Robotic Minimally Invasive Surgical skill assessment based on automated video-analysis motion...
7
Abstract²Assessment of surgical skill, arising from the synthesis of the cognitive and sensorimotor capabilities of the surgeon, has predominantly been a subjective task. Development of quantitative metrics-of-performance with clinical relevance and other desirable characteristics (repeatability and stability) has always lagged behind. New opportunities for objective and automated assessment frameworks have arisen by virtue of technological advances in computation, video-processing, and data-acquisition, especially in the robotic Minimally Invasive Surgical (rMIS) realm. Most efforts focus on semi-quantitative (Likert scale) or inadequately validated, spatially- or temporally-aggregated quantitative metrics derived from direct physical measurements. In this work we propose an automated surgical expertise evaluation method, by adapting well-established motion studies methodologies, especially for MIS evaluation. This method relies on segmenting a primary task into sub-tasks, which can be evaluated by statistical analyses of micromotions. Motion studies were developed by 2 methods: (A) manual annotation process by experts (to serve as a benchmark); and (B) automated kinematic-analysis-of-videos; for economy, repeatability as well as dexterity. The da Vinci SKILLS simulator was used to serve as a uniform testbed. Surgeons with varied levels of expertise were recruited to perform two representative simplified tasks (Peg Board and Pick & Place). The automated kinematic analysis of video was compared with the ground truth data (obtained by manual labeling) using misclassification rate and true classification confusion matrix. Future studies aimed towards analyzing real surgical procedures are already underway. I. INTRODUCTION Surgical proficiency engenders merger of sensorimotor and cognitive capabilities and its systematic assessment has been a topic of considerable importance. In the current 6HH RQH ’R RQH 7HDFK RQH¶ paradigm [1], novitiate clinicians typically learn to perform procedures by observing more experienced personnel actually performing them [2, 3]. The biggest challenges to assessment and accreditation of *This work was supported in part by the National Science Foundation under Grants, CNS 0751132 and CNS 1135660. S.-K. Jun, M. Sathianarayanan and P. Agarwal are PhD candidates in Dept of Mech. & Aero. Engg. at SUNY Buffalo, NY 14260 USA (e-mails: [email protected], [email protected], [email protected] ). A. Eddib, M.D. is the OB-GYN Robotic Fellow at Millard Fillmore Suburban Hospital, while P. Singhal, M.D., is a Director of Robotic Surgery Division for the Kaleida Health System, in Buffalo, NY 14221 USA (email: [email protected], [email protected]) S. Garimella, M.D., is a Clinical Asst. Prof. in Pediatrics Nephrology, SUNY Buffalo, NY 14260 USA (email: [email protected]) V. Krovi, is an Associate Professor with the Dept. of Mech. & Aero. Engg., SUNY Buffalo, NY 14260 USA (e-mail: [email protected]). surgeons include (i) creating appropriately rich and diverse clinical settings (real or virtual); as well as (ii) developing uniform, repeatable, stable, verifiable performance metrics; both at manageable financial levels for ever increasing cohorts of trainees. Due to significant diversity in training, surgical assessment can occur in different settings ranging from operations on live patients, to surrogate phantoms ranging from cadavers, animal models to plastic mannequins to most recently simulated/virtual environments. Current practice leverages an apprenticeship model and entails subjective or at best semi-objective (Likert-scale) evaluation of surgical performance by an expert surgeon [4, 5]. However, as Satava [6] notes, the concomitant revolutions of objective assessment of procedural skills and transition from an apprenticeship- to criterion-based model is revolutionizing medical training. Over the past decade, the ACGME (Accreditation Council for Graduate Medical Education) [7] has espoused development of a cost-efficient proficiency- based curriculum, with an emphasis on simulation methodologies and quantitative skills-assessment tools, to bypass the limitations in the current apprenticeship-based system. The growth of computer integration and data acquisition in the form of robotic Minimally Invasive Surgical (rMIS) now offers a unique set of opportunities to comprehensively address this situation. Quantitative metrics of surgical performance are not only critical for distinguishing novice from expert but can provide a gradated basis for expertise necessary to monitor performance. In conjunction with a well-structured curriculum, it would form the core of a comprehensive training program. While quantitative metrics are clearly superior to subjective assessment, it is unclear as to WHICH data, at WHAT spatial and temporal resolution needs to be collected from the vast choices of physical measurements possible. It is the improper understanding of the underlying relationships, coupled with insufficient computational support that has led to present system of quantitative metrics comprising of relatively simplistic metrics (spatial and temporal aggregated measures) for example, total-time-to- task completion (TTC) [8-10], total-tool-path-length (TPL) [11-13] etc). Even the commercial surgical simulators use only these metrics. For example, da Vinci Skills simulator (dVSS) uses a MScore TM evaluation system to evaluate robotic surgical expertise [14]. The principal issue in such a Robotic Minimally Invasive Surgical Skill Assessment based on Automated Video-Analysis Motion Studies Seung-Kook Jun, Madusudanan Sathia Narayanan, Priyanshu Agarwal, Abeer Eddib MD, Pankaj Singhal MD, Sudha Garimella MD and Venkat Krovi, Member, IEEE The Fourth IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics Roma, Italy. June 24-27, 2012 978-1-4577-1200-5/12/$26.00 ©2012 IEEE 25
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Robotic Minimally Invasive Surgical skill assessment based on automated video-analysis motion...

�
Abstract²Assessment of surgical skill, arising from the
synthesis of the cognitive and sensorimotor capabilities of the
surgeon, has predominantly been a subjective task.
Development of quantitative metrics-of-performance with
clinical relevance and other desirable characteristics
(repeatability and stability) has always lagged behind. New
opportunities for objective and automated assessment
frameworks have arisen by virtue of technological advances in
computation, video-processing, and data-acquisition, especially
in the robotic Minimally Invasive Surgical (rMIS) realm. Most
efforts focus on semi-quantitative (Likert scale) or inadequately
validated, spatially- or temporally-aggregated quantitative
metrics derived from direct physical measurements. In this
work we propose an automated surgical expertise evaluation
method, by adapting well-established motion studies
methodologies, especially for MIS evaluation. This method
relies on segmenting a primary task into sub-tasks, which can
be evaluated by statistical analyses of micromotions. Motion
studies were developed by 2 methods: (A) manual annotation
process by experts (to serve as a benchmark); and (B)
automated kinematic-analysis-of-videos; for economy,
repeatability as well as dexterity. The da Vinci SKILLS
simulator was used to serve as a uniform testbed. Surgeons
with varied levels of expertise were recruited to perform two
representative simplified tasks (Peg Board and Pick & Place).
The automated kinematic analysis of video was compared with
the ground truth data (obtained by manual labeling) using
misclassification rate and true classification confusion matrix.
Future studies aimed towards analyzing real surgical
procedures are already underway.
I. INTRODUCTION
Surgical proficiency engenders merger of sensorimotor
and cognitive capabilities and its systematic assessment has
been a topic of considerable importance. In the current µ6HH�
RQH��'R� RQH��7HDFK� RQH¶� paradigm [1], novitiate clinicians
typically learn to perform procedures by observing more
experienced personnel actually performing them [2, 3]. The
biggest challenges to assessment and accreditation of
*This work was supported in part by the National Science Foundation
under Grants, CNS 0751132 and CNS 1135660.
S.-K. Jun, M. Sathianarayanan and P. Agarwal are PhD candidates in
Dept of Mech. & Aero. Engg. at SUNY Buffalo, NY 14260 USA (e-mails:
[email protected], [email protected], [email protected] ).
A. Eddib, M.D. is the OB-GYN Robotic Fellow at Millard Fillmore
Suburban Hospital, while P. Singhal, M.D., is a Director of Robotic Surgery
Division for the Kaleida Health System, in Buffalo, NY 14221 USA (email:
[email protected], [email protected])
S. Garimella, M.D., is a Clinical Asst. Prof. in Pediatrics Nephrology,
SUNY Buffalo, NY 14260 USA (email: [email protected])
V. Krovi, is an Associate Professor with the Dept. of Mech. & Aero.
Engg., SUNY Buffalo, NY 14260 USA (e-mail: [email protected]).
surgeons include (i) creating appropriately rich and diverse
clinical settings (real or virtual); as well as (ii) developing
uniform, repeatable, stable, verifiable performance metrics;
both at manageable financial levels for ever increasing
cohorts of trainees.
Due to significant diversity in training, surgical
assessment can occur in different settings ranging from
operations on live patients, to surrogate phantoms ranging
from cadavers, animal models to plastic mannequins to most
recently simulated/virtual environments. Current practice
leverages an apprenticeship model and entails subjective or
at best semi-objective (Likert-scale) evaluation of surgical
performance by an expert surgeon [4, 5]. However, as
Satava [6] notes, the concomitant revolutions of objective
assessment of procedural skills and transition from an
apprenticeship- to criterion-based model is revolutionizing
medical training. Over the past decade, the ACGME
(Accreditation Council for Graduate Medical Education) [7]
has espoused development of a cost-efficient proficiency-
based curriculum, with an emphasis on simulation
methodologies and quantitative skills-assessment tools, to
bypass the limitations in the current apprenticeship-based
system. The growth of computer integration and data
acquisition in the form of robotic Minimally Invasive
Surgical (rMIS) now offers a unique set of opportunities to
comprehensively address this situation.
Quantitative metrics of surgical performance are not only
critical for distinguishing novice from expert but can provide
a gradated basis for expertise necessary to monitor
performance. In conjunction with a well-structured
curriculum, it would form the core of a comprehensive
training program. While quantitative metrics are clearly
superior to subjective assessment, it is unclear as to WHICH
data, at WHAT spatial and temporal resolution needs to be
collected from the vast choices of physical measurements
possible. It is the improper understanding of the underlying
relationships, coupled with insufficient computational
support that has led to present system of quantitative metrics
comprising of relatively simplistic metrics (spatial and
temporal aggregated measures) for example, total-time-to-
task completion (TTC) [8-10], total-tool-path-length (TPL)
[11-13] etc). Even the commercial surgical simulators use
only these metrics. For example, da Vinci Skills simulator
(dVSS) uses a MScoreTM
evaluation system to evaluate
robotic surgical expertise [14]. The principal issue in such a
Robotic Minimally Invasive Surgical Skill Assessment
based on Automated Video-Analysis Motion Studies
Seung-Kook Jun, Madusudanan Sathia Narayanan, Priyanshu Agarwal, Abeer Eddib MD,
Pankaj Singhal MD, Sudha Garimella MD and Venkat Krovi, Member, IEEE
The Fourth IEEE RAS/EMBS International Conferenceon Biomedical Robotics and BiomechatronicsRoma, Italy. June 24-27, 2012
978-1-4577-1200-5/12/$26.00 ©2012 IEEE 25

case is that the reliability, stability and relevance of these
measures have not been established [11-13] creating
lingering questions about the utility of the evaluation system
to support a pathway to accreditation [7, 15].
Clearly, a clinically-relevant scenario coupled with
automated and quantitative skill assessment system is the
need of the hour that would enable seamless skill evaluation
with minimal manual (expert surgeon) intervention. In this
work we propose to adapt and study a variant of motion
analysis, used frequently for evaluation of skill and efficacy
within the industrial engineering community, for use in the
context of robotic surgeries (RS). Within this larger context,
we wish to: (i) leverage machinery of motion studies and
process charts to aid characterization of the performance; (ii)
retain clinical significance in terms of creation of a catalog
of basic motion elements; (iii) begin the process of
automation of evaluation of such motion studies based on
3D motion-capture techniques; and (iv) examine self-
consistency and reliability of ensuring qualitative measures
to characterize skill levels of user population. In this
manuscript, we focus on the first three aspects principally
and work is currently underway to address the fourth.
II. BACKGROUND
A. Current Surgical Assessment
A range of techniques exist today based on manual
assessment of technical skills of surgeons. Yet they lack
consistency and reliability due to the subjective nature of
experts¶ intervention [4], such as: (a) procedure lists with
logs; (b) direct observation; (c) direct observation with
criteria; (d) video based assessment. Robust methods of
assessment of technical skills are sought to establish high-
standards required for modern surgical training programs.
These methods should be flexible and effective regardless of
modality of training used.
B. Objective Assessment
In recent times, standardized objective methods for
assessing technical skills were introduced and accepted for
use in surgical training programs. These include Objective
Structured Assessment of Technical Skills (OSATS) [16, 17]
as well as Objective Structured Clinical Examination
(OSCE) that emphasizes the quantitative assessment
processes. These methods require hardware (measurement
device) such as Imperial College Surgical Assessment
Device (ICSAD) and Advanced Dundee Endoscopic
Psychomotor Trainer (ADEPT) to perform surgical dexterity
analysis. New generation of virtual simulators now provide
the ability to: (1) Control presentation of stimuli to trainees:
Varying sets of exercises with increasing complexity and
clinical relevance are available ranging from relatively
simple peg-transfer and suturing exercises to realistic
clinical scenarios such as resections and anastomoses [10,
18]. (2) Accurately and transparently monitor user
responses: Physical measurements of a variety of quantities
(tool motions, completion times) can be done using data-
acquisition hardware in a transparent manner [13, 19].
C. Motion Studies
Within industrial engineering practice, motion studies are
a well-established method used to characterize, simplify and
improve the efficiency and effectiveness of manual tasks
[20, 21]. For over a half century now, such motion studies
have been employed to characterize expertise as well as to
eliminate inefficient motions. In this work, we seek to
examine the applicability and usefulness of such a technique
to assess surgical performance and help create a viable
quantitative basis for grounding the training process.
Frank Gilbreths cataloged a set of basic motion elements
FDOOHG� ³Therbligs´� WKDW� KDV� VHUYHG� DV�EXLOGLQJ�EORFNV�RI� Dll
manual manipulative activities especially in a factory shop
floor. At its core, these elements allow for decomposition of
a complex manual job sequence into sub-parts that could be
individually examined. This segmentation potentially allows
for a finite state automaton representation of a complex
activity that could form the discrete basis for linguistic
representation as well as fault-detection and correction
similar to the ones explained in [22-24].
However, the challenge remains in being able to systematically, consistently and automatedly achieve the temporal discretization in a generalized manner. Current practice is highly reliant on the expertise of the manual annotators. For example, multiple manual annotators may create similar but slightly differing process charts for the same task² the discretization remains unable to distinguish between the natural variability in task performance by the user and the capability of the trained annotator. Video-recording of task performance for subsequent manual activity labeling (and reviewing) alleviates some of the variability in the temporal discretization.
D. Automated Video Analysis
While markerless video analysis has been used to study
hand-gesturing and skill [25-27], tracking unconstrained
human motions in concise quantitative terms with the
precision and fidelity suitable for motion analysis remains a
challenging task. Several studies in the recent past showed
that segmenting the surgical videos into sub-tasks (defined
as surgemes in [24]) and identifying kinematic tool poses
[28] can aid in analyzing the performance and skill. The
basis and requirements of the surgical task segmentation has
not been dealt with necessary detail in most of these studies.
It is necessary as these subtasks are the building blocks on
top of which metrics for skill and expertise will be defined.
Nonetheless, the problem still remains highly complicated
due to high variability and dependence on multiple-
parameters involved in inter- and intra- subject studies.
III. MOTION STUDIES
A. Robotic Surgery Therbligs
In an effort to develop a specialized but well defined set
of Robotic Surgery (RS) Therbligs, we base the development
on already established set of the basic motion elements. In
26
VHOHFW� FDVHV�� VXFK� DV� µ8VH� 7RRO¶�� WKLV� action was expanded
LQWR� DOWHUQDWH� FODVVHV� VSHFLILFDOO\� DV� µ&XW� 7LVVXH¶�� µ2SHQ�
7LVVXH¶��µ6FLVVRUV¶�DQG�µ&DXWHUL]H�7LVVXH¶��$W�WKH�Vame time,
several of original Therblig series were deemed
inappropriate and not included (refer to Table 1).
B. Process Charts
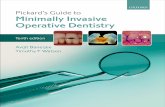
Traditional motion studies are captured in a process chart
where basic motion elements (Therbligs) are hierarchically
grouped into work elements and then ultimately into
meaningful tasks [29], which has proved adequate to offer a
primary discretization of industrial manipulation tasks. At its
core, the process chart consists of a table as shown in Fig. 1:
Fig. 1: Process Chart
A description of manipulation-related Therbligs can be
found in many standard textbooks [21, 29]. Enhancements to
this basic process chart now involve taking advantage of
bilateral symmetry (left/ right) or increased discretization or
agglomeration of tasks as well as performing varying levels
of statistical analyses for the collected information. The
principle of motion economy can then be applied to analyze,
assess, simplify and improve the efficiency and effectiveness
of a (hand-manipulable) manual task, as widely used by
industrial engineers. In this work, the same principle is
extended to analyze robotic surgical skill assessment.
C. Kinematic Motion Capture and Analysis
3D motion capture techniques are widely used in the
field of biomechanics [30] and robotics [31] to accurately
estimate the kinematics of a system especially, when
measurements from onboard sensing are inaccurate or
unavailable. Among the many methods, marker based video
motion analysis methods build upon availability of
synchronized video streams to estimate 3D motions of
moving objects within the scene. Virtual markers can be
potentially introduced via manual annotation (or template
matching image processing techniques) even if physical
markers are not explicitly present in the videos. However, a
minimum of 2 video streams with calibrated baseline are
required to estimate 3D coordinates with considerable
accuracy. In our analysis, the two endoscopic video feeds
from dVSS-Si serve for this purpose. In order to calibrate the
cameras in 2D and 3D prior to digitizing the videos,
inanimate objects present in the video feeds were used. In
this work, a motion analysis application (SIMIMotion [32])
was used to analyze the videos and estimate 3D positions,
velocities and accelerations (both linear and angular) of tool
motions (as will be discussed in Section V). This
information served as a basis to devise our algorithms for
automated recognition of Therblig elements, which are
presented in the following section.
TABLE 1: ROBOTIC SURGICAL THERBLIGS
Therbligs* Symbol Description
RE Reach Reaching for object with empty
hand.
G Grasp Moving an object using a hand
motion
M Move Grasping an object by contacting and
closing the finger of the active hand
RL Release Releasing control of an object
PP Pre-Position Positioning and/or orienting an
object for the next operation
P Position Positioning and/or orienting an
object in the defined location
U
Use
(UC, UO,
US, UZ)
Manipulating and/or applying a tool
in the intended way (UC- cutting
tissue, UO- cut-open tissues, US-
scissors cut, UZ- cauterize tissues)
A Assemble Joining the two parts together to
form an assembled entity
DA Disassemble Separating multiple components that
were previously joined in some way
H Hold Holding an object
SH Search Attempting to find an object using
the eyes or hand
SL Select Choosing an object from a group
I Inspect Determining the quality of
characteristic of an object
PL Plan Deciding a course of action
AD Avoidable
Delay :DLWLQJ� WKDW� LV� ZLWKLQ� WKH� ZRUNHU¶V�control
R
Rest to
overcome
Fatigue Rest to overcome fatigue
UD Unavoidable
Delay Wait due to the factors beyond the
control of the worker
Italicized: ineffective Therbligs, bold: used in the current study
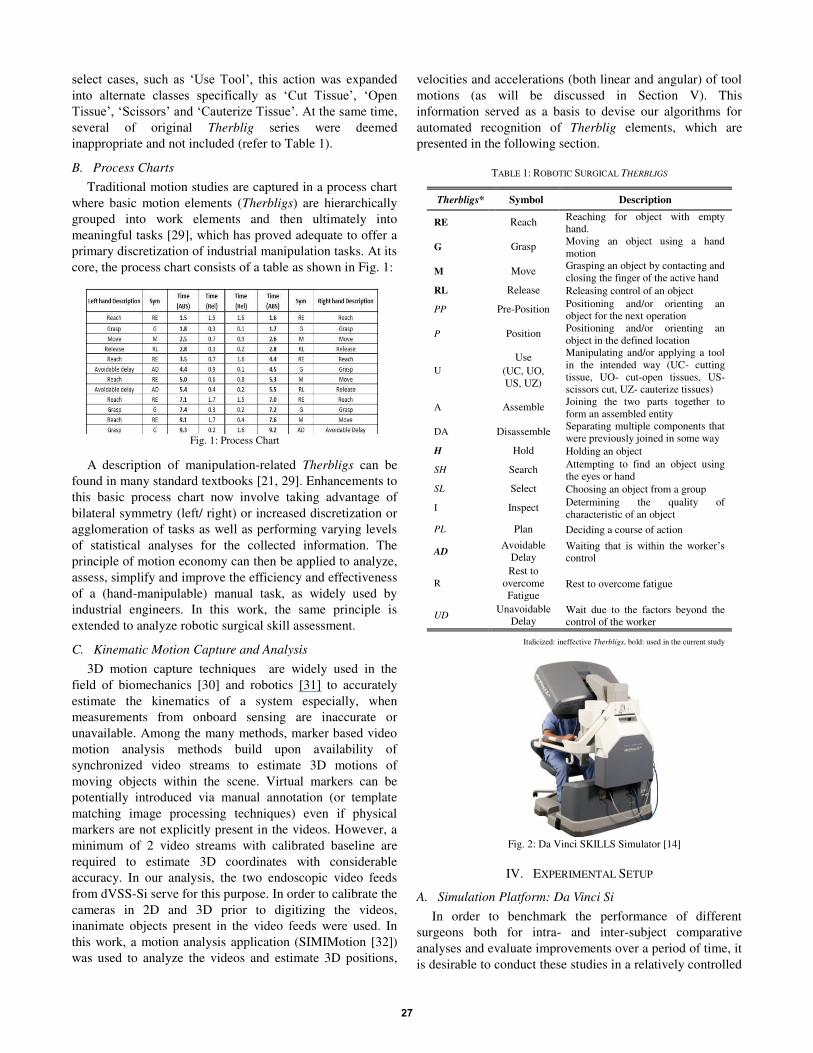
IV. EXPERIMENTAL SETUP
A. Simulation Platform: Da Vinci Si
In order to benchmark the performance of different
surgeons both for intra- and inter-subject comparative
analyses and evaluate improvements over a period of time, it
is desirable to conduct these studies in a relatively controlled
Fig. 2: Da Vinci SKILLS Simulator [14]
27
and standardized testbed. In this particular study, the dVSSSi was used along with its SKILLS simulator system [14] asin Fig. 2. In addition, using the dVSS-Si enabled recordingof stereoscopic video images for post -processing as eachtask was being performed. Since, our objective was todevelop a system skill assessment methods for a genericsurgical robotic device, only the video feeds were used asinput to our evaluation scheme.
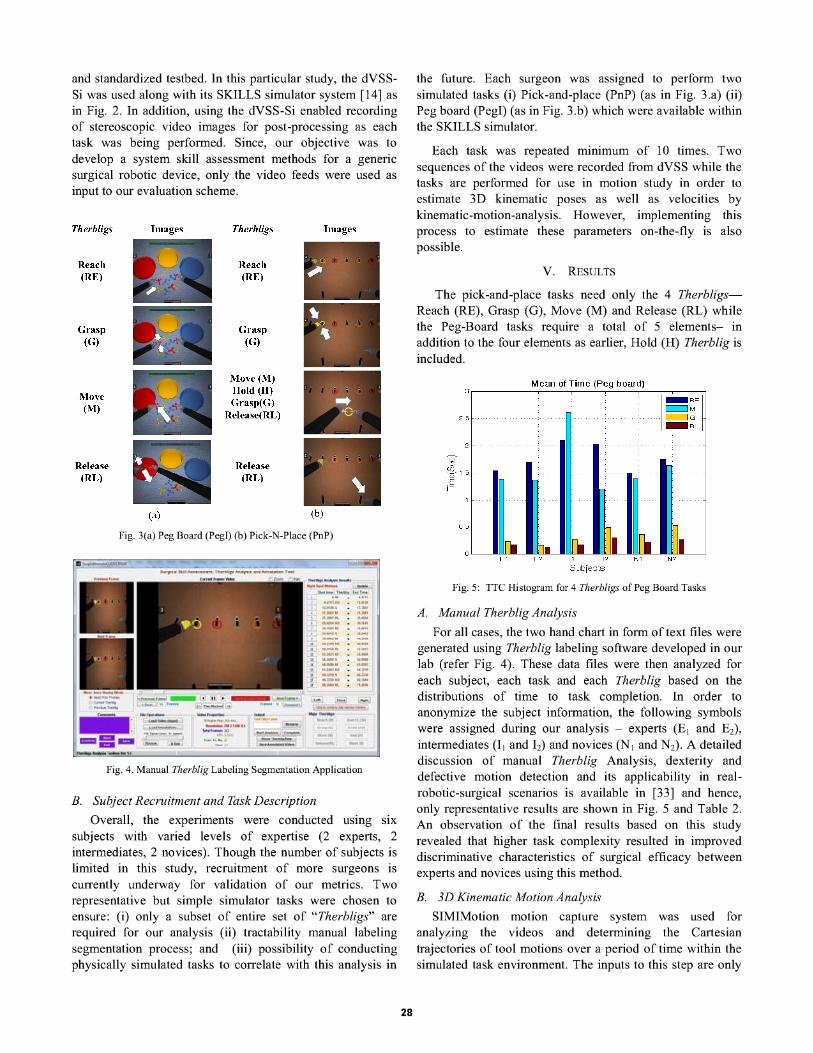
Fig. 3(a) Peg Board (PegI) (b) Pick-N-Place (PnP)
Fig. 4. Manual Therblig Labeling Segmentation Application
B. Subject Recruitment and Task Description
Overall, the experiments were conducted using sixsubjects with varied levels of expertise (2 experts, 2intermediates, 2 novices). Though the number of subjects islimited in this study, recruitment of more surgeons iscurrently underway for validation of our metrics. Tworepresentative but simple simulator tasks were chosen toensure: (i) only a subset of entire set of "Therbligs" arerequired for our analysis (ii) tractability manual labelingsegmentation process; and (iii) possibility of conductingphysically simulated tasks to correlate with this analysis in
28
the future. Each surgeon was assigned to perform twosimulated tasks (i) Pick-and-place (PnP) (as in Fig. 3.a) (ii)Peg board (Pegl) (as in Fig. 3.b) which were available withinthe SKILLS simulator.
Each task was repeated minimum of 10 times. Twosequences of the videos were recorded from dVSS while thetasks are performed for use in motion study in order toestimate 3D kinematic poses as well as velocities bykinematic-motion-analysis. However, implementing thisprocess to estimate these parameters on-the-fly is alsopossible.
V. RESULTS
The pick-and-place tasks need only the 4 TherbligsReach (RE), Grasp (G), Move (M) and Release (RL) whilethe Peg-Board tasks require a total of 5 elements- inaddition to the four elements as earlier, Hold (H) Therblig isincluded.
Fig. 5: TTC Histogram for 4 Therbligs of Peg Board Tasks
A. Manual Therblig Analysis
For all cases, the two hand chart in form of text files weregenerated using Therblig labeling software developed in ourlab (refer Fig. 4). These data files were then analyzed foreach subject, each task and each Therblig based on thedistributions of time to task completion. In order toanonymize the subject information, the following symbolswere assigned during our analysis - experts (E1 and E2) ,
intermediates (11 and 12) and novices (N 1and N2) . A detaileddiscussion of manual Therblig Analysis, dexterity anddefective motion detection and its applicability in realrobotic-surgical scenarios is available in [33] and hence,only representative results are shown in Fig. 5 and Table 2.An observation of the final results based on this studyrevealed that higher task complexity resulted in improveddiscriminative characteristics of surgical efficacy betweenexperts and novices using this method.
B. 3D Kinematic Motion Analysis
SIMIMotion motion capture system was used foranalyzing the videos and determining the Cartesiantrajectories of tool motions over a period of time within thesimulated task environment. The inputs to this step are only
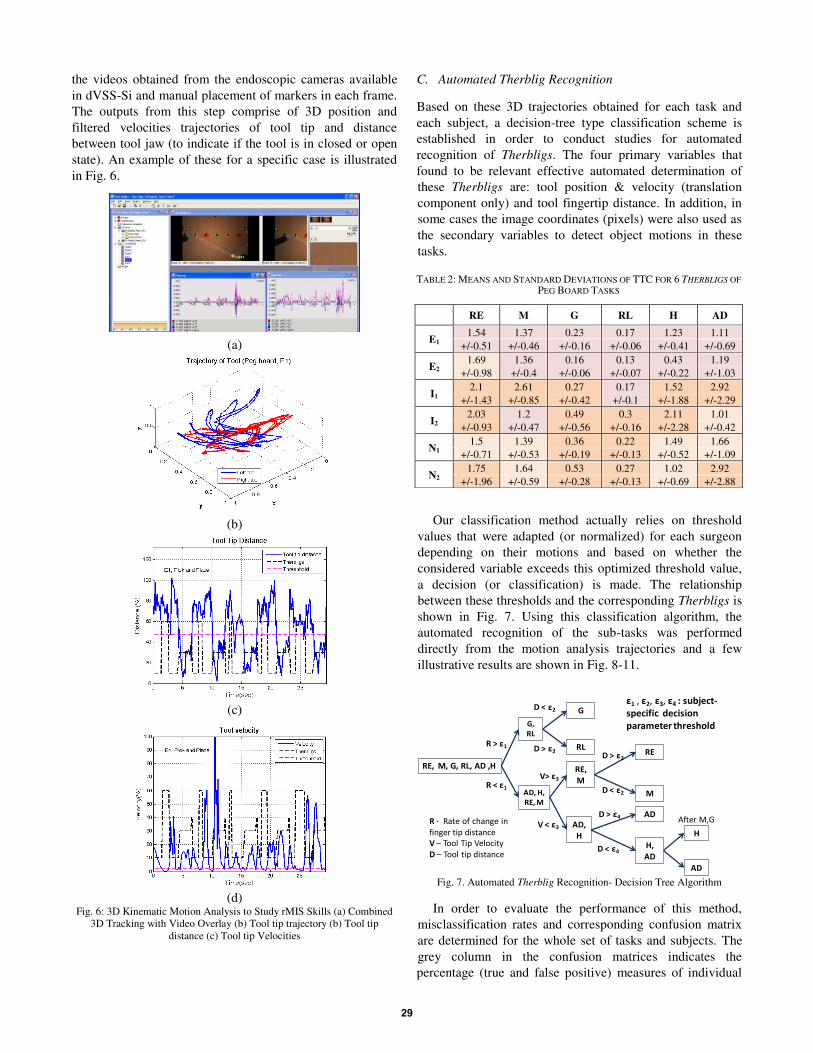
the videos obtained from the endoscopic cameras available
in dVSS-Si and manual placement of markers in each frame.
The outputs from this step comprise of 3D position and
filtered velocities trajectories of tool tip and distance
between tool jaw (to indicate if the tool is in closed or open
state). An example of these for a specific case is illustrated
in Fig. 6.
C. Automated Therblig Recognition
Based on these 3D trajectories obtained for each task and
each subject, a decision-tree type classification scheme is
established in order to conduct studies for automated
recognition of Therbligs. The four primary variables that
found to be relevant effective automated determination of
these Therbligs are: tool position & velocity (translation
component only) and tool fingertip distance. In addition, in
some cases the image coordinates (pixels) were also used as
the secondary variables to detect object motions in these
tasks.
Our classification method actually relies on threshold
values that were adapted (or normalized) for each surgeon
depending on their motions and based on whether the
considered variable exceeds this optimized threshold value,
a decision (or classification) is made. The relationship
between these thresholds and the corresponding Therbligs is
shown in Fig. 7. Using this classification algorithm, the
automated recognition of the sub-tasks was performed
directly from the motion analysis trajectories and a few
illustrative results are shown in Fig. 8-11.
In order to evaluate the performance of this method,
misclassification rates and corresponding confusion matrix
are determined for the whole set of tasks and subjects. The
grey column in the confusion matrices indicates the
percentage (true and false positive) measures of individual
(a)
(b)
(c)
(d)
Fig. 6: 3D Kinematic Motion Analysis to Study rMIS Skills (a) Combined
3D Tracking with Video Overlay (b) Tool tip trajectory (b) Tool tip
distance (c) Tool tip Velocities
TABLE 2: MEANS AND STANDARD DEVIATIONS OF TTC FOR 6 THERBLIGS OF
PEG BOARD TASKS
RE M G RL H AD
E1 1.54 1.37 0.23 0.17 1.23 1.11
+/-0.51 +/-0.46 +/-0.16 +/-0.06 +/-0.41 +/-0.69
E2 1.69 1.36 0.16 0.13 0.43 1.19
+/-0.98 +/-0.4 +/-0.06 +/-0.07 +/-0.22 +/-1.03
I1 2.1 2.61 0.27 0.17 1.52 2.92
+/-1.43 +/-0.85 +/-0.42 +/-0.1 +/-1.88 +/-2.29
I2 2.03 1.2 0.49 0.3 2.11 1.01
+/-0.93 +/-0.47 +/-0.56 +/-0.16 +/-2.28 +/-0.42
N1 1.5 1.39 0.36 0.22 1.49 1.66
+/-0.71 +/-0.53 +/-0.19 +/-0.13 +/-0.52 +/-1.09
N2 1.75 1.64 0.53 0.27 1.02 2.92
+/-1.96 +/-0.59 +/-0.28 +/-0.13 +/-0.69 +/-2.88
Fig. 7. Automated Therblig Recognition- Decision Tree Algorithm
RE, M, G, RL, AD ,H
R > x1
V < x3 AD,
H
AD, H,
RE, M
AD
H,
ADD < x4
D > x4
H
AD
After M,G
G,
RL
R < x1
V> x3
RE,
M
G
RL
D < x2
D > x2 RE
MD < x2
D > x2
R - Rate of change in
finger tip distance
V t Tool Tip Velocity
D t Tool tip distance
x1 , x2, x3, x4 : subject-
specific decision
parameter threshold
29
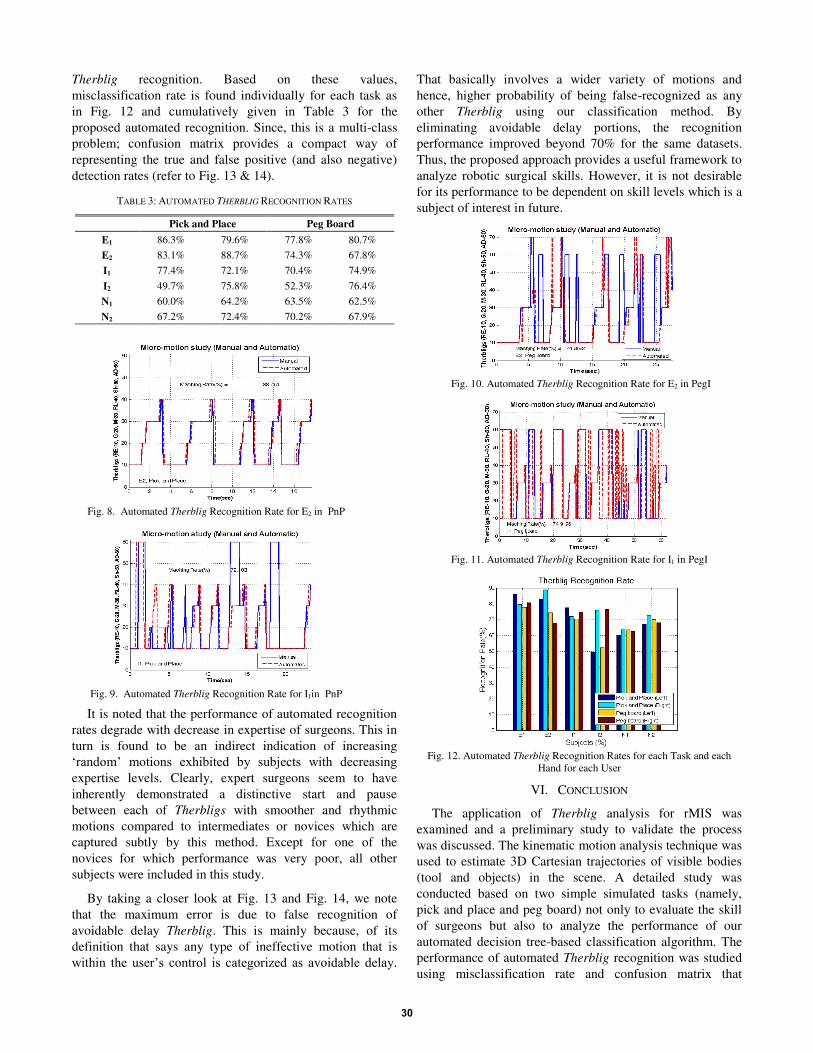
Therblig recognition. Based on these values,
misclassification rate is found individually for each task as
in Fig. 12 and cumulatively given in Table 3 for the
proposed automated recognition. Since, this is a multi-class
problem; confusion matrix provides a compact way of
representing the true and false positive (and also negative)
detection rates (refer to Fig. 13 & 14).
TABLE 3: AUTOMATED THERBLIG RECOGNITION RATES
Pick and Place Peg Board
E1 86.3% 79.6% 77.8% 80.7%
E2 83.1% 88.7% 74.3% 67.8%
I1 77.4% 72.1% 70.4% 74.9%
I2 49.7% 75.8% 52.3% 76.4%
N1 60.0% 64.2% 63.5% 62.5%
N2 67.2% 72.4% 70.2% 67.9%
It is noted that the performance of automated recognition
rates degrade with decrease in expertise of surgeons. This in
turn is found to be an indirect indication of increasing
µUDQGRP¶� PRWLRQV� H[KLELWHG� E\� VXEMHFWV� ZLWK� GHFUHDVLQJ�
expertise levels. Clearly, expert surgeons seem to have
inherently demonstrated a distinctive start and pause
between each of Therbligs with smoother and rhythmic
motions compared to intermediates or novices which are
captured subtly by this method. Except for one of the
novices for which performance was very poor, all other
subjects were included in this study.
By taking a closer look at Fig. 13 and Fig. 14, we note
that the maximum error is due to false recognition of
avoidable delay Therblig. This is mainly because, of its
definition that says any type of ineffective motion that is
ZLWKLQ� WKH� XVHU¶V� FRQWURO� LV� FDWHJRUL]HG� DV� DYRLGDEOH� GHOD\��
That basically involves a wider variety of motions and
hence, higher probability of being false-recognized as any
other Therblig using our classification method. By
eliminating avoidable delay portions, the recognition
performance improved beyond 70% for the same datasets.
Thus, the proposed approach provides a useful framework to
analyze robotic surgical skills. However, it is not desirable
for its performance to be dependent on skill levels which is a
subject of interest in future.
Fig. 10. Automated Therblig Recognition Rate for E2 in PegI
Fig. 11. Automated Therblig Recognition Rate for I1 in PegI
Fig. 12. Automated Therblig Recognition Rates for each Task and each
Hand for each User
VI. CONCLUSION
The application of Therblig analysis for rMIS was
examined and a preliminary study to validate the process
was discussed. The kinematic motion analysis technique was
used to estimate 3D Cartesian trajectories of visible bodies
(tool and objects) in the scene. A detailed study was
conducted based on two simple simulated tasks (namely,
pick and place and peg board) not only to evaluate the skill
of surgeons but also to analyze the performance of our
automated decision tree-based classification algorithm. The
performance of automated Therblig recognition was studied
using misclassification rate and confusion matrix that
Fig. 8. Automated Therblig Recognition Rate for E2 in PnP
Fig. 9. Automated Therblig Recognition Rate for I1in PnP
30

provided reasonable estimates for accuracy as well as
sensitivity of our algorithm. This classification method were
also found to be capable for in real surgical analyzes [33].
Collection of video data from comprehensive subject studies
will enable us to augment this classification method under
probabilistic framework as well as achieve more uniform
performance across different levels of expertise.
Fig. 13. Confusion Matrix (Recognition Rate) for E2 in Pick and Place
Fig. 14. Confusion Matrix (Recognition Rate) for N1 in Peg Board
REFERENCES
[1] J. Vozenilek, et al., "See One, Do One, Teach One: Advanced
Technology in Medical Education," Academic Emergency Medicine,
vol. 11, pp. 1149-1154, 2004.
[2] M. Bridges and D. L. Diamond, "The financial impact of teaching
surgical residents in the operating room," The American Journal of
Surgery, vol. 177, pp. 28-32, 1999.
[3] E. Harrison. (2006) The Cost of Surgical Training. Association of
Surgeons of Great Britain and Ireland Newsletter. 4-6.
[4] B. M. Schout, et al., "Validation and implementation of surgical
simulators: a critical review of present, past, and future," Surgical
Endoscopy, vol. 24, pp. 536-546, Mar 2010.
[5] J. A. Aucar, et al., "A Review of Surgical Simulation With Attention to
Validation Methodology," Surgical Laparoscopy Endoscopy &
Percutaneous Techniques, vol. 15, pp. 82-89, 2005.
[6] R. Satava, "Historical Review of Surgical Simulation²A Personal
Perspective," World Journal of Surgery, vol. 32, pp. 141-148, 2008.
[7] N. Brown, et al., "The revised ACGME laparoscopic operative
requirements: how have they impacted resident education?," Surgical
Endoscopy, pp. 1-7, Jan 2012.
[8] M. Pellen, et al., "Construct validity of the ProMIS laparoscopic
simulator," Surgical Endoscopy, vol. 23, pp. 130-139, 2009.
[9] K. Tanoue, et al., "Skills assessment using a virtual reality simulator,
/DS6LP���DIWHU�WUDLQLQJ�WR�GHYHORS�IXQGDPHQWDO�VNLOOV�IRU�HQGRVFRSLF�
surgery," Minimally Invasive Therapy & Allied Technologies, vol. 19,
pp. 24-29, 2010.
[10] P. Kanumuri, et al., "Virtual Reality and Computer-Enhanced Training
Devices Equally Improve Laparoscopic Surgical Skill in Novices,"
Journal of the Society of Laparoendoscopic Surgeons, vol. 12, pp. 219-
226, 2008.
[11] J. H. Chien, et al., "Accuracy and speed trade-off in robot-assisted
surgery," The International Journal Of Medical Robotics and Computer
Assisted Surgery, vol. 6, pp. 324-329, 2010.
[12] P. A. Kenney, et al., "Face, content, and construct validity of dV-
trainer, a novel virtual reality simulator for robotic surgery," Urology,
vol. 73, pp. 1288-92, Jun 2009.
[13] M. A. Lerner, et al., "Does training on a virtual reality robotic
simulator improve performance on the da Vinci surgical system?,"
Journal of Endourology, vol. 24, pp. 467-72, Mar 2010.
[14] Intuitive-Surgical and Inc. da Vinci Surgical Robot: Si and SKILLS
Simulator. Available: www.intuitivesurgical.com/
[15] D. Wagner and M. L. Lypson, "Centralized Assessment in Graduate
Medical Education: Cents and Sensibilities," Journal of Graduate
Medical Education, vol. 1, pp. 21-27, 2009.
[16] J. A. Martin, et al., "Objective structured assessment of technical skill
(OSATS) for surgical residents," British Journal of Surgery, vol. 84,
pp. 273-278, 1997.
[17] K. Moorthy, et al., "Objective assessment of technical skills in
surgery," BMJ, vol. 327, pp. 1032-1037, 2003.
[18] M. P. Fried, et al., "Identifying and reducing errors with surgical
simulation," Quality and Safety in Health Care, vol. 13, pp. i19-i26,
October 1 2004.
[19] J. D. Hernandez, et al., "Qualitative and quantitative analysis of the
learning curve of a simulated surgical task on the da Vinci system,"
Surgical Endoscopy, vol. 18, pp. 372-378, 2004.
[20] Handbook of Industrial Engineering: Technology and Operations
Management, 3rd ed.: John Wiley & Sons, 2001.
[21] Motion and Time Study: Design and Measurement of Work, 7th ed.
Univ. of California, Los Angeles: Wiley, August 1980.
[22] J. Rosen, et al., "Generalized approach for modeling minimally
invasive surgery as a stochastic process using a discrete Markov
model," Biomedical Engineering, IEEE Transactions on, vol. 53, pp.
399-413, 2006.
[23] J. Rosen, et al., "Markov modeling of minimally invasive surgery
based on tool/tissue interaction and force/torque signatures for
evaluating surgical skills," Biomedical Engineering, IEEE
Transactions on, vol. 48, pp. 579-591, 2001.
[24] H. C. Lin, et al., "Towards automatic skill evaluation: detection and
segmentation of robot-assisted surgical motions," Computer Aided
Surgery: Official Journal Of The International Society For Computer
Aided Surgery, vol. 11, pp. 220-230, 2006.
[25] G. Ye, et al., "Gesture Recognition Using 3D Appearance and Motion
Features," presented at the Conference on Computer Vision and
Pattern Recognition Workshop, 2004.
[26] J. Corso, et al., "Analysis of Composite Gestures with a Coherent
Probabilistic Graphical Model," Virtual Reality, vol. 8, pp. 242-52,
2005.
[27] N. Padoy, et al., "Statistical modeling and recognition of surgical
workflow," Medical Image Analysis, vol. 16, pp. 632-641, 2012.
[28] A. Jog, et al., "Towards integrating task information in skills
assessment for dexterous tasks in surgery and simulation," presented at
the 2011 IEEE International Conf. on Robotics & Automation,
Shangai, China, 2011.
[29] B. Niebel and A. Freivalds, Methods, Standards, and Work Design,
10th ed.: McGraw-Hill, 2003.
[30] M. S. Narayanan, et al., "Parallel Architecture Manipulators for Use in
Masticatory Studies," International Journal of Intelligent Mechatroncis
and Robotics, vol. 1, pp. 100-22, 2011.
[31] Q. Fu and V. Krovi, "Articulated Wheeled Robots: Exploiting
Reconfigurability and Redundancy," in 2008 ASME DSCC Dynamic
Systems and Control Conference, DSCC2008-130, Ann Arbor,
Michigan, USA., 2008.
[32] 3D-Motion-Capture. SIMI-Motion. Available:
http://www.simi.com/en/products/motion/overview/analysis/index.htm
[33] S.-K. Jun, et al., "Evaluation of Robotic Minimally Invasive Surgical
Skills using Motion Studies," in Performance Metrics for Intelligent
Systems Workshop (PerMIS'12), 2012.
31