Review of Non-physician Prescribing and Administration of ...
444
Review of Non-Physician Prescribing and Administration of Drugs Under the Regulated Health Professions Act 170 Bloor Street W. Suite 1001 Toronto, Ontario M5S 1T9 tel (416) 975-4353 fax (416) 975-4355 1 (800) 563-5847 www.cmrto.org To: Health Professions Regulatory Advisory Council By: College of Medical Radiation Technologists of Ontario Date: November 12, 2008
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Review of Non-physician Prescribing and Administration of ...
Review of Non-Physician Prescribing and Administration of Drugs Under the Regulated Health Professions Act
170 Bloor Street W. Suite 1001 Toronto, Ontario M5S 1T9 tel (416) 975-4353 fax (416) 975-4355 1 (800) 563-5847 www.cmrto.org
To: Health Professions Regulatory Advisory Council
By: College of Medical Radiation Technologists of Ontario
Date: November 12, 2008
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
Table of Contents
INTRODUCTION ............................................................................................3
PROFESSION INFORMATION........................................................................4
CURRENT AUTHORIZED ACTS AND REGULATIONS .....................................8
PROPOSED CHANGES TO AUTHORIZED ACTS AND REGULATIONS ..........13
RISK OF HARM ...........................................................................................13
EDUCATION AND CONTINUING COMPETENCY .........................................14
PUBLIC INTEREST........................................................................................16
PRESCRIBING: DRUG REGULATIONS UNDER PROFESSIONAL ACTS .........17
COLLABORATION .......................................................................................18
OTHER JURISDICTIONS...............................................................................18
COSTS AND BENEFITS ................................................................................19
CONCLUSION..............................................................................................19
November 12, 2008 Page 2
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
INTRODUCTION The College of Medical Radiation Technologists of Ontario (CMRTO), the regulatory body for more than 6,200 medical radiation technologists (MRTs) in Ontario, is pleased to respond to the request from the Health Professions Regulatory Advisory Council (HPRAC), dated October 2, 2008 inviting the CMRTO to make a submission regarding HPRAC’s Review of Non-Physician Prescribing and Administration of Drugs under the Regulated Health Professions Act. This submission by the CMRTO sets out the role of MRTs related to the administration of drugs and substances and responds to the HPRAC document “Review of Non-Physician Prescribing and Administration of Drugs under the Regulated Health Professions Act – Questionnaire for Health Professions”. MRTs are highly skilled and knowledgeable health care professionals who are an integral component of health care delivery to the public of Ontario. MRTs operate complex imaging and therapy equipment in the delivery of diagnostic and therapeutic services such as computed tomography (CT) scanners, single-photon emission computed tomography (SPECT) scanners, linear accelerators for the delivery of radiation treatments, and magnetic resonance (MR) scanners. MRTs work collaboratively with other health care practitioners. In particular, on a regular basis they consult with physicians, nurses, dietitians and respiratory therapists in the course of engaging in the practice of medical radiation technology. MRTs are authorized to perform four authorized acts, two of which relate to this submission. The first is administering substances by injection or inhalation and the second is administering contrast media through or into the rectum or an artificial opening into the body. CMRTO’s mission is to serve and protect the people of Ontario through the self-regulation of the profession. The practice of medical radiation technologists is guided by the profession’s scope of practice statement: “The practice of medical radiation technology is the use of ionizing radiation and other forms of energy prescribed under subsection 12(2) to produce diagnostic images and tests, the evaluation of the technical sufficiency of the images and tests, and the therapeutic application of ionizing radiation.” The CMRTO, in conjunction with the Ontario Association of Medical Radiation Technologists, has recently undertaken a review of the scope of practice of MRTs and has submitted a proposal to HPRAC which requests changes to the scope of practice to allow MRTs to practise to their full competency. The proposal does not suggest any changes to the current regulatory framework related to the substances that MRTs use and administer in their practice. The CMRTO supports the current regulatory framework which authorizes MRTs to administer or use any substance that is prescribed by a physician, as we feel it encourages collaborative and patient-centred care and promotes access to services and service efficiencies within the healthcare system. The current system ensures patient safety and we do not believe that restrictions on the drugs or substances that MRTs administer and use in practice are necessary. In fact, we are concerned that any attempt to specifically list in regulation the drugs or classes of drugs used by MRTs would create a barrier to collaborative practice and could also negatively impact access to services and system efficiencies.
November 12, 2008 Page 3
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
PROFESSION INFORMATION The name of the group making this submission is: College of Medical Radiation Technologists of Ontario (CMRTO) Registrar: Linda Gough 1. Address/website/email
The address and website of the group is as follows: College of Medical Radiation Technologists of Ontario 170 Bloor Street West, Suite 1001 Toronto, ON M5S 1T9 www.cmrto.org
2. Telephone and fax numbers
Telephone and facsimile numbers are as follows: College of Medical Radiation Technologists of Ontario Telephone: (416) 975-4353 Toll free: 1 (800) 563-5847 Facsimile: (416) 975-4355
3. Contact person (including day telephone numbers)
The contact person, the daytime telephone number and email address is as follows: Ms. Linda Gough CMRTO Registrar 416-975-4353 [email protected]
The following is a list of organizations and individuals that the CMRTO has collaborated with in a number of MRT related initiatives. Regulatory Bodies College of Nurses of Ontario Anne Coghlan, Executive Director 101 Davenport Road Toronto, ON M5R 3P1 Tel: 416-928-0900 ext. 7525
November 12, 2008 Page 4
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
College of Respiratory Therapists of Ontario Christine Robinson, Registrar 180 Dundas Street West, Suite 2103 Toronto, ON M5G 1Z8 Tel: (416) 591-7800
College of Physiotherapists of Ontario Jan Robinson, Registrar 375 University Avenue, Suite 901 Toronto, ON M5G 2J5 Tel: (416) 591-3834
College of Physicians and Surgeons of Ontario Dr. Rocco Gerace, Registrar 80 College Street Toronto, ON M5G 2E2 Tel: (416) 967-2600
Professional Associations Ontario Association of Medical Radiation Technologists (OAMRT) Craig Willson, Chair of the Board & President P.O. Box 1054 Station Main Brantford, ON N3T 5S7 Tel: (519) 753-6037 Canadian Association of Medical Radiation Technologists (CAMRT) Charles Shields Jr., Chief Executive Officer 1000 - 85 Albert Street Ottawa, ON K1P 6A4 Tel: (613) 234-0012 Ontario Association of Radiology Managers Debbie Wilson, President Alberta College of Medical Diagnostic and Therapeutic Technologists (ACMDTT) Kathy Hilsenteger, CEO/Registrar 501 - 5241 Calgary Trail NW Edmonton, AB T6H 5G8 Tel: (780) 487-6130
November 12, 2008 Page 5
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
Ordre des technologues en radiologie du Québec (OTRQ) Alain Cromp, Directeur general et secretaire 401 - 6455, rue Jean-Talon est Saint-Léonard, QC H1S 3E8 Tel: (514) 351-0052 ext. 222 Ontario Hospital Association Heather Stewart, Consultant, Health Professional Issues # 2800-200 Front Street West Toronto, ON M5V 3L1 Tel: (416) 205-1382
Ontario Medical Association Ada Maxwell, Senior Policy Analyst 525 University Ave, Suite 200 Toronto, ON M5G 2K7 Tel: (416) 599-2580
Ontario Association of Radiologists
Dr. Giuseppe Tarulli, President 245 Lakeshore Road East
Oakville, ON L6J 1J9 Tel: (905) 337-2680
Canadian Association of Radiologists Dr. David Vickar, President 377 Dalhousie Street, Suite 310 Ottawa, ON K1N 9N8 Tel: (613) 860-3111 Educational institutions which deliver CMRTO approved programs in medical radiation technology Confederation College of Applied Arts & Technology Michael Kelly, Program Coordinator, Health Sciences Division P.O. Box 398, 1450 Nakina Drive Thunder Bay, ON P7C 4W1 Tel: (807) 475-6142
November 12, 2008 Page 6
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
Fanshawe College of Applied Arts & Technology Jamie Kueneman, Program Coordinator, Health Sciences and Human Services Room D3024, 1460 Oxford Street East P.O. Box 7005 London, ON N5Y 5R6 Tel: (519) 452-4430 ext. 4207 Mohawk College of Applied Arts & Technology Diane Barrafato, Program Director Mohawk/McMaster Institute for Applied Health Sciences 1400 Main Street West Hamilton, ON L8S 1C7 Tel: (905) 540-4247 ext. 26745 Collège Boréal d’Arts Appliqués et de Technologie Marcel Bradley, Program Coordinator 21 boulevard Lasalle Sudbury, ON P3A 6B1 Tel: (705) 560-6673 ext. 4640 Eastern Ontario School of X-ray Technology Karen Pearson, Program Director c/o Kingston General Hospital Imaging Services 76 Stuart Street Kingston, ON K7L 2V7 Tel: (613) 549-6666 ext. 4054 Cambrian College of Applied Arts & Technology Brenda Cliff, Program Co-ordinator, Medical Radiation Technology 1400 Barrydowne Road Sudbury, ON P3A 3V8 The Michener Institute for Applied Health Sciences Fiona Cherryman, Chair, Medical Radiation Sciences 222 St. Patrick Street Toronto, ON M5T 1V4 Tel: (416) 506-3101
November 12, 2008 Page 7
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
CURRENT AUTHORIZED ACTS AND REGULATIONS MRTs are only permitted to perform a procedure falling within an authorized act if there is an order for performance of the procedure from a physician. We are not proposing any change to this condition.1 Under the MRT Act, MRTs are currently authorized to perform four authorized acts as follows: In the course of engaging in the practice of medical radiation technology, a member is authorized, subject to the terms, conditions and limitations imposed on his or her certificate of registration, to perform the following: 1. Taking blood samples from veins
Authorized Act 1 for MRTs falls within Controlled Act 2 of the RHPA: an example of a procedure falling within this authorized act would be taking blood samples for the purpose of assessing effective renal plasma flow
2. Administering substances by injection or inhalation Authorized Act 2 for MRTs is Controlled Act 5 of the RHPA: examples of procedures falling within this authorized act would be performing an intravenous, subcutaneous or intramuscular injection; or starting peripheral intravenous lines, or establishing saline locks for the purpose of administering substances such as radiopharmaceuticals or contrast media for the visualization of body organs, such as the kidneys or heart
3. Administering contrast media through or into the rectum or an artificial opening into the body Authorized Act 3 for MRTs falls within Controlled Act 6 of the RHPA: an example of a procedure falling within this authorized act would be inserting an enema tip and barium for an examination of the colon
4. Tattooing
Authorized Act 4 for MRTs falls within Controlled Act 2 of the RHPA: an example of a procedure falling within this authorized act would be marking the area of a patient’s body to receive radiation therapy for cancer treatment
Under the MRT Act, MRTs are only permitted to perform a procedure falling within an authorized act if there is an order for performance of the procedure from a physician. As mentioned previously, we are not proposing any change to this condition. 1 We have proposed that this condition be amended so that an MRT would also be authorized to perform an
authorized act on the order of prescribed regulated health professionals. This proposal recognizes the possibility that the scope of practice of other regulated health professions, such as nurse practitioners, may be expanded to authorize them to order certain procedures, such as the application of electromagnetism for magnetic resonance imaging.
November 12, 2008 Page 8
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
The practice of MRTs is also governed by the Healing Arts Radiation Protection Act (HARP Act). The HARP Act regulates the ordering and application of ionizing radiation through the regulation of the use and operation of X-ray machines and equipment. In the case of applying ionizing radiation under the HARP Act, it is a requirement that an MRT have an order from a physician or other regulated health professional named in the HARP Act.2 To review the College of Medical Radiation Technologists of Ontario Standards of Practice, please refer to Appendix 1. MRTs Use and Administration of Drugs and Substances The administration and use of drugs has almost always been an integral part of MRT practice. The substances administered by MRTs would be considered drugs as defined by the Drug and Pharmacies Regulations Act. MRTs administer substances including drugs through various methods including orally, topically, rectally as well as by injection and inhalation. This is done as part of a variety of diagnostic and therapeutic procedures and has long been included in the core competencies of an MRT. When William Conrad Röntgen discovered X-rays in 1895, this opened up a completely new perspective for medicine: the ability to look directly inside the human body without the need for surgery. In 1931 iodine-based contrast media was introduced to improve the quality of the images of body structure and function. It remained the standard for X-rays of the kidney, bladder and blood vessels for decades. Since then, countless innovative contrast media have been developed for diagnostic imaging and therapeutic procedures. Diagnostic imaging and radiation therapy has developed into a highly specialized field of medicine. Digital image acquisition has become the standard for modern equipment used in general radiography, mammography, angiography, computed tomography, magnetic resonance imaging, nuclear medicine, radiation therapy planning and image guided delivery of radiation therapy. Specific contrast media or radiopharmaceuticals are an integral part of many imaging procedures. For example, contrast media is injected into the patient’s veins to enhance the visualization of certain organs for a CT or MR scan on the resultant images. It is not uncommon for a physician (radiologist) who will be reading the resultant images to prescribe the contrast media according to his or her preference in order to acquire optimum image quality (sharp images and high resolution). This enables the radiologist to make a diagnosis based on optimum image quality. In a rapidly changing technological environment where innovative procedures are introduced into the practice of medical radiation technology to improve patient care outcomes, there are constant changes in equipment, contrast media and radiopharmaceuticals used in diagnostic imaging procedures.
2 Healing Arts Radiation Protection Act, section 6.
November 12, 2008 Page 9

CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
There is sometimes a need for the type of contrast media ordered by the physician and administered by the MRT to be altered or changed in a timely fashion based on research findings. This is exemplified by the recent negative impact on some patients who had received gadolinium administered for the purpose of magnetic resonance imaging examinations. In 2006, exposure to gadolinium-based contrast agents was implicated in the pathogenesis of nephrogenic systemic fibrosis (NSF), a rare and potentially fatal complication of certain gadolinium-based contrast agents for the purpose of magnetic resonance imaging, affecting patients with compromised renal function. It was crucial that the practice guidelines be altered and tailored to the individual patient via consultation with the referring physician, radiologist and, when necessary, a nephrologist. The widespread negative impact of this finding resulted in immediate changes being made to the screening protocols and management of patients with chronic kidney disease requiring a magnetic resonance imaging procedure. It was crucial that practice guidelines be developed by the radiologist that could be adapted to the individual patient’s specific clinical circumstances. Once the framework for the appropriate work-up and management of patients with chronic kidney disease presenting for a magnetic resonance imaging procedure had been developed, it was the role of the medical radiation technologist to work collaboratively with the physicians to implement the new practice guidelines. The gadolinium example illustrates why it is crucial for MRTs to be able to administer any substance ordered by a physician that may be necessary to allow a patient to undergo an imaging or therapeutic procedure. The substance that is ordered will vary depending on a number of factors which change rapidly based on advances in technology and research findings. Ensuring that all of the potential substances that might be needed for safe and effective practice are currently listed in a regulation would be impossible given the rapid pace of change. Even listing the categories of drugs or substances used would present a challenge in light of how quickly the technology and practice is evolving. What follows next is a brief description of just a few of the diagnostic and therapeutic procedures where, on the order of a physician, medical radiation technologists administer a substance to the patient. It is important to note that the order from a physician to administer a substance may be a medical directive or a direct order. The legal requirement for an order may be based on the condition set out in the MRT Act for the performance of an authorized act or the requirement for an order under the HARP Act or both. The order from the physician to administer a substance is usually found in the protocols that define the procedure. Procedure is a broad term that refers to procedures, treatments, interventions and professional services provided by a regulated health professional. MRTs in the specialty of nuclear medicine conduct nuclear medicine procedures based on departmental protocols that include an order from a physician for the administration by injection or inhalation of a radiopharmaceutical. Nuclear medicine technologists perform procedures that involve the administration of ionizing radiation only when the conditions under the federal Nuclear Safety and Control Act and its regulations and licenses have been met.
November 12, 2008 Page 10
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
MRTs in the specialty of nuclear medicine are expected to assess the nuclear medicine images and data related to the procedure and then to modify or optimize the nuclear medicine procedure to best visualize the physiological functioning of the patient’s body. “For patients undergoing a white blood cell study to determine the site of an infection, the nuclear medicine technologist will first check the white cell count from the blood test result of a patient and, depending on the white cell count, will then determine how much blood to draw from the patient in order to ensure an accurate study using a minimum amount of blood. A radiopharmaceutical is attached to the white cells of the patient’s blood and injected back into the patient. The MRT is then able to locate the site of the infection using the nuclear medicine camera, and produce images for reporting by the nuclear medicine radiologist”. M.R.T.(N.), Manager, Medical Imaging Department One of the best practices identified by the Ministry of Health and Long-Term Care in its Wait Time Strategy for CT and MRI for the administration of contrast media for patients undergoing CT and MRI scans, is for MRTs to perform the injection of the contrast media for patients at all times, including the evening and night shifts, when a radiologist is not present. The MRT must explain the procedure to the patient; identify any contraindications to the administration of the contrast media by reviewing the patient’s blood test results and obtaining a history of allergies. In this way, the MRT assesses whether the patient’s condition will allow the safe injection of the contrast media in accordance with the established protocols. If so, the MRT will proceed to start an intravenous line and will administer the contrast media at the appropriate time during the CT or MRI scan. As some patients may experience a severe allergic reaction to the contrast media, the MRT must constantly assess the condition of the patient, and initiate emergency response procedures if a patient suffers any adverse reaction.
November 12, 2008 Page 11
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
“In our computed tomography (CT) area, the MRTs are injecting contrast media into patients undergoing CTs, under medical directives, without the physician being present. This has helped reduce our waiting list for CT, as we can now schedule patients who require contrast in the evening when the radiologist is not available. When starting the procedure, the MRT interviews the patient and asks about his or her allergies, whether the patient has experienced any previous problems with contrast, and his or her medical conditions. The MRT performs an assessment of the patient and makes note of any pre-existing conditions that may be contraindications to the administration of the contrast. Further tests may be required which the MRT may order under a medical directive. For example, if a patient has a known renal problem, the MRT will arrange for a blood test to check the patient’s creatine levels. If the patient meets the criteria under the medical directive or protocol, the MRT will proceed with the injection of the contrast media. Immediately following the injection, the MRT carefully monitors the patient for any signs of allergic reaction. The MRT may take the patient’s blood pressure and check his or her blood oxygen levels. If the patient develops rashes or hives, the MRT will refer the patient to the radiologist (if available), or to the hospital’s emergency department. As our CT scanners are now so fast, the patient’s CT scan is often finished within a very short period of time. We often ask the patient to remain in the department for a few more minutes after the CT is completed, in order that the MRT can assess the condition of the patient prior to letting him or her go home.” M.R.T.(R.), Computed Tomography Department MRTs perform upper gastrointestinal procedures where the patient drinks barium or other contrast media to outline the upper gastrointestinal tract. A barium meal, also known as an upper gastrointestinal series, is a procedure in which images of the esophagus, stomach and duodenum are taken as and after barium sulfate or another contrast media is ingested by a patient. The barium shows the shape and details the lining of the esophagus, stomach and duodenum. MRTs also perform barium enema studies which are imaging procedures used to examine and diagnose conditions and diseases of the colon. To make the large intestine visible on an X-ray image, the colon is filled with a contrast material. The procedure involves the MRT inserting an enema tip into the rectum and administering barium sulfate, air or other contrast media to fill the colon. X-ray images are taken by the MRT while he or she performs the barium enema study.
November 12, 2008 Page 12
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
“MRTs in the specialty of radiography, who perform gastrointestinal procedures under medical directives, have the knowledge, skill and judgment to recognize pathology and know how to optimize visualization of the pathology for the diagnosis by a radiologist. For example, during a barium enema procedure, the MRT must be able to distinguish normal bowel from abnormal bowel. During each procedure, we as technologists look for filling defects and changes in mucosal patterns. Once pathology is noted, the technologist modifies the procedure by adding or changing the imaging to best visualize the pathology. For example, if the MRT identifies a polyp in the bowel of a patient, the MRT will turn the patient and image the polyp from different views to ensure we see the pathology in multiple dimensions to define the involvement, size and shape of the polyps. This is important as the radiologist will consider all these factors in order to make an accurate diagnosis of the patient’s disease.” M.R.T.(R.), Service Coordinator, Diagnostic Imaging PROPOSED CHANGES TO AUTHORIZED ACTS AND REGULATIONS The College of Medical Radiation Technologists of Ontario is not proposing any changes to current authorized acts and regulations as they relate to the administration and use of drugs by medical radiation technologists.3 RISK OF HARM The risk of harm clause of the RHPA states that: “No person, other than a member treating or advising within the scope of practice of his or her profession, shall treat or advise a person with respect to his or her health in circumstances in which it is reasonably foreseeable that serious physical harm may result from the treatment or advice or from an omission from them.” Effective June 4, 2009, "serious physical harm" will be amended to "serious bodily harm". As stated above, the administration and use of drugs has almost always been an integral part of MRT practice because they are necessary for many of the diagnostic imaging and radiation therapy procedures performed by MRTs. However, were an MRT to administer or use a drug outside of the scope of practice of the profession under circumstances where serious physical harm may result, such activity would be contrary to the harm clause.
3 Please refer to the Request for Change in Scope of Practice – Medical Radiation Technology dated June 30,
2008 made by the College of Medical Radiation Technologists of Ontario and the Ontario Association of Medical Radiation Technologists for the proposed changes to the authorized acts currently authorized to MRTs.
November 12, 2008 Page 13
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
The CMRTO has not proposed any changes to the current regulatory framework for the administration and use of drugs by MRTs in their practice. We believe that the current system appropriately addresses any potential risk of harm to the patient by ensuring that all substances administered to patients by MRTs are prescribed or ordered by a physician, whether as a result of the requirement for an order of a physician under the MRT Act, the HARP Act or both. EDUCATION AND CONTINUING COMPETENCY All MRT programs in Ontario teach the Canadian MRT core competencies which are linked to and support the acts authorized to MRTs. Each of the authorized acts relates directly to diagnostic imaging and radiation therapy procedures. They are currently taught and tested in the educational programs for medical radiation technology. In addition, the MRT competencies of the Canadian Association of Medical Radiation Technologists (CAMRT), which are the basis for the accreditation of MRT programs in Ontario and for the national certification examination, support the controlled acts authorized to MRTs. The CAMRT competency profiles for each of the specialties can be found in Appendix 2 Tabs 1, 2, 3 and 4. Set out below are examples of curricula from Ontario MRT educational programs which demonstrate that each of the authorized acts related to the use of drugs is being taught and tested in Ontario MRT educational programs.
1. Administering substances by injection or inhalation Authorized Act 2 for MRTs is Controlled Act 5 of the RHPA: examples of procedures falling within this authorized act would be performing an intravenous, subcutaneous or intramuscular injection; or starting peripheral intravenous lines, or establishing saline locks for the purpose of administering substances such as radiopharmaceuticals or contrast media for the visualization of body organs, such as the kidneys or heart. For examples of the curricula related to this authorized act, see Appendix 3, Tabs 1, 2, 3 and 4. 2. Administering contrast media through or into the rectum or an artificial opening into the body Authorized Act 3 for MRTs falls within Controlled Act 6 of the RHPA: an example of a procedure falling within this authorized act would be inserting an enema tip and barium for an examination of the colon For examples of the curricula related to this authorized act, see Appendix 4, Tabs 1 and 2. As demonstrated by the curricula and CAMRT competencies, each of the authorized acts are currently taught and tested in the educational programs for medical radiation technology and tested through the national certification examination.
November 12, 2008 Page 14
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
Continuing education programs on authorized acts also exist and are available for those existing practitioners who may not have received education in their original training, e.g. administering substances by injection offered to MRTs by the Michener Institute for Applied Health Sciences and by the OAMRT. A well-rounded, rigorous and comprehensive quality assurance program ensures continuing competency and public protection. The CMRTO quality assurance (QA) program includes self-assessment and continuous learning by each member and evaluation by the QA Committee of this self assessment and continuous learning.
The QA program requires that each member of the College do the following each year: • Complete a Self-Assessment Profile • Complete a Continuous Learning Portfolio • Complete and submit a Certificate of Competence (Quality Assurance Declaration) to the
College at the same time as payment of the annual fee.
The QA program also includes a practice assessment of members. The assessment conducted through a multi-source feedback system is a program designed to assess members’ knowledge, skills and judgment. The multi-source assessment process provides a means for peers (MRTs), co-workers, such as clerical staff or other health care providers, patients and the MRT who is being assessed to complete a survey focused on the standards of practice. The assessed MRT receives a performance assessment profile or feedback about his or her performance.
The multi-source feedback system provides a means to assess how members in the profession actually perform in practice. The assessment process is a formative evaluation which incorporates feedback regarding a MRT’s performance in the practice setting from those who are in the best position to provide feedback.
The questionnaires cover a number of norms drawn from the profession’s Standards of Practice as established by the CMRTO. The multi-source feedback assessment provides the MRT with a formative evaluation in the form of a report that compares the MRT clinical performance to that of other MRTs. The report is provided to the MRT and the Quality Assurance Committee.
Life-long learning is a professional obligation of all MRTs and is embedded in the CMRTO’s quality assurance program. The CMRTO expects that all MRTs will engage in continuous learning activities that are related to his or her individual practice and employment setting including continuous learning activities that may be a direct result of scope of practice changes.
November 12, 2008 Page 15
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
PUBLIC INTEREST The CMRTO believes that the current regulatory framework for the use and administration of drugs and substances by MRTs in their practice is in the public interest. It ensures patient safety while still allowing the system to be flexible and respond to change, allowing for access to services and system efficiencies and promoting interprofessional collaboration and patient-centred care. Promoting patient safety is a shared responsibility involving many parts of the health system. As the regulatory body for MRTs in Ontario, CMRTO’s role is to protect the public. This is achieved through: • Setting the criteria for entry to the profession; • Establishing practice standards; • Administering a Quality Assurance Program; and • Enforcement of practice standards.
By fulfilling this mandate, CMRTO strives to ensure the provision of safe and ethical practice of medical radiation technology by its members. In addition, employers, professional associations, unions, researchers, individual providers and health provider teams have key roles to play in promoting patient safety.
MRTs administer a wide array of substances in the course of their practice. The specific substance used depends on the nature of the procedure, the diagnostic or therapeutic outcome sought, the technology being used and the health status of the patient. Other factors which may influence the choice of substance used are potential side effects, contraindications, the comparative cost of the substance, and physician preference. What is common regardless of specialty, technology or patient is the fact that the substance in question has been ordered by a physician, in many cases a radiation oncologist, nuclear medicine radiologist or diagnostic imaging radiologist. MRTs are trained in the administration of substances related to diagnostic and therapeutic procedures and to deal with any potential adverse effects related to their administration, including initiating emergency response procedures. By having the substance prescribed by a physician or radiologist and administered by a qualified and trained MRT patient safety is ensured. The recent review of MRTs' scope of practice confirmed that MRTs safely administer substances in their practice and no change is being proposed to the existing regulatory structure. MRTs' practice is currently regulated by the requirement for an order for the diagnostic imaging or therapeutic procedure under the MRT Act, the HARP Act or both. Based on the order from the physician or radiologist relating to the diagnostic and therapeutic procedures, MRTs are able to deliver patient-centred care in a safe and efficient manner while practising to their full professional competency. The current system encourages collaboration between MRTs and physicians as the process of patient screening is a shared responsibility and the substance administered very dependent on the input of both professionals with the MRT often having the most direct patient contact.
November 12, 2008 Page 16
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
PRESCRIBING: DRUG REGULATIONS UNDER PROFESSIONAL ACTS The drugs and substances used and administered by MRTs in practice are prescribed by authorized and regulated prescribers in accordance with applicable provincial and federal statutes and regulations. Those drugs and substances that are radioactive carry an additional layer of federal regulation and the facilities where they are dispensed and administered are themselves regulated under federal laws. Contrast media and radiopharmaceuticals are purchased under the direction of the radiologist and Imaging or Radiation Therapy department manager and the administration of the hospital or independent health facility. Contrast media and radiopharmaceuticals are delivered directly to the specific department by the manufacturer and do not go through the hospital pharmacy. The protocol for storage and administration of the contrast media and radiopharmaceuticals in the Imaging or Radiation Therapy department is determined by the physician radiologist and the manager of the department and implemented by the MRTs in the department, in accordance with any statutory requirements (for example, the Nuclear Safety and Control Act) and applicable guidelines (for example, Health Canada or the manufacturer’s guidelines). As indicated above, the regulation of the practice of medical radiation technology with respect to the administration of substances is done through the requirement of an order in order to perform the authorized act of administering a substance by injection or inhalation under the MRT Act or an order under the HARP Act. The use of radiopharmaceuticals is also regulated under the Nuclear Safety and Control Act. We note that, with the exception of medicine and dentistry, the regulatory framework for the administration of substances by the use of lists of specific drugs and substances or through categories or classes tends to be linked to whether a regulated health profession has the authority to self-initiate its authorized acts and/or prescribe drugs for patients. For example, chiropody and registered nurses in the extended class do not require the order of another regulated health professional to perform the controlled acts authorized to them, which include prescribing drugs designated in the regulations. Medical radiation technologists neither have the authority to perform the controlled acts authorized to them without an order of a physician nor the authority to prescribe drugs. We believe that the current regulatory framework for medical radiation technology with respect to the use of substances reflects an appropriate balance of autonomy and regulation to ensure patient safety and would not recommend any change. Listing specific drugs or classes of drugs in regulation would pose a significant challenge to MRTs. Safe, efficient, patient centred care relies on an MRT’s ability to administer whatever substance has been prescribed for the procedure that has been ordered. Advances in technology and research related to contrast media and radiopharmaceuticals inform the choice of substance ordered and any form of restriction on what can be administered will negatively impact access to services and efficiencies in patient care and adversely affect the collaborative relationship currently enjoyed between MRTs and physician specialists. We would comment, however, that if HPRAC were to
November 12, 2008 Page 17
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
conclude that there is a need to include drugs in a regulation, it would seem unrealistic to expect to list specific drugs, given the rapid pace of change in healthcare. If HPRAC reaches such a conclusion, it would seem more logical to try to articulate classes or categories, thus allowing greater flexibility to account for changing practice and supply. Medical radiation technology is a rapidly evolving and exciting field of practice. Innovations quickly translate into patient care applications and regulation change could never hope to keep pace. Restricting the substances that may be used and administered in practice would seriously compromise MRTs’ ability to practise to their full scope. The current system allows patients to enjoy the benefits of research findings quickly and encourages a high level of collaboration and shared learning amongst the professionals involved in their care. Patient safety is ensured by the physician’s order which is specific to the patient and procedure. In addition, the substances used are the subject of federal regulation and facility specific requirements and oversight. COLLABORATION MRTs collaborate with a range of other health professionals in their practice. Physicians, nurses, respiratory therapists, dietitians, physiotherapists and medical laboratory technologists all play a role on the team. Collaboration is enhanced when each member of the team is able to optimize their skills to benefit the patient. The current regulatory structure that allows professions who have an order from another regulated health professional to administer substances (without the substances being restricted to a list in a regulation) maximizes access to services and efficiencies in patient care and improves wait times for patients. Restricting the substances that may be used and administered in practice would create a real barrier to inter-professional collaboration as each profession would need to keep abreast of one another’s authority and each profession’s regulations would need to be perfectly aligned with the team’s practice to ensure patient care would not be compromised. In light of the length of time the regulation-making process requires, this would simply not be a practical or workable framework. OTHER JURISDICTIONS MRTs enjoy a high degree of mobility across Canada as a result of a Mutual Recognition Agreement and national recognition of the CAMRT competency profile. There are currently no issues related to the use and administration of drugs or substances in MRT practice which affect mobility rights and use and administration of drug and substances are a part of practice for MRTs across Canada.
November 12, 2008 Page 18
CMRTO - Review of Non-physician Prescribing and Administration of Drugs Under the RHPA
November 12, 2008 Page 19
In terms of international experience, we are aware that radiographers in the UK have limited prescribing rights. This is not something that is currently part of the curriculum or routine expectations of practice for MRTs in Ontario or in the rest of Canada. COSTS AND BENEFITS The CMRTO supports the current regulatory framework for the use and administration of drugs and substances in MRT practice. This framework allows MRTs to administer and use drugs and substances that are prescribed for patients and allows the system to achieve the benefits of ordering what is most appropriate and cost effective without having to ensure that a specific substance is listed in a regulation. Restricting what can be administered or used in health care practice ties the hands of professionals. Regulations cannot quickly be changed to adapt to advances in technology and practice or unforeseen circumstances such as the shortages in radioisotopes caused by the temporary shutdown of the Chalk River Nuclear Reactor. The benefits of the current regulatory framework are its flexibility and adaptability to change, and its ability to ensure patient safety through the requirement for an order. We believe this is an ideal system to ensure maximum patient benefit at minimum system cost. CONCLUSION The CMRTO supports the current regulatory framework related to the use and administration of drugs and substances by MRTs. We believe that it strikes an appropriate balance and ensures patient safety while promoting system flexibility and efficiency. We do not feel it would be appropriate to restrict the substances that may be administered by MRTs and in fact believe it would impose artificial barriers to patient-centred care. If restrictions are considered necessary to ensure patient safety, they should be minimal and relate to categories or classes of drugs to allow for maximum flexibility and efficiency. HPRAC may also wish to review the June 30, 2008 joint submission by the CMRTO and OAMRT related to the scope of practice review for MRTs. Thank you for the opportunity to participate in this review and share with you the many ways that MRTs use and administer drugs and substances in their practice to advance patient care. We would be happy to provide any additional information you may require and look forward to the next phase of this consultation.
Appendix 1
Guidel ines And Standards
Tab Title Page No.
1 College of Medical Radiation Technologists of Ontario, Essential Competencies 2003.
1
2 College of Medical Radiation Technologists of Ontario, Addendum to Comprehensive Guidelines for acting in accordance with the Regulated Health Professions Act Scope of Practice/Controlled Acts Model, January 1, 2004.
13
3 College of Medical Radiation Technologists of Ontario, Comprehensive Guidelines for acting in accordance with the Regulated Health Professions Act Scope of Practice/Controlled Acts Model, 1999.
27

Essential Competencies
College of Medical RadiationTechnologists of Ontario
Page 1
Essential Competencies : Introduction and Background to the Essential Competencies
Page : i
Introduction and Background to theEssential Competencies1. Standards of Practice DefinedEffective January 1, 2004, medical radiation technologists in the specialties of radiography, nuclear medicine, radiation therapy and magnetic resonance have new standards of practice.
These standards of practice are composed of the Essential Competencies and theComprehensive Guidelines for acting in accordance with the Regulated HealthProfessions Act Scope of Practice/Controlled Acts Model, as amended by theAddendum to the Comprehensive Guidelines.
These standards of practice replace the documents titled “Standards of Practicefor Medical Radiation Technologists – Radiography”, “Standards of Practice forMedical Radiation Technologists – Radiation Therapy” and “Standards of Practice for Medical Radiation Technologists – Nuclear Medicine” published by the CMRTO in 1994.
Standards of Practice for:M.R.T.(R.)M.R.T.(N.)M.R.T.(T.)M.R.T.(M.R.)
Essential Competencies Comprehensive Guidelinefor acting in accordancewith the Regulated HealthProfessions Act Scope ofPractice/Controlled
Addendum to theComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
Addendum toComprehensiveGuidelines
Addendum to Comprehensive Guidelines For acting in
accordance with the Regulated Health Professions Act Scope
of Practice / Controlled Acts Model (January 1, 2004)
Standards of Practice forMedical RadiationTechnologists (1994)
Radiography
Standards of Practice forMedical RadiationTechnologists (1994)
Radiation Therapy
Standards of Practice forMedical RadiationTechnologists (1994)
Nuclear Medicine
20041994
Page 2
Essential Competencies : Introduction and Background to the Essential Competencies
Page : ii
2. Standards of Practice – The Heart of the CMRTO’s Mission Statement“The mission of the College of Medical Radiation Technologists of Ontario is to serveand protect the people of Ontario through self-regulation of the profession.” One ofthe ways the College meets its mission statement is by establishing and enforcingStandards of Practice for Medical Radiation Technologists (M.R.T.s).
3. Purpose of the Standards of PracticeThe Standards of Practice will assist M.R.T.s in understanding the College’s expectations with respect to the professional practice of medical radiation technology. They will help managers in making appropriate decisions regardingmanagement of the practice of M.R.T.s and in developing suitable policies and procedures. They will assist educators in developing curriculum and in providingappropriate instruction. Finally, they will assist the public in assessing quality of care.
The Standards of Practice will serve the College in all areas where criteria for professional performance are needed in making decisions. They will be used by the Complaints Committee, the Discipline Committee and the Fitness to PractiseCommittee in making their determinations regarding professional misconduct,incompetence or incapacity. They will also be used for other College processes suchas ascertaining entry-level requirements for registration and for evaluation of QualityAssurance records in the Quality Assurance Program.
In the event that the Standards of Practice set a standard that is higher than departmental policy or procedure, the M.R.T. must comply with the standard set by the Standards of Practice.
Page 3
Essential Competencies
Table of Contents
01 Introduction
02 1. Legislation, Standards and Ethics
02 2. Equipment and Materials
03 3. Diagnostic Examinations and Radiation Treatment
05 4. Safe Practice
06 5. Relationship with Patients
07 6. Records and Reporting
Page 4

I N T R O D U C T I O N
The Essential Competencies document has beendeveloped by the College of Medical RadiationTechnologists of Ontario (CMRTO) as a reference tool to determine whether a MedicalRadiation Technologist (M.R.T.) can perform atan acceptable level. The Essential Competenciesreflect the knowledge, skills and judgmentM.R.T.s need in order to perform the servicesand procedures that fall within the scope of practice of the profession.
In the Essential Competencies, there are references to the Comprehensive Guidelines.These refer to the Comprehensive Guidelines foracting in accordance with the Regulated HealthProfessions Act Scope of Practice/Controlled ActsModel (the Comprehensive Guidelines). TheEssential Competencies and the ComprehensiveGuidelines, as amended from time to time,replace the “Standards of Practice for MedicalRadiation Technologists” for radiography, nuclearmedicine and radiation therapy published by the CMRTO, and together constitute the new standards of practice for M.R.T.s.
In the Essential Competencies, there is also reference to the Code of Ethics. This refers to thecode of ethics for CMRTO members (the Codeof Ethics). It is intended that the EssentialCompetencies and Comprehensive Guidelines beused in conjunction with the Code of Ethics.Together, these documents provide a model forensuring safe, effective and ethical professionalperformance to ensure safe, effective and ethicaloutcomes for patients.
By providing objective criteria, the Essential Competencies will assist M.R.T.s in understanding the CMRTO’s expectations forprofessional practice. They will assist managers inmaking appropriate decisions regarding management of the practice of M.R.T.s and indeveloping appropriate policies and procedures.They will assist educators in curriculum development and in providing appropriateinstruction. Finally, they will assist the public inassessing quality of care.
The Essential Competencies document will serve the College in all areas where criteria for professional performance are needed in makingdecisions. It will be used by the ComplaintsCommittee, the Discipline Committee, and the Fitness to Practise Committee in making their determinations regarding professional misconduct, incompetence or incapacity. It will also be used for other College processes.
Some examples are:• Registration:
o ascertaining entry-level requirements• Quality Assurance:
o peer review of practiceo evaluation of QA recordso evaluation of self-assessment profiles.
The Essential Competencies are intended to be generic. The indicators following each competency are examples of the application of that competency in a specific dimension of practice. Most indicators refer to tasks that arecommon to all M.R.T.s. Indicators that refer totasks generally performed only by M.R.T.s in one of the specialties are listed under separate headings. The methods for implementing eachtask may be determined by departmental policiesand procedures. In the event that the EssentialCompetencies or Comprehensive Guidelines set standards that are higher than departmental policies or procedures, the M.R.T. must comply with the standards set by the EssentialCompetencies or Comprehensive Guidelines, asthe case may be. In the Essential Competencies,the term “legislation” refers to both statutes and regulations.
Essential Competencies
Page : 01 Page 5
Essential Competencies
Page : 02
1. Legislation, Standards and Ethics
M.R.T.s are members of the College of MedicalRadiation Technologists of Ontario. This ensuresthat they have met the professional educationrequirements of the College and that they continue to educate themselves about practical,legal, ethical and other matters pertaining to the profession.
E S S E N T I A L C O M P E T E N C Y:
M.R.T.s must understand, and adhere to, the legislation governing the practice of the profession, the standards of practice set by theCollege, and the Code of Ethics.
I N D I C AT O R S
All M.R.T.s must:a) maintain the knowledge, skills and judgment
to perform all procedures undertaken in thecourse of practising the profession;
b) adhere to all relevant provincial and federallegislation and guidelines governing the practice of the profession;
c) adhere to the standards of practice set by the College;
d) adhere to the Code of Ethics; ande) adhere to all regulations made under the
Medical Radiation Technology Act(MRT Act), including:i) quality assurance;ii) registration;iii) professional misconduct; andiv) advertising.
2. Equipment and Materials
The work of M.R.T.s entails the use of a widerange of equipment and materials. M.R.T.s must be cognizant of the functions, capabilities, specifications and hazards of materials and equipment being used in the course of their practice.
E S S E N T I A L C O M P E T E N C Y:
M.R.T.s must have the knowledge, skills and judgment to select the appropriate equipment andmaterials for procedures ordered by a physician (or other health care practitioners listed in the Healing Arts Radiation Protection Act), to make determinations as to their quality, serviceability,
and operability, and to take any corrective actionsrequired to meet standards set by legislation, facility policies and manufacturers’ guidelines.M.R.T.s must be able to prepare or construct personalized devices and materials where required. M.R.T.s must be skilled in making safe, efficient and effective use of resources to produce the desired examination information or treatment effects.
I N D I C AT O R S
All M.R.T.s must:a) ensure the room is prepared for the procedure
specified in the order;b) select and set up the equipment and materials
needed for the procedure specified in theorder;
c) select the correct substances to be administeredorally, by injection or inhalation, or throughor into the rectum or artificial opening of thebody, as required;
d) prepare diagnostic or therapeutic substances as required;
e) conduct or ensure that the required quality control tests on each piece of equipmentand any materials used in the ordered procedure have been conducted correctly,according to the applicable legislation and thefacility policies and manufacturers’ guidelines;
f ) determine if the results of the quality controltests are acceptable;
g) if quality control tests are not within acceptable limits, take corrective action toensure that the standards set by legislation,facility policies and manufacturers’ guidelines are met;
h) determine, set and verify the technique andprotocol to be used in the procedure;
i) verify all required immobilization and/or beam modification devices; and
j) make use of appropriate shielding devices;
In addition, all M.R.T.s in the specialties ofradiation therapy and nuclear medicine must:k) construct immobilization devices and/or
beam modification devices as required;
In addition, all M.R.T.s in the specialty of magnetic resonance must:l) administer and follow the necessary safety
precautions for entry to the magnet room;
Page 6
In addition, all M.R.T.s in the specialty ofnuclear medicine must:m)dispose of expired, unused or contaminated
eluate, radioactive materials and all administrative devices in accordance with legislation and established safety protocols; and
n) store radiopharmaceuticals according to manufacturers’ specifications.
3. Diagnostic Examinations andRadiation Treatment
M.R.T.s are health care professionals who employionizing radiation, radiopharmaceuticals, andelectromagnetism (static magnetic fields andradio frequencies) to create images that are partof diagnostic imaging examinations or that are used for defining and recording treatment parameters. These images may be dynamic, on film, digital displays, three-dimensional models or templates. M.R.T.s in the specialties of radiation therapy and nuclear medicine, administer ionizing radiation to treat cancer and other diseases.
M.R.T.s who apply ionizing radiation do so under the authority of, and in accordance with,the Healing Arts Radiation Protection Act and,where applicable, the Nuclear Safety and ControlAct and their respective regulations. M.R.T.s are permitted to apply electromagnetism for magnetic resonance imaging under an exemptionset out in a regulation made under the RegulatedHealth Professions Act.
M.R.T.s perform four controlled acts, which theyhave been authorized to perform under theMedical Radiation Technology Act. The four con-trolled acts that M.R.T.s are authorized toperform are:
1. taking blood samples from veins;2. administering substances by injection or
inhalation;3. administering contrast media through or
into the rectum or an artificial opening into the body; and
4. tattooing.
M.R.T.s may accept delegation of other procedures that are controlled acts under theRegulated Health Professions Act, provided theycomply with the Regulated Health Professions Actand the Comprehensive Guidelines.
E S S E N T I A L C O M P E T E N C Y:
M.R.T.s must be able to create images that aresufficiently accurate and clear for the diagnosticor treatment purposes that are ordered by aphysician (or other health care practitioner listedin the Healing Arts Radiation Protection Act),while using only the minimum amount of radiation or electromagnetism (radio frequency)necessary during the course of an examination or treatment. M.R.T.s must be proficient in evaluating the technical sufficiency of the images and tests to ensure that the images are satisfactory. M.R.T.s must be able to administerthe therapeutic application of ionizing radiationaccurately and in accordance with the treatmentprescription ordered by a physician under theHealing Arts Radiation Protection Act. M.R.T.smust not apply or administer ionizing radiationunless the conditions under the applicable legislation (including, without limitation, theHealing Arts Radiation Protection Act and its regulations, and the Nuclear Safety and ControlAct, its regulations and licences issued thereunder) have been met.
M.R.T.s must be able to perform the four controlled acts authorized to M.R.T.s (authorizedacts) as required in the course of engaging in thepractice of the profession. They must not perform the authorized acts, or any exemptedcontrolled act, unless the conditions under theRegulated Health Professions Act, the MedicalRadiation Technology Act, their respective regulations and the Comprehensive Guidelineshave been met. M.R.T.s must only perform delegated controlled acts in accordance with the conditions set out in the Regulated HealthProfessions Act and the Comprehensive Guidelines.
Essential Competencies
Page : 03 Page 7
Essential Competencies
Page : 04
I N D I C AT O R S
All M.R.T.s must:a) position the patient as required for
examination or treatment;b) perform procedures involving the application
or administration of ionizing radiation onlywhen the conditions under the applicable legislation (including, without limitation, theHealing Arts Radiation Protection Act and itsregulations, and the Nuclear Safety andControl Act, its regulations and licenses issuedthereunder) have been met;
c) perform only those controlled acts that havebeen authorized, or exempted or excepted underthe legislation, or delegated in accordance withthe legislation and the ComprehensiveGuidelines;
d) perform authorized acts, or delegated orexempted controlled acts, only when the conditions under the legislation andComprehensive Guidelines have been met;
e) not perform any procedure which may resultin serious physical harm, unless that procedure is within the scope of practice ofthe profession or the M.R.T. is authorized or permitted to do so by legislation;
f ) ensure the area to be diagnosed or treated willbe displayed on the exposed film or capturedelectronically;
g) use radiation protection devices and otherpatient protection devices as required;
h) instruct the patient on breathing and movement procedures;
i) ensure that the orientation of the body andother pertinent parameters are marked correctly on the image;
j) ensure the exposure provides optimum imagequality while using minimal radiation;
k) ensure examination results (film, electronicimage or other computer data input) provideall the information requested in the order;
l) carry out the procedures ordered; andm)assess the patient’s condition during the
course of treatment or procedures andrespond accordingly;
In addition, all M.R.T.s in the specialties ofradiography, nuclear medicine and magneticresonance must:n) determine if the image is of sufficient diagnostic
quality or if additional or repeat images are necessary;
In addition, all M.R.T.s in the specialty of magnetic resonance must:o) perform procedures involving the application
of electromagnetism (static magnetic fieldsand radio frequencies) only when the conditions under the Regulated HealthProfessions Act and its regulations have been met;
In addition, all M.R.T.s in the specialty of radiation therapy must:p) develop an optimal treatment distribution for
each patient;q) calculate treatment doses and duration of
administration;r) ensure use of record and verification systems;s) identify the treatment field and
treatment volumes;t) select and/or verify treatment parameters;u) administer treatment; andv) determine if the image verifies treatment
parameters or if a repeat image is necessary.
Page 8
4. Safe Practice
M.R.T.s operate equipment, apply ionizing radiation and electromagnetism (static magneticfields and radio frequencies) and administerradiopharmaceuticals, all of which could be dangerous if used incorrectly. Therefore, theyendeavour to reduce the risk of harm to theirpatients, to themselves, to their colleagues and toany other individuals who may be present in thepractice environment, at all times and in everyaspect of their practice.
E S S E N T I A L C O M P E T E N C Y:
M.R.T.s must have the knowledge, skills andjudgment to practise safely by adhering to all relevant provincial and federal legislation andguidelines, departmental protocols and policies,and manufacturers’ directions pertaining tohealth and safety. In the event of any unexpectedproblems or emergencies, M.R.T.s must be competent and prepared to handle or to assist inthe management of the situation.
I N D I C AT O R S
All M.R.T.s must:a) observe all departmental policies and relevant
provincial and federal legislation and guidelines pertaining to health and safety,such as the:i) Regulated Health Professions Act and its
regulations;ii) Medical Radiation Technology Act and
its regulations;iii) Public Hospitals Act and its regulations;iv) Independent Health Facilities Act and its
regulations;v) Healing Arts Radiation Protection Act
and its regulations;vi) Occupational Health and Safety Act and
its regulations;vii) Health and Welfare Canada Health
Protection Branch guidelines;viii) Nuclear Safety and Control Act and its
regulations and licenses issued there under;
ix) X-Ray Equipment in Medical Diagnosis Part A: Recommended Safety Procedures for Installation and Use (Safety Code 20A); and
x) As Low As Reasonably Achievable (ALARA) principle;
b) conduct appropriate quality control tests forall equipment and substances to be used in anexamination or treatment session;
c) take corrective action if quality control testsare not within acceptable limits;
d) only use substances before their expiry time ordate;
e) verify the patient’s identity for all treatmentprocedures and examinations;
f ) ascertain whether any female patient, age 10 –55, might be pregnant, and make necessaryexplanations, referrals or implement essentialrestrictions;
g) notify the patient’s physician, radiologist orradiation oncologist of any contraindicationsto the ordered procedure and obtain permission to proceed or halt the procedure;
h) take into account the patient’s physical andemotional limitations, and ensure that thepatient will not be expected to perform anytask or movement that would cause physicalharm;
i) ensure that no equipment can injure a patient;j) use the ALARA principle to minimize the
patient’s exposure to radiation and electromagnetism (static magnetic fields andradio frequencies) for any given examination or procedure;
k) use shielding/protective devices where indicated;
l) initiate emergency response procedures, notify a physician (if possible), and assist in or carry out emergency treatment as required, if a patient suffers any adverse reaction to treatment or to substances administered orally, by injection, inhalation or through or into the rectum or artificial opening into the body;
m)use appropriate aseptic techniques and infection control procedures in the course of examinations or treatment;
n) protect themselves, their colleagues, othermembers of the health care team, any otherindividuals who may be present, as well as anypatient, from any unnecessary exposure toradiation;
o) ensure all immobilization devices immobilizethe patient in the treatment or examinationposition appropriate to the procedure specified in the patient’s chart/order accordingto departmental policy;
Essential Competencies
Page : 05 Page 9
Essential Competencies
Page : 06
p) assess the patient’s condition during thecourse of treatment or procedure; and
q) remove all markers and all accessory equipment/devices before the patient is dismissed;
In addition, all M.R.T.s in the specialties ofradiography, nuclear medicine and magneticresonance must:r) ascertain whether any female patient, age 10 –
55, might be nursing, and make necessaryexplanations, referrals or implement essentialrestrictions;
In addition, all M.R.T.s in the specialty of magnetic resonance (MR) must:s) ensure that there are no contraindicators
present that could harm the patient or would exclude the patient from having the examination; and
t) ensure that all equipment and devices, bothpatient-specific and accessory, are MR compatible before being brought into the MR area;
In addition, all M.R.T.s in the specialty of radiation therapy must:u) label and orient all patient-specific ancillary
equipment.
5. Relationship with Patients
Medical radiation technology is a health care profession that has patient care as its main concern.
E S S E N T I A L C O M P E T E N C Y:
M.R.T.s must be able to accept the patient’sautonomy and the right of the patient, or thepatient’s substitute decision maker, to refuse service. M.R.T.s must treat all patients with dignity and respect. M.R.T.s must maintain clearand appropriate professional boundaries in the M.R.T.-patient relationship. M.R.T.s must havethe knowledge, skills and judgment to avoid placing patients at unnecessary risk of harm, pain or distress. M.R.T.s must be able to provideappropriate responses to the patient’s inquiriesabout procedures and related issues. M.R.T.smust understand how, and act, to protect theconfidentiality of all professionally acquiredinformation about patients.
I N D I C AT O R S
All M.R.T.s must:a) provide clear and understandable information
to the patient, or the patient’s substitute decision maker, prior to, during and aftertreatment, using an interpreter, if necessary;
b) give the patient, or the patient’s substitutedecision maker, an opportunity to ask questions;
c) provide the patient, or the patient’s substitutedecision maker, with answers to his or herquestions within the scope of the M.R.T.’sresponsibility;
d) refer questions of the patient, or the patient’ssubstitute decision maker, that are outside the scope of the M.R.T.’s responsibility to an appropriate health care professional for answers;
e) carry out examinations or treatment only withthe informed consent of the patient, or thepatient’s substitute decision maker;
f ) make modifications to procedures based onthe patient’s physical, medical and/or emotional status/needs;
g) instruct the patient to remove only the clothing and items that would interfere withthe examination or treatment procedures;
h) provide the patient with a gown/sheet to coverareas where clothing was removed;
i) explain to the patient when and where theM.R.T. might touch him/her and why;
j) touch the patient only in those areas neededto facilitate carrying out the procedure;
k) keep all patient information confidential,except when necessary to facilitate diagnosis ortreatment of the patient or when legally obligedor allowed to disclose such information;
l) observe all relevant legislation, such as theHealth Care Consent Act, and all CMRTOguidelines pertaining to consent; and
m)observe the Regulated Health Professions Actand all guidelines of the College of MedicalRadiation Technologists of Ontario pertainingto the prevention of sexual abuse.
Page 10
Essential Competencies
Page : 07
6. Records and Reporting
Creating and maintaining records and reports areessential components of the professional practiceof all M.R.T.s. M.R.T.s’ records and reports provide information to other health care professionals about relevant aspects of patientcare, treatment and assessment.
E S S E N T I A L C O M P E T E N C Y:
M.R.T.s must be proficient in creating records,charts, incident and other reports that attest tothe diagnostic, treatment, quality assurance,workplace and patient safety procedures thathave been carried out. M.R.T.s must have theknowledge, skills and judgment to record information that will adequately identify the subjects of all the images they create and treatments they administer. M.R.T.s must be skilful in producing records and reports that arealways accurate, complete, legible and timely.
I N D I C AT O R S
All M.R.T.s must:a) record results of quality control tests;b) record and report any equipment faults or
problems;c) record and notify the supervising (attending)
physician or radiologist of any allergies,abnormal test results or other contraindicationsto the ordered procedures;
d) mark all images with the patient’s identity;e) ensure all images are archived, according to
principles and guidelines established by theemployment facility;
f ) record the patient’s reactions to the treatmentor procedure or to any administered substances;
g) record all aspects of patient care and all procedures performed, including emergencytreatments and descriptions of, and reasonsfor, any deviations from standard procedureson order forms, treatment prescriptions,patient’s charts or other relevant documentation;
h) forward the patient’s records, images and pertinent data to appropriate recipients; and
i) record and inform patient and/or nursing staffof personal contact limitations and any otherspecial or follow-up care required;
In addition, all M.R.T.s in the specialties ofnuclear medicine and radiation therapy must:j) record results of radiopharmaceutical assays,
quality control and other tests, radioactivepreparations and disposal methods of radioactive pharmaceuticals;
In addition, all M.R.T.s in the specialty ofnuclear medicine must:k) record receipt and disposal of
radiopharmaceuticals and generators;l) label radiopharmaceutical preparations; andm)maintain radiopharmaceutical and
pharmaceutical dispensing records;
In addition, all M.R.T.s in the specialty of radiation therapy must:n) implement a medical directive for sample
analyses; ando) record and communicate any concerns
regarding the treatment or treatment prescription to the appropriate attending radiation oncology personnel.
Page 11

170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
2003 © COLLEGE OF MEDICAL RADIATION TECHNOLOGISTS OF ONTARIO Page 12
Sect ion 1 : Addendum to Comprehensive Guidel ines
a
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
Addendum toComprehensiveGuidelines
Addendum to Comprehensive Guidelines for acting in
accordance with the Regulated Health Professions Act Scope
of Practice / Controlled Acts Model (January 1, 2004)
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page a
Page 13
Introduct ion : Addendum to Comprehensive Guidel ines
1
Introduction
The purpose of the Addendum to the Comprehensive
Guidelines for acting in accordance with the Regulated Health
Professions Act Scope of Practice/Controlled Acts Model is:
> to establish the guidelines as part of the standards of practice
for medical radiation technologists;
> to explain the regulation of magnetic resonance technologists
with the College and how the scope of practice/controlled
acts model of the RHPA works in connection with applying
electromagnetism for MRI examinations;
> to provide other changes to the guidelines that result from
changes to certain regulations.
The Addendum is not intended to be an all-encompassing
revision of the Comprehensive Guidelines.
Terms used in the “Paragraph” column
“replacement” indicates that the text of the Addendum substitutes for the text of the Comprehensive Guidelines (or Condensed Guidelines) identified under the columns, “Page” and “Paragraph”
“addition” indicates that the text of the Addendum is to be added to an existing section of the Comprehensive Guidelines (or Condensed Guidelines) identified under the columns, “Page” and “Paragraph”
“change” indicates the modifications of existing text of the Comprehensive Guidelines (or Condensed Guidelines) identified under the columns, “Page” and “Paragraph”
“supplement” indicates the addition of a new section to the text of the Comprehensive Guidelines (or Condensed Guidelines) identified under the columns, “Page” and “Paragraph”
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page b
Page 14
2 Book Page Paragraph Text of Addendum
1 Book Page Paragraph Text of Addendum
Section 1 : Addendum to Comprehensive Guidel ines Sect ion 1 : Addendum to Comprehensive Guidel ines
32
Guidelines changed to Standards of Practice for Medical Radiation Technologists
Effective January 1, 2004, the Essential Competencies and the Comprehensive Guidelines, as amended from time to time, replace the “Standards of Practice for Medical Radiation Technologists” for radiography, nuclear medicine and radiation therapy published by the CMRTO and, together, constitute the new standards of practice for medical radiation technologists in the specialties of radiography, nuclear medicine, radiation therapy and magnetic resonance.
It is intended that the Essential Competencies and Comprehensive Guidelines be used in conjunctionwith the Code of Ethics for members of the CMRTO. Together, these documents provide a model forensuring safe, effective and ethical professional performance to ensure safe, effective and ethical outcomes for patients.
In the event that the Essential Competencies or Comprehensive Guidelines set a standard that is higherthan departmental policy or procedure, the MRT must comply with the standard set by the EssentialCompetencies or Comprehensive Guidelines, as the case may be.
Regulation of Magnetic Resonance Technologists with the College of Medical RadiationTechnologists of Ontario (CMRTO)
On May 29, 2003, the government brought into force two regulations under the Medical RadiationTechnology Act that have the effect of regulating MR technologists with the College. One regulation is anamendment to the registration regulation of the College that sets out the registration requirements inorder for a magnetic resonance (MR) technologist to be issued a certificate of registration by the Collegewhich authorizes the practice of the specialty of MR.
Medical Radiation Technology (MRT) Scope of Practice under the Medical Radiation TechnologyAct (MRTA), 1991
The other regulation changes the scope of practice of medical radiation technology so that the use ofelectromagnetism to produce diagnostic images and tests is included as part of the scope of practice.
In the MRTA, the scope of practice for MRTs is as follows:“The practice of medical radiation technology is the use of ionizing radiation and other forms of energy prescribed under subsection 12(2) to produce diagnostic images and tests, the evaluation of thetechnical sufficiency of the images and tests, and the therapeutic application of ionizing radiation.”
Ontario Regulation 226/03 made under the Medical Radiation Technology Act prescribes electromagnetismas a form of energy for the purpose of the scope of practice of medical radiation technology.
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-4355
1 (800) 563-5847
For acting in accordance with theRegulated Health Professions act scope ofpractice / controlled acts model
This publication contains the following sections:
1Overview
2Authorized
3Agency practices
4Delegation
CondensedGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-4355
1 (800) 563-5847
For acting in accordance with theRegulated Health Professions act scope ofpractice / controlled acts model
This publication contains the following sections:
1Overview
2Authorized
3Agency practices
4Delegation
CondensedGuidelines
Standards of Practice Replacement
(a) 4th paragraph on page 4; and (b) 1st sentence under the heading “Summary” onpage 31
Standards of PracticeReplacement
(a) last paragraph on page 4; and(b) 1st sentence under the heading “Summary” on page 24
MRT Scope of Practice Statement
Addition
MRT Scope of Practice Statement
Addition
431
424
935
8
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 2
Page 15
3 Book Page Paragraph Text of Addendum
Section 1 : Addendum to Comprehensive Guidel ines Sect ion 1 : Addendum to Comprehensive Guidel ines
54
Controlled Acts – Applying or Ordering the Application of Electromagnetism for MagneticResonance Imaging
One of the 13 procedures listed in the RHPA as a controlled act is applying or ordering the application of aform of energy prescribed by the regulations under the RHPA. Electromagnetism for magnetic resonanceimaging has been prescribed as a form of energy. (See Appendix C.) This means that applying or orderingthe application of electromagnetism for magnetic resonance imaging is a controlled act procedure.
Only those persons who are authorized to perform controlled act procedures, either through legislation ordelegation, may do so; however, there are limited exceptions and exemptions set out in the legislation. Onesuch exemption is provided in subsection 27(3) of the RHPA. This provision permits a controlled act procedure to be performed if the person is exempted by regulations under the RHPA, or if the act is donein the course of an activity exempted by the regulations under the RHPA.
On May 29, 2003, the government passed a regulation under the Regulated Health Professions Act, 1991(O. Reg. 228/03) which amends O. Reg. 107/96 made under the Regulated Health Professions Act, 1991.O. Reg. 107/96 as amended by O. Reg. 228/03 (the Controlled Acts Regulation) provides exemptions forcertain persons to apply electromagnetism for magnetic resonance imaging (MRI) in public hospitals andindependent health facilities if certain conditions are met.
Under the Controlled Acts Regulation, a member of the College of Physicians and Surgeons of Ontario ispermitted to apply or order the application of electromagnetism provided certain conditions are met. Seesubsection 5(2) of Appendix E.
Prior to June 18, 2004, any person is permitted to perform an MRI examination in a public hospital oran independent health facility, provided the examination is ordered by a member of the College ofPhysicians and Surgeons of Ontario (CPSO), and the other conditions set out in the Controlled ActsRegulation are met. (Refer to clause 7(d) of Appendix E.) The other conditions that apply to a personwho performs an MRI examination in a public hospital are described in subclause 7(d)(i) of Appendix E.The other conditions that apply to a person who performs an MRI examination in an independent healthfacility are described in subclauses 7(d)(ii) or 7(d)(iii) of Appendix E.
On or after June 18, 2004, only a member of the CMRTO (or a member of CPSO) will be permitted to perform an MRI examination in a public hospital or an independent health facility, provided the examination is ordered by a member of the CPSO, and the other conditions set out in the ControlledActs Regulation are met. The other conditions that apply to a member of the CMRTO who performs anMRI examination in a public hospital are described in clause 3.1(a) of Appendix E. The other conditionsthat apply to a member of the CMRTO who performs an MRI examination in an independent healthfacility are described in clauses 3.1(b) or (c) of Appendix E.
An MRT must ensure that the application of electromagnetism has been ordered by a member of CPSOand the other conditions set out in the Controlled Acts Regulation have been met before he or she applieselectromagnetism for an MRI, either in a public hospital or an independent health facility. See Appendix E.
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-4355
1 (800) 563-5847
For acting in accordance with theRegulated Health Professions act scope ofpractice / controlled acts model
This publication contains the following sections:
1Overview
2Authorized
3Agency practices
4Delegation
CondensedGuidelines
Controlled Acts – Applying or Ordering theApplication of Electromagnetism for MagneticResonance Imaging
Supplement (to follow page 18)
Controlled Acts – Applying or Ordering theApplication of Electromagnetism for MagneticResonance Imaging
Supplement (to follow page 13)
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 4
Page 16
7 Book Page Paragraph Text of Addendum
6 Book Page Paragraph Text of Addendum
5 Book Page Paragraph Text of Addendum
Section 1 : Addendum to Comprehensive Guidel ines
7
Sect ion 1 : Addendum to Comprehensive Guidel ines
6
Exceptions and Exemptions
For a description of the exemption that relates to the controlled act procedure of applying or orderingthe application of electromagnetism for magnetic resonance imaging, see “Controlled Acts – Applyingor Ordering the Application of Electromagnetism for Magnetic Resonance Imaging” of the Addendum.
Appendix E
Exemptions to Subsection 27(1) of RHPA(see attached Appendix E)
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
Exceptions and Exemptions
Addition
Appendix E
Replacement
Exemptions to Subsection 27(1) of RHPA
46
394041
GlossaryMedical Radiation Technology (MRT) Scope of Practice:
O. Reg. 226/03 made under the Medical Radiation Technology Act prescribes electromagnetism as a formof energy for the purpose of the scope of practice statement of medical radiation technology.
The four medical radiation technology specialties are:• Radiography• Radiation Therapy• Nuclear Medicine• Magnetic Resonance
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
(MRT) Medical Radiation Technology Scope of Practice
Addition and change46
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 6
Page 17
8 Book Page Paragraph Text of Addendum
Section 1 : Addendum to Comprehensive Guidel ines
9
Sect ion 1 : Addendum to Comprehensive Guidel ines
8
Glossary
Medical Radiation Technologist(s) (MRT or MRTs):member(s) of the College of Medical Radiation Technologists of Ontario. The title “medical radiation technologist” is a protected title and may only be used by those registered with theCollege of Medical Radiation Technologists of Ontario.
A member who holds a specialty certificate of registration listed in the first column of the Table belowmay use the title and the abbreviation set out opposite to the specialty in the second and third columnsof the Table:
Specialty Title AbbreviationRadiography Medical Radiation M.R.T.(R.)
Technologist – Radiography
Radiation Therapy Medical Radiation M.R.T.(T.)Technologist – Radiation Therapy; or Medical Radiation Technologist – Radiation Therapist
Nuclear Medicine Medical Radiation M.R.T.(N.)Technologist – Nuclear Medicine
Magnetic Resonance Medical Radiation M.R.T.(M.R.)Technologist – Magnetic Resonance
A member shall not use a title or abbreviation set out in the second or third column of the Table aboveunless the member holds a specialty certificate of registration listed in the first column of the Tableopposite the title or abbreviation.
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
Medical Radiation Technologist(s) (MRT or MRTs)
Replacement47
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 8
Page 18
Sect ion 1 : Addendum to Comprehensive Guidel ines
11
Sect ion 1 : Addendum to Comprehensive Guidel ines
10
Glossary
Order:
Under the Controlled Acts Regulation made under the RHPA, an order from a physician is necessary topermit MRTs to apply electromagnetism for magnetic resonance imaging.
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
Order
Addition47
Appendix F
Orders for Treatment – Section 24 of Revised Regulations of Ontario 1990, Regulation 965 (Hospital Management) made under the Public Hospitals Act. (See attached Appendix F.)
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
Appendix FOrders for Treatment
Replacement
Types of Orders
Direct order
Under the regulations made under the Public Hospitals Act (PHA), physicians (and dentists, midwives orregistered nurses in the extended class) may dictate an order for treatment or for a diagnostic procedureby telephone. The requirements respecting such orders include that they must be signed by the physician, dentist, midwife or registered nurse in the extended class who dictated the order on the firstvisit to the hospital after dictating the order.
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions Act Scope of Practice / Controlled Acts Model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-4355
1 (800) 563-5847
For acting in accordance with theRegulated Health Professions act scope ofpractice / controlled acts model
This publication contains the following sections:
1Overview
2Authorized
3Agency practices
4Delegation
CondensedGuidelines
What MRTs need to know about ordersand authorized acts
Addition of paragraph 3.1
Types of OrdersDirect order
Change (underlined text) 14
11
9 Book Page Paragraph
10 Book Page Paragraph Text of Addendum
11 Book Page Paragraph Text of Addendum
41
Text of Addendum
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 10
Page 19
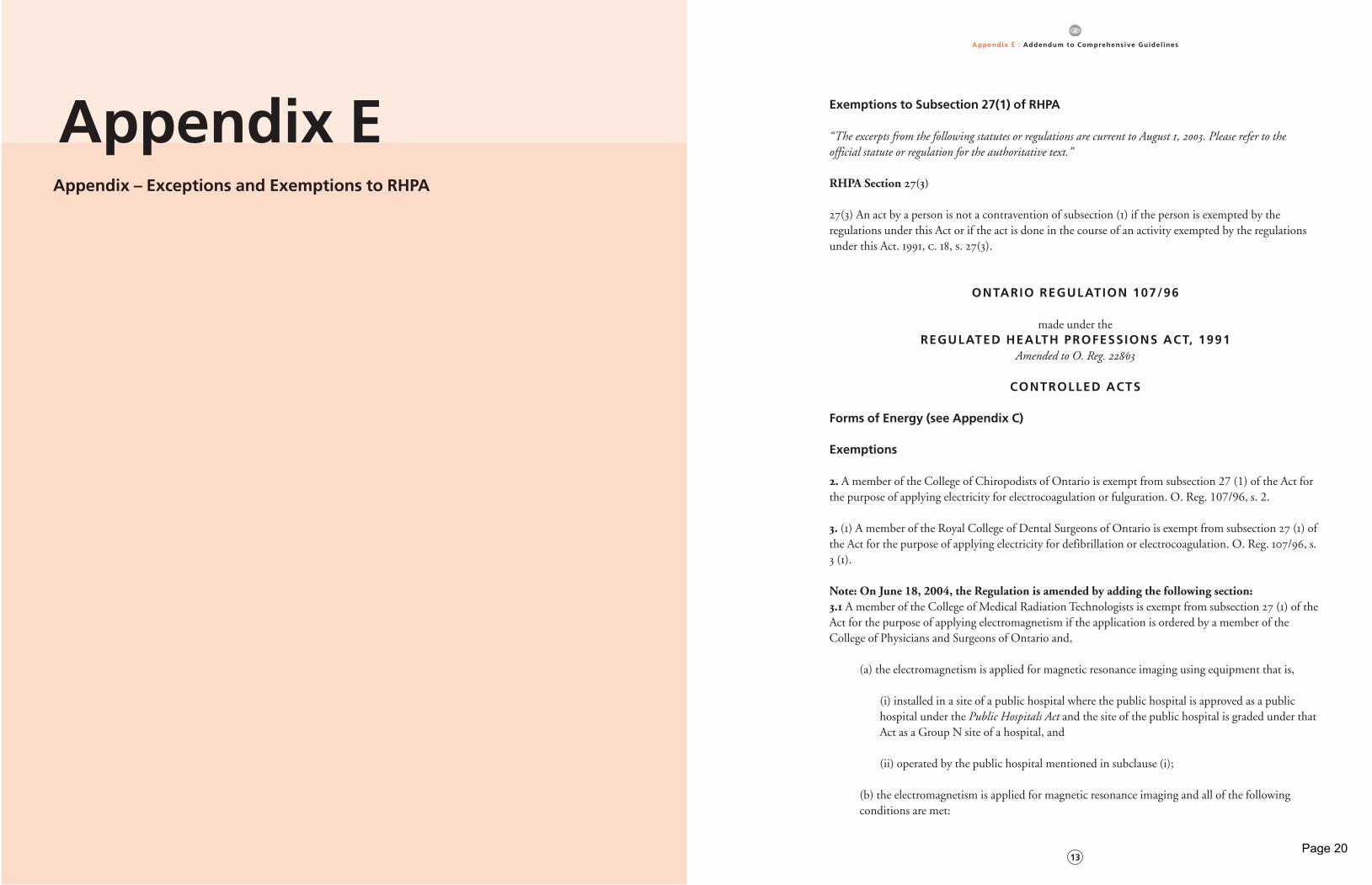
Appendix E : Addendum to Comprehensive Guidel ines
13
Sect ion 1 : Addendum to Comprehensive Guidel ines
12
Appendix – Exceptions and Exemptions to RHPA
Appendix E Exemptions to Subsection 27(1) of RHPA
“The excerpts from the following statutes or regulations are current to August , . Please refer to the official statute or regulation for the authoritative text.”
RHPA Section 27(3)
27(3) An act by a person is not a contravention of subsection (1) if the person is exempted by the regulations under this Act or if the act is done in the course of an activity exempted by the regulationsunder this Act. 1991, c. 18, s. 27(3).
ONTARIO REGULATION 107/96
made under theREGULATED HEALTH PROFESSIONS ACT, 1991
Amended to O. Reg. ⁄
CONTROLLED ACTS
Forms of Energy (see Appendix C)
Exemptions
. A member of the College of Chiropodists of Ontario is exempt from subsection 27 (1) of the Act forthe purpose of applying electricity for electrocoagulation or fulguration. O. Reg. 107/96, s. 2.
. (1) A member of the Royal College of Dental Surgeons of Ontario is exempt from subsection 27 (1) ofthe Act for the purpose of applying electricity for defibrillation or electrocoagulation. O. Reg. 107/96, s.3 (1).
Note: On June 18, 2004, the Regulation is amended by adding the following section: . A member of the College of Medical Radiation Technologists is exempt from subsection 27 (1) of theAct for the purpose of applying electromagnetism if the application is ordered by a member of theCollege of Physicians and Surgeons of Ontario and,
(a) the electromagnetism is applied for magnetic resonance imaging using equipment that is,
(i) installed in a site of a public hospital where the public hospital is approved as a public hospital under the Public Hospitals Act and the site of the public hospital is graded under thatAct as a Group N site of a hospital, and
(ii) operated by the public hospital mentioned in subclause (i);
(b) the electromagnetism is applied for magnetic resonance imaging and all of the following conditions are met:
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 12
Page 20

Appendix E : Addendum to Comprehensive Guidel ines
15
Appendix E : Addendum to Comprehensive Guidel ines
14
(i) the electromagnetism is used to support, assist and be a necessary adjunct, or any of them,to an insured service within the meaning of Health Insurance Act ;
(ii) the magnetic resonance imaging is provided to persons who are insured persons withinthe meaning of the Health Insurance Act ,
(iii) the electromagnetism is applied in an independent health facility licensed under theIndependent Health Facilities Act in respect of magnetic resonance imaging; or
(c) the electromagnetism is applied for magnetic resonance imaging and all of the following conditions are met:
(i) the electromagnetism is not used to support, assist and be a necessary adjunct, or any ofthem, to an insured service within the meaning of Health Insurance Act , or the magnetic resonance imaging is not provided to persons who are insured persons within the meaning ofthat Act, or both,
(ii) the electromagnetism is applied in a facility that is operated by an operator that holds alicence under the Independent Health Facilities Act in respect of magnetic resonance imaging,
(iii) the electromagnetism is applied in a facility that is operated on the same premises as theindependent health facility licensed under the Independent Health Facilities Act in respect ofmagnetic resonance imaging that is operated by the operator mentioned in subclause (ii),
(iv) the electromagnetism is applied using the same equipment that is used to provide magnetic resonance imaging in the independent health facility licensed under theIndependent Health Facilities Act in respect of magnetic resonance imaging that is operated bythe operator mentioned in subclause (ii),
(v) the operator of the facility in which the electromagnetism is applied is a party to a validand subsisting agreement with the Minister concerning the provision of magnetic resonanceimaging. O. Reg. 228/03, s. 1.
See: O. Reg. ⁄, ss. , ⁽⁾.
(2) A member of the Royal College of Dental Surgeons of Ontario is exempt from subsection 27 (1) ofthe Act for the purpose of applying electricity for electromyography or nerve conduction studies, in thecourse of conducting research. O. Reg. 107/96, s. 3 (2).
. A member of the College of Midwives of Ontario is exempt from subsection 27 (1) of the Act for thepurpose of ordering the application of soundwaves for pregnancy diagnostic ultrasound or pelvic diagnostic ultrasound. O. Reg. 107/96, s. 4.
. (1) A member of the College of Physicians and Surgeons of Ontario is exempt from subsection 27 (1)of the Act for the purpose of applying, or ordering the application of, electricity for a procedure listed inparagraph 1 of section 1 or soundwaves for a procedure listed in paragraph 3 of section 1.O. Reg. 107/96, s. 5 (1).
(2) A member of the College of Physicians and Surgeons of Ontario is exempt from subsection 27 (1) ofthe Act for the purpose of applying or ordering the application of electromagnetism if,
(a) the electromagnetism is applied for magnetic resonance imaging using equipment that is,
(i) installed in a site of a public hospital where the public hospital is approved as a public hospital under the Public Hospitals Act and the site of the public hospital is graded under thatAct as a Group N site of a hospital, and
(ii) operated by the public hospital mentioned in subclause (i);
(b) the electromagnetism is applied for magnetic resonance imaging and all of the following conditions are met:
(i) the electromagnetism is used to support, assist and be a necessary adjunct, or any of them,to an insured service within the meaning of Health Insurance Act ;
(ii) the magnetic resonance imaging is provided to persons who are insured persons withinthe meaning of the Health Insurance Act ,
(iii) the electromagnetism is applied in an independent health facility licensed under theIndependent Health Facilities Act in respect of magnetic resonance imaging; or
(c) the electromagnetism is applied for magnetic resonance imaging and all of the following conditions are met:
(i) the electromagnetism is not used to support, assist and be a necessary adjunct, or any ofthem, to an insured service within the meaning of Health Insurance Act , or the magnetic resonance imaging is not provided to persons who are insured persons within the meaning ofthat Act, or both,
(ii) the electromagnetism is applied in a facility that is operated by an operator that holds alicence under the Independent Health Facilities Act in respect of magnetic resonance imaging,
(iii) the electromagnetism is applied in a facility that is operated on the same premises as theindependent health facility licensed under the Independent Health Facilities Act in respect ofmagnetic resonance imaging that is operated by the operator mentioned in subclause (ii),
(iv) the electromagnetism is applied using the same equipment that is used to provide magnetic resonance imaging in the independent health facility licensed under theIndependent Health Facilities Act in respect of magnetic resonance imaging that is operated by the operator mentioned in subclause (ii),
(v) the operator of the facility in which the electromagnetism is applied is a party to a validand subsisting agreement with the Minister concerning the provision of magnetic resonanceimaging. O. Reg. 228/03, s. 2.
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 14
Page 21
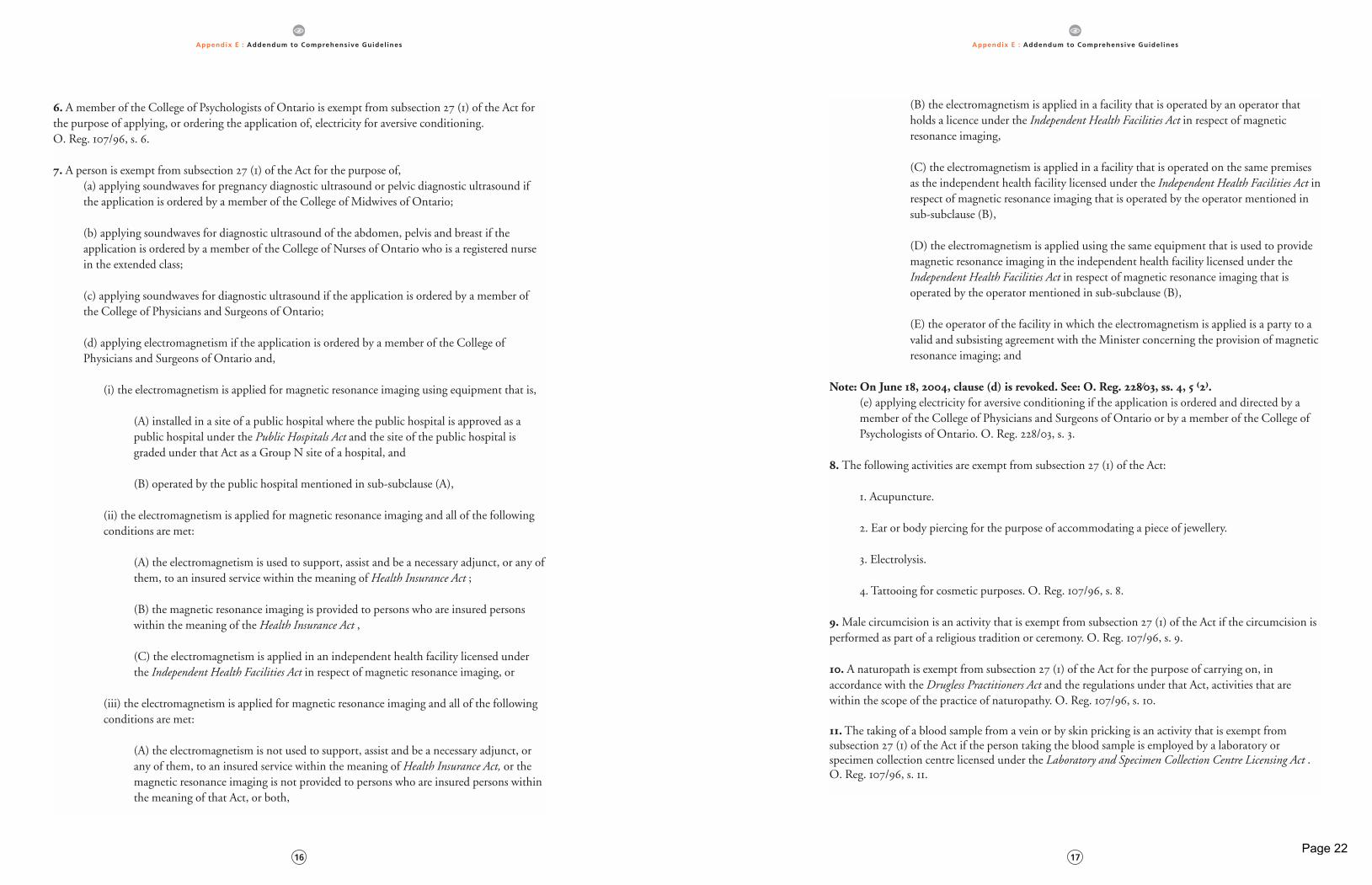
Appendix E : Addendum to Comprehensive Guidel ines
17
Appendix E : Addendum to Comprehensive Guidel ines
16
. A member of the College of Psychologists of Ontario is exempt from subsection 27 (1) of the Act forthe purpose of applying, or ordering the application of, electricity for aversive conditioning. O. Reg. 107/96, s. 6.
. A person is exempt from subsection 27 (1) of the Act for the purpose of, (a) applying soundwaves for pregnancy diagnostic ultrasound or pelvic diagnostic ultrasound ifthe application is ordered by a member of the College of Midwives of Ontario;
(b) applying soundwaves for diagnostic ultrasound of the abdomen, pelvis and breast if the application is ordered by a member of the College of Nurses of Ontario who is a registered nursein the extended class;
(c) applying soundwaves for diagnostic ultrasound if the application is ordered by a member ofthe College of Physicians and Surgeons of Ontario;
(d) applying electromagnetism if the application is ordered by a member of the College ofPhysicians and Surgeons of Ontario and,
(i) the electromagnetism is applied for magnetic resonance imaging using equipment that is,
(A) installed in a site of a public hospital where the public hospital is approved as apublic hospital under the Public Hospitals Act and the site of the public hospital is graded under that Act as a Group N site of a hospital, and
(B) operated by the public hospital mentioned in sub-subclause (A),
(ii) the electromagnetism is applied for magnetic resonance imaging and all of the followingconditions are met:
(A) the electromagnetism is used to support, assist and be a necessary adjunct, or any ofthem, to an insured service within the meaning of Health Insurance Act ;
(B) the magnetic resonance imaging is provided to persons who are insured personswithin the meaning of the Health Insurance Act ,
(C) the electromagnetism is applied in an independent health facility licensed underthe Independent Health Facilities Act in respect of magnetic resonance imaging, or
(iii) the electromagnetism is applied for magnetic resonance imaging and all of the followingconditions are met:
(A) the electromagnetism is not used to support, assist and be a necessary adjunct, orany of them, to an insured service within the meaning of Health Insurance Act, or themagnetic resonance imaging is not provided to persons who are insured persons withinthe meaning of that Act, or both,
(B) the electromagnetism is applied in a facility that is operated by an operator thatholds a licence under the Independent Health Facilities Act in respect of magnetic resonance imaging,
(C) the electromagnetism is applied in a facility that is operated on the same premisesas the independent health facility licensed under the Independent Health Facilities Act inrespect of magnetic resonance imaging that is operated by the operator mentioned insub-subclause (B),
(D) the electromagnetism is applied using the same equipment that is used to providemagnetic resonance imaging in the independent health facility licensed under theIndependent Health Facilities Act in respect of magnetic resonance imaging that is operated by the operator mentioned in sub-subclause (B),
(E) the operator of the facility in which the electromagnetism is applied is a party to avalid and subsisting agreement with the Minister concerning the provision of magneticresonance imaging; and
Note: On June , , clause (d) is revoked. See: O. Reg. ⁄, ss. , ⁽⁾.
(e) applying electricity for aversive conditioning if the application is ordered and directed by amember of the College of Physicians and Surgeons of Ontario or by a member of the College ofPsychologists of Ontario. O. Reg. 228/03, s. 3.
8. The following activities are exempt from subsection 27 (1) of the Act:
1. Acupuncture.
2. Ear or body piercing for the purpose of accommodating a piece of jewellery.
3. Electrolysis.
4. Tattooing for cosmetic purposes. O. Reg. 107/96, s. 8.
. Male circumcision is an activity that is exempt from subsection 27 (1) of the Act if the circumcision isperformed as part of a religious tradition or ceremony. O. Reg. 107/96, s. 9.
. A naturopath is exempt from subsection 27 (1) of the Act for the purpose of carrying on, in accordance with the Drugless Practitioners Act and the regulations under that Act, activities that are within the scope of the practice of naturopathy. O. Reg. 107/96, s. 10.
. The taking of a blood sample from a vein or by skin pricking is an activity that is exempt from subsection 27 (1) of the Act if the person taking the blood sample is employed by a laboratory or specimen collection centre licensed under the Laboratory and Specimen Collection Centre Licensing Act .O. Reg. 107/96, s. 11.
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 16
Page 22
Appendix E : Addendum to Comprehensive Guidel ines
18
. (1) A medical geneticist who holds a doctorate is exempt from subsection 27 (1) of the Act for thepurpose of communicating to an individual or his or her personal representative a diagnosis identifyinga genetic disease or genetic disorder as the cause of the symptoms of the individual in circumstances inwhich it is reasonably foreseeable that the individual or his or her personal representative will rely on thediagnosis, if,
(a) the disease or disorder identified is within the geneticist’s area of expertise; and
(b) the geneticist is employed by a university or a health care facility and the communication ofthe diagnosis is performed in accordance with the university’s or facility’s guidelines or protocols.O. Reg. 107/96, s. 12 (1).
(2) In this section,
“health care facility” means a facility governed by or funded under an Act set out in the Schedule.O. Reg. 107/96, s. 12 (2).
. A member of the College of Nurses of Ontario who holds a general certificate of registration as a registered nurse is exempt from subsection 27 (1) of the Act for the purpose of prescribing a solution ofnormal saline (0.9 per cent) for venipuncture performed to establish peripheral intravenous access andmaintain patency. O. Reg. 107/96, s. 13.
SCHEDULE
1. Alcoholism and Drug Addiction Research Foundation Act.2. Cancer Act.3. Charitable Institutions Act.4. Child and Family Services Act.5. Community Psychiatric Hospitals Act.6. Developmental Services Act. 7. General Welfare Assistance Act.8. Homes for Retarded Persons Act. 9. Homes for Special Care Act.10. Homes for the Aged and Rest Homes Act. 11. Independent Health Facilities Act. 12. Mental Health Act.13. Mental Hospitals Act. 14. Ministry of Community and Social Services Act. 15. Ministry of Correctional Services Act. 16. Ministry of Health Act.17. Nursing Homes Act.18. Ontario Mental Health Foundation Act.19. Private Hospitals Act.20. Public Hospitals Act.
O. Reg. 107/96, Sched.
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 18
Page 23
Appendix F : Addendum to Comprehensive Guidel ines
21
“The excerpts from the following statutes or regulations are current to August , . Please refer to the official statute or regulation for the authoritative text.”
Orders for Treatment – Section of Revised Regulations of Ontario , Regulation
(Hospital Management) made under the Public Hospitals Act
. (1) Every order for treatment or for a diagnostic procedure of a patient shall, except as provided insubsection (2), be in writing and shall be dated and authenticated by the physician, dentist, midwife orregistered nurse in the extended class giving the order. O. Reg. 64/03, s. 10.
(2) A physician, dentist, midwife or registered nurse in the extended class may dictate an order for treatment or for a diagnostic procedure by telephone to a person designated by the administrator to take such orders. O. Reg. 64/03, s. 10.
(3) Where an order for treatment or for a diagnostic procedure has been dictated by telephone,
(a) the person to whom the order was dictated shall transcribe the order, the name of the physician, dentist, midwife or registered nurse in the extended class who dictated the order, thedate and the time of receiving the order and shall authenticate the transcription; and
(b) the physician, dentist, midwife or registered nurse in the extended class who dictated the order shall authenticate the order on the first visit to the hospital after dictating the order. O. Reg. 761/93, s. 11; O. Reg. 45/98, s. 3.
Appendix F – Orders for Treatment under the Public Hospitals Acts
Appendix F
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 20
Page 24

Sect ion 1 : Addendum to Comprehensive Guidel ines
22
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
2178_CMRTO_Addendum_v2.qxd 11/26/03 12:03 AM Page 22
Page 25

Page 26
170 Bloor Street W.Suite 1001Toronto, OntarioM5S 1T9
tel (416) 975-4353fax (416) 975-43551 (800) 563-5847
www.cmrto.org
For acting in accordance with the Regulated Health Professions act scope of practice/controlled acts model
This publication contains the following sections:
1Overview
2Authorized Acts
3Delegation
4 Agency Practices
ComprehensiveGuidelines
cmrto - comprehensive.cov.qxd 6/25/04 5:55 AM Page 1
Page 27
Contents
1 Overview4 Purpose
4 A note on competencies to perform specific procedures
5 The Regulated Health Professions Act
5 Overall expectations for professional practice under the RHPA
6 Relationship between the RHPA and the HARP Act
6 Scope of practice/controlled acts model
7 Elements of the model
8 Risk of harm clause
8 Penalties for contravention
9 Scope of practice for MRTs
9 MRT scope of practice statement
9 What MRTs need to know about the scope of practice statement
2 Authorized Acts12 What MRTs need to know about authorized acts
12 Controlled acts authorized to MRTS (authorized acts)
12 MRT performance of an authorized act
13 What is an order ?
14 Authorized acts are ordered, not delegated
14 Types of orders
14 Direct order
14 Directive or protocol
15 When to use a directive or protocol
15 Procedures are ordered, not MRTS
16 What MRTs should do if they have concerns about an order or a
treatment plan
16 What MRTs should do if they are not competent to perform an
authorized act
17 Summary of Practice Guidelines for MRTs performing authorized acts
17 Recommended agency practices
3 Delegation20 What MRTs need to know about delegation
20 Definition of delegation
20 When delegation is and is not required
20 MRTs delegation of authorized acts to others
21 MRT acceptance of delegation
21 Deciding whether to accept delegation and perform a delegated act
21 Delegator qualifications
21 An order is necessary to perform delegated acts
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 1
Page 28

cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 2
Page 29
21 Delegation and consent
22 Acceptable delegation programs
23 MRT assistance in the delegation program
23 MRT responsibility and accountability when accepting delegation
23 Recommended agency practices
24 Summary of Practice Guidelines for MRTs accepting delegation
4 Agency Practices26 Deciding whether to perform procedures or services which do not fall
within principal expectations of MRT practice
26 Identifying the field: principal expectations of practice clarified
27 Overview of the decision-making guide
27 Assumptions underlying the decision-making guide
28 Applying the guide: case studies
29 Summary of practice guidelines for MRTs performing services or
procedures beyond principal expectations of practice
29 How quality practice settings support MRT practice
29 Recommended agency practices to support safe, effective and ethical
MRT practice in relation to performing authorized acts, using directives
or protocols accepting delegation and performing beyond principal
expectations of practice
31 What MRTS should do if agency practices compromise their ability to
practice safely, effectively and ethically
Appendices 34 Appendix A
Scope of practice statements for all regulated health professions
36 Appendix B
13 controlled acts
37 Appendix C
RHPA regulation defining the forms of energy and the controlled act of
applying or ordering the application of “energy”
38 Appendix D
Summary of controlled acts authorized for each profession under the
profession-specific acts
39 Appendix E
Exceptions and Exemptions to RHPA
41 Appendix F
Orders for treatment under the Public Hospitals Act
42 Appendix G
Decision-making guide for determining the appropriateness of
accepting delegation and performing services or procedures beyond
principal expectations of MRT practice
43 List of acronyms
43 Glossary
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 3
Page 30

Please note that the guidelines contain a description of certain provisions of the Regulated Health Professions Act and related health profession Acts.
The guidelines are not intended as a definitive legal analysis of the legislation nor to provide legal advice. The reader is advised to consult the
actual legislation for specific wording and terminology and, where appropriate, seek legal advice.
Published by the College of Medical Radiation Technologists of Ontario for technologists in the fields of
radiation therapy, nuclear medicine and radiography
Copyright © 1999 by the College of Medical Radiation Technologists of Ontario.
All Rights Reserved
Additional copies of these guidelines may be obtained by writing:
170 Bloor Street West, Suite 1001Toronto, Ontario
M5S 1T9
Tel: (416) 975-4353Fax: (416) 975-4355
1 (800) 563-5847
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 4
Page 31
2 •
5
2 •
5
2 •
In this section the following topics will be covered:
• The Regulated Health Professions Act
• Overall expectations for professional practice
under the RHPA
• Relationship between the RHPA and the HARP Act
• Scope of practice / controlled acts model
• What MRTs need to know about the scope of practice
statement
1 Overview
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 5
Page 32
1 • O V E RV I E W
4
The purpose of these practice guidelines is to establish:• a reference for medical radiation technologists (MRTs) performing controlled act procedures
authorized to MRTs and accepting delegation of controlled act procedures; and • a decision-making framework for determining the appropriateness of performing services or
procedures that are beyond the principal expectations of MRT practice.
In developing these guidelines, the College of Medical Radiation Technologists of Ontario (CMRTO) hopes to assist MRTs in:
• understanding how the scope of practice/controlled acts model of the Regulated Health Professions Act (RHPA) works and how it applies to practice;
• practicing safely, effectively and ethically when performing controlled act procedures;• responding appropriately to requests or proposals for providing procedures or services that are
beyond the principal expectations of MRT practice;• performing appropriately those services or procedures that are beyond principal expectations; and• taking appropriate action when unable to implement services or procedures safely, effectively and
ethically, in compliance with legislated and professional practice requirements.
These guidelines are also intended to assist managers with responsibility for MRT practice to understand MRT expectations for practice, to make appropriate decisions in relation to that practice, and to provide policies and procedures that support MRTs in providing safe, effective and ethical care.
The College will review these guidelines in 2001, evaluating a number of factors, including the implementation process, the decision-making models and the evolution of College approaches to delegation and front-line MRT practice. After this evaluation, the guidelines will be updated accordingly and, by 2002,will be incorporated into the Standards of Practice.
The CMRTO has developed two versions of the guidelines: this comprehensive version and a condensed version. The condensed version provides an overview of basic concepts to clarify practice expectations and the summaries of practice guidelines - an “at-a-glance” approach. This version provides more background information and full explanations of how to implement the practice guidelines, along with suggestions for agency practices. It will be useful to those who require more in-depth information to carry out their roles; for example, those involved in MRT administration, or front-line MRTs who wish to obtain more background information or who have a greater need for detail regarding the practice guidelines.
A note on competencies to perform specific proceduresDue to the ever-evolving nature of health care and the challenges in maintaining an accurate and up-to-date list of the competencies necessary to perform specific controlled act procedures, the CMRTO has opted to identify the conditions that must be met when performing procedures, instead of identifying the specific competencies.
It is expected that MRTs performing, or accepting delegation of, a procedure will maintain current competencies and best practice methods when implementing that procedure.
Purpose
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 4
Page 33
1 • O V E RV I E W
5
The Regulated Health Professions Act (RHPA) and the companion health profession Acts govern the practice of regulated health professions in Ontario. They protect the public through the regulation of those health professions. Proclaimed or enacted into law on December 31, 1993, they replaced the Radiological Technicians Act and other legislation, including the Health Disciplines Act. The RHPA introduces a number of reforms that deal with public protection and participation in health care and with competence, accountability and evolution of regulated professions. Chief amongst the reforms is the establishment of thescope of practice/controlled acts model, which is the focus of this publication.
Another aspect is the structure of the Act. The RHPA consists of different parts: a Main Part and a Procedural Code that includes the administering bodies, the controlled acts and requirements for all the Colleges. These parts constitute the RHPA proper and apply to, or are deemed to apply to, all the regulatedhealth professions. In addition, there are 21 health profession Acts that apply to specific regulated professions. The health profession Acts list profession-specific provisions, such as the profession’s scope of practice statement and authorized acts. The health profession Act for MRTs is the Medical Radiation Technology Act (MRTA).
The primary body responsible for administering the RHPA, and the companion health profession Acts, is the regulatory College of the profession. For MRTs, this is the College of Medical Radiation Technologists of Ontario (CMRTO).
Under the RHPA, regulated health professionals are expected to be:
Competent:i.e., to have the necessary knowledge, skills and judgement to perform safely, effectively and ethically and to apply that knowledge, skill and judgement to ensure safe, effective and ethical outcomes for the patient. This means that MRTs must maintain current competence in their area of practice, to refrain from acting if not competent and take appropriate action to address the situation.
Accountable: i.e., to take responsibility for decisions and actions, including those undertaken independently and collectively as a member of a team. This means that MRTs must accept the consequences of their decisions and actions and act on the basis of what they, in their clinical judgement, believe is in the best interests of the patient. MRTs must take appropriate action if they feel these interests are being unnecessarily and unacceptably compromised. This includes not implementing ordered procedures or treatment plans that, from their perspective, appear to be contraindicated, and taking appropriate action to address the situation.
Collaborative:i.e., to work with other members of the health care team to achieve the best possible outcomes for the patient. This means MRTs are responsible for communicating and coordinating care provision with other members of the team and taking the appropriate action to address gaps and differences in judgement about care provision.
The Regulated Health Professions Act
Overall expectations for professional practice under the RHPA
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 5
Page 34

1 • O V E RV I E W
6
Both the RHPA and the Healing Arts Radiation Protection Act (HARP Act) govern MRT practice. Both regulate applying or ordering the application of energy. However, they deal with different types of energy : the RHPA deals with energy as defined under its regulations and the HARP Act deals with ionizing radiation.
Under the RHPA, the application of energy falls within Controlled Act 7, “applying or ordering the application of a form of energy prescribed by regulation.” The regulations defining what constitutes energy, for purposes of the controlled act, can be found in Appendix C. To date, the list does not include ionizing radiation. That is because ionizing radiation is regulated under the HARP Act and other legislation. The manner in which the HARP Act regulates the ordering and application of ionizing radiation is through the regulation of the use and operation of X-ray machines and equipment. As a result, the application or ordering of the application of ionizing radiation is not a controlled act procedure, and it is not referred to in these terms.
Therefore, when looking at the list of controlled acts authorized to MRTs (i.e., taking blood samples from veins, administering substances by injection or inhalation, administering contrast media through or into the rectum or an artificial opening into the body, and tattooing), you will not see the application of ionizing radiation. However, for practical purposes, the rules governing MRTs when applying ionizing radiation are similar to those governing the performance of authorized act procedures: both require an order from an authorizing professional. (In the case of performing an authorized act procedure under the MRTA, the MRTneeds an order from a physician. In the case of applying ionizing radiation under the HARP Act, the MRT needs an order from a physician, dentist, designated chiropodist, chiropractor, osteopath or, under certain circumstances, a nurse who holds an extended certificate of registration). Failure to obtain a proper order, when performing an authorized act or applying ionizing radiation, constitutes professional misconduct.
There is one notable difference between the RHPA and the HARP Act. Under the RHPA, controlled acts can be performed if they have been properly delegated. There is no such provision under the HARP Act. Therefore, ionizing radiation can only be applied by those who are specifically named in the HARP Act.
For the remainder of this document, we will be referring only to the controlled acts under the RHPA, and not to ionizing radiation. Requirements and guidelines for the application of ionizing radiation can be found in the HARP Act and its regulations and guidelines and other legislation.
The scope of practice/controlled acts model is one of the main reforms and innovations under the RHPA. This model enhances public protection and choice by specifically identifying and controlling the performance of those procedures that pose risk of harm (the 13 controlled acts), without giving any profession an exclusive or licensed area of practice. Instead, each profession has a scope of practice statement, which describes in general terms what the profession does. The controlled act procedures are authorized for specific health professions. Procedures that are not controlled acts are in the “public domain” and may be performed by regulated health professions or by unregulated individuals. In this model, therefore, controlled act procedures may be likened to “licensed” procedures, because only persons authorized under the RHPA may perform them. The scope of practice statements, however, are not “licensed”, and elements of the scope statements may overlap between professions. The regulated health professions, therefore, are registered, not licensed.
Relationship between the RHPA and the HARP Act
Scope of practice / controlled acts model
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 6
Page 35

1 • O V E RV I E W
7
The intent of this model is to provide the public with protection and choice amongst regulated health care professions who may provide a range of health care services, subject to scope, standards and competence. A more detailed explanation of the model follows.
Elements of the modelThis model consists of a number of elements, the main ones being:
Scope of Practice Statement: A general statement describing what the profession does and the methods it uses (see Appendix A for a list of all the scope of practice statements of the regulated health professions). The scope of practice statement corresponds to what members of the profession learn in their programs of preparation and sets out the areas of expected competency. It establishes the foundation for the practice of the profession and serves as a frame of reference for such things as entry to practice requirements, the performance of authorized acts, the standards of practice of the profession and decision-making on responsibilities beyond principal expectations. The scope of practice statements do not establish a licensed area of practice (i.e., the area of practice is not restricted to a particular profession), and elements of the statements of the different health professions overlap, so that various professions may provide similar health care services. The MRT scope of practice statement is unique in that it identifies activities that may only be performed by those designated in the HARP Act, including MRTs. Therefore, under the RHPA, there are no “licensed” areas ofpractice; it is the controlled acts that are regulated or, in a manner of speaking, “licensed.”
Controlled Acts: 13 procedures, listed in the RHPA, that are deemed to pose risk of physical harm if performedby unqualified persons. (See Appendix B for a list of the 13 controlled acts). Under the profession-specific health profession Act, the professions are authorized to perform, either in fullor in part, the controlled acts, depending on the profession’s scope of practice and expected com-petencies. In addition to permitting performance of controlled act procedures, the RHPA alsogives the option to delegate or transfer the authority to perform the controlled acts from thoseauthorized to perform them under their health profession Act to others who are not. Therefore,professions have the option to delegate procedures within their authorized acts to others and toaccept delegation of controlled act procedures not authorized for them from others. Only thoseauthorized to perform controlled act procedures, either through legislation or delegation, may doso; however, there are limited exceptions set out in the legislation that identify circumstanceswhen someone who is not authorized may perform a controlled act (See Appendix E for a list of exceptions).
Authorized Act:Is a controlled act, or portion of a controlled act, that is authorized for a specific profession to
perform under its health profession Act. Each regulated health profession is authorized to perform from 0 to 12 of the 13 controlled acts, either in full or in part, depending on the scopeof practice and competencies of the profession. (See p.12 for MRT authorized acts and AppendixD for a summary of each profession’s authorized acts). As an example, in relation to ControlledAct 2, “performing a procedure on tissue below the dermis, below the surface of a mucous membrane, cornea, surfaces of the teeth, including scaling”: physicians are authorized to performall of this controlled act except for scaling; nurses are authorized to perform part of the controlled act (performing a procedure beneath the dermis or mucous membrane); and MRTs areauthorized to perform two specific procedures that fall within this controlled act (taking bloodsamples from veins and tattooing). MRTs may perform four authorized acts, which fall withinthree of the 13 controlled act procedures. (See p.12 for MRTs list of authorized acts). Some professions are authorized to perform procedures outright, without any conditions, while others[MRTs, Medical Laboratory Technologists (MLTs), Respiratory Therapists (RTs), DentalHygienists (DHs), Opticians, Registered Nurses (RNs) and Registered Practical Nurses (RPNs)]have additional requirements that must be met prior to implementation, such as the requirementfor an order or prescription from another profession or requirements set out in regulations.
Scope of Practice
Controlled Acts
Authorized Acts
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 7
Page 36
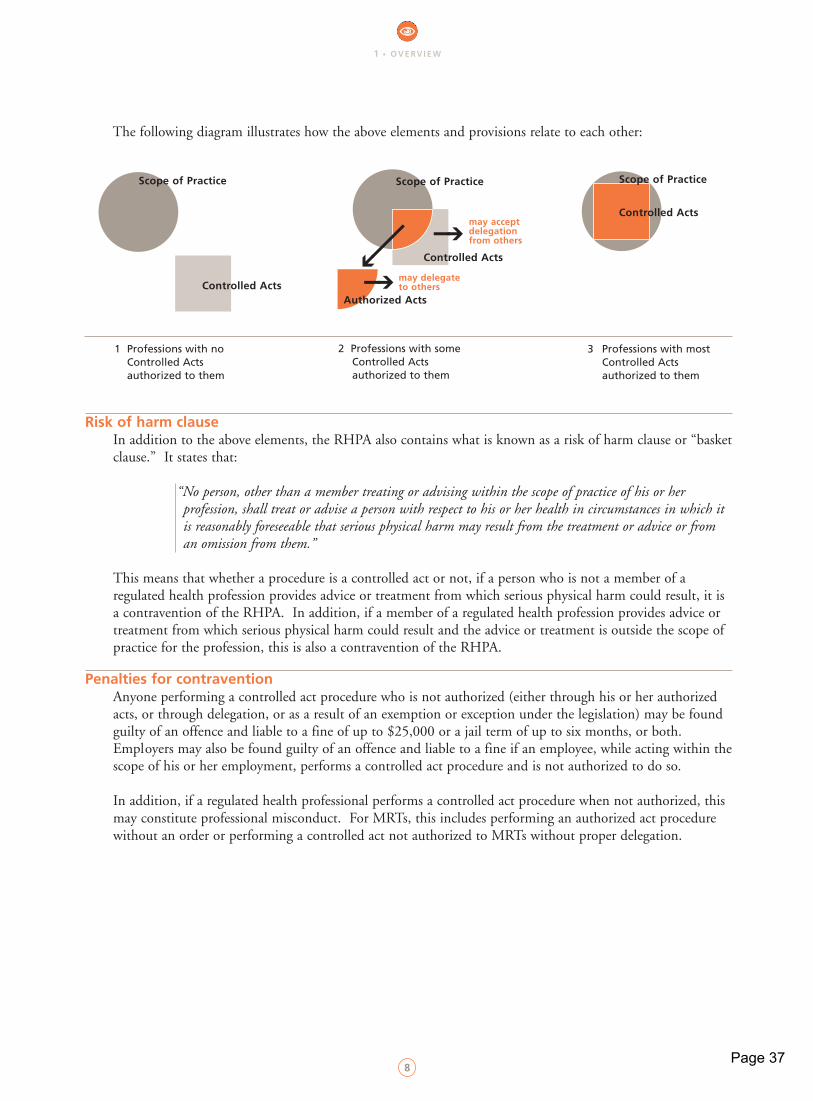
The following diagram illustrates how the above elements and provisions relate to each other:
Risk of harm clauseIn addition to the above elements, the RHPA also contains what is known as a risk of harm clause or “basketclause.” It states that:
“No person, other than a member treating or advising within the scope of practice of his or her profession, shall treat or advise a person with respect to his or her health in circumstances in which it is reasonably foreseeable that serious physical harm may result from the treatment or advice or from an omission from them.”
This means that whether a procedure is a controlled act or not, if a person who is not a member of a regulated health profession provides advice or treatment from which serious physical harm could result, it is a contravention of the RHPA. In addition, if a member of a regulated health profession provides advice or treatment from which serious physical harm could result and the advice or treatment is outside the scope of practice for the profession, this is also a contravention of the RHPA.
Penalties for contravention Anyone performing a controlled act procedure who is not authorized (either through his or her authorized acts, or through delegation, or as a result of an exemption or exception under the legislation) may be found guilty of an offence and liable to a fine of up to $25,000 or a jail term of up to six months, or both. Employers may also be found guilty of an offence and liable to a fine if an employee, while acting within thescope of his or her employment, performs a controlled act procedure and is not authorized to do so.
In addition, if a regulated health professional performs a controlled act procedure when not authorized, this may constitute professional misconduct. For MRTs, this includes performing an authorized act procedure without an order or performing a controlled act not authorized to MRTs without proper delegation.
1 • O V E RV I E W
8
Scope of Practice Scope of Practice Scope of Practice
Controlled Acts
Controlled Acts
may accept delegation from others
may delegate to others
Controlled Acts
Authorized Acts
1 Professions with no Controlled Acts authorized to them
2 Professions with someControlled Acts authorized to them
3 Professions with most Controlled Acts authorized to them
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 8
Page 37
1 • O V E RV I E W
9
MRT scope of practice statementIn the MRTA, the scope of practice statement for MRTs is as follows:
The practice of medical radiation technology is the use of ionizing radiation and other forms of energy prescribed under subsection 12(2) to produce diagnostic images and tests, the evaluation of the technical sufficiency of the images and tests, and the therapeutic application of ionizing radiation.
Subsection 12(2) of the MRTA states:
Subject to the approval of the Lieutenant Governor in Council, the Minister may make regulations prescribing forms of energy, other than ionizing radiation, for the purposes of section 3.
This provision was intended to enable the inclusion of other forms of energy under the MRT scope of practice statement, subject to approval by the Lieutenant Governor.
What MRTs need to know about the scope of practice statementThe scope of practice statement identifies what can be expected of MRTs in practice. It corresponds to what members of the profession learn in their programs of preparation and sets out the areas of expected competency. It establishes the foundation for the practice of the profession and serves as the frame of reference for such things as entry to practice requirements, the performance of authorized acts, the standards of practice of the profession and decision making regarding responsibilities beyond principal expectations of practice. As such, it clarifies MRT practice and provides a window for the evolution of that practice.
Scope of practice for MRTs
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 9
Page 38

cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 10
Page 39
2 • A U T H O R I Z E D A C T S
1111
2 • A U T H O R I Z E D A C T S
11
2 • A U T H O R I Z E D A C T S
2 Authorized Acts
In this section the following topics will be covered:
• What MRTs need to know about authorized acts
• What is an order?
• Procedures and concerns
• Recommended agency practices
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 11
Page 40
2 • A U T H O R I Z E D A C T S
12
Controlled acts authorized to MRTS (authorized acts)Under the MRTA, MRTs are authorized to perform four authorized acts (which fall within three of the 13 controlled acts) as follows:
In the course of engaging in the practice of medical radiation technology, a member is authorized, subject to the terms, conditions and limitations imposed on his or her certificate of registration, to perform the following:
1. Taking blood samples from veins (Authorized Act 1 for MRTs falls within Controlled Act 2 of RHPA: an example of a procedure falling within this authorized act would be taking blood samples for the purpose of assessing effective renal plasma flow).
2. Administering substances by injection or inhalation(Authorized Act 2 for MRTs falls within Controlled Act 5 of RHPA: examples of procedures falling within this authorized act include an intravenous, subcutaneous or intramuscular injection; starting peripheral intravenous lines; or establishing saline locks for the purpose of administering substances, such as radiopharmaceuticals or contrast media for IVPs. Procedures falling within Authorized Act 2 are not specifically defined in the legislation. In order to enable all the specialties to practice, CMRTO has interpreted the authorized act to include the aforementioned procedures).
3. Administering contrast media through or into the rectum or an artificial opening into the body(Authorized Act 3 for MRTs falls within Controlled Act 6 of RHPA: an example of a procedure falling within this authorized act would be inserting an enema tip into the rectum for a barium enema procedure).
4. Tattooing(Authorized Act 4 for MRTs falls within Controlled Act 2 of RHPA: an example of a procedure falling within this authorized act would be radiation therapy marking).
MRT performance of an authorized act1. There must be an order from a physician.
Under the MRTA, MRT are only permitted to perform a procedure falling within an authorized act if there is an order for the authorized act from a physician. The exact wording of this requirement is as follows:
“A member shall not perform a (authorized act) procedure…unless the procedure is ordered by a member of the College of Physicians and Surgeons of Ontario.”
In the practice of medical radiation technology, orders may also be known as requisitions and doctor’s notes. An order must be obtained for each procedure the MRT is to perform. For example, if an MRT is to administer contrast media and apply ionizing radiation, the MRT requires an order for each procedure. Exactly what constitutes a proper order is discussed in the following sections, along with a determination of which type of order - a direct order, a directive or protocol - is appropriate.
What MRTS need to know about authorized acts
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 12
Page 41
2 • A U T H O R I Z E D A C T S
13
In summary, members may not perform a procedure that falls within medical radiation technology’s four authorized acts unless there is an order from a physician. If an MRT performs an authorized act without an order, he or she has committed an act of professional misconduct and may be subject to disciplinary action by the College.
2. Authorized acts can only be performed in the course of engaging in the practice of medical radiation technology.MRTs are authorized to perform procedures falling within the four authorized acts in the course of engaging in the practice of the profession. MRTs are not authorized to perform authorized acts outside the course of practice of the profession. In this way, MRTs are only permitted to administer substances by injection or inhalation and establish IVs in the context of performing a radiological, nuclear medicine or radiation therapy procedure.
If an MRT is asked to perform an authorized act outside the practice of the profession, the MRT should refrain from performing the procedure and take the necessary action to address the situation. This may vary, but generally involves discussing any concerns with the person who hasrequested performance of the procedure to clarify and resolve the situation.
3. An MRT must not be acting contrary to terms, conditions and limitations placed upon his or her certificate of registration when performing authorized acts.If there are any terms, conditions or limitations placed upon an MRT’s certificate of registration that regulate the performance of authorized acts, such as restricting performance to certain circumstances or prohibiting performance outright, then these must be adhered to.
4. An MRT must be competent to perform the authorized act in light of the circumstances in the situation in which the procedure is to be performed. This includes having the ability tomanage the outcomes of performing the procedure.The legislation permits, but does not require performance of authorized acts. Having the authority to perform an authorized act does not automatically mean it is appropriate to do so. MRTs will have different competencies within the overall MRT scope of practice, depending on qualifications and practice setting requirements. MRTs may only perform authorized acts if there is an order from a physician and if they have the necessary knowledge, skills and judgementto perform the procedure safely, effectively and ethically, given the circumstances in the situation.
For further discussion and direction, see the section “What MRTs should do if they are not competent to perform an authorized act” on p. 16.
What is an order?An order is an authorizing statement, from a regulated health professional with prescribing authority, permitting an MRT to implement a procedure that falls within the MRT scope of practice. Under the MRTA, an order from a physician is necessary to permit MRTs to implement authorized act procedures. (Under the HARP Act, an order from a physician, dentist, chiropractor, designated chiropodist, osteopath or, under some circumstances, a nurse who holds an extended certificate of registration, is necessary to permit MRTs to apply or administer ionizing radiation).
An order may also be known as a:• Prescription• Requisition• Request for consultation• Doctor’s note
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 13
Page 42
2 • A U T H O R I Z E D A C T S
14
An order may be one of two types:1. Direct order (for one specific patient)2. Directive or protocol (for a number of patients under specific circumstances)
An order may also be used to prompt performance of a procedure that is neither a controlled act nor ionizing radiation, but which falls within patient procedures or treatments (e.g., taking blood pressure).
Authorized acts are ordered, not delegatedDelegation is the transfer of authority by a regulated health professional who is authorized to perform a controlled act procedure, to someone (another regulated health professional or an unregulated health care provider) who is not authorized to perform it. Since MRTs are already authorized under the MRTA toperform the four authorized acts, delegation to an MRT is not necessary and such procedures are ordered, not delegated.
Types of ordersDirect Order An order or prescription, for a specific procedure, treatment or intervention, for a specific patient, written byan individual physician directly in the patient record. To be complete, the order must include:
• Name of patient• Date and time• Name of procedure or substance being ordered; and, when a substance is being ordered, the order
must include:
• the dosage; • the route of administration; • the frequency with which
the substance is to be administered; and• the signature of the ordering physician.
Direct orders are generally written. Under the Public Hospitals Act (PHA), physicians (and dentists, midwives or registered nurses in the extended class) may dictate an order for treatment or for a diagnostic procedure by telephone. The requirements respecting such orders include that they must be signed by the physician on the first visit to the hospital after dictation. (See Appendix F, regulation 965/98 made under the Public Hospitals Act).
In order to deal properly with telephone orders or requests, MRTs are expected, if working in hospitals governed by the PHA, to:
• ensure they have been designated by the administrator as someone who can accept telephone orders;
• transcribe the order along with the name of the physician who dictated it, and the date and time of its reception;
• sign the order; • be reasonably assured that any physician who dictates an order will sign it on the first visit to the
hospital after dictation; and• ensure that if someone else has transcribed a telephone order, the person has the authority to
accept such orders before implementing them.
Directive or protocolAn order or prescription for a procedure, treatment or intervention for a range of patients who meet specific conditions (in some instances this may have been known as a “standing order”). Directives or protocols are always written and must contain:
• a standardized reference number;• identification of the specific procedure or treatment or range of treatments being ordered;• identification of who specifically may implement the procedure under the authority of and according
This information may appear in the written orderitself or it may exist in protocols, that have beendeveloped in the department by the appropriateauthorizing physician.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 14
Page 43
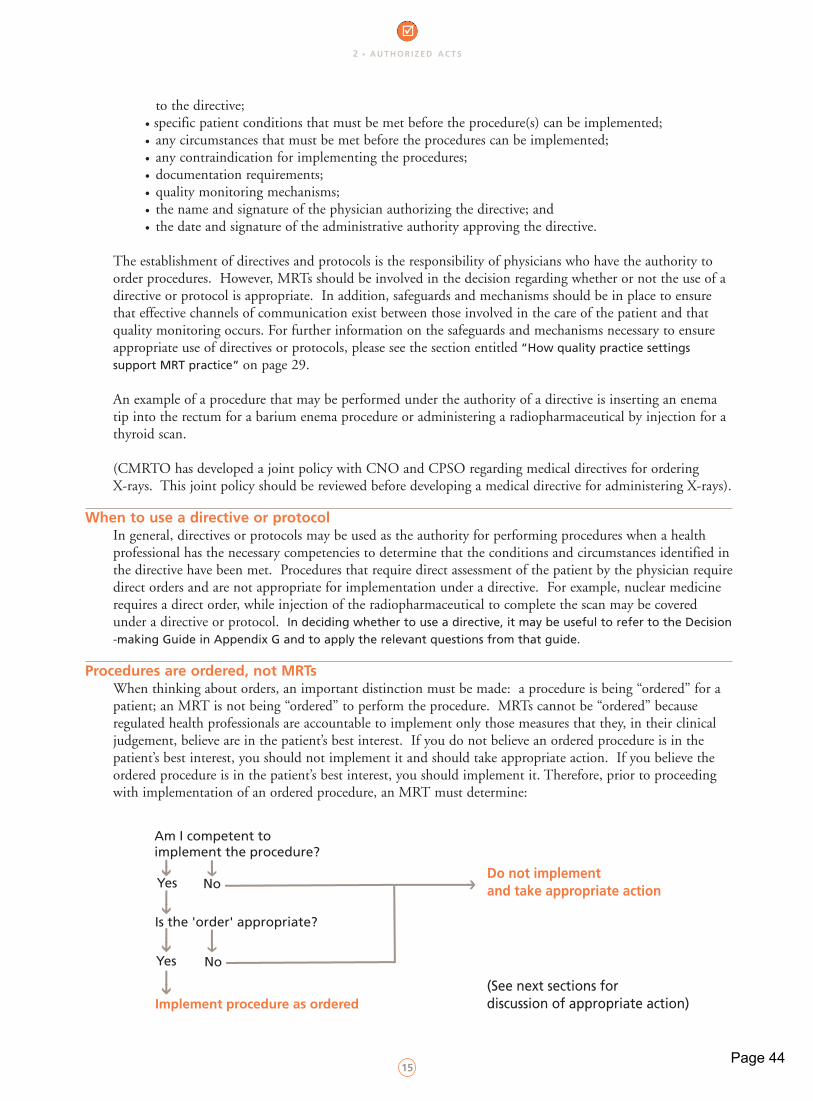
2 • A U T H O R I Z E D A C T S
15
to the directive;• specific patient conditions that must be met before the procedure(s) can be implemented;• any circumstances that must be met before the procedures can be implemented;• any contraindication for implementing the procedures;• documentation requirements;• quality monitoring mechanisms;• the name and signature of the physician authorizing the directive; and• the date and signature of the administrative authority approving the directive.
The establishment of directives and protocols is the responsibility of physicians who have the authority to order procedures. However, MRTs should be involved in the decision regarding whether or not the use of a directive or protocol is appropriate. In addition, safeguards and mechanisms should be in place to ensure that effective channels of communication exist between those involved in the care of the patient and that quality monitoring occurs. For further information on the safeguards and mechanisms necessary to ensure appropriate use of directives or protocols, please see the section entitled “How quality practice settings support MRT practice” on page 29.
An example of a procedure that may be performed under the authority of a directive is inserting an enema tip into the rectum for a barium enema procedure or administering a radiopharmaceutical by injection for a thyroid scan.
(CMRTO has developed a joint policy with CNO and CPSO regarding medical directives for ordering X-rays. This joint policy should be reviewed before developing a medical directive for administering X-rays).
When to use a directive or protocolIn general, directives or protocols may be used as the authority for performing procedures when a health professional has the necessary competencies to determine that the conditions and circumstances identified inthe directive have been met. Procedures that require direct assessment of the patient by the physician requiredirect orders and are not appropriate for implementation under a directive. For example, nuclear medicine requires a direct order, while injection of the radiopharmaceutical to complete the scan may be covered under a directive or protocol. In deciding whether to use a directive, it may be useful to refer to the Decision-making Guide in Appendix G and to apply the relevant questions from that guide.
Procedures are ordered, not MRTs When thinking about orders, an important distinction must be made: a procedure is being “ordered” for a patient; an MRT is not being “ordered” to perform the procedure. MRTs cannot be “ordered” because regulated health professionals are accountable to implement only those measures that they, in their clinical judgement, believe are in the patient’s best interest. If you do not believe an ordered procedure is in the patient’s best interest, you should not implement it and should take appropriate action. If you believe the ordered procedure is in the patient’s best interest, you should implement it. Therefore, prior to proceeding with implementation of an ordered procedure, an MRT must determine:
Am I competent to implement the procedure?
Yes
Yes
Is the 'order' appropriate?
Implement procedure as ordered
No
No
Do not implement and take appropriate action
(See next sections for discussion of appropriate action)
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 15
Page 44
2 • A U T H O R I Z E D A C T S
16
What MRTs should do if they have concerns about an order or a treatment planBecause MRTs are obliged to implement only those procedures and treatment plans which in their clinical judgement, are in the patient’s best interest, they should not implement any procedure they have concerns about and take appropriate action to address the situation. This may vary from situation to situation, but in general, if an MRT has concerns about an order or treatment plan, resolving the concern will involve the following steps:
1. The MRT should discusses the concern directly with the responsible health care provider to: a) identify the concern clearly and concisely;b) support it with a rationale and best practice evidence;c) identify outcomes desired for resolution; andd) use effective communication methods.
(This may follow consultation with the patient (as appropriate), MRT colleagues, other knowledgeable professionals, reference materials and any other resources necessary to clarify and verify the nature of the concern).
2. If unable to resolve the concern, the MRT should inform the responsible health provider and discuss the concern with his or her immediate manager.
3. If the manager shares the concern, a) the MRT should contact the responsible health care provider for further discussion, butb) if the health care provider remains decided about the original treatment plan, the MRT
should refer back to the manager and agency policy to determine how to bring the concernto the attention of a higher management authority in the agency.
4. If the manager does not share the concern and cannot provide information that will dispel it, the MRT should decide whether to report to a higher management authority.
5. The MRT should report to higher authorities in the facility until convinced of the appropriateness of treatment, or until the treatment is changed.
6. If the decision is to refuse to implement the ordered procedure or treatment plan, the MRT should inform the health care provider of the decision and the action taken to date.
7. The MRT should document the concern and the steps taken to resolve it that directly relate to patient care, in the health care record. If necessary, the MRT should refer to agency policy for the appropriate format to document information not directly related to patient care.
(Adapted from College of Nurses of Ontario materials -Standards for Nurses Disagreeing with the Multidisciplinary Plan of Care, 1997 )
What MRTs should do if they are not competent to perform an authorized actThe authorized acts enable all MRTs, across a broad range of practice settings, to provide procedures that fall within those authorized acts. This does not mean that all MRTs are expected to be competent to perform all the procedures that fall within the acts. On the contrary, it is acknowledged that MRTs will have different competencies within the overall MRT scope of practice, depending on qualifications and practice setting requirements. Therefore, if an MRT is not competent to perform an authorized act procedure, even though legally authorized to do so under the legislation, he or she must refrain from performing it and take the appropriate action to address the situation.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 16
Page 45
2 • A U T H O R I Z E D A C T S
17
The appropriate action will vary from situation to situation, as follows:• If performing the procedure is part of an MRT’s regular role expectations within a
practice setting, the MRT should obtain the competencies necessary to provide safe, effective and ethical services to patients in his or her care. The MRT may consult with his or her manager to determine how this may be achieved. In making this decision, the MRT is ultimately responsible to be competent to provide services required by patients within the practice setting. Quality practice settings foster the acquisition, maintenance and continuing improvement of competence.
• If performing the procedure is not part of an MRT’s regular role expectations, the appropriateness of obtaining the necessary competencies should be evaluated. In order toassist with such an evaluation, it may be useful to refer to the “Decision-making Guide for determining the appropriateness of accepting delegation and performing services or procedures beyond principal expectations of MRT practice” and apply the relevant questions from that guide.
Recommended agency practicesIn practice settings, where MRTs perform authorized acts, there should be mechanisms in place to enable MRTs to practice safely, effectively and ethically, according to the expectations identified above. Such mechanisms may include those that:
• ensure the requisites permitting performance of authorized acts by MRTs are in place (physician order, the MRT is performing the procedure in the course of engaging in the practice of medical radiation technology, in accordance with his or her certificate of registration, and is able to perform the procedure safely, effectively and ethically);
• ensure directives and protocols are established and used appropriately (see the section entitled “How quality practice settings support MRT practice” on page 29 for guidelines);
• establish agency practices or policies and procedures consistent with the expectations for MRT practice regarding dealing with concerns about an order or a treatment plan;
• establish agency practices or policies and procedures consistent with the expectations for dealing withsituations when an MRT identifies that he or she is not able to perform an authorized act safely, effectively and ethically, either because the MRT lacks the necessary competencies (as identified in the guidelines above) or because the circumstances in the situation or agency practices do not permit the MRT to implement the procedure safely, effectively and ethically (see the section entitled“How quality practice settings support MRT practice” on page 29 for guidelines).
An MRT may perform an authorized act procedure when all the following conditions have been met:
1. An appropriate order is in place from a physician authorizing performance of the procedure;
2. The procedure will be performed in the course of engaging in the practice of medical radiation technology;
3. Performance of the procedure is not restricted by the terms, conditions or limitations placed upon his or her certificate of registration;
4. The MRT ensures that he or she has and applies the necessary knowledge, skill and judgement toperform and manage the outcomes of performing the procedure safely, effectively and ethically;
5. Patient consent has been obtained;
Summary of Practice Guidelines for MRTs performing authorized acts
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 17
Page 46
2 • A U T H O R I Z E D A C T S
18
6. Responsibility and accountability for performing the procedure are accepted by the MRT, having considered:
a) the known risks to the patient in performing the procedure;b) the predictability of the outcomes in performing the procedure;c) whether the management of the possible outcomes is within the MRT's knowledge, skill
and judgement given the situation; andd) any other factors specific to the situation to ensure the procedure is implemented safely,
effectively and ethically;
7. Implementation of the procedure and/or actions taken is documented; and
8. The MRT refrains in from performing the procedure if the above conditions are not met andtakes appropriate action to address the situation.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 18
Page 47
2 • A U T H O R I Z E D A C T S
1919
authorized actstitle page
2 • A U T H O R I Z E D A C T S
19
2 • A U T H O R I Z E D A C T S
In this section the following topics will be covered:
• What MRTs need to know about delegation
• When delegation is and is not required
• Delegator qualifications
• Delegation and consent
• Recommended agency practices
3 Delegation
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 19
Page 48
3 • D E L E G AT I O N
20
Definition of delegationDelegation is the transfer of authority from a member of a regulated health profession, authorized by his or her health profession Act to perform a controlled act procedure, to someone who is not authorized, either another regulated health professional or an unregulated person. Only regulated health professionals, authorized under their health profession Act to perform a controlled act procedure, may delegate the procedure to another, subject to the standards and any applicable guidelines or regulations of the profession.
Delegation is a systematic process consisting of the following steps:• An initial evaluation of whether it is appropriate to consider delegation under the circumstances in
the situation;• Completion of a delegation program established by the delegator, which includes:
• a theoretical and practical educational component;• supervised practice (assisting and observing the person who will be performing the delegated
act to acquire the knowledge, skill and judgement necessary to perform the procedure safely and effectively); and
• a formal, written transfer of authority to perform the procedure; and• Ongoing evaluation of the appropriateness of delegation and performing a delegated act.
A delegated act is a procedure that falls within a controlled/authorized act that is performed under the authority of delegation. For example, if an MRT is authorized through delegation to perform the controlledact of urinary catheterization, then urinary catheterization becomes a delegated act procedure.
Under the RHPA, regulated health professionals are given the option of delegating or accepting delegation ofcontrolled act procedures.
When delegation is and is not requiredDelegation is required when:
• the procedure is a controlled act procedure and the person is not authorized to perform it under a health profession Act.
Delegation is not required when:• a procedure is not a controlled act;• the health professional is authorized to perform the controlled act in the health profession Act, with
or without an order; or• the procedure falls within one of the exemptions, exceptions, or the person is exempt
(see Appendix E for the list of exceptions and exemptions).
Therefore, in practice, if an MRT is assigned to work with a patient who requires a controlled act procedure that is not within the four controlled acts authorized to MRTs (e.g., urinary catheterization), the MRT must not accept the assignment unless the authority to perform the procedure has been delegated to him or her by a regulated health professional who is authorized to perform it (e.g., a physician or nurse).
MRT delegation of authorized acts to othersMRTs cannot delegate authorized acts at this time. This policy decision is based on public protection considerations and current practice patterns. As practice patterns evolve, this decision may be reviewed. If MRTs wish to discuss this further, they may contact the CMRTO.
What MRTS need to know about delegation
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 20
Page 49
3 • D E L E G AT I O N
21
MRT acceptance of delegationMRTs may accept delegation of controlled acts from another regulated health professional authorized to perform and delegate the procedure (most likely a physician or nurse), subject to the guidelines described below.
Deciding whether to accept delegation and perform a delegated actIn order to determine whether it is appropriate to accept delegation or perform a delegated act, MRTs and those making decisions about MRTs accepting delegation need to answer the following question:
Given the patient’s condition and needs and the circumstances, in the situation, is the MRT competent to perform the delegated act safely, effectively and ethically, in accordance with legal requirements and standards of practice?
To assist MRTs and those making such decisions, the CMRTO has developed a decision-making framework entitled the “Decision-making guide for determining the appropriateness of accepting delegation and performing services or procedures beyond principal expectations of MRT practice” (see Appendix G). MRTs and others may use the guide or another framework of their choice to address the question, as long asit covers the same factors set out in the guide. The guide is described in more detail in the section entitled “Deciding whether to perform procedures or services that do not fall within principal expectations of MRT practice.”
Delegator qualificationsIn order to accept delegation, MRTs must be certain the delegating regulated health professional is acting in accordance with any applicable guidelines, policies or regulations of his or her College or any other applicable legislative regulations to delegate the procedure. This includes confirming that the College of the delegator has not prohibited or restricted delegation.
The MRT must also reasonably believe that the delegator has the competence to delegate the procedure. Competence to delegate includes the competence both to perform and to delegate the procedure, and MRTsmust be reasonably assured of this prior to accepting delegation from a proposed delegator.
An order is necessary to perform delegated acts When MRTs have been authorized through delegation to perform a controlled act procedure, theremust be an order in place to permit them to perform the procedure. Whether the order is an individual order, a directive or protocol will depend on the situation (see the section above, “When to use a directive orprotocol,” for further discussion of when to use either individual orders or directives).
Delegation and consentAs stated in a March 1995 Ontario Hospital Association (OHA) fact sheet on delegation, under the Consent to Treatment Act (CTA), revised as the Health Care Consent Act (the HCCA), it is generally accepted that :
“The professional who delegates performance of the procedure will be the practitioner proposing the treatment to the patient. He or she will therefore be the practitioner responsible for ensuring that the CTA [now the HCCA] has been complied with in relation to rights notification and consent. However, the practitioner who has the authority to perform the act by means of delegation, may in some circumstances also be responsible for proposing the treatment to the patient...[and is] responsible for ensuring the act (CTA) [now the HCCA] has been complied with...In either case, the proposer must obtain an informed consent to the procedure... No health practitioner should begin aprocedure without prior discussion with the patient and confirming that the patient has consented and continues to consent.1 ’’
1 The rights notification requirements under the CTA were substantially amended by the HCCA.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 21
Page 50
3 • D E L E G AT I O N
22
If an MRT has accepted delegation of a controlled act procedure and is implementing a delegated act under the HCCA, the MRT may be responsible for confirming informed consent prior to the implementation of the procedure and for confirming that the patient continues to consent. (For example, if an MRT accepts delegation of urinary catheterization as part of a voiding cystourethrogram, then the MRT may be responsible for ensuring informed consent for the overall treatment, including the urinary catheterization component, and will be responsible for confirming that the patient continues to provide informed consent.)
If the patient does not have appropriate information to provide informed consent, and it is beyond anMRT’s your scope and competence to provide the information (for example, information regarding alternative diagnostic tests or treatments), then the MRT should refrain from administering the procedure and take the appropriate action to resolve the situation.
Acceptable delegation programsIt is the responsibility of the delegator to establish a delegation program, in accordance with any applicable guidelines, policies or regulations, having considered the condition and needs of the patient(s) and the competencies necessary to meet those needs under the circumstances in the situation.
From an MRT’s perspective, an acceptable delegation program enables the MRT to accept delegation and perform a delegated act according to the standards of practice of the profession. This means that the program enables an MRT to obtain the necessary theoretical and practical knowledge, skills and judgement to perform, and manage the outcomes of performing the delegated procedure safely, effectively and ethically, given the circumstances in the situation.
The content and extent of the program may vary, depending on the patient, circumstances and competenciesof the MRTs. Who teaches the program and how it is delivered may also vary (e.g. an authorized delegator may approve a program offered at a community college as the means of acquiring the necessary knowledge, skill and judgement). However, regardless of variances, the actual transfer of authority must come from an authorized delegator satisfied with the competency of the specific MRT to perform the delegated act, given the circumstances in the situation. The program or authorization process will consist of more than simply providing an order for performance of the delegated procedure. In general, acceptable programs will involve:
• provision of a theoretical and practical educational component;• provision of supervised practice (assistance with and observation of the acquisition of the knowledge,
skill and judgement necessary to perform the procedure safely and effectively); and• determination of the initial and the continuing delegation through:
• a formal decision by the delegator that each individual MRT is competent to perform theprocedure under the specified conditions (certification process); and
• a formal process and system for ensuring the continuing competence of each individual MRT to perform the delegated procedure (re-certification processes).
It is essential that the decision to transfer authority to the MRT be documented. The documentation is the basis for the MRT to demonstrate that he or she was properly authorized to perform the delegated act.
Ultimately, if MRTs do not believe they have the necessary competencies to perform the delegated act, they must refrain from accepting delegation.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 22
Page 51
3 • D E L E G AT I O N
23
MRT assistance in the delegation programSome Colleges have made provision for the members of the profession receiving delegation to assist in the delegation program by providing, either in whole or in part, the educational component of the program. The CMRTO has established the following position in relation to this practice:
The CMRTO will permit MRTs to assist in the delegation program as long as the MRT has acquired the necessary competencies, and the responsibility for the standards for certification of competence and the procedures for evaluating, whether or not the standards have been met, remain with the delegator.
These conditions are outlined below in the “Summary of Practice Guidelines for MRTs accepting delegation,” under the section on assisting in the delegator’s delegation program.
MRT responsibility and accountability when accepting delegationThe decision to delegate a controlled act procedure rests solely with the delegating health professional. When accepting delegation of a controlled act procedure, MRTs are responsible
• for the decision to accept delegation; • to have the knowledge, skill and judgement to perform the delegated procedure, given the
patient’s conditions and needs and the circumstances in the situation;• to act in accordance with the CMRTO professional practice guidelines; and• to act in accordance with any requirements imposed by the delegator as a condition of transferring
the authority to perform the delegated act.
Although the decision to delegate a controlled act procedure rests solely with the delegating health professional, any decisions about delegating to MRTs should be made in collaboration with MRTs. MRTs are responsible for determining whether or not accepting delegation lies within their practice and competencies, given the patient’s condition and needs as they know them, and the circumstances in the situation. This requires MRTs to know their limits of practice. Determining limits of practice includes an examination of the extent to which their foundation of knowledge, skills and judgement can support taking on additional acts.
Recommended agency practicesAgencies that are quality practice settings will provide structures and processes to support MRTs in acceptingdelegation safely, effectively and ethically. Such structures and processes include mechanisms to determine the appropriateness of delegation and to ensure that the appropriate people are involved in the decision, thateffective channels of communication exist between those involved in delegation and the performance of delegated acts, and that quality monitoring of delegation occurs. Please see the section entitled “How quality practice settings support MRT practice” on page 29.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 23
Page 52
3 • D E L E G AT I O N
24
An MRT may accept delegation of a controlled act procedure within the controlled acts not authorized to MRTs when all of the following conditions have been met:
1. It is appropriate to accept delegation given the factors identified in the “Decision-making guide for determining the appropriateness of accepting delegation and performing services or procedures beyond principal expectations of MRT practice;”
2. The delegator is acting in accordance with any applicable guidelines and policies of the regulatorybody or regulations under the specific health profession Act governing the delegator, and has not been restricted or prohibited from delegating the procedure;
3. The delegator has the knowledge, skill and judgement to perform and delegate the procedure;
4. The MRT has the knowledge, skill and judgement to perform the procedure safely, effectively and ethically, given the circumstances in the situation;
5. A written record of the transfer of authority and certification of the MRT’s competence is maintained;
6. The conditions established by the delegator for maintaining the authority to perform the delegated act are adhered to;
7. It is appropriate to perform the delegated act, given the factors identified in the “Decision-making guide for determining the appropriateness of accepting delegation and performing services or procedures beyond principal expectations of MRT practice;”
8. Patient consent has been obtained;
9. The MRT accepts full responsibility and accountability for accepting delegation and performing the delegated act;
10. Implementation of the delegated act and/or actions is documented; and
11. If any of the above conditions are not met, the MRT will refrain from accepting delegation and performing the delegated act.
Additionally, an MRT may assist in the delegation program established by the delegator, when all the following conditions have been met:
1. The MRT reasonably believes the delegation program has been developed and approved by a regulated health professional authorized by his or her health profession Act to perform the controlled act (e.g., a physician authorized by the Medicine Act) who has the knowledge, skill and judgement to perform and delegate the procedure safely, effectively and ethically in accordance with any applicable guidelines or regulations;
2. The MRT has the knowledge, skill and judgement to perform and teach the procedure safely, effectively and ethically, in consideration of the patient’s condition and needs and the circumstances in the situation;
3. The MRT assists in the educational component of the program, but does not become involved inthe determination of competence or transfer of authority to perform the delegated act, either during the initial delegation (certification) or subsequent determinations of competence to continue to perform the delegated act (re-certification); and
4. The MRT refrains from participating in the program if the above conditions are not met.
Summary of Practice Guidelines for MRTs accepting delegation
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 24
Page 53
2 • A U T H O R I Z E D A C T S
2525
2 • A U T H O R I Z E D A C T S
25
2 • A U T H O R I Z E D A C T S
In this section the following topics will be covered:
• Deciding whether to perform procedures or services which do
not fall within principal expectations of MRT practice
• Case studies
• How quality practice settings support MRT practice
4 AgencyPractices
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 25
Page 54
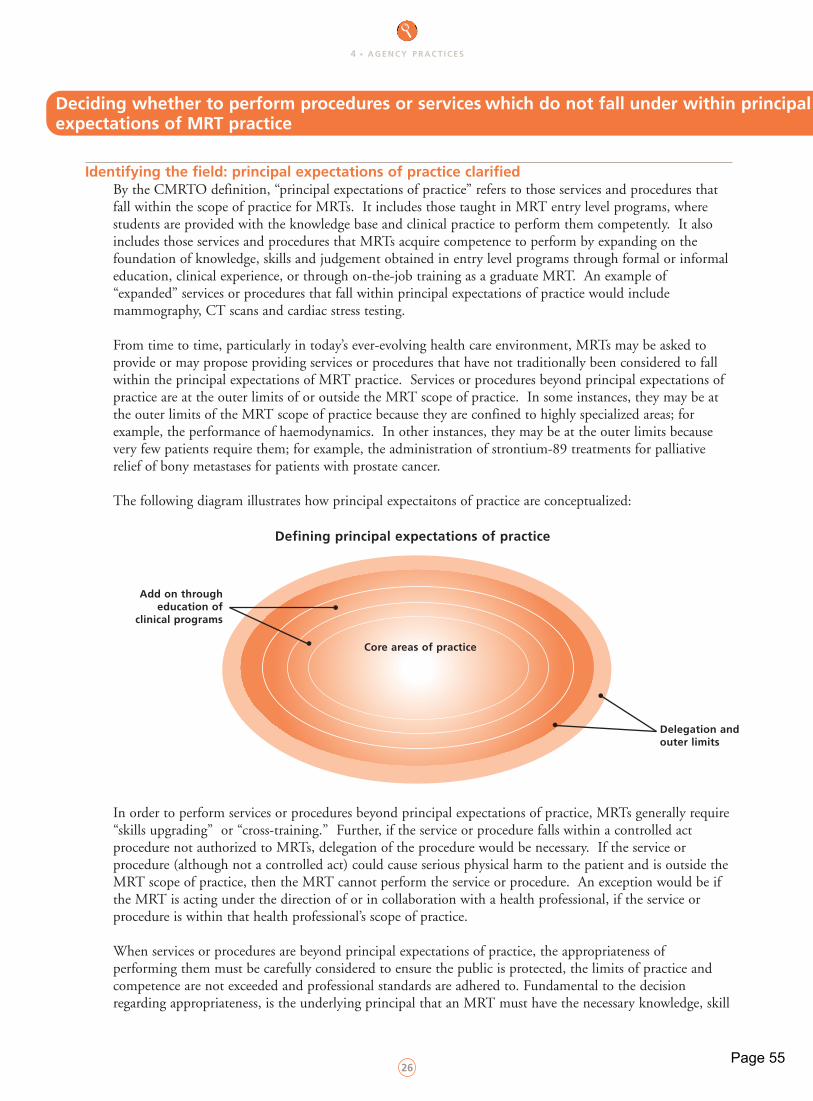
4 • A G E N C Y P R A C T I C E S
26
Identifying the field: principal expectations of practice clarifiedBy the CMRTO definition, “principal expectations of practice” refers to those services and procedures that fall within the scope of practice for MRTs. It includes those taught in MRT entry level programs, where students are provided with the knowledge base and clinical practice to perform them competently. It also includes those services and procedures that MRTs acquire competence to perform by expanding on the foundation of knowledge, skills and judgement obtained in entry level programs through formal or informal education, clinical experience, or through on-the-job training as a graduate MRT. An example of “expanded” services or procedures that fall within principal expectations of practice would include mammography, CT scans and cardiac stress testing.
From time to time, particularly in today’s ever-evolving health care environment, MRTs may be asked toprovide or may propose providing services or procedures that have not traditionally been considered to fall within the principal expectations of MRT practice. Services or procedures beyond principal expectations of practice are at the outer limits of or outside the MRT scope of practice. In some instances, they may be at the outer limits of the MRT scope of practice because they are confined to highly specialized areas; for example, the performance of haemodynamics. In other instances, they may be at the outer limits because very few patients require them; for example, the administration of strontium-89 treatments for palliative relief of bony metastases for patients with prostate cancer.
The following diagram illustrates how principal expectaitons of practice are conceptualized:
In order to perform services or procedures beyond principal expectations of practice, MRTs generally require“skills upgrading” or “cross-training.” Further, if the service or procedure falls within a controlled act procedure not authorized to MRTs, delegation of the procedure would be necessary. If the service or procedure (although not a controlled act) could cause serious physical harm to the patient and is outside theMRT scope of practice, then the MRT cannot perform the service or procedure. An exception would be if the MRT is acting under the direction of or in collaboration with a health professional, if the service or procedure is within that health professional’s scope of practice.
When services or procedures are beyond principal expectations of practice, the appropriateness ofperforming them must be carefully considered to ensure the public is protected, the limits of practice and competence are not exceeded and professional standards are adhered to. Fundamental to the decision regarding appropriateness, is the underlying principal that an MRT must have the necessary knowledge, skill
Deciding whether to perform procedures or services which do not fall under within principalexpectations of MRT practice
Add on through education of
clinical programs
Defining principal expectations of practice
Delegation and outer limits
Core areas of practice
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 26
Page 55
4 • A G E N C Y P R A C T I C E S
27
and judgement to perform an act safely and effectively before implementing any procedure or treatment plan.In order to assist MRTs and agencies to determine whether it is appropriate for MRTs to provide such services or procedures, a decision-making guide has been developed. The guide can be found in Appendix G and a description of it follows.
Overview of the decision-making guideWhen making decisions about whether to perform services or procedures beyond MRT principal expectations, the question is:
Given the patient’s condition and needs and the circumstances in the situation, does the MRT have thecompetence to perform the procedure or service safely, effectively and ethically, in accordance with legal requirements and standards of practice?
The factors to consider in answering this question have been incorporated into the “Decision-making guide for determining the appropriateness of accepting delegation and performing services or procedures beyond principal expectations of practice” found in Appendix G.
An overview of the factors is as follows: • What is the exact nature of the service or procedure being proposed and what are the circumstances
in which it would be performed?• Is providing the service or procedure possible, given legal requirements and MRT practice and
competence?• Is providing the service or procedure in the situation within an MRT’s practice, competencies and
the legal requirements, given the patient’s overall condition and care needs and the circumstances in the situation (such as the degree of independence of the MRT when performing the procedure and the safeguards in place to ensure safe, effective and ethical practice)?
• Does performance of the procedure by an MRT make sense?
Overall, when deciding whether to provide services or procedures beyond principal expectations of practice, MRTs must know the limits of their practice. Determining limits of practice includes examining the foundation for practice: one’s basic educational preparation and the extent to which one’s knowledge, skills and judgement can support taking on additional services and procedures that are at the outer limits or outside the MRT scope of practice, authorized acts and personal competencies.
Assumptions underlying the decision-making guideThe assumptions underlying the guide (found in Appendix G) include:
• Careful consideration and analysis before performing services or procedures beyond principal expectations of practice, in the interests of public protection;
• Analysis of any proposal to practice beyond principal MRT expectations;• Careful analysis of the appropriateness of performing such services or procedures,
supported by quality practice settings;• The outcomes of care for the patient should be the same, regardless of who provides it, in situations
where more than one health care provider is eligible to provide care;• Cost should not be a primary determinant of whether MRTs provide services or procedures beyond
principal expectations of practice. The primary determinant is whether the needs of the patient can be met safely, effectively and ethically. Cost may only be factored in after this initial determination; and
• The CMRTO’s role in clarifying scope of practice for MRTs and its availability to consult with MRTs, agencies and the public to assist in decision-making and clarification.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 27
Page 56
4 • A G E N C Y P R A C T I C E S
28
Applying the Guide: Case studiesThe following case studies are not intended to be a complete application of the decision-making guide in Appendix G; rather, they are examples of some of the questions to be considered in an analysis of the issues.
case study 1An MRT, working at night, has completed radiographs of an MVA victim’s cervical spine, along with other body parts. The patient is semi-conscious and has multiple injuries. The emergency physician has ordered supine flexion and extension views of the cervical spine to rule out vertebral subluxation. As the emergency department is very busy, the emergency physician has requested that the MRT move the patient’s head and neck to attain the required positions. Should the MRT position the patient’s head and neck to achieve the flexion and extension views, as requested?
Applying the decision-making guide in Appendix G and responding to the series of questions and considerations listed there might result in the following decision making process:
Positioning a patient to obtain the required radiographs is within an MRT’s scope and principal expectations of practice. Obtaining flexion and extension views are in the patient’s best interest, and an order is in place to authorize the procedure. However, positioning patients for flexion and extension views when they are unable to sit and move their own heads is not within principal expectations of practice. The risks of performing such a procedure are high, because the requested positioning and movement necessary to demonstrate or rule out a spinal cord injury put the spinal cord at risk and could produce permanent disability. In addition, the outcomes of performing such a procedure are unpredictable and the MRT does not have the knowledge, skill and judgement to manage the possible outcomes of the procedure.
Therefore, using the decision-making guide in this particular scenario, one would expect that the MRTwould conclude that it is not appropriate for the MRT to position the patient’s head and neck in orderto achieve the flexion and extension positions as requested. Instead, the MRT should speak with the physician requesting the procedure and take appropriate action to address the situation.
case study 2The radiological procedures of voiding cystography (to investigate recurrent urinary tract infections) and defecography (to investigate difficulties with bowel elimination) are provided ina Medical Imaging Department of a large tertiary care hospital. Both procedures require urinary catheterization to infuse contrast media into the bladder. In order to reduce the number of health care professionals involved in the care of the patients during the procedures, the department is investigating the possibility of an MRT catheterizing patients. Medical and nursing staff are available to delegate and provide back-up. Is it appropriate for an MRT to catheterize patients during these procedures?
Applying the decision-making guide in Appendix G and responding to the series of questions and considerations listed there might result in the following decision making process:
Urinary catheterization is a controlled act procedure not authorized to MRTs. However, it is being proposed to be implemented in the context of radiological procedures and may therefore bewithin the range of the MRT scope of practice; consideration may be given to accepting delegation. The goal of minimizing the number of staff involved in care is of benefit to patients.
Patients are assessed by physicians prior to undergoing the procedure. They are generally healthy,with anatomically predictable and structurally intact urinary tracts, and the outcomes of the procedure, when performed competently, are quite predictable. The risk factors include infection, misplaced insertion and damage to the urinary tract. MRTs have preparation in
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 28
Page 57
4 • A G E N C Y P R A C T I C E S
29
anatomy, physiology and aseptic technique that provides a foundation of knowledge to acquire the additional knowledge, skills and judgement necessary to safely and effectively catheterize such patients.The prevention and management of risks can be dealt with in a training program and by having nursing and medical back-up readily available (e.g., if any resistance is encountered when inserting the catheter, the MRT would not proceed and would obtain medical or nursing back-up). The proceduresare done often enough to enable designated MRTs to maintain competence. The medical and nursing authorities in the hospital have agreed in principal to delegation, and qualified and competent medical and nursing staff are available to implement delegation processes and provide readily available back-up.
Therefore, using the decision-making guide in this particular scenario, when patients are undergoing voidingcystography or defecography under the described circumstances, it may be appropriate for MRTs who have completed a delegation program to perform urinary catheterization, in accordance with the guidelines for accepting delegation set out in this publication.
An MRT may perform a service or procedure that does not fall within principal expectations of practice when all the following conditions have been met:
1. It is appropriate to perform the service or procedure given the factors identified in the “Guidelines for decision-making when determining the appropriateness of accepting delegation and providing services or procedures beyond principal expectations of practice (Appendix G)”;
2. If the service or procedure falls within a controlled act procedure not authorized to MRTs, the service or procedure has been delegated appropriately;
3. If the service or procedure (although not a controlled act) could cause serious physical harm to the patient and is outside the MRT scope of practice, then the service or procedure is not performed unless an exception to the ‘risk of harm’ clause applies;
4. The service or procedure is performed according to relevant practice guidelines; and
5. Performance of the service or procedure and/or action taken is documented.
The MRT refrains from performing the service or procedure if the above conditions are not met and takes appropriate action to address the situation.
Recommended agency practices to support safe, effective and ethical MRT practice in relation to performing authorized acts, using directives or protocols, accepting delegationand performing beyond principal expectations of practice
Agencies that are quality practice settings provide the structures and processes to enable MRTs to fulfill professional standards of practice and provide safe, effective and ethical care. In relation to performing authorized acts, using medical directives or protocols, accepting delegation from others, and performing services or procedures that do not fall within principal expectations of practice, the following mechanisms are recommended:
Summary of Practice Guidelines for MRTs performing services or procedures beyondprincipal expectations of practice
How quality practice settings support MRT practice
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 29
Page 58
4 • A G E N C Y P R A C T I C E S
30
1. Ensure appropriate health professionals are involved in the consideration and development of proposals and policies related to directives or protocols, delegation and performing beyond principal expectations. Generally:
a) The establishment of directives and protocols are the responsibility of physicians who have the authority to order procedures. The establishment of a delegation process is theresponsibility of the profession authorized to perform and delegate an authorized act procedure (e.g., medicine or nursing). However, a collaborative process enabling any health profession, affected directly or indirectly in the implementation of a directive or delegation, to be part of the decision making regarding establishing those directives or delegation practices is strongly encouraged; and
b) Those involved in making decisions about the establishment of directives and delegation practices must know how to analyze the fit between the patient’s condition and needs properly, have the competencies necessary to meet those needs in the given situation, and know which health care provider can be expected to have those competencies.
2. Establish a structure and process to determine the appropriateness of using a directive, accepting delegation, delegating to others or performing beyond principal expectations. The framework inthe “Decision-making guide for determining the appropriateness of accepting delegation and performing services or procedures beyond principal expectations of MRT practice” in Appendix Gsets out factors to take into account and offers a foundation to draw upon.
3. Ensure that all staff, particularly physicians involved in the care of patients who may receive MRT procedures or treatments on the authority of a directive or delegation, are aware exactly what procedures and treatments patients will be receiving. For example, under some agency directives or protocols, when a physician orders an upper gastrointestinal follow-through and small bowel series to rule out Crohn’s disease, this includes a pneumocolon.
4. Establish feedback mechanisms, including a defined communication path, to enable the MRT to identify and, if necessary, obtain clarification from the physician or other team members responsible for the care of the patient.
5. Establish quality monitoring systems to track the use of directives, the performance of delegated acts and performance beyond principal expectations, to determine when these practices are being implemented inappropriately or are resulting in unanticipated outcomes and to ensure practices are updated.
6. Ensure that when MRTs are performing procedures on the authority of a directive or delegation or are performing beyond principal expectations, agency practices are such that MRTs are able to fulfill standards of practice and provide safe, effective and ethical care (e.g., are able to appropriately monitor patients to manage outcomes and are able to adhere to practice guidelines).
7. Provide structures and processes to enable MRTs to advocate for agency practices that enable them to fulfill standards of practice and provide safe, effective and ethical care. The process set out below offers a framework to draw upon.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 30
Page 59
4 • A G E N C Y P R A C T I C E S
31
What MRTs should do if agency practices compromise their ability to practice safely,effectively and ethically
Agency practices may compromise an MRT’s ability to meet professional standards of practice and provide safe, effective and ethical care. Examples of possible situations that may give rise to concerns of this nature include inadequate or unavailable channels of communication to clarify concerns about orders, lack of appropriate back-up, inability to appropriately supervise unregulated care providers, or MRTs being asked toprovide services that are beyond principal expectations of practice with no evaluation of the appropriateness of doing so.
In such situations, MRTs are expected to advocate for changes that will enable the delivery of safe, effective and ethical care. The specific methods for doing this may vary from setting to setting, but in general will involve the following steps:
1. Identifying the concern and providing suggestions for dealing with it. The MRT consults and works with all relevant stakeholders (colleagues, patients, administrators) to address and resolve the concern;
2. Meeting with the immediate manager to identify:• the nature of, and rationale for, the concern;• the MRT’s suggestions for dealing with the concern; and• a mutually established date by which the concern should be addressed;
3. If the manager disagrees with the concern and is unable to dispel it or does not address it by the agreed date, scheduling a meeting to discuss why and to determine the next step, including a newtarget date for resolution;
4. If the new date passes and/or the issue is not resolved to the MRT’s satisfaction, forwarding the concern in writing to the manager, including the information in #2;
5. If the issue continues to remain unresolved, deciding whether to:• take the concern to a higher authority, informing the manager; or • implement other dispute resolution mechanisms; and
6. Maintaining a record of actions taken.
(Adapted from CNO materials)
SummaryThese guidlines are presented to assist MRTs to provide safe, effective and ethical care.
If there are any questions, please feel free to contact the College of Medical Radiation Technologists of Ontario at (416) 975-4353 or toll-free at 1-800-563-5847.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 31
Page 60

cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 32
Page 61
2 • A U T H O R I Z E D A C T S
333333
2 • A U T H O R I Z E D A C T S
In this section the following topics will be covered:
Appendix A – Scope of practice statements for all regulated
health professions
Appendix B – 13 controlled acts
Appendix C – RHPA regulation defining the forms of enegy and
the controlled act of applying or ordering the
application of “energy”
Appendix D – Summary of controlled acts authorized to each
profession under the profession-specific Acts
Appendix E – Exceptions and Exemptions under RHPA
Appendix F – Orders for treatment
Appendix G – Decision-making guide for determining the
appropriateness of accepting delegation and
performing services or procedures beyond principal
expectations of MRT practice
Appendices
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 33
Page 62
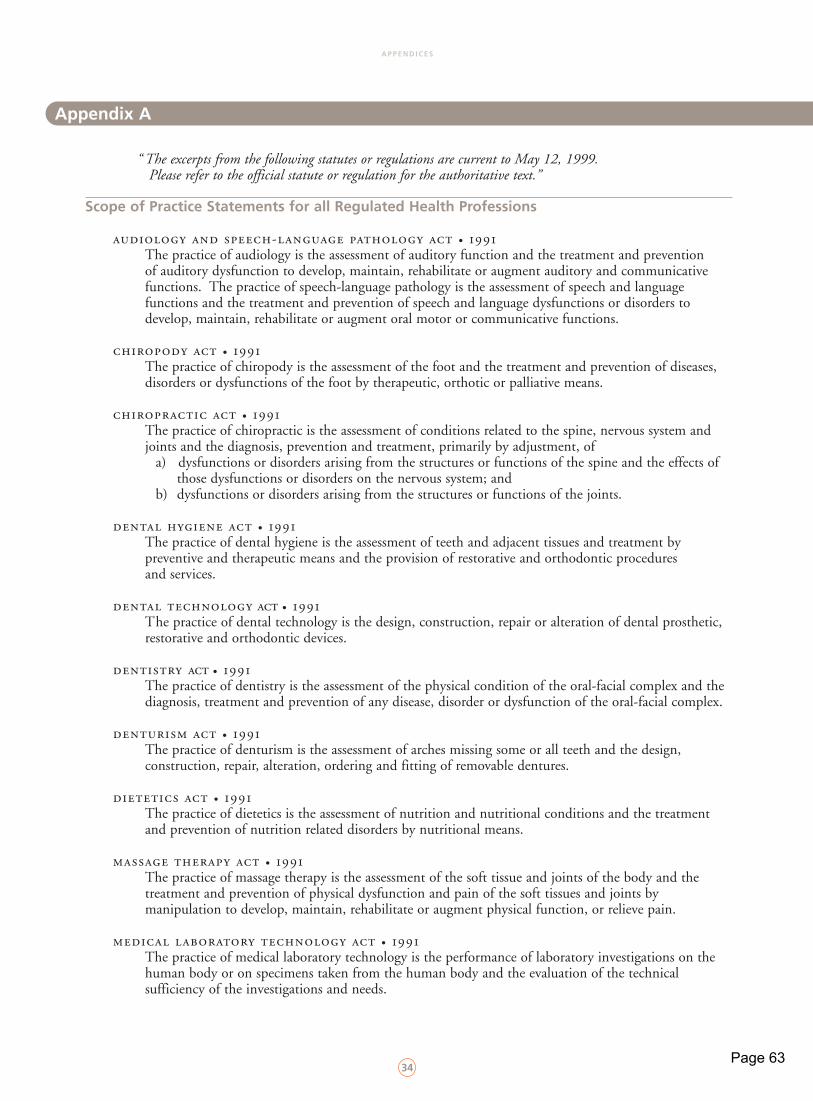
A P P E N D I C E S
34
“ The excerpts from the following statutes or regulations are current to May 12, 1999. Please refer to the official statute or regulation for the authoritative text.”
Scope of Practice Statements for all Regulated Health Professions
audiology and speech-language pathology act • 1991The practice of audiology is the assessment of auditory function and the treatment and prevention of auditory dysfunction to develop, maintain, rehabilitate or augment auditory and communicative functions. The practice of speech-language pathology is the assessment of speech and language functions and the treatment and prevention of speech and language dysfunctions or disorders to develop, maintain, rehabilitate or augment oral motor or communicative functions.
chiropody act • 1991The practice of chiropody is the assessment of the foot and the treatment and prevention of diseases, disorders or dysfunctions of the foot by therapeutic, orthotic or palliative means.
chiropractic act • 1991The practice of chiropractic is the assessment of conditions related to the spine, nervous system and joints and the diagnosis, prevention and treatment, primarily by adjustment, of
a) dysfunctions or disorders arising from the structures or functions of the spine and the effects of those dysfunctions or disorders on the nervous system; and
b) dysfunctions or disorders arising from the structures or functions of the joints.
dental hygiene act • 1991The practice of dental hygiene is the assessment of teeth and adjacent tissues and treatment by preventive and therapeutic means and the provision of restorative and orthodontic procedures and services.
dental technology act • 1991The practice of dental technology is the design, construction, repair or alteration of dental prosthetic, restorative and orthodontic devices.
dentistry act • 1991The practice of dentistry is the assessment of the physical condition of the oral-facial complex and the diagnosis, treatment and prevention of any disease, disorder or dysfunction of the oral-facial complex.
denturism act • 1991The practice of denturism is the assessment of arches missing some or all teeth and the design, construction, repair, alteration, ordering and fitting of removable dentures.
dietetics act • 1991The practice of dietetics is the assessment of nutrition and nutritional conditions and the treatment and prevention of nutrition related disorders by nutritional means.
massage therapy act • 1991The practice of massage therapy is the assessment of the soft tissue and joints of the body and the treatment and prevention of physical dysfunction and pain of the soft tissues and joints by manipulation to develop, maintain, rehabilitate or augment physical function, or relieve pain.
medical laboratory technology act • 1991The practice of medical laboratory technology is the performance of laboratory investigations on the human body or on specimens taken from the human body and the evaluation of the technical sufficiency of the investigations and needs.
Appendix A
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 34
Page 63
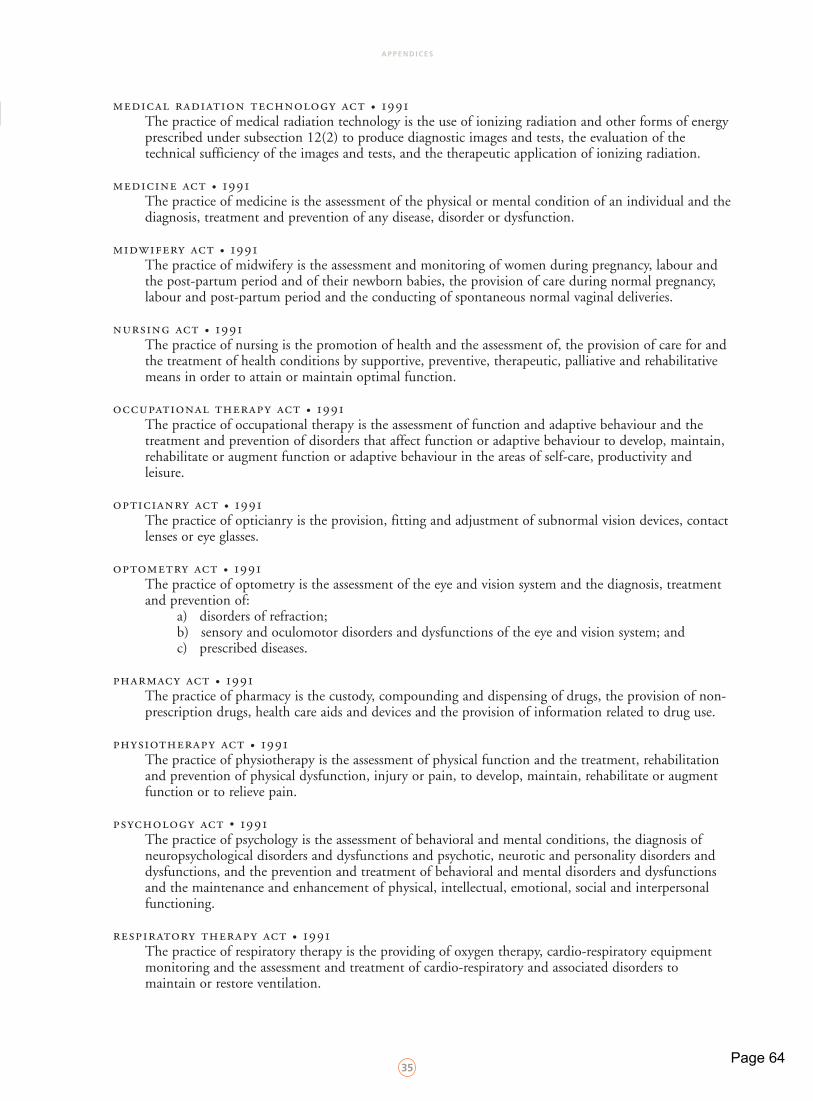
A P P E N D I C E S
35
medical radiation technology act • 1991The practice of medical radiation technology is the use of ionizing radiation and other forms of energy prescribed under subsection 12(2) to produce diagnostic images and tests, the evaluation of the technical sufficiency of the images and tests, and the therapeutic application of ionizing radiation.
medicine act • 1991The practice of medicine is the assessment of the physical or mental condition of an individual and thediagnosis, treatment and prevention of any disease, disorder or dysfunction.
midwifery act • 1991The practice of midwifery is the assessment and monitoring of women during pregnancy, labour and the post-partum period and of their newborn babies, the provision of care during normal pregnancy, labour and post-partum period and the conducting of spontaneous normal vaginal deliveries.
nursing act • 1991The practice of nursing is the promotion of health and the assessment of, the provision of care for and the treatment of health conditions by supportive, preventive, therapeutic, palliative and rehabilitative means in order to attain or maintain optimal function.
occupational therapy act • 1991The practice of occupational therapy is the assessment of function and adaptive behaviour and the treatment and prevention of disorders that affect function or adaptive behaviour to develop, maintain, rehabilitate or augment function or adaptive behaviour in the areas of self-care, productivity and leisure.
opticianry act • 1991The practice of opticianry is the provision, fitting and adjustment of subnormal vision devices, contact lenses or eye glasses.
optometry act • 1991The practice of optometry is the assessment of the eye and vision system and the diagnosis, treatment and prevention of:
a) disorders of refraction;b) sensory and oculomotor disorders and dysfunctions of the eye and vision system; andc) prescribed diseases.
pharmacy act • 1991The practice of pharmacy is the custody, compounding and dispensing of drugs, the provision of non-prescription drugs, health care aids and devices and the provision of information related to drug use.
physiotherapy act • 1991The practice of physiotherapy is the assessment of physical function and the treatment, rehabilitation and prevention of physical dysfunction, injury or pain, to develop, maintain, rehabilitate or augment function or to relieve pain.
psychology act • 1991The practice of psychology is the assessment of behavioral and mental conditions, the diagnosis of neuropsychological disorders and dysfunctions and psychotic, neurotic and personality disorders and dysfunctions, and the prevention and treatment of behavioral and mental disorders and dysfunctions and the maintenance and enhancement of physical, intellectual, emotional, social and interpersonal functioning.
respiratory therapy act • 1991The practice of respiratory therapy is the providing of oxygen therapy, cardio-respiratory equipment monitoring and the assessment and treatment of cardio-respiratory and associated disorders to maintain or restore ventilation.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 35
Page 64
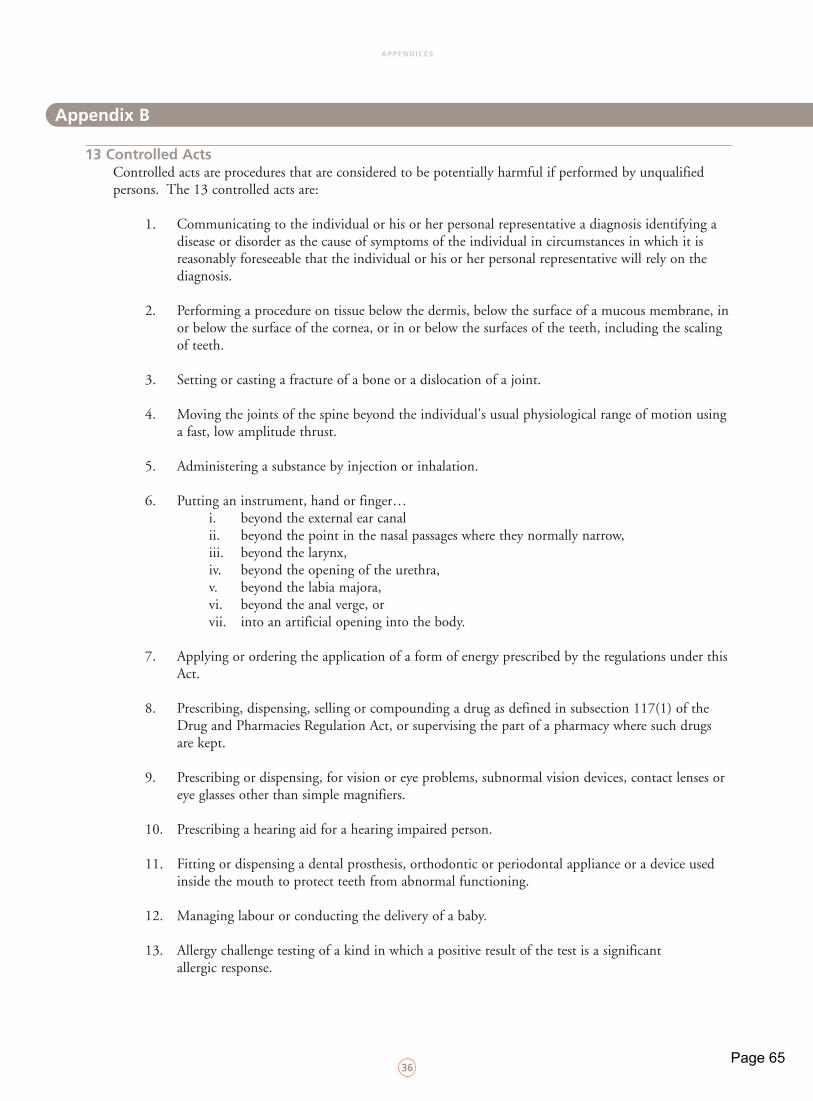
A P P E N D I C E S
36
13 Controlled ActsControlled acts are procedures that are considered to be potentially harmful if performed by unqualified persons. The 13 controlled acts are:
1. Communicating to the individual or his or her personal representative a diagnosis identifying a disease or disorder as the cause of symptoms of the individual in circumstances in which it is reasonably foreseeable that the individual or his or her personal representative will rely on the diagnosis.
2. Performing a procedure on tissue below the dermis, below the surface of a mucous membrane, inor below the surface of the cornea, or in or below the surfaces of the teeth, including the scaling of teeth.
3. Setting or casting a fracture of a bone or a dislocation of a joint.
4. Moving the joints of the spine beyond the individual's usual physiological range of motion using a fast, low amplitude thrust.
5. Administering a substance by injection or inhalation.
6. Putting an instrument, hand or finger…i. beyond the external ear canalii. beyond the point in the nasal passages where they normally narrow,iii. beyond the larynx,iv. beyond the opening of the urethra,v. beyond the labia majora,vi. beyond the anal verge, orvii. into an artificial opening into the body.
7. Applying or ordering the application of a form of energy prescribed by the regulations under this Act.
8. Prescribing, dispensing, selling or compounding a drug as defined in subsection 117(1) of the Drug and Pharmacies Regulation Act, or supervising the part of a pharmacy where such drugs are kept.
9. Prescribing or dispensing, for vision or eye problems, subnormal vision devices, contact lenses or eye glasses other than simple magnifiers.
10. Prescribing a hearing aid for a hearing impaired person.
11. Fitting or dispensing a dental prosthesis, orthodontic or periodontal appliance or a device used inside the mouth to protect teeth from abnormal functioning.
12. Managing labour or conducting the delivery of a baby.
13. Allergy challenge testing of a kind in which a positive result of the test is a significant allergic response.
Appendix B
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 36
Page 65
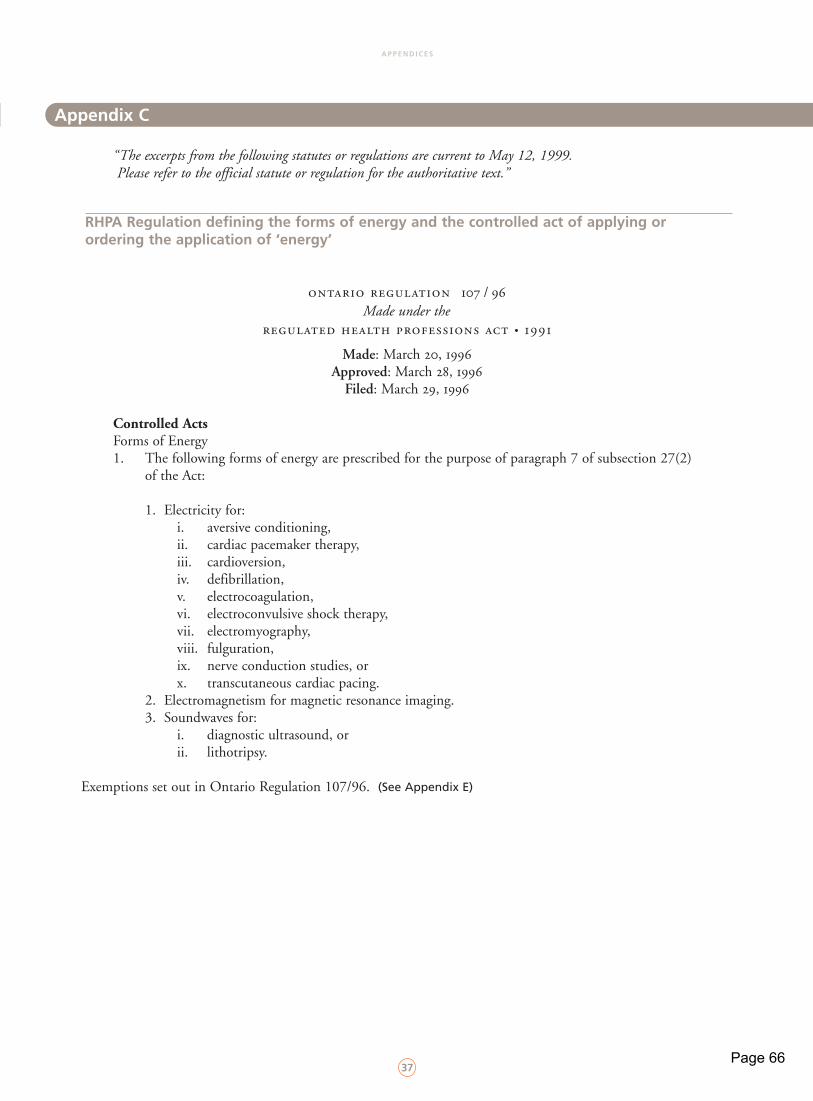
A P P E N D I C E S
37
“The excerpts from the following statutes or regulations are current to May 12, 1999. Please refer to the official statute or regulation for the authoritative text.”
RHPA Regulation defining the forms of energy and the controlled act of applying or ordering the application of ‘energy’
ontario regulation 107 / 96Made under the
regulated health professions act • 1991
Made: March 20, 1996Approved: March 28, 1996
Filed: March 29, 1996
Controlled ActsForms of Energy1. The following forms of energy are prescribed for the purpose of paragraph 7 of subsection 27(2)
of the Act:
1. Electricity for:i. aversive conditioning,ii. cardiac pacemaker therapy,iii. cardioversion,iv. defibrillation,v. electrocoagulation,vi. electroconvulsive shock therapy,vii. electromyography,viii. fulguration,ix. nerve conduction studies, orx. transcutaneous cardiac pacing.
2. Electromagnetism for magnetic resonance imaging.3. Soundwaves for:
i. diagnostic ultrasound, orii. lithotripsy.
Exemptions set out in Ontario Regulation 107/96. (See Appendix E)
Appendix C
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 37
Page 66
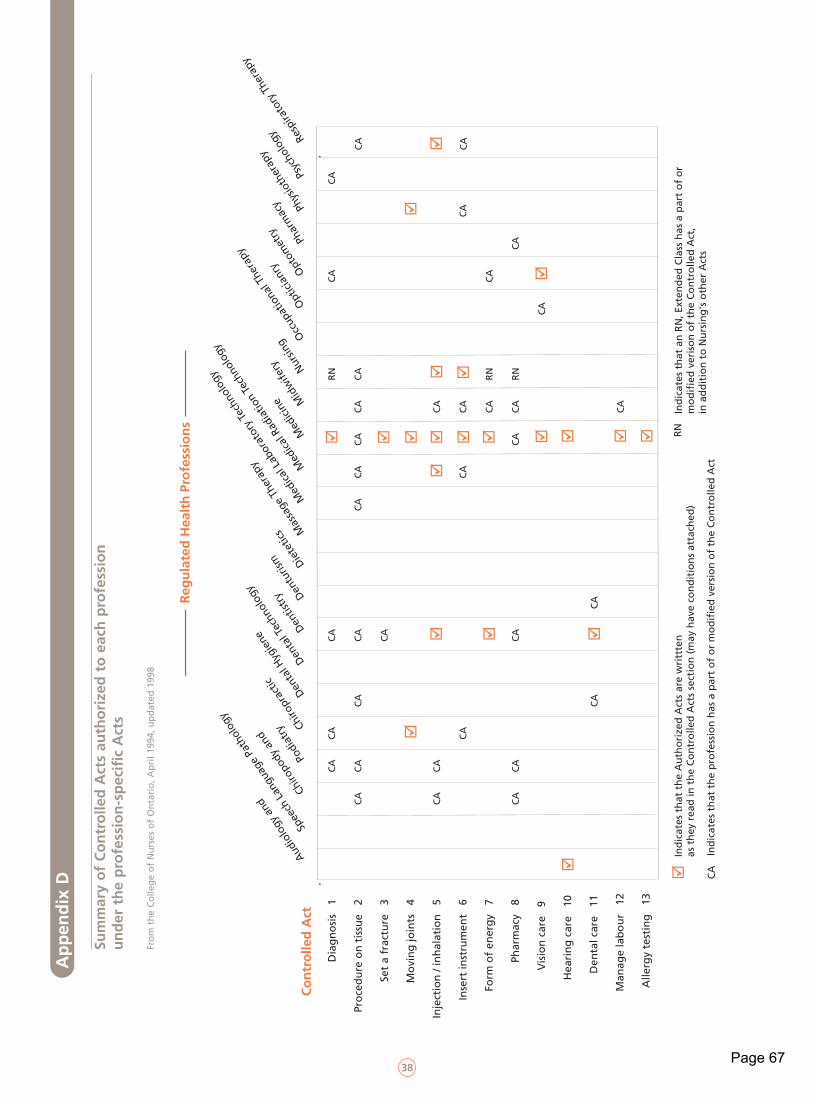
38
Dia
gn
osi
s 1
Pro
ced
ure
on
tis
sue
2
Set
a fr
actu
re
3
Mo
vin
g jo
ints
4
Inje
ctio
n /
inh
alat
ion
5
Inse
rt in
stru
men
t 6
Man
age
lab
ou
r 1
2
Alle
rgy
test
ing
13
Ind
icat
es t
hat
th
e A
uth
ori
zed
Act
s ar
e w
ritt
ten
as
th
ey r
ead
in t
he
Co
ntr
olle
d A
cts
sect
ion
(m
ay h
ave
con
dit
ion
s at
tach
ed)
Ind
icat
es t
hat
th
e p
rofe
ssio
n h
as a
par
t o
f o
r m
od
ifie
d v
ersi
on
of
the
Co
ntr
olle
d A
ct
Ind
icat
es t
hat
an
RN
, Ext
end
ed C
lass
has
a p
art
of
or
mo
dif
ied
ver
iso
n o
f th
e C
on
tro
lled
Act
, in
ad
dit
ion
to
Nu
rsin
g's
oth
er A
cts
Form
of
ener
gy
7
Phar
mac
y 8
Vis
ion
car
e 9
Hea
rin
g c
are
10
Den
tal c
are
11
Audi
olog
y an
d
Spe
ech
Lang
uage
Pat
holo
gy
Reg
ula
ted
Hea
lth
Pro
fess
ion
s
Chiro
pody
and
Podi
atry Ch
iropr
actic
Dent
al H
ygie
ne
Dent
istry
Dent
al T
echn
olog
y
Dent
urism Di
etet
ics
Mas
sage
The
rapy
Med
ical L
abor
ator
y Te
chno
logy
Med
ical R
adia
tion
Tech
nolo
gy
Med
icine M
idw
ifery
Nurs
ing
Occ
upat
iona
l The
rapy
Opt
ician
ry Opt
omet
ry Phar
mac
y Phys
ioth
erap
y
Resp
irato
ry T
hera
py
Psyc
holo
gy
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
CA
RN
CA
RN
RN
CA
CA
CA
CA
CA
CA
CA
CA
Co
ntr
olle
d A
ct
CA
RN
Ap
pen
dix
D
Sum
mar
y o
f C
on
tro
lled
Act
s au
tho
rize
d t
o e
ach
pro
fess
ion
u
nd
er t
he
pro
fess
ion
-sp
ecif
ic A
cts
Fro
m t
he
Co
lleg
e o
f N
urs
es o
f O
nta
rio
, Ap
ril 1
994,
up
dat
ed 1
998
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 38
Page 67
A P P E N D I C E S
39
Exceptions to Subsection 27(1) of RHPA
“The excerpt from the following statutes or regulations are current to May 12, 1999. Please refer to the official statute or regulation for the authoritative text.”
RHPA Section 29(1) and (2)
29(1) An act by a person is not a contravention of subsection 27(1) if it is done in the course of:a) rendering first aid or temporary assistance in an emergency;b) fulfilling the requirements to become a member of a health profession and the act is within the
scope of practice of the profession and is done under the supervision or direction of a member of the profession;
c) treating a person by prayer or spiritual means in accordance with the tenets of the religion of the person giving the treatment;
d) treating a member of the person's household and the act is a controlled act set out in paragraph 1, 5 or 6 of subsection 27(2); or
e) assisting a person with his or her routine activities of living and the act is a controlled act set out in paragraph 5 or 6 of subsection 27(2).
(2) Subsection 27(1) does not apply with respect to a communication made in the course of counseling about emotional, social, educational or spiritual matters as long as it is not a communication that a health profession Act authorizes members to make. 1991, c. 18, s. 29.
Exemptions to Subsection 27(1) of RHPA
“The excerpt from the following statutes or regulations are current to May 11, 1999. Please refer to the official statute or regulation for authoritative text.”
ontario regulation 107 / 96Made under the
regulated health professions act • 1991
Made: March 20, 1996Approved: March 28, 1996
Filed: March 29, 1996
Forms of Energy (See Appendix C)Exemptions
2. A member of the College of Chiropodists of Ontario is exempt from subsection 27(1) of the Act for the purpose of applying electricity for electrocoagulation or fulguration.
3. (1) A member of the Royal College of Dental Surgeons of Ontario is exempt from subsection 27(1) of the Act for the purpose of applying electricity for defibrillation or electrocoagulation.
(2) A member of the Royal College of Dental Surgeons of Ontario is exempt from subsection 27(1) of the Act for the purpose of applying electricity for electromyography or nerve conduction studies, in the course of conducting research.
4. A member of the College of Midwives of Ontario is exempt from subsection 27(1) of the Act for the purpose of ordering the application of soundwaves for pregnancy diagnostic ultrasound or pelvic diagnostic ultrasound.
Appendix E
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 39
Page 68
A P P E N D I C E S
40
5. (1) A member of the College of Physicians and Surgeons of Ontario is exempt from subsection 27(1) of the Act for the purpose of applying, or ordering the application of, electricity for a procedure listed in paragraph 1 of section 1 or soundwaves for a procedure listed in paragraph 3 of section 1.
(2) A member of the College of Physicians and Surgeons of Ontario is exempt from subsection 27(1) of the Act for the purpose of applying in a public hospital, or ordering the application in a public hospital of, electromagnetism for magnetic resonance imaging.
6. A member of the College of Psychologists of Ontario is exempt from subsection 27(1) of the Act for the purpose of applying, or ordering the application of, electricity for aversive conditioning.
7. A person is exempt from subsection 27(1) of the Act for the purpose of:a) applying soundwaves for diagnostic ultrasound if the application is ordered by a
member of the College of Physicians and Surgeons of Ontario;b) applying soundwaves for pregnancy diagnostic ultrasound or pelvic diagnostic ultrasound
if the application is ordered by a member of the College of Midwives of Ontario;c) applying electromagnetism for magnetic resonance imaging in a public hospital if the
application is ordered by a member of the College of Physicians and Surgeons of Ontario; and
d) applying electricity for aversive conditioning if the application is ordered and directed by a member of the College of Physicians and Surgeons of Ontario or by a member of the College of Psychologists of Ontario.
8. The following activities are exempt from subsection 27(1) of the Act:1. Acupuncture.2. Ear or body piercing for the purpose of accommodating a piece of jewelry.3. Electrolysis.4. Tattooing for cosmetic purposes.
9. Male circumcision is an activity that is exempt from subsection 27(1) of the Act if the circumcision is performed as part of a religious tradition or ceremony.
10. A naturopath is exempt from subsection 27(1) of the Act for the purpose of carrying on, in accordance with the Drugless Practitioners Act and the regulations under that Act, activities that are within the scope of the practice of naturopathy.
11. The taking of a blood sample from a vein or by skin pricking is an activity that is exempt from subsection 27(1) of the Act if the person taking the blood sample is employed by a laboratory or specimen collection centre licensed under the Laboratory and Specimen Collection Centre Licensing Act.
12. (1) A medical geneticist who holds a doctorate is exempt from subsection 27(1) of the Act for the purpose of communicating to an individual or his or her personal representative a diagnosis identifying a genetic disease or genetic disorder as the cause of the symptoms of the individual in circumstances in which it is reasonably foreseeable that the individual or his or her personal representative will rely on the diagnosis, if,
a) the disease or disorder identified is within the geneticist's area of expertise; andb) the geneticist is employed by a university or a health care facility and the
communication of the diagnosis is performed in accordance with the university's or facility's guidelines or protocols.
(2) In this section “health care facility” means a facility governed by or funded under an Act set out in the Schedule.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 40
Page 69
A P P E N D I C E S
41
13. A member of the College of Nurses of Ontario who holds a general certificate of registration as a registered nurse is exempt from subsection 27(1) of the Act for the purpose of prescribing a solution ofnormal saline (0.9 per cent) for venipuncture performed to establish peripheral intravenous access and maintain patency.
“ The excerpt from the following statutes or regulations are current to May 12, 1999. Please refer to the official statute or regulation for the authoritative text.”
Orders for Treatment - Section 24 of the Public Hospitals ActMade under the Public Hospitals Act, 1990, Ontario Regulation 965/98
24 (1) Every order for treatment or a diagnostic procedure of a patient shall, except as provided in subsection (2), be in writing and shall,
a) in the case of an order for treatment, be dated and authenticated by the physician, dentist or midwife giving the order; and
b) in the case of an order for a diagnostic procedure, be dated and authenticated by the physician, dentist, midwife or registered nurse in the extended class giving the order.
ont . reg. 518/88, s. 23, part ont . reg. 761/93, s. 11, part ont . reg. 45/98, s. 9(1)
(2) A physician, dentist or midwife may dictate an order for treatment or for a diagnostic procedure by telephone to a person designated by the administrator to take such orders and a registered nurse in the extended class may dictate an order for a diagnostic procedure by telephone to any such person.
ont . reg. 518/88, s. 23, part ont . reg. 761/93, s. 11, part ont . reg. 45/98, s. 9(2)
(3) Where an order for treatment or for a diagnostic procedure has been dictated by telephone,a) the person to whom the order was dictated shall transcribe the order, the name of the physician,
dentist, midwife or registered nurse in the extended class who dictated the order, the date and the time of receiving the order and shall authenticate the transcription; and
b) the physician, dentist, midwife or registered nurse in the extended class who dictated the order shall authenticate the order on the first visit to the hospital after dictating the order.
ont . reg. 518/88, s. 23, part ont . reg. 761/93, s. 11, part ont . reg. 45/98, s. 9(3,4)
Schedule1. Alcoholism and Drug Addiction Research
Foundation Act2. Cancer Act3. Charitable Institutions Act4. Child and Family Services Act5. Community Psychiatric Hospitals Act6. Developmental Services Act 7. General Welfare Assistance Act8. Homes for Retarded Persons Act9. Homes for Special Care Act10. Homes for the Aged and Rest Homes Act
11. Independent Health Facilities Act12. Mental Health Act13. Mental Hospitals Act14. Ministry of Community and Social
Services Act15. Ministry of Correctional Services Act16. Ministry of Health Act17. Nursing Homes Act18. Ontario Mental Health Foundation Act19. Private Hospitals Act20. Public Hospitals Act
Appendix F
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 41
Page 70
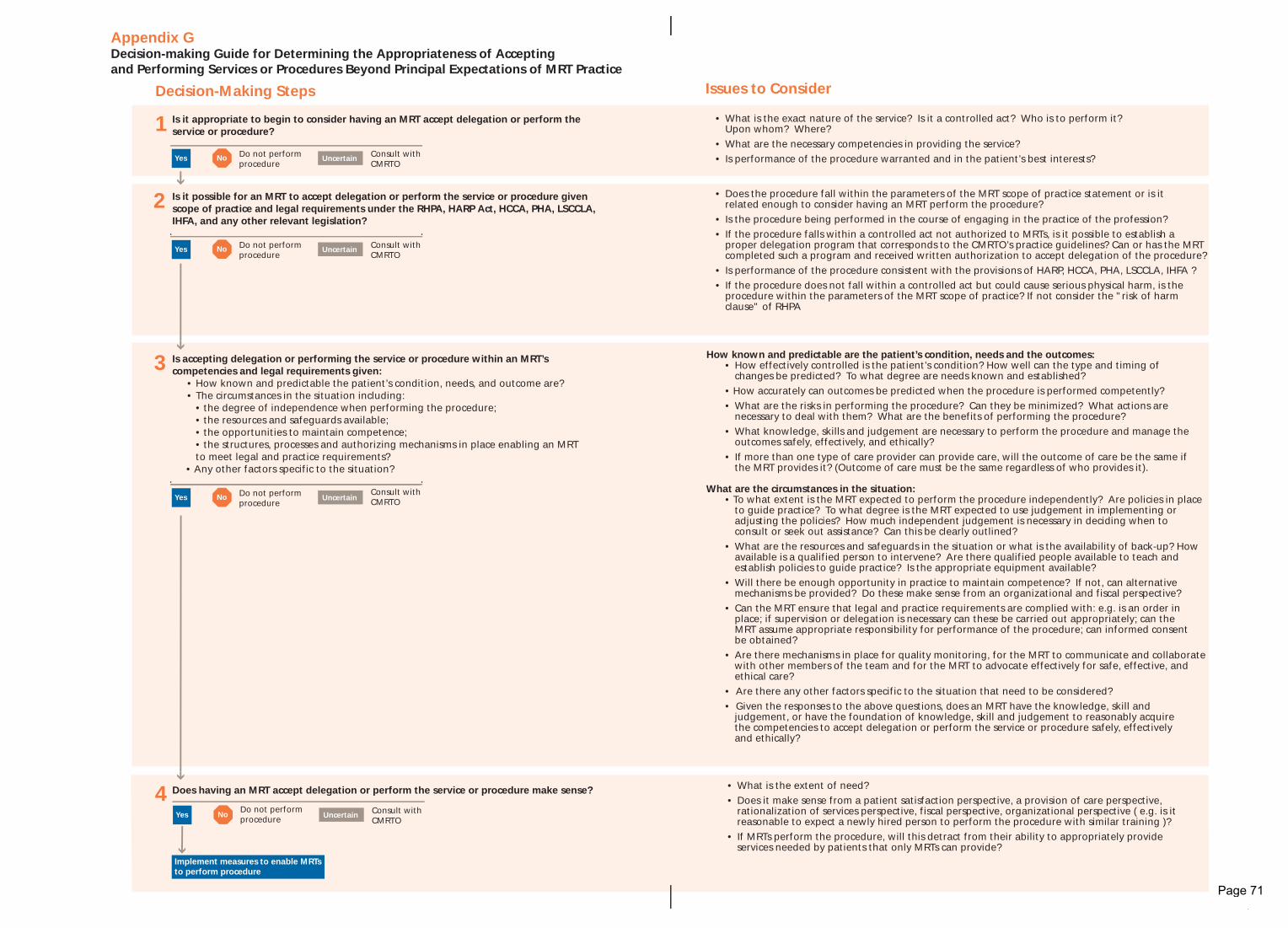
Issues to Consider
• What is the exact nature of the service? Is it a controlled act? Who is to perform it? Upon whom? Where?
• What are the necessary competencies in providing the service?• Is performance of the procedure warranted and in the patient’s best interests?
• Does the procedure fall within the parameters of the MRT scope of practice statement or is it
related enough to consider having an MRT perform the procedure? • Is the procedure being performed in the course of engaging in the practice of the profession?• If the procedure falls within a controlled act not authorized to MRTs, is it possible to establish a
proper delegation program that corresponds to the CMRTO’s practice guidelines? Can or has the MRT completed such a program and received written authorization to accept delegation of the procedure?
• Is performance of the procedure consistent with the provisions of HARP, HCCA, PHA, LSCCLA, IHFA ?• If the procedure does not fall within a controlled act but could cause serious physical harm, is the
procedure within the parameters of the MRT scope of practice? If not consider the "risk of harm clause" of RHPA
How known and predictable are the patient’s condition, needs and the outcomes: • How effectively controlled is the patient’s condition? How well can the type and timing of
changes be predicted? To what degree are needs known and established? • How accurately can outcomes be predicted when the procedure is performed competently? • What are the risks in performing the procedure? Can they be minimized? What actions are
necessary to deal with them? What are the benefits of performing the procedure? • What knowledge, skills and judgement are necessary to perform the procedure and manage the
outcomes safely, effectively, and ethically? • If more than one type of care provider can provide care, will the outcome of care be the same if
the MRT provides it? (Outcome of care must be the same regardless of who provides it).
What are the circumstances in the situation: • To what extent is the MRT expected to perform the procedure independently? Are policies in place
to guide practice? To what degree is the MRT expected to use judgement in implementing or adjusting the policies? How much independent judgement is necessary in deciding when to consult or seek out assistance? Can this be clearly outlined?
• What are the resources and safeguards in the situation or what is the availability of back-up? How available is a qualified person to intervene? Are there qualified people available to teach and establish policies to guide practice? Is the appropriate equipment available?
• Will there be enough opportunity in practice to maintain competence? If not, can alternative mechanisms be provided? Do these make sense from an organizational and fiscal perspective?
• Can the MRT ensure that legal and practice requirements are complied with: e.g. is an order in place; if supervision or delegation is necessary can these be carried out appropriately; can the MRT assume appropriate responsibility for performance of the procedure; can informed consent be obtained?
• Are there mechanisms in place for quality monitoring, for the MRT to communicate and collaborate with other members of the team and for the MRT to advocate effectively for safe, effective, and ethical care?
• Are there any other factors specific to the situation that need to be considered? • Given the responses to the above questions, does an MRT have the knowledge, skill and
judgement, or have the foundation of knowledge, skill and judgement to reasonably acquire the competencies to accept delegation or perform the service or procedure safely, effectively and ethically?
• What is the extent of need? • Does it make sense from a patient satisfaction perspective, a provision of care perspective,
rationalization of services perspective, fiscal perspective, organizational perspective ( e.g. is it reasonable to expect a newly hired person to perform the procedure with similar training )?
• If MRTs perform the procedure, will this detract from their ability to appropriately provide services needed by patients that only MRTs can provide?
Does having an MRT accept delegation or perform the service or procedure make sense?
Is it appropriate to begin to consider having an MRT accept delegation or perform the service or procedure?
Is it possible for an MRT to accept delegation or perform the service or procedure given scope of practice and legal requirements under the RHPA, HARP Act, HCCA, PHA, LSCCLA, IHFA, and any other relevant legislation?
Decision-Making Steps
Appendix G Decision-making Guide for Determining the Appropriateness of Accepting and Performing Services or Procedures Beyond Principal Expectations of MRT Practice
Is accepting delegation or performing the service or procedure within an MRT’s competencies and legal requirements given:
• How known and predictable the patient’s condition, needs, and outcome are?• The circumstances in the situation including:
• the degree of independence when performing the procedure; • the resources and safeguards available; • the opportunities to maintain competence; • the structures, processes and authorizing mechanisms in place enabling an MRT
to meet legal and practice requirements? • Any other factors specific to the situation?
1
2
3
4
No UncertainYes Do not perform procedure
Consult with CMRTO
No UncertainYes Do not perform procedure
Consult with CMRTO
No UncertainYesDo not perform procedure
Implement measures to enable MRTs to perform procedure
Consult with CMRTO
No UncertainYes Do not perform procedure
Consult with CMRTO
CMADFA~1.QXD 6/28/04 5:19 PM Page 4
Page 71
A P P E N D I C E S
43
List of acronyms
CMRTO College of Medical Radiation Technologists of Ontario
CNO College of Nurses of Ontario
CPSO College of Physicians and Surgeons of Ontario
DH Dental Hygienists
HARP Act Healing Arts Radiation Protection Act
HCCA Health Care Consent Act
IHFA Independent Health Facilities Act
IHF Independent Health Facility
IVP Intravenous Pyelogram
LSCCLA Laboratory and Specimen Collection Centre Licensing Act
MLT Medical Laboratory Technologist
MRT Medical Radiation Technologist
MRTA Medical Radiation Technology Act
OHA Ontario Hospital Association
PHA Public Hospitals Act
RHPA Regulated Health Professions Act
RN Registered Nurse
RNEC Registered Nurse, Extended Class
RPN Registered Practical Nurse
RT Respiratory Therapist
Glossary
Accountability:means being responsible for one’s decisions and actions, including those undertaken independently or collectively as a member of a team. This means that MRTs must accept the consequences of their decisions and actions and act on the basis of what they, in their clinical judgement, believe is in the best interests of the patient. MRTs must take appropriate action if they feel these interests are being unnecessarily and unacceptably compromised. This includes refusing to implement ordered procedures or treatment plans that, from the MRT’s perspective, appear to be contraindicated, and taking appropriate action to address the situation.
Competent: means having the necessary knowledge, skills and judgement to perform safely, effectively and ethically and applying that knowledge, skill and judgement to ensure safe, effective and ethical outcomes for the patient. MRTs must maintain current competence in their area of practice and, if not competent, refrain from acting and take appropriate action to address the situation.
Circumstances in the Situation: refers to those factors related to the patient and the environment, which affect one’s ability to perform an act safely and effectively. They include, but are not limited to, the patient's condition, the predictability of the outcomes of performing the procedure, the known risks and benefits to the patient, the patient's wishes, and the safeguards and resources available.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 43
Page 72
A P P E N D I C E S
44
College or Regulatory Body: is the organization responsible for governing a health profession under the Regulated Health Professions Act. For medical radiation technologists in Ontario, the governing body is the College of Medical Radiation Technologists of Ontario (CMRTO).
Controlled Acts: are the 13 procedures, listed in the RHPA, deemed to pose risk of physical harm to the public if performed by unqualified persons. Controlled act procedures can only be performed if the authority isgiven under a specific health profession Act or if the authority is delegated. The 13 controlled acts are listed in Appendix B.
Authorized Act: is a controlled act procedure, or a portion of a controlled act procedure, that is authorized to a specific profession to perform under the appropriate health profession Act. MRTs are permitted to perform the following authorized acts if there is an order in place from a physician:
1. Taking blood samples from veins;2. Administering substances by injection or inhalation;3. Administering contrast media through or into the rectum or an artificial opening into
the body; and4. Tattooing.
Delegated Act:a controlled act procedure, that is performed under the authority of delegation.
Delegation: is the transfer of authority from a member of a regulated profession, authorized by the specific health profession Act under RHPA to perform a controlled act procedure, to someone who is not authorized (another regulated health professional or an unregulated person). Delegation does not refer to instances when an MRT is authorized by the Medical Radiation Technology Act (MRTA) to perform acontrolled act on the order of a physician. In this case, no transfer of authority is required; the medicalradiation technologist has the authority to carry out the controlled act procedure on the condition of an order.
Exceptions and Exemptions: specific circumstances listed either in the regulations under the RHPA or in the RHPA, respectively, identifying when someone who is not authorized under subsection 27(1), may perform a controlled actprocedure and not be in contravention of the legislation. For the list of exceptions and exemptions, see Appendix E.
Medical Radiation Technology (MRT) Scope of Practice: “The practice of medical radiation technology is the use of ionizing radiation and other forms ofenergy prescribed under subsection 12(2) of the RHPA to produce diagnostic images and tests, the evaluation of the technical sufficiency of the images and tests, and the therapeutic application ofionizing radiation” (MRTA).
The three medical radiation technology specialties are:• Radiography• Radiation Therapy• Nuclear Medicine
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 44
Page 73
A P P E N D I C E S
45
Medical Radiation Technologist(s) (MRT or MRTs): member(s) of the College of Medical Radiation Technologists of Ontario. The title “medical radiation technologist” is a protected title and may only be used by those registered with the College of Medical Radiation Technologists of Ontario. The titles Medical Radiation Technologist - Radiography, or M.R.T.(R.), Medical Radiation Technologist - Radiation Therapist or M.R.T.(T.) and Medical Radiation Technologist - Nuclear Medicine, or M.R.T.(N.) are also protected. Previous titles, such as radiological technician, radiographer or radiological technologist no longer apply.
Order: an authorizing statement from a regulated health professional with prescribing authority permitting an MRT to implement a procedure. Under the MRTA, an order from a physician is necessary to permit MRTs to implement authorized act procedures. Under the HARP Act, an order from a physician, dentist, chiropractor, designated chiropodist, osteopath or, under some circumstances, a nurse who holds an extended certificate of registration, is necessary to permit MRTs to apply or administer ionizing radiation.
An order may also be known as a:• Prescription• Requisition• Request for consultation• Doctor’s note
An order may be one of two types:• Direct order (for one specific patient)• Directive or protocol (for a number of patients under specific circumstances)
An order may also be used to prompt performance of a procedure that is neither a controlled act nor ionizing radiation, but falls within patient procedures or treatments (e.g. taking blood pressure).
Principal Expectations of Practice:refers to services and procedures that clearly fall within the scope of practice for MRTs. It includes those taught in MRT entry level programs where students are provided with the knowledge base and clinical practice to perform them competently. It also includes those services and procedures which MRTs acquire competence to perform, by expanding on the foundation of knowledge, skills and judgement obtained in entry level programs through formal or informal education, clinical experience or on-the-job training as a graduate MRT. Examples of “expanded” services or procedures that fall within principal expectations of practice would include mammography, CT scan and cardiac stress testing. Services or procedures beyond principal expectations of practice are at the outer limits of or outside the MRT scope of practice. In some instances, they may be at the outer limits because they areconfined to highly specialized areas; for example, the performance of haemodynamics. In other instances, very few patients require the services or procedures; for example, the administration ofstrontium-89 treatments for palliative relief of bony metastases in patients with prostate cancer.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 45
Page 74
AcknowledgementsCreated by: Paula May Ponesse – Consultant, Health Care Policy and PracticeEdited by: Sharon Saberton – Registrar, College of Medical Radiation Technologists of OntarioDesigned by: Crescent Design Consultants Thanks to the College of Nurses of Ontario for its support and for the use of its materials.
cmrto - comprhensive.ins.qxd 6/25/04 5:58 AM Page 46
Page 75
Appendix 2
Competency Prof i les
Tab Title Page No.
1 Radiation Therapy 1
2 Nuclear Medicine 65
3 Radiological Technology (Radiography) 125
4 Magnetic Resonance 171

November 2006 Revised Feb 2008 (#29232)
Radiation Therapy
COMPETENCY PROFILE November 2006
Revised February 2008
Revised Profile for use with the development of the
September 2011 Certification exams
Prepared by the Radiation Therapy Competency Profile Task Group
© CANADIAN ASSOCIATION OF MEDICAL RADIATION TECHNOLOGISTS Suite 1000, 85 Albert Street, Ottawa, Ontario K1P 6A4
Tel: 1-800-463-9729 or (613) 234-0012 / Fax: (613) 234-1097 www.camrt.ca
Page 1

November 2006 Revised Feb 2008 (#29232)
© Copyright 2006 by Canadian Association of Medical Radiation Technologists All rights reserved. No part of this publication may be reproduced or transmitted in any form or by
any means, electronic or mechanical, including photocopy, recording, or any information storage or retrieval system, without the prior written permission of the Canadian Association of Medical Radiation Technologists.
Page 2
Nov 06
Revised Feb 2008 1
COMPETENCY PROFILE - RADIATION THERAPY Competencies for Entry Level Radiation Therapists This document describes the essential competencies required for an entry-level radiation therapist in Canada to provide best practice as defined by safe, competent and ethical practice of radiation therapy in a variety of clinical environments. The profile defines competencies reflecting the integration of knowledge, skills, attitudes and judgment necessary to practice in an environment that requires the therapist to use effective organizational skills and critical thinking. This requires the ability to assess, adapt, modify, analyse and evaluate in a variety of situations and environments in the practice of radiation therapy. Critical decision-making is, therefore, inherent to the practice of radiation therapy and is demonstrated in the competencies required of entry-to-practice therapists. The competency profile defines the standard for certification and registration of entry-level radiation therapists in Canada. The document is also used to: - provide direction to entry-level education programs to assist in developing curriculum; - inform Ministries of Health and Education of the standard expected from entry-level radiation
therapists; - inform the public and employers of the standard expected from entry-level radiation therapists; - assist CMA Conjoint Committee with accreditation of education programs; - provide guidance by identifying professional development needs for practicing radiation therapists - develop a blueprint for CAMRT certification examination. Accredited programs must ensure that their certification candidates possess all the competencies listed in the profile. Education programs are encouraged to include additional skills at their discretion. In the development of the competencies, the following assumptions have been made. That the Radiation Therapist: - has completed an accredited Canadian educational program, or is eligible for certification by another
recognized process; - has acquired the theoretical knowledge required to achieve a wide range of competencies; - has developed a broad knowledge base that has been assessed prior to the certification examination; - commits to the principle that their primary role and function is to serve the public interest; - is a member of the inter-professional health care team, collaborating with other health care
professionals to provide appropriate patient care in the planning and delivery of radiation therapy treatments;
- is responsible for the safe and effective application of ionizing radiation; - is responsible for the production, assessment, optimization and archiving of images; - is responsible for the performance of therapeutic planning and treatment procedures; - participates in interventional procedures; - is responsible for the education of patients, public and other health care providers regarding ionizing
radiation for medical use; - performs effectively encompassing physical, psychological, social, economic and cultural factors that
interact in predictable and unpredictable ways; - recognizes patients as unique individuals, treating them with dignity and respect;
Page 3
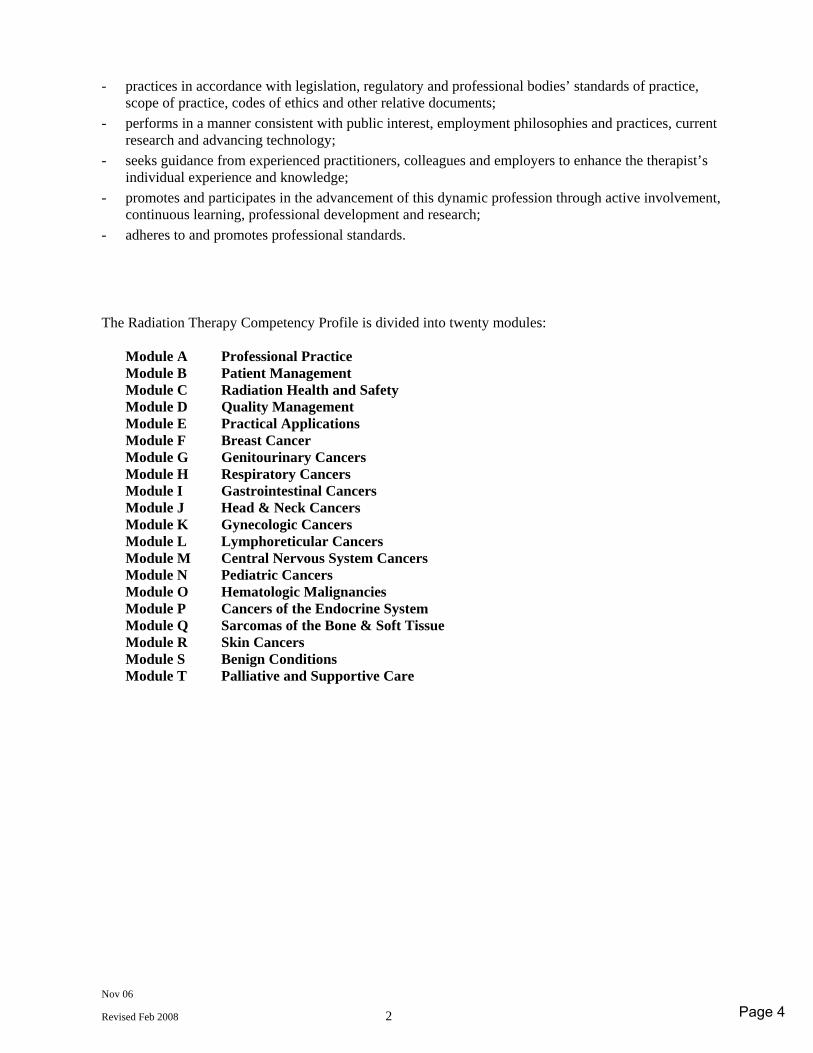
Nov 06
Revised Feb 2008 2
- practices in accordance with legislation, regulatory and professional bodies’ standards of practice, scope of practice, codes of ethics and other relative documents;
- performs in a manner consistent with public interest, employment philosophies and practices, current research and advancing technology;
- seeks guidance from experienced practitioners, colleagues and employers to enhance the therapist’s individual experience and knowledge;
- promotes and participates in the advancement of this dynamic profession through active involvement, continuous learning, professional development and research;
- adheres to and promotes professional standards. The Radiation Therapy Competency Profile is divided into twenty modules: Module A Professional Practice Module B Patient Management Module C Radiation Health and Safety Module D Quality Management Module E Practical Applications Module F Breast Cancer Module G Genitourinary Cancers Module H Respiratory Cancers Module I Gastrointestinal Cancers Module J Head & Neck Cancers Module K Gynecologic Cancers Module L Lymphoreticular Cancers Module M Central Nervous System Cancers Module N Pediatric Cancers Module O Hematologic Malignancies Module P Cancers of the Endocrine System Module Q Sarcomas of the Bone & Soft Tissue Module R Skin Cancers Module S Benign Conditions Module T Palliative and Supportive Care
Page 4
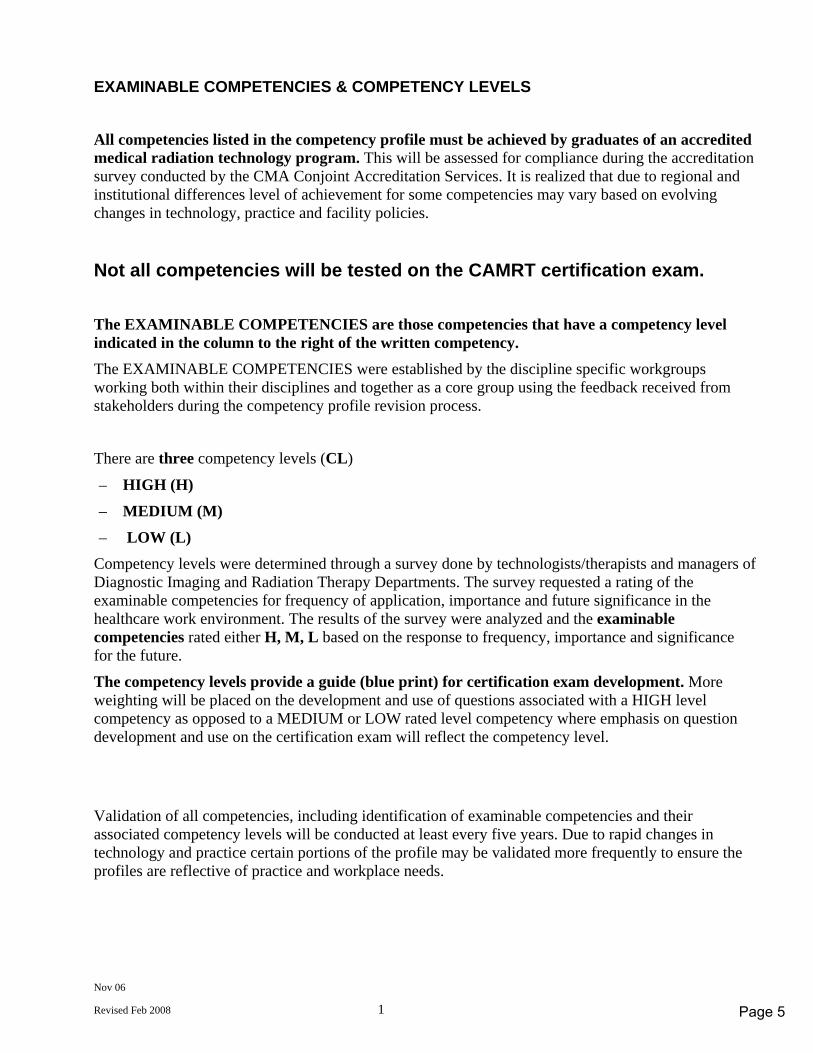
Nov 06
Revised Feb 2008 1
EXAMINABLE COMPETENCIES & COMPETENCY LEVELS
All competencies listed in the competency profile must be achieved by graduates of an accredited medical radiation technology program. This will be assessed for compliance during the accreditation survey conducted by the CMA Conjoint Accreditation Services. It is realized that due to regional and institutional differences level of achievement for some competencies may vary based on evolving changes in technology, practice and facility policies.
Not all competencies will be tested on the CAMRT certification exam.
The EXAMINABLE COMPETENCIES are those competencies that have a competency level indicated in the column to the right of the written competency. The EXAMINABLE COMPETENCIES were established by the discipline specific workgroups working both within their disciplines and together as a core group using the feedback received from stakeholders during the competency profile revision process.
There are three competency levels (CL)
– HIGH (H)
– MEDIUM (M)
– LOW (L) Competency levels were determined through a survey done by technologists/therapists and managers of Diagnostic Imaging and Radiation Therapy Departments. The survey requested a rating of the examinable competencies for frequency of application, importance and future significance in the healthcare work environment. The results of the survey were analyzed and the examinable competencies rated either H, M, L based on the response to frequency, importance and significance for the future.
The competency levels provide a guide (blue print) for certification exam development. More weighting will be placed on the development and use of questions associated with a HIGH level competency as opposed to a MEDIUM or LOW rated level competency where emphasis on question development and use on the certification exam will reflect the competency level.
Validation of all competencies, including identification of examinable competencies and their associated competency levels will be conducted at least every five years. Due to rapid changes in technology and practice certain portions of the profile may be validated more frequently to ensure the profiles are reflective of practice and workplace needs.
Page 5
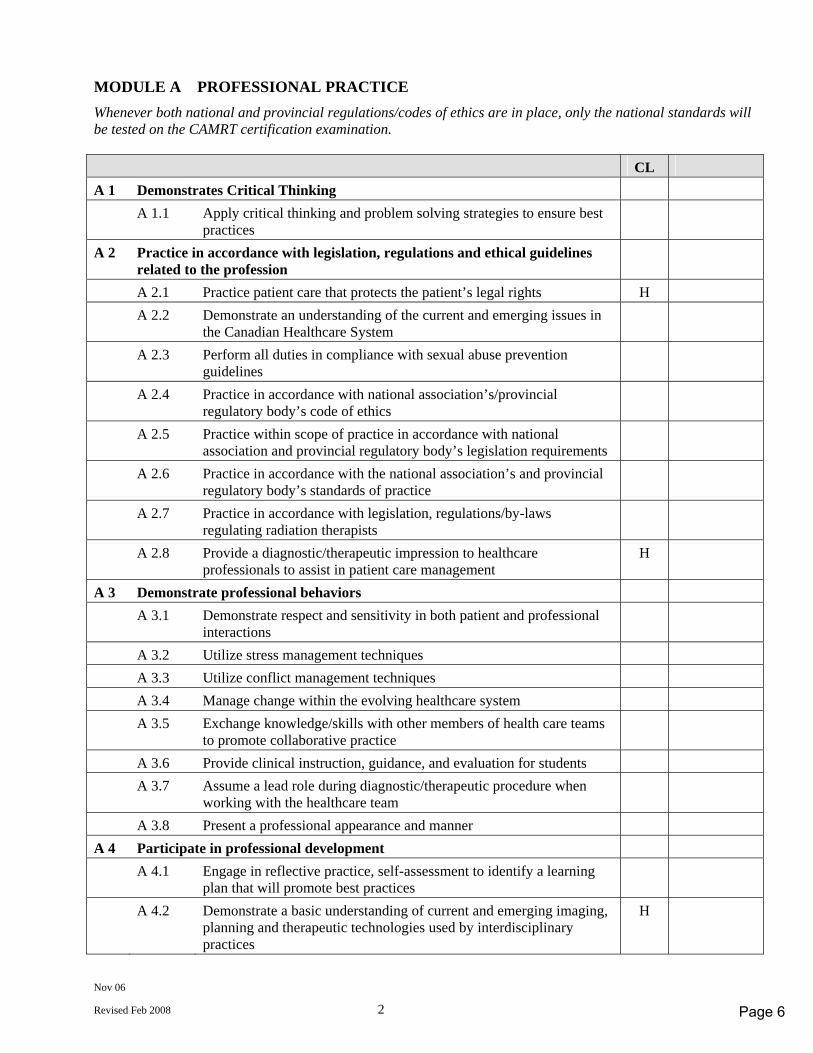
Nov 06
Revised Feb 2008 2
MODULE A PROFESSIONAL PRACTICE Whenever both national and provincial regulations/codes of ethics are in place, only the national standards will be tested on the CAMRT certification examination. CL A 1 Demonstrates Critical Thinking A 1.1 Apply critical thinking and problem solving strategies to ensure best
practices
A 2 Practice in accordance with legislation, regulations and ethical guidelines related to the profession
A 2.1 Practice patient care that protects the patient’s legal rights H A 2.2 Demonstrate an understanding of the current and emerging issues in
the Canadian Healthcare System
A 2.3 Perform all duties in compliance with sexual abuse prevention guidelines
A 2.4 Practice in accordance with national association’s/provincial regulatory body’s code of ethics
A 2.5 Practice within scope of practice in accordance with national association and provincial regulatory body’s legislation requirements
A 2.6 Practice in accordance with the national association’s and provincial regulatory body’s standards of practice
A 2.7 Practice in accordance with legislation, regulations/by-laws regulating radiation therapists
A 2.8 Provide a diagnostic/therapeutic impression to healthcare professionals to assist in patient care management
H
A 3 Demonstrate professional behaviors A 3.1 Demonstrate respect and sensitivity in both patient and professional
interactions
A 3.2 Utilize stress management techniques A 3.3 Utilize conflict management techniques A 3.4 Manage change within the evolving healthcare system A 3.5 Exchange knowledge/skills with other members of health care teams
to promote collaborative practice
A 3.6 Provide clinical instruction, guidance, and evaluation for students A 3.7 Assume a lead role during diagnostic/therapeutic procedure when
working with the healthcare team
A 3.8 Present a professional appearance and manner A 4 Participate in professional development A 4.1 Engage in reflective practice, self-assessment to identify a learning
plan that will promote best practices
A 4.2 Demonstrate a basic understanding of current and emerging imaging, planning and therapeutic technologies used by interdisciplinary practices
H
Page 6
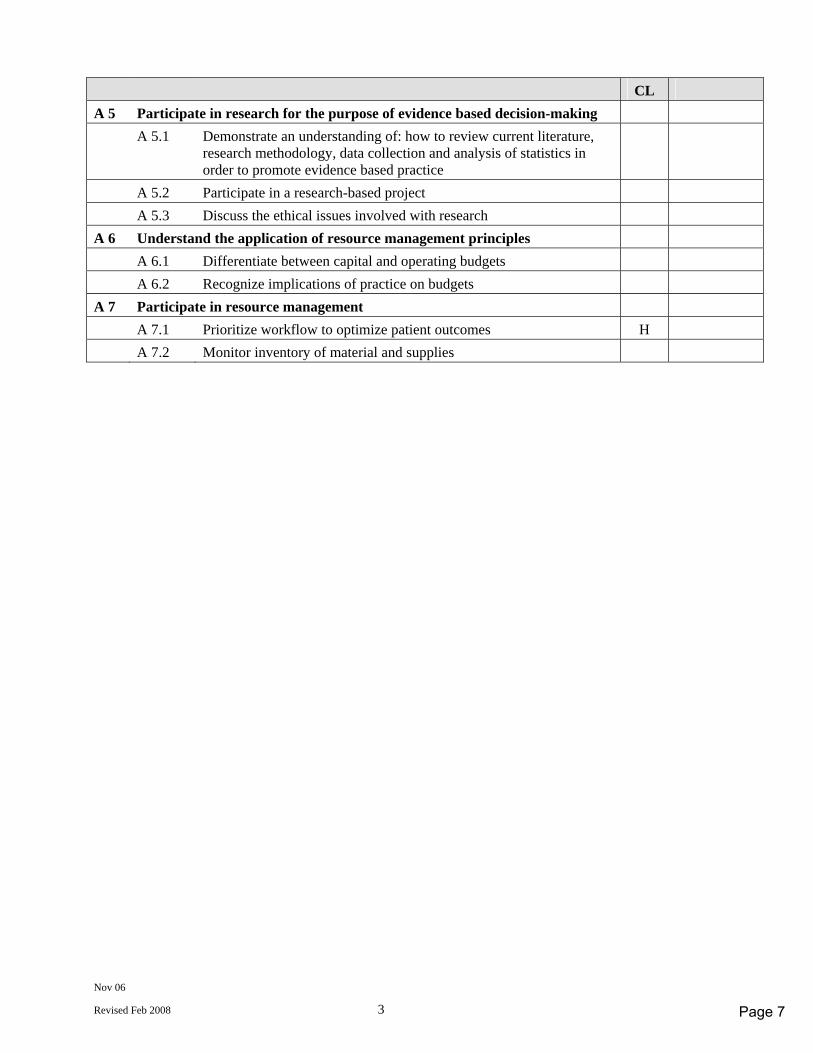
Nov 06
Revised Feb 2008 3
CL A 5 Participate in research for the purpose of evidence based decision-making A 5.1 Demonstrate an understanding of: how to review current literature,
research methodology, data collection and analysis of statistics in order to promote evidence based practice
A 5.2 Participate in a research-based project A 5.3 Discuss the ethical issues involved with research A 6 Understand the application of resource management principles A 6.1 Differentiate between capital and operating budgets A 6.2 Recognize implications of practice on budgets A 7 Participate in resource management A 7.1 Prioritize workflow to optimize patient outcomes H A 7.2 Monitor inventory of material and supplies
Page 7
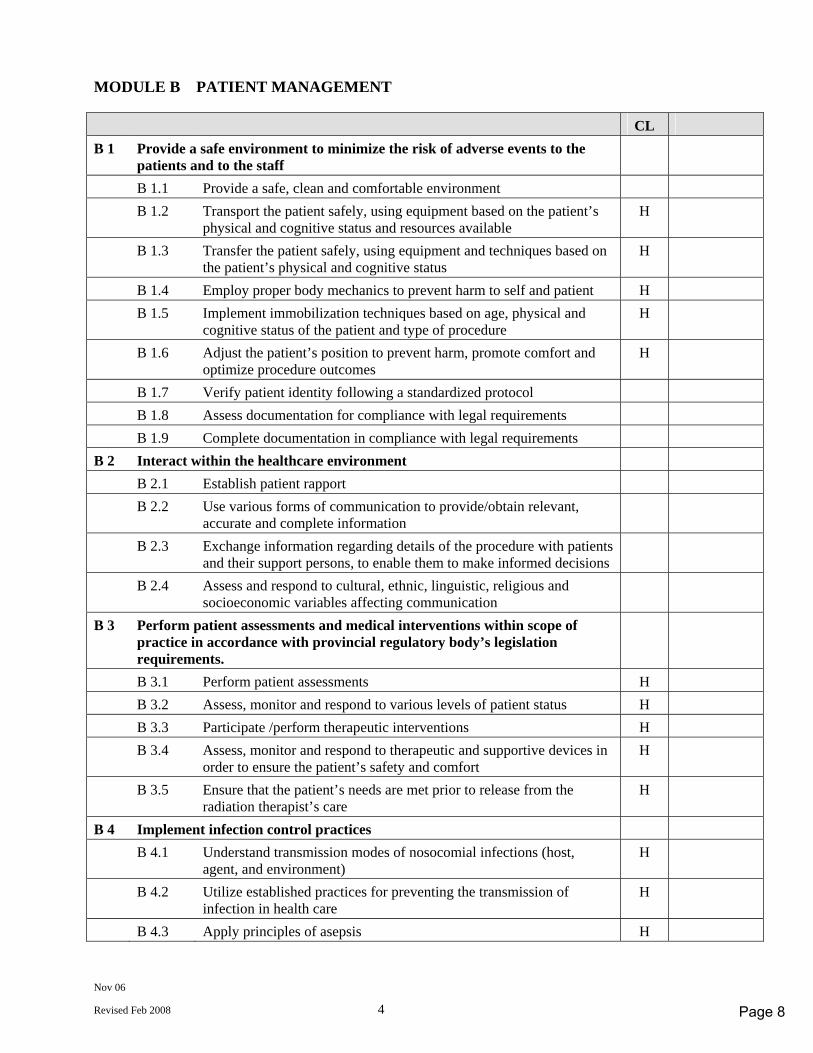
Nov 06
Revised Feb 2008 4
MODULE B PATIENT MANAGEMENT CL B 1 Provide a safe environment to minimize the risk of adverse events to the
patients and to the staff
B 1.1 Provide a safe, clean and comfortable environment B 1.2 Transport the patient safely, using equipment based on the patient’s
physical and cognitive status and resources available H
B 1.3 Transfer the patient safely, using equipment and techniques based on the patient’s physical and cognitive status
H
B 1.4 Employ proper body mechanics to prevent harm to self and patient H B 1.5 Implement immobilization techniques based on age, physical and
cognitive status of the patient and type of procedure H
B 1.6 Adjust the patient’s position to prevent harm, promote comfort and optimize procedure outcomes
H
B 1.7 Verify patient identity following a standardized protocol B 1.8 Assess documentation for compliance with legal requirements B 1.9 Complete documentation in compliance with legal requirements B 2 Interact within the healthcare environment B 2.1 Establish patient rapport B 2.2 Use various forms of communication to provide/obtain relevant,
accurate and complete information
B 2.3 Exchange information regarding details of the procedure with patients and their support persons, to enable them to make informed decisions
B 2.4 Assess and respond to cultural, ethnic, linguistic, religious and socioeconomic variables affecting communication
B 3 Perform patient assessments and medical interventions within scope of practice in accordance with provincial regulatory body’s legislation requirements.
B 3.1 Perform patient assessments H B 3.2 Assess, monitor and respond to various levels of patient status H B 3.3 Participate /perform therapeutic interventions H B 3.4 Assess, monitor and respond to therapeutic and supportive devices in
order to ensure the patient’s safety and comfort H
B 3.5 Ensure that the patient’s needs are met prior to release from the radiation therapist’s care
H
B 4 Implement infection control practices B 4.1 Understand transmission modes of nosocomial infections (host,
agent, and environment) H
B 4.2 Utilize established practices for preventing the transmission of infection in health care
H
B 4.3 Apply principles of asepsis H
Page 8
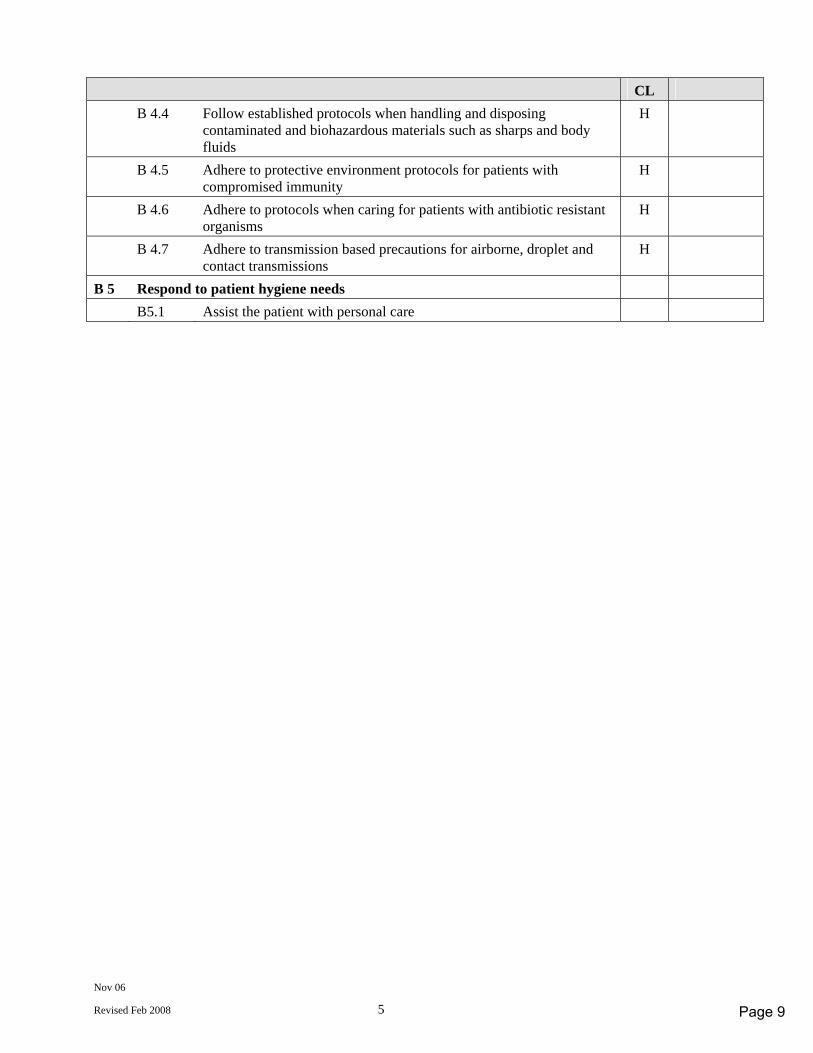
Nov 06
Revised Feb 2008 5
CL B 4.4 Follow established protocols when handling and disposing
contaminated and biohazardous materials such as sharps and body fluids
H
B 4.5 Adhere to protective environment protocols for patients with compromised immunity
H
B 4.6 Adhere to protocols when caring for patients with antibiotic resistant organisms
H
B 4.7 Adhere to transmission based precautions for airborne, droplet and contact transmissions
H
B 5 Respond to patient hygiene needs B5.1 Assist the patient with personal care
Page 9
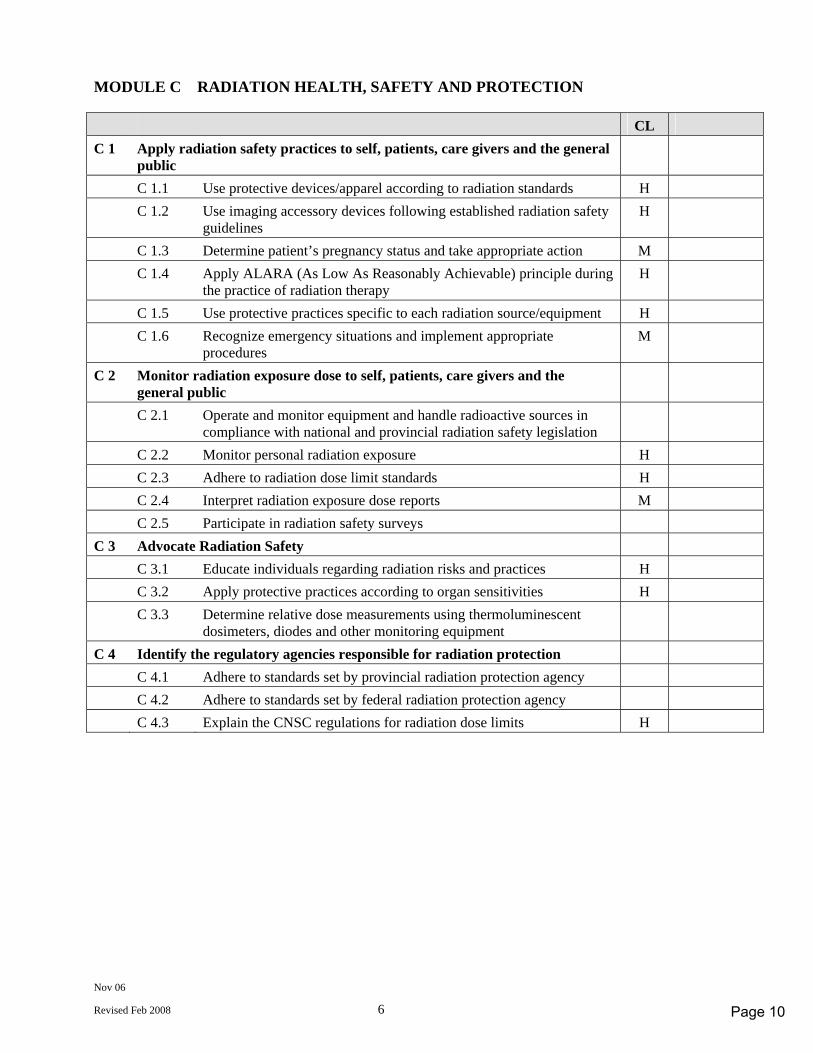
Nov 06
Revised Feb 2008 6
MODULE C RADIATION HEALTH, SAFETY AND PROTECTION CL C 1 Apply radiation safety practices to self, patients, care givers and the general
public
C 1.1 Use protective devices/apparel according to radiation standards H C 1.2 Use imaging accessory devices following established radiation safety
guidelines H
C 1.3 Determine patient’s pregnancy status and take appropriate action M C 1.4 Apply ALARA (As Low As Reasonably Achievable) principle during
the practice of radiation therapy H
C 1.5 Use protective practices specific to each radiation source/equipment H C 1.6 Recognize emergency situations and implement appropriate
procedures M
C 2 Monitor radiation exposure dose to self, patients, care givers and the general public
C 2.1 Operate and monitor equipment and handle radioactive sources in compliance with national and provincial radiation safety legislation
C 2.2 Monitor personal radiation exposure H C 2.3 Adhere to radiation dose limit standards H C 2.4 Interpret radiation exposure dose reports M C 2.5 Participate in radiation safety surveys C 3 Advocate Radiation Safety C 3.1 Educate individuals regarding radiation risks and practices H C 3.2 Apply protective practices according to organ sensitivities H C 3.3 Determine relative dose measurements using thermoluminescent
dosimeters, diodes and other monitoring equipment
C 4 Identify the regulatory agencies responsible for radiation protection C 4.1 Adhere to standards set by provincial radiation protection agency C 4.2 Adhere to standards set by federal radiation protection agency C 4.3 Explain the CNSC regulations for radiation dose limits H
Page 10
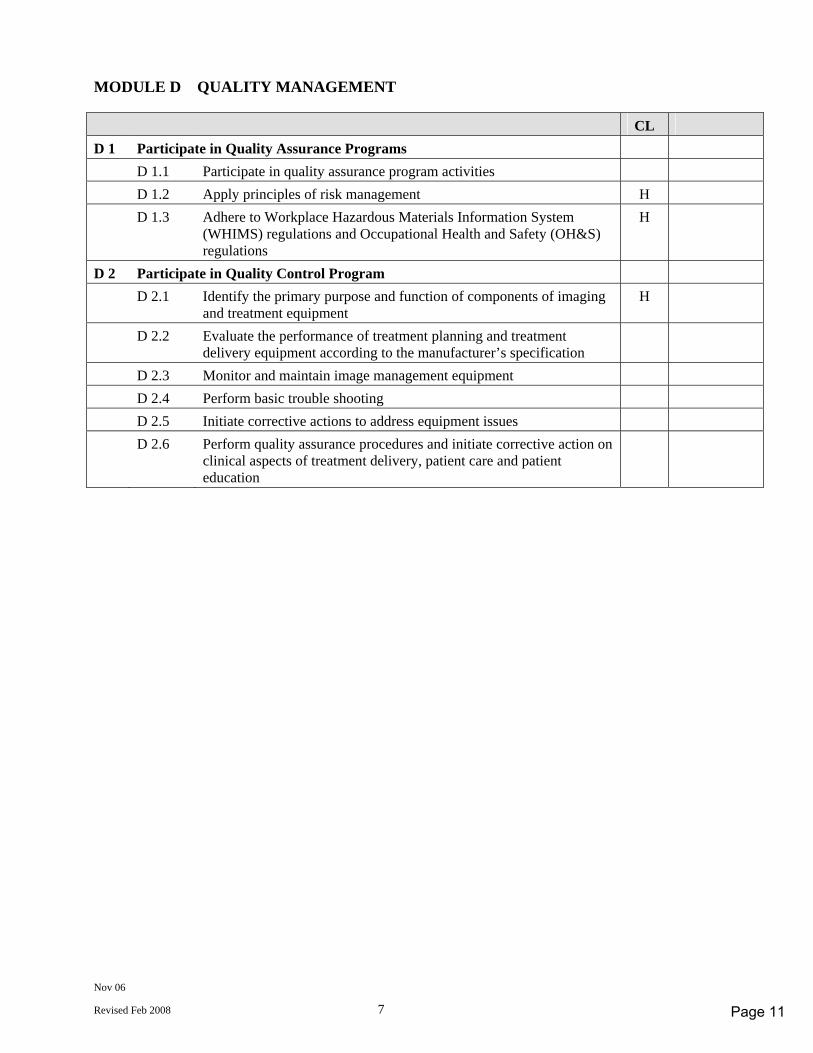
Nov 06
Revised Feb 2008 7
MODULE D QUALITY MANAGEMENT CL D 1 Participate in Quality Assurance Programs D 1.1 Participate in quality assurance program activities D 1.2 Apply principles of risk management H D 1.3 Adhere to Workplace Hazardous Materials Information System
(WHIMS) regulations and Occupational Health and Safety (OH&S) regulations
H
D 2 Participate in Quality Control Program D 2.1 Identify the primary purpose and function of components of imaging
and treatment equipment H
D 2.2 Evaluate the performance of treatment planning and treatment delivery equipment according to the manufacturer’s specification
D 2.3 Monitor and maintain image management equipment D 2.4 Perform basic trouble shooting D 2.5 Initiate corrective actions to address equipment issues D 2.6 Perform quality assurance procedures and initiate corrective action on
clinical aspects of treatment delivery, patient care and patient education
Page 11
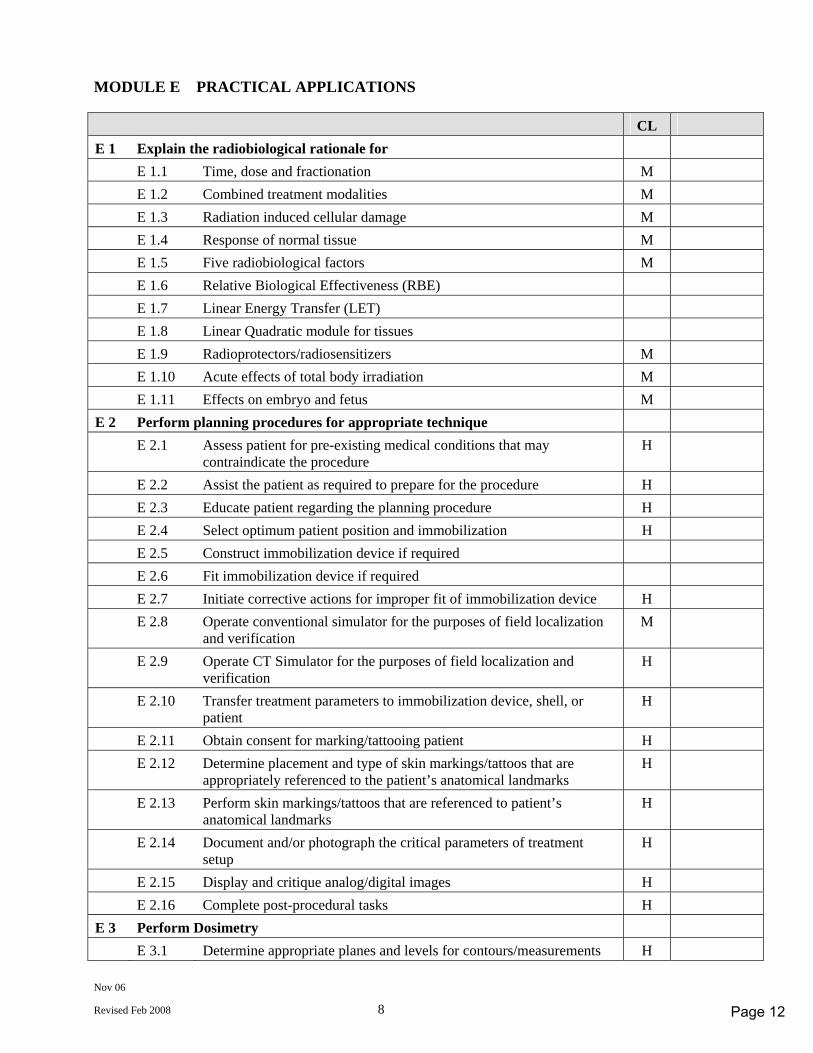
Nov 06
Revised Feb 2008 8
MODULE E PRACTICAL APPLICATIONS CL E 1 Explain the radiobiological rationale for E 1.1 Time, dose and fractionation M E 1.2 Combined treatment modalities M E 1.3 Radiation induced cellular damage M E 1.4 Response of normal tissue M E 1.5 Five radiobiological factors M E 1.6 Relative Biological Effectiveness (RBE) E 1.7 Linear Energy Transfer (LET) E 1.8 Linear Quadratic module for tissues E 1.9 Radioprotectors/radiosensitizers M E 1.10 Acute effects of total body irradiation M E 1.11 Effects on embryo and fetus M E 2 Perform planning procedures for appropriate technique E 2.1 Assess patient for pre-existing medical conditions that may
contraindicate the procedure H
E 2.2 Assist the patient as required to prepare for the procedure H E 2.3 Educate patient regarding the planning procedure H E 2.4 Select optimum patient position and immobilization H E 2.5 Construct immobilization device if required E 2.6 Fit immobilization device if required E 2.7 Initiate corrective actions for improper fit of immobilization device H E 2.8 Operate conventional simulator for the purposes of field localization
and verification M
E 2.9 Operate CT Simulator for the purposes of field localization and verification
H
E 2.10 Transfer treatment parameters to immobilization device, shell, or patient
H
E 2.11 Obtain consent for marking/tattooing patient H E 2.12 Determine placement and type of skin markings/tattoos that are
appropriately referenced to the patient’s anatomical landmarks H
E 2.13 Perform skin markings/tattoos that are referenced to patient’s anatomical landmarks
H
E 2.14 Document and/or photograph the critical parameters of treatment setup
H
E 2.15 Display and critique analog/digital images H E 2.16 Complete post-procedural tasks H E 3 Perform Dosimetry E 3.1 Determine appropriate planes and levels for contours/measurements H
Page 12
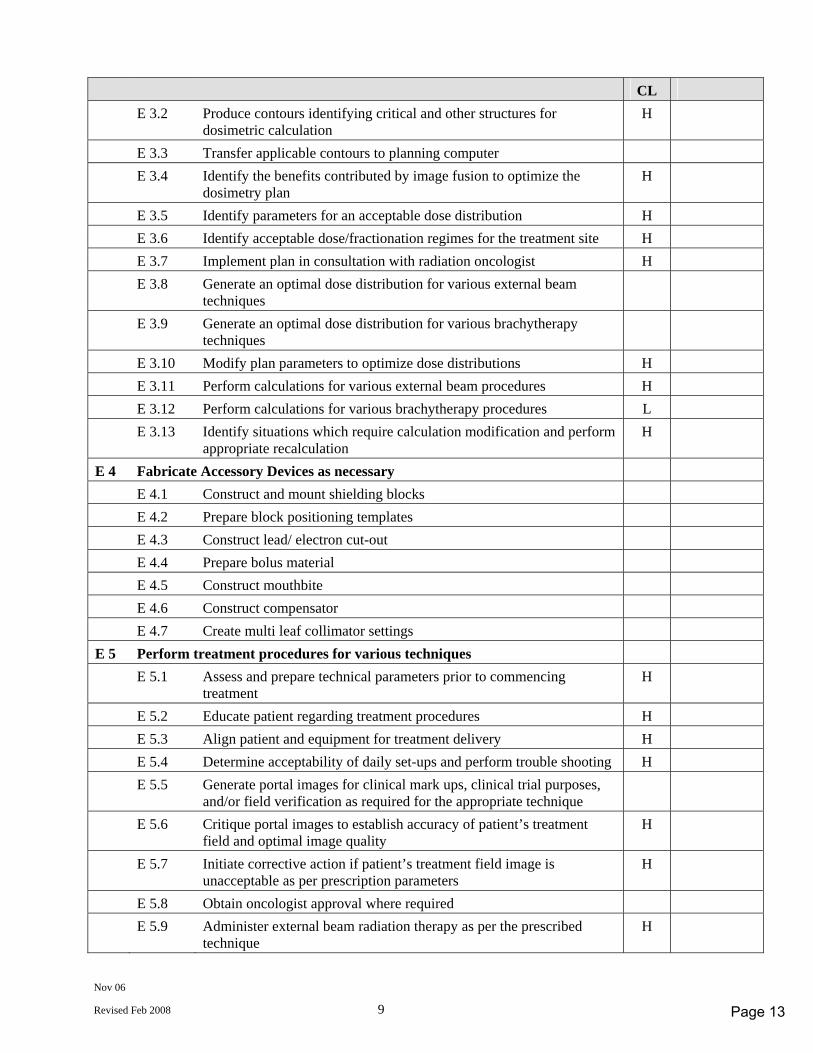
Nov 06
Revised Feb 2008 9
CL E 3.2 Produce contours identifying critical and other structures for
dosimetric calculation H
E 3.3 Transfer applicable contours to planning computer E 3.4 Identify the benefits contributed by image fusion to optimize the
dosimetry plan H
E 3.5 Identify parameters for an acceptable dose distribution H E 3.6 Identify acceptable dose/fractionation regimes for the treatment site H E 3.7 Implement plan in consultation with radiation oncologist H E 3.8 Generate an optimal dose distribution for various external beam
techniques
E 3.9 Generate an optimal dose distribution for various brachytherapy techniques
E 3.10 Modify plan parameters to optimize dose distributions H E 3.11 Perform calculations for various external beam procedures H E 3.12 Perform calculations for various brachytherapy procedures L E 3.13 Identify situations which require calculation modification and perform
appropriate recalculation H
E 4 Fabricate Accessory Devices as necessary E 4.1 Construct and mount shielding blocks E 4.2 Prepare block positioning templates E 4.3 Construct lead/ electron cut-out E 4.4 Prepare bolus material E 4.5 Construct mouthbite E 4.6 Construct compensator E 4.7 Create multi leaf collimator settings E 5 Perform treatment procedures for various techniques E 5.1 Assess and prepare technical parameters prior to commencing
treatment H
E 5.2 Educate patient regarding treatment procedures H E 5.3 Align patient and equipment for treatment delivery H E 5.4 Determine acceptability of daily set-ups and perform trouble shooting H E 5.5 Generate portal images for clinical mark ups, clinical trial purposes,
and/or field verification as required for the appropriate technique
E 5.6 Critique portal images to establish accuracy of patient’s treatment field and optimal image quality
H
E 5.7 Initiate corrective action if patient’s treatment field image is unacceptable as per prescription parameters
H
E 5.8 Obtain oncologist approval where required E 5.9 Administer external beam radiation therapy as per the prescribed
technique H
Page 13
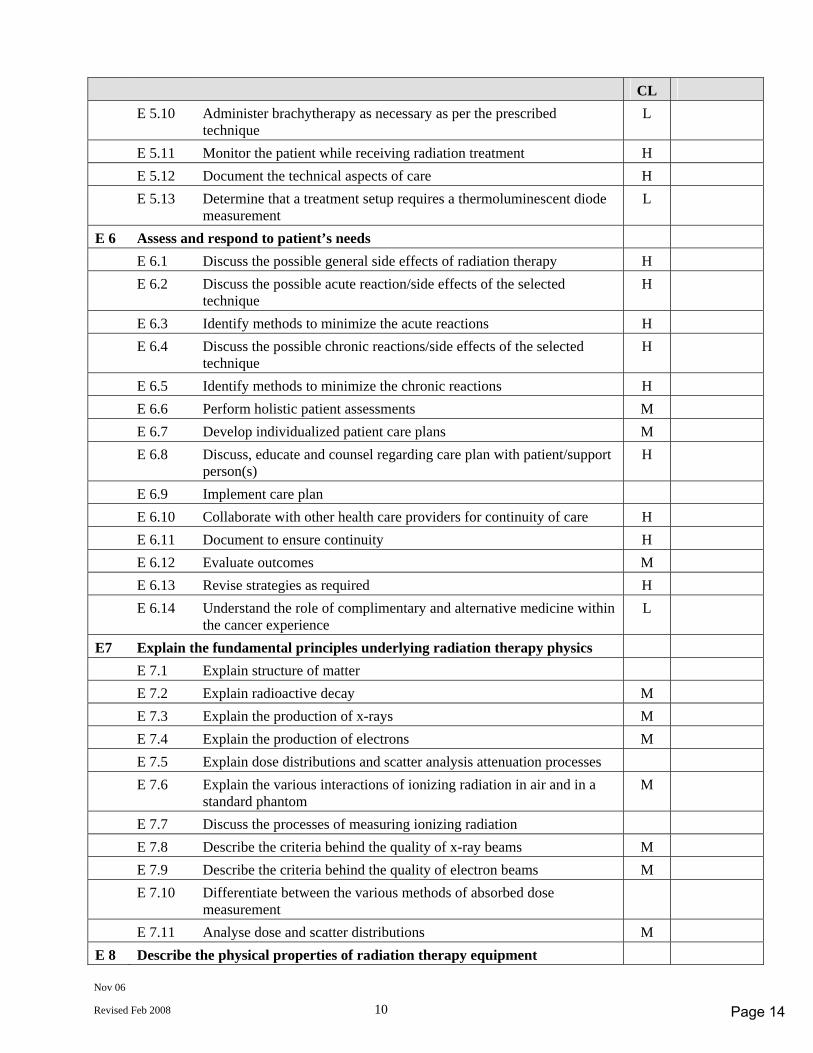
Nov 06
Revised Feb 2008 10
CL E 5.10 Administer brachytherapy as necessary as per the prescribed
technique L
E 5.11 Monitor the patient while receiving radiation treatment H E 5.12 Document the technical aspects of care H E 5.13 Determine that a treatment setup requires a thermoluminescent diode
measurement L
E 6 Assess and respond to patient’s needs E 6.1 Discuss the possible general side effects of radiation therapy H E 6.2 Discuss the possible acute reaction/side effects of the selected
technique H
E 6.3 Identify methods to minimize the acute reactions H E 6.4 Discuss the possible chronic reactions/side effects of the selected
technique H
E 6.5 Identify methods to minimize the chronic reactions H E 6.6 Perform holistic patient assessments M E 6.7 Develop individualized patient care plans M E 6.8 Discuss, educate and counsel regarding care plan with patient/support
person(s) H
E 6.9 Implement care plan E 6.10 Collaborate with other health care providers for continuity of care H E 6.11 Document to ensure continuity H E 6.12 Evaluate outcomes M E 6.13 Revise strategies as required H E 6.14 Understand the role of complimentary and alternative medicine within
the cancer experience L
E7 Explain the fundamental principles underlying radiation therapy physics E 7.1 Explain structure of matter E 7.2 Explain radioactive decay M E 7.3 Explain the production of x-rays M E 7.4 Explain the production of electrons M E 7.5 Explain dose distributions and scatter analysis attenuation processes E 7.6 Explain the various interactions of ionizing radiation in air and in a
standard phantom M
E 7.7 Discuss the processes of measuring ionizing radiation E 7.8 Describe the criteria behind the quality of x-ray beams M E 7.9 Describe the criteria behind the quality of electron beams M E 7.10 Differentiate between the various methods of absorbed dose
measurement
E 7.11 Analyse dose and scatter distributions M E 8 Describe the physical properties of radiation therapy equipment
Page 14
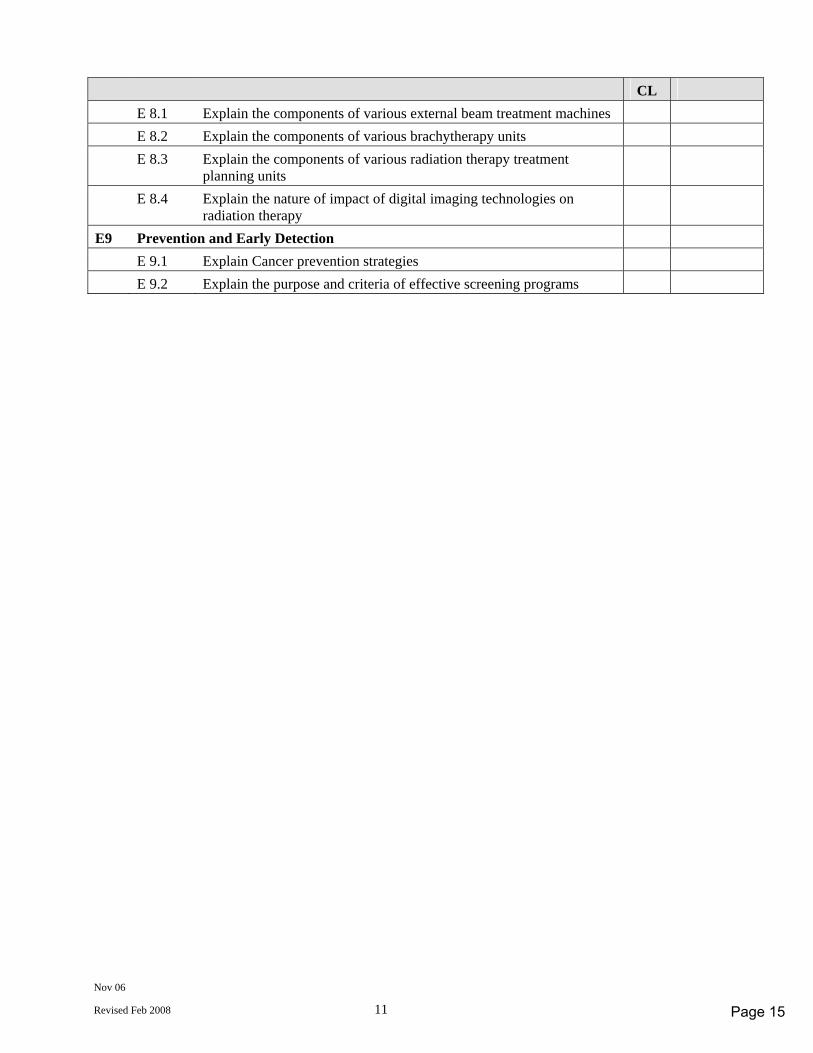
Nov 06
Revised Feb 2008 11
CL E 8.1 Explain the components of various external beam treatment machines E 8.2 Explain the components of various brachytherapy units E 8.3 Explain the components of various radiation therapy treatment
planning units
E 8.4 Explain the nature of impact of digital imaging technologies on radiation therapy
E9 Prevention and Early Detection E 9.1 Explain Cancer prevention strategies E 9.2 Explain the purpose and criteria of effective screening programs
Page 15
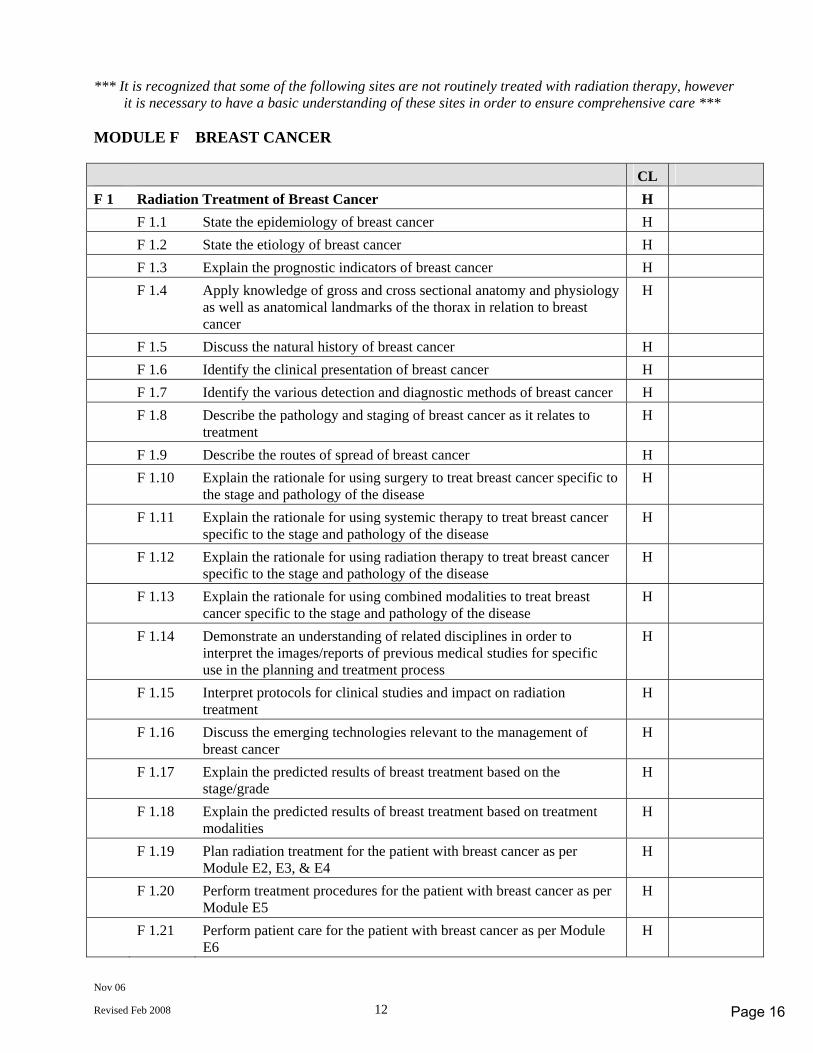
Nov 06
Revised Feb 2008 12
*** It is recognized that some of the following sites are not routinely treated with radiation therapy, however it is necessary to have a basic understanding of these sites in order to ensure comprehensive care ***
MODULE F BREAST CANCER CL F 1 Radiation Treatment of Breast Cancer H F 1.1 State the epidemiology of breast cancer H F 1.2 State the etiology of breast cancer H F 1.3 Explain the prognostic indicators of breast cancer H F 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the thorax in relation to breast cancer
H
F 1.5 Discuss the natural history of breast cancer H F 1.6 Identify the clinical presentation of breast cancer H F 1.7 Identify the various detection and diagnostic methods of breast cancer H F 1.8 Describe the pathology and staging of breast cancer as it relates to
treatment H
F 1.9 Describe the routes of spread of breast cancer H F 1.10 Explain the rationale for using surgery to treat breast cancer specific to
the stage and pathology of the disease H
F 1.11 Explain the rationale for using systemic therapy to treat breast cancer specific to the stage and pathology of the disease
H
F 1.12 Explain the rationale for using radiation therapy to treat breast cancer specific to the stage and pathology of the disease
H
F 1.13 Explain the rationale for using combined modalities to treat breast cancer specific to the stage and pathology of the disease
H
F 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
F 1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
F 1.16 Discuss the emerging technologies relevant to the management of breast cancer
H
F 1.17 Explain the predicted results of breast treatment based on the stage/grade
H
F 1.18 Explain the predicted results of breast treatment based on treatment modalities
H
F 1.19 Plan radiation treatment for the patient with breast cancer as per Module E2, E3, & E4
H
F 1.20 Perform treatment procedures for the patient with breast cancer as per Module E5
H
F 1.21 Perform patient care for the patient with breast cancer as per Module E6
H
Page 16
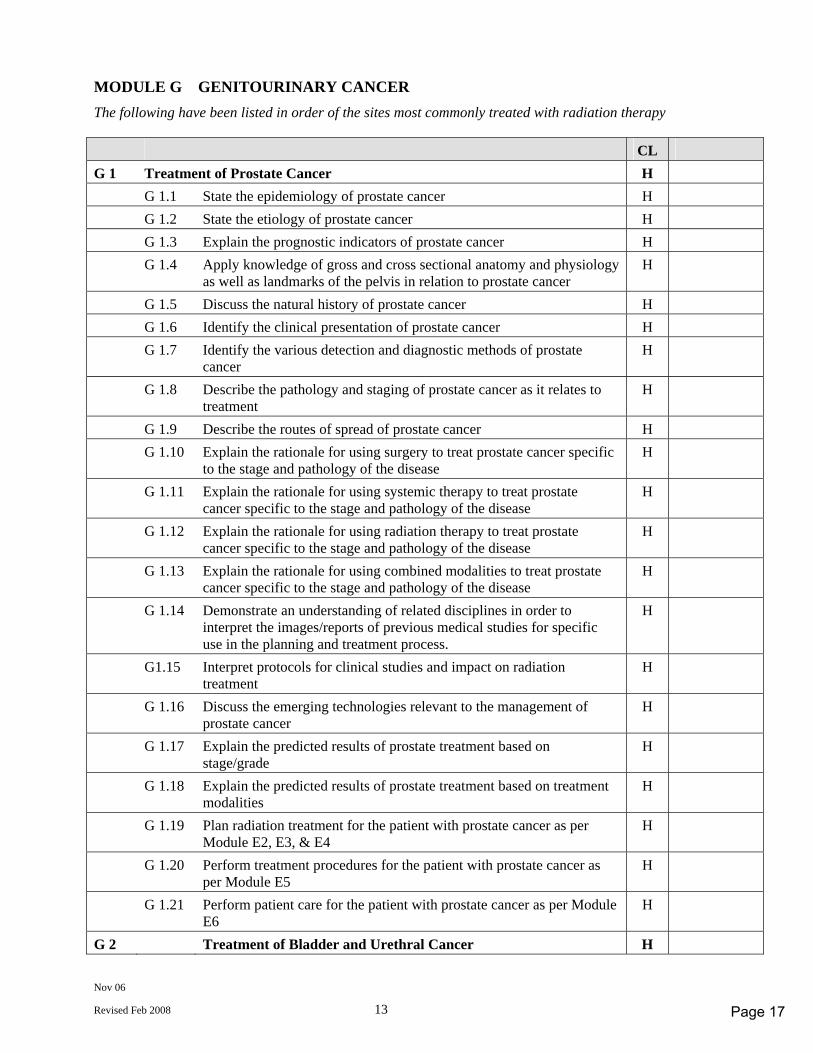
Nov 06
Revised Feb 2008 13
MODULE G GENITOURINARY CANCER The following have been listed in order of the sites most commonly treated with radiation therapy CL G 1 Treatment of Prostate Cancer H G 1.1 State the epidemiology of prostate cancer H G 1.2 State the etiology of prostate cancer H G 1.3 Explain the prognostic indicators of prostate cancer H G 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as landmarks of the pelvis in relation to prostate cancer H
G 1.5 Discuss the natural history of prostate cancer H G 1.6 Identify the clinical presentation of prostate cancer H G 1.7 Identify the various detection and diagnostic methods of prostate
cancer H
G 1.8 Describe the pathology and staging of prostate cancer as it relates to treatment
H
G 1.9 Describe the routes of spread of prostate cancer H G 1.10 Explain the rationale for using surgery to treat prostate cancer specific
to the stage and pathology of the disease H
G 1.11 Explain the rationale for using systemic therapy to treat prostate cancer specific to the stage and pathology of the disease
H
G 1.12 Explain the rationale for using radiation therapy to treat prostate cancer specific to the stage and pathology of the disease
H
G 1.13 Explain the rationale for using combined modalities to treat prostate cancer specific to the stage and pathology of the disease
H
G 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process.
H
G1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
G 1.16 Discuss the emerging technologies relevant to the management of prostate cancer
H
G 1.17 Explain the predicted results of prostate treatment based on stage/grade
H
G 1.18 Explain the predicted results of prostate treatment based on treatment modalities
H
G 1.19 Plan radiation treatment for the patient with prostate cancer as per Module E2, E3, & E4
H
G 1.20 Perform treatment procedures for the patient with prostate cancer as per Module E5
H
G 1.21 Perform patient care for the patient with prostate cancer as per Module E6
H
G 2 Treatment of Bladder and Urethral Cancer H
Page 17
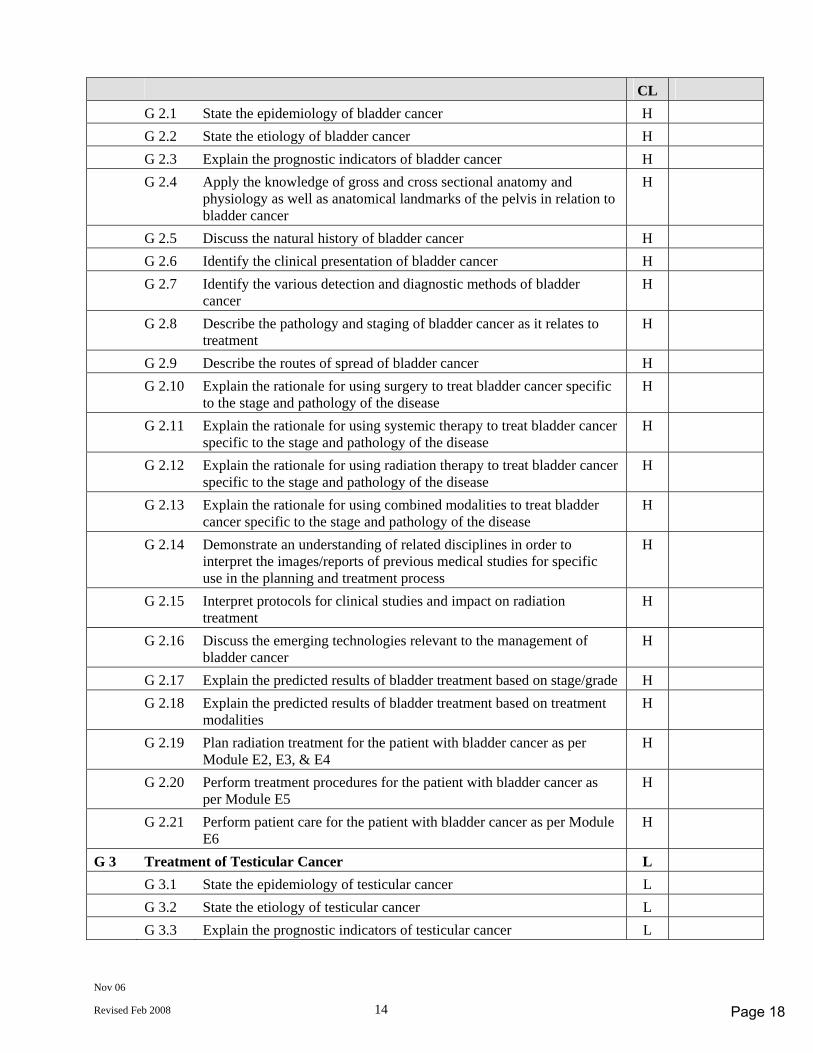
Nov 06
Revised Feb 2008 14
CL G 2.1 State the epidemiology of bladder cancer H G 2.2 State the etiology of bladder cancer H G 2.3 Explain the prognostic indicators of bladder cancer H G 2.4 Apply the knowledge of gross and cross sectional anatomy and
physiology as well as anatomical landmarks of the pelvis in relation to bladder cancer
H
G 2.5 Discuss the natural history of bladder cancer H G 2.6 Identify the clinical presentation of bladder cancer H G 2.7 Identify the various detection and diagnostic methods of bladder
cancer H
G 2.8 Describe the pathology and staging of bladder cancer as it relates to treatment
H
G 2.9 Describe the routes of spread of bladder cancer H G 2.10 Explain the rationale for using surgery to treat bladder cancer specific
to the stage and pathology of the disease H
G 2.11 Explain the rationale for using systemic therapy to treat bladder cancer specific to the stage and pathology of the disease
H
G 2.12 Explain the rationale for using radiation therapy to treat bladder cancer specific to the stage and pathology of the disease
H
G 2.13 Explain the rationale for using combined modalities to treat bladder cancer specific to the stage and pathology of the disease
H
G 2.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
G 2.15 Interpret protocols for clinical studies and impact on radiation treatment
H
G 2.16 Discuss the emerging technologies relevant to the management of bladder cancer
H
G 2.17 Explain the predicted results of bladder treatment based on stage/grade H G 2.18 Explain the predicted results of bladder treatment based on treatment
modalities H
G 2.19 Plan radiation treatment for the patient with bladder cancer as per Module E2, E3, & E4
H
G 2.20 Perform treatment procedures for the patient with bladder cancer as per Module E5
H
G 2.21 Perform patient care for the patient with bladder cancer as per Module E6
H
G 3 Treatment of Testicular Cancer L G 3.1 State the epidemiology of testicular cancer L G 3.2 State the etiology of testicular cancer L G 3.3 Explain the prognostic indicators of testicular cancer L
Page 18
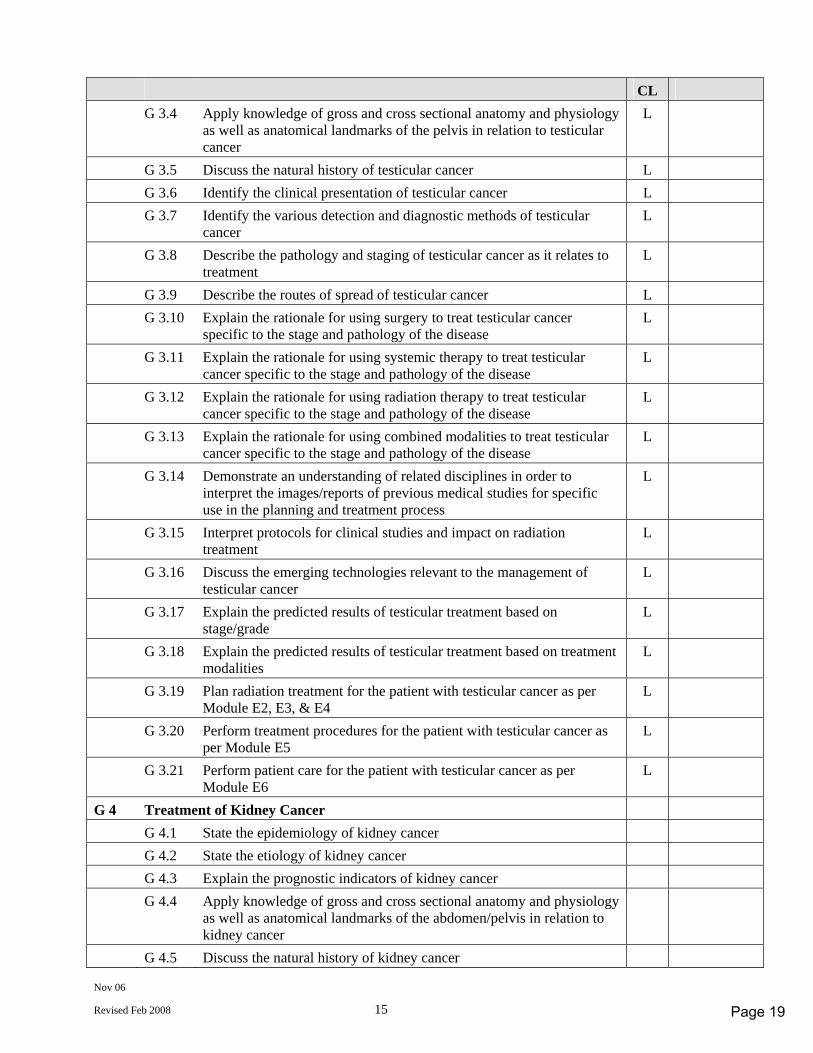
Nov 06
Revised Feb 2008 15
CL G 3.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the pelvis in relation to testicular cancer
L
G 3.5 Discuss the natural history of testicular cancer L G 3.6 Identify the clinical presentation of testicular cancer L G 3.7 Identify the various detection and diagnostic methods of testicular
cancer L
G 3.8 Describe the pathology and staging of testicular cancer as it relates to treatment
L
G 3.9 Describe the routes of spread of testicular cancer L G 3.10 Explain the rationale for using surgery to treat testicular cancer
specific to the stage and pathology of the disease L
G 3.11 Explain the rationale for using systemic therapy to treat testicular cancer specific to the stage and pathology of the disease
L
G 3.12 Explain the rationale for using radiation therapy to treat testicular cancer specific to the stage and pathology of the disease
L
G 3.13 Explain the rationale for using combined modalities to treat testicular cancer specific to the stage and pathology of the disease
L
G 3.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
L
G 3.15 Interpret protocols for clinical studies and impact on radiation treatment
L
G 3.16 Discuss the emerging technologies relevant to the management of testicular cancer
L
G 3.17 Explain the predicted results of testicular treatment based on stage/grade
L
G 3.18 Explain the predicted results of testicular treatment based on treatment modalities
L
G 3.19 Plan radiation treatment for the patient with testicular cancer as per Module E2, E3, & E4
L
G 3.20 Perform treatment procedures for the patient with testicular cancer as per Module E5
L
G 3.21 Perform patient care for the patient with testicular cancer as per Module E6
L
G 4 Treatment of Kidney Cancer G 4.1 State the epidemiology of kidney cancer G 4.2 State the etiology of kidney cancer G 4.3 Explain the prognostic indicators of kidney cancer G 4.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to kidney cancer
G 4.5 Discuss the natural history of kidney cancer
Page 19
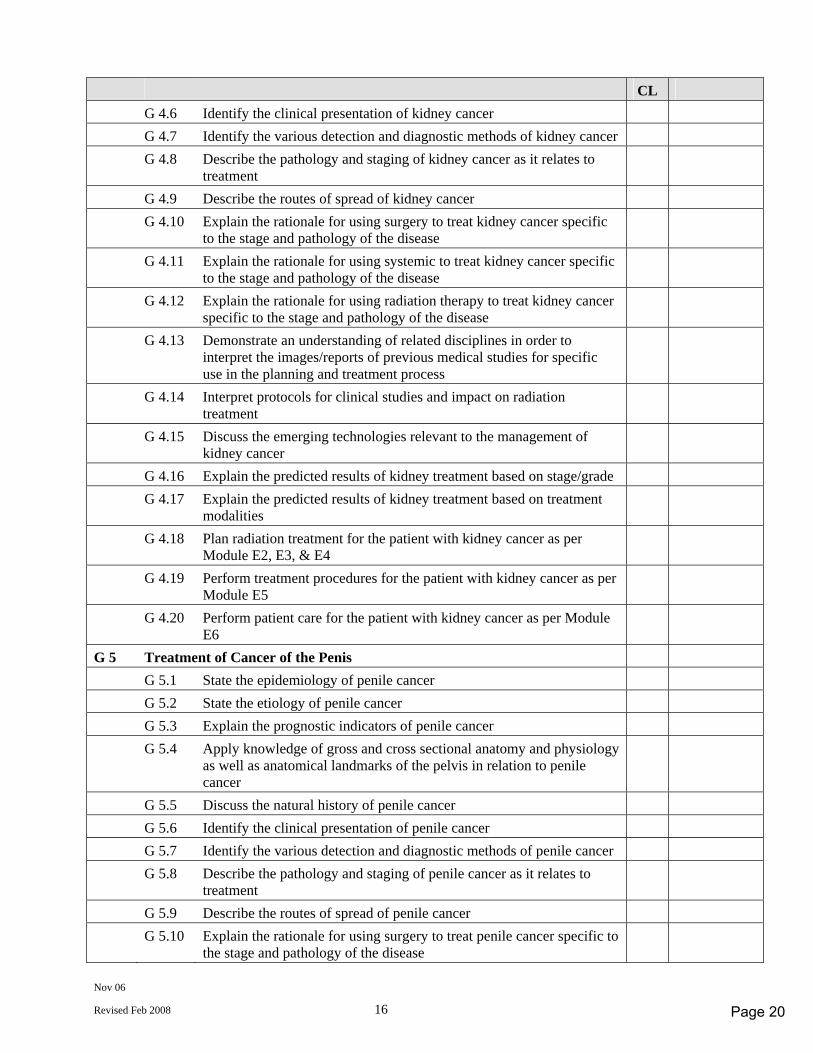
Nov 06
Revised Feb 2008 16
CL G 4.6 Identify the clinical presentation of kidney cancer G 4.7 Identify the various detection and diagnostic methods of kidney cancer G 4.8 Describe the pathology and staging of kidney cancer as it relates to
treatment
G 4.9 Describe the routes of spread of kidney cancer G 4.10 Explain the rationale for using surgery to treat kidney cancer specific
to the stage and pathology of the disease
G 4.11 Explain the rationale for using systemic to treat kidney cancer specific to the stage and pathology of the disease
G 4.12 Explain the rationale for using radiation therapy to treat kidney cancer specific to the stage and pathology of the disease
G 4.13 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
G 4.14 Interpret protocols for clinical studies and impact on radiation treatment
G 4.15 Discuss the emerging technologies relevant to the management of kidney cancer
G 4.16 Explain the predicted results of kidney treatment based on stage/grade G 4.17 Explain the predicted results of kidney treatment based on treatment
modalities
G 4.18 Plan radiation treatment for the patient with kidney cancer as per Module E2, E3, & E4
G 4.19 Perform treatment procedures for the patient with kidney cancer as per Module E5
G 4.20 Perform patient care for the patient with kidney cancer as per Module E6
G 5 Treatment of Cancer of the Penis G 5.1 State the epidemiology of penile cancer G 5.2 State the etiology of penile cancer G 5.3 Explain the prognostic indicators of penile cancer G 5.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the pelvis in relation to penile cancer
G 5.5 Discuss the natural history of penile cancer G 5.6 Identify the clinical presentation of penile cancer G 5.7 Identify the various detection and diagnostic methods of penile cancer G 5.8 Describe the pathology and staging of penile cancer as it relates to
treatment
G 5.9 Describe the routes of spread of penile cancer G 5.10 Explain the rationale for using surgery to treat penile cancer specific to
the stage and pathology of the disease
Page 20
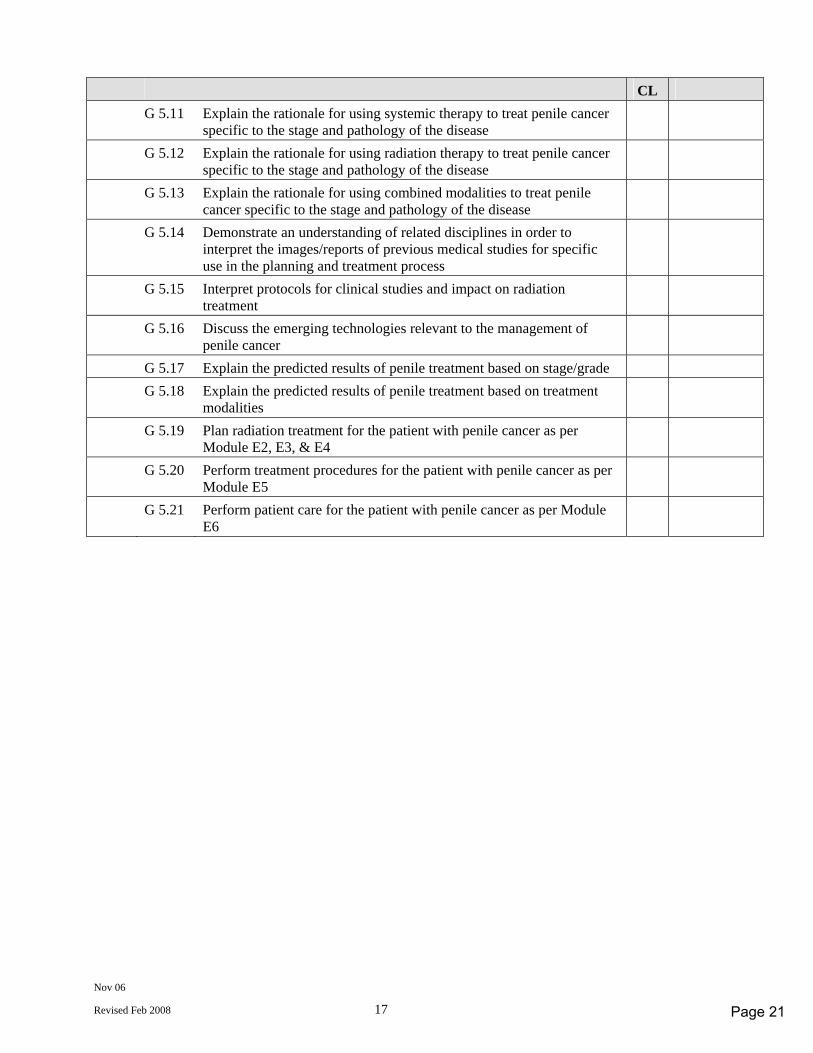
Nov 06
Revised Feb 2008 17
CL G 5.11 Explain the rationale for using systemic therapy to treat penile cancer
specific to the stage and pathology of the disease
G 5.12 Explain the rationale for using radiation therapy to treat penile cancer specific to the stage and pathology of the disease
G 5.13 Explain the rationale for using combined modalities to treat penile cancer specific to the stage and pathology of the disease
G 5.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
G 5.15 Interpret protocols for clinical studies and impact on radiation treatment
G 5.16 Discuss the emerging technologies relevant to the management of penile cancer
G 5.17 Explain the predicted results of penile treatment based on stage/grade G 5.18 Explain the predicted results of penile treatment based on treatment
modalities
G 5.19 Plan radiation treatment for the patient with penile cancer as per Module E2, E3, & E4
G 5.20 Perform treatment procedures for the patient with penile cancer as per Module E5
G 5.21 Perform patient care for the patient with penile cancer as per Module E6
Page 21
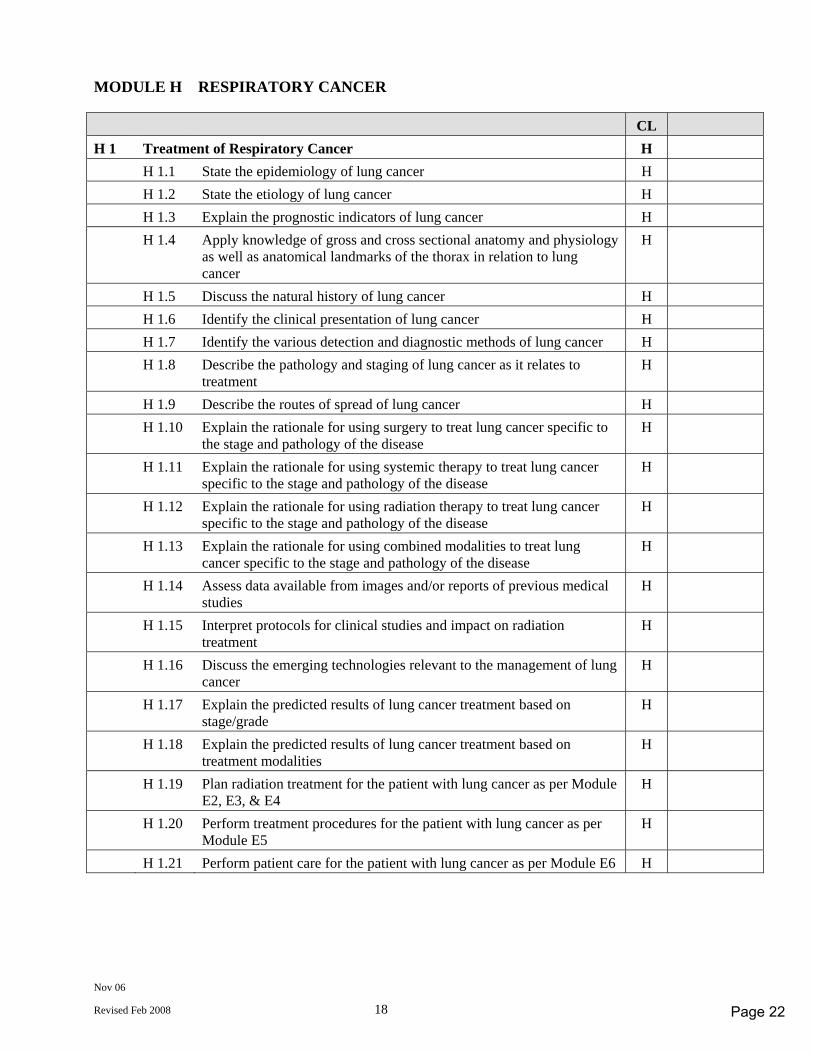
Nov 06
Revised Feb 2008 18
MODULE H RESPIRATORY CANCER CL H 1 Treatment of Respiratory Cancer H H 1.1 State the epidemiology of lung cancer H H 1.2 State the etiology of lung cancer H H 1.3 Explain the prognostic indicators of lung cancer H H 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the thorax in relation to lung cancer
H
H 1.5 Discuss the natural history of lung cancer H H 1.6 Identify the clinical presentation of lung cancer H H 1.7 Identify the various detection and diagnostic methods of lung cancer H H 1.8 Describe the pathology and staging of lung cancer as it relates to
treatment H
H 1.9 Describe the routes of spread of lung cancer H H 1.10 Explain the rationale for using surgery to treat lung cancer specific to
the stage and pathology of the disease H
H 1.11 Explain the rationale for using systemic therapy to treat lung cancer specific to the stage and pathology of the disease
H
H 1.12 Explain the rationale for using radiation therapy to treat lung cancer specific to the stage and pathology of the disease
H
H 1.13 Explain the rationale for using combined modalities to treat lung cancer specific to the stage and pathology of the disease
H
H 1.14 Assess data available from images and/or reports of previous medical studies
H
H 1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
H 1.16 Discuss the emerging technologies relevant to the management of lung cancer
H
H 1.17 Explain the predicted results of lung cancer treatment based on stage/grade
H
H 1.18 Explain the predicted results of lung cancer treatment based on treatment modalities
H
H 1.19 Plan radiation treatment for the patient with lung cancer as per Module E2, E3, & E4
H
H 1.20 Perform treatment procedures for the patient with lung cancer as per Module E5
H
H 1.21 Perform patient care for the patient with lung cancer as per Module E6 H
Page 22
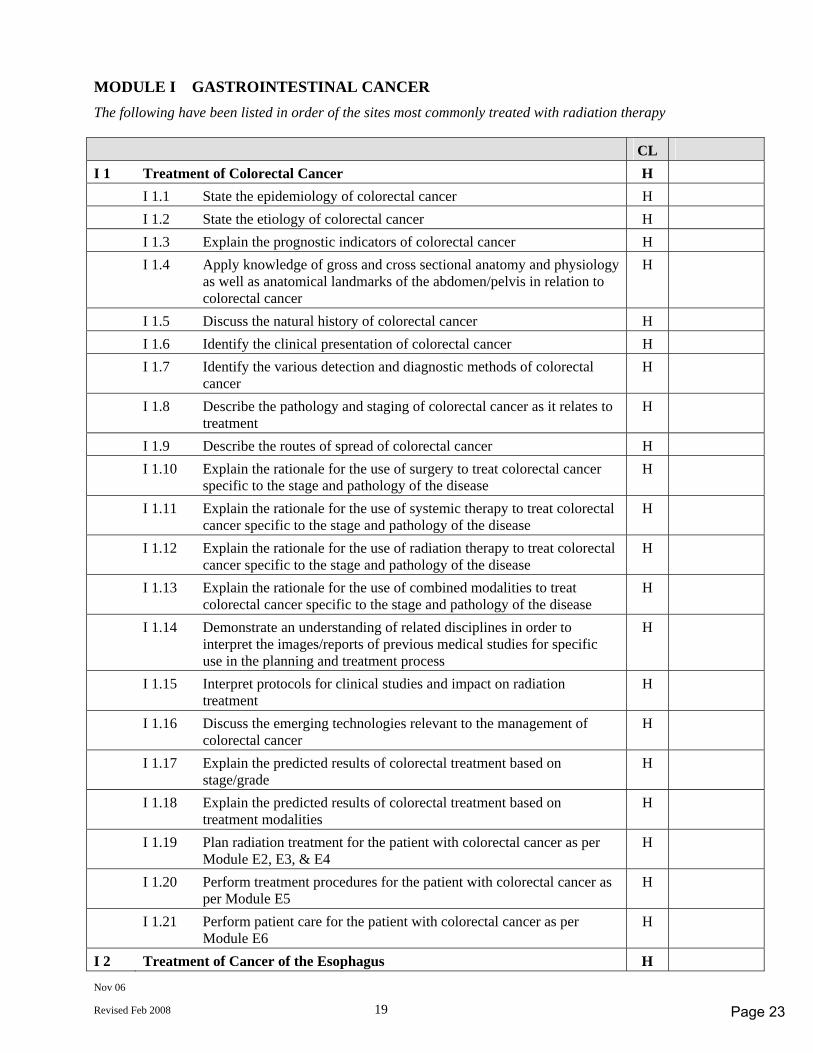
Nov 06
Revised Feb 2008 19
MODULE I GASTROINTESTINAL CANCER The following have been listed in order of the sites most commonly treated with radiation therapy CL I 1 Treatment of Colorectal Cancer H I 1.1 State the epidemiology of colorectal cancer H I 1.2 State the etiology of colorectal cancer H I 1.3 Explain the prognostic indicators of colorectal cancer H I 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to colorectal cancer
H
I 1.5 Discuss the natural history of colorectal cancer H I 1.6 Identify the clinical presentation of colorectal cancer H I 1.7 Identify the various detection and diagnostic methods of colorectal
cancer H
I 1.8 Describe the pathology and staging of colorectal cancer as it relates to treatment
H
I 1.9 Describe the routes of spread of colorectal cancer H I 1.10 Explain the rationale for the use of surgery to treat colorectal cancer
specific to the stage and pathology of the disease H
I 1.11 Explain the rationale for the use of systemic therapy to treat colorectal cancer specific to the stage and pathology of the disease
H
I 1.12 Explain the rationale for the use of radiation therapy to treat colorectal cancer specific to the stage and pathology of the disease
H
I 1.13 Explain the rationale for the use of combined modalities to treat colorectal cancer specific to the stage and pathology of the disease
H
I 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
I 1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
I 1.16 Discuss the emerging technologies relevant to the management of colorectal cancer
H
I 1.17 Explain the predicted results of colorectal treatment based on stage/grade
H
I 1.18 Explain the predicted results of colorectal treatment based on treatment modalities
H
I 1.19 Plan radiation treatment for the patient with colorectal cancer as per Module E2, E3, & E4
H
I 1.20 Perform treatment procedures for the patient with colorectal cancer as per Module E5
H
I 1.21 Perform patient care for the patient with colorectal cancer as per Module E6
H
I 2 Treatment of Cancer of the Esophagus H
Page 23
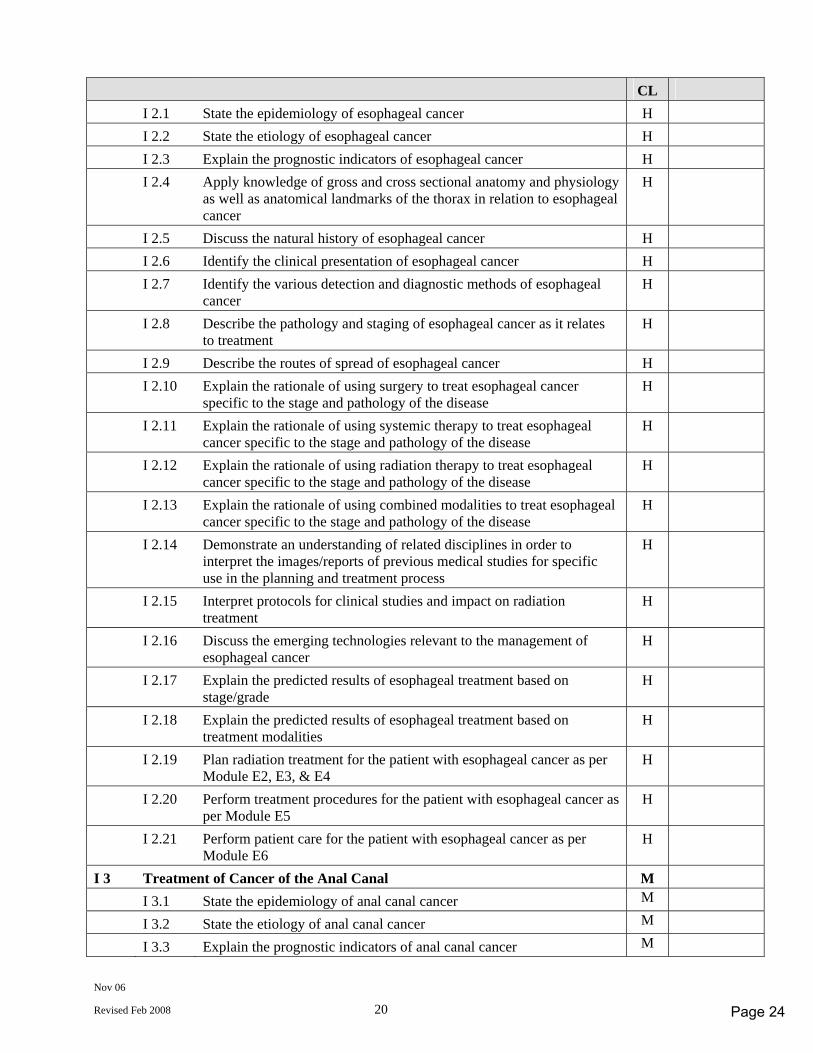
Nov 06
Revised Feb 2008 20
CL I 2.1 State the epidemiology of esophageal cancer H I 2.2 State the etiology of esophageal cancer H I 2.3 Explain the prognostic indicators of esophageal cancer H I 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the thorax in relation to esophageal cancer
H
I 2.5 Discuss the natural history of esophageal cancer H I 2.6 Identify the clinical presentation of esophageal cancer H I 2.7 Identify the various detection and diagnostic methods of esophageal
cancer H
I 2.8 Describe the pathology and staging of esophageal cancer as it relates to treatment
H
I 2.9 Describe the routes of spread of esophageal cancer H I 2.10 Explain the rationale of using surgery to treat esophageal cancer
specific to the stage and pathology of the disease H
I 2.11 Explain the rationale of using systemic therapy to treat esophageal cancer specific to the stage and pathology of the disease
H
I 2.12 Explain the rationale of using radiation therapy to treat esophageal cancer specific to the stage and pathology of the disease
H
I 2.13 Explain the rationale of using combined modalities to treat esophageal cancer specific to the stage and pathology of the disease
H
I 2.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
I 2.15 Interpret protocols for clinical studies and impact on radiation treatment
H
I 2.16 Discuss the emerging technologies relevant to the management of esophageal cancer
H
I 2.17 Explain the predicted results of esophageal treatment based on stage/grade
H
I 2.18 Explain the predicted results of esophageal treatment based on treatment modalities
H
I 2.19 Plan radiation treatment for the patient with esophageal cancer as per Module E2, E3, & E4
H
I 2.20 Perform treatment procedures for the patient with esophageal cancer as per Module E5
H
I 2.21 Perform patient care for the patient with esophageal cancer as per Module E6
H
I 3 Treatment of Cancer of the Anal Canal M I 3.1 State the epidemiology of anal canal cancer M I 3.2 State the etiology of anal canal cancer M I 3.3 Explain the prognostic indicators of anal canal cancer M
Page 24
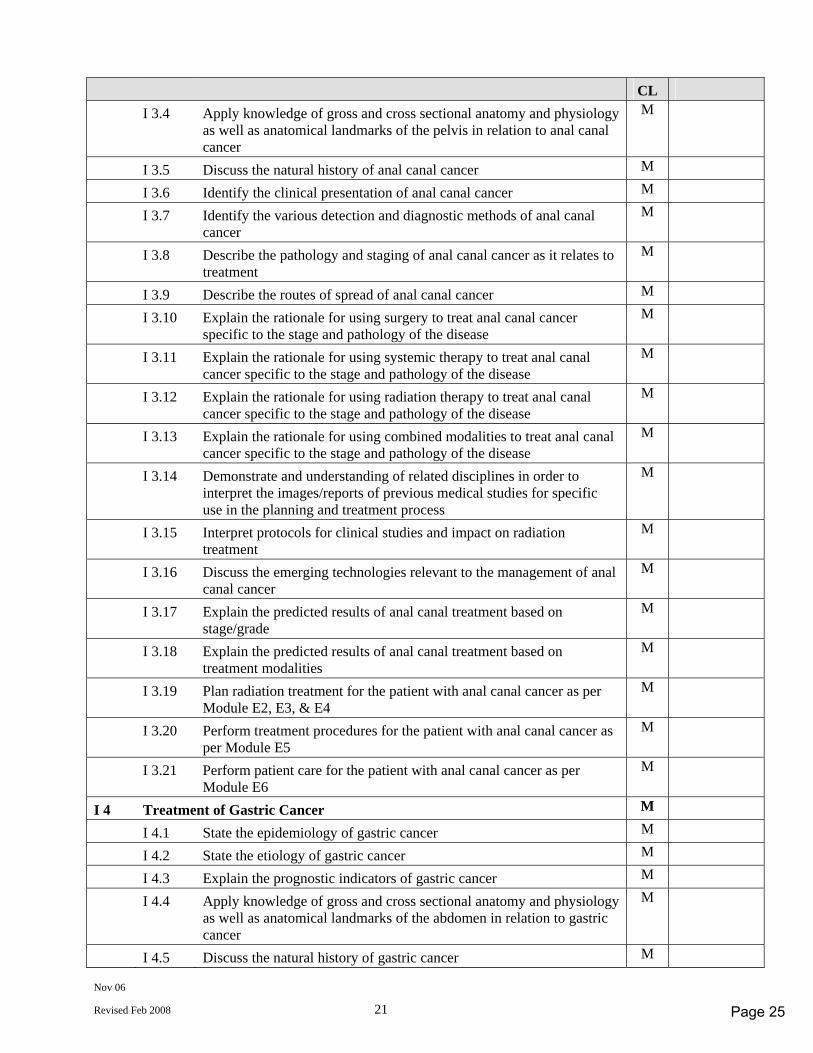
Nov 06
Revised Feb 2008 21
CL I 3.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the pelvis in relation to anal canal cancer
M
I 3.5 Discuss the natural history of anal canal cancer M I 3.6 Identify the clinical presentation of anal canal cancer M I 3.7 Identify the various detection and diagnostic methods of anal canal
cancer M
I 3.8 Describe the pathology and staging of anal canal cancer as it relates to treatment
M
I 3.9 Describe the routes of spread of anal canal cancer M I 3.10 Explain the rationale for using surgery to treat anal canal cancer
specific to the stage and pathology of the disease M
I 3.11 Explain the rationale for using systemic therapy to treat anal canal cancer specific to the stage and pathology of the disease
M
I 3.12 Explain the rationale for using radiation therapy to treat anal canal cancer specific to the stage and pathology of the disease
M
I 3.13 Explain the rationale for using combined modalities to treat anal canal cancer specific to the stage and pathology of the disease
M
I 3.14 Demonstrate and understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
M
I 3.15 Interpret protocols for clinical studies and impact on radiation treatment
M
I 3.16 Discuss the emerging technologies relevant to the management of anal canal cancer
M
I 3.17 Explain the predicted results of anal canal treatment based on stage/grade
M
I 3.18 Explain the predicted results of anal canal treatment based on treatment modalities
M
I 3.19 Plan radiation treatment for the patient with anal canal cancer as per Module E2, E3, & E4
M
I 3.20 Perform treatment procedures for the patient with anal canal cancer as per Module E5
M
I 3.21 Perform patient care for the patient with anal canal cancer as per Module E6
M
I 4 Treatment of Gastric Cancer M I 4.1 State the epidemiology of gastric cancer M I 4.2 State the etiology of gastric cancer M I 4.3 Explain the prognostic indicators of gastric cancer M I 4.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen in relation to gastric cancer
M
I 4.5 Discuss the natural history of gastric cancer M
Page 25
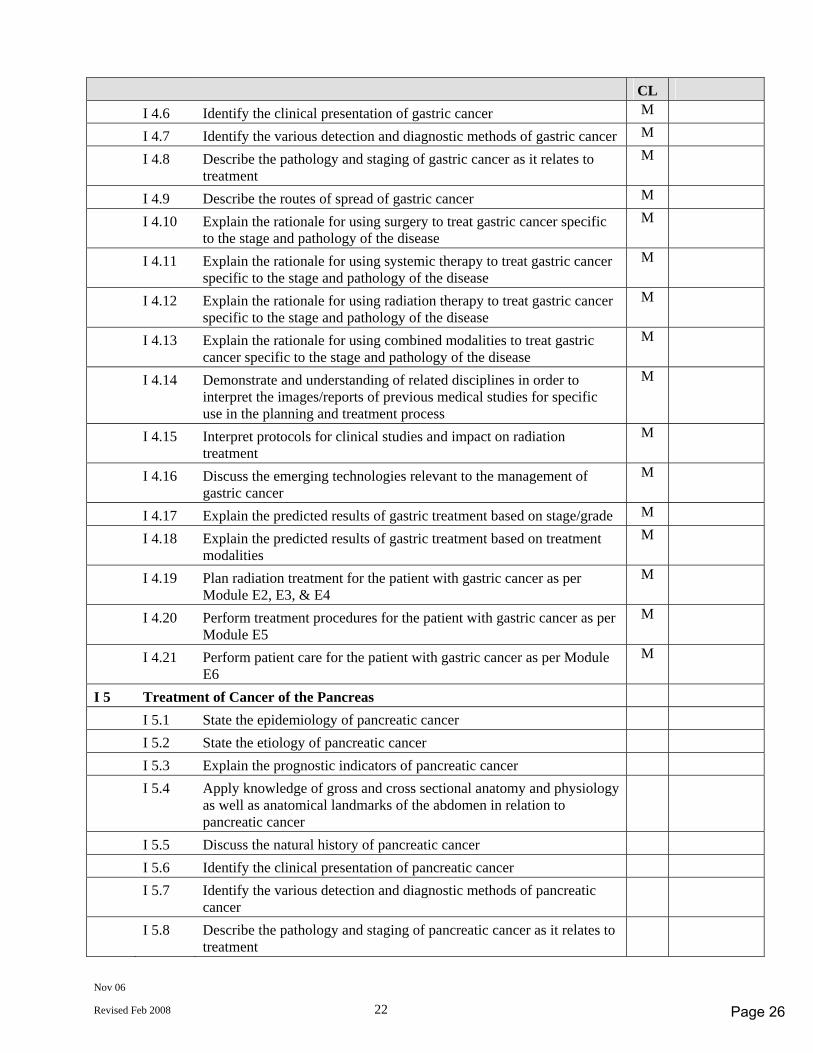
Nov 06
Revised Feb 2008 22
CL I 4.6 Identify the clinical presentation of gastric cancer M I 4.7 Identify the various detection and diagnostic methods of gastric cancer M I 4.8 Describe the pathology and staging of gastric cancer as it relates to
treatment M
I 4.9 Describe the routes of spread of gastric cancer M I 4.10 Explain the rationale for using surgery to treat gastric cancer specific
to the stage and pathology of the disease M
I 4.11 Explain the rationale for using systemic therapy to treat gastric cancer specific to the stage and pathology of the disease
M
I 4.12 Explain the rationale for using radiation therapy to treat gastric cancer specific to the stage and pathology of the disease
M
I 4.13 Explain the rationale for using combined modalities to treat gastric cancer specific to the stage and pathology of the disease
M
I 4.14 Demonstrate and understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
M
I 4.15 Interpret protocols for clinical studies and impact on radiation treatment
M
I 4.16 Discuss the emerging technologies relevant to the management of gastric cancer
M
I 4.17 Explain the predicted results of gastric treatment based on stage/grade M I 4.18 Explain the predicted results of gastric treatment based on treatment
modalities M
I 4.19 Plan radiation treatment for the patient with gastric cancer as per Module E2, E3, & E4
M
I 4.20 Perform treatment procedures for the patient with gastric cancer as per Module E5
M
I 4.21 Perform patient care for the patient with gastric cancer as per Module E6
M
I 5 Treatment of Cancer of the Pancreas I 5.1 State the epidemiology of pancreatic cancer I 5.2 State the etiology of pancreatic cancer I 5.3 Explain the prognostic indicators of pancreatic cancer I 5.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen in relation to pancreatic cancer
I 5.5 Discuss the natural history of pancreatic cancer I 5.6 Identify the clinical presentation of pancreatic cancer I 5.7 Identify the various detection and diagnostic methods of pancreatic
cancer
I 5.8 Describe the pathology and staging of pancreatic cancer as it relates to treatment
Page 26
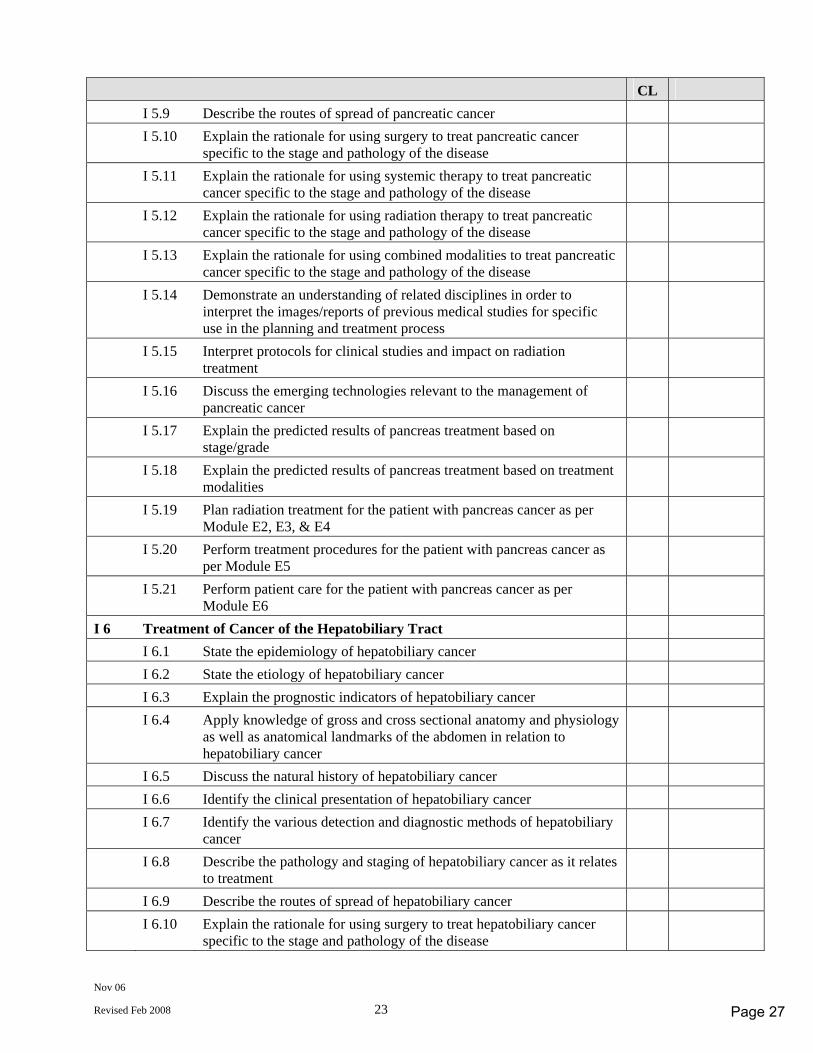
Nov 06
Revised Feb 2008 23
CL I 5.9 Describe the routes of spread of pancreatic cancer I 5.10 Explain the rationale for using surgery to treat pancreatic cancer
specific to the stage and pathology of the disease
I 5.11 Explain the rationale for using systemic therapy to treat pancreatic cancer specific to the stage and pathology of the disease
I 5.12 Explain the rationale for using radiation therapy to treat pancreatic cancer specific to the stage and pathology of the disease
I 5.13 Explain the rationale for using combined modalities to treat pancreatic cancer specific to the stage and pathology of the disease
I 5.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
I 5.15 Interpret protocols for clinical studies and impact on radiation treatment
I 5.16 Discuss the emerging technologies relevant to the management of pancreatic cancer
I 5.17 Explain the predicted results of pancreas treatment based on stage/grade
I 5.18 Explain the predicted results of pancreas treatment based on treatment modalities
I 5.19 Plan radiation treatment for the patient with pancreas cancer as per Module E2, E3, & E4
I 5.20 Perform treatment procedures for the patient with pancreas cancer as per Module E5
I 5.21 Perform patient care for the patient with pancreas cancer as per Module E6
I 6 Treatment of Cancer of the Hepatobiliary Tract I 6.1 State the epidemiology of hepatobiliary cancer I 6.2 State the etiology of hepatobiliary cancer I 6.3 Explain the prognostic indicators of hepatobiliary cancer I 6.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen in relation to hepatobiliary cancer
I 6.5 Discuss the natural history of hepatobiliary cancer I 6.6 Identify the clinical presentation of hepatobiliary cancer I 6.7 Identify the various detection and diagnostic methods of hepatobiliary
cancer
I 6.8 Describe the pathology and staging of hepatobiliary cancer as it relates to treatment
I 6.9 Describe the routes of spread of hepatobiliary cancer I 6.10 Explain the rationale for using surgery to treat hepatobiliary cancer
specific to the stage and pathology of the disease
Page 27
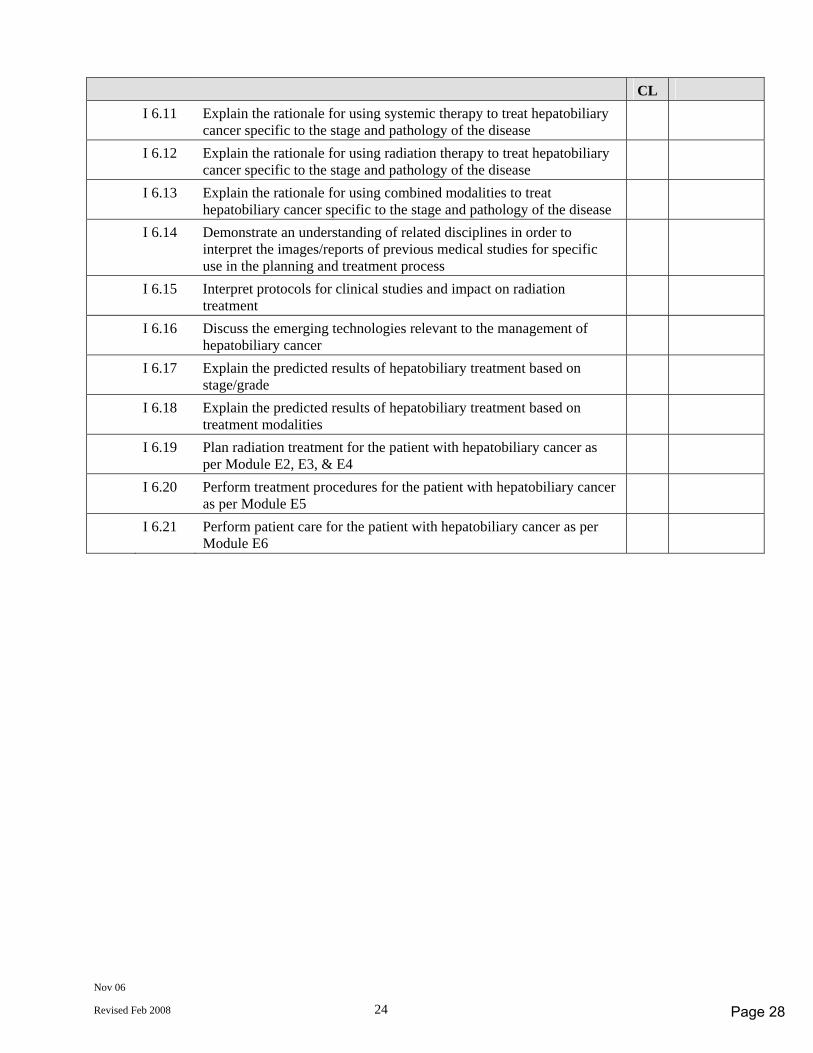
Nov 06
Revised Feb 2008 24
CL I 6.11 Explain the rationale for using systemic therapy to treat hepatobiliary
cancer specific to the stage and pathology of the disease
I 6.12 Explain the rationale for using radiation therapy to treat hepatobiliary cancer specific to the stage and pathology of the disease
I 6.13 Explain the rationale for using combined modalities to treat hepatobiliary cancer specific to the stage and pathology of the disease
I 6.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
I 6.15 Interpret protocols for clinical studies and impact on radiation treatment
I 6.16 Discuss the emerging technologies relevant to the management of hepatobiliary cancer
I 6.17 Explain the predicted results of hepatobiliary treatment based on stage/grade
I 6.18 Explain the predicted results of hepatobiliary treatment based on treatment modalities
I 6.19 Plan radiation treatment for the patient with hepatobiliary cancer as per Module E2, E3, & E4
I 6.20 Perform treatment procedures for the patient with hepatobiliary cancer as per Module E5
I 6.21 Perform patient care for the patient with hepatobiliary cancer as per Module E6
Page 28
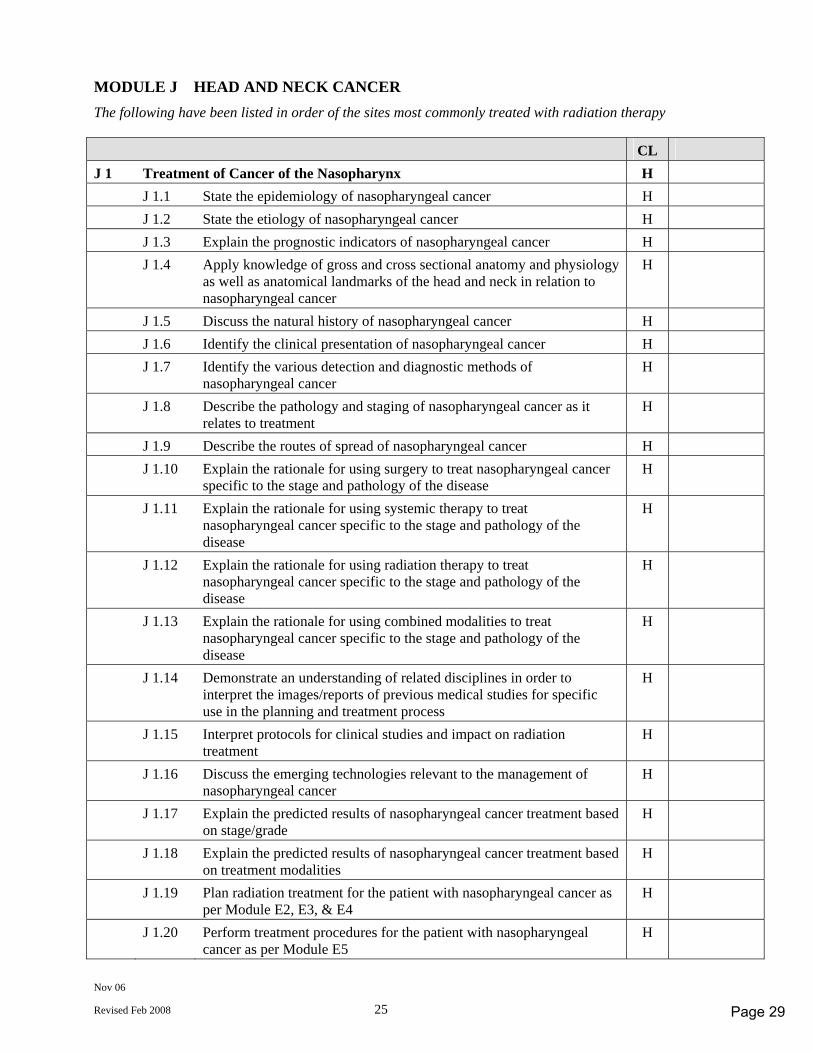
Nov 06
Revised Feb 2008 25
MODULE J HEAD AND NECK CANCER The following have been listed in order of the sites most commonly treated with radiation therapy CL J 1 Treatment of Cancer of the Nasopharynx H J 1.1 State the epidemiology of nasopharyngeal cancer H J 1.2 State the etiology of nasopharyngeal cancer H J 1.3 Explain the prognostic indicators of nasopharyngeal cancer H J 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to nasopharyngeal cancer
H
J 1.5 Discuss the natural history of nasopharyngeal cancer H J 1.6 Identify the clinical presentation of nasopharyngeal cancer H J 1.7 Identify the various detection and diagnostic methods of
nasopharyngeal cancer H
J 1.8 Describe the pathology and staging of nasopharyngeal cancer as it relates to treatment
H
J 1.9 Describe the routes of spread of nasopharyngeal cancer H J 1.10 Explain the rationale for using surgery to treat nasopharyngeal cancer
specific to the stage and pathology of the disease H
J 1.11 Explain the rationale for using systemic therapy to treat nasopharyngeal cancer specific to the stage and pathology of the disease
H
J 1.12 Explain the rationale for using radiation therapy to treat nasopharyngeal cancer specific to the stage and pathology of the disease
H
J 1.13 Explain the rationale for using combined modalities to treat nasopharyngeal cancer specific to the stage and pathology of the disease
H
J 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
J 1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
J 1.16 Discuss the emerging technologies relevant to the management of nasopharyngeal cancer
H
J 1.17 Explain the predicted results of nasopharyngeal cancer treatment based on stage/grade
H
J 1.18 Explain the predicted results of nasopharyngeal cancer treatment based on treatment modalities
H
J 1.19 Plan radiation treatment for the patient with nasopharyngeal cancer as per Module E2, E3, & E4
H
J 1.20 Perform treatment procedures for the patient with nasopharyngeal cancer as per Module E5
H
Page 29
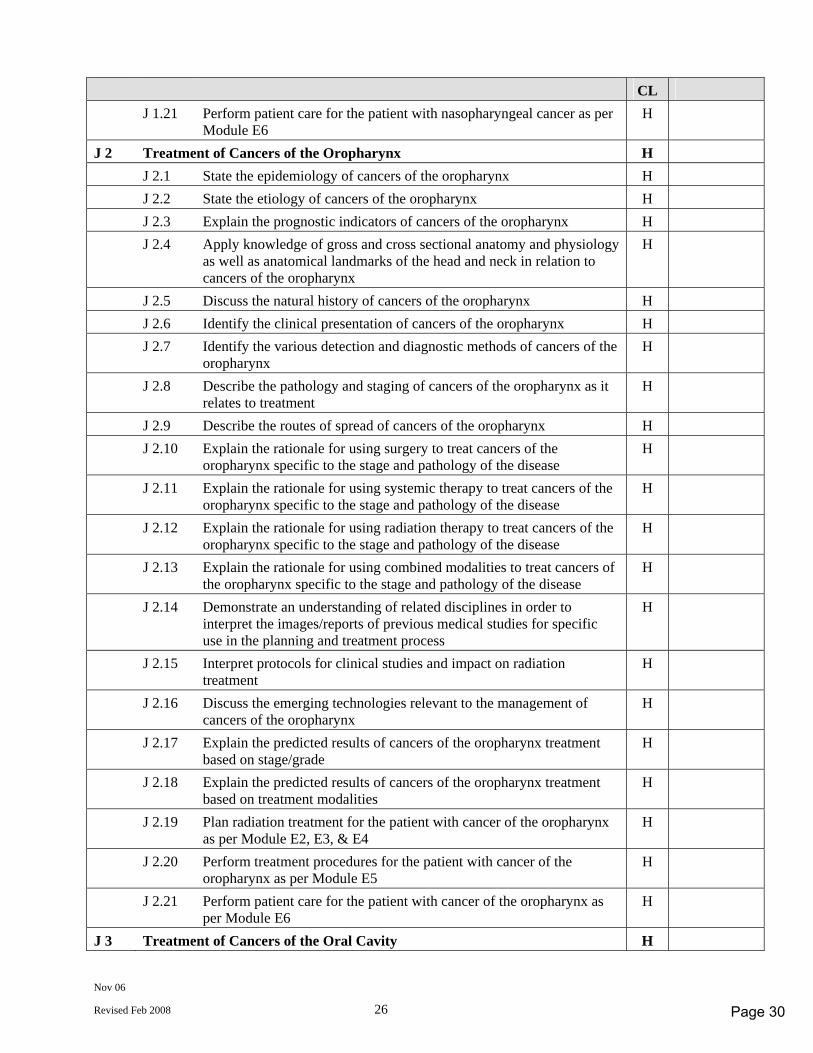
Nov 06
Revised Feb 2008 26
CL J 1.21 Perform patient care for the patient with nasopharyngeal cancer as per
Module E6 H
J 2 Treatment of Cancers of the Oropharynx H J 2.1 State the epidemiology of cancers of the oropharynx H J 2.2 State the etiology of cancers of the oropharynx H J 2.3 Explain the prognostic indicators of cancers of the oropharynx H J 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to cancers of the oropharynx
H
J 2.5 Discuss the natural history of cancers of the oropharynx H J 2.6 Identify the clinical presentation of cancers of the oropharynx H J 2.7 Identify the various detection and diagnostic methods of cancers of the
oropharynx H
J 2.8 Describe the pathology and staging of cancers of the oropharynx as it relates to treatment
H
J 2.9 Describe the routes of spread of cancers of the oropharynx H J 2.10 Explain the rationale for using surgery to treat cancers of the
oropharynx specific to the stage and pathology of the disease H
J 2.11 Explain the rationale for using systemic therapy to treat cancers of the oropharynx specific to the stage and pathology of the disease
H
J 2.12 Explain the rationale for using radiation therapy to treat cancers of the oropharynx specific to the stage and pathology of the disease
H
J 2.13 Explain the rationale for using combined modalities to treat cancers of the oropharynx specific to the stage and pathology of the disease
H
J 2.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
J 2.15 Interpret protocols for clinical studies and impact on radiation treatment
H
J 2.16 Discuss the emerging technologies relevant to the management of cancers of the oropharynx
H
J 2.17 Explain the predicted results of cancers of the oropharynx treatment based on stage/grade
H
J 2.18 Explain the predicted results of cancers of the oropharynx treatment based on treatment modalities
H
J 2.19 Plan radiation treatment for the patient with cancer of the oropharynx as per Module E2, E3, & E4
H
J 2.20 Perform treatment procedures for the patient with cancer of the oropharynx as per Module E5
H
J 2.21 Perform patient care for the patient with cancer of the oropharynx as per Module E6
H
J 3 Treatment of Cancers of the Oral Cavity H
Page 30
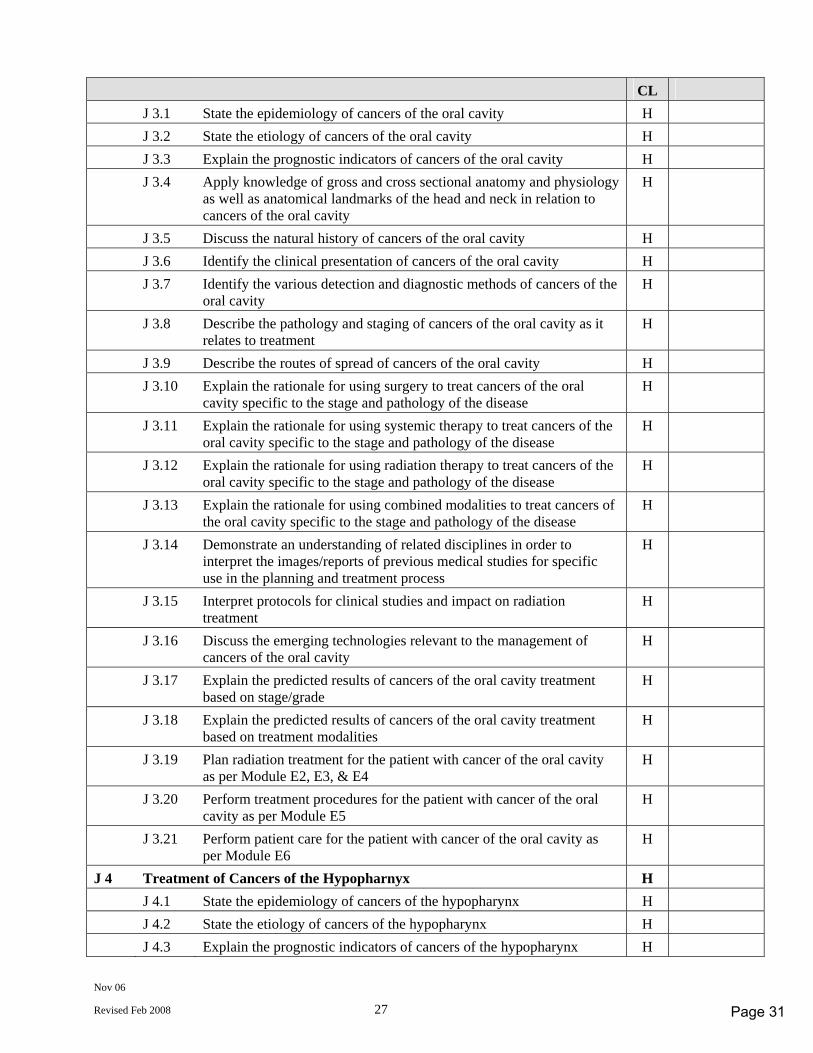
Nov 06
Revised Feb 2008 27
CL J 3.1 State the epidemiology of cancers of the oral cavity H J 3.2 State the etiology of cancers of the oral cavity H J 3.3 Explain the prognostic indicators of cancers of the oral cavity H J 3.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to cancers of the oral cavity
H
J 3.5 Discuss the natural history of cancers of the oral cavity H J 3.6 Identify the clinical presentation of cancers of the oral cavity H J 3.7 Identify the various detection and diagnostic methods of cancers of the
oral cavity H
J 3.8 Describe the pathology and staging of cancers of the oral cavity as it relates to treatment
H
J 3.9 Describe the routes of spread of cancers of the oral cavity H J 3.10 Explain the rationale for using surgery to treat cancers of the oral
cavity specific to the stage and pathology of the disease H
J 3.11 Explain the rationale for using systemic therapy to treat cancers of the oral cavity specific to the stage and pathology of the disease
H
J 3.12 Explain the rationale for using radiation therapy to treat cancers of the oral cavity specific to the stage and pathology of the disease
H
J 3.13 Explain the rationale for using combined modalities to treat cancers of the oral cavity specific to the stage and pathology of the disease
H
J 3.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
J 3.15 Interpret protocols for clinical studies and impact on radiation treatment
H
J 3.16 Discuss the emerging technologies relevant to the management of cancers of the oral cavity
H
J 3.17 Explain the predicted results of cancers of the oral cavity treatment based on stage/grade
H
J 3.18 Explain the predicted results of cancers of the oral cavity treatment based on treatment modalities
H
J 3.19 Plan radiation treatment for the patient with cancer of the oral cavity as per Module E2, E3, & E4
H
J 3.20 Perform treatment procedures for the patient with cancer of the oral cavity as per Module E5
H
J 3.21 Perform patient care for the patient with cancer of the oral cavity as per Module E6
H
J 4 Treatment of Cancers of the Hypopharnyx H J 4.1 State the epidemiology of cancers of the hypopharynx H J 4.2 State the etiology of cancers of the hypopharynx H J 4.3 Explain the prognostic indicators of cancers of the hypopharynx H
Page 31
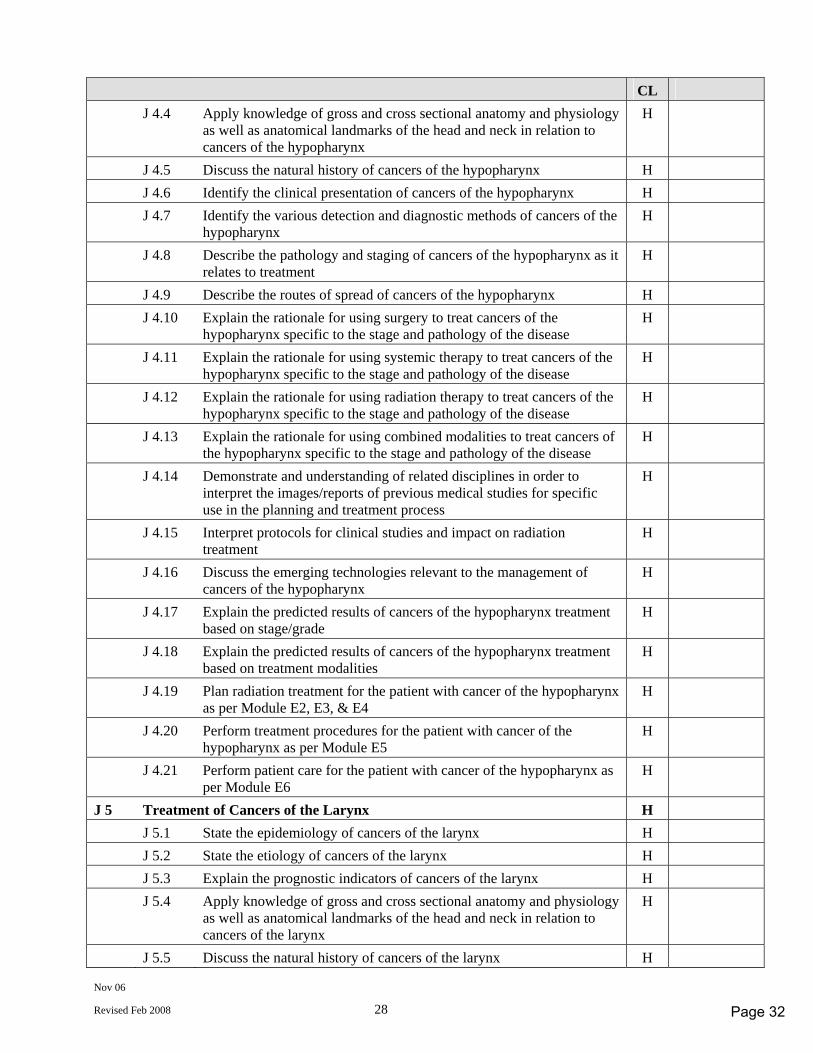
Nov 06
Revised Feb 2008 28
CL J 4.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to cancers of the hypopharynx
H
J 4.5 Discuss the natural history of cancers of the hypopharynx H J 4.6 Identify the clinical presentation of cancers of the hypopharynx H J 4.7 Identify the various detection and diagnostic methods of cancers of the
hypopharynx H
J 4.8 Describe the pathology and staging of cancers of the hypopharynx as it relates to treatment
H
J 4.9 Describe the routes of spread of cancers of the hypopharynx H J 4.10 Explain the rationale for using surgery to treat cancers of the
hypopharynx specific to the stage and pathology of the disease H
J 4.11 Explain the rationale for using systemic therapy to treat cancers of the hypopharynx specific to the stage and pathology of the disease
H
J 4.12 Explain the rationale for using radiation therapy to treat cancers of the hypopharynx specific to the stage and pathology of the disease
H
J 4.13 Explain the rationale for using combined modalities to treat cancers of the hypopharynx specific to the stage and pathology of the disease
H
J 4.14 Demonstrate and understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
J 4.15 Interpret protocols for clinical studies and impact on radiation treatment
H
J 4.16 Discuss the emerging technologies relevant to the management of cancers of the hypopharynx
H
J 4.17 Explain the predicted results of cancers of the hypopharynx treatment based on stage/grade
H
J 4.18 Explain the predicted results of cancers of the hypopharynx treatment based on treatment modalities
H
J 4.19 Plan radiation treatment for the patient with cancer of the hypopharynx as per Module E2, E3, & E4
H
J 4.20 Perform treatment procedures for the patient with cancer of the hypopharynx as per Module E5
H
J 4.21 Perform patient care for the patient with cancer of the hypopharynx as per Module E6
H
J 5 Treatment of Cancers of the Larynx H J 5.1 State the epidemiology of cancers of the larynx H J 5.2 State the etiology of cancers of the larynx H J 5.3 Explain the prognostic indicators of cancers of the larynx H J 5.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to cancers of the larynx
H
J 5.5 Discuss the natural history of cancers of the larynx H
Page 32
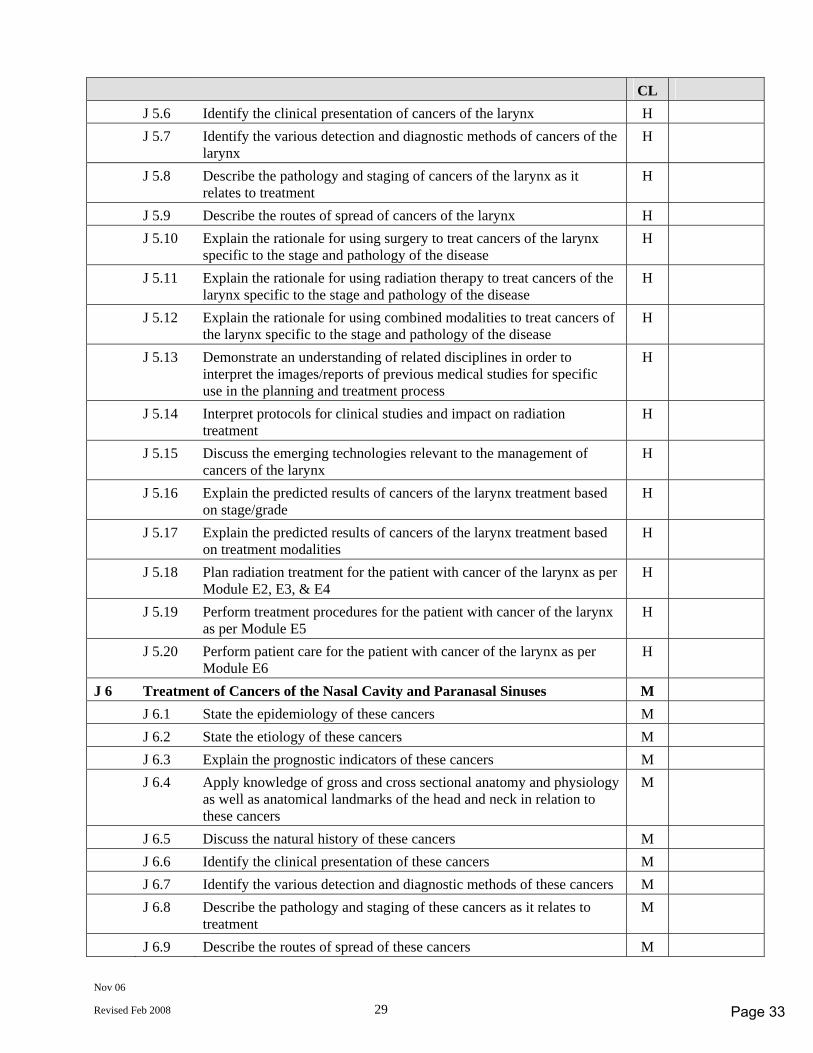
Nov 06
Revised Feb 2008 29
CL J 5.6 Identify the clinical presentation of cancers of the larynx H J 5.7 Identify the various detection and diagnostic methods of cancers of the
larynx H
J 5.8 Describe the pathology and staging of cancers of the larynx as it relates to treatment
H
J 5.9 Describe the routes of spread of cancers of the larynx H J 5.10 Explain the rationale for using surgery to treat cancers of the larynx
specific to the stage and pathology of the disease H
J 5.11 Explain the rationale for using radiation therapy to treat cancers of the larynx specific to the stage and pathology of the disease
H
J 5.12 Explain the rationale for using combined modalities to treat cancers of the larynx specific to the stage and pathology of the disease
H
J 5.13 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
J 5.14 Interpret protocols for clinical studies and impact on radiation treatment
H
J 5.15 Discuss the emerging technologies relevant to the management of cancers of the larynx
H
J 5.16 Explain the predicted results of cancers of the larynx treatment based on stage/grade
H
J 5.17 Explain the predicted results of cancers of the larynx treatment based on treatment modalities
H
J 5.18 Plan radiation treatment for the patient with cancer of the larynx as per Module E2, E3, & E4
H
J 5.19 Perform treatment procedures for the patient with cancer of the larynx as per Module E5
H
J 5.20 Perform patient care for the patient with cancer of the larynx as per Module E6
H
J 6 Treatment of Cancers of the Nasal Cavity and Paranasal Sinuses M J 6.1 State the epidemiology of these cancers M J 6.2 State the etiology of these cancers M J 6.3 Explain the prognostic indicators of these cancers M J 6.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to these cancers
M
J 6.5 Discuss the natural history of these cancers M J 6.6 Identify the clinical presentation of these cancers M J 6.7 Identify the various detection and diagnostic methods of these cancers M J 6.8 Describe the pathology and staging of these cancers as it relates to
treatment M
J 6.9 Describe the routes of spread of these cancers M
Page 33
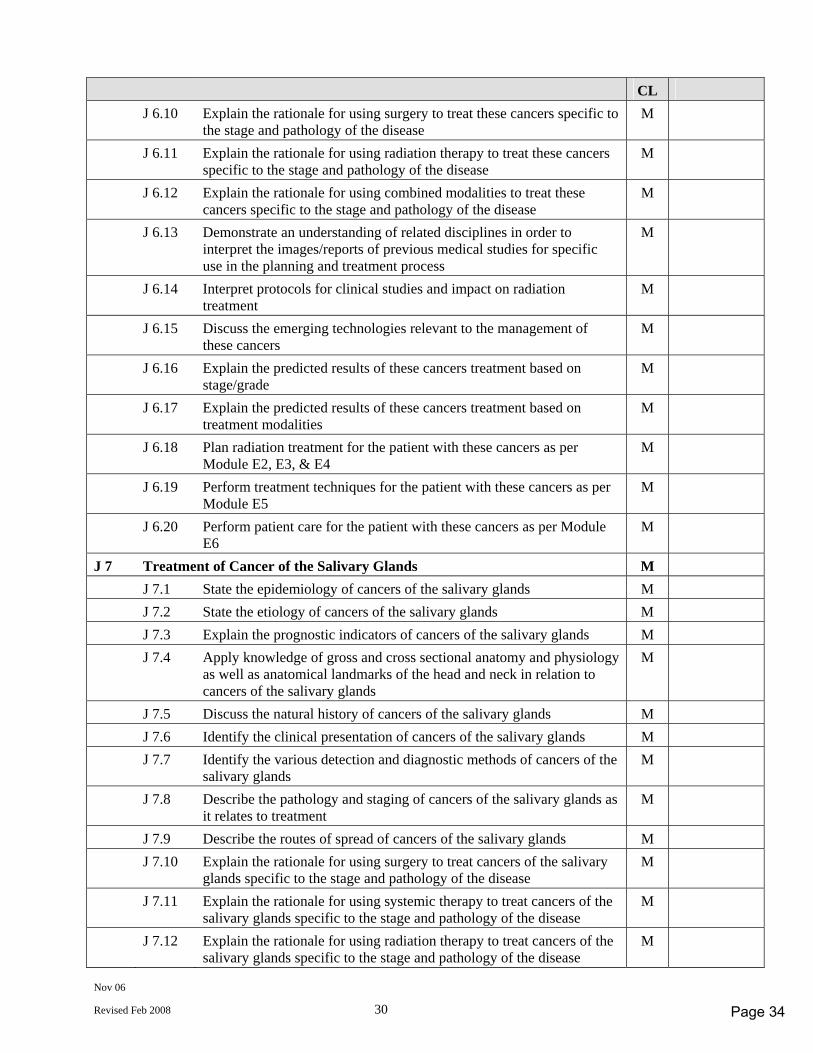
Nov 06
Revised Feb 2008 30
CL J 6.10 Explain the rationale for using surgery to treat these cancers specific to
the stage and pathology of the disease M
J 6.11 Explain the rationale for using radiation therapy to treat these cancers specific to the stage and pathology of the disease
M
J 6.12 Explain the rationale for using combined modalities to treat these cancers specific to the stage and pathology of the disease
M
J 6.13 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
M
J 6.14 Interpret protocols for clinical studies and impact on radiation treatment
M
J 6.15 Discuss the emerging technologies relevant to the management of these cancers
M
J 6.16 Explain the predicted results of these cancers treatment based on stage/grade
M
J 6.17 Explain the predicted results of these cancers treatment based on treatment modalities
M
J 6.18 Plan radiation treatment for the patient with these cancers as per Module E2, E3, & E4
M
J 6.19 Perform treatment techniques for the patient with these cancers as per Module E5
M
J 6.20 Perform patient care for the patient with these cancers as per Module E6
M
J 7 Treatment of Cancer of the Salivary Glands M J 7.1 State the epidemiology of cancers of the salivary glands M J 7.2 State the etiology of cancers of the salivary glands M J 7.3 Explain the prognostic indicators of cancers of the salivary glands M J 7.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head and neck in relation to cancers of the salivary glands
M
J 7.5 Discuss the natural history of cancers of the salivary glands M J 7.6 Identify the clinical presentation of cancers of the salivary glands M J 7.7 Identify the various detection and diagnostic methods of cancers of the
salivary glands M
J 7.8 Describe the pathology and staging of cancers of the salivary glands as it relates to treatment
M
J 7.9 Describe the routes of spread of cancers of the salivary glands M J 7.10 Explain the rationale for using surgery to treat cancers of the salivary
glands specific to the stage and pathology of the disease M
J 7.11 Explain the rationale for using systemic therapy to treat cancers of the salivary glands specific to the stage and pathology of the disease
M
J 7.12 Explain the rationale for using radiation therapy to treat cancers of the salivary glands specific to the stage and pathology of the disease
M
Page 34
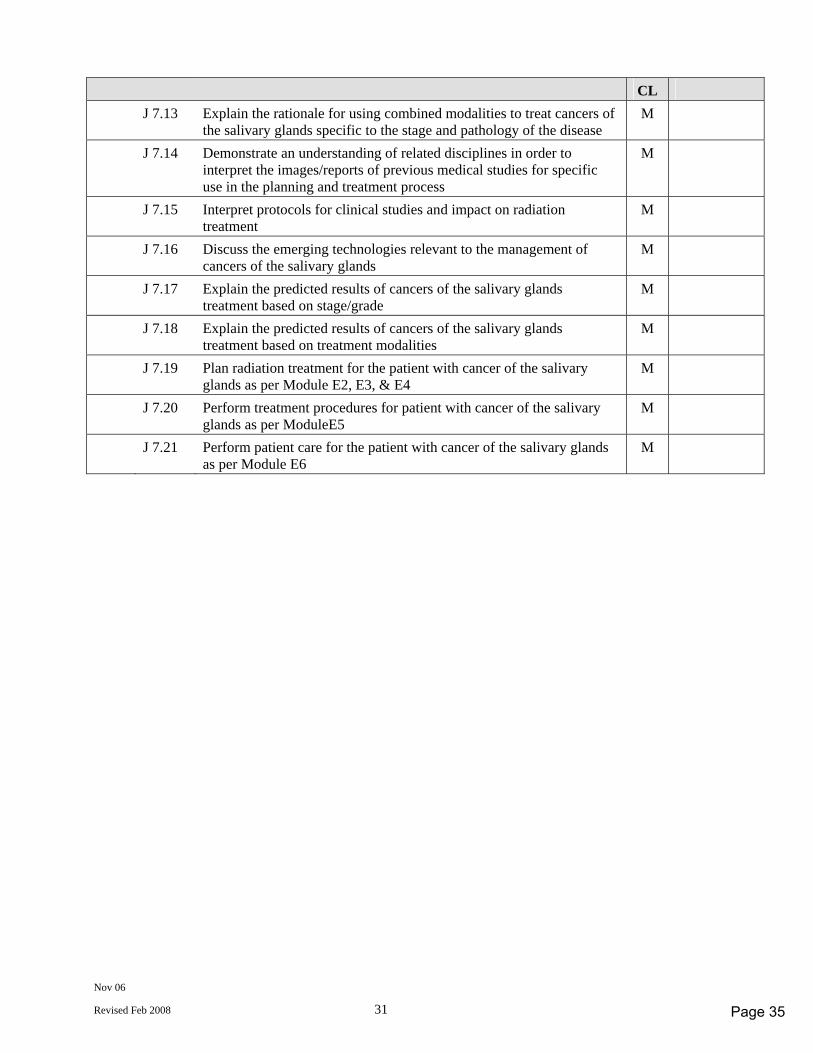
Nov 06
Revised Feb 2008 31
CL J 7.13 Explain the rationale for using combined modalities to treat cancers of
the salivary glands specific to the stage and pathology of the disease M
J 7.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
M
J 7.15 Interpret protocols for clinical studies and impact on radiation treatment
M
J 7.16 Discuss the emerging technologies relevant to the management of cancers of the salivary glands
M
J 7.17 Explain the predicted results of cancers of the salivary glands treatment based on stage/grade
M
J 7.18 Explain the predicted results of cancers of the salivary glands treatment based on treatment modalities
M
J 7.19 Plan radiation treatment for the patient with cancer of the salivary glands as per Module E2, E3, & E4
M
J 7.20 Perform treatment procedures for patient with cancer of the salivary glands as per ModuleE5
M
J 7.21 Perform patient care for the patient with cancer of the salivary glands as per Module E6
M
Page 35
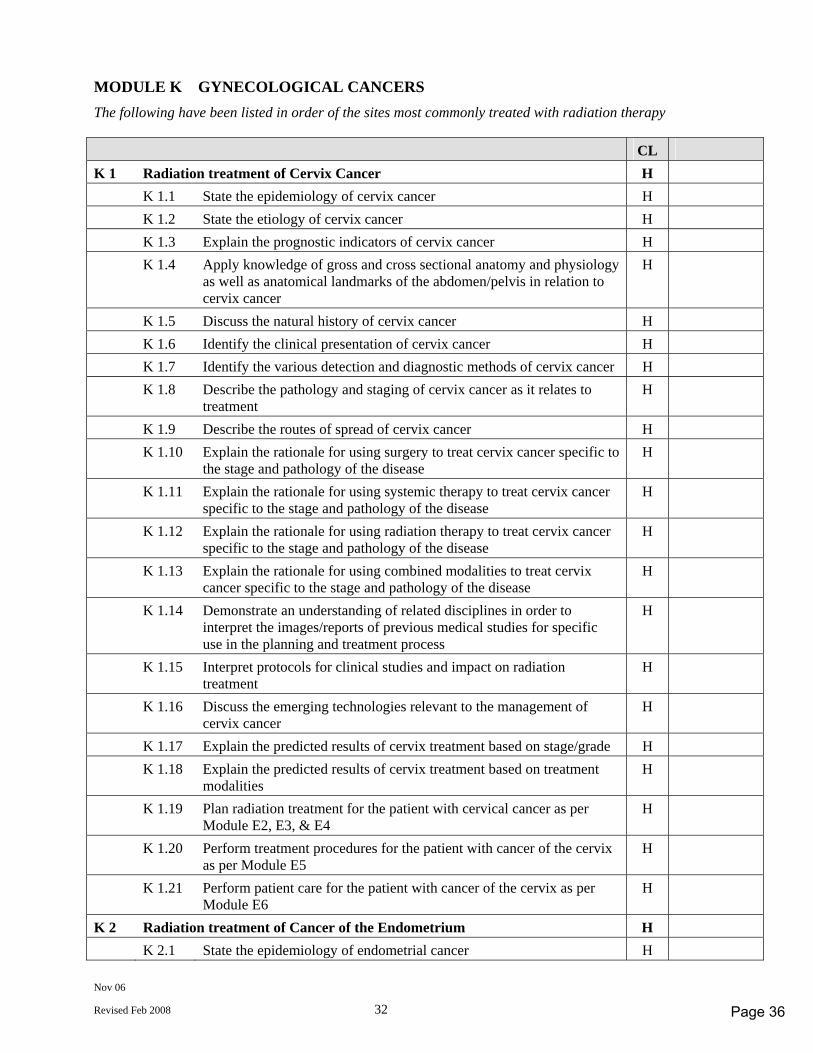
Nov 06
Revised Feb 2008 32
MODULE K GYNECOLOGICAL CANCERS The following have been listed in order of the sites most commonly treated with radiation therapy CL K 1 Radiation treatment of Cervix Cancer H K 1.1 State the epidemiology of cervix cancer H K 1.2 State the etiology of cervix cancer H K 1.3 Explain the prognostic indicators of cervix cancer H K 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to cervix cancer
H
K 1.5 Discuss the natural history of cervix cancer H K 1.6 Identify the clinical presentation of cervix cancer H K 1.7 Identify the various detection and diagnostic methods of cervix cancer H K 1.8 Describe the pathology and staging of cervix cancer as it relates to
treatment H
K 1.9 Describe the routes of spread of cervix cancer H K 1.10 Explain the rationale for using surgery to treat cervix cancer specific to
the stage and pathology of the disease H
K 1.11 Explain the rationale for using systemic therapy to treat cervix cancer specific to the stage and pathology of the disease
H
K 1.12 Explain the rationale for using radiation therapy to treat cervix cancer specific to the stage and pathology of the disease
H
K 1.13 Explain the rationale for using combined modalities to treat cervix cancer specific to the stage and pathology of the disease
H
K 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
K 1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
K 1.16 Discuss the emerging technologies relevant to the management of cervix cancer
H
K 1.17 Explain the predicted results of cervix treatment based on stage/grade H K 1.18 Explain the predicted results of cervix treatment based on treatment
modalities H
K 1.19 Plan radiation treatment for the patient with cervical cancer as per Module E2, E3, & E4
H
K 1.20 Perform treatment procedures for the patient with cancer of the cervix as per Module E5
H
K 1.21 Perform patient care for the patient with cancer of the cervix as per Module E6
H
K 2 Radiation treatment of Cancer of the Endometrium H K 2.1 State the epidemiology of endometrial cancer H
Page 36
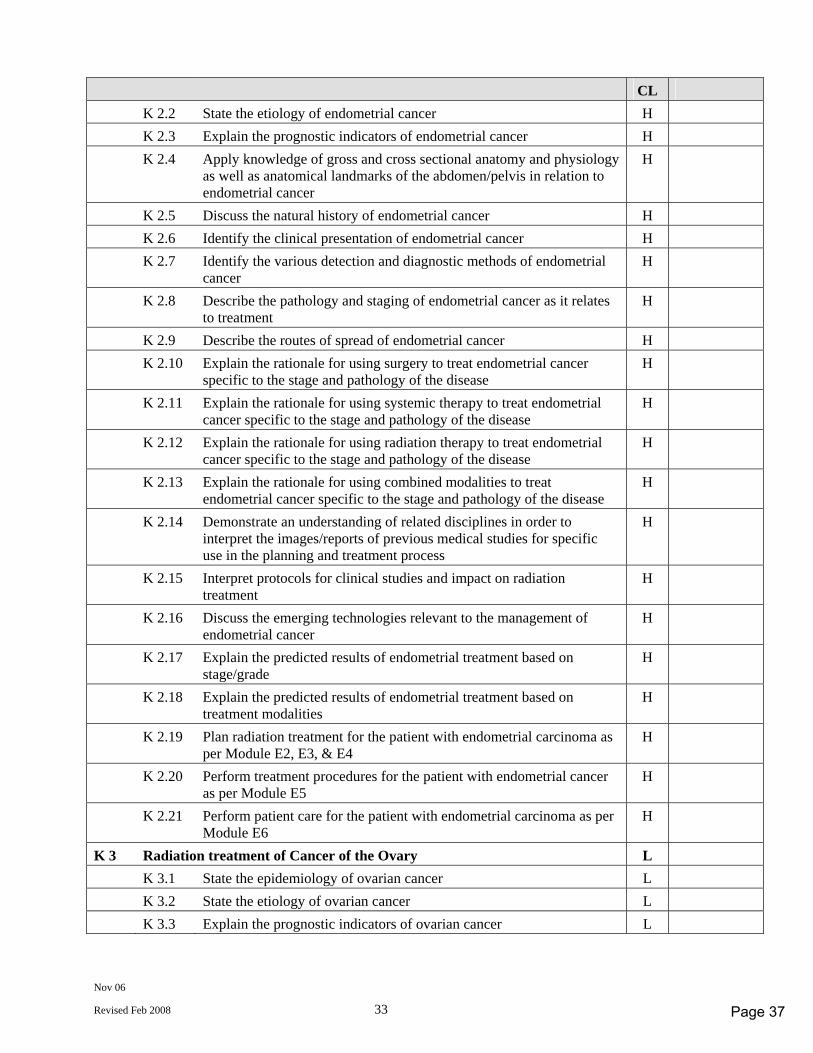
Nov 06
Revised Feb 2008 33
CL K 2.2 State the etiology of endometrial cancer H K 2.3 Explain the prognostic indicators of endometrial cancer H K 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to endometrial cancer
H
K 2.5 Discuss the natural history of endometrial cancer H K 2.6 Identify the clinical presentation of endometrial cancer H K 2.7 Identify the various detection and diagnostic methods of endometrial
cancer H
K 2.8 Describe the pathology and staging of endometrial cancer as it relates to treatment
H
K 2.9 Describe the routes of spread of endometrial cancer H K 2.10 Explain the rationale for using surgery to treat endometrial cancer
specific to the stage and pathology of the disease H
K 2.11 Explain the rationale for using systemic therapy to treat endometrial cancer specific to the stage and pathology of the disease
H
K 2.12 Explain the rationale for using radiation therapy to treat endometrial cancer specific to the stage and pathology of the disease
H
K 2.13 Explain the rationale for using combined modalities to treat endometrial cancer specific to the stage and pathology of the disease
H
K 2.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
K 2.15 Interpret protocols for clinical studies and impact on radiation treatment
H
K 2.16 Discuss the emerging technologies relevant to the management of endometrial cancer
H
K 2.17 Explain the predicted results of endometrial treatment based on stage/grade
H
K 2.18 Explain the predicted results of endometrial treatment based on treatment modalities
H
K 2.19 Plan radiation treatment for the patient with endometrial carcinoma as per Module E2, E3, & E4
H
K 2.20 Perform treatment procedures for the patient with endometrial cancer as per Module E5
H
K 2.21 Perform patient care for the patient with endometrial carcinoma as per Module E6
H
K 3 Radiation treatment of Cancer of the Ovary L K 3.1 State the epidemiology of ovarian cancer L K 3.2 State the etiology of ovarian cancer L K 3.3 Explain the prognostic indicators of ovarian cancer L
Page 37
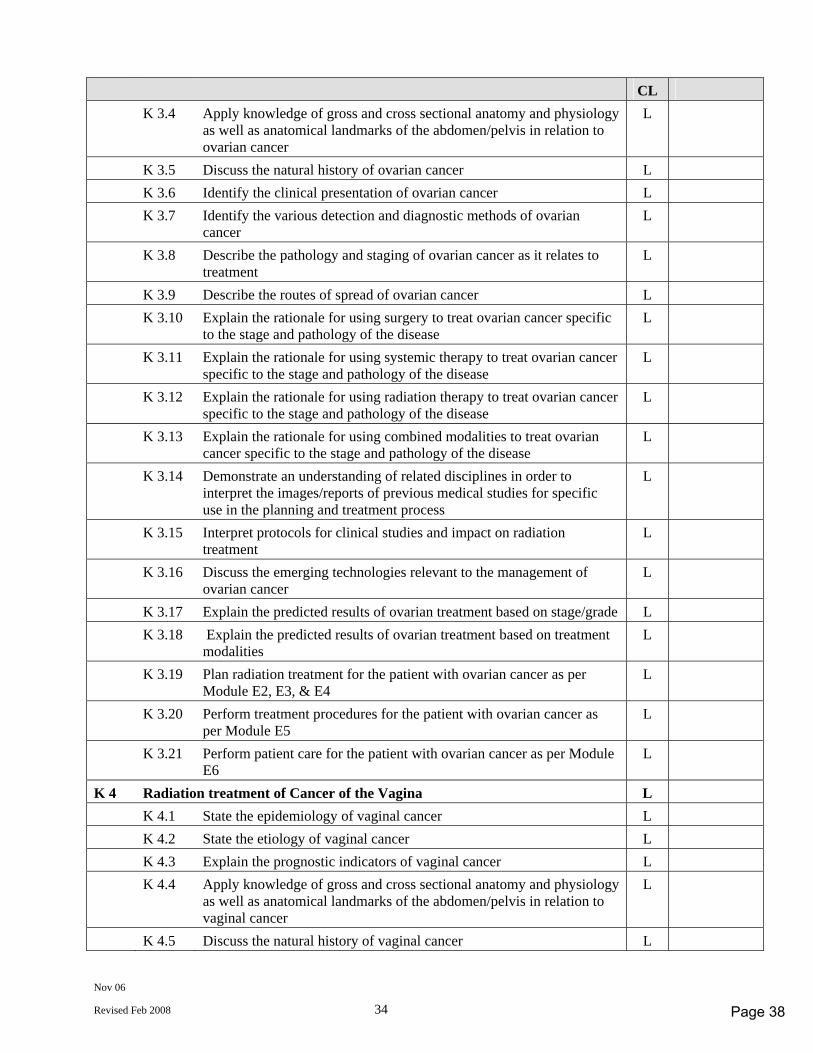
Nov 06
Revised Feb 2008 34
CL K 3.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to ovarian cancer
L
K 3.5 Discuss the natural history of ovarian cancer L K 3.6 Identify the clinical presentation of ovarian cancer L K 3.7 Identify the various detection and diagnostic methods of ovarian
cancer L
K 3.8 Describe the pathology and staging of ovarian cancer as it relates to treatment
L
K 3.9 Describe the routes of spread of ovarian cancer L K 3.10 Explain the rationale for using surgery to treat ovarian cancer specific
to the stage and pathology of the disease L
K 3.11 Explain the rationale for using systemic therapy to treat ovarian cancer specific to the stage and pathology of the disease
L
K 3.12 Explain the rationale for using radiation therapy to treat ovarian cancer specific to the stage and pathology of the disease
L
K 3.13 Explain the rationale for using combined modalities to treat ovarian cancer specific to the stage and pathology of the disease
L
K 3.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
L
K 3.15 Interpret protocols for clinical studies and impact on radiation treatment
L
K 3.16 Discuss the emerging technologies relevant to the management of ovarian cancer
L
K 3.17 Explain the predicted results of ovarian treatment based on stage/grade L K 3.18 Explain the predicted results of ovarian treatment based on treatment
modalities L
K 3.19 Plan radiation treatment for the patient with ovarian cancer as per Module E2, E3, & E4
L
K 3.20 Perform treatment procedures for the patient with ovarian cancer as per Module E5
L
K 3.21 Perform patient care for the patient with ovarian cancer as per Module E6
L
K 4 Radiation treatment of Cancer of the Vagina L K 4.1 State the epidemiology of vaginal cancer L K 4.2 State the etiology of vaginal cancer L K 4.3 Explain the prognostic indicators of vaginal cancer L K 4.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to vaginal cancer
L
K 4.5 Discuss the natural history of vaginal cancer L
Page 38
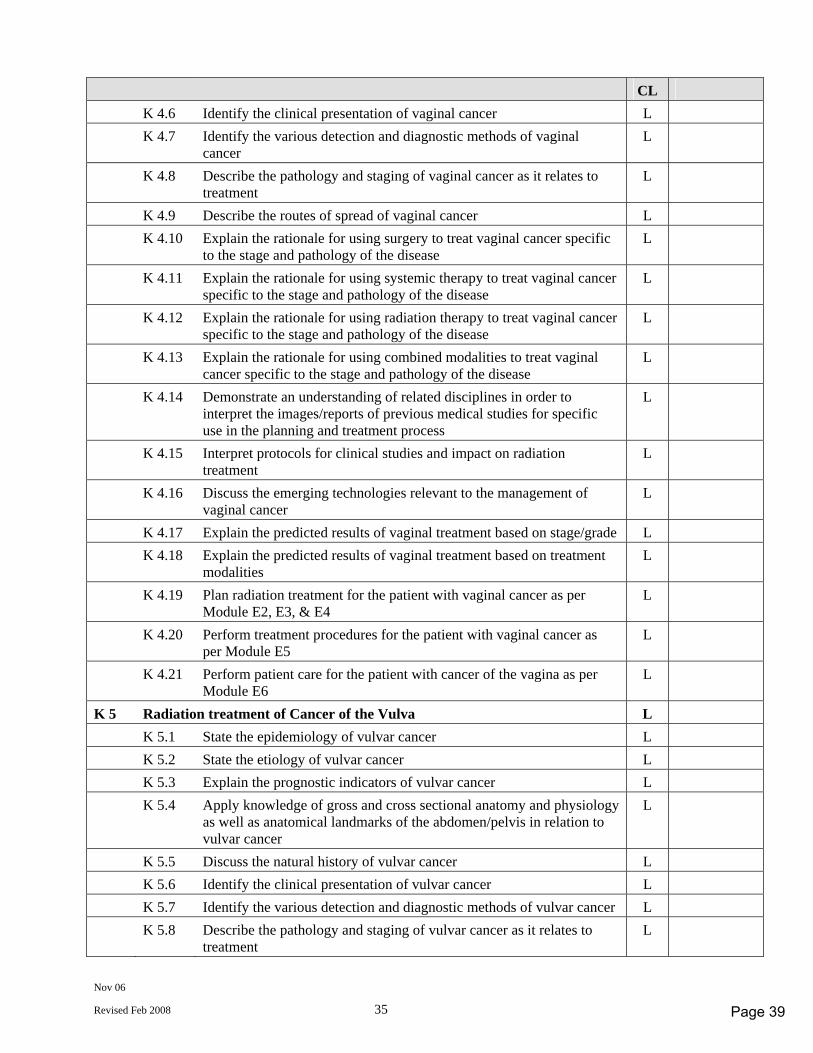
Nov 06
Revised Feb 2008 35
CL K 4.6 Identify the clinical presentation of vaginal cancer L K 4.7 Identify the various detection and diagnostic methods of vaginal
cancer L
K 4.8 Describe the pathology and staging of vaginal cancer as it relates to treatment
L
K 4.9 Describe the routes of spread of vaginal cancer L K 4.10 Explain the rationale for using surgery to treat vaginal cancer specific
to the stage and pathology of the disease L
K 4.11 Explain the rationale for using systemic therapy to treat vaginal cancer specific to the stage and pathology of the disease
L
K 4.12 Explain the rationale for using radiation therapy to treat vaginal cancer specific to the stage and pathology of the disease
L
K 4.13 Explain the rationale for using combined modalities to treat vaginal cancer specific to the stage and pathology of the disease
L
K 4.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
L
K 4.15 Interpret protocols for clinical studies and impact on radiation treatment
L
K 4.16 Discuss the emerging technologies relevant to the management of vaginal cancer
L
K 4.17 Explain the predicted results of vaginal treatment based on stage/grade L K 4.18 Explain the predicted results of vaginal treatment based on treatment
modalities L
K 4.19 Plan radiation treatment for the patient with vaginal cancer as per Module E2, E3, & E4
L
K 4.20 Perform treatment procedures for the patient with vaginal cancer as per Module E5
L
K 4.21 Perform patient care for the patient with cancer of the vagina as per Module E6
L
K 5 Radiation treatment of Cancer of the Vulva L K 5.1 State the epidemiology of vulvar cancer L K 5.2 State the etiology of vulvar cancer L K 5.3 Explain the prognostic indicators of vulvar cancer L K 5.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the abdomen/pelvis in relation to vulvar cancer
L
K 5.5 Discuss the natural history of vulvar cancer L K 5.6 Identify the clinical presentation of vulvar cancer L K 5.7 Identify the various detection and diagnostic methods of vulvar cancer L K 5.8 Describe the pathology and staging of vulvar cancer as it relates to
treatment L
Page 39
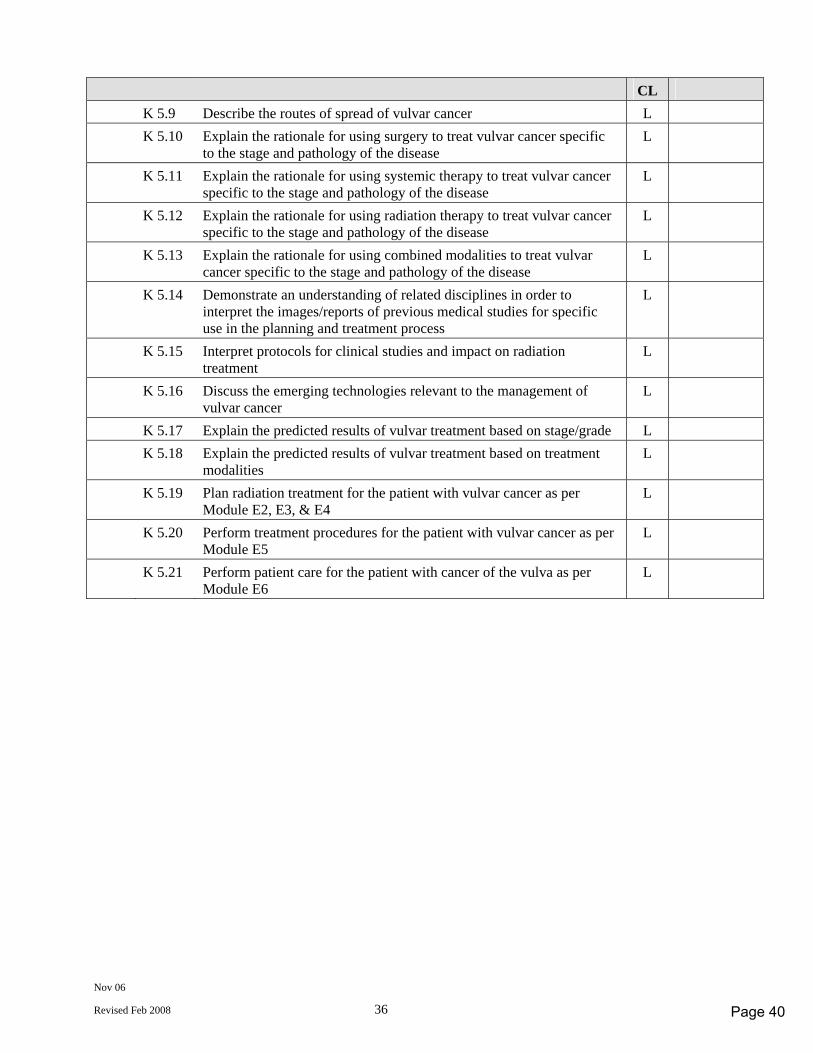
Nov 06
Revised Feb 2008 36
CL K 5.9 Describe the routes of spread of vulvar cancer L K 5.10 Explain the rationale for using surgery to treat vulvar cancer specific
to the stage and pathology of the disease L
K 5.11 Explain the rationale for using systemic therapy to treat vulvar cancer specific to the stage and pathology of the disease
L
K 5.12 Explain the rationale for using radiation therapy to treat vulvar cancer specific to the stage and pathology of the disease
L
K 5.13 Explain the rationale for using combined modalities to treat vulvar cancer specific to the stage and pathology of the disease
L
K 5.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
L
K 5.15 Interpret protocols for clinical studies and impact on radiation treatment
L
K 5.16 Discuss the emerging technologies relevant to the management of vulvar cancer
L
K 5.17 Explain the predicted results of vulvar treatment based on stage/grade L K 5.18 Explain the predicted results of vulvar treatment based on treatment
modalities L
K 5.19 Plan radiation treatment for the patient with vulvar cancer as per Module E2, E3, & E4
L
K 5.20 Perform treatment procedures for the patient with vulvar cancer as per Module E5
L
K 5.21 Perform patient care for the patient with cancer of the vulva as per Module E6
L
Page 40
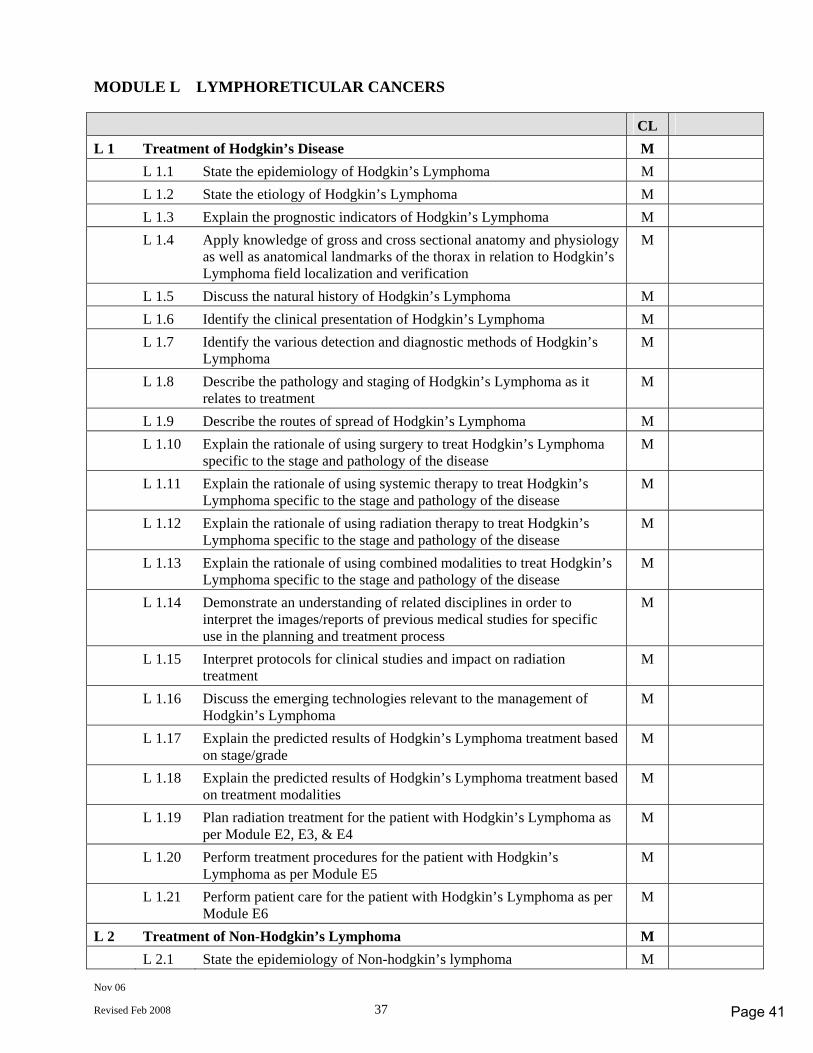
Nov 06
Revised Feb 2008 37
MODULE L LYMPHORETICULAR CANCERS CL L 1 Treatment of Hodgkin’s Disease M L 1.1 State the epidemiology of Hodgkin’s Lymphoma M L 1.2 State the etiology of Hodgkin’s Lymphoma M L 1.3 Explain the prognostic indicators of Hodgkin’s Lymphoma M L 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the thorax in relation to Hodgkin’s Lymphoma field localization and verification
M
L 1.5 Discuss the natural history of Hodgkin’s Lymphoma M L 1.6 Identify the clinical presentation of Hodgkin’s Lymphoma M L 1.7 Identify the various detection and diagnostic methods of Hodgkin’s
Lymphoma M
L 1.8 Describe the pathology and staging of Hodgkin’s Lymphoma as it relates to treatment
M
L 1.9 Describe the routes of spread of Hodgkin’s Lymphoma M L 1.10 Explain the rationale of using surgery to treat Hodgkin’s Lymphoma
specific to the stage and pathology of the disease M
L 1.11 Explain the rationale of using systemic therapy to treat Hodgkin’s Lymphoma specific to the stage and pathology of the disease
M
L 1.12 Explain the rationale of using radiation therapy to treat Hodgkin’s Lymphoma specific to the stage and pathology of the disease
M
L 1.13 Explain the rationale of using combined modalities to treat Hodgkin’s Lymphoma specific to the stage and pathology of the disease
M
L 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
M
L 1.15 Interpret protocols for clinical studies and impact on radiation treatment
M
L 1.16 Discuss the emerging technologies relevant to the management of Hodgkin’s Lymphoma
M
L 1.17 Explain the predicted results of Hodgkin’s Lymphoma treatment based on stage/grade
M
L 1.18 Explain the predicted results of Hodgkin’s Lymphoma treatment based on treatment modalities
M
L 1.19 Plan radiation treatment for the patient with Hodgkin’s Lymphoma as per Module E2, E3, & E4
M
L 1.20 Perform treatment procedures for the patient with Hodgkin’s Lymphoma as per Module E5
M
L 1.21 Perform patient care for the patient with Hodgkin’s Lymphoma as per Module E6
M
L 2 Treatment of Non-Hodgkin’s Lymphoma M L 2.1 State the epidemiology of Non-hodgkin’s lymphoma M
Page 41
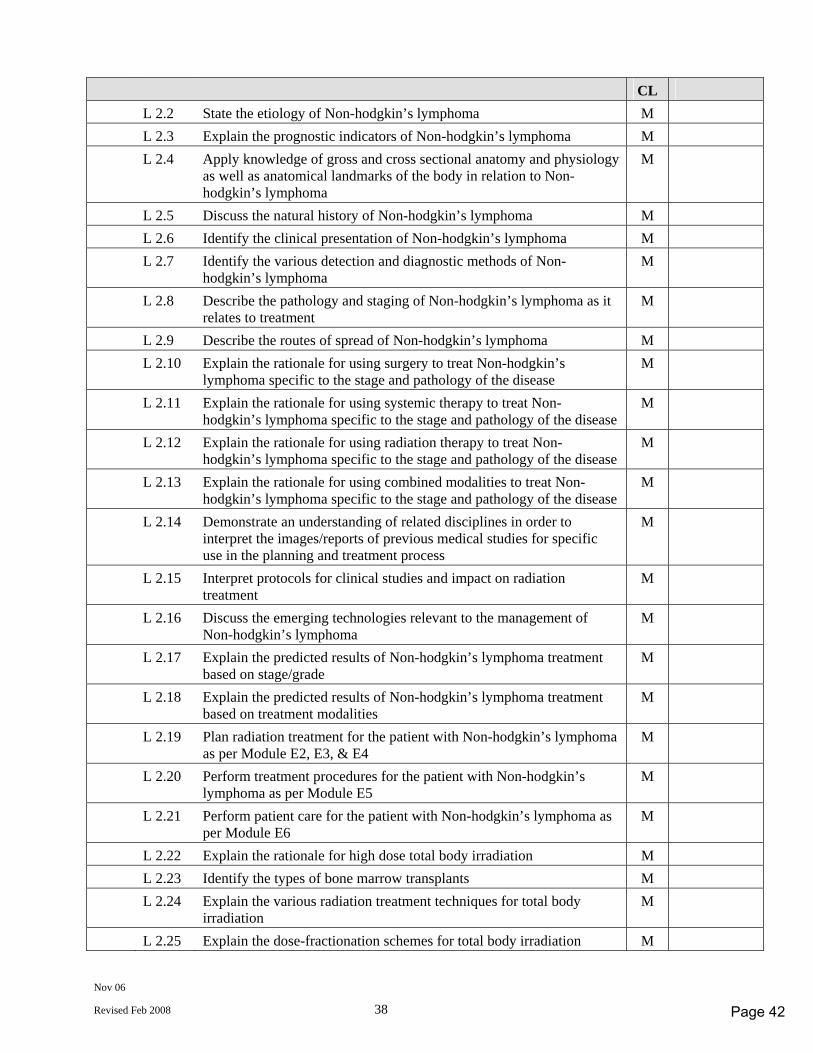
Nov 06
Revised Feb 2008 38
CL L 2.2 State the etiology of Non-hodgkin’s lymphoma M L 2.3 Explain the prognostic indicators of Non-hodgkin’s lymphoma M L 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to Non-hodgkin’s lymphoma
M
L 2.5 Discuss the natural history of Non-hodgkin’s lymphoma M L 2.6 Identify the clinical presentation of Non-hodgkin’s lymphoma M L 2.7 Identify the various detection and diagnostic methods of Non-
hodgkin’s lymphoma M
L 2.8 Describe the pathology and staging of Non-hodgkin’s lymphoma as it relates to treatment
M
L 2.9 Describe the routes of spread of Non-hodgkin’s lymphoma M L 2.10 Explain the rationale for using surgery to treat Non-hodgkin’s
lymphoma specific to the stage and pathology of the disease M
L 2.11 Explain the rationale for using systemic therapy to treat Non-hodgkin’s lymphoma specific to the stage and pathology of the disease
M
L 2.12 Explain the rationale for using radiation therapy to treat Non-hodgkin’s lymphoma specific to the stage and pathology of the disease
M
L 2.13 Explain the rationale for using combined modalities to treat Non-hodgkin’s lymphoma specific to the stage and pathology of the disease
M
L 2.14 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
M
L 2.15 Interpret protocols for clinical studies and impact on radiation treatment
M
L 2.16 Discuss the emerging technologies relevant to the management of Non-hodgkin’s lymphoma
M
L 2.17 Explain the predicted results of Non-hodgkin’s lymphoma treatment based on stage/grade
M
L 2.18 Explain the predicted results of Non-hodgkin’s lymphoma treatment based on treatment modalities
M
L 2.19 Plan radiation treatment for the patient with Non-hodgkin’s lymphoma as per Module E2, E3, & E4
M
L 2.20 Perform treatment procedures for the patient with Non-hodgkin’s lymphoma as per Module E5
M
L 2.21 Perform patient care for the patient with Non-hodgkin’s lymphoma as per Module E6
M
L 2.22 Explain the rationale for high dose total body irradiation M L 2.23 Identify the types of bone marrow transplants M L 2.24 Explain the various radiation treatment techniques for total body
irradiation M
L 2.25 Explain the dose-fractionation schemes for total body irradiation M
Page 42
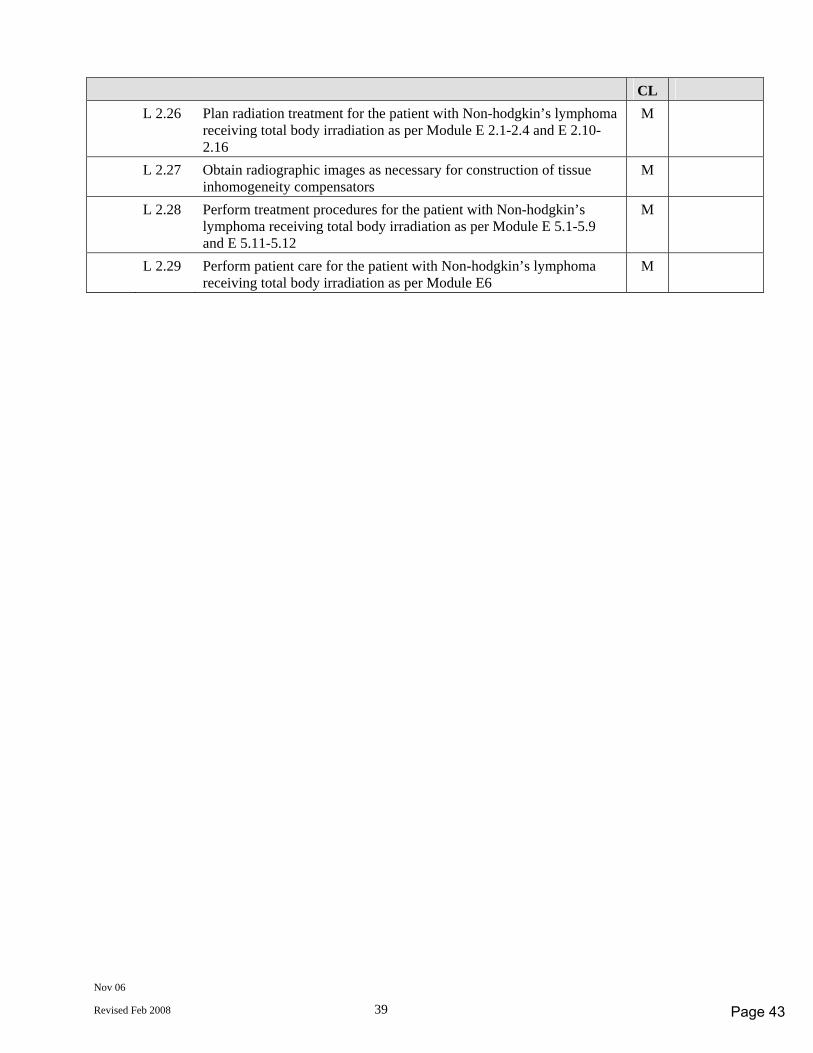
Nov 06
Revised Feb 2008 39
CL L 2.26 Plan radiation treatment for the patient with Non-hodgkin’s lymphoma
receiving total body irradiation as per Module E 2.1-2.4 and E 2.10-2.16
M
L 2.27 Obtain radiographic images as necessary for construction of tissue inhomogeneity compensators
M
L 2.28 Perform treatment procedures for the patient with Non-hodgkin’s lymphoma receiving total body irradiation as per Module E 5.1-5.9 and E 5.11-5.12
M
L 2.29 Perform patient care for the patient with Non-hodgkin’s lymphoma receiving total body irradiation as per Module E6
M
Page 43
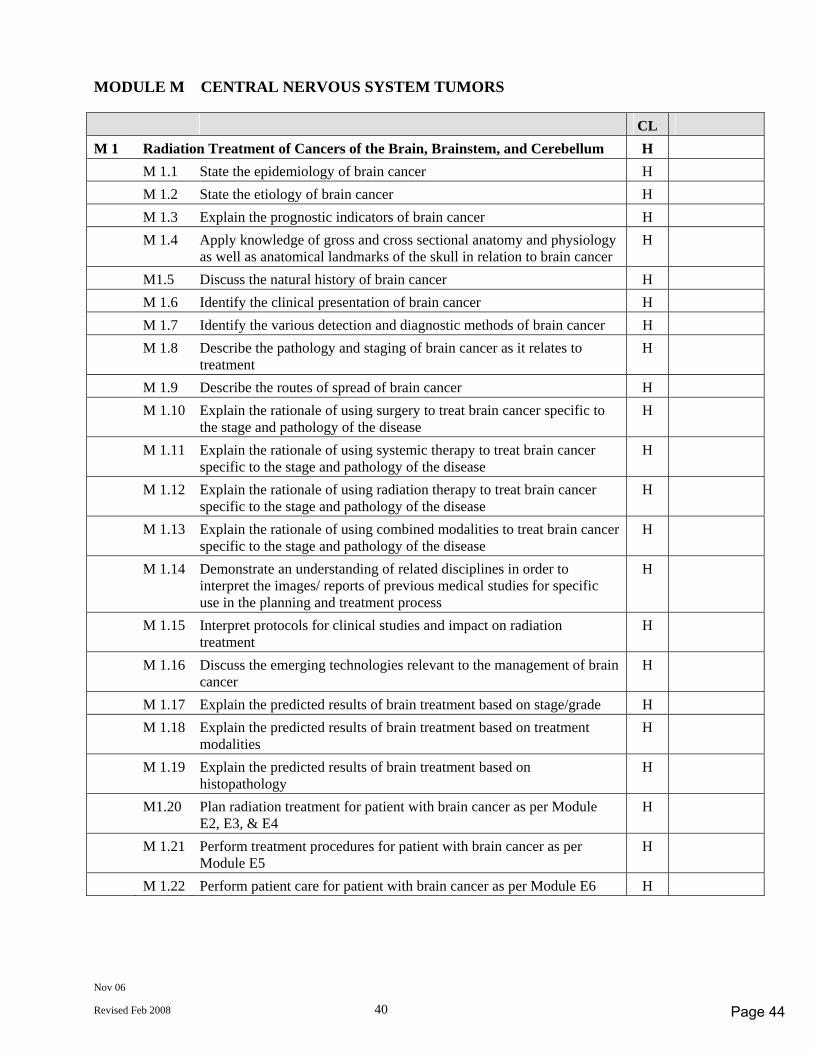
Nov 06
Revised Feb 2008 40
MODULE M CENTRAL NERVOUS SYSTEM TUMORS CL M 1 Radiation Treatment of Cancers of the Brain, Brainstem, and Cerebellum H M 1.1 State the epidemiology of brain cancer H M 1.2 State the etiology of brain cancer H M 1.3 Explain the prognostic indicators of brain cancer H M 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the skull in relation to brain cancer H
M1.5 Discuss the natural history of brain cancer H M 1.6 Identify the clinical presentation of brain cancer H M 1.7 Identify the various detection and diagnostic methods of brain cancer H M 1.8 Describe the pathology and staging of brain cancer as it relates to
treatment H
M 1.9 Describe the routes of spread of brain cancer H M 1.10 Explain the rationale of using surgery to treat brain cancer specific to
the stage and pathology of the disease H
M 1.11 Explain the rationale of using systemic therapy to treat brain cancer specific to the stage and pathology of the disease
H
M 1.12 Explain the rationale of using radiation therapy to treat brain cancer specific to the stage and pathology of the disease
H
M 1.13 Explain the rationale of using combined modalities to treat brain cancer specific to the stage and pathology of the disease
H
M 1.14 Demonstrate an understanding of related disciplines in order to interpret the images/ reports of previous medical studies for specific use in the planning and treatment process
H
M 1.15 Interpret protocols for clinical studies and impact on radiation treatment
H
M 1.16 Discuss the emerging technologies relevant to the management of brain cancer
H
M 1.17 Explain the predicted results of brain treatment based on stage/grade H M 1.18 Explain the predicted results of brain treatment based on treatment
modalities H
M 1.19 Explain the predicted results of brain treatment based on histopathology
H
M1.20 Plan radiation treatment for patient with brain cancer as per Module E2, E3, & E4
H
M 1.21 Perform treatment procedures for patient with brain cancer as per Module E5
H
M 1.22 Perform patient care for patient with brain cancer as per Module E6 H
Page 44
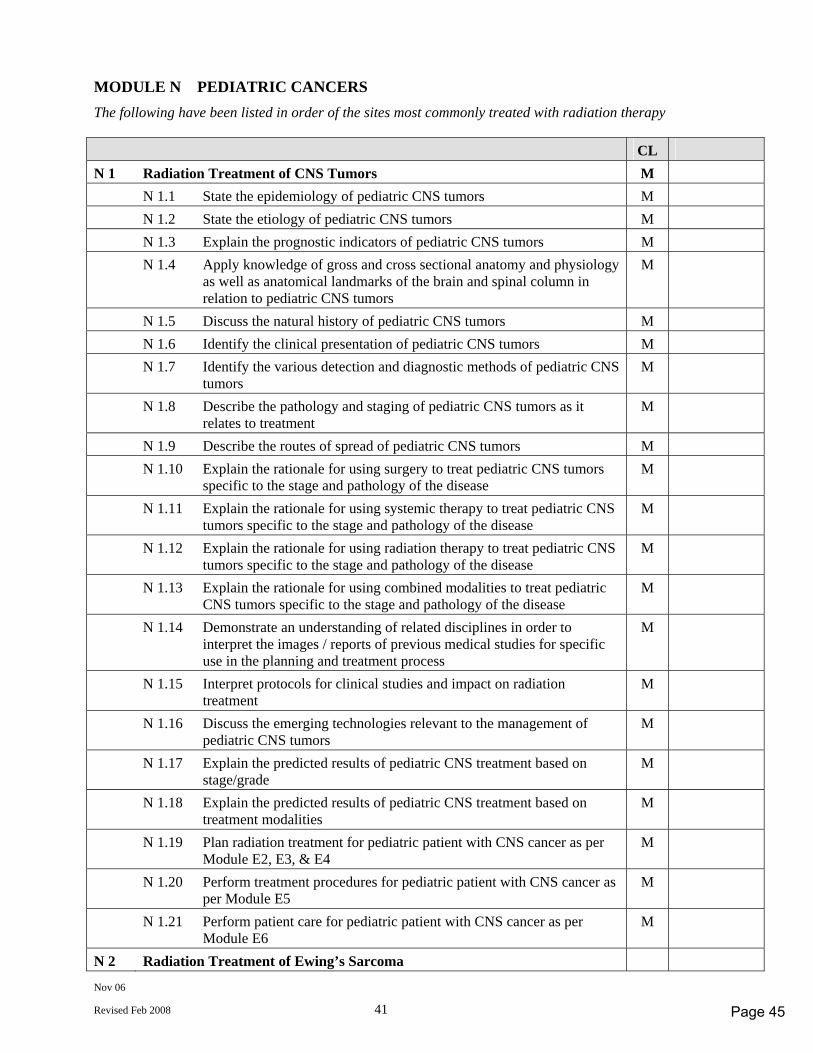
Nov 06
Revised Feb 2008 41
MODULE N PEDIATRIC CANCERS The following have been listed in order of the sites most commonly treated with radiation therapy CL N 1 Radiation Treatment of CNS Tumors M N 1.1 State the epidemiology of pediatric CNS tumors M N 1.2 State the etiology of pediatric CNS tumors M N 1.3 Explain the prognostic indicators of pediatric CNS tumors M N 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the brain and spinal column in relation to pediatric CNS tumors
M
N 1.5 Discuss the natural history of pediatric CNS tumors M N 1.6 Identify the clinical presentation of pediatric CNS tumors M N 1.7 Identify the various detection and diagnostic methods of pediatric CNS
tumors M
N 1.8 Describe the pathology and staging of pediatric CNS tumors as it relates to treatment
M
N 1.9 Describe the routes of spread of pediatric CNS tumors M N 1.10 Explain the rationale for using surgery to treat pediatric CNS tumors
specific to the stage and pathology of the disease M
N 1.11 Explain the rationale for using systemic therapy to treat pediatric CNS tumors specific to the stage and pathology of the disease
M
N 1.12 Explain the rationale for using radiation therapy to treat pediatric CNS tumors specific to the stage and pathology of the disease
M
N 1.13 Explain the rationale for using combined modalities to treat pediatric CNS tumors specific to the stage and pathology of the disease
M
N 1.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
M
N 1.15 Interpret protocols for clinical studies and impact on radiation treatment
M
N 1.16 Discuss the emerging technologies relevant to the management of pediatric CNS tumors
M
N 1.17 Explain the predicted results of pediatric CNS treatment based on stage/grade
M
N 1.18 Explain the predicted results of pediatric CNS treatment based on treatment modalities
M
N 1.19 Plan radiation treatment for pediatric patient with CNS cancer as per Module E2, E3, & E4
M
N 1.20 Perform treatment procedures for pediatric patient with CNS cancer as per Module E5
M
N 1.21 Perform patient care for pediatric patient with CNS cancer as per Module E6
M
N 2 Radiation Treatment of Ewing’s Sarcoma
Page 45
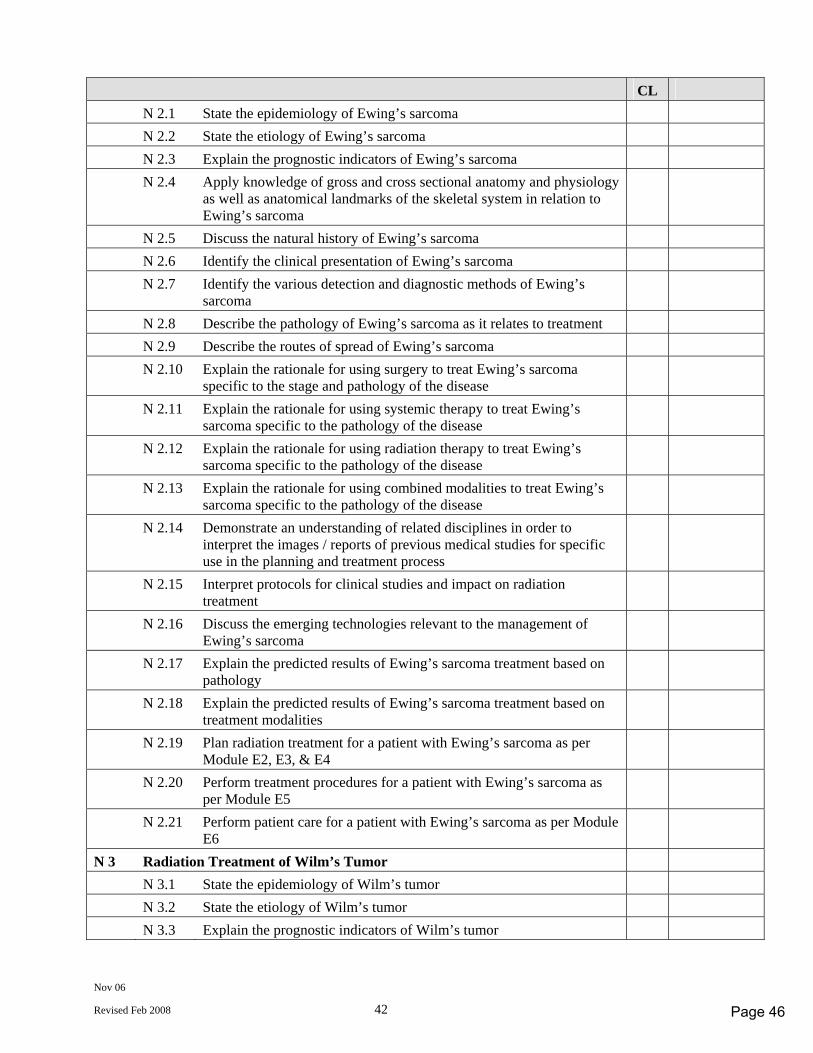
Nov 06
Revised Feb 2008 42
CL N 2.1 State the epidemiology of Ewing’s sarcoma N 2.2 State the etiology of Ewing’s sarcoma N 2.3 Explain the prognostic indicators of Ewing’s sarcoma N 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the skeletal system in relation to Ewing’s sarcoma
N 2.5 Discuss the natural history of Ewing’s sarcoma N 2.6 Identify the clinical presentation of Ewing’s sarcoma N 2.7 Identify the various detection and diagnostic methods of Ewing’s
sarcoma
N 2.8 Describe the pathology of Ewing’s sarcoma as it relates to treatment N 2.9 Describe the routes of spread of Ewing’s sarcoma N 2.10 Explain the rationale for using surgery to treat Ewing’s sarcoma
specific to the stage and pathology of the disease
N 2.11 Explain the rationale for using systemic therapy to treat Ewing’s sarcoma specific to the pathology of the disease
N 2.12 Explain the rationale for using radiation therapy to treat Ewing’s sarcoma specific to the pathology of the disease
N 2.13 Explain the rationale for using combined modalities to treat Ewing’s sarcoma specific to the pathology of the disease
N 2.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
N 2.15 Interpret protocols for clinical studies and impact on radiation treatment
N 2.16 Discuss the emerging technologies relevant to the management of Ewing’s sarcoma
N 2.17 Explain the predicted results of Ewing’s sarcoma treatment based on pathology
N 2.18 Explain the predicted results of Ewing’s sarcoma treatment based on treatment modalities
N 2.19 Plan radiation treatment for a patient with Ewing’s sarcoma as per Module E2, E3, & E4
N 2.20 Perform treatment procedures for a patient with Ewing’s sarcoma as per Module E5
N 2.21 Perform patient care for a patient with Ewing’s sarcoma as per Module E6
N 3 Radiation Treatment of Wilm’s Tumor N 3.1 State the epidemiology of Wilm’s tumor N 3.2 State the etiology of Wilm’s tumor N 3.3 Explain the prognostic indicators of Wilm’s tumor
Page 46
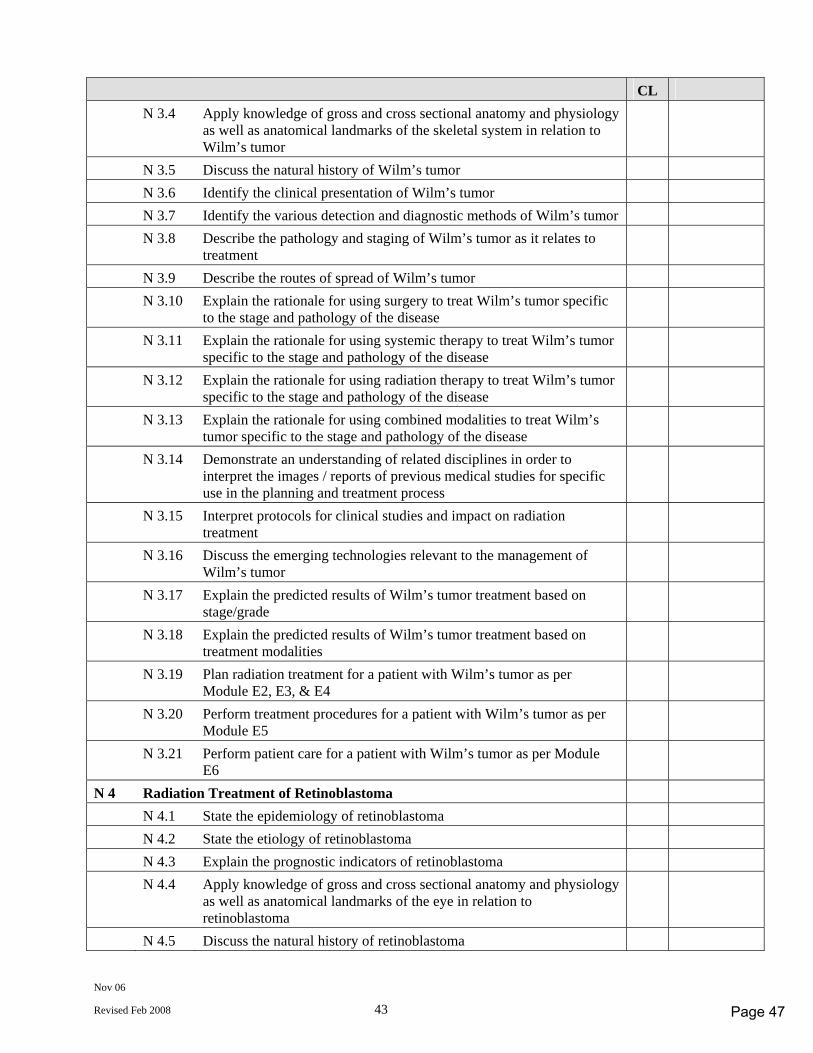
Nov 06
Revised Feb 2008 43
CL N 3.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the skeletal system in relation to Wilm’s tumor
N 3.5 Discuss the natural history of Wilm’s tumor N 3.6 Identify the clinical presentation of Wilm’s tumor N 3.7 Identify the various detection and diagnostic methods of Wilm’s tumor N 3.8 Describe the pathology and staging of Wilm’s tumor as it relates to
treatment
N 3.9 Describe the routes of spread of Wilm’s tumor N 3.10 Explain the rationale for using surgery to treat Wilm’s tumor specific
to the stage and pathology of the disease
N 3.11 Explain the rationale for using systemic therapy to treat Wilm’s tumor specific to the stage and pathology of the disease
N 3.12 Explain the rationale for using radiation therapy to treat Wilm’s tumor specific to the stage and pathology of the disease
N 3.13 Explain the rationale for using combined modalities to treat Wilm’s tumor specific to the stage and pathology of the disease
N 3.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
N 3.15 Interpret protocols for clinical studies and impact on radiation treatment
N 3.16 Discuss the emerging technologies relevant to the management of Wilm’s tumor
N 3.17 Explain the predicted results of Wilm’s tumor treatment based on stage/grade
N 3.18 Explain the predicted results of Wilm’s tumor treatment based on treatment modalities
N 3.19 Plan radiation treatment for a patient with Wilm’s tumor as per Module E2, E3, & E4
N 3.20 Perform treatment procedures for a patient with Wilm’s tumor as per Module E5
N 3.21 Perform patient care for a patient with Wilm’s tumor as per Module E6
N 4 Radiation Treatment of Retinoblastoma N 4.1 State the epidemiology of retinoblastoma N 4.2 State the etiology of retinoblastoma N 4.3 Explain the prognostic indicators of retinoblastoma N 4.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the eye in relation to retinoblastoma
N 4.5 Discuss the natural history of retinoblastoma
Page 47
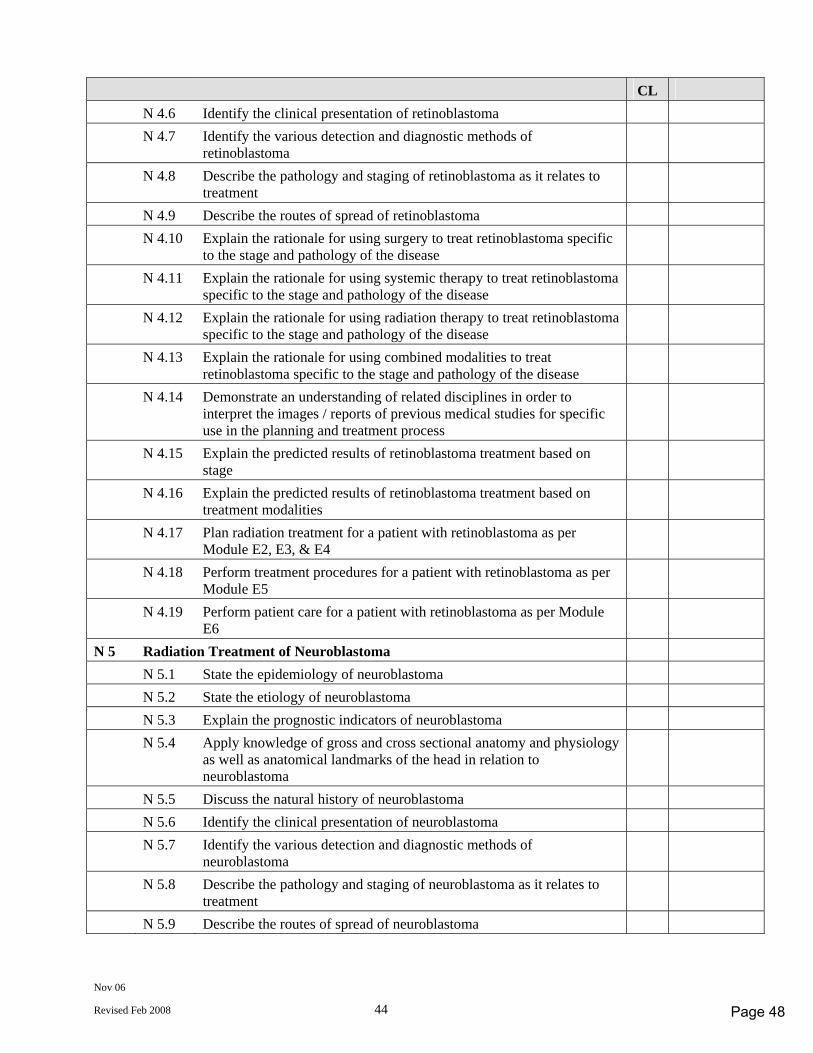
Nov 06
Revised Feb 2008 44
CL N 4.6 Identify the clinical presentation of retinoblastoma N 4.7 Identify the various detection and diagnostic methods of
retinoblastoma
N 4.8 Describe the pathology and staging of retinoblastoma as it relates to treatment
N 4.9 Describe the routes of spread of retinoblastoma N 4.10 Explain the rationale for using surgery to treat retinoblastoma specific
to the stage and pathology of the disease
N 4.11 Explain the rationale for using systemic therapy to treat retinoblastoma specific to the stage and pathology of the disease
N 4.12 Explain the rationale for using radiation therapy to treat retinoblastoma specific to the stage and pathology of the disease
N 4.13 Explain the rationale for using combined modalities to treat retinoblastoma specific to the stage and pathology of the disease
N 4.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
N 4.15 Explain the predicted results of retinoblastoma treatment based on stage
N 4.16 Explain the predicted results of retinoblastoma treatment based on treatment modalities
N 4.17 Plan radiation treatment for a patient with retinoblastoma as per Module E2, E3, & E4
N 4.18 Perform treatment procedures for a patient with retinoblastoma as per Module E5
N 4.19 Perform patient care for a patient with retinoblastoma as per Module E6
N 5 Radiation Treatment of Neuroblastoma N 5.1 State the epidemiology of neuroblastoma N 5.2 State the etiology of neuroblastoma N 5.3 Explain the prognostic indicators of neuroblastoma N 5.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head in relation to neuroblastoma
N 5.5 Discuss the natural history of neuroblastoma N 5.6 Identify the clinical presentation of neuroblastoma N 5.7 Identify the various detection and diagnostic methods of
neuroblastoma
N 5.8 Describe the pathology and staging of neuroblastoma as it relates to treatment
N 5.9 Describe the routes of spread of neuroblastoma
Page 48
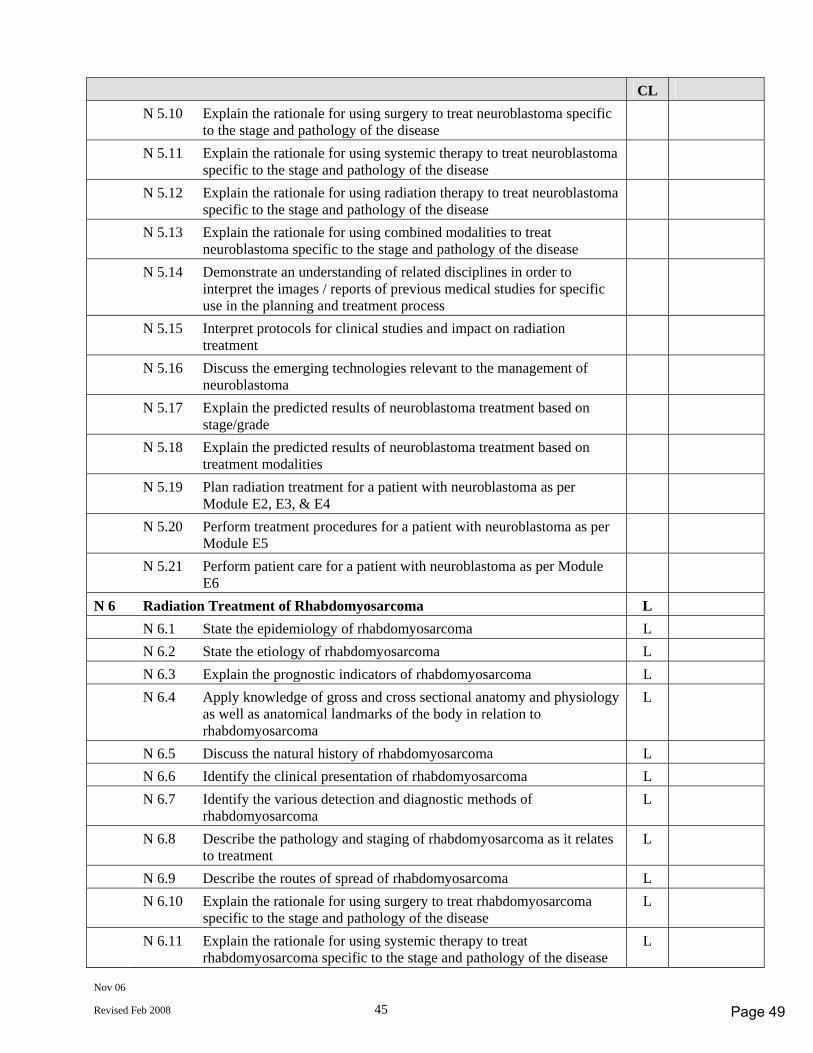
Nov 06
Revised Feb 2008 45
CL N 5.10 Explain the rationale for using surgery to treat neuroblastoma specific
to the stage and pathology of the disease
N 5.11 Explain the rationale for using systemic therapy to treat neuroblastoma specific to the stage and pathology of the disease
N 5.12 Explain the rationale for using radiation therapy to treat neuroblastoma specific to the stage and pathology of the disease
N 5.13 Explain the rationale for using combined modalities to treat neuroblastoma specific to the stage and pathology of the disease
N 5.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
N 5.15 Interpret protocols for clinical studies and impact on radiation treatment
N 5.16 Discuss the emerging technologies relevant to the management of neuroblastoma
N 5.17 Explain the predicted results of neuroblastoma treatment based on stage/grade
N 5.18 Explain the predicted results of neuroblastoma treatment based on treatment modalities
N 5.19 Plan radiation treatment for a patient with neuroblastoma as per Module E2, E3, & E4
N 5.20 Perform treatment procedures for a patient with neuroblastoma as per Module E5
N 5.21 Perform patient care for a patient with neuroblastoma as per Module E6
N 6 Radiation Treatment of Rhabdomyosarcoma L N 6.1 State the epidemiology of rhabdomyosarcoma L N 6.2 State the etiology of rhabdomyosarcoma L N 6.3 Explain the prognostic indicators of rhabdomyosarcoma L N 6.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to rhabdomyosarcoma
L
N 6.5 Discuss the natural history of rhabdomyosarcoma L N 6.6 Identify the clinical presentation of rhabdomyosarcoma L N 6.7 Identify the various detection and diagnostic methods of
rhabdomyosarcoma L
N 6.8 Describe the pathology and staging of rhabdomyosarcoma as it relates to treatment
L
N 6.9 Describe the routes of spread of rhabdomyosarcoma L N 6.10 Explain the rationale for using surgery to treat rhabdomyosarcoma
specific to the stage and pathology of the disease L
N 6.11 Explain the rationale for using systemic therapy to treat rhabdomyosarcoma specific to the stage and pathology of the disease
L
Page 49
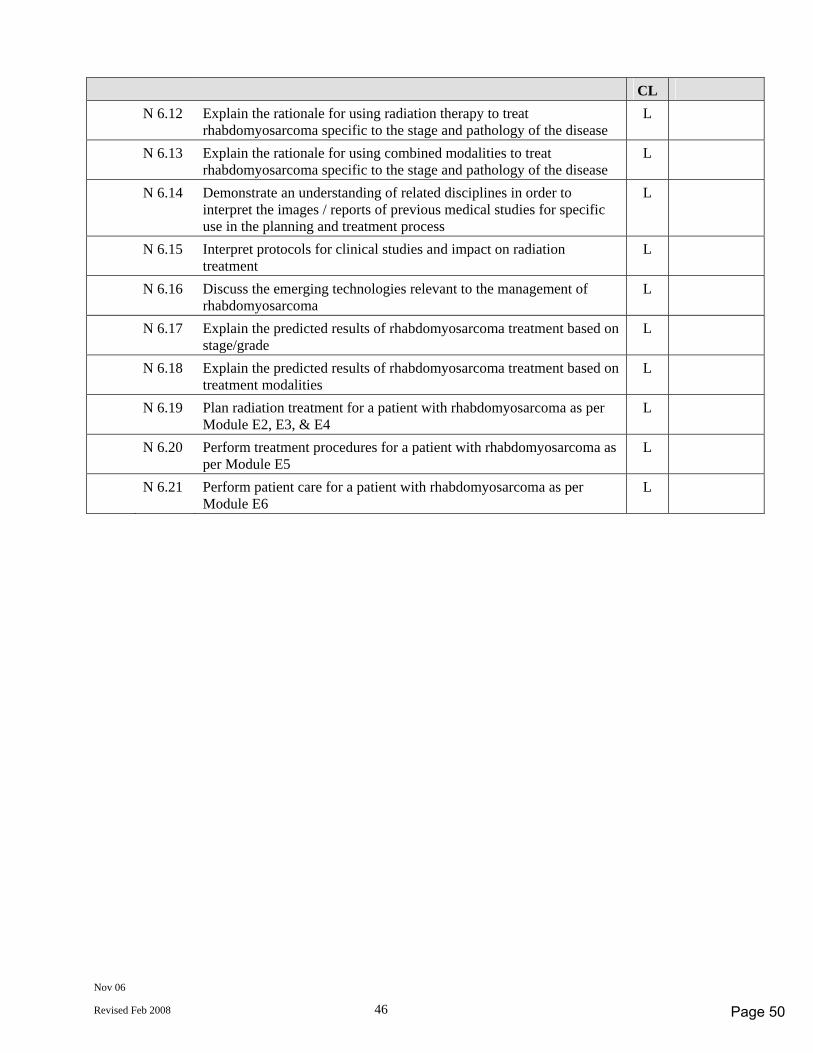
Nov 06
Revised Feb 2008 46
CL N 6.12 Explain the rationale for using radiation therapy to treat
rhabdomyosarcoma specific to the stage and pathology of the disease L
N 6.13 Explain the rationale for using combined modalities to treat rhabdomyosarcoma specific to the stage and pathology of the disease
L
N 6.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
N 6.15 Interpret protocols for clinical studies and impact on radiation treatment
L
N 6.16 Discuss the emerging technologies relevant to the management of rhabdomyosarcoma
L
N 6.17 Explain the predicted results of rhabdomyosarcoma treatment based on stage/grade
L
N 6.18 Explain the predicted results of rhabdomyosarcoma treatment based on treatment modalities
L
N 6.19 Plan radiation treatment for a patient with rhabdomyosarcoma as per Module E2, E3, & E4
L
N 6.20 Perform treatment procedures for a patient with rhabdomyosarcoma as per Module E5
L
N 6.21 Perform patient care for a patient with rhabdomyosarcoma as per Module E6
L
Page 50
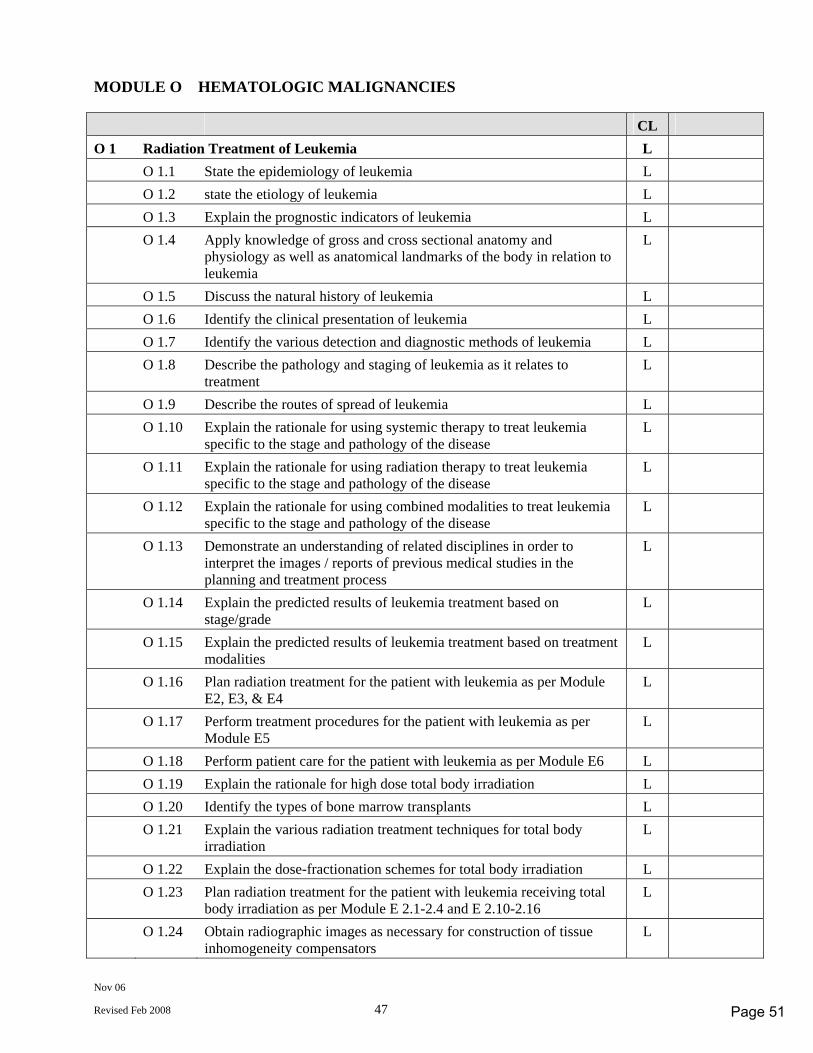
Nov 06
Revised Feb 2008 47
MODULE O HEMATOLOGIC MALIGNANCIES CL O 1 Radiation Treatment of Leukemia L O 1.1 State the epidemiology of leukemia L O 1.2 state the etiology of leukemia L O 1.3 Explain the prognostic indicators of leukemia L O 1.4 Apply knowledge of gross and cross sectional anatomy and
physiology as well as anatomical landmarks of the body in relation to leukemia
L
O 1.5 Discuss the natural history of leukemia L O 1.6 Identify the clinical presentation of leukemia L O 1.7 Identify the various detection and diagnostic methods of leukemia L O 1.8 Describe the pathology and staging of leukemia as it relates to
treatment L
O 1.9 Describe the routes of spread of leukemia L O 1.10 Explain the rationale for using systemic therapy to treat leukemia
specific to the stage and pathology of the disease L
O 1.11 Explain the rationale for using radiation therapy to treat leukemia specific to the stage and pathology of the disease
L
O 1.12 Explain the rationale for using combined modalities to treat leukemia specific to the stage and pathology of the disease
L
O 1.13 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies in the planning and treatment process
L
O 1.14 Explain the predicted results of leukemia treatment based on stage/grade
L
O 1.15 Explain the predicted results of leukemia treatment based on treatment modalities
L
O 1.16 Plan radiation treatment for the patient with leukemia as per Module E2, E3, & E4
L
O 1.17 Perform treatment procedures for the patient with leukemia as per Module E5
L
O 1.18 Perform patient care for the patient with leukemia as per Module E6 L O 1.19 Explain the rationale for high dose total body irradiation L O 1.20 Identify the types of bone marrow transplants L O 1.21 Explain the various radiation treatment techniques for total body
irradiation L
O 1.22 Explain the dose-fractionation schemes for total body irradiation L O 1.23 Plan radiation treatment for the patient with leukemia receiving total
body irradiation as per Module E 2.1-2.4 and E 2.10-2.16 L
O 1.24 Obtain radiographic images as necessary for construction of tissue inhomogeneity compensators
L
Page 51
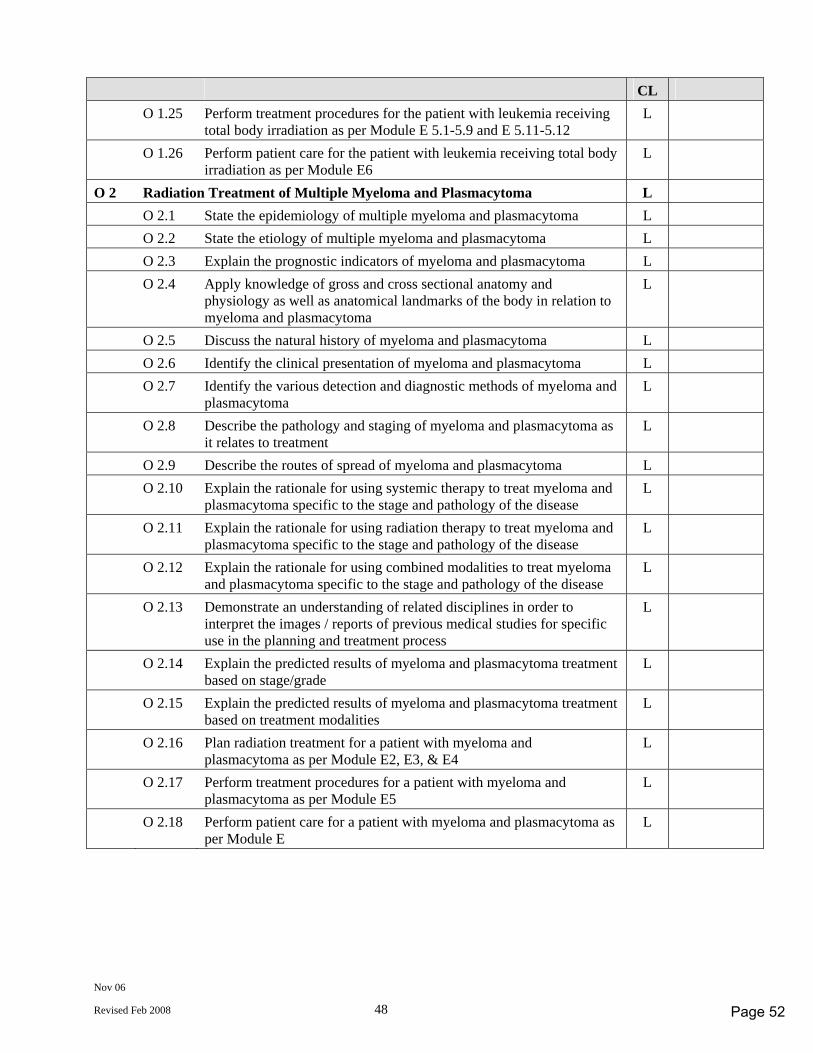
Nov 06
Revised Feb 2008 48
CL O 1.25 Perform treatment procedures for the patient with leukemia receiving
total body irradiation as per Module E 5.1-5.9 and E 5.11-5.12 L
O 1.26 Perform patient care for the patient with leukemia receiving total body irradiation as per Module E6
L
O 2 Radiation Treatment of Multiple Myeloma and Plasmacytoma L O 2.1 State the epidemiology of multiple myeloma and plasmacytoma L O 2.2 State the etiology of multiple myeloma and plasmacytoma L O 2.3 Explain the prognostic indicators of myeloma and plasmacytoma L O 2.4 Apply knowledge of gross and cross sectional anatomy and
physiology as well as anatomical landmarks of the body in relation to myeloma and plasmacytoma
L
O 2.5 Discuss the natural history of myeloma and plasmacytoma L O 2.6 Identify the clinical presentation of myeloma and plasmacytoma L O 2.7 Identify the various detection and diagnostic methods of myeloma and
plasmacytoma L
O 2.8 Describe the pathology and staging of myeloma and plasmacytoma as it relates to treatment
L
O 2.9 Describe the routes of spread of myeloma and plasmacytoma L O 2.10 Explain the rationale for using systemic therapy to treat myeloma and
plasmacytoma specific to the stage and pathology of the disease L
O 2.11 Explain the rationale for using radiation therapy to treat myeloma and plasmacytoma specific to the stage and pathology of the disease
L
O 2.12 Explain the rationale for using combined modalities to treat myeloma and plasmacytoma specific to the stage and pathology of the disease
L
O 2.13 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
O 2.14 Explain the predicted results of myeloma and plasmacytoma treatment based on stage/grade
L
O 2.15 Explain the predicted results of myeloma and plasmacytoma treatment based on treatment modalities
L
O 2.16 Plan radiation treatment for a patient with myeloma and plasmacytoma as per Module E2, E3, & E4
L
O 2.17 Perform treatment procedures for a patient with myeloma and plasmacytoma as per Module E5
L
O 2.18 Perform patient care for a patient with myeloma and plasmacytoma as per Module E
L
Page 52
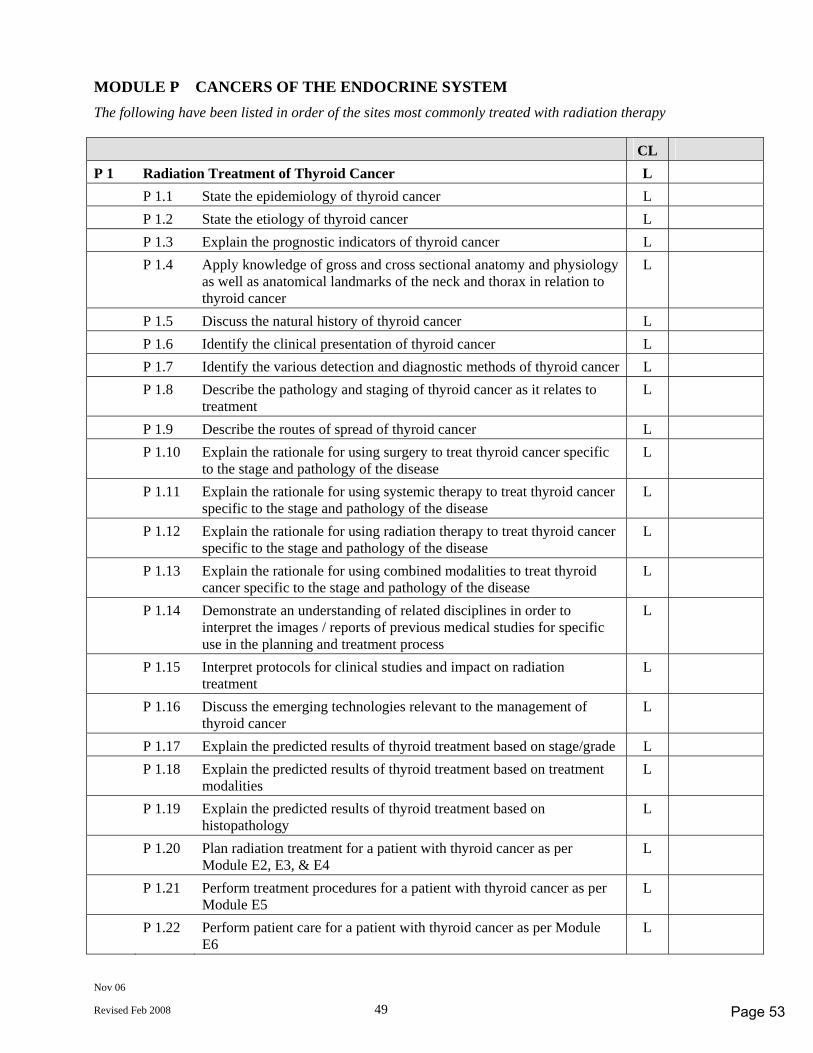
Nov 06
Revised Feb 2008 49
MODULE P CANCERS OF THE ENDOCRINE SYSTEM The following have been listed in order of the sites most commonly treated with radiation therapy CL P 1 Radiation Treatment of Thyroid Cancer L P 1.1 State the epidemiology of thyroid cancer L P 1.2 State the etiology of thyroid cancer L P 1.3 Explain the prognostic indicators of thyroid cancer L P 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the neck and thorax in relation to thyroid cancer
L
P 1.5 Discuss the natural history of thyroid cancer L P 1.6 Identify the clinical presentation of thyroid cancer L P 1.7 Identify the various detection and diagnostic methods of thyroid cancer L P 1.8 Describe the pathology and staging of thyroid cancer as it relates to
treatment L
P 1.9 Describe the routes of spread of thyroid cancer L P 1.10 Explain the rationale for using surgery to treat thyroid cancer specific
to the stage and pathology of the disease L
P 1.11 Explain the rationale for using systemic therapy to treat thyroid cancer specific to the stage and pathology of the disease
L
P 1.12 Explain the rationale for using radiation therapy to treat thyroid cancer specific to the stage and pathology of the disease
L
P 1.13 Explain the rationale for using combined modalities to treat thyroid cancer specific to the stage and pathology of the disease
L
P 1.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
P 1.15 Interpret protocols for clinical studies and impact on radiation treatment
L
P 1.16 Discuss the emerging technologies relevant to the management of thyroid cancer
L
P 1.17 Explain the predicted results of thyroid treatment based on stage/grade L P 1.18 Explain the predicted results of thyroid treatment based on treatment
modalities L
P 1.19 Explain the predicted results of thyroid treatment based on histopathology
L
P 1.20 Plan radiation treatment for a patient with thyroid cancer as per Module E2, E3, & E4
L
P 1.21 Perform treatment procedures for a patient with thyroid cancer as per Module E5
L
P 1.22 Perform patient care for a patient with thyroid cancer as per Module E6
L
Page 53
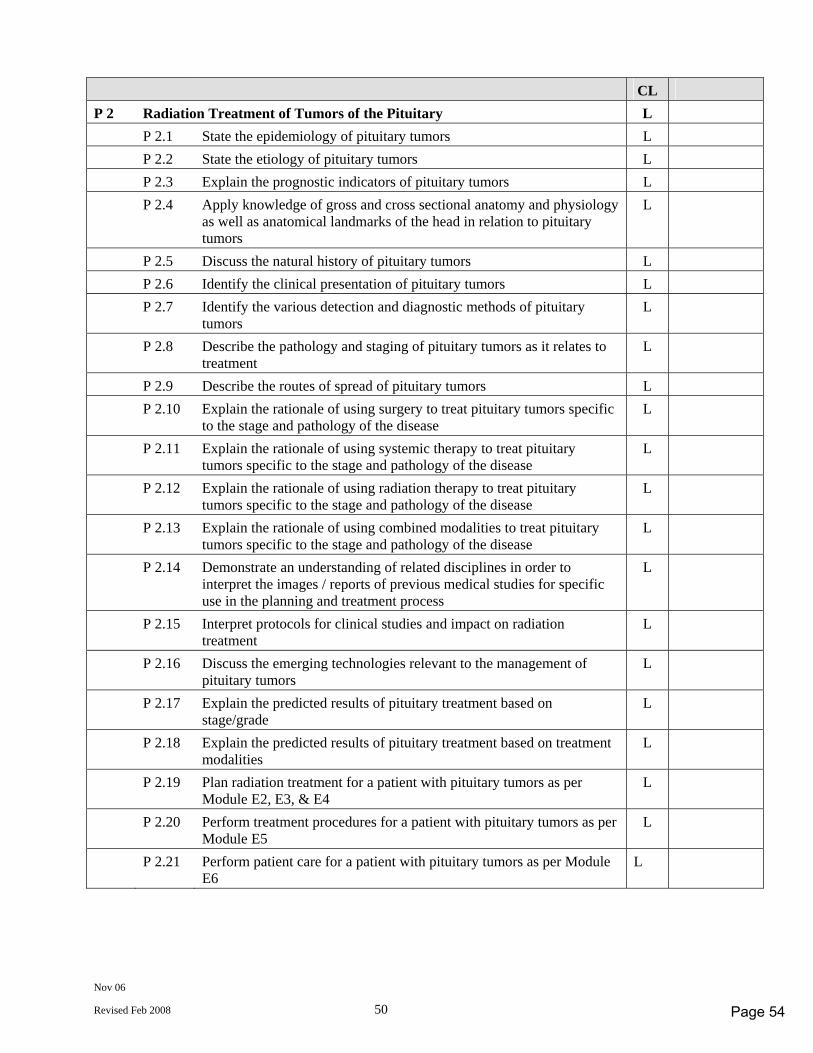
Nov 06
Revised Feb 2008 50
CL P 2 Radiation Treatment of Tumors of the Pituitary L P 2.1 State the epidemiology of pituitary tumors L P 2.2 State the etiology of pituitary tumors L P 2.3 Explain the prognostic indicators of pituitary tumors L P 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the head in relation to pituitary tumors
L
P 2.5 Discuss the natural history of pituitary tumors L P 2.6 Identify the clinical presentation of pituitary tumors L P 2.7 Identify the various detection and diagnostic methods of pituitary
tumors L
P 2.8 Describe the pathology and staging of pituitary tumors as it relates to treatment
L
P 2.9 Describe the routes of spread of pituitary tumors L P 2.10 Explain the rationale of using surgery to treat pituitary tumors specific
to the stage and pathology of the disease L
P 2.11 Explain the rationale of using systemic therapy to treat pituitary tumors specific to the stage and pathology of the disease
L
P 2.12 Explain the rationale of using radiation therapy to treat pituitary tumors specific to the stage and pathology of the disease
L
P 2.13 Explain the rationale of using combined modalities to treat pituitary tumors specific to the stage and pathology of the disease
L
P 2.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
P 2.15 Interpret protocols for clinical studies and impact on radiation treatment
L
P 2.16 Discuss the emerging technologies relevant to the management of pituitary tumors
L
P 2.17 Explain the predicted results of pituitary treatment based on stage/grade
L
P 2.18 Explain the predicted results of pituitary treatment based on treatment modalities
L
P 2.19 Plan radiation treatment for a patient with pituitary tumors as per Module E2, E3, & E4
L
P 2.20 Perform treatment procedures for a patient with pituitary tumors as per Module E5
L
P 2.21 Perform patient care for a patient with pituitary tumors as per Module E6
L
Page 54
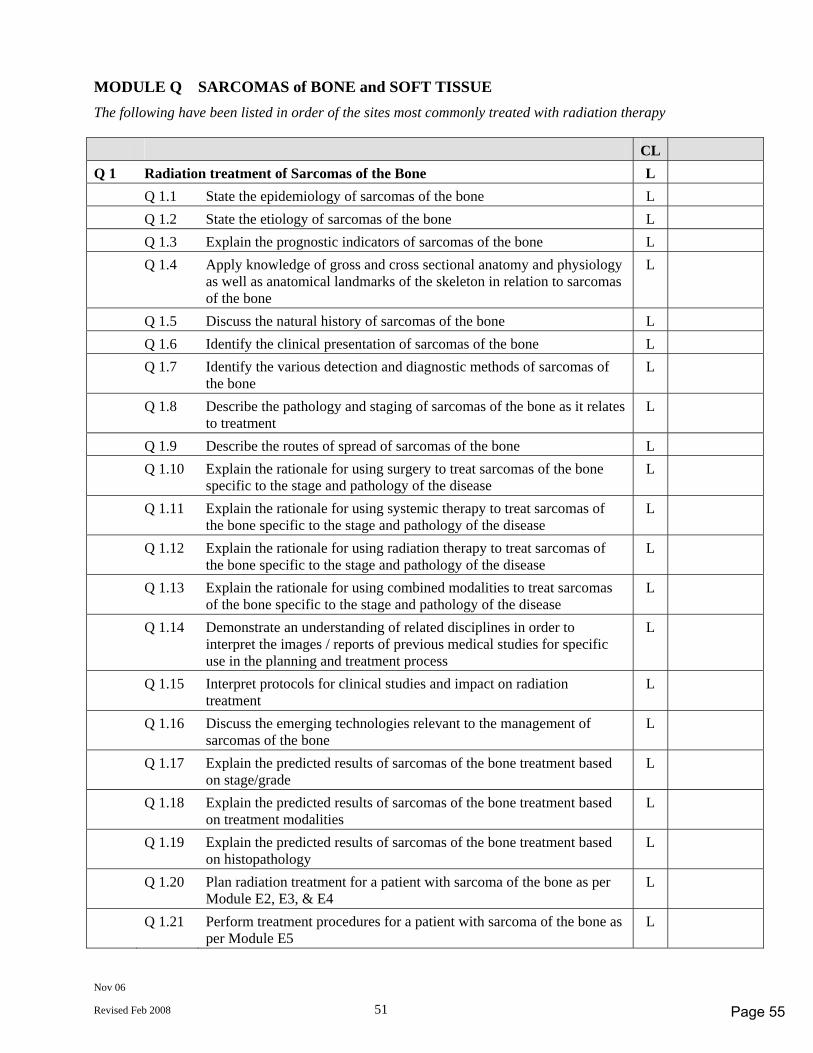
Nov 06
Revised Feb 2008 51
MODULE Q SARCOMAS of BONE and SOFT TISSUE The following have been listed in order of the sites most commonly treated with radiation therapy CL Q 1 Radiation treatment of Sarcomas of the Bone L Q 1.1 State the epidemiology of sarcomas of the bone L Q 1.2 State the etiology of sarcomas of the bone L Q 1.3 Explain the prognostic indicators of sarcomas of the bone L Q 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the skeleton in relation to sarcomas of the bone
L
Q 1.5 Discuss the natural history of sarcomas of the bone L Q 1.6 Identify the clinical presentation of sarcomas of the bone L Q 1.7 Identify the various detection and diagnostic methods of sarcomas of
the bone L
Q 1.8 Describe the pathology and staging of sarcomas of the bone as it relates to treatment
L
Q 1.9 Describe the routes of spread of sarcomas of the bone L Q 1.10 Explain the rationale for using surgery to treat sarcomas of the bone
specific to the stage and pathology of the disease L
Q 1.11 Explain the rationale for using systemic therapy to treat sarcomas of the bone specific to the stage and pathology of the disease
L
Q 1.12 Explain the rationale for using radiation therapy to treat sarcomas of the bone specific to the stage and pathology of the disease
L
Q 1.13 Explain the rationale for using combined modalities to treat sarcomas of the bone specific to the stage and pathology of the disease
L
Q 1.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
Q 1.15 Interpret protocols for clinical studies and impact on radiation treatment
L
Q 1.16 Discuss the emerging technologies relevant to the management of sarcomas of the bone
L
Q 1.17 Explain the predicted results of sarcomas of the bone treatment based on stage/grade
L
Q 1.18 Explain the predicted results of sarcomas of the bone treatment based on treatment modalities
L
Q 1.19 Explain the predicted results of sarcomas of the bone treatment based on histopathology
L
Q 1.20 Plan radiation treatment for a patient with sarcoma of the bone as per Module E2, E3, & E4
L
Q 1.21 Perform treatment procedures for a patient with sarcoma of the bone as per Module E5
L
Page 55
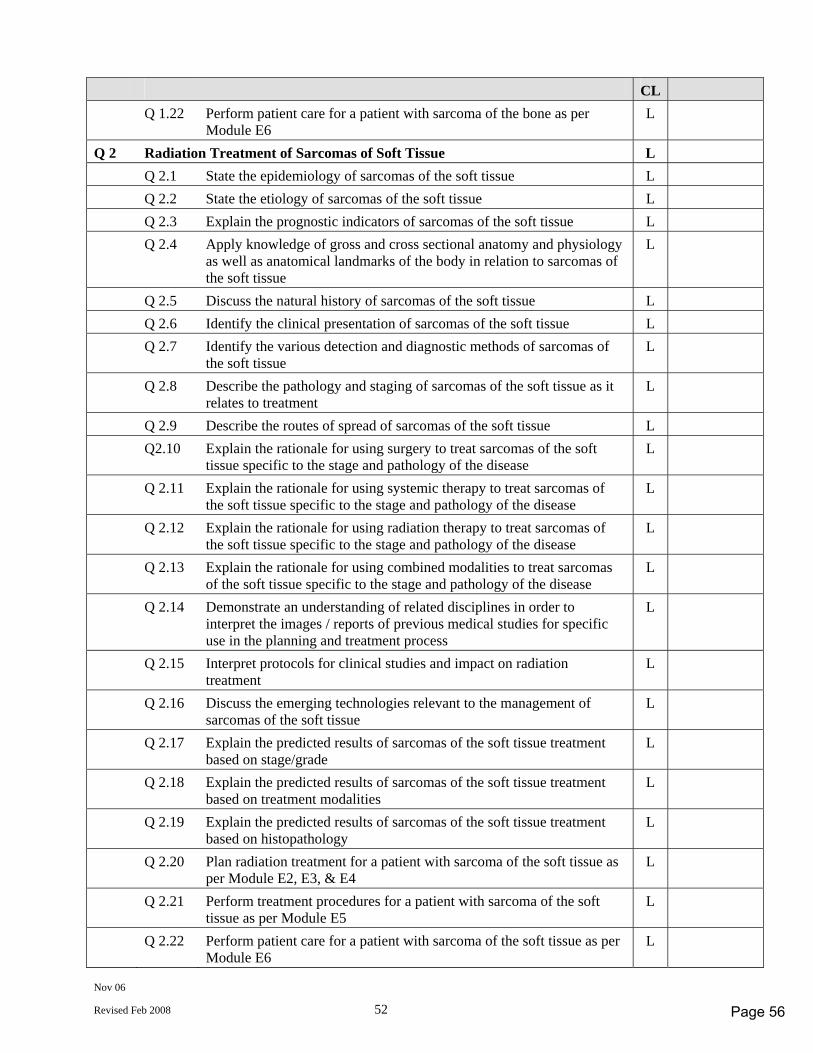
Nov 06
Revised Feb 2008 52
CL Q 1.22 Perform patient care for a patient with sarcoma of the bone as per
Module E6 L
Q 2 Radiation Treatment of Sarcomas of Soft Tissue L Q 2.1 State the epidemiology of sarcomas of the soft tissue L Q 2.2 State the etiology of sarcomas of the soft tissue L Q 2.3 Explain the prognostic indicators of sarcomas of the soft tissue L Q 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to sarcomas of the soft tissue
L
Q 2.5 Discuss the natural history of sarcomas of the soft tissue L Q 2.6 Identify the clinical presentation of sarcomas of the soft tissue L Q 2.7 Identify the various detection and diagnostic methods of sarcomas of
the soft tissue L
Q 2.8 Describe the pathology and staging of sarcomas of the soft tissue as it relates to treatment
L
Q 2.9 Describe the routes of spread of sarcomas of the soft tissue L Q2.10 Explain the rationale for using surgery to treat sarcomas of the soft
tissue specific to the stage and pathology of the disease L
Q 2.11 Explain the rationale for using systemic therapy to treat sarcomas of the soft tissue specific to the stage and pathology of the disease
L
Q 2.12 Explain the rationale for using radiation therapy to treat sarcomas of the soft tissue specific to the stage and pathology of the disease
L
Q 2.13 Explain the rationale for using combined modalities to treat sarcomas of the soft tissue specific to the stage and pathology of the disease
L
Q 2.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
Q 2.15 Interpret protocols for clinical studies and impact on radiation treatment
L
Q 2.16 Discuss the emerging technologies relevant to the management of sarcomas of the soft tissue
L
Q 2.17 Explain the predicted results of sarcomas of the soft tissue treatment based on stage/grade
L
Q 2.18 Explain the predicted results of sarcomas of the soft tissue treatment based on treatment modalities
L
Q 2.19 Explain the predicted results of sarcomas of the soft tissue treatment based on histopathology
L
Q 2.20 Plan radiation treatment for a patient with sarcoma of the soft tissue as per Module E2, E3, & E4
L
Q 2.21 Perform treatment procedures for a patient with sarcoma of the soft tissue as per Module E5
L
Q 2.22 Perform patient care for a patient with sarcoma of the soft tissue as per Module E6
L
Page 56
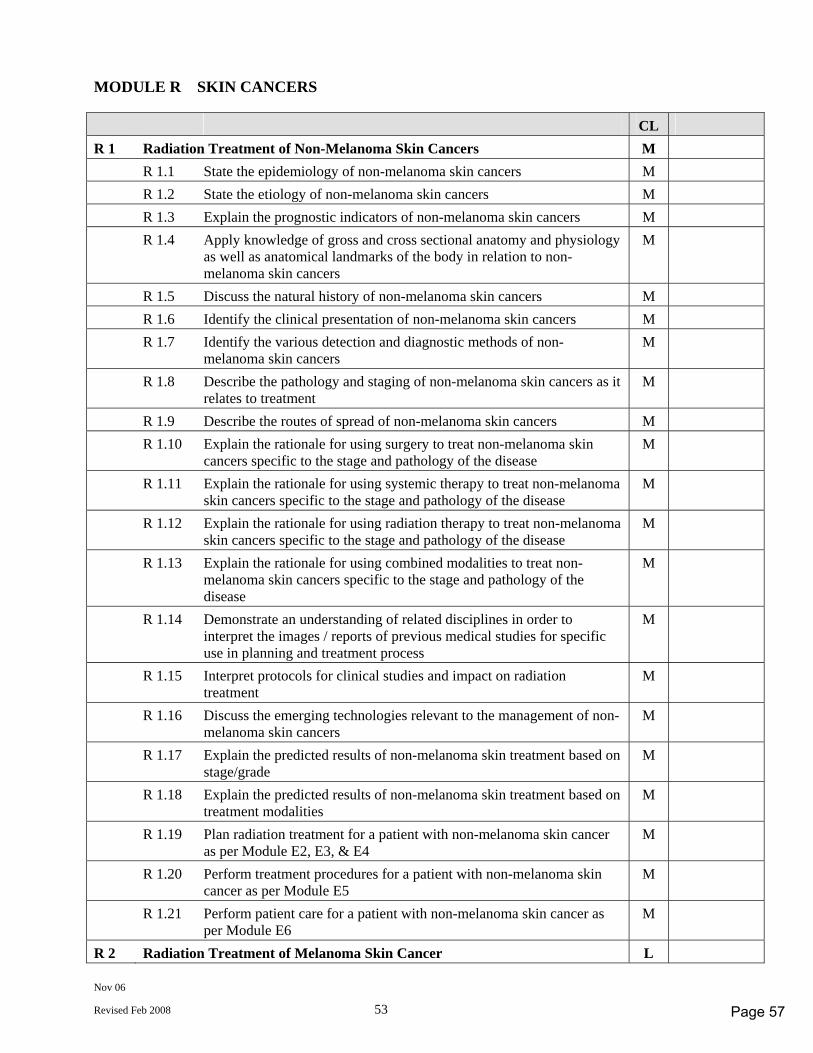
Nov 06
Revised Feb 2008 53
MODULE R SKIN CANCERS CL R 1 Radiation Treatment of Non-Melanoma Skin Cancers M R 1.1 State the epidemiology of non-melanoma skin cancers M R 1.2 State the etiology of non-melanoma skin cancers M R 1.3 Explain the prognostic indicators of non-melanoma skin cancers M R 1.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to non-melanoma skin cancers
M
R 1.5 Discuss the natural history of non-melanoma skin cancers M R 1.6 Identify the clinical presentation of non-melanoma skin cancers M R 1.7 Identify the various detection and diagnostic methods of non-
melanoma skin cancers M
R 1.8 Describe the pathology and staging of non-melanoma skin cancers as it relates to treatment
M
R 1.9 Describe the routes of spread of non-melanoma skin cancers M R 1.10 Explain the rationale for using surgery to treat non-melanoma skin
cancers specific to the stage and pathology of the disease M
R 1.11 Explain the rationale for using systemic therapy to treat non-melanoma skin cancers specific to the stage and pathology of the disease
M
R 1.12 Explain the rationale for using radiation therapy to treat non-melanoma skin cancers specific to the stage and pathology of the disease
M
R 1.13 Explain the rationale for using combined modalities to treat non-melanoma skin cancers specific to the stage and pathology of the disease
M
R 1.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in planning and treatment process
M
R 1.15 Interpret protocols for clinical studies and impact on radiation treatment
M
R 1.16 Discuss the emerging technologies relevant to the management of non-melanoma skin cancers
M
R 1.17 Explain the predicted results of non-melanoma skin treatment based on stage/grade
M
R 1.18 Explain the predicted results of non-melanoma skin treatment based on treatment modalities
M
R 1.19 Plan radiation treatment for a patient with non-melanoma skin cancer as per Module E2, E3, & E4
M
R 1.20 Perform treatment procedures for a patient with non-melanoma skin cancer as per Module E5
M
R 1.21 Perform patient care for a patient with non-melanoma skin cancer as per Module E6
M
R 2 Radiation Treatment of Melanoma Skin Cancer L
Page 57
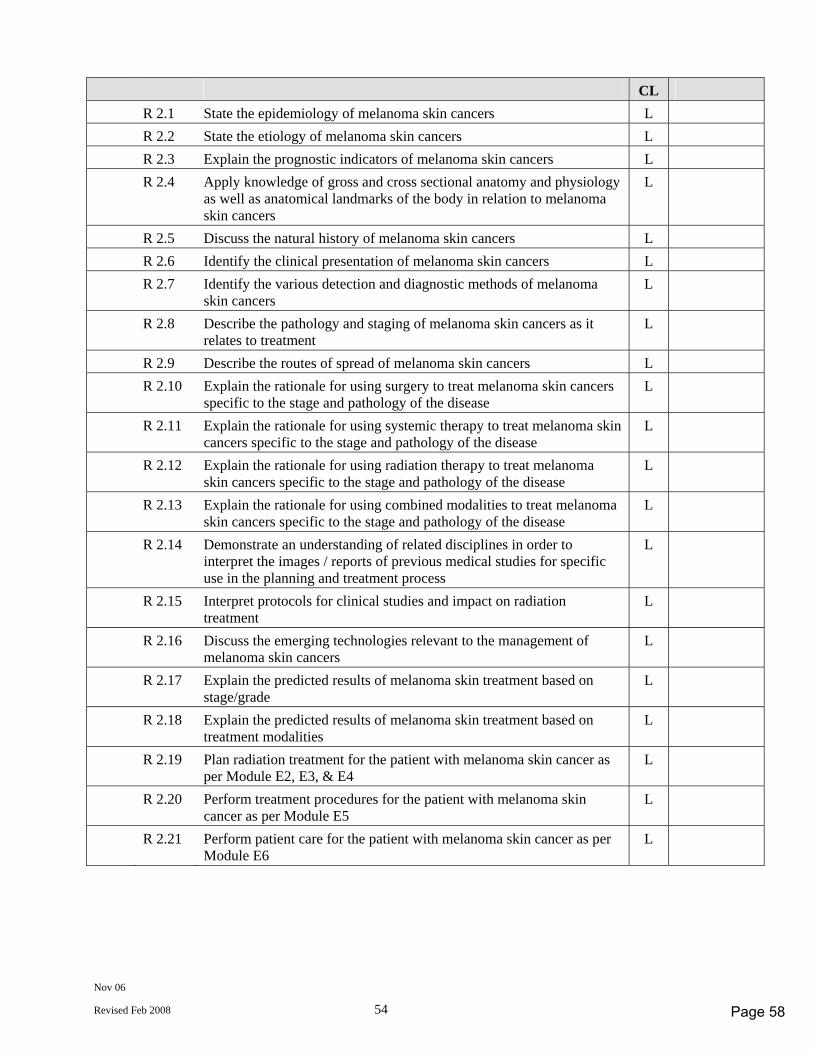
Nov 06
Revised Feb 2008 54
CL R 2.1 State the epidemiology of melanoma skin cancers L R 2.2 State the etiology of melanoma skin cancers L R 2.3 Explain the prognostic indicators of melanoma skin cancers L R 2.4 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to melanoma skin cancers
L
R 2.5 Discuss the natural history of melanoma skin cancers L R 2.6 Identify the clinical presentation of melanoma skin cancers L R 2.7 Identify the various detection and diagnostic methods of melanoma
skin cancers L
R 2.8 Describe the pathology and staging of melanoma skin cancers as it relates to treatment
L
R 2.9 Describe the routes of spread of melanoma skin cancers L R 2.10 Explain the rationale for using surgery to treat melanoma skin cancers
specific to the stage and pathology of the disease L
R 2.11 Explain the rationale for using systemic therapy to treat melanoma skin cancers specific to the stage and pathology of the disease
L
R 2.12 Explain the rationale for using radiation therapy to treat melanoma skin cancers specific to the stage and pathology of the disease
L
R 2.13 Explain the rationale for using combined modalities to treat melanoma skin cancers specific to the stage and pathology of the disease
L
R 2.14 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
L
R 2.15 Interpret protocols for clinical studies and impact on radiation treatment
L
R 2.16 Discuss the emerging technologies relevant to the management of melanoma skin cancers
L
R 2.17 Explain the predicted results of melanoma skin treatment based on stage/grade
L
R 2.18 Explain the predicted results of melanoma skin treatment based on treatment modalities
L
R 2.19 Plan radiation treatment for the patient with melanoma skin cancer as per Module E2, E3, & E4
L
R 2.20 Perform treatment procedures for the patient with melanoma skin cancer as per Module E5
L
R 2.21 Perform patient care for the patient with melanoma skin cancer as per Module E6
L
Page 58
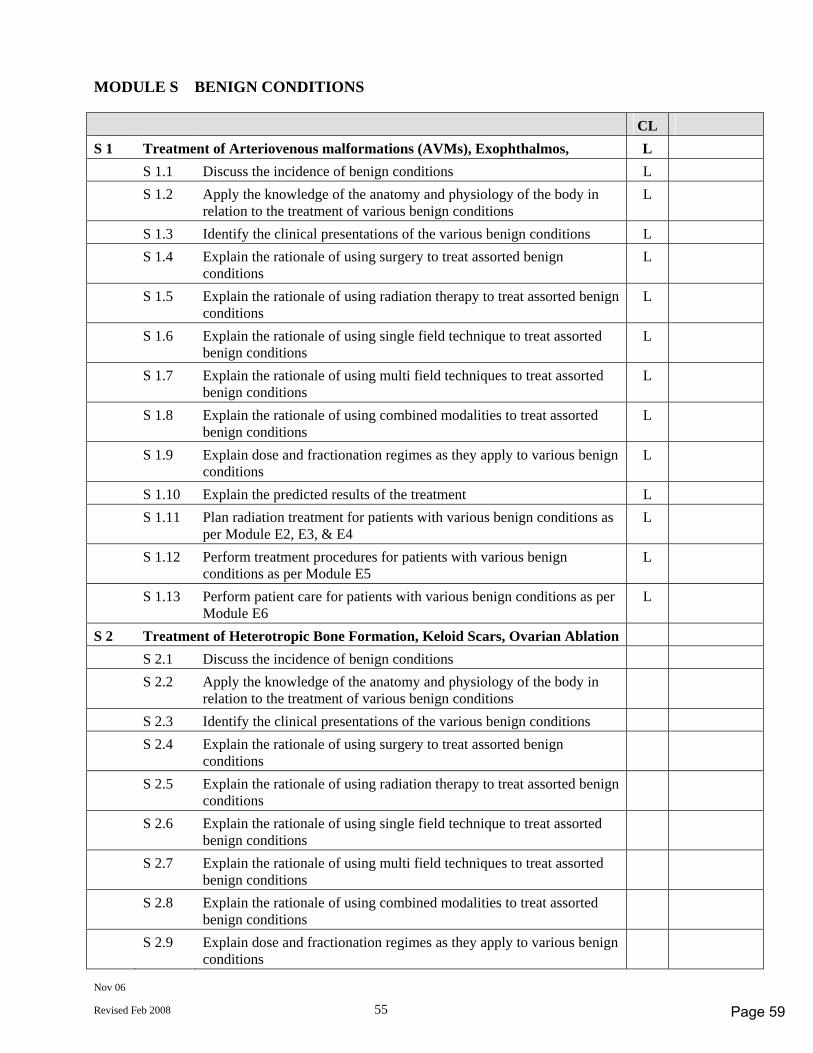
Nov 06
Revised Feb 2008 55
MODULE S BENIGN CONDITIONS CL S 1 Treatment of Arteriovenous malformations (AVMs), Exophthalmos, L S 1.1 Discuss the incidence of benign conditions L S 1.2 Apply the knowledge of the anatomy and physiology of the body in
relation to the treatment of various benign conditions L
S 1.3 Identify the clinical presentations of the various benign conditions L S 1.4 Explain the rationale of using surgery to treat assorted benign
conditions L
S 1.5 Explain the rationale of using radiation therapy to treat assorted benign conditions
L
S 1.6 Explain the rationale of using single field technique to treat assorted benign conditions
L
S 1.7 Explain the rationale of using multi field techniques to treat assorted benign conditions
L
S 1.8 Explain the rationale of using combined modalities to treat assorted benign conditions
L
S 1.9 Explain dose and fractionation regimes as they apply to various benign conditions
L
S 1.10 Explain the predicted results of the treatment L S 1.11 Plan radiation treatment for patients with various benign conditions as
per Module E2, E3, & E4 L
S 1.12 Perform treatment procedures for patients with various benign conditions as per Module E5
L
S 1.13 Perform patient care for patients with various benign conditions as per Module E6
L
S 2 Treatment of Heterotropic Bone Formation, Keloid Scars, Ovarian Ablation S 2.1 Discuss the incidence of benign conditions S 2.2 Apply the knowledge of the anatomy and physiology of the body in
relation to the treatment of various benign conditions
S 2.3 Identify the clinical presentations of the various benign conditions S 2.4 Explain the rationale of using surgery to treat assorted benign
conditions
S 2.5 Explain the rationale of using radiation therapy to treat assorted benign conditions
S 2.6 Explain the rationale of using single field technique to treat assorted benign conditions
S 2.7 Explain the rationale of using multi field techniques to treat assorted benign conditions
S 2.8 Explain the rationale of using combined modalities to treat assorted benign conditions
S 2.9 Explain dose and fractionation regimes as they apply to various benign conditions
Page 59
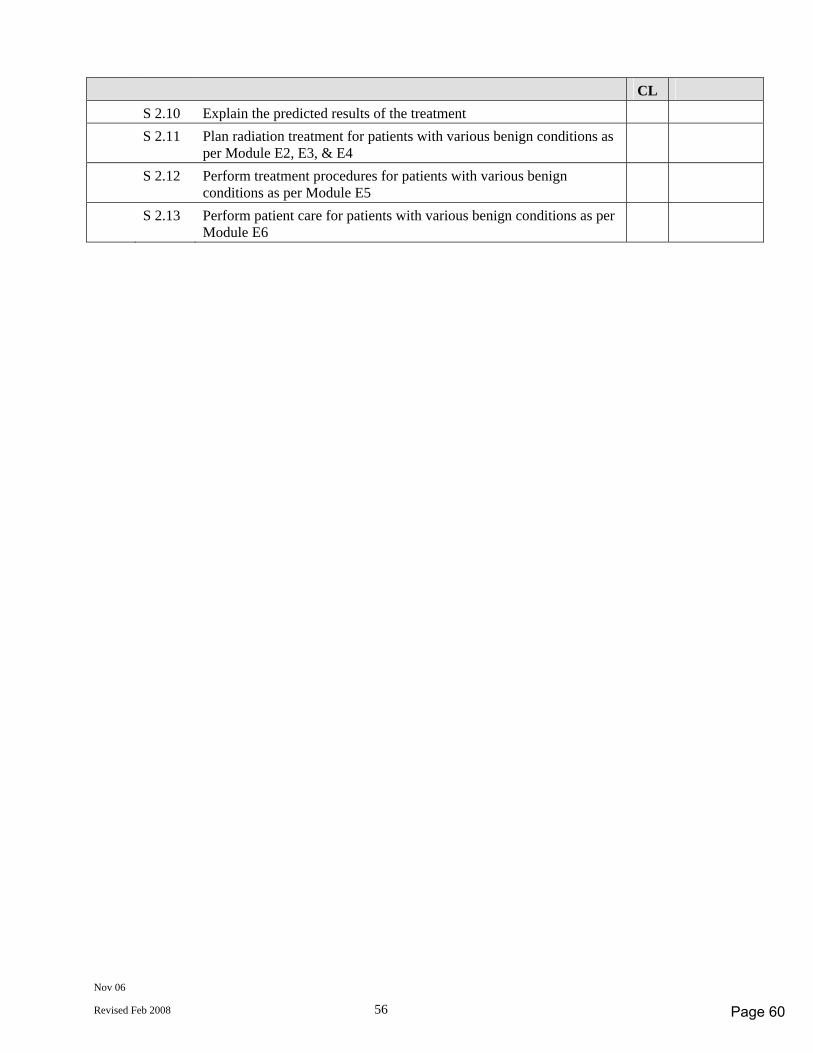
Nov 06
Revised Feb 2008 56
CL S 2.10 Explain the predicted results of the treatment S 2.11 Plan radiation treatment for patients with various benign conditions as
per Module E2, E3, & E4
S 2.12 Perform treatment procedures for patients with various benign conditions as per Module E5
S 2.13 Perform patient care for patients with various benign conditions as per Module E6
Page 60
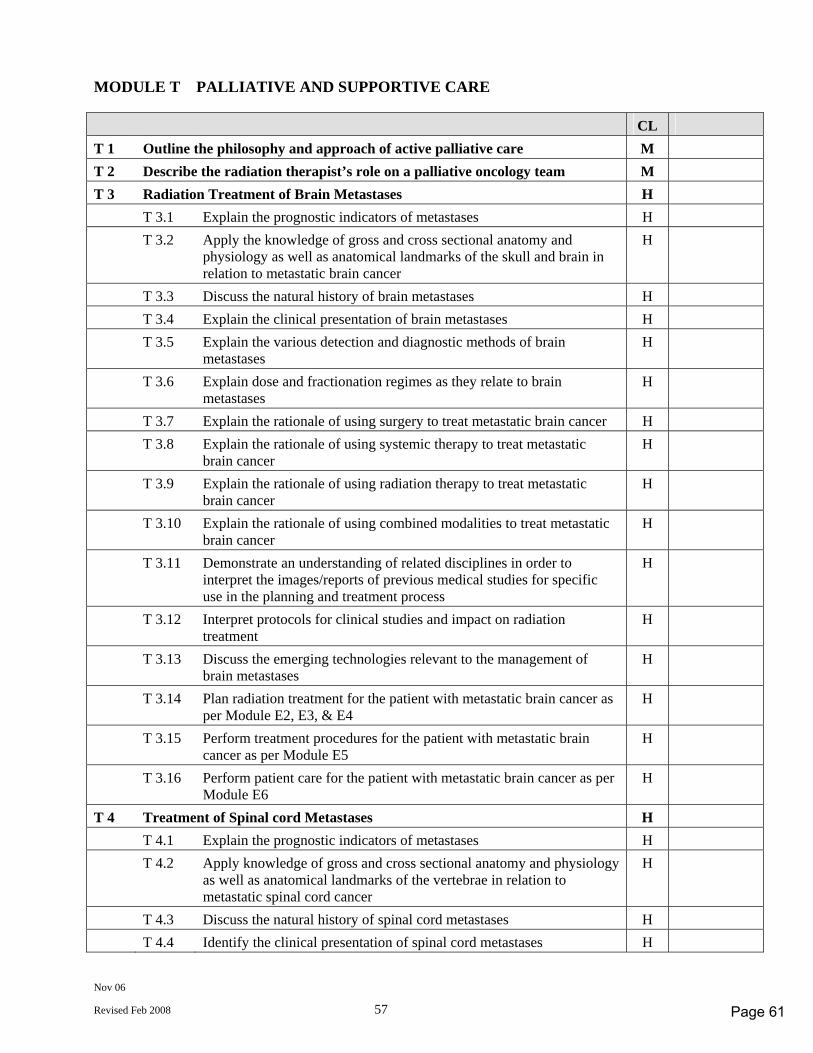
Nov 06
Revised Feb 2008 57
MODULE T PALLIATIVE AND SUPPORTIVE CARE CL T 1 Outline the philosophy and approach of active palliative care M T 2 Describe the radiation therapist’s role on a palliative oncology team M T 3 Radiation Treatment of Brain Metastases H T 3.1 Explain the prognostic indicators of metastases H T 3.2 Apply the knowledge of gross and cross sectional anatomy and
physiology as well as anatomical landmarks of the skull and brain in relation to metastatic brain cancer
H
T 3.3 Discuss the natural history of brain metastases H T 3.4 Explain the clinical presentation of brain metastases H T 3.5 Explain the various detection and diagnostic methods of brain
metastases H
T 3.6 Explain dose and fractionation regimes as they relate to brain metastases
H
T 3.7 Explain the rationale of using surgery to treat metastatic brain cancer H T 3.8 Explain the rationale of using systemic therapy to treat metastatic
brain cancer H
T 3.9 Explain the rationale of using radiation therapy to treat metastatic brain cancer
H
T 3.10 Explain the rationale of using combined modalities to treat metastatic brain cancer
H
T 3.11 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
T 3.12 Interpret protocols for clinical studies and impact on radiation treatment
H
T 3.13 Discuss the emerging technologies relevant to the management of brain metastases
H
T 3.14 Plan radiation treatment for the patient with metastatic brain cancer as per Module E2, E3, & E4
H
T 3.15 Perform treatment procedures for the patient with metastatic brain cancer as per Module E5
H
T 3.16 Perform patient care for the patient with metastatic brain cancer as per Module E6
H
T 4 Treatment of Spinal cord Metastases H T 4.1 Explain the prognostic indicators of metastases H T 4.2 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the vertebrae in relation to metastatic spinal cord cancer
H
T 4.3 Discuss the natural history of spinal cord metastases H T 4.4 Identify the clinical presentation of spinal cord metastases H
Page 61
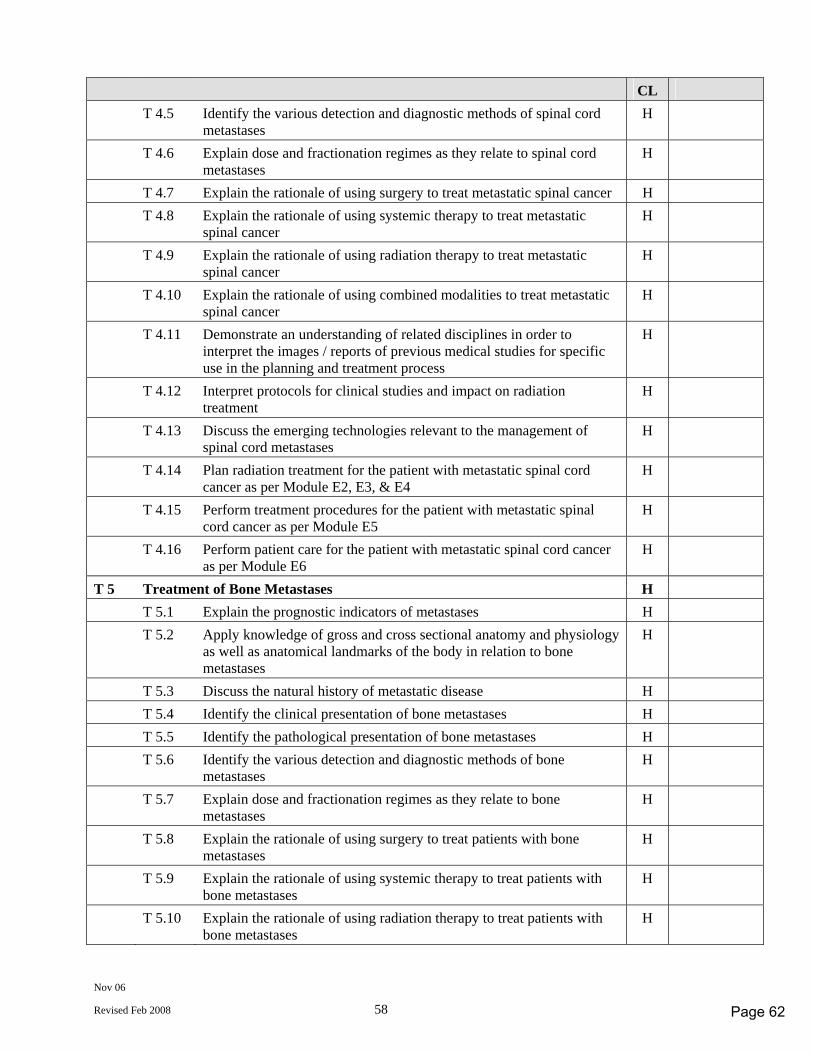
Nov 06
Revised Feb 2008 58
CL T 4.5 Identify the various detection and diagnostic methods of spinal cord
metastases H
T 4.6 Explain dose and fractionation regimes as they relate to spinal cord metastases
H
T 4.7 Explain the rationale of using surgery to treat metastatic spinal cancer H T 4.8 Explain the rationale of using systemic therapy to treat metastatic
spinal cancer H
T 4.9 Explain the rationale of using radiation therapy to treat metastatic spinal cancer
H
T 4.10 Explain the rationale of using combined modalities to treat metastatic spinal cancer
H
T 4.11 Demonstrate an understanding of related disciplines in order to interpret the images / reports of previous medical studies for specific use in the planning and treatment process
H
T 4.12 Interpret protocols for clinical studies and impact on radiation treatment
H
T 4.13 Discuss the emerging technologies relevant to the management of spinal cord metastases
H
T 4.14 Plan radiation treatment for the patient with metastatic spinal cord cancer as per Module E2, E3, & E4
H
T 4.15 Perform treatment procedures for the patient with metastatic spinal cord cancer as per Module E5
H
T 4.16 Perform patient care for the patient with metastatic spinal cord cancer as per Module E6
H
T 5 Treatment of Bone Metastases H T 5.1 Explain the prognostic indicators of metastases H T 5.2 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to bone metastases
H
T 5.3 Discuss the natural history of metastatic disease H T 5.4 Identify the clinical presentation of bone metastases H T 5.5 Identify the pathological presentation of bone metastases H T 5.6 Identify the various detection and diagnostic methods of bone
metastases H
T 5.7 Explain dose and fractionation regimes as they relate to bone metastases
H
T 5.8 Explain the rationale of using surgery to treat patients with bone metastases
H
T 5.9 Explain the rationale of using systemic therapy to treat patients with bone metastases
H
T 5.10 Explain the rationale of using radiation therapy to treat patients with bone metastases
H
Page 62
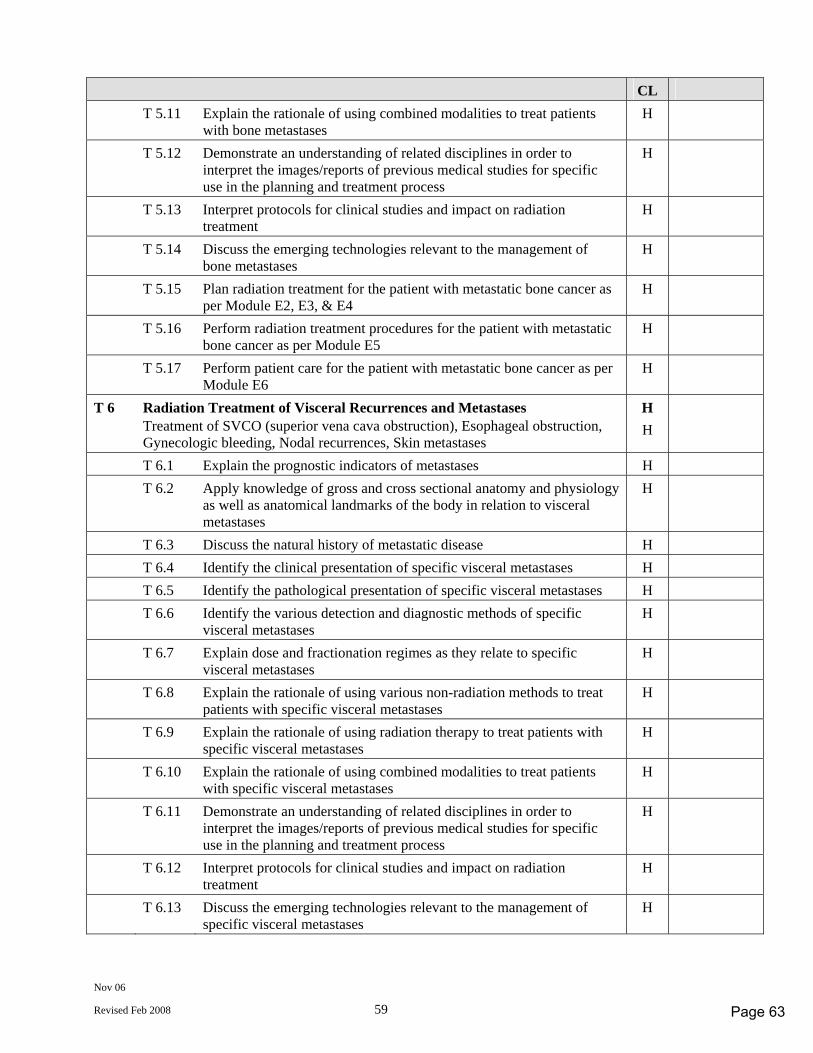
Nov 06
Revised Feb 2008 59
CL T 5.11 Explain the rationale of using combined modalities to treat patients
with bone metastases H
T 5.12 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
T 5.13 Interpret protocols for clinical studies and impact on radiation treatment
H
T 5.14 Discuss the emerging technologies relevant to the management of bone metastases
H
T 5.15 Plan radiation treatment for the patient with metastatic bone cancer as per Module E2, E3, & E4
H
T 5.16 Perform radiation treatment procedures for the patient with metastatic bone cancer as per Module E5
H
T 5.17 Perform patient care for the patient with metastatic bone cancer as per Module E6
H
T 6 Radiation Treatment of Visceral Recurrences and Metastases H Treatment of SVCO (superior vena cava obstruction), Esophageal obstruction,
Gynecologic bleeding, Nodal recurrences, Skin metastases H
T 6.1 Explain the prognostic indicators of metastases H T 6.2 Apply knowledge of gross and cross sectional anatomy and physiology
as well as anatomical landmarks of the body in relation to visceral metastases
H
T 6.3 Discuss the natural history of metastatic disease H T 6.4 Identify the clinical presentation of specific visceral metastases H T 6.5 Identify the pathological presentation of specific visceral metastases H T 6.6 Identify the various detection and diagnostic methods of specific
visceral metastases H
T 6.7 Explain dose and fractionation regimes as they relate to specific visceral metastases
H
T 6.8 Explain the rationale of using various non-radiation methods to treat patients with specific visceral metastases
H
T 6.9 Explain the rationale of using radiation therapy to treat patients with specific visceral metastases
H
T 6.10 Explain the rationale of using combined modalities to treat patients with specific visceral metastases
H
T 6.11 Demonstrate an understanding of related disciplines in order to interpret the images/reports of previous medical studies for specific use in the planning and treatment process
H
T 6.12 Interpret protocols for clinical studies and impact on radiation treatment
H
T 6.13 Discuss the emerging technologies relevant to the management of specific visceral metastases
H
Page 63
Nov 06
Revised Feb 2008 60
CL T 6.14 Plan radiation treatment for the patient with specific visceral
metastases as per Module E2, E3, & E4 H
T 6.15 Perform radiation treatment procedures for the patient with specific visceral metastases as per Module E5
H
T 6.16 Perform patient care for the patient with specific visceral metastases as per Module E6
H
Page 64
November 2006
(Revised Feb 2008) (#29260)
Nuclear Medicine
COMPETENCY PROFILE
November 2006 Revised February 2008
Revised Profile for use with the development of the
September 2011 Certification exams
Prepared by the Nuclear Medicine Competency Profile Task Group
© CANADIAN ASSOCIATION OF MEDICAL RADIATION TECHNOLOGISTS Suite 1000, 85 Albert Street, Ottawa, Ontario K1P 6A4
Tel: 1-800-463-9729 or (613) 234-0012 / Fax: (613) 234-1097 www.camrt.ca
Page 65

November 2006
(Revised Feb 2008) (#29260)
© Copyright 2006 by Canadian Association of Medical Radiation Technologists
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage or retrieval system, without the prior written permission of the Canadian Association of Medical Radiation Technologists.
Page 66
Nov 06
Revised Feb. 2008 1
COMPETENCY PROFILE – NUCLEAR MEDICINE Competencies for Entry Level Nuclear Medicine Technologists This document describes the essential competencies required for an entry-level nuclear medicine technologist in Canada to provide best practice as defined by safe, competent and ethical practice of medical radiation technology in a variety of clinical environments. The profile defines competencies reflecting the integration of knowledge, skills, attitudes and judgment necessary to practice in an environment that requires the technologist to use effective organizational skills and critical thinking. This requires the ability to assess, adapt, modify, analyse and evaluate in a variety of situations and environments in the practice of nuclear medicine technology. Critical decision-making is, therefore, inherent to the practice of nuclear medicine technology and is demonstrated in the competencies required of entry-to-practice technologists. The competency profile defines the standard for certification and registration of entry-level nuclear medicine technologists in Canada.
The document is also used to:
- provide direction to entry-level education programs to assist in developing curriculum - inform Ministries of Health and Education of the standard expected from entry-level nuclear
medicine technologists - inform the public and employers of the standard expected from entry-level nuclear medicine
technologists - assist CMA Conjoint Committee with accreditation of education programs - provide guidance by identifying professional development needs for practicing technologists - develop a blueprint for CAMRT certification examination Accredited programs must ensure that their certification candidates possess all the competencies listed in the profile. Education programs are encouraged to include additional skills at their discretion. In the development of the competencies, the following assumptions have been made. That the nuclear medicine technologist - has completed an accredited Canadian program, or other recognized program - has acquired the theoretical knowledge required to achieve a wide range of competencies - has developed a broad knowledge base that has been assessed prior to the certification examination - commits to the principle that their primary role and function is to serve the public interest - is a member of the inter-professional health care team collaborating with other health care
professionals to provide appropriate patient care in the delivery of diagnostic and therapeutic imaging services
is responsible for the safe and effective application of ionizing radiation - is responsible for the production, assessment, optimization and archiving of images - is responsible for the performance of diagnostic and therapeutic nuclear medicine procedures - is responsible for the education of patients, public and other health care providers regarding
ionizing radiation for medical use - performs effectively encompassing physical, psychological, social, economic and cultural factors
that interact in predictable and unpredictable ways
Page 67
Nov 06
Revised Feb. 2008 2
- recognizes patients as unique individuals, treating them with dignity and respect - practices in accordance with legislation, regulatory and professional bodies’ standards of practice,
scope of practice, codes of ethics and other relevant documents - performs in a manner consistent with public interest, employment philosophies and practices,
current research and advancing technology - seeks guidance from experienced practitioners, colleagues and employers to enhance the
technologist’s individual experience and knowledge - promotes and participates in the advancement of this dynamic profession through active
involvement, continuous learning, professional development and research - adheres to and promotes professional standards The Nuclear Medicine Technology Competency Profile is divided into fourteen modules: Module A Professional Practice Module B Patient Management Module C Radiation Health & Safety Module D Quality Management Module E Radiopharmacy and Laboratory Procedures Module F Clinical Procedures - Core Competencies Module G Clinical Procedures - Cardiovascular (CV) Module H Clinical Procedures - Gastrointestinal (GI) Module I Clinical Procedures - Genitourinary (GU) Module J Clinical Procedures - Skeletal (SK) Module K Clinical Procedures - Inflammatory Process/Tumor/Lymph (TU) Module L Clinical Procedures - Central Nervous System (CN) Module M Clinical Procedures - Endocrine (EN) Module N Clinical Procedures - Respiratory System (RE)
Page 68
Nov 06
Revised Feb. 2008 3
EXAMINABLE COMPETENCIES & COMPETENCY LEVELS
All competencies listed in the competency profile must be achieved by graduates of an accredited medical radiation technology program. This will be assessed for compliance during the accreditation survey conducted by the CMA Conjoint Accreditation Services. It is realized that due to regional and institutional differences level of achievement for some competencies may vary based on evolving changes in technology, practice and facility policies.
Not all competencies will be tested on the CAMRT certification exam. The EXAMINABLE COMPETENCIES are those competencies that have a competency level indicated in the column to the right of the written competency. The EXAMINABLE COMPETENCIES were established by the discipline specific workgroups working both within their disciplines and together as a core group using the feedback received from stakeholders during the competency profile revision process.
There are three competency levels (CL)
– HIGH (H)
– MEDIUM (M)
– LOW (L) Competency levels were determined through a survey done by technologists/therapists and managers of Diagnostic Imaging and Radiation Therapy Departments. The survey requested a rating of the examinable competencies for frequency of application, importance and future significance in the healthcare work environment. The results of the survey were analyzed and the examinable competencies rated either H, M, L based on the response to frequency, importance and significance for the future.
The competency levels provide a guide (blue print) for certification exam development. More weighting will be placed on the development and use of questions associated with a HIGH level competency as opposed to a MEDIUM or LOW rated level competency where emphasis on question development and use on the certification exam will reflect the competency level.
Validation of all competencies, including identification of examinable competencies and their associated competency levels will be conducted at least every five years. Due to rapid changes in technology and practice certain portions of the profile may be validated more frequently to ensure the profiles are reflective of practice and workplace needs.
Due to regional differences in the practice of nuclear medicine technology it is recognized that candidates may not be clinically competent in 100% of nuclear medicine clinical procedures. However candidates must demonstrate competency in a minimum of eleven (11) clinical procedures with a HIGH competency level plus a minimum of eleven (11) clinical procedures with a MEDIUM competency level.
Page 69
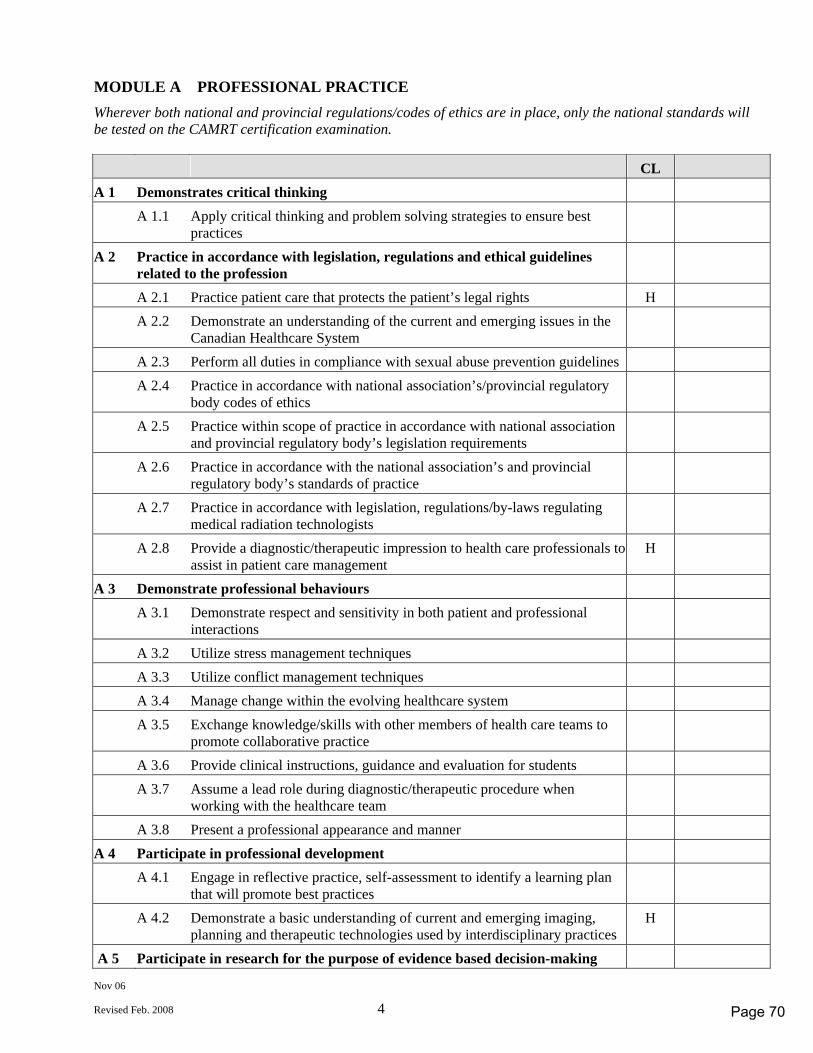
Nov 06
Revised Feb. 2008 4
MODULE A PROFESSIONAL PRACTICE Wherever both national and provincial regulations/codes of ethics are in place, only the national standards will be tested on the CAMRT certification examination. CL A 1 Demonstrates critical thinking A 1.1 Apply critical thinking and problem solving strategies to ensure best
practices
A 2 Practice in accordance with legislation, regulations and ethical guidelines related to the profession
A 2.1 Practice patient care that protects the patient’s legal rights H A 2.2 Demonstrate an understanding of the current and emerging issues in the
Canadian Healthcare System
A 2.3 Perform all duties in compliance with sexual abuse prevention guidelines A 2.4 Practice in accordance with national association’s/provincial regulatory
body codes of ethics
A 2.5 Practice within scope of practice in accordance with national association and provincial regulatory body’s legislation requirements
A 2.6 Practice in accordance with the national association’s and provincial regulatory body’s standards of practice
A 2.7 Practice in accordance with legislation, regulations/by-laws regulating medical radiation technologists
A 2.8 Provide a diagnostic/therapeutic impression to health care professionals to assist in patient care management
H
A 3 Demonstrate professional behaviours A 3.1 Demonstrate respect and sensitivity in both patient and professional
interactions
A 3.2 Utilize stress management techniques A 3.3 Utilize conflict management techniques A 3.4 Manage change within the evolving healthcare system A 3.5 Exchange knowledge/skills with other members of health care teams to
promote collaborative practice
A 3.6 Provide clinical instructions, guidance and evaluation for students A 3.7 Assume a lead role during diagnostic/therapeutic procedure when
working with the healthcare team
A 3.8 Present a professional appearance and manner A 4 Participate in professional development A 4.1 Engage in reflective practice, self-assessment to identify a learning plan
that will promote best practices
A 4.2 Demonstrate a basic understanding of current and emerging imaging, planning and therapeutic technologies used by interdisciplinary practices
H
A 5 Participate in research for the purpose of evidence based decision-making
Page 70
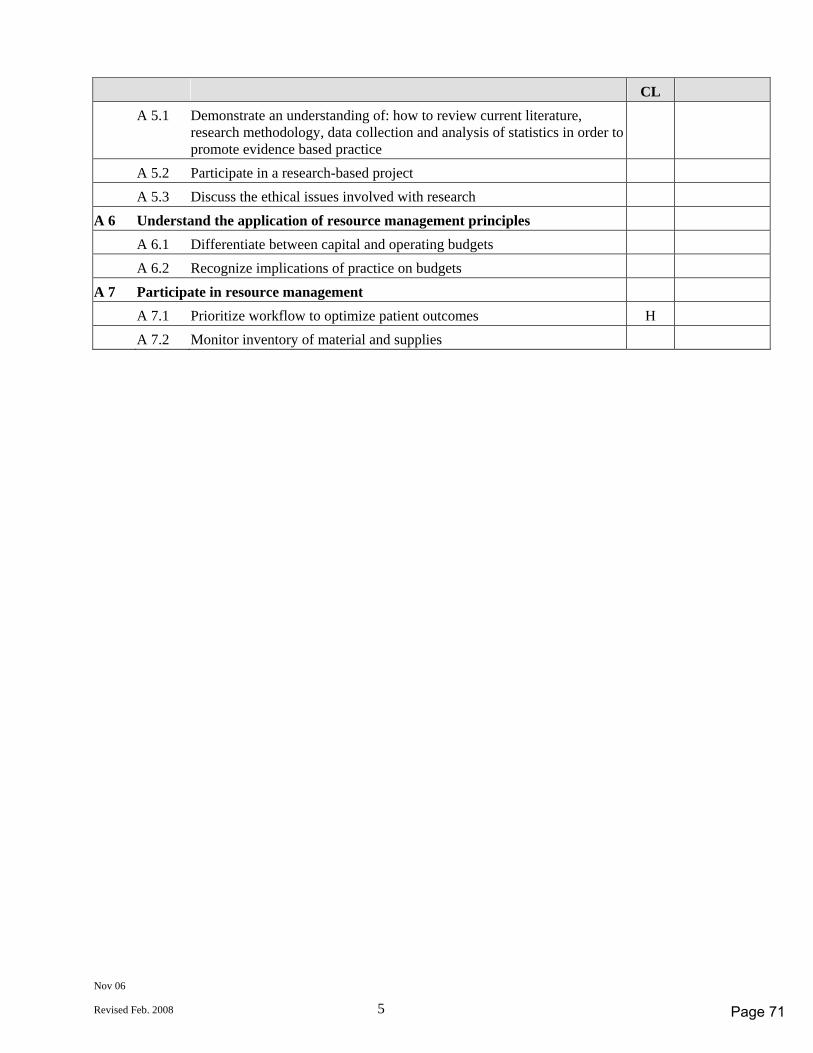
Nov 06
Revised Feb. 2008 5
CL A 5.1 Demonstrate an understanding of: how to review current literature,
research methodology, data collection and analysis of statistics in order to promote evidence based practice
A 5.2 Participate in a research-based project A 5.3 Discuss the ethical issues involved with research A 6 Understand the application of resource management principles A 6.1 Differentiate between capital and operating budgets A 6.2 Recognize implications of practice on budgets A 7 Participate in resource management A 7.1 Prioritize workflow to optimize patient outcomes H A 7.2 Monitor inventory of material and supplies
Page 71
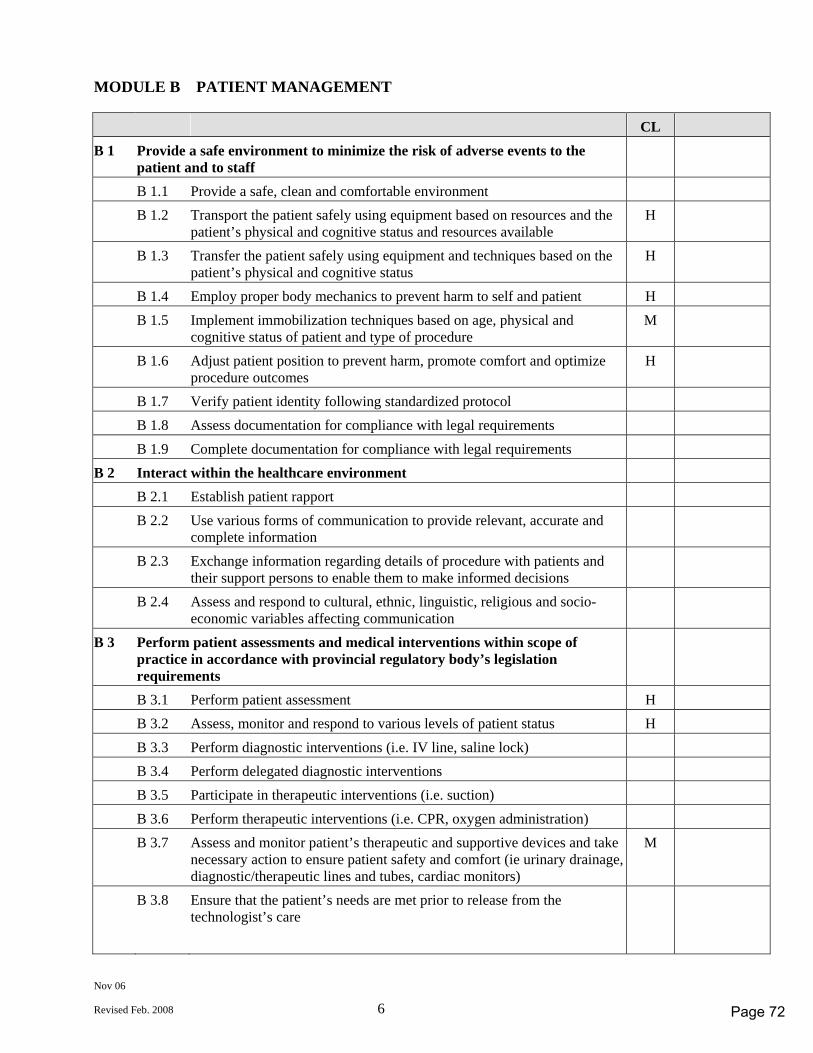
Nov 06
Revised Feb. 2008 6
MODULE B PATIENT MANAGEMENT CL B 1 Provide a safe environment to minimize the risk of adverse events to the
patient and to staff
B 1.1 Provide a safe, clean and comfortable environment B 1.2 Transport the patient safely using equipment based on resources and the
patient’s physical and cognitive status and resources available H
B 1.3 Transfer the patient safely using equipment and techniques based on the patient’s physical and cognitive status
H
B 1.4 Employ proper body mechanics to prevent harm to self and patient H B 1.5 Implement immobilization techniques based on age, physical and
cognitive status of patient and type of procedure M
B 1.6 Adjust patient position to prevent harm, promote comfort and optimize procedure outcomes
H
B 1.7 Verify patient identity following standardized protocol B 1.8 Assess documentation for compliance with legal requirements B 1.9 Complete documentation for compliance with legal requirements B 2 Interact within the healthcare environment B 2.1 Establish patient rapport B 2.2 Use various forms of communication to provide relevant, accurate and
complete information
B 2.3 Exchange information regarding details of procedure with patients and their support persons to enable them to make informed decisions
B 2.4 Assess and respond to cultural, ethnic, linguistic, religious and socio-economic variables affecting communication
B 3 Perform patient assessments and medical interventions within scope of practice in accordance with provincial regulatory body’s legislation requirements
B 3.1 Perform patient assessment H B 3.2 Assess, monitor and respond to various levels of patient status H B 3.3 Perform diagnostic interventions (i.e. IV line, saline lock) B 3.4 Perform delegated diagnostic interventions B 3.5 Participate in therapeutic interventions (i.e. suction) B 3.6 Perform therapeutic interventions (i.e. CPR, oxygen administration) B 3.7 Assess and monitor patient’s therapeutic and supportive devices and take
necessary action to ensure patient safety and comfort (ie urinary drainage, diagnostic/therapeutic lines and tubes, cardiac monitors)
M
B 3.8 Ensure that the patient’s needs are met prior to release from the technologist’s care
Page 72
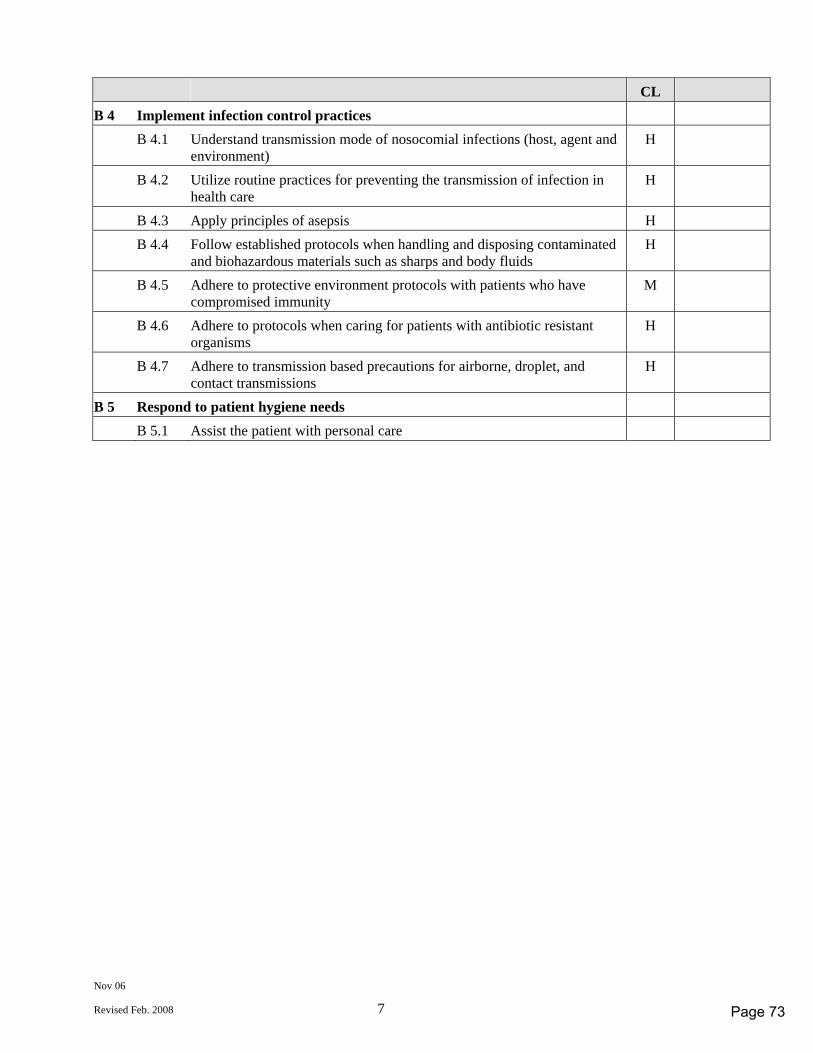
Nov 06
Revised Feb. 2008 7
CL B 4 Implement infection control practices B 4.1 Understand transmission mode of nosocomial infections (host, agent and
environment) H
B 4.2 Utilize routine practices for preventing the transmission of infection in health care
H
B 4.3 Apply principles of asepsis H B 4.4 Follow established protocols when handling and disposing contaminated
and biohazardous materials such as sharps and body fluids H
B 4.5 Adhere to protective environment protocols with patients who have compromised immunity
M
B 4.6 Adhere to protocols when caring for patients with antibiotic resistant organisms
H
B 4.7 Adhere to transmission based precautions for airborne, droplet, and contact transmissions
H
B 5 Respond to patient hygiene needs B 5.1 Assist the patient with personal care
Page 73
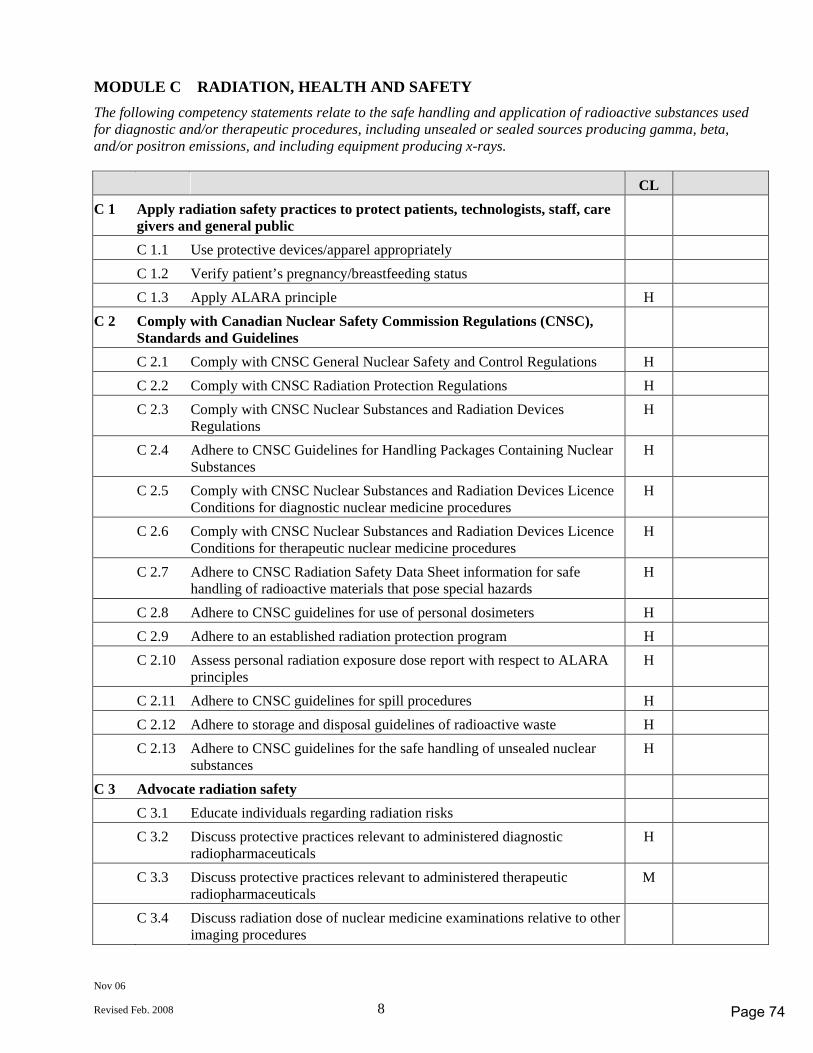
Nov 06
Revised Feb. 2008 8
MODULE C RADIATION, HEALTH AND SAFETY The following competency statements relate to the safe handling and application of radioactive substances used for diagnostic and/or therapeutic procedures, including unsealed or sealed sources producing gamma, beta, and/or positron emissions, and including equipment producing x-rays. CL C 1 Apply radiation safety practices to protect patients, technologists, staff, care
givers and general public
C 1.1 Use protective devices/apparel appropriately C 1.2 Verify patient’s pregnancy/breastfeeding status C 1.3 Apply ALARA principle H C 2 Comply with Canadian Nuclear Safety Commission Regulations (CNSC),
Standards and Guidelines
C 2.1 Comply with CNSC General Nuclear Safety and Control Regulations H C 2.2 Comply with CNSC Radiation Protection Regulations H C 2.3 Comply with CNSC Nuclear Substances and Radiation Devices
Regulations H
C 2.4 Adhere to CNSC Guidelines for Handling Packages Containing Nuclear Substances
H
C 2.5 Comply with CNSC Nuclear Substances and Radiation Devices Licence Conditions for diagnostic nuclear medicine procedures
H
C 2.6 Comply with CNSC Nuclear Substances and Radiation Devices Licence Conditions for therapeutic nuclear medicine procedures
H
C 2.7 Adhere to CNSC Radiation Safety Data Sheet information for safe handling of radioactive materials that pose special hazards
H
C 2.8 Adhere to CNSC guidelines for use of personal dosimeters H C 2.9 Adhere to an established radiation protection program H C 2.10 Assess personal radiation exposure dose report with respect to ALARA
principles H
C 2.11 Adhere to CNSC guidelines for spill procedures H C 2.12 Adhere to storage and disposal guidelines of radioactive waste H C 2.13 Adhere to CNSC guidelines for the safe handling of unsealed nuclear
substances H
C 3 Advocate radiation safety C 3.1 Educate individuals regarding radiation risks C 3.2 Discuss protective practices relevant to administered diagnostic
radiopharmaceuticals H
C 3.3 Discuss protective practices relevant to administered therapeutic radiopharmaceuticals
M
C 3.4 Discuss radiation dose of nuclear medicine examinations relative to other imaging procedures
Page 74
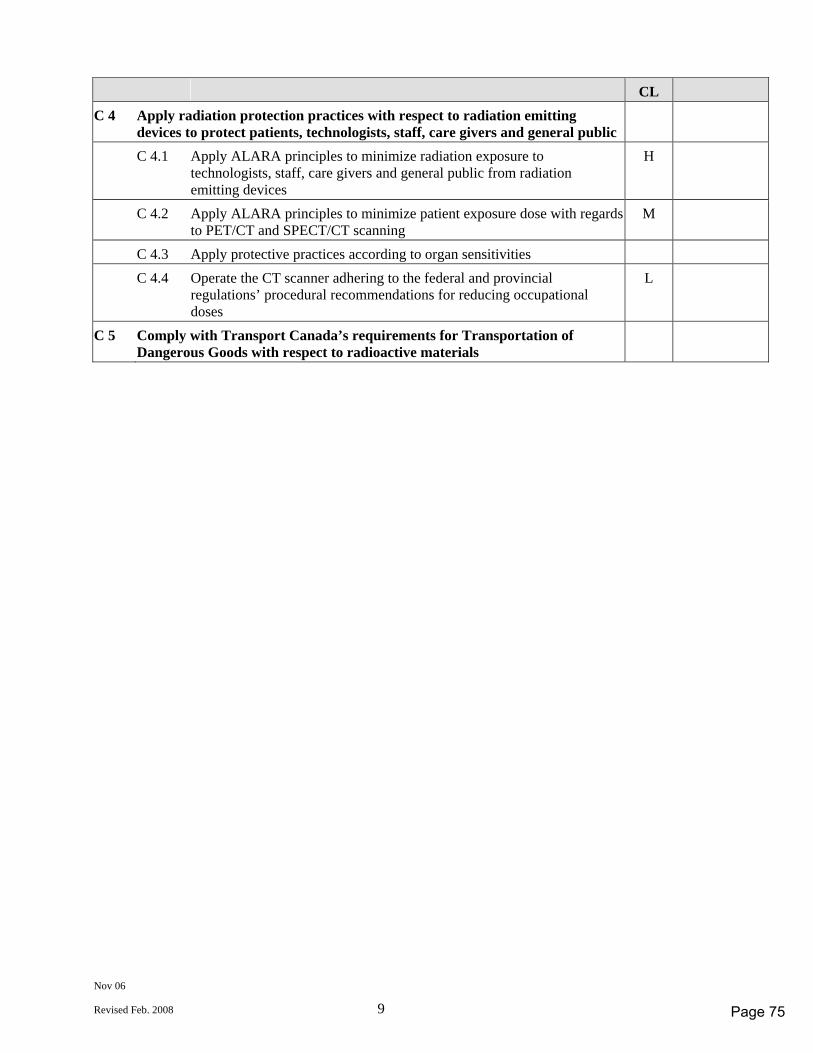
Nov 06
Revised Feb. 2008 9
CL C 4 Apply radiation protection practices with respect to radiation emitting
devices to protect patients, technologists, staff, care givers and general public
C 4.1 Apply ALARA principles to minimize radiation exposure to technologists, staff, care givers and general public from radiation emitting devices
H
C 4.2 Apply ALARA principles to minimize patient exposure dose with regards to PET/CT and SPECT/CT scanning
M
C 4.3 Apply protective practices according to organ sensitivities C 4.4 Operate the CT scanner adhering to the federal and provincial
regulations’ procedural recommendations for reducing occupational doses
L
C 5 Comply with Transport Canada’s requirements for Transportation of Dangerous Goods with respect to radioactive materials
Page 75
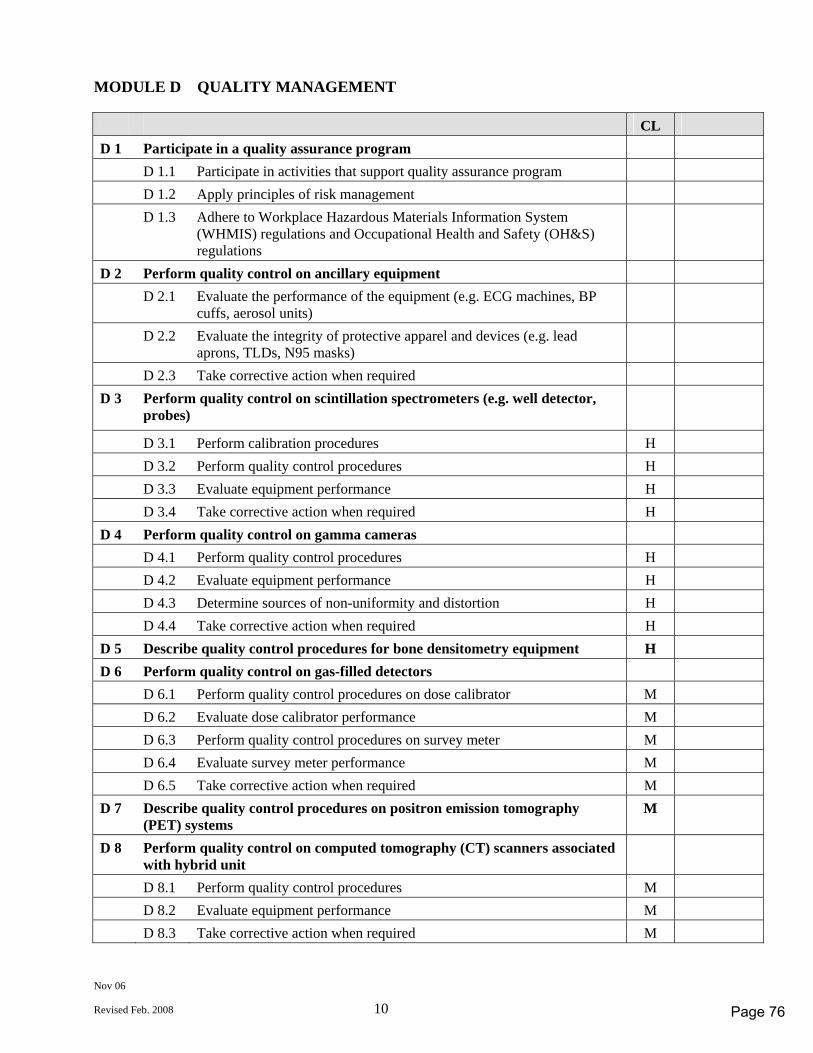
Nov 06
Revised Feb. 2008 10
MODULE D QUALITY MANAGEMENT CL D 1 Participate in a quality assurance program D 1.1 Participate in activities that support quality assurance program D 1.2 Apply principles of risk management D 1.3 Adhere to Workplace Hazardous Materials Information System
(WHMIS) regulations and Occupational Health and Safety (OH&S) regulations
D 2 Perform quality control on ancillary equipment D 2.1 Evaluate the performance of the equipment (e.g. ECG machines, BP
cuffs, aerosol units)
D 2.2 Evaluate the integrity of protective apparel and devices (e.g. lead aprons, TLDs, N95 masks)
D 2.3 Take corrective action when required D 3 Perform quality control on scintillation spectrometers (e.g. well detector,
probes)
D 3.1 Perform calibration procedures H D 3.2 Perform quality control procedures H D 3.3 Evaluate equipment performance H D 3.4 Take corrective action when required H D 4 Perform quality control on gamma cameras D 4.1 Perform quality control procedures H D 4.2 Evaluate equipment performance H D 4.3 Determine sources of non-uniformity and distortion H D 4.4 Take corrective action when required H D 5 Describe quality control procedures for bone densitometry equipment H D 6 Perform quality control on gas-filled detectors D 6.1 Perform quality control procedures on dose calibrator M D 6.2 Evaluate dose calibrator performance M D 6.3 Perform quality control procedures on survey meter M D 6.4 Evaluate survey meter performance M D 6.5 Take corrective action when required M D 7 Describe quality control procedures on positron emission tomography
(PET) systems M
D 8 Perform quality control on computed tomography (CT) scanners associated with hybrid unit
D 8.1 Perform quality control procedures M D 8.2 Evaluate equipment performance M D 8.3 Take corrective action when required M
Page 76
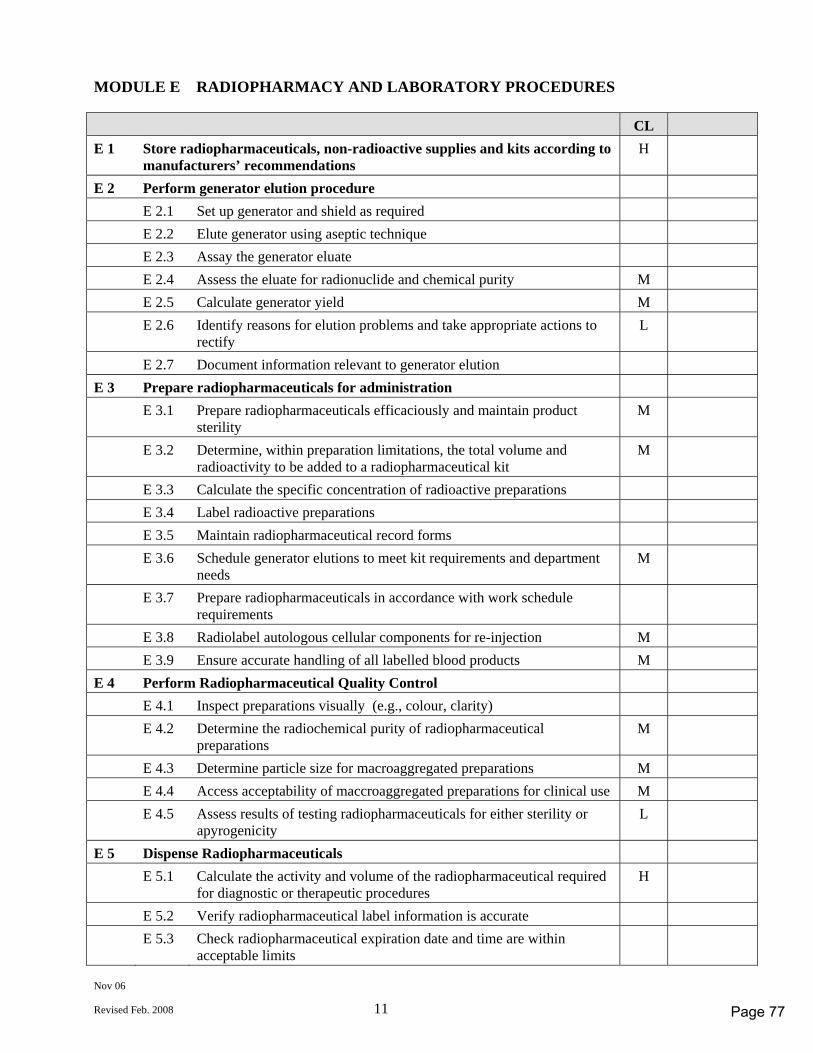
Nov 06
Revised Feb. 2008 11
MODULE E RADIOPHARMACY AND LABORATORY PROCEDURES CL E 1 Store radiopharmaceuticals, non-radioactive supplies and kits according to
manufacturers’ recommendations H
E 2 Perform generator elution procedure E 2.1 Set up generator and shield as required E 2.2 Elute generator using aseptic technique E 2.3 Assay the generator eluate E 2.4 Assess the eluate for radionuclide and chemical purity M E 2.5 Calculate generator yield M E 2.6 Identify reasons for elution problems and take appropriate actions to
rectify L
E 2.7 Document information relevant to generator elution E 3 Prepare radiopharmaceuticals for administration E 3.1 Prepare radiopharmaceuticals efficaciously and maintain product
sterility M
E 3.2 Determine, within preparation limitations, the total volume and radioactivity to be added to a radiopharmaceutical kit
M
E 3.3 Calculate the specific concentration of radioactive preparations E 3.4 Label radioactive preparations E 3.5 Maintain radiopharmaceutical record forms E 3.6 Schedule generator elutions to meet kit requirements and department
needs M
E 3.7 Prepare radiopharmaceuticals in accordance with work schedule requirements
E 3.8 Radiolabel autologous cellular components for re-injection M E 3.9 Ensure accurate handling of all labelled blood products M E 4 Perform Radiopharmaceutical Quality Control E 4.1 Inspect preparations visually (e.g., colour, clarity) E 4.2 Determine the radiochemical purity of radiopharmaceutical
preparations M
E 4.3 Determine particle size for macroaggregated preparations M E 4.4 Access acceptability of maccroaggregated preparations for clinical use M E 4.5 Assess results of testing radiopharmaceuticals for either sterility or
apyrogenicity L
E 5 Dispense Radiopharmaceuticals E 5.1 Calculate the activity and volume of the radiopharmaceutical required
for diagnostic or therapeutic procedures H
E 5.2 Verify radiopharmaceutical label information is accurate E 5.3 Check radiopharmaceutical expiration date and time are within
acceptable limits
Page 77
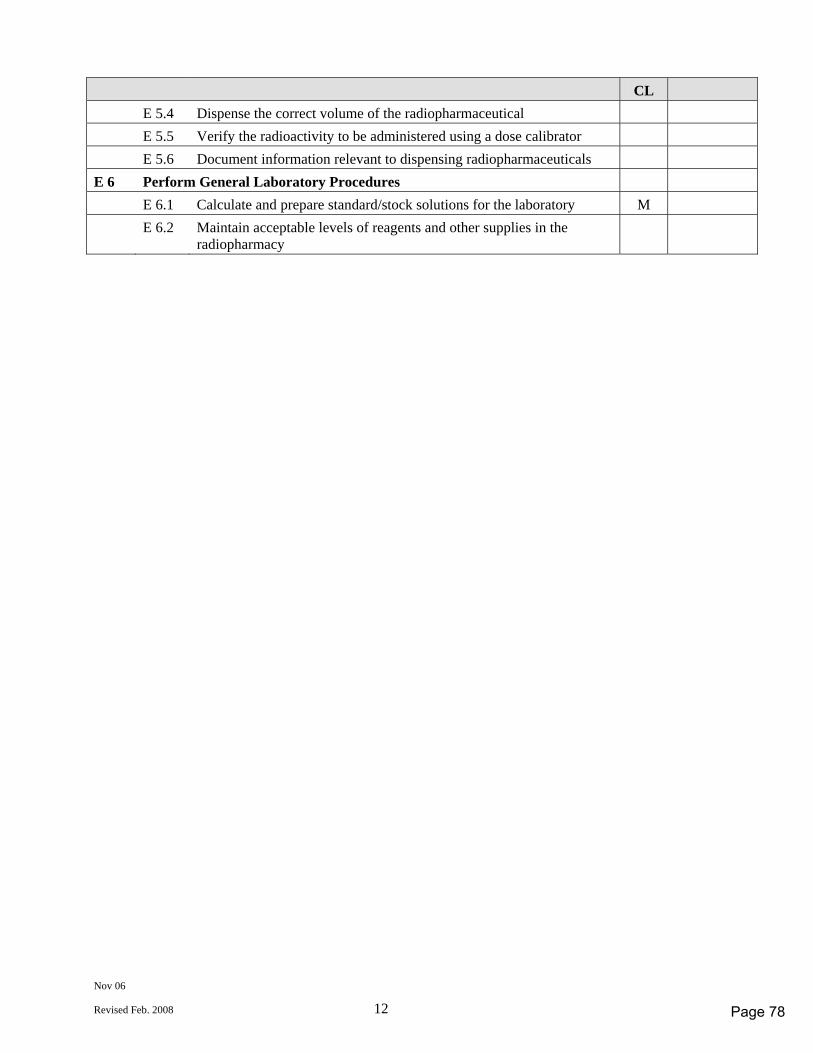
Nov 06
Revised Feb. 2008 12
CL E 5.4 Dispense the correct volume of the radiopharmaceutical E 5.5 Verify the radioactivity to be administered using a dose calibrator E 5.6 Document information relevant to dispensing radiopharmaceuticals E 6 Perform General Laboratory Procedures E 6.1 Calculate and prepare standard/stock solutions for the laboratory M E 6.2 Maintain acceptable levels of reagents and other supplies in the
radiopharmacy
Page 78
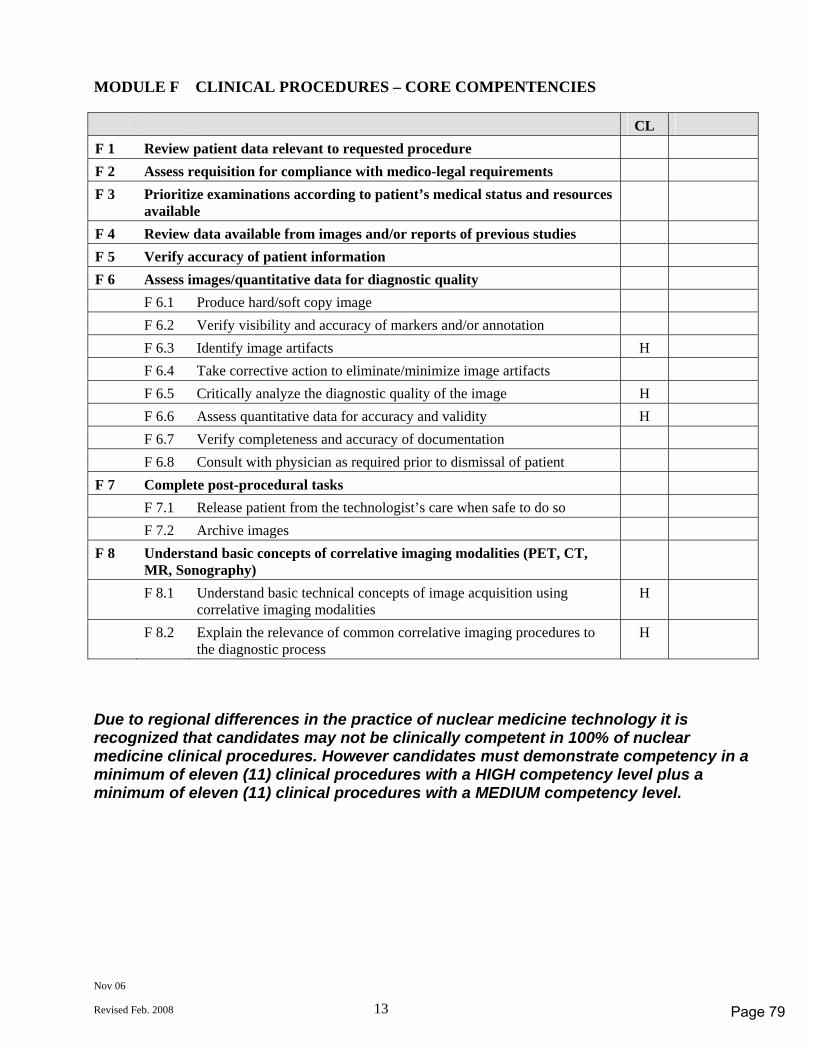
Nov 06
Revised Feb. 2008 13
MODULE F CLINICAL PROCEDURES – CORE COMPENTENCIES CL F 1 Review patient data relevant to requested procedure F 2 Assess requisition for compliance with medico-legal requirements F 3 Prioritize examinations according to patient’s medical status and resources
available
F 4 Review data available from images and/or reports of previous studies F 5 Verify accuracy of patient information F 6 Assess images/quantitative data for diagnostic quality F 6.1 Produce hard/soft copy image F 6.2 Verify visibility and accuracy of markers and/or annotation F 6.3 Identify image artifacts H F 6.4 Take corrective action to eliminate/minimize image artifacts F 6.5 Critically analyze the diagnostic quality of the image H F 6.6 Assess quantitative data for accuracy and validity H F 6.7 Verify completeness and accuracy of documentation F 6.8 Consult with physician as required prior to dismissal of patient F 7 Complete post-procedural tasks F 7.1 Release patient from the technologist’s care when safe to do so F 7.2 Archive images F 8 Understand basic concepts of correlative imaging modalities (PET, CT,
MR, Sonography)
F 8.1 Understand basic technical concepts of image acquisition using correlative imaging modalities
H
F 8.2 Explain the relevance of common correlative imaging procedures to the diagnostic process
H
Due to regional differences in the practice of nuclear medicine technology it is recognized that candidates may not be clinically competent in 100% of nuclear medicine clinical procedures. However candidates must demonstrate competency in a minimum of eleven (11) clinical procedures with a HIGH competency level plus a minimum of eleven (11) clinical procedures with a MEDIUM competency level.
Page 79
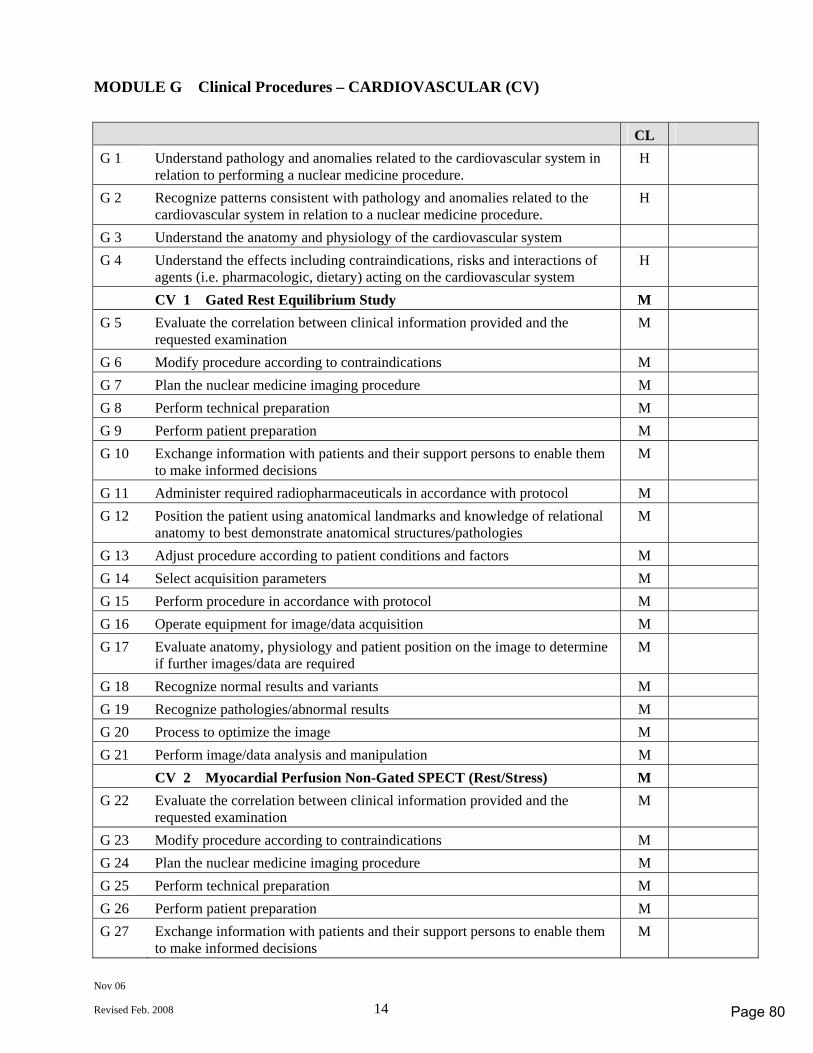
Nov 06
Revised Feb. 2008 14
MODULE G Clinical Procedures – CARDIOVASCULAR (CV)
CL G 1 Understand pathology and anomalies related to the cardiovascular system in
relation to performing a nuclear medicine procedure. H
G 2 Recognize patterns consistent with pathology and anomalies related to the cardiovascular system in relation to a nuclear medicine procedure.
H
G 3 Understand the anatomy and physiology of the cardiovascular system G 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the cardiovascular system H
CV 1 Gated Rest Equilibrium Study M G 5 Evaluate the correlation between clinical information provided and the
requested examination M
G 6 Modify procedure according to contraindications M G 7 Plan the nuclear medicine imaging procedure M G 8 Perform technical preparation M G 9 Perform patient preparation M G 10 Exchange information with patients and their support persons to enable them
to make informed decisions M
G 11 Administer required radiopharmaceuticals in accordance with protocol M G 12 Position the patient using anatomical landmarks and knowledge of relational
anatomy to best demonstrate anatomical structures/pathologies M
G 13 Adjust procedure according to patient conditions and factors M G 14 Select acquisition parameters M G 15 Perform procedure in accordance with protocol M G 16 Operate equipment for image/data acquisition M G 17 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required M
G 18 Recognize normal results and variants M G 19 Recognize pathologies/abnormal results M G 20 Process to optimize the image M G 21 Perform image/data analysis and manipulation M CV 2 Myocardial Perfusion Non-Gated SPECT (Rest/Stress) M G 22 Evaluate the correlation between clinical information provided and the
requested examination M
G 23 Modify procedure according to contraindications M G 24 Plan the nuclear medicine imaging procedure M G 25 Perform technical preparation M G 26 Perform patient preparation M G 27 Exchange information with patients and their support persons to enable them
to make informed decisions M
Page 80
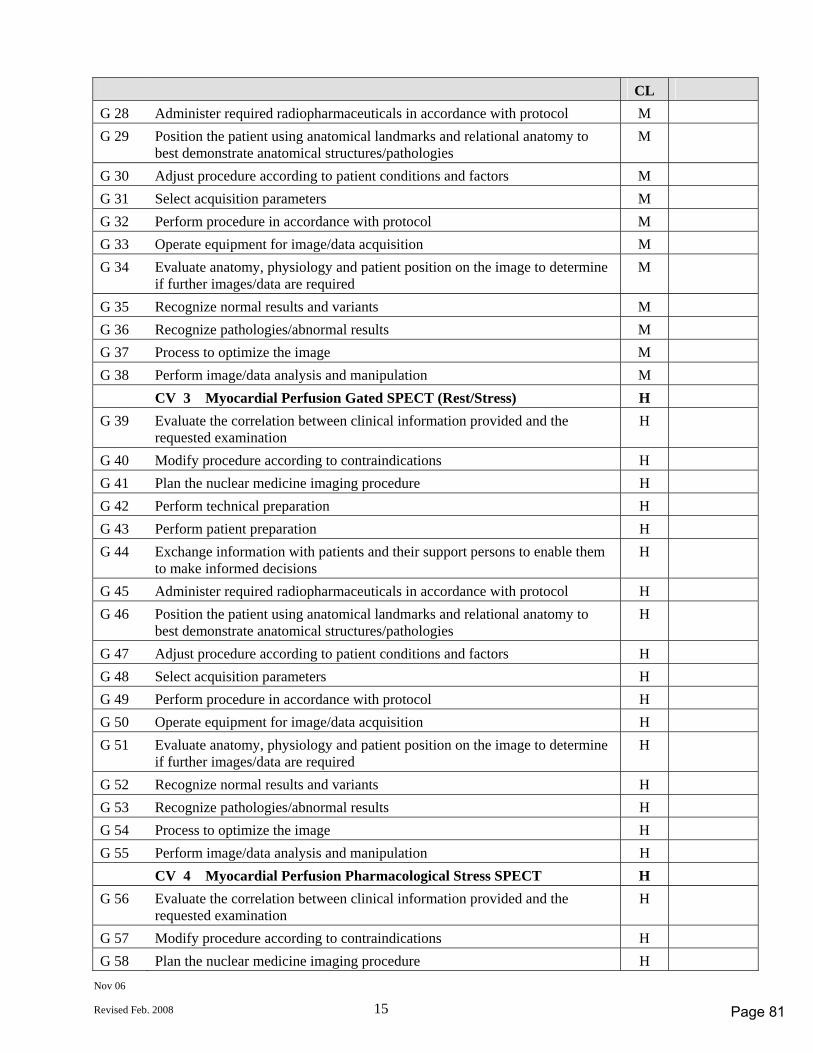
Nov 06
Revised Feb. 2008 15
CL G 28 Administer required radiopharmaceuticals in accordance with protocol M G 29 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies M
G 30 Adjust procedure according to patient conditions and factors M G 31 Select acquisition parameters M G 32 Perform procedure in accordance with protocol M G 33 Operate equipment for image/data acquisition M G 34 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required M
G 35 Recognize normal results and variants M G 36 Recognize pathologies/abnormal results M G 37 Process to optimize the image M G 38 Perform image/data analysis and manipulation M CV 3 Myocardial Perfusion Gated SPECT (Rest/Stress) H G 39 Evaluate the correlation between clinical information provided and the
requested examination H
G 40 Modify procedure according to contraindications H G 41 Plan the nuclear medicine imaging procedure H G 42 Perform technical preparation H G 43 Perform patient preparation H G 44 Exchange information with patients and their support persons to enable them
to make informed decisions H
G 45 Administer required radiopharmaceuticals in accordance with protocol H G 46 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies H
G 47 Adjust procedure according to patient conditions and factors H G 48 Select acquisition parameters H G 49 Perform procedure in accordance with protocol H G 50 Operate equipment for image/data acquisition H G 51 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required H
G 52 Recognize normal results and variants H G 53 Recognize pathologies/abnormal results H G 54 Process to optimize the image H G 55 Perform image/data analysis and manipulation H CV 4 Myocardial Perfusion Pharmacological Stress SPECT H G 56 Evaluate the correlation between clinical information provided and the
requested examination H
G 57 Modify procedure according to contraindications H G 58 Plan the nuclear medicine imaging procedure H
Page 81
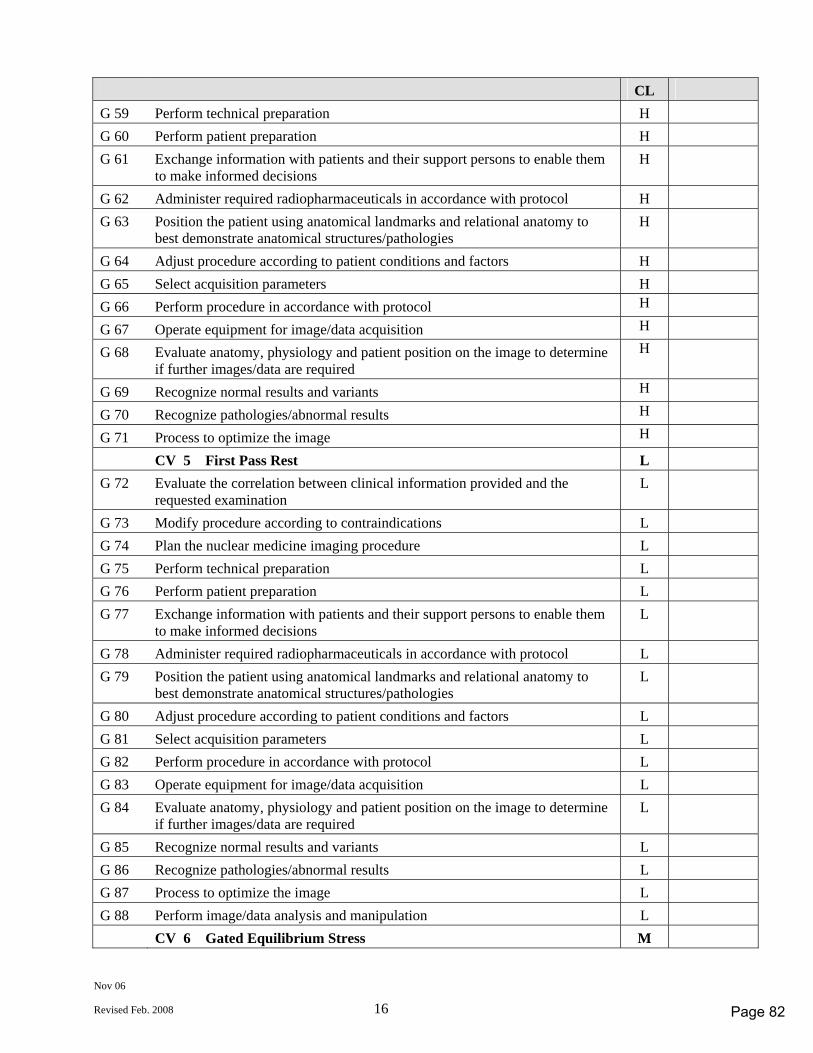
Nov 06
Revised Feb. 2008 16
CL G 59 Perform technical preparation H G 60 Perform patient preparation H G 61 Exchange information with patients and their support persons to enable them
to make informed decisions H
G 62 Administer required radiopharmaceuticals in accordance with protocol H G 63 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies H
G 64 Adjust procedure according to patient conditions and factors H G 65 Select acquisition parameters H G 66 Perform procedure in accordance with protocol H G 67 Operate equipment for image/data acquisition H G 68 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required H
G 69 Recognize normal results and variants H G 70 Recognize pathologies/abnormal results H G 71 Process to optimize the image H CV 5 First Pass Rest L G 72 Evaluate the correlation between clinical information provided and the
requested examination L
G 73 Modify procedure according to contraindications L G 74 Plan the nuclear medicine imaging procedure L G 75 Perform technical preparation L G 76 Perform patient preparation L G 77 Exchange information with patients and their support persons to enable them
to make informed decisions L
G 78 Administer required radiopharmaceuticals in accordance with protocol L G 79 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies L
G 80 Adjust procedure according to patient conditions and factors L G 81 Select acquisition parameters L G 82 Perform procedure in accordance with protocol L G 83 Operate equipment for image/data acquisition L G 84 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required L
G 85 Recognize normal results and variants L G 86 Recognize pathologies/abnormal results L G 87 Process to optimize the image L G 88 Perform image/data analysis and manipulation L CV 6 Gated Equilibrium Stress M
Page 82
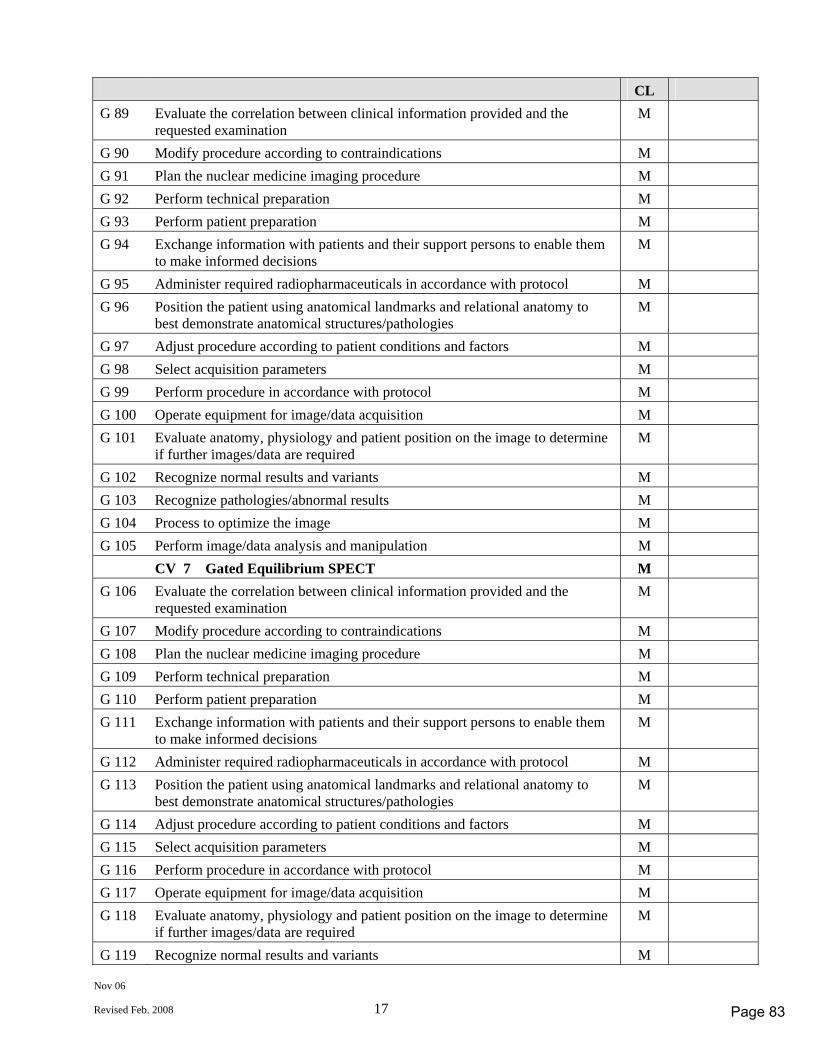
Nov 06
Revised Feb. 2008 17
CL G 89 Evaluate the correlation between clinical information provided and the
requested examination M
G 90 Modify procedure according to contraindications M G 91 Plan the nuclear medicine imaging procedure M G 92 Perform technical preparation M G 93 Perform patient preparation M G 94 Exchange information with patients and their support persons to enable them
to make informed decisions M
G 95 Administer required radiopharmaceuticals in accordance with protocol M G 96 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies M
G 97 Adjust procedure according to patient conditions and factors M G 98 Select acquisition parameters M G 99 Perform procedure in accordance with protocol M G 100 Operate equipment for image/data acquisition M G 101 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required M
G 102 Recognize normal results and variants M G 103 Recognize pathologies/abnormal results M G 104 Process to optimize the image M G 105 Perform image/data analysis and manipulation M CV 7 Gated Equilibrium SPECT M G 106 Evaluate the correlation between clinical information provided and the
requested examination M
G 107 Modify procedure according to contraindications M G 108 Plan the nuclear medicine imaging procedure M G 109 Perform technical preparation M G 110 Perform patient preparation M G 111 Exchange information with patients and their support persons to enable them
to make informed decisions M
G 112 Administer required radiopharmaceuticals in accordance with protocol M G 113 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies M
G 114 Adjust procedure according to patient conditions and factors M G 115 Select acquisition parameters M G 116 Perform procedure in accordance with protocol M G 117 Operate equipment for image/data acquisition M G 118 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required M
G 119 Recognize normal results and variants M
Page 83
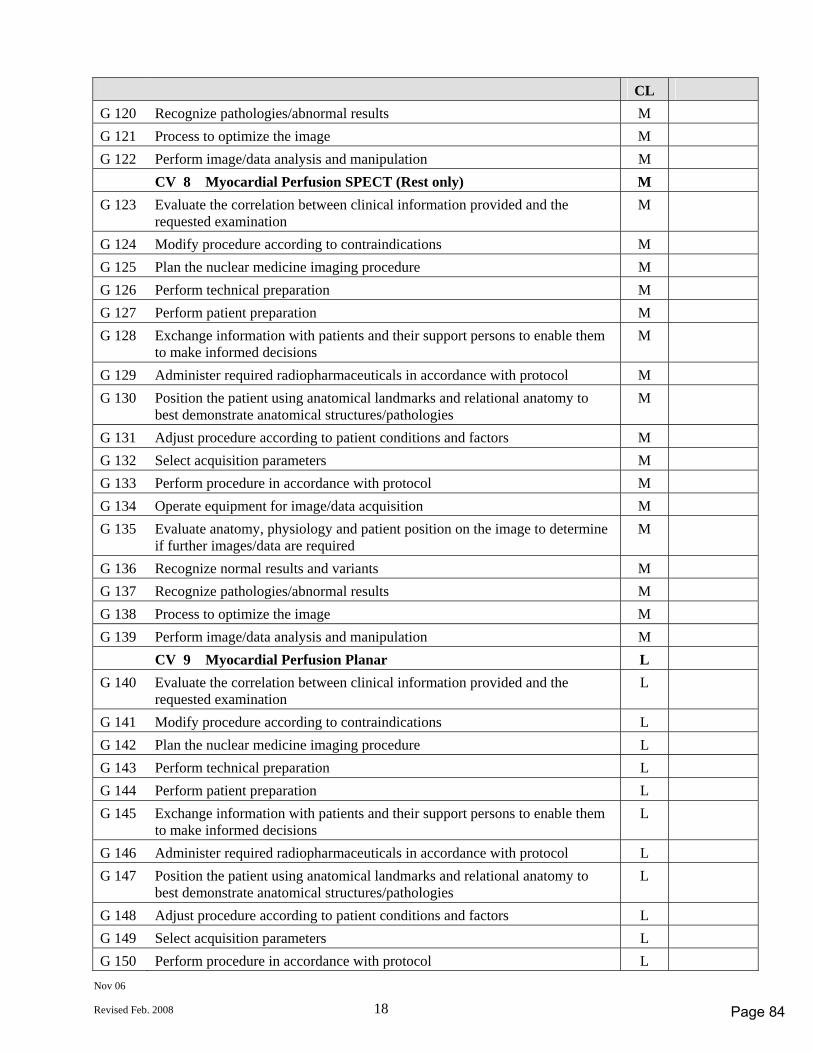
Nov 06
Revised Feb. 2008 18
CL G 120 Recognize pathologies/abnormal results M G 121 Process to optimize the image M G 122 Perform image/data analysis and manipulation M CV 8 Myocardial Perfusion SPECT (Rest only) M G 123 Evaluate the correlation between clinical information provided and the
requested examination M
G 124 Modify procedure according to contraindications M G 125 Plan the nuclear medicine imaging procedure M G 126 Perform technical preparation M G 127 Perform patient preparation M G 128 Exchange information with patients and their support persons to enable them
to make informed decisions M
G 129 Administer required radiopharmaceuticals in accordance with protocol M G 130 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies M
G 131 Adjust procedure according to patient conditions and factors M G 132 Select acquisition parameters M G 133 Perform procedure in accordance with protocol M G 134 Operate equipment for image/data acquisition M G 135 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required M
G 136 Recognize normal results and variants M G 137 Recognize pathologies/abnormal results M G 138 Process to optimize the image M G 139 Perform image/data analysis and manipulation M CV 9 Myocardial Perfusion Planar L G 140 Evaluate the correlation between clinical information provided and the
requested examination L
G 141 Modify procedure according to contraindications L G 142 Plan the nuclear medicine imaging procedure L G 143 Perform technical preparation L G 144 Perform patient preparation L G 145 Exchange information with patients and their support persons to enable them
to make informed decisions L
G 146 Administer required radiopharmaceuticals in accordance with protocol L G 147 Position the patient using anatomical landmarks and relational anatomy to
best demonstrate anatomical structures/pathologies L
G 148 Adjust procedure according to patient conditions and factors L G 149 Select acquisition parameters L G 150 Perform procedure in accordance with protocol L
Page 84
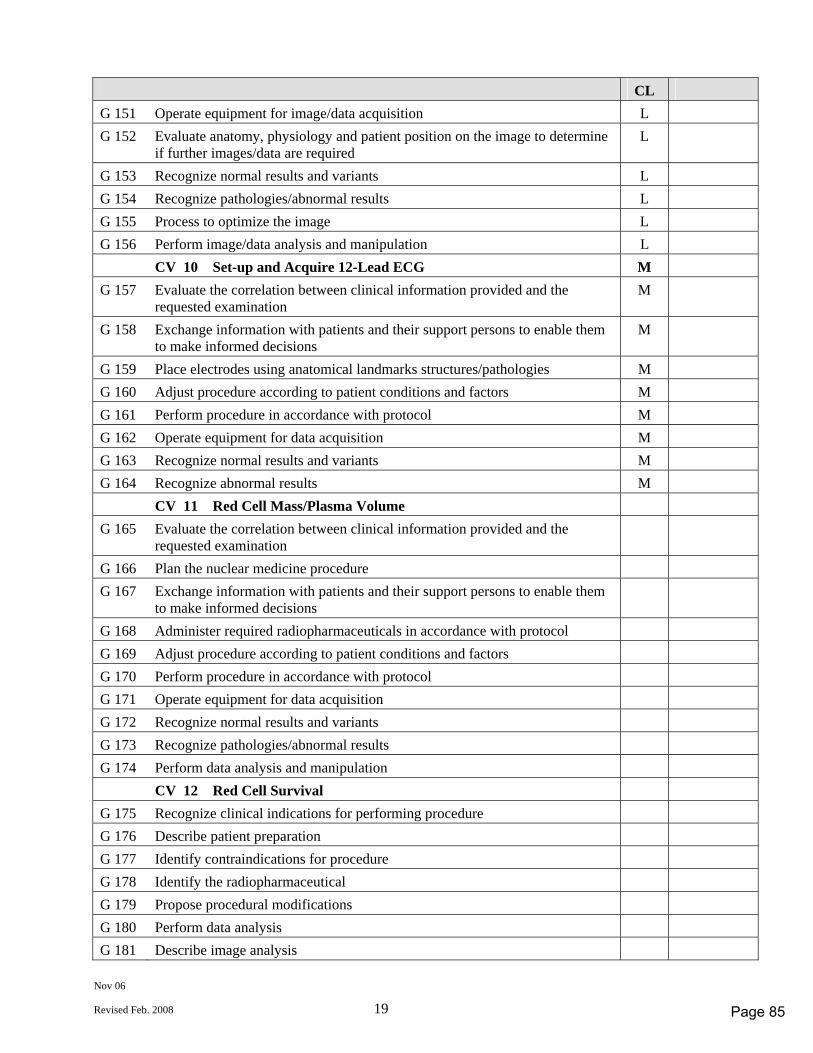
Nov 06
Revised Feb. 2008 19
CL G 151 Operate equipment for image/data acquisition L G 152 Evaluate anatomy, physiology and patient position on the image to determine
if further images/data are required L
G 153 Recognize normal results and variants L G 154 Recognize pathologies/abnormal results L G 155 Process to optimize the image L G 156 Perform image/data analysis and manipulation L CV 10 Set-up and Acquire 12-Lead ECG M G 157 Evaluate the correlation between clinical information provided and the
requested examination M
G 158 Exchange information with patients and their support persons to enable them to make informed decisions
M
G 159 Place electrodes using anatomical landmarks structures/pathologies M G 160 Adjust procedure according to patient conditions and factors M G 161 Perform procedure in accordance with protocol M G 162 Operate equipment for data acquisition M G 163 Recognize normal results and variants M G 164 Recognize abnormal results M CV 11 Red Cell Mass/Plasma Volume G 165 Evaluate the correlation between clinical information provided and the
requested examination
G 166 Plan the nuclear medicine procedure G 167 Exchange information with patients and their support persons to enable them
to make informed decisions
G 168 Administer required radiopharmaceuticals in accordance with protocol G 169 Adjust procedure according to patient conditions and factors G 170 Perform procedure in accordance with protocol G 171 Operate equipment for data acquisition G 172 Recognize normal results and variants G 173 Recognize pathologies/abnormal results G 174 Perform data analysis and manipulation CV 12 Red Cell Survival G 175 Recognize clinical indications for performing procedure G 176 Describe patient preparation G 177 Identify contraindications for procedure G 178 Identify the radiopharmaceutical G 179 Propose procedural modifications G 180 Perform data analysis G 181 Describe image analysis
Page 85
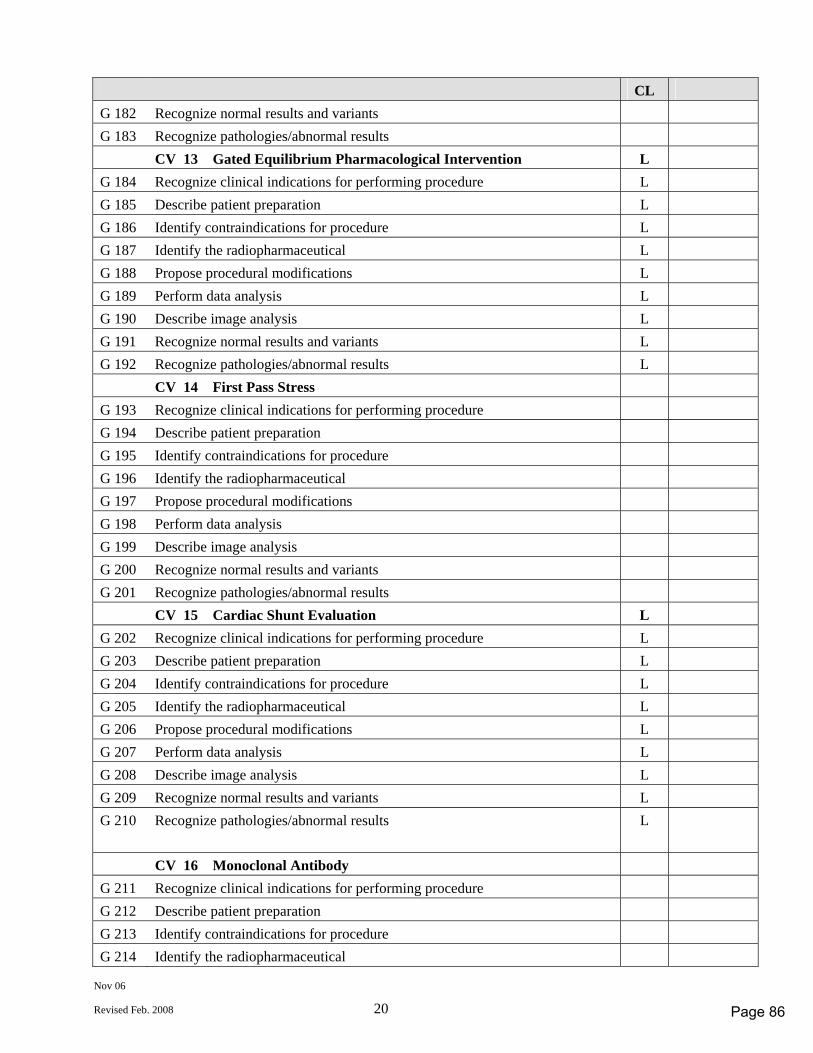
Nov 06
Revised Feb. 2008 20
CL G 182 Recognize normal results and variants G 183 Recognize pathologies/abnormal results CV 13 Gated Equilibrium Pharmacological Intervention L G 184 Recognize clinical indications for performing procedure L G 185 Describe patient preparation L G 186 Identify contraindications for procedure L G 187 Identify the radiopharmaceutical L G 188 Propose procedural modifications L G 189 Perform data analysis L G 190 Describe image analysis L G 191 Recognize normal results and variants L G 192 Recognize pathologies/abnormal results L CV 14 First Pass Stress G 193 Recognize clinical indications for performing procedure G 194 Describe patient preparation G 195 Identify contraindications for procedure G 196 Identify the radiopharmaceutical G 197 Propose procedural modifications G 198 Perform data analysis G 199 Describe image analysis G 200 Recognize normal results and variants G 201 Recognize pathologies/abnormal results CV 15 Cardiac Shunt Evaluation L G 202 Recognize clinical indications for performing procedure L G 203 Describe patient preparation L G 204 Identify contraindications for procedure L G 205 Identify the radiopharmaceutical L G 206 Propose procedural modifications L G 207 Perform data analysis L G 208 Describe image analysis L G 209 Recognize normal results and variants L G 210 Recognize pathologies/abnormal results L
CV 16 Monoclonal Antibody G 211 Recognize clinical indications for performing procedure G 212 Describe patient preparation G 213 Identify contraindications for procedure G 214 Identify the radiopharmaceutical
Page 86
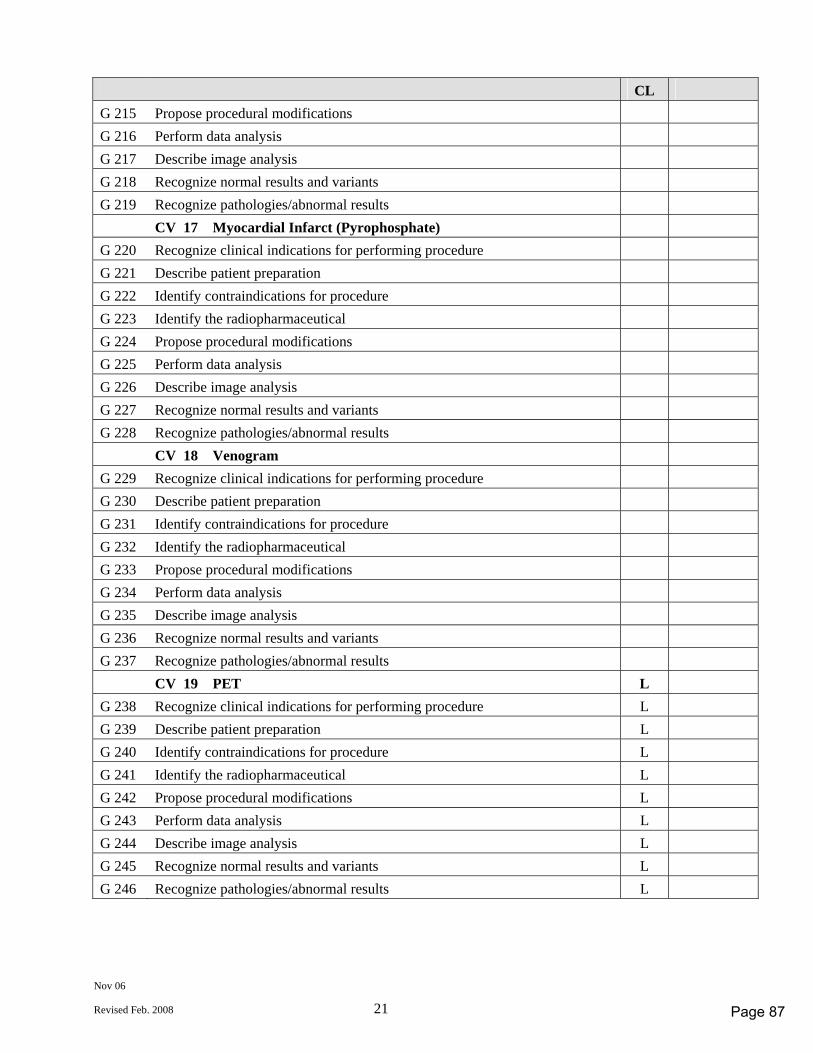
Nov 06
Revised Feb. 2008 21
CL G 215 Propose procedural modifications G 216 Perform data analysis G 217 Describe image analysis G 218 Recognize normal results and variants G 219 Recognize pathologies/abnormal results CV 17 Myocardial Infarct (Pyrophosphate) G 220 Recognize clinical indications for performing procedure G 221 Describe patient preparation G 222 Identify contraindications for procedure G 223 Identify the radiopharmaceutical G 224 Propose procedural modifications G 225 Perform data analysis G 226 Describe image analysis G 227 Recognize normal results and variants G 228 Recognize pathologies/abnormal results CV 18 Venogram G 229 Recognize clinical indications for performing procedure G 230 Describe patient preparation G 231 Identify contraindications for procedure G 232 Identify the radiopharmaceutical G 233 Propose procedural modifications G 234 Perform data analysis G 235 Describe image analysis G 236 Recognize normal results and variants G 237 Recognize pathologies/abnormal results CV 19 PET L G 238 Recognize clinical indications for performing procedure L G 239 Describe patient preparation L G 240 Identify contraindications for procedure L G 241 Identify the radiopharmaceutical L G 242 Propose procedural modifications L G 243 Perform data analysis L G 244 Describe image analysis L G 245 Recognize normal results and variants L G 246 Recognize pathologies/abnormal results L
Page 87
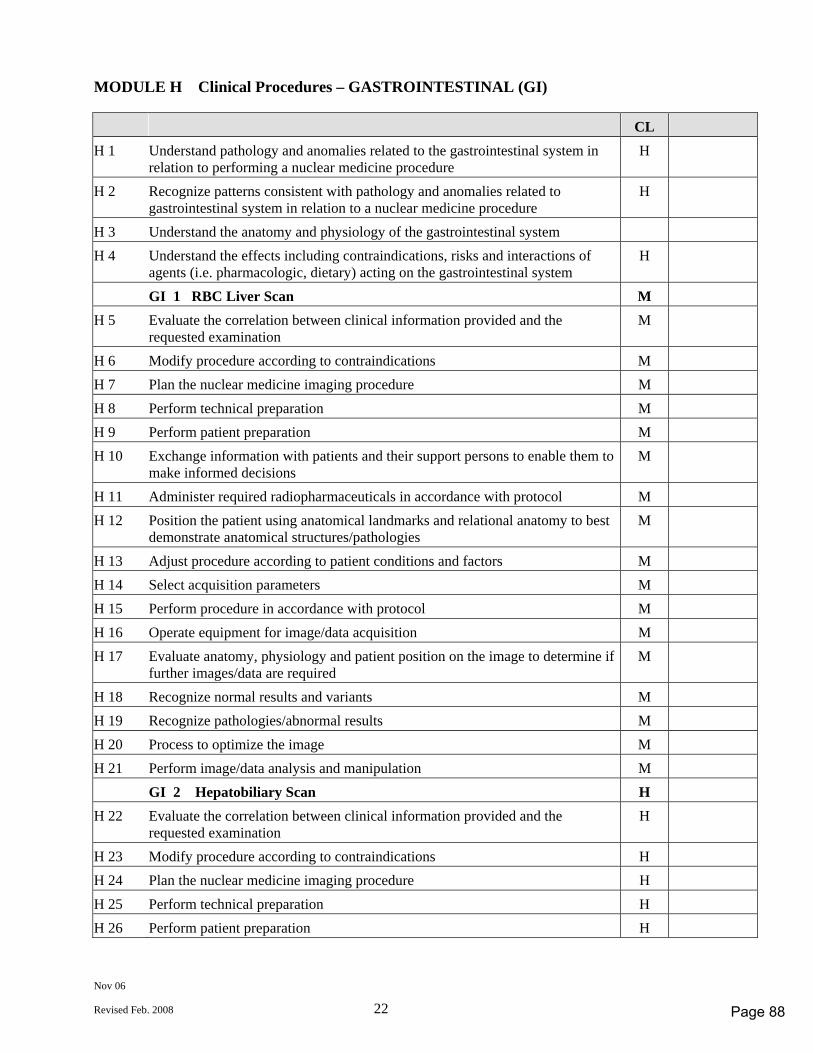
Nov 06
Revised Feb. 2008 22
MODULE H Clinical Procedures – GASTROINTESTINAL (GI) CL H 1 Understand pathology and anomalies related to the gastrointestinal system in
relation to performing a nuclear medicine procedure H
H 2 Recognize patterns consistent with pathology and anomalies related to gastrointestinal system in relation to a nuclear medicine procedure
H
H 3 Understand the anatomy and physiology of the gastrointestinal system H 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the gastrointestinal system H
GI 1 RBC Liver Scan M H 5 Evaluate the correlation between clinical information provided and the
requested examination M
H 6 Modify procedure according to contraindications M H 7 Plan the nuclear medicine imaging procedure M H 8 Perform technical preparation M H 9 Perform patient preparation M H 10 Exchange information with patients and their support persons to enable them to
make informed decisions M
H 11 Administer required radiopharmaceuticals in accordance with protocol M H 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
H 13 Adjust procedure according to patient conditions and factors M H 14 Select acquisition parameters M H 15 Perform procedure in accordance with protocol M H 16 Operate equipment for image/data acquisition M H 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
H 18 Recognize normal results and variants M H 19 Recognize pathologies/abnormal results M H 20 Process to optimize the image M H 21 Perform image/data analysis and manipulation M GI 2 Hepatobiliary Scan H H 22 Evaluate the correlation between clinical information provided and the
requested examination H
H 23 Modify procedure according to contraindications H H 24 Plan the nuclear medicine imaging procedure H H 25 Perform technical preparation H H 26 Perform patient preparation H
Page 88
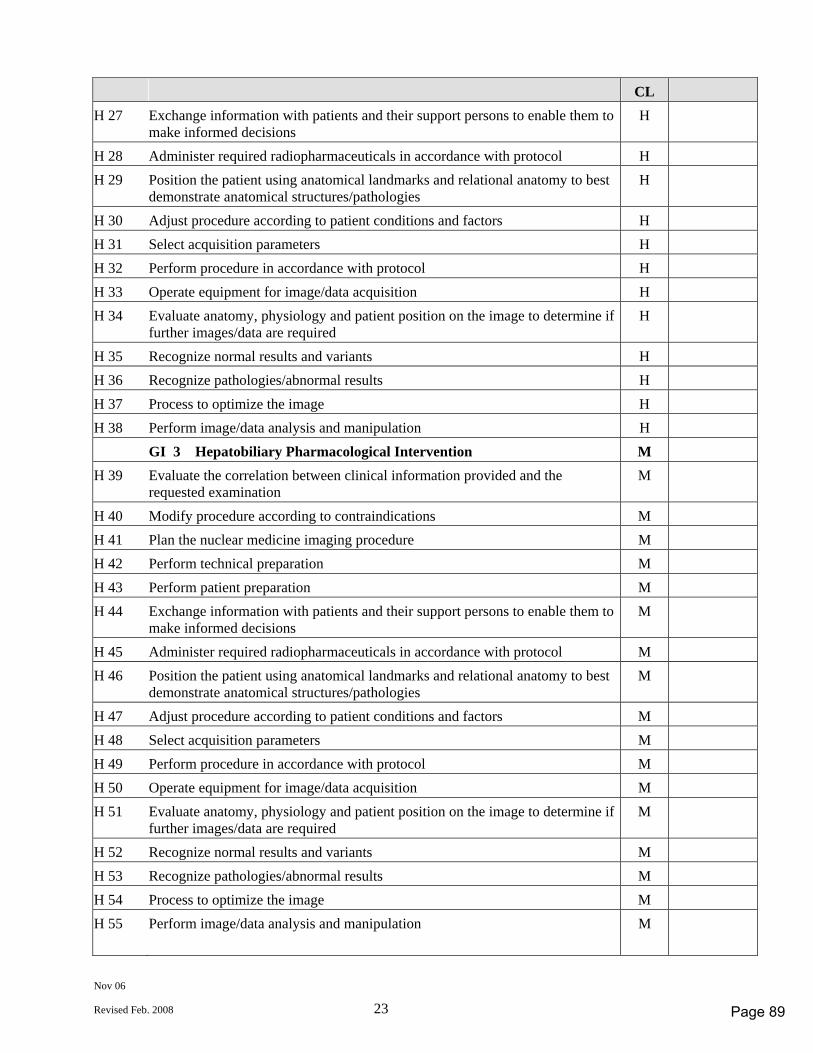
Nov 06
Revised Feb. 2008 23
CL H 27 Exchange information with patients and their support persons to enable them to
make informed decisions H
H 28 Administer required radiopharmaceuticals in accordance with protocol H H 29 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
H 30 Adjust procedure according to patient conditions and factors H H 31 Select acquisition parameters H H 32 Perform procedure in accordance with protocol H H 33 Operate equipment for image/data acquisition H H 34 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
H 35 Recognize normal results and variants H H 36 Recognize pathologies/abnormal results H H 37 Process to optimize the image H H 38 Perform image/data analysis and manipulation H GI 3 Hepatobiliary Pharmacological Intervention M H 39 Evaluate the correlation between clinical information provided and the
requested examination M
H 40 Modify procedure according to contraindications M H 41 Plan the nuclear medicine imaging procedure M H 42 Perform technical preparation M H 43 Perform patient preparation M H 44 Exchange information with patients and their support persons to enable them to
make informed decisions M
H 45 Administer required radiopharmaceuticals in accordance with protocol M H 46 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
H 47 Adjust procedure according to patient conditions and factors M H 48 Select acquisition parameters M H 49 Perform procedure in accordance with protocol M H 50 Operate equipment for image/data acquisition M H 51 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
H 52 Recognize normal results and variants M H 53 Recognize pathologies/abnormal results M H 54 Process to optimize the image M H 55 Perform image/data analysis and manipulation M
Page 89
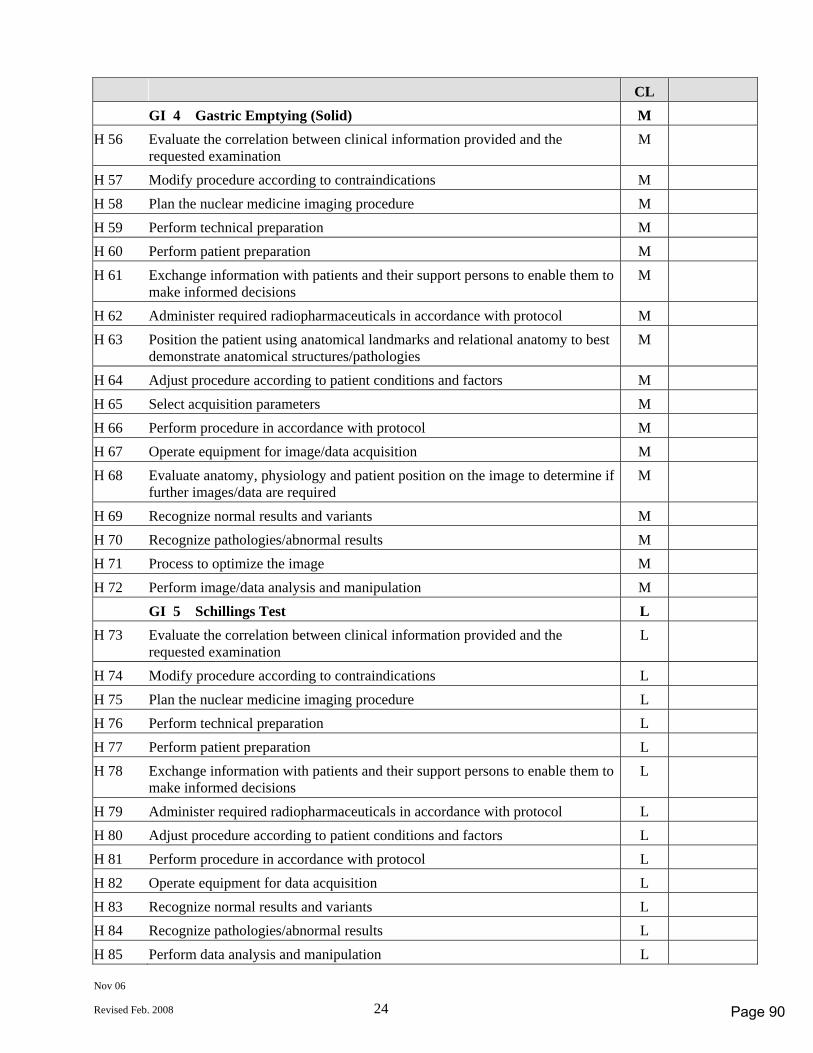
Nov 06
Revised Feb. 2008 24
CL GI 4 Gastric Emptying (Solid) M H 56 Evaluate the correlation between clinical information provided and the
requested examination M
H 57 Modify procedure according to contraindications M H 58 Plan the nuclear medicine imaging procedure M H 59 Perform technical preparation M H 60 Perform patient preparation M H 61 Exchange information with patients and their support persons to enable them to
make informed decisions M
H 62 Administer required radiopharmaceuticals in accordance with protocol M H 63 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
H 64 Adjust procedure according to patient conditions and factors M H 65 Select acquisition parameters M H 66 Perform procedure in accordance with protocol M H 67 Operate equipment for image/data acquisition M H 68 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
H 69 Recognize normal results and variants M H 70 Recognize pathologies/abnormal results M H 71 Process to optimize the image M H 72 Perform image/data analysis and manipulation M GI 5 Schillings Test L H 73 Evaluate the correlation between clinical information provided and the
requested examination L
H 74 Modify procedure according to contraindications L H 75 Plan the nuclear medicine imaging procedure L H 76 Perform technical preparation L H 77 Perform patient preparation L H 78 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 79 Administer required radiopharmaceuticals in accordance with protocol L H 80 Adjust procedure according to patient conditions and factors L H 81 Perform procedure in accordance with protocol L H 82 Operate equipment for data acquisition L H 83 Recognize normal results and variants L H 84 Recognize pathologies/abnormal results L H 85 Perform data analysis and manipulation L
Page 90
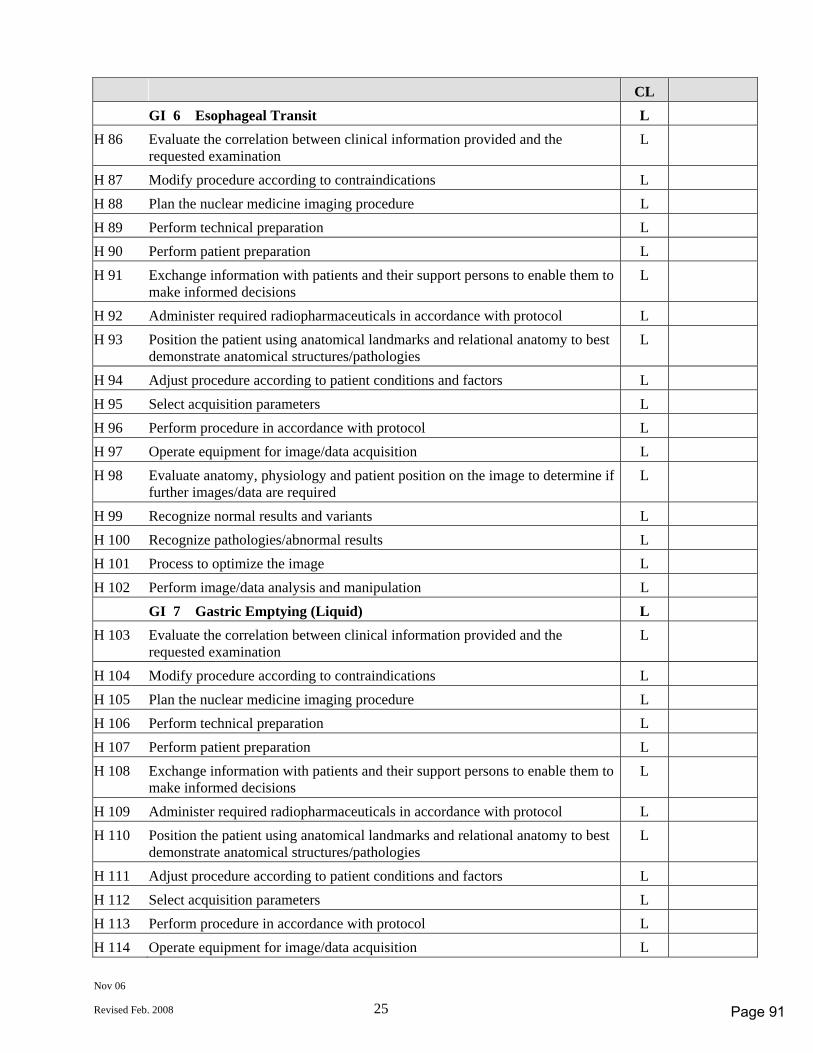
Nov 06
Revised Feb. 2008 25
CL GI 6 Esophageal Transit L H 86 Evaluate the correlation between clinical information provided and the
requested examination L
H 87 Modify procedure according to contraindications L H 88 Plan the nuclear medicine imaging procedure L H 89 Perform technical preparation L H 90 Perform patient preparation L H 91 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 92 Administer required radiopharmaceuticals in accordance with protocol L H 93 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
H 94 Adjust procedure according to patient conditions and factors L H 95 Select acquisition parameters L H 96 Perform procedure in accordance with protocol L H 97 Operate equipment for image/data acquisition L H 98 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
H 99 Recognize normal results and variants L H 100 Recognize pathologies/abnormal results L H 101 Process to optimize the image L H 102 Perform image/data analysis and manipulation L GI 7 Gastric Emptying (Liquid) L H 103 Evaluate the correlation between clinical information provided and the
requested examination L
H 104 Modify procedure according to contraindications L H 105 Plan the nuclear medicine imaging procedure L H 106 Perform technical preparation L H 107 Perform patient preparation L H 108 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 109 Administer required radiopharmaceuticals in accordance with protocol L H 110 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
H 111 Adjust procedure according to patient conditions and factors L H 112 Select acquisition parameters L H 113 Perform procedure in accordance with protocol L H 114 Operate equipment for image/data acquisition L
Page 91
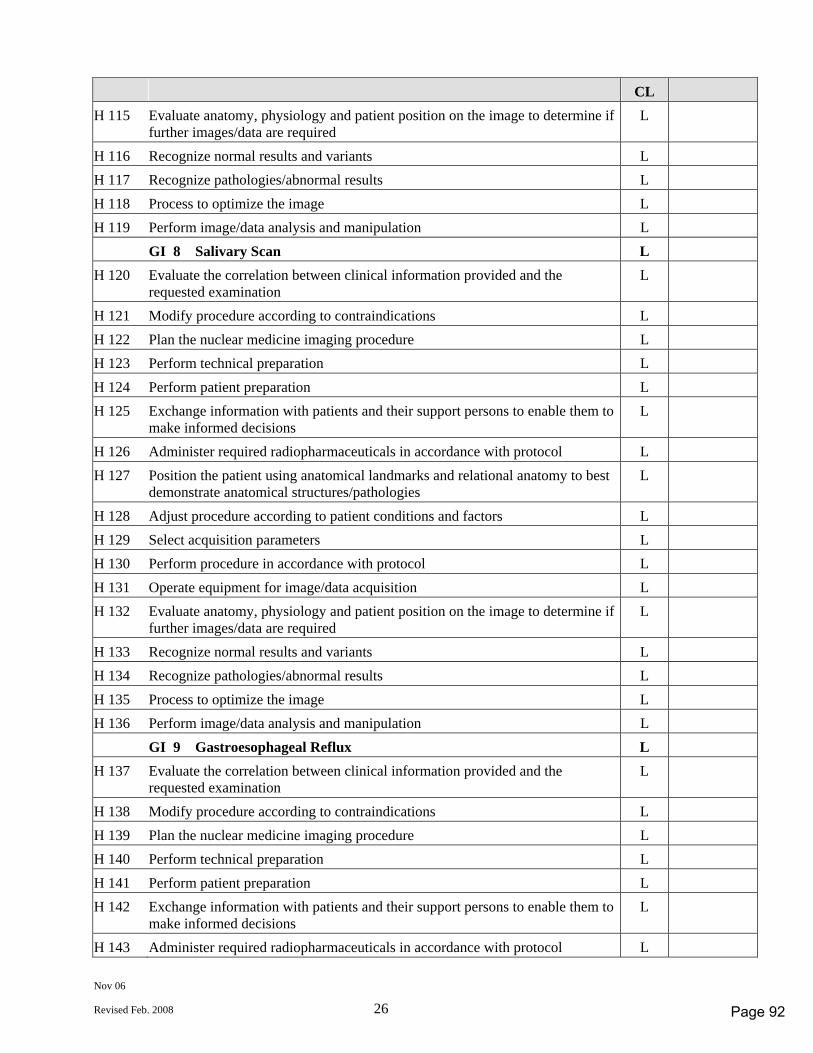
Nov 06
Revised Feb. 2008 26
CL H 115 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
H 116 Recognize normal results and variants L H 117 Recognize pathologies/abnormal results L H 118 Process to optimize the image L H 119 Perform image/data analysis and manipulation L GI 8 Salivary Scan L H 120 Evaluate the correlation between clinical information provided and the
requested examination L
H 121 Modify procedure according to contraindications L H 122 Plan the nuclear medicine imaging procedure L H 123 Perform technical preparation L H 124 Perform patient preparation L H 125 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 126 Administer required radiopharmaceuticals in accordance with protocol L H 127 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
H 128 Adjust procedure according to patient conditions and factors L H 129 Select acquisition parameters L H 130 Perform procedure in accordance with protocol L H 131 Operate equipment for image/data acquisition L H 132 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
H 133 Recognize normal results and variants L H 134 Recognize pathologies/abnormal results L H 135 Process to optimize the image L H 136 Perform image/data analysis and manipulation L GI 9 Gastroesophageal Reflux L H 137 Evaluate the correlation between clinical information provided and the
requested examination L
H 138 Modify procedure according to contraindications L H 139 Plan the nuclear medicine imaging procedure L H 140 Perform technical preparation L H 141 Perform patient preparation L H 142 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 143 Administer required radiopharmaceuticals in accordance with protocol L
Page 92
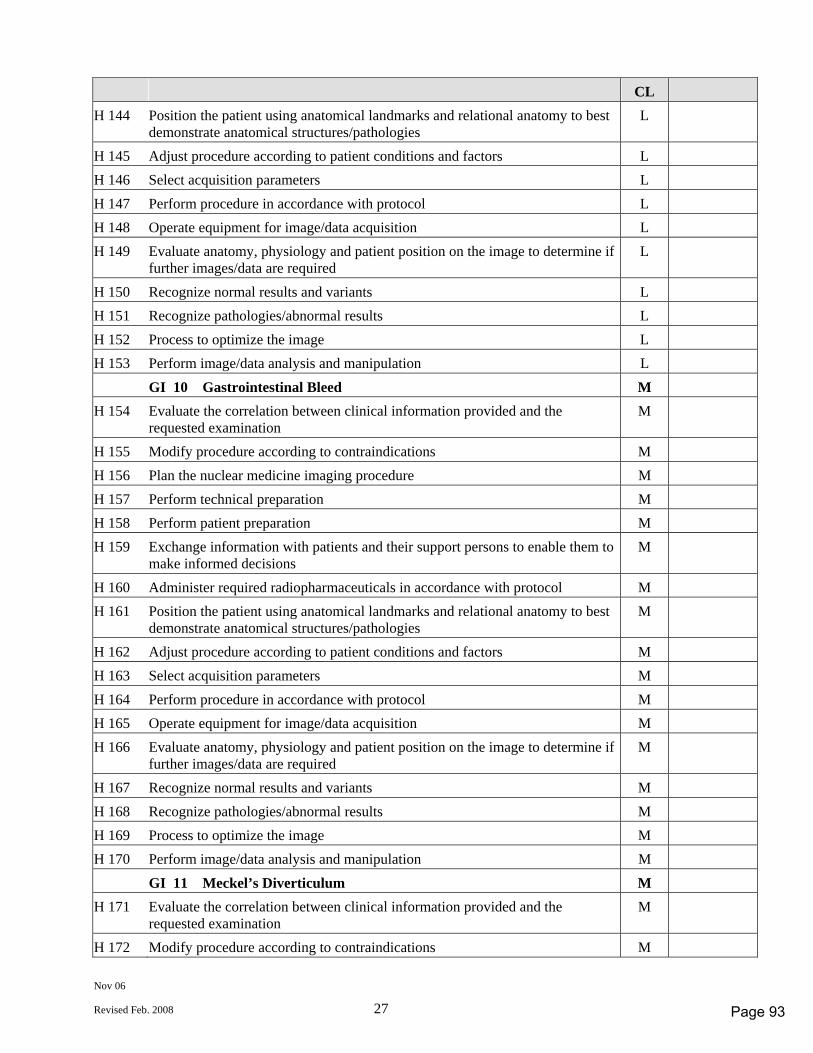
Nov 06
Revised Feb. 2008 27
CL H 144 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
H 145 Adjust procedure according to patient conditions and factors L H 146 Select acquisition parameters L H 147 Perform procedure in accordance with protocol L H 148 Operate equipment for image/data acquisition L H 149 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
H 150 Recognize normal results and variants L H 151 Recognize pathologies/abnormal results L H 152 Process to optimize the image L H 153 Perform image/data analysis and manipulation L GI 10 Gastrointestinal Bleed M H 154 Evaluate the correlation between clinical information provided and the
requested examination M
H 155 Modify procedure according to contraindications M H 156 Plan the nuclear medicine imaging procedure M H 157 Perform technical preparation M H 158 Perform patient preparation M H 159 Exchange information with patients and their support persons to enable them to
make informed decisions M
H 160 Administer required radiopharmaceuticals in accordance with protocol M H 161 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
H 162 Adjust procedure according to patient conditions and factors M H 163 Select acquisition parameters M H 164 Perform procedure in accordance with protocol M H 165 Operate equipment for image/data acquisition M H 166 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
H 167 Recognize normal results and variants M H 168 Recognize pathologies/abnormal results M H 169 Process to optimize the image M H 170 Perform image/data analysis and manipulation M GI 11 Meckel’s Diverticulum M H 171 Evaluate the correlation between clinical information provided and the
requested examination M
H 172 Modify procedure according to contraindications M
Page 93
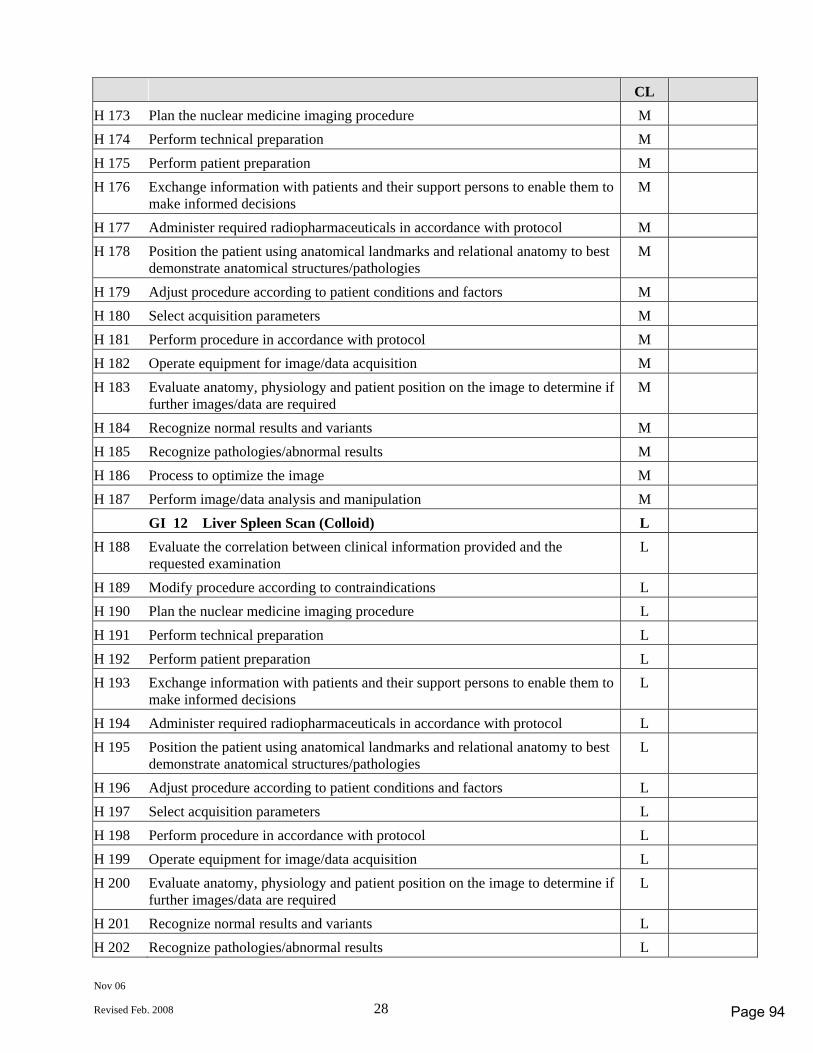
Nov 06
Revised Feb. 2008 28
CL H 173 Plan the nuclear medicine imaging procedure M H 174 Perform technical preparation M H 175 Perform patient preparation M H 176 Exchange information with patients and their support persons to enable them to
make informed decisions M
H 177 Administer required radiopharmaceuticals in accordance with protocol M H 178 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
H 179 Adjust procedure according to patient conditions and factors M H 180 Select acquisition parameters M H 181 Perform procedure in accordance with protocol M H 182 Operate equipment for image/data acquisition M H 183 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
H 184 Recognize normal results and variants M H 185 Recognize pathologies/abnormal results M H 186 Process to optimize the image M H 187 Perform image/data analysis and manipulation M GI 12 Liver Spleen Scan (Colloid) L H 188 Evaluate the correlation between clinical information provided and the
requested examination L
H 189 Modify procedure according to contraindications L H 190 Plan the nuclear medicine imaging procedure L H 191 Perform technical preparation L H 192 Perform patient preparation L H 193 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 194 Administer required radiopharmaceuticals in accordance with protocol L H 195 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
H 196 Adjust procedure according to patient conditions and factors L H 197 Select acquisition parameters L H 198 Perform procedure in accordance with protocol L H 199 Operate equipment for image/data acquisition L H 200 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
H 201 Recognize normal results and variants L H 202 Recognize pathologies/abnormal results L
Page 94
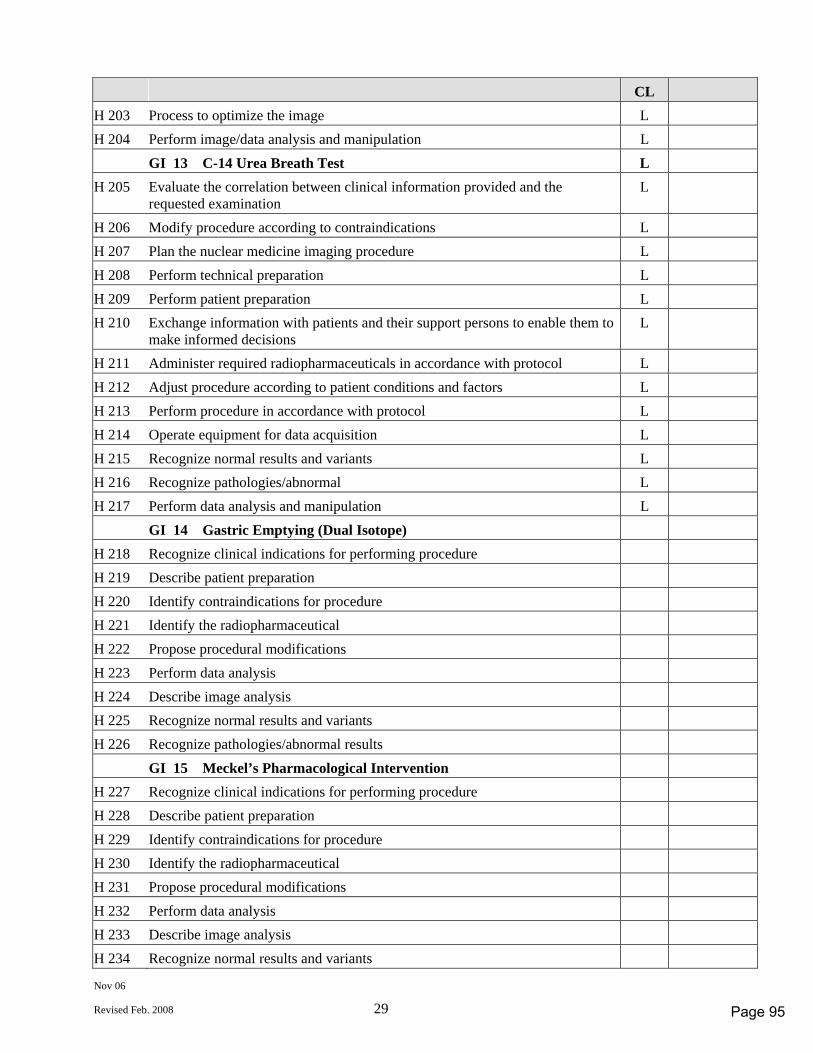
Nov 06
Revised Feb. 2008 29
CL H 203 Process to optimize the image L H 204 Perform image/data analysis and manipulation L GI 13 C-14 Urea Breath Test L H 205 Evaluate the correlation between clinical information provided and the
requested examination L
H 206 Modify procedure according to contraindications L H 207 Plan the nuclear medicine imaging procedure L H 208 Perform technical preparation L H 209 Perform patient preparation L H 210 Exchange information with patients and their support persons to enable them to
make informed decisions L
H 211 Administer required radiopharmaceuticals in accordance with protocol L H 212 Adjust procedure according to patient conditions and factors L H 213 Perform procedure in accordance with protocol L H 214 Operate equipment for data acquisition L H 215 Recognize normal results and variants L H 216 Recognize pathologies/abnormal L H 217 Perform data analysis and manipulation L GI 14 Gastric Emptying (Dual Isotope) H 218 Recognize clinical indications for performing procedure H 219 Describe patient preparation H 220 Identify contraindications for procedure H 221 Identify the radiopharmaceutical H 222 Propose procedural modifications H 223 Perform data analysis H 224 Describe image analysis H 225 Recognize normal results and variants H 226 Recognize pathologies/abnormal results GI 15 Meckel’s Pharmacological Intervention H 227 Recognize clinical indications for performing procedure H 228 Describe patient preparation H 229 Identify contraindications for procedure H 230 Identify the radiopharmaceutical H 231 Propose procedural modifications H 232 Perform data analysis H 233 Describe image analysis H 234 Recognize normal results and variants
Page 95
Nov 06
Revised Feb. 2008 30
CL H 235 Recognize pathologies/abnormal results
Page 96
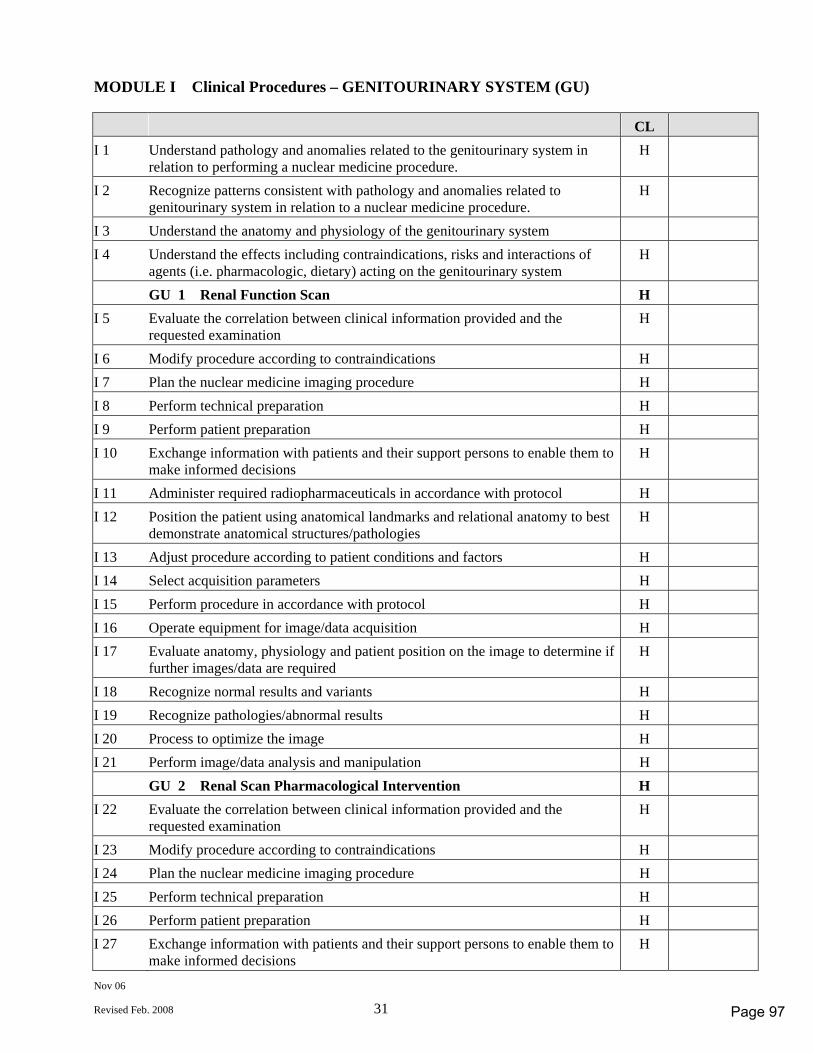
Nov 06
Revised Feb. 2008 31
MODULE I Clinical Procedures – GENITOURINARY SYSTEM (GU) CL I 1 Understand pathology and anomalies related to the genitourinary system in
relation to performing a nuclear medicine procedure. H
I 2 Recognize patterns consistent with pathology and anomalies related to genitourinary system in relation to a nuclear medicine procedure.
H
I 3 Understand the anatomy and physiology of the genitourinary system I 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the genitourinary system H
GU 1 Renal Function Scan H I 5 Evaluate the correlation between clinical information provided and the
requested examination H
I 6 Modify procedure according to contraindications H I 7 Plan the nuclear medicine imaging procedure H I 8 Perform technical preparation H I 9 Perform patient preparation H I 10 Exchange information with patients and their support persons to enable them to
make informed decisions H
I 11 Administer required radiopharmaceuticals in accordance with protocol H I 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
I 13 Adjust procedure according to patient conditions and factors H I 14 Select acquisition parameters H I 15 Perform procedure in accordance with protocol H I 16 Operate equipment for image/data acquisition H I 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
I 18 Recognize normal results and variants H I 19 Recognize pathologies/abnormal results H I 20 Process to optimize the image H I 21 Perform image/data analysis and manipulation H GU 2 Renal Scan Pharmacological Intervention H I 22 Evaluate the correlation between clinical information provided and the
requested examination H
I 23 Modify procedure according to contraindications H I 24 Plan the nuclear medicine imaging procedure H I 25 Perform technical preparation H I 26 Perform patient preparation H I 27 Exchange information with patients and their support persons to enable them to
make informed decisions H
Page 97
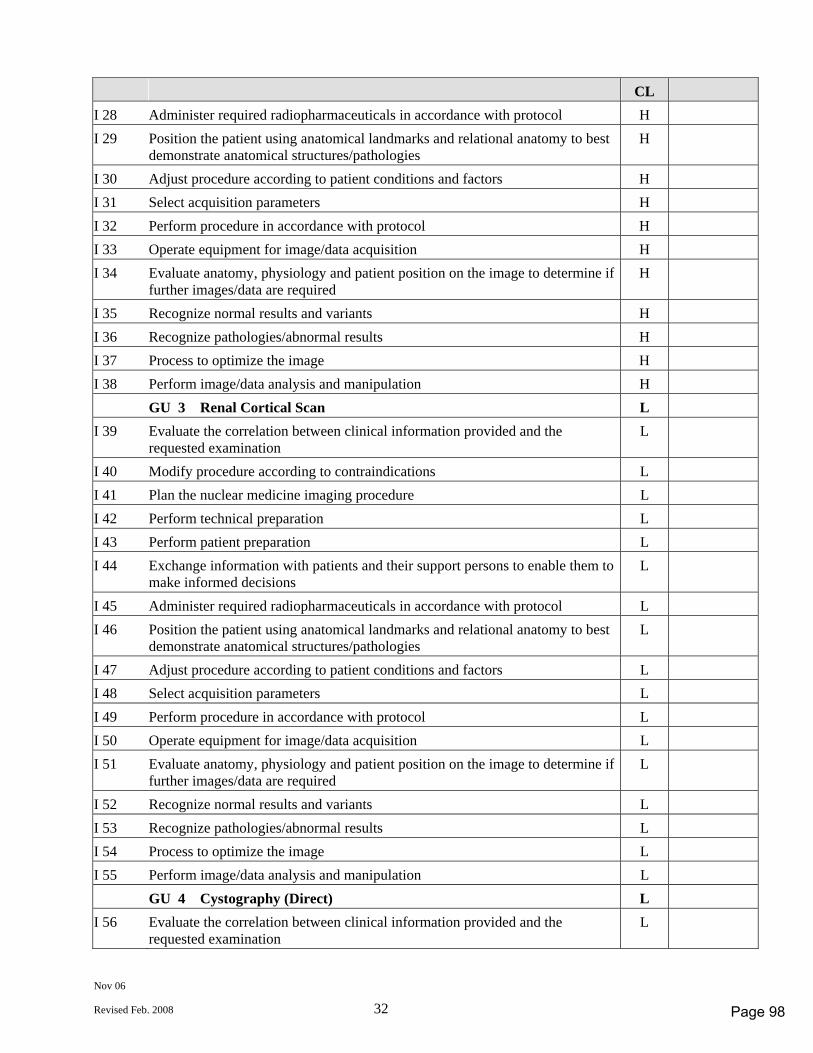
Nov 06
Revised Feb. 2008 32
CL I 28 Administer required radiopharmaceuticals in accordance with protocol H I 29 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
I 30 Adjust procedure according to patient conditions and factors H I 31 Select acquisition parameters H I 32 Perform procedure in accordance with protocol H I 33 Operate equipment for image/data acquisition H I 34 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
I 35 Recognize normal results and variants H I 36 Recognize pathologies/abnormal results H I 37 Process to optimize the image H I 38 Perform image/data analysis and manipulation H GU 3 Renal Cortical Scan L I 39 Evaluate the correlation between clinical information provided and the
requested examination L
I 40 Modify procedure according to contraindications L I 41 Plan the nuclear medicine imaging procedure L I 42 Perform technical preparation L I 43 Perform patient preparation L I 44 Exchange information with patients and their support persons to enable them to
make informed decisions L
I 45 Administer required radiopharmaceuticals in accordance with protocol L I 46 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
I 47 Adjust procedure according to patient conditions and factors L I 48 Select acquisition parameters L I 49 Perform procedure in accordance with protocol L I 50 Operate equipment for image/data acquisition L I 51 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
I 52 Recognize normal results and variants L I 53 Recognize pathologies/abnormal results L I 54 Process to optimize the image L I 55 Perform image/data analysis and manipulation L GU 4 Cystography (Direct) L I 56 Evaluate the correlation between clinical information provided and the
requested examination L
Page 98
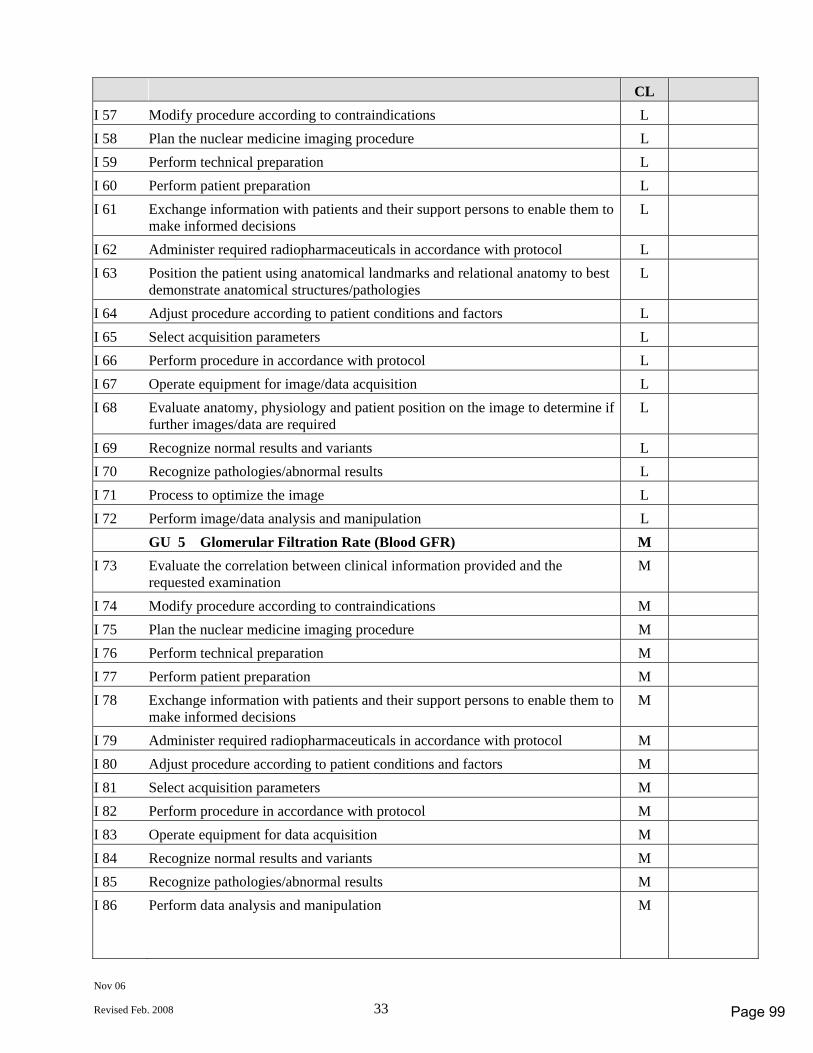
Nov 06
Revised Feb. 2008 33
CL I 57 Modify procedure according to contraindications L I 58 Plan the nuclear medicine imaging procedure L I 59 Perform technical preparation L I 60 Perform patient preparation L I 61 Exchange information with patients and their support persons to enable them to
make informed decisions L
I 62 Administer required radiopharmaceuticals in accordance with protocol L I 63 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
I 64 Adjust procedure according to patient conditions and factors L I 65 Select acquisition parameters L I 66 Perform procedure in accordance with protocol L I 67 Operate equipment for image/data acquisition L I 68 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
I 69 Recognize normal results and variants L I 70 Recognize pathologies/abnormal results L I 71 Process to optimize the image L I 72 Perform image/data analysis and manipulation L GU 5 Glomerular Filtration Rate (Blood GFR) M I 73 Evaluate the correlation between clinical information provided and the
requested examination M
I 74 Modify procedure according to contraindications M I 75 Plan the nuclear medicine imaging procedure M I 76 Perform technical preparation M I 77 Perform patient preparation M I 78 Exchange information with patients and their support persons to enable them to
make informed decisions M
I 79 Administer required radiopharmaceuticals in accordance with protocol M I 80 Adjust procedure according to patient conditions and factors M I 81 Select acquisition parameters M I 82 Perform procedure in accordance with protocol M I 83 Operate equipment for data acquisition M I 84 Recognize normal results and variants M I 85 Recognize pathologies/abnormal results M I 86 Perform data analysis and manipulation M
Page 99
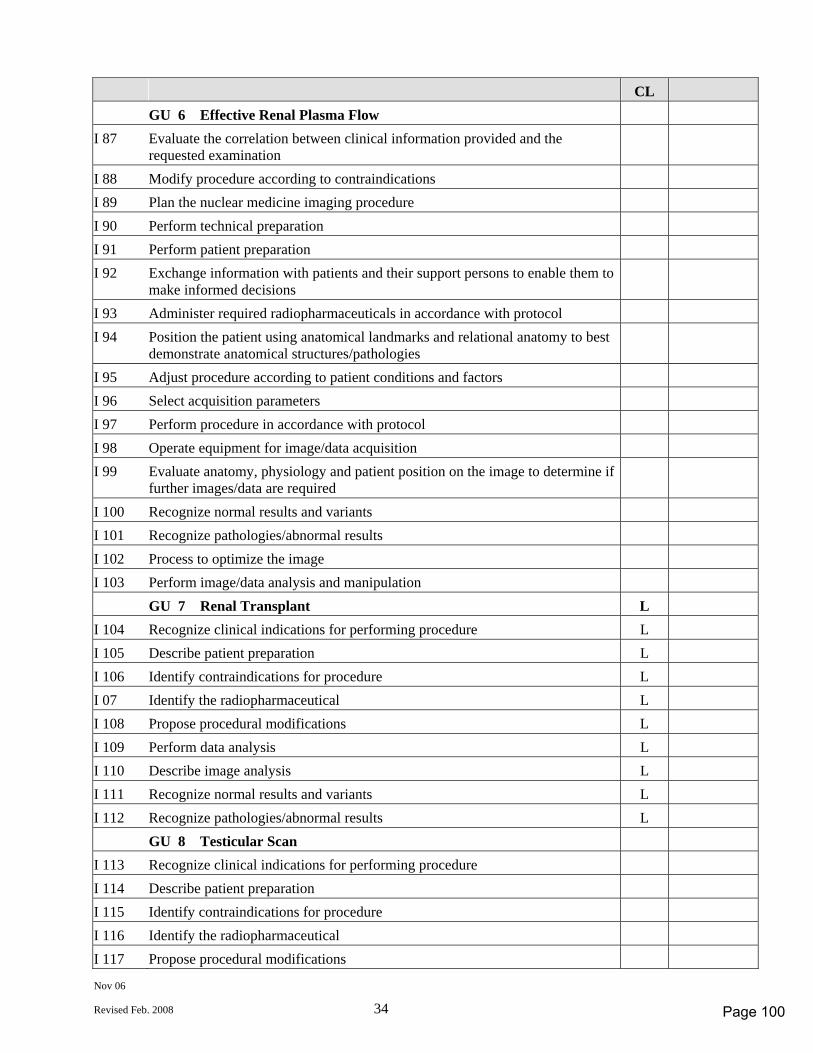
Nov 06
Revised Feb. 2008 34
CL GU 6 Effective Renal Plasma Flow I 87 Evaluate the correlation between clinical information provided and the
requested examination
I 88 Modify procedure according to contraindications I 89 Plan the nuclear medicine imaging procedure I 90 Perform technical preparation I 91 Perform patient preparation I 92 Exchange information with patients and their support persons to enable them to
make informed decisions
I 93 Administer required radiopharmaceuticals in accordance with protocol I 94 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies
I 95 Adjust procedure according to patient conditions and factors I 96 Select acquisition parameters I 97 Perform procedure in accordance with protocol I 98 Operate equipment for image/data acquisition I 99 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required
I 100 Recognize normal results and variants I 101 Recognize pathologies/abnormal results I 102 Process to optimize the image I 103 Perform image/data analysis and manipulation GU 7 Renal Transplant L I 104 Recognize clinical indications for performing procedure L I 105 Describe patient preparation L I 106 Identify contraindications for procedure L I 07 Identify the radiopharmaceutical L I 108 Propose procedural modifications L I 109 Perform data analysis L I 110 Describe image analysis L I 111 Recognize normal results and variants L I 112 Recognize pathologies/abnormal results L GU 8 Testicular Scan I 113 Recognize clinical indications for performing procedure I 114 Describe patient preparation I 115 Identify contraindications for procedure I 116 Identify the radiopharmaceutical I 117 Propose procedural modifications
Page 100
Nov 06
Revised Feb. 2008 35
CL I 118 Describe image analysis I 119 Recognize normal results and variants I 120 Recognize pathologies/abnormal results
Page 101
Nov 06
Revised Feb. 2008 36
MODULE J Clinical Procedures – SKELETAL SYSTEM (SK) CL J 1 Understand pathology and anomalies related to the skeletal system in relation to
performing a nuclear medicine procedure H J 2 Recognize patterns consistent with pathology and anomalies related to skeletal
system in relation to a nuclear medicine procedure H J 3 Understand the anatomy and physiology of the skeletal system J 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the skeletal system H SK 1 Three Phase Local Bone Scan H J 5 Evaluate the correlation between clinical information provided and the
requested examination H J 6 Modify procedure according to contraindications H J 7 Plan the nuclear medicine imaging procedure H J 8 Perform technical preparation H J 9 Perform patient preparation H J 10 Exchange information with patients and their support persons to enable them to
make informed decisions H J 11 Administer required radiopharmaceuticals in accordance with protocol H J 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H J 13 Adjust procedure according to patient conditions and factors H J 14 Select acquisition parameters H J 15 Perform procedure in accordance with protocol H J 16 Operate equipment for image/data acquisition H J 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H J 18 Recognize normal results and variants H J 19 Recognize pathologies/abnormal results H J 20 Process to optimize the image H J 21 Perform image/data analysis and manipulation H SK 2 Whole Body Bone Scan H J 22 Evaluate the correlation between clinical information provided and the
requested examination H J 23 Modify procedure according to contraindications H J 24 Plan the nuclear medicine imaging procedure H J 25 Perform technical preparation H J 26 Perform patient preparation H J 27 Exchange information with patients and their support persons to enable them to
make informed decisions H
Page 102
Nov 06
Revised Feb. 2008 37
CL J 28 Administer required radiopharmaceuticals in accordance with protocol H J 29 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H J 30 Adjust procedure according to patient conditions and factors H J 31 Select acquisition parameters H J 32 Perform procedure in accordance with protocol H J 33 Operate equipment for image/data acquisition H J 34 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H J 35 Recognize normal results and variants H J 36 Recognize pathologies/abnormal results H J 37 Process to optimize the image H J 38 Perform image/data analysis and manipulation H SK 3 Bone Scan SPECT H J 39 Evaluate the correlation between clinical information provided and the
requested examination H J 40 Modify procedure according to contraindications H J 41 Plan the nuclear medicine imaging procedure H J 42 Perform technical preparation H J 43 Perform patient preparation H J 44 Exchange information with patients and their support persons to enable them to
make informed decisions H J 45 Administer required radiopharmaceuticals in accordance with protocol H J 46 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H J 47 Adjust procedure according to patient conditions and factors H J 48 Select acquisition parameters H J 49 Perform procedure in accordance with protocol H J 50 Operate equipment for image/data acquisition H J 51 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H J 52 Recognize normal results and variants H J 53 Recognize pathologies/abnormal results H J 54 Process to optimize the image H J 55 Perform image/data analysis and manipulation H SK 4 Bone Mineral Density M J 56 Evaluate the correlation between clinical information provided and the
requested examination M
Page 103
Nov 06
Revised Feb. 2008 38
CL J 57 Modify procedure according to contraindications M J 58 Plan the nuclear medicine imaging procedure M J 59 Perform technical preparation M J 60 Perform patient preparation M J 61 Exchange information with patients and their support persons to enable them to
make informed decisions M J 62 Position the patient on bone mineral density scanning bed M J 63 Use anatomical landmarks and relational anatomy to best demonstrate
anatomical structures/pathologies M J 64 Adjust procedure according to patient conditions and factors M J 65 Select acquisition parameters M J 66 Perform procedure in accordance with protocol M J 67 Operate equipment for image/data acquisition M J 68 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M J 69 Recognize normal results and variants M J 70 Recognize pathologies/abnormal results M J 71 Perform image/data analysis and manipulation M SK 5 Bone Marrow Imaging L J 72 Evaluate the correlation between clinical information provided and the
requested examination L J 73 Modify procedure according to contraindications L J 74 Plan the nuclear medicine imaging procedure L J 75 Perform technical preparation L J 76 Perform patient preparation L J 77 Exchange information with patients and their support persons to enable them to
make informed decisions L J 78 Administer required radiopharmaceuticals in accordance with protocol L J 79 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L J 80 Adjust procedure according to patient conditions and factors L J 81 Select acquisition parameters L J 82 Perform procedure in accordance with protocol L J 83 Operate equipment for image/data acquisition L J 84 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L J 85 Recognize normal results and variants L J 86 Recognize pathologies/abnormal results L
Page 104
Nov 06
Revised Feb. 2008 39
CL J 87 Process to optimize the image L J 88 Perform image/data analysis and manipulation L
Page 105
Nov 06
Revised Feb. 2008 40
MODULE K Clinical Procedures – INFLAMMATORY PROCESS/TUMOR/LYMPH (TU) CL K 1 Understand pathology and anomalies related to the inflammatory
process/tumor, and lymph disorders in relation to performing nuclear medicine procedures
H
K 2 Recognize patterns consistent with pathology and anomalies related to inflammatory processes, tumors, and lymph disorders in relation to nuclear medicine procedures
H
K 3 Understand the anatomy and physiology of inflammatory processes, tumor, and lymph disorders
K 4 Understand the effects including contraindications, risks and interactions of agents (i.e. pharmacologic, dietary) acting on inflammatory processes, tumor, and lymph disorders
H
TU 1 Gallium Scan H K 5 Evaluate the correlation between clinical information provided and the
requested examination H
K 6 Modify procedure according to contraindications H K 7 Plan the nuclear medicine imaging procedure H K 8 Perform technical preparation H K 9 Perform patient preparation H K 10 Exchange information with patients and their support persons to enable them to
make informed decisions H
K 11 Administer required radiopharmaceuticals in accordance with protocol H K 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
K 13 Adjust procedure according to patient conditions and factors H K 14 Select acquisition parameters H K 15 Perform procedure in accordance with protocol H K 16 Operate equipment for image/data acquisition H K 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
K 18 Recognize normal results and variants H K 19 Recognize pathologies/abnormal results H K 20 Process to optimize the image H K 21 Perform image/data analysis and manipulation H TU 2 White Blood Cell Scan M K 22 Evaluate the correlation between clinical information provided and the
requested examination M
K 23 Modify procedure according to contraindications M K 24 Plan the nuclear medicine imaging procedure M
Page 106
Nov 06
Revised Feb. 2008 41
CL K 25 Perform technical preparation M K 26 Perform patient preparation M K 27 Exchange information with patients and their support persons to enable them to
make informed decisions M
K 28 Perform white cell labelling procedure according to procedure M K 29 Use equipment for white cell labelling M K 30 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
K 31 Adjust procedure according to patient conditions and factors M K 32 Select acquisition parameters M K 33 Perform procedure in accordance with protocol M K 34 Operate equipment for image/data acquisition M K 35 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
K 36 Recognize normal results and variants M K 37 Recognize pathologies/abnormal results M K 38 Process to optimize the image M K 39 Perform image/data analysis and manipulation M TU 3 Tumor Imaging (Iodine) M K 40 Evaluate the correlation between clinical information provided and the
requested examination M
K 41 Modify procedure according to contraindications M K 42 Plan the nuclear medicine imaging procedure M K 43 Perform technical preparation M K 44 Perform patient preparation M K 45 Exchange information with patients and their support persons to enable them to
make informed decisions M
K 46 Administer appropriate radionuclide agent M K 47 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
K 48 Adjust procedure according to patient conditions and factors M K 49 Select acquisition parameters M K 50 Perform procedure in accordance with protocol M K 51 Operate equipment for image/data acquisition M K 52 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
K 53 Recognize normal results and variants M K 54 Recognize pathologies/abnormal results M
Page 107
Nov 06
Revised Feb. 2008 42
CL K 55 Process to optimize the image M K 56 Perform image/data analysis and manipulation M TU 4 Gallium SPECT M K 57 Evaluate the correlation between clinical information provided and the
requested examination M
K 58 Modify procedure according to contraindications M K 59 Plan the nuclear medicine imaging procedure M K 60 Perform technical preparation M K 61 Perform patient preparation M K 62 Exchange information with patients and their support persons to enable them to
make informed decisions M
K 63 Administer required radiopharmaceuticals in accordance with protocol M K 64 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
K 65 Adjust procedure according to patient conditions and factors M K 66 Select acquisition parameters M K 67 Perform procedure in accordance with protocol M K 68 Operate equipment for image/data acquisition M K 69 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
K 70 Recognize normal results and variants M K 71 Recognize pathologies/abnormal results M K 72 Process to optimize the image M K 73 Perform image/data analysis and manipulation M TU 5 Somatostatin-Receptor Tumor Imaging L K 74 Evaluate the correlation between clinical information provided and the
requested examination L
K 75 Modify procedure according to contraindications L K 76 Plan the nuclear medicine imaging procedure L K 77 Perform technical preparation L K 78 Perform patient preparation L K 79 Exchange information with patients and their support persons to enable them to
make informed decisions L
K 80 Administer appropriate radionuclide agent L K 81 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
K 82 Adjust procedure according to patient conditions and factors L K 83 Select acquisition parameters L
Page 108
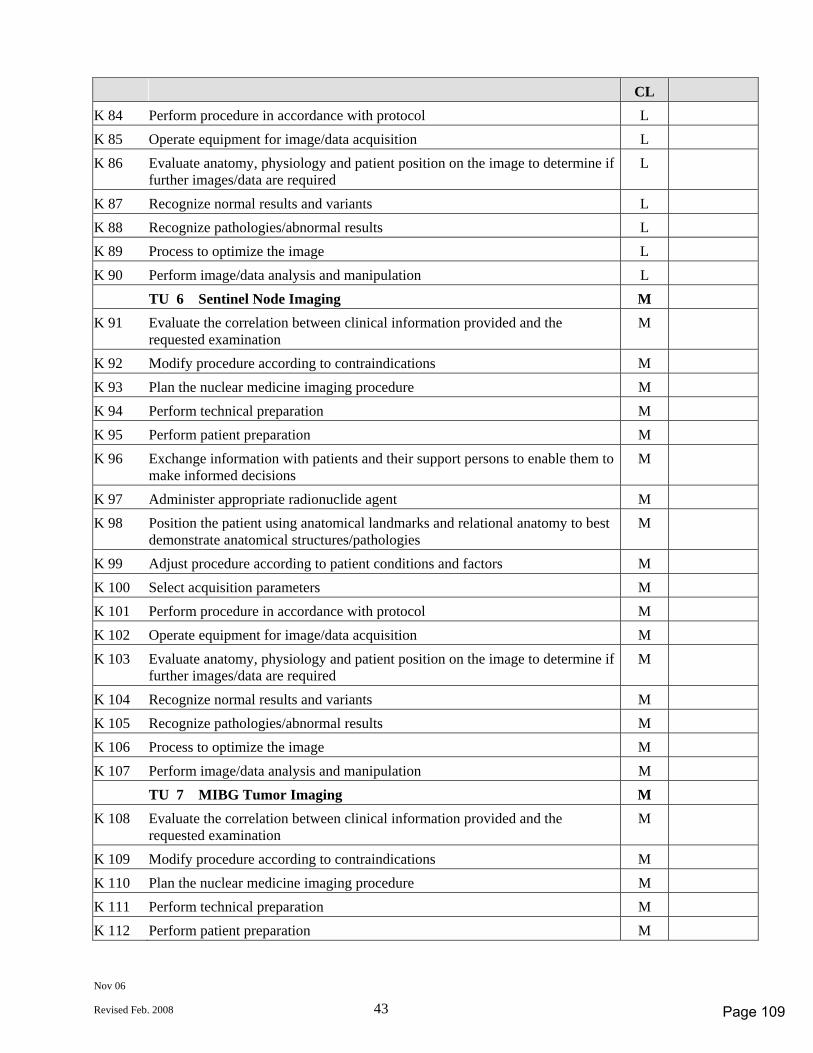
Nov 06
Revised Feb. 2008 43
CL K 84 Perform procedure in accordance with protocol L K 85 Operate equipment for image/data acquisition L K 86 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
K 87 Recognize normal results and variants L K 88 Recognize pathologies/abnormal results L K 89 Process to optimize the image L K 90 Perform image/data analysis and manipulation L TU 6 Sentinel Node Imaging M K 91 Evaluate the correlation between clinical information provided and the
requested examination M
K 92 Modify procedure according to contraindications M K 93 Plan the nuclear medicine imaging procedure M K 94 Perform technical preparation M K 95 Perform patient preparation M K 96 Exchange information with patients and their support persons to enable them to
make informed decisions M
K 97 Administer appropriate radionuclide agent M K 98 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
K 99 Adjust procedure according to patient conditions and factors M K 100 Select acquisition parameters M K 101 Perform procedure in accordance with protocol M K 102 Operate equipment for image/data acquisition M K 103 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
K 104 Recognize normal results and variants M K 105 Recognize pathologies/abnormal results M K 106 Process to optimize the image M K 107 Perform image/data analysis and manipulation M TU 7 MIBG Tumor Imaging M K 108 Evaluate the correlation between clinical information provided and the
requested examination M
K 109 Modify procedure according to contraindications M K 110 Plan the nuclear medicine imaging procedure M K 111 Perform technical preparation M K 112 Perform patient preparation M
Page 109
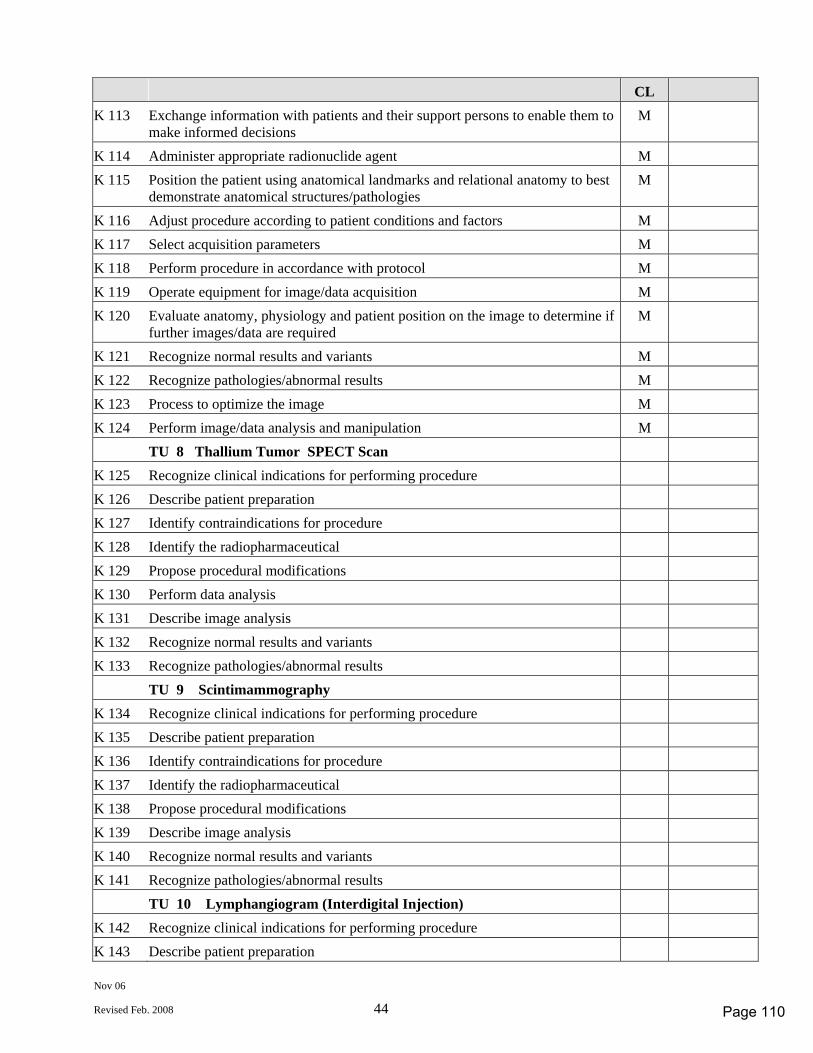
Nov 06
Revised Feb. 2008 44
CL K 113 Exchange information with patients and their support persons to enable them to
make informed decisions M
K 114 Administer appropriate radionuclide agent M K 115 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
K 116 Adjust procedure according to patient conditions and factors M K 117 Select acquisition parameters M K 118 Perform procedure in accordance with protocol M K 119 Operate equipment for image/data acquisition M K 120 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
K 121 Recognize normal results and variants M K 122 Recognize pathologies/abnormal results M K 123 Process to optimize the image M K 124 Perform image/data analysis and manipulation M TU 8 Thallium Tumor SPECT Scan K 125 Recognize clinical indications for performing procedure K 126 Describe patient preparation K 127 Identify contraindications for procedure K 128 Identify the radiopharmaceutical K 129 Propose procedural modifications K 130 Perform data analysis K 131 Describe image analysis K 132 Recognize normal results and variants K 133 Recognize pathologies/abnormal results TU 9 Scintimammography K 134 Recognize clinical indications for performing procedure K 135 Describe patient preparation K 136 Identify contraindications for procedure K 137 Identify the radiopharmaceutical K 138 Propose procedural modifications K 139 Describe image analysis K 140 Recognize normal results and variants K 141 Recognize pathologies/abnormal results TU 10 Lymphangiogram (Interdigital Injection) K 142 Recognize clinical indications for performing procedure K 143 Describe patient preparation
Page 110
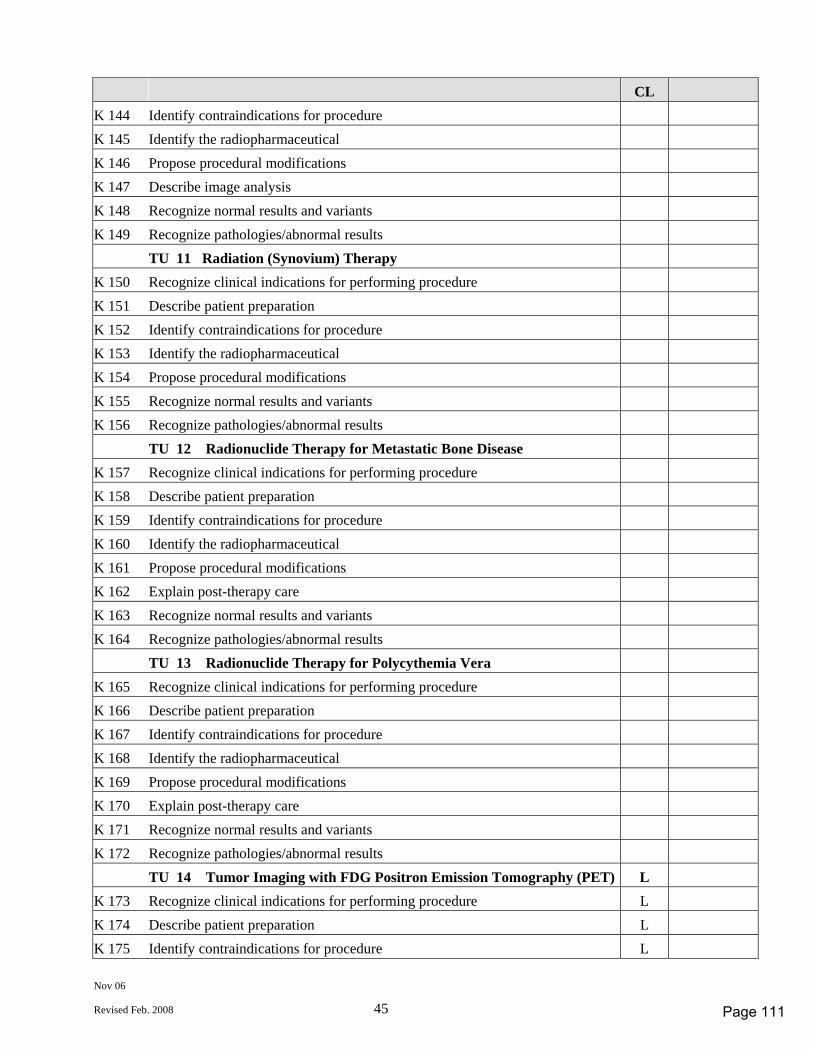
Nov 06
Revised Feb. 2008 45
CL K 144 Identify contraindications for procedure K 145 Identify the radiopharmaceutical K 146 Propose procedural modifications K 147 Describe image analysis K 148 Recognize normal results and variants K 149 Recognize pathologies/abnormal results TU 11 Radiation (Synovium) Therapy K 150 Recognize clinical indications for performing procedure K 151 Describe patient preparation K 152 Identify contraindications for procedure K 153 Identify the radiopharmaceutical K 154 Propose procedural modifications K 155 Recognize normal results and variants K 156 Recognize pathologies/abnormal results TU 12 Radionuclide Therapy for Metastatic Bone Disease K 157 Recognize clinical indications for performing procedure K 158 Describe patient preparation K 159 Identify contraindications for procedure K 160 Identify the radiopharmaceutical K 161 Propose procedural modifications K 162 Explain post-therapy care K 163 Recognize normal results and variants K 164 Recognize pathologies/abnormal results TU 13 Radionuclide Therapy for Polycythemia Vera K 165 Recognize clinical indications for performing procedure K 166 Describe patient preparation K 167 Identify contraindications for procedure K 168 Identify the radiopharmaceutical K 169 Propose procedural modifications K 170 Explain post-therapy care K 171 Recognize normal results and variants K 172 Recognize pathologies/abnormal results TU 14 Tumor Imaging with FDG Positron Emission Tomography (PET) L K 173 Recognize clinical indications for performing procedure L K 174 Describe patient preparation L K 175 Identify contraindications for procedure L
Page 111
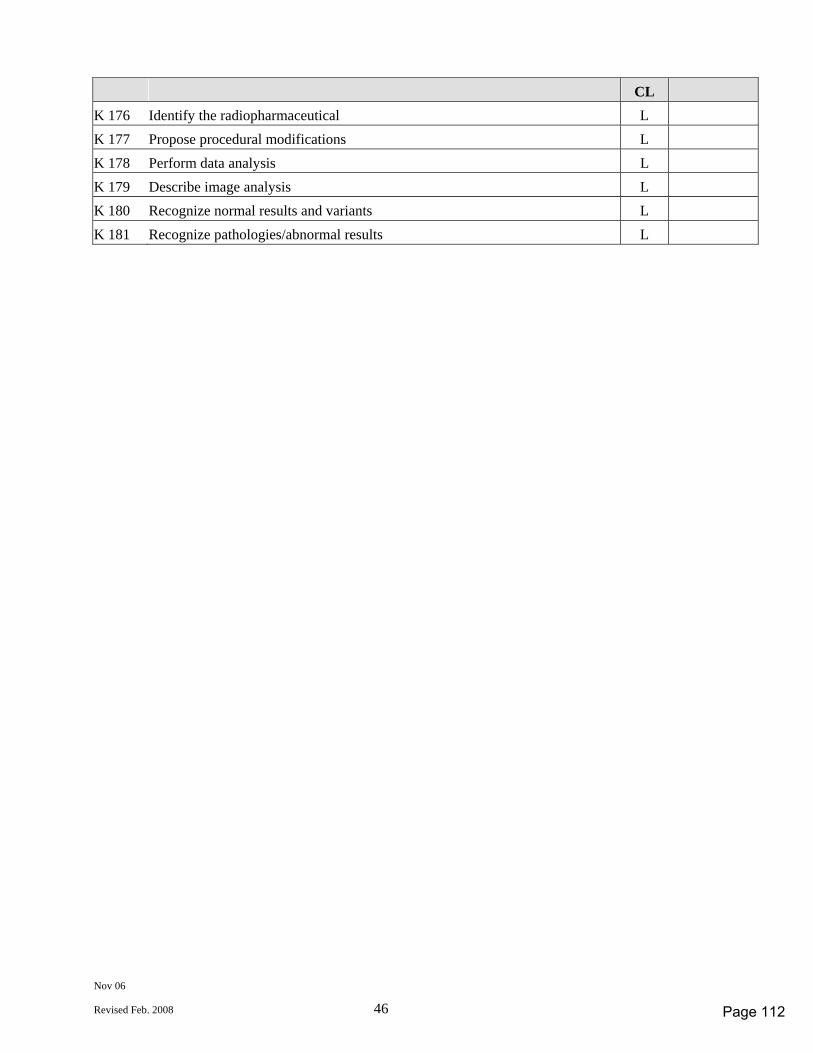
Nov 06
Revised Feb. 2008 46
CL K 176 Identify the radiopharmaceutical L K 177 Propose procedural modifications L K 178 Perform data analysis L K 179 Describe image analysis L K 180 Recognize normal results and variants L K 181 Recognize pathologies/abnormal results L
Page 112
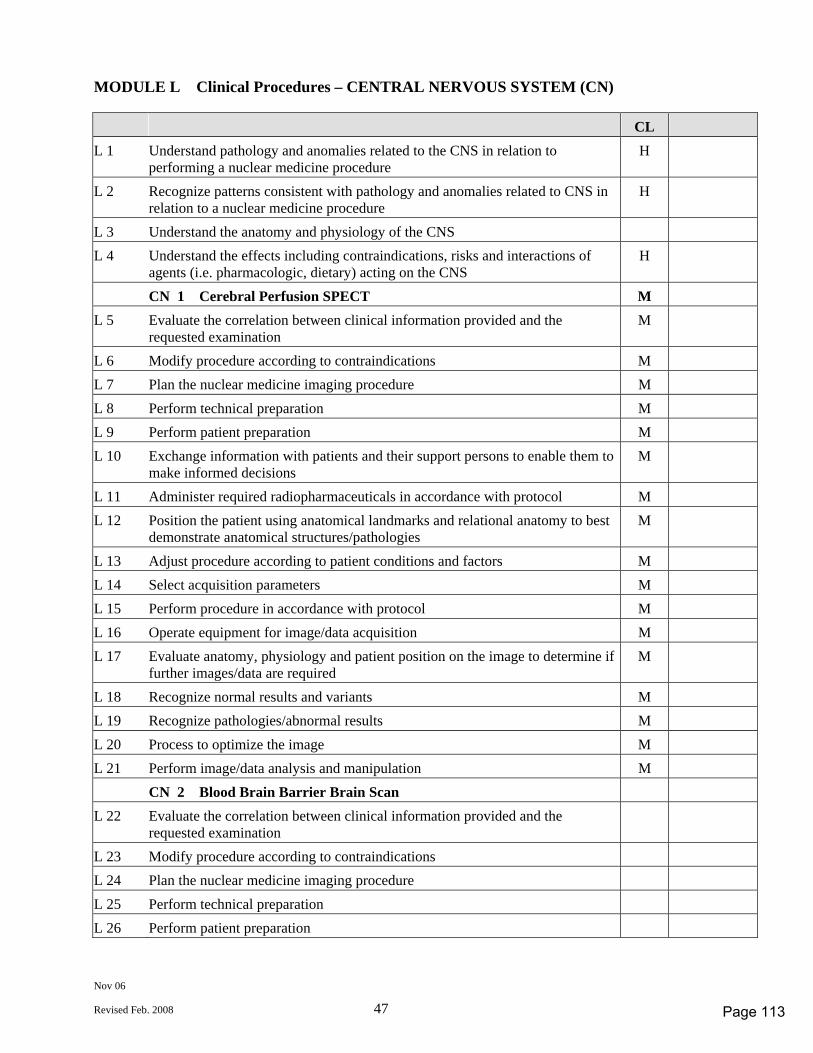
Nov 06
Revised Feb. 2008 47
MODULE L Clinical Procedures – CENTRAL NERVOUS SYSTEM (CN) CL L 1 Understand pathology and anomalies related to the CNS in relation to
performing a nuclear medicine procedure H
L 2 Recognize patterns consistent with pathology and anomalies related to CNS in relation to a nuclear medicine procedure
H
L 3 Understand the anatomy and physiology of the CNS L 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the CNS H
CN 1 Cerebral Perfusion SPECT M L 5 Evaluate the correlation between clinical information provided and the
requested examination M
L 6 Modify procedure according to contraindications M L 7 Plan the nuclear medicine imaging procedure M L 8 Perform technical preparation M L 9 Perform patient preparation M L 10 Exchange information with patients and their support persons to enable them to
make informed decisions M
L 11 Administer required radiopharmaceuticals in accordance with protocol M L 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
L 13 Adjust procedure according to patient conditions and factors M L 14 Select acquisition parameters M L 15 Perform procedure in accordance with protocol M L 16 Operate equipment for image/data acquisition M L 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
L 18 Recognize normal results and variants M L 19 Recognize pathologies/abnormal results M L 20 Process to optimize the image M L 21 Perform image/data analysis and manipulation M CN 2 Blood Brain Barrier Brain Scan L 22 Evaluate the correlation between clinical information provided and the
requested examination
L 23 Modify procedure according to contraindications L 24 Plan the nuclear medicine imaging procedure L 25 Perform technical preparation L 26 Perform patient preparation
Page 113
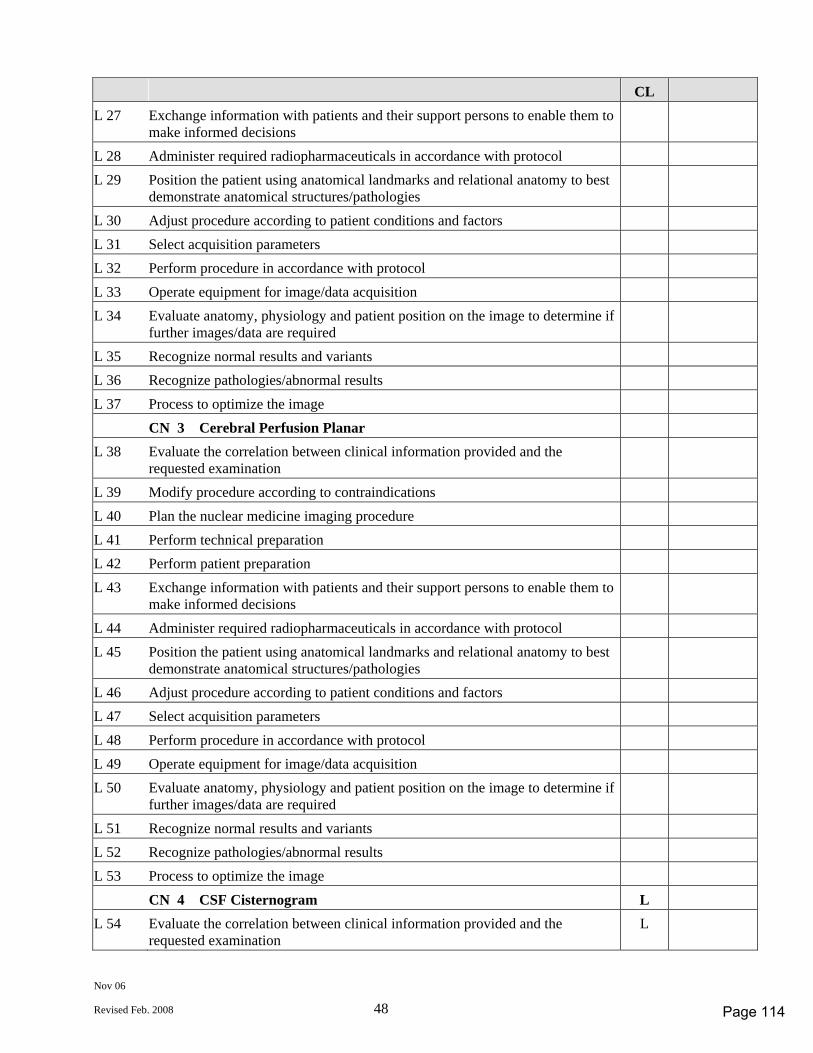
Nov 06
Revised Feb. 2008 48
CL L 27 Exchange information with patients and their support persons to enable them to
make informed decisions
L 28 Administer required radiopharmaceuticals in accordance with protocol L 29 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies
L 30 Adjust procedure according to patient conditions and factors L 31 Select acquisition parameters L 32 Perform procedure in accordance with protocol L 33 Operate equipment for image/data acquisition L 34 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required
L 35 Recognize normal results and variants L 36 Recognize pathologies/abnormal results L 37 Process to optimize the image CN 3 Cerebral Perfusion Planar L 38 Evaluate the correlation between clinical information provided and the
requested examination
L 39 Modify procedure according to contraindications L 40 Plan the nuclear medicine imaging procedure L 41 Perform technical preparation L 42 Perform patient preparation L 43 Exchange information with patients and their support persons to enable them to
make informed decisions
L 44 Administer required radiopharmaceuticals in accordance with protocol L 45 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies
L 46 Adjust procedure according to patient conditions and factors L 47 Select acquisition parameters L 48 Perform procedure in accordance with protocol L 49 Operate equipment for image/data acquisition L 50 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required
L 51 Recognize normal results and variants L 52 Recognize pathologies/abnormal results L 53 Process to optimize the image CN 4 CSF Cisternogram L L 54 Evaluate the correlation between clinical information provided and the
requested examination L
Page 114
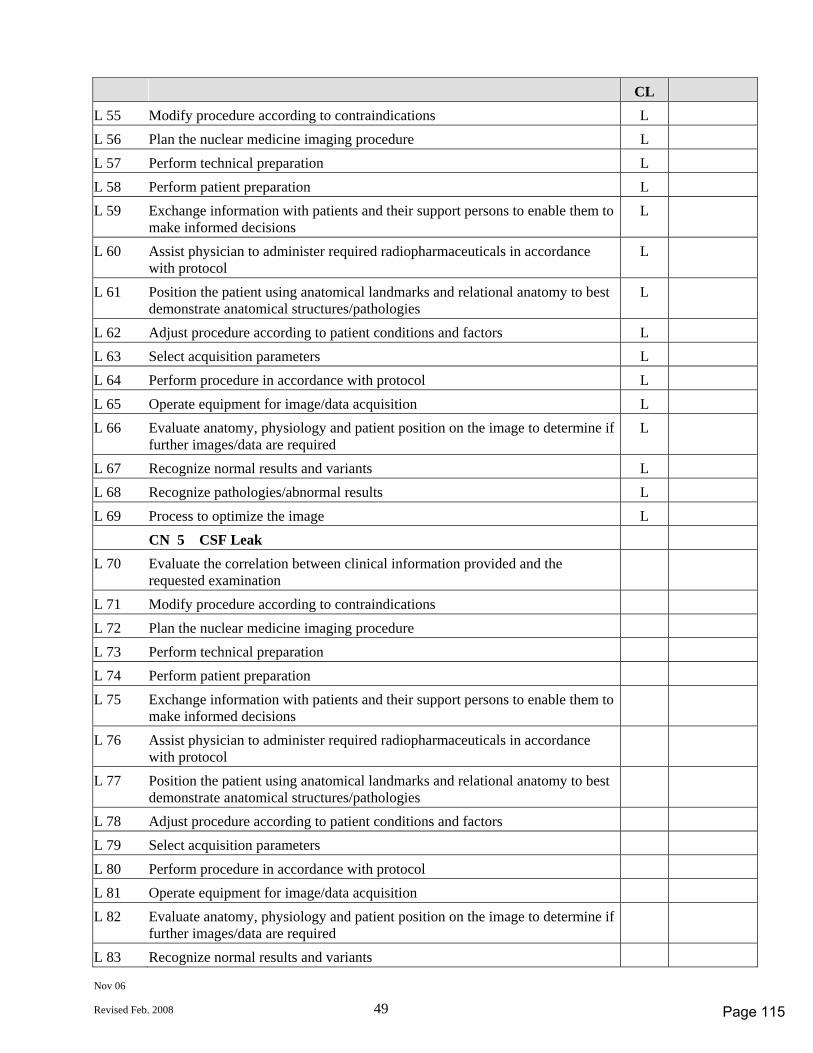
Nov 06
Revised Feb. 2008 49
CL L 55 Modify procedure according to contraindications L L 56 Plan the nuclear medicine imaging procedure L L 57 Perform technical preparation L L 58 Perform patient preparation L L 59 Exchange information with patients and their support persons to enable them to
make informed decisions L
L 60 Assist physician to administer required radiopharmaceuticals in accordance with protocol
L
L 61 Position the patient using anatomical landmarks and relational anatomy to best demonstrate anatomical structures/pathologies
L
L 62 Adjust procedure according to patient conditions and factors L L 63 Select acquisition parameters L L 64 Perform procedure in accordance with protocol L L 65 Operate equipment for image/data acquisition L L 66 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
L 67 Recognize normal results and variants L L 68 Recognize pathologies/abnormal results L L 69 Process to optimize the image L CN 5 CSF Leak L 70 Evaluate the correlation between clinical information provided and the
requested examination
L 71 Modify procedure according to contraindications L 72 Plan the nuclear medicine imaging procedure L 73 Perform technical preparation L 74 Perform patient preparation L 75 Exchange information with patients and their support persons to enable them to
make informed decisions
L 76 Assist physician to administer required radiopharmaceuticals in accordance with protocol
L 77 Position the patient using anatomical landmarks and relational anatomy to best demonstrate anatomical structures/pathologies
L 78 Adjust procedure according to patient conditions and factors L 79 Select acquisition parameters L 80 Perform procedure in accordance with protocol L 81 Operate equipment for image/data acquisition L 82 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required
L 83 Recognize normal results and variants
Page 115
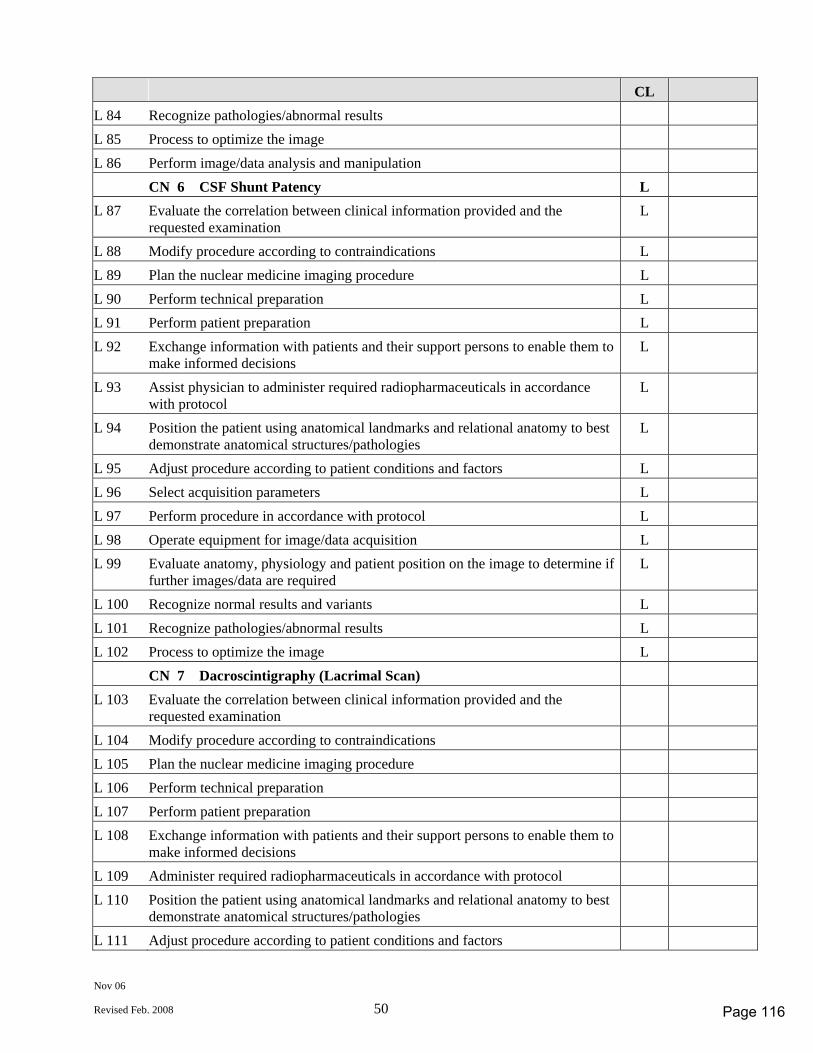
Nov 06
Revised Feb. 2008 50
CL L 84 Recognize pathologies/abnormal results L 85 Process to optimize the image L 86 Perform image/data analysis and manipulation CN 6 CSF Shunt Patency L L 87 Evaluate the correlation between clinical information provided and the
requested examination L
L 88 Modify procedure according to contraindications L L 89 Plan the nuclear medicine imaging procedure L L 90 Perform technical preparation L L 91 Perform patient preparation L L 92 Exchange information with patients and their support persons to enable them to
make informed decisions L
L 93 Assist physician to administer required radiopharmaceuticals in accordance with protocol
L
L 94 Position the patient using anatomical landmarks and relational anatomy to best demonstrate anatomical structures/pathologies
L
L 95 Adjust procedure according to patient conditions and factors L L 96 Select acquisition parameters L L 97 Perform procedure in accordance with protocol L L 98 Operate equipment for image/data acquisition L L 99 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
L 100 Recognize normal results and variants L L 101 Recognize pathologies/abnormal results L L 102 Process to optimize the image L CN 7 Dacroscintigraphy (Lacrimal Scan) L 103 Evaluate the correlation between clinical information provided and the
requested examination
L 104 Modify procedure according to contraindications L 105 Plan the nuclear medicine imaging procedure L 106 Perform technical preparation L 107 Perform patient preparation L 108 Exchange information with patients and their support persons to enable them to
make informed decisions
L 109 Administer required radiopharmaceuticals in accordance with protocol L 110 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies
L 111 Adjust procedure according to patient conditions and factors
Page 116
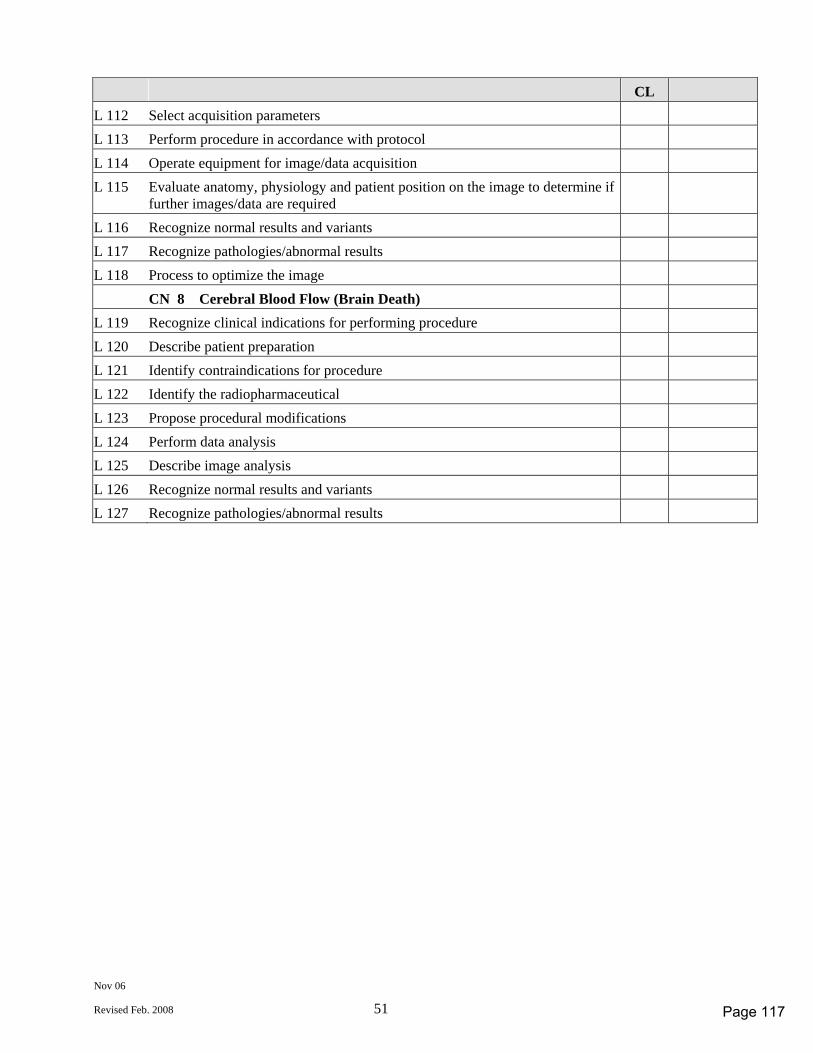
Nov 06
Revised Feb. 2008 51
CL L 112 Select acquisition parameters L 113 Perform procedure in accordance with protocol L 114 Operate equipment for image/data acquisition L 115 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required
L 116 Recognize normal results and variants L 117 Recognize pathologies/abnormal results L 118 Process to optimize the image CN 8 Cerebral Blood Flow (Brain Death) L 119 Recognize clinical indications for performing procedure L 120 Describe patient preparation L 121 Identify contraindications for procedure L 122 Identify the radiopharmaceutical L 123 Propose procedural modifications L 124 Perform data analysis L 125 Describe image analysis L 126 Recognize normal results and variants L 127 Recognize pathologies/abnormal results
Page 117
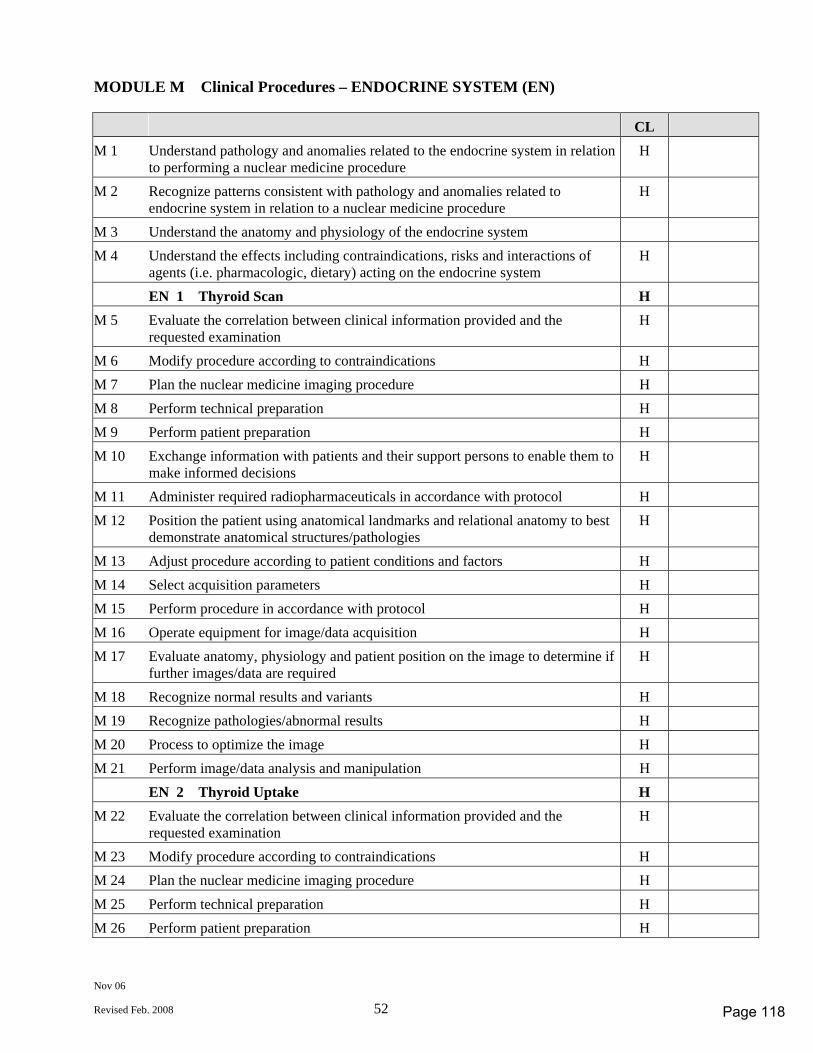
Nov 06
Revised Feb. 2008 52
MODULE M Clinical Procedures – ENDOCRINE SYSTEM (EN) CL M 1 Understand pathology and anomalies related to the endocrine system in relation
to performing a nuclear medicine procedure H
M 2 Recognize patterns consistent with pathology and anomalies related to endocrine system in relation to a nuclear medicine procedure
H
M 3 Understand the anatomy and physiology of the endocrine system M 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the endocrine system H
EN 1 Thyroid Scan H M 5 Evaluate the correlation between clinical information provided and the
requested examination H
M 6 Modify procedure according to contraindications H M 7 Plan the nuclear medicine imaging procedure H M 8 Perform technical preparation H M 9 Perform patient preparation H M 10 Exchange information with patients and their support persons to enable them to
make informed decisions H
M 11 Administer required radiopharmaceuticals in accordance with protocol H M 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
M 13 Adjust procedure according to patient conditions and factors H M 14 Select acquisition parameters H M 15 Perform procedure in accordance with protocol H M 16 Operate equipment for image/data acquisition H M 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
M 18 Recognize normal results and variants H M 19 Recognize pathologies/abnormal results H M 20 Process to optimize the image H M 21 Perform image/data analysis and manipulation H EN 2 Thyroid Uptake H M 22 Evaluate the correlation between clinical information provided and the
requested examination H
M 23 Modify procedure according to contraindications H M 24 Plan the nuclear medicine imaging procedure H M 25 Perform technical preparation H M 26 Perform patient preparation H
Page 118
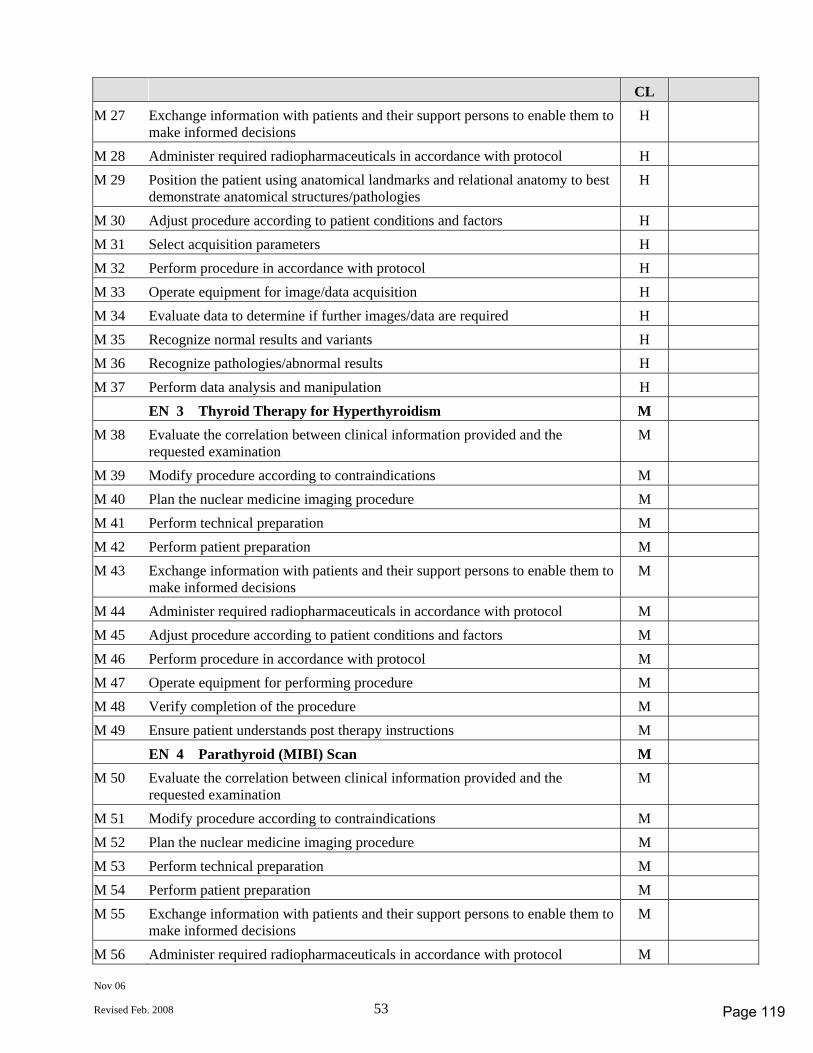
Nov 06
Revised Feb. 2008 53
CL M 27 Exchange information with patients and their support persons to enable them to
make informed decisions H
M 28 Administer required radiopharmaceuticals in accordance with protocol H M 29 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
M 30 Adjust procedure according to patient conditions and factors H M 31 Select acquisition parameters H M 32 Perform procedure in accordance with protocol H M 33 Operate equipment for image/data acquisition H M 34 Evaluate data to determine if further images/data are required H M 35 Recognize normal results and variants H M 36 Recognize pathologies/abnormal results H M 37 Perform data analysis and manipulation H EN 3 Thyroid Therapy for Hyperthyroidism M M 38 Evaluate the correlation between clinical information provided and the
requested examination M
M 39 Modify procedure according to contraindications M M 40 Plan the nuclear medicine imaging procedure M M 41 Perform technical preparation M M 42 Perform patient preparation M M 43 Exchange information with patients and their support persons to enable them to
make informed decisions M
M 44 Administer required radiopharmaceuticals in accordance with protocol M M 45 Adjust procedure according to patient conditions and factors M M 46 Perform procedure in accordance with protocol M M 47 Operate equipment for performing procedure M M 48 Verify completion of the procedure M M 49 Ensure patient understands post therapy instructions M EN 4 Parathyroid (MIBI) Scan M M 50 Evaluate the correlation between clinical information provided and the
requested examination M
M 51 Modify procedure according to contraindications M M 52 Plan the nuclear medicine imaging procedure M M 53 Perform technical preparation M M 54 Perform patient preparation M M 55 Exchange information with patients and their support persons to enable them to
make informed decisions M
M 56 Administer required radiopharmaceuticals in accordance with protocol M
Page 119
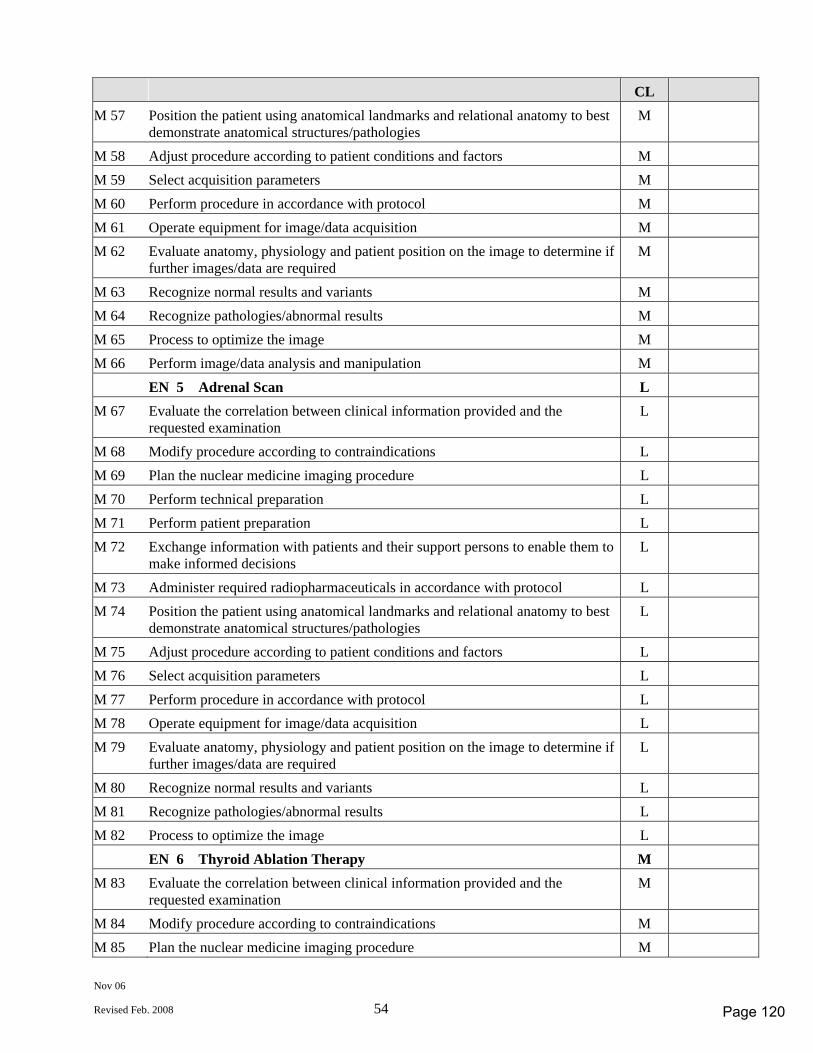
Nov 06
Revised Feb. 2008 54
CL M 57 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies M
M 58 Adjust procedure according to patient conditions and factors M M 59 Select acquisition parameters M M 60 Perform procedure in accordance with protocol M M 61 Operate equipment for image/data acquisition M M 62 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required M
M 63 Recognize normal results and variants M M 64 Recognize pathologies/abnormal results M M 65 Process to optimize the image M M 66 Perform image/data analysis and manipulation M EN 5 Adrenal Scan L M 67 Evaluate the correlation between clinical information provided and the
requested examination L
M 68 Modify procedure according to contraindications L M 69 Plan the nuclear medicine imaging procedure L M 70 Perform technical preparation L M 71 Perform patient preparation L M 72 Exchange information with patients and their support persons to enable them to
make informed decisions L
M 73 Administer required radiopharmaceuticals in accordance with protocol L M 74 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
M 75 Adjust procedure according to patient conditions and factors L M 76 Select acquisition parameters L M 77 Perform procedure in accordance with protocol L M 78 Operate equipment for image/data acquisition L M 79 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
M 80 Recognize normal results and variants L M 81 Recognize pathologies/abnormal results L M 82 Process to optimize the image L EN 6 Thyroid Ablation Therapy M M 83 Evaluate the correlation between clinical information provided and the
requested examination M
M 84 Modify procedure according to contraindications M M 85 Plan the nuclear medicine imaging procedure M
Page 120
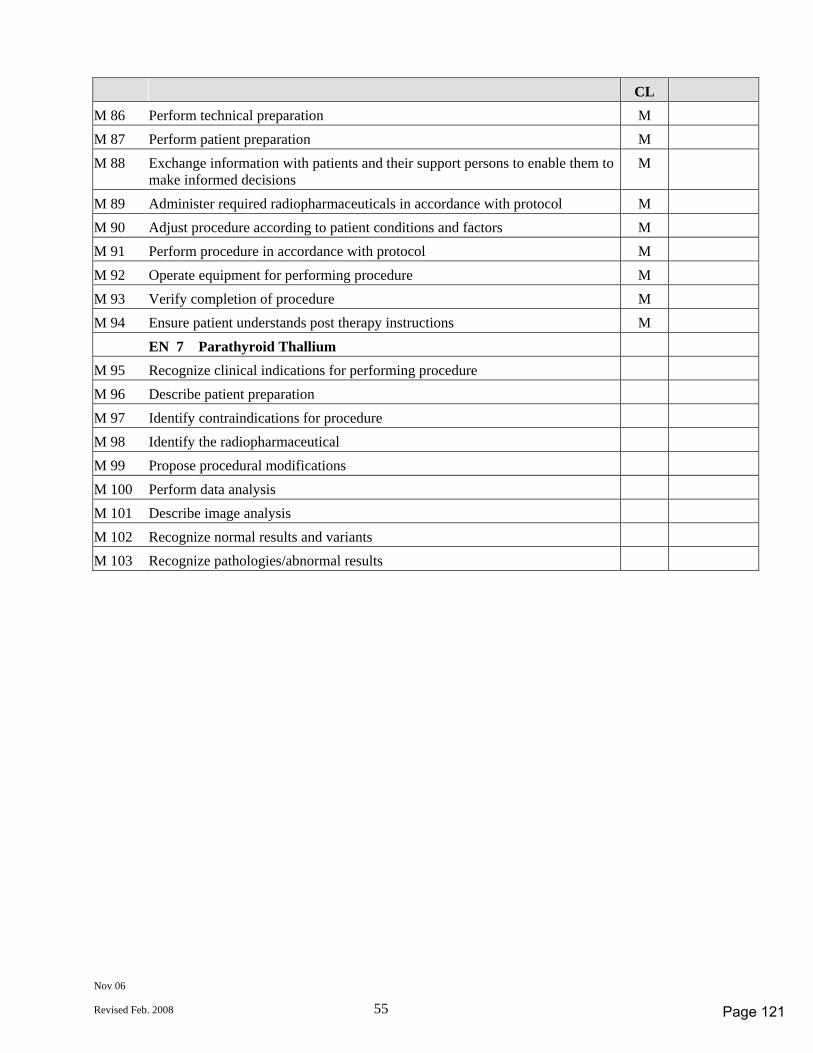
Nov 06
Revised Feb. 2008 55
CL M 86 Perform technical preparation M M 87 Perform patient preparation M M 88 Exchange information with patients and their support persons to enable them to
make informed decisions M
M 89 Administer required radiopharmaceuticals in accordance with protocol M M 90 Adjust procedure according to patient conditions and factors M M 91 Perform procedure in accordance with protocol M M 92 Operate equipment for performing procedure M M 93 Verify completion of procedure M M 94 Ensure patient understands post therapy instructions M EN 7 Parathyroid Thallium M 95 Recognize clinical indications for performing procedure M 96 Describe patient preparation M 97 Identify contraindications for procedure M 98 Identify the radiopharmaceutical M 99 Propose procedural modifications M 100 Perform data analysis M 101 Describe image analysis M 102 Recognize normal results and variants M 103 Recognize pathologies/abnormal results
Page 121
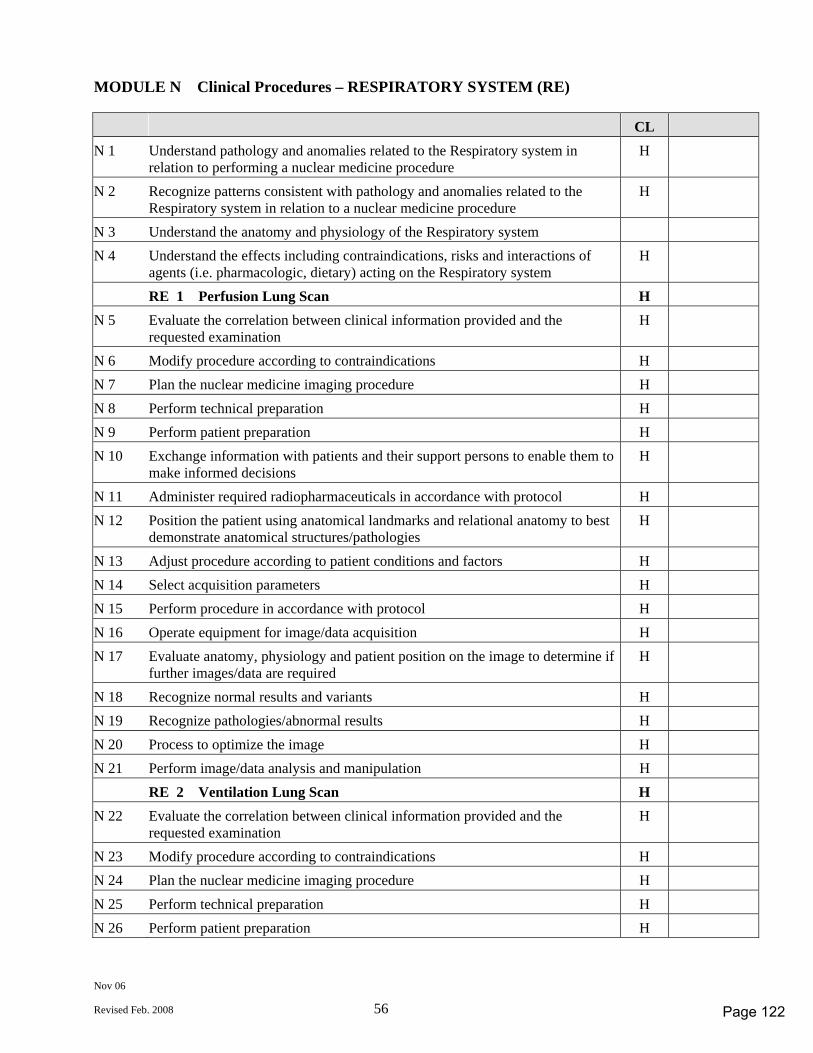
Nov 06
Revised Feb. 2008 56
MODULE N Clinical Procedures – RESPIRATORY SYSTEM (RE) CL N 1 Understand pathology and anomalies related to the Respiratory system in
relation to performing a nuclear medicine procedure H
N 2 Recognize patterns consistent with pathology and anomalies related to the Respiratory system in relation to a nuclear medicine procedure
H
N 3 Understand the anatomy and physiology of the Respiratory system N 4 Understand the effects including contraindications, risks and interactions of
agents (i.e. pharmacologic, dietary) acting on the Respiratory system H
RE 1 Perfusion Lung Scan H N 5 Evaluate the correlation between clinical information provided and the
requested examination H
N 6 Modify procedure according to contraindications H N 7 Plan the nuclear medicine imaging procedure H N 8 Perform technical preparation H N 9 Perform patient preparation H N 10 Exchange information with patients and their support persons to enable them to
make informed decisions H
N 11 Administer required radiopharmaceuticals in accordance with protocol H N 12 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
N 13 Adjust procedure according to patient conditions and factors H N 14 Select acquisition parameters H N 15 Perform procedure in accordance with protocol H N 16 Operate equipment for image/data acquisition H N 17 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
N 18 Recognize normal results and variants H N 19 Recognize pathologies/abnormal results H N 20 Process to optimize the image H N 21 Perform image/data analysis and manipulation H RE 2 Ventilation Lung Scan H N 22 Evaluate the correlation between clinical information provided and the
requested examination H
N 23 Modify procedure according to contraindications H N 24 Plan the nuclear medicine imaging procedure H N 25 Perform technical preparation H N 26 Perform patient preparation H
Page 122
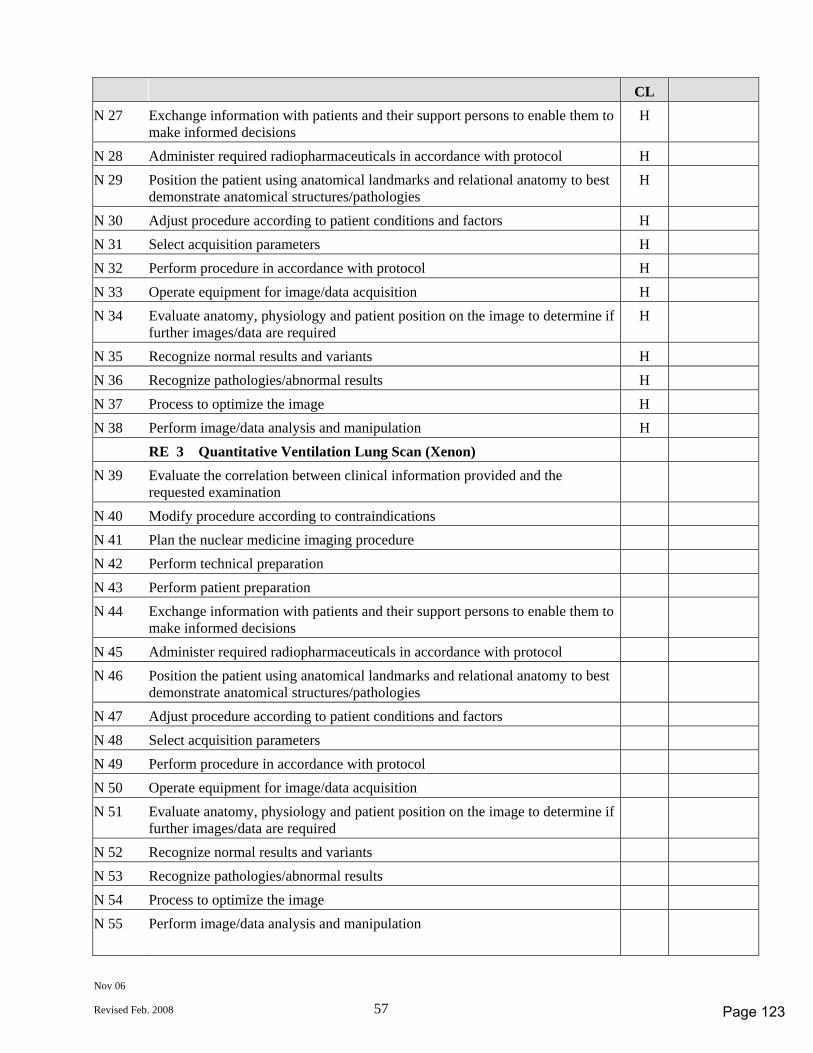
Nov 06
Revised Feb. 2008 57
CL N 27 Exchange information with patients and their support persons to enable them to
make informed decisions H
N 28 Administer required radiopharmaceuticals in accordance with protocol H N 29 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies H
N 30 Adjust procedure according to patient conditions and factors H N 31 Select acquisition parameters H N 32 Perform procedure in accordance with protocol H N 33 Operate equipment for image/data acquisition H N 34 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required H
N 35 Recognize normal results and variants H N 36 Recognize pathologies/abnormal results H N 37 Process to optimize the image H N 38 Perform image/data analysis and manipulation H RE 3 Quantitative Ventilation Lung Scan (Xenon) N 39 Evaluate the correlation between clinical information provided and the
requested examination
N 40 Modify procedure according to contraindications N 41 Plan the nuclear medicine imaging procedure N 42 Perform technical preparation N 43 Perform patient preparation N 44 Exchange information with patients and their support persons to enable them to
make informed decisions
N 45 Administer required radiopharmaceuticals in accordance with protocol N 46 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies
N 47 Adjust procedure according to patient conditions and factors N 48 Select acquisition parameters N 49 Perform procedure in accordance with protocol N 50 Operate equipment for image/data acquisition N 51 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required
N 52 Recognize normal results and variants N 53 Recognize pathologies/abnormal results N 54 Process to optimize the image N 55 Perform image/data analysis and manipulation
Page 123
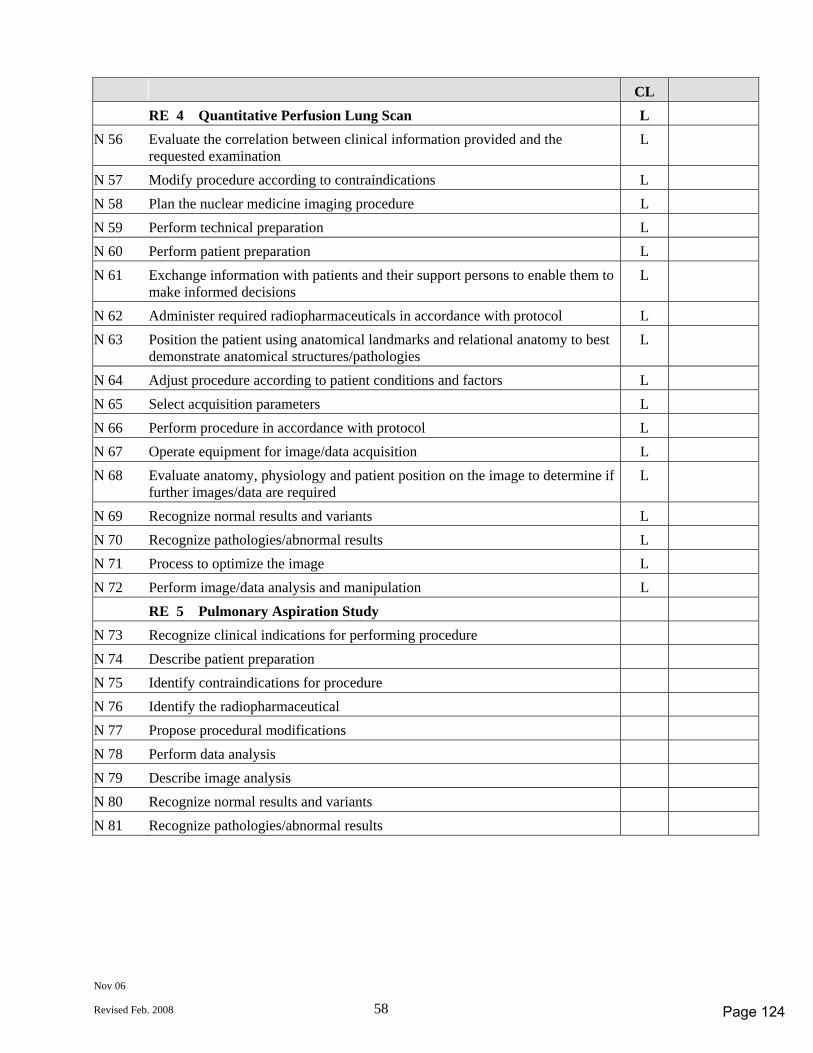
Nov 06
Revised Feb. 2008 58
CL RE 4 Quantitative Perfusion Lung Scan L N 56 Evaluate the correlation between clinical information provided and the
requested examination L
N 57 Modify procedure according to contraindications L N 58 Plan the nuclear medicine imaging procedure L N 59 Perform technical preparation L N 60 Perform patient preparation L N 61 Exchange information with patients and their support persons to enable them to
make informed decisions L
N 62 Administer required radiopharmaceuticals in accordance with protocol L N 63 Position the patient using anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
N 64 Adjust procedure according to patient conditions and factors L N 65 Select acquisition parameters L N 66 Perform procedure in accordance with protocol L N 67 Operate equipment for image/data acquisition L N 68 Evaluate anatomy, physiology and patient position on the image to determine if
further images/data are required L
N 69 Recognize normal results and variants L N 70 Recognize pathologies/abnormal results L N 71 Process to optimize the image L N 72 Perform image/data analysis and manipulation L RE 5 Pulmonary Aspiration Study N 73 Recognize clinical indications for performing procedure N 74 Describe patient preparation N 75 Identify contraindications for procedure N 76 Identify the radiopharmaceutical N 77 Propose procedural modifications N 78 Perform data analysis N 79 Describe image analysis N 80 Recognize normal results and variants N 81 Recognize pathologies/abnormal results
Page 124
December 2006
Revised Feb 2008 (#29222)
Radiological Technology
COMPETENCY PROFILE
November 2006 Revised February 2008
Revised Profile for use with the development of the
September 2011 Certification exams
Prepared by the Radiological Technology Competency Profile Task Group
© CANADIAN ASSOCIATION OF MEDICAL RADIATION TECHNOLOGISTS Suite 1000, 85 Albert Street, Ottawa, Ontario K1P 6A4
Tel: 1-800-463-9729 or (613) 234-0012 / Fax: (613) 234-1097 www.camrt.ca
Page 125

December 2006
Revised Feb 2008 (#29222)
© Copyright 2006 by Canadian Association of Medical Radiation Technologists
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage or retrieval system, without the prior written permission of the Canadian Association of Medical Radiation Technologists.
Page 126
Dec 06
Revised Feb 2008 1
COMPETENCY PROFILE - RADIOLOGICAL TECHNOLOGY Competencies for Entry Level Radiological Technologists This document describes the essential competencies required for an entry-level radiological technologist in Canada to provide best practice as defined by safe, competent and ethical practice of radiological technology in a variety of clinical environments. The profile defines competencies reflecting the integration of knowledge, skills, attitudes and judgment necessary to practice in an environment that requires the technologist to use effective organizational skills and critical thinking. This requires the ability to assess, adapt, modify, analyse and evaluate in a variety of situations and environments in the practice of radiological technology. Critical decision-making is, therefore, inherent to the practice of radiological technology and is demonstrated in the competencies required of entry-to-practice technologists. The competency profile defines the standard for certification and registration of entry-level radiological technologists in Canada. The document is also used to: - provide direction to entry-level education programs to assist in developing curriculum - inform Ministries of Health and Education of the standard expected from entry-level radiological
technologists - inform the public and employers of the standard expected from entry-level radiological technologists - assist CMA Conjoint Committee with accreditation of education programs - provides a guide to identify professional development needs for practicing technologists - develop a blueprint for CAMRT certification examination Accredited programs must ensure that their certification candidates possess all the competencies listed in the profile. Education programs are encouraged to include additional skills at their discretion. In the development of the competencies, the following assumptions have been made. That the Radiological Technologist: - has completed an accredited Canadian program, or other recognized program; - has acquired the theoretical knowledge required to achieve a wide range of competencies; - has developed a broad knowledge base that has been assessed prior to the certification examination; - commits to the principle that their primary role and function is to serve the public interest; - is a member of the inter-professional health care team, collaborating with other health care
professionals to provide appropriate patient care in the delivery of diagnostic imaging services; - is responsible for the safe and effective application of ionizing radiation; - is responsible for the production, assessment, optimization and archiving of images; - is responsible for the performance of diagnostic radiographic/fluoroscopic procedures; - participates in interventional procedures; - is responsible for the education of patients, public and other health care providers regarding ionizing
radiation for medical use;
Page 127
Dec 06
Revised Feb 2008 2
- performs effectively in all environments taking into consideration physical, psychological, social, economic and cultural factors that can occur in predictable and unpredictable ways ;
- recognizes patients as unique individuals, treating them with dignity and respect; - practices in accordance with legislation, regulatory and professional bodies’ standards of practice,
scope of practice, codes of ethics and other relative documents; - performs in a manner consistent with public interest, employment philosophies and practices,
current research and advancing technology; - seeks guidance from experienced practitioners, colleagues and employers to enhance the
technologist’s individual experience and knowledge; - promotes and participates in the advancement of this dynamic profession through active
involvement, continuous learning, professional development and research; - adheres to and promotes professional standards. The Radiological Technology Competency Profile is divided into 13 modules: Module A Professional Practice Module B Patient Management Module C Radiation Health and Safety Module D Quality Management Module E Operate Imaging Equipment Module F Skeletal System Module G Digestive System Module H Respiratory System Module I Urinary System Module J Reproductive System Module K Computed Tomography Module L Bone Mineral Densitometry Module M Vascular / Interventional Studies
Page 128
Dec 06
Revised Feb 2008 3
EXAMINABLE COMPETENCIES & COMPETENCY LEVELS
All competencies listed in the competency profile must be achieved by graduates of an accredited medical radiation technology program. This will be assessed for compliance during the accreditation survey conducted by the CMA Conjoint Accreditation Services. It is realized that due to regional and institutional differences level of achievement for some competencies may vary based on evolving changes in technology, practice and facility policies.
Not all competencies will be tested on the CAMRT certification exam.
The EXAMINABLE COMPETENCIES are those competencies that have a competency level indicated in the column to the right of the written competency. The EXAMINABLE COMPETENCIES were established by the discipline specific workgroups working both within their disciplines and together as a core group using the feedback received from stakeholders during the competency profile revision process.
There are three competency levels (CL)
– HIGH (H)
– MEDIUM (M)
– LOW (L) Competency levels were determined through a survey done by technologists/therapists and managers of Diagnostic Imaging and Radiation Therapy Departments. The survey requested a rating of the examinable competencies for frequency of application, importance and future significance in the healthcare work environment. The results of the survey were analyzed and the examinable competencies rated either H, M, L based on the response to frequency, importance and significance for the future.
The competency levels provide a guide (blue print) for certification exam development. More weighting will be placed on the development and use of questions associated with a HIGH level competency as opposed to a MEDIUM or LOW rated level competency where emphasis on question development and use on the certification exam will reflect the competency level.
Validation of all competencies, including identification of examinable competencies and their associated competency levels will be conducted at least every five years. Due to rapid changes in technology and practice certain portions of the profile may be validated more frequently to ensure the profiles are reflective of practice and workplace needs.
Page 129
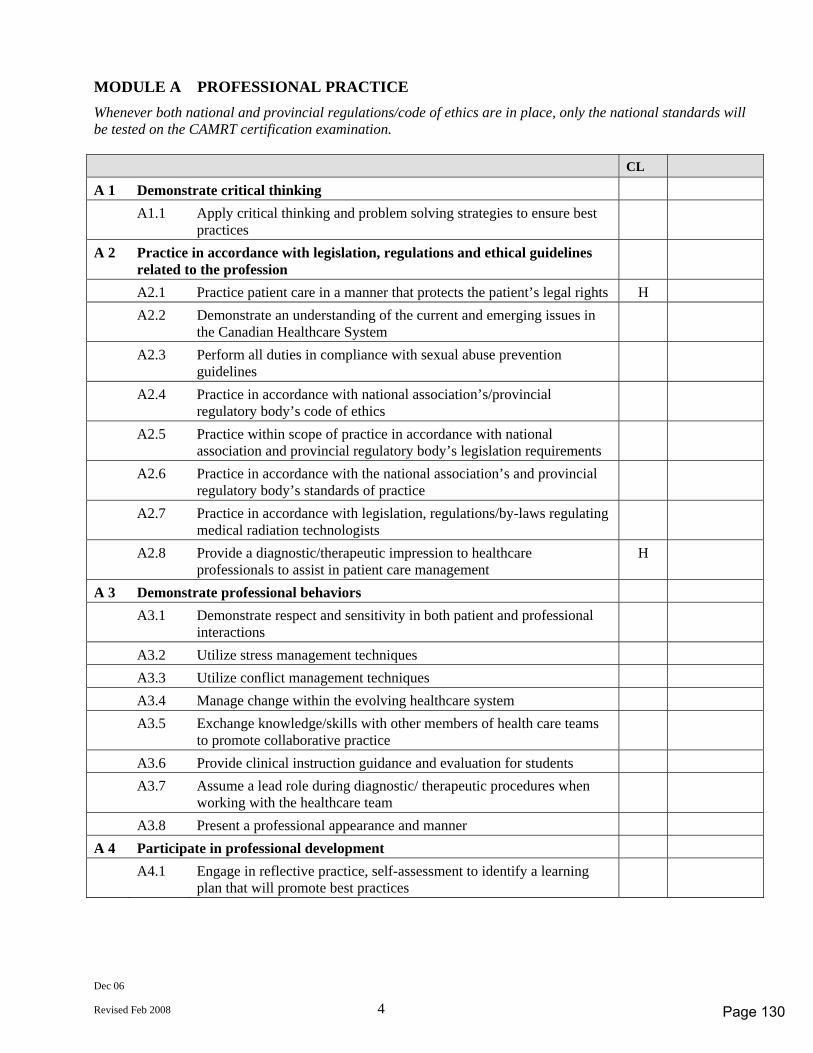
Dec 06
Revised Feb 2008 4
MODULE A PROFESSIONAL PRACTICE Whenever both national and provincial regulations/code of ethics are in place, only the national standards will be tested on the CAMRT certification examination. CL A 1 Demonstrate critical thinking A1.1 Apply critical thinking and problem solving strategies to ensure best
practices
A 2 Practice in accordance with legislation, regulations and ethical guidelines related to the profession
A2.1 Practice patient care in a manner that protects the patient’s legal rights H A2.2 Demonstrate an understanding of the current and emerging issues in
the Canadian Healthcare System
A2.3 Perform all duties in compliance with sexual abuse prevention guidelines
A2.4 Practice in accordance with national association’s/provincial regulatory body’s code of ethics
A2.5 Practice within scope of practice in accordance with national association and provincial regulatory body’s legislation requirements
A2.6 Practice in accordance with the national association’s and provincial regulatory body’s standards of practice
A2.7 Practice in accordance with legislation, regulations/by-laws regulating medical radiation technologists
A2.8 Provide a diagnostic/therapeutic impression to healthcare professionals to assist in patient care management
H
A 3 Demonstrate professional behaviors A3.1 Demonstrate respect and sensitivity in both patient and professional
interactions
A3.2 Utilize stress management techniques A3.3 Utilize conflict management techniques A3.4 Manage change within the evolving healthcare system A3.5 Exchange knowledge/skills with other members of health care teams
to promote collaborative practice
A3.6 Provide clinical instruction guidance and evaluation for students A3.7 Assume a lead role during diagnostic/ therapeutic procedures when
working with the healthcare team
A3.8 Present a professional appearance and manner A 4 Participate in professional development A4.1 Engage in reflective practice, self-assessment to identify a learning
plan that will promote best practices
Page 130
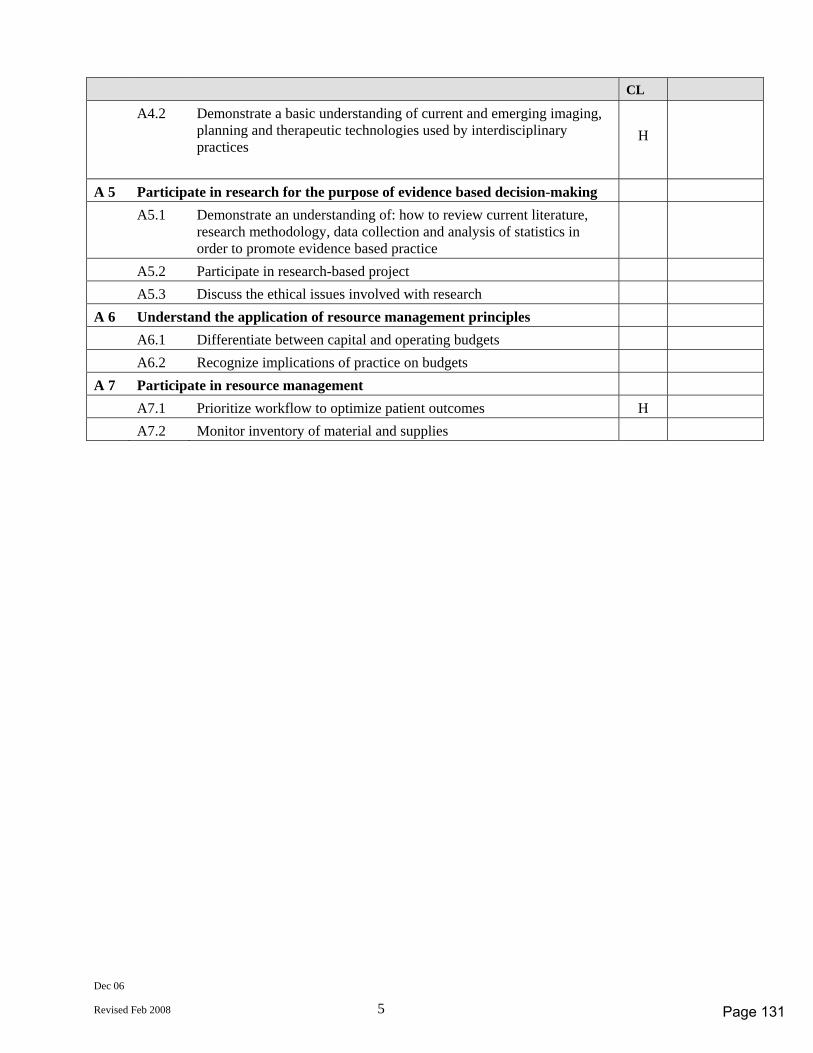
Dec 06
Revised Feb 2008 5
CL A4.2 Demonstrate a basic understanding of current and emerging imaging,
planning and therapeutic technologies used by interdisciplinary practices
H
A 5 Participate in research for the purpose of evidence based decision-making A5.1 Demonstrate an understanding of: how to review current literature,
research methodology, data collection and analysis of statistics in order to promote evidence based practice
A5.2 Participate in research-based project A5.3 Discuss the ethical issues involved with research A 6 Understand the application of resource management principles A6.1 Differentiate between capital and operating budgets A6.2 Recognize implications of practice on budgets A 7 Participate in resource management A7.1 Prioritize workflow to optimize patient outcomes H A7.2 Monitor inventory of material and supplies
Page 131
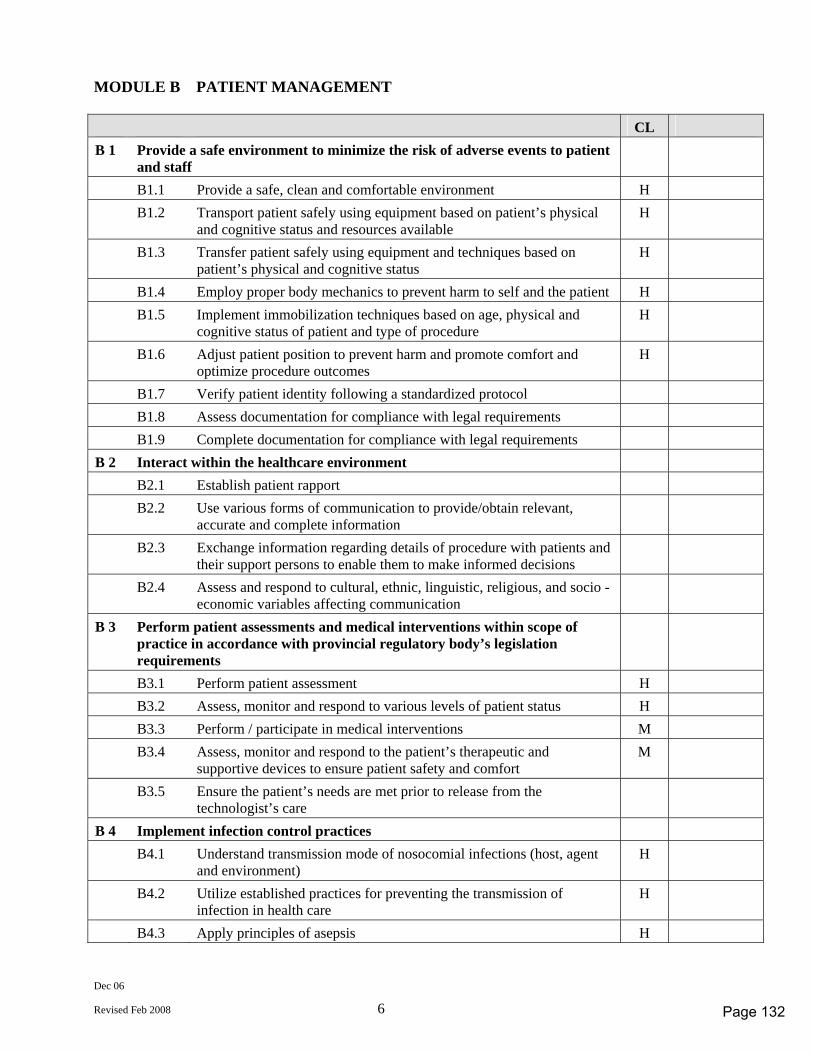
Dec 06
Revised Feb 2008 6
MODULE B PATIENT MANAGEMENT CL B 1 Provide a safe environment to minimize the risk of adverse events to patient
and staff
B1.1 Provide a safe, clean and comfortable environment H B1.2 Transport patient safely using equipment based on patient’s physical
and cognitive status and resources available H
B1.3 Transfer patient safely using equipment and techniques based on patient’s physical and cognitive status
H
B1.4 Employ proper body mechanics to prevent harm to self and the patient H B1.5 Implement immobilization techniques based on age, physical and
cognitive status of patient and type of procedure H
B1.6 Adjust patient position to prevent harm and promote comfort and optimize procedure outcomes
H
B1.7 Verify patient identity following a standardized protocol B1.8 Assess documentation for compliance with legal requirements B1.9 Complete documentation for compliance with legal requirements B 2 Interact within the healthcare environment B2.1 Establish patient rapport B2.2 Use various forms of communication to provide/obtain relevant,
accurate and complete information
B2.3 Exchange information regarding details of procedure with patients and their support persons to enable them to make informed decisions
B2.4 Assess and respond to cultural, ethnic, linguistic, religious, and socio - economic variables affecting communication
B 3 Perform patient assessments and medical interventions within scope of practice in accordance with provincial regulatory body’s legislation requirements
B3.1 Perform patient assessment H B3.2 Assess, monitor and respond to various levels of patient status H B3.3 Perform / participate in medical interventions M B3.4 Assess, monitor and respond to the patient’s therapeutic and
supportive devices to ensure patient safety and comfort M
B3.5 Ensure the patient’s needs are met prior to release from the technologist’s care
B 4 Implement infection control practices B4.1 Understand transmission mode of nosocomial infections (host, agent
and environment) H
B4.2 Utilize established practices for preventing the transmission of infection in health care
H
B4.3 Apply principles of asepsis H
Page 132
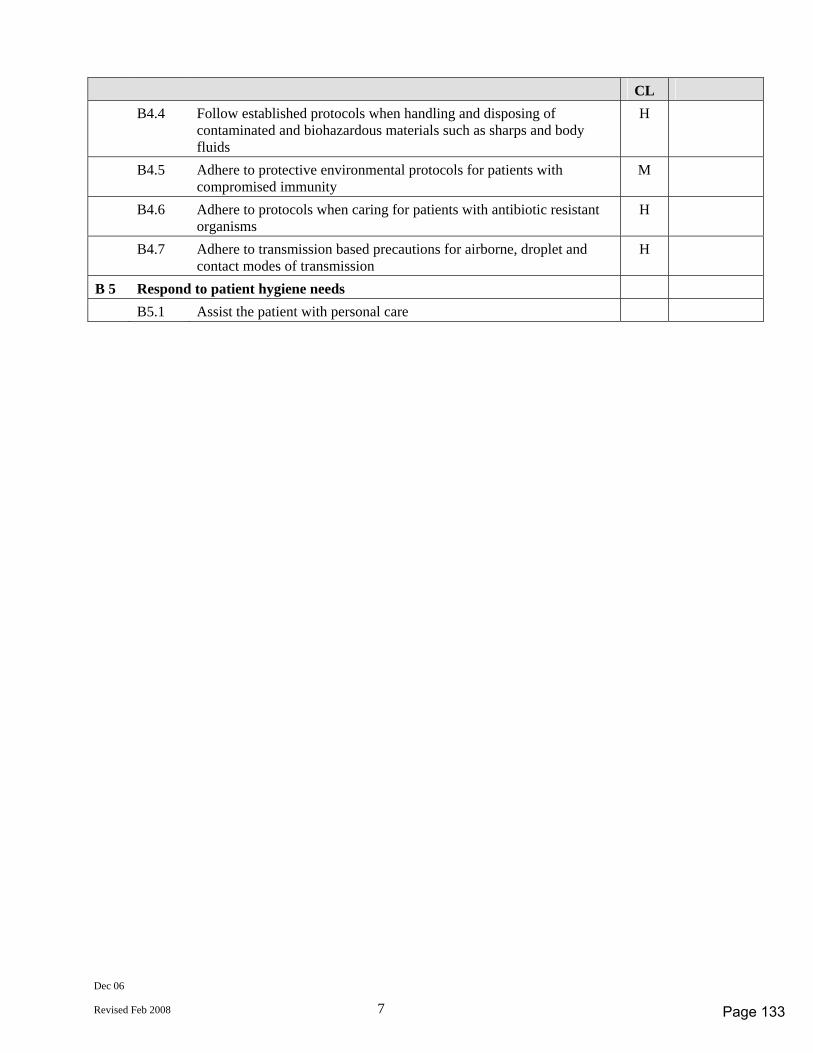
Dec 06
Revised Feb 2008 7
CL B4.4 Follow established protocols when handling and disposing of
contaminated and biohazardous materials such as sharps and body fluids
H
B4.5 Adhere to protective environmental protocols for patients with compromised immunity
M
B4.6 Adhere to protocols when caring for patients with antibiotic resistant organisms
H
B4.7 Adhere to transmission based precautions for airborne, droplet and contact modes of transmission
H
B 5 Respond to patient hygiene needs B5.1 Assist the patient with personal care
Page 133
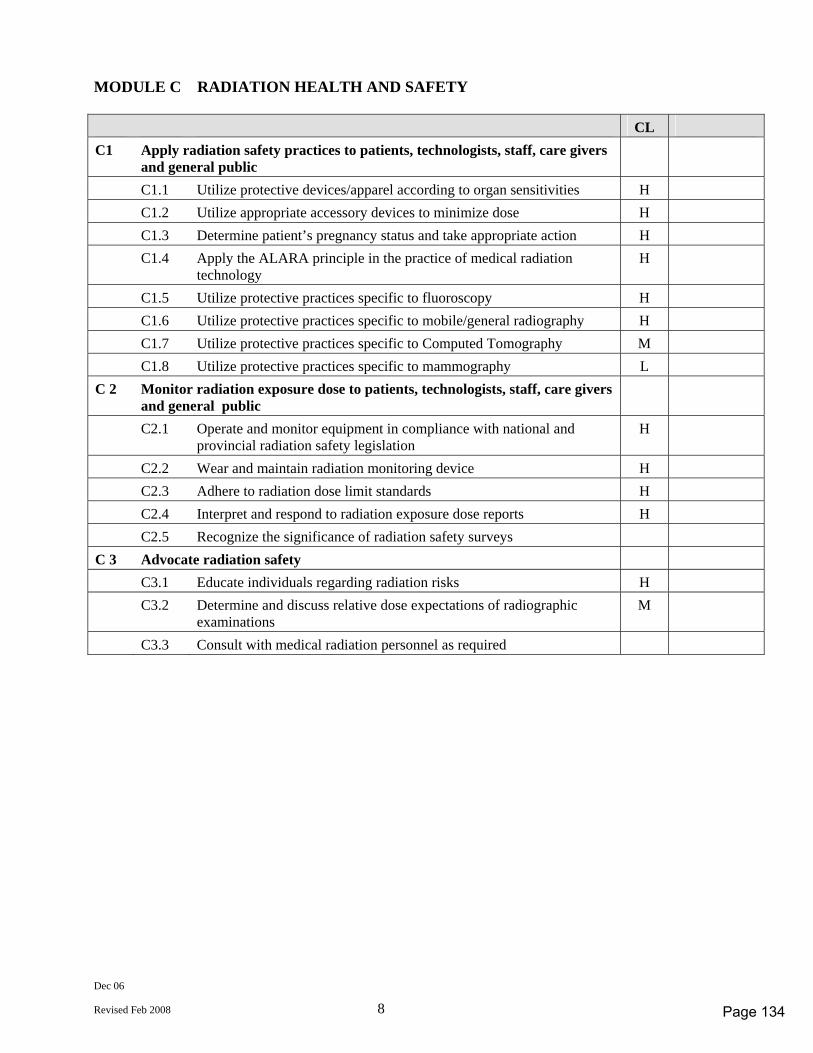
Dec 06
Revised Feb 2008 8
MODULE C RADIATION HEALTH AND SAFETY CL C1 Apply radiation safety practices to patients, technologists, staff, care givers
and general public
C1.1 Utilize protective devices/apparel according to organ sensitivities H C1.2 Utilize appropriate accessory devices to minimize dose H C1.3 Determine patient’s pregnancy status and take appropriate action H C1.4 Apply the ALARA principle in the practice of medical radiation
technology H
C1.5 Utilize protective practices specific to fluoroscopy H C1.6 Utilize protective practices specific to mobile/general radiography H C1.7 Utilize protective practices specific to Computed Tomography M C1.8 Utilize protective practices specific to mammography L C 2 Monitor radiation exposure dose to patients, technologists, staff, care givers
and general public
C2.1 Operate and monitor equipment in compliance with national and provincial radiation safety legislation
H
C2.2 Wear and maintain radiation monitoring device H C2.3 Adhere to radiation dose limit standards H C2.4 Interpret and respond to radiation exposure dose reports H C2.5 Recognize the significance of radiation safety surveys C 3 Advocate radiation safety C3.1 Educate individuals regarding radiation risks H C3.2 Determine and discuss relative dose expectations of radiographic
examinations M
C3.3 Consult with medical radiation personnel as required
Page 134
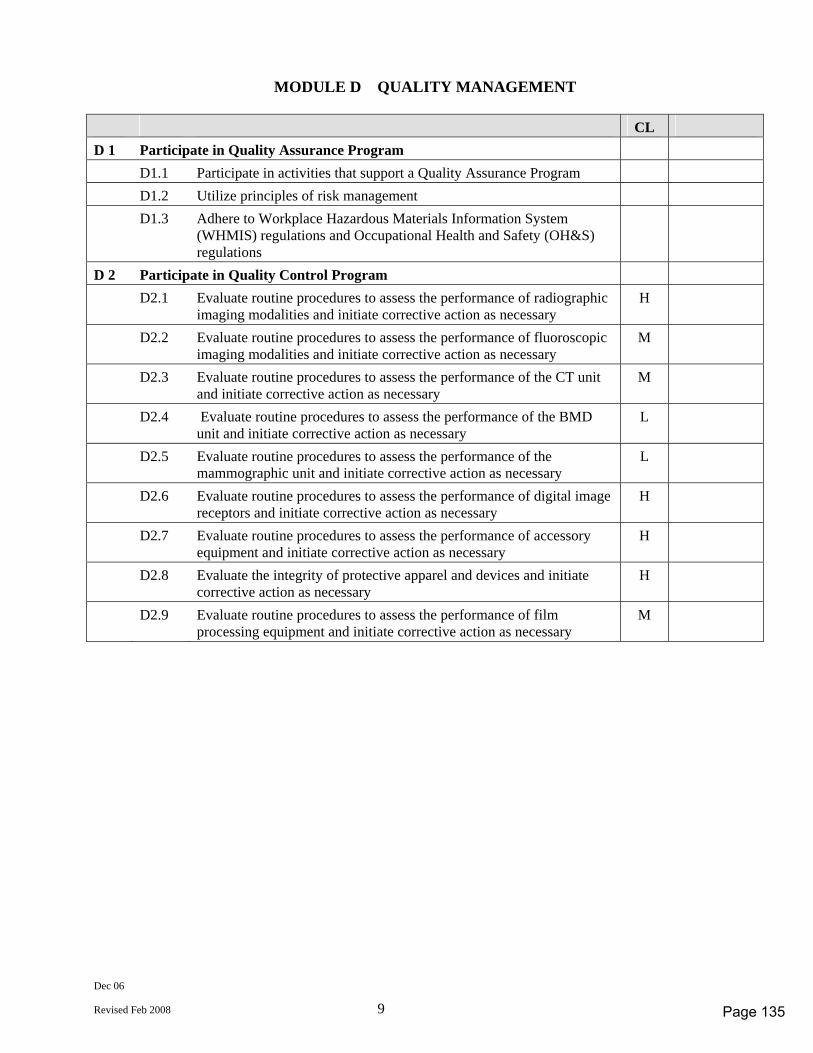
Dec 06
Revised Feb 2008 9
MODULE D QUALITY MANAGEMENT CL D 1 Participate in Quality Assurance Program D1.1 Participate in activities that support a Quality Assurance Program D1.2 Utilize principles of risk management D1.3 Adhere to Workplace Hazardous Materials Information System
(WHMIS) regulations and Occupational Health and Safety (OH&S) regulations
D 2 Participate in Quality Control Program D2.1 Evaluate routine procedures to assess the performance of radiographic
imaging modalities and initiate corrective action as necessary H
D2.2 Evaluate routine procedures to assess the performance of fluoroscopic imaging modalities and initiate corrective action as necessary
M
D2.3 Evaluate routine procedures to assess the performance of the CT unit and initiate corrective action as necessary
M
D2.4 Evaluate routine procedures to assess the performance of the BMD unit and initiate corrective action as necessary
L
D2.5 Evaluate routine procedures to assess the performance of the mammographic unit and initiate corrective action as necessary
L
D2.6 Evaluate routine procedures to assess the performance of digital image receptors and initiate corrective action as necessary
H
D2.7 Evaluate routine procedures to assess the performance of accessory equipment and initiate corrective action as necessary
H
D2.8 Evaluate the integrity of protective apparel and devices and initiate corrective action as necessary
H
D2.9 Evaluate routine procedures to assess the performance of film processing equipment and initiate corrective action as necessary
M
Page 135
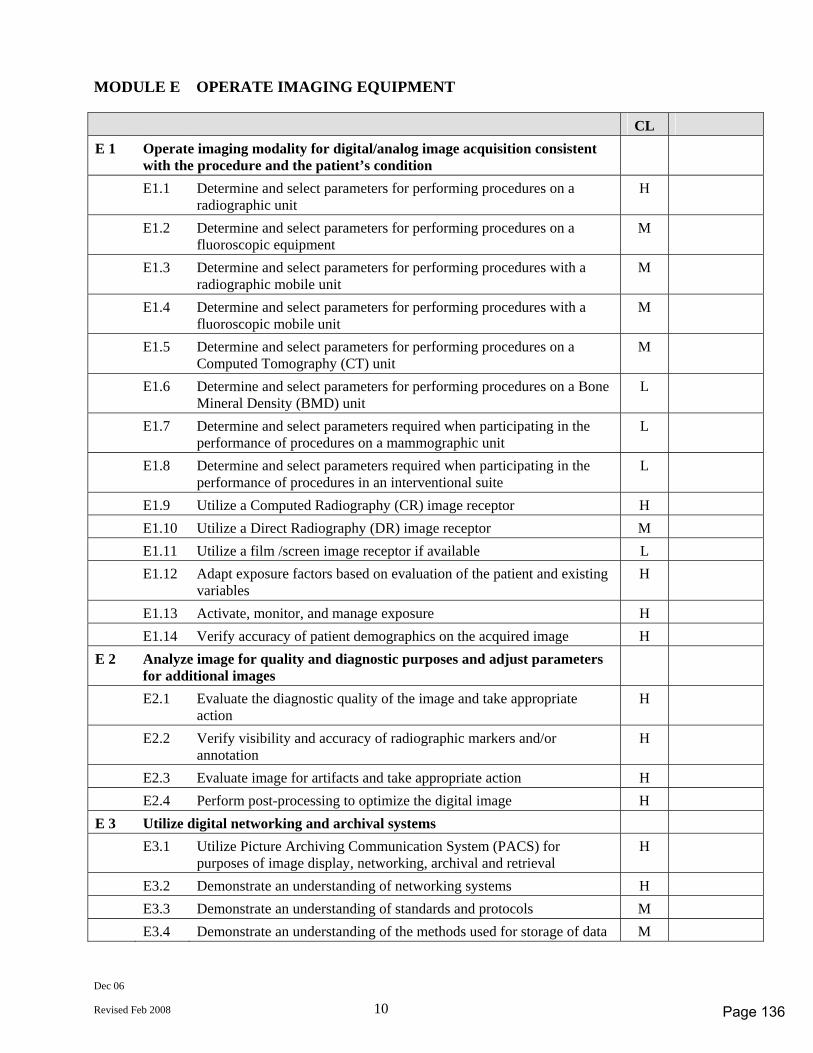
Dec 06
Revised Feb 2008 10
MODULE E OPERATE IMAGING EQUIPMENT CL E 1 Operate imaging modality for digital/analog image acquisition consistent
with the procedure and the patient’s condition
E1.1 Determine and select parameters for performing procedures on a radiographic unit
H
E1.2 Determine and select parameters for performing procedures on a fluoroscopic equipment
M
E1.3 Determine and select parameters for performing procedures with a radiographic mobile unit
M
E1.4 Determine and select parameters for performing procedures with a fluoroscopic mobile unit
M
E1.5 Determine and select parameters for performing procedures on a Computed Tomography (CT) unit
M
E1.6 Determine and select parameters for performing procedures on a Bone Mineral Density (BMD) unit
L
E1.7 Determine and select parameters required when participating in the performance of procedures on a mammographic unit
L
E1.8 Determine and select parameters required when participating in the performance of procedures in an interventional suite
L
E1.9 Utilize a Computed Radiography (CR) image receptor H E1.10 Utilize a Direct Radiography (DR) image receptor M E1.11 Utilize a film /screen image receptor if available L E1.12 Adapt exposure factors based on evaluation of the patient and existing
variables H
E1.13 Activate, monitor, and manage exposure H E1.14 Verify accuracy of patient demographics on the acquired image H E 2 Analyze image for quality and diagnostic purposes and adjust parameters
for additional images
E2.1 Evaluate the diagnostic quality of the image and take appropriate action
H
E2.2 Verify visibility and accuracy of radiographic markers and/or annotation
H
E2.3 Evaluate image for artifacts and take appropriate action H E2.4 Perform post-processing to optimize the digital image H E 3 Utilize digital networking and archival systems E3.1 Utilize Picture Archiving Communication System (PACS) for
purposes of image display, networking, archival and retrieval H
E3.2 Demonstrate an understanding of networking systems H E3.3 Demonstrate an understanding of standards and protocols M E3.4 Demonstrate an understanding of the methods used for storage of data M
Page 136
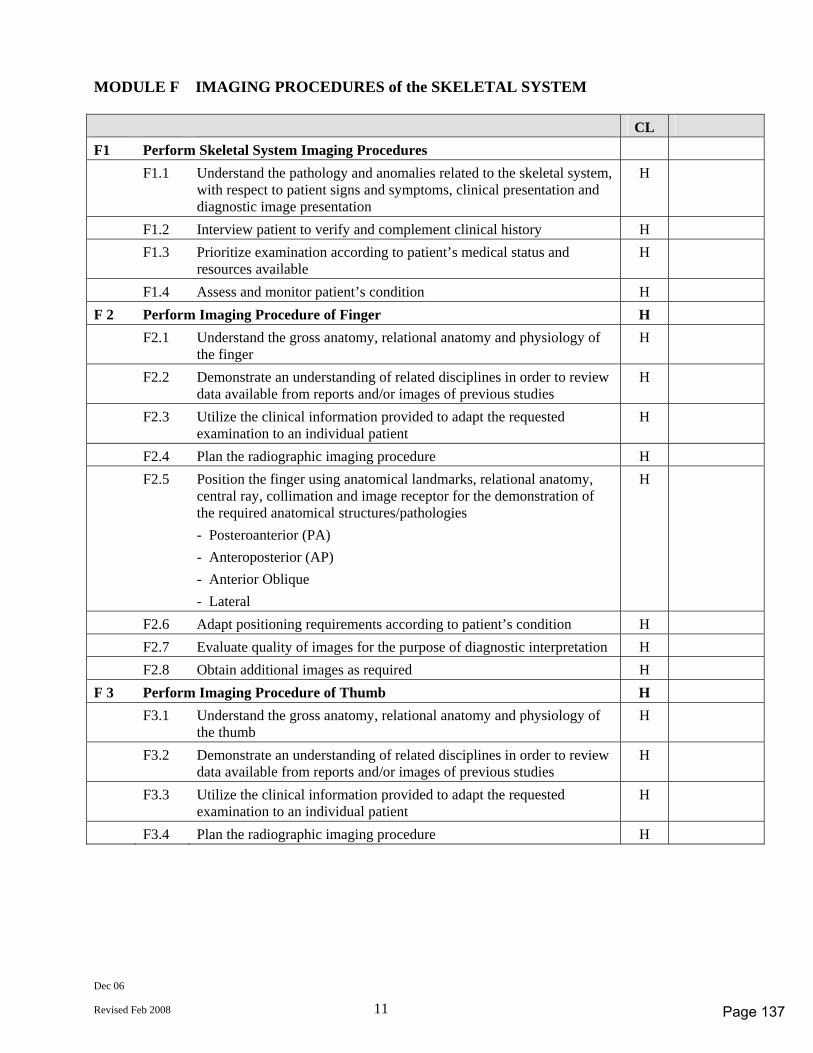
Dec 06
Revised Feb 2008 11
MODULE F IMAGING PROCEDURES of the SKELETAL SYSTEM CL F1 Perform Skeletal System Imaging Procedures F1.1 Understand the pathology and anomalies related to the skeletal system,
with respect to patient signs and symptoms, clinical presentation and diagnostic image presentation
H
F1.2 Interview patient to verify and complement clinical history H F1.3 Prioritize examination according to patient’s medical status and
resources available H
F1.4 Assess and monitor patient’s condition H F 2 Perform Imaging Procedure of Finger H F2.1 Understand the gross anatomy, relational anatomy and physiology of
the finger H
F2.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F2.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F2.4 Plan the radiographic imaging procedure H F2.5 Position the finger using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) - Anteroposterior (AP) - Anterior Oblique - Lateral
H
F2.6 Adapt positioning requirements according to patient’s condition H F2.7 Evaluate quality of images for the purpose of diagnostic interpretation H F2.8 Obtain additional images as required H F 3 Perform Imaging Procedure of Thumb H F3.1 Understand the gross anatomy, relational anatomy and physiology of
the thumb H
F3.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F3.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F3.4 Plan the radiographic imaging procedure H
Page 137
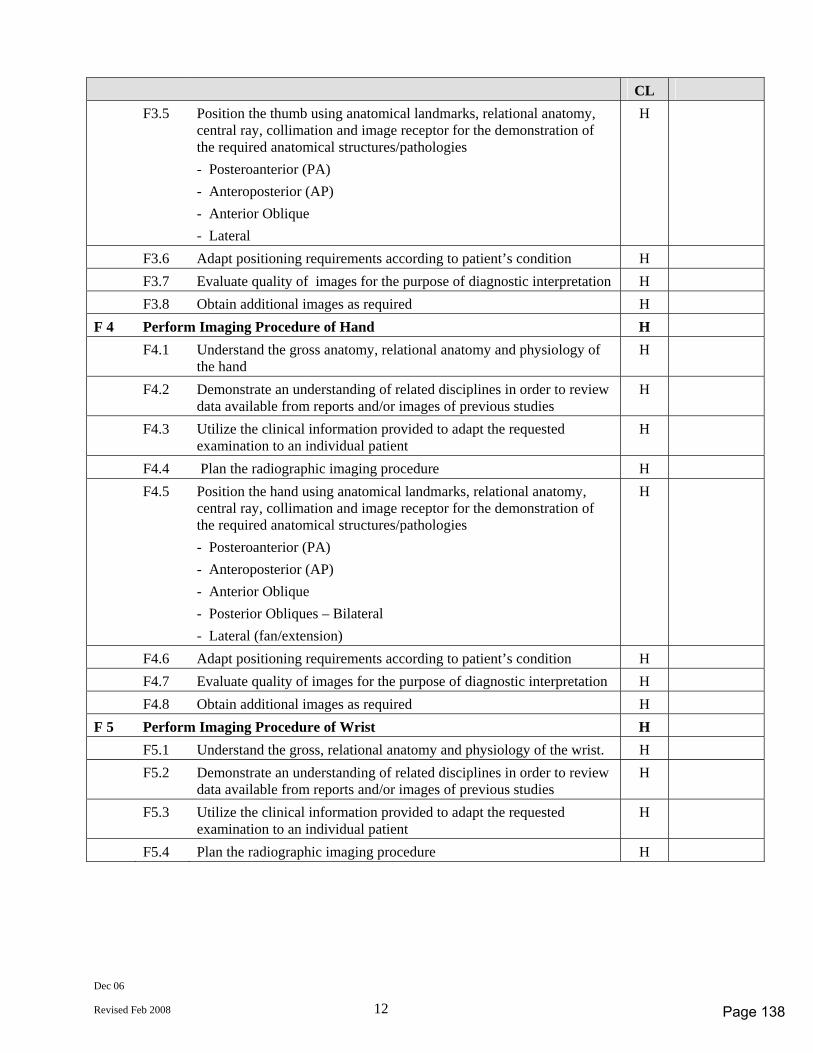
Dec 06
Revised Feb 2008 12
CL F3.5 Position the thumb using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) - Anteroposterior (AP) - Anterior Oblique - Lateral
H
F3.6 Adapt positioning requirements according to patient’s condition H F3.7 Evaluate quality of images for the purpose of diagnostic interpretation H F3.8 Obtain additional images as required H F 4 Perform Imaging Procedure of Hand H F4.1 Understand the gross anatomy, relational anatomy and physiology of
the hand H
F4.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F4.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F4.4 Plan the radiographic imaging procedure H F4.5 Position the hand using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) - Anteroposterior (AP) - Anterior Oblique - Posterior Obliques – Bilateral - Lateral (fan/extension)
H
F4.6 Adapt positioning requirements according to patient’s condition H F4.7 Evaluate quality of images for the purpose of diagnostic interpretation H F4.8 Obtain additional images as required H F 5 Perform Imaging Procedure of Wrist H F5.1 Understand the gross, relational anatomy and physiology of the wrist. H F5.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous studies H
F5.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F5.4 Plan the radiographic imaging procedure H
Page 138
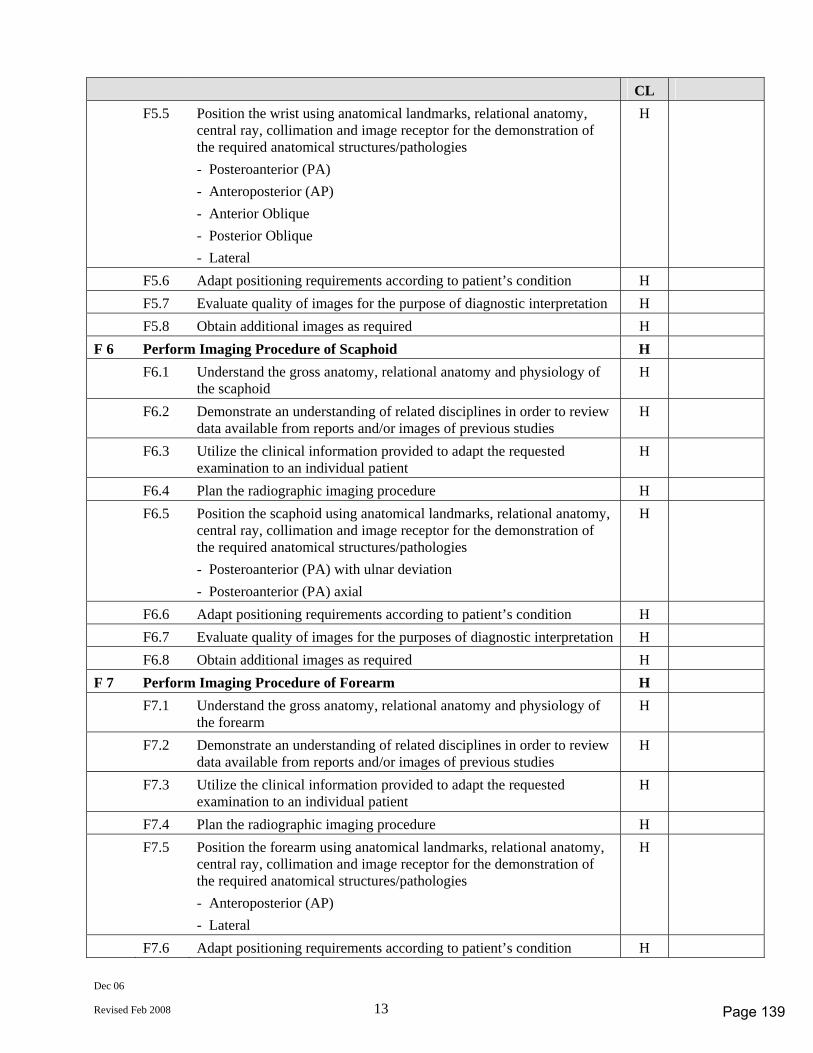
Dec 06
Revised Feb 2008 13
CL F5.5 Position the wrist using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) - Anteroposterior (AP) - Anterior Oblique - Posterior Oblique - Lateral
H
F5.6 Adapt positioning requirements according to patient’s condition H F5.7 Evaluate quality of images for the purpose of diagnostic interpretation H F5.8 Obtain additional images as required H F 6 Perform Imaging Procedure of Scaphoid H F6.1 Understand the gross anatomy, relational anatomy and physiology of
the scaphoid H
F6.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F6.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F6.4 Plan the radiographic imaging procedure H F6.5 Position the scaphoid using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) with ulnar deviation - Posteroanterior (PA) axial
H
F6.6 Adapt positioning requirements according to patient’s condition H F6.7 Evaluate quality of images for the purposes of diagnostic interpretation H F6.8 Obtain additional images as required H F 7 Perform Imaging Procedure of Forearm H F7.1 Understand the gross anatomy, relational anatomy and physiology of
the forearm H
F7.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F7.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F7.4 Plan the radiographic imaging procedure H F7.5 Position the forearm using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral
H
F7.6 Adapt positioning requirements according to patient’s condition H
Page 139
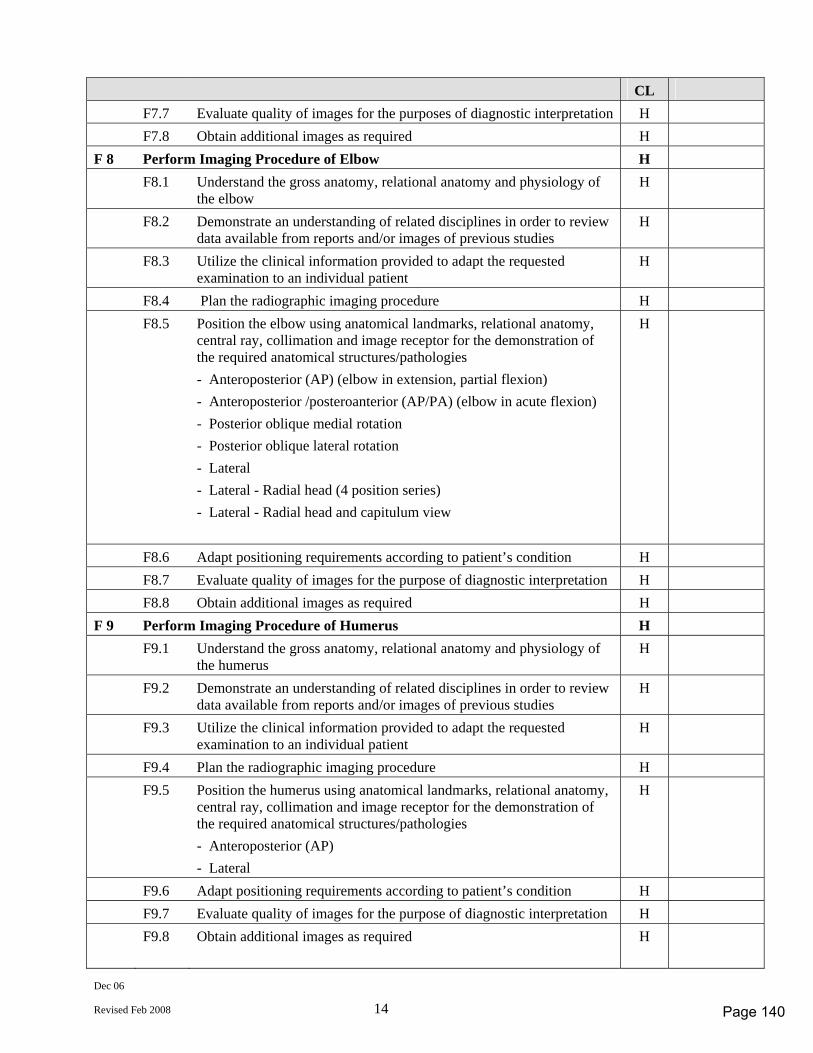
Dec 06
Revised Feb 2008 14
CL F7.7 Evaluate quality of images for the purposes of diagnostic interpretation H F7.8 Obtain additional images as required H F 8 Perform Imaging Procedure of Elbow H F8.1 Understand the gross anatomy, relational anatomy and physiology of
the elbow H
F8.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F8.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F8.4 Plan the radiographic imaging procedure H F8.5 Position the elbow using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) (elbow in extension, partial flexion) - Anteroposterior /posteroanterior (AP/PA) (elbow in acute flexion) - Posterior oblique medial rotation - Posterior oblique lateral rotation - Lateral - Lateral - Radial head (4 position series) - Lateral - Radial head and capitulum view
H
F8.6 Adapt positioning requirements according to patient’s condition H F8.7 Evaluate quality of images for the purpose of diagnostic interpretation H F8.8 Obtain additional images as required H F 9 Perform Imaging Procedure of Humerus H F9.1 Understand the gross anatomy, relational anatomy and physiology of
the humerus H
F9.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F9.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F9.4 Plan the radiographic imaging procedure H F9.5 Position the humerus using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral
H
F9.6 Adapt positioning requirements according to patient’s condition H F9.7 Evaluate quality of images for the purpose of diagnostic interpretation H F9.8 Obtain additional images as required H
Page 140
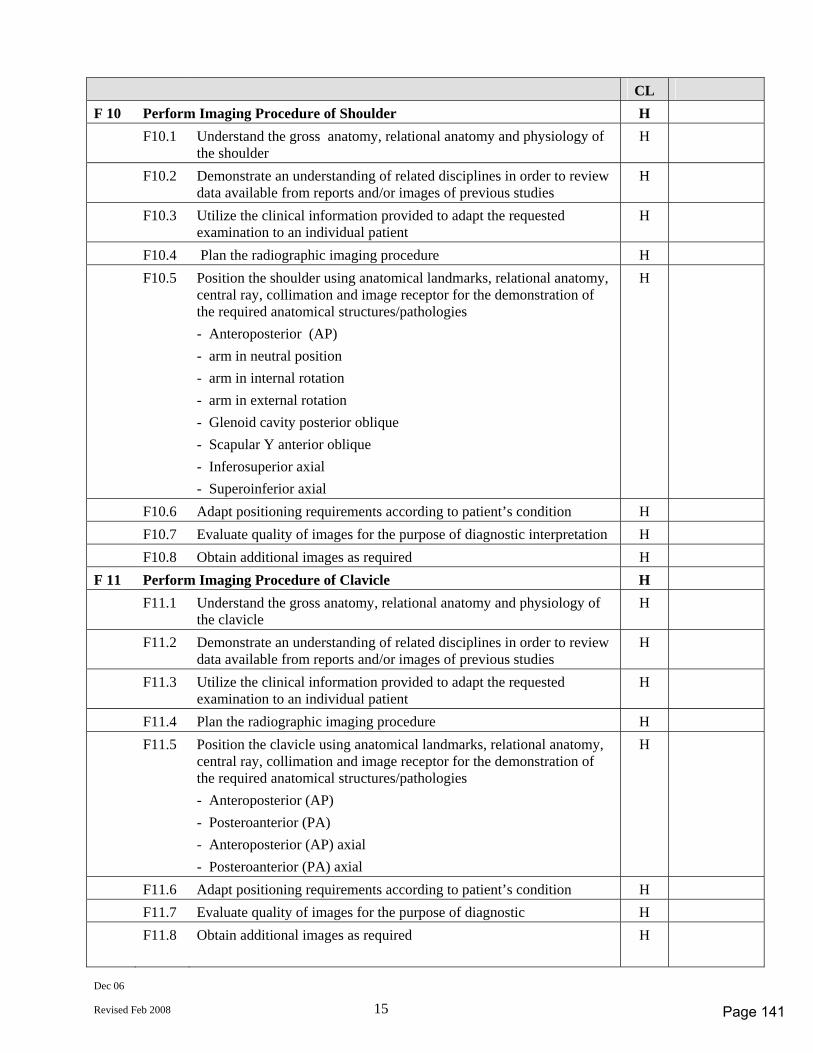
Dec 06
Revised Feb 2008 15
CL F 10 Perform Imaging Procedure of Shoulder H F10.1 Understand the gross anatomy, relational anatomy and physiology of
the shoulder H
F10.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F10.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F10.4 Plan the radiographic imaging procedure H F10.5 Position the shoulder using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - arm in neutral position - arm in internal rotation - arm in external rotation - Glenoid cavity posterior oblique - Scapular Y anterior oblique - Inferosuperior axial - Superoinferior axial
H
F10.6 Adapt positioning requirements according to patient’s condition H F10.7 Evaluate quality of images for the purpose of diagnostic interpretation H F10.8 Obtain additional images as required H F 11 Perform Imaging Procedure of Clavicle H F11.1 Understand the gross anatomy, relational anatomy and physiology of
the clavicle H
F11.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F11.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F11.4 Plan the radiographic imaging procedure H F11.5 Position the clavicle using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posteroanterior (PA) - Anteroposterior (AP) axial - Posteroanterior (PA) axial
H
F11.6 Adapt positioning requirements according to patient’s condition H F11.7 Evaluate quality of images for the purpose of diagnostic H F11.8 Obtain additional images as required H
Page 141
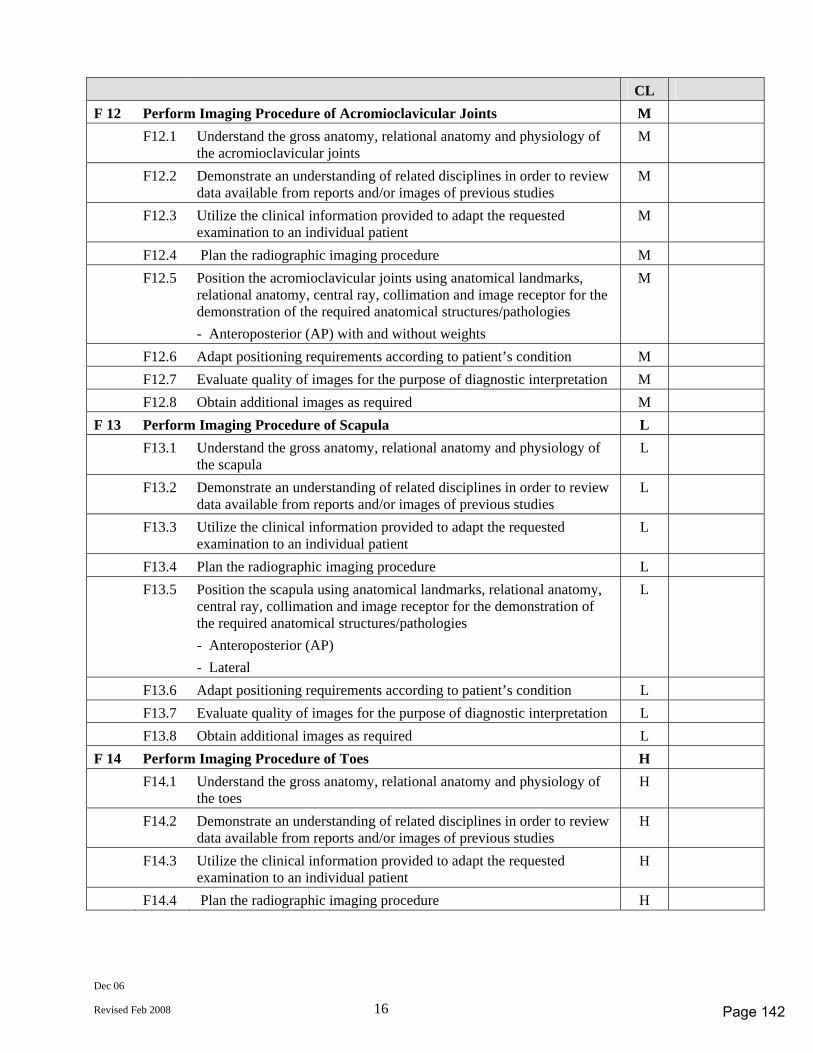
Dec 06
Revised Feb 2008 16
CL F 12 Perform Imaging Procedure of Acromioclavicular Joints M F12.1 Understand the gross anatomy, relational anatomy and physiology of
the acromioclavicular joints M
F12.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F12.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F12.4 Plan the radiographic imaging procedure M F12.5 Position the acromioclavicular joints using anatomical landmarks,
relational anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) with and without weights
M
F12.6 Adapt positioning requirements according to patient’s condition M F12.7 Evaluate quality of images for the purpose of diagnostic interpretation M F12.8 Obtain additional images as required M F 13 Perform Imaging Procedure of Scapula L F13.1 Understand the gross anatomy, relational anatomy and physiology of
the scapula L
F13.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
F13.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F13.4 Plan the radiographic imaging procedure L F13.5 Position the scapula using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral
L
F13.6 Adapt positioning requirements according to patient’s condition L F13.7 Evaluate quality of images for the purpose of diagnostic interpretation L F13.8 Obtain additional images as required L F 14 Perform Imaging Procedure of Toes H F14.1 Understand the gross anatomy, relational anatomy and physiology of
the toes H
F14.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F14.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F14.4 Plan the radiographic imaging procedure H
Page 142
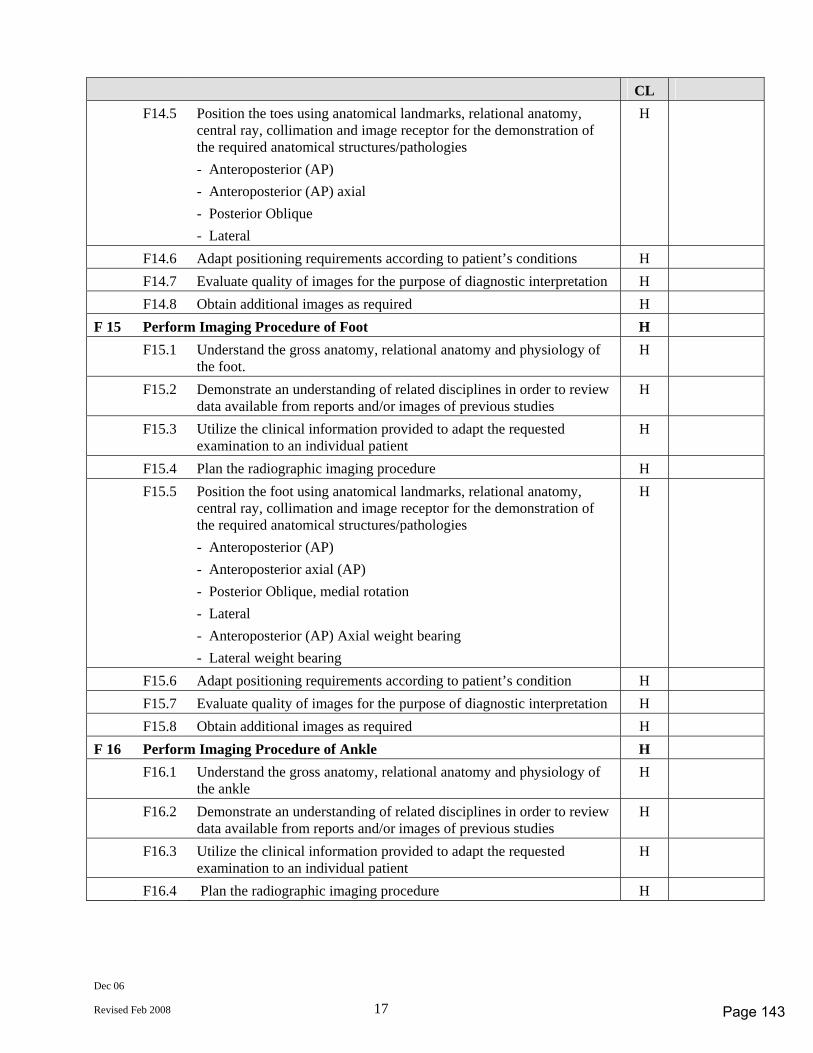
Dec 06
Revised Feb 2008 17
CL F14.5 Position the toes using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Anteroposterior (AP) axial - Posterior Oblique - Lateral
H
F14.6 Adapt positioning requirements according to patient’s conditions H F14.7 Evaluate quality of images for the purpose of diagnostic interpretation H F14.8 Obtain additional images as required H F 15 Perform Imaging Procedure of Foot H F15.1 Understand the gross anatomy, relational anatomy and physiology of
the foot. H
F15.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F15.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F15.4 Plan the radiographic imaging procedure H F15.5 Position the foot using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Anteroposterior axial (AP) - Posterior Oblique, medial rotation - Lateral - Anteroposterior (AP) Axial weight bearing - Lateral weight bearing
H
F15.6 Adapt positioning requirements according to patient’s condition H F15.7 Evaluate quality of images for the purpose of diagnostic interpretation H F15.8 Obtain additional images as required H F 16 Perform Imaging Procedure of Ankle H F16.1 Understand the gross anatomy, relational anatomy and physiology of
the ankle H
F16.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F16.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F16.4 Plan the radiographic imaging procedure H
Page 143
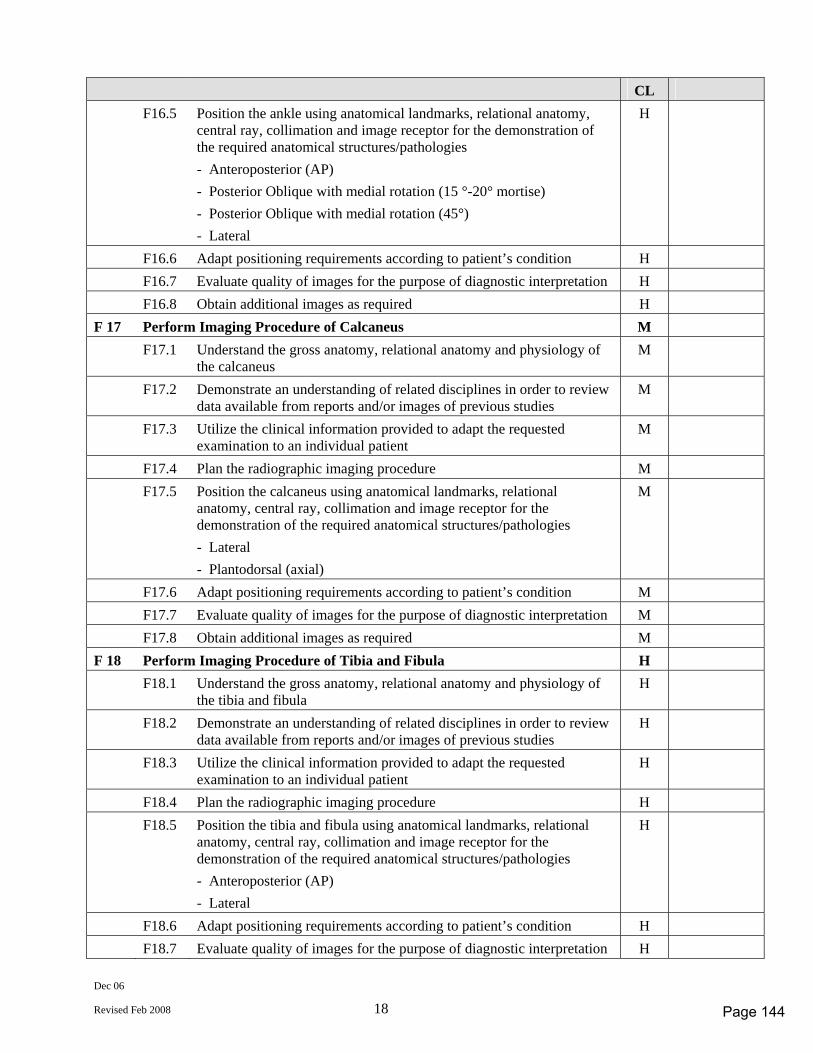
Dec 06
Revised Feb 2008 18
CL F16.5 Position the ankle using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posterior Oblique with medial rotation (15 °-20° mortise) - Posterior Oblique with medial rotation (45°) - Lateral
H
F16.6 Adapt positioning requirements according to patient’s condition H F16.7 Evaluate quality of images for the purpose of diagnostic interpretation H F16.8 Obtain additional images as required H F 17 Perform Imaging Procedure of Calcaneus M F17.1 Understand the gross anatomy, relational anatomy and physiology of
the calcaneus M
F17.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F17.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F17.4 Plan the radiographic imaging procedure M F17.5 Position the calcaneus using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Lateral - Plantodorsal (axial)
M
F17.6 Adapt positioning requirements according to patient’s condition M F17.7 Evaluate quality of images for the purpose of diagnostic interpretation M F17.8 Obtain additional images as required M F 18 Perform Imaging Procedure of Tibia and Fibula H F18.1 Understand the gross anatomy, relational anatomy and physiology of
the tibia and fibula H
F18.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F18.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F18.4 Plan the radiographic imaging procedure H F18.5 Position the tibia and fibula using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral
H
F18.6 Adapt positioning requirements according to patient’s condition H F18.7 Evaluate quality of images for the purpose of diagnostic interpretation H
Page 144
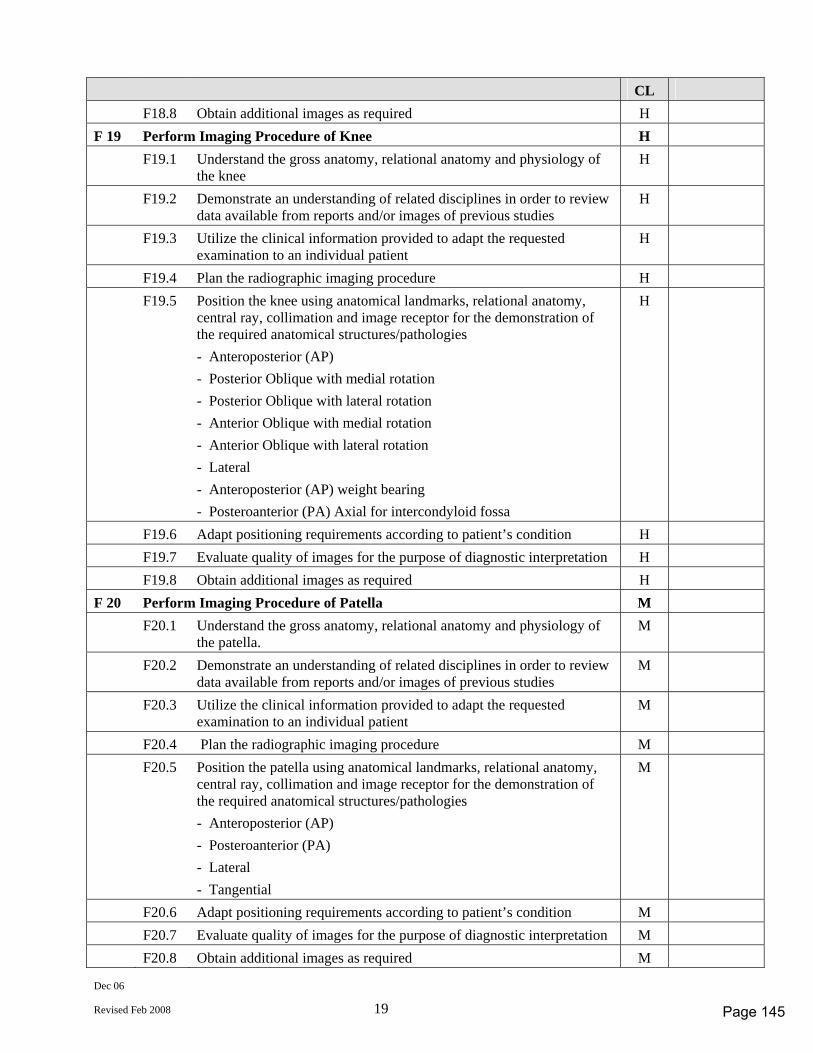
Dec 06
Revised Feb 2008 19
CL F18.8 Obtain additional images as required H F 19 Perform Imaging Procedure of Knee H F19.1 Understand the gross anatomy, relational anatomy and physiology of
the knee H
F19.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F19.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F19.4 Plan the radiographic imaging procedure H F19.5 Position the knee using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posterior Oblique with medial rotation - Posterior Oblique with lateral rotation - Anterior Oblique with medial rotation - Anterior Oblique with lateral rotation - Lateral - Anteroposterior (AP) weight bearing - Posteroanterior (PA) Axial for intercondyloid fossa
H
F19.6 Adapt positioning requirements according to patient’s condition H F19.7 Evaluate quality of images for the purpose of diagnostic interpretation H F19.8 Obtain additional images as required H F 20 Perform Imaging Procedure of Patella M F20.1 Understand the gross anatomy, relational anatomy and physiology of
the patella. M
F20.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F20.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F20.4 Plan the radiographic imaging procedure M F20.5 Position the patella using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posteroanterior (PA) - Lateral - Tangential
M
F20.6 Adapt positioning requirements according to patient’s condition M F20.7 Evaluate quality of images for the purpose of diagnostic interpretation M F20.8 Obtain additional images as required M
Page 145
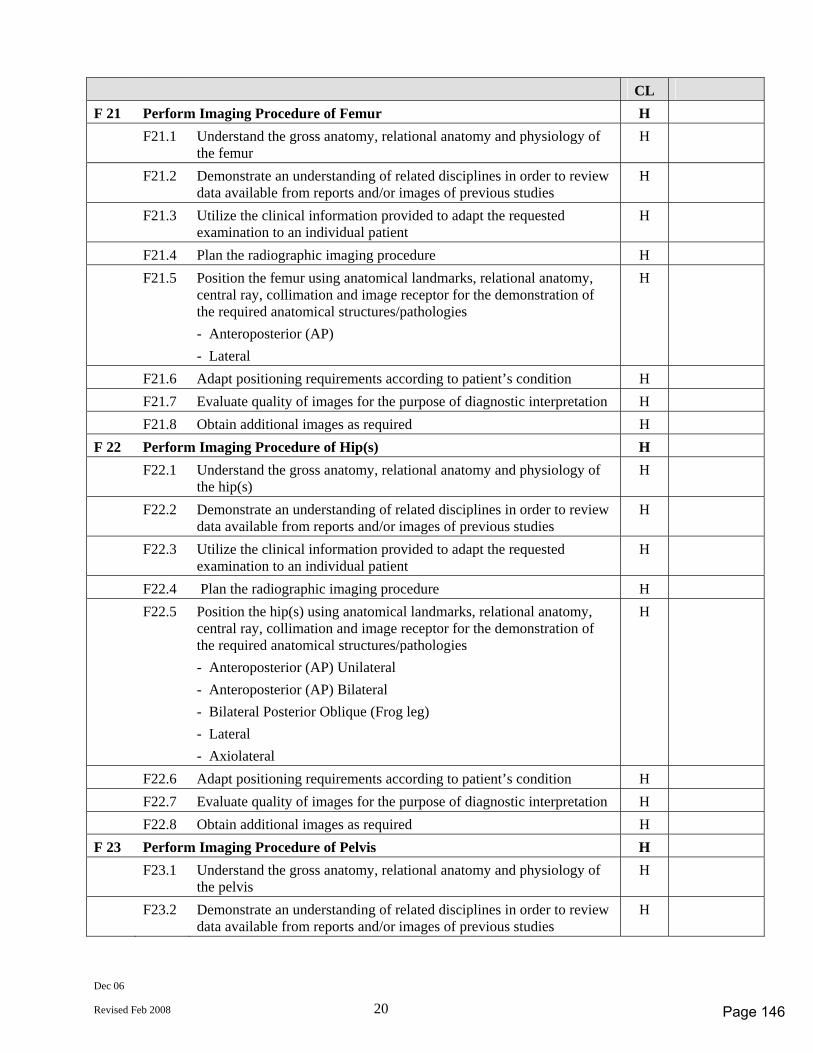
Dec 06
Revised Feb 2008 20
CL F 21 Perform Imaging Procedure of Femur H F21.1 Understand the gross anatomy, relational anatomy and physiology of
the femur H
F21.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F21.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F21.4 Plan the radiographic imaging procedure H F21.5 Position the femur using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral
H
F21.6 Adapt positioning requirements according to patient’s condition H F21.7 Evaluate quality of images for the purpose of diagnostic interpretation H F21.8 Obtain additional images as required H F 22 Perform Imaging Procedure of Hip(s) H F22.1 Understand the gross anatomy, relational anatomy and physiology of
the hip(s) H
F22.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F22.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F22.4 Plan the radiographic imaging procedure H F22.5 Position the hip(s) using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) Unilateral - Anteroposterior (AP) Bilateral - Bilateral Posterior Oblique (Frog leg) - Lateral - Axiolateral
H
F22.6 Adapt positioning requirements according to patient’s condition H F22.7 Evaluate quality of images for the purpose of diagnostic interpretation H F22.8 Obtain additional images as required H F 23 Perform Imaging Procedure of Pelvis H F23.1 Understand the gross anatomy, relational anatomy and physiology of
the pelvis H
F23.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
Page 146
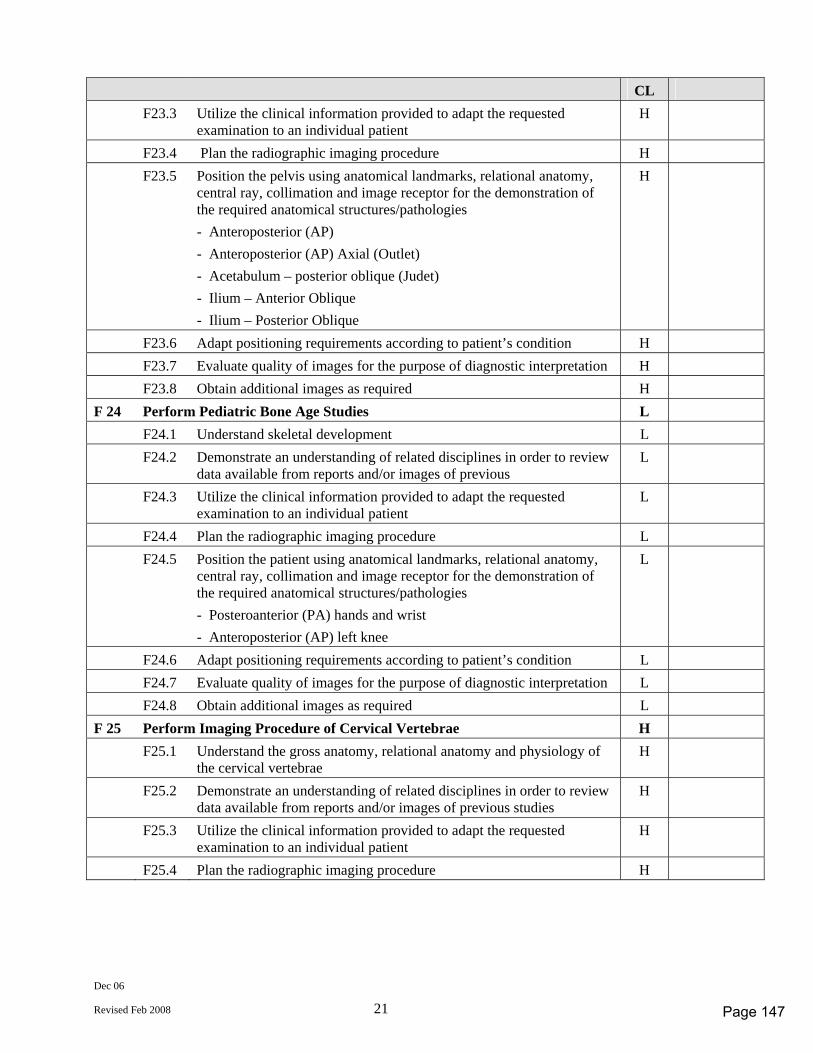
Dec 06
Revised Feb 2008 21
CL F23.3 Utilize the clinical information provided to adapt the requested
examination to an individual patient H
F23.4 Plan the radiographic imaging procedure H F23.5 Position the pelvis using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Anteroposterior (AP) Axial (Outlet) - Acetabulum – posterior oblique (Judet) - Ilium – Anterior Oblique - Ilium – Posterior Oblique
H
F23.6 Adapt positioning requirements according to patient’s condition H F23.7 Evaluate quality of images for the purpose of diagnostic interpretation H F23.8 Obtain additional images as required H F 24 Perform Pediatric Bone Age Studies L F24.1 Understand skeletal development L F24.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous L
F24.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F24.4 Plan the radiographic imaging procedure L F24.5 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) hands and wrist - Anteroposterior (AP) left knee
L
F24.6 Adapt positioning requirements according to patient’s condition L F24.7 Evaluate quality of images for the purpose of diagnostic interpretation L F24.8 Obtain additional images as required L F 25 Perform Imaging Procedure of Cervical Vertebrae H F25.1 Understand the gross anatomy, relational anatomy and physiology of
the cervical vertebrae H
F25.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F25.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F25.4 Plan the radiographic imaging procedure H
Page 147
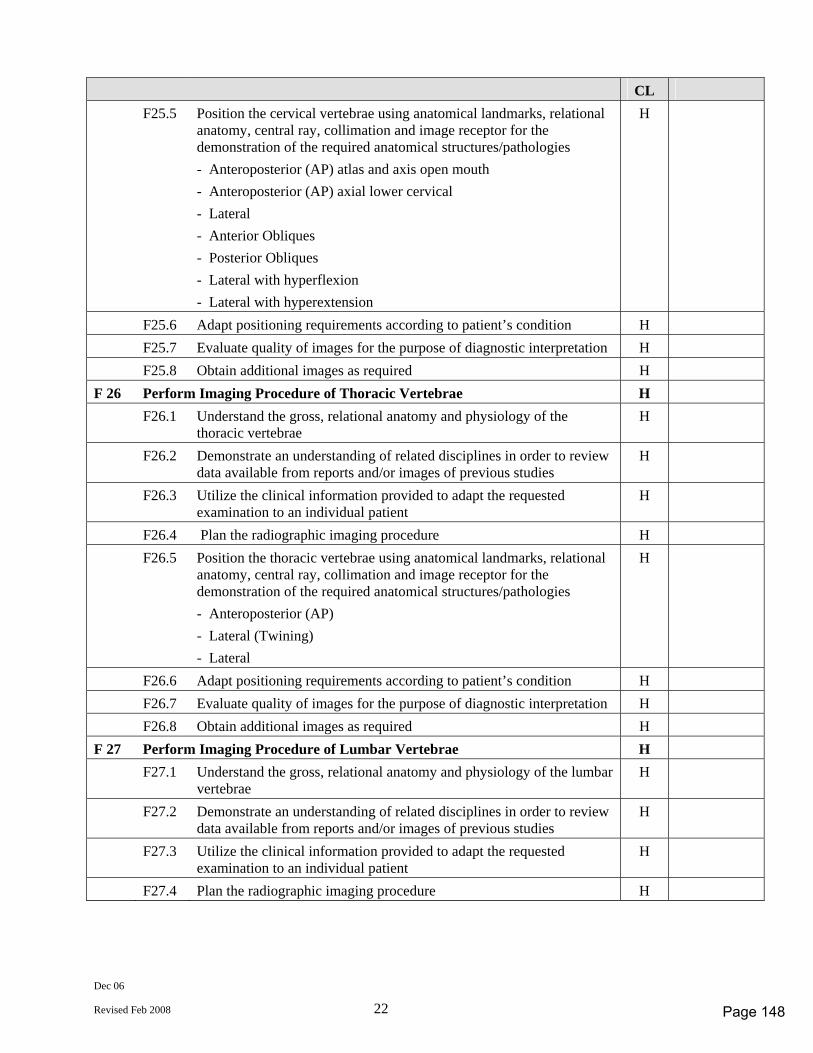
Dec 06
Revised Feb 2008 22
CL F25.5 Position the cervical vertebrae using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) atlas and axis open mouth - Anteroposterior (AP) axial lower cervical - Lateral - Anterior Obliques - Posterior Obliques - Lateral with hyperflexion - Lateral with hyperextension
H
F25.6 Adapt positioning requirements according to patient’s condition H F25.7 Evaluate quality of images for the purpose of diagnostic interpretation H F25.8 Obtain additional images as required H F 26 Perform Imaging Procedure of Thoracic Vertebrae H F26.1 Understand the gross, relational anatomy and physiology of the
thoracic vertebrae H
F26.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F26.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F26.4 Plan the radiographic imaging procedure H F26.5 Position the thoracic vertebrae using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral (Twining) - Lateral
H
F26.6 Adapt positioning requirements according to patient’s condition H F26.7 Evaluate quality of images for the purpose of diagnostic interpretation H F26.8 Obtain additional images as required H F 27 Perform Imaging Procedure of Lumbar Vertebrae H F27.1 Understand the gross, relational anatomy and physiology of the lumbar
vertebrae H
F27.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F27.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F27.4 Plan the radiographic imaging procedure H
Page 148
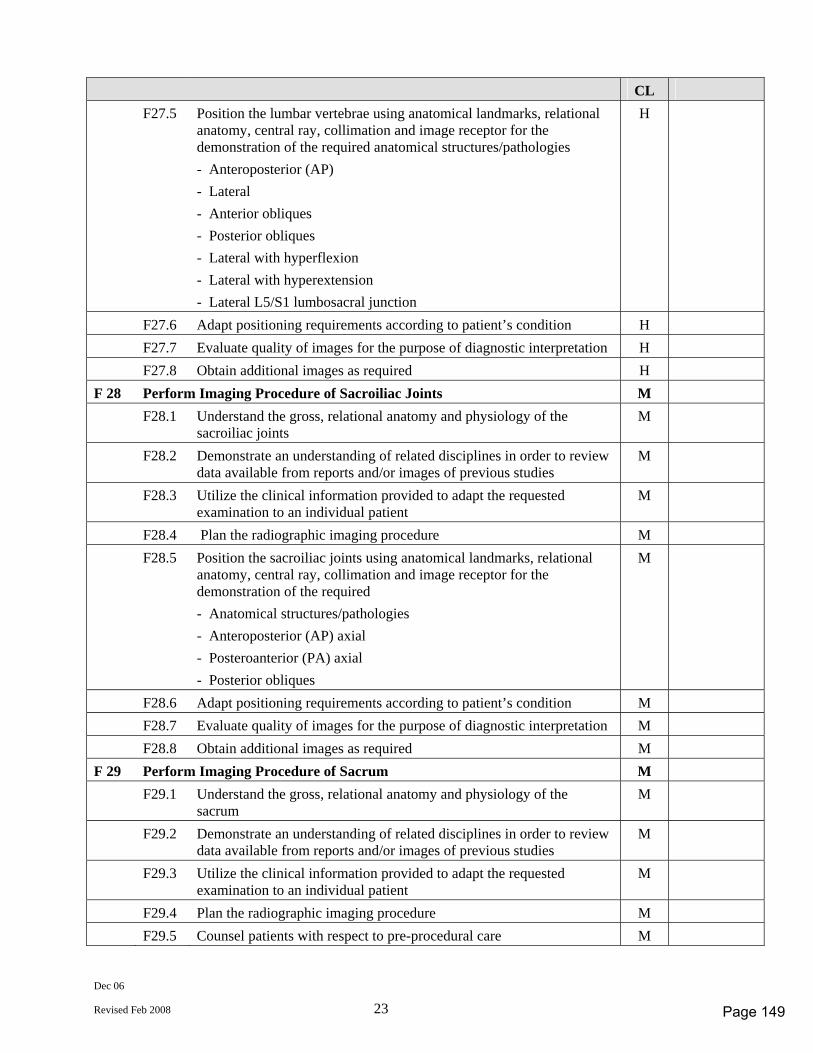
Dec 06
Revised Feb 2008 23
CL F27.5 Position the lumbar vertebrae using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral - Anterior obliques - Posterior obliques - Lateral with hyperflexion - Lateral with hyperextension - Lateral L5/S1 lumbosacral junction
H
F27.6 Adapt positioning requirements according to patient’s condition H F27.7 Evaluate quality of images for the purpose of diagnostic interpretation H F27.8 Obtain additional images as required H F 28 Perform Imaging Procedure of Sacroiliac Joints M F28.1 Understand the gross, relational anatomy and physiology of the
sacroiliac joints M
F28.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F28.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F28.4 Plan the radiographic imaging procedure M F28.5 Position the sacroiliac joints using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required - Anatomical structures/pathologies - Anteroposterior (AP) axial - Posteroanterior (PA) axial - Posterior obliques
M
F28.6 Adapt positioning requirements according to patient’s condition M F28.7 Evaluate quality of images for the purpose of diagnostic interpretation M F28.8 Obtain additional images as required M F 29 Perform Imaging Procedure of Sacrum M F29.1 Understand the gross, relational anatomy and physiology of the
sacrum M
F29.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F29.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F29.4 Plan the radiographic imaging procedure M F29.5 Counsel patients with respect to pre-procedural care M
Page 149
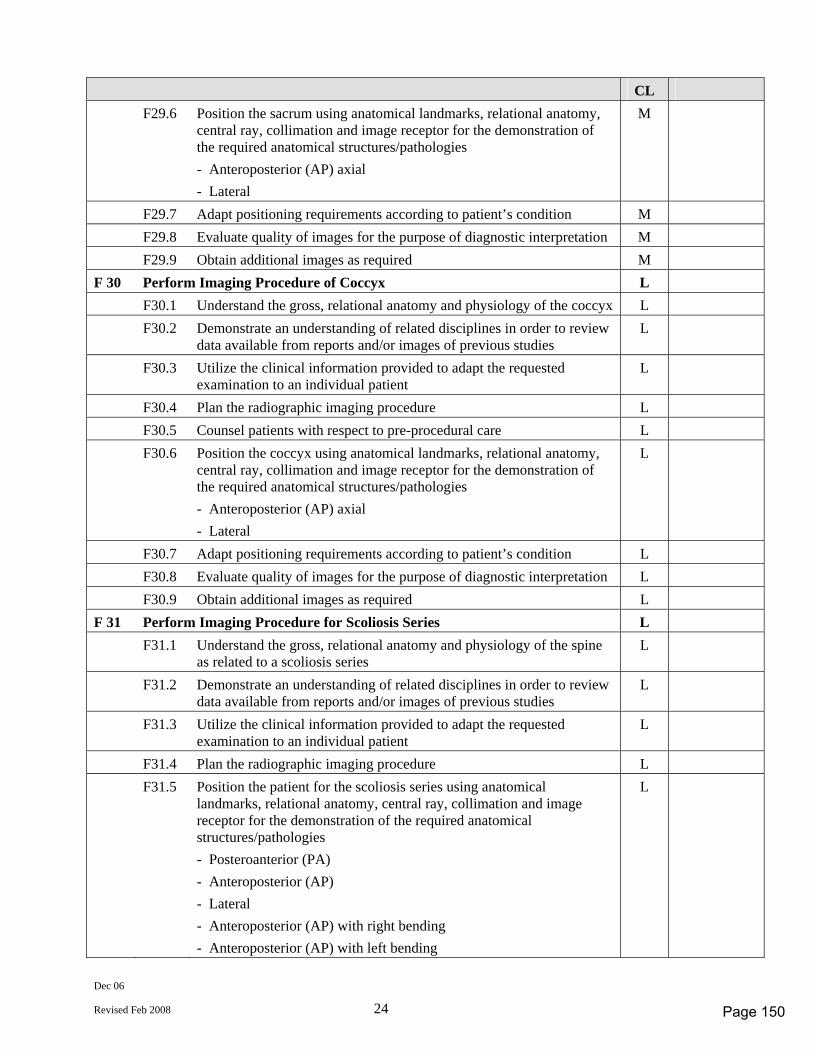
Dec 06
Revised Feb 2008 24
CL F29.6 Position the sacrum using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) axial - Lateral
M
F29.7 Adapt positioning requirements according to patient’s condition M F29.8 Evaluate quality of images for the purpose of diagnostic interpretation M F29.9 Obtain additional images as required M F 30 Perform Imaging Procedure of Coccyx L F30.1 Understand the gross, relational anatomy and physiology of the coccyx L F30.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous studies L
F30.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F30.4 Plan the radiographic imaging procedure L F30.5 Counsel patients with respect to pre-procedural care L F30.6 Position the coccyx using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) axial - Lateral
L
F30.7 Adapt positioning requirements according to patient’s condition L F30.8 Evaluate quality of images for the purpose of diagnostic interpretation L F30.9 Obtain additional images as required L F 31 Perform Imaging Procedure for Scoliosis Series L F31.1 Understand the gross, relational anatomy and physiology of the spine
as related to a scoliosis series L
F31.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
F31.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F31.4 Plan the radiographic imaging procedure L F31.5 Position the patient for the scoliosis series using anatomical
landmarks, relational anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) - Anteroposterior (AP) - Lateral - Anteroposterior (AP) with right bending - Anteroposterior (AP) with left bending
L
Page 150
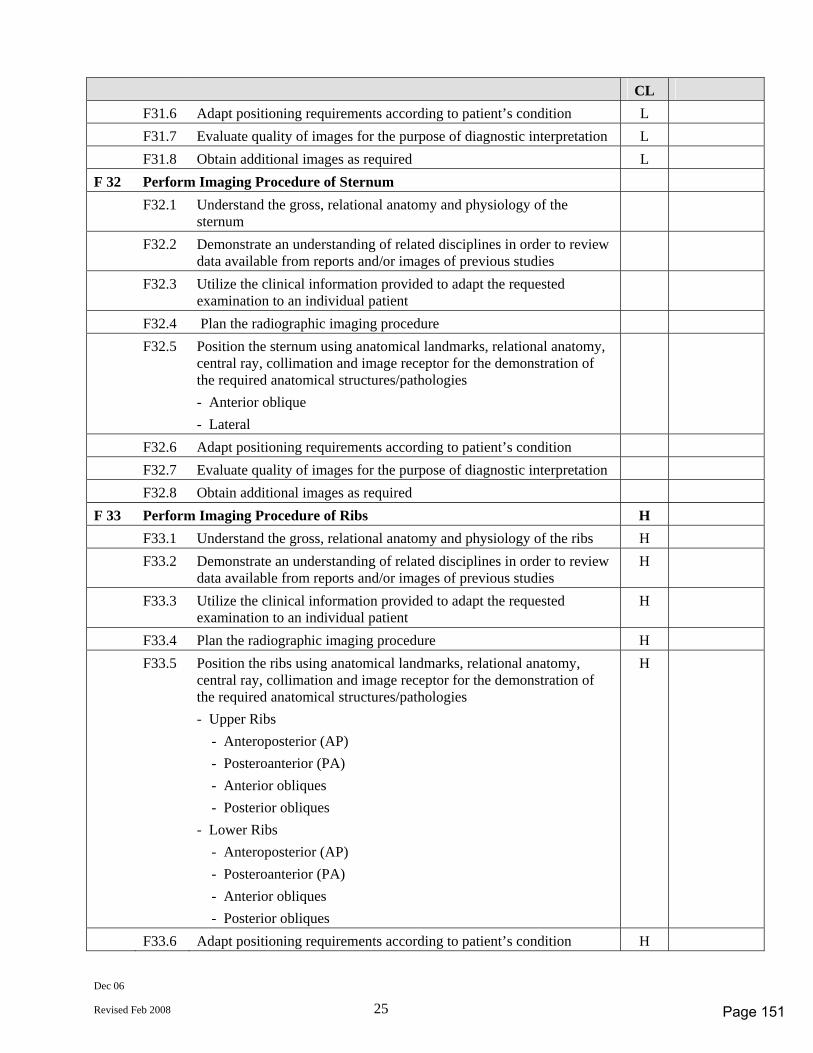
Dec 06
Revised Feb 2008 25
CL F31.6 Adapt positioning requirements according to patient’s condition L F31.7 Evaluate quality of images for the purpose of diagnostic interpretation L F31.8 Obtain additional images as required L F 32 Perform Imaging Procedure of Sternum F32.1 Understand the gross, relational anatomy and physiology of the
sternum
F32.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
F32.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
F32.4 Plan the radiographic imaging procedure F32.5 Position the sternum using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anterior oblique - Lateral
F32.6 Adapt positioning requirements according to patient’s condition F32.7 Evaluate quality of images for the purpose of diagnostic interpretation F32.8 Obtain additional images as required F 33 Perform Imaging Procedure of Ribs H F33.1 Understand the gross, relational anatomy and physiology of the ribs H F33.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous studies H
F33.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F33.4 Plan the radiographic imaging procedure H F33.5 Position the ribs using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Upper Ribs - Anteroposterior (AP) - Posteroanterior (PA) - Anterior obliques - Posterior obliques - Lower Ribs - Anteroposterior (AP) - Posteroanterior (PA) - Anterior obliques - Posterior obliques
H
F33.6 Adapt positioning requirements according to patient’s condition H
Page 151
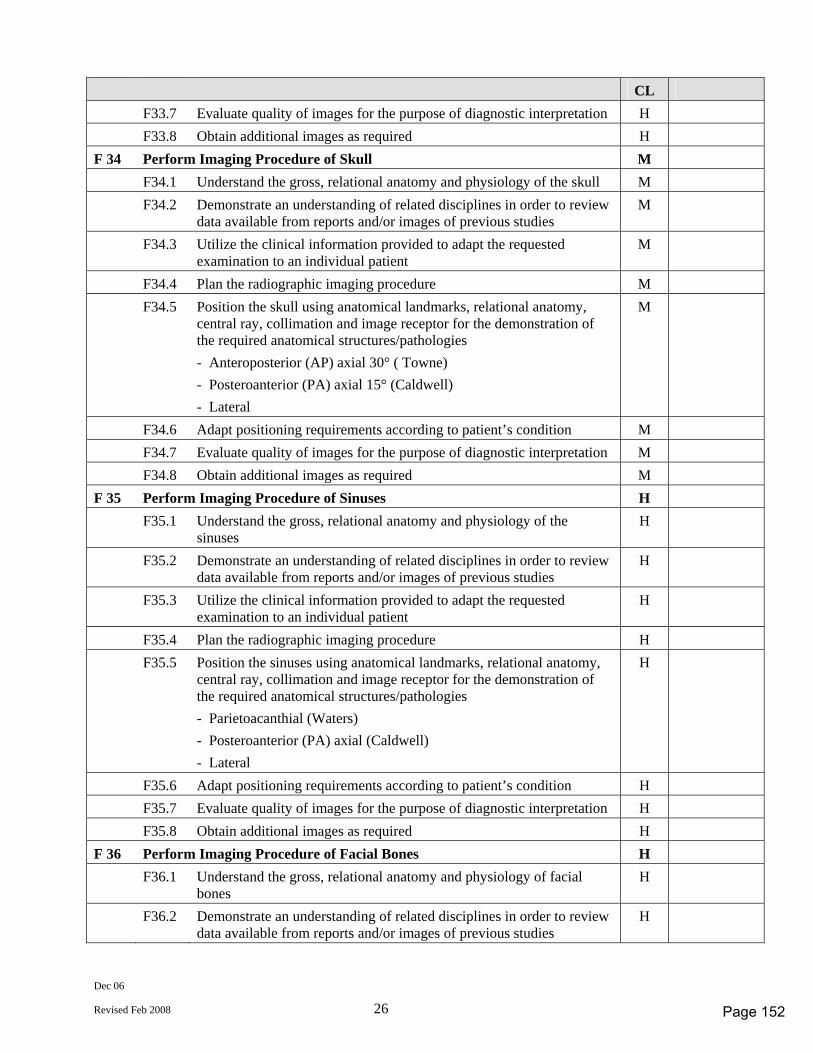
Dec 06
Revised Feb 2008 26
CL F33.7 Evaluate quality of images for the purpose of diagnostic interpretation H F33.8 Obtain additional images as required H F 34 Perform Imaging Procedure of Skull M F34.1 Understand the gross, relational anatomy and physiology of the skull M F34.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous studies M
F34.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F34.4 Plan the radiographic imaging procedure M F34.5 Position the skull using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) axial 30° ( Towne) - Posteroanterior (PA) axial 15° (Caldwell) - Lateral
M
F34.6 Adapt positioning requirements according to patient’s condition M F34.7 Evaluate quality of images for the purpose of diagnostic interpretation M F34.8 Obtain additional images as required M F 35 Perform Imaging Procedure of Sinuses H F35.1 Understand the gross, relational anatomy and physiology of the
sinuses H
F35.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
F35.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
F35.4 Plan the radiographic imaging procedure H F35.5 Position the sinuses using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Parietoacanthial (Waters) - Posteroanterior (PA) axial (Caldwell) - Lateral
H
F35.6 Adapt positioning requirements according to patient’s condition H F35.7 Evaluate quality of images for the purpose of diagnostic interpretation H F35.8 Obtain additional images as required H F 36 Perform Imaging Procedure of Facial Bones H F36.1 Understand the gross, relational anatomy and physiology of facial
bones H
F36.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
Page 152
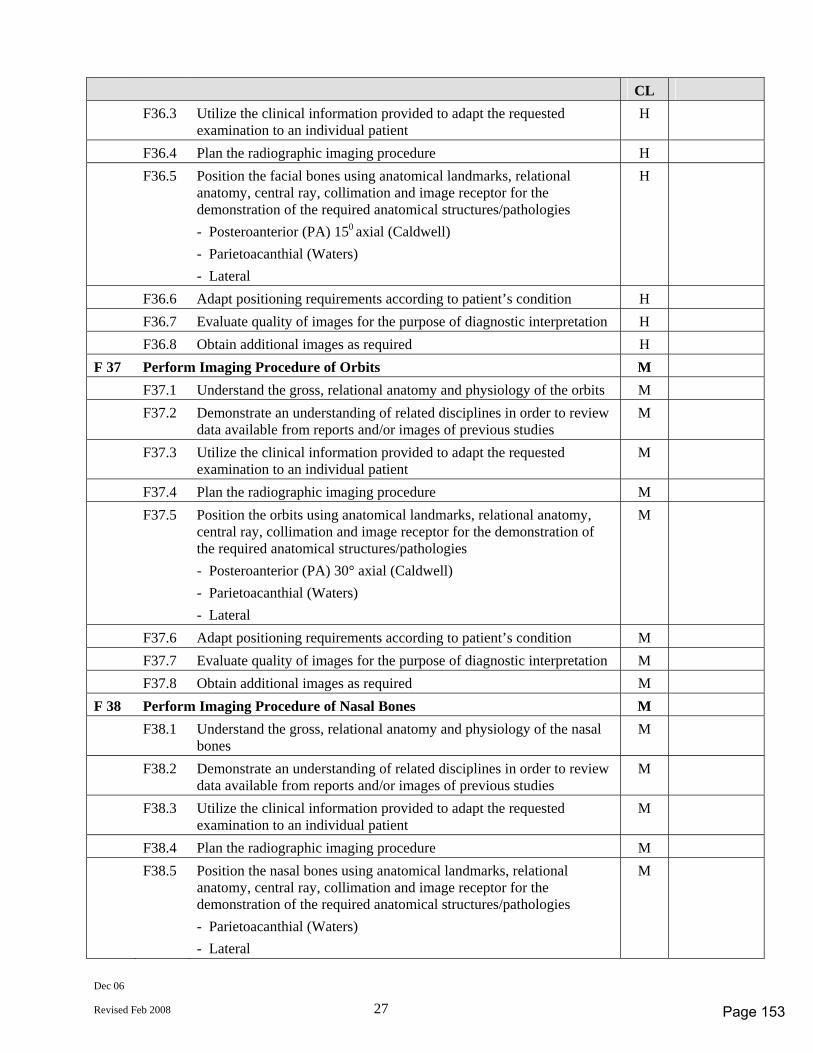
Dec 06
Revised Feb 2008 27
CL F36.3 Utilize the clinical information provided to adapt the requested
examination to an individual patient H
F36.4 Plan the radiographic imaging procedure H F36.5 Position the facial bones using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) 150 axial (Caldwell) - Parietoacanthial (Waters) - Lateral
H
F36.6 Adapt positioning requirements according to patient’s condition H F36.7 Evaluate quality of images for the purpose of diagnostic interpretation H F36.8 Obtain additional images as required H F 37 Perform Imaging Procedure of Orbits M F37.1 Understand the gross, relational anatomy and physiology of the orbits M F37.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous studies M
F37.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F37.4 Plan the radiographic imaging procedure M F37.5 Position the orbits using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Posteroanterior (PA) 30° axial (Caldwell) - Parietoacanthial (Waters) - Lateral
M
F37.6 Adapt positioning requirements according to patient’s condition M F37.7 Evaluate quality of images for the purpose of diagnostic interpretation M F37.8 Obtain additional images as required M F 38 Perform Imaging Procedure of Nasal Bones M F38.1 Understand the gross, relational anatomy and physiology of the nasal
bones M
F38.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F38.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F38.4 Plan the radiographic imaging procedure M F38.5 Position the nasal bones using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Parietoacanthial (Waters) - Lateral
M
Page 153
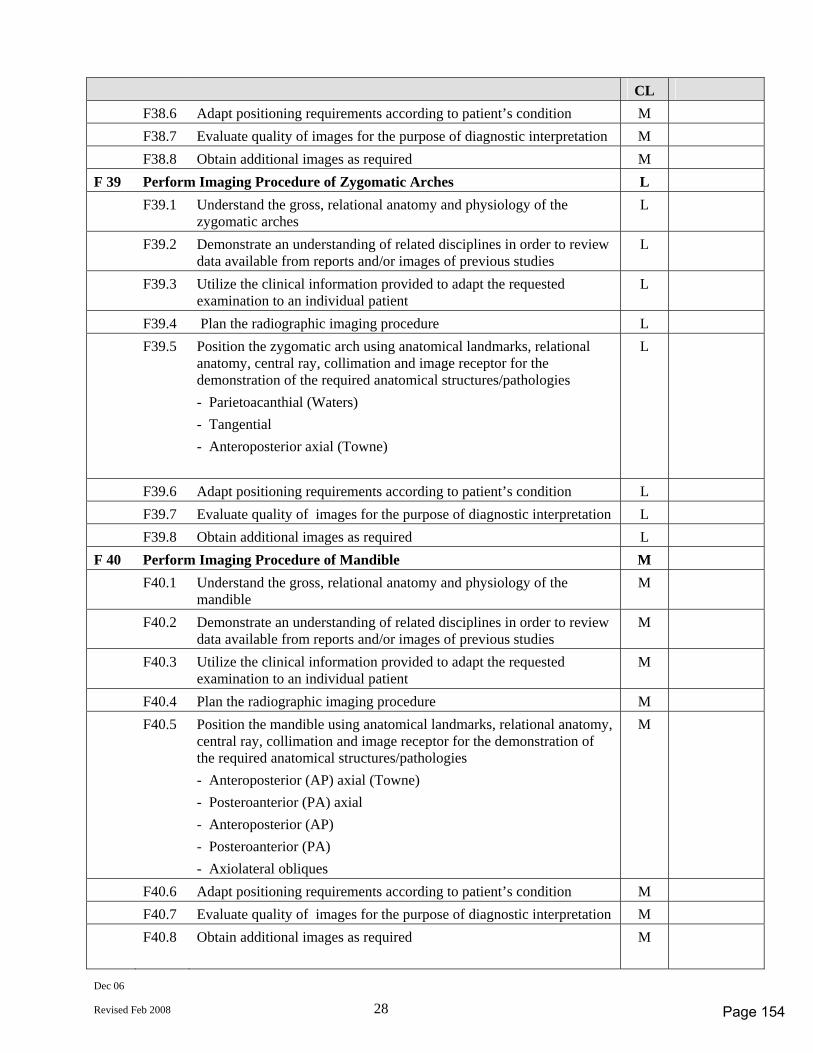
Dec 06
Revised Feb 2008 28
CL F38.6 Adapt positioning requirements according to patient’s condition M F38.7 Evaluate quality of images for the purpose of diagnostic interpretation M F38.8 Obtain additional images as required M F 39 Perform Imaging Procedure of Zygomatic Arches L F39.1 Understand the gross, relational anatomy and physiology of the
zygomatic arches L
F39.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
F39.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F39.4 Plan the radiographic imaging procedure L F39.5 Position the zygomatic arch using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Parietoacanthial (Waters) - Tangential - Anteroposterior axial (Towne)
L
F39.6 Adapt positioning requirements according to patient’s condition L F39.7 Evaluate quality of images for the purpose of diagnostic interpretation L F39.8 Obtain additional images as required L F 40 Perform Imaging Procedure of Mandible M F40.1 Understand the gross, relational anatomy and physiology of the
mandible M
F40.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
F40.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
F40.4 Plan the radiographic imaging procedure M F40.5 Position the mandible using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) axial (Towne) - Posteroanterior (PA) axial - Anteroposterior (AP) - Posteroanterior (PA) - Axiolateral obliques
M
F40.6 Adapt positioning requirements according to patient’s condition M F40.7 Evaluate quality of images for the purpose of diagnostic interpretation M F40.8 Obtain additional images as required M
Page 154
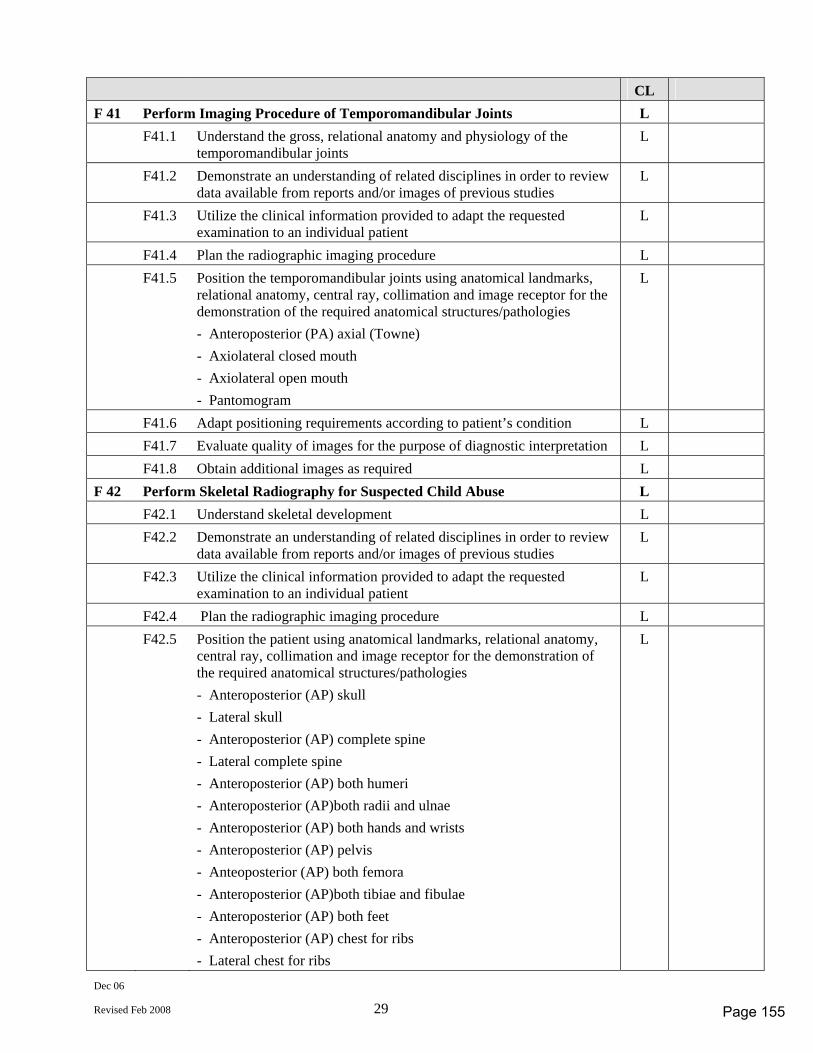
Dec 06
Revised Feb 2008 29
CL F 41 Perform Imaging Procedure of Temporomandibular Joints L F41.1 Understand the gross, relational anatomy and physiology of the
temporomandibular joints L
F41.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
F41.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F41.4 Plan the radiographic imaging procedure L F41.5 Position the temporomandibular joints using anatomical landmarks,
relational anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (PA) axial (Towne) - Axiolateral closed mouth - Axiolateral open mouth - Pantomogram
L
F41.6 Adapt positioning requirements according to patient’s condition L F41.7 Evaluate quality of images for the purpose of diagnostic interpretation L F41.8 Obtain additional images as required L F 42 Perform Skeletal Radiography for Suspected Child Abuse L F42.1 Understand skeletal development L F42.2 Demonstrate an understanding of related disciplines in order to review
data available from reports and/or images of previous studies L
F42.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
F42.4 Plan the radiographic imaging procedure L F42.5 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) skull - Lateral skull - Anteroposterior (AP) complete spine - Lateral complete spine - Anteroposterior (AP) both humeri - Anteroposterior (AP)both radii and ulnae - Anteroposterior (AP) both hands and wrists - Anteroposterior (AP) pelvis - Anteoposterior (AP) both femora - Anteroposterior (AP)both tibiae and fibulae - Anteroposterior (AP) both feet - Anteroposterior (AP) chest for ribs - Lateral chest for ribs
L
Page 155
Dec 06
Revised Feb 2008 30
CL F42.6 Adapt positioning requirements according to patient’s condition L F42.7 Evaluate quality of images for the purpose of diagnostic interpretation L F42.8 Obtain additional images as required L
Page 156
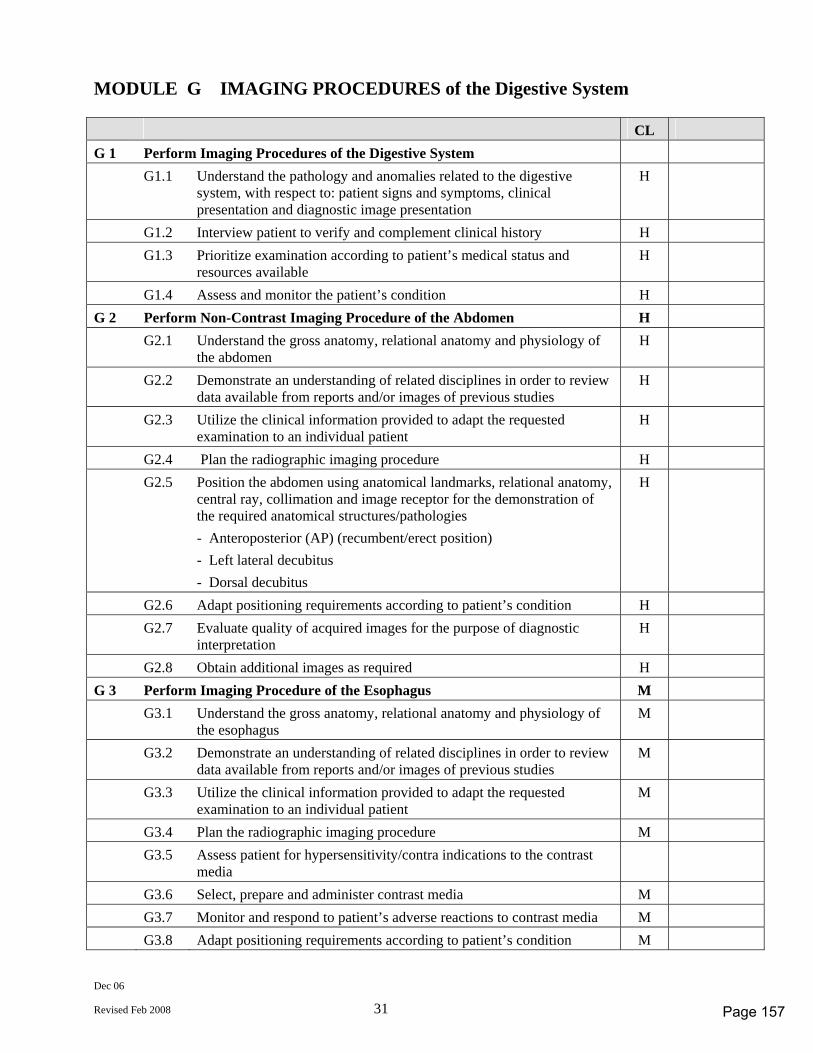
Dec 06
Revised Feb 2008 31
MODULE G IMAGING PROCEDURES of the Digestive System CL G 1 Perform Imaging Procedures of the Digestive System G1.1 Understand the pathology and anomalies related to the digestive
system, with respect to: patient signs and symptoms, clinical presentation and diagnostic image presentation
H
G1.2 Interview patient to verify and complement clinical history H G1.3 Prioritize examination according to patient’s medical status and
resources available H
G1.4 Assess and monitor the patient’s condition H G 2 Perform Non-Contrast Imaging Procedure of the Abdomen H G2.1 Understand the gross anatomy, relational anatomy and physiology of
the abdomen H
G2.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
G2.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
G2.4 Plan the radiographic imaging procedure H G2.5 Position the abdomen using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) (recumbent/erect position) - Left lateral decubitus - Dorsal decubitus
H
G2.6 Adapt positioning requirements according to patient’s condition H G2.7 Evaluate quality of acquired images for the purpose of diagnostic
interpretation H
G2.8 Obtain additional images as required H G 3 Perform Imaging Procedure of the Esophagus M G3.1 Understand the gross anatomy, relational anatomy and physiology of
the esophagus M
G3.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
G3.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
G3.4 Plan the radiographic imaging procedure M G3.5 Assess patient for hypersensitivity/contra indications to the contrast
media
G3.6 Select, prepare and administer contrast media M G3.7 Monitor and respond to patient’s adverse reactions to contrast media M G3.8 Adapt positioning requirements according to patient’s condition M
Page 157
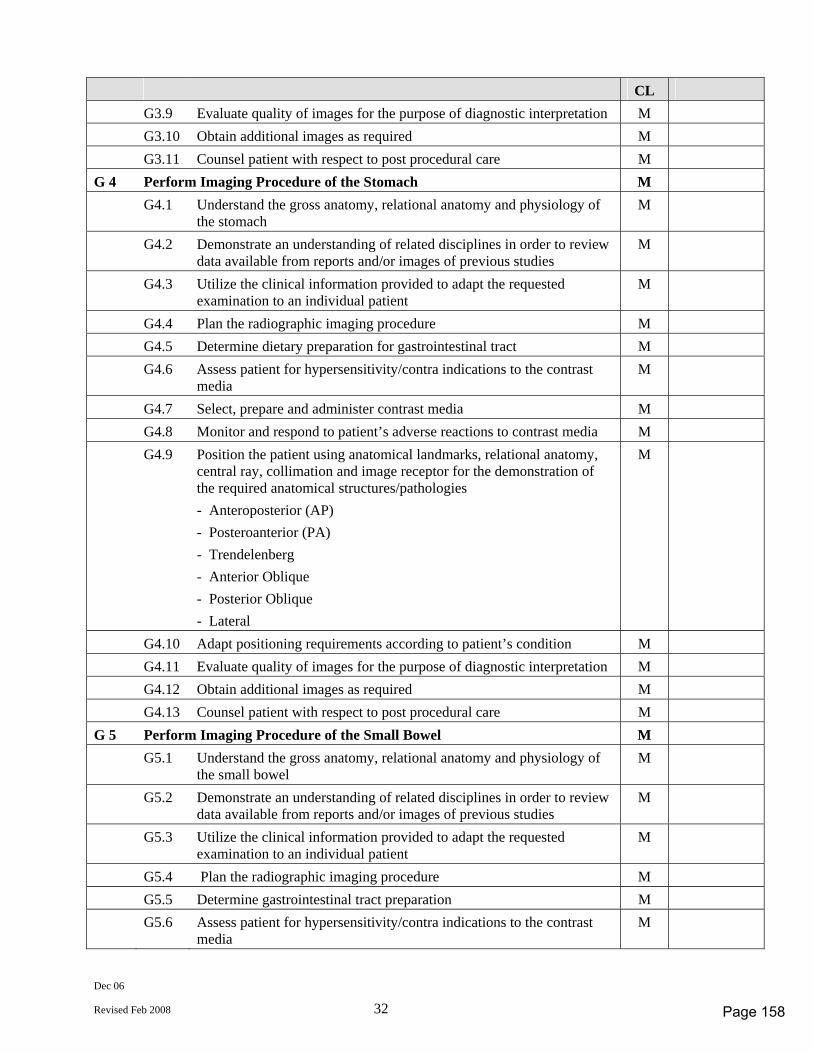
Dec 06
Revised Feb 2008 32
CL G3.9 Evaluate quality of images for the purpose of diagnostic interpretation M G3.10 Obtain additional images as required M G3.11 Counsel patient with respect to post procedural care M G 4 Perform Imaging Procedure of the Stomach M G4.1 Understand the gross anatomy, relational anatomy and physiology of
the stomach M
G4.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
G4.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
G4.4 Plan the radiographic imaging procedure M G4.5 Determine dietary preparation for gastrointestinal tract M G4.6 Assess patient for hypersensitivity/contra indications to the contrast
media M
G4.7 Select, prepare and administer contrast media M G4.8 Monitor and respond to patient’s adverse reactions to contrast media M G4.9 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posteroanterior (PA) - Trendelenberg - Anterior Oblique - Posterior Oblique - Lateral
M
G4.10 Adapt positioning requirements according to patient’s condition M G4.11 Evaluate quality of images for the purpose of diagnostic interpretation M G4.12 Obtain additional images as required M G4.13 Counsel patient with respect to post procedural care M G 5 Perform Imaging Procedure of the Small Bowel M G5.1 Understand the gross anatomy, relational anatomy and physiology of
the small bowel M
G5.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
G5.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
G5.4 Plan the radiographic imaging procedure M G5.5 Determine gastrointestinal tract preparation M G5.6 Assess patient for hypersensitivity/contra indications to the contrast
media M
Page 158
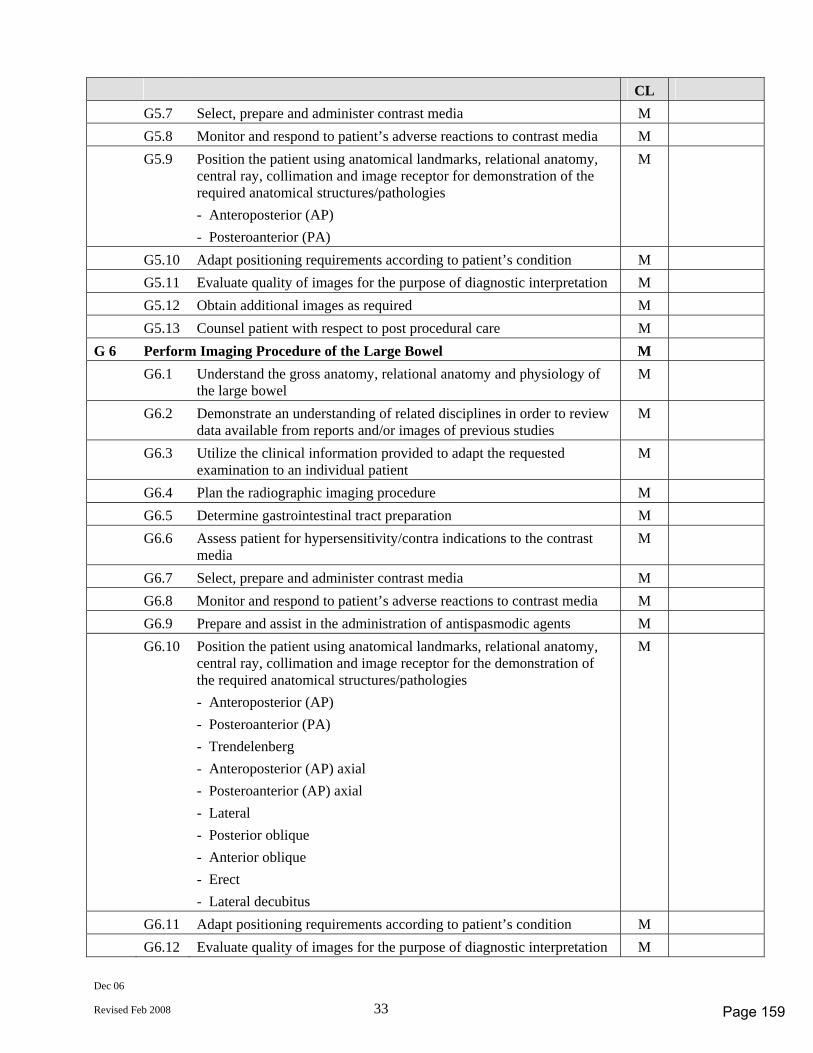
Dec 06
Revised Feb 2008 33
CL G5.7 Select, prepare and administer contrast media M G5.8 Monitor and respond to patient’s adverse reactions to contrast media M G5.9 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posteroanterior (PA)
M
G5.10 Adapt positioning requirements according to patient’s condition M G5.11 Evaluate quality of images for the purpose of diagnostic interpretation M G5.12 Obtain additional images as required M G5.13 Counsel patient with respect to post procedural care M G 6 Perform Imaging Procedure of the Large Bowel M G6.1 Understand the gross anatomy, relational anatomy and physiology of
the large bowel M
G6.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
G6.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
G6.4 Plan the radiographic imaging procedure M G6.5 Determine gastrointestinal tract preparation M G6.6 Assess patient for hypersensitivity/contra indications to the contrast
media M
G6.7 Select, prepare and administer contrast media M G6.8 Monitor and respond to patient’s adverse reactions to contrast media M G6.9 Prepare and assist in the administration of antispasmodic agents M G6.10 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posteroanterior (PA) - Trendelenberg - Anteroposterior (AP) axial - Posteroanterior (AP) axial - Lateral - Posterior oblique - Anterior oblique - Erect - Lateral decubitus
M
G6.11 Adapt positioning requirements according to patient’s condition M G6.12 Evaluate quality of images for the purpose of diagnostic interpretation M
Page 159
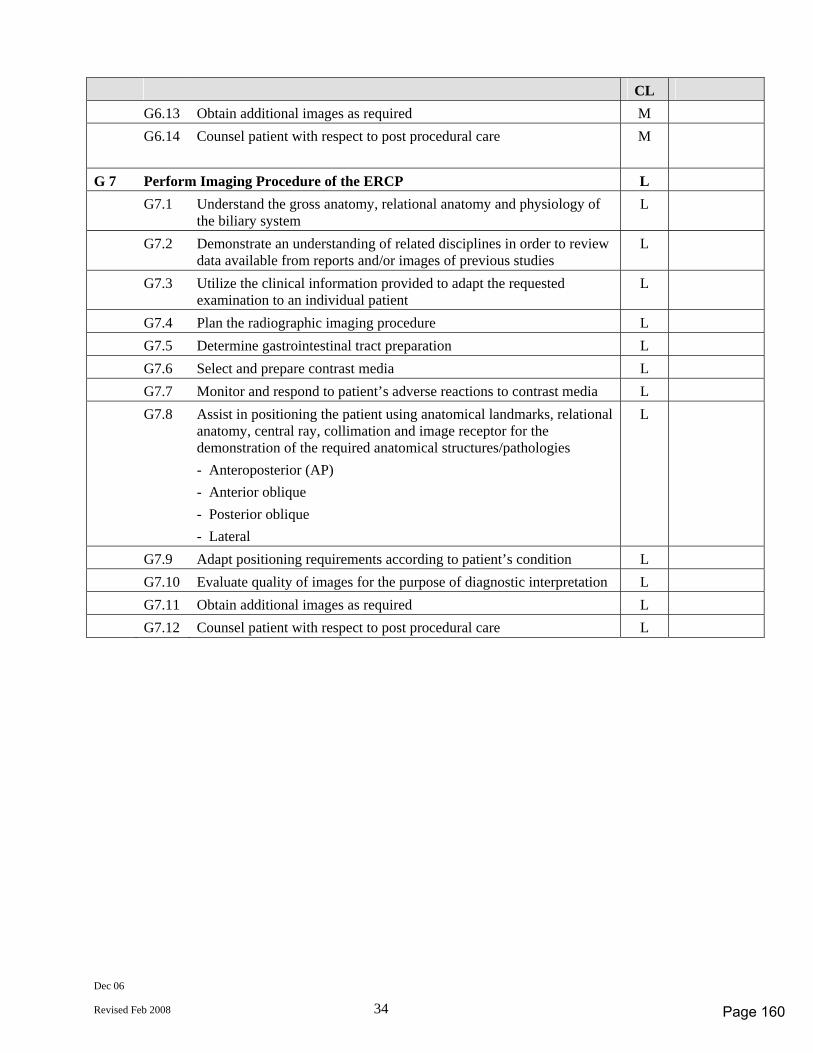
Dec 06
Revised Feb 2008 34
CL G6.13 Obtain additional images as required M G6.14 Counsel patient with respect to post procedural care M
G 7 Perform Imaging Procedure of the ERCP L G7.1 Understand the gross anatomy, relational anatomy and physiology of
the biliary system L
G7.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
G7.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
G7.4 Plan the radiographic imaging procedure L G7.5 Determine gastrointestinal tract preparation L G7.6 Select and prepare contrast media L G7.7 Monitor and respond to patient’s adverse reactions to contrast media L G7.8 Assist in positioning the patient using anatomical landmarks, relational
anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Anterior oblique - Posterior oblique - Lateral
L
G7.9 Adapt positioning requirements according to patient’s condition L G7.10 Evaluate quality of images for the purpose of diagnostic interpretation L G7.11 Obtain additional images as required L G7.12 Counsel patient with respect to post procedural care L
Page 160
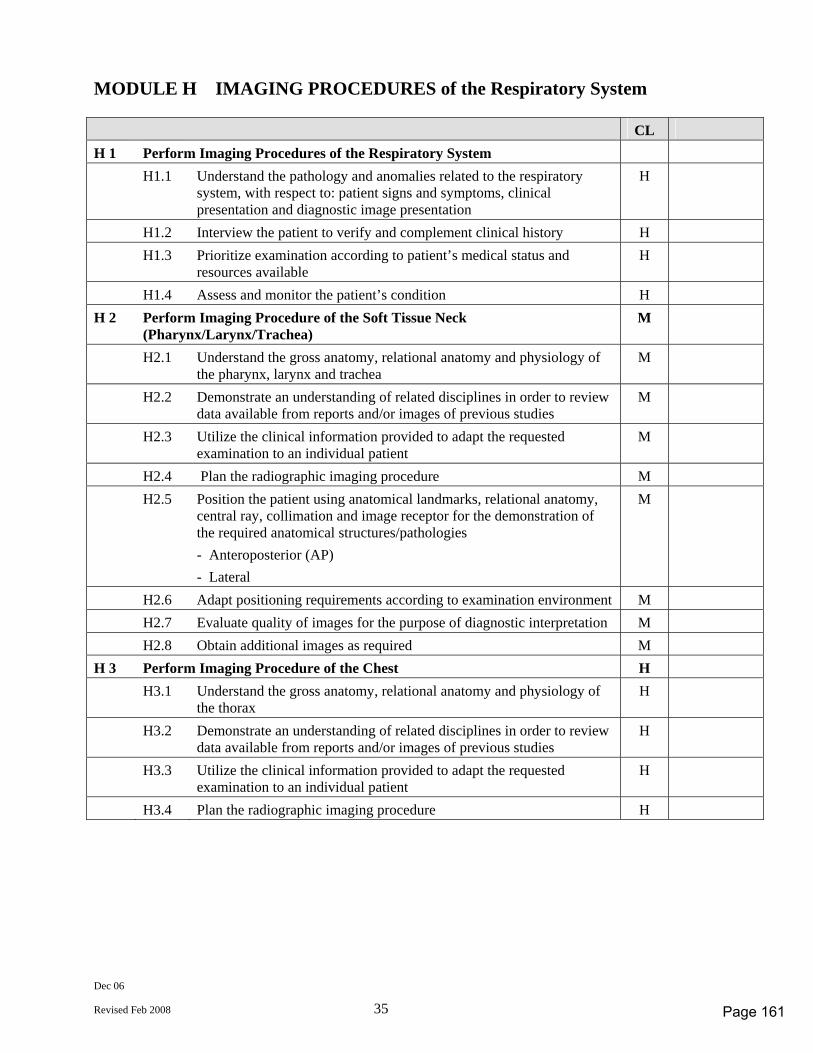
Dec 06
Revised Feb 2008 35
MODULE H IMAGING PROCEDURES of the Respiratory System CL H 1 Perform Imaging Procedures of the Respiratory System H1.1 Understand the pathology and anomalies related to the respiratory
system, with respect to: patient signs and symptoms, clinical presentation and diagnostic image presentation
H
H1.2 Interview the patient to verify and complement clinical history H H1.3 Prioritize examination according to patient’s medical status and
resources available H
H1.4 Assess and monitor the patient’s condition H H 2 Perform Imaging Procedure of the Soft Tissue Neck
(Pharynx/Larynx/Trachea) M
H2.1 Understand the gross anatomy, relational anatomy and physiology of the pharynx, larynx and trachea
M
H2.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
H2.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
M
H2.4 Plan the radiographic imaging procedure M H2.5 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Lateral
M
H2.6 Adapt positioning requirements according to examination environment M H2.7 Evaluate quality of images for the purpose of diagnostic interpretation M H2.8 Obtain additional images as required M H 3 Perform Imaging Procedure of the Chest H H3.1 Understand the gross anatomy, relational anatomy and physiology of
the thorax H
H3.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
H3.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
H3.4 Plan the radiographic imaging procedure H
Page 161
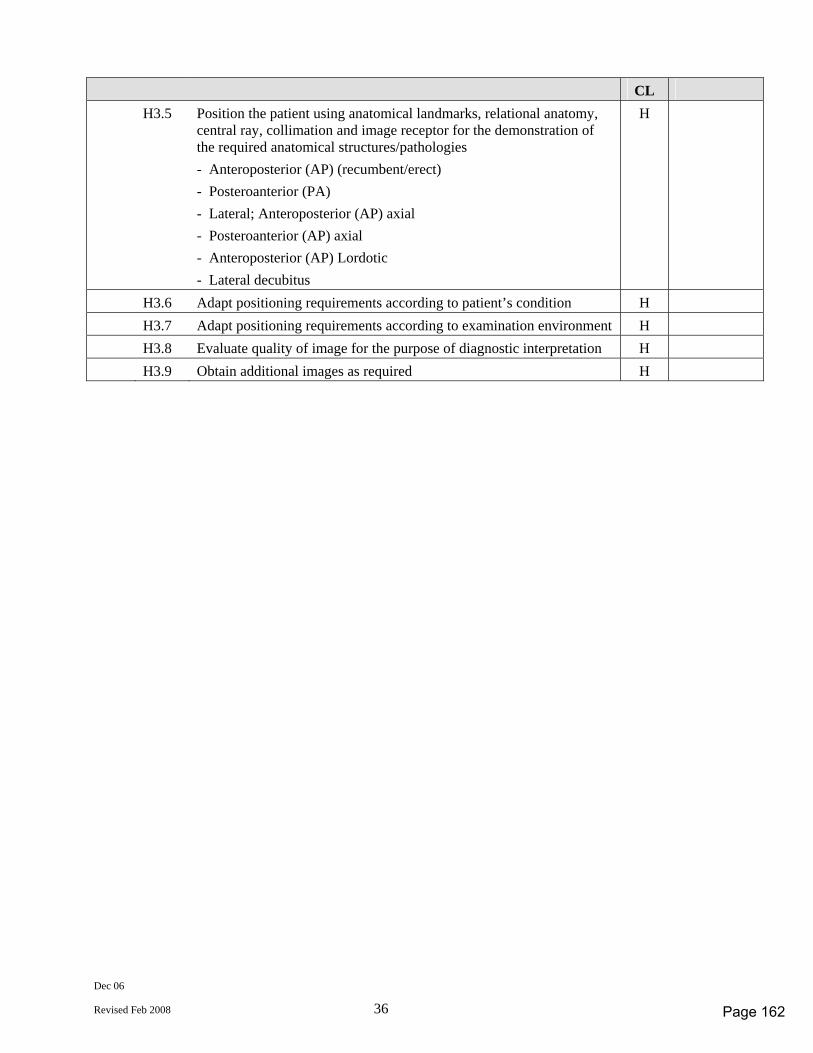
Dec 06
Revised Feb 2008 36
CL H3.5 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) (recumbent/erect) - Posteroanterior (PA) - Lateral; Anteroposterior (AP) axial - Posteroanterior (AP) axial - Anteroposterior (AP) Lordotic - Lateral decubitus
H
H3.6 Adapt positioning requirements according to patient’s condition H H3.7 Adapt positioning requirements according to examination environment H H3.8 Evaluate quality of image for the purpose of diagnostic interpretation H H3.9 Obtain additional images as required H
Page 162
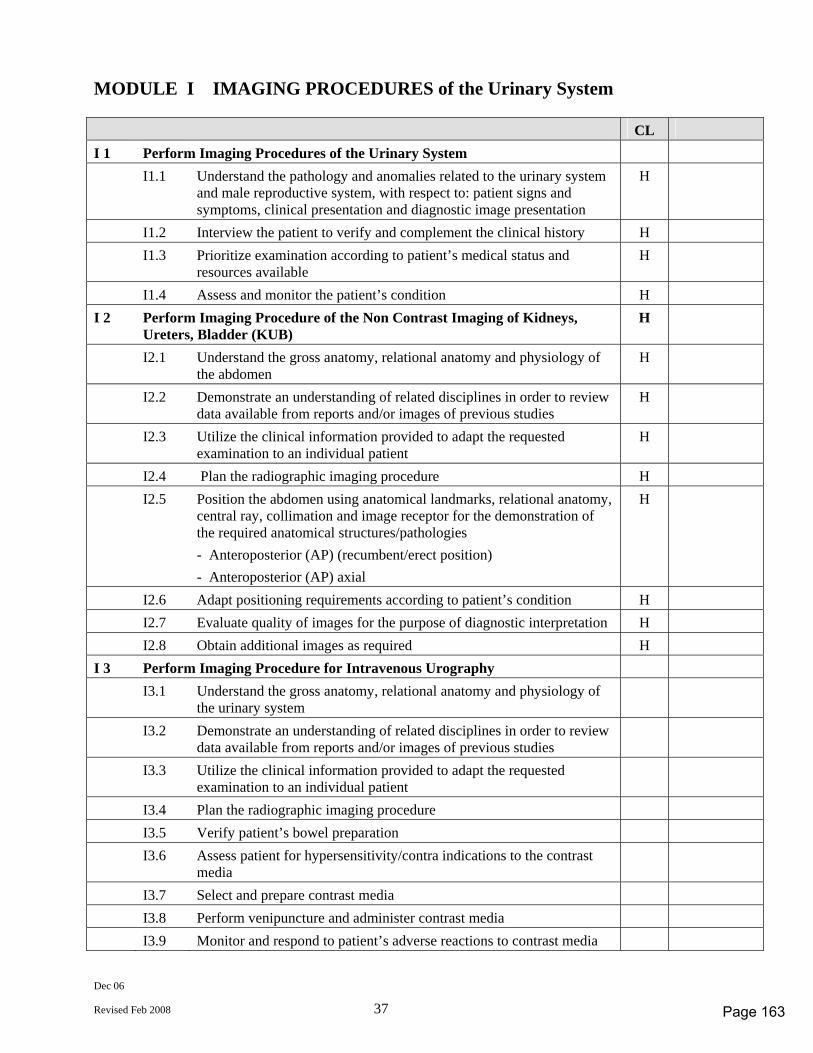
Dec 06
Revised Feb 2008 37
MODULE I IMAGING PROCEDURES of the Urinary System CL I 1 Perform Imaging Procedures of the Urinary System I1.1 Understand the pathology and anomalies related to the urinary system
and male reproductive system, with respect to: patient signs and symptoms, clinical presentation and diagnostic image presentation
H
I1.2 Interview the patient to verify and complement the clinical history H I1.3 Prioritize examination according to patient’s medical status and
resources available H
I1.4 Assess and monitor the patient’s condition H I 2 Perform Imaging Procedure of the Non Contrast Imaging of Kidneys,
Ureters, Bladder (KUB) H
I2.1 Understand the gross anatomy, relational anatomy and physiology of the abdomen
H
I2.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
H
I2.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
H
I2.4 Plan the radiographic imaging procedure H I2.5 Position the abdomen using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) (recumbent/erect position) - Anteroposterior (AP) axial
H
I2.6 Adapt positioning requirements according to patient’s condition H I2.7 Evaluate quality of images for the purpose of diagnostic interpretation H I2.8 Obtain additional images as required H I 3 Perform Imaging Procedure for Intravenous Urography I3.1 Understand the gross anatomy, relational anatomy and physiology of
the urinary system
I3.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
I3.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
I3.4 Plan the radiographic imaging procedure I3.5 Verify patient’s bowel preparation I3.6 Assess patient for hypersensitivity/contra indications to the contrast
media
I3.7 Select and prepare contrast media I3.8 Perform venipuncture and administer contrast media I3.9 Monitor and respond to patient’s adverse reactions to contrast media
Page 163
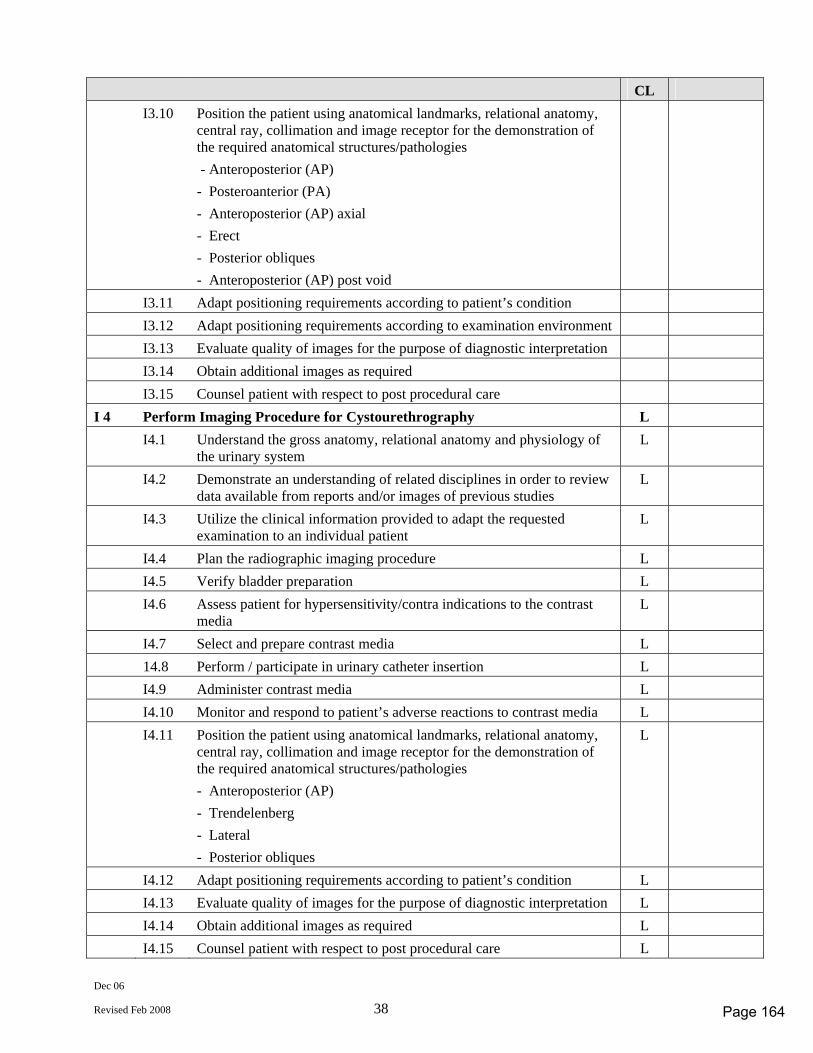
Dec 06
Revised Feb 2008 38
CL I3.10 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posteroanterior (PA) - Anteroposterior (AP) axial - Erect - Posterior obliques - Anteroposterior (AP) post void
I3.11 Adapt positioning requirements according to patient’s condition I3.12 Adapt positioning requirements according to examination environment I3.13 Evaluate quality of images for the purpose of diagnostic interpretation I3.14 Obtain additional images as required I3.15 Counsel patient with respect to post procedural care I 4 Perform Imaging Procedure for Cystourethrography L I4.1 Understand the gross anatomy, relational anatomy and physiology of
the urinary system L
I4.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
I4.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
I4.4 Plan the radiographic imaging procedure L I4.5 Verify bladder preparation L I4.6 Assess patient for hypersensitivity/contra indications to the contrast
media L
I4.7 Select and prepare contrast media L 14.8 Perform / participate in urinary catheter insertion L I4.9 Administer contrast media L I4.10 Monitor and respond to patient’s adverse reactions to contrast media L I4.11 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Trendelenberg - Lateral - Posterior obliques
L
I4.12 Adapt positioning requirements according to patient’s condition L I4.13 Evaluate quality of images for the purpose of diagnostic interpretation L I4.14 Obtain additional images as required L I4.15 Counsel patient with respect to post procedural care L
Page 164
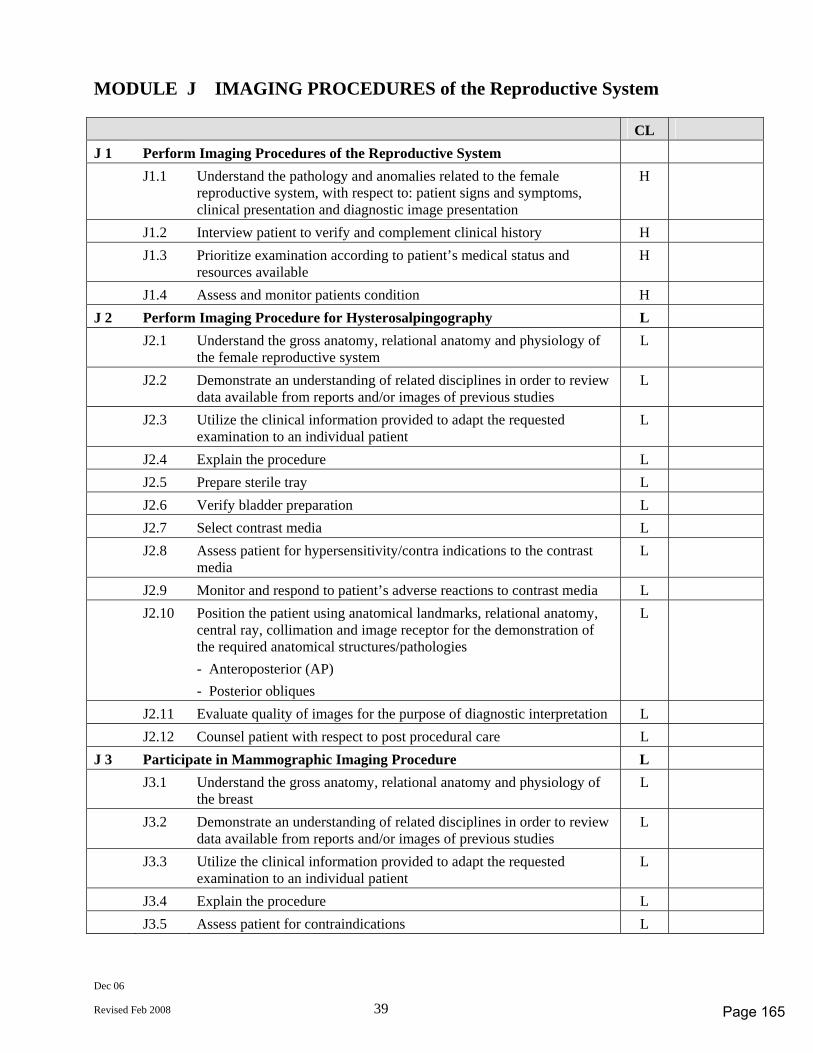
Dec 06
Revised Feb 2008 39
MODULE J IMAGING PROCEDURES of the Reproductive System CL J 1 Perform Imaging Procedures of the Reproductive System J1.1 Understand the pathology and anomalies related to the female
reproductive system, with respect to: patient signs and symptoms, clinical presentation and diagnostic image presentation
H
J1.2 Interview patient to verify and complement clinical history H J1.3 Prioritize examination according to patient’s medical status and
resources available H
J1.4 Assess and monitor patients condition H J 2 Perform Imaging Procedure for Hysterosalpingography L J2.1 Understand the gross anatomy, relational anatomy and physiology of
the female reproductive system L
J2.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
J2.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
J2.4 Explain the procedure L J2.5 Prepare sterile tray L J2.6 Verify bladder preparation L J2.7 Select contrast media L J2.8 Assess patient for hypersensitivity/contra indications to the contrast
media L
J2.9 Monitor and respond to patient’s adverse reactions to contrast media L J2.10 Position the patient using anatomical landmarks, relational anatomy,
central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Anteroposterior (AP) - Posterior obliques
L
J2.11 Evaluate quality of images for the purpose of diagnostic interpretation L J2.12 Counsel patient with respect to post procedural care L J 3 Participate in Mammographic Imaging Procedure L J3.1 Understand the gross anatomy, relational anatomy and physiology of
the breast L
J3.2 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
J3.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
J3.4 Explain the procedure L J3.5 Assess patient for contraindications L
Page 165
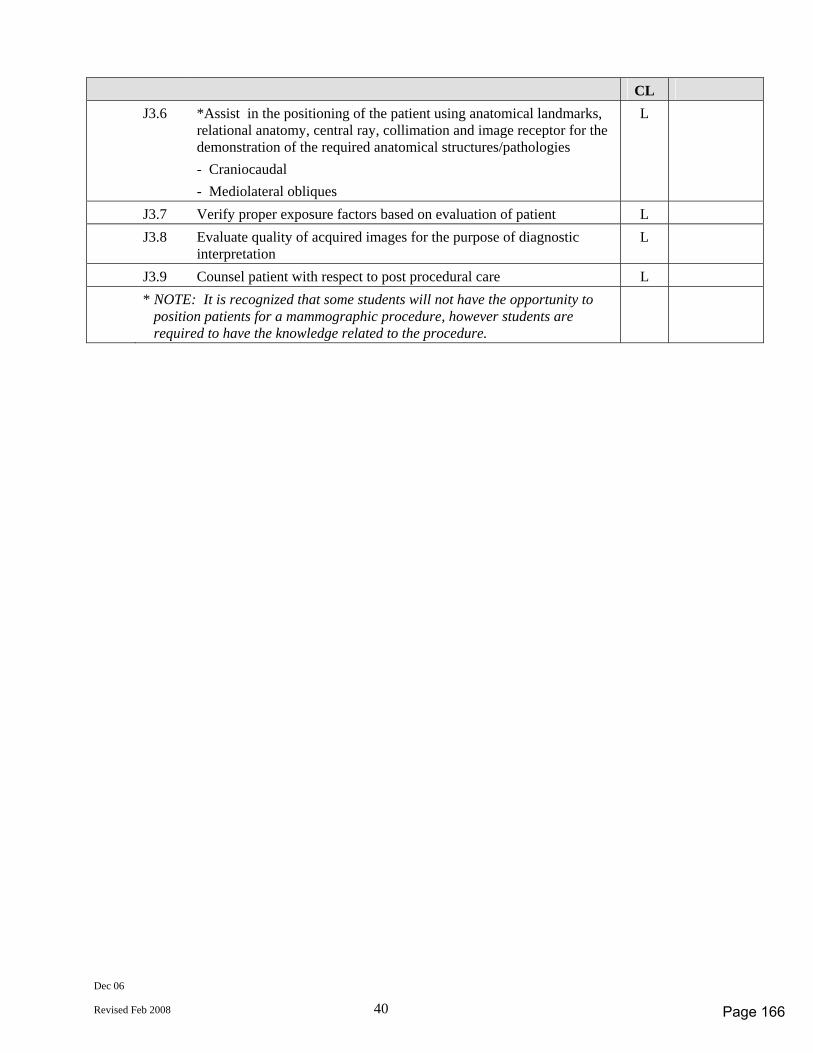
Dec 06
Revised Feb 2008 40
CL J3.6 *Assist in the positioning of the patient using anatomical landmarks,
relational anatomy, central ray, collimation and image receptor for the demonstration of the required anatomical structures/pathologies - Craniocaudal - Mediolateral obliques
L
J3.7 Verify proper exposure factors based on evaluation of patient L J3.8 Evaluate quality of acquired images for the purpose of diagnostic
interpretation L
J3.9 Counsel patient with respect to post procedural care L * NOTE: It is recognized that some students will not have the opportunity to
position patients for a mammographic procedure, however students are required to have the knowledge related to the procedure.
Page 166
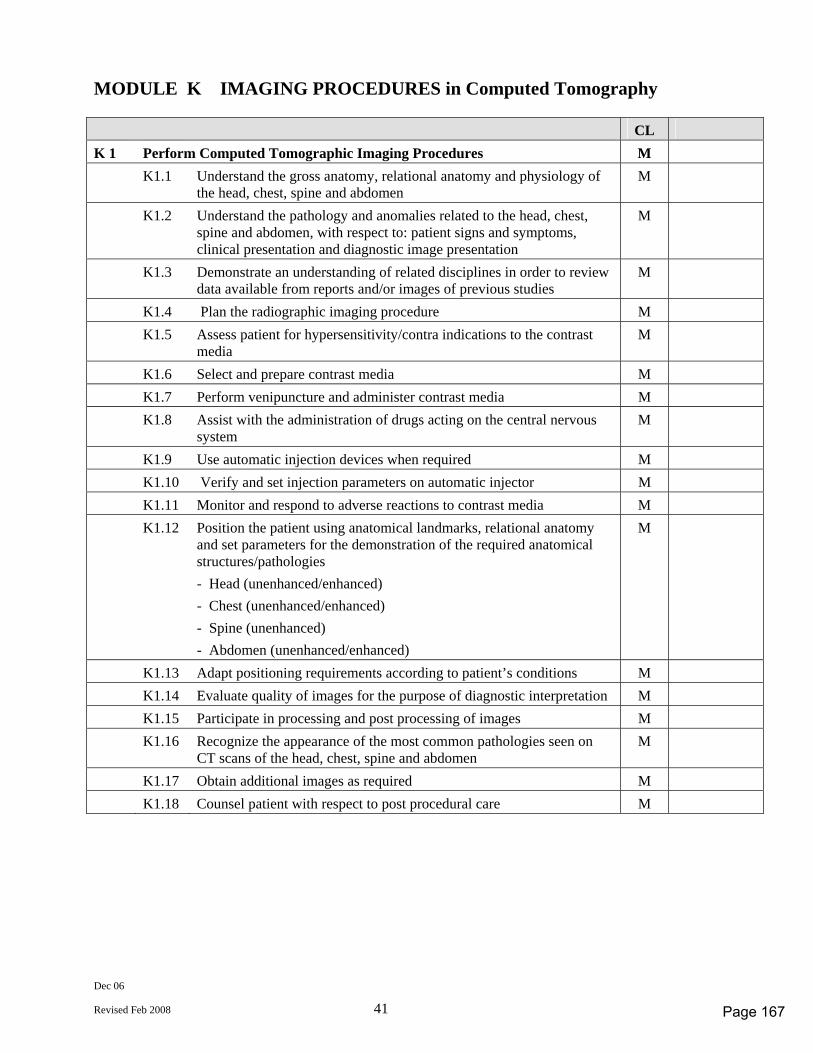
Dec 06
Revised Feb 2008 41
MODULE K IMAGING PROCEDURES in Computed Tomography CL K 1 Perform Computed Tomographic Imaging Procedures M K1.1 Understand the gross anatomy, relational anatomy and physiology of
the head, chest, spine and abdomen M
K1.2 Understand the pathology and anomalies related to the head, chest, spine and abdomen, with respect to: patient signs and symptoms, clinical presentation and diagnostic image presentation
M
K1.3 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
M
K1.4 Plan the radiographic imaging procedure M K1.5 Assess patient for hypersensitivity/contra indications to the contrast
media M
K1.6 Select and prepare contrast media M K1.7 Perform venipuncture and administer contrast media M K1.8 Assist with the administration of drugs acting on the central nervous
system M
K1.9 Use automatic injection devices when required M K1.10 Verify and set injection parameters on automatic injector M K1.11 Monitor and respond to adverse reactions to contrast media M K1.12 Position the patient using anatomical landmarks, relational anatomy
and set parameters for the demonstration of the required anatomical structures/pathologies - Head (unenhanced/enhanced) - Chest (unenhanced/enhanced) - Spine (unenhanced) - Abdomen (unenhanced/enhanced)
M
K1.13 Adapt positioning requirements according to patient’s conditions M K1.14 Evaluate quality of images for the purpose of diagnostic interpretation M K1.15 Participate in processing and post processing of images M K1.16 Recognize the appearance of the most common pathologies seen on
CT scans of the head, chest, spine and abdomen M
K1.17 Obtain additional images as required M K1.18 Counsel patient with respect to post procedural care M
Page 167
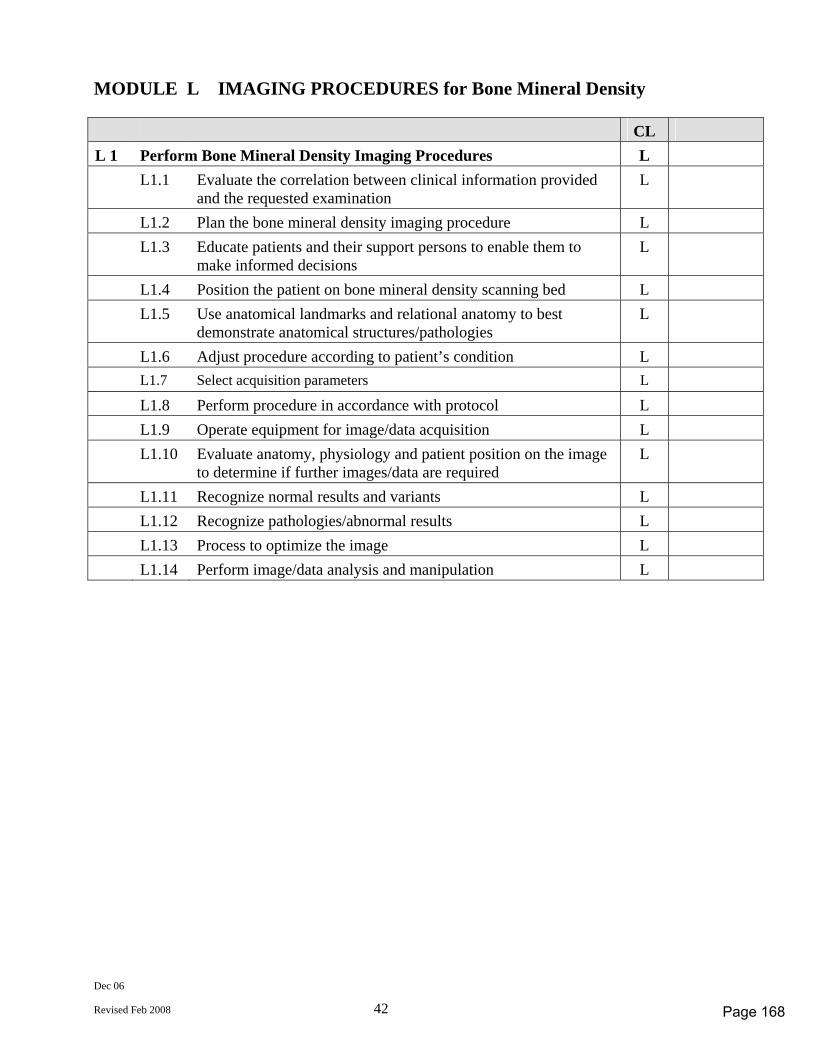
Dec 06
Revised Feb 2008 42
MODULE L IMAGING PROCEDURES for Bone Mineral Density CL L 1 Perform Bone Mineral Density Imaging Procedures L L1.1 Evaluate the correlation between clinical information provided
and the requested examination L
L1.2 Plan the bone mineral density imaging procedure L L1.3 Educate patients and their support persons to enable them to
make informed decisions L
L1.4 Position the patient on bone mineral density scanning bed L L1.5 Use anatomical landmarks and relational anatomy to best
demonstrate anatomical structures/pathologies L
L1.6 Adjust procedure according to patient’s condition L L1.7 Select acquisition parameters L
L1.8 Perform procedure in accordance with protocol L L1.9 Operate equipment for image/data acquisition L L1.10 Evaluate anatomy, physiology and patient position on the image
to determine if further images/data are required L
L1.11 Recognize normal results and variants L L1.12 Recognize pathologies/abnormal results L L1.13 Process to optimize the image L L1.14 Perform image/data analysis and manipulation L
Page 168
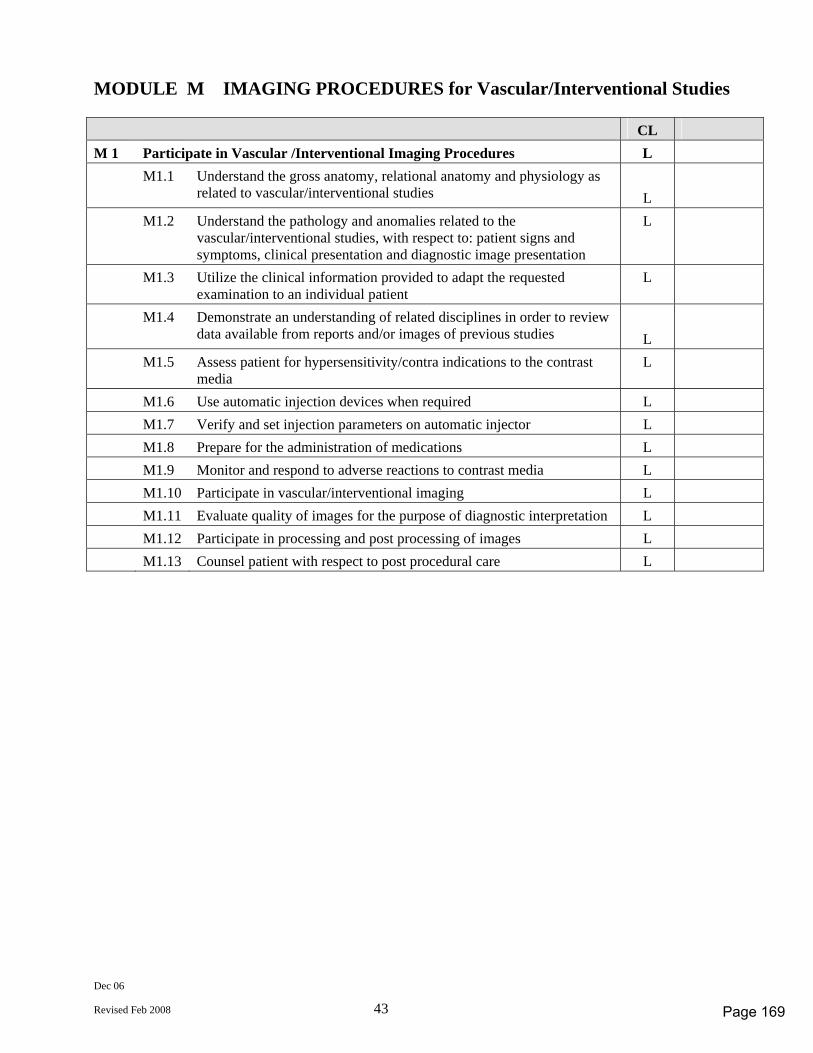
Dec 06
Revised Feb 2008 43
MODULE M IMAGING PROCEDURES for Vascular/Interventional Studies CL M 1 Participate in Vascular /Interventional Imaging Procedures L M1.1 Understand the gross anatomy, relational anatomy and physiology as
related to vascular/interventional studies
L
M1.2 Understand the pathology and anomalies related to the vascular/interventional studies, with respect to: patient signs and symptoms, clinical presentation and diagnostic image presentation
L
M1.3 Utilize the clinical information provided to adapt the requested examination to an individual patient
L
M1.4 Demonstrate an understanding of related disciplines in order to review data available from reports and/or images of previous studies
L
M1.5 Assess patient for hypersensitivity/contra indications to the contrast media
L
M1.6 Use automatic injection devices when required L M1.7 Verify and set injection parameters on automatic injector L M1.8 Prepare for the administration of medications L M1.9 Monitor and respond to adverse reactions to contrast media L M1.10 Participate in vascular/interventional imaging L M1.11 Evaluate quality of images for the purpose of diagnostic interpretation L M1.12 Participate in processing and post processing of images L M1.13 Counsel patient with respect to post procedural care L
Page 169

Page 170
January 2007
Revised Feb 2008 (#29261)
Magnetic Resonance
COMPETENCY PROFILE
November 2006 Revised February 2008
Revised Profile
for use with the development of the September 2011 Certification exams*
*EXCEPTION: FIRST DISCIPLINE MR PROGRAM EFFECTIVE for MAY 2007 Certification Exams
Prepared by the Magnetic Resonance Competency Profile Task Group
© CANADIAN ASSOCIATION OF MEDICAL RADIATION TECHNOLOGISTS Suite 1000, 85 Albert Street, Ottawa, Ontario K1P 6A4
Tel: 1-800-463-9729 or (613) 234-0012 / Fax: (613) 234-1097 www.camrt.ca
Page 171

January 2007
Revised Feb 2008 (#29261)
© Copyright 2006 by Canadian Association of Medical Radiation Technologists
All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage or retrieval system, without the prior written permission of the Canadian Association of Medical Radiation Technologists.
Page 172
Jan 07
Revised Feb 2008 1 Magnetic Resonance - 1
COMPETENCY PROFILE – Magnetic Resonance (MR)
Competencies for Entry Level Magnetic Resonance Technologists This document describes the essential competencies required for an entry-level magnetic resonance technologist in Canada to provide best practice as defined by safe, competent and ethical practice of magnetic resonance technology in a variety of clinical environments. The profile defines competencies reflecting the integration of knowledge, skills, attitudes and judgment necessary to practice in an environment that requires the technologist to use effective organizational skills and critical thinking. This requires the ability to assess, adapt, modify, analyse and evaluate in a variety of situations and environments in the practice of magnetic resonance. Critical decision-making is, therefore, inherent to the practice of magnetic resonance and is demonstrated in the competencies required of entry-to-practice technologists. The competency profile defines the standard for certification of entry-level magnetic resonance technologists in Canada. The document is also used to: - provide direction to entry-level education programs to assist in developing
curriculum; - inform Ministries of Health and Education of the standard expected from entry-level
magnetic resonance technologists; - inform the public and employers of the standard expected from entry-level magnetic
resonance technologists; - assist the Canadian Medical Association (CMA) Conjoint Committee with
accreditation of education programs; - provide a guide for identifying professional development needs for practicing
technologists; - develop a blueprint for CAMRT certification examination. Accredited programs must ensure their certification candidates possess all the competencies listed in the profile. Education programs are encouraged to include additional skills at their discretion. In the development of the competencies, the following assumptions have been made. That the Magnetic Resonance Technologist: - has completed an accredited Canadian program, or is eligible for certification by
another process - has acquired the theoretical knowledge required to achieve a wide range of
competencies - has developed a broad knowledge base that has been assessed prior to the certificate
examination - commits to the principle that their primary role and function is to serve the public
interest
Page 173
Jan 07
Revised Feb 2008 2 Magnetic Resonance - 1
- is a member of the inter-professional health care team collaborating with other health care professionals to provide appropriate patient care in the delivery of diagnostic imaging services
- is responsible for the safe and effective application of magnetic resonance - is responsible for the production, assessment, optimization and archiving of images - is responsible for the performance of diagnostic magnetic resonance procedures and
participates in interventional procedures - is responsible for the education of patients, public and other health care providers
regarding magnetic resonance for medical use - performs effectively encompassing physical, psychological, social, economic and
cultural factors that interact in predictable and unpredictable ways - recognizes patients as unique individuals, treating them with dignity and respect - practices in accordance with legislation, regulatory and professional bodies’ standards
of practice, scope of practice, codes of ethics and other relative documents - performs in a manner consistent with public interest, employment philosophies and
practices, current research and advancing technology - seeks guidance from experienced practitioners, colleagues and employers to enhance
the technologist’s individual experience and knowledge - promotes and participates in the advancement of this dynamic profession through
active involvement, continuous learning, professional development and research - adheres to and promotes professional standards The Magnetic Resonance Competency Profile is divided into twelve modules: Module A Professional Practice Module B Patient Management Module C MR Safety Module D Quality Management Module E MR Instrumentation and Image Quality Module F Core Competencies of Imaging Procedures Module G Musculoskeletal Imaging Procedures Module H Head and Neck Imaging Procedures Module I Spinal Imaging Procedures Module J Abdominal Imaging Procedures Module K Thorax Imaging Procedures Module L Pelvic Imaging Procedures
Page 174
Jan 07
Revised Feb 2008 3 Magnetic Resonance - 1
EXAMINABLE COMPETENCIES & COMPETENCY LEVELS
All competencies listed in the competency profile must be achieved by graduates of an accredited medical radiation technology program. This will be assessed for compliance during the accreditation survey conducted by the CMA Conjoint Accreditation Services. It is realized that due to regional and institutional differences level of achievement for some competencies may vary based on evolving changes in technology, practice and facility policies.
Not all competencies will be tested on the CAMRT certification exam.
The EXAMINABLE COMPETENCIES are those competencies that have a competency level indicated in the column to the right of the written competency. The EXAMINABLE COMPETENCIES were established by the discipline specific workgroups working both within their disciplines and together as a core group using the feedback received from stakeholders during the competency profile revision process.
There are three competency levels (CL)
– HIGH (H)
– MEDIUM (M)
– LOW (L) Competency levels were determined through a survey done by technologists/therapists and managers of Diagnostic Imaging and Radiation Therapy Departments. The survey requested a rating of the examinable competencies for frequency of application, importance and future significance in the healthcare work environment. The results of the survey were analyzed and the examinable competencies rated either H, M, L based on the response to frequency, importance and significance for the future.
The competency levels provide a guide (blue print) for certification exam development. More weighting will be placed on the development and use of questions associated with a HIGH level competency as opposed to a MEDIUM or LOW rated level competency where emphasis on question development and use on the certification exam will reflect the competency level.
Validation of all competencies, including identification of examinable competencies and their associated competency levels will be conducted at least every five years. Due to rapid changes in technology and practice certain portions of the profile may be validated more frequently to ensure the profiles are reflective of practice and workplace needs.
Page 175
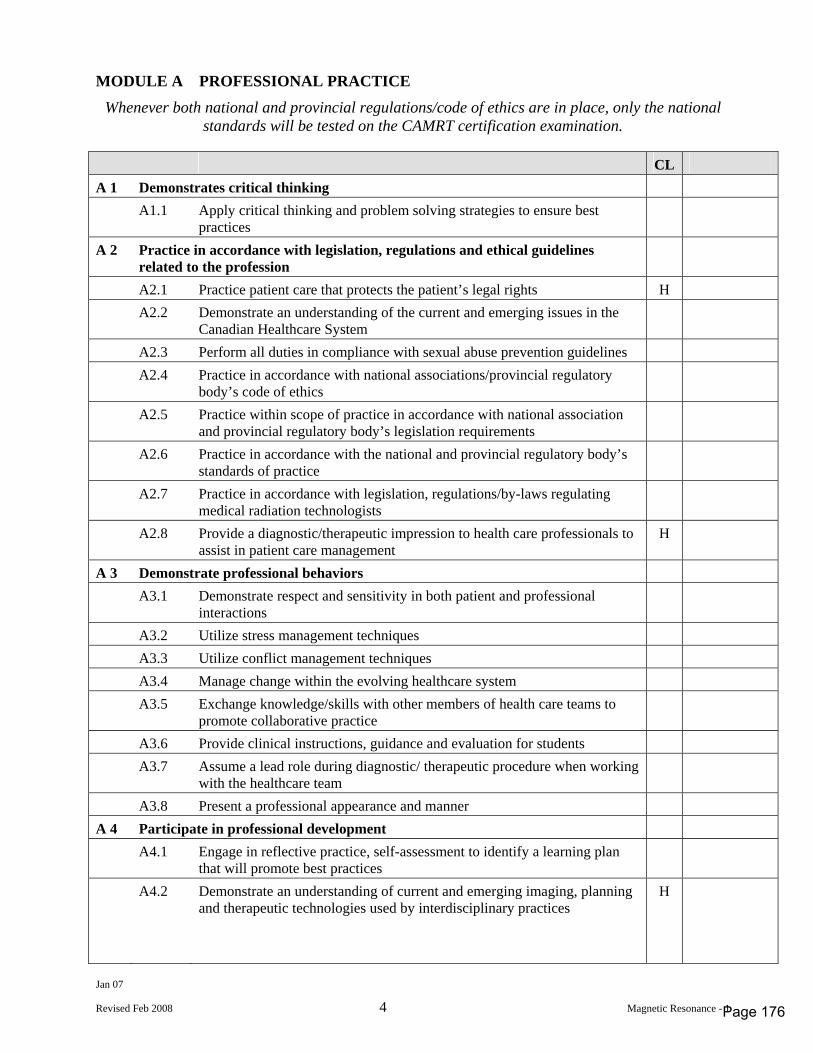
Jan 07
Revised Feb 2008 4 Magnetic Resonance - 1
MODULE A PROFESSIONAL PRACTICE
Whenever both national and provincial regulations/code of ethics are in place, only the national standards will be tested on the CAMRT certification examination.
CL A 1 Demonstrates critical thinking A1.1 Apply critical thinking and problem solving strategies to ensure best
practices
A 2 Practice in accordance with legislation, regulations and ethical guidelines related to the profession
A2.1 Practice patient care that protects the patient’s legal rights H A2.2 Demonstrate an understanding of the current and emerging issues in the
Canadian Healthcare System
A2.3 Perform all duties in compliance with sexual abuse prevention guidelines A2.4 Practice in accordance with national associations/provincial regulatory
body’s code of ethics
A2.5 Practice within scope of practice in accordance with national association and provincial regulatory body’s legislation requirements
A2.6 Practice in accordance with the national and provincial regulatory body’s standards of practice
A2.7 Practice in accordance with legislation, regulations/by-laws regulating medical radiation technologists
A2.8 Provide a diagnostic/therapeutic impression to health care professionals to assist in patient care management
H
A 3 Demonstrate professional behaviors A3.1 Demonstrate respect and sensitivity in both patient and professional
interactions
A3.2 Utilize stress management techniques A3.3 Utilize conflict management techniques A3.4 Manage change within the evolving healthcare system A3.5 Exchange knowledge/skills with other members of health care teams to
promote collaborative practice
A3.6 Provide clinical instructions, guidance and evaluation for students A3.7 Assume a lead role during diagnostic/ therapeutic procedure when working
with the healthcare team
A3.8 Present a professional appearance and manner A 4 Participate in professional development A4.1 Engage in reflective practice, self-assessment to identify a learning plan
that will promote best practices
A4.2 Demonstrate an understanding of current and emerging imaging, planning and therapeutic technologies used by interdisciplinary practices
H
Page 176
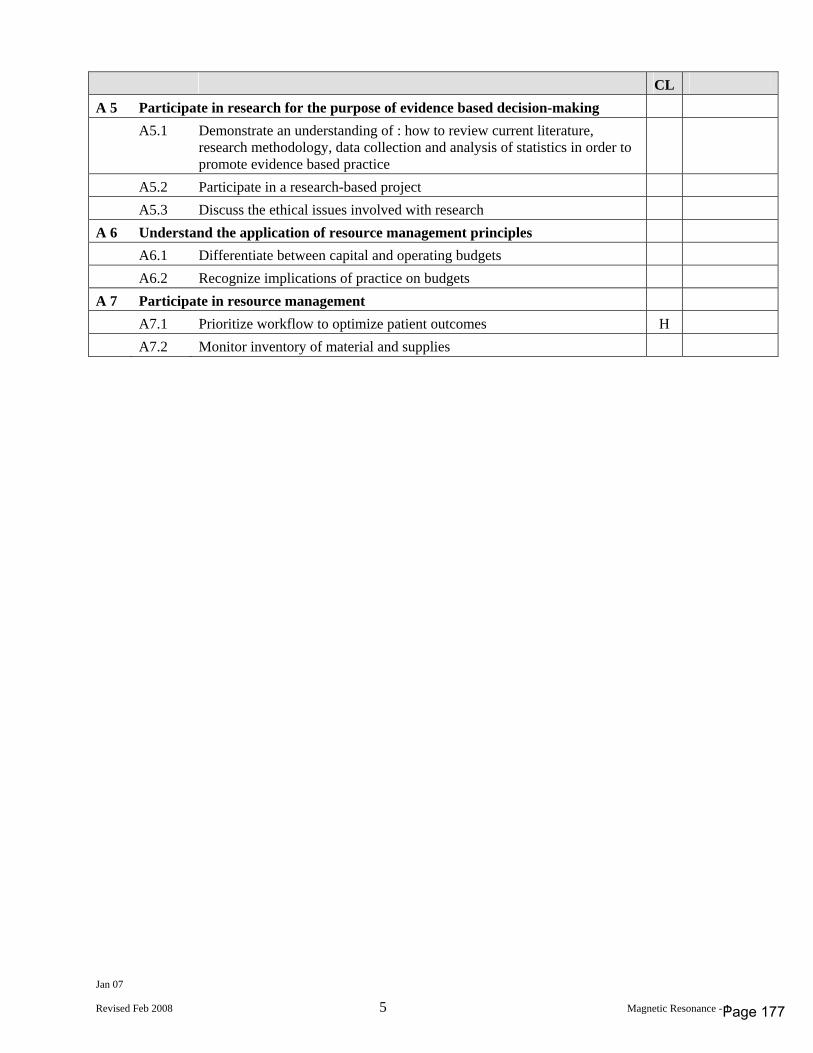
Jan 07
Revised Feb 2008 5 Magnetic Resonance - 1
CL A 5 Participate in research for the purpose of evidence based decision-making A5.1 Demonstrate an understanding of : how to review current literature,
research methodology, data collection and analysis of statistics in order to promote evidence based practice
A5.2 Participate in a research-based project A5.3 Discuss the ethical issues involved with research A 6 Understand the application of resource management principles A6.1 Differentiate between capital and operating budgets A6.2 Recognize implications of practice on budgets A 7 Participate in resource management A7.1 Prioritize workflow to optimize patient outcomes H A7.2 Monitor inventory of material and supplies
Page 177
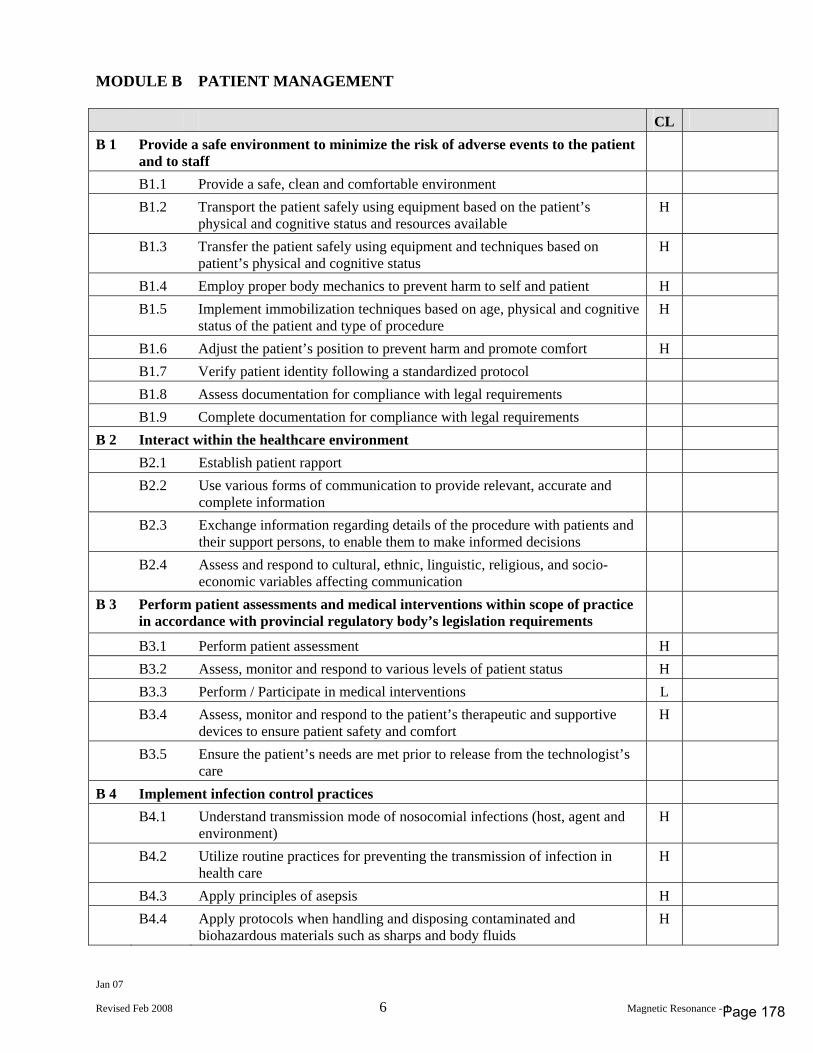
Jan 07
Revised Feb 2008 6 Magnetic Resonance - 1
MODULE B PATIENT MANAGEMENT CL B 1 Provide a safe environment to minimize the risk of adverse events to the patient
and to staff
B1.1 Provide a safe, clean and comfortable environment B1.2 Transport the patient safely using equipment based on the patient’s
physical and cognitive status and resources available H
B1.3 Transfer the patient safely using equipment and techniques based on patient’s physical and cognitive status
H
B1.4 Employ proper body mechanics to prevent harm to self and patient H B1.5 Implement immobilization techniques based on age, physical and cognitive
status of the patient and type of procedure H
B1.6 Adjust the patient’s position to prevent harm and promote comfort H B1.7 Verify patient identity following a standardized protocol B1.8 Assess documentation for compliance with legal requirements B1.9 Complete documentation for compliance with legal requirements B 2 Interact within the healthcare environment B2.1 Establish patient rapport B2.2 Use various forms of communication to provide relevant, accurate and
complete information
B2.3 Exchange information regarding details of the procedure with patients and their support persons, to enable them to make informed decisions
B2.4 Assess and respond to cultural, ethnic, linguistic, religious, and socio-economic variables affecting communication
B 3 Perform patient assessments and medical interventions within scope of practice in accordance with provincial regulatory body’s legislation requirements
B3.1 Perform patient assessment H B3.2 Assess, monitor and respond to various levels of patient status H B3.3 Perform / Participate in medical interventions L B3.4 Assess, monitor and respond to the patient’s therapeutic and supportive
devices to ensure patient safety and comfort H
B3.5 Ensure the patient’s needs are met prior to release from the technologist’s care
B 4 Implement infection control practices B4.1 Understand transmission mode of nosocomial infections (host, agent and
environment) H
B4.2 Utilize routine practices for preventing the transmission of infection in health care
H
B4.3 Apply principles of asepsis H B4.4 Apply protocols when handling and disposing contaminated and
biohazardous materials such as sharps and body fluids H
Page 178
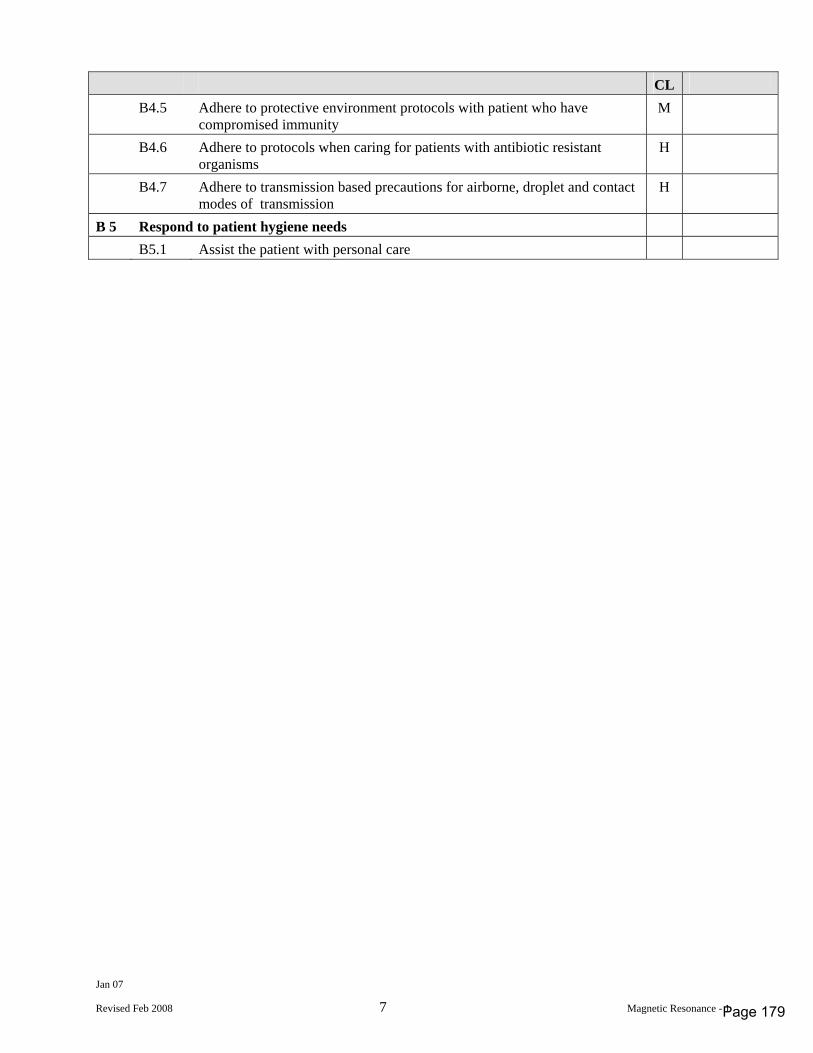
Jan 07
Revised Feb 2008 7 Magnetic Resonance - 1
CL B4.5 Adhere to protective environment protocols with patient who have
compromised immunity M
B4.6 Adhere to protocols when caring for patients with antibiotic resistant organisms
H
B4.7 Adhere to transmission based precautions for airborne, droplet and contact modes of transmission
H
B 5 Respond to patient hygiene needs B5.1 Assist the patient with personal care
Page 179
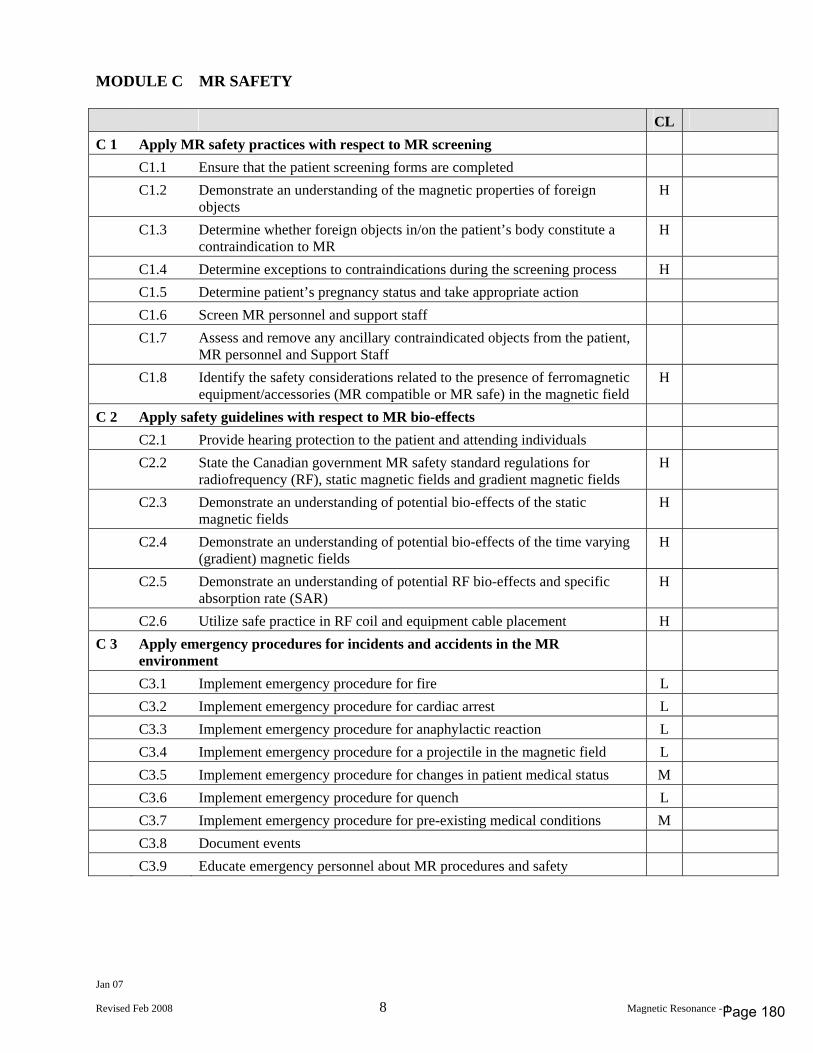
Jan 07
Revised Feb 2008 8 Magnetic Resonance - 1
MODULE C MR SAFETY CL C 1 Apply MR safety practices with respect to MR screening C1.1 Ensure that the patient screening forms are completed C1.2 Demonstrate an understanding of the magnetic properties of foreign
objects H
C1.3 Determine whether foreign objects in/on the patient’s body constitute a contraindication to MR
H
C1.4 Determine exceptions to contraindications during the screening process H C1.5 Determine patient’s pregnancy status and take appropriate action C1.6 Screen MR personnel and support staff C1.7 Assess and remove any ancillary contraindicated objects from the patient,
MR personnel and Support Staff
C1.8 Identify the safety considerations related to the presence of ferromagnetic equipment/accessories (MR compatible or MR safe) in the magnetic field
H
C 2 Apply safety guidelines with respect to MR bio-effects C2.1 Provide hearing protection to the patient and attending individuals C2.2 State the Canadian government MR safety standard regulations for
radiofrequency (RF), static magnetic fields and gradient magnetic fields H
C2.3 Demonstrate an understanding of potential bio-effects of the static magnetic fields
H
C2.4 Demonstrate an understanding of potential bio-effects of the time varying (gradient) magnetic fields
H
C2.5 Demonstrate an understanding of potential RF bio-effects and specific absorption rate (SAR)
H
C2.6 Utilize safe practice in RF coil and equipment cable placement H C 3 Apply emergency procedures for incidents and accidents in the MR
environment
C3.1 Implement emergency procedure for fire L C3.2 Implement emergency procedure for cardiac arrest L C3.3 Implement emergency procedure for anaphylactic reaction L C3.4 Implement emergency procedure for a projectile in the magnetic field L C3.5 Implement emergency procedure for changes in patient medical status M C3.6 Implement emergency procedure for quench L C3.7 Implement emergency procedure for pre-existing medical conditions M C3.8 Document events C3.9 Educate emergency personnel about MR procedures and safety
Page 180
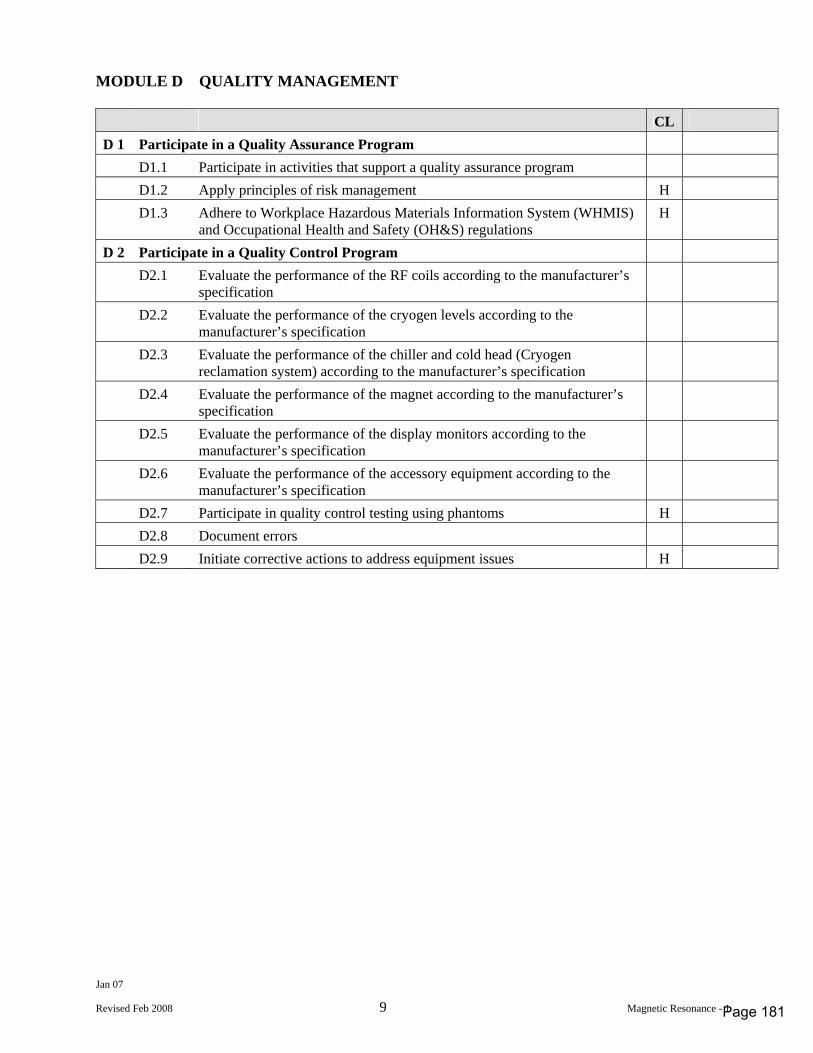
Jan 07
Revised Feb 2008 9 Magnetic Resonance - 1
MODULE D QUALITY MANAGEMENT CL D 1 Participate in a Quality Assurance Program D1.1 Participate in activities that support a quality assurance program D1.2 Apply principles of risk management H D1.3 Adhere to Workplace Hazardous Materials Information System (WHMIS)
and Occupational Health and Safety (OH&S) regulations H
D 2 Participate in a Quality Control Program D2.1 Evaluate the performance of the RF coils according to the manufacturer’s
specification
D2.2 Evaluate the performance of the cryogen levels according to the manufacturer’s specification
D2.3 Evaluate the performance of the chiller and cold head (Cryogen reclamation system) according to the manufacturer’s specification
D2.4 Evaluate the performance of the magnet according to the manufacturer’s specification
D2.5 Evaluate the performance of the display monitors according to the manufacturer’s specification
D2.6 Evaluate the performance of the accessory equipment according to the manufacturer’s specification
D2.7 Participate in quality control testing using phantoms H D2.8 Document errors D2.9 Initiate corrective actions to address equipment issues H
Page 181
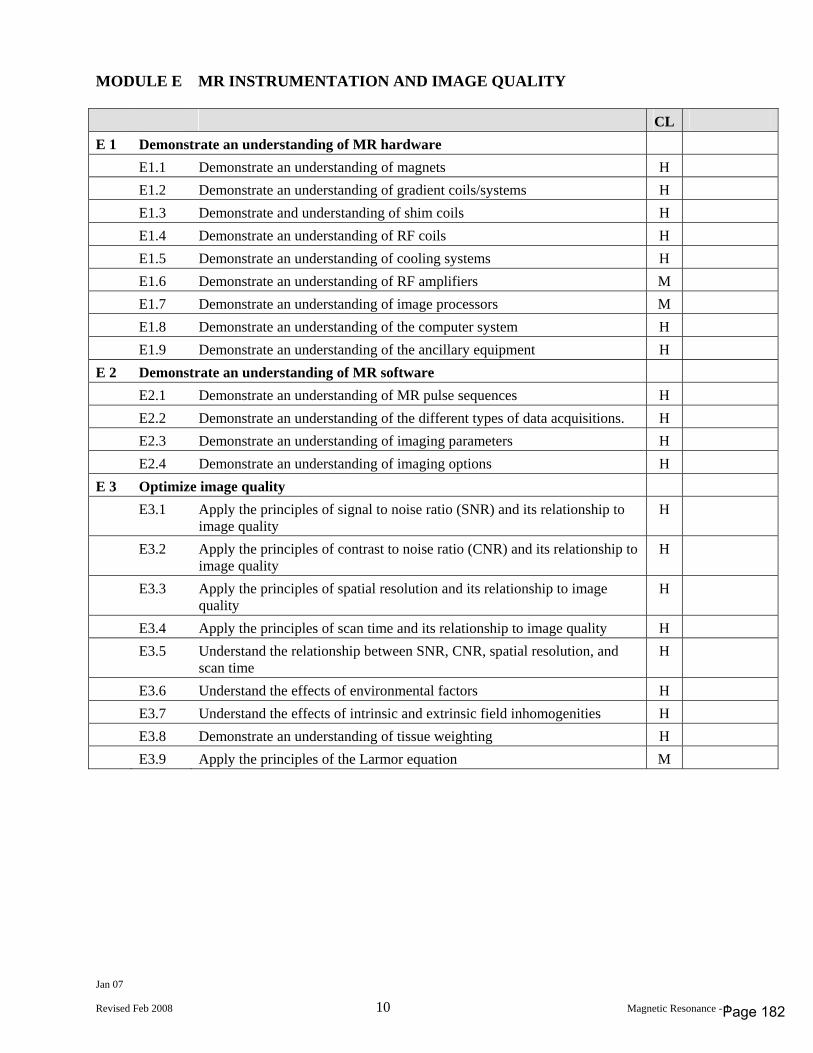
Jan 07
Revised Feb 2008 10 Magnetic Resonance - 1
MODULE E MR INSTRUMENTATION AND IMAGE QUALITY CL E 1 Demonstrate an understanding of MR hardware E1.1 Demonstrate an understanding of magnets H E1.2 Demonstrate an understanding of gradient coils/systems H E1.3 Demonstrate and understanding of shim coils H E1.4 Demonstrate an understanding of RF coils H E1.5 Demonstrate an understanding of cooling systems H E1.6 Demonstrate an understanding of RF amplifiers M E1.7 Demonstrate an understanding of image processors M E1.8 Demonstrate an understanding of the computer system H E1.9 Demonstrate an understanding of the ancillary equipment H E 2 Demonstrate an understanding of MR software E2.1 Demonstrate an understanding of MR pulse sequences H E2.2 Demonstrate an understanding of the different types of data acquisitions. H E2.3 Demonstrate an understanding of imaging parameters H E2.4 Demonstrate an understanding of imaging options H E 3 Optimize image quality E3.1 Apply the principles of signal to noise ratio (SNR) and its relationship to
image quality H
E3.2 Apply the principles of contrast to noise ratio (CNR) and its relationship to image quality
H
E3.3 Apply the principles of spatial resolution and its relationship to image quality
H
E3.4 Apply the principles of scan time and its relationship to image quality H E3.5 Understand the relationship between SNR, CNR, spatial resolution, and
scan time H
E3.6 Understand the effects of environmental factors H E3.7 Understand the effects of intrinsic and extrinsic field inhomogenities H E3.8 Demonstrate an understanding of tissue weighting H E3.9 Apply the principles of the Larmor equation M
Page 182
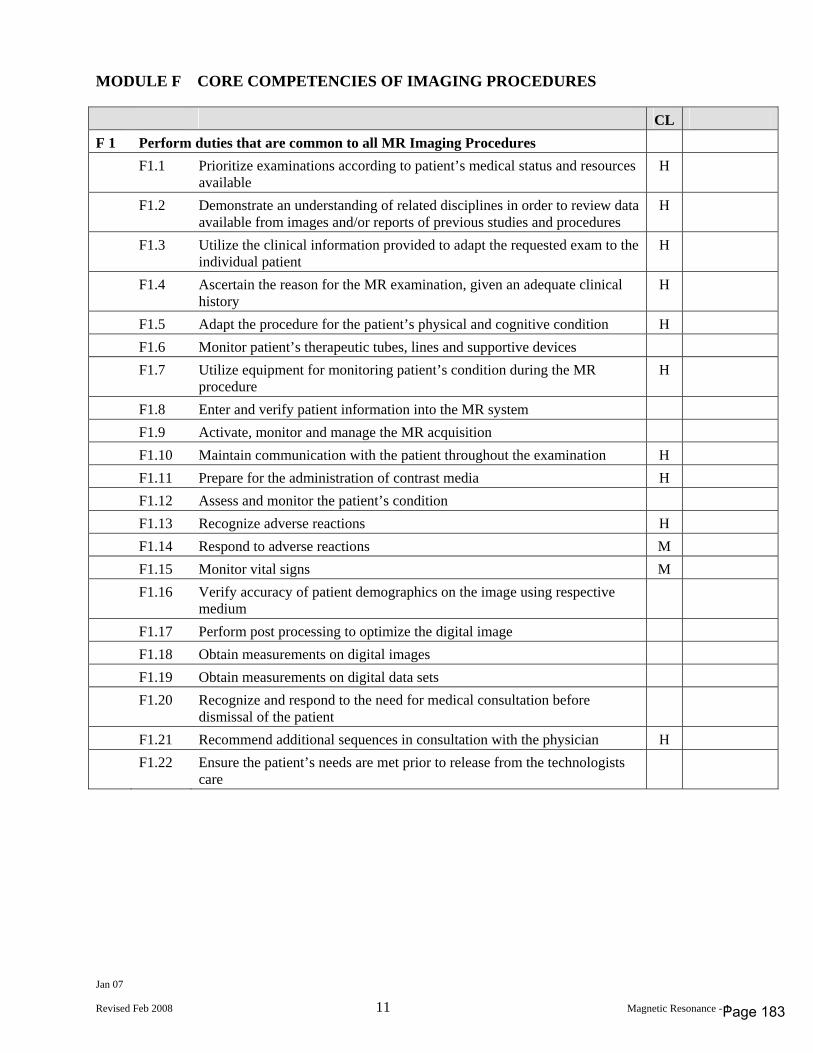
Jan 07
Revised Feb 2008 11 Magnetic Resonance - 1
MODULE F CORE COMPETENCIES OF IMAGING PROCEDURES CL F 1 Perform duties that are common to all MR Imaging Procedures F1.1 Prioritize examinations according to patient’s medical status and resources
available H
F1.2 Demonstrate an understanding of related disciplines in order to review data available from images and/or reports of previous studies and procedures
H
F1.3 Utilize the clinical information provided to adapt the requested exam to the individual patient
H
F1.4 Ascertain the reason for the MR examination, given an adequate clinical history
H
F1.5 Adapt the procedure for the patient’s physical and cognitive condition H F1.6 Monitor patient’s therapeutic tubes, lines and supportive devices F1.7 Utilize equipment for monitoring patient’s condition during the MR
procedure H
F1.8 Enter and verify patient information into the MR system F1.9 Activate, monitor and manage the MR acquisition F1.10 Maintain communication with the patient throughout the examination H F1.11 Prepare for the administration of contrast media H F1.12 Assess and monitor the patient’s condition F1.13 Recognize adverse reactions H F1.14 Respond to adverse reactions M F1.15 Monitor vital signs M F1.16 Verify accuracy of patient demographics on the image using respective
medium
F1.17 Perform post processing to optimize the digital image F1.18 Obtain measurements on digital images F1.19 Obtain measurements on digital data sets F1.20 Recognize and respond to the need for medical consultation before
dismissal of the patient
F1.21 Recommend additional sequences in consultation with the physician H F1.22 Ensure the patient’s needs are met prior to release from the technologists
care
Page 183
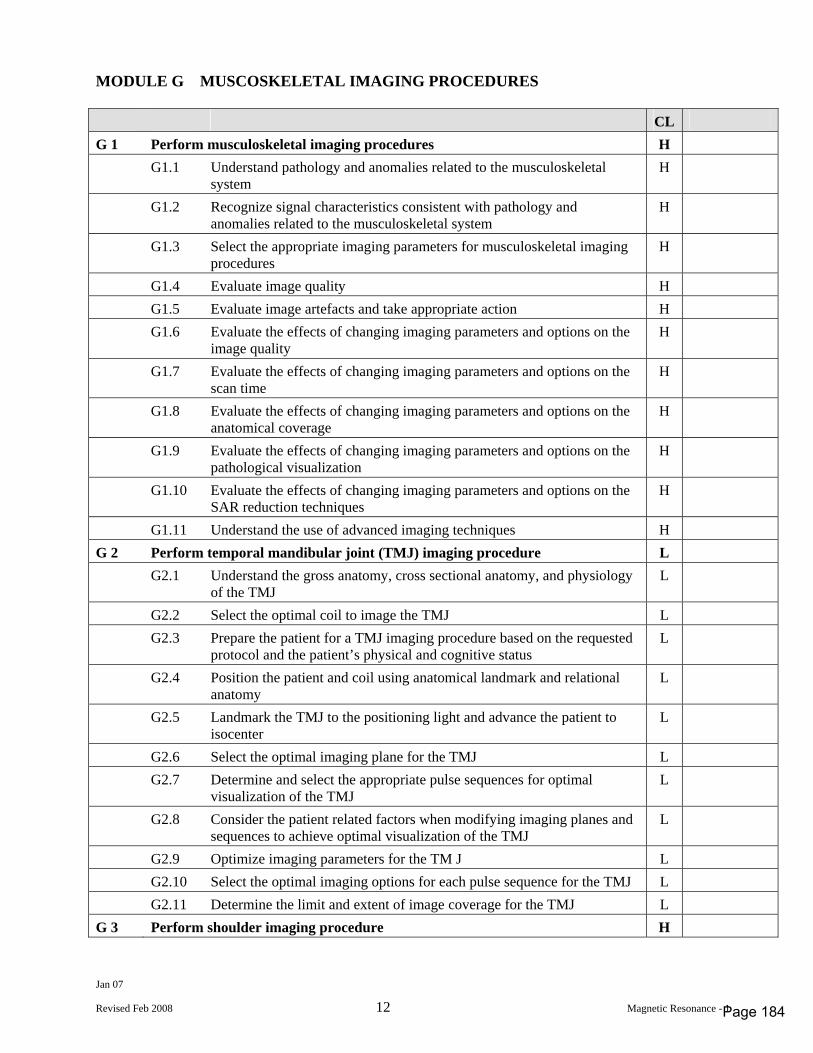
Jan 07
Revised Feb 2008 12 Magnetic Resonance - 1
MODULE G MUSCOSKELETAL IMAGING PROCEDURES CL G 1 Perform musculoskeletal imaging procedures H G1.1 Understand pathology and anomalies related to the musculoskeletal
system H
G1.2 Recognize signal characteristics consistent with pathology and anomalies related to the musculoskeletal system
H
G1.3 Select the appropriate imaging parameters for musculoskeletal imaging procedures
H
G1.4 Evaluate image quality H G1.5 Evaluate image artefacts and take appropriate action H G1.6 Evaluate the effects of changing imaging parameters and options on the
image quality H
G1.7 Evaluate the effects of changing imaging parameters and options on the scan time
H
G1.8 Evaluate the effects of changing imaging parameters and options on the anatomical coverage
H
G1.9 Evaluate the effects of changing imaging parameters and options on the pathological visualization
H
G1.10 Evaluate the effects of changing imaging parameters and options on the SAR reduction techniques
H
G1.11 Understand the use of advanced imaging techniques H G 2 Perform temporal mandibular joint (TMJ) imaging procedure L G2.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the TMJ L
G2.2 Select the optimal coil to image the TMJ L G2.3 Prepare the patient for a TMJ imaging procedure based on the requested
protocol and the patient’s physical and cognitive status L
G2.4 Position the patient and coil using anatomical landmark and relational anatomy
L
G2.5 Landmark the TMJ to the positioning light and advance the patient to isocenter
L
G2.6 Select the optimal imaging plane for the TMJ L G2.7 Determine and select the appropriate pulse sequences for optimal
visualization of the TMJ L
G2.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the TMJ
L
G2.9 Optimize imaging parameters for the TM J L G2.10 Select the optimal imaging options for each pulse sequence for the TMJ L G2.11 Determine the limit and extent of image coverage for the TMJ L G 3 Perform shoulder imaging procedure H
Page 184
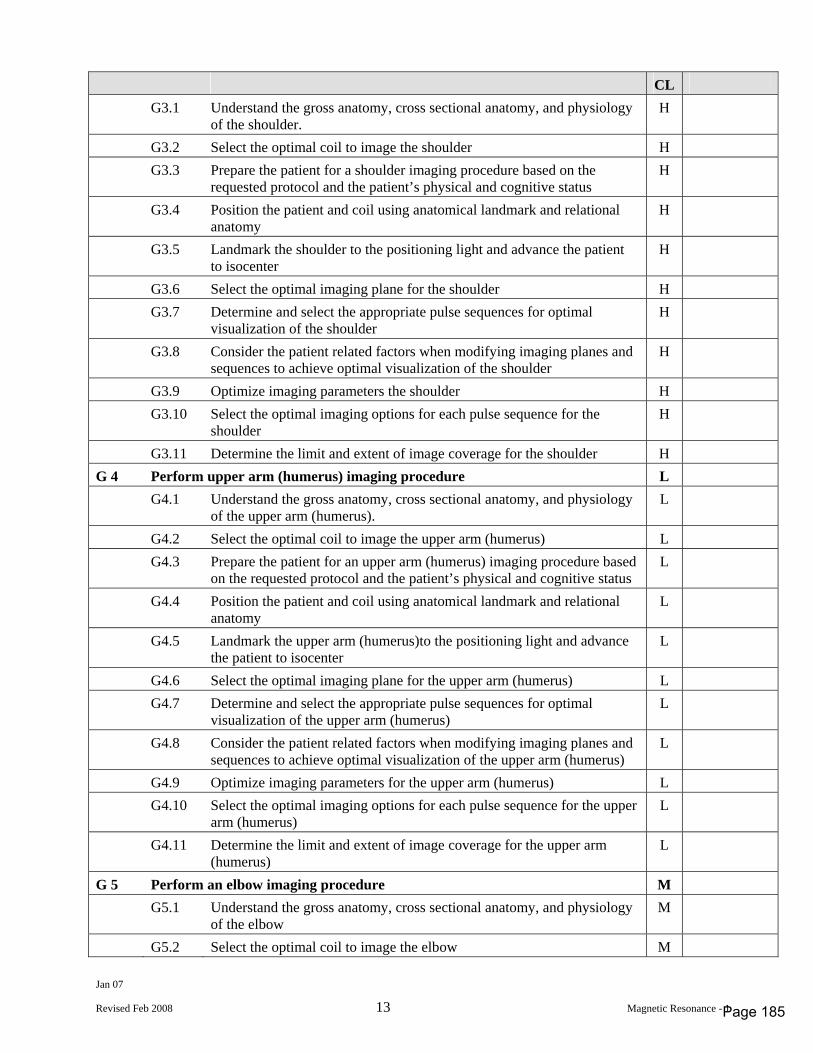
Jan 07
Revised Feb 2008 13 Magnetic Resonance - 1
CL G3.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the shoulder. H
G3.2 Select the optimal coil to image the shoulder H G3.3 Prepare the patient for a shoulder imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
G3.4 Position the patient and coil using anatomical landmark and relational anatomy
H
G3.5 Landmark the shoulder to the positioning light and advance the patient to isocenter
H
G3.6 Select the optimal imaging plane for the shoulder H G3.7 Determine and select the appropriate pulse sequences for optimal
visualization of the shoulder H
G3.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the shoulder
H
G3.9 Optimize imaging parameters the shoulder H G3.10 Select the optimal imaging options for each pulse sequence for the
shoulder H
G3.11 Determine the limit and extent of image coverage for the shoulder H G 4 Perform upper arm (humerus) imaging procedure L G4.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the upper arm (humerus). L
G4.2 Select the optimal coil to image the upper arm (humerus) L G4.3 Prepare the patient for an upper arm (humerus) imaging procedure based
on the requested protocol and the patient’s physical and cognitive status L
G4.4 Position the patient and coil using anatomical landmark and relational anatomy
L
G4.5 Landmark the upper arm (humerus)to the positioning light and advance the patient to isocenter
L
G4.6 Select the optimal imaging plane for the upper arm (humerus) L G4.7 Determine and select the appropriate pulse sequences for optimal
visualization of the upper arm (humerus) L
G4.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the upper arm (humerus)
L
G4.9 Optimize imaging parameters for the upper arm (humerus) L G4.10 Select the optimal imaging options for each pulse sequence for the upper
arm (humerus) L
G4.11 Determine the limit and extent of image coverage for the upper arm (humerus)
L
G 5 Perform an elbow imaging procedure M G5.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the elbow M
G5.2 Select the optimal coil to image the elbow M
Page 185
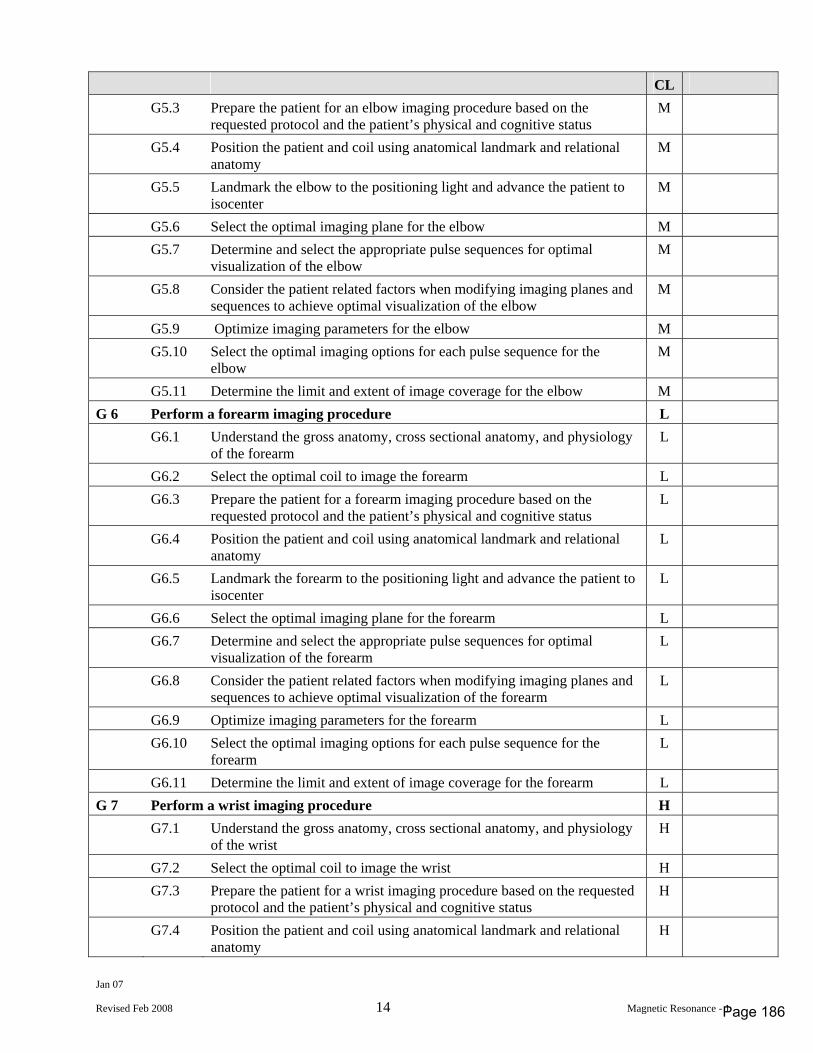
Jan 07
Revised Feb 2008 14 Magnetic Resonance - 1
CL G5.3 Prepare the patient for an elbow imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
G5.4 Position the patient and coil using anatomical landmark and relational anatomy
M
G5.5 Landmark the elbow to the positioning light and advance the patient to isocenter
M
G5.6 Select the optimal imaging plane for the elbow M G5.7 Determine and select the appropriate pulse sequences for optimal
visualization of the elbow M
G5.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the elbow
M
G5.9 Optimize imaging parameters for the elbow M G5.10 Select the optimal imaging options for each pulse sequence for the
elbow M
G5.11 Determine the limit and extent of image coverage for the elbow M G 6 Perform a forearm imaging procedure L G6.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the forearm L
G6.2 Select the optimal coil to image the forearm L G6.3 Prepare the patient for a forearm imaging procedure based on the
requested protocol and the patient’s physical and cognitive status L
G6.4 Position the patient and coil using anatomical landmark and relational anatomy
L
G6.5 Landmark the forearm to the positioning light and advance the patient to isocenter
L
G6.6 Select the optimal imaging plane for the forearm L G6.7 Determine and select the appropriate pulse sequences for optimal
visualization of the forearm L
G6.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the forearm
L
G6.9 Optimize imaging parameters for the forearm L G6.10 Select the optimal imaging options for each pulse sequence for the
forearm L
G6.11 Determine the limit and extent of image coverage for the forearm L G 7 Perform a wrist imaging procedure H G7.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the wrist H
G7.2 Select the optimal coil to image the wrist H G7.3 Prepare the patient for a wrist imaging procedure based on the requested
protocol and the patient’s physical and cognitive status H
G7.4 Position the patient and coil using anatomical landmark and relational anatomy
H
Page 186
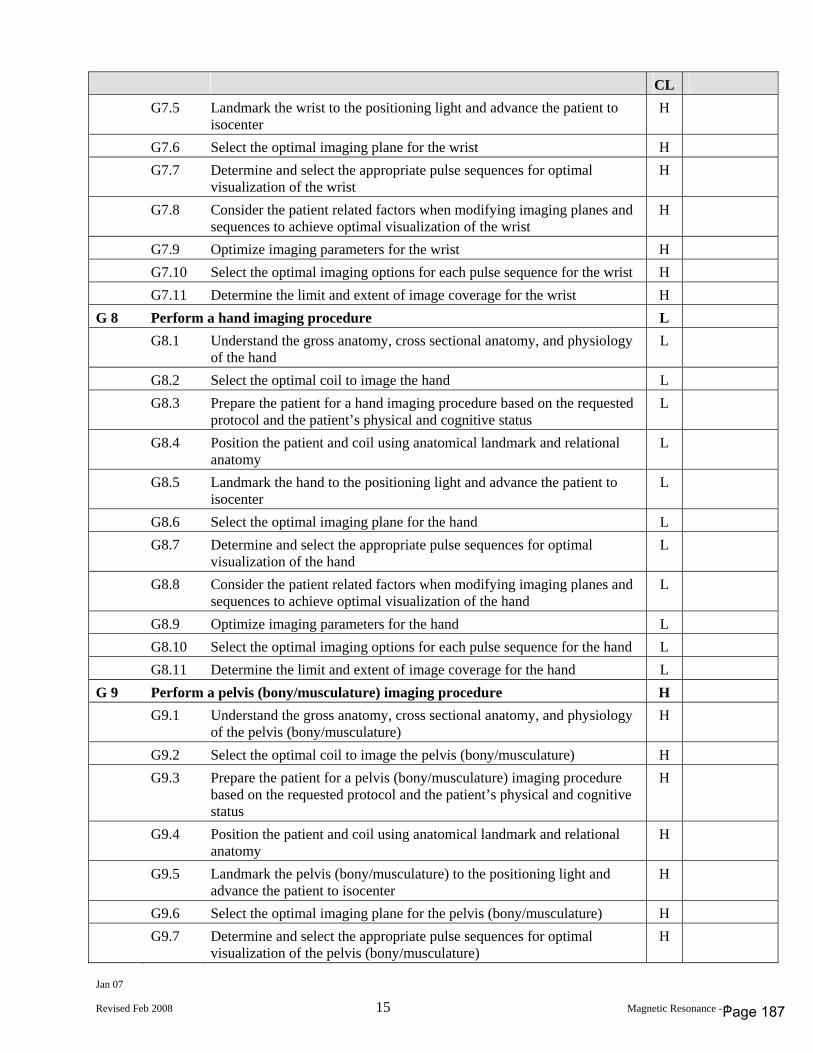
Jan 07
Revised Feb 2008 15 Magnetic Resonance - 1
CL G7.5 Landmark the wrist to the positioning light and advance the patient to
isocenter H
G7.6 Select the optimal imaging plane for the wrist H G7.7 Determine and select the appropriate pulse sequences for optimal
visualization of the wrist H
G7.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the wrist
H
G7.9 Optimize imaging parameters for the wrist H G7.10 Select the optimal imaging options for each pulse sequence for the wrist H G7.11 Determine the limit and extent of image coverage for the wrist H G 8 Perform a hand imaging procedure L G8.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the hand L
G8.2 Select the optimal coil to image the hand L G8.3 Prepare the patient for a hand imaging procedure based on the requested
protocol and the patient’s physical and cognitive status L
G8.4 Position the patient and coil using anatomical landmark and relational anatomy
L
G8.5 Landmark the hand to the positioning light and advance the patient to isocenter
L
G8.6 Select the optimal imaging plane for the hand L G8.7 Determine and select the appropriate pulse sequences for optimal
visualization of the hand L
G8.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the hand
L
G8.9 Optimize imaging parameters for the hand L G8.10 Select the optimal imaging options for each pulse sequence for the hand L G8.11 Determine the limit and extent of image coverage for the hand L G 9 Perform a pelvis (bony/musculature) imaging procedure H G9.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the pelvis (bony/musculature) H
G9.2 Select the optimal coil to image the pelvis (bony/musculature) H G9.3 Prepare the patient for a pelvis (bony/musculature) imaging procedure
based on the requested protocol and the patient’s physical and cognitive status
H
G9.4 Position the patient and coil using anatomical landmark and relational anatomy
H
G9.5 Landmark the pelvis (bony/musculature) to the positioning light and advance the patient to isocenter
H
G9.6 Select the optimal imaging plane for the pelvis (bony/musculature) H G9.7 Determine and select the appropriate pulse sequences for optimal
visualization of the pelvis (bony/musculature) H
Page 187
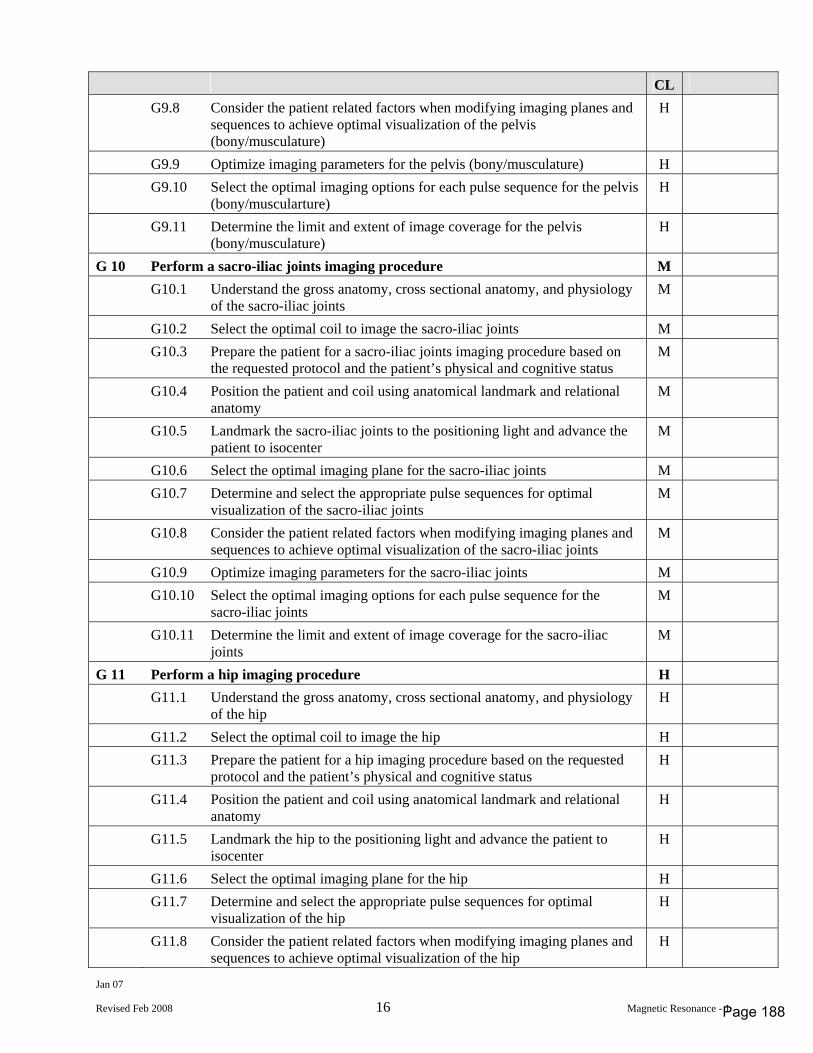
Jan 07
Revised Feb 2008 16 Magnetic Resonance - 1
CL G9.8 Consider the patient related factors when modifying imaging planes and
sequences to achieve optimal visualization of the pelvis (bony/musculature)
H
G9.9 Optimize imaging parameters for the pelvis (bony/musculature) H G9.10 Select the optimal imaging options for each pulse sequence for the pelvis
(bony/muscularture) H
G9.11 Determine the limit and extent of image coverage for the pelvis (bony/musculature)
H
G 10 Perform a sacro-iliac joints imaging procedure M G10.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the sacro-iliac joints M
G10.2 Select the optimal coil to image the sacro-iliac joints M G10.3 Prepare the patient for a sacro-iliac joints imaging procedure based on
the requested protocol and the patient’s physical and cognitive status M
G10.4 Position the patient and coil using anatomical landmark and relational anatomy
M
G10.5 Landmark the sacro-iliac joints to the positioning light and advance the patient to isocenter
M
G10.6 Select the optimal imaging plane for the sacro-iliac joints M G10.7 Determine and select the appropriate pulse sequences for optimal
visualization of the sacro-iliac joints M
G10.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the sacro-iliac joints
M
G10.9 Optimize imaging parameters for the sacro-iliac joints M G10.10 Select the optimal imaging options for each pulse sequence for the
sacro-iliac joints M
G10.11 Determine the limit and extent of image coverage for the sacro-iliac joints
M
G 11 Perform a hip imaging procedure H G11.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the hip H
G11.2 Select the optimal coil to image the hip H G11.3 Prepare the patient for a hip imaging procedure based on the requested
protocol and the patient’s physical and cognitive status H
G11.4 Position the patient and coil using anatomical landmark and relational anatomy
H
G11.5 Landmark the hip to the positioning light and advance the patient to isocenter
H
G11.6 Select the optimal imaging plane for the hip H G11.7 Determine and select the appropriate pulse sequences for optimal
visualization of the hip H
G11.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the hip
H
Page 188
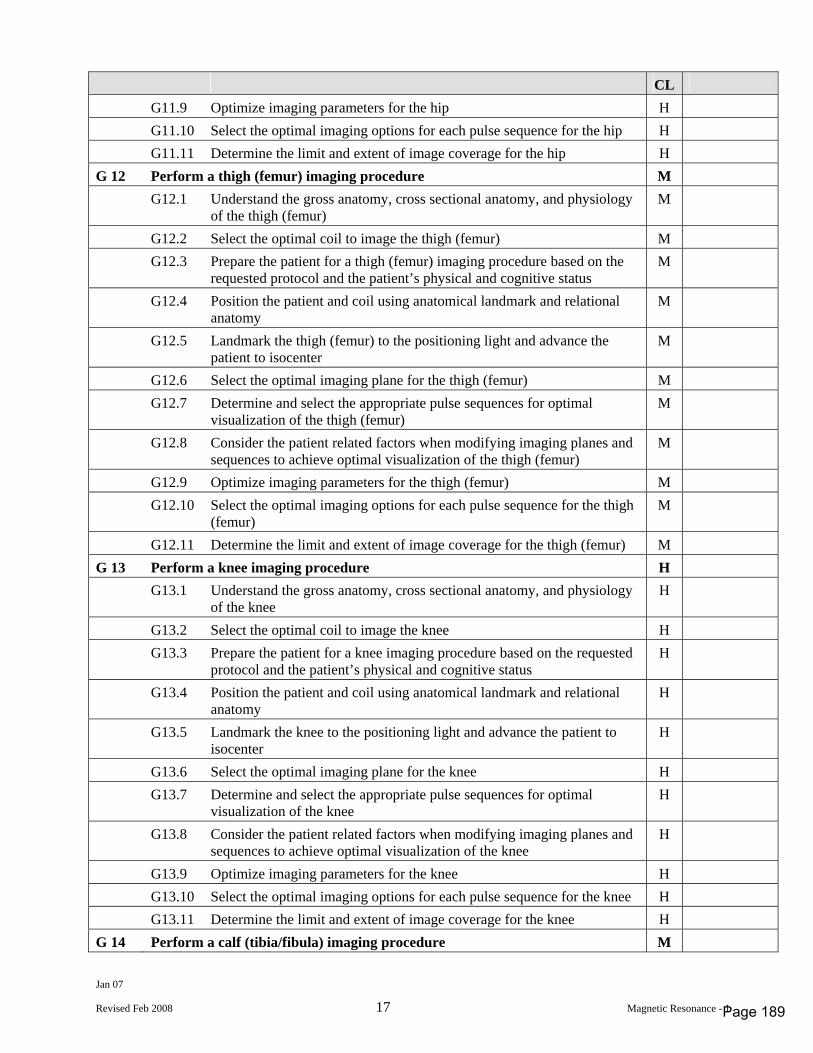
Jan 07
Revised Feb 2008 17 Magnetic Resonance - 1
CL G11.9 Optimize imaging parameters for the hip H G11.10 Select the optimal imaging options for each pulse sequence for the hip H G11.11 Determine the limit and extent of image coverage for the hip H G 12 Perform a thigh (femur) imaging procedure M G12.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the thigh (femur) M
G12.2 Select the optimal coil to image the thigh (femur) M G12.3 Prepare the patient for a thigh (femur) imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
G12.4 Position the patient and coil using anatomical landmark and relational anatomy
M
G12.5 Landmark the thigh (femur) to the positioning light and advance the patient to isocenter
M
G12.6 Select the optimal imaging plane for the thigh (femur) M G12.7 Determine and select the appropriate pulse sequences for optimal
visualization of the thigh (femur) M
G12.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the thigh (femur)
M
G12.9 Optimize imaging parameters for the thigh (femur) M G12.10 Select the optimal imaging options for each pulse sequence for the thigh
(femur) M
G12.11 Determine the limit and extent of image coverage for the thigh (femur) M G 13 Perform a knee imaging procedure H G13.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the knee H
G13.2 Select the optimal coil to image the knee H G13.3 Prepare the patient for a knee imaging procedure based on the requested
protocol and the patient’s physical and cognitive status H
G13.4 Position the patient and coil using anatomical landmark and relational anatomy
H
G13.5 Landmark the knee to the positioning light and advance the patient to isocenter
H
G13.6 Select the optimal imaging plane for the knee H G13.7 Determine and select the appropriate pulse sequences for optimal
visualization of the knee H
G13.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the knee
H
G13.9 Optimize imaging parameters for the knee H G13.10 Select the optimal imaging options for each pulse sequence for the knee H G13.11 Determine the limit and extent of image coverage for the knee H G 14 Perform a calf (tibia/fibula) imaging procedure M
Page 189
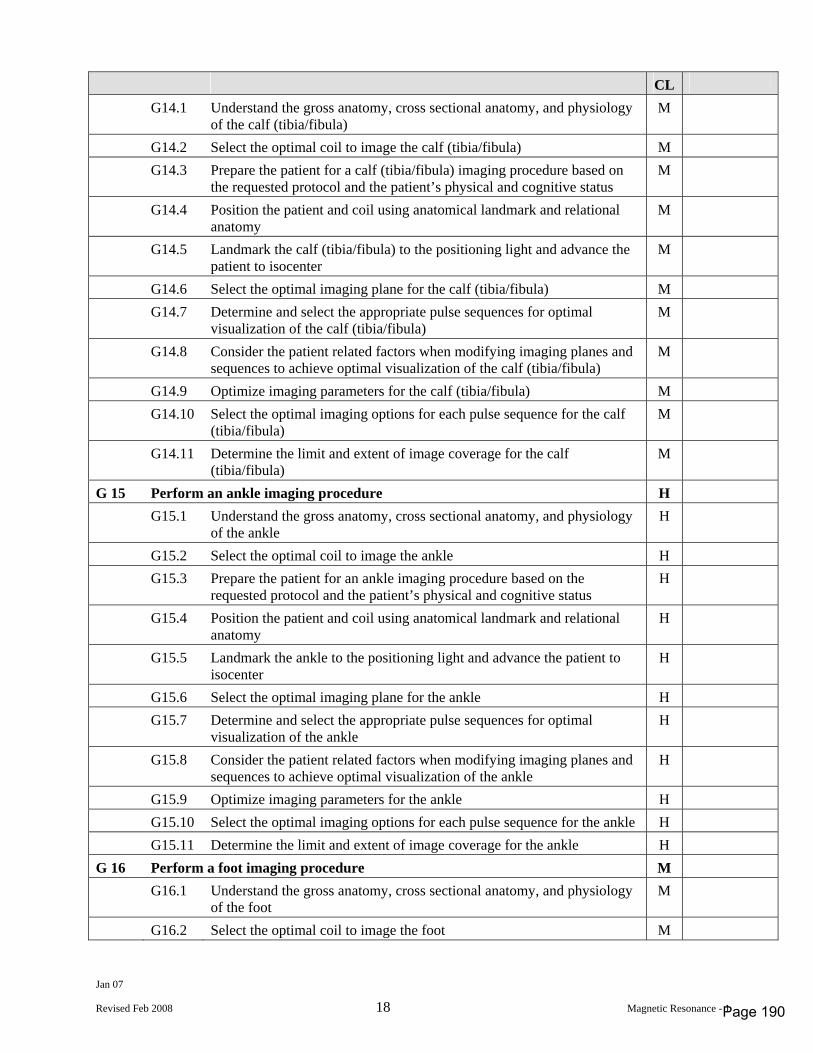
Jan 07
Revised Feb 2008 18 Magnetic Resonance - 1
CL G14.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the calf (tibia/fibula) M
G14.2 Select the optimal coil to image the calf (tibia/fibula) M G14.3 Prepare the patient for a calf (tibia/fibula) imaging procedure based on
the requested protocol and the patient’s physical and cognitive status M
G14.4 Position the patient and coil using anatomical landmark and relational anatomy
M
G14.5 Landmark the calf (tibia/fibula) to the positioning light and advance the patient to isocenter
M
G14.6 Select the optimal imaging plane for the calf (tibia/fibula) M G14.7 Determine and select the appropriate pulse sequences for optimal
visualization of the calf (tibia/fibula) M
G14.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the calf (tibia/fibula)
M
G14.9 Optimize imaging parameters for the calf (tibia/fibula) M G14.10 Select the optimal imaging options for each pulse sequence for the calf
(tibia/fibula) M
G14.11 Determine the limit and extent of image coverage for the calf (tibia/fibula)
M
G 15 Perform an ankle imaging procedure H G15.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the ankle H
G15.2 Select the optimal coil to image the ankle H G15.3 Prepare the patient for an ankle imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
G15.4 Position the patient and coil using anatomical landmark and relational anatomy
H
G15.5 Landmark the ankle to the positioning light and advance the patient to isocenter
H
G15.6 Select the optimal imaging plane for the ankle H G15.7 Determine and select the appropriate pulse sequences for optimal
visualization of the ankle H
G15.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the ankle
H
G15.9 Optimize imaging parameters for the ankle H G15.10 Select the optimal imaging options for each pulse sequence for the ankle H G15.11 Determine the limit and extent of image coverage for the ankle H G 16 Perform a foot imaging procedure M G16.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the foot M
G16.2 Select the optimal coil to image the foot M
Page 190
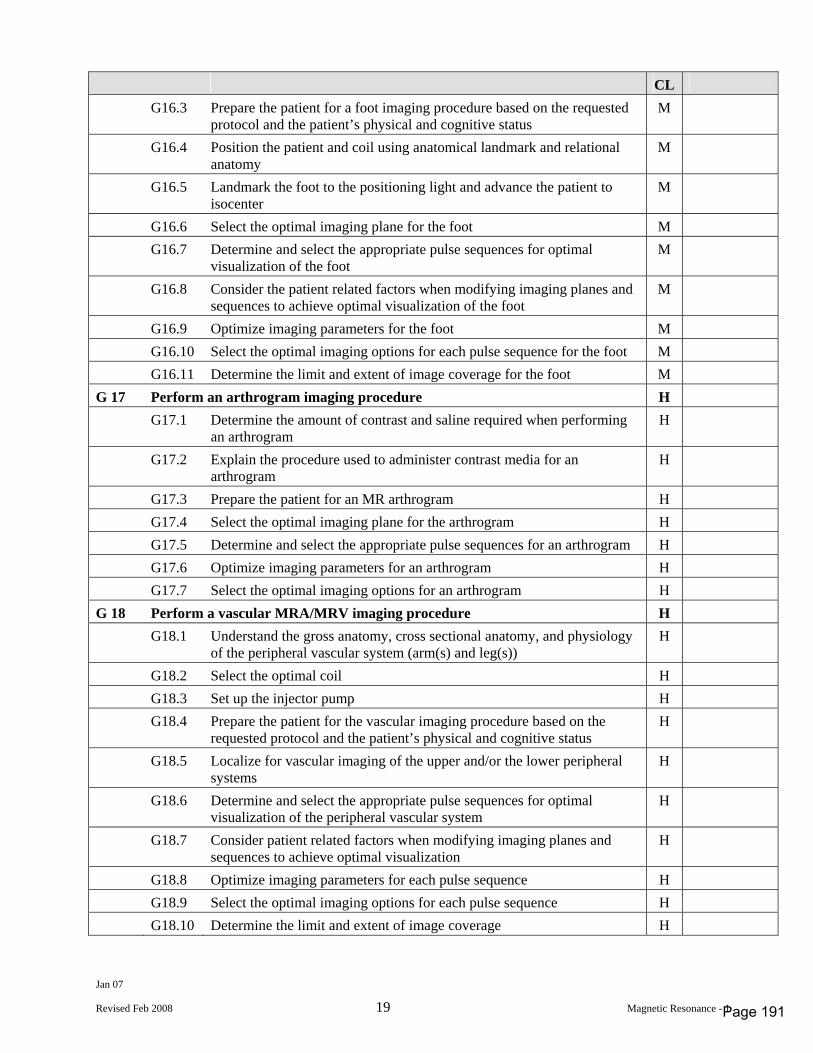
Jan 07
Revised Feb 2008 19 Magnetic Resonance - 1
CL G16.3 Prepare the patient for a foot imaging procedure based on the requested
protocol and the patient’s physical and cognitive status M
G16.4 Position the patient and coil using anatomical landmark and relational anatomy
M
G16.5 Landmark the foot to the positioning light and advance the patient to isocenter
M
G16.6 Select the optimal imaging plane for the foot M G16.7 Determine and select the appropriate pulse sequences for optimal
visualization of the foot M
G16.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the foot
M
G16.9 Optimize imaging parameters for the foot M G16.10 Select the optimal imaging options for each pulse sequence for the foot M G16.11 Determine the limit and extent of image coverage for the foot M G 17 Perform an arthrogram imaging procedure H G17.1 Determine the amount of contrast and saline required when performing
an arthrogram H
G17.2 Explain the procedure used to administer contrast media for an arthrogram
H
G17.3 Prepare the patient for an MR arthrogram H G17.4 Select the optimal imaging plane for the arthrogram H G17.5 Determine and select the appropriate pulse sequences for an arthrogram H G17.6 Optimize imaging parameters for an arthrogram H G17.7 Select the optimal imaging options for an arthrogram H G 18 Perform a vascular MRA/MRV imaging procedure H G18.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the peripheral vascular system (arm(s) and leg(s)) H
G18.2 Select the optimal coil H G18.3 Set up the injector pump H G18.4 Prepare the patient for the vascular imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
G18.5 Localize for vascular imaging of the upper and/or the lower peripheral systems
H
G18.6 Determine and select the appropriate pulse sequences for optimal visualization of the peripheral vascular system
H
G18.7 Consider patient related factors when modifying imaging planes and sequences to achieve optimal visualization
H
G18.8 Optimize imaging parameters for each pulse sequence H G18.9 Select the optimal imaging options for each pulse sequence H G18.10 Determine the limit and extent of image coverage H
Page 191
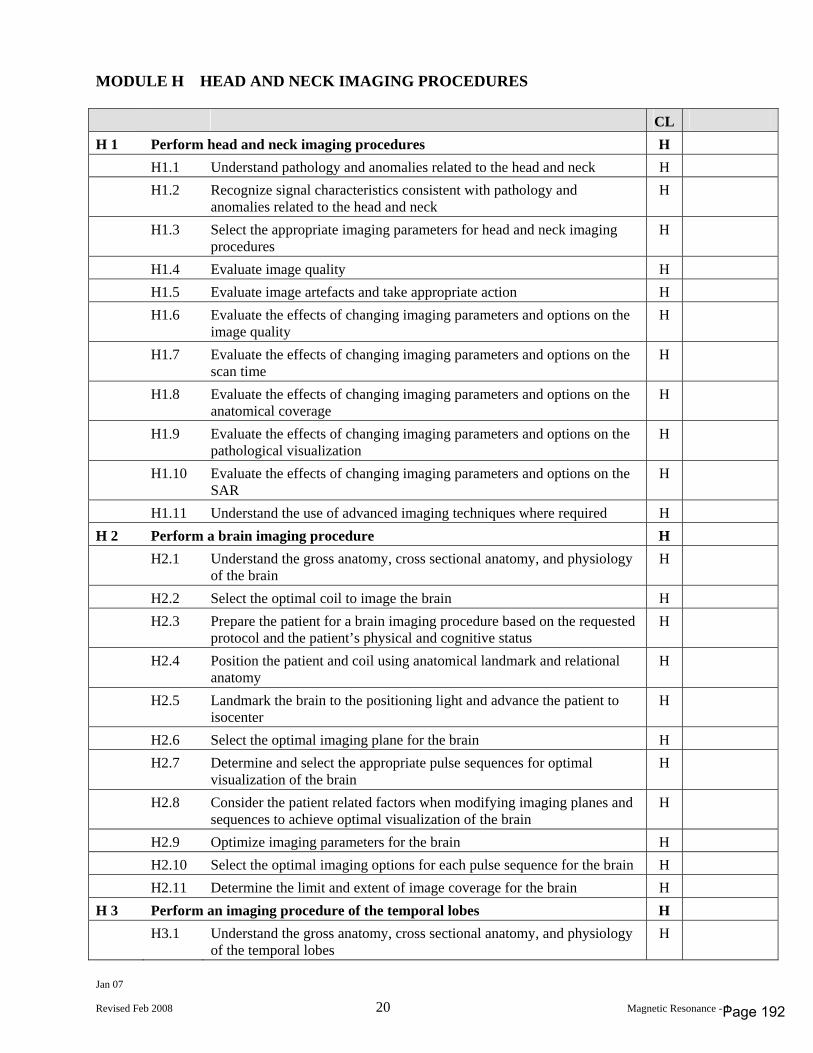
Jan 07
Revised Feb 2008 20 Magnetic Resonance - 1
MODULE H HEAD AND NECK IMAGING PROCEDURES CL H 1 Perform head and neck imaging procedures H H1.1 Understand pathology and anomalies related to the head and neck H H1.2 Recognize signal characteristics consistent with pathology and
anomalies related to the head and neck H
H1.3 Select the appropriate imaging parameters for head and neck imaging procedures
H
H1.4 Evaluate image quality H H1.5 Evaluate image artefacts and take appropriate action H H1.6 Evaluate the effects of changing imaging parameters and options on the
image quality H
H1.7 Evaluate the effects of changing imaging parameters and options on the scan time
H
H1.8 Evaluate the effects of changing imaging parameters and options on the anatomical coverage
H
H1.9 Evaluate the effects of changing imaging parameters and options on the pathological visualization
H
H1.10 Evaluate the effects of changing imaging parameters and options on the SAR
H
H1.11 Understand the use of advanced imaging techniques where required H H 2 Perform a brain imaging procedure H H2.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the brain H
H2.2 Select the optimal coil to image the brain H H2.3 Prepare the patient for a brain imaging procedure based on the requested
protocol and the patient’s physical and cognitive status H
H2.4 Position the patient and coil using anatomical landmark and relational anatomy
H
H2.5 Landmark the brain to the positioning light and advance the patient to isocenter
H
H2.6 Select the optimal imaging plane for the brain H H2.7 Determine and select the appropriate pulse sequences for optimal
visualization of the brain H
H2.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the brain
H
H2.9 Optimize imaging parameters for the brain H H2.10 Select the optimal imaging options for each pulse sequence for the brain H H2.11 Determine the limit and extent of image coverage for the brain H H 3 Perform an imaging procedure of the temporal lobes H H3.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the temporal lobes H
Page 192
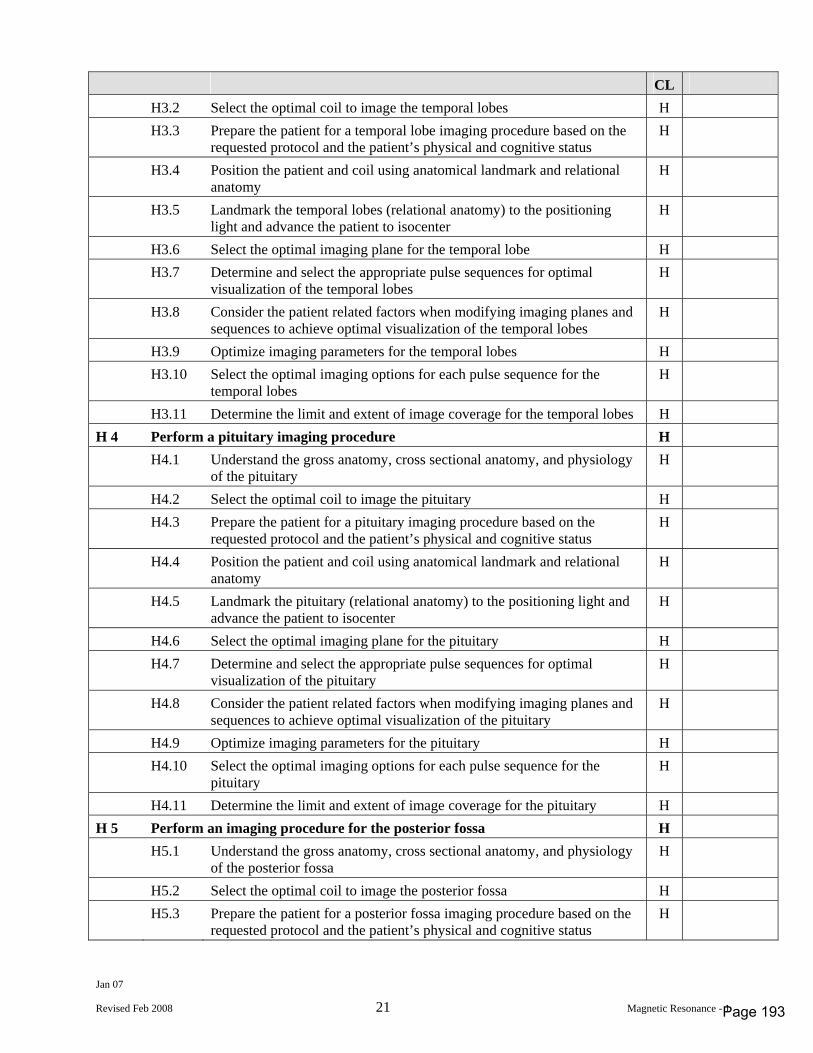
Jan 07
Revised Feb 2008 21 Magnetic Resonance - 1
CL H3.2 Select the optimal coil to image the temporal lobes H H3.3 Prepare the patient for a temporal lobe imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
H3.4 Position the patient and coil using anatomical landmark and relational anatomy
H
H3.5 Landmark the temporal lobes (relational anatomy) to the positioning light and advance the patient to isocenter
H
H3.6 Select the optimal imaging plane for the temporal lobe H H3.7 Determine and select the appropriate pulse sequences for optimal
visualization of the temporal lobes H
H3.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the temporal lobes
H
H3.9 Optimize imaging parameters for the temporal lobes H H3.10 Select the optimal imaging options for each pulse sequence for the
temporal lobes H
H3.11 Determine the limit and extent of image coverage for the temporal lobes H H 4 Perform a pituitary imaging procedure H H4.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the pituitary H
H4.2 Select the optimal coil to image the pituitary H H4.3 Prepare the patient for a pituitary imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
H4.4 Position the patient and coil using anatomical landmark and relational anatomy
H
H4.5 Landmark the pituitary (relational anatomy) to the positioning light and advance the patient to isocenter
H
H4.6 Select the optimal imaging plane for the pituitary H H4.7 Determine and select the appropriate pulse sequences for optimal
visualization of the pituitary H
H4.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the pituitary
H
H4.9 Optimize imaging parameters for the pituitary H H4.10 Select the optimal imaging options for each pulse sequence for the
pituitary H
H4.11 Determine the limit and extent of image coverage for the pituitary H H 5 Perform an imaging procedure for the posterior fossa H H5.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the posterior fossa H
H5.2 Select the optimal coil to image the posterior fossa H H5.3 Prepare the patient for a posterior fossa imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
Page 193
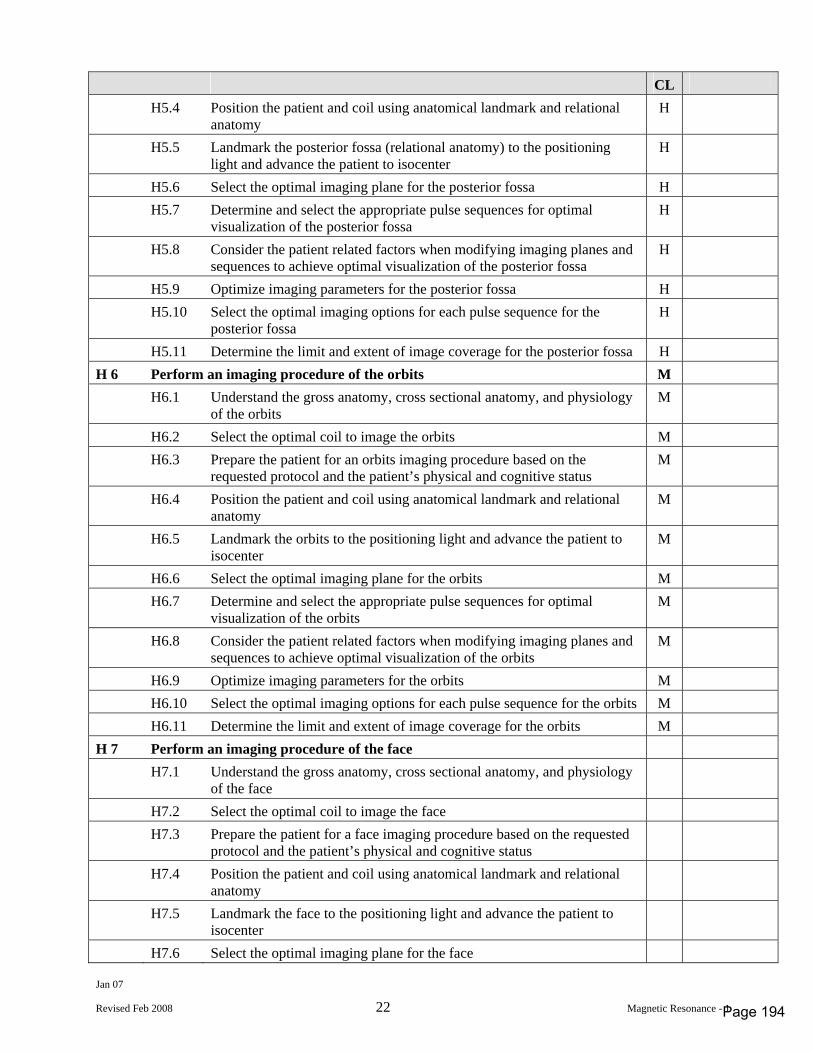
Jan 07
Revised Feb 2008 22 Magnetic Resonance - 1
CL H5.4 Position the patient and coil using anatomical landmark and relational
anatomy H
H5.5 Landmark the posterior fossa (relational anatomy) to the positioning light and advance the patient to isocenter
H
H5.6 Select the optimal imaging plane for the posterior fossa H H5.7 Determine and select the appropriate pulse sequences for optimal
visualization of the posterior fossa H
H5.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the posterior fossa
H
H5.9 Optimize imaging parameters for the posterior fossa H H5.10 Select the optimal imaging options for each pulse sequence for the
posterior fossa H
H5.11 Determine the limit and extent of image coverage for the posterior fossa H H 6 Perform an imaging procedure of the orbits M H6.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the orbits M
H6.2 Select the optimal coil to image the orbits M H6.3 Prepare the patient for an orbits imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
H6.4 Position the patient and coil using anatomical landmark and relational anatomy
M
H6.5 Landmark the orbits to the positioning light and advance the patient to isocenter
M
H6.6 Select the optimal imaging plane for the orbits M H6.7 Determine and select the appropriate pulse sequences for optimal
visualization of the orbits M
H6.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the orbits
M
H6.9 Optimize imaging parameters for the orbits M H6.10 Select the optimal imaging options for each pulse sequence for the orbits M H6.11 Determine the limit and extent of image coverage for the orbits M H 7 Perform an imaging procedure of the face H7.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the face
H7.2 Select the optimal coil to image the face H7.3 Prepare the patient for a face imaging procedure based on the requested
protocol and the patient’s physical and cognitive status
H7.4 Position the patient and coil using anatomical landmark and relational anatomy
H7.5 Landmark the face to the positioning light and advance the patient to isocenter
H7.6 Select the optimal imaging plane for the face
Page 194
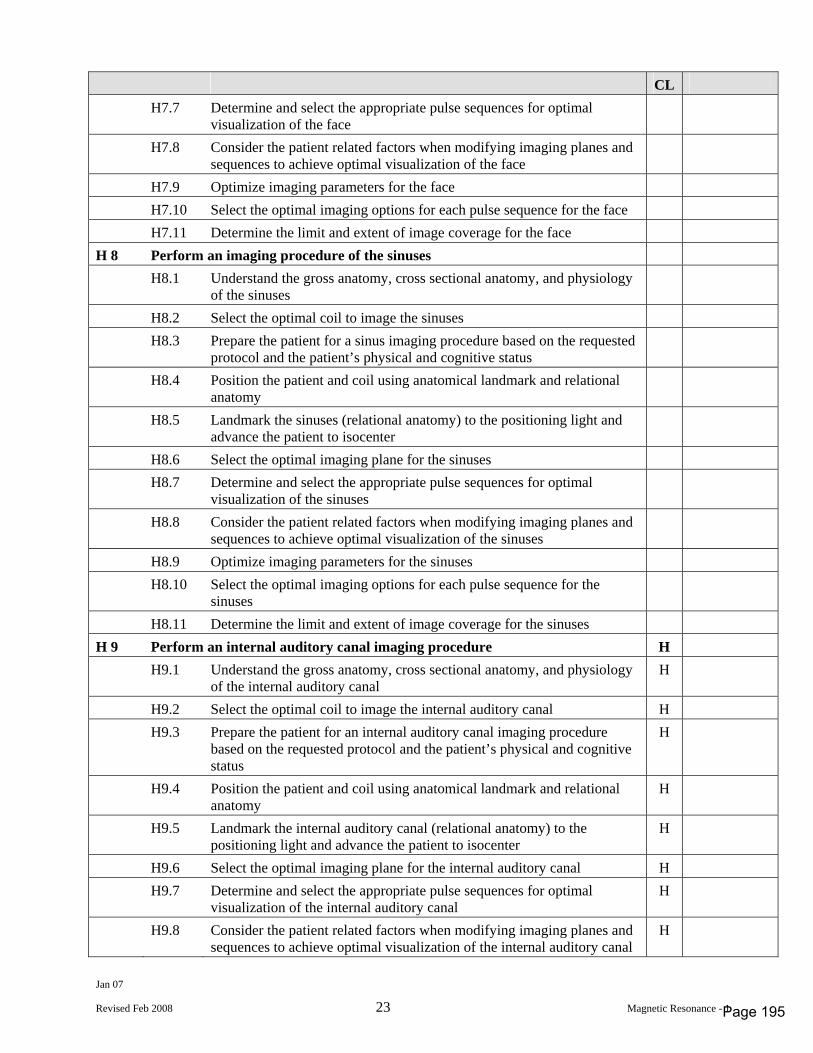
Jan 07
Revised Feb 2008 23 Magnetic Resonance - 1
CL H7.7 Determine and select the appropriate pulse sequences for optimal
visualization of the face
H7.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the face
H7.9 Optimize imaging parameters for the face H7.10 Select the optimal imaging options for each pulse sequence for the face H7.11 Determine the limit and extent of image coverage for the face H 8 Perform an imaging procedure of the sinuses H8.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the sinuses
H8.2 Select the optimal coil to image the sinuses H8.3 Prepare the patient for a sinus imaging procedure based on the requested
protocol and the patient’s physical and cognitive status
H8.4 Position the patient and coil using anatomical landmark and relational anatomy
H8.5 Landmark the sinuses (relational anatomy) to the positioning light and advance the patient to isocenter
H8.6 Select the optimal imaging plane for the sinuses H8.7 Determine and select the appropriate pulse sequences for optimal
visualization of the sinuses
H8.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the sinuses
H8.9 Optimize imaging parameters for the sinuses H8.10 Select the optimal imaging options for each pulse sequence for the
sinuses
H8.11 Determine the limit and extent of image coverage for the sinuses H 9 Perform an internal auditory canal imaging procedure H H9.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the internal auditory canal H
H9.2 Select the optimal coil to image the internal auditory canal H H9.3 Prepare the patient for an internal auditory canal imaging procedure
based on the requested protocol and the patient’s physical and cognitive status
H
H9.4 Position the patient and coil using anatomical landmark and relational anatomy
H
H9.5 Landmark the internal auditory canal (relational anatomy) to the positioning light and advance the patient to isocenter
H
H9.6 Select the optimal imaging plane for the internal auditory canal H H9.7 Determine and select the appropriate pulse sequences for optimal
visualization of the internal auditory canal H
H9.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the internal auditory canal
H
Page 195
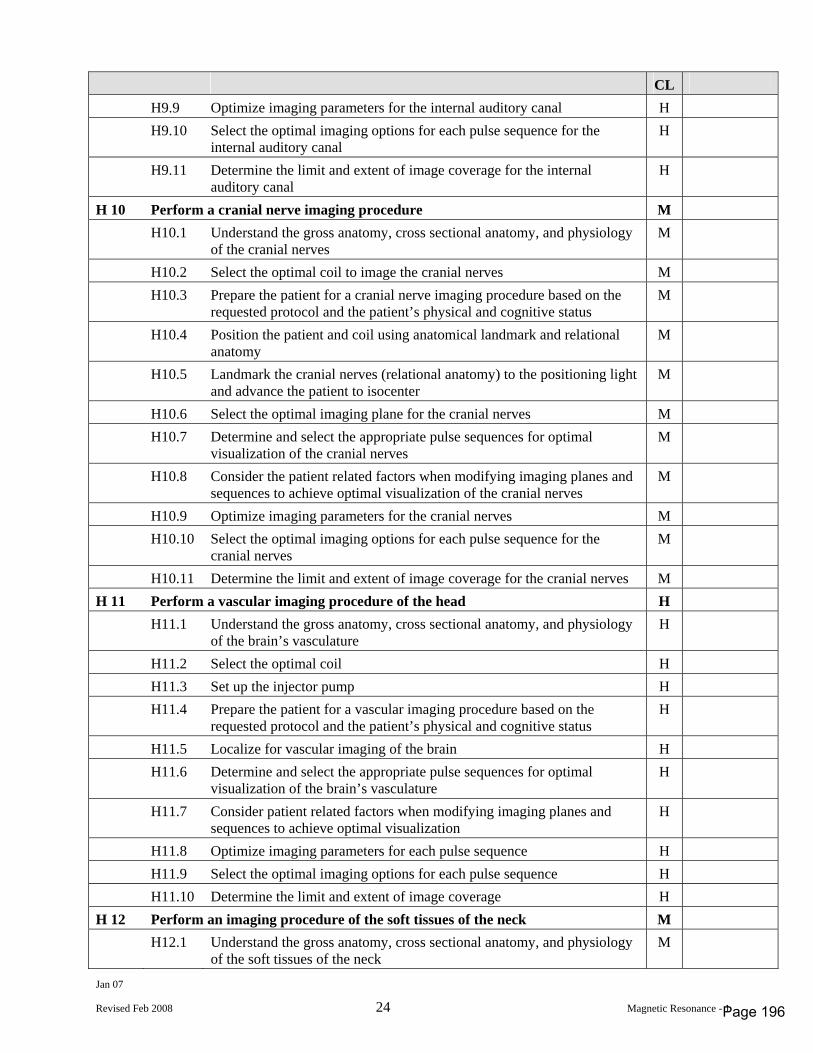
Jan 07
Revised Feb 2008 24 Magnetic Resonance - 1
CL H9.9 Optimize imaging parameters for the internal auditory canal H H9.10 Select the optimal imaging options for each pulse sequence for the
internal auditory canal H
H9.11 Determine the limit and extent of image coverage for the internal auditory canal
H
H 10 Perform a cranial nerve imaging procedure M H10.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the cranial nerves M
H10.2 Select the optimal coil to image the cranial nerves M H10.3 Prepare the patient for a cranial nerve imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
H10.4 Position the patient and coil using anatomical landmark and relational anatomy
M
H10.5 Landmark the cranial nerves (relational anatomy) to the positioning light and advance the patient to isocenter
M
H10.6 Select the optimal imaging plane for the cranial nerves M H10.7 Determine and select the appropriate pulse sequences for optimal
visualization of the cranial nerves M
H10.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the cranial nerves
M
H10.9 Optimize imaging parameters for the cranial nerves M H10.10 Select the optimal imaging options for each pulse sequence for the
cranial nerves M
H10.11 Determine the limit and extent of image coverage for the cranial nerves M H 11 Perform a vascular imaging procedure of the head H H11.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the brain’s vasculature H
H11.2 Select the optimal coil H H11.3 Set up the injector pump H H11.4 Prepare the patient for a vascular imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
H11.5 Localize for vascular imaging of the brain H H11.6 Determine and select the appropriate pulse sequences for optimal
visualization of the brain’s vasculature H
H11.7 Consider patient related factors when modifying imaging planes and sequences to achieve optimal visualization
H
H11.8 Optimize imaging parameters for each pulse sequence H H11.9 Select the optimal imaging options for each pulse sequence H H11.10 Determine the limit and extent of image coverage H H 12 Perform an imaging procedure of the soft tissues of the neck M H12.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the soft tissues of the neck M
Page 196
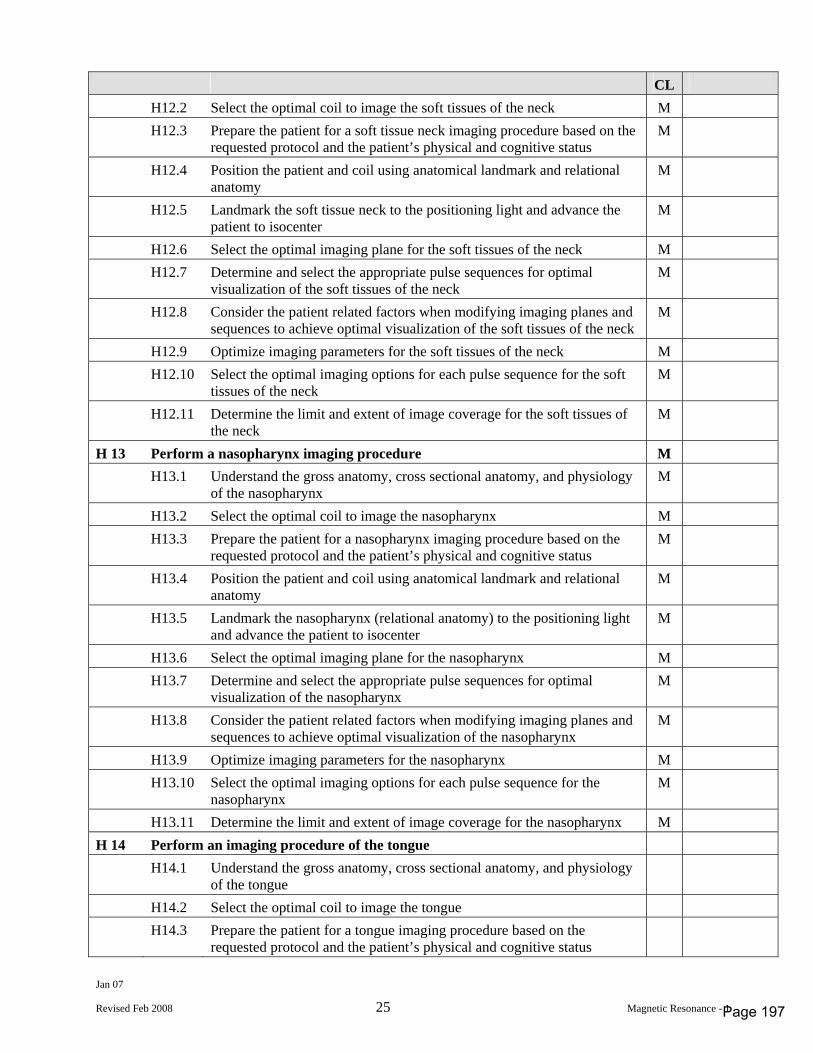
Jan 07
Revised Feb 2008 25 Magnetic Resonance - 1
CL H12.2 Select the optimal coil to image the soft tissues of the neck M H12.3 Prepare the patient for a soft tissue neck imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
H12.4 Position the patient and coil using anatomical landmark and relational anatomy
M
H12.5 Landmark the soft tissue neck to the positioning light and advance the patient to isocenter
M
H12.6 Select the optimal imaging plane for the soft tissues of the neck M H12.7 Determine and select the appropriate pulse sequences for optimal
visualization of the soft tissues of the neck M
H12.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the soft tissues of the neck
M
H12.9 Optimize imaging parameters for the soft tissues of the neck M H12.10 Select the optimal imaging options for each pulse sequence for the soft
tissues of the neck M
H12.11 Determine the limit and extent of image coverage for the soft tissues of the neck
M
H 13 Perform a nasopharynx imaging procedure M H13.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the nasopharynx M
H13.2 Select the optimal coil to image the nasopharynx M H13.3 Prepare the patient for a nasopharynx imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
H13.4 Position the patient and coil using anatomical landmark and relational anatomy
M
H13.5 Landmark the nasopharynx (relational anatomy) to the positioning light and advance the patient to isocenter
M
H13.6 Select the optimal imaging plane for the nasopharynx M H13.7 Determine and select the appropriate pulse sequences for optimal
visualization of the nasopharynx M
H13.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the nasopharynx
M
H13.9 Optimize imaging parameters for the nasopharynx M H13.10 Select the optimal imaging options for each pulse sequence for the
nasopharynx M
H13.11 Determine the limit and extent of image coverage for the nasopharynx M H 14 Perform an imaging procedure of the tongue H14.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the tongue
H14.2 Select the optimal coil to image the tongue H14.3 Prepare the patient for a tongue imaging procedure based on the
requested protocol and the patient’s physical and cognitive status
Page 197
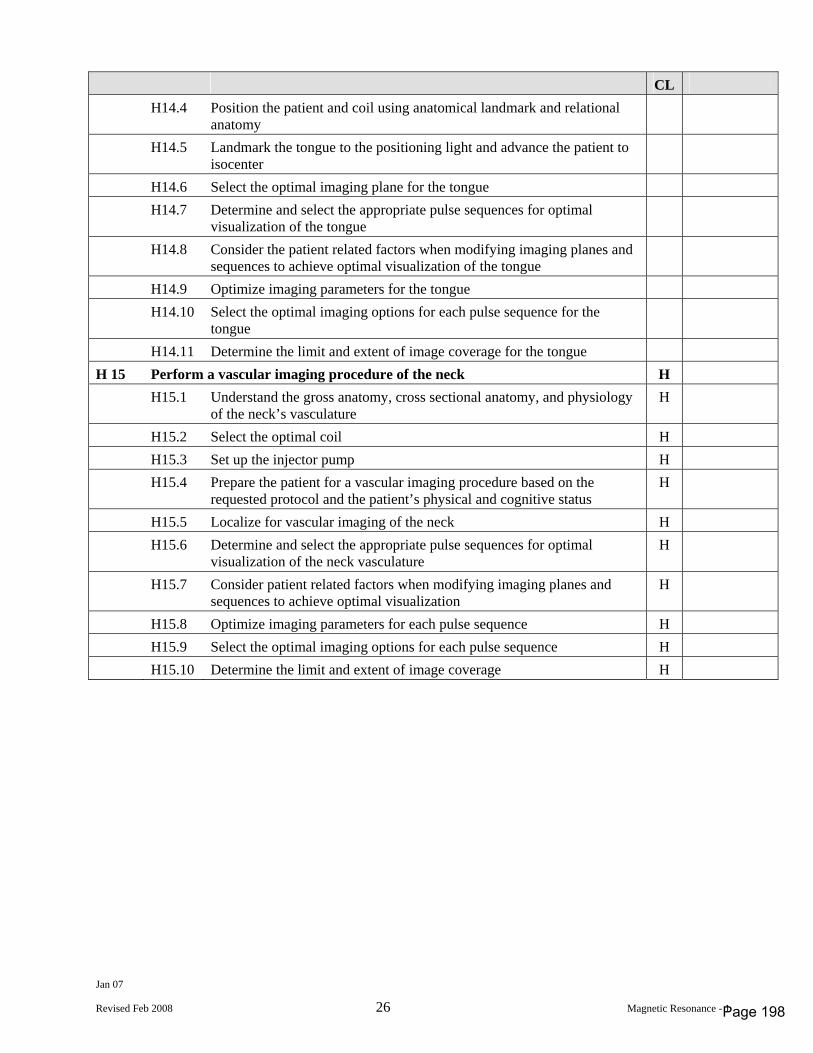
Jan 07
Revised Feb 2008 26 Magnetic Resonance - 1
CL H14.4 Position the patient and coil using anatomical landmark and relational
anatomy
H14.5 Landmark the tongue to the positioning light and advance the patient to isocenter
H14.6 Select the optimal imaging plane for the tongue H14.7 Determine and select the appropriate pulse sequences for optimal
visualization of the tongue
H14.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the tongue
H14.9 Optimize imaging parameters for the tongue H14.10 Select the optimal imaging options for each pulse sequence for the
tongue
H14.11 Determine the limit and extent of image coverage for the tongue H 15 Perform a vascular imaging procedure of the neck H H15.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the neck’s vasculature H
H15.2 Select the optimal coil H H15.3 Set up the injector pump H H15.4 Prepare the patient for a vascular imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
H15.5 Localize for vascular imaging of the neck H H15.6 Determine and select the appropriate pulse sequences for optimal
visualization of the neck vasculature H
H15.7 Consider patient related factors when modifying imaging planes and sequences to achieve optimal visualization
H
H15.8 Optimize imaging parameters for each pulse sequence H H15.9 Select the optimal imaging options for each pulse sequence H H15.10 Determine the limit and extent of image coverage H
Page 198
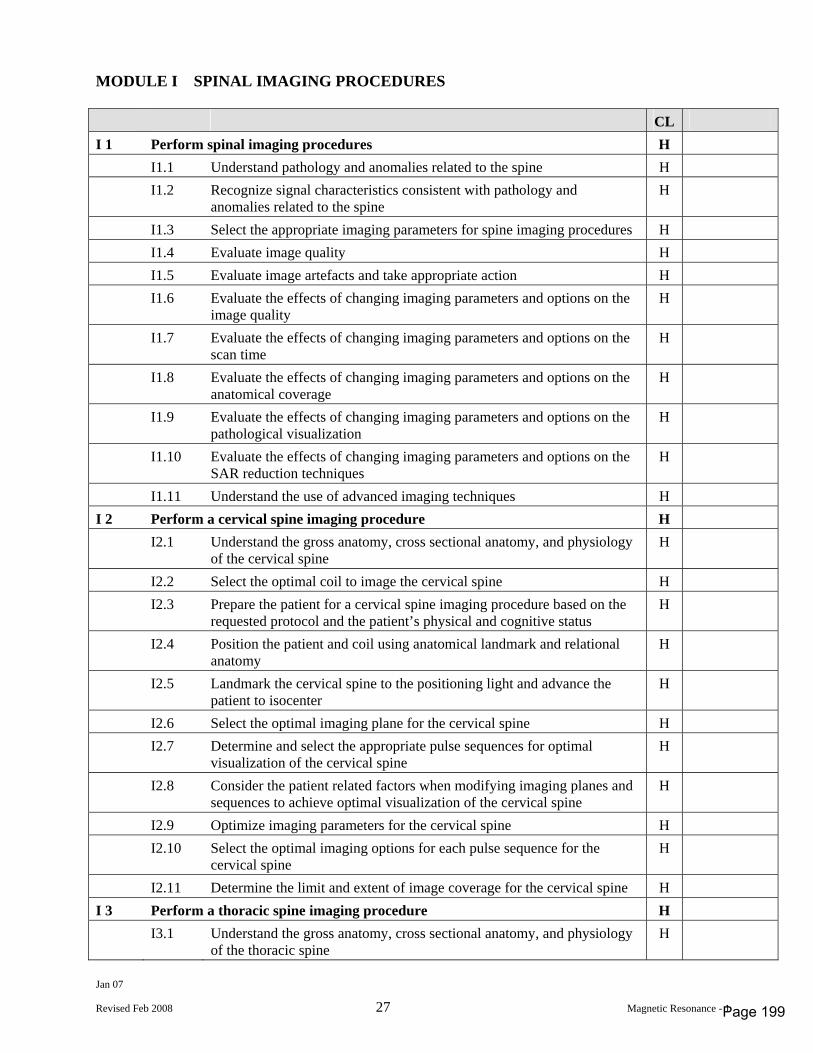
Jan 07
Revised Feb 2008 27 Magnetic Resonance - 1
MODULE I SPINAL IMAGING PROCEDURES CL I 1 Perform spinal imaging procedures H I1.1 Understand pathology and anomalies related to the spine H I1.2 Recognize signal characteristics consistent with pathology and
anomalies related to the spine H
I1.3 Select the appropriate imaging parameters for spine imaging procedures H I1.4 Evaluate image quality H I1.5 Evaluate image artefacts and take appropriate action H I1.6 Evaluate the effects of changing imaging parameters and options on the
image quality H
I1.7 Evaluate the effects of changing imaging parameters and options on the scan time
H
I1.8 Evaluate the effects of changing imaging parameters and options on the anatomical coverage
H
I1.9 Evaluate the effects of changing imaging parameters and options on the pathological visualization
H
I1.10 Evaluate the effects of changing imaging parameters and options on the SAR reduction techniques
H
I1.11 Understand the use of advanced imaging techniques H I 2 Perform a cervical spine imaging procedure H I2.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the cervical spine H
I2.2 Select the optimal coil to image the cervical spine H I2.3 Prepare the patient for a cervical spine imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
I2.4 Position the patient and coil using anatomical landmark and relational anatomy
H
I2.5 Landmark the cervical spine to the positioning light and advance the patient to isocenter
H
I2.6 Select the optimal imaging plane for the cervical spine H I2.7 Determine and select the appropriate pulse sequences for optimal
visualization of the cervical spine H
I2.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the cervical spine
H
I2.9 Optimize imaging parameters for the cervical spine H I2.10 Select the optimal imaging options for each pulse sequence for the
cervical spine H
I2.11 Determine the limit and extent of image coverage for the cervical spine H I 3 Perform a thoracic spine imaging procedure H I3.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the thoracic spine H
Page 199
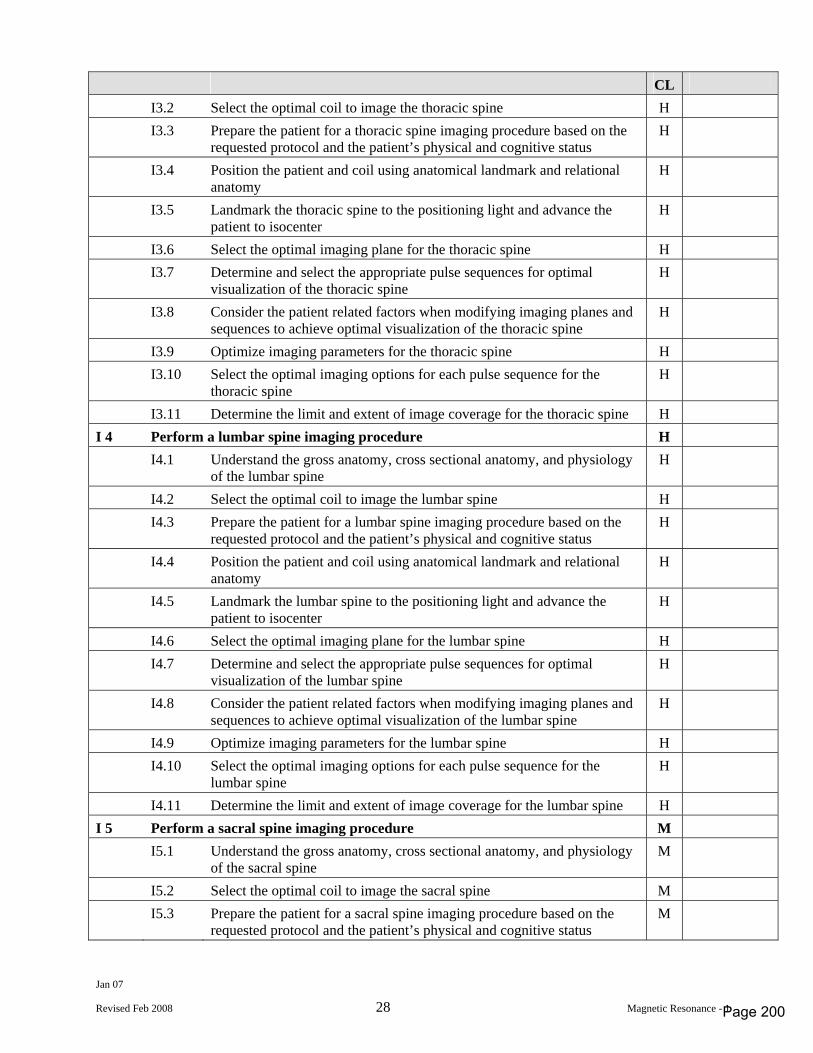
Jan 07
Revised Feb 2008 28 Magnetic Resonance - 1
CL I3.2 Select the optimal coil to image the thoracic spine H I3.3 Prepare the patient for a thoracic spine imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
I3.4 Position the patient and coil using anatomical landmark and relational anatomy
H
I3.5 Landmark the thoracic spine to the positioning light and advance the patient to isocenter
H
I3.6 Select the optimal imaging plane for the thoracic spine H I3.7 Determine and select the appropriate pulse sequences for optimal
visualization of the thoracic spine H
I3.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the thoracic spine
H
I3.9 Optimize imaging parameters for the thoracic spine H I3.10 Select the optimal imaging options for each pulse sequence for the
thoracic spine H
I3.11 Determine the limit and extent of image coverage for the thoracic spine H I 4 Perform a lumbar spine imaging procedure H I4.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the lumbar spine H
I4.2 Select the optimal coil to image the lumbar spine H I4.3 Prepare the patient for a lumbar spine imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
I4.4 Position the patient and coil using anatomical landmark and relational anatomy
H
I4.5 Landmark the lumbar spine to the positioning light and advance the patient to isocenter
H
I4.6 Select the optimal imaging plane for the lumbar spine H I4.7 Determine and select the appropriate pulse sequences for optimal
visualization of the lumbar spine H
I4.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the lumbar spine
H
I4.9 Optimize imaging parameters for the lumbar spine H I4.10 Select the optimal imaging options for each pulse sequence for the
lumbar spine H
I4.11 Determine the limit and extent of image coverage for the lumbar spine H I 5 Perform a sacral spine imaging procedure M I5.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the sacral spine M
I5.2 Select the optimal coil to image the sacral spine M I5.3 Prepare the patient for a sacral spine imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
Page 200
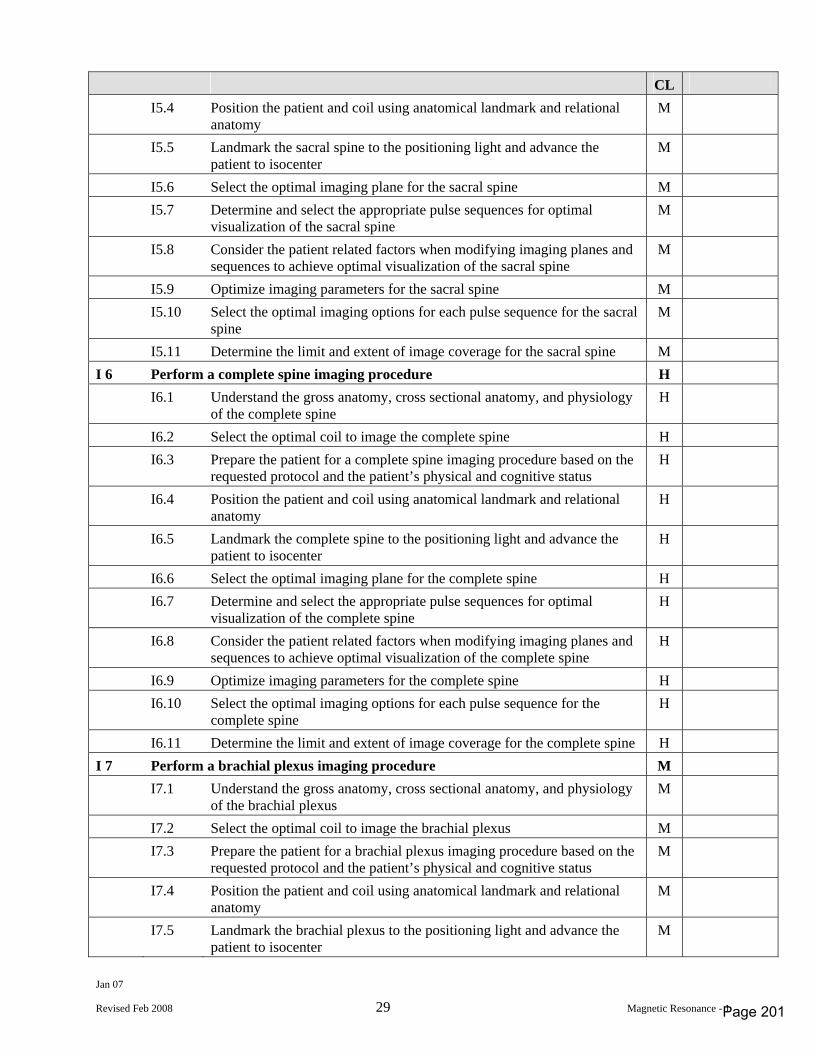
Jan 07
Revised Feb 2008 29 Magnetic Resonance - 1
CL I5.4 Position the patient and coil using anatomical landmark and relational
anatomy M
I5.5 Landmark the sacral spine to the positioning light and advance the patient to isocenter
M
I5.6 Select the optimal imaging plane for the sacral spine M I5.7 Determine and select the appropriate pulse sequences for optimal
visualization of the sacral spine M
I5.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the sacral spine
M
I5.9 Optimize imaging parameters for the sacral spine M I5.10 Select the optimal imaging options for each pulse sequence for the sacral
spine M
I5.11 Determine the limit and extent of image coverage for the sacral spine M I 6 Perform a complete spine imaging procedure H I6.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the complete spine H
I6.2 Select the optimal coil to image the complete spine H I6.3 Prepare the patient for a complete spine imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
I6.4 Position the patient and coil using anatomical landmark and relational anatomy
H
I6.5 Landmark the complete spine to the positioning light and advance the patient to isocenter
H
I6.6 Select the optimal imaging plane for the complete spine H I6.7 Determine and select the appropriate pulse sequences for optimal
visualization of the complete spine H
I6.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the complete spine
H
I6.9 Optimize imaging parameters for the complete spine H I6.10 Select the optimal imaging options for each pulse sequence for the
complete spine H
I6.11 Determine the limit and extent of image coverage for the complete spine H I 7 Perform a brachial plexus imaging procedure M I7.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the brachial plexus M
I7.2 Select the optimal coil to image the brachial plexus M I7.3 Prepare the patient for a brachial plexus imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
I7.4 Position the patient and coil using anatomical landmark and relational anatomy
M
I7.5 Landmark the brachial plexus to the positioning light and advance the patient to isocenter
M
Page 201
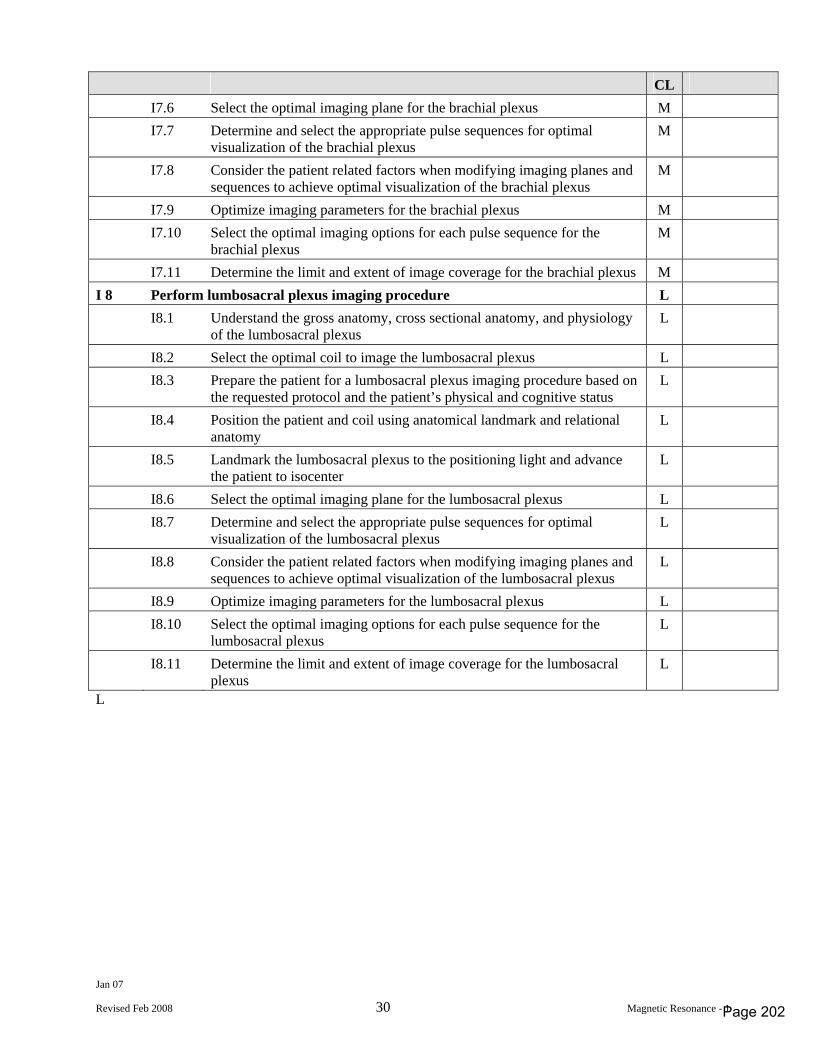
Jan 07
Revised Feb 2008 30 Magnetic Resonance - 1
CL I7.6 Select the optimal imaging plane for the brachial plexus M I7.7 Determine and select the appropriate pulse sequences for optimal
visualization of the brachial plexus M
I7.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the brachial plexus
M
I7.9 Optimize imaging parameters for the brachial plexus M I7.10 Select the optimal imaging options for each pulse sequence for the
brachial plexus M
I7.11 Determine the limit and extent of image coverage for the brachial plexus M I 8 Perform lumbosacral plexus imaging procedure L I8.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the lumbosacral plexus L
I8.2 Select the optimal coil to image the lumbosacral plexus L I8.3 Prepare the patient for a lumbosacral plexus imaging procedure based on
the requested protocol and the patient’s physical and cognitive status L
I8.4 Position the patient and coil using anatomical landmark and relational anatomy
L
I8.5 Landmark the lumbosacral plexus to the positioning light and advance the patient to isocenter
L
I8.6 Select the optimal imaging plane for the lumbosacral plexus L I8.7 Determine and select the appropriate pulse sequences for optimal
visualization of the lumbosacral plexus L
I8.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the lumbosacral plexus
L
I8.9 Optimize imaging parameters for the lumbosacral plexus L I8.10 Select the optimal imaging options for each pulse sequence for the
lumbosacral plexus L
I8.11 Determine the limit and extent of image coverage for the lumbosacral plexus
L
L
Page 202
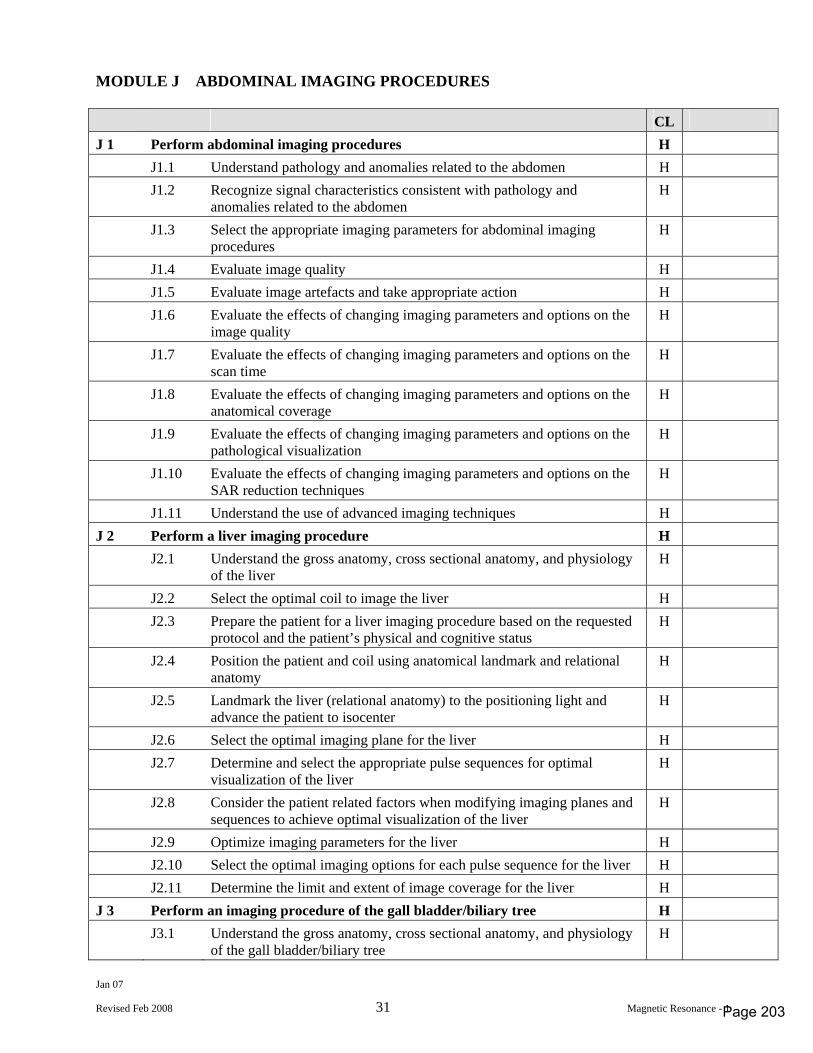
Jan 07
Revised Feb 2008 31 Magnetic Resonance - 1
MODULE J ABDOMINAL IMAGING PROCEDURES CL J 1 Perform abdominal imaging procedures H J1.1 Understand pathology and anomalies related to the abdomen H J1.2 Recognize signal characteristics consistent with pathology and
anomalies related to the abdomen H
J1.3 Select the appropriate imaging parameters for abdominal imaging procedures
H
J1.4 Evaluate image quality H J1.5 Evaluate image artefacts and take appropriate action H J1.6 Evaluate the effects of changing imaging parameters and options on the
image quality H
J1.7 Evaluate the effects of changing imaging parameters and options on the scan time
H
J1.8 Evaluate the effects of changing imaging parameters and options on the anatomical coverage
H
J1.9 Evaluate the effects of changing imaging parameters and options on the pathological visualization
H
J1.10 Evaluate the effects of changing imaging parameters and options on the SAR reduction techniques
H
J1.11 Understand the use of advanced imaging techniques H J 2 Perform a liver imaging procedure H J2.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the liver H
J2.2 Select the optimal coil to image the liver H J2.3 Prepare the patient for a liver imaging procedure based on the requested
protocol and the patient’s physical and cognitive status H
J2.4 Position the patient and coil using anatomical landmark and relational anatomy
H
J2.5 Landmark the liver (relational anatomy) to the positioning light and advance the patient to isocenter
H
J2.6 Select the optimal imaging plane for the liver H J2.7 Determine and select the appropriate pulse sequences for optimal
visualization of the liver H
J2.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the liver
H
J2.9 Optimize imaging parameters for the liver H J2.10 Select the optimal imaging options for each pulse sequence for the liver H J2.11 Determine the limit and extent of image coverage for the liver H J 3 Perform an imaging procedure of the gall bladder/biliary tree H J3.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the gall bladder/biliary tree H
Page 203
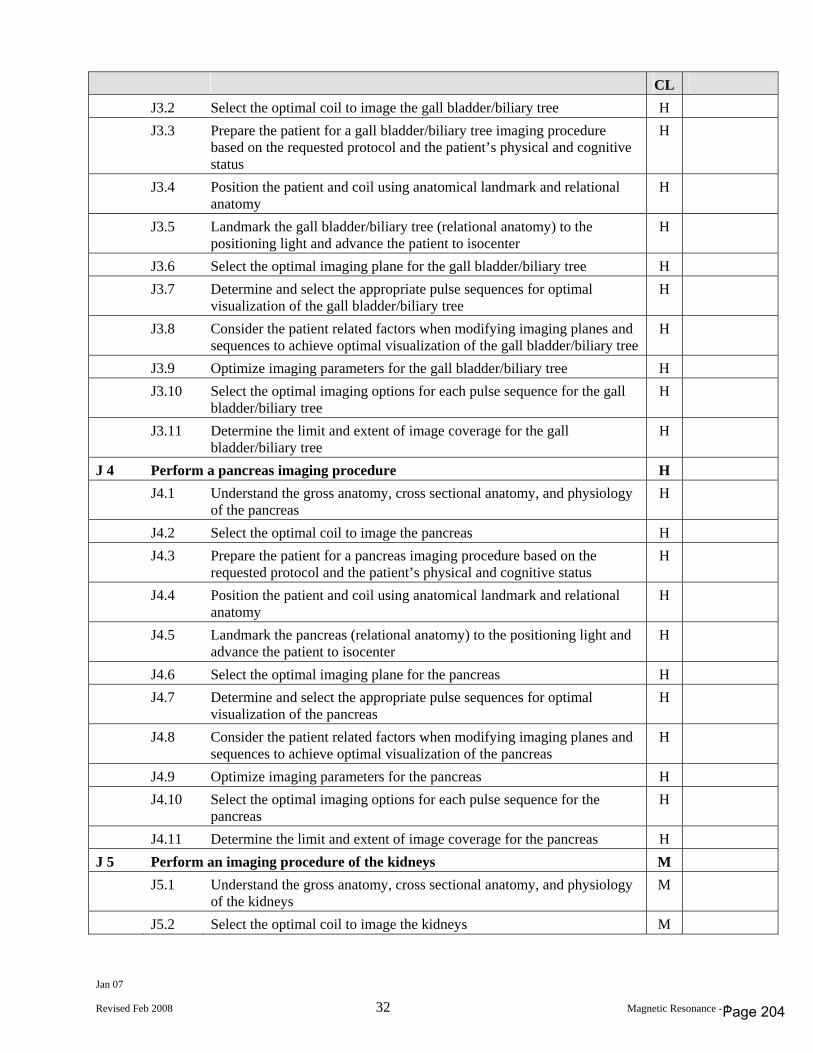
Jan 07
Revised Feb 2008 32 Magnetic Resonance - 1
CL J3.2 Select the optimal coil to image the gall bladder/biliary tree H J3.3 Prepare the patient for a gall bladder/biliary tree imaging procedure
based on the requested protocol and the patient’s physical and cognitive status
H
J3.4 Position the patient and coil using anatomical landmark and relational anatomy
H
J3.5 Landmark the gall bladder/biliary tree (relational anatomy) to the positioning light and advance the patient to isocenter
H
J3.6 Select the optimal imaging plane for the gall bladder/biliary tree H J3.7 Determine and select the appropriate pulse sequences for optimal
visualization of the gall bladder/biliary tree H
J3.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the gall bladder/biliary tree
H
J3.9 Optimize imaging parameters for the gall bladder/biliary tree H J3.10 Select the optimal imaging options for each pulse sequence for the gall
bladder/biliary tree H
J3.11 Determine the limit and extent of image coverage for the gall bladder/biliary tree
H
J 4 Perform a pancreas imaging procedure H J4.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the pancreas H
J4.2 Select the optimal coil to image the pancreas H J4.3 Prepare the patient for a pancreas imaging procedure based on the
requested protocol and the patient’s physical and cognitive status H
J4.4 Position the patient and coil using anatomical landmark and relational anatomy
H
J4.5 Landmark the pancreas (relational anatomy) to the positioning light and advance the patient to isocenter
H
J4.6 Select the optimal imaging plane for the pancreas H J4.7 Determine and select the appropriate pulse sequences for optimal
visualization of the pancreas H
J4.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the pancreas
H
J4.9 Optimize imaging parameters for the pancreas H J4.10 Select the optimal imaging options for each pulse sequence for the
pancreas H
J4.11 Determine the limit and extent of image coverage for the pancreas H J 5 Perform an imaging procedure of the kidneys M J5.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the kidneys M
J5.2 Select the optimal coil to image the kidneys M
Page 204
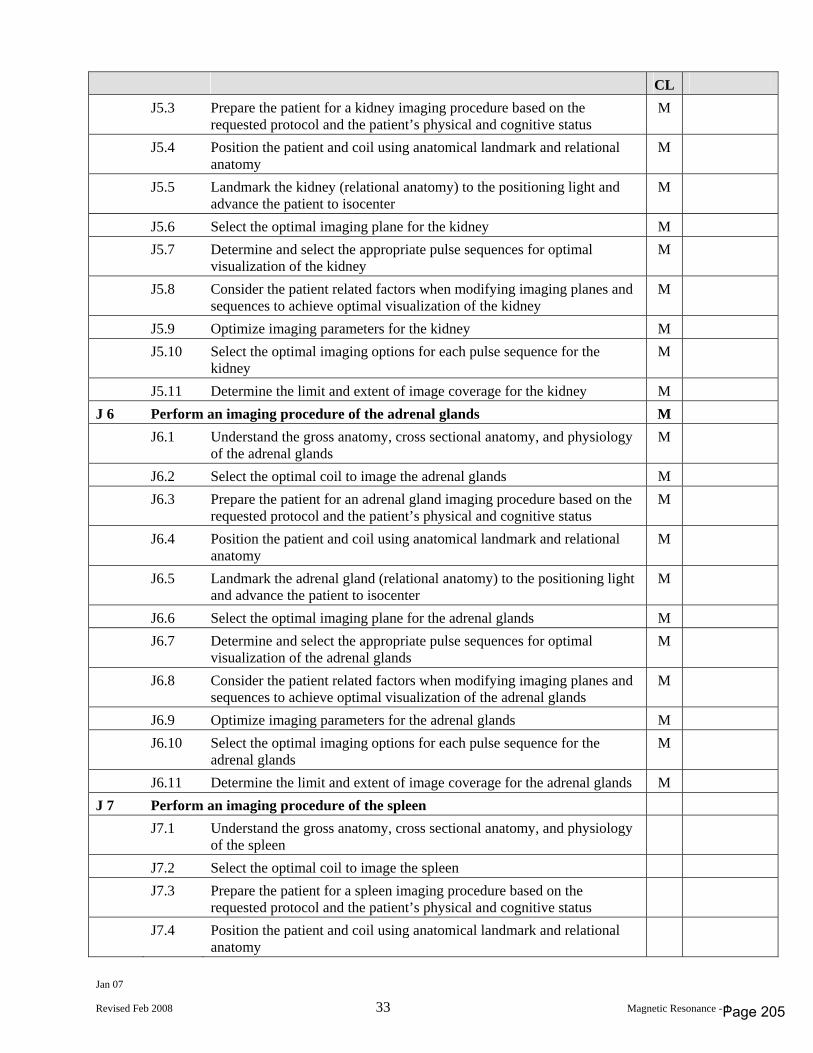
Jan 07
Revised Feb 2008 33 Magnetic Resonance - 1
CL J5.3 Prepare the patient for a kidney imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
J5.4 Position the patient and coil using anatomical landmark and relational anatomy
M
J5.5 Landmark the kidney (relational anatomy) to the positioning light and advance the patient to isocenter
M
J5.6 Select the optimal imaging plane for the kidney M J5.7 Determine and select the appropriate pulse sequences for optimal
visualization of the kidney M
J5.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the kidney
M
J5.9 Optimize imaging parameters for the kidney M J5.10 Select the optimal imaging options for each pulse sequence for the
kidney M
J5.11 Determine the limit and extent of image coverage for the kidney M J 6 Perform an imaging procedure of the adrenal glands M J6.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the adrenal glands M
J6.2 Select the optimal coil to image the adrenal glands M J6.3 Prepare the patient for an adrenal gland imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
J6.4 Position the patient and coil using anatomical landmark and relational anatomy
M
J6.5 Landmark the adrenal gland (relational anatomy) to the positioning light and advance the patient to isocenter
M
J6.6 Select the optimal imaging plane for the adrenal glands M J6.7 Determine and select the appropriate pulse sequences for optimal
visualization of the adrenal glands M
J6.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the adrenal glands
M
J6.9 Optimize imaging parameters for the adrenal glands M J6.10 Select the optimal imaging options for each pulse sequence for the
adrenal glands M
J6.11 Determine the limit and extent of image coverage for the adrenal glands M J 7 Perform an imaging procedure of the spleen J7.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the spleen
J7.2 Select the optimal coil to image the spleen J7.3 Prepare the patient for a spleen imaging procedure based on the
requested protocol and the patient’s physical and cognitive status
J7.4 Position the patient and coil using anatomical landmark and relational anatomy
Page 205
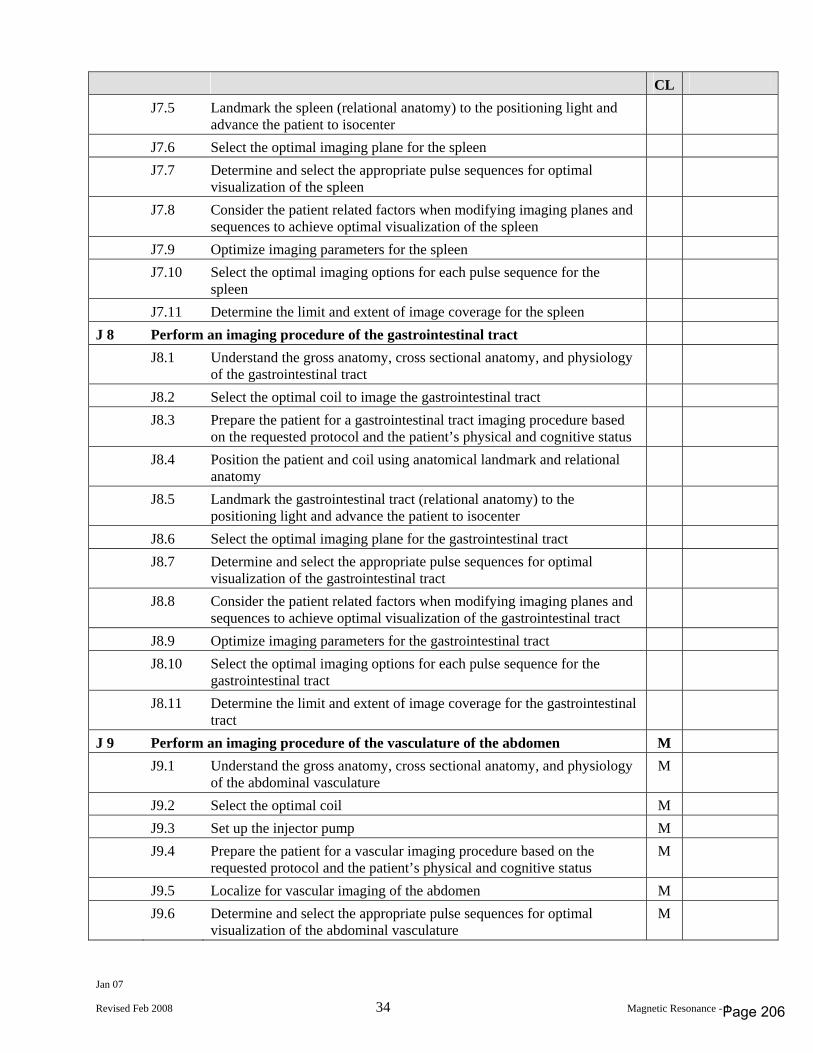
Jan 07
Revised Feb 2008 34 Magnetic Resonance - 1
CL J7.5 Landmark the spleen (relational anatomy) to the positioning light and
advance the patient to isocenter
J7.6 Select the optimal imaging plane for the spleen J7.7 Determine and select the appropriate pulse sequences for optimal
visualization of the spleen
J7.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the spleen
J7.9 Optimize imaging parameters for the spleen J7.10 Select the optimal imaging options for each pulse sequence for the
spleen
J7.11 Determine the limit and extent of image coverage for the spleen J 8 Perform an imaging procedure of the gastrointestinal tract J8.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the gastrointestinal tract
J8.2 Select the optimal coil to image the gastrointestinal tract J8.3 Prepare the patient for a gastrointestinal tract imaging procedure based
on the requested protocol and the patient’s physical and cognitive status
J8.4 Position the patient and coil using anatomical landmark and relational anatomy
J8.5 Landmark the gastrointestinal tract (relational anatomy) to the positioning light and advance the patient to isocenter
J8.6 Select the optimal imaging plane for the gastrointestinal tract J8.7 Determine and select the appropriate pulse sequences for optimal
visualization of the gastrointestinal tract
J8.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the gastrointestinal tract
J8.9 Optimize imaging parameters for the gastrointestinal tract J8.10 Select the optimal imaging options for each pulse sequence for the
gastrointestinal tract
J8.11 Determine the limit and extent of image coverage for the gastrointestinal tract
J 9 Perform an imaging procedure of the vasculature of the abdomen M J9.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the abdominal vasculature M
J9.2 Select the optimal coil M J9.3 Set up the injector pump M J9.4 Prepare the patient for a vascular imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
J9.5 Localize for vascular imaging of the abdomen M J9.6 Determine and select the appropriate pulse sequences for optimal
visualization of the abdominal vasculature M
Page 206
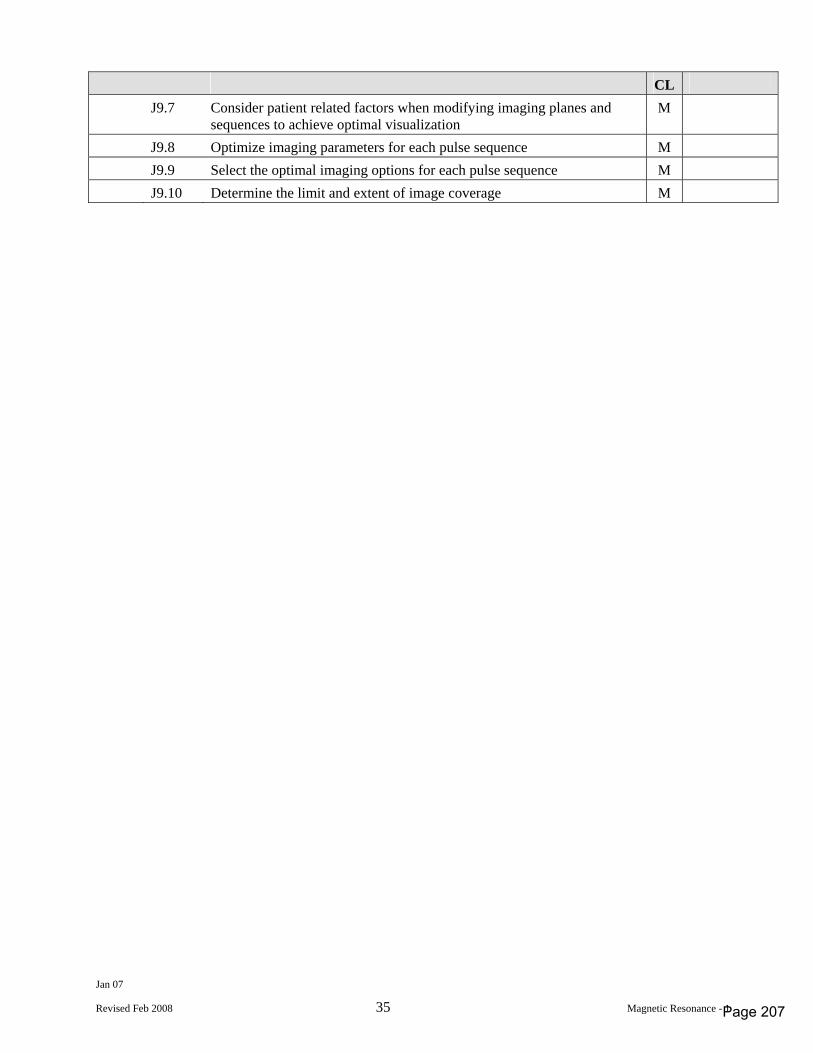
Jan 07
Revised Feb 2008 35 Magnetic Resonance - 1
CL J9.7 Consider patient related factors when modifying imaging planes and
sequences to achieve optimal visualization M
J9.8 Optimize imaging parameters for each pulse sequence M J9.9 Select the optimal imaging options for each pulse sequence M J9.10 Determine the limit and extent of image coverage M
Page 207
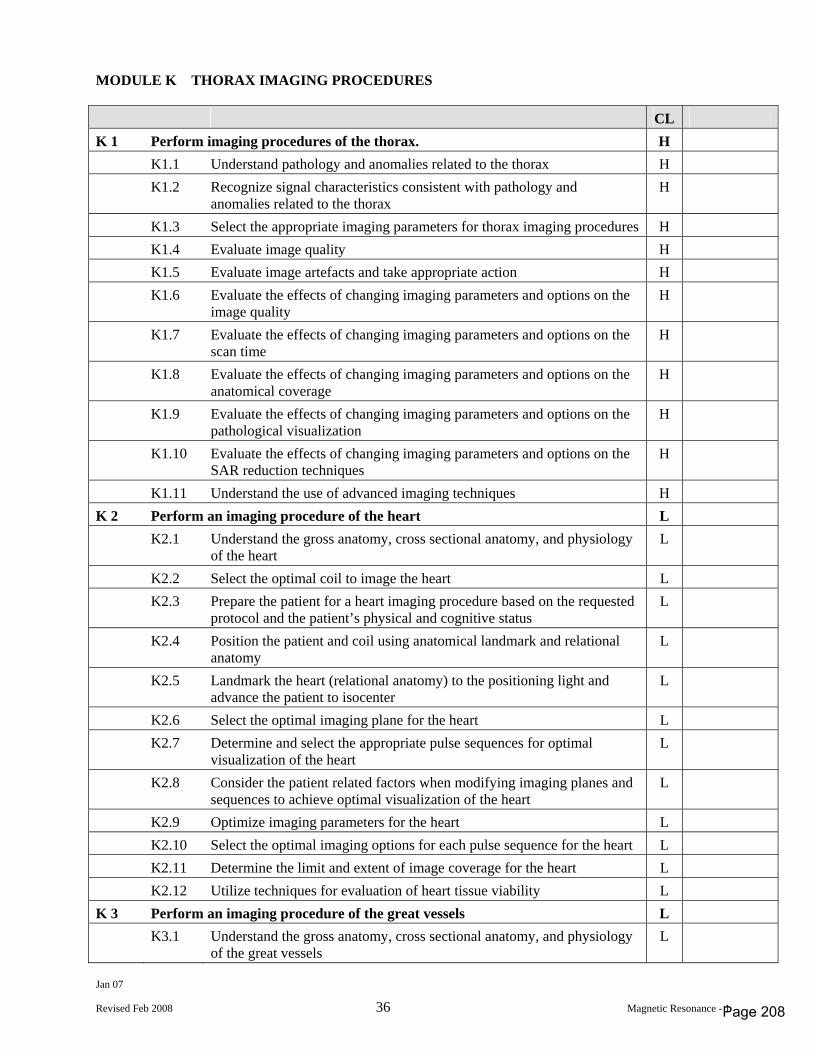
Jan 07
Revised Feb 2008 36 Magnetic Resonance - 1
MODULE K THORAX IMAGING PROCEDURES CL K 1 Perform imaging procedures of the thorax. H K1.1 Understand pathology and anomalies related to the thorax H K1.2 Recognize signal characteristics consistent with pathology and
anomalies related to the thorax H
K1.3 Select the appropriate imaging parameters for thorax imaging procedures H K1.4 Evaluate image quality H K1.5 Evaluate image artefacts and take appropriate action H K1.6 Evaluate the effects of changing imaging parameters and options on the
image quality H
K1.7 Evaluate the effects of changing imaging parameters and options on the scan time
H
K1.8 Evaluate the effects of changing imaging parameters and options on the anatomical coverage
H
K1.9 Evaluate the effects of changing imaging parameters and options on the pathological visualization
H
K1.10 Evaluate the effects of changing imaging parameters and options on the SAR reduction techniques
H
K1.11 Understand the use of advanced imaging techniques H K 2 Perform an imaging procedure of the heart L K2.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the heart L
K2.2 Select the optimal coil to image the heart L K2.3 Prepare the patient for a heart imaging procedure based on the requested
protocol and the patient’s physical and cognitive status L
K2.4 Position the patient and coil using anatomical landmark and relational anatomy
L
K2.5 Landmark the heart (relational anatomy) to the positioning light and advance the patient to isocenter
L
K2.6 Select the optimal imaging plane for the heart L K2.7 Determine and select the appropriate pulse sequences for optimal
visualization of the heart L
K2.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the heart
L
K2.9 Optimize imaging parameters for the heart L K2.10 Select the optimal imaging options for each pulse sequence for the heart L K2.11 Determine the limit and extent of image coverage for the heart L K2.12 Utilize techniques for evaluation of heart tissue viability L K 3 Perform an imaging procedure of the great vessels L K3.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the great vessels L
Page 208
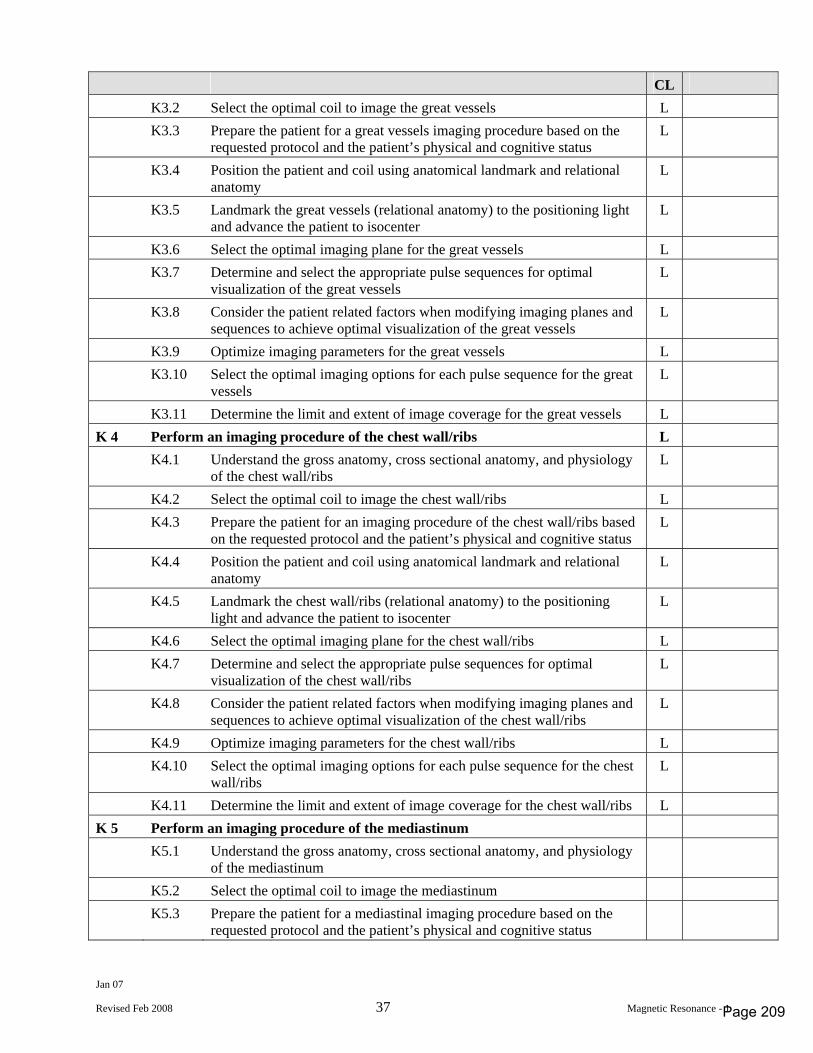
Jan 07
Revised Feb 2008 37 Magnetic Resonance - 1
CL K3.2 Select the optimal coil to image the great vessels L K3.3 Prepare the patient for a great vessels imaging procedure based on the
requested protocol and the patient’s physical and cognitive status L
K3.4 Position the patient and coil using anatomical landmark and relational anatomy
L
K3.5 Landmark the great vessels (relational anatomy) to the positioning light and advance the patient to isocenter
L
K3.6 Select the optimal imaging plane for the great vessels L K3.7 Determine and select the appropriate pulse sequences for optimal
visualization of the great vessels L
K3.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the great vessels
L
K3.9 Optimize imaging parameters for the great vessels L K3.10 Select the optimal imaging options for each pulse sequence for the great
vessels L
K3.11 Determine the limit and extent of image coverage for the great vessels L K 4 Perform an imaging procedure of the chest wall/ribs L K4.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the chest wall/ribs L
K4.2 Select the optimal coil to image the chest wall/ribs L K4.3 Prepare the patient for an imaging procedure of the chest wall/ribs based
on the requested protocol and the patient’s physical and cognitive status L
K4.4 Position the patient and coil using anatomical landmark and relational anatomy
L
K4.5 Landmark the chest wall/ribs (relational anatomy) to the positioning light and advance the patient to isocenter
L
K4.6 Select the optimal imaging plane for the chest wall/ribs L K4.7 Determine and select the appropriate pulse sequences for optimal
visualization of the chest wall/ribs L
K4.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the chest wall/ribs
L
K4.9 Optimize imaging parameters for the chest wall/ribs L K4.10 Select the optimal imaging options for each pulse sequence for the chest
wall/ribs L
K4.11 Determine the limit and extent of image coverage for the chest wall/ribs L K 5 Perform an imaging procedure of the mediastinum K5.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the mediastinum
K5.2 Select the optimal coil to image the mediastinum K5.3 Prepare the patient for a mediastinal imaging procedure based on the
requested protocol and the patient’s physical and cognitive status
Page 209
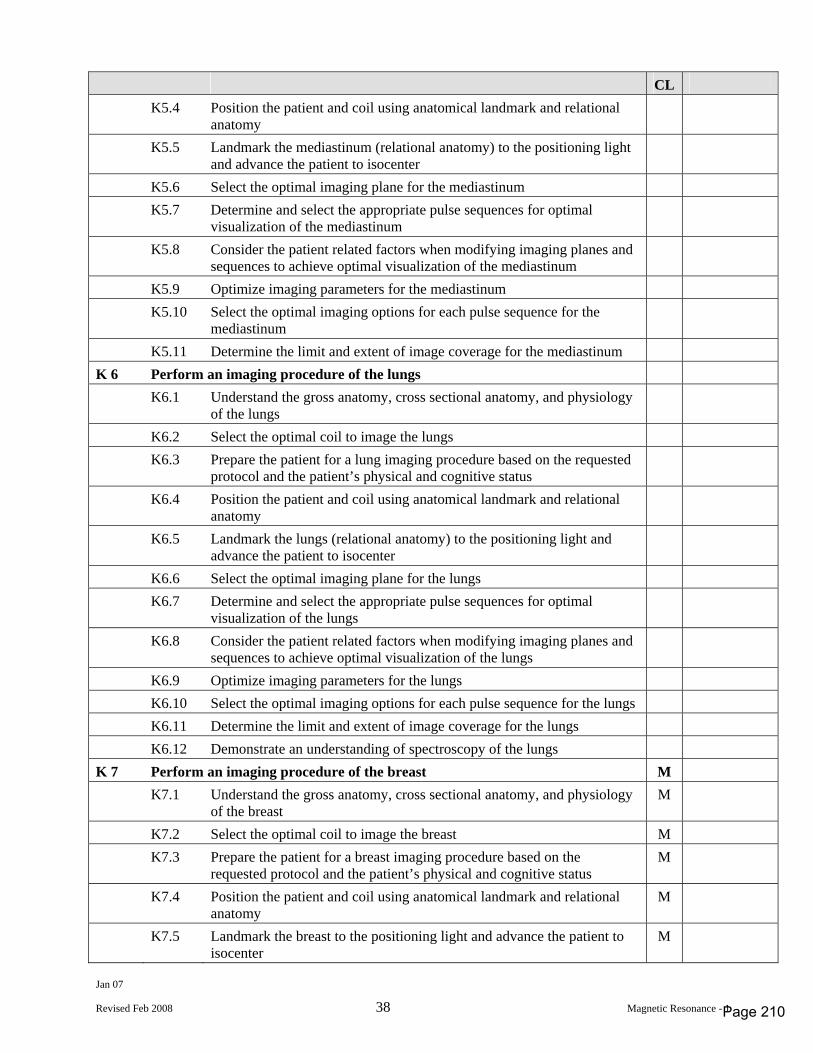
Jan 07
Revised Feb 2008 38 Magnetic Resonance - 1
CL K5.4 Position the patient and coil using anatomical landmark and relational
anatomy
K5.5 Landmark the mediastinum (relational anatomy) to the positioning light and advance the patient to isocenter
K5.6 Select the optimal imaging plane for the mediastinum K5.7 Determine and select the appropriate pulse sequences for optimal
visualization of the mediastinum
K5.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the mediastinum
K5.9 Optimize imaging parameters for the mediastinum K5.10 Select the optimal imaging options for each pulse sequence for the
mediastinum
K5.11 Determine the limit and extent of image coverage for the mediastinum K 6 Perform an imaging procedure of the lungs K6.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the lungs
K6.2 Select the optimal coil to image the lungs K6.3 Prepare the patient for a lung imaging procedure based on the requested
protocol and the patient’s physical and cognitive status
K6.4 Position the patient and coil using anatomical landmark and relational anatomy
K6.5 Landmark the lungs (relational anatomy) to the positioning light and advance the patient to isocenter
K6.6 Select the optimal imaging plane for the lungs K6.7 Determine and select the appropriate pulse sequences for optimal
visualization of the lungs
K6.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the lungs
K6.9 Optimize imaging parameters for the lungs K6.10 Select the optimal imaging options for each pulse sequence for the lungs K6.11 Determine the limit and extent of image coverage for the lungs K6.12 Demonstrate an understanding of spectroscopy of the lungs K 7 Perform an imaging procedure of the breast M K7.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the breast M
K7.2 Select the optimal coil to image the breast M K7.3 Prepare the patient for a breast imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
K7.4 Position the patient and coil using anatomical landmark and relational anatomy
M
K7.5 Landmark the breast to the positioning light and advance the patient to isocenter
M
Page 210
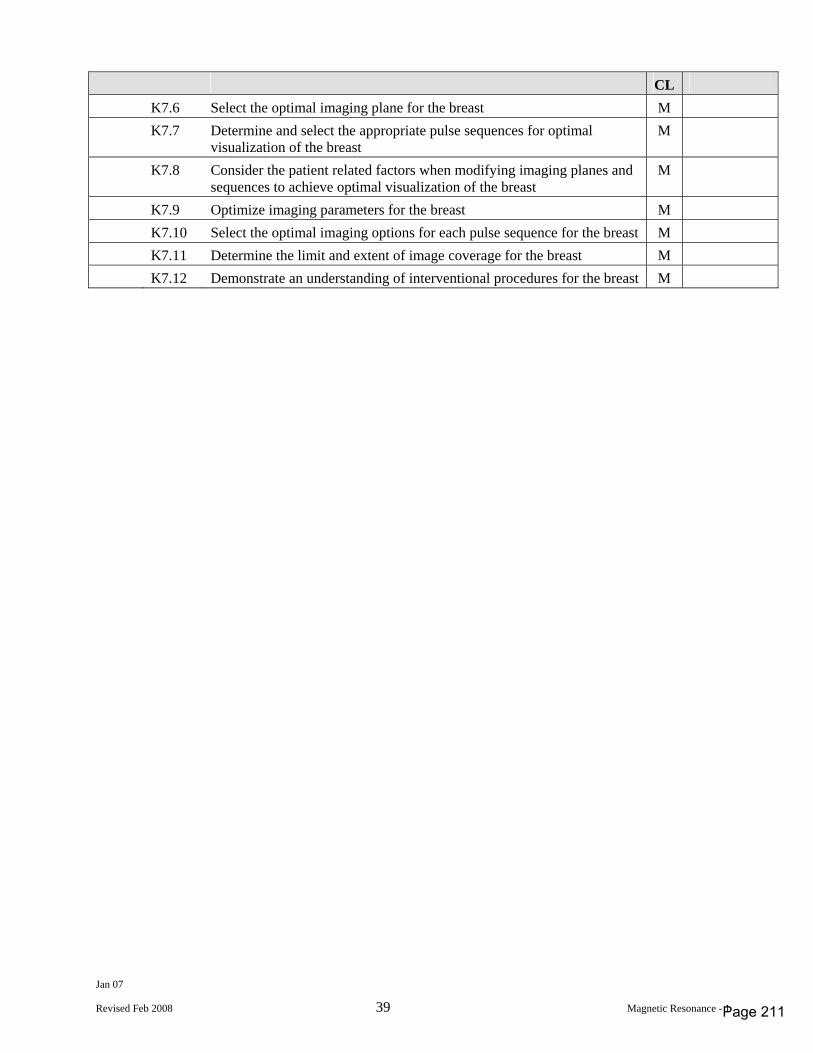
Jan 07
Revised Feb 2008 39 Magnetic Resonance - 1
CL K7.6 Select the optimal imaging plane for the breast M K7.7 Determine and select the appropriate pulse sequences for optimal
visualization of the breast M
K7.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the breast
M
K7.9 Optimize imaging parameters for the breast M K7.10 Select the optimal imaging options for each pulse sequence for the breast M K7.11 Determine the limit and extent of image coverage for the breast M K7.12 Demonstrate an understanding of interventional procedures for the breast M
Page 211
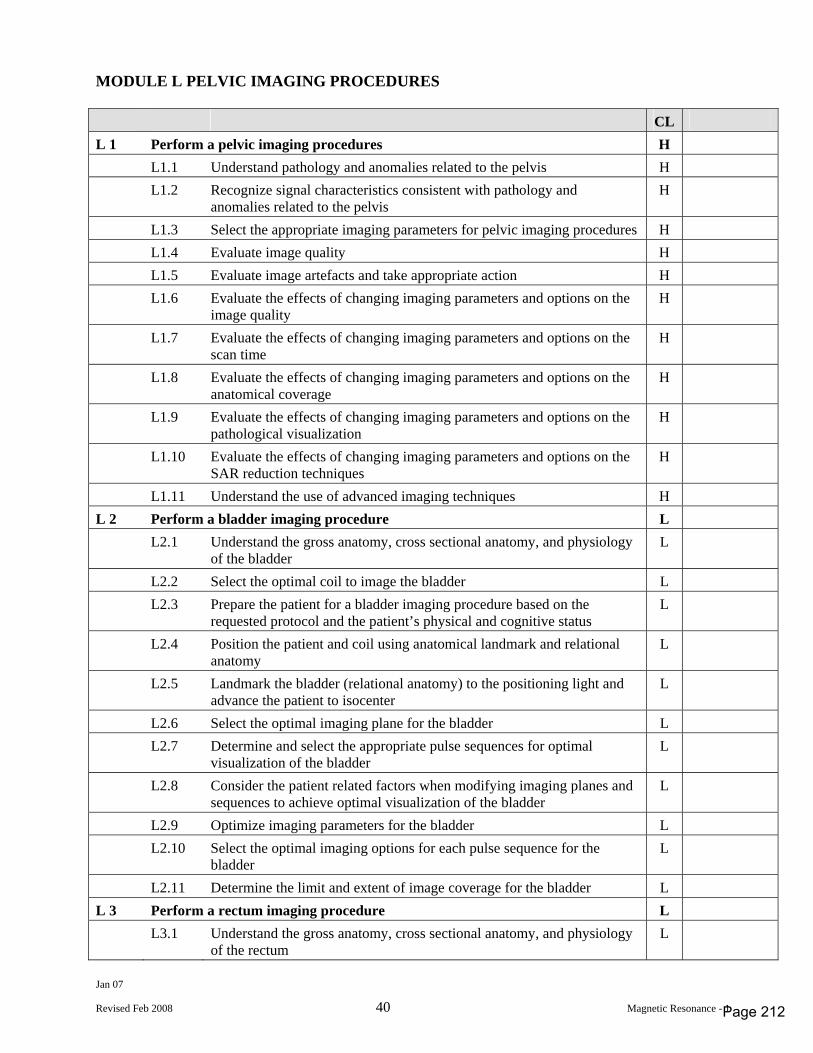
Jan 07
Revised Feb 2008 40 Magnetic Resonance - 1
MODULE L PELVIC IMAGING PROCEDURES CL L 1 Perform a pelvic imaging procedures H L1.1 Understand pathology and anomalies related to the pelvis H L1.2 Recognize signal characteristics consistent with pathology and
anomalies related to the pelvis H
L1.3 Select the appropriate imaging parameters for pelvic imaging procedures H L1.4 Evaluate image quality H L1.5 Evaluate image artefacts and take appropriate action H L1.6 Evaluate the effects of changing imaging parameters and options on the
image quality H
L1.7 Evaluate the effects of changing imaging parameters and options on the scan time
H
L1.8 Evaluate the effects of changing imaging parameters and options on the anatomical coverage
H
L1.9 Evaluate the effects of changing imaging parameters and options on the pathological visualization
H
L1.10 Evaluate the effects of changing imaging parameters and options on the SAR reduction techniques
H
L1.11 Understand the use of advanced imaging techniques H L 2 Perform a bladder imaging procedure L L2.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the bladder L
L2.2 Select the optimal coil to image the bladder L L2.3 Prepare the patient for a bladder imaging procedure based on the
requested protocol and the patient’s physical and cognitive status L
L2.4 Position the patient and coil using anatomical landmark and relational anatomy
L
L2.5 Landmark the bladder (relational anatomy) to the positioning light and advance the patient to isocenter
L
L2.6 Select the optimal imaging plane for the bladder L L2.7 Determine and select the appropriate pulse sequences for optimal
visualization of the bladder L
L2.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the bladder
L
L2.9 Optimize imaging parameters for the bladder L L2.10 Select the optimal imaging options for each pulse sequence for the
bladder L
L2.11 Determine the limit and extent of image coverage for the bladder L L 3 Perform a rectum imaging procedure L L3.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the rectum L
Page 212
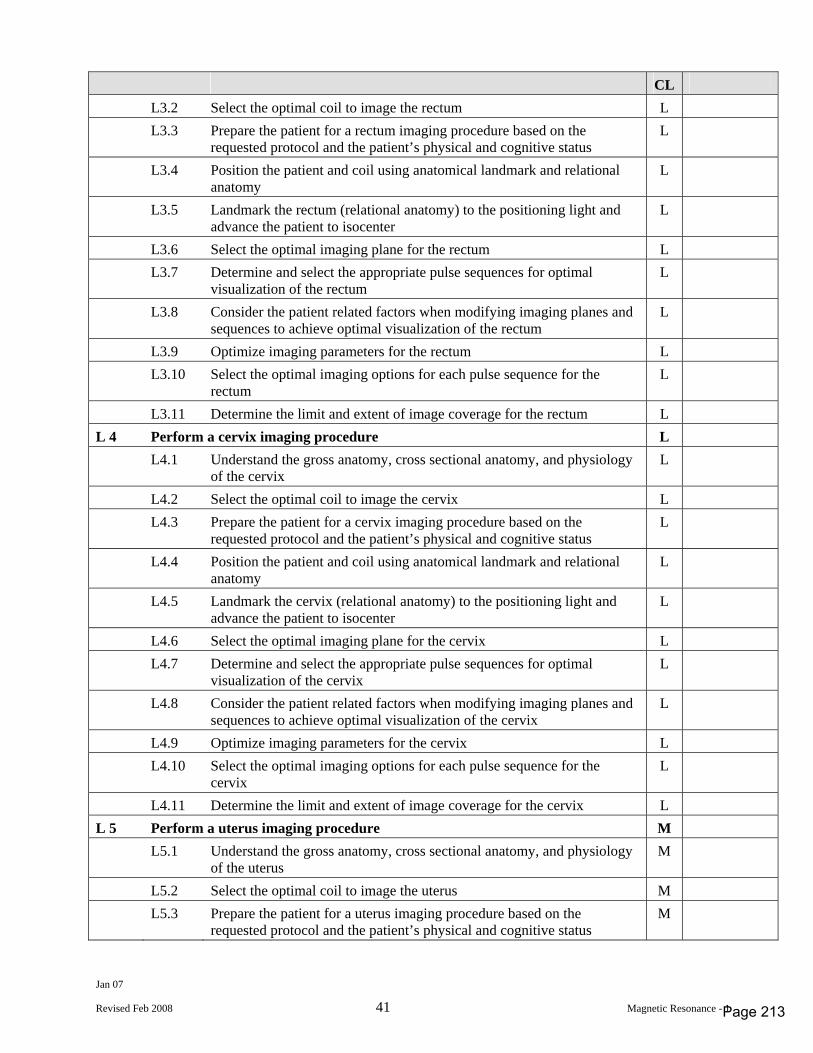
Jan 07
Revised Feb 2008 41 Magnetic Resonance - 1
CL L3.2 Select the optimal coil to image the rectum L L3.3 Prepare the patient for a rectum imaging procedure based on the
requested protocol and the patient’s physical and cognitive status L
L3.4 Position the patient and coil using anatomical landmark and relational anatomy
L
L3.5 Landmark the rectum (relational anatomy) to the positioning light and advance the patient to isocenter
L
L3.6 Select the optimal imaging plane for the rectum L L3.7 Determine and select the appropriate pulse sequences for optimal
visualization of the rectum L
L3.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the rectum
L
L3.9 Optimize imaging parameters for the rectum L L3.10 Select the optimal imaging options for each pulse sequence for the
rectum L
L3.11 Determine the limit and extent of image coverage for the rectum L L 4 Perform a cervix imaging procedure L L4.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the cervix L
L4.2 Select the optimal coil to image the cervix L L4.3 Prepare the patient for a cervix imaging procedure based on the
requested protocol and the patient’s physical and cognitive status L
L4.4 Position the patient and coil using anatomical landmark and relational anatomy
L
L4.5 Landmark the cervix (relational anatomy) to the positioning light and advance the patient to isocenter
L
L4.6 Select the optimal imaging plane for the cervix L L4.7 Determine and select the appropriate pulse sequences for optimal
visualization of the cervix L
L4.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the cervix
L
L4.9 Optimize imaging parameters for the cervix L L4.10 Select the optimal imaging options for each pulse sequence for the
cervix L
L4.11 Determine the limit and extent of image coverage for the cervix L L 5 Perform a uterus imaging procedure M L5.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the uterus M
L5.2 Select the optimal coil to image the uterus M L5.3 Prepare the patient for a uterus imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
Page 213
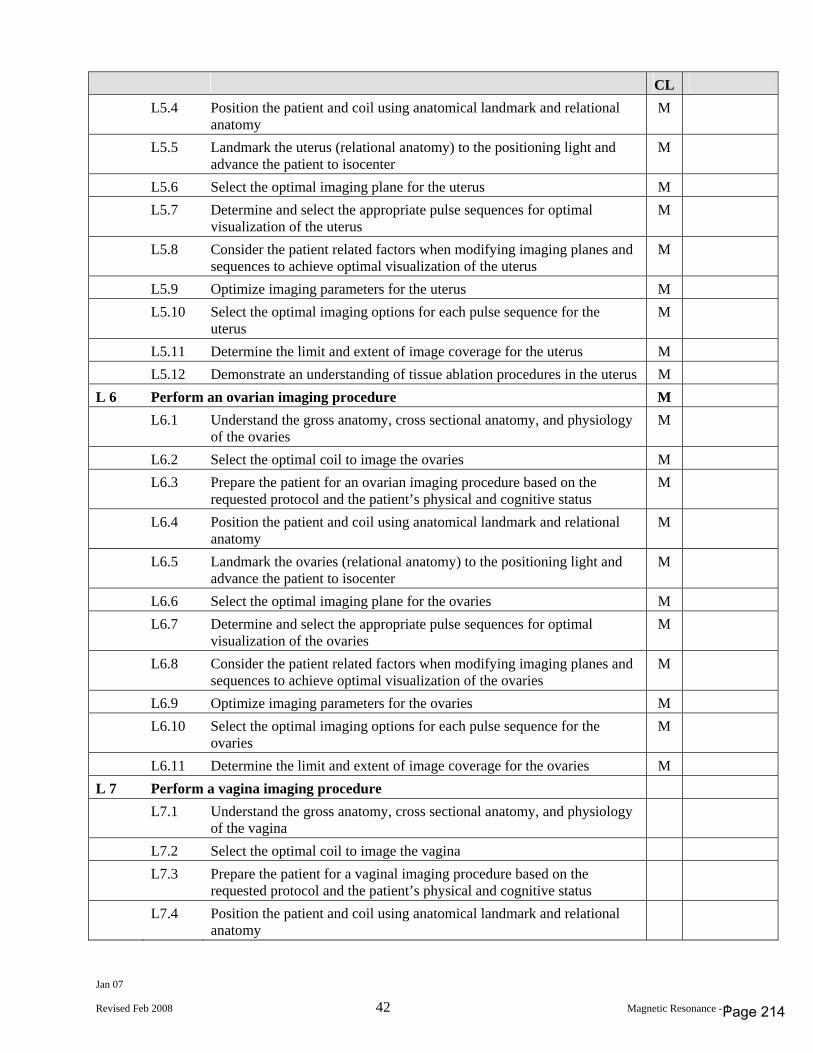
Jan 07
Revised Feb 2008 42 Magnetic Resonance - 1
CL L5.4 Position the patient and coil using anatomical landmark and relational
anatomy M
L5.5 Landmark the uterus (relational anatomy) to the positioning light and advance the patient to isocenter
M
L5.6 Select the optimal imaging plane for the uterus M L5.7 Determine and select the appropriate pulse sequences for optimal
visualization of the uterus M
L5.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the uterus
M
L5.9 Optimize imaging parameters for the uterus M L5.10 Select the optimal imaging options for each pulse sequence for the
uterus M
L5.11 Determine the limit and extent of image coverage for the uterus M L5.12 Demonstrate an understanding of tissue ablation procedures in the uterus M L 6 Perform an ovarian imaging procedure M L6.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the ovaries M
L6.2 Select the optimal coil to image the ovaries M L6.3 Prepare the patient for an ovarian imaging procedure based on the
requested protocol and the patient’s physical and cognitive status M
L6.4 Position the patient and coil using anatomical landmark and relational anatomy
M
L6.5 Landmark the ovaries (relational anatomy) to the positioning light and advance the patient to isocenter
M
L6.6 Select the optimal imaging plane for the ovaries M L6.7 Determine and select the appropriate pulse sequences for optimal
visualization of the ovaries M
L6.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the ovaries
M
L6.9 Optimize imaging parameters for the ovaries M L6.10 Select the optimal imaging options for each pulse sequence for the
ovaries M
L6.11 Determine the limit and extent of image coverage for the ovaries M L 7 Perform a vagina imaging procedure L7.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the vagina
L7.2 Select the optimal coil to image the vagina L7.3 Prepare the patient for a vaginal imaging procedure based on the
requested protocol and the patient’s physical and cognitive status
L7.4 Position the patient and coil using anatomical landmark and relational anatomy
Page 214
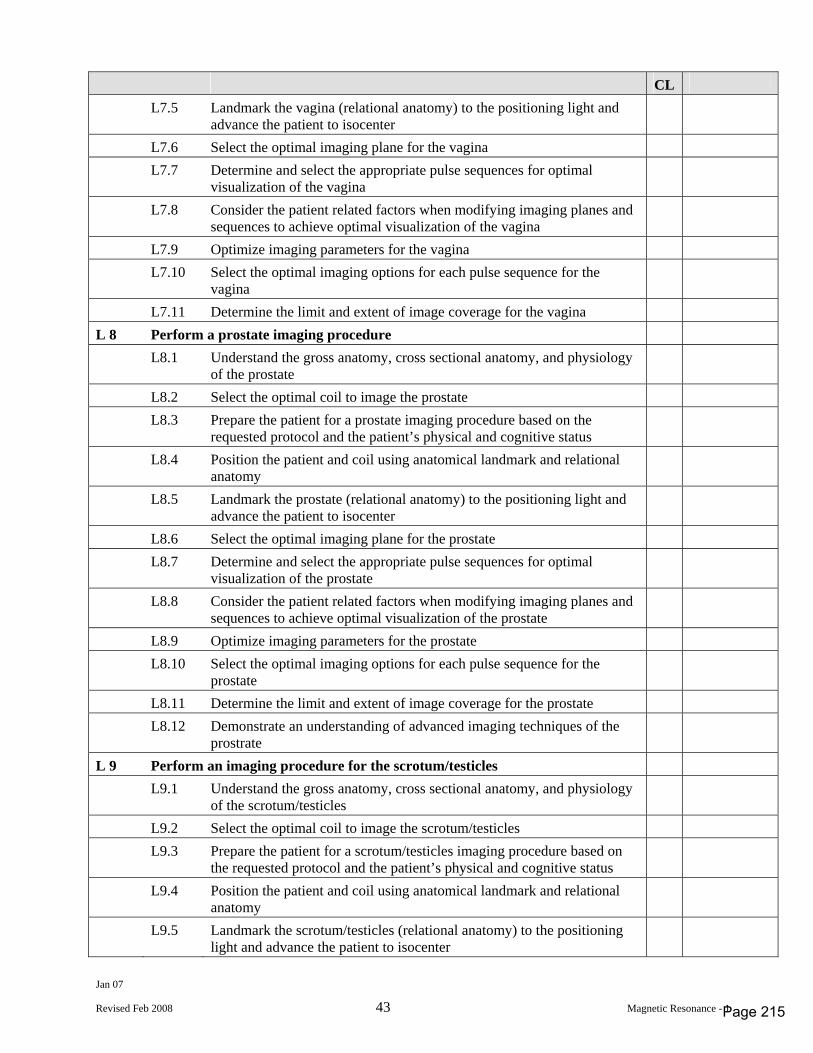
Jan 07
Revised Feb 2008 43 Magnetic Resonance - 1
CL L7.5 Landmark the vagina (relational anatomy) to the positioning light and
advance the patient to isocenter
L7.6 Select the optimal imaging plane for the vagina L7.7 Determine and select the appropriate pulse sequences for optimal
visualization of the vagina
L7.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the vagina
L7.9 Optimize imaging parameters for the vagina L7.10 Select the optimal imaging options for each pulse sequence for the
vagina
L7.11 Determine the limit and extent of image coverage for the vagina L 8 Perform a prostate imaging procedure L8.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the prostate
L8.2 Select the optimal coil to image the prostate L8.3 Prepare the patient for a prostate imaging procedure based on the
requested protocol and the patient’s physical and cognitive status
L8.4 Position the patient and coil using anatomical landmark and relational anatomy
L8.5 Landmark the prostate (relational anatomy) to the positioning light and advance the patient to isocenter
L8.6 Select the optimal imaging plane for the prostate L8.7 Determine and select the appropriate pulse sequences for optimal
visualization of the prostate
L8.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the prostate
L8.9 Optimize imaging parameters for the prostate L8.10 Select the optimal imaging options for each pulse sequence for the
prostate
L8.11 Determine the limit and extent of image coverage for the prostate L8.12 Demonstrate an understanding of advanced imaging techniques of the
prostrate
L 9 Perform an imaging procedure for the scrotum/testicles L9.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the scrotum/testicles
L9.2 Select the optimal coil to image the scrotum/testicles L9.3 Prepare the patient for a scrotum/testicles imaging procedure based on
the requested protocol and the patient’s physical and cognitive status
L9.4 Position the patient and coil using anatomical landmark and relational anatomy
L9.5 Landmark the scrotum/testicles (relational anatomy) to the positioning light and advance the patient to isocenter
Page 215
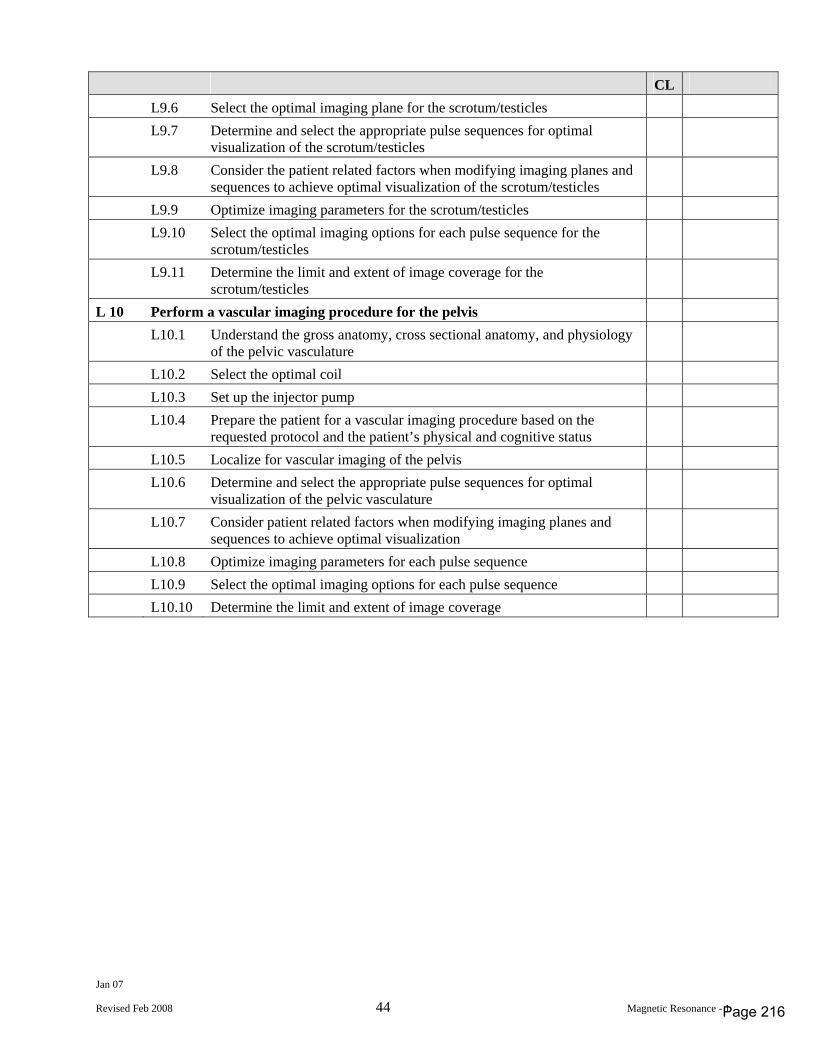
Jan 07
Revised Feb 2008 44 Magnetic Resonance - 1
CL L9.6 Select the optimal imaging plane for the scrotum/testicles L9.7 Determine and select the appropriate pulse sequences for optimal
visualization of the scrotum/testicles
L9.8 Consider the patient related factors when modifying imaging planes and sequences to achieve optimal visualization of the scrotum/testicles
L9.9 Optimize imaging parameters for the scrotum/testicles L9.10 Select the optimal imaging options for each pulse sequence for the
scrotum/testicles
L9.11 Determine the limit and extent of image coverage for the scrotum/testicles
L 10 Perform a vascular imaging procedure for the pelvis L10.1 Understand the gross anatomy, cross sectional anatomy, and physiology
of the pelvic vasculature
L10.2 Select the optimal coil L10.3 Set up the injector pump L10.4 Prepare the patient for a vascular imaging procedure based on the
requested protocol and the patient’s physical and cognitive status
L10.5 Localize for vascular imaging of the pelvis L10.6 Determine and select the appropriate pulse sequences for optimal
visualization of the pelvic vasculature
L10.7 Consider patient related factors when modifying imaging planes and sequences to achieve optimal visualization
L10.8 Optimize imaging parameters for each pulse sequence L10.9 Select the optimal imaging options for each pulse sequence L10.10 Determine the limit and extent of image coverage
Page 216
Appendix 3
Administer ing substances by in ject ion or inhalat ion
Tab Title Page No.
1 The Michener Institute for Applied Health Sciences, Course outline, Special Topics in Patient Care 1
1
2 The Michener Institute for Applied Health Sciences, Contrast Injection for Radiographers
12
3 The Michener Institute for Applied Health Sciences, Course outline, Principles of Pharmacology for Radiation Sciences
73
4 Mohawk College of Applied Arts and Technology, Course outlines, Radiation Therapy Skills II and Patient Care, includes venipuncture skills
102

MEDICAL RADIATION SCIENCES Joint Degree / Diploma Program
COURSE OUTLINE/SYLLABUS
Course Title: Special Topics in Patient Care I The Michener Institute Course Code University of Toronto Course Code PCRD120 MRS264H1 Program Chair: Fiona Cherryman, Chair MRS
Course Start Date: January 2008 Revision Date: October 2007
Page 1
PROGRAM: MRS Radiological Technology COURSE NUMBER: PCRD120/MRS264H1
COURSE TITLE: Special Topics in Patient Care I
SEMESTER OFFERING: Semester1/Year2
CHAIR APPROVAL:
2 of 7
Course Information Course Title Special Topics in Patient Care I
Description This quarter credit (0.25) course examines the use of contrast media agents for the purpose of diagnostic and interventional medical imaging. Learners will examine the rationale for the use of different types of contrast media agents available, the complications and adverse reactions that can result from the use of contrast agents, and the legal implications of contrast media administration. Learners will also gain practical skills in performing intravenous injections using both angiocatheters and butterfly needles.
Grading Information: 1. Checklist assignment (week 4) - 10% 2. Group assignment Reaction Flowchart (week 6)-10% 3. Written Assessment (week 11) - 40% 4. Skills Assessment (week 13) - 40%
Teaching Faculty Bonnie Sands Additional Instructors TBA
Organization The University of Toronto/Michener Institute for Applied Health Sciences Course Number PCRD120/MRS264H1 Credits 0.25 Contact Hours 26 Instructor Bonnie Sands, Additional Instructors TBA Course/Faculty Website Blackboard Site Campus The Michener Institute of Applied Health Sciences Address 222 St Patrick Street City/State/Zip Toronto, Ontario Office Hours Available upon request. Office Phone (416) 596-3101 ext. 3416 Beginning Date January 7, 2008 Number of Weeks 13 Meeting Times/Location Room 741 (Patient Care Lab)
Lecture room TBA
Page 2
PROGRAM: MRS Radiological Technology COURSE NUMBER: PCRD120/MRS264H1
COURSE TITLE: Special Topics in Patient Care I
SEMESTER OFFERING: Semester1/Year2
CHAIR APPROVAL:
3 of 7
Prerequisites Introduction to Patient Care in the Medical Radiation Sciences Fundmentals of Interprofessional Collaboration I: Communication Textbooks
Torres LS, Norcutt T LW, Dutton AG. Basic Medical Techniques and Patient Care in Imaging Technology. Lippincott Williams & Wilkins. 2003. Edition: sixth. ISBN: 0-7817-3101-7. Learner Supplies
Lab Coat. Manufacturer: Any. Quantity: 1. Price: Any. Source: Any. Core Abilities A. Exhibit Professional Behaviour B. Demonstrate positive attitudes and behaviors C. Communicate clearly and effectively D. Evaluate his/her own thinking throughout the steps and processes used in problem solving and
decision making. E. Take responsibility for his/her own actions. F. Work effectively in teams Competencies 1. Explore the indications for and types of contrast media agents used for diagnostic and
interventional imaging purposes Learning Objectives a. Explain how contrast media agents afford greater visualization of soft-tissue
structures/organs b. Differentiate the following: positive versus negative contrast media agents; double versus
single contrast studies; ionic versus non-ionic contrast agents; high versus low-osmolar agents c. Summarize the common indications for using contast media agents to visualize the
following systems: (a) intrathecal, (b) gastric, (c) vascular/arterial d. Identify the appropriate contrast agents for visualizing the following systems: (a)
intrathecal, (b) gastric, (c) vascular/arterial 2. Obtain informed consent to perform contrast media administration Learning Objectives a. Describe the potential risks associated with contrast media administration
Page 3
PROGRAM: MRS Radiological Technology COURSE NUMBER: PCRD120/MRS264H1
COURSE TITLE: Special Topics in Patient Care I
SEMESTER OFFERING: Semester1/Year2
CHAIR APPROVAL:
4 of 7
b. Ascertain that the patient understands the potential risks associated with contrast media administration
c. Conduct a patient history to determine contraindications to contrast media use 3. Perform venipuncture for the purpose of administering radiographic contrast media. Learning Objectives a. Select the correct equipment for the administration of an intravenous solution as per
physicians orders. b. List the anatomical sites commonly used for contrast media venipucture. c. Demonstrate the correct methods for cannulating a vessel using an angiocatheter. d. Demonstrate the correct method for cannulating a vessel using a Butterfly-needle set. e. Demonstrate the correct method for removing and disposing of venipuncture equipment. f. Demonstrate the correct method for filling a syringe from an ampule or vial. g. Describe the rationale for and benefits of using an autoinjector for administering contrast
media versus hand-injection h. Explain the precautions that must be taken when using an autoinjector for contrast media
administration 4. Manage intravenous therapy set-ups. Learning Objectives a. Identify possible intravenous complications. b. Demonstrate knowledge in monitoring IV pumps. c. Demonstrate the correct method for starting and stopping an intravenous drip. d. Identify how flow rates are determined in intravenous administration. 5. Determine potential adverse reactions/events specific to the injection of radiographic contrast
media agents, and appropriate management of such events Learning Objectives a. Differentiate between a normal side-effect of contrast media injection and an abnormal
reaction or event. b. Identify prescription drugs which would contraindicate the administration of radiographic
contrast media. c. State which medical conditions inherently increase the risk of an adverse contrast media
reaction/event occuring. d. Differentiate between the terms "Anaphylactoid" and "Anaphylactic" e. Describe "extravasation" and its harmful effects. f. List the items that comprise a contrast media injection reaction-kit. 6. Summarize the legal implications of contrast media injection as they pertain to Medical
Radiation Technologists.
Page 4
PROGRAM: MRS Radiological Technology COURSE NUMBER: PCRD120/MRS264H1
COURSE TITLE: Special Topics in Patient Care I
SEMESTER OFFERING: Semester1/Year2
CHAIR APPROVAL:
5 of 7
Learning Objectives a. Cite the guidelines for delegating the act of contrast media injection from Radiologist to
Medical Radiation Technologist. b. Describe the requirements for legal consent. c. Define what makes a patient capable to provide legal consent. d. Summarize the events to be followed when a patient is not capable of providing legal
consent. e. Define "Therapeutic Privilege" and its impact on the practice of medicine in Canada. f. List the three requirements for a plaintiff to present a successful "tort" case. g. Describe how health care practitioners can help ensure they are not found guilty of
professional neglect. Grading Information Grading Rationale Evaluations will be both applied and theoretical in nature. Skills must be successfully demonstration to pass the course. Students must achieve a minimum of 60%
Grading Scale 10% Reflection on Learning: Correctly sequence checklist for autoinjector 10% Contrast Media Reaction Flowchart Group Assignment 40% Written Examination: Contrast Media and Related Skills 40% Venipuncture Skills Demonstration Guidelines for Success Safety In this course, learners will be working with sterile needles which have the potential to transmit blood borne diseases. As such, any horse-play in the laboratory setting will result in the student(s) being immediately removed from the session. Students must be aware of the correct manner of disposing of sharp items; failure to do so could result in harm to the student or others in the labs. Digital Courtesy Many students like to tape lectures but it is important to obtain the instructor's permission before doing so. If you obtain permission to tape, you should do so in an unobtrusive manner to avoid distracting your classmates. Copyrighted material cannot be taped, eg videotapes, etc. If you carry a cell phone to class, convert it to vibration mode or turn it off for the duration of the class. This is especially critical during tests.
Page 5
PROGRAM: MRS Radiological Technology COURSE NUMBER: PCRD120/MRS264H1
COURSE TITLE: Special Topics in Patient Care I
SEMESTER OFFERING: Semester1/Year2
CHAIR APPROVAL:
6 of 7
Guidelines for Mutual Respect This course is designed for collaboration rather than competition. That means that each member of the class supports the others in their efforts to succeed. Be sure to come to each class prepared to: 1. Listen with respect. 2. Speak with respect. 3. Contribute actively to the work of your team both in the classroom and the laboratory setting.
Page 6
PROGRAM: MRS Radiological Technology COURSE NUMBER: PCRD120/MRS264H1
COURSE TITLE: Special Topics in Patient Care I
SEMESTER OFFERING: Semester1/Year2
CHAIR APPROVAL:
7 of 7
Schedule Session Notes Week 1 Lecture
Introduction to Contrast Media Legal aspects of Contrast Media injection Informed Consent
Week 2 Lab
Examine different types of intravenous setups Standard precautions and Sharps/Ampule disposal Informed Consent
Week 3 Lecture
IV Contrast- LOMC/HOCM, Ionic vs nonionic Uses
Week 4 Lab
Draw up contrast media Intro to venipuncture Auto-injectors and IV pumps *Checklist Assignment Due
Week 5 Lecture
Complications and adverse reactions to Radiographic contrast media agents
Week 6 Lab
IV solutions and setups *Flowchart Assignment Due
Week 7 Lecture
Management of reactions
Week 8 Lab
Angiocath and butterfly neeedles
Week 9 Lecture
Specialty contrast agents Intrathecal injections Intracavitary injection
Week 10 Lab:
Skills Practice
Week 11 Written Exam Week 12 Lab
Skills Practice
Week 13 Lab
Practical Assessment of injection skills
Page 7
© Michener/University of Toronto Medical Radiation Sciences Program Jan 2008
Performance Assessment Task Flowchart - Contrast Media Reactions
Target Competencies Determine potential adverse reactions/events specific to the injection of radiographic contrast media agents, and appropriate management of such events Linked Core Abilities Evaluate his/her own thinking throughout the steps and processes used in problem solving and
decision making. Take responsibility for his/her own actions. Directions For this performance assessment your group will create a flowchart depicting the steps involved in dealing with a contrast media reaction. You will be assigned a set of signs and symptoms.
Group A 1 Warmth, flushing and anxiety 2 Cardiopulmonary Arrest 3 Bronchospasm Group B 1 Laryngeal Edema 2 Hypotension 3 Nausea/Vomiting, Pallor and Sweating
Group C 1 Tachycardia/Bradycardia 2 Shaking, Itching and Rash 3 Convulsions 1. Determine all of the steps in the process. Write them down. 2. Create a flowchart of the process. Make sure your flowchart meets the criteria on the scoring guide. 3. Submit your flowchart to your instructor for evaluation. 4. Submit your completed peer-evaluation to your instructor. The peer evaluation will be used as a factor to calculate your final mark. For example if your combined average score from your group peer evaluation is 80% then you will receive 80% of the group mark. This assignment is scheduled during week 6 of the course and the mark will contribute towards 10% of your final grade for this course. Scenario/Prompt Your group should be comprised of students from each of the MRS disciplines and have a maximum of six (6) members. You will need to meet outside of class time to coordinate your assignment. Your flowchart needs to be submitted in electronic format to the course supervisor on the due date. You will need to complete and submit a confidential peer assessment for each of your team members.
Page 8
© Michener/University of Toronto Medical Radiation Sciences Program Jan 2008
Rating Scale 0 Did not meet criterion 1 Met most criterion - more detail required 2 Satisfied criterion expectations 3 Exceeded criterion with a high level of creativity, accuracy, and attention to detail Scoring Guide Criteria Ratings 1. flowchart depicts all of the items in the process 3 2 1 0 2. flowchart classifies the severity of the signs/symptoms and type of
reaction 3 2 1 0
3. flow chart identifies possible treatment options 3 2 1 0 4. flowchart differentiates between the roles and responsibilities of
the health care team members 3 2 1 0
5. flowchart identifies the types of prescription drugs which should be available for treatment of the reaction
3 2 1 0
6. flowchart shows the relationship of one step to another and possible progression/complications of the reaction
3 2 1 0
7. flowchart shows a clear understanding of the topic 3 2 1 0 8. flowchart is neat and well organized 3 2 1 0 9. Resources used are listed 3 2 1 0
Total Points ___________ Peer Assessment Factor (PAF) ____________
Grade __________ (mark x PAF)
Name _________________________________________ Date ____________ Evaluator's Signature _________________________________ Date ____________ Comments:
Page 9
© Michener/University of Toronto Medical Radiation Sciences Program Revised Mar 2008
Performance Assessment Task Venipuncture Skills Demonstration
Target Competencies Perform venipuncture for the purpose of administering radiographic contrast media. Linked Core Abilities Exhibit Professional Behaviour Demonstrate positive attitudes and behaviors Communicate clearly and effectively Evaluate his/her own thinking throughout the steps and processes used in problem solving and
decision making. Take responsibility for his/her own actions. Work effectively in teams Directions For this performance assessment you will demonstrate a technical skill required to perform a task. You will work in a laboratory or simulated work environment. Equipment, instruments, tools, supplies, materials that you need will be provided, but you will be required to select the appropriate items need to complete the task. Practice the skill, self-assessing according the scoring guide. Schedule your skill assessment with your instructor as directed. If necessary, arrange for a role-play client or patient. Bring any personal protective equipment and tools that are required to perform the task. Bring any job aids that are permitted. A. At the time of performance be sure that you: 1. Gather the required tools, equipment, instruments, materials or supplies. 2. Don the appropriate personal safety clothing and equipment. 3. Provide for the comfort and safety of your client or patient. 4. Perform each step of the task. 5. Follow all safety procedures. 6. Explain that steps of the tasks as you perform them. (what, why, how, precautions) 7. Answer any questions posed by the evaluator or your client/patient.
Scenario/Prompt EQUIPMENT Biohazard bags Cannula (angiocatheter) set 22- 25 G Patient Consent Form Tourniquet (non-latex) Needles: 21G, 25G 5/8 in. Sensitive tape Sharps containers Venipuncture arms IV poles Gauze squares (2 x 2) or cotton balls Basic admin-type IV tubing Sterile sodium chloride bags (250 mL) Scoring Standard You must earn a 2 or higher on each criterion in order to earn credit for this assessment. This Assessment is worth 40 % of the final grade.
Rating Scale 0 Fails to perform skill adequately or does not attempt to perform skill. 1 Attempts to perform the skill, but makes one or more critical mistakes and/or multiple minor
mistakes that go unrecognized. Explanation is inaccurate or does not occur. Fails to provide adequate answers to questions or reveals critical misunderstanding.
2 Performs adequately, with no more than one minor prompt, and without critical mistakes. May fail to recognize minor mistakes. Explains what and how, but fails to explain why. Answers to questions about the process may reveal minor misunderstandings.
3 Performs confidently with only minor hesitation, without prompting, and with no critical mistakes. Recognizes and corrects minor mistakes in safe and appropriate manner if they occur. Explains what and how, but may need prompting to explain why. Answers questions about the process accurately revealing no significant misunderstandings.
4 Performs confidently, without prompting, and without mistakes. Clearly explains what, why, how, and any precautions. Answers questions about the process accurately and insightfully.
Page 10
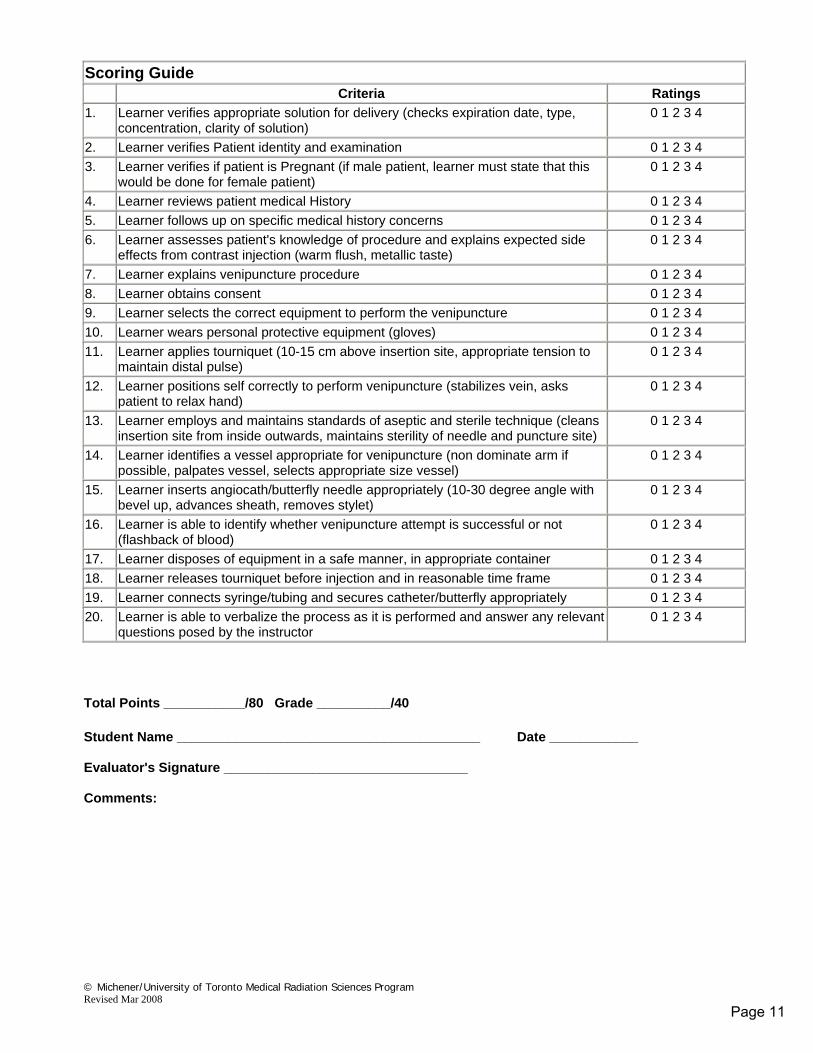
© Michener/University of Toronto Medical Radiation Sciences Program Revised Mar 2008
Scoring Guide Criteria Ratings 1. Learner verifies appropriate solution for delivery (checks expiration date, type,
concentration, clarity of solution) 0 1 2 3 4
2. Learner verifies Patient identity and examination 0 1 2 3 4 3. Learner verifies if patient is Pregnant (if male patient, learner must state that this
would be done for female patient) 0 1 2 3 4
4. Learner reviews patient medical History 0 1 2 3 4 5. Learner follows up on specific medical history concerns 0 1 2 3 4 6. Learner assesses patient's knowledge of procedure and explains expected side
effects from contrast injection (warm flush, metallic taste) 0 1 2 3 4
7. Learner explains venipuncture procedure 0 1 2 3 4 8. Learner obtains consent 0 1 2 3 4 9. Learner selects the correct equipment to perform the venipuncture 0 1 2 3 4 10. Learner wears personal protective equipment (gloves) 0 1 2 3 4 11. Learner applies tourniquet (10-15 cm above insertion site, appropriate tension to
maintain distal pulse) 0 1 2 3 4
12. Learner positions self correctly to perform venipuncture (stabilizes vein, asks patient to relax hand)
0 1 2 3 4
13. Learner employs and maintains standards of aseptic and sterile technique (cleans insertion site from inside outwards, maintains sterility of needle and puncture site)
0 1 2 3 4
14. Learner identifies a vessel appropriate for venipuncture (non dominate arm if possible, palpates vessel, selects appropriate size vessel)
0 1 2 3 4
15. Learner inserts angiocath/butterfly needle appropriately (10-30 degree angle with bevel up, advances sheath, removes stylet)
0 1 2 3 4
16. Learner is able to identify whether venipuncture attempt is successful or not (flashback of blood)
0 1 2 3 4
17. Learner disposes of equipment in a safe manner, in appropriate container 0 1 2 3 4 18. Learner releases tourniquet before injection and in reasonable time frame 0 1 2 3 4 19. Learner connects syringe/tubing and secures catheter/butterfly appropriately 0 1 2 3 4 20. Learner is able to verbalize the process as it is performed and answer any relevant
questions posed by the instructor 0 1 2 3 4
Total Points ___________/80 Grade __________/40
Student Name _________________________________________ Date ____________ Evaluator's Signature _________________________________ Comments:
Page 11
RA815
CONTRAST INJECTION FOR RADIOGRAPHERS 2008
THE MICHENER INSTITUTE for Applied Health Sciences
Page 12
RA 815
CONTRAST INJECTION FOR RADIOGRAPHERS
CONTENTS PAGE CONTRAST MEDIA 1 STARTING AN INTRAVENOUS LINE 13 BASIC IV MAINTENANCE 28 INJECTING INTO AN EXISTING LINE 49
Page 13
RA815 1383PTSPC
RADIOPAQUE CONTRAST MEDIA History Contrast agents are used in radiography because some organs and tissues do not have sufficient density to provide adequate contrast with adjacent tissue to be visualized. Visualization of the vasuclar system, kidneys, colon and GU system requires the introduction of a radiopaque medium or contrast agent. Early contrast media included bismuth in oil, iodized oil, organic iodides and strontium bromide. The very first contrast examination was attempted only one month after the discovery of x-rays in 1895. It was a mixture of cinnibar, vaseline, and gypsum injected into the vessels of a cadaver arm. The procedure took 57 minutes. However a successful contrast agent for use on living humans was not discovered for another 30 years. In 1923 it was discovered that sodium iodide (inorganic iodide) made an excellent contrast but the physiological effects were so dangerous that most patients died. Interaction of Contrast Media with X-rays The most commonly used radiopaque contrast media are Barium and Iodine. These are used because their atomic number and mass density are higher than the tissues being imaged. Their atomic numbers are 56 and 53 respectively, while human tissue has an average atomic number of 18. Iodine is the most widely used injectable agent as iodine absorbs x-ray photons and this limits the amount of photons that pass through the body and reach the image receptor. The higher the iodine concentation the greater the absorption. The result is higher opacification on the image. Structure of Iodinated Radiography Media Advancement in the finding of a suitable contrast occurred with the development of the water-soluble organic iodide compounds. These compounds are triiodinated compounds derived from the benzoic acid ring structure Iodine, the opacifying portion of the structure is located at the 2nd, 4th, & 6th, parts of the ring. The anion is located at the 3rd & 5th position. The salt or cation (positively charged ion) is located on the first portion. The salts most commonly used for water-soluble organic iodides are sodium and meglamine. They are responsible for the solubility of the medium.
Page 14
RA815 2 1383PTSPC
There are three main anions (negatively charged particles) employed today. They are diatrizoate, iothalamate, and metrizoate. The anions are responsible for stabilizing and detoxifying the contrast medium. The generic name of a contrast medium is derived from the cation and anion, for example sodium diatrizoate (Sodium Hypaque). The development of Low Osmolality Contrast Media (LOCM) both ionic and non-ionic has steadily improved safety and toxicity of contrast since the 1970’s. The toxicity of an ionic monomer is the result of the Osmolality and ionicity of the contrast agent. In the non-ionic agents, the cation was eliminated, as it was responsible for most of the osmotic effect of the agent. The ionizing carboxyl group (COO-) of high Osmolality agents is replaced with a non-dissociating group such as amide or glucose. When dissolved in water a non-ionic compound forms a molecule not an ionizing solution. First and second Generation Triiodinated Contrast Agents IONIC MONOMER DIMER Generic Name Trade Name Generic Name Trade Name Diatrizoate Hypaque Ioxaglate- Hexabrix Iothalamote Conray Metrizoate Isopaque Acetrizoate Diaginol Ioglicate Rayvist NON IONIC MONOMER DIMER Generic Name Trade Name Generic Name Trade Name Metrizamide Amipaque Iodixanol Visipaque Iohexon Omnipaque Iotrolan Isovist Iopamidol Isovue Isomin* Ioversol Optiray Iopromide Ultravist Iopentol Imagopaque * still in clinical trials
Page 15
RA815 3 1383PTSPC
Magnetic Resonance Contrast Gadolinuim is a rare earth element. Its ion (Gd+) has 7 unpaired electrons and therefore shows paramagnetic properties. It has a strong effect on the hydrogen-proton spin-lattice relaxation time (t1) which causes the contrast enhancement in MRI scans. Gadopentetate Dimeglumine (Magnevist) is excreted in the urine. Ultrasound Contrast Agents Many substances may act as contrast in ultrasound and Doppler. The altered echo amplitude due to changes in absorption, reflection and/or refraction causes the contrast. Echo free fluids such as water or saline, distends body cavities to improve visualization of the luminal walls. The newer contrast media, designed for vascular work are intended to increase Doppler signals from blood or the echogenicity of tissue. They are based on either micorbubble solutions or solid particles suspended in solutions or emulsions. Gas bubbles in liquid are capable of strong oscillatory motion. Depending upon bubble size and the mechanical properties of the bubble capsule, some microbubble contrast media may have resonance frequencies close to the transmitted ultrasound frequency. In an ultrasound field they will start to oscillate thus actively transmitting ultrasound. Some contrast depends upon gas bubble rupture. This contrast media (gas microbubbles) is taken up by the reticuloendolthelial cells of liver and spleen. When imaged by Doppler, the pressure waves caused by the bubble rupturing creates a coloured mosaic pattern in tissue. Tumors devoid of reticuloendolthelial tissue such as metastases stands out as dark, non coloured regions. What causes the undesirable physioloigcal effects of Contrast Media? The osmolality (concentration) and the chemical nature of these agents are believed to be the major factors responsible for the “side-effects” experienced with intravascular contrast administration. The osmolality of contrast media used today is two to three times greater than that of blood. Remembering the concept of osmosis (passage of water from a weaker solution to a more concentrated solution until equilibrium is established on both sides of the membrane), when contrast media is injected into the vasculature, a rapid movement of water occurs. Water moves into the vessels both from the extravascular tissues and from the red blood cells. The red blood cells begin to shrink or crenate. As a result, the circulating blood volume and peripheral blood flow increases and systemic vascular resistance decreases, as does the blood pressure. All this occurs because of the introduction of a solution with a higher concentration than that of blood. Vasodilation produced by the injection of a contrast medim is thought to be the primary cause of the accompanying pain, discomfort and flushing.
Page 16
RA815 4 1383PTSPC
The pain and discomfort are similar in concept to swimming in the ocean with your eyes open – the hypertonic salt water flows over your eyes drawing water out of the conjunctiva, thus you experience pain in your eyes often with an associated burning sensation. In angiography, a hypertonic contrast media flowing over endothelial cells of the vessels draws water out of the vessel wall and causes pain. Fluid drawn from the red blood cells distort their shape and result in difficult passage of oxygen through the capillaries, potentially causing trauma at the pulmonary, renal and cerebral capillary beds. This interruption of oxygen exchange at the peripheral capillary level results in the tingling, uncomfortable sensation that patients often report with contrast injections. Many of the adverse physiological effects of contrast media can be related directly to osmolality. With the development of the low osmolality contrats media (LOCM) the incidence of reaction has been reduced as we get closer to the osmolality of blood. Contrast media are excreted mainly through the kidneys. Approximely 85% of the injected dose is excreted with 24 to 48 hours. The thyroid and liver retains about 1.5% which can result in blood tests being elevated after a procedure. Nuclear Medicine scans of the thyroid should not be attempted after a contrast injection, as the results will be inaccurate. Dehydration is dangerous and may contribute to acute renal failure in patients with pre-existing renal insufficiency, diabetes or advanced vascular disease. Before contrast is injected, an adequate history should be obtained to determine who is most likely to experience a reaction. Patients with a history of allergies are twice as likely and those with a previous reaction history are three times more likely to react than the general population. Manufacturers of contrast media consider the following patient groups to be in a “high risk” cataegory: a) patients with a history of previoius contrast reactions b) patients with allergies c) patients with liver disease d) patients with kidney disease In any high-risk patients, the benefits of the procedure should be evaluated and contrast given only if the benefits outweigh the risks involved. Contrast agents passively cross the placental barrier and should be used only if absoluately imperature in the treatment of the mother. X-ray procedures also present a risk related to the exposure of the fetus to radiation. Contrast is secreted in human milk. Nursing should be suspended for a mimimum ofe 48 hours post contrast injection. Any woman of childbearing age should be questioned as to the possibility of pregnancy before a radiological procdure.
Page 17
RA815 5 1383PTSPC
Serious and fatal reations have been associated with the administration of contrast and it is vital that you are prepared to treat reactions of any severity. a) Ensure that a skilled and experienced physician is in the radiology department should
intervention be required. b) Have a fully stocked emergency cart and personnel familiar with the equipment readily
available. c) An emergency drug box should be in each injection room. d) Familiarize yourself with the location of all emergency equipment, emergency call
alarms, oxygen, suction, ambubags and oral airways. e) Cardiac arrest number should be posted on or near the phone. In the event of a severe reaction, discontinue administration of the contrast medium and summon assistance. Do not remove the needle from the arm. Most adverse reactions appear within thirty minutes after the start of the injection. Delayed reactions have been reported and patients should be advised to contract their physician or present to their local emergency department should any problems arise after they leave your department.
Page 18
RA815 6 1383PTSPC
Adverse reactions
These are specific for Opitray. CPS inserts for Omnipaque, Isovue and Hexabrix are included in the teaching package.
Page 19
RA815 7 1383PTSPC
Treatment of Adverse Reactions: For minor allergic reactions such as hives, facial edema, etc. (see allergic-type reactions), IV or IM administration of an antihistamine such as Bendadryl is recommended. This medication can cause drwsiness and therefore it is imperative that outpatients do not drive or return home unaccompanied. A major reaction may manifest by signs and symptoms of cardiovascular collapse (shock), severe respiratory difficulty and nervous system dysfunction. Convulsions, com and cardio-respiratory arrest may ensue. The following measures should be taken: 1. Summon assistance - do not leave patient unattended.
2. Maintain an airway – if the patient has vomited, roll onto his/herside to rpevent
aspiration (called shock position). • Suction may be necessary if gurgling is audible and/or oral secretions are
accumulating. • If the patient becomes unconscious, roll onto is/her side to prevent airway
obstruction by the tongue. • If an oral airway is available, insert in any patient who appears to be having
difficulty guarding his/her airway, i.e. semi-comatose. 3. Monitor vital signs.
• Take pulse (take not of strength of pulse) • Take blood pressure.
4. Apply 02 as instructed – familiarize yourself with 02 set-ups, regulating flow, loction of
flow-meters in your area. 5. Any further resuscitation should be continued under the physician’s supervision. You
may be required to commence artificial respiration and/or external cardiac massage until the arrest team arrives.
• Familiarize yourself with the ambubag and/or pocket-mask with one-way valve depending upon what is available in your department.
• Ask about CPR update if not currently available.
Page 20
RA815 8 1383PTSPC
6. Set up an IV of D/W for medication infusion. 7. Record as per hospital policy.
Medications Most Frequently Used: The following medications should be contained in your emergency drug box. Familiarize yourself with location and contents of the drug box just in case you are asked to provide them. Restocking and replacing expired medications is usually the responsibility of the pharmacy department or department nurse(s). Check this, however, to ensure patient safety. Soluble Hydocortisone (SoluCortef) - used for acute, allergic anaphylactic reactions. Adrenalin/Epinephrine - for severe allergic, anaphylactic reactions (this is the subcutaneous medication contained in "Bee-Sting Kits"). - Intravenous administration produces a rapid rise in BP by direct stimulation of the heart. - Increase heart rate. - Relaxes smooth muscle of bronchi and therefore relieves severe bronchospasm (asthma
attacks) not controlled by inhalation therapy. Levophed - for severe hypotension. Atropine - increases heart rate in severe bradycardia (vaso-vagal attacks). Phenobarb - control convulsions. Valium - control convulsions. Chlortripolon - antihistamine for treatment of minor/moderate reactions such as hives. Ventolin - bronchodilator. - Often used daily by asthmatics to relieve bronchospasm (puffer). - Also used via inhalation therapy for more severe bronchospasm. Aminophylline - bronchodilator. - Generally administered for long-term sustained bronchodilation. - Mixed in an intravenous, volume controlled drip via pump or Buretrol. Benadryl - used for mild allergic reactions such as hives.
Page 21
RA815 9 1383PTSPC
Administration of Contrast Media - General Recommendations: 1. Patients may be instructed to omit the meal immediately prior to the procedure, however,
they should not be fluid restricted. Diabetic patients may require some appointment time adjustment to facilitate their insulin regime.
2. Before withdrawing contrast, inspect the container for particulate matter and/or
discolouration. The solution should be clear and colourless - if not, discard. 3. Check the expiry date and discard outdated contrast. 4. Once the seal has been punctured or removed, the contrast should be transferred into the
delivery system(s) and used immediately. Contrast media does not contain preservatives and therefore should not be stored for later use.
5. Contrast media should be at or close to body temperature when injected. Cold solutions
increase the likelihood of cardiovascular collapse. Warm solutions decrease the viscosity and are easier to inject.
6. Contrast media may be injected into solutions of NS, D/W, R/L and 2/3 & 1/3 with
manufacturers added KCl (bright red printing on right hand side of IV solution bag). 7. Other medications should never be administered concomitantly in the same syringe or IV
administration set because of the potential for incompatibility. 8. Between injections, aspirate the syringe slightly to ensure patency of the needle/cannula
and proper positioning. 9. In the case of a reaction, stop injecting and summon assistance immediately.
Page 22
RA815 10 1383PTSPC
Sample Interview: Obtaining Consent "All medical procedures carry an element of risk and this procedure is no exception. Your doctor has considered these risks before recommending this examination and believes that the diagnostic benefits far outweigh the risks involved. The use of intravenous contrast dye will help provide better pictures and will give us more information in helping diagnose or evaluate your problem. Minor allergic reactions to intravenous contrast occur in about 1-3% of patients in the form of itching, sneezing or hives. Less common minor reactions include slight wheezing and slight swelling of the eyes. Serious complications may also occur in 1-3% of the population and can include serious allergic reactions; fall in blood pressure, shortness of breath, seizures, kidney damage and even death. Certain conditions may make you more susceptible to an allergic reaction to the contrast dye. For this reason, I need to ask you a few questions regarding your past health." 1. Do you have any allergies? If so, to what? What happens? (Ask about seafood allergies as many patients do not correlate the importance of
reporting what they may consider a "minor food allergy".) 2. Do you have a history of asthma? 3. Are you diabetic? 4. Do you have any kidney or liver disease? 5. Have you ever had X-ray dye in the past? Any problems? If so, what were they? 6. Are you being treated for any medical problems? What are they? 7. What medications are you on currently? Are you taking aspirin or ‘blood thinners’ ? Selective Questions: 8. Is there any possibility of you being pregnant? 9. Have you ever been tested for the sickle cell trait? Are you positive? For patients already admitted to hospital, check the chart for the following information: 1. BUN and Creatinine - are they elevated? 2. Allergy history 3. Diagnosis - why is the procedure being done?
Page 23
RA815 11 1383PTSPC
The following list is a review of patient conditions that may predispose them to experiencing a reaction: 1. renal impairment or failure 2. liver disease 3. known hypersensitivity to contrast media 4. allergies especially those with allergies to shellfish 5. asthmatics 6. known pheochromocytoma 7. hyperthyroidism 8. cardiac conditions 9. elderly, debilitated and/or severely ill 10. multiple myeloma 11. sickle cell positive In summary, contrast media, like any medication must be administered with caution. Although the incidence of reaction in the general population is low (about 1-3%), especially since the introduction of low osmolality contrast media, you should never allow yourself to become complacent with its administration. Reactions can occur quickly and without warning. Most of these reactions can be reversed with immediate and proper intervention and potentially fatal reactions can, fortunately, be resuscitated with quick, aggressive treatment. Being prepared to handle the worst case scenario will ensure that appropriate intervention is available for the patient in the event of an emergency. This knowledge also instills staff confidence, which is reflected to the patient, and assures everyone that they are working under conditions of optimum safety. MODERATE RISK PATIENTS - Caution Required - Consult Radiologist 1. Asthmatics 2. Elderly, severely ill and/or debilitated 3. Known cardiac conditions 4. Known pheochromocytoma 5. Known hyperthyroidism 6. Multiple myeloma 7. Positive sickle cell trait 8. Diabetics
Page 24
RA815 12 1383PTSPC
HIGH RISK PATIENTS - Consult Radiologist - Radiologist Should inject 1. History of allergies Ä incidence of reaction is twice that of general population 2. History of previous contrast reactions Ä incidence is three times that of general
population 3. Renal patients 4. Liver disease
Page 25
RA815 13 1383PTSPC
STARTING AN INTRAVENOUS LINE Initiating intravenous (IV) therapy is a specialized technique requiring technical skill, knowledge and communication skills. Since it involves the introduction of a sterile catheter or cannula into the vascular system, it requires consistent aseptic technique to prevent or minimize risks and complications. The technique itself varies slightly with different types of sets available. Both the insertion of "winged sets" (see Figure 4) and "catheters or cannula sets" (see Figure 3) will be instructed and lab time available for practice. Proficiency with venipuncture is only a matter of repetition. As with any new skill, the more practice you have, the more confident and accurate you become, and the easier this new skill will seem.
Venipuncture Sites Veins of the forearm present the most accessible route because they are numerous and relatively easy to locate. Knowledge of the basic anatomy and physiology of veins and arteries allows one to distinguish the two and to safely choose appropriate veins for IV therapy. Median, cephalic and basilic veins - found in the antecubital fossa (see Figure 1). These veins are large, easily palpable and accept the pressure exerted when viscous contrast media is injected quickly, directly via syringe or pump. These veins are safe to use for oneÄtime injection, however, ensure that the patient keeps his/her elbow straight to prevent kinking of the catheter, extravasation of dye into surrounding tissues or damage to underlying arteries and nerves. Smaller veins (see Figure 2) in the hands, provide more resistance when injecting and may "blow" under pressure causing extravasation at the site. This is common with very ill or elderly patients whose venous integrity is compromised.
Page 26
RA815 14 1383PTSPC
FIGURE 1: Superficial Veins Of The Arm
87/00168R
Superficial Veins Of The Upper Extremities Metacarpal veins - formed by the union of digital veins on the back of the hand (Figure 2), including the metacarpal arch. These veins are ideal for IV therapy, as they are usually visible, lie flat, and are splinted naturally by the metacarpal bones.
Page 27
RA815 15 1383PTSPC
Cephalic vein - runs upward along the radial border of the forearm. (Avoid using this vein in the "watchstrap" area over the radius; there is a risk of hitting an aberrant radial nerve here.) It is often visible, readily accommodates large catheters or cannulas, and can be entered between the wrist and upper arm. Basilic vein - originates in the ulnar portion of the dorsal venous network and ascends the ulnar surface of the forearm. Below the elbow, it curves toward the inside of the forearm to meet the median cubital vein. It is often inconspicuous and, therefore, overlooked. It is very prominent in males. Both cephalic and basilic sites will easily accept a "Butterfly" needle or large-bore cannula, and are usually large enough to withstand the sudden increased pressure exerted with direct injection of contrast media. Because these veins lie more superficially than do the veins at the antecubital fossa area, your angle of insertion will need to be altered to avoid perforating the far wall of the vessel. FIGURE 2: Superficial Veins of the Hand
87/00167R
Addressing the Patient Your approach to patients has a direct bearing on their acceptance of IV therapy. The conscious patient has the right to know what you are doing and why. A careful, simple explanation takes only seconds to convey and establishes the patient's trust in you and your ability to provide care.
Page 28
RA815 16 1383PTSPC
You may also be required to obtain the consent for the procedure and for the injection of contrast media. Your professional and confident approach will help alleviate the patients anxiety and will facilitate a better understanding of what is to happen during the procedure. In essence, you are creating optimum conditions for obtaining a fully informed consent - that being patient understanding and compliance - whereby you may now legally proceed according to the policies and guidelines of your department. Here are some practical suggestions: • Indicate that the physician has requested you to carry out his order. • Give the patient a simple reason for the therapy. • Explain step-by-step what will happen next. • Explain that the insertion is painful but only briefly. Once the insertion is complete, it is
no longer uncomfortable. • Tell them when the painful part is finished. • Patients displaying extreme anxiety may benefit from some distraction, such as taking a
deep breath in through the mouth and exhaling slowly. A prepared, relaxed patient has skin that is easier to penetrate and veins which accept cannulation more readily. Anxiety causes vasoconstriction making venous palpation difficult. Venipunctures should always be performed with the patient supine and the limb well supported. Vagal (fainting) episodes are not uncommon; watch the patient and be prepared, regardless of their apparent comfort level with the procedure. If an intravenous line is being established, explain to the patient that they may experience a cool sensation as the solution initially infuses. This is normal. When they receive the contrast injection, they may experience a warm, flushing sensation (expand on other side effects just prior to injection). This is also normal. Before you perform your first venipuncture, prepare in advance what you will tell the patient if you are unsuccessful and require a second attempt. For example, you may say: "On occasion, veins collapse or constrict, which is a normal response brought on by the anxiety experienced prior to any medical procedure. This makes my job more difficult as it is more difficult to access a small vein. If I am unsuccessful initially, I may have to try again in another location."
Page 29
RA815 17 1383PTSPC
Equipment
Catheter, Cannula, Needle Devices Catheters or cannulas are made of flexible TeflonTm or plastic with a silicone coating. Both are radio-opaque. Catheter hubs are colour-coded for size, but the code varies with the manufacturer. You will need to be aware of the code for your setting. Most clinical settings have policies and usual practices for sizing. Number 20 angiocathsTm are generally large enough to allow injection of contrast media with minimal resistance. Occasionally, patients with extremely small or fragile veins may require a smaller, shorter size #22 to be inserted. It is possible to inject the viscous contrast through such a small diameter however, you will notice a definite increase in the resistance, resulting in a much slower injection rate. Observe these sites closely for infiltration. The parts of a catheter or cannula set (Figure 3) include: • A needle or stylet, with a bevelled tip and flashback chamber. Blood appears in the
chamber when the stylet tip has entered the vein. • A catheter or cannula, with a colour-coded hub. The tip is tapered to facilitate insertion
and prevent trauma to the vein while in place. The stylet is situated inside the catheter; it is removed when insertion is complete.
• A protective cap, covering all of the catheter and hub. Only the flashback chamber is
exposed. The protected areas are considered to be sterile.
Page 30

RA815 18 1383PTSPC
FIGURE 3: The Catheter/Cannula Set A. Before Insertion 87/00529 B. In Situ
Page 31
RA815 19 1383PTSPC
Winged Needle Sets These devices include an inflexible metal needle of differing gauges, about 2 cm long with plastic "wing-like" handles for insertion and anchoring. The length of attached tubing can be subsequently connected to an IV infusion or to a syringe for direct injection. The parts of a winged needle include: • Needle (metal) • Bevelled tip • Wings, which provide handles for insertion and some stability after insertion • Tubing • Protective cap • Needle sheath. There are no separate or detachable parts to this set. Only the needle, underneath the sheath is sterile. FIGURE 4: Winged Needle Set
89/04333R Winged needles are inflexible and will readily pierce the vein wall, causing extravasation. They are used only for short-term therapy (or for children in scalp veins).
Page 32
RA815 20 1383PTSPC
Other Equipment • Tourniquet of soft rubber tubing or a blood pressure cuff inflated to 60-70 mm Hg.
(Tourniquets should be wiped with alcohol or replaced frequently.) • Non-allergenic tape, to secure the needle device. Dry gauze sponges. • Alcohol wipes (70% isopropyl alcohol) and/or crushable iodophor capsules. Clinical
policy will specify the skin preparation to be used. • IV standard or pole. • Clean gloves to protect you from the patient's blood. • Disposable arm-boards or splints for use when the veins used are over areas of flexion,
e.g. the wrist or the antecubital fossa. (Not usually required for short-term infusions.)
Initiating An IV Infusion 1. Maintain aseptic technique throughout. Keep in mind the parts of your equipment which
are sterile. 2. Explain the procedure to the patient. 3. Check the administration set and the solution against the physician's order, or as per
hospital policy. 4. Hang the prepared bag and tubing on an IV standard (pole) approximately one metre
above the patient's chest. 5. Prime the tubing; prepare your tape. 6. Select an appropriate vein, considering: • The size, condition and location of veins • The patient's age, size, comfort and condition • The purpose of IV therapy.
Page 33
RA815 21 1383PTSPC
Palpate the vein:
• To determine its depth, size, length and resiliency. The vein should be long and
straight enough to accept the catheter; it should feel wide enough for blood flow to continue around the catheter after insertion.
• To distinguish a vein from an artery, aberrant artery or AV fistula. Veins are never
pulsatile.
An AV fistula is a surgically created anastomosis between an artery and a vein. They usually involve the cephalic vein and provide circulatory access for patients receiving hemodialysis (during which a machine removes waste normally removed by the kidney, from the blood). They are easily recognizable by a surgical scar over a dilated, pulsatile vessel. Never put a tourniquet on this arm or attempt venipuncture on this arm. These vessels are accessed only by specially trained hemodialysis nurses and physicians.
Where possible, avoid veins:
• In the inner aspect of the wrist, in order to avoid radial nerve damage • Hardened or scarred from previous use • Which are inflamed or infected • In an area over a joint.
7. Apply a tourniquet by placing it about 10Ä15 cm above intended site. Distend the veins,
via:
• Proper application of the tourniquet. Too tight an application will restrict arterial flow; check by feeling for a radial pulse. If it is absent, release the tourniquet and reapply.
• Gentle tapping of the intended puncture area after applying the tourniquet. • Alternate clenching and relaxing of the patient's fist.
If a vein is difficult to find:
• Ensure adequate light. • Try leaving the tourniquet on a few moments longer than you normally would,
without of course, causing discolouration or loss of sensation to the arm. • Try looking on the opposite arm. • Massage the arm from wrist to elbow (assisting with venous return).
Page 34
RA815 22 1383PTSPC
• Remove the tourniquet, have patient move his/her arm (flex and extend) with fist
clenched, then reapply tourniquet. • Have patient dangle arm over side of bed/stretcher/ table. • Apply warm compresses. • Ask the patient if, in his experience, one arm seems better than the other. It is
surprising how many patients are aware of idiosyncrasies in their venous anatomy but are reluctant to say anything unless asked. Often, their information is helpful and it gives the patient a sense of control over the situation and a feeling of contribution.
8. Put a clean glove onto one or both of your hands, to protect yourself from the patient's
blood. 9. Cleanse the area with alcohol or iodophor, using a friction rub. Once prepared, do not
touch the area. 10. Anchor the vein by holding the patient's arm and stretching the skin taut with the thumb
of your nondominant hand. This is important to prevent rolling of the vein while you insert the catheter (or cannula). Do not release this tension until after venipuncture is completed (Figure 5).
Page 35
RA815 23 1383PTSPC
FIGURE 5: Technique For IV Insertion
87/00578R 11. Grasp the catheter by the flashback chamber only. Do not touch the hub. 12. Holding the catheter set at a 30-45° angle with the bevel up, pierce the skin quickly and
firmly, one-half to one centimetre below where you intend to enter the vein (Figure 5). 13. Immediately lower the catheter until it is almost parallel to the skin. Aim directly at the
vein. You may or may not feel a snap or pop when you enter the vein. 14. When blood appears in the flashback chamber, withdraw the inner stylet very slightly
while advancing the catheter completely into the vein. Withdrawal of the stylet allows you to observe the flashback up into the catheter while advancing with the softer, more flexible catheter tip. Accidental perforation of the far wall of the vessel is diminished.
15. Release the tourniquet. 16. Apply securing piece of tape or dressing. 17. Grasp the hub of the catheter and remove the stylet, pressing lightly on the area above
the catheter tip to prevent backflow of blood while you are connecting the tubing.
Page 36
RA815 24 1383PTSPC
18. Once the stylet is pulled back or removed, do not attempt to readvance or reinsert for
any reason. Readvancing or reinserting could shear the catheter tip introducing it into the systemic circulation.
19. If you have entered the tissue and have not entered the vein, you may be able to "catch"
it by refeeling for the vein, restabilizing the skin below the insertion point and angling the needle toward where you palpated the vein. Essentially, you are relocating the vein with your fingertip(s) and aiming the needle toward that point.
Depending upon the patient, this may or may not be uncomfortable. If the patient is
uncomfortable, do not attempt this technique. Instead, remove the tourniquet and needle, apply a Band-AidTm or gauze dressing to the site and attempt again. If the patient seems unduly upset, summon assistance. After two unsuccessful attempts, definitely summon assistance.
If you inadvertently enter an artery (evidenced by the flashback being bright red, frothy
and pulsatile), DO NOT PANIC! Remove the tourniquet, remove the needle and apply firm pressure over the site with a sterile gauze. Do not relieve the pressure until after approximately 10 minutes at which time hemostasis should have occurred. (This means no peeking under the gauze!)
Explain to the patient that an artery was inadvertently "nicked" and that you will be
compressing the site for 10 minutes to prevent bruising. 20. Second attempts should be made ideally on the opposite arm. Reapplying the tourniquet
to the same arm even after application of pressure, could result in rebleeding at the original site thus causing a painful hematoma.
21. Once the cannulation is successful and the tubing connected, open the roller clamp fully
to establish patency of the line and observe for infiltration at or above the site. 22. Adjust flow rate TKVO (to keep vein open). 23. Secure the catheter and tubing with tape. 24. Commence with the contrast media injection inspecting the site frequently for
infiltration.
Page 37
RA815 25 1383PTSPC
Documentation is specific for and usually different with each institution. The basic, necessary information is standard however and should contain: • Date and time of insertion • Site, gauge and type of needle device • Type, amount of solution hung and the rate of infusion • Additives, i.e. contrast amount and type • Any untoward reactions and treatment if required.
Insertion T For Winged Needles, I.E. Butterfly, Scalp-Vein Sets The needle is held bevel-up by grasping one or both of the wings. The approach to the vein is identical to that of the angiocath, i.e. 30° to 45° depending upon the depth of the vein. Remember, cephalic and basilic veins that are observed superficially on the forearm, require a more shallow angle of insertion than do deeper veins at the antecubital fossa. Penetration of the skin and vein is generally easier with winged sets as the metal needles are extremely sharp. Before inserting the needle, loosen the cap over the end of the tubing just to loosen. This will "break the vacuum" that may occur during manufacturing and therefore will facilitate a flashback once the vein is entered. Flashback should appear about 2 cm along the proximal tubing. Outflow of blood does not continue until the cap is removed. Larger veins such as those at the antecubital fossa are large enough to accept complete cannulation, however, because the needle is rigid and therefore inflexible, there presents a risk of perforating the far wall of the vein. For this reason, it is acceptable to secure the needle once flashback is observed, without attempting to advance it further into the vessel. After flashback is seen release the tourniquet and tape the needle over the winged parts to secure. Remove the cap. Blood should flow freely to the distal end of the tubing. If not, reapply the tourniquet and if again, freely flowing blood return is not apparent, consider the venipuncture unsuccessful. Remove the needle, apply pressure with a sterile gauze and attempt again once hemostasis has occurred. Small amounts of air that remain in the tubing may be aspirated with a syringe prior to direct injection. Otherwise, blood should be allowed to flow back to the hub completely before attaching to an IV set. Coil the tubing as seen in Figure 6 to secure.
Page 38
RA815 26 1383PTSPC
FIGURE 6: Taping the Winged Needle
89/07878R
Discontinuing an Intravenous Line
Equipment Clean gloves Sterile gauze (2×2 or 4×4) Tape (one piece, 4-6" length) Procedure 1. Tell the patient that the procedure is completed and that you will now be removing the
catheter/needle. 2. Open the sterile gauze and have the tape cut and accessible. 3. Put on gloves. 4. Carefully remove the existing tape so as to not dislodge the needle accidentally.
Unfortunately, removing tape slowly can be painful for the patient. Explain to them why you must remove it in this seeming barbaric manner.
5. If an IV is infusing, clamp it off. 6. Apply light pressure with the gauze directly over the site with your non-dominant hand.
Page 39
RA815 27 1383PTSPC
7. Grasp the hub of the cannula or wings of the needle device with your dominant hand and
withdraw the cannula/needle slowly, in line with the vein. Increase the pressure over the site immediately upon removal and maintain steady pressure until hemostasis is achieved Ä again, no peeking underneath the dressing!
If a needle has been used, dispose of it in a "sharps" container (avoiding accidental
needle sticks). If a cannula has been used, check to ensure that the entire catheter has remained intact. If a portion of the catheter appears to be missing, reapply the tourniquet well above the antecubital fossa area and summon assistance immediately.
8. Once hemostasis is complete, fold the gauze into quarters and tape securely so as to make a "pressure dressing". Instruct the patient to leave the
dressing on for a few hours and if bleeding should recur, reapply pressure for at least ten minutes. Patients should avoid carrying heavy objects, i.e. handbags, with this arm until complete hemostasis has occurred (usually, a few hours is adequate).
Generally, continuous pressure for two or three minutes following the removal of a
cannula or needle is sufficient to stop bleeding. Some patients may require longer compression time to achieve hemostasis. For example:
• Elderly patients • Patients on anticoagulant therapy • Patients on ASA • Patients receiving steroid therapy, i.e. Prednisone • Patients with platelet disorders. Careful prescreening of the patient should alert you to those who may present a problem
with hemostasis. This does not warrant cancellation of the procedure, only that extra time and monitoring will be required post procedure.
9. Dispose of all used equipment according to your hospital policy. 10. Wash your hands. 11. Document according to your hospital policy.
Page 40
RA815 28 1383PTSPC
BASIC IV MAINTENANCE Intravenous (IV) lines are common among hospitalized patients. They provide access to the venous side of the cardiovascular system. An IV setup (Figure 1) typically comprises a clear plastic bag containing a sterile solution ordered by the physician. This connects to tubing designed to deliver either very small or large volumes of fluid. The interior of the tubing is sterile, as are all parts of connections. This connects to the patient by way of a needle made of flexible material or metal. It is inserted into the patient's vein, usually in the arm (peripheral IV therapy). Other setups may insert elsewhere in the body, e.g. central venous lines, or include special equipment, e.g. infusion pumps. Lines introduced into the arterial system appear identical to IV setups and often use identical equipment, i.e. angiographic procedures whereby continuous flushing of the catheter(s) is required. Any arterial line is recognized by the fact that the solution bag (which is always Normal Saline) must be constantly under external pressure by means of either a pressure bag or box that encloses the entire solution bag.
Peripheral Intravenous Therapy Peripheral IV lines can be required: • To maintain access to the venous circulation, should it be necessary. These are ordered
"to keep vein open" (TKVO), and run very slowly. • To administer replacement fluid, blood, or electrolytes. They may be used to prevent or
correct volume depletion in patients who are not allowed (NPO) or not able to drink or eat. These flow more rapidly.
• To administer medication, radiopharmaceuticals, or contrast media directly into the
circulatory system, either intermittently (by injection into the system) or by continuous infusion. The rate of flow varies with the nature of the substance administered.
Initiation always requires a physician's order, which states the solution, concentration and rate of administration. (Discontinuing an IV also requires a physician's order.) The order may be carried out by personnel who have been taught and certified. No physician's order is required to stop or restart a troublesome line, as long as this is done promptly.
Page 41
RA815 29 1383PTSPC
FIGURE 1: The Intravenous Setup
88/01360R
Role of the Technologist The goals for technologists caring for patients are to maintain the infusion by: • Monitoring or regulating the flow • Preventing dislodgement of the needle • Preventing the introduction of air or contaminants into the system • Identifying and reporting any problems encountered. Additional skills now include establishing intravenous lines for purposes of contrast dye administration.
Page 42
RA815 30 1383PTSPC
Assembling an Intravenous Line
The Bag Of Solution Bags of fluid are all very similar in appearance. Their contents are identified by name and concentration of the solution. The name, unfortunately, states the chemical constituents of the contents of the bag; however, clinical jargon is frequently used in verbal references. Some examples of common solution names and clinical translations are presented in Table 1.
TABLE 1 IV Solution Nomenclature
BAG READS CLINICAL TERM
0.9% Sodium Chloride Normal saline
3.3% Dextrose and 0.3% Sodium Chloride 2/3 and 1/3
5% Dextrose in Water D5W or 5DW
Page 43
RA815 31 1383PTSPC
Bags are supplied in sizes of 250 mL, 500 mL, and 1000 mL (1 L), sealed in a translucent outer wrapper for protection. The wrapper is removed by holding it firmly in one hand while sharply ripping downward from one of the notches at the top edge (Figure 2). FIGURE 2: Removing the Wrapper
89/04340R The presence of some moisture inside the wrapper is not abnormal. Next, check the bag for: • Correctness of solution and concentration. • Clarity and colour. Solutions must be crystal-clear and colourless. Discard any that are
otherwise. • Expiry date (never use past the date). • Leaks. Uncommonly found, but do not use if leaking. The solution is sterile and safe for both intravenous and intra-arterial use. Any bag having a leak cannot be considered sterile. Any contamination during connection or flushing of the IV setup warrants discarding of all equipment to ensure the safety of the patient.
Page 44
RA815 32 1383PTSPC
Hang the bag on the IV pole or stand, by the hanger hole at the top. You can freely handle the entire bag or even drop it without risking contamination (not recommended for glass IV bottles however!). Features of the IV bag (Figure 3): • The scale on the edge of the bag, which indicates the volume infused into the patient. • The medication injection port - a self-sealing latex nipple that allows for adding solutions
to the bag via needle and syringe. • The spike insertion port, which is covered to maintain sterility. This cover is removed to
connect the tubing. Inside this port is a diaphragm, which prevents leakage until it is punctured by the spike of the tubing.
FIGURE 3: The IV Bag 87/00525
Page 45
RA815 33 1383PTSPC
• The solution, concentration and rate of infusion are determined and ordered by the physician. It is the responsibility of the individual preparing the IV setup to ensure that the correct solution is used and it is the responsibility of the individual performing the venipuncture to double-check that the solution is as ordered.
For most of your procedures in radiology, Normal Saline is the solution most commonly
used for contrast media injection. • When establishing the intravenous for purposes of contrast injection, running TKVO (to
keep vein open) is adequate and safest for the patient.
Administration Sets All IV administration sets include these parts: • A spike (with protective cap) for bag insertion • A drip chamber for inspection of flow rate • Tubing • One or two regulator (roller) clamps, to adjust the flow rate • A needle adapter (with protective cap), which fits any needle. The sets are supplied in boxes and carefully coiled to prevent kinking of the tubing. Only the interior of the tubing and the ends (covered by caps) are sterile. The sets can be freely handled until assembly. Although tubing varies somewhat in appearance among manufacturers, there are three general types for use in different clinical situations: • Straight or plain tubing • Y-tubing or blood tubing • Minidrip tubing, with and without a flow-control chamber. Some tubings have injection sites to allow for the administration of medication or contrast media, via a needle and syringe.
Y-Tubing This type of IV tubing (Figure 4) is used: • For all blood transfusions • For infusions of maintenance or large volumes of fluid, e.g. for patients in shock • Any time that longer tubing is desirable, e.g. OR settings.
Page 46
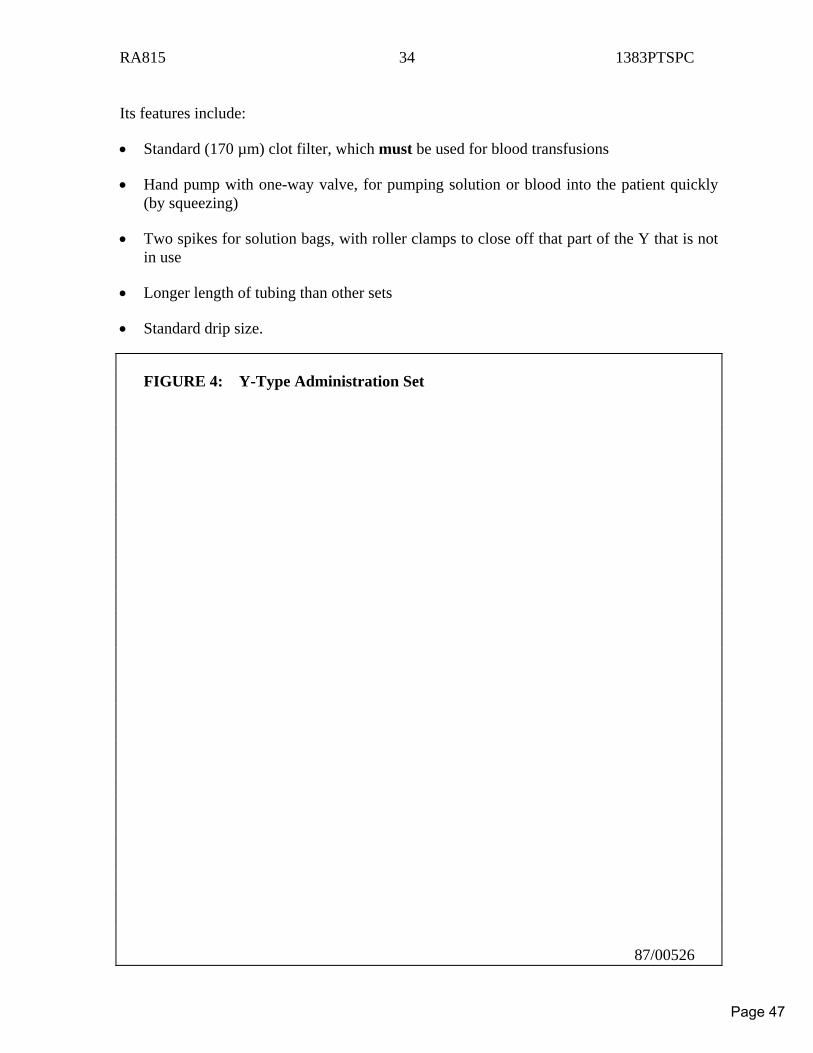
RA815 34 1383PTSPC
Its features include: • Standard (170 µm) clot filter, which must be used for blood transfusions • Hand pump with one-way valve, for pumping solution or blood into the patient quickly
(by squeezing) • Two spikes for solution bags, with roller clamps to close off that part of the Y that is not
in use • Longer length of tubing than other sets • Standard drip size. FIGURE 4: Y-Type Administration Set 87/00526
Page 47
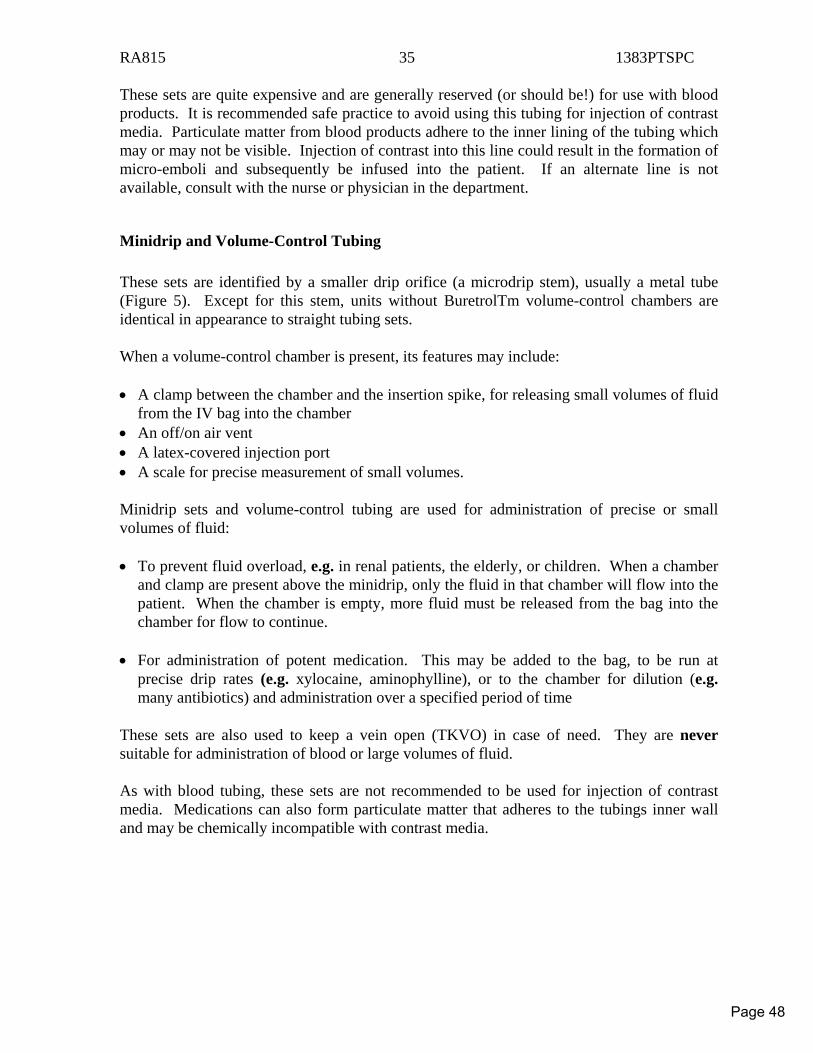
RA815 35 1383PTSPC
These sets are quite expensive and are generally reserved (or should be!) for use with blood products. It is recommended safe practice to avoid using this tubing for injection of contrast media. Particulate matter from blood products adhere to the inner lining of the tubing which may or may not be visible. Injection of contrast into this line could result in the formation of micro-emboli and subsequently be infused into the patient. If an alternate line is not available, consult with the nurse or physician in the department.
Minidrip and Volume-Control Tubing These sets are identified by a smaller drip orifice (a microdrip stem), usually a metal tube (Figure 5). Except for this stem, units without BuretrolTm volume-control chambers are identical in appearance to straight tubing sets. When a volume-control chamber is present, its features may include: • A clamp between the chamber and the insertion spike, for releasing small volumes of fluid
from the IV bag into the chamber • An off/on air vent • A latex-covered injection port • A scale for precise measurement of small volumes. Minidrip sets and volume-control tubing are used for administration of precise or small volumes of fluid: • To prevent fluid overload, e.g. in renal patients, the elderly, or children. When a chamber
and clamp are present above the minidrip, only the fluid in that chamber will flow into the patient. When the chamber is empty, more fluid must be released from the bag into the chamber for flow to continue.
• For administration of potent medication. This may be added to the bag, to be run at
precise drip rates (e.g. xylocaine, aminophylline), or to the chamber for dilution (e.g. many antibiotics) and administration over a specified period of time
These sets are also used to keep a vein open (TKVO) in case of need. They are never suitable for administration of blood or large volumes of fluid. As with blood tubing, these sets are not recommended to be used for injection of contrast media. Medications can also form particulate matter that adheres to the tubings inner wall and may be chemically incompatible with contrast media.
Page 48
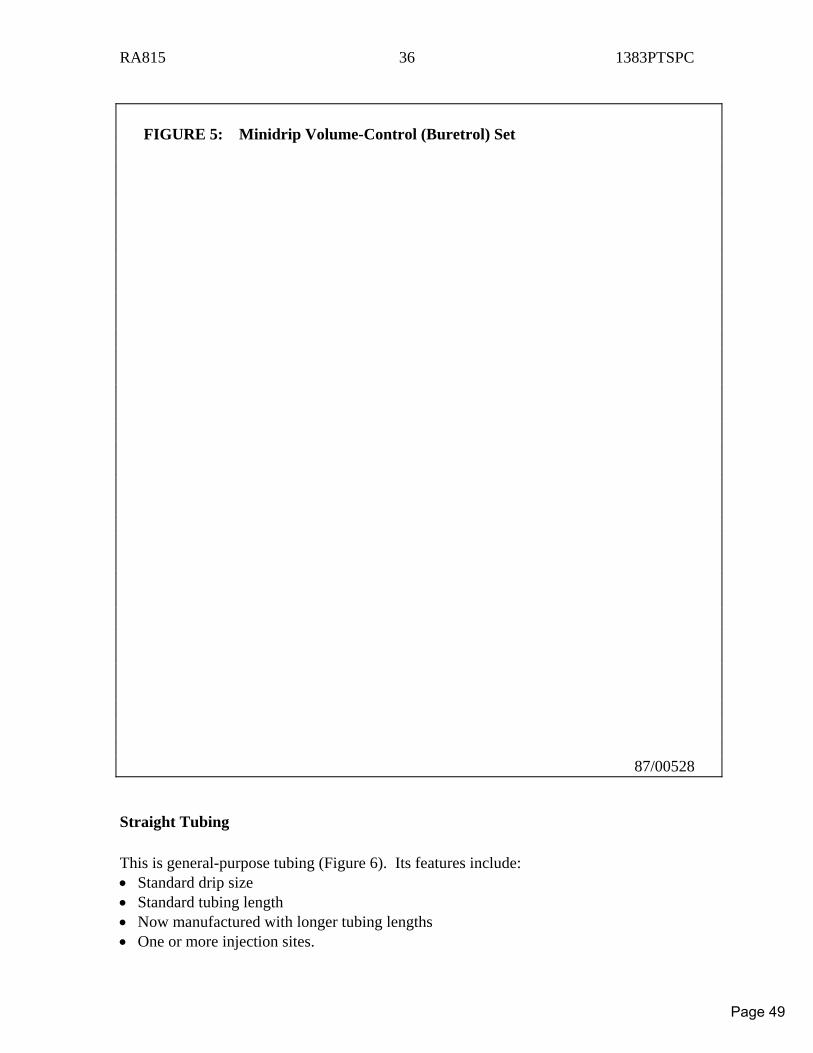
RA815 36 1383PTSPC
FIGURE 5: Minidrip Volume-Control (Buretrol) Set 87/00528
Straight Tubing This is general-purpose tubing (Figure 6). Its features include: • Standard drip size • Standard tubing length • Now manufactured with longer tubing lengths • One or more injection sites.
Page 49
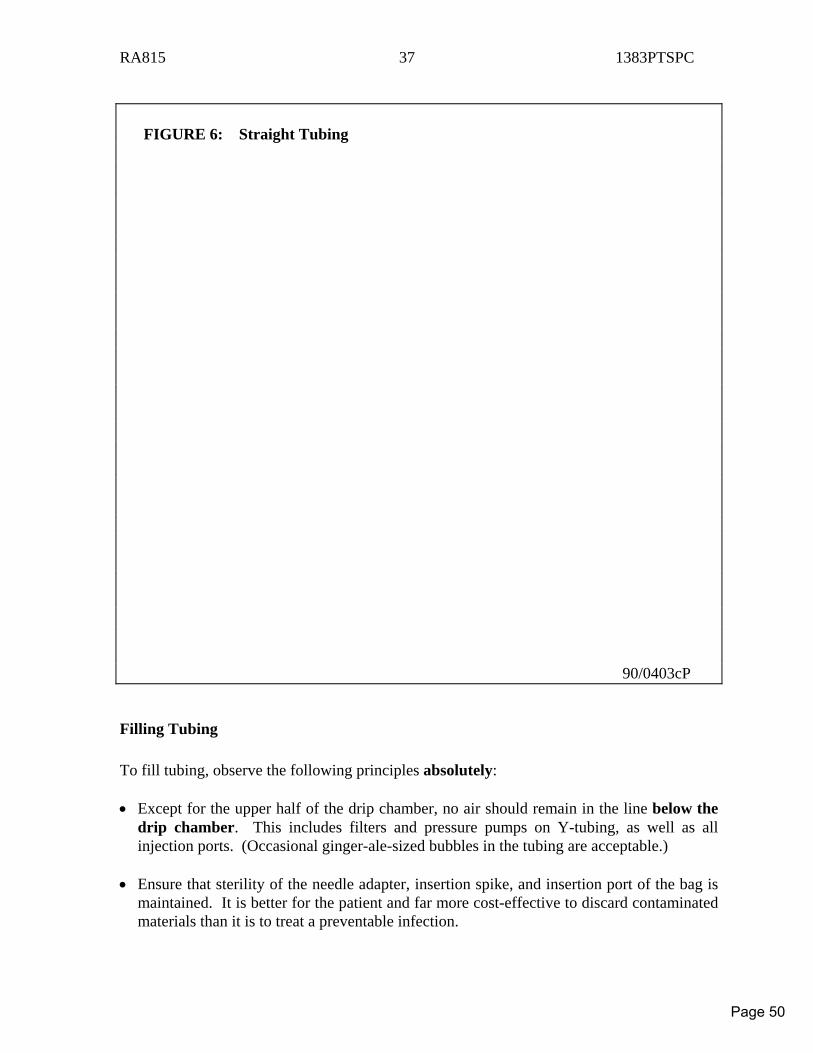
RA815 37 1383PTSPC
FIGURE 6: Straight Tubing 90/0403cP
Filling Tubing To fill tubing, observe the following principles absolutely: • Except for the upper half of the drip chamber, no air should remain in the line below the
drip chamber. This includes filters and pressure pumps on Y-tubing, as well as all injection ports. (Occasional ginger-ale-sized bubbles in the tubing are acceptable.)
• Ensure that sterility of the needle adapter, insertion spike, and insertion port of the bag is
maintained. It is better for the patient and far more cost-effective to discard contaminated materials than it is to treat a preventable infection.
Page 50
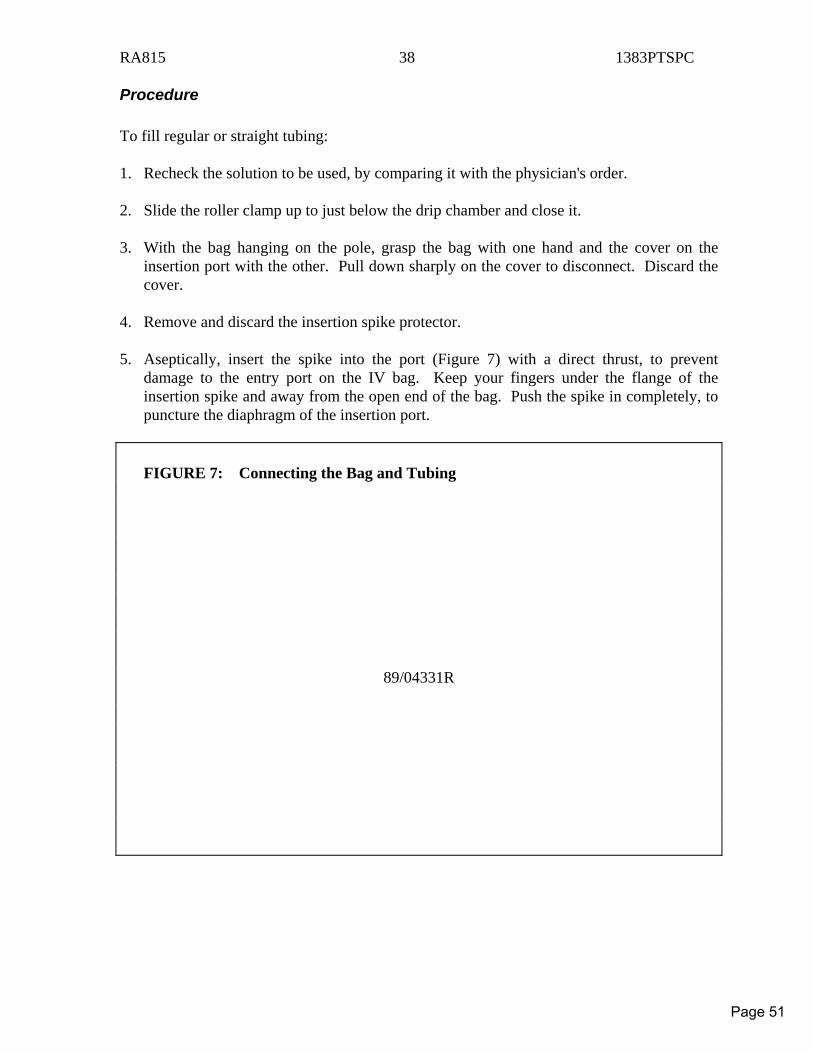
RA815 38 1383PTSPC
Procedure To fill regular or straight tubing: 1. Recheck the solution to be used, by comparing it with the physician's order. 2. Slide the roller clamp up to just below the drip chamber and close it. 3. With the bag hanging on the pole, grasp the bag with one hand and the cover on the
insertion port with the other. Pull down sharply on the cover to disconnect. Discard the cover.
4. Remove and discard the insertion spike protector. 5. Aseptically, insert the spike into the port (Figure 7) with a direct thrust, to prevent
damage to the entry port on the IV bag. Keep your fingers under the flange of the insertion spike and away from the open end of the bag. Push the spike in completely, to puncture the diaphragm of the insertion port.
FIGURE 7: Connecting the Bag and Tubing
89/04331R
Page 51
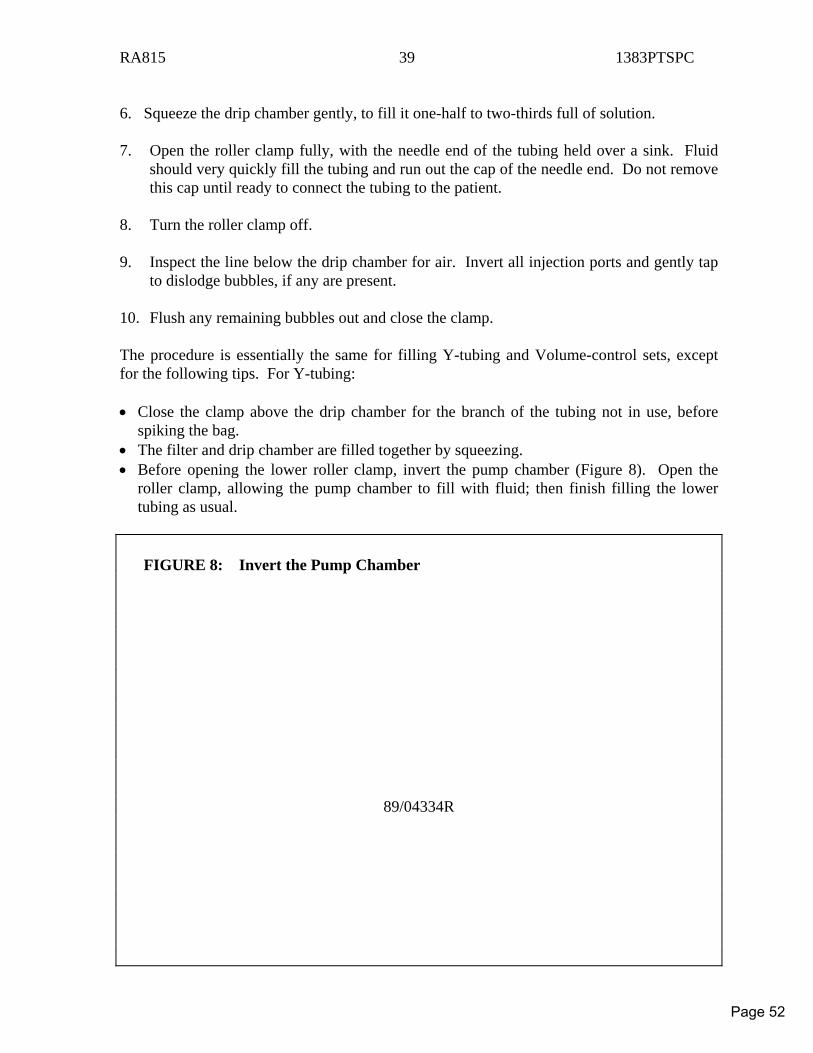
RA815 39 1383PTSPC
6. Squeeze the drip chamber gently, to fill it one-half to two-thirds full of solution. 7. Open the roller clamp fully, with the needle end of the tubing held over a sink. Fluid
should very quickly fill the tubing and run out the cap of the needle end. Do not remove this cap until ready to connect the tubing to the patient.
8. Turn the roller clamp off. 9. Inspect the line below the drip chamber for air. Invert all injection ports and gently tap
to dislodge bubbles, if any are present. 10. Flush any remaining bubbles out and close the clamp. The procedure is essentially the same for filling Y-tubing and Volume-control sets, except for the following tips. For Y-tubing: • Close the clamp above the drip chamber for the branch of the tubing not in use, before
spiking the bag. • The filter and drip chamber are filled together by squeezing. • Before opening the lower roller clamp, invert the pump chamber (Figure 8). Open the
roller clamp, allowing the pump chamber to fill with fluid; then finish filling the lower tubing as usual.
FIGURE 8: Invert the Pump Chamber
89/04334R
Page 52
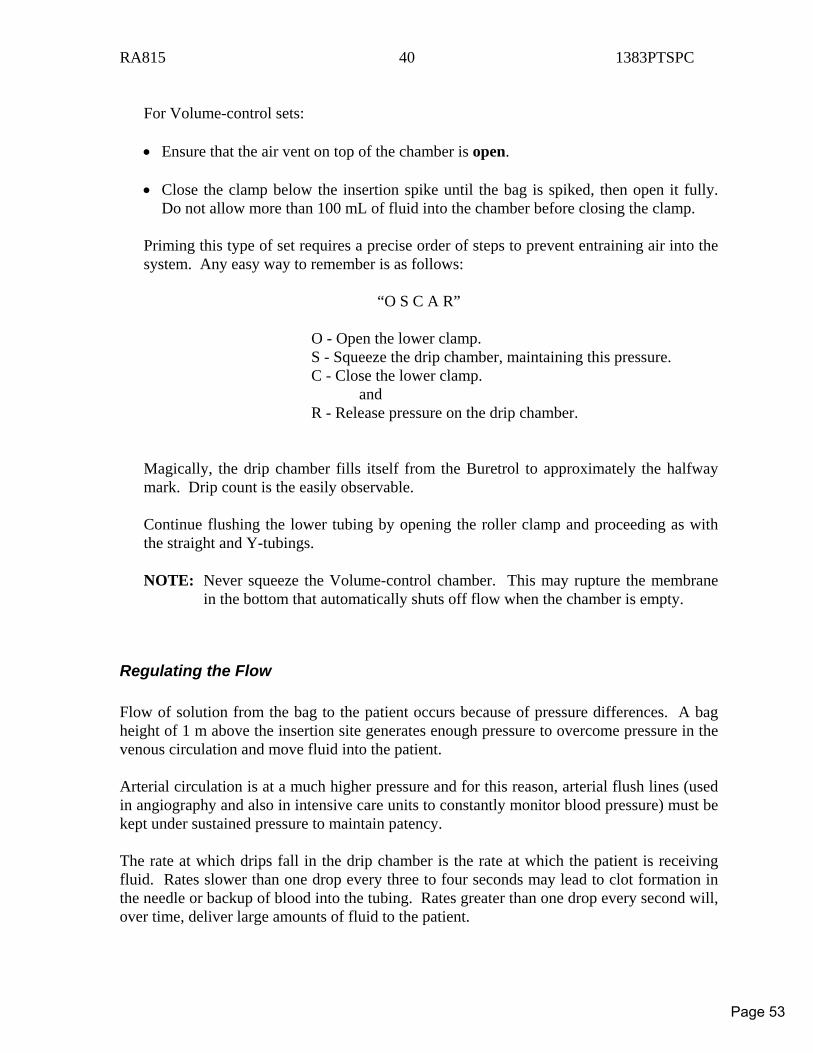
RA815 40 1383PTSPC
For Volume-control sets: • Ensure that the air vent on top of the chamber is open. • Close the clamp below the insertion spike until the bag is spiked, then open it fully.
Do not allow more than 100 mL of fluid into the chamber before closing the clamp. Priming this type of set requires a precise order of steps to prevent entraining air into the system. Any easy way to remember is as follows:
“O S C A R”
O - Open the lower clamp. S - Squeeze the drip chamber, maintaining this pressure. C - Close the lower clamp. and R - Release pressure on the drip chamber.
Magically, the drip chamber fills itself from the Buretrol to approximately the halfway mark. Drip count is the easily observable. Continue flushing the lower tubing by opening the roller clamp and proceeding as with the straight and Y-tubings. NOTE: Never squeeze the Volume-control chamber. This may rupture the membrane
in the bottom that automatically shuts off flow when the chamber is empty.
Regulating the Flow Flow of solution from the bag to the patient occurs because of pressure differences. A bag height of 1 m above the insertion site generates enough pressure to overcome pressure in the venous circulation and move fluid into the patient. Arterial circulation is at a much higher pressure and for this reason, arterial flush lines (used in angiography and also in intensive care units to constantly monitor blood pressure) must be kept under sustained pressure to maintain patency. The rate at which drips fall in the drip chamber is the rate at which the patient is receiving fluid. Rates slower than one drop every three to four seconds may lead to clot formation in the needle or backup of blood into the tubing. Rates greater than one drop every second will, over time, deliver large amounts of fluid to the patient.
Page 53
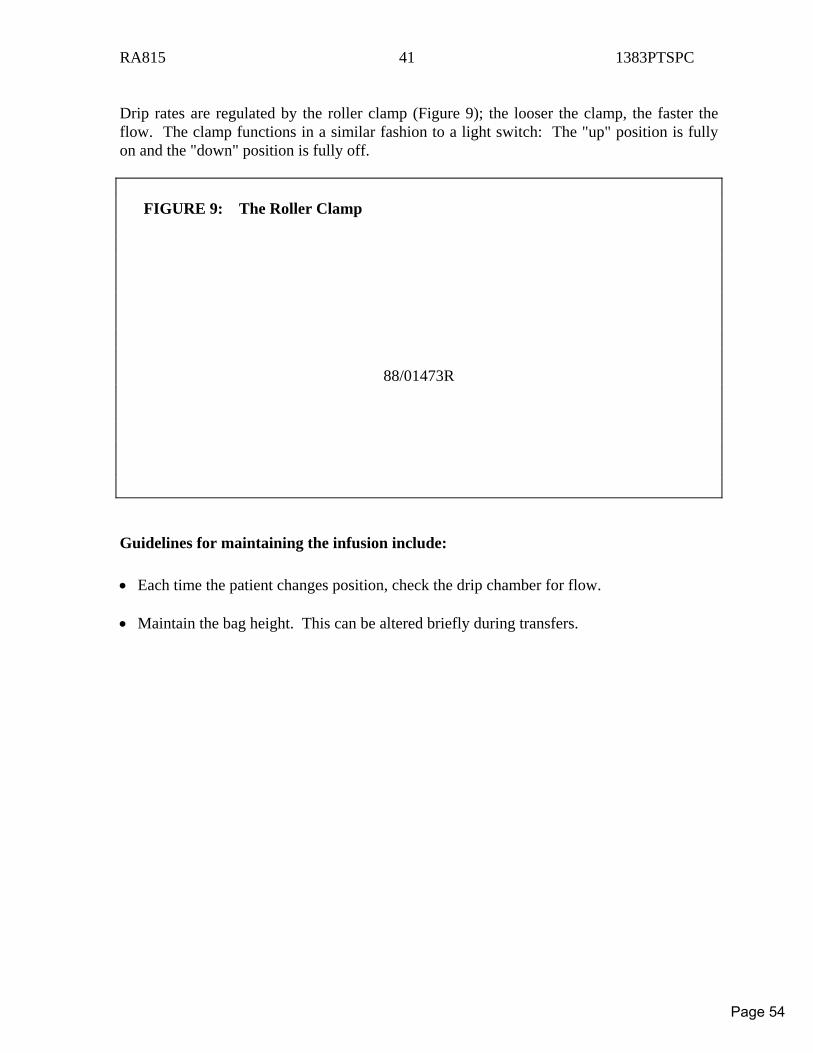
RA815 41 1383PTSPC
Drip rates are regulated by the roller clamp (Figure 9); the looser the clamp, the faster the flow. The clamp functions in a similar fashion to a light switch: The "up" position is fully on and the "down" position is fully off. FIGURE 9: The Roller Clamp
88/01473R
Guidelines for maintaining the infusion include: • Each time the patient changes position, check the drip chamber for flow. • Maintain the bag height. This can be altered briefly during transfers.
Page 54
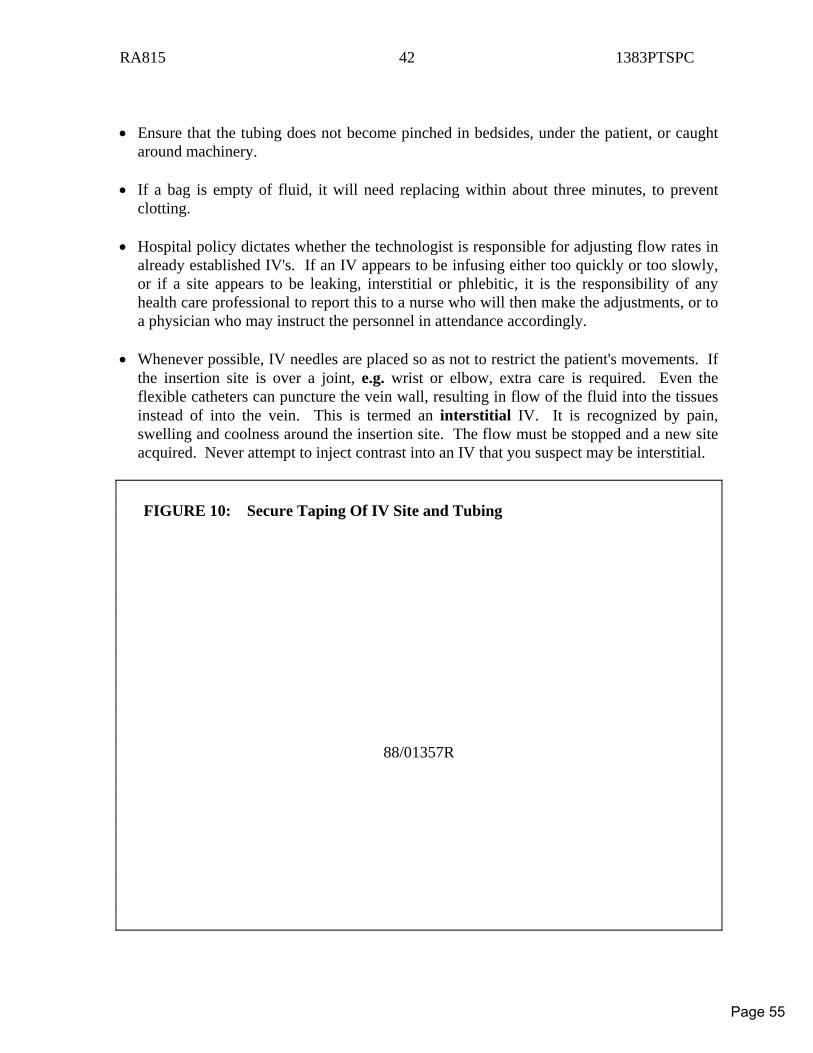
RA815 42 1383PTSPC
• Ensure that the tubing does not become pinched in bedsides, under the patient, or caught
around machinery. • If a bag is empty of fluid, it will need replacing within about three minutes, to prevent
clotting. • Hospital policy dictates whether the technologist is responsible for adjusting flow rates in
already established IV's. If an IV appears to be infusing either too quickly or too slowly, or if a site appears to be leaking, interstitial or phlebitic, it is the responsibility of any health care professional to report this to a nurse who will then make the adjustments, or to a physician who may instruct the personnel in attendance accordingly.
• Whenever possible, IV needles are placed so as not to restrict the patient's movements. If
the insertion site is over a joint, e.g. wrist or elbow, extra care is required. Even the flexible catheters can puncture the vein wall, resulting in flow of the fluid into the tissues instead of into the vein. This is termed an interstitial IV. It is recognized by pain, swelling and coolness around the insertion site. The flow must be stopped and a new site acquired. Never attempt to inject contrast into an IV that you suspect may be interstitial.
FIGURE 10: Secure Taping Of IV Site and Tubing
88/01357R
Page 55
RA815 43 1383PTSPC
The insertion site should be well taped and the tubing looped and taped again (Figure 10) to prevent, not only needle dislodgement, but also accidental disconnection of tubing from the needle. Accidental dislodgement of tubing and/or catheter does unfortunately occur. The site may bleed profusely depending upon the catheter size, blood pressure, location and patient's position. If this occurs, calmly apply pressure to the area with a sterile gauze pad folded into quarters. Keep applying pressure for at least 2Ä3 minutes and then tape the folded gauze firmly to the site (thus creating a "pressure dressing").
Always inspect the insertion site for possible problems before using an existing IV for contrast injection: • If a site appears to be insecure or insufficiently taped, add some tape before moving the
patient. Always use non-allergenic tape. Never encircle the arm with tape or apply tape tightly; you could stop the infusion.
• If moisture (either blood or IV fluid) is present around the site, suspect a leak and inspect
for disconnection. If the tubing is completely disconnected from the needle, the tubing is considered to be contaminated and must be replaced. If it is only leaking, grasp the hub of the needle (being careful not to contaminate the connection or needle puncture site) and the tubing, and press the tubing into the needle. Wet tape should be replaced with fresh non-allergenic tapes.
• Sites that are red, swollen, or painful often need to be changed. These should not be
used for injection. Have the site checked by a physician or nurse in your department, or call the patient's nursing unit if the patient is returning to his or her room shortly.
• Never attempt to advance a needle or catheter that has been partially dislodged. Summon
assistance. An intravenous line is a closed, sterile system. Any interruption in this system other than through aseptic intervention will result in contamination of the line. The line should be discontinued to provide optimum safety for the patient. It is our responsibility to provide safe and cost-effective health care. It is safer and less expensive to discard a contaminated IV set than it is to risk introducing a preventable infection. Prevent contamination and risk of infection by: • Observing recommended aseptic technique when setting up and/or establishing an
intravenous. • Maintaining aseptic technique during bag changes. • Using sterile technique when injecting into intravenous lines. • Promptly tightening leaking lines. • Assuming responsibility for removing disconnected lines. • Summoning assistance for further assessment of suspected infiltrated or phlebitic IV's.
Page 56
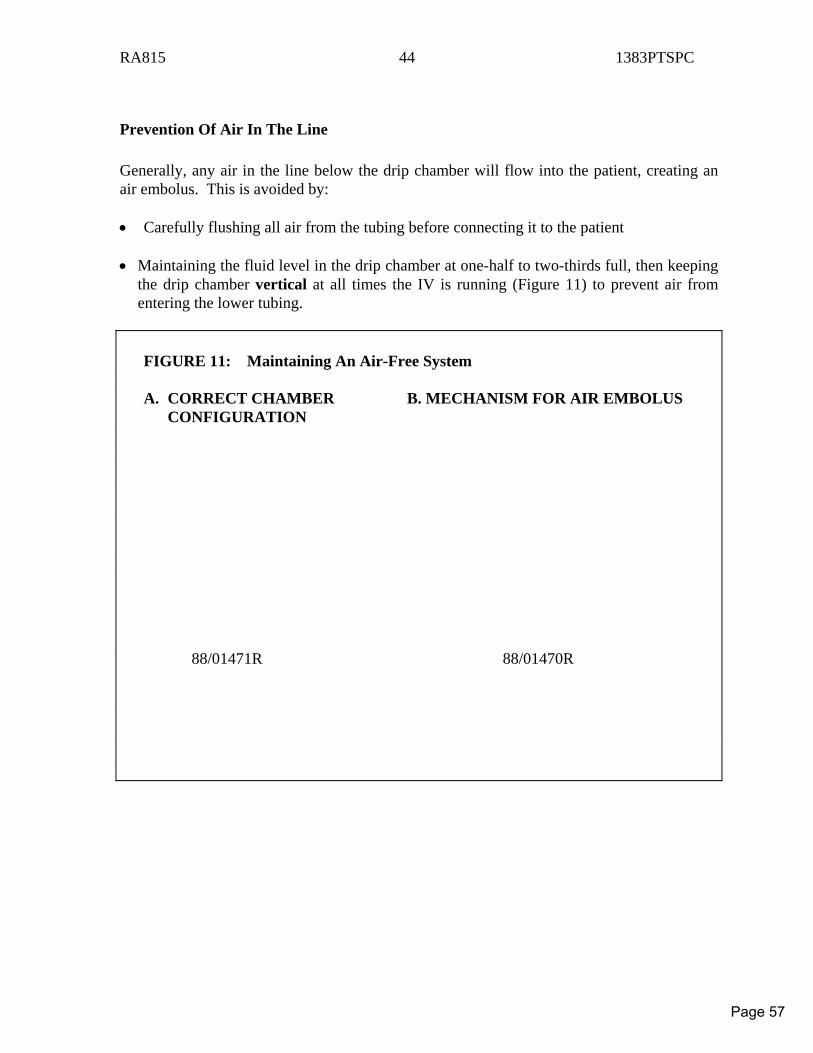
RA815 44 1383PTSPC
Prevention Of Air In The Line Generally, any air in the line below the drip chamber will flow into the patient, creating an air embolus. This is avoided by: • Carefully flushing all air from the tubing before connecting it to the patient • Maintaining the fluid level in the drip chamber at one-half to two-thirds full, then keeping
the drip chamber vertical at all times the IV is running (Figure 11) to prevent air from entering the lower tubing.
FIGURE 11: Maintaining An Air-Free System A. CORRECT CHAMBER B. MECHANISM FOR AIR EMBOLUS CONFIGURATION 88/01471R 88/01470R
Page 57
RA815 45 1383PTSPC
In practice, this means not putting flowing bags and tubing in bed with the patient during transfers. If this must be done, the roller clamp should be shut off until the bag is vertical again. Ensure that the lower line is free of air before re-establishing the flow. If the bag runs dry, air will enter the lower tubing; this will not flow into the patient, however, due to pressure in the venous system. This air will have to be removed by a qualified person when a new bag is hung.
Central Venous Lines Although the external apparatus for central IV setups (Figure 12) is similar to that of peripheral IVs, they are very different. The internal portion of the equipment is a long catheter, the tip of which rests in the right atrium of the patient's heart. Central venous lines are used: • For measurement of venous pressure • To prevent or treat circulatory overload • When peripheral veins are inaccessible. Central IVs may also be connected to a column (manometer) for measuring central venous pressure. The catheter is secured in position and covered with a sterile dressing at the insertion site, usually at the subclavian vein (under the clavicle) or the antecubital fossa. All connections should be securely taped. Permanent central lines are seen: • For chronically ill patients who require frequent venous access, e.g. for chemotherapy • For total parenteral nutrition (TPN) in patients with non-functioning digestive tracts. Between uses, permanent lines are sealed, filled with anticoagulant and disconnected, so that only a dressing and short tubing are visible externally.
Page 58
RA815 46 1383PTSPC
FIGURE 12: Central Venous Line
88/01359R
Personnel Qualified to Initiate Only physicians with special skills may insert central lines, utilizing strict aseptic technique. Line placement must be confirmed radiographically after insertion. Bag changes and regulation of flow are the responsibility of nurses and some respiratory therapists.
Role of the Technologist Accidental disconnection of these lines is accompanied by a greater risk of air embolus. Pinch the tubing as close to the patient as possible and summon immediate help. Avoid adjusting flow rate or changing bags for these lines. If the IV bag is almost empty, summon a qualified person. No tension should be placed on these lines. Removal of the line may precipitate cardiac dysrhythmias. A physician with special skills must reinsert.
Page 59
RA815 47 1383PTSPC
Clotting of blood in these lines must be prevented. When a line must be reinserted due to an empty bag or flow that has stopped, the procedure is uncomfortable and involves risk for the patient, i.e. pneumothorax. Be certain that you do not alter the position of the stopcock at the base of the pressure manometer; this changes the direction of flow of the IV fluid. These lines usually do not become interstitial with patient movement. Never inject routine medications, contrast media or radiopharmaceuticals into a central line. If no other access is possible, the physician may elect to use this line.
Infusion Pumps An infusion pump is a mechanical device that precisely regulates IV flow to the patient. Tubing from the IV bag passes through the machine and is compressed by it. These pumps operate from a wall plug or via internal rechargeable batteries, good for 3Ä4 hours of operation. They are equipped with an audible alarm and a light display panel to indicate problems, e.g. low battery, empty IV bag, increased pressure in the line, or air in the tubing. (These functions differ somewhat among manufacturers.) All pumps display the amount of solution infused into the patient. Most have their own wheeled stands; all have IV tubing longer than standard to allow the patient to move about. Infusion pumps can be attached to central or peripheral lines. They are used for administration of medication that must be delivered at a precise rate over an exact period of time, e.g. medication which raises or lowers blood pressure or that controls heart rate or rhythm (called "critical drips"). They are also used frequently to maintain infusions of a less critical nature, e.g. anticoagulants, aminophylline. Hospital policy usually dictates which medication infusions must be regulated by pumps.
Personnel Qualified to Initiate Special inservicing is required to initiate and maintain these pumps. Physicians rarely, if ever, operate them. Most nursing staff have some orientation to infusion pumps and should be able to assist you. Also, many ambulatory patients are now being instructed on how to care for the pump when they are away from the unit.
Role of the Technologist
Page 60

RA815 48 1383PTSPC
Patients receiving critical drips will always be accompanied by a qualified person. Patients with other kinds of drips might not be. As a technologist, you will not be required to plug in the unit unless the "low battery" alarm sounds. Attendants with patients on critical drips will usually request a power source. Never attempt to dismantle a pump to transfer a patient. It is not considered good practice to place the device in the patient's bed; tubing should be long enough for all situations. IV sites connected to these pumps are subject to the same problems as any IV, e.g. the site becoming interstitial or painful. Summon help as necessary. Never use a line on a pump for injection of medication or contrast materials. A separate site should be used. The physician may elect to utilize this line if other veins are inaccessible. Never adjust the roller clamp. When an alarm sounds and no attendant is present: • Leave the alarm on until the problem is resolved • Look at the display panel to ascertain the problem • If the "low battery" light is on, plug the pump in • For other problems, seek qualified assistance.
Page 61
RA815 49 1383PTSPC
INJECTING INTO AN EXISTING LINE Injection of any substance, e.g. medication, radiopharmaceuticals, or contrast media, is considered to be a delegated medical act, to be performed by the technologist only after training and written certification in each clinical setting. Principles involved include: • Maintaining sterility of the line • Maintaining an air-free line • Utilizing the injection site, needle size, and speed of injection most suited to the purpose
of that injection • Maintaining the integrity of the patient's tissues at the needle insertion site.
INJECTION SITES
Characteristics You can recognize these sites by the presence of latex at various positions on the tubing. Careful scrutiny will reveal one or a number of small circles (Figure 1). Injections may be done only within these circles, as they are specially designed to be self-sealing after repeated needle punctures. This prevents leakage and entry of microorganisms. FIGURE 1: Injection Sites A. SINGLE B. MULTIPLE 89/04337R 89/04338R
Page 62
RA815 50 1383PTSPC
Multiple injection ports (Figure 1B) should not be used for contrast media injection. These ports tend to leak after punctures (especially with the large bore needles required to infuse the viscons contrast media) thus risking infection of the site. These ports are used primarily for "IV push" medications in emergency situations and in fact many hospitals are choosing to substitute "Luer lock" tubing with multiple single-injection sites instead of the flashball tubing set. Use the site closest to the patient for contrast injection. Use a size 18 gauge needle to allow injection with minimal resistance, without causing damage to the latex port. Any intravenous solution may be used with IV contrast media injection and manufacturers added KCl solutions are also acceptable if no other line is available. No other additives should be present in the set that you use for contrast media injection as chemical incompatibility may result in particulate matter forming in the line. Check the insertion site for redness, swelling and/or coolness. Never inject into a line where the site is potentially phlebitic or interstitial. Always summon assistance ("second opinion") if you are unsure of line patency or integrity!
THE INJECTION PROCEDURE 1. Prepare the patient for the injection (ensure that he or she consents) and tell him or her
what sensations to expect at the site and as a result of the injection. 2. Using a disposable alcohol wipe, firmly disinfect the injection port and allow it to air-dry. 3. Stabilize the site with your non-dominant hand, keeping your fingers clear of the path of
the needle. 4. With your dominant hand, direct the needle into and through the latex circle until a
decrease in resistance is felt or the needle bevel is seen to be in the lumen. The needle tip is directed to go with the IV flow, not against it.
5. If dilution is not required, pinch the IV tubing above the injection site and inject while
watching the IV site for deformity. The speed of injection of the substance (push) is determined by the recommendations associated with the substance injected. (Consider that too rapid or too forceful an injection can explode the vein.) Release the tubing when the injection is complete.
If dilution is desirable, increase the flow rate of the IV and inject slowly without
pinching the tubing. If the level of fluid in the drip chamber rises, you are pushing too fast.
Page 63
RA815 51 1383PTSPC
6. Remove the needle, being careful not to bend it. It is possible to break needles off in the
tubing. 7. Ensure that the flow rate of the IV returns to the original rate. 8. Watch the patient for effects. 9. Dispose of the needle and syringe according to clinical policy. Document your injection according to hospital policy.
REFERENCES 1. Michener Institute: Starting An Intravenous Line, 880-099. 2. Michener Institute: Additional Needle Insertion Techniques, 880-099-1. 3. Michener Institute: Basic IV Maintenance, 880-133. 4. Michener Institute: IV-Related Skills, 880-098. 5. Mallinckrodt Canada:: Optiray Insert (Excerpts from Clinical Supplement).
Page 64
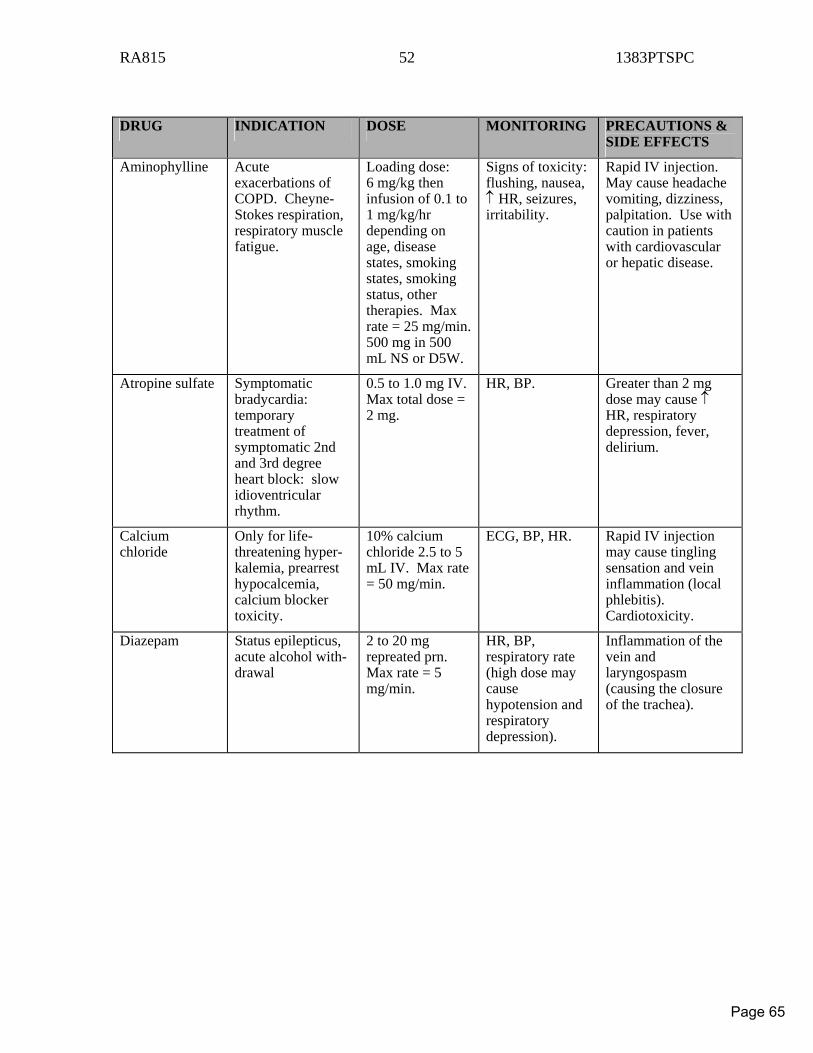
RA815 52 1383PTSPC
DRUG INDICATION DOSE MONITORING PRECAUTIONS &
SIDE EFFECTS
Aminophylline Acute exacerbations of COPD. Cheyne-Stokes respiration, respiratory muscle fatigue.
Loading dose: 6 mg/kg then infusion of 0.1 to 1 mg/kg/hr depending on age, disease states, smoking states, smoking status, other therapies. Max rate = 25 mg/min. 500 mg in 500 mL NS or D5W.
Signs of toxicity: flushing, nausea, ↑ HR, seizures, irritability.
Rapid IV injection. May cause headache vomiting, dizziness, palpitation. Use with caution in patients with cardiovascular or hepatic disease.
Atropine sulfate Symptomatic bradycardia: temporary treatment of symptomatic 2nd and 3rd degree heart block: slow idioventricular rhythm.
0.5 to 1.0 mg IV. Max total dose = 2 mg.
HR, BP. Greater than 2 mg dose may cause ↑ HR, respiratory depression, fever, delirium.
Calcium chloride
Only for life-threatening hyper-kalemia, prearrest hypocalcemia, calcium blocker toxicity.
10% calcium chloride 2.5 to 5 mL IV. Max rate = 50 mg/min.
ECG, BP, HR. Rapid IV injection may cause tingling sensation and vein inflammation (local phlebitis). Cardiotoxicity.
Diazepam Status epilepticus, acute alcohol with-drawal
2 to 20 mg repreated prn. Max rate = 5 mg/min.
HR, BP, respiratory rate (high dose may cause hypotension and respiratory depression).
Inflammation of the vein and laryngospasm (causing the closure of the trachea).
Page 65
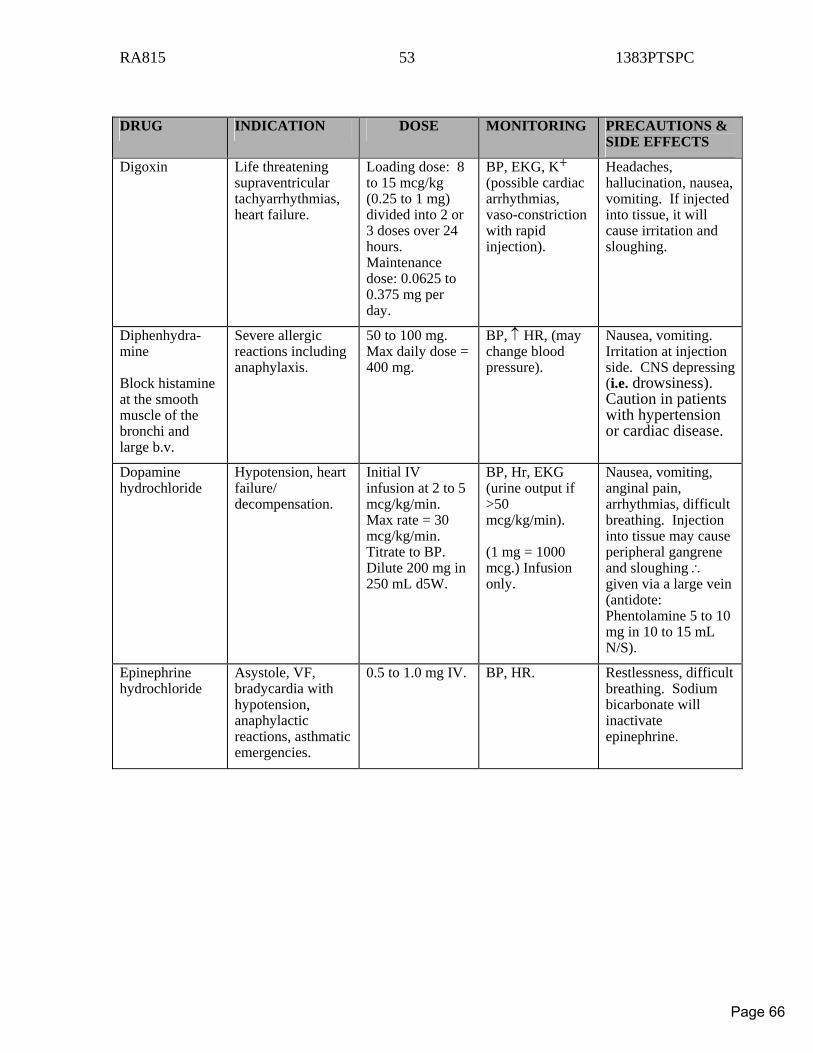
RA815 53 1383PTSPC
DRUG INDICATION DOSE MONITORING PRECAUTIONS &
SIDE EFFECTS
Digoxin Life threatening supraventricular tachyarrhythmias, heart failure.
Loading dose: 8 to 15 mcg/kg (0.25 to 1 mg) divided into 2 or 3 doses over 24 hours. Maintenance dose: 0.0625 to 0.375 mg per day.
BP, EKG, K+ (possible cardiac arrhythmias, vaso-constriction with rapid injection).
Headaches, hallucination, nausea, vomiting. If injected into tissue, it will cause irritation and sloughing.
Diphenhydra-mine Block histamine at the smooth muscle of the bronchi and large b.v.
Severe allergic reactions including anaphylaxis.
50 to 100 mg. Max daily dose = 400 mg.
BP, ↑ HR, (may change blood pressure).
Nausea, vomiting. Irritation at injection side. CNS depressing (i.e. drowsiness). Caution in patients with hypertension or cardiac disease.
Dopamine hydrochloride
Hypotension, heart failure/ decompensation.
Initial IV infusion at 2 to 5 mcg/kg/min. Max rate = 30 mcg/kg/min. Titrate to BP. Dilute 200 mg in 250 mL d5W.
BP, Hr, EKG (urine output if >50 mcg/kg/min). (1 mg = 1000 mcg.) Infusion only.
Nausea, vomiting, anginal pain, arrhythmias, difficult breathing. Injection into tissue may cause peripheral gangrene and sloughing ∴ given via a large vein (antidote: Phentolamine 5 to 10 mg in 10 to 15 mL N/S).
Epinephrine hydrochloride
Asystole, VF, bradycardia with hypotension, anaphylactic reactions, asthmatic emergencies.
0.5 to 1.0 mg IV. BP, HR. Restlessness, difficult breathing. Sodium bicarbonate will inactivate epinephrine.
Page 66
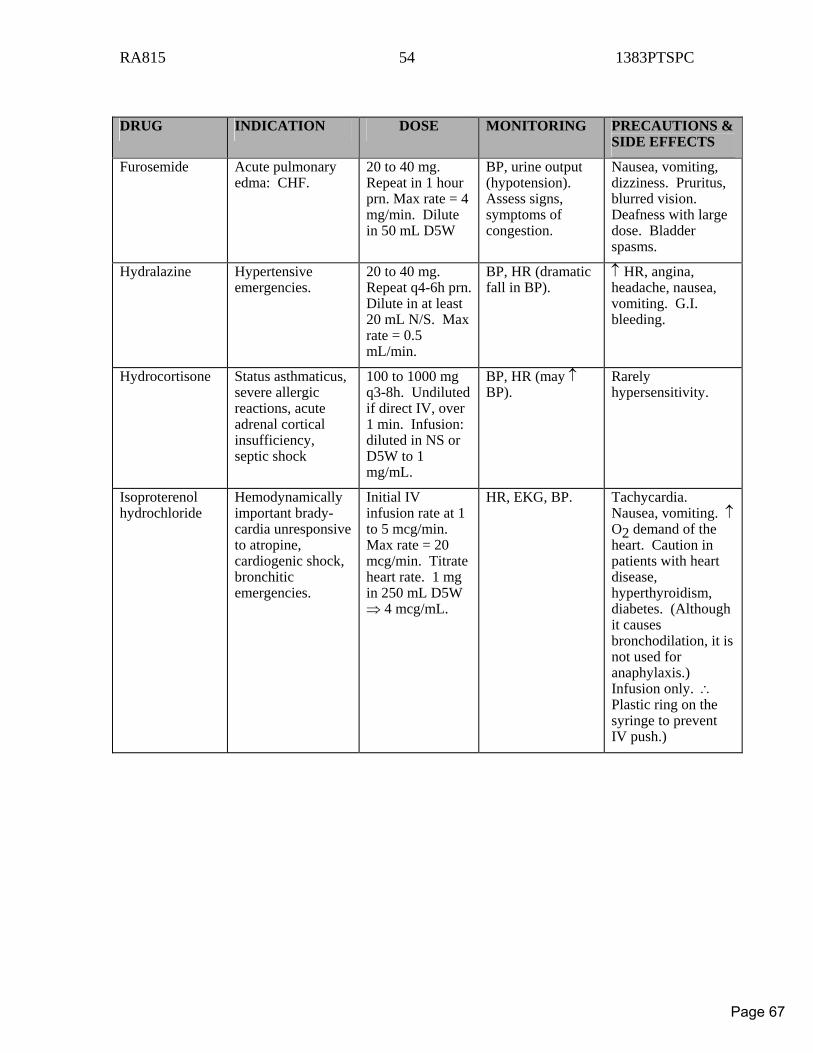
RA815 54 1383PTSPC
DRUG INDICATION DOSE MONITORING PRECAUTIONS &
SIDE EFFECTS
Furosemide Acute pulmonary edma: CHF.
20 to 40 mg. Repeat in 1 hour prn. Max rate = 4 mg/min. Dilute in 50 mL D5W
BP, urine output (hypotension). Assess signs, symptoms of congestion.
Nausea, vomiting, dizziness. Pruritus, blurred vision. Deafness with large dose. Bladder spasms.
Hydralazine Hypertensive emergencies.
20 to 40 mg. Repeat q4-6h prn.Dilute in at least 20 mL N/S. Max rate = 0.5 mL/min.
BP, HR (dramatic fall in BP).
↑ HR, angina, headache, nausea, vomiting. G.I. bleeding.
Hydrocortisone Status asthmaticus, severe allergic reactions, acute adrenal cortical insufficiency, septic shock
100 to 1000 mg q3-8h. Undiluted if direct IV, over 1 min. Infusion: diluted in NS or D5W to 1 mg/mL.
BP, HR (may ↑ BP).
Rarely hypersensitivity.
Isoproterenol hydrochloride
Hemodynamically important brady-cardia unresponsive to atropine, cardiogenic shock, bronchitic emergencies.
Initial IV infusion rate at 1 to 5 mcg/min. Max rate = 20 mcg/min. Titrate heart rate. 1 mg in 250 mL D5W ⇒ 4 mcg/mL.
HR, EKG, BP. Tachycardia. Nausea, vomiting. ↑ O2 demand of the heart. Caution in patients with heart disease, hyperthyroidism, diabetes. (Although it causes bronchodilation, it is not used for anaphylaxis.) Infusion only. ∴ Plastic ring on the syringe to prevent IV push.)
Page 67
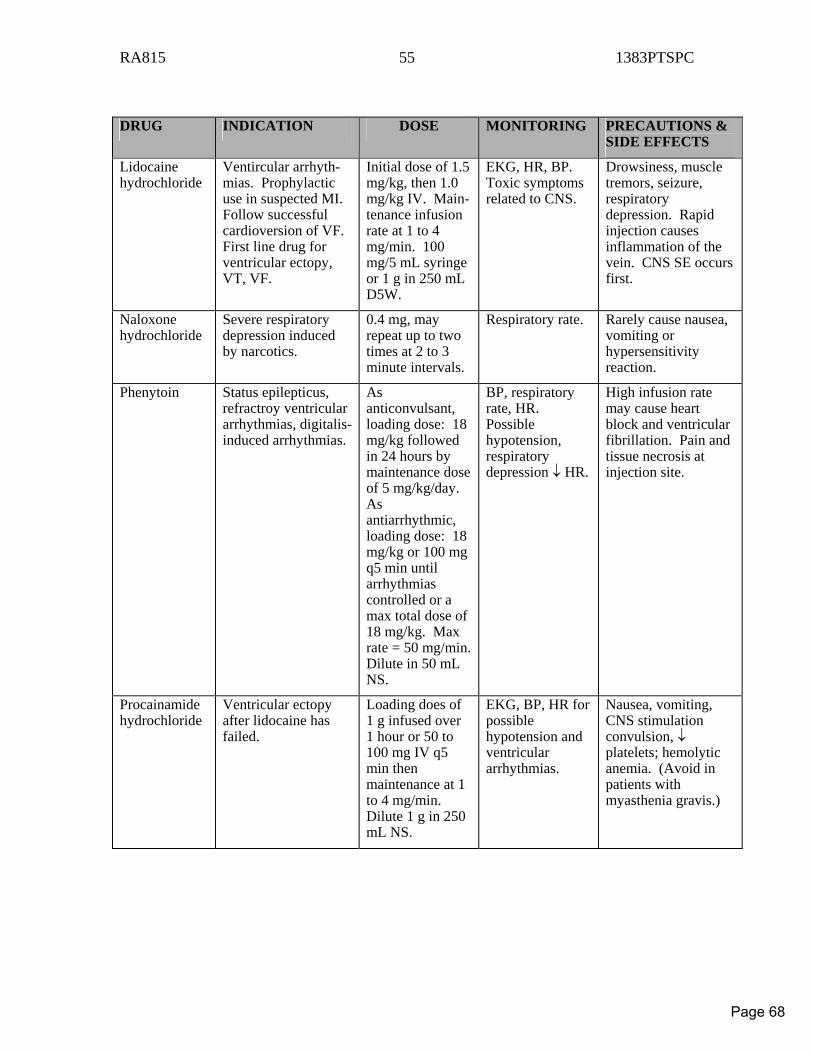
RA815 55 1383PTSPC
DRUG INDICATION DOSE MONITORING PRECAUTIONS &
SIDE EFFECTS
Lidocaine hydrochloride
Ventircular arrhyth-mias. Prophylactic use in suspected MI. Follow successful cardioversion of VF. First line drug for ventricular ectopy, VT, VF.
Initial dose of 1.5 mg/kg, then 1.0 mg/kg IV. Main-tenance infusion rate at 1 to 4 mg/min. 100 mg/5 mL syringe or 1 g in 250 mL D5W.
EKG, HR, BP. Toxic symptoms related to CNS.
Drowsiness, muscle tremors, seizure, respiratory depression. Rapid injection causes inflammation of the vein. CNS SE occurs first.
Naloxone hydrochloride
Severe respiratory depression induced by narcotics.
0.4 mg, may repeat up to two times at 2 to 3 minute intervals.
Respiratory rate. Rarely cause nausea, vomiting or hypersensitivity reaction.
Phenytoin Status epilepticus, refractroy ventricular arrhythmias, digitalis-induced arrhythmias.
As anticonvulsant, loading dose: 18 mg/kg followed in 24 hours by maintenance dose of 5 mg/kg/day. As antiarrhythmic, loading dose: 18 mg/kg or 100 mg q5 min until arrhythmias controlled or a max total dose of 18 mg/kg. Max rate = 50 mg/min. Dilute in 50 mL NS.
BP, respiratory rate, HR. Possible hypotension, respiratory depression ↓ HR.
High infusion rate may cause heart block and ventricular fibrillation. Pain and tissue necrosis at injection site.
Procainamide hydrochloride
Ventricular ectopy after lidocaine has failed.
Loading does of 1 g infused over 1 hour or 50 to 100 mg IV q5 min then maintenance at 1 to 4 mg/min. Dilute 1 g in 250 mL NS.
EKG, BP, HR for possible hypotension and ventricular arrhythmias.
Nausea, vomiting, CNS stimulation convulsion, ↓ platelets; hemolytic anemia. (Avoid in patients with myasthenia gravis.)
Page 68
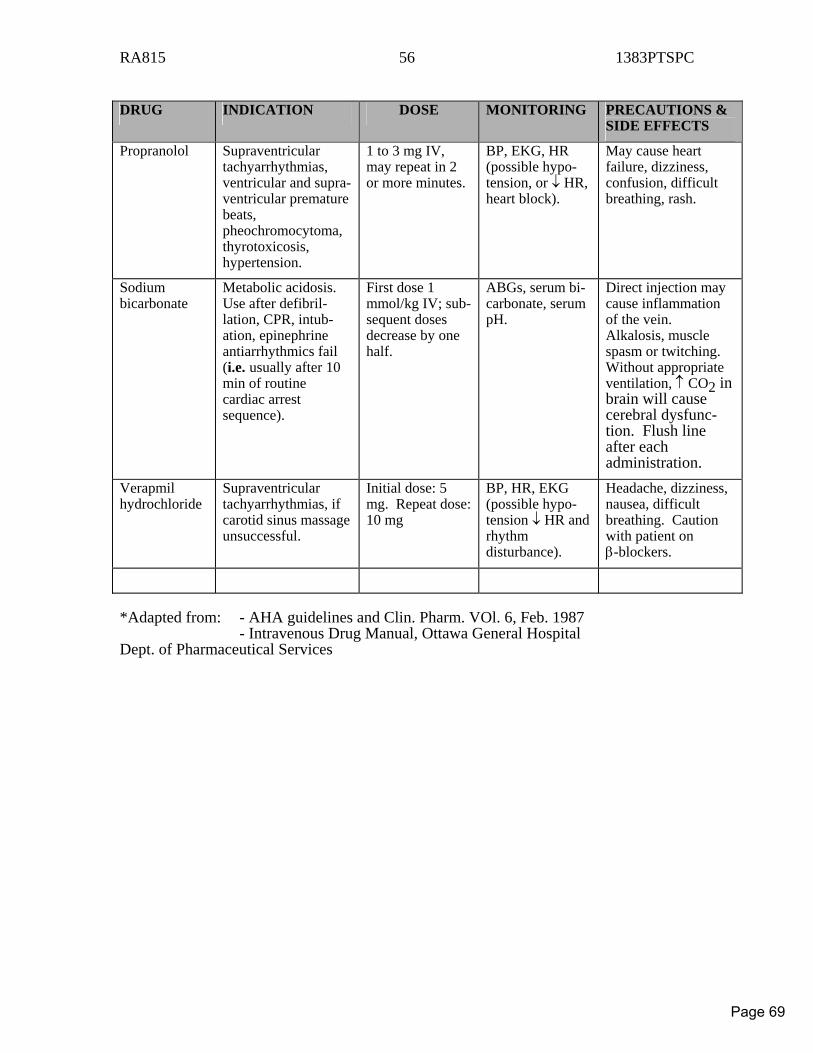
RA815 56 1383PTSPC
DRUG INDICATION DOSE MONITORING PRECAUTIONS &
SIDE EFFECTS
Propranolol Supraventricular tachyarrhythmias, ventricular and supra-ventricular premature beats, pheochromocytoma, thyrotoxicosis, hypertension.
1 to 3 mg IV, may repeat in 2 or more minutes.
BP, EKG, HR (possible hypo-tension, or ↓ HR, heart block).
May cause heart failure, dizziness, confusion, difficult breathing, rash.
Sodium bicarbonate
Metabolic acidosis. Use after defibril-lation, CPR, intub-ation, epinephrine antiarrhythmics fail (i.e. usually after 10 min of routine cardiac arrest sequence).
First dose 1 mmol/kg IV; sub-sequent doses decrease by one half.
ABGs, serum bi-carbonate, serum pH.
Direct injection may cause inflammation of the vein. Alkalosis, muscle spasm or twitching. Without appropriate ventilation, ↑ CO2 in brain will cause cerebral dysfunc-tion. Flush line after each administration.
Verapmil hydrochloride
Supraventricular tachyarrhythmias, if carotid sinus massage unsuccessful.
Initial dose: 5 mg. Repeat dose: 10 mg
BP, HR, EKG (possible hypo-tension ↓ HR and rhythm disturbance).
Headache, dizziness, nausea, difficult breathing. Caution with patient on β-blockers.
*Adapted from: - AHA guidelines and Clin. Pharm. VOl. 6, Feb. 1987 - Intravenous Drug Manual, Ottawa General Hospital Dept. of Pharmaceutical Services
Page 69
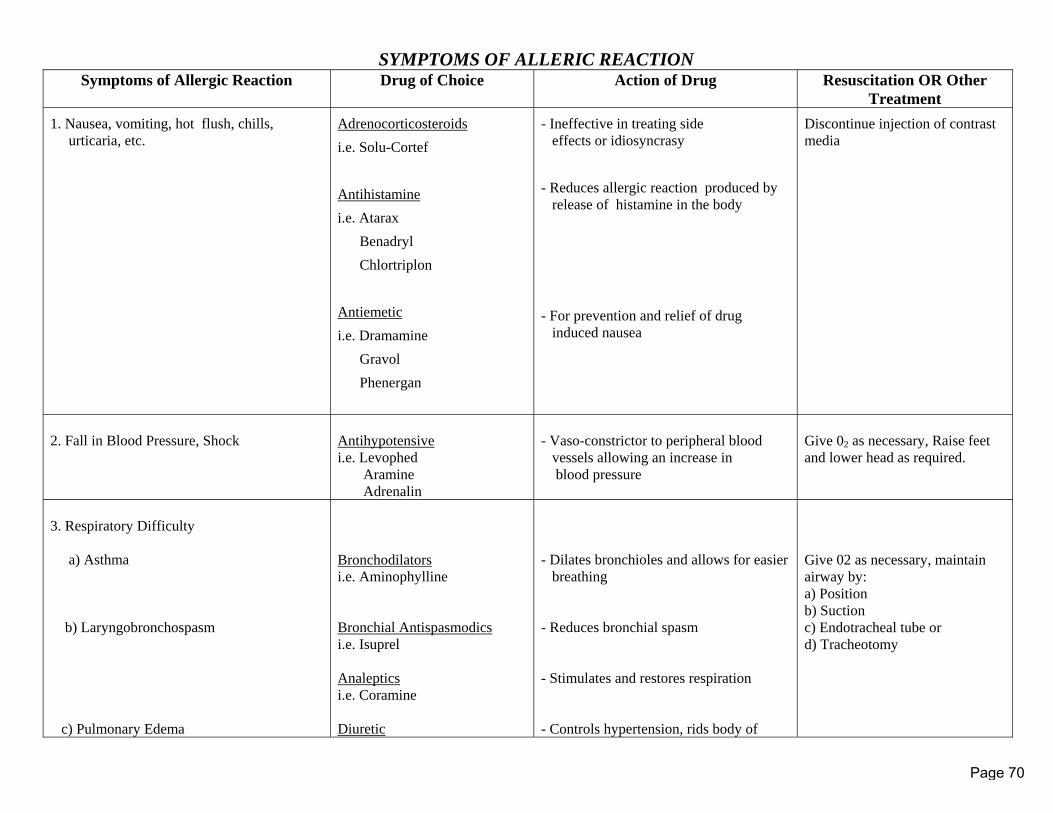
SYMPTOMS OF ALLERIC REACTION
Symptoms of Allergic Reaction Drug of Choice Action of Drug Resuscitation OR Other Treatment
1. Nausea, vomiting, hot flush, chills, urticaria, etc.
Adrenocorticosteroids i.e. Solu-Cortef Antihistamine i.e. Atarax Benadryl Chlortriplon Antiemetic i.e. Dramamine Gravol Phenergan
- Ineffective in treating side effects or idiosyncrasy - Reduces allergic reaction produced by release of histamine in the body - For prevention and relief of drug induced nausea
Discontinue injection of contrast media
2. Fall in Blood Pressure, Shock
Antihypotensive i.e. Levophed Aramine Adrenalin
- Vaso-constrictor to peripheral blood vessels allowing an increase in blood pressure
Give 02 as necessary, Raise feet and lower head as required.
3. Respiratory Difficulty a) Asthma b) Laryngobronchospasm c) Pulmonary Edema
Bronchodilators i.e. Aminophylline Bronchial Antispasmodics i.e. Isuprel Analeptics i.e. Coramine Diuretic
- Dilates bronchioles and allows for easier breathing - Reduces bronchial spasm - Stimulates and restores respiration - Controls hypertension, rids body of
Give 02 as necessary, maintain airway by: a) Position b) Suction c) Endotracheal tube or d) Tracheotomy
Page 70
SYMPTOMS OF ALLERIC REACTION
i.e. Lasix excess fluid in tissue
Page 71
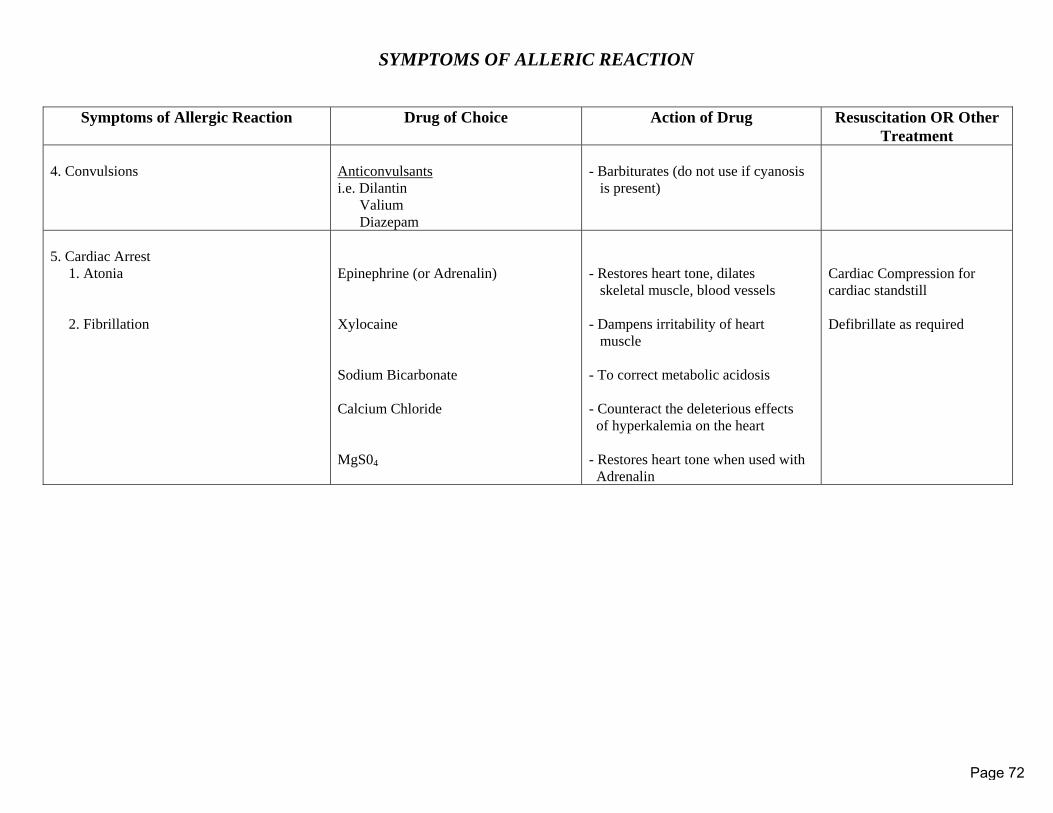
SYMPTOMS OF ALLERIC REACTION
Symptoms of Allergic Reaction Drug of Choice Action of Drug Resuscitation OR Other Treatment
4. Convulsions
Anticonvulsants i.e. Dilantin Valium Diazepam
- Barbiturates (do not use if cyanosis is present)
5. Cardiac Arrest 1. Atonia 2. Fibrillation
Epinephrine (or Adrenalin) Xylocaine Sodium Bicarbonate Calcium Chloride MgS04
- Restores heart tone, dilates skeletal muscle, blood vessels - Dampens irritability of heart muscle - To correct metabolic acidosis - Counteract the deleterious effects of hyperkalemia on the heart - Restores heart tone when used with Adrenalin
Cardiac Compression for cardiac standstill Defibrillate as required
Page 72

MEDICAL RADIATION SCIENCES Joint Degree / Diploma Program
COURSE OUTLINE/SYLLABUS
Course Title: Principles of Pharmacology for Radiation Sciences
The Michener Institute Course Code University of Toronto Course Code PRRD240 MRS267H1 Program Chair: Susan Weltz, Chair, MRS
Course Start Date: September 2008 Revision Date: August 2008
Page 73
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
2
Course Director: Dr. Jose Lança, MD, PhD Department of Pharmacology and Toxicology Faculty of Medicine and Faculty of Dentistry University of Toronto
E-Mail: [email protected] Tel: (416) 979-4900 x4609 Address:
Faculty of Dentistry (Room #258) University of Toronto 124 Edward Street Toronto ON M5G 1G6
COURSE PRESENTATION This fifty-two (52) hour course is delivered by the Department of Pharmacology and Toxicology - Faculty of Medicine, University of Toronto. It is taught in the Medical Sciences Building - Faculty of Medicine and follows the academic guidelines and principles applicable to the Undergraduate Programs offered through the Faculty of Arts & Sciences. The general objectives of this course are threefold: (1) Introduce the students to the basic concepts of pharmacology; (2) develop a multidisciplinary and integrated approach to systems pharmacology; and (3) apply knowledge in a critical manner as members of a patient centered health care team. TARGET POPULATION Principles of Pharmacology for Radiation Sciences (MRS267H1/PRRD240) is a 0.5 credit course presented at the introductory and intermediated levels to second year students enrolled in Nuclear Medicine Technology and Radiological Technology.
Note: Special assistance programs (e.g., alternative arrangements for tests and examinations, academic skills development) are offered to students with documented special needs by the UofT Student Services - Accessibility Services. Students enrolled in
Page 74
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
3
this course that may require special assistance must contact and register with UofT Accessibility Services at least 14 days prior to requiring assistance. For additional information contact the UofT Accessibility Services (416-978-8060 or http://studentlife.utoronto.ca/accessibility.htm). LEARNING GOALS
1. Define the concept of drug as a compound used in the treatment, diagnostic or
prevention of disease and understand the functional interactions between drugs and the body (i.e., pharmacokinetics).
2. Understand the biological mechanisms underlying drug actions on biological targets (i.e., pharmacodynamics).
3. Apply principles of pharmacokinetics and pharmacodynamics to clinical situations. 4. Develop an integrated view of the pathophysiology underlying diseases as the basis
for the understanding of therapeutic drug administration (i.e., systems pharmacology).
5. Understand and apply pharmacological principles to contrast media and radiopharmaceuticals and explore their diagnostic and therapeutic applications.
6. Identify emergency situations (e.g., cardiac and respiratory arrest), recognize adverse reactions resulting from the administration of contrast media (e.g., anaphylaxis and anaphylactoid reactions, renal failure, vasovagal reaction) implement therapeutic management as part of the health care team.
7. Understand and discuss the process of drug development, drug safety and pharmacovigilance.
Page 75
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
4
CORE ABILITIES A. Exhibit professional behaviour B. Demonstrate positive attitudes and behaviours C. Communicate clearly and effectively D. Manage the use of time and other resources to complete tasks and attain goals. E. Solve problems using a variety of strategies. F. Evaluate his/her own thinking throughout the steps and processes used in problem solving and decision making. G. Take responsibility for his/her own actions. H. Work effectively in teams I. Use a variety of computer and other tools appropriate and necessary to the performance of tasks. J. Apply a wide variety of mathematical techniques with the degree of accuracy required to solve problems and make decisions. K. Adapt to new situations and demands. L. Act as a patient advocate COURSE DESCRIPTION This course is primarily a lecture-based pharmacology course common to both Nuclear Medicine Technology and Radiological Technology Programs. The interdisciplinary nature of pharmacology is approached in an integrated manner. The course (a) builds on the understanding of the pharmacological principles of drug/body interactions as a prerequisite to (b) develop an evidence-based approach to drug action, and (c) apply knowledge to the clinical use of drugs in the prevention, diagnosis and treatment of diseases. This course also includes small-group analysis and discussion of case-studies. This learning tool provides the students with opportunities to develop strategies to build team-work, problem solving and apply pharmacological principles to clinical diagnostic and therapeutic settings. The course begins with the presentation of the general principles of pharmacology and includes a series of lectures on the following topics:
• drug groups and classification systems
Page 76
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
5
• pharmacokinetics
o drug absorption and distribution o drug biotransformation o drug clearance o drug bioavailability
• quantification of drug action and clinical outcomes
o agonist vs antagonist o specific vs nonspecific binding o competitive vs non-competitive and uncompetitive antagonists o dose-response studies o potency and efficacy o time-course studies o normal and cumulative distribution o median effective dose (ED50) o median lethal dose (LD50) o median toxic dose (TD50) o therapeutic index (TI= TD50/ED50) o therapeutic window
• pharmacodynamics
o molecular targets o channels, transporters and pumps o receptor mediated events o ionotropic, metabotropic, enzyme-linked and nuclear receptors o drug actions and measurements of their effects
• contrast media (CM) pharmacology
o classification and pharmacokinetics of CM o pharmacodynamics o adverse reactions and drug interactions
• therapeutic agents in nuclear medicine
o pharmacokinetic implications o pharmacodynamics and practical functional applications o implications on diagnostic outcomes
• pharmacology of the autonomic nervous system
Page 77
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
6
o adrenergic and cholinergic pharmacology o clinical outcomes
• systems pharmacology
o drugs acting on the respiratory system o drugs acting on the cardiovascular system o drugs acting on the renal system o drugs acting on the central nervous system o drugs acting on the endocrine system o drugs acting on the gastrointestinal system o drugs acting on the skeletal system o drugs acting on the neuromuscular junction and muscle relaxants o anti-inflammatory and analgesic drugs
• cancer pharmacotherapy and radiopharmaceuticals
• clinical pharmacology of emergency situations in radiation sciences
• drug development and postmarketing surveillance
o principles of drug development o drug safety and efficacy
• adverse drug reactions and drug interactions COURSE OBJECTIVES A - Principles of Pharmacology 1. Define the term pharmacology and outline the scope and subdivisions of
pharmacology. 2. Explain the following terms as they apply to drugs:
• indications • contraindications • precautions • adverse reactions • dosage • formulation
Page 78
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
7
3. Classify drugs using a standard classification system. 4. Describe and use various drug nomenclatures. 5. Describe the various routes of drug delivery and outline the different formulations
that may be used to deliver drugs. 6. Define pharmacokinetics and describe its principles in terms of the following:
• dose administration • drug dissolution • drug absorption • drug distribution • drug bioavailability / bioequivalence • duration of action • drug metabolism • drug elimination / clearance
7. Discuss the routes of drug administration including advantages, disadvantages,
dose form, factors affecting rate of absorption, and pharmacological and clinical factors that influence route of drug administration.
8. Outline the molecular mechanisms of drug absorption and the major factors that
regulate drug absorption. 9. Define drug distribution, outline factors that influence drug distribution for an
intravenously- and an orally-administered drug, and discuss clinical implications. 10. Outline the processes of drug binding to plasma proteins and importance on drug
distribution and bioavailability. 11. Define drug metabolism and biotransformation. 12. Outline the major pathways and the consequences of drug biotransformation or
metabolism. 13. Briefly describe “phase 1” and “phase 2” drug biotransformation reactions.
Page 79
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
8
14. Discuss the factors that can influence drug biotransformation and briefly explain their clinical relevance.
15. Describe the major routes of drug elimination. 16. Outline factors that influence rates of drug elimination by different routes and
explain clinical relevance. 17. Define basic pharmacodynamic concepts and outline the principles of drug
receptor theory. 18. Define the following terms and apply concept:
• agonist • antagonist • partial agonist • irreversible antagonist
19. Define the following terms and discuss relevance:
• drug efficacy • potency • intrinsic activity • median effective dose (ED50) • median lethal dose (LD50) • median toxic dose (TD50) • therapeutic index (TI= TD50/ED50) • therapeutic window
20. Describe dose-response studies, and apply concepts to relevant clinical situations. 21. Describe the following molecular targets of drug action,
• channel • transporter • pump • receptor • ionotropic receptor
Page 80
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
9
• G protein-coupled receptor • enzyme-linked receptor • cytoplasmic/nuclear receptors • transduction pathway • second messengers • receptor regulation
22. Outline the factors that influence drug specificity and selectivity. 23. Compare the specific intracellular mechanisms of drug-target interaction and apply
to regulation of physiological responses and pharmacological actions of drugs: 24. Define systems pharmacology. 25. Describe the pharmacology of the autonomic nervous system. 26. Compare the pharmacology of the adrenergic and cholinergic divisions of the
autonomic nervous system and discuss clinical relevance. 27. Develop an integrated and interdisciplinary approach to the pharmacology of the
following sytems and drug groups:
• respiratory system • cardiovascular system • renal system • central nervous system • endocrine system • cancer pharmacotherapy • gastrointestinal system • skeletal system • neuromuscular junction and muscle relaxants • anti-inflammatory and analgesic drugs
28. Apply pharmacological principles to contrast media (CM) and their clinical applications
• classification and pharmacokinetics of CM: • pharmacodynamics • adverse reactions and drug interactions
Page 81
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
10
29. Apply pharmacological principles to therapeutic agents in nuclear medicine:
• pharmacokinetic implications • pharmacodynamics and practical functional applications • implications on diagnostic outcomes • adverse drug reactions and drug interactions
30. Classify mechanisms of drug interaction. 31. Outline the principles of each class of drug interaction. 32. Classify mechanisms of drug toxicity. 33. Outline the principles of drug toxicity. B - Pharmacology of Drug Groups Related to Nuclear Medicine and Radiology Upon completion of the course as described above, the student should be able to outline and explain the characteristics and role in Nuclear Medicine or Radiology of the drug groups listed below. Examples of drugs related to Nuclear Medicine and Radiology will be provided during the presentation and discussion of the different topics listed above, and will also be included in case studies (please see Course Evaluation). The student should (a) be aware of the indications for the use of a drug in Nuclear Medicine or Radiology, (b) apply knowledge in a critical and professional manner, (c) use the drugs according to the recommended information provided by the manufacturer, and (d) follow the protocols developed by the health care facility where they exerting their profession. At all times they must follow professional and ethical principles in their interactions with patients and other members of the health care team. The use of drugs in the context of Nuclear Medicine and Radiology must take into account special requirements regarding:
• dosages and dosage forms • indications • contraindications • drug effects on target and critical organs • therapeutic effects
Page 82
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
11
• side effects / toxicity • adverse effects • applications in Nuclear Medicine or Radiology
Relevant Drug Groups
Note: that drugs marked with asterisks (*) require special emphasis. The information required for each of these drug groups is the following:
• Respiratory Drugs:
• bronchodilators • xanthines/inotropic agents (see cardiovascular drugs)* • steroids (e.g. puffers)
• Cardiovascular and Renal Drugs:
• beta blockers* • calcium channel blockers* • angiotensin converting enzyme (ACE) inhibitors* • diuretics* • furosemide • acetazolamide • vasodilators* • dipyridimole (e.g. Persantine)* • adenosine* • dobutamide • xanthines/aminophylline* • antiarrhythmics • nitrates • others • fluids (saline versus dextrose) • cardiac glycosides (digoxin) • other antihypertensives
• Endocrine Drugs: • thyroxine/thyroid stimulating hormone*
Page 83
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
12
• anti-thyroid medications* • cholecystokinin (CCK)* • steroids* • estrogens
• Central Nervous System Drugs:
• sedatives • antidepressants • antiepileptics • antipsychotics • others • analgesics • acetazolamide (cerebrovascular dilation)*
• Gastrointestinal System Drugs:
• H2 blockers* • cimetidine • ranitidine • others • CCK* • glucagon/pentagastrin • morphine* • laxatives • phenobarbital.
• Therapeutic Agents:
• chemotherapeutic agents • doxorubicin (adriamycin) • bone mineral therapy • hormone replacement therapy
Competencies Radiological Technology
1. Describe the pharmacological properties of contrast media used in Radiological
Page 84
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
13
Technology. 2. Determine potential adverse reactions/events specific to the injection of
radiographic contrast media agents. 3. Describe the drugs used in the treatment of adverse drug reactions 4. Implement appropriate response processes in the event of a contrast media
reaction.
Competencies Nuclear Medicine Technology
1. Describe therapeutic agents used to augment Nuclear Medicine procedural protocols.
2. Describe how a therapeutic agent affects the biodistribution of the radiopharmaceutical agent in a given procedure.
3. Describe how the use of the therapeutic agent affects the diagnostic outcomes of the Nuclear Medicine study.
4. Describe how the use of therapeutic agents alter the quality of the diagnostic outcomes of the Nuclear Medicine study.
INSTRUCTIONAL STRATEGIES Academic success results from the learning/teaching interaction in a learning environment that encourages professional excellence, inter-professional collaboration and personal integrity. Although the institutional and instructional components are in place, they cannot assure a student’s academic success if there is not commitment and involvement on the learner’s part. Ultimately, it is the student’s responsibility to achieve the learning objectives of the course. Systems Pharmacology and Clinical Pharmacology require the understanding of basic principles of pharmacokinetics and pharmacodynamics, and builds upon the understanding of physiological and pathophysiological mechanisms. Students’s are advised to become involved in the learning process from the very beginning.. A timely preparation will easily provide a solid foundation required to successfully meet the objectives.
Page 85
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
14
This course is primarily presented in lecture format. Lecture Notes are posted in the University of Toronto (Uof T) Libraries “Exam and Courses” website. This is a “password-protected” website. Detailed information on how to log in the UofT course website will be provided in the first lecture. Students are responsible for (1) the material presented in the Lectures, and related material presented in the (2) Lecture Notes and (3) Required Textbook (Page et al., Integrated Pharmacology, 3rd ed., 2006), and (4) Readings . Students are expected to be prepared to participate in the class by asking and answering questions. Students will also participate in small group discussions applied to case studies (see section on Performance Assessments). REQUIRED RESOURCES 1. Textbook Title: Integrated Pharmacology. Editors: Page C., Curtis M., Walker M., Hoffmann B. Edition: 3rd edition Year: 2006 ISBN: 0-323-04080-2 Pages: 675 Publisher: Mosby – Elsevier 2. Lecture Notes Title: Principles of Pharmacology for Radiation Science (PCLRSR410) Author: Lança, A.J. Year: 2008 Publisher: The Lecture Notes are available for download from the University of Toronto (Uof T), Libraries - ERes Course Collections.
Page 86
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
15
(http://eres.library.utoronto.ca/courseindex.asp) The UofT Course Website is password protected, and in agreement with the policies of the UofT.
“All course materials are the copyrighted property of their authors, unless otherwise stated, and are published for course use only, as authorized by your instructor. All other rights reserved”. UofT Libraries website.
3. Readings Readings are required for special topics (see schedule below). They will be posted on the course website prior to lecture day. SUGGESTED ADDITIONAL SOURCES (NOT required. For consultation only.) Title: Principles of Medical Pharmacology Editors: Kalant H, Grant DM, Mitchell J Edition: Seventh edition Year: 2007 ISBN: 0-7796-9945-9 Pages: 1022 Publisher: Elsevier Title: Basic and Clinical Pharmacolgy Editor: Katzung B Edition: Tenth edition Year: 2007 ISBN: 0-07-145155-2 Pages: 1179 Publisher: McGraw-Hill Title: Rang and Dale’s Pharmacology Editors: Rang, H.P., Dale, M.M., Ritter, J.M. and Flower R.J.
Page 87
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
16
Edition: 6th edition Year: 2007 ISBN: 0-8089-2354-4 Pages: 829 Publisher: Churchill Livingstone - Elsevier Title: Compendium of Pharmaceuticals and Specialties (CPS) / or its electronic version (e-CPS). Ottawa: Canadian Pharmaceutical Association, (43th edition) 2008. PERFORMANCE ASSESSMENTS AND MARKING SCHEME An overall course mark of 60% must be obtained to successfully complete MRS267H. Evaluation Date Final Mark Weight (%) Eval. 1 - Case Study 1 Thurs, Sept 25 10% of Final Mark Eval. 2 - Midterm Test Thurs, Oct 16 30% of Final Mark Eval. 3 – Case Study 2 Thurs, Nov 6 10% of Final Mark Eval. 4 – Case Study 3 Thurs, Nov 20 10% of Final Mark Eval. 5 – Final Examination Examination Period (TBA) 40% of Final Mark
Page 88
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
17
Faculty of Medicine – Medical Radiations Sciences
Principles of Pharmacology for Radiation Sciences
Course Director: Dr. A. J. Lança, MD, PhD
2008-2009 Tuesdays: 9-11- Medical Sciences Building, Room 3163
Thursdays: 9-11 Medical Sciences Building, Room 3154
Required Readings: 1. Textbook: Integrated Pharmacology. Page et al. 3rd ed., 2006 2. Additional Readings 3. Lecture Notes
Date
Topic
Chapters
Sept 9 Introduction 1 ” Pharmacokinetics I – Drug Delivery and Drug Formulation 4
Sept 11 Pharmacokinetics II - Absorption 4 ” Pharmacokinetics III – Distribution 4
Sept 16 Pharmacokinetics IV - Biotransformation 4 ” Pharmacokinetics V – Clearance 2
Sept 18 Quantification of Drug Action 2 ” Pharmacology - Clinical Outcomes 2
Sept 23 Pharmacodynamics I – Channels, Transporters and Pumps 2 ” Pharmacodynamics II – Receptors 2
Sept 25 (2 hours)
Evaluation – Case Study #1 (10% of Final Mark) MSB Room 31542
Sept 30 Pharmacodynamics III - Receptors 2 ” Pharmacodynamics III - Receptors 2
Oct 2 Contrast Media Pharmacology Reading Autonomic Nervous System I Reading
Oct 7 Autonomic Nervous System II Reading ” Autonomic Nervous System III Reading
Page 89
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
18
Oct 9 Respiratory System I 14 ” Respiratory System II 14
Oct 14 CVS I - Introduction 13 ” Review 13
Oct 16 (2 hours)
Evaluation – MIDTERM TEST (30% of Final Mark) MSB Room 31542
Oct 21 CVS II – Heart Failure 13 ” CVS IIl – Coronary Heart Disease 13
Oct 23 CVS IV - Arrhythmias 13 ” CVS V - Hypertension 13
Oct 28 Renal System 12 ” CNS I - Introduction 8
Oct 30 CNS II - Depression 8 ” CNS III - Anxiety 8
Nov 4 CNS IV - Schizophrenia 8 ” CNS V – Motor Diseases 8
Nov 6 (2 hours)
Evaluation – Case Study #2 (10% of Final Mark) MSB Room 3154
Nov 11 Endocrine System I - Introduction 11 ” Endocrine System II - Pituitary Gland 11
Nov 13 Endocrine System III - Thyroid Gland 11 ” Endocrine System IV - Adrenal Gland 11
Nov 18 Endocrine V - Pancreas 11 ” Cancer Pharmacotherapy and Radiopharmaceuticals 7
Nov 20 (2 hours)
Evaluation – Case Study #3 (10% of Final Mark) MSB Room 31542
Nov 25 Gastrointestinal System I 16 ” Gastrointestinal System II 16
Nov 27 Skeletal System 9, 15 ” NMJ/Muscle Relaxants 15
Dec 2 Anti-inflammatory and Analgesic Drugs 9,15 ” Pharmacology of Pain Management 8
Dec 4 Clinical Pharmacology of Emergency Situations in Rad Sci Reading ” Drug Development, Drug Safety and Pharmacovigilance 3
Examination Period
FINAL EXAMINATION (40% of Final Mark) (Date and location to be announced by TMI)
Page 90
PROGRAM: Medical Radiation Sciences COURSE NUMBER:
PRRD240/MRS267H1 COURSE TITLE: Principles of Pharmacology for Radiation Sciences
DATE: September 2008
TEACHING FACULTY: Dr. A. J. Lança, MD, PhD REVISED: August 2008
CHAIR SIGNATURE:
© Michener/University of Toronto Medical Radiation Sciences Program
19
Contact Information
Dr. Jose Lança
E-mail: [email protected] Tel: 416-979-4900 x4609
Faculty of Dentistry (Room #258) University of Toronto 124 Edward Street Toronto ON M5G 1G6
Page 91
1
November, 2008 CURRICULUM VITAE
A. JOSÉ LANÇA University Degrees M.D. - Faculty of Medicine, University of Coimbra, Coimbra, Portugal (1977). Ph.D. – Neurosciences, with highest distinction (summa cum laude) (1991). Faculty of Medicine, University of Coimbra, Portugal / University of Toronto, Canada
Citizenship: Canadian Written and Spoken Languages: English, Portuguese, French and Spanish.
University Address Faculty of Dentistry
University of Toronto, 124 Edward Street, Room 258 Toronto, ON, M5G 1G6
e-mail: [email protected] Tel: (416) 979-4900 x4609 or (416) 830-8313 Fax: (416) 979 4936
Home Address 24, Crendon Drive Toronto. Ontario M9C 3G4 Tel: (H) (416) 620-7998 ___________________________________________________________________ Current Academic Positions and Responsibilities Assistant Professor – Faculty of Medicine, Dept. of Pharmacology and Toxicology
University of Toronto, Toronto, ON, Canada (Feb. 2000/present) Assistant Professor – Faculty of Dentistry
University of Toronto, Toronto, ON, Canada (September 2006/present)
Curriculum and course development Current coordination and/or teaching of the following Pharmacology courses:
o Pharmacology (DEN212Y) – Faculty of Dentistry, University of Toronto o International Dentist Advanced Placement Program (IDAPP) – Faculty of
Dentistry, University of Toronto o Pharmacology – Graduate Program, Faculty of Dentistry, University of Toronto o Principles of Pharmacology for Radiation Sciences – Faculty of Medicine,
University of Toronto (MRS267H) o Clinical Pharmacology (PMCH121) – The Michener Institute for Applied Health
Sciences/University of Toronto
Page 92
2
Career Experience
Educational/Academic Experience
Coordination or lecturing in the following Courses:
Pharmacology (DEN212Y) – Faculty of Dentistry, University of Toronto. This is a 78 lecture course with an enrollment of 70 students (2006-present)
Graduate Pharmacology – Faculty of Dentistry, University of Toronto (2006-present). Principles of Pharmacology for Radiation Sciences (PRNU320 – Faculty of Medicine,
University of Toronto/Michener Institute for Applied Medical Sciences). This is a 50 lecture course with an enrollment of 80 students (2000-present)
International Dentist Advanced Placement Program (IDAPP) – Faculty of Dentistry, University of Toronto (2006-present)
Clinical Pharmacology (PMCH121) – Chiropody Program – The Michener Institute for Applied Health Sciences/University of Toronto. This is a 65 lecture course with an enrollment of 30 students (2006-present)
Physiological Sciences II (PSCV120) – Cardiovascular Perfusion Program – The Michener Institute for Applied Health Sciences with an enrollment of 10 students (2007- present)
Systems Pharmacology (PCL470Y - Faculty of Arts and Sciences, PCL361Y - Faculty of Pharmacy and PCL1001Y – School of Graduate Studies). This is a full-year course (78 Lectures), with an enrollment of 250 students, including students enrolled in the Graduate Program of the Department of Pharmacology (2000-2005)
Course and Program Development: Herbal Medications – Relevance to Dental Practice. A Certified Continuing Education
Course for Dentists and Allied Professions. Faculty of Dentistry, University of Toronto.
Herbal Medications – An Evidence-Based Review. A Post-Graduate Certified Continuing Medical Education Course (CME) for Physicians, Dentists, Pharmacists and other Health Care Professionals, U.S.A.
Pharmacology - Faculty of Dentistry, University of Toronto (DEN212Y) Principles of Pharmacology for Radiation Sciences – The Michener Institute for
Applied Health Sciences/University of Toronto (MRS267H) Clinical Pharmacology – Chiropody Program - The Michener Institute for Applied
Health Sciences/University of Toronto (PMCH121) Systems Pharmacology (PCL470Y - Faculty of Arts and Sciences, PCL361Y -
Faculty of Pharmacy and PCL1001Y – School of Graduate Studies) – University of Toronto
Physiological Sciences II – Cardiovascular Perfusion Program - The Michener Institute for Applied Health Sciences (PSCV120)
Undergraduate Education: Major Programs in Pharmacology and Toxicology (Hon. B.Sc.) – Department of Pharmacology and Toxicology, University of Toronto
Undergraduate Coordinator/Undergraduate Program Director – Dept. of Pharmacology, University of Toronto (2000-2005).
Responsible for the Academic Coordination of three Undergraduate Specialist Programs (Hon. B.Sc.) in Pharmacology, Toxicology and Double Specialist (Pharmacology and Toxicology).
Development of two Major Programs (Hon. B.Sc.) – Major in Pharmacology and Major in Toxicology
Page 93
3
Additional teaching for Graduate Programs and Health Professions: Medical Curriculum - Neuropharmacology, Histology and Embryology, University of
Coimbra and University of Toronto Dentistry Curriculum (DDS) – Pharmacology, UofT Graduate Dentistry - Pharmacology –, UofT Pharmacology – International Program (IDAPP) – Faculty of Dentistry, UofT Clinical Pharmacology – Medical Resident Program and Motherisk Program, Hospital
for Sick Children, UofT Graduate Course on “Drug Addiction From Cells to Society” – CAMH, UofT Graduate Course on “Molecular and Applied Pharmacology” – University of Santiago, Chile Continuing Education - Herbal Medications. Relevance to Dental Practice, Faculty of
Dentistry, UofT
Professional development, including courses on: Teaching, Technology and Inclusive Learning Teaching Large University Classes Public Relations – Media Skills Training Instructional Strategies and Problem Based Learning and Teaching Carving New Pathways I and II – Learning-Centered Journeys Psychological Principles and Methods in Pedagogy Professional Teaching Advancement
Other Academic Service: Chair, Undergraduate Education Committee - Department of Pharmacology, Faculty
of Medicine, University of Toronto Member, Basic Medical Sciences Undergraduate Program Decanal Advisory
Committee - Faculty of Medicine, University of Toronto Member, Ad-hoc Committee on Development of New Major Programs, Faculty of
Medicine, University of Toronto Member, Faculty of Pharmacy Curriculum Committee - University of Toronto. Member, Departments of Physical Therapy and Occupational Therapy Board of
Examiners - Faculty of Medicine, University of Toronto. Member, IPE Global Health Working Group, IPE Program University of Toronto Co-supervision of Graduate Students (PhD Program) in the Department of
Pharmacology, University of Toronto. Supervision of fourth year Pharmacology Project students (PCL472Y and PCL474Y,
Undergraduate Project), Dept. Pharmacology, University of Toronto. Faculty Member Radiation Sciences Program and Chiropody Program – University of
Toronto and The Michener Institute for Applied Health Sciences Alberta Heritage Foundation for Medical Research, Grant Reviewer Development of interdepartmental contacts aimed at implementing institutional
interchanges and curricular development
Additional Professional Experience
Medical Practice (1977-1989) Independent Medical Consultant (2004-present) Professional affiliation and specialization in Neuropharmacology and Clinical Pharmacology
(1989- present)
Page 94
4
Previous Positions
Feb. 2000/June 2005: Assistant Professor and Undergraduate Coordinator Department of Pharmacology, University of Toronto, Toronto, Ontario, Canada
Academic Coordination of three Undergraduate Specialist Programs (Hon. B. Sc. in Pharmacology, Toxicology and Double-Specialist Program).
Curriculum development and implementation of two Major Programs (Hon B.Sc. in Pharmacolgy and Toxicology).
Coordination and teaching of two Pharmacology courses. Participation in research programs aimed at elucidating the neuropharmacological basis
of drug addiction.
Oct. 1995/Jan. 2000: Assistant Professor, Department of Pharmacology, University of Toronto, Toronto, Ontario, Canada
Sept. 1993/ Sept 1995: Special Lecturer, Department of Psychology, University of Toronto, Toronto, Ontario, Canada.
Aug. 1989/Sept. 1993: Scientist, Department of Primary Mechanisms, Addiction Research Foundation, Toronto, Ontario, Canada.
Oct. 1984/Aug.1989: Assistant Professor (Senior Level), Department of Histology and Embryology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
Sept. 1982/Oct. 1984: Visiting Scientist in the laboratory of Dr. Derek van der Kooy,
Neurobiology Research Group, Department of Anatomy and Cell Biology, University of Toronto, Toronto, Canada.
Jan. 1980/Sept. 1982: Assistant Professor (Junior Level), Department of Histology and Embryology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
Oct. 1977/Jan. 1980: Medical Internship, University Hospital, University of Coimbra. Cross-appointed Assistant Professor (Junior Level) in the Department of Histology and Embryology, Faculty of Medicine, University of Coimbra, Coimbra, Portugal.
Selected Invited Lectures and Seminars
Lança, A.J. Herbal Medications - Relevance to Dental Practice. Continuing Education, Faculty of Dentistry, University of Toronto, Toronto, Canada (October, 2008)
Lança, A.J. Cellular and Molecular Mechanisms of Drug Addiction. Faculty of Chemical
and Pharmaceutical Sciences, University of Chile, Santiago, Chile (August, 2004) Lança, A.J. Advanced Topics in Neuropharmacology. A series of Lectures, Discussion
Groups in the Graduate Course “Molecular and Applied Pharmacology” - PhD Program in Pharmacology, Faculty of Chemical and Pharmaceutical Sciences, University of Chile, Santiago, Chile (July 23 to August 3, 2004)
Page 95
5
Lança, A.J. Nicotine Induction of fos expression in the PMT. Mechanisms and possible implications on nicotine dependence. 49th National Congress of Physiological Sciences, Symposium on: Nicotine from Cell to Clinical Practice. Monterrey, Mexico (August 26-30, 2001)
Lança, A.J. Cell transplantation and pharmacological approaches to the dopaminergic
modulation of alcohol intake. International Conference on Drugs of Abuse. Madeira, Portugal (April 29 - May 3, 1995)
Wu, P.H., Lança, A.J*. and Kalant, H. Vasopressinergic and serotonergic regulation of
tolerance to alcohol: neuroanatomical and molecular studies. International Conference on Drugs of Abuse. Madeira, Portugal (April 29 - May 3, 1995)
Lança, A.J. Distribution of mu-opiate receptor binding in rat cerebral cortex. 7th
International Meeting of the International Society for Developmental Neuroscience – Symposium on Opiate System Pharmacology. Jerusalem, Israel (June 19-24, 1989)
Academic Awards
1994-1996: Young Investigator Award. National Alliance for Research on Schizophrenia and Depression (NARSAD). United States of America.
1982-1984: Research Award. Calouste Gulbenkian Foundation, Lisbon, Portugal and Department of Anatomy and Cell Biology, University of Toronto. Toronto, ON, Canada.
Membership in Scientific Societies
Society for Neuroscience, USA Canadian Society of Pharmacology and Therapeutics International Brain Research Association European Neuroscience Association
Page 96
6
Publications Book Chapters
1. A.J. Lança Chapter 11: Autonomic Nervous System Neurotransmitters. In: Kalant, H., Grant, D.,
and Mitchell, J.A. eds. Principles of Medical Pharmacology, 7th edition, Elsevier Canada: 2007, 107-120.
2. A.J. Lança Chapter 13: Adrenergic Agonists, Direct and Indirect. In: Kalant, H., Grant, D., and
Mitchell, J.A. eds. Principles of Medical Pharmacology, 7th edition, Elsevier Canada: 2007, 121-136.
3. A.J. Lança Chapter 14: Adrenergic Antagonists, Direct and Indirect. In: Kalant, H., Grant, D., and
Mitchell, J.A. eds. Principles of Medical Pharmacology, 7th edition, Elsevier Canada: 2007, 137-155.
4. A.J. Lança Chapter 16: Functional and Neurochemical Organization of the Central Nervous
System. In: Kalant, H., Grant, D., and Mitchell, J.A. eds. Principles of Medical Pharmacology, 7 th edition, Elsevier Canada, 2007, 187-210.
5. A.J. Lança Chapter 17: Drugs Modifying Movement Control. In: Kalant, H., Grant, D., and
Mitchell, J.A. eds. Principles of Medical Pharmacology, 7th edition, Elsevier Canada, 2007, 211-222.
6. Lança, A.J. Chapter 20: Functional organization of the central nervous system. In: Kalant, H.
and Roschlau, W.H.E. eds. Principles of Medical Pharmacology, 6th ed., New York, Oxford University Press: 1998, 217-240.
Peer Reviewed Publications 1. Lanca, A. J. Herbal Medications: An Evidence-Based Review. CME Resource, Sacramento CA,
USA: (http://www.netce.com/425/Course_9838.pdf) 2007, 48 pages. 2. Lee, S.P., So, C.H., Rashid, A.J., Varghese, G., Cheng, R., Lança, A.J., O’Dowd, B.F. and
George, S.R. Dopamine D1 and D2 Receptor co-activation generates a novel phospholipase C-mediated calcium signal. Journal of Biological Chemistry (2004) 279/34, 35671-35678.
3. 2. Lee, D.K., Lança, A.J., Cheng, R., Nguyen, T., Ji, X.D., Gobeil Jr., F., Chemtob, S., George, S.R., O’Dowd, B.F.
Agonist-independent nuclear localization of the apelin, angiotensin AT1 and Bradykinin B2 receptors. Journal of Biological Chemistry (2004) 279/9, 7901-7908.
4. Lança, A.J., Sanelli, T. R., and Corrigall, W.A.
Nicotine-induced Fos expression in the pedunculopontine mesencephalic tegmentum in the rat. Neuropharmacology (2000) 39, 2808-2817.
5. Lança, A.J., Adamson, K.L., Coen, M.K., Chow, B.L.C. and Corrigall, W.A.
Page 97
7
The pedunculopontine tegmental nucleus and the role of cholinergic neurons in nicotine self-administration in the rat: A correlative neuroanatomical and behavioral study. Neuroscience (2000) 96, 735-742.
6. Lança, A.J., Wu, P.H., Jung, B., Liu, J.-F., Ng, V. and Kalant, H.
Differential increase in Fos immunoreactivity in hypothalamic and septal nuclei by arginine-8-vasopressin and desglycinamide-9-arginine-8-vasopressin. Neuroscience (1999) 91, 1331-1341.
7. Lança, A.J., De Cabo, C., Arifuzzaman, A.I., Vaccarino, F.J.
Cholecystokinergic innervation of nucleus accumbens subregions. Peptides (1998) 19, 859-868.
8. Lança, A.J.
Functional and Neuropharmacological Organization of the Central Nervous System. in: Principles of Medical Pharmacology - 6th Edition, Edited by H. Kalant and W. Roschlau. Oxford University Press, pp. 217-240, 1998.
9. Wu, P.H., Liu, J.F., Wu, W.L., Lança, A.J. and Kalant, H.
Development of alcohol tolerance in the rat after a single exposure to combined treatment with arginine8-vasopressin and ethanol. Journal of Pharmacology and Experimental Therapeutics (1996) 276, 1283-1291.
10. Wu, P.H., Lança, A.J., Liu, J.-F., Man, C.-F. and Kalant, H.
Peripheral injection of arginine-8-vasopressin increases Fos in specific brain areas. European Journal of Pharmacology (1995) 281, 263-269.
11. Wu, P.H., Liu, J.F., Lança, A.J. and Kalant, H.
Selective involvement of central 5-HT2 receptors in the maintenance of tolerance to ethanol by arginine8-vasopressin. Journal of Pharmacology and Experimental Therapeutics (1994) 270, 802-808.
12. Niemella, O., Parkkila, S., Yla-Herttuala, S., Halsted, C., Witztum, J.L., Lança, A.J., Israel, Y.
Covalent protein adducts in the liver as a result of ethanol metabolism and lipid peroxidation. Laboratory Investigation (1994) 70, 537-546.
13. Lança, A.J.
Reduction of voluntary alcohol intake in the rat by modulation of the dopaminergic mesolimbic system:Tansplantation of ventral mesencephalic cell suspensions. Neuroscience (1994) 58, 359-369.
14. Lança, A.J., Grupp, L.A. and Y. Israel, Y.
Reduction of voluntary alcohol consumption in the rat by transplantation of hypothalamic grafts. Brain Research (1993) 632, 287-295.
15. Israel, Y., Speisky, H., Lança, A.J., Iwamura, S., Irai, M. and Varghese, G.
Metabolism of hepatic glutathione and its relevance in alcohol induced liver damage. in: Cellular and Molecular Aspects of Cirrhosis. Eds. B. Clément and A. Guillouzo.
Colloque INSERM/John Libbey Eurotext Ltd., vol.216, pp.25-37, 1992. 16. Lança, A.J. and Y. Israel, Y.
Histochemical demonstration of sinusoidal gamma-glutamyltransferase activity by substrate protection fixation: Comparative studies in rat and guinea pig liver.
Hepatology (1991) 14, 857-863. 17. Lança, A.J.
Page 98
8
The brain renin-angiotensin system. Review and personal contribution. University of Coimbra, 1991.
18. Lança, A.J.
Ontogenetic development of the neostriatum. An experimental model of morphofunctional compartmentation of the telencephalon. Doctoral Dissertation. University of Coimbra, Coimbra, Portugal, 1991.
19. Lança, A.J., Boyd, S., Kolb, B.E. and van der Kooy, D.
The development of a patchy organization in the rat striatum. Developmental Brain Research (1986) 27, 1-10
20. Lança, A.J. and van der Kooy, D. A serotonin-containing pathway from the are postrema to the parabrachial nucleus in the rat. Neuroscience (1985) 14, 1117-1126
Selected Abstracts Presented at Scientific Meetings
1. So, C.H., Rashid, A.J., Varghese, G., Lança, A.J., O’Dowd, B.F., George, S.R. Dopamine D1 and D2 receptor co-activation generates a novel phospholipase C-mediated calcium signal. Visions in Pharmacology Research Symposium, Toronto (2005) 2. Lee, D.K., Lança, A.J., Saldivia V.R., Cheng, R., George, S.R and O’Dowd, B.F. Investigations of ligand-dependent and independent trafficking of the apelin receptor and the
design of a novel apelin antagonist. Visions in Pharmacology Research Symposium, Toronto (2005) 3. Lee, D.K., Lança, A.J., Cheng, R., Nguyen, T., Gobeil, F., Chemtob, S., George, S.R and
O’Dowd, B.F. Nuclear localization of apelin receptor oligomers in human brain. Visions in Pharmacology Research Symposium, Toronto, (2004) 4. So, C.H., Rashid, A.J., Varghese, G., Lança, A.J., Cheng, R., Lee, S.L., O’Dowd, B.F., George,
S.R. Dopamine D1 and D2 receptors traffic together in cells and co-localize in human and rodent striatal neurons. Soc. Neurosci. Abstr. (2003)
5. Lee, DK., Lança, A.J., Cheng, R., Nguyen, T., Ji, X.D., George, S.R., O’Dowd, B.F.
Nuclear localization of the apelin, bradikynin B2 and angiotensin AT1 receptors. Soc. Neurosci. Abstr. (2003)
6. So, C.H., Varghese, G., Lança, A.J., Cheng, R., Lee, S.L., Fan, T., O’Dowd, B.F., George, S.R.
Dopamine D1 and D2 receptors traffic together and co-localize in neurons. Soc. Neurosci. Abstr. (2002)
7. Lee, D.K., Lança, A.J., Cheng, R., Gobeil, F. Jr., Chemtob, S., George, S.R. and O’Dowd, B. A novel nuclear localization of the G protein-coupled receptor for apelin in human brain and cultured cells. Soc. Neurosci. Abstr. (2002)
Page 99
9
8. Lança, A.J., Martens, D.J., Sanelli, T.R. and Corrigall, W.A. Nicotine induction of immediate early gene expression in the rat pedunculopontine mesencephalic tegmentum.
Drug and Alcohol Dependence (2001) 63, Suppl. 1, S86/343
9. Lança, A.J., Sanelli, T.R. and Corrigall, W.A. Nicotine-induced Fos expression in the pedunculopontine mesencephalic tegmentum in the rat.
Soc. Neurosci. Abstr. (2000) 26, 1575.
10. Lança, A.J., Adamson, K.L., Coen, K.M., Chow, B.L.C. and Corrigall, W.A. Cholinergic regulation of nicotine self-administration in the rat - a correlative neuroanatomical and behavioral study.
Soc. Neurosci. Abstr. (1999) 25, 1068. 11. Elmhurst, J.L., Lee, S.P., Lança, A.J., Ng, G.Y.-K., O'Dowd, B.F. and George, S.R. Characterization of the dopamine D3 receptor and a D3 splice variant, D3nf, in SF9 cells. Soc. Neurosci. Abstr. (1998) 24, 1360.
12. Lança, A.J., Manklow, C., de Cabo, C., Vaccarino, F.J. and Arifuzzaman, A.I. Increase in dopaminergic innervation of the cingulate cortex induced by chronic, but not acute, neuroleptic administration in the rat. Soc. Neurosci. Abstr. (1996) 22, 1188.
13. Cormier, H., Tran, M., Lança, A.J. and Ralph, M.R. Regulation of locomotor behavior by vasopressin and the circadian system in hamsters. Soc. Neurosci. Abstr. (1996) 22, 2053.
14. Wu, P.H., Liu, J.F., Lança, A.J., Arifuzzaman, A.I., Grupp, L.A. and Kalant, H. N-methyl-D-aspartate (NMDA)-induced septal lesion prevents the retention of tolerance to ethanol by desglycinamide-[Arg8]-vasopressin (DGAVP). Soc. Neurosci. Abstr. (1995) 21, 1339.
15. Lança, A.J., Wu. P.H., Liu,J.F., Jung, B. and Kalant, H. Differential increases of c-fos expression in the septum and hypothalamus by exogenous arginine-8-vasopressin (AVP) and desglycinamide-arg-8-vasopressin (DGAVP). Soc. Neurosci. Abstr. (1995) 21,507.
16. DeSousa, N., Lança, A.J., Coscina, D.V., and Vaccarino, F.J.
Blockade of CCKA receptors does not affect amphetamine- or dark phase-induced locomotor activity. Soc. Neurosci. Abstr. (1994) 20, 380.
17. Vaccarino, F.J., Westwood, R. and Lança, A.J.
The effects of blockade of CCKB receptors in the nucleus accumbens on amphetamine- induced locomotor activity.
Soc. Neurosci. Abstr. (1994) 20, 380. 18. Berns, T.A., Ekholm, S., Adamson,L. Gurevich, N. and Lança,A.J.
Selective lesions of the mesencephalic compartments of the dopaminergic system or of the nucleus accumbens reduce voluntary alcohol intake in the rat. Soc. Neurosci. Abstr. (1994) 20, 859.
Page 100
10
19. Lança, A.J., Irving, W.J., Wu, P.W., Kalant, H. and Saint-Cyr*, J.A. Ascending projections from the dorsal (DR) and median raphe (MR) nuclei: Possible functional implications with respect to ethanol tolerance. Soc. Neurosci. Abstr. (1993) 1059.
20. Lança, A.J. Autoradiographic distribution of the opiate receptor binding in rat thalamus. Journal of Neurochemistry (1989) 52, Suppl.S149.
21. Lança, A.J.
Distribution of the mu-opiate receptor binding in rat cerebral cortex. International Journal of Developmental Neuroscience(1988) 7th Meeting ISDN, 63.
22. Lança, A.J. Influence of the nigrostriatal pathway on the cholinergic population of the rat caudate nucleus. Neurosci. Lett. (1986) Suppl.26, S169.
Page 101

Course Outline
1.0 IDENTIFICATION
COURSE INFORMATION
Course Name RADIATION THERAPY SKILLS IICourse Code 3W03Course Classification Specialized – Radiation TherapyCourse Type Core Program Code and Name MedRadSci Medical Radiation SciencesTotal Course Hours 65Credit Value 3 unitsDevelopment School Health SciencesAcademic Year 2007-2008 Approving Associate Dean Diane Barrafato
2.0 LEARNING OVERVIEW
SUBSECTION VALUE
Course Description
This course builds on Radiation Skills I and is designed to further develop the radiation therapy student’s critical thinking, psychomotor and problem solving skills required in the simulation and treatment of radiation therapy patients. An emphasis is placed on professional behaviours, teamwork and communication throughout the course. Working in small groups students will practice and ultimately perform a series of simulations and radiation therapy treatment set-ups. Skills II will draw on the student’s knowledge and understanding of their previous didactic/clinical courses within the core curriculum.
Status of Resources
REQ= RequiredREC= RecommendedREF= Reference
Type of Resources
Text Book OR Supply
Codeor
ISBNName or Title Author/Publisher
or Vendor Version/ Edition
Type Status
0-323-01748-7
Principles and Practice of Radiation Therapy
Washington C.M. & Leaver D./Mosby
Second Textbook REQ
The Lymphatic System Barker et al The Michener Institute for Applied Health Sciences and the University of Toronto
Second TextbookREQ
Treatment Planning in Radiation Oncology
Khan, F.M./ Lippincott Williams & Wilkins
Second Textbook REQ
Cross-sectional Nodal Atlas: A Tool for the Definition of Clinical Target Volumes in Three-Dimensional Radiation Therapy Planning
Martinez-Monge, R., et al.
- Article supplied previous course (Treatment Planning)
REQ
Tolerance of Normal Tissue to Therapeutic Irradiation. International Journal of Radiation Oncology, Biology, Physics
Emami, B. et al. 1991 Article supplied previous course (Treatment Planning)
SUP
Blue scrubs - - Supply REQ
1Page 102
Course Outline
Pre-requisite(s) Successful completion in Radiation Skills I (2U03), Treatment Planning II (3V03) and Registration in Level 3 of the Medical Radiation Sciences Therapy Specialization.
3.0 COURSE CONTENTTopics
This course will cover an introduction to simulations and treatment set-ups for Parallel Opposed Pairs, 3-Field Technique, 4-Field Box Technique and 3-Field Head and Neck Technique. The disease sites discussed will be lung cancer, gastrointestinal cancers, genitourinary cancers, gynecological cancers, and head and neck cancers.
4.0 COURSE LEARNING OUTCOMES Upon successful completion of the course learning outcomes, the student will reliably demonstrate the ability to:
LO01 Exhibit professional behaviours Learning ElementsDemonstrate professional conduct Maintain patient confidentialityPractice informed consent Illustrate reflective practice
LO02 Demonstrate effective written, verbal and non-verbal communication skillsLearning ElementsDemonstrate listening skills with colleagues and patients Demonstrate appropriate tone of voice, facial expressions, posture and eye contactDemonstrate a respect for personal spaceDemonstrate ability to speak clearly and conciselyDemonstrate ability to articulate and pronounce words clearlyDemonstrate ability to use an appropriate rate of speechDemonstrate ability to deliver information clearly
LO03 Demonstrate effective teamwork skillsLearning ElementsDemonstrate collaborationDemonstrate respect Contribute equallyDemonstrate active listening
LO04 Perform radiation therapy treatment set-ups and simulations Learning ElementsDemonstrate technical skills required to perform a variety of treatment set-upsDemonstrate technical skills required to perform a variety of simulations Complete required documentation Interpret documentationApply theoretical principles and knowledge to treatment set-ups and simulationsInvestigate advancements in imaging and treatment Demonstrate ability to safely and effectively handle radiation therapy equipmentAdhere to radiation protection requirements
2Page 103
Course Outline
5.0ASSESSMENTAssessment Method Weight
Skills Testing (Test 1 or Test 2 best score out of first two tests) 15%
Final Skills Test (Test 3) 30%
Assignment 15%
Final Written Exam 25%
Professional Behaviours (including reflective practice submissions) 15%
TOTAL
100%
The final course grade will be reported as a PASS/FAIL. In order to achieve a PASS grade the student must achieve:- A minimum of 70% weighted average on two Skills Tests (Test 1 and 3 or 2 and 3)- A minimum of 70% on each of the Final Skills Tests (Simulation and Set-up). Individual marks for the simulation and set-
up tests will be totaled to determine the weighted average for the Final Skills Test.- A minimum of 70% on totaled overall raw score
A student who does not meet these requirements will be assigned an ‘F’ grade for the course
Note: In the event of an appeal of a skills test mark, a remark of Tests 1 or 2 will not be an available option. In the event of an appeal following the final grade, a remark of Test 3 may be considered.
ADDITIONAL REQUIREMENTS:
DRESS CODE FOR LABSFor security reasons students must wear their program specialization scrubs for all labs and practice sessions. For safety students are required to wear shoes with closed toes and heels and tie long hair back. Students are expected to have a clean and neat appearance at all times and their photo ID must be visible. Students are expected to wear their JCC photo for the labs scheduled at JCC. Failure to comply with the dress code will result in the student being immediately required to leave the lab area. Repeated non-compliance will result in application of the McMaster Disruptive Behavior policy.
POLICY PERSONAL APPEARANCE HAMILTON HEALTH SCIENCES It is expected if students are not in their scrubs when they arrive at the JCC that they adhere to the Policy on Personal Appearance (posted on WebCT).
ATTENDANCESuccessful learning is dependent on the involvement of each member of the group. Therefore, students must participate in all scheduled labs. Labs are scheduled at the Juravinski Cancer Centre (JCC). Students are expected to arrive a minimum of 10 minutes before their scheduled lab time. Students should report to either Simulator A or Linear Accelerator 6A/B according to their schedule and wait outside the treatment/simulator room.
1. Students will be scheduled to attend two labs per week, one in the simulator and one on the linear accelerator. Students must attend both labs. The labs are scheduled on Tuesday, Wednesday or Thursday evenings; however in the event of an unforeseen circumstance and/or during skills testing, an alternate evening may be required. It is expected that students be available if an alternate evening must be scheduled.
2. Skills testing may be conducted during the lab times or scheduled during at alternative times.3. Attendance at all labs is mandatory. A deduction of 2 marks from the total possible 15 course marks allocated for
“Professional Behaviours” will be applied for each missed lab. A deduction of 2 marks from the total possible 15 course marks allocated for “Professional Behaviours” will be applied for each late arrival. Late arrivals of more than 15 minutes will not be permitted into the lab and this will be considered a missed lab.
4. Attendance at all skills tests is mandatory. Any student absent (without proper notification) for a skills test will receive a mark of zero for that test.
3Page 104
Course Outline
PROFESSIONAL BEHAVIOURSThe instructor will use a skills checklist to evaluate the professional skills, technical skills and applied knowledge of each student during the labs and at the time of skills testing. For details refer to the appropriate skills checklist.
REFLECTIVE PRACTICEStudents will be required to complete 3 reflective journal assignments throughout the course. For details refer to the reflective journal assignment.
LABSLabs will be held at the Juravenski Cancer Centre on Tuesday, Wednesday and Thursday evenings from 4:30 .pm. – 8:00 p.m. In the event of an unforeseen circumstance and/or during skills testing, alternate evenings may be required. It is expected that students be available if an alternate evening must be scheduled.
EMERGENCY PATIENTSIn the event that there is an emergency patient to be treated after hours using the conventional simulator, it may be necessary to delay and/or re-schedule the lab.
RADIATION PROTECTION REQUIREMENTSStudents will be issued a TLD badge by the Juravinski Cancer Centre (JCC) and must wear this TLD for all lab sessions. TLD badges must be left after lab in the student classroom at JCC. Students are expected to review their Radiation Protection notes prior to the first laboratory session. Students must adhere at all times to the policy that under nocircumstances is any living person to be irradiated.
GENERAL SAFETYCare must be taken in order to prevent any injury when placing a fellow student on the treatment table. Any problems with the equipment must be reported to your instructor immediately, in order that corrective action may be taken. Students must be aware of the location of fire exits and of Hamilton Health Sciences policies and procedures regarding fire safety. Students are expected to review their Code Red Fire Education Guide (Hamilton Health Sciences) issued last year.
6.0 STUDENT SUCCESS – POLICIES AND PROCEDURESRELATED POLICIES AND PROCEDURES:All policies guiding the Medical Radiation Sciences program must be adhered to at all times. It is the student’s responsibility to familiarize his or herself with these policies. Examples are as follows:
Rules for Written TestsPlease refer to pages 17 and 18 of the MRSc Program Handbook for policy and procedures.
Missed Tests/ExamsPlease refer to page 25 of the McMaster University Undergraduate Calendar 2007/08, General Academic Regulations, Petitions for Relief for Missed Term Work and for Deferred Examinations.
AssignmentsPlease refer to page 25 of the McMaster University Undergraduate Calendar 2007/08, General Academic Regulations, Petitions for Relief for Missed Term Work and for Deferred Examinations.
Review of Term Tests Prior to Final ExaminationsPlease refer to page 18 of the MRSc Program Handbook for policy. In the event of a supplemental examination, the same policy applies for viewing a final examination.
Academic IntegrityBe sure to review the policy regarding academic integrity available at the website: http://www.mcmaster.ca/policy/ac_ethics.htm
4Page 105
Course Outline
1.0 IDENTIFICATION
COURSE INFORMATION
Course Name Patient Care Course Code MEDRADSC 2A03 Course Classification Foundation Revision date February 5, 2008 Course Type Core Program Code and Name Medical Radiation Sciences: 1410 Total Course Hours 52 Credit Value 3 units Development School Health Sciences Academic Year 2007/2008 Approving Associate Dean Diane Barrafato
2.0 LEARNING OVERVIEW
SUBSECTION VALUE
Course Description
Theoretical foundation and skills development to enable the student to meet the physical and emotional needs of patients in the clinical setting while utilizing self-care concepts and safe practices.
Status of
Resources
Code
or ISBN
Name or Title Author/Publisher or Vendor
Version/ Edition
Type
Status
0-7817-3191-7
Basic Medical Techniques and Patient Care in Imaging Technology
Lillian S Torres, TerriAnn Linn-Watson Norcutt, Andrea Guillen Dutton, publ 2003 Lippincott, Williams and Wilkins
6th ed T Req
Patient Care Course Notes Mohawk College S Req
Medical Dictionary Any T Req Internet Access S Req
Patient Care in Radiography
Ehrlich, RA, publ 2004 by Mosby 6th ed T Ref
Page 106
2
Pre-requisite(s)
Course Code
Course Name Details
Registration in Level II of a Medical Radiation Sciences Specialization
3.0 COURSE CONTENT
Topics Module 1-Safe Practices: infection control, isolation precautions, aseptic technique, administration of pharmaceuticals and contrast media Module 2- Applied Patient Care: body mechanics lifts and transfers, vital signs, cavity insertions and tattooing, oxygen and suction administration, emergency medicine and pharmacology, specialized tubes, lines and indwelling catheters
4.0 REFERENCE TO STANDARDS 5.0 COURSE LEARNING OUTCOMES Upon successful completion of the course learning outcomes, the student will reliably demonstrate the ability to:
LO01 Practice effective communication in a professional manner Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability to communicate effectively with various types of patients through lectures and labs.
LO02 Demonstrate specified patient care skills in a simulated clinical environment
Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability to perform the following the skills; proper aseptic hand wash, sterile gowning and gloving, setting up and tearing down a sterile tray, syringe preparation using both a vial and an ampule, venipuncture using an angiocath and butterfly needle, transfer a patient from a wheelchair to a bed and return and a transfer from a stretcher to bed and return, blood pressure measurement, and a cavity insertion (enema tip for radiography specialization and transvaginal probe insertion for radiography specialization) or tattooing for radiation therapy specialization.
LO03 Provide an environment of safety and comfort for the patient
Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability to safely care for a patient through lectures and simulated labs.
SAFE PRACTICES Unit 1: INFECTION CONTROL
Upon successful completion of this unit, the student will be able to: 1. Define the basic terminology used in the practice of infection control
2. Identify the component elements of the “Chain of Infection” 3. List and describe the four known microorganisms that may cause infection and their portals of
entry
Page 107
3
4. List and define the factors that contribute to the process of infection 5. List the signs and symptoms commonly exhibited by a patient with an infection 6. Discuss nosocomial infection 7. Describe standard precautions and identify the two main impetuses leading to the “Blood and Body Fluid Precaution” standard 8. Differentiate between “Universal Precautions” and “Body Substance Isolation”. 9. Identify the body substance isolation procedures that should be a routine
part of every procedure a medical imaging technologist performs
ASEPTIC TECHNIQUE Upon completion of this unit, the student will be able to:
2. Define the basic terminology used in the practice of aseptic technique 3. Differentiate between medical and surgical asepsis
3. List the basic rules for surgical aseptic technique 4. Identify methods of sterilization 5. Identify materials which are suitable for sterilization
6. Distinguish between a disposable and non-disposable sterile tray
7. Don and remove a sterile gown 8. Perform the steps required to:
complete an aseptic handwash correctly don and remove sterile gloves and a face mask open and set up a disposable sterile tray
ADMINISTRATION OF PHARMACEUTICALS AND CONTRAST MEDIA Upon completion of this unit, the student will be able to:
1. Define the medical terminology used in the practice of medication administration 2. discuss basic pharmacology and basic emergency medications 3. Identify types and parts of a: syringe, needle, intravenous infusion setup 4. Identify injection/infusion sites for adults and infants.
5. Manage contaminated and biohazardous materials 6. List the steps to be followed when setting up an intravenous infusion 7. Identify the veins suitable for intravenous injections
8. Demonstrate how to establish and discontinue intravenous access 9. Discuss post-puncture care 10. Correctly perform the following: prepare a syringe for injection handle the filled syringe demonstrate venipuncture technique using two types of needles
MODULE 2: APPLIED PATIENT CARE Unit 1: BODY MECHANICS, LIFTS & TRANSFERS Upon successful completion of this unit, the student will be able to:
1. Define the basic terminology used in the practice of correct body mechanics 2. Discuss methods of preventing personal injury when lifting and moving patients and medical
imaging equipment. 3. Discuss ways of assessing a patient’s need for assistance when preparing them for a medical
imaging examination 4. Describe how to perform the following procedures: Log Roll
transfer using a Gait or Transfer belt
Page 108
4
sheet transfer sliding board transfer
5. Perform the steps required to safely transfer a patient: into and out of a wheelchair from stretcher to bed and back
Unit 2: VITAL SIGNS Upon successful completion of this unit, the student will be able to: 1. Define the terminology used in the practice of assessing vital signs
2. Demonstrate knowledge of how to assess and record normal and abnormal: pulse rate respiration body temperature blood pressure for: adults, children and infants 3. Discuss factors which can cause variations in characteristics of the vital
signs listed in #2 above 4. Define and discuss Cheyne-Stokes Respiration 5. State the pressure ranges where “hypotension” and “hypertension” occur
6. Explain how to recognize and respond to medical Unit 3: CAVITY INSERTIONS Upon successful completion of this unit, the student will be able to: ALL STREAMS:
1. Define the related terminology 2. Describe any special considerations required with elderly or pediatric patients, or patients with an
altered body image with respect to endorectal or endovaginal insertions. 3. Demonstrate correct patient communication prior to, during and after an endovaginal and/or
endorectal scan. 4. Identify the risks and complications for both endorectal and endovaginal insertions. 5. Discuss aseptic practices to be used with respect to endorectal or endovaginal tip/probe insertions
RADIOGRAPHY/ STREAM: 1. List 3 types of cleansing enema utilized in conjunction with radiographic examinations
2. State the common reason for the use of each type of cleansing enema. 3. Discuss the patient preparation required prior to a barium enema examination. 4. Describe the method of administration of:
(a) single contrast barium enema (b) double contrast barium enema (c) barium enema via colostomy
4. List the steps to be followed with respect to the endorectal insertion of a barium enema tip. 5. Describe the correct procedure for disposing of the enema apparatus following a barium enema
exam. 6. Perform a endorectal tube insertion (barium enema tip insertion) correctly SONOGRAPHY STREAM: 1. Describe the patient preparation for both an endovaginal and endorectal scan 2. State the procedure for preparing, cleaning and storing the transducer 3. List the steps to be followed with respect to the probe insertion for an endorectal or endovaginal scan. 4. Perform an endovaginal probe insertion correctly.
Page 109
5
RADIATION THERAPY STREAM: TATTOOING 1. List 3 reasons to tattoo patients who require Radiation Therapy. 2. Discuss other options for marking in Radiation Therapy. 3. List all equipment required for tattooing. 4. Describe dangers to therapists when tattooing and precautions taken. 5. Describe the correct procedure for tattooing. 6. Perform s tattooing procedure correctly including patient education and documentation.
LO04 Work effectively in small groups in a simulated clinical environment
Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability through lab participation.
5.0 ASSESSMENT Assessment Method Weight Associated Outcome(s)
Attendance and Participation 5% Midterm test 20% Final Exam 45% Skills Assessments 5% X 6
TOTAL 100% "The overall term score is calculated using the weighting shown above. The final grade for the course will be PASS/FAIL, with 50% as the minimum required term score to achieve a PASS grade. Any student with a final term score of less than 50% will receive a FAIL grade." In the case of a discrepancy, course textbooks and power point content will be considered correct. RELATED POLICIES AND PROCEDURES Rules for Written Tests Please refer to pages 16 and 17 in the MRSc Program Handbook for policy and procedures. Missed Tests/Exams/Labs Please refer to page 24 of the McMaster University Undergraduate Calendar 2006/07, General
Academic Regulations, Petitions for Relief for Missed Term Work and for Deferred Examinations. Review of Term Tests Prior to Final Examinations
Please refer to page 17 of the MRSc Program Handbook for policy. In the event of a supplemental examination, the same policy applies for viewing a final examination.
Academic Integrity
Be sure to review the policy regarding academic integrity available at the website, http://www.mcmaster.ca/policy/ac_ethics.htm
Page 110
Appendix 4
Administer ing contrast media through or into the rectum or an art i f i c ia l opening into the body
Tab Title Page No.
1 The Michener Institute for Applied Health Sciences, Learning plan, rectal tube insertion
1
2 Mohawk College of Applied Arts and Technology, Course outline, Radiation Therapy Skills II, and Patient Care, cavity insertion to include rectal tube insertion
5

The Michener Institute for Applied Health Sciences & The University of Toronto Faculty of Medicine - 1 - Equal Opportunity Employer and Educator Detailed Performance Assessment Task Systems Methodology RARA410 © Copyright 2005 Development Date: 05/02/2005 Current Date: 09/12/07
Systems Methodology Performance Assessment Task 2 Skill Demonstration: Rectal Tube Insertion Information Developer(s) Lori L Hill/Nathalie Machabée Environment Lab Strategy Skill Demonstration Evaluators Instructor
Target Competency and Linked Exit Learning Outcomes Competency 8. Demonstrate the correct method for inserting a rectal tube for contrast enema purposes
using a simulated patient. Linked External Standards Responsibility to Patients (CMRTO Code of Ethics, p. 1, January 1, 2004) Equipment and Materials (CMRTO Essential Competencies, p. 2, January 1, 2004) Safe Practice (CMRTO Essential Competencies, p. 5, January 1, 2004) Linked Program Outcomes A. Develop transferable radiological technology skill sets that are transferable across health care and
professional environments Linked Core Abilities * Exhibit Professional Behavior * Demonstrate positive attitudes and behaviors * Communicate clearly and effectively * Adapt to new situations and demands * Act as a patient advocate Directions For this performance assessment you will demonstrate the correct method for inserting a rectal tube for the purpose of performing a contrast enema procedure. You will perform this competency in the laboratory environment. Equipment, instruments, tools, supplies, materials that you need will be provided, but you will be required to select the appropriate items need to complete the task. Practice the skill, self-assessing according the scoring guide. Schedule your skill assessment with your instructor as directed. At the time of performance be sure that you: 1. Gather the required tools, equipment, instruments, materials or supplies. 2. Don the appropriate personal safety clothing and equipment. 3. Provide for the comfort and safety of your client or patient. 4. Perform each step of the task. 5. Follow all safety procedures. 6. Explain that steps of the tasks as you perform them. (what, why, how, precautions) 7. Answer any questions posed by the evaluator or your client/patient.
Page 1
The Michener Institute for Applied Health Sciences & The University of Toronto Faculty of Medicine - 2 - Equal Opportunity Employer and Educator Detailed Performance Assessment Task Systems Methodology RARA410 © Copyright 2005 Development Date: 05/02/2005 Current Date: 09/12/07
Skill Demonstration: Rectal Tube Insertion Scoring Standard You must earn a rating of 'Satisfactory' on each criterion in order to earn credit for this assessment. You must pass this evaluation in order to complete the course. Rating Scale Unsatisfactory Fails to perform skill adequately or does not attempt to perform skill. Satisfactory Performs adequately, with no more than one minor prompt, and without critical mistakes.
May fail to recognize minor mistakes. Explains what and how, but fails to explain why. Answers to questions about the process may reveal minor misunderstandings.
Scoring Guide
Criteria Ratings 1. you select the correct materials satisfactory unsatisfactory 2. you employ the principles of medical asepsis satisfactory unsatisfactory 3. you position the patient correctly satisfactory unsatisfactory 4. you lubricate the rectal tube prior to insertion satisfactory unsatisfactory 5. you insert the tube at the correct angle and in the correct direction
satisfactory unsatisfactory
6. you perform the procedure in a safe manner satisfactory unsatisfactory 7. you verbalize an explanation of the process to the patient as you perform it
satisfactory unsatisfactory
8. your explanation presents sound reasoning as you describe the decisions you make throughout the process
satisfactory unsatisfactory
Grade____________
Student Name ____________________________ Date _______________ Evaluator's Signature ____________________________ Date_______________ Comments:
Page 2
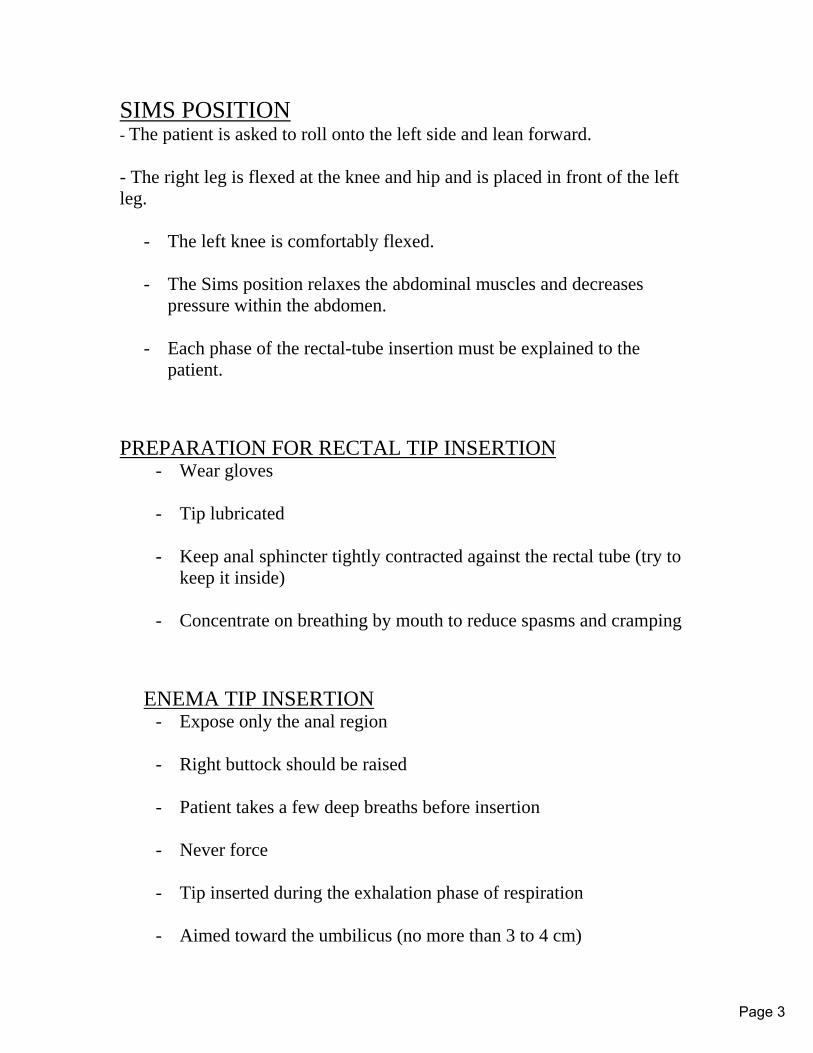
SIMS POSITION - The patient is asked to roll onto the left side and lean forward. - The right leg is flexed at the knee and hip and is placed in front of the left leg.
- The left knee is comfortably flexed. - The Sims position relaxes the abdominal muscles and decreases
pressure within the abdomen. - Each phase of the rectal-tube insertion must be explained to the
patient. PREPARATION FOR RECTAL TIP INSERTION
- Wear gloves
- Tip lubricated
- Keep anal sphincter tightly contracted against the rectal tube (try to keep it inside)
- Concentrate on breathing by mouth to reduce spasms and cramping
ENEMA TIP INSERTION
- Expose only the anal region
- Right buttock should be raised
- Patient takes a few deep breaths before insertion
- Never force
- Tip inserted during the exhalation phase of respiration
- Aimed toward the umbilicus (no more than 3 to 4 cm)
Page 3

Page 4
Course Outline
1.0 IDENTIFICATION
COURSE INFORMATION
Course Name RADIATION THERAPY SKILLS IICourse Code 3W03Course Classification Specialized – Radiation TherapyCourse Type Core Program Code and Name MedRadSci Medical Radiation SciencesTotal Course Hours 65Credit Value 3 unitsDevelopment School Health SciencesAcademic Year 2007-2008 Approving Associate Dean Diane Barrafato
2.0 LEARNING OVERVIEW
SUBSECTION VALUE
Course Description
This course builds on Radiation Skills I and is designed to further develop the radiation therapy student’s critical thinking, psychomotor and problem solving skills required in the simulation and treatment of radiation therapy patients. An emphasis is placed on professional behaviours, teamwork and communication throughout the course. Working in small groups students will practice and ultimately perform a series of simulations and radiation therapy treatment set-ups. Skills II will draw on the student’s knowledge and understanding of their previous didactic/clinical courses within the core curriculum.
Status of Resources
REQ= RequiredREC= RecommendedREF= Reference
Type of Resources
Text Book OR Supply
Codeor
ISBNName or Title Author/Publisher
or Vendor Version/ Edition
Type Status
0-323-01748-7
Principles and Practice of Radiation Therapy
Washington C.M. & Leaver D./Mosby
Second Textbook REQ
The Lymphatic System Barker et al The Michener Institute for Applied Health Sciences and the University of Toronto
Second TextbookREQ
Treatment Planning in Radiation Oncology
Khan, F.M./ Lippincott Williams & Wilkins
Second Textbook REQ
Cross-sectional Nodal Atlas: A Tool for the Definition of Clinical Target Volumes in Three-Dimensional Radiation Therapy Planning
Martinez-Monge, R., et al.
- Article supplied previous course (Treatment Planning)
REQ
Tolerance of Normal Tissue to Therapeutic Irradiation. International Journal of Radiation Oncology, Biology, Physics
Emami, B. et al. 1991 Article supplied previous course (Treatment Planning)
SUP
Blue scrubs - - Supply REQ
1Page 5
Course Outline
Pre-requisite(s) Successful completion in Radiation Skills I (2U03), Treatment Planning II (3V03) and Registration in Level 3 of the Medical Radiation Sciences Therapy Specialization.
3.0 COURSE CONTENTTopics
This course will cover an introduction to simulations and treatment set-ups for Parallel Opposed Pairs, 3-Field Technique, 4-Field Box Technique and 3-Field Head and Neck Technique. The disease sites discussed will be lung cancer, gastrointestinal cancers, genitourinary cancers, gynecological cancers, and head and neck cancers.
4.0 COURSE LEARNING OUTCOMES Upon successful completion of the course learning outcomes, the student will reliably demonstrate the ability to:
LO01 Exhibit professional behaviours Learning ElementsDemonstrate professional conduct Maintain patient confidentialityPractice informed consent Illustrate reflective practice
LO02 Demonstrate effective written, verbal and non-verbal communication skillsLearning ElementsDemonstrate listening skills with colleagues and patients Demonstrate appropriate tone of voice, facial expressions, posture and eye contactDemonstrate a respect for personal spaceDemonstrate ability to speak clearly and conciselyDemonstrate ability to articulate and pronounce words clearlyDemonstrate ability to use an appropriate rate of speechDemonstrate ability to deliver information clearly
LO03 Demonstrate effective teamwork skillsLearning ElementsDemonstrate collaborationDemonstrate respect Contribute equallyDemonstrate active listening
LO04 Perform radiation therapy treatment set-ups and simulations Learning ElementsDemonstrate technical skills required to perform a variety of treatment set-upsDemonstrate technical skills required to perform a variety of simulations Complete required documentation Interpret documentationApply theoretical principles and knowledge to treatment set-ups and simulationsInvestigate advancements in imaging and treatment Demonstrate ability to safely and effectively handle radiation therapy equipmentAdhere to radiation protection requirements
2Page 6
Course Outline
5.0ASSESSMENTAssessment Method Weight
Skills Testing (Test 1 or Test 2 best score out of first two tests) 15%
Final Skills Test (Test 3) 30%
Assignment 15%
Final Written Exam 25%
Professional Behaviours (including reflective practice submissions) 15%
TOTAL
100%
The final course grade will be reported as a PASS/FAIL. In order to achieve a PASS grade the student must achieve:- A minimum of 70% weighted average on two Skills Tests (Test 1 and 3 or 2 and 3)- A minimum of 70% on each of the Final Skills Tests (Simulation and Set-up). Individual marks for the simulation and set-
up tests will be totaled to determine the weighted average for the Final Skills Test.- A minimum of 70% on totaled overall raw score
A student who does not meet these requirements will be assigned an ‘F’ grade for the course
Note: In the event of an appeal of a skills test mark, a remark of Tests 1 or 2 will not be an available option. In the event of an appeal following the final grade, a remark of Test 3 may be considered.
ADDITIONAL REQUIREMENTS:
DRESS CODE FOR LABSFor security reasons students must wear their program specialization scrubs for all labs and practice sessions. For safety students are required to wear shoes with closed toes and heels and tie long hair back. Students are expected to have a clean and neat appearance at all times and their photo ID must be visible. Students are expected to wear their JCC photo for the labs scheduled at JCC. Failure to comply with the dress code will result in the student being immediately required to leave the lab area. Repeated non-compliance will result in application of the McMaster Disruptive Behavior policy.
POLICY PERSONAL APPEARANCE HAMILTON HEALTH SCIENCES It is expected if students are not in their scrubs when they arrive at the JCC that they adhere to the Policy on Personal Appearance (posted on WebCT).
ATTENDANCESuccessful learning is dependent on the involvement of each member of the group. Therefore, students must participate in all scheduled labs. Labs are scheduled at the Juravinski Cancer Centre (JCC). Students are expected to arrive a minimum of 10 minutes before their scheduled lab time. Students should report to either Simulator A or Linear Accelerator 6A/B according to their schedule and wait outside the treatment/simulator room.
1. Students will be scheduled to attend two labs per week, one in the simulator and one on the linear accelerator. Students must attend both labs. The labs are scheduled on Tuesday, Wednesday or Thursday evenings; however in the event of an unforeseen circumstance and/or during skills testing, an alternate evening may be required. It is expected that students be available if an alternate evening must be scheduled.
2. Skills testing may be conducted during the lab times or scheduled during at alternative times.3. Attendance at all labs is mandatory. A deduction of 2 marks from the total possible 15 course marks allocated for
“Professional Behaviours” will be applied for each missed lab. A deduction of 2 marks from the total possible 15 course marks allocated for “Professional Behaviours” will be applied for each late arrival. Late arrivals of more than 15 minutes will not be permitted into the lab and this will be considered a missed lab.
4. Attendance at all skills tests is mandatory. Any student absent (without proper notification) for a skills test will receive a mark of zero for that test.
3Page 7
Course Outline
PROFESSIONAL BEHAVIOURSThe instructor will use a skills checklist to evaluate the professional skills, technical skills and applied knowledge of each student during the labs and at the time of skills testing. For details refer to the appropriate skills checklist.
REFLECTIVE PRACTICEStudents will be required to complete 3 reflective journal assignments throughout the course. For details refer to the reflective journal assignment.
LABSLabs will be held at the Juravenski Cancer Centre on Tuesday, Wednesday and Thursday evenings from 4:30 .pm. – 8:00 p.m. In the event of an unforeseen circumstance and/or during skills testing, alternate evenings may be required. It is expected that students be available if an alternate evening must be scheduled.
EMERGENCY PATIENTSIn the event that there is an emergency patient to be treated after hours using the conventional simulator, it may be necessary to delay and/or re-schedule the lab.
RADIATION PROTECTION REQUIREMENTSStudents will be issued a TLD badge by the Juravinski Cancer Centre (JCC) and must wear this TLD for all lab sessions. TLD badges must be left after lab in the student classroom at JCC. Students are expected to review their Radiation Protection notes prior to the first laboratory session. Students must adhere at all times to the policy that under nocircumstances is any living person to be irradiated.
GENERAL SAFETYCare must be taken in order to prevent any injury when placing a fellow student on the treatment table. Any problems with the equipment must be reported to your instructor immediately, in order that corrective action may be taken. Students must be aware of the location of fire exits and of Hamilton Health Sciences policies and procedures regarding fire safety. Students are expected to review their Code Red Fire Education Guide (Hamilton Health Sciences) issued last year.
6.0 STUDENT SUCCESS – POLICIES AND PROCEDURESRELATED POLICIES AND PROCEDURES:All policies guiding the Medical Radiation Sciences program must be adhered to at all times. It is the student’s responsibility to familiarize his or herself with these policies. Examples are as follows:
Rules for Written TestsPlease refer to pages 17 and 18 of the MRSc Program Handbook for policy and procedures.
Missed Tests/ExamsPlease refer to page 25 of the McMaster University Undergraduate Calendar 2007/08, General Academic Regulations, Petitions for Relief for Missed Term Work and for Deferred Examinations.
AssignmentsPlease refer to page 25 of the McMaster University Undergraduate Calendar 2007/08, General Academic Regulations, Petitions for Relief for Missed Term Work and for Deferred Examinations.
Review of Term Tests Prior to Final ExaminationsPlease refer to page 18 of the MRSc Program Handbook for policy. In the event of a supplemental examination, the same policy applies for viewing a final examination.
Academic IntegrityBe sure to review the policy regarding academic integrity available at the website: http://www.mcmaster.ca/policy/ac_ethics.htm
4Page 8
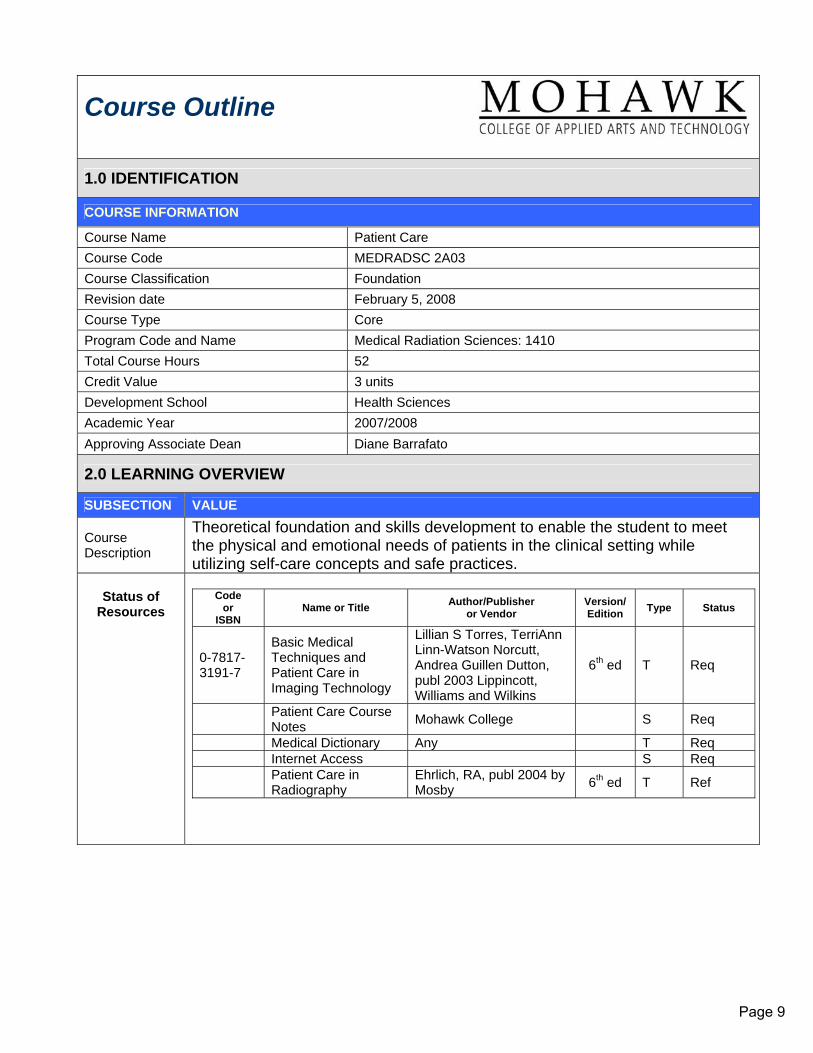
Course Outline
1.0 IDENTIFICATION
COURSE INFORMATION
Course Name Patient Care Course Code MEDRADSC 2A03 Course Classification Foundation Revision date February 5, 2008 Course Type Core Program Code and Name Medical Radiation Sciences: 1410 Total Course Hours 52 Credit Value 3 units Development School Health Sciences Academic Year 2007/2008 Approving Associate Dean Diane Barrafato
2.0 LEARNING OVERVIEW
SUBSECTION VALUE
Course Description
Theoretical foundation and skills development to enable the student to meet the physical and emotional needs of patients in the clinical setting while utilizing self-care concepts and safe practices.
Status of
Resources
Code
or ISBN
Name or Title Author/Publisher or Vendor
Version/ Edition
Type
Status
0-7817-3191-7
Basic Medical Techniques and Patient Care in Imaging Technology
Lillian S Torres, TerriAnn Linn-Watson Norcutt, Andrea Guillen Dutton, publ 2003 Lippincott, Williams and Wilkins
6th ed T Req
Patient Care Course Notes Mohawk College S Req
Medical Dictionary Any T Req Internet Access S Req
Patient Care in Radiography
Ehrlich, RA, publ 2004 by Mosby 6th ed T Ref
Page 9
2
Pre-requisite(s)
Course Code
Course Name Details
Registration in Level II of a Medical Radiation Sciences Specialization
3.0 COURSE CONTENT
Topics Module 1-Safe Practices: infection control, isolation precautions, aseptic technique, administration of pharmaceuticals and contrast media Module 2- Applied Patient Care: body mechanics lifts and transfers, vital signs, cavity insertions and tattooing, oxygen and suction administration, emergency medicine and pharmacology, specialized tubes, lines and indwelling catheters
4.0 REFERENCE TO STANDARDS 5.0 COURSE LEARNING OUTCOMES Upon successful completion of the course learning outcomes, the student will reliably demonstrate the ability to:
LO01 Practice effective communication in a professional manner Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability to communicate effectively with various types of patients through lectures and labs.
LO02 Demonstrate specified patient care skills in a simulated clinical environment
Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability to perform the following the skills; proper aseptic hand wash, sterile gowning and gloving, setting up and tearing down a sterile tray, syringe preparation using both a vial and an ampule, venipuncture using an angiocath and butterfly needle, transfer a patient from a wheelchair to a bed and return and a transfer from a stretcher to bed and return, blood pressure measurement, and a cavity insertion (enema tip for radiography specialization and transvaginal probe insertion for radiography specialization) or tattooing for radiation therapy specialization.
LO03 Provide an environment of safety and comfort for the patient
Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability to safely care for a patient through lectures and simulated labs.
SAFE PRACTICES Unit 1: INFECTION CONTROL
Upon successful completion of this unit, the student will be able to: 1. Define the basic terminology used in the practice of infection control
2. Identify the component elements of the “Chain of Infection” 3. List and describe the four known microorganisms that may cause infection and their portals of
entry
Page 10
3
4. List and define the factors that contribute to the process of infection 5. List the signs and symptoms commonly exhibited by a patient with an infection 6. Discuss nosocomial infection 7. Describe standard precautions and identify the two main impetuses leading to the “Blood and Body Fluid Precaution” standard 8. Differentiate between “Universal Precautions” and “Body Substance Isolation”. 9. Identify the body substance isolation procedures that should be a routine
part of every procedure a medical imaging technologist performs
ASEPTIC TECHNIQUE Upon completion of this unit, the student will be able to:
2. Define the basic terminology used in the practice of aseptic technique 3. Differentiate between medical and surgical asepsis
3. List the basic rules for surgical aseptic technique 4. Identify methods of sterilization 5. Identify materials which are suitable for sterilization
6. Distinguish between a disposable and non-disposable sterile tray
7. Don and remove a sterile gown 8. Perform the steps required to:
complete an aseptic handwash correctly don and remove sterile gloves and a face mask open and set up a disposable sterile tray
ADMINISTRATION OF PHARMACEUTICALS AND CONTRAST MEDIA Upon completion of this unit, the student will be able to:
1. Define the medical terminology used in the practice of medication administration 2. discuss basic pharmacology and basic emergency medications 3. Identify types and parts of a: syringe, needle, intravenous infusion setup 4. Identify injection/infusion sites for adults and infants.
5. Manage contaminated and biohazardous materials 6. List the steps to be followed when setting up an intravenous infusion 7. Identify the veins suitable for intravenous injections
8. Demonstrate how to establish and discontinue intravenous access 9. Discuss post-puncture care 10. Correctly perform the following: prepare a syringe for injection handle the filled syringe demonstrate venipuncture technique using two types of needles
MODULE 2: APPLIED PATIENT CARE Unit 1: BODY MECHANICS, LIFTS & TRANSFERS Upon successful completion of this unit, the student will be able to:
1. Define the basic terminology used in the practice of correct body mechanics 2. Discuss methods of preventing personal injury when lifting and moving patients and medical
imaging equipment. 3. Discuss ways of assessing a patient’s need for assistance when preparing them for a medical
imaging examination 4. Describe how to perform the following procedures: Log Roll
transfer using a Gait or Transfer belt
Page 11
4
sheet transfer sliding board transfer
5. Perform the steps required to safely transfer a patient: into and out of a wheelchair from stretcher to bed and back
Unit 2: VITAL SIGNS Upon successful completion of this unit, the student will be able to: 1. Define the terminology used in the practice of assessing vital signs
2. Demonstrate knowledge of how to assess and record normal and abnormal: pulse rate respiration body temperature blood pressure for: adults, children and infants 3. Discuss factors which can cause variations in characteristics of the vital
signs listed in #2 above 4. Define and discuss Cheyne-Stokes Respiration 5. State the pressure ranges where “hypotension” and “hypertension” occur
6. Explain how to recognize and respond to medical Unit 3: CAVITY INSERTIONS Upon successful completion of this unit, the student will be able to: ALL STREAMS:
1. Define the related terminology 2. Describe any special considerations required with elderly or pediatric patients, or patients with an
altered body image with respect to endorectal or endovaginal insertions. 3. Demonstrate correct patient communication prior to, during and after an endovaginal and/or
endorectal scan. 4. Identify the risks and complications for both endorectal and endovaginal insertions. 5. Discuss aseptic practices to be used with respect to endorectal or endovaginal tip/probe insertions
RADIOGRAPHY/ STREAM: 1. List 3 types of cleansing enema utilized in conjunction with radiographic examinations
2. State the common reason for the use of each type of cleansing enema. 3. Discuss the patient preparation required prior to a barium enema examination. 4. Describe the method of administration of:
(a) single contrast barium enema (b) double contrast barium enema (c) barium enema via colostomy
4. List the steps to be followed with respect to the endorectal insertion of a barium enema tip. 5. Describe the correct procedure for disposing of the enema apparatus following a barium enema
exam. 6. Perform a endorectal tube insertion (barium enema tip insertion) correctly SONOGRAPHY STREAM: 1. Describe the patient preparation for both an endovaginal and endorectal scan 2. State the procedure for preparing, cleaning and storing the transducer 3. List the steps to be followed with respect to the probe insertion for an endorectal or endovaginal scan. 4. Perform an endovaginal probe insertion correctly.
Page 12
5
RADIATION THERAPY STREAM: TATTOOING 1. List 3 reasons to tattoo patients who require Radiation Therapy. 2. Discuss other options for marking in Radiation Therapy. 3. List all equipment required for tattooing. 4. Describe dangers to therapists when tattooing and precautions taken. 5. Describe the correct procedure for tattooing. 6. Perform s tattooing procedure correctly including patient education and documentation.
LO04 Work effectively in small groups in a simulated clinical environment
Learning Elements Upon successful completion of this outcome, the student will have demonstrated the ability through lab participation.
5.0 ASSESSMENT Assessment Method Weight Associated Outcome(s)
Attendance and Participation 5% Midterm test 20% Final Exam 45% Skills Assessments 5% X 6
TOTAL 100% "The overall term score is calculated using the weighting shown above. The final grade for the course will be PASS/FAIL, with 50% as the minimum required term score to achieve a PASS grade. Any student with a final term score of less than 50% will receive a FAIL grade." In the case of a discrepancy, course textbooks and power point content will be considered correct. RELATED POLICIES AND PROCEDURES Rules for Written Tests Please refer to pages 16 and 17 in the MRSc Program Handbook for policy and procedures. Missed Tests/Exams/Labs Please refer to page 24 of the McMaster University Undergraduate Calendar 2006/07, General
Academic Regulations, Petitions for Relief for Missed Term Work and for Deferred Examinations. Review of Term Tests Prior to Final Examinations
Please refer to page 17 of the MRSc Program Handbook for policy. In the event of a supplemental examination, the same policy applies for viewing a final examination.
Academic Integrity
Be sure to review the policy regarding academic integrity available at the website, http://www.mcmaster.ca/policy/ac_ethics.htm
Page 13