Macadamia oil supplementation attenuates inflammation and adipocyte hypertrophy in obese mice
Upload
khangminh22Category
view
2download
0
1
Role of Adipocyte Impairment in Heart Failure Induction in Subjects thatare Obese along with Prediabetes and Overt Diabetes Mellitus - A Systematic
ReviewInternational Journal of Cardiology and Cardiovascular Disorder Review Article
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
Kulvinder Kochar Kaur M.D1*, Gautam Allahbadia M.D(Obstt&Gynae) D.N.B2, Mandeep Singh M.D.DM.(Std)(Neurology)3
1Scientific Director, Dr Kulvinder Kaur Centre For Human Reproduction, 721,G.T.B. Nagar, Jalandhar-144001, Punjab, India
2Scientific Director, Ex-Rotunda-A Centre for Human Reproduction, 672, Kalpak Garden, Perry Cross Road, Near Otter’s Club, Bandra(W)-400040, Mumbai, India
3Consultant Neurologist, Swami Satyanand Hospital, Near Nawi Kachehri, Baradri, Ladowali road, Jalandhar, Punjab, India
*Correspondence authorKulvinder Kochar Kaur M.DScientific DirectorDr Kulvinder Kaur Centre For Human Reproduction PunjabIndia
Submitted : 27 Apr 2021 ; Published : 1 Jul 2021
AbstractEarlier we have extensively reviewed the etiopathogenesis of obesity, role of white adipose tissue (WAT), brown AT (BAT), transcription factors involved like PRDM 16 associated with development of beige/brite AT, role of mirabegron and development of therapies for obese patients with or without diabetes. Here we aimed to study how AT impairment might be an anticipator of cardiovascular (CV) processes heart failure (HF), in patient population with obesity, MetS, in addition to known cases of overt type 2 diabetes mellitus (DM) in view of contradictory observations in association with collection of AT of separate kinds in CV risk along with HF-associated clinical results in obese subjects. Thus here we conducted a systematic review utilizing search engine pubmed; google scholar; web of science; embase; Cochrane review library utilizing the MeSH terms like AO; WAT; BAT; Visceral AT; Epicardial AT (EAT); Obesity; BMI; WC; DM; HFpEF; HFrEF; Atrial fibrillation; Adipocytokines; Adiponectin; Leptin; Resistin; Visfatin; Omentin; Zinc—α-2glycoprotein; Angiopoietin like protein 2; Cardiac remodeling; Renin-Angiotensin –aldosterone System (RAAS); Brain natriuretic peptide; Sympathetic nervous system (SNS); Oxidative stress (OS); Insulin resistance (IR) from 1950 to 2021 till date. We found a total of 550 articles out of which we selected 195 articles for this review. No meta-analysis was done. Proof exists that direct influence of epicardial adipocytes into the underlying myocardium resulting in stimulation of worst cardiac remodeling along with modulating HF generation in addition to AF. Further peri vascular collection of adipocytes, leads to liberation of proinflammatory adipocytokines (adiponectin, leptin, resistin) OS stimulation, switching of phenotypes of macrophages in addition to poor vascular repair, all of which result in microvascular inflammation, endothelial impairment, Atherosclerosis exaggeration, and finally escalation of CV mortality. Nevertheless, systemic actions of WAT and BAT might be separate, with adipogenesis in addition to browning of AT and deficient antiinflammatory adipocytokines (visfatin, omentin, zinc—α-2glycoprotein, glypican 4) were usually correlated withadipose triglyceride lipase escalation, changed glucose homeostasis, IR of skeletal muscles, escalation of cardiomyocyte apoptosis, decreased survival and poor progenitor endothelial cell function that could have a significant Impact on HF generation along with cardiac fibrosis. Thus here we have summarized all these along with how better diagnosis of HFpEF might be feasible with echocardiography. The pro and anti-inflammatory profiles act as good biomarkers for HF risk stratification.
Keywords: AT; HF; Cardiac Remodeling; Vascular Remodeling; T2DM; Biomarkers; AO.
IntroductionEarlier we have been working on the aetiopathogenesis of obesity and have reviewed the role of different adipose tissue depots like white adipose tissue (WAT) and brown adipose tissue (BAT) specifically visceral AT effects on obesity, various parameters of measurement (like body mass index [BMI], waist circumference [WC]) and therapy for obesity including various drugs including thylakoids, glucagon like agonists and why it is significant to treat obesity and diabetes mellitus together as diabesity and different aetiopathogenic factors for type1 Diabetes mellitus (T1D) and type2 Diabetes mellitus (T2D)
and how we can prevent development of T1D with improved aetiopathogenesis like role of gut microbiota in obesity along with T1D and how with bariatric surgery it is easier to control DM besides morbid obesity along with novel ways of utilizing plant products [1-15, besides lot more]. At present abdominal obesity (AO) as well as type2 diabetes mellitus (T2DM), continue to be a global public health challenge, correlated with an escalation of preterm mortality along with other physical complications in the general population [16]. This Global AO along with T2DM epidemic has been impacting

2
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
2 billion individuals as well 415 Million individuals all over the world [16]. There is a constant escalation of prevalence of both that imposes a greater burden on exaggeration of cardiovascular disease (CVD) secondary to exaggeration of atherosclerosis, endothelial impairment, cells along with microvascular inflammation [17]. A lot of observational studies have demonstrated that AO along with T2DM correlated with an escalation of chances of heart failure (HF), presentations irrespective of the other conventional CV risk factors [18]. The Framingham heart study have revealed that the population-ascribed risk of HF associated with AO was 5% for men as well as 7% for women for every enhancement of 1 in the body mass index (BMI) along with DM was 6% in males in addition to 12% in females [19]. The National Health and Nutritional Examination Survey (NHANES) epidemiological follow up study has demonstrated that DM by itself anticipated HF [20]. Furthermore mild escalation of fasting glucose amounts as well as insulin resistance (IR) aberrations, despite lack of overt DM had great correlation with a drastically escalated risk of HF generation [21]. A Metaanalysis of 77 prospective studies, that incorporated patients with DM, AO along with HF has illustrated that subjects with DM, possessed an escalated risk of generation of HF, besides there was proof of escalated risk of HF in prediabetic patients possessing a prediabetic range of blood glucose in AO patients [22].
Inspite of both AO along with T2DM mainly were compatible with HF with conserved (≥50%) ejection fraction (HFpEF), the prevalence of problems in subjects with HF with decreased (<40%) ejection fraction (HFrEF) is relatively great. The inter action of mortality among with AO along with T2DM in patients possessing different phenotypes of HF continues to be controversial. Despite 90 days post discharge accumulated all cause mortality in case of HFrEF patients possessing DM was greater than those possessing HFpEF, although no significant variations in the total accumulated all cause mortality in patients possessing DM with different phenotypes of HF [23]. Nevertheless, in non DM subjects presenting with HFrEF, all cause mortality was greater in contrast to those having HFpEF or HF with midrange (40-49%), ejection fraction [23, 24]. In addition patients with HF in contrast to patients possessing known DM along with microvascular complications possessed an escalated risk of hospitalization, as well as prognostic significance of DM for complications that are Diabetic Nephropathy (DN), Diabeticperipheral neuropathy (DPN), as well as retinopathy was greater in subjects with HFpEF in contrast to those with HFrEF [25].
Thus we decided to conduct a systematic review on role of adipose tissue (AT) impairment, in view of contradicting findings on prior preclinical and clinical studies on effect of collection of AT in different kinds of cardiovascular risk along with HF-associated results clinically in obese subjects.
MethodsHere we conducted a systematic review utilizing search engine pubmed, google scholar; web of science; embase; Cochrane review library utilizing the MeSH terms like AO;
WAT; BAT; Visceral AT; Epicardial AT (EAT); Obesity; BMI; WC; DM; HFpEF; HFrEF; Atrial fibrillation; Adipocytokines; adiponectin; leptin; resistin; visfatin; omentin; zinc—α-2glycoprotein; angiopoietin like protein 2; cardiac remodeling; Renin-Angiotensin–Aldosterone System (RAAS); Brain Natriuretic Peptide (BNP); Sympathetic Nervous System (SNS); Insulin Resistance (IR) from 1950 to 2021 till date.
Results We found a total of 550 articles out of which we selected 195 articles for this review. No meta-analysis was done. Additionally, earlier overweight along with AO were observed to be correlated with significantly escalated survival in HF subjects in contrast to normal weight HF subjects [16]. This process has been termed the ‘obesity paradox’, which was seen for ‘all cause mortality’ [26]. Despite ‘obesity paradox’ having been proved in various ranges of CVD, that are stable angina, Atrial Fibrillation, along with hypertension; this process has got detected in retrospective studies where AO was decided as per the body mass index (BMI) criteria, but not with other indices correlated with adiposity like dual–energy Xray absorptiometry (DEXA) [27, 28]. Possibly AO in patients might manifest to the practitioner before the HF got initiated resulting in lag-time bias. Nevertheless AO in patients might illustrate significant differences in the CV risk factor profile along with possess an ameliorated neurohormonal stimulation[Renin-Angiotensin-aldosterone System (RAAS), Natriuretic peptides (NP)], that could prefer a more advantageous long term prognosis. A meta-analysis of 29 clinical trials later had documented that overweight correlated with lesser CV mortality, Nevertheless there were no significant variations in mortality in case of AO subjects with HFpEF or HFrEF [28].
Inspite of contradiction as per the involvement of AO with regards to mortality in HF subjects [26, 27] significant escalation of AO prevalence is correlated with an escalating incidence of prediabetes as well as DM and thus subsequently results in escalated CV risk in all people groups with varying ages, in both sexes, each racial along with ethnic groups [28]. AO that were in conformity to over expression along with liberation of adipocytokines like adiponectin, leptin, resistin, visfatin, omentin, zinc—α-2 glycoprotein along with glypican-4, in white adipose tissue (WAT) as well as brown adipose tissue (BAT), has been correlated with DM as well as insulin resistance (IR) [29]. Hence the systemic actions of WAT as well as BAT can be variable, along with adipogenesis that includes browning of adipose tissue (AT) along with deficit of anti inflammatory adipocytokines had a robust correlation with adipose triglyceride lipase escalation along with changed glucosehomeostasis, resistance towards insulin of skeletal muscles, escalated cardiac myocyte apoptosis as well as lesser survival along with function of progenitor endothelial cells that could have a significant impact on HF generation along with end-organ fibrosis, besides a lot of comorbidities [30]. Nevertheless, if the adipocytokine impairment is key for bad non adaptive cardiac as well as vascular remodeling along with generation of various phenotypes of HF is not certain as

3
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
well as in under evaluation till now [31, 32]. Ultimately that part of adipocyte Impairment in correlation with AO as well as survival benefit in HF is not clear. Here the proof demonstrating that adipocyte impairment might stimulate the initiation of HF via various biological modes implicating inflammation, epicardial in addition to perivascular AT collection, bad as well as electrical cardiac refashioning along with skeletal muscle Impairment.
Abdominal obesity along with AT Collection; Concentration on HF generationAs per the earlier thinking, AT Collection occurs secondary to an imbalance among energy intake along with its expenditure. A lot of depots make up the AT like the WAT, BAT as well as other ectopic AT that are epicardial, abdominal, retroperitoneal along with perivascular AT. The phenotype of thoracic along with epicardial AT simulates BAT, while with regards to both molecular as well as functional aspects of abdominal, retroperitoneal along with perivascular AT do not discriminate WAT [32, 33].
Generation of AO is equivalent to the conversion of fat collecting WAT towards energy liberating functional BAT [33] Conversely,the interaction among sympathetic nervous system (SNS), RAAS, endothelin as well as NP system in addition to thyroid-adrenal gland axis are robust constituents of the adaptive haemodynamic responses by which control of cardiac output blood pressure (BP), peripheral vascular resistance, fluid retaining, water as well as afterload [rev in ref 34] (Figure 1). Secondly, these neurohormonal modes modulates the physiological BAT associated thermogenesis, EnergyExpenditure (EE), along with WAT→ BAT conversion in case of pathophysiological situations, resulting in conversion of metabolically nonactive obesity towards metabolically active obesity [35] Furthermore Adipose –obtained Angiotensin II aids in the circulating RAAS, Kidney Function, electrolytes as well as water homeostasis, besides blood pressure (BP) control [35].
Figure 1: Courtesy ref no-34-The interplay between metabolic derangements and heart failure development. BAT, brown adipose tissue; BP, blood pressure; ET, endothelin-1; HFpEF, heart failure with preserved ejection fraction; HFmrEF, heart failure with midrange ejection fraction; HFrEF, heart failure with reduced ejection fraction; NPs, natriuretic peptides; RAAS, renin–angiotensin–aldosterone system; SNS, sympathetic nervous system; PPAR-γ, peroxisome proliferator-activated receptor
coactivator-1γ; WAT, white adipose tissue.

4
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
Additionally, IR occurs secondary to change of insulin along with 5’ AMP-activated protein kinase (AMPK) signaling pathways, that control the use of glucose along with free fatty acids (FFA). AMPK stimulation results in phosphorylation of AKT phosphatidylatidylinositide 3-kinase (PI3K), which recruits the AKT kinase, phospoinositide-dependent–kinase 1 as well as subsequently Thr 308. The Akt phosphorylates various molecular targets like caspase9, proapoptotic B cell-leukemia/lymphoma2 along with ribosomal 70S subunits-6 protein kinase that controls cell growth, differentiation as well as survival [36]. Lastly insulin working via the insulin receptor kinase manages to negatively control signal transduction
along with IR [36]. Hence a lot of modes that are equivalent to AMPK’s capacity to repress cell growth, tissues differentiation, besides repair. Actually AMPK indirectly reduces the action as well as generation of various biosynthetic enzymes in addition to directly blocking phosphorylation of p70S6K via targeting the tuberous sclerosis complex 2 as well as rapamycin complex 1 (TORC1) raptor. Subsequently, the stimulation of AMPK escalates double metabolic along with cellular responses from target organs, like amelioration of cell metabolism along with repression of cell differentiation as well as growth [36]. Figure 2 documents the part of insulin as well as AMPK in growth, differentiation, as well as survival of cells.
Figure 2: Courtesy ref no-34-The role of insulin and AMPK in growth, differentiation, and survival of cells. AMPK, 5′-AMP–activated protein kinase; IRK, insulin receptor kinase; PI3K, phosphatidylinositol 3-kinase; CAP–CBL–TC10, the Cb1-associated protein (CAP)–casitas B-lineage lymphoma (CBL)–ras-like protein TC10; PKC, protein kinase C; JNK-1, c-Jun N-terminal
kinase 1; SIK2, salt-inducible kinase 2.White adipose tissue(WAT) vis a vis brown adipose tissue (BAT)By definition WAT comprises of a heterogenous tissues possessing greater metabolic along with regenerative plasticity. WAT comprises of subcutaneous as well as visceral AT, besides possessing lipid collected adipocytes along with a lot of non adipocytes population that has mature as well as progenitor endothelial cells, stromal cell whose properties have not been labeled, precursors cells of adipocytes, fibroblasts, peripheral blood cells along with that has various populations of Antigen presenting cells (APC) like T-lymphocytes, mononuclear cells along with macrophages [37]. Despite metabolic (lipogenesis, lipolysis FA oxidation, amino acid as well as sex steroid metabolism) in addition to endocrine, paracrine (generation of adipocytokine as well as NP) actions of WAT are from adipocytes, non adipocytes population have illustrated a key part in sustenance, growth along with function of WAT, along with in metabolic along with structural remodeling of distant organs (heart, skeletal muscles, liver, pancreas) along with tissues (perivascular as well as pericardiac AT) [38].
In reaction to proper stimuli, WAT might get converted into BAT. Usually BAT is implicated in adaptive sympathetically stimulated thermogenesis along with energy homeostasis at the time of cold exposure as well as subsequent to hyperphagia [39]. Since it is active metabolically, it modulates thermogenesis via expression on their surfaces of UCP1 possessing various phenotypes in both typical brown adipocytes as well as beige/brite adipocytes [40, rev by us in ref 1, 2]. Nevertheless, thermogenesis activation might take place by different stimuli like cold exposure, adrenergic substances or genetic changes. Under normal circumstances an inverse association is present among energy liberating action of uncoupling protein 1 (UCP1) in adult human beige/brite adipocytes as well as BAT collection. Further, amounts of UCP1 mRNA, along with other transcriptional controllers [PPAR –gamma coactivator-1α along with PR domain containing 16 [PRDM 16] in beige/brite adipocytes have been escalated in association with PPAR –gamma presentation [41]. This observation pointed that the metabolic action of BAT provides protective influence on body fat collection, glucose tolerance as well as IR [41]. Hence SNS,

5
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
RAAS, as well as certain adipocytokine (adiponectin, visfatin, fetuin) have further illustrated robust potency for stimulation as well as recruitment of beige/brite adipocytes as well as subsequent sustenance of metabolic homeostasis as well as lipid metabolism [42]. Facilitation of BAT action or browning of WAT is correlated with in vivo cold tolerance, enhancement of energy expenditure (EE), as well as confers protection against obesity as well as T2DM [43, 44]. In toto, lesser BAT action or which is commonly detailed as BAT impairment has been observed to be a central actor in control of metabolic homeostasis, being key in etiopathogenesis of AO, T2DM, as well as, of CV complications that are poor cardiac remodeling as well as HF [38, 44].
Adiposity and HFpEF or HFrEFDespite AO represents a risk factor for HF, there is discriminative crosstalk of AO with the initiation of HFpEF as well as HFrEF [45]. Actually the MESA (Multi-ethnic Study of Atherosclerosis Study) had documented that the adiposity that got measured with utilization of anthropometrics (body mass index (BMI) as well as waste circumference [WC]) along with an abdominal computer tomography did not correlate with HFrEF but VAT collection had a robust association with HFpEF. Furthermore, HFpEF patients possessed significantly greater intramyocardial fat in contrast to HFrEF patients or non HF controls. Intriguingly, intramyocardial fat possessed robust association with left ventricular (LV) diastolic impairment parameters (mainly echocardiographic E/e’ ratio) in HFpEF patients, in contrast to HFrEF patients which was not dependent on age –comorbidities, BMI, gender along with myocardial fibrosis [46]. Nevertheless, AO through myocardial steatosis, IR, as well as endothelial impairment implicates cardiomyocytes hypertrophy along with cardiac systolic as well as diastolic impairment [47]. Actually insulin in the form of a stimulator of PI3K/AKT changes titin isoform of constituents as well as titin dependent rigidness as well as might further aid to changed cardiac diastolic function in case of patients with AO along with DM [48].
Actually AO is correlated with a systemic proinflammatory condition which stimulates OS along with results in coronary microvascular as well as vasculature rectification. Additionally, OS impacts on nitric oxide (NO) biopresence, amount of cyclic guanoside monophosphate along with protein kinaseG action in the neighbouring cardiomyocytes [49]. However low action of protein kinaseG as well as escalation modulates the generation of cardiac hypertrophy along with resting tension secondary to hyper phosphorylation of titin as well as collection of collagen extracellular matrix [ECM] [49]. Furthermore proof exists that hyper phosphorylation of myofilament proteins as well as escalation of calcium sensitivity represent the molecular processes at the start of generation of HFpEF [50]. Subsequently rigidity of myocardium along with interstitial fibrosis confirms the diastolic filling aberration along withHF [51].
Hence cardiac remodeling in HFpEF varies from HFrEF, where remodeling is directly stimulated by primary deletion
of myocytes. The variation in the molecular mode of the generation of HF phenotypes is equivalent to the observation that give a reasoning in detail of fast stimulation of actin following ionotropic stimulation in HFpEF secondary to hypo phosphorylation of Ca2+-based thin filaments [52].
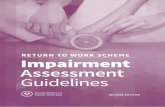
Phenotypes of Adipocytes Macrophage, Phenotypes as well as Changed WAT/BAT ActionMarked plastic characteristics of mature WAT/BAT adipocytes get validated by different stimuli like lipolysis, lipoliberation, low grade inflammation, growth factors (FGF) (fibroblast growth factor, transforming growth factor beta (TGF-β) that modulate survival, migration along with trans differentiation of stromal cells, like pre adipocytes, endothelial cells fibroblasts, lymphocytes, macrophages along with immune cells. There is proof that the adult adipocytes of WAT get converted to fibroblast like structures (rainbow adipocytes). Besides modulation of macrophage polarization of the macrophages possessing anti-inflammatory characteristics to classical M1 macrophages [53]. Nevertheless macrophages possessing proinflammatory characteristics get lured by WAT secondary to AT-associated cytokines [adiponectin, tumor necrosis factor alpha(TNFα), as well as interleukin-6 (IL-6) along with growth factors like, transforming growth factor beta (TGF-β) [53]. M1 macrophages generate as well as liberate lot of proinflammatory cytokines, like TNFα, IL-6 as well as monocytechemoattractant protein1 (MCP-1), hence aid in the generation of microvascular inflammation, IR, skeletal muscles Impairment as well as exaggerating atherosclerosis. Hence the inflassome system getting stimulated under stress adipocytes of WAT control transdifferentiation of ATmacrophages [rev by1-3], with nonclassical Phenotypes to classical macrophages along with, thus stimulates apoptosis of mature adipocytes [53, 54]. The remnants of apoptotic AT get resorbed by adipocytes macrophages as well as stimulate chronic low grade inflammation, that aids in low BAT action, low amount of BAT mass due to its conversion to WAT, generation of IR along with DM (Figure 3). In contrast to nonclassical-anti-inflammatory macrophages, adipose tissue manipulates tissue dendritic cells to take care of the adaptive immune response along with pro apoptotic action via TH 2/TH 17 polarization. M2 macrophages in addition have the capacity of induction of regulatory Tcells as well as generation of IL-10, aiding in tolerance to TH 1 activation [55]. In total, the percentage of the classic as well as nonclassic proinflammatory macrophages in AT in obese patients are greater in contrast to lean healthy subjects who possess WAT that has escalated macrophage amounts, with a lower inflammatory phenotype.
6
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
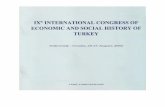
Figure 3: Courtesy ref no-194-Diagram illustrating hypothetical pathological link between excecssive EAT, A-FABP, and HFpEF. In HFpEF, myocardial remodeling and diastolic dysfunction are driven by endothelial inflammation, a physical constriction effect limiting myocardial relaxation during diastolic phase caused by EAT, and EAT-related paracrine signaling/cytokines from oxidative stress and lipotoxicity (FFA hyper-influx). A-FABP, a main mediator enriched in and released from visceral adipose tissue, is believed to elicit downstream pro-inflammatory cascades, has been proposed as part of the “visceral adiposity syndrome”. Deteriorating microvascular/endothelial function accompanying diverse metabolic syndrome-related comorbidities and systemic pro-inflammatory signaling, leading to excessive extracellular matrix turnover/fibrosis, structural remodeling, impaired cardiac lusitropic/contractile properties with increased myocardial stiffness predisposing to HFpEF, and co-morbid renovascular dysfunction. A-FABP, adipocyte fatty acid-binding protein; HFpEF, heart failure with preserved ejection fraction.

7
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
Intriguingly, great quantities of macrophages get collected in WAT/BAT in obese as well as lean subjects by various modes. AT macrophage (ATM) differentiation is controlled via WAT through MCP1/C-C chemokine receptor 2 (CCR2) pathways, but BAT modulates macrophages get collected through TNFα/MAPK/NFκB signaling, whereas the stimuli for the event can be equivalent [56]. Actually escalated local extracellular lipid amounts are believed to be significant molecular stimuli for macrophages get collected in WAT. The stromal AT cells are further implicated in metabolic alterations in AT function. Like in animal models of obesity have documented that once there is expansion of ectopic AT there was escalated ketone bodies amounts in circulation with diminished ratio of M1-like AT macrophages: M2 like macrophages [55]. Furthermore certain crucial signal transducers which were presented on the surface of macrophages implicate variables based on the macrophage phenotypes. Noticeably G- protein coupled receptor-43 (GPR43) transduces local TNFα signaling obtained from the steady state AT to macrophages. Actually M2 macrophages that got activated via TNFα that implicated GPR43 mode, validated WAT homeostasis as well as escalated metabolic action, nevertheless, M1 macrophages did not [56]. Possibly functional heterogeneity of main as well as ectopic kinds of AT that includes perivascular as well as pericardiac existence
might be in context with different manifestations of molecular receptor signal transductors [57]. Nevertheless, AT impairment as well as escalated amounts of TNFα get coordinated with macrophages that are polarized [58, 59].
The crosstalk among WAT adipocytes as well as macrophages work via autocrine as well as paracrine modes that include FFA –associated activation of p53 in addition to local generation of TNFα that which causes the generation of a vicious cycle accelerating inflammatory implications on target organs like analysis heart, skeletal muscles, liver, kidney vasculature, as well as AT, (Figure 4). Actually FFA collected in WAT, secondary to lipolysis stimulates GPR43 induction, toll like receptor 4 ( TLR4) as well as activates c-jun N terminal kinase janus kinase (JAK)- associated proinflammatory pathways in APC’s that include CD 11c+ macrophages, that is correlated with WAT inflammation [60]. Mature adipocytes get degraded by macrophages, thus act as liberators of proinflammatory cytokines, besides stimulation for adipocytokines liberation, free radical generation along with oxidized phospholipid generation [61]. Nevertheless, dysfunctional macrophage autophagy was seen to be a central actor in macrophage polarization which downregulates the local inflammation in WAT [62].
Figure 4: Courtesy ref no-34-The role of free fatty acids–related stimulation of p53 and local production of adipocytokines in pathogenesis of HF. TLR4, toll-like receptor-4; NF-κB, nuclear factor κβ; TNF-α, tumor necrosis factor α; WAT, white adipose tissue; BAT, brown adipose tissue; IL, interleukin; RBP4, retinol-binding protein-4; ANGPTL2, angiopoietin-related protein 2.

8
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
Adipocyte-particular-caspase 1 that gets locally generated via M1 macrophages along with proinflammatory cytokines (IL-6 as well as IL-1β) via stimulation of nuclear factor κ(NFκB) have an impact on the endothelial progenitor cells along with fibroblast precursors as well as change the endogenous repair of the vasculature. Hence proinflammatory cytokines have a direct impact on the metabolic status of the skeletal muscles resulting in stimulation the generation of IR as well as subsequently the skeletal muscles Impairment [63]. Conversely polarized macrophages robustly aid in molecular biology in addition to metabolic Impairment of AT via interference with both its function along with its capacity of transdifferentiating [64].
Rest of Non AT Cells along with inflammation in WAT Adipose tissue (AT) further posseses Non AT Cells, like endothelial cells along with their precursors, fibroblasts, pro fibroblasts, epithelial cells vascular smooth muscle cells (VSMC’s), along with immune in addition to APC’s, that modulates WAT inflammation, regeneration, along with stromal conversion, besides resulting in pleiotropic or multiple actions on adipocytes. WAT stroma is basically generated by fibroblasts, that generates as well as liberates various constituents of of ECM, like collagen, elastin fibres in addition to fibronectins laminin, tenascin as well as proteoglycans [65].The matrix structure yields mechanical strength of WAT as well as makes sure of the endocrine function of adipocytes via controlling matrix metalloproteinases (MMP’s) action along with expansion of Non AT Cells that are APC’s, effector Tcells, natural killer cells (NKcells), interleukin-10 (IL-10) generating Fox P3+ T Regulatory cells, mononuclear cells/macrophages, along with different progenitor resident cells of various origins [66]. Actually effector TH 1 Cells that are CD8+ Cytotoxic T cells that are regulated by adipose resident M1 macrophages generate Interferon γ(IFN-γ) as well as induce generation along with liberation of TNFα, the janus kinase (JAK) Signal Transducers and Activators of Transcription (STAT3) signaling pathway [67]. Further in addition, the amount of WAT Regulatory T cells directly hampers WAT infiltration of TH 1 Cells as well as ameliorates the reconversion of M1 to M2 phenotypes of AT macrophages [68].
In toto Tcells possess a significant part in the origin along with propagation of inflammation in AT [69]. Despite that macrophages are observed within AT, T cells liberate proinflammatory cytokines which can be observed locally within the AT, as well as these cells aid in further stimulation of inflammatory cells. On the other hand, an escalated infiltration of Tcells along with macrophages into AT, further has an impact on adipocyte functions by controlling the liberation of adipokines [70]. During this immunological reaction TH 1 Cells as well as TH 2 Cells liberate cytokines like IFN-γ as well as IL-4 which influence T cell subset differentiation. Moreover TH 17 cells are robust mediators during local tissue inflammation as well as liberate IL-17,besides further cytokines like IL-21, IL-22, IL-23 [71]. Stimulation of TH 17 cells activates inflammation that is long lasting [72] as well as liberate cytokines, despite part of some of these cytokines
is illunderstood in obesity particularly during its initial stages when subjects still are young. Animal studies demonstrated that high fat diet (HFD) intake stimulated a short term escalation of IL-17 along with TH 17- correlated cytokines. Nevertheless, over a longer duration HFD caused a reduction in IL-17, IL-22, IFN-γ, TNFα as well as IL-4 [73]. Greater amount of IL-17, also got documented in obese adults [73]. IL-17, IL-22, IFN-γ, TNFα TH 1 Cells. Additionally, Peroxisome Proliferator Activated Receptor-γ (PPAR-γ). PPAR-γ stimulated lipolysis, that escalates free radical generation by adipocytokines, that work through toll like receptor (TLR) signaling as well as netrin-1 based mode hampers the capacity of repair of the residential endothelial progenitor cells as well as mesenchymal stem cells (MSC’s) which further results in deterioration of the Vascular structure along with function, microvascular inflammation, as well as ultimately APC infiltration of WAT [63, 74]. In total adipose-resident immune cells facilitating the proliferation as well as differentiation of other non- adipose tissue cells see to it that significant escalation as well as refashioning of Clinical extracellular matrix [ECM] that results in adipose tissue Impairment along with unproportional generation of anti inflammatory as well as proinflammatory adipocytokines [75]. Secondary to these events, the infiltration of WAT by inflammatory cells is the place that generates inflammatory cytokines as well as Oxidative stress (OS) factors resuting in peri vascular inflammation, cardiac along with vascular remodeling as well as endothelial Impairment with dysfunctional bioavailability of NO, aiding in Atherosclerosis exaggeration unstable plaque, target organ perfusion aberration as well as HF presentations [76].
Adipose Tissue (AT) Impairment as well as HFAT acts in the form of a critical endocrine organ by liberation of a lot of adipocytokines possessing proinflammatory or anti inflammatory actions. Impairment in generation or liberation of adipocytokines secondary to Impairment of WAT might aid in the etiopathogenesis of obesity as well as HF [77]. Conversely Free fatty acids (FFA) leaking from the adipocytes secondary to lipolysis aids directly in apoptosis of non AT cells, microvascular inflammation, changed perfusion of the AT, resulting in hypoxia/ischemia as well as necrosis, hence governs a lot of proinflammatory signaling pathway in adipocytes, fibroblasts as well as immune cells [78]. Whereas hypoxia, that gets generated secondary torelative diminished perfusion of the adipocytes that are hypertrophic as well as excessive AT stroma or an escalation in O2 utilization in AO, gets generated in the form of a stimulus for inflammation of WAT. Actually hypoxia is correlated with proinflammatory genes getting overexpressed that includes Hypoxia inducible factor 1 (HIF 1) gene, free radical generation, OS, along with lipotoxicity in AT, as well as influences changed adipocytokines liberation, resulting in a vicious cycle along with facilitation of IR, wasting of skeletal muscles, cardiac along with vascular remodeling, endothelial Impairment, as well as ultimately HF [79].

9
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
Besides, liberation of adipocytokines, the secretome of adipocytes possesses extracellular vesicles (ECV’s), that shift a wide range of controlling molecules that are coding in addition to non coding RNA which have a key part in the intraorgan crosstalk among AT as well as CVS [80, reviewed by us ref 15]. Despite existence of cell free RNAs in human serum in greater amount in contrast to ECV, 50% of the biotypes of coding in addition to non coding RNA (mi RNA, transfer RNA, small γ RNA, circular RNA as well as long non coding RNA (lnc RNA) get shifted with ECV’s. Proof exists that various phenotypes of HF occur secondary to changed cardiac along with vascular rectification secondary to some epigenetic reactions that get parted by AO to as well as DM [32]. The genetic material in addition to active molecules, present in ECV represent to be Transducters of epigenetics signals as well as hence control remodeling [81]. Additionally, adipocytes, cardiac myocytes along with the whole vasculature, besides immune cells in case of AO as well as DM have an interaction with each other via particular ECV’s, that are transporting nucleic acids, proteins, lipids as well as cellular metabolites [82]. Despite the of different subtypes of ECV’s, specifically getting origin from endothelial cells were associated with BMI along with homeostasis model assessment of insulin resistance (HOMA-IR)well [83], a few lncRNA’ like hsa-miR-423-5p, rno- miR-16, rno- miR-93, rno- miR-106b, rno- miR-223, hsa-miR-660-3p, hsa-miR-660-3p, hsa-miR-1285-3p, along with hsa-miR-4491, having robust association with the generation of HFpEF [84]. Certain of the muscles particular circulating miRNA (hsa-miR-423-5p, rno- miR-16, as well as rno- miR-20b) along with others aid in interstitial fibrosis (hsa-miR-665, hsa-miR-1285-3p, as well as hsa-miR-4491) IR (miR-141-3p), along with Inflammation (miR-4763-3p) [32]. On the basis of our present insight on RNA controlling networks, a lot of ECV-obtained ncRNA’s for sure see to it that cell-cell crosstalk, besides modulates tissues reaction, like cardiac along with vascular remodeling, endothelial Impairment, along with browning of adipose tissue. Nevertheless, the practical advantages of these observations is not totally understood, needing deep probe in future.
Circulating AdipocytokinesThe maximum Adipocytokine significant in the context of WAT Impairment correlated with clinical results in heart failure patients are adiponectin, leptin, resistin, visfatin, omentin, angiopoietin like protein, zinc—α-2glycoprotein, glypican 4, lipocalin 2, secreted frizzled – related protein, retinol binding protein-4, TNFα, IL-6 as well as IL-18.
m Role of AdiponectinAdiponectin represents one of the adipocytokine that exists in large quantities, circulating in large amounts in the peripheral blood [85]. Normally adiponectin, gets liberated by adipocytes, being present in a lot of isoforms (multimeric as well as monomeric forms possessing full length as well as globular subforms, along with certain oligomers) as well as facilitates insulin sensitivity of liver, skeletal muscles, as well as adipose tissue that includes the ectopic components along with influence conferring protection to cardiac tissue [86]. The
biological part of adiponectin has been proved a lot, which is correlated with escalation of FFA β-oxidation, glucose transport getting activated gluconeogenesis getting hampered in target organs like liver, heart, skeletal muscles, white adipose tissue via activation of AMPK, p38-MAPK, as well as Peroxisome Proliferator Activated Receptor (PPAR-α), PPAR-α, thus ameliorate IR [87]. This biological reaction gets modulated via presentation of particular receptors (AdipoR1 as well as AdipoR2). Nevertheless, a broad spectrum of adiponectin-associated multiple phenotypic functions like anti diabetic, anti atherosclerosis, anti inflammatory, antiProliferative, as well as antiischemic characteristics [88]. It has been pointed that adiponectin facilitates the expression of anti inflammatory IL-10 along with thus represses the nuclear factor κ(NFκB) signaling pathway, resulting in down regulation of (TNFα –associated inflammatory reactions [88]. The antagonist of maximum significance of adiponectin are leptin as well as resistin, whose biological influence on energy homeostasis in addition to target tissue metabolism is just reverse of adiponectin [89].
The circulating amounts of adiponectin in obese patients as well as patients with diabetes mellitus are lesser in contrast to healthy subjects [90]. Actually, greater, total along with high molecular weight adiponectin amounts have been correlated with significantly lesser risk of T2DM [89, 90]. Prior Clinical studies have demonstrated that high molecular weight adiponectin oligomers had an inverse correlation with BMI, fasting, triglyceride amounts, HOMA-IR, in addition to visceral fat collection [91]. Hence lesser circulating amounts of adiponectin (<12.4mg/L) have illustrated a robust association with the conventional cardiovascular risk factors, like smoking a as well as hypertension [92].
Intriguingly, patients presenting with LV hypertrophy along with asymptomatic diastolic Impairment as well as subjects with HFpEF [93-95]. Escalated amounts of circulating adiponectin along with enhanced adiponectin expression in skeletal muscles have been observed in HFrEF subjects but it was a paradox that escalated adiponectin amounts were equivalent to bad clinical results, CV along with all cause mortality [96]. These observation were associated with lesser tissue expression of the major adiponectin receptor as well as genes implicated in the downregulation of lipids as well as glucose metabolism [97]. In view of these metabolic aberrations (like IR), aerobic ability, submaximal exercise manifestation, muscles intolerance correlated with exercise in addition to how much muscles possessed strength in case of HF patients had a robust correlation with circulating adiponectin amounts, thus posit that adiponectin in addition to its receptors might be critical actors in the generation along with progression of HF myopathy [98]. A positive association with plasma amounts of brain NP (BNP) as well as adiponectin in patients possessing generated HFrEF in addition to those at greater risk of generation of HF was observed [99]. Furthermore BNP was seen to be the major infuencer of circulating adiponectin in case of AO subjects manifesting coronary artery disease (CAD), irrespective of HF [100]. Depending on these outcomes it has been pointed

10
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
that escalated amounts of circulating adiponectin in HFrEF in patients represent adaptative modes as a compensation for metabolic Impairment aiding in getting over this metabolic Impairment as well as resistance to adiponectin for avoid HF advancement. Actually HF associated dysfunction of target organs perfusion like skeletal muscles, heart, liver, kidney along with vasculature is correlated with uncoupling of G-protein which gets included in the adiponectin Receptor’s structure AdipoR1 (skeletal muscles, heart, kidney along with vasculature), as well as AdipoR2 (in liver). AdipoR1 is a strong controller of Peroxisome Proliferator Activated Receptor (PPAR γ) coactivator -1α, besides Ca2+ based ionic channels along with AMPK/SIRT signaling pathway [101]. In contrast to that expression of AdipoR2 sees to it that transduction of tissue protective signaling via ubiquitin-proteasome pathway as well as insulin Receptor tyrosine phosphorylation as well as miR-150, that counterwork the G-subunit of AdipoR2, might aid in adiponectin resistance HF [102]. Hence, expression of AdipoR2 in tissue in case of extensive HF was observed to be significantly diminished [103].
The impairment of both Receptors ,ameliorates the capacity of adiponectin of binding them as well as escalate lipids as well as glucose metabolism which results in shifting of aerobic glucose metabolism to anaerobic type of glucose metabolism along with changes in FFA uptake by skeletal muscles, lipid peroxidation, mitochondrial impairment as well as ultimately generation of IR [104]. Despite adiponectin having the capacity of mitochondrial biogenesis, oxidative as well as metabolic stress decreases the capacity of adiponectin to escalate glucose getting utilizated besides escalation of FA-β oxidation [105]. Hence, adiponectin resistance seems to be the etiological factor in cardiac contractility Impairment along with skeletal muscles weakness [106]. Though precise molecular modes via which adiponectin resistance leads to cardiac as well as skeletal muscles Impairment is not clear, adiponectin amounts in peripheral blood remain as significant biomarkers with regards to metabolic aberrations in HFrEF patients robustly association with clinical results as well as survival.
LeptinLeptin represents an adipocyte generated hormone possessing a lot of functions, having their receptors broadly expressed in umpteen peripheral tissues in addition to the hypothalamus but none in adipose tissue [107]. The basic work of leptin is control of body weight, food consumption behavior as well as energy metabolism [108]. This hormone works as a functional antagonist to adiponectin via binding to proper receptors along with, stimulation of JAK-STAT3 signaling transduction pathway. In case of females circulating leptin amounts are normally greater in females in contrast to males, whereas there is a robust positive association of leptin in addition to AT mass, along with obese subjects mostly display greater amounts of leptin as compared to healthy subjects [108]. Nevertheless, the generation of AO as well as MetS relates to hyperleptinemia in addition to leptintolerance [109]. Delivery of leptin correlated with hyperleptinemia as well as tissue leptin tolerance. Proof exists that escalation of hypothalamic amounts of leptin
promote cognition in addition to synaptic plasticity, but in contrast resistance to leptin escalates the risk of depression in subjects with AO as well as T2DM [109]. Delivery of leptin correlated with the enhancement of peripheral tissues insulin sensitivity along with mitigation of energy homeostasis [110].
In the form of a cytokine possessing a structural similarity to IL-2 as well as growth hormone 1(GH1) leptin mediates both innate as well as adaptive immune responses, in addition to antiproliferative proinflammatory ability of TH 1 lymphocytes as well as macrophages working as activators of JAK2-STAT3 pathway as well as thus escalates the generation of various proinflammatory cytokines like IL-2, IFN-γ, TNFα a along with C-C- chemokine ligands (CCL3, CCL4 as well as CCL5) [110, 111]. Hence leptin escalates at a significant amounts both proliferation, as well as migration capacity of mononuclear Cells along with monocytes, besides stimulation of liberation of free radicals resulting in escalated OS [112]. Despite proof of leptin acting directly as well as indirectly in controlling cardiac function, the precise insight if leptin possesses harmful or beneficial actions is not clear [113]. Whereas leptin in animal models illustrated a proinflammatory action, that was correlated with remodeling of extracellular matrix [ECM], WAT inflammation, endothelial impairment [114]. Conversely proof exists that leptin could hamper apoptosis of cardiac myocytes along with decreased the degree of robustness of myocardial impairment in acute myocardial infarction (MI) model, seeing to it that the antiproliferative action via activation of cardiac STAT-3, physiology phosphatidylinositide 3-kinase (PI3K) as well as Akt action along with mitochondrial function, besides leptin activation of vascular repair via through nitric oxide (NO),-p-38MAP Kinase –based mode [115]. Besides that non-canonical leptin signaling pathway that has been observed to be the pathway by which leptin impacts the epidermal growth factor receptor (EGFR) as well as thus results in the antiproliferative action [116].
The patients who had earlier HF demonstrated escalated amounts of leptin, based on sodium getting retained, besides expansion of the plasma, while a lot of outcomes of the serum leptin measures have been contradictory [117]. A posit has been that the generation of leptin in case of HF subjects is secondary to cardiac as well as renal fibrosis, besides WAT along with microvascular inflammation in addition to leptin modulated neurohormonal as well as proinflammatory stimulation might escalate the expression of SGLT2 in kidney tubules Hence Sodium–glucose cotransporter 2 (SGLT2) inhibitors confers protection against tissues by causing reduction of leptin associated inflammation along with repression of generation of leptin in WAT, although not via natriuretic effects [118, 119]. Another reasoning given for leptin etiopathogenesis in HF is the harmful crosstalk Leptin-aldosterone-neprilysin in HF subjects possessing AO or T2DM [120]. Possibly, SNS, along with neprilysin overaction in obese patients escalates the generation of leptin along with other proinflammatory adipokines, besides being correlated with changed natriuretic peptide (NP) getting cleared along with adiponectin generation which aids in HF advancement [121]. Further a posit is given

11
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
that leptin acts as a prohypertrophic factor that confers cardiac protection, as well as its liberation from adipcytes signifies a maladaptive reaction from HF- associated stimulation [122]. Nevertheless, leptin acting as an association among AO, T2DM. HF, represents a CV biomarker needing a clear insight on these correlations.
ResistinResistin represents a low molecular weight adipcytokine that aids in IR, inflammation as well as Oxidative stress (OS) [123]. The basic biological actions of Resistin get manifested via different molecular targets (like FFA transport protein 1, acetyl-CoA–Carboxylase, as well as AMPK, CD36) along with get influenced by the amelioration of glucose metabolism, hampering of FFA β-Oxidation, along with uptake [29]. Resistin gets expressed mainly, besides getting liberated by macrophages secondary to activation by proinflammatory cytokines [124]. Hence Resistin was observed to facilitate microvascular inflammation, endothelial impairment, VSMC proliferation in addition to plaque generation [125]. Despite serum resistin amounts did not illustrate an association with a risk of non fatal MI in CAD patients, besides not decreasing the infarct size, the greatest quartile of resistin amounts a were observed to be an independent anticipator of an escalated risk of HF generation [126]. The multi-ethnic study of Atherosclerosis (MESA) Study has documented that incidence of CVD, CAD as well as HF illustrated robust, independent correlation with resistin amounts in general population [126].
Prior Studies have demonstrated that escalated serum amounts of resistin were correlated with IR, T2DM, AO as well as CVD [127], whereas no significant association with resistin amounts as well as echocardiographic parameters that were LVEF, Gensini score index tissue in addition to angiographic reports along with robustness of atherosclerosis [128]. The The Framingham offspring study as well as the Health ABC Study have documented that The serum amounts of resist in were independently associated with a high risk of poor CVS results along with deterioration of kidney function in the patients with HF, but adiponectin amounts were not [95]. Furthermore the deterioration of kidney function was the chief etiology of the escalated circulating resistin amounts rather than reducing cardiac pump HF action [129]. Contradictory outcomes of clinical studies related to the correlation of resistin amounts, as well as HF- associated results along with all cause as well as CV mortality. Patients presenting with non-ischemic dilated as well as inflammatory cardiomyopathy, resistin independently anticipated the incidence of HF [130]. Additionally, resistin possesses the anticipating capacity for HFrEF, but not with regards to HFpEF, as far as morbidity as well as mortality [131]. A crosstalk among serum amounts of resistin as well as HFrEF clinical results in the BioSHiFT Study demonstrated that in the 2.2yr follow up was not observed [132]. As compared to that serum amounts of resistin illustrated robust association with serum markers of ECMs (typeIII amino terminal peptide of procollagen, MMP2, TIMP1), BNP, apelin as well as mortality in HFrEF individuals [133]. Hence resistin reasons out a crosstalk among metabolic co morbidities, inflammation as well as HF as compared to independent influence on a natural
evolution of HF [134].VisfatinVisfatin represents an inflammatory adipokine enzyme (alias nicotinamide phospho ribosyl transferase as well as pre B cell colony enhancing factor) that possesses growth factor action that is implicated in the generation pathway of NAD+ [135]. It gets liberated actively by both adipocytes as well as macrophages, also observed in the circulation as well as in ECM, where it controls the OS, immune response, apoptosis inflammation via Sirt-1 based as well as MAP-Kinase (ERK1/2 – associated pathways [136]. The translocation of nuclear factor κ(NFκB) MAP-Kinase (ERK1/2 in addition to repression of NFκB, Visfatin significantly declined the generation of MMP-8 as well as hence reduced the remodeling of ECM [137]. Under physiological situations Visfatin controls thermogenesis in BAT through escalation of UCP1 amounts in BAT adipocytes [138]. Hence Visfatin binds to insulin Receptor-1 as well as thus influences insulin like actions [139]. Belonging to the adipocytokine class, possessing different multiple actions, Visfatin causes IR, hampers WAT Oxidative stress along with inflammation, facilitates vascular repair along with represses ischemia stimulation of apoptosis of cardiomyocytes basically via upregulation of proinflammatory cytokines like TNFα as well as monocyte chempoattractant protein 1(MCP1) [140]. Conversely, Visfatin further upregulates NFκB, in endothelial progenitor cells resulting in apoptosis stimulation of these precursors, causing a reduction in the circulating endothelial progenitor cells amounts possessing angiopoietic action [141]. The serum amounts of Visfatin escalation occurred significantly in patients with T2DM, AO, metabolic syndrome (MetS), acute MI, as well as HFpEF, while reducing in patients with HFrEF [142, 143]. Of the patients with acute ST elevation MI, escalation of serum amounts of Visfatin anticipated total main CV side effects [144]. Further more proof exists with regards to escalation of serum Visfatin anticipated restenosis Subsequent to implantation of drug eluting stent [145]. Moreover, a positive association among plasma Visfatin amounts with triglycerides along with inverse association with high density lipoprotein (HDL) Cholesterol amounts of omentin-1 in CAD patients with HFpEF [146].
Generation of Visfatin in patients with HF has been pointed to be an adaptive reaction, that is directly against the dysfunction of mitochondrial ultrastructure, stimulation of Oxidative stress as well as free radical generation along with cell death in the myocardium [147]. Nevertheless, serum Visfatin amounts in HFrEF patients was equivalent to the NewYork Heart Association Classes, as well as they being significantly lesser in contrast to healthy volunteers irrespective of age anthropometric parameters along with metabolic features [148]. In total, if Visfatin has a potential advantageous actions on myocardium, vasculature along with AT in HF is not totally clear as well as needs to be evaluated in larger controlled trials in coming future.
Omentin Omentin gets liberated from AT of the omentum, that is

12
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
34KD protein, implicated in controlling the adipocytes differentiation, maturation, energy metabolism, immune response, inflammation, as well as insulin sensitivity [149]. 2 homologous isoforms (Omentin 1 as well as Omentin 2) exist in the circulation, with Omentin 1 being the major isoform [150]. Omentin 1 works with utilization of AMPK/Akt/NFκB/MAP-Kinase (extracellular signal kinase1/2[ERK1/2], JNK as well as p38) signaling systems via which anti proliferative, anti inflammatory, anti oxidative as well as angiopoietic action [151]. It has been observed that omentin 1 confers protection besides the direct cardiac myocytes protection in addition to modulating crosstalk among WAT as well as myocardium [151]. Omentin 1 illustrated enough action against Oxidation of low density lipoprotein (LDL) cholesterol as well as avoided generation of foam cells through down regulation of CD36, scavenger Receptor class A in addition to acyl CoA- cholesterol transferase-1, besides up regulation of neutral cholesterol ester hydrolase in case of activated macrophages [152]. Further Omentin 1 diminished angiotensin stimulated migration of monocyte/macrophages in addition to platelet derived growth factor receptor (PDGFR) BB- stimulated proliferation of VSMC’s [146]. Noticeably Omentin 1 amounts had significantly less expression in coronary artery endothelium, as well as epicardial adipose tissue, whereas circulating Omentin 1 amounts in addition to its expression in plaques were escalated [153].
Possibly lesser Omentin 1 amounts as well as escalated amounts of visfatin might have a role in the generation of coronary artery disease (CAD) in AO patients [153, 154]. The population-dependent EPIC-Potsdam study has demonstrated that serum Omentin 1 amounts did not possess significant association with HF chance, nevertheless they had a correlation with a risk of CAD in the general population [153]. Intriguingly, patients with HFrEF illustrated greater Omentin 1 amounts in contrast to those having HFpEF [154]. Hence the escalated circulating Omentin 1 amounts had a mild along with positive correlation with cardiac volume along with systolic function in addition to negative association with adiponectin, high sensitivity C Reactive Protein (hsCRP), as well as N-terminal pro-BNP (NT-pro-BNP) in HF patients [154]. Additionally, the escalated circulating Omentin 1 amounts were an independent anticipator of weight gain in patients with decompensated as well as chronic HF who possessed lesser mortality along with hospital readmission irrespective of leptin as well as NT- pro-BNP amounts [155]. Nevertheless, the primary etiology of positive influence of omentin 1 on mortality in HF patients is not clear.
Zinc—α-2glycoproteinZinc—α-2glycoprotein, anadipocytokine, belonging to MHC I protein class gets liberated by epithelial cells along with adipocytes [156]. It binds with the dansylated C11 FA11 (dansyloamino) undecanoic acid on the surface target cells (like adipocytes, skeletal muscles) in addition to controlling lipid metabolism, along with insulin sensitivity [157]. Zinc—α-2glycoprotein exerts its pleiotropic actions in association with the negative controlling of fibrosis in addition to repressing generation of various proinflammatory cytokines like S100A1
[158].It is implicated in the generation of AO as well as T2DM. Prior studies demonstrated that Zinc—α-2glycoprotein had a better anticipation capacity for IR in contrast to HOMA-IR Index [159]. Mechanistically It works through crosstalk with p- ERK as well as transforming growth factor beta (TGF-β) that facilitates proliferation of endothelial precursors, repression of low grade inflammation, controlling of metabolism of ketone bodies in addition to escalation of expression of visfatin in target cells [160]. Proof exists that Zinc—α-2glycoprotein avoids cardiac hypertrophy along with enhances diastolic outcomes possibly secondary to amelioration of cardiac fibrosis [161]. How this adipocytokine confers cardiac protection needs to be evaluated thoroughly.
Lipocalin 2Lipocalin 2 (neutrophil gelatinase-associated Lipocalin) gets liberated by different cell kinds, belonging to the Lipocalin protein super family [162]. Broad expression occurs in AT, resulting in inflammation in addition to fibrosis. There is proof with regards to over expression of Lipocalin2 in WAT gets regulated by up regulation of IL-1β [163]. There is a positive association of Lipocalin2 with adiposity, hyperglycemia, IR, ECM remodeling, MMP action along with high sensitivity CRP (hsCRP) [164]. Despite resulting in inflammatory, Proliferative as well as fibrotic reaction in myocardium, kidney [165], its part as biomarker in poor cardiac remodeling along with HF taking place is not understood. That Lipocalin aids in priming along with stimulation of NLRP3 inflassome as well as liberation of HMGB1 from cells, resulting in escalation of circulating amounts of IL-1β, IL-18, as well as caspase 1 stimulation [166, 167]. Microvascular inflammation along with cardiac fibrosis are the maximum etiologies resulting in decreasing influence of Lipocalin2 on myocardial structure as well as kidney function.
Angiopoietin–Like Protein-2Angiopoietin–Like Protein-2 represents a proinflammatory adipocytokine possessing lot of functions which facilitates IR as well as gets broadly expressed in WAT [168]. Escalated circulating amounts as well as over expression of Angiopoietin–Like Protein-2 were observed in patients with AO as well as T2DM [169]. The capacity of this adipocytokine to mediate vascular permeability as well as stimulate microvascular inflammation regarding HF generation is getting evaluated.
Secreted frizzled–related protein 5Secreted frizzled–related protein 5 represents an innovative adipocytokine that gets expressed in cardiomyocytes, adipocytes as well as fibroblasts [170]. It represses Wnt/β-catenin signaling pathway in addition to embryonic generation, proliferation, vascular permeability, atherosclerosis along with adipocytes [171]. Secreted frizzled–related protein 5 gets down regulated in case of HF patients, playing a key part in HF stimulated skeletal muscle impairment, cardiac fibrosis along with ECM remodeling via crosstalk with TGF-β1 [171, 172]. This biomarker seems to be attractive for further evaluation with regards to poor cardiac remodeling as well as prognosis

13
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
with regards to HF generation.Glypican 4Glypican 4 represents another innovative adipocytokine, belonging to the heparin sulfate proteoglycan family that gets liberated by adipocytes. It participates in controlling glucose tolerance (GT), besides escalation of insulin signaling [173]. Glypican 4 in myogenic regulatory factor causes skeletal muscle hyperplasia as well as hypertrophy, besides cardiac remodeling, along with myocardial hypertrophy [174]. Furthermore Glypican 4 has a role in controlling Rac stimulation for sustenance of polarized actin rich lamellipodia in ECM’s, being key for good migration of endodermal cells into ECM’s [175].
The serum amounts of Glypican 4 get escalated in subjects with AO, MetS, T2DMin a progressive manner in relation to escalation of BMI, WC, Waist to hip ratio along with total WAT mass [176]. Measurement of serum Glypican 4 has been pointed for anticipation of CVrisk [177]. In HF patients serum amounts of Glypican 4 anticipated endurance training, hence it could be an innovative target for biomarker dependent treatment of HF [178].
Retinol binding protein-4 Retinol binding protein-4 represents an AT-obtained protein possessing pro diabetogenic action that gets liberated by adipocytes along with hepatocytes [179]. Contradictory results are existing in association among serum amounts of Retinol binding protein-4, in addition to IR, T2DM, AO as well as CV complications that includes HF. Like Ulgen et al. [180], did not observe the correlation of Retinol binding protein-4 amounts with IR as well as a other constituents of MetS. Conversely Lee et al [181], documented that significant correlated with existed among fasting blood glucose amounts, insulin amounts, HOMA-IR in addition to Retinol binding protein-4 in AO patients. It has been the implication of Retinol binding protein-4 in WAT/BAT distribution among obese subjects, although this presumption needs wide exploration.
Serum amounts of Retinol binding protein-4 were significantly greater in HF patients in contrast to healthy subjects [182]. The role of Retinol binding protein-4 as an anticipator of HF nature evolution or HF- associated risks is not clear.
Tumor necrosis factor alpha (TNFα)Tumor necrosis factor alpha (TNFα) is a well accepted adipocytokine that gets generated by the VSMC’s, adipocytes along with APC’s, that is implicated in the controlling of local in addition to systemic inflammation, immune response as well as IR [183]. Generated by cardiac myocytes or macrophages Secondary to volume overload, or get shifted in cardiac tissue from distant areas of generation like WAT [184]. Since it represents being a central inflammatory mediator, it directly stimulates cardiac remodeling a along with results in cardiac impairment in case of T2DM, in addition to AO patients, whereas in directly by stimulation of nitric oxide synthase (NOS) [185]. Nevertheless, no well demonstrated proof of any part of anti TNFα treatment in avoidance of HF in case
of AO patients having well generated rheumatoid arthritis [186]. Actually certain huge, international randomized, placebo controlled (Clinical trial (RECOVER [Research into Etanacerpt cytokine antagonism in ventricular dysfunction] and RENAISSANCE [Randomized Etanacerpt North American Strategy to Study Antagonism of Cytokine] did not illustrate a robust positive action of anti TNFα treatment vis a vis placebo on clinical results in case of HF patients [187]. At present anti TNFα treatment is not advocated in all HF patients [188].
Conversely, muscle wasting as well as cardiac cachexia aid in HF propagation, in addition to concomitantly stimulated by systemic inflammation validated by TNFα [189]. Prior Clinical Studies have illustrated that circulating TNFα amounts in addition to its secondary mediators, like IL6 as well as IL-18 were significantly greater observed in HFrEF patients in contrast to HFpEF patients as well as healthy subjects. Hence TNFα, IL6 as well as IL-18 possess significantly greater amounts in ischemia–stimulated HF in contrast to HF caused secondary to valvular heart disease in addition to hypertension [190]. Despite a robust association among mortality rate along with serum TNFα as well as IL6 amounts in HFrEF patients, still proper insight with regards to how these cytokines aid in HF as well as modulates their interaction with sympathetic nervous system (SNS) in addition to WAT impairment [191]. Lastly TNFα represents possibly an attractive biomarkers for anticipation of skeletal muscle weakness at the time of personalizing HF treatment.
Crosstalk among adipocytes impairment, AO along with Survival Benefit in HFRecent clinical work has illustrated that irregularity of adipocytokines generation is a key factor in aiding in presentation along with propagation of metabolic as well as cardiovascular complications that includes HF [178, 180, 185, 191, 192]. The influence of changed adipocytokines profile on cardiovascular remodeling in patients possessing variety of phenotypes of HF is significantly different in addition to is not always associated with induction of inflammatory stimulation. The mode which links AO along with HFpEF differ from obesity stimulated haemodynamic alterations to significant biohumoral systems like adipocytokines, RAAS, SNS, NP in addition to Oxidative stress. [Probably, changes in adipocytokines might anticipate the precipation of HFpEF along with HFrEF, despite the aetiogical association of AO to a chance of Clinical results in HFrEF still needs to be properly evaluated in depth. Nevertheless still no consensus as per survival benefit in AO patients manifesting HFrEF or HFpEF depending on adipocytokines impairment exists [193]. Further Lin et al. conducted a prospective cohort study with prospectively recruited subjects as healthy (n=40), high risk (n=161), or HFpEF (n=51). Epicardial adipose tissue (EAT) was evaluated with utilization of ECHO and comparison done among 3 groups along with associated with Adipocyte-Fatty acid binding protein (FABP), cardiac structural along with functional evaluation with utilization of myocardial deformations in the form 0f stress/strain rates illustrated in addition to HF results. Maximum EAT thickness was existing

14
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
in subjects with HFpEF (9.7_1,7mm) in addition to high risk (8.2_1,5mm), whereas least in healthy controls (6.4_1.9mm.p<0.001). Greater EAT was associated with the existence of cardiometabolic syndrome, Diabetes mellitus along with renal problems irrespective ofBMI, WC (pinteractionfor all>0.1), besides being correlated with decreased LV global longitudinal strain (GLS) as well as LV mass that was not based on the systolic /diastolic strainrate (SRs/SRe) (allp<0.05). Greater FABP amounts were correlated with higher EAT thickness (pinteractionl>0.1), along with significantly, in the combined control cohort, FABP amounts modulated the correlation among EAT in addition to new onset HF. Escalated EAT was independently correlated with MetS, renal inefficiency along with Greater FABP amounts, pointing to a metabolic association among EAT in addition to HF [194]. Further Zhou et al. [195] conducted a study with the objective to evaluate the functional changes, diagnostic usage, in addition to prognostic significance of carotid arterial deformations in subjects with CVrisk factors and HF with preserved ejection fraction (HFpEF). In a prospective study 251 participants (mean age 66.0 ± 9.8 years, 65.7% female)from a single centre between December 2011 and September 2014, carotid artery deformations including circumferential strain (CCS)/strain rate radial strain were analysed by two-dimensional speckle tracking. They further associated these carotid artery deformation indicesto HF biomarkers and cardiac structure and function by echocardiography and explored their prognostic values. Significant decrease of CCS, circumferential strain rate, and circumferential radial strain were seen across control (n = 52), high risk (n = 147), and HFpEF (n = 52) (trend P ≤ 0.001). Aging, hypertension, HFpEF, and higher pulse rate demonstrated independent correlations with decreased CCS by stepwise multivariate regressions (all P < 0.05). Greater CCS was inversely associated with better cardiac remodelling and functional indices, and lower multiple HF biomarkers (all P ≤ 0.005). After adjustment, higher CCS was independently associated with better global ventricular longitudinal strain/early diastolic strain rate, lower matrixmetalloproteinase-2, and Nterminal propeptide of procollagen type III levels (adjusted coef: _0.08 and _19.9, allP < 0.05). During a median follow-up of 1406 days (interquartile range: 13421720 days), CCS less than 3.28% as a cut-off had markedly higher HF events [Harrell’s C: 0.72, adjusted HR: 2.20 (95% confidence interval: 1.24, 3.16), P = 0.008]. CCS also showed significantly improved risk prediction for HF over global ventricular longitudinal strain (net reclassification index: 48%,P = 0.001; integrated discrimination improvement: 1.8%, P < 0.001).Thus concluding that Carotid artery deformations using two-dimensional speckle-tracking imaging showed novel mechanistic insights on functional arterial alterations reflecting coupled arterial-ventricular pathophysiology. Utilization of such methods might further yield extra prognostic value to enhanced myocardial functional evaluation [195].
ConclusionsHF is a usual outcome of AO in addition to T2DM, usually presenting secondary to adipocytes impairment along with expansion of adipose tissue. There is involvement of
adipocytokines in the complicated cascade of reversible HF metabolic impairments potentially, that can be treated with efficacy, besides correct anticipation by circulating biomarkers. The balance among pro in addition to anti inflammatory cytokines which are implicated in the metabolic controlling of WA/BAT is a necessary element in getting insight of the key part of adipocytokine impairment in HF presentation in obese patients in addition to patients with Diabetes mellitus. Proper molecular along with functional mode of adipose tissue impairment needs to be evaluated in large Clinical trials for getting unfolded novel perspectives in anticipation of HF presence along with generation among AO in addition to T2DM patients.
References1. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2015).
Therapeutic Applications of the Recent Understanding of Brown or “Beige” Adipocyte Physiology. Adv Tech Biol Med, 3(2). doi: http://dx.doi.org/10.4172/2379-1764.1000128
2. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2018). Advances in BAT physiology for understanding and translating into Pharmacotherapies for obesity and comorbidities. MOJ Drug Des Develop Ther, 2(5), 166‒176. doi: 10.15406/mojddt.2018.02.00057
3. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2015). An Update on Microrna’s and Metabolic Regulation with Future Therapeutic Potentials Regarding Diagnosis and Treatment of Obesity, Metabolic Syndrome and Other Related Disorders. J HealthMed Informat, 6, 184. doi: 10.4172/2157-7420.1000184
4. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2016). “An Update on a Etiopathogenesis and Management of Obesity”. Obesity and Control Therapies, 3(1), 1-17. doi: http://dx.doi.org/10.15226/2374-8354/2/2/00123
5. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2017). An Update on Etiopathogenesis and Management of Type 1 Diabetes Mellitus. J Endocrinol, 1(2), 1-23.
6. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2017). A Review of Nutrient Metabolism in Obesity with Special Emphasis on Fatty Acid Metabolism. BAOJ Food Sci & Tec, 1, 1.
7. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2018). Existing and prospective pathways for intervention in treatment of obesity in a novel way‒a review. MOJ Drug Des Develop Ther, 2(3), 95‒105. doi: 10.15406/mojddt.2018.02.00035
8. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2018). Weight Loss Associated with High Protein Diet Intake in Obesity: Interactions of Gut Microbiota in Protein Sources Influencing this Positive Effect”. Acta Scientific Nutritional Health, 2(7), 80-89.
9. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2019). Importance of simultaneous treatment of obesity and diabetes mellitus: A sequelae to the understanding of diabesity-A review. Obes Res Open J, 6(1), 1-10. doi: 10.17140/OROJ-6-136
10. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2019).

15
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
Have Probiotics and Synbiotics passed the test of time to be implemented in management of obesity and related metabolic disorders-a comprehensive review. Adv Obes Weight Manag Control, 9(1), 21‒28.
11. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2020). The association of dietary fatty acids and gut microbiota alterations in the development of neuropsychiatric diseases: A systematic review. Obes Res Open J, 7(1), 19-45. doi: 10.17140/OROJ-7-143
12. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2020). Attempting Getting Insulin Independent Immunotherapies in Type 1 Diabetes Mellitus (T1D) in the PreStage 1 (BeforeIslet Autoantibodies)”. Acta Scientific Paediatrics, 3(6), 01-04.
13. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2020). Path Directed towards a Stage when we almost Cure Type1 Diabetes Mellitus (T1dm) after a Century of Insulin Advent”. EC Diabetes and Metabolic Research, 4(6), 37-46.
14. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2021). Are we any close to unraveling the mechanisms of interactions among Susceptibility genes towards type 1 Diabetes, Gut Microbiota along with Environmental factors –Specifically Early Diet patterns –A Systematic Review. Endocrinology and Surgical Endocrinology, 2(1), 1-20. doi: http;//doi.org/03.2021/1.1005
15. Kulvinder Kochar Kaur, Allahbadia GN, Singh M (2020). Utilization of Extracellular Vesicles for Treatment of Type 1 Diabetes Mellitus (T1DM) Along with Type 2 Diabetes Mellitus (T2DM) besides Complications Associated with Diabetes- A Systematic Review. J Clin Diabetes Obes, 1, 001-013. doi: 10.47755
16. GBD2015. Disease and injury incidence and Prevalence Collaborators. Global, regional, and national incidence, Prevalence and years lived with disability for310 Diseases and injuries.1990-2015, a systematic analysis for the Global burden of Disease study 2015.Lancet, 388, 1545-602.
17. Mobasseri M, Shirmohammadi M, Amiri T, Vahed N, Hosseini Fard H, Ghoja zadeh M (2020). Prevalence and incidence of type1 diabetes mellitus in the world: a systematic review and meta-analysis. Health Promot Perspect, 10, 98-115.
18. DeiCas A, Fonarow GC, Gheorghiade M, Butler J (2015). Concomitant diabetes mellitus and heart failure. Curr Probl Cardiol, 40, 7-43.
19. Butler J, Kalogeropoulos AP, Georgiopoulos VV, Bibbins Domingo K, Najjar SS, Sutton Tyrrell KC et al (2011). Systolic blood pressure and incident heart failure in the elderly. The cardiovascular health study and the health, ageing and body composition study. Heart, 97, 1304-11.
20. He J, Ogden LG, Bazzano LA, Vupputuri S, Loria C, Whelton PK (2001). Risk factors for congestive incident heart failure in US men and women: NHANESI epidemiologic follow up study. Ann Intern Med, 161, 996-1002.
21. Matsushita K, Blecker S, Pazin –Filho A, Bertoni A, Chang PP, Coresh J et al (2010). The association of hemoglobin
A1 C with incident heart failure among people without diabetes: the Atherosclerosis risk in communities study. Diabetes, 59, 2020-6.
22. Aune D, Schlesinger S, Neuen schwander M, Feng T, Janszky I, Noral T et al (2018). Diabetes mellitus, blood glucose and the risk of heart failure: A systematic review and meta-analysis of prospective studies. Nutr Metab Cardiovasc Dis, 28, 1081-91.
23. Bozkurt B, Aguilar D, Deswal A, Dunbar SB, Francis GS, Horwich T et al (2016). American heart association heart failure and transplantation committee of the council on Clinical cardiology, council on cardiovascular surgery and anaesthesia, council on cardiovascular and stroke nursing, council onhypertension and council on quality and outcomes research, contributory risk and management of co morbidities of hypertension, obesity, diabetes, and metabolic syndrome in chronic heart failure, a scientific statement from the American heart association. Circulation, 134, e535-78.
24. Al Jarallah M, Rajan R, AlZ akwani I, Dashti R, Bulbanat R, Ridha M et al (2020). Mortality and morbidity in HFrEF, HFmEF, HFpEF patients with diabetes in the middle east. Oman Med J, 35, e99.
25. Sandesara PB, O’Neil WT, Kelli HM, Samman-Tahhan A, Hammadah M, Quyyami AA et al (2018). The prognostic significance of Diabetes and micro vascular complications in patients with heart failure and preserved ejection fraction. Diabetes Care, 41, 150-5.
26. Nagarajan v, Kohan I, Holland E, Keeley EC, Mazimba S (2016). Obesity paradox in heart failure: a heavy matter. ESC Heart Fail, 3, e227-34.
27. Mahajan R, Strokes M, Elliot A, Munawar DA, Khokhar KB, Thiyagarajah A et al (2020). Complex interaction of Obesity, intentional weight loss and heart failure: a systematic review and meta-analysis. Heart, 106, 58-68.
28. Iorio A, Senni M, Barbati G, Greene SJ, Poli SA, Zambon E et al (2018). Prevalence and prognostic impact of noncardiac co morbidities in heart failure out patients with preserved and reduced ejection fraction:a community based study. Eur J Heart Fail, 20, 1257-66.
29. Park HK, Kwak MK, Kim HJ, Ahima RS (2017). Linking resistin, inflammation and cardio metabolic diseases. Korean J Intern Med, 32, 239-47.
30. Yazizadeh H, Setayesh I, Askarpoor M, Pooyan S, Sajjadi SF, Badrooj N et al (2020). Principal component analysis of adipocytokines and insulin associate with risk factors of cardiovascular diseases. BMC Res Notes, 13, 212.
31. Basma H, Johanson AN, Dhar K, Anderson D, Qiu F, Rennard S et al (2019). TGF-β induces a heart failure pheno type via fibroblast exosome signaling. Heliyon, m5, e02633.
32. Berezin AE, Berezin AA (2020). Extracellular endothelial cells-derived vesicles: emerging role in cardiac and Vascular remodeling in heart failure. Front Cardiovasc Med, 7, 47.
33. Montanari T, Poscic N, Collitti M (2017). Factors involved in white to brown adipose tissue conversion and in thermogenesisa review. Obes Rev, 18, 495-513.

16
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
34. Berezin AE, Berezin AA, Lichtenaur M (2020). Emerging role of adipocytes dysfunction in inducing heart failure among obese patients with pre diabetes and known diabetes mellitus. Front Cardiovasc Med, 583175.
35. Pahlavani M, Kalupahana NS, Ramalingam I, Moustaid-Moussa N (2017). Regulation and functions of the Renin-Angiotensin-aldosterone System in White and brown adipose tissue. Compr Physiol , 7, 1, 137-50.
36. Chopra I, Li HF, Wang H, Webster KA (2012). Phosphorylation of the insulin receptor by AMP-activated protein kinase (AMPK)-promotes ligand independent activation of the insulin signaling pathway in rodent muscles. Diabetologia, 55, 783-94.
37. Saely CH, Geiger K, Drexel H (2012). Brown versus White adipose tissue: a mini review. Gerontology, 58, 15-23
38. Kaisanlahti A, Glumofft (2019). Browning of White fatand implications for beige adipose tissue in type 2 diabetes mellitus. J Physiol Biochem, 75, 1-10.
39. Lo KA, Sun L (2013). Turning WAT into BAT: A review on regulators controlling the White and Brown adipocytes. Biosci Rep, 33, e00065.
40. Fenzl A, Kiefer FW (2014). Brown adipose tissue and thermogenesis. Horm Mol Biol Clin Invest, 19, 12-37.
41. Jankovic A, Golic I, Markelic M, Stancic A, Otasevic V, Buzadzic B et al (2015). Twokey temporally distinguishable molecular and cellular components of White adipose tissue browning during cold acclimation. J Physiol, 593, 3267-80.
42. Lu H, Cassis LA, Kool CW, Daugherty A (2016). Structure and functions of angiotensinogen. Hypertens Res, 39, 492-500.
43. Bahler L, Holleman F, Booij J, Hoekstra JB, Verberne HJ (2017). Hot head sand cool bodies: the conundrums of human Brown adipose tissue (BAT)activity research. Eur J Intern Med, 40, 26-9.
44. Vijgen GH, Bouvy ND, Teule GJ, Brans B, Schrauwen P, Van Marken Lichtenbelt WT (2011). Brown adipose tissue in morbidly obese patients. PLoS ONE, 6, e17247.
45. Rao VN, Zhao D, Allison MA, Guallar E, Sharma K, Criqui MH et al (2018). Adiposity and incident heart failure and its subtypes: MESA (Multiethnic study of Atherosclerosis. JACC Heart Fail, 6, 999-1007.
46. Wu CK, Lee JK, Hsu JC, Su MM, Wu YF, Lin TT et al (2020). Myocardial adipose deposition and the development of Heart Failure with preserved ejection fraction. Eur J Heart Fail, 22, 445-54.
47. Kruger M, Babicz K, Von Frieling Salewsky M, Linke WA (2010). Insulin signaling regulates cardiac titin properties in Heart development and diabetic cardiomyopathy. J Mol Cell Cardiol, 48, 910-16.
48. Fukuda N, Terui T, Ishiwata S, Kurihara S (2010). Titin based regulations of diastolic and systolic functions of mammalian cardiac muscle. J Mol Cell Cardiol, 48, 876-81.
49. Van Hweerebeek L, Hamdani N, Falcao Pires I, Beigineman MP, Bronzwaer JG et al (2012). Low Myocardial protein kinase G activity in Heart Failure with preserved ejection
fraction. Circulation, 126, 830-9. 50. Hamdani N, Bishu KG, Von –Frieling Salewsky M,
Redfield MM, Linke WA (2013). Deranged myofilament phosphorylation and function in experimental heart failure with preserved ejection fraction. Cardiovasc Res, 97, 464-71.
51. Borbely A, Falcao Pires I, Van Hweerebeek L, Hamdani N, Edis I, Gavina C et al (2009). Hypo phosphorylation of the Stiff N2B titin isoforms raises cardiomyocyte resting tension in failing human Myocardium. Cardiovasc Res, 104, 780-6.
52. Careman M, Pinzauti F, Powers JD, Governali S, Naraynan T, Stienen GJM et al (2019). Inotropic interventions do change the resting state of myosin motors during cardiac diastole. J Gen Physiol, 151, 53-65.
53. Cinti S (2018). Adipose organ development and remodeling. Compr Physiol, 8, 1357-431.
54. Kotzbeck P, GiordanoA, Mondini E, Murano I, Severi I, Venema W et al (2018). Brown adipose tissue whitening leads to Brown adipocyte death and adipose tissue inflammation. J Lipid Res, 59, 784-94.
55. Appari M, Channon KM, Mcneil E (2018). Metabolic regulation of adipose tissue macrophages function in obesity and diabetes. Antioxid Redox Signal, 29, 97-312.
56. Ghosh EE, Cassado AA, Govoni GR, Fukuhara T, Yang Y, Monack DM et al (2010). Two physically, functionally and developmentally distinct peritoneal macrophage subsets. Proc Natl Acad Sci USA, 107, 2568-73.
57. Esser N, Legrand-Poels S, Piette J, Scheen AJ, Paquot N (2014). Inflammation as a link between obesity, Metabolic syndrome and type2 diabetes. Diabetes Res Clin Pract, 105, 41-50.
58. Parmeswaran N, Patial S (2010). Tumor necrosis factor alpha signaling in macrophages. Crit Rev Eukaryot Gene Expr, 20, 87-103.
59. Engin AB (2017). Adipocyte- macrophage cross talk in obesity. Adv Exp Med Biol, 960, 327-43.
60. Serbulea V, Upchurch CM, Schappe MS, Voigt P, DeWeese DE, Desai BN et al (2018). Macrophage phenotype and bioenergetics are controlled by oxidized phospholipids defined in lean and obese adipose tissue. Proc Natl Acad Sci USA, 115, E6254-63.
61. Liu K, Zhao E, Ilyas G, Lalazar G, Lin Y, Haseeb M et al (2015). Impaired Macrophage autophagy increases the immune response in obese mice by promoting proinflammatory macrophage polarization. Autophagy, 11, 271-84.
62. Zhang Y, Bose T, Unger RE, Jansen JA, Kirkpatrick CJ, VanDen Beucken JJJP (2017). Macrophage type modulates osteogenic differentiation of adipose tissue MSC’s. Cell Tissue Res, 369, 273-86.
63. Zhu F, Wang A, Li Y, Liang R, Li D, Li B (2017). Adipose tissue resident regulatory T cells. Adv Exp Med Biol, 1011, 153-62.
64. Ouchi N, Parker L, Lugus JJ, Walsh K (2011). Adipokines in inflammation and metabolic disease. Nat Rev Immunol, 11, 85-97.
65. Tang LL, Tang XH, Li X, Yu HB, Xie ZG, Liu XY et al

17
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
(2014). Effect of high fat or high glucose diet on obesity and visceral adipose tissue in mice. Zhongguo Yi Xue Ke Xue Yuan Xue Bao, 36, 614-9.
66. Jaiswal A, Reddy S, Maurya M, Maurya P, Barthwal MK (2019). Micro RNA-99a mimics inhibit M1 Macrophage phenotype and adipose tissue inflammation by targeting TNFα. Cell Mol Immunol, 16, 495-507.
67. Periyalil HA, Wood LG, Wright TA, Karihaloo C, Staarkey MR, Miu AS et al (2007). Obese asthmatics are characterized by altered adipose tissue Macrophage activation and improves insulin resistance. Nature, 447, 1116-20.
68. Guzik TJ, Skiba DS, Touyz RM, Harrison DG (2017). The role of infiltrating immune cells in dysfunctional adipose tissue. Cardiovasc Res, 113, 1009-23.
69. Seijkens T, Kusters P, Chatzigeorgiou A, Chakris T, Lutgens E (2014). Immune cells crosstalk in obesity:a key role for co stimulation. Diabetes, 63, 3982-9.
70. Kintscher U, Hartge M, Hess K, Foryst-Ludwig A, Clemenz M et al (2008). T-Lymphocytes infiltration in visceral adipose tissue:a primary event in adipose tissue inflammation and the development of obesity mediated insulin resistance. Arterioscler Thromb Vasc Biol, 28, 1304-10.
71. Korn T, Betelli E, Oukka M (2009). Kuchroo VK.IL-17 and Th17cells. Annu Rev Immunol, 27, 485-517.
72. Shi G, Ramaswamy M, Vistica BP, Cox CA, Tan C et al (2009). UnlikeTh1, Th17cells mediate sustained autoimmune inflammation and are highly resistant to restimulation induced cell death. J Immunol, 183, 7547-56.
73. Jung C, Lichtenaur M, Strodthoff D, Winkels H, Wernly B et al (2017). Alterations in systemic levels of Th1, Th2 and Th17 cytokines in overweight adolescents and obese mice. Pediatr Diabetes, 18, 714-21.
74. Berezin AE (2014). Diabetes mellitus and cellular replacement therapy: expected clinical potential and perspectives. World J Diabetes, 5, 777-86.
75. Kanemastu Y, Kanemastu M, Kurihara C, Tada Y, Tsou TL, Van Rooijen N et al (2011). Critical roles of macrophages in the formation of intracranial aneurysm. Stroke, 42, 173-8.
76. Berg AH, Scherer PE (2005). Adipose tissue, inflammation and cardiovascular disease. Circ Res, 96, 939-49
77. Longo M, Zatterale F, Naderi J, Parrilo L, Formisano P, Raciti GA et al (2019). Adipose tissue dysfunction as determinants of obesity associated metaboliscomplications. Int J Mol Sci, 20, 2358.
78. Lee YS, Kim JW, Osborne O, Oh DY, Sasik R, Schenk S et al (2014). Increased adipocyte O2 consumption triggers HIF 1 causing inflammation and insulin resistance in obesity. Cell, 157, 1339-52.
79. Muir LA, Neeley CK, Meyer KA, Baker NA, Brosius AM, WashabaughAR et al (2016). Adipose tissue fibrosis, hypertrophy, and hyperplasia correlation with Diabetes in human obesity. Obesity, 24, 597-605.
80. Stepien E, Costa MC, Kurc S, Drosdz A, Cortez-Dias N, Enquita FJ (2018). The circulating long non coding RNA
landscape for biomarker research: lessons and prospects from cardiovascular diseases. Acta Pharmacol Sin, 39, 1085-99.
81. Kobayashi Y, Eguchi A, Tempaku M, Honda T, Togashi K, Iwasa M et al (2018). Circulating extracellular vesicles are associated with lipid and insulin metabolism. Am J Physiol Endocrinol Metab, 315, E574-82.
82. Zhou Y, Tan C (2020). mi RNA in Adipocyte-derived extracellular vesicles: multiple roles in development of obesity- associated- diseases. Front Mol Biosci, 7, 171.
83. Eguchi A, Lazic M, Armando AM, Phillips SA, Katebian R, Maraka S et al (2016). Circulating Adipocyte-derived extracellular vesicles are novel, markers of metabolic stress. J Mol Med, 94, 1241-53.
84. Tang R, Long T, Lui KO, Chen Y, Huang ZP (2020). A roadmap for fixing the heart: RNA regulatory networks in cardiac disease. Mol Ther Nucleic Acids, 20, 673-86.
85. Shehzad A, Iqbal W, Shehzad O, LeeYS (2012). Adiponectin: Regulation of its production and its role in human diseases. Hormones, 11, 8-20.
86. Kadowaki T, Yamuchi T (2005). Adiponectin and Adiponectin Receptors. EndocrRev, 26, 439-51.
87. Yamuchi T, Kadowaki T (2008). Physiological and pathophysiological role of Adiponectin and Adiponectin Receptors in the integrated Regulation of metabolic and cardiovascular diseases. Int J Obese, 32(Suppl 7), S13-S18.
88. Ouchi N, Walsh K (2007). Adiponectin As an antiinflammatory factor. Clin Chim Acta, 380, 24-30.
89. Heidemann C, Sun Q, Van dan RamRM, Meigs JB, Zhang C, Tworoger SS et al (2008). Total and high adiponectin and resistin in relation to the risk for type 2 diabetes in women. Ann Intern Med, 149, 307-16.
90. Nigro E, Schudiero O, Monaco ML, Mazzarella G, Costagliola C et al (2014). New insights into Adiponectin role in obesity and obesity-related diseases. BioMed Res Med, 2014, 658913.
91. De Rosa A, Monaco ML, Forestieri P, Pilone V, Nardelli C et al (2013). Adiponectin oligomers as as potential indicators of adipose tissue improvement in obese subjects. Eur J Endocrinol, 169, 37-43.
92. Hashimoto N, Kanda J, Nakamura T, Horis A, Kurosawa H, Hashimoto T et al (2006). Association between Adiponectin and early heart disease and multiple coronary heart stenosis. Metabolism, 355, 1653-7.
93. Djousse L, Wilk JB, Hanson NQ, Glynn RJ, Tsai MY, Gaziano JM (2013). Association of hypo Adiponectinemia in men and Heart Failure risks in the physician’s health study. Obesity, 21, 831-4.
94. Karas MG, Benkeser S, Arnold AM, Batz TM, Djousse L, Mukamal KJ et al (2013). Relations of plasma total and high molecular weight Adiponectin to new onset Heart Failure in adults≥65 years of age (from the cardiovascular health study. Am J Cardiol, 113, 28-34.
95. Frankel DS, Vasan RS, D’Agostino RBSr, Benjamin EJ, Levy D, Wang TJ et al (2009). Resistin and adiponectin, and risk of Heart Failure: The Framingham offspring heart study. J Am Coll Cardiol, 53, 74-62.

18
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
96. Van Berendoncks AM, Garnier A, Ventura –Clapier R,Conraads VM (2013). Adiponectin: key role and potential targets to reverse energy wasting in chronic Heart Failure. Heart Fail Rev, 18, 557-66.
97. Shibata R, Ouchi N, Murohara T Adiponectin and cardiovascular disease (2009). Circ J, U73, 608-14.
98. Van Berendoncks AM, Garnier A, Beckers P, Hoymans VY, Possemeirs N, Fortin D et al (2011). Exercise training reverses Adiponectin Resistance in skeletal muscles of patients with chronic Heart Failure. Heart, 97, 1403-9
99. Inglesson R, Riserus U, Berne C, Frystyk U, Flyvjberg a, Axelsson T et al (2006). Adiponectin and risk of congestive Heart Failure. JAMA, 295, 1772-4.
100. Antonopoulos AS, Margritis M, Coutinho P, Digby J, Patel R, Psarros C et al (2014). Reciprocal effects of systemic inflammationand brain natriuretic peptideon Adiponectin biosynthesis in adipose tissue of patients with ischaemic heart disease. Arterioscler Thromb Vasc Biol, 34, 2151-9.
101. Iwabu M, Yamuchi T, Okada- Iwabu M, Sato K, Nakagawa T, Funata M et al (2010). Adiponectin and AdipoR1 by PGC-1 alpha and mitochondria by Ca2+ and AMPK/SIRT. Nature, 464, 1313-9
102. Wang X, Hu Z, Hu J, Du J, Mitch WE (2006). Insulin resistance accelerates muscle protein degradation: activation of ubiquitin proteasome pathway by defects in muscle cell signaling. Endocrinology, 147, 4160-8
103. Stefan N, Vozarova B, Funa hashi T, Matsuzawa Y, Weyer C, Lindsay RC et al (2002). Plasma Adiponectin concentration is associated with skeletal muscle insulin Receptor tyrosine phosphorylation and low Plasma concentration precedes a decrease in whole body insulin sensitivity in humans. Diabetes, 51, 1884-8.
104. Qiao L, Kinney B, YooHS, LeeB, Schaak K (2012). Adiponectin increases skeletal muscle mitochondrial biosynthesis by suppressing mitogen Activated protein kinase phosphatase1. Diabetes, 61, 1463-70.
105. Szabo T, Scher bakov N, Sandek A, Kung T, Von Haehling S, Lainscak M et al (2014). Plasma Adiponectin in heart failure with and without cachexia: catabolic signal linking catabolism, symptomatic, status and prognosis. Nutr Metab Cardiovasc Dis, 24, 50-6.
106. Krause MP, Liu Y, Vu V, Chan L, Xu A, Riddell MC et al (2008). Adiponectin is expressed by skeletal muscle fibers and influences muscle phenotype and function. Am J Physiol Cell Physiol, 295, C203-12.
107. Zhang Y, Chua SJr (2017). Leptin function and regulation. Compr Physiol, 8, 351-69.
108. Triantafyllou GA, Paschou SA, Mantzoros CS (2016). Leptin and hormones: energy homeostasis. Endocrinol Metab ClinNorth Am, 45, 633-45.
109. Farr OM, Gavrieli A, Mantzoros CS (2015). Leptin applications in 2015: what have we learned about Leptin and obesity. Curr Opin Endocrinol Diabetes Obes, 22, 353-9.
110. Reid IR, Baldock PA, Cornish J (2018). Effects of Leptin on skeleton. Endocr Rev, 39, 938-59.
111. Wabitsch M, Funcke JB, Lennerz B, Kuhnle –Krahl U, Debatin KM et al (2015). Biologically inactive Leptin and
early onset extreme obesity. N Engl J Med, 372, 48-54112. Lord GM, Matarese G, Howard JK, Baker RJ, Bloom
SR, Lechler RJ (1998). Leptin modulates the T Cells immune response and reverses starvation –induced immunosuppression. Nature, 394, 897-901.
113. Feijoo-Bandin S, Portoles M, Rosello –Lleti E, Rivera M, Gonzalez-Juanatey JR, Lago F (2015).20years of Leptin: role of Leptin in Cardiomyocyte physiology and physiopathology Life Sci, 140, 10-8.
114. Dobaczewski M, Frango giannis NG (2011). The cellular specificity of leptin mediated action in the infarcted heart. Cardiovasc Res, 89, 9-11.
115. William W, Yester K, O’Donnell CP, McGaffin KR (2012). Restoration of glucose metabolism in leptin resistant mouse hearts after patients through the activation of survival kinase pathways. J Mol Cell Cardiol, 53, 91-100.
116. Zabeau L, Wauman J, Dam J, Van Lint S, Burg E, DeGeest J et al (2019). A novel leptin Receptors antagonist uncouples leptin’s metabolic and immune functions. Cell Mol Life Sci, 76, 1201-14.
117. Kamimura D, Suzuki D, Wang W, DeShazo M, Hall JF, Winniford MD et al (2018). Higher Plasma leptinlevels are associated with reduced left ventricular mass and left ventricular diastolic stiffness in black women: insights from genetic epidemiology network of arteriopathy(GENOA) Study. Hypertens Res, 41, 629-38.
118. Packer M (2018). Do Sodium –glucose cotransporter 2 inhibitors prevent Heart Failure with a preserved ejection fraction by counterbalancing the effects of leptin? a novel hypothesis. Diabetes Obes Metab, 20, 1361-6.
119. Packer M (2018). Leptin - aldosterone-neprilysin axis: identification of the distinctive role of in the pathogenesis of the three phenotypes of Heart Failure in people with obesity. Circulation, 137, 1614-31.
120. Shimada YJ (2019). Is Leptin protective against Heart Failure with preserved ejection fraction? a complex interrelationship among Leptin, obesity, and left ventricular hypertrophy. Hypertens Res, 42, 141-2.
121. Karmazyn M, Raja purohitam V (2014). Leptin asa cardiac pro-hypertrophic factor and its potential role in the development of Heart Failure. Curr Pharm Dis, 20, 646-51.
122. Bhalla V, Kalogeropoulos G, Georgi opoulos V, Butler J (2010). Serum resistin: Physiology pathophysiology and implications for Heart Failure. Biomark Med, 4, 445-52.
123. au WB, Ohashi K, Wang Y, Ogawa H, Murohara T, Ma XL et al (2017). Role of Adipokines in cardiovascular disease. Circ J, 81, 920-8.
124. Acquarone E, Monacelli E, Borghi R, Nencioni A, Oderi P (2019). Resistin: A Reappraisal. Mech Ageing Dev, 178, 46-63.
125. Zhang MH, Na B, Schiller NB, Whooley MA (2011). Association of resistin with Heart Failure: data from the heart and soul study. J Card Fail, 17, 24-30.
126. Muse ED, Feldman DI, Blaha MJ, Dardari ZA, Blumenthal RS, Budoff MJ et al (2015). The Association of resistin with cardiovascular diseasein the multi-ethnic study of Atherosclerosis. Atherosclerosis, 239, 101-8.

19
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
127. Saeedi Borujeni MJ, Esfandiary E, Taheripak G, Codoner Franch P, Alonso-Iglesias E, Mirzael H (2018). Molecular aspects of Diabetes mellitus, Resistin, microRNA and exosome. J Cell Biochem, 119, 1257-72.
128. Turgay Yildirim O, Yildirir A, Sade LE, Has Hasirci S, Kozan H, Ozcalik E et al (2018). Ia there a relationship between Resistin levels and left ventricular end diastolic pressure? Anatol J Cardiol, 19, 267-72.
129. Baldasseroni S, Mannucci E, DeSerio C, Orso F, Bartoli N, Mosello E et al (2013). Resistin level in coronary artery disease and heart Failure: the central role of kidney function. J Cardiovasc Med, 14, 150-7.
130. Bobbert P, Jenke A, Bobbert T, Kuhl U,Rauch U, Lassner D et al (2012). High Leptin and Resistin expression in chronic Heart Failure: Adverse outcomes in patients with dilated and inflammatory cardiomyopathy. Eur J Heart Fail, 14, 1265-75.
131. Cheng M, Akkerhuis KM, Battes LC, Van Vark LC, Hillege HL, Paulus WJ et al (2013). Biomarkers of Heart Failure with normal ejection fraction; a systematic review. Eur J Heart Fail, 15, 1350-62.
132. Brankovic M, Akkerhuis KM, Mouthaan H, Brugts JL, Maninveld OC, Ramshorst J et al (2018). Cardiometabolic biomarkers of Heart Failure and their temporal patterns predict poor outcome in chronic Heart Failure (BioSHiFT)Study. J Clin Endocrinol Metab, 103, 3954-64.
133. Ho YL, Lin YH, Lee CM, Hsu RB, Ting HT, Chou NK et al (2009). Prognostic significance of adipocytokines and extracellular matrix activity in Heart Failure patients with high B type natriuretic peptide. Clin Biochem, 42, 1407-12.
134. Kaplon –Clepslicka A, Tyminska A, Rosiak M, Ozieranski K, Peller M, Eyileten C et al (2019). Resistin is a Prognostic factor for death in type2 Diabetes. Diabetes Metab Res Rev, 35, e3098.
135. Carbone F, Liberale L, Bonaventura A, Vecchie A, Casula M, Cea M et al (2017). Regulation and function of extracellular nicotinamide phosphoribosyltransferase/ visfatin. Compr Physiol, 7, 603-21.
136. Svoboda P, KriZova E, Cenkova K, Vapenkova K, Zidkova J, Zidek V et al (2017). Visfatin is actively secreted in vitro from U-937 macrophages but only passively released from 3T3-L1 adipocytes and HepG2 hepatocytes. Physiol Res, 66, 709-14.
137. Li B, Zhao Y, Liu H, Meng B, Wang J, QiT et al (2016). Visfatin destabilizes Atherosclerotic plaques in apolipoprotein E-deficient mice. PLoS ONE, 11, e0148273.
138. Dimitradis GK, Adya R, Tan BK, Jones TA, Menon VS, Ramajaneya M et al (2019). Effects of Visfatinon brown adipose tissue energy regulation using T37i cells. Cytokine, 113, 248-55.
139. Radzica S, Piettryga M, Iciek R, Brazert J (2018). The role of Visfatin in gestational diabetes mellitus (GDM). Ginekol Pol, 89, 518-21.
140. Qu S, Mo L, Niu Y, Sun X, Li H, Wang Z et al (2016). Expression of Visfatin in the diabetic rat retina. ClinExp Ophthalmol, 44, 251-9.
141. Sun L, Chen S, Gao H, Ren L, Song G (2017). Visfatin induces the apoptosis of endothelial progenitor cells via the induction of proinflammatory mediators through the NFκB pathway. Int J Mol Med, 40, 637-46.
142. Kumari B, Yadav UCS (2018). Adipokine Visfatin’s role in the pathogenesis of diabesity and related metabolic derangements. Curr Mol Med, 18, 116-25.
143. Kocelak P, Olszanecka-Glini anowicz M, Owczarek AJ, Krupa W, Obirek P, Bozentowicz –Wikarek M et al (2015). Plasma visfatin/nicotinamide phosphoribosyltransferase (visfatin/NAMPT) concentration in dearly subjects with metabolic syndrome. Pol Arch Med Wewn, 125, 402-13.
144. Hung WC, YuTH, Hsu CC, Lu LF, Chung FM, Tsai IT et al (2015). Plasma visfatin levels are associated with major cardiovascular events in patients with acute ST elevation myocardial infarction. Clin Invest Med, 38, E100-9.
145. Wu XA, Xie G, LiXQ, Wu HT, Wang X (2018). The value of serum Visfatinin predicting in-stent restenosis of drug –eluting stents. Clin Chem Acta, 479, 20-24.
146. Wang X H, Dou LZ, Gu C, Wang XQ (2014). Plasma levels of Omentin 1 and visfatinin senile patients with) coronary artery disease and Heart Failure. Asian Pac J Trop Med, 55-62.
147. Diguet N, TrammellSAJ, Tannous C, Deloux R, Piquereau J, Mougenot N et al (2018). Nicotinamide Riboside prevents cardiac function in a mouse model of dilated cardiomyopathy. Circulation, 137, 2256-73.
148. Straburzyriska –Migaj E, Pilaczynska –Szczesniak I, Nowak A, Straburzyriska-Lupa A, Silwica E, Grajek S (2012). Serum concentration of visfatin is decreased in patients with chronic Heart Failure. Acta Biochim Pol, 59, 339-43.
149. Watanabe T, Watanabe-Kominato K, Takahashi Y, Kojima M, Watanabe R (2017). Adipose tissue-derived Omentin 1 function and regulation. Compr Physiol, 7, 765-81.
150. Escote X, Gomez-Zorita S, Lopez –Yoldi M, Milton-Laskibar I, Fernandez –Quintela A, Martinez JA et al (2017). Role of Omentin, vaspin, cardiotrophin-1, TWEAK and NOV/CCN3 in obesity and Diabetes development. Int J Mol Sci, 18, 1770.
151. Li F, Pang LZ, Zhang I, Zhang Y, Zhang YY, Yu BY et al (2019). Yi1QiFuMai powder injection ameliorates chronic Heart Failure through crosstalk between adipose tissue and cardiomyocyte via up regulation of circulating adipokine Omentin. Bio Med Pharmacotherap, 119, 109418.
152. Watanabe K, Watanabe R, Konii H, Shirai R, Sato K, Matsuyama TA et al (2016). Counteractive effects of Omentin 1 against atherogenesis. Cardiovasc Res, 110, 118-28.
153. Menzel J, DiGiuseppe R, Biemann R, Witten becher C, Aleksandrova K, Eichelmann F et al (2017). Association between chimerin, Omentin 1 and risk of Heart Failure in the population-based EPIC-Potsdam study. Sci Rep, 7, 14171.
154. Jiang H, Zhao G, Li X, Jin H, Yang G, Jin K et al (2017). Association between Omentin and echopatterns in patients with Heart Failure. Minerva Cardioangiol, 65, 8-15.
155. Agra –Bermejo RM, Gonzalez-Ferreiro R, Lopez-Canoa

20
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
JN, Varela-Roman A, Gomez-Otero I, Eiras S et al (2019). Long term weight gain is associated with high Omentin 1 levels at hospital discharge improves prognosis of patients following acute Heart Failure. J Cardiovasc Transl Res, 12, 231-9.
156. Wei X, Liu X, Tan C, Mo L, Wang H, Peng X et al (2019). Expression and function of zinc—α-2glycoprotein. Neurosci Bull, 35, 540-50.
157. Zahid H, Miah L, Lau AM, Brochard L, Hati D, Bui TT et al (2016). Zinc induced polymerization of Zinc—α-2glycoprotein reveals multiple fatty acid binding sites. Biochem J, 473, 43-54.
158. Ebrahim E, Kheirouri S, Alizadeh M (2017). Down regulation of S100A1 protein in patients with metabolic syndrome and its e association with Zinc—α-2glycoprotein. Scott Med J, 62, 88-95. Positive
159. Severo JS, Morais JBS, Bessera JB, Dos Santos LR, De SousaMelo SR, De Sousa JS et al (2020). Role of Zinc in Zinc—α-2glycoprotein metabolism in obesity: A review of literature. Biol Trace Elem Res, 193, 81-88.
160. Liu Y, Wang T, Liu X, Wei X, Xu T, Yin M et al (2017). Neuronal Zinc—α-2glycoprotein is decreased in temporal lobe epilepsy in patients and rats. Neuroscience, 357, 56-66.
161. Bilovol OM, Knyazkova II, Al-Travneh OV, Bogun MV, Berezin AE (2020). Altered adipocytokine profile predicts early stage of left ventricular remodeling in hypertensive patients with type2 Diabetes mellitus. Diabetes Metab Syndr, 14, 109-16.
162. Moschen AR, Adolph TE, Gerner RR, Wieser V, Tilg H (2017). Lipocalin 2: A master mediator of intestinal and metabolic inflammation. Trends Endocrinol Metab, 28, 388-97.
163. Cowland JB, Muta T, Borregard N (2006). IL-1beta specific up regulation of neutrophil gelatinase-associated Lipocalin is controlled by Ikappa –B-zeta. J Immunol, 176, 5559-66.
164. Law IK, Xu A, Lam KS, Berger T, Mak TW, Vanhoutte PM et al (2010). Increased adipose tissue expression of Lipocalin 2 in obesity is related to inflammation and matrix metalloproteinase -2 and metalloproteinase -9 activities in humans. Diabetes, 59, 872-82.
165. Marques FZ, Prestes MR, Byars SG, Ritchie SC, Wurtz P, Patel SK et al (2017). Experimental and human evidence for Lipocalin 2(neutrophil gelatinase-associated Lipocalin) [NGAL]in the development of cardiac hypertrophy and Heart Failure. J Am Heart Assoc, 6, e005971.
166. Song E, Jahng W, Chong LP, Sung HK, Han M, Luo C et al (2017). Lipocalin 2 induces NLRP3 inflassome activation via HMGB1induced TLR4 signaling in Heart tissue of mice under pressure overload challenge. Am J Transl Res, 9, 2723-35.
167. Ahmad T, Jackson K, Rao V, Tang WHW, Brisco-Bacic M, Chen HH et al (2018). Worsening renal function in patients with acute Heart Failure undergoing aggressive diuresis is not associated with tubular injury. Circulation, 137, 2016-28.
168. Tabata M, Kadimatso T, Fukuhara S, Miyata K, Ito Y, Endo
M et al (2009). Angiopoietin –Like Protein-2 promotes chronic adipose tissue inflammation and obesity related systemic insulin resistance. Cell Metab, 10, 178-88.
169. Thorin-Trescases N, Thorin E (2014). Angiopoietin –Like 2: A multifaceted Protein- with pathophysiological and pathological properties. Expert Rev Mol Med, 16, e17.
170. Jin X, Guo B, Yan J, Yang R, Chang L, Wang Y et al (2015). Angiopoietin II increases Secreted frizzled – related protein 5(sFRP5) expression through AT1 Receptor/Rho/ROCK/JNK signaling in cardiomyocytes. Mol Cell Biochem, 408, 215-22.
171. Lin H, Angeli M, Chung KJ, Ejimadu C, Rosa AR, LeeT (2016). sFRP5 activates Wnt/β-catenin signaling n cardiac fibroblasts: differential roles in cell growth, energy metabolism and extracellular matrix remodeling. Am J Physiol Cell Physiol, 311, C710-9.
172. Zhu X, Koy M, Schmidt F, Hahn A, Wollersheim T, Kleber C et al (2017). Secreted frizzled – related protein 2 and inflammation induced skeletal muscle atrophy. Crit Care Med, 45, e169-83.
173. Abdomaleki F, Heidarianpour A (2018). The response of serum Glypican 4 levels and its potential regulatory mechanisms to endurance training and chamomile flowers hydroethanolic extract in streptozocin- Nicotinamide-inuced Diabetic rats. Acta Diabetol, 55, 935-42.
174. Harthan LB, McFarland DC Velleman SG (2013). The effect of syndecan 4 and Glypican 4 expression on age –related changes in myogenic satellite cell proliferation, differentiation and blast growth factor 2 responsiveness. Comp Biochem Physiol A Mol Integr Physiol, 166, 590-602.
175. Hu B, Gao Y, Davies L, Woo S, Topczewski J, Jessen JR et al (2018). Glypican 4 and Mmp4 interact in regulating the migration of anterior endodermal cells by limiting extracellular matrix deposition. Development, 145, dev163303.
176. Ning DP, Xu K, Zhu HJ, Shan GL, Wang DM, Ping B et al (2019). Serum Glypican 4 levels are associated with metabolic syndrome in a han population from guizhou province. China Biomed Environ Sci, 32, 383-8.
177. Jed rzejuk D, Lwow F, Kuliczkowska –Plaksej J, Hirnle L, Trzmiel –Bira A, Lenarcic –Kabza A et al (2016). Association of Serum Glypican 4 levels with cardiovascular risk predictors in women with Polycystic ovary syndrome-a pilot study. Gynecol Endocrinol, 32, 223-6.
178. Christensen G, Herum KM, Lunde IG (2019). Sweet yet unappreciated: Proteglycans and extracellular matrix remodeling in Heart disease. Matrix Biol, 75-76,286-99.
179. Lu HY, Li XF, Mu PW, Jiang W, Zeng LY (2010). Depot specific expression of Retinol binding protein-4 in human adipose tissue and their relationship with obesity and insulin resistance. Zhongua Yi Xue Za Zhi, 90, 3395-8.
180. Ulgen F, Herder C, Kuhn MC, Willenberg HS, Schott M, Scherbaum WA et al (2010). Association of Serum levels of Retinol binding protein-4 with male sex but not with insulin resistance in obese patients. Arch Physiol Biochem, 116, 57-62.

21
Volume 2 | Issue 2 I J cardio & card diso; 2021 www.unisciencepub.com
181. Lee DC, Lee JW, Im JA (2007). Association of Serum Retinol binding protein-4 and insulin resistance in apparently healthy adolescents. Metabolism, 56, 327-31.
182. Chavarria N, Kato TS, Khan R, Chokshi A, Collado E, Akashi H et al (2012). Increased levels of Retinol binding protein-4 in patients with advanced Heart Failure correct after haemodynamic improvement through ventricular assist device placement. Circ J, 76, 2148-52.
183. Pedersen BK (2017). Anti inflammatory effects of exercise: role in Diabetes and cardiovascular disease. Eur J Clin Invest, 47, 600-11.
184. Negrusz-Kawecka M, Udzial W (2002). TNFα etiopatogegenezie niewydolnosci serca the role of TNF-alpha in the etiopathogenesis of Heart Failure. Pol Mercur Lekarski, 12, 69-72.
185. Mann DL (2015). Innate immunity and the falling heart: the cytokine hypothesis revisited. Circ J 116, 1254-68.
186. 1arzi –Puttini P, Atzeni F, Scoenfield Y, Ferrancioli G (2005). TNF-alpha, rheumatoid arthritis: A rheumatological dilemma. Autoimmun Rev, 4, 153-61.
187. Mousa SA, Gondcharuk O, Miller D (2007). Recent advances of TNF-alpha, antagonists in rheumatoid arthritisand chronic Heart Failure. Expert Opin Biol Therap, 7, 617-25.
188. Kotyla PI (2018). Bimodal function of anti TNFα treatment: shall we be concerned about anti TNFα treatment in patients with rheumatoid arthritis and Heart Failure. Int J Mol Sci, 19, 1739.
189. Rahman A, Jafry S, Jeejee bhoy K, Nagpal AD, Pisani B, Agarwala R (2016). Malnutrition and cachexia in Heart Failure. JPEN J Parenteral Enterol Nutr, 40, 475-86.
190. Fedacko J, Singh RB, Gupta A, Hristova K, Toda E, Kumar A et al (2014). Inflammatory Mediators in chronic Heart Failure in North India. Acta Cardiol, 69, 391-8.
191. Schumacher SM, Naga Prasad SV (2018). Tumor necrosis factor-α in Heart Failure: An updated review. Curr Cardiol Rep, 2, 117.
192. Chandramouli C, Tay WT, Bamdhaj NS, Trump J, Teng TK, Yap JJL et al (2019). ASIAN –HF Investigators: Association ofobesity with Heart Failure outcomes in 11Asian regions: a cohort study. PLoS Med, 16, e1002916.
193. Tadic M, Cuspidi C (2019). Obesity and Heart Failure with preserved ejection fraction. Heart Fail Rev, 24, 379-85.
194. Lin JL, Sung KT, Lai YH, Yen CH, Yun CH, Su CH et al (2021). Epicardial adiposity in relation to metabolic abnormality, circulating adipocyte FABP and with preserved ejection fraction Heart Failure. Diagnostics, 11, 397.
195. Zhou KN, Sung KT, Sung KT, Yen CH, Su CH, Lee PY, Hung CH et al (2020). Carotid arterial biomechanics as useful biomarkers for extracellular matrix turnover and preserved ejection fraction Heart Failure. ESC Heart Failure, 7, 1615-625.
Copyright: ©2021 Kulvinder Kochar Kaur M.D. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in anymedium, provided the original author and source are credited.
Copyright © 2022 FDOKUMEN