reSpOrT GUiDELinES U d E I P S r - European Commission
105
re Sp O GU i Li n ES European ReSport Guidelines For implementation Of ReSport Activities European sports network for rehabilitation of persons with disabilities reSpOrT GUiDELinES U d E I P S r
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of reSpOrT GUiDELinES U d E I P S r - European Commission

re SpOrT GUiDE Li nES
European ReSport Guidelines
For implementation
Of ReSport Activities
European sports network
for rehabilitation of persons
with disabilities
reSpOrT GUiDELinESU d EI
PS r

reSpOrT GUiDELinESU d EI
PS r

Maribor 2019
European ReSport Guidelines
For implementation
Of ReSport Activities
European sports network
for rehabilitation of persons
with disabilities
reSpOrT GUiDELinESU d EI
PS r
EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES
ReSport Guidelines
European ReSport Guidelines for implementation of ReSport Activities
Jasna Vešligaj Damiš, Yoana Filipic, Vladimir Jaćević, Ladislav Mesarič, Zvonka Novak, Valentina
Bolšec, Danijela Majcenovič Cipot, Zsuzsanna Kovács, Zsuzsana Antal, Dr Mohammed Mammad, Mireille
Boucher, Nihat Yıldız, Mehmet Afşin Güven, Gökhan Bahçecik, Melik Bingöl, Eduardo Borges Pereira,
Raúl Candido, Carlota Cunha, Michele Lepori, Alessandro Munarini, Silvia Noci, Paolo Zarzana, Ilona
Koval Grubišić, Michael Lamont, Fiona Mc Cabe, Treasa Rice.
Editor and foreword: Jasna Vešligaj Damiš
Proof reading: Brain Injury Matters
Technical editor, design and illustrations: Marko Damiš
Dtp: Marko Damiš & Kostja Bras
Publisher: Center Naprej, Maribor
centre for persons with acquired brain injury
Maribor 2019 www.resport.si
1st edition - 125 copies
Guidelines were published with the support of the Erasmus+ programme of the European Union.
The authors take sole responsibility for the content. The copyright is owned by partners and authors
in the project. Copying and reproduction without written permission is prohibited and is punishable
under the Copyright Act.
CIP - Kataložni zapis o publikaciji
Narodna in univerzitetna knjižnica, Ljubljana
796.034-056
RESPORT guidelines : European Resport guidelines
for implementation of Resport activities / [Jasna
Vešligaj Damiš ... [et al.] ; editor and foreword
Jasna Vešligaj Damiš ; illustrations Marko Damiš]. -
1st ed. - Maribor : Center Naprej, 2019
ISBN 978-961-290-436-4
1. Vešligaj Damiš, Jasna
COBISS.SI-ID 301584896
European sports network
for rehabilitation of persons
with disabilities
1. INTRODUCTION 9
FOREWORD 11
PARTNERS IN THE EU PROJECT ERASMUS + SPORT “EUROPEAN SPORTS
NETWORK FOR REHABILITATION OF PERSONS WITH DISABILITIES – RESPORT” 17
AUTHORS OF RESPORT GUIDELINES 18
1.1. TERMINOLOGY IN THE GUIDELINES 22
1.2. ADAPTED PHYSICAL ACTIVITY 24
1.3. DECLARATION ON THE SPECIFIC CHARACTERISTICS OF 26
SPORT AND ITS SOCIAL FUNCTION IN EUROPE (NICE 2000)
2. THE ROLE OF ORGANIZATIONS IN THE PROCESS OF INCLUSION 29
2.1. EXCLUSION, SEGREGATION, INTEGRATION AND INCLUSION 30
2.2. EFFECTIVE IMPLEMENTATION OF INCLUSION FOR VOLUNTEERS 32
2.3. RAISING AWARENESS OF INCLUSION 35
2.4. THE ROLE OF RESPORT PROJECT PARTNERS ORGANIZATIONS IN THE PROCESS OF INCLUSION 37
2.4.1. THE ROLE OF CENTER NAPREJ IN THE PROCESS OF COMMUNITY INCLUSION OF 37
PERSONS WITH ACQUIRED BRAIN INJURY
2.4.2. CENTRO SPORTIVO ITALIANO 41
2.4.3. RIJEKA DISABILITY SPORTS ASSOCIATION - THE ROLE OF ORGANIZATION 42
IN THE PROCESS OF INCLUSION
2.4.4. THE ROLE OF FPDD IN THE PROCESS OF INCLUSION 44
2.4.5. THE ROLE OF BRAIN INJURY MATTERS IN THE PROCESS OF COMMUNITY 44
INCLUSION OF PERSONS WITH ACQUIRED BRAIN INJURY
2.4.6. KEÇIÖREN MUNICIPALITY AND ITS ROLE IN THE PROCESS OF INCLUSION 45
2.4.7. THE ROLE OF HUMAN PROFESS NON-PROFIT LTD. IN THE 46
PROCESS OF INCLUSION OF PEOPLE WITH DISABILITIES
2.4.8. THE ROLE OF CIF FRANCE IN THE PROCESS OF INCLUSION 47
3. DISABILITY AND HEALTH 49
3.1. DEFINITIONS OF DISABILITY 50
3.2. CLASSIFICATION OF DISABILITY 52
3.3. HEALTH CONCERNS 55
3.3.1. THE HEALTH OF PEOPLE WITH DISABILITIES 55
3.3.2. MENTAL HEALTH 56
3.3.3. DISABILITY AND OBESITY 58
3.3.4. HARMFUL HABITS 59
3.3.5. 21ST CENTURY - VIDEO GAMES OR TRADITIONAL SPORT DISCIPLINES 62
3.3.6. DOPING IN THE SPORT FOR PERSONS WITH DISABILITY 65
4. BENEFITS OF PHYSICAL ACTIVITY 69
4.1. BENEFITS FOR THE PSYCHOLOGICAL AND SOCIAL FUNCTIONING 70
4.2. SPORTS AND PHYSICAL ACTIVITY AS REHABILITATION 76
ConTEnTS

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES
5. PLANNING AN ADAPTIVE PHYSICAL ACTIVITY 87
5.1. HOW TO PLAN ADAPTIVE PHYSICAL ACTIVITY 88
5.2. COMPETITION IN SPORTS 93
5.3. RISKS IN ADAPTED PHYSICAL ACTIVITY 98
5.4. THE ROLE OF ADAPTED PHYSICAL ACTIVITY EDUCATION 104
5.4.1. CHANGING TRADITIONAL ATTITUDES, BELIEFS AND ASSUMPTIONS 104
5.4.2. BUILDING SAFE RELATIONSHIPS 106
5.4.3. PSYCHOLOGICAL PREPARATION OF ATHLETES WITH DISABILITIES AND CHALLENGES WE FACE 108
5.4.4. PHYSICAL ACTIVITY RECOMMENDATIONS 116
5.4.5. CHALLENGES FOR FACILITATORS AND SERVICE USERS 118
5.4.6. EQUIPMENT AND TECHNOLOGY 120
6. APPLICATION OF ADAPTED PHYSICAL ACTIVITY PROGRAMMES 125
6.1. SWIMMING 126
6.2. NORDIC WALKING AND GYMSTICK - GNW PROGRAM 129
6.3. STAND UP PADDLE BOARDING (SUP) AS A NEW FORM 134
OF REHABILITATION OF INDIVIDUALS WITH ACQUIRED BRAIN INJURY (ABI)
6.4. SLACKLINING OR WALKING ON FLAT WEBBING 141
6.5. CROSSBOCCIA 146
6.6. SKIING 150
6.7. FOOTGOLF 155
6.8. SNOWSHOEING 158
6.9. NETBALL 162
6.10. SPORT ORIENTATION 165
6.11. TABLE TENNIS 169
6.12. CHEERLEADING 172
7. EVALUATION OF SPORT PROGRAMMES 177
7.1. THE PURPOSE OF MONITORING AND EVALUATING SPORTS PROGRAMMES 179
7.2. THE SPORT FOR DEVELOPMENT COLLATION OUTCOMES MODEL 182
7.3. SPECIFIC OUTCOME MEASURES 186
8. LONGEVITY AND QUALITY OF LIFE 191
8.1. REGULAR PHYSICAL ACTIVITY 195
8.2. COMMUNITY ACTIVE LIVING PROGRAMMES 199

inTRo DUc tIon

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 11
ForewOrD
Sport represents a great part of human interest and life. His-
torically sport activities and other similar activities have
attracted huge interest since ancient times. Current evidence
can be traced back to 30,000 years as examples of paintings in
caves originating from prehistoric periods.
Sport activities in the form of rehabilitation originate from
the Greek, Roman, and Chinese empires. Then they already knew
that physical activity was an excellent media for rehabilita-
tion, since they also dealt with the physical, mental, emotion-
al, social and spiritual elements of a person.
The basic goal of physical activity is to optimize the psycho-
somatic condition of the individual, make effective use of the
leisure time, preventive health care procedures and improve
health, well-being and recovery.
Sport is an area of human activity, which is important for all
citizens of the European Union with an exceptional potential
for unifying people. It concerns everyone, regardless of age,
social status, disability, race or gender. However, we face the
fact that people with disabilities are physically less active
than their peers, and consequently 38% are overweight (53% more
than people without disability). Physical inactivity is the
fourth most common risk factor for premature mortality. At the
same time, we must be aware that every sixth person in the Eu-
ropean Union suffers from a mild or severe form of disability,
which means approximately 80 million individuals. Many European
countries are aware of this problem and act accordingly.
Sports activities represent an effective method for rehabil-
itation of persons with disabilities. Taking part in sporting
activities helps people with disabilities to achieve greater
quality of life and greater social inclusion. For this pur-
pose, they need to be able to participate in sports events and
appropriate sports programs, where they can engage equally and
access sports and recreational areas. Sports activities must
also become an integral part of the rehabilitation of people
with disabilities, regardless of the type or level of their
disability, age and level of physical fitness.
These facts are the reason that 8 partners from 8 European
countries gathered within the framework of the Erasmus + Sport
with a project entitled “European sports network for rehabili-
tation of persons with disabilities “ReSport”, connecting many
organizations, professionals, people with disabilities and
their relatives, volunteers and all who have a common goal of
11

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 1312
equal opportunities. We decided to follow this goal and join in
the preparation of comprehensive sports solutions in the field
of physical activities with rehabilitation effects for persons
with disabilities. Therefore, after a long planning process and
discussion, we created and published European ReSport Guide-
lines for the implementation of “ReSport Activities”.
As project partners we are aware of the importance of ensur-
ing equal access and equal opportunities for all and promoting
healthy physical activity for all, especially for people with
disabilities. It is believed that patterns of physical activi-
ty are fundamental to lifelong physical activity and health in
the future and that they represent an important part of every
individual’s life.
The Guidelines is a result of the team work of the interdis-
ciplinary team of all partners in the project. The members of
the working group have made an enormous contribution in terms
of time, effort, knowledge and experience in shaping the guide-
lines, and this is why we are extremely grateful to the whole
team.
The Guidelines contain a number of directions and examples of
good practice that will help all readers - employees, thera-
pists, trainers, people with disabilities, their relatives and
interested members of society - in deciding and preparing pro-
grams of adaptive and integrated sports activities for people
with disabilities. Following the guidelines allow us to take
appropriate actions and monitor users in various adapted sports
activities, timely identification and prevent possible compli-
cations, and thus carry out sports and recreational programs
smoothly.
According to the data of international and national health
and sports organizations, physical activity is very important
factor in maintaining health. Indeed, persons with disabili-
ties, representing almost 15% of the world’s population, rarely
participate in sport and physical activity.
At the same time, we understand that, like everyone else, they
have to fight more and more for their rights, and always look
for optimal solutions for rightful development. Based on the
Convention on the Rights of Persons with Disabilities adopted
in 2006, the signatory countries of the Convention committed to
ensure appropriate conditions for the development of sports for
persons with disabilities, especially with regards to sports
facilities, financing, school system and education, both at
state level and in the local community, and introduce appro-
priate actions to enable persons with disabilities, as well as
others, to participate in recreational, leisure and sporting
activities.
Nevertheless, we still notice that there are too few existing
programs and organizations that allow them to exercise prop-
erly. It is of utmost importance that we encourage and raise
awareness both among state and experts at all levels about the
need to increase the chances of including people with disabil-
ities in various sports and recreational programs. “Re Sport”
Guidelines are designed to promote awareness of the importance
of the physical activity of people with disabilities, to trans-
fer knowledge at European level and to inspire as many of them
as possible to be active in their life.
Sport and recreation have many other positive outcomes, and
one of these is certainly connecting people with and without
disabilities. It is an excellent opportunity for integration,
overcoming prejudices and creating a tolerant society. And the
authors of the ReSport Guidelines hope that it will serve this
purpose!
JASNA VEŠLIGAJ DAMIŠ
PROJECT MANAGER

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 15
Photo: Center Naprej, Expert meeting, March 2017, Planica Slovenija

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 1716
UK
FR
IT
SI
HR
HU
TRPT
SI - PARTNER 1 – coordinator and lead partner
CENTER NAPREJ Maribor
Slovenia
IT - PARTNER 2
CSI - Centro sportivo Italiano
Italy
HR - PARTNER 3
Rijeka Disability Sport Center Association
Croatia
PT - PARTNER 4
Federação Portuguesa de Desporto para pessoas
com Deficiência
Portugal
UK - PARTNER 5
Brain Injury Matters
United Kingdom
TR - PARTNER 6
Keçiören Municipality
Turkey
HU - PARTNER 7
Human Profess Közhasznú Nonprofit Kft
Hungary
FR - PARTNER 8
CIF France
France
Figure 1: Partners in the EU project Erasmus + Sport “European sports network for rehabilitation
of persons with disabilities – ReSport”.
Partners in the EU project Erasmus + Sport “European sports network
for rehabilitation of persons with disabilities – ReSport”.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 1918
Jasna Vešligaj Damiš, MA Psychology and licensed psychodrama
psychotherapist with extensive experience as Director of
Center Naprej providing long-term rehabilitation of persons
with acquired brain injury (ABI). She has completed the
course of dr. Sarah McKay in neuroscience and brain health:
The Neuroscience Academy Certificate of Completion in Applied
Neuroscience and Brain Health. She is also the project
manager of ReSport project. Leader of several rehabilitation
sports summer and winter events for people with ABI. She
offers psychological preparation for professional athletes
at international and world competitions in athletics - Ath-
letics Club Slovenska Bistrica, Jitai Maribor. She developed
a number of training programs for long-term ABI caregivers.
She is also an expert in management and co-ordination of EU
projects, national projects, realization of good practices,
networking with schools, companies and institutions and
dissemination of the project products and outcomes.
Yoana Filipic, MA Psychology and DBT skills coach currently
works at Center Naprej providing long-term psychological
rehabilitation of persons with acquired brain injury (ABI).
She has facilitated and provided support in the process of
crisis intervention of persons with disabilities and persons
with psychiatric disorders. Her professional interests are
focused in the area of counseling, goal setting and motiva-
tion of persons with disabilities and exploring challenges
facilitators of adapted physical activity programs face.
Vladimir Jaćević, BA Physiotherapy is certified for Bobath
problem-solving neuro-developmental approach and Cyriax
method. He currently works at Center Naprej providing long-
term rehabilitation of persons with acquired brain injury
(ABI). He facilitates a number of adapted sports programs.
His professional interests include assessment and treatment
of individuals with cerebral palsy, stroke and brain injury
and other allied neurological conditions, and incorporating
various techniques in the process of treatment.
Ladislav Mesarič, MSc Physical education, Sport and Kinesio-
therapy, Olympic coach in athletics, strength and condition-
ing coach of Taekwondo federation of Slovenia. He has more
than thirty years of experience coaching and training numer-
ous successful sportsmen, representatives of various sports.
With his primary sport - athletics he has been coaching
three Olympic athletes. He is an external collaborator of
Center Naprej in the preparation and evaluation of adapted
sports programs for persons with acquired brain injury.
Zvonka Novak, MA Social Work, licensed mediator and paedi-
atric nurse. She is currently employed as Head of unit at
Center Naprej in Maribor providing long-term rehabilitation
of persons with acquired brain injury (ABI). She has worked
as a paediatric nurse at Intensive therapy in Paediatrics
Unit of University Medical Centre Maribor. She has got vast
experience in the field of social welfare, managing dislo-
cated units, leadership in numerous camps and other group
activities for people with intellectual disabilities. Zvonka
has incorporated MATP (motor activity training program) in
different activities for people with severe disorders and
she has participated in Special Olympics with them. She has
participated in the project Happy Farm (Leonardo da Vinci)
and Grundtvig (Socrates).
Valentina Bolšec, MA Psychology currently works at Center
Naprej providing long-term psychological rehabilitation of
persons with acquired brain injury (ABI). Her work is based
on providing emotional and psychological support for people
with disability. She also focuses on providing cognitive re-
habilitation and encouragement of motivation and achievement
of goals for individuals with ABI.
Danijela Majcenovič Cipot, B.A. Sociology, as sociolo-
gist passed professional examinations on a field of public
administration and welfare. She worked on various fields (Law
enforcement, Military, Social Welfare, Long-term unemploye-
ment). She is currently working as group facilitator provid-
ing long-term rehabilitation of persons with acquired brain
injury (ABI). She is also Head of unit in Murska Sobota. She
participated in many international and national conferences
as attendee and also author of papers and gave preventive
workshops to various target groups. She has experience with
various projects on national and international level.
Zsuzsanna Kovács, she is 32 years old. She graduated at
the Faculty of Economics of West Hungarian University. Her
thesis focuses on equal chances and disadvantaged social
groups. She lives with a locomotory disability; she has been
swimming and cycling since childhood. She has always been
striving to help her fellow sufferes as much as she can.
She is aware of the opportunities provided by local sport
associations. She knows the system of national para sport
organizations, she is informed about the regularly orga-
nized programs and events, and she continuously follows the
changes. Along with her job, she completed a course entitled
„Enforcement of equal treatment and development of social
awareness”, organized by Equal Treatment Authority. Cur-
rently she has been working for Human Profess Public Benefit
Nonprofit Ltd. Her task is, among others, to organize sport
activity of disabled people.
Zsuzsana Antal, she is a certified adult training manager -
teacher. She has 20 years experience in the field of social
and labour market rehabilitation of disadvantaged groups and
people living with a brain injury. In her job, she primarily
deals with the development of international training mate-
rials. She used to work in the framework of a Slovenian-Hun-
garian project on the development of sport opportunities for
disabled people. Working together with a medical and dive
master team, she took part in the adaptation of the method
of diving, so that it can become a sport that is available
for disabled people. She took part in the development of the
ABI training manual, as well as the preparation of the Study
entitled Long-term rehabilitation of people living with an
acquired brain injury.
Dr Mohammed Mammad, Born on 11/07/1965 in Oran –Algeria,
Dentist surgeon since 1988, French License 200, Magister of
French, option: Sciences of the Literary Texts 2008, Doc-
torate of French, option: Sciences of Literary Texts, Jury
in 2019, Training in Mediation and Conflict Management from
2012 to 2014 in Algeria, France and Germany, Head of the IEC
(Information - Education - Communication) unit at the Hai
El Ghoualem Public Health Establishment in Oran, Training
in Montpellier for one month in 2001 on “Teaching French
as a Foreign Language”, 4 internships (2 in Lyon and 2 in
Oran) for the development of the university manual on oral
methodology in 2010, 2017 Social Action Program CIF France
in Bourges Saint Florent sur Cher, 2018 Training ANPAA (ad-
dictology) Bourges. Dr. Mammad takes part in a weekly radio
show “Tips on Health”, Trainer, communicator and trainer
of trainers. He joined the CIF France team as an expert for
actions around people with disabilities.
Mireille BOUCHER, Born April 11, 1951 Bourges, Retired
social worker director. Training: specialized educator.
President CIF France, CIF International Association inter-
national of social workers. Deputy Mayor school affairs and
early childhood in Saint Florent sur Cher Vice President of
the Local Mission (Insertion 16-25 years people) Competence
in the field of social action and integration. Trainer for
fosters families. Expert on insertion, animation of collec-
tive actions for people with disabilities.
AUThors oF Re-SPOrt guIDelINes

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 2120
Nihat Yıldız, Deputy Mayor of Keçiören Municipality. He is
responsible for Sports and Youth Department of Municipality
and Sports Centres. He temporarily serves as rapporteur in
various commissions established by the Ministry of Interior
in the budget and accounting systems of the municipalities,
State Tender and Public Procurement Legislation, Personnel
Legislation, Public Financial Management System and Public
Audit. He is lecturer in seminars and training programmes
organized by the Ministry of Interior, Turkish Municipal-
ities Union, Konya Municipal Union, Aegean Municipalities
Union, Marmara and Boğazlar Municipalities Union, Black
Sea and Mediterranean Municipalities Associations, TODAİE,
Governorships, municipalities, foundations and universities.
He is member, founder or manager in various non-governmental
organizations.
Mehmet Afşin Güven, computer engineer and biologist. He
has got experience in EU Projects, preparation of Technical
Handbook, testing reports and evaluation. He is an expert
in EU Projects for disabled people, developing skills of
young disabled people, development of vocational suitabil-
ity for disabled adults and parental training in families
of children with disabilities. He has got experience in
web site design and management, software design, testing,
data analysis and management. He is a professional computer
programmer.
Gökhan Bahçecik, manager and head of Department of Youth
and Sports. He worked on several European Union Leonardo Da
Vinci Action Programmes related to local municipalities. He
participated in various seminars, meetings, symposiums and
training programmes regarding Turkish politics and local
government.
Melik Bingöl, manager and head of IT Department. He is a
computer engineer. He has many experience with various
projects (project partner and manager of EMPATHY Project,
Parental Training in Families of Children with Disabilities
and of DEVOMDA project - Development Of Vocational Suitabil-
ity for Disabled Adults, project coordinator of Developing
Skills of Young Disabled People DESYODIP, LLP –Leonardo
– TOI. He has got experience in preparation of Training
Modules for Disabled, Preparing Technical Handbook, Country
Analysis Reports, Expert Platforms, Dissemination of Proj-
ects and Mobility Tools.
Eduardo Borges Pereira, Sports Manager.
• National Technical Director of FPDD since 2017.
• Board of Directors Chairman and Sports Director at the
municipal town hall company “Palmela Desporto, EM” (Sport
Palmela) for five years – 2011 to 2016.
• Portuguese Sports Institute Vice-President of the Board
between 2003 and 2005.
• Sports Coordinator at the municipal town hall of Palmela,
from 1996 to 2011 (except from 2003 to 2005).
Raúl Candido, Sports Technician at FPDD Portugal since 1999.
• Adapted Sport Coach.
• Work in the technical area of Disability Sports since
1991.
• Technical support to several Paralympic Missions at
Portugal team.
CUNHA, Carlota, Sports Technician at FPDD Portugal since 2015
• 2 years work experience as physical teacher for disabled
people at Ginásio Clube Português.
• Technical Officials Coordinator in Paralympic Games Rio 2016.
• Boccia International Referee.
• 2 years work experience as Personal Trainer at Health
Club Solinca Vasco da Gama.
• Goalball National Referee.
• Coach of Boccia in the Cerebral Palsy Association of
Lisbon.
• Participation as National Technical Official at the Boccia
World Cup 2011 organized by the Cerebral Palsy Interna-
tional Sports & Recreation Association (CRISRA).
Michele Lepori, CSI ReSport project handler. He has twen-
ty years of experience in the field of sports associations
and in organizing events in the field of sport for disabled
people. For 10 years he has been a provincial councilor and
a member of the Paralympic commission of the Lombardy re-
gion of CSI, where he obtained the qualification of Paralym-
pic coach. Thanks to the experience he has acquired, he has
also obtained a CONI high-level diploma.
Alessandro Munarini, CSI referente nazionale attività
disabili. He obtained his magistral diploma, and for 15
years worked as a social worker in a cooperative, providing
assistance and support to disabled people. In the 90’s he
obtained the requalification on the job, acquiring the qual-
ification of professional educator. After a break in which he
carried out various jobs (building trade and agriculture) he
returned, from 2015, to work as a professional educator in
a cooperative, always in relationship with disabled people,
both minors and adults. In terms of volunteering, it has
given rise to and developed a sports club in the municipali-
ty of Reggio Emilia; he was president of this sports company
for 30 years. Also at the level of the Sports Center, he
performed, always free of charge, various tasks: provincial
councilor, head of training, regional councilor and gener-
al manager of the committee. He is currently President and
general manager of the Reggio Emilia committee, national
representative of the Sports Center for disabled persons and
professional educators (part-time) in a cooperative with
disabled people.
Silvia Noci, CSI National Technical Commission for disabled
people. She is a federal swimming technician. He is the
director of the CO.G.IS swimming facility and coordinator
of the swimming school. Swimming instructor, water fitness,
water pilates, bike and treadmill. Specializing in water
sports for infants and disabled people, she has worked in
this sector since 1992. She collaborates with local health
authorities and schools for inclusion and self-development
projects for disabled people, through physical activity in
the water. He currently manages the AcquaInsieme project
with the Centro Toscana Toscana which involves around 25
children from 20 months to 15 years.
Paolo Zarzana, CSI national trainer, CT of Italian Nation-
al amputee soccer team. He works at the CSI of Modena with
the role of Vice President, responsible for school projects
and activities for disabled athletes. In addition, he is a
councilor of the Municipality of Formigine (Mo). Graduated
in Educational Sciences, he is the Vice CT of the Italian
Soccer Amputation Team, which he has been following since
2012. With this team he participated in a European and 2
world championship. He currently works with the CSI in the
Technical School.
Ilona Koval Grubišić, Ph.D., associate professor, master of
physiotherapy
Michael Lamont, BSc Psychology has recently moved on from
his role as Associate Psychologist with Brain Injury Matters
(NI). Michael coordinated the Youth Matters Programme pro-
viding 1:1 and group based support services to young people
(13-25 years) across Northern Ireland, who have experience
of an acquired brain injury. Michael provided psychologic
input based on the individuals needs of the young people
involved in the programme.
Fiona Mc Cabe, Brain Injury Matters Ireland.
Treasa Rice, Community Engagement Officer, Brain Injury
Matters. Treasa Rice, BSc Environmental Health, MSc Health
Promotion currently works at Brain Injuri Matters (NI) coor-
dinating youth and adult services for persons with acquired
brain injury within their local community. She has facil-
itated support groups, sports interventions and one to one
sessions within her role as community engagement officer.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 2322
1.1.TerMinoLOGY in the gUIDeLiNES
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: handicapped, disability, disabled person
For the purpose of these guidelines we used the
terms person with disability and athlete with
disability. Athletes with disability are peo-
ple with a disability who engage in sports and
are able to compete in sports at elite levels.
They can also practice almost any sports and
sometimes need adapted equipment (Ferrara &
Peterson, 2000). As we realize that the language
used is very important in terms of attitudes and
beliefs we chose to emphasise the person rath-
er than the disability placing the word person
first.
We also present a table differentiating the
terms disabled and handicapped person. We did
not decide to use the term handicapped for the
reasons stated in the table on the right page.
A disability is an impairment that may be cogni-
tive, developmental, intellectual, mental, phys-
ical, sensory, or some combination of these. It
substantially affects a person’s life activities
and may be present from birth or occur during a
person’s lifetime (Tanaka & Seals, 2003).
We refer to disability as normal part of human
life and experience that can occur. However
there are many definitions and different ways of
describing the term. We have chosen the World
Health Organization (2018) definition: “Disabil-
ity is an umbrella term, covering impairments,
activity limitations, and participation restric-
tions. Impairment is a problem in body function
or structure; an activity limitation is a diffi-
culty encountered by an individual in executing
a task or action; while a participation restric-
tion is a problem experienced by an individual
in involvement in life situations. Disability is
thus not just a health problem. It is a complex
phenomenon, reflecting the interaction between
features of a person’s body and features of the
society in which he or she lives.” — World Health
Organization, Disabilities. Writing these Guide-
lines we have followed the description of WHO
as this is the definition we support and think is
the most appropriate and politically correct. It
gives a vast and correct perception of the topic
and issues explored.
Reference
Ferrara M.S. & Peterson C.L. (2000). Injuries to athletes
with disabilities: identifying injury patterns. Sports Medi-
cine; 30(2):137-43.
Tanaka, H. & Seals, D. (2003). Invited Review: Dynamic
exercise performance in Masters athletes: insight into the
effects of primary human aging on physiological functional
capacity. J Appl Physiol.; 95(5): 2152–2162. pmid: 14555676
https://en.wikipedia.org/wiki/Disability “Disabilities”.
World Health Organization. Retrieved 6.5.2018
http://www.differencebetween.info/difference-between-disabil-
ity-and-handicap. Retrieved 18.9.2018
Disability Handicap
Meaning Disability means the inabil-ity of a person to perform his/her routine actions.
Handicap means the difficulty experienced by a person in performing his/her tasks.
Core difference
Disability is being completely unable to perform a function.
Handicap is a partial disability.
Applicability Disability is mostly as-sociated with the medi-cal condition of not being able to perform a task.
Handicap could also mean a disadvan-tage imposed in a professional sport.
Variants Disabilities of various kinds such as physical, sen-sory, intellectual, men-tal, emotional, etc.
Handicap related to medical condi-tions such as being physically, mental-ly handicapped et al., and handicap in terms of sports such as golf handicap, chess handicap, tennis handicap, etc.
Diplomatic accuracy
More acceptable as com-pared to ‘handicap’.
Regarded as being offensive to peo-ple suffering from conditions of im-pairment or disability.
Table 1: Difference between Disability and Handicap (http://www.differencebetween.info/difference-between-disabili-
ty-and-handicap, 18.9.2018)

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 2524
1.2.ADApted PhySIcAL AcTIvity
AUTHORS: YOANA FILIPIC, JASNA VEŠLIGAJ DAMIŠ
Key words: adapted physical activity, EUSAPA, EUFAPA
Adapted physical activity (APA) is an extremely
broad concept. Therefore, we cannot give a sin-
gle exclusive definition. Opinions and views in
this area are quite different. Greg Reid (2003)
believes that the main problem lies in the word
“adapted”. Most of us have some ideas about what
physical activity means, however the word adapt-
ed is sometimes problematic. So, an immediate
response is often: “It’s physical activity for
people with special needs.” The APA description
in terms of activity for people with disabili-
ties gives us a perspective, but this is by no
means a complete definition or more precisely a
limited view of this concept (Reid, 2003). The
development of APA for people with disabilities
has gone through various stages of implementa-
tion and overcoming difficulties, due to dif-
ferences in understanding in various paradigms
- philosophical, kinesiological, psychological,
and social. EUFAPA (European Federation of
Adapted Physical Activity) defines APA as a cross
disciplinary field of knowledge and research
directed towards identification and solution of
individual differences in physical activity. It
is a service delivery profession and an academ-
ic field of study that supports an approach that
promotes acceptance of differences among indi-
viduals, advocates improving access to an active
lifestyle and sport activities and encourages
innovation and cooperative service delivery and
empowering systems (EUFAPA, 2018). The purpose
of adapted physical activity is to promote human
health, independence, quality of life and social
inclusion. APA is an area of interdisciplinary
expertise, which includes: rehabilitation and
therapy; physical education and sport; recre-
ation, competition and recreational activities;
sport in all its dimensions (Ninor & Partyka,
2007, Mälkiä, 2002).
EUSAPA - European Standards in Adapted Physical
Activities is a project that strives to devel-
op and research adapted physical activity at a
European level. It defines three areas of adapted
physical activity - 1 - adapted physical edu-
cation, 2 - adapted sports and recreation, and
3 - adapted physical activities in rehabilita-
tion. The Finnish expert Mälkiä shares a similar
opinion and states that apart from the implemen-
tation of adapted physical activity in sport,
recreation and education, it is also important
in rehabilitation of persons with disabili-
ties or people with chronic diseases. Physical
activity is crucial part of all areas of life
- health, knowledge, social inclusion, educa-
tion and rehabilitation. Adaptation of physical
activity may also involve technical adjustments,
such as using technical adaptation, adapting
sports equipment and structural changes. For
example in adapting rules and instructions of
the game or in developing training, which means
adapting professional approaches and methods and
methods of exercise and teaching (Mälkiä, 1991).
References
EUFAPA - European Federation of Adapted Physical Activity,
http://www.eufapa.eu/index.php/apa.pdf, Retrieved 2.2.2018
EUSAPA -European Standards in Adapted Physical Activities.
http://eacea.ec.europa.eu/LLp/project_reports/documents/
erasmus/multilateral_actions_2008/eras_emhe_142271_eusapa.pdf
Retrieved on 12.3.2018
Mälkiä, E. Puolanne, M. & Palosuo, M. (1991). Special Ex-
ercise 1: Appropriate Exercise basics. Jyväskylä. Gummerus
Kirjapaino Oy.
Mälkiä, E. & Rintala, P. (2002). New Special Movement. Exer-
cise facilitation for special groups Tampere. Tammer-paino
Oy.
Ninot, G. & Partyka, M. (2007). 50 good practices for teaching
APAs, REVUE EPS n°73, p.65
Reid, G. (2003). Defining Adapted Physical Activity. In R.D.
Steadward, G.D. Wheeler, & E.J. Watkinson (Eds.), Adapted
Physical Activity (pp. 11-25).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 2726
1.3.DeclaratIOn on the spECIfic Char-acteriStics of sP•Ort aNd its s•O-Cial FUnCTion in EurOPe (NICE 2000)
AUTHORS : ZSUZSANNA KOVÁCS, ZSUZSANNA ANTAL
Key words: declaration, sport for all, protection of young sportsmen and – women, solidarity
Introduction
The European Council has noted the report on
sport submitted to it by the European Commis-
sion in Helsinki in December 1999 with a view
to safeguarding current sports structures and
maintaining the social function of sport within
the European Union.
The European Council hopes in particular that
the cohesion and ties of solidarity binding the
practice of sports at every level, fair competi-
tion and both the moral and material interests
and the physical integrity of those involved in
the practice of sport, especially minors, may be
preserved.
Sport for all - ANNEX IV (Declaration, 2018)
- DECLARATION ON THE SPECIFIC CHARACTERISTICS
OF SPORT AND ITS SOCIAL FUNCTION IN EUROPE, OF
WHICH ACCOUNT SHOULD BE TAKEN IN IMPLEMENTING
COMMON POLICIES
Sport is a human activity resting on fundamental
social, educational and cultural values. It is
a factor making for integration, involvement in
social life, tolerance, acceptance of differenc-
es and playing by the rules.
Sporting activity should be accessible to every
man and woman, with due regard for individual
aspirations and abilities, throughout the whole
gamut of organized or individual competitive or
recreational sports.
For the physically or mentally disabled, the
practice of physical and sporting activities
provides a particularly favourable opening for
the development of individual talent, rehabili-
tation, social integration and solidarity and,
as such, should be encouraged.
The Member States encourage voluntary services
in sport, by means of measures providing ap-
propriate protection for and acknowledging the
economic and social role of volunteers, with the
support, where necessary, of the Community in
the framework of its powers in this area.
1.3.1. Role of sports federations
The European Council stresses its support for
the independence of sports organizations and
their right to organize themselves through ap-
propriate associative structures. It recognizes
that, with due regard for national and Community
legislation and on the basis of a democratic
and transparent method of operation, it is the
task of sporting organizations to organize and
promote their particular sports, particularly
as regards the specific sporting rules applica-
ble and the make-up of national teams, in a way
which they think best reflects their objectives.
It notes that sports federations have a central
role in ensuring the essential solidarity be-
tween the various levels of sporting practice,
from recreational to top-level sport, which
co-exist there; they provide the possibility of
access to sports for the public at large, human
and financial support for amateur sports, promo-
tion of equal access to every level of sporting
activity for men and women alike, youth train-
ing, health protection and measures to combat
doping, acts of violence and racist or xenopho-
bic occurrences.
These social functions entail special responsi-
bilities for federations and provide the basis
for the recognition of their competence in orga-
nizing competitions.
While taking account of developments in the
world of sport, federations must continue to be
a key feature of a form of organization provid-
ing a guarantee of sporting cohesion and partic-
ipatory democracy.
1.3.2. Protection of young
sportsmen and women
The European Council underlines the benefits
of sport for young people and urges the need
for special heed to be taken, in particular by
sporting organizations, to the education and
vocational training of top young sportsmen and
women, in order that their vocational integra-
tion is not jeopardized because of their sport-
ing careers, to their psychological balance and
family ties and to their health, in particular
the prevention of doping. It appreciates the
contribution of associations and organizations
which minister to these requirements in their
training work and thus make a valuable contribu-
tion socially.
1.3.3. Economic context of
sport and solidarity
The sale of television broadcasting rights is
one of the greatest sources of income today for
certain sports. The European Council thinks that
moves to encourage the mutualisation of part of
the revenue from such sales, at the appropriate
levels, are beneficial to the principle of soli-
darity between all levels and areas of sport.
Reference
European Council – Nice, 7-10 DECEMBER 2000, Declaration on
the specific characteristics of sport and its social function
in Europe, of which account should be taken in implementing
common policies. Retrieved from:
http://www.europarl.europa.eu/summits/nice2_en.htm?textMod-
e=on, 2018.02.08
Draft declaration on the specific characteristics of sport
and its social function in Europe, of which account should be
taken in implementing common policies. Retrieved from:
http://data.consilium.europa.eu/doc/document/ST-13948-2000-
INIT/en/pdf, 2018.02.08)
Incorporating the specific characteristics of sport and its
social functions into the implementation of common policies.
Retrieved from:
http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=LEGIS-
SUM:l35007, 2018.02.08

Learning outcomes:
• Familiarise readers with the differ-
ence between exclusion, segregation,
integration and inclusion and the devel-
opment of the concepts in the society.
• Effective implementation of in-
clusion for volunteers.
• An understanding of how organizations can
raise awareness to promote inclusion.
• The benefits of volunteering for generat-
ing equal opportunities for participation.
• Familiarise readers with the role of each
partner country in the process of inclusion.
• Familiarise reader with the differ-
ent approaches and ways of imple-
menting inclusive programmes.
2. The Role of Or gani zati•Ons in the ProcESs of InCl UsiOn
EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 3130
2.1.ExCLusI•ON, seGre-gatIon, INtegRati•On anD inclUSIOnAUTHORS: JASNA VEŠLIGAJ DAMIŠ, YOANA FILIPIC
Key words: inclusion, integration, segregation, exclusion, disability, education, employment
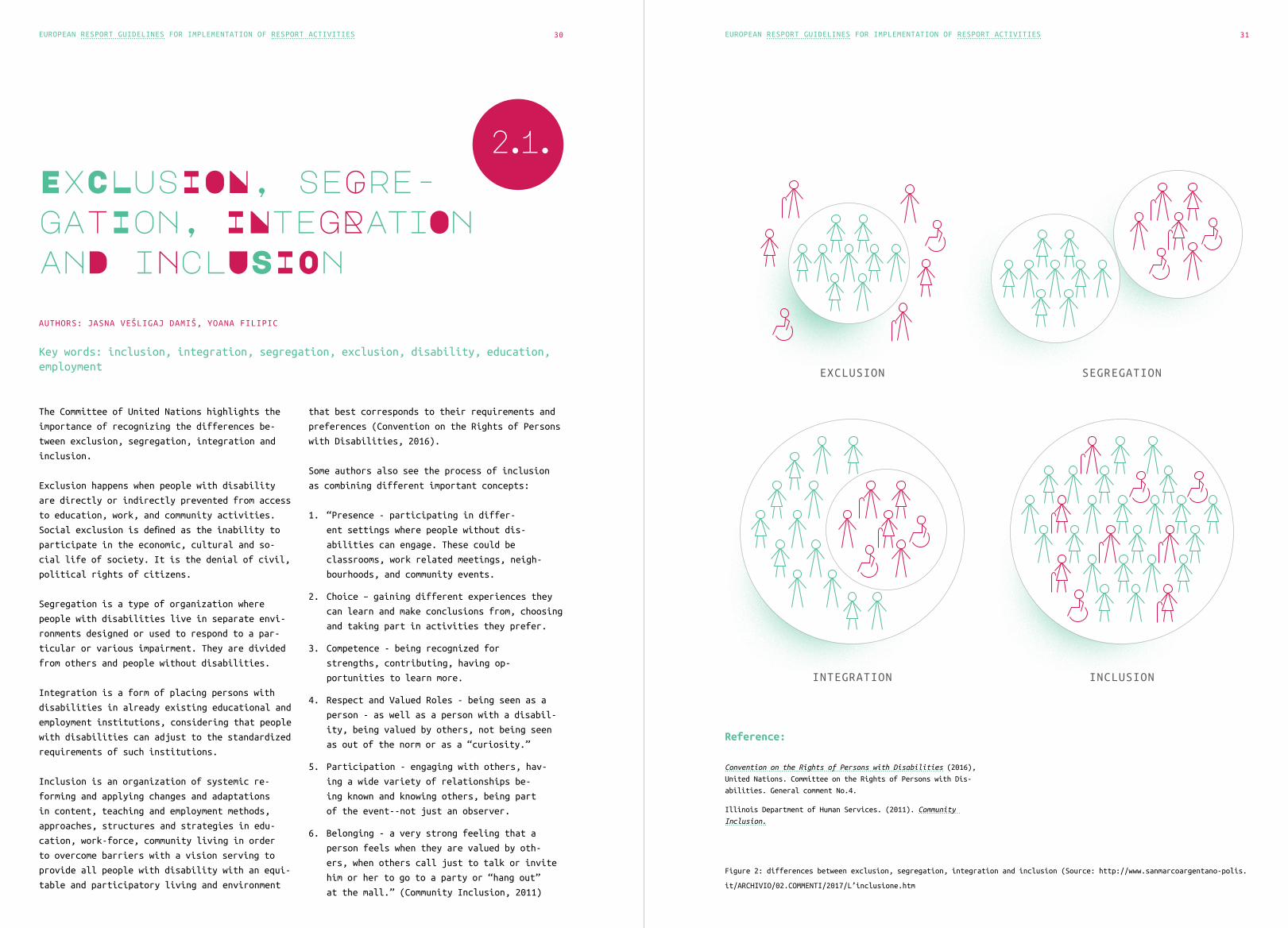
The Committee of United Nations highlights the
importance of recognizing the differences be-
tween exclusion, segregation, integration and
inclusion.
Exclusion happens when people with disability
are directly or indirectly prevented from access
to education, work, and community activities.
Social exclusion is defined as the inability to
participate in the economic, cultural and so-
cial life of society. It is the denial of civil,
political rights of citizens.
Segregation is a type of organization where
people with disabilities live in separate envi-
ronments designed or used to respond to a par-
ticular or various impairment. They are divided
from others and people without disabilities.
Integration is a form of placing persons with
disabilities in already existing educational and
employment institutions, considering that people
with disabilities can adjust to the standardized
requirements of such institutions.
Inclusion is an organization of systemic re-
forming and applying changes and adaptations
in content, teaching and employment methods,
approaches, structures and strategies in edu-
cation, work-force, community living in order
to overcome barriers with a vision serving to
provide all people with disability with an equi-
table and participatory living and environment
that best corresponds to their requirements and
preferences (Convention on the Rights of Persons
with Disabilities, 2016).
Some authors also see the process of inclusion
as combining different important concepts:
1. “Presence - participating in differ-
ent settings where people without dis-
abilities can engage. These could be
classrooms, work related meetings, neigh-
bourhoods, and community events.
2. Choice – gaining different experiences they
can learn and make conclusions from, choosing
and taking part in activities they prefer.
3. Competence - being recognized for
strengths, contributing, having op-
portunities to learn more.
4. Respect and Valued Roles - being seen as a
person - as well as a person with a disabil-
ity, being valued by others, not being seen
as out of the norm or as a “curiosity.”
5. Participation - engaging with others, hav-
ing a wide variety of relationships be-
ing known and knowing others, being part
of the event--not just an observer.
6. Belonging - a very strong feeling that a
person feels when they are valued by oth-
ers, when others call just to talk or invite
him or her to go to a party or “hang out”
at the mall.” (Community Inclusion, 2011)
Reference:
Convention on the Rights of Persons with Disabilities (2016),
United Nations. Committee on the Rights of Persons with Dis-
abilities. General comment No.4.
Illinois Department of Human Services. (2011). Community
Inclusion.
EXCLUSION
INTEGRATION
SEGREGATION
INCLUSION
Figure 2: differences between exclusion, segregation, integration and inclusion (Source: http://www.sanmarcoargentano-polis.
it/ARCHIVIO/02.COMMENTI/2017/L’inclusione.htm

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 3332
2.2.Effective im-plemeNTAtion Of inclusIOn fOR VOLunteers
AUTHOR: TREASA RICE
Key words: inclusion, volunteers, Raising Awareness, Barriers
Introduction
There are around 11 million disabled people in
the UK. Only two in ten disabled people in En-
gland are currently active. A lack of knowledge
and awareness of opportunities that are avail-
able to disabled people is a major factor in the
lack of disabled people participating in sports
(The Association of Paediatric Chartered Physio-
therapists, 2014).
Sport Scotland (2001) outlined that some people
were simply unaware of the existence of facil-
ities or activities that could cater for the
needs of an individuals with a disability. They
had no knowledge of sports (at any level) that
was available and that they felt they would be
able to take part in. As such, they were pre-
vented from even considering taking in sport.
Sport, as an option, had no profile in the con-
text of their life (Sport Scotland, 2001).
Women are generally less inclined than men to do
sport, and ethnic minorities, people with dis-
abilities and other socially vulnerable groups
are also under represented (EU,2014).
For people with a disability sport can play a
key role; both as regards its value for social
inclusion and for activating health-enhancing
physical activity (European Paralympic Commit-
tee, 2015).
2.2.1. Impact of volunteering
The Department for Social Development (2012)
highlighted that volunteering is at the heart of
a vibrant society where people can contribute to
social change giving their time. Volunteers are
central in delivering the many things we take for
granted such as youth activities, sports clubs,
faith based activities, arts festivals, etc.
In 2002 research for Sport England identified 5.7
million sport volunteers and the National Survey
of Volunteering estimated a similar number in
1997 (Taylor et al., 2003; Davis Smith, 1998).
The Active People Survey conducted by Sport En-
gland in 2005-06 suggested a lower figure – more
than 2.7 million (Sport England, 2006).
Sport England’s 2002 National Population Survey
estimated that volunteers contribute 1.2 billion
hours each year to sport, with a value of over
£14 billion and equivalent to 720,000 additional
full-time paid workers (Taylor et al., 2003).
Volunteering in sport has an impact on clubs,
members and players, the community, and volun-
teers themselves. Sport England notes that the
community sport sector “can make increasingly
vital contributions to the health of the nation,
community regeneration and cohesion, community
safety and educational attainment” (Taylor et
al., 2003).
2.2.2. Characteristics
of volunteering
Ibsen (1992) defined volunteering by five central
characteristics:
• Voluntary activities
The activities are undertaken free-
ly without physical force, legal coer-
cion or financial pressure, and “retiring”
from voluntary work does not threat-
en the livelihood of volunteers.
• Which are unpaid or paid with a symbolic
amount
Volunteers may only receive reimburse-
ment of costs connected to the voluntary
work and symbolic fees for their work.
• The voluntary activities must be carried out
for other people than the family
This distinguishes voluntary work from
ordinary domestic activities and the in-
formal care for family members.
• For the benefit of other people
The value that the work done by the vol-
unteers has for other people is a con-
stitutive element of volunteering.
• And have a formal character (organized or
agreed)
Volunteering can take place in a voluntary
organization, but it can also be performed
outside of the voluntary organizations as
long as it is “agreed’ upon between the
person(s) doing the voluntary work and the
person(s) benefiting from it. Ordinary helpful-
ness of a spontaneous and informal character
is, however not considered volunteering.
2.2.3. Benefits of Volunteering
Gaskin (2008) highlighted that volunteers are
the lifeblood of sport in local communities;
the presence of volunteers in clubs and groups
enables them to function successfully and to
exist at all. Volunteers keep clubs and groups
going, and provide good quality services for
members and users. The opportunities that they
provide enable people to have fun, make friends,
improve fitness and health, and develop confidence
and skills. Volunteers themselves benefit from a
sense of satisfaction and the social aspects of
their volunteering.
2.2.4. Implementing
inclusion as a volunteer
Youth Sport Trust – Lead your gen-eration – An Inclusive Future
The Youth Sport Trust (2013) developed train-
ing courses for volunteers who work with people
with disabilities or additional support needs in
their local communities.
They use the STEP Model, developed by Black and
Stevenson (2011). This can be used to change the
way an activity is delivered so it can be made
in one or more STEP areas (Space, Task, Equip-
ment, People).
STEP Model (Black & Stevenson, 2011)
Space examples:
• Increase or decrease the size
of the playing area.
• Use zoning. e.g. where children are
matched by ability and therefore have
more opportunity to participate.
Task examples:
• Break down complex skills into small-
er component parts if this helps
to develop skills more easily.
• Ensure there is adequate opportunity for
players to practice skills or components
individually or with a partner before in-
cluding in a small-sided team game.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 3534
Equipment examples:
• In ball games, increase or decrease
the size of the ball to suit the abil-
ity of the participants, or on the
kind of skill being practised.
• The use of bell or rattle balls can as-
sist the inclusion of some players.
People examples:
Match players of similar ability in small-sided
or close marking activities.
• Balance team numbers to the over-
all ability of the group.
Youth Sport Trust (2013) provides some top tips
for volunteers to ensure they are implementing
inclusive practice:
• Focus on the participant is able to do – don’t
worry about the detail of their impairment.
Take the time to get to know what the partic-
ipant can do and plan activities around this.
• Ask – don’t be afraid to ask the individual
what works best for them and involve them in
the planning stage of the activity/session.
• Sometimes things don’t work – don’t be wor-
ried if something doesn’t work – not ev-
erything you have planned will work. Keep
communication open with participants during
the session and adapt when necessary.
• Use appropriate language – aim to always
give short, clear instructions and pro-
vide a demonstration where possible.
2.3.rAIsiNg AwAre-NEsS of IncLUsioN
AUTHOR: TREASA RICE
Key words: inclusion, volunteers, Raising Awareness, Barriers
2.3.1. Inclusion in sport
The European Paralympic Committee (2015) refers
to inclusion as a sense of belonging, which in-
cludes respecting feelings, being valued for who
you are, and a level of supportive energy and
commitment from others.
The concept of inclusion is particularly im-
portant in the sport realm, because in adapting
sport it is important to gain as much knowledge
from those that are directly playing it as they
are able to comment on their own capabilities as
well as providing great insight into any adapta-
tions or limitations etc. (Conroy, 2007).
Within a sport atmosphere persons with disabil-
ities are presented with a space that they can
develop skills such as teamwork, respect, commu-
nication and confidence which are all skills that
are important in everyday living (U.N Task Force
Report, 2003). Sport can also represent a form
of low-cost physiotherapy in that it allows in-
dividuals to work on mobility, balance, strength
etc. (Roy, 2006).
2.3.2. Barriers to inclusion
Conroy (2007) highlighted that there are major
difficulties in getting those with disabilities
to take part in sport, due to several reasons
including discriminatory attitudes of family
members who view those with disabilities as an
embarrassment, thus depriving them of access to
their local communities and facilities.
Conroy (2007) goes on the say that sport is an
excellent arena to raise awareness. Sport also
provides spectators the opportunity to break
their stereotypical beliefs about those with
disabilities because the spectators frequently
are surprised by those with disabilities exceed-
ing their expectations (Conroy, 2007).
2.3.3. Raising Awareness
There is still a great lack of awareness and
knowledge around the abilities of individuals
with disabilities. By raising awareness you can
provide people with information about the per-
sonal backgrounds of those with disabilities,
subsequently helping to overcome attitudinal
barriers (The European Paralympic Committee,
2015). By creating a barrier-free environment
for everybody you can ensure that persons with
any type of disability are able to have access
to all activities (The European Paralympic Com-
mittee, 2015).
England Athletics raise awareness by ensuring
that all their employees receive up to date
training on Equality, Diversity and Inclusion,
as well as providing information for clubs,
coaches, officials and members to help them tack-
le inequality and discrimination in athletics
(England Athletics, 2018).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 3736
Major events, such as the International Day of
Disabled Persons and European Week of Sport,
can provide great opportunities for raising
awareness, from national to local level, about
the need for inclusive recreation and sporting
activities. These events often attract posi-
tive media attention, which can raise awareness
across a wide audience (Khasnabis et al., 2010).
Case Studies
Alana, 25 Wellbeing Programme Volunteer
In 2012, Alana experienced a neurotoxic reaction
to medication and had to leave university. She
made a good recovery but through her experience
she learnt how isolating an illness can be, es-
pecially as brain injury has many symptoms that
are not visible to others and therefore wanted
to volunteer with brain injury survivors to help
others.
Through her volunteer role, Alana has developed
skills such as being flexible, creative, and pa-
tient, having an encouraging attitude and being
a good communicator. Alana assists the project
officer with setting up arts workshops, having
conversations with services users, helping them
to complete the arts activities, helping them
with their lunch and cleaning and tidying up
after the workshop. Alana also helps service
users with physical activity programs in the
gym; making sure they are completing the cor-
rect movements; helping them with their balance;
encouraging them to take part and assisting them
when they need help with specific exercises.
“Brain Injury Matters is a great place where
people with different brain injuries and from
different backgrounds can meet together to have
fun, learn new skills, and make friends. I love
getting to know the service users and see them
enjoy themselves and grow in confidence.”
“I hope to become an Occupational Therapist.
Through volunteering I gained experience of
working with people with brain injuries and have
observed how the well-being program can improve
their quality of life.”
“Volunteering is a great way to help improve the
quality of life of people with brain injuries,
to meet new people and learn new skills. Brain
Injury Matters is a great cause and I would en-
courage anyone who wants to help those affected
by a brain injury to get involved.”
Reference:
Association of Paediatric Chartered Physiotherapists. (2014).
Disability Sport. Retrieved from: http://apcp.csp.org.uk/
publications/disability-sport-0
Black, K., & Stevenson, P. (2011). The inclusion club.
Conroy, E. C. (2007). Aiming for Inclusive Sport: the Legal
and Practical Implications of the United Nation’s Disability
Convention for Sport, Recreation and Leisure for People with
Disabilities. The Entertainment and Sports Law Journal, 5(1),
4.
England Athletics. (2018). Equality, Diversity and Inclusion.
Retrieved from: https://www.englandathletics.org/about-en-
gland-athletics/equality--inclusion, Retrieved 3.9.2018.
EU. (2014). Special Eurobarameter 412. Sport and Physical
activity. Brussels: TNS Opinion and Social.
European Paralympic Committee. (2015). A Toolkit for Disabil-
ity – and Para – Sports. Retrieved from: http://be-inclusive.
eu/wp-content/uploads/2016/06/BeInclusive_Handbook.pdf,
3.9.2018.
Gaskin, K. (2008). A Winning Team? The Impact of Volunteers
in Sport. London: The Institute for Volunteering Research and
Volunteering England.
Isben, B. (1992). Frivilligt arbejde I idraetsforeninger
[Voluntary work in sports clubs]. Copenhegan: DHL.
Khasnabis, C., Heinicke Motsch, K., & Achu K. (2010). Com-
munity-Based Rehabilitation: CBR Guidelines. Geneva: World
Health Organization; 2010.
Roy, E. (2006). The Development of the Human Rights of Indi-
viduals with Disabilities in Sport at the United Nations and
Beyond. International Council of Sport Science and Physical
Education 48.
Sport Scotland. (2001). Sport and People with a Disability:
Aiming at Social Inclusion. Research Report No.77. Sport
Scotland.
The Department for Social Development. (2011). Join In, Get
Involved: Build a Better Future. The Volunteering Strategy
for Northern Ireland. The Department of Social Development.
Taylor, P., Nichols, G., Holmes, K., James, M., Gratton, C.,
Garrett, R., Kokolakakis, T., Mulder, C., & King, L. (2003).
Sports Volunteering in England. London: Sports England.
United Nations Inter-Agency Task Force for Sport Development
and Peace. (2003). Sport for Development and Peace: Towards
Achieving the Millennium Goals’ United Nations.
Youth Sport Trust. (2013). Lead your generation. An Inclusive
Future. Inclusive Futures. Volunteer Toolkit. Retrieved from:
https://www.youthsporttrust.org/sites/yst/files/resources/doc-
uments/IF%20Toolkit%20-%20volunteers%20FINAL.pdf, Retrieved
3.9.2018.
2.4.The ROle of Re-Sp•Ort Project ParTNers •OrgAni-zaTi•ONS in the ProcesS of In-cluSIOn
2.4.1. The Role of Center Naprej in the Process of Community Inclusion of Persons with Acquired Brain Injury
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: Center Naprej, inclusion in sports, acquired brain injury, rehabilitation
NAPREJ, Centre for Persons with Acquired Brain
Injury is a non-profit organization from Slove-
nia. Our field of expertise is long-term psycho-
social and health rehabilitation after acquired
brain injury. All the services and programmes
that we deliver (occupational therapy, physio-
therapy, psychological, social and health care,
employment under special conditions) are de-
signed to increase active participation of users
in society and to raise the quality of their
lives as well as the lives of their families. An
important field of our work are various preven-
tive, counselling, and educational programmes
taegeted at special groups and the general pub-
lic. Besides our users we devote special care to
their families – we include them in all phases
of the rehabilitation process, providing them
with counselling and support. The rehabilitation
programmes take place at two different units in
Maribor and Murska Sobota.
Our service users are people who have experi-
enced severe brain injury, have a disability
status, and need different type of assistance
for daily living.
2.4.1.1. Center Naprej as an inclusive institution
Center Naprej holds an important role through
its work and implementation of services, the
role of integrating people with acquired brain
injury (hereinafter referred to as ABI) in the

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 3938
local and wider social environment. Definite-
ly, this is a very sensitive area, since we
are talking about the people who are the most
vulnerable and threatened part of humanity in
the provision of declared rights, because they
themselves most often cannot defend and demand
their own rights.
Since most of our users need help of another
person, it is important who and what are the
organizations who provide this assistance. It is
important to support employees with appropriate
counselling, professional help, education and
training, supervision and intervision. Appro-
priate learning and technical tools are also
essential.
Center Naprej as an inclusive institution:
• emphasises/encourages partici-
pation, not competition,
• searches for solutions that are beneficial
to all, considering their impairments,
• prepares for relationships and
life in the community,
• establishes new relationships, con-
nects an individual with others,
• enhances respect and under-
standing of one another,
• it is directed towards the needs of the
individual – satisfying what is possi-
ble within or outside the institution.
2.4.1.2. The regulation of inte-gration of persons with disabil-ities as a mirror of society
The regulation of the integration of persons
with disabilities in the community is undoubt-
edly a mirror of the society as a whole (Šte-
fančič, 2002) and a society that wants to enable
people with disabilities to have better oppor-
tunities for development and that wish to accept
them as equal members of the community must, to
the greatest possible extent create suitable
environment for their social integration and
inclusion.
Joining the European Union, Slovenia has commit-
ted to following democratic values on equal op-
portunities and independent life of persons with
special needs. The country is responsible for
ensuring equal opportunities. It is especially
important to think about professional and ethi-
cal responsibilities, responsibility for ensur-
ing equal opportunities for all, which we have
signed as a country with numerous conventions
and wrote in the Constitution of the Republic of
Slovenia. To achieve this, a proper professional
and legal basis that allows it must be adopted.
There are many arguments in the professional
literature that confirm this hypothesis, but un-
fortunately in practice it often turns out to be
different (Bužan, 2011).
Persons with disabilities are an important
social subsystem, representing a significant
proportion of the total population: about 10%
worldwide, about 15% in the EU, in Slovenia
numbers are similar (Kresal Šoltes, 2006). The
Convention on the Rights of Persons with Dis-
abilities, which was ratified by the Republic of
Slovenia in 2008, has contributed significantly
to the recognition of their rights. This has
supported the greater realization of the objec-
tives of the Action Programme for Persons with
Disabilities 2014–2021 and the European Disabil-
ity Strategy 2010-2020: A Renewed Commitment to
a Barrier-Free Europe at the national and local
level in the everyday life of people with dis-
abilities in the Republic of Slovenia.
People with disabilities have the same needs as
all other people. In order to meet these, it is
necessary to support them, help them recognize
their needs, and even demand them. Every indi-
vidual needs to be paid attention to his special
features (Bužan, 2011). The Convention on the
Rights of Persons with Disabilities (http://
www.mddsz.gov.si) in its Article 30 regulates
this area of rights - the right to participate
in cultural life, recreation, leisure activities
and sports.
Individuals with disabilities can experience a
number of challenges in the process of inclusion
in the community. They also often face isolation
due to a narrowed social network, despite the
fact that nowadays the whole developed world
accepts the idea and the paradigm of inclusion.
2.4.1.3. What does “inclu-sion in sports” mean?
Often, in our work enabling our users (ABI sur-
vivors) to participate in sports, we encounter
various obstacles, such as:
1. lack of awareness of inclusion amongst people
without disabilities and how to properly
engage people with disabilities in groups;
2. lack of opportunities and sports programs;
3. lack of training programs for profession-
als and providers of assistance in the field
of sports for persons with disabilities;
4. limited access to some facili-
ties due to physical obstacles;
5. limited information, access to pro-
grams, facilities, assistants,
etc. (DePauw and Gavron, 2005)
Sport and recreation can be a great medium that
supports an active lifestyle and the development
of healthy relationships between people with
disabilities and people without disabilities,
as they offer many opportunities for communica-
tion and rich social experience. Adapted sports
activities carried out in the community promote
and facilitate the full participation of people
with disabilities in the real life.
Although sport activities can vary greatly (e.g.
skiing, stand-up paddle boarding, horseback
riding, biking, climbing, etc.), success depends
not only on the characteristics of an individ-
ual with disabilities, but also on the skills
and knowledge of professionals, assistants and
volunteers who collaborate with them. These
individuals spontaneously become partners in
communication as a result of a shared activity.
Thus, through active sports and recreational ex-
periences we encourage communication and social
relationships. Groups cooperate to be success-
ful and make the most of the experience of all
interested parties. Sports should not be the ex-
clusive right of a particular social group, but
an opportunity for everyone to develop oneself
through movement and mental activity according
to their abilities. (Mihorko, 2014)
Sport can be perceived as concept defined by the
President of UNESCO as “all forms of physical
activity that contribute to physical fitness,
mental well-being and social interaction, such
as playing, recreation, organized or competi-
tive sports and indigenous sports and games” (UN
Inter -Agency Task Force, 2003).
Over the past few decades, UNESCO has devoted
many efforts to implementing the principle of
inclusion at all levels in education systems
around the world. The idea that they must “pro-
vide a system of inclusive education at all
levels” is also a central objective of the UN
Convention on the Rights of Persons with Dis-
abilities. These questions about the principles
of inclusion are especially important in our
work, when we support our service users in their
return back to community.
2.4.1.4. Sports programs in Cen-ter Naprej - inclusive and adapt-ed physical activities
When integrating people with ABI into sports
programs, we are focused on two important as-
pects: the aspect of integration in general and
the real value of sports activities. Sports must
represent a way of social inclusion. Sports
activities are introduced as a training content
where, unlike educational activities, individ-
ual choice of sports activities can be made on
a large scale, ranging from separate activities
intended for people with disabilities to modi-
fied or adapted activities that are intended for
everyone. However, it should be emphasized that
each approach is equally important and valid,
and there is no need to discredit the separate
structures and to praise the role of the persons
with disabilities involved.
We focus our attention on the importance of the
processes and mechanisms of integration that
happen in the area of sports, and on the ques-
tions what happens or could happen to ABI survi-
vors when they enter sports settings. Involving
disabled athletes in sports in the community
helps overcoming prejudice, stereotypes and
fears. The latters tends to occur most often
as a result of lack of information about the
life of people with disabilities, their needs
and abilities. This is why this often leads to
social isolation of children, adolescents and
adults with disabilities.
The mechanisms of integration through sports
allow them to socialize, meet and communicate
in social settings. Sports activities can be
adapted for each individual according to his
abilities and capabilities and to the greatest
possible extent; they are adapted for people
with disabilities. Appropriate sports activi-
ties can be found for each individual, whether
for recreational, rehabilitation or competitive
purposes.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 4140
We include people with ABI in sports activities.
Survivors may be:
1. physically impaired,
2. blind or visually impaired,
3. deaf, hard of hearing,
4. cognitively-impaired,
5. speech-impaired,
6. individuals with mental health and/
or neurological disorders,
7. individuals with emotional and/
or behavioural problems,
8. multiple impairments – combined impairments.
Examples of sports programs that we perform for
rehabilitation, recreational or / and competi-
tive purposes in the Center Naprej:
1. rehabilitation exercise with or with-
out accessories, fitness;
2. water sports: rehabilitation swim-
ming, swimming using Halliwick con-
cept, water games, stand up paddle
boarding, rowing, snorkelling;
3. ball games (small, big, sound): football,
basketball, netball, foot golf, tennis,
table tennis, volleyball, crossboccia,
bowling, boccia, badminton, speedminton;
4. walking, Nordic walking, hiking,
slack line, orienteering, running;
5. winter sports: alpine skiing, snow
shoeing, sledding, skiing;
6. sports with animals: rehabilitation horse-
back riding, rehabilitation fishing;
7. dancing, cheer leading.
If we are committed to work promoting the health
of our users, we need to think about ways to
increase their physical activity considering
their individual differences. Consequently this
could be an important contribution to achieving
a healthier lifestyle. Participation in sport
can significantly improve their health, well-be-
ing and quality of life.
When adding sports programs into rehabilitation,
we are aware that for people with ABI sports may
impact physical condition in different ways -
good blood circulation, stronger muscles, im-
proved balance and coordination, etc. But sports
can offer much more. People who engage in sports
also benefit from a number of psychological
benefits, such as improved self-esteem, self-dis-
cipline and self-confidence, and confidence in
their abilities and capabilities. We also notice
an improved anger management and the ability to
deal with stressful situations more effectively
than those ABI survivors who are less active.
They are more cooperative and interactive with
others. They have more opportunities to gain a
sense of responsibility towards themselves and
others. Sport provides them with something to
looking forward to.
After suffering a brain injury, individuals may
find it difficult to cope in ordinary situations
and activities of daily living, so they experi-
ence many losses in their new lives. Therefore
it is very important that we help them find some-
thing they cannot only cope with but also enjoy.
Sport can give them a reason to live.
Therefore, we can state that sport is a platform
for acquiring knowledge and life skills as well
as an opportunity for social inclusion.
Reference
Bužan V. (2011). Uvod, Usposabljanje strokovnih delavcev za
uspešno vključevanje otrok in mladostnikov s posebnimi po-
trebami v vzgojo in izobraževanje v letih 2008, 2009, 2010 in
2011, Skupnost organizacij za usposabljanje oseb s posebnimi
potrebami v Republiki Sloveniji, Ljubljana
DePauw, K. P., and S. J. Gavron (2005). Disability and Sport.
Champaign, IL: Human Kinetics.
Konvencija o pravicah invalidov, Retrieved from http://www.
mddsz.gov.si/fileadmin/mddsz.gov.si/pageuploads/dokumenti__
pdf/konvencija_o_pravicah_invalidov.pdf, 8.6.2018
Kresal Šoltes,K., Novak, M., Kresal,B., Kalčič, M., Zaviršek,
D., Invalidi med socialnim varstvom in trgom dela (ekspertiza
– pravni in mednarodni vidik), Ministrstvo za delo, družino
in socialne zadeve, Ljubljana, 2006, Retrieved from http://
www.mddsz.gov.si/fileadmin/mddsz.gov.si/pageuploads/dokumen-
ti__pdf/invalidi_soc_varstvo_trg_dela.pdf, 10.6.2018
Mihorko, B., Štrumbej, B., Čander, J., Cimerman Sitar, M.
(2014). Smernice za šport in rekreacijo invalidov Operativni
program Slovenija-Avstrija 2007-2013, Maribor
Stevenson, P. (2009). “The Pedagogy of Inclusive Youth Sport:
Working towards Real Solutions.” In Disability and Youth
Sport, edited by H. Fitzgerald, 119–131. London: Routledge.
Štefančič, Z. (2002). Vizija preobrazbe specializiranih in-
stitucij – zavodov za vzgojo in izobraževanje oseb z zmerno,
težjo in težko in najtežjo motnjo v duševnem razvoju. V:
Destovnik (ur). Osebe s posebnimi potrebami v procesu inklu-
zije ter vloge defektologov in specializiranih institucij.
Društvo defektologov Slovenije.
UN Inter-Agency Task Force on Sport for Development and Peace.
(2003), Why Sport? Paris: UNESCO. Retrieved from http://www.
un.org/wcm/content/site/sport/home/sport on 20.6.2018
2.4.2. Centro Sportivo Italiano
AUTHORS : CENTRO SPORTIVO ITALIANO-WELFARE AND SOCIAL PROMOTION OFFICE
Key words: Centro Sportivo Italiano, non-profit association, voluntary work, promot-ing sport, educating through sports
Introduction
CSI - Centro Sportivo Italiano is a non-profit
association, based on voluntary work, promot-
ing sport as a moment of education, growth,
social engagement and aggregation, prompted by
the Christian vision of man and history at the
service of the people and the territory. Among
the most ancient sports promoting associations
in our country, CSI meets the demand of a sport
that is not only numerical, but also qualified on
the professional, human and social level. Young
people always make up our main reference point,
even if the promoted sports activities are de-
voted to any age bracket.
2.4.2.1. CSI mission and vision
Educating through sports is the mission of CSI.
This is consolidated in the procedure and con-
science of the association on all levels. Sport
facilitated by CSI can also be a preventative
instrument for particular social pathologies
such as loneliness, fears, dreads, doubts, devi-
ance of young people.
CSI is a sports promoting institution spread all
over the national territory acknowledged by the
Italian Olympic Committee (CONI). It is recog-
nized by the Italian Episcopal Conference as a
Christian inspired association. It is recognized
by the Interior Department as a national insti-
tution with charitable aims. It is registered in
the national register of Social Promotion Asso-
ciations, recognized by the Ministry of Work and
Social Policies.
CSI is recognized by the Department of Educa-
tion, University and Scientific Research as an
accredited institution for the formation of
school staff. It has stipulated an understanding
protocol for the organization and promotion of
sensitization and information actions devoted to
students, teachers and parents on the value of
sports practice as well as formation, updating
pathways and meeting occasions for teachers and
parents. It has an understanding protocol with
the Ministry of Justice to promote reinsertion
and social inclusion activities devoted to young
people moving around in the external penal area.
It is an institution accredited by the Nation-
al Office for Civil Service to manage projects
of voluntary civil service. It is a member of
the National Court of Laical Aggregation (Cnal)
it represents Italy internationally within the
Fédération Internationale Catholique d’Educa-
tion Physique et Sportive (Ficep), gathering
the catholic sports associations from Austria,
Belgium, Czech Republic, France, Germany, Italy,
Holland, Poland, Slovak Republic, Switzerland at
present, besides some sports groups from Mada-
gascar and the former Yugoslavia.
It is a member of the Permanent Forum in the
Third Sector and has signed cooperation conven-
tions with the Italian Parents Association, with
the Childline, etc.
THE NUMBERS OF CSI
• 1.152.000 Athletes
• 13.000 Sports clubs
• 42.000 Teams
• 100 sports disciplines
• 8.000 Tournaments per year

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 4342
• 300.000 Competitions per year
• 139 Territorial gatherings
• 21 Regional gatherings
• 135.000 Trainers, animators, ref-
erees, judges and executives
• 12.000.000 Yearly hours of free en-
gagement and voluntary work
2.4.3. Rijeka Disability Sports Association - the role of organization in the process of inclusion
AUTHOR: ILONA KOVAL GRUBIŠIĆ,
Key words: sports association, sports clubs for persons with disabilities, inclu-sion, adaptive physical culture, adaptive sports, Paralympics sport.
The growth of disability is a world trend. In
total there are about 650 million officially reg-
istered disabled people in the world. According
to the World Health Organization, people with
disabilities make up about 10% of the world’s
population. Despite the success of medicine,
their number is slowly but steadily growing,
especially among children and adolescents. For
comparison: in the US - 54 million disabled, or
19%, in China - 60 million, or 5%. Until recent-
ly, the problems of this fairly large group of
people were ignored, and yet, as a result of the
gradual humanization of society, the Universal
Declaration of Human Rights, the World Program
of Action concerning Disabled Persons and the
United Nations Standard Rules on the Implemen-
tation of Equal Opportunities for Persons with
Disabilities were adopted. In many countries,
legislative acts have been adopted that reflect
the problems of disabled people. From year to
year, the number of children with developmen-
tal disorders increases. The number of children
with developmental disabilities and poor health
reaches 85% of the total number of new-borns.
Only some of these children will later become
the object of correctional work, but the number
of children who need such work is quite large.
According to foreign statistics, it is 9-11% of
the total child population (Sunagatova, 2012,
Dyachenko, Rzyankina, Solokhina, 2010)
Working with children with developmental disabilities in sports clubs (guidelines)
The Rijeka Sports Association for Persons with
Disabilities provides equal opportunities for
sports and recreation for all persons with
disabilities in the Rijeka area, regardless of
age, gender, socio-economic status or type of
disability.
The aim of the Association is to create a net-
work of sports clubs for persons with disabil-
ities in the Rijeka area, which will provide a
wide range of sports for people with disabil-
ities, as well as engagement and training of
skilled professionals to work with people with
disabilities. Such a bid will encourage and at-
tract many people with disabilities, and espe-
cially youth with disabilities to sports.
2.4.3.1. Basic programs of the association
Promotion of sports for per-sons with disabilities
The level of knowledge regarding the sport of
people with disabilities is very low in our
society. Reasons for this are numerous, but the
main cause is poor media coverage (below 2% of
total media coverage). In 2011 and 2012, the
Association made the project “Paralympics School
Day”, in cooperation with the HPO, which proved
to be extremely successful. The Association is
actively participating in the media promotion
of all sports and sports competitions for per-
sons with disabilities in the area of Rijeka, in
cooperation with all relevant media. The Associ-
ation communicates with the public through the
website.
Sports games for children with difficulties
The Rijeka sports games for children with dis-
abilities – launched in 2009, have transcended
their initial form and expanded so that now they
include a new Educational-Sport program for
children and young people. GAMES are held for
the 8th time in a row, and the Rijeka Sports As-
sociation for Persons with Disabilities took an
active part in the project. This year’s program
consisted of a series of games involving chil-
dren with developmental difficulties as well as
their friends without any difficulties in devel-
opment, and in this way, through the program “My
Friend and Me”, inclusion through sports was
presented.
The goal of Rijeka’s sports games is to enable
children with developmental difficulties to have
the best effect of physical activity, improving
self-confidence, positive perception, improving
sensory abilities, developing self-reliance and
helping in the group, socializing and joys, and
acceptance in the community.
Inclusion of new people with dis-abilities and new coaches in sport of people with disabilities
The success of any sports club in the long run
is based on the ability of the club to keep
current members and to attract new ones. At-
tracting new members to clubs has proved to be
the biggest problem of some member clubs of the
Association.
The key to recruiting new members - the op-
tion to include new people with disabilities
in sporting activities is to “reach” the right
people, especially the parents of young people
with disabilities. Therefore, the Association
regularly carries out workshops on the sport of
people with disabilities and actively promotes
sports for persons with disabilities in schools
health organizations, hospitals and healthcare
institutions.
As is common knowledge in our society, very
few people with disabilities are involved in
active sports and recreation, which is very
important in rehabilitation as well as social-
ization in society. In order to include people
with disabilities in sports and recreation, it
is necessary to organize effectively: clubs,
trainers, adapted facilities where people with
disabilities can have easy access, organize
seminars, promotion of available sports activ-
ities, organize promotional tournaments, and
tour of various institutions. The inclusion in
sports and recreation depends primarily on the
active participation of people with disabilities
and their primary environment (family, friends)
where they cease to be passive observers and be-
gin to actively participate in the creation and
upgrading of the system of their service.
By conducting sports and recreational activities
of people with disabilities, as well as accompa-
nying media coverage, the perception in society
of people with disabilities as passive social
entities will also change.
By actively engaging in sports, people with
disabilities will also gain new skills and in
doing so, will challenge community to respond
with new, different expectations, which will
in turn start the unstoppable process of social
evolution.
The employment program of city sports instruc-
tors for the sport of people with disabilities
will enable the creation of a special data bank
of one portion of the population with disabil-
ities, which will bring about new public in-
terest, and in particular the inclusion of a
greater number of young people with disabilities
in sport.
The program also includes ongoing openness to
the health system, its members and their ideas,
and cooperation with the families of people with
disabilities that, due to the many experiences
they have had, need to be actively involved in
the system. Since sport has a particular place
in the social hierarchy, it is logical to choose
this activity as the primary means of sensitiz-
ing our public, because of its social, public,
medical and emotional reasons.
References
Sunagatova LV, Marchenkova UA Influence of adaptive sports on
social adaptation of invalids // Young scientist. - 2012. - №
12. - P. 603-607. - URL https://moluch.ru/archive/47/5856/.
Retrieved 15.10.2018.
Dyachenko, VG, Rzyankina MF, Solokhina LV A guide to social
paediatrics. Under. Ed. V.G. Dyachenko / V.G. Dyachenko, M.F.
Rzyankina, L.V. Solokhin - Khabarovsk: Publishing house of
the Far-Eastern State Medical University, 2010, - 124 p.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 4544
2.4.4. The Role of FPDD in the Process of Inclusion
AUTHOR: EDUARDO BORGES PEREIRA
Key words: sport development; inclusion of people with disabilities through sport; disability areas.
FPDD – Portuguese Federation for Disability
Sports has 30 years of contribution for develop-
ment of sport in Portugal, especially for people
with disabilities.
FPDD and his four associates (there were five un-
til 2017) – the National Associations for sports
are specialized for disability area: blind,
cerebral palsy, deaf, intellectual and motor
impairment. They have had a major contribution
to bring more people with disabilities to sport,
having “sport for all” as the main mission and
competition sports, national teams and high per-
formance as second goal.
Our mission is to provide to all persons, in-
dependently of their functional capacity,
opportunities of sport practice and physical
activity through life, according with the level
of involvement required by each one, in their
community.
Our organization develops many projects in
partnership with other organizations, focusing
on disabled people, especially children and
youngsters, and on training of professionals
and teachers. We support the organization and
participation in international competitions by
some national teams, such as Boccia and Goal-
ball. This is a continuous process of inclusion
through sport and physical activities with very
good results in Portugal.
References:
http://fpdd.org/
2.4.5. The Role of Brain Injury Matters in the Process of Community Inclusion of Persons with Acquired Brain Injury
AUTHOR: FIONA MC CABE
Key words: Brain Injury Matters NI, inclusion, acquired brain injury, rehabilitation
2.4.5.1. Brain Injury Matters NI; organisational overview
Brain Injury Matters (NI) is a non-profit or-
ganisation aiming to help rebuild the lives of
children and adults living with Acquired brain
injury (ABI) to enable them to reach their full
potential in family and community life in North-
ern Ireland. Our purpose is to support people
living with brain injury, help develop the
skills and confidence to optimise their function-
ing and access a positive quality of life.
A considerable number of people with ABI will
have executive functioning impairments and ex-
perience a greatly reduced capacity to problem
solve, plan, organise and make decisions etc.
This can have a major impact on their ability to
manage everyday living, educational, employment
and inter-personal situations which many people
take for granted.
Brain Injury Matters (NI) delivers age-appro-
priate, needs-led support services designed to
minimize the impact of acquired brain injury on
the person and their wider network and reduce
the onset of secondary problems as a result of
the initial injury or illness. Our programmes
aim to help individuals achieve self-identified
goals, promote age appropriate independence,
maximise social and educational engagement,
promote psychological adjustment post-ABI and
improve overall well-being.
Services offering social, sports, exercise and
recreational activity, skills development,
counselling, information and support are now
recognised as an essential element in the range
of services required to support people with ABI
and their carers. They can influence recovery
and outcomes, in that they support and promote
the long-term adjustment and seek to help the
family unit manage stress, establish meaningful
activities, positive relationships and a valued
lifestyle.
2.4.5.2. Brain Injury Matters NI as an inclusive organisation
Inclusion of people with disabilities in society
means involving them in every aspect of social
participation and maximising a person’s quality
of life. This is a key principle underlying the
work of Brain Injury Matters. The principle of
inclusion is reflected in our organisational vi-
sion of a society where those with brain injury
can live a full and meaningful life. It also is
central to our three core organizational values:
Rights & Responsibilities Where everyone is
actively involved in creating solutions, encour-
aged & supported to take responsibility
Innovation Where we will not be satisfied with
the status quo and continually strive to deliver
the best evidence-based services
Respect for All Where we will treat everyone,
people affected by ABI, their families, staff
and stakeholders with equal respect and honesty,
listening and paying attention to feedback about
our services
References:
www.braininjurymatters.org.uk
2.4.6. Keçiören Municipality and its role in the process of inclusion
AUTHOR: KEÇIÖREN MUNICIPALITY
Key words: Keçiören, Keçiören Municipality
Keçiören Municipality is the biggest district in
Turkey by area and population density. Keçiören
Municipality is a local government unit which
uses its authorities to improve the economic,
social and cultural status of its residents in a
way that encourages them to participate in the
management of the district.
The services provided by Keçiören Belediyesi to
the residents are:
• Development and construction of pub-
lic facilities and infrastructures
• Develop geographical and city man-
agement information systems
• Provide recycling and environmental cleaning
• Provide municipal police, fire depart-
ment, ambulance, emergency assistance
• Forestation, parks and recreation areas
• Cultural activities, education, tour-
ism and publicity, sports activities
• Social services and care for dis-
abled and other disadvantaged people
• Protective services for children and women
Keçiören dates back to 1983 when it became a
separate municipal constituency. It comprises 51
Precincts and covers the area of 190 square km.
It is situated about 13 km from the city centre
with altitude of 1075 m above sea level. It is
the largest Municipality in Ankara with over
900,000 residents.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 4746
Our Values:
• Transparency
• Accessibility
• Productivity
• Participation
• Ecological Awareness
• Honesty
• Innovative Approach
2.4.7. The role of Human Profess Non-profit Ltd. in the process of inclusion of people with disabilities
AUTHOR: ZSUZSANNA KOVÁCS
Keywords: Human Profess, inclusion, disabled people
Human Profess Non-profit Ltd. is offering – among
other things – project management and labour
market services, training for NGOs, governments
and for-profit companies in Hungary. Activities
of the company also include services that pre-
serve, improve and assist the living and health
conditions of workers with disabilities.
Human Profess is an accredited employer where
they provide work for 24 workers with disabil-
ities: from simple, easily acquirable, semi-
skilled work through project administrators to
trainer tasks.
Their experts have many years of experience
in the fields of rehabilitation, labour market
services, adult education, and international
practices. Professional experience and knowledge
provides a safe base for the organisation to be
able to offer long-term assistance for people
with disabilities regarding their rehabilita-
tion employment. Methods and practices employed
in international projects are also incorporated
into the improvement process of employees. They
provide a complex service to their employees
with disabilities (job opportunity, training
opportunity, mentor support) in the interest of
their successful rehabilitation.
The long-term goal of Human Proffes is to assist
in the employment of workers with disabilities
and to provide them with an occupation suitable
to their education, existing skills and health
conditions. The company’s further goals involve
contributing to the improvement of their adap-
tion skills, to ensure their permanent employ-
ment, and to motivate and support their entry
into the open labour market. They also provide
regular sport activities for colleagues with
disabilities. Posts are regularly available on
their Facebook-site. They continuously share
articles and videos that are related to people
living with various diseases and impairments.
2.4.8. The role of CIF France in the process of inclusion
AUTHOR: DR MOHAMMED MAMMAD, MIREILLE BOUCHER
Key words: people with disabilities
CIF France contributes to the integration of
people with disabilities, which are excluded
from social interactions, with its continuously
organized programs in France for profession-
als and volunteers from different countries,
who work on the social field and socio-cultural
animation.
CIF France organizes multicultural international
programs in coordination with other branches in
25 countries around the world.
CIF France continues its integration actions
with its local, regional, national and inter-
national partners. Through its expertise, CIF
France has participated in several European
programs.
As part of the ReSport project, they contribute
to the integration by mobilizing local partners
with or without disabilities. They have devel-
oped partnerships by integrating people with
disabilities with people without disabilities.
The vision and fundamental goal of CIF France is
inclusion and in pursuit of this goal they have
made several visits to specialized centres for
the disabled. In order to carry out this project
well, they thought it would be better to include
young people and people with disabilities, they
also had the idea of giving them training in
communication and speaking to convey a message.
Inclusion was not just a theory but the action
of a whole group who saw this project as a step
to continuous working together and developing
new actions.

Learning Outcomes:
• to outline different definitions of disability
• to highlight the importance of focusing on
functional abilities and not on disability
• familiarising readers with general in-
formation about what disability is and
certain types of disabilities
• information on the specialties in the men-
tal health of people with disabilities
• familiarising readers with the risk
of obesity and preventing obesity
• to highlight the impact of harm-
ful habits for people with disabil-
ity and how to deal with them
• to get to know advantages and disadvantag-
es of video games, the usefulness of vid-
eo games for people with disabilities
• to highlight the problem of dop-
ing of people with disability
3. Dis aBil iTy and hEaLTh

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 5150
3.1.DefinItions •Of DisabILiTy
AUTHOR: DANIJELA MAJCENOVIČ CIPOT
Keywords: Disability, models, interpretation
Disability is a concept that has during the
years and different cultures been described from
various perspectives. Although the authors of
these perspectives use the same term, the mean-
ing differs. This caused various interpretations
of the term, what is not good from the person
attached point of view – if these different
interpretations cause deprivation of rights in
one field, a person with disability is quickly
in a subordinate position. “The lack of consis-
tency is most dramatic when a person is defined
as disabled in one context and not another, such
that she or he receives therapies for serious
impairments but does not qualify for certain
disability-related benefits provided by his or
her employer or by the government” (Altman,
2011:98). In her research of different models
and concepts Altman produced a table, in which
she summarized the differences in understanding
of the term disability, that are most commonly
used.
Model Disability (A) Disability (B) Disability (C) Disability (D) Disability (E)
Social model ICIDH-1 model Nagi model Verbrugge and
Jette model
IOM-1 and IOM-
2 models
Definition Limit or loss of
opportunities
to take part
in community
life because of
physical and
social barriers
In the context of
health experience,
any restriction
or lack (re-
sulting from an
impairment) of
ability to perform
an activity in
the manner or
within the range
considered normal
for a human being
Pattern of
behaviour that
evolves in situa-
tions of long-term
or continued
impairments that
are associated
with functional
limitations
Disability is
experiencing
difficulty doing
activities in any
domain of life
due to a health or
physical problem
The expression
of a physical or
mental limita-
tion in a social
context-the gap
between a person’s
capabilities and
the demands of
the environment
Table 2: Variety of Meanings Given the Term Disability in Five Theoretical Models (Altman, B. M.: Disability Definitions,
Models, Classification Schemes, and Applications. 2001).
Use of these contexts differs from one public
sphere to another. Where rights and benefits of
special groups is in sight, legal and adminis-
trative spheres tend to categorise disabled in
groups granting them special rights, what can
cause differences and unequal treatment and
therefore inequalities between them. Social
definitions are usually not considered a medi-
cal point of view and vice versa. In a medical
context a person is seen in the light of his/her
boundaries deriving from their disability and
does not consider individuality. And there is
always personal view of the usage of the right
term – some people prefer the term handicapped
for this relates to their ability to work, other
prefer term person with disability or person
with special needs. This always differs from how
a person sees and defines him/herself.
All classification and categorisation of dis-
ability have special aspects on the person they
refer to. Thus they are all imperfect and incom-
plete, because they do not emphasize a person
as an individual, but tend to point out only
certain aspects. In the light of adapted physi-
cal activities the most useful classification is
based on functional level – what a person can do
without or with different levels of assistance.
Nowadays it is customary to describe the person
first and then state the disability – ex. child
with learning disability, person with multiple
sclerosis…. what gives emphasis on the indi-
vidual and doesn’t point out their disability.
But still we must recognize that categorizing
gives us fundamental knowledge about general
characteristics of disability types and there-
fore it is useful in planning adaptive activi-
ties. It can provide a wider framework because
it is essential to be aware of the fundamental
characteristics of conditions as described in
traditional disability classification and then
take into account the unique characteristics
(physiological and psychological) and functional
abilities of a person with disability.
Reference
Altman, B. M. (2001). Disability Definitions,
Models, Classification Schemes, and Applications.
Published in: Albrecht, G.L., Seelman K., Bury
M. (ed.), Handbook of Disability Studies (97-
122). Thousand Oaks – London – New Delhi: Sage
Publications Inc.
Squair, L., Groeneveld, H.J. (2003): Disability
Definitions. Published in: R. D. Steadward, G.
D. Wheeler and E. J. Watkinson (ed.), Adapted
Physical Activity (45-64). Canada: The Univerity
of Alberta Press

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 5352
3.2.CLaSsiFIcaTIon oF DisabILIty
AUTHOR: VALENTINA BOLŠEC
Keywords: disability, mental illness, physical disabilities, sensory disabilities, learning disabilities, developmental disabilities, recommendations
People differ from each other according to their
physical, sensory, and other abilities. Also,
the types of disability are different, covering
all long-term physical, mental and sensory im-
pairments and mental disorders that disable the
person in order to function fully and partici-
pate in society. Persons with disabilities are
classified in categories of disability according
to impairments and other indicators. Since peo-
ple differ from each other, we must never equate
two people with the same disability category;
each person functions in his/her own way and at
his/her best (Squair and Groeneveld, 2003). From
the perspective of its etiology and basic under-
standing, we can place disability in the follow-
ing classification:
Mental disorders
Mental disorder is a medical condition that
includes changes in thinking, emotions and
behaviour or a combination of all and is asso-
ciated with distress or difficulties in the field
of social life, work, and family. It can occur
anytime and anywhere, regardless of age, gender,
financial and social status, race, ethnicity, re-
ligion, sexual orientation or cultural identity.
It can occur in different intensities and can
even cause a person to require hospital treat-
ment (Parekh, 2018). Mental disorders are often
the cause of stigma due to a lack of knowledge
and awareness amongst the public. Patients are
afraid to seek help due to shame, which can, of
course, cause the situation to worsen. Mental
disorders that cause impairment are: mood dis-
orders (depression, bipolar disorder), anxiety,
phobia, panic disorder, obsessive compulsive
disorder, schizophrenia, eating disorders, per-
sonality disorders, multiple personality disor-
ders, etc. (Squair and Groeneveld, 2003).
Recommendations: persons with mental disorders
may often have difficulty participating in phys-
ical activity due to feelings of worthlessness,
helplessness and/or hopelessness. Individuals
may need prompting or motivational tips to
attend a program or activity. It is also recom-
mended that they are accompanied by a friend/
carer/support worker and transported to the
activity location. They need to feel comfort-
able and safe in the environment (Squair and
Groeneveld, 2003).
Physical Disabilities
Physical disability can cause problems in vari-
ous areas such as neuromuscular, cardiovascular,
orthopaedic and pulmonary areas, and limit a
person’s movement, swallowing, breathing and/or
speech (Nkabinde, Obiakor, Offor & Smith, 2010).
People with physical disabilities tend to rely
on devices such as wheelchairs, crutches, walk-
ing frames, rods or artificial limbs. Disability
can be congenital or acquired, which is devel-
oped after birth and is not hereditary, degen-
erative, or induced by birth trauma (O’Reilly
et al., 2015). In the category of physical
disability, we include conditions such as ar-
thritis, asthma, amputation, amyotrophic lateral
sclerosis (ALS), arthrogryposis, brain injury,
cerebral palsy (spastic CP, athetoid CP, ataxic
CP), congenital hip dislocation, cystic fibrosis,
diabetes mellitus, epilepsy, Friedreich’s atax-
ia, Guillain-Barre syndrome, hemophilia, multi-
ple sclerosis, muscular dystrophy, osteogenesis
imperfecta, osteomyelitis, osteoporosis, paral-
ysis, Parkinson’s diesase, polyomyelitis, spina
bifida, spinal cord injury, Tourette syndrome and
tuberculosis (Squair and Groeneveld, 2003).
Recommendations: it is important that we adapt
activities to individual abilities and needs
of the person and to take into account all the
barriers which may occur. We need to ensure the
safety and protection for persons, especially
when they have problems maintaining balance.
Sensory Disabilities
We get to know the world around us through our
senses, which enable us to collect and under-
stand information and connect with people and
our surroundings. As much as 95% of all envi-
ronmental information is obtained through hear-
ing and sight, therefore, the failure of these
senses greatly affects the way a person collects
information about the environment (Types of
sensory disabilities, 2019). It is not necessary
for a person to completely lose hearing or sight
to be regarded as a disabled person with sensory
deficits. Sensory deficits include a partial or
complete loss of hearing, vision, or a combina-
tion of both. Squair and Groeneveld (2003) claim
that hearing loss can be divided into three
categories: conductive, sensory-neural and mixed
hearing loss. Visual impairments can be caused
by albinism, cataracts, glaucoma, retinal blas-
toma and rubella.
Recommendations: individuals, who have a vi-
sual disability, may need orientation of the
area where the activity is taking place. For
partially sighted, colour contrasts might be
appropriate. We can provide auditory cues, where
descriptive language is used. Individual can
be also guided or moved by another person. For
persons with hearing disability it is important
that instructions are given face to face. Also
visible signals and demonstrations should be
used (Squair and Groeneveld, 2003).
Learning Disabilities
We talk about learning disabilities when one or
more of the basic psychological processes in-
volving understanding or using spoken or writ-
ten language exist. Individuals with a learning
disability may have difficulty with input of
information to the brain, organizing and under-
standing information, storing information in
memory, communicating through language or motor
output. Learning disabilities can be broken down
into attention deficiency-hyperactivity disorder
(ADHD) and developmental coordination disorder
(DCD) (Squair and Groeneveld, 2003).
Recommendations: when planning physical activity
for people with learning disabilities, we must
take into account the difficulties of learning
cognitive information and some motor coordina-
tion difficulties. For individuals with ADHD, who
have very little patience, it is very important,
that we set an environment with few distrac-
tions. The activity should be consistent and
structured (Squair and Groeneveld, 2003).
Developmental Disabilities
Developmental disability is defined as severe,
chronic disability attributable to mental and/or
physical impairments that are likely to continue
indefinitely; resulting in substantial functional
limitations in three or more major life activity
areas: self-care, receptive or expressive lan-
guage, learning, self-direction, capacity for
independent living and economic self-sufficiency
and requiring care, treatment or other services
of lifelong or extended duration. (Larson et
al., 2001, p. 231-232). Squair and Groeneveld
(2003) divide developmental disabilities into:
Asperger’s disorder, autism, Alzheimer’s dis-
ease/dementia/senility, Down’s syndrome, fetal
alcohol syndrome (FS), fetal alcohol effects
(FAE) and intellectual disability.
Recommendations: for persons with developmen-
tal disabilities directions and instructions
should be clear, brief, concise, with appropri-
ate vocabulary and simple language that suits
the level of understanding. It is recommended
that in order to ascertain participant’s lev-
el of understanding the facilitator should get
the participants to repeat the instructions
or demonstrate them. Also the use of pictures,
videos, other visual aids, games and repetitions

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 5554
are very effective. Instructions can be broken
into sequential steps for successful learning.
The use of a buddy system is also recommended
(Squair and Groeneveld, 2003).
References:
Larson, S. A., Lakin, K. C., Anderson, L., Kwak Lee, N.,
Lee, J. H., & Anderson, D. (2001). Prevalence of mental
retardation and developmental disabilities: estimates from
the 1994/1995 National Health Interview Survey Disability
Supplements. American Journal on Mental Retardation, 106(3),
231-252
Nkabinde, Z. P., Obiakor, F. E., Offor, M. T., & Smith, D. J.
(2010). Educating Children with Physical Disabilities
O’Reilly, M. F., Sammarco, N., Kuhn, M., Gevarter, C.,
Watkins, L., Gonzales, H. K.,... & Lang, R. (2015). Inborn
and Acquired Brain and Physical Disabilities. In Clinical and
Organizational Applications of Applied Behavior Analysis (pp.
179-193). Academic Press
Parekh, R. (2018). What Is Mental Illness? Retrieved
20.5.2019 from https://www.psychiatry.org/patients-families/
what-is-mental-illness
Squair, L., Groeneveld, H. J. (2003). Disability Definitions.
In R. D. Steadward, G. D. Wheeler and E. J. Watkinson (ed.),
Adapted Physical Activity (11-25). Canada: The Univerity of
Alberta Press
Types of sensory disabilities, 2019. Retrieved 21.5.2019
from https://www.hwns.com.au/about-us/about-disability/
types-of-disabilities/types-of-sensory-disabilities/
3.3.hEaLth COnCerns
3.3.1. The health of people with disabilities
AUTHOR: JASNA VEŠLIGAJ-DAMIŠ
Key words: health condition, disability
An individual’s health status is crucial for
experiencing a better quality of life, indepen-
dence and full participation in society. The
central mission of public health is to improve
the health of all inhabitants. It can be ob-
served that, compared to the general population,
individuals with disabilities often have worse
health and higher levels of chronic illnesses,
such as diabetes, obesity and depression. At the
same time, we can see that persons with disabil-
ities are less involved in organized preven-
tive health activities and often develop a less
healthy lifestyle. (Kasser, Lytle, 2013)
Over a billion people are estimated to live
with some form of disability. This corresponds
to about 15% of the world’s population. Between
110 million (2.2%) and 190 million (3.8%) people
15 years and older have significant difficulties
in functioning. Furthermore, the rates of dis-
ability are increasing in part due to ageing
populations and an increase in chronic health
conditions (“WHO: Disability and health”, 2019).
Disability is extremely diverse. While some
health conditions associated with disability
result in poor health and extensive health care
needs, others do not. However all people with
disabilities have the same general health care
needs as everyone else, and therefore need ac-
cess to mainstream health care services. Article
25 of the UN Convention on the Rights of Persons
with Disabilities (CRPD) reinforces the right of
persons with disabilities to attain the highest
standard of health care, without discrimination
(“WHO: Disability and health”, 2019).
In the case of persons with disabilities, a
number of health problems can be detected due to
secondary health conditions that overlap with
their primary disability as they are very sus-
ceptible to them. For example, in people with a
spinal cord injury or cerebral palsy, a number
of secondary health conditions such as osteo-
porosis, osteoarthritis, increased spasticity,
depression, etc. can be detected, and at the
same time lower balance, muscular strength, en-
durance, mobility and general fitness are common.
All this can significantly affect their daily
activities and the quality of life.
With a good health plan, people with disabili-
ties can improve their health and functionality.
A person, who has suffered a spinal cord injury
and takes good care of his health, eats well,
exercises physically and mentally, goes on reg-
ular medical examinations, prevents ulcers and
maintains appropriate body weight, will certain-
ly maintain good health. In cases were he/she
does not adopt a healthy lifestyle, health will
more than likely deteriorate and “unhealthy”
habits will be adopted, like smoking, alcohol
and drug consumption, which may have additional
unwanted consequences.
Because of all that, people with disabilities
often have more needs for health services,
but are also limited in access to them due to
disability (architectural barriers, necessary
escorts, communication barriers etc).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 5756
In some groups of people with disabilities we
can observe that ageing process begins earlier
than in the rest of the population. For example
some people with developmental disabilities show
signs of premature ageing in their 40s and 50s
(“WHO: Disability and health”, 2019).
In addition to early ageing, some people with
disabilities also notice a higher rate of pre-
mature death or lower life expectancy, what is
also connected to their general health condi-
tion. Overall, the life expectancy of people
with mental disorders is increasing (Coppus,
2013), but their health is still worse than in
the general population (Emerson et al, 2012),
and their life expectancy is still lower than
the life expectancy of their peers without
disability (Heslop et al., 2013; Hosking et al.,
2016).
In the case of individuals with disabilities
that belong to specific racial, ethnic and other
groups, who have a higher degree of disability
and a lower level of participation in the health
care system, we see even more health problems.
In these groups risky behaviour, such as physi-
cal inactivity and obesity are even greater.
It is important that we are aware that the
health of people with disabilities is equal-
ly important and has equal decisive influence
on their quality of life compared with others.
It is therefore necessary to provide them with
equal opportunities, conditions and access to
health services.
References
Coppus, A.M.W. (2013) People with intellectual disability:
what do we know about adulthood and life expectancy? Develop-
mental Disabilities Reviews, 18, 6 – 16
Emerson, E., Baines, S., Allerton, L., Welch, V. (2012)
Health Inequalities and People with Learning Disabilities in
the UK: 2012, Lancaster: Improving Health and Lives
Heslop, P. Blair, P. Fleming, P., Hoghton, M., Marriott, A.,
Russ, L. (2013) Confidential Inquiry into Premature Deaths
of People with Learning Disabilities, Bristol: Norah Fry
Research Centre, University of Bristol
Hosking, F.J., Carey, I.M., Shah, S., Harris, T., DeWilde,
S., Beighton, C., Cook, D.G. (2016) Mortality among adults
with intellectual disability in England: comparisons with the
general population, American Journal of Public Health, d.o.i.
10.2105/AJPH.2016.303240
Kasser, S.L., Lytle R.K., 2013, Inclusive physical activity:
Promoting Health for Lifetime, 2nd ed., Human Kinetics (8-9).
Konvencija o pravicah invalidov (2003). Uradni list RS, št.
37 (10. 4. 2008) Pridobljeno s http://www.mddsz.gov.si/
fileadmin/mddsz.gov.si/pageuploads/dokumenti__pdf/konvenci-
ja_o_pravicah_invalidov.pdf, 2018.02.08.
WHO: Disability and health, 2019: Retrieved from: https://
www.who.int/news-room/fact-sheets/detail/disabili-
ty-and-health, 2019.01.21.
3.3.2. Mental Health
AUTHORS: ILONA KOVAL GRUBIŠIĆ, VALENTINA BOLŠEC
Key words: mental health, mental disorders, mental disabilities, mental health and disability
Mental health is more than the absence of mental
disorders. Mental health is an integral part
of health; indeed, there is no health without
mental health. Mental health is determined by a
range of socio-economic, biological and envi-
ronmental factors. Cost-effective public health
and inter sectoral strategies and interventions
exist to promote, protect and restore mental
health (“WHO: Mental health: strengthening our
response”, 2018).
Mental health is an integral and essential com-
ponent of health. The WHO constitution states:
“Health is a state of complete physical, mental
and social well-being and not merely the absence
of disease or infirmity.” An important implica-
tion of this definition is that mental health is
more than just the absence of mental disorders
or disabilities (“WHO: Mental health: strength-
ening our response”, 2018).
Mental health is a state of well-being in which
an individual realizes his or her own abilities,
can cope with the normal stresses of life, can
work productively and is able to make a contri-
bution to his or her community. Mental health
and well-being are fundamental to our collec-
tive and individual ability as humans to think,
emote, interact with each other, earn a living
and enjoy life. On this basis, the promotion,
protection and restoration of mental health can
be regarded as a vital concern of individuals,
communities and societies throughout the world
(“WHO: Mental health: strengthening our re-
sponse”, 2018).
3.3.2.1. Determinants of mental health
Multiple social, psychological, and biological
factors determine the level of mental health
of a person at any point of time. For example,
persistent socio-economic pressures are recog-
nized risks to mental health for individuals and
communities. The clearest evidence is associated
with indicators of poverty, including low levels
of education.
Poor mental health is also associated with rapid
social change, stressful work conditions, gen-
der discrimination, social exclusion, unhealthy
lifestyle, risks of violence, physical ill-
health and human rights violations (“WHO: Mental
health: strengthening our response”, 2018).
There are also specific psychological and per-
sonality factors that make people vulnerable
to mental disorders. Lastly, there are some
biological causes of mental disorders including
genetic factors which contribute to imbalances
in chemicals in the brain (“WHO: Mental health:
strengthening our response”, 2018).
3.3.2.2. Disability and Mental Health
Disability undoubtedly presents a dimension that
increases risk for negative outcomes in mental
health and stress. Results of studies provide
evidence of a linkage between disability and
risk for impairments in mental health. Nearly
4 of 10 individuals with disability have faced
problems in mental health, which is almost dou-
ble the rate observed for non-disabled. There is
also higher risk for men than for women and for
the young than for the old (Turner, Lloyd and
Taylor, 2006).
Significant research has highlited that depres-
sion is commonly associated with impairment
or disability. Increased rates of depression
amongst people with disability are often a
consequence of experience of impairment and
functional limitations in the coexistence of
social and economic factors that may accompany
disability (Morris 2004). Causal link between
impairment and depression also often rests on
the assumption that acquisition of impairment
is an experience of traumatic loss. Person with
disability has to go through various stages of
grieving before becoming psychologically whole
again (Siller, 1969, p. 292 in Morris, 2004).
Sometimes disability can also be benefit-finding
and post-traumatic growth. Many individuals
believe that their disabilities have helped them
to find meaning or take a more adaptive perspec-
tive to life. These individuals reported they
appreciate personal worth regardless of appear-
ance or ability, they value time spent in family
activities and they became more thoughtful and
understanding. Persons who have developed great-
er acceptance of disability will value their
selfhood and maintain positive beliefs about
themselves (Wright 1983, Taylor 1983 in Elliot,
Kurylo and Rivera, 2002).
Individuals with a disability who have effec-
tive social-problem-solving skills and who have
positive orientations toward solving problems
are more assertive, more psychosocially mo-
bile, more accepting of their disability, and
less depressed than their counterparts who lack
these skills (Elliott, Godshall, Herrick, Witty,
& Spruell, 1991 in Elliot, Kurylo and Rivera,
2002). It is also very important for persons
with disabilities that they are goal-oriented.
Higher goal orientation is definitely associated
with lower levels of depression, greater accep-
tance of disability and increased life satisfac-
tion. We must also not forget the importance of
social support which is crucial for people with
disability.
References
WHO: Mental health: strengthening our response, 2018:
https://www.who.int/news-room/fact-sheets/detail/men-
tal-health-strengthening-our-response
retrieved 12.2.2019 11:48
Elliott, T. R., Kurylo, M., & Rivera, P. (2002). Positive
growth following acquired physical disability. Handbook of
positive psychology, 687-699.
Morris, J. (2004). People with physical impairments and men-
tal health support needs: A critical review of the litera-
ture. Joseph Rowntree Foundation.
Turner, R. J., Lloyd, D. A., and Taylor, J. (2006). Physical
disability and mental health: An epidemiology of psychiatric and
substance disorders. Rehabilitation Psychology, 51(3), 214.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 5958
3.3.3. Disability and Obesity
AUTHORS: LADISLAV MESARIČ, ILONA KOVAL GRUBIŠIĆ
Keywords: obesity, sports activities, healthy food, body mass index (BMI).
Obesity is one of the world’s greatest health
problems. Since 1975, the number of obese peo-
ple in the world has almost tripled. In 2016,
there were more than 1.9 billion adults with
overweight. Of these, more than 650 million were
obese (WHO, 2018). Research shows that obesity
among people with disabilities is significant-
ly higher than for the rest of the population
(Liou, 2005). For people with physical disabil-
ities, obesity is twice as distracting. It is
associated with potential chronic diseases and,
in linkage with existing limits, prevents or
aggravates active participation in sports and
social activities (Liou, 2005).
Obesity is a medical condition in which an
excess of body fat has accumulated to such an
extent that it could have a negative effect on
health (Sackett et al., 1996).
According to the WHO definitions, adults are
considered as obese if their body mass index
(BMI - is defined as the body mass divided by
the square of the body height, and is universal-
ly expressed in units of kg/m2) exceeds 30 kg /
m2. For weight gain, it is considered if the in-
dex is greater than 25 (Swinburn et al., 2005).
BMI is the most useful measure of overweight and
obesity at the population level, since it is the
same for both sexes and for all ages of adults.
However, it should be treated with caution be-
cause it may not correspond to the same degree
of obesity in different individuals.
In children, age should be taken into account
when determining overweight and obesity (Lob-
steinin sod, 2004). Research has shown that BMI
also may not be the best method for some people
with disabilities. BMI can underestimate the
amount of fat in people with spinal cord in-
juries that have less muscle mass. Different
measurement methods should be used for these
individuals, or the BMI value that determines
obesity should be lower (Liou et al., 2005).
The cause of obesity and overweight is most
often the energy imbalance between consumed and
spent calories. At the global level, there has
been an increase in the intake of energy (rich
foods that are high in fat and sugar); reducing
physical activity due to the increasingly sed-
entary nature of many forms of work, changing
modes of transport and increasing urbanization.
The genesis of obesity in people with physical
disability is unclear. There are several risk
factors as they are: type of injury, severity
and duration of injury or illness and sex and
age. More than 50% of youngsters with muscular
dystrophy are obese. As with a healthy popula-
tion, obesity is more susceptible to women than
men. Physical inactivity and consequently mus-
cular atrophy are very characteristic for people
with disabilities (Liou et al., 2005).
Obesity (elevated BMI) is one of the major risk
factors for diseases such as:
• Cardiovascular diseases (especially car-
diovascular disease and stroke)
• Diabetes
• Musculoskeletal disorders (especially os-
teoarthritis - degenerative joint disease)
• Some types of cancer (including endo-
metrium, breast, ovary, prostate, liv-
er, gall bladder, kidneys and colon).
One of the leading causes of disability is the
weakening of the muscular skeletal system caused
by overweight. In this case, this is a vicious
circle. The sedentary lifestyle causes obesi-
ty and obesity aggravates disability. The role
of physical inactivity in the development of
obesity is significantly higher in persons with
disabilities. There is plenty of evidence to
show that obesity can aggravate the state of
disability and that many disorders accompanying
disability cause a risk of obesity. (Ells et
al., 2006)
Illness associated with excessive weight and
obesity can be avoided. The choice of healthy
food and regular physical activity is essential.
This can be achieved by creating an appropriate
support environment and informing people.
Each individual can take care for himself by:
• limit the intake of foods contain-
ing high saturated fat and sugar,
• limit the intake of alcoholic beverages,
• increases the consumption of vege-
tables, legumes, nuts and fruit
• is regularly physical active (60 minutes per
day for children and 150 minutes for adults).
Sports activities can greatly improve motor
skills, improve quality of life and represent
prevention against obesity. In order to reduce
weight, it is necessary to take into account
nutrition laws (Mesarič, 2017).
References
Ells, L. J., Lang, R., Shield, J. P., Wilkinson, J. R.,
Lidstone, J. S., Coulton, S. and Summerbell, C. D. (2006),
Obesity and disability – a short review. Obesity Reviews, 7:
341-345.
Liou, T., Pi-Sunyer, F. X. and Laferrere, B. (2005), Physical
Disability and Obesity. Nutrition Reviews, 63: 321-331.
Lobstein, T., Baur, L., Uauy, R. (2004): Obesity in children
and young people: a crisis in public health. Obes Rev.,5 Suppl
1:4-104.
Mesarič, L. (2017): Adaptirano fizičko vežbanje za osobe sa
traumatskom povredom mozga (master rad). Fakultet za sport i
turizam, Novi Sad
Sackett, D., Rosenberg W.M., Gray, J.A., Haynes, R.B., Rich-
ardson, W.S. (1996) Evidence based medicine: What it is and
what it isn’t. BMJ. 13; 312(7023): 71-2.
Swinburn, B., Gill, T., Kumanyika, S. (2005): Obesity pre-
vention: a proposed framework for translating evidence into
action. Obes Rev., 6 (1): 23-33.
WHO Helth Topics, Obesity. Prevzeto 21. decembra 2018 s stra-
ni: http://www.who.int/topics/obesity/en
3.3.4. Harmful habits
AUTHORS: DANIJELA MAJCENOVIČ CIPOT, ILONA KOVAL GRUBIŠIĆ
Keywords: harmful habits and disability, drugs, nicotine, alcohol, prevention
Harmful habits of a person are actions that
automatically repeat a large number of times
and can harm the health of a person or those
around him/her. If he/she cannot force them-
selves to stop doing certain actions that may
harm the health in the future, then gradually
it becomes a habit, which is quite difficult to
get rid of. What are bad habits? The influence
of bad habits on the life and health of a person
can be different. Some of them (alcoholism, drug
addiction) are considered by modern medicine
as a disease. Others are classified as unneces-
sary actions caused by imbalance of the nervous
system. Below the main bad habits of modern man
are listed:
• smoking;
• drug addiction;
• alcoholism;
• game dependence;
• shopaholism;
• internet and television dependency;
• binge eating;
• the habit of picking your skin or gnaw-
ing your nails; flicking the joints.
The main causes of bad habits
Most often, the causes of development of bad
habits in humans are:
• social coherence: if in the social group to
which a person belongs is considered a norm,
this or that behaviour pattern, for example,
smoking, then most likely he will also fol-
low it to prove his belonging to this group,
hence the fashion for bad habits arises;
• disorder in life and alienation;
• pleasure is one of the main reasons why
the influence of bad habits is so great, it
is constant enjoyment that leads to peo-
ple becoming alcoholics or drug addicts;
• idleness, inability to correct-
ly dispose of free time;

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 6160
• curiosity;
• avoiding stress.
Harmful habits and their im-pact on human health
All bad habits can have a direct or indirect
effect on human health. The most severe conse-
quences are the habits of using drugs, nicotine
and alcohol, which quickly develop into addic-
tion and can lead to the development of a number
of complications, even to death.
As we stated in previous articles, people with
disabilities experience poorer health than those
in the general population with delays in access
to diagnosis, investigations and treatment.
Consequently they are particularly vulnerable
to the harmful impact of bad habits on their
health, and also on their financial and social
well-being. Despite this, indulging in bad hab-
its among people with disabilities has received
little research attention therefore there is
little known facts about this behaviour.
Next, we will examine in more detail some of
these harmful habits and their effect on human
health.
Tobacco smoking. Risks from smoking include:
• The risk of developing cancer and re-
spiratory system pathologie;
• Calcium is washed out from the body, the
skin of the face grows old, fingers be-
come yellow, the teeth become damaged, the
structure of hair and nails is destroyed;
• The work of the gastrointesti-
nal tract worsens, the develop-
ment of peptic ulcer is possible;
• Vessels become brittle and
weak, lose elasticity;
• Supply of the brain with oxygen dete-
riorates, hypertension develops.
The percentage of adults who smoke cigarettes is
higher among people with disabilities than peo-
ple without disabilities. For example, in 2014,
cigarette smoking was significantly higher among
those who reported having any disability (more
than 1 in 5 were smokers) compared to those who
reported having no disability (about 1 in 6 were
smokers) (CDC, 2017).
Smoking is especially common in people with
mental health difficulties. Around 33% of people
with mental health difficulties, such as schizo-
phrenia, and approximately 70% of patients in
psychiatric inpatient units, smoke. People with
a mental health difficulty die 10-20 years ear-
lier, on average, than people in the general
population, and smoking is the single biggest
factor contributing to this difference. Further-
more, smoking exacerbates poverty and social
stigma of people with a mental health difficulty
(UH, 2016).
Alcoholism is nothing more than a drug depen-
dence of the body, in which a person feels a
painful craving for alcohol. With this disease
develops not only the mental dependence, but
also the physical dependence of a person on al-
cohol (WHO, 2010, 2014). With alcoholism, severe
damage to the internal organs (especially the
liver) and degradation of personality occurs.
The systematic use of alcohol leads to the fol-
lowing consequences:
• The immune defence of the body decreas-
es thus the person is often unwell;
• Gradual destruction of the liver occurs;
• Increases the glucose level in the blood
thus leading to increased risk of Diabetes;
• Among alcoholics, the mortality rate is
higher due to accidents, suicides, poi-
soning with low-quality alcohol;
• Loss of memory (ASSIST, 2010).
Drug addiction is perhaps the most powerful and
dangerous bad habit that has long been rec-
ognised as a disease. Addiction is the depen-
dence of a person on the use of narcotic drugs.
The disease has several phases of the course and
staged syndromes. The harm that drugs do to the
human body is great. The following are the most
serious consequences of drug addiction:
• a significant reduction in life expectancy;
• an increased risk of contracting dangerous and
often incurable diseases (HIV, hepatitis);
• high mortality among drug addicts from acci-
dents, suicides, overdoses and drug poisoning;
• rapid ageing of the body;
• development of mental and so-
matic abnormalities;
• the strongest degradation of the in-
dividual (ASSIST, 2010).
Substance abuse (drugs, alcohol) is also a
problem for people with physical, cognitive, or
psychological disabilities. There is very little
research data to indicate frequency, however, in
2011 the United States Department of Health and
Human Services Office on Disability reported that
nearly 75 million people in the United States
have some form of disability. In addition,
nearly 5 million adults have both a disability
and a co-occurring substance use disorder. Based
on these figures, about 7 percent of people with
disabilities struggles with substance abuse
(Alcohol.org, 2018).
Other research showed that people with disabil-
ities use drugs and alcohol at least as often
as the general population and perhaps even more
often; however, they have less access to treat-
ment, even though treatment outcomes are similar
to those in the general population (Alcohol.org,
2018). Alcohol is one of the most common sub-
stances of abuse among people with disabilities
because of its availability, social acceptance,
and central nervous system depressant effects.
Use of other types of substances depends on type
of disability.
The risk factors associated with the development
of a substance use disorder among people with
disabilities include:
• Unemployment and low income
• Chronic pain and other chronic physical issues
• Mental illness, which is always a risk fac-
tor for developing a substance use disorder
• Easier access to prescription medications
• Less access to education
• Social isolation
• Physical abuse and sexual abuse
• Enabling behaviours by caregiv-
ers (Alcohol.org, 2018).
How to deal with bad habits of people with disabilities
What are the methods and ways to combat bad
habits, and which one is the most effective?
There is no unambiguous answer to this question.
Everything depends on many factors - the degree
of dependence, the willpower of a person and
individual characteristics of the organism. But
the most important is the person’s desire to
start a new life without bad habits, being with
or without disability. As we mentioned so many
times before, people with disabilities are even
more vulnerable when it comes to fighting a bad
habit or addiction.
They face:
1. Attitudinal barriers;
2. Communication barriers;
3. Discriminatory practices and procedures;
4. Architectural barriers.
Therefore it is of the utmost importance that we
have competent trained professionals that will
understand functional limitations and help over-
come these barriers regarding the specific types
of disabilities require specific adjustments to
the treatment program (deaf, blind, with cog-
nitive deficits, etc.). All treatment should
be inclusive, not only for people from diverse
racial and ethnic groups, but also for people
with disabilities. Inclusive programs need to
be accessible to those who want to participate
and in some cases adapted to address the needs
and expectations of the target population and
adjusted to suit the needs of the individual
included in the treatment.
Prevention of bad habits
Unfortunately, till now the prevention of bad
habits amongst people with disabilities has
not been given adequate attention. Due to the
architectural barriers they face, prevention
campaigns don’t reach them or they are excluded
because they are dependent on the help of an-
other person or cannot get to the program. In
some cases they don’t understand the topics or
they don’t have adequate support or understand-
ing environment to exercise changes in life.
They face financial deficit and therefore cannot
afford to live healthier. But most of all they
already face stress by struggling with disabil-
ity and therefore have additional psychological
problems, which make harder for them to face and
fight bad habits.
EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 6362
References
Alcohol.org, 2018. Treating an Alcoholic Who Is Differently
Abled. Retrieved from: https://www.alcohol.org/disabled/,
accessed 2019 02 16, 23:37.
ASSIST: The Alcohol, Smoking and Substance Involvement
Screening Test. Manual for use in primary care. Geneva, 2010.
Retrieved from: (http://www.who.int/substance_abuse/publica-
tions/assist/en/, accessed 31 March 2017.
CDC, 2017. How to Help People with Disabilities Quit Smoking.
Centers for Disease Control and Prevention. Retrieved from:
https://www.cdc.gov/features/disability-quit-smoking/index.
html, accessed 2019 02 16, 23:05.
UH, 2016. Smoking and People with an Intellectual Disabili-
ty. University of Hertfordshire. Retrieved from: http://www.
intellectualdisability.info/physical-health/articles/smok-
ing-and-people-with-an-intellectual-disability, accessed 2019
02 16, 23:16.
WHO. Set of recommendations on the marketing of foods and
non-alcoholic beverages to children. Geneva, 2010. Retrieved
from: https://www.who.int/dietphysicalactivity/publications/
recsmarketing/en/, accessed 31 March 2017.
WHO. Global status report on alcohol and health 2014.
Retrieved from: https://apps.who.int/iris/bitstream/
handle/10665/112736/9789240692763_eng.pdf;jsession-
id=B1AD972DD48280A38DD796C57AB86FF7?sequence=1, accessed 31
March 2017.
WHO. European Food and Nutrition Action Plan 2015-2020.
Regional Committee for Europe, 64th session; Copenhagen,
Denmark, 15-18 September 2014. Retrived from: http://www.
euro.who.int/__data/assets/pdf_file/0008/253727/64wd14e_Food-
NutAP_140426.pdf, accessed 31 March 2017.
WHO. HEARTS Technical package for cardiovascular disease
management in primary health care: healthy-lifestyle counsel-
ling; Geneva. Retrieved from: https://www.who.int/cardiovas-
cular_diseases/hearts/Hearts_package.pdf, accessed 31 March
2017.
WHO. Global strategy on diet, physical activity and health,
the 57th World Health Assembly, 2004. Retrieved from:
https://www.who.int/dietphysicalactivity/strategy/eb11344/
strategy_english_web.pdf, accessed 31 March 2017.
3.3.5. 21st Century - Video Games or Traditional Sport Disciplines
AUTHORS: LADISLAV MESARIČ
Keywords: video games, benefits, bad sides, health, physical activity
Introduction
Nowadays, video gaming is a highly popular and
prevalent entertainment option; its use is no
longer limited to children and adolescents.
Demographic data on video gaming shows that the
mean age of video game players is 31 years old
and has been on the rise in recent decades. It
is a common activity among young adults (Palaus
et al., 2016).
New research from innovation charity Nesta re-
veals that those who play video games are better
educated, no less wealthy and more likely than
non-games players to participate actively in
culture. The findings also turn the gamer stereo-
type on its head, with women more likely to play
than men do and the average gamer being aged 43.
However, among those that play, females do so
less often than men do. (Nesta, 2017) Gaming is
broad and complex. A ‘typical’ gamer may not ex-
ist. Based on the written, we can conclude that
video games are not just for young people.
In our perception, video games still have some-
thing bad. Against this backdrop of nearly ubiq-
uitous play, the popular press regularly pulses
out urgent warnings against the perils of addic-
tion to these games and their inevitable link to
violence and aggression, especially in children
and adolescents (Granic et al., 2016).
Video games are changing and the approach has
changed. The more balanced perspective, consid-
ers not only the possible negative effects but
also the benefits of playing these games.
3.3.5.1. The Benefits of Play-ing Video Games
According to meta study (Granic et al., 2016)
video games provide people with compelling so-
cial, cognitive, and emotional experiences and
can potentially boost mental health and well-be-
ing. Authors find the following benefits:
Cognitive development
Research into action games shows enhanced mental
rotation abilities, faster and more accurate
attention allocation, higher spatial resolution
in visual processing. Meta-analysis studies
showed that spatial skills can be learned in a
relatively brief time by playing video games and
that the results are often comparable to train-
ing in formal courses designed to enhance those
same skills. Cognitive advantages from video
games also appear to produce greater neural
processing and efficiency, improve attention
functioning and help with pattern recognition.
Interactive games also appear to improve cre-
ativity as well. Although it is still not clear
how well the skills learned from video games
generalize to real-world situations, early
research results seem promising (Granic et al.,
2016).
Emotion
Most gamers play video games for enjoyment and
to help improve their mood. Along with distract-
ing them from real-world problems (a special
concern for young people looking for escape from
bullying or other negative life situations),
succeeding in video games can lead to positive
feelings, reduced anxiety, and becoming more
relaxed.
Motivation
By setting specific tasks and allowing people to
work through obstacles to achieve those tasks,
video games can help boost self-esteem and
help people to learn the value of persistence.
By providing immediate feedback as video game
players solve problems and achieve greater
expertise, players can learn to see themselves
as having skills and intelligence they might not
otherwise realize they possess. Gaming helps
people realize that intelligence can increase
with time and effort rather than being fixed.
Social activity
Perhaps more than ever before, video games have
become an intensely social activity. Instead
of the stereotypical gaming nerd who uses video
games to shun social contact, over 70 percent of
gamers play with friends, whether as part of a
team or in direct competition. Social and pro-
social activities are an intrinsic part of the
gaming experience with gamers rapidly learning
social skills that could generalize to social
relationships in the real world.
The vast majority of reviewed studies revealed
positive health outcomes for older adults asso-
ciated with digital video game play, especially
related to mental and physical health benefits.
Significant mental health positive outcomes,
such as cognitive improvement, were reported in
multiple digital video game interventions, which
used measures such as working memory, focused
attention, fluid intelligence, scales for demen-
tia, scales for depression, information process-
ing, enjoyment of physical exercise, and balance
confidence to assess cognitive improvement. The
most frequently reported significant health out-
come among digital game interventions for older
adults were mental health outcome factors (Hall
et al., 2016).
Video games have been used as a form of physio-
therapy or occupational therapy in many differ-
ent groups of people. Such games focus attention
away from potential discomfort and, unlike more
traditional therapeutic activities; they do not
rely on passive movements and sometimes painful
manipulation of the limbs. Therapeutic benefits
have also been reported for a variety of adult
populations including wheelchair users with spi-
nal cord injuries, people with severe burns, and
people with muscular dystrophy (Griffiths, 2005).
Video games have many positive effects and are
appropriate for people with disabilities. Howev-
er, consideration should be given to suitability
of some games for special groups of people. In
addition to the above mentioned positive sides,
video games also have many negative sides.
3.3.5.2. The bad sides of video game
Muscle pain, Obesity, Sleep Deprivation
Though the activity level needed to play Wii or
Xbox Kinect are a step in the right direction,
a majority of video games still involve sitting
in front of a screen, often with poor posture.
Excessive screen game playing leads to increased
levels of muscle stiffness, especially in the
shoulders, which can be caused by poor posture.
Sedentary lifestyles and bad diets are directly
linked to obesity. Playing too many video games

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 6564
has been associated with changes in physical
appearance. Increased gaming can cause sleep
deprivation and gamers can develop black rings
in the skin under the eyes (Tazawa & Okada,
2001).
According to a report in Paediatrics, seven out
of 10 children are vitamin D deficient. Vitamin
D, of course, is commonly absorbed from expo-
sure to sunlight. Unfortunately, being holed up
in front of video games console does not afford
the same exposure to sunlight as being outside
(Misra et.all 2008).
Negative aspects include the risk of video game
addiction (although the prevalence of true ad-
diction, rather than excessive use, is very low)
and increased aggressiveness. There have been
numerous reports of other adverse medical and
psycho-social effects. For instance, the risk of
epileptic seizures whilst playing video games in
photosensitive individuals with epilepsy is well
established (Griffiths 2005).
3.3.5.3. Answer to the main question
In accordance with the text above, video games
have a lot of space in our field of operation.
However, we have to answer the main question:
21st Century - Video Games or Traditional Sport
Disciplines?
The answer is both. While video games show their
advantages having regard to all the weaknesses
traditional games are another story.
People have many different reasons for exercis-
ing. Sport activities provide the health related
benefits. The main goals are to lower the risk
of developing health problems and preventable
disease. A person can be well even if he or she
has differences in movement capabilities, wheth-
er these are caused by a particular experience
or factors such as cerebral palsy, injury to
the spinal cord and paralysis, or advanced age.
Disabilities are not considered illnesses or
deficiencies. Regardless of ability level, age or
level of experience, exercise benefits can lead
to wellness. (Kasser & Lytle, 2013).
For adapted physical activity, it is considered
that it is one of the most sustainable support
systems for promoting physical activity for peo-
ple with different forms of disability and for
the continuous development of scientific knowl-
edge, based on the support of applied practice
and human rights (Aleksandrović et al., 2016).
Video games can be used for special purposes,
taking into account advantages and disadvantag-
es, but they cannot replace traditional sports
activities. We need to adapt physical activities
so people with disabilities can participate and
gain benefits.
Man was made to move. This is a biological fact
that no video game can substitute. But even from
video games we will have more if we play them in
good physical condition.
References
Bakhshi, H. (2017). New research proves cultural val-
ue of video gaming. (https://www.nesta.org.uk/news/
new-research-proves-cultural-value-of-video-gaming/)
Brown, A. (2017) Younger men play video games, but so do a
diverse group of other Americans. (http://www.pewresearch.
org/fact-tank/2017/09/11/younger-men-play-video-games-but-so-
do-a-diverse-group-of-other-americans/)
Granic, I., Lobel, A., & Engels, R. C. M. E. (2014). The
benefits of playing video games. American Psychologist, 69(1),
66-78.
Griffiths, M. (2005). Video games and health: Video gaming is
safe for most players and can be useful in health care. BMJ :
British Medical Journal, 331(7509), 122–123.
Hall, A.K., Chavarria,E., Maneeratana, V., Chaney, B.H., M.
Bernhardt J.M. (2012). Health Benefits of Digital Videogames
for Older Adults: A Systematic Review of the Literature.
Games for Health Journal 1:6, 402-410
Kaminsky, L. A. (2010) ACSM Priručnik za procenu fizičke forme
povezane sa zdravjem, Data Staus, Beograd
Kasser, S.L., Lytle R.K., (2013), Inclusive Physical Activ-
ity-2nd Edition, Human Kinetics, Human Kinetics Europe Ltd,
United Kingdom
Misra, M., Pacaud, D., Petryk A., Collett-Solberg P.F.,
Kappy, M. (2008) Vitamin D Deficiency in Children and Its
Management: Review of Current Knowledge and Recommendations.
Pediatrics, Volume 122 / Issue 2
Palaus, M., Marron, E. M., Viejo-Sobera, R., & Redolar-Rip-
oll, D. (2017). Neural Basis of Video Gaming: A Systematic
Review. Frontiers in Human Neuroscience, 11, 248. http://doi.
org/10.3389/fnhum.2017.00248
Tazawa, Y. and Okada, K. (2001), Physical signs associ-
ated with excessive television-game playing and sleep
deprivation. Paediatrics International, 43: 647-650.
doi:10.1046/j.1442-200X.2001.01466.x
3.3.6. Doping in the sport for persons with disability
AUTHOR: LADISLAV MESARIČ
Key words: doping, technodoping, bosting, self-harm
Most athletes who take part in adapted sports
activities compete ethically and use the ap-
proved methods to improve sports performance.
Improving the results is achieved through train-
ing that takes into account scientific knowledge
in the field of sports training. People, like in
all areas of life, as well as in adapted sports,
are looking for shortcuts to succeed. The rea-
sons for this are recognition and publicity (in
particular, the Olympic Games), financial benefits
from sponsors and state grants, and the human
desire to be better than others, albeit in an
illegal way.
There are many known cases of doping. In par-
allel with the development of methods for the
detection of doping in sport, even in the ear-
ly 1980s, doping controls were also conducted
in competitions for persons with disabilities
(Hale, 2016).
The use of doping in the Olympic and Paralym-
pic athletes does not differ significantly. As a
rule, there is an increase in power and endur-
ance. There are also similar sanctions, which
include disqualification, repossession of awards
and all the benefits that they have been given
after winning the medal (Collier, 2008)
However, in adapted sports activities, there are
certain characteristics that are specific for
athletes with physical and mental disabilities.
3.3.6.1. Different technology
Athletes from countries with advanced technology
and better economic standards have access to a
better technology that allows them greater com-
petitiveness. This can lead to an unequal posi-
tion among competitors (Guerrero et al., 2018).
Some people call it techno doping (Bolta, 2016).
3.3.6.2. Increasing of blood pressure (Bosting)
Another form of “cheating” is encountered in
some athletes with spinal cord injuries who want
to increase their blood pressure and thereby
improve their performance. Due to the nature
of the spinal cord injury, some athletes do
not feel the parts of their body. If the body
is damaged in areas where there is no sense,
a physiological response, known as autonomic
dyslexia, is triggered. In order to speed up
this response, some athletes deliberately harm
themselves. Self-harm is, for example, fracture,
causing pressure due to very tight clothing,
overload of the bladder or in male sport - too
tight clothing in the area of pelvis. These are
very extreme behaviours, but they point to what
all para athletes are willing to do to reach the
desired result or success (Bolta 2016, Guerrero
et al., 2018).
Different qualification systems are available
in the sport of persons with disabilities. That
enables equal and fair competitions for persons
with different types and degrees of disabili-
ty (Aleksandrović et al., 2016). Although the
system is constantly improving, it may be con-
troversial, because in some cases individuals
simulate a lower level of ability. A well-known
example is the Spanish basketball team where
people without disabilities appeared and entered
the competition due to inconsistent classifica-
tion procedures (Bolta, 2016).
References
Aleksandrović, M., Jorgić, B., Mirić, F. (2016). Holistički
pristup adaptivnom fizičkom vežbanju, učbenik za studente
master akademskih studija. Fakultet sporta i fizičkog vaspi-
tanja Niš
Bolta T.(2016) Paraolimpijske igre in Slovenci. Diplomsko
delo, Fakulteta za šport, Ljubljana
EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 66
Collier, R. (2008). Most Paralympians inspire, but others
cheat. CMAJ : Canadian Medical Association Journal, 179(6),
524. http://doi.org/10.1503/cmaj.081279
Guerrero L.A., Drakes S., De Luigi A.J. (2018) Controversies
in Adaptive Sports. In: De Luigi A. (eds) Adaptive Sports
Medicine. Springer, Cham
Hale L. (2016) A brief history of doping in disability sport.
Retrieved from http://www.parasport-news.com/a-brief-history-
of-doping-in-disability-sport/10515/ on 15.5.2018

4.
Learning outcomes:
• to outline Physiological and So-
cial benefit of Physical activity
• recommendation for physical activi-
ty in different stages of life
• an understanding of Adapted Phys-
ical Activities (APA).
• familiarizing reader with the benefits
of sport and APA in rehabilitation.
BeNe fITs of PhySI cAL AcTIv ITy

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 7170
4.1.BENefiTS fOr thE PSYcholOGIcal aND SoCial FUNctIONingAUTHORS : MICHELE LEPORI, ALESSANDRO MUNARINI, SILVIA NOCI, PAOLO ZARZANA
Key Words: Well being; physical activity; muscular fitness; self-esteem; self-confi-dence; social relationship;
Introduction
There are many publications in the field of mo-
tor sciences and the promotion of health; many
studies have been carried out to state both the
value and the importance of motor activity,
physical activity and sports on the psychophysi-
cal well-being of any individual.
WHO guidelines (2010) provide recommendations
on Physical Activity specific for each age
group (following) and concepts and technical
terminologies.
5–17 years
For children and young people physical activity
includes play, games, sports, transportation,
recreation, physical education or planned ex-
ercise, in the context of family, school, and
community activities. Physical activity benefits
include cardiorespiratory and muscular fitness,
bone health, cardiovascular and metabolic health
biomarkers and reduced symptoms of anxiety and
depression.
18–64 years old
For adults of this age group, physical activity
includes recreational or leisure-time physi-
cal activity, transportation (e.g. walking or
cycling), occupational (i.e. work), household
chores, play, games, sports or planned exercise,
in the context of daily, family, and community
activities in order to improve cardiorespiratory
and muscular fitness, bone health and to reduce
the risk of Non-Communicable diseases NCD’s
(e.g. Parkinson’s disease, stroke, and cancer)
and depression.
Adults aged 18–64 years should aim to do at
least 150 minutes of moderate-intensity aerobic
physical activity throughout the week, or at
least 75 minutes of vigorous-intensity aerobic
physical activity throughout the week, or an
equivalent combination of moderate- and vigor-
ous-intensity activity.
65 years old and above
For adults of this age group, physical activity
includes recreational or leisure-time physi-
cal activity, transportation (e.g. walking or
cycling), occupational (if the person is still
engaged in work), household chores, play, games,
sports or planned exercise, in the context of
daily, family, and community activities in order
to improve cardiorespiratory and muscular fit-
ness, bone and functional health, and reduce the
risk of NCD’s, depression and cognitive decline.
In 2008 the U.S. Department Health and Hu-
man Services published the Physical Activity
Guidelines for Americans - Be Active, Healthy,
and Happy! (www.health.gov/paguidelines) that
provide achievable steps for youth, adults and
seniors, as well as people with special condi-
tions to live healthier and longer lives.
Key Guidelines for Adults with Disabilities
• Adults with disabilities, who are able to,
should get at least 150 minutes a week of
moderate-intensity, or 75 minutes a week
of vigorous-intensity aerobic activity, or
an equivalent combination of moderate- and
vigorous-intensity aerobic activity. Aero-
bic activity should be performed in episodes
of at least 10 minutes, and preferably, it
should be spread throughout the week.
• Adults with disabilities, who are able
to, should also do muscle-strengthening
activities of moderate or high intensi-
ty that involve all major muscle groups
on 2 or more days a week, as these activi-
ties provide additional health benefits.
• When adults with disabilities are not able
to meet the Guidelines, they should engage
in regular physical activity according to
their abilities and should avoid inactivity.
• Adults with disabilities should consult their
health-care provider about the amounts and
types of physical activity that are appro-
priate for their abilities (ODPHP, 2008).
In addition, it is important to note that sport
has an important social role, not only does it
help to improve the physical and psychological
recovery, but it also helps to develop social
relationships regardless of the age, the social
origin or the physical difficulties. It is a
source of important values such as team spirit,
solidarity, tolerance and fair play, contribut-
ing to personal development and fulfilment.
Sport is an important means of social integra-
tion by which the person increases social inter-
actions which subedequently improve self-esteem.
Benefits for the Psychologi-cal and Social Functioning
Sports activity, in general, assumes, of course,
a role of “privileged context” within which to
foster relationships and to counter the risk of
isolation, which weighs heavily on certain cate-
gories of citizens, such as, for example, people
with disabilities.
The UN Convention on the Rights of Persons
with Disabilities suggests a set of rights,
including:
a. to encourage and promote the widest possible
participation of persons with disabilities in
mainstream sports activities at all levels;
b. ensure that they have access to plac-
es that host sports activities
c. to ensure that minors with disabilities can
participate, on an equal basis with oth-
er minors, in recreational activities,
leisure and sport, including the activi-
ties provided for by the school system.
As the Ministry of Health confirms, sporting
activity produces, a beneficial effect on the
physical and mental health.
It is well known that the benefits of sport are
undeniable. Those who play sports live longer
because they protect their health better example
prevents muscle and bone decline. The calming
action of sports activity should not be forgot-
ten. Doing sports allows you to disconnect from
everyday problems and recharge yourself. Sport
makes it possible to become not only stronger
physically but also mentally, giving greater
motivation to achieve increased self-esteem,
confidence and optimism.
All these considerations can thus safely be
transported to the world of sports for persons
with a disability; we always tend to think of
disabled people as sick, steady, immobile peo-
ple, but if we look at them engaged in sports we
find them to be tenacious, determined and con-
centrated people. This is because practising a
sport and trying to reach a goal creates import-
ant motivations. Through the sporting activi-
ty the disabled person has the possibility to
improve in different aspects, in particular on
the psychological, social and educational level
increasing their autonomy, encouraging commit-
ment during training and respect for opponents,

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 7372
teaching courage, promoting loyalty; encourag-
ing socialization, integration, thus overcoming
fears, prejudices and isolation. We must there-
fore always put the person at the centre of our
project. Sport has some peculiarities that we
must always be able to exploit: managing emo-
tions, collaborating with others, feeling part
of a team, respecting the rules and learning to
accept their limits, not without trying to go
further. All these benefits affect all people,
disabled or not (Munarini A., CSI referente
nazionale attività disabili CSI).
4.1.1. Motivation
One of the most influential internal barriers
addressed in the literature is the attitudes and
motivations of people with a disability, par-
ticularly self-consciousness and low levels of
confidence. This lack of confidence and self-es-
teem has been reported to manifest itself in the
following ways:
• Feeling different from the ma-
jority of the population.
• Feeling unable to fit in at
a sporting facility.
• Self-consciousness or lack of confi-
dence in asking for help and assis-
tance in a sporting environment.
• A fear of failure on the part of the per-
son with the disability can present another
type of internal barrier, particularly in
the case of people who have newly acquired
their disability and with low self-esteem.
Motivation is essential for physical activity
in the general population and among individuals
with disabilities. Self-determination theory
(SDT) divides motivation into 2 components.
Controlled motivation is derived from exter-
nal sources, such as physicians, trainers or
media, while autonomous motivation is derived
from oneself across 3 basic psychological needs:
autonomy, relatedness and competence. Recent
research has shown the importance of autonomous
motivation for adherence to physical activi-
ty, and that it is associated with increased
activity in people with physical disabilities
(Saebu M. et al.; 2013). It is also noteworthy
that maintenance of behaviours over time re-
quires autonomous motivation for that behaviour.
Conversely, controlled motivation is unrelated
to long-term adherences and is less malleable
(Bean J. Et al., 2007). Autonomous motivation
is closely associated with motivation for a
change in behaviour, and is a person’s confidence
in the ability to perform new activities. This
notion is often termed “self-efficacy” and is
defined by Bandura (Bean J. Et al., 2007) as the
perceived capability of a person to perform a
specific action required to achieve a concrete
goal. Self-efficacy has been shown to be a strong
predictor of physical activity in individuals
with disabilities (Hutzler Y. Et al.; 2007). In
addition, the degree of impairment is close-
ly related to physical activity in individuals
with disabilities. However, it is challenging to
reach a common assessment of impairment across
different diseases and disabilities. Pain and
fatigue are associated with disability, but may
play a unique role for motivation in physical
activity. Adapted Physical Activity (APA)-based
rehabilitation includes physical activities
adapted to the specific needs of each individual
with a disability. The goal is to enhance the
subject’s autonomy, motivation and ability to
engage in physical activities, and ultimately
increase physical activity over time. Although
this type of rehabilitation is beneficial with
respect to pain and functioning, we have less
knowledge about its influence on motivation and
physical activity levels over time (van Mid-
delkoop M. et al. ; 2011).
4.1.2. Self-Esteem
Practising sport helps to develop and enhance
the potential and autonomy of the disabled
person in respect of the evolutionary process:
through motor sports activities aimed at the
well-being of the disabled person, it contrib-
utes to the increase of specific skills to be
carried out by increasing the opportunities
for social integration, using it as a tool for
growth and enhancement of personal skills (Noci
S., CSI National technical commission for dis-
abled people).
Individuals with disabilities who participate
in sports have higher self-esteem, better body
images and higher rates of academic success;
are more confident and more likely to gradu-
ate from high school and enrolling in college.
Furthermore, sport is where skills like team-
work, goal-setting, the pursuit of excellence in
performance and other achievement-oriented be-
haviours necessary for success in the workplace
are developed (Richman, E. L.; 2000).
An adapted physical activity helps to achieve a
good autonomy in the game and changing room en-
vironment, to develop a gradual transition from
not knowing one’s body to the elaboration of the
body schema; to find a balance between mind and
body; to reach a personal balance, to improve
co-ordinative and conditional skills, to develop
laterality, to better perceive one’s own body
through the elaboration of motor and perceptual
experiences (Noci S., CSI commissione tecnica
Nazionale disabili)
4.1.3. Emotional Well-Being
Sports Reduce Stress and Depression
Those who practice sport prevent bone and mus-
cle decline, protect their health, recharge by
detaching their mind from everyday problems and
focusing on movement. The sporting motion pro-
duces endorphins, substances that stimulate the
body to react positively to situations of anxi-
ety and stress. The movement not only enhances
the physical, but also strengthens the mind,
increasing self-esteem, optimism and self-con-
fidence. On the sporting level, the technical
knowledge of the sports disciplines is acquired,
the respect of the rules and the collaboration
are encouraged, communication is encouraged. On
the psychological level we work on the contain-
ment of emotions and on increasing the capacity
for self-control. (Noci S., CSI National techni-
cal commission for disabled people).
When you are physically active, your mind is
distracted from daily stressors. This can help
avoid getting bogged down by negative thoughts.
Exercise reduces the levels of stress hormones
in your body. At the same time, it stimulates
production of endorphins. These are natural mood
lifters that can help keep stress and depression
at bay. Endorphins may even leave you feeling
more relaxed and optimistic after a hard workout
on the field. Experts agree that more quality
research is needed to determine the relationship
between sports and depression.
4.1.4. Attention
Regular physical activity helps keep your key
mental skills sharp as you age. This includes
sharp thinking, learning, and using good judge-
ment. Research has shown that doing a mix of
aerobic and muscle strengthening activities
is especially helpful. Thanks to the sporting
performance a return is achieved in terms of
improving the strength of determination, vital
energy and passion in everyone.
4.1.5. Social encounters
and Social Skills
The relationship with the sports opponent or
with the teammate, stimulates interaction with
the other, promotes socialization and social
integration, offering valuable help to the
prevention of isolation and overcoming fears and
false judgements (Noci S., CSI National tech-
nical commission for disabled people). If the
physical benefits are evident and known, perhaps
the psychological benefits of sport, are less
experienced, and are a secondary and not very
visible aspect.
Sport, on the other hand, produces decidedly
positive and important effects on a psychologi-
cal level. Physical activity allows the athlete
with a disability to gain greater confidence in
the things they do, helping to restore confidence
in their potential.
In addition, the athlete is able to test their
skills and abilities, their possibilities and
limits, thus acquiring a greater awareness of
them.
Sports practice is very important, because it
allows individuals to be inserted or reinserted
in a healthy and suitable social context. By
coming into contact with the outside world, an
athlete with a disability discovers a healthy
collaboration, one that goes beyond personal
benefits, and savours the joy of human relation-
ships. Within the sports world the interactions
that are established are, in fact, multiple
and of different types; for example, you get in
touch with the coach, with the teammates, in the
case of team sports, and with opponents.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 7574
These connections allow individuals to experi-
ence a wide range of feelings and emotions, to
manage any relationship conflicts and to learn
how to adapt relationships dependent on who they
are interacting with. In the interpersonal re-
lationships to the subject, goals and a specific
role are recognized, thus enhancing the process
of building his personal identity (Zarzana P.,
CSI National trainer and CSI formatori nazi-
onali, Italian National amputee football team
coach).
The power of sport as a transformative tool is
of particular importance for women as women
with disabilities often experience double dis-
crimination on the basis of their gender and
disability. It is reported that 93% of women
with disabilities are not involved in sport and
women comprise only one-third of athletes with
disabilities in international competitions. By
providing women with disabilities the opportu-
nity to compete and demonstrate their physical
ability, sport can help to reduce gender stereo-
types and negative perceptions associated with
women with disabilities.
Moreover, by improving the inclusion and
well-being of persons with disabilities, sport
can also help to advance the Millennium Devel-
opment Goals (MDGs). For example, sports-based
opportunities can help achieve the goal of
universal primary education (MDG2) by reducing
stigma preventing children with disabilities
from attending school; promote gender equality
(MDG3) by empowering women and girls with dis-
abilities to acquire health information, skills,
social networks, and leadership experience; and
lead to increased employment and lower levels of
poverty and hunger (MDG1) by helping to reduce
stigma and increase self-confidence.
The UN Convention on the Rights of Persons with
Disabilities is the first legally binding inter-
national instrument to address the rights of
persons with disabilities and sport. Article 30
of the Convention addresses both mainstream and
disability-specific sport and stipulates that
“States Parties shall take appropriate measures
to encourage and promote the participation, to
the fullest extent possible, of persons with
disabilities in mainstream sporting activities
at all levels”. It also calls upon Governments,
States party to the Convention, to ensure that
persons with disabilities have access to sport
and recreational venues — as spectators and as
active participants. This also requires that
children with disabilities be included in phys-
ical education within the school system “to the
fullest extent possible” and enjoy equal access
to “play, recreation and leisure and sporting
activities” (Convention on the Rights of Persons
with Disabilities Article 30); (General Assembly
Resolution: Sport as a means to promote educa-
tion, health, development and peace A/RES/69/6);
(International Disability in Sport Working
2018).
Case studies
Background Although the promotion of social
inclusion through sports has received increased
attention with other disadvantaged groups, this
is not the case for children and adults with
intellectual disability who experience marked
social isolation. The study evaluated the out-
comes from one sports programme with particular
reference to the processes that were perceived
to enhance social inclusion.
Method The Youth Unified Sports programme of Spe-
cial Olympics combines players with intellectual
disabilities (called athletes) and those without
intellectual disabilities (called partners) of
similar skill level in the same sports teams for
training and competition. Alongside the devel-
opment of sporting skills, the programme offers
athletes a platform to socialise with peers and
to take part in the life of their community.
Unified football and basketball teams from five
countries – Germany, Hungary, Poland, Serbia and
Ukraine – participated. Individual and group
interviews were held with athletes, partners,
coaches, parents and community leaders: total-
ling around 40 participants per country.
Results Qualitative data analysis identified
four thematic processes that were perceived
by participants across all countries and the
two sports to facilitate social inclusion of
athletes. These were: (World Health Organiza-
tion 2010 “Global Recommendations on Physical
Activity for Health”) the personal development
of athletes and partners; (Richman, E. L., &
Shaffer, D. R.; 2000) the creation of inclusive
and equal bonds; (Saebu M.; 2013) the promo-
tion of positive perceptions of athletes; and
(Bean JF, 2007) building alliances within local
communities.
Conclusions Unified Sports does provide a vehicle
for promoting the social inclusion of people
with intellectual disabilities that is theoreti-
cally credible in terms of social capital schol-
arship and which contains lessons for advancing
social inclusion in other contexts. Nonetheless,
certain limitations are identified that require
further consideration to enhance athletes’ so-
cial inclusion in the wider community
References
Bean JF, Bailey A, Kiely DK, Leveille SG. Do attitudes toward
exercise vary with differences in mobility and disability
status? – a study among low-income seniors. Disabil Rehabil
2007; 29: 1215–1220.
Chapter Five: Sport and Persons with Disabilities: Fostering
Inclusion and Well-Being. 2008, p.167-175. International
network of sport and development consultants (INSDC).
Ilias, Bantekas & Chow, Pok Yin & Karapapa, Stavroula &
Polymenopoulou, Eleni. (2018). Art.30 Participation in
Cultural Life, Recreation, Leisure, and Sport. 10.1093/
law/9780198810667.003.0031.
United Nations General Assembly – Seventy-first session Agenda
item 11 - Sport as a means to promote education, health,
development and peace, 7 December 2016.
Hutzler Y, Sherrill C. Defining adapted physical activity:
international perspectives. Adapt Phys Activ Q 2007; 24: 1–20
International Disability in Sport Working Group Sport in
the United Nations Convention on the Rights of Persons with
Disabilities International Platform on Sport and Development;
2008.
Frances Hannon, National Disability Authority. “Promoting the
Participation of People with Disabilities in Physical Activi-
ty and Sport in Ireland”. October 2005
Office of Disease Prevention and Health Promotion (ODPHP),
2008. 2008 Physical Activity Guidelines for Americans – Be
Active, Healthy and Happy! retrieved from: https://health.
gov/paguidelines/2008/chapter7.aspx
Richman, E. L., & Shaffer, D. R. (2000). ‘If you let me play
sport’: How might sport participation influence the self-es-
teem of adolescent females? Psychology of Women Quarterly,
24:189-199.
Saebu M, Sørensen, M, Halvari, H. Motivation for physical
activity in young adults with physical disabilities during a
rehabilitation stay: a longitudinal test of self-determina-
tion theory. J App Soc Psychol 2013; 43: 612–625.
Sport for Development and Peace-International Working Group,
“Harnessing the Power of Sport for Development and Peace:
Recommendations to Government” (2008). Author: Right To Play
on behalf of the Sport for Development and Peace Internation-
al Working Group (SDPIWG).
Van Middelkoop M, Rubinstein SM, Kuijpers T, Verhagen AP, Os-
telo R, Koes BW, et al. A systematic review on the effective-
ness of physical and rehabilitation interventions for chronic
non-specific low back pain. Eur Spine J 2011; 20: 19–39.
World Health Organization-“Young People with Disability in
Physical Education/ Physical Activity/Sport In and Out of
Schools: Technical Report for the World Health Organization”.
C.Sherrill; International Federation of Adapted Physical
Activity (IFAPA), 2004.
World Health Organization, 2010 “Global Recommendations on
Physical Activity for Health”, 7-8 and c.4 – 16-33.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 7776
4.2.Sports and Phys-ical Activity as RehabilitationAUTHOR: MICHAEL LAMONT
Key Words: sport, rehabilitation, persons with disabilities, Adapted Physical Activities
Introduction
Sport is a cultural phenomenon and an integral
part of society. It is highly visible and touch-
es almost everyone as participants, spectators
and consumers - DePauw & Gavron (2005).
Sport represents an efficient rehabilitation
method for persons with disabilities. Through
regular sporting activity persons with dis-
abilities can achieve greater quality of life
and improved social inclusion. For this purpose
persons with disabilities need to be provided
with the possibility of participating in appro-
priate sport programme, where they can equally
participate. Sporting activities need to become
a component of rehabilitation of persons with
disabilities regardless of the nature or degree
of their disability, age and level of physical
competence.
4.2.1. Definition of
Rehabilitation
The World Health Organisation
The WHO (2011) defined rehabilitation as “a set
of measures that assist individuals who expe-
rience, or are likely to experience disability,
to achieve and maintain optimal functioning
in interaction with their environments. Reha-
bilitation provides disabled people with the
tools they need to attain independence and
self-determination.”
The European Standards in Adapt-ed Physical Activities
The EUSAPA (2010) stated that “Rehabilitation
is concerned with identifying and maximising
quality of life and movement potential within
the spheres of promotion, prevention, treatment/
intervention, habilitation and rehabilitation,
encompassing physical, psychological, emotional,
and social well-being.”
The United Nations Convention on the Rights of Persons with Disabilities
The UNCRPD (2007) outlined the responsibility of
states to provide “appropriate measures, includ-
ing through peer support, to enable persons with
disabilities to attain and maintain their maxi-
mum independence, full physical, mental, social
and vocational ability, and full inclusion and
participation in all aspects of life.”
4.2.2. Definition of
Adapted Physical Activity
– Play, Game Sport
Sport
Sport is defined as “all forms of physical activ-
ity which, through casual or organised partici-
pation, aim at expressing or improving physical
fitness and mental well-being, forming social
relationships or obtaining results in competi-
tion at all levels.” (European Sports Charter
1992; revised 2001).
Adapted Physical Activity (APA)
APA can be defined as the provision of physical
activity services and programmes to persons of
all ages with special needs (Hutzler & Sherrill,
2007). APA includes, but is not limited to,
physical education, sport, recreation, and reha-
bilitation of people with disabilities (EUFAPA,
2006, article 5).
According to the International Federation of
Adapted Physical Activity (IFAPA), APA means:
• A service-oriented profession
• An academic specialisation or field of study
• A cross disciplinary body of knowledge
• An emerging discipline or subdiscipline
• A philosophy or set of be-
liefs that guides practices
• An attitude of acceptance that pre-
disposes behaviours
• A dynamic system of interwo-
ven theories and practices
• A process and a product (i.e. pro-
grammes in which adaptation occurs)
• An advocacy network for disabili-
ty rights to physical activity of par-
ticipants with disability
4.2.3. The benefits of Sports in
the Process of Rehabilitation
The history of Sport in Rehabilitation
Although the use of physical activity in re-
habilitation can be traced as far back as 3000
B.C. in ancient China (EUSAPA, 2010), the modern
evolution of physical activity and sports as a
means of rehabilitation is attributed, among
others, to the Swedish scholar Per Henrik Ling
(1776-1839). Ling established a system of medi-
cal gymnastics in the University of Stockholm,
Sweden after curing himself from rheumatism and
paralysis through practising fencing and gymnas-
tics (Hutzler, 2010).
The inclusion of sport and organised competi-
tion in rehabilitation is associated with Sir
Ludwig Guttmann, founder of the International
Stoke Mandeville Games in 1948, followed by the
first Paralympics in 1960 and the Special Olym-
pics in 1968. Since the 1970s there has been a
dramatic increase in the number of international
organisations/associations serving athletes with
disabilities (De Pauw & Gavron, 2005).
EUSAPA
The European Standards in Adapted Physical
Activities (EUSAPA, 2010) identifies three main
areas of benefit of APA for rehabilitation:
1. Adapted physical activities during, but
also after the rehabilitation phase have a
beneficial effect on an individual’s general
physical fitness level, their functional-
ity, and performance of activities of daily
living. Research suggests that physiotherapy
programmes often pay insufficient attention to
these domains, therefore implementing adapted
physical activities within the rehabilitation
programme may result in an enhanced qual-
ity and successfulness of rehabilitation,
while also reducing the risk of relapse.
2. Adapted physical activities have a beneficial
effect on the patient’s/client’s psycho-
social well-being, reducing isolation and
sedentary lifestyle. Adapted physical ac-
tivities offer opportunities to share expe-
riences and to learn how to accept or come
to terms with an impairment, disorder, etc.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 7978
3. In addition, individuals experience the
benefits of physical activity and sports
with respect to their physical and men-
tal and psychosocial well-being, enhanced
quality of life and the improved execu-
tion of activities of daily living.
APA vs Physical Therapy (PT)
Hutzler (2010) highlighted that the differences
between physical therapy (PT) and APA suggested
by Lorenzen (1961) are still evident today:
• A medical orientation in PT, compared
to a pedagogical orientation in APA;
• Intervention goals mostly refer to the
impairment in PT compared to the whole
person and participation in APA;
• Activity is typically prescribed in PT,
compared to self-motivation in APA;
• The participant is passive and ac-
tive in PT but only active, most-
ly in group settings, in APA;
• The goal in PT is mostly restricted to specif-
ic biological changes, while in APA the goal
is promoting activity across the lifespan;
• The intervention is mostly identi-
fied as treatment in PT, compared to
self-determined action in APA.
The Benefits of Sport and APA in Rehabilitation
As with the general population, physical activ-
ity reduces the risk for chronic illnesses and
secondary conditions for persons with disabil-
ities (Durstine et al., 2000; Heath & Fentem,
1997). However the benefits of participation in
sports and APA reach beyond physical rehabil-
itation (Parnes and Hashemi, 2007), improving
independence and empowerment, increasing social
integration and inclusion, and helping to change
attitudes among members of the society in gen-
eral (Burchell, 2006; Capella-McDonnall, 2007;
Sherrill, 2004).
APA and sport promotes rehabilitation through
social networks between those who share simi-
lar life experiences and through teaching how
to function with relative autonomy (Lindemann
& Cherney, 2008), this happens in both causal
recreational activity as well as elite disabil-
ity sport (Cherney, Lindemann & Hardin, 2015).
Social networks can help people negotiate con-
straints to participation, including lack of
knowledge about an activity or lack of motiva-
tion to participate (Jackson, Crawford, & God-
bey, 1993; Jackson & Scott, 1999). Both children
(Seymour, Reid, & Bloom, 2009), and adults with
disabilities report developing friendships as
one of the benefits of participation in sport and
APA (Ashton-Shaeffer, Gibson, Autry, & Hanson,
2001; Lindemann & Cherney, 2008).
4.2.4. Opportunities
for Participation
UNCRPD, Article 30
Article 30 addresses equal participation of per-
sons with disabilities in recreational, leisure
and sporting activities and states that State
Parties shall take appropriate measures:
• To encourage and promote the participa-
tion, to the fullest extent possible, of
persons with disabilities in mainstream
sporting activities at all levels;
• To ensure that persons with disabilities
have an opportunity to organize, devel-
op and participate in disability-specific
sporting and recreational activities and,
to this end, encourage the provision, on
an equal basis with others, of appropri-
ate instruction, training and resources;
• To ensure that persons with disabil-
ities have access to sporting, rec-
reational and tourism venues;
• To ensure that children with disabilities
have equal access with other children to
participation in play, recreation and lei-
sure and sporting activities, including
those activities in the school system;
• To ensure that persons with disabilities have
access to services from those involved in
the organization of recreational, tourism,
leisure and sporting activities (UN, 2006).
APA and the International Classification of Functioning, Disability and Health
APA is strongly associated with an understanding
of the interrelationship between the person, the
environment and the task (Kiphard 1983; Newell
1986; Reed 1988). In 2007, Hutzler and Sherrill
proposed the WHO’s International Classification
of Functioning, Disability and Health (ICF: WHO
2001) as a conceptual framework for the planning
and implementation of APA.
ICF is a comprehensive classification system
designed to capture aspects of human functioning
in the context of a health condition. The sys-
tem consists of a hierarchy of classifications
for each of its domains: Body Functions and
Structures, Activities and Participation, and
Environmental Factors (See figure 3. below) and
has been widely accepted among rehabilitation
services worldwide (Hutzler, 2010). Codes can be
recorded for each classified item within a domain
to indicate the extent of ‘problem’ with any
of these aspects of functioning. Environmental
Factors can be recorded as being either barriers
to or facilitators of a person’s functioning
(Bufka, 2009).
Helpful resources explaining how to use the ICF
are available from the website:
http://www.who.int/classifications/icf/en/
PARTICIPATION
(Restriction) (work, social,
athletic, etc roles)
PERSONAL FACTORS
(age, comorbidities, person-
ality, etc)
HEALTH CONDITION
ACTIVITY
(Limitation) (speaking, walk-
ing, jumping, etc)
ENVIROMENT FACTORS
(living conditions, occu-
pational situation, social
circumstances, climate, etc)
BODY FUNCTIONS & STRUCTURES
(Impairments) (bones, liga-
ments, muscles, sensation,
circulation, etc.)
Figure 3: ICF example adopted from ‘WHO, How to use the ICF: A practical manual for using the ICF’ (2013).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 8180
EUSAPA Functional MAP - Rehabilitation
The EUSAPA (2010) developed functional guidance
for the design and implementation of APA in re-
habilitation, consisting of four key areas:
Key Area Key Role Key Functions
A. Planning A.1. Assess the role and
added value of an Adapted
Physical Activity programme
within the multidisci-
plinary character of the
rehabilitation programme.
A.1.1. Identify the responsibilities of the APA programme
as a complementary part of the rehabilitation programme.
A.1.2. Identify the strengths and weaknesses of the cur-
rently used rehabilitation and APA programme.
A.1.3. Identify the available and required resources (fa-
cilities, equipment) to implement the APA programme.
A.1.4. Develop a structured Adapted Physical Activity pro-
gramme in collaboration with rehabilitation team.
A.1.5. Identify the short and long term aims of
the Adapted Physical Activity programme.
A.2. Assess the (dis)
abilities, risk factors,
needs and potential of
the patient / client.
A.2.1. Understand the condition of the patients / cli-
ents and its consequences in terms of function-
al (dis)abilities, health conditions, etc...
A.2.2. Understand clinical investigation data (e.g. X-rays,
gait analyses, cardiorespiratory tests) and the conclu-
sions and recommendations of rehabilitation specialists.
A.2.3. Assess the patient’s / client’s cur-
rent and potential level of functioning.
A.2.4. Understand the patient’s / client’s response to
physical activity; identify and remediate potential con-
traindications, health risks and risk factors.
B. Education &
Information
B.1. Educate patients /
clients about their (dis)
abilities and potential
through physical activity.
B.1.1. Educate the patient / client about his/her functional (dis)
abilities, response to exercise, potential health risks, risk
factors and contraindications with regards to physical activity.
B.1.2. Educate the patient / client about the recog-
nition and remediation of symptoms that potential-
ly lead to health risks, injuries, etc...
B.1.3. Educate patients / clients about the APA pro-
gramme and its benefits during rehabilitation.
B.2. Provide the appro-
priate information to
guarantee a continuation
of an active lifestyle
post rehabilitation.
B.2.1. Inform the patient / client about communi-
ty based physical activity programmes, and the short
and long term benefits of physical activity.
B.2.2. Provide a database with information regarding com-
panies and community based organisations to ensure a con-
tinuation of an active life style post rehabilitation.
B.2.3. Provide information regarding legislation about possible
benefits from national, regional and local governing bodies with
respect to physical activity and sports post rehabilitation.
C. Implementation C.1. Implement an individual-
ised Adapted Physical Activi-
ty programme complementary to
the other disciplines within
the rehabilitation programme.
C.1.1. Develop a structured and individualised APA pro-
gramme in collaboration with the multidisciplinary team.
C.1.2. Facilitate and optimise participation
through adaptation of the instructions, encourage-
ments, rules and settings when appropriate.
C.1.3. Initiate community based physical activity.
Key Area Key Role Key Functions
D. Assessment
& Evaluation
D.1. Evaluate the effects
of the Adapted Physical
Activity programme as a part
of the rehabilitation and
post-rehabilitation process.
D.1.1. Monitor the long term health related out-
comes of the Adapted Physical Activity programme.
D.1.2. Determine the effects of the Adapted Physical Ac-
tivity programme on functional ability of the patients/
clients in collaboration with rehabilitation team.
D.2. Evaluate the pa-
tient’s/client’s response
to physical activity, his/
her progress, and compare
with the preset goals.
D.2.1. Assess and evaluate the patient’s / client’s physical and psy-
chological well being and its progress, and remediate if necessary.
D.2.2. Assess the motivation of the patient/client toward the
Adapted Physical Activity programme, and remediate if necessary.
D.2.3. Monitor and assess the responses to physical ac-
tivity to ensure safe and successful participation.
D.2.4. Document individual development and progress accord-
ing to the aims of the rehabilitation and the APA programme.
D.2.5. Identify tools, methods, etc… to optimise the patient’s / cli-
ent’s functional abilities in daily life and in physical activity.
Table 3: EUSAPA Functional Map – Rehabilitation, adapted from EUSAPA (2010) Appendix 3.
European Opportunities for Participation
A detailed list of European organisations,
campaigns and initiatives providing people with
disabilities opportunities to participate in
sport can be found in the Council of Europe’s
‘Good Practice Handbook, No. 3 – Disability
Sport in Europe, Learning from experience’:
http://unescoittralee.com/wp-content/
uploads/2015/04/Disability-Sport-in-Eu-
rope-Good-practice-handbook.pdf
4.2.5. Challenges that
Organisations Face
Some common barriers to inclusion in sporting
activities for people with disabilities have
been identified as (DePauw & Gavron, 2005; Hut-
zler & Sherrill, 2007):
• Lack of early experiences in sport (this var-
ies between individuals and whether a disabil-
ity is from birth or acquired later in life)
• Lack of understanding and awareness of how to
include people with a disability in sport
• Limited opportunities and programmes for
participation, training and competition
• Lack of accessible facilities, such
as gymnasiums and buildings
• Limited accessible transportation
• Limiting psychological and sociological
factors including attitudes towards dis-
ability of parents, coaches, teachers and
even people with disabilities themselves
• Limited access to information and resources
Different. Just like you. A psychosocial ap-
proach promoting the inclusion of persons with
disabilities.
This Danish Red Cross handbook (2015) provides
practical guidance for organisations and profes-
sionals on how to facilitate safe and inclusive
sport and APA:
https://www.icsspe.org/sites/default/files/Dif-
ferent.%20Just%20like%20you.pdf
Safety
• Wherever possible, select locations that
are screened off from the general public.
• Before activities begin, all facilita-
tors, helpers and participants should do
a safety check on the playing field. Dan-
gers might include glass, garbage, plas-
tic bags and wrappings, animal excrement,
sharp rocks, wood or any other debris that
could cause injury to participants.
• Use locations that are safe for all us-
ers (e.g. stay away from rivers, em-
bankments, cliffs, roads, etc).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 8382
• Make sure there is enough space for all
of the participants to do the activity.
• Make sure there is enough equipment for
everyone and that it is the correct equip-
ment for the activity wherever possible.
• Make sure it is safe to get to and from the
playing field, if a sports activity is held
outside (e.g. no travelling in the dark).
• Changing rooms and bathrooms should
be available, wherever possible.
• First aid kits should be available and
all facilitators trained in using them.
• Be aware of participant’s pre-existing
health conditions (e.g. asthma, diabe-
tes), psychological/emotional problems or
current illnesses or risk conditions.
• Always plan each session and ensure that the
activities are suitable for the participants.
• Rival groups should not be involved in
competitive games. If competitive games
are played, rival group members could
play in mixed teams. Choose activi-
ties carefully to promote cooperation.
• Make sure that participants choose team
members in a fair way and in a manner that
does not demean anyone. For example, if
two team captains choose team members in
turn, someone will be left at the end, feel-
ing they are not wanted in any team.
• Be sure that there are enough facilita-
tors and helpers for each session so that
the participants are supervised well and
are not at risk of harm. Facilitators
should be trained in risk management.
Inclusion
Organisers promote inclusion by building on in-
dividuals’ strengths and interests, rather than
focusing on their impairments.
The key elements in this approach are:
• Do not underestimate the person’s abilities.
• Have a plan for positive experiences by
setting challenging but achievable goals.
• Have a flexible approach to coach-
ing and communication that recog-
nizes individual differences.
• Be creative and explore new and unconven-
tional methods to ensure that every ses-
sion is fun and rewarding for all.
• Be aware that there are different impair-
ment groups (blind, deaf, learning disabled
and physically disabled) that need dif-
ferent adaptations and that safety, (both
physical and mental), is very important.
The Inclusion Spectrum
Developed by Black and Stevenson (2011), this
model (figure 2.) is now widely used for the de-
sign and implementation of inclusion for all in
physical education and sport.
The model classifies activities into 5 differ-
ent groups based on the level of adaptation
required:
1. Open – minimal or no adaptations to the
environment or equipment; open activi-
ties are by their nature inclusive so that
the activity suits every participant.
2. Modified - everyone plays the same game or
performs the same activity but the rules,
equipment or area of activity are adapt-
ed to promote the inclusion of all indi-
viduals regardless of their abilities.
3. Parallel - although participants fol-
low a common activity theme, they do so
at their own pace and level by working
in groups based on their abilities.
4. Separate/Alternate - emphasises that,
on occasions, it may be better for a
person to practice sports individual-
ly or with their disabled peers.
5. Disability/APA - ‘reverse integration’ where
non disabled people are included in disabil-
ity sports together with disabled peers.
STEP tool - enables organisers to adapt the
activity across the key areas of Space, Task,
Equipment and People.
Figure 4: The Inclusion Spectrum incorporating STEP
(Black & Stevenson, 2012) adapted from England Athlet-
ics: https://www.englandathletics.org/shared/get-file.
ashx?itemtype=document&id=10176
4.2.6. Development of
preventative and health
conscious habits
Persons with disabilities have lower levels of
physical activity than their peers, consequently
38% of the population is obese (53% more than
people without disabilities), and engage in low-
er levels of physical activity. High costs for
health services caused by overweight (increased
blood pressure, diabetes Type 2, Hypercholes-
terolemia, stroke, osteoarthritis, sleep apnea,
etc.) are a huge problem for the European tax
payers.
A review of the literature (Zakus, Njelesani &
Darnell, 2007) on sport, physical activity and
health demonstrated:
• Cardiovascular health benefits occur at
moderate levels of physical activity and
increase at higher levels of physical ac-
tivity and fitness (General, 1996).
• Exercise is effective in the manage-
ment of diabetes, as it has been shown
to improve glucose homeostasis (War-
burton, Nichol & Bredin, 2006).
• Both obesity and physical inactivi-
ty have similar patterns of associa-
tion with clinical risk factors, such as
blood pressure (Blair & Church, 2004).
• Obese individuals with at least moderate
cardio respiratory fitness have lower rates of
cardiovascular disease (Blair & Church, 2004).
• 40% of all cancers may be prevent-
ed by a healthy diet, physical ac-
tivity and not using tobacco.
• Regular physical activity is an effective sec-
ondary prevention strategy for osteoporosis,
as well as the maintenance of bone health.
• Exercise can be effective in improving men-
tal well-being largely through improved mood
and physical self-perception (Fox, 1999).
Parnes & Hashemi (2007) highlighted the health
benefits of physical activity specifically for
persons with disabilities:
• Persons with Disabilities share many traits
with the general population, suggesting that
the positive effects of physical activity on
cardiovascular diseases are also attributable.
• Individuals disabled by osteoarthritis
of the knee may benefit from aerobic and/
or resistance exercise programs in the
areas of physical performance and pain
management (Ettinger et al., 1999).
• Physical activity and sport participation re-
sult in improved functional status and quality
of life among persons with selected impair-
ments and disabilities (Heath & Fentem, 1997).
• Children and adolescents with cerebral
palsy may benefit from physical activity
through improvements in strength and abil-
ity to walk, run, jump and climb stairs
after participating in a strength-training
program (Dodd, Taylor & Graham, 2003).
• Aerobic dance may affect cardiovascular
endurance of adults with intellectual dis-
abilities (Cluphf, O’Connor & Vanin, 2001).
• Physical activity may lead to improvements
in physical health and well-being. Spe-
cifically, improvements have been noted in
coordination, postural alignment and nor-
malization of muscle tone, improved sitting
balance and strength and rhythmical move-
ments of the upper body (DePauw, 1986).
• Aerobic (endurance training) exercise is
effective in improving general mood and
depressive and anxiety disorders in se-
lect psychiatric patients. There is no
harm associated with participation in
STEPAdaptation tool
DI
SABIL
ITY SPORTAdapted physical a
ctiv
ity
everyone can play
OPEN
ability groupsPARALLEL
MODIFIED
change to includeS
EPARATE/
ALTERNATE

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 8584
physical activity and exercise in these
populations (Meyer & Broocks, 2000).
• Participation in sports and physical fitness
activities has been associated with three em-
powerment outcomes: perceived competence as a
social actor; facilitation of goal attainment
(including setting and pursuing goals, deter-
mination, and competitiveness); and social
integration (including bonding, broadening
social skills and experiences, and increased
social inclusiveness) (Blinde & Taub, 1999).
Romano-Spica et al., (2015) highlighted that
advances in APA technologies and the scientific
evidence to date indicates physical activity is
a priority tool in the prevention of multifacto-
rial diseases and sedentary lifestyle.
Incorporating sport and APA into rehabilitation
services as well as post-rehabilitation com-
munity services, as outlined in this chapter,
provides an effective means of improving the
physical activity levels of persons with dis-
abilities, ultimately improving the health and
well-being of this population.
Case studies
Tom, 64
In 2016, Tom suffered a brain injury and un-
derwent two brain surgeries. As a result he
initially lost all mobility and suffered facial
paralysis, affecting his ability to swallow. Tom
spent 5 months as an inpatient in hospital. When
being discharged from hospital Tom was able to
walk with support for very short periods of time
in the home, but required the use of a wheel-
chair when travelling outside.
As a result of his injury Tom experienced left-
side weakness and had difficulties with memory,
concentration and fatigue. He now needed support
in performing everyday tasks such as getting
dressed, cutting food and tying his shoe laces.
“I was motivated to improve my mobility as I
have two sons who live abroad that I would like
to be able to visit… but I lacked the confidence
to engage in physical activity.”
The Community Brain Injury Team Physiotherapist
informed Tom of Brain Injury Matters’ Sports 4
U programme. Sports 4 U involves a Physiothera-
pist-led exercise programme specifically designed
for people with acquired brain injury, followed
by workshops aimed at improving overall health
and well-being.
Tom’s wife describe the timing of the programme
as “a god send, both physically and mentally for
Tom.” Since starting the programme Tom has made
tremendous progress and reports enjoying “being
part of a group that share similar experiences.”
Having just been signed off to walk up and down
the stairs independently before commencing the
programme, Tom is now jogging for the first time
since his injury and reports using the ‘SMART’
goals discussed in the Sports 4 U workshops to
increase the distance he walks outside of the
programme.
“I now have the confidence to go places we hav-
en’t been since my injury, like the cinema… and
to sign up for another physical activity pro-
gramme with the GP.”
“We were able to visit our son in Scotland,
our next goal is to visit our son who lives in
America.”
Tom’s wife said “we couldn’t speak highly enough
of Brain Injury Matters and the work they have
been doing; we would thoroughly recommend the
Sports 4 U programme to anyone in a similar
situation.”
Reference
Ashton-Shaeffer, C., Gibson, H. J., Autry, C. E., & Hanson, C.
S. (2001). Meaning of sport to adults with physical disabili-
ties: A disability sport camp experience. Sociology of Sport
Journal, 18(1), 95-114.
Black, K., & Stevenson, P. (2011). The inclusion club.
Blair, S. N., & Church, T. S. (2004). The fitness, obesity, and
health equation: is physical activity the common denomina-
tor?. Jama, 292(10), 1232-1234.
Blinde, E., & Taub, D. (1999). Personal empowerment through
sport and physical fitness activity: Perspectives from
male college students with physical and sensory disabili-
ties. Journal of Sport Behavior, 22(2), 181.
Burchell, A. (2006). The Importance of Sport to the Disabled.
The Commonwealth Health Minister’s Book, 2006.
Bufka, L. (2009). International Classification of Functioning,
Disability and Health: APA Update. Spotlight on Disability
Newsletter, May 2009. Retrieved from:
http://www.apa.org/pi/disability/resources/publications/news-
letter/2009/05/icf.aspx
Capella-McDonnall, M. (2007). The need for health promotion
for adults who are visually impaired. Journal of Visual Im-
pairment & Blindness, 101(3), 133.
Cherney, J. L., Lindemann, K., & Hardin, M. (2015). Research
in communication, disability, and sport. Communication &
Sport, 3(1), 8-26.
Cluphf, D., O’Connor, J., & Vanin, S. (2001). Effects of
aerobic dance on the cardiovascular endurance of adults with
intellectual disabilities. Adapted Physical Activity Quarter-
ly, 18(1), 60-71.
CRPD, U. (2007). United Nations Convention on the Rights of
Persons with Disabilities. UN, New York.
Council of Europe. (1992). The European Sport’s Charter.
Brussels: Council of Europe.
Council of Europe. (2001). The European Sport’s Charter (re-
vised). Brussels: Council of Europe.
DePauw, K. P. (1986). Research on sport for athletes with
disabilities. Adapted physical activity quarterly, 3(4),
292-299.
DePauw, K. P., & Gavron, S. J. (2005). Disability sport. Human
Kinetics.
Dodd, K. J., Taylor, N. F., & Graham, H. K. (2003). A random-
ized clinical trial of strength training in young people with
cerebral palsy. Developmental medicine and child neurolo-
gy, 45(10), 652-657.
Durstine, J. L., Painter, P., Franklin, B. A., Morgan, D.,
Pitetti, K. H., & Roberts, S. O. (2000). Physical activity
for the chronically ill and disabled. Sports Medicine, 30(3),
207-219.
Ettinger, B., Black, D. M., Mitlak, B. H., Knickerbocker, R.
K., Nickelsen, T., Genant, H. K.,... & Glüer, C. C. (1999).
Reduction of vertebral fracture risk in postmenopausal women
with osteoporosis treated with raloxifene: results from a
3-year randomized clinical trial. Jama, 282(7), 637-645.
EUFAPA (2006). Bye-laws. Retrieved from: http://www.eufapa.
eu/index.php/eufapa/bylaws, 15.8.2018
Fox, K. R. (1999). The influence of physical activity on mental
well-being. Public health nutrition, 2(3a), 411-418.
General, S. (1996). Physical Activity and Health: A Report
of the Surgeon General. Atlanta, GA: US Department of Health
and Human Services, Centers for Disease Control and Preven-
tion. National Center for Chronic Disease Prevention and
Health Promotion.
Heath, G. W., & Fentem, P. H. (1997). Physical activity among
persons with disabilities--a public health perspective. Exer-
cise and sport sciences reviews, 25, 195-234.
Hutzler, Y. (2010). Adapted Physical Activity and Sport in
Rehabilitation. International Encyclopedia of Rehabilitation,
2010.
Hutzler, Y., & Sherrill, C. (2007). Defining adapted physical
activity: International perspectives. Adapted Physical Activ-
ity Quarterly, 24(1), 1-20.
Jackson, E. L., Crawford, D. W., & Godbey, G. (1993). Negotia-
tion of leisure constraints. Leisure sciences, 15(1), 1-11.
Jackson, S., & Scott, S. (1999). Risk anxiety and the social
construction of childhood. Risk and sociocultural theory: New
directions and perspectives, 86-107.
Kiphard, E. (1983). Mototherapie–Teil I. Modernes Lernen,
Dortmund.
Kudláček, M., Morgulec-Adamowicz, N., & Verellen, J. (2010).
European Standards in Adapted Physical Activities, 2010.
Lee, J., & Haegele, J. A. (2015). A cross-disciplinary
comparison of published articles: Adapted physical activity
and special education. European Journal of Adapted Physical
Activity, 8(1).
Lindemann, K., & Cherney, J. L. (2008). Communicating in
and through “Murderball”: Masculinity and disability in
wheelchair rugby. Western Journal of Communication, 72(2),
107-125.
Lorenzen H. (1961). Lehrbuch des Versehrtensport [Textbook of
disabled sports] Stuttgart (Germany): Enke Verlag.
Meyer, T., & Broocks, A. (2000). Therapeutic impact of
exercise on psychiatric diseases. Sports Medicine, 30(4),
269-279.
Newell, K. (1986). Constraints on the development of coordi-
nation. Motor development in children: Aspects of coordina-
tion and control.
Parnes, P., & Hashemi, G. (2007). Sport as a means to foster
inclusion, health and well-being of people with disabili-
ties. Literature Reviews on Sport for Development and Peace,
124.
Rasmussen, T. J., Wiedemann, N., Kryger, L. S., Koenen, K.,
Trimmel, J. & Boersma, M. (2015). Different. Just like you: A
psychosocial approach promoting the inclusion of persons with
disabilities. International Federation of Red Cross and Red
Crescent Societies Reference Centre for Psychosocial Support
(PS Centre). Retrieved at: http://www.attiva-mente.info/1.
pdf, 15.8.2018
Romano-Spica, V., Macini, P., Fara, G. M., & Giammanco, G.
(2015). Adapted Physical Activity for the Promotion of Health
and the Prevention of Multifactorial Chronic Diseases: the
Erice Charter. Ann Ig, 27(2), 406-14.
Seymour, H., Reid, G., & Bloom, G. A. (2009). Friendship in
inclusive physical education. Adapted Physical Activity Quar-
terly, 26(3), 201-219.
Reed, E. S. (1988). James J. Gibson and the psychology of
perception. Yale University Press.
Sherrill, C. (2004). Young people with disability in physi-
cal education/physical activity/sport in and out of schools:
technical report for the world health organization. Geneva:
The World Health Organization.
Sherrill, C., & Hutzler, Y. (2008). Adapted physical activity
sciences. Directory of sport science, 89-103.
Warburton, D. E., Nicol, C. W., & Bredin, S. S. (2006). Health
benefits of physical activity: the evidence. Canadian medical
association journal, 174(6), 801-809.
World Health Organization. (2011). World report on disabili-
ty: World Health Organization.
World Health Organization. (2013). How to use the ICF. A
practical Manual for using the International Classification of
Functioning Disability. Health. Geneva.
Zakus, D., Njelesani, D., & Darnell, S. (2007). The use
of sport and physical activity to achieve health objec-
tives. Literature reviews on sport for development and Peace,
48.

5.
Learning outcomes:
• Familiarise readers with what needs
to be focused on when planning APA
• Familiarise readers with common principles
of preparation for competitive sports
• Gain knowledge of recommendations for
managing risks in adapted sports
• Highlight and understand risk factors when
planning APA for people with disability
• Recognise professionals assump-
tions, attitudes and beliefs, ana-
lysing them and challenging them
• Practical examples and strategies in the
process of maintaining boundaries
• Familiarise readers with the importance of
psychological preparation and strategies
to prepare athletes with disabilities
• Define the importance of motivation and goal
setting in the process of mental preparation
• Familiarise readers with the importance of fa-
cilitating physical activities for people with
disabilities and identify obstacles they face
• Getting familiar with devices and equip-
ment used by persons with disabilities
when performing physical activity
• Defining the impact of technological de-
velopment and the use of modern devic-
es and equipment on the integration
of people with disabilities into var-
ious adapted sports activities
Pla nniNg aN adaptiVE PhySIcal ACTiviTy

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 8988
5.1.hOW tO plan ADAptIVe Phys-ICal ActivITy
AUTHORS: VALENTINA BOLŠEC, JASNA VEŠLIGAJ DAMIŠ
Key words: physical activity, adaptation, persons with disability, sports, barriers
Active living means integrating physical activ-
ity into daily routines. Our body was meant to
move and be physically active. Physical activ-
ity includes walking or cycling for transport,
dancing, traditional games and pastimes, garden-
ing and housework as well as sport or deliberate
exercise (Edwards and Tsouros, 2008).
Any physical activity, movement and participa-
tion in sports can be beneficial as it has posi-
tive effects on our health which is particularly
important for people with disabilities. When we
are planning physical activity for people with
disability, we refer to it as adapted physical
activity (Reid, 2003).
When we are planning physical activity for peo-
ple with disability particular attention must be
paid to the adaptation of certain areas.
Persons with a disability can participate in sports for able bodied persons but they may need addi-
tional equipment or adaptations. Not all sports are appropriate for everyone. Certain sports can be
recommended and appropriate for certain disability. We can also find sports developed specially for
people with certain disability, for example goalball for blind (Burger, 2010).
5.1.1. How to choose sports?
In the “Participation possibility chart” we can find some of the major physical disabilities and
major sporting activities. It was developed by The American Academy of Orthopaedic Surgeons (Adams
1991, v Burger 2010). There are very few sports where adaptations are not possible and people with
disabilities will not be able to participate.
PARTICIPATION
POSSIBILITY
CHART
Archery
Bicycling
Tricyclinh
Bowling
Canoeing/kayaking
Diving
Fencing
Field events*
Fishing
Golf
Horseback riding
Rifle shooting
Sailing
Scuba diving
Skating (roller & ice)
Skiing (downhill)
Skiing (cross-country)
Swimming
Table tennis
Tennis
Tennis (wheelchair)
Track
Track (wheelchair)
Weight lifting
Wheelchair poling
Baseball
Softball
Basketball
Basketball (wheelchair)
Football (tackle)
Football (touch)
Football (Whellchair)
Ice hockey
Sledge hockey
Soccer
Soccer (wheelchair)
Volleyball
AMPUTATIONS
Upper Extremity RA R R R RA R R R R RA R A R R R R R R R R R R R R R R R R R R
Lower Extremity (AK) R R R R R R I R R R R R R R I RA RA R R I R R R R RA RA R I I R R I R R
Lower Extremity (BK) R R R R R R R R R R R R R R R R R R R R I R I R I R R R I R R I I I R I R
CEREBRAL PALSY
Ambulatory R R R R R R I R R R R R R I R RA RA R R R R R R R I I I I R R
Wheelchair R I I R R I I I R I I R R I R R R R R I I R R I R I
SPINAL CORD DISRUPTION
Cervical RA RA RA IA I R X RA R IA IA R RA IA R I I I I IA
High-thoracic (T1-T5) R R R R RA R R RA I R R R IA IA R R R R R R RA RA R R R R RA
Low thoracolumbar (T6-L3) R R R R RA R R RA R R R R RA RA R R R R R R RA RA R R R R RA
Lumbosacral (L4-sarcal) R R R R R R R R R R R R R I R R R R R R R R R R R I I R I I R R
NEUROMUSCULAR DISORDERS
Muscular dystrophy RA I R R I I R R R I RA R I I I I R R I I I I R I I I I I I I I I I
Spinal muscular atrophy RA I R R I I R R R I RA R I I I I R R I I I I R I I I I I I I I I I
Charcot-Marie-Tooth R R R R R R R R R R R R R R R R R R R R R R R R R R R I R R
Ataxias R I I R I I R R I I R R I I I R R R R R I R I R I I I R I I I I I R I
OTHERS
Osteogenesis imperfecta R I R R R I R R R I I R R I I I R R R R R R R I R I I I R X I I X X X R I
Arthrogryposis R I I R R I I R R I R R R I I I R R R R R I R R R X R I I I R
Juvenile rheumatoid arthritis RA I I RA R I I I R I I R R I I I I R R I I I I I I I I I I I I I I I I I I
Hemophilia RA R R R R R R R R R R R R R I I R R R I R I I R R X I X I R
Skeletal dysplasias R R R R R R R R R R R R R R R RA R R R R R I R R R I R R R R
* Clubthrow, discus, javel, shotput
R = Recomemended
I = Individualized
A = Adapted
X = Not Recommended
Table 4: Participation possibility chart. Adams, 1991
Figure 5: https://www.birmingham.ac.uk/Documents/college-les/
sportex/Physical-Activity-Disability-Infographic.pdf
5.4.7. What do we adapt?
• Environment
• Equipment
• Sport/play games
• Rules
• Exercises
• Age adaptation – early childhood to
elderly (Wittmannová, 2018).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 9190
5.1.2. Barriers
When planning sports activities for persons with
disabilities, we also have to refer to different
barriers. Bragaru et al, 2013, exposed some fac-
tors that are negatively associated with partic-
ipation in sports:
• Technical barriers can include fac-
tors related to transportation, pros-
thesis, information etc.
• Social barriers include lack of sup-
port in interactions with so-
cial groups or sports partners
• Personal barriers include factors re-
lated to physical health or psychologi-
cal attributes and even time management
• There are also many other barriers that
influence participation in sports: older
age, poor weather, high cost and others.
A more detailed description and distribution
of barriers can be found in the chapter 5.3.5.
Challenges for Facilitators and Service Users.
5.1.3. How to Plan an Adaptive
Physical Activity?
Planning an Adaptive Physical Activity can be
demonstrated using a cyclic model:
Figure 6: PAIE model for planning an Adaptive Physical Ac-
tivity (Vešligaj Damiš, 2018)
The first component of the PAIE model is plan-
ning of a sports program or sports activities.
It involves making decisions about the choice
of sport - according to the wishes of the ath-
lete with disabilities and according to his/
her abilities and consideration of the personal
characteristics of an athlete with disabilities,
decisions about necessary adaptations, manage-
ment of obstacles and risk analysis.
When planning a sports program or sports activ-
ities we must take into account the specifics of
the individual disability as well as the recom-
mendations for prescribing exercise (frequency,
intensity, duration). In addition to general
knowledge in the field of sports, trainers must
also be equipped with knowledge of the specific-
ities of people with disabilities and know the
importance and possibilities of physical exer-
cise for persons with disabilities.
If sport activities for people with disabilities
are well planned, they are safe and appropriate
for them and what is important, athletes show
personal satisfaction in achieving personal
goals in sports. For athletes with disabilities,
sport activity is planned according to their
functional abilities, physical capacity, inter-
est and accessibility. It can take place in the
gym or outdoors, individually or in groups.
When planning a sports program, we are looking for answers to a num-ber of important questions, such as:
• What are the current competencies of an
individual - an athlete with a disability?
• What kind of activity is appro-
priate for this individual?
• What skills and abilities need to be
evaluated for this individual?
• What kind of interests does an ath-
lete with disabilities now have and
what will he have in the future?
• How effective is the program in satis-
fying the needs of this individual?
• Will the individual achieve any bene-
fits from participating in this program?
PROGRAM
PLANNING
ASSESSINGPERSON WITH
DISABILITY
IMPLEMENTA-
TION PLANING
AND TEACHING
EVALUATION -
PERSON, PROGRAM
• What new skills will an individ-
ual learn in this program?
• Is it possible and needed to improve the in-
structions for an individual in this program?
• How will his/her quality of life be im-
proved after joining the program?
It is necessary to take into account that we
can achieve a better motivation of athletes
with disabilities by including new activities,
working with athletes without disabilities or
practicing with music. Greater persistence in
training can be promoted by the fact that the
participant receives admiration and award when
he reaches the goal or we can help ourselves
with modern technology, for example, interac-
tive computer games involving physical activity
(Saunders, 2016).
Regular physical exercise of the appropriate
intensity and frequency in people with disabil-
ities may be hampered by a number of factors.
Personal factors include depression, fatigue,
lack of interest, poor perception, inadequate
self-assessment of one’s own abilities, negative
values related to physical exercise, fear (from
falling, to defeat, etc.). Among environmental
factors it is very important that the individual
has family and social support. It is also im-
portant that training centers are available and
that transport and exercise costs are low.
Sports training also bring a certain risk for
people with disabilities. Therefore, it is
important to make a risk analysis in prepara-
tion of the sports program, which covers all
the possible dangers of the sporting, physical
exercise for people with disabilities. We base
our assumption on the fact that the benefits of
sports activities outweigh the risk.
The second component of the PAIE model is the
assessment, which includes the systematic pro-
cess of observing the athlete with disabilities,
on the basis of which his needs and progress are
determined. It is a multi-faceted approach of
gathering information on the success and ability
of an individual. It is an integral part of the
effective implementation of physical activity.
This is a continuous process that takes place
before, during and after the implementation of
the program (Kasser & Lytle, 2013).
The assessment covers several areas: screening,
decision about support, planning and develop-
ment, assessment of progress and testing for
classification in sport (Kasser & Lytle, 2013).
Evaluation can be performed by standardized
tests (tests, questionnaires or scales) or by
non-formal testing (recording, task analysis,
behavioral observation, communication, use of
support technology, etc.).
The third component of the PAIE model is the
implementation of sports programs and learning.
Athletes with disabilities actively carry out
the chosen sports activity and gain experi-
ence based on their assessed needs. In the case
of involvement in sport, we are talking about
choosing: today, participants should have the
option of choosing, and the disabled person has
the opportunity to participate in sports activ-
ities and sports together with peers without
disabilities and competitors or in separate
environments. Accessible activities cover a
range of opportunities ranging from “involvement
in conventional circumstances” to “inclusion
in opportunities for specific disabled people”
(Kiuppis, 2018).
The last component is an evaluation that is done
for both athletes with disabilities as well
as for sports programs and activities. It is
important to check if the program is appropri-
ate, satisfies the athlete with disabilities and
allows him/her to achieve their set goals. On
the basis of the evaluation, proposals for the
necessary changes will be made.
Reference
Bragaru, M., Van Wilgen, C. P., Geertzen, J. H., Ruijs, S. G.,
Dijkstra, P. U., & Dekker, R. (2013). Barriers and facili-
tators of participation in sports: a qualitative study on
Dutch individuals with lower limb amputation. PLoS One, 8(3),
e59881.
Burger, H. (2010). Sport for disabled. In M. Kovač, G. Jurak
and G. Starc (ed.), Proceedings of the 5th International Con-
gress Youth Sport 2010 (29-30). Ljubljana: Faculty of Sport,
University of Ljubljana
Edwards P, Tsouros AG. (2008). A healthy city is an active
city: a physical activity planning guide. World Health Orga-
nization Europe.
Kasser, S.L., Lytle R.K., (2013), Inclusive Physical Activ-
ity-2nd Edition, Human Kinetics, Human Kinetics Europe Ltd,
United Kingdom)
Kiuppis, F., & Kurzke - Maasmeier, S. (2012). Sport Im
Spiegel Der UN-Behindertenrechtskonvention [Sports Reflected
in the UN-Convention on the Rights of Persons with Disabili-
ties: Interdisciplinary Approaches and Political Positions].
Stuttgart: Kohlhammer.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 9392
Reid, G. (2003). Defining Adapted Physical Activity. In R. D.
Steadward, G. D. Wheeler and E. J. Watkinson (ed.), Adapted
Physical Activity (11-25). Canada: The Univerity of Alberta
Press
Saunders, D.H., Sanderson, H., Hayes, S., Kilrane, M., Greig,
C.A., Brazelli, M., Mead, Ge. Physical fitness training for
stroke patients. Cochrane Database of Systematic Reviews
2016: CD003316. DOI: 10.1002/14651858.CD003316.pub6.
Wittmannová, J. (2018). Šport za vse: opolnomočenje
strokovnih kompetenc z izobraževanjem o prilagojenih športnih
aktivnostih. In M. Pajek (ed.), 13. kongres športa za vse,
športna rekreacija invalidov (17-22). Ljubljana: Olimpijski
komite Slovenije–Združenje športnih zvez
Figure 5: https://www.birmingham.ac.uk/Documents/college-les/
sportex/Physical-Activity-Disability-Infographic.pdf Re-
trieved 12.2.2019 at 9:25
Table 4: Adams R.C., Mc Cubbin J.A. (1991). Games sport, and
exercise for the physically disabled. London: Lea & Febiger
5.2.CompetITiON iN SpoRTs
AUTHOR: LADISLAV MESARIČ
Key words: competition, weather conditions, overload, principle of specifici-ty, principle of progressive development, continuity principle, principle of individuality
Experts acknowledge the importance of sports
and recreation in the successful rehabilitation
of people with different types of disabilities.
Adapted sports and recreational activities offer
an opportunity for success in a very short time.
Success has a positive impact on self-esteem
and focus on opportunities, rather than dealing
with what is no longer possible. The ability
to participate in sport offers the opportunity
to reunite with family and friends in a joint
venture (Sherrill, 2003).
People get engaged in various sports activities
in order to improve their health, well-being and
working abilities. Many of them are not satisfied
with just being active. They want to compare
their abilities with others at sports compe-
titions. Increased interest in sports has led
to the development of competitive systems for
people with disabilities. Different regulations
and classifications have been developed for indi-
vidual sports, enabling people with disabilities
to compete under the same conditions. The clas-
sification of disability is numerous and diverse,
some are based on the cause of disability,
others on the affected body parts such as arms,
legs, heart etc. (Aleksandrović, 2016).
Dealing with competitive sports irrespective of
gender and age requires proper preparation for
competition. In the case of persons with dis-
abilities, specific limitations arising from the
nature of their disability should be taken into
account. These limitations must be taken into
account both in the choice of sport and in the
choice of training assets. Every chosen sport
has its own laws and necessary adjustments.
In any case, the general principles of sports
training apply to all athletes, with or without
disability.
Many authors have defined different principles
that basically overlap. As a rule, they refer to
the frequency, intensity, duration and type of
sports activity. Frequency describes how often
a person deals with a certain sport activity.
The intensity of the exercise is the strength
with which the individual perform a sport. It
represents a key point in training planning.
It depends on the maturity of the individuals
involved, the current form, the personal goals
of athletes and many other factors. The duration
describes how long the training should last to
get the proper results. The duration is inverse-
ly proportional to the intensity of training. We
cannot train for a long time at a high level of
intensity. However, the development of aerobic
abilities requires a longer duration with an
appropriate lower intensity. The type of exer-
cise relates to the way or form of how a sports
exercise is performed. Aerobic abilities can be
practised by walking, cycling and other contin-
uous activities. We can gain power with weights,
exercises with our own weight, and other exer-
cises where we overcome external resistance.
Different types of exercise are crucial for
involving different people into sports activi-
ties, each meeting their own needs and goals. Of

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 9594
course, different sports disciplines have their
own specific features. However, this principle
is well established (Ayers & Sariscsany, 2013;
Bompa & Haff, 2009).
The most common are the following principles
(Ayers & Sariscsany, 2013):
The overload principle
The principle of overload refers to the fact
that the individual needs to be burdened more
than usual for it to make changes or positive
adaptation to the training. Progress is achieved
by the gradual burden of physical systems with
specific exercises and training schedule. Over-
load is a positive stress, which is achieved by
increasing the intensity of training, increasing
the number of training sessions, increasing the
duration of each training.
The principle of
progressive development
Good sports condition cannot be achieved in a
short time. Body systems have their own lim-
itations in terms of the speed of adapting to
the training load. Loads must be gradual. If
a load increases in a short time, it can lead
to fatigue and damage. By contrast, insisting
on a certain degree of burden without a gradu-
al increase leads to stagnation as a result of
reduced adaptation to training.
Principle of specificity
The sports training program must be adapted to
the desired result. Training improves only those
skills that we train and have a slight influence
on other abilities. We need to choose the ap-
propriate exercises. It does matter, however,
which exercises we perform. If we want to im-
prove the strength of the hands, we will choose
strengthening hand exercises, we will increase
the mobility by stretching the part of the body,
where the mobility is reduced, and the aerobic
abilities will be trained with long-term contin-
uous activities.
Continuity principle
Sports training should be carried out regularly
so that we can get proper results. As the organ-
ism gradually adjusts to the load and reaches
the appropriate fitness level, at reduced activi-
ty body is adapted to it and the fitness reduces.
This training principle helps to understand why
lifelong sport activities are so important.
Principle of individuality
People who are involved in sports have different
physical characteristics and biological poten-
tials for change. Coaching takes into account a
variety of factors and has different objectives.
Opportunity for individually selecting a sports
program is crucial for creating lifelong habits
of engaging in sports.
Recommendations for
physical activity
Regardless of the above recommendations, it is
necessary to know how many physical activities
we need in order to achieve our goals and conse-
quently adjust our training plan accordingly.
Physical activity that provides a variety of
health benefits consists of dynamic and rhythmic
contractions of large muscle groups that trans-
mit the body at a distance or act against gravi-
ty with moderate intensity over a long period of
time in which the body consumes 200 to 400 kilo
calories (or 4 kilo calories per kilogram of
body weight). For optimal health benefits, such
(aerobic) activity should be carried out every
day or at least every other day, and should be
supplemented by strength and mobility exercises
(Haskell et al., 1985).
Competitors with higher ambitions need to find
appropriate professional help.
Recommendations for exercising
individual motor skills
in an adaptive sports
exercise programme
The following tables describe the application of
training principles for flexibility, strength and
aerobic endurance.
The mobility and extent of movement depend on
various factors. These may be anatomical (joint
shape, tendon characteristics) or are condi-
tioned by neuromuscular factors. The latter
are common in adapted sports practice (e.g.,
spasticity). The usual exercises for flexibility
are performed in the form of static stretching
(Kasser, 2013)
Training
variables
General recommendation
Frequency Before and after activi-
ty, minimum 3x per week
Intensity Individually depending on the abil-
ities, should not cause pain
Duration 10-30 seconds, 2-3 repeti-
tion of each exercise
Type Static stretching, dimanic stretching
as preparation for sports training
Overload Careful movement of the stretching
points, increasing of the number of
repetition and duration of stretching
Progress Slow and easy progress, first big-
ger muscle groups, then extreme
and small muscle groups.
Application of training principles for flexibility (Kasser,
2013)
Training
variables
General recommendation
Frequency 3-4 x per week with one day break
during the exercise days
Intensity Easy or medium 40-0% of the maximum effort
Duration 3-5 series, 3-7 repetition for strength
and 12-20 repetition for endurance
Type Exercises with own weight, ex-
ercises with resistance
Overload For strength we gradually increase
the resistance, for endurance in-
crease the number of repetition or
duration of repetition or decrease the
duration of break between series
Progress Gradually as trying to avoid injuries
Application of training principles for muscular strength and
endurance in strength (Kasser, 2013)
Training
variables
General recommendation
Frequency 3-5 per week
Intensity 55-90% of maximum heart rate (de-
pending on the abilities)
Duration 15-60 minutes (in time it
could be increased)
Type Walking, running, swimming …
continuous activities
Overload Increased speed, time or temp
Progress We predict gradual prog-
ress in the individual plan.
Application of training principles for training aerobic
abilities (Kasser, 2013)
Less is more
Successful training is not just the final goal.
The aim is to achieve optimal results with opti-
mum amount of training. We do not need to train
until pain and injuries occur. Training is usu-
ally strenuous and often unpleasant, but pain is
not a regular companion. If it occurs regular-
ly, it should be treated seriously. Unpleasant
feelings in particular parts of the training may
occur due to the release of lactic acid, which
monitors anaerobic activity, weight lifting and
interval training. Fatigue and pain may also oc-
cur due to micro-lesions in the muscles. Delayed
muscular fatigue and pain that occur 24 hours or
more after activity are not a result of lactic
acid. Lactic acid is removed rapidly by the
blood circulation quickly after the activity.
Activity-related pain usually occurs after new
activities and in when some activities have not
been performed for a long time and are probably
related to the micro traumas of the muscles and
connective tissue.
Organization of training hours
Each training session must be systematically or-
ganized and consist of a warm-up, main training
activity and cool down. This approach helps the
athlete to gradually prepare for the main loads
and gradually reduce the load before the end of
the training so that there are no fast transi-
tions from one part to another.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 9796
Warm-up
Warm-up is a low-intensity sports activity
that takes place before an intense main part of
the training and serves for preparation of the
body and mind to what follows in the main part.
Regular and thorough implementation of warm-up
can significantly reduce the likelihood of sport
related injuries.
The main part of the training
The main part of the training is the key part
in which we acquire new knowledge and improve
one or more components of the sports shape. By
following the basic principles of training we
develop motor skills and elements of sports
games. The main part can have one or two main
contents.
Final part of the
training (cooling)
The final part of the training consists of
low-intensity activities and rests. It usually
consists of continuous low-intensity aerobic
activity. Sometimes stretching is also included.
It is also recommended to do a short analysis of
the work done and to help further training.
Exaggeration and
exercise dependence
Although inactivity is a far greater problem,
overloading during training can lead to over-
training in active people. This is the state
of the reduced ability of the immune system to
resist infection. Symptoms of overtraining are
low motivation, fatigue, insomnia, poor results,
loss of appetite and poor health. Symptoms come
gradually, so overtraining is difficult to de-
tect. The reasons may be the following: boring
and overloaded training, rapid weight loss,
inadequate nutrition and inadequate hydration.
Overtraining is treated by reducing the volume
and intensity of training, and in many cases
with complete rest.
The influence of the environment
on the training process
Environmental effects, such as heat, cold, hu-
midity, altitude and poor air, can have a strong
impact on health and sports achievement. If we
do not pay attention to the environment, serious
problems can arise, which may end up with death.
On the other hand, we can adapt to the circum-
stances, which makes it easier for us to work,
improves the effect, and helps us to survive
comfortably in different circumstances (Sharkey
et al., 2008).
Sport activity in high-er outdoor temperature
During sports activity at high temperatures, we
can only regulate the temperature balance with
circular adaptation and sweating mechanisms for
a short time. The body absorbs heat when the
outside temperature exceeds the temperature of
the skin. When the air humidity is low, the heat
balance is controlled by sweating, and when the
humidity is high, the sweat does not evaporate
quickly enough, the heat is not released quickly
enough, the temperature of the body grows and
endangers the working abilities and in extreme
cases the life of the athlete. Therefore, it
follows from this that there is a logical advice
to avoid great efforts at high outdoor tempera-
tures. If we cannot avoid high temperatures
and moisture, we must adapt to such situation.
People who live in such environment are usually
adapted to these conditions. People from dif-
ferent backgrounds usually adapt within five to
ten days. The key principal is hydration and the
input of minerals. Liquids need to be introduced
several times during the activity. Minerals can-
not be compensated by the introduction of clean
water. Water rinses the minerals from the body.
We can help with sports drinks rich in carbohy-
drates and electrolytes.
Activities in the cold
Since the metabolic processes of the human body
produce heat during sport activities, low tem-
peratures are not as dangerous as high. If ath-
letes are exposed to low temperatures for a long
time, frostbite can occur, and extreme exposures
may lead to hyperthermia and death. The intense
muscular activity in cold weather consumes
significantly more energy than in the normal
environment. Individuals who train in the cold
weather should have enough energy when they are
at risk. The feeling of fatigue is the first step
to hypothermia. Cold wind increases the rate of
heat loss. Athletes can themselves cause the ef-
fect of cold wind, when on skies, skates as they
are rapidly moving towards the wind. In cases
where you are dealing with sports in a cool
environment, you should be adequately protected,
especially the distal parts of the body, eyes
and nose. People who regularly engage in sports
activities in the cold are psychologically and
physiologically adapted to low temperatures and
enjoy winter activities despite the cold. It is
especially important that during winter activ-
ities, due to sweating and breathing fluids lost
are always replaced. For longer activities, it
is also necessary to have an appropriate amount
of calories from snacks and energy drinks.
Activities at a higher altitude
Although a healthy person may not notice this;
saturation of arterial oxygen decreases already
at an altitude of 1500 m. But as we climb more,
the pressure of oxygen in the lungs decreases as
air pressure decreases. Under such conditions,
oxygen cannot be properly attached to the blood,
only a small amount of oxygen is transferred to
the tissues, and these are forced to adapt to
the new conditions. As a result, aerobic abili-
ties associated with endurance are always re-
duced at higher altitudes.
Athletes who train and live at normal altitudes
must prepare properly for performance at higher
altitudes. They can do this by spending time in
“climatic chambers”. These are rooms or chambers
that simulate high-altitude conditions. Athletes
should be at the competition location at least
three weeks prior to the competition in order to
adapt to the conditions properly.
Avoiding bad air
Sport activity increases the amount of air we
breathe. Injuries due to bad air are propor-
tional to the amount of exposure time to the
polluted air; therefore, they need to reduce the
time of activity in a polluted environment or to
avoid such activities completely and find another
option. Air pollution is different in many areas
and depends heavily on traffic, industry and
season. In large cities with constant pollution,
an adequate alternative is indoor exercise with
an appropriate air purification system. Although
polluted air is a serious problem in some plac-
es, cigarette smoke contains the highest amount
of harmful substances. This irritates bronchial
pathways, reduces resistance to bronchial in-
fections, causes bronchitis and hinder oxygen
transportation, causes lung disease, cardiovas-
cular problems, and many other problems. Smok-
ing unlike industrial pollution, is a matter of
personal choice.
Reference
Aleksandrović, M., Jorgić, B., Mirić, F. (2016). Holistički
pristup adaptivnom fizičkom vežbanju, učbenik za studente mas-
ter akademskih studija. Fakultet sporta i fizičkog vaspitanja,
Niš.
Ayres, S.F. & Sariscsany, M.J. (2013) Fizičko vaspitanje za
celoživotnu formu. Data Staus, Beograd
Cox, H.R. (2005). Psihologija sporta, konceoti i prmjene,
Naklada Slap, Jastrebarsko
Haskell, W.L., Montoye, H.J., Orenstein, D. (1985). Activity
and Exercise o Achieve Health-Related Physical Fitness Com-
ponents. Published in: Public Health Reports 100(2):202-12.
March 1985.
Kasser, S.L. & Lytle R. K. (2013). Inclusive Physical Activi-
ty: Promoting Helth for Lifestyle, Human Kinetics, Montgomery
Sharkey, J.B. & Gaskill, S. E. (2008). Vežbanje i zdravlje,
Data Staus, Beograd
Sherrill, C.(2003). Adapted Physical Activity, Recreation,
and Sport: Crossdisciplinary and Lifespan, Mc Graw Hill, New
York

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 9998
5.3.risKS iN ADAptED PhYsICal ACTivITy
AUTHOR: LADISLAV MESARIČ, JASNA VEŠLIGAJ DAMIŠ, ZVONKA NOVAK
Key words: risk factors, prevention of injuries, regulation of temperature, risk assessment, risk management plan
Fifteen percent of the world’s population lives
with disabilities, many of whom decide to en-
gage in sports. There are numerous obstacles to
the participation of athletes with disabilities
in sports activities, and sports injuries can
have a major impact on everyday life. Therefore,
prevention of their sports injuries is extremely
important (Weiler, Van Mechelen, Fuller & Verha-
gen, 2016). The number of athletes with disabil-
ities who participate in organized sports and
the popularity of the Paralympic Games are con-
stantly increasing all over the world. Despite
the growing interest and the fact that partic-
ipation in sports exposes athletes to certain
risks of injury, there is little research about
the types of injuries, risk factors and injury
prevention strategies for athletes with disabil-
ities (Fagher & Lexell, 2014)
5.3.1. Risk factors and injuries
Traditionally, risk factors are divided into
two main categories: internal risk factors and
external environmental risk factors. It is im-
portant that we can divide the risk factors into
dependent and independent variables or factors.
Although independent factors such as gender
and age can be interesting, it is important to
consider factors that can change with exercise,
such as power, balance or mobility. However,
this is not enough to determine internal and
external risk factors for sports injuries. For a
complete understanding of the causes, the mech-
anisms of occurring must be identified. Sports
injuries are due to the complex interaction of
several risk factors and events, of which only
some are known (Bahr, Holme, 2003).
Therefore, studies on sports injuries require
a dynamic model that takes into account several
factors of sports injuries, and considers the
sequence of events that eventually lead to an
injury. One of these dynamic models, describing
how injuries occur as a result of several fac-
tors, is the one adapted according to Meeuwisse
1994 (Bahr & Holme, 2003). The model is tested
on population without disability, but without
special adaptations can be used for the popula-
tion of athletes with disabilities. Only specific
definitions of individual expressions are needed.
The internal risk factors for persons with
disabilities are mainly the type and degree of
disability. This defines the choice of sports
activities and risk prevention measures during
sports activity. Among the external risk factors
is sports equipment. For persons with disabili-
ties, the risk factor is the adequacy of equip-
ment adjustments. During the activity, it is
necessary to pay due attention to the adapted
program of sports training and competitions.
5.3.2. Prevention of injuries
Many factors influence the prevention of injury
or reduce the risk of injury. Some are general
and do not depend on the type and degree of dis-
ability. The instructions for Special Olympics
contain the following actions:
• An appropriate assessment of the fitness
of athletes - the coaching staff must de-
termine the baseline for each athlete es-
tablished on his/her fitness and skill. The
type and complexity of the sport activities
that are taking place depends on this.
• The sports performance must be the backbone of
the appropriate long-term preparation of ath-
letes. The coach cooperates with the athlete,
healthcare staff, the family and other factors
that influence the long-term development of
the athlete. Individual must develop specif-
ic skills and fitness for the chosen sport.
• Special healthcare guidelines and co-
ordinated activities must be avail-
able for each individual.
• A first aid kit should always be avail-
able at all trainings and competitions.
• It is recommended for the athlete to adapt
to the environment. Athletes must gradually
adapt to exercise at an elevated temperature.
At the beginning, they should practice in
light clothing in the cooler parts of the day.
They gradually expose themselves to heat for
a short time and carry out activities even
in the hotter part of the day, at the time
when the competition takes place. If sport
involves the use of heavier clothing and
equipment, they must first adapt to wearing
clothing under normal conditions only then
in hot conditions. For all games and compe-
titions proper hydration must be maintained.
• They should also get gradually adapt-
ed to low temperatures. They must learn
to layer their clothes so that they can
adjust their outfit to the temperature.
If necessary, wear caps and gloves.
• Competitions at higher altitudes require grad-
ual adjustment that lasts 10 to 14 days. Exer-
cise should be gradually increased in duration
and intensity. Without gradual adaptation
they may experience altitude sickness, such
as nausea, dizziness and shortness of breath.
• In order to prevent sun and snow blind-
ness due to strong sun athletes need
PREDISPOSED
ATHLETE
SUSCEPTIBLE
ATHLETE INJURY
Internal risk factors:
• Age (maturation, aging)
• Gender
• Body composition (eg
body weight, fat mass,
BMD, anthropometry)
• Health (eg history of previous
injury, joint instability)
• Physical fitness (eg mus-
cle strength/power, maxi-
mal O2 uptake, joint ROM)
• Anatomy (eg alignment in-
tercondylar notch width)
• Skill level (eg sport, specific
technique, postural stability)
RISK FACTORS FOR INJURY
(DISTANT FROM OUTCOME)
INJURY MECHANISMS
(PROXIMAL TO OUTCOME)
Exposure to external risk factors:
• Human factors (eg team
mates, opponents, referee)
• Protective equipment (eg
helmet, shin guards)
• Sports equipment (eg skis)
• Enviroment (eg weather, snow
and ice conditions, floor and
turf type, maintenance)
Inciting event:
• Joint motion (eg kinematics,
joint forces and moments)
• Playing situation (eg
skill performed)
• Training programme
• Match schedule
Figure 7 : Risk factors for injury (Meeuwisse, 1994)

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 101100
to wear dark glasses with side shields
during outdoor activities. Glass-
es must have an ultraviolet blockade.
• If during sports activity athletes are exposed
to the sun, they must wear shades and t-shirts
with long sleeves. On exposed parts of the
body, such as the nose, ears, face, bald-
ness, lips, sun protection must be applied.
Temperature Regulation
Dysfunction of the sympathetic nervous system,
especially important for athletes with spinal
cord injury above the eighth thoracic vertebra,
can cause significant problems in regulating
internal body temperature. These athletes cannot
sweat effectively or have difficulty in vasodila-
tion below the level of injury. This can lead to
difficult body thermoregulation, or the body is
more difficult to cool by sweating or warm up by
shaking and vasodilation.
Athletes with a significantly reduced body sur-
face, such as those with bilateral amputation,
should also be considered. Medicines commonly
used by individuals with disabilities, such as
anticholinergics, sympathomimetics, diuretics,
muscle relaxants, and medicines that improve
thyroid function, can cause greater sensitivity
to heat (Richter, Sherrill, McCann, Mushett and
Kaschalk, 1998).
5.3.3. Risks related to sports
activities by type of disability
Different types of disability are classified into
wider categories, such as motor impairment,
sensory impairment, and intellectual disability.
Disability can be congenital (present at birth)
or acquired (not present at birth resulting from
acquired injury or disease). Coaches should try
to understand the disability of athletes they
train.
A plan or risk assessment should be made for
each athlete, including one’s disability, ill-
ness, relevant characteristics and behavioural
disorders (e.g. epileptic seizures) and other
important information which may have a signif-
icant impact on the sport performance of the
persons involved.
Basic information about specific safety aspects
according to the type of disability (Coaching
Association of Canada, 2005)
Athletes with intellectual disabilities
Close co-operation between athletes, parents,
guardians, trainers and assisting staff regard-
ing the characteristics and needs of the athlete
is crucial. People with Down’s syndrome often
have orthopaedic problems due to too much loose
joint envelopes and reduced normal muscular ten-
sion (i.e., muscle tone). People with DS often
have foot problems. Hallux valgus is 2.5 times
more common than in the general population and
presents an increased risk of subsequent arthro-
sis of the underlying joint of the thumb. Due to
the flat feet of 2- 6% of children with DS, they
are more likely to get tired of walking, report-
ing pain in the tibia. Difficulties can occur on
all joints due to increased mobility for exam-
ple on knee joint, unstable kneecap, hip, spine
(Leshing, 2003). It is necessary to determine if
they have atlanto-axial instability. The insta-
bility in the joints between the nasal bone and
the first and second cervical vertebrae is due
to loss of bonds. It is present in 80% of people
with DS, but for the vast majority of them (90%)
it does not cause any problems. If they have not
performed this examination or if instability is
found, it is necessary to avoid activities such
as contact sport, diving, gymnastics, especially
sports activities with intense neck movements
(Büchler, 2003). Congenital heart defects, un-
derdeveloped vascular system and low respiratory
capacity are also possible.
Athletes with physical disabilities
These are athletes with impaired mobility
caused by a spinal cord injury that prevents
the transmission of nerve signals below the
level of injury. Spinal cord injury is usually
due to traumatic injury. The trainers must pay
attention to their feet and toes while pulling
on various surfaces because people with this
type of injury feel poorly or do not feel legs.
For the same reasons, we must be mindful of the
surface on which activities are taking place.
Particular care must be taken that the surface
is not too hot (in the summer) or too cold (in
the winter). Individuals with tetraplegia have
limited ability to control body temperature, so
they need to be protected against heat and cold.
Due to limited access to sanitary facilities
they have difficult access to water. Assisting
staff must ensure adequate hydration during
sports activity.
Athletes with mobility disad-vantages (amputated limbs)
This group includes athletes with amputated
limbs and athletes born without limbs. Caring
for the remaining part of the limb is the key
daily activity of athletes with amputated limbs.
Sport activity can cause additional wear on the
remaining limb and orthosis. In particular, it
is necessary to monitor the skin of the wound to
prevent possible infections. Suitable socks must
be used for remaining limb to keep it dry and to
prevent irritation, scabies and other injuries.
Athletes in wheelchairs should use helmets when
beginning with sport.
Athletes with cerebral palsy
Injuries to different parts of the brain during
pregnancy, at birth or in childhood are mani-
fested in muscle weakness, paralysis, poor coor-
dination and uncontrolled movement of the limbs.
Individuals may also have intellectual disabil-
ities. As there are usually balance problems,
falls are a common risk that we must consider.
It is necessary to remove all potential obsta-
cles from the environment in which they are
moving. We need to avoid situations requiring
demanding movement control, and avoid contact
with other people and objects or perform these
with the extreme attention of the trainer. We
approach slowly to activities, such as climbing,
bicycle riding and similar consistently using
protective equipment.
Athletes with sensory impairments
Athletes with vision or hearing impairment need
accurate and well-established instructions
in case of a danger. In particular, they must
clearly understand the signal for the immediate
cessation of the activity that will protect them
from continuing and reduce the possibility of
injury. Athletes with hearing impairment cannot
receive verbal instructions from the trainer
or co-athletes. Therefore it is necessary to
establish an appropriate alternative communica-
tion strategy. For activities starting with an
acoustic signal, it is necessary to replace the
acoustic signal with a visual one.
Athletes with acquired brain injury (ABI)
The consequences of traumatic or non-traumatic
brain injuries are manifested in different ways.
Because, as a rule, two people do not have the
same abilities, it is the task of the coach /
facilitator of the sports activities to deter-
mine what a person can or cannot do. Activities
are carried out slowly by gradually increasing
the intensity, duration and complexity of the
exercise. It is important to follow the needs,
abilities and wishes of individual athletes
with ABI, and that we can adapt the activities
accordingly during the activity. In the chronic
period after brain injury, the lack of aware-
ness and insight often impedes the involvement
in activities. However this should not be an
obstacle to one’s cooperation, as it can reason-
ably be expected that the state of awareness and
insight can be improved over time. Together with
an athlete with ABI, we shape realistic expec-
tations during setting goals that he/she can
actually achieve. We must also consider all the
clinical problems and disorders that are pres-
ent in people who suffer from brain damage. For
this purpose in Center Naprej, we have designed
recommendations for sports activities (with-
in the framework of the ReSport project) and a
risk assessment form, which we complete prior to
including an athlete with ABI in sports activity
(Vešligaj Damiš, 2017). It is important for all
facilitators to familiarize themselves with ABI
athletes and consider them during all sports
activities.
5.3.4. Risk assessment in
Adapted Physical Activity
An example of a risk assessment for people with brain injury in the Center Naprej
When we include users with ABI in sports ac-
tivities, we must be aware that the latter are
often accompanied by various risks of someone or
something get injured, of a physical or emotion-
al nature, etc. To this end, we complete a risk
assessment process.
When making a risk assessment, we identify all

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 103102
the hazards and anything that could cause dam-
age. Based on this, we decide how serious the
risks are and how we will manage these risks. We
assess the risk for each sport activity for all
athletes with disabilities in order to prevent
possible complications or negative impacts of
the sport to the individual. The benefits of
sports activities must be greater than the risks
that sport presents to the person. The facilita-
tor of sports activities must know and respect
the limitations of each individual - athlete
with disabilities.
The risks that we know and are aware of can be
assumed as part of the real possibilities. It is
important that we understand the risk as some-
thing that is not negative. We are not at risk
because we expect negative outcomes and conse-
quences, as we expect positive results involving
people with disabilities in sports activities.
In order to complete a risk assessment, we
prepared a risk assessment form at the Center
Naprej. It assesses the risk areas with a risk
matrix, which helps us to evaluate the degree of
risk with regard to the impact of the threat in
relation to the likelihood of the risk.
If the risk or impact of the threat and the
likelihood of risk is high (the red field), we
should ask ourselves whether it is worth risk-
ing or whether such a high risk for the user
is still appropriate. Therefore, for such an
area / areas we prepare a RISK MANAGEMENT PLAN,
which reduces the risk and damage and protects
the athletes with disabilities. The plan must
include measures to reduce the risk. There are a
number of measures that we need to define clear-
ly: how, who and what we will do to reduce the
risk.
In the process of risk assessment and the prepa-
ration of a risk management plan, an individual
who is included in sports activity (athlete with
disabilities) must be actively involved. We help
him/her to understand the risks and take re-
sponsibility for his/her actions. If necessary,
relevant expert people are included in the Risk
Management Plan. If the risk of inclusion of a
disabled athlete is greater than his benefit of
sports activities, if it is harming the ath-
lete or others, and also with various measures
and adjustments, we do not achieve sufficient
safety for all, we do not include him in sports
activity.
The problem arises when an individual (athlete
with a disability) wants to make a decision
without consent of facilitator and latter thinks
that the individual who has made such a decision
does not fully understand the decisions and its
consequences. The task of the sports activities
facilitator and other participating experts is
to ensure that the athlete fully understands
the consequences of his/her decision and that
such decisions can lead him to a situation in
which he/she can be emotionally and physically
injured. It is important that we work together
with an athlete with disabilities in looking for
suitable solutions to the situation, consid-
ering different options, goals or find possible
adaptations.
Figure 8: Risk assessment form (Center Naprej)
Reference
Bahr, R., Holme, I. (2003). Risk factors for sports injuries
— a methodological approach. British Journal of Sports Medi-
cine, 37(5), 384–392. http://doi.org/10.1136/bjsm.37.5.384
Büchler, G. (2003),Atlanto-axiale Instabilität Leben mit
Down-Syndrom Nr. 43, September 2003 https://www.ds-infocen-
ter.de/downloads/lmds_44_sept2003.pdf
Coaching Association of Canada (2005). Coaching Athletes with
a Disabilityhttps://www.coach.ca/files/Coaching_Athletes_Dis-
ability_update2016.pdf
Fagher K1, Lexell J. (2014). Sports-related injuries
in athletes with disabilities. Scand J Med Sci Sports.
Oct;24(5):e320-31. https://onlinelibrary.wiley.com/doi/
abs/10.1111/sms.12175
Leshing, L. (2003) Orthopädische Probleme. Leben mit
Down-Syndrom Nr. 43, September 2003 https://www.ds-infocen-
ter.de/downloads/lmds_44_sept2003.pdf
Richter K.J., Sherrill C, McCann C.B., Mushett C.A. &
Kaschalk S. (1998). Recreation and sport for people with
disabilities. In JA DeLisa and B Gans (Eds.). Rehabilitation
Medicine: Principles and Practice. Third Edition (pp. 853-
871). Philadelphia, Lippincott-Raven
Special Olympics (2003) COACHING GUIDE Sport Safety and Risk
Management for Coaches http://media.specialolympics.org/soi/
files/resources/Sports-Rules-Competitions/Sport_Safety-Risk-
Management.pdf
Vešligaj Damiš, J., Čeh, M., Majcenovič Cipot, D. (2017),
Priporočila izvajalcem »ReSport« aktivnosti, interno gradivo
Center Naprej, Maribor
Weiler, R., Van Mechelen, W., Fuller, C., & Verhagen, E.
(2016). Sport Injuries Sustained by Athletes with Disability:
A Systematic Review. Sports Medicine (Auckland, N.z.), 46,
1141–1153. http://doi.org/10.1007/s40279-016-0478-0
AREAS OF RISK
RISK RELATED TO: Risk level RISK RELATED TO: Risk level RISK RELATED TO: Risk level
Falling Breathing problems Alcohol abuse
Balance problems Cognitive problems Swallowing harmful substances
Movement control Special disorientation Depression, Anxiety
Illness and injury of locomotor system
Time disorientation Suicide
Sensory impairments Leave without informing Other mental health problems
Chronic illnesses and conditions Vanish and get lost Aggression towards self
Amputated/missing limbs Use of staircase/ liftAggression towards others verbal (threads)
Problems with cardio vascular system (high blood pressure, Cardiac rhythm disturbances…)
Use of equipment/ devices Aggression towards others – physical
Bladder and bowel dysfunction Eating disturbances (exaggerated eating)
Self – neglecting
AlergiesEating characteristics – diet, avoiding particular food
Socialy inappropriate behaviour
Epilepsy seizures Swallowing Sexually inappropriate behaviour – towards self
Problems with thermoregulation Smoking Sexually inappropriate behaviour – towards others
Other Other Other
Risk Assessment Form - Center Naprej Risk Assessment In The Rehabilita-tion Plan For Sports Activities
Date of assessment
Name and surname of the user
Facilitator of sports activities
Sports activity
Use of supporting accessories (wheelchair, walking stick, orthoses, prostheses etc.) during the sports activity
RISKS MATRIX
Omitted Small Medium High Catastrophic
Rare 1 2 3 4 5
Less probable 2 4 6 8 10
Probable 3 6 9 12 15
More probable 4 8 12 16 20
Almost certain 5 10 15 20 25
Risk level
Very small Small Medium High
Annex 1
AREA OF HIGHEST RISK (red areas)
Impact on the physical activity and impact of the sports with regards to the risk, warnings:
RISK MANAGEMENT PLAN:
NOTES, EXPLANATORY STATEMENTS (and other relevant characteristics regarding the individual):
RISK ASSESSMENT UPDATED WITH CHANGES
Updated by: Signature:
Date:
Changes:
RISK ASSESSMENT COMPLETED
Assessment
completed by:
Signature:
Date:
Impact of the risk
Proba-bility of the risk
Footnote:It is very important to prepare a risk management plan for each area with the highest level of risk (red areas) - Appendix 1.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 105104
5.4.The ROLe oF adaPt-Ed PhySICal AcTIvity EduCAtiOn
5.4.1. Changing traditional attitudes, beliefs and assumptions
AUTHOR: YOANA FILIPIC
Key words: assumptions, attitudes, beliefs
Attitudes, assumptions and beliefs are important
concepts in understanding facilitators’ thought
processes, classroom practices, change, and
learning to teach. In such adapted programs,
beliefs and attitudes of facilitators and ser-
vice users affect what they perform and how they
practice sports activities (Sikula, 1996).
Allport (1967) describes attitudes as “a mental
and neural state of readiness, organized through
experience, exerting directive or dynamic influ-
ence upon the individual’s response to all ob-
jects and situations with which it is related”.
Therefore attitudes could be predispositions
that consistently affect actions and consequent-
ly strongly influence facilitating activities.
Assumptions are something taken for granted;
a supposition. It is something that you accept
as true without question or proof (Cambridge
Dictionary, 2018). It represents preconceived
notions about what is good or bad, what is pos-
sible or impossible.
Goodenough (1963) defines beliefs as proposi-
tions that are held to be true and are “accepted
as guides for assessing the future, are cited
in support of decisions, or are referred to in
passing judgement on the behaviour of others”.
Multiple studies have examined those concepts
and how these beliefs affect facilitators’ con-
ceptions of their role. In a study of teachers’
theories of learning, Anning (1988) stated that
the theories about student’s learning in her
study were determined “by their own particular
previous experiences of teaching and learning
in their classrooms”. Debora Britzman (1991)
has wrote useful case studies of two student
educators that indicated that they held power-
ful conceptions of the role of educators --both
positive and negative--gained from observing
teaching models. Britzman prompted the consider-
ation that these conceptions profoundly affected
the student teachers’ classroom behaviours.
All facilitators hold beliefs, about their work,
their students, service users, their activity,
and their roles and responsibilities. For ex-
ample, Clark (1988) suggested that their use is
not at all consistent with what one might find in
textbooks or professors’ lecture notes, for they
“tend to be eclectic aggregations of cause-ef-
fect propositions from many sources, rules of
thumb, generalizations drawn from personal ex-
perience, beliefs, values, biases, and prejudic-
es”. These predispositions and beliefs include
questions about the purpose of implementing ac-
tivities, about facilitators responsibility for
achieving specific goals, and about beliefs that
users are capable of achieving these goals.
In another study Fitzgerald and Kirk (2009)
have prepared an analysis of the experience of
the persons with disability of physical educa-
tion and disability sport. They emphasised some
of the primary concerns when using disability
sports as a tool for change. Considering having
a disability is often associated with a deficit
perspective, by default then, disability sports
is thought to be a lesser form of sport. Con-
sequently disability sports could be viewed as
either accommodating basic principles inherent
to mainstream sport or as sports activities
suitable only for persons with disabilities.
Research that focused on experience of teachers
within a teacher education program that en-
courages reflective teaching, Korthagen (1988)
came to important conclusions in relation to
attitudes in the education process. He suggest-
ed that some teachers varied in terms of their
learning orientations from those who learn with-
in an internal orientation (reflection) to those
who have an external orientation (just tell me
what I should do). As a result of different ori-
entations, Korthagen found that they may relate
to their beliefs and theories about how students
learn. Many students, whose approaches were not
reflective and therefore not in tune with the
orientations represented in the program, dropped
out after one year, suggesting to Korthagen that
educators should understand both their students’
learning orientations and those of the program.
These findings definitely lead to useful impli-
cation for our programmes in terms of exploring
our attitudes and beliefs and those of our users
who join the programmes.
In their study of 2006 Smith and Thomas implied
that some educators support segregation by
engaging students with a disability in differ-
ent activities to mainstream students, which
“appears to be strongly associated with the
‘privileging’ of competitive teams sports over
more individualized physical activities”. Jer-
linder et al. (2009) declared that “disability
ought not to matter”, but also concluded that
“it paradoxically seems to matter very much …
particularly, in the specific context of sports
activities for individuals with physical impair-
ments” who were often judged against “normative
aspects of parity of participation.” Researchers
noted that students with physical disabilities
were often denied participation, not purely
because of a lack of resources, but also because
individuals’ abilities and desires were not
explored and recognised. Slee (2001) drew on the
notion of identity and stated that “inclusive
education has been framed as a field for special
educational research, training and bureaucratic
intervention”, in which such perceptions have
inhibited inclusion in mainstream schools. He
suggested that students with a disability were
often denied their individuality as it was be-
lieved that physical activity may be dangerous
and may cause more complications than benefits.
On the other hand authors like Sharma et al.
(2008) suggest that educators’ attitudes needed
to evolve. In their review of literature, Sharma
et al. (2008) outlined that ‘disability physi-
cal education’ was the single common variable
that influenced educators to be more positive
about physical education. Slee (2001) hoped that
pre-service teachers might be the innovators of
future solutions to inclusive education.
Nevertheless, there are a number of characteris-
tics that a successful facilitator should hold;
particularly those related to the exploration
of his/her own attitudes (who am I, what is my
goal as a facilitator, what am I able to do) and
the students’ own beliefs (of their identity and
abilities) as well as alternative beliefs and
practices. In addition, facilitators should have
the opportunity to engage extensively in the
active exploration of different living contexts
of persons with disabilities. This process may
promote the first stages in the acquisition of
practical knowledge.
Discussing and evaluating our work and approach-
es opens opportunities for new ideas and more
creative approaches to planning adapted physical
activity. Therefore we all would benefit from
on-going learning, searching new ways of imple-
menting programmes, differentiate facts from
opinions search for information that will enrich
our professional learning and discussions with
those we work with.
Reference
Allport, G. (1967). Attitudes. In M. Fishbein (Ed.), Readings
in attitude theory and measurement (pp. 1-13). New York: John
Wiley & Sons.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 107106
Anning, A. (1988). Teachers’ theories about children’s learn-
ing. In J. Calderhead (Ed.), Teachers’ professional learning
(pp. 128-145). London: Falmer.
Britzman, D. (1991). Practice makes practice: A critical
study of learning to teach. Albany: State University of New
York Press.
Clark, C. M. (1988). Asking the right questions about teacher
preparation: Contributions of research on teaching thinking.
Educational Researcher, 17(2), 5-12.
Goodenough, W. (1963). Cooperation in change. New York: Rus-
sell Sage Foundation.
Korthagen, F. A. J. (1988). The influence of learning ori-
entations on the development of reflective teaching. In J.
Calderhead (Ed.), Teachers’ professional learning (pp.35-50).
Philadelphia: Falmer.
Mauerberg-de Castro, E., de Souza Paiva, A.C., Figueredo,
G.A., Ayres de Costa, T.D., Rodrigues de Castro, M., Frances
Campbell, D. (2013). Attitudes about inclusion by educators
and physical educators: Effects of participation in an inclu-
sive adapted physical education program. Mortis, Rio Claro,
vol. 19 n. 3, p.649 – 661.
Porter, A. C, & Freeman, D. J. (1986). Professional orienta-
tions: An essential domain for teacher testing. Journal of
Negro Education, 55, 284-292.
Sharma U, Forlin C & Loreman T (2008). Impact of training on
pre-service teachers’ attitudes and concerns about inclusive
education and sentiments about persons with disabilities.
Disability & Society, 23 (7), pp. 773-785.
Slee R (2001). Social justice and the changing directions in
educational research: the case of inclusive education. Inter-
national Journal of Inclusive Education, 5 (2), pp. 167-177.
Smith A & Thomas N (2006). Including pupils with special
educational needs and disabilities in National Curriculum
Physical Education: a brief review. European Journal of Spe-
cial Needs Education, 21 (1), pp. 69-83.
Fitzgerald H (2005). Still feeling like a spare piece of
luggage? Embodied experiences of (dis) ability in physical
education and school sport. Physical Education & Sport Peda-
gogy, 10 (1), pp. 41-59.
Richardson, V. (1996). The role of attitudes and beliefs in
learning to teach. In J. Sikula (Ed.), Handbook of research
on teacher education (2nd ed., pp. 102–119). New York:
Macmillan.
5.4.2. Building Safe Relationships
AUTHOR: YOANA FILIPIC
Key words: safe relationships, boundaries, maintaining boundaries
Extending beyond education building safe re-
lationships has been a topic of intense theo-
retical and empirical interest within teaching
and counselling. The collaborative relationship
between facilitator and service user in the
teaching setting is definitely a predictor of
programme outcomes. This research area raises
the question of why sport psychology researchers
have not considered examining the “we” of the
relationship, in addition to the two separate
“I”s or the two separate individuals in the dyad
relationship.
The basis for the professional relationship is
the respect for the dignity, worth and rights
of the client. Facilitators demonstrate respect
when they maintain “appropriate boundaries and
ensure their relationships are always for the
benefit of the persons with disability. Another
important characteristic of the relationship
is trust. Therefore it is the belief that the
facilitators possess the knowledge and skills
required for particular programme, that they
will keep confidentiality if shared a personal
experience. Boundaries are a very important part
of the relationship as an appropriate emotional
and physical distance is required in order to
stay objective and professional while teach-
ing service users. This is also related to the
imbalance of power and facilitator must remain
mindful of the goal of the relationship in order
to prevent abuse. What is needed is the sense of
closeness and empathy that is needed to under-
stand and react adequately when a person with
disability is anxious and experiencing distress
(Papouli, 2014; Reamer, 2003).
A sample list of tips to create a safe
relationship:
1. Honour each member’s style of interaction
2. Invite users to share experience and
thoughts with regards to the program
3. Show gratefulness when lis-
tened to and respected
4. Invite families of other profession-
als to participate in special events
5. Create time when you see a user in
distress and speak to him/her
6. Respect individual cultur-
al and familial differences
Professional boundaries are a key component of
any professional ethics. Not all issues related
to these boundaries are necessarily unethical,
but many of them are (Reamer, 2003). Factors
such as emotional involvement with a service
user, a desire to religiously indoctrinate him
or her, potential financial gain, and a desire
to exploit the user in other ways can sometimes
lead to crossing these boundaries in an unethi-
cal manner (Papouli, 2014; Reamer, 2003).
This means that maintaining professional bound-
aries can sometimes mean balancing personal and
professional codes of ethics (Reamer, 2003).
Bowler and Nash’s (2014) training framework
includes discussions on the differences be-
tween two types of relationship – professional
and personal. In terms of behaviour they set
few important categories - remuneration, pur-
pose of the relationship, balance of power in
the relationship, and responsibility for the
relationship. These categories are very dif-
ferent considering their implication in profes-
sional and personal relationship. With regards
to behaviour, professional relationships are
regulated by professional standards and codes
of ethics, on the other hand personal relation-
ships are guided by personal beliefs and values.
In personal relationships, no remuneration is
required, whereas in professional relationships
the facilitator is paid for providing education
to the client. There is an employment contract
that states the terms for this payment.
We have provided you with a sample scenario so
that this could be useful for helping facilita-
tors understand how to differentiate between the
two types of relationships in real-world situ-
ations, and how they could benefit from doing so
in an effective manner.
Situation: You are a facilitator of sports ac-
tivities working in a centre for rehabilitation
of persons with acquired brain injury. A person
with a traumatic injury was admitted a month ago
and you have become particularly attached to him
while spending time on the playground. His fami-
ly is distant and not particularly interested in
his success in sports. On his win at a competi-
tion you buy him a present costing 30€ and make
a cake. He is excited. You feel satisfied.
Should you do this, if so why, if not why?
Answer: In your excitement to do something spe-
cial for the person with an injury, you inde-
pendently singled out an individual client. You
did not carefully consider the broader meaning
of giving a gift to this person. As a result,
another client in the physical activity group
may have felt excluded. Also the giving of a
gift can be seen as an attempt by you to cre-
ate a special, personal relationship beyond the
boundaries of the professional relationship. The
reaction of the person may create an element of
attachment and hope for friendship and socializ-
ing outside the centre.
Smith et al (1997) have provided us with a sam-
ple list of warning signs for facilitators that
their behaviour has crossed the boundaries of a
professional relationship (Smith et al 1997).
The list is not exhaustive but it gives a view
of some common situations when our relationship
with a user has become confused:
• Frequently thinking of the
user when away from work
• Frequently planning other users’ ac-
tivities around that user’s needs
• Seeking social contact with or spend-
ing free time with the client
• Sharing personal information or work concerns
with the client that can cause user see you
as friend, not as professional any more
• Feeling so strongly about the client’s goals
that colleagues’ comments or the client’s
or their family’s wishes are disregarded
• Hiding aspects of the relation-
ship with the client from others
• More physical touching than is appro-
priate or required for the situation
• Romantic or sexual thoughts about the client
Reference
Bowler, M. & Nash, P. (2014). Professional Boundaries in
Learning Disability Care. Nursing Times, 110, 12-15.
Papouli, E. (2014). The Development of Professional Social
Work Values and Ethics in the Workplace: A Critical Inci-
dent Analysis from the Students’ Perspective. Retrieved from
http://sro.sussex.ac.uk/48325/1/Papouli%2C_Eleni.pdf on
29.6.2018
Reamer, F. (2003). Boundary Issues in Social Work: Managing
Dual Relationships. Social Work, 48 (1). 121-133.
Smith, L.L., Taylor, B.B., Keys, A.T. & Gornto, S.B. (1997).
Nurse-patient boundaries: Crossing the line. American Journal
of Nursing, 97 (12), 26-32.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 109108
5.4.3. Psychological Preparation of athletes with disabilities and challenges we face
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: psychological preparation, relaxation, motivation, goal setting, commu-nication, self-esteem
In modern sports, appropriate psychological
preparation has become more and more important
in order to achieve good, excellent results. The
purpose of this preparation is improvement of
results, which the individual is able to achieve
only if he/she is well psychologically prepared
for all the distress he faces in sports.
Good psychological preparation of the athlete
means strong motivation, high concentration,
high self-esteem and good emotion management.
An athlete who has received good psychological
preparation works better, reaches ones potential
and top results.
However, in order to become a successful ath-
lete, you do not need to be a professional
athlete or an Olympic champion. You do not need
to have many trophies or cups, you do not need
to win at the national championship or be on the
cover of a sports magazine.
It is essential for an athlete that the sport
he/she chooses is important to him/her and he/
she is dedicated to it, regardless of the fact
if he/she is a top athlete or a recreational
player, an athlete with disability or no dis-
ability, a Paralympic or an Olympic athlete who
uses sports as a means of rehabilitation.
It is important that an athlete develops desired
realistic goals that are sufficiently high and
realistic according to his/her own abilities. It
is important for the goals to be in accordance
with ones limitations such as, daily life obli-
gations, finances, time, disability, etc. Conse-
quently sport participation enriches the life
of an athlete, and if he/she values what he/she
receives, it is worth the resources he/she has
invested in sports.
At the same time, psychological work for an
athlete can be of much broader significance since
the same mental abilities that athletes use to
achieve success in sport can also be used to
achieve success in other areas of life.
Sports psychologists thus help athletes improve
their motivation, increase self-confidence, in-
crease team cohesion, and concentration (Kajtna
and Jeromen, 2013). If a sports psychologist
cooperates with a disabled athlete, it is im-
portant to focus on the individual’s abilities
rather than on his disabilities (Hanrahan,
2007).
The goal of professional psy-chological preparation
Through psychological characteristics for an
athlete with a disability, we encourage the
improvement of the performance of the activity,
the achieving of better results and significant
success in competition. Therefore, we discover
the causes of:
• fluctuations in implementation, motiva-
tion for sports activities, etc.,
• managing crisis, stress,
• setting limits (how much he/she is
able to perform, where is his/her lim-
it, or limits can be improved);
• differences in performance, when he/
she works better or worse,
• slow progress - the athlete progress-
es steadily, but much slower than he/
she wants or imagines he/she could.
5.4.3.1. Practical aspects of men-tal preparations for work with athletes with disabilities
In general, psychological skills programs for
athletes with disabilities are not very differ-
ent from those for athletes without disabili-
ties. Nevertheless, there are some adaptations
to be taken into account (Hanrahan, 2014).
The main adaptations that are normally required
in the work of people with disabilities are most
often related to communication issues and other
specific adjustments resulting from disabili-
ty. Working with individuals with disabilities
requires appropriate assistance, communication
adaptation and creativity. (Hanrahan, 2015).
The mental preparation of an athlete with dis-
abilities, like an athlete without disabilities,
helps him/her to focus, to be self-confident
and to have a positive mindset. General mental
preparation consists of:
• creating a positive philosophical, moral
and ethical attitude towards the world,
• creating a positive attitude towards sport,
• Creating a high level of motivation,
self-motivation (internal motivation),
• creating appropriate, realistic goals,
• managing effectively anxi-
ety, emotions and stress,
• maintaining good and focused concentration,
• creating a stimulating social envi-
ronment where appropriate atmosphere
and support must be established,
• learning effective patterns of behaviour
towards self, situations and others,
• learning and using different psy-
chological techniques.
Psychological preparation involves learning
psychological techniques that allow an athlete
to recognize his or her abilities. This process
requires of him/her many hours of training and
persistence. Among the most popular and most
frequently used techniques are (Tušak, Misja and
Vičič, 2003):
• Relaxation techniques,
• Visualization, sensory,
• Concentration techniques,
• Self-speech techniques,
• Breathing techniques,
• And techniques of positive think-
ing and hypnosis.
All these techniques can also be used for ath-
letes with disabilities, if necessary, modified
according to their abilities or skills and spe-
cific limitations.
Relaxation training
Progressive muscle relaxation (PMR) may be prob-
lematic for some individuals with physical dis-
orders. For example, clinical observation shows
that individuals with cerebral palsy who have
higher level of spasticity may skip the phase of
tension of PMR and focus only on relaxation, as
the tension phase may increase spasticity (Han-
rahan, 2015).
Alternatively, these athletes may want to con-
sider alternative ways of relaxation, such as
autogenic training.
Athletes with amputated limbs or those in
wheelchairs are given the option of selecting
the PMR script: the relaxation is performed on
individual parts of the body, where the muscles
are in place and leave the amputated limbs or
body parts that are affected by the spinal cord
lesion. Hanrahan (1995) found that the ath-
letes with physical difficulties decided about
50:50 with regards to the mentioned relaxation
scripts.
It should be noted that abdominal breathing as
a relaxing exercise can enhance relaxation and
concentration in athletes who do not use abdomi-
nal muscles (Hanrahan, 1995).
Visualization and sensory training
The technique of visualization, which is a
form of mental representation, is very often
used in sports. It helps to learn new motor-
ic functions and movement elements, eliminates
negative thoughts and feelings and improves
concentration.
Visualization technique or presentation of
motoric images can be an extremely useful
technique for athletes with physical disabili-
ties, and can be used as mental preparation for
training physical skills. Because athletes with
disabilities often have limited opportunities

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 111110
and certain training problems that are difficult
to overcome compared to their healthy colleagues
(due to problems such as transport, accessibil-
ity, poor equipment etc.), mental exercise can
become extremely important. In addition, exer-
cise for visual motoric behaviour is helpful for
athletes with cerebral palsy, because the relax-
ation component can reduce spasticity (Martin,
2013).
It also assists with preparation for stressful
events and sports performance, as with mental
imaging the automation and optimization of the
performance is increased.
The visualization technique can be effective
for athletes with physical disabilities. It is
important that athletes see themselves as they
are and how they do sports (Hanrahan, 1995). For
example: swimmers with one foot do not swim with
prosthetic devices, so prosthesis is not part of
the image they represent.
It is important to ensure that images of visu-
alization are precise in terms of what is or
what is not included and physically match the
real situation (for example, if a sportsman uses
prosthesis in sport, this prosthesis should also
be part of the visualization image).
The clarity of the motoric images (visualiza-
tion) of affected limbs after complete damage to
the spinal cord is maintained, but is weaker af-
ter loss of the limb (Malouin & Richards, 2010).
Short-term physical disorders, such as broken
legs, can lead to reduced clarity of motoric
images, for example those that include the leg.
Immobilisation of the ankle in only 2-4 weeks
leads to a significant reduction in the clarity
of motoric images in movement of the foot (Mal-
ouin et al., 2009).
Of course in athletes who have acquired physical
disorders (as opposed to those who have genetic
disorders), the use of visualization techniques
can lead to frustrations that originates mainly
from the relationship between the image itself
and image before the injury. For example: a
swimmer who has an amputated hand, swims with
only one hand, and visualizing themselves in the
picture with both hands as before the injury.
This can lead to anger, frustration, split image
of oneself, etc. This is why we must be very
careful when we guide such an athlete through a
visualisation technique. It is important that
we build on the clarity of the imagined image of
himself, the image control (swim with one hand)
and in this way we form an effective strate-
gy for improving his technique, preparing for
competition and strengthening his own confidence
(Hanrahan, 2014).
Similar to visualization is sensory technique in
which athlete imagines ones sport performance
but it also contains kinesthesia, voices and
other sensory performances that occur during the
sport performance (Tušak & Tušak, 2003).
People with mild mental disorders have improved
their performances in cognitive and motoric
tasks through visualization (Screws & Surburg,
1997). The combination of physical training and
visualization in people with mental disorders
has shown to be more effective compared to only
physical exercise (Surburg, Porretta & Sutlive,
1995).
Positive thinking training
During mental preparation we also include the
technique control of positive thinking. It is
important that we guide an athlete with a dis-
ability to positive thoughts and self-managing
them. This can be achieved by training positive
thoughts and positive self-talking. The conse-
quences of negative thinking cause low self-es-
teem, increase anxiety and worsen performance.
The athlete uses different autosuggestion during
the training of positive thinking, which is also
the most important part of the positive think-
ing. Suggestions must be realistic and specific,
some are focused on correcting problems that
arise from negative thoughts, and some sugges-
tions prevent misconception. Important are also
the suggestions that improve self-confidence and
self-esteem of the athlete.
Routine
When developing preliminary routines for ath-
letes with physical problems, it is important
to pay attention to the problems associated
with accessories for example wheelchairs and
allow longer time for transportation and solving
problems with accessibility at the competition
location (De Bress, De Guast et al., 2013).
5.4.3.2. Communication as a chal-lenge for facilitators and per-sons with disabilities
When working with athletes with disabilities,
communication is extremely important. For ex-
ample, it is important that a psychologist, as
well as a coach or assistant talk with an ath-
lete in a wheelchair on the same level.
As cerebral palsy often affects muscle control,
which is necessary for a clear speech (Nordberg,
Miniscalco, Lohmander & Himmelmann, 2013), it is
sometimes difficult to understand athletes, who
are strongly affected by it. Some athletes have
assistants who can take part in sports events
and training with them. If assistants play
together with an athlete, make sure that you
continue to maintain eye contact and communicate
with athlete not with the assistant. When commu-
nicating with a disabled person, be patient when
they speak and avoid finishing their sentences.
When communicating with athletes with disabil-
ities, it is always important that we are aware
of the extent to which individuals can see or
hear, and what forms of communication are best
for them (for example, reading from lips, large
fonts…). It is also useful to establish methods
for gaining attention (eg. flashing lights, touch
on the shoulder, beeping).
When working with athletes who have vision or
hearing disorders, it is important to reduce
background noise. Individuals with visual im-
pairments rely on hearing aids and those with
hearing impairments (but they are not completely
deaf) will struggle if the voice overlies noise
from the background.
We must consider that the level of communication
and understanding is adapted to the abilities of
athlete with intellectual disabilities. If nec-
essary, give the athlete more time to understand
and respond, talk slowly using short sentences
and wait long enough before asking a new ques-
tion. Ensure our sentences are clear and we need
to speak to them gradually, it may be neces-
sary to clarify and explain multiple times the
purpose of the tasks and the instructions for
work. We combine verbal instructions with other
ways of providing information. The instructions
should be simple, short and accurate. Longer and
more complex instructions should be divided into
shorter sequences or steps.
When working with people with mental disorders
it is important to provide additional time for
mental training and gradually prepare them for
particular mental ability, each one according to
the situation and behaviour. Learning and train-
ing more than one mental skill at a time can be
too difficult for them (Gregg et al., 2004). This
is the most common mistake sports psychologists,
trainers and assistants are dealing with. For
example: to play tennis, they may explicitly
learn to avoid going on the other side of the
field during the game to get the ball.
If a person with intellectual disability is il-
literate, we should consider using audio records
or drawings instead of writing when setting
goals or performing other activities that usual-
ly involve writing (Hanrahan, 2004).
Often, creativity is needed to pass the messag-
es effectively to individuals with intellectual
disabilities. It is also important to make sure
that the messages are correctly understood.
As people with mental disorders often agree or
accept positive answers (Gregg, 2013), it is
better to avoid asking yes/no questions (because
the answer will likely be ‘’no’’, regardless of
the question). Instead, we ask questions that
require an individual to show understanding of
the answer, or ask the athlete to repeat infor-
mation or message.
In the case where a sport psychologist has
limited contact with a team or the athlete, it
is useful to explain to the coach or to other
relevant professionals what the team or indi-
vidual athlete has learned from psychological
preparation or intervention (Gregg, 2013), to
repeat, train and strengthen it during exercises
and competitions. Patience and numerous repe-
titions are important when working with people
with intellectual disabilities.
When working with people with acquired brain
injury (ABI), facilitators of the sports ac-
tivities should be aware of the numerous
consequences caused by ABI and abide by the rec-
ommendations of the professional body according-
ly. The consequences of the brain injury, which
may affect the sport activity of an athlete with
ABI, can influence the physical activity perfor-
mance as well as mental functioning. Thus, we
have to devote special attention to the problems
in executive functioning, motivation, confron-
tation, problems of setting goals and creating
realistic expectations etc…

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 113112
Athletes with ABI often have difficulty in plan-
ning and organizing their activities. Problems
have been identified in determining the steps
required to achieve the goal and their order
(what happens sooner or later). They initiate an
activity with difficulty and often need detailed
or additional instructions before performing the
activity.
After brain injury, injured victims face a range
of memory problems. The most common and highly
unpleasant form of memory disorder is a problem
with short-term or ‘’working’’ memories. This
means that it is difficult to remember new facts,
new names, faces, agreements, forget where they
left belongings, obligations they have.
When working with athletes with ABI it is im-
portant (as with people with developmental
disorders etc.) to avoid excessive stimulation,
such as several people speaking at the same
time, and address him/her directly, slowly,
clearly and comprehensively. It is crucial to
eliminate as much as possible stimuli in terms
of sounds from the background or environment
(radio, noise in the room, etc.). We need to
carry out numerous repetitions and behavioural
trainings due to user’s memory problems and
diminished learning ability.
5.4.3.3. Motivation and set-ting goals techniques
Practical approaches to motivating athletes with
disabilities derive from different theoreti-
cal directions, similar to those for athletes
without disabilities (for example, productiv-
ity motivation theory, theoretical directions
explained by behaviour, theories based on incen-
tive motivation, goal setting theory, etc…).
The basic characteristics of motivation are
encouraging and guidance (Kajtna & Jeromen,
2013). One of the most important factors in the
process of motivation is setting goals. It is a
planned choice of specified goals, which must be
precisely defined, realistic and achievable. This
technique is used in sports most of the time.
An athlete sets goals and tries to achieve them
with appropriate behaviour. Goals should meet
athlete’s needs. Motives are goal focused rea-
sons for behaviour. Needs arise and maintain mo-
tives until satisfaction occurs (Tušak & Tušak,
2003).
Specific goals affect activity more accurately
than general goals. The coach sets them up with
the athlete, and they have to define strategies
for achieving the set goals. In this approach
the feedback given by the coach to the athlete
after the analysis play an important role. If it
shows positive progress, the technique will be
more successful.
Setting short-term and long-term goals has a
significant impact on maintaining motivation.
Sub- targets (sub-goals) lead to the main goal
and when one of them is not achieved, this is
a sign of the need to change the strategy to
achieve an ultimate goal.
The athlete must believe that he/she is able to
achieve set goals. Setting goals does not only
serve as a tool to increase motivation, but also
to improve concentration and effective time man-
aging (Tušak, Misja & Vičič, 2003).
This technique of setting goals in sport is
equally applicable in sports for people with
disabilities, regardless of whether it is a
competitive sport, recreational sport or reha-
bilitation. At the same time it is important to
understand why an athlete with disabilities is
attracted by sport. Disabled and healthy ath-
letes have similar incentive systems (incentive
are attractive goals). According to Tušak and
Tušak (2013), from existing research we can
recognize 7 incentive systems that explain the
motivation of the athlete to participate in
sports:
• Desires for achievement and success,
• Desire for socialising,
• Desires for sensual satisfaction,
excitement,
• Curiosity
• Aggression
• Power
• Independence.
The importance of certain incentives varies
from individual to individual. The first two are
extremely important for everyday life, social-
ization, entertainment and achievements. We
can connect them with the individual’s need for
experience and activation.
5.4.3.4. Self-concept and self-con-fidence of an athlete with disabili-ties as challenge for facilitators
Self-confidence is by definition an athlete’s
conviction or a sense of confidence about the
possibility of successful performance. It is a
subjective factor that arises from an athlete
and has a major impact on his sports engagement.
In some sports studies of people with disabil-
ities, the positive benefits of sports partic-
ipation have been identified to include better
self-image, feelings of belonging and many
benefits to health (DePauw & Gavon, 2005).
Sports psychologist can help both athletes with
disabilities or those without with psychologi-
cal preparation to develop psychological resis-
tance and build self-confidence and appropriate
motivation.
The process of achieving high self-confidence
in an athlete with disabilities can last for
many years and the psychologist has a role of
counsellor. An athlete must set an environment
around him/her that includes people who always
believe in him/her. Repeated positive sport
experiences can contribute greatly for achiev-
ing global and balanced self-confidence (Tušak,
2001).
By analysing the self-confidence of an athlete,
we can determine his/her personality. Indi-
viduals with low self-confidence are afraid of
defeats, have negative thoughts, doubt their
abilities and feel that they will not succeed.
Those with too high self-confidence do not see
their mistakes and do not want to fix them, they
think they are better than they really are, and
in case of failure always find excuses. Such
problems can often be faced by athletes with
ABI, as a result of the injury and inability to
create a real image of oneself and one’s abili-
ties (Žini, 2018).
Parents, relatives, coaches and personal as-
sistants have the strongest influence on the
individual’s self-confidence and self-esteem.
The right approach includes positive encourage-
ment, praise, positive experience and emotional
support.
Self-concept is a set of individual’s opinions
and attitudes towards oneself based on experi-
ence and beliefs, reflected in the individual’s
relationship with oneself. As a consequence one
forms values about oneself and the environment
he/she lives in. The one with good self-concept
has high self-confidence and vice versa, low
self-concept comes from low self-esteem.
Self-concept depends on the perception and
knowledge of one’s own strengths and weaknesses,
depends on the individual’s opinion of his/hers
abilities and the people the individual compares
with. We separate physical, social and academic
self-concept.
The physical self-concept of an athlete with a
disability can be largely influenced by sports
activities. Sport can be an important stimulus,
which increases the competence of their perfor-
mance and improves their physical abilities. Un-
fortunately, in practice, it often happens that
poorly coordinated individuals with disabilities
are less active in sports and recreation, spend
more time watching other better coordinated
individuals with disabilities, consequently
limiting their chances of improvement.
5.4.3.5. Coping with stress
A successful athlete must have the ability to
effectively cope with stress, and this also
applies to athletes with disabilities. Several
techniques are known to adequately solve prob-
lems caused by stressors.
In order to reduce stress we introduce training,
which include a program for reducing the harmful
effects of stress. It involves learning self-
talk, observing one’s thoughts, problem solving
skills and focusing attention.
It has three phases:
• Education about this principle of training,
• Multiple exercises that involve plan-
ning and problem solving, relaxation
and changing thinking patterns.
• Testing of acquired skills in a controlled
environment (Tušak, Misja and Vičič, 2003).
Sport as an environment where a person with
disabilities can develop connections and reduce
loneliness can be described as an extremely
positive activity and a tool for improving the
quality of life. However, in everyday life they
may be limited by their disability due to their

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 115114
physical abilities and consequently experience
stress and low self-confidence.
5.4.3.6. Coping with stress in paralympic sports
The Paralympic Games, like the Olympic Games,
are considered to be the highest level of compe-
tition an athlete with a disability can aim for.
The increased attention paid to the Paralympic
Games and the importance that society, coaches
and support staff all attribute to the winners
of the Paralympic Games, therefore influence
the experience of the Paralympic Games as very
exciting and stressful. Athletes with disabil-
ities experience similar pressures as athletes
without disabilities to achieve victory. First
often experience increased stress as a result of
increased attention of media and family (Dis-
ability and Sport, 2018)
In addition to related sources of stress ex-
perienced by both athletes with disabilities
or without disabilities, we can identify some
are unique to disabled athletes, e.g. those in
wheelchairs or with prosthetics, such as: prob-
lems travelling to the competition, how to get
on the plane, transfers from seat to wheelchair
to toilets and back and personal care, how to
proceed from a long evening trip to competi-
tion, gastrointestinal problems, etc. Often, a
longer absence from home can also be stressful.
Athletes with disabilities miss their important
ones who help them and support them socially
(Disability and Sport, 2018).
Paralympic athletes spend considerable time in
the Paralympic village. Athletes, who compete
at the end of games, have to spend a critical
amount of time in an unknown environment. They
sleep in a bed they are not used to. A study on
Brazilian Paralympic athletes who participated
in the Paralympic Games in Beijing, shows that
most of them had poor quality of sleep. Anxiety
was associated with poor sleep, 72% of athletes
had a medium degree of anxiety, while only 28%
of athletes who were sleeping well were less
anxious. Members of the British team also re-
ported that they were dealing with issues about
room sharing and how well they would compete
after a poor sleep (Martin & Wheeler, 2011).
Athletes with disabilities often have less
access to sports psychologists and coaches
compared to athletes without disabilities. Sim-
ilarly, access to doctors, therapists, masseurs
and athletic trainers is also limited. They usu-
ally have only coaches and assistants available.
Athletes with disabilities are ranked by func-
tionality and competitors are also assigned in
this way. Ranking that occurs before the compe-
tition can be stressful as athletes may expect
classification at a different level. If athletes
reclassify, they will have to compete with bet-
ter athletes. It is clear that such a scenario
can reduce confidence and increase anxiety in key
times (Disability and Sport, 2018).
Drug testing has also become an essential part
of the Paralympic Games and can be a new and
therefore stressful experience. Testing in
Paralympic Games may be more complicated com-
pared to the testing of healthy athletes. For
example, many athletes urinate with catheters.
Some may need to ask for exceptions to the use
of illicit substances as part of their treatment
in relation to their disability.
Some suffer chronic pain and can be treated with
medical marijuana, which can be legally per-
mitted at home, but is prohibited in Paralympic
Games.
Most elite athletes are influenced by the events
and conditions of their sports world. However,
Paralympic athletes must deal with a number of
unique conditions and challenges that can hinder
their optimal functioning.
Well-developed psychological abilities help
disabled athletes cope with stress. Furthermore
sports psychologists play an important role in
the psychological preparation and training.
Reference
De Bressy de Guast, V., Golby, J., Van Wersch, A., & d’Ar-
ripe-Longueville, F. (2013). Psychological skills training
of an elite wheelchair water-skiing athlete: A single-case
study. Adapted Physical Activity Quarterly,30, 351–372
Disability in Sport, pridobljeno junij 2018 iz http://
psychology.iresearchnet.com/sports-psychology/
disability-in-sport/
Gregg, M. (2013). Working with athletes with intellectual
disabilities. In S. J. Hanrahan & M. B. Andersen (Eds.), Rout-
ledge handbook of applied sport psychology: A comprehensive
guide for students and practitioners, (pp. 441–449). London:
Routledge
Gregg, M. J., Hrycaiko, D., Mactavish, J. B., & Martin, G. L.
(2004). Amental skills training package for Special Olym-
pic athletes: Apreliminary study. Adapted Physical Activity
Quarterly,21, 4–18.
Hanrahan, S. J. (2004). Sport psychology and athletes
with disabilities. In T. Morris & J. Summers (Eds.), Sport
psychology: Theory, applications and issues (2nd ed., pp.
572–583). Milton, Queensland: John Wiley & Sons.
Hanrahan, S. J. (2007). Athletes with disabilities. In G.
Tenenbaum & R. C. Eklund (Eds.), Handbook of sport psychology
(3rd ed., pp. 845–858). Hoboken, NJ: Wiley.
Hanrahan, Stephanie J., Psychological Skills Training for
Athletes With Disabilities, First published: 09 March 2015,
https://doi.org/10.1111/ap.12083
James H. Rimmer, PhD, Barth Riley, PhD, Edward Wang, PhD,
Amy Rauworth, MS, Janine Jurkowski, PhD, Physical activity
participation among persons with disabilities: Barriers and
facilitators. Available from: https://www.researchgate.net/
publication/8540158_Physical_activity_participation_among_
persons_with_disabilities_Barriers_and_facilitators [accessed
Jul 05 2018].
Kajtna, T. in Jeromen, T. (2013). Šport z bistro glavo –
utrinki iz športne psihologije za mlade
Malouin, F., & Richards, C. L. (2010). Mental practice for
relearning locomotor skills.Physical Therapy, 90, 240–251.
doi:10.2522/ptj.20090029
Malouin, F., Richards, C. L., Durand, A., Descent, M., Poire,
D., Fremont, P., Doyon, J. (2009). Effects of practice, vi-
sual loss, limb amputation, and disuse on motor imagery viv-
idness. Neurorehabilitation and Neural Repair, 23, 449–467.
doi:10.1177/1545968308328733
Martin, J. J. (2013). Athletes with physical disabilities. In
S. J. Hanrahan &M. B. Andersen (Eds.), Routledge handbook of
applied sport psychology: A comprehensive guide for students
and practitioners (pp. 432–440). London: Routledge.
Martin, J. J., & Wheeler, G. (2011). Psychology. In Y. Van-
landewijck & W. Thompson (Eds.), The Paralympic athlete (pp.
116–136). London: International Olympic Committee)
Screws, D. P., & Surburg, P. R. (1997). Motor performance of
children with mild mental disabilities after using mental
imagery. Adapted Physical Activity Quarterly, 14, 119–130.
Stephanie J Hanrahan, (2014), Psychological Skills Train-
ing for Athletes With Disabilities, Schools of Human Move-
ment Studies and Psychology, The University of Queensland,
Australia.
Tušak, M., Misja, R. in Vičič, A. (2003). Psihologija ekipnih
športov. Ljubljana: Fakulteta za šport, Inštitut za šport.
Tušak, M.[Maks]in Tušak, M. [Matej](2003). Psihologija špor-
ta. Ljubljana: Znanstveni inštitut Filozofske fakultete
Vešligaj Damiš, J., Majcenovič Cipot D., Čeh, M., (2017).
PRIPOROČILA IZVAJALCEM »ReSport« aktivnosti, Center Naprej
(Internal book), Maribor
Žilni, S., 2018. PSIHOLOŠKA PRIPRAVA V KONJENIŠTVU, DIPLOMSKO
DELO, UNIVERZA V LJUBLJANI, FAKULTETA ZA ŠPORT, Kineziologi-
ja, Ljubljana

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 117116
5.4.4. Physical Activity Recommendations
AUTHOR: VLADIMIR JAĆEVIĆ
Key words: recommendations for facilitators, education of professionals, professionals
The importance of regular movement activities
for persons with disabilities and the factors
that impede their inclusion and implementation
Physical activities are defined as physical move-
ments that are produced by skeletal musculature
and require energy consumption. They include
activities that are carried out during work,
travel, play, housework and recreation. The
World Health Organization advises 150 minutes of
moderate physical activity per week (WHO, 2017).
In comparison with persons performing physical
activities in this range, inactive persons have
a 20-30% higher risk of mortality due to various
causes (WHO, 2017).
When talking about persons with disabilities, it
is essential to put the individual first. Dis-
ability does not define the person and is only
a medical diagnosis. According to the medical
model, disability is defined as a medical and
biological problem, the emphasis is on treatment
compared to prevention and promotion of health.
On the other hand, the social model presents
disability as a uniqueness, without condemna-
tion, and highlights deficiencies in the system
and discriminatory behavior as an obstacle to
the integration of people with disabilities into
motor activities (Martin, 2013).
For people with disabilities, physical activity
is extremely important due to the high degree of
influence on chronic diseases, due to the posi-
tive effect on cognitive, emotional and social
difficulties, psychological benefits in terms of
improving self-image in positive experiences
during exercise, stress reduction, reduction of
pain, improvement of depressive symptoms, due
to the social benefits - better social integra-
tion, improved communication skills, networking
through communication with professionals and
other participants (Jaarsma, 2014).
Despite these benefits, there are obstacles to
the integration of people with disabilities into
physical activities related to their age and
type of disability. Obstacles can be individual
- lack of knowledge about opportunities engaging
in physical activity, fears, nature of deficits
and pain, lack of energy. There are also social
barriers, such as the lack of properly trained
professionals (eg gym trainers, sports education
professors with special skills in activities
adapted for people with disabilities), lack of
necessary equipment for adapted sports practice,
underestimation of the ability of persons with
disabilities by health professionals and other
experts. Obstacles may also be environmental
when locations for physical activities are not
adapted for use by persons with disabilities.
(Martin, 2013).
5.4.4.1. Professional recommen-dation and guidelines for facil-itating physical activities
Physical activities are one of the most import-
ant factors for improving the health status of
people of all ages. Therefore, the recommenda-
tions and guidelines that the general population
receives from experts is very important. For
example, in the US, the US Physical Activity
Guidelines 2008 (2008 Physical Activity Guide-
lines for Americans) are applied. The guidelines
contain guidance based on scientific evidence
to help people aged over 6 years to improve
their health by appropriate physical activity.
This is even more important for people with
disabilities, as they tend to have less active
lifestyle. According to US data, almost half of
the people with disabilities who are capable of
physical activities do not even perform aerobic
exercise. On the other hand, disability should
not be equated with poor health, since most
people with disabilities are able to engage in
regular physical activities. Therefore, there
are special guidelines for persons with dis-
abilities in the USA that include the following
recommendations:
• Adults with disabilities should practice at
least 150 minutes of weekly moderate exercise
activity or 75 minutes of more intense aero-
bic activity or an equivalent combination of
moderate and intense motor activity. Aerobic
activity should be performed in episodes of at
least 10 minutes, best spread over the week.
• Adults with disabilities should also per-
form twice a week activities of moder-
ate or higher intensities, which involve
bigger muscle groups to increase muscu-
lar strength. These activities bring ad-
ditional positive health effects.
• In case persons with disabilities are
not able to adhere to these guidelines,
they should be involved in physical ac-
tivities according to their abilities
and avoid physically inactive life.
• They should consult an expert about
the quantity, type and intensi-
ty of physical activities.
• Also, children and adolescents with dis-
abilities should adhere to specific
guidelines for physical activity appro-
priate for their age and abilities.
It has been proven that physical activities play
an important role in the maintenance of health,
well-being and quality of life. They can help
maintain adequate body weight, improve mental
functioning, reduce the risk of premature death,
heart disease, type 2 diabetes, and certain
types of cancer. Physical activities are very
helpful for improving day-to-day functioning
and for increasing the autonomy of persons with
disabilities (CDC, 2014).
5.4.4.2. The role of healthcare and other professionals who treat peo-ple with disabilities in the pro-motion of physical activities
Healthcare workers significantly influence the
amount of physical activity persons with dis-
abilities engage in as they are more likely to
contact them than other experts. It is also more
likely for people with disabilities to be more
active if they are recommended by experts.
In order to appropriately encourage people with
disabilities to perform physical activities,
experts can follow these steps:
• Physical activities are recommend-
ed for all persons with disabilities.
• When performing physical activi-
ties, persons with disabilities fol-
low general recommendations.
• Persons with disabilities are led and
asked by experts on specific issues, such
as how often they are active in the week,
what is the duration of activities, what
is the intensity, what activities they
perform, how to incorporate more physi-
cal activities into their life, etc.
• Experts encourage persons with disabil-
ities to talk about their obstacles and
limitations when performing physical ac-
tivities. Thus obtain information about
the individual and his/her ability needed
to prepare an appropriate program, appro-
priate preparation of the venue, necessary
adjustments, necessary assistance from the
experts and the extent of social support.
• Experts need to know the particular opportu-
nities for physical activity of persons with
disabilities and provide them with appropri-
ate instructions and guidance for partici-
pation in various physical activities and
in various organized programs (CDC, 2014).
5.4.4.3. The importance of edu-cating professionals in the field of adapted physical activities for people with disabilities
Nowadays, the term is adapted physical activi-
ty. It refers to movement, physical activities
and sports activities, with special emphasis on
the interests and abilities of individuals with
different limitations such as disability, health
problems and age. This growing field requires
the integrated treatment of people with dis-
abilities, which includes a multidisciplinary
approach and professionals from various fields
(occupational therapists, physiotherapists,
social workers, psychologists, coaches, sports
instructors, sports education professors, etc.).
The technological development and accessibility
of modern equipment makes it easier to include
more and more people with disabilities not only
in recreational but also in competitive sports
activities. Therefore, continuous professional
training is necessary as well as developing and
learning new methods and approaches. Experts

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 119118
with appropriate knowledge and approach can
encourage people with disabilities in performing
physical activities, monitoring them and pro-
viding necessary support resulting in positive
effects on their health and functioning.
Reference
CDC Centers for Disease Control and Prevention. Adults with
Disabilities - Physical activity is for everybody. 2014
[cited 01/08/2018]. Retrieved from: https://www.cdc.gov/vi-
talsigns/disabilities/ on 20.6.2018
Jaarsma EA, Dijkstra PU, Geertzen JHB, Dekker R. Barriers
to and facilitators of sports participation for people with
physical disabilities: A systematic review. (2014) Scandina-
vian Journal of Medicine & Science in Sports, 24 (6), 871-881
Martin JJ. (2013). Benefits and barriers to physical activ-
ity for individuals with disabilities: a social-relational
model of disability perspective Disability Rehabilita-
tion. ;35(24):2030-7. doi: 10.3109/09638288.2013.802377. Epub
2013 Jun 19.
US Department of Health and Human Services. 2008 Physical
Activity Guidelines for Americans, 2008. Retrieved from
https://health.gov/paguidelines/pdf/paguide.pdf on 20.6.2018
WHO. Physical Activity Fact sheet [Internet]. 2017 [cited
01/08/2018]. Retrieved from: http://www.who.int/mediacentre/
factsheets/fs385/en/ on 20.6.2018
WHOa. Prevalence of insufficient physical activity [Internet].
2017 [cited 01/08/2018]. Retrieved from: http://www.who.int/
gho/ncd/risk_factors/physical_activity_text/en/ on 20.6.2018
5.4.5. Challenges for Facilitators and Service Users
AUTHORS: JASNA VEŠLIGAJ DAMIŠ, YOANA FILIPIC
Key words: location, facilities, communication, perception
This chapter draws on the research and experi-
ence of facilitators in order to outline the
challenges that facilitators/coaches/ trainers
and persons with disabilities themselves face
when planning or participating in physical ac-
tivity. Many authors describe multiple specific
characteristics and challenges they face when
organizing adapted physical activity programmes
(Bodde and Dong-Chul, 2009; Frey et al., 2005)
What we first observe is the learning of mo-
tor skills, which should be taken into account
during the implementation of the activity. We
plan more time for consolidation of skills -
the more complex the skill, the harder it is to
acquire. The degree of flexibility is reduced,
and in the activities where coordination is
needed, the rigidity of the muscles is visible.
During the performing of the new skill, there
are excessive movements that are present for a
long time and are difficult to eliminate. People
with special needs often strain the wrong mus-
cles, hyperactivity or muscle hypoactivity also
occurs.
The challenges are organized according to B.
Horne´s criteria in “Making Sport and Physical
Activity Inclusive for Disabled People, 2016”
(in Clemete 2017) and Dowling’s criteria in
Sport, Coaching and Intellectual Disability. So
we divided bridges and challenges into two main
categories:
Environmental:
• Facility: No accessible build-
ings/facilities, waiting lists
• Equipment: Lack of accessible exercise
equipment, lack of suitable equipment
• Health and safety: Pain, lack of energy,
health conditions, lack of strength, fatigue,
longer to develop skills, obesity, decreased
ability to understand rules and interpret
instructions, poor motor skills, prosthesis
(which can cause corns or blisters during
walking or running so a number of athletes
chose to take part in wheelchair sports or
another type of sports in which the prosthe-
sis was not required) (Bragaru et al, 2013).
• Location: Lack of transportation, build-
ings or facilities located far away.
• Expense: Programme and equip-
ment costs, complicated family situa-
tion due to high extra costs for taking
care of person with disability
• Support from others: Unqualified staff that
cannot modify or adapt individual and group
exercise classes for people with disabilities,
not having necessary staff or support, not
having knowledgeable staff, lack of interest
from the administration to adapt activities
• Communication: Lack of specific knowledge
about the benefits of physical activity, lack
of knowledge about how to exercise, lack of
information about physical activity, no coun-
selling, limited partnerships between sectors
• Suitability: High level competition, em-
phasis on winning, no facilities adapt-
ed for a person with disability.
Psychological:
• Personal perceptions: Lack of motivation, lack
of self-confidence about exercising in public,
perception that exercise is too difficult,
negative mood, depression, anxieties, fears,
frustration and even time management (a busy
schedule or a busy daily life, taking care of
children, daily household activities or work
were can be a barrier) (Bragaru et al, 2013).
• Attitudes from others: Discriminatory prac-
tices at fitness centres and other recreational
venues, other people´s negative attitudes,
not having a role model, overprotecting
parents, parental exhaustion and there-
fore, the parents themselves discourage
5.4.5.1. Bridges to over-come those barriers
In the second part of this article we would like
to suggest possible encouraging factors and
changes that may enable involvement in sports
and physical activities (Heller et al., 2002;
Howie et al., 2012; Messent et al., 1999; Rob-
ertson & Emerson, 2010; Temple, 2007).
Environmental:
• Facility: Accessible facilities to physical
activity or sports in the community, good
surface for walking or running, parks and
playgrounds available in the community,
• Equipment: Direct exercise equip-
ment, adapted exercise equipment
• Health and safety: Maintenance of fitness/
muscle strength, maintenance of functional
independence, walking ability, wheelchair
skills, perceiving health benefits, physi-
cal appearance, weight loss, endurance.
• Location: Transportation, Good weather
• Expense: Better funding of pro-
grammes and play areas
• Support from others: Social support, having
a good trainer, friends are supportive or
physically active, family is supportive or
physically active, doing chores at home.
• Communication: Awareness of opportuni-
ties for sport and physical activity,
good communication between coaches, so-
cial contact, asking for help, collabo-
rative approach between organisations.
• Suitability: Training in small groups,
playing individual/dual sports, playing
team sport, involving favourite figures/
interests, programme emphasis on improve-
ment of social skills and self-confidence.
Psychological:
• Personal perceptions: Perception of relaxation
and fun, attitude that exercise has health
benefits, desire to be active, positive at-
titude towards being challenged, acceptance
of the disability, view of sports and phys-
ical activity as an opportunity for social
encounters, feeling accepted as part of a
group, feeling recognized, feeling rewarded.
• Attitudes from others: Important others
awareness of the benefits of physical activ-
ity, relatives’ perseverance, relatives’
assertiveness, being accepted by peers.
Aside from the practical strategies, and to
support people with disability access to sports
activities there is need to encourage government
for wider access to many other kinds of opportu-
nities within individuals’ communities. Limited
by dependency on the attitudes of carers people
with disability remain subject to significant
discrimination.
Reference
Bode, A.E. & Dong-Chul, S. (2009) A review of social and
environmental barriers to physical activity for adults with

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 121120
intellectual disabilities. Disability and Health Journal, 2,
57–66
Bragaru, M., Van Wilgen, C. P., Geertzen, J. H., Ruijs, S. G.,
Dijkstra, P. U., & Dekker, R. (2013). Barriers and facili-
tators of participation in sports: a qualitative study on
Dutch individuals with lower limb amputation. PLoS One, 8(3),
e59881.
Clemente, I. (2017) Barriers and facilitators to participa-
tion in physical activity for children with disabilities A
systematic literature review. (Master Thesis) Retrieved from
http://www.diva-portal.org/smash/get/diva2:1107967/FULL-
TEXT01.pdf
Frey, G.C., Buchanan, A.M. & Rosser Sandt, D.D. (2005) ‘I’d
Rather Watch TV’: An examination of physical activity in
adults with mental retardation. Mental Retardation, 43,
241–254.
Hassan, D., Dowling, S., & McConkey, R. (2014). Sport, Coach-
ing and Intellectual Disability. London: Routledge.
Heller, T., Hsieh, K. & Rimmer, J. (2002) Barriers and
supports for exercise participation among adults with Down
syndrome. Journal of Gerentological Social Work, 38, 161–177.
Howie, E.K., Barnes, T.L., McDermott, S., Mann, J.R., Clark-
son, J. & Meriwether, R.A. (2012) Availability of physi-
cal activity resources in the environment for adults with
intellectual disabilities. Disability Health Journal, 5 (1),
41–48.
Mahy, J., Sheilds, N., Taylor, N.F. & Dodd, K.J. (2010) Iden-
tifying facilitators and barriers to physical activity for
adults with Down syndrome. Journal of Intellectual Disability
Research, 54 (9), 795–805.
Messent, P.R., Cooke, C.B. & Long, J. (1999) Primary and sec-
ondary barriers to physically active healthy lifestyles for
adults with learning disabilities. Disability and Rehabilita-
tion, 9, 409–419.
Robertson, J. & Emerson, E. (2010) Participation in sports
by people with intellectual disabilities in England: A brief
report. Journal of Applied Research in Intellectual Disabili-
ties, 23, 616–622.
Temple, V.A. (2007) Barriers, enjoyment and preference for
physical activity among adults with intellectual disabili-
ty. International Journal of Rehabilitation Research, 30,
281–287.
5.4.6. Equipment and Technology
AUTHOR: VLADIMIR JAĆEVIĆ
Key words: support technology, prostheses, orthoses
For persons with disabilities it is common to
be poorly included in physical activities than
for the general population and consequently
first have more health problems. At the same
time, there are fewer programs for recreation
and sports education available for adults with
disabilities. (Rimmer et al., 2014). Technologi-
cal development of sports activities for persons
with disabilities enables more and more people
to be involved in sports activities using vari-
ous devices and tools. The development of tech-
nology, especially in the field of materials for
the manufacture of devices, allows people with
disabilities with specially designed prostheses
or other adapted equipment to participate in a
variety of sports, individual and collective
(Steadward, Wheeler and Watkinson, 2003)
5.4.6.1. Definition of technology in relation to the physical activi-ties for persons with disabilities
According to one of the definitions, the technol-
ogy is “the application of science for industri-
al and commercial purposes” (American Heritage
Dictionary). This very broad definition neverthe-
less points to the connection between technology
and functionality. In the field of adapted physi-
cal activity for persons with disabilities, the
primary goal is to improve the functionality of
individuals. So, in this case, the term technol-
ogy refers to the use of science for manufactur-
ing devices - orthoses and prostheses in order
to achieve greater functionality for the users.
All devices, equipment, tools, and product
systems used to maintain and improve the ability
of people with disabilities are referred to as
the common term supportive technology. Simi-
larly, term adaptive technology is also in use,
and relates primarily to the use of electronic
devices and information technology and devices
that are intended and designed exclusively for
people with disabilities (“Assistive and Adap-
tive Technologies for HIE”, 2018)
5.4.6.2. Definitions of basic con-cepts in the field of equipment and devices for adapted physical activi-ties for persons with disabilities
In this chapter, we will focus primarily on
equipment designed to establish, improve and
maintain the functionality of the loco motor
system of persons with disabilities or devices,
common for general use - prostheses, orthoses
and wheelchairs.
Prostheses are devices that replace missing
parts of the body due to trauma, illness or con-
genital conditions. The purpose of using pros-
theses is to restore the function of the missing
parts. (“How artificial limb is made,”, 2018).
Orthoses are defined as external mechanical de-
vices that modify the structural and functional
characteristics of the neuromuscular system.
These are external devices that help individu-
al parts of the body to overcome motor deficits
and problems. The orthoses are used for various
parts of the body such as belts and bandages.
(Redford et al., 1995)
A special area dedicated to prescribing, making,
adjusting and maintaining orthoses and prosthe-
ses is called orthotics and prosthetics. It is
a science that links knowledge in the field of
anatomy, physiology, pathophysiology, biomechan-
ics and engineering, and professionals in this
field need special education.
A wheelchair is a commonly used device that is
used when walking is difficult or impossible due
to illness, injury, or disability.
5.4.6.3. The impact of the develop-ment of technology on the use of or-thoses, prostheses and wheelchairs
Due to technological development, in the area of
the manufacturing of prostheses, orthoses and
wheelchair, three fundamental changes occurred
that influenced the use and functionality. The
devices have become significantly lighter, more
complex and with the possibility of external
regulation. One of the most important technolog-
ical changes in the sports activities of people
with disabilities is the use of more modern
materials such as polymers, ceramics, carbon
fibres, for making devices. These materials have
mechanical and physical characteristics substan-
tially better than conventional materials such
as steel and aluminium. Another essential change
is the use of computers in the manufacture of
prostheses and wheelchairs. Computer chips
built into devices can help control the walking
(Steadward, Wheeler and Watkinson, 2003).
The first records of iron prostheses were written
between 3500 and 1800 BC. Knights who used heavy
iron prostheses were unable to carry out daily
activities. The first aluminium prosthesis was
made in 1912. When the materials became lighter,
the functionality of the user’s prosthesis was
extensively improved. Similar changes have oc-
curred throughout history in the field of wheel-
chair manufacturing. Progress in biomechanics
and kinematics influenced the development of ar-
ticulated and more complex devices. In 1980, the
first sports wheelchair was manufactured. With
the development of specialized sports activities
for wheelchair users, arouse the need for spe-
cialized sports wheelchairs (e.g. basketball,
races, etc.) (Steadward, Wheeler and Watkinson,
2003).
For walking or running, we do not usually need
to focus attention on physical activity, as it
is automated patterns. In old times, the use of
prostheses and wheelchairs for movement involved
cognitive activity, attention and regulation
by the user. The use of modern gadgets still
requires a degree of regulation by the user,
but so-called “intelligent devices” allow more
effective walking for people after amputation
using a built-in computer chip. Similarly, the
use of electric wheelchairs with the possibili-
ty of external regulation and control (e.g. use
in adapted sports activities for children with
cerebral palsy) (Steadward, Wheeler and Watkin-
son, 2003).
5.4.6.4. Use of technological achieve-ments and involvement of people in adapted sports activities
In contemporary world, people with disabilities
have a full range of specific sports activities
they can engage in. Therefore, they can join
recreational activities, participate in various
organized programs and groups or actively com-
pete at international level.
Organized sport for people with disabilities
has existed for more than 100 years, the first
sports clubs for people with hearing impairments
existed in Berlin in 1888. Nevertheless, adapted
sports activities became more widely available
after World War II. The purpose was to help
a large number of war veterans and civilians
who suffered injuries during the war. In 1944,
at the request of the British Government, Dr.
Ludwig Guttman opened a centre for spinal cord

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 123122
injury at Stoke Mandewille Hospital in Great
Britain. Dr. Guttman promoted the idea of using
sports for rehabilitation purposes (“Paralympics
History - History of the Paralympic Movement”,
2018). After this, numerous studies have con-
firmed the positive impact of sports activi-
ties on the physical, psychological and social
functioning of persons with disabilities. In
addition to the improvements in the affected
functions, a positive impact on self-esteem,
mood, social inclusion and employability, is
essential. Long-term physiological adjustments,
as a result of long-term intensive training in
athletes with disabilities, among other positive
effects, lead to a better respiratory volume,
reaction time and improvement of executive func-
tions (Lastuka, Cottingham 2015).
Over time, sports activities part for rehabili-
tation developed first into recreational and then
into competitive sport. Increasing involvement
in a wide variety of sports activities is accom-
panied by the development of technology for the
production of various accessories or customized
equipment and equipment for individual sports.
With appropriate education people with disabil-
ities can also use recreational facilities that
are generally used, such as different poles
(e.g. Nordic walking, gymstick, balance boards,
balls of different sizes and different materi-
als). In addition, the use of modern materials
in production eases adaptation to the needs of
the individual.
In 1948, on the day of the opening ceremony of
the London Olympics, Sir Guttman organized the
first international wheelchair sports competi-
tion called Stoke Mandewill Games. These games
later became the Paralympic Games, which first
took place in Rome in 1960 and were attended by
athletes of 23 countries (“Paralympics History -
History of the Paralympic Movement”, 2018).
People with disability can compete in various
sports disciplines in modern times. Most sports
disciplines are existing sports, adapted to the
needs and abilities of people with disabilities.
One of the main disciplines is athletics. We
would also mention adapted swimming, wheelchair
basketball, sitting volleyball, shooting, and
table tennis. Contemporary sports as curling,
bowling, and netball are somewhat less preva-
lent. These activities include the use of specif-
ic equipment that can be specifically designed or
slightly adapted for persons with disabilities.
Some disciplines and sports are designed espe-
cially for people with disabilities. An example
is the discipline boccia (Italian word, bullet)
developed for people with cerebral palsy and
first presented at the Paralympics in New York in
1984. Discipline is now practised in more than
50 countries by people with cerebral palsy or
various neurological conditions involving the
use of a wheelchair. The rules and equipment are
adapted to the specific abilities of people with
different levels of disability (people can move
balls with a hand or foot, they can throw them
or roll them through specially designed ramp
(“fusion ramp”) (“Boccia - Disabled Sports USA”,
2018).
The development of sports disciplines and the
inclusion of more and more people with disabil-
ities are accompanied by the rapid development
of technology in the field of the production of
accessories and equipment. As an illustration,
athletes who competed on Stoke Mandewille games
used trolleys weighing approximately 22 kg. Con-
temporary adapted trolleys for competitions are
roughly 5 kg. Three-wheel wheelchairs are often
used for competitions, and five wheel wheelchairs
are used for ball games. Nowadays athletes in
wheelchairs can ski, bake, play hockey, cycle.
For persons after amputation of legs and arms,
there are special devices adapted to be used in
specific sports activities (for example, swing-
ing prostheses, climbing prostheses, basketball
prostheses). The use of modern technology in
competitive sports opens up new ethical ques-
tions about the impact of equipment on sporting
results. (Steadward, Wheeler and Watkinson,
2003).
5.4.6.5. The importance of the mul-tidisciplinary team and the impact of specialized education in work-ing with people with disabilities
The use of modern equipment undoubtedly results
in improving the quality of life of people with
disabilities, as well as in the field of daily
activities and implementation of adapted phys-
ical activities. On the other hand, users need
professional treatment and a complex approach
when choosing, using and maintaining various
technology and equipment.
Rapid technological development in the field
of prosthetics and orthotics and the use of
increasingly demanding devices requires addi-
tional assistance and involvement of profes-
sionals working with persons with disabilities.
The choice and prescription of the appropriate
device is definitely highly individualized ac-
cording to the characteristics and needs of each
user (it is about the motor, health, psychologi-
cal, social and other factors). All profession-
als of different profiles involved in disability
treatment programs (selected doctors, sports
education professors, trainers, physiothera-
pists, work therapists, nurses, psychologists,
social workers) need additional knowledge of
the equipment and devices used by the persons
concerned, where they can provide users with
help and support. It is a field in which there
is a trend of very rapid changes. Due to all of
this, cooperation and knowledge sharing within
multidisciplinary teams is essential. It is also
important to regularly train all team members in
terms of specific know-how in the field of orthot-
ics and prosthetics, and in general the use of
science and technology achievements to improve
the functionality of people with disabilities.
Reference
Rimmer, J. H., Riley, B., Wang, E., Rauworth, A., & Jurkows-
ki, J. (2004). Physical activity participation among per-
sons with disabilities: Barriers and facilitators. American
Journal of Preventive Medicine, 26, 419–425. http://dx.doi.
org/10.1016/j.amepre.2004.02.002
Fox, K. R., & Hillsdon, M. (2007). Physical activity and
obesity. Obesity Reviews, 8, 115–121.
Steadward, R., Wheeler, G., & Watkinson, E. (2003). Adapted
physical activity (1st ed., pp. 541-557). The University of
Alberta Press, Steadward Centre.
Parant, Aymeric; Schiano-Lomoriello, Sandrine; March-
an, Francis (October 2017). “How would I live with
a disability? Expectations of bio-psychosocial con-
sequences and assistive technology use”. Disabili-
ty and Rehabilitation. Assistive Technology. 12 (7):
681–685. doi:10.1080/17483107.2016.1218555. ISSN 1748-
3115. PMID 27677931
How artificial limb is made - material, manufacture, making,
used, parts, components, structure, procedure. (2018). Re-
trieved from http://www.madehow.com/Volume-1/Artificial-Limb.
html on 20.6.2018
Redford, John B.; Basmajian, John V.; Trautman, Paul
(1995). Orthotics: clinical practice and rehabilitation tech-
nology. New York: Churchill Livingstone Inc. pp. 11–12.
Assistive and Adaptive Technologies for HIE. (2018).
Retrieved from https://hiehelpcenter.org/treatment/
assistive-adaptive-technologies/
Company, H. (2018). The American Heritage Dictionary entry:.
Retrieved from http://ahdictionary.com/ on 20.6.2018
Paralympics History - History of the Paralympic Movement.
(2018). Retrieved from https://www.paralympic.org/the-ipc/
history-of-the-movement on 20.6.2018
Lastuka, Amy & Cottingham, Michael. (2015). The ef-
fect of adaptive sports on employment among people with
disabilities. Disability and rehabilitation. 38. 1-7.
10.3109/09638288.2015.1059497.
Boccia - Disabled Sports USA. (2018). Retrieved from https://
www.disabledsportsusa.org/sport/boccia/ on 20.6.2018

6.
Learning outcomes:
• Familiarizing readers with the programmes
we implement in the ReSport Project
• Present useful information about
adapting rules, equipment and ter-
rain for persons with disabilities
Adapted Physical Activity Programmes
Based on the developed and performed activities
in the framework of the ReSport project, test-
ing results, evaluation and consultations with
experts from different sport and rehabilitation
fields we prepared a number of adapted physical
programmes. We facilitated those sports in dif-
ferent locations and settings in the three years
of the project and researched its implications
for persons with disabilities.
aPpliCa ti•On •Of ADaPTeD PhySicaL ACTivIty Pr•OgramMEs

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 127126
6.1.SwimMING
AUTHOR: ILONA KOVAL GRUBIŠIĆ
Key words: swimming, adapted aquatics, aquatic activities, therapeutic water exer-cise, swimmers with disabilities, Halliwick
Swimming and aquatic activities for children
with disabilities can foster physical fitness and
motor skill development within a physical educa-
tion program and during recreational pursuits.
In the opening scenario, Jack’s parents are
within their legal rights to request swimming
as part of their son’s IEP because aquatics is
listed as a component of physical education un-
der the Individuals with Disabilities Education
Act (IDEA). Aquatics instruction for students
with disabilities is neither a luxury nor a
therapeutic (related) service. Adapted aquatics
means modifying the aquatic teaching environ-
ment, skills, facilities, equipment and instruc-
tional strategies for people with disabilities.
It can include aquatic activities of all types,
including instructional and competitive swim-
ming, small-craft boating, water aerobics, and
skin diving or scuba diving (AAHPERD-AAALF,
1996).
Physical educators, school administrators,
parents, related service personnel, and special
education teachers must be educated about the
benefits of aquatics and its role in a child’s
physical education. The physical and psycho-
social benefits of aquatics for students with
disabilities are more pronounced and significant
than for students without disabilities. Because
of the buoyancy afforded by water, many people
whose disabilities impair mobility on land can
function independently in an aquatic environ-
ment without the assistance of braces, crutch-
es, walkers, or wheelchairs. Although adapted
aquatics does not focus on therapeutic water
exercise, warm water facilitates muscle relax-
ation, joint range of motion (ROM), and improved
muscle strength and endurance (Koury, 1996).
Swimming strengthens muscles that enhance the
postural stability necessary for locomotor and
object-control skills. Water supports the body,
enabling a person to possibly walk for the first
time, thus increasing strength for ambulation
on land. Adapted aquatics also enhances breath
control and cardiorespiratory fitness. Blowing
bubbles, holding one’s breath, and inhalation
and exhalation during the rhythmic breathing of
swimming strokes improve respiratory function
and oral motor control, aiding in speech devel-
opment (Martin, 1983).
Benefits are not limited to the physical realm.
Water activities that are carefully planned and
implemented to meet individual needs provide an
environment that contributes to psychosocial
and cognitive development. As a student with
a physical disability learns to move through
the water without assistance, self-esteem and
self-awareness improve. Moreover, the freedom
of movement made possible by water boosts morale
and provides an incentive to maximize potential
in other aspects of rehabilitation.
The Swimming-Therapeutic Club Forca is the first
such club in our area and one of the few clubs
in Croatia whose members are children with
developmental disabilities and persons with
disabilities - persons with physical disabili-
ties, impaired sight and hearing and those with
learning disabilities. The club was founded with
the basic aim of promoting and developing the
sport of people with disabilities in Rijeka and
the region.
Club activities:
• planning of the work and development of
swimming sport of persons with disabilities
• organizing and conducting regular system-
atic training sessions for learning and
improving swimming skills of its members
and preparing them for competitions
• teaching and training of children and youth
• preparing its members for participation
in the city, county or state selection
• care for the health and health pro-
tection of club members
• the overall club activities aim to fos-
ter understanding and adoption of ethi-
cal values through sporting activities
• kinesiotherapy
In the SC Forca, we gather 120 members with whom
we regularly work at the Kantrida pools and in
summer on the disability beach in Kostabela.
In addition to regular activities in summer
schools, more than 200 children and young people
have been trained.
We are a sports club in the County with the
most highly educated staff that we have further
educated at the Halliwick courses. The club is
operated by kinesiologists, physiotherapists,
defectologists, educators all of whom are former
swimmers or athletes. The volunteers are the
students of the Physiotherapy Studies at the
Faculty of Medicine in Rijeka. The main goal is
to teach children to swim regardless of their
disability, ie, they are literally learning
about their motor abilities.
There are five sections in the club:
1. Therapeutic section
2. School for non-swimmers
3. Swimming School
4. Competitors
5. Recreation
With our program we want to improve the biopsy-
chosocial development of the child. The program
is implemented by a multidisciplinary team of
kinesiologists-kinesitherapists, physiothera-
pists, educators and trainers.
The Halliwick concept is widely used in the club
program. The Halliwick concept is the approach
to teaching of all people, especially those with
physical disabilities and / or learning disabil-
ities, to be able to take part in activities in
the water, to move independently and swim. (IHA
- Halliwick Concept 2000).
Photo, Center Naprej, rehabilitation in the water, summer camp in Moščenička Draga, 2018

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 129128
At first, Halliwick was called the method. The
International Halliwick Organization (IHA) was
founded in 1994 with the goals of promoting and
developing Halliwick around the world. IHA has
chosen to use the term Halliwick concept as
the word ‘concept’ because it suggests a wider
framework within which different practitioners
can apply Halliwick in different contexts.
The concept influenced the traditional ways of
teaching swimming and hydrotherapy techniques.
At the same time it developed into a special
therapeutic activity in water.
The Halliwick concept recognizes the benefits
that can be derived from water activity, and
sets out the basics needed for teaching and
learning in this environment. These benefits are
holistic and include physical, personal, recre-
ational, social and therapeutic aspects.
Therefore, Halliwick can have a significant
impact on the quality of life of people. The
holistic Halliwick approach encourages people to
take part in water activities, to float and swim
independently, and it fits well within the ICF.
Therapists who want to solve certain limita-
tions can use Halliwick’s structure with special
emphasis on areas such as movement (including
range of movement, coordination and planning),
strength, endurance, respiratory capacity, oral
control, fitness etc. Water also promotes sensory
integration.
Halliwick helps develop social skills, commu-
nication, learning abilities, psychological
well-being and self-esteem. Working in a group
further promotes the development of these abili-
ties. (Lambeck, Stanat, 2001).
Swimming can be an important activity in pro-
moting quality of life. As mentioned earlier,
swimming as a therapeutic tool plays an import-
ant role in improving and maintaining health.
At the swimming school, by methodical approach
and the appropriate props, we approach the
teaching of all swimming techniques: the front
crawl (freestyle stroke), the breaststroke, the
backstroke, and the butterfly stroke. The aim is
for the participants to adopt basic swimming
techniques and to start participating in local
and regional competitions. Attendees of the
swimming school are children ranging 4-12 years
of age.
In the club, we gathered a special social
group, children with intellectual impairments,
who attend a swimming school 3 times a week on
recreational and rehabilitation levels, but at
the same time, for the interested and serious
participants, there are opportunities to compete
at local, regional and state level.
Photo, Center Naprej, rehabilitation in the water with aqua
gymstick, 2018
The program consists of a swimming school –
teaching and perfecting basic swimming tech-
niques – front crawl, backstroke, breaststroke
and butterfly stroke. With regular trainings, we
raise the level of fitness for the participants,
influence the morphological characteristics of
the body, teach new motor skills and raise the
overall level of motor skills.
Reference
Koury, Joanne M. (1996). Aquatic therapy programming: guide-
lines for orthopedic rehabilitation. Champaign, IL: Human
Kinetics, 280 p.
Martin, K. (1983). Therapeutic pool activities for young
children in a community facility. Physical and Okkupational
Therapy in Pediatrics, 3, 59-74.
Lambeck, J., Stanat, F.C. (2001). The Halliwick method. Part
1and Part 2. AKMA, 15, 39-41.
6.2.NoRDic Walk-iNG aND GyMSTick - GNW PROGRAMAUTHOR: JASNA VEŠLIGAJ DAMIŠ, LADISLAV MESARIČ
Key words: nordic walking, gymstick, bands, nordic walking poles, gymstick exercise bands
Introduction
With Nordic Walking Gym exercise bands we can
modify our walking, cross country or alpine
poles into a Gymstick exercise bar in just a few
seconds by attaching the NW Gym bands on them.
The combination of poles and bands will allow
you to perform a complete workout improving your
muscle strength, balance and mobility. You can
choose to exercise in between your walking pro-
gram in the open air or at home. This allows you
to do both walking cardio exercise and muscle
condition training anywhere, anytime!
6.2.1. GNW program -
who is it for?
The program is intended for those who are
attracted to this kind of physical activi-
ty, but especially adapted for persons with
disabilities.
Persons with disabilities are those who devi-
ate from the expected features and capabilities
defined in a particular environment, and require
extra attention and care, like:
• Persons with acquired brain injury (ABI),
• Persons with intellectual disabilities (ID),
• Visually impaired,
• Hearing impaired,
• Persons with speech and language disorders,
• Physically handicapped persons,
• Long-term sick persons,
• Persons with learning difficulties,
• Persons with emotional and be-
havioral disorders,
• Persons with autism spectrum disorders,
• Talented person.
The program was developed by the Centre Naprej
as part of rehabilitation programs to include
users who all experienced severe brain damage.
6.2.2. Why gnw program for
people with disabilities or
for persons with ABI?
Good physical condition allows welfare. The re-
sult of a systematic and continuous work is also

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 131130
a consequence of mental attitude to live healthy
and active, which also increases confidence.
Being fit does not mean only physical ability,
but it touches all areas of our lives. It helps
to purify negative patterns, traumas from past,
frustrations and focus on what really counts in
life. Physical activities are critical to main-
taining an active and independent lifestyle. A
man aged between 30 and 70 years losses about a
quarter of his muscle strength, a man who ex-
periences 90 years more than half. Movement is
the key to maintaining the health, welfare and
working capabilities.
Physical/sport activity may be an important
factor in the social life of a person. It allows
him to have fun in the company of others, make
acquaintances and friendships, and feel part of
the group.
All individuals with special needs can have a
variety of problems in the field of physical dis-
abilities. Despite this, they must be physically
active within their capabilities, because the
lack of movement leads to new complications that
prevent a better quality of life. People with
traumatic head and brain injury, which usually
occurs as a result of a traffic accident, fall,
etc., the basic physical exercises affect the
improvement of motor functions, functions of the
locomotor system, relaxation of muscle tone and
stimulate the equilibrium reaction.
Walking is man’s elemental movement and efficient
movement workout. It is suitable for all people
who can walk and is a completely natural and
safe recreation that can be performed anywhere,
anytime. It does not require expensive equipment
or special facilities, but only the time and
the will. Regular walking improves both mental
as well as physical health as it strengthens
each and every muscle in the body, while not
overloading the joints. In addition, the body
after thirty minutes of walking begins with the
secretion of serotonin, the hormone of happi-
ness, and endorphin, thus largely contributing
to a good and a lot less stressful mood. Due to
release tension, walking has a beneficial effect
on sleep.
The first step towards improving the efficiency
of walking is walking with poles (more common-
ly known as Nordic walking). Poles have always
been a device for walking. The poles evenly
distribute loads which occur during walking.
They redistribute part of the weight that would
otherwise put pressure on the hips and knees,
on the hands. Thus, with each step, we are
strengthening the hands. The intensive work
period also strengthens the cardio-respiratory
function. Poles provide additional stability
when walking which is especially important for
people with impaired balance.
However, exercising only through walking is
not sufficient to prevent the loss of muscle
strength. Without strength training the muscles
still become weake and less functional. Ef-
fective training has duration of not more than
twenty minutes and requires little effort. The
key is to use the exercises in which muscles
work against an external resistance, and to in-
clude all parts of the body. Methods of strength
training include the use of free weights, fitness
equipment, rubber bands, balls and exercis-
es with its own weight. To avoid injury start
slowly and build up exercise strengths where
appropriate.
Poles also serve as requisite and support for
exercises for flexibility. The combination of
walking with poles, exercises for power with
elastics and exercises for flexibility with
poles, gives an ideal combination, which meets
all the basic requirements of natural (physical)
fitness related to health. The American College
of Sports Medicine has defined adequate physical
fitness related to health, as a set of five dif-
ferent measurable elements.
Cardio respiratory capacity is defined as the
ability of the heart, circulatory and respira-
tory system that efficiently supplies the active
muscles with oxygen at the time of continuous
muscle activity. The structure of the body
usually refers to the percentage of muscle, bone
and fat mass in the body. Normally we monitor
the percentage of fatty tissue. Physique is an
organism’s ability to perform activities re-
quiring a high level of generation of muscular
force.
Muscle endurance is the ability of a muscle or
muscle group to perform repeated muscular con-
traction for a long time, or to retain a high
level of development of muscular force for a
long time.
Especially important is to maintain muscle mass,
that is, if it is inactive, subjected to rapid
atrophy. Both parameters can be in dealing with
the physical form and health considered together
as muscle strength.
Mobility is the ability to perform large ampli-
tude movements in a certain order or a certain
plane.
All of the above mentioned areas effectively
improve due to appropriate exercise at all ages.
6.2.3. Gymstick nordic
walking – adaptations for
persons with disabilities
Adjustments to the program in terms of age
Implementation of the program is not limited
by age; it can be implemented in all stages of
life. Therefore it is wrong to think that this
kind of physical activity cannot be carried out
by elderly. Ageing is a gradual reduction of
biological functions, and the ability of the
organism. During this process an individual
is facing deterioration of his working, repro-
ductive and creative functions. During ageing
changes can be seen at the level of cells,
tissues and the organism itself. Many years of
research confirmed the fact that in the process
of ageing regular and balanced aerobic physical
activity has a significant impact on the preser-
vation and enhancement of physical and mental
abilities. So it is never too late to start with
exercising regularly.
Regular exercise can effectively reduce or
prevent a number of functional problems asso-
Photo: Jasna Vešligaj Damiš, users of Center Naprej, Piramida, Maribor, 2017
CARDIO-
RESPIRATORY
BODY
COMPOSITION
MUSCLE
STRENGTH
PHYSICAL FITNESS RELATED TO HEALTH
MUSCULAR
ENDURANCEFLEXIBILITY
Figure 9: Physical fitness related to health (Source: American College of Sport Medicine)

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 133132
135
130
125
120
115
110
105
100
6’5” 200
6’3” 190
6’1” 185
5’11” 180
5’9” 175
5’7” 170
5’5” 165
5’3” 160
5’1” 155
4’11” 150
4’9” 145
ciated with ageing. Strength training helps to
delay the reduction of muscle mass and strength,
which is typical for ageing. This type of ex-
ercise improves the bone structure, and there-
by reduces the risk of osteoporosis, improves
the balance and thereby minimizes the risk of
falling, consequently associated with injuries
and fractures, and also improves flexibility and
range of motion. Physical activity has a favour-
able effect on the cardiovascular and respirato-
ry systems. Regular exercise is also connected
with the maintenance of cognitive function,
reducing depression and improving self-esteem.
In addition to these, regular physical activity
enriches the elderly with positive emotion and
welfare, reduces nervousness and mental stress,
maintains the mental and spiritual balance,
improves sleep, maintains and creates new
friendships.
Adjustments to the pro-gram in terms of gender
This program is suitable for both men and women
and there is no need for adjustments regarding
gender. There are also no restrictions in terms
of physical, cognitive and sensory deficits.
Quite the contrary - appropriately selected
physical activities that improve flexibility,
muscle strength, aerobic capacity and other
physical aspects, allow better rehabilitation of
people with various deficits.
For the implementation of the program for per-
sons with different limitations two conditions
must be provided: trainers must know the par-
ticularities of the population they are dealing
with and must be specially trained to adapt the
exercise to the remaining physical and cognitive
abilities of users. Therefore an
individual training can be ac-
complished, completely balanced
on the personal aims. An import-
ant part is also risk assessment
of the program because in ev-
ery training there must be full
safety measures provided for all
included.
6.2.4. Equipment for gnw programme
Nordic Walking Poles
Nordic Walking poles differ from regular trek-
king or alpine skiers poles in one main area:
the grips and straps. The Nordic Walking straps
stay wrapped snugly round the hands and are
clipped to the slimmer grip of the pole. This
allows the pole to be swung from the hand, with
the downward pressure from the arms quickly
applied to the pole when it reaches the desired
position. Carbon is best for pole composition
but it costs more and other compounds are en-
tirely suitable for the recreational Nordic
Walker.
Select the correct Length of Poles
To choose the right length poles, first determi-
nate the proper pole by multiplying your height
by 0,68 or by referring to the chart down. As a
rule of thumb, the elbow should be at 90 degree
angle to the surface when the poles in a relaxed
grip on the ground. For beginners it is recom-
mended to start with a shorter pole.
Use the following table to select the correct
length of the poles:
Photo: Zvonka Novak, users of Center Naprej, Kalvarija,
Maribor, 2017
Figure 10: Gymstick Nordic
Walking poles
Nordic Walking Gym Exercise Bands
The Nordic Walking Gym Exercise bands are avail-
able in any of the three resistance levels
below:
• Light/Green - for rehabilitation workouts and
exercise for the elderly. The resistance of
green exercise bands ranges from 1 to 10 kg.
• Medium/Blue - for junior athletes and women
who want to start exercising. The resistance
of blue exercise bands ranges from 1 to 15 kg.
• Strong/Black - for fit women, men who
want to start exercising, and ath-
letes. The resistance of black exer-
cise bands ranges from 1 to 20 kg.
Photo: Zvonka Novak, users of Center Naprej, Piramida,
Maribor, 2017
How to use the Exercise Bands
Transforming the poles to a Gymstick and adjust-
ing the resistance
• Take bands from handbag.
• Put the poles next to each other, han-
dles pointing to opposite directions,
with the paw-part extending further out
than the handle of the other pole.
• Tighten the poles to each oth-
er with the Velcro.
• Set the loops on both feet, in the middle of
the sole, roll the elastic band around the
bar (both poles) a couple of times and you are
ready to begin a Gymstick exercise routine.
• In the beginning of each movement the ex-
ercise band must be straight but not
stretched. You can increase the resis-
tance by rolling the bands around the
poles and decrease the resistance by re-
leasing the bands from around the poles.
• When you have adjusted a suitable resis-
tance, remember to grip the stick with a
relaxed but firm grip to avoid slipping.
• Do not stretch the bands over four times
their original length when exercising
Appropriate clothing and footwear
In order to feel good during the training and to
maintain obtain safety we have to pay special
attention on proper footwear and clothing. We
should never put on new shoes or hiking boots
for the first long hike. Footwear must be suited
to activities carried out in nature. We can use
running shoes, trekking shoes or light hiking
boots. Hiking boots shouldn’t be too high, as
this prevents proper technical implementation
of Nordic walking. It is important that the shoe
offers good support and has non-slip soles.
We can engage in GNW in all seasons, but we
must always dress according to the weather
conditions, because the cold contributes to
exhaustion. In the case of variable weather
conditions, we have to wear several layers of
clothing, which can be, if necessary, removed.
Clothing should be light, sporty. Too loose
clothing can hinder us in the activities. If we
are too hot and we face excessive sweating, we
need to make sure our body gets enough fluids. In
the backpack, which should not be too heavy, we
carry only the necessary things. We have to make
sure that our back and neck are protected from
the cold and wind. Therefore, we should have a
spare T-shirt to be able to change clothes.
Reference
Retrieved from manual for rehabilitation of persons with
disabilities: Vešligaj Damiš, J., Mesarič, L., Mesarič, P.
GNW- Gymstick – Nordic walking program
Table 5: Measure of Poles

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 135134
6.3.stand UP paddle Boarding (SUP) as a NEw form of RE-haBILitaTIOn Of iNDivIDUals With ACqUiREd BRAin iNJurY (aBI)
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: swimming, adapted aquatics, aquatic activities, therapeutic water exer-cise, swimmers with disabilities
Introduction
Stand up paddle boarding, otherwise known as
SUP, once an ancient method of transportation
is now a sport that is easy and appropriate for
everyone who wants to explore the nature pad-
dling. Nevertheless, it is also a unique oppor-
tunity for developing a rehabilitation program,
practising interesting sports, rehabilitation
exercise for the whole body, exploring nature
and way of meeting new people and sharing expe-
rience (Hammer, 2011, Walker, Nichols, & Forman,
2010).
It is sports enjoyed by young kids, men, women,
older adults and people of all sizes, disabled
and everyone in between. Saying it is appropri-
ate for the whole family we should not forget
our four-legged companions as paddle boarding is
a fun way to spend time with our dogs.
Standing, paddling and taking the pleasure in
observing the nature we were honestly surprised
that our users got used to balancing and gained
control over the paddle boards very quickly.
Even though having fun is important, safety is
always our priority as any sport may lead to
injuries (Walker, Nichols, & Forman, 2010).
Boards should be appropriate length and width,
hull type and we should have accessories like a
paddle, PFDs (Personal flotation devices) and a
leash. Our service users were capable to learn
how to maintain control of the boards and confi-
dently floated around in just half an hour. With
a lower centre of gravity and a life vest on,
which adds buoyancy they did not fear much and
falling in off a board when they lost balance
was the best thing they could possibly do. As
they fell on the soft life vest they faced their
fear of water and slowly overcame it and en-
joyed, even more, when they got on the board the
next time.
And last but not least SUP stands out amongst
sports for being a very sociable, calming and
engaging with nature activity (Hammer, 2011,
Schram, Hing, Climstein, 2016). As we quietly
float together crossing lakes we have the unique
opportunity to explore and learn about the beau-
tiful nature of Slovenia.
6.3.1. Why is stand up paddle
boarding appropriate for persons
with acquired brain injury (ABI)?
1. Because SUP is a fun full body workout ac-
tivity (Green, 2016, Ruess et al., 2013).
2. It is a great sport for everyone.
3. We can stimulate brain activity ex-
ploring rivers, lakes, sea bays...
4. We have an opportunity to observe the lo-
cal scenery from a new angle. SUP gives us
a wider view than we would get on land so
we can see and experience the hidden side
of the rivers and lakes we already know.
5. Lying on the board with eyes closed,
listening to the sounds of the sea al-
lows us to escape the urban con-
fines and reconnect with nature.
6. Service users with severely impaired vi-
sion and those with other disabilities
that prevent them from standing, go on
the board with assistants who choose an
appropriate size of board for two.
7. It offers a very effective workout. The
constant wobbling of the board means that all
our muscles are working to keep the balance
of our body (Schram, Hing, Climstein, 2016).
It’s also good for rehabilitation of our
service users, to offset the loss of balance
which often comes with acquired brain injury.
8. It is a fantastic full-body workout. We
practice relaxation and at the same time we
facilitate injury rehabilitation. Almost
every muscle in the body is working during
paddle boarding. Because of the balance re-
quired, leg muscles are struggling attempting
to stabilize our centre of gravity, while the
arms, back, shoulders and higher abdominal
muscles are used to push the paddle in the
water. The core, back and abdominal mus-
cles are constantly at work to maintain our
balance. Therefore paddle boarding increases
our strength; improve our balance and endur-
ance (Schram, Hing, Climstein, 2016, Vojska,
2017). If we spend enough time in the water
paddling quickly we would get a good car-
dio workout. It is also a good way to burn
off excess weight and build lean muscles
that would help us in reducing strain on the
Photo: Jasna V.D., users of Center Naprej, Hoška gramoznica, 2017

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 137136
lower back and the knees (Green, 2016).
9. SUP is an extremely fun and enjoy-
able activity that could replace in
some ways therapeutic work indoors
(Schram, Hing, Climstein, 2016).
10. We can go paddle boarding alone or with
friends. It’s very easy to chat to
friends paddling alongside.
11. We would never forget the unique expe-
rience while boarding as a group.
12. Stand up paddle boarding may reduce stress.
Floating on water naturally, soothes the
body, it is an exercise for mind and mus-
cles. That is why we would recommend
this powerful natural stress buster.
13. We gain a completely different and more
beautiful perspective of the nature
around us when we stand on the board.
14. It is quite a “green” activity as we need
just a board and a paddle. We do not need an
engine, fuel and we do not make noise or dis-
turb wild creatures in their natural habitat.
15. SUP offers us a lot of opportuni-
ties – to engage in conversation with
friends, to exercise outdoors or even
get an adrenaline adventure.
16. It is relatively easy to learn and practice,
and it is probably the only activity which
can be equally enjoyable for everyone.
6.3.2. General advice and
instructions for stand up paddle
boarding with individuals
with acquired brain injury
Preparation
• Start out in flat, calm water – the most
appropriate locations are lakes, sea sur-
face without waves or safe gravel pits.
• Safety check access to the water as it
should enable us to go in and out safely.
• Prepare the service users appropriately for
the activity (what is expected to happen,
safety instructions, accessories etc.) Pre-
pare a risk assessment for the activity.
• Prepare the equipment. We should be care-
ful when choosing a proper board (all round,
solid). We should adapt the volume in or-
der to fit our weight – we should add 110 to
our weight and we would get the appropri-
ate volume for us. We should not forget the
accessories such as paddle, PFD (personal
floatation device), leash and proper clothes
(t-shirt, baseball cap, sunscreen) and fluids.
Basic Paddle Board Equipment
• Stand up paddle board
• Leash
• Paddle
• Sunscreen
• Baseball cap
• UV protection t-shirt
• Water bottle
• Dry bag
• PFD (personal floatation device)
6.3.3. Educational approach
1. Teaching service users how to stand up on the paddle board their first time out
• First, we have to teach the service us-
ers how to step on the board, how to at-
tach their leash, to squat on the board
in order for them to be able to stand.
• Gradually we teach service users how to
stand up, how to gain balance and after
they have developed these skills we fo-
cus on teaching them how to paddle and
turn the board in the desired direction.
• We always teach our service users where
the water is deep enough (at least 80cm)
to prevent them from hitting the bot-
tom when they fall. They start out on
their knees and take a few strokes on each
side of the board until they reach deep-
er water, then they slowly stand up with
one foot at a time trying to balance.
2. Teaching service users to stand on the paddleboard
• The right combination for gaining balance
- being upright on the board, feet shoul-
der width apart, knees slightly bent plac-
ing our head in the centre of the board.
• We should balance with our hips, so head
and shoulders stay still, keeping eyes
on the horizon, not on our feet.
• We should be careful positioning our service
users on the board as they should not place
their body in the front of the board as the
nose will drop in the water and as soon as
they start paddling they will fall. If they
stand far back on the board, the tail will
drop into the water and the speed will de-
crease. They should stay in the middle of the
board with their feet parallel to the string-
er – about shoulder width apart with knees
slightly bent, and back completely upright.
3. Teaching service users to pad-dle (stroke techniques)
• As soon as service users feel com-
fortable on the board we start teach-
ing them how to use the paddle
• We use adjustable paddles, take the rid-
er’s height and add 15 - 20cm to de-
termine the correct paddle length.
• They paddle as they grip the top of the paddle
with one hand and place their other hand at
a comfortable distance about one - third
down the paddle. They should keep their arms
straight as they extend the paddle forward
for each stroke. When paddling on the right
side of the board right hand stays lower when
switching sides we reverse our hand position.
• They should start paddling keeping their lower
shoulder to the front and the top shoulder
back in order to reach far out to the front,
preferably – 30 – 50cm ahead as it is the most
important thing for making a good stroke. They
push the paddle down with their whole upper
body moving it from the nose to the tail and
then as it reaches the point of their an-
kles they take the paddle out, quickly put
their body upright again, throwing their hips
forward and shoulder backwards. They should
not use their arms but use the whole upper
body to push the blade deep into the water and
pull through. Using upper body and shoulder
rotation for power would make the board move
faster. They should keep the paddle upright
and closer to the sides of the board, moving
their core forward using hips and legs to
pull the paddle. As hips move forward board
slides faster. This technique is appropriate
for those who are physically and mentally
capable of completing it. Otherwise, we can
simplify it in order to ensure the safety of
the users and let them enjoy the paddling.
Photo: Jasna Vešligaj Damiš, users of Center Naprej, Drage, Croatia, 2017

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 139138
• In order to paddle in a straight line, they
should take a few strokes (3-5) on one side
then switch to the same number of strokes
on the other. Usually, in the beginning we
are able to complete fewer strokes that
are also shorter. At this point in time,
the most important tasks are keeping bal-
ance and getting used to the board.
And a frequently asked question: How to hold a sup paddle properly?
We should hold the paddle so that its angle
should face away from us. As there are many
kinds of paddles with differently placed angles
we provide you with a simple way to show you the
correct way. When faced the right way the blade
will lift and allow us to move faster with less
effort (derived from https://www.justpaddle-
board.com/proper-paddle-form/). Please see the
photos below:
Figure 11 and 12: Paddle height and paddle position. Adappt-
ed from: https://www.justpaddleboard.com/proper-paddle-form/
Falling into the water
• Spend time to prepare the users for the
possibility of falling into the water.
Give them instructions when losing bal-
ance to try falling into the water rath-
er than on the boards as it is safer.
• Users have their boards attached to them
using a leash. In the event of fall, they
should release the paddle for safety rea-
sons, swim back to the board and then push
the board forward with hands to the paddle.
Turning the board
Once users are able to paddle forward and keep
the balance we move on to turning the board.
This is an important lesson as they need to know
how to go back to the shore. We start lessons
when the board is still, making a 180-degrees
turn as this is the easiest turn. They should
keep a low stance and pull, towards the tail or
backwards, while twisting and leaning to the de-
sired side with their torso. The important thing
is keeping the balance and the core still as the
board may become unstable.
Paddling faster
If the service users are successful in learning
the basic stroke techniques and safety measures
we continue the learning process with teaching
them how to paddle faster completing more and
longer strokes (3-5 on the left side and 3-5 on
the right side).
These are the basic lessons that we teach our
users. We could always upgrade our knowledge to
knee paddling, advanced turn techniques, one-
leg, squat paddling, squat paddling, exercising
on the board.
We focus on the learning techniques finding a
calm body of water, once we have learned to pad-
dle there we could explore seas where the waves
are slightly bigger.
Photo: Jasna Vešligaj Damiš, users of Center Naprej, Gams
Bad, Austria, 2017
Always remember: Start with providing a thorough
stand up paddle boarding and swimming training
for your assistants before teaching your users.
Photo: Jasna Vešligaj Damiš, users of Center Naprej, Velen-
jska plaža, 2018
6.3.4. The Benefits of Stand
up Paddle Boarding
• SUP is having fun outdoors: a little safe
sun exposure is great for our body’s need
of vitamin D. Our body needs vitamin D that
keeps our bones strong by helping our body
absorb calcium and phosphorus (Green, 2016).
• We can practice stand up paddle board-
ing almost everywhere: in the sea (near
the coast, in lagoons, bays, in the open
sea...), in lakes, gravel pits, rivers, wa-
tercourses, streams, ponds and even pools.
• It is an extraordinary activity that en-
ables paddlers to get the benefits of
a full-body workout (Schram, 2015).
• SUP improves our overall fitness, it is
great workout, which is one of the rea-
sons that top athletes involved in various
sports practice it as part of their routine
or as part of the rehabilitation process.
• When paddling we train our muscles,
“burn” calories, increase our heart rate.
Movement relaxes muscles, and releas-
es endorphins (pleasure hormone) in the
body, which alleviates the effects of
stress and makes us feel better (Schram,
Hing, Climstein, 2016, Green, 2016).
• SUP is a full-body workout. As paddlers
we use different muscle groups. We need to
learn to balance which trains core mus-
cles and fingers. SUP strokes require move-
ments of hips and shoulders similar to
those in golf, tennis or baseball.
• The back muscles are of crucial impor-
tance and constantly at work as they
maintain the posture and stabilize the up-
per part of the body (Schram, 2015).
• The abdominal muscles are at work when pad-
dling, they are used to propel the paddle-
board into the water and work together with
the back muscles attempting to maintain our
balance (Schram, Hing, Climstein, 2016).
• Paddling strengthens and trains the mus-
cles of the spine, as well as the triceps
and biceps. Our buttocks, thigh and calf
muscles are also working hard in order to
keep our body upright (Schram, 2015).
• SUP improves our motor skills,
strength, endurance, coordina-
tion and mobility (Schram, 2015).
• SUP activates both sides of the body. Thus,
the users (persons with acquired brain injury)
also activate their weaker (affected) side
of the body, as a result of that they extend
the shortened muscles of this side and rotate
the core, which is extremely important for
their rehabilitation (Ruess et al., 2013).
• SUP as mental training. Practicing SUP af-
fects our mental health and mental fitness
(Schram, Hing, Climstein, 2016). Stand up
paddle boarding can alleviate stress levels
and mental tension. On the boards we can get
closer to nature and its beauty as it is sci-
entifically proven to have a relaxing effect.
SUP enables our overwhelming mind to rest.
The released endorphins improve our mood.
• Stand up paddle boarding stands out as
a very sociable activity. This is a fun
and safe way to spend time with friends
(Schram, Hing, Climstein, 2016).
• SUP is a great opportunity to find adventures,
explore and discover wilderness and reconnect
with nature. It is a way of travelling and
conquering interesting places (Green, 2016).
• SUP is also a popular activity for compe-
titions (Schram, Hing, Climstein, 2016).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 141140
• Age is not a barrier for those who want to
stand up paddle board. It does not matter
whether we are young or old, it is suit-
able for everyone. It offers relaxed rec-
reation and everyone can learn to do it.
We can see children, teenagers, pregnant
women or our grandparents on the boards.
• SUP is also appropriate for practis-
ing by persons with disabilities, and
we do practice SUP at Center Naprej!
Reference
Green, D. (2016). “ACE-Sponsored Research: Can Stand-Up
Paddleboarding Stand Up To Scrutiny?” ProSource. American
Council On Exercise. August 2016.
Hammer, S. (2011). Catch the wave of stand-up paddling The
Providence Journal, Sep. 5, 3.
Maja Vojska (2017). Aktivnosti, ki ti učinkovito pomagajo
izboljšati ravnotežje. derived from https://www.bananaway.
si/7-aktivnosti-ki-ti-ucinkovito-pomagajo-izboljsevati-rav-
notezje/
Ruess C, Kristen KH, Eckelt M, Mally F, Litzenberger S, et al.
(2013) Stand up Paddle Surfing-An Aerobic Workout and Balance
Training. Procedia Engineering 60: 62-66.
Schram B. (2015). Stand up paddle boarding : an analysis of a
new sport and recreational activity. PhD Thesis. Gold Coast:
Bond University.
Schram B, Hing W, Climstein M. (2016) The physiological,
musculoskeletal and psychological effects of stand up paddle
boarding. BMC Sports Science, Medicine and Rehabilitation 8:
32.
Walker, C., Nichols, A., & Forman, T. (2010). A survey of
injuries and medical conditions affecting stand-up paddle
surfboarding participants. Clinical Journal of Sports Medi-
cine, 20(2), 144.
https://www.justpaddleboard.com/proper-paddle-form/
Photo: Zvonka Novak, users of Center Naprej, Velenjska plaža, 2018
Figure 13: SUP - complete workout Adapted: http://www.serenapaddlesports.com/blog/standup-paddleboardinga-complete-workout
6.4.SlACkliniNG OR walking On flAT webBINgAUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: slackline, balance, basic positions and movement, outdoor sports activities
The introduction of a novelty, especially new
sports activities, such as slackline or walking
on flat webbing is always challenging but at the
same time exciting. When users perform something
new as part of their rehabilitation, they do not
know whether they will succeed or not, regard-
less of the experience - if they have already
tried it before the injury or not, it causes an
increased level of stress for them.
The introduction of novelties is also a partic-
ular challenge for employees. The employees of
Center Naprej tried first themselves walking on
flat webbing. They tested their balance, focus,
giving and receiving feedback, managing waves
on the webbing, managing fear of falling, per-
sistence, and so on. When they had familiarized
themselves with the various aspects, possibil-
ities and critical points of slacklining, and
gained the appropriate skills and knowledge, we
started introducing users to this interesting
but also challenging sports activity.
6.4.1. What is slackline?
Slackline is a suspended length of flat web-
bing that is tensioned between two anchors.
It is most often tensioned between two strong
trees about 30 - 50 cm above the ground. We can
tension it just above the ground or above water
surface, and we can stand on it, walk, jump,
perform tricks, do yoga, etc. It differs from
the ordinary rope because slackline is more
elastic therefore it can function similarly to a
narrow trampoline.
In the beginning, we try to keep the balance on
the tape, and from time to time, we try to take
a step across the whole length or even make a
more demanding exercise.
6.4.2. Why slacklining
with persons with acquired
brain injury (ABI)?
Walking along the nylon tape is a sports ac-
tivity with multiple aspects, where awareness
of one’s own body, balance and coordination is
extremely important, and at the same time it
influences a wide spectrum of other human psycho-
physical abilities. While slacklining, people
with ABI develop different abilities:
Sense of the position of one’s own parts of the body - proprioception
Proprioception is the perception of motion and
the positions of the body parts. While slacklin-
ing, we perceive the movement, the positions of
the limbs, the pressure on the feet, the speed
BODY EXERCISE CARDIO EXERCISE
SHOULDER MUSCLES
CHEST MUSCLES
ARM MUSCLES
ABDOMINALS
THIGH MUSCLES
LOWER LEG MUSCLES
TRAOEZIUS MUSCLES
LOWER BACK MUSCLES
GLUTEAL MUSCLES
LOWER LEG MUSCLES
• HEART
• LUNGS

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 143142
of movement and the force of inertia that arise
during the activity. Thus they improve their
proprioception. It is important to focus the
sight to the horizon. For even more propriocep-
tive challenges, we close our eyes and try to
stand and walk on the mice tape.
Balance
Slacklining is a test of balance. Some users’
goal is to remain on the webbing, others’ to
take a few steps or to move from one end to the
other, others to stretch on the tape. While
slacklining, we are constantly trying to hold
our body in a stable position and are constantly
on the border between stable and unstable state.
When we step onto the webbing we leave the
ground (the comfort zone) which we are used to,
and enter the state of uncertainty (no comfort).
The line swings. The main problems are caused
by the body and the mind that like known situ-
ations. Let’s confront the unknown, which is a
good training for all and it is happening to us
in everyday life. In fact we are never sure how
the day will end. Therefore, slacklining can be
said to be an ‘’ out of comfort zone ‘’ activity
or opportunity to cross the threshold of our own
uncertainties.
Stabilization and strength-ening of the core
Slacklining requires a fairly tight central part
of the body (the core), the upper part of the
legs, while the arms are released. In this way,
we stabilize the transverse bandwidth of the
tape.
A social and healthy entertain-ment for everyone and psycho-phys-ical abilities training
Slacklining is a social and healthy entertain-
ment for anyone who is able to stand upright and
take a step on solid ground. It is a good phys-
ical as well as mental exercise that improves
the management and stabilization of the body and
helps to cope with feelings (fear, excitement).
In addition to the above mentioned positive
effects, it is observed to help improving body
posture, reaction time, concentration, focus and
perception. It can be a relaxation technique and
help with remaining calm in difficult situations
and in achieving greater determination. It is
a preventive activity and helps the treatment
of joint damage. It is a good workout for the
ankles, knees or hips and strengthen the whole
body.
6.4.3. Tips before starting your
employment with persons with ABI
First, let’s get familiar with the rules import-
ant for all aspects of slacklining. They are
especially useful for beginners (Nahtigal, 2012)
and of course when working with our users - ath-
letes with acquired brain injury.
Preparation of the surface
• We select and prepare the surface: the ground
should be flat, preferably grass, prefera-
bly we placed a thin protective pad under
the line, for safety in case of fall.
• Select the appropriate tension points - the
distance of the tensioning. We have to se-
cure enough space around the line (at
least 5 meters on each side of the line)
to prevent damage in the event of fall.
• Tension the tape to fixing points (e.g.
two trees). The best fit is with origi-
nal clips. We must not forget to pro-
tect the trees so they do not get damaged
(e.g. wrap them with a foam sponge).
• The distance from the ground should be big
so that the tape in the middle at the largest
part is just above the ground (10 to 20 cen-
timeters), and the distance between the fixing
points should be short, 5 to 10 steps, to be
as close as possible to the ground to jump.
• Stretch the webbing to the desired extend
(the shorter and more tense it is, smaller and
faster is the wavelength of the oscillation).
• On both sides of the tension point
(i.e. on both trees), we mark the
point of sight (the horizon).
Preparing the users
• Before commencing slacklining it is import-
ant to prepare the users appropriately psy-
chophysically: we perform various exercises
for balance training and coordination, teach
them relaxation with breathing, managing
emotions, awareness of body parts, etc.
• Users have to take off their shoes before
slacklining. They are barefoot on the tape.
Bare feet improve the feeling for the line
and help them to start balancing faster.
• Before users start the activity, we
calm them down and make them relax and
gain control of their breathing. If he/
she is appropriately prepared, his/her
legs on the tape will be less shaky.
• Before slacklining, they need to be lead
as to how to step on it, to focus eye-
sight on the indicated point on the tree.
Some general instructions
• The recommended width of the line
is 3.5 cm and the length for be-
ginners is between 4 and 8 m.
• We start with demonstration of each exercise.
• Often, the first attempts to tackle the
tape are unsuccessful and the user can-
not stand alone on the tape. That is why
we offer him support and encouragement
to persistently repeat the exercise.
• When stepping down from the tape, make
sure that the user does not jump quick-
ly from the line. The line is dynamic and
will respond to the jump with stretch, and
consequently the user will lose control
and fall uncontrollably from the tape.
• It is best to start in the centre of the
tape, especially for safety reasons. It is
more likely to hit and get injured in case
of a fall near the tension point. In the
middle, the tape is at the lowest point
and thus reduces the height of any fall.
• When slacklining, the user will initially be
most hindered by the fluctuation of the tape,
but continuous exercising may improve con-
trol or even eliminate the fluctuation over
time. The tension of the line depends on the
distance between the fixing points. The wave-
length of the oscillation in the middle is
the largest and slowest; when approaching the
fixing points, the wavelength of the vibration
is always short and quick. The fluctuation
also depends on the length of the tape and
the force with which the tape is tensed.
• The line is very tense, so care should
be taken to ensure that in case of fall-
ing line does not hit the user.
• Even if the line is only a few centime-
ters above the ground, the fall can cause
injury (strains, bumps). Injury depends
on the surface under the webbing and the
type of fall. Therefore, a protective lin-
ing is recommended under the tape.
Photo: Center Naprej, 2017
6.4.4. Basic exercises
Exercises with assis-tance while slacklining:
• Exercises with assistant (hold-
ing the user for the hips).
• The assistant sits on the tape.
• The user is holding the assistant’s shoulder.
Practical exercises
• Training with running poles (2 poles, one
pole, the length of the poles is approx-
imately to the shoulders of the user)

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 145144
Examples of exercises for prepar-ing users for walking along the tape with various forms of assistance
Exercises on the ground:
• walking along the line with
open / closed eyes,
• walking on a low bench, low lath
• exercises on soft surfaces - soft pillows
• exercises on sticks, walking, squats, turns
• exercises on balance boards
• breathing exercises, relaxation exercises
Exercises for getting used to the webbing - we start all exercises in a way that the user is placed in front of the tape:
• with one foot on the line and push-
ing it in all directions;
• with one foot on the line, swings, so that
the tape pushes the foot back to the ground;
• with one foot jump on the line, so that
the line pushes foot back to the ground;
• with one foot on the line and
cross it with the other foot.
Exercises for balance position on the line - all exercises are performed while the assistant is sitting on the line.
We start with the exercises as we are about 2
meters away from the user. Later this distance
between the user and the assistant sitting on
the webbing is increasing. We can perform:
• walking with the help of poles,
• walking with the help of an assistant.
6.4.5. Movements - basic
instructions for implementation
1. Stepping on the line
Start position: Basic start position.
Implementation: We focus our weight directly on
the leg on the line, and then with a calm and
balanced motion we step on it. Keep the body
upright throughout the movement. Finish in the
basic position on the tape with one leg on.
Note: Do not press down on the foot on the tape,
as the tape is moving away and the pressure is
higher, feet are shaking quicker. In order to
get on the tape, you need some determination.
Photo: Center Naprej, 2017
2. Walking forward - backwards
Start position: Basic start position.
Implementation: From a balanced basic position,
we begin to move the body’s center of gravity to
the foreleg. Gradually we begin raising the heel
of the leg behind. When the body’s center of
gravity is already completely on the front leg,
we make a steady step forward with the rear. The
foot leaves the tape with the fingers, we step on
the whole foot, and the center of gravity of the
body rests on both feet. The body is upright all
the time while the arms are in a slightly bent
position. The joints of the feet, the knee and
hip joint are slightly bent.
Exercises:
• Get on the line.
• Stand on the line on one leg.
• Stand on the line on the other leg.
• Stand on the strap on both legs,
one leg should be behind the oth-
er, then replace the legs.
• Stand on both legs to swing the tape
in the direction up - down.
• Stand on both feet to carry the center
of gravity from one leg to the other.
• Stand on the line on one leg; touch the
line with the other foot first in front
of the holding led then behind it.
• Take a short step forward.
• Take a short step backward.
• Stand on the line with your eyes closed.
• Stand on the line with your
hands on your body.
• Take a few steps forward.
• Take a few steps backwards.
• Step on the line side laterally (the shoul-
ders parallel to the tape) with both legs on.
• Try to make a turn on the tape.
Reference
Nahtigal, A. (2012), Učenje hoje po najlonskem traku,
Diplomska naloga, Univerza v Ljubljani, Fakulteta za šport,
Specialna športna vzgoja, Gorništvo z dejavnostmi v naravi,
Ljubljana

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 147146
6.5.CrOssBOCCIa
AUTHOR: RAÚL CANDIDO
Keywords: Cross Boccia as a trendy sport; physical adapted activity; sport for all.
We are in an age where the participation of
communities is of the utmost importance for the
societies. Sport is a factor that ensures equi-
table conditions and has been one of the stron-
gest tools for people with disabilities to take
an active role by creating close links in their
communities.
The sports phenomenon, when valued by a signif-
icant number of people, allows minorities, in
this case people with disabilities, a kind of
affirmation that will pose new challenges, which
will tend to find new answers in search of an
increasingly inclusive participation. Cross Boc-
cia, as a group game, can be a friendly instru-
ment for socialization, establishing group and
family ties, which can help draw attention to
physical, psychological or group culture bar-
riers, which at first sight are not visible, or
when they exist seem insurmountable.
Some dilemmas put on people with disabilities,
such as those that follow, may seem outdated,
but in unfortunately, they are not.
Because I use a wheelchair I can´t play, or
cannot throw the balls with enough strength for
more distance I can never play Cross Boccia.
Because I have visual difficulties I do not
know my street, my neighborhood, I cannot have
friends to play Cross Boccia.
Because I do not understand all the Cross Boc-
cia rules, or I find it difficult to learn some
things on a daily basis, or do not have much
concentration, I will therefore be condemned to
being trapped in a life, like a force jacket,
that will not let me make friends and relate to
others, and enter the game.
As I do not hear, I cannot even speak, I am only
isolated in my corner, because sports are not
for me, because most people do not understand
me.
In a time of such sophisticated conquests these
questions are still of the daily life of those
who have some kind of disability. It is true
that adapted sport has grown in implementation
in several countries and the number of informal
or federated practitioners has increased, but it
is not enough and we must continue to affirm the
need for regular sports to maintain the neces-
sary stabilization and progression of physical
adapted activity and sport for all.
The Cross Boccia is a trend sport that takes ad-
vantage of the basics of traditional boccia and
boules, but adds some aspects to it. The Cross
Boccia, also called soft boccia, is therefore
an additional development of boccia sport and
therefore equates to sports formats like BMX,
snowboard, parkour or headis, known as radical
sports, which also expanded the game principles
to create a new sport.
The fact is that Cross Boccia can be played ev-
erywhere, especially in the aspects of freedom,
spontaneity and creativity. In February 2010,
the sport was for the first time in the largest
global start-up competition, “Brand New Award”,
in the international recognition of the brand.
Cross Boccia is the new freedom. With the
free-style variant of the well-known boccia or
boules, you make the world the playing field.
With the flexible balls, you can now, for exam-
ple, play on the stairs, in the teams or on the
10th floor of the yard. Your creativity knows no
bounds!
The idea of playing Cross Boccia also “crossed”,
that is, in three-dimensional space, is much
longer than the term boccia in street itself.
For example, the use of plastic balls has been
used to bring more movement into the game. The
problem, however, was that the balls jumped and
the control needed to play the game was no lon-
ger guaranteed.
The Cross Boccia as another sport that can be
practiced outdoors by everyone, so the inclusive
aspect of the game is very important. People
with any type of disability can play it, and it
is advisable that this participation has the
greatest possible autonomy for the practitioner,
attending naturally to the minimum safety mea-
sures for their practice, in the chosen space.
Just like a game that is fashionable, we set out
to further develop this opportunity for inclu-
sive sports practice. It provides group inter-
vention strategies, space and time structuring,
strategic reasoning, movement skills develop-
ment, body notion, abstract thinking and group
notions. GET THE FUNSPORT!
6.5.1. Rules of CROSS BOCCIA
Overall characterization:
The game consists of sets of three (3) balls of
the same color / designs / patterns and a main
ball, the target ball, which is smaller and
different from all the others. It can be prac-
ticed by players individually or in teams with
three (3) players. In this variant there must be
two sets of three (3) equal balls per team and
each player has two balls at his disposal. It
is played on any terrain, indoors or outdoors,
without space limitations.
Goal:
The objective of the game is to reach / stay in
contact with the target ball or place the balls
as close as possible to to target closer to the
opponent’s balls and thus score points.
Development of the game:
Each player, in the individual variant, has
three (3) equal balls (colors / drawings /
patterns) to play; in games between teams,
each player only has two (2) balls. A player /
team is drawn or selected to start the game by
throwing the target ball from a starting point
he chooses. All other players also have to play
from this same location. The target ball can be
played anywhere; there is no special or delim-
ited play area. The player who threw the target
ball must start the game by throwing his first
ball. All other players then play their first
ball as well. The player having the ball far-
thest from the target ball must play the second
ball and, if not closer to the target ball, the
third ball. All other players also have to play
their second and third game balls, according to
the distance to the target ball. When all the
balls are played, the points must be counted.
The player who won the game begins the next game
by throwing the target ball to a place he choos-
es. If in a game set two or more players are
tied in number of points, the player who won the
previous game starts to throw in the next game.
Points:
Each game ball that is closer to the target than
any opponent’s ball counts a point. If in any of
the two or more opponents’ throws, the balls are
the same distance to the target ball, then each
game ball scores with one point each. If a ball
falls on an opponent’s ball and overlaps it,
this is called “KO / kill” and the opponent’s
ball is not counted. The game ends as soon as a
player or team reaches 13 points, but there has
to be a two-point advantage, for example, 13-11,
12-14, 15-13, etc.
Note: in these rules, the player who throws the
target ball first and then the first ball of the
game did not take it into account, that the op-
posing player had to reproduce the same type of
gesture, and other conditions determined.
Examples: the ball must be thrown between the
legs, the ball has to make two tables on the
walls, before going to the target ball, we have
to throw on our back, we have to throw with the
left hand, etc…
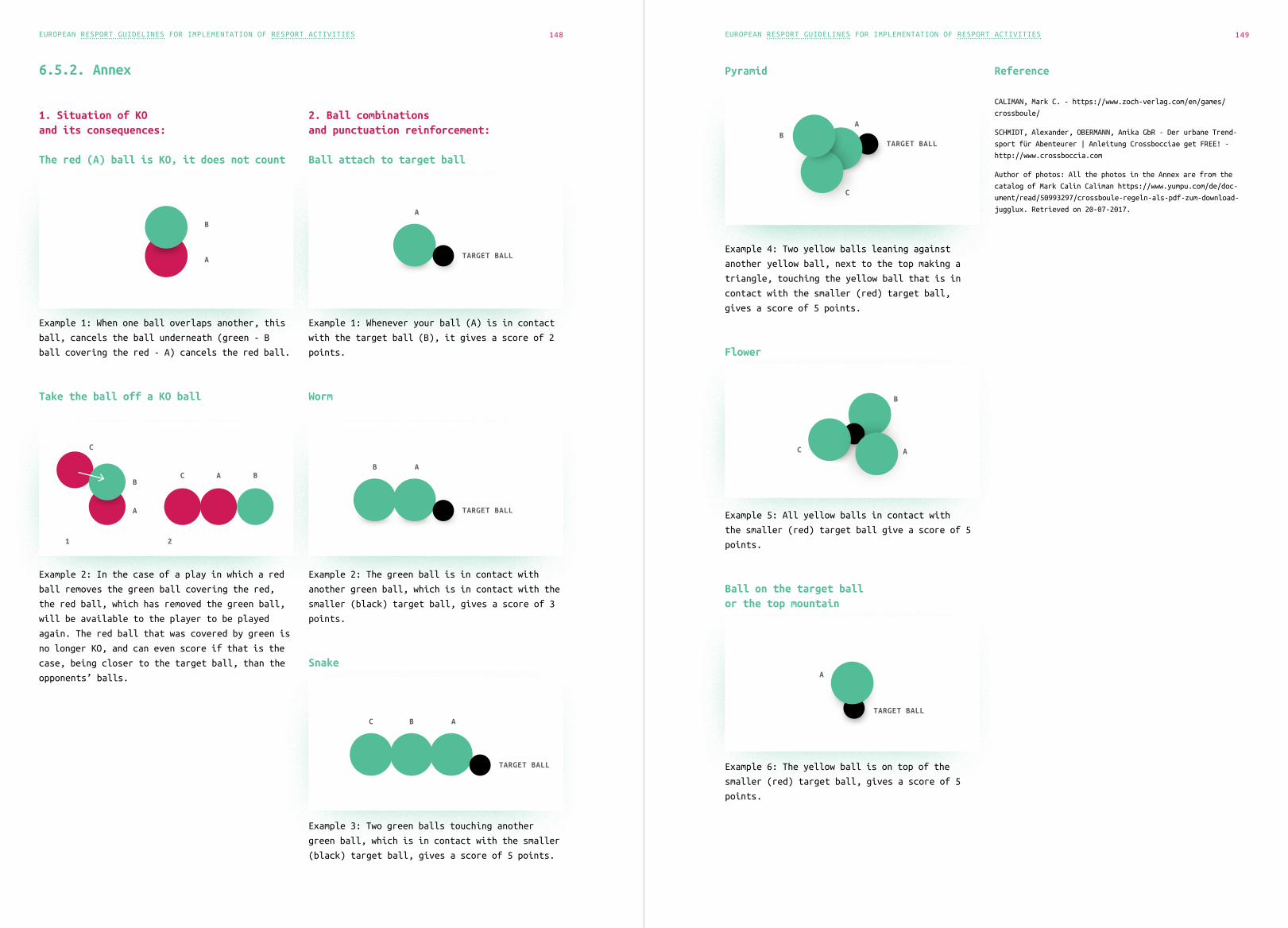
EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 149148
6.5.2. Annex
1. Situation of KO and its consequences:
The red (A) ball is KO, it does not count
Example 1: When one ball overlaps another, this
ball, cancels the ball underneath (green - B
ball covering the red - A) cancels the red ball.
Take the ball off a KO ball
Example 2: In the case of a play in which a red
ball removes the green ball covering the red,
the red ball, which has removed the green ball,
will be available to the player to be played
again. The red ball that was covered by green is
no longer KO, and can even score if that is the
case, being closer to the target ball, than the
opponents’ balls.
2. Ball combinations and punctuation reinforcement:
Ball attach to target ball
Example 1: Whenever your ball (A) is in contact
with the target ball (B), it gives a score of 2
points.
Worm
Example 2: The green ball is in contact with
another green ball, which is in contact with the
smaller (black) target ball, gives a score of 3
points.
Snake
Example 3: Two green balls touching another
green ball, which is in contact with the smaller
(black) target ball, gives a score of 5 points.
A
TARGET BALL
A
TARGET BALL
B
A
TARGET BALL
BC
A
B
Pyramid
Example 4: Two yellow balls leaning against
another yellow ball, next to the top making a
triangle, touching the yellow ball that is in
contact with the smaller (red) target ball,
gives a score of 5 points.
Flower
Example 5: All yellow balls in contact with
the smaller (red) target ball give a score of 5
points.
Ball on the target ball or the top mountain
Example 6: The yellow ball is on top of the
smaller (red) target ball, gives a score of 5
points.
Reference
CALIMAN, Mark C. - https://www.zoch-verlag.com/en/games/
crossboule/
SCHMIDT, Alexander, OBERMANN, Anika GbR - Der urbane Trend-
sport für Abenteurer | Anleitung Crossboccia® get FREE! -
http://www.crossboccia.com
Author of photos: All the photos in the Annex are from the
catalog of Mark Calin Caliman https://www.yumpu.com/de/doc-
ument/read/50993297/crossboule-regeln-als-pdf-zum-download-
jugglux. Retrieved on 20-07-2017.
A
TARGET BALLB
C
A
TARGET BALL
A
B
CC
B
A
C A B
1 2

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 151150
6.6.SkIINg
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: skiing, balance, safety measures, outdoor sports activities
Alpine skiing is one of the most popular winter
sports. It is accessible to a wider audience of
people who poses the appropriate mobility skills
and ski equipment. Alpine skiing is sliding on
the snow, with ski on your feet. Usually, the
skier also has sticks in his/her hands. Anyone
who likes winter sports and is not afraid of
cold can do skiing. Alpine skiing means white
slopes, low temperatures and great pleasure.
6.6.1. Who is the program
appropriate for and why we are
skiing in Center Naprej?
Alpine skiing is one of the important programs
we have included in our sports rehabilitation
programs, which we use for training and testing
the balance of users. It is a comprehensive and
very demanding activity with a high level of
risk for our users. As part of the risk assess-
ment, we identified weak balance as a major risk
factor in the rehabilitation skiing program
that causes a high level of risk of a fall and,
consequently, a risk of a new brain injury or
a bone fracture. Activity, focusing on bal-
ance training presents great importance for all
day-to-day activities, including self-care and
walking.
The Alpine skiing program is intended for skiers
with disabilities with acquired brain injury,
who have at least basic ski knowledge that they
had acquired before the brain injury. Skiing
belongs to a very complex physical activity,
and it would be very difficult and risky to learn
after such heavy injuries suffered by our us-
ers. Learning is one of the most complex higher
mental processes that the brain performs, and
any disturbance or damage to the brain causes a
change in this process.
In Center Naprej, we started skiing with us-
ers who had already skied before the injury
and wanted to reacquire and improve their ski
skills. Skiing is a great challenge for us,
because besides pleasure it also has a certain
risk.
Photo: Center Naprej, Weinebenne 2017
6.6.2. Some tips and instructions
for alpine skiing with our users
or persons with disability
In order to be able to perform alpine skiing,
the skier must have:
• good preparation and physical fitness (aer-
obically sufficient muscular strength
and an aerobic ability, especially mus-
cles of the legs, abdomen and back),
• ability to maintain balance.
The ski training consists of two parts:
1. physical preparation for ski-
ing and fitness training,
2. ski training, skiing and racing.
At the same time, all the above conditions are
necessary to be integrated for a harmonised
programme. Only then a specific movement, such as
skiing, would be harmonized - thus recognized as
good or successful. This can be achieved through
a well-planned ski preparation program and care-
ful implementation of this. Only in this way,
we can expect a successful snow movement, which
will be pleasant and safe for the user. Without
good preparation, skiing will not be successful.
It includes fitness training, skiing “gymnastics”
and maintenance of the motor fitness throughout
the year. We also help with the ProSki simulator
training.
Each disabled skier has his companion. For bet-
ter orientation and improved visibility on the
track, we use visual support and signs. Proper
preparation and adequate knowledge of skiing of
the companion and good competence for working
with people with disability are important. In
order to work with our users, knowledge of the
field of work and rehabilitation of persons with
acquired brain injury (limitations, specifici-
ties, rules) is required.
Skiing with users is usually individual or
maximum in pairs - up to 2 users per trainer.
Particular emphasis is placed on the safety of
users, so it is extremely important that we pre-
pare a risk assessment for the location and all
skiers before the skiing starts.
6.6.3. Special features for
skiing with persons with
acquired brain injury
In the case of skiers - persons with acquired
brain injury - we must pay attention to the
following:
1. choose appropriate ski slopes and ski trails
according to the individual’s capabilities
(physical and cognitive) and knowledge;
2. the load during exercise should not ex-
ceed the individual’s ability,
3. users must be appropriately dressed,
Photo: Center Naprej, 2017

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 153152
so that they can move properly, that
they are not cold or hot and that this
does not hinder their activity;
4. due to cold, we must pay atten-
tion to the skin care and the prob-
lem of thermoregulation;
5. brain injury can damage the centre of bal-
ance, which affects the balance of the
individual. In case of weak balance, the
risk of a fall and new brain damage or
bone fracture is very high. Therefore it
is important to make an appropriate risk
assessment and prepare actions to cope
with these problems before skiing.
6. We need to be alert to the visibility an-
gle of persons with neglect (where part of
the visual field fail) and to take appro-
priate safety measures at the ski track.
7. We must take into account and anticipate
users’ needs and physical comfort. Users
can become agitated and restless when they
are tired, hungry or feel pain, often fail-
ing to recognize latter. We must determine
the breaks during the activity and the
length of skiing individually, depending on
fatigue, attention deficit and other abil-
ities. Fatigue consequently affects both
physical and cognitive ability, and in-
creases the risk of injury and accidents.
8. When preparing for skiing with users, it is
important that we form realistic expecta-
tions setting goals that users can achieve.
9. Avoid excessive stimulation in the ski
track. We give short, clear instructions.
10. We use learning by model: we teach our
users giving example and thus provide
them with adequate patterns of behaviour
and consistency in various (burdensome)
situations. Demonstration: Sometimes
it takes several demonstrations to un-
derstand; let the person do the exer-
cise; repeat the necessary steps, etc.
11. Users need a lot of directions, di-
rectives and guidance. The least em-
phasis should be on errors. We focus
on encouraging achieving success.
12. The skiing needs to be planned well, because
ABI users can have problems with the sim-
plest tasks due to problems with executive
functions and motivation, rather than as-
suming that he/she does not want to do this.
The fact is that the affected part of the
brain may disable initiating, motivation and
planning capability. It is sometimes very
difficult to distinguish between these dis-
turbances and non-cooperation on purpose.
13. Skiing should be a fun and pleasant activity.
Photo: Jasna Vešligaj Damiš, 2018, Weinebene
6.6.4. Advantages, positive
effects and goals of the program
Exercise has many positive effects on the human
organism including a number of disease preven-
tion effects. The most important thing is that
activities are carried out in nature in the
winter, in the fresh air.
The main goals of the program are to improve or
maintain physical fitness, to improve and promote
a healthy lifestyle, to develop an appropriate
attitude towards nature, to use its properties
for a healthy lifestyle, to promote positive
self-image and personal satisfaction in life, to
increase the self-confidence in performing tasks,
acquire knowledge and skills.
Some of the health and psychosocial benefits that
skiing brings to our users:
• improves general fitness be-
cause the whole body works,
• improves flexibility of joints, mobility,
• has a positive impact on raising gen-
eral motivation due to activation and
achievement of success in sports,
• strengthens the abdominal muscles,
• improves functioning of the car-
diovascular system,
• positively affects cardiorespiratory
health and increase aerobic capacity,
• increases anaerobic abilities - muscle
strength of the legs, back and abdomen,
• improves balance and coordination - coordi-
nates the movement of all large muscle groups,
• outdoor skiing in nature im-
proves stress management,
• enables learning, renewal and main-
tenance of ski skills,
• allows you to compete and entertain,
• provides training in social skills
and group activities,
• provides training for receiving and performing
instructions and executing functions training,
• provides memory and communication training.
For our users, it is a unique effort to try to
stay upright while skiing. They must work with
the abdominal muscles to remain balance, with
those abdominal muscles located deeper and begin
on each side of the spine, swirl around the body
and end up in the pelvis. These are the key ab-
dominal muscles that shortened act as a “corset”
and squeezing the lower abdomen. Other abdomi-
nal muscles also strengthen and stabilize the
spine, so it does not bend when leaning forward
or falling. Improving the strength of the abdom-
inal muscles helps them to improve balance and
coordination.
Half an hour of skiing without breaks is a
good exercise for the cardiovascular system,
no matter how you ski, that means an increased
heartbeat, increased blood circulation, and more
intense nutrients and oxygen flow through the
body, extra substances discharged. At the same
time, more calories are burnt when skiing, mus-
cles are prepared for more oxygen and blood, the
capillaries are more loaded and the muscles are
able to stretch. Skiing strengthens the entire
body and is good for all the main muscle groups.
The inner and outer muscles of the thigh, mus-
cles bending knees, the muscles of the buttocks
are most affected.
Skiing is also good for managing body weight.
The steeper the terrain is, the more calories
you burn. Greater inclination of the ski slope
requires investing more efforts to balance and
using more energy. The reason for losing weight
is also the low temperature in the environment,
if it is below zero body causes body tempera-
ture to rise and you spend more calories. All
this also applies to our users, although we do
not ski with them on very steep and demanding
ski slopes, but carefully choose the difficul-
ty of the route according to their skills and
knowledge.
6.6.5. Skiing equipment
Technical equipment
• alpine skis, which must be properly pre-
pared and ready for snow with bindings,
• ski poles.
For seated skiing, we use: “biski, monoski,
kartski, tandemski” and stabilizers with skis
(instead of sticks) - which we have not prac-
ticed so far in our centre, because there have
not been similar needs or opportunities.
Personal equipment
• personal clothing: jacket and ski pants
Jacket should be warm, waterproof. The ski pants
must be extremely warm so people do not get cold
in the legs.
• mandatory helmet
The helmet must allow the user comfort from the
inside, especially in the area of the ears, and
at the same time strength from the outside to
protect the head from possible hits. Also im-
portant is the locking system of the helmet,
which keeps the helmet stable in case of fall.
• ski gloves
Ski gloves must be warm and at the same time

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 155154
provide good grip on the stabilizer. For people
with impaired motoric hand functions, they use
gloves for one finger, due to the difficulty in
using gloves.
• ski shoes
Ski boots, like other equipment, must keep feet
warm but at the same time they must have appro-
priate hardness and not be too demanding.
• a reflective jacket
The reflective jacket is highly recommended,
especially in ski resorts where there are more
people, as the skier and skier’s reactions are
longer than in individual skiing. With this, we
remind other skiers to pay more attention to us
at the ski resort.
• ski goggles or sunglasses
They are recommended mainly due to the reflec-
tion of light from the snow cover. They are also
important in case of bad weather and fog.
Personal equipment of the trainer / assistant
• alpine skis
Usually we recommend shorter skis (slalom), for
easier handling and medium hardness. Assistants
must have skis light enough to make them swiv-
el, and at the same time must be able to manage
themselves and the skier.
• ski shoes
They are usually softer, because preparation and
heating require a lot of work without skis for
the trainer, walking in ski shoes, opening and
closing the skis, track assistance, etc.
• personal clothing and helmet
The gloves should be thin but warm, with good
grip, so that they are not a hinder.
Accessories for making ski-ing more appealing
• cones,
• flags,
• flex poles, etc.
Reference
Alpsko smučanje za osebe s pridobljeno možgansko poškodbo
v Centru Naprej. Interno gradivo Centra Naprej. Maribor,
oktober 2014.
6.7.F•O•OTgoLF
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: footgolf, footgolf rules, outdoor sports activities
6.7.1. What is footgolf and
for whom is it appropriate?
Footgolf is a sport where we replace the golf
ball with a soccer ball. It is played by golf
rules. This represents a unique and fun sport
that combines the passion of football and the
precision of golf and is a unique opportunity
to socialize in a slightly different way. It’s
an easy and fun sport for everyone who is able
to kick the ball. According to the tactics, the
footgolf is similar to playing golf, but the
players kick the ball with their leg. It can be
played as a group activity or individually. The
advantage of this fairly new sport is in its
simplicity. After acquiring basic knowledge of
the rules and the good manners on the footgolf
course, we can very quickly start enjoying the
game. It is suitable for individuals from all
generations.
Footgolf offers us:
• a pleasant environment and the possibili-
ty of socializing over fun activities,
• a competitive spirit in a green environment,
and in the winter time on a snowy slope,
• interesting recreation and intense play,
• a football spirit on the golf course
for an unforgettable entertainment,
• relaxation from everyday worries.
The classic footgolf course has 18 holes, which
can also be scribbled. There is a flag on each
hole. The size of the holes must be adapted to
the size of the ball. Each player has his own
ball. Footgolf can be played individually or in
small groups. The group consists of a maximum
of 4 players who count the number of theirs and
others hits. During the entire game, the player
can use 72 shots. If a player moves his own ball
while searching or preparing for a shot, he gets
a penalty spot. During the game, it is necessary
to wait until the ball stops completely be-
fore the player kicks it. The footgolf match is
shorter than the match of golf, and it usually
lasts for more than two hours.
6.7.2. Why are we playing
footgolf with the users
of Center Naprej?
People with acquired brain injury (ABI) suf-
fer from serious consequences that permanently
affect their daily functioning and their sur-
roundings. Although the person with ABI can ex-
perience various chronic physical disabilities,
it is generally the cognitive, emotional and be-
havioural disorders that restrict the individual
the most resulting in many problems in interper-
sonal relationships, creating and maintaining a
social network, integrating into daily leisure
activities, sports activities and employment.
These disorders most often change lives of indi-
viduals completely, affect their family life and
their integration into the community.
In Center Naprej, therefore, we are constantly
looking for new ways to encourage users to join

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 157156
activities that would be fun on the one hand,
and on the other hand have rehabilitation ef-
fects in order to manage more effectively their
limitation. At the same time, we want to encour-
age them to improve their strong areas.
That’s exactly why we started with this com-
pletely new for us sport, footgolf, that com-
bines fun and recreation. It is an activity
where users can relax, have fun, and at the same
time have to follow certain rules, improve their
physical as well as mental abilities, and learn
to improve their tolerance levels. Users have
learned how to play footgolf very quickly, they
enjoyed playing and had fun.
6.7.3. Some tips and instructions
for playing footgolf with our
users or people with disabilities
When we started playing footgolf with our users,
we did not have the right course available. We
made the course on a grass surface, and in the
winter on a snowy terrain, where we marked the
course and made large enough holes in the snow
for the balls to fit in. The holes were marked
with flags or cones, in order to be well visible
to users with vision disturbances.
We took care of appropriate clothing and foot-
wear depending on the weather. In the winter,
we were dressed in comfortable warm clothes and
suitable hiking boots, and in warmer months more
loose clothing (T-shirt, shorts). Appropriate
footwear is important.
In case you play footgolf outside of the official
course (if you do not have a footgolf course
nearby), be careful where making holes and ar-
ranging the terrain so that it is properly pre-
pared (remove branches, obstacles, litter etc.).
The rules of footgolf have to be well presented
to the users (counting shots, penalty points,
when the ball can be hit) so that there will be
no complications.
6.7.4. Advantages and positive
effects of playing footgolf
1. improving fitness
2. improving balance,
3. learn to transfer and take weight to
the weaker (affected) side and ac-
tivate that part of the body
Photo: Center Naprej, 2018
4. improvement of visual - motor coordination
5. improving the functional body position
6. activation of proprioception
7. activation of several muscle groups
8. socializing while having fun in the nature
9. encouraging a competitive spirit
10. relaxation in the nature and
in pleasant company
11. training precision, patience, memory, pos-
itive behavioural patterns and clothing
12. training acceptance and implementa-
tion of precise instructions.
6.7.5. Necessary equipment
for footgolf
The mandatory equipment of the player includes:
• appropriate clothing and footwear (rec-
ommendations: shirt with a collar or
polo shirt, short trousers to the knees,
suitable footwear as indoor soccer
shoes or shoes for artificial grass)
• ball.
If you do not play footgolf on a footgolf
course, you can prepare it on your own because
there is no footgolf without a course!
Reference
http://www.footgolf.si/footgolf-pravila/, retrieved on
18.10.2018
https://en.wikipedia.org/wiki/Footgolf, retrieved on
18.10.2018
https://www.golftrnovo.si/kaj-ponujamo/footgolf, retrieved on
18.10.2018

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 159158
6.8.SnowShOEiNg
AUTHOR: JASNA VEŠLIGAJ DAMIŠ
Key words: showshoeing, safety measures, outdoor sports activities
6.8.1. Snowshoeing – lost in the
beauty of the white wilderness
There is nothing more beautiful than spending
an active sunny winter day in nature. Take the
snowshoes and go on a hike. Snowshoeing can be a
particularly magical experience: walking through
the white winter landscape, spending the day in
the nature, filling your lungs with fresh win-
ter air, and at the same time doing some good
exercise.
Considering this, it is necessary also to pro-
vide good protection for the face against sun
rays, since the sun is reflected from the snow
cover and therefore is even more intense. It is
also advisable to wear a hat and gloves, because
regardless of how sunny and warm the day is in
the snow your body begin to cool down.
6.8.2. What is snowshoeing?
Snowshoeing is walking on snow-covered surface
with snowshoes, attached to winter hiking boots.
Snowshoes, due to their shape and surface, pre-
vent you from sinking in the snow, thus enabling
walking safely on it. Snowshoeing is an ancient
way of walking in the snowy landscape, as snow-
shoes were used by our ancestors when hunting.
Snowshoeing is very similar to walking or run-
ning, but doing it in the snow - where you can
enjoy the wonderful winter day. In this form of
recreation, everyone can experience something
nice, because it is an undemanding, interesting
form of movement that can be learned by everyone
with a little exercise. Above all, it is import-
ant that, when walking with snowshoes, you move
as naturally as possible, and enjoy it.
6.8.3. How it looks?
Snowshoeing is, in fact, walking in the snow,
with specially adapted footwear, which has a
large surface area, so during the walk, the foot
does not sink into the snow. It is also possible
to walk across very deep and soft snow cover-
ings with snowshoes - in the snowy provinces of
Canada and Alaska, this was once the main way to
go from place to place. Snowshoes were also used
in Scandinavian and some Asian countries. Today,
snowshoeing is especially popular as a form of
recreation. We activate the whole body during
the activity, so this excellent winter exercise
ensures higher heart rate and intense muscle
strengthening. And the most beautiful thing is
that at the same time, you can enjoy the view of
snow-covered nature around you.
6.8.4. What are snowshoes?
Snowshoes are a kind of footwear that we attach
to hiking shoes in order to make it easier to
walk on the snow. They work on the principle
of allocating an individual’s weight over the
entire surface of the snowshoes, which prevents
sinking in the snow. Therefore walking on the
snow is much easier and more energy saving and
it is also supported by functional ties and free
heel, which can be fixed if necessary. When snow-
shoeing, it is advisable to use walking poles
to improve the balance, while at the same time
doing exercise for the entire body.
6.8.5. Who is the program
intended for and why are we
snowshoeing in Center Naprej?
The program of snowshoeing is intended for users
of the Center Naprej - people with acquired
brain injury who can walk or move with the sup-
port of others or a crutch.
It is an easy and safe way of walking and run-
ning across the snowy surface. The technique of
walking or running is not demanding, which is
why users learn it very quickly. It is one of
the most popular winter activities, which pro-
vides excellent exercise for the cardiovascular
system; it is suitable for people with little
physical fitness, for the elderly and people
after injuries.
You can snowshoe by yourself or accompanied by
friends, you can discover the unknown landscape;
you can take part in guided hikes. In the Cen-
ter, we do it in small groups, organize a compe-
tition and have fun in the nature.
Snowshoeing is fun for people of all ages, even
for the youngest. Older users can also join
the hike, because they can learn the skills
relatively quickly, and at the same time, walk-
ing will not pose a dangerous burden on their
joints. We can snowshoe during the daytime, but
we can also go on night walks.
6.8.6. Some advice and
instructions or preparation
for safe snowshoeing
Although exercise at first glance may seem com-
pletely simple and undemanding, snowshoeing
can replace intense cardiovascular training by
activating most of the body’s muscles. However,
when snowshoeing with users (people with ABI),
you need to be particularly careful about the
following:
• Select a safe location and select the
difficulty of the route according to
the individual’s capabilities or lim-
itations (physical and cognitive).
• Choose a location and terrain that match-
es the competence of people with dis-
ability. The load during exercise should
not exceed the individual’s ability.
• Remove larger objects from the sur-
face for walking.
• Practice on trodden trails, such as cycling
trails or trail routes closed for traffic.
• Check the route before starting the activ-
ity. Avoid narrow paths dense with trees
and ice paths that allow high speeds.
• Check all equipment before ex-
ercise or competition.
• Check the first-aid kit and com-
plete it if needed.
• Assume emergency procedures (haz-
ards). Teach all participants how
to act in case of emergency.
• If necessary use helmets.
Photo: Center Naprej, 2018

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 161160
• Have mobile phones and drinks with you.
• Train and compete on windless terrain.
• Attach the snowshoes properly to the
feet and check the fasteners.
• The user must be adequately dressed so
that he7she does not overheat while walk-
ing and his/her clothes do not pre-
vent him/her performing the activity.
• Pay attention to skin care and the problem
of thermoregulation due to cold and freez-
ing in the snow or due to the strong sun.
• Because of the brain injury, the centre of
balance can be damaged, which affects the
balance of the individual. In case of a
poor balance, the risk of a fall, another
brain injury or bone fracture is high, so
it is important that we do an appropriate
risk assessment and prepare actions to cope
with these problems before snowshoeing.
6.8.7. Trainers / assistants
safety checks
The safety and well-being of people with ac-
quired brain injury are the most important.
Snowshoeing is not a dangerous sport, but it
includes speed and variety of conditions that
require caution. Accidents can happen. The main
task and responsibility of the trainer/coach
assistant is to reduce the chance of accidents
to a minimum.
What is necessary for suc-cessful snowshoeing:
• During exercise and competition, introduce
clear behavioural rules from the beginning.
• No one should hike alone.
• Encourage disabled athletes to wear ap-
propriate clothing and shoes.
• Pay attention to changes in weather.
• Ensure that disabled athletes per-
form appropriate stretching exercis-
es before and after the activity.
6.8.8. Dry training -
preparation of disabled
athletes for snowshoeing
In order to successfully carry out the activity,
it is necessary to:
• have good physical fitness (suffi-
cient aerobic muscular strength, an-
aerobic ability in particular muscles
of the legs, abdomen and back),
• be able to maintain balance.
Athletes should be prepared for snowshoeing
appropriately and in time – enable them to try
activities for improving their psychophysical
fitness. This can be achieved through a well-
planned fitness training program and its cautious
implementation. Only in this way can we expect
and provide a successful movement on the snow,
which will be pleasant and safe for the user
(person with disability).
Type of training:
1. exercise for training specific mus-
cle groups (lower limb muscles, ten-
dons in the knee, hip flexor and
quadriceps - four-head thigh muscles),
2. walking and / or running according to
the length of the snowshoe trail,
3. specific exercises in the phys-
iotherapy cabinet,
4. aerobic exercises and stretching.
Every person with disability, who does the
activity, has an assistant. In order for users
to orientate better and to increase visibility
on the track we use visual support and signs. We
provide users with individual guidance and help.
6.8.9. Positive effects
of snowshoeing and goals
of the program
Snowshoeing has many positive effects on the hu-
man body and at the same time health prevention
and effects. It is important that the activity
is carried out in nature breathing fresh air.
Although it is known that anyone who can walk
can snowshoe, this activity nevertheless re-
quires some skills, such as the basic elements
of this sport: hiking uphill, hiking downhill,
walking in an arc, so that no unnecessary prob-
lems and falls occur during a serious hike.
Snowshoeing is very similar to cross-country
skiing or Nordic walking, as it is highly in-
tense, but less burdensome to your joints than
many other winter activities.
Some of the benefits that snowshoeing brings to
our users (ABI people):
1. Improving fitness.
2. Improving balance and coordination.
3. Improving joint flexibility.
4. Social skills training and group activities.
5. Acceptance training and implementing in-
structions and executing functions.
6. Communication and memory training.
7. Competition and fun.
8. Physical activity in nature.
6.8.10. Necessary equipment
for snowshoeing
For this unique sport you need:
• a pair of snowshoes,
• waterproof hiking shoes,
• walk bars,
• appropriate suit for movement in win-
ter conditions, gloves and hat,
• a headlamp (in the case of night hiking),
• helmet (in the case of a user with
a weaker mobility or balance).
And of course, snowshoeing is not possible with-
out a large amount of snow.
Reference
Priročnik Krpljanje: Krpljanje, hoja in tek s krpljami, Spe-
cialna olimpiada Slovenije -SOS, http://www.specialna-olimpi-
ada.si/si/za-clanice/knjiznica/, Pridobljeno 17.9.2017

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 163162
6.9.NeTBaLL
AUTHORS: RAÚL CÂNDIDO, CARLOTA CUNHA
6.9.1. Rules of the game
Netball, mainly practised in England and the
United States of America, initially began to be
played by men and women. However this sport has
always been more popular among female players.
Today it is practised in some European countries
such as England, Holland and Germany, but mainly
in the United States of America and Australia,
but only in the female variant.
We do not know an inclusive version with the
adaptations for people with disabilities, a
solution that we will propose later after a sum-
mary characterization of the game in its formal
aspect.
Netball is a collective sport, consisting of
teams of seven elements, played in a sport pa-
vilion. The goal is to score in a basket; this
is achieved through passes between the players,
who occupy specific and pre-defined zones in the
field. It is in these areas that the players have
their action in the game. The objective of the
game is to score more points than the opposing
team, and the players who occupy the attack
zone, the semicircle or the launch area that is
closest to the basket, positions occupied by
the pivot and the attacker, can only score the
points.
In order for the positions of
each player to be perceptible
in the field, the shirts they
wear have the initials of the
positions they occupy on the
playing field.
WA - Wing Attack - Can move within the attacking
third and center third, with the exception of
the shooting circle – lateral forward;
GK - Goal Keeper - Can move anywhere within the
defensive third of the court, but cannot leave
it – goalkeeper;
GA - Goal Attack - Can move anywhere within the
attacking third and the center third of the
court – forward;
WD - Wing Defense - Can move within the center
third and the defensive third, with the excep-
tion of the shooting circle – lateral defense;
GS - Goal Shooter - Can move anywhere within the
attacking third of the court, but cannot leave
it – pivot;
C - Centre - Can move anywhere across the court,
apart from either of the shooting circles – mid-
dle field;
GD - Goal Defense - Can move anywhere within
the attacking third and the center third of the
court – defense. Only the ‘Goal Shooter’ and
‘Goal Attack’ of a team are allowed to score di-
rectly, and can only do so when they are in the
position’s goal circle.
The basket is similar to that of korfball, has
no table and is on a pole 3 meters from the
ground.
The ball used is specific to Netball.
The dimensions of the field are 35 meters length
by 20 meters wide, being divided by 3 zones,
defense, central and attack.
The players cannot dribble or run with the ball.
As already said, this is a positional game above
all, in which the passes are decisive, since
it is from these that the teams try to progress
WA
in the field, attack and score through basket,
avoiding the interception of the players of
the opposing team. The player who receives and
passes the ball shall, at least, always have one
foot in contact with the ground.
Each player must have the ball in his / her pos-
session for a maximum of 3 seconds, after which
he / she must have executed a pass or throw
into play zone. The player of the team that is
defending, that is that does not have the pos-
session of the ball, must maintain the distance
of about one meter of its opponent that has the
ball. Contact is not allowed in the game.
The infractions / fouls occurring when there is
contact between players, offside (player who
invades another position in the field, other than
their zone), or dribbling, give place to the
loss of ball, or placement of the missing player
in a position, behind the player who can receive
the ball.
The players of the two teams are distributed
in the field by doubles, in situation of oppo-
sition 1 to 1, according to the pre-determined
positions.
The winning team will be the one that scores the
most points. The game is played in four parts
of 15 minutes each, without stopping the game’s
timer.
6.9.2. Inclusive / adapted
netball proposal
Netball’s adaptation proposal for players with locomotor disabili-ties and other disabilities
We have tried to adapt this sport to an inclu-
sive version for athletes with locomotor and
other disabilities. The game is intended for
players who have locomotor disability, wheel-
chairs users or not, intellectual disabilities
and able-bodied, playing on the same team. We
used identical approach to the original game,
with some adaptations according to the athletes
and their functional capacity, mainly for loco-
motor disabilities.
Physical Rehabilitation Centers and other dis-
ability support institutions are target groups
which allows both disabled and non-disabled
players to interact, so that the physical ther-
apists, physicians, other staff at the Center
and the players’ families and friends can be
involved. Our formula that consists of the use
of this sport as rehabilitation, and can later
explored more formally, as a regular practice
variant, and that they can play it in full in-
clusion with other potential players. The game
is mixed can be played by athletes with and
without disabilities. They are eligible for the
game, players with locomotor disabilities, upper
and lower limbs, intellectually handicapped and
able-bodied players, making it an all-inclusive
sport.
DEFENSE/ATTACK ZONE CENTRAL ZONE ATTACK/DEFENSE ZONE
WD
WD
C
GK
GKWA
WA
C
GS
GSGA
GA
GD
GD

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 165164
In each team there must have, at least, two
players who use a wheelchair. In terms of ad-
aptation of the game, players who play in a
wheelchair can only be marked / striking by
opposing players who also has this device of
compensation. Wheelchair players will be allowed
to dribble (hit the ball on the ground) at least
once and move with the ball in the lap. The
type of wheelchairs can be sporty, like basket-
ball-style, or simple daily wheelchairs, while
not ideal, but make the practice possible and
more accessible with more rudimentary materials
and then less high equipment costs.
Adapted game
As players distributed by zones according to
rules of the regular Netball, this is a game
that privilege the ball pass, strategic place-
ment and field positions, marking the zone of the
opponent, for the conquest of the ball through
movements of defence and attack, with which it
is possible to get to score. The movements in
the wheelchair in the zone of action and the
accurate and speed in the pass, are fundamental
for the success in the game.
1. Game of 40 minutes with four
parts of 10 minutes.
2. The game starts in the center with
player C (center) passing the ball.
When you score a point the game re-
turns to the center of the field.
3. Wheelchair players can move with
the ball within their zone.
4. Wheelchair players can propel the chair with
the ball on your legs; you can only rotate
the chair with the ball on your legs.
5. There is no contact with oth-
er players or chair.
6. The chair of a defending play-
er must be away one meter from the
other player with the ball.
7. Player only being allowed 5 seconds with the
ball in the hands; if it exceeds 5 sec-
onds the ball is passed to the opponent.
8. Only GS and GA can score goals while
still within the throwing circle.
9. Penalties are scored when there is contact
with the player or wheelchair, or obstruc-
tion of the player who has the ball.
10. Remaining fouls, the ball passed
to the opposing team.
11. Only GS and GA can score every time
they are inside the throwing circle.
12. Each goal is worth one point
for the team that scores.
13. The height of the basket may be
3 or 2 meters off the floor.
Reference
Netball, http://www.educacaofisica.seed.pr.gov.br/modules/con-
teudo/conteudo.php?conteudo=212. Retrieved 12.2.2019.
6.10.SpORT OriENTATioN
AUTHOR: RAÚL CANDIDO
Keywords: A Sport for Intellectual Disability; Sport for all; Alternative communication.
6.10.1. Adapted Orienteering
– A sport for all
Adapted Orienteering (a variation of Sport
Orienteering) is a sport that, above all, pro-
motes a fruition of outdoor spaces, removing
people with intellectual disabilities, but also
children, young and old participants of a cer-
tain passivity, bringing them into contact with
nature, in an active and interplay with others
and with the environment in a playful way.
When we are sharing the activity with people
with intellectual disabilities, we must take
into account some strategies so that activity
can proceed without precariousness and keep the
participants interested and involved.
Is important:
• If possible, a previous approach
with educators or monitors to mea-
sure the types of needs of the group.
• If possible, request previously for
global group characterization.
• Participants with total need of sup-
port to do the activity;
• Partial need for support to do the activity;
• Almost independent to do the activity.
• Make prior recognition of the space when-
ever possible, while marking the course.
This may help to predict some less “friendly”
situations and create strategies for greater
and better involvement, but also the safety of
participants. Thus, aspects like the signaliza-
tion and the marking of the route can bring many
advantages.
6.10.2. Building the
circuit for the game:
Nature walks adapted for more participants
that are elderly, young children or people with
disabilities. It is a type of “vulnerable”
participants, with losses of balance, or high-
er levels of fatigue, intolerance to heat and
cold. It is necessary to avoid sharp gradients
in the terrain of the course; to prevent fatigue
that can compromise the success of the game,
with negative consequences for the rest of the
participants, as well as for the most vulnera-
ble participants. Concern about travel course
time and hydration should be quite compensated
factors.
In case of need, delimit the route / trail
for orientation reasons and safety of the
participants.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 167166
Simple elements and reference points should be
considered so that participants with more lim-
itations can be able to identify them. One of
the characteristics that present a significant
part of the participants with moderate or even
severe intellectual disability is related to the
decoding of the symbols. Thus, the greater the
possibility of association with known elements,
symbols and codes, the greater will be the ten-
dency towards a more autonomous exploration.
Seek to use simple messages in communication.
The instruction must be detailed, and must
tell what the activity consists of, such as the
course and the necessary safety measures.
You should be patient and make sure that the
participant understands and memorizes the in-
structions, as the attention and interest in the
instructions, is usually low. It is necessary
to use simple and pragmatic messages during
communication. There may need to receive re-
inforcement in the repetition of messages and
instructions.
Before the orienteering trail, a body warming
should be done, using music or dancing in a
combination of fitness. Through augmentative lan-
guage, schematics or three-dimensional models,
you can help to structure the adventure of what
will be found in the trail route, bringing to
the choreography elements of increased communi-
cation, with the symbols of the cards, maps and
the colours that will appear on the course.
The spots on the map of course must be easy to
relate to elements that the participants can
make simple association: ex. doghouse, water
well, flower beds, mill, lake, etc.
For this purpose, several strategies can be
used, such as:
• Words with rhyme; Sounds; Graphics; Move-
ments, facial and body expressions.
Endow the educators / monitors of groups with
extended versions of the elements of the game.
Such elements would be provided separately in
order that different puzzle sets can be made.
For example: color plates, symbols, and numbers,
like the Bliss symbols, which are shown on the
game cards.
A map in A3 format allows a short story to be
devised making use of the symbols and creating
associations for example the food chain. An area
with games that can help you relate to elements
and objects that you find along the trail will be
available.
Use exercises / games like: Stone, scissors,
paper; Boxes of different sizes for a color
puzzle.
Identification of groups: With t-shirts, vests,
badges, bracelets, etc. to ensure that the par-
ticipant does not get lost and is not endangered
by rough terrain which gives security to educa-
tors and monitors.
Adapted Orienteering is mainly a game that
should help to achieve situations of autonomy,
in terms of space and time for people with in-
tellectual disabilities. For example, for those
participants who do not know the letters and
numbers and even some colors, we can use tex-
tures so that they can make associations to the
images / pictograms in the cards and the plates
in order to achieve the combinations for the
answers.
6.10.3. Brief history and
basic rules of the sport
Orienteering is a competitive sport, practised
in many countries, particularly popular in
Northern Europe.
In Portugal, Mr. Joaquim Margarido, blogger,
photographer, a nurse practitioner, in the
Prelada Hospital, in the Oporto region, and pas-
sionate about nature and orienteering, has been
linked to this sport for several years, decided,
to make a variant in which all people with and
without disabilities of all ages could partici-
pate, he created Adapted Orienteering in 2014.
He created a simple scheme with the use of maps
of basic routes, with cards where basic colors,
red, green and blue are used, together with
effective language pictures or symbols invented
by Charles Bliss, so that people with more deep
disabilities, can use for a basic communication.
Based on his work, we create these guidelines,
which can help all to perceive this variant of
this sport and enjoy it as an activity practised
outdoors, in contact with nature.
Let us get started!
6.10.4. Activity development
and materials:
Adapted Orienteering is a game which runs along
a route drawn on a map. In the map are marked
spots / points, that we call beacons, that must
be found and visited in a sequential way; It
must start at the first point on the map and
finish at the last one that is proposed. When we
draw the map we can choose the number of points
that we will have on route and that are marked
on the map.
1. At the place of departure, which will also be
that of the arrival, the judges give each player
or team, a map and control card, with the number
of points that we must visit in our route, (fig-
ure 1). Each player or team will have a map with
different routes. Near the map, we have a card
drawn that has three colors and numbers that are
the various points / beacons, through which we
will have to go through, to do the course. Next
to the colors, there is an empty square, where
there should be a symbol / picture.
2. On the control card with symbols (figure 2),
that is given with the map to each player or
team, can also place your name/team name and
the hour and minutes of your departure. The
card will serve to mark the passage through the

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 169168
points indicated on the map, attesting that
you have found the various points noted on your
route map.
3. Each point on the map signalled with a bea-
con, which we see in the next image, will have a
check punch attached that will be used to per-
forate our control card in the square to confirm
completion of the points.
4. Each point on the course will be allocated
with one number, 4 stakes, 4 plates with the
colors, red, green or blue, which may be in
another order, and one of the symbols we have
already talked about.
5. Then we look at the plates, to choose the one
that has the right answer following the correct
sequence of colors plus the corresponding pic-
ture. Next we mark the picture on the control
card with check punch marking what we think is
right and move on to another point. If none of
the color matches the desired sequence, mark
square with X.
6. When we finish our course after visiting all
the points, we return to the starting point and
deliver our card with all answers perforated.
Judges of the game, who have a card with all the
correct answers, color sequence and pictures
will compare with yours and provide a score for
all correct answers.
7. If players or teams tie, in the number of
correct answers, the team who take the least
time to complete the entire course will win
overall.
Reference
Margarido, Joaquim in http://orientovar.blogspot.com/2012/10/
orientacao-adaptada-um-desporto-para.html Retrieved on
02-10-2018
Figures and photos from: Joaquim Margarido’s Blog
6.11.TABle TenNIs
AUTHOR: MICHELE LEPORI
Key words: Tennis table, Adapted sport activity, Equipments and rules
Introduction
Table tennis training can be very flexible and
can satisfy a wide range of needs. Adding a
warm-up and improvement of resistance skills,
in addition to training specific skills, can
give life to a complete routine that improves
balance, coordination, mobility and muscle
strength. Speaking of activities for rehabili-
tation purposes they do not necessarily require
expensive materials and, with simple precau-
tions, you can adapt the workouts to your needs.
Orienteering is a very common sport in Europe
and is increasingly gaining ground.
6.11.1. Table tennis
- Who is it for?
Table tennis is a sport that lends itself to
many types of disability, both physical and
intellectual relational. For physical disability
there are specific measures and regulations, de-
veloped by the high level activity, which cover
practically the whole range of possibilities.
Even for the most serious cases it is possible
to find ad hoc solutions.
The most difficult case is for people with visual
impairments. These limit the ability to see the
ball, already small in itself, to make it impos-
sible in the event of complete blindness. For
this type of disability we advise against table
tennis.
6.11.2. Why Table Tennis?
Table tennis can be interesting for a number of
factors. Like all sports, it brings benefits to
the physical condition that has already been
stated in these guidelines. Specifically, it is
very challenging in the eye-hand coordination
skills and in the ability to perceive one’s own
spatiality, that is, to manage one’s movements
coherently with the environment around us.
However, the greatest benefits are in terms of
integration. In many institutions, especially
for youth, you can find a table tennis table,
bats and balls. This gives the opportunity to
have the tools available to play, without having
to purchase expensive materials. In addition
you can play in the same places and schedules
of able-bodied boys, by reacquiring the dis-
abled boys their qualification of athletes in all
respects. Joint training and integrated activi-
ties between able-bodied and disabled people are
to be encouraged and can also be used to create
real tournaments (for example in double).
Accessibility of table tennis tables in common
areas will help to integrate the boys socially.
They will be able to practice table tennis even
outside of training facilities, public gathering
centres, parks...
6.11.3. How to adapt the activity
The table tennis practice does not discrimi-
nate against age and gender. Indeed, it is easy

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 171170
even in high-level federal tournaments, to find
athletes of very different ages in the same
category.
For wheelchair athletes (category 1-5 according
to the criteria of the international federa-
tion - ITTF site citation) or with other types
of motor disabilities (6-10) there are minor
regulatory adaptations, which do not specifically
affect our rehabilitation activities.
Obviously athletes with amputations, paralysis
or similar to the upper limbs, have the possi-
bility to use special bats. They may use velcro
bands to secure the racket to the hand or to the
prosthesis.
For athletes with intellectual-relational
disabilities (class 11 according to ITTF clas-
sification) there are no particular general adap-
tations, we will proceed to train progressively,
reacting to the specific needs of children.
For all three groups, preparation is necessary
before moving on to the actual practice.
In the case where athletes have difficulty co-
ordinating and hitting the ball in flight, you
can proceed as follows. Mount the side barriers
to the table, lift the net, and use soft rub-
ber balls (of decreasing size depending on the
skills) with special bats (or even the hands).
In this case the ball will be slid on the sur-
face of the table, rather than bounced.
It is an exercise that can be quite challenging
for some types of disability (those with the
greatest impact on the abilities of the boys),
but also a good exercise of introduction to more
advanced training levels.
6.11.4. Equipment
To proceed with the activity of table tennis we
need: a table, a net, bats and balls.
TABLES: Approved tables can be costly and
heavy, but offer the possibility to train at
the highest level and to be able to organize
competitions approved in the future. From that
point of view all the intermediate solutions are
possible, with non-approved tables (lighter and
cheaper), up to adapt to alternative solutions
(see chapter nets).
NETS: There are different types and prices. Al-
most all of them consist of two clamps that hook
to the table and support the net. Those approved
by the international federation are of very
resistant material, they allow to control many
variables (height of the net, tension, length),
obviously they are more expensive and do not
always adapt to any type of table. Other cheaper
solutions are based on the same principle, vary-
ing only the reliability of the materials. They
are specifically created to adapt to any type of
table, even kitchen tables, desks etc.
BATS: the costs vary a lot. In this case, how-
ever, we suggest the economic solution. The
benefits of high-cost bats are not understood
by the athlete until he/she has developed some
experience. In addition to each frame and each
rubber correspond some specific characteris-
tics. These are used by coaches to support
the athlete’s type of game at a higher level.
Therefore, for the bats, you can easily use the
cheaper solution. Different specifications for
the various disabilities that affect the upper
limbs. Those who have difficulty in shaking a bat
can use special accessories (extended handles,
velcro strips...). These are solutions that must
be evaluated on a case-by-case basis, almost
tailor-made for each athlete. The general rule
is that adaptations do not interfere with the
part of the bat covered by rubber or increase
the surface.
BALLS: There are also different types and pric-
es. It makes no sense to start with the expen-
sive balls of competition grade (which could
become useful only after a certain technical
level acquired by the boys). The most economi-
cal solution is valid, especially taking into
account the fact that many will be broken during
training.
To decrease the breakage of many balls it is
useful to give only one / two to the table, or
have a supervisor to help you collect them.
Photos: Center Naprej, 2018

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 173172
6.12.CheeRLeadINg
AUTHORS: MICHELE LEPORI, ZVONKA NOVAK
Keywords: cheerleading, fun, balance, cooperation, support, affiliation.
Introduction
Cheerleading is a very common sport especially
in the United States. In Europe it is catching
on, thanks to a movement that is gaining more
and more competence and professionalism, coming
out of an initial phase of improvisation. The
goal of cheerleading is to combine choreography
composed of elements of gymnastics, dance and
acrobatics, to create routines. Cheerleading is
designed to encourage teams on the playing field
during matches. For this reason, an element of
excitment and encouragement to the public is
never missing in the choreography, to increase
its involvement during the performance.
6.12.1. Cheerleading - What is it?
Cheerleading is a routine of dance. This is a
group dance that includes cheering, aerobics,
gymnastics and more. It began to develop in the
19th century in the United States as a support-
ive activity in other sports (»rtv slo: otroški
portal - Navijanje«, 2019).
There are 2 types of cheerleading: the first is
competitive cheerleading, and the other is the
pom pom groups (Cheerleading, 2018).
It is common for both of them that their main
purpose is to enhance the sporting atmosphere
at competitions and to represent the society,
school or institution. Choreographies are made
up of dance steps performed with rhythmic music,
and is very cheerful, where the vocal power of
performers, their energetic and originality ap-
pear. Groups can make use of boards with signs,
coffees (pom poms), megaphones, flags and other.
Cheerleaders include choreographers with rather
difficult acrobatic elements (jumping, pyramid),
but choreographies of pom pom groups should not
contain acrobatic elements. Important part of
the choreography is the clothes that need to be
matched in color. In the pom pom dance groups,
the pom poms need to be matched in color also
(Zveza znps: Navijaške in plesne skupine, 2019).
6.12.2. Cheerleading
- Who is it for?
Cheerleading is very versatile and, working on
the complexity of the choreography, it is possi-
ble to adapt it to almost all types of disabili-
ty. For example, there are integrated teams with
physical and intellectual relational disabili-
ties, which perform with great ease.
Obviously the basic level will be composed
mainly by elements of dance, leaving the parts
of artistic gymnastics (flip, wheels...) or
acrobatic (jumps, stunt...) only to athletes
whose disabilities allow it. The element of
spectacularisation that cheerleading brings
with it should not be underestimated. It is not
by chance that the term “exhibition” is used.
The choreography is made to bring attention to
the guys who are doing it, to engage the public
on an extrovert and energizing way. That is an
aspect that could help young people to relate to
a more or less extensive public.
6.12.3. Why do it?
Energy, excitment, involvement. These are three
key words in cheerleading. This allows the wall
of pietism and sadness to be more effective-
ly eliminated, which too often accompanies the
activities of disabled children. Even public
accustomed to contact with the Paralympic ac-
tivity will be infected by the choreography, the
invitation to action and rhythmic music.
Furthermore, cheerleading is not just a compe-
tition sport. Born as a “sideline” activity,
that is to say the field of a sporting event, to
entertain the public and encourage it to cheer.
It’s a component that can still be exploited
today, leading the team to perform at large or
small events in the area and help promote and
raise awareness of the sport.
6.12.4. How to adapt the activity
The activity is adapted, as already underlined,
depends on the difficulty of the choreography.
The simplest elements are those of the dance
that should be well exploited with intelli-
gence. The routine must be simple enough for the
kids to perform but interesting enough for the
audience.
If for the users with relational intellectual
disability coordination, memory and spatiality
should be taken into account, for the Paralym-
pics users others factors must be taken into
account.
Artificial arts may not be a problem in the sim-
plest choreography, but they could become a risk
in the more complex ones, becoming blunt ob-
jects. Always pay close attention. Wheelchairs,
on the other hand, are not an insurmountable
obstacle. There are also many examples in the
dance world, from which it is possible to take a
cue.
When athletes have more physical possibilities,
they can include elements of artistic gymnastics
or even acrobatics. Recall that these elements
should be well considered and evaluated on a
case-by-case basis. In addition, you should
devote much effort and introduce them gradual-
ly, so as to make them as perfect as possible
(during the performance the emotion could play
tricks).
6.12.5. Equipment
Cheerleading, in its less demanding form, does
not require special equipment:
Clothing
The impact of a uniform is fundamental, at least
during performances. Various solutions are
possible. An equal suit for everyone is a good
starting point, up to the professional uniforms
(which require an important budget).
Pom poms
Old-fashioned in the collective imagination, they
are not absolutely necessary elements in sports
cheerleading. Also in this case there are cheaper
“training” versions up to the professional ones.
Audio system
The choreography is designed based on a musi-
cal composition. This must be played during the
tests. It will therefore be necessary to equip
oneself with a system to reproduce the chosen
track. This is what is needed to carry out a
very basic choreography, composed of elements of
pure dance. As training difficulties increase,
other equipment will also be needed. Mattress-
es and artistic stripes are essential to train
stunt and artistic gymnastics safely.
6.12.6. Example - cheerleading
in Center Naprej
In Center Naprej, we offered users the oppor-
tunity to join the pom pom dance group. We made
two groups of users who expressed their desire
to participate in the group. Different mov-
able structures, jumps, dance steps and spatial
changes affect the balance, coordination, flexi-
bility and memory of the involved users. Because
the activity is group-based and requires cooper-
ation and consistency, we also actively work on
social skills like cooperation, customization,
acceptance...
We adapt choreographies to the abilities and
limitations of the users involved (problems with
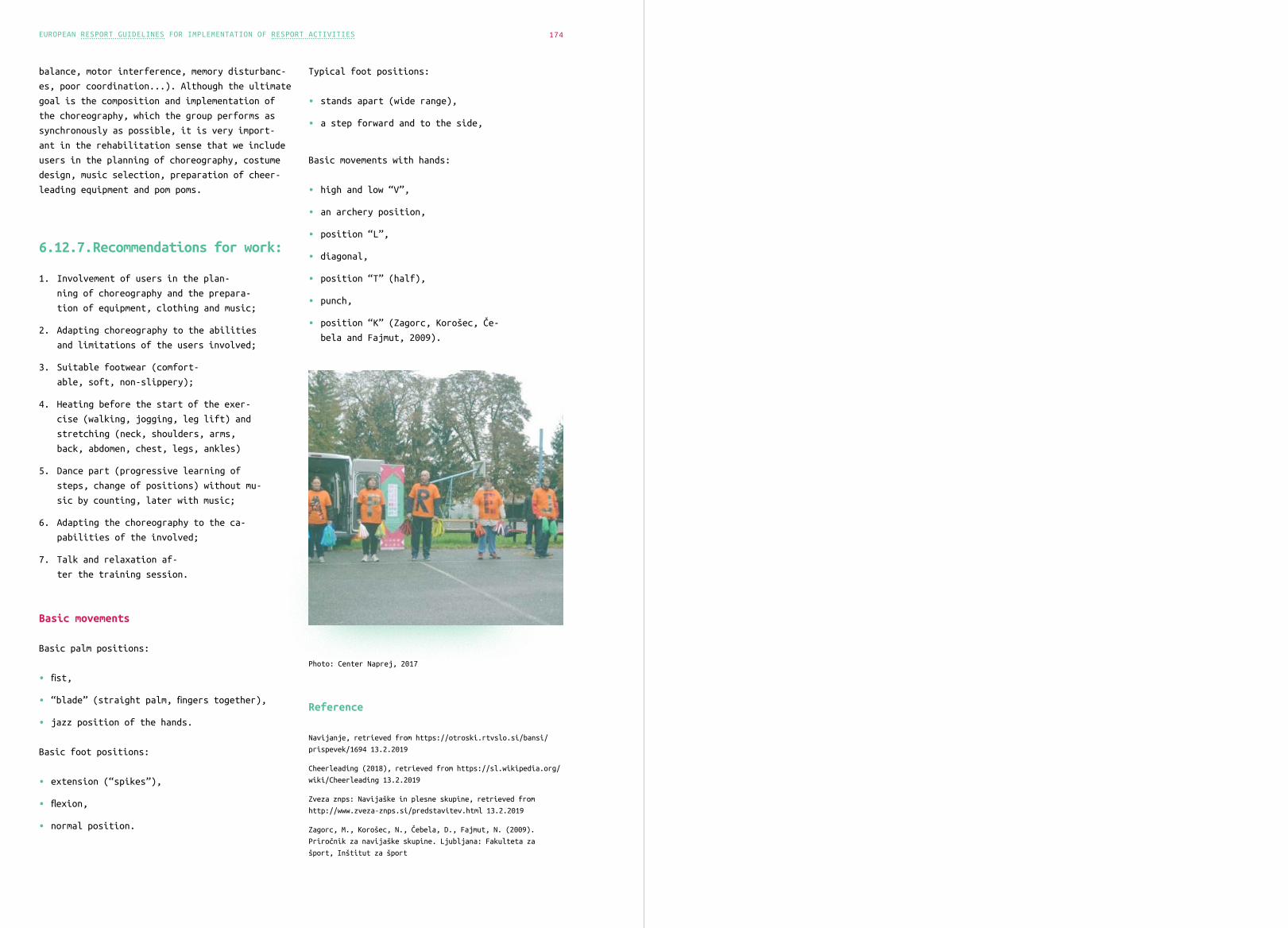
EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 174
balance, motor interference, memory disturbanc-
es, poor coordination...). Although the ultimate
goal is the composition and implementation of
the choreography, which the group performs as
synchronously as possible, it is very import-
ant in the rehabilitation sense that we include
users in the planning of choreography, costume
design, music selection, preparation of cheer-
leading equipment and pom poms.
6.12.7. Recommendations for work:
1. Involvement of users in the plan-
ning of choreography and the prepara-
tion of equipment, clothing and music;
2. Adapting choreography to the abilities
and limitations of the users involved;
3. Suitable footwear (comfort-
able, soft, non-slippery);
4. Heating before the start of the exer-
cise (walking, jogging, leg lift) and
stretching (neck, shoulders, arms,
back, abdomen, chest, legs, ankles)
5. Dance part (progressive learning of
steps, change of positions) without mu-
sic by counting, later with music;
6. Adapting the choreography to the ca-
pabilities of the involved;
7. Talk and relaxation af-
ter the training session.
Basic movements
Basic palm positions:
• fist,
• “blade” (straight palm, fingers together),
• jazz position of the hands.
Basic foot positions:
• extension (“spikes”),
• flexion,
• normal position.
Typical foot positions:
• stands apart (wide range),
• a step forward and to the side,
Basic movements with hands:
• high and low “V”,
• an archery position,
• position “L”,
• diagonal,
• position “T” (half),
• punch,
• position “K” (Zagorc, Korošec, Če-
bela and Fajmut, 2009).
Photo: Center Naprej, 2017
Reference
Navijanje, retrieved from https://otroski.rtvslo.si/bansi/
prispevek/1694 13.2.2019
Cheerleading (2018), retrieved from https://sl.wikipedia.org/
wiki/Cheerleading 13.2.2019
Zveza znps: Navijaške in plesne skupine, retrieved from
http://www.zveza-znps.si/predstavitev.html 13.2.2019
Zagorc, M., Korošec, N., Čebela, D., Fajmut, N. (2009).
Priročnik za navijaške skupine. Ljubljana: Fakulteta za
šport, Inštitut za šport

7.
Learning outcomes:
• An understanding of monitoring and evaluation.
• An understanding of why it is import-
ant to evaluate sports programmes.
• How to plan effective evalua-
tion of sports programmes.
• Examples of physical, psychological and so-
cial outcome measures used in evaluation.
EvalUa ti•On of Sp•Ort Pr•O GramMEs

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 179
7.1.ThE PUrpOse Of mOnitORIng anD evalUating sPOrTs ProgrammEs
AUTHOR: MICHAEL LAMONT
Key Words: monitoring, evaluation, outcome measures and tools
Introduction
What is monitoring and evaluation?
The online platform Sportanddev.org (2013)
defines monitoring as the systematic and routine
collection of information from projects and pro-
grammes for four main purposes:
• To learn from experiences to improve prac-
tices and activities in the future;
• To have internal and external ac-
countability of the resources used
and the results obtained;
• To take informed decisions on the fu-
ture of the programme;
• To promote empowerment of bene-
ficiaries of the programme.
Monitoring is defined as a periodically recurring
task which begins in the planning stage of a
programme. Monitoring allows results, processes
and experiences to be documented and used as a
basis to steer decision-making and learning pro-
cesses. Monitoring is checking progress against
plans. The data acquired through monitoring is
used for evaluation.
Evaluation is systematically assessing a
completed or phase of an ongoing programme.
Evaluations appraise the collected data and
information, informing strategic decisions and
thus improving the programme and outcomes in
the future. Evaluation is made up of a number of
progressive steps, the most important of which
is the collection of appropriate data that is
subsequently used to make a judgment about the
value of a programme (Dugdill & Stratton, 2007).
Sportanddev.org (2013) states an evaluation
should help to draw conclusions about five main
aspects of the programme:
• Relevance of the programme to pre-
determined goals.
• Effectiveness of the programme.
• Efficiency of the implementa-
tion of the programme.
• Impact of the programme.
• Sustainability of running the programme.
Information gathered during the monitoring
process provides the basis for the evaluation.
The evaluation process is an analysis of the
collected information which looks at the rela-

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 181180
tionships between the results, the effects and
overall impact of the programme (“Sportanddev.
org”, 2013).
The World Health Organisation recommends that
between 10-20% of the total intervention costs
should be spent on evaluation (Dugdill & Strat-
ton, 2007). However, evaluation can be seen as
problematic, time consuming and can take lower
priority compared to delivery of the programme
(Stratton et al., 2005).
A recent review (Sport England, 2017) assessed
the evidence to date supporting the impact of
sports programmes on 5 key areas:
• Physical Wellbeing
• Mental Wellbeing
• Individual development
• Social and community development
• Economic development
The review outlined the evidence supporting the
positive benefits of sports and physical activity
programmes in each of these areas, including:
7.1.1. Physical wellbeing
Good evidence for the prevention of illness,
increased therapeutic and management effects
in rehabilitation, improvements in strength,
balance, gait and motor skills, and maintaining
a healthy weight. Other outcomes include im-
proved sleep, increased energy, healthy early
year’s development, reduced engagement in risk
behaviours such as smoking, reduced mortality,
effective pain management and improved quality
of life in ageing.
7.1.2. Mental Well-being
There is a strong association between taking
part in sport and physical activity and posi-
tive mental wellbeing outcomes, but the causal
mechanisms are less well understood. There are
challenges around the varied definitions used in
the field, and the subjective nature of measures.
There is much evidence that sport and physical
activity contributes to enjoyment, happiness,
and life satisfaction. Social interaction ap-
pears to be central to this. Self-esteem and
confidence can increase through the opportunity
to develop new skills and relationships. There
is potential for sports and physical activity
programmes to reduce the symptoms of anxiety
and depression in participants. Other outcomes
include improved cognitive functioning, benefits
for people with dementia, and impacts around
emotion regulation.
7.1.3. Individual development
To date substantial evidence indicates the po-
tential for positive outcomes from taking part
or volunteering, particularly for young peo-
ple, but the wider set of circumstances around
an individual will determine effectiveness in
relation to these outcomes. Evidence was identi-
fied for improved educational attainment, either
directly (improved grades and behaviour) or
indirectly (enhanced skills like concentration
and teamwork).
There are positive impacts on employability
(employment opportunities, earnings, job per-
formance and satisfaction), including (limited)
evidence for younger people ‘not in education,
employment or training’ (NEETS). Sport can
promote self-efficacy (motivation and commit-
ment), for groups including elderly people and
disaffected young people. Other outcomes are
an increased willingness to volunteer and the
development of soft skills (such as integrity,
responsibility and leadership).
7.1.4. Social and
Community Development
Outcomes can be defined in relation to a range of
concepts that are often challenging to evidence
(such as social capital, trust and networks).
Many of which are positively associated with
participation or volunteering, but the effec-
tiveness of any intervention is dependent on
a broader set of conditions. Sport acts as a
conduit for people of different backgrounds to
interact, can bridge divides between groups such
as men and women and people with different em-
ployment backgrounds, and play a key role in the
integration of migrants. A small body of lit-
erature on bonding capital suggests that sport
helps to build relationships within communities.
For volunteers, motivations and outcomes over-
lap at the personal and the community level (for
example, bonding with others increases a sense
of community and citizenship).
7.1.5. Economic development
The sources reviewed use a wide variety of tech-
niques to calculate economic value and it was
not possible to accurately assess the strength
of the evidence base without a critically ap-
praising the full range of these methods.
There was some evidence on the direct impact
of the sport sector on the economy, largely in
terms of gross value added and job creation.
There was more evidence on the indirect impacts,
including reduced healthcare costs due to a
healthier population, reduced crime and improved
employability.
This review concluded that:
The evidence base is strongest for the physical
and mental well-being outcomes, then the indi-
vidual development outcome. It is weaker for
the social and community development and econom-
ic development outcomes.
More longitudinal studies could help strengthen
the evidence base by identifying the longer-term
effects on mental well-being, individual devel-
opment and social and community development.
The main focus of this review was examining
the evidence of the impact of sports programmes,
rather than how to design programmes to ef-
fectively achieve outcomes. A number of other
working groups have focused on developing a
framework for identifying, monitoring and eval-
uating outcomes of sports programmes, including
The Sport for Development Collation (2013).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 183182
7.2.ThE SPort fOR DeveLOpmENt CoLLaTIon Out-cOMes MoDEl
The focus of the Sport for Development Colla-
tion is to define a collective and sector-led
understanding of how to improve the outcomes
of sports programmes, provide advice on how to
design programmes and promote the use of shared
and consistent measurements of impact in an
attempt to further strengthen the evidence base
in this area (Sport for Development Collation,
2015).
The Sport for Development Collation Outcomes
Model (2015) defines outcomes across two contin-
uous sequences - from intrinsic to extrinsic,
and from individual to social. The two sequences
reflect the strong evidence that links emotional
skills and behaviours to positive outcomes in
other areas of life.
Sport programme outcomes can either be in-
trinsic or extrinsic, for example a programme
can support a person to increase essential and
intrinsic elements of their nature (self-esteem,
managing emotions, motivation), and also support
them to develop certain extrinsic behaviours
(play sport, be active and healthy, learn and
have a job).
Sports programmes deliver outcomes for the in-
dividual person or for social groups and commu-
nities. For example, a programme can change an
individual’s emotional skills and behaviours,
and as a result influence their family lives,
communities and wider society.
The model identifies four distinct groups of
outcomes:
• Social, emotional and cognitive capabilities
• Individual achievements and behaviours
• Inter-personal relationships
• Benefits to society
Definitions of the outcomes identified in each section can be found below:
Social, emotional and cognitive skills
Self-efficacy* Perceived self-confidence in their current abilities and future tasks.
It is task specific; a person can view themselves as good at one task but not another.
A person’s sense of self-efficacy can play a major role in how they approach goals, tasks
and challenges. It involves recognition that they can make a difference to their own life
Self- esteem An individual’s overall sense of self-worth (personal value), self-re-
spect, selfperception and self-awareness. It involves beliefs about the
self, such as appearance (body image), emotions and behaviours
Motivation The process that initiates, guides and maintains an individual’s goal oriented behaviour.
Motivation is what causes a person to act and achieve something:
a person’s ambitions and aspirations. Sometimes individuals are motivated by per-
sonal gratification and other times for external rewards (such as money, recog-
nition or praise). Motivation involves initiating action (active initiative)
and continued effort even though obstacles may exist (determination)
Managing emotions An individual’s ability to recognise their emotions and their effects (self-
awareness) by examining and regulating emotions, thoughts and resulting ac-
tions (self-reflection, self-management) and keeping disruptive emotions and
impulses in check (self-control, self-regulation, self-discipline)
Resilience An individual’s perseverance and persistence when faced with obsta-
cles (grit) and their flexibility in handling change (adapting, coping)
Social skills How an individual interacts and relates to others. It can apply to simple social contexts
and work environments. It relates to confidence in social interactions (social competence),
forming relationships, working effectively in teams and interpreting others. It includes
the ability to lead peers and be a role model, and to empathise and motivate others.
It also includes communication skills such as expressing, presenting and listening
Cognitive functioning The mental processes (such as perception, attention, memory and deci-
sionmaking) involved in an individual’s problem-solving, time manage-
ment, critical thinking, creativity and intellectual flexibility
Benefits to society
• Less need for health services
• Contribution to economy through par-
ticipation to the labour market
• Less dependence on welfare
• Not subject to the criminal justice system
• Strengthened community through leader-
ship and democratic participation
• Increased fairness and equality
Individual achievements and behaviours
• Increased physical wellbeing*
• Improved mental wellbeing*
• Sustained participation in sport
and physical activities*
• Positive health behaviour
• Reduced anti-social behaviour
• Improved attitudes to learning and attendance to school
• Improved educational attain-
ment and achieving qualifications
• Enhanced career prospects
• More securely housed
Social, emotional and cognitive capabilities
• Self-efficacy*
• Self- esteem
• Motivation
• Managing emotions
• Resilience
• Social skills
• Cognitive functioning
Inter-personal relationships
• Increased social capital and trust*
• Increased volunteering
• Increased community cohesion and spirit
• Positive parenting
Figure 15: The Sport for Development Collation Outcomes Model (2015, adapted from: https://londonfunders.org.uk/sites/de-
fault/files/images/SfD%20Framework_0.pdf)
EXTRINSIC
INTRINSIC

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 185184
Individual achievements and behaviours
Increased physical
wellbeing
Improved functional fitness, cardio respiratory fitness, muscular strength, adiposity/ body
composition; cholesterol levels, bone health, joint health and immune system function
Improved mental wellbeing Improved mood, feelings of happiness and life satisfac-
tion, and reduced levels of stress and anxiety
Sustained participation in
sport/physical activity
Increased intrinsic motivation for physical activity; cre-
ation of sporting habits; and belief that ‘sport is for them’
Positive health behaviour Improved diet (healthy eating), safe sex, reduced substance misuse, and smoking cessation
Reduced anti-
social behaviour
Improved pro-social values and reduction of behaviour likely to cause harass-
ment, alarm or distress to others. Increased positive social interactions
Improved attitudes
to learning and
attendance to school
Improved engagement with school; improved behaviour in school; reduced abenteeism
Improved educational
attainment and achieving
qualifications
Improved learning, academic performance, attain-
ment at school and achievement of qualifications
Enhanced career prospects In a secure job or accessing training opportunity; improved skills and experience
More securely housed Adequate and sustained accommodation
Inter-personal relationships
Increased social cap-
ital and trust*
Social capital describes the pattern and intensity of formal and informal networks among
people and the shared values which arise from those networks. Aspects of social capital
include increased levels of trust, increased membership of various groups and improved
access to networks and amount of social contact individuals have in their lives. Differ-
ent types of social capital can be described in terms of different types of networks:
• Bonding social capital describes closer connections be-
tween people and is characterised by strong bond
• Bridging social capital describes more distant connections between peo-
ple and is characterised by weaker, but more cross-cutting ties
• Linking social capital describes connections with people in posi-
tions of power and is characterised by relations between those with-
in a hierarchy where there are differing levels of power
Increased volunteering Frequent activity that involves spending time, unpaid, doing something that aims to
benefit the environment or someone (individuals or groups) other than, or in addition
to, close relatives. Volunteering must be a choice freely made by each individual
Increased community
cohesion and spirit
A cohesive community is one where there is a common vision and a sense of be-
longing for all communities; the diversity of people’s different back-
grounds and circumstances is appreciated and positively valued; and those
from different backgrounds have similar life opportunities
Positive parenting Improved parenting skills and styles, improved parent men-
tal well-being, reduced behaviour difficulties in children
Benefits to society
Less need for
health services
Improvement in physical health by increasing fitness and reducing obesity; pre-
venting a number of chronic diseases (cardiovascular disease, coronary heart dis-
ease, diabetes, some cancers, strokes, osteoporosis, hypertension); and providing
therapeutic benefits for the management of existing diseases and illnesses. Im-
provement in mental health by lowering the risk of depression; managing anxiety
and stress; increasing an overall sense of wellbeing; and helping with some sys-
tems of clinically diagnosed personality disorders (such as schizophrenia)
Contribution to econo-
my through participation
in the labour market
Healthy employment market; increased productivity for goods and services; increased
innovation and new businesses; and increased revenue gerenated through taxable income
Less dependance on welfare More people better able to meet the expenses of daily living for a prolonged pe-
riod of time and not be reliant on government welfare benefits (such as heat-
ing and housing benefits, Jobseeker’s Allowance and low-income benefits)
Benefits to society
Not subject to the crim-
inal justice system
Improvement in pro-social behaviour, reduction in crime and reduction in anti-social
behaviour particularly through lower levels of recidivism, drunk driving, use of illegal
drugs, crime and suspension from school, property crime, shoplifting and juvenile crime
Strengthened community
through leadership and
democratic participation
Increased civic engagement (citizens participate in the life of a com-
munity in order to improve conditions for others or to help shape
the community’s future); and greater social cohesion
Increased fair-
ness and equality
Improved equality of opportunity and reduced stigma and discrimination for all,
at work, in public, social and political life, and in people’s life chances
Figure 16:. (i-iv) Definitions of the Sport for Development Collation Outcomes (2015, retrieved from: https://londonfunders.
org.uk/sites/default/files/images/SfD%20Framework_0.pdf)
Dugdill & Stratton (2007) highlighted the RE-
AIM framework planning tool as a useful way for
practitioners to think about structuring their
evaluation:
• Reach - Who did the intervention reach?
– e.g. monitoring of participant num-
bers through registers, post codes,
questionnaires, facility usage.
• Effectiveness - How effective was the inter-
vention at meeting its aims and objectives?
– e.g. physical activity increase, decrease
in body mass index or increasing the con-
templation to become physically active.
• Adoption – Have significant parts of
the intervention been adopted else-
where? -e.g. programme has been ad-
opted by other organisations.
• Implementation - How was the intervention
implemented and managed? How was the interven-
tion funded? What skills did the staff have?
• Monitoring: What were the monitoring
and evaluation strategies used to as-
sess the quality of the intervention?
Is the intervention sustainable?

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 187186
7.3.SPEcific OUt-cOme MEaSUresAs the resources and skills available for eval-
uations are often limited, it is important to
decide at the planning stage of a programme what
will be measure and why (Dugdill & Stratton,
2007). For the purpose of these guidelines we
have categorised outcome measures into three
categories:
• Physical outcome measures
• Psychological outcome measures
• Social functioning outcome measures
7.3.1. Physical outcome measures
There are a variety of methods available for
measuring sport/physical activity levels but
there is no gold standard (Welk, 2002).
Key parameters for physical activity measurement
include:
• Frequency (when/how often does it occur)
• Intensity (how hard is the activity)
• Time (the duration)
• Type of activity (walking, run-
ning, swimming etc.).
Dugdill & Stratton (2007) stated the challenge
is selecting a measure that is valid, accurate
and reliable, defining a valid instrument as one
that measures what it purports to measure and
a reliable measure as one that produces stable
and repeatable results when used under the same
conditions.
Self-report tools
Self-report tools are one of the most commonly
used outcome measure as they are less time con-
suming than other measures and are easily ad-
ministered. Self-report tools can take the form
of diaries, questionnaires or interviews. They
can be completed both by the participant and by
another person significant in the participant’s
life e.g. parent, carer, sibling or child.
A person’s ability to understand a survey ques-
tion and their ability to accurately recall and
communicate their activity pattern will affect
the reliability and validity of their self-re-
port, therefore the most reliable tools tend to
be 3 day or 7 day recall tools (e.g. a partic-
ipant recalling and communicating their level
of physical activity participation over past
3 or 7 days) (Dugdill & Stratton, 2007). These
self-report tools are recommended as they have
shown adequate reliability and validity in large
populations (Welk, 2002).
International Physical Activity Questionnaire
Revised (IPAQ): The IPAQ (Booth, 2002) comprises
a set of 4 questionnaires. The purpose of the
questionnaires is to provide common instru-
ments that can be used to obtain international-
ly comparable data on health–related physical
activity.
Global Physical Activity Questionnaire (GPAQ)
(“WHO: GPAQ Questionnaire): The GPAQ covers sev-
eral components of physical activity including
intensity, duration, and frequency.
The Active Lives Questionnaire (“Sport England”,
2015): The Active Lives Questionnaire collects
data on demongraphics, geography and engagement
in sport/physical activity and takes roughly
15 minutes to complete.
The Physical Activity Questionnaire for Old-
er Children (PAQ-C) and Adolescents (PAQ-A)
(Crocker et al., 1997): The PAQ-C and PAQ-A are
Self-administered 7 day recall questionnaires,
assessing general levels of physical activity
in 9 to 15 year old children using 10 questions.
There are no valid questionnaires for children
under the age of 9.
The Borg Scale of Perceived Exertion (Borg,
1982): The Borg RPE scale is a self-report rat-
ing scale assessing a participant’s level
of perceived exertion during physical activity.
Heart rate Monitors
Heart rate monitoring usually come in the form
of a belt that fits around the chest and detects
electrical impulses from the heart and converts
these to beats per minute. These data are either
stored in the belt or transmitted to a receiver
in the form of a wristwatch. Heart rate monitors
can be programmed to record heart rate second to
second or minute to minute (recording interval
is called an epoch) continuously for weeks. The
main advantage of heart rate monitoring is the
relatively low participant burden and ease with
which data is collected and analysed. The in-
struments require a PC for collected data to be
downloaded. Although these tools provide objec-
tive measures of physical activity, the cost and
technical expertise required for use and data
analysis may restrict the feasibility of use
for evaluation purposes.
Accelerometers
These small devices are usually placed on the
waistband or the wrist in wheelchair users and
record the vertical (uni-axial) or vertical,
horizontal and diagonal (tri-axial) accelera-
tion of the body. These accelerations are then
converted to gravitational counts per epoch
duration. These instruments can record in second
by second or minute-by-minute epochs (Dugdill
& Stratton 2007). As with heart rate monitors,
the cost and technical expertise required for
the use and data analysis of accelerometers may
restrict the feasibility of their use for evalu-
ation purposes.
Pedometers
Pedometers provide information on walking.
A person’s individual data such as stride
length, body weight and age can be input into
some pedometers. The in correct input of stride
length is arguably the largest cause of error in
estimating physical activity energy expenditure
and distances covered during walking. The best
use of pedometers is for recording steps and
pedometers should always be manually checked for
counts by using a calibrated shaker table or by
hand (by counting each shake 1, 2, 3 etc. and
checking against the device) (Dugdill & Stratton
2007). For representative data to be obtained
participants it is advised participants wear a
pedometer for 3 days (Tudor-Locke et al., 2005).
Pedometers are a low cost method of generating
accurate and reliable data (depending on the
quality of the pedometer; Schneider et al.,
2004). The daily target for physical activity
is 10,000 steps per day (Tudor-Locke and Bas-
sett, 2004) for persons without physical dis-
abilities. However 15,000 and 12,000 steps have
been recommended for male and female adoles-
cents, respectively (Tudor Locke et al., 2004).
The key aspect for activity intervention is not
necessarily the debate over number of steps but
whether total steps increase as a result
of engaging in an activity intervention. Recent
pedometer evaluations in schools have suggest-
ed that pedometers work as motivational tools
(Butcher et al., 2007) and stimulate increases
in physical activity (Dugdill & Stratton 2007).
Berg balance scale (BBS) (Berg, Wood-Dauphinée,
Williams & Maki, 1992)
The BBS is a qualitative measure that assess-
es balance via performing functional activi-
ties such as reaching, bending, transferring,
and standing that incorporates most components
of postural control: sitting and transferring
safely between chairs; standing with feet apart,
feet together, in single-leg stance, and feet
in the tandem Romberg position with eyes open
or closed; reaching and stooping down to pick
something off the floor. Each item is scored
along a 5-point scale, ranging from 0 to 4,
each grade with well-established criteria. Zero
indicates the lowest level of function and 4
the highest level of function. The total score
ranges from 0 to 56. The BBS is reliable (both
inter- and intratester) and has concurrent and
construct validity.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 189188
Systemic Observation
Systematic observation involves a trained per-
son observing and coding predetermined physical
activity behaviours of participants over a set
period of time, e.g. sitting, walking, running
etc. The SPACES system (Systematic Pedestrian
and Cycling Environmental Scan, Pikora et al.,
2002) is an example of a comprehensive observa-
tion tool used to assess walking and cycling.
Systematic observation requires observers to
have undertaken specific training and can be used
to assess participants in real time or video
recordings. Although providing vaild data, the
time and specific training required for this
technique may reduce its feasibility for evalua-
tion purposes.
7.3.2. Psychological
outcome measures
The Warwick-Edinburgh Mental Well-being Scale
(WEMWBS) (Tennant et al., 2007): The WEMWBS was
developed to enable the monitoring of mental
wellbeing in the general population and the
evaluation of projects, programmes and pol-
icies which aim to improve mental wellbeing.
SWEMWBS is a shortened version of WEMWBS. This
is a 7 item scale for which item scores need
transforming.
Rosenberg Self-esteem Scale (RSES) (Rosenberg,
1965): The RSES is a 10-item scale that measures
global self-worth by measuring both positive
and negative feelings about the self. The scale
is believed to be uni-dimensional. All items
are answered using a 4-point Likert scale for-
mat ranging from strongly agree to strongly
disagree.
General Self-Efficacy Scale (GSE) (Schwarzer
& Jerusalem, 2010): This scale was created to
assess a general sense of perceived self-effica-
cy with the aim in mind to predict coping with
daily hassles as well as adaptation after ex-
periencing all kinds of stressful life events.
The scale is designed for the general adult
population, including adolescents. Persons below
the age of 12 should not be tested. The measure
has been used internationally with success for
two decades. It is suitable for a broad range of
applications. It can be taken to predict adapta-
tion after life changes, but it is also suitable
as an indicator of quality of life at any point
in time
The Life Satisfaction Questionnaire (LISAT)
(Fugl-Maeyer et al. 1991): The LISAT is a self
or interviewer-administered rating scale,
taking approximately 5 minutes to administer.
The LISAT-9 has 9 items; one is a global item
for ‘life as a whole’ and 8 are domain-spe-
cific items for ‘vocational situation’, ‘finan-
cial situation’, ‘leisure’, ‘contact friends’,
‘sexual life’, ‘activities of daily living’,
‘family life’, and ‘partnership relationship’.
The LISAT-11 has 11 items, which includes the
same items as the LISAT-9 but with two additions
evaluating ‘physical health’ and ‘psychological
health’.
World Health Organization Quality of Life In-
strument (WHOQOL-BREF) (WHO, 1998): The WHO-
QOL-BREF instrument comprises 26 items, which
measure the following broad domains: physical
health, psychological health, social relation-
ships, and environment. The WHOQOL-BREF is a
shorter version of the original instrument that
may be more convenient for use in large research
studies or clinical trials. The questionnaire
captures many subjective aspects of quality of
life (QOL) and is one of the best known instru-
ments for cross-cultural comparisons of QOL and
is available in many languages.
The Beck Depression Inventory (BDI) (Steer,
Beck, Brown, 1996): BDI is a 21-item self-re-
porting questionnaire for evaluating the se-
verity of depression in normal and psychiatric
populations. A shorter version of the question-
naire, the BDI Fast Screen for Medical Patients
(BDI-FS), is available for primary care use.
That version contains seven self-reported items
each corresponding to a major depressive symptom
in the preceding 2 weeks.
7.3.3. Evaluation of
Social Functioning
The New Philanthropy Capital’s Outcomes Map:
Personal and Social Well-being (Copps and Plim-
mer, 2013).
In this NPC publication, Copps & Plimmer (2013)
defined personal and social well-being as a per-
son’s state of mind, relationship with the world
around them, and the fulfilment they get from
life. It can be understood as how people feel
and how they function, both on a personal and a
social level, and how they evaluate their lives
as a whole. It is linked to a range of other
outcomes, including mental health.
Copps & Plimmer (2013) divided the measurement
of personal and social well-being into on 3
categories:
1. Feelings about self.
2. Relationships with family and friends.
3. Perception and connected-
ness to the community.
1. Improved feelings of self
Examples of valid outcome measures discussed in
Psychological Outcome Measures section. Other
examples include:
• The Self-concept Scale
(10-items) (Marsh, 1992).
• The Resilience Scale (14-item) (Wag-
nild and Young, 1987).
• The Children’s Society’s Wellbeing In-
dex (Rees, Goswami & Bradshaw, 2010).
2. Improved relationships with family and friends
Examples of valid outcome measures included:
The Multidimensional Students’ Life Satisfaction
Scale (MSLSS) (Huebner, 2001)
The MSLSS is designed to provide a profile of
children’s life satisfaction across key domains.
The 40-item scale is completed by children and
young people and captures information on five
domains:
• Family (7 items)
• Friends (9 items)
• School (8 items)
• Living Environment (9 items)
• Self (7 items)
• There is also a 6-item Brief Multidimen-
sional Students’ Life Satisfaction Scale.
The Friendship Scale (Hawthorne 2006)
This short, user-friendly 6 item scale measures
6 of the 7 important dimensions that contribute
to social isolation and its opposite, social
connection.
Lubben Social Network Scale–Revised (LSNS-R)
(Lubben et al., 2002)
The LSNS-R is designed to gauge social isolation
in older adults by measuring perceived social
support received by family, friends and mutual
supports (eg. neighbours), including confidant
relationships. The tool has an abbreviated
version (LSNS-6) and an expanded version (LSNS-
18) and takes approximately 5-10 minutes to
administer.
UCLA Loneliness Scale – Revised (Russell, Pep-
lau, & Cutrona, 1980)
This 20-item scale is designed to measure a
person’s subjective feelings of loneliness and
social isolation.
3. Improved perceptions of and con-nectedness to the community
Copps & Plimmer (2013) defined this as a per-
son feeling part of a meaningful community or
communities, feeling connected to the envi-
ronment around them, and feeling included and
involved. Approaches to measuring these aspects
of well-being tend to be survey-based and depend
on the responses of individuals to questions
about their feelings and perceptions. Many of
the tools tend to be very similar and are often
derived from the same research base but differ
slightly in length and emphasis. Overall, there
is no firm consensus on what the best tools are.
In practice, where they are in use, well-being
approaches tend to be combined with measures
specific measures tailored to the intervention.
As in many areas of measurement, there remains a
skills gap in analysing and interpreting data.
There is a clear need to create tools that are
practical and can be applied by non-experts
(Copps & Plimmer, 2013).

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 190
Reference
Berg K, Wood-Dauphinee S, Williams JI, Maki, B: Measuring
balance in the elderly: Validation of an instrument. Can. J.
Pub. Health, supplement 2:S7-11, 1992.
Borg, G. A. (1982). Psychophysical bases of perceived exer-
tion. Med sci sports exerc, 14(5), 377-381.
Butcher, Z. Fairclough, S. Stratton, G. & Richardson, D.
(2007) The Effect of Feedback and Information on Children’s
Pedometer Step Counts at School. Pediatric Exercise Science,
19(1).
Copps, J. & Plimmer, D. (2013). Outcomes Map: Personal and
Social Well-being. NPC, retrieved from: https://www.thinknpc.
org/?s=OUTCOMES+MAP%3A+PERSONAL+AND+SOCIAL+WELL-BEING.
Dugdill, L. & Stratton, G. (2007). Evaluating sport and
physical activity interventions: a guide for practitioners.
University of Salford.
Fugl-Meyer, A. R. Eklund, M. & Fugl-Meyer, K. S. (1991).
Vocational rehabilitation in northern Sweden. III. Aspects
of life satisfaction. Scandinavian journal of rehabilitation
medicine, 23(2), 83-87.
Hawthorne, G. (2006). Measuring social isolation in older
adults: development and initial validation of the friendship
scale. Social Indicators Research, 77(3), 521-548.
Huebner, E. S. (2001). Manual for the multidimensional
students’ life satisfaction scale. SC: University of South
Carolina (unpublished paper provided by the author).
Lubben, J. (2002). Lubben Social Network Scale–Revised.
Retrieved from: https://instruct.uwo.ca/kinesiology/9641/
Assessments/Social/LSNS-R.html
Sportanddev.org, (2013). Retrieved from: https://www.
sportanddev.org/en/toolkit/monitoring-and-evaluation/
what-monitoring-and-evaluation-me.
Sport England: The Active Lives Questionnaire, 2015, re-
trieved from: http://www.activelivessurvey.org/main/)
Sport England, (2017). Review of Evidence on the Outcomes
of Sport and Physical Activity – A Rapid Evidence Review.
Retrieved from: https://www.sportengland.org/media/11719/
sport-outomes-evidence-review-report.pdf.
Pikora, T. J. Bull, F. C. L. Jamrozik, K. Knuiman, M. Giles-
Cortie, B. & Donovan, R. J. (2002). Developing a reliable
audit instrument to measure the physical activity environment
for physical activity. American Journal of Preventive Medi-
cine, 23 (3), 187-194.
Sport for Development Coalition, (2015). Sport for Devel-
opment outcomes and measurement framework. Retrieved from:
https://londonfunders.org.uk/sites/default/files/images/SfD%20
Framework_0.pdf
Steer R.A., Beck A.T. & Garrison B (1986). Applications of
the Beck Depression Inventory. In: Sartorius N, Ban TA, eds.
Assessment of Depression. Geneva, Switzerland: World Health
Organization, 121–142.
Stratton, G. Ridgers, N.D. Gobbii, R. & Tocque, K. (2005)
Physical Activity Exercise, Sport and Health: Regional Map-
ping for the North-West. Retrieved from: www.nwph.net/pad/
accessed.
Schwarzer, R. & Jerusalem, M. (2010). The general self-effica-
cy scale (GSE). Anxiety, Stress, and Coping, 12, 329-345.
RE-AIM, (2014). RE-AIM as a planning tool. Retrieved from:
http://www.re-aim.org/re-aim-as-a-planning-tool/.
Rosenberg, M. (1965). Rosenberg self-esteem scale (RSE).
Acceptance and commitment therapy. Measures package, 61, 52.
Russell, D. Peplau, L. A. & Cutrona, C. E. (1980). The revised
UCLA Loneliness Scale: Concurrent and discriminant validi-
ty evidence. Journal of personality and social psychology,
39(3), 472-480.
Tennant, R. Hiller, L. Fishwick, R. Platt, S. Joseph, S.
Weich, S. & Stewart-Brown, S. (2007). The Warwick-Edinburgh
mental well-being scale (WEMWBS): development and UK valida-
tion. Health and Quality of life Outcomes, 5(1), 63.
World Health Organization: GPAQ Questionnaire http://www.who.
int/ncds/surveillance/steps/GPAQ/en/) Retrieved 12.11.2018
Welk, G. J. (2002). Physical activity assessments for
health-related research. Human Kinetics.
World Health Organization, (1998). World Health Organization
Quality of Life Instrument (WHOQOL-BREF). Retrieved from:
http://www.who.int/substance_abuse/research_tools/whoqolbref/
en/.

8. LonGEV itY aND QUal ItY of LiFELearning outcomes:
• what regular physical activi-
ty means and how important it is
• how and in what ways people with phys-
ical disability can be motivat-
ed to do exercises regularly
• what the expert can do according to the lev-
els of physical condition and motivation
• Factors influencing the participation of
people with disabilities in community sport
• What can the trainer do?
• What is team sport and community sport?

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 195194
InTroDUctioN
AUTHORS: ZSUZSANNA KOVÁCS, ZSUZSANNA ANTAL
Suppositions, studies and questions about qual-
ity of life and longevity are not new at all.
Perhaps it is one of the most ancient questions
of mankind: the question of what makes a human
satisfied, what makes life meaningful and happy,
and what is the secret to have a full and good
life. The basic aim of human existence is to
practise human functions as fully as possible.
The living conditions of mankind have changed
to a great extent, but the final aim remained the
same - reaching happiness and integrity.
There are many conditions influencing one’s qual-
ity of life. Including, but not limited to: cul-
ture and leisure activities, economic situation,
environmental conditions, infrastructure, secure
and health state. These factors are of course
all related to each other, and they cannot be
examined on their own. Just a simple example:
financial wealth influences the consumption rate
of healthy food as well as the total spent on
health insurance. The quality of our nutrition
and the money spent on relaxation and recreation
influences our health state, etc.
Life length and life quality cannot be separated
from each other, either. The higher our quality
of life is, the more likely that we will live to
a higher age. If we spend the last 5-10 years of
our life ill, then we speak about a lower life
quality.
8.1.rEGuLar PhYSi-CaL ACTIvity
AUTHOR: ZSUZSANNA KOVÁCS, ZSUZSANNA ANTAL
Keywords: disability/impairment, physical condition, motivation, guiding
It is useful to consider factors affecting life
quality in terms of those ones we can influence.
Our health state is such a factor. If you think
that we are merely passive sufferers of the na-
ture of our genetic map that is not necessarily
true. We can do against the encumbered gene pool
for example by attending regular screenings or
by doing regular physical activity and sport.
8.1.1. Conceptual definition
Advantages of regular physical activity are
well-known, “regardless of sex and age”. Beyond
the general, favourable impacts of physical
training and sport, it can be applied in the
prevention, treatment and rehabilitation of some
illnesses. Based on the stand of several Hun-
garian and international statements it can be
stated that:
• Regular physical activity reduces the
number of illnesses and early deaths
due to hypertonia, diabetes, coro-
nary-artery disease and obesity.
• Its advantageous impact at-
tunes the motoric system.
• The regulation of central ner-
vous system improves.
• The capacity of the endocrine system grows.
• The metabolism will become more economical.
• It affects the function of the im-
mune system advantageously.
• It prevents obesity and ill-
nesses connected to it.
• The oxygen supply of the organism improves.
As a bonus, regular physical activity also has a
good impact on our psychological well-being:
• It reduces anxiety and depression.
• It maintains memory.
• It increases self-esteem and self-confidence.
• It stimulates endorphin production that brings
about the growth of long-term happiness.
• It increases libido.
Even a moderately intensive and a moderate time
of physical activity has a positive impact (e.g.
30 minutes of walk done 4-5 times a week) as it
is able to improve one’s state of health and
quality of life.
Regular physical activity and recreation-
al sport activity are an important element of
health behaviour as it has an important role
in the prevention and intervention of several
chronic illnesses. Regular physical activity
has a significant life quality-raising impact
both among healthy people, those suffering from
chronic illnesses and those with disabilities.
It improves corporal and mental health, as well
as psychosocial well-being and the ability of
coping with stress.

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 197196
In places where there is lower economic depri-
vation, the frequency of doing regular sport
activity decreases, thereby contributing to
lower health indicators of these groups. How-
ever, there are unexploited health development
opportunities that could be addressed by move-
ment intervention programmes that could target
these groups. With the use of adequate tools
and measures this could provide a cost-efficient
solution to increase the physical and mental
health of this population.
The question of social responsibility has been
brought into the foreground, according to which
sport has a positive impact on the individual
and on wider society. Higher economically and
socially developed countries have already rec-
ognized that quality of life in society contrib-
utes to the economic success of the individual,
his/her broader surroundings as well as to that
of the country. On the contrary, where people
are struggling with illnesses and psychological
disorders this can place a large burden on the
social security of the given country.
8.1.2. What can regular
physical activity mean to
people with disability?
Photo: Zsuzsanna Antal, Boccia, Human Profess, Szombathely,
2017
Irrespective of having physical, intellectual,
mental, psychosocial or sensory disabilities,
regular physical activity can create stability
in the individual’s life. Not only because this
can contribute to the development of a routine,
but also because certain exercises contribute to
the production of endorphins, thus promoting the
feeling of happiness.
8.1.3. Models and methods
Here, the physically injured have to be empha-
sized since for them, regular physical activity
means life itself. Therefore, this is the only
means by which self-care may be promoted or
facilitated.
There are several models (ICF, IMAPA) and
methods (Dévény Anna, Pető András) which aim
to improve the state of people with physical
injuries.
However, it is well-known that models only serve
as a theoretical basis as they often simplify
reality. On the other hand, methods only provide
solutions for certain types of diseases. Conse-
quently, the combination of different methods or
modified versions may be the solution.
8.1.4. Individualised physical
training/physiotherapy for
physically injured people
Before creating a training plan, the charac-
teristic features and the symptoms of a disease
have to be studied, in addition to its develop-
ment. This information is important as it can
influence and explain how unmotivated or motivat-
ed the individual is and influences the end re-
sult to be achieved. In addition to this, family
background is also of great importance. The key
to regular physical training/physiotherapy is to
continuously set achievable goals and promote a
sense of achievement.
8.1.5. Relationships and guiding in the interest of the
successful training of people with disabilities
Table 1: The relation between the type of physical impairment and the main goal of physical train-ing/adapted physical education
The type of impairment Goal
Physical impairment
acquired by stroke
Restoring former phys-
ical condition
Cerebral palsy acquired
during/after childbirth
Achieving the possible
highest level of self-care
Person suffering from
muscular atrophy
Delaying the impair-
ment of condition at the
possible highest level
Injury or limb loss
acquired by accident
Restoring former phys-
ical condition
Person with multi-
ple impairments
At least maximising
physical condition
Source: Data colection of Zsuzsanna Kovács made among her
disabled sport mates, 2018
Table 2: Different life stag-es and motivational strength
Life stage Motivation
Child Acquiring reward
Teenager Reducing dependen-
cy on parents
Unmarried Starting an inde-
pendent life
Married Commitment in a rela-
tionship and family
Divorced/ Widowed/ El-
derly single people
Preserving the abil-
ity of self-care as
long as possible.
Source: Data colection of Zsuzsanna Kovács made among her
disabled sport mates, 2018
Table 3: What the expert can do according to the lev-el of physical condition and motivation
Physical condition Intrinsic motivational level What can the sport expert do?
The development of
physical condition has
just started (child)
Very motivated (from instinct) Diversified exercise series, maintenance
of interest/curiosity is essential,
Rehabilitation fol-
lowing an accident
Very motivated (from instinct) Diversified exercise series, maintenance
of interest/curiosity is essential
Rehabilitation following
a reconstructive sur-
gery correcting former
injury/impairment
Motivated, (the hope of a physical con-
dition being better than the previous),
however, this can diminish quickly if
there are no small senses of achieve-
ment since it may happen that the physi-
cal condition has to be improved from the
lowest level as a result of the surgery.
Not only a diversified exercise series, but
also a diversified environment (background
music, exercises done outdoors, diversified
training program (floor exercises – swim-
ming – horse-riding) is necessary.
Physical condition
that has been stagnat-
ing for a long time
Unmotivated (It may have been triggered
by the same exercises that had to be done
too many times and also by little sense of
achievement or by too great goals or the lack
of goals together. Respectively, the individ-
ual is satisfied with their state and thinks
that it is enough to take actions if the next
stage of the impairment of condition begins.)
In the first case, diversified training
program, exercise series, environment, and
surmountable challenges are essential. In
the second case, motivating conversations
supported by powerful arguments are necessary
(With physical training the next stage of the
impairment of condition can be delayed and/
or its degree can be decreased. The de-
crease/termination of possible pains or the
control or termination of the assuaging of
pain with medicine can also be achieved.)
Continuously deteriorat-
ing physical condition
Unmotivated (embittered, tired of, re-
signed themselves to their condition)
Combination of various methods, devel-
oping new methods in close collaboration
with the individual in order to stop or
reverse physical deterioration or showing
a tiny ray of hope regularly in any way.
Source: Data colection of Zsuzsanna Kovács made among her disabled sport mates, 2018

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 199198
To achieve and maintain the demand for regu-
lar physical activity, we have to continuous-
ly affect the individual’s emotions either by
encouraging, praising, warning, or sanctioning
which depends on the individual’s personality to
a large extent.
Reference
DSGM Retrieved from: http://www.dsgm.eu/index.php?option=com_
content&view=article&id=20&Itemid=2&lang=en (2018. 07.26)
Meet the needs of all individuals with IMAPA Retrieved from:
https://uk.humankinetics.com/blogs/excerpts/meet-the-needs-
of-all-individuals-with-imapa (2018. 07.26)
Method by Pető András Retrieved from:http://semmelweis.hu/
pak/en/ (2018. 07.26)
The International Classification of Functioning, Disability
and Health (ICF) Retrieved from: http://www.rehab-scales.
org/international-classification-of-functioning-disabili-
ty-and-health.html (2018. 07.26)
8.2.COmmuNItY acTIVE liVINg pROgraMmEs
AUTHOR: ZSUZSANNA KOVÁCS
KEYWORDS: INDIVIDUALIZED CONDITIONS, TYPES AND ADVICE OF TEAM/COMMUNITY SPORT
8.2.1. It’s better to
sport in a community!
Community sport goes beyond what exercising
means in order to preserve one’s health. Exer-
cising in a team, or even together at the same
space creates a community: it helps you to make
new relationships, it strongly motivates you,
it inspires you and it fills you up emotional-
ly. It strengthens the social network around
the people, it motivates for playing, it in-
spires, and participants thereby can reach a
“flow”-experience.
If we do sports in a team, then the good partic-
ipation of the team depends on the cooperation
of the individuals. It is a common interest of
every team member; let it be either an occasion-
al leisure community, or a permanent one, not
to speak about athletes involved in top-level
sport, to be part of the game and of a poten-
tially winning match. For this, it is necessary
to have the skill of cooperative behaviour,
the altruistic cooperation built on realistic
self-knowledge, the humility and the effort
towards the common aim. The feeling of group
identity and belonging together, which provides
security, can be established based on these val-
ues. (Rétsági, 2015)
In the publication entitled White Paper on sport
(2007:7), made by the Committee of European
Communities, we can read that belonging to a
team, the fair competition, keeping the rules,
respecting others, solidarity, principles of
discipline all foster active citizenship, social
integration, and they discourage from crime.
Photo: Zsuzsanna Antal, Gymstick-Nordic walking, Human Pro-
fess, Szombathely, 2017
8.2.2. Factors influencing the
participation of people with
disabilities in community sport
• Personality (how motivated a person is, at-
titude, determination – impressionability)

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 201200
• The character and degree of impairment
(physical and intellectual condition, ac-
cess to the establishment and to the scene)
• Living conditions, financial situation
(travel expenses, purchase of equip-
ment’s, activity that can be performed
in parallel with learning or work)
• Access to the establishment, its facilities
and degree of accessibility with wheel-
chair, (Zsuzsanna Kovács, own experience)
8.2.3. The trainer has to be
aware of the following things:
For what reason does the indi-vidual choose the sport?
a. external pressure: it was recommended
by a doctor or the person was persuad-
ed by family, friends and acquaintances
b. own decision
What is the primary goal of doing sports?
a. to gain community experiences
b. preserving or developing health/
physical condition/appearance
c. proof, self-realisation, competing
What kind of ideas does the individu-al have on their own sport facilities?
a. has no idea
b. has an idea at large, but it is not realistic
c. has a realistic idea at large
d. has a concrete idea, but is not realizable
e. has a concrete, realistic idea
To what extent can the individual be influenced or guided? What is their at-titude? What is their habitus like?
a. does not accept help either from
helpers or volunteers
b. accepts help from helpers and volunteers
c. does not accept either instructions or advice
d. carries out instructions, but
does not accept advice
e. is a pessimistic or optimistic person
f. is an introvert or extrovert person
g. is an unmotivated or persuad-
able or suitably motivated person
h. is a person who easily runs away from
problems or is a persistent one
What are the individual’s liv-ing conditions like? What about their financial situation?
a. is it or is it not a problem for the in-
dividual and for their relatives to en-
sure the conditions of doing sports?
What are the most important cri-teria, symptoms and consequenc-es of the individual’s disease?
Zsuzsanna Kovács, own experience
8.2.4. As a trainer what can
I do with knowledge of the
above mentioned things?
Based on the cause, the aim, the personality,
on the individual’s idea and disease, it has to
be decided whether I am able to choose the right
type of sport, the suitable training method and
the appropriate motivational tools thus, the
strategy either individually or with assistance.
8.2.5. Educational methods:
Typical methodical procedures
• Verbal methodical procedure: explanation,
instruction, word of command, exhortation,
stimulation, encouragement Take the indi-
vidual’s age, preliminary training and dis-
ease into consideration. There is a great
emphasis on employing explanation, exhor-
tation, stimulation and encouragement.
• Visual methodical procedure: direct and
indirect demonstration. The basic criteri-
on of direct demonstration is exemplariness
and faultlessness. Therefore, demonstration
performed by the trainer seems to be more
effective. However, it is possible that a
greater stimulating effect can be achieved
if demonstration is done by an experienced
fellow sufferer. The tools of direct demon-
stration are: drawings on board, magnetic
board, pictures, videos, common match, vis-
iting competitions.The greatest motivating
power is embodied by the two latter tools.
• Practical methodical procedure: providing
and ensuring assistance, and exercising. In
case of assistance, if it is not provided
by the trainer, but it is given by a vol-
unteer, it is important that expertise of
a certain degree is necessary in this case
too, and they also have to know the train-
er’s and the individual’s all vibration.
Assistance shall only be provided if the indi-
vidual needs it. However, assistance should be
continuously guaranteed.
Exercising: Depending on the aim of doing sports
and on the individual’s disease, either the
quality or the quantity is a priority.
8.2.6. If necessary, I have to
decide, to whom I turn for help.
For example: The individual’s family, friends,
or a doctor, a physiotherapist, a masseur,
(sport) psychologist, a social expert.
If it is required by the living conditions and
the financial situation, we have to try to create
an optimal condition more carefully than usual,
either by ensuring accessibility with wheelchair
or providing ideal training time and occasion or
simply by providing the available information.
(Zsuzsanna Kovács, own experience)
8.2.7. Team sport and
community sport
The good participation of a team depends on the
cooperation of the individuals constituting
the team. It is a common interest of every team
member regarding either occasional or permanent
leisure communities, not to mention partici-
pants of high-performance sports and first-class
sports, that they should be participants of
games involving experience and possibly of a
winning match. For this, the skill of cooper-
ative behaviour, the altruistic cooperation
based on realistic self-knowledge, humility, and
effort toward a common aim are essential. Team
identity and belonging together which gives the
feeling of security may develop based on these
values. (Rétsági, 2015)
In the publication entitled White Paper on Sport
(2007:7) made by the Commission of the Europe-
an Communities, we can read that belonging to
a team, fair competition, following the rules,
respecting others, solidarity, principles of
discipline all promote active citizenship, so-
cial integration and discourage from crimes.
Proposals of the White Paper (2007:7) aim at the
improvement of the situation:
‘The Commission furthermore encourages Member
States and sport organisations to adapt sport
infrastructure to take into account the needs
of people with disabilities. Member States and
local authorities should ensure that sport ven-
ues and accommodations are accessible for people
with disabilities. Specific criteria should be
adopted for ensuring equal access to sport for
all pupils, and specifically for children with
disabilities. Training of monitors, volunteers
and host staff of clubs and organisations for
Photo: Zsuzsanna Antal, Nordic walking training, Human Pro-
fess, Szombathely, 2017

EUROPEAN RESPORT GUIDELINES FOR IMPLEMENTATION OF RESPORT ACTIVITIES 202
the purpose of welcoming people with disabili-
ties will be promoted. In its consultations with
sport stakeholders, the Commission takes special
care to maintain a dialogue with representatives
of sportspeople with disabilities.’
Photo: Zsuzsanna Antal, Netball training, Human Profess,
Szombathely, 2018
Reference
Bíróné Nagy, E. (2011): Sportpedagógia. Dialóg Campus Kiadó.
Commission of the European Communities: White Paper on Sport
Retrieved from: https://eur-lex.europa.eu/legal-content/EN/
TXT/?uri=celex:52007DC0391 (2018. 07 23.)
Kristonné dr. Bakos, M.: Testneveléstanítás és módszertan.
Retrieved from: http://uni-eszterhazy.hu/public/uploads/
testneveles-tanitas-es-modszertan_544f3a032bdb9.pptx (2018.
07 23.)
Rétsági, E. (2015): Sport szerepe a szocializációban és a
pedagógiában. In Laczkó, T. – Rétsági, E. (Eds.), A sport
társadalmi aspektusai. (pp.51-61).
Pécs: Pécsi Tudományegyetem Egészségtudományi Kar.
Vincze, T.: A testnevelés tanítása. Retrieved from: https://
uni-eszterhazy.hu/public/uploads/a-testneveles-tanita-
sa-2-_5538f30805117.pptx (2018. 07 23.)


re SpOrT GUiDE Li nES
ISBN 978-961-290-436-4
www.resport.si