Role of diffusion-weighted MR imaging in cervical lymphadenopathy
10
Eur Radiol (2006) 16: 1468–1477 DOI 10.1007/s00330-005-0133-x HEAD AND NECK Ahmed Abdel Khalek Abdel Razek Nermin Yehia Soliman Sahar Elkhamary Mousa K. Alsharaway Ali Tawfik Received: 23 December 2004 Revised: 9 November 2005 Accepted: 12 December 2005 Published online: 24 March 2006 # Springer-Verlag 2006 Role of diffusion-weighted MR imaging in cervical lymphadenopathy Abstract The role of diffusion- weighted magnetic resonance imaging (MRI) for differentiation between various causes of cervical lymphade- nopathy was evaluated. In a prospec- tive study, 31 untreated patients (22 males and nine females, aged 5– 70 years) with 87 cervical lymph nodes underwent diffusion-weighted MRI before performance of neck dissection (n=14), surgical biopsy (n=9) or core biopsy (n=8). Diffusion- weighted MR images were acquired with a b factor of 0 and 1,000 s/mm 2 using single-shot echo-planar se- quence. Apparent diffusion coefficient (ADC) maps were reconstructed for all patients. The signal intensity of the lymph nodes was assessed on images obtained at b=0 or 1,000 s/mm 2 and from the ADC maps. The ADC value of lymph nodes was also calculated. On the ADC map, malignant nodes showed either low (n=52) or mixed (n=20) signal intensity and benign nodes revealed high (n=13) or low (n=2) signal intensity. The mean ADC value of metastatic (1.09±0.11× 10 -3 mm 2 /s) and lymphomatous (0.97±0.27×10 -3 mm 2 /s) lymph nodes was significantly lower than that of benign (1.64±0.16×10 -3 mm 2 /s) cervi- cal lymph nodes (P<0.04). When an ADC value of 1.38×10 -3 mm 2 /s was used as a threshold value for differ- entiating malignant from benign lymph nodes, the best results were obtained with an accuracy of 96%, sensitivity of 98%, specificity of 88%, positive predictive value of 98.5% and negative predictive value of 83.7%. The smallest detected lymph node was 0.9 cm. In conclusion, diffusion-weighted MRI with ADC mapping is a new promising technique that can differentiate malig- nant from benign lymph nodes and delineate the solid viable part of the lymph node for biopsy. This technique provides additional useful physiologi- cal and functional information regard- ing characterization of cervical lymph nodes. Keywords Diffusion MR imaging . Cervical lymph nodes . Head and neck Introduction Evaluation of cervical lymph nodes represents one of the most challenging problems for radiologists. Although morphological imaging with computed tomography (CT) and magnetic resonance (MR) allows the detection of enlarged cervical nodes, neither method can accurately differentiate benign from malignant lymph nodes. Meta- bolic imaging with single photon emission CT (SPECT) and photon emission tomography (PET) can help this differentiation, but they are expensive, less available and have low spatial resolution. Ultrasound (US) and US- guided fine-needle aspiration cytology (FNAC) have been extensively used in Europe, but this technique is invasive and operator-dependent with high incidence of false negative results that might result from aspiration of the wrong node or the wrong part of the correct node (sampling error) [1–4]. M. K. Alsharaway . A. Tawfik ENT & Head & Neck Surgery Departments, Faculty of Medicine, Mansoura University, Mansoura, Egypt A. A. K. Abdel Razek (*) . N. Y. Soliman . S. Elkhamary Diagnostic Radiology Department, Faculty of Medicine, Mansoura University, Mansoura, Egypt e-mail: [email protected] Tel.: +20-50-231505
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Role of diffusion-weighted MR imaging in cervical lymphadenopathy

Eur Radiol (2006) 16: 1468–1477DOI 10.1007/s00330-005-0133-x HEAD AND NECK
Ahmed Abdel Khalek Abdel RazekNermin Yehia SolimanSahar ElkhamaryMousa K. AlsharawayAli Tawfik
Received: 23 December 2004Revised: 9 November 2005Accepted: 12 December 2005Published online: 24 March 2006# Springer-Verlag 2006
Role of diffusion-weighted MR imagingin cervical lymphadenopathy
Abstract The role of diffusion-weighted magnetic resonance imaging(MRI) for differentiation betweenvarious causes of cervical lymphade-nopathy was evaluated. In a prospec-tive study, 31 untreated patients (22males and nine females, aged 5–70 years) with 87 cervical lymphnodes underwent diffusion-weightedMRI before performance of neckdissection (n=14), surgical biopsy(n=9) or core biopsy (n=8). Diffusion-weighted MR images were acquiredwith a b factor of 0 and 1,000 s/mm2
using single-shot echo-planar se-quence. Apparent diffusion coefficient(ADC) maps were reconstructed forall patients. The signal intensity of thelymph nodes was assessed on imagesobtained at b=0 or 1,000 s/mm2 andfrom the ADC maps. The ADC valueof lymph nodes was also calculated.On the ADC map, malignant nodesshowed either low (n=52) or mixed(n=20) signal intensity and benignnodes revealed high (n=13) or low(n=2) signal intensity. The mean ADCvalue of metastatic (1.09±0.11×
10−3 mm2/s) and lymphomatous(0.97±0.27×10−3 mm2/s) lymph nodeswas significantly lower than that ofbenign (1.64±0.16×10−3 mm2/s) cervi-cal lymph nodes (P<0.04). When anADC value of 1.38×10−3 mm2/s wasused as a threshold value for differ-entiating malignant from benign lymphnodes, the best results were obtainedwith an accuracy of 96%, sensitivity of98%, specificity of 88%, positivepredictive value of 98.5% and negativepredictive value of 83.7%. The smallestdetected lymph node was 0.9 cm. Inconclusion, diffusion-weighted MRIwith ADCmapping is a new promisingtechnique that can differentiate malig-nant from benign lymph nodes anddelineate the solid viable part of thelymph node for biopsy. This techniqueprovides additional useful physiologi-cal and functional information regard-ing characterization of cervical lymphnodes.
Keywords Diffusion MR imaging .Cervical lymph nodes . Head andneck
Introduction
Evaluation of cervical lymph nodes represents one of themost challenging problems for radiologists. Althoughmorphological imaging with computed tomography (CT)and magnetic resonance (MR) allows the detection ofenlarged cervical nodes, neither method can accuratelydifferentiate benign from malignant lymph nodes. Meta-bolic imaging with single photon emission CT (SPECT)
and photon emission tomography (PET) can help thisdifferentiation, but they are expensive, less available andhave low spatial resolution. Ultrasound (US) and US-guided fine-needle aspiration cytology (FNAC) have beenextensively used in Europe, but this technique is invasiveand operator-dependent with high incidence of falsenegative results that might result from aspiration of thewrong node or the wrong part of the correct node (samplingerror) [1–4].
M. K. Alsharaway . A. TawfikENT & Head & Neck SurgeryDepartments, Faculty of Medicine,Mansoura University,Mansoura, Egypt
A. A. K. Abdel Razek (*) .N. Y. Soliman . S. ElkhamaryDiagnostic Radiology Department,Faculty of Medicine,Mansoura University,Mansoura, Egypte-mail: [email protected].: +20-50-231505

Malignant lymph nodes, often, but not always, showcertain characteristic changes that help to differentiatethem from benign nodes. Nodal metastases are detectedwith imaging modalities on the basis of the size and shapeof the node, extracapsular tumor spread, and abnormalityof internal architecture, including necrosis. The detec-tion of nodal necrosis in patients with a primary head andneck tumor is the most reliable sign of a metastatic node[5–8].
Diffusion of water protons in biologic tissue derivesfrom the diffusion of extracellular water protons, transportof water protons through the cell membranes, and diffusionof intracellular water protons. The motion is disturbed byintra-cellular organelles and macromolecules located in thetissue. Any architectural changes in the proportion ofextracellular to intracellular water protons will alter thediffusion coefficient of the tissue. Thus, the signal intensityof diffusion-weighted MR images and the apparent diffu-sion coefficient of the tissues vary according to themicrostructure and physiologic state of the tissue [9–11].
The aim of this work was to evaluate the role ofdiffusion-weighted MR imaging (MRI) for differentiationbetween various causes of cervical lymphadenopathy.
Materials and methods
This prospective study was performed on 31 consecutivepatients (22 males and nine females) who presented andenlarged cervical lymph nodes clinically suggestive ofmalignancy. Their age ranged between 5–70 years (mean,49.5±11.7 years). The approval of the hospital’s reviewboard was obtained and an informed written consent wasalso obtained from all patients before the study.
All MR studies were performed with a 1.5 Tesla MRmachine (Symphony; Siemens Medical Systems, Erlangen,Germany) using a head and/or neck circular polarizationsurface coil. The machine is equipped with a self-shieldedgradient set (30 mT/m maximum gradient strength and120 T/m/s slew rate) for echo-planar imaging. All patients
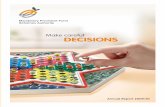
Fig. 1a–d Metastatic cervicallymph node. a Axial T2-weighted MR image showingmultiple enlarged cervicallymph nodes at level of IIB thatexhibit high SI. The largest oneis seen on the left side.b Diffusion-weighted MR imageat b=0 s/mm2 shows the en-larged lymph nodes show highSI. c Diffusion-weighted MRimages at b=1,000 s/mm2 showsthe lymph nodes show high SI.d ADC map showing that thelymph nodes exhibit low SI. Themean ADC value of the largestleftsided lymph node is 0.91±0.12×10−3 mm2/s
1469

underwent conventional T1-weighted images (TR/TE of800/15 ms) and T2-weighted fast spin-echo images (TR/TEof 6,000/80 ms) with a section thickness of 4 mm, aninterslice gap of 1–2 mm, a field of view (FOV) of 25–30 cm and an acquisition matrix of 256×224. Images wereobtained in the axial plane.
Diffusion- weighted images were obtained using amultislice, single-shot, spin-echo, echo-planar imagingsequence. A set of multiple axial scans (average 15 slices)of the head and neck were obtained to cover the area ofinterest. Section thickness was 4 mm with interslice gap of1 mm. Imaging parameters were: TR=10,000 ms,TE=108 ms, bandwidth=125 kHz, matrix 256×128 andFOV=25–30 cm. The diffusion gradients were applied inthree orthogonal directions (X, Y and Z). Diffusion-weighted MR images were acquired with a diffusionfactor, b, of 0 or 1,000 s/mm2 and ADC maps werereconstructed in all cases. Diffusion MR scanning time wasless than 2 min.
Final diagnosis for all lymph nodes was made byhistopathological examination after neck dissection for 14
patients, surgical biopsy for nine patients or core biopsy foreight patients. To ensure that the node removed surgicallyduring neck dissection was the same node as seen at MRI,the lymph nodes were excised en block along with adjacentreference structures to determine the relationship betweenthe excised nodes and the surrounding structures (such asmuscles, salivary gland or veins). The size of the excisednode was also compared with the size of the node on thediffusion-weighted MR images. Correlation between thediffusion MR findings and the histopathologic reports forthese excised lymph nodes was done.
MR studies were read independently by three blindedobservers. Each observer was not aware of the location ofthe primary tumor, its histologic type or clinical stage. Thesignal intensity of the lesions were graded as high, mixedor low signal intensity, on images obtained with b values of0 and 1,000 s/mm2 and the ADC maps, compared with theadjacent muscle on the basis of visual analysis findings. Inthe homogenously enlarged lymph nodes, a region ofinterest (ROI) was placed around the margin of the lymphnode and the ADC value was measured. When heteroge-
Fig. 2a–d Metastatic cervicallymph node. a Axial T2-weighted MR image showsmultiple enlarged cervicallymph nodes at level of IIB thatexhibit high SI. b Diffusion-weighted MR image at b=0s/mm2 showing that the en-larged lymph nodes exhibit highSI. c Diffusion-weighted MRimages at b=1,000 sc/mm2
showing the lymph nodes ex-hibit high SI. d ADC mapshowing that the lymph nodesexhibit low SI. The mean ADCvalue of the lymph node is0.121±0.11×10−3 mm2/s
1470

neity in signal intensity was observed, a larger ROI (meanvalue) and several smaller ROIs were placed within thecross section of the node. The mean ADC values of lowand high signal intensity regions within the nodes werecalculated separately.
Statistical analysis was done by using the SPSS(“Statistical Package for Social Science”) program softwarepackage for Windows. One-way ANOVA test was done tocompare more than two groups and Student’s t-test tocompare between two groups. A value of P<0.05 wasconsidered significant. We used a receiver operating char-acteristic (ROC) curve to evaluate the diagnostic capabilityof the ADC value and to determine the cutoff value fordifferentiating malignant from benign lymph nodes.
Results
Eighty-seven enlarged cervical lymph nodes were de-tected in 31 untreated patients. The causes of cervicallymphadenopathy in our study were: metastasis from headand neck malignancy (n=51), lymphoma (n=21), benignlymphadenopathy (n=15). Metastatic lymph nodes had
originated from squamous cell carcinoma of the larynx(n=21), oropharynx (n=12), hypopharynx (n=10) and oralcavity (n=8). Among 20 patients with squamous cellcarcinoma, nine patients were well differentiated (27nodes), two moderately differentiated (six nodes) and ninepoorly differentiated (18 nodes). Lymphomatous nodesincluded non-Hodgkin lymphoma (n=18) and Hodgkindisease (n=3). Benign nodes were reactive lymphoidhyperplasia (n=5), lymphadenitis (n=2), cat scratchlymphadenitis (n=1), sarcoidosis (n=4) and tuberculouslymphadenitis (n=3). Diffusion-weighted MR imagesdepicted all lymph nodes larger than 0.9 cm.
The enlarged lymph nodes showed different signalintensity on diffusion-weighted MR images dependingupon the selected b value. Metastatic lymph nodes showedeither homogenous (n=31) or heterogonous (n=20) signalintensity. The homogenous signal intensity seen in 31 ofthe metastatic lymph nodes was in the form of high signalintensity on images obtained at b value of 0 s/mm2 and at bvalue of 1,000 s/mm2 and low signal intensity on ADCmap(Figs. 1 and 2). The remaining metastatic lymph nodes(n=20), showed mixed signal intensity at different b valuesand high signal intensity at ADC map. The ADC map better
Fig. 3a–d Metastatic necroticcervical lymph nodes. a AxialT2-weighted MR image show-ing multiple enlarged cervicallymph nodes at level of II on theright side that exhibit mixed SI.The posterior node is homoge-nous, while the anterior one isnecrotic with high signal inten-sity. There are associated lymphnodes on the left side.b,c Diffusion-weighted MR im-ages at b=0 and 1,000 s/mm2
show the lymph nodes haveinhomogenous SI. d ADC mapshowing that the anterior lymphnode exhibits high SI representnecrotic node and the posteriorlymph node exhibits low SIrepresent tumor cells. Therefore,biopsieswere selected from theposterior located lymph nodes.The mean ADC value of theposterior lymph node is 1.11±0.23×10−3 mm2/s and of theanterior lymph node is 1.85±0.27×10−3 mm2/sec. Also, thereis mass in the right side of thepharynx that represent the pri-mary site
1471

delineates the solid part (low signal intensity) from thenecrotic part (high signal intensity) of the node than on T2-weighted MR images (Figs. 3 and 4). Biopsies from lowsignal intensity regions revealed tumor cells and from highsignal intensity regions showed areas of necrosis. Inlymphoma, there were multiple bilateral enlarged upperdeep cervical lymph nodes that showed high signal intensityin diffusion-weighted MR images obtained at b=0 s/mm2 andb=1,000 s/mm2. At ADCmap, they showed homogenous lowsignal intensity (Figs. 5 and 6). Benign lymph nodes wereseen in 15 patients. As regard benign nodes, 13 nodes showedhomogenous high signal intensity at images at b=0 s/mm2,low signal intensity at b=1,000 s/mm2 and high signalintensity on ADC map (Fig. 7). While the remaining twonodes showed low signal intensity on ADC map.
The ADC value of metastatic lymph nodes rangedbetween 0.77×10−3 mm2/s and 1.24×10−3 mm2/s (mean1.09±0.11±10−3 mm2/s). The ADC value of the metastaticlymph node varied according to degree of differentiation.Poorly differentiated metastatic lymph nodes showed lowerADC values (mean 0.89±0.12×10−3 mm2/s) than well andmoderately differentiated lesions (mean 1.13±0.11×10−3
mm2/s). The ADC value of poorly differentiated squamouscell carcinomas is statistically different (P<0.02) from welldifferentiated nodes. The mean ADC value for the necrotic
part of lymph nodes was 1.96± 0.33×10−3 mm2/s. Inlymphoma, the ADC value of the lymph nodes ranged from0.88×10−3 mm2/s to 1.13×10−3 mm2/s (mean 0.97±0.27×10−3 mm2/s). The mean ADC value was lower in patientwith non-Hodgkin lymphoma (mean 0.93±0.07×10−3 mm2/s)compared with patients with Hodgkin disease (mean 1.03±0.07×10−3 mm2/s). The ADC values of benign lymph nodesranged from 1.34×10−3 mm2/s to 1.92×10−3 mm2/s (mean1.64±0.16×10−3 mm2/s). No benign lymph nodes had ADCvalues less than 1.34×10−3 mm2/s.
The mean ADC value of metastatic and lymphomatousnodes was statistically different from (P<0.04) to that forbenign nodes. Table 1 shows the mean ADC value ofcervical lymphadenopathy. Figure 8 is box and Whiskerplot that compares the mean ADCs of metastatic, lympho-matous and benign nodes.
When an ADC value of 1.38×10−3 mm2/s was used as athreshold value for differentiating malignant from benignlymph nodes, the best results were obtained with anaccuracy of 96%, sensitivity of 98%, specificity of 88%,positive predictive value of 98.5% and negative predictivevalue of 83.7%. Figure 9 is the receiver operating char-acteristic (ROC) curve of the ADC value used for dif-ferentiating benign from malignant lymph nodes. The areaunder the curve was 0.955.
Fig. 4a–d Metastatic necroticcervical lymph nodes. a AxialT2-weighted MR image show-ing enlarged cervical lymphnodes at level II on the left sidethat exhibit high SI. b,c Diffu-sion-weighted MR images atb=0 and 1,000 s/mm2 show thelymph node has high SI. d ADCmap showing that the anteriorlymph node exhibits high SIrepresent necrotic tumor. Themean ADC value of the lymphnode is 1.89±0.11×10−3 mm2/s
1472

Discussion
Detection of cervical lymph nodes and differentiationbetween benign and malignant nodes is essential fordiagnosis of malignancy, tumor staging, therapy planningand follow-up, during and after therapy. CT and MRI arelimited by the fact that normal sized nodes may harbortumor foci, while enlarged lymph nodes may be reactiverather than neoplastic [1, 4, 12].
The performance of currently available techniques (US,CT and MR) for characterization of cervical lymph nodesremains, however, unsatisfactory. The use of conventionalMRI sequences does not seem to have any value over CTscan in this respect. However, the use of new MR pulsesequences, such as magnetization transfer imaging, diffu-sion-weighted imaging or dynamic enhanced MR imaging(using gadolinium or superparamgnetic iron oxide ascontrast medium), may improve the performance of MRI[10, 13, 15]. We evaluated the potential to use echo-planardiffusion-weighted MRI in the characterization of enlargedcervical lymph nodes by determining their ADC values. To
our knowledge, only a limited number of reports studiedthe characterization of head and neck lesions with diffu-sion-weighted MRI [10, 11, 14] and described the role ofdiffusion-weighted MRI in cervical lymph nodes [16, 17].
Diffusion-weighted MRI is a non-invasive techniquethat measures the diffusion and motion of water protons. Itrepresents a major advance in the evolution of pulsesequences that can make subtle abnormality more obviousand can provide better characterization of tissue and theirpathological processes as it reflects the random motion ofwater protons in tissue, including extra-, intra- andtranscellular motion. Diffusion imaging enables thecharacterization of tissue at microscopic level, emphasizinga mechanism that is different from T1 and T2 relaxation[10, 18].
Sumi et al. [16] reported that diffusion-weighted MRIsuccessfully depicted the metastatic nodes, benign lymph-adenopathy and nodal lymphomas and they added that withincreasing the b value, the signal intensity from the nodesgradually decreased, while the node contour was readilydetectable even at a b factor of 1,000 s/mm2. In our study,
Fig. 5a–d Non-Hodgkin lym-phoma. a Axial T2-weightedMR image showing multipleenlarged cervical lymph nodeson both sides at level IIA and Bthat show homogenous high SI.b,c Diffusion-weighted MR im-ages at b=0 and 1,000 s/mm2
show that the lymph nodes havehigh SI. d ADC map showinglow SI of lymphomatous nodes.The mean ADC value of thelymph node is 0.89±0.11×10−3 mm2/s
1473

the signal intensity of the lymph nodes varied according tothe selected b value and histopathological type of thelymph nodes. Images obtained with different b values ofecho-planar diffusion-weighted MR images may beassociated with susceptibility artifacts and T2 shine-through effect, and therefore they are less accurate thanADC map in characterization of the lymph node. To ourknowledge, appearance of cervical lymph nodes on theADC map has not been described. On ADC map, the signalintensity of the lymph nodes correlated with histopatho-logical changes. Metastatic and lymphomatous nodesshowed low signal intensity on ADC map compared withhigh signal intensity of the reactive and granulomatouslymph nodes. The smallest cervical lymph node detectedwith diffusion-weighted MRI was 0.9 cm.
In this study, the mean ADC value of malignant nodeswas lower than that of benign nodes, but overlap wasencountered in some cases. Benign nodes usually haveADC values higher than 1.34×10−3 mm2/s. The mean ADCvalue of metastatic and lymphomatous nodes was sig-nificantly lower than that of reactive and granulomatousnodes (P<0.04). If an ADC value of 1.3×10−3 mm2/s waschosen as a threshold value to differentiate benign frommalignant nodes, the best results would have been achieved
with high accuracy. This preliminary study indicates thatdiffusion-weighted MRI can distinguish benign frommalignant lymph nodes with a high degree of accuracy.Sumi et al. [16] reported that diffusion-weighted MRI candifferentiated reactive from metastatic lymph nodes inpatients with head and neck cancer (P<0.01). Also,Herneth et al. [17] reported that the mean ADC value ofmetastatic lymph nodes (0.59±0.27×10−3 mm2/s) wasstatistically different from regular lymph nodes (1.21±0.24×10−3 mm2/s) in head and neck cancer patients(P<0.04). Chang et al. [7] reported that a threshold ADCvalue of 1.22×10−3 mm2/s has an 86% accuracy, 84%sensitivity and 91% specificity, 93% positive predictivevalue and 78% negative predictive value for differentiatingbenign and malignant tumors of the head and neck.
There is a difference in the histopathologic features ofboth benign and malignant tumors. The difference in ADCvalue and signal intensity on ADC map of cervical lymphnodes reflects the difference in cellularity and histopatho-logical features of benign and malignant nodes. Malignantnodes have increased cellularity compared with benignnodes with subsequent reduction of the ADC value.Anderson [19] reported that malignant tumors have enlargednuclei and hyperchromatism. These histopathologic char-
Fig. 6a–d Non-Hodgkin lym-phoma. a Axial T2-weightedMR image showing multipleenlarged cervical lymph nodeson the left side at level III thatshow homogenous low SI.b,c Diffusion-weighted MR im-ages at b=0 and 1,000 s/mm2
show that the lymph nodesexhibit high SI. d ADC mapshowing low SI of lymphoma-tous lymph node. The meanADC value of the lymph node is1.01±0.17×10−3 mm2/s
1474

acteristics reduce the extra-cellular dimension that results ina decrease in the ADC values of malignant lymph nodes.
The ADC value of poorly differentiated squamous cellcarcinoma is statistically different (P<0.04) from welldifferentiated nodes. Sumi et al. [16] reported that the ADCvalue of metastatic nodes from well or moderatelydifferentiated cancers was significantly greater than thatfrom poorly differentiated cancers (P<0.01). Wang etal. [10] reported that histopathologic changes explain thedifference in ADCs among benign solid lesions, carcino-mas, and malignant lymphomas. Malignant lymphomasand poorly differentiated carcinomas have much incommon in histologic and cytologic features. These tumorshave more cellularity, larger nuclei with more abundantmacromolecular proteins, and less extracellular space thanwell or moderately differentiated carcinomas.
Mixed or heterogeneous signal intensity on T2-weightedMR images is suggestive of metastatic lymph nodes.Presence of non-contrast enhancement or irregular contrastenhancement is attributed to tumor necrosis, tumorkeratinzation or cystic areas inside the tumor [4, 6, 7].Curtin et al. [1] found that CT is more sensitive andaccurate than MR imaging in depicting nodal necrosis.
Fig. 7a–d Sarciodosis of thecervical lymph node. a AxialT2-weighted MR image show-ing enlarged cervical lymphnode at level III that exhibit highSI. b Diffusion-weighted MRimages at b=0 s/mm2 show thelymph nodes have high SI.c Diffusion-weighted MR im-ages at b=1,000 s/mm2 show thelymph nodes have high SI.d ADC map showing highsignal intensity of the lymphnode. The mean ADC value ofthe lymph node is 1.79±0.18×10−3 mm2/s
Fig. 8 Box and whisker plot comparing the mean ADCs ofmetastatic, lymphomatous and benign nodes. The horizontal line isthe median (50th percentile) of the measured values, the top andbottom of the box represent the 25th and 75th percentiles,respectively, and whiskers indicate the range from the largest tosmallest observed data points. Note that despite the overlap betweenthe ADC values of different groups, the ADCs of benign nodes aresignificantly higher than those of malignant nodes
1475

Contrast-enhanced MRI is certainly more sensitive indetecting necrosis than unenhanced MRI [7]. In this study,the ADC map could delineate and differentiate between thenecrotic and solid part of the tumor much better than T2-weighted images. The mean ADC value of the solid partsof metastatic nodes that exhibited low signal intensity was1.09±0.11×10−3 mm2/s. The mean ADC value of thehyperintense cystic or necrotic part was 1.96±0.33×10−3 mm2/s. This can help to select the biopsy sitefrom the solid part of the lymph nodes. Abdel Razeket al. [20] reported that the mean ADC of the viablepart (1.17±0.33×10−3 mm2/s) was less than that of thenecrotic part of the tumor (2.11±0.58×10−3 mm2/s). Thus,ADC map can differentiate the viable from the necroticpart of head and neck tumors.
Two benign nodes showed a relatively low ADC valueand were falsely mistaken for malignant nodes. One lymphnode was in a sarcoid patient and the other node in a patientwith Cat scratch disease. Histopathological analysis ofthese two nodes revealed that the dominant reaction wasdense fibrous reaction with restriction of water diffusion.The contributions of different components, such as fibrousscar tissue and granulation tissue, may alter the ADC value.This could explain the variability of ADC values foundamong our patients with benign lymph nodes and accountfor the relatively low ADC values found in two nodes.
The potential contribution of echo-planar diffusion-weighted imaging in the head and neck is still limited bytechnical problems regarding susceptibility artifacts, spatialresolution and motion artifact due to swallowing, respira-tion or blood flow. Susceptibility artifacts either at an air/tissue interface or due to incomplete filling of the coil (bulksusceptibility) are an additional source of artifacts whichcan hamper image quality of T2*-echo-planar imaging[21]. In this study, two benign lymph nodes showed lowsignal intensity on ADC map. These nodes were small andlocated in the lower part of the neck and were associatedwith susceptibility artifact. The detection of small-sizednodes less than 9 mm or abnormal internal texture of smalllymph nodes is still limited by imaging spatial resolution.A potential problem with the use of ADC value fordetection of metastases is that a necrotic area seen inmetastatic nodes exhibit high ADC value due to freediffusion. To avoid bias from a high ADC value of thenecrotic part of the lymph node, the ADC value wascalculated from the solid and necrotic part of the lymphnodes separately.
Conclusion
Diffusion-weighted MRI with ADC map is a newpromising technique that can help the differentiation ofnon-necrotic malignant from benign lymph node, delinea-
ROC Curve
Diagonal segments are produced by ties.
1 - Specificity
1.00.75.50.250.00
Sen
sitiv
ity1.00
.75
.50
.25
0.00
Fig. 9 Receiver operating characteristic (ROC) curve of the ADCvalue used for differentiating benign from malignant lymph nodes.The area under the curve is 0.955
Table 1 Causes and mean ADCvalue of cervicallymphadenopathy
Pathology Number Mean ADC value
Metastatic 1.09±0.11×10−3 mm2/sPoorly differentiated 18 0.89±0.12×10−3 mm2/sWell and moderately differentiated 33 1.13±0.11×10−3 mm2/sLymphoma 0.97±0.27×10−3 mm2/sNon-Hodgkin lymphoma 18 0.93±0.07×10−3 mm2/sHodgkin lymphoma 3 1.03±0.07×10−3 mm2/sBenign 1.64±0.16×10−3 mm2/sChronic inflammatory (reactive) 5 1.75±0.16×10−3 mm2/sTuberculous node 3 1.62±0.11×10−3 mm2/sCat scratch disease 1 1.41±0.0810−3 mm2/sSarcoidosis 4 1.81±0.12×10−3 mm2/s
1476

tion of the solid viable part of the lymph node and evenallows detecting small adenopathies. The addition ofdiffusion-weighted MRI to routine MRI provides addi-tional useful physiological and functional information
regarding characterization of the cervical lymph nodes.Recent advances and further refinement of diffusion MRtechniques and diffusion tensor MRI will improve theimage quality and accuracy of this technique.
References
1. Curtin HD, Ishwaran H, MancousoAA, Dalley RW, Caudry DJ, McNeil BJ(1998) Comparison of CT and MRimaging in staging of neck metastsis.Radiology 207:123–130
2. Castelijns JA, van den Brekel MW(2002) Imaging of lymphadenopathy inthe neck. Eur Radiol 12:727–738
3. Kaji A, Mohuchy T, Swartz JD (1997)Imaging of cervical lymphadenopathy.Semin Ultrasound CT MR 18:220–249
4. Fischbein N, Noworolski S, Herny R,Kaplan M, Dillon W, Nelson S (2003)Assessment of metastatic cervical ad-enopathy using dynamic contrast-en-hanced MR imaging. AJNR AmJ Neuroradiol 24:301–311
5. Ishikawa M, Anzai Y (2004) MRimaging of lymph nodes in the headand neck. Neuroimag Clin North Amer14:679–694
6. King AD, Tse GM, Ahuja AT, YuenEH, Vlantis AC, To EW, van HasseltAC (2004) Necrosis in metastatic necknodes: diagnostic accuracy of CT, MRimaging, and US. Radiology 230:720–726
7. Chang VF, Fan YF, Khoo JB (1996)MRI features of central necrosis inmetastatic disease. Clin Radiol 51:103–109
8. Ferreira T (2003) Comments on Cas-telijns and van den Brekel: Imaging oflymphadenopathy in the neck. EurRadiol 13:2236
9. Rowley H, Grant E, Roberts T (1999)Diffusion MR imaging. Theory andapplication. Neuroimag Clin NorthAmer 9:343–361
10. Wang J, Takashima S, Takayama Fet al (2001) Head and neck lesions:characterization with diffusion-weighted echoplanar MR imaging.Radiology 220:621–630
11. Sumi M, Takagi Y, Uetani Met al (2002) Diffusion-weighted echo-planar MR imaging of the salivaryglands. AJR Am J Roentgenol178:959–965
12. Sakai O, Curtin HD, Romo LV, SomPM (2000) Lymph node pathology.Benign proliferative, lymphoma andmetastatic disease. Radiol Clin NorthAmer 38:979–998
13. Markkola AT, Aronen HJ, Paavonen Tet al (1996) Spin lock and magnetiza-tion transfer imaging of head and necktumors. Radiology 200:369–375
14. Yoshino N, Yamada I, Ohbayashi Net al (2001) Salivary gland and lesions:evaluation of apparent diffusion coef-ficient with split echo diffusionweighted MT imaging-initial results.Radiology 211:837–842
15. Hudgins PA, Anzai Y, Morris M, LucasM (2002) Ferumoxtran-10, a super-paramagentic iron oxide as a magneticresonance enhancement agent for im-aging lymph nodes: a phase 2 dosestudy. AJNR Am J Neuroradiol23:649–656
16. Sumi M, Sakiham N, Sumi Tet al (2003) Discrimination of meta-static lymph nodes with diffusion MRimaging in patients with head and neckcancer. AJNR Am J Neuroradiol24:1627–1634
17. Herneth AM, Czerny C, Krestan C(2003) Role of diffusion weighted MRIin the characterization of lymph nodemetastasis. XVI International Congressof Head and Neck Radiology, Frankfurt(Abstract)
18. Gray L, MacFall J (1998) Overview ofdiffusion imaging. MR Clin NorthAmer 6:125–138
19. Anderson JR, Tumours I ( 1985) Gen-eral features, types and examples. In:Anderson JR (ed) Muir’s textbook ofpathology, 20th edn. Edward Arnold,London, pp. 121–149
20. Abdel Razek A, Tawfik A, Rizk N(2002) Role of diffusion trace MRimaging in differentiation between via-ble and necrotic head and neck tumors.Abstracts of the 88th Scientific As-sembly and Annual Meeting of theRadiologic Society of North America,Chicago, p. 431
21. Sigal R, Vogl T, Casselman J et al(2002) Lymph node metastasis fromhead and neck squamous cell carcinoma:MR imaging with ultrasmall superpar-amagnetic iron oxide particles (SireremMR)—results of a phase-III multicenterclinical trial. Eur Radiol 12:1104–1113
1477