
Religiosity and treatment response to antidepressant medication: a prospective multi-site clinical...
16
Religiosity and treatment response to antidepressant medication: A prospective multi-site clinical trial Jonathan R. Schettino a , Natasha T. Olmos a , Hector F. Myers a,* , Nataria T. Joseph a , Russell E. Poland b , and Ira M. Lesser c a Department of Psychology, University of California at Los Angeles, Los Angeles, CA, USA b Cedars Sinai Medical Center, Los Angeles, CA, USA and Meharry Medical Center, Nashville, TN, USA c Harbor-UCLA Medical Center, Torrance, USA and the Los Angeles Biomedical Research Institute, Torrance, USA Abstract The present study examined the relationship between religiosity/spirituality and treatment response to antidepressant medication (citalopram). One-hundred and forty-eight Caucasian and African-American adults with uncomplicated major depression were treated with citalopram (20– 60mg/day) over an 8-week period in a prospective multi-site clinical trial. Treatment response was assessed weekly with the Hamilton Rating Scale for Depression. Religiosity (i.e., religious behaviours) and spirituality (i.e., spiritual well-being) were assessed at Week 3. No significant associations between spirituality and treatment response were found; however, there was a strong curvilinear relationship between religiosity and treatment response. Compared to lower or higher levels of religiosity, a moderate level of religiosity was significantly associated with a higher likelihood of remission and greater reduction in severity of depression. This association was independent of social support, ethnicity, gender, education, and baseline depression severity. A moderate amount of religiosity appears to be independently associated with an enhanced treatment response to citalopram. Keywords religiosity; spirituality; depression; antidepressant; citalopram Introduction Over the past two decades, the relationship between religiosity, spirituality 1 and mental health has become an increasingly important topic of scientific inquiry. Specifically, * Correspondence concerning this manuscript should be addressed to Hector F. Myers, Ph.D., Department of Psychology, UCLA, 1285 Franz Hall, Los Angeles, CA 90095-1563, [email protected], Tel: 310.825.1813. Jonathan R. Schettino, Department of Psychology, University of California, Los Angeles 1285 Franz Hall, Los Angeles, CA 90095-1563, [email protected] Natasha T. Olmos, Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Los Angeles, CA 90095-1563, [email protected] Hector F. Myers, Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Los Angeles, CA 90095-1563, [email protected] Nataria T. Joseph, Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Los Angeles, CA 90095-1563, [email protected] Russell E. Poland, Meharry Medical College, 1005 Dr. D.B. Todd Jr. Blvd., Nashville, TN 37208, [email protected] Ira M. Lesser, Department of Psychiatry, Harbor-UCLA Medical Center, Box 8, 1000 W. Carson Street, Torrance, CA 90509, [email protected] NIH Public Access Author Manuscript Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21. Published in final edited form as: Ment Health Relig Cult. 2011 January 1; 14(8): 805–818. doi:10.1080/13674676.2010.527931. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Religiosity and treatment response to antidepressant medication: a prospective multi-site clinical...

Religiosity and treatment response to antidepressantmedication: A prospective multi-site clinical trial
Jonathan R. Schettinoa, Natasha T. Olmosa, Hector F. Myersa,*, Nataria T. Josepha, RussellE. Polandb, and Ira M. Lesserc
aDepartment of Psychology, University of California at Los Angeles, Los Angeles, CA, USAbCedars Sinai Medical Center, Los Angeles, CA, USA and Meharry Medical Center, Nashville,TN, USAcHarbor-UCLA Medical Center, Torrance, USA and the Los Angeles Biomedical ResearchInstitute, Torrance, USA
AbstractThe present study examined the relationship between religiosity/spirituality and treatmentresponse to antidepressant medication (citalopram). One-hundred and forty-eight Caucasian andAfrican-American adults with uncomplicated major depression were treated with citalopram (20–60mg/day) over an 8-week period in a prospective multi-site clinical trial. Treatment response wasassessed weekly with the Hamilton Rating Scale for Depression. Religiosity (i.e., religiousbehaviours) and spirituality (i.e., spiritual well-being) were assessed at Week 3. No significantassociations between spirituality and treatment response were found; however, there was a strongcurvilinear relationship between religiosity and treatment response. Compared to lower or higherlevels of religiosity, a moderate level of religiosity was significantly associated with a higherlikelihood of remission and greater reduction in severity of depression. This association wasindependent of social support, ethnicity, gender, education, and baseline depression severity. Amoderate amount of religiosity appears to be independently associated with an enhanced treatmentresponse to citalopram.
Keywordsreligiosity; spirituality; depression; antidepressant; citalopram
IntroductionOver the past two decades, the relationship between religiosity, spirituality1 and mentalhealth has become an increasingly important topic of scientific inquiry. Specifically,
*Correspondence concerning this manuscript should be addressed to Hector F. Myers, Ph.D., Department of Psychology, UCLA, 1285Franz Hall, Los Angeles, CA 90095-1563, [email protected], Tel: 310.825.1813.Jonathan R. Schettino, Department of Psychology, University of California, Los Angeles 1285 Franz Hall, Los Angeles, CA90095-1563, [email protected] T. Olmos, Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Los Angeles, CA 90095-1563,[email protected] F. Myers, Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Los Angeles, CA 90095-1563,[email protected] T. Joseph, Department of Psychology, University of California, Los Angeles, 1285 Franz Hall, Los Angeles, CA 90095-1563,[email protected] E. Poland, Meharry Medical College, 1005 Dr. D.B. Todd Jr. Blvd., Nashville, TN 37208, [email protected] M. Lesser, Department of Psychiatry, Harbor-UCLA Medical Center, Box 8, 1000 W. Carson Street, Torrance, CA 90509,[email protected]
NIH Public AccessAuthor ManuscriptMent Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
Published in final edited form as:Ment Health Relig Cult. 2011 January 1; 14(8): 805–818. doi:10.1080/13674676.2010.527931.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
researchers have examined whether religiosity and spirituality enhance psychologicalresilience under high stress and whether either serve to protect against the onset ofpsychiatric disorders or facilitate recovery from these disorders. Although findings aremixed, evidence has begun to emerge suggesting that religiosity and spirituality mightpromote mental health by protecting against the onset of depression in populationscontending with both acute and chronic stressors (see Idler et al. 2003 for review; Smith,McCullough & Poll, 2003).
In studies of heart surgery patients, patients diagnosed with a terminal illness, men withsevere disabilities, recent widowers, and parents who had lost a child, those with spiritualresources had lower levels of depression than those without such resources (Ai, Dunkle,Peterson, & Bolling., 1998; Nelson, Rosenfeld, Breitbart & Galietta, 2002; Idler & Kasl,1992; Siegel & Kuykendall, 1990; McIntosh, Silver & Wortman, 1993). Additionally, in alarge community sample of older adults, greater religiosity was associated with lower levelsof depression (Roff, Kelmmack, Parker, et al., 2004). Husaini, Baqar & Miller (1999) founda similar negative association between religiosity and levels of depression in older adults,but this relationship was fully mediated by social support. In addition, several systematicreviews of the literature have concluded that religiosity and spirituality measured in variousways are reliably associated with lower levels of depression, at least in cross-sectionalanalysis (McCullough & Larson, 1999; Koenig, McCullough & Larson, 2001). Finally, in alarge meta-analysis (174 studies, N = 98,975), religiosity/spirituality was modestly, butreliably associated with lower severity of depressive symptoms (omnibus effect size = −.096) (Smith, McCullough & Poll, 2003).
A comparatively small body of research has examined the roles that religiosity andspirituality play in recovery from depression. In a sample of elderly individuals (N = 177),the relative importance of religion in one’s life (i.e., religious salience) was positivelyassociated with improvement of depression over a 1 year period for those who wereclinically depressed at baseline (Braam, Beekman, Deeg, Smit & van Tilburg, 1997). In a48-week longitudinal study with medically-ill, older patients (N = 94), intrinsic religiosity(i.e., the degree to which one believes that their religiousness has value in and of itself)(Allport & Ross, 1967), but not religious behaviours (e.g., church attendance, prayer), waspredictive of more rapid remission of depression (Koenig, George & Peterson, 1998). Intheir sample, every 10-point increase in intrinsic religiosity was associated with a 70%increase in speed of remission. These results were independent of quality of life, change infunctional status during follow-up, family psychiatric history, number of medical diagnoses,social support, and treatment with antidepressant medication. Based on the results of thesestudies, the association between religiosity, spirituality and improvement of depressionmight depend in part on the operational definition of these constructs and the characteristicsof the population being studied, but overall, evidence suggests that both resources mightpromote improvement.
Although the evidence for an association between religiosity, spirituality and lower levels ofdepression is compelling, there is a dearth of research examining potential mediators of thisrelationship. Many theorists have advanced social support as a mechanism that might be aprimary mediator of the relationship between religiosity, spirituality, and mental healthoutcomes (Joiner, Perez & Walker, 2002). Social support is known to have a positiveinfluence on psychological well-being (Cohen & Wills, 1985) and many individuals might
1Researchers have yet to agree upon standard operational definitions for the constructs of religiosity and spirituality and there is stillsome debate as to whether these are distinct or overlapping constructs (Hall, Meador & Koenig, 2008). In order to avoid confusion inthis paper, religiosity is being defined here as behaviours and practices associated with religion (e.g., prayer, church attendance, etc.)and spirituality is being defined here as the existential aspects of religion (e.g., spiritual beliefs, faith, spiritual well-being).
Schettino et al. Page 2
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

access this resource through religious involvement. Most major world religions promotepro-social behaviour and the cultivation of harmonious, supportive relationships with others(Roberts & Robins, 200; Saroglou et al., 2004). In addition to religious doctrines thatencourage supportive relationships, religion might provide direct access to social support viathe local religious congregation. For example, the local congregation often providesfellowship opportunities for believers and might serve as a source of emotional andinstrumental social support in times of hardship. In the case of the major organized religions,the faithful are given access to a vast, sometimes international, network of individuals whoshare a world-view, have similar values, and could potentially provide support (see Hill &Pargament, 2003 for a review). Although, social support appears to be an importantmediator between religiosity, spirituality and psychological adjustment, these resourcesmight still have salutary effects even when social support is controlled (Levin, Markides &Rav, 1996).
The relationship between religiosity, spirituality and depression might be moderated byethnicity. It is well-attested in the literature that African-Americans tend to be morereligiously active than Caucasian-Americans (Ellison, 1995). Indeed, some researchsuggests that the relationship between religiosity, spirituality and lower levels of depressionmight be stronger for African-Americans than Caucasian-Americans (Musick, Koenig, Hays& Cohen, 1998); however, a large meta-analysis of the literature linking religiosity andspirituality to depression failed to find significant moderation of this relationship byethnicity (Smith, McCullough & Poll, 2003). If ethnicity does moderate this relationship,perhaps the observed moderation is the result of between-group differences in the practice ofcertain salutary religious behaviours or differential exposure to spiritual beliefs that mightserve as a protective factor against depression.
The empirical evidence suggests that religiosity and spirituality have a robust cross-sectionalassociation with lower levels of depression and these resources might also play a role inspeeding up recovery from depression. Additionally, these relationships are likely to be atleast partially mediated by social support and might be moderated by ethnicity (Caucasian-Americans as compared to African-Americans). However, surprisingly little is known aboutwhether and how religiosity and spirituality might affect treatment response toantidepressant medication. In fact, to our knowledge, there are no studies that have directlyexamined whether religiosity and/or spirituality are associated with the effectiveness ofpharmacotherapy for depression. Since religiosity/spirituality are important coping resourcesfor a large percentage of Americans (see Idler et al. 2003 for a review), it is important tounderstand whether and how these resources might enhance or interfere with the efficacy ofantidepressant medication.
The purpose of the present study is to investigate whether spirituality and/or religiosity areassociated with treatment response to an antidepressant medication (citalopram; CIT) inCaucasian-Americans and African-Americans who were enrolled in a highly structured 8-week clinical trial. We hypothesized, consistent with the evidence of the salutary effects ofreligiosity and spirituality, that both will be associated with better response to CIT (e.g.,greater reduction in the severity of depression symptoms and higher rates of remission).Additionally, since research has demonstrated that increased access to social support mightbe one mechanism through which religiosity and spirituality affect mental health outcomes(see Hill & Pargament, 2003 for review; Husaini, Baqar & Miller, 1999), we alsohypothesized that the relationship between religiosity/spirituality and treatment responsewill be at least partially mediated by social support. Finally, because there is some evidencethat African-Americans and Caucasian-Americans respond differently to antidepressantmedication (Lin, Poland & Nakasaki, 1993) and the literature suggests that these two mightdiffer in the salience of spirituality and the frequency of certain religious behaviours, we
Schettino et al. Page 3
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

explored whether ethnicity moderates the relationship between religiosity, spirituality andtreatment response.
MethodsParticipants
The present study uses a sub-sample of African-American and Caucasian-American adultswith non-psychotic major depressive disorder who enrolled in a multi-site, non-randomizedclinical trial of CIT and were part of the intent-to-treat group (i.e. participants who returnedfor the screening visit, and received at least one dose of medicine). The purpose of the mainclinical trial was to examine whether there were significant ethnic differences in treatmentresponse to CIT. The sub-sample used in the present study (N = 148) consists of only thoseparticipants from the intent-to-treat group of the main trial who completed the religiosity andspirituality inventories. Participants in the main trial were recruited at each of three mentalhealth clinics enrolling treatment seeking patients as well as those responding toadvertisements. To qualify, participants had to: be men and women between 18 – 70 years ofage; self-identified as African-American or Caucasian-Americans, and report that both oftheir parents and all four of their grandparents also self-identified with the same ethnicgroup; meet DSM-IV criteria for current major depression; have a Hamilton Rating Scale ofDepression (21-item HRDS) (Hamilton, 1960) score of ≥ 17; if of child-bearing potential,women agreed to use effective contraception; and were capable of giving written informedconsent.
Additionally, prospective participants were excluded if they reported: a current or lifetimediagnosis of schizophrenia, schizophreniform or schizoaffective disorder, psychoticdepression or bipolar disorder; current drug or alcohol abuse or dependence or history ofdrug or alcohol abuse or dependence within the past 6 months; unstable medical orneurological conditions that were likely to interfere with the treatment of depression; historyof allergic reaction to CIT; history of failure of response to CIT, as documented by anadequate trial of the medication defined as having been treated with the medication at a doselevel of at least 40 mg of CIT per day for at least 6 weeks; history of or current seizuredisorder; pregnancy or breast-feeding; currently on psychotropic medications includingantidepressants, antipsychotics, benzodiazepines, or opiates; treatment with fluoxetine orMAOIs in the previous two months; active suicidal ideation of at least a moderate degree, orother safety issues determined by the clinician to not be suitable for inclusion in the study;or currently receiving ongoing psychotherapy.
More than 1000 potential subjects were screened by telephone or face-to-face interview forthe main clinical trial and a total of 327 subjects were enrolled, including 184 AfricanAmericans and 143 Caucasians-Americans. The most likely reasons for non-enrolmentwere: not meeting criteria for major depression; reported significant substance abuse; takingmedication not allowed by the protocol; did not want to enrol in a clinical trial; were ofmixed race. The intent to treat group consisted of 301 participants: 168 African-Americansand 133 Caucasian-Americans.
The sub-sample used in the present study consisted of only those participants from theintent-to-treat group who completed both the religiosity and spirituality measures (N = 148)(mean age = 43, SD = 10.7). The sub-sample was predominantly female (64%), African-American (64%), unmarried/not cohabitating (79%), reasonably well-educated (mean yearsof education = 14, SD = 2.4) and approximately half were employed. Compared to thosewho did not complete the religiosity and spirituality inventories, those who did weresignificantly more likely to be African-American, more likely to be living with a significantother, and more likely to receive dose escalations of CIT during the clinical trial.
Schettino et al. Page 4
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

ProceduresAfter describing the study to the participants, written informed consent was obtained.Demographic information, medical and psychiatric history, and physical examination andlaboratory tests (complete blood counts, EKG, thyroid and liver function tests, pregnancytest (when appropriate), and urine toxicology screen were obtained at screening. Psychiatricdiagnoses were obtained by clinically-trained interviewers using the Structured ClinicalInterview for DSM-IV Disorders (SCID) (First, Spitzer, Gibbon & Williams, 1995).
After screening, participants returned for a baseline visit which included a comprehensivebattery of clinical and psychosocial measures administered by trained staff in face-to-faceprivate interviews. Severity of depression was assessed at baseline and at weekly intervalsthroughout the study using the HRSD (Hamilton, 1960). All participants were placed on aplacebo for a one week “washout” period following the baseline assessment and then wereplaced on CIT for 8 weeks. A placebo control group was not included here, because thepurpose of the main trial was to investigate possible ethnic differences in response to CITdue to genetic and/or psychosocial factors, not to determine the efficacy of CIT in thetreatment of depression. The effectiveness of CIT has been consistently demonstrated inprevious research (see Keller, 2000 for a review).
All participants received an initial dose of 20 mg/day of CIT, which could be increased to 40mg at week 4 and to 60 mg/day at week 7 if there was lack of efficacy and tolerable sideeffects. Participants remained free of non-study psychoactive medication throughout the trialexcept for zolpidem 5 mg, which could be prescribed occasionally for insomnia (not toexceed 2 nights per week). To monitor compliance with the protocol, pill counts were madeat each visit. Participants were compensated up to $320, with the amount of pay prorated bynumber of sessions attended.
MeasuresSpirituality—Spirituality (i.e., spiritual well-being) was assessed during week 3 of thestudy using the Religious Well-being subscale of the SWB (Paloutzian & Ellison, 1982).This scale consists of 10 items that assess the perceived quality of one’s relationship withGod/Higher Being. The items are scored on a 6-point Likert-type scale from “stronglydisagree” to “strongly agree”, and scores range from 10 – 60. Factor analyses of thismeasure identify two distinct, but highly correlated factors (affiliation with God/HigherBeing and alienation from God/Higher Being) (Scott, Agresti & Fitchett, 1998). Theaffiliation items assess one’s perceived positive relationship with God/Higher Being (e.g., Ibelieve that God/Higher Being loves me and cares about me). The alienation items assessone’s perceived distance from God/Higher Being (e.g., I believe that God/Higher Being isimpersonal and is not interested in my daily situations). Since these factors were negativelycorrelated in the current sample (r = −.68), a reliable (Cronbach α =.95) sum score wascalculated by adding the total score on the affiliation items to the reverse-coded total scoreof the alienation items.
Religiosity—Religiosity (i.e., religious behaviours) was assessed at week 3 of the studyusing The Personal Faith subscale of the Religious Involvement Inventory (RII) (Hilty,Morgan & Burns, 1984). This scale consists of 5 items that assess the frequency with whichparticipants engage in religious practices (e.g., prayer, attending worship services, etc.). Theitems are rated on a 4-point Likert-type scale from “seldom/never” to “regularly”, and yieldsa reliable sum score (Cronbach α = .86) that ranges from 5 – 20.
Social Support—Social support was measured at baseline and post-treatment using ashort (5-item) version of a social support scale used by Vinokur and Vinokur-Kaplan (1990),
Schettino et al. Page 5
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
which was adapted from a scale developed by Abbey, Abramis, and Caplan (1985).Participants were asked to list the 4 most important people to them and to rate each on a 5-point scale (1 = not at all to 5 = a great deal) on the degree to which they received each ofthe following 5 aspects of social support: giving useful information or advice, listening,showing care, providing help with specific problems, and providing needed resources. Theresponses were summed to create a reliable composite score (Cronbach α = .90).
Depression—Severity of depression was the primary outcome and was assessed eachweek using the Hamilton Rating Scale for Depression (HRSD) (Hamilton, 1960). This is awidely used interview measure completed by clinically-trained interviewers who receivedstandardized training and rated participants on a 24-item version of the measure. Only thecore 17 items that were common across study sites were used in the analyses. Item ratingscales are based on either a 3 or 5 point Likert scale, with a rating of 0 indicating that thesymptom is absent or within normal limits and the highest rating indicating that thesymptom is present and severe. Ratings were summed to form a composite score. Cronbachalpha and inter-rater reliability have been found to be within appropriate range (e.g.,Cronbach α = .82). For purpose of analysis, an HRSD change score (HRSD at their last visit– pre-treatment HRSD) was calculated.
Data AnalysisAll data were verified and screened for outliers. In order to identify possible covariates, aseries of ANOVA and Pearson Correlation analyses were conducted to determine whetherdemographic and medical/psychiatric history variables co-varied with religiosity orspirituality and the treatment outcome measures. No covariates were identified; thus thefindings reported below are independent of age, gender, ethnicity, SES (e.g., employmentstatus, years of education), history of diagnosed physical or psychiatric illness, currentphysical or psychiatric illness, severity of depression at study entry, final dose of CIT, andrate of attrition from the study.
ResultsSpirituality Predicting Treatment Outcomes
The SWB, our measure of spirituality, was administered to 148 participants (M = 41.2, SD =15.45). A linear regression revealed that spirituality did not significantly predict reduction inseverity of depression (i.e., change in HRSD score from pre-treatment to post-treatment) (R2
= .001, β = −.038, p = .639). Binary logistic regressions revealed that spirituality was not asignificant predictor of being a treatment responder (i.e., HRSD pre-post change greater than50%) (B = .014, Exp(B) = 1.014, p = .195) or a remitter (i.e., post-treatment HRSD score ≤7) (B = .019, Exp(B) = 1.019, p = .074).
SWB was converted into tertiles to test for a possible curvilinear relationship with treatmentresponse, but no significant curvilinear relationship was obtained. Transformations alsowere attempted to see if alternative ways of measuring spirituality made relationshipsbetween SWB and treatment response more apparent, but none of these transformationsresulted in any significant results. Therefore, spirituality appears to have no directrelationship with any of the treatment outcomes studied in this sample.
Religiosity Predicting Treatment OutcomesThe RII, our measure of religiosity, was administered to 148 participants (M = 11.9, SD =4.44). A linear regression revealed that there was no significant linear relationship betweenreligiosity and reduction in severity of depression (R2 = .011, β = −.103, p = .212). Binarylogistic regressions revealed that religiosity was not a significant predictor of either being a
Schettino et al. Page 6
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

treatment responder (B = .065, Exp(B) = 1.068, p = .112) or a remitter (B = .058, Exp(B) =1.060, p = .131).
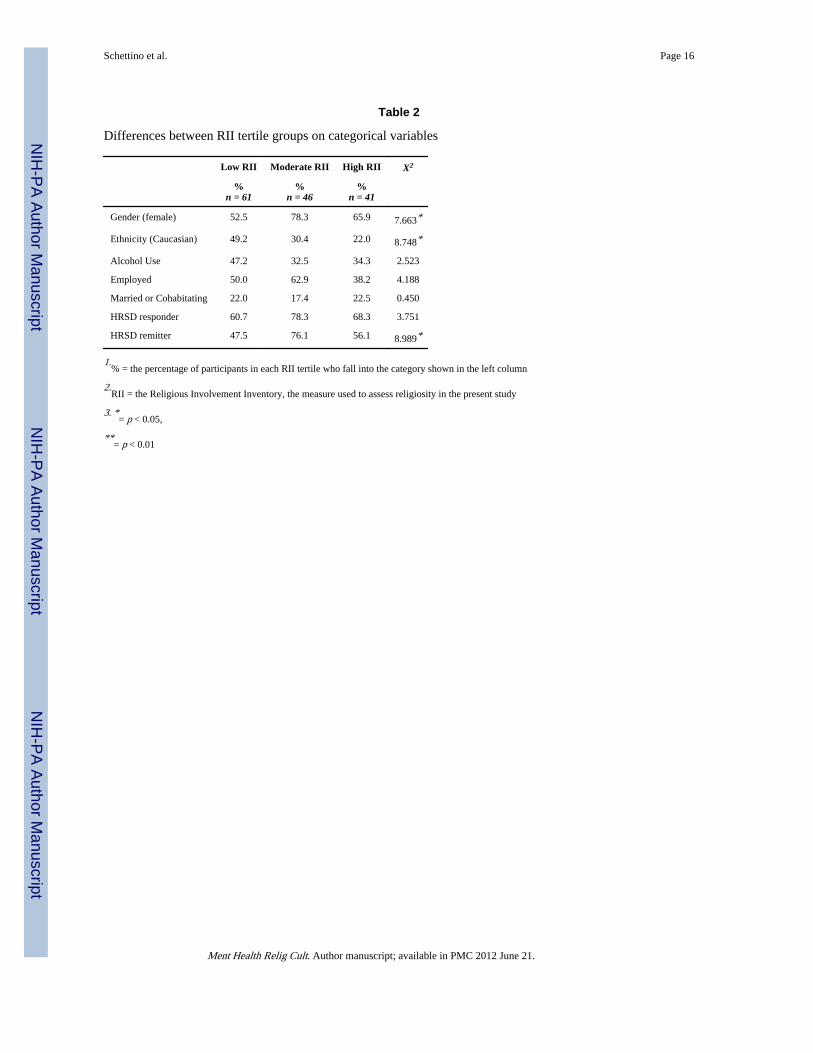
However, when RII was converted into a categorical variable by dividing its scores intotertiles, significant relationships were found between religiosity and the outcomes. Aunivariate ANOVA revealed that religiosity tertile was significantly associated withreduction in severity of depression (F(2, 145) = 5.483, p = .005, R2 = .07). Chi-square testsrevealed that religiosity tertile was also significantly associated with remission (X2(2, N =148) = 8.989, p = .011), but not with being a treatment responder (X2(2, N = 148) = 3.751, p= .153). For more detailed information on the relationship between religiosity tertile anddemographic, psychosocial, and outcome variables see Tables 1 and 2.
Post-hoc analyses revealed that participants who were in the middle tertile for religiosityevidenced significantly greater reduction in severity of depression than in participants inboth the lower tertile (t(105) = −3.204, p = .002) and the higher tertile (t(85) = −2.200, p = .031) (see Figure 1). This indicates that the relationship between religiosity and reduction inseverity of depression is curvilinear, which was partially supported by the results of aquadratic regression which yielded a marginally significant curvilinear relationship (R2 = .037, F(2, 145) = 2.808, p = .064).
Post-hoc analyses revealed that participants who were in the middle tertile for religiositywere also significantly more likely to remit than participants in the lower tertile (X2(1, N =107) = 8.890, p = .003) and the higher tertile (X2(1, N = 87) = 3.898, p = .048) (see Figure2).
When religiosity was coded as a dummy variable with two levels (“membership in themiddle tertile” and “membership in the other tertiles”), binary logistic regressions revealedthat participants who scored in the middle tertile had approximately 3 times greater odds ofremitting than participants in the other tertiles (B = 1.118, Exp(B) = 3.059, p = .005).Additionally, individuals who were in the middle tertile were 50% more likely to remit thanindividuals in the other tertiles. Finally, membership in the middle tertile accounted forapproximately 7% of the variance in pre-post HRSD change (R2 = .066, β = −.257, p = .000).
Analysis of MediationAnalyses were conducted to test whether the relationship between religiosity and theoutcome measures was mediated by social support. In order to test the first step of mediationas established by Baron & Kenney (1986), univariate ANOVA analyses were conducted todetermine whether religiosity, as categorized using the aforementioned tertile procedure,was significantly associated with social support. Results showed that religiosity was notsignificantly associated with social support measured at baseline or post-treatment (F(2,140) = 0.817, p = .444; F(2, 111) = 2.488, p = .088); therefore, social support does notmediate the relationship between religiosity and treatment response.
Analysis of Ethnicity as a Possible ModeratorWe found no ethnic differences (African-American vs. Caucasian-American) in any of theindicators of treatment response to antidepressant medication in our sample as reported inthe main trial (Lesser et al., 2010). However, since religiosity was significantly associatedwith ethnicity in the present study (See Table 2), and some research has shown that ethnicitymight moderate the association between religiosity and depression (Musick, Koenig, Hays &Cohen, 1998), we explored whether ethnicity moderated the relationship between religiosityand treatment response to CIT. A univariate ANOVA revealed that ethnicity was not asignificant moderator of the relationship between religiosity and reduction in severity of
Schettino et al. Page 7
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
depression, F(2, 143) = 0.189, p = .828. A series of Chi-Square tests also revealed thatethnicity was not significantly associated with treatment response in either the lowest RIItertile (X 2(1, N = 61) = .794, p = .373), the middle RII tertile (X2(1, N = 46) = 3.111, p = .078, or the highest RII tertile (X2(1, N = 41) = .523, p = .470). Therefore, ethnicity was not asignificant moderator of the relationship between religiosity and overall treatment responsein our sample.
We also tested whether ethnicity moderated the relationship between spirituality andtreatment response by testing the interaction term (spirituality × ethnicity) using linearregression. Results from this analysis revealed that spirituality × ethnicity was notsignificantly associated with HRSD change after controlling for the independent effects ofspirituality and ethnicity, R2 = .004, β = .299, p = .437. Thus, regardless of how it wastested, ethnicity did not moderate the relationship between spirituality and treatmentresponse.
DiscussionThese results show mixed support for our hypotheses. Contrary to expectations, spirituality(i.e., spiritual well-being) was not significantly associated with pre-post reduction in severityof depression, remission from depression or with significant treatment response (≥ 50%reduction in HRSD score). Therefore, level of spirituality was not significantly associatedwith treatment response to antidepressant medication in this sample.
On the other hand, religiosity was significantly associated with treatment response in thissample; however, this relationship was more complex than we initially hypothesized.Contrary to the linear relationship that we predicted, we found a curvilinear relationshipbetween these two variables. That is, participants in the study who had moderate levels ofreligiosity responded significantly better to treatment than those who had either lower orhigher levels of religiosity. Specifically, participants who had moderate levels of religiositywere significantly more likely to remit by the end of the clinical trial (50% more likely inthis sample) and evidenced significantly greater reduction in severity of their depression,with religiosity accounting for 7% of the variance. This strong relationship appears to beindependent of baseline severity of depression, final CIT dose, rate of attrition from study,age, gender, ethnicity, and SES. In addition, ethnicity (African-American vs. Caucasian-American) did not moderate the association between religiosity and treatment response toantidepressant medication in our sample which is consistent with evidence suggesting thatethnicity also does not moderate the relationship between religiosity/spirituality and severityof depression (Smith, McCullough & Poll, 2003). Finally, and contrary to expectation, socialsupport did not mediate this relationship.
Based on the results of this study, it appears that engaging in a moderate amount of religiousbehaviour might be associated with an enhanced treatment response to antidepressantmedication. Some researchers posit that religiosity might have positive effects on mentalhealth outcomes because it is associated with increased access to social support andexposure to spiritual beliefs that aid in benefit finding and positive reappraisal coping (Hill& Pargament, 2003); however, religiosity does not appear to be operating through these twomechanisms because religiosity was not associated with social support and spiritual-well-being was not associated with the treatment outcomes in this study. Perhaps religiosity aidsin treatment response by increasing behavioural activation and/or providing additionalmeans (e.g., prayer, meditation, worship service attendance, etc) to cope with negative moodstates. Additionally, some religious practices, such as meditation or prayer, might directlyaid in stress reduction by eliciting the “relaxation” response, which is antagonistic to thestress response of the hypothalamic-pituitary-adrenal (HPA) axis (Delmonte, 1985; Ai et al.,
Schettino et al. Page 8
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

1998). Finally, individuals who are more religious might have greater expectancy thatmedical treatment, including treatment with antidepressants, will be more effective (e.g., abelief that God is working through the medication).
If this finding is replicated, it raises the question as to why a moderate level of religiosity isassociated with an enhanced treatment response, but higher or lower levels provide noadditive benefit. Since this is the first study of its kind, the literature does not offer a directanswer to this question. We propose two non-mutually exclusive explanations for thisrelationship.
First, it might be that a greater percentage of participants who reported a higher level ofreligiosity also belong to religious traditions that passively or actively discourage medicaltreatments for depression. Thus, these participants might not have derived additionalbenefits from religious practice because practice itself might expose them to informationabout their disorder that conflicts with information they receive from their healthcareproviders and thereby reduce their expectation that the treatment will be effective and/orelicit feelings of guilt or shame about treating their depression with medication. Forexample, individuals in the higher religiosity group might be more likely to belong totraditions that believe that depression is a “spiritual” disease as opposed to a psychologicaldisorder. In the Apostle Paul’s epistle to the Galatians, he writes that “joy” is one indicatorof spiritual health (Galatians 5:19–23, New King James Version). Thus, adherents toreligious traditions that interpret this or similar passages literally might believe that theabsence of joy (i.e., depression) is an indicator of their “spiritual deficiency” and this beliefmight promote negative affective states. Unfortunately, this hypothesis could not be testedhere, because data on participants’ religious beliefs related to depression and religiousdenomination membership were not collected.
Alternatively, it could be that many individuals who reported higher religiosity in this studymight only exhibit high religiosity during times of stress, but return to a low baseline ofreligious activity after the stress has abated. Thus, these individuals might appear to behighly religious in a cross-sectional design; however, longitudinal research designs wouldreveal that these individuals exhibit low stable levels of religiosity. Gall, Kristjannson,Charbonneau & Florack (2009) argue that individuals who exhibit this pattern might notderive benefits from religiosity, because their religious resources are only utilized duringtimes of stress, and are consequently not developed enough to effectively cope with stressorswhen they arise. In a study of women undergoing biopsies for breast cancer with low pre-morbid spiritual salience, they found that activation of spiritual resources post-diagnosispredicted poorer psychological adjustment 6 months later. Based on these results, they arguethat mobilization of spiritual resources to cope with a stressor might only be effective if anindividual maintains high levels of religious/spiritual salience in the absence of stress.Therefore, it is possible that the higher religiosity group failed to exhibit an enhancedresponse to treatment because many individuals in this group might have been attempting toactivate religious resources that were underdeveloped and ineffective due to infrequent use.Of course, this hypothesis rests upon the assumption that individuals who fit this religiousprofile are over-represented in the higher religiosity group. Unfortunately, since religiositywas assessed cross-sectionally in this study, we are unable to test this assumption becausewe cannot distinguish between individuals who exhibit high temporary religiosity and thosewho exhibit high stable levels of religiosity.
Another surprising finding was the lack of an association between scores on the SWB (ourmeasure of spirituality) and treatment response to antidepressant medication; however, thisfinding does not necessarily mean that spirituality has no association with treatmentresponse. The SWB assesses only one dimension of spirituality (the quality of one’s
Schettino et al. Page 9
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
relationship with God/Higher Being). Although relationship with and attachment to God/Higher Being has been found to be associated with health (see Hill & Pargament, 2003 for areview), it is possible that this dimension of spirituality is not as relevant to pharmacologicaltreatment response as some other dimensions might be (e.g., spiritual meaning and purpose,health-related faith, etc.). Thus, if a comprehensive, multi-dimensional measure ofspirituality were used, an association between some facet of spirituality and treatmentresponse might have been obtained.
Although the results of this study are suggestive, there are several limitations that areimportant to note. First, because religiosity was assessed cross-sectionally and was notmanipulated in this design, we cannot make conclusions about causal relationships. Thus,we can only claim that a moderate amount of religiosity appears to be associated with anenhanced response to antidepressant medication. Second, religiosity was assessed at week 3instead of at baseline; this methodological limitation introduces the possibility that treatmentresponse might have affected religious behaviour rather than the converse. Third, since thisstudy did not include a placebo control group, it is possible, though unlikely, that theobserved “treatment response” (e.g., reduction in symptoms, remission) was not due totreatment with CIT, but to some unknown third variable (e.g., spontaneous recovery). Inaddition, because the study did not include a placebo control group, we cannot conclusivelydetermine from our data whether religiosity is specifically associated with improvedresponse to antidepressant medication or just generally associated with improved recoveryfrom depression. Fourth, since only African-Americans and Caucasians were recruited inthis study, it is unknown whether these results will generalize to other ethnic groups. Fifth,the relatively small sample size might have limited power to detect some effects. Finally,since this is the first study to examine the relationship between religiosity, spirituality andtreatment response to antidepressant medication, our findings should be replicated beforefirm conclusions are made from these results.
In conclusion, a moderate amount of religiosity appears to be associated with improvedtreatment response to antidepressant medication. The results of the present study highlightthe importance of understanding religiosity within the context of treatment for depression. Ifreplicated, these findings could have important implications for clinical practice. Forexample, clinicians could assess patients’ religiosity prior to prescribing antidepressantmedication and address religious concerns that might interfere with treatment or promotepre-existing religious behaviour that might benefit treatment. Additional research is alsoneeded to identify some of the biological and psychosocial mechanisms that mediate ormoderate this relationship. In future research, religiosity should be assessed longitudinally todetermine the direction of causality and to distinguish the effect of acutely activatedreligiosity (i.e., increase in religious behaviour in response to a crisis) from stable religiosity(i.e. regular religious practices). It is also recommended that researchers employ multi-dimensional measures of religiosity/spirituality to more accurately pinpoint the specificdimensions of religiosity/spirituality that have the strongest associations with treatmentresponse. Finally, additional studies are needed to investigate whether religiosity/spiritualityenhances or interferes with treatment response to psychotherapy for depression.
AcknowledgmentsThe authors would like to acknowledge with appreciation the significant contributions of the research staff andclinical research coordinator staff at each of the three study sites, as well as all of the patients who participated inthe trial. The study is registered on ClinicalTrials.gov (ID# NCT00047671) and was supported by NIMH GrantsR01MH62675, R01MH62676, R01MH62677, and M01RR00425.
Schettino et al. Page 10
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
ReferencesAbbey A, Abramis DJ, Caplan RD. Effects of difference sources of social support and social conflict
on emotional well-being. Basic and Applied Social Psychology. 1985; 6(2):111–129.
Ai AL, Dunkle RE, Peterson C, Bolling SF. The role of private prayer in psychological recoveryamong midlife and aged patients following cardiac surgery. Gerontologist. 1998; 38(5):591–601.[PubMed: 9803647]
Allport GW, Ross JM. Personal religious orientation and prejudice. Journal of Personality and SocialPsychology. 1967; 5:432–443. [PubMed: 6051769]
Baron RM, Kenny DA. The moderator/mediator variable distinction in social psychological research:Conceptual, strategic and statistical considerations. Journal of Personality and Social Psychology.1986; 51:1173–1182. [PubMed: 3806354]
Braam AW, Beekman AT, Deeg DJ, Smit JH, van Tilburg W. Religiosity as a protective or prognosticfactor of depression in later life: results from a community survey in the Netherlands. ActaPsychiatrica Scandinavica. 1997; 96:199–205. [PubMed: 9296551]
Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98:310–357. [PubMed: 3901065]
Delmonte MM. Biochemical indices associated with meditation practice: A literature review.Neuroscience & Biobehavioral Reviews. 1985; 9(4):557–561. [PubMed: 2867509]
Ellison CG. Race, religious involvement and depressive symptomatology in a southeastern U.S.community. Social Science and Medicine. 1995; 40:1561–1572. [PubMed: 7667660]
First, BM.; Spitzer, RL.; Gibbon, M.; Williams, JBW. User’s guide for the Structured ClinicalInterview for DSM–IV Axis I Disorders: SCID-I Clinician Version. Washington, DC: AmericanPsychiatric Press; 1995.
Gall TL, Kristjansson E, Charbonneau C, Florack P. A longitudinal study on the role of spirituality inresponse to the diagnosis and treatment of breast cancer. Journal of Behavioral Medicine. 2009;32:174–186. [PubMed: 18982441]
Hall DE, Meador KG, Koenig HG. Measuring religiousness in health research: Review and critique.Journal of Religion & Health. 2008; Vol 47(2):134–163. [PubMed: 19105008]
Hamilton M. A rating scale for depression. Journal of Neurology. 1960; 23:56–62.
Hill PC, Pargament KI. Advances in the conceptualization and measurement of religion andspirituality. Implications for physical and mental health research. American Psychologist. 2003;58(1):64–74. [PubMed: 12674819]
Hilty DM, Morgan RL, Burns JE. King and Hunt revisited: Dimensions of religious involvement.Journal for the Scientific Study of Religion. 1984; 23:252–266.
Husiani B, Blasi A, Miller O. Does public and private religiosity have a moderating effect ondepression? A bi-racial study of elders in the American South. International Journal of Aging &Human Development. 1999; 48(1):63–72. [PubMed: 10363560]
Idler EL, Kasl SV. Religion, disability, depression, and the timing of death. American Journal ofSociology. 1992; 97(4):1052–1079.
Idler EL, Musick MA, Ellison CG, George LK, Krause N, Ory MG. Measuring multiple dimensions ofreligion and spirituality for health research. Research on Aging. 2003; 25:327–365.
Joiner TE Jr, Perez M, Walker RL. Playing devil’s advocate: Why not conclude that the relation ofreligiosity to mental health reduces to mundane mediators? Psychological Inquiry. 2002; 13:214–216.
Keller MB. Citalopram therapy for depression: a review of 10 years of European experience and datafrom U.S. clinical trials. Journal of Clinical Psychiatry. 2000; 61:896–908. [PubMed: 11206593]
Koenig HG, George LK, Peterson B. Religiosity and remission of depression in medically ill olderpatients. American Journal of Psychiatry. 1998; 155:536–542. [PubMed: 9546001]
Koenig, HG.; McCullough, ME.; Larson, DB. Handbook of religion and health. New York: OxfordUniversity Press; 2001.
Lesser IM, Myers HF, Lin KM, Bingham MC, Joseph NT, Olmos NT, Schettino J, Poland RE. Ethnicdifferences in antidepressant response: a prospective multi-site clinical trial. Depression andAnxiety. 2010; 27:56–62. [PubMed: 19960492]
Schettino et al. Page 11
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Levin JS, Markides KS, Ray LA. Religious attendance and psychological well being in MexicanAmericans: a panel analysis of three-generations data. Gerontologist. 1996; 36(4):454–463.[PubMed: 8771973]
Lin, KM.; Poland, RE.; Nakasaki, G. Psychopharmacology and Psychobiology of Ethnicity.Washington, DC: American Psychiatric Press; 1993. 1993.
McCullough ME, Larson DB. Religion and depression: A review of the literature. Twin Research.1999; 2:126–136. [PubMed: 10480747]
McIntosh DN, Silver RC, Wortman CB. Religion's role in adjustment to a negative life event: Copingwith the loss of a child. Journal of Personality & Social Psychology. 1993; 65(4):812–821.[PubMed: 8229652]
Musick MA, Koenig HG, Hays JC, Cohen HJ. Religious activity and depression among community-dwelling elderly persons with cancer: The moderating effect of race. Journals of GerontologySeries B: Psychological Sciences and Social Sciences. 1998; 53B:S218–S227.
Nelson C, Rosenfeld B, Breitbart W, Galietta M. Spirituality, religion, and depression in the terminallyill. Psychosomatics. 2002; 43:213–220. [PubMed: 12075036]
Paloutzian, RF.; Ellison, CW. Loneliness, spiritual well-being, and quality of life. In: Peplau, LA.;Perlman, D., editors. Loneliness: A sourcebook for current theory, research, and therapy. NewYork: Wiley Interscience; 1982.
Roberts BW, Robins RW. Broad dispositions, broad aspirations: The intersection of personality traitsand major life goals. Personality and Social Psychology Bulletin. 2000; 26:1284–1296.
Roff LL, Kelmmack DL, Parker M, Koenig HG, Crowther M, Baker PS. Depression and religiosity inAfrican American and White community-dwelling older adults. Journal of Human Behavior in theSocial Environment. 2004; 10:175–189.
Saroglou V, Delpierre V, Dernelle R. Values and religiosity: A meta-analysis of studies usingSchwartz’s model. Personality and Individual Differences. 2004; 37:721–734.
Scott EL, Agresti AA, Fitchett G. Factor analysis of the 'Spiritual Well-Being Scale' and its clinicalutility with psychiatric inpatients. Journal for the Scientific Study of Religion. 1998; 37:314–321.
Siegel JM, Kuykendall DH. Loss, widowhood, and psychological distress among the elderly. Journalof Consulting & Clinical Psychology. 1990; 58(5):519–524. [PubMed: 2254497]
Smith TB, McCullough ME, Poll J. Religiousness and depression: Evidence for a main effect and themoderating influence of stressful life events. Psychological Bulletin. 2003; 129:614–636.[PubMed: 12848223]
Vinokur AD, Vinokur-Kaplan D. “In sickness and in health”: patterns of social support andundermining in older married couples. Journal of Aging and Health. 1990; 2:215–241.
Schettino et al. Page 12
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
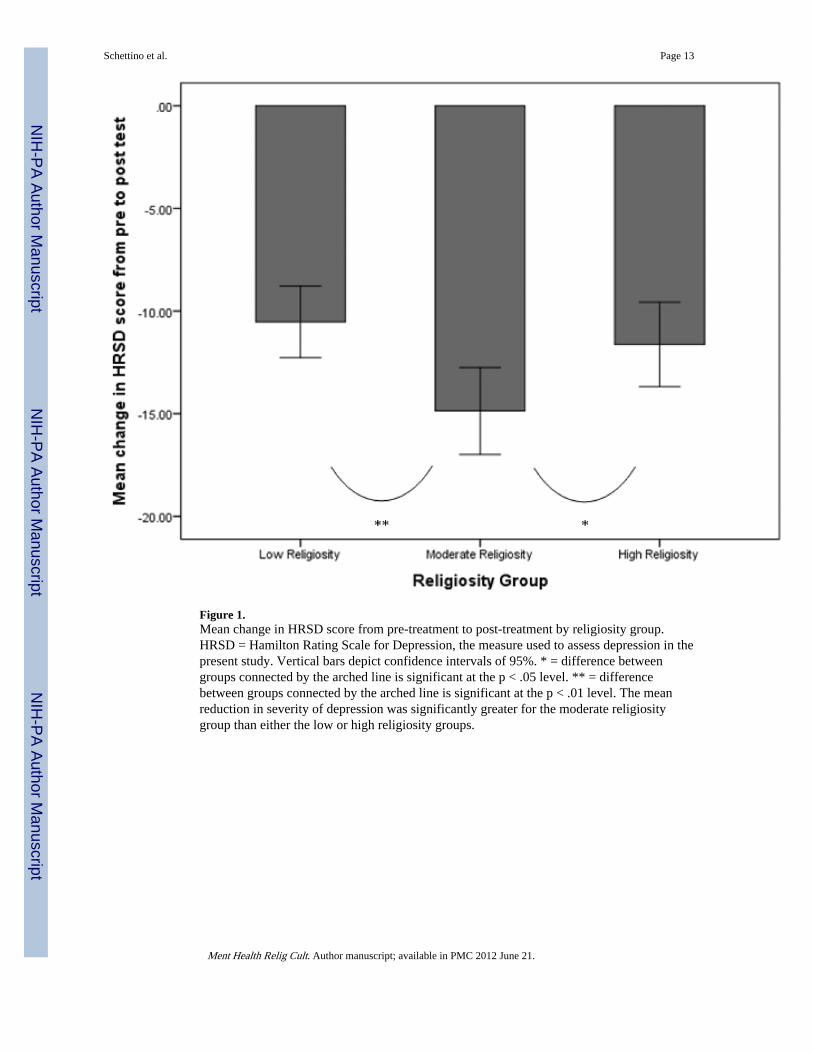
Figure 1.Mean change in HRSD score from pre-treatment to post-treatment by religiosity group.HRSD = Hamilton Rating Scale for Depression, the measure used to assess depression in thepresent study. Vertical bars depict confidence intervals of 95%. * = difference betweengroups connected by the arched line is significant at the p < .05 level. ** = differencebetween groups connected by the arched line is significant at the p < .01 level. The meanreduction in severity of depression was significantly greater for the moderate religiositygroup than either the low or high religiosity groups.
Schettino et al. Page 13
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
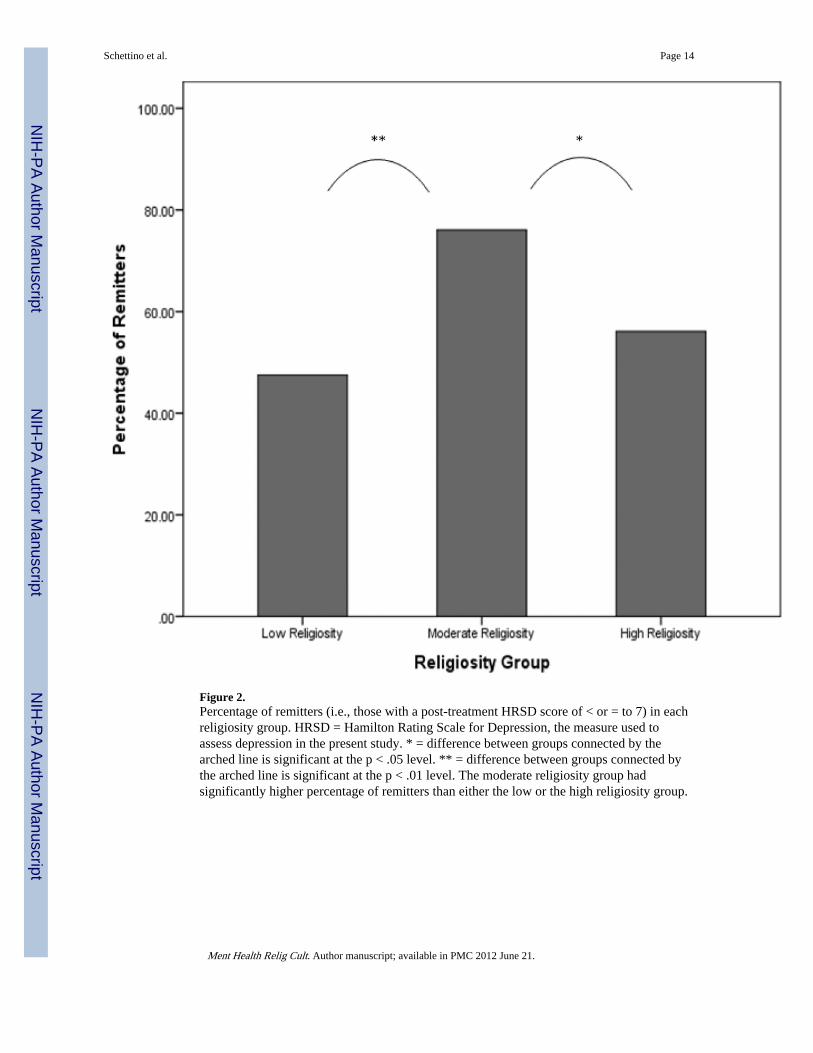
Figure 2.Percentage of remitters (i.e., those with a post-treatment HRSD score of < or = to 7) in eachreligiosity group. HRSD = Hamilton Rating Scale for Depression, the measure used toassess depression in the present study. * = difference between groups connected by thearched line is significant at the p < .05 level. ** = difference between groups connected bythe arched line is significant at the p < .01 level. The moderate religiosity group hadsignificantly higher percentage of remitters than either the low or the high religiosity group.
Schettino et al. Page 14
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Schettino et al. Page 15
Table 1
Differences between RII tertile groups on continuous variables
Low RII Moderate RII High RII F
VariableM (SD)n = 61
M (SD)n = 46
M (SD)n = 41
Age 42.0 (11.77) 44.3 (10.29) 44.5 (9.41) 0.91
Years of Education 13.7 (2.44) 13.9 (2.43) 14.0 (2.41) 1.09
Chronic Burden 35.9 (8.88) 36.9 (8.23) 37.2 (9.09) 1.91
Spirituality (SWB) 35.6 (12.04) 46.4 (14.29) 44.1 (18.42) 8.04**
Baseline HRSD 20.1 (4.53) 21.6 (5.12) 21.1 (5.68) 1.12
# of Tx Weeks Completed 7.6 (1.32) 7.7 (1.05) 7.8 (0.88) 0.54
Baseline Soc. Undermining 20.5 (8.24) 21.2 (7.96) 21.0 (9.11) 0.10
Post-Tx Soc. Undermining 18.6 (7.04) 19.7 (7.79) 19.8 (7.66) 0.32
Baseline Soc. Support 65.1 (21.60) 67.5 (21.11) 70.5 (19.48) 0.82
Post-Tx Soc. Support. 65.9 (21.14) 74.6 (20.72) 73.8 (16.11) 2.49
HRSD Change −10.5 (6.79) −14.9 (7.14) −11.6 (6.53) 5.48**
1.RII = the Religious Involvement Inventory, the measure used to assess religiosity in the present study
2. *= p < 0.05,
**= p < 0.01
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Schettino et al. Page 16
Table 2
Differences between RII tertile groups on categorical variables
Low RII Moderate RII High RII X2
%n = 61
%n = 46
%n = 41
Gender (female) 52.5 78.3 65.9 7.663*
Ethnicity (Caucasian) 49.2 30.4 22.0 8.748*
Alcohol Use 47.2 32.5 34.3 2.523
Employed 50.0 62.9 38.2 4.188
Married or Cohabitating 22.0 17.4 22.5 0.450
HRSD responder 60.7 78.3 68.3 3.751
HRSD remitter 47.5 76.1 56.1 8.989*
1.% = the percentage of participants in each RII tertile who fall into the category shown in the left column
2.RII = the Religious Involvement Inventory, the measure used to assess religiosity in the present study
3. *= p < 0.05,
**= p < 0.01
Ment Health Relig Cult. Author manuscript; available in PMC 2012 June 21.




















