
Right and access to healthcare for undocumented children: Addressing the gap between international...
8
Right and access to healthcare for undocumented children: Addressing the gap between international conventions and disparate implementations in North America and Europe Mo ´ nica Ruiz-Casares a, b, * , Ce ´ cile Rousseau a, b , Ilse Derluyn c , Charles Watters d , François Cre ´ peau e a Faculty of Medicine, McGill University, Montre ´al, Canada b Sante´ Mentale Jeunesse, CSSS de la Montagne, Montre ´al, Canada c Department of Orthopedagogics, Ghent University, Gent, Belgium d School of Social Policy, Sociology and Social Research, University of Kent, Canterbury, UK e Faculty of Law, McGill University, Montre ´al, Canada article info Article history: Available online xxx Keywords: Undocumented children Illegal immigrant Right to health Healthcare access International policy USA Canada Europe abstract Limited access to healthcare for vulnerable immigrant children in Europe and North America is increasingly worrisome as immigration policies harden. This paper analyzes the gap between States’ obligations under international human rights law and the disparate local implementations in diverse countries. Studies that are both multidisciplinary and incorporate micro and macro level indicators are needed to reveal discrepancies between entitlements and access. It is argued that the lack of available data on the magnitude of the problem and on its individual and public health consequences stems from the conflicting situation faced by health institutions required to simultaneously protect the best interest of each child and allocate limited resources. Collaboration in research is urgently needed to assist policy- makers and institutions make informed decisions. Ó 2009 Elsevier Ltd. All rights reserved. Introduction Of the more than 200 million migrants in the world, 60.5 percent reside in the more developed regions, particularly North America and Europe, and 10–15 percent or 20–30 million migrants are estimated to be undocumented (United Nations, 2009). Increasingly concerned with the social, economic, and political consequences of high levels of immigration, North American and European governments are tightening their immigration laws in an effort to lower the levels of immigration and to adjust the status of those already residing in their territory (e.g., through the imposi- tion of numerous restrictions to enter or extend their stay indefi- nitely) (Cre ´ peau & Nakache, 2006). In consequence, countless migrants are entering and remaining in the host country without legal documents or staying longer or on different terms than their temporary permits allowed (e.g., when the asylum claim has failed) (Derluyn & Broekaert, 2005; Derluyn, Lippens, et al., in press; Lindert, Schouler-Ocak, et al., 2008; Passel, 2006; Ter Kuile, Rous- seau, et al., 2007). Of these millions of undocumented migrants (12 million for the USA alone), a small but significant number (esti- mated at between 800,000 and 2.4 million people worldwide yearly, 80 percent of whom are women and girls and up to 50 percent are minors, and most of whom are improperly docu- mented) are especially vulnerable as they have been trafficked and are subsequently exploited (United Nations, 2005; USDS, 2008). Recent immigration policy changes and increasing weight of unremunerated medical services on hospital budgets have rekin- dled the debate about what medical services should be provided to undocumented migrants and who should pay for those services (Ellis, 2006). Obliged to never disclose their presence to the host country’s authorities, undocumented migrants are generally only entitled to emergency care or ‘immediately necessary’ services. Faced with widespread use of healthcare as an immigration policy tool, researchers, medical professionals and national associations in the UK, Sweden, and the US have expressed their concern about increasing restrictions of access to primary healthcare by failed asylum seekers and other undocumented migrants (Arnold, Chalmers, et al., 2008; BMA, 2008; Committee on Community Health Services, 1997; Hjern & Bouvier, 2004). To support their claim, they allege not only humanitarian and public health reasons, * Corresponding author. McGill University/CSSS de la Montagne, Psychiatry, 7085, Hutchinson, Office 204.2.14, Montre ´al, QC Canada H3N 1Y9. Tel.: þ1 514 273 3800x6579. E-mail address: [email protected] (M. Ruiz-Casares). Contents lists available at ScienceDirect Social Science & Medicine journal homepage: www.elsevier.com/locate/socscimed ARTICLE IN PRESS 0277-9536/$ – see front matter Ó 2009 Elsevier Ltd. All rights reserved. doi:10.1016/j.socscimed.2009.10.013 Social Science & Medicine xxx (2009) 1–8 Please cite this article in press as: Ruiz-Casares, M., et al., Right and access to healthcare for undocumented children: Addressing the gap between..., Social Science & Medicine (2009), doi:10.1016/j.socscimed.2009.10.013
-
Upload
universidadlagrancolombia -
Category
Documents
-
view
1 -
download
0
Transcript of Right and access to healthcare for undocumented children: Addressing the gap between international...

lable at ScienceDirect
ARTICLE IN PRESS
Social Science amp Medicine xxx (2009) 1ndash8
Contents lists avai
Social Science amp Medicine
journal homepage wwwelsevier comlocatesocscimed
Right and access to healthcare for undocumented children Addressing the gapbetween international conventions and disparate implementations in NorthAmerica and Europe
Monica Ruiz-Casares ab Cecile Rousseau ab Ilse Derluyn c Charles Watters d Franccedilois Crepeau e
a Faculty of Medicine McGill University Montreal Canadab Sante Mentale Jeunesse CSSS de la Montagne Montreal Canadac Department of Orthopedagogics Ghent University Gent Belgiumd School of Social Policy Sociology and Social Research University of Kent Canterbury UKe Faculty of Law McGill University Montreal Canada
a r t i c l e i n f o
Article historyAvailable online xxx
KeywordsUndocumented childrenIllegal immigrantRight to healthHealthcare accessInternational policyUSACanadaEurope
Electronic Electronic
Corresponding author McGill UniversityCSSS d7085 Hutchinson Office 204214 Montreal QC Cana3800x6579
E-mail address monicaruizcasaresmailmcgillca
0277-9536$ ndash see front matter 2009 Elsevier Ltddoi101016jsocscimed200910013
Please cite this article in press as Ruiz-Casbetween Social Science amp Medicine (2009
a b s t r a c t
Limited access to healthcare for vulnerable immigrant children in Europe and North America isincreasingly worrisome as immigration policies harden This paper analyzes the gap between Statesrsquoobligations under international human rights law and the disparate local implementations in diversecountries Studies that are both multidisciplinary and incorporate micro and macro level indicators areneeded to reveal discrepancies between entitlements and access It is argued that the lack of availabledata on the magnitude of the problem and on its individual and public health consequences stems fromthe conflicting situation faced by health institutions required to simultaneously protect the best interestof each child and allocate limited resources Collaboration in research is urgently needed to assist policy-makers and institutions make informed decisions
2009 Elsevier Ltd All rights reserved
Introduction
Of the more than 200 million migrants in the world 605percent reside in the more developed regions particularly NorthAmerica and Europe and 10ndash15 percent or 20ndash30 million migrantsare estimated to be undocumented (United Nations 2009)Increasingly concerned with the social economic and politicalconsequences of high levels of immigration North American andEuropean governments are tightening their immigration laws in aneffort to lower the levels of immigration and to adjust the status ofthose already residing in their territory (eg through the imposi-tion of numerous restrictions to enter or extend their stay indefi-nitely) (Crepeau amp Nakache 2006) In consequence countlessmigrants are entering and remaining in the host country withoutlegal documents or staying longer or on different terms than theirtemporary permits allowed (eg when the asylum claim has failed)(Derluyn amp Broekaert 2005 Derluyn Lippens et al in press
copy available at httpcopy available at http
e la Montagne Psychiatryda H3N 1Y9 Tel thorn1 514 273
(M Ruiz-Casares)
All rights reserved
ares M et al Right and ac) doi101016jsocscimed20
Lindert Schouler-Ocak et al 2008 Passel 2006 Ter Kuile Rous-seau et al 2007) Of these millions of undocumented migrants (12million for the USA alone) a small but significant number (esti-mated at between 800000 and 24 million people worldwideyearly 80 percent of whom are women and girls and up to 50percent are minors and most of whom are improperly docu-mented) are especially vulnerable as they have been trafficked andare subsequently exploited (United Nations 2005 USDS 2008)
Recent immigration policy changes and increasing weight ofunremunerated medical services on hospital budgets have rekin-dled the debate about what medical services should be provided toundocumented migrants and who should pay for those services(Ellis 2006) Obliged to never disclose their presence to the hostcountryrsquos authorities undocumented migrants are generally onlyentitled to emergency care or lsquoimmediately necessaryrsquo servicesFaced with widespread use of healthcare as an immigration policytool researchers medical professionals and national associations inthe UK Sweden and the US have expressed their concern aboutincreasing restrictions of access to primary healthcare by failedasylum seekers and other undocumented migrants (ArnoldChalmers et al 2008 BMA 2008 Committee on CommunityHealth Services 1997 Hjern amp Bouvier 2004) To support theirclaim they allege not only humanitarian and public health reasons
ssrncomabstract=1513419ssrncomabstract=1513419cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash82
ARTICLE IN PRESS
but also find it lsquolsquomore cost-effective to provide on-going supportrather than to wait until emergency treatment is requiredrsquorsquo (BMA2008)
Access to healthcare for children is of special concern because ofthe long lasting consequences of inadequate care on developmentas well as the State duty of protection of the most vulnerableIndeed there is growing recognition of the far reaching impact ofgood health during pregnancy and childhood on adult health (LuLin et al 2000) Underutilization of preventive care has also beenassociated with poorer health outcomes such as longer stays inhospitals more acute health crises and higher mortality rates(Hadley 2003 Ter Kuile et al 2007) This has lead inter alia to thecreation of special public healthcare programs for undocumentedchildren andor pregnant women in Sweden and several stateswith large immigrant populations in the USA (Hill Dubay et al2008 Hjern amp Bouvier 2004)
This paper raises a profound ethical and public health questionWhich children (should) have the right to healthcare Afterreviewing international human rights instruments addressing theright to health and which have been endorsed by most Europeanand North American countries this paper provides legal and ethicalarguments for extending full coverage to all children withoutregard to their immigration status To illustrate the disconnectbetween international obligations and their national implementa-tion we then compare entitlements to healthcare by undocu-mented migrants in a selected group of countries with specialattention to children This lsquodisconnectrsquo is however but one aspectof the lsquogaprsquo highlighted in this paper Research in the field ofmigration and health is all too frequently confined to a macro levelof analysis with an overriding emphasis on comparing countries onthe level of entitlement alone without an examination of theproblems of access faced by migrants at ground level (Watters2008) This analysis groups countries on the basis of theirsubscription to international conventions and the development ofnational laws and policies It has well established precedents ininternational and comparative social policy in which macro levelanalysis of the features of specific welfare states have given rise tohighly influential typologies such as the lsquothree worlds of welfarecapitalismrsquo proposed by Esping-Andersen (1990)
However the confining of the field of inquiry to laws and poli-cies may we argue generate a potentially misleading impression ofthe localized implementation of such regulations and of the livedexperience of migrants The investigation of these aspects requiresan approach that engages with both macro and micro dimensionsand explores the relationship between these levels (Castles 2003Watters 2008) A bridging of these levels of analysis is suggested byCastles and Miller (2003) in their articulation of lsquomigration systemstheoryrsquo the basic principle of which is that any migratory move-ment can be seen as the result of interacting macro- (ie lsquothe lawsstructures and practicesrsquo established by states) and micro-struc-tures (ie informal social networks developed by migrants them-selves) (p 27) Here we argue that a micro level of investigation isnot confined to relations between migrants but includes theinterpretation and implementation of laws and policies at a locallevel Examples of this approach include the work of NGOs con-cerned with the documentation of human rights abuses withincountries that are signatories to relevant human rights instruments(eg AI 2005 HRW 2008) Another significant illustrationcombining both the macro level of laws and policies and the microlevel of local implementation is the detailed study of unaccompa-nied children in the US UK and Australia undertaken by Bhabhaand Crock (2007) These examples highlight the need forapproaches to research in this field that are both multidisciplinaryand offer multilevel examination incorporating micro and macrolevels The discussion proposes a research agenda and advocates for
Electronic copy available at httpElectronic copy available at httpPlease cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
collaboration of health providers and institutions to ensure thegenuine realization of the right to health for all children Weacknowledge that the right to health contains a variety of freedomsand entitlements yet our discussion will focus on equality of accessto health facilities goods and services because guaranteeingprimary healthcare is an essential intervention to prevent child-hood poor health outcomes and maternal complications Althoughrelevant to all countries receiving immigrants we will illustrate thisdiscussion with legislation and implementation practices in Europeand North America as these regions represent the highest propor-tion of international migrants worldwide as well as a diversity ofhealthcare systems (ie universal and non-universal coverage)
The international legal framework for the right to health
International human rights law sets the boundaries of the rightto health The Constitution of the World Health Organization (WHO1946) adopted by 193 countries recognizes the fundamental rightof every human being to the enjoyment of the highest attainablestandard of health (Preamble) Also widely accepted the UniversalDeclaration of Human Rights (UDHR) (United Nations 1948)proclaims the right of everyone to lsquolsquoa standard of living adequate forthe health and well-being of himself and of his family including() medical care and necessary social servicesrsquorsquo especially duringchildhood and motherhood (art 25) The principles included in theUDHR inspired the development of numerous legally bindinguniversal and regional human rights treaties (Table 1) as well as theinclusion of the right to health healthcare andor health-relatedrights in national constitutions Subsequently case law and otherjurisprudence continue to clarify the scope of the right to health
Among the legally binding international treaties the right tohealth has been more extensively codified in the InternationalCovenant on Economic Social and Cultural Rights (1966) and in theConvention on the Rights of the Child (UNCRC) (United Nations1989)In accordance with article 121 of the Covenant States Partiesrecognize lsquolsquothe right of everyone to the enjoyment of the highestattainable standard of physical and mental healthrsquorsquo while article122 enumerates lsquolsquosteps to be taken by the States Parties () toachieve the full realization of this rightrsquorsquo In the UNCRC ratified todate by all States except two (Somalia and the USA) States Partiesrecognize lsquolsquothe right of the child to the enjoyment of the highestattainable standard of healthrsquorsquo and commit to making every effort lsquolsquotoensure that no child is deprived of his or her right of access to suchhealthcare servicesrsquorsquo (art 241) through inter alia the provision oflsquolsquonecessary medical assistance and healthcare to all childrenrsquorsquo andlsquolsquoappropriate pre-natal and post-natal healthcare for mothersrsquorsquo (art242) Besides the right to healthcare contained in article 24 theUNCRC urges State parties to respect among others the right toprotection (art 19) periodic review of treatment (art 25) andrehabilitation (art 39) with special provisions for children seekingrefugee status (art 22) and those suffering all sorts of exploitation(art 32ndash35) Article 2 of the UNCRC also specifies that the promotionof all these rights should be irrespective of the origin or status of thechild parent(s) or legal guardians Additionally the right to health isrecognized in article 5(e) (iv) of the International Convention on theElimination of All Forms of Racial Discrimination (1965) and in articles111(f) and 12 of the International Convention on the Elimination of AllForms of Discrimination Against Women (1979) The right to healthhas also been proclaimed in regional human rights instruments suchas the European Social Charter (1961) as revised (arts 11 13 and 17the latter dealing more specifically with the protection of mothersand children) and the Additional Protocol to the American Conventionon Human Rights in the Area of Economic Social and Cultural Rights(lsquolsquoProtocol of San Salvadorrsquorsquo) (1988 art10) The right to health has alsobeen specifically protected for migrants in the International
ssrncomabstract=1513419ssrncomabstract=1513419cess to healthcare for undocumented children Addressing the gap0910013
Table 1Status of membership and ratification of international and regional human rights provisions relevant to the right to health by selected countries 2008
Treaty amp opening date of the treaty for signature or adoption North America Europe
Canada USA Sweden Germany UK Belgium Spain
International treatiesa
WHO constitution (22 Jul 1946)d Member Member Member Member Member Member MemberUDHR Universal declaration of human rights (10 Dec 1948)e 10 Dec
194810 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
CERD International convention on the elimination ofall forms of racial discrimination (21 Dec 1965)
14 Oct1970
21 Oct1994
6 Dec1971
16 May1969
7 Mar1969
7 Aug1975
13 Sep1968 a
ICESCR International covenant on economic social andcultural rights (16 Dec 1966)
19 May1976 a
5 Oct1977 s
6 Dec1971
17 Dec1973
20 May1976
21 Apr1983
27 Apr1977
CEDAW International convention on the elimination of all formsof discrimination against women (18 Dec 1979)
10 Dec1981
17 Jul1980 s
2 Jul1980
10 Jul1985
7 Apr1986
10 Jul1985
5 Jan1984
UNCRC UN convention on the rights of the child (20 Nov 1989) 13 Dec1991
16 Feb1995 s
29 Jun1990
6 Mar1992
16 Dec1991f
16 Dec1991
6 Dec1990
CMW International convention on the protection of therights of all migrant workers and members of theirfamilies (18 Dec 1990)
No action No action No action No action No action No action No action
CDP Convention on the rights of persons with disabilities(13 Dec 2006)
30 march2007 s
No action 30 Mar2007 s
30 Mar2007 s
30 March2007 s
30 March2007 s
3 Dec2007
Regional treatiesbc
ECHR ETS No 005 Convention for the protection of human rightsand fundamental freedoms or Europeanconvention on human rights (4 Nov 1950)
na na 4 Feb1952
5 Dec1952
8 Mar1951
14 Jun1955
4 Oct1979
ETS No 14 amp 14A European convention on social and medical assistanceand its protocol (11 December 1953)
na na 2 Sep1955
24 Aug1956
7 Sep1954
24 Jul1956
21 Nov1983
ETS No 035 European social charter (18 Oct 1961) na na 17 Dec1962
27 Jan1965
11 Nov1962
16 Oct1990
6 May1980
ETS No 163 European social charter (revised) (3 May 1996) na na 29 May1998
29 Jun2007 s
7 Nov1997 s
2 Mar2004
23 Oct2000 s
P ACHR OASTS No 69
Additional protocol to the American convention onhuman rights in the area of economic social andcultural rights (lsquolsquoprotocol of San Salvadorrsquorsquo) (17 Nov 1988)
No action No action na na na na na
ETS No 177 Protocol no 12 to the convention for the protection ofhuman rights and fundamental freedoms (4 Nov 2000)
na na No action 4 Nov2000 s
No action 4 Nov2000 s
13 Feb2008
Sources aOHCHR (2008) bCouncil of Europe (2008) cOAS (2008)Notes Dates listed refer to the date of ratification unless followed by an lsquolsquoarsquorsquo which signifies accession or lsquolsquosrsquorsquo which signifies signature only lsquolsquoNo actionrsquorsquo means that country is neither signatory nor party lsquolsquonarsquorsquo (not applicable)means that the instrument is not open to signature for certain states
d All countries which are members of the United Nations may become members of WHO by accepting its Constitutione Adopted and proclaimed by the General Assembly of the United Nations in which all countries listed are representedf Article 22 of the CRC guarantees the protection of children seeking refugee status In the interests of effective immigration control the UK entered a general reservation to the CRC as regards the entry stay in and departure
from the UK of those children subject to immigration control and the acquisition and possession of citizenship The UN Committee on the Rights of the Child as well as the UK Joint Committee on Human Rights have repeatedlydenounced that this exclusion results in lsquolsquounjustified discrimination against asylum-seeking children on the grounds of nationalityrsquorsquo and have recommended that the government should withdraw the immigration andnationality reservation to the CRC (JCHR 2005) Joint Committee On Human RightsdSeventeenth Report London House of Lords and House of Commons
MR
uiz-Casareset
alSocial
Scienceamp
Medicine
xxx(2009)
1ndash83
AR
TIC
LE
INP
RE
SS
Pleasecite
this
articlein
pressas
Ruiz-Casares
M
etal
Righ
tan
daccess
toh
ealthcare
forun
documen
tedch
ildren
Addressin
gth
egap
between
SocialScience
ampM
edicine
(2009)doi101016jsocscim
ed200910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash84
ARTICLE IN PRESS
Convention on the Protection of the Rights of All Migrant Workers andMembers of their Families (1990 in force 2003) all migrant workersand members of their families regardless of their administrativestatus or lack of have a right to lsquolsquoreceive any medical care that isurgently required for the preservation of their life or the avoidanceof irreparable harm to their health on the basis of equality oftreatment with nationals of the State concernedrsquorsquo (art 28) The sameConvention provides that migrant workers in a regular situationhave access to healthcare on a par with nationals Unfortunately thisconvention has been ratified by none of the countries of the GlobalNorth presumably because it specifically recognizes minimal rightsfor undocumented migrants and their families Nonetheless thisdoes not alter their commitments under other instruments
On May 11 2000 the Committee on Economic Social andCultural Rights (CESCR) adopted a General Comment on the right tothe highest attainable standard of health a summary of thedoctrine developed over the years by the Committee on Article 12of the Covenant All State signatories are hence obliged to takewhatever steps are necessary to ensure that everyone has access toavailable healthcare programs and that they can exercise their rightto health without discrimination States parties are under a legalobligation to respect protect and fulfill the right to the highestattainable standard of health for all States must refrain frominterfering directly or indirectly with the enjoyment of the right tohealth (respect) and prevent third parties from doing it too (protect)In this sense the CESCR (2000 para 34) has clarified that the dutyto respect includes abstaining from discriminatory practices anddenying or restricting equal access to healthcare for all personswith special attention to those belonging to especially disadvan-taged groups such as asylum seekers and illegal immigrants Healthsystems must also be responsive to the particular health needs ofchildren adolescents women and other especially vulnerableindividuals and communities (HRC 2008) To fulfill (ie facilitateprovide and promote) this obligation States must take all legisla-tive administrative budgetary judicial and other measuresnecessary for the realization of the lsquolsquoright to the enjoyment ofa variety of facilities goods services and conditions necessary forthe realization of the highest attainable standard of healthrsquorsquo (CESCR2000 para 9 and 33) In the provision of health facilities goods andservices both the CESCR (2000) and the Committee on the Rights ofthe Child (CRC 2003) have urged States parties to pay attention to
a availabilityb accessibility (economically physically and socially) to all chil-
dren without discriminationc acceptability (ie gender sensitive respectful of cultural values
and medical ethicsconfidentiality) andd quality (ie scientifically appropriate facilities drugs methods
and trained personnel)
Human rights law acknowledges that States must addresslegitimate public health safety and other concerns and that theright to health is subject to progressive realization and resourceavailability States are not expected to realize the right to healthimmediately rather they have lsquolsquoa legal obligation to take lsquodelib-erate concrete and targetedrsquo steps towards the realization of theright to health for allrsquorsquo (HRC 2007 para 66) However States mustact in ways that are consistent with obligations acquired underinternational law and always respectful of human dignity and theprinciples of equality and non-discrimination In fact the obligationto avoid de jure and de facto discrimination has an immediate effectgenerating immediate obligations that are subject to neitherprogressive realization nor resource availability (HRC 2007 para63) Moreover a special effort must be made to safeguard the rightsof vulnerable groups
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Legal moral and prudential claims for children
Arguments in favour of comprehensive healthcare for all chil-dren regardless of their immigration status are legal moral andprudential in nature The previous section presented North Amer-ican and European countries as bound by international HumanRights instruments and in many cases their own (constitutional-ized) bills of rights to achieve real equality in access to care andhealth status for all children By becoming a lsquolsquoState partyrsquorsquo thesecountries accepted a legal as well as a moral obligation to promoteand protect human rights and fundamental freedoms voluntarilyundertaking to implement its norms and provisions and to becomeaccountable for so doing to the international community to otherState members and to their own people
Moral claims whether considered a matter of charity or rightsdo not only appeal to humanitarian grounds but are further sup-ported by migrantsrsquo contribution in work and taxes That isundocumented migrants are morally entitled to healthcare andother social services because lsquolsquoall persons have moral claims againstothers to needed assistance in obtaining the requirements ofsurvival and a decent life These claims will obligate others who areable to help and can do so without imposing a harmful burden onthemselves or othersrsquorsquo (Nickel 1986 22) Additionally migrantworkers and their families should benefit from the welfare systembecause they contribute to the economy through work and taxation(eg through income property and sales taxes) Ultimatelywhether we respond to moral claims out of charity or rightslsquolsquodepends not on the nature of the claim but rather on what sorts ofresponses are likely to be affordable and effective in circumstancesrsquorsquo(Nickel 1986 22) While moral claims are binding on all agents(including individuals charitable organizations national govern-ments and international agencies) generally States can respondmore effectively though existing structures such as public schoolsand hospitals (Kuiper Richwald et al 1999 Nickel 1986)
As Nickel (1986) showed in his persuasive rendering of undoc-umented migrantsrsquo entitlement to healthcare there are alsoprudential reasons to provide medical care (BMA 2008 Chang2005 Costich 2001ndash2002 Kaiser Commission on Medicaid andthe Uninsured 2003) These lsquolsquoreasons appealing to the interests oflegal residents of the countryrsquorsquo include
e Public health concerns Excluding children from medical carewould expose others to communicable diseases (eg TB orhepatitis) and jeopardize the effectiveness of outreachparticularly since undocumented migrants are not screenedbefore entering the country
f Lasting impact on individuals and societies Appropriatesupport is needed to ensure childrenrsquos healthy developmentand social integration Denying services to undocumentedmigrants is counterproductive as if they get sick or disabled theywill need more public services and support whereas allowingthem to lead economically independent lives will benefit thesociety at large and prevent higher lsquolsquocosts of unemploymentwelfare and crimersquorsquo (Plyer v Doe 457 US 202 1982) Pre-natalcare and services during birth and early childhood are essentialto prevent or mitigate many long-term disabilities and theirassociated costs This argument is further enhanced if we takeinto account that undocumented immigrant children may stayindefinitely in the country by becoming lawful residents orcitizens (Plyer v Doe 457 US 202 226 230 1982)
g Efficiency and quality of the health system services to eligiblechildren would suffer as a result of lsquolsquoredirecting resources fromproviding services to sorting and enforcement of more restrictiveeligibility standardsrsquorsquo (Committee on Community HealthServices1997) Denying access to preventive care also leads to an
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 5
ARTICLE IN PRESS
inefficient and costly use of other services (such as emergencycare) Although the exact cost of providing care to undocu-mented immigrant children is unknown given the relativelysmall proportion of undocumented children and their under-utilization of services providing them with free preventive andprimary caredrather than with delayed emergency inter-ventiondmay actually lower the costs of the health system
h Limited or no responsibility Children should not be punishedfor their irregular immigration status Whether some contendthat host governments are not obliged to uphold undocu-mented rights of migrants who entered or remained in thecountry illegally it is not fair to apply this argument to chil-dren as they did not chose their place of residence
i Denying healthcare to children is an ineffective method ofdeterring illegal immigration as most individuals migrate foreconomic reasons (Berk Schur et al 2000 Chang 2005)
Although some authors allege distributive justice to defenda very limited access to healthcare for undocumented migrantsnobody to our knowledge has used this argument to justifydepriving children from benefits that are essential to their healthydevelopment In practice however there is a vast discrepancybetween international legal standards and moral and legal nationalframeworks of child protection on the one hand and their actualimplementation in the field of healthcare on the other
Undocumented migrants and access to healthcare in Europeand North America
Wide gaps in implementation of legal obligations to providehealthcare to all children exist both in countries with no universalhealthcare system such as the United States as well as countrieswith public healthcare coverage for all (eg Europe and Canada)Our emphasis on State protection and obligations which originatesin the fact that we live in universal healthcare system environ-ments should not be interpreted however as an endorsement ofexclusive responsibility on the part of the government On thecontrary the assignment of responsibility among stakeholders iscomplex and should consider their relative levels of power
Healthcare for undocumented immigrant children in theUnited States
The March 2005 Current Population Survey in the US shows thatthere were 18 million undocumented children and 31 millionchildren who are US citizens by birth living in families in which thehead of the family or a spouse was undocumented (Passel 2006)Most children in undocumented familiesdparticularly youngerchildrendare eligible for the full range of state and federal publicbenefits because they are USA citizens Many of these childrenhowever may not be receiving the benefits available to thembecause of their parentsrsquo reluctance to approach the government(Fortuny Capps et al 2007 28) Undocumented migrant childrenface the highest barriers to care In 2004 59 percent of undocu-mented migrant adults lacked health insurance in the US with 35percent of their children following that pattern too (Fortuny et al2007) Following the enactment of the Personal Responsibility andWork Opportunity Reconciliation Act (PRWORA) of 1996 all undocu-mented children and those legal migrant children in the UnitedStates for less than five years are ineligible for the two largestfederally-funded health insurance programs for low-income chil-dren ie Medicaid and the State Childrenrsquos Health InsuranceProgram (SCHIP) Medical treatment provided to an undocumentedmigrant child is only covered under Medicaid for immuni-zations treatment of communicable diseases (8 USC xx 1611(b)
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
(1) 1621(b)) and lsquoemergency medical conditionsrsquo (42 USC x1396b(v)(2)(A)) The vagueness of this term however has lead todivergent interpretations by the Courts generating unpredictabilityand inequity (McKeefery 2007) Although some states and countieswithin states have created programs for low-income undocumentedchildren and Federally Qualified Health Centers provide careregardless of ability to pay and de facto immigration status manychildren are still not enrolled and undocumented pregnant womengenerally only receive emergency services Federal and state statutesdenying healthcare benefits to undocumented immigrant childrenare likely to prevail on constitutional grounds yet strong policyarguments have been built on Supreme Court rulings (Chang 2005)
Healthcare for undocumented immigrant children in Canada
Whereas in the United States and in most European countriesimmigrants account for 12 percent or less of the populationimmigrants made up 19 percent of Canadarsquos population (Dumont ampLemaıtre 2005) However estimates of undocumented migrants areparticularly vague with 200000 being the conservative figure mostoften used (Jiminez 2006 Keung 2008) Recent studies conductedin Toronto and Montreal two of the three largest immigrant desti-nations in Canada raised important questions regarding theaccessibility of basic services such as education and healthcare forchildren who are undocumented or whose parents lack legalimmigration status in Canada (Caulford amp Vali 2006 Sidhu 2008Ter Kuile et al 2007) Even if children are born in Canada and qualifyfor provincial coverage parents often find it difficult to obtaindocumentation or are fearful of the consequences that seekinghealthcare might have on their immigration status A number ofwrongful deaths related to immigration status concerns occur everyyear according to a coroner interviewed For refugee claimants withpapers the Interim Federal Health Program (IFHP) only coverslsquoemergency health concernsrsquo (although other services are some-times provided by willing providers) (Ter Kuile et al 2007)
Ever since Singh (1985) Canadian courts have consistentlyrecognized that most provisions of the Canadian Charter of Rightsand Freedoms (1982) including the equality rights guaranteed bysection 15 apply to non-citizens present on Canadian territory Inpractice however policies and government procedures restrictaccess to healthcare for many children including those withprecarious status As a result the Committee on the Rights of theChild (2003) has voiced concerns about the lack of universal accessto quality health services across provinces the increase of traffickedforeign children into Canada and the absence of a national policyon unaccompanied asylum-seeking children Healthcare beingunder provincial jurisdiction the Canadian Coalition for the Rightsof Children (2003) has also called for a review of provincial andterritorial compliance with the Canada Health Act (1984)dparticu-larly itsrsquo two main principles of universality and accessibilitydandrecalled that all provinces are responsible for providing consistentand adequate services to every child Operating out of this mandateto protect children the provincial government of Quebec passedthe Loi sur la Protection de la Jeunesse [Youth Protection Act](Gouvernement du Quebec 2006) which emphasizes the parentalobligation to ensure children safety and development throughlsquoappropriate carersquo Conflicting situations may emerge when parentsare unable to ensure childrenrsquos access to healthcare and educationdue to limitations imposed by their immigration status
Healthcare for undocumented immigrant children in theEuropean Union
It is estimated that 60 million migrants and 8 million undocu-mented migrants are living in the European region (Lancet 2007)
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash86
ARTICLE IN PRESS
Policies on migrationdincluding access to healthcaredremaindiverse in European countries and are strongly influenced by thedifferences in the countryrsquos historical context of migration A recentreport by the Platform for International Cooperation on Undocu-mented Migrants (PICUM 2007) suggests five different systems ofaccess to healthcare for undocumented migrants in Europe
a Countries such as Sweden and Austria where undocumentedmigrants are not entitled to benefit from the public healthsystem They may only access emergency care but have to payfor the incurred medical expenses Notable exceptions are freehealthcare to children of rejected asylum seekers in Swedenand free testing (eg HIV) and treatment of some contagiousdiseases (eg TB) in Austria
b Countries such as Germany and Hungary where undocu-mented migrants do not have access to any publicly subsidizedhealthcare besides emergency care and a limited number ofservices In Germany these include accidents in the workplacecounselling and testing for infectious diseases (eg TB andSTIs) and maternity care and healthcare for children and forundocumented women from 6 weeks prior to delivery to 8ndash12weeks after delivery only and for asylum-seeking pregnantwomen In Germany however public institutions are obligedby law to denounce undocumented migrants seeking health-care to the Foreignersrsquo Office hence deterring them fromexercising their entitlements In Hungary undocumentedmigrants may access other medical services on a paymentbasis
c Countries such as the United Kingdom and Portugal offeringwider health coverage but whose highly ambiguous regula-tions and complicated procedures (eg required registration inPortugal) interfere with the enjoyment of these entitlementsUndocumented migrants may consult a general practitioner inthe UK yet secondary care is usually not covered (ChauvinParizot et al 2007 Cole 2007) Undocumented pregnantwomen and children are charged for services rendered otherthan lsquolsquourgentrsquorsquo healthcare In Portugal undocumented migrantsproving residence for more than 90 days may access publichealthcare upon payment of a fee except in cases of infectiousdiseases maternity care vaccination and family planningOtherwise they may only access emergency care on a paymentbasis Undocumented children may access public healthcareand education like national and documented children
d Countries such as Belgium France and the Netherlands whereundocumented migrants are treated in the mainstream healthsystem yet services are processed through a lsquolsquoparallelrsquorsquo admin-istrative andor payment system In Belgium undocumentedmigrants have free access to lsquolsquourgent medical assistancersquorsquo whichencompasses a broad range of care provisions (eg medicalexaminations childbirth and medications) Under certainconditions undocumented migrants may receive healthinsurance In France undocumented migrants and their fami-lies may access publicly subsidized healthcare after residing inthe country for 3 months and proving minimum income levelsOtherwise they may only access free emergency care treat-ment for contagious diseases all types of healthcare for chil-dren maternity care and abortion for medical reasons Since1998 undocumented migrants in the Netherlands may onlyreceive lsquolsquocare that is medically necessaryrsquorsquo (including maternitycare and preventive care and vaccinations for children) or maylsquolsquojeopardize public healthrsquorsquo If unable to pay a special fund willreimburse the healthcare provider
e Countries such as Spain and Italy offering free access tohealthcare to all including undocumented migrants Undocu-mented minors and pregnant women can access the Spanish
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
national health system free of charge under the same condi-tions as nationals Since 2002 other undocumented migrantsmay access free health services upon registering in the localcivil registry of their usual residence and obtaining a healthcard however variations exist across autonomous communi-ties and lsquofear ignorance and administrative obstaclesrsquo detersome from registering (Ingleby amp Watters 2005 PICUM 2007)In Italy undocumented migrants may access certain freeservices such as emergency care maternity care and any carefor children younger than 6 years lsquolsquoSpecialized carersquorsquo andoutpatient treatment of contagious and chronic diseases are inmost cases subject to a fee
Among European countries access to healthcare for undocu-mented migrants is generally limited to emergencies or to treatconditions jeopardizing public health (Romero-Ortuno 2004)Hereto related Romero-Ortuno (2004) distinguishes two possibleapproaches in Europe concerning the access to healthcare forundocumented migrants the lsquohumanitarianrsquo (or human rights-based) approach as seen in Spain and the lsquoutilitarianrsquo (or negativeexternalities-based) approach as seen in Germany and even in theUK which covers undocumented migrants in order to lsquoprotectrsquo thehost populationrsquos health Finally Belgium and the Netherlandsillustrate a lsquosoftenedrsquo case of the lsquoutilitarianrsquo approach
While the frameworks offered here by PICUM and Romero-Ortuno may be helpful in identifying differences between countrieswith respect to entitlements to healthcare they may say little aboutthe extent to which undocumented migrants can actually gainaccess to health services As Watters (2008) has argued it isimportant to distinguish analytically between entitlement andaccess The former relates to questions at a macro level concerninglaws and policies and can be answered with reference to officialliterature By contrast questions of access can only be answeredadequately through investigating the implementation of laws andpolicies at lsquostreet levelrsquo (p 157) Indeed Romero-Ortuno (2004)notes the distinction between laws and their implementation in hisown research arguing that if a lsquobiased perspective is to be avoided itis necessary to question beforehand whether undocumentedmigrants can actually enjoy the entitlements that all those laws arecurrently providing for (or in other words whether these provi-sions can actually reach the IMs [illegal immigrants])rsquo (p 263) Hegoes on to make the interesting observation that in the UK forexample there is in practice an emphasis on humanitarian practiceat the micro level coexisting with a utilitarian approach at a macroand meso levels
A further weakness of approaches that focus solely on the levelof entitlements is that they can pay scant regard to the widercontexts in which undocumented migrants live For examplerecent reports on the situation of immigrants arriving in theSpanish territory of the Canary Islands have highlighted the plightof migrant children Human Rights Watch (HRW 2007) reports thathundreds of unaccompanied migrant children are held in severelyovercrowded and ill equipped centres where they are at risk ofviolence and ill treatment These examples suggest the importanceof multidisciplinary and multilevel approaches to the investigationof healthcare for undocumented children where legal and policyoriented analysis is combined with the collection and collation ofevidence at a micro level
Improving accountability for the implementation ofhealthcare standards for undocumented migrant children
The full enjoyment of the right to health still remains a distantgoal for millions of migrant children throughout the world Theincreasing use of healthcare access as a weapon in immigration
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013

M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash82
ARTICLE IN PRESS
but also find it lsquolsquomore cost-effective to provide on-going supportrather than to wait until emergency treatment is requiredrsquorsquo (BMA2008)
Access to healthcare for children is of special concern because ofthe long lasting consequences of inadequate care on developmentas well as the State duty of protection of the most vulnerableIndeed there is growing recognition of the far reaching impact ofgood health during pregnancy and childhood on adult health (LuLin et al 2000) Underutilization of preventive care has also beenassociated with poorer health outcomes such as longer stays inhospitals more acute health crises and higher mortality rates(Hadley 2003 Ter Kuile et al 2007) This has lead inter alia to thecreation of special public healthcare programs for undocumentedchildren andor pregnant women in Sweden and several stateswith large immigrant populations in the USA (Hill Dubay et al2008 Hjern amp Bouvier 2004)
This paper raises a profound ethical and public health questionWhich children (should) have the right to healthcare Afterreviewing international human rights instruments addressing theright to health and which have been endorsed by most Europeanand North American countries this paper provides legal and ethicalarguments for extending full coverage to all children withoutregard to their immigration status To illustrate the disconnectbetween international obligations and their national implementa-tion we then compare entitlements to healthcare by undocu-mented migrants in a selected group of countries with specialattention to children This lsquodisconnectrsquo is however but one aspectof the lsquogaprsquo highlighted in this paper Research in the field ofmigration and health is all too frequently confined to a macro levelof analysis with an overriding emphasis on comparing countries onthe level of entitlement alone without an examination of theproblems of access faced by migrants at ground level (Watters2008) This analysis groups countries on the basis of theirsubscription to international conventions and the development ofnational laws and policies It has well established precedents ininternational and comparative social policy in which macro levelanalysis of the features of specific welfare states have given rise tohighly influential typologies such as the lsquothree worlds of welfarecapitalismrsquo proposed by Esping-Andersen (1990)
However the confining of the field of inquiry to laws and poli-cies may we argue generate a potentially misleading impression ofthe localized implementation of such regulations and of the livedexperience of migrants The investigation of these aspects requiresan approach that engages with both macro and micro dimensionsand explores the relationship between these levels (Castles 2003Watters 2008) A bridging of these levels of analysis is suggested byCastles and Miller (2003) in their articulation of lsquomigration systemstheoryrsquo the basic principle of which is that any migratory move-ment can be seen as the result of interacting macro- (ie lsquothe lawsstructures and practicesrsquo established by states) and micro-struc-tures (ie informal social networks developed by migrants them-selves) (p 27) Here we argue that a micro level of investigation isnot confined to relations between migrants but includes theinterpretation and implementation of laws and policies at a locallevel Examples of this approach include the work of NGOs con-cerned with the documentation of human rights abuses withincountries that are signatories to relevant human rights instruments(eg AI 2005 HRW 2008) Another significant illustrationcombining both the macro level of laws and policies and the microlevel of local implementation is the detailed study of unaccompa-nied children in the US UK and Australia undertaken by Bhabhaand Crock (2007) These examples highlight the need forapproaches to research in this field that are both multidisciplinaryand offer multilevel examination incorporating micro and macrolevels The discussion proposes a research agenda and advocates for
Electronic copy available at httpElectronic copy available at httpPlease cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
collaboration of health providers and institutions to ensure thegenuine realization of the right to health for all children Weacknowledge that the right to health contains a variety of freedomsand entitlements yet our discussion will focus on equality of accessto health facilities goods and services because guaranteeingprimary healthcare is an essential intervention to prevent child-hood poor health outcomes and maternal complications Althoughrelevant to all countries receiving immigrants we will illustrate thisdiscussion with legislation and implementation practices in Europeand North America as these regions represent the highest propor-tion of international migrants worldwide as well as a diversity ofhealthcare systems (ie universal and non-universal coverage)
The international legal framework for the right to health
International human rights law sets the boundaries of the rightto health The Constitution of the World Health Organization (WHO1946) adopted by 193 countries recognizes the fundamental rightof every human being to the enjoyment of the highest attainablestandard of health (Preamble) Also widely accepted the UniversalDeclaration of Human Rights (UDHR) (United Nations 1948)proclaims the right of everyone to lsquolsquoa standard of living adequate forthe health and well-being of himself and of his family including() medical care and necessary social servicesrsquorsquo especially duringchildhood and motherhood (art 25) The principles included in theUDHR inspired the development of numerous legally bindinguniversal and regional human rights treaties (Table 1) as well as theinclusion of the right to health healthcare andor health-relatedrights in national constitutions Subsequently case law and otherjurisprudence continue to clarify the scope of the right to health
Among the legally binding international treaties the right tohealth has been more extensively codified in the InternationalCovenant on Economic Social and Cultural Rights (1966) and in theConvention on the Rights of the Child (UNCRC) (United Nations1989)In accordance with article 121 of the Covenant States Partiesrecognize lsquolsquothe right of everyone to the enjoyment of the highestattainable standard of physical and mental healthrsquorsquo while article122 enumerates lsquolsquosteps to be taken by the States Parties () toachieve the full realization of this rightrsquorsquo In the UNCRC ratified todate by all States except two (Somalia and the USA) States Partiesrecognize lsquolsquothe right of the child to the enjoyment of the highestattainable standard of healthrsquorsquo and commit to making every effort lsquolsquotoensure that no child is deprived of his or her right of access to suchhealthcare servicesrsquorsquo (art 241) through inter alia the provision oflsquolsquonecessary medical assistance and healthcare to all childrenrsquorsquo andlsquolsquoappropriate pre-natal and post-natal healthcare for mothersrsquorsquo (art242) Besides the right to healthcare contained in article 24 theUNCRC urges State parties to respect among others the right toprotection (art 19) periodic review of treatment (art 25) andrehabilitation (art 39) with special provisions for children seekingrefugee status (art 22) and those suffering all sorts of exploitation(art 32ndash35) Article 2 of the UNCRC also specifies that the promotionof all these rights should be irrespective of the origin or status of thechild parent(s) or legal guardians Additionally the right to health isrecognized in article 5(e) (iv) of the International Convention on theElimination of All Forms of Racial Discrimination (1965) and in articles111(f) and 12 of the International Convention on the Elimination of AllForms of Discrimination Against Women (1979) The right to healthhas also been proclaimed in regional human rights instruments suchas the European Social Charter (1961) as revised (arts 11 13 and 17the latter dealing more specifically with the protection of mothersand children) and the Additional Protocol to the American Conventionon Human Rights in the Area of Economic Social and Cultural Rights(lsquolsquoProtocol of San Salvadorrsquorsquo) (1988 art10) The right to health has alsobeen specifically protected for migrants in the International
ssrncomabstract=1513419ssrncomabstract=1513419cess to healthcare for undocumented children Addressing the gap0910013
Table 1Status of membership and ratification of international and regional human rights provisions relevant to the right to health by selected countries 2008
Treaty amp opening date of the treaty for signature or adoption North America Europe
Canada USA Sweden Germany UK Belgium Spain
International treatiesa
WHO constitution (22 Jul 1946)d Member Member Member Member Member Member MemberUDHR Universal declaration of human rights (10 Dec 1948)e 10 Dec
194810 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
CERD International convention on the elimination ofall forms of racial discrimination (21 Dec 1965)
14 Oct1970
21 Oct1994
6 Dec1971
16 May1969
7 Mar1969
7 Aug1975
13 Sep1968 a
ICESCR International covenant on economic social andcultural rights (16 Dec 1966)
19 May1976 a
5 Oct1977 s
6 Dec1971
17 Dec1973
20 May1976
21 Apr1983
27 Apr1977
CEDAW International convention on the elimination of all formsof discrimination against women (18 Dec 1979)
10 Dec1981
17 Jul1980 s
2 Jul1980
10 Jul1985
7 Apr1986
10 Jul1985
5 Jan1984
UNCRC UN convention on the rights of the child (20 Nov 1989) 13 Dec1991
16 Feb1995 s
29 Jun1990
6 Mar1992
16 Dec1991f
16 Dec1991
6 Dec1990
CMW International convention on the protection of therights of all migrant workers and members of theirfamilies (18 Dec 1990)
No action No action No action No action No action No action No action
CDP Convention on the rights of persons with disabilities(13 Dec 2006)
30 march2007 s
No action 30 Mar2007 s
30 Mar2007 s
30 March2007 s
30 March2007 s
3 Dec2007
Regional treatiesbc
ECHR ETS No 005 Convention for the protection of human rightsand fundamental freedoms or Europeanconvention on human rights (4 Nov 1950)
na na 4 Feb1952
5 Dec1952
8 Mar1951
14 Jun1955
4 Oct1979
ETS No 14 amp 14A European convention on social and medical assistanceand its protocol (11 December 1953)
na na 2 Sep1955
24 Aug1956
7 Sep1954
24 Jul1956
21 Nov1983
ETS No 035 European social charter (18 Oct 1961) na na 17 Dec1962
27 Jan1965
11 Nov1962
16 Oct1990
6 May1980
ETS No 163 European social charter (revised) (3 May 1996) na na 29 May1998
29 Jun2007 s
7 Nov1997 s
2 Mar2004
23 Oct2000 s
P ACHR OASTS No 69
Additional protocol to the American convention onhuman rights in the area of economic social andcultural rights (lsquolsquoprotocol of San Salvadorrsquorsquo) (17 Nov 1988)
No action No action na na na na na
ETS No 177 Protocol no 12 to the convention for the protection ofhuman rights and fundamental freedoms (4 Nov 2000)
na na No action 4 Nov2000 s
No action 4 Nov2000 s
13 Feb2008
Sources aOHCHR (2008) bCouncil of Europe (2008) cOAS (2008)Notes Dates listed refer to the date of ratification unless followed by an lsquolsquoarsquorsquo which signifies accession or lsquolsquosrsquorsquo which signifies signature only lsquolsquoNo actionrsquorsquo means that country is neither signatory nor party lsquolsquonarsquorsquo (not applicable)means that the instrument is not open to signature for certain states
d All countries which are members of the United Nations may become members of WHO by accepting its Constitutione Adopted and proclaimed by the General Assembly of the United Nations in which all countries listed are representedf Article 22 of the CRC guarantees the protection of children seeking refugee status In the interests of effective immigration control the UK entered a general reservation to the CRC as regards the entry stay in and departure
from the UK of those children subject to immigration control and the acquisition and possession of citizenship The UN Committee on the Rights of the Child as well as the UK Joint Committee on Human Rights have repeatedlydenounced that this exclusion results in lsquolsquounjustified discrimination against asylum-seeking children on the grounds of nationalityrsquorsquo and have recommended that the government should withdraw the immigration andnationality reservation to the CRC (JCHR 2005) Joint Committee On Human RightsdSeventeenth Report London House of Lords and House of Commons
MR
uiz-Casareset
alSocial
Scienceamp
Medicine
xxx(2009)
1ndash83
AR
TIC
LE
INP
RE
SS
Pleasecite
this
articlein
pressas
Ruiz-Casares
M
etal
Righ
tan
daccess
toh
ealthcare
forun
documen
tedch
ildren
Addressin
gth
egap
between
SocialScience
ampM
edicine
(2009)doi101016jsocscim
ed200910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash84
ARTICLE IN PRESS
Convention on the Protection of the Rights of All Migrant Workers andMembers of their Families (1990 in force 2003) all migrant workersand members of their families regardless of their administrativestatus or lack of have a right to lsquolsquoreceive any medical care that isurgently required for the preservation of their life or the avoidanceof irreparable harm to their health on the basis of equality oftreatment with nationals of the State concernedrsquorsquo (art 28) The sameConvention provides that migrant workers in a regular situationhave access to healthcare on a par with nationals Unfortunately thisconvention has been ratified by none of the countries of the GlobalNorth presumably because it specifically recognizes minimal rightsfor undocumented migrants and their families Nonetheless thisdoes not alter their commitments under other instruments
On May 11 2000 the Committee on Economic Social andCultural Rights (CESCR) adopted a General Comment on the right tothe highest attainable standard of health a summary of thedoctrine developed over the years by the Committee on Article 12of the Covenant All State signatories are hence obliged to takewhatever steps are necessary to ensure that everyone has access toavailable healthcare programs and that they can exercise their rightto health without discrimination States parties are under a legalobligation to respect protect and fulfill the right to the highestattainable standard of health for all States must refrain frominterfering directly or indirectly with the enjoyment of the right tohealth (respect) and prevent third parties from doing it too (protect)In this sense the CESCR (2000 para 34) has clarified that the dutyto respect includes abstaining from discriminatory practices anddenying or restricting equal access to healthcare for all personswith special attention to those belonging to especially disadvan-taged groups such as asylum seekers and illegal immigrants Healthsystems must also be responsive to the particular health needs ofchildren adolescents women and other especially vulnerableindividuals and communities (HRC 2008) To fulfill (ie facilitateprovide and promote) this obligation States must take all legisla-tive administrative budgetary judicial and other measuresnecessary for the realization of the lsquolsquoright to the enjoyment ofa variety of facilities goods services and conditions necessary forthe realization of the highest attainable standard of healthrsquorsquo (CESCR2000 para 9 and 33) In the provision of health facilities goods andservices both the CESCR (2000) and the Committee on the Rights ofthe Child (CRC 2003) have urged States parties to pay attention to
a availabilityb accessibility (economically physically and socially) to all chil-
dren without discriminationc acceptability (ie gender sensitive respectful of cultural values
and medical ethicsconfidentiality) andd quality (ie scientifically appropriate facilities drugs methods
and trained personnel)
Human rights law acknowledges that States must addresslegitimate public health safety and other concerns and that theright to health is subject to progressive realization and resourceavailability States are not expected to realize the right to healthimmediately rather they have lsquolsquoa legal obligation to take lsquodelib-erate concrete and targetedrsquo steps towards the realization of theright to health for allrsquorsquo (HRC 2007 para 66) However States mustact in ways that are consistent with obligations acquired underinternational law and always respectful of human dignity and theprinciples of equality and non-discrimination In fact the obligationto avoid de jure and de facto discrimination has an immediate effectgenerating immediate obligations that are subject to neitherprogressive realization nor resource availability (HRC 2007 para63) Moreover a special effort must be made to safeguard the rightsof vulnerable groups
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Legal moral and prudential claims for children
Arguments in favour of comprehensive healthcare for all chil-dren regardless of their immigration status are legal moral andprudential in nature The previous section presented North Amer-ican and European countries as bound by international HumanRights instruments and in many cases their own (constitutional-ized) bills of rights to achieve real equality in access to care andhealth status for all children By becoming a lsquolsquoState partyrsquorsquo thesecountries accepted a legal as well as a moral obligation to promoteand protect human rights and fundamental freedoms voluntarilyundertaking to implement its norms and provisions and to becomeaccountable for so doing to the international community to otherState members and to their own people
Moral claims whether considered a matter of charity or rightsdo not only appeal to humanitarian grounds but are further sup-ported by migrantsrsquo contribution in work and taxes That isundocumented migrants are morally entitled to healthcare andother social services because lsquolsquoall persons have moral claims againstothers to needed assistance in obtaining the requirements ofsurvival and a decent life These claims will obligate others who areable to help and can do so without imposing a harmful burden onthemselves or othersrsquorsquo (Nickel 1986 22) Additionally migrantworkers and their families should benefit from the welfare systembecause they contribute to the economy through work and taxation(eg through income property and sales taxes) Ultimatelywhether we respond to moral claims out of charity or rightslsquolsquodepends not on the nature of the claim but rather on what sorts ofresponses are likely to be affordable and effective in circumstancesrsquorsquo(Nickel 1986 22) While moral claims are binding on all agents(including individuals charitable organizations national govern-ments and international agencies) generally States can respondmore effectively though existing structures such as public schoolsand hospitals (Kuiper Richwald et al 1999 Nickel 1986)
As Nickel (1986) showed in his persuasive rendering of undoc-umented migrantsrsquo entitlement to healthcare there are alsoprudential reasons to provide medical care (BMA 2008 Chang2005 Costich 2001ndash2002 Kaiser Commission on Medicaid andthe Uninsured 2003) These lsquolsquoreasons appealing to the interests oflegal residents of the countryrsquorsquo include
e Public health concerns Excluding children from medical carewould expose others to communicable diseases (eg TB orhepatitis) and jeopardize the effectiveness of outreachparticularly since undocumented migrants are not screenedbefore entering the country
f Lasting impact on individuals and societies Appropriatesupport is needed to ensure childrenrsquos healthy developmentand social integration Denying services to undocumentedmigrants is counterproductive as if they get sick or disabled theywill need more public services and support whereas allowingthem to lead economically independent lives will benefit thesociety at large and prevent higher lsquolsquocosts of unemploymentwelfare and crimersquorsquo (Plyer v Doe 457 US 202 1982) Pre-natalcare and services during birth and early childhood are essentialto prevent or mitigate many long-term disabilities and theirassociated costs This argument is further enhanced if we takeinto account that undocumented immigrant children may stayindefinitely in the country by becoming lawful residents orcitizens (Plyer v Doe 457 US 202 226 230 1982)
g Efficiency and quality of the health system services to eligiblechildren would suffer as a result of lsquolsquoredirecting resources fromproviding services to sorting and enforcement of more restrictiveeligibility standardsrsquorsquo (Committee on Community HealthServices1997) Denying access to preventive care also leads to an
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 5
ARTICLE IN PRESS
inefficient and costly use of other services (such as emergencycare) Although the exact cost of providing care to undocu-mented immigrant children is unknown given the relativelysmall proportion of undocumented children and their under-utilization of services providing them with free preventive andprimary caredrather than with delayed emergency inter-ventiondmay actually lower the costs of the health system
h Limited or no responsibility Children should not be punishedfor their irregular immigration status Whether some contendthat host governments are not obliged to uphold undocu-mented rights of migrants who entered or remained in thecountry illegally it is not fair to apply this argument to chil-dren as they did not chose their place of residence
i Denying healthcare to children is an ineffective method ofdeterring illegal immigration as most individuals migrate foreconomic reasons (Berk Schur et al 2000 Chang 2005)
Although some authors allege distributive justice to defenda very limited access to healthcare for undocumented migrantsnobody to our knowledge has used this argument to justifydepriving children from benefits that are essential to their healthydevelopment In practice however there is a vast discrepancybetween international legal standards and moral and legal nationalframeworks of child protection on the one hand and their actualimplementation in the field of healthcare on the other
Undocumented migrants and access to healthcare in Europeand North America
Wide gaps in implementation of legal obligations to providehealthcare to all children exist both in countries with no universalhealthcare system such as the United States as well as countrieswith public healthcare coverage for all (eg Europe and Canada)Our emphasis on State protection and obligations which originatesin the fact that we live in universal healthcare system environ-ments should not be interpreted however as an endorsement ofexclusive responsibility on the part of the government On thecontrary the assignment of responsibility among stakeholders iscomplex and should consider their relative levels of power
Healthcare for undocumented immigrant children in theUnited States
The March 2005 Current Population Survey in the US shows thatthere were 18 million undocumented children and 31 millionchildren who are US citizens by birth living in families in which thehead of the family or a spouse was undocumented (Passel 2006)Most children in undocumented familiesdparticularly youngerchildrendare eligible for the full range of state and federal publicbenefits because they are USA citizens Many of these childrenhowever may not be receiving the benefits available to thembecause of their parentsrsquo reluctance to approach the government(Fortuny Capps et al 2007 28) Undocumented migrant childrenface the highest barriers to care In 2004 59 percent of undocu-mented migrant adults lacked health insurance in the US with 35percent of their children following that pattern too (Fortuny et al2007) Following the enactment of the Personal Responsibility andWork Opportunity Reconciliation Act (PRWORA) of 1996 all undocu-mented children and those legal migrant children in the UnitedStates for less than five years are ineligible for the two largestfederally-funded health insurance programs for low-income chil-dren ie Medicaid and the State Childrenrsquos Health InsuranceProgram (SCHIP) Medical treatment provided to an undocumentedmigrant child is only covered under Medicaid for immuni-zations treatment of communicable diseases (8 USC xx 1611(b)
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
(1) 1621(b)) and lsquoemergency medical conditionsrsquo (42 USC x1396b(v)(2)(A)) The vagueness of this term however has lead todivergent interpretations by the Courts generating unpredictabilityand inequity (McKeefery 2007) Although some states and countieswithin states have created programs for low-income undocumentedchildren and Federally Qualified Health Centers provide careregardless of ability to pay and de facto immigration status manychildren are still not enrolled and undocumented pregnant womengenerally only receive emergency services Federal and state statutesdenying healthcare benefits to undocumented immigrant childrenare likely to prevail on constitutional grounds yet strong policyarguments have been built on Supreme Court rulings (Chang 2005)
Healthcare for undocumented immigrant children in Canada
Whereas in the United States and in most European countriesimmigrants account for 12 percent or less of the populationimmigrants made up 19 percent of Canadarsquos population (Dumont ampLemaıtre 2005) However estimates of undocumented migrants areparticularly vague with 200000 being the conservative figure mostoften used (Jiminez 2006 Keung 2008) Recent studies conductedin Toronto and Montreal two of the three largest immigrant desti-nations in Canada raised important questions regarding theaccessibility of basic services such as education and healthcare forchildren who are undocumented or whose parents lack legalimmigration status in Canada (Caulford amp Vali 2006 Sidhu 2008Ter Kuile et al 2007) Even if children are born in Canada and qualifyfor provincial coverage parents often find it difficult to obtaindocumentation or are fearful of the consequences that seekinghealthcare might have on their immigration status A number ofwrongful deaths related to immigration status concerns occur everyyear according to a coroner interviewed For refugee claimants withpapers the Interim Federal Health Program (IFHP) only coverslsquoemergency health concernsrsquo (although other services are some-times provided by willing providers) (Ter Kuile et al 2007)
Ever since Singh (1985) Canadian courts have consistentlyrecognized that most provisions of the Canadian Charter of Rightsand Freedoms (1982) including the equality rights guaranteed bysection 15 apply to non-citizens present on Canadian territory Inpractice however policies and government procedures restrictaccess to healthcare for many children including those withprecarious status As a result the Committee on the Rights of theChild (2003) has voiced concerns about the lack of universal accessto quality health services across provinces the increase of traffickedforeign children into Canada and the absence of a national policyon unaccompanied asylum-seeking children Healthcare beingunder provincial jurisdiction the Canadian Coalition for the Rightsof Children (2003) has also called for a review of provincial andterritorial compliance with the Canada Health Act (1984)dparticu-larly itsrsquo two main principles of universality and accessibilitydandrecalled that all provinces are responsible for providing consistentand adequate services to every child Operating out of this mandateto protect children the provincial government of Quebec passedthe Loi sur la Protection de la Jeunesse [Youth Protection Act](Gouvernement du Quebec 2006) which emphasizes the parentalobligation to ensure children safety and development throughlsquoappropriate carersquo Conflicting situations may emerge when parentsare unable to ensure childrenrsquos access to healthcare and educationdue to limitations imposed by their immigration status
Healthcare for undocumented immigrant children in theEuropean Union
It is estimated that 60 million migrants and 8 million undocu-mented migrants are living in the European region (Lancet 2007)
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash86
ARTICLE IN PRESS
Policies on migrationdincluding access to healthcaredremaindiverse in European countries and are strongly influenced by thedifferences in the countryrsquos historical context of migration A recentreport by the Platform for International Cooperation on Undocu-mented Migrants (PICUM 2007) suggests five different systems ofaccess to healthcare for undocumented migrants in Europe
a Countries such as Sweden and Austria where undocumentedmigrants are not entitled to benefit from the public healthsystem They may only access emergency care but have to payfor the incurred medical expenses Notable exceptions are freehealthcare to children of rejected asylum seekers in Swedenand free testing (eg HIV) and treatment of some contagiousdiseases (eg TB) in Austria
b Countries such as Germany and Hungary where undocu-mented migrants do not have access to any publicly subsidizedhealthcare besides emergency care and a limited number ofservices In Germany these include accidents in the workplacecounselling and testing for infectious diseases (eg TB andSTIs) and maternity care and healthcare for children and forundocumented women from 6 weeks prior to delivery to 8ndash12weeks after delivery only and for asylum-seeking pregnantwomen In Germany however public institutions are obligedby law to denounce undocumented migrants seeking health-care to the Foreignersrsquo Office hence deterring them fromexercising their entitlements In Hungary undocumentedmigrants may access other medical services on a paymentbasis
c Countries such as the United Kingdom and Portugal offeringwider health coverage but whose highly ambiguous regula-tions and complicated procedures (eg required registration inPortugal) interfere with the enjoyment of these entitlementsUndocumented migrants may consult a general practitioner inthe UK yet secondary care is usually not covered (ChauvinParizot et al 2007 Cole 2007) Undocumented pregnantwomen and children are charged for services rendered otherthan lsquolsquourgentrsquorsquo healthcare In Portugal undocumented migrantsproving residence for more than 90 days may access publichealthcare upon payment of a fee except in cases of infectiousdiseases maternity care vaccination and family planningOtherwise they may only access emergency care on a paymentbasis Undocumented children may access public healthcareand education like national and documented children
d Countries such as Belgium France and the Netherlands whereundocumented migrants are treated in the mainstream healthsystem yet services are processed through a lsquolsquoparallelrsquorsquo admin-istrative andor payment system In Belgium undocumentedmigrants have free access to lsquolsquourgent medical assistancersquorsquo whichencompasses a broad range of care provisions (eg medicalexaminations childbirth and medications) Under certainconditions undocumented migrants may receive healthinsurance In France undocumented migrants and their fami-lies may access publicly subsidized healthcare after residing inthe country for 3 months and proving minimum income levelsOtherwise they may only access free emergency care treat-ment for contagious diseases all types of healthcare for chil-dren maternity care and abortion for medical reasons Since1998 undocumented migrants in the Netherlands may onlyreceive lsquolsquocare that is medically necessaryrsquorsquo (including maternitycare and preventive care and vaccinations for children) or maylsquolsquojeopardize public healthrsquorsquo If unable to pay a special fund willreimburse the healthcare provider
e Countries such as Spain and Italy offering free access tohealthcare to all including undocumented migrants Undocu-mented minors and pregnant women can access the Spanish
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
national health system free of charge under the same condi-tions as nationals Since 2002 other undocumented migrantsmay access free health services upon registering in the localcivil registry of their usual residence and obtaining a healthcard however variations exist across autonomous communi-ties and lsquofear ignorance and administrative obstaclesrsquo detersome from registering (Ingleby amp Watters 2005 PICUM 2007)In Italy undocumented migrants may access certain freeservices such as emergency care maternity care and any carefor children younger than 6 years lsquolsquoSpecialized carersquorsquo andoutpatient treatment of contagious and chronic diseases are inmost cases subject to a fee
Among European countries access to healthcare for undocu-mented migrants is generally limited to emergencies or to treatconditions jeopardizing public health (Romero-Ortuno 2004)Hereto related Romero-Ortuno (2004) distinguishes two possibleapproaches in Europe concerning the access to healthcare forundocumented migrants the lsquohumanitarianrsquo (or human rights-based) approach as seen in Spain and the lsquoutilitarianrsquo (or negativeexternalities-based) approach as seen in Germany and even in theUK which covers undocumented migrants in order to lsquoprotectrsquo thehost populationrsquos health Finally Belgium and the Netherlandsillustrate a lsquosoftenedrsquo case of the lsquoutilitarianrsquo approach
While the frameworks offered here by PICUM and Romero-Ortuno may be helpful in identifying differences between countrieswith respect to entitlements to healthcare they may say little aboutthe extent to which undocumented migrants can actually gainaccess to health services As Watters (2008) has argued it isimportant to distinguish analytically between entitlement andaccess The former relates to questions at a macro level concerninglaws and policies and can be answered with reference to officialliterature By contrast questions of access can only be answeredadequately through investigating the implementation of laws andpolicies at lsquostreet levelrsquo (p 157) Indeed Romero-Ortuno (2004)notes the distinction between laws and their implementation in hisown research arguing that if a lsquobiased perspective is to be avoided itis necessary to question beforehand whether undocumentedmigrants can actually enjoy the entitlements that all those laws arecurrently providing for (or in other words whether these provi-sions can actually reach the IMs [illegal immigrants])rsquo (p 263) Hegoes on to make the interesting observation that in the UK forexample there is in practice an emphasis on humanitarian practiceat the micro level coexisting with a utilitarian approach at a macroand meso levels
A further weakness of approaches that focus solely on the levelof entitlements is that they can pay scant regard to the widercontexts in which undocumented migrants live For examplerecent reports on the situation of immigrants arriving in theSpanish territory of the Canary Islands have highlighted the plightof migrant children Human Rights Watch (HRW 2007) reports thathundreds of unaccompanied migrant children are held in severelyovercrowded and ill equipped centres where they are at risk ofviolence and ill treatment These examples suggest the importanceof multidisciplinary and multilevel approaches to the investigationof healthcare for undocumented children where legal and policyoriented analysis is combined with the collection and collation ofevidence at a micro level
Improving accountability for the implementation ofhealthcare standards for undocumented migrant children
The full enjoyment of the right to health still remains a distantgoal for millions of migrant children throughout the world Theincreasing use of healthcare access as a weapon in immigration
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013
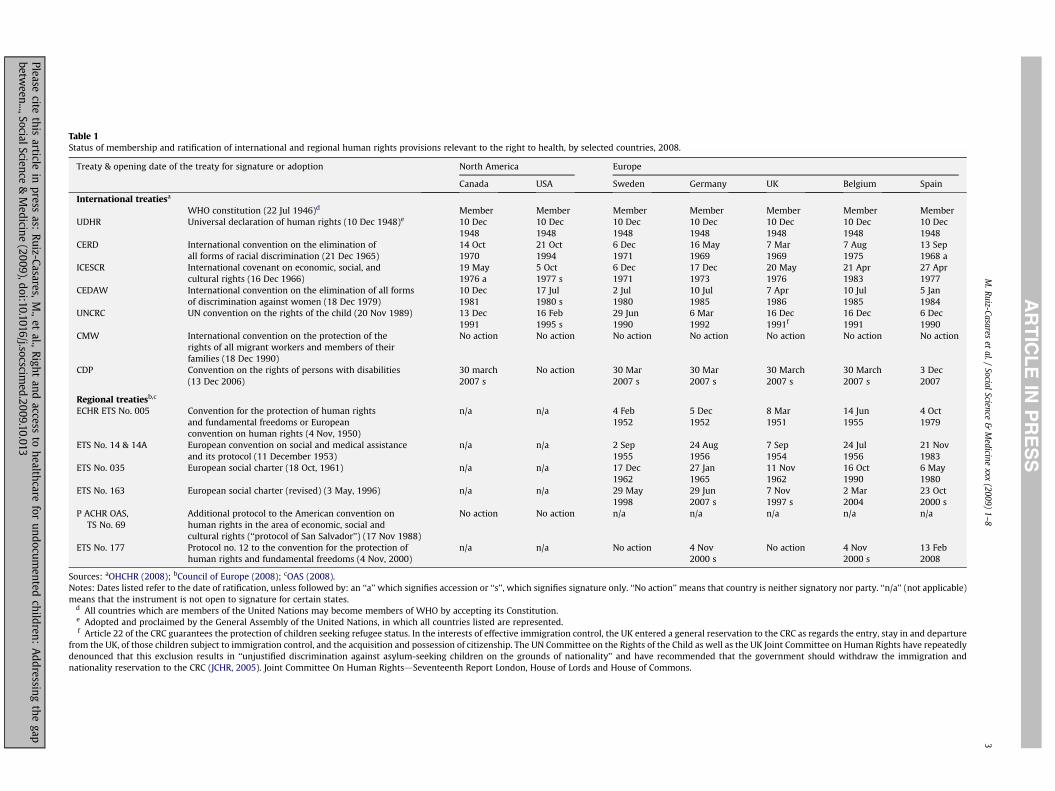
Table 1Status of membership and ratification of international and regional human rights provisions relevant to the right to health by selected countries 2008
Treaty amp opening date of the treaty for signature or adoption North America Europe
Canada USA Sweden Germany UK Belgium Spain
International treatiesa
WHO constitution (22 Jul 1946)d Member Member Member Member Member Member MemberUDHR Universal declaration of human rights (10 Dec 1948)e 10 Dec
194810 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
10 Dec1948
CERD International convention on the elimination ofall forms of racial discrimination (21 Dec 1965)
14 Oct1970
21 Oct1994
6 Dec1971
16 May1969
7 Mar1969
7 Aug1975
13 Sep1968 a
ICESCR International covenant on economic social andcultural rights (16 Dec 1966)
19 May1976 a
5 Oct1977 s
6 Dec1971
17 Dec1973
20 May1976
21 Apr1983
27 Apr1977
CEDAW International convention on the elimination of all formsof discrimination against women (18 Dec 1979)
10 Dec1981
17 Jul1980 s
2 Jul1980
10 Jul1985
7 Apr1986
10 Jul1985
5 Jan1984
UNCRC UN convention on the rights of the child (20 Nov 1989) 13 Dec1991
16 Feb1995 s
29 Jun1990
6 Mar1992
16 Dec1991f
16 Dec1991
6 Dec1990
CMW International convention on the protection of therights of all migrant workers and members of theirfamilies (18 Dec 1990)
No action No action No action No action No action No action No action
CDP Convention on the rights of persons with disabilities(13 Dec 2006)
30 march2007 s
No action 30 Mar2007 s
30 Mar2007 s
30 March2007 s
30 March2007 s
3 Dec2007
Regional treatiesbc
ECHR ETS No 005 Convention for the protection of human rightsand fundamental freedoms or Europeanconvention on human rights (4 Nov 1950)
na na 4 Feb1952
5 Dec1952
8 Mar1951
14 Jun1955
4 Oct1979
ETS No 14 amp 14A European convention on social and medical assistanceand its protocol (11 December 1953)
na na 2 Sep1955
24 Aug1956
7 Sep1954
24 Jul1956
21 Nov1983
ETS No 035 European social charter (18 Oct 1961) na na 17 Dec1962
27 Jan1965
11 Nov1962
16 Oct1990
6 May1980
ETS No 163 European social charter (revised) (3 May 1996) na na 29 May1998
29 Jun2007 s
7 Nov1997 s
2 Mar2004
23 Oct2000 s
P ACHR OASTS No 69
Additional protocol to the American convention onhuman rights in the area of economic social andcultural rights (lsquolsquoprotocol of San Salvadorrsquorsquo) (17 Nov 1988)
No action No action na na na na na
ETS No 177 Protocol no 12 to the convention for the protection ofhuman rights and fundamental freedoms (4 Nov 2000)
na na No action 4 Nov2000 s
No action 4 Nov2000 s
13 Feb2008
Sources aOHCHR (2008) bCouncil of Europe (2008) cOAS (2008)Notes Dates listed refer to the date of ratification unless followed by an lsquolsquoarsquorsquo which signifies accession or lsquolsquosrsquorsquo which signifies signature only lsquolsquoNo actionrsquorsquo means that country is neither signatory nor party lsquolsquonarsquorsquo (not applicable)means that the instrument is not open to signature for certain states
d All countries which are members of the United Nations may become members of WHO by accepting its Constitutione Adopted and proclaimed by the General Assembly of the United Nations in which all countries listed are representedf Article 22 of the CRC guarantees the protection of children seeking refugee status In the interests of effective immigration control the UK entered a general reservation to the CRC as regards the entry stay in and departure
from the UK of those children subject to immigration control and the acquisition and possession of citizenship The UN Committee on the Rights of the Child as well as the UK Joint Committee on Human Rights have repeatedlydenounced that this exclusion results in lsquolsquounjustified discrimination against asylum-seeking children on the grounds of nationalityrsquorsquo and have recommended that the government should withdraw the immigration andnationality reservation to the CRC (JCHR 2005) Joint Committee On Human RightsdSeventeenth Report London House of Lords and House of Commons
MR
uiz-Casareset
alSocial
Scienceamp
Medicine
xxx(2009)
1ndash83
AR
TIC
LE
INP
RE
SS
Pleasecite
this
articlein
pressas
Ruiz-Casares
M
etal
Righ
tan
daccess
toh
ealthcare
forun
documen
tedch
ildren
Addressin
gth
egap
between
SocialScience
ampM
edicine
(2009)doi101016jsocscim
ed200910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash84
ARTICLE IN PRESS
Convention on the Protection of the Rights of All Migrant Workers andMembers of their Families (1990 in force 2003) all migrant workersand members of their families regardless of their administrativestatus or lack of have a right to lsquolsquoreceive any medical care that isurgently required for the preservation of their life or the avoidanceof irreparable harm to their health on the basis of equality oftreatment with nationals of the State concernedrsquorsquo (art 28) The sameConvention provides that migrant workers in a regular situationhave access to healthcare on a par with nationals Unfortunately thisconvention has been ratified by none of the countries of the GlobalNorth presumably because it specifically recognizes minimal rightsfor undocumented migrants and their families Nonetheless thisdoes not alter their commitments under other instruments
On May 11 2000 the Committee on Economic Social andCultural Rights (CESCR) adopted a General Comment on the right tothe highest attainable standard of health a summary of thedoctrine developed over the years by the Committee on Article 12of the Covenant All State signatories are hence obliged to takewhatever steps are necessary to ensure that everyone has access toavailable healthcare programs and that they can exercise their rightto health without discrimination States parties are under a legalobligation to respect protect and fulfill the right to the highestattainable standard of health for all States must refrain frominterfering directly or indirectly with the enjoyment of the right tohealth (respect) and prevent third parties from doing it too (protect)In this sense the CESCR (2000 para 34) has clarified that the dutyto respect includes abstaining from discriminatory practices anddenying or restricting equal access to healthcare for all personswith special attention to those belonging to especially disadvan-taged groups such as asylum seekers and illegal immigrants Healthsystems must also be responsive to the particular health needs ofchildren adolescents women and other especially vulnerableindividuals and communities (HRC 2008) To fulfill (ie facilitateprovide and promote) this obligation States must take all legisla-tive administrative budgetary judicial and other measuresnecessary for the realization of the lsquolsquoright to the enjoyment ofa variety of facilities goods services and conditions necessary forthe realization of the highest attainable standard of healthrsquorsquo (CESCR2000 para 9 and 33) In the provision of health facilities goods andservices both the CESCR (2000) and the Committee on the Rights ofthe Child (CRC 2003) have urged States parties to pay attention to
a availabilityb accessibility (economically physically and socially) to all chil-
dren without discriminationc acceptability (ie gender sensitive respectful of cultural values
and medical ethicsconfidentiality) andd quality (ie scientifically appropriate facilities drugs methods
and trained personnel)
Human rights law acknowledges that States must addresslegitimate public health safety and other concerns and that theright to health is subject to progressive realization and resourceavailability States are not expected to realize the right to healthimmediately rather they have lsquolsquoa legal obligation to take lsquodelib-erate concrete and targetedrsquo steps towards the realization of theright to health for allrsquorsquo (HRC 2007 para 66) However States mustact in ways that are consistent with obligations acquired underinternational law and always respectful of human dignity and theprinciples of equality and non-discrimination In fact the obligationto avoid de jure and de facto discrimination has an immediate effectgenerating immediate obligations that are subject to neitherprogressive realization nor resource availability (HRC 2007 para63) Moreover a special effort must be made to safeguard the rightsof vulnerable groups
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Legal moral and prudential claims for children
Arguments in favour of comprehensive healthcare for all chil-dren regardless of their immigration status are legal moral andprudential in nature The previous section presented North Amer-ican and European countries as bound by international HumanRights instruments and in many cases their own (constitutional-ized) bills of rights to achieve real equality in access to care andhealth status for all children By becoming a lsquolsquoState partyrsquorsquo thesecountries accepted a legal as well as a moral obligation to promoteand protect human rights and fundamental freedoms voluntarilyundertaking to implement its norms and provisions and to becomeaccountable for so doing to the international community to otherState members and to their own people
Moral claims whether considered a matter of charity or rightsdo not only appeal to humanitarian grounds but are further sup-ported by migrantsrsquo contribution in work and taxes That isundocumented migrants are morally entitled to healthcare andother social services because lsquolsquoall persons have moral claims againstothers to needed assistance in obtaining the requirements ofsurvival and a decent life These claims will obligate others who areable to help and can do so without imposing a harmful burden onthemselves or othersrsquorsquo (Nickel 1986 22) Additionally migrantworkers and their families should benefit from the welfare systembecause they contribute to the economy through work and taxation(eg through income property and sales taxes) Ultimatelywhether we respond to moral claims out of charity or rightslsquolsquodepends not on the nature of the claim but rather on what sorts ofresponses are likely to be affordable and effective in circumstancesrsquorsquo(Nickel 1986 22) While moral claims are binding on all agents(including individuals charitable organizations national govern-ments and international agencies) generally States can respondmore effectively though existing structures such as public schoolsand hospitals (Kuiper Richwald et al 1999 Nickel 1986)
As Nickel (1986) showed in his persuasive rendering of undoc-umented migrantsrsquo entitlement to healthcare there are alsoprudential reasons to provide medical care (BMA 2008 Chang2005 Costich 2001ndash2002 Kaiser Commission on Medicaid andthe Uninsured 2003) These lsquolsquoreasons appealing to the interests oflegal residents of the countryrsquorsquo include
e Public health concerns Excluding children from medical carewould expose others to communicable diseases (eg TB orhepatitis) and jeopardize the effectiveness of outreachparticularly since undocumented migrants are not screenedbefore entering the country
f Lasting impact on individuals and societies Appropriatesupport is needed to ensure childrenrsquos healthy developmentand social integration Denying services to undocumentedmigrants is counterproductive as if they get sick or disabled theywill need more public services and support whereas allowingthem to lead economically independent lives will benefit thesociety at large and prevent higher lsquolsquocosts of unemploymentwelfare and crimersquorsquo (Plyer v Doe 457 US 202 1982) Pre-natalcare and services during birth and early childhood are essentialto prevent or mitigate many long-term disabilities and theirassociated costs This argument is further enhanced if we takeinto account that undocumented immigrant children may stayindefinitely in the country by becoming lawful residents orcitizens (Plyer v Doe 457 US 202 226 230 1982)
g Efficiency and quality of the health system services to eligiblechildren would suffer as a result of lsquolsquoredirecting resources fromproviding services to sorting and enforcement of more restrictiveeligibility standardsrsquorsquo (Committee on Community HealthServices1997) Denying access to preventive care also leads to an
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 5
ARTICLE IN PRESS
inefficient and costly use of other services (such as emergencycare) Although the exact cost of providing care to undocu-mented immigrant children is unknown given the relativelysmall proportion of undocumented children and their under-utilization of services providing them with free preventive andprimary caredrather than with delayed emergency inter-ventiondmay actually lower the costs of the health system
h Limited or no responsibility Children should not be punishedfor their irregular immigration status Whether some contendthat host governments are not obliged to uphold undocu-mented rights of migrants who entered or remained in thecountry illegally it is not fair to apply this argument to chil-dren as they did not chose their place of residence
i Denying healthcare to children is an ineffective method ofdeterring illegal immigration as most individuals migrate foreconomic reasons (Berk Schur et al 2000 Chang 2005)
Although some authors allege distributive justice to defenda very limited access to healthcare for undocumented migrantsnobody to our knowledge has used this argument to justifydepriving children from benefits that are essential to their healthydevelopment In practice however there is a vast discrepancybetween international legal standards and moral and legal nationalframeworks of child protection on the one hand and their actualimplementation in the field of healthcare on the other
Undocumented migrants and access to healthcare in Europeand North America
Wide gaps in implementation of legal obligations to providehealthcare to all children exist both in countries with no universalhealthcare system such as the United States as well as countrieswith public healthcare coverage for all (eg Europe and Canada)Our emphasis on State protection and obligations which originatesin the fact that we live in universal healthcare system environ-ments should not be interpreted however as an endorsement ofexclusive responsibility on the part of the government On thecontrary the assignment of responsibility among stakeholders iscomplex and should consider their relative levels of power
Healthcare for undocumented immigrant children in theUnited States
The March 2005 Current Population Survey in the US shows thatthere were 18 million undocumented children and 31 millionchildren who are US citizens by birth living in families in which thehead of the family or a spouse was undocumented (Passel 2006)Most children in undocumented familiesdparticularly youngerchildrendare eligible for the full range of state and federal publicbenefits because they are USA citizens Many of these childrenhowever may not be receiving the benefits available to thembecause of their parentsrsquo reluctance to approach the government(Fortuny Capps et al 2007 28) Undocumented migrant childrenface the highest barriers to care In 2004 59 percent of undocu-mented migrant adults lacked health insurance in the US with 35percent of their children following that pattern too (Fortuny et al2007) Following the enactment of the Personal Responsibility andWork Opportunity Reconciliation Act (PRWORA) of 1996 all undocu-mented children and those legal migrant children in the UnitedStates for less than five years are ineligible for the two largestfederally-funded health insurance programs for low-income chil-dren ie Medicaid and the State Childrenrsquos Health InsuranceProgram (SCHIP) Medical treatment provided to an undocumentedmigrant child is only covered under Medicaid for immuni-zations treatment of communicable diseases (8 USC xx 1611(b)
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
(1) 1621(b)) and lsquoemergency medical conditionsrsquo (42 USC x1396b(v)(2)(A)) The vagueness of this term however has lead todivergent interpretations by the Courts generating unpredictabilityand inequity (McKeefery 2007) Although some states and countieswithin states have created programs for low-income undocumentedchildren and Federally Qualified Health Centers provide careregardless of ability to pay and de facto immigration status manychildren are still not enrolled and undocumented pregnant womengenerally only receive emergency services Federal and state statutesdenying healthcare benefits to undocumented immigrant childrenare likely to prevail on constitutional grounds yet strong policyarguments have been built on Supreme Court rulings (Chang 2005)
Healthcare for undocumented immigrant children in Canada
Whereas in the United States and in most European countriesimmigrants account for 12 percent or less of the populationimmigrants made up 19 percent of Canadarsquos population (Dumont ampLemaıtre 2005) However estimates of undocumented migrants areparticularly vague with 200000 being the conservative figure mostoften used (Jiminez 2006 Keung 2008) Recent studies conductedin Toronto and Montreal two of the three largest immigrant desti-nations in Canada raised important questions regarding theaccessibility of basic services such as education and healthcare forchildren who are undocumented or whose parents lack legalimmigration status in Canada (Caulford amp Vali 2006 Sidhu 2008Ter Kuile et al 2007) Even if children are born in Canada and qualifyfor provincial coverage parents often find it difficult to obtaindocumentation or are fearful of the consequences that seekinghealthcare might have on their immigration status A number ofwrongful deaths related to immigration status concerns occur everyyear according to a coroner interviewed For refugee claimants withpapers the Interim Federal Health Program (IFHP) only coverslsquoemergency health concernsrsquo (although other services are some-times provided by willing providers) (Ter Kuile et al 2007)
Ever since Singh (1985) Canadian courts have consistentlyrecognized that most provisions of the Canadian Charter of Rightsand Freedoms (1982) including the equality rights guaranteed bysection 15 apply to non-citizens present on Canadian territory Inpractice however policies and government procedures restrictaccess to healthcare for many children including those withprecarious status As a result the Committee on the Rights of theChild (2003) has voiced concerns about the lack of universal accessto quality health services across provinces the increase of traffickedforeign children into Canada and the absence of a national policyon unaccompanied asylum-seeking children Healthcare beingunder provincial jurisdiction the Canadian Coalition for the Rightsof Children (2003) has also called for a review of provincial andterritorial compliance with the Canada Health Act (1984)dparticu-larly itsrsquo two main principles of universality and accessibilitydandrecalled that all provinces are responsible for providing consistentand adequate services to every child Operating out of this mandateto protect children the provincial government of Quebec passedthe Loi sur la Protection de la Jeunesse [Youth Protection Act](Gouvernement du Quebec 2006) which emphasizes the parentalobligation to ensure children safety and development throughlsquoappropriate carersquo Conflicting situations may emerge when parentsare unable to ensure childrenrsquos access to healthcare and educationdue to limitations imposed by their immigration status
Healthcare for undocumented immigrant children in theEuropean Union
It is estimated that 60 million migrants and 8 million undocu-mented migrants are living in the European region (Lancet 2007)
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash86
ARTICLE IN PRESS
Policies on migrationdincluding access to healthcaredremaindiverse in European countries and are strongly influenced by thedifferences in the countryrsquos historical context of migration A recentreport by the Platform for International Cooperation on Undocu-mented Migrants (PICUM 2007) suggests five different systems ofaccess to healthcare for undocumented migrants in Europe
a Countries such as Sweden and Austria where undocumentedmigrants are not entitled to benefit from the public healthsystem They may only access emergency care but have to payfor the incurred medical expenses Notable exceptions are freehealthcare to children of rejected asylum seekers in Swedenand free testing (eg HIV) and treatment of some contagiousdiseases (eg TB) in Austria
b Countries such as Germany and Hungary where undocu-mented migrants do not have access to any publicly subsidizedhealthcare besides emergency care and a limited number ofservices In Germany these include accidents in the workplacecounselling and testing for infectious diseases (eg TB andSTIs) and maternity care and healthcare for children and forundocumented women from 6 weeks prior to delivery to 8ndash12weeks after delivery only and for asylum-seeking pregnantwomen In Germany however public institutions are obligedby law to denounce undocumented migrants seeking health-care to the Foreignersrsquo Office hence deterring them fromexercising their entitlements In Hungary undocumentedmigrants may access other medical services on a paymentbasis
c Countries such as the United Kingdom and Portugal offeringwider health coverage but whose highly ambiguous regula-tions and complicated procedures (eg required registration inPortugal) interfere with the enjoyment of these entitlementsUndocumented migrants may consult a general practitioner inthe UK yet secondary care is usually not covered (ChauvinParizot et al 2007 Cole 2007) Undocumented pregnantwomen and children are charged for services rendered otherthan lsquolsquourgentrsquorsquo healthcare In Portugal undocumented migrantsproving residence for more than 90 days may access publichealthcare upon payment of a fee except in cases of infectiousdiseases maternity care vaccination and family planningOtherwise they may only access emergency care on a paymentbasis Undocumented children may access public healthcareand education like national and documented children
d Countries such as Belgium France and the Netherlands whereundocumented migrants are treated in the mainstream healthsystem yet services are processed through a lsquolsquoparallelrsquorsquo admin-istrative andor payment system In Belgium undocumentedmigrants have free access to lsquolsquourgent medical assistancersquorsquo whichencompasses a broad range of care provisions (eg medicalexaminations childbirth and medications) Under certainconditions undocumented migrants may receive healthinsurance In France undocumented migrants and their fami-lies may access publicly subsidized healthcare after residing inthe country for 3 months and proving minimum income levelsOtherwise they may only access free emergency care treat-ment for contagious diseases all types of healthcare for chil-dren maternity care and abortion for medical reasons Since1998 undocumented migrants in the Netherlands may onlyreceive lsquolsquocare that is medically necessaryrsquorsquo (including maternitycare and preventive care and vaccinations for children) or maylsquolsquojeopardize public healthrsquorsquo If unable to pay a special fund willreimburse the healthcare provider
e Countries such as Spain and Italy offering free access tohealthcare to all including undocumented migrants Undocu-mented minors and pregnant women can access the Spanish
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
national health system free of charge under the same condi-tions as nationals Since 2002 other undocumented migrantsmay access free health services upon registering in the localcivil registry of their usual residence and obtaining a healthcard however variations exist across autonomous communi-ties and lsquofear ignorance and administrative obstaclesrsquo detersome from registering (Ingleby amp Watters 2005 PICUM 2007)In Italy undocumented migrants may access certain freeservices such as emergency care maternity care and any carefor children younger than 6 years lsquolsquoSpecialized carersquorsquo andoutpatient treatment of contagious and chronic diseases are inmost cases subject to a fee
Among European countries access to healthcare for undocu-mented migrants is generally limited to emergencies or to treatconditions jeopardizing public health (Romero-Ortuno 2004)Hereto related Romero-Ortuno (2004) distinguishes two possibleapproaches in Europe concerning the access to healthcare forundocumented migrants the lsquohumanitarianrsquo (or human rights-based) approach as seen in Spain and the lsquoutilitarianrsquo (or negativeexternalities-based) approach as seen in Germany and even in theUK which covers undocumented migrants in order to lsquoprotectrsquo thehost populationrsquos health Finally Belgium and the Netherlandsillustrate a lsquosoftenedrsquo case of the lsquoutilitarianrsquo approach
While the frameworks offered here by PICUM and Romero-Ortuno may be helpful in identifying differences between countrieswith respect to entitlements to healthcare they may say little aboutthe extent to which undocumented migrants can actually gainaccess to health services As Watters (2008) has argued it isimportant to distinguish analytically between entitlement andaccess The former relates to questions at a macro level concerninglaws and policies and can be answered with reference to officialliterature By contrast questions of access can only be answeredadequately through investigating the implementation of laws andpolicies at lsquostreet levelrsquo (p 157) Indeed Romero-Ortuno (2004)notes the distinction between laws and their implementation in hisown research arguing that if a lsquobiased perspective is to be avoided itis necessary to question beforehand whether undocumentedmigrants can actually enjoy the entitlements that all those laws arecurrently providing for (or in other words whether these provi-sions can actually reach the IMs [illegal immigrants])rsquo (p 263) Hegoes on to make the interesting observation that in the UK forexample there is in practice an emphasis on humanitarian practiceat the micro level coexisting with a utilitarian approach at a macroand meso levels
A further weakness of approaches that focus solely on the levelof entitlements is that they can pay scant regard to the widercontexts in which undocumented migrants live For examplerecent reports on the situation of immigrants arriving in theSpanish territory of the Canary Islands have highlighted the plightof migrant children Human Rights Watch (HRW 2007) reports thathundreds of unaccompanied migrant children are held in severelyovercrowded and ill equipped centres where they are at risk ofviolence and ill treatment These examples suggest the importanceof multidisciplinary and multilevel approaches to the investigationof healthcare for undocumented children where legal and policyoriented analysis is combined with the collection and collation ofevidence at a micro level
Improving accountability for the implementation ofhealthcare standards for undocumented migrant children
The full enjoyment of the right to health still remains a distantgoal for millions of migrant children throughout the world Theincreasing use of healthcare access as a weapon in immigration
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013

M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash84
ARTICLE IN PRESS
Convention on the Protection of the Rights of All Migrant Workers andMembers of their Families (1990 in force 2003) all migrant workersand members of their families regardless of their administrativestatus or lack of have a right to lsquolsquoreceive any medical care that isurgently required for the preservation of their life or the avoidanceof irreparable harm to their health on the basis of equality oftreatment with nationals of the State concernedrsquorsquo (art 28) The sameConvention provides that migrant workers in a regular situationhave access to healthcare on a par with nationals Unfortunately thisconvention has been ratified by none of the countries of the GlobalNorth presumably because it specifically recognizes minimal rightsfor undocumented migrants and their families Nonetheless thisdoes not alter their commitments under other instruments
On May 11 2000 the Committee on Economic Social andCultural Rights (CESCR) adopted a General Comment on the right tothe highest attainable standard of health a summary of thedoctrine developed over the years by the Committee on Article 12of the Covenant All State signatories are hence obliged to takewhatever steps are necessary to ensure that everyone has access toavailable healthcare programs and that they can exercise their rightto health without discrimination States parties are under a legalobligation to respect protect and fulfill the right to the highestattainable standard of health for all States must refrain frominterfering directly or indirectly with the enjoyment of the right tohealth (respect) and prevent third parties from doing it too (protect)In this sense the CESCR (2000 para 34) has clarified that the dutyto respect includes abstaining from discriminatory practices anddenying or restricting equal access to healthcare for all personswith special attention to those belonging to especially disadvan-taged groups such as asylum seekers and illegal immigrants Healthsystems must also be responsive to the particular health needs ofchildren adolescents women and other especially vulnerableindividuals and communities (HRC 2008) To fulfill (ie facilitateprovide and promote) this obligation States must take all legisla-tive administrative budgetary judicial and other measuresnecessary for the realization of the lsquolsquoright to the enjoyment ofa variety of facilities goods services and conditions necessary forthe realization of the highest attainable standard of healthrsquorsquo (CESCR2000 para 9 and 33) In the provision of health facilities goods andservices both the CESCR (2000) and the Committee on the Rights ofthe Child (CRC 2003) have urged States parties to pay attention to
a availabilityb accessibility (economically physically and socially) to all chil-
dren without discriminationc acceptability (ie gender sensitive respectful of cultural values
and medical ethicsconfidentiality) andd quality (ie scientifically appropriate facilities drugs methods
and trained personnel)
Human rights law acknowledges that States must addresslegitimate public health safety and other concerns and that theright to health is subject to progressive realization and resourceavailability States are not expected to realize the right to healthimmediately rather they have lsquolsquoa legal obligation to take lsquodelib-erate concrete and targetedrsquo steps towards the realization of theright to health for allrsquorsquo (HRC 2007 para 66) However States mustact in ways that are consistent with obligations acquired underinternational law and always respectful of human dignity and theprinciples of equality and non-discrimination In fact the obligationto avoid de jure and de facto discrimination has an immediate effectgenerating immediate obligations that are subject to neitherprogressive realization nor resource availability (HRC 2007 para63) Moreover a special effort must be made to safeguard the rightsof vulnerable groups
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Legal moral and prudential claims for children
Arguments in favour of comprehensive healthcare for all chil-dren regardless of their immigration status are legal moral andprudential in nature The previous section presented North Amer-ican and European countries as bound by international HumanRights instruments and in many cases their own (constitutional-ized) bills of rights to achieve real equality in access to care andhealth status for all children By becoming a lsquolsquoState partyrsquorsquo thesecountries accepted a legal as well as a moral obligation to promoteand protect human rights and fundamental freedoms voluntarilyundertaking to implement its norms and provisions and to becomeaccountable for so doing to the international community to otherState members and to their own people
Moral claims whether considered a matter of charity or rightsdo not only appeal to humanitarian grounds but are further sup-ported by migrantsrsquo contribution in work and taxes That isundocumented migrants are morally entitled to healthcare andother social services because lsquolsquoall persons have moral claims againstothers to needed assistance in obtaining the requirements ofsurvival and a decent life These claims will obligate others who areable to help and can do so without imposing a harmful burden onthemselves or othersrsquorsquo (Nickel 1986 22) Additionally migrantworkers and their families should benefit from the welfare systembecause they contribute to the economy through work and taxation(eg through income property and sales taxes) Ultimatelywhether we respond to moral claims out of charity or rightslsquolsquodepends not on the nature of the claim but rather on what sorts ofresponses are likely to be affordable and effective in circumstancesrsquorsquo(Nickel 1986 22) While moral claims are binding on all agents(including individuals charitable organizations national govern-ments and international agencies) generally States can respondmore effectively though existing structures such as public schoolsand hospitals (Kuiper Richwald et al 1999 Nickel 1986)
As Nickel (1986) showed in his persuasive rendering of undoc-umented migrantsrsquo entitlement to healthcare there are alsoprudential reasons to provide medical care (BMA 2008 Chang2005 Costich 2001ndash2002 Kaiser Commission on Medicaid andthe Uninsured 2003) These lsquolsquoreasons appealing to the interests oflegal residents of the countryrsquorsquo include
e Public health concerns Excluding children from medical carewould expose others to communicable diseases (eg TB orhepatitis) and jeopardize the effectiveness of outreachparticularly since undocumented migrants are not screenedbefore entering the country
f Lasting impact on individuals and societies Appropriatesupport is needed to ensure childrenrsquos healthy developmentand social integration Denying services to undocumentedmigrants is counterproductive as if they get sick or disabled theywill need more public services and support whereas allowingthem to lead economically independent lives will benefit thesociety at large and prevent higher lsquolsquocosts of unemploymentwelfare and crimersquorsquo (Plyer v Doe 457 US 202 1982) Pre-natalcare and services during birth and early childhood are essentialto prevent or mitigate many long-term disabilities and theirassociated costs This argument is further enhanced if we takeinto account that undocumented immigrant children may stayindefinitely in the country by becoming lawful residents orcitizens (Plyer v Doe 457 US 202 226 230 1982)
g Efficiency and quality of the health system services to eligiblechildren would suffer as a result of lsquolsquoredirecting resources fromproviding services to sorting and enforcement of more restrictiveeligibility standardsrsquorsquo (Committee on Community HealthServices1997) Denying access to preventive care also leads to an
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 5
ARTICLE IN PRESS
inefficient and costly use of other services (such as emergencycare) Although the exact cost of providing care to undocu-mented immigrant children is unknown given the relativelysmall proportion of undocumented children and their under-utilization of services providing them with free preventive andprimary caredrather than with delayed emergency inter-ventiondmay actually lower the costs of the health system
h Limited or no responsibility Children should not be punishedfor their irregular immigration status Whether some contendthat host governments are not obliged to uphold undocu-mented rights of migrants who entered or remained in thecountry illegally it is not fair to apply this argument to chil-dren as they did not chose their place of residence
i Denying healthcare to children is an ineffective method ofdeterring illegal immigration as most individuals migrate foreconomic reasons (Berk Schur et al 2000 Chang 2005)
Although some authors allege distributive justice to defenda very limited access to healthcare for undocumented migrantsnobody to our knowledge has used this argument to justifydepriving children from benefits that are essential to their healthydevelopment In practice however there is a vast discrepancybetween international legal standards and moral and legal nationalframeworks of child protection on the one hand and their actualimplementation in the field of healthcare on the other
Undocumented migrants and access to healthcare in Europeand North America
Wide gaps in implementation of legal obligations to providehealthcare to all children exist both in countries with no universalhealthcare system such as the United States as well as countrieswith public healthcare coverage for all (eg Europe and Canada)Our emphasis on State protection and obligations which originatesin the fact that we live in universal healthcare system environ-ments should not be interpreted however as an endorsement ofexclusive responsibility on the part of the government On thecontrary the assignment of responsibility among stakeholders iscomplex and should consider their relative levels of power
Healthcare for undocumented immigrant children in theUnited States
The March 2005 Current Population Survey in the US shows thatthere were 18 million undocumented children and 31 millionchildren who are US citizens by birth living in families in which thehead of the family or a spouse was undocumented (Passel 2006)Most children in undocumented familiesdparticularly youngerchildrendare eligible for the full range of state and federal publicbenefits because they are USA citizens Many of these childrenhowever may not be receiving the benefits available to thembecause of their parentsrsquo reluctance to approach the government(Fortuny Capps et al 2007 28) Undocumented migrant childrenface the highest barriers to care In 2004 59 percent of undocu-mented migrant adults lacked health insurance in the US with 35percent of their children following that pattern too (Fortuny et al2007) Following the enactment of the Personal Responsibility andWork Opportunity Reconciliation Act (PRWORA) of 1996 all undocu-mented children and those legal migrant children in the UnitedStates for less than five years are ineligible for the two largestfederally-funded health insurance programs for low-income chil-dren ie Medicaid and the State Childrenrsquos Health InsuranceProgram (SCHIP) Medical treatment provided to an undocumentedmigrant child is only covered under Medicaid for immuni-zations treatment of communicable diseases (8 USC xx 1611(b)
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
(1) 1621(b)) and lsquoemergency medical conditionsrsquo (42 USC x1396b(v)(2)(A)) The vagueness of this term however has lead todivergent interpretations by the Courts generating unpredictabilityand inequity (McKeefery 2007) Although some states and countieswithin states have created programs for low-income undocumentedchildren and Federally Qualified Health Centers provide careregardless of ability to pay and de facto immigration status manychildren are still not enrolled and undocumented pregnant womengenerally only receive emergency services Federal and state statutesdenying healthcare benefits to undocumented immigrant childrenare likely to prevail on constitutional grounds yet strong policyarguments have been built on Supreme Court rulings (Chang 2005)
Healthcare for undocumented immigrant children in Canada
Whereas in the United States and in most European countriesimmigrants account for 12 percent or less of the populationimmigrants made up 19 percent of Canadarsquos population (Dumont ampLemaıtre 2005) However estimates of undocumented migrants areparticularly vague with 200000 being the conservative figure mostoften used (Jiminez 2006 Keung 2008) Recent studies conductedin Toronto and Montreal two of the three largest immigrant desti-nations in Canada raised important questions regarding theaccessibility of basic services such as education and healthcare forchildren who are undocumented or whose parents lack legalimmigration status in Canada (Caulford amp Vali 2006 Sidhu 2008Ter Kuile et al 2007) Even if children are born in Canada and qualifyfor provincial coverage parents often find it difficult to obtaindocumentation or are fearful of the consequences that seekinghealthcare might have on their immigration status A number ofwrongful deaths related to immigration status concerns occur everyyear according to a coroner interviewed For refugee claimants withpapers the Interim Federal Health Program (IFHP) only coverslsquoemergency health concernsrsquo (although other services are some-times provided by willing providers) (Ter Kuile et al 2007)
Ever since Singh (1985) Canadian courts have consistentlyrecognized that most provisions of the Canadian Charter of Rightsand Freedoms (1982) including the equality rights guaranteed bysection 15 apply to non-citizens present on Canadian territory Inpractice however policies and government procedures restrictaccess to healthcare for many children including those withprecarious status As a result the Committee on the Rights of theChild (2003) has voiced concerns about the lack of universal accessto quality health services across provinces the increase of traffickedforeign children into Canada and the absence of a national policyon unaccompanied asylum-seeking children Healthcare beingunder provincial jurisdiction the Canadian Coalition for the Rightsof Children (2003) has also called for a review of provincial andterritorial compliance with the Canada Health Act (1984)dparticu-larly itsrsquo two main principles of universality and accessibilitydandrecalled that all provinces are responsible for providing consistentand adequate services to every child Operating out of this mandateto protect children the provincial government of Quebec passedthe Loi sur la Protection de la Jeunesse [Youth Protection Act](Gouvernement du Quebec 2006) which emphasizes the parentalobligation to ensure children safety and development throughlsquoappropriate carersquo Conflicting situations may emerge when parentsare unable to ensure childrenrsquos access to healthcare and educationdue to limitations imposed by their immigration status
Healthcare for undocumented immigrant children in theEuropean Union
It is estimated that 60 million migrants and 8 million undocu-mented migrants are living in the European region (Lancet 2007)
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash86
ARTICLE IN PRESS
Policies on migrationdincluding access to healthcaredremaindiverse in European countries and are strongly influenced by thedifferences in the countryrsquos historical context of migration A recentreport by the Platform for International Cooperation on Undocu-mented Migrants (PICUM 2007) suggests five different systems ofaccess to healthcare for undocumented migrants in Europe
a Countries such as Sweden and Austria where undocumentedmigrants are not entitled to benefit from the public healthsystem They may only access emergency care but have to payfor the incurred medical expenses Notable exceptions are freehealthcare to children of rejected asylum seekers in Swedenand free testing (eg HIV) and treatment of some contagiousdiseases (eg TB) in Austria
b Countries such as Germany and Hungary where undocu-mented migrants do not have access to any publicly subsidizedhealthcare besides emergency care and a limited number ofservices In Germany these include accidents in the workplacecounselling and testing for infectious diseases (eg TB andSTIs) and maternity care and healthcare for children and forundocumented women from 6 weeks prior to delivery to 8ndash12weeks after delivery only and for asylum-seeking pregnantwomen In Germany however public institutions are obligedby law to denounce undocumented migrants seeking health-care to the Foreignersrsquo Office hence deterring them fromexercising their entitlements In Hungary undocumentedmigrants may access other medical services on a paymentbasis
c Countries such as the United Kingdom and Portugal offeringwider health coverage but whose highly ambiguous regula-tions and complicated procedures (eg required registration inPortugal) interfere with the enjoyment of these entitlementsUndocumented migrants may consult a general practitioner inthe UK yet secondary care is usually not covered (ChauvinParizot et al 2007 Cole 2007) Undocumented pregnantwomen and children are charged for services rendered otherthan lsquolsquourgentrsquorsquo healthcare In Portugal undocumented migrantsproving residence for more than 90 days may access publichealthcare upon payment of a fee except in cases of infectiousdiseases maternity care vaccination and family planningOtherwise they may only access emergency care on a paymentbasis Undocumented children may access public healthcareand education like national and documented children
d Countries such as Belgium France and the Netherlands whereundocumented migrants are treated in the mainstream healthsystem yet services are processed through a lsquolsquoparallelrsquorsquo admin-istrative andor payment system In Belgium undocumentedmigrants have free access to lsquolsquourgent medical assistancersquorsquo whichencompasses a broad range of care provisions (eg medicalexaminations childbirth and medications) Under certainconditions undocumented migrants may receive healthinsurance In France undocumented migrants and their fami-lies may access publicly subsidized healthcare after residing inthe country for 3 months and proving minimum income levelsOtherwise they may only access free emergency care treat-ment for contagious diseases all types of healthcare for chil-dren maternity care and abortion for medical reasons Since1998 undocumented migrants in the Netherlands may onlyreceive lsquolsquocare that is medically necessaryrsquorsquo (including maternitycare and preventive care and vaccinations for children) or maylsquolsquojeopardize public healthrsquorsquo If unable to pay a special fund willreimburse the healthcare provider
e Countries such as Spain and Italy offering free access tohealthcare to all including undocumented migrants Undocu-mented minors and pregnant women can access the Spanish
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
national health system free of charge under the same condi-tions as nationals Since 2002 other undocumented migrantsmay access free health services upon registering in the localcivil registry of their usual residence and obtaining a healthcard however variations exist across autonomous communi-ties and lsquofear ignorance and administrative obstaclesrsquo detersome from registering (Ingleby amp Watters 2005 PICUM 2007)In Italy undocumented migrants may access certain freeservices such as emergency care maternity care and any carefor children younger than 6 years lsquolsquoSpecialized carersquorsquo andoutpatient treatment of contagious and chronic diseases are inmost cases subject to a fee
Among European countries access to healthcare for undocu-mented migrants is generally limited to emergencies or to treatconditions jeopardizing public health (Romero-Ortuno 2004)Hereto related Romero-Ortuno (2004) distinguishes two possibleapproaches in Europe concerning the access to healthcare forundocumented migrants the lsquohumanitarianrsquo (or human rights-based) approach as seen in Spain and the lsquoutilitarianrsquo (or negativeexternalities-based) approach as seen in Germany and even in theUK which covers undocumented migrants in order to lsquoprotectrsquo thehost populationrsquos health Finally Belgium and the Netherlandsillustrate a lsquosoftenedrsquo case of the lsquoutilitarianrsquo approach
While the frameworks offered here by PICUM and Romero-Ortuno may be helpful in identifying differences between countrieswith respect to entitlements to healthcare they may say little aboutthe extent to which undocumented migrants can actually gainaccess to health services As Watters (2008) has argued it isimportant to distinguish analytically between entitlement andaccess The former relates to questions at a macro level concerninglaws and policies and can be answered with reference to officialliterature By contrast questions of access can only be answeredadequately through investigating the implementation of laws andpolicies at lsquostreet levelrsquo (p 157) Indeed Romero-Ortuno (2004)notes the distinction between laws and their implementation in hisown research arguing that if a lsquobiased perspective is to be avoided itis necessary to question beforehand whether undocumentedmigrants can actually enjoy the entitlements that all those laws arecurrently providing for (or in other words whether these provi-sions can actually reach the IMs [illegal immigrants])rsquo (p 263) Hegoes on to make the interesting observation that in the UK forexample there is in practice an emphasis on humanitarian practiceat the micro level coexisting with a utilitarian approach at a macroand meso levels
A further weakness of approaches that focus solely on the levelof entitlements is that they can pay scant regard to the widercontexts in which undocumented migrants live For examplerecent reports on the situation of immigrants arriving in theSpanish territory of the Canary Islands have highlighted the plightof migrant children Human Rights Watch (HRW 2007) reports thathundreds of unaccompanied migrant children are held in severelyovercrowded and ill equipped centres where they are at risk ofviolence and ill treatment These examples suggest the importanceof multidisciplinary and multilevel approaches to the investigationof healthcare for undocumented children where legal and policyoriented analysis is combined with the collection and collation ofevidence at a micro level
Improving accountability for the implementation ofhealthcare standards for undocumented migrant children
The full enjoyment of the right to health still remains a distantgoal for millions of migrant children throughout the world Theincreasing use of healthcare access as a weapon in immigration
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013

M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 5
ARTICLE IN PRESS
inefficient and costly use of other services (such as emergencycare) Although the exact cost of providing care to undocu-mented immigrant children is unknown given the relativelysmall proportion of undocumented children and their under-utilization of services providing them with free preventive andprimary caredrather than with delayed emergency inter-ventiondmay actually lower the costs of the health system
h Limited or no responsibility Children should not be punishedfor their irregular immigration status Whether some contendthat host governments are not obliged to uphold undocu-mented rights of migrants who entered or remained in thecountry illegally it is not fair to apply this argument to chil-dren as they did not chose their place of residence
i Denying healthcare to children is an ineffective method ofdeterring illegal immigration as most individuals migrate foreconomic reasons (Berk Schur et al 2000 Chang 2005)
Although some authors allege distributive justice to defenda very limited access to healthcare for undocumented migrantsnobody to our knowledge has used this argument to justifydepriving children from benefits that are essential to their healthydevelopment In practice however there is a vast discrepancybetween international legal standards and moral and legal nationalframeworks of child protection on the one hand and their actualimplementation in the field of healthcare on the other
Undocumented migrants and access to healthcare in Europeand North America
Wide gaps in implementation of legal obligations to providehealthcare to all children exist both in countries with no universalhealthcare system such as the United States as well as countrieswith public healthcare coverage for all (eg Europe and Canada)Our emphasis on State protection and obligations which originatesin the fact that we live in universal healthcare system environ-ments should not be interpreted however as an endorsement ofexclusive responsibility on the part of the government On thecontrary the assignment of responsibility among stakeholders iscomplex and should consider their relative levels of power
Healthcare for undocumented immigrant children in theUnited States
The March 2005 Current Population Survey in the US shows thatthere were 18 million undocumented children and 31 millionchildren who are US citizens by birth living in families in which thehead of the family or a spouse was undocumented (Passel 2006)Most children in undocumented familiesdparticularly youngerchildrendare eligible for the full range of state and federal publicbenefits because they are USA citizens Many of these childrenhowever may not be receiving the benefits available to thembecause of their parentsrsquo reluctance to approach the government(Fortuny Capps et al 2007 28) Undocumented migrant childrenface the highest barriers to care In 2004 59 percent of undocu-mented migrant adults lacked health insurance in the US with 35percent of their children following that pattern too (Fortuny et al2007) Following the enactment of the Personal Responsibility andWork Opportunity Reconciliation Act (PRWORA) of 1996 all undocu-mented children and those legal migrant children in the UnitedStates for less than five years are ineligible for the two largestfederally-funded health insurance programs for low-income chil-dren ie Medicaid and the State Childrenrsquos Health InsuranceProgram (SCHIP) Medical treatment provided to an undocumentedmigrant child is only covered under Medicaid for immuni-zations treatment of communicable diseases (8 USC xx 1611(b)
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
(1) 1621(b)) and lsquoemergency medical conditionsrsquo (42 USC x1396b(v)(2)(A)) The vagueness of this term however has lead todivergent interpretations by the Courts generating unpredictabilityand inequity (McKeefery 2007) Although some states and countieswithin states have created programs for low-income undocumentedchildren and Federally Qualified Health Centers provide careregardless of ability to pay and de facto immigration status manychildren are still not enrolled and undocumented pregnant womengenerally only receive emergency services Federal and state statutesdenying healthcare benefits to undocumented immigrant childrenare likely to prevail on constitutional grounds yet strong policyarguments have been built on Supreme Court rulings (Chang 2005)
Healthcare for undocumented immigrant children in Canada
Whereas in the United States and in most European countriesimmigrants account for 12 percent or less of the populationimmigrants made up 19 percent of Canadarsquos population (Dumont ampLemaıtre 2005) However estimates of undocumented migrants areparticularly vague with 200000 being the conservative figure mostoften used (Jiminez 2006 Keung 2008) Recent studies conductedin Toronto and Montreal two of the three largest immigrant desti-nations in Canada raised important questions regarding theaccessibility of basic services such as education and healthcare forchildren who are undocumented or whose parents lack legalimmigration status in Canada (Caulford amp Vali 2006 Sidhu 2008Ter Kuile et al 2007) Even if children are born in Canada and qualifyfor provincial coverage parents often find it difficult to obtaindocumentation or are fearful of the consequences that seekinghealthcare might have on their immigration status A number ofwrongful deaths related to immigration status concerns occur everyyear according to a coroner interviewed For refugee claimants withpapers the Interim Federal Health Program (IFHP) only coverslsquoemergency health concernsrsquo (although other services are some-times provided by willing providers) (Ter Kuile et al 2007)
Ever since Singh (1985) Canadian courts have consistentlyrecognized that most provisions of the Canadian Charter of Rightsand Freedoms (1982) including the equality rights guaranteed bysection 15 apply to non-citizens present on Canadian territory Inpractice however policies and government procedures restrictaccess to healthcare for many children including those withprecarious status As a result the Committee on the Rights of theChild (2003) has voiced concerns about the lack of universal accessto quality health services across provinces the increase of traffickedforeign children into Canada and the absence of a national policyon unaccompanied asylum-seeking children Healthcare beingunder provincial jurisdiction the Canadian Coalition for the Rightsof Children (2003) has also called for a review of provincial andterritorial compliance with the Canada Health Act (1984)dparticu-larly itsrsquo two main principles of universality and accessibilitydandrecalled that all provinces are responsible for providing consistentand adequate services to every child Operating out of this mandateto protect children the provincial government of Quebec passedthe Loi sur la Protection de la Jeunesse [Youth Protection Act](Gouvernement du Quebec 2006) which emphasizes the parentalobligation to ensure children safety and development throughlsquoappropriate carersquo Conflicting situations may emerge when parentsare unable to ensure childrenrsquos access to healthcare and educationdue to limitations imposed by their immigration status
Healthcare for undocumented immigrant children in theEuropean Union
It is estimated that 60 million migrants and 8 million undocu-mented migrants are living in the European region (Lancet 2007)
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash86
ARTICLE IN PRESS
Policies on migrationdincluding access to healthcaredremaindiverse in European countries and are strongly influenced by thedifferences in the countryrsquos historical context of migration A recentreport by the Platform for International Cooperation on Undocu-mented Migrants (PICUM 2007) suggests five different systems ofaccess to healthcare for undocumented migrants in Europe
a Countries such as Sweden and Austria where undocumentedmigrants are not entitled to benefit from the public healthsystem They may only access emergency care but have to payfor the incurred medical expenses Notable exceptions are freehealthcare to children of rejected asylum seekers in Swedenand free testing (eg HIV) and treatment of some contagiousdiseases (eg TB) in Austria
b Countries such as Germany and Hungary where undocu-mented migrants do not have access to any publicly subsidizedhealthcare besides emergency care and a limited number ofservices In Germany these include accidents in the workplacecounselling and testing for infectious diseases (eg TB andSTIs) and maternity care and healthcare for children and forundocumented women from 6 weeks prior to delivery to 8ndash12weeks after delivery only and for asylum-seeking pregnantwomen In Germany however public institutions are obligedby law to denounce undocumented migrants seeking health-care to the Foreignersrsquo Office hence deterring them fromexercising their entitlements In Hungary undocumentedmigrants may access other medical services on a paymentbasis
c Countries such as the United Kingdom and Portugal offeringwider health coverage but whose highly ambiguous regula-tions and complicated procedures (eg required registration inPortugal) interfere with the enjoyment of these entitlementsUndocumented migrants may consult a general practitioner inthe UK yet secondary care is usually not covered (ChauvinParizot et al 2007 Cole 2007) Undocumented pregnantwomen and children are charged for services rendered otherthan lsquolsquourgentrsquorsquo healthcare In Portugal undocumented migrantsproving residence for more than 90 days may access publichealthcare upon payment of a fee except in cases of infectiousdiseases maternity care vaccination and family planningOtherwise they may only access emergency care on a paymentbasis Undocumented children may access public healthcareand education like national and documented children
d Countries such as Belgium France and the Netherlands whereundocumented migrants are treated in the mainstream healthsystem yet services are processed through a lsquolsquoparallelrsquorsquo admin-istrative andor payment system In Belgium undocumentedmigrants have free access to lsquolsquourgent medical assistancersquorsquo whichencompasses a broad range of care provisions (eg medicalexaminations childbirth and medications) Under certainconditions undocumented migrants may receive healthinsurance In France undocumented migrants and their fami-lies may access publicly subsidized healthcare after residing inthe country for 3 months and proving minimum income levelsOtherwise they may only access free emergency care treat-ment for contagious diseases all types of healthcare for chil-dren maternity care and abortion for medical reasons Since1998 undocumented migrants in the Netherlands may onlyreceive lsquolsquocare that is medically necessaryrsquorsquo (including maternitycare and preventive care and vaccinations for children) or maylsquolsquojeopardize public healthrsquorsquo If unable to pay a special fund willreimburse the healthcare provider
e Countries such as Spain and Italy offering free access tohealthcare to all including undocumented migrants Undocu-mented minors and pregnant women can access the Spanish
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
national health system free of charge under the same condi-tions as nationals Since 2002 other undocumented migrantsmay access free health services upon registering in the localcivil registry of their usual residence and obtaining a healthcard however variations exist across autonomous communi-ties and lsquofear ignorance and administrative obstaclesrsquo detersome from registering (Ingleby amp Watters 2005 PICUM 2007)In Italy undocumented migrants may access certain freeservices such as emergency care maternity care and any carefor children younger than 6 years lsquolsquoSpecialized carersquorsquo andoutpatient treatment of contagious and chronic diseases are inmost cases subject to a fee
Among European countries access to healthcare for undocu-mented migrants is generally limited to emergencies or to treatconditions jeopardizing public health (Romero-Ortuno 2004)Hereto related Romero-Ortuno (2004) distinguishes two possibleapproaches in Europe concerning the access to healthcare forundocumented migrants the lsquohumanitarianrsquo (or human rights-based) approach as seen in Spain and the lsquoutilitarianrsquo (or negativeexternalities-based) approach as seen in Germany and even in theUK which covers undocumented migrants in order to lsquoprotectrsquo thehost populationrsquos health Finally Belgium and the Netherlandsillustrate a lsquosoftenedrsquo case of the lsquoutilitarianrsquo approach
While the frameworks offered here by PICUM and Romero-Ortuno may be helpful in identifying differences between countrieswith respect to entitlements to healthcare they may say little aboutthe extent to which undocumented migrants can actually gainaccess to health services As Watters (2008) has argued it isimportant to distinguish analytically between entitlement andaccess The former relates to questions at a macro level concerninglaws and policies and can be answered with reference to officialliterature By contrast questions of access can only be answeredadequately through investigating the implementation of laws andpolicies at lsquostreet levelrsquo (p 157) Indeed Romero-Ortuno (2004)notes the distinction between laws and their implementation in hisown research arguing that if a lsquobiased perspective is to be avoided itis necessary to question beforehand whether undocumentedmigrants can actually enjoy the entitlements that all those laws arecurrently providing for (or in other words whether these provi-sions can actually reach the IMs [illegal immigrants])rsquo (p 263) Hegoes on to make the interesting observation that in the UK forexample there is in practice an emphasis on humanitarian practiceat the micro level coexisting with a utilitarian approach at a macroand meso levels
A further weakness of approaches that focus solely on the levelof entitlements is that they can pay scant regard to the widercontexts in which undocumented migrants live For examplerecent reports on the situation of immigrants arriving in theSpanish territory of the Canary Islands have highlighted the plightof migrant children Human Rights Watch (HRW 2007) reports thathundreds of unaccompanied migrant children are held in severelyovercrowded and ill equipped centres where they are at risk ofviolence and ill treatment These examples suggest the importanceof multidisciplinary and multilevel approaches to the investigationof healthcare for undocumented children where legal and policyoriented analysis is combined with the collection and collation ofevidence at a micro level
Improving accountability for the implementation ofhealthcare standards for undocumented migrant children
The full enjoyment of the right to health still remains a distantgoal for millions of migrant children throughout the world Theincreasing use of healthcare access as a weapon in immigration
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013

M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash86
ARTICLE IN PRESS
Policies on migrationdincluding access to healthcaredremaindiverse in European countries and are strongly influenced by thedifferences in the countryrsquos historical context of migration A recentreport by the Platform for International Cooperation on Undocu-mented Migrants (PICUM 2007) suggests five different systems ofaccess to healthcare for undocumented migrants in Europe
a Countries such as Sweden and Austria where undocumentedmigrants are not entitled to benefit from the public healthsystem They may only access emergency care but have to payfor the incurred medical expenses Notable exceptions are freehealthcare to children of rejected asylum seekers in Swedenand free testing (eg HIV) and treatment of some contagiousdiseases (eg TB) in Austria
b Countries such as Germany and Hungary where undocu-mented migrants do not have access to any publicly subsidizedhealthcare besides emergency care and a limited number ofservices In Germany these include accidents in the workplacecounselling and testing for infectious diseases (eg TB andSTIs) and maternity care and healthcare for children and forundocumented women from 6 weeks prior to delivery to 8ndash12weeks after delivery only and for asylum-seeking pregnantwomen In Germany however public institutions are obligedby law to denounce undocumented migrants seeking health-care to the Foreignersrsquo Office hence deterring them fromexercising their entitlements In Hungary undocumentedmigrants may access other medical services on a paymentbasis
c Countries such as the United Kingdom and Portugal offeringwider health coverage but whose highly ambiguous regula-tions and complicated procedures (eg required registration inPortugal) interfere with the enjoyment of these entitlementsUndocumented migrants may consult a general practitioner inthe UK yet secondary care is usually not covered (ChauvinParizot et al 2007 Cole 2007) Undocumented pregnantwomen and children are charged for services rendered otherthan lsquolsquourgentrsquorsquo healthcare In Portugal undocumented migrantsproving residence for more than 90 days may access publichealthcare upon payment of a fee except in cases of infectiousdiseases maternity care vaccination and family planningOtherwise they may only access emergency care on a paymentbasis Undocumented children may access public healthcareand education like national and documented children
d Countries such as Belgium France and the Netherlands whereundocumented migrants are treated in the mainstream healthsystem yet services are processed through a lsquolsquoparallelrsquorsquo admin-istrative andor payment system In Belgium undocumentedmigrants have free access to lsquolsquourgent medical assistancersquorsquo whichencompasses a broad range of care provisions (eg medicalexaminations childbirth and medications) Under certainconditions undocumented migrants may receive healthinsurance In France undocumented migrants and their fami-lies may access publicly subsidized healthcare after residing inthe country for 3 months and proving minimum income levelsOtherwise they may only access free emergency care treat-ment for contagious diseases all types of healthcare for chil-dren maternity care and abortion for medical reasons Since1998 undocumented migrants in the Netherlands may onlyreceive lsquolsquocare that is medically necessaryrsquorsquo (including maternitycare and preventive care and vaccinations for children) or maylsquolsquojeopardize public healthrsquorsquo If unable to pay a special fund willreimburse the healthcare provider
e Countries such as Spain and Italy offering free access tohealthcare to all including undocumented migrants Undocu-mented minors and pregnant women can access the Spanish
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
national health system free of charge under the same condi-tions as nationals Since 2002 other undocumented migrantsmay access free health services upon registering in the localcivil registry of their usual residence and obtaining a healthcard however variations exist across autonomous communi-ties and lsquofear ignorance and administrative obstaclesrsquo detersome from registering (Ingleby amp Watters 2005 PICUM 2007)In Italy undocumented migrants may access certain freeservices such as emergency care maternity care and any carefor children younger than 6 years lsquolsquoSpecialized carersquorsquo andoutpatient treatment of contagious and chronic diseases are inmost cases subject to a fee
Among European countries access to healthcare for undocu-mented migrants is generally limited to emergencies or to treatconditions jeopardizing public health (Romero-Ortuno 2004)Hereto related Romero-Ortuno (2004) distinguishes two possibleapproaches in Europe concerning the access to healthcare forundocumented migrants the lsquohumanitarianrsquo (or human rights-based) approach as seen in Spain and the lsquoutilitarianrsquo (or negativeexternalities-based) approach as seen in Germany and even in theUK which covers undocumented migrants in order to lsquoprotectrsquo thehost populationrsquos health Finally Belgium and the Netherlandsillustrate a lsquosoftenedrsquo case of the lsquoutilitarianrsquo approach
While the frameworks offered here by PICUM and Romero-Ortuno may be helpful in identifying differences between countrieswith respect to entitlements to healthcare they may say little aboutthe extent to which undocumented migrants can actually gainaccess to health services As Watters (2008) has argued it isimportant to distinguish analytically between entitlement andaccess The former relates to questions at a macro level concerninglaws and policies and can be answered with reference to officialliterature By contrast questions of access can only be answeredadequately through investigating the implementation of laws andpolicies at lsquostreet levelrsquo (p 157) Indeed Romero-Ortuno (2004)notes the distinction between laws and their implementation in hisown research arguing that if a lsquobiased perspective is to be avoided itis necessary to question beforehand whether undocumentedmigrants can actually enjoy the entitlements that all those laws arecurrently providing for (or in other words whether these provi-sions can actually reach the IMs [illegal immigrants])rsquo (p 263) Hegoes on to make the interesting observation that in the UK forexample there is in practice an emphasis on humanitarian practiceat the micro level coexisting with a utilitarian approach at a macroand meso levels
A further weakness of approaches that focus solely on the levelof entitlements is that they can pay scant regard to the widercontexts in which undocumented migrants live For examplerecent reports on the situation of immigrants arriving in theSpanish territory of the Canary Islands have highlighted the plightof migrant children Human Rights Watch (HRW 2007) reports thathundreds of unaccompanied migrant children are held in severelyovercrowded and ill equipped centres where they are at risk ofviolence and ill treatment These examples suggest the importanceof multidisciplinary and multilevel approaches to the investigationof healthcare for undocumented children where legal and policyoriented analysis is combined with the collection and collation ofevidence at a micro level
Improving accountability for the implementation ofhealthcare standards for undocumented migrant children
The full enjoyment of the right to health still remains a distantgoal for millions of migrant children throughout the world Theincreasing use of healthcare access as a weapon in immigration
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013

M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash8 7
ARTICLE IN PRESS
control by European and North American countries lsquolsquomakes a farceof the UN conventions that they have all ratifiedrsquorsquo (Lancet 2007 2070)Human rights violations are justified as an inevitable consequenceof irregular migration and limited resources yet nobody dares toopenly defend this position vis-a-vis children Undocumentedchildren are a particularly vulnerable group and their human rightsassume a greater importance as a result The UN interprets basichuman rightsdincluding the right to the highest attainable stan-dard of healthdas inherent to the human dignity of all humanbeings indivisible and interdependent all needed to ensure theprotection of people as full persons If weighted against the stan-dards set by international human rights instruments and moni-toring bodies local situations concerning access to healthcare forundocumented migrants reveal a breach requiring urgentattention
In order to guarantee the improvement of health systems andthe progressive realization of the right to health for all monitoringand accountability play a key role The lack of adequate dis-aggregated data on the situation of disadvantaged individuals andcommunities such as undocumented migrants interferes with theeffective monitoring of Statesrsquo obligations (HRC 2008) and opensa door for escaping responsibility Likewise absence of reliablefigures on the costs of unreimbursed medical care to undocu-mented migrants hinders policy development and the planningand provision of public services The Special Rapporteur (HRC2007 2008) calls for a range of effective and accessible account-ability mechanisms including the development of appropriateindicators and the involvement of civil society organizations andhealth professionals At this time we face a generalized resistanceto open discussion on the ethical stance that underlies ourresponsibility in providing care to precarious status children and itsrelationship to citizenship status and health insurance As a firststep information should be provided to healthcare professionalsand other stakeholders regarding childrenrsquos right to healthcareunder local national and international law and the usefulness ofthe human rights framework to advance the right to health Theidea proposed by Watters (2007) of a moral economy of care inrelation to refugees provides an interesting frame of analysis tounderstand the way in which some humanitarian and compas-sionate measures are highlighted while othersdas in the case ofthe care to children with precarious immigration statusdaresilenced As conceptualized here a moral economy has consider-able historical precedent and echoes earlier distinctions betweenlsquodeserving and undeserving poorrsquo as can be traced back for exampleto England in the 16th century Moreover the idea of the moraleconomy raises important questions as to the contexts in whichsome migrant and refugee children are deemed worthy of societyrsquosprotection and support while the presence of others engenderspractices of disengagement and exclusion
To address these questions researchers have an important roleto play in breaking the silence around the question of healthcareaccess for undocumented migrant children In order to makeinformed decisions stakeholders at all levelsdgovernment healthinstitutions and civil societydneed to understand the physical andmental short and long-term consequences of the present limita-tions in access as well as the specific obstacles that undocumentedfamilies encounter to access healthcare for their children It is alsocrucial to examine the impact of legal changes on access tohealthcare for undocumented children in the line of the studyconducted by Torres-Cantero Miguel et al (2007) analyzing theintroduction of individual health cards and free medical care forundocumented migrants in Spain Interdisciplinarity and collabo-ration are needed to combine legal and ethical monitoring ofnational laws institutional regulations and the position ofprofessional associations It is also needed to reveal the gaps that
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
exist between the formal positions taken by governments andorganisations and implementation at street level This requiresmultilevel approaches that engage with both the macro and microlevel of analysis
In our judgment legal provisions as well as institutional andindividual practices should ensure an unqualified respect forhuman rights Specific examples of good practices in countriesreceiving large numbers of undocumented children do exist andshould be studied in order to explore conditions of feasibility Tolimit the provision of true universal health coverage for all childrenis therefore not acceptable particularly for countries able to ensurethe availability of basic medical services to their own citizens(Nickel 1986 23) Beyond its health and development conse-quences access to healthcare and education are some of the mostbasic and powerful manifestations of equity in a society Formigrant children this is often an experience of belonging orexclusion The right to health for all children is thus a foundingstone of solidarity and peace
Acknowledgements
We thank the participants in the Seminaire sur lrsquoacces aux soinsde sante des personnes a statut migratoire precaire held in January2008 at the Centre drsquoetudes et de recherches internationales(CERIUM) at the Universite de Montreal We are also grateful toAnne-Claire Gayet Sarah Curtis and three anonymous reviewersfor their input This article was written while Monica Ruiz-Casareswas a Richard H Tomlinson Postdoctoral Fellow at McGillUniversity
References
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1611(b)(1) (2007a)
Aliens who are not qualified aliens or nonimmigrants ineligible for state and localpublic benefits 8 USC xx 1621(b) (2007b)
AI (2005) Spain The southern border London Amnesty InternationalArnold F Chalmers I Herxheimer A Lewith G Kennedy S Kandela P et al
(2008) Medical justice for undocumented migrants The Lancet 371(no 9608)201
Bhabha J amp Crock M (2007) Seeking asylum alone A comparative study of lawspolicy and practice in Australia the UK the US Sydney Themis Press
Berk Marc L Schur C L Chavez L R amp Frankel M (2000) Health care use amongundocumented Latino immigrants Is free health care the main reason whyLatinos come to the United States A unique look at the facts Health Affairs19(4) 51ndash64
BMA (2008) Asylum Seekers and Their Health London British Medical AssociationCastles S (2003) Towards a sociology of forced migration and social trans-
formation Sociology 37(1) 13ndash34Castles S amp Miller M (2003) The age of migration Basingstoke Palgrave
MacmillanCaulford P amp Vali Y (2006) Providing health care to medically uninsured immi-
grants and refugees Canadian Medical Association Journal 174(9) 1253ndash1254CCRC (2003) The UN convention on the rights of the child How does Canada measure
up 2003 Update to Canadarsquos report to the UN committee for the rights of childrenOttawa ON Canadian Coalition for the Rights of Children
CESCR (2000) The right to the highest attainable standard of health [Article 12 of theInternational Covenant on Economic Social and Cultural Rights] GeneralComment No 14 EC1220004 Committee on Economic Social and CulturalRights
Chang C (2005) Health care for undocumented immigrant children specialmembers of an underclass Washington University Law Quarterly 83 1271ndash1294
Chauvin P Parizot I Drouot N Simonnot N amp Tomasino A (2007) EuropeanSurvey on undocumented migrantsrsquo access to health care Medecins du Monde
Cole P (2007) Human rights and national interest migrants healthcare and socialjustice Journal of Medical Ethics 33 269ndash272
Committee on Community Health Services (1997) American academy of pediat-rics health care for children of immigrant families Pediatrics 100 153ndash156
Costich J F (2001ndash2002) Legislating a public health nightmare the anti-immi-grant provisions of the lsquocontract with Americarsquo congress Kentucky Law Journal90 1043ndash1070
Crepeau F amp Nakache D (2006) Controlling irregular migration in CanadaReconciling security concerns with human rights protection In Shaping CanadarsquosFuture Immigration and Refugee Policy Paper Series Montreal Institute for
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013
M Ruiz-Casares et al Social Science amp Medicine xxx (2009) 1ndash88
ARTICLE IN PRESS
Research on Public Policy February Online httpwwwirpporgchoicesarchivevol12no1pdf
CRC (2003) Concluding observations of the committee on the rights of the childCanada Geneva Switzerland Committee on the Rights of the Child
Derluyn I amp Broekaert E (2005) On the way to a better future Belgium as transitcountry for trafficking and smuggling of unaccompanied minors InternationalMigration 43 31ndash56
Derluyn I V Lippens T Verachtert W Bruggeman and E Broekaert (2009)Minors Travelling Alone A Risk Group for Human Traffickingrsquorsquo InternationalMigration in press doi101111j1468-2435200900548x)
Dumont J-C amp Lemaıtre G (2005) Counting immigrants and expatriates in OECDCountries a new perspective OECD social employment and migration workingpapers No 25 Paris OECD Publishing
Ellis C (2006) Assessing hospitalsrsquo responsibility to provide unremuneratedservices Healthcare Management Forum 19(3) 6ndash12
Esping-Andersen G (1990) The three worlds of welfare capitalism CambridgePolity Press
Fortuny K Capps R amp Passel J S (2007) The characteristics of unauthorizedimmigrants in California Los Angeles County and the United States WashingtonDC The Urban Institute
Gouvernement du Quebec (2006) Loi sur la Protection de la Jeunesse LRQ c P-341
Hadley J (2003) Sicker and poorer ndash the consequences of being uninsured ndasha review of the research on the relationship between health insurance medicalcare use health work and income Medical Care Research amp Review 60(2Suppl) 3Sndash75S
Hill I Dubay L Kenney G M Howell E M Courtot B amp Palmer L (2008)Improving coverage and access for immigrant Latino children the Los Angeleshealthy kids program Health Affairs 27(2) 550ndash559
Hjern A amp Bouvier P (2004) Migrant children a challenge for European paedi-atricians Acta Paediatrica 93 1535ndash1539
HRC (2007) Report of the special Rapporteur on the right of everyone to the enjoymentof the highest attainable standard of physical and mental health Paul Hunt NewYork Human Rights Council United Nations AHRC428
HRC (2008) Report of the Special Rapporteur on the right of everyone to the enjoy-ment of the highest attainable standard of physical and mental health Paul HuntNew York Human Rights Council United Nations AHRC711
HRW (2007) Unwelcome responsibilities Spainrsquos failure to protect the rights ofunaccompanied migrant children in the Canary islands New York Human RightsWatch 19
HRW (2008) Left to survive Systematic failure to protect unaccompanied migrantchildren in Greece New York Human Rights Watch
Ingleby D amp Watters C (2005) Mental health and social care for asylum seekersand refugees A comparative study In D Ingleby (Ed) Forced migration andmental health Rethinking the care of refugees and displaced persons (pp 193ndash212) Dordrecht Springer
JCHR (2005) Joint Committee on Human Rights ndash Seventeenth Report London Houseof Lords and House of Commons
Jiminez M (2006) Ottawa rules out amnesty for 200000 illegal workers Theunderground economy Construction industry hit hard by decision Toronto Globeand Mail
Kaiser Commission on Medicaid and the Uninsured (2003) The uninsured and theiraccess to health care Washington DC The Henry J Kaiser Family Foundation
Keung N (2008) lsquolsquoDonrsquot Askrsquorsquo policy urged for children of migrants Toronto Star
Please cite this article in press as Ruiz-Casares M et al Right and acbetween Social Science amp Medicine (2009) doi101016jsocscimed20
Kuiper H Richwald G A Rotblatt H amp Asch S (1999) The communicable diseaseimpact of eliminating publicly funded prenatal care for undocumented immi-grants Maternal and Child Health Journal 3(1) 39ndash52
Lancet (2007) Access to health care for undocumented migrants in Europe Lancet370(9605) 2070
Lindert J Schouler-Ocak M Heinz A amp Priebe S (2008) Mental health healthcare utilisation of migrants in Europe European Psychiatry 23 S14ndashS20
Lu M C Lin Y G Prietto N M amp Garite T J (2000) Elimination of public fundingof prenatal care for undocumented immigrants in California a costbenefitanalysis American Journal of Obstetrics and Gynecology 182(1 Part 1) 233ndash239
McKeefery M J (2007) A call to move forward pushing past the unworkablestandard that governs undocumented immigrantsrsquo access to health care undermedicaid The Journal of Health Care Law amp Policy 10(2) 391ndash419
Nickel J W (1986) Should undocumented aliens be entitled to health care TheHastings Center 16(6) 19ndash23
OAS (2008) A-52 Additional protocol to the American convention on human rights inthe area of Economic social and cultural rights lsquolsquoProtocol of San Salvadorrsquorsquo Wash-ington DC Department of International Law Organization of American States
OHCHR (2008) Ratifications and reservations Office of the UN High Commissionerfor Human Rights
Passel J S (2006) Size and characteristics of the unauthorized migrant population inthe US Estimates based on the march 2005 current population survey Wash-ington DC Pew Hispanic Center
Payment to States 42 USC x 1396b(v)(2)(A) (2006)PICUM (2007) Access to health care for undocumented migrants in Europe Brussels
Platform for International Cooperation on Undocumented MigrantsPlyer v Doe 457 US 202 (1982)Romero-Ortuno R (2004) Access to health care for illegal immigrants in the EU
should we be concerned European Journal of Health Law 11 245ndash272Sidhu N (2008) The right to learn Access to public education for non-status immi-
grants Toronto Community Social Planning Council of TorontoSingh C Ministre De Lrsquoemploi Et De Lrsquoimmigration (1985) (Vol 1 RCS 177)Ter Kuile S Rousseau C Munoz M Nadeau L amp Ouimet M J (2007) The
universality of the Canadian health care system in question barriers to servicesfor immigrants and refugees International Journal of Migration Health and SocialCare 3(1) 15ndash26
Torres-Cantero A M Miguel A G Gallardo C amp Ippolito S (2007) Health careprovision for illegal migrants may health policy make a difference EuropeanJournal of Public Health 17(5) 483ndash485
Treaty Office (2008) Complete list of the council of Europersquos treaties Council of EuropeUnited Nations (1948) Universal Declaration of Human Rights New York UNUnited Nations (1989) Convention on the Rights of the Child New York UNUnited Nations (2005) More than 12 million people are victims of forced labour
UN labour agency says UN News ServiceUnited Nations (2009) Trends in total migrant stock The 2005 revision Population
Division Department of Economic and Social Affairs United Nations Secretariathttpesaunorgmigration Accessed 190409
USDS (2008) Trafficking in persons report Washington DC United States Depart-ment of State
Watters C (2007) Refugees at Europersquos borders the moral economy of careTranscultural Psychiatry 44 394ndash417
Watters C (2008) Refugee children Towards the next horizon London RoutledgeWHO (1946) Constitution of the World Health Organization Geneva World Health
Organization
cess to healthcare for undocumented children Addressing the gap0910013



















