Minimally assistive robot training for proprioception enhancement
13
RESEARCH ARTICLE Minimally assistive robot training for proprioception enhancement Maura Casadio Pietro Morasso Vittorio Sanguineti Psiche Giannoni Received: 23 August 2008 / Accepted: 4 December 2008 / Published online: 13 January 2009 Ó Springer-Verlag 2008 Abstract In stroke survivors, motor impairment is fre- quently associated with degraded proprioceptive and/or somatosensory functions. Here we address the question of how to use robots to improve proprioception in these patients. We used an ‘assist-as-needed’ protocol, in which robot assistance was kept to a minimum and was conti- nuously adjusted during exercise. To specifically train proprioceptive functions, we alternated blocks of trials with and without vision. A total of nine chronic stroke survivors participated in the study, which consisted of a total of ten 1-h exercise sessions. We used a linear mixed-effects sta- tistical model to account for the effects of exercise, vision and the degree of assistance on the overall performance, and to capture both the systematic effects and the indi- vidual variations. Although there was not always a complete recovery of autonomous movements, all subjects exhibited an increased amount of voluntary control. Moreover, training with closed eyes appeared to be bene- ficial for patients with abnormal proprioception. Our results indicate that training by alternating vision and no-vision blocks may improve the ability to use proprioception as well as the ability to integrate it with vision. We suggest that the approach may be useful in the more general case of motor skill acquisition, in which enhancing proprioception may improve the ability to physically interact with the external world. Keywords Robot training Haptic interaction Proprioception Stroke patients Neuro-rehabilitation Introduction During the last two decades, robots have been widely used to investigate the mechanisms underlying the acquisition of novel motor skills. Furthermore, starting with early experiments based on the MIT-Manus system (Aisen et al. 1997), robots have proven effective in promoting the recovery of sensorimotor functions in persons with neu- romotor impairments (Prange et al. 2006; Kwakkel et al. 2007). As regards motor learning, in a seminal paper (Shad- mehr and Mussa-Ivaldi 1994) used a manipulandum-type robot to simulate a dynamic environment that systemati- cally perturbed arm motion. With practice, subjects gradually recovered their original performance, by learning to predict the disturbance. Vision and proprioception are known to be equally important in skill acquisition (Battig 1954), but in these experiments adaptation still occurred in absence of visual feedback (Franklin et al. 2007), thus suggesting a crucial role for proprioception in developing an internal model of the disturbance. The nervous system uses flexible strategies while inte- grating visual and proprioceptive information (Sober and Sabes 2005). However, when both sources of information are available, vision tends to dominate (Wolpert et al. 1994; van Beers et al. 1996, 1998; Botvinick and Cohen 1998; Smeets et al. 2006). M. Casadio (&) P. Morasso V. Sanguineti Department of Informatics, Systems and Telematics (DIST), University of Genoa, Via Opera Pia 13, 16145 Genoa, Italy e-mail: [email protected] M. Casadio P. Morasso Italian Institute of Technology (IIT), Genoa, Italy P. Giannoni ART Education and Rehabilitation Center, Genoa, Italy 123 Exp Brain Res (2009) 194:219–231 DOI 10.1007/s00221-008-1680-6
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Minimally assistive robot training for proprioception enhancement

RESEARCH ARTICLE
Minimally assistive robot training for proprioceptionenhancement
Maura Casadio Æ Pietro Morasso ÆVittorio Sanguineti Æ Psiche Giannoni
Received: 23 August 2008 / Accepted: 4 December 2008 / Published online: 13 January 2009
� Springer-Verlag 2008
Abstract In stroke survivors, motor impairment is fre-
quently associated with degraded proprioceptive and/or
somatosensory functions. Here we address the question of
how to use robots to improve proprioception in these
patients. We used an ‘assist-as-needed’ protocol, in which
robot assistance was kept to a minimum and was conti-
nuously adjusted during exercise. To specifically train
proprioceptive functions, we alternated blocks of trials with
and without vision. A total of nine chronic stroke survivors
participated in the study, which consisted of a total of ten
1-h exercise sessions. We used a linear mixed-effects sta-
tistical model to account for the effects of exercise, vision
and the degree of assistance on the overall performance,
and to capture both the systematic effects and the indi-
vidual variations. Although there was not always a
complete recovery of autonomous movements, all subjects
exhibited an increased amount of voluntary control.
Moreover, training with closed eyes appeared to be bene-
ficial for patients with abnormal proprioception. Our results
indicate that training by alternating vision and no-vision
blocks may improve the ability to use proprioception as
well as the ability to integrate it with vision. We suggest
that the approach may be useful in the more general case of
motor skill acquisition, in which enhancing proprioception
may improve the ability to physically interact with the
external world.
Keywords Robot training � Haptic interaction �Proprioception � Stroke patients � Neuro-rehabilitation
Introduction
During the last two decades, robots have been widely used
to investigate the mechanisms underlying the acquisition of
novel motor skills. Furthermore, starting with early
experiments based on the MIT-Manus system (Aisen et al.
1997), robots have proven effective in promoting the
recovery of sensorimotor functions in persons with neu-
romotor impairments (Prange et al. 2006; Kwakkel et al.
2007).
As regards motor learning, in a seminal paper (Shad-
mehr and Mussa-Ivaldi 1994) used a manipulandum-type
robot to simulate a dynamic environment that systemati-
cally perturbed arm motion. With practice, subjects
gradually recovered their original performance, by learning
to predict the disturbance. Vision and proprioception are
known to be equally important in skill acquisition (Battig
1954), but in these experiments adaptation still occurred in
absence of visual feedback (Franklin et al. 2007), thus
suggesting a crucial role for proprioception in developing
an internal model of the disturbance.
The nervous system uses flexible strategies while inte-
grating visual and proprioceptive information (Sober and
Sabes 2005). However, when both sources of information
are available, vision tends to dominate (Wolpert et al.
1994; van Beers et al. 1996, 1998; Botvinick and Cohen
1998; Smeets et al. 2006).
M. Casadio (&) � P. Morasso � V. Sanguineti
Department of Informatics, Systems and Telematics (DIST),
University of Genoa, Via Opera Pia 13, 16145 Genoa, Italy
e-mail: [email protected]
M. Casadio � P. Morasso
Italian Institute of Technology (IIT), Genoa, Italy
P. Giannoni
ART Education and Rehabilitation Center, Genoa, Italy
123
Exp Brain Res (2009) 194:219–231
DOI 10.1007/s00221-008-1680-6

A consequence of visual dominance is that vision may
mask proprioceptive impairments. In fact, in stroke survi-
vors motor impairment is frequently associated with
degraded proprioceptive and/or somatosensory functions
(Tyson et al. 2007), with negative consequences for func-
tional outcome (Carey et al. 1993). These subjects may
have difficulties in estimating the position of their arm in
absence of vision. In addition, they may be unable to
integrate visual and proprioceptive information. Further-
more, they may not be able to detect the presence,
magnitude and direction of external forces.
As a consequence, impaired proprioception may affect
not only motor performance, but also neuromotor recovery.
On the other hand, repeated, active exercise is known to
have a positive influence not only on motor deficits, but on
defective proprioception as well (Dechaumont-Palacin
et al. 2007).
Robot therapy exercises for neuromotor rehabilitation
usually consist of video games with a predominantly visual
component, which tends to hide the proprioceptive com-
ponent of interaction. However, robots might be potentially
beneficial for promoting the recovery of impaired
proprioception and/or visuo-proprioceptive integration in
addition to that of motor functions.
In most cases, robot therapy protocols for neuromotor
rehabilitation use a combination of different exercises
(Prange et al. 2006; Kwakkel et al. 2007)—passive, active-
assisted and/or active-resistive—and it is difficult to draw
solid conclusions on which technique is more effective.
However, the most recent studies (Takahashi and Rein-
kensmeyer 2003; Patton and Mussa-Ivaldi 2004; Patton
et al. 2006b) suggest that therapy protocols should explicitly
take the adaptive nature of the nervous system into con-
sideration. More specifically, Emken et al. (2007) suggested
that sensorimotor adaptation is driven by the optimization of
a cost function which accounts for both effort and position
error. Accordingly, the motor system would behave as a
‘greedy’ optimizer, exploiting the assistive forces generated
by the robot to reduce the degree of voluntary control (and
therefore muscle activation), while keeping the position
error small. A similar situation is likely to occur during
active-assisted exercises (and, even more, during passive
training), so that an assistive force with constant magnitude
would progressively depress voluntary control rather than
promoting its increase. To prevent this, the degree of
assistance should be continuously adjusted as training pro-
ceeds, and ideally kept to the minimum amount that is
necessary to achieve the goal. As a consequence, in robot-
assisted motor rehabilitation (as well as motor skill learning)
it is crucial to design interaction schemes that are capable of
delivering a minimum amount of assistance (Casadio et al.
2009). This principle of interaction is often referred as
‘assist-as-needed’ (Trombly 1995; Emken et al. 2007).
Here we investigate, in a pilot study, the potential
benefit of a form of active-assisted training that emphasizes
the role of proprioception and keeps assistance to a mini-
mum, in the recovery of arm movements after stroke.
Chronic stroke survivors performed reaching movements
with their affected arm, under the influence of robot-gen-
erated assistive forces. Subjects were initially unable to
complete the task without assistance. The therapist initially
set the magnitude of the assistive force provided by the robot
so that assistance allowed patients to initiate the movements,
but in no way imposed the trajectory, the reaching time, and
the speed profile. Whenever patient performance improved,
in the subsequent blocks of trials force magnitude was
reduced; however, each session included trials with all the
previously experienced levels of assistance. In summary, we
used an adaptive, ‘assist-as-needed’ protocol.
Across sessions, trials were performed with open or
closed eyes, in alternation. In closed eyes trials, subjects
were forced to rely on proprioception alone to successfully
achieve the movement goal.
A problem of the protocols based on variable degrees of
assistance for severely impaired subjects is that the amount
of voluntary control (i.e., the performance in absence of
assistance), as well as its change due to exercise, is not
immediately observable when looking at performance in
assisted trials (Colombo et al. 2005). Moreover, if assis-
tance is tailored on individual subjects and is decreased as
subjects improve, treatment protocols tend to vary widely
across subjects, which makes comparisons difficult.
A similar problem occurs if therapy protocols include
both open and closed eyes training. The effect may be
highly variable from subject to subject, depending on the
nature of their impairment. Subjects with impaired pro-
prioception may perform better in presence of vision.
Subjects with problems in integration of proprioceptive and
visual information may perform better in absence of vision.
In these different situations, open and closed eyes training
is likely to have different effects.
To allow the exploration of this form of between-sub-
jects variability, we used a mixed-effects statistical model,
which separately accounts for the effects of exercise, vision
and degree of assistance on the overall performance. At the
same time, the model allows to analyze inter-subject
variability.
Materials and methods
Subjects
Nine stroke survivors (2 males, 7 females, age 52 ± 14)
participated in this study. Subjects were recruited among
those followed as outpatients of the ART Rehabilitation
220 Exp Brain Res (2009) 194:219–231
123

and Educational Center, Genova. All patients were treated
regularly on a weekly basis for at least 6 months before
entering the study.
The inclusion criteria were: chronic conditions (at least
1 year after stroke), stable clinical conditions for at least
1 month before entering robot therapy. The exclusion cri-
teria were inability to understand instructions about the
exercise protocol and other neuro-cognitive problems.
Preference was given to patients with a high degree of
motor impairment.
Disease duration was 34 ± 19 months (range 12–76),
with a majority of ischemic etiology (7/9). Patient
impairment was evaluated by means of the Fugl-Meyer
score, limited to the arm section (FMA) (Gladstone et al.
2002; Platz et al. 2005). Four subjects had a severe
impairment (FMA \ 10/66); three patients had an impair-
ment of intermediate level (10 \ FMA \ 20); two patients
had a mild impairment (FMA [ 20). The average FMA
score was 15 ± 13 (range 5–41). The average Ashworth
score of muscle spasticity (Bohannon and Smith 1987) was
1.9 ± 0.9 (range 1–3). Table 1 reports the demographic
and clinical data for all the subjects.
Due to the small size of the population of subjects, this
study cannot be considered a clinical trial but, rather, a
feasibility study for the proposed robot-therapy approach
(assist-as-needed and proprioceptive training) and a dem-
onstration of the application of the related analytical tools.
The research conforms to the ethical standards laid
down in the 1964 Declaration of Helsinki, which protect
research subjects, and to ethical bylaws of the International
Association of Bobath Instructors (IBITA). Each subject
signed a consent form that conforms to these guidelines.
Experimental apparatus
The robot—Braccio di Ferro (BdF)—is a planar manipu-
landum with 2 degrees of freedom (Fig. 1), which has been
described elsewhere (Casadio et al. 2006). The subjects sit
in a chair, with their chest and wrist restrained by means of
suitable holders, and grasp the handle of the manipulan-
dum. A light, soft support is connected to the forearm that
allows low-friction sliding of the hand on the horizontal
surface of a table, with no influence of gravity. The posi-
tion of the seat can be adjusted in such a way that the
farthest targets (see the next section) can only be reached
with an almost extended arm. A 1900 LCD screen is posi-
tioned right in front of the patients at a distance of about
1 m in order to display the positions of hand and target (see
below) by means of circles of different colors, with a
diameter of 2 cm. The visual scale factor is 1:1.
Training protocol
The training protocol specifically focuses on facilitating
active execution of outward movements. The task consists
of hitting a set of targets, arranged in the horizontal plane
(Fig. 1) according to three layers: inner (A, 3 targets),
middle (B, 3 targets), and outer (C, 7 targets); reaching the
outer targets requires an almost full arm extension. The
distance between adjacent layers is 10 cm; the distance
between targets on the same layer is, respectively, 6.26 cm
(layer A), 8.77 cm (layer B), 5.65 cm (layer C). A target is
reached when its distance from the hand is less than 2 cm.
The training movements are performed either with
open eyes (vision condition) or closed eyes (no-vision
Table 1 Subjects’ demographic and clinical data
Subjects Sex Age (years) Paretic hand Etiology Disease
duration (months)
Site of
lesion
FMA
(0–66)
Ashworth
(0–4)
S1 M 72 L PACI 28 FTP 6 3
S2 F 59 R TACI 39 FTP 5 3
S3 F 69 R PACI 25 FL-PR 12 1?
S4 M 57 L PACI 40 FTP 17 3
S5 F 34 R PACI 24 FTP 13 1?
S6 F 30 L TACI 12 FTO 6 2
S7 F 46 R ICH 26 F-PR 6 2
S8 F 53 R SAH 39 FTN 41 1
S9 F 55 L SAH 76 IPO 36 1
Mean 52.78 34.33 15.78 1.88
SD 14.19 18.08 13.56 0.92
Disease duration refers to the time of start of the robot therapy protocol. Etiology is expressed according to the classification of (Bamford et al.
1991). Arm portion of Fugl-Meyer score (FMA), and Ashworth scale of muscle spasticity, both at the beginning of robot therapy
Site of lesion: FTP, fronto-temporo-parietal; FT-PR, fronto-temporal ? pre-rolandic; FTO, fronto-temporo-occipital; FTN, fronto-temporo-
nuclear; IPO, intra-parenchimal occipital; TACI, total anterior circulation infarct; PACI, partial anterior circulation infarct; ICH, intracerebral
hemorrhagic; SAH, subarachnoid hemorrhagic
Exp Brain Res (2009) 194:219–231 221
123

condition). Target sequences are generated according to
the following scheme: A ? C ? B ? A in order to
emphasize the training of wide, outward movements with
respect to the return to the initial flexed posture. In the
vision condition, targets are presented to the subjects
simultaneously in two ways, visual and haptic: (1) visu-
ally, by means of a circle on the computer screen; (2)
haptically, by means of an assistive force field, i.e., a force
vector directed toward the current target, xT whatever the
current position of the hand. This field was designed in
order to fulfill two requirements: (1) to have a ‘gentle’
interaction with the patient, (2) to be effective even in
absence of vision, in order to focus the patient’s attention
on proprioceptive informations. For these reasons, the
assistive force is not activated abruptly at target presen-
tation but with a ramp-and-hold profile R(t): rise time of
1 s and saturation to a force magnitude, FA, which is set
by the therapist as the minimum value that evokes a
functional response, i.e., a (possibly incomplete) move-
ment in the intended direction. The force is switched off as
soon as the subject hits the target. The next target is
presented after a pause of 1 s. It should be noted that the
chosen assistive field does not emulate the behavior of an
ordinary linear spring but rather a constant-force spring. In
both cases it is possible to define a potential function with
a point attractor. In a linear spring, the potential function
grows in a quadratic way with respect to the distance from
the target whereas, in the constant-force spring, it only
grows linearly. In this application, a constant-force spring
is a better assistive mechanism because it provides a
uniform assistance throughout the whole movement, irre-
spective of the distance to the target. In contrast, a linear
spring would provide an assistive force that vanishes as
one approaches the target and is very large when far from
the target.
In addition to the assistive force component, the haptic
control of the robot includes a mild viscous force field
(viscosity coefficient: 12 Ns/m), intended to damp occa-
sional hand oscillations without significantly affecting the
voluntary reaching patterns, and a virtual ‘wall’ (stiffness:
1,000 N/m) which prevents subjects to go beyond the C
layer of targets and provides an additional feedback about
the successful achievement of the outward target.
The force field generated by the robot is summarized as
follows:
FðtÞ ¼ FA
ðxT � xHÞxT � xHj j � RðtÞ � B _xH
� KWðxW � xHÞ step ðxW � xHÞ ð1Þ
where xT is the vector that identifies the target position in
the plane; xH and _xH are, respectively, the hand position
and speed vectors; xW indicates the projection of hand
position on the wall; B is the viscous coefficient; KW is the
stiffness coefficient of the wall; step identifies a step
function, in order to allow the ‘‘wall’’ term to be one-sided.
Considering that subjects were simply instructed to
reach the targets as soon as possible, it should be noted that
the above scheme of assistance does not explicitly specify
the timing of the reaching movement and/or the trajectory
that subjects have to follow in order to reach the target,
except for the occasional ‘sliding’ movements along the
virtual wall. In other words, the robot does not ‘‘guide’’ the
subject’s hand along a fixed trajectory, and does not
enforce a fixed reaching time. This was done on purpose,
together with the choice of keeping the level of robotic
assistance as low as possible, in order to make sure that the
observed responses were mainly driven by active motor
control, not robot action.
The protocol started with a test phase, in which indi-
vidual subjects familiarized with the apparatus and the
range of assistive forces. This phase was supervised by a
physical therapist, who observed the subjects’ response to
the different force levels and selected the minimum level
Ftest capable to induce at least a hint of active response in
the direction of the target.
One block of trials included repetitions of the
A ? C ? B ? A sequence with different targets in ran-
dom order, for a total of 3 9 3 9 7 = 63 movements; 21
of them were large amplitude, outward movements and 42
movements had smaller amplitude and were directed
inward. The protocol, for each session, is then defined by
the following pseudo-code:
Fig. 1 A view from above of a subject holding the manipulandum.
The subject’s shoulders are strapped to a chair; the forearm is attached
to a sliding support; the wrist is stabilized by means of a skateboard
wrist brace and the hand grasp by means of a Velcro holder. The
targets are arranged on three layers: A, B, C. The C layer is placed in
front of a virtual wall. The basic sequence of target activation is
A ? C ? B ? A and it is repeated 3 9 7 9 3 = 63 times in a
random order. Note that the target distance in the figure is twice the
real distance for graphical reasons
222 Exp Brain Res (2009) 194:219–231
123

Session: set F = Ftest
Train: perform 1 block with assistive field intensity F,
Vision condition
if patient is fatigued or time is over then stop
otherwise perform 1 block with assistive field intensity
F, No-vision condition
if patient is fatigued or time is over then stop
else
if performance over threshold then reduce F by 10–20%
go to Train.
Fatigue was ascertained verbally, by asking the patient
at the end of each session. The ‘Time over’ threshold was
set to 1 h (±5 min). Performance was measured as the
mean speed within the session. The performance threshold
for force decrease was empirically set to 10%.
A consequence of the protocol is that, as training pro-
ceeded, the number of blocks increased and the minimum
assistance level decreased. Moreover, in each session
subjects experienced all the assistance levels used in the
previous sessions, plus some additional ones if they were
not fatigued and time was not over. In other words, the
overall pattern of variation of the assistive force during the
training procedure is nonmonotonic: at the beginning of
each session it goes back to the initial force, selected in the
test session; then it is reduced in steps down to a minimum
value that sometimes is lower than the value reached in the
previous session and sometimes is not. The rationale
is double: (1) to help consolidate the memory of the
learned patterns; (2) to adapt the assistance to the actual
performance.
If subjects reached a level of assistance with a force
below 4 N, the no-vision blocks were eliminated because
that level of force is quite close to the acknowledged per-
ceptual threshold and thus is insufficient for allowing the
subjects to perceive target direction without vision.
The robot training protocol consisted of ten sessions (1
session/week), plus the initial test session. Each session did
not last more that 1 h.
Data analysis
Hand trajectories and the forces generated by the robot
were recorded at a sampling rate of 100 Hz. Hand position
was measured from the 17-bit encoders of the motors, with
a precision better than 0.1 mm in the whole workspace.
Hand speed was estimated by using a 4th order Savitzky–
Golay smoothing filter (with an equivalent cut-off
frequency of 6 Hz).
The analysis focused on the outward movements
(A ? C). In particular, we defined four performance
indicators:
• Mean speed: average hand speed, computed from the
time of target presentation to the time at which the
subject reaches the target. This indicator is expected to
increase as training proceeds.
• Number of sub-movements, identified by the number of
peaks in the speed profile. The output of the smoothing
filter may contain a few spurious velocity peaks. We
eliminated them by means of two criteria: (1) a
threshold on the speed (0.01 m/s), (2) a threshold on
the time interval between one peak and the next one
(0.3 s). Normal reaching movements are characterized
by a single-peaked, bell-shaped speed profile (Morasso
1981) and thus this indicator should approach 1, as
training proceeds.
• T-ratio, defined as the ratio between the duration of the
first sub-movement and the total time required for
reaching the target. The corresponding sub-movement
duration is identified by two consecutive points of
minimum in the speed profile, one before and the other
after the point of peak. As training proceeds, this
indicator should go up to 1 (or 100%).
• Endpoint error, defined as the distance from the target
of the hand position at the end of the firs sub-
movement. As training proceeds, this indicator should
decrease to 0.
The first indicator is a global performance parameter.
The second and third indicators express, in different ways,
the degree of smoothness of the movements. This choice is
motivated by the fact that studies on the recovery from
neural injury suggested that smoothness is a result of a
learned, coordinative process rather than a natural conse-
quence of the structure of the neuromuscular system. The
fourth indicator is related to accuracy.
Statistical analysis
As stated in ‘‘Introduction’’, we are interested in assessing
the overall effect of the treatment (number of sessions,
degree of assistance, presence–absence of vision) on
movement performance. However, this same effect may
differ in individual subjects and, within the same subject,
for different target directions. To account for this, we used
a multilevel mixed-effects model (Laird and Ware 1982),
with three fixed factors (session, force, vision) plus an
interaction term (session 9 vision) and two (nested) ran-
dom factors (subject and target). This allows to properly
account for the correlations among repeated measures from
the same subject and within the same target (Murdoch et al.
1998), and at the same time to analyze inter-subject vari-
ability, i.e., how performance and the effect of treatment
varies in different subjects and, for the same subject, in
different movement directions.
Exp Brain Res (2009) 194:219–231 223
123

For each indicator, the model is defined as:
indicatorijk ¼ B0ij þ B1ij � Sijk þ B2ij � Fijk þ B3ij � Fijk
þ B4ij � ðSijk � VijkÞ þ eijk ð2Þ
where Sijk (session) is the session number (from 0 to 9), Fijk
(force) is the intensity of the assistive force (in N), and Vijk
(vision) is the absence (0) or presence (1) of vision,
respectively for the ith subject (i = 1,…,9), the jth target
(j = 1,…,7) and the kth outward trial (k = 1,…,3). The
residual eijk is the portion of the indicator that is explained
by neither of the above factors.
Model coefficients may be interpreted as follows. The
intercept, B0ij, is the estimated baseline performance level,
i.e., the performance at the initial session, with zero as-
sistive force; this can be interpreted as the initial degree of
voluntary control. Parameter B1ij is the between-session
rate of improvement. Parameter B2ij is a ‘compliance’
component, measuring the dependence of performance on
the assistance level. Parameter B3ij is the ‘vision’ compo-
nent, which denotes the contribution to the performance
provided by presence of vision. Finally, parameter B4ij is
the ‘session 9 vision’ component, which accounts for the
differences in the session effect that are due to vision. In
other words, B4ij accounts for the different behaviors, in
terms of between-session improvement, of the vision and
no-vision trials.
The presence of random factors implies that each of the
above parameters can be seen as having a fixed component
(the same for all subjects and targets), and a random
component (different for each subject and, within each
subject, for each target). For instance:
B0ij ¼ b0 þ b0i þ b0i;j ð3Þ
where b0 is the ‘fixed’ portion of the parameter, common to
all subjects and targets; b0i is the portion of the parameter
which relates to the ith subject, and b0i,j is the portion of the
parameter related to the jth target within the ith subject.
These components can be estimated separately. Testing
the significance of the ‘fixed’ components (e.g., b0) cor-
respond to hypothesis testing as in ANOVA. For instance,
asking like whether the therapy produces a significant
improvement would correspond to testing the significance
of the session effect, i.e., b1.
Moreover, if we look at the random parameters (e.g., b0i
and b0i,j) we can analyze inter-subject (and possibly inter-
target) variability. For instance, for the ith subject we may
look at the relationship between the baseline performance
(b0i) and the subsequent improvement (b1i) in the no-vision
condition. Or, we may look at the difference of baseline
performance between vision and no-vision trials (b3i) and
the corresponding difference in improvement between the
same trials (b4i). For each indicator, we fitted the model to
the data by using a restricted maximum-likelihood proce-
dure, which provided estimates of the coefficients that
account for both the fixed and the random components, as
well as the corresponding significance scores. For all sta-
tistical calculations, we used the R statistical package and
specifically the ‘lme’ function library implementation of
mixed-effect models (Bates and Pinheiro 1998).
Results
Overall evolution of the training sessions
In the early sessions, the outward reaching movements
were typically segmented into a sequence of sub-move-
ments. The first sub-movement only covered part of the
total distance, possibly with a directional error, thus
requiring the subjects to make subsequent corrections. In
contrast, inward movements were usually characterized by
a single, higher peak in the speed profile. As a conse-
quence, outward movements tend to have a greater duration
than inward ones. Figure 2 shows, for all the subjects, the
evolution of the speed profile from the initial to the final
session in the two experimental conditions, vision and no
vision, respectively. In general, all the subjects were
characterized by a trend to quicker and smoother reaching
movements in spite of the fact that the level of the assis-
tance force was progressively reduced.
The evolution of the assistance level is summarized in
Table 2. Table 2 shows that the initial assistance level,
which matched the subjects’ degree of impairment, ranged
between 5 and 25 N; this range was reduced to 0–10 N in
the final session.
It should be noted that the less severe patients (S8, S9)
could carry out the task without assistance. The corre-
sponding number of blocks of trials was increased from an
initial range of 3–8 to a final range of 8–12, while keeping
the same total duration of the therapy sessions.
The evolution of the four performance indicators, from
the initial to the final session, in the two experimental
conditions (vision vs. no vision), is reported in Tables 3
(mean speed), 4 (number of sub-movements), 5 (T-ratio),
and 6 (end point error after the first sub-movement).
Fixed effects
Movement performance is affected by repeated training
(the session factor), by the magnitude of assistive force (the
force factor) and by the experimental condition (vision vs.
no vision). In the same session we used different levels of
assistive force, and for a specific subject the same assistive
force was applied throughout the training protocol in a
variable number of blocks.
224 Exp Brain Res (2009) 194:219–231
123

Force
As regards the level of assistance, we found a significant
effect of force—b2 coefficient—on peak speed
(P \ 0.0001), number of peaks (P = 0.0026), endpoint
error (P = 0.0003) and T-ratio (P \ 0.0001). This is no
surprise, as it is the mere confirmation that assistance has a
beneficial effect on performance.
Session
We found highly significant effects of session for the mean
speed (P = 0.0076), the number of sub-movements
(P \ 0.0001), the T-ratio (P = 0.0001), and the endpoint
error (P = 0.0308).
The b1 coefficient—session, systematic part—is positive
for the two indicators (mean speed, T-ratio) for which the
improvement corresponds to an increase of the indicator
(0.335 ± 0.096 cm/s per session and 2.70 ± 0.659% per
session, respectively), and negative for the two indicators
(number of sub-movements and endpoint error) for which
improvement is denoted by a decrement (-0.369 ± 0.098
peaks per session and -0.316 ± 0.088 cm per session,
respectively). This means that the significant effects of
session in fact correspond to improved performance.
Vision
As regards the effect of vision, in no indicator we found
significant vision and session 9 vision effects. This means
that the presence of vision did not have a systematic effect.
Again, this is hardly surprising, as subjects are likely to
differ widely in their sensory impairment as regards its
relationship with the underlying motor impairment: some
subjects strongly rely on vision because proprioception is
poor; in other subjects proprioception is good enough to
take the place of vision; in some case there may even be a
conflict between vision and proprioception.
Random effects
The model of Eq. 2 can be used to identify the individual
variations—subjects by subject and target by target—in the
contributions of each factor (session, force, vision) to each
indicator. Here we only discuss the variability across
subjects.
Fig. 2 Speed profile of the typical movement in the first and the last
session, for each subject and for the same movement (from the central
position of the A layer to the central position of the C layer). The plots
refer to the vision (open eyes, black) and non vision (closed eyes,
gray) conditions, respectively
c
Exp Brain Res (2009) 194:219–231 225
123
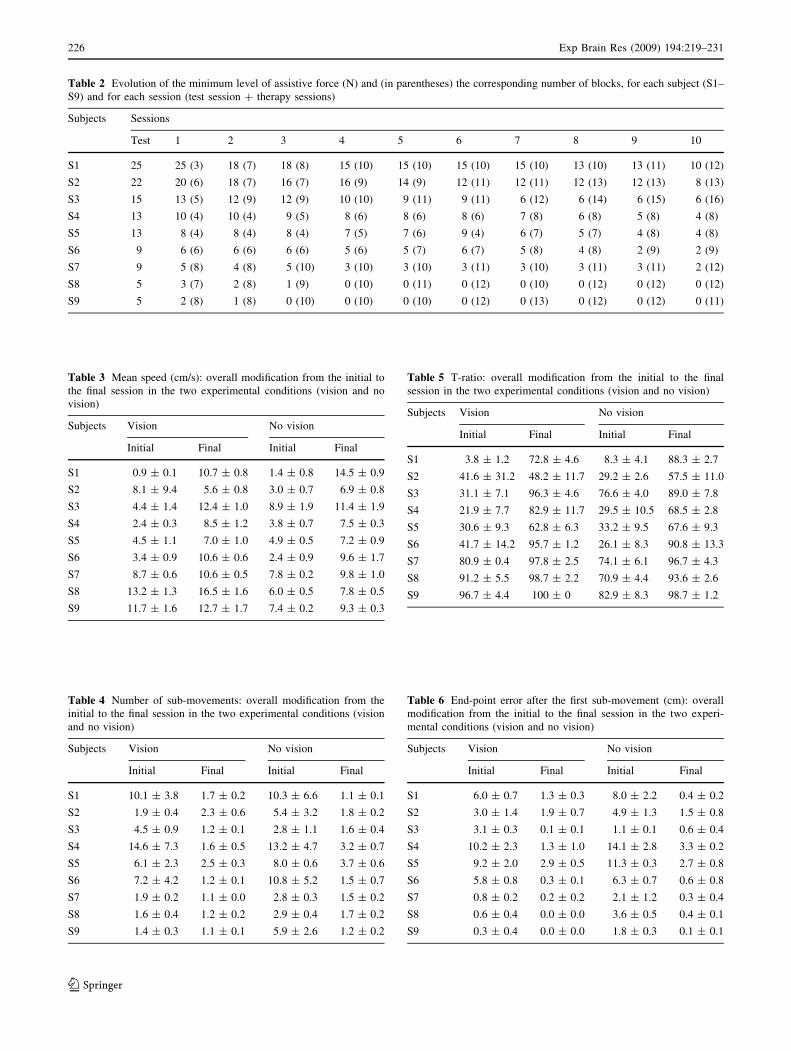
Table 2 Evolution of the minimum level of assistive force (N) and (in parentheses) the corresponding number of blocks, for each subject (S1–
S9) and for each session (test session ? therapy sessions)
Subjects Sessions
Test 1 2 3 4 5 6 7 8 9 10
S1 25 25 (3) 18 (7) 18 (8) 15 (10) 15 (10) 15 (10) 15 (10) 13 (10) 13 (11) 10 (12)
S2 22 20 (6) 18 (7) 16 (7) 16 (9) 14 (9) 12 (11) 12 (11) 12 (13) 12 (13) 8 (13)
S3 15 13 (5) 12 (9) 12 (9) 10 (10) 9 (11) 9 (11) 6 (12) 6 (14) 6 (15) 6 (16)
S4 13 10 (4) 10 (4) 9 (5) 8 (6) 8 (6) 8 (6) 7 (8) 6 (8) 5 (8) 4 (8)
S5 13 8 (4) 8 (4) 8 (4) 7 (5) 7 (6) 9 (4) 6 (7) 5 (7) 4 (8) 4 (8)
S6 9 6 (6) 6 (6) 6 (6) 5 (6) 5 (7) 6 (7) 5 (8) 4 (8) 2 (9) 2 (9)
S7 9 5 (8) 4 (8) 5 (10) 3 (10) 3 (10) 3 (11) 3 (10) 3 (11) 3 (11) 2 (12)
S8 5 3 (7) 2 (8) 1 (9) 0 (10) 0 (11) 0 (12) 0 (10) 0 (12) 0 (12) 0 (12)
S9 5 2 (8) 1 (8) 0 (10) 0 (10) 0 (10) 0 (12) 0 (13) 0 (12) 0 (12) 0 (11)
Table 3 Mean speed (cm/s): overall modification from the initial to
the final session in the two experimental conditions (vision and no
vision)
Subjects Vision No vision
Initial Final Initial Final
S1 0.9 ± 0.1 10.7 ± 0.8 1.4 ± 0.8 14.5 ± 0.9
S2 8.1 ± 9.4 5.6 ± 0.8 3.0 ± 0.7 6.9 ± 0.8
S3 4.4 ± 1.4 12.4 ± 1.0 8.9 ± 1.9 11.4 ± 1.9
S4 2.4 ± 0.3 8.5 ± 1.2 3.8 ± 0.7 7.5 ± 0.3
S5 4.5 ± 1.1 7.0 ± 1.0 4.9 ± 0.5 7.2 ± 0.9
S6 3.4 ± 0.9 10.6 ± 0.6 2.4 ± 0.9 9.6 ± 1.7
S7 8.7 ± 0.6 10.6 ± 0.5 7.8 ± 0.2 9.8 ± 1.0
S8 13.2 ± 1.3 16.5 ± 1.6 6.0 ± 0.5 7.8 ± 0.5
S9 11.7 ± 1.6 12.7 ± 1.7 7.4 ± 0.2 9.3 ± 0.3
Table 4 Number of sub-movements: overall modification from the
initial to the final session in the two experimental conditions (vision
and no vision)
Subjects Vision No vision
Initial Final Initial Final
S1 10.1 ± 3.8 1.7 ± 0.2 10.3 ± 6.6 1.1 ± 0.1
S2 1.9 ± 0.4 2.3 ± 0.6 5.4 ± 3.2 1.8 ± 0.2
S3 4.5 ± 0.9 1.2 ± 0.1 2.8 ± 1.1 1.6 ± 0.4
S4 14.6 ± 7.3 1.6 ± 0.5 13.2 ± 4.7 3.2 ± 0.7
S5 6.1 ± 2.3 2.5 ± 0.3 8.0 ± 0.6 3.7 ± 0.6
S6 7.2 ± 4.2 1.2 ± 0.1 10.8 ± 5.2 1.5 ± 0.7
S7 1.9 ± 0.2 1.1 ± 0.0 2.8 ± 0.3 1.5 ± 0.2
S8 1.6 ± 0.4 1.2 ± 0.2 2.9 ± 0.4 1.7 ± 0.2
S9 1.4 ± 0.3 1.1 ± 0.1 5.9 ± 2.6 1.2 ± 0.2
Table 5 T-ratio: overall modification from the initial to the final
session in the two experimental conditions (vision and no vision)
Subjects Vision No vision
Initial Final Initial Final
S1 3.8 ± 1.2 72.8 ± 4.6 8.3 ± 4.1 88.3 ± 2.7
S2 41.6 ± 31.2 48.2 ± 11.7 29.2 ± 2.6 57.5 ± 11.0
S3 31.1 ± 7.1 96.3 ± 4.6 76.6 ± 4.0 89.0 ± 7.8
S4 21.9 ± 7.7 82.9 ± 11.7 29.5 ± 10.5 68.5 ± 2.8
S5 30.6 ± 9.3 62.8 ± 6.3 33.2 ± 9.5 67.6 ± 9.3
S6 41.7 ± 14.2 95.7 ± 1.2 26.1 ± 8.3 90.8 ± 13.3
S7 80.9 ± 0.4 97.8 ± 2.5 74.1 ± 6.1 96.7 ± 4.3
S8 91.2 ± 5.5 98.7 ± 2.2 70.9 ± 4.4 93.6 ± 2.6
S9 96.7 ± 4.4 100 ± 0 82.9 ± 8.3 98.7 ± 1.2
Table 6 End-point error after the first sub-movement (cm): overall
modification from the initial to the final session in the two experi-
mental conditions (vision and no vision)
Subjects Vision No vision
Initial Final Initial Final
S1 6.0 ± 0.7 1.3 ± 0.3 8.0 ± 2.2 0.4 ± 0.2
S2 3.0 ± 1.4 1.9 ± 0.7 4.9 ± 1.3 1.5 ± 0.8
S3 3.1 ± 0.3 0.1 ± 0.1 1.1 ± 0.1 0.6 ± 0.4
S4 10.2 ± 2.3 1.3 ± 1.0 14.1 ± 2.8 3.3 ± 0.2
S5 9.2 ± 2.0 2.9 ± 0.5 11.3 ± 0.3 2.7 ± 0.8
S6 5.8 ± 0.8 0.3 ± 0.1 6.3 ± 0.7 0.6 ± 0.8
S7 0.8 ± 0.2 0.2 ± 0.2 2.1 ± 1.2 0.3 ± 0.4
S8 0.6 ± 0.4 0.0 ± 0.0 3.6 ± 0.5 0.4 ± 0.1
S9 0.3 ± 0.4 0.0 ± 0.0 1.8 ± 0.3 0.1 ± 0.1
226 Exp Brain Res (2009) 194:219–231
123

Session
To look at the session effect on each individual subject, for
each indicator we compared the model coefficients (both
the systematic and the random part), namely b0 ? b0i
(baseline performance) and b1 ? b1i (session effect, i.e.,
the change over sessions), for each individual subject. This
allowed to assess, across subjects, the relationship between
initial performance and the magnitude of the session effect
(i.e., the change in performance due to training).
These results are displayed in Fig. 3. All indicators
display a strong negative correlation between the baseline
performance, b0 ? b0i and the change over sessions,
b1 ? b1i: r = -0.89 for the mean speed; r = -0.75 for the
number of peaks; r = -0.68 for the T-ratio; r = -0.95 for
the endpoint error. This indicates that subjects with poorer
initial performance tend to improve more. Although this
result can be partly attributed to a ‘ceiling’ effect—in less
severe subjects the initial values of the indicators are closer
to the ‘ceiling’—it also suggests that, irrespective of the
initial conditions, all subjects have a potential for
improvement that is enhanced by the assist-as-needed
protocol. Figure 3 specifically refers to the session effect in
the ‘no-vision’ case. Similar results were found in the
‘vision’ case.
Vision
The model also allows to assess the effect of vision on the
individual subjects. A crucial question is how the different
subjects compare in terms of their initial performance with
open or closed eyes. Another question, similar to the one
we asked before for the ‘session’ effect, is whether there is
any systematic relationship between the difference in the
vision and no-vision baseline behavior and the differential
change in vision and no-vision trials.
The former question can be addressed by comparing, for
each subject, the baseline performance without vision
(b0 ? b0i) and with vision (b0 ? b0i ? b3 ? b3i). For all
four indicators, the comparison is shown in Fig. 4.
The figure indicates that some subjects (namely, S1 and
S3) have a better initial performance with closed eyes (data
points below the diagonal line in the speed and T-ratio
plots). In contrast, other subjects (S8, S9) have a better
performance with open eyes (data points above the diag-
onal). The remaining subjects have similar performances
Fig. 3 Relationship between
the baseline performance (the
b0 ? b0i parameter in the
model) and the change over
sessions (the b1 ? b1i parameter
in the model), relative to the no
vision (closed eyes) case. All
plots display a strong negative
correlation, indicating that
improvement is greater in
subjects with poorer initial
performance. Negative values of
the baseline parameters denote
that these subjects are unable to
move without assistance. For
clarity, the ‘change’ parameter
has been projected over the set
of sessions (i.e., what is shown
is b1 ? b1i multiplied by 9)
Exp Brain Res (2009) 194:219–231 227
123

under both conditions. Moreover, the same figure suggests
that, whatever the initial state of each subject as regards the
relationship between vision and no-vision performance, the
final performance in both conditions improves for all
subjects and all indicators.
Figure 5 complements the above picture by displaying
how the initial performance compares with the change over
sessions. More specifically, it depicts, for each subject, the
relationship between the difference in the baseline perfor-
mance with and without vision (i.e., parameter b3 ? b3i)
and the difference in the performance change over sessions
between trials with and without vision (i.e., parameter
b4 ? b4i).
Figure 5 indicates a strong negative correlation among
these parameters. For speed, number of peaks, T-ratio and
endpoint error, the correlation coefficients are -0.36,
-0.96, -0.88, and -0.81, respectively. This means that
subjects with an initial more severe impairment with closed
eyes (negative b3 ? b3i) result in a greater improvement in
closed eyes trials (negative b4 ? b4i), and vice versa.
Discussion
Subjects improve their motor performance
Analysis of the results suggests that the proposed robot
therapy exercise, based on an assist-as-needed paradigm, is
capable of improving the ability to perform outward
movements in chronic stroke survivors.
Improved performance was characterized by a general
regularization of the movements. In particular, we observed
a remarkable reduction in the degree of segmentation into
sub-movements and the emergence of normal reaching
patterns—straight paths and bell-shaped velocity profiles
(Morasso 1981). As training proceeded, kinematic indica-
tors showed a trend toward movements that were faster,
smoother, and with more symmetric speed profiles. It may
be asked to what extent such improvements are also
indicative of functional recovery. Studies on stroke recov-
ery (Rohrer et al. 2002) have suggested that smoothness is a
result of a learned, coordinative process rather than a natural
Fig. 4 Differential effect of
open eyes (vision) and closed
eyes (no vision) training. For
each subject, filled circlesindicate the baseline
performance in vision and no
vision trials. Circles below thediagonal denote subjects with
better performance (or greater
error, depending on the
indicator) in absence of vision;
circles above the diagonalindicate better performance (or
greater error) in presence of
vision. The lines indicate the
direction and the magnitude of
improvement. Subjects display a
strong trend toward improving
most in the modality in which
they are initially more defective
so that the final performance is
closer to the diagonal. For
clarity, the ‘change’ parameter
(i.e., the length of the line) has
been projected over the set of
sessions
228 Exp Brain Res (2009) 194:219–231
123

consequence of the structure of the neuromuscular system.
Additionally, there is some evidence that the segmented
structure of arm movements in stroke patients can be
attributed to a deficit of inter-joint coordination (Levin
1996). Therefore, smooth movements result from an
improved coordination, which is a necessary condition for
functional recovery.
Minimally assistive training
A peculiar feature of our proposed approach is that
assistance is kept at a minimum, thus preventing move-
ments, as much as possible, from being performed
passively. In other words, movements are assisted, not
enforced by the robot therapist. In contrast, in other more
common approaches the level of assistance is increased if
subjects are unable to reach the target, up to a value that
allows to reach it in one way or another. The difference is
that in our case robot assistance focuses on movement
initiation whereas in other approaches it focuses on
movement termination.
It is interesting to note that after training, the subjects
generally reported mental, not physical tiredness. This
occurs, in particular, when subjects have great difficulties
in reaching the target, in spite of robot assistance. In this
case, they tend to stop temporarily their effort to generate
the appropriate command. To do this, they may carry out
some kind of mental simulation, in which they ‘imagine’
how to reach it. In conclusion, the proposed minimally
assistive strategy may incorporate an element of ‘mental
practice’, facilitated by the fact that movement termination
is not enforced by the robot. This speculation motivates the
design of specific future experiments aimed at the incor-
poration of mental practice in human–robot interaction.
Robot therapy is still effective in severely impaired
subjects
Our results suggest that even severely impaired patients
benefit from robot therapy, to an extent that is at least
comparable to those with mild to intermediate levels of
impairment. This is partly in contrast with other studies,
Fig. 5 Relationship between
the differential effect of training
with open eyes (vision) and
closed eyes (no vision) in the
baseline performance (the
b3 ? b3i parameter in the
model) and in the change over
sessions (the b4 ? b4i parameter
in the model). For the number of
peaks and endpoint error
indicators, subjects with an
initial more severe impairment
in the no-vision condition
(negative b4 ? b4i) result in a
greater improvement in the
same condition
Exp Brain Res (2009) 194:219–231 229
123

which suggest a greater benefit for mildly impaired sub-
jects (Fasoli et al. 2003; Colombo et al. 2005; Patton et al.
2006a). This is a contribution to an open debate, about the
extent to which physical therapy (by either human or robot
therapists) may contribute to the functional recovery of
severe, chronic patients. At least, our results provide some
evidence for a positive prognostic outcome.
The importance of proprioceptive training
Our results suggest that at least a significant part of stroke
survivors may benefit more from proprioception-enhancing
therapy sessions (the ‘no-vision’ condition) than from tra-
ditional visually guided training. In particular, subjects
who initially had problems with closed eyes tend to benefit
most from this training modality (the inverse is true for
subjects who initially displayed more problems with
movements performed in presence of vision). Although this
observation is not conclusive from a strictly clinical point
of view, it strongly motivates future controlled clinical
trials based on this working hypothesis.
In conclusion, we suggest that robots may be useful in
neuromotor rehabilitation not only because they combine
in the same device a capability of delivering interactive and
repeatable sensorimotor exercises and continuously moni-
toring the actual motor performance, but also because they
allow to create new and ‘controlled’ haptic environments in
which patients can learn to move by only using proprio-
ceptive information. We also believe that robot-controlled,
rich, haptic virtual environments may be powerful tools for
a better understanding of the role of proprioception during
acquisition of novel sensorimotor skills and, possibly, for
designing effective robot trainers which are capable to
improve subjects’ performance in skill acquisition.
Acknowledgments This work was supported by two Research
Projects of National Relevance (PRIN) grants awarded by the Italian
Ministry of University and Research to P. Morasso and V. Sanguineti.
We thank Ms. Liliana Zerbino, PT, for the help in the selection of the
patients and the evaluation of the FMA score.
References
Aisen ML, Krebs HI, Hogan N, McDowell F, Volpe BT (1997) The
effect of robot-assisted therapy and rehabilitative training on
motor recovery following stroke. Arch Neurol 54:443–446
Bamford J, Sandercock P, Dennis M, Burn J, Warlow C (1991)
Classification and natural history of clinically identifiable
subtypes of cerebral infarction. Lancet 337:1521–1526
Bates DM, Pinheiro JC (1998) lme and nlme—mixed-effects methods
and classes for S and S-PLUS, Version 3.0. In: Bell Labs, Lucent
Technologies, University of Wisconsin, Madison
Battig WF (1954) The effect of kinesthetic, verbal, and visual cues on
the acquisition of a lever-positioning skill. J Exp Psychol
47:371–380
Bohannon RW, Smith MB (1987) Interrater reliability of a modified
Ashworth scale of muscle spasticity. Phys Ther 67:206–207
Botvinick M, Cohen J (1998) Rubber hands ‘feel’ touch that eyes see.
Nature 391:756
Carey LM, Matyas TA, Oke LE (1993) Sensory loss in stroke
patients: effective training of tactile and proprioceptive discrim-
ination. Arch Phys Med Rehabil 74:602–611
Casadio M, Morasso PG, Sanguineti V, Arrichiello V (2006) Braccio
di Ferro: a new haptic workstation for neuromotor rehabilitation.
Technol Health Care 13:1–20
Casadio M, Giannoni P, Morasso P, Sanguineti V (2009) A proof of
concept study for the integration of robot therapy with physio-
therapy in the treatment of stroke patients. Clin Rehabil (in press)
Colombo R, Pisano F, Micera S, Mazzone A, Delconte C, Carrozza
MC, Dario P, Minuco G (2005) Robotic techniques for upper
limb evaluation and rehabilitation of stroke patients. IEEE Trans
Neural Syst Rehabil Eng 13:311–324
Dechaumont-Palacin S, Marque P, De Boissezon X, Castel-Lacanal
E, Carel C, Berry I, Pastor J, Albucher JF, Chollet F, Loubinoux
I (2007) Neural correlates of proprioceptive integration in the
contralesional hemisphere of very impaired patients shortly after
a subcortical stroke: an fMRI study. Neurorehabil Neural Repair
22(2):154–165
Emken JL, Benitez R, Sideris A, Bobrow JE, Reinkensmeyer DJ
(2007) Motor adaptation as a greedy optimization of error and
effort. J Neurophysiol 97:3997–4006
Fasoli SE, Krebs HI, Stein J, Frontera WR, Hogan N (2003) Effects of
robotic therapy on motor impairment and recovery in chronic
stroke. Arch Phys Med Rehabil 84:477–482
Franklin DW, So U, Burdet E, Kawato M (2007) Visual feedback is
not necessary for the learning of novel dynamics. PLoS ONE
2:e1336
Gladstone DJ, Danells CJ, Black SE (2002) The Fugl-Meyer assessment
of motor recovery after stroke: a critical review of its measurement
properties. Neurorehabil Neural Repair 16:232–240
Kwakkel G, Kollen BJ, Krebs HI (2007) Effects of robot-assisted
therapy on upper limb recovery after stroke: a systematic review.
Neurorehabil Neural Repair 22(2):111–121
Laird NM, Ware JH (1982) Random-effects models for longitudinal
data. Biometrics 38:963–974
Levin MF (1996) Interjoint coordination during pointing movements
is disrupted in spastic hemiparesis. Brain 119(Pt 1):281–293
Morasso P (1981) Spatial control of arm movements. Exp Brain Res
42:223–227
Murdoch IE, Morris SS, Cousens SN (1998) People and eyes:
statistical approaches in ophthalmology. Br J Ophthalmol
82:971–973
Patton JL, Mussa-Ivaldi FA (2004) Robot-assisted adaptive training:
custom force fields for teaching movement patterns. IEEE Trans
Biomed Eng 51:636–646
Patton JL, Kovic M, Mussa-Ivaldi FA (2006a) Custom-designed
haptic training for restoring reaching ability to individuals with
poststroke hemiparesis. J Rehabil Res Dev 43:643–656
Patton JL, Stoykov ME, Kovic M, Mussa-Ivaldi FA (2006b)
Evaluation of robotic training forces that either enhance or
reduce error in chronic hemiparetic stroke survivors. Exp Brain
Res 168:368–383
Platz T, Pinkowski C, van Wijck F, Kim IH, di Bella P, Johnson G
(2005) Reliability and validity of arm function assessment with
standardized guidelines for the Fugl-Meyer Test, Action
Research Arm Test and Box and Block Test: a multicentre
study. Clin Rehabil 19:404–411
Prange GB, Jannink MJ, Groothuis-Oudshoorn CG, Hermens HJ,
Ijzerman MJ (2006) Systematic review of the effect of robot-
aided therapy on recovery of the hemiparetic arm after stroke.
J Rehabil Res Dev 43:171–184
230 Exp Brain Res (2009) 194:219–231
123

Rohrer B, Fasoli S, Krebs HI, Hughes R, Volpe B, Frontera WR, Stein
J, Hogan N (2002) Movement smoothness changes during stroke
recovery. J Neurosci 22:8297–8304
Shadmehr R, Mussa-Ivaldi FA (1994) Adaptive representation of
dynamics during learning of a motor task. J Neurosci 14:3208–
3224
Smeets JB, van den Dobbelsteen JJ, de Grave DD, van Beers RJ,
Brenner E (2006) Sensory integration does not lead to sensory
calibration. Proc Natl Acad Sci USA 103:18781–18786
Sober SJ, Sabes PN (2005) Flexible strategies for sensory integration
during motor planning. Nat Neurosci 8:490–497
Takahashi CD, Reinkensmeyer DJ (2003) Hemiparetic stroke impairs
anticipatory control of arm movement. Exp Brain Res 149:131–
140
Trombly (1995) Occupational therapy for dysfunction. Williams and
Wilkins, Baltimore
Tyson S, Hanley M, Chillala J, Selley AB, Tallis RC (2007) Sensory
loss in hospital-admitted people with stroke: characteristics,
associated factors and relationship with function. Neurorehabil
Neural Repair 22(2):166–172
van Beers RJ, Sittig AC, Denier van der Gon JJ (1996) How humans
combine simultaneous proprioceptive and visual position infor-
mation. Exp Brain Res 111:253–261
van Beers RJ, Sittig AC, Denier van der Gon JJ (1998) The precision
of proprioceptive position sense. Exp Brain Res 122:367–377
Wolpert DM, Ghahramani Z, Jordan MI (1994) Perceptual distortion
contributes to the curvature of human reaching movements. Exp
Brain Res 98:153–156
Exp Brain Res (2009) 194:219–231 231
123