Physician vs. Patient Incentives in Prescription Drug Choice
Accepted Manuscript
Disaggregating ethnoracial disparities in physician trust
Abigail A. Sewell
PII: S0049-089X(15)00132-5
DOI: http://dx.doi.org/10.1016/j.ssresearch.2015.06.020
Reference: YSSRE 1820
To appear in: Social Science Research
Received Date: 17 June 2014
Revised Date: 31 May 2015
Accepted Date: 25 June 2015
Please cite this article as: Sewell, A.A., Disaggregating ethnoracial disparities in physician trust, Social Science
Research (2015), doi: http://dx.doi.org/10.1016/j.ssresearch.2015.06.020
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers
we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and
review of the resulting proof before it is published in its final form. Please note that during the production process
errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
DISAGGREGATING ETHNORACIAL DISPARITIES IN PHYSICIAN TRUST
Abigail A. Sewell
Emory University & University of Pennsylvania
RUNNING HEAD: Disaggregating Trust
WORD COUNT: 11,019 Words, 4 Tables, and 1 Appendix
KEYWORDS: race, trust, patient-physician relationship, medicine, doctors, medical sociology
CORRESPONDING AUTHOR: Abigail A. Sewell; Emory University; Department of Sociology; 204
Tarbutton Hall; 1555 Dickey Drive; Atlanta, GA 30322; [email protected]
1
ABSTRACT
Past research yields mixed evidence regarding whether ethnoracial minorities trust physicians
less than Whites. Using the 2002 and 2006 General Social Surveys, variegated ethnoracial
differences in trust in physicians are identified by disaggregating a multidimensional physician
trust scale. Compared to Whites, Blacks are less likely to trust the technical judgment and
interpersonal competence of doctors. Latinos are less likely than Whites to trust the fiduciary
ethic, technical judgment, and interpersonal competence of doctors. Black-Latino differences in
physician trust are a function of ethnoracial differences in parental nativity. The ways ethnoracial
hierarchies are inscribed into power-imbalanced clinical exchanges are discussed.
KEYWORDS: race, trust, patient-physician relationship, medicine, doctors, medical sociology
2
The patient-physician relationship is inherently unequal given the status differences
between clinicians and help-seekers (Gilson 2003; Kramer and Cook 2004; Mechanic 1998;
Parsons 1951). The absence of physician trust on behalf of ethnoracial (i.e., racial/ethnic)
minorities is considered to be a key mechanism underlying health care disparities (LaVeist,
Nickerson, and Bowie 2000; Smedley, Stith, and Nelson 2003). In fact, ample evidence shows
that Blacks and Latinos hold less trust towards medical research, pharmaceuticals, health care
facilities, and health care providers than Whites (Armstrong et al. 2006; Boulware et al. 2003;
Corbie-Smith et al. 2002; Freimuth et al. 2001; Hughes-Halbert et al. 2006; Stepanikova et al.
2006). Lack of trust in physicians and health care matters in a broader sense because trust in
medical actors is considered a contributing factor to help-seeking behavior when one becomes ill
and to compliance behavior as one navigates the medical institution (Mechanic 1998; Whetten et
al. 2006). High levels of trust, moreover, have been linked to better self-rated health and more
positive functional health across the life course (Barefoot et al. 1998). Inequalities in trusting
medical actors by race and ethnicity, then, may partly contribute to ethnoracial inequalities in
morbidity, mortality, and health care service use (Smedley, Stith, and Nelson 2003).
Yet, research evaluating ethnoracial differences in trusting personal physicians provides
mixed evidence regarding both the magnitude and substantive nature of ethnoracial differences
in physician trust. For instance, on one hand, unidimensional studies examining the perceived
willingness of doctors to put their patients’ needs above all other considerations show Blacks are
substantially less likely than Whites to trust personal physicians (Ahern and Hendryx 2003;
Doescher et al. 2000; Levinson et al. 2005; Patel and Chernew 2007; Schnittker 2004;
Stepanikova et al. 2006). On the other hand, studies employing multi-dimensional scales of
trusting personal physicians do not show evidence of less trusting affect towards medical doctors
3
among Blacks compared to Whites (Benjamins 2006; Guffey and Yang 2012; Musick and
Whorten 2008; Tai-Seale and Pescosolido 2003). Meanwhile, Latino-White differences in
physician trust have been found in unidimensional studies (Stepanikova et al. 2006) but have not
been evaluated in multidimensional studies. These divergent sets of findings prompt an
important question: Why do multidimensional studies of physician trust not detect ethnoracial
differences in physician trust? If ethnoracial minorities are so overwhelmingly distrustful of
medicine and, arguably by extension, physicians, then ethnoracial gaps should be evident
regardless of the instrument employed.
This ethnoracial physician trust paradox is the concern of this study. Recent studies argue
that (dis)trust in the health care system cannot be translated to (dis)trust in physicians (Shoff and
Yang 2012). I argue that ethnoracial differences in medical system trust do not necessarily
translate to ethnoracial differences in physician trust. The perspective that ethnoracial minorities
are culturally predisposed to distrust must be questioned. Rather, as stated by Benjamin (2013) in
a study of stem cell research, “distrust is socially produced in the everyday experiences of patient
families in and outside of the clinic” (115). The approach taken to elucidating this paradox is
primarily methodological, with substantive and theoretical implications, as it highlights the
utility of disaggregating multidimensional physician trust scales.
Using data from English-speaking respondents of the 2002 and 2006 General Social
Surveys, this study adjudicates among the disparate findings of physician trust studies by
evaluating measurement variance in a shortened form of a standard multi-dimensional “Trust in
Physician” scale and its constituent disaggregated items (Anderson and Dedrick 1990). Five
dimensions of the patient-physician relationship are considered: honesty, fiduciary ethics (i.e.,
commitment to uphold the Hippocratic Oath), technical expertise, cultural authority, and
4
interpersonal competence (Mechanic 1998; Pescosolido, Tuch, and Martin 2001). A commonly-
used measure of confidence in medicine is employed as a comparison measure to capture social
attitudes towards the larger health care system. Ethnoracial differences in the form of physician
trust are evaluated both naïvely and holding constant sociodemographic factors. The ways
ethnoracial hierarchies are inscribed into power-imbalanced clinical exchanges are discussed.
1. LITERATURE REVIEW
1.1 Trust in the Health Care System
Trust is an essential ingredient of social interactions characterized by high levels of
uncertainty and vulnerability (Smith 2010), such as those within the medical institution (Cook et
al. 2004; Hall et al. 2001; Mechanic 1998; Pearson and Raeke 2000). Social conditions, such as
race and ethnicity, constrain and shape the contour of interactions within and across ethnoracial
groups (Ross, Mirowsky, and Pribesh 2001). Race, in particular, influences the relationships
people form with others (Link and Phelan 1995). Racism creates dissimilarities in the life
opportunities, lived experiences, and collective interests of individuals marked indelibly by
phenotype (Bonilla-Silva 1997; Omi and Winant 1996). Moreover, racial stratification intensifies
power imbalances already present in the interactions between patients and physicians (King
1996). Racial stratification fosters racially distinct attitudinal profiles towards institutional
gatekeepers of the goods and services of society (Bonilla-Silva 1997), including towards the
medical and scientific enterprises (Benjamin 2013).
Processes of inequality within and tangential to the medical system have placed racial
and ethnic minorities in a position of high vulnerability to medical actors (Smedley et al. 2003;
Whaley 1998). For instance, the misuse and abuse of Black bodies in medical science is
considered to have incited general mistrust and anxiety among Blacks towards medicine
(Gamble 1997; Thomas and Curran 1999; White 2005). Such mistrust and anxiety reflects a
5
history of exploitation and benign neglect that Blacks have experienced at the hands of actors
across the medical hierarchy (Beardsley 1987; Jones 1981; Nelson 2011; Washington 2006. In
characterizing the medical attitudes of Blacks, Gamble (1997) suggests there is a spillover effect
from Black’s general beliefs that their lives are devalued: “They perceive, at times correctly, that
they are treated differently in the health care system solely because of their race, and such
perceptions fuel mistrust of the medical profession” (1775-6).
Social processes of inequality also place Latinos at a disadvantage in medical encounters.
Recent studies indicate that experiments such as Tuskegee also occurred among Guatemaleans
during the 1940s (Reverby 2011), suggesting that Latinos may also have a collective memory of
medical abuse and benign neglect. Moreover, Latinos have more limited English proficiency
than non-Latinos (Betancourt et al. 2004; McGorry 1999). One study found that 82 percent of
Latinas who participated in a focus group study cited language problems as a reason to withhold
information from their physicians (Julliard et al. 2008). Because the presence of a third party
heightens feelings of discomfort, fear, and vulnerability in a relationship that is already power-
imbalanced, interpreters may create more barriers to establishing trust between Latino patients in
their doctors. In fact, Latinos may experience cultural dissonance with Western medical practices
that mandate patients disclose confidential information and personal problems with clinicians
(Echeverry 1997).
Still, researchers have not provided a systematic examination of how pan-ethnic
inequalities influence the extension of trust to physicians within the medical encounters. For
instance, research often lumps Latinos into the “Other” category or omits them from analysis
altogether. Furthermore, among demographically-similar adults, no ethnoracial differences have
been found in prior studies examining ethnoracial differences in confidence in leaders of
6
medicine or general confidence in physicians (e.g., Alesina and La Ferrara 2002; Benjamins
2006). These findings call into question the assumption that ethnoracial inequalities in physician
trust are ubiquitous and/or are a ready reflection of ethnoracial inequalities in medical distrust.
1.2 Trust in Personal Physicians
Still, research has suggested that processes of social distance negate the positive impact
that high-quality physician behavior (thoroughness of physical exams, attentiveness during visit,
clarity of medical explanations) have on Blacks trusting their physicians (Schnittker 2004). For
instance, even upon accessing health services, minorities – directly through personal contact and
indirectly through networks of friends and family – report more negative interactions with health
care professionals than do Whites (Diala et al. 2005; Lillie-Blanton et al. 2000;). Minority
patients also report less participatory visits and more verbally dominant encounters with their
physicians than do White patients (Cooper-Patrick et al. 1999; Saha et al. 1999). Minority
patients in racially-discordant relationships report poorer clinical encounters in the health care
system and express more concerns with unfair treatment in medicine than do minority patients in
racially-concordant relationships (Cooper-Patrick et al. 1999; Saha et al. 1999; Schnittker and
Liang 2006). Yet, ethnoracial differences in physician trust persist despite the racial concordance
of the patient-physician relationship (Schnittker and Liang 2006; Sohler et al. 2007).
While a good deal of research supports the claim that ethnoracially marginalized people
are less trusting of medicine than Whites, research on whether such distrust/mistrust extends to
personal physicians presents equivocal results. Two bodies of research have emerged. The first
body of research draws mainly, but not exclusively, from fiduciary trust data, while the second
body of research draws from multidimensional trust data. The remainder of this section reviews
the evidence provided by each body of research and concludes with a critique of extant research.
Due to the limited availability of physician trust research on Latinos, the review examined
7
focuses primarily on Black-White differences in physician trust; however, research on Latino-
White differences in physician trust is also considered, where available.
1.2.1 Support for Ethnoracial Differences in Trusting Personal Physicians
Given past histories of abuse and exploitation toward Black patients by medical actors
(e.g., Tuskegee Syphilis Study, Henrietta Lacks, the Mississippi Appendectomy, gynecological
experiments on slaves), ethnoracial differences in perceptions of the honesty of physicians are
expected to be substantial. Blacks have been found to be less trusting of medical actors’ honesty
about a range of ethical and privacy issues, including blood tests, experimentation, medication,
public health information, and mistakes made during medical care (Armstrong et al. 2006;
Armstrong et al. 2008; Whetten et al. 2006). Assessments of honesty with measures of mistrust
in hospitals suggest that Blacks, more so than Whites, often perceive violations of their privacy
(LaVeist et al. 2000). Honesty is reported to be an issue for Latinos also – specifically, focus
groups of Latinas reported not trusting that their doctor would keep their medical information
confidential (Julliard et al. 2008). Still, no research is available that assesses ethnoracial
differences in trusting the honesty of one’s personal physician.
Furthermore, the rise of managed care has fostered concerns with whether physicians are
able to attend to institutionally-motivated fiscal concerns while placing their patients’ needs first
(Caronna 2011; Mechanic 1998). Researchers suggest that concerns with increasing health care
costs and the dominance of managed care system models may disproportionately impinge upon
the health care experiences of minorities because they are often uninsured or underinsured
(Schlesinger 1987). For example, an early study reported that Blacks are more likely than Whites
to believe the duration of their hospitalization is too short (Blendon et al. 1989).
Recent studies of ethnoracial differences in trusting a physician’s fiduciary ethic suggests
that minorities are concerned about the implications of managed care. Specifically, Levinson and
8
colleagues (2005) find that Blacks and Latinos are less likely than Whites to believe that
physicians prioritize patients over financial costs. However, the lower levels of fiduciary trust
among Latinos documented in this study were only marginally significant. Using scales that
aggregate measures of the fiduciary ideal of medicine with measures of more specific physician
behaviors (e.g., whether one’s physician will provide references to a specialist, is influenced by
health insurance rules, and might perform unnecessary tests or procedures), studies indicate that
Blacks and Latinos are less trusting than Whites (Ahern and Hendryx 2003; Doescher et al.
2000; Patel and Chernew 2007; Schnittker 2004). Yet, a study that disaggregates items of
fiduciary trust scales indicates that Blacks and Whites are equally likely to trust in the fiduciary
ideal of medicine (Stepanikova et al. 2006). Moreover, lower levels of fiduciary trust among
Latinos compared to Whites are less pronounced for those surveyed in English than for those
surveyed in Spanish. This study also indicates that no Latino-White fiduciary trust differences
occurred once sociodemographic differences in correlates of trust are taken into consideration.
1.2.2 Lack of Support for Ethnoracial Differences in Trusting Personal Physicians
Evidence of negative affect towards medicine among minorities has been difficult to
replicate when scholars employ multidimensional trust in physician scales (Benjamins 2006;
Guffey and Yang 2012; Tai-Seale and Pescosolido 2003). Some studies suggest that Blacks may
be more trusting of some medical actors than others. For instance, recent studies suggest that
Blacks’ negative evaluations of medicine may be more related to concerns about the health care
system rather than concerns about one’s personal physician (Armstrong et al. 2006; LaVeist et al.
2000). One study even suggests that non-Black minorities display more trust in their personal
physician than Whites (Benjamins 2006). However, this study aggregates all non-Black
minorities into an ambiguous “Other” category that combines ethnoracial groups with diverse
attachments to physicians and different resources to navigate the health care system. It is
9
therefore unclear what proportion of this category is Latino, Asian, multiracial, or some other
ethnoracial group.
Less pronounced ethnoracial differences also have been found regarding trusting another
ideal of medicine – that is, the belief that providers have an excellent sense of judgment
(technical judgment) and are scientific experts (cultural authority). Studies of distrust in the
health care system reveal no Black-White differences in assessments of the technical judgments
physicians display during medical visits (Armstrong et al. 2008). In fact, during a period when
the cultural authority of physicians declined rapidly for the general population, researchers
revealed that Blacks held more favorable views of doctors in the 1990s than in the 1970s
(Pescosolido, Tuch, and Martin 2001). These findings provide additional evidence that there may
be dimensions of the patient-physician relationship where Blacks and Latinos demonstrate more
trust than comparable Whites. However, no studies have shown that Latinos do in fact exhibit
more trust in physicians than Whites.
1.2.3 Critique of Extant Research
When assessing ethnoracial differences in trusting personal physicians, most studies do
not assess multiple dimensions of patient-physician relationship as independent constructs.
Instead, studies often employ scales that treat multi-dimensional items of the patient-physician
relationship as reflecting a unidimensional trust construct (Anderson and Dedrick 1990; Hall,
Camacho et al. 2002; Kao et al. 1998). Multidimensional physician trust scales include
evaluations of both the technical and interpersonal aspects of the patient-physician. While such
evaluations may be tightly bound (Hall et al. 2001; Hall, Zheng, et al. 2002; Mechanic 1998;
Pearson and Raeke 2000), the social conditions of race independently shape the socioemotional
cues exchanged between practitioner and patient (Johnson et al. 2004). Race also differentiates
the likelihood that patients evaluate trust as a reflection of physician’s behaviors (Schnittker
10
2004). Thus, minorities may hold a great deal of respect for their doctors yet still not feel as if
their doctors really care about them.
In alignment with this critique, a number of researchers note that there may be
measurement variance across ethnoracial groups in the form of the underlying construct of trust
(Hall, Zheng et al. 2002; Perreira et al. 2003). In the case of physician trust, the form of an
underlying construct refers to the manifest indicators of physician trust that constitute the
standard Trust in Physician scale, which is multidimensional in nature and includes items tapping
both the values and competence ideals of the patient-physician relationship. This insight lays
open the possibility that specific dimensions of physician scales might evidence ethnoracial
differences in trust, even when scales as a whole do not (Hall, Camacho, et al. 2002). Notably,
Armstrong and colleagues (2008) show that the disaggregation thesis is useful for understanding
Black-White differences in trusting the health care system. They show that Blacks are less
trusting than Whites in the values of the health care system (e.g., whether the health care system
lies to make money and experiments on patients without them knowing) but equally trusting as
Whites are in the competence of the health care system. This kind of material/sociocultural
bifurcation is also evident in studies of patient satisfaction. For example, a study disaggregating
patient satisfaction scales illustrates that ethnoracial differences are most pronounced in
interpersonal assessments of the patient-physician relationship that reflect a physician’s
compassion for the patient rather than technical assessments of physicians (Jackson and George
1998). Yet, no studies have indicated that such a divide exists in studies of physician trust.
While no quantitative studies to date have assessed the role that ethnoraciality may have
on trusting the interpersonal component of the patient-physician relationship, there is ample
reason to believe that such a gap exists in regards to physician trust. First, focus group studies
11
suggest that the ability of physicians to demonstrate empathy and caring contributes to whether
Blacks and Latinos trust their physicians and view them as trustworthy (Jacobs et al. 2006;
Julliard et al 2008; Kaplan et al. 2006; Tucker et al. 2003). Second, Blacks and Latinos are more
likely than Whites to report they feel disrespected by their health care providers (Blanchard and
Lurie 2004). Third, studies indicate that Blacks and Latinos are less satisfied with the quality of
the care they receive from doctors (Doescher et al. 2003; LaVeist et al. 2000; Saha et al. 1999).
Fourth, studies show that minorities receive less quality communication than Whites: Physicians
are more likely to dominate conversations, less likely to speak of socioemotional topics, and less
likely to exchange positive affective tones with minority patients than with White patients
(Johnson et al. 2004; see also Cooper-Patrick et al. 1999; Julliard et al. 2008; Morales et al.
1999). Studies have shown that Latinos, particularly those with limited English proficiency, also
report poorer communication with regards to providers explaining things clearly, showing
respect, and spending time with a patient (Stepanikova et al. 2006; Tucker et al. 2003; Weech-
Maldonado et al. 2003). Fifth and finally, medical encounters with minority patients display less
signs of participatory decision-making than do medical encounters with White patients (Cooper-
Patrick et al. 1999).
1.3 Expected Relationships
This study expects that ethnoracial differences in trusting physicians and the health care
system should persist holding constant sociodemographic characteristics. Still, these cleavages
could partially account for ethnoracial differences in physician trust, since they serve as
resources that can be deployed to more effectively navigate medical encounters (Andersen and
Newman 1973). For example, male gender, lower socioeconomic status, and younger age are
linked to lower levels of trust in physicians (Doescher et al. 2000; Pearson and Raeke 2000; Tai-
Seale and Pescosolido 2003). A measure of parental nativity is employed to proxy the effects of
12
language problems and cultural dissonance (Stepanikova et al. 2006). Persons with two native
parents are expected to have higher levels of trust than persons with more than one non-native
parent. Engagement in religious and political organizations taps the extent to which individuals
are connected to and willing to seek help from institutions. For example, regular religious service
attendance and voluntary civic engagement are positively associated with both utilizing health
services and trusting physicians (Ahern and Hendryx 2003; Benjamins 2006; Hendryx et al.
2002). Demographic, religious, and political attributes are considered controls in the analyses.
Focusing on the English-speaking population, this study analyzes constituent items of a
standard Trust in Physician scale separately to characterize ethnoracial differences in medical
trust. Given past research suggesting that Blacks may display more negative affect towards the
disembodied health care system than to embodied personal physicians, this study hypothesizes
that Black-White differences in trusting the health care system will be larger than Black-White
differences in trusting personal physicians. Given the language and cultural barriers that Latinos
face and ethnoracial differences in demographic factors, this study hypothesizes that Latinos will
be less trusting than Whites of all aspects of the medical encounter – including extending trust to
physicians and the health care system. This study will also explore the extent to which Blacks
and Latinos hold dissimilar attitudes towards their physicians and the medical institution and the
factors responsible for Black-Latino trust differences. It is expected that Blacks and Latinos hold
similar trust views towards personal physicians; however, differences that may exist between the
groups should be an artifact of sociodemographic differences between the groups (e.g., Blacks
are less likely to have immigrant parents and therefore may hold more favorable attitudes
towards personal physicians than Latinos).
13
2. MATERIALS AND METHODS
2.1 Data
Data for this study come from the 2002 and 2006 General Social Surveys (GSS) conducted by
the National Opinion Research Center (Davis and Smith 2009). The 2002 and 2006 GSS used a
full probability sample of persons of 18 years of age or over living in non-institutional
arrangements within the 48 contiguous states of the U.S. In 2002, GSS only sampled English-
speaking persons. In 2006, GSS also sampled Spanish-speaking persons. Face-to-face interviews
of approximately 1½ hours were conducted between March and May of 2002 and 2006.
Assessments of general physicians are derived from a random sub-sample of 2,728 respondents
given questions from the Mental Health Module. An assessment of social attitudes towards
medicine is derived from random sub-samples of 2,792 respondents given rotating core questions
from the GSS Base Module. Final sample sizes are 2,558 for physician trust items (93.8% of
original sample) and 2,715 for the confidence in medicine item (97.2% of original sample).
Respondents with invalid data on the dependent and independent variables are excluded across
the two survey years. Respondents dropped from the analysis have less years of education and
are more likely to identify as Democrats (analysis available upon request). The response rate for
the 2002 GSS is 70.1 percent, while the response rate for the 2006 GSS is 71.2 percent.
2.1.1 Dependent Variables
Trust in physicians is measured by asking a series of statements about the medical care they are
receiving now (or would expect if they sought care). These are adapted from Anderson and
Dedrick’s (1990) Trust in Physician scale. A shortened scale is employed because only a limited
number of items gauging attitudes towards general physicians are asked in multiple years of the
GSS. Five conceptual dimensions of the patient-physician relationship are considered: Honesty;
Fiduciary Ethic; Technical Judgment; Cultural Authority; and Interpersonal Competence. The
14
Honesty dimension is assessed by agreement with the statement, “I trust my doctor to tell me if a
mistake was made about my treatment.” The Fiduciary Ethic dimension is assessed by agreement
with the statement, “I trust my doctor to put my medical needs above all other considerations
when treating my medical problem.” The Technical Judgment dimension is assessed by
agreement with the statement, “I trust my doctor’s judgment about my medical care.” The
Cultural Authority dimension is assessed by agreement with the statement, “My doctor is a real
expert in taking care of medical problems like mine.” The Interpersonal Competence dimension
is assessed by disagreement with the statement, “I doubt my doctor really cares about me as a
person.” Respondents were asked to answer questions concerning their primary care physicians,
as such it can be assumed that respondents answered questions about physician trust concerning
health care primarily for physical health conditions.
Each physician trust statement was coded originally on a 5-point scale (1=strongly agree,
2=agree, 3=neither agree nor disagree, 4=disagree, and 5=strongly disagree). Respondents’
answers were coded “don’t know” if they volunteered this response. Hence, these respondents
are dropped from subsequent analyses. Respondents who refused to provide a response to the
statements are also dropped from the analyses. Items are coded so that more positive responses
reflect more trust in physicians. Factor analysis of the five items does, in fact, indicate a single
underlying dimension with little variation in the factor loadings (Cronbach’s alpha (α) = .75). A
summary scale was constructed by dividing the sum of responses by five.
Evaluations of confidence in medicine are used to capture social attitudes towards the
health care system. GSS prompts [coding in brackets]: “I am going to name some institutions in
this country. As far as the people running these institutions are concerned, would you say you
have a great deal of confidence [3: High Trust], only some confidence [2: Middle Trust], or
15
hardly any confidence at all [1: Low Trust] in them?” Prior studies have employed GSS
confidence items to evaluate social attitudes towards institutions (Alesina and La Ferrara 2002;
Pescosolido et al. 2001). Table 1 presents descriptive statistics for all dependent variables.
[Table 1 about here]
2.1.2 Ethnoracial Group Membership
Racial group membership is measured by two mutually-exclusive dummy indicator variables –
Black non-Latino (herein referred to as “Black”) and any race Latino (herein referred to as
“Latino”). The reference category for each race dummy is White non-Latino. Ethnoracial group
membership is classified by the respondent using procedures followed in the decennial U.S.
Census. Fifteen percent of the sample is classified as Black, and eight percent of the sample is
classified as Latino.
2.1.3 Control Variables
To account for the time elapsed between survey years and for sources of measurement error
associated with differences in the coding of trust responses between the two surveys, a dummy
indicator for the 2002 survey year is included as a control variable (reference category = 2006
survey year) in all analyses. In the 2002 Mental Health module, the middle response category of
the trust statements was labeled “neither agree nor disagree” (instead of “uncertain”), and both
“agree” and “disagree” categories were preceded by “somewhat” (e.g., “somewhat agree”).
Supplemental analyses indicate that the survey year indicator could capture the effects of time
and survey measurement error. Though the effect of year was significant (F = 20.04, p < .001),
the effects of correlates of trust were consistent across years of the GSS (F = 0.67, p = .733).
Thus, the 2002 and 2006 GSS samples are pooled for the following analyses.
To assess the role of ethnoracial differences in sociodemographic correlates of trust,
covariates measured consistently for marital, work, and parental status, household size, gender,
16
age, education, subjective class identification, region, parental nativity, religious service
attendance, voting behavior, and political party affiliation are included (see Table 1). Measures
that tap sociodemographic differences between Blacks and Whites include marital status
(1=married, 0=other); work status (1=full-time worker, 0=other); parental status (1=have
children, 0=no children); household size (family sizes more than 10 collapsed into highest
category); gender (1=females, 0=males); age (1st and 2
nd order polynomial term for years of life
lived); education (years of school completed); a categorical measure of lower or working class
identification (reference category = middle or upper class); region (1=Southerner, 0=non-
Southerner); and parental nativity (1= has two native parents, 0 = has one or two non-native
parents). Ethnoracial differences in religiosity are measured using a 9-category ordinal variable
assessing frequency of religious service attendance (0=never, 1=less than one time a year,
2=about 1-2 times a year, 3=several times a year, 4=about once a month, 5=2-3 times a month,
6=nearly every week, 7=every week, 8=several times a week). Ethnoracial differences in
political factors are measured by voting behavior (1=ever voted, 0=never voted) and a
categorical measure of Democratic or Republican political party affiliation (reference category =
Independent or Other party). Sociodemographic variables are included as they may be
confounders of ethnoracial differences in physician trust (see Expected Relationships section of
Literature Review).
2.2 Methods of Analysis
This study examines ethnoracial differences in trust towards physicians using a shortened Trust
in Physician Scale and its constituent items (Anderson and Dedrick 1990). Trust in the health
care system is evaluated using a measure of confidence in leaders of institutions. Models for
ordered limited dependent variables are employed to hold constant the effects of ethnoracial
differences in demographic, political, and religious characteristics on the Trust in Physician
17
scale, the five (5) Trust in Physician items, and trust in the health care system medicine. Case
weights are used to adjust for differential sampling probabilities among individuals across survey
year (WTSSALL). Estimation procedures and hypothesis testing account for both probability
weights and robust standard errors.
First, this study examines unadjusted ethnoracial differences (Black non-Latino vs. White
non-Latino; any race Latino vs. White non-Latino) in trusting physicians and the health care
system with the dummy indicators for Black and Latino respondents. To compare the magnitude
of ethnoracial differences across trust items, the likelihood of affirming trust in physicians and
confidence in medicine is considered. The Unadjusted model includes an indicator of racial
group membership for Blacks and Latinos (Reference category: Whites). Second, ethnoracial
differences in trusting physicians and the health care system are examined, holding constant
sociodemographic characteristics. The Adjusted model includes controls for survey year, marital
status, full-time worker status, number of people in household, parental status, female sex, age &
age squared, years of education, subjective class status, Southern region, parental nativity,
religious service attendance, voting behavior, and political party affiliation. For the analytical
sample, listwise deletion on dependent and control variables are applied. The sample size for the
trust in physician items is 2,558, while the sample size for the trust in the health care system item
is 2,715. Sample sizes vary because the trust in the health care system item is a part of the
rotating core of the GSS and, thus, is not asked of all respondents in the topical modules.
Since the response categories for the trust outcomes are ordered, the appropriateness of
using nominal regression models is considered (Agresti 2010). A Brant test indicated that the
ordinal model violated the parallel regression assumption when assessing proportional odds due
to race (Long and Freese 2006) with regards to multiple dimensions of the patient-physician
18
relationship in one or both of the models considered. Accordingly, this study provides estimates
of racial differences in physician trust using a partial parallel lines regression model – otherwise
known as a partial generalized ordered logit model (Williams 2006) or the partial proportional
odds model (Peterson and Harrell 1990). Odds ratios are shown, where values above 1 indicate
more trust and values below 1 indicate less trust. T-statistics are in parentheses. Weighted
parameters are provided. Consistent parameters across comparison categories indicate that the
parallel lines assumption is not violated. Inconsistent parameters across comparison categories
indicate that the parallel lines assumption is violated and, thereby, suggests that an ordinal model
is inappropriate for analyzing a particular outcome.
The equation for the partial parallel lines regression model is:
where the β1 are the parallel line (equal slope) parameters, the β21…β1k are k vectors of
unequal slope (unconstrained) parameters, and the β3 are the constrained slope parameters
whose constraints are provided by the diagonal Γi matrix. According to this specification, the
parameters for ethnoraciality (coefficients indicating Black/White and Latino/White differences
in affirmative responses) can be either unconstrained or constrained. Consistent parameters
across comparison categories indicate that the parallel lines assumption is not violated at a 0.05
statistical significance level.
3. RESULTS
3.1 A Standard Scaling Approach
Table 2 provides estimates of ethnoracial differences in trust using a standard approach – the
Trust in Physician scale. The three ethnoracial groups assessed are referred to as Blacks (Black
non-Latinos), Whites (White non-Latinos), and Latinos (Latinos of any racial/ethnic group).
19
Weighted least squares regression provides mean differences in the scores from the trust scale
between Blacks and Whites and between Latinos and Whites. Using a standard scaling approach,
both Black-White and Latino-White differences in trust are in the expected direction – negative.
On average, Latinos and Blacks are less trusting of physicians than Whites. However, only
Latino-White trust differences are statistically significant (β=-0.20; p<0.001). The standard
scaling approach suggests that the Black-White trust gap is minute (less than a tenth of a
standard deviation change in the Trust in Physician scale), while the Latino-White gap is
substantial (almost a third of a standard deviation change in the Trust in Physician scale).
[Table 2 about here]
3.2 Disaggregation Approach
Table 2 also provides estimates of ethnoracial differences in trust using a disaggregation
approach – five Trust in Physician items. The Confidence in Medicine measure is a comparison
item that allows a reasonable expectation of what ethnoracial differences should look like were
(dis)trust in personal physicians to follow (dis)trust in the health care system. Using a
disaggregation approach, Black-White trust differences are in various directions; mostly, Black-
White trust differences are not statistically significant. The Black-White trust gap is significant
for two of the five dimensions of trust in physicians – fiduciary ethic and interpersonal
competence — and for the confidence in medicine measure. For each of these items, the parallel
lines assumption is violated. The violation of the parallel lines assumptions means that racial
gaps in physician trust are particularly salient for certain response categories in ways that refute a
linear representation of racial trust differences.
Overall, Blacks are less trusting than Whites that their physician will put their needs
above all else and that their physician cares about them as a person. They are also less likely than
Whites to affirm that leaders of the health care system should be extended confidence. The
20
violation of the parallel lines assumption indicates that Black-White differences in
trust/confidence are not consistent across all response categories – for example, Blacks are not
equally less likely to respond with “strong disagreement” in a physician’s fiduciary ethic as they
are “disagreement”. With regards to fiduciary ethic, for instance, Blacks are 63 percent less
likely than Whites to strongly disagree with the medical ideal that physicians put their patients
needs above all else. The implications of the parallel lines violation are important to consider.
Specifically, this substantial Black-White difference in the likelihood of strongly disagreement
with the fiduciary ethic of the patient-physician relationship is masked in traditional ordinal
models, as Black-White differences in affirming more positively worded response categories
(e.g., “disagreement”) are smaller in magnitude. Assumptions that the Black-White gap in
fiduciary ethic is the same regardless of what response categories are compared, then, would
result in an interpretation that Blacks and Whites emit similar views concerning this ideal of
medicine – a pattern that has been noted in previous research (Stepanikova et al. 2006).
Similarly, Black-White differences in the interpersonal confidence ideal of the patient-
physician relationship and in confidence towards leaders of medicine are largest along the most
negative category affirming trust. Together, these findings might suggest that Blacks are more
likely to express extreme negative responses in regards to specific medical ideals – that is, the
interpersonal efficaciousness of personal physicians and assessments of the overall health care
system. However, given that gaps in “strong agreement” are absent, these findings do not suggest
that Blacks are simply more likely to respond at the extreme ends of a response scale, as is
suggested might be an underlying phenomenon by Doescher and colleagues (2000). Rather, I
would conclude that they strongly disagree that physicians can be trusted in regards to aspects of
the patient-physician relationship that represent key faultlines of race and medicine. In other
21
words, these category-specific findings represent substantive realities, rather than mere
methodological constructions.
Using a disaggregation approach, most Latino-White trust differences are in the expected
direction. In fact, the Latino-White trust gap is significant for four of the five dimensions of
physician trust evaluated – fiduciary ethic, technical judgment, cultural authority, and
interpersonal competence. Yet, Latinos exhibit similar confidence levels towards leaders of
medicine as do Whites.
For the most part, Latino-White physician trust differences do not violate the parallel
lines assumptions. Regardless of the response category comparison, Latinos are less trusting than
Whites that their physicians put their needs above all else (OR = 0.62; Z = -3.57), that their
physician’s judgment is sound (OR = 0.59; Z = -3.66), and that their physician cares about them
as a person (OR = 0.51; Z = -4.54). The differences between Latinos and Whites along these
dimensions of the patient-physician relationship are large and substantial: Latinos are at least 40
percent less likely than Whites to exhibit trusting attitudes in these 3 ideals of the patient-
physician relationship.
Latinos’ views of the cultural authority of physicians, however, are more variegated.
Latinos are more likely than their White counterparts to express at least neutral/uncertain affect
about whether their personal physician is a scientific expert. However, they are less likely to
express strong affirmation for this aspect of the patient-physician relationship. A comparison of
the most extreme category of affirmation (“strongly agree”) indicates that Latino-White
differences in cultural authority are most similar to Latino-White differences in fiduciary ethic,
albeit more positive (Table 2). Overall, the parallel lines regression parameters speak to lower
levels of trust in the cultural authority of physicians among Latinos than among Whites.
22
Nonetheless, Latinos’ view the cultural authority of physicians more favorably than they do their
physicians’ fiduciary ethic, technical judgment, and interpersonal competence.
3.3 The Role of Ethnoracial Differences in Sociodemographic Correlates of Trust
Ethnoracial differences in sociodemographic characteristics play an important role in Latino-
White trust differences (Table 3). Together, Latinos’ younger age, lower levels of parental
nativity, and lower levels of civic participation situate Latinos as less trusting than Whites in the
omnibus physician trust scale and in affirmations that their physician will put their needs above
all else (fiduciary ethic). Once such factors are considered, Latino-White differences in trusting
the fiduciary ethic of personal physicians are reduced to non-significance.
[Table 3 about here]
Likewise, Black-White differences in having confidence in medicine are a function of
ethnoracial differences in sociodemographic factors. Specifically, Blacks’ lower levels of
education and lower likelihood of identifying as middle/upper class situate Blacks as less
confident in leaders of medicine than Whites. Once such factors are considered, Black-White
differences in trusting the health care system are reduced to non-significance.
However, ethnoracial differences in sociodemographic factors are not completely
responsible for ethnoracial differences in trusting medicine. For instance, while the Latino-White
gap in trusting whether one’s physician really cares about a patient as a person is reduced by
30%, the Latino-White gap remains significant (OR = 0.63; Z = -2.85). Similarly, the Latino-
White technical judgment gap is reduced by considering sociodemographic correlates of trust but
remains statistically significant (OR = 0.69; Z = -2.12).
Moreover, neither the magnitude nor significance of the Black-White interpersonal
competence gap is affected by ethnoracial differences in sociodemographic factors. Blacks
remain over 30 percent less likely to strongly affirm that their doctors really care about them as a
23
person. Furthermore, Blacks remain much less likely than Whites to endorse positive attitudes
towards the fiduciary ethic of the patient-physician relationship. For this dimension of physician
trust, the Black coefficient continues to violate the parallel lines assumption, which suggest that
the substantial gap between Blacks and Whites on this aspect of the medical encounter is not a
result of ethnoracial differences in sociodemographic factors.
In some aspects of the medical encounter, however, ethnoracial differences in trusting
physicians are more pronounced among sociodemographically-similar respondents. Holding
constant ethnoracial differences in demographic, religious, and political correlates of trust,
Blacks are less trusting of their physician’s technical judgment than Whites (OR = 0.67; Z = -
2.57). Among sociodemographically-similar respondents (especially, Blacks and Whites with
similar parental nativity status, Southern geographical residence, religious service attendance,
and political party affiliation), Blacks are 33 percent less likely than Whites to trust the technical
judgment of personal physicians. A summary of the effects of sociodemographic factors on
Black-White and Latino-White trust differences can be found in Table 4.
[Table 4 about here]
Supplementary analysis (available upon request) indicates that sociodemographic factors
account for differences in physician trust among ethnoracial minorities. Latinos are less trusting
of physicians than Blacks for the general Trust in Physician scale and for two of the five
dimensions of physician trust evaluated – fiduciary ethic and cultural authority. Yet, Latinos
exhibit more confidence in medicine than Blacks. The supplemental analysis indicates that
Black-Latino differences in trusting physicians and having confidence in medicine are a function
of ethnoracial differences in parental nativity. Specifically, Blacks and Latinos with two parents
born in the U.S. exhibit similar trust levels towards physicians and similar confidence levels
24
towards medicine. However, Latinos with one or more non-native parents report significantly
less trust and confidence than comparable Blacks. Thus, even differences in trust among
minorities are a function of factors related to ethnoracial stratification.
4. CONCLUSIONS
This study finds that ethnoracial physician trust gaps are variegated: They are contingent upon
the item used to epitomize the patient-physician relationship. The paper identifies assorted
Black-White and Latino-White differences in trusting personal physicians that obscures
ethnoracial differences in physician trust when standard scaling approaches are employed. While
ethnoracial inequalities and sources of identity are implicated in medical exchanges and
outcomes, past research offers mixed evidence for the direction and magnitude of the Black-
White and Latino-White gaps in trusting physicians and the health care system. No evidence for
the direction and magnitude of Black-Latino gaps in trusting such medical actors has been
provided. The findings reported here take the standard scale approach into consideration but
augments such analysis with a disaggregation approach. Overall, the paper speaks to the
importance of disaggregating physician trust scales to improve researchers’ abilities to
characterize ethnoracial gaps in trusting medical actors. Three findings are of import.
First, ethnoracial differences in trusting physicians have been thwarted by standard use of
a scaling approach. Primarily, a scaling approach aggregates dimensions of the patient-physician
relationship that evidenced countervailing directions for the Black-White trust in physicians gap.
In fact, the overall effect of Black ethnoracial group membership on physician trust was thwarted
by non-significant parameters, such as those represented by the dimensions of cultural authority,
technical judgment, and honesty. Moreover, overall Black-White differences are thwarted by
variance in the ethnoracial gap across ordered response categories, as was shown in the case of
25
the fiduciary ethic dimension. Higher levels of uncertainty/ambivalence among Blacks along the
fiduciary ethic and interpersonal competence dimensions of the patient-physician relationship
appear, in the linear model, as more positive affect. Yet, uncertainty/ambivalence itself is a
troubling indicator of disconnect between patient and physician – one that is more likely to occur
along certain dimensions for Blacks than for Whites. This study, then, is in line with, but
extends, a recent study of the GSS (Zheng 2015) showing that racial differences in attitudes
towards doctors are contingent upon the underlying issue scale items tap: Minorities are less
likely to believe that doctors are ethical but, depending on the measures employed, more or
equally likely to believe in the authority of doctors (Zheng 2015).
Second, aggregating dimensions of the patient-physician relationship disallows
researchers from identifying the domains of the medical encounter that are made problematic by
ethnoracial stratification. Similarly, given lower levels of trust in the health care system among
Blacks, compared to Whites, aggregating attitudes towards different medical stimuli also works
to obscure important information about how Blacks deploy trust as they navigate the health care
system. Importantly, Blacks and Latinos are less likely than Whites to believe that their doctors
really care about them as a person. Prior studies demonstrate that social distance processes
negatively influence the extent of mutual communication and understanding that occurs in cross-
racial patient-physician relationships with Black patients (Cooper-Patrick et al. 1999; Johnson et
al. 2004; Saha et al. 1999). However, no studies of trusting medical actors have assessed the
Black-White and Latino-White gaps along this dimension of the medical encounter. This study
indicates that minorities’ reduced trust in this aspect of the patient-physician relationship
represents a salient point of contention within medical exchanges. This study is in alignment
with studies reporting the disrespect minorities convey they feel from authority figures of
26
medicine (Blanchard and Lurie 2004). Moreover, this study is also in alignment with historical
studies that note that the expressive needs of Black patients are not met within the confines of the
traditional patient-physician relationship (Skipper, Wooldridge, and Leonard 1968).
Third, Latino-White differences in trusting physicians are substantial. They are even
more substantial than Black-White differences in trusting physicians. The Latino-White trust gap
is found consistently to be larger than the Black-White gap. Moreover, this study shows that
Black-Latino trust gaps are a function of ethnoracial differences in parental nativity, which is an
understudied component of ethnoracial stratification. These findings are in alignment with prior
studies that illustrate Latino-White fiduciary trust differences are larger among Spanish-speaking
respondents than among English-speaking respondents. These findings extend such research to
other dimensions of the medical encounter. These findings, particularly those regarding the
multivariate effect of parental nativity, are in alignment with scholars who note that linguistic
and cultural barriers serve to increase the social distance of Latinos from their physicians and
cultivate dissatisfaction with the quality of services (Julliard et al. 2008; Tucker et al. 2003).
Yet, these findings in regards to Latinos are surprising given extant research. Much of the
existing literature only discusses why minorities are less trusting than Whites, primarily focusing
on Black-White differences, and assumes consistency in distrust across dimensions of the
patient-physician relationship. In doing so, the previous literature has created homogenous non-
White ethnoracial groups (e.g., Zheng 2015), whereas the results of this study show important
forms of heterogeneity among minorities. These assumptions are, in part, an artifact of research
design, as most studies include only 2 or 3 ethnoracial groups or attend to ethnic differences
among racialized groups (e.g., the effect of language on Latino-White differences [Stepanikova
et al. 2006]). This study takes the perspective that ethnoracial differences in trust may exist for
27
different reasons for different ethnoracial groups (i.e., a legacy of historical abuse for Blacks and
cultural reasons for Latinos). In fact, Latino-White differences in physician trust may be larger
because Latinos are affected by the same factors as Blacks (e.g., deprived socioeconomic status),
as well as cultural factors mentioned in the manuscript (e.g., language). Overall, however, there
is no a priori reason in the extant literature to expect differences among ethnoracial minorities
nor is there a priori reason in the extant literature to expect inconsistencies in the ethnoracial
trust gap across dimensions of the patient-physician relationship. Previous research does,
however, find evidence of non-significant effects on specific dimensions of physician trust, such
as cultural authority (Pescosolido et al. 2001), and preliminary evidence that Latino-White
differences in fiduciary trust are larger than Black-White differences (Stepanikova et al. 2006).
This study, then, serves to buttress research that indicates similarities between ethnoracial
minorities and White and formally examines the magnitude of, and rationale for, the Black-
Latino gap in physician trust for an array of trust ideals. These non-differences and intragroup
minority gaps reflect substantive realities rather than pure methodological issues or spurious
effects.
There are several limitations to this study. First, the GSS includes a limited set of
variables to measure physician trust. For instance, a shortened Trust in Physician scale must be
employed, as only five items are asked in more than one wave of the GSS. These five items,
thus, can only provide singular indicators of the five dimensions of physician trust evaluated in
this study. Research would benefit from having multiple indicators of each of the five
dimensions of physician trust examined. Moreover, among these five items, only one of the
items was negatively worded – interpersonal competence, which is the dimension where the
largest ethnoracial differences were found. Perhaps, a scale that included more negatively
28
worded items would produce larger ethnoracial differences in physician trust, reflecting greater
affirmations of distrust rather than lower affirmations of trust among ethnoracial minorities.
Second, the GSS has traditionally been a sample of English-speaking adults. However, in
2006, the Spanish-speaking population was also sampled. Research indicates that physician trust
levels are lower among Latinos who are Spanish-speaking (Stepanikova et al. 2006). A similar
relationship may also exist among non-English speaking Blacks. For instance, it is possible that
lower levels of trust among Latinos are a function of the fact that they are more likely to be
Spanish-speaking. The fact that Black-Latino differences in trust were found to be a function of
parental nativity speaks to this possibility somewhat. Latinos with one or more parents born
outside the U.S. may be more likely to speak Spanish. However, neither of these patterns could
be evaluated with this study, as a Spanish-speaking indicator could only be ascertained in one of
the two waves of the GSS assessed.
Third, while the GSS does have indicators of nationality that would allow a
disaggregation of both ethnoracial groups along this important dimension of ethnicity, sample
sizes are too small to evaluate ethnoracial group by nation-state background. For instance, there
are less than 200 Latinos in the final sample of this study, which covers two waves of the GSS.
While Latinos can be further classified by whether they are descendants of Cuba, Mexico, Puerto
Rico, or another Latin American country, any further disaggregation of this ethnoracial group by
nation-state background reduces the power to detect differences substantially. Research would
benefit from having a larger sample of ethnoracial minorities assessed Trust in Physician items.
Fourth, there are a number of missing variables of importance to a study of ethnoracial
differences in physician trust. Namely, affirmations of physician trust vary by type of health
insurance, usual source of care, continuity of care, and health literacy (Doescher et al. 2000; Hall
29
et al. 2001; Hall, Zheng et al. 2002; Kao et al. 1998; Lee and Lin 2010). For instance, the insured
tend to report higher levels of trust in physicians and the health care system, but ethnoracial
minorities are less likely to be insured (Doescher et al. 2000; Smedley, Stith, and Nelson 2003).
Accordingly, the ethnoracial differences in trust identified through the disaggregation approach
could, in fact, represent ethnoracial differences in health insurance status. However, the GSS did
not ascertain health insurance information from the sample of respondents asked the physician
trust. Moreover, the GSS does not ascertain usual source of care, the recentness/frequency of
visits to a personal physician in the past year, or health literacy of the same respondents who
were provided physician trust items. As such, the analysis is limited by the larger research
design. Research would benefit from examining whether health care quality, broadly speaking,
or health literacy are mediating factors of ethnoracial differences in physician trust.
In sum, this analysis uncovers a notable degree of complexity in ethnoracial trust gaps
among Whites, Blacks, and Latinos. A theory of race and trust is proposed based on the findings
of the study: The presence of ethnoracial differences along specific dimensions of the patient-
physician relationship reflects the ways that ethnoracial stratification transform standard health
care processes. Studies indicate that power-imbalances within most medical encounters are most
likely to impact interpersonal aspects of the medical visit that hinge upon the communication
skills of physicians. Trust is developed only in the presence of mutual respect and personalizing
interactions that demonstrate a physician cares about a minority patient and has compassion for
the social problems he or she is encountering (Kaplan et al. 2006; Sheppard, Zambrana, and
O’Malley 2004). The hierarchical nature of medical encounters makes communication a key
component of the patient-physician relationship that can build or destroy trust (Cook et al. 2004;
van Ryn 2002). The implications of these findings for understanding power-imbalanced
30
dynamics in other institutions that rely on communication (e.g., pedestrian-policeman, student-
teacher, defendant-judge) are important to explore.
What do the findings mean as it relates to improving racial disparities in health care
utilization? A key point made by Bonilla-Silva (1997) is extended to the study of physician trust:
Since a racialized social system fosters distinct ideological and cultural meanings of institutions
and individuals, ethnoracial inequality is inscribed into institutional processes through the
manners in which race shapes components of interaction. Notably so, ethnoracial differences in
physician trust were largest along the interpersonal competence dimension of the medical
encounter. Accordingly, these findings suggest that patients’ perceptions of the interpersonal
competence of physicians are a key contributor to ethnoracial inequities in utilization. Because
ethnoracial minorities are more likely to believe that physicians do not care about them as a
person, they may be less likely to seek help for medical problems, comply and adhere to
physician’s orders, and persist with difficult treatments. In this way, ethnoracial differences in
utilization patterns may reflect the disconnection minority patients feel from their doctor, rather
than mere cultural beliefs. To alleviate the disconnection that ethnoracial minorities exhibit with
the health care system, attention must be paid not only to developing cultural-sensitivity among
doctors, but also to developing an anti-racist praxis from which physicians treat patients.
How ethnoracial minority patients navigate the health care system reflects how they
perceive the interactions within the health care system. The patient-physician relationship is not
unlike intergroup interactions that may occur outside of the medical system, which suffer from
miscues and biases that concretize the social distance between minorities and whites. Future
research would benefit from employing stratified samples and/or interaction terms to assess
heterogeneity among Blacks and Latinos in both levels of trust and factors that mediate trust.
31
Future research would also benefit from methodological designs that ascertain both physician
race and multi-dimensional trust. Research designs should also include a larger sample of Blacks
and Latinos to assess multi-dimensional trust scales. Moreover, future research would benefit by
more clearly delineating the ways that the interpersonal competence of doctors can be improved
using a culturally-sensitive, anti-racist lens towards the care of the ethnoracially marginalized.
ACKNOWLEDGMENTS: The paper was supported by a National Science Predoctoral Fellowship, a
Ford Foundation Predoctoral Fellowship, and a Ronald E. McNair Graduate Fellowship to the author while in the Department of Sociology at Indiana University and a Vice Provost’s Postdoctoral Fellowship
to the author while in the Population Studies at the University of Pennsylvania. A previous draft of this
paper was the winner of the 2008 Graduate Student Paper Competition for the Health, Health Policy, and Health Services Division of the Society for the Study of Social Problems (SSSP).
32
5. REFERENCES
Agresti, Alan. 2010. Analysis of Ordinal Categorical Data, 2nd Edition. New York: John Wiley &
Sons.
Ahern, Melissa M., and Michael S. Hendryx. 2003. "Social Capital and Trust in Providers." Social
Science and Medicine 57:1195-203.
Alesina, Alberto, and Eliana La Ferrara. 2002. "Who Trusts Others?" Journal of Public Economics
85:207-234.
Andersen, Ronald and John F. Newman. 1973. "Societal and Individual Determinants of Medical
Care Utilization in the United States." The Milbank Memorial Fund Quarterly 51:95-124.
Anderson, Lynda A., and Robert F. Dedrick. 1990. "Development of the Trust in Physician Scale: A
Measure to Assess Interpersonal Trust in Patient-Physician Relationships." Psychological
Reports 67:1091-100.
Armstrong, Katrina, Suzanne McMurphy, Lorraine Dean, Ellyn Micco, Mary Putt, Chanita Halbert,
J. Schwartz, Pamela Sankar, Reed Pyeritz, Barbara Bernhardt, and Judy Shea. 2008.
"Differences in the Patterns of Health Care System Distrust Between Blacks and Whites."
Journal of General Internal Medicine 23:827-833.
Armstrong, Katrina, Abigail Rose, Nikki Peters, Judith A. Long, Suzanne McMurphy, and Judy A.
Shea. 2006. "Distrust of the Health Care System and Self-Reported Health in the United
States." Journal of General Internal Medicine 21:292-297.
Barefoot, John C., Kimberly E. Maynard, Jean C. Beckham, Beverly H. Brummett, Karen Hooker,
Ilene C. Siegler. 1998. “Trust, Health, and Longevity.” Journal of Behavioral Medicine
21:517-526.
Beardsley, Edward H. 1987. A History of Neglect: Health Care for Blacks and Mill Workers in the
33
Twentieth-Century South. Knoxville: University of Tennessee Press.
Benjamin, Ruha. 2013. People’s Science: Bodies and Rights on the Stem Cell Frontier. Stanford,
CA: Stanford University Press.
Benjamins, Maureen R. 2006. "Religious Influences on Trust in Physicians and the Health Care
System." International Journal of Psychiatry in Medicine 36:69-83.
Betancourt, Joseph R., Alexander R. Green, J. Emilio Carrillo, and Owusu Ananeh-Firempong, II.
2003. "Defining Cultural Competence: A Practical Framework for Addressing Racial/Ethnic
Disparities in Health and Health Care." Public Health Reports 118:293-302.
Blanchard, Janice, and Nicole Lurie. 2004. "R-E-S-P-E-C-T: Patient Reports of Disrespect in the
Health Care Setting and Its Impact on Care." Journal of Family Practice 53:721-30.
Blendon, Robert J., Linda H. Aiken, Howard E. Freeman, and Christopher R. Corey. 1989. “Access
to Medical Care for Black and White Americans: A Matter of Continuing Concern.” JAMA
261:278-281.
Bonilla-Silva, Eduardo. 1997. "Rethinking Racism: Toward a Structural Interpretation." American
Sociological Review 62:465-480.
Boulware, L. Ebony, Lisa A. Cooper, Lloyd E. Ratner, Thomas A. LaVeist, and Neil R. Powe. 2003.
"Race and Trust in the Health Care System." Public Health Reports 118:358-65.
Caronna, Carol A. 2011. "Clash of Logics, Crisis of Trust: Entering the Era of Public For-Profit
Health Care?" Pp. 255-270 in Handbook of the Sociology of Health, Illness, and Healing,
Handbooks of Sociology and Social Research, edited by Bernice A. Pescosolido, Jack K.
Martin, Jane D. McLeod, and Anne Rogers. New York: Springer.
Cook, Karen S., Roderick M. Kramer, David H. Thom, Irena Stepanikova, Stefanie B. Mollborn, and
Robin M. Cooper. 2004. "Trust and Distrust in Patient-Physician Relationships: Perceived
34
Determinants of High- and Low-Trust Relationships in Managed-Care Settings." Pp. 65-98 in
Trust and Distrust in Organizations: Dilemmas and Approaches, edited by Roderick M.
Kramer and Karen S. Cook. New York: Russell Sage Foundation.
Cooper-Patrick, Lisa, Joseph J. Gallo, Junius J. Gonzales, Hong T. Vu, Neil R. Powe, Christine
Nelson, and Daniel E. Ford. 1999. "Race, Gender, and Partnership in the Patient-Physician
Relationship." JAMA: The Journal of the American Medical Association 282:583-9.
Corbie-Smith, Giselle, Stephen B. Thomas, and Diane Marie St. George. 2002. "Distrust, Race, and
Research." Archives of Internal Medicine 162:2458-2463.
Davis, James Allan, and Tom W. Smith. 2009. General Social Surveys, 1972-2008. Chicago:
National Opinion Research Center.
Diala, Chamberlain, Carles Muntaner, Christine Walrath, Kim J. Nickerson, Thomas A. LaVeist, and
Philip J. Leaf. 2000. "Racial Differences in Attitudes toward Professional Mental Health Care
and in the Use of Services." American Journal of Orthopsychiatry 70:455-464.
Doescher, Mark P., Barry G. Saver, Peter Franks, and Kevin Fiscella. 2000. "Racial Disparities in
Perceptions of Physician Style and Trust." Archives of Family Medicine 9:1156-1163.
Echeverry, John J. 1997. "Treatment Barriers: Accessibility and Accepting of Professional Help." Pp.
94-107 in Psychological interventions and research with Latino populations, edited by Jorge
G. García and Maria C. Zea. Boston: Allyn and Bacon.
Freimuth, Vicki S., Sandra C. Quinn, Stephen B. Thomas, Galen Cole, Eric Zook, and Ted Duncan.
2001. “African Americans’ Views on Research and the Tuskegee Syphilis Study.” Social
Science and Medicine 52:797-808.
Gamble, Vanessa N. 1997. "Under the Shadow of Tuskegee: African Americans and Health Care."
American Journal of Public Health 87:1773-1778.
35
Gilson, Lucy. 2003. "Trust and the Development of Health Care as a Social Institution." Social
Science and Medicine 56:1453-1468.
Guffey, Thomas and Philip Q. Yang. 2012. “Are African Americans Less Likely to Trust Their
Doctors Than Whites?” SAGE Open 2: DOI: 10.1177/2158244012466092
Hall, Mark A., Fabian Camacho, Elizabeth Dugan, and Rajesh Balkrishnan. 2002. "Trust in the
Medical Profession: Conceptual and Measurement Issues." Health Services Research 37:1419-
39.
Hall, Mark A., Elizabeth Dugan, Beiyao Zheng, and Aneil K. Mishra. 2001. "Trust in Physicians and
Medical Institutions: What Is It, Can It Be Measured, and Does It Matter?" The Milbank
Memorial Fund Quarterly 79:613-639.
Hall, Mark A., Fabian Camacho, Elizabeth Dugan, and Rajesh Balkrishnan. 2002. “Trust in the
Medical Profession: Conceptual and Measurement Issues.” Health Services Research 37:1419-
39.
Hall, Mark A., Beiyao Zheng, Elizabeth Dugan, Fabian Camacho, Kristin E. Kidd, Aneil Mishra, and
Rajesh Balkrishnan. 2002. "Measuring Patients’ Trust in their Primary Care Providers."
Medical Care Research and Review 59:293-318.
Hendryx, Michael S., Melissa M. Ahern, Nicholas P. Lovrich, and Arthur H. McCurdy. 2002.
"Access to Health Care and Community Social Capital." Health Services Research 37:87-103.
Hughes-Halbert, Chanita, Katrina Armstrong, Oscar H. Gandy, Jr, and Lee Shaker. 2006. "Racial
Differences in Trust in Health Care Providers." Archives of Internal Medicine 166:896-901.
Jackson, Pamela Braboy, and Linda K. George. 1998. "Racial Differences in Satisfaction with
Physicians: A Study of Older Adults." Research on Aging 20:298-316.
Jacobs, Elizabeth A., Italia Rolle, Carol Estwing Ferrans, Eric E. Whitaker, and Richard B.
36
Warnecke. 2006. "Understanding African Americans' Views of the Trustworthiness of
Physicians." Journal of General Internal Medicine 21:642-647.
Johnson, Rachel L., Debra Roter, Neil R. Powe, and Lisa A. Cooper. 2004. "Patient Race/Ethnicity
and Quality of Patient-Physician Communication During Medical Visits." American Journal of
Public Health 94:2084-2090.
Jones, James H. 1981. Bad Blood: The Tuskegee Syphilis Experiment. New York: Free Press.
Julliard, Kell, Josefina Vivar, Carlos Delgado, Eugenio Cruz, Jennifer Kabak, and Heidi Sabers.
2008. "What Latina Patients Don't Tell Their Doctors: A Qualitative Study." Annals of Family
Medicine 6:543-549.
Kao, Audiey C., Diane C. Green, Alan M. Zaslavsky, Jeffrey P. Koplan, and Paul D. Cleary. 1998.
"The Relationship Between Method of Physician Payment and Patient Trust." JAMA: The
Journal of the American Medical Association 280:1708-1714.
Kaplan, Sue A., Neil S. Calman, Maxine Golub, Joyce H. Davis, Charmaine Ruddock, and John
Billings. 2006. "Racial Disparities in Health: A View from the South Bronx." Journal of
Health Care for the Poor and Underserved 17:116-127.
King, Gary. 1996. "Institutional Racism and the Medical/Health Complex: A Conceptual Analysis."
Ethnicity and Disease 6:30-46.
Kramer, Roderick Moreland, and Karen S. Cook. 2004. Trust and Distrust in Organizations:
Dilemmas and Approaches. New York: Russell Sage Foundation.
LaVeist, Thomas A., Kim J. Nickerson, and Janice V. Bowie. 2000. "Attitudes about Racism,
Medical Mistrust, and Satisfaction with Care among African American and White Cardiac
Patients." Medical Care Research and Review 57:146-161.
Lee, Yin-Yang and Julia L. Lin. 2010. “Do Patient Autonomy Preferences Matter? Linking Patient-
37
Centered Care to Patient-Physician Relationships and Health Outcomes.” Social Science and
Medicine 71:1811-1818.
Levinson, Wendy, Audiey Kao, Alma M. Kuby, and Ronald A. Thisted. 2005. "The Effect of
Physician Disclosure of Financial Incentives on Trust." Archives of Internal Medicine
165:625-630.
Lillie-Blanton, Marsha, Mollyann Brodie, Diane Rowland, Drew Altman, and Mary McIntosh. 2000.
"Race, Ethnicity, and the Health Care System: Public Perceptions and Experiences." Medical
Care Research and Review 57:218-235.
Link, Bruce G., and Jo Phelan. 1995. "Social Conditions As Fundamental Causes of Disease."
Journal of Health and Social Behavior 35:80-94.
Long, J. Scott, and Jeremy Freese. 2006. Regression Models for Categorical Dependent Variables
Using Stata. College Station, TX: Stata Press.
McGorry, Susan Y. 1999. "An Investigation of Expectations and Perceptions of Health-Care
Services with a Latino Population." International Journal of Health Care Quality Assurance
12:190-198.
Mechanic, David. 1998. "The Functions and Limitations of Trust in the Provision of Medical Care."
Journal of Health Politics, Policy and Law 23:661-86.
Morales, Leo S., William E. Cunningham, Julie A. Brown, Honghu Liu, and Ron D. Hays. 1999.
"Are Latinos Less Satisfied with Communication by Health Care Providers?" Journal of
General Internal Medicine 14:409-417.
Musick, Mark A. and Meridith G. Worthen. 2008. “The Social Underpinnings of Trust.” Research in
the Sociology of Health Care 25:97-123.
Omi, Michael, and Howard Winant. 1994. Racial Formation in the United States: From the 1960s to
38
the 1990s. New York: Routledge.
Nelson, Alondra. 2011. Body and Soul: The Black Panther Party and the Fight Against Medical
Discrimination. Minneapolis, MN: University of Minnesota Press.
Parsons, Talcott. 1951. The Social System. New York: Free Press.
Patel, Mitesh S., and Michael E. Chernew. 2007. "The Impact of the Adoption of Gag Laws on Trust
in the Patient-Physician Relationship." Journal of Health Politics, Policy and Law 32:819-42.
Pearson, Steven D., and Lisa H. Raeke. 2000. "Patients' Trust in Physicians: Many Theories, Few
Measures, and Little Data." Journal of General Internal Medicine 15:509-513.
Perreira, Krista M., Natalia Deeb-Sossa, Kathleen Mullan Harris, and Kenneth Bollen. 2005. "What
Are We Measuring? An Evaluation of the CES-D across Race/Ethnicity and Immigrant
Generation." Social Forces 83:1567-1601.
Pescosolido, Bernice A., Steven A. Tuch, and Jack K. Martin. 2001. "The Profession of Medicine
and the Public: Examining Americans' Changing Confidence in Physician Authority from the
Beginning of the 'Health Care Crisis' to the Era of Health Care Reform." Journal of Health and
Social Behavior 42:1-16.
Peterson, Bercedis L. and Harrell, Frank E., Jr. 1990. “Partial Proportional Odds Models for Ordinal
Response Variables.” Journal of the Royal Statistical Society, Series B 39:205–217.
Reverby, Susan M. 2011. “ ‘Normal Exposure’ and Inoculation Syphilis: A PHS ‘Tuskegee’ Doctor
in Guatemala, 1946-1948.” Journal of Policy History 23:6-28.
Ross, Catherine E., John Mirowsky, and Shana Pribesh. 2001. "Powerlessness and the Amplification
of Threat: Neighborhood Disadvantage, Disorder, and Mistrust." American Sociological
Review 66:568-591.
Saha, Somnath, Miriam Komaromy, Thomas D. Koepsell, and Andrew B. Bindman. 1999. "Patient-
39
Physician Racial Concordance and the Perceived Quality and Use of Health Care." Archives of
Internal Medicine 159:997-1004.
Schlesinger, Mark. 1987. "Paying the Price: Medical Care, Minorities, and the Newly Competitive
Health Care System." The Milbank Quarterly 65:270-296.
Schnittker, Jason. 2004. "Social Distance in the Clinical Encounter: Interactional and
Sociodemographic Foundations for Mistrust in Physicians." Social Psychology Quarterly
67:217-235.
Schnittker, Jason, and Ke Liang. 2006. "The Promise and Limits of Racial/Ethnic Concordance in
Physician-Patient Interaction." Journal of Health Politics, Policy and Law 31(4):811-38.
Sheppard, Vanessa B, Ruth E. Zambrana, and Ann S. O'Malley. 2004. "Providing Health Care to
Low-Income Women: A Matter of Trust." Family Practice 21:484-491.
Shoff, Carla and Tse-Chuan Yang. 2012. “Untangling the Associations among Distrust, Race, and
Neighborhood Social Environment: A Social Disorganization Perspective.” Social Science and
Medicine 74: 1342-1352.
Skipper, James K., Powhatan J. Wooldridge, and Robert C. Leonard. 1968. “Race, Status, and
Interaction between Patients and Hospital Personnel.” The Sociological Quarterly 9:35-46.
Smedley, Brian D., Adrienne Y. Stith, and Alan R. Nelson. 2003. Unequal Treatment: Confronting
Racial Disparities in Health Care. Washington, D.C.: National Academy Press.
Smith, Sandra S. 2010. "Race and Trust." Annual Review of Sociology 36:453-475.
Sohler, Nancy Lynn, Lisa K. Fitzpatrick, Rebecca G. Lindsay, Kathryn Anastos, and Chinazo O.
Cunningham. 2007. “Does Patient-Provider Racial/Ethnic Concordance Influence Ratings of
Trust in People with HIV Infection?” AIDS and Behavior 11:884-896.
Stepanikova, Irena, Stefanie Mollborn, Karen S. Cook, David H. Thom, and Roderick M. Kramer.
40
2006. "Patients' Race, Ethnicity, Language, and Trust in a Physician." Journal of Health and
Social Behavior 47:390-405.
Tai-Seale, Ming, and Bernice A. Pescosolido. 2003. "The Public's Opinions of Physicians: Do
Perceived Choice and Exercised Choice Matter?" American Journal of Managed Care 9:631-
8.
Thomas, Stephen B. and James W. Curran. 1999. “Tuskegee: From Science to Conspiracy to
Metaphor.” American Journal of Medical Sciences 317:1-4.
Tucker, Carolyn M., Keith C. Herman, Tyler R. Pedersen, Brian Higley, May Montrichard, and
Phyllis Ivery. 2003. "Cultural Sensitivity in Physician-Patient Relationships: Perspectives of an
Ethnically Diverse Sample of Low-Income Primary Care Patients." Medical Care 41:859-870.
van Ryn, Michelle. 2002. "Research on the Provider Contribution to Race/Ethnicity Disparities in
Medical Care." Medical Care 40:I140-I151.
Washington, Harriet A. 2006. Medical Apartheid: The Dark History of Medical Experimentation on
Black Americans from Colonial Times to the Present. New York: Doubleday.
Weech-Maldonado, Robert, Leo S. Morales, Marc Elliott, Karen Spritzer, Grant Marshall, and Ron
D. Hays. 2003. "Race/Ethnicity, Language, and Patients' Assessments of Care in Medicaid
Managed Care." Health Services Research 38:789-808.
Whaley, Arthur L. 1998. "Cross-Cultural Perspective on Paranoia: A Focus on the Black American
Experience." Psychiatric Quarterly 69:325-343.
Whetten, Kathryn, Jane Leserman, Rachel Whetten, Jan Ostermann, Nathan Thielman, Marvin
Swartz, and Dalene Stangl. 2006. "Exploring Lack of Trust in Care Providers and the
Government as a Barrier to Health Service Use." American Journal of Public Health 96:716-
721.
41
White, Robert M. 2005. “Misinformation and Misbeliefs in the Tuskegee Study of Untreated
Syphilis Fuel Mistrust in the Healthcare System.” Journal of the National Medical Association
97:1566-1573.
Williams, Richard. 2006. “Generalized Ordered Logit/Partial Proportional Odds Models for Ordinal
Dependent Variables.” Stata Journal 6: 58–82.
Zheng, Hui. 2015. "Losing Confidence in Medicine in an Era of Medical Expansion?" Social Science
Research 52:701-15.
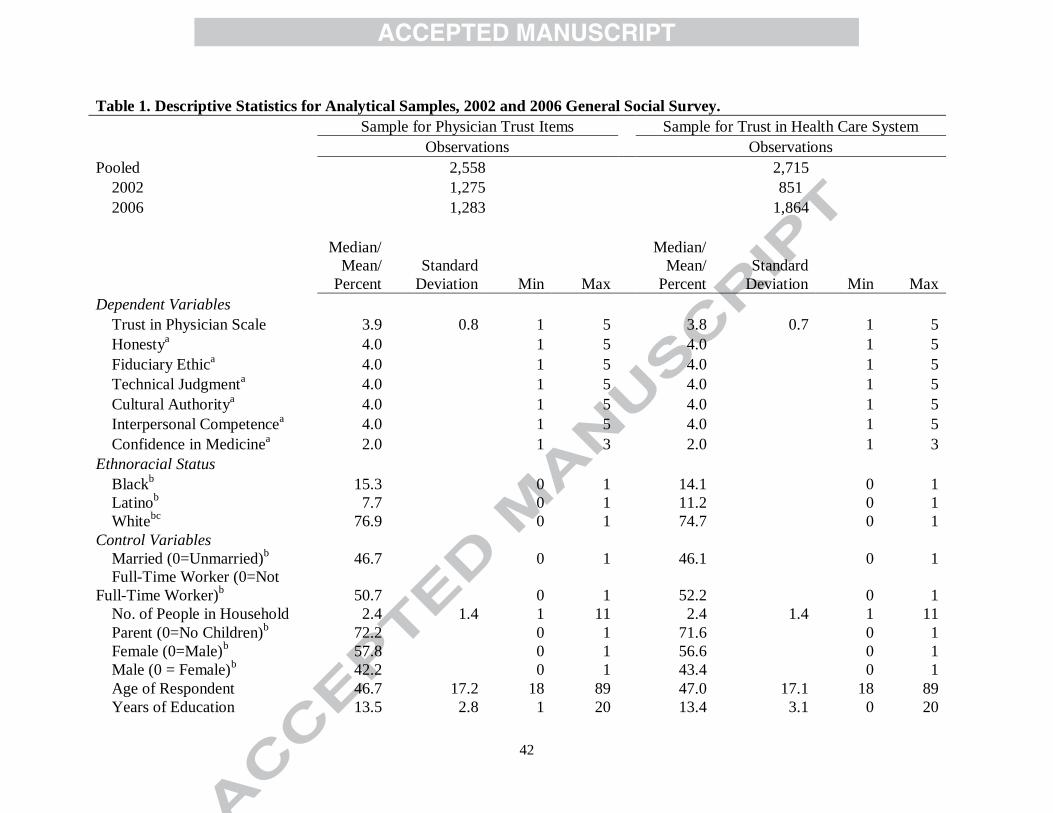
42
Table 1. Descriptive Statistics for Analytical Samples, 2002 and 2006 General Social Survey.
Sample for Physician Trust Items
Sample for Trust in Health Care System
Observations Observations
Pooled 2,558
2,715
2002 1,275
851
2006 1,283
1,864
Median/
Mean/
Percent
Standard
Deviation Min Max
Median/
Mean/
Percent
Standard
Deviation Min Max
Dependent Variables
Trust in Physician Scale 3.9
0.8
1
5
3.8
0.7
1
5
Honestya 4.0
1
5
4.0
1
5
Fiduciary Ethica 4.0
1
5
4.0
1
5
Technical Judgmenta 4.0
1
5
4.0
1
5
Cultural Authoritya 4.0
1
5
4.0
1
5
Interpersonal Competencea 4.0
1
5
4.0
1
5
Confidence in Medicinea 2.0
1
3
2.0
1
3
Ethnoracial Status
Blackb 15.3
0
1
14.1
0
1
Latinob 7.7
0
1
11.2
0
1
Whitebc
76.9
0
1
74.7
0
1
Control Variables
Married (0=Unmarried)b 46.7
0
1
46.1
0
1
Full-Time Worker (0=Not
Full-Time Worker)b 50.7
0
1
52.2
0
1
No. of People in Household 2.4
1.4
1
11
2.4
1.4
1
11
Parent (0=No Children)b 72.2
0
1
71.6
0
1
Female (0=Male)b 57.8
0
1
56.6
0
1
Male (0 = Female)b 42.2
0
1
43.4
0
1
Age of Respondent 46.7
17.2
18
89
47.0
17.1
18
89
Years of Education 13.5
2.8
1
20
13.4
3.1
0
20
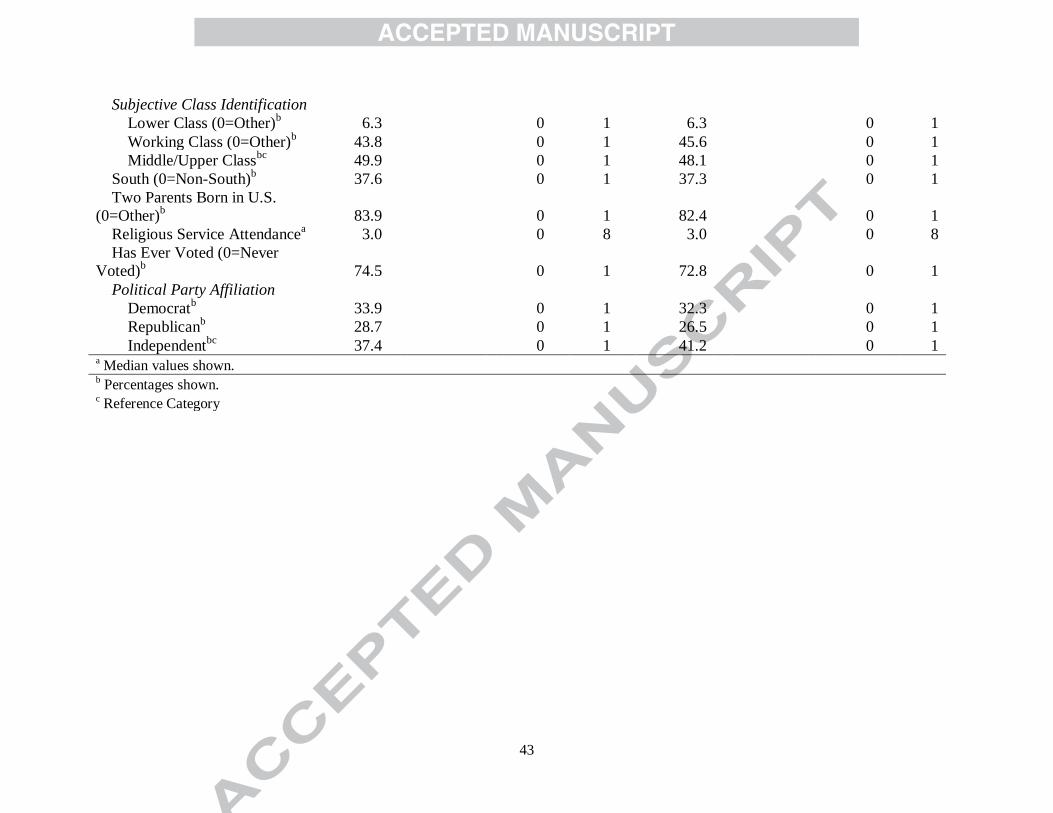
43
Subjective Class Identification
Lower Class (0=Other)b 6.3
0
1
6.3
0
1
Working Class (0=Other)b 43.8
0
1
45.6
0
1
Middle/Upper Classbc
49.9
0
1
48.1
0
1
South (0=Non-South)b 37.6
0
1
37.3
0
1
Two Parents Born in U.S.
(0=Other)b 83.9
0
1
82.4
0
1
Religious Service Attendancea 3.0
0
8
3.0
0
8
Has Ever Voted (0=Never
Voted)b 74.5
0
1
72.8
0
1
Political Party Affiliation
Democratb 33.9
0
1
32.3
0
1
Republicanb 28.7
0
1
26.5
0
1
Independentbc
37.4
0
1
41.2
0
1 a Median values shown.
b Percentages shown.
c Reference Category

44
Table 2. Regression of Trust in Medical Actors on Ethnoracial Group Status: 2002 and 2006 General Social Survey.
Unadjusted
Beta/SE
Trust in Physician Scale (N = 2,558)
Black -0.06
(0.04)
Latino -0.23 *
(0.05)
Greater than Strongly Disagree Greater than Disagree
Greater than Neither/Uncertain Greater than Agree
OR/Z OR/Z OR/Z OR/Z
Trust in Physician Items (N = 2,558)
Honesty Black 1.02
1.02
1.02
1.02
(0.15)
(0.15)
(0.15)
(0.15)
Latino 0.79
0.79
0.79
0.79
(-1.52)
(-1.52)
(-1.52)
(-1.52)
Fiduciary Ethic
Black 0.37 * 0.89
0.78
0.96
(-2.52)
(-0.50)
(-1.40)
(-0.26) Latino 0.62 *** 0.62 *** 0.62 *** 0.62 ***
(-3.57)
(-3.57)
(-3.57)
(-3.57)
Technical Judgment Black 0.78
0.78
0.78
0.78
(-1.82)
(-1.82)
(-1.82)
(-1.82)
Latino 0.59 *** 0.59 *** 0.59 *** 0.59 ***
(-3.66)
(-3.66)
(-3.66)
(-3.66)
Cultural Authority
Black 1.15
1.15
1.15
1.15
(1.16)
(1.16)
(1.16)
(1.16) Latino 1.42
2.51 * 1.14
0.65 *
(0.48)
(2.36)
(0.68)
(-2.10)
Interpersonal Competence
Black 0.44 *** 0.72 * 0.66 ** 0.72 *
(-3.56)
(-2.14)
(-3.10)
(-2.28)
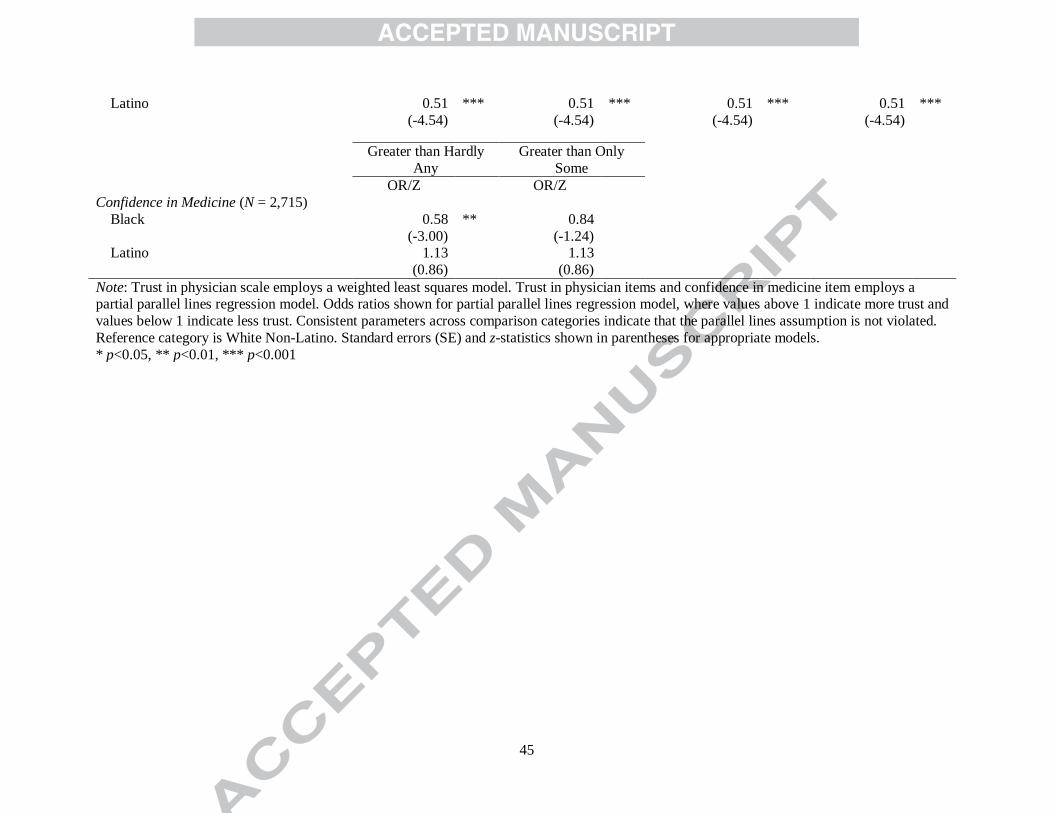
45
Latino 0.51 *** 0.51 *** 0.51 *** 0.51 ***
(-4.54)
(-4.54)
(-4.54)
(-4.54)
Greater than Hardly
Any
Greater than Only
Some
OR/Z
OR/Z
Confidence in Medicine (N = 2,715)
Black 0.58 ** 0.84
(-3.00)
(-1.24) Latino 1.13
1.13
(0.86)
(0.86)
Note: Trust in physician scale employs a weighted least squares model. Trust in physician items and confidence in medicine item employs a partial parallel lines regression model. Odds ratios shown for partial parallel lines regression model, where values above 1 indicate more trust and
values below 1 indicate less trust. Consistent parameters across comparison categories indicate that the parallel lines assumption is not violated.
Reference category is White Non-Latino. Standard errors (SE) and z-statistics shown in parentheses for appropriate models.
* p<0.05, ** p<0.01, *** p<0.001
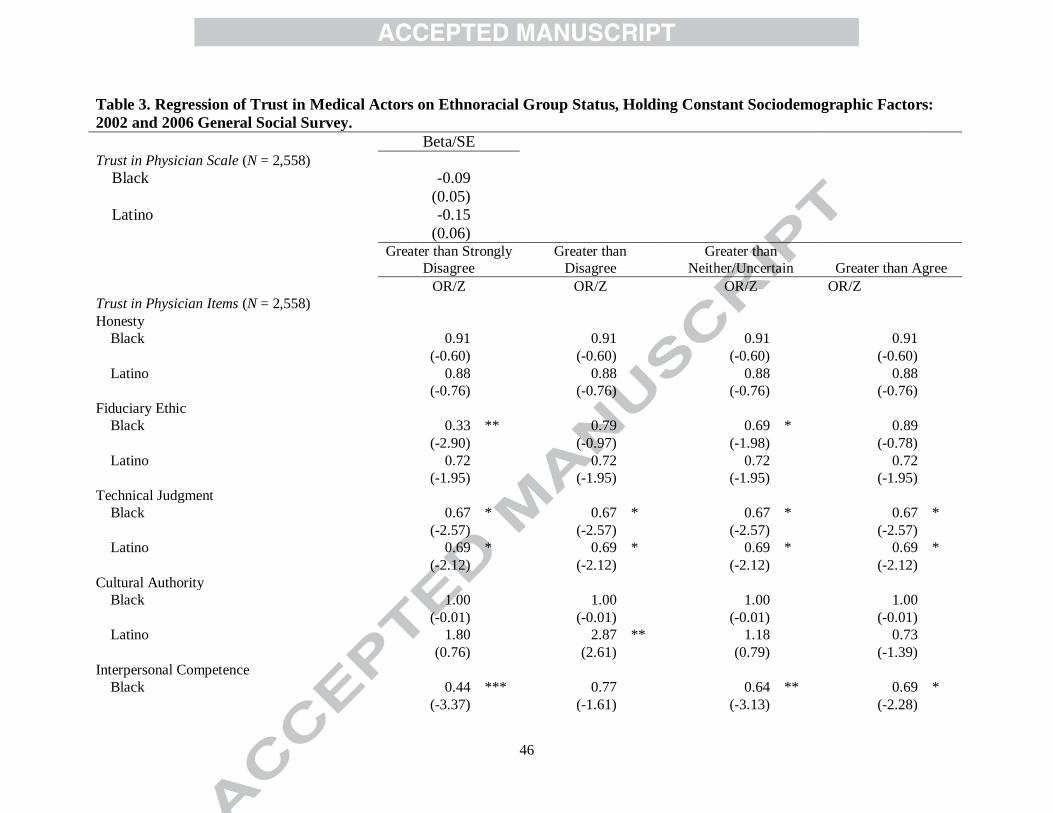
46
Table 3. Regression of Trust in Medical Actors on Ethnoracial Group Status, Holding Constant Sociodemographic Factors:
2002 and 2006 General Social Survey.
Beta/SE
Trust in Physician Scale (N = 2,558)
Black -0.09
(0.05)
Latino -0.15
(0.06)
Greater than Strongly
Disagree
Greater than
Disagree
Greater than
Neither/Uncertain Greater than Agree
OR/Z OR/Z OR/Z OR/Z
Trust in Physician Items (N = 2,558)
Honesty
Black 0.91
0.91
0.91
0.91
(-0.60)
(-0.60)
(-0.60)
(-0.60)
Latino 0.88
0.88
0.88
0.88
(-0.76)
(-0.76)
(-0.76)
(-0.76)
Fiduciary Ethic
Black 0.33 ** 0.79
0.69 * 0.89
(-2.90)
(-0.97)
(-1.98)
(-0.78)
Latino 0.72
0.72
0.72
0.72
(-1.95)
(-1.95)
(-1.95)
(-1.95)
Technical Judgment
Black 0.67 * 0.67 * 0.67 * 0.67 *
(-2.57)
(-2.57)
(-2.57)
(-2.57)
Latino 0.69 * 0.69 * 0.69 * 0.69 *
(-2.12)
(-2.12)
(-2.12)
(-2.12)
Cultural Authority
Black 1.00
1.00
1.00
1.00
(-0.01)
(-0.01)
(-0.01)
(-0.01)
Latino 1.80
2.87 ** 1.18
0.73
(0.76)
(2.61)
(0.79)
(-1.39)
Interpersonal Competence
Black 0.44 *** 0.77
0.64 ** 0.69 *
(-3.37)
(-1.61)
(-3.13)
(-2.28)
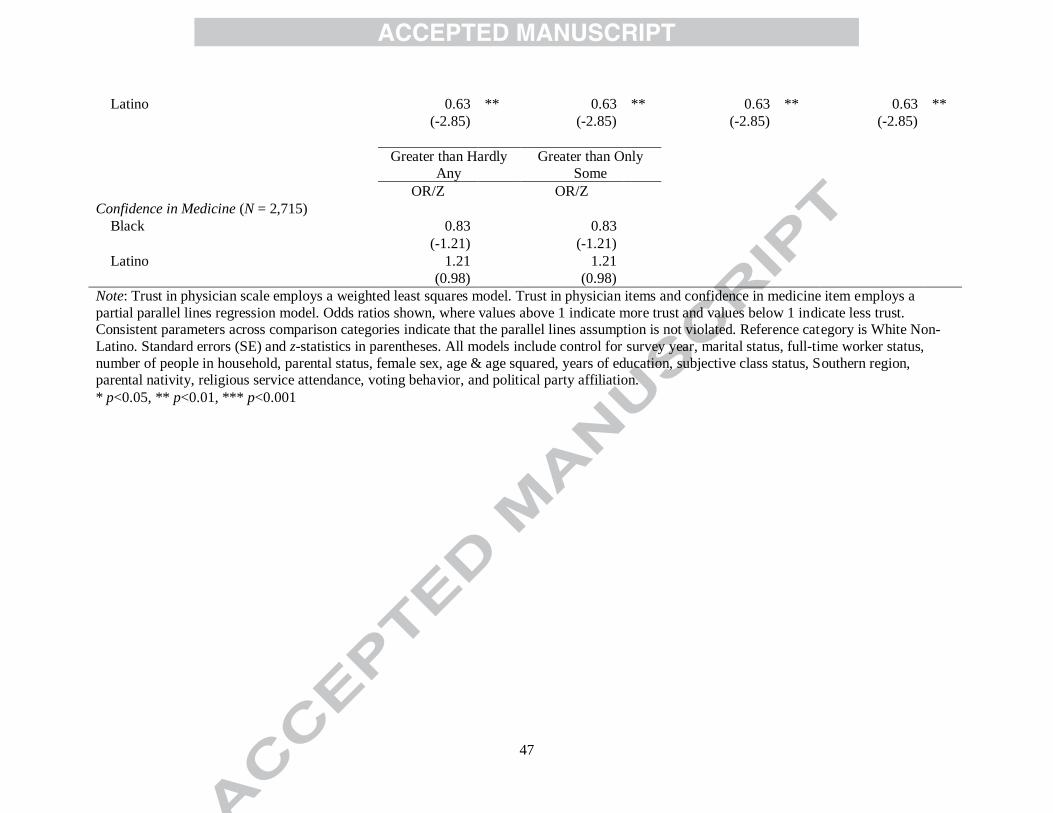
47
Latino 0.63 ** 0.63 ** 0.63 ** 0.63 **
(-2.85)
(-2.85)
(-2.85)
(-2.85)
Greater than Hardly
Any
Greater than Only
Some
OR/Z
OR/Z
Confidence in Medicine (N = 2,715)
Black 0.83
0.83
(-1.21)
(-1.21)
Latino 1.21
1.21
(0.98)
(0.98)
Note: Trust in physician scale employs a weighted least squares model. Trust in physician items and confidence in medicine item employs a
partial parallel lines regression model. Odds ratios shown, where values above 1 indicate more trust and values below 1 indicate less trust. Consistent parameters across comparison categories indicate that the parallel lines assumption is not violated. Reference category is White Non-
Latino. Standard errors (SE) and z-statistics in parentheses. All models include control for survey year, marital status, full-time worker status,
number of people in household, parental status, female sex, age & age squared, years of education, subjective class status, Southern region, parental nativity, religious service attendance, voting behavior, and political party affiliation.
* p<0.05, ** p<0.01, *** p<0.001
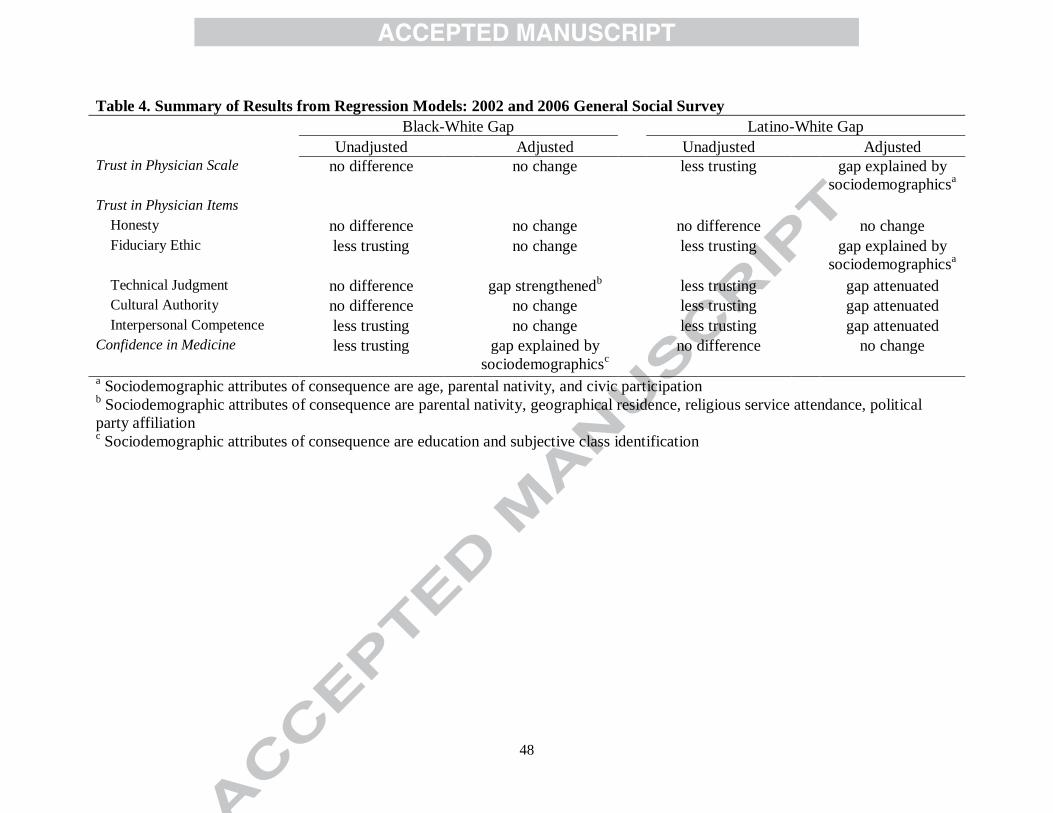
48
Table 4. Summary of Results from Regression Models: 2002 and 2006 General Social Survey
Black-White Gap
Latino-White Gap
Unadjusted Adjusted Unadjusted Adjusted Trust in Physician Scale no difference no change less trusting gap explained by
sociodemographicsa
Trust in Physician Items
Honesty no difference no change no difference no change
Fiduciary Ethic less trusting no change less trusting gap explained by
sociodemographicsa
Technical Judgment no difference gap strengthenedb less trusting gap attenuated
Cultural Authority no difference no change less trusting gap attenuated
Interpersonal Competence less trusting no change less trusting gap attenuated
Confidence in Medicine less trusting gap explained by
sociodemographicsc
no difference no change
a Sociodemographic attributes of consequence are age, parental nativity, and civic participation
b Sociodemographic attributes of consequence are parental nativity, geographical residence, religious service attendance, political
party affiliation c Sociodemographic attributes of consequence are education and subjective class identification
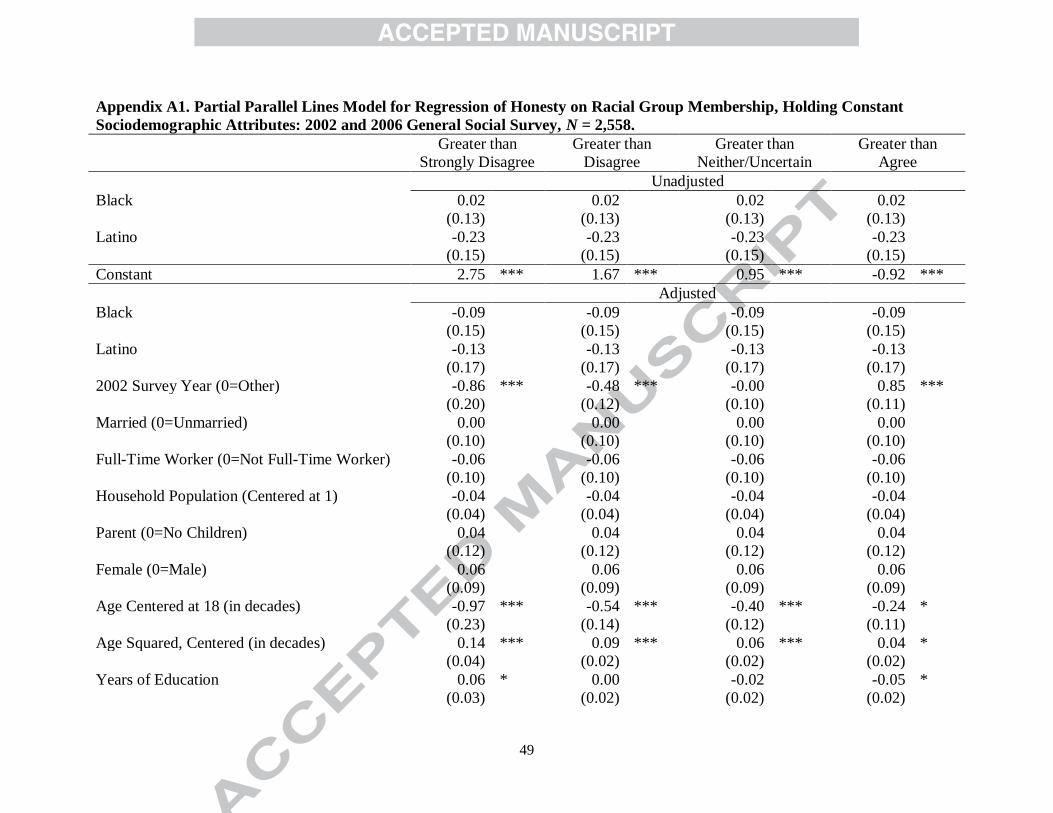
49
Appendix A1. Partial Parallel Lines Model for Regression of Honesty on Racial Group Membership, Holding Constant
Sociodemographic Attributes: 2002 and 2006 General Social Survey, N = 2,558.
Greater than
Strongly Disagree
Greater than
Disagree
Greater than
Neither/Uncertain
Greater than
Agree
Unadjusted
Black 0.02
0.02
0.02
0.02
(0.13)
(0.13)
(0.13)
(0.13)
Latino -0.23
-0.23
-0.23
-0.23
(0.15)
(0.15)
(0.15)
(0.15)
Constant 2.75 *** 1.67 *** 0.95 *** -0.92 ***
Adjusted
Black -0.09
-0.09
-0.09
-0.09
(0.15)
(0.15)
(0.15)
(0.15)
Latino -0.13
-0.13
-0.13
-0.13
(0.17)
(0.17)
(0.17)
(0.17)
2002 Survey Year (0=Other) -0.86 *** -0.48 *** -0.00
0.85 ***
(0.20)
(0.12)
(0.10)
(0.11)
Married (0=Unmarried) 0.00
0.00
0.00
0.00
(0.10)
(0.10)
(0.10)
(0.10)
Full-Time Worker (0=Not Full-Time Worker) -0.06
-0.06
-0.06
-0.06
(0.10)
(0.10)
(0.10)
(0.10)
Household Population (Centered at 1) -0.04
-0.04
-0.04
-0.04
(0.04)
(0.04)
(0.04)
(0.04)
Parent (0=No Children) 0.04
0.04
0.04
0.04
(0.12)
(0.12)
(0.12)
(0.12)
Female (0=Male) 0.06
0.06
0.06
0.06
(0.09)
(0.09)
(0.09)
(0.09)
Age Centered at 18 (in decades) -0.97 *** -0.54 *** -0.40 *** -0.24 *
(0.23)
(0.14)
(0.12)
(0.11)
Age Squared, Centered (in decades) 0.14 *** 0.09 *** 0.06 *** 0.04 *
(0.04)
(0.02)
(0.02)
(0.02)
Years of Education 0.06 * 0.00
-0.02
-0.05 *
(0.03)
(0.02)
(0.02)
(0.02)
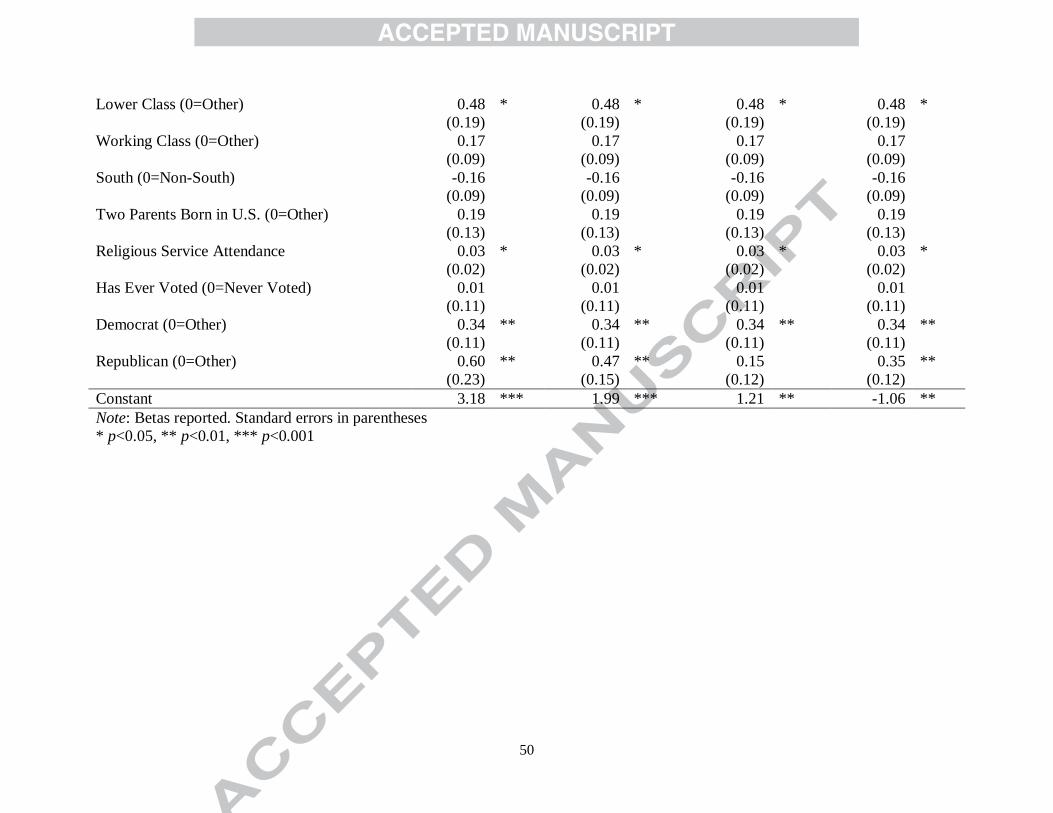
50
Lower Class (0=Other) 0.48 * 0.48 * 0.48 * 0.48 *
(0.19)
(0.19)
(0.19)
(0.19)
Working Class (0=Other) 0.17
0.17
0.17
0.17
(0.09)
(0.09)
(0.09)
(0.09)
South (0=Non-South) -0.16
-0.16
-0.16
-0.16
(0.09)
(0.09)
(0.09)
(0.09)
Two Parents Born in U.S. (0=Other) 0.19
0.19
0.19
0.19
(0.13)
(0.13)
(0.13)
(0.13)
Religious Service Attendance 0.03 * 0.03 * 0.03 * 0.03 *
(0.02)
(0.02)
(0.02)
(0.02)
Has Ever Voted (0=Never Voted) 0.01
0.01
0.01
0.01
(0.11)
(0.11)
(0.11)
(0.11)
Democrat (0=Other) 0.34 ** 0.34 ** 0.34 ** 0.34 **
(0.11)
(0.11)
(0.11)
(0.11)
Republican (0=Other) 0.60 ** 0.47 ** 0.15
0.35 **
(0.23)
(0.15)
(0.12)
(0.12)
Constant 3.18 *** 1.99 *** 1.21 ** -1.06 **
Note: Betas reported. Standard errors in parentheses
* p<0.05, ** p<0.01, *** p<0.001
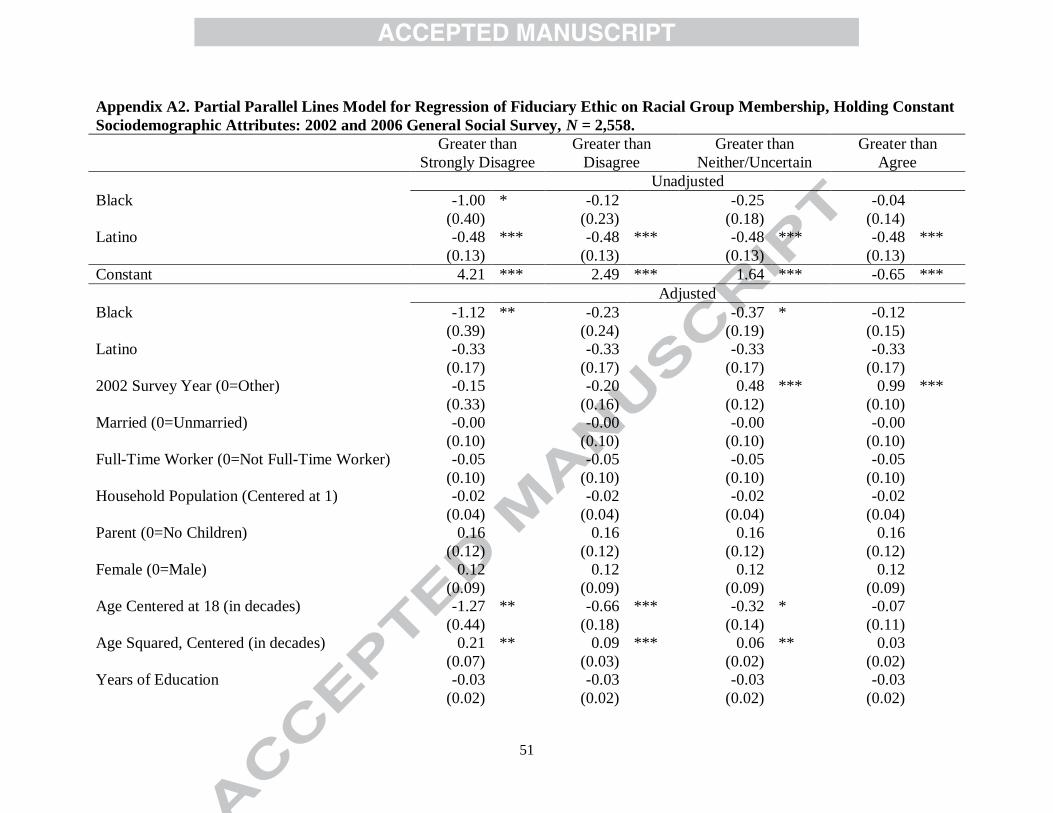
51
Appendix A2. Partial Parallel Lines Model for Regression of Fiduciary Ethic on Racial Group Membership, Holding Constant
Sociodemographic Attributes: 2002 and 2006 General Social Survey, N = 2,558.
Greater than
Strongly Disagree
Greater than
Disagree
Greater than
Neither/Uncertain
Greater than
Agree
Unadjusted
Black -1.00 * -0.12
-0.25
-0.04
(0.40)
(0.23)
(0.18)
(0.14)
Latino -0.48 *** -0.48 *** -0.48 *** -0.48 ***
(0.13)
(0.13)
(0.13)
(0.13)
Constant 4.21 *** 2.49 *** 1.64 *** -0.65 ***
Adjusted
Black -1.12 ** -0.23
-0.37 * -0.12
(0.39)
(0.24)
(0.19)
(0.15)
Latino -0.33
-0.33
-0.33
-0.33
(0.17)
(0.17)
(0.17)
(0.17)
2002 Survey Year (0=Other) -0.15
-0.20
0.48 *** 0.99 ***
(0.33)
(0.16)
(0.12)
(0.10)
Married (0=Unmarried) -0.00
-0.00
-0.00
-0.00
(0.10)
(0.10)
(0.10)
(0.10)
Full-Time Worker (0=Not Full-Time Worker) -0.05
-0.05
-0.05
-0.05
(0.10)
(0.10)
(0.10)
(0.10)
Household Population (Centered at 1) -0.02
-0.02
-0.02
-0.02
(0.04)
(0.04)
(0.04)
(0.04)
Parent (0=No Children) 0.16
0.16
0.16
0.16
(0.12)
(0.12)
(0.12)
(0.12)
Female (0=Male) 0.12
0.12
0.12
0.12
(0.09)
(0.09)
(0.09)
(0.09)
Age Centered at 18 (in decades) -1.27 ** -0.66 *** -0.32 * -0.07
(0.44)
(0.18)
(0.14)
(0.11)
Age Squared, Centered (in decades) 0.21 ** 0.09 *** 0.06 ** 0.03
(0.07)
(0.03)
(0.02)
(0.02)
Years of Education -0.03
-0.03
-0.03
-0.03
(0.02)
(0.02)
(0.02)
(0.02)
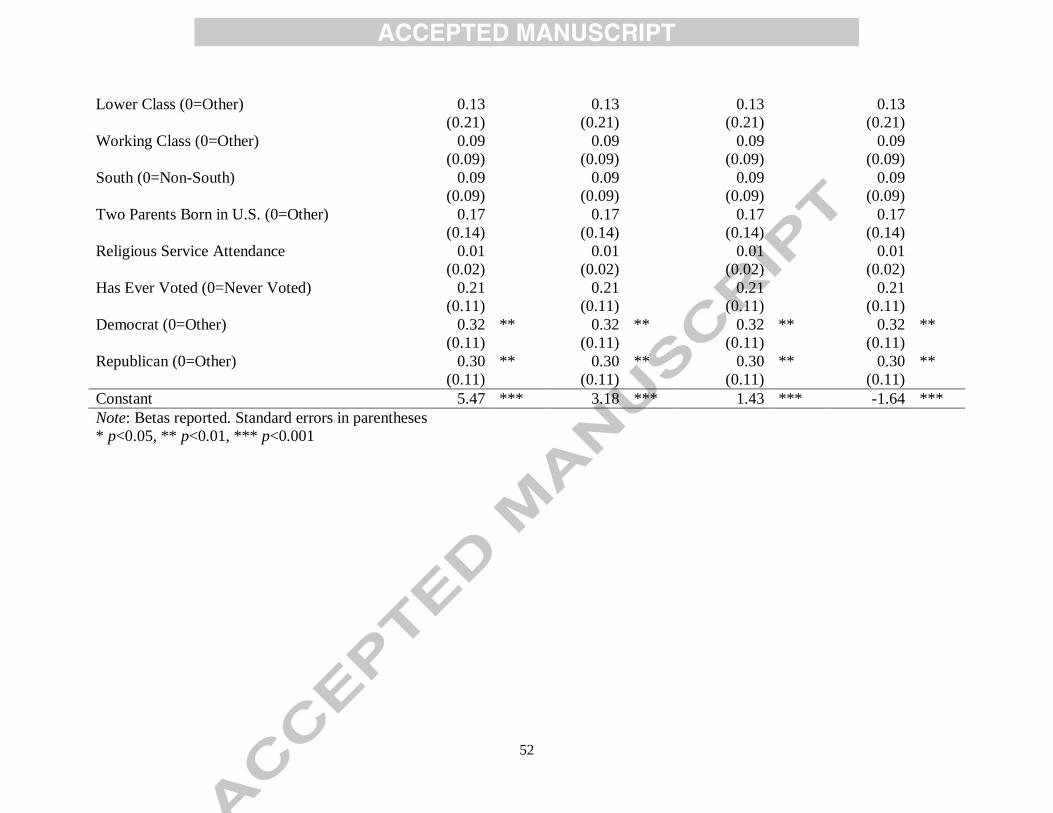
52
Lower Class (0=Other) 0.13
0.13
0.13
0.13
(0.21)
(0.21)
(0.21)
(0.21)
Working Class (0=Other) 0.09
0.09
0.09
0.09
(0.09)
(0.09)
(0.09)
(0.09)
South (0=Non-South) 0.09
0.09
0.09
0.09
(0.09)
(0.09)
(0.09)
(0.09)
Two Parents Born in U.S. (0=Other) 0.17
0.17
0.17
0.17
(0.14)
(0.14)
(0.14)
(0.14)
Religious Service Attendance 0.01
0.01
0.01
0.01
(0.02)
(0.02)
(0.02)
(0.02)
Has Ever Voted (0=Never Voted) 0.21
0.21
0.21
0.21
(0.11)
(0.11)
(0.11)
(0.11)
Democrat (0=Other) 0.32 ** 0.32 ** 0.32 ** 0.32 **
(0.11)
(0.11)
(0.11)
(0.11)
Republican (0=Other) 0.30 ** 0.30 ** 0.30 ** 0.30 **
(0.11)
(0.11)
(0.11)
(0.11)
Constant 5.47 *** 3.18 *** 1.43 *** -1.64 ***
Note: Betas reported. Standard errors in parentheses
* p<0.05, ** p<0.01, *** p<0.001
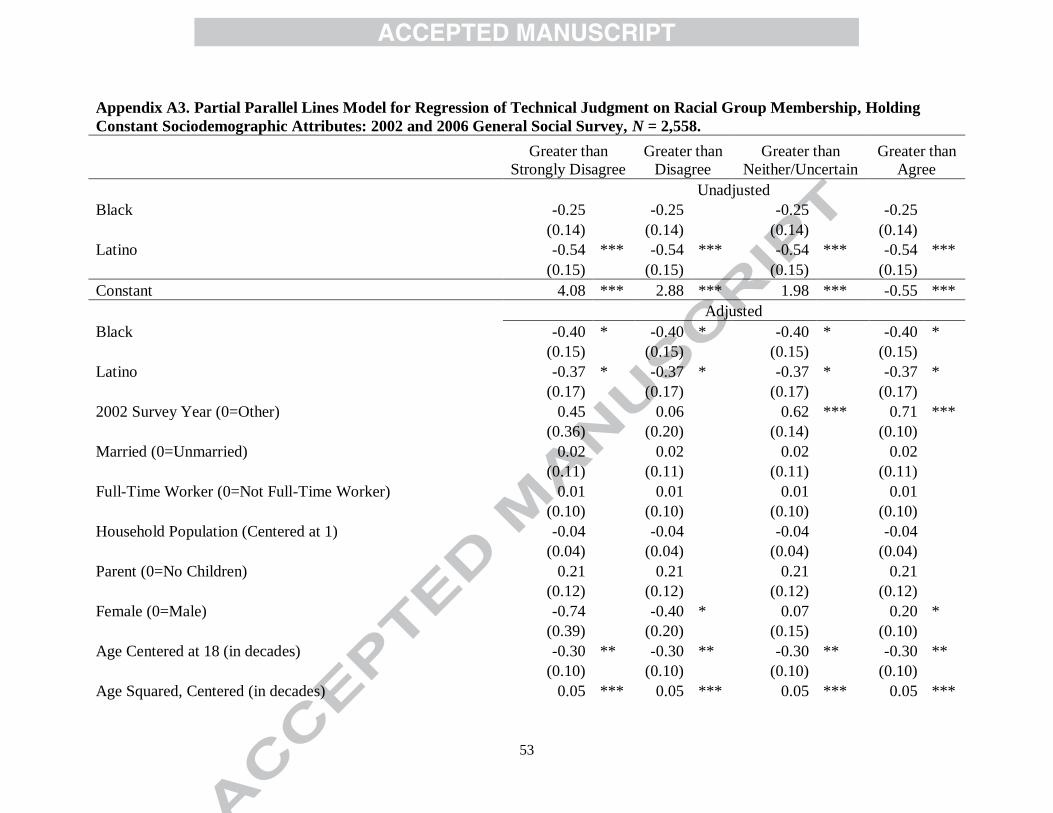
53
Appendix A3. Partial Parallel Lines Model for Regression of Technical Judgment on Racial Group Membership, Holding
Constant Sociodemographic Attributes: 2002 and 2006 General Social Survey, N = 2,558.
Greater than
Strongly Disagree
Greater than
Disagree
Greater than
Neither/Uncertain
Greater than
Agree
Unadjusted
Black -0.25
-0.25
-0.25
-0.25
(0.14)
(0.14)
(0.14)
(0.14)
Latino -0.54 *** -0.54 *** -0.54 *** -0.54 ***
(0.15)
(0.15)
(0.15)
(0.15)
Constant 4.08 *** 2.88 *** 1.98 *** -0.55 ***
Adjusted
Black -0.40 * -0.40 * -0.40 * -0.40 *
(0.15)
(0.15)
(0.15)
(0.15)
Latino -0.37 * -0.37 * -0.37 * -0.37 *
(0.17)
(0.17)
(0.17)
(0.17)
2002 Survey Year (0=Other) 0.45
0.06
0.62 *** 0.71 ***
(0.36)
(0.20)
(0.14)
(0.10)
Married (0=Unmarried) 0.02
0.02
0.02
0.02
(0.11)
(0.11)
(0.11)
(0.11)
Full-Time Worker (0=Not Full-Time Worker) 0.01
0.01
0.01
0.01
(0.10)
(0.10)
(0.10)
(0.10)
Household Population (Centered at 1) -0.04
-0.04
-0.04
-0.04
(0.04)
(0.04)
(0.04)
(0.04)
Parent (0=No Children) 0.21
0.21
0.21
0.21
(0.12)
(0.12)
(0.12)
(0.12)
Female (0=Male) -0.74
-0.40 * 0.07
0.20 *
(0.39)
(0.20)
(0.15)
(0.10)
Age Centered at 18 (in decades) -0.30 ** -0.30 ** -0.30 ** -0.30 **
(0.10)
(0.10)
(0.10)
(0.10)
Age Squared, Centered (in decades) 0.05 *** 0.05 *** 0.05 *** 0.05 ***
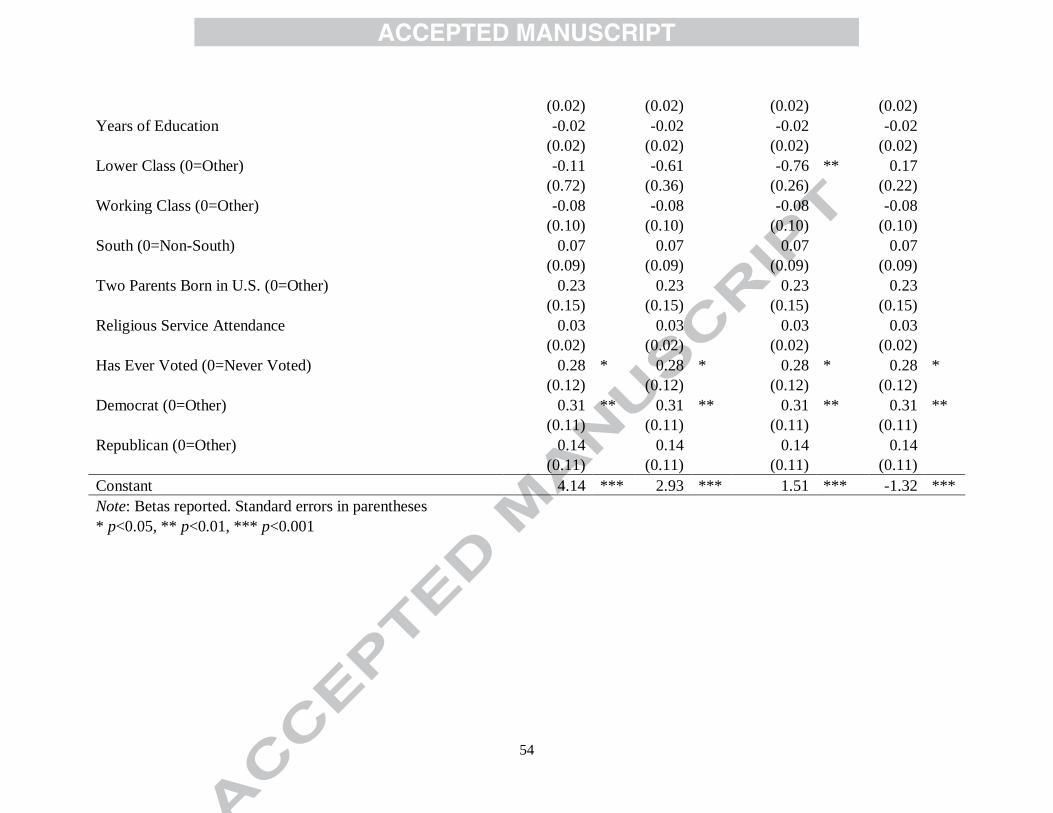
54
(0.02)
(0.02)
(0.02)
(0.02)
Years of Education -0.02
-0.02
-0.02
-0.02
(0.02)
(0.02)
(0.02)
(0.02)
Lower Class (0=Other) -0.11
-0.61
-0.76 ** 0.17
(0.72)
(0.36)
(0.26)
(0.22)
Working Class (0=Other) -0.08
-0.08
-0.08
-0.08
(0.10)
(0.10)
(0.10)
(0.10)
South (0=Non-South) 0.07
0.07
0.07
0.07
(0.09)
(0.09)
(0.09)
(0.09)
Two Parents Born in U.S. (0=Other) 0.23
0.23
0.23
0.23
(0.15)
(0.15)
(0.15)
(0.15)
Religious Service Attendance 0.03
0.03
0.03
0.03
(0.02)
(0.02)
(0.02)
(0.02)
Has Ever Voted (0=Never Voted) 0.28 * 0.28 * 0.28 * 0.28 *
(0.12)
(0.12)
(0.12)
(0.12)
Democrat (0=Other) 0.31 ** 0.31 ** 0.31 ** 0.31 **
(0.11)
(0.11)
(0.11)
(0.11)
Republican (0=Other) 0.14
0.14
0.14
0.14
(0.11)
(0.11)
(0.11)
(0.11)
Constant 4.14 *** 2.93 *** 1.51 *** -1.32 ***
Note: Betas reported. Standard errors in parentheses
* p<0.05, ** p<0.01, *** p<0.001
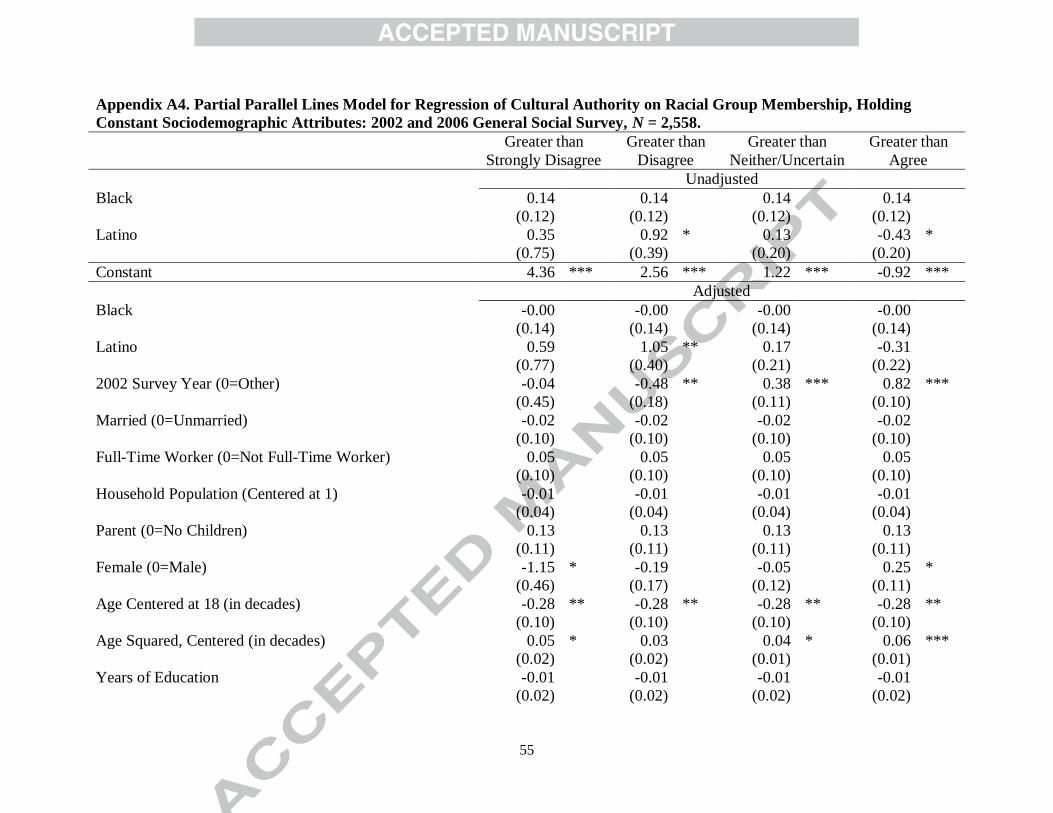
55
Appendix A4. Partial Parallel Lines Model for Regression of Cultural Authority on Racial Group Membership, Holding
Constant Sociodemographic Attributes: 2002 and 2006 General Social Survey, N = 2,558.
Greater than
Strongly Disagree
Greater than
Disagree
Greater than
Neither/Uncertain
Greater than
Agree
Unadjusted
Black 0.14
0.14
0.14
0.14
(0.12)
(0.12)
(0.12)
(0.12)
Latino 0.35
0.92 * 0.13
-0.43 *
(0.75)
(0.39)
(0.20)
(0.20)
Constant 4.36 *** 2.56 *** 1.22 *** -0.92 ***
Adjusted
Black -0.00
-0.00
-0.00
-0.00
(0.14)
(0.14)
(0.14)
(0.14)
Latino 0.59
1.05 ** 0.17
-0.31
(0.77)
(0.40)
(0.21)
(0.22)
2002 Survey Year (0=Other) -0.04
-0.48 ** 0.38 *** 0.82 ***
(0.45)
(0.18)
(0.11)
(0.10)
Married (0=Unmarried) -0.02
-0.02
-0.02
-0.02
(0.10)
(0.10)
(0.10)
(0.10)
Full-Time Worker (0=Not Full-Time Worker) 0.05
0.05
0.05
0.05
(0.10)
(0.10)
(0.10)
(0.10)
Household Population (Centered at 1) -0.01
-0.01
-0.01
-0.01
(0.04)
(0.04)
(0.04)
(0.04)
Parent (0=No Children) 0.13
0.13
0.13
0.13
(0.11)
(0.11)
(0.11)
(0.11)
Female (0=Male) -1.15 * -0.19
-0.05
0.25 *
(0.46)
(0.17)
(0.12)
(0.11)
Age Centered at 18 (in decades) -0.28 ** -0.28 ** -0.28 ** -0.28 **
(0.10)
(0.10)
(0.10)
(0.10)
Age Squared, Centered (in decades) 0.05 * 0.03
0.04 * 0.06 ***
(0.02)
(0.02)
(0.01)
(0.01)
Years of Education -0.01
-0.01
-0.01
-0.01
(0.02)
(0.02)
(0.02)
(0.02)
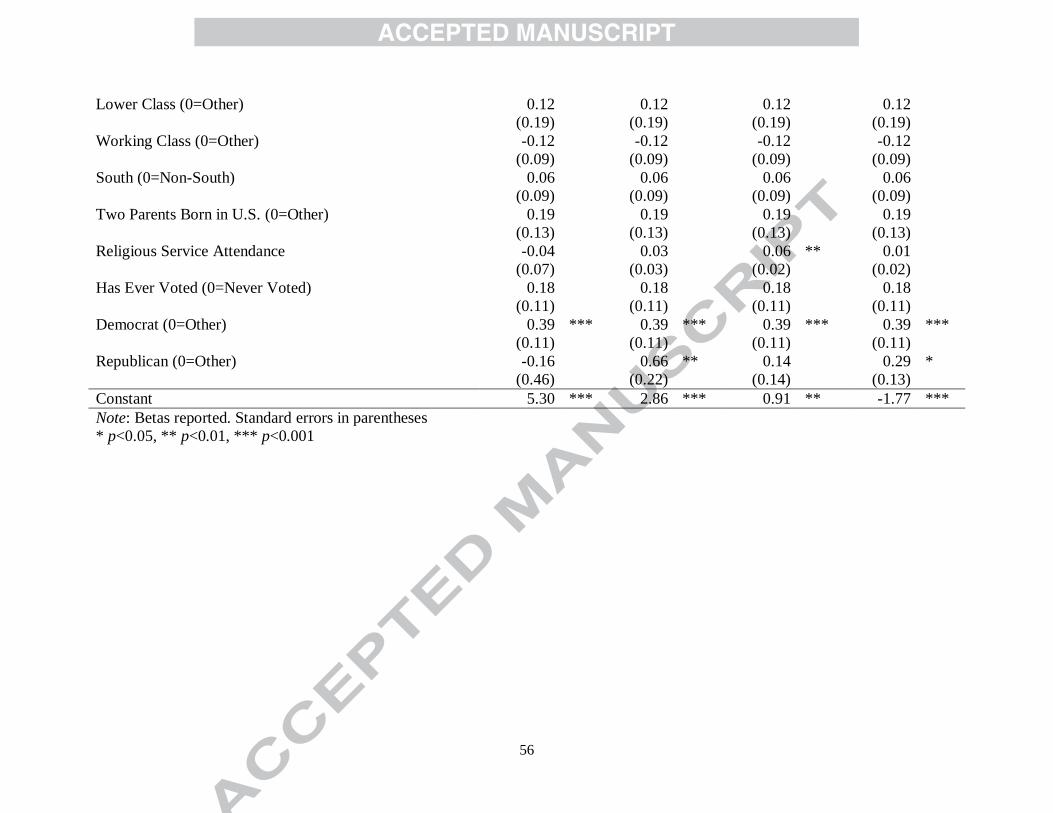
56
Lower Class (0=Other) 0.12
0.12
0.12
0.12
(0.19)
(0.19)
(0.19)
(0.19)
Working Class (0=Other) -0.12
-0.12
-0.12
-0.12
(0.09)
(0.09)
(0.09)
(0.09)
South (0=Non-South) 0.06
0.06
0.06
0.06
(0.09)
(0.09)
(0.09)
(0.09)
Two Parents Born in U.S. (0=Other) 0.19
0.19
0.19
0.19
(0.13)
(0.13)
(0.13)
(0.13)
Religious Service Attendance -0.04
0.03
0.06 ** 0.01
(0.07)
(0.03)
(0.02)
(0.02)
Has Ever Voted (0=Never Voted) 0.18
0.18
0.18
0.18
(0.11)
(0.11)
(0.11)
(0.11)
Democrat (0=Other) 0.39 *** 0.39 *** 0.39 *** 0.39 ***
(0.11)
(0.11)
(0.11)
(0.11)
Republican (0=Other) -0.16
0.66 ** 0.14
0.29 *
(0.46)
(0.22)
(0.14)
(0.13)
Constant 5.30 *** 2.86 *** 0.91 ** -1.77 ***
Note: Betas reported. Standard errors in parentheses
* p<0.05, ** p<0.01, *** p<0.001
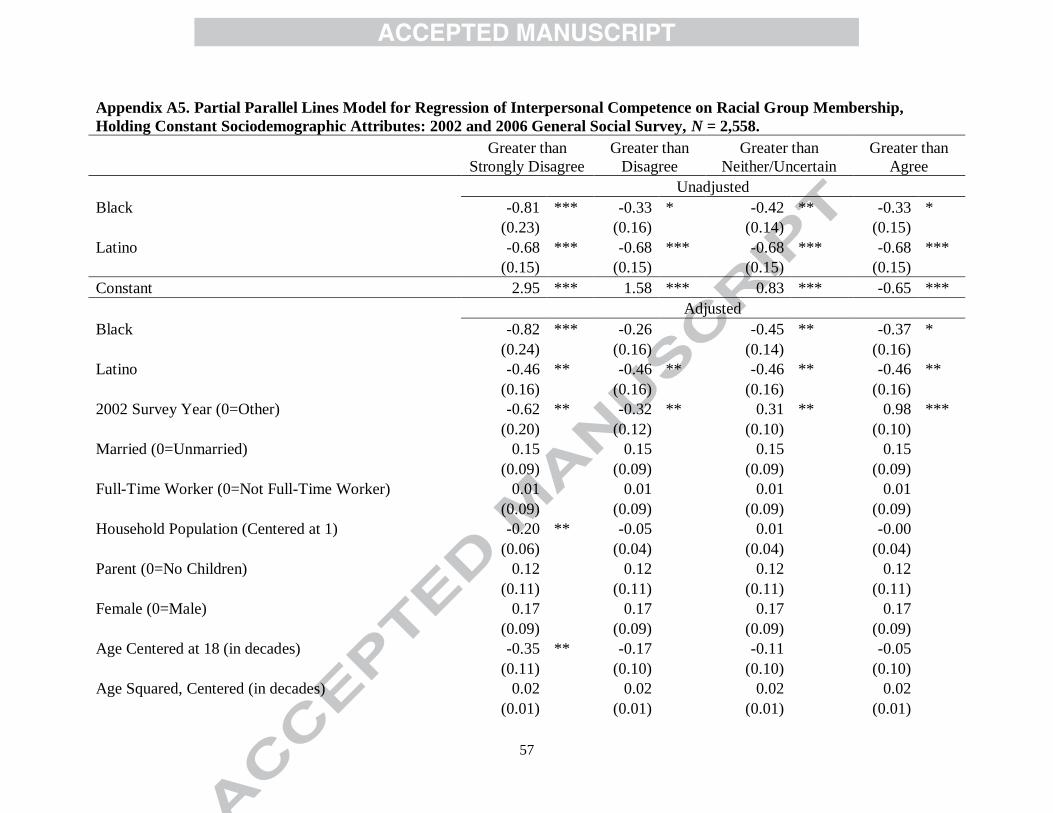
57
Appendix A5. Partial Parallel Lines Model for Regression of Interpersonal Competence on Racial Group Membership,
Holding Constant Sociodemographic Attributes: 2002 and 2006 General Social Survey, N = 2,558.
Greater than
Strongly Disagree
Greater than
Disagree
Greater than
Neither/Uncertain
Greater than
Agree
Unadjusted
Black -0.81 *** -0.33 * -0.42 ** -0.33 *
(0.23)
(0.16)
(0.14)
(0.15)
Latino -0.68 *** -0.68 *** -0.68 *** -0.68 ***
(0.15)
(0.15)
(0.15)
(0.15)
Constant 2.95 *** 1.58 *** 0.83 *** -0.65 ***
Adjusted
Black -0.82 *** -0.26
-0.45 ** -0.37 *
(0.24)
(0.16)
(0.14)
(0.16)
Latino -0.46 ** -0.46 ** -0.46 ** -0.46 **
(0.16)
(0.16)
(0.16)
(0.16)
2002 Survey Year (0=Other) -0.62 ** -0.32 ** 0.31 ** 0.98 ***
(0.20)
(0.12)
(0.10)
(0.10)
Married (0=Unmarried) 0.15
0.15
0.15
0.15
(0.09)
(0.09)
(0.09)
(0.09)
Full-Time Worker (0=Not Full-Time Worker) 0.01
0.01
0.01
0.01
(0.09)
(0.09)
(0.09)
(0.09)
Household Population (Centered at 1) -0.20 ** -0.05
0.01
-0.00
(0.06)
(0.04)
(0.04)
(0.04)
Parent (0=No Children) 0.12
0.12
0.12
0.12
(0.11)
(0.11)
(0.11)
(0.11)
Female (0=Male) 0.17
0.17
0.17
0.17
(0.09)
(0.09)
(0.09)
(0.09)
Age Centered at 18 (in decades) -0.35 ** -0.17
-0.11
-0.05
(0.11)
(0.10)
(0.10)
(0.10)
Age Squared, Centered (in decades) 0.02
0.02
0.02
0.02
(0.01)
(0.01)
(0.01)
(0.01)
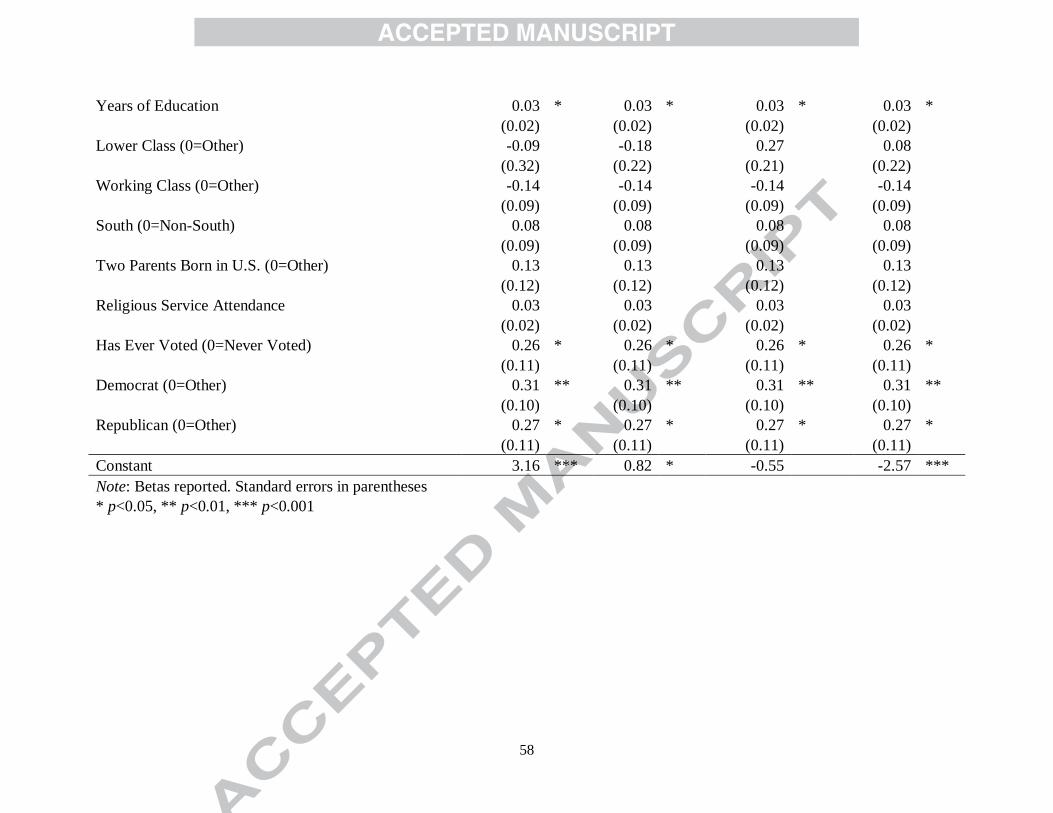
58
Years of Education 0.03 * 0.03 * 0.03 * 0.03 *
(0.02)
(0.02)
(0.02)
(0.02)
Lower Class (0=Other) -0.09
-0.18
0.27
0.08
(0.32)
(0.22)
(0.21)
(0.22)
Working Class (0=Other) -0.14
-0.14
-0.14
-0.14
(0.09)
(0.09)
(0.09)
(0.09)
South (0=Non-South) 0.08
0.08
0.08
0.08
(0.09)
(0.09)
(0.09)
(0.09)
Two Parents Born in U.S. (0=Other) 0.13
0.13
0.13
0.13
(0.12)
(0.12)
(0.12)
(0.12)
Religious Service Attendance 0.03
0.03
0.03
0.03
(0.02)
(0.02)
(0.02)
(0.02)
Has Ever Voted (0=Never Voted) 0.26 * 0.26 * 0.26 * 0.26 *
(0.11)
(0.11)
(0.11)
(0.11)
Democrat (0=Other) 0.31 ** 0.31 ** 0.31 ** 0.31 **
(0.10)
(0.10)
(0.10)
(0.10)
Republican (0=Other) 0.27 * 0.27 * 0.27 * 0.27 *
(0.11)
(0.11)
(0.11)
(0.11)
Constant 3.16 *** 0.82 * -0.55 -2.57 ***
Note: Betas reported. Standard errors in parentheses
* p<0.05, ** p<0.01, *** p<0.001
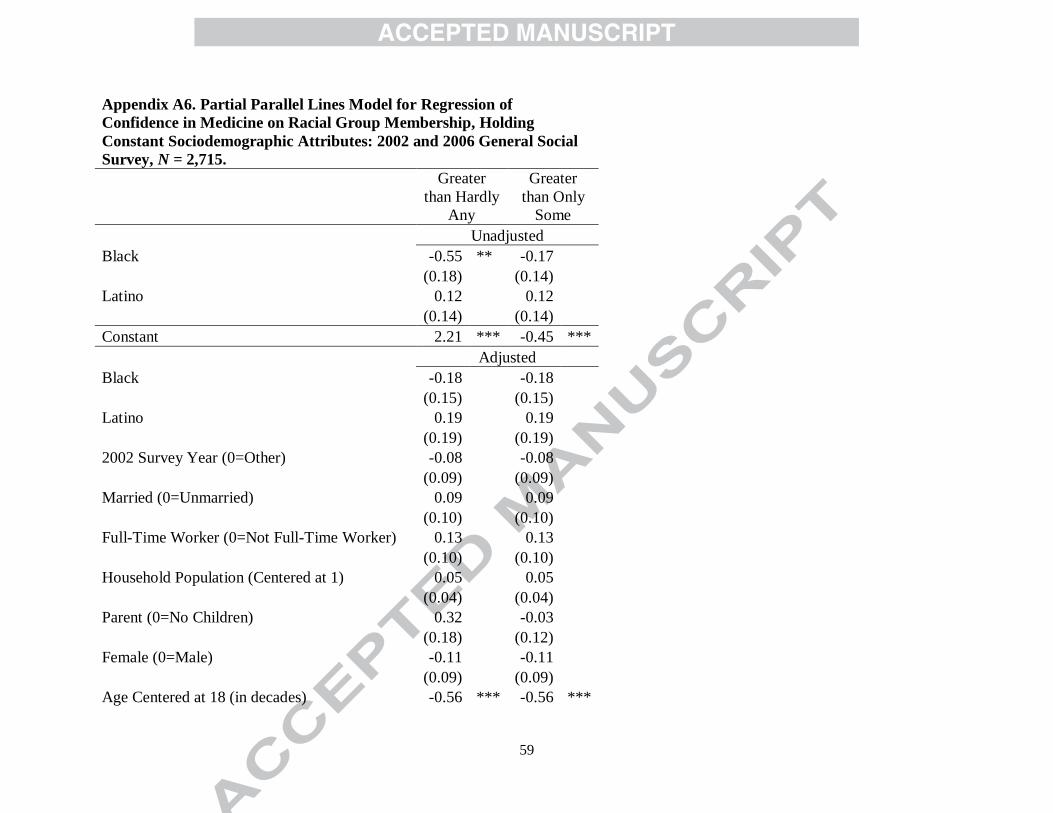
59
Appendix A6. Partial Parallel Lines Model for Regression of
Confidence in Medicine on Racial Group Membership, Holding
Constant Sociodemographic Attributes: 2002 and 2006 General Social
Survey, N = 2,715.
Greater
than Hardly
Any
Greater
than Only
Some
Unadjusted
Black -0.55 ** -0.17
(0.18)
(0.14)
Latino 0.12
0.12
(0.14)
(0.14)
Constant 2.21 *** -0.45 ***
Adjusted
Black -0.18
-0.18
(0.15)
(0.15)
Latino 0.19
0.19
(0.19)
(0.19)
2002 Survey Year (0=Other) -0.08
-0.08
(0.09)
(0.09)
Married (0=Unmarried) 0.09
0.09
(0.10)
(0.10)
Full-Time Worker (0=Not Full-Time Worker) 0.13
0.13
(0.10)
(0.10)
Household Population (Centered at 1) 0.05
0.05
(0.04)
(0.04)
Parent (0=No Children) 0.32
-0.03
(0.18)
(0.12)
Female (0=Male) -0.11
-0.11
(0.09)
(0.09)
Age Centered at 18 (in decades) -0.56 *** -0.56 ***
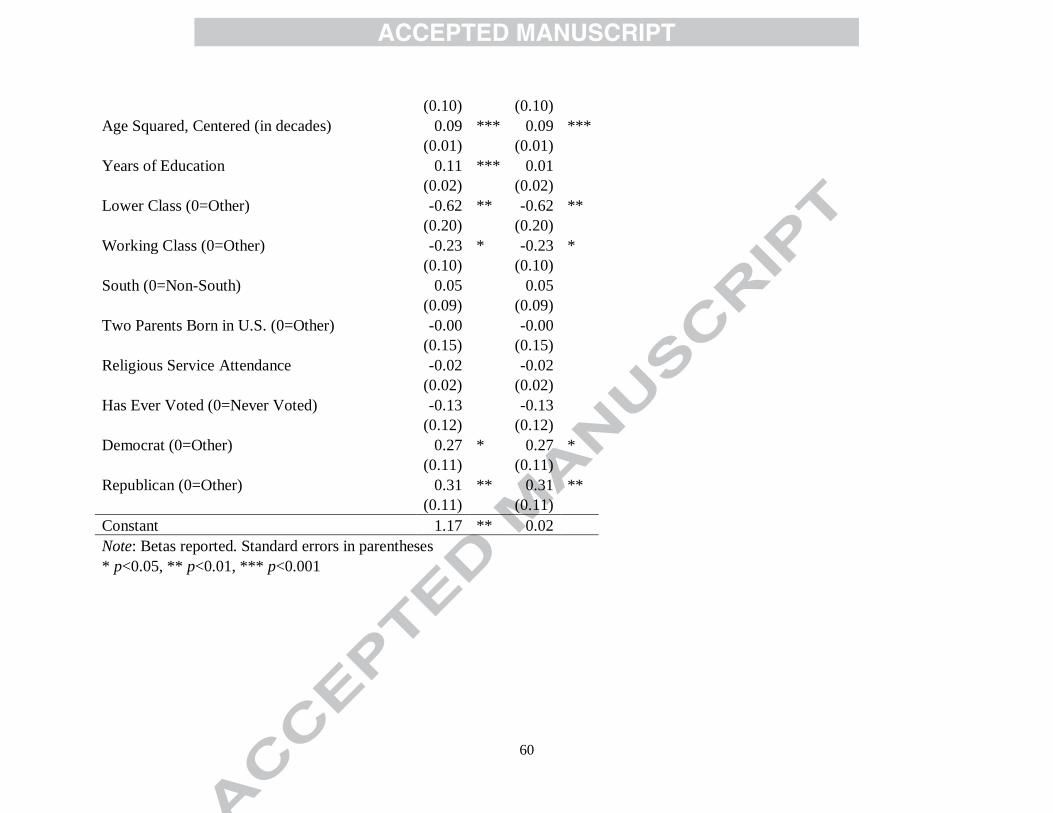
60
(0.10)
(0.10)
Age Squared, Centered (in decades) 0.09 *** 0.09 ***
(0.01)
(0.01)
Years of Education 0.11 *** 0.01
(0.02)
(0.02)
Lower Class (0=Other) -0.62 ** -0.62 **
(0.20)
(0.20)
Working Class (0=Other) -0.23 * -0.23 *
(0.10)
(0.10)
South (0=Non-South) 0.05
0.05
(0.09)
(0.09)
Two Parents Born in U.S. (0=Other) -0.00
-0.00
(0.15)
(0.15)
Religious Service Attendance -0.02
-0.02
(0.02)
(0.02)
Has Ever Voted (0=Never Voted) -0.13
-0.13
(0.12)
(0.12)
Democrat (0=Other) 0.27 * 0.27 *
(0.11)
(0.11)
Republican (0=Other) 0.31 ** 0.31 **
(0.11)
(0.11)
Constant 1.17 ** 0.02
Note: Betas reported. Standard errors in parentheses
* p<0.05, ** p<0.01, *** p<0.001
61
HIGHLIGHTS
Standard physician trust scales obfuscate ethnoracial differences in trust.
Blacks are less likely than Whites to trust doctor’s interpersonal competence.
Latinos are less likely than Whites to trust doctor’s interpersonal competence.
Black-Latino differences in physician trust are a function of parental nativity.
Copyright © 2022 FDOKUMEN