘a facility based in either primary or secondary health
care that administers services to individuals with the purpose of
preventing falls, and involves qualified health professionals in the
delivery of some or all of the assessment and intervention’ (based on
the Oxford Medical Dictionary’s definition of a clinic). Our intention
was to review the scope of this definition as the project evolved, and
as we progressed we became aware that the predominant
characteristic of a fallers’ clinic in the UK was that it was an
environment in which health professionals undertook multi-factorial
fall risk assessment, followed by some form of linked intervention.
This was consistent with the NICE guideline.
1.4 Overview of methods
In formulating our methods, we considered fallers’ clinics as complex
interventions that would potentially comprise a number of variables
affecting clinical effectiveness and cost-effectiveness. These variables
include:
• staffing and organisation;
• the population targeted, in particular the baseline risk of falling;
• local organisational issues that might influence participant
selection, for example, whether referrals are from emergency
departments or from primary care alone;
• the screening strategy used to identify participants, and whether
any targeting is used to direct intervention and resource to those
at highest risk of injury or falling;

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 11
• treatments provided: interventions may be low intensity (e.g.
group or home exercise programmes, advice- and knowledge-
based activities) or high intensity (e.g. tailored exercise
supervised individually by a health professional, home visits,
substantial home modifications, cardiac pacing, cataract surgery).
Our aim was to design a survey to capture the breadth of these
variations in service provision, and to determine the extent to which
we could identify a typical service configuration. It was intended that
this typical configuration (which we term a pathway) would inform the
basic structure of any economic model, and indicate key variables that
should be considered.
The next step of the project was to identify what evidence is available
to parameterise each significant variable on the pathway, including an
assessment of the quality of that evidence and its relevance for the UK
NHS. A priori, we intended that this quality appraisal would encompass
a systematic review of the effectiveness of multi-factorial
interventions, screening tools and cost estimates. In addition to
utilising usual methods for synthesising effectiveness of interventions,
we intended to extract detailed information on the interventions that
have been tested in published trials. This would enable us to judge the
extent to which parameters derived from the published literature could
be used to inform a robust model of the cost-effectiveness of fallers’
clinics. We intended to model the effectiveness of clinics, in
comparison with normal care, which we assumed to consist of
responsive treatment to clinical events associated with a fall. These
would include, but not be limited to, the probability of falls, probability
of fall-related injury; costs and impact on physical activity and quality
of life associated with each fall-related event; effect of prevention
clinic on various event rates including additional service utilisation and
the cost of fall-prevention interventions delivered. We anticipated
exploring the impact of clinic skill mix and characteristics of population
within the economic model.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 12
Section 2 National survey of fallers’ clinics and services
2.1 Introduction
The aim of the survey was to map the current organisational structure
and process of falls clinics/units in the UK that provide falls
assessment and or intervention. The rationale was to use the
frequency of various structures and functions estimated from the
survey to identify the most commonly occurring service-delivery
model in the UK. The profile of the model could then be compared with
interventions of known effectiveness to assess the extent to which
current practice replicates evidence-based models (see below), and to
determine the extent to which the evidence base could provide robust
estimates to model commonly used service-delivery models.
2.2 Methods
2.2.1 Methodology
A nationally representative telephone-based survey was conducted. All
reported falls services were contacted by telephone. The nature of the
study was explained and services were asked to participate in the
survey. Telephone interviews were chosen as they allow clarification of
detail more readily, particularly where organisational structures cannot
be anticipated, and help to ensure complete data capture.
2.2.2 Sampling
We sampled all fallers’ clinics in the UK. From experience, we
anticipated that the clinics may be nested in various different
organisations and as no directory of services is available, would be
difficult to locate. We utilised a number of different strategies to
ensure we had, as far as possible, complete sampling. Our aim was to
map the provisions of publicly funded fallers’ services within each
Primary Care Trust or health board including those provided by social
services. Therefore, as the first stage of sampling a letter explaining
the survey of practice and a contact form requesting contact details
for clinics were sent to the lead clinicians/managers/directors of all
UK:
• Primary Care Trusts,
• physiotherapy departments,
• gerontology (or equivalent) departments,
• emergency departments,
• social services.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 13
We supplemented this with a number of additional information
sources. The recently completed Department of Health/British
Association of Emergency Medicine-funded survey of emergency
department services in the UK was able to identify all emergency
departments that were providing fallers’ services. A request for
contact details of clinics/units was also posted on the following
websites:
• the Interactive Chartered Society of Physiotherapy website,
www.interactivecsp.org.uk;
• the Fallers’ Project website, www.warwick.ac.uk/go/fallers.
2.2.3 Data capture
We used a standardized template for data capture in the survey of
fallers’ clinics in the UK. This template was based on a taxonomy of
fall-prevention interventions developed by the Prevention of Falls
Network Europe (ProFANE). Full details are available at
www2warwick.ac.uk/fac/med/research/hsri/emergencycare/research/f
alls_clinics_project/taxonomy/. A taxonomy is a classification system
that identifies characteristics of a system or group of systems that can
be measured objectively, and are meaningful in terms of
distinguishing important differences between systems. The ProFANE
taxonomy was developed by international practice and academic
experts in fall prevention and is designed to improve the reporting and
design of fall-prevention interventions. It identifies the various
components of a fall-prevention intervention, and provides a uniform
method of coding and describing variables. It has been used
successfully in a number of meta-analytic projects where details of
interventions have been extracted retrospectively. This was its first
application in a prospective study.
In brief, components of the ProFANE data-extraction tool are:
• approach used by the clinic [its aims, selection and exclusion
criteria (screening tools) and referral routes];
• base and characteristics (site, geographical location, responsible
organisation, size and clinical lead);
• assessments undertaken to determine treatment plan and who
performs the assessment;
• interventions used, including the type, frequency, who provides
the treatment (single/multiple/multi-factorial, exercise,
medication, surgery, psychological, environmental, social
environment, knowledge, group-based interventions, method of
follow-up/promoting adherence).
We collected a number of additional items not included in the
taxonomy. These were the organisation overseeing the clinics’
activities, the relationship with other service providers, referral routes
into the clinic and onward, relationships with other local amenities and
services, and information about process, financial and outcome data

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 14
that might be collected routinely. NHS Trust reports were used to
estimate the base population of services: the ethnic and age mix of
the local population, the sociodemographic index and whether the
clinic was based in a rural, urban or mixed area. A full list of all
variables collected is given in Table 1.
Table 1 Variables collected in the survey of 231 UK fallers’ services
Category Item
Demographics The name of the service
The name of the NHS Trust/Primary Care Trust
Number of new attendances per year
Population size of the catchments area
Location of the service
Aims Primary aims of the service
Referrals/ eligibility
Who refers to the service
Where referrals are taken from
Eligibility criteria for referral
Eligibility criteria for attendance
Who undertakes eligibility screening
Eligibility screening tools used
Client group(s) excluded
Age range of attendees
Gender of attendees
Who undertakes the eligibility screening
Assessment Geriatric assessment
Medication assessment
Gait, balance and/or mobility assessment
Environment assessment (housing, personal mobility, personal care and protection, aids for communication)
Cardiovascular
Vision and hearing
Surgery
Urinary incontinence
Dietary
Foot
Other
Psychosocial
Functional
Psychological
Who undertakes the assessments and interventions
Assessment tools used
Intervention Geriatric assessment
Medication assessment
Gait and balance assessment
Environment assessment (housing, personal mobility, personal care and protection, aids for communication)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 15
Cardiovascular
Vision and hearing
Surgery
Urinary incontinence
Dietary
Foot
Other
Psychosocial
Functional
Psychological
Who undertakes the interventions
What resources they use
Follow-up of any interventions
What onward referrals are made and by whom
Economic How many FTE/WTE staff members work in the service and their grade
How patients are transported to the service
The eligibility for transport
Whether patients are provided with written, audio or video material
Floor area of the service? (m2/ft2)
Total overall budget
Drug budget
Equipment budget
Consumables budget
Provision of lunch
FTE/WTE, full-time equivalent/whole-time equivalent.
2.2.4 Analysis
The data were collated and analysed using the SPSS statistical
software package. The majority of the analysis is based on frequency
counts. We compared service profiles across three settings: acute
care, community settings and emergency departments by analysis of
descriptive data supplemented by a Chi-squared (χ2) test. Data from
these tests are presented only where statistically significant
differences were observed. Missing data were minimal (<30% for the
worst-case variable), and occurred only in the more detailed aspects
of the survey. Most often, missing data were attributable to the
member of staff we interviewed not being full aware of all aspects of
the service. Where data were missing we dealt with it in the most
conservative manner, by making the assumption that if the
respondent did not know, or did not report the variable in response to
questioning, the service was coded as not providing that service.
Overall, as missing data were on average less than 5% our results are
not likely to be significantly biased in this respect.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 16
2.2.5 Ethical approval
Due to recent changes in the UK Central Research Ethics Code of
Practice (COREC), ethical approval is no longer required for service-
evaluation projects. COREC confirmed that ethics approval was not
required for this study.
2.3 Results
2.3.1 Sample
We mailed a total of 2744 introduction letters and forms requesting
contact details of falls-prevention services and key personnel, between
1 June and 31 July 2006. A second letter and request form was sent to
non-responders after 6 weeks. Returns reporting falls-prevention
services were received from 597 respondents (shown in Table 2). The
clinics/units that responded were from every region across the UK.
The majority of returns were derived through the mail shot
(n=453/597, 75.8%), but additional returns were identified from the
Interactive Chartered Society of Physiotherapy website, and through
our own Fallers’ Project website (n=144/597, 24.1%).
Table 2 The number of returns and the total number of units of service
provision identified and surveyed
Returns Number
Total returns
postal
electronic
597
453
144
Ineligible
duplicates
from countries outside the UK
no clinic
services had closed in the preceding 18 months
undergoing re-organisation, due to open in 2007
not publicly funded
245
7
27
8
6
1
Eligible
declined to take part in the survey
3 were currently undertaking a research audit
2 do not participate in surveys
classed as non-responders after multiple contacts
303
3
2
67
Total available for analysis 231
Of the 303 services identified, 231 (76%) agreed to participate in the
survey. Three units declined as they were already taking part in a
research audit, and two had a policy not to participate in surveys.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 17
2.3.2 Site of the clinic
The majority of services were located in an urban area (n=142/231,
61.5%). Rural services were much less frequent (n=48/231, 20.8%)
and mixed rural/urban services were reported by 41/231 (17.7%).
The name of units varied widely across the sites; most units included
mention of falls or fallers in their title, with only nine (25.7%) services
not mentioning falls or fallers in their title. Not all services called
themselves a clinic.
The site of the service was defined as the place in which the first
contact occurred with the service unit. The most common base was a
hospital (n=222/231, 96%), with a near-equal division between
community and acute hospitals (Table 3).
Table 3 Point of contact with falls-prevention team (all categories)
Point of contact with falls prevention team Number (%)
Community hospital 107 (46.3%)
Primary care 2 (0.9%)
Community based (social services) 1 (0.4%)
Community based (other) 6 (2.6%)
Acute hospital 105 (45.5%)
Acute hospital (emergency department) 5 (2.2%)
Intermediate care hospital 5 (2.2%)
Total 231
Primary care-based services were surprisingly infrequent, as were
services based in emergency departments. To simplify further data
presentation, the categories of service-unit providers were collapsed
into three main categories and the remainder of the analysis are
based on these (Table 4):
1 community (the majority of which were community hospitals),
2 acute (including intermediate care facilities),
3 emergency department.
Table 4 Summary of point of contact with falls-prevention teams
collapsed into three categories (acute, community and emergency
departments)
Point of contact with falls-prevention team Number (%)
Community (community hospital, primary care, social services, other)
116 (50.2%)
Acute (including intermediate care) 110 (47.6%)
Emergency department 5 (2.2%)
Total 231

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 18
Emergency DepartmentCommunity Acute
80
60
40
20
0
Count
0
26
15
0
31
17
5
59
78
Urban and Rural
Rural
Urban
LocArea
Figure 1 First point of contact with the falls-prevention service by
location (n=231)
The first points of contact with the falls-prevention service are broken
down by type of location in Figure 1.
2.3.3 Aims of the service
The most commonly cited primary aims for falls-prevention services
were reducing falls (n=127/231, 55.0%), reducing health and social
care resource use (n=58/231, 25.1%). Only 19.5% of clinics reported
reducing injuries to be part of their aim (Table 5).
Table 5 Primary aims of the falls-prevention service
Aim Percentage (n)
To reduce falls 55.0 (n=127/231)
To reduce heath and social care use including hospitalisation
25.1 (n=58/231)
To reduce fall-related injuries including fractures 19.5 (n=45/231)
To improve quality of life 12.6 (n=29/231)
To increase physical activity 7.8 (n=18/231)
To reduce fear of falling 10.0 (n=23/231)
To improve function 7.4 (n=17/231)
The total number of primary aims cited exceeds the number of services as some
services cited more than one primary aim.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 19
2.3.4 Referral to the service
The most frequent method of entry into a service was referral from a
health or social care professional (n=143/231, 62%) (see Figure 2).
Some services operated a more open referral system, accepting in
addition to health or social care referral, self-referral (n=73/231,
32%), family referral and referral from nursing homes, voluntary
agencies and care and home support services. Eight of the services
required a referral from or approval by a doctor (n=8/231, 3%). Who
can refer to a falls service is broken down by point of contact in
Figure 3.
Other (nursing homes/voluntary services)
Doctor only
Open
Health and social care professional only
Who can refer to to your unit (collapsed)
140120100806040200
5
8
143
73
Figure 2 Who can refer to the falls service
Emergency DepartmentCommunity Acute
80
60
40
20
0
032
0
44 5
60
78
0
48
25
Other (nursing homes/voluntary services)
Doctor only
Health and social care professional only
Open
ReferWhoCate
__
Figure 3 Who can refer to the falls service by first point of contact

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 20
2.3.5 Eligibility criteria
The majority of clinics (n=212/231, 91.8%) used some form of criteria
to determine entry into the service (inclusion or exclusion). Of those
clinics using eligibility criteria, 183/231 (79.2%) used more than one
criterion (Figure 4).
Multiple criteriaSingle criteriaNo criteria
200
150
100
50
0
Count
183
2118
Figure 4 Services using multiple and single criteria for eligibility to the
service
The most common inclusion criteria were:
• falls, near falls or fear of falling (n=170/231, 73.6%),
• a published or unpublished screening tool (n=141/231, 61%),
• age (n=82/231, 35.5%),
• taking three or more medications (n=58/231, 25.1%).
Only 7.8% (n=18/231) of clinics used no criteria. None of the services
used gender as an eligibility criterion.
Published screening tools were used by 51/231 (22.1%) clinics, and
the remainder of clinics using screening tools used their own tool
(88/231, 38.1%) (Figure 5).

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 21
Own toolNonePublished tool
100
80
60
40
20
0
Count
51
8886
Figure 5 Utilisation of published screening tools
The most commonly reported published screening tool was the Falls
Risk Assessment Tool (FRAT), which was reported to be used in 29
clinics (Table 6).
Table 6 Screening tools
Tool Frequency
Fall Risk Assessment Tool (FRAT) (Nandy et al., 2004) 29
Performance-Oriented Mobility Assessment (POMA) (Tinetti 1986) 1
NICE guidelines (National Institute for Clinical Excellence, 2004) 4
Falls Risk Assessment Score for the Elderly (FRASE) (Cannard, 1996)
7
Timed Up and Go (TUAG) test (Podsiallo and Richardson, 1991) 4
BERG balance test (Berg et al., 1992) 4
Confidence balance (CONFbal) (Simpson et al., 1998) 3
Fear of Falling Scale (FFS) (Wolpe and Lang, 1964) 1
Mini Mental Score (Folstein et al., 1975) 3
MORSE scale (Morse et al., 1989b) 1
Survey of Activities and Fear of Falling in the Elderly (SAFFE) (Lachman et al., 1998)
1
Other 3
The total number of published screening tools exceeds the number used as some
services utilised more than one published tool.
2.3.6 Age
The age range for clients attending the service was wide, from 16 to
105 years. The majority of services were limited to clients over

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 22
60 years (n=145/231, 62.8%) but over one-third of services could be
attended by people aged 15 or over (n=82/231, 35.5%).
2.3.7 Attendances
The number of new attendances per year was reported by 142/231
services (61.5%) (see Figure 6). Two services were unable to report
attendance statistics for the year as they had only opened recently.
The median number of new attendances per year was 180 (range 10–
1700).
2000150010005000
Attend
50
40
30
20
10
0
Frequency
Mean =265.426Std. Dev. =283.3856
N =142
Figure 6 Reported attendance at falls clinics able to provide this
information
2.3.8 Staffing
The predominant staffing structure comprised a multi-disciplinary
team (n=212/231, 91.8%). The remaining services were
uni-disciplinary (n=18/231, 7.8%).
There was considerable diversity in team structure. Disciplines
mentioned included doctor, nurse, occupational therapist,
physiotherapist, postural instructor, technical instructor, rehabilitation
and physiotherapy assistants, exercise instructor, clinical exercise
specialist, generic technician, podiatrist, falls co-ordinator, pharmacist,
psychologist, social worker, speech and language therapists, dietician,
local government officer, advisor, handy person, falls-prevention
advisor (age concern) and health visitor.
Physiotherapists were the most frequently mentioned member of staff,
followed by nurse, occupational therapist and doctor. Of the 212
multi-disciplinary teams 187/212 (88.2%) included a physiotherapist,
163/212 (76.9%) included a nurse, 162/212 (76.4%) included an
occupational therapist and 123/212 (58%) included a doctor.
All four disciplines (physiotherapist, nurse, occupational therapist and
doctor) were found to comprise 70/231 (30.3%) of teams. Teams

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 23
were more likely to have this configuration if they were based in an
acute-sector hospital (Figure 7).
Figure 7 Skills mix by setting
2.3.9 Assessment
Multi-factorial assessment was undertaken by 228/231 (98.7%) of
services. The components of the assessment varied across services.
The most common assessments were gait and balance (n=210/231,
90.9%), environment (n=176/231, 76.2%), medication review
(n=167/231, 72.3%), cardiovascular (n=160/231, 69.3%), vision
(n=135/231, 58.4%), cognitive function (n=124/231, 53.6%), foot
(n=123/231, 53.2%), nutrition (n=118/231, 51.1%), bone health
(n=107/231, 46.3%) and hearing (n=80/231, 34.6%).
Gait and balance assessment
The majority of services undertook a gait and balance assessment
(n=210/231, 90.9%). There were a wide variety of measures used
(Table 7). However, many measures failed to meet the criteria for the
definition of a gait and balance test as they were not observed tests of
performance of function, gait analysis, balance and/or strength (Lamb
et al., 2005).
Emergency Department
Community Acute
100
80
60
40
20
0
Count
5
90
65
0
26
44
Other skill mix
All four disciplines
Skill Mix

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 24
Table 7 Gait and balance assessment tools
Assessment tools
180° Turn Elderly Mobility Score
Outside Mobility
1-leg stand Morse fall scale
BERG balance test Posture
Exercise tolerance Physiological Profile Approach
Flexibility Romberg
Falls Risk Assessment Score for the Elderly (FRASE)
Strength
Falls Risk Assessment Tool (FRAT) Tandem Stand
Functional reach Tinetti
Gait analysis Timed walk
3-metre
10-metre
Guide to Action Transfers
Hip fracture scale Timed Up and Go test (TUG test)
Internal and external shoulder rotation Timed Unsupported Stand (TUS)
Environment assessment
An environment assessment is designed to determine hazards in a
person’s home environment including inside and outside the home,
aids for personal mobility and communication and signalling, and for
personal care and protection (Lamb et al., 2005). The majority of
services undertake this assessment (n=176/231, 76.2%).
Foot assessment
A foot assessment was undertaken by 123/231 services (53.2%).
Vision assessment
The majority of services undertook an assessment of the patient’s
vision (n=135/231, 58.8%) either informally by asking clients whether
they were having difficulty seeing or when they last had their eyes
examined, or formally using an assessment tool. Of services that
utilised an assessment tool the most commonly used was the Snellen
chart (n=29/231, 12.6%).
Medication assessment
An assessment of the client’s medication was undertaken by 167/231
services (72.3%).

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 25
Cardiovascular assessment
A cardiovascular assessment was undertaken at 160/231 services
(69.3%). Components of the assessment mentioned by the services
are listed in Table 8.
Table 8 Cardiovascular procedures
Cardiovascular assessment
Blood pressure
lying and standing
lying and sitting
24-hour monitoring
ambulatory assessment
Electrocardiogram
Echocardiogram
Tilt table testing
Sinus carotid massage
Listen to heart
24-tape
Incontinence assessment
Incontinence was assessed by 124/231 services (53.7%).
Cognitive and mental health assessment
Cognition was assessed by 124/231 services (53.5%). Commonly
used tools are shown in Table 9.
Table 9 Tests used to measure cognition and mental health
Assessment Number (%)
Cognitive
mini-mental
Mini Mental State Examination (MMSE)
Abbreviated mental test (AMT) score
Geriatric Depression Scale
Middlesex Elderly Assessment of Mental State (MEAMS)
Hospital Anxiety and Depression Scale (HADS)
124/231 (53.6%)
Comprehensive geriatric assessment
A total of 120/231 services (51.9%) reported undertaking an
assessment which was consistent with the definition of a
comprehensive geriatric assessment.
Nutrition
Over half the clinics assessed nutritional status (n=118/231, 51.1%).

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 26
Bone health assessment
Fewer than half of the units reported undertaking an assessment of
bone health (n=107/231, 46.3%).
Hearing assessment
An assessment of the patients’ hearing was undertaken by 80/231
services (34.6%). Assessments of hearing were more likely to be
undertaken in the community setting (n=51/80) than in an acute
setting (n=26/80).
Other assessments
Other less commonly used assessments included daily functioning and
fear of falling.
2.3.10 Interventions
Most clinics utilised the traditional formulation of a multi-factorial
intervention; that is, multiple interventions matched to the findings of
the risk assessments undertaken (n=192/231, 83.1%). The most
commonly used intervention components were:
• knowledge: information provision (94% of clinics),
• exercise (89% of clinics),
• medication review (66% of clinics).
Knowledge: information and/or educational provision
Almost all services (n=215/231, 93.2%) provided information to
clients. The most common format was written, and some clinics
provided information in more than one format (Table 10). The topics
most commonly addressed were exercise, alcohol, benefits and
services available, bone health, continence, diet, environmental
hazards, foot care, getting up off the floor, medication and vision care.
This was in addition to published materials by the Department of
Health and voluntary organisations such as Age Concern (Table 11).
Table 10 Information format
Information Number (%)
No information provided 13/231 (5.6%)
Written information provided 215/231 (93.2%)
Video information provided 26/231 (11.3%)
Audio information provided 22/231 (9.6%)
The total number of types of information provided exceeds the number of
services as some services issued information in more than one format.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 27
Table 11 Topics for information leaflets
Written information leaflets
Staying steady
General health care
Osteoporosis
Benefits available
Avoiding slips, trips and broken hips
Safety in the home
Message in a bottle
Lighting in the home; changing lights bulbs, etc.
Some services also ran a formal educational programme (n=112/231,
48.5%). Typically sessions are run parallel to an exercise intervention
and cover the following topics:
• environmental hazards, home safety,
• lighting,
• flooring,
• vision, eye care,
• footwear, foot care,
• general health,
• continence,
• alcohol,
• medication,
• nutrition.
The most common format for formal educational interventions were
talks (n=109/231, 47.1%), given either by members of the team or
by invited external speakers such as a pharmacist or podiatrist. Other
speakers included representatives of Help the Aged and Age Concern.
A video was used by 3/231 services (1.3%).
Exercise intervention
Use of an exercise intervention was reported by 188/231 services
(81.4%). The majority of exercise programmes were undertaken at
the service location with some undertaken either at home and/or in
the community (note that the total number of exercise venues
exceeds 100% as some services offer more than one type of exercise
programme):
• supervised in the service location (n=182/231, 78.8%),
• in the client’s home (n=104/231, 45%),
• based in the community (n=48/231, 38.4%).
Exercise provision was varied, with some services combining
supervised and unsupervised home programmes, or unsupervised
home exercise, and some using a combination of an initial supervised
programme with progression to community-based programmes. The

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 28
mean number of sessions per week was 1 (standard deviation
±0.04 weeks). The length of the programme varied from 2 to 24
weeks with a mean of 8 weeks (standard deviation ±2.96 weeks).
Four services (4/231, 1.7%) did not specify an end point to the
programme as it was dependent on the client’s progress.
Improving gait, balance, co-ordination and function (n=132/231,
57.1%), strength and resistance (n=73/231, 31.6%) and flexibility
(n=45/231, 19.5%) were the three most frequently cited purposes of
the exercise intervention. Others were improving endurance
(n=18/231, 7.8%), general physical activity (n=12/231, 5.2%) and a
practical demonstration of getting up off the floor (n=14/231, 6.0%).
Medication intervention
Following medication review, the majority of services (n=61/231,
26.5%) undertook a direct intervention to alter a prescription by
either modifying or removing medications (Table 12). A smaller
number of services (n=38/231, 16.5%) undertook an indirect
intervention (Table 12), referring patients to their GP (n=32/231,
13.9%), a pharmacist (n=4/231, 1.7%) or consultant (n=2/231,
1.4%) for the prescription modification. Just over 20% of services did
not intervene on medication.
Table 12 Intervention options following medication assessment
Medication intervention Number (%)
No intervention 48/231 (20.8%)
Direct intervention, including
withdrawing medication
reducing medication
substituting medication
provision of medication
advice
61/231 (26.5%)
Indirect intervention, including
doctor recommends changes to GP
pharmacist recommends changes to GP
referral to GP
referral to pharmacist
referral to consultant
38/231 (16.5%)
Bone health intervention
Fifty-five services (55/231, 23.8%) reported using an intervention
following a bone health assessment. Thirty services reported making
direct changes to prescriptions (30/231, 13.0%), including
commencing calcium, vitamin D and bisphosphates. Twenty-five clinics
(n=25/231, 18.5%) referred on to the client’s GP, consultant, or
pharmacist.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 29
Vision intervention
Following vision assessment, the most common management strategy
was onward referral to the optometrist or ophthalmologist (n=63/231,
27.2%), with 10/231 (4.3%) referring clients to their GP and 8/231
(3.5%) undertaking a vision intervention within the clinic. The
remainder did not report an intervention on vision, despite reporting
undertaking assessments in this domain.
Hearing intervention
The majority (n=37/231, 16.0%) of services referred on to an
audiology clinic, day hospital or GP following a hearing assessment.
Only 8/231 (3.5%) services undertook direct intervention (removal of
ear wax).
Environmental, personal mobility, prevention and signalling
interventions
The most commonly reported interventions were modifications to the
internal dwelling (n=80/231, 34.6%). The types of modification
undertaken were provision of bath/hand rails, raised toilets seats,
toilet frames, removal of rugs, cooking aids, lighting and trolleys.
Some services undertook these modifications themselves, with the
remainder referring on to social services, community occupational
therapist or a handy person.
Very few services (n=10/231, 4.3%) dealt with major external
modifications or substantial changes to lighting, flooring or bathrooms,
or with the provision of ramps or external rails. Just over 100 services
(n=102/231, 44.2%) referred these modifications to social services,
community occupational therapists or the Handy Man service. The
remainder made no intervention on the external dwelling.
Surprisingly, only a minority of services reported dealing with aids for
personal mobility. Interventions reported were prescription of walking
aids and provision of wheelchairs (n=77/231, 33.3%). Referral was
used where large aids such as electric wheelchairs were indicated
(n=67/231, 29%).
Only a minority of clinics reported intervening in the area of
protection. Interventions under this category were hip protectors
and/or safe footwear. Only a minority of services provided hip
protectors or safe footwear (n=39/231, 16.9%), with 67/231 services
(29%) either referring the client onwards or providing advice and
recommendations about hip protectors or safe footwear.
Only a minority of services reported addressing the need for signalling
devices. Twenty-five services (25/231, 10.8%) provided signalling
devices, and 72/231 (31.2%) either referred on or provided advice
about signalling devices. Onward referral was usually to home care
managers for community alarms. The information leaflets provided
were for LifeLine or CareLine.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 30
Incontinence intervention
The majority of services made an onward referral following an
incontinence assessment (n=74/231, 32.0%). The remaining either
undertook an intervention (n=15/231, 6.5%), including pelvic floor
exercises, the provision of incontinence items such as urinary bottles
and pads, and treatment of urinary-tract infections, or some other
treatment (n=11/231, 7.6%) (Table 13).
Table 13 Referral/intervention options following incontinence
assessment
Referral/intervention options
Refer to disciplines
urology (retention, spasms)
Interventions
medicate, antibiotics for urinary-tract infections
provide bottles
pads
incontinence pack
physiotherapy, exercises
Investigations
bladder scanner
MSU
Refer to health professionals
district nurse
GP
incontinence specialist team/nurse
occupational therapist
MSU, mid-stream urine specimen.
Surgery intervention
Surgical interventions included treatment for cataracts, pacemakers
and urinary-tract surgery. The majority of services made an onward
referral (n=62/231, 26.9%), either directly (n=47/231, 20.2%) or via
the client’s GP (n=15/231, 6.5%). Podiatry was offered by 20/231
(8.7%) of clinics, with some services referring on (n=48/231, 20.3%).

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 31
Other interventions
Other interventions mentioned by the services sampled are listed in
Table 14.
Table 14 Other interventions
Item Number (%)
Practices (getting up off, travelling on the bus ) 14/231 (6.0%)
Outside walking 9/231 (3.9%)
Falls workbook 4/231 (1.7%)
Risky movements (carrying objects, etc.) 3/231 (1.3%
Peer mentors 1/231 (0.4%)
2.3.11 Post-intervention follow-up
Follow-up was undertaken by 118/231 services (51.1%). The
approach taken by the majority of services (75/231, 75%) was face-
to-face follow-up, either bringing clients back to the service or visiting
them at home. One service used written follow-up (1/231, 0.4%),
28/231 (12.1%) followed-up clients by telephone and the remainder
9/231 (3.9%) varied their approach, using either telephone or face-to-
face depending on the client. The length of the follow-up period varied
across services from 2 to 52 weeks; the mean number of weeks
follow-up was 21 (standard deviation ±16.9 weeks). The minimum
number of follow-up sessions was one and the maximum four. For
those providing follow-up, the usual mode of provision was one
session (56/231, 24.2%).
2.3.12 Cost of services and economic data available
Cost data are provided in Appendix 1. The average cost of providing
services in the acute sector was estimated to be £171,340 per annum
(p.a.) based on 79 services reporting these data. The average cost of
community services was £109,691 p.a. based on 78 services. The
average cost of emergency-based services was £175,430 p.a. based
on four services. The estimated grand total cost of fallers’ clinics is
£32,448,847 p.a.
2.4 Summary
The main components of a fallers’ clinic provided in the UK can be
described from this survey. The most common patient pathway is:
• access to the service is via referral from a health or social care
professional;
• a falls clinic based in a community or secondary care hospital;
there are likely to be some differences in costs between these two
environments;

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 32
• most services utilise eligibility criteria; the most common criteria
are previous falls and/or a published or unpublished screening
instrument;
• the most frequently used screening instrument is the FRAT;
• all clients undergo multiple assessments;
• these assessments will be undertaken predominantly in the
service setting;
• Allied Health Professionals are the most commonly cited members
of the falls-prevention team; about half of the services utilise a
physician;
• the assessments used vary substantially between services, in
terms of number, combination and type.
• nearly all use an assessment of gait and balance, although the
quality of the assessments used is questionable; thereafter,
common assessments are environment, medication review,
cardiovascular and vision;
• assessments of bone health are surprisingly few, suggesting a
poor link-up to bone health services;
• interventions are most likely to be multiple, and the most
commonly reported combination of treatments is knowledge-
based interventions, exercise and medication review;
• the number of exercise sessions offered is low;
• onward referral is used in a number of models;
• follow-up is implemented by approximately 50% of services;
• routine data collection is poor.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 33
Section 3 Estimates of the effectiveness of fallers’ clinics
3.1 Introduction
There are some good-quality reviews of the effectiveness of fall-
prevention interventions available (e.g. Gillespie et al., 2003; Chang
et al., 2004), but none evaluates fallers’ clinics per se. All needed to
be updated to include recent evidence. There were a number of new
trials that needed to be considered. Our objectives were as follows.
1 To update the evidence relating to fallers’ clinics.
2 To determine whether any interventions currently included in the
review are similar to existing models of fallers’ clinics, and
whether they could provide robust estimates for economic
modelling. This involved an appraisal of intervention content that
was undertaken using the taxonomy tool, allowing us to link the
results of the survey and review more closely.
3 To conduct stratified meta-analyses to give estimates of
interventions’ effectiveness in different groups of patients
targeted by existing settings of fallers’ clinics, screening strategy
(low versus high risk) and intensity of intervention (characterised
by whether or not a medical doctor was included in the team).
4 Outcome measures were extended beyond current reviews to
consider fall-related injury, medical care and death, institutional
care and health-related quality of life.
5 To identify areas where there is insufficient information on
important outcomes.
3.2 Eligibility criteria
3.2.1 Types of study
Randomised controlled trials (RCTs; both individually and cluster-
randomised) and quasi-randomised studies were included.
Non-randomised studies such as cohort studies were excluded because
of their increased risk of bias.
3.2.2 Population
The population covered was older people (using any definition) living
in the community, not in nursing homes or hospitals. Studies of
particular patient groups (e.g. people who have had a stroke) were
included.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 34
3.2.3 Types of intervention
Studies were included if they evaluated an intervention fulfilling the
definition of a fallers’ clinic compared with a control treatment (most
often usual care) or compared with another intervention.
There is no definition of the term fallers’ clinic in the literature. In the
initial phases of the project we developed a broad definition of a
fallers’ clinic: ‘A facility based in either primary or secondary health
care that administers health services to individuals with the purpose of
preventing falls, and involves qualified health professionals in the
delivery of some or all of the assessment and intervention’ (based on
the Oxford Medical Dictionary definition of a clinic). Our intention was
to review the scope of this definition as the project evolved. For this
systematic review we included studies of interventions that fulfilled the
following criteria:
1 multi-factorial falls risk assessment; that is, assessment of more
than one risk factor for falling, undertaken with a view to either
predicting the likelihood of falling and/or identifying potentially
modifiable risk factors;
2 interventions to reduce the risk of falls are provided or arranged
by the clinic;
3 intervention is delivered to individuals, not at community or
population level;
4 comparator was either usual care or a control intervention (as
opposed to a second experimental treatment).
Studies were included regardless of whether the risk assessment and
delivery of interventions was undertaken in peoples’ homes or in a
central clinic.
3.2.4 Outcomes
Studies were included if they reported quantitative data on one or
more of the following outcomes:
• number of fallers or falls;
• recurrent falls (two or more falls in a 12-month period);
• fall-related injury:
• peripheral fractures;
• soft-tissue injuries (as defined by individual studies).
In addition, the following secondary outcomes were recorded:
• hospitalisation;
• unscheduled health service contacts;
• death;
• move to institutional care;
• health-related quality of life;
• physical activity/mobility.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 35
Studies were not included if they did not provide any data on any of
the falls outcomes, or they reported only surrogate outcomes such as
balance or strength.
3.3 Search strategy for eligible studies
Multiple search strategies were used to locate eligible studies for the
review.
3.3.1 Cochrane review
All studies located by the Cochrane review of Interventions for
preventing falls in elderly people (as published in The Cochrane
Library, Issue 3, 2006, last updated July 2003; Gillespie et al., 2003)
were considered for inclusion in this review. We considered all studies
included, excluded, ongoing and awaiting assessment.
3.3.2 Update of the Cochrane review’s searches to
2003–2006
We repeated the search strategy used by the Cochrane review,
covering the years 2003–2006, including seven electronic databases
(CENTRAL, MEDLINE, EMBASE, CINAHL, National Research Register,
PsycINFO, Social Sciences Citation Index). The search strategy was
used as published in the Cochrane review for MEDLINE, EMBASE and
CINAHL, with the correction of one typographic error. It was
translated into the correct syntax for PsycINFO, Social Sciences
Citation Index and CENTRAL.
The Cochrane review also searched the Cochrane Bone, Joint and
Muscle Trauma Group’s register, but this is not a publicly available
resource so it was not possible to repeat this search. All of the entries
in this database are ultimately transferred to CENTRAL, but the
group’s register is more up to date. Its omission therefore may
exclude some recent studies that are not indexed in other databases.
3.3.3 Specific search for studies of falls clinics
A specific search for studies of falls clinics was conducted in MEDLINE
and EMBASE, to determine whether searching using additional terms
specifically describing falls clinics would locate any additional studies
(see Appendix 2).
3.4 Review methods
The results of the searches were assessed by two authors of this
study, and potentially eligible papers were obtained as full reports.
These were evaluated further against the eligibility criteria, and
decisions were made about inclusion of each study. Disagreements
were referred to a third author and resolved by discussion.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 36
We extracted data from each included study onto a form designed for
this review. This included characteristics of the study, quality
assessment and outcome data. Characteristics of the interventions
were extracted using the ProFANE taxonomy for studies of fall
prevention. Quality assessment used the tool used in the Cochrane
review, with the addition of two questions specifically about cluster-
randomised trials (Appendix 3).
We used random-effects analysis for statistical combination of the
results of studies, because there was substantial heterogeneity
between studies in their populations, the interventions they evaluated,
the definitions of the outcomes used and the duration of follow-up. We
measured statistical heterogeneity in all analyses using the I2 statistic.
For studies that followed up participants for more than 12 months, we
used data collected at 12 months if they were available. For studies
with less than 12 months of follow-up, we used the longest duration
reported. We performed three subgroup analyses, stratifying by:
1 hospital-based versus primary care-/community-based;
2 high-risk population versus unselected population;
3 falls clinic team including a doctor versus not including a doctor.
For the third subgroup analysis, studies were classified as including a
doctor if a doctor was involved performing assessments or delivering
interventions that were provided by the clinic. Interventions were
classified as not including a doctor if treatments recommended as a
result of assessments were delivered by the participant’s GP or other
doctors not involved in the clinic. We performed interaction tests as
described by Deeks (2001) to investigate whether there was evidence
of differences in treatment effects between the subgroups. We did not
calculate interaction test statistics when one of the subgroups
contained only one or no trials.
Cluster-randomised trials were included in the analyses along with
individually randomised trials. To do this, the number of outcomes and
the denominator were adjusted to account for clustering by dividing by
the design effect. If the reports of the cluster-randomised trials gave
an estimate of the intracluster correlation coefficient (ICC), this was
used to calculate the design effect. If not, we used a value of 0.01 for
the ICC to include these studies in the figures, and we performed
sensitivity analyses assuming a range of ICC values from 0.001 to 0.1
to assess their effect on the results.
3.5 Included and excluded studies
The updated electronic search covering 2003–2006 retrieved 1087
records. Two hundred and nine studies from the Cochrane review were
considered for inclusion; however, seven studies listed as ongoing in
this review could not be located and were therefore not considered.
The specific searches for falls clinic studies retrieved 142 and 217
studies from MEDLINE and EMBASE respectively. No additional eligible

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 37
studies were retrieved from the searches; therefore, we did not
extend the searches to other databases.
After screening of the titles and abstracts, 43 full papers were
obtained and considered in detail for eligibility. Of these, 18 were
comparisons of eligible interventions with a control group or usual
care, and hence were included. Twenty-five were excluded. Reasons
for exclusion are given in Appendix 4.
Characteristics of the 18 included studies are summarised in Table 15.
Fifteen studies randomised participants to receive some form of multi-
factorial risk assessment followed by individualised interventions
based on its findings, compared with usual care, which involved no
specific falls risk assessment or intervention. Three studies made a
slightly different comparison (Tinetti et al., 1994; Shaw et al., 2003;
Lord et al., 2005); they performed multi-factorial risk assessment on
all participants, who were then randomised either to receive
interventions to address the risk factors discovered by the
assessment, or to receive no interventions. Hence in these three
studies the control group received the assessments. These three
studies are included in analyses with the other studies because it was
considered unlikely that assessment alone would have an appreciable
effect on outcomes such as falls.
Two studies were cluster-randomised (Tinetti et al., 1994; Coleman et
al., 1999). One used physicians as the unit of randomisation (Tinetti)
and included 16 clusters with an average size of 18.8 participants.
Coleman et al. (1999) used the physician practice as the unit of
randomisation and included nine clusters with the same average size,
18.8 participants. The design effect assumed for presentation of these
studies in the figures (using an ICC of 0.01) was therefore 1.18. The
other 16 studies were individually randomised.
Two studies (Wagner et al., 1994, Coleman et al., 1999) did not
provide information on the number of participants included in
analyses, giving only the percentage with each outcome. For inclusion
in analyses we have assumed that there were no missing data and the
denominator is the number randomised. It is likely that there were in
fact some missing data in these studies and that the denominators we
have used are slightly too large. We contacted the first author of each
study to request the denominator data but did not receive any replies.
The characteristics of the interventions used in the included studies
are summarised using the ProFANE taxonomy in Tables 16 and 17.
3.6 Methodological quality of included studies
The methodology of the studies and the results of the quality
assessment are summarised in Table 18.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 38
3.6.1 Randomisation
Only five of the 16 individually randomised studies reported methods
of random allocation that had secure allocation concealment, and one
of these stated that allocations were concealed but did not describe
how. The other 11 studies did not report adequate information to
allow assessment of their randomisation methods. No studies reported
quasi-random allocation or any other methods that were clearly
inadequate.
3.6.2 Blinding
Blinding of participants and personnel delivering the interventions was
generally not possible in these trials. One study (van Haastregt et al.,
2000) achieved partial blinding of care providers by ensuring that
doctors were not aware of patients’ allocations; however, the nurses
who provided the intervention were not blinded.
Several trials used partial blinding of outcome assessment by ensuring
that personnel who were reviewing outcomes or interviewing
participants were not aware of allocations (i.e. investigator blinded).
3.6.3 Losses and exclusions
The proportion of randomised participants excluded from analyses
varied widely between trials. In five studies, losses and exclusions by
the end of follow-up were more than 20%. Principles of intention to
treat (i.e. that all participants are included in the analysis, and that
participants are analysed in the groups to which they were
randomised) were adhered to poorly in a number of studies. For
example, Hogan et al. (2001) excluded participants who did not
adhere to the protocol or were admitted to institutional care, and
Close et al. (1999) omitted those who did not complete the 12-month
follow-up. Where possible, we have restored participants
inappropriately excluded.
3.6.4 Follow-up
Follow-up duration was very variable, ranging from 2 months (Huang
and Acton, 2004) to 3 years (Jitapunkul, 1998). Thirteen studies
reported outcomes for a 12-month follow-up period, and three of
these studies performed a longer follow-up. Three studies presented
data for 6-month follow-up only (Gallagher and Brunt, 1996;
Lightbody et al., 2002; Whitehead et al., 2003), Huang and Acton
(2004) only for 2-month follow-up and Jitapunkul (1998) for 3-year
follow-up only. The variation in follow-up duration is likely to introduce
heterogeneity to the results. One study (Fabacher et al., 1994) used
different methods for follow-up of the two trial arms; for the
intervention group follow-up data were collected at a home visit, but
the control group were interviewed by telephone. This has the
potential to produce spurious differences between the groups.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 39
3.6.5 Recording of falls outcomes
Eleven studies used reliable methods to collect information on falls;
most used a diary or calendar to be returned at predefined intervals,
plus telephone contact if a calendar was not returned or if a fall was
reported. Three studies recorded falls only at intervals during
follow-up, and four studies collected falls data only at the end of the
follow-up period. These are likely to be significantly less accurate
methods.
3.6.6 Cluster-randomised trials
Of the two cluster-randomised trials included in the review, one
(Coleman et al., 1999) reported the use of adequate analytical
methods to take clustering into account but the other (Tinetti et al.,
1994) did not.
Overall, the mean quality score for studies was 21.3 out of a possible
maximum of 33, ranging from 16 to 26 (data shown in Table 18).
3.7 Results
The results of meta-analyses are summarised as forest plots (Figures
8–11), and statistics for interaction tests for the subgroup analyses
are given in Table 19.
3.7.1 Falls
Data on the number of fallers or the number of falls were available
from 18 studies. One study (Gallagher and Brunt, 1996) gave only the
mean number of falls in each group (intervention 1.7 compared with
control 2.1) but no standard deviations, and hence this study could
not be included in any meta-analysis.
Seventeen studies reported the number of people in each group who
experienced one or more falls. The overall analysis of the number of
fallers suggests a small reduction in the intervention group [relative
risk (RR) 0.9, 95% confidence interval (CI) 0.8–1.0], but there is
considerable heterogeneity between the studies (I2=59.5%). None of
the stratified analyses showed a statistically significant difference in
effect between the subgroups; there is therefore no evidence that the
location of the clinic, whether or not the population has risk factors for
falls or whether or not the team includes a doctor have any effect on
the number of participants that will fall.
We intended to include analysis of the fall rate (i.e. number of falls per
unit time of follow-up), but this was not possible for two reasons.
First, only two studies provided accurate data on the overall duration
of follow-up for each group. Second, the results were extremely
heterogeneous and statistical combination of them would not be
meaningful. These data were therefore omitted.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 40
3.7.2 Recurrent falls
Four studies reported recurrent falls. Close et al. (1999) and Hogan et
al. (2001) reported the number of participants who reported three or
more falls, whereas Lord et al. (2005) and van Haastregt et al. (2000)
reported those who had two or more falls. The overall analysis
suggested a reduction in recurrent falls in the intervention group
(RR 0.76, 95% CI 0.58–0.99), but again there was considerable
heterogeneity (I2=76%). Interaction statistics could not be calculated
for any of the stratified analyses because one of the subgroups
contained only one trial. The effect was larger (RR 0.44, 95% CI 0.28–
0.69) in the one hospital-based study that included a doctor in the
team (Close et al., 1999) than in the three other studies (RR 0.98,
95% CI 0.77–1.24).
3.7.3 Fall-related injury
Eight studies reported fall-related injury. Heterogeneity was
substantial (I2=55.7%), but there was no suggestion of an overall
treatment effect (RR 0.90, 95% CI 0.68–1.20). The heterogeneity
may be partly due to the differences in the outcomes recorded by the
different studies (Table 20); there were substantial differences
between studies in the types of injuries that were reported. There was
no evidence of any differences between the subgroups in the stratified
analyses.
3.7.4 Hospitalisation
Nine studies reported hospitalisation. Overall, there was very low
heterogeneity (I2=0%) and no evidence of a treatment effect
(RR 0.82, 95% CI 0.63–1.07). There was no evidence of a difference
between the subgroups in any of the stratified analyses.
3.7.5 GP attendance
This outcome was reported by one study (Lightbody et al., 2002),
which showed an increase in fall-related GP attendance in the
intervention group (RR 1.39, 95% CI 1.11–1.74).
3.7.6 Emergency department attendance
Fall-related emergency department attendance was reported by four
studies. Heterogeneity was moderate (I2=39%) and there was no
evidence of an overall effect (RR 0.96, 95% CI 0.72–1.27). There was
no evidence of a different effect in the subgroup of interventions that
included a doctor, in the one stratified analysis for which an
interaction statistic could be calculated.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 41
3.7.7 Death
Fourteen studies reported the number of participants that died during
follow-up. Overall, there was no evidence of a difference between the
groups (RR 0.96, 95% CI 0.73–1.27), and heterogeneity was very low
(I2=0%). The stratified analyses showed no evidence of any difference
between the subgroups.
3.7.8 Move to institutional care
Five studies reported the number of participants who moved to
institutional care during follow-up. Overall, there was no evidence of a
difference between the groups (RR 0.92, 95% CI 0.59–1.43; I2=0%),
and there was no evidence of any difference between the subgroups in
two stratified analyses.
3.7.9 Health-related quality of life and physical
activity
These outcomes were not reported by any studies.
3.7.10 Sensitivity analysis for inclusion of
cluster-randomised trials
Using values between 0.001 and 0.1 for the ICC for the two cluster-
randomised trials made very little difference to the analyses, and for
no outcome were the conclusions changed.
3.8 Discussion
The research literature has grown substantially since the last update
of the Cochrane review of fall-prevention effectiveness, and of the
literature review informing the NICE guideline on fall prevention.
Unfortunately, the quality of some of the more recent studies is poor.
The overall quality of the existing evidence from RCTs is not high. The
majority were small, and many had methodological drawbacks that
may leave them open to bias. For example, only five out of 18 studies
reported secure methods of allocation concealment. The sample sizes
of most studies were relatively small, and were insufficient to detect
modest but potentially clinically important differences. None of the
trials incorporate an estimate of the multi-factorial programmes on
health-related quality of life, or other metrics commonly utilised in
health economic appraisal. Only one study reported a parallel
economic evaluation that collected costs of the intervention and
resource in a methodological acceptable format. Unfortunately this
study was based in the USA, making it difficult to generalise to the UK
setting and health service system. No large-scale, high-quality RCTs
have yet been conducted, and there is therefore scope for such
studies to resolve the uncertainty about the effectiveness of this type
of intervention.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 42
The evidence to support the effectiveness of multi-factorial
fall-prevention interventions from existing studies is inconclusive.
There is substantial statistical heterogeneity between the trials. This
means that, in terms of reducing the number of fallers, the estimate of
effectiveness is uncertain, and not robust. The range of possibilities
spans from multi-factorial interventions being no more effective than
control interventions, or alternatively, that they may reduce falls by as
much as 20%. The average estimate of effectiveness is a 10%
reduction in the number of people falling. The overall analysis is of
borderline statistical significance in favour of multi-factorial fall
prevention being effective, and if a figure were to be selected for
economic analysis, the overall estimate of RR 0.9 (95% CI 0.8–1.0) is
the most robust. However, use of this estimate would require
knowledge of the cost implication of falls in general as opposed to falls
that result in injury.
There were no clear differences in effectiveness between hospital- and
primary care-based studies, populations with risk factors and
unselected populations and interventions that included a doctor.
The heterogeneity in falls outcomes is likely to be partly due to the
differences between studies in the populations they recruited and the
assessments and interventions that they provided. Studies varied in
the exact set of assessments of fall risks that they performed, and in
the interventions that were provided to address these risk factors.
Methodological heterogeneity is also likely to play a part; studies were
variable in their methodological quality and duration of follow-up.
Analysis of the fall rate ratio was expected to control for differences in
the follow-up duration and hence reduce heterogeneity; however, in
fact heterogeneity was highest in this analysis. Data to calculate rates
were available in only a small sub-set of papers, and hence are not
presented.
There were no clear effect on fall-related injury and use of health care
services. No effect was seen on analysis of fall-related injury, although
there was substantial heterogeneity in this analysis, which may have
been partly due to differing definitions of this outcome. Injury rates
could be estimated from these studies, both within- and between-
group differences. However, there are substantial differences in the
way that injuries have been reported, and these should be considered.
A recent international consensus conference concluded that the only
robust method of measuring injury was to estimate the rate of
peripheral fracture. None of the studies reported these rates.
One study suggested that GP attendance was increased by a multi-
factorial intervention, whereas the analysis of emergency department
attendance suggested no effect. Three studies report the effect on
unspecified medical care, but these data are of little use to economic
modelling, because the costs of different types of medical care can
vary substantially. These results appear to be inconsistent, but the
differences may be due to chance or methodological heterogeneity.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 43
Table 15 Characteristics of included studies
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
Close et al. 1999
(UK)
ED; day hospital and home
Age: 78.2 (SD 7.6)
Sex: 68% female
Cognition: not stated
Aged ≥65
Presented to ED after a fall
Excluded if cognitive impairment and no regular carer, or non-English speaking
Medical and OT assessment and referral compared with no assessment
Medical assessment (day hospital):
Comprehensive general examination
Visual acuity
Balance
Cognition
Affect
Prescribing practice
OT assessment (home):
Functional independence
Environmental hazards
Psychological consequences of fall
Interventions to modify risk factors if possible
Referral to relevant services or day hospital
Advice and education about home safety
Minor home modifications made
Minor equipment supplied by OT
Referral to social or hospital services
Falls
Recurrent falls
Fall-related injury
Death
Move to institutional care
Coleman et al. 1999
(USA)
Primary care; primary care
Age: 77.3 (SD not given)
Sex: 48.5% female
Cognition: not
Aged ≥65
Patients of 9 practices; those with highest risk
Half-day chronic care clinics every 3–4 months compared with
Four-part assessment: 1. Physician and nurse assessment for planning chronic
Not specified Falls
Health-related quality of life

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 44
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
stated scores for functional decline in each practice selected
Exclusions: too ill to participate, moderate to severe dementia, residence in nursing home, terminal illness
usual care disease management
2. Pharmacist assessment
3. Self-management group session
4. provision of health status assessment information to the practice team
Davison et al. 2005
(UK)
ED; hospital and home
Age: 77 (SD 7)
Sex: 72.2% female
Cognition: MMSE median 28.5
Aged ≥65
Presenting to ED with a fall or fall-related injury
At least one additional fall in previous year
Exclusions: cognitively impaired, >1 previous episodes of
Multi-factorial assessment and intervention compared with usual care
Medical assessment (hospital):
Vision
Neurological examination
Cardiovascular assessment
Laboratory blood tests
Physiotherapy assessment (home):
Referral to optician or ophthalmologist
Advice on avoidance of factors precipitating orthostatic hypotension
Modification of medication
Compression stockings
Fludrocortisone
Falls
Fall-related injury
Hospitalisation
Death

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 45
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
syncope, immobile, lived >15 miles from hospital, registered blind, aphasic, clear medical explanation for fall
Gait and balance (Performance Oriented Mobility Score)
Feet, footwear and assistive devices
OT assessment (home):
Home environmental hazards
and midodrine
Dual chamber cardiac pacing
β-Adrenergic antagonists
Gait re-education and functional training programme
Provision of assistive devices
Footwear modification
Referral to chiropody
Interventions for home hazards
Fabacher et al. 1994
(USA)
Community; home
Age 72.7 (SD 5.8)
Sex: 2.3% female
Cognition: not given
US veterans aged ≥70, not currently enrolled in a Veterans Association outpatient clinic
Exclusions: terminal disease, dementia
Home Assessment Program for Successful Aging (HAPSA) compared with no intervention
Home assessment by physician’s assistant or nurse:
Medical history
Medication review
Hearing
Vision
Height and
Personalised letter to each participant detailing findings and recommendations
Follow-up visits by volunteers or staff at 4-month intervals, to assist in carrying out
Falls
Hospitalisation
Move to institutional care
Death

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 46
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
weight
Blood pressure
Oral inspection
Health behaviour
Mental status
Depression
ADL/IADLs
Gait and balance
Blood tests
Home environment
recommendations
Gallagher and Brunt 1996
(Canada)
Community; home
Age: 74.6 (SD not given)
Sex: approx 80% female
Cognition: not stated
Aged ≥60
Fall in previous 3 months
No exclusions specified
Comprehensive falls risk assessment, counselling and motivational video compared with usual care
Nurse home assessment:
Physical health (checklist of 26 problems)
IADLs
Sickness Impact Profile
Blood pressure
Vision
Cognition (Folstein’s MMSE)
Gait
Total number of faults in gait
Counselling session providing feedback about result of risk assessment
Falls
Unscheduled health service contacts
Death
Health-related quality of life

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 47
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
Static balance
Handgrip dynamometry
Chair stand
Medications
Home safety checklist
Gill et al. 2002
(USA)
Primary care; home
Age: 83.2 (SD 5.1)
Sex: 79.8% female
Cognition: MMSE mean 26.5 (SD 6.3)
Aged ≥75
Physically frail (more than 10 seconds to perform rapid gait test or could not stand from seated position with arms folded)
Excluded if unable to walk, undergoing physical therapy, did not speak English, diagnosis of dementia or scored <20
Home assessment by physical therapist followed by interventions compared with
health educational program (six monthly home visits) plus six monthly phone calls
Home assessment by physical therapist (average of 16 visits), assessed:
Impaired ability to move in bed or outdoors, to transfer from one position to another or indoor gait
Impairment in balance or range of motion
Presence of environmental hazards
Instruction in techniques to facilitate activity
Training in use of assistive devices
Removal of environmental hazards
Exercises
Removal of hazards
Repairs and installation of equipment and lighting
Falls
Death
Move to institutional care
Physical activity (disability score)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 48
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
on MMSE, life expectancy <12 months, had stroke, myocardial infarction, hip fracture or hip or knee replacement surgery within last 6 months
Hogan et al. 2001
(Canada)
Community; home
Age: 77.7 (SD 6.8)
Sex: 71.8% female
Cognition: MMSE mean 27.7 (SD 2.0)
Aged ≥65
Fall within past 3 months
Qualifying fall not during high-risk activity, in hospital or because of syncope or stroke, and not resulting in lower-extremity fracture
In-home assessment and development of individualised treatment plan compared with usual care
Home assessment by geriatric medicine specialist, nurse, OT or PT. Assessed:
Environmental hazards
Balance and mobility
Neurological and sensory impairment
Behaviour
Leg disability
Drug and alcohol use
Advice on environmental hazards
Referral to PT or exercise programme
Advice on assistive devices
Referral to optometrist or ophthalmologist
Behavioural advice
Exercises for leg disability or referral to exercise programme
Falls
Recurrent falls
Time to first fall
Fall-related injury
Fall-related hospitalisation

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 49
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
Postural hypotension
Suggestions for drugs, alcohol and postural hypotension
Treatment plan to decrease fall risk devised
Recommendations in writing to participants, attending physician and referral source
Huang and Acton 2004
(Taiwan)
Community; home
Age: 72.0 (SD 5.7)
Sex: 45.8% female
Cognition: not stated
Aged ≥ 65
Community living
Living in registered households
No exclusions specified
Standard and individualized fall prevention compared with standard fall prevention (written information) only
Home visits by researcher:
Gait and balance (Tinetti mobility scale)
Family support (Family APGAR scale)
Fear of falling (Falls Efficacy Scale)
Medications
Environmental safety
Individualised teaching and brochure based on subject’s risk factors
Falls
Jitapunkul 1998
Community; home
Age: 75.6 (SD 5.8)
Aged ≥70
Interviewed
Home visit and screening
Home visit by non-professional
Appropriate action taken,
Falls
Hospitalisatio
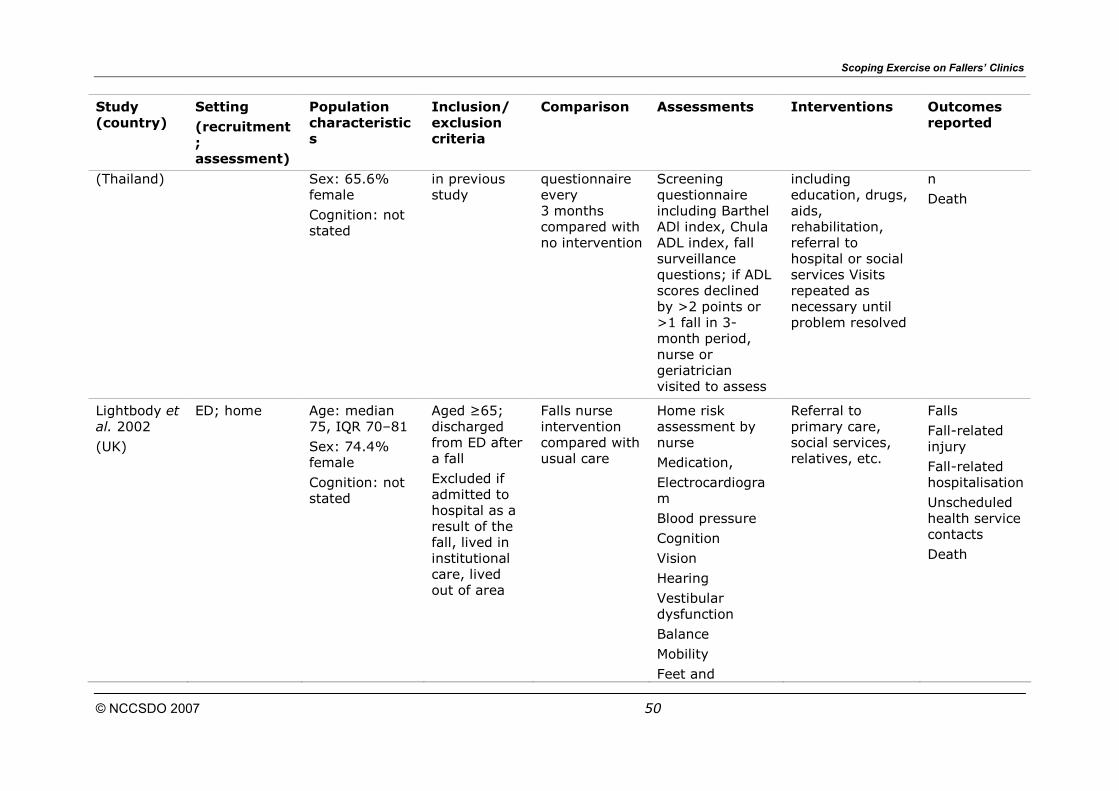
Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 50
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
(Thailand) Sex: 65.6% female
Cognition: not stated
in previous study
questionnaire every 3 months compared with no intervention
Screening questionnaire including Barthel ADl index, Chula ADL index, fall surveillance questions; if ADL scores declined by >2 points or >1 fall in 3-month period, nurse or geriatrician visited to assess
including education, drugs, aids, rehabilitation, referral to hospital or social services Visits repeated as necessary until problem resolved
n
Death
Lightbody et al. 2002
(UK)
ED; home
Age: median 75, IQR 70–81
Sex: 74.4% female
Cognition: not stated
Aged ≥65; discharged from ED after a fall
Excluded if admitted to hospital as a result of the fall, lived in institutional care, lived out of area
Falls nurse intervention compared with usual care
Home risk assessment by nurse
Medication,
Electrocardiogram
Blood pressure
Cognition
Vision
Hearing
Vestibular dysfunction
Balance
Mobility
Feet and
Referral to primary care, social services, relatives, etc.
Falls
Fall-related injury
Fall-related hospitalisation
Unscheduled health service contacts
Death

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 51
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
footwear
Environmental hazards
Lord et al. 2005
(Australia)
Community; home
Age: 80.3 (SD 4.5)
Sex: 67.9% female
Cognition: not stated
Aged ≥75
Randomly drawn from health insurance database
Excluded if minimal English, blind, Parkinson’s disease, Short Portable Mental Status Questionnaire score less than 7
PPA plus extensive intervention compared with PPA plus minimal intervention compared with PPA plus no intervention
PPA performed on all participants Unclear who performed assessments
Extensive intervention: PPA report, profile of test results and specific written recommendations. Counselling session to explain report
Individualised exercises, referral to eye specialist, eye surgery, counselling for strategies to compensate for reduced peripheral sensation, as appropriate
Minimal intervention
Report outlining falls risk, profile of test results, specific recommendations
Falls
Recurrent falls
Fall-related injury
Death

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 52
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
Instruction sheets for home exercises and brief training session; list of exercise groups provided; written advice about vision and peripheral sensation
Newbury et al. 2001
(Australia)
Primary care; home
Age: mean 79.3
Sex: 63% female
Cognition: not stated
Aged ≥75
Community living
Recruited from GP lists
No exclusions specified
75+ health assessment compared with usual care
Home visit from nurse assessed:
Hearing
Vision
Physical condition
Medication
Compliance
Vaccination, alcohol and tobacco use
Cognition
Depression
ADL
Mobility
Nutrition
Social
Housing
Problems found outlined in letter to GP
Falls
Death
Move to institutional care

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 53
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
Pardessus et al. 2002
(France)
ED; home
Age: 83.2 (SD 7.8)
Sex: 78.3% female
Cognition: not stated
Aged ≥65.
Able to return home after hospitalisation for falling
Excluded: cognitive impairment (mini mental test <24), no phone, lived >30 km from hospital, fall secondary to cardiac, neurologic, vascular or therapeutic problems
Home visit and assessment compared with usual care
Home visit from physical medicine and rehabilitation doctor and ergotherapist
ADL
Some IADLs
Transfers
Mobility
Environmental hazards
Environmental hazards modified where possible or advice given if modification impossible Hospital social worker contacted to discuss problems after visit
Falls
Hospitalisation
Death
Move to institutional care
Shaw et al. 2003
(UK)
ED; hospital
Age: 84 (SD 6.6)
Sex: 80% female
Cognition: MMSE median 13
Aged ≥65
Cognitive impairment and dementia (MMSE <24), presented to ED after a fall
Excluded if unable to walk, medical diagnosis that
Multi-factorial assessment and intervention compared with assessment followed by usual care
Multi-factorial clinical assessment for all participants at baseline, performed by doctor, PT and OT:
Medical history
Drugs
Management of untreated medical problems
Medication review
Referral to optician or ophthalmologist
Psychogeriatric assessment
Compression
Falls
Time to first fall
Fall-related injury
Hospitalisation
Unscheduled health service contacts

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 54
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
was likely cause of fall, unfit for investigation within 4 months, unable to communicate, lived more than 15 miles from site of recruitment, no person in regular contact
Vision
Electrocardiogram
Depression
Cardiovascular
Performance- oriented mobility assessment
Walking aids, feet and footwear
Environmental hazards
hosiery, fludrocortisone or midodrine
Pacemaker
Supervised home exercise programme
Provision of walking aids and footwear
Chiropody referral
Home hazard modification
Death
Tinetti et al. 1994
(USA)
Primary care; home
Age: 77.9 (SD 5.3)
Sex: 69% female
Cognition: MMSE score ≥25, 84%
Aged ≥70
Enrolees of health maintenance organisation, independent ambulation, residence outside nursing home, score of ≥20 on MMSE, no participation in vigorous
Multi-factorial assessment and intervention compared with assessment followed by usual care
Multi-factorial assessments done for all participants
Home assessment by nurse/PT; nurse assessed:
History of falls
Medication
Depressive symptoms
Chronic diseases
Behavioural recommendations or medication changes for postural hypotension
Education about sedative-hypnotic agents
Nonpharmacologic treatment of sleep problems
Medication review with physician
Falls
Fall-related injury
Hospitalisation
Unscheduled health service contacts
Death

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 55
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
sports or walking in month before enrolment, at least one risk factor
No exclusions specified
ADL
Falls efficacy scale
Sickness Impact Profile (ambulation and mobility)
Vision
Hearing
Home hazards
PT assessed:
Strength and joint impairment
Balance and transfer skills
Walking and stability
Transfer skills training
Environmental alterations
Gait training
Balance or strength exercises
van Haastregt et al. 2000
(The Netherlands)
Primary care; home
Age: 77.2 (SD 5.1)
Sex: 66% female
Cognition: not stated
Aged ≥70
Community living
Two or more falls in previous 6 months or score ≥3 on Sickness Impact Profile mobility
Nurse home visits compared with usual care
Nurse home assessment on 5 occasions over 1 year:
Fear of falling
Mobility
Physical health
Drugs
ADL
Social functioning
Advice, referral and other actions aimed at dealing with observed problems
Falls
Recurrent falls
Fall-related injury
Unscheduled health service contacts

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 56
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
control scale
Excluded if bedridden, wheelchair-dependent, terminally ill, on waiting list for nursing home or receiving home care from community nurse
Cognitive functioning
Psychosocial functioning
Home safety
Wagner et al. 1994
(USA)
Primary care; primary care
Age: mean 72.5
Sex: 60% female
Cognition: not stated
Aged ≥65
Ambulatory and independent in ADL
Sampled from people receiving care from Seattle Group Health Cooperative clinics
Excluded if too ill to participate
Disability and fall-prevention nurse visit and interventions compared with chronic disease prevention visit versus usual care
All participants had baseline assessment, nurse visit reviewed risk factors at baseline assessment and also assessed:
Hearing
Blood pressure
Specific interventions for six risk factors as needed:
Inadequate exercise, high-risk alcohol use, increased fall risk, high-risk prescription drug use, impaired vision, impaired hearing.
Exercise class
Referral to alcohol treatment
Falls
Fall-related injury
Hospitalisation for falls
Medically attended falls

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 57
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
programme
Home safety inspections, drug review by pharmacist, referral to audiological evaluation, information about community resources to allow poor vision to
maintain activity
Whitehead et al. 2003
(Australia)
ED; home Age: 77.8 (SD 7.0)
Sex: 71.4% female
Cognition: not stated
Aged ≥65
Fall-related presentation to ED
Excluded if living in nursing home, cognitive impairment (MMSE <25/30) without resident carer, could not speak English,
Fall risk profile and individualised risk-reduction strategy compared with usual care
Authors’ own fall risk screening questionnaire (questions not specified in paper); fall risk profile derived from this Questionnaire administered during home visit by researcher
Customised strategy devised based on fall risk profile; GP sent letter highlighting risk factors and suggesting interventions:
Review of medication
Home assessment by OT
Participation in exercise programme
Assessment at interdisciplinary
Falls

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 58
Study (country)
Setting
(recruitment; assessment)
Population characteristics
Inclusion/ exclusion criteria
Comparison Assessments Interventions Outcomes reported
severe or terminal illness
fall and balance clinic
Assessment of osteoporosis risk
ADL, Activities of Daily Living; ED, emergency department; IADL, Instrumental Activities of Daily Living; IQR, interquartile range; MMSE,
Mini Mental State Examination; OT, occupational therapy or therapist; PPA, physiological profile assessment; PT, physical
therapist; SD, standard deviation.
57

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 59
Table 16 Characteristics of interventions in emergency department-based studies
Close et al. 1999
Davison et al. 2005
Lightbody et al. 2002
Pardessus et al. 2002
Shaw et al. 2003
Whitehead et al. 2003
Age X X X X X X
Demographics
Previous falls X X X X X X
Chronic diseases/symptoms X
Medication
Screening tool
Selection
Specific exclusions X X X X
Hospital (emergency department)
X X X X X X
Residential care
Primary care
Site of recruitment
Community (home)
Hospital X X X
Residential care
Primary care
Site of delivery
Community (home) X X X X X
Doctor X X X X
Nurse X X
Physiotherapist X X
Occupational therapist X X X
Delivered by
Pharmacist

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 60
Non-professionals X
Geriatric assessment X
Validated fall risk
Gait and balance X X X X X
Cardiovascular assessment X X X X
Medication review X X X
Vision X X X X
Foot assessment X X X
Psychological assessment X X X
Environment (dwelling units) X X X X X
Environment (public outdoor)
Environment (aids for personal care and protection)
X X X
Assessments
Other X X
Exercise (supervised) X X
Exercise (unsupervised) X
Medication X X X
Surgery X X
Psychological X
Environment/assistive devices X X X X X
Social environment
Knowledge X X X
Interventions
Referral X X X X X

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 61
Table 17 Characteristics of interventions in primary care/community based studies
Coleman
et al.
1999
Fabacher
et al.
1994
Gallagher
and
Brunt
1996
Gill
et al.
2002
Hogan
et al.
2001
Huang
and
Acton
2004
Jitapunkul
1998
Lord
et al.
2005
Newbury
et al.
2001
Tinetti
et al.
1994
van
Haastregt
et al.
2000
Wagner
et al.
1994
Age X X X X X X X X X X X X
Demographics
Previous falls X X X
Chronic diseases/
symptoms
X X
Medication
Screening tool
Selection
Specific exclusions X X X X X X
Hospital (emergency
department)
Residential care
Primary care X X X X X X
Site of recruitment
Community (home) X X X X X X
Hospital
Residential care
Primary care X X
Site of delivery
Community (home) X X X X X X X X X X
Doctor X X X
Nurse X X X X X X X X X
Delivered by
Physiotherapist X X X

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 62
Occupational
therapist
X
Pharmacist X
Non-professionals X X
Geriatric assessment X
Validated fall risk X
Gait and balance X X X X X X
Cardiovascular
assessment
X X X X
Medication review X X X X X X X X X
Vision X X X X X
Foot assessment
Psychological
assessment
X X X X X
Environment
(dwelling units)
X X X X X X X X X
Environment (public
outdoor)
Environment (aids for
personal care and
protection)
Assessments
Other X X X X X X X X X X X
Exercise (supervised) X X X X
Exercise
(unsupervised)
X X X X
Medication X X X
Interventions
Surgery
Unclear
X

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 63
Psychological
Environment/assistive
devices
X X X X
Social environment
Knowledge X X X X X X X X X X
Referral
X X X X X X X

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 64
Table 18 Methodology and methodological quality of included studies
Quality-assessment scores Study Randomisation Number randomi-sed
Blinding Losses/
exclusions
Follow-up
Notes
A B C D E F G H J K L X Y
Close et al. 1999
Individually randomised by random-number table held independently of the investigators (no further information)
397 No blinding 93 (23.4%)
No falls data included for those who died or moved to institutional care
12 months
Fairly large difference in numbers randomised between groups (184 and 213); stated to be attributable to chance when no mechanism for balancing numbers used
Analyses restricted to those who completed study
2 2 1 3 1 1 1 3 3 3 3 – –
Coleman et al. 1999
Cluster-randomised by physician practice
9 clusters
169 participants
No blinding 12 months: 27 (16.0%)
24 months: 42 (24.9%)
12 and 24 months
2 3 1 3 1 1 3 2 1 1 3 Yes No
Davison et Individually 313 Outcomes 31 (9.9%) 12 1 2 2 3 1 1 1 3 3 3 3 – –

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 65
Quality-assessment scores
al. 2005 randomised States ‘computer-generated block randomisation’ but no information on how it was used
self-reported but processed blinded Participants clinicians not blinded
months
Fabacher et al. 1994
Individually randomised Cards in sealed envelopes, done over phone by study personnel Numbering not mentioned
254 No blinding 59 (23.2%) 12 months
Follow-up done in different ways for the two groups; home visit for intervention group, phone for control group
2 2 1 2 1 1 1 3 1 2 3 – –
Gallagher and Brunt 1996
Individually randomised. No information on methods
100 No blinding 0 (0%) 6 months
1 3 1 2 1 1 1 3 1 3 2 – –
Gill et al. 2002
Individually randomised ‘Computer-generated algorithm’ but no information
188 No blinding 10 (5.3%) 12 months
1 3 1 3 1 1 1 3 3 2 3 – –

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 66
Quality-assessment scores
on how it was used
Hogan et al. 2001
Individually randomised States allocation sequence concealed in locked cabinet prior to allocation but no further information on methods
152 Research assistant contacting participants about falls blinded Participants and caregivers not blinded
13 (8.6%) 12 months
Participants who did not adhere to protocol or were admitted to an institution were excluded from analysis
2 2 2 3 1 1 1 3 3 3 3 – –
Huang and Acton 2004
Individually randomised
No information on methods
120 No blinding 7 (5.8%) 2 months
1 1 1 3 1 1 1 3 1 3 2 – –
Jitapunkul 1998
Individually randomised
No information on methods
160 No blinding 44 (27.5%) 3 years 1 2 1 2 1 1 1 1 2 1 3 – –
Lightbody et al. 2002
Individually randomised Unclear whether allocations concealed before assignment
348 No blinding 34 (9.8%) 6 months
1 2 1 2 1 1 1 3 3 3 2 – –

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 67
Quality-assessment scores
Lord et al. 2005
Individually randomised States allocations were concealed but no information on how this was implemented
620 No blinding 42 (6.8%) 12 months
Falls data available for more participants than completed 12-month follow-up Suggests follow-up was incomplete for some
3 2 1 3 1 1 3 3 3 3 3 – –
Newbury et al. 2001
Individually randomised by sealed numbered envelopes
100 Researchers blind to intervention status when assessing patients Patients and caregivers not blinded
11 (11%) 12 months
3 2 2 1 1 1 1 3 1 1 3 – –
Pardessus et al. 2002
Individually randomised by random-number table
No information on methods
60 No blinding 0 (0%) 12 months
1 3 1 3 1 1 1 3 1 2 3 – –
Shaw et Individually 308 Blinded outcome
34 (11.0%) 12 3 2 3 3 1 1 1 3 3 3 3 – –

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 68
Quality-assessment scores
al. 2003 randomised
Computer- generated random numbers, assignment done by independent researcher blind to baseline data
assessment
(216/308 completed follow-up; 70.1%)
months
Tinetti et al. 1994
Cluster-randomised by physician
16 clusters
301 participants
Blinded interviewers assessed falls
Participants and caregivers not blinded
10 (3.3%) 12 months
3 2 2 3 1 1 1 3 3 3 3 No No
van Haastregt et al. 2000
Individually randomised ‘Computer generated random numbers’
No information on method of assignment
316 Doctors blinded; nurses doing home visits not blinded Participants not blinded
12 months: 64 (20.3%)
18 months: 81 (25.6%)
12 and 18 months
1 2 1 3 1 2 1 3 2 3 3 – –
Wagner et al. 1994
Individually randomised
No information
1559 No blinding 89 (5.7%) 12 and 24 months
Numbers analysed in each group
1 1 1 3 1 1 1 2 3 1 3 – –

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 69
Quality-assessment scores
on methods not given; outcomes reported as percentages only
Whitehead et al. 2003
Individually randomised Numbered, sealed opaque envelopes
140 No blinding 17 (12.1%) 6 months
3 1 1 3 1 1 1 3 3 3 2 – –
See Appendix 3 for the quality-assessment tool used.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 70
Table 19 Results of interaction tests
Hospital×community Risk factors×unselected Doctor×no doctor Outcome
χ2 P χ2 P χ2 P
Fallers 0 1 2.61 0.11 0 1
Fall-related injury 0.1 0.75 0.42 0.52 0.1 0.75
Hospitalisation 0.75 0.39 0.06 0.81 1.12 0.29
ED attendance – – – – 2.8 0.09
Death 1.47 0.23 1.58 0.21 0.19 0.66
Move to institutional care 0.3 0.58 – – 0.3 0.58
ED, emergency department.
Table 20 Details of fall-related injuries included in outcomes
Study Injuries reported
Close et al. 1999 Serious injury (fracture or dislocation)
Davison et al. 2005 Fractured neck of femur, other fracture
Gill et al. 2002 Fall-related fracture (fractures were of hand, hip, coccyx, shoulder)
Lord et al. 2005 Falls resulting in injury (self report, no definition)
Shaw et al. 2003 Major injury (not defined)
Tinetti et al. 1994 Serious injury due to fall: fracture, head injury requiring hospitalisation, joint dislocation or severe sprain, lacerations requiring suturing
van Haastregt et al. 2000
Injurious fall (not defined)
Wagner et al. 1994 Injurious falls (self reported, no definition given)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 71
Figure 8 Analyses including all studies

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 72

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 73

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 74
Figure 9 Analyses stratified by location of clinic

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 75

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 76

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 77

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 78
Figure 10 Analyses stratified by whether or not population was selected
for risk factors

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 79

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 80

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 81

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 82
Figure 11 Analyses stratified by whether or not the team included a
doctor

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 83

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 84

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 85
Section 4 Systematic review of screening instruments to predict fallers among community-living older people
4.1 Introduction
Identification of older people at high risk of falling would theoretically
allow targeting of fall-prevention interventions to those most likely to
benefit from them. A large number of possible screening instruments
have been proposed that may be able to predict fallers, including tests
of balance and gait, and scores based on a person’s risk factors for
falls. In this review we aim to assess the evidence about the accuracy
of screening tests for predicting fallers, and indicate where more
research is needed.
4.2 Methods
4.2.1 Eligibility
Studies were included if they satisfied the following eligibility criteria:
1 prospective cohort studies that evaluated the performance of one
or more screening tests for predicting fallers;
2 the population was elderly people living in the community;
3 falls were recorded prospectively; that is, participants were
followed-up for falls occurring after the screening test was
performed;
4 follow-up was at least 3 months;
5 data were presented on sensitivity, specificity, positive predictive
value (PPV), negative predictive value (NPV) or receiver operating
characteristics (ROC) curves, for falls or fall-related injuries.
We included studies of older people living in the community and in
residential care environments where they were substantially
independent. We excluded hospital populations and residential care
situations where participants were not independent. A few studies
which recruited participants in hospital but followed them up after
discharge (hence recording falls among people living in the
community) were included.
We excluded studies that used a screening test to ‘predict’ falls that
had already occurred. In these retrospective studies performance on
the screening test is related to a patient’s history of falls. This study
design may give misleading results because past falls may affect test
performance, and hence overestimate the accuracy of screening
instruments. Moreover, this design does not represent a real-life
clinical situation, in which clinicians need to predict future falls.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 86
We included studies that assessed the performance of tests that have
been proposed or are used for prediction of fallers in clinical practice.
Studies that built a multivariate model and then assessed its
performance were not included. Some individual risk factors; for
example, previous falls, could be used clinically for prediction of falls.
However, it was not possible to include them in this review because
most of the studies that have evaluated them were risk-factor studies
that analysed their data using multiple-regression techniques and did
not report the relevant data or summary statistics.
Studies had to report the number of people positive and negative on
the screening test (or a range of cut-off values if appropriate), and the
number of people with falls or fall-related injuries within a specified
duration of follow-up for each of these groups, or summary statistics
such as the sensitivity and specificity. Studies were not included if
they reported results as odds ratios or risk ratios, without the raw
data from which sensitivity, specificity, PPV and NPV could be
calculated. A duration of follow-up of at least 3 months was required
for inclusion, although reliable identification of fallers requires much
longer follow-up than this. This was reflected in the quality
assessment, where 12 months or more of follow-up was required for
the highest-quality grading.
4.2.2 Search strategy
Electronic search
We searched MEDLINE (1966 to July 2006), EMBASE (1980 to July
2006), PsycINFO (1975 to July 2006), CINAHL, Social Science Citation
Index and Social Science Citation Index Expanded (all 1970 to July
2006). Searches were conducted in July 2006.
We based the search strategy on the search strategy of van der
Weijden et al. (1997), which was found to be the most effective in a
recent review (Leeflang et al., 2006). We added extra terms to this
search strategy, because it is likely that eligible studies for this review
would not use terms usually associated with diagnostic studies in their
title or abstract. The extra terms were ‘risk assessment’ or
‘assessment tool’, and the names of known possible screening
instruments. The search strategies used for each database are given
in Appendix 5.
Review articles and reference lists
We considered for inclusion all studies included in four earlier reviews
(Perell et al., 2001; Jarnlo, 2003; Myers, 2003; Oliver et al., 2004).
We also inspected the reference lists of all eligible studies to identify
any further studies that were cited by them.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 87
Hand searching
We conducted a hand search of two volumes of two journals, to
estimate the number of eligible articles that might have been missed
by the electronic search. The two journals were selected at random
from the last six volumes of journals with five or more papers in the
list of papers to be considered for inclusion. The volumes searched
were Journal of the American Geriatrics Society, volume 50 (2002),
and Physical Therapy, volume 83 (2003). The hand search found no
additional eligible articles.
4.2.3 Data extraction
Data were extracted by two reviewers independently, and
discrepancies resolved by discussion or by reference to a third
reviewer.
4.2.4 Quality assessment of included studies
We used a modified version of the QUADAS quality-assessment tool
(Whiting et al., 2003). Three items (numbers 4, 7 and 10) were
omitted as they were not applicable to this review and other questions
were rephrased to be relevant to this review. The quality-assessment
tool is given in Appendix 6.
4.3 Statistical analysis
For each study, the specificity, sensitivity, PPV and NPV were either
extracted from the paper or calculated from the data extracted from
the paper, where this was possible. We planned to carry out
meta-analyses combining the results of independent studies that used
the same screening test with the same cut-off point to determine
positive tests, measured the same outcome and used similar
populations. In fact there were only a few studies that could be
combined, and excessive heterogeneity among them meant that this
would not be meaningful. Hence, no meta-analyses were performed.
Results were tabulated, giving the sensitivity, specificity, PPV, NPV and
95% CI for each screening test in each study.
4.4 Results
4.4.1 Searches
The electronic search yielded 3028 citations. Of these, 116 were
selected for further consideration based on their title and abstract, and
full reports obtained. The search of the reference lists of the review
articles and all selected studies yielded an additional nine potentially
eligible studies, which were also obtained as full reports. One hundred
and twenty five full reports were considered (Table 21). Twenty-three
studies were eligible and included in the review. Studies excluded from

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 88
the review are given in Appendix 7. Thirty-three studies included
ineligible populations, which were either hospital patients (31 studies)
or populations including all age groups (two studies). Falls data were
not collected prospectively in 19 studies, and 11 studies did not
provide information on falls. Many of these assessed the relationship
of a screening test with another marker of falls risk, often another
screening test. Twenty-four studies did not report relevant data; these
included multiple-regression analyses of risk factors, and studies that
evaluated screening tests but did not present the required statistics or
the raw data.
Nineteen of 23 included studies were located by the electronic search,
three from reference lists of other studies that were considered for
inclusion, and one from a previous review article.
4.4.2 Characteristics of studies
Of the 23 eligible studies (Table 22), 19 either presented quantitative
data for 2×2 tables of the numbers of fallers and non-fallers who were
positive and negative for one or more screening tests, or these data
could be calculated from information given. Two studies (Nandy et al.,
2004; Smith et al., 2006) presented sensitivity, specificity, PPV and
NPV, and two (Stel et al., 2003; Lin et al., 2004) reported the area
under the ROC curve for the tests they included.
In the majority of studies (17) participants were community residents,
but in six they were living in residential care or retirement
communities. They were stated to be substantially independent in all
studies. Three studies (Hyndman and Ashburn, 2004; Andersson et
al., 2006; Smith et al., 2006) recruited patients who had recovered
from a stroke, and one (Bloem et al., 2001) studied patients with
Parkinson’s disease. These studies were considered separately from
the studies of the general population as their risks of falling are
substantially different. The remainder of the studies (19) recruited
unselected populations of elderly people, although many excluded
those with cognitive impairment or specific diagnoses.
In total the 23 included papers reported data for 28 different
screening tests. The tests assessed by the most studies were: Tinetti
mobility scale (including studies using just the balance component; six
studies), the Stops Walking When Talking test (SWWT test; four
studies) and the Timed Up and Go test (TUG test; four studies).
However, in most cases even where studies used the same test, there
were differences in the cut-off value used to determine a positive test,
or in the way the test was performed (see Discussion, section 4.5).
Also, the definitions of falls outcomes differed between studies. Some
studies reported all falls, but others reported recurrent falls or
excluded some types of fall from their outcome (Table 22). These
differences are likely to introduce heterogeneity into the comparisons
between studies.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 89
4.4.3 Methodological quality
Table 23 gives the quality-assessment scores for the 23 studies.
Follow-up period
Follow-up periods were variable, from 3 months to 5 years. Only two
studies had less than 6 months’ follow-up, and 11 had 12 months or
more.
Recording of falls
Only 9/23 studies (39%) used falls diaries, calendars or other
prospective methods of recording falls. The remainder either used
participant recall at predefined intervals or at the end of the follow-up
period only. With long follow-up periods these methods may lead to
under-reporting.
Reporting of tests
The majority of studies (18/23, 78%) reported screening tests in
sufficient detail or gave references to a description elsewhere. In some
cases, where several studies evaluated the same test, it was not
possible to be sure that the test was performed in the same way in
different studies. For example, four studies evaluated SWWT, but two
of them gave insufficient detail about implementation of the screening
tests, so it is possible that it was performed in a different way from
the other studies. In the case of the Tinetti balance and gait scales,
there were differences in scoring and the number of assessments
performed between studies.
Blinding
Only a few studies reported measures to ensure that assessment of
falls outcomes was not influenced by knowledge of the screening test
results. In most studies falls were self-reported and it was not clear
whether participants knew whether their test result had classified
them as high or low risk for falls. In the studies that reported blinding
methods, it was the clinicians who assessed falls and decided whether
they qualified as outcomes who were blinded.
Losses and exclusions
In most studies (17/23, 74%) losses and exclusions were fewer than
20%. A few had greater than 30% losses and exclusions, leading to a
possibility of bias in these studies.
4.4.4 Measurement performance
Table 24 includes results for studies of populations not selected for a
particular disease that provided raw data, or the values of sensitivity,
specificity, PPV and NPV. Table 25 includes the results for studies that
presented results as ROC curves. Results are tabulated separately for

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 90
studies of Parkinson’s disease (Table 26) and post-stroke (Table 27)
populations.
Tinetti mobility test
Six studies evaluated the Tinetti mobility score, and/or its balance and
gait components. All of them were studies of unselected populations,
and one (Lin et al., 2004) presented results only as an ROC curve.
Four studies provided data on the balance scale, two on the gait scale
and three on the combined mobility scale. The number of assessments
performed and scoring systems varied between studies. One study
(Tinetti et al, 1986) analysed recurrent falls rather than all falls, so its
results are incompatible with the others. No two studies used the
same cut-off point and scoring system so no meta-analysis was
performed.
For the three studies that provided data on the overall mobility scale,
the sensitivities varied between 0.27 (Hale et al., 1992) and 0.76
(Tinetti et al, 1986), whereas the specificities were from 0.52 (Raiche
et al., 2000) to 0.83 (Tinetti et al 1986, 1986; Hale et al., 1992). Two
out of three studies had sensitivity greater than 70% and two had
specificity over 80%. The PPVs were between 0.31 and 0.68, and
NPVs between 0.67 and 0.88.
For the balance scale alone, three studies provided data (Tinetti et al,
1986; Trueblood et al., 2001; Verghese et al., 2002). Tinetti et al
(1986) found a high sensitivity of 0.80 (for recurrent falls), and
Verghese et al. (2002) similarly found a fairly high sensitivity (0.62)
when using a cut-off value of 10/16. Trueblood et al. (2001), using a
higher cut-off value of 12/16, found a sensitivity of only 0.23. All of
these tests had a specificity of greater than 0.70. NPVs were uniformly
high (78–89%), but PPVs were lower than those for the combined
mobility scale, ranging from 0.20 to 0.59.
One study (Lin et al., 2004) reported results for the balance scale
using ROC curve statistics. The area under the ROC curve was 0.559
(no CI given), suggesting that the test was not good at predicting
fallers.
Two studies provide data on the gait scale alone (Tinetti, 1986;
Trueblood et al., 2001), but used different cut-off values and
outcomes. Their results were inconsistent for sensitivity and
specificity, but similar for PPV (0.43 and 0.46) and NPV (0.86 and
0.81).
Stops Walking When Talking (SWWT)
Four studies evaluated this test, one of which (Hyndman and Ashburn,
2004) assessed its relationship to both falls and recurrent falls. Two of
the studies were in post-stroke populations (Hyndman and Ashburn,
2004; Andersson et al., 2006), one in Parkinson’s disease (Bloem et
al., 2001), and the fourth used an unselected population

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 91
(Lundin-Olsson et al., 1997). As the populations and ways in which the
test was implemented varied, no meta-analysis has been conducted.
In an unselected population, the test appeared to have high PPV
(83%) and NPV (76%), although sensitivity was low (48%).
In post-stroke populations, both studies had PPV and NPV for falls of
around 60%, although sensitivities and specificities were variable. In
the one study of a Parkinson’s disease population, the SWWT test was
not good at predicting recurrent fallers (sensitivity of 12% and PPV of
29%).
Timed Up and Go (TUG)
Three studies assessed the TUG test, using different cut-off values
(from 14 to 20 seconds) and different populations and durations of
follow-up. Hence no meta-analysis was conducted. One study
(Andersson et al., 2006) assessed the test in a post-stroke population.
The two studies in unselected populations (Okumiya et al., 1998;
Trueblood et al., 2001) used different cut-off values (16 and 20
seconds respectively). The longer cut-off in Trueblood et al. (2001)
performed very poorly (sensitivity 10% and PPV 27%).
One other study (Lin et al., 2004) reported the ROC area under the
curve as 0.61 (no CI given), but there was no information on the best
performing cut-off value. It was the best-performing of four screening
tests in this study.
Berg Balance Scale
The Berg Balance Scale was assessed by two studies, one conducted
in a post-stroke population. Both studies used a cut-off of 45/56 for
considering a test positive (i.e. high risk), but differences in their
populations mean that meta-analyses were not possible. Andersson et
al. (2006) found that sensitivity, specificity, PPV and NPV were similar
(between 58 and 69%) in a population of recovering stroke patients,
but Bogle Thorbahn and Newton (1996) found sensitivity of 53% and
specificity of 92% in an unselected population. PPV was 73% and NPV
was 84% in this study, although CIs were wide because of its small
size.
Mobility Interaction Fall (MIF) chart
This screening test was evaluated in two studies by Lundin-Olsson et
al. (2000, 2003). There was considerable heterogeneity between the
results, however, so they have not been combined. The earlier study
found high values of sensitivity and specificity (0.85 and 0.82
respectively), which were not confirmed by the later and larger study
(0.43 and 0.69). PPV and NPV were similarly higher in the earlier
study.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 92
Other tests
Twenty-one other tests were assessed by only one included study. Of
the studies of unselected populations, the best results were the
Coalition for Community Falls Prevention (CCFP screen; Killough,
2005) and the Downton Index (Rosendahl et al., 2003), which both
had a sensitivity of over 80%, with a PPVs of 51 and 68%
respectively.
4.5 Discussion
There was not adequate evidence to determine with any confidence
how good any screening test was at predicting fallers. Only a few tests
were evaluated by several studies, and differences among them in the
performance of the tests, populations, cut-off values and outcomes
meant that no meta-analyses were possible. At present, therefore, it is
not possible to provide a quantitative summary of the accuracy of any
fall-risk screening tool. For robust determination of the accuracy of
screening tests, further high-quality studies are needed. These should
seek to use compatible study designs to allow pooling of their results
in future systematic reviews.
There is currently very little good-quality evidence about the
performance of any of the screening tools most commonly used by
falls clinics in the UK. The FRAT was evaluated by only one study
(Nandy et al., 2004). Although this study had a reasonably large
sample size it suffered from high loss to follow-up, use of only a
6-month follow-up period and not using the most reliable method for
collecting falls data. Data for three cut-off points were presented. They
all had high specificity and NPV, but sensitivity varied from 59% with
two risk factors as the cut-off to 15% with four risk factors.
Conversely, PPV was 43% with two risk factors and 58% with four.
The Tinetti balance, gait and mobility scales were evaluated by the
most studies, but differences among the cut-off points and outcomes
used precluded any combination of results. Moreover, it was clear that
the test procedures differed between studies. Tinetti (1986) described
the screening tool as comprising 13 balance assessments and nine gait
assessments, without any description of the scoring system to be
used. In a different paper (Tinetti et al., 1986) the scale is described
as consisting of eight balance tests with a maximum score of 15 and
eight gait tests with a maximum score of 13, giving a total maximum
score of 28. Of the studies that used both balance and gait
assessments, Raiche et al. (2000) had 14 balance items (scored out of
24) and 10 gait items (scored out of 16), to give a total score out of
40. Hale et al. (1992) similarly had a total score of 40, but gave no
information about the numbers of items assessed, and used a different
cut-off value for determining a positive test (30/40 compared with
36/40). Trueblood et al. (2001) had a total of 16 items in the gait and
balance subscales, with maximum scores of 12 and 16 respectively, to
give a maximum total of 28. Two studies used only the balance

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 93
assessments. Verghese et al. (2002) used a nine-item balance and
mobility scale, scored from 0 to 16 (the paper stated that gait
assessment was not used), and Lin et al. (2004) had a 13-item
balance scale, scored 0–26. Because of the variation in the
assessments performed, the cut-off values used and the outcomes
recorded, it was not possible to combine any of these results in
meta-analyses.
4.5.1 Design, reporting and methodological quality
of existing studies
A large number of studies were excluded from this review because
they used poor study designs. Nineteen studies evaluated screening
tools but did not collect falls data prospectively. Instead, they
performed screening tests and evaluated their relationship with
historical falls. This study design may give quite different results from
use of the tests in clinical practice, where prediction of future falls is
the aim. For example, Shumway-Cook et al. (2000) used a
retrospective design to assess the performance of the TUG test, and
found a sensitivity and specificity of 87%. In contrast, the two
prospective studies included in this review found considerably lower
sensitivities of 54 and 10%.
Some other excluded studies assessed the relationship of a screening
test to a ‘gold standard’ (usually another screening test) rather than
measuring falls. This is potentially misleading; no screening test is
perfect for measuring falls and agreement between two tests does not
necessarily mean that they will be good at predicting falls. At present
there is no screening test that has been shown to be accurate enough
to be regarded as a gold standard. For example, Whitney et al. (2005)
analysed correlations of TUG with the Physiological Profile Assessment
(PPA), a comprehensive falls risk assessment. They found that TUG
performance was related to PPA falls risk measured by PPA, but this
does not give an assessment of the accuracy of TUG for predicting
falls.
There were methodological drawbacks to many of the existing studies.
The most common problem was poor recording of falls outcomes; the
majority of studies did not use the most reliable methods. Many
follow-up periods were too short; less than half of the included studies
(11/23) followed participants for 12 months or more. Losses to
follow-up were also an issue in some studies, with 30% or more lost
by some studies. Reporting of results was in some cases poor; in
some cases the raw data for 2×2 tables of test results against falls
could be deduced, but in others they could not. Some relevant studies
were excluded because they reported the results as odds ratios or
other statistics.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 94
4.5.2 Searching for relevant studies
Studies relevant to this review may have been difficult to locate
because they may not have included search terms for diagnostic
studies in their title and abstract. We tested the accuracy of our
search strategy against two earlier reviews that included studies
relevant to this review (Perell et al., 2001; Jarnlo, 2003). It located
16/21 studies included in Perell et al. (2001) and 15/23 included in
Jarnlo (2003). Examination of the studies not located revealed that
none of them was eligible for this review. They were generally poorly
described in their titles and abstracts, without any terms describing
their population or methodology, and hence would be difficult to locate
with any electronic search strategy. This emphasised the importance
of additional searching of reference lists to locate relevant studies for
this review.
A question that has not yet been answered is how good does a
screening test need to be to be useful in assessing people for falls
risk? The answer will depend on the use to which it is to be put. As a
first screen to identify people who may benefit from more detailed
assessment, it may be sufficient to have a high NPV, so that people
not at high risk for falls are excluded from further assessment.
Modelling studies may help to determine what are the most important
features of a test for these purposes.
Table 21 Inclusion and exclusion of studies
Number of studies
Included 23
Non-eligible population (hospital or non-elderly) 33
No falls outcome 11
Not prospective falls data 19
Relevant data not reported 25
Non-English language 6
Study could not be located 3*
Duplicate publication 1
Discussion paper; no data 3
Insufficient duration of follow-up 1
*One conference abstract, reference apparently incorrect; one error in electronic
database (wrong year; correct reference was considered for eligibility);
one journal could not be located.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 95
Table 22 Characteristics of included studies
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
Andersson et al. 2006
Community living discharged stroke patients
First ever stroke
Treated in Orebro University Hospital
Excluded: subarachnoid haemorrhage
Age: mean 73.4, range 33–94
Sex: 55% male
Prev. falls: ?
Cognitive impairment: 38%
Visual impairment: 34%
BBS
SWWT
TUG
diffTUG
All self- reported falls
196 55 (28%) 6/12 months
(50% followed up at 6 months and 50% at 12 months)
Selection of patients for treatment in stroke unit
A few non-old people included
Bergland and Laake 2005
Female ≥75 years
Randomly selected from Oslo census file
Excluded: Unable to get to research office
Major cognitive impairment
Unable to stand for >60 seconds
Age: mean 80.3, range 75–93
Sex: 0% male
Prev falls: 41%
Cognitive impairment: ?
Visual impairment:?
Getting up from lying on the floor
All falls
Falls with serious injuries: fractures, joint dislocations, lacerations requiring sutures, other high-impact soft-tissue injuries
328 21 (6%) 12 months
Bloem et al. 2001
59 Parkinson’s disease patients with good response to
Age: 60.2, SD 9.1
Sex: 49% male
Retropulsion test
Romberg test
Recurrent falls: ≥2 falls (self-reported)
114 0 6 months Population was a mixture of Parkinson’s
89

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 96
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
treatment and 55 age-matched controls
Ambulant community resident
MMSE ≥24
Excluded: Other neurological disorder, visual or orthopaedic problems interfering with balance
Prev. falls: 33.3%
Cognitive impairment: MMSE 28.6 SD 1.7
Visual impairment: ?
Tandem stance (eyes closed)
Tandem stance (eyes open)
SWWT
disease patients and non-Parkinson’s ‘controls’
Bogle Thorbahn and Newton 1996
Volunteer independent-living residents of two life care communities
Excluded if unable to follow directions of test
Age: mean 79.2, SD 6.2
Sex: 24% male
Prev falls: ?
Cognitive impairment: ?
Visual impairment: ?
BBS All self- reported falls
66 12 (18%) 6 months
Cwikel et al. 1998
Aged ≥60, functional independence, able to be interviewed
Age: mean 71.5
Sex: 42% male
Prev falls: 20.6%
Cognitive impairment: ?
Visual impairment: ?
Elderly Fall Screening Test (EFST)
All falls (self-reported)
361 78 (22%) 12 months

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 97
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
Hale et al. 1992
Community living consecutive patients of a family practice Aged ≥65, ambulatory, mentally competent (no dementia and able to answer questions), not acutely ill
Age: mean 74.7
Sex: 19.6% male
Prev falls 27.5%
Cognitive impairment: 0%
Visual impairment: ?
Tinetti mobility test
Physician mobility score estimate
Physician fall risk estimate
All falls 120 18 (15%) 12 months
Hyndman and Ashburn 2004
Diagnosis of stroke
Independently mobile (with walking aid if used)
‘Oriented to place and time’
Able to complete questionnaires
Excluded: bed or chair bound
Required assistance to mobilise
Other neurological conditions
Acute conditions impeding mobility or
Age: Mean 68, range 42–84
Sex: 57% male
Prev falls: ?
Cognitive impairment: Middlesex Elderly Assessment of mental state score median 12 (range 8–12)
Visual impairment: ?
SWWT Falls not as a result of major intrinsic event or overwhelming hazard
65 2 (3%) 6 months Small number of non-elderly people included

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 98
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
balance (lower limb amputation or joint replacement)
Killough 2001
Community-dwelling
Age ≥65
Ability to walk for 6 m
Could follow directions and answer survey questions
No information CCFP fall risk screen
All falls 122 0 (0%) 12 months
Reported as abstract only
Lin et al. 2004
Aged ≥65
Living in one of six rural villages
Not hospitalised or bed-ridden
Age: mean 73.4
Sex: 59.1% male
Prev falls: 10.6%
Cognitive impairment: 53.6% (mild or severe)
Visual impairment: ?
TUG
Functional reach
One leg stance
Tinetti balance
All falls 1200 402 (33.5%) 12 months
Results given as odds ratio and AUC
Lundin-Olsson et al. 1997
Living in sheltered accommodation
Able to walk without aids
Able to follow simple instructions
Age: mean 80.1, SD 6.1
Sex: 28% male
Cognitive impairment: MMSE median
SWWT Falls indoors 58 0 (0%) 6 months

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 99
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
21.5, IQR 18–26
Visual impairment: ?
Lundin-Olsson et al. 2000
Residents of a residential care facility aged ≥65
Age: median 82, range 66–99
Sex: 39.3% male
Prev falls: 47%
Cognitive impairment: MMSE median 21, range 12–26
Visual impairment: 21.8%
MIF chart Falls indoors 78 0 6 months
Lundin-Olsson et al. 2003
Residents of four residential care facilities aged ≥65
No exclusions specified
Age: 83.2, SD 6.8
Sex: 30.3% male
Prev falls: ?
Cognitive impairment: ?
Visual impairment:
MIF
Staff judgement
Falls indoors including those resulting form acute medical events
208 0 (0%) 6 months

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 100
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
22.1%
Nandy et al. 2004
Random sample of people aged over 65
living in one primary care group area contacted
Age: mean 74.4, SD 6.4
Sex: 45% male
Prev falls: 25.4%Cognitive impairment: ?
Visual impairment: ?
FRAT part 1 All falls 510 165 (32.4%) 6 months
Okumiya et al. 1998
Participants in Kahoku Longitudinal Aging Study; non-fallers at start of study
Age: ?
Sex: ?
Prev falls: ?
Cognitive impairment: ?
Visual impairment: ?
TUG All falls 278 35 (12.6%) 5 years Results also presented as odds ratio for Button score and visuospatial cognitive performance test
Raiche et al. 2000
Participants in control group of RCT
Random sample of 225 from electoral list over 75
Age: mean 80.0, SD 4.4
Tinetti balance scale
All falls 225 0 (0%) 12 months
Rosendahl et al. 2003
Residents of one residential care facility in Feb 1994 or moved in during
Age: mean 81, SD 6
Sex: 28% male
Downton index
Indoor falls
Falls not caused by acute illness
78 0 (0%) 12 months

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 101
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
subsequent year
Aged ≥65
No exclusions specified
Prev falls: ?
Cognitive impairment: MMSE median 21, IQR 12–26
Visual impairment: ?
or drug side effects
Smith et al. 2006
All patients with diagnosis of acute stroke admitted to six participating stroke rehabilitation units
Age: median 78, range 34–100
Sex: 49% male
Prev falls: 18%
Cognitive impairment: Abbreviated mental test ≤6: 23%
Visual impairment: 12.4%
STRATIFY All falls 284 50 (17.6%) 3 months Small number of non-elderly people included
Population characteristics include 75 people included in inpatient study
Stel et al. 2003
Subset of participants in LASA cohort study Random sample of elderly people in three regions of The Netherlands
328 participants who fell in previous year
Age: mean 78.3, SD 6.2
Sex: 45.4% male
Prev falls: 15.9%
Cognitive
Mediolateral sway
Handgrip strength
Leg extension strength
Tandem stand
Recurrent falls ≥2 falls
439 21 (4.8%) 12 months
Results given as ROC AUC

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 102
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
plus random sample of 196 of 746 who did not fall were invited
impairment: ?
Visual impairment: ?
Studenski et al. 1994
Aged ≥70
Lived within 30 mile radius of Durham Veterans Affairs hospital
Receive care in ambulatory care clinics
Excluded: Terminal illness
Blindness
Acute illness
Severe cognitive impairment (MMSE <18) and no caregiver to assist with falls monitoring
Age: mean 74.3, SD 5.1
Sex: 100% male
Prev falls: 50.6%
Cognitive impairment: ?
Visual impairment: ?
Mobility screen (6 item, high/low risk)
Mobility skills assessment (13 item)
Risk preference (3 item)
Environmental threat (not clear how scored)
Recurrent falls: two or more falls not due to loss of consciousness, acute illness, unusual activities or unusually hazardous environment
325 19 (5.8%) 6 months
Tinetti 1986
First-time admissions to intermediate care
Excluded: <60 years old
Did not walk as a means of transportation
Age: mean 79, range 61–92
Sex: 32% male
Prev falls: ?
Cognitive impairment: ?
Visual
Balance score (0–28)
Gait score (0–13)
Mobility score (0–28)
Recurrent falls (≥2 falls under circumstances in which a fit person could have resisted the external
79 0 3 months

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 103
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
Admitted for less than 3 months
Unable to participate
impairment: ? hazard if there was one)
Trueblood et al. 2001
Living in community and retirement centres. Aged ≥60
Able to stand for at least 5 minutes
Able to walk at least 40 feet
Excluded: Cognitive deficit (MMSE ≤24)
Underlying neurological problems (Parkinson’s or cerebral vascular accident)
Age: mean 78.1, SD 8.2
Sex: 19.2% male
Prev falls: 50%
Cognitive impairment: ?
Visual impairment:?
Tinetti POMA
TUG
Modified CTSIB
Limits of Stability (LOS)
All falls 198 18 (9.1%) 6 months
Vellas et al. 1997
Participants in Albuquerque Falls Study: volunteers >60 years old, no serious medical conditions
No exclusions specified
Age: mean 72.7, SD 6.1
Sex: 41% male
Prev falls: ?
Cognitive impairment (MMSE <30): 45.6%
Visual impairment: ?
One leg balance
Falls not as a result of violent blow, loss of consciousness or sudden onset of paralysis
Falls for which medical attention was
364 48 (13.2%) 3 years

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 104
Study Inclusion/exclusion Population Screening tests
Outcomes Number recruited
Losses/exclusions Follow-up duration
Notes
sought
Verghese et al. 2002
Participants in Einstein Aging Study – randomly selected Medicare recipients in the Bronx
Aged ≥65
Excluded: Severe visual loss interfering with completion of tests
Not speaking English or Spanish
institutionalisation
Age: mean 79.6, SD 6.4
Sex: 43% male
Prev falls: 28%
Cognitive impairment: ?
Visual impairment: 0%
Tinetti balance and mobility screen
Timed gait
Walking while talking tasks (WWT simple and WWT complex)
All falls 60 1 (1.7%) 12 months
?, data not given; AUC, area under the curve; BBS, Berg Balance Scale; CCFP, Coalition for Community Falls Prevention; CTSIB, Clinical
Test for Sensory Interaction in Balance; diffTUG, difference between times for TUG with and without carrying a glass of water;
IQR, interquartile range; MIF, Mobility Interaction Fall; MMSE, Mini Mental State Examination; POMA, Performance-Oriented
Mobility Assessment; STRATIFY, St Thomas’s Risk Assessment Tool in Falling Elderly Inpatients; SWWT, Stops Walking When
Talking; TUG, Timed Up and Go.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 105
Table 23 Quality-assessment scores
Quality-assessment criteria Study
1 2 3a 3b 5 6 8 9 11 12 13 14a 14b 15 16
Andersson et al. 2006
2 2 2 1 3 3 2 3 2 3 1 2 2 3 3
Bergland and Laake 2005
3 3 3 3 3 3 3 3 2 2 3 3 3 3 3
Bloem et al. 2001
1 2 2 3 3 3 3 3 1 3 3 3 3 3 2
Bogle Thorbahn and Newton 1996
3 2 2 2 3 3 3 3 1 3 2 3 3 3 3
Cwikel et al. 1998
3 3 3 1 1 3 3 3 3 2 2 2 3 3 2
Hale et al. 1992
3 3 3 3 3 3 3 3 2 2 3 3 3 3 2
Hyndman and Ashburn 2004
2 3 2 3 3 3 3 3 2 3 2 3 3 3 3
Killough 2001 2 2 3 2 2 2 1 3 2 1 3 3 2 3 1
Lin et al. 2004
3 3 3 2 1 3 3 3 2 2 1 1 1
2 1
Lundin-Olsson et al. 1997
2 1 2 1 3 3 2 1 2 3 3 3 3 3 3
Lundin-Olsson et al. 2000
3 3 2 2 3 3 3 2 2 3 3 3 3 3 3
Lundin-Olsson et al. 2003
3 3 2 3 3 3 3 3 2 3 2 3 3 3 3
Nandy et al. 2004
3 3 2 1 3 3 3 3 2 2 1 3 3 3 2
Okumiya et al. 1998
2 1 3 1 2 3 2 3 2 1 2 3 1 1 2
Raiche et al. 2000
3 1 3 3 2 3 2 3 2 2 3 3 3 3 3
Rosendahl et al. 2003
3 2 3 3 3 3 3 3 2 3 3 3 2 3 3
Smith et al. 2006 3 3 1 1 2 3 3 3 2 3 3 3 3 3 3
Stel et al. 2003
1 2 3 3 3 3 3 3 2 2 1 1 3 2 3
Studenski et al. 1994
2 3 2 3 3 3 3 3 3 3 3 3 3 1 3
Tinetti 1986 3 2 1 3 3 3 3 3 3 2 3 3 3 3 3
Trueblood et al. 2001
3 3 2 1 3 3 3 3 2 2 2 3 3 3 2
Vellas et al. 1997 3 3 3 2 3 3 3 2 2 1 1 3 2 3

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 106
Quality-assessment criteria Study
1 2 3a 3b 5 6 8 9 11 12 13 14a 14b 15 16
Verghese et al. 2002
3 3 3 2 3 3 3 3 3 3 3 3 3 3 3

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 107
Table 24 Results for sensitivity, specificity, positive predictive value and negative predictive value
Screening tool/study Outcome Cut-off value used Sensitivity (95% CI)
Specificity
(95% CI)
PPV
(95% CI)
NPV
(95%
Berg Balance Scale (BBS)
Bogle Thorbahn and Newton 1996 Falls 45/56 0.53
(0.27, 0.79)
0.92
(0.79, 0.98)
0.73
(0.43, 0.90)
0.84
(0.70, 0.92)
Coalition for Community Fall Prevention Screen
Killough 2005 Falls Not stated 0.83
(0.69, 0.92)
0.51
(0.39, 0.62)
0.51
(0.40, 0.62)
0.83
(0.69, 0.91)
Downton index
All falls ≥3/11 0.81
(0.67, 0.91)
0.4
(0.23, 0.59)
0.68
(0.56, 0.79)
0.57
(0.37, 0.76)
Rosendahl et al. 2003
Falls not due to illness or drugs
≥3/11 0.77
(0.60, 0.90)
0.3
(0.17, 0.46)
0.47
(0.35,0.60)
0.62
(0.41, 0.79)
Elderly Fall Screening Test (EFST)
Cwikel et al. 1998 Falls ≥2/5 0.49
(0.38, 0.61)
0.83
(0.77, 0.89)
0.62
(0.49, 0.72)
0.75
(0.68, 0.81)
FRAT
2 risk factors 0.59
(0.48, 0.70)
0.80
(0.74, 0.84)
0.43
(0.34, 0.53)
0.88
(0.84, 0.92)
3 risk factors 0.42
(0.32, 0.54)
0.92
(0.88, 0.94)
0.57
(0.43, 0.69)
0.86
(0.83, 0.89)
Nandy et al. 2004
Falls
4 risk factors 0.15
(0.09, 0.26)
0.97
(0.94, 0.99)
0.58
(0.37, 0.77)
0.82
(0.77, 0.86)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 108
Screening tool/study Outcome Cut-off value used Sensitivity (95% CI)
Specificity
(95% CI)
PPV
(95% CI)
NPV
(95%
Getting up from lying on the floor
Falls 0.2
(0.14, 0.27)
0.77
(0.69, 0.83)
0.46
(0.35, 0.58)
0.49
(0.42, 0.55)
Bergland and Laake 2005
Fall-related injury 0.33
(0.21, 0.46)
0.81
(0.76, 0.86)
0.3
(0.20, 0.42)
0.83
(0.78, 0.87)
75% Limits of Stability
Reaction time
Trueblood et al. 2001
Falls 0.43
(0.26, 0.63)
0.56
(0.48, 0.64)
0.16
(0.10, 0.26)
0.83
(0.75, 0.89)
End-point excursion
Trueblood et al. 2001
Falls 0.6
(0.41, 0.77)
0.55
(0.46, 0.63)
0.21
(0.14, 0.31)
0.87
(0.79, 0.93)
Maximum excursion
Trueblood et al. 2001
Falls 0.63
(0.44, 0.80)
0.46
(0.38, 0.54)
0.19
(0.13, 0.28)
0.86
(0.77, 0.92)
Movement velocity
Trueblood et al. 2001
Falls 0.33
(0.17, 0.53)
0.76
(0.68, 0.83)
0.22
(0.12, 0.36)
0.85
(0.78, 0.90)
Directional control
Trueblood et al. 2001
Falls
>1 SD from age-based mean
0.43
(0.26, 0.63)
0.54
(0.46, 0.62)
0.16
(0.10, 0.25)
0.83
(0.74, 0.89)
Mobility Interaction Fall chart
Lundin-Olsson et al. 2000 Falls 0.85
(0.68, 0.95)
0.82
(0.68, 0.92)
0.78
(0.62, 0.88)
0.88
(0.75, 0.95)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 109
Screening tool/study Outcome Cut-off value used Sensitivity (95% CI)
Specificity
(95% CI)
PPV
(95% CI)
NPV
(95%
Lundin-Olsson et al. 2000 Falls 0.43
(0.34, 0.53)
0.69
(0.59, 0.78)
0.58
(0.47, 0.69)
0.55
(0.46, 0.63)
Mobility screen
Falls 0.74
(0.64, 0.83)
0.57
(0.50, 0.63)
0.40
(0.32, 0.47)
0.85
(0.78, 0.90)
Studenski et al. 1994
Recurrent falls 0.84
(0.70, 0.93)
0.53
(0.47, 0.60)
0.23
(0.17, 0.30)
0.95
(0.90, 0.98)
Modified CTSIB
Firm surface eyes closed
Trueblood et al. 2001
Falls >1 SD from age-based mean
0.43
(0.26, 0.63)
0.61
(0.52, 0.69)
0.18
(0.11, 0.28)
0.84
(0.76, 0.90)
Firm surface eyes open Trueblood et al. 2001
Falls >1 SD from age-based mean
0.20
(0.08, 0.39)
0.93
(0.87.0.96)
0.35
(0.17, 0.59)
0.85
(0.79, 0.90)
Foam surface eyes closed
Trueblood et al. 2001
Falls >1 SD from age-based mean
0.13
(0.04, 0.31)
0.81
(0.73, 0.87)
0.12
(0.05, 0.27)
0.82
(0.75, 0.88)
Foam surface eyes open
Trueblood et al. 2001
Falls >1 SD from age-based mean
0.37
(0.20, 0.56)
0.66
(0.58, 0.74)
0.18
(0.10, 0.29)
0.84
(0.76, 0.89)
One leg balance
Vellas et al. 1997 Injurious falls 0.36
(0.25, 0.48)
0.77
(0.72, 0.82)
0.31
(0.22, 0.42)
0.81
(0.75, 0.85)
Stops walking when talking
Lundin-Olsson et al. 1997 Falls 0.48
(0.26, 0.70)
0.95
(0.82, 0.99)
0.83
(0.55, 0.95)
0.76
(0.62, 0.86)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 110
Screening tool/study Outcome Cut-off value used Sensitivity (95% CI)
Specificity
(95% CI)
PPV
(95% CI)
NPV
(95%
Timed gait
≥12 s 1.00
(0.75, 1.0)
0.24
(0.13, 0.39)
0.27
(0.17, 0.48)
1.00
(0.74, 1.00)
≥14 s 0.77
(0.46, 0.95)
0.57
(0.41, 0.71)
0.33
(0.19, 0.51)
0.9
(0.74, 0.96)
Verghese et al. 2002
Falls
≥18 s 0.39
(0.14, 0.68)
0.85
(0.71, 0.94)
0.42
(0.19, 0.68)
0.83
(0.70, 0.91)
Tinetti balance scale
Tinetti et al 1986 Recurrent falls <10/15 0.8
(0.59, 0.93)
0.74
(0.60, 0.85)
0.59
(0.42, 0.74)
0.89
(0.77, 0.95)
Trueblood et al. 2001 Falls <12/16 0.23
(0.10, 0.42)
0.91
(0.85, 0.95)
0.33
(0.17, 0.55)
0.86
(0.79, 0.90)
<8/16 0.08
(0.00, 0.36)
0.91
(0.79, 0.98)
0.20
(0.04, 0.62)
0.78
(0.65, 0.87)
<9/16 0.23
(0.05, 0.54)
0.8
(0.66, 0.91)
0.25
(0.09, 0.53)
0.79
(0.65, 0.88)
Verghese et al. 2002
Falls
<10/16 0.62
(0.32, 0.86)
0.7
(0.54, 0.82)
0.36
(0.20, 0.57)
0.86
(0.72, 0.94)
Tinetti gait scale
Tinetti et al 1986 Recurrent falls <9/13 0.68
(0.47, 0.85)
0.63
(0.49, 0.76)
0.46
(0.31, 0.62)
0.81
(0.67, 0.90)
Trueblood et al. 2001 Falls <8/12 0.2 0.95 0.43 0.86

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 111
Screening tool/study Outcome Cut-off value used Sensitivity (95% CI)
Specificity
(95% CI)
PPV
(95% CI)
NPV
(95%
(0.08, 0.39) (0.90, 0.98) (0.21, 0.67) (0.79, 0.90)
Tinetti mobility scale
Hale et al. 1992 Falls <30/40 0.27
(0.14, 0.44)
0.83
(0.72, 0.91)
0.48
(0.28, 0.68)
0.67
(0.56, 0.76)
≤33/40 0.51
(CI not reported)
0.74
(CI not reported)
Not reported Not reportedRaiche et al. 2000
Falls
≤36/40 0.7
(0.56, 0.82)
0.52
(0.44, 0.59)
0.31
(0.23, 0.40)
0.85
(0.77, 0.90)
Tinetti 1986 Recurrent falls <19/28 0.76
(0.55, 0.91)
0.83
(0.71, 0.92)
0.68
(0.49, 0.82)
0.88
(0.77, 0.94)
Timed Up and Go (TUG)
Okumiya et al. 1998 Falls 16s 0.54
(0.42, 0.67)
0.73
(0.65, 0.79)
0.44
(0.34, 0.55)
0.8
(0.73, 0.86)
Trueblood et al. 2001 Falls 20s 0.1
(0.02, 0.27)
0.95
(0.90, 0.98)
0.27
(0.10, 0.57)
0.84
(0.78, 0.89)
WWT complex
≥26 s 0.54
(0.25, 0.81)
0.85
(0.71, 0.94)
0.5
(0.27, 0.73)
0.87
(0.74, 0.94)
≥30 s 0.39
(0.14, 0.68)
0.91
(0.79, 0.98)
0.56
(0.27, 0.81)
0.84
(0.71, 0.92)
Verghese et al. 2002
Falls
≥33 s 0.39
(0.14, 0.68)
0.96
(0.85, 1.00)
0.71
(0.36, 0.92)
0.85
(0.72, 0.92)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 112
Screening tool/study Outcome Cut-off value used Sensitivity (95% CI)
Specificity
(95% CI)
PPV
(95% CI)
NPV
(95%
WWT simple
≥16 s 0.54
(0.25, 0.81)
0.61
(0.45, 0.75)
0.28
(0.14, 0.48)
0.82
(0.66, 0.92)
≥18 s 0.46
(0.19, 0.75)
0.76
(0.61, 0.87)
0.35
(0.17, 0.59)
0.83
(0.69, 0.92)
Verghese et al. 2002
Falls
≥20 s 0.46
(0.19, 0.75)
0.89
(0.76, 0.96)
0.55
(0.28, 0.79)
0.85
(0
WWT, walking while talking tasks.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 113
Table 25 Results reported as summary ROC curves or similar
Study Screening test Outcome ROC AUC
95% CI
TUG 0.610 Not given
One-leg standing 0.527 Not given
Functional reach 0.509 Not given
Lin and Wang 2004
Tinetti balance
Falls
0.559 Not given
Mediolateral sway (n=161)
0.67 (0.57, 0.77)
Tandem stand (n=161) 0.61 (0.49, 0.73)
Leg extension strength (n=419)
0.58 (0.51, 0.64)
Stel et al. 2003
Handgrip strength (n=419)
Recurrent falls
0.57 (0.51, 0.64)
AUC, area under the curve.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 114
Table 26 Results for Parkinson’s disease population
Test Outcome Sensitivity Specificity PPV NPV
Retropulsion test 0.29
(0.10, 0.56)
0.89
(0.81, 0.94)
0.31
(0.14, 0.56)
0.88
(0.80,0.93)
Romberg test 0.18
(0.04, 0.43)
1
(0.96, 1.00)
1
(0.44, 1.00)
0.87
(0.80, 0.92)
Tandem stance (eyes closed) 0.88
(0.64, 0.99)
0.46
(0.36, 0.57)
0.22
(0.14, 0.34)
0.96
(0.86, 0.99)
Tandem stance (eyes open) 0.53
(0.28, 0.77)
0.84
(0.75, 0.91)
0.36
(0.20, 0.55)
0.91
(0.84, 0.95)
Bloem et al. 2001
SWWT
Recurrent falls
0.12
(0.02, 0.36)
0.95
(0.88, 0.98)
0.29
(0.08, 0.64)
0.86
(0.78, 0.91)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 115
Table 27 Results for post-stroke populations
Test Outcome Cut off Sensitivity Specificity PPV NPV
BBS 45/56 0.63
(0.50, 0.75)
0.65
(0.53, 0.75)
0.58
(0.46, 0.69)
0.69
(0.58, 0.78)
SWWT 0.15
(0.06, 0.28)
0.97
(0/90, 1.00)
0.78
(0.45, 0.94)
0.61
(0.52, 0.70)
TUG 14 s 0.5
(0.34, 0.66)
0.79
(0.66, 0.88)
0.59
(0.42, 0.74)
0.72
(0.60, 0.81)
Andersson et al. 2006
diffTUG
Falls
4.5 s 0.17
(0.06, 0.36)
0.95
(0.86, 0.99)
0.63
(0.31, 0.86)
0.70
(0.59, 0.79)
Falls 1 s 0.53
(0.34, 0.72)
0.70
(0.51, 0.84)
0.62
(0.43, 0.78)
0.62
(0.46, 0.76)
Hyndman and Ashburn 2004
SWWT
Recurrent falls
1 s 0.73
(0.45, 0.92)
0.69
(0.54, 0.81)
0.42
(0.26, 0.61)
0.89
(0.75, 0.96)
Smith et al. 2004 STRATIFY Falls ≥2 0.16
(0.09, 0.26)
0.86
(0.81, 0.92)
Not calculable
Not calculable
BBS, Berg Balance Scale.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 116
Section 5 Cost-effectiveness systematic review
5.1 Introduction
In 2003 the economic costs of falls in the UK was estimated to be
£981 million (Scuffham et al., 2003). The majority of costs were
incurred for inpatient admissions and long-term care costs for patients
75 years and older. Given the expected increase in the over 65-year-
old population these costs are likely to increase the ‘burden’ on the
NHS and personal social services attributable to falls in older people
(Scuffham et al., 2003). Reducing falls that may result in inpatient
admissions and or long-term care costs is a key aim set out in the
National Service Framework for Older People (Department of Health,
2001).
NICE guidance for the assessment and prevention of falls in older
people (National Institute for Clinical Excellence, 2004) explored
factors that increase peoples’ risk of falling, assessment methods for
identifying people at risk of falling, the effectiveness of hip protectors,
the user experience of falls-prevention services and the clinical
effectiveness and cost-effectiveness for preventing falls, preventing
further falls and rehabilitation. Although cost-effectiveness data for
falls prevention were reviewed, this reflected an international
perspective, and included studies from New Zealand, Australia and the
USA; no data were obtained on the cost-effectiveness of interventions
for the prevention of falls in older people in the UK (National Institute
for Clinical Excellence, 2004).
NICE have proposed the provision of additional guidance from the
Technology Appraisal programme that aims ‘to appraise the clinical
and cost-effectiveness of fallers’ clinics for the assessment and
prevention of falls’. However, the appraisal was suspended due to
insufficient evidence and the lack of a definition of a fallers’ clinic.
Preparatory work has been commissioned, designed to underpin the
continuance of the planned guideline by NICE, and this update of the
cost-effectiveness systematic review forms part of the commissioned
programme.
5.2 Methods
This review explored whether any new evidence on the resources
utilised in the provision of FPPs for older people, reflecting the UK
perspective, has been published since the completion of the NICE
guideline review in 2004.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 117
5.2.1 Selection criteria
Types of study
All types of cost and cost-effectiveness study designs were considered.
Types of participant and setting
Older people, women and men, who had fallen or were at risk of
falling, living in the community and participating in a falls-prevention
intervention programme in the UK were included.
Types of intervention
Any interventions comparing the cost and cost-effectiveness of falls
prevention compared with control intervention, usual care, or no
intervention were included.
Types of outcome
Cost-benefit, cost-effectiveness and/or cost utility outcomes in terms
of health-care resource utilisation resulting from a falls-related
diagnosis were included:
• treatment cost in primary and secondary care,
• diagnostic cost in primary and secondary care,
• hospital admission,
• quality-of-life measures,
• mortality.
Additional resource use resulting from the implementation of
interventions was also included.
5.2.2 Search strategy
The search strategies (Appendix 8) utilised by NICE were modified (by
C. McCabe) to include variants of Short-form 36 and Quality Of
Wellbeing, and the addition of the following search terms: vas, hrqol,
utility, preference and value, and are given in Appendix 8.
In this update of the NICE guideline for the assessment and
prevention of falls in older people we searched:
• MEDLINE, Ovid 1966 to August week 3 2006;
• CINAHL, Ovid 1982 to August week 3 2006;
• EMBASE, Ovid 1996 to week 34 2006;
• NHS EED, from 2003 to August 2006;
• OHE HEED, from 2003 to August 2006;
• National Research Register (www.nrr.nhs.uk/search.htm),
relevant ongoing projects;
• reference-list search of retrieved and relevant articles.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 118
5.3 Results
The results of the search and the sifting process are summarised in
Figure 12. Data extraction and appraisal were undertaken using a
modified version of the Drummond and Jefferson framework (shown in
Appendix 9; Drummond and Jefferson, 1996). Excluded studies are
given in Appendix 10.
Figure 12 The sifting process
Although 242 articles contained key terms including cost, cost-
effectiveness, economic or economic evaluation, falls prevention and
falls there where no additional studies of community-dwelling older
people who had fallen or were at risk of falling participating in falls-
prevention interventions that was the subject of a cost-effectiveness
analysis published in the UK in the intervening period since the
publication of the NICE systematic review in 2004.
The implementation of well-designed trials of FPPs with effective
evaluation, including an economic evaluation, is costly in terms of time
and money and may account for the lack of subsequent evidence. The
need for cost-effectiveness analysis of FPPs is widely acknowledged
within the falls-prevention community. However, of the four ongoing
falls-prevention studies reported on the National Research Register
only one is reporting that they intend to undertake a cost-
effectiveness analysis of their programme.
A large UK study (Masud et al., 2006) of community-dwelling, high-
risk older women and men participating in a multi-factorial
intervention designed to reduce the incidence of falls is currently being
undertaken; the study is expected to take 3 years to complete and is
due to report at the end of 2007. However, it is not possible to
Electronic database search n=3942 (854 duplicates) Reference list search n=77
Titles screened for relevance (n=1740 rejected)
Full papers screened for relevance n=62
Titles and abstracts screened for relevance (n=1363 rejected)
Studies included n=0
Total articles retrieved: N=3165

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 119
comment on whether these studies will provide sufficient quality
evidence required for the construction of a UK cost-effectiveness
model for effective falls prevention in older people.
Cost-effectiveness analyses of FPPs have been undertaken
internationally, including in Australia (Beard et al., 2006), New
Zealand (Campbell et al., 2005) and Denmark. In addition, a FPP
study with cost-effectiveness analysis is currently being undertaken in
The Netherlands (Hendriks et al., 2005).
5.4 Discussion
At this time there are no published cost-effectiveness studies of falls-
intervention programmes, to inform the policy question of whether
falls-intervention programmes for older community-dwelling
population are cost-effective in the UK NHS.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 120
Section 6 Feasibility of constructing a cost-effectiveness model of multi-factorial interventions for falls prevention
6.1 Background
The National Service Framework for Older People (Department of
Health, 2001) and the NICE guideline on falls prevention (National
Institute for Clinical Excellence, 2004) both recommended that
Primary Care Trusts in the UK should implement FPPs. However,
neither document provided detailed guidance on the organisation or
content of these programmes.
In 2004, a proposed Appraisal of Fallers Clinics as part of the NICE
Technology Appraisal Programme was suspended because of a lack of
information necessary to produce a scope for the document; most
notably, the inability to describe current service provision.
This project was commissioned, in part, to establish whether it was
feasible to provide the evidence base necessary for the appraisal of
fallers clinics to be recommenced. To this end, we have surveyed NHS
organisations to provide a detailed description of the falls-prevention
activities currently ongoing and the resources required. We have also
undertaken a systematic review of the evidence for the performance of
screening tools and the effectiveness of interventions for falls
prevention.
In this section we describe the evidence required to undertake a
robust cost-effectiveness analysis of FPPs and consider whether the
evidence matches this specification. We then consider whether further
research is required before a robust cost-effectiveness analysis is
feasible, and if so, what that research should be.
6.2 Structure and parameter specification
for a cost-effectiveness model
The proposed model considers the cost-effectiveness of a FPP in a
community-dwelling population; that is, it excludes older people living
in residential and/or nursing homes.
The first decision to be made in specifying the model structure is how
patients present to the service. Are they identified opportunistically
when they contact another NHS service or is there a pro-active search
process? The results of the survey suggest that the majority of
services operating in the NHS identify participants opportunistically
when they contact another NHS service.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 121
Once candidates for the service have been identified the next decision
to be made in specifying the model structure is whether the
candidates are subject to triage to establish eligibility prior to further
assessment and/or the preventive intervention. The survey
demonstrates that this process varies in content and format, with
some services using a screening tool and others using more simple
criteria. Where there is initial triage prior to intervention, data on the
performance of the triage criteria are required. The information
required is the sensitivity and specificity of the screening tool and/or
triage factors as the expected health outcomes and resource utilisation
differ between the four groups of true negative, true positive, false
negative and false positive. It will also be necessary to identify the
resource utilisation associated with the triage process used.
For each group of patients in the treated arm and the patients in the
untreated arm it will be necessary to identify the expected resource
use and event rate over time. This will include the resources used for
the intervention and the resources used in treating fall-related events.
Given that the argument for falls prevention is that falls are a
significant cause of major injury in the elderly, which is associated
with substantial morbidity and mortality, the appropriate time horizon
is a lifetime one. Failure to adopt a lifetime horizon will produce a
biased estimate of the cost-effectiveness of the intervention. Thus,
event-rate data will be required for sufficient follow-up to allow a
reliable estimate of event rates out to 20 years, assuming that
participants are aged 65 years or more at the time of the intervention.
As fall-related events range from extremely minor to fatal, with an
associated difference in their resource implications, the event-rate
data will have to be at a sufficient level of disaggregation to allow an
accurate representation of these differential impacts. At a minimum it
will be necessary to differentiate fall-related injuries into peripheral
fractures, hip fractures and head injuries.
Depending upon the severity of the fall-related injury, the individual
may or may not be fit to return to independent living. The model will
therefore have to capture the resource, morbidity and mortality
implications of being discharged to different residential settings
including home, residential care and nursing care.
In addition to the implications for resource utilisation of the different
fall-related events it would be desirable to attach quality-of-life
weights (utilities) to each category of event. Where events are known
to increase the subsequent mortality risk, the post-event mortality will
be required.
In the next section we summarise the findings of the review with
regard to the evidence needs of the model.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 122
6.3 Evidence on parameters in cost-effectiveness models
6.3.1 Patient identification and eligibility
The majority of falls-prevention services required a referral from
another NHS or social service. Approximately 25% of services that
provided information on this to the survey operated an open referral
process. The remainder required referral from a health professional,
although there was some variation in the categories of health
professional who could refer. None of the services operated a
pro-active identification processes.
The survey found that the approximately 90% of falls-prevention
services operated eligibility criteria. The most common criteria used
were previous falls or ‘near falls’, age, a short screening tool and/or
polypharmacy. Most falls-prevention services used more than one
criterion.
Only a minority (33%) of falls-prevention services used a published
screening tool to assess a risk of falling. A third used a screening tool
of their own devising and a third did not use any screening tool
beyond the referral eligibility criteria. The systematic review of
published screening tools established that ‘At present it is not possible
to provide a quantitative summary of the accuracy of any fall-risk
screening tool.’ The review of the screening instruments found no
evidence that quantified the relationship between screening tools and
the underlying risk of fall or fall-related injury.
If it is impossible to identify the baseline risk of falling – the proportion
of patients who will be correctly and incorrectly allocated to the four
groups of false positive, false negative, true positive and true negative
– then it is impossible to establish the incremental outcomes or costs
associated with an effective falls-prevention treatment even when
there is evidence of its relative effectiveness from an RCT. Research in
this area should be a priority.
6.3.2 Effectiveness
There is a substantial literature reporting RCTs of falls-prevention
interventions, although there are methodological limitations to most of
the studies. This report presents an exhaustive set of meta-analyses.
Whether falls have a significant effect depends upon which outcome
measure is considered. The meta-analyses suggest that, using
conventional standards of evidence, FPPs may have a small impact
upon the incidence of falls in the follow-up period (RR 0.9, 95% CI
0.8–1.0). However, the evidence does not support a conclusion that
FPPs impact upon fall-related injuries (RR 0.97, 95% CI 0.73–1.28),
mortality (RR 1.0, 95% CI 0.78–1.27) or the transition to institutional
care (RR 0.92, 95% CI 0.66–1.29), nor that FPPs impact upon
emergency department attendance (RR 0.98, 95% CI 0.74–1.29) or

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 123
hospital admissions (RR 0.85, 95% CI 0.69–1.04). They may,
however, lead to increased GP attendances (RR 1.39, 95% CI 1.11–
1.74).
As the rationale for FPPs is that they will impact upon the morbidity,
mortality and resource use associated with falls (NICE Falls Guideline
Scope; www.nice.org.uk/page.aspx?o=30591), whereas the evidence
base on effectiveness is sufficient to parameterise these parts of a
cost-effectiveness model, it is possible to draw the conclusion that
FPPs are as likely to exacerbate as ameliorate the problems that they
are designed to address. In this context, the value of constructing a
cost-effectiveness model may be less than originally expected.
6.3.3 Resource utilisation
The published literature is of very little use in identifying the resource
implications of falls and fall-prevention programmes in the UK. None of
the published economic evaluations were of UK NHS FPPs and thus the
resource use and unit costs cannot be easily generalised to the UK
NHS. Some studies provide top-down estimates of the total cost of
falls to the UK NHS – notably Scuffham et al. (2003) – but these
estimates do not provide the level of detail required to characterise
the cost parameters in a cost-effectiveness model.
The detailed survey of FPPs undertaken as part of this study provides
the most detailed description of the resource use in an NHS context to
date. It is clear that there is substantial variation in the resources
consumed by FPPs in different settings: in terms of the staffing
requirements, accommodation and the combination of assessments
and interventions provided. From the survey we cannot conclude that
there is any degree of consensus as to the model of FPP that should be
utilised in the NHS, nor can we confidently link the majority of the
FPPs we have identified to interventions for which there is RCT
evidence.
It would be possible to specify resource use of some of the
interventions reported in published RCTs by contacting authors for
additional data, and to utilise unit-cost data collected in the survey.
However, there are two significant limitations. First, there is
considerable disparity between the interventions reported in the
survey and those described adequately in the literature. Second, it
would be necessary to undertake further data collection to attach
resource-use and unit-cost data to the post-intervention events (e.g.
fall-related injuries, admission to hospital, referral to residential care)
that would also be an important element of any cost-effectiveness
analysis.
6.4 Discussion
There is a large volume of NHS activity that falls under the umbrella of
falls prevention. However, the degree of variation in content of this

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 124
activity and the evidence base for its effectiveness is even greater.
The limitations of the evidence base for FPPs are such that it would not
allow us to confidently differentiate between what works and does not
work within the portfolio of FPPs. This is perhaps unsurprising given
the mandate to provide FPPs from both the National Service
Framework for Older People (Department of Health, 2001) and the
NICE guideline on falls prevention (National Institute for Clinical
Excellence, 2004) without detailed direction. Against this background
it would not be possible to construct a cost-effectiveness model that
was representative of current falls-prevention activity in the NHS.
The review of the evidence base identifies a number of challenges to
the construction of a cost-effectiveness model of ideal practice in falls
prevention. The first of these is the lack of reliable validated tools for
identification of the baseline risk of falling. Without this it is impossible
to identify the magnitude of benefit from the FPP; and identifying the
magnitude of benefit from the treatment is essential to calculating an
incremental cost-effectiveness ratio.
Whereas there are a number of RCTs of FPPs the duration of follow-up
for the trials is generally short and there are concerns regarding the
robustness of the follow-up in some of the studies. To establish the
cost-effectiveness of the interventions in the long term it is important
to know whether the effects are sustained or not, and whether repeat
intervention can maintain the effectiveness in the longer term. The
evidence base is weak in this regard, although extrapolations from this
type of data can be, and often are, made.
Arguably the most important finding of the effectiveness review is that
the FPPs that have been subject to an RCT do not have a significant
effect on the outcomes which provide the policy basis for
recommending their implementation in the NHS; that is, falls-related
injuries, hospitalisation and emergency department attendance. We
can speculate as to why this may be the case; for example, it might
be that the factors that predispose towards sustaining an injury in fall
are likely to represent a barrier to engagement in a clinical trial, or it
might be that the FPP tests do not act on the factors that predispose
to an injury from fall. Whatever the explanation, the current evidence
base cannot be interpreted as a foundation for the widespread
implementation of the FPPs to reduce the incidence of falls-related
injuries and the associated morbidity, mortality and resource use.
The RCTs identified in this review are relatively small and of short
duration. It may be that the underlying event rate of interest, falls-
related injury, is too small for them to have provided strong evidence
for an effect. Thus, there may be value in undertaking a much larger
trial powered to identify a difference in fall-related injury. However,
researchers may also need to revisit the underlying aetiological model
of fall-related injuries and establish a firm evidence base on the
causes of fall-related injuries prior to designing interventions that
clearly address those causes.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 125
Any future trial of an FPP should be designed to ensure that it provides
unbiased and robust evidence on the following:
1 the untreated risk of falls and fall-related injuries;
2 the sensitivity and specificity of screening tools used to determine
eligibility for services;
3 the impact of the intervention on falls, fall-related injuries,
mortality, health-related quality of life and utilisation of health
and social care resources in primary, secondary and community
care;
4 the resource utilisation associated with the intervention;
5 the impact of the intervention on health-related quality of life.
Of particular importance is the use of a published and validated risk-
assessment tool delivered in a standardised manner and interpreted
according to standard and validated rules.
6.5 Conclusion
At the present time, the evidence base is insufficient to support the
construction of a cost-effectiveness model to assess the question of
what is the incremental cost-effectiveness of a FPP in the prevention
and management of fall-related injuries and the associated morbidity
and mortality, for a community-dwelling UK population, from the
perspective of the NHS and social services.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 126
References
Ahmad Hasali MA, Mohamed Ibrahim MI, Syed Sulaiman SA, Ahmad Z,
Ahmad Hasali JB. 2005. A clinical and economic study of
community-acquired pneumonia between single versus
combination therapy. Pharmacy World and Science 27(3): 249–
53.
Alexander NB, Goldberg A. 2005. Gait disorders: search for multiple
causes. Cleveland Clinic Journal of Medicine 72(7): 586, 589–90,
592–4, 597–600.
Allum JH, Carpenter MG. 2005. A speedy solution for balance and gait
analysis: angular velocity measured at the centre of body mass.
Current Opinion in Neurology 18(1): 15–21.
Andersson AG, Kamwendo K, Seiger A, Appelros P. 2006. How to
identify potential fallers in a stroke unit: validity indexes of 4 test
methods. Journal of Rehabilitation Medicine 38(3): 186–91.
Anonymous. 2003. Burden of falls in older people. Pharmaceutical
Journal 271(7264): 258.
Anonymous. 2005. Fall prevention programmes in older people.
Evidence-based Healthcare & Public Health 9(5): 343–8.
Ashton J, Gilbert D, Hayward G, O'Dell C, Rogowski B. 1989.
Predicting patient falls in an acute care nursing setting. Kansas
Nurse 64(10): 3–5.
Asplund R. 2004. Nocturia, nocturnal polyuria, and sleep quality in the
elderly. Journal of Psychosomatic Research 56(5): 517–25.
Avdic D, Pecar D. 2006. Significance of specificity of Tinetti B-POMA
test and fall risk factor in third age of life. Bosnian Journal of Basic
Medical Sciences 6(1): 50–7.
Bagust A, Grayson AD, Palmer ND, Perry RA, Walley T. 2006. Cost
effectiveness of drug eluting coronary artery stenting in a UK
setting: cost-utility study. Heart 92(1): 68–74.
Ballard C, Cream J. 2005. Drugs used to relieve behavioral symptoms
in people with dementia or an unacceptable chemical cosh?
Argument. International Psychogeriatrics 17(1): 4–12.
Barnett A, Smith B, Lord SR, Williams M, Baumand A. 2003.
Community-based group exercise improves balance and reduce
falls in at-risk older people: a randomised controlled trial. Age and
Ageing 32: 407–14.
Barr RJ, Stewart A, Torgerson DJ, Seymour DG, Reid DM. 2005.
Screening elderly women for risk of future fractures - participation
rates and impact on incidence of falls and fractures. Calcified
Tissue International 76(4): 243–8.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 127
Beard J, Rowell D, Scott D, van Beurden E, Barnett L, Hughes K, et al.
2006. Economic analysis of a community-based falls prevention
program. Public Health 120(8): 742–51.
Becker C, Loy S, Sander S, Nikolaus T, Rimann U, Kron M. 2005. An
algorithm to screen long-term care residents at risk for accidental
falls. Aging Clinical & Experimental Research 17(3): 186–92.
Beer C, Giles E. 2005. Hip fracture–challenges in prevention and
management. Australian Family Physician 34(8): 673–6.
Beghe C, Wilson A, Ershler WB. 2004. Prevalence and outcomes of
anemia in geriatrics: a systematic review of the literature.
American Journal of Medicine 116 (Suppl 7A): 3S–10S.
Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. 1992. Measuring
balance in the elderly: validation of an instrument. Canadian
Journal of Public Health. Revue Canadienne de Sante Publique 83
Suppl 2: S7–11.
Bergland A, Laake K. 2005. Concurrent and predictive validity of
"getting up from lying on the floor". Aging Clinical & Experimental
Research 17(3): 181–5.
Bergland A, Jarnlo GB, Laake K. 2002. Validity of an index of self-
reported walking for balance and falls in elderly women. Advances
in Physiotherapy 4(2): 65–73.
Bergland A, Jarnlo GB, Wyller TB. 2006. Self-reported walking,
balance testing and risk of fall [Norwegian]. Tidsskrift for Den
Norske Laegeforening 126(2): 176–8.
Berryman E, Gaskin D, Jones A, Tolley F, MacMullen J. 1989. Point by
point: predicting elders' falls. Geriatric Nursing 10(4): 199–201.
Billek-Sawhney B, Holbein-Jenny MA, Beckman E, Smith T. 2002.
Reliability of the activities-specific balance Confidence Inventory,
the Berg Balance Score and the Multidirectional Reach Test in
personal care home residents. Journal of Geriatric Physical
Therapy 25(3): 34–5.
Birks Y, Porthouse J, Torgerson DJ. 2003. Regarding the systematic
review of hip protectors undertaken by Waldegger et al.
Osteoporosis International 14(10): 868–9.
Birks YF, Hildreth R, Campbell P, Sharpe C, Torgerson DJ, Watt I.
2003. Randomised controlled trial of hip protectors for the
prevention of second hip fractures. Age and Ageing 32(4): 442–4.
Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Johnson BE. 2004.
Review: prophylactic use of vitamin D reduces falls in older
persons. Evidence Based Medicine 9(6): 169.
Bischoff-Ferrari HA, Dawson-Hughes B, Willett WC, Staehelin HB,
Bazemore MG, Zee RY, et al. 2004. Effect of vitamin D on falls: a
meta-analysis. Journal of the American Medical Association
291(16): 1999–2006.
Bischoff-Ferrari HA, Willett WC, Wong JB, Giovannucci E, Dietrich T,
Dawson-Hughes B. 2005. Fracture prevention with vitamin D

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 128
supplementation: a meta-analysis of randomized controlled trials.
Journal of the American Medical Association 293(18): 2257–64.
Black A, Wood J. 2005. Vision and falls. Clinical & Experimental
Optometry 88(4): 212–22.
Bloem BR, Grimbergen YAM, Cramer M, Valkenburg VV. 2000. 'Stops
walking when talking' does not predict falls in Parkinson's disease
[1]. Annals of Neurology 48(2): 268.
Bloem BR, Grimbergen YAM, Cramer M, Willemsen M, Zwinderman AH.
2001. Prospective assessment of falls in Parkinson's disease.
Journal of Neurology 248(11): 950–8.
Bogle Thorbahn LD, Newton RA. 1996. Use of the Berg Balance Test to
predict falls in elderly persons. Physical Therapy 76(6): 576–83.
Bosma H, Sanderman R, Scaf-Klomp W, van Eijk JTM, Ormel J,
Kempen GIJ. 2004. Demographic, health-related and psychosocial
predictors of changes in depressive symptoms and anxiety in late
middle-aged and older persons with fall-related injuries.
Psychology and Health 19(1): 103–15.
Boulgarides LK, McGinty SM, Willett JA, Barnes CW. 2003. Use of
clinical and impairment-based tests to predict falls by community-
dwelling older adults. Physical Therapy 83(4): 328–39.
Boustani M, Sloane PD. 2003. Should residential care/assisted living
facilities institute falls prevention programs for their residents?
Annals of Long-Term Care 11(2): 39–44.
Braithwaite RS, Col NF, Wong JB. 2003. Estimating hip fracture
morbidity, mortality and cross. Journal of the American Geriatric
Society 51(3): 364–70.
Brauer SG, Burns YR, Galley P. 2000. A prospective study of
laboratory and clinical measures of postural stability to predict
community-dwelling fallers. Journals of Gerontology Series A-
Biological Sciences & Medical Sciences 55(8): M469–76.
Brennan nee Saunders J, Johansen A, Butler J, Stone M, Richmond P,
Jones S, et al. 2003. Place of residence and risk of fracture in
older people: a population-based study of over 65-year-olds in
Cardiff. Osteoporosis International 14(6): 515–9.
British Association of Emergency Medicine. 2005. National Survey of
Emergency Secondary Care.
www2.warwick.ac.uk/fac/med/research/hsri/emergencycare/resea
rch/survey2005/.
Broadhurst C, Wilson KCM, Kinirons MT, Wagg A, Dhesi JK. 2003.
Clinical pharmacology of old age syndromes. British Journal of
Clinical Pharmacology 56(3): 261–72.
Brown DS. 2004. Do leaves have to fall in their autumn? A falls
prevention strategy in action in the south east of South Australia.
Rural and Remote Health 4(1).
Bruyere O, Wuidart M-A, Di Palma E, Gourlay M, Ethgen O, Richy F, et
al. 2005. Controlled whole body vibration to decrease fall risk and

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 129
improve health-related quality of life of nursing home residents.
Archives of Physical Medicine & Rehabilitation 86(2): 303–7.
Burl JB, Centola J, Bonner A, Burque C. 2003. Hip protector
compliance: a 13-month study on factors and cost in a long-term
care facility. Journal of the American Medical Directors Association
4(5): 245–50.
Bush T. 2003. More than gravity – falls in the elderly mentally ill
patient with dementia – increasing nurses' awareness of the risk
factors. Nurse 2 Nurse 3(9): 36–8.
Campbell AJ, Robertson MC, La Grow SJ, Kerse NM, Sanderson GF,
Jacobs RJ, et al. 2005. Randomised controlled trial of prevention
of falls in people aged > or=75 with severe visual impairment:
the VIP trial. British Medical Journal 331: 817–20.
Cannard, G. 1996. Falling trend. Nursing Times 92: 36–7.
Carpenter I. 2004. Aging and community care. Aging Clinical &
Experimental Research 16(4): 257–8.
Carroll NV, Slattum PW, Cox FM. 2005. The cost of falls among the
community-dwelling elderly. Journal of Managed Care Pharmacy
11(4): 307–16.
Chandler JM, Duncan PW, Weiner DK, Studenski SA. 2001. Special
feature: the Home Assessment Profile – a reliable and valid
assessment tool. Topics in Geriatric Rehabilitation 16(3): 77–88.
Chang JT, Morton SC, Rubenstein LZ, Mojica WA. 2004. Interventions
for the prevention of falls in older adults: systematic review and
meta-analysis of randomised clinical trials. British Medical Journal
328(7441): 680.
Chappel NL, Havens B, Hollander MJ, Miller JA, McWilliam C. 2004.
Comparative costs of home care and residential care. The
Gerontologist 44(3): 389–400.
Chiari P, Mosci D, Fontana S. 2002. Comparison of two scales for the
assessment of the risk of falls in hospitalised patients [Italian].
Assistenza Infermieristica e Ricerca 21(3): 117–24.
Chiu AYY, Au-Yeung SSY, Lo SK. 2003. A comparison of four functional
tests in discriminating fallers from non-fallers in older people.
Disability & Rehabilitation 25(1): 45–50.
Clark DO, Callahan CM, Counsell SR. 2005. Reliability and validity of a
steadiness score. Journal of the American Geriatrics Society
53(9): 1582–6.
Clemson L, Cumming RG, Kendig H, Swann M, Heard R, Taylor K.
2004. The effectiveness of a community-based program for
reducing the incidence of falls in the elderly: a randomized trial.
Journal of the American Geriatrics Society 52(9): 1487–94.
Close JCT. 2005. Prevention of falls-a time to translate evidence into
practice. Age and Ageing 34: 98–100.
Close JCT, McMurdo MET. 2003. Falls and bone health services for
older people. Age and Ageing 32(5): 494–6.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 130
Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C, et al.
1999. Prevention of falls in the elderly trial (PROFET): a
randomised controlled trial. The Lancet 353: 93–7.
Coker E, Oliver D. 2003. Evaluation of the STRATIFY falls prediction
tool on a geriatric unit. Outcomes Management 7(1): 8–14.
Coleman EA, Grothaus LC, Sandhu N, Wagner EH. 1999. Chronic care
clinics: a randomized controlled trial of a new model of primary
care for older frail adults. Journal of the American Geriatrics
Society 47: 775–83.
Collins JW, Wolf L, Bell J, Evanoff B. 2004. An evaluation of a "best
practices" musculoskeletal injury prevention program in nursing
homes. Injury Prevention 10(4): 206–11.
Colon-Emeric CS. 2002. Falls in older adults: assessment and
intervention in primary care. Hospital Physician 38(4): 55–66.
Colon-Emeric CS, Datta SK, Matchar DB. 2003. An economic analysis
of external hip protector use in ambulatory nursing facility
residents. Age and Ageing 32(1): 47–52.
Conley DM. 2005. Specificity and sensitivity of the Morse Fall Scale on
three medical surgical units. Geriatric Nursing 26(6): 353–4.
Conley D, Schultz AA, Selvin R. 1999. The challenge of predicting
patients at risk for falling: development of the Conley Scale.
MEDSURG Nursing 8(6): 348–54.
Consortium KCHNTRD. 1997. Can the Incidence of Falls in the Elderly
be Reduced by a Secondary Falls Prevention Protocol? National
Research Register; www.nrr.nhs.uk/default.htm.
Cornali C, Franzoni S, Stofler PM, Trabucchi M. 2004. Mental functions
and physical performance abilities as predictors of falling in a
geriatric evaluation and rehabilitation unit. Journal of the
American Geriatrics Society 52(9): 1591–2.
Costa JC, Hesselbo B, Poulsen I, Norregard JC, Schroll M, Kirchhoff M.
2006. [The significance of cataract surgery and balance function
of the elderly]. Ugeskrift for Laeger 168(11): 1124–8.
Covinsky KE, Kahana E, Kahana B, Kercher K, Schumacher JG, Justice
AC. 2001. History and mobility exam index to identify community-
dwelling elderly persons at risk of falling. Journals of Gerontology
Series A-Biological Sciences & Medical Sciences 56(4): M253–9.
Cowper PA, Weinberger M, Hanlon JT, Landsman PB, Samsa GP,
Uttech KM, et al. 1998. The cost-effectiveness of a clinical
pharmacist intervention among elderly outpatients.
Pharmacotherapy 18(2): 327–32.
Cravens DD. 2006. Comprehensive geriatric assessment for non-
geriatricians. Missouri Medicine 103(2): 157–60.
Crome P. 2003. What's different about older people. Toxicology
192(1): 49–54.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 131
Crome P, Hill S, Mossman J, Stockdale P. 2000. A randomised
controlled trial of a nurse-led falls prevention clinic (abstract).
Journal of the American Geriatrics Society 48(8): S78.
Cumming RG, Thomas M, Szonyi G, Salkeld G, O'Neill E, Westbury C.
1999. Home visits by an occupational therapist for assessment
and modification of environmental hazards: a randomized trial of
falls prevention. Journal of the American Geriatrics Society
47(12): 1397–1402.
Cwikel JG, Fried A, Biderman A, Galinsky D. 1998. Validation of a fall-
risk screening test, the Elderly Fall Screening Test (EFST), for
community-dwelling elderly. Disability and Rehabilitation: An
International Multidisciplinary Journal 20(5): 161–7.
Dargent-Molina P, Schott AM, Hans D, Favier F, Grandjean H, Baudoin
C, et al. 1999. Separate and combined value of bone mass and
gait speed measurements in screening for hip fracture risk:
Results from the EPIDOS study. Osteoporosis International 9(2):
188–92.
Darkow T, Fontes CL, Williamson TE. 2005. Costs associated with the
management of overactive bladder and related comorbidities.
Pharmacotherapy 25(4): 511–9.
Davison J, Bond J, Dawson P, Steen IN, Kenny RA. 2005. Patients with
recurrent falls attending accident & emergency benefit from
multifactorial intervention – a randomised controlled trial. Age
and Ageing 34(2): 162–8.
Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S. 2002.
Randomised factorial trial of falls prevention among older people
living in their own homes. British Medical Journal 325(7356): 128.
Deeks JJ, Altman DG, Bradburn MJ. 2001. Statistical methods for
examining heterogeneity and combining results from several
studies in meta-analysis. In: Egger M, Davey Smith G, Altman DG
(eds), Systematic Reviews in Health Care: Meta-Analysis in
Context (2nd edn). London: BMJ Publication Group.
Dejaeger E. 2003. Falls in the elderly: any use of a special clinic for
falls? [Dutch]. Tijdschrift voor Gerontologie en Geriatrie 34(1): 3–
5.
Delbaere K, Van den Noortgate N, Bourgois J, Vanderstraeten G, Tine
W, Cambier D. 2006. The Physical Performance Test as a
predictor of frequent fallers: a prospective community-based
cohort study. Clinical Rehabilitation 20(1): 83–90.
De Moraes Barros GDV. 2006. Falls in elderly people The Lancet
367(9512): 729–30.
Department of Health. 2001. National Service Framework for Older
People. London: The Stationery Office.
Department of Veterans Affairs. 1999–2002. Effects of Functional
Incidental Training in VA NHCU Residents. www.Clinical Trials.gov.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 132
Dharmarajan TS, Norkus EP. 2004. Mild anemia and the risk of falls in
older adults from nursing homes and the community. Journal of
the American Medical Directors Association 5(6): 395–400.
Di Fabio RP, Anacker SL. 1996. Identifying fallers in community living
elders using a clinical test of sensory interaction for balance.
European Journal of Physical Medicine & Rehabilitation 6(2): 61–
6.
Di Fabio RP, Seay R. 1997. Use of the "fast evaluation of mobility,
balance, and fear" in elderly community dwellers: validity and
reliability. Physical Therapy 77(9): 904–17.
Dite W, Temple VA. 2002. A clinical test of stepping and change of
direction to identify multiple falling older adults. Archives of
Physical Medicine & Rehabilitation 83(11): 1566–71.
Dowse J. 2003. Risk awareness can contribute to optimal health.
Nursing Times 99(40): 33.
Drummond MF, Jefferson TO. 1996. Guidelines for authors and peer
reviewers of economic submissions to the BMJ. British Medical
Journal 313(7052): 275–83.
Dubey C, Terme A. 2004. [Fewer falls thanks to nursing research].
Krankenpflege - Soins Infirmiers 97(12): 10–14.
Duncan PW, Studenski S, Chandler J, Prescott B. 1992. Functional
reach: predictive validity in a sample of elderly male veterans.
Journal of Gerontology 47(3): M93–8.
Dutcher JA, Miller SW. 2003. Overactive bladder: definition, etiology,
prevalence, and cost. Consultant Pharmacist 18 (Suppl B): 4–12.
Eagle DJ, Salama S, Whitman D, Evans LA, Ho E, Olde J. 1999.
Comparison of three instruments in predicting accidental falls in
selected inpatients in a general teaching hospital. Journal of
Gerontological Nursing 25(7): 40–5.
Edwards N. 2003. Older people. Shifting the balance. Health Service
Journal 113(5883): 28–9.
Eldridge S, Spencer A, Cryer C, Parsons S, Underwood M, Feder G.
2005. Why modelling a complex intervention is an important
precursor to trial design: lessons from studying an intervention to
reduce falls-related injuries in older people. Journal of Health
Service Research and Policy 10(3): 133–42.
Ellis A, Trappes-Lomax T, Fox M, Taylor R, Power M, Stead J, et al.
2006. Buying time II: an economic evaluation of a joint
NHS/Social Services residential rehabilitation unit for older people
on discharge from hospital. Health & Social Care in the
Community 14(2): 95–106.
Eng JJ, Chu KS, Kim CM, Dawson AS, Carswell A, Hepburn KE. 2003. A
community-based group exercise program for persons with
chronic stroke. Medicine & Science in Sports & Exercise 35(8):
1271–8.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 133
Esquenazi A. 2004. Falls and fractures in older post-stroke patients
with spasticity: consequences and drug treatment considerations.
Clinical Geriatrics 12(8): 27–35.
Ettinger MP. 2003. Aging bone and osteoporosis. Archives of Internal
Medicine 163: 2237–46.
Evans BJW, Rowlands G. 2004. Correctable visual impairment in older
people: a major unmet need. Ophthalmic & Physiological Optics
24(3): 161–80.
Fabacher D, Josephson K, Pietruszka F, Linderborn K, Morley JE,
Rubenstien LZ. 1994. An in-home preventive assessment program
for independent older adults: a randomized controlled trial.
Journal of the American Geriatrics Society 42: 630–8.
Fayad R, Nuwayhid I, Tamim H, Kassak K, Khogali M. 2003. Cost of
work-related injuries in insured workplaces in Lebanon. Bulletin of
the World Health Organization 81(7): 509–16.
Feinberg JL, Cameron KA, Lapane KL, Allsworth JE. 2004. The use of
GRAM software to improve patient safety in nursing facilities.
Consultant Pharmacist 19(5): 398–413.
Finkelstein EA, Chen H, Miller TR, Corso PS, Stevens JA. 2005. A
comparison of the case-control and case-crossover designs for
estimating medical costs of nonfatal fall-related injuries among
older Americans. Medical Care 43(11): 1087–91.
Folstein MF, Folstein SE, McHugh PR. 1975. Mini Mental State - a
practical guide for grading the cognitive state of patients for the
clinician. Journal of Psychiatric Research 12(3): 189–98.
Forrester DA, McCabe-Bender J, Tiedeken K. 1999. Fall risk
assessment of hospitalized adults and follow-up study. Journal for
Nurses in Staff Development - JNSD 15(6): 251–8.
Fosnight SM, Holder CM, Allen KR, Hazelett S. 2004. A strategy to
decrease the use of risky drugs in the elderly. Cleveland Clinic
Journal of Medicine 71(7): 561–8.
Franzen H, Hunter H, Landreth C, Beling J, Greenberg M, Canfield J.
1998. Comparison of functional reach in fallers and nonfallers in
an independent retirement community. Physical and Occupational
Therapy in Geriatrics 15(4): 33–40.
Fritz SL, Kornetti DL, Prieto-Lewis N, Light KE. 2001. Use of the Timed
Up and Go as a screening tool for prediction of falls and its
correlation with the Dynamic Gait Index and Berg Balance Test in
the geriatric population. Journal of Geriatric Physical Therapy
24(3): 21.
Galinsky D, Fried V, Biderman A, Cwikel J, Ben Moshe Y. 2000.
[Identifying the elderly at risk for falling and accompanying
protocols]. Harefuah 138(3): 189–94.
Gallagher EM, Brunt H. 1996. Head over heels: impact of a health
promotion program to reduce falls in the elderly. Canadian Journal
on Aging 15(1): 84–96.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 134
Gass M, Dawson-Hughes B. 2006. Preventing osteoporosis-related
fractures: an overview. American Journal of Medicine 119 (4
Suppl 1): S3–11.
Gaugler JE, Zarit SH, Townsend A, Stephens MAP, Greene R. 2003.
Evaluating community-based programs for dementia caregivers:
the cost implications of adult day services. Journal of Applied
Gerontology 22(1): 118–33.
Gerdhem P, Ringsberg KAM, Akesson K, Obrant KJ. 2005. Clinical
history and biologic age predicted falls better than objective
functional tests. Journal of Clinical Epidemiology 58(3): 226–32.
Gill TM, Baker DI, Gottschalk M, Peduzzi PN, Allore H, Byers A. 2002.
A program to prevent functional decline in physically frail, elderly
persons who live at home. New England Journal of Medicine
347(14): 1068–74.
Gill-Body KM, Murphy MP, Sullivan PE. 2002. Concurrent validity of the
Dynamic Gait Index in community dwelling elderly... Platform &
poster presentations for CSM 2003. Neurology Report 26(4): 194.
Gillespie LD, Gillespie WJ, Robertson MC, Lamb SE, Cumming RG,
Rowe BH. 2003. Interventions for preventing falls in elderly
people [update of Cochrane Database of Systematic Reviews
2001, 3: CD000340]. Cochrane Database of Systematic Reviews
4: CD000340.
Gitlin LN, Winter L, Dennis MP, Corcoran M, Schinfeld S, Hauck WW.
2006. A randomized trial of a multicomponent home intervention
to reduce functional difficulties in older adults. Journal of the
American Geriatrics Society 54(5): 809–16.
Grandjean CK, McMullen PC, Miller KP, Howie WO, Ryan K, Myers A.
2006. Severe occupational injuries among older workers:
demographic factors, time of injury, place and mechanism of
injury, length of stay, and cost data. Nursing & Health Sciences
8(2): 103–7.
Grant AM, Avenell A, Campbell MK, McDonald AM, MacLennan GS,
McPherson GC, et al. 2005. Oral vitamin D3 and calcium for
secondary prevention of low-trauma fractures in elderly people
(Randomised Evaluation of Calcium Or vitamin D, RECORD): a
randomised placebo-controlled trial. The Lancet 365(9471):
1621–8.
Grigor C, Capell H, Stirling A, McMahon AD, Lock P, Vallance R, et al.
2004. Effect of a treatment strategy of tight control for
rheumatoid arthritis (the TICORA study): a single-blind
randomised controlled trial. The Lancet 364(9430): 263–9.
Guimarães JMN, Farinatti Pde TV. 2005. Descriptive analysis of
variables theoretically associated to the risk of falls in elder
women. Revista Brasileira de Medicina do Esporte 11(5): 280e-
286e.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 135
Gulich M, Zeitler HP. 2000. Walking and counting test for assessing
the risk of falling in the elderly. Deutsche Medizinische
Wochenschrift 125(9): 245–8.
Gunther JS, Kolodziej TA, Nyquist K, Sakamoto Y. 2002. Validity of the
Standardized Walking Obstacle Course (SWOC) as a functional
balance and Mobility Assessment tool in frail elderly persons.
Journal of Geriatric Physical Therapy 25(3): 34.
Haines TP, Bennell KL, Osborne RH, Hill KD. 2004. Effectiveness of
targeted falls prevention programme in subacute hospital setting:
randomised controlled trial. British Medical Journal 328(7441):
676–9.
Haines TP, Bennell KL, Osborne RH, Hill KD. 2006. A new instrument
for targeting falls prevention interventions was accurate and
clinically applicable in a hospital setting. Journal of Clinical
Epidemiology 59(2): 168–75.
Hale WA, Delaney MJ, McGaghie WC. 1992. Characteristics and
predictors of falls in elderly patients. Journal of Family Practice
34(5): 577–81.
Hall N, De Beck P, Johnson D, Mackinnon K, Gutman G, Glick N. 1992.
Randomized trial of a prevention program for frail elders.
Canadian Journal on Aging 11: 72–91.
Hall SE, Hendrie DV. 2003. A prospective study of the costs of falls in
older adults living in the community. Australian & New Zealand
Journal of Public Health 27(3): 343–51.
Hanssens L, Reginster JY. 2003. Relevance of bone mineral density,
bone quality and falls in reduction of vertebral and non-vertebral
fractures. Journal of Musculoskeletal Neuronal Interactions 3(3):
189–93.
Harada N, Chiu V, Damron-Rodriguez J, Fowler E, Siu A, Reuben DB.
1995. Screening for balance and mobility impairment in elderly
individuals living in residential care facilities. Physical Therapy
75(6): 462–9.
Harwood RH, Foss AJE, Osborn F, Gregson RM, Zaman A, Masud T.
2005. Falls and health status in elderly women following first eye.
cataract surgery: a randomised controlled trial. British Journal of
Ophthalmology 89: 53–9.
Haumschild MJ, Karfonta TL, Haumschild MS, Phillips SE. 2003. Clinical
and economic outcomes of a fall-focused pharmaceutical
intervention program. American Journal of Health-System
Pharmacy 60(10): 1029–32.
Hausdorff J, Rios D, Edelberg H. 2000. Fall risk assessment: a
prospective study of the relationship between gait instability and
falls in older adults. Journal of the American Geriatrics Society
48(8): S3.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 136
Hausdorff JM, Rios DA, Edelberg HK. 2001. Gait variability and fall risk
in community-living older adults: a 1-year prospective study.
Archives of Physical Medicine & Rehabilitation 82(8): 1050–6.
Haya J, Castelo-Branco C. 2003. Is it possible to prevent and treat
osteoporosis: How? [Spanish] Revista de Iberoamericana de
Revisiones en Menopausia 5(2): 12–19.
Hayes N. 2004. Hip protectors: interpreting the evidence and
addressing practicalities. Nursing Older People 16(3): 15–6.
Hebert R, Robichaud L, Roy PM, Bravo G, Voyer L. 2001. Efficacy of a
nurse-led multidimensional preventive programme for older
people at risk of functional decline. A randomized controlled trial.
Age and Ageing 30: 147–53.
Heinze C. 2002. [Preventing the risks of accidental falls. The Hendrich
Accidental Falls Risk Scale]. Pflege Aktuell 56(3): 174–6.
Helbostad JL. 2005. [Physical training for nursing home residents–has
it any effect?]. Tidsskrift for Den Norske Laegeforening 125(9):
1195–7.
Hellstrom K, Lindmark B, Fugl-Meyer A. 2002. The Falls-Efficacy Scale,
Swedish version: does it reflect clinically meaningful changes after
stroke? Disability and Rehabilitation 24(9): 471–81.
Hendrich A, Nyhuis A, Kippenbrock T, Soja ME. 1995. Hospital falls:
development of a predictive model for clinical practice. Applied
Nursing Research 8(3): 129–39.
Hendrie D, Hall SE, Arena G, Legge M. 2004. Health system costs of
falls of older adults in Western Australia. Australian Health Review
28(3): 363–73.
Hendriks MRC, van Haastregt JCM, Diederiks JPM, Evers SMAA,
Crebolder HFJM, van Eijk JTM. 2005. Effectiveness and cost-
effectiveness of a multidisciplinary intervention programme to
prevent new falls and functional decline among elderly persons at
risk: design of a replicated randomised controlled trial
[ISRCTN64716113]. BMC Public Health 5: 6.
Hill K, Schwarz J, Flicker L, Carroll S. 1999. Falls among healthy,
community-dwelling, older women: a prospective study of
frequency, circumstances, consequences and prediction accuracy.
Australian & New Zealand Journal of Public Health 23(1): 41–8.
Hill K, Vrantsidis F, Jessup R, McGann A, Pearce J, Collins T. 2004.
Validation of a falls risk assessment tool in the sub-acute hospital
setting: a pilot study. Australasian Journal of Podiatric Medicine
38(4): 99–108.
Hofmann MT, Bankes PF, Javed A, Selhat M. 2003. Decreasing the
incidence of falls in the nursing home in a cost-conscious
environment: a pilot study. Journal of the American Medical
Directors Association 4(2): 95–7.
Hogan DA, MacDonald FA, Betts J, Bricker S, Ebly EM, Delarue B, et al.
2001. A randomized controlled trial of a community-based

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 137
consultation service to prevent falls. Canadian Medical Association
Journal 165(5): 537–43.
Honkanen L. 2003. Preventing hip fractures with external hip
protectors. Family Practice Recertification 25(7): 28–32.
Honkanen L. 2004. An overview of hip fracture prevention. Topics in
Geriatric Rehabilitation 20(4): 285–96.
Honkanen LA, Schackman BR, Mushlin AI, Lachs MS. 2005. A cost-
benefit analysis of external hip protectors in the nursing home
setting. Journal of the American Geriatrics Society 53(2): 190–7.
Hopley C, Salkeld G, Mitchell P. 2004. Cost utility of photodynamic
therapy for predominantly classic neovascular age related macular
degeneration. British Journal of Ophthalmology 88(8): 982–7.
Hornbrook MC, Stevens VJ, Wingfield DJ, Hollis JF, Greenlick MR, Ory
MG. 1994. Preventing falls among community-dwelling older
persons: results from a randomized trial. Gerontologist 34: 16–
23.
Hotchkiss A, Fisher A, Robertson R, Ruttencutter A, Schuffert J, Barker
DB. 2004. Convergent and predictive validity of three scales
related to falls in the elderly. American Journal of Occupational
Therapy 58(1): 100–3.
Hu T-W, Wagner TH. 2005. Health-related consequences of overactive
bladder: an economic perspective. BJU International 96 (Suppl 1):
43–5.
Huang G. 2003. Designing exercise protocol for patients with
osteoporosis: an evidence-based nursing approach [Chinese].
Journal of Nursing (China) 50(1): 21–8.
Huang T-T, Acton GJ. 2004. Effectiveness of home visit falls
prevention strategy for Taiwanese community-dwelling elders:
randomized trial. Public Health Nursing 21(3): 247–56.
Hulme C, Long AF, Kneafsey R, Reid G. 2004. Using the EQ-5D to
assess health-related quality of life in older people. Age and
Ageing 33(5): 504–7.
Hyndman D, Ashburn A. 2004. "Stops walking when talking" as a
predictor of falls in people with stroke living in the community.
Journal of Neurology, Neurosurgery and Psychiatry 75(7): 994–7.
Irwin D, Skelton D, Dinan S. 2004. Exercise and falls. SportEX Health
20: 11–13.
Iyer P. 2004. Liability in the care of the elderly. JOGNN: Journal of
Obstetric, Gynecologic, and Neonatal Nursing 33(1): 124–31.
Izumi K, Makimoto K, Kato M, Hiramatsu T. 2002. Prospective study of
fall risk assessment among institutionalized elderly in Japan.
Nursing & Health Sciences 4(4): 141–7.
Jansson B, Stenbacka M, Leifman A, Romelsjo A. 2004. A small
fraction of patients with repetitive injuries account for a large
portion of medical costs. European Journal of Public Health 14(2):
161–7.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 138
Jarnlo GB. 2003. Functional balance tests related to falls among
elderly people living in the community. European Journal of
Geriatrics 5: 7–14.
Jester R, Wade S, Henderson K. 2005. A pilot investigation of the
efficacy of falls risk assessment tools and prevention strategies in
an elderly hip fracture population. Journal of Orthopaedic Nursing
9(1): 27–34.
Jitapunkul S. 1998. A randomised controlled trial of regular
surveillance an Thai elderly using a simple questionnaire
administered by non-professional personnel. Journal of the
Medical Association of Thailand 81(5): 352–6.
Johansson C. 2003. Rising with the fall: addressing quality of life in
physical frailty. Topics in Geriatric Rehabilitation 19(4): 239–48.
Jones D, Perese EF. 2003. Promoting self-management of urinary
incontinence in a geropsychiatric day treatment program. Journal
of Psychosocial Nursing & Mental Health Services 41(5): 38–43.
Jonsson B, Christiansen C, Johnell O, Hedbrandt J. 1995. Cost-
effectiveness of fracture prevention in established osteoporosis.
Osteoporosis International 5: 136–42.
Kahnert E, Fellman P, Di Fabio R. 2004. Saccade step latency identifies
high risk community-dwelling elderly. Journal of Geriatric Physical
Therapy 27(3): 105–6.
Kai MC, Anderson M, Lau EMC. 2003. Exercise interventions: defusing
the world's osteoporosis time bomb. Bulletin of the World Health
Organization 81(11): 827–30.
Kannus P, Parkkari J, Khan K. 2003. Hip protectors need an evidence
base. The Lancet 362(9391): 1168–9.
Kannus P, Sievanen H, Palvanen M, Jarvinen T, Parkkari J. 2005.
Prevention of falls and consequent injuries in elderly people. The
Lancet 366(9500): 1885–93.
Kapp MB. 2003. "At least Mom will be safe there": the role of resident
safety in nursing home quality. Quality & Safety in Health Care
12(3): 201–4.
Kelly A, Dowling M. 2004. Reducing the likelihood of falls in older
people. Nursing Standard 18(49): 33–40.
Keys PA, Tress DR. 2004. Preventing falls in the elderly: the role of
the pharmacist. Journal of Pharmacy Practice 17(2): 149–52.
Killough J. 2005. Validity of a new fall risk screen. Journal of Geriatric
Physical Therapy 28(3): 119.
Kingston P, Jones M, Lally F, Crome P. 2001. Older people and falls: a
randomized controlled trial of a health visitor (HV) intervention.
Reviews in Clinical Gerontology 11: 209–14.
Kinirons MT. 2003. Randomised controlled trial of a nurse-led falls
prevention programme. Age and Ageing 32(3): 361–2.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 139
Kinn S, Hood K. 2001. A falls risk-assessment tool in an elderly care
environment. British Journal of Nursing 10(7): 440, 442, 444–9.
Kobelt G, Lindgren P, Singh A, Klareskog L. 2005. Cost effectiveness
of etanercept (Enbrel) in combination with methotrexate in the
treatment of active rheumatoid arthritis based on the TEMPO trial.
Annals of the Rheumatic Diseases 64(8): 1174–9.
Kolanowski AM, Fick D, Waller JL, Shea D. 2004. Spouses of persons
with dementia: their healthcare problems, utilization, and costs.
Research in Nursing & Health 27(5): 296–306.
Kooijman AC, Cornelissen FW, De Boer MR, Pluijm SMF, Lips P, Moll
AC, et al. 2005. Better lighting to reduce falls and fracture? A
comment on de Boer et al. (2004): Different aspects of visual
impairment as risk factors for falls and fractures in older men and
women (multiple letters). Journal of Bone & Mineral Research
20(11): 2061–3.
Kuchynka J, Kaser L, Wettstein A. 2004. [Can falls in nursing homes
be avoided?]. Schweizerische Rundschau fur Medizin Praxis
93(37): 1503–8.
Kuh D, Bassey EJ, Butterworth S, Hardy R, Wadsworth MEJ. 2005.
Grip strength, postural control, and functional leg power in a
representative cohort of British men and women: associations
with physical activity, health status, and socioeconomic
conditions. Journals of Gerontology Series A-Biological Sciences &
Medical Sciences 60(2): 224–31.
Lachman ME, Howland J, Tennstedt S, Jette A, Assman S, Peterson E.
(1998). Fear of Falling and Activity Restriction: The Survey of
Activities and Fear of Falling in the Elderly. Journal of
Gerontology: Psychological Sciences, 53B:43-50.
Lafont C, Costes-Salon MC, Dupui P, Nourhashemi F, Vellas B,
Albarede JL. 1998. The timed "up & go" test is a useful predictor
of falls in community-dwelling older people. Journal of the
American Geriatrics Society 46(7): 929–30.
Lamb SE, Jorstad-Stein EC, Hauer K, Becker C. 2005. Development of
a common outcome data set for fall injury prevention trials: the
Prevention of Falls Network Europe consensus. Journal of the
American Geriatrics Society 53(9): 1618–22.
Landis DM. 2005. Fracture risk in postmenopausal women. Nurse
Practitioner: American Journal of Primary Health Care 30(11): 48.
Lansley P, McCreadie C, Tinker A. 2004. Can adapting the homes of
older people and providing assistive technology pay its way? Age
and Ageing 33(6): 571–6.
Large J, Gan N, Basic D, Jennings N. 2006. Using the timed up and go
test to stratify elderly inpatients at risk of falls. Clinical
Rehabilitation 20(5): 421–8.
Lasagna L, Baloh RW, Berg K, Maki B, Nevitt M, Wolfson L, et al. 1997.
Clinical relevance of postural stability measures to an assessment

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 140
of risk of falling in most elderly. Journal of the American Geriatrics
Society 45(9): P176.
LaStayo PC, Ewy GA, Pierotti DD, Johns RK, Lindstedt S. 2003. The
positive effects of negative work: increased muscle strength and
decreased fall risk in a frail elderly population. Journals of
Gerontology Series A-Biological Sciences & Medical Sciences
58(5): M419–24.
Latham NK, Anderson CS, Lee A, Bennett DA, Moseley A, Cameron ID,
et al. 2003a. A randomized, controlled trial of quadriceps
resistance exercise and vitamin D in frail older people: the Frailty
Interventions Trial in Elderly Subjects (FITNESS). Journal of the
American Geriatrics Society 51(3): 291–9.
Latham NK, Anderson CS, Lee A, et al. 2003b. Resistance exercises or
vitamin D did not improve physical health or reduce falls in frail
older people. Evidence Based Nursing 6: 116–17.
Lawrence TM, White CT, Wenn R, Moran CG. 2005. The current
hospital costs of treating hip fractures. Injury 36(1): 88–91.
Leeflang MMG, Scholten RJPM, Rutjes AWS, Reitsma JB, Bossuyt PMM.
2006. Use of methodological filters to identify diagnostic accuracy
studies can lead to the omission of relevant studies. Journal of
Clinical Epidemiology 59: 234–40.
Leslie WD, Roe EB, Szul M, LoGerfo JP, Rubenstein LZ, Tinetti ME.
2003. Preventing falls in elderly persons (multiple letters). New
England Journal of Medicine 348(18): 1816–18.
Lightbody E, Watkins C, Leathley M, Sharma A, Lye M. 2002.
Evaluation of a nurse-led falls prevention programme versus usual
care: a randomized controlled trial. Age and Ageing 31: 203–10.
Lin MR, Wang YW. 2004. Risk factors and prevention of falls among
community-dwelling older people [Chinese]. Chinese Journal of
Public Health 23(4): 259–71.
Lin M, Hwang H, Hu M, Wu HI, Wang Y, Huang F. 2004. Psychometric
comparisons of the timed up and go, one-leg stand, functional
reach, and Tinetti balance measures in community-dwelling older
people. Journal of the American Geriatrics Society 52(8): 1343–8.
Lindsay R, James EL, Kippen S. 2004. The Timed Up and Go Test:
unable to predict falls on the acute medical ward. Australian
Journal of Physiotherapy 50(4): 249–51.
Lipscomb HJ, Li L, Dement J. 2003. Work-related falls among union
carpenters in Washington State before and after the Vertical Fall
Arrest Standard. American Journal of Industrial Medicine 44(2):
157–65.
Liu JH. 2006. The WHI and Postmenopausal Women: no Magic Bullet.
http://womens-health.jwatch.org/cgi/content/full/2006/502/1
Journal watch: Medicine that matters.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 141
Ljung R, Peterson S, Hallqvist J, Heimerson I, Diderichsen F. 2005.
Socioeconomic differences in the burden of disease in Sweden.
Bulletin of the World Health Organization 83(2): 92–9.
Lord SR, Clark RD. 1996. Simple physiological and clinical tests for the
accurate prediction of falling in older people. Gerontology 42(4):
199–203.
Lord SR, Dayhew J. 2001. Visual risk factors for falls in older people.
Journal of the American Geriatrics Society 49(5): 508–15.
Lord SR, Castell S, Corcoran J, Dayhew J, Matters B, Shan A, et al.
2003. The effect of group exercise on physical functioning and
falls in frail older people living in retirement villages: a
randomized, controlled trial. Journal of the American Geriatrics
Society 51(12): 1685–92.
Lord SR, Tiedemann A, Chapman K, Munro B, Murray SM, Gerontology
M, et al. 2005. The effect of an individualized fall-prevention
program on fall risk and falls in older people: a randomized,
controlled trial. Journal of the American Geriatrics Society 53(8):
1296–1304.
Lotrich FE, Pollock BG. 2005. Aging and clinical pharmacology:
Implications for antidepressants. Journal of Clinical Pharmacology
45(10): 1106–22.
Lubbeke A, Stern R, Grab B, Herrmann F, Michel J-P, Hoffmeyer P.
2005. Upper extremity fractures in the elderly: consequences on
utilization of rehabilitation care. Aging Clinical & Experimental
Research 17(4): 276–80.
Lundin-Olsson L, Jensen J, Nyberg L, Gustafson Y. 2003. Predicting
falls in residential care by a risk assessment tool, staff judgement,
and history of falls. Aging Clinical & Experimental Research 15(1):
51–9.
Lundin-Olsson L, Nyberg L, Gustafson Y. 1997. "Stops walking when
talking" as a predictor of falls in elderly people. Lancet
349(9052): 617.
Lundin-Olsson L, Nyberg L, Gustafson Y. 2000. The Mobility
Interaction Fall chart. Physiotherapy Research International 5(3):
190–201.
MacAvoy S, Skinner T, Hines M. 1996. Fall risk assessment tool.
Applied Nursing Research 9(4): 213–8.
Macrae PG, Lacourse M, Moldavon R. 1992. Physical performance-
measures that predict faller status in community-dwelling older
adults. Journal of Orthopaedic & Sports Physical Therapy 16(3):
123–8.
Magnus A, Carr V, Mihalopoulos C, Carter R, Vos T. 2005. Assessing
cost-effectiveness of drug interventions for schizophrenia.
Australian & New Zealand Journal of Psychiatry 39(1–2): 44–54.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 142
Maki BE. 1997. Gait changes in older adults: predictors of falls or
indicators of fear? Journal of the American Geriatrics Society
45(3): 313–20.
Maki BE, Holliday PJ, Topper AK. 1994. A prospective study of postural
balance and risk of falling in an ambulatory and independent
elderly population. Journal of Gerontology 49(2): M72–84.
Maly RC, Hirsch SH, Reuben DB. 1997. The performance of simple
instruments in detecting geriatric conditions and selecting
community-dwelling older people for geriatric assessment. Age
and Ageing 26(3): 223–31.
Mamun K, Goh-Tan CYE, Ng LL. 2003. Prescribing psychoactive
medications in nursing homes: current practice in Singapore.
Singapore Medical Journal 44(12): 625–9.
Marks R, Allegrante JP. 2004. Falls-prevention programs for older
ambulatory community dwellers: from public health research to
health promotion policy. Sozial- und Praventivmedizin 49(3):
171–8.
Marks R, Allegrante JP, Ronald MacKenzie C, Lane JM. 2003. Hip
fractures among the elderly: causes, consequences and control.
Ageing Research Reviews 2(1): 57–93.
Masud T, Coupland C, Drummond A, Gladman J, Kendrick D, Sach T,
et al. 2006. Multifactorial day hospital intervention to reduce falls
in high risk older people in primary care: a multi-centre
randomised controlled trial. Trials 27(7): 5.
Maurer MS, Cohen S, Cheng H. 2004. The degree and timing of
orthostatic blood pressure changes in relation to falls in nursing
home residents. Journal of the American Medical Directors
Association 5(4): 233–8.
McCarthy C, Mills PM, Pullen P, Richardson G, Hawkins N, Roberts CR,
et al. 2004. Supplementation of a Home-based Exercise
Programme with a Class-based Programme for People with
Osteoarthritis of the Knees: a Randomised Controlled Trial and
Health Economic Analysis. Health Technology Assessment 8(46):
iii–iv, 1–61.
McClung MR. 2003. Effective strategies for the prevention of hip
fractures. Managed Care Consultant 3(2): 17–23.
McClure R, Turner C, Peel N, Spinks A, Eakin E, Hughes K. 2006.
Population-based interventions for the prevention of fall-related
injuries in older people (Cochrane Review). From The Cochrane
Library. Chichester: John Wiley & Sons.
McCreadie C, Tinker A. 2005. The acceptability of assistive technology
to older people. Ageing and Society 25: 91–110.
McDonald L, Robb AL. 2004. The economic legacy of divorce and
separation for women in old age. Canadian Journal on Aging 23
(Suppl 1): S83-S97.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 143
McEwan RT, Davison N, Forster DP, Pearson P, Stirling E. 1990.
Screening elderly people in primary care: a randomized controlled
trial. British Journal of General Practice 40: 94–7.
McLean RR, Jacques PF, Selhub J, Tucker KL, Samelson EJ, Broe KE, et
al. 2004. Homocysteine as a predictive factor for hip fracture in
older persons. New England Journal of Medicine 350: 2042–9.
McMurdo MET, Harper JR. 2004. Institutional falls: quality not
quantity. Age and Ageing 33(4): 399–404.
Meerding WJ, Mulder S, Van Beeck EF. 2006. Incidence and costs of
injuries in The Netherlands. European Journal of Public Health
16(3): 271–7.
Melton III LJ, Johnell O, Lau E, Mautalen CA, Seeman E. 2004.
Osteoporosis and the global competition for health care resources.
Journal of Bone and Mineral Research 19(7): 1055–8.
Meyer G, Warnke A, Muhlhauser I. 2003. Fall and fracture prevention
in the elderly. Geriatrics and Aging 6(7): 12–14.
Meyer G, Kopke S, Bender R, Muhlhauser I. 2005a. Predicting the risk
of falling–efficacy of a risk assessment tool compared to nurses'
judgement: a cluster-randomised controlled trial
[ISRCTN37794278]. BMC Geriatrics 5: 14.
Meyer G, Wegscheider K, Kersten JF, Icks A, Muhlhauser I. 2005b.
Increased use of hip protectors in nursing homes: economic
analysis of a cluster randomized, controlled trial. Journal of the
American Geriatrics Society 53(12): 2153–8.
Millward LM, Morgan A, Kelly PK. 2003. Prevention and reduction of
accidental injury in children and older people. NHS Health
Development Agency.
http://www.nice.org.uk/aboutnice/whoweare/aboutthehda/hdapu
blications/prevention_and_reduction_of_accidental_injury_in_chil
dren_and_older_people_evidence_briefing_summary.jsp.
Mitani T, Komatsu T. 2004. [Osteoporosis and living of residents in a
nursing home]. Clinical Calcium 14(3): 389–96.
Moller J. 2005. Current costing models: are they suitable for allocating
health resources? The example of fall injury prevention in
Australia. Accident Analysis & Prevention 37(1): 25–33.
Montgomery AA, Fahey T, Ben-Shlomo Y, Harding J. 2003. The
influence of absolute cardiovascular risk, patient utilities, and
costs on the decision to treat hypertension: a Markov decision
analysis. Journal of Hypertension 21(9): 1753–9.
Moore T, Martin J, Stonehouse J. 1996. Predicting falls: risk
assessment tool versus clinical judgement. Perspectives 20(1): 8–
11.
Morgan RO, Virnig BA. 2004. Low-intensity exercise and reduction of
the risk for falls among at-risk elders. Journal of Gerontology
Series A: Biological Sciences and Medical Sciences 59A(10):
1062–72.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 144
Morse JM, Black C, Oberle K, Donahue P. 1989a. A prospective study
to identify the fall-prone patient. Social Science & Medicine 28(1):
81–6.
Morse JM, Morse RM, Tylko SJ. 1989b. Development of a scale to
identify the fall-prone patient. Canadian Journal on Aging 8(4):
366–77.
Murray KJ, Hill K, Phillips B, Waterston J. 2005. A pilot study of falls
risk and vestibular dysfunction in older fallers presenting to
hospital emergency departments. Disability and Rehabilitation
27(9): 499–506.
Myers AM, Fletcher PC, Myers AH, Sherk W. 1998. Discriminative and
evaluative properties of the Activities-specific Balance Confidence
(ABC) scale. Journals of Gerontology Series A-Biological Sciences
& Medical Sciences 53: M287–94.
Myers H. 2003. Hospital fall risk assessment tools: a critique of the
literature. International Journal of Nursing Practice 8: 223–35.
Myers H, Nikoletti S. 2003. Fall risk assessment: a prospective
investigation of nurses' clinical judgement and risk assessment
tools in predicting patient falls. International Journal of Nursing
Practice 9(3): 158–65.
Nagata-Kobayashi S, Shimbo T, Fukui T. 2002. Cost-effectiveness
analysis of screening for osteoporosis in postmenopausal
Japanese women. Journal of Bone and Mineral Metabolism 20(6):
350–7.
Nandy S, Parsons S, Cryer C, Underwood M, Rashbrook E, Carter Y, et
al. 2004. Development and preliminary examination of the
predictive validity of the Falls Risk Assessment Tool (FRAT) for
use in primary care. Journal of Public Health 26(2): 138–43
[erratum appears in Journal of Public Health 2005, 27(1): 129–
30].
National Center for Injury Prevention and Control (NCIPC). 2006. Falls
and Hip Fractures Among Older Adults. http://0-
www.cdc.gov.mill1.sjlibrary.org/ncipc/default.htm.
National Institute for Clinical Excellence. 2004. Clinical Practice
Guideline for the Assessment and Prevention of Falls in Older
People. Royal College of Nursing. London: National Institute for
Clinical Excellence.
Neubauer DN. 2004. Introduction. Clinical Cornerstone 6 (Suppl 1A):
S5–6.
Newbury J, Marley JE, Beilby JJ. 2001. A randomised controlled trial of
the outcome of health assessment of people aged 75 years and
over. Medical Journal of Australia 175: 104–7.
Newton JL, Kenny RA, Frearson R, Francis RM. 2003. A prospective
evaluation of bone mineral density measurement in females who
have fallen. Age and Ageing 32(5): 497–502.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 145
Newton JL, Jones DEJ, Wilton K, Pairman J, Parry SW, Francis RM.
2006. Calcaneal bone mineral density in older patients who have
fallen. QJM: Monthly Journal of the Association of Physicians
99(4): 231–6.
Newton RA, Warren RS, Barhameen AY, McGinnis P, Cutillo-Schmitter
T. 2002. Timed up and go and timed up and go-manual as a
measure of dual processing in institutionalized older adults.
Journal of Geriatric Physical Therapy 25(3): 38.
Neyens JCL, Dijcks BPJ, van Haastregt JCM, de Witte LP, van den
Heuvel WJA, Crebolder HFJM, et al. 2006. The development of a
multidisciplinary fall risk evaluation tool for demented nursing
home patients in the Netherlands. BMC Public Health 6: 74.
NHS Executive South East. 1995–1997. Can the Incidence of Falls in
the Elderly be Reduced by a Secondary Prevention Protocol?
National Research Register. www.blackwell-synergy.com/doi/abs/
10.1046/j.1532-5415.2003.51102.x
Nikolaus T, Bach M. 2003. Preventing falls in community-dwelling frail
older people using a home intervention team (HIT): results from
the Randomized Falls-HIT Trial. Journal of the American Geriatrics
Society 51(3): 300–5.
Noyes K, Dick AW, Holloway RG, Parkinson Study Group. 2004.
Pramipexole v. levodopa as initial treatment for Parkinson's
disease: a randomized clinical-economic trial. Medical Decision
Making 24: 472–85.
Nyberg L, Gustafson Y. 1996. Using the Downton index to predict
those prone to falls in stroke rehabilitation. Stroke 27(10): 1821–
4.
O'Connell B, Wellman D, Cockayne M, Baker L. 2005. Fall risk factors
and the nature of falls in inpatient oncology and palliative care
settings. Contemporary Nurse 18(3): 247–57.
Odegard PS. 2006. Geriatric pharmacotherapy update: New
medications, recent releases, and coming attractions. Annals of
Long Term Care 14(5): 20–7.
Ohsfeldt RL, Gavin NI, Thorp JM. 2004. Medical care costs associated
with postmenopausal estrogen plus progestogen therapy. Value in
Health 7(5): 544–53.
Okumiya K, Matsubayashi K, Nakamura T, Fujisawa M, Osaki Y, Doi Y,
et al. 1998. The timed "up & go" test is a useful predictor of falls
in community-dwelling older people. Journal of the American
Geriatrics Society 46(7): 928–9.
Oliver D, Britton M, Seed P, Martin FC, Hopper AH. 1997. Development
and evaluation of evidence based risk assessment tool (STRATIFY)
to predict which elderly inpatients will fall: case-control and
cohort studies. British Medical Journal 315(7115): 1049–53.
Oliver D, Connelly J, Allain T. 2005. Economic modeling on cost-
effectiveness of hip protectors in institutionalized older people

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 146
based on contentious interpretation of original effectiveness data.
Journal of the American Geriatrics Society 53(12): 2241–2.
Oliver D, Daly F, Martin FC, McMurdo MET. 2004. Risk factors and risk
assessment tool for falls in hospital: a systematic review. Age and
Ageing 33: 122–30.
Olsson E, Lofgren B, Gustafson Y, Nyberg L. 2005. Validation of a fall
risk index in stroke rehabilitation. Journal of Stroke and
Cerebrovascular Diseases 14(1): 23–8.
O'Mahony D. 2006. Falls and fracture prevention in older people: Time
for action. Irish Journal of Medical Science 175(2): 10.
O'Sullivan J, Wakai A, O'Sullivan R, Luke C, Cusack S. 2004. Ladder
fall injuries: patterns and cost of morbidity. Injury 35(4): 429–31.
Owen CG, Fletcher AE, Donoghue AR, Rudnicka AR. 2003. How big is
the burden of visual loss caused by age related macular
degeneration in the United Kingdom. British Journal of
Ophthalmology 87: 312–17.
Owens DK, Sanders GD, Harris RA, McDonald KM, Heidenreich PA,
Dembitzer AD, et al. 1997. Cost-effectiveness of implantable
cardioverter defibrillators relative to amiodarone for prevention of
sudden cardiac death. Annals of Internal Medicine 126(1): 1–12.
Ozcan A, Donat H, Gelecek N, Ozdirenc M, Karadibak D. 2005. The
relationship between risk factors for falling and the quality of life
in older adults. BMC Public Health 5: 90.
Pal J, Hale LA, Skinner MA. 2005. Investigating the reliability and
validity of two balance measures in adults with stroke... including
commentary by Tyson S and MacKintosh S. International Journal
of Therapy and Rehabilitation 12(7): 308–15.
Panneman MJM, Goettsch WG, Kramarz P, Herings RMC. 2003. The
costs of benzodiazepine-associated hospital-treated fall Injuries in
the EU: a Pharmo study. Drugs & Aging 20(11): 833–9.
Papaioannou A, Adachi JD, Winegard K, Ferko N, Parkinson W, Cook
RJ, et al. 2003. Efficacy of home-based exercise for improving
quality of life among elderly women with symptomatic
osteoporosis-related vertebral fractures. Osteoporosis
International 14(8): 677–82.
Papaioannou A, Parkinson W, Cook R, Ferko N, Coker E, Adachi JD.
2004. Prediction of falls using a risk assessment tool in the acute
care setting. BMC Medicine 2: 1.
Pardessus V, Puisieux F, BDi Pompeo C, Gaudefroy C, Thevenon A,
Dewailly P. 2002. Benefits of home visits for falls and autonomy in
the elderly. A randomized trial study. American Journal of Physical
Medicine and Rehabilitation 81(4): 247–52.
Parker MJ, Gillespie WJ, Gillespie LD. 2006. Effectiveness of hip
protectors for preventing hip fractures in elderly people:
systematic review. British Medical Journal 332(7541): 571–4.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 147
Parsons S, Cryer C, Eldridge S, Nandy S, Taylor M, Underwood M, et
al. 2001. Implementation of Multi-disciplinary Guidelines for the
Prevention of Falls in Older People: a Pilot Study.
www.ihse.qmul.ac.uk/chs/research/gppc/Download%20Report/im
plementationreport.pdf.
Paterson H, Marshall A, Hawley R. 2003. The effectiveness of hip
protectors in preventing hip fractures in older people: utilising
research to guide nursing practice. Geriaction 21(3): 19–23.
Perell KL, Nelson A, Goldman RL, Luther SL, Prieto-Lewis N,
Rubenstein LZ. 2001. Fall risk assessment measures: an analytic
review. Journal of Gerontology Medical Science 56A: M761–6.
Pils K, Neumann F, Meisner W, Schano W, Vavrovsky G, Van der
Cammen TJM. 2003. Predictors of falls in elderly people during
rehabilitation after hip fracture–who is at risk of a second one?
Zeitschrift fur Gerontologie und Geriatrie 36(1): 16–22.
Pluijm SMF, Smit JH, Tromp EAM, Stel VS, Deeg DJH, Bouter LM, et al.
2006. A risk profile for identifying community-dwelling elderly
with a high risk of recurrent falling: results of a 3-year
prospective study. Osteoporosis International 17(3): 417–25.
Podsiadlo D, Richardson S. 1991. The timed "Up & Go": a test of basic
functional mobility for frail elderly persons. Journal of the
American Geriatric Society 39: 142–8.
Porath M, Brunner S, Schiowitz R, Sigman B, Hayes S, Costello E.
2002. Assessing the validity of the Timed Up and Go Test, and its
ability to predict falls in the ALS population... Platform & poster
presentations for CSM 2003. Neurology Report 26(4): 208–9.
Powell MW, Carnegie DH, Burke TJ. 2006. Reversal of diabetic
peripheral neuropathy with phototherapy (MIRE) decreases falls
and the fear of falling and improves activities of daily living in
seniors. Age and Ageing 35(1): 11–6.
Price C, Suddes M, Maguire L, Harrison S, O'Shea D. 1998. Single
assessment of risk predicted which elderly patients would fall.
British Medical Journal 316(7146): 1750.
Prosser L, Canby A. 1997. Further validation of the Elderly Mobility
Scale for measurement of mobility of hospitalized elderly people.
Clinical Rehabilitation 11(4): 338–43.
Raiche M, Hebert R, Prince F, Corriveau H. 2000. Screening older
adults at risk of falling with the Tinetti balance scale. Lancet
356(9234): 1001–2.
Ranson DL, Emmett SL. 2003. Falls and fall-related injuries: far-
reaching implications. Journal of Law & Medicine 11(1): 16–7.
Resnick NM. 1995. Urinary incontinence. The Lancet 346: 94–9.
Reuben DB, Frank JC, Hirsch SH, McGuigan KA, Maly RC. 1999. A
randomized clinical trial of outpatient comprehensive geriatric
assessment coupled with an intervention to increase adherence to

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 148
recommendations. Journal of the American Geriatrics Society 47:
269–76.
Reuben DB, Roth C, Kamberg C, Wenger NS. 2003. Restructuring
primary care practices to manage geriatric syndromes: the
ACOVE-2 intervention. Journal of the American Geriatrics Society
51(12): 1787–93.
Richardson B, Shepstone L, Poland F, Mugford M, Finlayson B,
Clemence N. 2005. Randomised controlled trial and cost
consequences study comparing initial physiotherapy assessment
and management with routine practice for selected patients in an
accident and emergency department of an acute hospital.
Emergency Medicine Journal 22(2): 87–92.
Robinson B. 2003. Cost of anemia in the elderly. Journal of the
American Geriatrics Society 51(3 Suppl): S14–7.
Robson E, Edwards J, Gallagher E, Baker D. 2003. Steady as you go
(SAYGO): a falls-prevention program for seniors living in the
community. Canadian Journal on Aging 22(2): 207–16.
Rollins G. 2003. Pharmacists can help reduce falls in the elderly
through medication management. Report on Medical Guidelines &
Outcomes Research 14(12): 9–10.
Romeo R, Knapp M. 2006. Economic cost of severe antisocial
behaviour in children - and who pays it. British Journal of
Psychiatry 188 (June): 547–53.
Rose DJ, Jones CJ, Lucchese N. 2002. Predicting the probability of falls
in community-residing older adults using the 8-foot up-and-go: a
new measure of functional mobility. Journal of Aging and Physical
Activity 10(4): 466–75.
Rosendahl E, Lundin-Olsson L, Kallin K, Jensen J, Gustafson Y, Nyberg
L. 2003. Prediction of falls among older people in residential care
facilities by the Downton index. Aging Clinical & Experimental
Research 15(2): 142–7.
Roudsari BS, Ebel BE, Corso PS, Molinari N-AM, Koepsell TD. 2005.
The acute medical care costs of fall-related injuries among the
U.S. older adults. Injury 36(11): 1316–22.
Rubenstein LZ, Josephson KR. 2005. Interventions to reduce the
multifactorial risks for falling [Spanish]. Revista Espanola de
Geriatria y Gerontologia 40 (Suppl 2): 45–53.
Rubenstein LZ, Robbins AS, Josephson KR, Schulman BL, Osterweil D.
1990. The value of assessing falls in an elderly population. Annals
of Internal Medicine 113: 308–16.
Ruchinskas R. 2003. Clinical prediction of falls in the elderly. American
Journal of Physical Medicine & Rehabilitation 82(4): 273–8.
Rucker D, Rowe BH, Johnson JA, Steiner IP, Russell AS, Hanley DA, et
al. 2006. Educational intervention to reduce falls and fear of
falling in patients after fragility fracture: Results of a controlled
pilot study. Preventive Medicine 42(4): 316–19.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 149
Runge M, Schacht E. 2005. Multifactorial pathogenesis of falls as a
basis for multifactorial interventions. Journal of Musculoskeletal
Neuronal Interactions 5(2): 127–34.
Satterwhite LG, Pickelsimer KD, Riolo L. 2002. Using the Dynamic Gait
Index and activities specific balance confidence scale to identify
older adults at risk for falls. Journal of the American Geriatrics
Society 50(4): S96.
Sawka AM, Boulos P, Beattie K, Thabane L, Papaioannou A, Gafni A, et
al. 2005. Do hip protectors decrease the risk of hip fracture in
institutional and community-dwelling elderly? A systematic review
and meta-analysis of randomized controlled trials. Osteoporosis
International 16: 1461–74.
Scaf-Klomp W, Sanderman R, Ormel J, Kempen GIJM. 2003.
Depression in older people after fall-related injuries: a prospective
study. Age and Ageing 32(1): 88–94.
Schacht E, Richy F, Reginster JY. 2005. The therapeutic effects of
alfacalcidol on bone strength, muscle metabolism and prevention
of falls and fractures. Journal of Musculoskeletal Neuronal
Interactions 5(3): 273–84.
Schnelle JF, Kapur K, Alessi C, Osterweil D, Beck JG, Al-Samarrai NR,
et al. 2003. Does an exercise and incontinence intervention save
healthcare costs in a nursing home population? Journal of the
American Geriatrics Society 51: 161–8.
Schousboe JT, Ensrud KE, Nyman JA, Melton LJ, Kane RL. 2005.
Universal bone densitometry screening combined with
alendronate therapy for those diagnosed with osteoporosis is
highly cost-effective for elderly women. Journal of the American
Geriatrics Society 53(10): 1697–1704.
Schuffham P, Chaplin S, Legood R. 2003. Incidence and costs of
unintentional falls in older people in the United Kingdom. Journal
of Epidemiology and Community Health 57: 740–4.
Schulman CC, Asplund R, Desgrandchamps F, Jonas U. 2005. The
impact of nocturia on health status and quality of life in patients
with lower urinary tract symptoms suggestive of benign prostatic
hyperplasia (LUTS/BPH). European Urology Supplements 4(2): 1–
8.
Schwendimann R, De Geest S, Milisen K. 2006. Evaluation of the
Morse Fall Scale in hospitalised patients. Age and Ageing 35(3):
311–13.
Scranton RE, Young M, Lawler E. 2005. Statins reduce fracture risk in
elderly male veterans. Journal of Clinical Outcomes Management
12(11): 555.
Scuffham P, Chaplin S, Legood R. 2003. Incidence and costs of
unintentional falls in older people in the United Kingdom. Journal
of Epidemiology and Community Health 57(9): 740–4.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 150
Segal E, Zinnman C, Raz B, Tamir A, Gurevich B, Siebzehner MI, et al.
2005. Second hip fracture in elderly hip fracture patients: cost
and effectiveness of fracture prevention treatment. Age and
Ageing 34(5): 507–10.
Sharma S, Brown GC, Brown MM, Hollands H, Shah GK. 2001. The
cost-effectiveness of photodynamic therapy for fellow eyes with
subfoveal choroidal neovascularization secondary to age-related
macular degeneration. Ophthalmology 108(11): 2051–9.
Shaw FE, Bond J, Richardson DA, Dawson P, Steen IN, McKeith IG, et
al. 2003. Multifactorial intervention after a fall in older people with
cognitive impairment and dementia presenting to the accident and
emergency department: randomised controlled trial. British
Medical Journal 326(7380): 73.
Shaw FE, Richardson DA, Dawson P, Steen IN, McKeith IG, Bond J, et
al. 2000. Can multi-disciplinary intervention prevent falls in
patients with cognitive impairment and dementia attending an
accident and emergency facility? Age and Ageing 29 (Suppl 2):
S16 P18.
Shea B, Wells G, Cranney A, Zytaruk N, Robinson V, Griffith L, et al.
2006. Calcium supplementation on bone loss in postmenopausal
women. Cochrane Database of Systematic Reviews 4: CD004526
(status: withdrawn).
Sherritze S. 2003. Generating germane geriatrics. Pharmacy &
Therapeutics 28(11): 693.
Shumway-Cook A, Brauer S, Woollacott M. 2000. Predicting the
probability for falls in community-dwelling older adults using the
Timed Up & Go Test. Physical Therapy 80(9): 896–903.
Sieri T, Beretta G. 2004. Fall risk assessment in very old males and
females living in nursing homes. Disability & Rehabilitation
26(12): 718–23.
Simons AM, Dowell CJ, Bryant CM, Prashar S, Moore KH. 2001. Use of
the Dowell Bryant Incontinence Cost Index as a post-treatment
outcome measure after non-surgical therapy. Neurourology and
Urodynamics 20(1): 85–93.
Simpson JM, Jones F. 2004. Physical or psychological change? Which is
the most important rehabilitation outcome for older people who
fall? Age and Ageing 33(2): 204–5.
Simpson JM, Worsfold C, Hawke J. Balance confidence in elderly
people: the CONFbal scale. Age and Ageing 1998;27 (Suppl
2):57.
Siris ES, Chen Y-T, Abbott TA, Barrett-Connor E, Miller PD, Wehren LE,
et al. 2004. Bone mineral density thresholds for pharmacological
intervention to prevent fractures. Archives of Internal Medicine
164(10): 1108–12.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 151
Sitoh YY, Lau TC, Zochling J, Cumming RG, Lord SR, Schwarz J, et al.
2003. Proxy assessment of health-related quality of life in the frail
elderly. Age and Ageing 32(4): 459–61.
Smith DH, Fenn P, Drummond M. 2004. Cost effectiveness of
photodynamic therapy with verteporfin for age related macular
degeneration: the UK case. British Journal of Ophthalmology
88(9): 1107–12.
Smith J, Forster A, Young J. 2006. Use of the 'STRATIFY' falls risk
assessment in patients recovering from acute stroke. Age and
Ageing 35(2): 138–43.
Solomon DH, Finkelstein JS, Katz JN, Mogun H, Avorn J. 2003.
Underuse of osteoporosis medications in elderly patients with
fractures. American Journal of Medicine 115(5): 398–400.
Sorensen SV, De Lissovoy G, Kunaprayoon D, Resnick B, Rupnow MFT,
Studenski S. 2006. A taxonomy and economic consequences of
nursing home falls. Drugs & Aging 23(3): 251–62.
Southard V, Dave M, Davis MG, Blanco J, Hofferber A. 2005. The
Multiple Tasks Test as a predictor of falls in older adults. Gait &
Posture 22(4): 351–5.
Spillman BC. 2004. Changes in elderly disability rates and the
implications for health care utilization and cost. Milbank Quarterly
82(1): 157–94.
Spottke AE, Reuter M, Machat O, Bornschein B, von Campenhausen S,
Berger K, et al. 2005. Cost of illness and its predictors for
Parkinson's disease in Germany. Pharmacoeconomics 23(8): 817–
36.
Stalenhoef PA, Diederiks JPM, Knottnerus JA, Kester ADM, Crebolder
HFJM. 2002. A risk model for the prediction of recurrent falls in
community-dwelling elderly: a prospective cohort study. Journal
of Clinical Epidemiology 55(11): 1088–94.
Steadman J, Donaldson N, Kalra L. 2003. A randomized controlled trial
of an enhanced balance training program to improve mobility and
reduce falls in elderly patients. Journal of the American Geriatrics
Society 51(6): 847–52.
Steinberg M, Cartwright C, Peel N, Williams G. 2000. A sustainable
programme to prevent falls and near falls in community dwelling
older people: results of a randomised trial. Journal of
Epidemiology and Community Health 54: 227–32.
Stel VS, Pluijm SMF, Deeg DJH, Smit JH, Bouter LM, Lips P. 2003. A
classification tree for predicting recurrent falling in community-
dwelling older persons. Journal of the American Geriatrics Society
51(10): 1356–64.
Stevens JA. 2005. Falls among older adults–risk factors and
prevention strategies. Journal of Safety Research 36(4): 409–11.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 152
Stevens M, Holman CDJ, Bennett N, de Klerk N. 2001. Preventing falls
in older people: outcome evaluation of a randomized controlled
trial. Journal of the American Geriatrics Society 49: 1448–55.
Stokes EK, Bourke A, Monaghan F, Scully C. 2005. Hip protectors--a
survey of practice in Ireland. Irish Medical Journal 98(1): 21–3.
Stretanski M, Lusardi M, Dumont L, Evans L. 2002. CSM 2001 poster
presentation. Predicting risk of future falls among residents of
health care facilities: Berg Balance Scale and Fall Risk Assessment
Tool. Journal of Geriatric Physical Therapy 25(1): 22.
Studenski S, Duncan PW, Chandler J, Samsa G, Prescott B, Hogue C,
et al. 1994. Predicting falls: the role of mobility and nonphysical
factors. Journal of the American Geriatrics Society 42(3): 297–
302.
Swanenburg J, Mulder T, De Bruin ED, Uebelhart D. 2003.
[Physiotherapy interventions in osteoporosis]. Zeitschrift fur
Rheumatologie 62(6): 522–6.
Sweeney MA, Chiriboga DA. 2003. Evaluating the effectiveness of a
multimedia program on home safety. Gerontologist 43(3): 325–
34.
Swinburn B, Sager R. 2003. Promotion of exercise prescriptions in
general practice for older populations. Geriatrics and Aging 6(7):
20–3.
Swithinbank LV, Vestey S, Abrams P. 2004. Nocturnal polyuria in
community-dwelling women. BJU International 93(4): 523–7.
Talley K, Wyman J, Gross C. 2003. Validity of The Activities-Specific
Balance Confidence (ABC) scale and the Survey of Activities and
Fear of Falling in the Elderly (SAFE). Gerontologist 43: 381.
Taylor AH, Cable NT, Faulkner G, Hillsdon M, Narici M, Van Der Bij AK.
2004. Physical activity and older adults: a review of health
benefits and the effectiveness of interventions. Journal of Sports
Sciences 22(8): 703–25.
Taylor-Piliae RE. 2003. Tai Chi as an adjunct to cardiac rehabilitation
exercise training. Journal of Cardiopulmonary Rehabilitation
23(2): 90–6.
Thames Valley Primary Care Research Partnership. 1999. A study into
the prediction and prevention of disability and falls in the over 75
year population. National Research Register.
www.nrr.nhs.uk/default.htm.
Thapa PB, Gideon P, Brockman KG, Fought RL, Ray WA. 1996. Clinical
and biomechanical measures of balance as fall predictors in
ambulatory nursing home residents. Journals of Gerontology
Series A-Biological Sciences & Medical Sciences 51(5): M239–46.
Theodos P. 2003. Fall prevention in frail elderly nursing home
residents: a challenge to case management: part I. Lippincott's
Case Management 8(6): 246–51.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 153
Thomas DR. 2003. Wearing the hip protector. Journal of the American
Medical Directors Association 4(5): 281–2.
Thomas JI, Lane JV. 2005. A pilot study to explore the predictive
validity of 4 measures of falls risk in frail elderly patients. Archives
of Physical Medicine & Rehabilitation 86(8): 1636–40.
Tinetti ME. 1986. Performance oriented assessment of mobility
problems in elderly patients. Journal of the American Geriatrics
Society 34: 119–26.
Tinetti ME. 2003. Preventing falls in elderly persons. New England
Journal of Medicine 348(1): 42–9.
Tinetti ME, Williams TF, Mayewski R. 1986. Fall risk index for elderly
patients based on the number of chronic disabilities. American
Journal of Medicine 80: 429–34.
Tinetti ME, Baker DI, McAvay G, Claus EB, Garrett P, Gottschalk M, et
al. 1994. A multifactorial intervention to reduce the risk of falling
among elderly people living in the community. New England
Journal of Medicine 331(13): 821–7.
Tinker A. 2004. Introducing Assistive Technology Into Older People's
Homes: Feasibility, Acceptability, Costs And Outcomes. London:
Institute of Gerontology, King’s College.
Titler M, Dochterman J, Picone DM, Everett L, Xie X-J, Kanak M, et al.
2005. Cost of hospital care for elderly at risk of falling. Nursing
Economics 23(6): 290–306.
Todd C, Skelton D. 2004. What are the Main Risk Factors for Falls
Amongst Older People and What are the Most Effective
Interventions to Prevent these Falls? Copenhagen: World Health
Organization.
Topper A, Maki B, Holliday P. 1993. Are activity-based assessments of
balance and gait in the elderly predictive of risk of falling and/or
type of fall? Journal of the American Geriatrics Society 41(5):
479–87.
Toulotte C, Fabre C, Dangremont V, Lensel G, Thévenon A. 2003.
Effects of physical capacity of frail, demented patients with a
history of falling: a randomised controlled trial. Age and Ageing
32: 67–73.
Trivedi DP, Doll R, Khaw KT. 2003. Effect of four monthly oral vitamin
D3 (cholecalciferol) supplementation on fractures and mortality in
men and women living in the community: randomised double
blind controlled trial. British Medical Journal 326(7387): 469.
Tromp AM, Pluijm SM, Smit JH, Deeg DJ, Bouter LM, Lips P. 2001.
Fall-risk screening test: a prospective study on predictors for falls
in community-dwelling elderly. Journal of Clinical Epidemiology
54(8): 837–44.
Trueblood PR, Hodson-Chennault N, McCubbin A, Youngclarke D.
2001. Performance and impairment-based assessments among

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 154
community dwelling elderly: sensitivity and specificity. Issues on
Aging 24(1): 2–6.
Turnbull GB. 2003. Foresight. Fall update. Ostomy/Wound
Management 49(10): 20–1.
Vaillant J, Martigne P, Vuillerme N, Caillat-Miousse JL, Parisot J, Juvin
R, et al. 2006. Prediction of falls with performance on Timed 'Up-
and-Go' and one-leg-balance tests and additional cognitive tasks
[French]. Annales de Readaptation et de Medecine Physique
49(1): 1–7.
van der Weijden T, Ijzermans CJ, Dinant GJ, van Duijn NP, de Vet R,
Buntinx F. 1997. Identifying relevant diagnostic tests in Medline:
the diagnostic value of the erythrocyte sedimentation rate (ESR)
and dipstick as an example. Family Practice 14: 204–8.
van Haastregt JCM, Diedericks JPM, van Rossum E, de Witte LP,
Voorhoeve PM, Crebolder HFJM. 2000. Effects of a programme of
multifactorial home visits on falls and mobility impairments in
elderly people at risk: randomised controlled trial. British Medical
Journal 321: 994–8.
van Heuvelen M, Hochstenbach J, de Greef M, Brouwer W, Mulder T,
Scherder E. 2005. Is the Activities-specific Balance Confidence
Scale suitable for Dutch older persons living in the community?
Tijdschrift voor Gerontologie en Geriatrie 36(4): 146–54.
van Rossum E, Frederiks CMA, Philipsen H, Portengen K, Wiskerke J,
Knipschild P. 1993. Effects of preventive home visits to elderly
people. British Medical Journal 307: 27–32.
Van Schoor N, Smit JH, Twisk JWR. 2003. Prevention of hip fractures
by external hip protectors. Journal of the American Medical
Association 289(15): 1957–62.
VanSwearingen JM, Paschal KA, Bonino P, Chen T. 1998. Assessing
recurrent fall risk of community-dwelling, frail older veterans
using specific tests of mobility and the Physical Performance Test
of function. Journals of Gerontology Series A-Biological Sciences
and Medical Sciences 53(6): M457–64.
Van Vaerenbergh J, Broos P. 1990. [Positive Romberg test and the
probability of falls in the aged]. Tijdschrift voor Gerontologie en
Geriatrie 21(2): 71–4.
Vassallo M, Stockdale R, Sharma JC, Briggs R, Allen S. 2005. A
comparative study of the use of four fall risk assessment tools on
acute medical wards. Journal of the American Geriatrics Society
53(6): 1034–8.
Vellas BJ, Wayne SJ, Romero L, Baumgartner RN, Rubenstein LZ,
Garry PJ. 1997. One-leg balance is an important predictor of
injurious falls in older persons. Journal of the American Geriatrics
Society 45(6): 735–8.
Verghese J, Buschke H, Viola L, Katz M, Hall C, Kuslansky G, et al.
2002. Validity of divided attention tasks in predicting falls in older

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 155
individuals: a preliminary study. Journal of the American
Geriatrics Society 50(9): 1572–6.
Vladeck BC. 2005. Economic and policy implications of improving
longevity. Journal of the American Geriatrics Society 53 (9 Suppl):
S304–7.
von Renteln-Kruse W, Krause T. 2004. When do elderly in-hospital
patients fall? Age and Ageing 33(4): 413.
Vu HTV, Keeffe JE, McCarty CA, Taylor HR. 2005. Impact of unilateral
and bilateral vision loss on quality of life. British Journal of
Ophthalmology 89(3): 360–3.
Wagg A. 2004. Urinary incontinence - older people: where are we
now? BJOG International Journal of Obstetrics & Gynaecology 111
(Suppl 1): 15–19.
Wagner EH, LaCroix AZ, Grothaus LC, Leveille SG, Hecht JA, Artz K, et
al. 1994. Preventing disability and falls in older adults: a
population-based randomized trial. American Journal of Public
Health 84(11): 1800–6.
Wanless D. 2004. Securing Good Health for the Whole Population.
London: HMSO.
Warnke A, Meyer G, Bott U, Muhlhauser I. 2004. Validation of a quality
of life questionnaire measuring the subjective fear of falling in
nursing home residents. Zeitschrift fur Gerontologie und Geriatrie
37(6): 459–66.
Weatherall M. 2004. Prevention of falls and fall-related fractures in
community-dwelling older adults: a meta-analysis of estimates of
effectiveness based on recent guidelines. Internal Medicine
Journal 34(3): 102–8.
Webster B, Giunti G, Young A, Pransky G, Nesathurai S. 2004. Work-
related tetraplegia: cause of injury and annual medical costs.
Spinal Cord 42(4): 240–7.
Weir E, Culmer L. 2004. Fall prevention in the elderly population.
Canadian Medical Association Journal 171(7): 724-.
West J, Hippisley-Cox J, Coupland CAC, Price GM, Groom LM, Kendrick
D, et al. 2004. Do rates of hospital admission for falls and hip
fracture in elderly people vary by socio-economic status? Public
Health 118(8): 576–81.
Whitehead C, Wundke R, Crotty M, Finucane P. 2003. Evidence-based
clinical practice in falls prevention: a randomised controlled trial of
a falls prevention service. Australian Health Review 26(3): 88–97.
Whiting P, Rutjes AWS, Reitsma JB, Bossuyt PMM, Kleijnen J. 2003.
The development of QUADAS, a tool for the quality assessment of
studies of diagnostic accuracy included in systematic reviews.
BMC Medical Research Methodology 3: 25.
Whitney JC, Lord SR, Close JCT. 2005. Streamlining assessment and
intervention in a falls clinic using the Timed Up and Go Test and
Physiological Profile Assessments. Age and Ageing 34(6): 567–71.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 156
Wijnia JW, Ooms ME, van Balen R. 2006. Validity of the STRATIFY risk
score of falls in nursing homes. Preventive Medicine 42(2): 154–
7.
Wilson CJ, Datta SK. 2001. Tai chi for the prevention of fractures in a
nursing home population: an economic analysis. Journal of Clinical
Outcomes Management 8(3): 19–27.
Wolf SL, Sattin RW, Kutner M, O'Grady M, Greenspan AI, Gregor RJ.
2003. Intense tai chi exercise training and fall occurrences in
older, transitionally frail adults: a randomized, controlled trial.
Journal of the American Geriatrics Society 51(12): 1693–1701.
Wolpe J, Lang PJ (1964). A fear survey schedule for use in behaviour
therapy. Behav. Res. Ther. 2:27-30.
Wong JB, Singh G, Kavanagh A. 2002. Estimating the cost-
effectiveness of 54 weeks of infliximab for rheumatoid arthritis.
American Journal of Medicine 113(5): 400–8.
Woo J, Ho SC, Yu ALM. 1999. Walking speed and stride length predicts
36 months dependency, mortality, and institutionalization in
chinese aged 70 and older. Journal of the American Geriatrics
Society 47(10): 1257–60.
Woolf AD, Akesson K. 2003. Preventing fractures in elderly people.
British Medical Journal 327(7406): 89–95.
Yates SM, Dunnagan TM. 2001. Evaluating the effectiveness of a
home-based fall risk reduction program for rural community
dwelling older adults. Journal of Gerontology: Medical Sciences
56A(4): M226–30.
Yauk S, Hopkins BA, Phillips CD, Terrelu S, Bennion J, Riggs M. 2005.
Predicting in-hospital falls: development of the Scott and White
Falls Risk Screener. Journal of Nursing Care Quality 20(2): 128–
33.
Ytterstad B. 1996. The Harstad injury prevention study: community
based prevention of fall-fractures in the elderly evaluated by
means of a hospital based injury recording system in Norway.
Journal of Epidemiology and Community Health 50: 551–8.
Zaloshnja E, Miller TR, Lawrence BA, Romano E. 2005. The costs of
unintentional home injuries. American Journal of Preventive
Medicine 28(1): 88–94.
Zisselman PM, Robinson JP. 1998. Assessment of fall risk and
prevention of injurious falls. In Strumpf NE, Robinson JP, Wagner
JS and Evans LK (eds), Restraint Free Care: Individualized
Approaches for Frail Elders, pp. 60–83. New York: Springer.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 157
Appendices
Appendix 1 Summary economic data
Service Point of contact with falls-prevention team, location, new attendances p.a. (population size of catchment area)
Breakdown of cost: budget hospital transport cost*
beverages provided floor space staff costs
Total cost
1 Community, urban, 180
Budget: ‘Comes with the day hospital budget’
Clinic transport: 85% (£15,300)
Lunch§: Yes @£1.70 (£306) Partial staff information
Consultant†: £10,376.60
£25,982.60
2 Community, urban, 242
Clinic transport: 100% patients transported
Transported for assessment (£24,200) Transport for exercise**: £32,000
Floor space††: 371.61 m2
(£61,070.39)
No staff information
£117,270.39
3 Community, rural, 440
Clinic transport: 75% (£33,000) Exercise transport**: £25,200
Floor space††: 355 m2 (£58,340.70) £24,019.60 Consultant‡: £5534.32 Partial staff information
£146,094.62
4 Community, urban, 186 (390,000)
Budget: overall £7380 (this is for 2006 and is not recurrent)
Clinic transport: by mini bus (community transport) Partial staff information: £49,705.04
£57,085.04
5 Community, urban, 360 (330,000)
Salary full £100,673.10
£100,673.10
6 Community, rural, 108 (150,000)
Budget: ‘Part of overall day hospital budget’
Clinic transport: own transport
£32,365.74

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 158
or we provide hospital transport Salary full: £21,649.10 Consultant‡: £10,716.64
7 Community, urban, 93 (250,000)
Budget: consumables budget, £5000
Equipment budget (not delineated from overall budget) Drug budget (not allowed to prescribe)
Cost of falls work undertaken by generalists is unknown
Clinic transport: 50% (£4650)
Floor space††: 31.56m2
(£5186.57) Partial staff information: £73,000.00 Consultant‡: £11,068.64 SPR¶: £5144.48
£104,049.69
8 Community, urban and rural, 82
Budget: ‘We don’t have any budget. We are all ward based and all lose time on the ward as a result of the clinic. We use the same equipment as we use for our ward patient.’
Clinic transport: they have to make their own way, which means that many patients lose out; no funding for transport
Salary full: £87,814.19
£87,814.19
9 Community, urban and rural, 40 (122,725)
Budget: overall £130,000 Salary full: 155,705.08
£285,705.08
10 Community, rural, 154
Clinic transport: 80% (£12,320)
Exercise transport cost**: £23,040 Floor space††: 43.19 m2 (£7097.84) Salary full £46,768.21
£89,226.05
11 Community, urban and rural (157,050)
Budget: overall £78,903 Equipment: 0 Consumables: £4000 Drugs: 0 Clinic transport: staff visit the patients in their own homes
Floor space††: 30.66 m2 (£5038.66) Partial staff information
£83,941.66
12 Community, urban, 300 (25,100)
Budget: £58,000 for salaries covers the satellite clinics and additional integrated working
£84,928.75

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 159
across services some staff seconded free from services
Clinic transport: 10% (£3000) hospital taxis used for health clinic venue; mainly public transport/friends and family
Salary full: £22,821.92 Consultant‡: £1106.83
13 Community, urban, 196 (21,700)
Salary full: £154,435.40 Consultant‡: £51,883
£206,318.40
14 Community, urban, 557
Budget: £149,760
Clinic transport: social services transport
Floor space††: 42 m2 (£6902.28) Partial staff information: £118,026.80
£274,689.08
15 Community, urban, 260 (273,000)
Budget: overall: As part of 11PA job plan (approx 1 PA per week) Consumables: outpatient budget
Clinic transport: hospital transport/own transport
Consultant‡: £103,766
£103,766
16 Community, urban, 900 (208,465)
Partial staff information Consultant‡: £8297.52
£8297.52
17 Community, urban, 200
Clinic transport: hospital transport, voluntary agency
Floor space††: 12 m2 (£1972.08)
£1972.08
18 Community, urban Partial staff information Consultant†: £10,376.60
£10,376.60
19 Community, urban, 84 (239,000)
Budget: overall £116,000 Equipment: £2000
Clinic transport: by ambulance or voluntary car
Floor space††: 242 m2 (£39,770.28) Partial staff information £24,456.30
£182,226.58
20 Community, rural, 64 (122,725)
Budget: overall £130,000 £50,060.56
£180,060.56
21 Community, urban (500,000)
Salary full: £28,218.96 £28,218.96
22 Community, urban (500,000)
Partial staff information £24,301.16
£24,301.16

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 160
23 Community, urban, 641
Budget: overall £160,000 Equipment: £20,000 Drugs: nil
Clinic transport: people visited at home; for falls programme transport is by community transport, paid for by the service
Salary full: £106,054.10
£266,054.10
24 Community, urban, 66
Clinic transport: hospital transport 75% (£4950) Partial staff information Consultant‡: £8301.48
£13,251.48
25 Community, urban and rural, 31 (72,000)
Budget: staff costs, each from individual budget relating to OT (£5000), physiotherapist (£7700) and nursing (£7700) Transport costs to bring patients to hospital, part of larger transport budget, minimal admin/postage costs absorbed in whole hospital budget
Clinic transport: own transport, ambulance
Floor space††: 40 m2
(£6573.60) Salary full: £15,255.90
£42,229.50
26 Community, urban and rural
Budget: overall £30,000 Consumables: £500
Clinic transport: mostly by relatives or by subsidised volunteer driver service
Hospital transport difficult to access Partial staff information Consultant‡: £6037.44
£36,537.44
27 Community, urban, 708 (167,759)
Budget: overall £259,000 Equipment: £9000 Drugs: nil
Clinic transport: patients provide their own transport; where a person is house-bound either a home visit is offered or we have access to ambulance transport provided through another intermediate care team; this has very strict criteria Salary full: £259,714.60
£518,714.60

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 161
28 Community, urban, 300
Salary full: £86909.94 £86,909.94
29 Community, rural, 125 (120,000)
Floor space††: 64 m2 (£10517.76) Salary full: £26811.84
£37,329.60
30 Community, urban Partial staff information Consultant†: £10,376.60
£10,376.60
31 Community, rural, 10 (2400)
Budget: overall £600
Clinic transport: three came in hospital transport, last group (the rest came on their own)
Floor space††: 25 m2 (£4108.50) Salary full: £4624.40
£9332.90
32 Community, rural, 30
Clinic transport: own or hospital transport
Floor space††: 66 m2 (£10,846.44) Salary full: £34,298.88
£45,145.32
33 Community, urban, 600 (240,000)
Partial staff information Consultant‡: £6037.44
£6037.44
34 Community, urban and rural, 46 (46,000)
Budget: FPP budget within whole physiotherapist budget
Clinic transport: transport for those with none available
Floor space††: 100 m2
(£16,434) Partial staff information £12,220.76
Consultant‡: £5537.32
£34,192.08
35 Community, urban and rural, 46 (46,000)
Budget: FPP budget within whole physiotherapist budget
Clinic transport: transport for those with none available
Floor space††: 100 m2
(£16,434) Partial staff information £12,220.76
Consultant‡: £5537.32
£34,192.08
36 Community, rural, 150
Budget: £2000
Equipment: £200
Consumables: nil
Drugs: nil
Clinic transport: own transport, occasionally hospital transport booked
Floor space††: 89.19 m2
£32,625.52

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 162
(£14,657.48) Salary full: £15,968.04
37 Community, urban Clinic transport: hospital transport 75% Exercise transport cost**: £21,600 Salary full: £117,715.73
£139,315.73
38 Community, rural, 216 (65,028)
Clinic transport: hospital transport 80% (£33,600)
Floor space††: 157.07 m2
Partial staff information (£25,812.88) £76,022.18
£135,435.06
39 Community, urban and rural (163,000)
Salary full: £198,471.40 £198,471.40
40 Community, rural, 278 (110,000)
Budget: £50,000
Clinic transport: hospital transport, voluntary schemes, fairly occasional, they can drive Partial staff information £72,559.26
Consultant†: £10,376.60
£132,935.86
41 Community, urban Salary full: £40,573.99 £40,573.99
42 Community, urban Salary full: £145,756.80 £145,756.80
43 Community, urban, 416
Budget: overall £71,000 Consumables: £400
Clinic transport: hospital transport 95% (£39,520) Exercise transport cost**: £53,200
Floor space††: 375 m2
(£61,627.50) Salary full: £75,482.44
£300,829.94
44 Community, urban, 416
Budget: overall £71,000 Consumables: £400
Clinic transport: hospital transport 95% (£39,520) Exercise transport cost**: £53,200
Floor space††: 187.50 m2 Salary full: £75,482.44
£270,016.19
45 Community, urban, 336
Budget: overall £21,841
Clinic transport: hospital or private transport Salary full: £165,174.90
£187,015.90
46 Community, rural, 240
Salary full: £57,842.20 Consultant‡: 41,507.40
£99,349.60

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 163
47 Community, urban, 70 (49,500)
Budget: £15,000 total funding level 1
Clinic transport: either make their own way to the class or we can provide dial-a-ride buses to transport them to and from the classes
£15,000
48 Community, urban, 410 (27,500)
Salary full: £38,877.11
Consultant‡: £15,564.90
£54,442.01
49 Community, rural, 47 (3713)
Floor space††: 227.40 m2
(£37,370.92) Salary full: £95,820.73
£133,191.65
50 Community, rural, 60 (3672)
Floor space††: 161 m2
(£26,458.74) £26,458.74
51 Community, rural, 72 (32,421)
Budget: overall £1200
Clinic transport: patient transport service; ambulance service; voluntary car/bus; own transport
Floor space††: 121.15 m2
(£19,909.79)
£21,109.79
52 Community, urban, 1,300 (35,000)
Partial staff information £38,877.11
£38,877.11
53 Community, rural, 208
Budget: £84,000 integrated into ward budget
Clinic transport: hospital transport 50% (£10,400)
Floor space††: 34.75 m2
(£5710.81) Partial staff information £40,567.56 Consultant†: £10,376.60
£151,054.97
54 Community, urban and rural, 300
Floor space††: 55.74 m2
(£9160.31) Partial staff information £10,366.40
£19,526.71
55 Community, urban, 275 (244,424)
Salary full: £4541.46 Consultant†: £9685.06 SPR¶: £4501.42
£18,727.94
56 Community, rural, 135 (39,438)
‘Only budget available is for 371/2 hours band 7 falls co-ordinator.’
Clinic transport: own transport and hospital transport
Floor space††: 52.86 m2
(£8687.01) Salary full: £4146.56
£23,210.17

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 164
Consultant†: £10,376.60
57 Community, urban, 130 (196,121)
Partial staff information Consultant†: £10,376.60
£10,376.60
58 Community, urban, 104
Clinic transport: hospital transport 25% (£2600)
Exercise transport cost**: £800
Floor space††: 78.78 m2
(£12,946.71) Salary full: £86,615.42
£102,962.13
59 Community, urban, 24,116
Floor space††: 148.39 m2
(£24,386.41)
Partial staff information £71,363.80 Consultant‡: £103,766
£199,516.21
60 Community, urban, 216
Salary full: £61,190.80 £61,190.80
61 Community, rural Budget: overall £79,206
Partial staff information £69,648.32
£148,854.32
62 Community, urban, 252
Partial staff information £69,648.32
£69,648.32
63 Community, urban, 70 (31,182)
Partial staff information £4909.52 Consultant†: £10,376.60
£30,798.17
64 Community, urban and rural, 300
Floor space††: 53.75m2
(£8833.26) Salary full: £88,909.95
£97,743.21
65 Community, urban, 42 (150,000)
Floor space††: 42 m2
(£6902.28) £6902.28
66 Community, urban £169,240.60 £169,240.60
67 Community, urban, 48 (70,000)
Salary full: £169,240.60 Consultant†: £10,376.60
£179,617.20
68 Community, rural, 36
Budget: ‘Don’t have one specifically for falls clinic. Annual cost is approx £20,000.’
Clinic transport: via Primary Care Trust in-house transport system, escorted by physiotherapist assistant
Floor space††: 200m2 (£32,868) Salary full: £22,984.02
£75,852.02
69 Community, urban, 400 (90,000)
Budget: overall £25,000
Clinic transport: own this is an area of concern but no budget for this
£46,626.58

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 165
Floor space††: 72.46 m2
(£11,908.08) Partial staff information £9718.50
70 Community, urban and rural
£162,427.70 £162,427.70
71 Community, urban, 50 (350,000)
Floor space††: 10.41 m2 (£1710.78) Partial staff information £61,597.29
Consultant†: £10,376.60
£73,684.67
72 Community, rural, 30
Partial staff information £61,597.29
£61,597.29
73 Community, urban and rural, 69 (141,000)
Partial staff information £18,659.52 Consultant†: £10,376.60
£29,036.12
74 Community, urban, 43 (26,000)
Budget: overall £21,855
Clinic transport: hospital transport 65% (£2795) Exercise transport cost**: £35,100
£59,750
75 Community, urban, 110,091
Overall budget: £21,855 Partial staff information £20,732.80
£42,587.80
76 Community, rural, 540
Budget: overall £362,000
Clinic transport: hospital transport 75% dedicated ambulance (£40,500) Exercise transport cost**: £25,200 Salary full: £156,043.20
£583,743.72
77 Community, urban and rural, 50 (6654)
Budget: overall £247,377
Clinic transport: patients are encouraged to make their own transport arrangements however transport can be arranged via the ambulance service patient transport
Floor space††: 81.10 m2
(£13,327.97) Partial staff information Consultant‡: £3018.72
£263,723.69
78 Community, urban Budget: overall £79,206
Clinic transport: usually take approx. five new patients per clinic with approximately three follow-ups Partial staff information
£520,487.20

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 166
£441,281.20
Total £8,555,958.64/78=£109,691.78
1 Acute, urban, 210 (250,000)
Budget: ‘Linked budget with the day hospital so not able to separate.’
Clinic transport: 60–70% (£13,650)
£13,650
2 Acute, urban, 240 (230,500)
Floor space††: 5.57 m2 (£915.37) Partial staff information Consultant†: £10,376.60
£11,291.97
3 Acute, urban, 180 (300,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
4 Acute, urban, 180 (300,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
5 Acute, rural, 180 (300,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
6 Acute, urban and rural, 255
Partial staff information £137,851.40
£137,851.40
7 Acute, urban, 50 (69,000)
Floor space††: 600 m2 (£98,604) Partial staff information Consultant‡: £311,329.80
£409,933.80
8 Acute, urban, 550 (191,151)
Salary full: £149,597.40 Consultant‡: £20,753.20
£170,350.60
9 Acute, urban, 1700 (260,000)
Budget: £328,045.00 (overall)
£12,446.00 (equipment)
£7164.00 (consumables)
£745.00 (drugs)
Clinic transport: ambulance transport (£56,700)
Exercise transport cost**: £29,400
Lunch: not available
Floor space††: 451.1m2
(£74,133.77) Salary full: £158,988 Consultants†: £77,305.67 SPR¶: £337,708
£1,062,280.44
10 Acute, urban, 72 (250,000)
Budget: £420,000 (falls clinic shared budget with rapid access for the elderly clinic)
£420,000
11 Acute, urban, 312 (3,200,000)
Transport: 1 in 6 (52) (£5200) £5200
12 Acute, urban, 80 (200,000)
Budget: overall, as part of 11PA job plan (approx 1 PA per
£10,376.60

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 167
week) Consumables: outpatient budget
Salary full: Consultant†: £10,376.60
13 Acute, combination, 384 (225,000)
No specific budget
Transport: 10% (£3840)
Exercise cost**: £2520 Partial staff information Consultant‡: £10,376.60
SPR¶: £3858.36
£20,594.96
14 Acute, combination, 384 (225,000)
Partial staff information Consultant‡: £10,376.60
SPR¶: £3858.36
£14,234.96
15 Acute, urban (35,500)
Budget: £400,000
Clinic transport: 0% Exercise transport: 0
£400,000
16 Acute, urban, 208 Clinic transport: 60% ambulance (£12,480) Exercise transport cost**: £24,000
Floor space††: 240 m2 (£39,441.60) Salary full: £38,681.40
Consultant‡: £11,068.64
SPR¶: £2572.24
£128,243.88
17 Acute, urban, 50 Budget of from general elderly fund
Clinic transport: hospital transport: 75% (£3750) Salary full: £63,310.28 Consultant‡: £11,068.64
£78,128.92
18 Acute, urban (240,000)
Budget: £160,000 Equipment: £6000 revenue, however most equipment Is purchased on capital as opposed to revenue; capital funding is held centrally in the Trust and not just for this unit Consumables: £4000 Drug: £7000 ward budget
However, consultants also have associated drug budget and drugs can be requested for the unit on this budget as well
Clinic transport: patients are either transported to the hospital by ambulance or make their own arrangements to
£222,253.96

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 168
come either by car, taxi or public transport
Floor space††: 150 m2 (£45,651) Partial staff information Consultant‡: £16,602.96
19 Acute, rural, 50 (26,765)
Budget: overall £361,493
Clinic transport: hospital transport 50% (£2500)
Floor space††: 370 m2
(£60,805.80) Partial staff information £2726.79 Consultant‡: £8301.48
£435,827.07
20 Acute, urban, 92 (240,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
21 Acute, urban, 700 (330,000)
Budget: overall: £344,640
Equipment: £7035 Consumables: £1016
Clinic transport: ambulance service from day unit, own transport
Floor space††: 472 m2 (£77,568.48) Partial staff information Consultants‡: £171,213.90
Registrar¶: £5146.03
£598,568.41
22 Acute, urban and rural, 332 (250,000)
Transport: pay nominal amount for transport supplied by the unit
Floor space††: 148.64 m2 Partial staff information (£24,427.50) £65,177.81
£89,605.31
23 Acute, urban (300,000)
Salary full: consultant‡: £121,755.04
£121,755.04
24 Acute, urban and rural
Salary full: £43,216.80 Consultant‡: £19,370.12
£62,586.92
25 Acute, urban, 440 (180,000)
Clinic transport: hospital transport 2/3 (£29,333) Exercise transport cost**: £21,333 Partial staff information Consultant†: £10,376.60
£61,042.60
26 Acute, urban and rural, 200
Floor space††: 60.03 m2 (£9865.33) Salary full: £34,531.42
£44,396.75
27 Acute, urban and No budget £36,000

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 169
rural, 72 Clinic transport: hospital transport 100% (£7200) Exercise transport cost**: £28,800
28 Acute, urban, 79 (144,477)
Budget: overall £159,983 This does not include management costs from community rehabilitation services; also does not include doctor and pharmacist Falls equipment budget is under the Integrated Community equipment service and there for does not have a separate budget
Consumables: non-pay budget £8747 Drugs: nil
Transport: some patients make their own way, others are offered hospital transport
Floor space††: 15 m2 (£2465.10) Partial staff information £120,851.90 Consultant‡: £10,376.85 SPR¶: £4822.95
£298,499.80
29 Acute, urban, 144 (250,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
30 Acute, urban, 150 (300,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
31 Acute, urban, 100 No specific budget
Clinic transport: ambulance service where appropriate Partial staff information Consultant‡: £103,766
£103,766
32 Acute, urban, 50 (500,000)
Falls budget works within a larger budget
Clinic transport: own or hospital transport Partial staff information Consultant‡: £103,766
£10,376.60
33 Acute, urban Partial staff information Consultant†: £10,376.60
£10,376.60
34 Acute, rural, 40 (12,000)
Partial staff information Consultant†: £10,376.60
£10,376.60
35 Acute, urban, 144 (300,000)
Partial staff information Consultant†: £10,376.60
£10,376.60

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 170
36 Acute, urban, 350 (24,800)
Floor space††: 216 m2
(£35,497.44) Salary full: £59,343.85 Consultant‡: £103,766
£198,607.29
37 Acute, urban Partial staff information Consultant†: £10,376.60
£10,376.60
38 Acute, urban, 90 Floor space††: 184 m2
(£30,238.56) Partial staff information £32,486.69
£62,725.25
39 Acute, urban, 450 (200,000)
Lunch§: £1336.20
Consultant†:
£10,376.60
£11,712.80
40 Acute, urban, 120 (90,000)
Budget: overall £100,000 £100,000
41 Acute, urban, 1000 (300,000)
Clinic transport: hospital transport 91% (£9100) Salary full: £134,803.20
£143,903.20
42 Acute, urban, 420 (130,000)
Partial staff information £217,801.90 Consultant‡: £415,064
£632,865.90
43 Acute, urban, 420 (130,000)
Clinic transport: hospital transport 80% (£33,600) Exercise transport cost**: £40,000 Partial staff information £217,801.90 Consultant‡: £415,064
£706,465.90
44 Acute, rural, 60 (3672)
Floor space††: 161 m2
(£26,458.74) £26,458.74
45 Acute, urban, 336 Budget: overall £21,841
Salary full: £165,174.90
£187,015.90
46 Acute, urban, 174 (53,226)
Budget: overall £2404
Clinic transport: mostly ambulance transport but patients encouraged to arrange own transport
Floor space††: 4560.33 m2
(£749,444.63) Salary full: £69,790.80 Consultant‡: £51,884.25
£873,523.68
47 Acute, urban, 70 Clinic transport: hospital transport 90% (£6300) Exercise transport cost**: £60,480
Floor space††: 1500 m2
(£246,510)
£354,797.40

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 171
Partial staff information Consultant‡: £41,507.40
48 Acute, urban, 62 Salary full: £341,027.70 £341,027.70
49 Acute, rural, 655 Salary full: £152,001.90 £152,001.90
50 Acute, urban Budget: overall £181,628
Salary full: £211,196.40
£392,824.40
51 Acute, rural, 180 Budget: overall £37,987
Clinic transport: hospital transport 60%(£10,800)
Floor space††: 900 m2
(£147,906) Partial staff information £45,689.60 Consultant†: £10,376.60
£252,759.20
52 Acute, urban, 605 Clinic transport: hospital transport 100%
50% Ambulance £30,250 50% Voluntary transport‡‡: £907.50 Exercise transport cost¶¶: £18,540
Floor space††: 106 m2
(£17,420.04) Salary full: £21,509.84
£88,627.38
53 Acute, urban, 468 Partial staff information £60,609.33 Consultant‡: £69,608.99
£130,218.32
54 Acute, urban, 500 Floor space††: 14.86 m2
(£2242.09) Partial staff information £26,300.61 Consultant†: £103,766
£132,308.70
55 Acute, urban, 162 (210,000)
Budget: £1000 equipment budget
Floor space††: 73.60 m2
(£12,095.42) Partial staff information Consultant†: £10,376.60
£23,472.02
56 Acute, urban and rural, 80
Clinic transport: hospital transport 50% (£4000)
Exercise transport cost**: £16,800
£20,800
57 Acute, urban and rural, 80
Clinic transport: hospital transport 50% (£4000) Exercise transport cost**: £16,800
£20,800
58 Acute, urban, 1446 Budget: clinic held within £67,863.29

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 172
general hospital department
Physiotherapist
Consumables budget: hip protectors £25,000 Transport: Self-arranged via GP/ambulance service Partial staff information £32,486.69 Consultant†: £10,376.60
59 Acute, urban, 156 Floor space††: 23.06 m2
(£3789.68) Partial staff information Consultant†: £10,376.60
£14,166.28
60 Acute, urban (180,000)
Budget: overall £143,951 Equipment budget: £1795 Consumables: no budget Drug budget: £360.00
Clinic transport: hospital transport 45% Exercise transport cost**: £360 Salary full: £143,875.20 Consultant†: £10,376.60
£298,562.80
61 Acute, urban, 90 (248,700)
Clinic transport: hospital transport 100% (£9000) Exercise transport cost**: £3200 Partial staff information £143,875.20 Consultant†: £10,376.60
£166,451.80
62 Acute, urban, 160 Budget: overall £247,377
Clinic transport: hospital transport 100%, patient transport service (£1600) Exercise transport cost**: £28,800
Lunch§: £761.60
Floor space††: 148.39 m2
(£24,386.41) Salary full: £66,167.20 SPR¶: £1929.18
£371,021.39
63 Acute, urban, 100 (1100)
Partial staff information Consultant‡: £103,766
£103,766
64 Acute, urban, 200 (216,905)
Total overall budget for day hospital: £247,377
Equipment: £645.00 Consumables: £525.00
Drug budget: £7000
Clinic transport: hospital transport 65%, patients utilise
£463,027.15

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 173
hospital transport (£13,000)
Floor space††: 94.39 m2
(£15,512.05) Partial staff information £118,140.90 Consultant‡: £20,753.20
SPR¶: £48,244
65 Acute, urban, 24 (22,000)
Budget: overall £79,206 Equipment: £1300 Consumables: £840 Drugs: none
Clinic transport: community car scheme
Floor space††: 71.54 m2
(£11,756.88)
£90,962.88
66 Acute, urban Lunch§: £544
Partial staff information Consultant†: £10,376.60 SPR¶: £48,244
£59,164.60
67 Acute, urban Budget: £20,000
Floor space††: 41 m2
(£6737.94)
£26,737.94
68 Acute, urban, 42 (150,000)
Floor space††: 41 m2
(£6737.94) £6737.94
69 Acute, urban and rural, 150 (100,000)
Budget: ‘1 PA a week of consultant time.’
Clinic transport: hospital or own transport Partial staff information Consultant†: £10,376.60
£10,376.60
70 Acute, urban (500,000)
Floor space††: 12.07 m2
(£1983.58) Salary full: consultants‡: £9056.16
£11,039.74
71 Acute, urban, 360 Floor space††: 12.07 m2
(£1983.58) £1983.58
72 Acute, rural, 63 Clinic transport: hospital transport 98% (£6100)
Hospital transport**: £28,224 Salary full: £162,427.70
£196,751.70
73 Acute, urban Floor space††: 650 m2
(£106,821) £106,821
74 Acute, urban, 416 Clinic transport: hospital transport 60%(£24,960)
Exercise transport cost**: £28,224
Lunch§: £1278.40
£175,556.62

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 174
Floor space††: 650 m2
(£106,821) Partial staff information £3896.62 Consultant†: £10,376.60
75 Acute, urban, 352 Lunch§: £1088
Partial staff information £3896.62 Consultant†: £10,376.60
£153,612.22
76 Acute, urban, 200 (550,000)
Partial staff information £3896.62 Consultant‡: £8301.48
£12,198.10
77 Acute, urban, 282 (144,477)
Budget: overall £159,983 This does not include management costs from community rehabilitation services; also does not include doctor and pharmacist Falls equipment budget is under the Integrated Community equipment service and there for does not have a separate budget
Consumables: non-pay budget is £8747 Drugs: nil
Clinic transport: 100% community transport
Floor space††: 15 m2
(£2465.10) Salary full: £441,281.20 £120,851.90 Consultant‡: £10,376.60 SPR¶: £4822.95
£739,780.75
78 Acute, rural, 27 (32,428)
Floor space††: 2000 m2
(£328,680) Salary full: £21,627.76
£350,307.76
79 Acute, urban (1,000,000)
Salary full: £71,363.80
Consultant‡: £103,766 Consultant†: £10,376.60
£185,506.40
Total £13,535,894.20/79=£171,340.43
1 Emergency department, urban, 1100
Floor space††: 6800 m2
[caution: this seems to be referring to whole of emergency department] (£111,7512)§§
£111,7512.00
2 Emergency department, urban
Salary full: £326,822.90 £326,822.90
3 Emergency Salary full: £326,822.90 £326,822.90

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 175
department, urban
4 Emergency department, urban, 980
Floor space††: 7.5 m2
(£1232.55) Partial staff information £22,806.08
£24,038.63
5 Emergency department, urban, 980
Floor space††: 7.5 m2
(£1232.55) Partial staff information £22,806.08
£24,038.63
Total: £1,819,235.06/5=£363,847.01
Total excluding emergency department 1: £701,723.06/4=£175,430.77
Acute: (mean cost per service £171,340.43 based on 79 acute services reporting
data)*(110 acute services)=£18,847,447.30 grand total for acute
services. Community: (mean cost per service £109,691.78 based on 78
services reporting data)*(116 community services)=12,724,246.48 grand
total for community services. Emergency department: (mean cost per
service £175,430.77 based on four services reporting data)*(five
emergency departments reporting data)=£877,153.85 grand total for
emergency departments. Grand total=£32,448,847.63.
ED, emergency department; OT, occupational therapist; PA, physician assistant;
SPR, specialist registrar.
*The cost of a one-way journey is £50.13. (Curtis L, Netten A. Unit Costs of
Health and Social Care: PSSRU University of Kent: available from
http://www.pssru.ac.uk/uc/uc2006contents.htm, 2006.)
†Consultant hours unspecified based on 1PA, annual salary equates to
£10,376.60.
‡Annual salary estimated mid-point of consultant grade (£103,766).
¶Average estimated salary of a Specialist Registrar, excluding other increments,
£48,244.
§Lunch calculated from the number of new attendances and average number of
patients that would attend exercise sessions during the year.
**Exercise transport cost calculated £100 per each patient, based on the
percentage reported to use hospital transport.
†† Estimated cost of maintenance per floor space, obtained from Estates Return
Information Collection (ERIC) – The Department of Health (June 2006).
‡‡Maximum charge £3.00.
¶¶Exercise transport cost calculated on 50% using hospital transport per £100
and 50% using voluntary transport per £3.00.
§§Floor space for entire ward and does not reflect the size used for falls.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 176
Appendix 2 Search strategies for systematic review of effectiveness of fallers’ clinics
Replication of the Cochrane review’s search for 2003–2006
MEDLINE, EMBASE and CINAHL
As published in Cochrane review with correction to error.
PsycINFO
1 exp Clinical Trials/
2 exp placebo/
3 ((clinical or controlled or comparative or placebo or prospective$
or random$) adj (trial or study)).mp. [mp=title, abstract, subject
headings, table of contents, key concepts]
4 (random$ adj (allocat$ or allot$ or assign$ or basis$ or divid$ or
order$)).mp. [mp=title, abstract, subject headings, table of
contents, key concepts]
5 ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).mp.
[mp=title, abstract, subject headings, table of contents, key
concepts]
6 (cross?over$ or (cross adj over$)).mp. [mp=title, abstract,
subject headings, table of contents, key concepts]
7 ((allocat$ or allot$ or assign$ or divid$) adj (condition$ or
experiment$ or intervention$ or treatment$ or therap$ or
control$ or group$)).mp. [mp=title, abstract, subject headings,
table of contents, key concepts]
8 1 or 2 or 3 or 4 or 5 or 6 or 7
9 exp Falls/
10 (falls or faller$ or falling).mp. [mp=title, abstract, subject
headings, table of contents, key concepts]
11 9 or 10
12 exp Aging/
13 (elderly or senior$ or older or geriatric or old people).mp.
[mp=title, abstract, subject headings, table of contents, key
concepts]
14 12 or 13
15 8 and 11 and 14
Social Science Citation Index
1 TS=(accidental AND fall*)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 177
2 TS=(fall*)
3 TS=(falls or faller* or falling)
4 TS=(aged or older or elderly or senior* or geriatric* or old
people)
5 #4 AND #3
6 TS=((clinical or controlled or comparative or placebo or
prospective* or random*) AND (trial or study))
7 TS=(random* AND (allocat* or allot* or assign* or basis* or
divid* or order*))
8 TS=((singl* or doubl* or trebl* or tripl*) AND (blind* or mask*))
9 TS=(crossover* or (cross AND over))
10 TS=((allocat* or allot* or assign* or divid*) AND (condition* or
experiment* or intervention* or treatment* or therap* or
control* or group*))
11 #10 OR #8 OR #7 OR #6
12 #11 AND #5
CENTRAL
1 exp accidental falls/ (MeSH term)
2 (falls or faller*)
3 1 or 2
4 exp aged/ (MeSH term)
5 (older or senior* or elderly)
6 4 or 5
7 3 and 6
Additional searches extending to include additional terms for population and specific terms for falls clinics
Additional terms for falls clinics:
Fall$ clinic
Fall$ service
Fall$ and (risk assess$ or multifactorial or interdisciplinary or
multidisciplinary or multifacet$ or multicomponent)
Additional terms for old people:
older or senior$ or elderly or old people or geriatric$
MEDLINE
1 randomized controlled trial.pt.
2 controlled clinical trial.pt.
3 randomized controlled trials.sh.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 178
4 random allocation.sh.
5 double blind method.sh.
6 single blind method.sh.
7 1 or 2 or 3 or 4 or 5 or 6
8 (animals not human).sh.
9 7 not 8
10 clinical trial.pt.
11 exp clinical trials/
12 (clin$ adj trial$).ti,ab.
13 ((singl$ or doubl$ or trebl$ or tripl$) adj (blind$ or mask$)).ti,ab.
14 placebos.sh.
15 placebo$.ti,ab.
16 random$.ti,ab.
17 research design.sh.
18 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17
19 18 not 8
20 19 not 9
21 comparative study.sh.
22 exp evaluation studies/
23 follow up studies.sh.
24 prospective studies.sh.
25 (control$ or prospectiv$ or volunteer$).ti,ab.
26 21 or 22 or 23 or 24 or 25
27 26 not 8
28 27 not (9 or 20)
29 exp accidental falls/
30 (falls or faller$).tw.
31 29 or 30
32 exp aged/
33 (older or senior$ or elderly).tw.
34 32 or 33
35 (old people or geriatric$).mp. [mp=title, abstract, subject
headings, heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
36 34 or 35
37 9 or 20
38 31 and 36 and 37
39 limit 38 to yr="2003 - 2006"

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 179
40 (fall$ adj clinic).mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
41 (fall$ adj service).mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
42 (fall$ and (risk assessment or multifactorial$ or interdisciplinary
or multidisciplinary or multifacet$ or multicomponent)).mp.
[mp=title, abstract, subject headings, heading word, drug trade
name, original title, device manufacturer, drug manufacturer
name]
43 40 or 41 or 42
44 37 and 38 and 43
45 34 and 37 and 43
46 44 or 45
47 31 and 34 and 37
48 39 not 47
49 46 or 48
EMBASE
1 exp Randomized controlled trial/
2 exp Double Blind Procedure/
3 exp Single Blind Procedure/
4 exp Crossover Procedure/
5 1 or 2 or 3 or 4
6 ((clinical or controlled or comparative or placebo or prospective$
or randomi#ed) adj3 (trial or study)).tw.
7 (random$ adj7 (allocat$ or allot$ or assign$ or basis$ or divid$ or
order$)).tw.
8 ((singl$ or doubl$ or trebl$ or tripl$) adj7 (blind$ or mask$)).tw.
9 (cross?over$ or (cross adj1 over$)).tw.
10 ((allocat$ or allot$ or assign$ or divid$) adj3 (condition$ or
experiment$ or intervention$ or treatment$ or therap$ or
control$ or group$)).tw.
11 6 or 7 or 8 or 9 or 10
12 5 or 11
13 Animal/ not Human/
14 12 not 13
15 Falling/
16 (falls or fallers).tw.
17 15 or 16
18 exp Aged/

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 180
19 (elderly or senior$ or older).tw.
20 18 or 19
21 17 and 20
22 14 and 21
23 (old people or geriatric$).mp. [mp=title, abstract, subject
headings, heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
24 (fall$ adj clinic).mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
25 (fall$ adj service).mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
26 (fall$ and (risk assessment or multifactorial$ or interdisciplinary
or multidisciplinary or multifacet$ or multicomponent)).mp.
[mp=title, abstract, subject headings, heading word, drug trade
name, original title, device manufacturer, drug manufacturer
name]
27 24 or 25 or 26
28 20 or 23
29 14 and 17 and 28
30 limit 29 to yr="2003 - 2006"
31 14 and 20 and 27
32 14 and 28 and 27
33 31 or 32
34 30 not 22
35 33 or 34

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 181
Appendix 3 Quality-assessment tool for systematic review of effectiveness in fallers’ clinics
Score Comments
A Was the assigned treatment adequately concealed prior to allocation?
3=Method did not allow disclosure of
assignment
2=Small but possible chance of
disclosure of assignment
1=States random, but no description or
quasi-randomised
B Were the outcomes of patients who withdrew described and included in the analysis (intention to treat)?
3=Intention to treat analysis based on
all cases randomised possible or
carried out
2=States number and reasons for
withdrawal but intention-to-treat
analysis not possible
1=Inadequate detail
C Were the outcome assessors blinded to treatment status?
3=Effective action taken to blind
assessors
2=Small or moderate chance of
unblinding of assessors
1=Not mentioned or not possible
D Were the treatment and control group comparable at entry?
3=Good comparability of groups, or
confounding adjusted for in analysis
2=Confounding small; mentioned but
not adjusted for
1=Large potential for confounding, or
not discussed
E Were the subjects blind to assignment status after allocation?
3=Effective action taken to blind
subjects
2=Small or moderate chance of
unblinding of subjects

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 182
1=Not possible, or not mentioned
(unless double-blind), or possible,
but not done
F Were the treatment providers blind to assignment status?
3=Effective action taken to blind
treatment providers
2=Small or moderate chance of
unblinding of treatment providers
1=Not possible, or not mentioned, or
possible, but not done
G Were care programmes, other than the trial options, identical?
3=Care programmes clearly identical
2=Clear but trivial differences
1=Not mentioned, or clear and
important differences in care
programmes
H Were the inclusion and exclusion criteria clearly defined?
3=Clearly defined
2=Poorly defined
1=Not defined
J Were the outcome measures used clearly defined?
3=Clearly defined
2=Poorly defined
1=Not defined
K Was ascertainment of fall and other outcomes reliable?
3=Diary or active registration
2=Interval recall
1=Participant recall at end of study
period
L Was the duration of surveillance clinically appropriate?
3=1 year or more (duration of stay for
hospital studies)
2=Less than 1 year
1=Not defined
X Cluster-randomised studies only. Did analysis adjust for clustering correctly?
Yes/No
Y Cluster-randomised studies only. Were estimates of ICCs presented?
All outcomes/Some outcomes/No

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 183
Appendix 4 Studies excluded from the systematic review of effectiveness of fallers’ clinics
Study Reason for exclusion
Barr et al. 2005 RCT of fracture risk screening
Campbell et al. 2005 RCT of exercise and home hazard modification; not multi-factorial assessment and intervention
Clemson et al. 2004 RCT of Stepping on, a small group-based educational programme; non-eligible intervention
Crome et al. 2000 Published as abstract only
Cumming et al. 1999 RCT of environmental hazard assessment and modification; other risk factors not assessed
Day et al. 2002 RCT; three interventions each targeting single risk factor (vision, home hazards, exercise); non-eligible interventions
Gitlin et al. 2006 RCT of multi-component intervention to reduce functional difficulties, fear of falling and home hazards; falls not reported; fear of falling only
Haines et al. 2004 RCT of multi-factorial risk assessment and intervention in subacute hospital ward population; non-eligible population
Hall et al. 1992 RCT of nurse home visits and personal care plan; no falls outcome reported
Hebert et al. 2001 RCT of nurse-led multi-dimensional preventive programme to prevent functional decline; main outcome was functional decline, defined as increase of ≥5 points on SMAF score, admission to nursing home or long-term care, or death; no falls outcome reported
Hendriks et al. 2005 Ongoing study
Hornbrook et al. 1994 RCT of home safety assessment and weekly group meetings; not individualised fall-prevention interventions; non-eligible comparison
Jitapunkul 1998 RCT of 3-monthly home visits; non-eligible comparison
Kingston et al. 2001 Numerical data on falls not reported
Masud et al. 2006 Ongoing study
McEwan et al. 1990 RCT of nurse home assessment and intervention; no falls outcome reported
Nikolaus and Bach 2003
RCT comparing CGA plus diagnostic home visit and home intervention with CGA with recommendation and usual care at home; both groups received multi-factorial assessment and intervention
Reuben et al. 1999 RCT of outpatient CGA plus intervention to improve adherence to recommendations; no falls outcome reported.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 184
Robson et al. 2003 RCT of Steady as you go (SAYGO); a two group session intervention; non-eligible intervention
Rubenstein et al. 1990 RCT of post-fall assessment and preventive and therapeutic interventions, in long-term residential care; non-eligible population
Steadman et al. 2003 RCT of balance training
Steinberg et al. 2000 RCT of multi-component intervention targeting fall risk factors; cluster-randomised by National Seniors Association branches, but apparently no replication within arms (one cluster per arm); excluded on methodological grounds
Stevens et al. 2001 RCT of home hazard assessment compared with no home hazard assessment
van Rossum et al. 1993
RCT of preventive home visits by nurses; no quantitative data on falls reported
Yates et al. 2001 RCT of fall risk reduction programme; no falls outcome reported
CGA, Comprehensive Geriatric Assessment.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 185
Appendix 5 Search strategies for the systematic review of screening instruments
MEDLINE
1 exp accidental falls/
2 (falls or faller$).tw.
3 1 or 2
4 exp aged/
5 (older or senior$ or elderly).tw.
6 4 or 5
7 (old people or geriatric$).mp. [mp=title, original title, abstract,
name of substance word, subject heading word]
8 6 or 7
9 (risk assessment or assessment tool).mp.
10 (POMA or B-POMA or performance orient$ mobility).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
11 STRATIFY.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
12 FRHOP.mp. [mp=title, original title, abstract, name of substance
word, subject heading word]
13 falls risk for hospitalised older people.mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
14 (PPA or physiological profile assessment).mp. [mp=title, original
title, abstract, name of substance word, subject heading word]
15 (FSST or four square step test).mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
16 Functional reach test.mp. [mp=title, original title, abstract, name
of substance word, subject heading word]
17 ((timed up and go) or TUG or TUGT or timed up & go).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
18 berg balance scale.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
19 dynamic gait index.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
20 (((one leg or one-leg) and (stand or stance)) or OLST).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 186
21 (Peter James Centre Fall Risk assessment tool or PJC-FRAT).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
22 (falls risk assessment tool or FRAT).mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
23 activities-specific balance confidence.mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
24 (downton fall risk index or downton index).mp. [mp=title, original
title, abstract, name of substance word, subject heading word]
25 ((home falls and accidents screening tool) or HOME FAST).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
26 (activities of daily vision scale or ADVS).mp. [mp=title, original
title, abstract, name of substance word, subject heading word]
27 morse fall scale.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
28 elderly fall screening test.mp. [mp=title, original title, abstract,
name of substance word, subject heading word]
29 (tinetti balance and (score or scale)).mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
30 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or
21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29
31 (specificity or screening or false positive or false negative or
accuracy or (predictive and value$) or reference value$ or ROC or
likelihood ratio).mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
32. 9 or 30 or 31
33 3 and 8 and 32
EMBASE
1 falling/
2 (falls or faller$).tw.
3 1 or 2
4 exp aged/
5 (older or senior$ or elderly).tw.
6 4 or 5
7 (old people or geriatric$).mp. [mp=title, abstract, subject
headings, heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
8 6 or 7
9 (risk assessment or assessment tool).mp.
10 (POMA or B-POMA or performance orient$ mobility).mp.
[mp=title, abstract, subject headings, heading word, drug trade

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 187
name, original title, device manufacturer, drug manufacturer
name]
11 STRATIFY.mp. [mp=title, abstract, subject headings, heading
word, drug trade name, original title, device manufacturer, drug
manufacturer name]
12 FRHOP.mp. [mp=title, abstract, subject headings, heading word,
drug trade name, original title, device manufacturer, drug
manufacturer name]
13 falls risk for hospitalised older people.mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
14 (PPA or physiological profile assessment).mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
15 (FSST or four square step test).mp. [mp=title, abstract, subject
headings, heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
16 Functional reach test.mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
17 ((timed up and go) or TUG or TUGT or timed up & go).mp.
[mp=title, abstract, subject headings, heading word, drug trade
name, original title, device manufacturer, drug manufacturer
name]
18 berg balance scale.mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
19 dynamic gait index.mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
20 (((one leg or one-leg) and (stand or stance)) or OLST).mp.
[mp=title, abstract, subject headings, heading word, drug trade
name, original title, device manufacturer, drug manufacturer
name]
21 (Peter James Centre Fall Risk assessment tool or PJC-FRAT).mp.
[mp=title, abstract, subject headings, heading word, drug trade
name, original title, device manufacturer, drug manufacturer
name]
22 (falls risk assessment tool or FRAT).mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
23 activities-specific balance confidence.mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 188
24 (downton fall risk index or downton index).mp. [mp=title,
abstract, subject headings, heading word, drug trade name,
original title, device manufacturer, drug manufacturer name]
25 ((home falls and accidents screening tool) or HOME FAST).mp.
[mp=title, abstract, subject headings, heading word, drug trade
name, original title, device manufacturer, drug manufacturer
name]
26 (activites of daily vision scale or ADVS).mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
27 morse fall scale.mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
28 elderly fall screening test.mp. [mp=title, abstract, subject
headings, heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
29 (tinetti balance and (score or scale)).mp. [mp=title, abstract,
subject headings, heading word, drug trade name, original title,
device manufacturer, drug manufacturer name]
30 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or
21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29
31 (specificity or screening or false positive or false negative or
accuracy or (predictive and value$) or reference value$ or ROC or
likelihood ratio).mp. [mp=title, abstract, subject headings,
heading word, drug trade name, original title, device
manufacturer, drug manufacturer name]
32 9 or 30 or 31
33 3 and 8 and 32
CINAHL
1 exp accidental falls/
2 (falls or faller$).tw.
3 1 or 2
4 exp aged/
5 (older or senior$ or elderly).tw.
6 4 or 5
7 (old people or geriatric$).mp. [mp=title, original title, abstract,
name of substance word, subject heading word]
8 6 or 7
9 (risk assessment or assessment tool).mp.
10 (POMA or B-POMA or performance orient$ mobility).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 189
11 STRATIFY.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
12 FRHOP.mp. [mp=title, original title, abstract, name of substance
word, subject heading word]
13 falls risk for hospitalised older people.mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
14 (PPA or physiological profile assessment).mp. [mp=title, original
title, abstract, name of substance word, subject heading word]
15 (FSST or four square step test).mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
16 Functional reach test.mp. [mp=title, original title, abstract, name
of substance word, subject heading word]
17 ((timed up and go) or TUG or TUGT or timed up & go).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
18 berg balance scale.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
19 dynamic gait index.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
20 (((one leg or one-leg) and (stand or stance)) or OLST).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
21 (Peter James Centre Fall Risk assessment tool or PJC-FRAT).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
22 (falls risk assessment tool or FRAT).mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
23 activities-specific balance confidence.mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
24 (downton fall risk index or downton index).mp. [mp=title, original
title, abstract, name of substance word, subject heading word]
25 ((home falls and accidents screening tool) or HOME FAST).mp.
[mp=title, original title, abstract, name of substance word,
subject heading word]
26 (activities of daily vision scale or ADVS).mp. [mp=title, original
title, abstract, name of substance word, subject heading word]
27 morse fall scale.mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
28 elderly fall screening test.mp. [mp=title, original title, abstract,
name of substance word, subject heading word]
29 (tinetti balance and (score or scale)).mp. [mp=title, original title,
abstract, name of substance word, subject heading word]
30 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or
21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 190
31 (specificity or screening or false positive or false negative or
accuracy or (predictive and value$) or reference value$ or ROC or
likelihood ratio).mp. [mp=title, original title, abstract, name of
substance word, subject heading word]
32 9 or 30 or 31
33 3 and 8 and 32
PsycINFO
1 exp falls/
2 (falls or faller$ or falling).tw.
3 1 or 2
4 exp Aging/
5 (older or senior$ or elderly).tw.
6 4 or 5
7 (old people or geriatric$).mp. [mp=title, abstract, heading word,
table of contents, key concepts]
8 6 or 7
9 (risk assessment or assessment tool).mp.
10 (POMA or B-POMA or performance orient$ mobility).mp.
[mp=title, abstract, heading word, table of contents, key
concepts]
11 STRATIFY.mp. [mp=title, abstract, heading word, table of
contents, key concepts]
12 FRHOP.mp. [mp=title, abstract, heading word, table of contents,
key concepts]
13 falls risk for hospitalised older people.mp. [mp=title, abstract,
heading word, table of contents, key concepts]
14 (PPA or physiological profile assessment).mp. [mp=title, abstract,
heading word, table of contents, key concepts]
15 (FSST or four square step test).mp. [mp=title, abstract, heading
word, table of contents, key concepts]
16 Functional reach test.mp. [mp=title, abstract, heading word, table
of contents, key concepts]
17 ((timed up and go) or TUG or TUGT or timed up & go).mp.
[mp=title, abstract, heading word, table of contents, key
concepts]
18 berg balance scale.mp. [mp=title, abstract, heading word, table
of contents, key concepts]
19 dynamic gait index.mp. [mp=title, abstract, heading word, table
of contents, key concepts]
20 (((one leg or one-leg) and (stand or stance)) or OLST).mp.
[mp=title, abstract, heading word, table of contents, key
concepts]

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 191
21 (Peter James Centre Fall Risk assessment tool or PJC-FRAT).mp.
[mp=title, abstract, heading word, table of contents, key
concepts]
22 (falls risk assessment tool or FRAT).mp. [mp=title, abstract,
heading word, table of contents, key concepts]
23 activities-specific balance confidence.mp. [mp=title, abstract,
heading word, table of contents, key concepts]
24 (downton fall risk index or downton index).mp. [mp=title,
abstract, heading word, table of contents, key concepts]
25 ((home falls and accidents screening tool) or HOME FAST).mp.
[mp=title, abstract, heading word, table of contents, key
concepts]
26 (activites of daily vision scale or ADVS).mp. [mp=title, abstract,
heading word, table of contents, key concepts]
27 morse fall scale.mp. [mp=title, abstract, heading word, table of
contents, key concepts]
28 elderly fall screening test.mp. [mp=title, abstract, heading word,
table of contents, key concepts]
29 (tinetti balance and (score or scale)).mp. [mp=title, abstract,
heading word, table of contents, key concepts]
30 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or
21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29
31 (specificity or screening or false positive or false negative or
accuracy or (predictive and value$) or reference value$ or ROC or
likelihood ratio).mp. [mp=title, abstract, heading word, table of
contents, key concepts]
32 9 or 30 or 31
33 3 and 8 and 32
Social Science Citation Index and Social Science Citation Index Expanded 1970–July 2006
#28 #27 AND #26 AND #3
#27 #25 OR #24 OR #23 OR #22 OR #21 OR #20 OR #19 OR #18
OR #17 OR #16 OR #15 OR #14 OR #13 OR #12 OR #11 OR
#10 OR #9 OR #8 OR #7 OR #6 OR #5 OR #4
#26 #2 OR #1
#25 TS=(tinetti balance and (score or scale))
#24 TS=elderly fall screening test
#23 TS=morse fall scale
#22 TS=(activites of daily vision scale or ADVS)
#21 TS=((home falls and accidents screening tool) or HOME FAST)
#20 TS=(downton fall risk index or downton index)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 192
#19 TS=activities-specific balance confidence
#18 TS=(falls risk assessment tool or FRAT)
#17 TS=(Peter James Centre Fall Risk assessment tool or PJC-FRAT)
#16 TS=(((one leg or one-leg) and (stand or stance)) or OLST)
#15 TS=dynamic gait index
#14 TS=berg balance scale
#13 TS=((timed up and go) or TUG or TUGT or timed up & go)
#12 TS=Functional reach test
#11 TS=(FSST or four square step test)
#10 TS=(PPA or physiological profile assessment)
#9 TS=(falls risk for hospitalised older people)
#8 TS=FRHOP
#7 TS=STRATIFY
#6 TS=(POMA or B-POMA or performance orient* mobility)
#5 TS=(specificity or screening or false positive or false negative or
accuracy or (predictive and value*) or reference value* or ROC
or likelihood ratio)
#4 TS=(risk assessment or assessment tool)
#3 TS=(aged or older or elderly or senior* or geriatric* or old
people)
#2 TS=(falls or faller* or falling)
#1 TS=(accidental AND fall*)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 193
Appendix 6 Quality-assessment tool for the systematic review of screening instruments
QUADAS criterion Interpretation for this review
Scoring
1 Was the spectrum of patients representative of the patients who will receive the test in practice?
1 Was the spectrum of patients representative of the patients who will receive the test in practice?
3: Consecutive series or random selection of eligible people
2: Unclear
1: Not consecutive or random series
2 Were selection criteria clearly described?
2 Were selection criteria clearly described?
3: Sufficient detail that selection process could be replicated
2: Incomplete information
1: No information
3a Did recording of falls use adequate follow-up period?
3: At least 12 months
2: 6–12 months
1: Less than 6 months
3 Is the reference standard likely to classify the target condition correctly?
3b Did recording of falls use an accurate method?
3: Prospective data collection; falls diary or calendar
2: Data collected at intervals
1: Recall at end of follow-up only
4 Is the period between reference standard and index test short enough to be reasonably sure that the target condition did not change between the two tests?
4 Is the period between reference standard and index test short enough to be reasonably sure that the target condition did not change between the two tests?
Not used: not relevant to this review
5 Did the whole sample, or a random selection of the sample, receive verification using a reference standard of diagnosis?
5 Was falls data recorded for all participants?
3: If it was clear that there was no selection of patients to be followed up for falls

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 194
2: Possibility of selection
1: Clear selection
6 Did patients receive the same reference standard regardless of the index test result?
6 Was falls data collected in the same way for all participants regardless of screening test result?
3: Clear that methods of data collection did not differ
2: Unclear: no information
1: Clear differences
7 Was the reference standard independent of the index test (i.e. the index test did not form part of the reference standard)?
7 Was the reference standard independent of the index test (i.e. the index test did not form part of the reference standard)?
Not used: not relevant to this review
8 Was the execution of the index test described in sufficient detail to permit replication of the test?
8 Was the screening test described in sufficient detail to permit replication of the test?
3: Details of exactly how test was implemented
2: Partial information
1: Insufficient information
9 Was the execution of the reference standard described in sufficient detail to permit its replication?
9 Was the duration of follow-up and method of ascertainment of falls status reported in sufficient detail to permit replication?
3: Sufficient detail
2: Partial information
1: Insufficient information
10 Were the index test results interpreted without knowledge of the results of the reference standard?
10 Were the index test results interpreted without knowledge of the results of the reference standard?
Not used: not relevant to this review because falls data always collected after screening tests
11 Were the reference standard results interpreted without knowledge of the results of the index test?
11 Was assessment of falls done without knowledge of the screening test results?
3: Reliable measures reported to ensure that participants and clinicians assessing falls were unaware of screening test results
2: Possible blinding but insufficient detail
1: Not done or not mentioned
12 Were the same clinical data 12 Were data on age, sex 3: All reported

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 195
available when test results were interpreted as would be available when the test is used in practice?
and diagnoses reported?
2: Only one or two reported
1: None reported
13 Were uninterpretable/intermediate test results reported?
13 Were test results reported for all participants (including unclear/uninterpretable test results)?
3: All participants accounted for in screening test results
2: Partial explanation
1: Insufficient or no information
14a Were screening test and falls reported for all participants who entered the study?
3: >80%
2: 70–80%
1: <70%
14 Were withdrawals from the study explained?
14b Were withdrawals from the study explained?
3: Complete statement of losses and withdrawals
2: Partial explanation
1: Insufficient or no information
Additional (non-QUADAS) criteria
15 Were data presented for all screening tests performed?
3: Results for all screening tests
1: One or more screening tests omitted from results
16 Were methods of analysis adequately described and free from error?
3: Correct analysis and sufficient detail
2: Appears correct but insufficient detail to be sure
1: Errors in analytical method

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 196
Appendix 7 Studies excluded from the systematic review of screening instruments
Study Reason for exclusion
Ashton et al. 1989 Hospital
Avdic and Pecar 2006 Relevant data not presented
Becker et al. 2005 Relevant data not presented
Berg et al. 1992 Relevant data not presented
Bergland et al. 2002 Relevant data not presented
Bergland et al. 2006 Non-English
Berryman et al. 1989 Hospital
Billek-Sawhney et al. 2002 No falls outcome
Bloem et al. 2000 Duplicate publication
Boulgarides et al. 2003 Relevant data not presented
Brauer et al. 2000 Relevant data not presented
Chandler et al. 2001 Relevant data not presented
Chiari et al. 2002 Hospital
Chiu et al. 2003 Not prospective
Clark et al. 2005 Relevant data not presented
Coker and Oliver 2003 Hospital
Colon-Emeric 2002 No falls outcome
Conley et al. 1999 Hospital
Conley 2005 Hospital
Cornali et al. 2004 Hospital
Covinsky et al. 2001 Relevant data not presented
Dargent Molina et al. 1999 No falls outcome
Delbaere et al. 2006 Not prospective
Di Fabio and Anacker 1996 Not prospective
Di Fabio and Seay 1997 No falls outcome
Dite and Temple 2002 Not prospective
Duncan et al. 1992 Relevant data not presented
Eagle et al. 1999 Hospital
Forrester et al. 1999 Hospital
Franzen et al. 1998 Not prospective
Fritz et al. 2001 Not prospective
Galinsky et al. 2000 Non-English

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 197
Gerdhem et al. 2005 Relevant data not presented
Gill-Body et al. 2002 Not prospective
Gulich and Zeitler 2000 Non-English
Gunther et al. 2002 Not prospective
Haines et al. 2006 Hospital
Harada et al. 1995 No falls outcome
Hausdorff et al. 2000 Not located
Hausdorff et al. 2001 Relevant data not presented
Heinze 2002 Non-English
Hellstrom et al. 2002 No falls outcome
Hendrich et al. 1995 Hospital
Hill et al. 1999 Relevant data not presented
Hill et al. 2004 Hospital
Hotchkiss et al. 2004 Not prospective
Izumi et al. 2002 Follow-up too short
Jester et al. 2005 Hospital
Kahnert et al. 2004 Not prospective
Kinn and Hood 2001 Hospital
Lafont et al. 1998 Discussion
Large et al. 2006 Hospital
Lasagna et al. 1997 Discussion
Lindsay et al. 2004 Hospital
Lord and Clark 1996 Relevant data not presented
Lord and Dayhew 2001 Not prospective
MacAvoy et al. 1996 Hospital
Macrae et al. 1992 Not prospective
Maki et al. 1994 Relevant data not presented
Maki 1997 Relevant data not presented
Maly et al. 1997 No falls outcome
Moore et al. 1996 Hospital
Morse et al. 1989a Hospital
Morse et al. 1989b Not prospective
Myers et al. 1998 No falls outcome
Myers 2003 Hospital
Newton et al. 2002 No falls outcome
Nyberg et al. 1996 Hospital
O'Connell et al. 2002 Hospital
Oliver et al. 1997 Hospital

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 198
Olsson et al. 2005 Hospital
Pal et al. 2005 Relevant data not presented
Papaioannou et al. 2004 Hospital
Porath et al. 2002 Non-eligible population
Price et al. 1998 Hospital
Prosser and Candy 1997 Hospital
Rose et al. 2002 Not prospective
Ruchinskas 2003 Relevant data not presented
Satterwhite et al. 2002 Not prospective
Schwendimann et al. 2006 Hospital
Shumway-Cook et al. 2000 Not prospective
Southard et al. 2005 No falls outcome
Stalenhoef et al. 2002 Relevant data not presented
Stel et al. 2003 Relevant data not presented
Stretanski et al. 2002 Relevant data not presented
Talley et al. 2003 Not located
Thapa et al. 1996 Relevant data not presented
Thomas and Lane 2005 Not prospective
Tinetti 1986 Discussion
Topper et al. 1993 Relevant data not presented
Tromp et al. 2001 Relevant data not presented
Vaillant et al. 2006 Not prospective
van Heuvelen et al. 2005 Non English
Van Swearingen et al. 1998 Not prospective
van Vaerenbergh and Broos 1990 Non English
Vassallo et al. 2005 Hospital
von Renteln-Kruse and Krause 2004 Hospital
Whitney et al. 2005 No falls outcome
Wijnia et al. 2006 Non-eligible population
Woo et al. 1999 Relevant data not presented
Yauk et al. 2005 Hospital
Zisselman and Robinson 1998 Not located

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 199
Appendix 8 Search strategy for systematic review of cost-effectiveness of fallers’ clinics
1 exp Aged/
2 Geriatrics/
3 (old or older or elder or elderly or senior or geriatric$ or aged).tw.
4 1 or 2 or 3
5 Accidental Falls/
6 (fall or falls or falling or fallen or fell or faller or fallers or slip or
slipped or trip or tripped).tw.
7 5 or 6
8 4 and 7
9 Economics.mp. or Economics/
10 exp "Costs and Cost Analysis"/
11 economic value of life.mp. or "Value of Life"/
12 exp Economics, Hospital/
13 exp Economics, Medical/
14 exp Economics, Nursing/
15 exp Models, Economic/
16 Economics, Pharmaceutical/
17 exp "Fees and Charges"/
18 exp Budgets/
19 ec.fs.
20 (cost or costs or costed or costly or costing$).mp. [mp=title,
subject heading word, abstract, instrumentation]
21 (Economic$ or Pharmaeconomic$ or price$ or pricing$).mp.
[mp=title, subject heading word, abstract, instrumentation]
22 Quality-Adjusted Life Years/
23 Economic burden.tw.
24 "Cost of Illness"/
25 exp "Quality of Life"/
26 Quality of Life.tw.
27 Life Quality.tw.
28 hql.tw.
29 (sf 36 or sf36 or sf thirtysix or sf thirty six or short form 36 or
short form thirtysix or short form thirty six or shortform 36).tw.
30 qol.tw.
31 (euroqol or eq5d or eq 5d).tw.
32 qaly$.tw.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 200
33 quality adjusted life year$.tw.
34 hye$.tw.
35 health$ year$ equivalent$.tw.
36 health utilit$.tw.
37 hui.tw.
38 (health$ adj2 year$ adj2 equivalent$).tw.
39 quality of wellbeing$.tw.
40 (quality adj2 of adj2 wellbeing$).tw.
41 ((quality adj2 of adj2 wellbeing$) or (quality adj2 of adj2 well-
being$) or (quality adj2 of adj2 well adj being$)).mp. [mp=title,
subject heading word, abstract, instrumentation]
42 ((quality adj2 of adj2 wellbeing$) or (quality adj2 of adj2 well-
being$)).mp. or (quality adj2 of adj2 well adj being$).tw.
[mp=title, subject heading word, abstract, instrumentation]
43 41 or 42
44 qwb.tw.
45 quality of well being.tw.
46 (qald$ or qale$ or qtime$).tw.
47 vas.tw.
48 hrqol.tw.
49 utility.tw.
50 preference.tw.
51 value.tw.
52 9 or 10 or 11 or 12 or 13 or 14 or 15 or 16 or 17 or 18 or 19 or
20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 30 or
31 or 32 or 33 or 34 or 35 or 36 or 37 or 38 or 39 or 40 or 43 or
44 or 45 or 46 or 47 or 48 or 49 or 50 or 51
53 8 and 52
54 limit 53 to (yr="2003 - 2006")

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 201
Appendix 9 Quality-assessment tool used for the systematic review of economic studies
1 Study question: what is the research question?
Is the economic importance of the research question adequately outlined? Yes No Not Clear Not appropriate
Is the hypothesis being tested, or question being addressed, clearly stated? Yes No Not Clear Not appropriate
Have all viewpoint(s) for the analysis been clearly stated? Yes No Not Clear Not appropriate
Have all viewpoint(s) for the analysis been adequately justified? Yes No Not Clear Not appropriate
2 Selection of alternatives
Is the rationale for choice of the alternative programmes or
intervention/s for comparison clearly stated? Yes No Not
Clear Not appropriate
Is the rationale for choice of the alternative programme/s or
intervention/s for comparison adequately justified? Yes No Not
Clear Not appropriate
Is the alternative intervention/s described in sufficient detail to enable the reader to assess the relevance?
Yes No Not Clear
Not appropriate
3 Form of evaluation
Is the form/s of evaluation used clearly stated? Yes No Not Clear
Not appropriate
Is a clear justification given for the form/s of evaluation chosen in relation to the question/s being addressed?
Yes No Not Clear
Not appropriate
4 Effectiveness data
Is economic evaluation based on a single effectiveness study, e.g. clinical RCT?
Yes No Not Clear
Not appropriate
Is economic evaluation based on a multiple effectiveness studies? Yes No Not Clear
Not appropriate
Was the selection of the study population adequately described? Yes No Not Clear
Not appropriate

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 202
Was the selection of the study population appropriate? Yes No Not Clear
Not appropriate
Was the method of allocation adequately described?
Yes No Not Clear
Not appropriate
Was the method of allocation appropriate? Yes No Not Clear
Not appropriate
Was the data analysed by intention to treat? Yes No Not Clear
Not appropriate
Was the data analysed by evaluable cohort? Yes No Not Clear
Not appropriate
Were effect size/s with confidence intervals reported? Yes No Not Clear
Not appropriate
If CIs were not reported, how was uncertainty on effectiveness parameters described?
Described Not described
See comment
Was the method of data synthesis adequately reported? Yes No Not Clear
Not appropriate
5 Benefit measurement and valuation
Was the primary outcome measure/s for the economic evaluation
clearly stated? Yes No Not
Clear Not appropriate
If health benefits analysis has been undertaken, have details of the methods used been clearly reported?
Yes No Not Clear
Not appropriate
If changes in productivity analysis have been undertaken, what method was used?
Human-Capital
Friction-Cost
Other
If changes in productivity analysis have been undertaken, have they been reported separately?
Yes No Not Clear
Not appropriate
If changes in productivity analysis have been undertaken, has their relevance to the study question been discussed?
Yes No Not Clear
Not appropriate
6 Costing
Have the quantities of resources been reported separately from
the prices (unit costs) of those resources? Yes No Not
Clear Not appropriate

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 203
Have the methods for the estimation of both quantities and prices (unit costs) been clearly reported?
Yes No Not Clear
Not appropriate
Have the methods for the estimation of both quantities and prices (unit costs) been justified?
Yes No
Has the currency and price date been reported? Yes No Not Clear
Not appropriate
Have details of adjustment for inflation been reported? Yes No Not Clear
Not appropriate
Have details of currency conversion been reported? Yes No Not Clear
Not appropriate
7 Modelling
If data modelling was undertaken, was the method reported? Yes No Not Clear
Not appropriate
Were the key parameters clearly stated? Yes No Not Clear
Not appropriate
Was the choice of the model adequately justified? Yes No Not Clear
Not appropriate
8 Adjustments for timing of costs and benefits
Has the time frame for which the costs and benefits are considered been reported?
Yes No Not Clear
Not appropriate
Have the discount rate/s been reported? Yes No Not Clear
Not appropriate
Has choice of discount rate/s been justified? Yes No Not Clear
Not appropriate
If costs or benefits are not discounted, has this been adequately justified?
Yes No Not Clear
Not appropriate
9 Allowance for uncertainty
Have details of all statistical analysis undertaken been adequately described?
Yes No Not Clear
Not appropriate
Have confidence intervals around the main variables been Yes No Not Not

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 204
reported? Clear appropriate
Has a sensitivity analysis been performed? Yes No Not Clear
Not appropriate
If yes, what type of sensitivity analysis was used? 1-way Multi-way
Probabilistic
Other
Has the sensitivity analysis been adequately described? Yes No Not Clear
Not appropriate
10 Presentation of results
Has an incremental analysis been reported? Yes No Not Clear
Not appropriate
Have all relevant comparisons been reported? Yes No Not Clear
Not appropriate
Have major outcomes been presented in an aggregated form? Yes No Not Clear
Not appropriate
Have major outcomes been presented in a disaggregated form? Yes No Not Clear
Not appropriate
Has the uncertainty on the ICER been reported? Yes No
If uncertainty on the ICER has been reported what method was used?
CI CEAC Scatter plot on the cost effectives plane
Other
Are comparisons with other health care interventions appropriately similar in study methods and settings?
Yes No Not Clear
Not appropriate
Has the answer to the original study question been given? Yes No Not Clear
Not appropriate
Are the conclusions drawn appropriate given the data reported? Yes No Not Clear
Not appropriate
CEAC, cost-effectiveness acceptability curve; ICER, incremental cost-effectiveness ratio.

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 205
Appendix 10 Studies excluded from the economic systematic review
Study Reason for exclusion
Dejaeger 2003 Article in Dutch
Haya and Castelo-Branco 2003
Article in Spanish
Panneman et al. 2003 Costs of accidental fall injuries in the EU resulting from the use of benzodiazepines; not fall prevention
Robinson 2003 Description of cost
Dutcher and Miller 2003 Description of cost relating to the USA
McClure et al. 2006 Description of costs
Anonymous 2003 Description of costs
Schuffham et al. 2003 Description of costs
Todd and Skelton 2004 Description of costs
Paterson et al. 2003 Description of costs
Robinson 2003 Description of costs
Lawrence et al. 2005 Description of hip-fracture costs
Lansley et al. 2004 Designed to enable independent living, not fall prevention
Schousboe et al. 2005 Economic study undertaken in the USA
Masud et al. 2006 In progress, data available 2008
Thomas 2003 Individual study, do not meet criteria
Tinker 2004 No account of the benefits of falls prevention
Wolf et al. 2003 No cost data
Landis et al. 2005 No cost data
Kannus et al. 2005 No cost data
Davison et al. 2005 No cost data
Sitoh et al. 2003 No cost data
Evans and Rowlands 2004 No cost data
Parker et al. 2006 No cost data
Meyer et al. 2003 No cost data
Melton III et al. 2004 No cost data
Bischoff-Ferrari et al. 2005 No cost data
Irwin et al. 2004 No cost data
Gass and Dawson-Hughes 2006
No cost data

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 206
Kannus et al. 2003 No cost data
O'Mahony 2006 No cost data
Birks et al. 2003 No cost data
Kooijman et al. 2005 No cost data
Simpson and Jones 2004 No cost data
Bischoff-Ferrari et al. 2004 No cost data
Leslie et al. 2003 No cost data
Birks et al. 2003 No cost data
Liu 2006 No cost data
Hulme et al. 2004 No cost data
Broadhurst et al. 2003 No cost data
Thames Valley Primary Care Research Partnership 1999
No cost data
Consortium KCHNTRD 1997 No cost data
NHS Executive South East 1995–1997
No cost data
Taylor-Piliae 2003 No cost data
Kinirons 2003 No cost data
Shaw et al. 2003 No cost data
Latham et al. 2003a No cost data
Marks and Allegrante 2004 No cost data
Tinetti 2003 No cost data
Morgan and Virnig 2004 No cost data
Clemson et al. 2004 No cost data
Steadman et al. 2003 No cost data
Parker et al. 2006 No cost data
Woolf and Akesson 2003 No cost data
Van Schoor et al. 2003 No cost data; non-UK
Taylor et al. 2004 No cost-effectiveness data for falls prevention
Grant et al. 2005 No cost-effectiveness data for falls prevention
Lotrich and Pollock 2005 No cost-effectiveness data for falls prevention
Weatherall 2004 No cost-effectiveness data for falls prevention
Harwood et al. 2005 No cost-effectiveness data for falls prevention
Weir and Culmer 2004 No cost-effectiveness data for falls prevention
Close and McMurdo 2003 No cost-effectiveness data for falls prevention
Newton et al. 2003 No cost-effectiveness data for falls prevention
Close 2005 No cost-effectiveness data for falls prevention
Chang et al. 2004 No cost-effectiveness data for falls prevention

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 207
McCreadie and Tinker 2005 No cost-effectiveness data for falls prevention
Owen et al. 2003 No cost-effectiveness data for falls prevention
Trivedi et al. 2003 No cost-effectiveness data for falls prevention
Ettinger 2003 No cost-effectiveness data for falls prevention
Runge and Schacht 2005 No cost-effectiveness data for falls prevention
Schacht et al. 2005 No cost-effectiveness data for falls prevention
Schulman et al. 2005 No cost-effectiveness data for falls prevention
Magnus et al. 2005 No cost-effectiveness data for falls prevention
De Moraes Barros 2006 No cost-effectiveness data for falls prevention
Wagg 2004 No cost-effectiveness data for falls prevention
Swithinbank et al. 2004 No cost-effectiveness data for falls prevention
Sherritze 2003 No cost-effectiveness data for falls prevention
Shaw et al. 2000 No cost-effectiveness data for falls prevention
Edwards 2003 No cost-effectiveness data for falls prevention
Carpenter 2004 No cost-effectiveness data for falls prevention
Crome 2003 No cost-effectiveness data for falls prevention
Anonymous 2005 No cost-effectiveness data for falls prevention
Beghe et al. 2004 No cost-effectiveness data for falls prevention
British Association of Emergency Medicine 2005
No cost-effectiveness data for falls prevention
Toulotte et al. 2003 No cost-effectiveness data for falls prevention; non-UK
Solomon et al. 2003 No cost-effectiveness data for falls prevention; non-UK
Bischoff-Ferrari et al. 2004 No cost-effectiveness data for falls prevention
Sawka et al. 2005 No cost-effectiveness data for falls prevention
Wanless 2004 No cost-effectiveness data for falls prevention
Scaf-Klomp et al. 2003 No cost-effectiveness data for falls prevention; non-UK
Hayes 2004 No cost-effectiveness data for falls prevention
Nandy et al. 2004 No cost-effectiveness data for falls prevention
Ruchinskas 2003 No cost-effectiveness data for falls prevention
Pils et al. 2003 No cost-effectiveness data for falls prevention
Myers and Nikoletti 2003 No cost-effectiveness data for falls prevention
Roudsari et al. 2005 No cost-effectiveness data for falls prevention; non-UK (USA)
Pluijm et al. 2006 No cost-effectiveness data for falls prevention; non-UK
Rucker et al. 2006 No cost-effectiveness data for falls prevention; non-UK (Canada)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 208
Richardson et al. 2005 No cost-effectiveness data for falls prevention
Ozcan et al. 2005 No cost-effectiveness data for falls prevention
Becker et al. 2005 No cost-effectiveness data for falls prevention
Lubbeke et al. 2005 No cost-effectiveness data for falls prevention
Keys and Tress 2004 No cost-effectiveness data for falls prevention
Hanssens and Reginster 2003 No cost-effectiveness data for falls prevention
McClung 2003 No cost-effectiveness data for falls prevention
Swanenburg et al. 2003 No cost-effectiveness data for falls prevention
Millward et al. 2003 No cost-effectiveness data for falls prevention
Montgomery et al. 2003 No falls data
Smith et al., 2004 No falls data
McCarthy et al. 2004 No falls data
Hopley et al. 2004 No falls data
Spillman 2004 No falls data (changes in chronic disability among the elderly in USA)
Eng et al. 2003 Non-UK
Brennan nee Saunders et al. 2003
Non-community-dwelling population
Meyer et al. 2005a Non-community-dwelling population
Oliver et al. 2005 Non-community-dwelling population
Ellis et al. 2006 Non-community-dwelling population
Chappel et al. 2004 Non-community-dwelling population
Honkanen et al. 2005 Non-community-dwelling population
Hofmann et al. 2003 Non-community-dwelling population
Honkanen 2003 Non-community-dwelling population
Kapp 2003 Non-community-dwelling population
Kuchynka et al. 2004 Non-community-dwelling population
Warnke et al. 2004 Non-community-dwelling population
Mitani and Komatsu 2004 Non-community-dwelling population
Maurer et al. 2004 Non-community-dwelling population
Sieri and Beretta 2004 Non-community-dwelling population
Boustani and Sloane 2003 Non-community-dwelling population
Theodos 2003 Non-community-dwelling population
Mamun et al. 2003 Non-community-dwelling population
Helbostad 2005 Non-community-dwelling population
Collins et al. 2004 Non-community-dwelling population
Bruyere et al. 2005 Non-community-dwelling population
Lubbeke et al. 2005 Non-community-dwelling population; non-UK

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 209
McMurdo and Harper 2004 Non-community-dwelling population
Neyens et al. 2006 Non-community-dwelling population; non-UK
Schnelle et al. 2003 Non-community-dwelling population; non-UK
Barnett et al. 2003 Non UK
Sorensen et al. 2006 Non-community-dwelling population
Lord et al. 2003 Non-UK
Costa et al. 2006 Non-UK
Fosnight et al. 2004 Non-UK
Scranton et al. 2005 Non-UK
Stevens 2005 Non-UK
Latham et al. 2003b Non-UK
Murray et al. 2005 Non-UK
McLean et al. 2004 Non-UK
Moller 2005 Non-UK
Titler et al. 2005 Non-UK; descriptions of cost of hospitalisation following a fall
Asplund 2004 Non-UK; no cost-effectiveness data for falls prevention
Papaioannou et al. 2003 Non-UK; no cost-effectiveness data for falls prevention
Izumi et al. 2002 Non-UK
Dharmarajan and Norkus 2004
Non-UK
Moller 2005 Non-UK (Australia)
Day et al. 2002 Non-UK (Australia)
Hu and Wagner 2005 Non-UK (cost related to USA)
Spottke et al. 2005 Non-UK (Germany)
Segal et al. 2005 Non-UK (Israel)
Fayad et al. 2003 Non-UK (Lebanon)
Hendriks et al. 2005 Non-UK (Maastricht, The Netherlands)
Vu et al. 2005 Non-UK (Melbourne, Australia)
Bosma et al. 2004 Non-UK (The Netherlands)
Meerding et al. 2006 Non-UK (The Netherlands)
Beard et al. 2006 Non-UK (NSW, Australia)
Hall and Hendrie 2003 Non-UK (Perth, Australia)
Guimarães and Farinatti 2005 Non-UK (Rio de Janeiro)
Brown 2004 Non-UK (South Australia)
The National Center for Injury Prevention and Control 2006
Non-UK (USA)

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 210
Siris et al. 2004 Non-UK (USA)
Department of Veterans Affairs 1999–2002
Non-UK (USA)
Braithwaite et al. 2003 Non-UK (USA)
Reuben et al. 2003 Non-UK (USA)
Powell et al. 2006 Non-UK (USA)
Vladeck 2005 Non-UK (USA)
Darkow et al. 2005 Non-UK (USA)
Finkelstein et al. 2005 Non-UK (USA)
Sweeney and Chiriboga 2003 Non-UK (USA); no falls/cost data
Haumschild et al. 2003 Non-UK (USA)
LaStayo et al. 2003 Non-UK (USA)
Lipscomb et al. 2003 Non–UK (USA)
Carroll et al. 2005 Non-UK (USA) estimate of the direct medical costs of falls
Marks et al. 2003 Non-UK (USA) description of costs
Hendrie et al. 2004 Non-UK (Western Australia)
Meyer et al. 2005b Non-UK; non-community-dwelling population
Rollins 2003 Non-UK study
Swinburn and Sager 2003 Non-UK study (Australia)
O'Sullivan et al. 2004 Non-UK study (Dublin, Ireland)
Stokes et al. 2005 Non-UK study (Ireland)
Colon-Emeric et al. 2003 Non-community-dwelling participants; non-UK
Bush 2003 Non-community population
Johansson 2003 Not cost-effectiveness data
Honkanen 2004 Not cost-effectiveness study
Dubey and Terme 2004 Not cost-effectiveness study
Dowse 2003 Not cost-effectiveness study
Jansson et al. 2004 Not falls prevention
Smith et al., 2004 Not falls prevention
Montgomery et al. 2003 Not falls prevention
Grandjean et al. 2006 Not falls prevention
Ohsfeldt et al. 2004 Not falls prevention
Kolanowski et al. 2004 Not falls prevention
Beer and Giles 2005 Not falls-prevention intervention
Tinker 2004 Not related to falls
Ballard and Cream 2005 Not relevant
Alexander and Goldberg 2005 Not relevant

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 211
Burl et al. 2003 Not relevant
Odegard 2006 Not relevant
Newton et al. 2006 Not relevant
Neubauer 2004 Not relevant
Grigor et al. 2004 Not relevant
Esquenazi 2004 Not relevant
Allum and Carpenter 2005 Not relevant
Lamb et al. 2005 Not relevant
Kobelt et al. 2005 Not relevant; non-UK
West et al. 2004 Not relevant
Kuh et al. 2005 Not relevant
Ljung et al. 2005 Not relevant
Noyes et al. 2004 Not relevant
Romeo and Knapp 2006 Not relevant
Iyer 2004 Not relevant
Cravens 2006 Not relevant
Lipscomb et al. 2003 Not relevant
McDonald and Robb 2004 Not relevant
Ranson and Emmett 2003 Not relevant
Turnbull 2003 Not relevant
Feinberg et al. 2004 Not relevant
Jones and Perese 2003 Not relevant
Kelly and Dowling 2004 Not relevant
Kai et al. 2003 Not relevant
Black and Wood 2005 Not relevant
Bagust et al. 2006 Not relevant (coronary artery stenting)
Ahmad Hasali et al. 2005 Not relevant to falls
Huang 2003 Not relevant
Spottke et al. 2005 Non-UK (Germany)
Webster et al. 2004 Non-UK (USA)
Resnick 1995 Pre-2003
Wilson and Datta 2001 Pre-2003
Wong et al. 2002 Pre-2003
Ytterstad 1996 Pre-2003
Simons et al. 2001 Pre-2003
Sharma et al. 2001 Pre-2003
Owens et al. 1997 Pre-2003
Nagata-Kobayashi et al. 2002 Pre-2003

Scoping Exercise on Fallers’ Clinics
© NCCSDO 2007 212
Jonsson et al. 1995 Pre-2003
Cowper et al. 1998 Pre-2003
Eldridge et al. 2005 Reports a cost-effectiveness model to inform the design of a future trial
Parsons et al. 2001 Pre-2003 pilot study for the Eldridge (2005) paper
Rubenstein and Josephson 2005
Article in Spanish
Gillespie et al. 2003 Studies that incorporated an economic review; pre-2003
Gaugler et al. 2003 The economic study was undertaken in New Jersey/Ohio, USA
Noyes et al. 2004 The economic study was undertaken in the USA
Zaloshnja et al. 2005 Unintentional home-injuries cost for USA
Shea et al. 2006 Withdrawn

This document was published by the National Coordinating Centre for the Service Delivery and Organisation (NCCSDO) research programme, managed by the London School of Hygiene & Tropical Medicine.
The management of the Service Delivery and Organisation (SDO) programme has now transferred to the National Institute for Health Research Evaluations, Trials and Studies Coordinating Centre (NETSCC) based at the University of Southampton. Prior to April 2009, NETSCC had no involvement in the commissioning or production of this document and therefore we may not be able to comment on the background or technical detail of this document. Should you have any queries please contact [email protected].

Disclaimer: This report presents independent research commissioned by the National Institute for Health Research (NIHR). The views and opinions expressed therein are those of the authors and do not necessarily reflect those of the NHS, the NIHR, the SDO programme or the Department of Health.