
Requesting a Change in Training Requirements in Pediatrics ...
198
1 COS Application - Requesting a Change in Training Requirements in Pediatrics, with Implications on Length of Training Report Produced by the Preparedness for Practice in Pediatrics Working Group, Specialty Committee in Pediatrics Submitted August 31, 2018 (Revised January 7, 2019) Table of Contents Table of Contents 1 Working Group Members 3 Glossary 4 Executive Summary and Key Recommendations 5 Introduction 8 Background 9 Current Models of Pediatric Training in Canada 9 Historical Review 10 Jurisdictional Review 11 United States Model 11 United Kingdom Model 11 Australasian Model 12 Literature Review 12 ‘Preparedness for Practice in Pediatrics’ Survey 12 Rationale for Change in Training Requirements 14 Impact of Modification on Medical Education System 14 Consideration of Scope and Nature of Discipline 17 Level of Support for Modification 18 Royal College Committee on Specialties 18 Program Directors (Subspecialty) 19 Residents (Pediatrics) 21 Residents (Subspecialty) 21
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Requesting a Change in Training Requirements in Pediatrics ...

1
COS Application - Requesting a Change in Training Requirements in Pediatrics, with
Implications on Length of Training
Report Produced by the Preparedness for Practice in Pediatrics Working Group, Specialty Committee in Pediatrics
Submitted August 31, 2018 (Revised January 7, 2019)
Table of Contents Table of Contents 1
Working Group Members 3
Glossary 4
Executive Summary and Key Recommendations 5
Introduction 8
Background 9
Current Models of Pediatric Training in Canada 9
Historical Review 10
Jurisdictional Review 11
United States Model 11
United Kingdom Model 11
Australasian Model 12
Literature Review 12
‘Preparedness for Practice in Pediatrics’ Survey 12
Rationale for Change in Training Requirements 14
Impact of Modification on Medical Education System 14
Consideration of Scope and Nature of Discipline 17
Level of Support for Modification 18
Royal College Committee on Specialties 18
Program Directors (Subspecialty) 19
Residents (Pediatrics) 21
Residents (Subspecialty) 21

2
Department Chairs 22
Associate Deans 22
Canadian Paediatric Society 22
Ministries of Health 23
Support of New Training Models and Response to Emerging Issues in Health Care and Education Systems 23
Economic implications of the proposed change 24
Increased Productivity and Value 25
Better-Trained Pediatricians Provide Better Care: Better Care Reduces Overall Economic and Other Costs 25
Summary of Economic Implications 26
Table 1: Estimated Salary and Benefit Costs of Residents 26
Summary 27
References 27
Appendices Appendix A: Historical Review Appendix B: Jurisdictional Review Appendix C: Literature Review Appendix D: ‘Preparedness for Practice in Pediatrics” Survey Questions Appendix E: Letter from Pediatric Program Directors Appendix F: Minutes from May 29, 2018 Meeting with Pediatric Subspecialties
and Briefing Note Summary Appendix G: Pediatric Competencies draft (previously Objectives of Training) Appendix H: Required Training Experiences draft (previously Specialty Training Requirements) Appendix I: Specialty Specific Standards of Accreditation Appendix J: Submission of projected number of residents affected by this change Appendix K: Independent Cost Analysis

3
Working Group Members
Dr. Catherine Farrell Chair, Specialty Committee in Pediatrics, Royal College; Associate Clinical Professor, Pediatrics (Pediatric Critical Care), Université de Montreal
Dr. Adelle Atkinson Vice-Chair, Specialty Committee in Pediatrics, Royal College; Pediatric Program Director, University of Toronto
Dr. Karen Gripp Chair, Canadian Pediatric Program Directors; Director, Pediatric Postgraduate Medical Education, University of Manitoba
Dr. Robert Connelly President, Paediatric Chairs of Canada; Head of the Department of Pediatrics and Program Medical Director of Pediatrics, Queens University
Dr. Michael Dickinson President, Canadian Paediatric Society; Associate Professor, Dalhousie University
Dr. Ellen Wood Chair, Canadian Pediatric Society Education Subcommittee and Chair, Royal College Pediatrics Examination Committee; Division Head of Pediatric Neurology, Dalhousie University
Dr. Jonathan Kronick Former Chair of the RCPSC Pediatric Examination Board; Past-President of the Canadian Paediatric Society; Professor of Pediatrics, SickKids, University of Toronto
Dr. Susanna Martin Member, Pediatrics General Examination Board, Royal College; Region 2 Representative, Specialty Committee in Pediatrics; Associate Professor, General Pediatrics, University of Saskatchewan
Dr. Gina Neto Chair, Specialty Committee in Pediatric Emergency Medicine; Department of Pediatrics, University of Ottawa
Dr. Jayson Stoffman Program Director, Pediatrics Hematology/Oncology, University of Manitoba
Dr. Brie Yama Chief Resident at ICRE; Past Chief Resident at Sick Kids, University of Toronto
Dr. Jason Frank Director, Specialty Education, Strategy and Standards, Office of Specialty Education, Royal College
Ms. Sarah Taber
Associate Director, Education Strategy and Accreditation, Royal College
Ms. Jennifer Stewart Manager, Specialties Unit, Royal College
Ms. Lisa Gorman Manager; Educational Strategy, Innovations, and Development Unit; Royal College
Ms. Josée Conway Policy Analyst; Educational Strategy, Innovations, and Development Unit; Royal College
Ms. Shannon Elliot Policy Analyst; Educational Strategy, Innovations, and Development Unit; Royal College
Ms. Emma Huck Junior Policy Analyst;, Educational Strategy, Innovations and Development Unit; Royal College

4
Glossary
CanMEDS Educational framework designed by the RCPSC for residency education, focusing on the seven Roles of Medical Expert, Collaborator, Communicator, Leader, Health Advocate, Scholar and Professional
CBD Competence by Design CBME Competency-Based Medical Education CC Competence Committee COS Committee on Specialties (RCPSC) CPS Canadian Pediatric Society EMR Electronic Medical Record EPA Entrustable Professional Activity GIM General Internal Medicine ICRE International Conference on Medical Education IM Internal Medicine OSCE Objective Structured Clinical Examination PD Program Director PGME Postgraduate Medical Education PGY Postgraduate Year PPP Preparedness for Practice in Pediatrics survey RCPSC Royal College of Physicians and Surgeons (Canada) Royal College Royal College of Physicians and Surgeons (Canada) RPC Residency Program Committee RTE Required Training Experience STR Specialty Training Requirements TTD Transition to Discipline (Stage 1 of Competence by Design) TTP Transition to Practice (Stage 4 of Competence by Design) UGME Undergraduate Medical Education

5
Executive Summary and Key Recommendations The Royal College Specialty Committee in Pediatrics has examined the various components of Pediatric training in Canada on a regular basis in recent years. Inadequacies in the current training model have led us to recommend that changes should be made in order to best prepare Canadian pediatricians for the realities of practice in their specialty. The transition to competency-based medical education with the Competence by Design (CBD) process has provided the opportunity to clearly define the competencies to be demonstrated by residents upon completion of their training in Pediatrics, following a continuum of EPAs and associated milestones over four stages. During this process it has once again become clear to the Specialty Committee in Pediatrics that all residents must be provided the opportunity to achieve the EPAs reflecting the essential competencies of pediatricians practicing in Canada before they go on to further training in a pediatric subspecialty or Area of Focused Competence, or into practice in any setting. The Current Context of Pediatric Training In the current training system, certification in Pediatrics requires the successful completion of a Royal College accredited program in Pediatrics, the completion of a scholarly project and successful completion of the certification examination in Pediatrics. While the major, “core” part of Pediatric residency is explicitly mandated and includes a broad range of clinical experiences in academic, community and remote settings, the final, advanced phase of Pediatric residency allows some flexibility, the aim being to reflect a resident’s career plans and future practice setting, when this is known. This flexibility has extended to allowing residents to complete their residency in Pediatrics while being enrolled in a clinical residency in any of the subspecialty areas of Pediatrics. In the past two decades, two separate applications to the Committee on Specialties (COS) have outlined concerns about the adequacy of the “core” component of Pediatric training in preparing pediatricians for all aspects of general pediatric practice, especially given that many subspecialists also practice general pediatrics. At the time of the most recent prior application, the COS deferred a decision in the context of the impending transition to CBD and asked the Specialty Committee in Pediatrics to reframe the proposal in this new setting. Project Approach The Preparedness for Practice in Pediatrics Working Group (PPP WG) was formed in August 2017 with inclusive membership from across the country, representing postgraduate medical education expertise, academic leadership, the national specialty society for Pediatrics, with support from the Royal College Educational Strategy, Innovations and Development (ESID) Unit. This group completed a number of reviews—historical, other jurisdictions and the literature—related to the current model of training. In addition, a survey of Pediatric certificants who had completed Pediatric training as well as those who had completed subspecialty training was conducted in January 2018. Finally, an economic analysis of the impact of the proposed change to the requirements of certification in Pediatrics was performed. Key Findings The literature review revealed a relative dearth of any evaluations of the Canadian Pediatric training model with respect to its ability to adequately prepare pediatricians for general practice. While there are many studies in other jurisdictions on the preparedness of pediatricians for general pediatric practice, there have only been twelve relevant studies in the Canadian setting over the last twenty years. This review indicated that further data was needed regarding preparedness for practice, the

6
impact of overlap training and the current practice patterns of pediatric subspecialists after completion of training. The jurisdictional review examined three training systems globally that are similar to the Canadian model. In the United States, Pediatric training lasts for three years but has a different end-goal: the generation of general pediatricians practicing primary care but typically not as consultants, and also with no expectation of providing neonatal care. Subspecialty fellowships are usually of three years’ duration and include EPAs which would be considered part of Pediatric Core and Transition-To-Practice training in the Canadian system. In the United Kingdom, future general pediatricians train for at least seven years after medical school before they can practice independently. Prospective subspecialists must be certified in Pediatrics prior to commencing subspecialty training. In Australia and New Zealand, pediatricians must complete three years of basic training and then three years of additional training in either General Pediatrics or a subspecialty program to become fully certified. In the survey conducted by the working group, 34% of RCPSC subspecialty certificant respondents indicated their practice includes general pediatrics; of this group, 40% spend more than 40% of their overall clinical time in general pediatrics, yet 60% of those who practice any aspect of general pediatrics completed only three years of Pediatric training in a Pediatrics program. These findings reinforce the recommendation that all pediatricians have a solid general pediatric base in their training, before subspecialty training. The implications for funding the implementation of this proposal were also explored. The benefits of the proposed model are deemed to justify the cost of salaries for the completion of Pediatric residency training for those few residents who would require them. The additional clinical services provided by these senior residents are a tangible benefit to health care systems which currently compensates for resident shortages by paying for services provided by clinical assistants or in-house attending staff. What is more difficult to calculate is the ultimate economic benefit of the provision of care to pediatric patients in a broad range of settings by pediatricians who have all benefited from enhanced, comprehensive generalist training. Considerations The Specialty Committee in Pediatrics has recognized several training gaps of concern, which can be corrected in the new competency-based model of training. This includes increased emphasis in a variety of areas, including behavioral and developmental pediatrics, neonatology, mental health, advanced care planning and support, practice management, and medicolegal issues. This training is essential for all future pediatricians, including those who may go on to train in a subspecialty of Pediatrics. The re-design of Pediatric residency in the context of CBD makes it extremely challenging for pediatric subspecialty programs to provide the training experiences and evaluate the attainment of Pediatric EPAs within their programs. Thus, the recommendation is that training in Pediatrics should be completed within a Pediatric program before any further training begins. Support and Concerns There has been broad support from a number of stakeholders for this recommendation. The Program Directors (PDs) in Pediatrics have voiced unanimous support for including all components of Pediatric training, including the CBD Transition to Practice phase, within Pediatric programs. Similarly, subspecialty program directors have expressed concern about how subspecialty programs would assess EPAs from Pediatrics, which Competence Committee would have oversight of these trainees, and how to

7
ensure access to all Required Training Experiences, given they largely exist in the realm of general pediatrics. Both general and subspecialty Pediatric certificants have suggested a preference for completing all their Pediatric training before subspecialty training. Currently, the choices made by residents across Canada are often constrained by the length of training limits imposed in order to be eligible for Ministry-funded subspecialty training positions in Ontario, which offers by far the largest number of positions. They thus find themselves obliged to leave their Pediatric residency program having only completed the core components, even if they would prefer to complete their residency program first. The chairs of the Departments of Pediatrics recognize the considerable diversity in practice patterns across Canada as well as the need to support academic career training as part of a residency in Pediatrics; much of this advanced training occurs in the latter part of a Pediatrics residency. The PGME Associate Deans are aware of the decision to delay implementation of CBD and the reasons for doing so. The Canadian Pediatric Society supports the provision of the best possible training to meet the ever evolving and complex needs of Canadian children and youth. Recommendation Residency programs have a responsibility to patients, families and the greater community to train well-qualified specialist pediatricians, able to perform skills for which they are certified, and who are also sufficiently trained for all aspects of general pediatric practice. In the near future, certification in Pediatrics should be contingent upon the demonstration of competence through the completion of all EPAs within a Pediatrics residency program, in addition to passing the certification exam. This new model responds to emerging issues in the health care system by increasing skills and confidence, enhancing workforce flexibility, improving outcomes, and taking better care of children and youth. Given the breadth and depth of the practice of Pediatrics and the identification of gaps in training, providing equal opportunity for training of all pediatricians becomes the obvious path to meet the needs of Canadian children for decades to come. The working group proposes that subspecialty training can only begin once all of the clinical components of training in Pediatrics have been completed.

8
Introduction
Describe the rationale for a change in length of training for this discipline and specific educational objectives that are not being currently met. The transition to CBD has provided a new lens to examine the various components of Pediatric training in Canada, from the granular details to the far-reaching implications of how well pediatricians are prepared for practice during residency training. This process has highlighted, once again, inadequacies of the current model. Through the process of establishing EPAs and associated milestones for the four stages of Pediatric training, the Specialty Committee in Pediatrics and the larger CBD Working Group have unequivocally confirmed that it is highly desirable, indeed imperative, that all residents achieve the EPAs reflecting the essential competencies of pediatricians practicing in Canada in order to be certified as pediatricians. These competencies include the first three stages (TTD, Foundations and Core) as well as the final stage (TTP) EPAs that equip all pediatricians with the competencies they need for future practice in Canada, regardless of their practice environment. Currently, some pediatric residents enter subspecialty training after completing only the “core” portion of Pediatric residency training, as allowed by the Royal College and mandated by three provinces that do not provide funding to allow residents to complete all their Pediatric training before beginning subspecialty training. At the present time, for these residents, the final, advanced part of their Pediatric training is replaced by the initial phase of their training in a subspecialty of Pediatrics. However in a recent survey, 34% of RCPSC subspecialty certificant respondents stated their practice includes general pediatrics; of this group, 40% spend more than 40% of their overall clinical time in general pediatrics. Reasons for this choice included subspecialty job availability, desired location, lifestyle, changing scope of practice throughout their career trajectory, health and/or family issues. Of note, 60% of subspecialists who practice some aspect of general pediatrics completed only the “core” component of Pediatric training. This significant degree of combined general and subspecialty practice is not always anticipated by trainees; thus, it is essential that these pediatricians have the opportunity to complete their initial training in a Pediatrics program before embarking on further training in a subspecialty. The highly-detailed and specific nature of EPAs and milestones addresses deficiencies in current training in Pediatrics with increased emphasis on behavioral and developmental pediatrics, neonatology, mental health, advanced care planning and support, management of increasingly medical complex patients, practice management, and medicolegal issues. Some of these issues are contained within EPAs in the Core stage, which expands considerably the scope of the current “core” years. Others are part of the Transition to Practice phase, which does allow some degree of flexibility for residents to address specific learning goals related to their future career plans, while retaining specific training experiences in a general pediatric setting. Certification in Pediatrics would require the completion of all Pediatric EPAs within a residency program in Pediatrics. Trying to maintain the current pattern and timelines of “core” and “advanced” training in the CBD model has proved to be challenging. Royal College stipulations require that residents must complete at least the first three stages of specialty training (TTD, Foundation and Core) before starting subspecialty training, and some specialties may choose to design their model so that these three stages “fit” the way “core” training does now. But to condense the EPAs for these first three CBD stages to “fit” the existing model in Pediatrics would negate the benefit of the changes that have been made, and not truly address the requirements of pediatric practice, compromising the training of all Pediatric residents. In any

9
circumstance, we view Pediatric training as a continuum where the Transition to Practice phase builds on the first three stages, allowing residents to gain the maturity and skills they need for independent practice. There are four principles that form the basis of this analysis and subsequent recommendations: ● First, training experiences should be designed to achieve competencies in relation to
educational and career goals, not hospital service demands. This may require restructuring as to how care is delivered to pediatric patients.
● Second, the focus, especially with CBD, should be on achieving competencies for each certified
specialty or subspecialty using time as a resource and not as the driver of the curriculum.
● Third, the funding implications of the proposed change must be balanced with the overarching goals of improvement and achieving excellence.
● Finally and perhaps most importantly, our responsibility toward patients, families and the
greater community is to use our national and local resources to train well-qualified specialist pediatricians, able to perform skills for which they are certified and who are all adequately trained for all aspects of general pediatric practice.
Background
Current Models of Pediatric Training in Canada All residency programs must meet the Royal College Specialty Training Requirements (STR) for Pediatrics, with local variation to adapt to individual settings and resources. The current STR is relatively prescriptive with respect to the number and nature of rotations in the “core” component of specialty training. The final, advanced phase of training is designed to consolidate knowledge, especially in the key areas of general pediatrics outline above, further explore subspecialties, participate in electives outside one’s primary program, work in a longitudinal continuity clinic, gain administrative and managerial experience, and prepare for the transition to practice as a consultant general pediatrician. The current STR does allow the possibility that this final, advanced phase of Pediatric training may take place within a training program of a subspecialty of Pediatrics. This practice has occurred for at least 40 years with the assent of the RCPSC, based on the assumed premise of equivalency between the final phase of Pediatric residency and the initial phase of all subspecialty training programs. This proposal recognizes that this training is not equivalent when competencies are compared across the Pediatric subspecialty programs. In order to describe current practice, for the purpose of this document, residents whose final year of Pediatric residency takes place within their first year of subspecialty training are referred to as “3+2 residents” (signifying three years of Pediatrics and two years subspecialty training); “4+2 residents” are those who complete all of their Pediatrics residency before proceeding to subspecialty training. Several subspecialty programs, such as Hematology-Oncology and Cardiology, require more than two years of training, but for the purpose of this application, these residents will be considered as part of either the

10
3+2 or 4+2 group, based on whether or not Pediatrics residency is completed before starting subspecialty training. Currently, Ministry-funded subspecialty positions in Ontario, Quebec and Nova Scotia are essentially restricted to 3+2 candidates, with limited, non-guaranteed, non-Ministry of Health funding available for occasional 4+2 candidates who take the risk of not finding a training position if they choose to complete their Pediatric residency before entering subspecialty training. Historical Review (please see Appendix A for a more exhaustive summary) In the past two decades, two separate applications to the COS have outlined concerns about the adequacy of preparation of those residents who only completed three years of specialty training in Pediatrics. In 2003, the Pediatric Stream Model proposed a minimum of five years of training for general pediatricians as well as subspecialists, with the final two years to be focused on either Pediatrics or a subspecialty. This was similar to changes made in Pediatric training in Quebec by the Collège des Médecins du Québec beginning in 2000. While the RCPSC supported the proposal, residents and practicing pediatricians surveyed at that time felt adequately prepared for general pediatric practice with four years of training. Also, subspecialists were concerned they would not be allowed to practice any aspect of general pediatrics, as only those completing the five-year General Pediatrics track would be eligible for certification. Of note, only 2% of pediatricians felt that three years of training was sufficient to practice Pediatrics; 78% supported four years and 20% felt five years were required in order to practice as a general pediatrician. Liberman and Hilliard (2006) summarized much of the evidence gathered in support of the 2003 application. Areas in which respondents felt less adequate were similar to those identified in more recent surveys, and included mental health/behavioral issues (a growing part of a general consulting pediatrician’s practice), palliative care and bereaved parents, manager/office practice administration, and non-accidental trauma. At that time, concern was already being expressed following changes in duty hours and the consequent decrease in clinical exposure residents receive during their training. While the general consensus remains that duty hour limitations were and are necessary, evidence suggests that the overall competency of graduates has not improved and perhaps has even decreased, likely due to less “time in the trenches”. More post-call days and time away from rotations for mandatory formal teaching, as well as the increasing use of complex EMR systems, have resulted in decreasing continuity of care and opportunities to build clinical experience. Unpublished data suggests that residents now spend up to 25% fewer hours in direct patient contact than before implementation of duty hour limitations. Additionally, the delegation of tasks to other professionals such as nurse practitioners and physician assistants may also impact resident autonomy and decision-making. While some degree of skill acquisition has transitioned from the bedside to simulation centres, the need for “hands-on” experience in providing direct care for patients remains a fundamental part of residency training. In 2013, a second application was submitted to the COS, stating that three years is inadequate for ensuring core competencies for practice in Pediatrics. While the proposal had support from stakeholders, including residents and practicing pediatricians as well as the COS, there were concerns regarding the lack of evidence and funding implications. The COS deferred approval at that time, given the imminent plans for moving to a competency-based educational model, and recommended that the

11
Specialty Committee in Pediatrics reframe the discussion in the context of CBD and re-submit the application in the future. In May 2018, the Postgraduate Deans accepted the Specialty Committee in Pediatrics’ recommendation to delay the introduction of CBD in Pediatrics until July 2020 to allow for a comprehensive review of how to best plan Pediatric residency training. Jurisdictional Review (Please see Appendix B for a more exhaustive summary) What is the required length of training for this discipline in other jurisdictions? Please list a detailed comparison of training. Training systems in comparable jurisdictions across the globe were examined. Three pathways were identified with similarities to the Canadian model: the United States, the United Kingdom and the Australasian models. United States Model In the United States, Pediatric training lasts for three years and all requirements for general pediatric certification must be met prior to commencement of subspecialty training. Subspecialty fellowships are generally three years in duration and include EPAs which would be considered part of Pediatric Core and TTP training in Canada. Of note, Pediatric Hospital Medicine now offers subspecialty certification, acknowledging the need for additional experience, beyond that provided in specialty training, in the management of acutely ill in-patients and coordination of care of patients with unclear diagnoses and/or medical complexity. The distinction between training in the U.S. and Canada is not in quality, but in the final product. General pediatricians south of the border usually practice primary care pediatrics (without the requirement of neonatology) and not the consultant model found across Canada. Many EPAs expected of Canadian pediatricians would only be attained during fellowship training in the US, and for most, to complete training as a pediatric subspecialist (with eligibility for both general Pediatric and subspecialty certification) requires a total of six years. United Kingdom Model In the United Kingdom, pediatricians practice in a consultant model. A somewhat different pathway takes residents through an initial two-year foundation program following medical school graduation. Thereafter, residents selected as future pediatric consultants complete an additional 5–8 years of training before they can practice independently. As the U.K. uses a competency-based rather than a time-based system, a resident may finish specialty training in as little as five years (in addition to the two foundation years) as an absolute minimum, though the average is seven years (plus two foundation years). Training includes three stages of which the final stage is either General Pediatrics specialization or focus on a subspecialty. From the website of the Royal College of Paediatrics and Child Health: “All paediatric trainees achieving a Certificate of Completion of Training (CCT) in the UK receive accreditation in paediatrics, and so must be competent in delivering acute paediatric and neonatal care. While trainees in many subspecialties may not anticipate performing general paediatric on-call duties once qualified as a consultant, it is important that they recognise the value of these competencies in ensuring they can deliver safe care to the children for whom they are responsible.”

12
Australasian Model In the Australasian model, used by both Australia and New Zealand, pediatricians must complete three years of basic training and then three years of additional training in either General Pediatrics or a subspecialty program to become fully certified. With approval, overlap is allowed between two select subspecialty programs but not with General Pediatrics. In summary, one of three similar training models allows completion of Pediatrics training in three years but requires additional training to achieve many of the EPAs included in the Canadian Pediatric residency model. Both of the overseas models train consultant pediatricians, analogous to Canada, and require a minimum of six or seven years to do so. Literature Review (please see Appendix C for a more exhaustive summary) A literature review conducted in context of survey preparation attempted to determine the answers to three main questions. Are Pediatric residents prepared for practice upon graduation? What is the support for length of specialty training? And how many subspecialists practice general pediatrics in some capacity? With regard to preparedness for practice, Canadian pediatricians have consistently expressed concerns in several main areas including behavioural and developmental pediatrics, mental health, neonatology, and adolescent medicine. Various studies show strong support for four (or more) years of Pediatric training. While this support must now be interpreted in the context of a CBD non-time-based model, the objectives of specialty and subspecialty training remain sufficiently different that a fourth year of Pediatric training and the first year of subspecialty training should not be considered compatible. The literature also documents an increasing number of subspecialists who currently or are anticipated to practice general pediatrics. Additionally, multiple reports comment on the need for increased staffing with resident extenders, at a significant additional cost, to make up for the lost time due to resident duty hour limitations. Concerns exist among mental health, behavioural and developmental specialists that pediatricians currently practicing general pediatrics do not have an adequate foundation of knowledge and experience to cost-effectively manage the increasing number of patients with complex and/or mental health conditions. One author documents that approximately “20% of children have mental health diagnoses, which are now the “most costly chronic conditions of children.” (Stein, 2015). The review showed significant research gaps in the evaluation of Pediatric training in Canada and led to creation of a survey of all Pediatric specialty and subspecialty certificants, including different perspectives from those who had completed all four dedicated years of training versus subspecialists whose final year of training in Pediatrics was replaced by the first year of subspecialty training. ‘Preparedness for Practice in Pediatrics’ Survey In light of the Pediatric discipline’s upcoming transition to a competency-based curriculum, and with support from the Royal College, the ‘Preparedness for Practice in Pediatrics’ (PPP) Working Group conducted an in-depth review of the current configuration of Pediatric training. This study aimed to develop a comprehensive understanding of the current state of Pediatric training in Canada to help

13
determine whether the current training model provides trainees with the opportunity to acquire the skills required for independent practice in general pediatrics. To accomplish this objective, the PPP Working Group distributed self-report surveys to Pediatric certificants who had completed Pediatric training as well as those who had also completed subspecialty training. The survey also included Pediatric specialty and subspecialty program directors and provided opportunities for residents to share their perspectives through focus groups and interviews. Questions asked in this survey are included as Appendix D. [Of note, a certificant is an individual that has passed the Royal College of Physicians and Surgeons of Canada examinations and is certified to practice in the specific area. The General Pediatric Certificants Survey (GPCS) included two branches of certificants: Pediatric certificants and Pediatric certificants that are currently in subspecialty training. The Pediatric Subspecialties Certificants Survey (PSCS) was distributed to all Pediatric subspecialists.] Findings from the historical, jurisdictional and literature review identified three domains of information for data collection: the training model, career decision-making, and practice. The collection of demographic information helped group and compare responses of pediatricians with a similar training background. Information on the training model and the practice of participants was essential to understand the strengths and weaknesses of the current model in relation to the scope and nature of pediatric practice, while information about participants’ career decision-making revealed interrelated challenges that impacted training and practice context. The research design utilized a convergent mixed methods design, comprising both quantitative and qualitative methods of data collection, with the aim of qualitative methods to provide enhanced context to the quantitative results. Owing to design and practical considerations, quantitative and qualitative research occurred simultaneously, rather than consecutively, and asked two key questions: are all pediatricians adequately prepared for all aspects of general pediatric practice, regardless of the training model? Are there other interrelated challenges or considerations in this context that may be impacting training and practice? The quantitative analysis of responses supplied by program directors (PDs) with regards to residents’ management of general pediatric conditions demonstrated that PDs agreed that, with regard to managing several general pediatric conditions, trainees that left Pediatrics residency to pursue subspecialty training are less prepared than their counterparts who completed residency training in Pediatrics prior to subspecialty training. These results were statistically significant. The qualitative analysis assisted with providing context and developing an understanding of the perceived ‘preparedness for practice’ of residents from PDs perspective. PDs reported seeing similar challenges and offered similar solutions. Subspecialty and specialty PDs were more likely to raise challenges that related directly to the realities of subspecialty training and specialty training respectively. The findings indicated that subspecialists may be called upon to do general pediatric work even in academic centres, with the percentage of time spent in general pediatrics varying widely across sites and subspecialties, ranging from <10% of time to 55% of their time in the PPP study. Moreover, beyond the time spent in activities that are "labelled" as being general pediatrics, subspecialists still encounter issues in their patients that are not directly related to their subspecialty, as many subspecialists reported having to address more general pediatrics cases and conditions than anticipated. When comparing subspecialists who did or did not first complete their residency in a Pediatrics program, the difference in their perceived preparedness to handle a wide range of pediatric problems did not reach statistical significance. However, the proportion who expressed lack of readiness was twice as

14
high as the proportion of general pediatricians. Given that all subspecialists will be confronted with some general pediatric issues in their patients, and that some subspecialists will actually be responsible for a general pediatric patient population at least some of the time, these results support our conclusion that it is our responsibility to give them the training they need to be able to do this work as effectively as their general pediatrician colleagues.
Rationale for Change in Training Requirements
Impact of Modification on Medical Education System Outline of the implementation issues and funding implications for universities. Description of the role of post-certification fellowships in contrast to specialty residency training. This proposal separates training of defined competencies into two distinct and sequential pathways, with the first pathway consisting of residency training in Pediatrics. For some residents, this training can then be followed by further training in one or more subspecialty programs. In this model, the subspecialty training program, generally considerably shorter in duration than the Pediatrics residency, can focus on that specific area with its specific competencies. When comparing potential models for overlap training in the context of CBD, there are some EPAs, particularly in TTP, which appear similar, whether in Pediatrics or a Pediatric subspecialty. However, looking beyond the titles of these TTP EPAs, it becomes clear that the clinical context and assessment criteria (e.g. management of an office-based practice versus management of an Intensive Care Unit) are quite different. This juxtaposition applies to all subspecialties, even those not primarily hospital-based such as Developmental Pediatrics and Adolescent Medicine. The incompatibility is even more striking when comparing the TTP EPAs in Pediatrics with the Transition-to-Discipline/Foundation EPAs of subspecialties, although this corresponds to the period which would currently be considered equivalent if training is overlapped. The COS defines length of training as the “designated amount of time residents spend […] to be considered eligible for certification […] as based upon the stipulated Specialty Training Requirements of the discipline.” The COS also delegates authority to the relevant Specialty Committee for development of a national curriculum for the discipline. In this light, the Specialty Committee in Pediatrics feels strongly that eligibility for certification in Pediatrics must include completion of all the EPAs in Pediatrics through completion of the RTEs within the setting of a residency in Pediatrics. The Specialty Committee for Internal Medicine had similar discussions regarding the adequacy of training in general Internal Medicine (IM). This resulted in the creation of a two-year program in General Internal Medicine (GIM). Residents who choose to train in a subspecialty may be certified in IM after completing their first year of subspecialty training. However, in many jurisdictions it is now only those who have completed the core IM plus GIM program who can obtain positions to practice as internists. The CBD working group for IM chose to maintain the status quo by creating a three-stage core IM program feasible for completion in three years (including an exam similar to the current certification exam), with the assumption that all residents would proceed to further training before practice. The final stage of training is essentially delegated to the subspecialty the resident then enters, which may be GIM, although technically residents who go on to subspecialty training will also be able to be certified in Internal Medicine (but uncommonly practice IM in addition to their subspecialty).

15
Designing an additional “General Pediatrics” residency similar to GIM has been considered (as outlined in the 2003 proposal described previously), but the pediatric landscape differs from IM in several important ways. Pediatricians who practice both general pediatrics and a subspecialty require training and certification in both areas. Most Internal Medicine specialists are trained in and practice either GIM or a highly-focused Medicine subspecialty but rarely both. At least in medium-sized and many small communities, there are usually more IM subspecialists compared with few (if any) Pediatric subspecialists, so that community general pediatricians must have the competencies to manage patients with subspecialty-related disorders. The practice of Internal Medicine focuses on the care of adults, including geriatric patients. Pediatricians provide care to patients from many age groups with unique pathologies, as well as varying presentations of diseases, within the spectrum from newborns to late adolescents. As is the case with some IM physicians, pediatricians practice in ambulatory and community clinics, hospital inpatient units, emergency departments, rural towns, remote locations and First Nations reserves, as well as academic urban tertiary centres, with the added responsibilities of pediatric coverage of Level 1 and 2 nurseries, on-call services for obstetric deliveries, and the stabilization and management of sick newborns. Many pediatricians serve in two or more of these areas, and a substantial number move between different practice arenas as their career evolves. Finally, the high-volume service delivery model in IM means that trainees see relatively rare cases more frequently. This contrasts with Pediatrics, in which high-stakes diagnoses, such as meningitis and leukemia, are seen relatively infrequently and therefore trainees may take longer to gain sufficient clinical exposure and learning. It could thus be argued that those entering general pediatric practice could benefit from even more training than they currently receive. The financial implication of prolonging training for each and every pediatric resident would be substantial. The Specialty Committee in Pediatrics feels that the improvements made to training in Pediatrics in the CBD model are sufficient, as long as all residents are able to complete all components of this training, and with the move away from time based training providing the opportunity to ensure competencies are achieved. Offering certification in either Pediatrics OR a Pediatric subspecialty (and not with Pediatrics) is not an option, in accordance with Royal College policy that all Pediatric subspecialists be also certified in Pediatrics and because of the clear reality that many subspecialists practice both general pediatrics as well as their subspecialty. Nevertheless, we have considered the possible ways in which training in Pediatrics and training in a pediatric subspecialty could overlap, in the CBD model. Our conclusion is that these options present many challenges when the following factors are considered:
1. Each of the 17 RCPSC-accredited pediatric subspecialties would have to design its program in such a way that each of the Pediatrics TTP EPAs could be assessed within the subspecialty program. For some subspecialties, a few EPAs have a natural degree of overlap, such as management of “an outpatient consultative practice”. For many other subspecialties, the EPAs are more dissimilar and incompatible with general Pediatrics, such as acute care subspecialties like Pediatric Critical Care Medicine and Neonatal and Perinatal Medicine.
2. To ensure adequate training, the Pediatrics Core stage as currently designed is likely to extend
into what would currently be the PGY4 year. This creates obvious logistical challenges for the initiation of subspecialty training if a fixed July 1 start date is retained. Currently the Royal College requires that residents in any CBD program must complete the Core stage before advancing to subspecialty training. But even greater challenges would exist if the subspecialty program was charged with evaluating their new residents on the remaining Core EPAs in
16
Pediatrics, while concurrently trying to teach and evaluate those residents in their subspecialty Transition to Discipline and Foundations stage EPA’s.
3. Required training experiences, such as Continuity Clinics and the Pediatric Junior Attending role,
would be difficult to organize and evaluate during subspecialty training. The challenge becomes even more complicated if the resident undertakes subspecialty training in a different location.
4. Since Competence Committees (CC) will still need to make decisions about resident progress,
the Royal College has suggested three possible models for overlap training.
In a delegated model, the subspecialty CC will need to evaluate its subspecialty residents on Pediatric residual Core (if applicable) and TTP EPAs. This would require the subspecialty faculty to be competent to teach, coach and evaluate the Pediatric specialty TTP EPAs, a proportion of which are required to be evaluated in Pediatric training sites.
In a conjoint or facilitated model, a Pediatrics CC could maintain oversight on the
Pediatrics EPAs while the subspecialty CC oversees the subspecialty EPAs. This presents challenges if the resident moves to a different centre for subspecialty training, as the original CC no longer has jurisdiction over the resident and additionally has no control over assessments and training experiences at the new centre. Potentially, the Pediatrics CC at the new centre could become involved, necessitating a detailed transfer of information from the original centre. Technology such as ePortfolio could make some information easily accessible, but the resident file (with STACERs, in-training exams, etc.) from the first three years would remain at the original centre. This would place a substantial burden on centres that have a large number of subspecialty training programs and trainees. Furthermore, the various centers have not adopted uniform technology, posing additional challenges with compatibility and access to information.
With any of these models, a fundamental question remains: which CC has, or should have, the ultimate authority for recommending certification in Pediatrics for a resident who begins training in a subspecialty prior to completing their training in Pediatrics?
Another possibility is to assume that the TTP stages in Pediatrics and the pediatric subspecialty are equivalent. However, as discussed above, the EPAs and required training experiences and settings may not be equivalent. Moreover, the TTP stage in Pediatrics is anticipated to last for six to eight months, longer than the anticipated three to four months in most subspecialties.
5. The written certifying examination for Pediatrics which currently occurs at the end of PGY4 will likely move to the end of the Core stage, with the in-person OSCE examination taking place at the end of the TTP stage. This reduces but does not eliminate the concern of most subspecialty PDs who note the distraction of exam preparation in their trainees who have not completed the exam process prior to beginning subspecialty training. A few quotes from subspecialty program directors from our PPP survey:
“Most trainees admit that they do not study for their subspecialty until they have
completed their Pediatrics exam.”

17
“Many subspecialty groups now don’t expect much from their first years, recognizing that they are preparing for Pediatrics exams.”
“Subspecialty residents also express that they feel they wasted a year of potential
subspecialty training studying for the exam.” Consideration of Scope and Nature of Discipline How would a change in length of training for this discipline affect the delivery of medical care and meet community needs? Over the last 20 years, some elements of the practice of pediatric medicine have remained stable. General pediatricians are expected to provide care for a wide range of ages and developmental levels, including patients with delayed development. Pediatricians practice in many different settings and locales, from isolated rural areas to urban centres, as consultants and hospitalists and providers of primary care, in acute access departments and long-term clinics, providing a medical home for patients with chronic conditions. Many pediatricians have a mix of settings and patient populations in their own practice, including those in academic positions who do follow-up clinics or outreach clinics in outlying regions. However, much has changed. Thanks to rapid advances in technology and other health care modalities and resources, children with higher complexity live longer and more active lives, while still requiring ongoing monitoring and care. Their care has shifted from primarily inpatient to predominantly outpatient settings, so that both subacute and chronic issues are more often managed within the community, thanks to the expertise of general pediatricians. As many acute infectious pathologies such as meningitis and epiglottitis have decreased in frequency thanks to effective immunizations, the role of the pediatrician in diagnosing and managing complex behavioural, developmental and mental health issues has grown. And as tertiary care neonatology expands its horizons to the limits of viability, many regional centres now assume the care of younger and smaller premature infants beyond the acute phase. This poses challenges to pediatricians, and some universities, in an effort to ensure a skilled workforce for the care of sick newborns, are now offering a one-year fellowship to enhance these neonatal skills which are not felt to be acquired adequately during specialty training in Pediatrics. The content of pediatric training has continued to expand to address this reality as well as the needs of the greater medical system, hospitals and medical schools. Pediatric residency now must incorporate education in areas such as patient safety, quality assurance and quality improvement, working within interprofessional care teams, leadership skills, and physician wellness. Concurrent with these changes in the pediatric landscape, time spent in the training setting has decreased. As noted earlier, duty hours policies have significantly impacted the amount of time spent in direct patient care and other clinical experiences. Many curriculum topics cannot be adequately covered in the current “core” years, and the current survey demonstrates that pediatric graduates still feel unprepared to manage a number of conditions independently, such as behavioral issues/autism, mental health disorders, suspected abuse, advanced care planning and support, office management and billing, and medico-legal issues. Taking these into consideration means adding content to training, enhancing rather than replacing what is already there. Many programs presently face challenges in providing the content of the current Pediatric specialty program as laid out in the Specialty Training

18
Requirements, let alone adding additional areas. In all Pediatrics programs, the final, advanced phase of training, although not explicitly described in the Specialty Training Requirements, is structured to provide opportunities to allow residents to develop greater competency in these advanced areas. Thus, residents leaving a Pediatrics program before this phase have and will continue to have significant gaps in their training. Level of Support for Modification Many stakeholders provide oversight and support of Pediatric training in Canada, each playing a vital role in the training process. The level of support of each key stakeholder is reviewed below. Royal College Committee on Specialties COS policy defines specialties and subspecialties as clearly demarcated entities, with specialties providing training for a broad-based body of knowledge and a foundation for additional competencies. In contrast, a subspecialty consists of a more focused and advanced scope of practice, building upon the fundamental knowledge defined in a parent specialty. These criteria infer that subspecialties should build upon training and experience previously acquired. Pediatrics and its subspecialties are designed to follow these principles: Pediatric subspecialty training is intended to add an advanced and complementary skill set to training in Pediatrics. However, the current training model with the option to omit the final phase of residency in Pediatrics and replace it with training in a subspecialty reduces the quantity and quality of training in Pediatrics for residents following this model. There are certainly pediatric subspecialists who completed a 3+2 pathway and now practice general pediatrics proficiently and capably, often learning “on-the-job” the necessary skills and abilities that should have been acquired during the final phase of training in Pediatrics. This proposal does not intended to cast doubt on their skills and abilities but seeks to improve the current state of training by providing equal opportunities for all who are to be certified in Pediatrics to gain the competencies they require during residency. In Canada, a sustainable practice base for Pediatrics across the country currently depends on subspecialists providing general pediatric care, although practices vary with geographic location and setting. Even in settings where subspecialists can limit their patient population, they are frequently called upon to address the more general pediatric issues their patients present. The Royal College has promoted the concept of generalism, as “a philosophy of care that is distinguished by a commitment to the breadth of practice within each discipline and collaboration within the larger health care team in order to respond to patient and community needs” (Final Report of the Generalism and Generalist Task Force, 2013). It is in this spirit that the Specialty Committee in Pediatrics feels that it is essential for pediatric subspecialists and the patients they serve to have acquired the full range of competencies in Pediatrics before embarking upon focused training in the subspecialty. As previously stated, the Specialty Committee in Pediatrics has examined this issue on several occasions in the past two decades and firmly believes that this proposal is essential to ensuring the best possible provision of pediatric care in Canada. Program Directors (Pediatrics) All Pediatric Program Directors (PDs) unanimously support this proposal (Appendix E). As the individuals closest to the residents making these difficult career decisions and also as the overseers of the four stages of Pediatric training in CBD, program directors know most intimately the challenges of fitting
19
every needed component into a limited period of time. Additionally, PDs each have a finger on the pulse of newly-graduated residents, providing anecdotal yet valuable evidence to support a united desire to see all residents able to benefit from all stages of Pediatric training in their programs once CBD is launched. The PPP study findings indicated an important difference in trainees’ abilities to manage general pediatric conditions based on whether they overlapped training or not. These conditions included ADHD, behavioral issues such as autism, newborn resuscitation, mental health disorders, suspected abuse, anticipatory guidance, and children with medical complexity. In the PPP survey, when asked to suggest changes to the current training model, PDs suggested the following:
● Increased responsibility and more independence in training ● Enhanced and more comprehensive curriculum to include additional:
○ continuity clinic experience ○ rotations (or rotations of longer duration in some instances) ○ focus on NICU/neonatal care, mental health and psychiatry, acute and complex care,
and adolescent medicine ● Increase in exposure to community, rural and regional experiences ● Better balance between patient and outpatient exposure.
Quotes from the study include the following:
“In general, I would have more trainees out in the community, and support those hosting practitioners more to have them. Living the reality is the only way to wrestle with this work and understand the scope of it all. Too much developmental peds is taught in the tertiary care ("one patient all day") model that is not reality. Neonates are not seen enough, mental health is woefully underserviced.”
“It would be good to have longer rotations in Developmental Pediatrics later in training so that the generalist feels comfortable seeing a range of issues. Also recommend more mental health training since mental health issues are so common in Pediatrics.”
Program Directors (Subspecialty) Subspecialty program directors and Specialty Committees were asked how the EPAs for Pediatrics align with the EPAs for each program and how they envision resolving the question around assessment and competence committees. A dedicated Specialty Committee meeting was convened in May 2018 to discuss this proposal with subspecialty representatives. Those unable to attend in person or via teleconference provided briefing notes based on specific questions. The meeting minutes and the briefing note summary are attached (Appendix F). To date, only one subspecialty felt that retaining the 3+2 model is preferable, with the primary reason given that 95% of practitioners in this subspecialty enter academic practices without providing additional general pediatrics coverage. An additional reason is concern for funding reallocation from subspecialty positions in order to finance extra Pediatrics training. A third concern heard from subspecialty PDs is that fewer applicants will choose subspecialties because of the longer length of training. However, data from resident interviews suggests that a slightly longer training pathway will not change career plans.

20
Subspecialty PDs echo many of the concerns about overlap training previously identified. In general, PDs identified that a real difference exists in general pediatric knowledge and skill between 3+2 and 4+2 residents. Residents entering subspecialty training without having completed their Pediatrics residency have fewer opportunities to learn about the subspecialty as they focus on studying for the Pediatrics exam. In the recent survey, only 12% of subspecialty PDs stated they would feel comfortable assessing residents on EPAs belonging to Pediatrics. Subspecialty programs must also take into account the possibility that in the CBD version of Pediatrics their residents may not be ready to start subspecialty training on July 1 of their fourth year, as currently occurs, because they are unlikely to have completed all the Pediatric Core EPAs. This has obvious implications for staffing on various subspecialty services, depending on the provision-of-care model. Making this proposal operational would imply that each subspecialty that currently allows residents to begin training in the subspecialty while concurrently completing their Pediatric residency would have to change their entry requirements. Presently, they all require residents to be certified in Pediatrics as one of the criteria for certification in the subspecialty. This proposal would clarify that certification in Pediatrics implies having completed all of the Pediatric EPAs, within a Pediatric residency program. Quotes from the survey highlight the reasons for support from subspecialty PDs:
“[The subspecialty residents] all hate it. The ones who do four years of Peds worry about applying to our subspecialty because of funding. The ones who overlap feel like the overlap year is too stressful and an inefficient use of their training.” “They find the first year hugely challenging and then realize how much they have to catch up on in the second year.” “Overwhelmingly they wish they could do four years and then subspecialize.” “Trainees who complete a 3+2 model have a much less mature approach to managing pediatric patients, which would have a significant impact should they plan to work in Gen Peds.” “All pediatric residents should have to do four years of Pediatrics before a subspecialty.” “Make four-year training mandatory! There is insufficient time and supervision when overlapping. This is a detriment to both the pediatric and subspecialty training.” “Four years in general Pediatrics prior to subspecialty training [...] provides residents to enter fellowship programs with a more mature/ better developed set of consultancy skills [...] stronger fellows with refined clinical skills.” “Three years is not adequate to include all the general pediatric training that is very important for a sub-specialist to have. Parents and patients expect subspecialists to also be able to address general pediatric issues.” “Three years of general pediatrics is not enough to teach and assess the core competencies of general paediatrics. Pediatrics has continued to evolve to become more complex, and graduates who choose to do a subspecialty and ultimately practice general pediatrics and their subspecialty

21
feel, and are, unprepared for the general pediatric component, particularly around care of the sick newborn, as well as pediatric mental health, etc.” “I don't feel that three years of core Pediatrics training is sufficient to be able to consider oneself to be a Pediatrician, especially for practice outside of an acute care hospital setting. The increasing complexity of patients, as well as the many other demands on resident's time for academic pursuits, in a context of reduced duty hours, means that residents have much less clinical exposure in those three years than I did during my residency [...] The subspecialty programs cannot or will not offer these residents the same opportunities to consolidate their Pediatric knowledge and skills as the residents who continue for four years have.” “The objectives of PGY-4 in Pediatrics are completely different from the objectives of any of the subspecialty training programs at my institution.”
Residents (Pediatrics) What would residents choose if given the option of three versus four years of training prior to subspecialty residency? As part of the CBD planning workshops, chief resident representatives from the provinces with the 3+2 model were asked about a possible decision to make completion of Pediatric residency prior to beginning subspecialty training mandatory. The response indicated overwhelming support to do so. Data for the past four years in provinces which allow completion of Pediatric training prior to subspecialty training shows that a significant majority (59%) of residents chose to complete their residency in Pediatrics prior to starting subspecialty training. Program directors across the country have confirmed that many of the residents who transitioned into subspecialty training earlier, and were therefore not counted in the 59%, left their programs not because they wished to do so, but in order to have better access to a subspecialty position in Ontario (which offers the largest number and variety of subspecialty training positions in Canada). Mandating that all residents complete Pediatric training prior to subspecialty training would “level the playing field” with regard to applying for subspecialty positions through the Canadian Resident Matching Service (CaRMS) and will thus create a more fair, transparent and deeper applicant pool. Residents (Subspecialty) In the PPP survey, only just over a third of residents currently enrolled in subspecialty training would have chosen a 3+2 model if funding was not an issue. The main factors in their decision regarding the timing of the start of subspecialty training included funding (most had no choice), ability to focus on exam preparation, and adequate preparation in general pediatrics. Our survey indicated that the majority of the 3+2 residents in Canada considered funding restrictions as a significant factor in their decision-making. Both Pediatrics and Pediatric subspecialty certificants were asked about strengths and challenges of the current model. Those who volunteered comments on the desired length of base specialty training suggested that four years is the preferred length for all pediatricians who will have a general pediatric component to their practice. Practically, this applies as well to pediatric subspecialists, as most will encounter general pediatric issues within their subspecialty practice as well.

22
Department Chairs The chairs of Departments of Pediatrics across Canada play a major role in mediating the disparities between training positions and workforce needs. The need for general pediatric care by consultant pediatricians continues to grow, with recently published acknowledgement that Canada faces a countrywide shortage of pediatric generalists (Tithecott, 2018). Career opportunities for pediatric subspecialists do exist, especially in certain areas, and finding the right balance is not an easy task. If funding a potential increase in final-year Pediatric residency positions, is accompanied by a reduction in the number of funded subspecialty training positions, there is a risk of a detrimental pendulum swing, potentially training insufficient numbers of subspecialists to meet the demand. The Pediatric Chairs also feel strongly that preparation for an academic career should be part of Pediatric training. Providing all Pediatric residents with the final phase of training allows more in-depth focus on scholarly activity with the opportunity for advanced research projects and exploration. There is considerable variety across centres as to the component of their subspecialty faculty members’ practice which would be considered to be general pediatrics. This does potentially colour each Chair’s opinion regarding the pertinence of completing training in Pediatrics prior to starting subspecialty training. The Chairs share concerns about the incompatibility of fitting the first three stages of the Pediatrics CBD program into three years and acknowledge the major difficulties in scheduling that could ensue if the start dates for subspecialty residents no long fit the July 1 model. Associate Deans The PGME Associate Deans remain aware of our concerns and play a vital role as stakeholders in balancing the fiduciary relationships between educational needs and funding sources. At their request, a Working Group was struck in 2016 to evaluate the current CaRMS pediatric subspecialty match process using a mixed-methods approach. The Working Group identified as problematic the confusion between 3+2 and 4+2 applicants with different and non-guaranteed funding models. Of even more concern was the timing of the match, which forces residents to make crucial career decisions before the midpoint of their second year, in order to conform to the 3+2 model that is imposed to conform to the jurisdictions with the most subspecialty positions to offer. While not directly related to the current proposal, this unease suggests a desire to allow residents time for broader exposure and maturation before making definitive choices about their career path. Canadian Paediatric Society The Canadian Paediatric Society (CPS) fully supports the notion of providing the best possible training to meet the needs of all Canadian children and youth. One of the missions of the CPS is to support all of its members, including residents and early-career pediatricians and those who will be implementing CBD, as well as community preceptors, through its range of educational opportunities. A recent (2018) CPS survey of early-career pediatricians, defined as certificants from the years 2010–2016, provided additional clear evidence of gaps in current postgraduate training, particularly for those skills that will be acquired in the ‘Transition to Practice’ stage after implementation of Competency by Design. Survey results showed that early-career pediatricians are largely satisfied with their practice type and setting, but desire more support prior to, and during, their transition to practice. The most common specific identified challenges of transition to practice included:
1. Billing, financial, and practice management 2. Completing non-clinical activities (administrative, electronic health records)

23
3. Adjusting to a different scope of practice and learning local resources 4. Managing comfort level and stress associated with newfound responsibility 5. Achieving work-life balance
The main skills that early-career pediatricians wish they had acquired prior to starting practice were as follows: billing/office financial management; recognizing the significant volume of paperwork/ administrative tasks; establishing work-life balance; navigating competing professional demands; and understanding and negotiating employment contracts. Early-career pediatricians recommended further postgraduate training in the following areas: billing information and financial seminars; practice management; mentorship; orientation to job opportunities and pediatric practice types; career counselling; and understanding continuing professional development expectations. The results from this survey are similar to the American Academy of Pediatrics early-career pediatrician survey of April 2018. Of similar questions asked in the PPP survey, the vast majority of certificants reported that medicolegal issues as well as office management and billing were new to them at the beginning of independent practice or that they had minimal exposure and was not ready to manage it independently. Ministries of Health Any proposal to change the length of training has funding implications. Consideration of these concerns must include a strong justification of additional funding if necessary. The explanations given thus far do justify any extra cost for the training of a small number of residents. It is of note that it is already possible in a number of jurisdictions to complete residency training in Pediatrics prior to beginning subspecialty training. The overall benefit to the health care system in the long run, although difficult to anticipate with precision, is well worth the investment in improved training of Canada’s future pediatricians. Support of New Training Models and Response to Emerging Issues in Health Care and Education Systems Retaining the current model could provide some benefits. There would be no perceived “new money” to be found to pay for an additional year of residency training for approximately 35 individuals per year (although this expense is offset by savings in other areas). For some residents, family and/or financial reasons may motivate them to finish training as quickly as possible. Other residents may intend to practice exclusively in their subspecialty area, but past experience indicates that even these residents may have no choice but to accept positions with a general pediatrics component. A model where everyone completes their residency in a Pediatrics program provides more flexibility in the workforce if subspecialists choose to practice general pediatrics for one or more of many reasons mentioned earlier. This can help increase coverage in rural and remote areas. The challenges and flaws of retaining the 3+2 model once CBD is implemented overwhelm any potential benefits—but this is not the only reason for this proposal. The Pediatrics CBD program is designed as a continuum whose first three stages are unlikely to fit into the traditional three year “core” training model, unless substantial changes are made which would remove the enhancements that have been made. In addition, each subspecialty would have to individually negotiate a model of overlap with Pediatrics, including how the subspecialty program would ensure both the provision of Pediatric RTEs and the appropriate assessment of TTP EPAs. Each subspecialty program must also then maintain enormous flexibility, as residents may well not have completed the requirements to enter subspecialty training on July 1 of their fourth year.

24
The benefits to completing all stages of training in a Pediatrics program for all those seeking certification in Pediatrics are evident. Better-trained pediatricians who have the time to acquire the all Pediatric competencies prior to practice or any further training will be better equipped to meet the health care needs of Canadian children and youth. Structuring of CBD stages with transition between the Core and TTP stages during the final year will allow a natural and adequate progression of competency training and assessment. Delaying entry into subspecialty training will result in a better-trained subspecialist, one who can focus entirely on their chosen area for the relatively short duration of their subspecialty residency. As tentatively planned, the written examination will occur at the end of Core (mid-PGY4) prior to moving on to the TTP stage. Subspecialists will have a better foundation in Pediatrics and be better prepared for the rigours and focus of subspecialty training. When subspecialist certificants and residents were canvassed in the PPP survey, those who overlapped were less confident in general pediatrics than those who did not overlap. Outcomes are also key. Expert opinion from leaders in Neonatology states that those who practice general pediatrics after having completed a full residency in a Pediatrics program have better outcomes in the area of neonatal resuscitation. Community hospital chiefs share that 3+2 physicians practicing general neonatal care are not as comfortable and often decline to cover call for neonatal units, with resultant workforce implications. Better-trained general pediatricians have improved ability to care for earlier premature infants and sicker children who can then stay in the community longer, decreasing costs of transfer to tertiary centres and keeping families together when possible. More thorough training and experience in the area of mental health will result in decreased referrals to mental health providers, an area of significant unmet need with waiting lists often exceeding 6-12 months. As the proportion of children with complex chronic conditions grows, there is strong impetus to develop local health care teams, led by a highly competent pediatrician who has acquired experience and confidence in managing such conditions.
Economic implications of the proposed change Outline the implementation issues and funding implications for governments. Currently, all but three provinces (Ontario, Quebec and Nova Scotia) provide funding for four years of training in Pediatrics before entering subspecialty training. Appendix J outlines data obtained from program directors and CAPER regarding Pediatrics residents in these three provinces who leave their programs after the PGY-3 year to undertake subspecialty training. The data from the past 3 to 4 years suggest that an average of 40 residents fall into this group. It is estimated that this number will remain stable or decrease slightly in the coming years due to a decrease in the number of funded subspecialty positions, particularly in Québec, and in the overall number of residents in training. This implies that there are approximately 25-28 residents from Ontario, 8-10 residents from Québec and 1-2 residents from Nova Scotia who would remain in their Pediatric programs until their completion prior to commencing subspecialty training. Because of current restrictions, at least 50% of the residents from Québec who pursue subspecialty training leave the province to do so. For these residents, there should be no additional cost burden as they would have been funded to complete their pediatric residency if they had chosen to stay and

25
practice as a general pediatrician. There are a small number of residents from other provinces (< 5) who currently leave their programs after PGY-3 in order to conform with the requirements for training in a sub-specialty in Ontario, Québec or Nova Scotia, but funding currently exists for them to complete their Pediatrics training in their province. Thus, given the data obtained and current trends, it is expected that the financial burden associated with this proposal would involve the final year salaries for approximately 35 residents, two thirds of them enrolled in programs in Pediatrics in Ontario. This is a small proportion of the approximately 180 residents who complete training in Pediatrics each year. There are two main areas in which this proposal may result in a cost savings to the Ministries of Health from a government perspective. Increased Productivity and Value Residents receive lower pay and work longer hours than faculty attending physicians and other licensed independent providers The retention of all residents in Pediatric programs until completion would solve a problem of clinical service that early departure to subspecialty training creates. The deficit in call shifts, created when residents leave their programs to pursue subspecialty training, is often covered by paid substitutes such as House Medical Officers (HMOs), Clinical Associates, departmental fellows or even attending physicians providing in-house call, all at a significantly higher cost than a senior resident’s salary. Studies evaluating the impact of duty hour changes on children’s hospitals have indicated a consistent cost increase to meet workforce needs and ensure patient safety. With the overall reduction of resident hours, hospitals often hire staff hospitalists, nurse practitioners and physician assistants to assist with patient care at a much higher cost per full-time equivalent (Freed, 2012). The retention of the most senior residents who are in the final phase of training would not only provide quantitative benefit in terms of number of hours worked, but qualitative benefits due to their high level of skills. The skills and autonomy of these senior residents contribute to clinical productivity and efficiency without significantly increasing costs, particularly where faculty remuneration follows an Alternate Funding Plan. More patients may be seen in a timely manner, reducing wait times and outside referrals, without a significance increase in total billings. As well, it should be noted that postponing the entry of a resident into practice as an attending physician leads to significant cost savings with respect to physician remuneration. Although we believe there may be savings in these areas, we cannot accurately assign a monetary sum to each factor and changes in costs may affect budgets outside of the PGME. An independent analysis of the projected costs of this proposal is outlined in Appendix K. Better-Trained Pediatricians Provide Better Care: Better Care Reduces Overall Economic and Other Costs The quality of care provided by a physician will be higher with appropriate training and preparation for independent practice. Additional training and better qualifications can reduce referrals to other specialists, which positively affects waitlist time and overall efficiency of the health care system. As an

26
example, the Pediatric Urology group at the Hospital for Sick Children in Toronto recently approached the Pediatrics program director for assistance in developing a core curriculum for Pediatric residents, as a review of the referral patterns to Urology indicated 80% of referrals received by their group from general pediatricians could have been managed in the community.
Additional training can also lessen medicolegal liability and improve quality of care. Increased exposure during residency, leading to increased comfort with the management of children with higher acuity, such as mildly or moderately premature neonates, will reduce the number of referrals for transport from regional hospitals to tertiary care centres. Not only are the costs of providing the same level of care lower in a regional centre, the economic and psychosocial burdens placed on patients and their families by hospitalizations away from home are reduced. These changes in practice patterns can and should be measured. Together with the Pediatric program directors, the Specialty Committee in Pediatrics intends to study the impact of completion of all Pediatric training within a Pediatrics program on issues such as referral patterns, with a goal to inform ongoing curriculum development. Such feedback will help teaching programs to monitor gaps in training and assess improvements over time. In addition, an application currently in process to the Ontario-based Institute for Clinical Evaluative Sciences will look at practice characteristics, such as billing and referral patterns, in the context of length of training. Summary of Economic Implications It is recognized that allowing all residents to complete their training in Pediatrics prior to entering subspecialty training has financial implications, in the provinces where funding for post-graduate medical education is limited to the shortest possible time frame allowed under the current Specialty Training Requirements in Pediatrics. Nevertheless, there are tangible financial benefits to the health care system as a whole, by retaining a larger general pediatric resident workforce in pediatric hospitals, and postponing their entry into independent practice. The qualitative benefits of improved training leading to greater autonomy and broader scope of practice, as pediatricians and as pediatric subspecialists, will translate into cost savings to the global health care budget by changes in referral patterns and resource utilization. It is essential that this longer-term gain be balanced with the more immediate impact on budgets for postgraduate medical training. Table 1: Estimated Salary and Benefit Costs of Residents
Province # PGY6 Salary Salary + 30% Total Nova Scotia 1.25 87,829 114,178 142,723
Ontario 26.5 86,411 112,334 2,976,851 Quebec 7 74,082 96,307 674,149
Total 34.75 109,172 (average) 3,793,723

27
Summary
In summary, given the breadth and depth of Pediatrics and the identification of current gaps in training, allowing all residents to complete all components of training in a Pediatric program becomes the obvious and wise choice. As one anonymous survey participant commented:
“Three years of training is not sufficient for core Pediatrics. As a subspecialist, I have at times worked as a general pediatrician (as a locum in rural hospital) and also as an academic pediatrician on the general pediatric ward and I have felt incompetent and at times uncomfortable working as a pediatrician. I had wished I had an extra year of core pediatrics in my 4th year to have additional training in development, pediatric psychiatry, newborn care [...] When you are training, you also just don’t know what the job market will be like 4-5 years down the road and you have to be prepared in every way to practice as a general pediatrician first.”
There is an initial cost to this process, but this is far outweighed by both the financial savings and the cost of not effectively training all pediatricians for the type of work they may ultimately end up doing, given current practice patterns of specialists and societal needs. Now is the time to acknowledge the gaps in training and to adjudicate in favour of comprehensive education of pediatricians to meet the needs of Canadian children for decades to come. Thank you for your consideration.
References
AAP study on Early Career Providers: http://www.aappublications.org/news/2018/04/05/research040518 Final Report of the Generalism and Generalist Task Force, Royal College of Physicians and Surgeons of Canada, 2013. Freed G, Dunham K, Moran L, Spera L. Resident work hour changes in Children’s Hospitals: Impact on staffing patterns and workforce needs. Pediatrics, 2012; 130(4):700-704. Lieberman L, Hilliard RI. How well do paediatric residency programmes prepare residents for clinical practice and their future careers? Medical Education, 2006; 40(6):539–546. Stein REK. Are we on the right track? Examining the role of developmental behavioral pediatrics. Pediatrics, 2015; 135(4):589-591. Table A.5.1: Average gross fee-for-service payment per physician who received at least $60,000 in payments by physician specialty and province, 2015-2016. National Physician Database 2015-2016 data release, Canadian Institute for Health Information. Tithecott G, Levin S, Filler G. Innovating to educate paediatric consultant generalists for the new Canadian health care. Paediatrics and Child Health, 2018:122-124.

28

Historical Review
The aim of this historical review is to explore the context of ‘double-counting’ and rationale
for reform in Canadian pediatric residency training. More specifically, the review aims to
answer the following key question: How has ‘double-counting’ evolved in pediatric residency
programs and what was the rationale behind previous efforts to reform its practice?
In order to create an overview of the practice of double-counting in the context of pediatric
residency training, past editions of the Specialty Training Requirements (STRs) for pediatrics
and its various subspecialties were examined over a period of forty (40) years, from 1975 to
2017. Minutes and documents from any interaction between the Special Committee in
Pediatrics and the Committee on Specialties were then reviewed to identify proposed
changes to the program and the rationale behind these propositions.
Key Findings and Summary
‘Double-counting’, the practice of concurrently training in two programs, has existed
between Canadian pediatric specialty and subspecialty programs throughout the scope of
this historical review. Pediatric residents have been able to overlap the final fourth (4th) year
of primary training and the first (1st) year of training in a pediatric subspecialty, with little
change to the process over the last forty (40) years. There is also evidence that credit for
training in other primary programs, such as Family Medicine, was applied to the certification
of the pediatrics specialty, which is a form of ‘double-counting’. It is significant to note that
there is also a history of resistance to double-counting, although pediatricians are not united
on this issue. There have been two proposals made by the Specialty Committee in Pediatrics
to eradicate the practice since 2000.
Arguments both for and against the continuance of double-counting in pediatric training
programs have been framed as time-based and centred exclusively on whether the length of
the primary training program should be increased or decreased. Given the Royal College’s
transition to a competency-based model of educating specialty residents, there is an
opportunity to reframe the discussion of overlapped and double-counted training in pediatric
training and shift the focus away from program length and towards the recognition of
achievement of required competencies for practice.
The Evolution of Double-Counting
Pediatric residents have been able to overlap the final fourth (4th) year of primary training
and the first (1st) year of training in a pediatric subspecialty, with little change to the
process throughout the scope of this review. The 1975 Pediatrics Specialty Training
Requirements (STRs) outlines that the residency program may include:
2(b)ii) One or more years of approved resident training or fellowship (clinical or
research) in pediatrics or a special branch of pediatrics in a fully approved program.
STRs from subspecialties around this time confirm that one year of approved primary
specialty training or fellowship could concurrently be applied towards the certification of a
subspecialty. The Rheumatology STR from 1981, for example, requires:

2. Two years of approved training in rheumatology, not more than one of which may
be undertaken during training for Certification in Pediatrics or Internal Medicine.
Overlapped training has remained a component of the pediatrics’ STR throughout major
changes to the curriculum, including the application of the CanMEDs framework to the
program in 1998 and the shift to a core training model in 2008. The current wording of the
STR remains similar to that of the 1975 document as the final year of pediatric residency
may consist of:
2.1 Up to one (1) year further residency in Pediatrics, designed by the resident and
program director to reflect the resident’s career plans and future practice setting
2.2 Up to one (1) year of clinical residency in any of the subspecialty areas of
Pediatrics
Prior to 1998, residents who had previously studied Family Medicine could also receive up to
six (6) months of credit towards their certification in pediatrics. Before 2008, pediatrics
residents could also complete their fourth (4th) year in Internal Medicine or another
‘approved course of study and training, relevant to the objectives of pediatrics’. A precedent
therefore exists for applying credit from another specialty towards a certification in
pediatrics. This is significant as the jurisdictional review revealed that versions of this type
of ‘double-counting’ exist in current comparable contexts outside of Canada.
Challenges to Double-Counting
There have been repeated attempts to reform the pediatrics residency program and
eradicate double-counting since the year 2000. The rationale for reform centred on concerns
that overlapping training effectively reduces the primary training program from four (4)
years to three (3). Three (3) years of training is not perceived to be enough time for
residents to gain the skills necessary to become a competent general pediatrician. Since
2000, the Committee on Specialties examined two proposed reforms to the pediatric
residency program: the Pediatric Stream Model between 2001 and 2004, and an application
for training length modification in 2013.
Pediatric Stream Model
In 2003 a pediatric task group presented the ‘Pediatric Stream Model’ to the Committee on
Specialties. The model required three (3) ‘core’ years of pediatric training and an additional
two (2) years of training in either general pediatrics or one of its subspecialties. At the end
of this program, residents would have received a single certificate as a Pediatrician /
General Pediatrician or a Pediatrician / Subspecialty Pediatrician. This model removed the
ability of a resident to overlap primary and subspecialty training, and ensured that all
residents received five years of training. It is notable that the Pediatric Stream Model was
similar to the system in Quebec at the time.
Rationale
The pediatric task group were worried that the volume and complexity of pediatric training
had increased and felt that three (3) years of training in general pediatrics was no longer
sufficient for residents to gain the skills necessary to practice as a general pediatrician. Dr.
RI Hilliard raised explicit concerns about the ability of a pediatric subspecialist to perform
the same level of care as a pediatrician, who had received four (4) years of general training,
to developmental/behavioural patients and patients with physical and psychological
challenges. Other members of the task group were concerned that subspecialist residents
were distracted during the first year of their subspecialty training by the need to study for
the primary pediatrics exam which occurred during the year of overlapped training.
Outcome
The proposed changes had support from the Committee on Specialties; however it failed to
gain the approval of residents and practicing pediatricians. The results of a broad
consultation revealed that both general and subspecialist pediatricians were opposed to an
increase in the length of the residency training program. Subspecialists were also concerned
that the changes would prevent them from working as general pediatricians as they would
not have a certificate in general pediatrics. Significantly, the consultation revealed that
newly qualified pediatricians felt prepared for independent practice and so there was a lack
of evidence to support a major change in the structure of the residency program.
Application for Training Length Modification
The Special Committee in Pediatrics brought a proposal to the Committee on Specialties in
fall 2013 which sought to establish pediatrics residency training as a four (4) year, stand-
alone program. This proposal sought to remove the ability to overlap the final year of
primary pediatrics and the first year of subspecialty training. The proposal was clear that it
was not requesting a change to the length of residency training, but rather a confirmation
that the core pediatric competencies require four (4) years, rather than three (3), to
complete.
Rationale
The Special Committee in Pediatrics heard concerns that reduced work hours, academic half
(½) days, and an increasing volume of ‘core’ tasks to be completed had resulted in a
decrease in residents’ ability to competently perform procedural skills. Informal consultation
with residents and practicing pediatricians revealed a multitude of concerns regarding the
structure of the current program. Subspecialist residents felt that they had not received
enough training in general pediatrics before entering a subspecialty; however they also
raised concerns that an overlap in the training programs meant that they were unable to
focus on the first year of subspecialty training. Community pediatricians also expressed
concern that residents were not well prepared for community practice. The Specialty
Committee in Pediatrics thought that an additional year of general training would allow
residents to take more selective rotations that would enhance their procedural skills and be
beneficial in their future careers.
Outcome
The Committee on Specialties did not approve the proposal. This decision was based on the
proposal’s emphasis on time-based training, its rationale regarding a decrease in resident
duty hours, a lack of evidence concerning the need to increase training length, and the
funding implications of the proposed change. The Specialty Committee in Pediatrics,

however, was encouraged to re-frame and resubmit their proposal after taking into account
the Competence by Design framework, a competency-based model of training to which the
pediatrics discipline, along with all other disciplines in Canada, would transition.
Reflections for the Present
The objective of this historical review was to explore the key question: How has ‘double-
counting’ training evolved in pediatric residency programs and what was the rationale
behind previous efforts to reform its practice?
Findings from this historical review revealed that although ‘double-counting’ is firmly
entrenched in the history of pediatric training, there is also an established case for reform of
the program. There have been two attempts to extend the program length and remove the
ability to overlap the final year of primary training with the first year of subspecialty training
in the last fifteen years. Although both of these attempts at reform were unsuccessful, it is
important to note that the Committee on Specialties’ response to the 2013 proposal was not
a definitive rejection of the need for reform. Rather, the Committee on Specialties requested
that the proposal be re-framed after consideration of the Competency by Design framework.
In the past, opposition to reform was grounded in a reluctance to extend the overall length
of training. In shifting the dialogue surrounding reform to centre on outcomes, there is
opportunity to explore potential variations in the structure of the pediatrics program,
including the eradication of ‘double-counting’. If it is decided that the current model, which
overlaps primary and subspecialty training, is abandoned, this historical review reveals a
precedent for two other models of training.
1. Reform double-counting in a competency-based system
First is the option to ‘double-count’ or provide credit for competencies between
specialties that have been achieved between disciplines. In the past, residents could
apply credit from training in Family Medicine and Internal Medicine, as well as other
courses ‘relevant to the objectives of Pediatrics’, towards the completion of their primary
Pediatrics certificate.
2. Remove double-counting from the pediatric discipline
Second is the possibility to separate primary and subspecialty training programs and
eradicate the ability to overlap training. This model has not been practiced in the scope
of this historical review; however an aversion to overlapped training drove movements
for reform of the pediatrics program in both 2004 and 2013.
It is also notable that, in the rejection of both models of reform, a lack of evidence needed
to create major change was cited. It may be useful to conduct a study to establish if there
are concerns, and the causes of these concerns, with the current training model.
As the Canadian specialty medical education system shifts from a time-based to a
competency-based system, there is opportunity to explore new models of ‘double-counting’,
as well as its eradication. It is important, however, that any future proposal is framed with a
focus on competency and outcome rather than training length.

References
Royal College of Physicians and Surgeons of Canada (Royal College). (1975). Specialty
Training Requirements in Pediatrics from Royal College archives.
Royal College. (1979). Specialty Training Requirements in Pediatrics from Royal College
archives.
Royal College. (1986). Specialty Training Requirements in Pediatrics from Royal College
archives.
Royal College. (1989). Specialty Training Requirements in Pediatrics from Royal College
archives.
Royal College. (1998). Objectives of Training and Specialty Training Requirements in
Pediatrics from Royal College archives.
Royal College. (2008). Specialty Training Requirements in Pediatrics from Royal College
archives.
Royal College. (2015). Specialty Training Requirements in Pediatrics from
http://www.royalcollege.ca/rc/faces/oracle/webcenter/portalapp/pages/ibd.jspx?_adf.ctrl-
state=12uvj3ishv_4&_afrLoop=17076195542289680&_afrWindowMode=0&_afrWindowId=
12uvj3ishv_14#!
Royal College. (1981). Specialty Training Requirements in Rheumatology from Royal College
archives.
Royal College. (2013). Specialty Committee in Pediatrics: Minutes June 18th Meeting from
Royal College archives.
Royal College. (2013). Specialty Committee in Pediatrics: Minutes April 15th Meeting from
Royal College archives.
Royal College. (2012). Specialty Committee in Pediatrics: Minutes June 5th Meeting from
Royal College archives.
Royal College. (2012). Specialty Committee in Pediatrics: Minutes June 9-10th Meeting from
Royal College archives.
Royal College. (2002). Committee on Specialties: Minutes October 3rd-4th Meeting from
Royal College archives.
Royal College. (2004). Committee on Specialties Briefing Note: Update from Pediatrics from
Royal College archives.
Royal College. (2013). Committee on Specialties Supporting Materials: Pediatrics Application
for Change from Royal College archives.

Jurisdictional Review: Double-Counting in Other Comparable Contexts Double-counting or overlapped training are design features of the current configuration of primary pediatrics training and its subspecialties in Canada. In double counting, a postgraduate medical trainee may apply to have a past completed credit count towards their current program of study. Similarly, overlapped training refers to when a trainee is completing both his/her primary and subsequent subspecialty programs, using common overlapping requirements to concurrently complete both programs, and to shorten the time spent in training. For the purpose of simplicity, the term ‘double-counting’ will encompass both double-counting and overlapped training for the remainder of this report. Given the questions and concerns that have been raised surrounding the preparedness of pediatric subspecialists for general pediatric practice, a jurisdictional review was performed to compare and contrast the current design of primary pediatric and pediatric subspecialties in Canada to the configurations in other comparable contexts. More specifically, the aim of this jurisdictional review was to review the scope of pediatric training and the existence of double-counting training in other contexts and to answer this key question: Is the practice of “double counting” and the model of training (scope of training) comparable within other jurisdictions outside of Canada? Given the vast variability of health care and training systems around the world, only jurisdictions with similar approaches to postgraduate medical education were selected to increase case comparability: the United States, the United Kingdom, and Australia and New Zealand. Each country’s training system was reviewed on the basis of the following topics: pediatric subspecialties, typical training pathways, and offered variations in training pathways, including the practice of double-counting, should it exist. Key Findings and Summary This jurisdictional review revealed that double counting, as specifically practiced in Canada as one transitions from a primary to sub specialty, does not identically exist in comparable jurisdictions. With the exception of subspecialty “fast-tracking” in the United States, it is important to note that while integrative training programs and accelerated pathways may exist in other international contexts, these pathways are not necessarily targeted towards primary pediatrics training as it interfaces with pediatrics subspecialty training. Significantly, the design of double-counting in the United Kingdom demonstrates how this practice may possibly be a feasible option in a competency-based model. As such, findings from the jurisdictional review may inspire considerations that may be applicable to the Canadian context.

The following table provides a succinct summary of double counting as it exists in other jurisdictions: Table 1: Summary and Comparison of Double-Counting Findings in Other Jurisdictions
Canada Pediatric Subspecialties In Canada, the Royal College of Physicians and Surgeons of Canada (Royal College) recognizes the pediatric specialty and its subspecialties, establishes the minimum training requirements for pediatric residency training, accredits residency training programs based upon those requirements, writes and administers Royal College examinations and certifies pediatric specialists and subspecialists on completion of their training (Royal College (RC), 2017).
The Royal College currently recognizes 17 subspecialties of Pediatrics (Royal College 2015): Adolescent Medicine Pediatric Cardiology Pediatric Clinical Immunology and
Allergy Clinical Pharmacology and
Toxicology Critical Care Medicine
Developmental Pediatrics Neonatal Perinatal Medicine Pediatric Emergency Medicine Pediatric Endocrinology and
Metabolism Pediatric Gastroenterology Pediatric Hematology/Oncology
Double Counting /Overlap?
How? Notes
Can
ada
Yes Primary Subspecialty
Overlap of training requirements, or Application of past credits to complete current program of study
Un
ited
Sta
tes
Yes
Primary Subspecialty
Trainees who have demonstrated accomplishments in research may petition to have their research requirement waived thereby shortening the length of training
Subspecialty Subspecialty
Integrative program permits trainees to receive certification in two pediatric subspecialties in as little as four years. Proposals must be developed, submitted, and approved by the committees of both subspecialties.
Un
ited
K
ing
dom
Yes Primary Subspecialty
Double counting is unique in this context given that it is practiced in a competency-based model, versus the conventional time-based model. Nonetheless, approval is needed from the CSAC to double count already possessed competencies to shorten length of training.
Au
stra
lia
&
New
Ze
alan
d
Yes Subspecialty Subspecialty
Trainees have the option to overlap of training requirements and assessments in multiple subspecialties. Trainees must satisfy the minimum requirements of the supervising committees of both subspecialties.

Pediatric Infectious Diseases Pediatric Medical Biochemistry Pediatric Nephrology
Pediatric Palliative Medicine Pediatric Respirology Pediatric Rheumatology
Pediatric Training Pathways Currently, pediatric specialty training has been organized as a four (4) year program. The first three (3) years are designated to primary pediatrics, with the final fourth (4th) year consisting of advanced pediatrics training. In this final fourth (4th) year, trainees may choose to advance their residency in primary pediatrics by increasing their independence and leadership in generalist pediatric training, or pursue any of its subspecialty areas. In order to pursue subspecialty training during this year, the trainee must be granted approval from the director of the residency program and the trainee must be provided with opportunities that align with the requirements of both programs as well as with his/her personal educational and learning objectives (Royal College, 2015). Typically, Pediatric subspecialty programs are completed within two to three (2-3) years. Variations in Training Pathways Within the current configuration and interface between the primary pediatric specialty and its subspecialties, trainees are allowed to double count the final fourth (4th) year of primary pediatric training and the first (1st) year of training in any of the aforementioned pediatric subspecialties in one single year with the approval from all required program directors. In other words, the trainee effectively shortens the length of their primary pediatric training if they overlap primary and subspecialty training (Royal College, 2015). United States Pediatric Subspecialties In the United States, postgraduate medical education training is accredited by the Accreditation Council for Graduate Medical Education (ACGME) (ACGME, 2017a). Certification requirements and examination standards for primary pediatrics and the majority of its branching pediatric subspecialties are developed by the American Board of Pediatrics (ABP) (ABP, 2017a). The ABP is one of the 24 certifying boards of the American Board of Medical Specialties (ABMS). The ABP structures its certified programs according to the minimum educational requirements outlined by the ACGME. The ACGME accredits the listed 20 pediatric subspecialties (ACGME, 2017b):
Adolescent Medicine Child Abuse Pediatrics Clinical Informatics Developmental-Behavioral
Pediatrics Hospice and Palliative Medicine Internal Medicine-Pediatrics Neonatal-Perinatal Medicine Pediatric Cardiology Pediatric Critical Care Medicine Pediatric Emergency Medicine
Pediatric Endocrinology Pediatric Gastroenterology Pediatric Hematology Oncology Pediatric Infectious Diseases Pediatric Nephrology Pediatric Pulmonology Pediatric Rheumatology Pediatric Transplant Hepatology Sleep Medicine Sports Medicine
The ABP provides certification for 14 of the pediatric subspecialty programs accredited by the ACGME which are listed below (ABP, 2017b). Certifications for the remaining accredited Pediatric subspecialties are either co-sponsored by the ABP and another ABMS certifying board, or by other ABMS boards on their own.

Adolescent Medicine Pediatric Cardiology Child Abuse Pediatrics Pediatric Critical Care Medicine Developmental-Behavioural
Pediatrics Pediatrics Emergency Medicine Pediatric Endocrinology
Pediatric Gastroenterology Pediatric Hematology-Oncology Pediatric Infectious Diseases Neonatal-Perinatal Medicine Pediatric Nephrology Pediatric Pulmonology Pediatric Rheumatology
Additionally, the ABP offers certification for combined programs, which have been designed to allow trainees to pursue training in pediatrics and in another specialty in less time than it would conventionally take to complete both specialty programs sequentially. These programs are normally completed in four to five (4-5) years and this reduction in time is made possible due to the overlap of the curriculum and experience required for each discipline (ABP, 2017c). The following combined programs are offered by the ABP in collaboration with other ABMS Boards (ABP, 2017c; ABP, 2017d):
Pediatrics-Neurology Pediatrics-Neurodevelopmental
disabilities Allergy and Immunology Internal Medicine-Pediatrics Medicine-Pediatrics Pediatrics-Anesthesiology
Pediatrics-Emergency Medicine Pediatrics-Medical Genetics Pediatrics-Physical Medicine and
Rehabilitation Pediatrics-Psychiatry/Child and
Adolescent Psychiatry
As an example, trainees enrolled in the Pediatrics-Anesthesiology program will complete five (5) years of training, instead of the six (6) years that would be required if training in both specialties were completed sequentially (ABP, 2009). More specifically, “[t]he reduction of [six] 6 months of the standard 36 months of pediatric training is met by 30 months of training in the pediatric component of the combined residency and [six] 6 months of credit granted for training appropriate to pediatrics obtained during the 30 months of anesthesiology residency” (ABP, 2009). Although this form of double-counting is not identical to the training model in Canada, in that the Royal College allows for the overlap of the final year of primary pediatric training and the first year of pediatric subspecialty training, combined training programs are comparable to the Canadian context in that the shared competencies and training requirements that exist between two specialties are overlapped to minimize any existing redundancies and reduce length of training. It illustrates how double-counting can be practiced and incorporated in various ways, going beyond the interface between primary pediatrics and its subspecialties. Pediatric Training Pathways – Primary Subspecialty Requirements for ACGME accredited programs outline pediatric specialty training as a three (3) year program (ACGME, 2017c). Subspecialty programs are also three (3) years in length. In other words, trainees typically complete primary pediatric and pediatric subspecialty training in a total of six (6) years. Variations in Training Pathways Primary Subspecialty Subspecialty “fast-tracking” allows a trainee to complete training in a subspecialty in up to one year less by waiving the scholarly activity requirement (ABP, 2015a). Trainees who have demonstrated accomplishments in research, such as a PhD degree or other sustained research, may petition to have the requirement waived. An important caveat is that the trainee must have satisfactorily completed three (3) core years of pediatrics or approved

combined pediatrics and other specialty training in an accredited program, and at least two (2) years of subspecialty training, with one (1) year of broad-based clinical training. Additionally, all requirements for general pediatrics certification must be fulfilled without exception (ABP, 2015a). Graduates of combined training programs in internal medicine and general pediatrics may pursue training in a subspecialty program of each board (internal medicine and pediatrics) in one year less than would have been conventionally required (ABP, 2014). Similar to the subspecialty “fast-tracking” pathway described above, this reduction in total training time is due to the double-counting of scholarly activity required in both programs. Subspecialty Subspecialty Dual training permits trainees to receive certification in two pediatric subspecialties in as little as four (4) years, which is typically shorter than completing two subspecialty programs consecutively. However it must be noted that this allotted timeframe may not be feasible for some pediatric subspecialties (ABP, 2015b). Both fellowship programs must be offered in the same institution, and must be accredited by ACGME. The level of program integration must also be approved by the Credentials Committees of both pediatric subspecialties through the submission of a proposal detailing how the integrated program satisfies all of the eligibility requirements for certification in both subspecialties. Although dissimilar to the configuration of overlapping training in Canada, this training pathway accentuates the prevalence of double-counting through the mapping of similar training requirements and illustrates another configuration in which double-counting can take. This may have implications in the Canadian context as the pediatric discipline transitions to competency-based education. This transformational period presents an advantageous opportunity to review the competency requirements between multiple pediatric subspecialties, and consider a new approach to double-counting, should this practice continue to exist in the discipline of pediatrics in the future. United Kingdom Pediatric Subspecialties In the United Kingdom (UK), the Royal College of Child Health and Paediatrics (RCPCH) delivers and monitors postgraduate training and the examination of pediatricians and pediatrician subspecialties (RCPCH, 2017a). These programs and their curriculums are approved and accredited by the General Medical Council (GMC) of the UK. Pediatric subspecialties that are currently offered in the UK are (General Medical Council, 2017):
Pediatric Allergy, Immunology and Infectious Disease
Child Mental Health Pediatric Clinical Pharmacology Community Child Health Pediatric Diabetes and
Endocrinology Pediatric Emergency Medicine Pediatric Gastroenterology,
Hepatology and Nutrition
Pediatric Inherited Metabolic Medicine
Pediatric Intensive Care Medicine Neonatal Medicine Pediatric Nephrology Pediatric Neurodisability Pediatric Neurology Pediatric Oncology Pediatric Palliative Medicine Pediatric Respiratory Medicine Pediatric Rheumatology

Pediatrics Training Pathways – Primary Subspecialty Pediatric medical training is organized into three competency-based levels, sequentially increasing in specialization as a trainee progresses through the pathway. Level 1 (ST1-3) and level 2 (ST4-5) training are generally completed within three to five (3-5) years and consists of core and specialty training in general pediatrics, neonatal medicine, community pediatrics, and training in acute settings (RCPCH, 2017b). Prior to commencing Level 2 and Level 3 training, trainees are required to successfully complete all exams to receive Membership of the Royal College of Paediatrics and Child Health (MRCPCH). Trainees are able to specialize in a pediatric subspecialty in Level 3 training (ST6-8) through the National Trainee Number (NTN) Grid Scheme (RCPCH, 2017c). The NTN Grid Scheme is used for health human resource planning to avoid the oversaturation of trainees in one pediatric subspecialty. Level 3 training is typically two-three (2-3) years in duration, depending on the subspecialty and on the progression of the trainee through the required competencies. Successful completion of Level 3 training awards trainees with the Certificate of Completion of Training (CCT) and permits them to register with the General Medical Council (GMC) as pediatricians with subspecialty recognition (RCPCH, 2017c). Variations in Training Pathways1 During Level 3 training, individuals are given the option to continue training in primary pediatrics or to immediately begin subspecialty training (RCPCH, n.d.a). Trainees who continue general pediatrics training have the possibility of spending the last year training in a subspecialty. Any trainee desiring to complete subspecialty training in less time than outlined by the guide for reasons such as feeling as if they already possess a number of subspecialty competencies, are required to seek approval from the College Specialty Advisory Committee (CSAC) (RCPCH, n.d.b). However, trainees are generally expected to gain the necessary skills and competencies within the proposed timeline of the desired subspecialty. Given that this training program is competency-based, as opposed to time-based, this variation in training may be relevant in the Canadian context. Since Canada currently allows trainees to overlap the final year of primary pediatrics and the first year of its subspecialties, this similar feature offered during Level 3 training reinforces that there are some commonalities that exist between primary and subspecialty pediatrics, facilitating double-counting credit for competencies achieved. Furthermore, given the competency-based direction in which Canada is traveling, this pathway highlights how on a case by case basis, double-counting may still be a feasible design feature to offer moving forward. Nonetheless, more exploration is needed to assess the qualifications for certification and the level of preparedness of pediatric subspecialists to independently practice general pediatrics. Australia and New Zealand Pediatric Subspecialties In Australia and New Zealand, the Royal Australasian College of Physicians (RACP) trains, supports, and establishes standards for an array of specialties, including pediatrics and pediatric subspecialties (RACP, 2016a).
1 1 A request for clarification has been extended to the RCPCH to determine whether trainees who continue general pediatrics training in Level 3 are recognized as General Pediatricians with subspecialty interest or whether they are considered Pediatric Subspecialists and if these options are possible due to overlapped training.

The RACP accredits 26 Division Training Programs in both Adult Internal Medicine and Pediatrics and Child Health (RACP, 2016b). Listed below are the training programs that may be pursued after completing basic training in Pediatrics and Child Health (RACP, 2016c):
Cardiology Clinical Genetics Clinical Hematology Clinical Immunology and Allergy Clinical Pharmacology Community Child Health Dermatology Endocrinology Gastroenterology General Pediatrics
Infectious Diseases Medical Oncology Neonatal/Perinatal Medicine Nephrology Neurology Nuclear Medicine Palliative Medicine Respiratory Medicine Rheumatology Sleep Medicine
Joint training programs include:
Pediatric Rehabilitation Medicine Endocrinology and Chemical
pathology Hematology
Immunology and Allergy Infectious Disease and Microbiology Pediatric Emergency Medicine
Pediatric Training Pathways To begin, trainees must complete three (3) years of basic training in either Adult Internal Medicine or Pediatrics and Child Health (RACP, 2016b). Basic training is in itself not a qualification, but it is a base requirement to complete advanced training through a division training program or a joint training program, thereby gaining specialty recognition (E. Francis, personal communication, July 7, 2017). In other words, trainees are only eligible to practice as qualified physicians once they have successfully completed both basic and advanced training. Advanced training programs are normally completed in three (3) years (RACP, 2016c). In sum, pediatric subspecialists are required to undergo a total of six (6) years of training. To specialize as a pediatrician, trainees are required to successfully complete basic training in Pediatric and Child Health, and subsequently pursue an advanced training program in General Pediatrics (E. Francis, personal communication, July 7, 2017). Pediatrics and Child Health basic training involves certified training time in various pediatric areas such as general pediatric medicine, pediatric emergency medicine, and the perinatal unit (RACP, 2017). It is important to recognize that the framing of General Pediatrics within this jurisdiction is different when compared to that of the Royal College. In Canada, trainees holding a medical doctorate may not only practice as general physicians after certification, but they also have the opportunity to pursue training in the specialty of pediatrics, whereas in Australia and New Zealand, only those with basic training in Pediatrics and Child Health are eligible to enroll in General Pediatrics. A Joint Training Program is a “single, cohesive Advanced Training Program that results in the trainee being awarded more than one Fellowship” (RACP, 2016d). These programs are designed and conducted in conjunction with other postgraduate medical colleges such as the Australasian Faculty of Rehabilitation Medicine and the Royal College of Pathologists Australasia. Due to their design, trainees are able to complete a joint training program in less time when compared with the time it would take to pursue both fellowships separately. Variations in Training Pathways Trainees have the option to dual train in multiple specialties once they commence advanced training. In dual training, trainees must satisfy the minimum requirements of the

supervising committees of both specialties (RACP, 2016d). To do so, the trainee must complete the greater number of teaching, learning and formative assessment tools required by each committee. Completed tools can count towards the completion of both programs. “If the trainee is undertaking training rotations which count towards only one training program, they must complete the minimum requirements of that program only” (RACP, 2016d). In some cases, training will count concurrently for two (2) programs which reduces overall training time (E. Francis, personal communication, July 5, 2017). The trainee is awarded FRACP once the requirements of one (1) training program have been completed and will be considered a post-FRACP trainee for the remainder of their second specialty training. As an example, a trainee desiring to practice pediatric cardiology would first need to complete the basic training program in Pediatrics and Child Health and once achieved, the trainee may concurrently train in the two required specialties, General Pediatrics and Cardiology. Without the ability to dual train, it is assumed that trainees would need to complete a total of nine (9) years of training – three (3) years in basic training, (3) years for General Pediatric training, and the final three (3) years for Cardiology. Reflections for Canada To reiterate, the main objective of this jurisdictional review was to explore the key question: Is the practice of “double counting” and the model of training (scope of training) comparable within other jurisdictions outside of Canada? This key question stems from the greater objective of the ‘Preparedness for Practice’ Pediatrics Project which seeks to evaluate whether the current model of training, specifically the interface between primary pediatric training and pediatric subspecialty training, is optimally configured to ensure that all pediatricians are adequately prepared to practice all aspects of general pediatrics. Findings from this jurisdictional review revealed that double-counting, as specifically practiced in Canada as one transitions from primary to subspecialty, does not identically exist in the comparable jurisdictions chosen for this review. Rather, there are variations in how overlapped training and double-counting itself is configured such as overlapped training between specialties (i.e. Pediatrics and Anesthesiology) and between subspecialties (i.e. Pediatric Cardiology and Pediatric Pulmonology). These differences in the practice of double-count are rather significant to note. This dissimilarity suggests that there are competencies and training requirements that are unique to primary pediatric residency training which may not be achieved during pediatric subspecialty training. As such, the current configuration of overlapped training as a trainee transitions from primary pediatrics to a subspecialty program may be difficult. Additionally, it may also result in a decrease in the trainee’s preparedness to practice general pediatrics at an advanced level given that final year of primary pediatrics training focuses on increased independence and leadership. This opportunity to assume a senior mentorship role in general pediatrics may be lost as double-counting occurs, hindering readiness for independent practice in general pediatrics. Nonetheless, these variations may be worthy for consideration and further exploration in the Canadian context. As the future of specialty medical education in Canada navigates towards a competency based approach through the introduction of Competence by Design (CBD), the possibility to cross train in multiple pediatric subspecialties may be achieved through double-counting credit for competencies achieved between subspecialties. The existence of this training model in other jurisdictions speaks to the probability that there may be more comparable competencies between pediatric subspecialties than there are between primary

pediatrics and its branching subspecialties. This form of double-counting may be advantageous in ensuring that trainees are given a sufficient amount of time to adequately complete primary pediatric training prior to beginning subspecialty training. On the other hand, the current design of pediatrics training in the United Kingdom suggests that perhaps double-counting credit for competencies achieved is easier to facilitate between primary and subspecialty in a competency-based model as opposed to a time-based model. The number of competencies that can be double-counted may be less than is expected of the trainee during the current configuration of training. However, further evaluation is needed to explore how these alternative forms of double-counting influence the preparedness of pediatric subspecialists to perform general pediatric competencies. In sum, as the Canadian specialty medical education system shifts from a time-based approach to a competency, outcomes based system, there are potential opportunities for redesign and adaptations that may be inspired by other jurisdictions. Nevertheless, it must be recognized that the health and medical education systems in these jurisdictions are unique and are not identical to Canadian systems. References Accreditation Council for Graduate Medical Education (ACGME). (2017a). What We Do. Retrieved from http://www.acgme.org/What-We-Do/Overview ACGME. (2017b). Pediatrics Program Requirements and FAQS. Retrieved from http://www.acgme.org/Specialties/Program-Requirements-and-FAQs-and-Applications/pfcatid/16/Pediatrics ACGME. (2017c). ACGME Program Requirements for Graduate Medical Education in Pediatrics. Retrieved from http://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/320_pediatrics_2017-07-01.pdf American Board of Pediatrics (ABP). (2009). Pediatrics-Anesthesiology Program. Retrieved from https://www.abp.org/content/pediatrics-anesthesiology-program ABP. (2014). Combined Training in Adult and Pediatric Subspecialties. Retrieved from https://www.abp.org/content/combined-training-adult-and-pediatric-subspecialties ABP. (2015a). Subspecialty Fast-Tracking. Retrieved from https://www.abp.org/content/subspecialty-fast-tracking ABP. (2015b). Dual Subspecialty Certification. Retrieved from https://www.abp.org/content/dual-subspecialty-certification ABP. (2017a). About Us. Retrieved from https://www.abp.org/content/about-us ABP. (2017b). Subspecialty Certifications & Admission Requirements. Retrieved from https://www.abp.org/content/subspecialty-certifications-admission-requirements ABP. (2017c). Combined Programs. Retrieved from https://www.abp.org/content/combined-programs ABP. (2017d). Non-Standard Pathways and Combined Programs. Retrieved from https://www.abp.org/content/non-standard-pathways-and-combined-programs

General Medical Council (GMC). (2017). Pediatrics curriculum. Retrieved from http://www.gmc-uk.org/education/paediatrics.asp Royal Australasian College of Physicians (RACP). (2016a). About the RACP. Retrieved from https://www.racp.edu.au/about/about-the-racp RACP. (2016b). Basic Training. Retrieved from https://www.racp.edu.au/trainees/basic-training RACP. (2016c). Advanced Training. Retrieved from https://www.racp.edu.au/trainees/advanced-training RACP. (2016d). Variations in training. Retrieved from https://www.racp.edu.au/trainees/variations-in-training RACP. (2017). Basic Training in Paediatrics & Child Health 2017-18 Program Requirements Handbook. Retrieved from https://www.racp.edu.au/docs/default-source/default-document-library/bt-paediatrics-child-health-handbook-2017-18265d58afbbb261c2b08bff00001c3177.pdf?sfvrsn=10 Royal College of Paediatrics and Child Health (RCPCH). (2017a). About the College. Retrieved from http://www.rcpch.ac.uk/about RCPCH. (2017b). General paediatrics training. Retrieved from http://www.rcpch.ac.uk/training-examinations-professional-development/postgraduate-training/general-paediatrics-training/ge RCPCH. (2017c). Sub-specialty training (NTN grid scheme). Retrieved from http://www.rcpch.ac.uk/training-examinations-professional-development/paediatric-recruitment/sub-specialty-training-ntn-gri RCPCH. (n.d.a). The Paediatric Training Pathway. Retrieved from http://www.rcpch.ac.uk/system/files/protected/page/Paediatric%20Training%20Pathway_1.pdf RCPCH. (n.d.b). Sub-specialty training programmes – Training requirements. Retrieved from http://www.rcpch.ac.uk/system/files/protected/page/Sub-specialty%20training%20requirements%202017_0.pdf Royal College of Physicians and Surgeons of Canada (RC). (2017). What we do. Retrieved from http://www.royalcollege.ca/rcsite/about/what-we-do-e Royal College. (2015). Specialty Training Requirements in Pediatrics. Retrieved from http://www.royalcollege.ca/cs/groups/public/documents/document/mdaw/mdkx/~edisp/091601.pdf

Literature Review
The aim of this literature review is to examine the current body of research on the Canadian pediatric training model and determine its ability to prepare all trainees (general and subspecialties) for independent practice in general pediatrics. More specifically, the review aims to answer the following key questions: are all pediatricians adequately prepared for all aspects of general pediatric practice, regardless of training model? Are there other interrelated challenges that may be impacting upon this context of training and impact?
Methodology
PubMed and Medline were the principal databases used for this review. To ensure that all articles in the review evaluated the same training model, only studies published after 1998 were reviewed as the pediatric discipline moved to a curriculum based on the CanMEDs framework in this year. The literature review also focused only on research on Canadian pediatrics training as the jurisdictional review revealed that there is no identical context of health systems and medical training abroad. The methodology involved the following process: search strategies and terms were created, and searches were run on the two databases, as well as through individual journals, grey literature, position papers and reports. Each citation was reviewed using the inclusion and exclusion criteria outlined in the table below. A second level review was conducted of each article to extract information. From an initial result of 266 articles, twelve (12) articles fit all criteria for inclusion.
Include Exclude Topics Relevant to Canadian pediatric and
subspecialty training model, residency reform, the practice of double-counting, or preparedness to practice
North American and US-specific articles; articles about specific conditions, pediatric surgery, exam timing, general internal medicine.
Date After 1998 (CanMEDS-present) Before 1998
Databases PubMed MEDLINE
Journals and Grey Literature Search
Pediatrics and Child Health Medical Education Canadian Pediatric Society Canadian Pediatric Program Directors Canadian Pediatric Surveillance Program
Search terms ‘Pediatric Residency’ AND ‘Canada’ AND: ‘double-counting’, ‘overlap training’, ‘general training’, ‘preparedness to practice’, ‘PGY4’, ‘subspecialty training’, ‘specialty training’, ‘education’, and ‘knowledge gap’

Key Findings and Summary
There are three main themes explored within the current body of research relating to the Canadian pediatric training model:
1) Preparedness for Practice The review highlighted several clinical skills and areas of general pediatrics in which all pediatric residents and recent certificants do not feel adequately prepared for practice upon graduation. Developmental and behavioural pediatrics are cited most often as areas in which pediatricians do not feel prepared for practice.
2) Training Length The literature shows that pediatricians tend to support four or more years of specialty training in pediatrics.
3) Areas of Practice A significant percentage of subspecialist certificants ultimately practice general pediatrics in some capacity.
Importantly, the review exposes large research gaps in the evaluation of pediatric training in Canada. Despite the insights noted above and detailed in this review, the current body of research fails to answer the key research question: are all pediatricians adequately prepared for all aspects of general pediatric practice, regardless of training model? It is necessary to collect data on pediatricians’ perspectives of overlapped training, on the frequency of which subspecialists practice general pediatrics, and compare updated perspectives on the preparedness of general pediatric certificants who completed four dedicated years of training against those who completed only three ‘core’ years of training before beginning a subspecialty program.
Preparedness for Practice
Overview Canadian pediatricians have self-reported that, in certain areas of general pediatric practice, they were inadequately prepared for practice upon certification. Graduates of the University of British Colombia pediatrics program felt that there was a relative lack of education in behavioural/development/adolescent medicine, and well-child care (Macnab et al., 1998). Similarly, general and subspecialty pediatrics certificants across Canada, who were surveyed by Lieberman and Hilliard (2006), felt ‘less than adequately trained’ in gynaecology, child psychiatry, behaviour, surgical subspecialties, adolescent medicine, dermatology, nutrition, allergy and immunology, metabolic diseases, and genetics. Although Lieberman and Hilliard compared the preparedness of general pediatric and pediatric subspecialty trainees, they found that the difference between the two samples was not statistically significant. Grant and Macnab (2007), who surveyed graduates’ preparedness to treat neurological and neurobehavioral issues, reported that a greater emphasis on common neurobehavioral conditions is also needed during residency training. Studies into resident’s abilities to perform clinical skills corroborate the reports of inadequate preparedness for practice in similar areas. Levy et al. (2004) discovered that residents felt ‘somewhat prepared’ or ‘not at all prepared’ to perform twenty-three (23) of forty (40) procedural skills as set out in the

Royal College’s Specialty Training Requirements. Notably, residents are more prepared to perform skills taught through formal curricula than through the informal curriculum (Bismilla et al., 2015). Interestingly, Piedboeuf et al. (2012) note that there are not enough trainees to fill the number of jobs available in many of the identified areas: adolescent medicine, allergy-immunology, developmental paediatrics, endocrinology, gastroenterology, infectious diseases, and respiratory medicine.
There is also a positive correlation between the perceived importance of a skill and preparedness. Residents place less importance on core competencies in which they also felt unprepared (Amin et al., 2011; Kumar et al., 2012). This research corroborates Lieberman and Hilliard’s findings as trainees reported feeling unprepared in similar areas: mental health, development/behaviour, acute care, continuing care, surgery/trauma/MSK, CNS, cardiovascular, renal/GU, and adolescent medicine (Amin et al., 2011). Conversely, a study of pediatric program directors noted that, in areas that program directors rank as important, residents are less than prepared (Bismilla et al., 2015). There is a discrepancy, therefore, between the skills on which program directors place importance and the skills that residents think are valuable.
Limitations While these studies are helpful in identifying areas of practice in which pediatric specialists and subspecialists felt inadequately prepared for practice, these studies are limited in answering the key questions of this review. Only two of the studies compare the preparedness of general pediatricians and of subspecialist pediatricians for independent practice in general pediatrics (Lieberman and Hilliard, 2006; Grant and Macnab, 2007). Amin et al. (2011) note that subspecialist and general pediatric trainees reported differences in preparedness for practice, but the responses of subspecialist trainees were not used in the article. Furthermore, there is no study which compares the preparedness of subspecialists who consolidated their training by completing only three years of general pediatric training and other subspecialist trainees who completed four dedicated years of training in general pediatrics.
Training Length
Overview In a report on Child Health in the 21st Century (2006), the length of pediatric training is described as ‘being both too long and too short by various interested parties’. Lieberman and Hilliard’s (2006) self-report survey shows that this is indeed true. 78% of general and subspecialty pediatricians agreed that 4 years of training was adequate, whilst 20% thought that training should last five years. Interestingly, only 2% of respondents felt that 3 years of training was adequate. Recent graduates appear to prefer four or more years of mandatory training and this is corroborated by a resident representative at the Canadian Pediatric Society who stated that residents feel ‘a minimum of four years of training is required’ (Benchimol, 2004). This evidence, however, is now over a decade old and needs to be updated.

Limitations Although, as the pediatric discipline transitions to a competency-based model of postgraduate education, training length becomes a less important factor in preparedness for practice, these findings should not be ignored. Key stakeholders have stated that the objectives of primary and subspecialty training in pediatrics are entirely different during a year of overlapped training. It is likely, therefore, that residents who overlap their primary and subspecialty programs miss out on the skills specific to the fourth year of general pediatric training.
Areas of Practice
Overview The review indicated that subspecialist certificants do not always practice in an area related to their subspecialty training. Of the participants in the Macnab et al. survey, 79% of respondents completed subspecialty training, yet only 41% currently practice in a subspecialty area (1998). Similarly, 35% of respondents in the Grant and Macnab survey who had undertaken subspecialty training eventually practiced as general pediatricians (2007). Hameed and Lawrence suggest that, given an increase in the number of residents training in a subspecialty, the number of subspecialists working as general pediatricians will also increase due to a scarcity of jobs (2016). Piedboef et al. (2012), however, demonstrate that there are not enough trainees to fill the number of jobs available in a range of subspecialties. Shamseer et al. (2007) note a decrease in the proportion of respondents who planned to spend a majority of their time in general pediatrics but this is not shown to be statistically significant. If there are not enough jobs for subspecialist certificants, this may have implications for trainees who plan to work in a subspecialty and may prioritise subspecialty training during an overlapped year, but are forced to work as a general pediatrician.
Limitations In this review there is no study which specifically examines the degree of a subspecialist’s practice that is dedicated to general pediatrics. Subspecialist certificants are also certified general pediatricians, yet may have completed a year less general pediatric training than their colleagues. This data would be useful in order to analyse the preparedness of this group for practice in general pediatrics.
Commentary
The review highlighted three main themes of the current body of research: 1) preparedness for practice; 2) training length; and 3) areas of practice. It failed, however, to answer the key questions: are all pediatricians adequately prepared for all aspects of general pediatric practice, regardless of training model? Are there other interrelated challenges that may be impacting upon this context of training and impact?
There is an overall lack of evaluation of the Canadian pediatric training model and its ability to prepare pediatricians for general practice as there have only been twelve (12) relevant studies in the last twenty (20) years. Although there are many studies in other jurisdictions on the preparedness of pediatricians for general pediatric practice, these studies are not

generalizable. It is necessary to gain an updated perspective on the ability of the Canadian pediatric training model to prepare trainees for practice in Canada.
Lieberman and Hilliard (2006) reveal that there had been only one attempt by a pediatric residency program, prior to their research, to evaluate its graduates (Macnab et al., 1998). To date, there have only been two studies in which Canadian pediatricians were asked about their perceptions of their preparedness for practice. The utility of these studies to this current project, however, is limited as they did not touch on overlapped training, they did not isolate the perceptions of subspecialists who completed only three years of general pediatric training, and, as they are both over ten years old, they may not reflect current training or practice contexts.
There are also research gaps in the areas necessary to answer the key questions of this review. Studies tend to focus on either primary training or subspecialty training, or a specific aspect of a program. There is no study which seeks to evaluate the entire pediatric training model at a national level or examine the way in which pediatric primary and subspecialty training interface. Moreover, data is not collected on how frequently subspecialist certificants practice general pediatrics and if they were missing any skills necessary for practice.
In order to answer the key questions of the ‘Preparedness for Practice’ Pediatric Project, it is necessary to collect data on the areas in which this review has identified a lack of information:
1) Preparedness for Practice An updated perspective on pediatric training in Canada is necessary to evaluate whether the current configuration of training optimally prepares pediatricians for independent practice in general pediatrics. This data is essential to compare the preparedness of subspecialist certificants who completed three years of pediatric specialty training with pediatricians who dedicated four years of training to general pediatrics. If there is a reported difference in the abilities of these two groups, then it will be clear that the current training model does not adequately prepare all pediatricians for general pediatric practice.
2) Overlapped Training There is currently no national, Canadian data available on pediatrician’s perceptions of overlapped training between specialty and subspecialty programs, or on trainees’ rationale for opting to overlap the two programs. Collection of this data is necessary to identify strengths and weaknesses of the current training model in preparing pediatricians for independent practice in general pediatrics, and to subsequently inform recommendations regarding reform. This information should also help to identify any other factors that impact on the current context of training and practice.
3) Practice Patterns of Pediatric Subspecialists The goal of pediatric training is to prepare pediatricians for all aspects of practice. It is necessary to know how many, and how often, pediatric subspecialty certificants practice in general pediatrics to ensure that those who have followed this training pathway have the skills necessary for independent practice.

References
Amin, H.J., N. Singhal, and G. Cole. (2011). Validating objectives and training in Canadian paediatrics residency training programmes. Medical Teacher, 33(3), 131-144.
Benchimol, E.I. (2004). The common postgraduate year 1: A paediatric perspective. Paediatrics and Child Health, 9(9), 625-626.
Bismilla, Z., A. Dubrowski, and H. Amin. (2015). Program directors’ perceptions of importance of pediatric procedural skills and resident preparedness. British Medical Council Research Notes, 8(550). Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4600326/
Grant, E., A. Macnab, and K. Wambera. (2007). The Effectiveness of Pediatric Residency Education in Preparing Graduates to Manage Neurological and Neurobehavioural Issues in Practice. Academic Medicine, 82(3), 304-309.
Hameed, T. and S. Lawrence. (2016). The Training Paths and Practice Patterns of Canadian Paediatric Residency Graduates, 2004-2010. Paediatric Child Health, 12(3), 123-126.
Kumar, G., A. Ni, S.E. Lawrence, A. Doja. (2012). Incorporating CanMEDS and subspecialty training into paediatric residency programs: Why are we still deficient? Paediatrics and Child Health, 17(1) 7-11.
Levy, R., A. Dubrowski, H. Amin, and Z. Bismilla. (2014). Procedural skills in paediatric residency: Re-evaluating the competencies. Paediatrics and Child Health, 19(4), 180-184.
Lieberman, L., and R.I. Hilliard. (2006). How well do paediatric residency programmes prepare residents for clinical practice and their future careers? Medical Education, 40, 539-546.
Macnab, A., J. Martin, D. Duffy, and G. Murray. (1998). Measurement of how well a paediatric training programme prepares graduates for their chosen career paths. Medical Education, 32, 362-66.
Piedboeuf, B., S. Jones, E. Orrbine, and G. Filler. (2012). Are the career choices of paediatric residents meeting the needs of academic centres in Canada. Pediatric and Child Health, 17(1), 17-20.
Shamseer, L., D. Roth, S. Tallett, R. Hilliard, and S. Vohra. (2007). A Comparison of Canadian Pediatric Resident Career Plans in 1998 and 2006. Pediatrics, 112(6), 1202-1209.
Tallett, S. (2006). Educator’s Perspective. Child Health in the 21st Century: The Role of the Paediatrician in an Inter-Professional Environment. Invitational Workshop and Symposium: Proceedings and Recommendations, 15-16.

'Preparedness for Practice' Pediatric Postgraduate EducationStudy, 2018
Consent Disclosure
Page exit logic: Skip / Disqualify LogicIF: Question "Do you consent to participate in the study?" is one of the following answers("No") THEN: Jump to page 27 - Thank You!
Study Title: ‘Preparedness for Practice’: Pediatric Postgraduate Education Study,
2018
Principal Investigator: Dr. Karen Gripp, Pediatrics and Child Health, Faculty of
Medicine, University of Manitoba, on behalf of the Royal College of Physicians and
Surgeons of Canada.
Co-investigators: Dr. Jason Frank, Dr. Catherine Farrell, Ms. Sarah Taber, and
Ms. Lisa Gorman, on behalf of the Royal College of Physicians and Surgeons of
Canada
Thank you for considering participation in the ‘Preparedness for Practice’: Pediatric
Postgraduate Education Study, 2018. You are invited to participate in a study
conducted by the ‘Preparedness for Practice’ Pediatric Working Group (referred to
as "PPP Working Group"), with support from the Royal College of Physicians and
Surgeons of Canada (referred to as "Royal College"). This survey is part of an in-
depth review of the current configuration of pediatric training in Canada and
whether it adequately prepares pediatricians for independent general practice.
Your participation is important to us and the results of the study will be used to
develop recommendations regarding the current configuration of pediatric training
in Canada.
This study seeks to answer two key research questions:

1. Are pediatricians adequately prepared for all aspects of general pediatric practice?2. Are there other interrelated challenges or considerations that may be impacting upon
this context of training and practice?
The study consists of two surveys, interviews, and focus group discussions. The
participant populations are comprised of current trainees in and above their fourth
year of postgraduate studies, general pediatricians Certificants, pediatric
subspecialist Certificants, and Program Directors of pediatric disciplines. The study
focuses on four critical areas related to participants’ pediatric training and practice:
1) demographics; 2) the current training model; 3) career decision-making; and 4)
practice.
Your feedback will be collected through an online survey which will ask you a
series of questions and should take about twenty minutes to complete. At the end
of the survey, you will also be asked if you wish to participate in an interview.
Your participation in this study is completely voluntary. You are not required to
provide personal information such as your name, address or telephone number
during the survey, and you don’t have to answer any questions you don’t want to.
The survey system will not record your e-mail address or IP (Internet protocol)
address. You have the right to refuse to participate, to omit any questions, and/or
to stop participating at any time.
The risks of participating are low. All data collected in this survey will be kept
entirely confidential and anonymous. The potentially identifying information
collected by the survey Preparedness for Practice: Pediatrics Postgraduate
Education Study, 2018 Online Survey Consent Disclosure is minimal and the
research team will not be able to track individual responses. In order to keep
anonymity, the results will be presented in aggregate form and if we use
quotations, they will not be attributed to an individual. All information will be stored
on an encrypted, password-protected computer in a locked office. Only research
members of the Educational Strategy, Innovations and Development Unit at the
Royal College will have access to the data. Importantly, Department Chiefs and
Program Directors will not be informed on participation.

Please note that some questions may prompt you to reflect on past experiences in
practice that may be upsetting. You do not have to answer any questions that
make you feel uncomfortable. Should you require support, you can seek physician
support in your province here: https://www.cma.ca/En/Pages/physician-health.aspx
If you agree to participate in the survey, please note that you must complete the
survey in one sitting as the system will not let you save your survey responses and
return to complete them later. You will not be able to withdraw your responses
once submitted as the survey is anonymous and will not be able to link the survey
responses back to you.
The Principal Investigator and members of the ‘Preparedness for Practice’
Pediatric (PPP) Working Group practice pediatric medicine and their colleagues
are included in the participant population. The PPP Working Group was formed to
examine whether the current configuration of pediatric training optimally prepares
pediatricians for independent general practice and is supported by the Royal
College. Analysis of the study results will be undertaken by the Royal College of
Physicians and Surgeons of Canada Educational Strategy Unit, which is an
unbiased research unit housed by the Royal College’s Office of Specialty
Education. The data collected in this study will help inform the working group
discussion and the development of recommendations, with the input of the
Educational Strategy unit to ensure all results are displayed in an objective
manner.
If you have any questions about this survey study, please do not hesitate to
contact the principal investigator, Dr. Karen Gripp at [email protected] or (204)
787-2466, or the study coordinator, Ms. Lisa Gorman at [email protected]
or 613-730-8177 x467.
This study has been approved by the University of Manitoba Health Research
Ethics Board.
Thank you.

Demographics
Do you consent to participate in the study? *
Yes
No
Did you complete both pediatric specialty and subspecialty training inCanada? *
Yes
No
Show/hide trigger exists.Do you currently practice in Canada? *
Yes
No
AlbertaBritish ColumbiaManitobaNew BrunswickNewfoundland and LabradorNorthwest TerritoriesNova ScotiaNunavutOntarioPrince Edward IslandQuebecSaskatchewanYukonOther
Hidden unless: Question "Do you currently practice in Canada?" is one of the followinganswers ("Yes")In which Province / Territory do you currently practice?
Max = 2017 Must be numeric Whole numbers only Max character count = 4 Mincharacter count = 4In what year did you begin training in general pediatrics?

AlbertaBritish ColumbiaManitobaNew BrunswickNewfoundland and LabradorNova ScotiaOntarioQuebecSaskatchewanOther
Demographics
In what province/territory did you complete your core pediatric training (firstthree years)?
‘Overlap training’ occurs when a resident’s first year of subspecialty trainingis undertaken at the same time as their final year of residency in pediatrics.
Did you overlap your training? *
Yes
No
Max = 2017 Must be numeric Whole numbers only Max character count = 4 Mincharacter count = 4In what year did you begin pediatric subspecialty training?

AlbertaBritish ColumbiaManitobaNew BrunswickNova ScotiaOntarioQuebecOther
Adolescent MedicineClinical Pharmacology and ToxicologyCritical Care MedicineDevelopmental PediatricsMedical Genetics/MetabolicsNeonatal Perinatal MedicinePediatric CardiologyPediatric Clinical Immunology and AllergyPediatric Emergency MedicinePediatric Endocrinology and MetabolismPediatric GastroenterologyPediatric Hematology/OncologyPediatric Infectious DiseasesPediatric Medical BiochemistryPediatric NephrologyPediatric NeurologyPediatric Palliative MedicinePediatric RespirologyPediatric RheumatologyOther
In what province/territory did you complete pediatric subspecialty training? *
Show/hide trigger exists.In what subspecialty did you train? *

Demographics
Page exit logic: Skip / Disqualify LogicIF: Question "Did you complete both pediatric specialty and subspecialty training inCanada?" is one of the following answers ("No") THEN: Jump to page 27 - Thank You!
Hidden unless: Question "In what subspecialty did you train?" is one of the followinganswers ("Other")Please specify
Did you complete / are you currently completing a post-residency fellowship(not subspecialty training)?
Yes - Please specify
No
Show/hide trigger exists.Do you currently hold any of the following positions (you may select morethan one)? *
Pediatric Specialty Program Director
Pediatric Subspecialty Program Director
Academic Staff in Pediatrics (e.g. Lecturer, Instructor, Professor, etc.)
Department Chief
Not applicable

Hidden unless: Question "Do you currently hold any of the following positions (you mayselect more than one)?" is one of the following answers ("Department Chief")Do you expect subspecialty staff to provide general pediatric care?
Yes
No
Min = 0 Max = 100 Must be percentage Hidden unless: ( Question "Do you expect subspecialty staff to provide general pediatric
care?" is one of the following answers ("Yes") AND Question "Do you currently hold any ofthe following positions (you may select more than one)?" is one of the following answers("Department Chief"))What percentage of their overall work time do you expect subspecialty staffto provide general pediatric care on average?
Min = 0 Max = 100 Must be percentageWhat percentage of your overall clinical work time is spent in each capacity?
General Pediatrics
Subspecialty Pediatrics
0 out of 100% Total

Training Model
Page exit logic: Skip / Disqualify LogicIF: Question "Do you currently practice in Canada?" is one of the following answers ("No")THEN: Jump to page 27 - Thank You!
Min = 0 Max = 100 Must be percentageWhat percentage of your overall clinical work time is spent in each type ofmedical setting?
Urban, tertiary care university teaching hospital
Urban community hospital (e.g. may provide teaching but withoutresearch programs)
Rural community hospital (e.g. may provide teaching but withoutresearch programs)
Community office-based practice
Other
N/A
0 out of 100%Total
In your own opinion, what are the strengths of the current training model?

Career Decision-Making
Page entry logic:This page will show when: Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("Yes")
In your own opinion, what are the challenges of the current training model?

Not afactor
Minorfactor
Majorfactor
Idon'tknow
The subspecialty program to which I wanted to applywould not accept students who completed four yearsof training in pediatrics prior to entry.
There were limited training positions in mysubspecialty.
Funding in my province did not allow for four years ofpediatric residency and subspecialty training.
I felt that I would be adequately prepared in generalpediatrics after three years of core pediatrics.
I thought that I would only need three years of corepediatric training for my chosen career path.
Below is a list of some of the reasons why trainees overlapped the final yearof specialty training in pediatrics and the first year of a subspecialty program.
To what degree was each of these statements a factor in your own decision-making process?
Please list any other factors in your decision-making process:

Career Decision-Making
Page entry logic:This page will show when: Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("Yes")
I am verydissatisfied
with mydecision.
I am somewhatdissatisfied
with mydecision. I don’t know
I amsomewhat
satisfied withmy decision.
I am verysatisfied withmy decision.
Hidden unless: (( Question "The subspecialty program to which I wanted to apply wouldnot accept students who completed four years of training in pediatrics prior to entry." is one ofthe following answers ("Not a factor","I don't know") OR Question "There were limited trainingpositions in my subspecialty." is one of the following answers ("Not a factor","I don't know"))OR Question "Funding in my province did not allow for four years of pediatric residency andsubspecialty training." is one of the following answers ("Not a factor","I don't know"))If funding and admission criteria were no longer concerns during yourdecision-making, would you have made the same decision to overlap yourpediatric specialty and subspecialty training?
Yes
No
I don't know
In the context of your current practice, are you satisfied with your decision tooverlap specialty and subspecialty training?

Career Decision-Making
Page entry logic:This page will show when: Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("No")
Show/hide trigger exists.In the context of your current practice, do you think that it would have beenbeneficial to have had more training in general pediatrics?
Yes
No
I prefer not to say
Hidden unless: Question "In the context of your current practice, do you think that itwould have been beneficial to have had more training in general pediatrics?" is one of thefollowing answers ("Yes")Why do you think that additional general pediatric training would have beenbeneficial?

Not afactor
Minorfactor
Majorfactor
Idon'tknow
I did not feel adequately prepared in generalpediatrics after three years.
I had not fully decided on a subspecialty prior toentering my fourth year of residency in pediatrics.
I felt that I would be a more competitive applicant if Ichose to complete all four years of residency beforeentering a subspecialty.
I was worried that I would not be able to focus onpreparing for the pediatrics certification exam whiledoing my first year of training in a subspecialty.
I was unsuccessful in my application to entersubspecialty training after three years of pediatricresidency.
Below is a list of some of the reasons why trainees completed four years ofspecialty training in pediatrics before beginning a subspecialty program.
To what degree was each of these statements a factor in your own decision-making process?
Please list any other factors in your decision-making process:

I am verydissatisfied
with mydecision
I am somewhatdissatisfied
with mydecision I don't know
I amsomewhat
satisfied withmy decision
I am verysatisfied withmy decision
Practice
In the context of your current practice, are you satisfied with your decisionnot to overlap training in pediatrics and a pediatric subspecialty?
How long did it take you to find a job related to your subspecialty training?
Upon completion of my training
Within six months of completing my training
Within a year of completing my training
Within five years of completing my training
Longer than five years after completing my training
I have not worked in a job related to my training but I would like to.
I have not worked in a job related to my training but I chose not to.
Show/hide trigger exists.How often do you practice in general pediatrics (any clinical activity with orwithout on-call duties in general pediatrics)? *
1 or more times a week
1 or more times a month
Never

Practice
Thiscondition orprocedurewas new to
me onbeginning
independentpractice.
I had minimalexposure to
this conditionor procedure
during mytraining anddid not feel
ready tomanage it
independently.
I managed thiscondition orprocedure
multiple timesduring my
training but didnot feel readyto manage it
independently.
I was able toindependentlymanage thiscondition or
procedure onbeginning
independentpractice.
I don’tremember.
ADHD
Behavioralissues/autisticspectrumdisorders
Mental healthdisorders
Care ofacutely bornnewborn(Newbornresuscitation)
How often do you provide acute care for neonatal patients?
1 or more times a week
1 or more times a month
Never
Below is a list of general pediatric conditions and procedures.
Please indicate which response best describes your ability to manage thefollowing conditions and procedures upon graduation (ie. for the first patientyou saw after certification).

This aspectof practicewas new to
me onbeginning
independentpractice.
I had minimalexposure to
this aspect ofpractice during
my trainingand did notfeel ready tomanage it
independently.
I managed thisaspect ofpractice
multiple timesduring my
training but didnot feel readyto manage it
independently.
I was able toindependentlymanage this
aspect ofpractice onbeginning
independentpractice.
I don’tremember.
Medicolegalissues
OfficeManagementand Billing
Practice
Please indicate which response best describes your ability to manage thefollowing non-clinical aspects of practice.

This areasof practicewas new to
me onbeginning
independentpractice.
I had minimalexposure tocases in this
area ofpractice during
my trainingand did notfeel ready tomanage it
independently.
I managedcases in this
area ofpractice
multiple timesduring my
training but didnot feel readyto manage it
independently.
I was able toindependently
managecases in this
area ofpractice onbeginning
independentpractice.
I don’tremember.
Nutrition
Suspectedphysical orother abuse
Anticipatoryguidanceand wellchild care
Transitionto adultcare
Advancedcareplanningand support
Childrenwithmedicalcomplexity
Practice
Below is a list of areas of general pediatric practice.
Please indicate which response best describes your ability to manage thefollowing cases upon graduation (ie. for the first patient you saw aftercertification).

I stronglydisagree
I somewhatdisagree
I have noopinion
I somewhatagree
I stronglyagree
Veryunconfident
Somewhatunconfident
I don'tremember
Somewhatconfident
Veryconfident
Notapplicable -
I did notparticipate
in thematch
process
Hidden unless: Question "How often do you practice in general pediatrics (any clinicalactivity with or without on-call duties in general pediatrics)?" is one of the following answers("1 or more times a week","1 or more times a month")Using the following scale, please respond to the statement:
‘I was prepared to provide care for the range of patients that I saw when Istarted doing work in general pediatrics (clinical activity including on-callactivities in general pediatrics).’
Show/hide trigger exists.During the time of the subspecialty match, how confident did you feel in yourdecision?
Hidden unless: Question "During the time of the subspecialty match, how confident did you feel in your decision?" is one of the following answers ("Very unconfident","Somewhat unconfident","Somewhatconfident","Very confident")Why did you feel this way?

Program Director Perspective
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
Show/hide trigger exists.Did you switch disciplines during subspecialty training?
I switched to another subspecialty program
I switched back into general pediatrics
I did not switch
Hidden unless: Question "Did you switch disciplines during subspecialty training?" isone of the following answers ("I switched to another subspecialty program","I switched backinto general pediatrics")Why did you switch disciplines?
Show/hide trigger exists.How long have you been a faculty member?
0-5 years
6-10 years
11+ years

How long have you been a program director?
0-5 years
6-10 years
11+ years
Hidden unless: Question "How long have you been a faculty member?" is one of thefollowing answers ("6-10 years","11+ years")What have been some of the changes to the training model over the last fiveyears in your program?
Hidden unless: Question "How long have you been a faculty member?" is one of thefollowing answers ("11+ years")What have been some of the changes to the training model over the last tenyears in your program?

Show/hide trigger exists.Is there a formal curriculum for the fourth-year residents in pediatrics, differentfrom the core curriculum?
Yes
No
I don't know
Hidden unless: Question "Is there a formal curriculum for the fourth-year residents inpediatrics, different from the core curriculum?" is one of the following answers ("Yes")Please describe the curriculum.
Show/hide trigger exists.Do the objectives of fourth year of training in your pediatrics program alignwith those of the first year of subspecialty training?
The objectives are generally well-aligned
It depends on the subspecialty
The objectives are not well aligned
I don't know
I prefer not to say

Program Director Perspectives
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
Hidden unless: Question "Do the objectives of fourth year of training in your pediatricsprogram align with those of the first year of subspecialty training?" is one of the followinganswers ("The objectives are generally well-aligned","It depends on the subspecialty","Theobjectives are not well aligned")Please explain your response.
After four years of postgraduate training, please rate the ability of a traineewho did not overlap their specialty and subspecialty training to managecases in the following areas of general pediatric practice:

Traineesare notable to
managecases in
this area ofpractice
Traineesrequire a lot ofsupervision to
managecases in this
area ofpractice
Traineesrequire somesupervision to
managecases in this
area ofpractice
Trainees areready to
independentlymanage casesin this area of
practice
Idon'tknow
ADHD
Behavioralissues/autisticspectrumdisorders
Mental healthdisorders
Care of theacutely bornnewborn(Newbornresuscitation)
Nutrition
Suspectedphysical orother abuse
Anticipatoryguidance andwell childcare
Transition toadult care
Advancedcare planningand support
Children withmedicalcomplexity
Medicolegalissues
Officemanagementand billing

Program Director Perspectives
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
After four years of postgraduate training, please rate the ability of a traineewho overlapped their specialty and subspecialty training to manage casesin the following areas of general pediatric practice:

Traineesare notable to
managecases in
this area ofpractice
Traineesrequire a lot ofsupervision to
managecases in this
area ofpractice
Traineesrequire somesupervision to
managecases in this
area ofpractice
Trainees areready to
independentlymanage casesin this area of
practice
Idon'tknow
ADHD
Behavioralissues/autisticspectrumdisorders
Mental healthdisorders
Care of theacutely bornnewborn(Newbornresuscitation)
Nutrition
Suspectedphysical orother abuse
Anticipatoryguidance andwell childcare
Transition toadult care
Advancedcare planningand support
Children withmedicalcomplexity
Medicolegalissues
Officemanagementand billing

Program Director Perspectives
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
Never Rarely I don't know Sometimes Frequently
Program Director Perspectives
Must be percentage Whole numbers only Positive numbers onlyIn your opinion, what percentage of subspecialist trainees who overlappedspecialty and subspecialty training are satisfied with their experience of thetraining model?
Do recently certified subspecialty trainees who overlapped specialty andsubspecialty programs request additional training (ie. electives, prolongedtraining) in general pediatrics?
What feedback do you receive from trainees about the current configurationof pediatric specialty and subspecialty training?

Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SubspecialtyProgram Director")
Show/hide trigger exists.How long have you been a faculty member?
0-5 years
6-10 years
11+ years
How long have you been a program director?
0-5 years
6-10 years
11+ years
Hidden unless: Question "How long have you been a faculty member?" is one of thefollowing answers ("6-10 years","11+ years")What have been the changes to the training model over the last five years inyour program?

I stronglydisagree
I somewhatdisagree
I have noopinion
I somewhatagree
I stronglyagree
Hidden unless: Question "How long have you been a faculty member?" is one of thefollowing answers ("11+ years")What have been the changes to the training model over the last ten years inyour program?
Must be percentageIn your opinion, what percentage of subspecialist trainees who overlappedspecialty and subspecialty training are satisfied with their experience of thetraining model?
Using the following scale, please respond to the following statement:
‘I feel that I can adequately evaluate the competencies in pediatrics of first-year trainees who have overlapped their training, as required in order tocomplete the FITER for pediatrics.’
What feedback do you receive from trainees about the current configurationof pediatric specialty and subspecialty training?

Conclusion
Phone Interview
Page entry logic:This page will show when: ( Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("Yes") AND Question "Howoften do you practice in general pediatrics (any clinical activity with or without on-call duties ingeneral pediatrics)?" is one of the following answers ("1 or more times a week","1 or moretimes a month"))
Page exit logic: Redirect to phone interview surveyIF: Question "Would you like to participate in a phone interview?" is one of the followinganswers ("Yes") THEN: Flag response as complete Redirect to:ca.surveygizmo.com/s3/50016921/PPP-Study-Interview
Thank You!
What, if any changes, would you make in the current training model to betterprepare trainees for general pediatric practice?
Would you like to participate in a phone interview?
Yes
No

Thank you for taking the time to complete this survey. Your input is valuable and
will contribute to recommendations made on the optimal training model for
pediatric specialists and subspecialists in Canada.

'Preparedness for Practice' Pediatric Postgraduate EducationStudy, 2018
Consent Disclosure
Page exit logic: Skip / Disqualify LogicIF: Question "Do you consent to participate in the study?" is one of the following answers("No") THEN: Jump to page 24 - Thank You!
Study Title: ‘Preparedness for Practice’: Pediatric Postgraduate Education Study,
2018
Principal Investigator: Dr. Karen Gripp, Pediatrics and Child Health, Faculty of
Medicine, University of Manitoba, on behalf of the Royal College of Physicians and
Surgeons of Canada.
Co-investigators: Dr. Jason Frank, Dr. Catherine Farrell, Ms. Sarah Taber, and
Ms. Lisa Gorman, on behalf of the Royal College of Physicians and Surgeons of
Canada
Thank you for considering participation in the ‘Preparedness for Practice’: Pediatric
Postgraduate Education Study, 2018. You are invited to participate in a study
conducted by the ‘Preparedness for Practice’ Pediatric Working Group (referred to
as "PPP Working Group"), with support from the Royal College of Physicians and
Surgeons of Canada (referred to as "Royal College"). This survey is part of an in-
depth review of the current configuration of pediatric training in Canada and
whether it adequately prepares pediatricians for independent general practice.
Your participation is important to us and the results of the study will be used to
develop recommendations regarding the current configuration of pediatric training
in Canada.
This study seeks to answer two key research questions:

1. Are pediatricians adequately prepared for all aspects of general pediatric practice?2. Are there other interrelated challenges or considerations that may be impacting upon
this context of training and practice?
The study consists of two surveys, interviews, and focus group discussions. The
participant populations are comprised of current trainees in and above their fourth
year of postgraduate studies, general pediatricians Certificants, pediatric
subspecialist Certificants, and Program Directors of pediatric disciplines. The study
focuses on four critical areas related to participants’ pediatric training and practice:
1) demographics; 2) the current training model; 3) career decision-making; and 4)
practice.
Your feedback will be collected through an online survey which will ask you a
series of questions and should take about twenty minutes to complete. At the end
of the survey, you will also be asked if you wish to participate in an interview.
Your participation in this study is completely voluntary. You are not required to
provide personal information such as your name, address or telephone number
during the survey, and you don’t have to answer any questions you don’t want to.
The survey system will not record your e-mail address or IP (Internet protocol)
address. You have the right to refuse to participate, to omit any questions, and/or
to stop participating at any time.
The risks of participating are low. All data collected in this survey will be kept
entirely confidential and anonymous. The potentially identifying information
collected by the survey Preparedness for Practice: Pediatrics Postgraduate
Education Study, 2018 Online Survey Consent Disclosure is minimal and the
research team will not be able to track individual responses. In order to keep
anonymity, the results will be presented in aggregate form and if we use
quotations, they will not be attributed to an individual. All information will be stored
on an encrypted, password-protected computer in a locked office. Only research
members of the Educational Strategy, Innovations and Development Unit at the
Royal College will have access to the data. Importantly, Department Chiefs and
Program Directors will not be informed on participation.

Please note that some questions may prompt you to reflect on past experiences in
practice that may be upsetting. You do not have to answer any questions that
make you feel uncomfortable. Should you require support, you can seek physician
support in your province here: https://www.cma.ca/En/Pages/physician-health.aspx
If you agree to participate in the survey, please note that you must complete the
survey in one sitting as the system will not let you save your survey responses and
return to complete them later. You will not be able to withdraw your responses
once submitted as the survey is anonymous and will not be able to link the survey
responses back to you.
The Principal Investigator and members of the ‘Preparedness for Practice’
Pediatric (PPP) Working Group practice pediatric medicine and their colleagues
are included in the participant population. The PPP Working Group was formed to
examine whether the current configuration of pediatric training optimally prepares
pediatricians for independent general practice and is supported by the Royal
College. Analysis of the study results will be undertaken by the Royal College of
Physicians and Surgeons of Canada Educational Strategy Unit, which is an
unbiased research unit housed by the Royal College’s Office of Specialty
Education. The data collected in this study will help inform the working group
discussion and the development of recommendations, with the input of the
Educational Strategy unit to ensure all results are displayed in an objective
manner.
If you have any questions about this survey study, please do not hesitate to
contact the principal investigator, Dr. Karen Gripp at [email protected] or (204)
787-2466, or the study coordinator, Ms. Lisa Gorman at [email protected]
or 613-730-8177 x467.
This study has been approved by the University of Manitoba Health Research
Ethics Board.
Thank you.
Demographics
Do you consent to participate in the study? *
Yes
No
Did you complete training in general pediatrics in Canada? *
Yes
No
Show/hide trigger exists.Do you currently practice in Canada? *
Yes
No
I am currently in training

AlbertaBritish ColumbiaManitobaNew BrunswickNewfoundland and LabradorNorthwest TerritoriesNova ScotiaNunavutOntarioPrince Edward IslandQuebecSaskatchewanYukonOther
Hidden unless: Question "Do you currently practice in Canada?" is one of the followinganswers ("Yes")In which Province / Territory do you currently practice?
Max = 2017 Must be numeric Whole numbers only Max character count = 4 Mincharacter count = 4In what year did you begin training in general pediatrics?

AlbertaBritish ColumbiaManitobaNew BrunswickNewfoundland and LabradorNova ScotiaOntarioQuebecSaskatchewanOther
Demographics
In what province/territory did you complete your core pediatric training (firstthree years)?
Show/hide trigger exists.Are you currently completing subspecialty training in Canada? *
Yes
No
Hidden unless: Question "Are you currently completing subspecialty training inCanada?" is one of the following answers ("Yes")‘Overlap training’ occurs when a resident’s first year of subspecialty trainingis undertaken at the same time as their final year of residency in pediatrics.
Did you overlap your training? *
Yes
No

AlbertaBritish ColumbiaManitobaNew BrunswickNova ScotiaOntarioQuebecOther
Max = 2017 Must be numeric Whole numbers only Max character count = 4 Mincharacter count = 4
Hidden unless: Question "Are you currently completing subspecialty training inCanada?" is one of the following answers ("Yes")In what year did you begin pediatric subspecialty training?
Hidden unless: Question "Are you currently completing subspecialty training inCanada?" is one of the following answers ("Yes")In what province/territory are you completing pediatric subspecialty training?*

Adolescent MedicineClinical Pharmacology and ToxicologyCritical Care MedicineDevelopmental PediatricsMedical Genetics/MetabolicsNeonatal Perinatal MedicinePediatric CardiologyPediatric Clinical Immunology and AllergyPediatric Emergency MedicinePediatric Endocrinology and MetabolismPediatric GastroenterologyPediatric Hematology/OncologyPediatric Infectious DiseasesPediatric Medical BiochemistryPediatric NephrologyPediatric NeurologyPediatric Palliative MedicinePediatric RespirologyPediatric RheumatologyOther
Demographics
Page exit logic: Skip / Disqualify LogicIF: Question "Did you complete training in general pediatrics in Canada?" is one of thefollowing answers ("No") THEN: Jump to page 24 - Thank You!
Show/hide trigger exists. Hidden unless: Question "Are you currently completingsubspecialty training in Canada?" is one of the following answers ("Yes")In what subspecialty are you training? *
Hidden unless: Question "In what subspecialty are you training?" is one of the followinganswers ("Other")Please specify

Did you complete / are you currently completing a post-residency fellowship(not subspecialty training)?
Yes - Please specify
No
Show/hide trigger exists.Do you currently hold any of the following positions (you may select morethan one)? *
Pediatric Specialty Program Director
Pediatric Subspecialty Program Director
Academic Staff in Pediatrics (e.g. Lecturer, Instructor, Professor, etc.)
Department Chief
Not applicable
Hidden unless: Question "Do you currently hold any of the following positions (you mayselect more than one)?" is one of the following answers ("Department Chief")Do you expect subspecialty staff to provide general pediatric care?
Yes
No

Min = 0 Max = 100 Must be percentage Hidden unless: ( Question "Do you expect subspecialty staff to provide general pediatric
care?" is one of the following answers ("Yes") AND Question "Do you currently hold any ofthe following positions (you may select more than one)?" is one of the following answers("Department Chief"))What percentage of their overall work time do you expect subspecialty staffto provide general pediatric care on average?
Min = 0 Max = 100 Must be percentageWhat percentage of your overall clinical work time is spent in each capacity?
General Pediatrics
Subspecialty Pediatrics
0 out of 100% Total
Min = 0 Max = 100 Must be percentageWhat percentage of your overall clinical work time is spent in each type ofmedical setting?
Urban, tertiary care university teaching hospital
Urban community hospital (e.g. may provide teaching but withoutresearch programs)
Rural community hospital (e.g. may provide teaching but withoutresearch programs)
Community office-based practice
Other
N/A
0 out of 100%Total

Training Model
Page exit logic: Skip / Disqualify LogicIF: Question "Do you currently practice in Canada?" is one of the following answers ("No")THEN: Jump to page 24 - Thank You!
Career Decision-Making
Page entry logic:This page will show when: Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("Yes")
In your own opinion, what are the strengths of the current training model?
In your own opinion, what are the challenges of the current training model?

Not afactor
Minorfactor
Majorfactor
Idon'tknow
The subspecialty program to which I wanted to applywould not accept students who completed four yearsof training in pediatrics prior to entry.
There were limited training positions in mysubspecialty.
Funding in my province did not allow for four years ofpediatric residency and subspecialty training.
I felt that I would be adequately prepared in generalpediatrics after three years of core pediatrics.
I thought that I would only need three years of corepediatric training for my chosen career path.
Below is a list of some of the reasons why trainees overlapped the final yearof specialty training in pediatrics and the first year of a subspecialty program.
To what degree was each of these statements a factor in your own decision-making process?
Please list any other factors in your decision-making process:

Career Decision-Making
Page entry logic:This page will show when: Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("Yes")
I am verydissatisfied
with mydecision.
I am somewhatdissatisfied
with mydecision. I don’t know
I amsomewhat
satisfied withmy decision.
I am verysatisfied withmy decision.
Hidden unless: (( Question "The subspecialty program to which I wanted to apply wouldnot accept students who completed four years of training in pediatrics prior to entry." is one ofthe following answers ("Major factor","I don't know") OR Question "There were limited trainingpositions in my subspecialty." is one of the following answers ("Major factor","I don't know"))OR Question "Funding in my province did not allow for four years of pediatric residency andsubspecialty training." is one of the following answers ("Major factor","I don't know"))If funding and admission criteria were no longer concerns during yourdecision-making, would you have made the same decision to overlap yourpediatric specialty and subspecialty training?
Yes
No
I don't know
In the context of your current practice, are you satisfied with your decision tooverlap specialty and subspecialty training?

Career Decision-Making
Page entry logic:This page will show when: Question "‘Overlap training’ occurs when a resident’s first year ofsubspecialty training is undertaken at the same time as their final year of residency inpediatrics.
Did you overlap your training?" is one of the following answers ("No")
Show/hide trigger exists.In the context of your current practice, do you think that it would have beenbeneficial to have had more training in general pediatrics?
Yes
No
I prefer not to say
Hidden unless: Question "In the context of your current practice, do you think that itwould have been beneficial to have had more training in general pediatrics?" is one of thefollowing answers ("Yes")Why do you think that additional general pediatric training would have beenbeneficial?

Not afactor
Minorfactor
Majorfactor
Idon'tknow
I did not feel adequately prepared in generalpediatrics after three years.
I had not fully decided on a subspecialty prior toentering my fourth year of residency in pediatrics.
I felt that I would be a more competitive applicant if Ichose to complete all four years of residency beforeentering a subspecialty.
I was worried that I would not be able to focus onpreparing for the pediatrics certification exam whiledoing my first year of training in a subspecialty.
I was unsuccessful in my application to entersubspecialty training after three years of pediatricresidency.
Below is a list of some of the reasons why trainees completed four years ofspecialty training in pediatrics before beginning a subspecialty program.
To what degree was each of these statements a factor in your own decision-making process?
Please list any other factors in your decision-making process:

I am verydissatisfied
with mydecision
I am somewhatdissatisfied
with mydecision I don't know
I amsomewhat
satisfied withmy decision
I am verysatisfied withmy decision
Practice
In the context of your current practice, are you satisfied with your decisionnot to overlap training in pediatrics and a pediatric subspecialty?

Thiscondition orprocedurewas new to
me onbeginning
independentpractice.
I had minimalexposure to
this conditionor procedure
during mytraining anddid not feel
ready tomanage it
independently.
I managed thiscondition orprocedure
multiple timesduring my
training but didnot feel readyto manage it
independently.
I was able toindependentlymanage thiscondition or
procedure onbeginning
independentpractice.
I don’tremember.
ADHD
Behavioralissues/autisticspectrumdisorders
Mental healthdisorders
Care ofacutely bornnewborn(Newbornresuscitation)
Below is a list of general pediatric conditions and procedures.
Please indicate which response best describes your ability to manage thefollowing conditions and procedures upon graduation (ie. for the first patientyou saw after certification).

This aspectof practicewas new to
me onbeginning
independentpractice.
I had minimalexposure to
this aspect ofpractice during
my trainingand did notfeel ready tomanage it
independently.
I managed thisaspect ofpractice
multiple timesduring my
training but didnot feel readyto manage it
independently.
I was able toindependentlymanage this
aspect ofpractice onbeginning
independentpractice.
I don’tremember
Medicolegalissues
Officemanagementand Billing
Practice
Please indicate which response best describes your ability to manage thefollowing non-clinical aspects of practice.

This areasof practicewas new to
me onbeginning
independentpractice.
I had minimalexposure tocases in this
area ofpractice during
my trainingand did notfeel ready tomanage it
independently.
I managedcases in this
area ofpractice
multiple timesduring my
training but didnot feel readyto manage it
independently.
I was able toindependently
managecases in this
area ofpractice onbeginning
independentpractice.
I don’tremember.
applicable
in training
Nutrition
Suspectedphysical orother abuse
Anticipatoryguidanceand wellchild care
Transitionto adultcare
Advancedcareplanningand support
Childrenwithmedicalcomplexity
Practice
Below is a list of areas of general pediatric practice.
Please indicate which response best describes your ability to manage thefollowing cases upon graduation (ie. for the first patient you saw aftercertification).

I stronglydisagree
I somewhatdisagree
I have noopinion
I somewhatagree
I stronglyagree
Notapplicable - Iam currentlyin training
Veryunconfident
Somewhatunconfident
I don'tremember
Somewhatconfident
Veryconfident
Notapplicable -
I did notparticipate
in thematch
process
Using the following scale, please respond to the statement:
‘I was prepared to provide care for the range of patients that I saw when Istarted doing work in general pediatrics (clinical activity including on-callactivities in general pediatrics).’
During the time of the subspecialty match, how confident did you feel in yourdecision?
Why did you feel this way?

Program Director Perspective
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
Show/hide trigger exists.Did you switch disciplines during subspecialty training?
I switched to another subspecialty program
I switched back into general pediatrics
I did not switch
Hidden unless: Question "Did you switch disciplines during subspecialty training?" isone of the following answers ("I switched to another subspecialty program","I switched backinto general pediatrics")Why did you switch disciplines?
Show/hide trigger exists.How long have you been a faculty member?
0-5 years
6-10 years
11+ years

How long have you been a program director?
0-5 years
6-10 years
11+ years
Hidden unless: Question "How long have you been a faculty member?" is one of thefollowing answers ("6-10 years","11+ years")What have been some of the changes to the training model over the last fiveyears in your program?
Hidden unless: Question "How long have you been a faculty member?" is one of thefollowing answers ("11+ years")What have been some of the changes to the training model over the last tenyears in your program?

Show/hide trigger exists.Is there a formal curriculum for the fourth-year residents in pediatrics, differentfrom the core curriculum?
Yes
No
I don't know
Hidden unless: Question "Is there a formal curriculum for the fourth-year residents inpediatrics, different from the core curriculum?" is one of the following answers ("Yes")Please describe the curriculum.
Show/hide trigger exists.Do the objectives of fourth year of training in your pediatrics program alignwith those of the first year of subspecialty training?
The objectives are generally well-aligned
It depends on the subspecialty
The objectives are not well aligned
I don't know
I prefer not to say

Program Director Perspectives
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
Hidden unless: Question "Do the objectives of fourth year of training in your pediatricsprogram align with those of the first year of subspecialty training?" is one of the followinganswers ("The objectives are generally well-aligned","It depends on the subspecialty","Theobjectives are not well aligned")Please explain your response.
After four years of postgraduate training, please rate the ability of a traineewho did not overlap their specialty and subspecialty training to managecases in the following areas of general pediatric practice:

Traineesare notable to
managecases in
this area ofpractice
Traineesrequire a lot ofsupervision to
managecases in this
area ofpractice
Traineesrequire somesupervision to
managecases in this
area ofpractice
Trainees areready to
independentlymanage casesin this area of
practice
Idon'tknow
ADHD
Behavioralissues/autisticspectrumdisorders
Mental healthdisorders
Care of theacutely bornnewborn(Newbornresuscitation)
Nutrition
Suspectedphysical orother abuse
Anticipatoryguidance andwell childcare
Transition toadult care
Advancedcare planningand support
Children withmedicalcomplexity
Medicolegalissues
Officemanagementand billing

Program Director Perspectives
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
After four years of postgraduate training, please rate the ability of a traineewho overlapped their specialty and subspecialty training to manage casesin the following areas of general pediatric practice:

Traineesare notable to
managecases in
this area ofpractice
Traineesrequire a lot ofsupervision to
managecases in this
area ofpractice
Traineesrequire somesupervision to
managecases in this
area ofpractice
Trainees areready to
independentlymanage casesin this area of
practice
Idon'tknow
ADHD
Behavioralissues/autisticspectrumdisorders
Mental healthdisorders
Care of theacutely bornnewborn(Newbornresuscitation)
Nutrition
Suspectedphysical orother abuse
Anticipatoryguidance andwell childcare
Transition toadult care
Advancedcare planningand support
Children withmedicalcomplexity
Medicolegalissues
Officemanagementand billing

Program Director Perspectives
Page entry logic:This page will show when: Question "Do you currently hold any of the following positions(you may select more than one)?" is one of the following answers ("Pediatric SpecialtyProgram Director")
Never Rarely I don't know Sometimes Frequently
Conclusion
Must be percentage Whole numbers only Positive numbers onlyIn your opinion, what percentage of subspecialist trainees who overlappedspecialty and subspecialty training are satisfied with their experience of thetraining model?
Do recently certified subspecialty trainees who overlapped specialty andsubspecialty programs request additional training (ie. electives, prolongedtraining) in general pediatrics?
What feedback do you receive from trainees about the current configurationof pediatric specialty and subspecialty training?

Focus Group
Page entry logic:This page will show when: Question "Are you currently completing subspecialty training inCanada?" is one of the following answers ("Yes")
Page exit logic: Redirect to phone interview surveyIF: Question "Would you like to participate in a focus group?" is one of the following answers("Yes") THEN: Flag response as complete Redirect to:ca.surveygizmo.com/s3/50016931/PPP-Study-Focus-Group
Thank You!
Thank you for taking the time to complete this survey. Your input is valuable and
will contribute to recommendations made on the optimal training model for
pediatric specialists and subspecialists in Canada.
What, if any changes, would you make in the current training model to betterprepare trainees for general pediatric practice?
Would you like to participate in a focus group?
Yes
No

August 31, 2018 Committee on Specialties Royal College of Physicians and Surgeons of Canada 774 Echo Drive Ottawa, ON. K1S 5N8 Dear Colleagues: As the national group of Pediatric program directors in Canada, we write this letter in support of the Specialty Committee (Pediatrics) application for a mandatory four years of training for all pediatricians. The many reasons for this application are well-summarized in the main document, including our strong and unanimous recommendation that all residents complete their entire Pediatrics training prior to entering a subspecialty. As members of both our Specialty Committee and the Competence by Design working group for Pediatrics, and more importantly as supervisors for the 670 residents currently in specialty training in Pediatrics, we give our highest possible endorsement of this proposal. In support thereof, we have affixed our signatures below. Thank you for your time and consideration. Sincerely,
Karen E. Gripp, MD, FAAP, FRCPC Chair, Canadian Pediatric Program Directors University of Manitoba
Janet Greenman, MD, FRCPC, FAAP University of British Columbia
Mia Remington, MD, FRCPC University of British Columbia
Jennifer Balfour, MD, FRCPC University of British Columbia
Amonpreet Sandhu, MD, MSc (Med Ed), FRCPC University of Calgary
Marielena DiBartolo, MD, FRCPC University of Calgary
Mark Belletrutti, MD, MSc, FRCPC University of Alberta

Jessica Foulds, MD, FRCPC University of Alberta
Maryam Mehtar, MBBCh, FRCPC University of Saskatchewan
Ayisha Kurji, MD, FRCPC University of Saskatchewan
Elisabete Doyle, MD, FRCPC, FAAP University of Manitoba
Tara Baron, MD, FRCPC Northern Ontario School of Medicine
Tamara Van Hooren University of Western Ontario
Andrea Hunter, MD, FRCPC McMaster University
Quang Ngo, MD, FRCPC McMaster University
Bojana Babic, MD, FRCPC, FAAP McMaster University
Kirk Leifso, MD, FRCPC Queens University
Adelle R. Atkinson, MD, FRCPC University of Toronto
Hilary Writer, MD, FRCPC University of Ottawa
Kristy Parker, MD, FRCPC University of Ottawa
Robert Sternszus, MD, FRCPC McGill University
Olivia Tse, MD, FRCPC McGill University
Catherine Hervouet-Zeiber, MD, FRCPCq Université de Montréal

Genevieve Benoit, MD, FRCPC Université de Montréal
Miriam Santschi, MD, FRCPC Université de Sherbrooke
Sylvie Belanger, MD, FRCPC Université Laval
Sarah Manos, MD, FRCPC Dalhousie University
John Martin, MD, FRCPC Memorial University
Lynette Bowes, MD, FRCPC Memorial University

Specialty Committee in Pediatrics Pediatrics’ Consultation Meeting
Minutes
Tuesday, May 29, 2018 12:00 – 2:00 pm Eastern Time
La salle de la communauté - Le Monastère des Augustines, Québec City, Québec
1. Call to order and introductions The meeting was called to order and a round of introductions was made. A list of those in attendance both in person and remotely is included at the end of this document. The meeting was facilitated by Catherine Farrell, MD, FRCPC, chair of the Specialty Committee in Pediatrics, Adelle Atkinson MD, FRCPC, vice-chair of the Specialty Committee in Pediatrics, and Karen Gripp, MD, FRCPC, chair of the Canadian Pediatric Program Directors (CPPD). The goal of the meeting was to hold a robust discussion with all pediatric subspecialties regarding the possible models for overlap in training between the primary discipline of Pediatrics and the subspecialties, in the context of Competence by Design (CBD) 2. Review of Briefing Note Highlights from the briefing note included in the agenda package were reviewed:
Pediatrics’ CBD launch has been delayed to 2020 because of the need to come to a resolution regarding training duration/overlap training/etc. between the primary discipline and the pediatric subspecialties.
There was unanimous agreement among the Pediatrics’ CBD workshop participants that trainees would not be able to meet Entrustable Professional Activities (EPAs) and training experiences for the first three stages of CBD [Transition to Discipline (TTD), Foundations and Core] within the 36 months’ time period that a three-year training program would allow. This is a major limitation to maintaining the model of three years of general Pediatrics training followed by two to three years of subspecialty training, which currently exists in some jurisdictions. The Pediatrics CBD workshop participants unanimously endorsed the concept of all residents needing to complete all the requirements of training in Pediatrics, in a Pediatrics program, before going on the subspecialty training.
History and assumptions Need to train pediatricians who can meet needs of the Canadian population:
this is the premise of the move to CBD. The possibility of overlap between the primary discipline and the subspecialties
has existed for 40 years. This is the third attempt over the last 20 years aiming to eliminate overlap. All previous attempts were rejected.
Gaps identified in current training which need to be incorporated now include: Increased emphasis on behavior and development; mental health; advanced care planning; practice management and complex medical issues.
Pediatrics Transition to Practice (TTP) EPAs would be challenging to meet within subspecialty training programs
Increased cost for mandatory additional year of training; however, having more residents in the fourth year of training in the system will offset some expenses as senior trainees will do call. Additionally, incentive programs which already exist may

Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 2 of 8
become unnecessary. Also, better training for all pediatricians may lead to a possible decrease in medicolegal issues
Other stakeholders appear to be in agreement with the move. All Pediatric program directors unanimously agreed that residents reported preferring a four-year training program if possible. The Paediatric Chairs of Canada (PCC) have also discussed this issue and agree that a fourth training year would be best. The postgraduate (PG) deans are aware of the current consultation; however no formal discussions have yet been arranged between members of the Specialty Committee in Pediatrics and the PG deans.
Advantages with a new training model: Would better support the four stages of CBD training Excellence in training Excellence in clinical care Flexibility in workforce
3. Consultation Attendees were asked to considering the following questions:
If there is no overlap training – do all residents complete the four CBD stages of training prior to moving to a subspecialty?
If the concept of overlap training is accepted at what point should the overlap occur? Should overlap training be possible in all subspecialties? Or only in some? If overlap remains, how will the TTP and residual Core EPAs be taught/assessed? Who
is responsible for the final certification in Pediatrics? How will training experiences be achieved? How will communication work between the sending and receiving programs? How will off-cycle starts be managed?
On May 28, 2018, there was a joint meeting between the Canadian Paediatric Society (CPS) Board of Directors and the PCC. At this meeting, mental health was identified as a key component currently lacking in training, both clinically and pedagogically. This is an excellent example of an issue that doesn’t clearly look like it belongs to a subspecialty; however there is no subspecialty that doesn’t see mental health issues in patients. Emphasis being placed on training in mental health within general Pediatrics training serves all Pediatricians, including pediatric subspecialists. This issue highlights that gaps already exist in training, that adequate training is not being accomplished in the current three year training system model. The TTP EPAs for Pediatrics may superficially seem similar to subspecialty training (ex. managing a Pediatric Intensive Care Unit (PICU) vs. managing a general Pediatric practice). However, there are key differences that a number of subspecialists have very clearly indicated would pose problems such that such an EPA could not be accomplished within the subspecialty context. It was agreed that these issues have not been created by the move to CBD, but rather CBD has provided a framework and a lens to highlight problems that have existed for years. It was further emphasized that the problem will continue to exist and only become worse in years to come; this is also an opportunity to predict long-term trends, and whether the current practice model is appropriate and will meet the needs of the population in years to come. It was acknowledged that these conversations are taking place at a time when there are already constraints in subspecialty positions. All are aware and sensitive to this fact, that there are issues not just around funding, but also career opportunities for subspecialty trainees.

Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 3 of 8 Attendees asked the following questions: Q: Have there been any parallel discussions ongoing in Internal Medicine (IM), given it is
similar? A: It was reported that IM’s training looks superficially similar to Pediatrics, but it is different
in a number of ways. The way in which Pediatrics’ conducts training and the expectations for outcome are both very different from the other primary discipline. IM previously decided to create the subspecialty of General Internal Medicine (GIM) and went through a similar consultation process to put it in place. Virtually all trainees who start in IM training now go into a subspecialty, whether it is GIM or an alternate subspecialty. So there are two parallel pathways to become an “internist”: the “three year plus one year” model, the last year being within a subspecialty, and the “three year plus two year” GIM model. Since the creation of the subspecialty of GIM, it has actually become the accepted standard in many places for the practice of Internal Medicine, so much so that residents entering IM training who plan to take subspecialty training, but would like to still have option of doing general IM work in their practice, are now being told that practice in general IM is not possible without being certified in GIM. For the purposes of CBD, the assumption in IM is that trainees would go through three years of primary training (corresponding to the first three stages in CBD) and have a final year of TTD delegated to the subspecialties. The exact model of overlap will be determined in consultation with each subspecialty discipline separately. Internal Medicine recognizes that there will be residents that will not complete all of the EPAs for the first three CBD stages within three years. IM will be implementing CBD in 2019.
The differences between practicing IM and Pediatrics include: IM is much more homogeneous versus Pediatrics’ training is more heterogeneous (ex. age range, pathology presents differently across ages); high-stakes diagnoses (lower frequency of these in Pediatrics, therefore less opportunity to encounter than in IM), locale (IM typically does more training connected to academic centers versus Pediatrics that has a wide variety of practice environments); subspecialists certified IM are less likely to practice general IM vs. Pediatrics subspecialists who are more likely to also practice general Pediatrics (40% of respondents to the survey prepared by the members of the Working Group on the ‘Preparedness for Practice in Pediatrics” (PPP working group) indicated that general Pediatrics accounts for at least 40% of their practice – either voluntarily or by necessity of job availability, etc.)
Q: Why did Pediatrics historically not follow the same the path with overlap as IM? A: Beginning with the 2000 cohort of residents, the Collège des Médecins du Québec (CMQ)
mandated a “three year plus two year” model of training in Pediatrics, including general Pediatrics , In 2009, they transitioned back to four years in order to harmonize their requirements with those of the Royal College. Starting around 2002, there was serious consideration by the Royal College Specialty Committee in Pediatrics to move to five years of training nationally. Consultation took place, and continued for about two to three years ending with the decision not to transition to a longer training system, because it did not meet with broad support. The consensus was that as long as Pediatrics’ training programs provide the best four years of training possible, then the training is adequate. It is now recognized that there have been changes since, not in quality of training, but as a result of changes in the population needs, residents and outcomes. Is the training we are providing now adequate for current Pediatric practice? It became very clear that there are gaps in preparedness for practice and the EPAs for Pediatrics were drafted to address these gaps across the four stages of training.

Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 4 of 8 Q: Could following the path of IM and requesting residents identify a career path (e.g. only
academic practice in a specific subspecialty) be manageable /beneficial? A: In order to make such a change the Royal College would have to change the Pediatric
standards, and those of the subspecialties who require certification in Pediatrics prior to certification in the subspecialty. Pediatric subspecialists would also need to be discouraged from practicing general Pediatrics. It would be difficult to make this change at this time. A resident’s career path is often unpredictable and can change.
Q: Have the pediatric subspecialty disciplines discussed the overlap issue in their
meetings/workshops? A: Preliminary discussions are being held between subspecialty committee members. The
Specialty Committee in Neonatal-Perinatal Medicine reported the following concerns with continuing with a three plus two overlap training system:
If core EPAs are not completed in Pediatrics training, the Neonatal-Intensive Care Unit (NICU) does not have the ability to provide the expertise to assess these EPAs
The appropriate patient population to assess Pediatric EPAs does not exist in the subspecialty.
Where would the Pediatrics training experiences fit into their subspecialty program schedule?
Pediatric Respirologists indicated that there is no desire in their discipline to take on the assessment of Pediatrics EPAs in the midst of two years of subspecialty training, because the program will already be full. The Specialty Committee in Gastroenterology is concerned with the prospect of having to assess TTP EPAs within the subspecialty, keeping in mind that it also might include overseeing residual Core stage EPAs in addition to those from TTP Pediatrics. As a specialty implementing in 2019, if subspecialty program directors have to assess general Pediatrics TTP EPAs within early subspecialty training, that will have significant impact on the proposed training plan already being developed for CBD. The Specialty Committee in Adolescent Medicine also agreed that a four year training program for Pediatrics would be ideal with subspecialty training occurring after Pediatrics training is complete. Pediatric Rheumatologists reported that it would be difficult to fit Pediatrics TTP EPAs and residual core EPAs into the current subspecialty programs. A number of pediatric disciplines submitted feedback via briefing note ahead of the meeting. Such feedback was received from members of the following specialty committees: Developmental Pediatrics, Critical Care Medicine, Endocrinology and Metabolism, Gastroenterology, Medical Biochemistry, Nephrology and Rheumatology. A summary of these comments is appended at the end of the minutes.
Q: Should the pediatric subspecialties be delaying CBD rollout until this issue has been decided by the primary discipline of Pediatrics?
A: Jolanta Karpinski, MD, FRCPC, associate director, Specialties, Royal College indicated that
subspecialties should not delay CBD document design or implementation due to this issue. All disciplines are moving through the CBD process independently from each other. There are even some pediatric subspecialties, such as Critical Care Medicine, that are expected to launch CBD ahead of Pediatrics. It will take three or four years after CBD is implemented in Pediatrics’ training before subspecialties will be receiving trainees into their programs that have gone through training entirely in the CBD system. Until then, subspecialties will continue to use the traditional requirements.

Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 5 of 8 Q: Have the PCC provided feedback? And what is it? A: Members of the PCC brought forward the following issues:
Workforce report – the committee is in the in process of re-evaluating processes based on the results of this report. A lot of work was done with not an entirely satisfying result; a review is underway to see if more complete data can be gathered.
A few members thought four years of training might not be enough and asked why Pediatrics does not use the IM training model with a two-year general Pediatrics subspecialty
Credentialing trainees from outside Canada – outside scope of this work, but related – potential impacts of CBD environment on the Royal College credentialing process. This is currently time based and compared to the Specialty Training Requirements (STR) for Pediatrics. Additionally , this is separate from licensure credentialing as it only addresses eligibility to challenge the Royal College exams
Consideration of having patients/families (ex. adolescent, parent of patient with developmental delay, etc.) involved as stakeholder in this decision-making process. Is this possible or desired?
Important point – it is clear that there are difficulties in finding adequate care in adulthood for patients with complexity and/or developmental delay, including barriers of time, expertise, etc., thus these transitions should be a focus of training and advocacy in Pediatrics
Q: Some provinces supply only five years of funding for training in total; would extending
general Pediatrics training then reduce the amount of funding provided for the pediatric subspecialty programs?
A: Overall, the difference required to fund one year versus two is not that much money;
there are opportunities for savings. The problem is the funding comes from different sources. The bottom line is, the right thing should be done. It is expected that over time, things should balance out like in IM.
The provinces that don’t currently fund a fourth year of training in Pediatrics for those doing subspecialty training are Ontario, Québec and Nova Scotia. It is anticipated the cost would be about $2.4 million without accounting for any savings in other areas. The PPP working group arrived at this number by determining approximately how many residents were expected to do an extra year of training, resident salaries in those provinces, and the costs of community preceptors and other postgraduate year (PGY)4 requirements. Potential savings with this system include: more residents taking call that in some places would be covered by others that are higher paid; better trained general Pediatricians who may transfer fewer patients to higher level centers; may ultimately have fewer provincial College complaints/Canadian Medical Protective Association (CMPA) claims, etc. In conclusion, while there will be a cost to it, there would also be a cost to not changing the system; by not training all Pediatricians adequately. The PPP working group would welcome anyone able to provide further references or quantitative data on financial considerations.
Q: If the proposed change in length of training is approved, won’t the residents in those three provinces be at a disadvantage if their provinces choose not to provide the additional funding?
A: The current situation takes into account this issue. If residents in other provinces apply
through the CaRMS subspecialty match to programs in the provinces of Ontario, Québec or Nova Scotia, it can only be for entry after three years of training. But there are other

Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 6 of 8
positions made available using alternate funding sources. It remains to be seen what the impact of a decision for all residents to do 4 years of Pediatric residency prior to subspecialty would be, but it would have to be equitable, not just for residents but for programs.
Q: Is there not a risk of creating greater imbalance throughout the country, if the provinces
of Ontario, Québec and Nova Scotia, further restrict subspecialty positions, then residents will leave for other provinces, and be less likely to return?
A: This is certainly a possibility, but would be hard to predict. Q: At what level do the provincial funding bodies get involved in this discussion? A: When a discipline goes through the approval process for a change in the length of training
several steps need to take place. First, the initial proposition goes to the Royal College Committee on Specialties (COS), which requires a detailed package of information (re: rationale and impacts). Approval from stakeholders is not required at this point. Once the COS approves the application to move ahead, then a consultation with broader stakeholders is enacted. It was reiterated that the Pediatrics discipline made it very clear in their application that the decision to change the length of training is dissociated from the financial discussion.
Q: How will residents trained in the three year program in the United States of America
(USA) be dealt with? A: Pediatrics’ training in the United States has different goals and scope of practice. Training
in the USA is three years in length and focuses on producing competent primary care pediatricians. Canadian training is more comparable to Pediatrics’ training in the United Kingdom, Australia and New Zealand. Subspecialty training in the USA is three years and many of the Canadian general Pediatrics’ EPAs are incorporated in it.
4. Next steps In summary, it was concluded that the majority of subspecialists agree that changing Pediatrics training to a four-year model with no overlap would be best. Dr. Farrell acknowledged the tremendous assistance provided by the Royal College since last spring when the PPP working group was struck. When analyzing the data gathered by the survey, a “missing piece” was identified , as there appeared to be a disconnect between the perceived preparedness for practice between graduating residents and the program directors, and the input of subspecialty program directors and specialty committees was lacking. There a few more things to do before the submission of a proposal to change the length of training for Pediatrics is submitted to the COS for review. Individual stakeholder groups will be contacted ahead of time for feedback. How the proposal document is prepared and presented will be a key factor. The submission deadline is September 1, 2018, in order to be considered at the December 2018 meeting of the COS.
Name Position Notes Attendance
yes no
Specialty Committee in Pediatrics Farrell, Catherine Chair 1
Atkinson, Adelle Chair-Elect & PD Toronto 1
Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 7 of 8 Gervais, Pascale Region 4 1 Lynk, Andrew Region 5 1
Rowan-Legg, Anne Community-Based Representative 1
Wood, Ellen Chair, Exam Board 1
Amin, Harish Chair, SC in Neonatal-Perinatal Medicine
1
Fehlings, Darcy Chair, SC in Developmental Pediatrics Web/teleconference 1
Belletrutti, Mark John PD - Alberta 1 Bélanger, Sylvie PD - Laval 1 DiBartolo King, Marielena Linda PD - Calgary 1 Doyle, Elisabete Co-PD - Manitoba 1 Greenman, Janet Elizabeth PD - British Columbia 1 Gripp, Karen Elisabeth PD - Manitoba 1 Hunter, Andrea Jane PD - McMaster Web/teleconference 1 Leifso, Kirk Ryan PD - Queen's 1 Manos, Sarah Helen PD - Dalhousie 1 Martin, John Howard PD - Memorial 1 Mehtar, Maryam PD - Saskatchewan 1 Sandhu, Amonpreet Co-PD - Calgary 1 Santschi, Miriam PD - Sherbrooke 1 Sternszus, Robert PD - McGill 1 Baron, Tara PD - NOSM 1 Van Hooren, Tamara Angela PD - Western University 1 Writer, Hilary Kathryn PD - Ottawa 1
Total Committee 25 0 Members of pediatric subpecialty committees
Lane, Margo Alison Vice-Chair & Region 2 & NSS Observer - CPS
Adolescent Medicine 1
Fournier, Anne Region 4 Cardiology Web/teleconference 1
Duff, Jonathan PD - Alberta (P) Critical Care Medicine Web/teleconference 1
Kawamura, Anne NSS Observer & PD - Toronto Developmental Pediatrics 1
Francoeur, Emmett PD - McGill Developmental Pediatrics 1
Harman, Karen PD - McMaster Developmental Pediatrics Web/teleconference 1
Bassilious, Ereny PD - McMaster (P) Endocrinology & Metabolism Web/teleconference 1
Walsh, Catharine Chair-elect Gastroenterology
Web/teleconference 1
Top, Karina PD - Dalhousie Infectious Diseases 1
Nadeau, Sophie PD - Laval Neonatal-Perinatal Medicine 1
Leung, Elaine PD - Ottawa Pediatric Hematology/Oncology Web/teleconference 1

Pediatrics’ Consultation Meeting Minutes – May 29, 2018 Page 8 of 8 Yang, Connie PD - UBC Respirology 1
Rosie Scuccimarri PD - McGill (P) Rheumatology
Web/teleconference 1
Total Members of Related SCs 13 0 Pediatrics CBD & PPP Guests
Robert Connelly PPP Member Vice-chair and Region 3 rep.
Neonatal-Perinatal Medicine 1
Jonathan Kronick PPP Member Web/teleconference 1 Amy Acker CBD Particpant Web/teleconference 1 Ming-ka Chan CBD Particpant Web/teleconference 1 Ayisha Kirji CBD Particpant Web/teleconference 1 Total Guests 5 0 Royal College Representatives
Gorman, Lisa Manager, Educational Strategy, Innovations and Development (ESID)
Web/teleconference 1
Conway, Josée Educational Strategy Policy Analyst, ESID Web/teleconference 1
Elliot, Shannon Educational Strategy Policy Analyst, ESID Web/teleconference 1
Karpinski, Jolanta Associate Director, Specialties Web/teleconference 1
Stewart, Jennifer Manager, Specialties Web/teleconference 1 Marrello, Anna Administrator, Specialties 1 Total Staff 6/ 6 0
TOTAL ATTENDEES 49 0
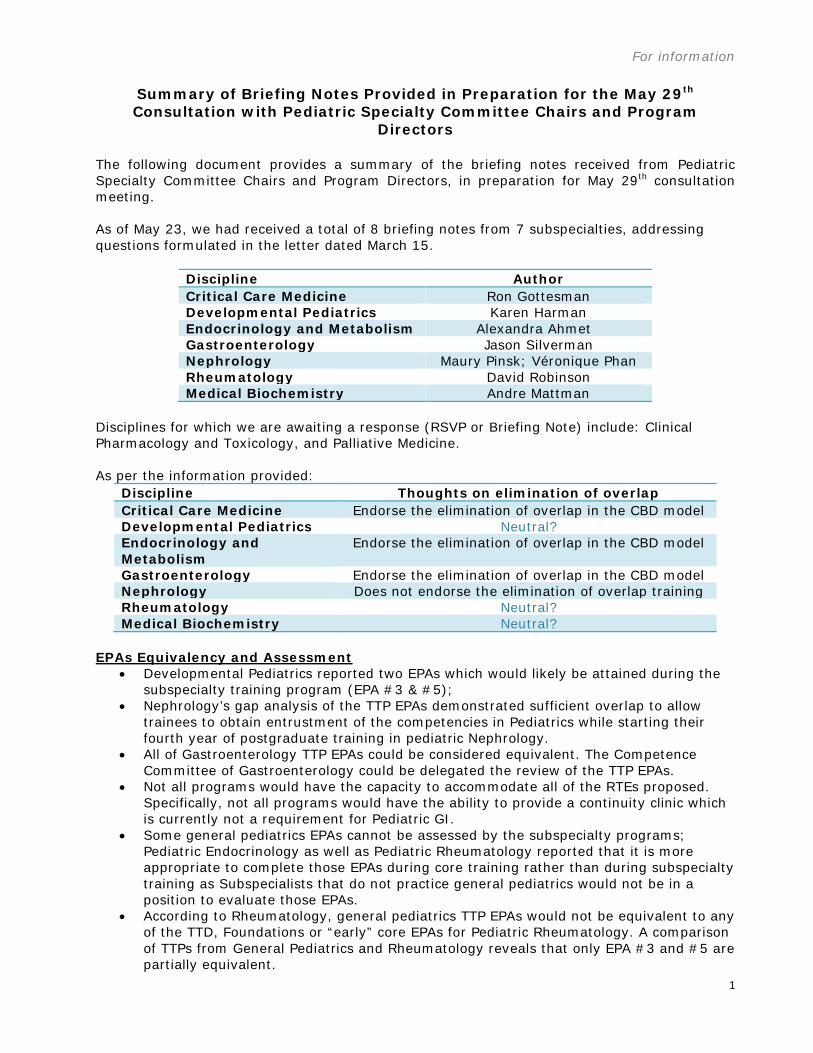
For information
1
Summary of Briefing Notes Provided in Preparation for the May 29th Consultation with Pediatric Specialty Committee Chairs and Program
Directors
The following document provides a summary of the briefing notes received from Pediatric Specialty Committee Chairs and Program Directors, in preparation for May 29th consultation meeting. As of May 23, we had received a total of 8 briefing notes from 7 subspecialties, addressing questions formulated in the letter dated March 15.
Discipline Author Critical Care Medicine Ron Gottesman Developmental Pediatrics Karen Harman Endocrinology and Metabolism Alexandra Ahmet Gastroenterology Jason Silverman Nephrology Maury Pinsk; Véronique Phan Rheumatology David Robinson Medical Biochemistry Andre Mattman
Disciplines for which we are awaiting a response (RSVP or Briefing Note) include: Clinical Pharmacology and Toxicology, and Palliative Medicine. As per the information provided:
Discipline Thoughts on elimination of overlap Critical Care Medicine Endorse the elimination of overlap in the CBD model Developmental Pediatrics Neutral? Endocrinology and Metabolism
Endorse the elimination of overlap in the CBD model
Gastroenterology Endorse the elimination of overlap in the CBD model Nephrology Does not endorse the elimination of overlap training Rheumatology Neutral? Medical Biochemistry Neutral?
EPAs Equivalency and Assessment
• Developmental Pediatrics reported two EPAs which would likely be attained during the subspecialty training program (EPA #3 & #5);
• Nephrology’s gap analysis of the TTP EPAs demonstrated sufficient overlap to allow trainees to obtain entrustment of the competencies in Pediatrics while starting their fourth year of postgraduate training in pediatric Nephrology.
• All of Gastroenterology TTP EPAs could be considered equivalent. The Competence Committee of Gastroenterology could be delegated the review of the TTP EPAs.
• Not all programs would have the capacity to accommodate all of the RTEs proposed. Specifically, not all programs would have the ability to provide a continuity clinic which is currently not a requirement for Pediatric GI.
• Some general pediatrics EPAs cannot be assessed by the subspecialty programs; Pediatric Endocrinology as well as Pediatric Rheumatology reported that it is more appropriate to complete those EPAs during core training rather than during subspecialty training as Subspecialists that do not practice general pediatrics would not be in a position to evaluate those EPAs.
• According to Rheumatology, general pediatrics TTP EPAs would not be equivalent to any of the TTD, Foundations or “early” core EPAs for Pediatric Rheumatology. A comparison of TTPs from General Pediatrics and Rheumatology reveals that only EPA #3 and #5 are partially equivalent.

For information
2
• Medical biochemistry EPAs are not yet developed but are expected to overlap substantially with four of the Pediatrics EPAs. This said, the focus on performing these EPA’s in the context of pediatric practice will not be possible given the requirement to train in a laboratory-based context during the subspecialty.
Non-Equivalent TTP EPAs
• The Competency Committee Developmental Pediatrics is not willing and able to attest to the completion of the non-equivalent TTP EPAs from Pediatrics. Therefore the completion of non-equivalent TTP would require adjustment of the current training rotation schedule and planning.
• Nephrology recognizes that some unique Core EPAs or training experiences cannot be offered in Pediatric Nephrology such as cannulation of umbilical arteries or community-based general pediatric EPAs.
• From Developmental Pediatrics’ perspective, some general pediatrics EPAs cannot be assessed by the subspecialty program because they do not have an inpatient portion and some issues are of very rare occurrence (such as patient safety issues). Some TTP EPA’s could be partially, not fully, achieved (such as TTP EPA #1 & #6). While some aspects of the milestones are part of the subspecialty program, the depth and breadth of knowledge is greater than what would be expected in general pediatrics.
• In Gastroenterology, EPAs that may not be encountered in routine practice (particularly around advanced care planning and QA/QI EPA) may represent a challenge as it would require involving trainees with core pediatric OSCEs and other services to gain the required exposure during subspecialty training.
• Gastroenterology competence committee would likely only be able to attest to the completion of the EPAs with the defined support and involvement of the local General Pediatrics program.
• The scope of practice, patient population and required expertise to achieve EPAs in the first year is not possible and unsafe. Completion of the non-equivalent TTP EPAs from Pediatrics will not be attainable in Pediatric Rheumatology and the competence committees will not be willing to attest nor complete those TTP EPAs.
• It would not be possible to complete general Pediatrics EPAs during Medical Biochemistry subspecialty; an additional period of training (and funding) would be required to practice in a pediatric setting that would allow proper completion of these EPAs.
Timing of the Examination • Endocrinology and Metabolism, Gastroenterology, Developmental Pediatrics, and
Rheumatology reported that residents should have met all requirements for certification in Pediatrics before joining subspecialty training. Two reasons were presented in support of this argument:
o 1) to allow for greater focus, full commitment and attention on the content of the subspecialty training program, which is comprehensive and rigorous;
o 2) if subspecialty examination (in Developmental Pediatrics and Rheumatology) occur prior the TTP stage of training, it might result in trainees having two certification examination in a small window of time.
• From Medical Biochemistry’s perspective, it is feasible and acceptable for a resident to begin training in the subspecialty while challenging their Pediatric exam.
Other Comments:
• Endocrinology and Metabolism reported noticing a significant difference in general pediatric skill and knowledge between the residents who completed 4 versus 3 years of the general pediatric training.

For information
3
• Nephrology support four years of general pediatric training specifically for individuals aspiring to practice general pediatrics post-completion of training as well as those who wish to moonlight during the subspecialty training.
• Possible negative consequences in terms of funding and CARMS positions are a concern mentioned by Nephrology and Critical Care Medicine.
• Nephrology reported that greater than 95 percent of practicing pediatric Nephrologists in Canada are practicing in academic centers with no general Pediatric practice as a component of their daily work. This said, individuals aspiring to academic Nephrology careers should not complete four years of Pediatrics training.
Suggestions: The Specialty Committee in Nephrology suggest to consider the General Internal Medicine (GIM) model for Pediatrics, by scheduling TTD, Foundations and Core Pediatrics to occur in three years, with a fourth year reserved for TTP.
• This would enable the examinations in Pediatrics to be completed by the end of the third year and allow trainees to enter subspecialty training unencumbered by examination preparation for Pediatrics.
• This would allow Pediatric trainees to focus their final year of training on competencies necessary for TTP, unencumbered by examination preparation as well.
• Doing so would harmonize a process for Nephrology and pediatric Nephrology, so that adult and pediatric trainees sitting the examination in Nephrology would have equal opportunities to complete training unencumbered by parent specialty exam preparation.
The GIM model was informally referenced by Rheumatology as a potential training model for Pediatrics during their CBD Workshop. While they believed EPAs should take place during the core stage of general pediatrics, they did not formally endorse or oppose the elimination of overlap training in Pediatrics.

© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved. This document may be reproduced for educational purposes only provided that the following phrase is included in all related materials: Copyright © 20xx The Royal College of Physicians and Surgeons of Canada. Referenced and produced with permission. Please forward a copy of the final product to the Office of Specialty Education, attn: Associate Director, Specialties. Written permission from the Royal College is required for all other uses. For further information regarding intellectual property, please contact: [email protected]. For questions regarding the use of this document, please contact: [email protected].
Page 1 of 35
Pediatrics Competencies
20xx VERSION x.x
Effective for residents who enter training on or after July 1, 20xx. (NOTE: Throughout this document, each reference to “children” includes infants, children, and youth.) DEFINITION
Pediatrics is that branch of medicine concerned with the study and care of children in health and disease, their growth and development, and their opportunity to achieve full potential as adults. A Pediatrician is a specialist trained in the diagnosis and treatment of a broad range of diseases involving children based on a sound knowledge of normal growth and development and of the wide range of clinical conditions encountered in children. PEDIATRIC PRACTICE
Pediatricians provide care for healthy children, between infancy and adolescence, as well as those that have acute presentations of illness, and/or who have chronic medical conditions, including acute exacerbation or decompensation of these conditions. They, therefore, manage a broad range of surgical and medical conditions with varying levels of acuity and complexity, involving all organ systems, establishing a shared patient-and family-centred care plan. The practice of Pediatrics includes resuscitation, medical and surgical treatment as well as preventative medicine and health promotion, and palliative care when appropriate. Children, especially early in life, present substantial anatomic and physiologic differences from adults, so pediatric practice must take into account these differences, across the developmental continuum. Congenital defects, genetic variance, behavioural and developmental issues are of concern to pediatricians. In most jurisdictions children cannot make decisions for themselves. The issues of guardianship, privacy, legal responsibility and informed consent and assent must be considered in every pediatric encounter. Pediatricians practice in a wide variety of clinical settings, ranging from hospital inpatient units, intensive care units and emergency departments, to ambulatory care settings, in hospitals and in the community. These settings may be urban, rural, or remote. They may practice in an academic health care centre or participate in medical education as a preceptor in a community setting. Those that practice in a pediatric subspecialty are more likely to practice in an academic health care centre, but not universally so, and their role may include general pediatric practice. Pediatricians act as consultants for patients referred by family physicians, emergency physicians, surgeons and other specialists, and may also act as primary care physicians in some settings. Pediatricians collaborate within an interprofessional team , including but not limited to nurses, pharmacists, dieticians, respiratory therapists, physiotherapists, occupational therapists, speech and language therapists, psychologists, Child Life specialists

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 2 of 35
and social workers, working together in the diagnosis and treatment of children, in partnership with families. They may interact with schools and social agencies to coordinate the services provided for their patients. Pediatricians play a major role in ensuring a harmonious transition of care of their adolescent patients to general physicians and specialists in the adult health care system. Residency training in Pediatrics provides physicians with the competencies required for general pediatric practice in diverse settings. Pediatric residency training may be followed by residency training in a subspecialty of Pediatrics or by focused training in a specific field pertinent to Pediatrics. PEDIATRIC COMPETENCIES
Medical Expert Definition: As Medical Experts, Pediatricians draw upon an evolving body of medical knowledge, their clinical skills, and their professional values in their provision of high-quality and safe patient- and family centred care. Medical Expert is the central physician Role in the CanMEDS Framework and defines the physician’s clinical scope of practice.
Key and Enabling Competencies: Pediatricians are able to…
Practise medicine within their defined scope of practice and expertise 1.
Demonstrate a commitment to high-quality care of their patients 1.1.
Identify that the health care needs of children are distinct from 1.1.1.
those of adults, and are changing throughout the developmental
continuum
Integrate the CanMEDS Intrinsic Roles into their practice of Pediatrics 1.2.
Apply knowledge of the clinical and biomedical sciences relevant to Pediatrics 1.3.
The normal healthy state, the natural course of pediatric problems, 1.3.1.
and variations in and departure from the normal
Anatomy of the internal organs and neuro-musculoskeletal system, 1.3.2.
including surface anatomy.¸
Physiology as it applies to the cardiac, vascular, pulmonary, 1.3.3.
gastrointestinal and hepatobiliary, renal, endocrine, neurological,
musculoskeletal, hematologic and immunologic systems,
throughout the continuum from fetal life to adulthood.
Epidemiology of common acute and chronic medical conditions in 1.3.4.
children
Microbiology of community and hospital acquired infections in 1.3.5.
children

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 3 of 35
Principles of immunity and immune dysfunction, either congenital 1.3.6.
or acquired, including autoimmune disorders
Pharmacologic principles including pharmacokinetics, 1.3.7.
pharmacodynamics, mechanism of action, routes of delivery and
elimination, use of therapeutic drug monitoring, and adverse effects
of medication, across the developmental continuum, and with
respect to the following classes of medication:
Analgesics 1.3.7.1.
Antimicrobials 1.3.7.2.
Cardiovascular medications 1.3.7.3.
Endocrine medications 1.3.7.4.
Immune modulating therapies used in children 1.3.7.5.
Neuropsychiatric medications, including anti-convulsants, 1.3.7.6.
central nervous system stimulant and anti-depressants
Respiratory medications 1.3.7.7.
Common, systemic therapies for childhood cancers 1.3.7.8.
Drugs commonly used recreationally to which children may be 1.3.7.9.
exposed
Supplementary and complementary medications 1.3.7.10.
Pharmacological principles to the following clinical contexts 1.3.8.
In newborns, issues related to placental transfer and breast milk 1.3.8.1.
excretion of drugs
Modifications of drug dosing required in altered pathophysiologic 1.3.8.2.
states including renal and liver dysfunction
Principles of screening, as well as of primary and secondary 1.3.9.
prevention
Immunizations 1.3.9.1.
Pharmacologic principles used in the following clinical contexts: 1.3.10.
Drug withdrawal 1.3.10.1.
Sedation, including procedural 1.3.10.2.
Apply knowledge of the following systems, clinical scenarios, conditions, diseases 1.4.
and therapies applicable to Pediatrics, including the manifestations,

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 4 of 35
investigation, and management
Cardiovascular system 1.4.1.
Fetal circulation and changes in circulation at birth 1.4.1.1.
Pre- and post-operative needs of the pediatric patient with 1.4.1.2.
heart disease, and long-term complications
Investigations, including but not limited to of: 1.4.1.3.
Echocardiogram 1.4.1.3.1.
Other cardiac imaging: computerized tomography, magnetic 1.4.1.3.2.
resonance imaging, radioisotope studies
Diagnostic and interventional cardiac catheterization and 1.4.1.3.3.
angiography
Electrocardiogram and Holter monitor 1.4.1.3.4.
Common syndromes and associated cardiac defects; genetic 1.4.1.4.
testing in cardiac disease in children
Symptoms 1.4.1.5.
Cardiac arrhythmia 1.4.1.5.1.
Cardiac murmers 1.4.1.5.2.
Chest pain 1.4.1.5.3.
Syncope 1.4.1.5.4.
Disorders 1.4.1.6.
Common forms of cyanotic and acyanotic congenital heart disease 1.4.1.6.1.
Congestive heart failure, acute and chronic 1.4.1.6.2.
Cor pulmonale/pulmonary hypertension 1.4.1.6.3.
Endocarditis, myocarditis, and pericarditis 1.4.1.6.4.
Kawasaki disease 1.4.1.6.5.
Rheumatic fever 1.4.1.6.6.
Respiratory system 1.4.2.
Investigations, including but not limited to: chest X-ray, 1.4.2.1.
bronchoscopy, lung biopsy, lung scintigraphy, sleep studies,
apnea monitors, pulmonary function studies, sweat test, and CT
scan of the chest
Signs and symptoms 1.4.2.2.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 5 of 35
1.3.2.2.1 Hypoxemia
1.3.2.2.2 Cough, acute and chronic
1.3.2.2.3 Dyspnea
1.3.2.2.4 Hemoptysis
1.3.2.2.5 Wheezing
Disorders 1.4.2.3.
Acute and chronic aspiration 1.4.2.3.1.
Acute lung injury/acute respiratory distress syndrome 1.4.2.3.2.
Bronchioleiti 1.4.2.3.3.
Cystic Fibrosis Mediastinal and intrathoracic masses 1.4.2.3.4.
Pleural effusions 1.4.2.3.5.
Pneumothorax 1.4.2.3.6.
Sleep apnea 1.4.2.3.7.
Asthma, including the use of respiratory devices such as spacers 1.4.2.3.8.
and metered dose inhalers
Gastrointestinal, hepatic, and biliary systems; 1.4.3.
nutrition and growth
Investigations, including but not limited to: 1.4.3.1.
Endoscopy 1.4.3.1.1.
Imaging including, plain abdominal X-rays, upper gastrointestinal 1.4.3.1.2.
and small bowel X-rays, contrast enema, abdominal ultrasound, CT
of abdomen, and radionuclide scans
Tests that assess gastrointestinal, pancreatic, and liver function 1.4.3.1.3.
Symptoms and signs 1.4.3.2.
Abdominal pain, acute and chronic 1.4.3.2.1.
Constipation/encopresis 1.4.3.2.2.
Dysphagia and feeding difficulties 1.4.3.2.3.
Enlargement of liver 1.4.3.2.4.
Intestinal bleeding 1.4.3.2.5.
Jaundice 1.4.3.2.6.
Vomiting and regurgitation 1.4.3.2.7.
Disorders 1.4.3.3.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 6 of 35
Abdominal masses 1.4.3.3.1.
Coeliac disease 1.4.3.3.2.
Hepatitis 1.4.3.3.3.
Inflammatory bowel disease 1.4.3.3.4.
Liver dysfunction/failure 1.4.3.3.5.
Liver transplantation, including long term health sequelae 1.4.3.3.6.
Malabsorption 1.4.3.3.7.
Short gut syndrome/intestinal failure 1.4.3.3.8.
Nutrition 1.4.4.
Recommended nutritional requirements for the infant, child, and 1.4.4.1.
adolescent
Nutritional assessment, including effect of disease states on 1.4.4.2.
nutritional requirements
Breast feeding 1.4.4.3.
Formula feeding 1.4.4.4.
Parenteral and enteral nutrition 1.4.4.5.
Health implications of restricted diets, fad diets, diets 1.4.4.6.
determined by custom, or socioeconomic situation
Disorders 1.4.4.7.
Failure to thrive 1.4.4.7.1.
Obesity and the metabolic syndrome 1.4.4.7.2.
Nutritional deficiencies and excesses 1.4.4.7.3.
Renal and genitourinary system 1.4.5.
Fluid and electrolyte requirements in normal and abnormal 1.4.5.1.
states
Normal mechanisms of acid-base balance 1.4.5.2.
Investigations 1.4.5.3.
Imagining, including but not limited to renal ultrasound, 1.4.5.3.1.
radioisotope scans, renal angiography
Urodynamic studies, including voiding cystourethrogram 1.4.5.3.2.
Renal function tests, including renin studies 1.4.5.3.3.
Urine microscopy 1.4.5.3.4.
Indications, complications, and contraindications of dialysis and 1.4.5.4.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 7 of 35
renal transplantation
Symptoms and signs 1.4.5.5.
1.4.5.5.1.1. Abdominal and pelvic mass
1.4.5.5.1.2. Enuresis and urinary incontinence
1.4.5.5.1.3. Hematuria
1.4.5.5.1.4. Hypertension
Disorders 1.4.5.6.
Acute and chronic renal failure 1.4.5.6.1.
Congenital and acquired hydronephrosis 1.4.5.6.2.
Congenital structural anomalies of the urinary tract 1.4.5.6.3.
Issues affecting the male and female external genitalia 1.4.5.6.4.
1.4.5.6.4.1. Circumcision
Undescended testes, swelling or pain in testes 1.4.5.6.5.
Nephritic syndromes 1.4.5.6.6.
Hypercalcemia, hypocalcemia, and rickets 1.4.5.6.7.
Hyperkalemia 1.4.5.6.8.
Hypernatremia, hyponatremia 1.4.5.6.9.
Proteinuria and nephrotic syndromes 1.4.5.6.10.
Renal stones 1.4.5.6.11.
Renal tubular disorders, Fanconi syndrome 1.4.5.6.12.
Urinary tract infection 1.4.5.6.13.
Vesico-uretal reflux and obstructive uropathies 1.4.5.6.14.
Endocrinology and metabolism 1.4.6.
Normal physical growth for the infant, child and adolescent 1.4.6.1.
Physiology of normal and abnormal puberty 1.4.6.2.
Investigations 1.4.6.3.
Common tests of endocrine function 1.4.6.3.1.
Symptoms, signs and findings 1.4.6.3.2.
Growth failure/short stature 1.4.6.3.3.
Ambiguous genitalia (cf. Renal/Genitourinary) 1.4.6.3.4.
Hypoglycemia 1.4.6.3.5.
Disorders 1.4.6.4.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 8 of 35
Adrenal disease 1.4.6.4.1.
Diabetes insipidus 1.4.6.4.2.
Disorders of sexual development 1.4.6.4.3.
Hyperlipidemia 1.4.6.4.4.
Hypo/hypercalcemia 1.4.6.4.5.
Hypoglycemia 1.4.6.4.6.
Inappropriate antidiuretic hormone (ADH) secretion 1.4.6.4.7.
Metabolic bone disease and osteoporosis 1.4.6.4.8.
Pituitary disorders 1.4.6.4.9.
Precocious and delayed puberty 1.4.6.4.10.
Thyroid disease: goiter, hypo/hyperthyroidism, thyroid nodules 1.4.6.4.11.
Type 1 and type 2 diabetes mellitus, diabetic ketoacidosis 1.4.6.4.12.
Neurologic system 1.4.7.
Investigations: 1.4.7.1.
Cerebral and spinal imaging including plain X-Rays, ultrasound, 1.4.7.1.1.
CT/MRI scans
Electroencephalogram (EEG) 1.4.7.1.2.
Evoked potentials 1.4.7.1.3.
Lumbar puncture including interpretation of cerebrospinal fluid 1.4.7.1.4.
analysis
Nerve conduction studies and electromyography 1.4.7.1.5.
Symptoms and signs 1.4.7.2.
Developmental regression 1.4.7.2.1.
Headache 1.4.7.2.2.
Nystagmus, dizziness and vertigo 1.4.7.2.3.
Positional plagiocephaly and torticollis 1.4.7.2.4.
Raised intracranial pressure 1.4.7.2.5.
Seizures and sudden loss of consciousness 1.4.7.2.6.
Tics 1.4.7.2.7.
Disorders 1.4.7.3.
Congenital malformations of the nervous system, including the 1.4.7.3.1.
PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 9 of 35
skull
Cerebral palsy 1.4.7.3.2.
Cerebrovascular disease, including intracranial hemorrhage and 1.4.7.3.3.
strokes
Diseases of muscle, including muscular dystrophies, myopathies 1.4.7.3.4.
Disorders of peripheral nerves 1.4.7.3.5.
Head trauma and sequelae 1.4.7.3.6.
Infections of the central nervous system (CNS): meningitis, 1.4.7.3.7.
encephalitis, abscess; and sequelae
Movement disorders 1.4.7.3.8.
Neurocutaneous syndromes 1.4.7.3.9.
Neuromuscular manifestations of common systemic 1.4.7.3.10.
infections/diseases
Non-epileptic events mimicking seizures, including breath-holding 1.4.7.3.11.
spells
Hematology and oncology 1.4.8.
Principles underlying transfusion of blood and blood products 1.4.8.1.
Issues related to oncology: 1.4.8.2.
Techniques for safe administration of chemotherapy 1.4.8.2.1.
Common side effects of chemotherapy and radiotherapy and their 1.4.8.2.2.
management
Management of the immunocompromised oncology patient 1.4.8.2.3.
Social, familial and personal effects of childhood cancer 1.4.8.2.4.
Late effects of cancer therapy 1.4.8.2.5.
Principles of palliative care 1.4.8.2.6.
Investigations 1.4.9.
Indications for and interpretation of common hematological tests 1.4.9.1.
Disorders 1.4.10.
Anemia 1.4.10.1.
Bleeding and clotting disorders, congenital and acquired 1.4.10.2.
Cytopenias 1.4.10.3.
Hemoglobinopathies and red cell disorders 1.4.10.4.
Lymphadenopathy 1.4.10.5.
Hepatosplenomegaly 1.4.10.6.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 10 of 35
Acute leukemias and common tumours of childhood 1.4.10.7.
Allergy and clinical immunology 1.4.11.
Investigations 1.4.11.1.
Indications for and limitations of skin testing, including prick and 1.4.11.1.1.
intradermal testing, radioallergosorbent test (RAST)/serum
immunoglobulin E (IgE) testing, and food/drug challenge testing
Basic diagnostic laboratory techniques for testing involving the 1.4.11.1.2.
immune system, including evaluation for primary
immunodeficiency diseases
Treatment options for patients with a primary 1.4.11.2.
immunodeficiency disease, including but not limited to
antimicrobials, antibody replacement therapy including
immunoglobulin products, and bone marrow transplantation
Antibiotics 1.4.11.2.1.
Disorders 1.4.11.3.
Recurrent infections and immunodeficiency syndromes, including B 1.4.11.3.1.
cell, T cell, combined B and T cell, phagocytic, and complement
problems
Allergic conditions including but not limited to allergic rhinitis, 1.4.11.3.2.
reactions to drugs and biologics, vaccine allergy, food allergy and
reaction to insect stings and bites
Anaphylaxis and non-IgE mediated anaphylaxis 1.4.11.3.3.
Acute and chronic urticaria/angioedema 1.4.11.3.4.
Serum sickness 1.4.11.3.5.
Musculoskeletal system/rheumatology 1.4.12.
Mechanisms of immune responses in rheumatic disease 1.4.12.1.
Investigations 1.4.12.2.
Indications for and interpretation of laboratory tests on blood and 1.4.12.2.1.
synovial fluid
Imaging, including X-rays, radioisotope studies, magnetic 1.4.12.2.2.
resonance imaging and ultrasound
Effects of chronic rheumatic diseases on physical growth and 1.4.12.3.
social developments
Symptoms and signs 1.4.12.4.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 11 of 35
Joint and limb pain 1.4.12.4.1.
Joint deformities including pes planus, hypermobility, and 1.4.12.4.2.
hypomobility
Disorders 1.4.12.5.
Acute/chronic arthritis 1.4.12.5.1.
Bone tumors 1.4.12.5.2.
Common fractures, dislocations or injuries, and osteochondroses, 1.4.12.5.3.
including Osgood-Schlatter disease, Legg-Calvé- Perthes disease,
Sever’s disease
Common gait disorders, including limp, and torsional and angular 1.4.12.5.4.
deformities of lower limbs
Common vasculitidies, including Henoch-Schönlein purpura and 1.4.12.5.5.
Kawasaki disease
Congenital abnormalities of the musculoskeletal system 1.4.12.5.6.
Non-inflammatory connective tissue diseases, including Marfan 1.4.12.5.7.
syndrome and Ehlers-Danlos syndrome
Scoliosis 1.4.12.5.8.
Septic arthritis and osteomyelitis 1.4.12.5.9.
Systemic rheumatologic diseases, including systemic lupus 1.4.12.5.10.
erythematosis, juvenile idiopathic (rheumatoid) arthritis, juvenile
dermatomyositis, and periodic fever syndromes
Demonstrate an understanding of the principles and 1.4.12.6.
applications of physical and occupational therapy for
musculoskeletal diseases
Skin/dermatology 1.4.13.
Classification and pharmacology of common topical medications 1.4.13.1.
Recognition of cutaneous findings in systemic disorders, 1.4.13.2.
including auto-immune and metabolic diseases, and hereditary
conditions
Disorders 1.4.13.3.
Acne 1.4.13.3.1.
Common autoimmune conditions in the skin, including vitiligo and 1.4.13.3.2.
alopecia areata
Common conditions of hair and nails 1.4.13.3.3.
Common papulosquamous eruptions, including psoriasis, pityriasis 1.4.13.3.4.
PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 12 of 35
rosea, and nummular dermatitis
Common pigmentary or vascular congenital lesions, including nevi, 1.4.13.3.5.
café au lait macules, hemangiomas, and simple vascular
malformations
Common skin infections/infestations 1.4.13.3.6.
Eczema and other dermatitides 1.4.13.3.7.
Skin exposures to physical and chemical factors 1.4.13.3.8.
Vesiculobullous diseases 1.4.13.3.9.
Specific contexts potentially involving multiple organ systems 1.5.
Acute care (encompassing emergencies and critical care) 1.5.1.
Principles of invasive and non-invasive mechanical ventilation 1.5.1.1.
Principles, techniques, advantages, and limitations of invasive 1.5.1.2.
and non-invasive cardiorespiratory monitoring
Fluid and electrolyte management in the acutely ill patient 1.5.1.3.
Principles, role, and logistics of both inter- and intra-hospital 1.5.1.4.
transport of acutely ill infants and children
Neurologic determination of death and principles of organ 1.5.1.5.
donation
Challenges of the child with special needs and/or technology 1.5.1.6.
dependence
Life-threatening cardiac, respiratory, gastrointestinal, metabolic, 1.5.1.7.
neurologic or other organ system dysfunction and abnormalities,
including but not limited to:
Acute severe vomiting and dehydration 1.5.1.7.1.
Brief resolved unexplained events (BRUE) 1.5.1.7.2.
Cardiorespiratory arrest and resuscitation 1.5.1.7.3.
Coma 1.5.1.7.4.
Electrolyte imbalance and acid base abnormality 1.5.1.7.5.
Foreign body aspiration 1.5.1.7.6.
Hepatic failure 1.5.1.7.7.
Hypothermia and hyperthermia 1.5.1.7.8.
Metabolic crises, including diabetic ketoacidosis, hyperammonemia, 1.5.1.7.9.
and metabolic acidosis

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 13 of 35
Near drowning 1.5.1.7.10.
Poisonings and drug overdoses requiring cardiovascular monitoring 1.5.1.7.11.
Renal failure and dialysis 1.5.1.7.12.
Sepsis 1.5.1.7.13.
Severe burn management 1.5.1.7.14.
Shock 1.5.1.7.15.
Status epilepticus 1.5.1.7.16.
Trauma: multi-system and single-system trauma 1.5.1.7.17.
Traumatic brain injury, both inflicted and accidental 1.5.1.7.18.
Infectious diseases 1.6.
Prevention of congenital and perinatal infections 1.6.1.
Nosocomial infections and infection control 1.6.2.
Use of antimicrobial agents, including interpretation of sensitivity 1.6.3.
tests and antimicrobial resistance
Investigations 1.6.4.
Bacterial and viral cultures, microscopy, serology and 1.6.4.1.
polymerase chain reaction (PCR)
Disorders: 1.6.5.
Common infectious diseases: viral, bacterial, fungal, parasitic, 1.6.5.1.
and protozoan infections
Fever of unknown origin (FUO) 1.6.5.2.
Fever without a focus 1.6.5.3.
Human immunodeficiency virus (HIV) infection 1.6.5.4.
Infection in the immunocompromised host 1.6.5.5.
Infectious issues relating to travel and immigration 1.6.5.6.
Life-threatening infection 1.6.5.7.
Non-immunized/under-immunized child 1.6.5.8.
Occult bacteremia 1.6.5.9.
Perinatal/congenital infections 1.6.5.10.
Genetics, teratology, and metabolics 1.7.
Modes, principles, and molecular basis of Mendelian and non-1.7.1.
Mendelian inheritance
Embryological basis of malformations, deformations, disruptions, 1.7.2.
and dysplasias

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 14 of 35
Environmental factors in fetal development 1.7.3.
Investigations 1.7.4.
Application and limitations of cytogenetics, including karyotype, 1.7.4.1.
and molecular cytogenetics, specifically fluorescence in situ
hybridization (FISH) and microarray
Applications and limitations of molecular diagnosis 1.7.4.2.
Indications, principles, and limitations of prenatal diagnosis and 1.7.4.3.
screening
Indications, principles, and limitations of screening for genetic 1.7.4.4.
disease
Principles of assessment of dysmorphology and syndrome 1.7.4.5.
identification
First-line investigation for a suspected inborn error of 1.7.4.6.
metabolism including collection of a critical sample
Ethical issues related to genetic testing of children 1.7.4.7.
Disorders: 1.7.5.
Common genetic syndromes, including Down syndrome, Turner 1.7.5.1.
syndrome, and fragile x syndrome
Exposure to a possible teratogen 1.7.5.2.
Inborn errors of metabolism, including the initial management of 1.7.5.3.
a metabolic crisis
The dysmorphic child 1.7.5.4.
Child maltreatment 1.8.
Social factors placing children at risk 1.8.1.
Impact of violence and maltreatment on health 1.8.2.
Laws relating to child protection including professional 1.8.3.
requirements in managing victims of maltreatment such as
mandatory reporting
Issues arising with children in care, including foster care, group 1.8.4.
homes, or incarceration
Disorders: 1.8.5.
Shaken baby syndrome 1.8.5.1.
Physical abuse 1.8.5.2.
Emotional abuse and neglect 1.8.5.3.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 15 of 35
Sexual abuse 1.8.5.4.
1.4.1 Issues related to international adoptions
Surgical conditions 1.9.
General principles 1.9.1.
Indications for surgical referral 1.9.2.
Principles of pre-operative assessment 1.9.3.
Principles of perioperative management, including type of 1.9.4.
anesthesia/sedation, fluid administration, antibiotic prophylaxis
Principles of post-operative management, including pain control 1.9.5.
General surgery 1.10.
Abdominal masses 1.10.1.
Acute abdomen 1.10.2.
Acute scrotal pain 1.10.3.
Appendicitis 1.10.4.
Bowel obstruction/ileus 1.10.5.
Hernias 1.10.6.
Multiple trauma 1.10.7.
Surgical problems of the newborn 1.10.8.
Ophthalmology 1.11.
Basic anatomy, embryology, and physiology of the eye, ocular 1.11.1.
muscles, and visual pathways
Screening procedures for vision 1.11.2.
Congenital and acquired abnormalities of the eye and ocular 1.11.3.
muscles, including but not limited to cataracts, glaucoma, refractive
errors
Ocular manifestations of systemic diseases and syndromes 1.11.4.
Common ophthalmologic disorders in children 1.11.5.
Conjunctival disorders: conjunctivitis, mucocutaneous diseases 1.11.5.1.
Disorders of orbit, including orbital cellulitis 1.11.5.2.
Nasolacrimal duct obstruction 1.11.5.3.
Ocular findings of non-accidental injuries 1.11.5.4.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 16 of 35
Ocular injuries 1.11.5.5.
Red eye 1.11.5.6.
Retinopathy of prematurity 1.11.5.7.
Strabismus/amblyopia 1.11.5.8.
Otolaryngology 1.12.
Embryology, anatomy, and pathophysiology of the ear, nose, 1.12.1.
throat, and upper airway
Indications and limitations of diagnostic imaging of the upper 1.12.2.
airway
Normal and abnormal dentition, including dental caries and dental 1.12.3.
trauma
Symptoms and signs: 1.12.4.
Congenital and acquired nasal obstruction 1.12.4.1.
Congenital and acquired neck masses 1.12.4.2.
Congenital and acquired stridor, hoarseness and voice 1.12.4.3.
abnormalities
Deformities of the ear 1.12.4.4.
Epistaxis 1.12.4.5.
Hearing loss 1.12.4.6.
Disorders: 1.12.5.
Cleft lip and palate 1.12.5.1.
Feeding and swallowing issues 1.12.5.2.
Deafness 1.12.5.3.
Mastoiditis and sinusitis 1.12.5.4.
Otitis media/otitis externa 1.12.5.5.
Retropharyngeal abscess; supraglottitis, epiglottitis 1.12.5.6.
Tonsillitis and complications 1.12.5.7.
Upper airway abnormalities 1.12.5.8.
Apply knowledge of the clinical and biomedical sciences applicable to pediatric 1.13.
patients at a specific period of life
Neonatal-perinatal medicine 1.13.1.
Fetal growth, development, and physiology, including the role 1.13.1.1.
of the placenta
Aspects of pregnancy, labour, and delivery that affect the 1.13.1.2.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 17 of 35
neonate
Effect of maternal systemic disease on the fetus and newborn 1.13.1.3.
Demographic, medical, and psychosocial factors that influence 1.13.1.4.
perinatal mortality and morbidity, including conditions associated
with high-risk pregnancies
Process of neonatal adaptation to extrauterine life 1.13.1.5.
Neonatal growth, nutrition, metabolic problems, feeding 1.13.1.6.
problems
Aspects of clinical pharmacology and drug therapy unique to 1.13.1.7.
the newborn, include choice of medication, dosing, and
monitoring
General principles of care of the newborn, including skin care, 1.13.1.8.
temperature regulation, feeding, fluid and metabolic
homeostasis, and pain management
Newborn screening, metabolic and clinical Principles and 1.13.1.9.
algorithms for neonatal resuscitation
Outcomes for survival and factors influencing outcome, in the 1.13.1.10.
term and preterm neonate
Care and followup of the premature infant and high-risk baby 1.13.1.11.
after discharge
Disorders: 1.13.1.12.
Abnormal fetal growth: growth retardation and macrosomia 1.13.1.12.1.
Birth trauma, including brachial plexus injuries, cephalhematoma, 1.13.1.12.2.
subgaleal hemorrhages, and fractures
Apnea 1.13.1.12.3.
Asphyxia and perinatal distress, including standardized 1.13.1.12.4.
assessment for therapeutic hypothermia initiation
Chronic lung disease 1.13.1.12.5.
Cyanosis 1.13.1.12.6.
Drug withdrawal 1.13.1.12.7.
Feeding difficulties/vomiting 1.13.1.12.8.
Hematologic conditions presenting in the newborn, including 1.13.1.12.9.
anemia, hemolytic disease, thrombocytopenia and abnormal bleeding
Hyperbilirubenemia, indirect and direct 1.13.1.12.10.
Intraventricular and intracranial hemorrhage 1.13.1.12.11.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 18 of 35
Metabolic abnormalities, including hypoglycemia, 1.13.1.12.12.
hypo/hypercalcemia, and hypermagnesemia
Neurologic issues, including but not limited to seizures and 1.13.1.12.13.
hypotonia
Prematurity, including extreme and late prematurity 1.13.1.12.14.
Respiratory distress 1.13.1.12.15.
Retinopathy of prematurity 1.13.1.12.16.
Seizures 1.13.1.12.17.
Sepsis 1.13.1.12.18.
Stridor and abnormal airways 1.13.1.12.19.
Surgical problems of the newborn including but not limited to: 1.13.1.13.
necrotizing enterocolitis, diaphragmatic hernia, gastroschisis,
omphalocoele
Adolescent health care 1.13.2.
Normal psychological and cognitive development, including 1.13.2.1.
resilience theory and practice
Normal social development, including peer relationships and 1.13.2.2.
parent-adolescent relationships
Normal adolescent behavior 1.13.2.3.
Impact of mental health on adolescent development and 1.13.2.4.
overall health
Adolescents and society: influencing factors and social 1.13.2.5.
determinants of health, including access and barriers to
adolescent health care
Developmentally appropriate approaches to adolescent care 1.13.2.6.
Transition of youth with chronic conditions to adult care 1.13.2.7.
Disorders: 1.13.2.8.
1.13.2.8.1.1. Behavioural problems
1.13.2.8.1.2. Chronic diseases and adherence
1.13.2.8.1.3. Eating disorders and obesity
1.13.2.8.1.4. Fatigue
1.13.2.8.1.5. Gynecological problems and disorders of menstruation
1.13.2.8.1.6. Psychosomatic conditions
1.13.2.8.1.7. School problems
1.13.2.8.1.8. Sleep problems

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 19 of 35
1.13.2.8.1.9. Substance use and abuse
1.13.2.8.1.10. Unintended pregnancy, contraception, sexually transmitted
infections
Apply knowledge of issues relating to behavior, development and mental health 1.14.
across the continuum from infant to child to adolescent
Development and behaviour 1.14.1.
Normal and abnormal development: gross motor, fine motor, 1.14.1.1.
language, personal-social, and behavioural
Biological and psychosocial factors affecting development and 1.14.1.2.
behaviour
Application of psychological and education testing 1.14.1.3.
Disorders 1.14.2.
Attention deficit disorders, with or without hyperactivity 1.14.2.1.
Common behavioural problems 1.14.2.2.
Crying infant, infantile colic, sleep disorders, nightmares and 1.14.2.3.
night terrors
Developmental delay and mental retardation 1.14.2.4.
Fetal alcohol spectrum disorder 1.14.2.5.
Learning disabilities 1.14.2.6.
Pervasive developmental disorders/autism spectrum disorders 1.14.2.7.
School avoidance 1.14.2.8.
Mental health 1.15.
Non-pharmacological approaches to management of mental 1.15.1.
health issues
Biological, psychosocial, and socioeconomic factors affecting 1.15.2.
mental health
Impact of having a parent with mental illness or substance abuse 1.15.3.
on child well-being
Community-based mental health resources and indications for 1.15.4.
hospitalization
Disorders: 1.15.5.
Adjustment to life stresses, including chronic illness 1.15.5.1.
Anxiety disorders, including separation anxiety, social phobia, 1.15.5.2.
post-traumatic stress disorder (PTSD), panic, generalized

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 20 of 35
anxiety
Attempted suicide or suicidal ideation 1.15.5.3.
Conduct disorders, oppositional defiant behaviour 1.15.5.4.
Conversion disorder 1.15.5.5.
Emotional abuse/bullying 1.15.5.6.
Family dynamics and psychological adjustment to family stress 1.15.5.7.
Mood disorders/depression 1.15.5.8.
Obsessive compulsive disorder 1.15.5.9.
Personality traits 1.15.5.10.
Psychoses 1.15.5.11.
Psychosomatic disorder 1.15.5.12.
Violent behaviour 1.15.5.13.
Perform appropriately timed clinical assessments with recommendations that 1.16.
are presented in an organized manner
Carry out professional duties in the face of multiple, competing demands 1.17.
Recognize and respond to the complexity, uncertainty, and ambiguity inherent 1.18.
in Pediatric practice
Establish management plans despite limited, non-diagnostic or conflicting 1.19.
clinical information
Perform a patient-centred clinical assessment and establish a management 2.
plan
Prioritize issues to be addressed in a patient encounter 2.1.
Recognize medical instability and establish priorities in 2.1.1.
resuscitation
Elicit a history, perform a physical exam, select appropriate investigations, and 2.2.
interpret their results for the purpose of diagnosis and management, disease
prevention, and health promotion
Elicit information relevant to the risk profile for specific disease 2.2.1.
processes, according to symptom pattern and past medical history.
Obtain relevant information from the family history, including 2.2.2.
where appropriate, the construction of a pedigree.
Use a systematic approach to the biopsychosocial assessment of 2.2.3.
the adolescent patient (e.g. HEADSSS)

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 21 of 35
Where appropriate, use screening tools for attention deficit disorder 2.2.4.
(ADD) and autism spectrum disorder (ASD)
Where appropriate, use screening tools, including the Swanson, 2.2.5.
Nolan and Pelham Scale, version IV (SNAP-IV)
Perform a physical examination which may include the following: 2.2.6.
Proper technique of height/length measurement 2.2.6.1.
Use of growth charts, including those of the World Health 2.2.6.2.
Organization and the Centers for Disease Control
Assessment of psychomotor development 2.2.6.3.
Tanner staging, including orchidometry 2.2.6.4.
In adolescent patients, breast examination, pelvic examination 2.2.6.5.
in females and testicular examination in males
In newborns, Apgar scores and estimation of gestational age 2.2.6.6.
Appropriate procurement of child maltreatment evidence, 2.2.6.7.
including documentation and specimen collection
Select investigation strategies, demonstrating awareness of the 2.2.7.
availability and access to resources in various clinical settings
Apply criteria for use of diagnostic imaging and nuclear medicine 2.2.7.1.
examinations, including their short- and long-term risks and
complications
2.2.3.2. Interpret reports of medical imaging and pathology in the context of the patient’s age and
clinical condition
Establish goals of care in collaboration with patients and their 2.2.8.
families*, which may include slowing disease progression, treating
symptoms, achieving cure, improving function, and palliation
Recognize and respond to changes in patient status that indicate a 2.2.9.
need to reassess goals of care
Establish a patient-centred management plan, in collaboration 2.2.10.
with the family
Develop and implement plans for 2.2.11.
* Throughout this document, references to the patient’s family are intended to include all those who are personally significant to the patient and are concerned with his or her care, including, according to the patient’s circumstances, family members, partners, caregivers, legal guardians, and substitute decision-makers.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 22 of 35
Hospitalized patients with acute illness, or acute exacerbations 2.2.11.1.
of chronic illness
Ambulatory patients with common acute presentations and/or 2.2.11.2.
chronic medical conditions
Patients with multiple medical conditions, including 2.2.11.3.
consideration of competing priorities, conditions or treatments as
well as potential drug interactions
Critically ill patients, including resuscitation and stabilization of 2.2.11.4.
hemodynamic or respiratory instability
Safe transition to another health care setting, including 2.2.11.5.
anticipation, prevention, and management of changes in health
status during transition or transport.
Safe discharge of patients with acute and chronic conditions, 2.2.11.6.
including referral to comprehensive or interprofessional care
services
Implementation of primary and secondary prevention 2.2.11.7.
strategies as part of the overall management plan
Incorporate consultant recommendations, as well as those from 2.2.11.8.
other health care professionals, into diagnostic and treatment
plans.
Provide initial management of a positive result of newborn 2.2.11.9.
screening
Plan and perform procedures and therapies for the purpose of assessment 3.
and/or management
Determine the most appropriate procedures or therapies 3.1.
3.1.1. Prioritize procedures or therapies, taking into account clinical urgency and available resources.
Obtain and document informed consent, explaining the risks and benefits of, and 3.2.
the rationale for, a proposed procedure or therapy
Demonstrate an understanding of the distinction between assent and consent 3.3.
and how this applies to pediatric patients.
Ensure appropriate pain management and patient comfort for procedures, 3.4.
including choice of non-pharmaocologic approaches, pharmacologie agent,
appropriate monitoring and surveillance, and non-invasive airway support.
Perform procedures in a skilful and safe manner, adapting to unanticipated 3.5.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 23 of 35
findings or changing clinical circumstances
Airway management, which includes bag-mask ventilation, tracheal 3.5.1.
intubation and tracheostomy tube change (neonatal and pediatric)
Intravenous access and blood-drawing 3.5.2.
Umbilical venous catheterization 3.5.3.
Intraosseous insertion 3.5.4.
Arterial puncture 3.5.5.
Bedside measurement of glucose 3.5.6.
Lumbar puncture, neonatal and pediatric 3.5.7.
Bladder catheterization and/or suprapubic aspiration 3.5.8.
Curettage of the ear under direct visualization 3.5.9.
Subcutaneous, intradermal, and intramuscular injections, 3.5.10.
including immunizations
Tuberculin skin testing: performance and interpretation 3.5.11.
Gastric tube placement (oro- or nasogastric) 3.5.12.
Needle thoracentesis and chest tube placement 3.5.13.
Foreign body removal from eye, nose, and upper airway 3.5.14.
Assessment of the traumatized eye, including eye irrigation, and 3.5.15.
the use of dilating drops, topical fluorescein, and topical anesthetics
Immobilization of acute limb injury, including fractures 3.5.16.
Cervical spine immobilization 3.5.17.
Simple wound closure, including suture laceration, and use of 3.5.18.
adhesive strips, staples, and tissue sealant
Establish plans for ongoing care and, when appropriate, timely consultation 4.
Implement a patient-centred care plan that supports ongoing care, follow-up on 4.1.
investigations, response to treatment, and further consultation
Anticipate, recognize, and manage complications of therapy and/or 4.1.1.
the underlying condition of the patient
Formulate and implement plans for discharge or transfer of care 4.1.2.
that include appropriate ongoing care, arrangement for relevant
community support, and follow up on investigations
Coordinate investigation, treatment and follow-up when multiple 4.1.3.
physicians and other health care professionals are involved

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 24 of 35
In appropriate circumstances, ensure patients and families receive 4.1.4.
palliative and end-of-life care
Actively contribute, as an individual and as a member of a team providing care, 5.
to the continuous improvement of health care quality and patient safety
Recognize and respond to harm from health care delivery, including patient 5.1.
safety incidents
Intervene to mitigate further injury 5.1.1.
Identify the clinical circumstances , and human and systems factors 5.1.2.
contributing to an adverse event
Report patient safety incidents to the appropriate institutional 5.1.3.
representative
Inform patients and families about patient safety incidents that 5.1.4.
arise, according to local and legislative guidelines
Adopt strategies that promote patient safety and address human and system 5.2.
factors
Use cognitive aids to enhance patient safety 5.2.1.
Communicator
Definition:
As Communicators, Pediatricians form relationships with patients and their families that
facilitate the gathering and sharing of essential information for effective health care.
Key and Enabling Competencies: Pediatricians are able to…
Establish professional therapeutic relationships with patients and their families 1.
Communicate using a patient- and family-centred approach that encourages 1.1.
patient trust and autonomy and is characterized by empathy, respect, and
compassion
Demonstrate an appreciation of the parents' perspective with 1.1.1.
regard to concerns for a child's health, and the impact of a child's
illness on family relationships

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 25 of 35
Demonstrate an understanding of the principles and limits related 1.1.2.
to age, maturity and capacity, with respect to patient confidentiality
Demonstrate an understanding of the issues related to assent and 1.1.3.
informed consent in children as well as in mature minors, as
defined by professional practice and the law
Optimize the physical environment for patient comfort, dignity, privacy, 1.2.
engagement, and safety
Recognize when the perspectives, values, or biases of patients, physicians, or 1.3.
other health care professionals may have an impact on the quality of care, and
modify the approach to the patient accordingly
Respect diversity and differences, including the impact of age, 1.3.1.
gender, abilities, disabilities, religion, language, cultural beliefs,
social support, and emotional influences on decision-making,
effective communication considering the patient’s illness
Immigrant children and their families 1.3.1.1.
Indigenous children and their families 1.3.1.2.
Demonstrate open-mindedness to the consideration of 1.3.1.3.
alternative health care practices
Respond to a patient’s non-verbal behaviours to enhance communication 1.4.
Manage disagreements and emotionally charged conversations 1.5.
Support and counsel a child and his/her family with chronic and/or 1.5.1.
catastrophic illness and/or impending death and provide
bereavement counseling
Provide support at the time of a sudden, unexpected death or 1.5.2.
other crisis situation
Adapt to the unique needs and preferences of each patient and to his or her 1.6.
clinical condition and circumstances
Elicit and synthesize accurate and relevant information, incorporating the 2.
perspectives of patients and their families
Use patient-and family-centred interviewing skills to effectively gather relevant 2.1.
biomedical and psychosocial information
Provide a clear structure for and manage the flow of an entire patient encounter 2.2.
PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 26 of 35
Seek and synthesize relevant information from other sources, including , with 2.3.
the patient and family’s consent
2 Share health care information and plans with patients and their families
Share information and explanations that are clear, accurate, and timely, while 2.4.
assessing for patient and family understanding
Disclose harmful patient safety incidents to patients and their families accurately 2.5.
and appropriately
3 Engage patients and their families in developing plans that reflect the patient’s
health care needs and goals
Facilitate discussions with patients and their families in a way that is respectful, 2.6.
non-judgmental, and culturally safe
Assist patients and their families to identify, access, and make use of 2.7.
information and communication technologies to support their care and manage
their health
Use communication skills and strategies that help patients and their families 2.8.
make informed decisions regarding their health
4 Document and share written and electronic information about the medical
encounter to optimize clinical decision-making, patient safety, confidentiality,
and privacy
Document clinical encounters in an accurate, complete, timely, and accessible 2.9.
manner, in compliance with regulatory and legal requirements
Communicate effectively using a written health record, electronic medical 2.10.
record, or other digital technology
Share information with patients, families and others in a manner that respects 2.11.
patient privacy and confidentiality, and enhances understanding

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 27 of 35
Collaborator
Definition:
As Collaborators, Pediatricians work effectively with other health care professionals to
provide safe, high-quality patient-centred care.
Key and Enabling Competencies: Pediatricians are able to…
Work effectively with physicians and other colleagues in the health care 1.
professions
Establish and maintain positive relationships with physicians and other 1.1.
colleagues in the health care professions to support relationship-centred
collaborative care
Negotiate overlapping and shared responsibilities with physicians and other 1.2.
colleagues in the health care professions in episodic and ongoing care
Take responsibility effectively in the organization and leadership of 1.2.1.
multidisciplinary teams
Utilize the unique skills and competencies of team members 1.2.2.
effectively to achieve optimal patient care
Engage in respectful shared decision-making with physicians and other 1.3.
colleagues in the health care professions
Consult as needed with other pediatricians, pediatric subspecialists 1.3.1.
or other consultants
Work with teachers, social workers, community leaders, child 1.3.2.
protection workers, and other non-health professionals to assess,
plan, provide, and integrate care for individuals and groups of
patients
Work with physicians and other colleagues in the health care professions to 2.
promote understanding, manage differences, and resolve conflicts
Show respect toward collaborators 2.1.
Implement strategies to promote understanding, manage differences, and 2.2.
resolve conflict in a manner that supports a collaborative culture

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 28 of 35
Hand over the care of a patient to another health care professional to facilitate 3.
continuity of safe patient care
Determine when care should be transferred to another physician or health care 3.1.
professional
Demonstrate safe handover of care, using both oral and written communication, 3.2.
during a patient transition to a different health care professional, setting, or
stage of care
Leader
Definition:
As Leaders, Pediatricians engage with others to contribute to a vision of a high-quality
health care system and take responsibility for the delivery of excellent patient care through
their activities as clinicians, administrators, scholars, or teachers.
Key and Enabling Competencies: Pediatricians are able to…
Contribute to the improvement of health care delivery in teams, organizations, 1.
and systems
Apply the science of quality improvement to contribute to improving systems of 1.1.
patient care
Apply a systems-based approach to address quality improvement 1.1.1.
and patient safety issues
Apply quality improvement tools to identify gaps in patient care 1.1.2.
and develop solutions
Contribute to a culture that promotes patient safety 1.2.
Promote and follow policies which create a just culture of patient 1.2.1.
safety
Analyze patient safety incidents to enhance systems of care 1.3.
Participate in reviews of mortality, morbidity and critical events 1.3.1.
Use health informatics to improve the quality of patient care and optimize 1.4.
patient safety

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 29 of 35
Engage in the stewardship of health care resources 2.
Allocate health care resources for optimal patient care 2.1.
Demonstrate an understanding of the importance of just and 2.1.1.
ethical allocation of health care resources, balancing effectiveness,
efficiency, and access with optimal patient care
Apply evidence and management processes to achieve cost-appropriate care 2.2.
Demonstrate leadership in professional practice 3.
Demonstrate leadership skills to enhance health care 3.1.
Demonstrate knowledge of the administrative structure of the 3.1.1.
health care system in which they practice
Facilitate change in health care to enhance services and outcomes 3.2.
Demonstrate an understanding of the organization of effective and 3.2.1.
efficient service delivery models for the care of children, at the
local, regional, and provincial levels
Manage career planning, finances, and health human resources in a practice 4.
Set priorities and manage time to integrate practice and personal life 4.1.
Develop strategies to achieve a balance between patient care, 4.1.1.
practice requirements, outside activities, personal life and family
responsibilities, and career goals
Manage a career and a practice 4.2.
Manage a practice ethically and efficiently, including finances and 4.2.1.
human resources
Implement processes to ensure personal practice improvement 4.3.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 30 of 35
Health Advocate
Definition:
As Health Advocates, Pediatricians contribute their expertise and influence as they work
with communities or patient populations to improve health. They work with those they serve
to determine and understand needs, speak on behalf of others when required, and support
the mobilization of resources to effect change.
Key and Enabling Competencies: Pediatricians are able to…
Respond to an individual patient’s health needs by advocating with the patient 1.
within and beyond the clinical environment
Work with patients to address determinants of health that affect them and their 1.1.
access to needed health services or resources
Identify determinants pertaining to an individual pediatric patient 1.1.1.
and family
Demonstrate an understanding of the importance of community 1.1.2.
services, including school, recreation, and appropriate
transportation, in the health of the pediatric patient
Determine a patient and family’s ability to access various services 1.1.3.
in the health and social systems
Work with patients and their families to increase opportunities to adopt healthy 1.2.
behaviours
Incorporate disease prevention, health promotion, and health surveillance into 1.3.
interactions with individual patients, including but not limited to the following
areas:
Attainment of developmental milestones 1.3.1.
Immunization 1.3.2.
Injury prevention 1.3.3.
Nutrition 1.3.4.
Physical activity 1.3.5.
Prevention of communicable diseases 1.3.6.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 31 of 35
Respond to the needs of the communities or populations they serve by 2.
advocating with them for system-level change in a socially accountable manner
Work with a community or population to identify the determinants of health that 2.1.
affect them
Identify the determinants of health of children, including barriers to 2.1.1.
access to care and resources, including those faced by the
vulnerable populations listed below
Describe how public policy impacts on child health 2.1.2.
Identify vulnerable or marginalized populations within those served 2.1.3.
and respond appropriately, including homeless children, children
living in poverty, victims of child abuse or neglect, Indigenous
children, and immigrant children
Improve clinical practice by applying a process of continuous quality 2.2.
improvement to disease prevention, health promotion, and health surveillance
activities
Contribute to a process to improve health in the community or population they 2.3.
serve
Implement measures to make a positive change in a determinant 2.3.1.
of health of children
Participate on committees or in other group settings when there is 2.3.2.
an opportunity to advocate for health care needs of pediatric
patients
Identify the role of Pediatricians in societal and governmental 2.3.3.
aspects of health care provision to children, including the role of
child protection agencies, policies related to infection control, and
safety issues

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 32 of 35
Scholar
Definition:
As Scholars, Pediatricians demonstrate a lifelong commitment to excellence in practice
through continuous learning, and by teaching others, evaluating evidence, and contributing
to scholarship.
Key and Enabling Competencies: Pediatricians are able to…
Engage in the continuous enhancement of their professional activities through 1.
ongoing learning
Develop, implement, monitor, and revise a personal learning plan to enhance 1.1.
professional practice
Identify opportunities for learning and improvement by regularly reflecting on 1.2.
and assessing their performance using various internal and external data
sources
Engage in collaborative learning to continuously improve personal practice and 1.3.
contribute to collective improvements in practice
Teach students, residents, the public, and other health care professionals 2.
Recognize the influence of role-modelling and the impact of the formal, informal, 2.1.
and hidden curriculum on learners
Promote a safe learning environment 2.2.
Ensure patient safety is maintained when learners are involved 2.3.
Plan and deliver learning activities 2.4.
Provide feedback to enhance learning and performance 2.5.
Assess and evaluate learners, teachers, and programs in an educationally 2.6.
appropriate manner
Integrate best available evidence into practice 3.
Recognize practice uncertainty and knowledge gaps in clinical and other 3.1.
professional encounters and generate focused questions that can address them
Identify, select, and navigate pre-appraised resources 3.2.
PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 33 of 35
Critically evaluate the integrity, reliability, and applicability of health-related 3.3.
research and literature
Integrate evidence into decision-making in their practice 3.4.
Contribute to the creation and dissemination of knowledge and practices 4.
applicable to health
Demonstrate an understanding of the scientific principles of research and 4.1.
scholarly inquiry and the role of research evidence in health care
Identify ethical principles for research and incorporate them into obtaining 4.2.
informed consent, considering potential harms and benefits, and considering
vulnerable populations
Contribute to the work of a research program 4.3.
Pose questions amenable to scholarly investigation and select appropriate 4.4.
methods to address them
Participate in the execution of scholarly work 4.4.1.
Conduct and complete a scholarly research, quality assurance, or 4.4.2.
educational project relevant to Pediatrics, demonstrating primary
responsibility for at least one of the following elements of the
project
Summarize and communicate to professional and lay audiences, including 4.5.
patients and their families, the findings of relevant research and scholarly inquiry
Professional
Definition:
As Professionals, Pediatricians demonstrate ethical practice, high personal standards of
behaviour, accountability to the profession and society, physician-led regulation, and
maintenance of personal health.
Key and Enabling Competencies: Pediatricians are able to…

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 34 of 35
Demonstrate a commitment to patients by applying best practices and adhering 1.
to high ethical standards
Exhibit appropriate professional behaviours and relationships in all aspects of 1.1.
practice, demonstrating honesty, integrity, humility, commitment, compassion,
respect, altruism, respect for diversity, and maintenance of confidentiality
Recognize the principles and limits of patient confidentiality as 1.1.1.
defined by professional practice standards and the law
Demonstrate an understanding of the cultural differences relevant 1.1.2.
to patient confidentiality
Demonstrate knowledge of the issues relating to assent and 1.1.3.
informed consent by children and mature minors.
Demonstrate a commitment to excellence in all aspects of practice 1.2.
Recognize and respond to ethical issues encountered in practice 1.3.
Apply the principles of biomedical ethics focusing on the "best 1.3.1.
interest" of the child
Recognize and manage conflicts of interest 1.4.
Exhibit professional behaviours in the use of technology-enabled communication 1.5.
Demonstrate a commitment to society by recognizing and responding to 2.
societal expectations in health care
Demonstrate accountability to patients, society, and the profession by 2.1.
responding to societal expectations of physicians
Demonstrate a commitment to patient safety and quality improvement 2.2.
Demonstrate a commitment to the profession by adhering to standards and 3.
participating in physician-led regulation
Fulfil and adhere to the professional and ethical codes, standards of practice, 3.1.
and laws governing practice
Demonstrate knowledge of obligations applicable to pediatrics, 3.1.1.
including notification of coroner, reporting of suspected physical or
sexual abuse, and public health issues
Abide by accepted guidelines of ethical interactions with industry, including the 3.2.

PEDIATRICS COMPETENCIES (20xx)
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 35 of 35
pharmaceutical industry, with respect to research, education, and clinical care
Demonstrate expertise by providing legal testimony or advising 3.2.1.
governments and governing bodies, as needed
Recognize and respond to unprofessional and unethical behaviours in physicians 3.3.
and other colleagues in the health care professions
Participate in peer assessment and standard setting 3.4.
Demonstrate a commitment to physician health and well-being to foster 4.
optimal patient care
Exhibit self-awareness and manage influences on personal well-being and 4.1.
professional performance
Manage personal and professional demands for a sustainable practice throughout 4.2.
the physician life cycle
Promote a culture that recognizes, supports, and responds effectively to 4.3.
colleagues in need
This document is to be reviewed by the Specialty Committee in [INSERT NAME OF DISCIPLINE] by [INSERT DATE]. Template document: Revised – Office of Specialty Education – January 2017 Revised – Specialty Standards Review Committee – September 2017; November 2017

© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved. This document may be reproduced for educational purposes only provided that the following phrase is included in all related materials: Copyright © 20xx The Royal College of Physicians and Surgeons of Canada. Referenced and produced with permission. Please forward a copy of the final product to the Office of Specialty Education, attn: Associate Director, Specialties. Written permission from the Royal College is required for all other uses. For further information regarding intellectual property, please contact: [email protected]. For questions regarding the use of this document, please contact: [email protected].
Page 1 of 8
Pediatrics Training Experiences
20xx VERSION x.x
These training requirements apply to those who begin training on or after July 1, 20xx. ELIGIBILITY REQUIREMENTS Royal College certification in Pediatrics, or enrolment in a Royal College-accredited residency program in these areas (see requirements for these qualifications). All candidates must be Royal College certified in their primary specialty in order to be eligible to write the Royal College examination in [INSERT SUBSPECIALTY NAME]. The following training experiences are required or recommended, as indicated. TRANSITION TO DISCIPLINE (TTD) The purpose of this stage is to confirm the knowledge and skills achieved in medical school, with a focus on conducting a pediatric-oriented history and physical examination in a variety of settings, as well as communicating a specific patient-centred plan. Residents will receive comprehensive orientation to institutional policies, programs, systems, and healthcare teams, and will be provided with resources that will help guide their training. Required training experiences (TTD stage):
1. Clinical training experiences 1.1. Exposure to neonates/infants, and children/adolescent 1.2. Exposure to outpatient (e.g. ambulatory, ER, community) or inpatient pediatrics or
both 1.3. On-call coverage (participate in providing care for sick children with support)
2. Other training experiences
2.1. Orientation (policies, resident resources, health and wellness, program portfolios, learning resources, assessment system, admitting and discharge process, information systems, technology)
2.2. Formal instruction in: 2.2.1. Patient safety (e.g. handover, infection control) 2.2.2. Diagnosis and management of common medical emergencies (on-call
readiness) 2.2.3. NRP or local equivalent 2.2.4. PALS or local equivalent
PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 2 of 8
Recommended training experiences (TTD stage):
3. Clinical training experiences 3.1. xxx
4. Other training experiences 4.1. Formal instruction in:
4.1.1. Writing orders (including intravenous fluids, medications/prescriptions, nutrition needs, investigations, monitoring requirements)
4.1.2. History and physical (age-specific) 4.1.3. Teaching more junior learners
. FOUNDATIONS OF DISCIPLINE (F) During this stage, residents will perform patient assessments, and initiate, communicate and document management plans for common pediatric presentations. In addition to experience with to toddlers, children and adolescents, they will provide neonatal care, including initiating resuscitation at low risk deliveries. Residents will teach trainees and team members, as well as patients and families, particularly with respect to preventative health care. They will perform common procedures and coordinate transition of care. They will gain exposure to a variety of settings including inpatient, outpatient, ambulatory care, acute care in the emergency room, and after-hours coverage.
Required training experiences (Foundations stage):
1. Clinical training experiences 1.1. Exposure to neonates/infants, toddlers, and children/adolescent 1.2. Inpatient clinical experience in general pediatrics 1.3. Ambulatory care clinics in general pediatrics 1.4. Acute care experience with patients presenting to emergency department 1.5. Clinical exposure to adolescents 1.6. After-hours coverage with opportunity to be first ‘assessor’ of pediatric patients of
all ages 1.7. Exposure to NICU II 1.8. Attendance at deliveries 1.9. Well-newborn care unit (postpartum/mother-baby unit, pediatric inpatient unit
providing neonatal care (ex. hyperbilirubinemia), community practice, ER
For SSRC reference only:
Entrustable professional activities (TTD stage):
TTD 1. Completing, presenting, and documenting a basic history and physical TTD 2. Composing and communicating pediatric-specific orders

PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 3 of 8
2. Other training experiences
2.1. Structured academic curriculum training 2.2. Teaching skills and clinical supervision of more junior learners 2.3. Training in procedural skills (may be in simulation) 2.4. Simulation when inadequate clinical exposure
Recommended training experiences (Foundations stage):
3. Clinical training experiences 3.1. Exposure to a minimum of 3 pediatric subspecialties (inpatient and outpatient) 3.2. Pediatrics in a community-based setting
4. Other training experiences
4.1. Formal instruction in critical appraisal, such as journal club 4.2. Introduction to research methodology/scholarly work 4.3. Formal instruction in patient handover
Optional training experiences (Foundation stage): 5. Clinical training experiences
5.1. Exposure to critically ill patients (PICU or level 3 NICU) 5.2. Longitudinal continuity clinic exposure
6. Other training experiences
6.1. Formative OSCE
For SSRC reference only:
Entrustable professional activities (Foundations stage):
F 1. Assessing, diagnosing, and initiating management of patients with common pediatric problems
F 2. Communicating, presenting, and documenting patient’s findings and plan F 3. Initiating neonatal resuscitation at low-risk deliveries F 4. Providing care for neonates F 5. Recognizing deteriorating patients and initiating stabilization and management F 6. Teaching trainees, patients, families, and team members F 7. Identifying unsafe situations involving self or others and seeking/offering
assistance F 8. Providing primary and secondary preventative health care across the age
spectrum F 9. Coordinating transitions of care for non-complex pediatric patients F 10. Performing simple procedural skills in either patients or simulation F 11. Developing a professional learning plan/engaging in regular goal-directed
professional activities

PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 4 of 8
CORE OF DISCIPLINE (C) The main focus of the Core of Discipline stage is to strengthen the skills required to practice as a competent Pediatrician. Residents will advance through this stage with a progressively increasing level of autonomy, managing pediatric patients with any degree of disease complexity, including acute critical illness or requiring episodic or longitudinal care. They will engage effectively with patients and families, communicating difficult or sensitive issues including mental health, behavioral and developmental concerns, as well as child maltreatment and neglect. They will manage patients in a variety of settings including inpatient, outpatient, ambulatory care, acute care in the emergency room, and after-hours coverage. They will lead interprofessional teams, supervise junior learners, provide consultation services to other disciplines, and transition care of complex patients, effectively.
Required training experiences (Core stage):
1. Clinical training experiences 1.1. Exposure to critically ill neonates (attending high-risk deliveries, level 3 NICU) 1.2. Pediatric inpatient CTU (or equivalent) – this experience must include being the
team leader 1.3. Ambulatory care, including experience with a broad spectrum of conditions as well
as patients with complex or undifferentiated disorders (Respirology, Neurology, Cardiology, Endocrinology, GI, Nephrology, Hematology/Oncology, Genetics, Adolescent Medicine, Rheumatology, Mental Health, Social Pediatrics)
1.4. Service providing pediatric consultations to other disciplines 1.5. After-hours coverage for a broad spectrum of inpatients and pediatric consultation
to the emergency department 1.6. Experience with critically ill patients – this must include PICU 1.7. Pediatric medicine in a community-based setting 1.8. Exposure to vulnerable/marginalized/at risk patients 1.9. Exposure to children in foster care, refugee/new immigrant populations, first
peoples, socially marginalized populations, culturally diverse populations, 1.10. Exposure to children and adolescents with developmental, behavioural, and
mental health concerns 1.11. PALS or APLS 1.12. NRP 1.13. PEM
2. Other training experiences
2.1. Structured academic curriculum: 2.1.1. Participation in a scholarly project 2.1.2. Experience in patient safety/quality improvement
2.2. Small group facilitated teaching sessions Recommended training experiences (Core stage):
3. Clinical training experiences 3.1. Continuity clinic

PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 5 of 8
3.2. Rural/remote, community clinics 3.3. NICU or PICU transport 3.4. Social pediatrics rotation 3.5. Sexual assault team training (including relevant procedural skills)
4. Other training experiences
4.1. Procedural skills workshop 4.2. ADHD workshop 4.3. Workshop on transitions to adult care 4.4. Communication workshop (conflict resolution, breaking bad news, communicating
in a cultural competent and patient centred fashion, effective electronic communication)
4.5. Ethics, medicolegal training/workshops 4.6. Mandatory reporting policies, multidisciplinary roles/responsibilities in child
protection 4.7. Formal teaching on recognizing/assessing/managing child maltreatment (such as
iLearn-Peds) 4.8. Online learning modules/curricula including aboriginal health, refugee/immigrant
health, health policy/social determinants of health, working with an interpreter, training in population and system advocacy, cultural sensitivity
TRANSITION TO PRACTICE (TTP) This stage is an opportunity for residents to refine and polish their skills as independent medical decision-makers, and to prepare for the next stage of their career as a Pediatrician. During this stage, residents integrate their prior learning to provide comprehensive pediatric care in any practice setting for common, complex, acute, and chronic patient presentations on a episodic or longitudinal basis. They will address complex issues such as supportive care for pediatric patients with life-limiting conditions. Residents will learn the principles of
For SSRC reference only:
Entrustable professional activities (Core stage):
C 1. Assessing patients of increased complexity C 2. Resuscitating and stabilizing critically ill neonates/infants/children/youth C 3. Managing acute illness in neonates/infants/children/youth C 4. Managing episodic and longitudinal care of infants/children/adolescents with
increased complexity C 5. Managing mental health, behavioral, developmental and school issues C 6. Discharging, handing over, and transferring care of complex patients safely and
effectively C 7. Conducting significant communications with patients/caregivers C 8. Leading interdisciplinary teams C 9. Managing child maltreatment and neglect

PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 6 of 8
practice management and participate in a system level safety or quality improvement initiative.
Required training experiences (TTP stage):
1. Clinical training experiences 1.1. Continuity clinic 1.2. Junior attending on inpatient ward 1.3. Junior attending in an ambulatory/emerg room setting 1.4. On-call 1.5. Home call
2. Other training experiences
2.1. Resource stewardship 2.2. Serving on committees? 2.3. Formal instruction in Medical Assistance in Dying 2.4. Discussion of initiation or withdrawal of treatment, including DNR 2.5. Personal learning plan? 2.6. QI/QA? 2.7. M&M rounds
Recommended training experiences (TTP stage):
3. Clinical training experiences 3.1. Community Pediatric experience 3.2. Neonatal 3.3. Mental health 3.4. IPE settings
4. Other training experiences
4.1. Wellness? 4.2. Delivery of teaching in the community (lay audience and/or HCPs) 4.3. Learning plan? 4.4. Participation in hospital committees or other administrative responsibilities 4.5. Legal aspects of transition to adult care (LTD, POA) 4.6. Holland Bloorview.ca (chronic pain assessment toolbox for children with disabilities) 4.7. Canadian modules for complex care (CPS) and Palliative care webinars (CAPHC)
including initiation or withdrawal of treatment, DNR 4.8. Education in Palliative and End of Life Care – Pediatric (EPEC) 4.9. Formal instruction in Medical Assistance in Dying (assisted suicide and euthanasia)
For SSRC reference only:
Entrustable professional activities (TTP stage):
TTP 1. Leading the management and operations of pediatric practice TTP 2. Leading consultation and ongoing management of pediatric inpatients TTP 3. Leading consultation and longitudinal management of pediatric outpatients TTP 4. Identifying and analyzing individual patient and system-level safety, quality
concerns in health care delivery
PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 7 of 8
CERTIFICATION REQUIREMENTS Royal College certification in Pediatrics requires all of the following:
1. Successful completion of the Royal College examination in Pediatrics; and
2. Successful completion of the Pediatrics Portfolio.
NOTES: This section should outline any exceptional or extraordinary clauses to the training requirements (e.g., other training options, agreements with American certification boards, discretion of a program director to extend length of training, etc.). The Pediatrics Portfolio refers to the list of entrustable professional activities across all four stages of the residency Competence Continuum, and associated national standards for assessment and achievement.
MODEL DURATION OF TRAINING Progress in training occurs through demonstration of competence and advancement through the stages of the Competence Continuum. Pediatrics is planned as an [x]-year residency program. There is no mandated period of training in each stage. Individual duration of training may be influenced by many factors, which may include but are not limited to the student’s singular progression through the stages [and/or overlap training], the availability of teaching and learning resources, and/or differences in program implementation. Duration of training in each stage is therefore at the discretion of the Faculty of Medicine, the Competence Committee, and the program director. Guidance for postgraduate medical education offices
The stages of the Competence Continuum in Pediatrics are generally no longer than Transition to Discipline – [xx weeks or months or blocks] Foundations of Discipline – [xx] Core of Discipline – [xx] Transition to Practice – [xx] Total duration of training – [xx]

PEDIATRICS TRAINING EXPERIENCES 20xx
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Page 8 of 8
*One block is equal to 4 weeks Guidance for programs
The Royal College Specialty Committee in Pediatrics’ suggested course of training, for the purposes of planning learning experiences and schedules, is as follows:
[xx weeks or months or blocks] in Transition to Discipline [xx] in Foundations of Discipline [xx] in Core of Discipline [xx] in Transition to Practice *One block is equal to 4 weeks This document is to be reviewed by the Specialty Committee in Pediatrics by [INSERT DATE]. Template document: Revised – Office of Specialty Education – January 2017 Revised – Office of Specialty Education – October 2017; November 2017

___________________________________________________________________________________________ © 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved. This document may be reproduced for educational purposes only provided that the following phrase is included in all related materials: Copyright © 20xx The Royal College of Physicians and Surgeons of Canada. Referenced and produced with permission. Please forward a copy of the final product to the Office of Specialty Education, attn: Associate Director, Specialties. Written permission from the Royal College is required for all other uses. For further information regarding intellectual property, please contact: [email protected]. For questions regarding the use of this document, please contact: [email protected].
Effective date: [Month day, year]
INTRODUCTION The Standards of Accreditation for Residency Programs in Pediatrics1 are a national set of standards maintained by the Royal College, for the evaluation and accreditation of Pediatrics residency programs. The standards aim to provide an interpretation of the General Standards of Accreditation for Residency Programs as they relate to the accreditation of residency programs in Pediatrics, and to ensure these programs adequately prepare residents to meet the health care needs of their patient population(s), upon completion of training. The standards include requirements applicable to residency programs and learning sites2 and have been written in alignment with a standards organization framework, which aims to provide clarity of expectations, while maintaining flexibility for innovation. These standards are intended to be read in conjunction with the General Standards of Accreditation for Residency Programs, as well as the discipline-specific documents for Pediatrics. In instances where the indicators reflected in the General Standards of Accreditation for Residency Programs have been modified within this document to reflect a discipline-specific expectation, the indicator as reflected in this document takes precedence.
1 Pediatrics is that branch of medicine concerned with the study and care of infants, children, and youth in health and disease, their growth and development, and their opportunity to achieve full potential as adults. Throughout this document, each reference to “child” or “children” includes infants, children, and youth. 2 Note: The General Standards of Accreditation for Institutions with Residency Programs also include standards applicable to learning sites.
Standards of Accreditation for Residency Programs in Pediatrics

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
1 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
STANDARDS
DOMAIN: PROGRAM ORGANIZATION The Program Organization domain includes standards focused on the structural and functional aspects of the residency program, which support and provide structure to meet the General Standards of Accreditation for Residency Programs. The Program Organization domain standards aim to
• ensure the organizational structure and personnel are appropriate to support the residency program, teachers, and residents;
• define the high-level expectations of the program director and residency program committee(s); and
• ensure the residency program and its structure are organized to meet and integrate the requirements for the Education Program; Resources; Learners, Teachers and Administrative Personnel; and Continuous Improvement domains.
STANDARD 1: There is an appropriate organizational structure, with leadership and administrative personnel to effectively support the residency program, teachers, and residents.
Refer to Standard 1 and its various components within the General Standards of Accreditation for Residency Programs, in addition to elements, requirements, and indicators detailed below.
Element 1.2: There is an effective and functional residency program committee structure to support the program director in planning, organizing, evaluating, and advancing the residency program.
Requirement(s) Indicator(s)
1.2.2: The residency program committee has a clear mandate to manage and evaluate key functions of the residency program.
1.2.2.4 [Modified]3: The residency program committee structure includes a competence committee responsible for reviewing and making recommendations regarding residents’ readiness for increasing professional responsibility, progress in achieving the national standards of Pediatrics, promotion, and transition to independent practice. 1.2.2.5: The frequency of competence committee meetings is sufficient for the committee to fulfil its mandate (at least twice a year).
3 “[Modified]” identifies an indicator from the General Standards of Accreditation for Residency Programs that has been modified with discipline-specific content.

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
2 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
STANDARD 2: All aspects of the residency program are collaboratively overseen by the program director and the residency program committee.
Refer to Standard 2 and its various components within the General Standards of Accreditation for Residency Programs, in addition to elements, requirements, and indicators detailed below. Element 2.2: Resources and learning sites are organized to meet the requirements of the discipline.
Requirement(s) Indicator(s)
2.2.2: Each learning site has an effective organizational structure to facilitate education and communication.
2.2.2.3: Community-based learning sites have appropriate administrative support and linkages with the residency program.

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
3 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
DOMAIN: EDUCATION PROGRAM
The Education Program domain includes standards focused on the planning, design, and delivery of the residency program, with the overarching outcome to ensure that the residency program prepares residents to be competent to begin independent practice.
NOTE: Time-based residency programs are planned and organized around educational objectives linked to required experiences, whereas Competency Based Medical Education (CBME) residency programs are planned and organized around competencies required for practice. The Education Program domain standards in the General Standards of Accreditation for Residency Programs have been written to accommodate both.
STANDARD 3: Residents are prepared for independent practice.
Refer to Standard 3 and its various components within the General Standards of Accreditation for Residency Programs, in addition to elements, requirements, and indicators detailed below. Element 3.1: The residency program’s educational design is based on outcomes-based competencies and/or objectives that prepare residents to meet the needs of the population(s) they will serve in independent practice. Requirement(s) Indicator(s)
3.1.1: Educational competencies and/or objectives are in place to ensure residents progressively meet all required standards for the discipline and address societal needs.
3.1.1.1 [Modified]: The competencies and/or educational objectives meet the specialty-specific requirements for Pediatrics, as outlined in the Pediatrics Competencies and the Pediatrics Training Experiences.

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
4 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
Element 3.2: The residency program provides educational experiences designed to facilitate residents’ attainment of the outcomes-based competencies and/or objectives. Requirement(s) Indicator(s)
3.2.1: The residency program’s competencies and/or objectives are used to guide the educational experiences while providing residents with opportunities for increasing professional responsibility at each stage or level of training.
3.2.1.2 [Modified]: The educational experiences meet the specialty-specific requirements for Pediatrics, as outlined in the Pediatrics Competencies and the Pediatrics Training Experiences. 3.2.1.3 [Modified]: The educational experiences and supervision are appropriate for residents’ stage or level of training and support residents’ achievement of increasing professional responsibility specific to Pediatrics. 3.2.1.5: The educational experiences include opportunities for residents to complete all mandatory rotations, as well as subspecialty and selective rotations. 3.2.1.6: The educational experiences include opportunities for electives made available throughout residency, with a maximum of three blocks in the core three years of residency. 3.2.1.7: The educational experiences include community-based learning outside of the academic learning centre. 3.2.1.8: The educational experiences during the final period of training include increasing professional responsibility and the opportunity to consolidate skills and competencies required for transition to independent practice in Pediatrics. 3.2.1.9: The educational experiences during the final year of training are approved by the program director, and provide the resident with opportunities to meet his/her personal educational/learning objectives related to his/her field of practice. 3.2.1.10: The educational experiences include opportunities for residents to develop skills as a consultant to other Pediatricians and to other health care professionals throughout the program. 3.2.1.11: The educational experiences include both organized clinical as well as formal instruction in pediatric and neonatal critical care medicine. 3.2.1.12: The educational experiences include initial management of all types of emergencies involving children, including injuries, poisoning, and violence, under appropriate supervision. 3.2.1.13: The educational experiences include opportunities for learning about child maltreatment pediatrics.

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
5 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
3.2.2: The residency program uses a comprehensive curriculum plan, which is specific to the discipline and addresses all of the CanMEDS/CanMEDS FM Roles.
3.2.2.7: The curriculum plan includes definitive, organized teaching in the basic sciences and in the advanced clinical and scientific knowledge essential to an understanding of those areas of Pediatrics outlined in the preceding sections, with special attention to instruction in genetics, growth and development, the provision of health care, and the social aspects of Pediatrics (Medical Expert). 3.2.2.8: The curriculum plan includes each resident’s participation in a scholarly research, quality assurance, or educational project. (Scholar). 3.2.2.9: The curriculum plan includes the provision of experience in critical appraisal and basic study design/statistics, through the academic half day or other educational activities (Scholar). 3.2.2.10 [Exemplary]: The residency program incorporates the Pediatrics Pathway to Competence in its curriculum plan.
3.2.5: The educational environment supports and promotes resident learning in an atmosphere of scholarly enquiry.
3.2.5.2 [Modified]: Residents are provided with protected time to participate in scholarly activities, including participation in a scholarly research, quality assurance, or educational project.
Element 3.4: There is an effective, organized system of resident assessment
Requirement(s) Indicator(s)
3.4.1: The residency program has a planned, defined, and implemented system of assessment.
3.4.1.8: The system of assessment requires the completion of an independent assessment as recorded on an In-training Evaluation Report (ITER) for longitudinal educational experiences (rotations).
3.4.3: There is a well-articulated process for decision-making regarding resident progression, including the decision on satisfactory completion of training.
3.4.3.1 [Modified]: The competence committee regularly reviews (at least twice a year, or once per stage, whichever is more frequent) residents’ readiness for increasing professional responsibility, promotion, and transition to independent practice, based on demonstrated achievement of expected competencies and/or objectives for each level or stage of training. 3.4.3.5 [Exemplary]: The competence committee’s recommendations regarding learner status are consistent with the Royal College’s guidelines for Competence by Design.

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
6 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
3.4.4: The system of assessment allows for timely identification of and support for residents who are not attaining the required competencies as expected.
3.4.4.2 [Modified]: Residents who are not progressing as expected are provided with the required support and opportunity to improve their performance, as appropriate.
DOMAIN: RESOURCES
The Resources domain includes standards focused on ensuring resources are sufficient for the delivery of the education program and to ultimately ensure that residents are prepared for independent practice. The Resources domain standards aim to ensure the adequacy of the residency program’s clinical, physical, technical, human and financial resources.
STANDARD 4: The delivery and administration of the residency program is supported by appropriate resources.
Refer to Standard 4 and its various components within the General Standards of Accreditation for Residency Programs, in addition to elements, requirements, and indicators detailed below. Element 4.1: The residency program has the clinical, physical, technical, and financial resources to provide all residents with the educational experiences needed to acquire all competencies. Requirement(s) Indicator(s)
4.1.1: The patient population is adequate to ensure that residents experience the breadth of the discipline.
4.1.1.3: The diversity and volume of patients consistently available to the residency program are sufficient to meet the educational needs of residents and to specifically provide
• support for residents’ acquisition of knowledge, skills, and behaviours relating to population aspects of age, gender, culture, and ethnicity, appropriate to Pediatrics;
• experience in the diagnosis and management of the wide variety of clinical problems seen in pediatric practice;
• support for the teaching of residents in the following specialized areas of pediatric medicine: adolescent medicine, cardiology, child and adolescent psychiatry, child maltreatment pediatrics, social pediatrics, clinical immunology and allergy, complex care, developmental pediatrics, endocrinology and metabolism, gastroenterology, genetics/metabolics,

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
7 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
hematology/oncology, infectious diseases, nephrology, palliative medicine, pediatric neurology, respirology, and rheumatology;
• full training in the clinical and technical skills associated with the management of normal and special-care newborn infants in newborn nurseries (level I) and intensive care units (level II/III); and
• full training in the clinical and technical skills associated with the management of those requiring pediatric critical care and emergency care.
4.1.2: Clinical and consultative services and facilities are organized and adequate to ensure that residents experience the breadth of the discipline.
4.1.2.4: The residency program has access to adequate resources to ensure full training for each resident in all branches of Pediatrics. 4.1.2.5: The residency program has access to newborn nurseries (level I) and intensive care units (level II/III), under the direction of qualified Pediatricians. 4.1.2.6: The residency program has access to Pediatric critical care and emergency care facilities, under the direction of qualified specialists. 4.1.2.7: The residency program’s pediatric services are organized into one or more formal inpatient clinical teaching units, each with an adequate number of patients available for teaching, and administered by a chief-of-service to whom the senior resident is directly responsible. 4.1.2.8: The residency program has access to ambulatory care facilities to provide learning opportunities in the management of patients with complex needs, including palliative care. 4.1.2.9: The residency program has access to emergency departments that are organized so as to ensure that residents in Pediatrics obtain experience in initial patient assessment, in addition to acting as consultants. 4.1.2.10: The residency program has access to the following special facilities and services that are closely coordinated with the overall residency program:
• an active psychiatric service with adequate arrangements for the training of Pediatrics residents in child and adolescent psychiatry, under the supervision of qualified teaching staff;
• facilities for the study and management of behavioural problems in infants, children, and adolescents;
• facilities for the comprehensive assessment and care of mentally and physically handicapped children;
• active obstetrical and pediatric surgical services, preferably in the same institutions as the general
STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
8 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
pediatric and neonatal teaching units; and • facilities and resources to provide an opportunity for all
residents in the program to receive appropriate training in pediatric advanced life support.
4.1.2.11 [Exemplary]: Inpatient and outpatient teaching services are integrated in order to provide continuity of observation of patients both in and out of hospital.
4.1.4: The residency program has the necessary financial, physical and technical resources.
4.1.4.6: The residency program has access to appropriate resources to support resident research, including participation in a scholarly research, quality assurance, or educational project.
4.1.5: There is appropriate liaison with other programs and teaching services to ensure that residents experience the breadth of the discipline.
4.1.5.2: The residency program has appropriate liaison with teaching services in anatomical pathology, anesthesiology, dermatology, diagnostic imaging, obstetrics and gynecology, psychiatry, and surgery. 4.1.5.3 [Exemplary]: Hospitals with a major role in the Pediatrics program are also engaged in medical undergraduate teaching. 4.1.5.4 [Exemplary]: Consultation services are coordinated with various subspecialties, including those of surgical and psychiatric clinics.
Element 4.2: The residency program has the appropriate human resources to provide all residents with the required educational experiences. Requirement(s) Indicator(s)
4.2.1: The number, credentials, competencies, and duties of the teachers are appropriate to teach the residency curriculum, supervise and assess trainees, contribute to the program, and role model effective practice.
4.2.1.1 [Modified]: The number, credentials, and competencies of the teachers are sufficient to provide the required clinical teaching, academic teaching, assessment, and feedback to residents, including teaching in the basic and clinical sciences related to Pediatrics. 4.2.1.2 [Modified]: The number, credentials, competencies, and scope of practice of the teachers are sufficient to provide appropriate supervision, based on stage or level of training, for training and teaching in the basic and clinical sciences related to Pediatrics, as well as in all clinical environments, including when residents are on-call and when providing care to patients, as part of the residency program, outside of a learning site. 4.2.1.5: There are sufficient competent individual supervisors to support a variety of resident scholarly activities, including resident participation in a scholarly research, quality

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
9 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
assurance, or educational project. 4.2.1.6: Teachers are sufficient to provide teaching of research methodology and critical appraisal. 4.2.1.7: Teachers are supported with adequate resources in order to carry out their teaching responsibilities, including coverage for clinical duties when teaching, and with appropriate resources for the development of teaching materials. 4.2.1.8: The program director has Royal College certification in Pediatrics.
DOMAIN: LEARNERS, TEACHERS, AND ADMINISTRATIVE PERSONNEL
The Learners, Teachers, and Administrative Personnel domain includes standards focused on supporting teachers, learners, and administrative personnel–“people services and supports.” The Learners, Teachers, and Administrative Personnel domain program standards aim to ensure
• a safe and positive learning environment for all (i.e., residents, teachers, patients, and administrative personnel); and
• value of and support for administrative personnel. STANDARD 5: Safety and wellness is promoted throughout the learning environment. Refer to Standard 5 and its various components within the General Standards of Accreditation for Residency Programs, in addition to elements, requirements, and indicators detailed below.
Element 5.1: The safety and wellness of patients and residents are actively promoted.
Requirement(s) Indicator(s)
5.1.1: Residents are appropriately supervised.
5.1.1.1 [Modified]: Residents and teachers follow the centralized and any program-specific policies regarding supervision of residents, including ensuring the physical presence of the appropriate supervisor, when mandated, during acts or procedures performed by the resident, as appropriate to their stage or level of training.
STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
10 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
STANDARD 6: Residents are treated fairly and adequately supported throughout their progression through the residency program. Refer to Standard 6 and its various components within the General Standards of Accreditation for Residency Programs, in addition to elements, requirements, and indicators detailed below.
Element 6.1: The progression of residents through the residency program is supported, fair, and transparent.
Requirement(s) Indicator(s)
6.1.1: There are effective, clearly defined, transparent, formal processes for the selection and progression of residents.
6.1.1.3: The residency program has effective policies and procedures, or complies with and effectively implements centralized policies and procedures, to address residents who are not progressing as expected through the stages of training.
STANDARD 7: Teachers effectively deliver and support all aspects of the residency program. Refer to Standard 7 and its various components within the General Standards of Accreditation for Residency Programs.
STANDARD 8: Administrative personnel are valued and supported in the delivery of the residency program. Refer to Standard 8 and its various components within the General Standards of Accreditation for Residency Programs.

STANDARDS OF ACCREDITATION FOR RESIDENCY PROGRAMS IN [DISCIPLINE NAME] (20xx VERSION x.x)
11 ___________________________________________________________________________________________
© 20xx The Royal College of Physicians and Surgeons of Canada. All rights reserved.
DOMAIN: CONTINUOUS IMPROVEMENT
The Continuous Improvement domain includes standards focused on ensuring a culture of continuous improvement is present throughout the residency program, with the aim of ensuring continuous improvement of residency programs.
NOTE: To reinforce and create clarity with respect to the expectations related to continuous improvement, the requirements under the element mimic the continuous improvement cycle (Plan, Do, Study, Act). STANDARD 9: There is continuous improvement of the educational experiences to improve the residency program and ensure residents are prepared for independent practice. Refer to Standard 9 and its various components within the General Standards of Accreditation for Residency Programs.
Drafted – Specialty Committee & Office of Specialty Education – Month Year Approved – Specialty Standards Review Committee – Month Year

Appendix J Submission of projected number of residents affected by this change The following information was provided in the submission to the Committee on Specialties in August 2018: “Currently, all but three provinces (Ontario, Quebec and Nova Scotia) provide funding for four years of training in Pediatrics before entering subspecialty training. Data from these three provinces over the last four years shows that approximately 39 additional residents each year (averages are 26.5 for Ontario, 11 for Quebec and 1.25 for Nova Scotia) would have done a fourth year of Pediatric training if it was required. Given the current and future restrictions on access to subspecialty training in Quebec, the projected total number of residents training in these three provinces for whom a fourth year of funding for Pediatric residency would be needed is approximately 35 residents annually, a small proportion of the approximately 180 residents who complete training in Pediatrics each year.” This appendix describes the method by which these numbers were obtained and then confirmed by external data. Program directors from all 18 Royal College-accredited Pediatric training programs were solicited for data on the residents who left their programs in the years 2015, 2016, 2017 and 2018. Residents were divided into three categories: those who completed four years of Pediatrics and did not proceed to subspecialty training, those who commenced subspecialty training after three years of Pediatrics, and those who did so after all four years of Pediatrics residency. These raw numbers have recently been updated by program directors to provide data regarding residents who left in 2018 and to ensure the accuracy of the data. It is important to note that these numbers may include residents leaving after three years who have obtained non-Ministry of Health (MOH)-funded positions for their subspecialty training. As well, this data does not include visa-sponsored trainees. Our initial focus was on trainees in Ontario, Quebec and Nova Scotia as these provinces do not currently provide funding for residents to complete the PGY-4 year in Pediatrics prior to entering subspecialty training. This is the data shown in the table below. While there is considerable fluctuation from year to year, the average number of residents from these three provinces who started subspecialty training in any province after three years of training was 40.25 over the four years. The situation for Québec residents is evolving as the number of funded positions for subspecialty training has been increasingly restricted, as well as the specific subspecialties whose positions are funded. This has actually led to some funded positions going unmatched. The change is dramatic: 20 funded positions for beginning subspecialty training in 2013-2014, but only four in 2017-2018, and five announced as available for those starting in 2020. The proportion of residents pursuing subspecialty training has decreased, particularly in the francophone universities, but some residents have exercised the option to pursue their training outside of Québec, the vast majority in Ontario. Ultimately, assuming the number of funded positions does not increase in other provinces, the overall number of residents entering subspecialty training in Canada should continue to fall if positions are further reduced in Québec. And thus, the number of trainees who would be remaining in these provinces to complete their PGY-4 year prior to subspecialty training should decrease to less than 40. Residents from provinces which allow completion of a Pediatrics residency prior to entering subspecialty training may not always do so, if the subspecialty program to which they are matched is one which requires entry after PGY-3 (usually in Ontario). While their departure currently represents a cost savings for their province, this would be negated if they were to all to complete their PGY-4 year prior to

subspecialty training. However, as the number of funded subspecialty positions in these provinces seems to have risen slightly in recent years, the number of residents choosing to stay and enter subspecialty training after PGY-4 should be on the rise, regardless of the outcome of this proposal. External data from the Canadian Post-M.D. Education Registry (CAPER) was also analyzed. This exercise tracked resident numbers over five years of training (2013-2018) and centered on PGY4 residents who were in an MOH-funded subspecialty training program anywhere in Canada. Data was compared for the three years which corresponded to those of the program director survey, so that PGY4 subspecialty residents training in 2015-2016, 2016-2017 and 2017-2018 were linked with residents leaving Pediatrics programs after PGY3 in 2015, 2016 and 2017 respectively. The CAPER results indicate an average of 40 residents leaving Pediatrics programs after PGY-3 per year, closely matching the information from program directors. Provincial cross-pollination may limit interpretation of the CAPER data, as residents may complete three years of training outside of Ontario, Quebec and Nova Scotia and then move to these three provinces for subspecialty training, or vice versa. In conclusion, data from recent years provided by Pediatric program directors as well as from CAPER indicate that on average, no more than 40, and probably 35-40, residents from Ontario, Quebec and Nova Scotia leave Pediatrics programs after their PGY-3 year in order to begin subspecialty training. These residents would require funding for the final phase of the training in Pediatrics under this proposal, the current PGY-4 year.


APPENDIX K: INDEPENDENT COST ANALYSIS
Background
The Committee on Specialties (COS) requested an independent cost analysis of the Pediatrics
application as part of their decision at Part I. The committee’s request was largely motivated by the
savings highlighted in the original proposal, owing to the complexity and degree of uncertainty
associated with such calculations. In their revised application, however, the applicant has refrained
from assigning specific monetary figures to these savings. As a result, the findings of this
independent cost analysis are largely consistent with those in the Pediatrics proposal.
Summary
If approved, resident salaries will need to accommodate an additional year of training for those
residents no longer permitted to overlap their training year. The estimated financial impact of this
proposal is approximately $5,854,713/year increase across Canada. Most of this sum is concentrated
in Ontario, Québec, and the Maritimes ($4,624,500). The latter figure is slightly higher than the one
presented by the applicant in the same three jurisdictions (applicant’s total: $3,793,723, difference of
-$830,777). The discrepancy between the two anticipated costs can be explained by:
A decreased number of PGY4 residents
o The applicant took into account a predicted decrease in the number of residents
from QC
o The applicant used a different methodology to gain an average number of trainees,
resulting in ten less trainees across ON, QC, and NS in their analysis.
Availability of more up-to-date resident salary figures
o There have been resident wage increases in several jurisdictions since the Pediatrics
application.
There are a number of potential savings, but quantifying the exact amounts remains challenging:
Calls covered by highly skilled PGY4s, rather than a certified Pediatrician.
Reduced provincial billing by certified Pediatricians due to cases seen by highly skilled PGY4
residents.
Better trained residents may provide better care, reducing cost of referrals and medicolegal
liability.
The remainder of this document details the methodology of the economic analysis as it was
undertaken by the Royal College’s Education Strategy, Innovations, and Development Unit.
Methodology
Number of Additional Trainees
In the 2017/8 academic year, there were a total of 64 PGY4 trainees completing subspecialty
training. Of this total, 48 received funding from the Ministries of Health and 16 received no
government funding. The costs will largely be to support the trainees who receive funding from the
Ministries of Health. This analysis therefore focuses on trainees who receive funding from the

Ministries of Health. There may also be an additional cost of teaching PGY4 trainees; however this
cost will likely be negligible.
There is an average of 56 Pediatrics trainees who entered subspecialty training in PGY4 across
Canada over the last 5 years. Saskatchewan and Newfoundland and Labrador do not currently offer
Pediatric subspecialty programs. 44.6 of these trainees were located in the three jurisdictions which
do not currently offer funding for four full years of training in Pediatrics, if the trainee also wishes to
pursue subspecialty training:
Maritimes Quebec Ontario Manitoba Alberta BC Total
Averages Totals: 1.4 13 30.2 1.8 6.8 2.8 56
Three Provinces: 1.4 13 30.2 - - - 44.6
These numbers are a high estimate, given the current and future restrictions on subspecialty
training in Quebec (minus around 4 trainees per year).
Cost of Salaries
Based on the last five years, there is an average of 56 PGY4 residents nationally in Pediatric
subspecialty programs who receive government funding. The additional cost of the change across
Canada will be $5,854,713:
Province
Number of
additional
residents
Annual salary per
PGY6 ($)
Salary +30%
(Benefits)
Total Cost Additional
PGY6
British
Columbia1
2.8 79,400.34 103,220.44 289,017.24
Alberta2 6.8 84,067 109,287.10 743,152.28
Saskatchewan3 0 85,879 111,642.70 0.00
Manitoba4 1.8 84,634 110,024.20 198,043.56
Ontario5 30.2 85,218.75 110,784.38 3,345,688.13
Quebec6 13 66,069 85,889.70 1,116,566.10
Maritimes7 1.4 89,146 115,889.80 162,245.72
1 https://residentdoctorsbc.ca/bargaining-benefits/collective-agreement/#Article21
2 https://para-ab.ca/wp-content/uploads/2017/10/Monetary-increases-summary-revised.pdf
3 http://www.residentdoctorssk.ca/contract/payroll/salaries
4 http://www.parim.org/wp-content/uploads/2015/06/PARIM-Collective-Agreement-2014-2018-OSB
5 http://www.myparo.ca/during-residency/#salary-and-benefits
6 http://www.myparo.ca/during-residency/#salary-and-benefits
7 http://www.myparo.ca/during-residency/#salary-and-benefits

Newfoundland
and Labrador8
0 74,823 97,269.90 0.00
Totals 56 5,854,713.02
Three jurisdictions (ON, QC, and the Maritimes) only provide funding for three years of Pediatrics if a
trainee also wishes to complete subspecialty training. Based on the average number of PGY4
trainees in Pediatric subspecialty disciplines from the last five years, the additional cost of the
change in these three jurisdictions will be $4,624,500:
Province
Number of
additional
residents
Annual salary per
PGY6
Salary +30%
(Benefits)
Total Cost Additional
PGY6
Ontario 30.2 85,218.75 110,784.38 3,345,688.13
Quebec 13 66,069 85,889.70 1,116,566.10
Maritimes 1.4 89,146 115,889.80 162,245.72
Totals 44.6 4,624,499.95
A small number of PGY4 trainees in jurisdictions that do provide funding for four full years of
Pediatrics training choose to overlap their primary and subspecialty programs, entering
subspecialty training after only three years of primary training. Based on the average number of
PGY4 trainees in Pediatric subspecialty disciplines from the last five years, the total cost of additional
PGY4 Pediatrics trainees in all other jurisdictions (BC, AB, SK, MB, NL) will be $1,230,213:
Province
Number of
additional
residents
Annual salary per
PGY6
Salary +30%
(Benefits)
Total Cost Additional
PGY6
British
Columbia
2.8 79,400.34 103,220.44 289,017.24
Alberta 6.8 84,067 109,287.10 743,152.28
Saskatchewan 0 85,879 111,642.70 0.00
Manitoba 1.8 84,634 110,024.20 198,043.56
Newfoundland
and Labrador
0 74,823 97,269.90 0.00
Totals 11.4 1,230,213.08
8 https://www.med.mun.ca/PGME/Current-Residents/PAIRN.aspx
10.October.2018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Clinical Immunology and Allergy, I would hereby like to voice our support for the proposed changes to the training requirements in Pediatrics. As proposed, we agree that the practice of “double-counting” be eliminated and that subspecialty training only start after the Transition-to-Practice Entrustable Professional Activities (EPAs) in Pediatrics have been completed. As such, we undesrstand that all residents should be required to complete 4 years of Pediatrics training before entering into a pediatric subspecialty training program.
In the eyes of our Committee members, were this change to take effect, issues that might affect our subspecialty are,:
•Extending training to 4+2 for all pediatric subspecialties may act as a deterrent for residents to pursue allergy training with subsequent negative impact on patient accessibility to CIA specialists. Alternately, medical students interested in CIA may choose the path of IM to reach their desired subspecialty.
•Last but not least, funding does not appear to meet consensus (e.g. in Quebec) and accepting disparities in training around Canada would be contrary to the nation-wide perspective that the Royal College fosters in our medical education system.
Of course, the ultimate forum to decide what your specialty requires is your Committee and we wish you success with the implementation of a change seen as beneficial to your residency training and the resolution of corollary problems.
Yours sincerely,
Fanny Silviu-Dan, MD, FRCPC
Chair, Specialty Committee in Clinical Immunology and Allergy
Royal College of Physicians and Surgeons of Canada

October 19, 2018 Dr. Catherine Farrell, MD, FRCPC Chair, Specialty Committee in Pediatrics Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Endocrinology and Metabolism I would like to voice our views on the proposed changes to the training requirements in Pediatrics. I understand that the Specialty Committee in Pediatrics is purposing that the practice of “double-counting” be eliminated and that subspecialty training only start after the Transition-to-Practice Entrustable Professional Activities (EPAs) in Pediatrics have been completed. As such, all residents will be required to complete 4 years of Pediatrics training before entering into a pediatric subspecialty training program. Our committee respects the decision of the Pediatric Specialty Committee that this change in the required years of training is necessary in order to meet the requirements of training in Pediatrics. However, we wish to express our concerns about the impact of this change on subspecialty training in Pediatric Endocrinology and Metabolism. At the present time, provincial funding is typically available for 5 years of training post medical school (“R5”). If core pediatric training requires 4 years, this will have profound and devastating effects on training in pediatric endocrinology and metabolism as funding will not be available to complete the 2 year Royal College approved training program in Pediatric Endocrinology and Metabolism. There must be an increase in provincial funding for training to 6 years (“R6”) if the requirement for Pediatric training is increased to 4 years.
We look forward to further discussion related to this issue as we move towards a positive solution that will meet the needs of both Pediatric and Pediatric Endocrinology and Metabolism training requirements. Yours sincerely,
Elizabeth AC Sellers MD MSc FRCPC Chair, Specialty Committee Endocrinology and Metabolism Royal College of Physicians and Surgeons of Canada

September 24th, 2018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Adolescent Medicine I would hereby like to
voice our support for the proposed changes to the training requirements in Pediatrics.
As proposed, we agree that the practice of “double-counting” be eliminated and that
subspecialty training only start after the Transition-to-Practice Entrustable Professional
Activities (EPAs) in Pediatrics have been completed. As such, all residents should be
required to complete 4 years of Pediatrics training before entering into a pediatric
subspecialty training program.
Please do not hesitate to contact me if you require any further information.
We look forward to hearing the final outcome of this proposal by the
Specialty Committee in Pediatrics to the Committee on Specialties.
Yours sincerely,
Sheri Findlay, MD, FRCPC
Associate Professor Pediatrics, McMaster University
Chair, Specialty Committee in Adolescent Medicine
Royal College of Physicians and Surgeons of Canada

Division of Pediatric Critical Care Section des soins intensifs pédiatriques
Intensivists/Intensivistes
Intensivists/Intensivistes
Saleem Razack, M.D. Director/Chef de Section
Vice-Chair Education
Ronald D. Gottesman, M.D. Medical Simulation/Simulation médicale
Sam D. Shemie, M.D.
Organ Donation/Transplantation
Davinia Withington, M.D. Critical Care Anesthesiology
Soins critiques en anesthésie
Pramod Puligandla, M.D. Surgical Critical Care
Soins critiques en chirurgie
Farhan Bhanji, M.D. Emergency Medicine/Médecine d’urgence
Samara Zavalkoff, M.D.
Extracorporeal Life Support Oxygénation extracorporelle par membrane
Fellowship Training Program Programme de formation en
éducation médicale postdoctorale
Patricia Fontela, M.D., Ph.D. Critical Care Research
Recherche en soins critiques
Tanya Di Genova, M.D. Rotation Coordinator
Coordinatrice de rotations
Christos Calaritis CPC CCP FFP ECMO Coordinator
Cordonnateur d’oxygénation extracorporelle
Fellows Fawaz Alanzi, M.D.
Nada Aljassim, M.D. Mohammed Al-Mazyad, M.D.
Razan Babakr, M.D. Christina Maratta, M.D.
Allison Shevell, M.D.
Associate Members Membres associés
Franco A. Carnevale, R.N., Ph.D. Janet Rennick, R.N., Ph.D.
Matthew Park, BSW
Margaret Ruddy, N., M. Mgmt(A) Nurse manager/
Infirmière gestionnaire
Marie Antonacci, N., B.Sc.N. Assistant nurse manager/
Assistante infirmière gestionnaire
Margaret Powell, N., MEd Nurse Educator/
Infirmière éducatrice
Maryse Dagenais, N.M.Sc.(A),CNCCP(C) Linda Massé, N,MSc.N(A),LL.M.,CNCCP(C)
Advanced Practice Nurses / Conseillères en soins spécialisés
Administrative Officer 1/
Agent administratif 1 Kerry Phillips
Administrative Officer 2/ Agent administratif 2
Tel:(514) 412-4400, ext: 22696 Fax:(514) 412-4205
Soins intensifs pédiatriques Pediatric Intensive Care Adresse / Address
B 06.3718
Dr. Catherine Farrell Chair, Specialty Committee in Pediatrics The Royal College of Physicians and Surgeons of Canada September 24, 2018 Re: Proposed changes in the length of training in Pediatrics / Perspective from Critical Care Medicine Dear Dr. Farrell, As per your request to the Committee on Specialties regarding the proposed changes of the length of training in Pediatrics, the Specialty Committee in Critical Care Medicine wholeheartedly endorses this change. Our previous written and verbal communications with your committee and the COS strongly identified the benefits of removing the current overlap year that exists purely as a legacy of expediting the 3+2 years framework. Our position has maintained that residents who complete a four year General Pediatrics program are better prepared for entry into Critical Care Medicine and do not have the distraction of writing their pediatric fellowship exams during the first year of subspecialty training. We concur that with the operationalization of CBD, the General Pediatrics’ Transition to Practice phase aligns well with our entry requirements to Critical Care Medicine’s Transition to Discipline phase. Clearly this change in policy will require assurances that interested trainees will not be penalized for changing to a 4+2 years framework. The necessary CARMS training places for Critical Care Medicine would need to be maintained as would ministerial funding for the entire duration of training (6 years). With warm regards,
Ronald D. Gottesman MD,CM,FRCPC(Founder-Critical Care Medicine),FAAP,FCCM The Wendy MacDonald Chair in Pediatric Medical Education Pediatric Critical Care Medicine Professor of Pediatrics McGill University Member, McGill Centre for Medical Education

Sept 14th, 2018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Developmental Pediatrics, I would hereby like to
voice our support for the proposed changes to the training requirements in Pediatrics. As
proposed, we agree that the practice of “double-counting” be eliminated and that
subspecialty training only start after the Transition-to-Practice Entrustable Professional
Activities (EPAs) in Pediatrics have been completed. As such, all residents should be required
to complete 4 years of Pediatrics training before entering into a pediatric subspecialty
training program.
There is strong support for this from our program directors and specialty committee
representatives across Canada. However, we do think is important to highlight that paired
with this requirement of completing all EPAs in Pediatrics prior to starting subspecialty
training, that their be strong advocacy for all provincial health authorities to review and
adequately fund positions for subspecialty training to avoid any potential negative impact on
recruitment into the subspecialty positions. This is particularly relevant to the provinces of
Ontario and Quebec.
We look forward to hearing the final outcome of this proposal by the Specialty
Committee in Pediatrics to the Committee on Specialties.
Yours sincerely,
Darcy L. Fehings MD MSc FRCPC
Chair, Specialty Committee in Developmental Pediatrics
Royal College of Physicians and Surgeons of Canada

September 25, 3018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Gastroenterology, I would hereby like to voice
unanimous support from the pediatric Gastroenterology program directors for the proposed
changes to the training requirements in Pediatrics. As proposed, we unanimously agree that
the practice of “double-counting” be eliminated and that subspecialty training only start after
the Transition-to-Practice Entrustable Professional Activities (EPAs) in Pediatrics have been
completed. As such, all residents should be required to complete 4 years of Pediatrics
training before entering into a pediatric subspecialty training program.
Please do not hesitate to contact me if you require any further information.
We look forward to hearing the final outcome of this proposal by the Specialty Committee
in Pediatrics to the Committee on Specialties.
Yours sincerely,
Catharine Walsh, MD, MEd, PhD, FAAP, FRCPC Chair, Specialty Committee in Gastroenterology
Royal College of Physicians and Surgeons of Canada
Education Researcher, Learning Institute
Scientist, Research Institute
Staff Gastroenterologist, Division of Gastroenterology, Hepatology & Nutrition
Department of Paediatrics, Hospital for Sick Children
Scientist, The Wilson Centre for Research in Education
Faculty of Medicine, University of Toronto
Assistant Professor, Department of Paediatrics, Faculty of Medicine
Assistant Professor, Institute of Health Policy, Management and Evaluation
University of Toronto
Sickkids PGCRL, 686 Bay Street | Room 11.9719 | Toronto ON M5G 0A4
T: 416.818.3578 | F: 416.813.6531| E: [email protected]

September 17, 2018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Infectious Diseases, I would hereby like to
voice our support for the proposed changes to the training requirements in Pediatrics.
As proposed, we agree that the practice of “double-counting” be eliminated and that
subspecialty training only start after the Transition-to-Practice Entrustable
Professional Activities (EPAs) in Pediatrics have been completed. As such, all
residents should be required to complete 4 years of Pediatrics training before entering
into a pediatric subspecialty training program.”
Please do not hesitate to contact me if you require any further information.
We look forward to hearing the final outcome of this proposal by the
Specialty Committee in Pediatrics to the Committee on Specialties.
Yours sincerely,
Cheryl Main, MD, FRCPC
Chair, Specialty Committee in Infectious Diseases
Royal College of Physicians and Surgeons of Canada

11th September 2018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Neonatal-Perinatal Medicine, I would hereby
like to voice our support for the proposed changes to the training requirements in
Pediatrics. As proposed, we agree that the practice of “double-counting” be eliminated
and that subspecialty training only start after the Transition-to-Practice Entrustable
Professional Activities (EPAs) in Pediatrics have been completed. As such, all residents
should be required to complete 4 years of Pediatrics training before entering into a
pediatric subspecialty training program.”
Please do not hesitate to contact me if you require any further information.
We look forward to hearing the final outcome of this proposal by the
Specialty Committee in Pediatrics to the Committee on Specialties.
Yours sincerely,
Harish Amin, FRCPC
Chair, Specialty Committee in Neonatal-Perinatal Medicine
Royal College of Physicians and Surgeons of Canada

September 12, 2018
Dr. Catherine Farrell, MD, FRCPC
Chair, Specialty Committee in Pediatrics
Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Respirology, I would hereby like to voice our
support for the proposed changes to the training requirements in Pediatrics. As
proposed, we agree that the practice of “double-counting” be eliminated and that
subspecialty training only start after the Transition-to-Practice Entrustable
Professional Activities (EPAs) in Pediatrics have been completed. As such, all
residents should be required to complete 4 years of Pediatrics training before entering
into a pediatric subspecialty training program.”
Please do not hesitate to contact me if you require any further information.
We look forward to hearing the final outcome of this proposal by the
Specialty Committee in Pediatrics to the Committee on Specialties.
Yours sincerely,
Dr. Gregg Eschun
Chair, Specialty Committee in Respirology
Royal College of Physicians and Surgeons of Canada

September 25, 2018 Dr. Catherine Farrell, MD, FRCPC Chair, Specialty Committee in Pediatrics Royal College of Physicians and Surgeons of Canada
Subject: Proposed Change in Pediatrics Training
Dear Dr. Farrell,
On behalf of the Specialty Committee in Pediatric Emergency Medicine, I would hereby like to voice our support for the proposed changes to the training requirements in Pediatrics. As proposed, we agree that the practice of “double-counting” be eliminated and that subspecialty training only start after the Transition-to-Practice Entrustable Professional Activities (EPAs) in Pediatrics have been completed. As such, all residents should be required to complete 4 years of Pediatrics training before entering into a pediatric subspecialty training program.
Please do not hesitate to contact me if you require any further information. We look forward to hearing the final outcome of this proposal by the Specialty Committee in Pediatrics to the Committee on Specialties. Yours sincerely,
Tim Lynch, MD, FRCPC Chair, Specialty Committee in Pediatric Emergency Medicine Royal College of Physicians and Surgeons of Canada

1
May 14, 2018 Dr. Catherine Farrell, MD, FRCPC Chair, Specialty Committee in Pediatrics Dear Dr. Farrell, Thank you for the opportunity to participate in the dialogue on the proposed mandatory four years of training in general Pediatrics before subspecialty training. The Specialty Committee in Nephrology met on May 3, 2018 to review the proposal from the Specialty Committee in Pediatrics. As a committee with stakeholder interests in this policy, we discussed the proposal, supported by a gap analysis completed between our currently published entrustable professional activities (EPAs), milestones, and required clinical experience documents, and the draft documents that were provided from Pediatrics in your correspondence. The following is the distillation of the discussion: While the Specialty Committee in Nephrology appreciates that some subspecialties are accepting of mandated four years of Pediatrics training before entering subspecialty training, Nephrology does not believe that our prospective trainees would benefit from such a policy. This is based on two observations:
1. A gap analysis of the EPAs in Pediatrics and those in pediatric Nephrology for Core and Transition to Practice (TTP) shows that there is sufficient overlap to allow a trainee to obtain entrustment of the overlapping competencies in Pediatrics while starting their fourth year of postgraduate training in pediatric Nephrology.
2. Because the Specialty Committee in Pediatrics has not stated the timelines for Core and TTP, there is some uncertainty as to where some EPAs would fall in the timing of training. We recognize that some of the procedures that are currently listed as unique Core EPAs or as unique training experiences in Core cannot be offered in pediatric Nephrology; our committee would like to work with you to ensure that these EPAs are placed in the sequence of training so that they are completed by the end of the third year, to ensure entrustment occurs while a trainee completes Pediatrics training. Examples of this include cannulation of umbilical arteries or community-based general pediatric EPAs.

2
Ideally, the Specialty Committee in Nephrology would like to see Pediatrics move to a similar training pattern as General Internal Medicine (GIM). That is, we would like to see Pediatrics schedule TTD, Foundations and Core Pediatrics to occur in three years, with a fourth year reserved for TTP. This would also enable the examinations in Pediatrics to be completed by the end of third year, and allow trainees to enter subspecialty training unencumbered by examination preparation for Pediatrics. This would also allow Pediatric trainees to focus their final year of training on competencies necessary for TTP, unencumbered by examination preparation as well. Doing so would harmonize a process for Nephrology and pediatric Nephrology, so that adult and pediatric trainees sitting the examination in Nephrology would have equal opportunities to complete training unencumbered by parent specialty exam preparation. We do agree that those aspiring to practice some general Pediatrics post-completion of training should complete four years of general Pediatrics before entering subspecialty training. Similarly, those who wish to moonlight during subspecialty training should complete four years of general Pediatrics before entering subspecialty residency. However, we note that greater than 95 percent of practicing pediatric Nephrologists in Canada are practicing in academic centers with no general Pediatric practice as a component of their daily work, so practically, we would not encourage individuals aspiring to academic Nephrology careers to complete four years of Pediatrics training. Additionally, The Specialty Committee in Nephrology felt that there is sufficient uncertainty in the current funding model that a required fourth year in Pediatrics (i.e.: three plus two model) could have negative effects on the ability to secure adequate funding from the provincial Ministries of Health (MOH) if there was a mandated fourth year of pediatrics (i.e.: four plus two model). We do not believe that the provincial MOHs will be willing to increase education budgets to accommodate an additional year of training. We are grateful for the opportunity to participate in the consultation process on a mandatory fourth year of training in Pediatrics and welcome the discussion of the impact on examination placement and transition to subspecialty training. We hope that this synopsis of the Specialty Committee in Nephrology discussion is helpful in moving forward to a decision on this matter. Sincerely, Maury Pinsk, MD, FRCPC Chair, Specialty Committee in Nephrology On behalf on the Specialty Committee in Nephrology CC: Dr. Jason Frank, MD, FRCPC, director, Specialty Education, Strategy and Standards The Royal College of Physicians and Surgeons of Canada
Dr. Farhan Bhanji, MD, FRCPC, associate director, Assessment The Royal College of Physicians and Surgeons of Canada




















