Religion Religious beliefs Mental health Emotions
13
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution and sharing with colleagues. Other uses, including reproduction and distribution, or selling or licensing copies, or posting to personal, institutional or third party websites are prohibited. In most cases authors are permitted to post their version of the article (e.g. in Word or Tex form) to their personal website or institutional repository. Authors requiring further information regarding Elsevier’s archiving and manuscript policies are encouraged to visit: http://www.elsevier.com/copyright
Transcript of Religion Religious beliefs Mental health Emotions

This article appeared in a journal published by Elsevier. The attachedcopy is furnished to the author for internal non-commercial researchand education use, including for instruction at the authors institution
and sharing with colleagues.
Other uses, including reproduction and distribution, or selling orlicensing copies, or posting to personal, institutional or third party
websites are prohibited.
In most cases authors are permitted to post their version of thearticle (e.g. in Word or Tex form) to their personal website orinstitutional repository. Authors requiring further information
regarding Elsevier’s archiving and manuscript policies areencouraged to visit:
http://www.elsevier.com/copyright

Author's personal copy
Blessed assurance: Religion, anxiety, and tranquility among US adults q
Christopher G. Ellison a, Amy M. Burdette b, Terrence D. Hill c,*
a Department of Sociology, University of Texas, Austin, USAb Department of Sociology, Mississippi State University, MS, USAc Department of Sociology, University of Miami, P.O. Box 248162, Coral Gables, FL 33124, USA
a r t i c l e i n f o
Article history:Available online 24 February 2009
Keywords:ReligionReligious beliefsMental healthEmotionsAnxiety
a b s t r a c t
A growing body of research investigates the possible relationships between religion andmental health. After developing a series of arguments linking various aspects of religionwith anxiety and tranquility, we test relevant hypotheses using data from the 1996 GeneralSocial Survey. Results show that frequency of religious attendance and the belief in anafterlife are inversely associated with feelings of anxiety and positively associated withfeelings of tranquility. However, frequency of prayer has no direct association with eitheroutcome. Strong beliefs in the pervasiveness of sin are positively linked with anxiety butunrelated to tranquility. Finally, belief in an afterlife and frequency of prayer buffer theadverse effects of poor health and financial decline on anxiety. Implications of these find-ings are discussed along with study limitations and promising directions for futureresearch.
� 2009 Elsevier Inc. All rights reserved.
1. Introduction
Over the past two decades, a burgeoning literature has explored the relationships between religion and mental health.While a long tradition of theoretical and case-based work suggests that religious involvement may be antithetical to psycho-logical well-being (e.g., Ellis, 1962; Branden, 1994; Watters, 1992), recent analyses of clinical and population-based sampleshave often reached a more favorable conclusion. Indeed, while the findings are not unanimous, mounting evidence indicatesthat religious involvement tends to be associated with better mental health (Levin and Chatters, 1998; Koenig et al., 2001;Hackney and Sanders, 2003). Although this area began as the province of other disciplines—notably psychiatry, psychology,gerontology, and public health—sociologists have also made significant contributions to this area, as exemplified by a num-ber of recent studies (e.g., Ellison et al., 2001; Schnittker, 2001; Nooney and Woodrum, 2002; Schieman et al., 2003; Jang andJohnson, 2004, 2005).
Despite the recent advances in this area, several key issues remain unresolved. First, while researchers have concentratedheavily on certain outcomes, such as depression and life satisfaction, surprisingly few studies have probed the links betweenreligion and other important emotional states, such as anxiety and tranquility, and the results of those investigations havebeen decidedly mixed (Koenig et al., 2001; Shreve-Neiger and Edelstein, 2004). Second, although it is widely recognized thatreligion is a multidimensional phenomenon (Stark and Glock, 1968; Williams, 1994; Idler et al., 2003), there is little agree-ment on which aspects (e.g., which behaviors, beliefs, experiences, etc.) are most closely related with anxiety. Indeed, the use
0049-089X/$ - see front matter � 2009 Elsevier Inc. All rights reserved.doi:10.1016/j.ssresearch.2009.02.002
q This research was supported by a Grant from the National Institute on Aging (R01 AG18432) to the lead author. An earlier version of this study waspresented at the 2004 meetings of the Association for the Sociology of Religion, San Francisco. The authors thank Robert Hummer, Neal Krause, MarcMusick, Kenneth Pargament, Mark Regnerus, and Catherine Ross for helpful comments and suggestions. However, the authors are solely responsible for anyerrors of fact or interpretation that remain.
* Corresponding author. Fax: +1 305 284 5310.E-mail address: [email protected] (T.D. Hill).
Social Science Research 38 (2009) 656–667
Contents lists available at ScienceDirect
Social Science Research
journal homepage: www.elsevier .com/locate /ssresearch

Author's personal copy
of inconsistent measures of religion may contribute to the discrepant findings concerning anxiety (Shreve-Neiger and Edel-stein, 2004). Third, the processes linking religion with anxiety and other mental health outcomes are not well understood.For example, one promising theoretical direction suggests that religious practices and cognitions can mediate or moderatethe effects of stressors on mental health (e.g., Ellison et al., 2001). However, the links between religion, stress, and mentalhealth remain understudied, particularly with regard to anxiety. Finally, the widespread use of small, localized, and evennon-random sampling in studies of religion and anxiety and other mental health outcomes limits generalizability andmay contribute to discrepant findings (Shreve-Neiger and Edelstein, 2004).
Our study contributes to the literature on religion and mental health in several ways. We begin by outlining theoreticallinks between multiple dimensions of religious involvement and feelings of anxiety and tranquility. In contrast to the bulk ofprevious research, we direct attention to the possible role of religious beliefs—especially belief in the afterlife and in humansinfulness—in shaping these outcomes. Hypotheses derived from this discussion are then tested using data from the 1996NORC General Social Survey, a nationally representative sample of community-dwelling US adults. Following the presenta-tion of results, the implications of our findings for theoretical perspectives on religion and mental health are discussed, studylimitations are noted, and promising directions for future investigation are identified.
2. Theoretical background and hypotheses
A long tradition of theory and research in the sociology of religion recognizes that religious involvement is a complex,multidimensional phenomenon (e.g., Stark and Glock, 1968; Levin et al., 1995). Nevertheless, issues of conceptualizationand measurement remain contentious in the religion-health literature, and three key points deserve special mention. First,there is little agreement on which aspects of religious involvement are most germane to the study of mental and/or physicalhealth; although many studies in this area continue to focus mainly on religious practices, especially organizational involve-ment (e.g., frequency of attendance at services), it is widely noted that other specific religious domains warrant consider-ation (Williams, 1994; Idler et al., 2003). Because this literature has generally neglected the belief dimension of religion,some researchers now advocate closer attention to core tenets of the major faith traditions, such as belief in an afterlife(e.g., Ellison et al., 2001). Second, although most published studies report salutary associations between religious involve-ment and health/well-being, it is also evident that certain types or facets of religious engagement (e.g., maladaptive religiouscoping, negative interactions, chronic doubting) are linked with undesirable outcomes (Pargament, 1997; Krause et al., 1999;Musick, 2000). Consequently, there is mounting interest in a more balanced approach that examines both positive and neg-ative implications of religion for health/well-being. Third, additional work is needed to clarify the various possible mecha-nisms that link religious involvement with well-being (Ellison and George, 1994; Idler et al., 2003). For example, it has beensuggested that the established concepts and models of the life-stress tradition offer a useful theoretical starting point for thiswork. Of particular interest are potential stress-moderating (i.e., -buffering and -exacerbating) effects of religious involve-ment (e.g., Ellison et al., 2001). Mindful of these important issues, in the section below we outline theoretical links betweenmultiple aspects of religious involvement and the outcomes of interest in this study, anxiety and tranquility.
2.1. Organizational religious involvement
How and why might organizational religious participation be linked with anxiety and/or tranquility? Prior theory andempirical research suggest several possible reasons to expect such a relationship (Ellison and Levin, 1998; Ellison et al.,2001; Koenig et al., 2001). First, regular participation in congregational life may influence individual lifestyles and behaviorsin ways that are likely to reduce cumulative exposure to social stressors, i.e., problematic events and conditions. For example,most religious groups discourage certain types of conduct—such as alcohol, tobacco, and drug use/abuse, risky sexual behav-ior, gambling, carousing, and other behaviors (Hill et al., 2006, 2007) that might foster or exacerbate feelings of anxiety. Bypromulgating ethical norms and guidance for the conduct of personal and family affairs, involvement in religious commu-nities may reduce the likelihood of family conflicts, health problems, economic and legal hassles, and other chronic and acutestressors (Grasmick and Bursik, 1991; Koenig et al., 1994, 1998; Hoffmann, 2000).
Second, religious institutions may provide social and psychological resources that reduce anxiety and promote feelings ofcalmness and tranquility among their members. Briefly, religious communities offer opportunities for the formation offriendships and the pursuit of common social activities among like-minded persons (Ellison and George, 1994; Bradley,1995). Most religious groups also encourage informal supportive exchanges among members, fostering access to social re-sources, and enhancing the perception of support network reliability among churchgoers (Taylor and Chatters, 1988; Wuth-now, 1994; Krause, 2002a,b). Further, religious organizations sponsor a wide array of formal support mechanisms includingchurch programs and outreach efforts, classes and seminars, and clergy assistance (Chaves and Higgins, 1992; Neighborset al., 1998; Tsitsos, 2001). Social bonds within religious communities may also foster feelings of self-worth, through positivereflected appraisals, and self-confidence, through congregational activities and leadership roles (Ellison, 1993; Krause, 1995).
Third, regular participation in congregational life may provide spiritual nourishment, and this collective experience mayreinforce religious plausibility structures (Berger, 1967). Persons who enjoy interaction with others who share their religiouscommitment and core theological convictions are likely to have their faith deepened and strengthened (e.g., Cornwall, 1987).This may occur in a number of ways: (a) religious education classes or informal conversations; (b) exchanges of stories and
C.G. Ellison et al. / Social Science Research 38 (2009) 656–667 657

Author's personal copy
personal anecdotes with other members; and (c) direct messages from the clergy or church. And the actual worship expe-rience (e.g., preaching, singing, ritual participation) may also nurture individual faith, stimulate religious cognitions, anddeepen faith journeys and encounters with the sacred. This discussion suggests the following hypothesis:
H1: The frequency of attendance at religious services will be inversely associated with feelings of anxiety, and positivelyassociated with feelings of calmness or tranquility.
2.2. Non-organizational religious involvement
Religious devotional practices, such as prayer or meditation, may be related to anxiety and tranquility for several reasons.First, individuals may construct relationships with perceived divine other(s) in much the same way that they build bondswith social others, i.e., through regular and ongoing patterns of interaction (Pollner, 1989). They believe that, through prayeror meditation, they can engage divine other(s) (i.e., God, Jesus, saints, etc.) in a quest for solace or guidance, and many per-sons come to experience divine other(s) as intimate members of their personal networks. Recent applications of attachmenttheory to the study of religion have underscored the fact that God is an important attachment figure for many believers. Con-sistent with the tenets of attachment theory, religious individuals (a) seek to maintain close proximity to God, and Godserves alternately as (b) a ‘‘haven of safety” and (c) a ‘‘secure base” that facilitates their confident engagement with, andexploration, of the wider environment (Kirkpatrick, 2004). This is borne out by qualitative accounts of the rich interior spiri-tual lives of many persons, and the strength with which they confront personal adversity (e.g., Black, 1999; Poindexter et al.,1999).
Viewed from this perspective, persons who regularly engage in prayer and other devotional practices may enjoy animportant mental health resource (Poloma and Gallup, 1991; Krause et al., 2000, Krause, 2004). Because individuals expe-rience a personal relationship with a powerful divine other, from whom they are able to seek aid and comfort directly, theymay find the demands of daily living—as well as personal problems—easier to manage (Pargament, 1997). They may antic-ipate and believe they are navigating their earthly existence with the help of a valued advisor, potent advocate, and trustedfriend. Such beliefs may foster hopefulness and optimism, and other healthy beliefs and emotions (Poloma and Gallup,1991). These theoretical insights suggest the following hypotheses regarding prayer and mental health:
H2a: The frequency of private prayer will be inversely association with feelings of anxiety and positively associated withfeelings of tranquility.H2b: The detrimental effects of stressful conditions (i.e., health problems, financial decline) on anxiety and tranquility willbe moderated or buffered by prayer.
2.3. Key religious beliefs: afterlife and sin
Despite the centrality of faith and belief in religious life, surprisingly few studies have explored the links between reli-gious beliefs and mental health outcomes. Although the domain of religious belief is complex and multifaceted, here we fo-cus on the role of two specific beliefs that are important in the Judeo-Christian tradition, which has shaped the dominantreligious ethos in the United States. These are (a) the belief in an afterlife, and (b) the belief in human sinfulness. The neglectof afterlife belief in religion-health research is particularly striking (Ellison et al., 2001) given that the prospect or promise oflife after death plays a pivotal role in major theoretical treatises on religion. These classic works range from Pascal’s wager, toseminal discussions of religious otherworldliness by Marx and Engels, Weber, and others, and to the ideas about religiouscompensators articulated by rational choice theorists, such as Stark and Bainbridge (1996). In the contemporary US, trendstudies show that the percentage of persons who believe in an afterlife is rising over time, and across birth cohorts (Harleyand Firebaugh, 1993; Greeley and Hout, 1999).
Individuals who believe in an afterlife may adopt a distinctive perspective on the world and their place within it. Such an‘‘eternal perspective” may provide a coherent framework within which to interpret daily affairs and personal problems alike(Berger, 1967; Idler, 1987; Antonovsky, 1987). Persons who are convinced that temporal earthly existence is not all there ismay experience feelings of calmness, as well as less tension, worry, fear, and anger. It is plausible that this may carry overinto their dealings with others, their attachment to status and material wealth, and their need to compete with others or toenact their own desires or plans. For many individuals, personal issues such as health problems or long-term financial de-clines often pose fundamental challenges for the sense of self, which require adjustments in lifestyles and future expecta-tions. These developments—however unpleasant—may be experienced as less threatening to the core identities ofbelievers (Ellison, 1993; Idler, 1995). The distinctive meanings that may be associated with human suffering, as well asthe promise of future spiritual rewards, may make these difficulties easier to bear (Foley, 1988; Pargament, 1997). This dis-cussion suggests the following hypotheses:
H3a: Belief in an afterlife will be inversely associated with feelings of anxiety, and positively associated with feelings oftranquility.H3b: The detrimental effects of stressful conditions (i.e., health problems, financial decline) on anxiety and tranquility willbe moderated or buffered by belief in an afterlife.Not all aspects of religious belief may have such favorable implications for emotional states. For example, critics of reli-
gion have long argued that beliefs in human sinfulness can undermine well-being. Albert Ellis (1962), the founder of Ra-tional-Emotive Therapy, asserted bluntly: ‘‘The concept of sin is the direct and indirect cause of virtually all neurotic
658 C.G. Ellison et al. / Social Science Research 38 (2009) 656–667

Author's personal copy
disturbance” (p. 146). Ellis (1962, 1980) and others (e.g., Branden, 1994; Watters, 1992) have insisted that notions of the sin-fulness of human nature have a number of specific pathological sequelae. In particular, they claim that individuals who be-lieve they are sinful experience: (a) lower self-esteem, or feelings of self-worth; (b) reduced feelings of mastery, or the abilityto control their own affairs and behavior; (c) and increased feelings of guilt and shame. Further, this focus on individualfaults may divert attention from constructive efforts to cope with personal problems or eliminate negative behaviors. Sinbeliefs are often accompanied by notions of divine judgment and punishment, which may increase feelings of external threatand fearfulness (Musick, 2000). Finally, to the extent that notions of sin promote blaming and moral critique, they may fosteranger and hostility toward others as well (Ellis, 1962). Despite the potential importance of these ideas, however, few inves-tigators have tested these claims empirically (for a partial exception, see Watson et al., 1988a,b). Nevertheless, the foregoingdiscussion suggests our final hypothesis:
H4: Belief in the ubiquity of sin will be positively associated with feelings of anxiety and inversely associated with feelingsof tranquility.
3. Materials and methods
3.1. Data
To test these hypotheses, we analyze data from the 1996 General Social Survey (GSS), conducted by the Chicago-basedNational Opinion Research Center (Davis and Smith, 1996).1 Between 1972 and 1993, the GSS was conducted annually (ex-cept for 1979, 1981, and 1992, when no surveys were fielded). Beginning in 1994, the GSS has been conducted in even-num-bered years only, but has involved larger samples than in the pre-1994 years. This is a valuable data source for severalreasons: (a) the GSS is a nationally representative sample of US adults residing in the lower 48 states; (b) the GSS routinelyincludes a number of relevant religious items; and (c) the 1996 edition also contains a special module of items on emotions,including appropriate measures of anxiety and tranquility (Schieman et al., 2001).
Since 1987, the GSS has used a split-ballot design in data collection, to maximize the number of items included in eachyear. As a result of this design, however, many items (except for a group of ‘‘core” questions that are included on all surveys)have been asked of only a randomly selected subset of GSS respondents. For instance, because the module on emotions—inwhich our control items were included—was asked of only approximately one-half of the respondents, the size of our avail-able sample is reduced from 2904 to 1460. In addition, our effective sample size is further reduced to 921 as a result of thesplit ballot design on select independent variables (e.g., items on belief in the afterlife and frequency of prayer were asked ofonly two-thirds of the remaining 1460 respondents), as well as the use of listwise deletion where appropriate. Although thissplit-ballot design reduces the available N for our analyses, the fact that these ballots are randomly assigned minimizes thepotential for sample bias.
3.2. Dependent variables: anxiety and tranquility
Anxiety is measured via a mean index based on responses to four items. Respondents were asked, ‘‘How many of the lastseven days have you. . .” (1) ‘‘felt so restless that you couldn’t sit long in a chair?”; (2) ‘‘felt anxious and tense?”; (3) ‘‘feltfearful about something that might happen to you?”; and, (4) ‘‘worried a lot about little things?”. Response categories foreach of these items range from 0 to 7 days in the past week. These items are then combined into an index ranging from0 (no anxiety) to 7 (high anxiety), for which the alpha was calculated to be .66.
Tranquility is also measured using a mean index based on responses to three items. As with items measuring anxiety,respondents were asked, ‘‘How many of the last seven days have you. . .” (1) ‘‘felt at ease?”; (2) ‘‘felt contented?”; and, (3)‘‘felt calm?” Response categories for each of these items range from 0 to 7 days in the past week (a = .73). Again, lower scoreson the index refer to lower levels of tranquility, and higher scores refer to higher levels of tranquility. The zero-order cor-relation between the two dependent variables, anxiety and tranquility, is .46.
3.3. Key independent variables: religious involvement
To model the ideas outlined above, we measure several distinct aspects of religious involvement. GSS respondents wereasked to place their views of human nature on a scale from 1 to 7, between two statements that represent polar opposites:(1) ‘‘Human nature is basically good” and (7) Human nature is fundamentally perverse and corrupt.” This item was subse-quently recoded so that higher scores reflect stronger sin beliefs, and then summed create an index ranging from 1 to 7.
Afterlife belief is measured via responses to the item, ‘‘Do you believe there is a life after death?” Responses included: yes(1) no (2) and undecided (8).2 This item was recoded into a dummy variable that identifies persons who clearly expressed beliefin an afterlife, versus those who do not or are undecided. Two aspects of religious practice are considered as well. The frequency
1 There were no substantial differences between our actual sample (N = 921) and the total GSS for 1996 (N = 2904). The make up of our sub-sample was notsignificantly different from the overall GSS sample for that year with regard to all of our major demographic controls.
2 Results suggest that there are no real differences in anxiety or tranquility between persons who do not believe in an afterlife and persons who areundecided.
C.G. Ellison et al. / Social Science Research 38 (2009) 656–667 659

Author's personal copy
of church attendance is gauged via the following item: ‘‘How often do you attend religious services?” Responses range fromnever (0) to several times a week (8). The frequency of prayer is measured using the following item: ‘‘About how often doyou pray?” Responses are recoded so that higher scores denote more frequent prayer; revised coding ranges from never (1)to several times a day (6).3
3.4. Chronic stressors
In order to evaluate our stress-buffering hypotheses, we examine two commonly experienced stressors, poor health andfinancial decline. Research shows that poor health (Farmer and Ferraro, 1997) and financial disadvantage (Mirowsky andRoss, 2003) are positively associated with anxiety. Health status is measured using the question, ‘‘Would you say yourown health in general, is excellent, good, fair or poor?” This item was recoded into a dichotomous variable to contrast thosein fair or poor health versus those in good or excellent health. Financial decline is measure via the following item: ‘‘Duringthe last few years, has your financial situation been getting better, worse, or has it stayed the same?” Responses to this itemwere recoded to identify those respondents who stated that their financial situation had gotten worse verses those who im-proved or stayed the same.
3.5. Background factors
Numerous background factors have been identified as significant correlates of anxiety. Anxiety is associated with beingyounger (Drentea, 2000), female (Mirowsky and Ross,1995, 2003), white (Ross and Van Willigen, 1997; Barrett, 2000), poorlyeducated (Ross and Van Willigen, 1997; Mirowsky and Ross, 2003), unmarried (Ross and Van Willigen, 1997), and less so-cially integrated (Williams et al., 1981; Thoits, 1995). Therefore, our analyses include controls for the following variables:gender (1 = female, 0 = male); race and/or ethnicity (1 = African American, 1 = other minority, 0 = non-Hispanic white); age(measured in single years); education (measured in years); household income (continuous imputed family income in$10,000s), and marital status (1 = married 0 = other status). Social integration is measured via a mean index based on re-sponses to three items. Respondents were asked how often they spend a social evening with (1) relatives; (2) someonewho lives in their neighborhood; and, (3) friends who live outside of the neighborhood. Revised response categories for eachof these items range from (1) never to (8) almost every day. Thus, higher values on this index refer to higher levels of secularsocial integration.
4. Analytic strategy
Our analysis proceeds in several stages. First, we provide descriptive statistics—means, standard deviations, minimum,and maximum values—for all variables used in our analyses (Table 1). Next we estimate a series of multivariate ordinaryleast squares (OLS) regression models to gauge the net effect of religious variables and covariates on anxiety (Table 2)and tranquility (Table 3). For each outcome, models are organized as follows: Model 1 (the baseline model) includes non-religious predictors, such as sociodemographic factors and key stressors. Model 2 adds measures of organizational religiousinvolvement (frequency of attendance) and non-organizational practice (frequency of prayer). Model 3 replaces these mea-sures of religious practice with two measures of religious beliefs (belief in an afterlife and in human sinfulness). Model 4 (thefull model) includes all predictors simultaneously. This sequence of models allows us to test hypotheses 1, 2a, 3a, and 4, andalso (b) to compare the estimated net effects of standard measures of religious practice with those of two key aspects of be-lief, which have been neglected in most previous studies of religion and mental health. In the final stage of our analysis, weadd cross-product (i.e., religion � stressor) interaction terms to the full models (Model 4) for anxiety and tranquility, to testhypotheses 2b and 3b, which suggest that frequency of prayer and afterlife belief will buffer the estimated net effects ofstressors on these mental health outcomes.
5. Results
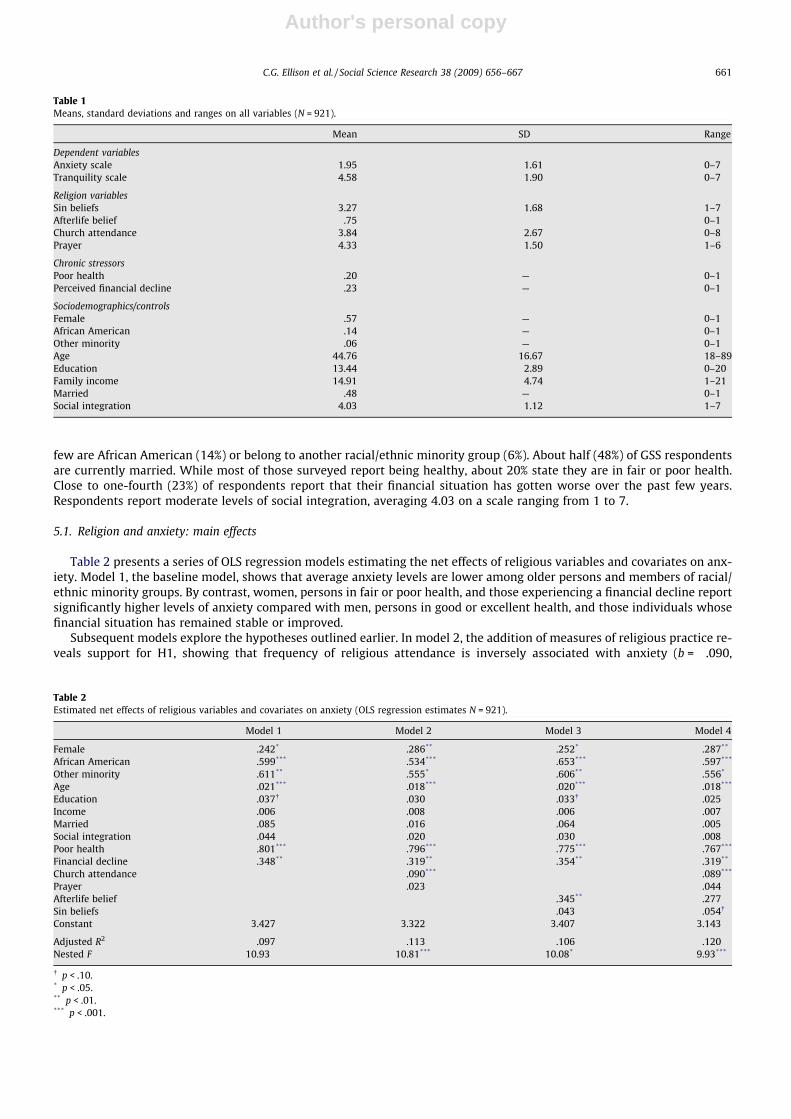
Descriptive statistics on all variables used in our analyses are displayed in Table 1. GSS respondents report relatively lowlevels of anxiety, scoring an average of 1.95 on a scale that ranges from 0 to 7. Those surveyed report moderate levels of tran-quility, scoring 4.58 on a scale ranging from 0 to 7. With regard to religious involvement, approximately 75% of GSS respon-dents believe in an afterlife. On average, they report attending religious services roughly once per month (3.84), and prayingat least once per week (4.33). GSS respondents display some skepticism about the pervasiveness of human sin. The averagescore on our measure of sin beliefs (3.27) is slightly below the midpoint of the scale, which ranges from 1 to 7. The average1996 GSS respondent is about 45 years of age, with a year and a half of post-secondary education (13.44 total years com-pleted), and a 1995 pre-tax family income of approximately $25,000. The majority of respondents are female (57%), while
3 Initial models also included controls for religious affiliation; however, these variables were not significant in any models and were therefore removed fromfurther analysis. The religious composition of the 1996 GSS sample is approximately 30% conservative Protestant (Southern Baptists, Pentecostals, Evangelicals),16% moderate Protestant (Lutherans, Methodists), 7% liberal Protestant (Presbyterians, Episcopalians), 24% Catholic, 12% other faiths (Buddhists, Mormons,Jews), and 13% non-affiliate.
660 C.G. Ellison et al. / Social Science Research 38 (2009) 656–667
Author's personal copy
few are African American (14%) or belong to another racial/ethnic minority group (6%). About half (48%) of GSS respondentsare currently married. While most of those surveyed report being healthy, about 20% state they are in fair or poor health.Close to one-fourth (23%) of respondents report that their financial situation has gotten worse over the past few years.Respondents report moderate levels of social integration, averaging 4.03 on a scale ranging from 1 to 7.
5.1. Religion and anxiety: main effects
Table 2 presents a series of OLS regression models estimating the net effects of religious variables and covariates on anx-iety. Model 1, the baseline model, shows that average anxiety levels are lower among older persons and members of racial/ethnic minority groups. By contrast, women, persons in fair or poor health, and those experiencing a financial decline reportsignificantly higher levels of anxiety compared with men, persons in good or excellent health, and those individuals whosefinancial situation has remained stable or improved.
Subsequent models explore the hypotheses outlined earlier. In model 2, the addition of measures of religious practice re-veals support for H1, showing that frequency of religious attendance is inversely associated with anxiety (b = �.090,
Table 2Estimated net effects of religious variables and covariates on anxiety (OLS regression estimates N = 921).
Model 1 Model 2 Model 3 Model 4
Female .242* .286** .252* .287**
African American �.599*** �.534*** �.653*** �.597***
Other minority �.611** �.555* �.606** �.556*
Age �.021*** �.018*** �.020*** �.018***
Education �.037� �.030 �.033� �.025Income �.006 �.008 �.006 �.007Married �.085 �.016 �.064 �.005Social integration �.044 �.020 �.030 �.008Poor health .801*** .796*** .775*** .767***
Financial decline .348** .319** .354** .319**
Church attendance �.090*** �.089***
Prayer .023 .044Afterlife belief �.345** �.277Sin beliefs .043 .054�
Constant 3.427 3.322 3.407 3.143
Adjusted R2 .097 .113 .106 .120Nested F 10.93 10.81*** 10.08* 9.93***
� p < .10.* p < .05.** p < .01.*** p < .001.
Table 1Means, standard deviations and ranges on all variables (N = 921).
Mean SD Range
Dependent variablesAnxiety scale 1.95 1.61 0–7Tranquility scale 4.58 1.90 0–7
Religion variablesSin beliefs 3.27 1.68 1–7Afterlife belief .75 0–1Church attendance 3.84 2.67 0–8Prayer 4.33 1.50 1–6
Chronic stressorsPoor health .20 — 0–1Perceived financial decline .23 — 0–1
Sociodemographics/controlsFemale .57 — 0–1African American .14 — 0–1Other minority .06 — 0–1Age 44.76 16.67 18–89Education 13.44 2.89 0–20Family income 14.91 4.74 1–21Married .48 — 0–1Social integration 4.03 1.12 1–7
C.G. Ellison et al. / Social Science Research 38 (2009) 656–667 661
Author's personal copy
p < .001). Contrary to H2a, however, frequency of prayer is unrelated to anxiety among GSS respondents. When measures ofreligious practice are replaced by theological convictions in model 3, belief in an afterlife is inversely related to anxiety(b = �.345, p < .01), as predicted by H3a, while belief in human sinfulness is not associated with anxiety. When all variablesare included simultaneously in model 4, the estimated net effect of afterlife belief on anxiety is diminished somewhat, byapproximately 20%, but it remains robust (b = �.277, p < .05); the net effect of sin belief becomes marginally significant(b = .054, p < .10), providing some support for H4. The estimated net effect of attendance remains virtually unchanged in thisfinal model.
5.2. Religion and tranquility: main effects
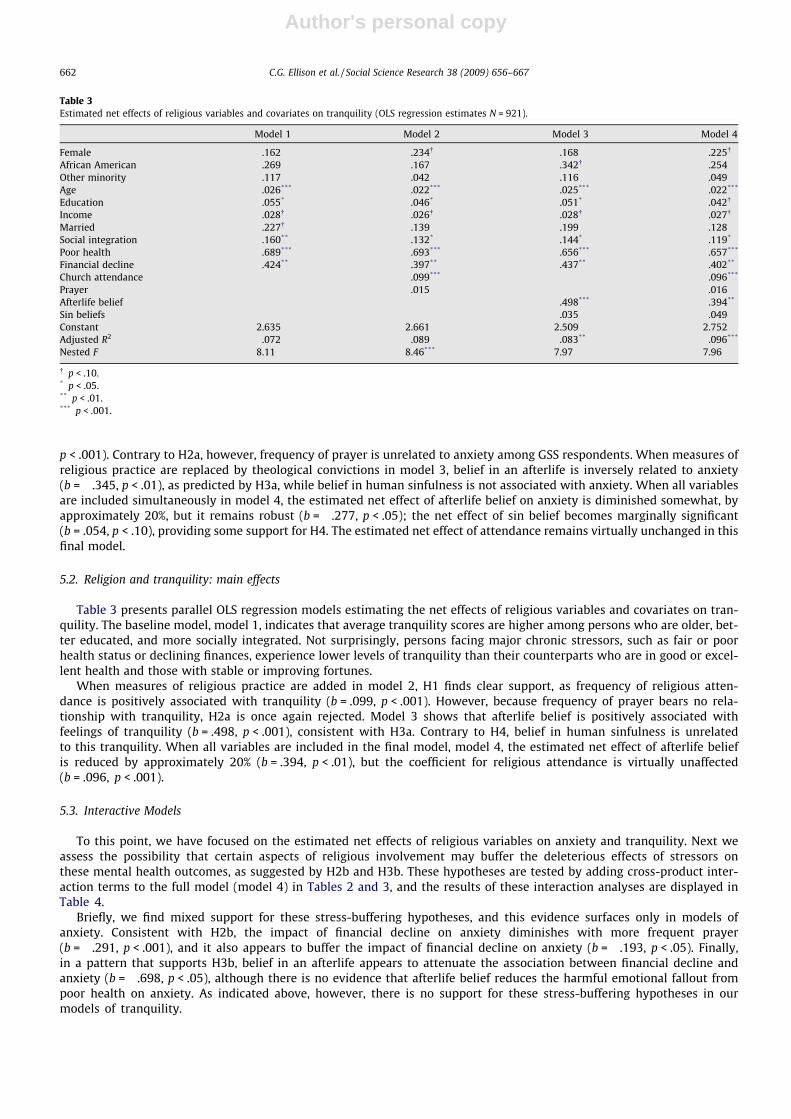
Table 3 presents parallel OLS regression models estimating the net effects of religious variables and covariates on tran-quility. The baseline model, model 1, indicates that average tranquility scores are higher among persons who are older, bet-ter educated, and more socially integrated. Not surprisingly, persons facing major chronic stressors, such as fair or poorhealth status or declining finances, experience lower levels of tranquility than their counterparts who are in good or excel-lent health and those with stable or improving fortunes.
When measures of religious practice are added in model 2, H1 finds clear support, as frequency of religious atten-dance is positively associated with tranquility (b = .099, p < .001). However, because frequency of prayer bears no rela-tionship with tranquility, H2a is once again rejected. Model 3 shows that afterlife belief is positively associated withfeelings of tranquility (b = .498, p < .001), consistent with H3a. Contrary to H4, belief in human sinfulness is unrelatedto this tranquility. When all variables are included in the final model, model 4, the estimated net effect of afterlife beliefis reduced by approximately 20% (b = .394, p < .01), but the coefficient for religious attendance is virtually unaffected(b = .096, p < .001).
5.3. Interactive Models
To this point, we have focused on the estimated net effects of religious variables on anxiety and tranquility. Next weassess the possibility that certain aspects of religious involvement may buffer the deleterious effects of stressors onthese mental health outcomes, as suggested by H2b and H3b. These hypotheses are tested by adding cross-product inter-action terms to the full model (model 4) in Tables 2 and 3, and the results of these interaction analyses are displayed inTable 4.
Briefly, we find mixed support for these stress-buffering hypotheses, and this evidence surfaces only in models ofanxiety. Consistent with H2b, the impact of financial decline on anxiety diminishes with more frequent prayer(b = �.291, p < .001), and it also appears to buffer the impact of financial decline on anxiety (b = �.193, p < .05). Finally,in a pattern that supports H3b, belief in an afterlife appears to attenuate the association between financial decline andanxiety (b = �.698, p < .05), although there is no evidence that afterlife belief reduces the harmful emotional fallout frompoor health on anxiety. As indicated above, however, there is no support for these stress-buffering hypotheses in ourmodels of tranquility.
Table 3Estimated net effects of religious variables and covariates on tranquility (OLS regression estimates N = 921).
Model 1 Model 2 Model 3 Model 4
Female �.162 �.234� �.168 �.225�
African American .269 .167 .342� .254Other minority .117 .042 .116 .049Age .026*** .022*** .025*** .022***
Education .055* .046* .051* .042�
Income �.028� �.026� �.028� �.027�
Married .227� .139 .199 .128Social integration .160** .132* .144* .119*
Poor health �.689*** �.693*** �.656*** �.657***
Financial decline �.424** �.397** �.437** �.402**
Church attendance .099*** .096***
Prayer .015 �.016Afterlife belief .498*** .394**
Sin beliefs �.035 �.049Constant 2.635 2.661 2.509 2.752Adjusted R2 .072 .089 .083** .096***
Nested F 8.11 8.46*** 7.97 7.96
� p < .10.* p < .05.** p < .01.*** p < .001.
662 C.G. Ellison et al. / Social Science Research 38 (2009) 656–667

Author's personal copy
6. Discussion
We began this study by noting that, despite the growing body and increased sophistication of studies on religion andmental health, several important issues remain in need of clarification. After identifying key gaps in this body of research,we outlined theoretical links between aspects of religious practice and belief, on the one hand, and anxiety and tranquilityon the other. And we tested a series of hypotheses based on these arguments, using data from a nationwide (US) survey ofadults. Overall, our analyses indicate support for 5 of the 6 hypotheses developed, and many of the key findings are similaracross the two dependent variables.
First, organizational religious involvement, gauged in terms of the frequency of religious attendance, is consistently asso-ciated with salutary outcomes. There are several possible explanations for this finding. Ritual participation and collectiveworship activities may enhance the experience of the sacred. By strengthening religious plausibility structures and meaningsystems, regular group worship may reduce feelings of uncertainty and fearfulness, and promote a sense of inner peace andharmony (Berger, 1967; Petersen and Roy, 1985; Idler, 1987). In addition, fellowship with like-minded others—ideally occur-ring in an atmosphere of trust and mutuality—may foster feelings of relaxation and assurance. And more intimate spiritualencounters, such as those in religious small groups, may provide valuable guidance on how to live out the precepts of one’sfaith (Wuthnow 1994; Krause et al. 2001). By supplying positive feedback and favorable comparisons, these interactions mayreduce feelings of uncertainty and self-doubt, e.g., by clarifying moral standards and role identities, and by affirming thatone’s lifestyles, beliefs, and judgments are reasonable and appropriate (Ellison 1993).
In a more speculative vein, some have suggested that the worship services themselves may direct and concentrate theenergies and attention of parishioners, engaging cognitions, senses, and the body (e.g., through ritual content, sermons, vi-sual and other sensory experiences, singing and praying, etc.) in ways that encourage the cathartic release of negative emo-tions (Griffith et al., 1984; Idler and Kasl, 1992; Williams, 1994). Given the common finding that (self-reported) religiousattendance is related to positive outcomes, including reduced anxiety and greater tranquility, it is increasingly importantto identify the specific mechanisms and processes that underlie these salutary patterns.
A second key set of findings concerns non-organizational (private) devotional activity, gauged here in terms of the fre-quency of prayer. In our main effects models, prayer frequency is unrelated to anxiety or tranquility. However, frequentprayer buffers the deleterious effects of poor health and financial decline on anxiety but not on tranquility. This is consistentwith other findings that prayer is an important coping resource for persons facing high levels of emotional distress, and thisis particularly the case when other possible coping responses are inaccessible or ineffective (Koenig et al., 1988; Ellison andTaylor, 1996; Pargament, 1997). And frequent prayer clearly appears to alleviate anxiety for persons under stress from prob-lems that require major long-term adjustments of behavior or expectation (e.g., poor health, financial decline). This salutarypattern may result from several factors. For example, religious cognitions and perceived interaction with a divine other canoffer a valuable source of meaning for those enduring personal pain. Religious explanations for suffering may reduce the neg-ative emotional fallout—e.g., (a) by affirming or restoring a sense of vicarious (divine) control over those problems; (b) byrestoring faith that personal suffering is part of a greater divine plan or purpose, and is not endured in vain; (c) by recallingand identifying with the suffering of scriptural figures (e.g., Jesus, Job, etc.) or more contemporary figures; or other cognitiveprocesses (Foley, 1988; Pargament, 1997). Many of the individuals who pray when facing major problems—and thus mayhave experience and efficacy in prayer—may benefit from the kinds of constructive, collaborative coping practices identifiedby Pargament (1997). Such practices involve the experience of working together with God in handling their problems, a cop-ing style exemplified by the popular epigram, ‘‘God is my copilot.”
Although this pattern of results is intriguing, and we believe important, the GSS item on the frequency of prayer does notprovide does not offer information about the varieties of prayer activities and experiences. In light of the range of ways inwhich people engage in prayer (Poloma and Gallup, 1991; Krause (2000)), it would be useful to know whether certain types
Table 4Interaction effects of religious involvement and stressors on anxiety and tranquility: stress buffering effects (N = 921).
Stressor/dependent variable Main effects: prayer Main effects: afterlife belief Main effects: stressor Interaction term: religion � stressor
Poor health/anxiety .096* — .839*** �.291***
Poor health/anxiety — �.268* .797*** �.041Financial decline/anxiety .086� — .338** �.193*
Financial decline/anxiety — �.134 .850*** �.698*
Poor health/tranquility �.047 — �.699*** .171Poor health/tranquility — .324* �.880** .311Financial decline/tranquility �.008 — �.398** �.037Financial decline/tranquility — .346* �.579� .233
Note: Interactive models control for all covariates included in the full model (Tables 2 and 3 model 4). All components of interaction terms are zero-centered, as recommended by Aiken and West (1991).� p < .10* p < .05.** p < .01.*** p < .001.
C.G. Ellison et al. / Social Science Research 38 (2009) 656–667 663

Author's personal copy
or modes of prayer yield greater reductions in anxiety than others. Given a number of experimental studies indicating thatmeditation induces physiological changes, such as lowered somatic arousal and shifts in brain function, it is important toinvestigate the extent to which prayer and meditation engage the same mechanisms, and the extent to which this may fosterstates of relaxation outside laboratory settings (Holmes, 1984; Brown, 2002). Finally, researchers should probe the role ofexpectancies, or beliefs about the effects and/or helpfulness of prayer, in shaping mental and physical health outcomes.In one recent example, Krause (2004) has shown that two specific prayer expectancies—having to do with (a) the timingof answers to prayers, and (b) the ways in which prayers are/will be answered—are linked with self-esteem among olderadults, and particularly among elderly African Americans.
Third, although religious practices are clearly linked with anxiety and tranquility, so too are beliefs. In particular, the be-lief in an afterlife—even measured very simply, as in the GSS data—bears a direct positive relationship to tranquility, and aninverse association with anxiety. It also seems to reduce the deleterious effects of financial decline on anxiety. Given suchfindings, as well as the centrality of belief in scholarly and lay understandings of (Judeo-Christian) religious culture, thehealth implications of belief in an afterlife merit careful attention. These apparent benefits may result from a sense of cos-mic/divine justice, and the promise of future spiritual rewards that surpass those available in this life. Further, with thepromise of afterlife may come less reason for self-doubt, anger, or recrimination, as well as reduced feelings of urgency tomaximize benefits and minimize costs in this life. To the extent that the afterlife is understood, as in orthodox Christianteaching, as a gift of divine grace, there may be an impetus toward gratitude and forgiveness, which may reduce or forestallnegative emotional states (Thoresen et al., 2000; Krause and Ellison, 2003). However, the impact of afterlife beliefs on mentalhealth no doubt varies by whether one believes that he or she is destined for a positive outcome, or has doubts about his orher prospects in the afterlife. Simply believing in an afterlife is likely unbeneficial for emotional wellbeing if an individualbelieves that he or she is fated for a negative experience (e.g., hell). How one envisions the afterlife also likely conditionsthe relationship between afterlife belief and mental health. Although this topic has been surprisingly understudied, recentstudies indicate that: (a) belief in an afterlife is inversely associated with a number of types of psychopathology among USadults (Flannelly et al., 2006); and (b) the nature of these links depend upon the content of specific beliefs or images regard-ing the afterlife (Flannelly et al., 2008). Clearly the psychosocial correlates and sequelae of afterlife beliefs warrant closerinvestigation in the future.
One intriguing possibility has been suggested in recent research (Schieman et al., 2006): To press): to the extent thatafterlife belief involves a sense of vicarious, or secondary (i.e., divine) control over one’s affairs and problems, it is theoret-ically plausible that the benefits from this belief are greater for persons who lack a sense of direct mastery or control, e.g.,persons from low-SES and/or racial/ethnic minority backgrounds. Indeed, recent studies conducted among older adults haveshown that the psychological implications of divine control tend to vary according to the race and socioeconomic status(SES) of the individual (Krause, 2005; Schieman et al., 2005), with the greatest emotional benefits accruing to lower-SES Afri-can Americans (Schieman et al., 2006). These and other possible contingent relationships deserve consideration from futureresearchers.
Our results also indicate that strong beliefs about human sinfulness are positively associated with anxiety, but unrelatedto feelings of tranquility. Although this pattern is marginally statistically significant, the effects are very modest and incon-sistent across models and outcomes. Nevertheless, this finding offers a glimmer of empirical support for claims that havelong been advanced by psychological critics of religious belief (e.g., Ellis, 1962, 1980). As we noted earlier, these critics haveargued that notions of original sin may: (a) erode positive psychological resources such as self-esteem and mastery; (b) fos-ter negative feelings such as guilt and shame; and (c) divert energy and attention from constructive efforts at personalchange and growth. In addition, strong beliefs about sinfulness may also promote hypervigilance over the threat of moraltemptation and divine judgment (Musick, 2000), and may also encourage mistrust of others, which has been associated withpsychological distress (Mirowsky and Ross, 1986). Given the limitations of our data, further work is needed to examine theseand other possible linkages between sin beliefs and anxiety. Further, this empirical finding also illustrates a broader point,i.e., that while certain aspects of religious practice and belief have salutary implications for health and well-being, the ‘‘sha-dow side” of religion deserves more investigation (Exline, 2002; Pargament, 2002). In addition to sin beliefs, other promisingthemes in this area include spiritual struggles, such as chronic religious doubting, troubled relationships with God, and neg-ative social relations within religious communities, as well as antipathy toward secular sources of psychological and physicalhealth care within some religious groups (Koenig et al., 2001; Krause et al., 1999; Pargament,1997; Pargament et al., 2001a).
Although the links between religion, anxiety, and tranquility are interesting and important in their own right, our findingsmay also have implications for physical health. When individuals are overcome by anxiety, the brain has the capacity to acti-vate bodily responses that are consistent with one’s worries and fears. The mere anticipation of what might happen is en-ough for the autonomic nervous system to flood the blood stream with adrenaline and noradrenaline, the principlechemicals that ready the body for fight-or-flight (Karren et al., 2002; McEwen, 2000a,b). When individuals are kept in a con-stant state of arousal, the hypothalamic–pituitary–adrenal axis increases circulation levels of corticotrophin-releasing hor-mone, adrenocorticotropic hormone, and cortisol (Seeman et al., 1997; Kiecolt-Glaser et al., 2002). This puts a heavy burdenon the body’s ability to properly restore itself. Soon the body may literally short-circuit or gradually become overwhelmed bythe physiological effects of stress. For example, when stress hormones are not metabolized in an efficient manner, chronicarousal may lead to disorders of the autonomic nervous system, causing headaches, irritable bowel syndrome, high bloodpressure, atherosclerosis, and eventually coronary artery disease. Chronic stress may also disrupt proper immune function,thus increasing susceptibility to infection and autoimmune diseases like allergies, arthritis, and lupus. In sum, this raises an
664 C.G. Ellison et al. / Social Science Research 38 (2009) 656–667

Author's personal copy
intriguing possibility that clearly merits additional research: Perhaps the role of religious practice and belief in reducing anx-iety, and fostering tranquility, may help to explain observed relationships between religious involvement and physicalhealth outcomes, including mortality risk (Ellison and Levin, 1998; Chatters, 2000; Koenig et al., 2001).
All research is characterized by limitations, and this is true of the present study as well. Although our analyses are basedon data from a nationally representative cross-sectional sample of US adults, it will be desirable for future studies to explorethese relationships using longitudinal data. As it stands, our inferences about causal order—i.e., that religion affects anxietyand tranquility—are based on cross-sectional associations and theoretical interpretation. However, it is conceivable thatthese relationships are more complex (e.g., bidirectional), and only multiple waves of prospective data can clarify that issue.Likewise, poor physical health may act as a source of stress, increasing levels of anxiety, yet health status may also deteri-orate as the result of chronic stress. To our knowledge, however, there are no longitudinal datasets currently available that(a) are based on nationally representative samples, (b) include appropriate multidimensional measures of religious practiceand belief (including afterlife and sin beliefs), and (c) contain appropriate measures of anxiety and tranquility as well asother relevant items.
Future research might also profitably examine several additional questions. For example, as suggested earlier it would beinstructive to explore possible subgroup differences in the links between religious involvement and anxiety and tranquility,e.g., race/ethnic, gender, age, and socioeconomic variations in the role of religion. It would also be useful to investigate therole of religious practices and beliefs in moderating the deleterious effects of other stressors—such as bereavement, familyconflict, work and unemployment—on anxiety and tranquility. This would help to clarify whether prayer and afterlife beliefscan buffer the impact of a broader constellation of personal problems. And finally, although our focus has been on an over-whelmingly Judeo-Christian population, i.e., US adults, it would be valuable to modify and extend these analyses to includeother religious and spiritual traditions in the future, a direction of several recent works (Pargament et al., 2001b; Tarakesh-war et al., 2003).
These limitations notwithstanding, we believe this study has made a worthwhile contribution to the literature on religionand mental health by: (a) focusing on anxiety and tranquility, which have received less scholarly attention than some others,such as depression and life satisfaction; (b) theorizing and examining the implications of multiple dimensions of religiouspractice and belief, particularly the neglected role of belief in eternal life; (c) presenting new information on the mainand stress-moderator effects of these various aspects of religious involvement vis-a-vis anxiety and tranquility; and (d) iden-tifying several important, understudied areas that warrant further investigation. Additional research along these linessketched above will expand our understanding of the complex relationships and relationships between religion and mentalhealth.
References
Aiken, Leona, West, Stephen G., 1991. Multiple Regression: Testing and Interpreting Interactions. Sage Publications, Newbury Park, CA.Antonovsky, Aaron, 1987. Unraveling the Mystery of Health. Jossey-Bass, San Francisco, CA.Barrett, Anne, 2000. Marital trajectories and mental health. Journal of Health and Social Behavior 41, 451–464.Berger, Peter, 1967. The Sacred Canopy. Doubleday, Garden City, NY.Black, Helen K., 1999. Poverty and prayer: spiritual narratives of elderly African American women. Review of Religious Research 40, 359–374.Bradley, Don E., 1995. Religious involvement and social resources: evidence from the dataset ‘Americans’ changing lives’. Journal for the Scientific Study of
Religion 34, 259–267.Branden, Nathaniel, 1994. The Six Pillars of Self-Esteem. Bantam Books, New York.Brown, Warren S., 2002. PNI and Western Religious Traditions. In: Koenig, H.G., Cohen, H.J. (Eds.), The Link Between Religion and Health. Oxford University
Press, New York, pp. 262–274.Chatters, Linda, 2000. Religion and health: public health research and practice. Annual Review of Public Health 21, 335–367.Chaves, Mark, Higgins, Lynn H., 1992. Comparing the community involvement of Black and White congregations. Journal for the Scientific Study of Religion
31, 425–440.Cornwall, Marie, 1987. The social bases of religion: a study of the factors influencing religious belief and commitment. Review of Religious Research 29, 44–
56.Davis, James A., Smith, Tom W., 1996. General Social Surveys, 1972–1996: Cumulative Codebook [and MRDF]. National Opinion Research Center, Chicago.Drentea, Patricia, 2000. Age, debt, and anxiety. Journal of Health and Social Behavior 41, 437–450.Ellis, Albert, 1962. Reason and Emotion in Psychotherapy. Citadel Press, Secaucus, NJ.Ellis, Albert, 1980. Psychotherapy and atheistic values: a response to A. E. Bergin’s ‘‘Psychotherapy and Religious Values”. Journal of Consulting and Clinical
Psychology 48, 635–639.Ellison, Christopher G., 1993. Religious involvement and self-perception among Black Americans. Social Forces 71, 1027–1055.Ellison, Christopher G., Boardman, Jason D., Williams, David R., Jackson, James S., 2001. Religious involvement, stress, and mental health: findings from the
1995 Detroit area study. Social Forces 80, 215–249.Ellison, Christopher G., George, Linda K., 1994. Religious involvement, social ties, and social support in a southeastern community. Journal for the Scientific
Study of Religion 33, 46–61.Ellison, Christopher G., Levin, Jeffrey S., 1998. The religion-health connection: evidence, theory, and future directions. Health Education and Behavior 25,
700–720.Ellison, Christopher G., Taylor, Robert J., 1996. Turning to prayer: social and situational antecedents of religious coping among African Americans. Review of
Religious Research 38, 111–131.Exline, Julia Juola, 2002. Stumbling blocks on the religious road: fractured relationships, nagging vices, and the inner struggle to believe. Psychological
Inquiry 13, 182–189.Farmer, Melissa, Ferraro, Kenneth, 1997. Distress and perceived health: mechanisms of health decline. Journal of Health and Social Behavior 38, 298–311.Flannelly, Kevin J., Koenig, Harold G., Ellison, Christopher G., Galek, Kathleen, Krause, Neal, 2006. Belief in life after death and mental health: findings from a
national survey. Journal of Nervous and Mental Disease 194, 524–529.Flannelly, Kevin J., Ellison, Christopher G., Galek, Kathleen, Koenig, Harold G., 2008. Beliefs about life-after-death, psychiatric symptomology, and cognitive
theories of psychopathology. Journal of Psychology and Theology 36, 94–103.
C.G. Ellison et al. / Social Science Research 38 (2009) 656–667 665

Author's personal copy
Foley, Daniel P., 1988. Eleven interpretations of personal suffering. Journal of Religion and Health 27, 321–328.Grasmick, Harold G., Bursik Jr., Robert J., 1991. Render unto Caesar what is Caesar’s’: religiosity and taxpayers’ inclinations to cheat. The Sociological
Quarterly 32, 251–266.Greeley, Andrew, Hout, Michael, 1999. Americans’ increasing belief in life after death: competition and assimilation. American Sociological Review 65, 813–
836.Griffith, Ezra E.H., Young, John L., Smith, Dorothy L., 1984. An analysis of the therapeutic elements in a Black church service. Hospital and Community
Psychiatry 35, 464–469.Hackney, Charles H., Sanders, Glenn S., 2003. Religiosity and mental health: a meta-analysis of recent studies. Journal for the Scientific Study of Religion 42,
43–55.Harley, Brian, Firebaugh, Glenn, 1993. Americans’ belief in an afterlife: trends over the past two decades. Journal for the Scientific Study of Religion 32, 269–
278.Hill, Terrence, Burdette, Amy, Ellison, Christopher, Music, Marc, 2006. Religious attendance and the health behaviors of Texas adults. Preventive Medicine
42, 309–312.Hill, Terrence, Burdette, Amy, Ellison, Christopher, Music, Marc, 2007. Religious involvement and healthy lifestyles: evidence from the survey of Texas
adults. Annals of Behavioral Medicine 34, 217–222.Hoffmann, John P., 2000. Religion and problem gambling in the US. Review of Religious Research 41, 488–509.Holmes, David S., 1984. Meditation and somatic arousal reduction: a review of the experimental evidence. American Psychologist 39, 1–10.Idler, Ellen L., 1987. Religious involvement and the health of the elderly: some hypotheses and an initial test. Social Forces 66, 226–238.Idler, Ellen L., 1995. Religion, health, and nonphysical senses of self. Social Forces 74, 683–704.Idler, Ellen L., Kasl, Stanislav V., 1992. Religion, disability, depression, and the timing of death. American Journal of Sociology 97, 1052–1079.Idler, Ellen L., Musick, Marc A., Ellison, Christopher G., George, Linda K., Krause, Neal, Levin, Jeffrey S., Ory, Marcia, Pargament, Kenneth I., Powell, Lynda,
Gordon, Lynn Underwood, Williams, David R., 2003. NIA/Fetzer measure of religiousness and spirituality: conceptual background and findings from the1998 general social survey. Research on Aging 25, 327–366.
Jang, Sung Joon, Johnson, Byron R., 2004. Explaining religious effects on distress among African Americans. Journal for the Scientific Study of Religion 43,239–260.
Jang, Sung Joon, Johnson, Byron R., 2005. Gender, religiosity, and reactions to strain among African Americans. The Sociological Quarterly 46, 323–357.Karren, Keith, Hafen, Brent, Smith, Lee, Frandsen, Kathryn, 2002. Mind/Body Health: The Effects of Attitudes, Emotions, and Relationships. Benjamin
Cummings, San Francisco.Kiecolt-Glaser, Janice, McGuire, Lyanne, Robles, Theodore, Glaser, Ronald, 2002. Emotions, morbidity, and mortality: new perspectives from
psychoneuroimmunology. Annual Review of Psychology 53, 83–107.Kirkpatrick, Lee, 2004. Attachment, Evolution, and the Psychology of Religion. Guilford Press, New York.Koenig, Harold G., George, Linda K., Cohen, Harvey J., Hays, Judith C., Larson, David B., Blazer, Dan G., 1998. The relationship between religious activities and
cigarette smoking in older adults. Journal of Gerontology: Medical Sciences 53A, M426–M434.Koenig, Harold G., George, Linda K., Meador, Keith G., Blazer, Dan G., Ford, S.M., 1994. The relationship between religion and alcoholism in a sample of
community-dwelling adults. Hospital and Community Psychiatry 45, 225–231.Koenig, Harold G., George, Linda K., Siegler, Ilene C., 1988. The use of religion and other emotion-regulating coping strategies among older adults. The
Gerontologist 28, 303–310.Koenig, Harold G., McCullough, Michael, Larson, David B., 2001. Handbook of Religion and Health. Oxford University Press, New York.Krause, Neal, 1995. Religiosity and self-esteem among older adults. Journal of Gerontology: Psychological Sciences 50, P236–P246.Krause, Neal, 2002a. Exploring race differences in a comprehensive battery of church-based social support measures. Review of Religious Research 44, 126–
149.Krause, Neal, 2002b. Church-based social support and health in old age: exploring variations by race. Journals of Gerontology Series B: Psychological
Sciences & Social Sciences 57B, S332–S348.Krause, Neal, 2004. Assessing the relationships among prayer expectancies, race, and self-esteem in late life. Journal for the Scientific Study of Religion 43,
393–406.Krause, Neal, 2005. God-mediated control and psychological well-being in late life. Research on Aging 27, 136–164.Krause, Neal, Ellison, Christopher G., 2003. Forgiveness by god, forgiveness of others, and psychological well-being in late life. Journal for the Scientific Study
of Religion 42, 77–93.Krause, Neal, Ellison, Christopher G., Shaw, Benjamin A., Marcum, Jack P., Boardman, Jason D., 2001. Church-based social support and religious coping.
Journal for the Scientific Study of Religion 40, 637–656.Krause, Neal, Ingersoll-Dayton, Berit, Ellison, Christopher G., Wulff, Keith H., 1999. Aging, religious doubt, and psychological well-being. The Gerontologist
39, 525–533.Krause, Neal, Morgan, David L., Chatters, Linda M., Tina, Meltzer, 2000. Using focus groups to explore the nature of prayer in late life. Journal of Aging Studies
14, 191–212.Levin, Jeffrey S., Chatters, Linda M., 1998. Research on religion and mental health: a review of empirical findings and theoretical issues. In: Koenig, H.G. (Ed.),
Handbook of Religion and Mental Health. Academic Press, San Diego, CA, pp. 33–50.Levin, Jeffrey S., Taylor, Robert J., Chatters, Linda M., 1995. A multidimensional measure of religious involvement for African Americans. The Sociological
Quarterly 36, 157–173.McEwen, Bruce, 2000a. Allostasis and allostatic load: implications for neuropsychopharmacology. Neuropsychopharmacology 22, 108–124.McEwen, Bruce, 2000b. The neurobiology of stress: from serendipity to clinical relevance. Brain Research 886, 172–189.Mirowsky, John, Ross, Catherine, 1986. Social patterns of distress. Annual Review of Sociology 12, 23–45.Mirowsky, John, Ross, Catherine, 1995. Sex differences in distress: real or artifact? American Sociological Review 60, 449–468.Mirowsky, John, Ross, Catherine, 2003. Social Causes of Psychological Distress. Aldine de Gruyter, Hawthorne, NY.Musick, Marc A., 2000. Theodicy and life satisfaction among Black and White Americans. Sociology of Religion 61, 267–287.Neighbors, Harold W., Musick, Marc A., Williams, David R., 1998. The African American minister as a source of help for serious personal crises: bridge or
barrier to mental health care? Health Education and Behavior 25, 759–777.Nooney, Jennifer, Woodrum, Eric, 2002. Religious coping and church-based support as predictors of mental health outcomes: testing a conceptual model.
Journal for the Scientific Study of Religion 41, 359–368.Pargament, Kenneth I., 1997. The Psychology of Religion and Coping. Guilford Press, New York.Pargament, Kenneth I., 2002. The bitter and the sweet: an evaluation of the costs and benefits of religiousness. Psychological Inquiry 13, 168–181.Pargament, Kenneth I., Koenig, Harold G., Tarakeshwar, Nalini, Hahn, June, 2001a. Religious struggle as a predictor of mortality among medically-Ill elderly
patients: a two-year longitudinal study. Archives of Internal Medicine 161, 1881–1885.Pargament, Kenneth I., Poloma, Margaret, Tarakeshwar, Nalini, 2001b. Spiritual healing, karma, and the bar Mitzvah: methods of coping from the religions
of the world. In: Snyder, C.R. (Ed.), Coping and Copers: Adaptive Process and People. Oxford University Press, New York, pp. 259–284.Petersen, Larry A., Roy, Anita, 1985. Religiosity, anxiety, and meaning and purpose: religion’s consequences for psychological well-being. Review of
Religious Research 27, 49–62.Poindexter, Cynthia Cannon, Linsk, Nathan L., Stephen Warner, R., 1999. ‘He Listens... and Never Gossips’: spiritual coping without church support among
older, predominantly African American caregivers of persons with HIV. Review of Religious Research 40, 230–243.Pollner, Melvin, 1989. Divine relations, social relations, and well-being. Journal of Health and Social Behavior 30, 92–104.
666 C.G. Ellison et al. / Social Science Research 38 (2009) 656–667

Author's personal copy
Poloma, Margaret, Gallup Jr., George, 1991. Varieties of Prayer: A Survey Report. Trinity Press International, Philadelphia.Ross, Catherine, Van Willigen, Marieke, 1997. Education and the subjective quality of life. Journal of Health and Social Behavior 38, 275–297.Schieman, Scott H., Nguyen, Kim, Elliot, Diana, 2003. Religiosity, socioeconomic status, and the sense of mastery. Social Psychology Quarterly 66, 202–221.Schieman, Scott, Pudrovska, Tetyana, Milkie, Melissa, 2005. The sense of divine control and the self-concept: a study of race differences in late-life. Research
on Aging 27, 165–196.Schieman, Scott H., Pudrovska, Tetyana, Pearlin, Leonard I., Ellison, Christopher G., 2006. The sense of divine control and mental health in late life:
moderating effects of race and socioeconomic status. Journal for the Scientific Study of Religion 45, 529–549.Schieman, Scott, Van Gundy, Karen, Taylor, John, 2001. Status, role and resource explanations for age patterns in psychological distress. Journal of Health
and Social Behavior 42, 80–96.Schnittker, Jason, 2001. When is faith enough? The effects of religious involvement on depression. Journal for the Scientific Study of Religion 40, 393–412.Seeman, Teresa, Burton, Singer, John, Rowe, Ralph, Horwitz, Bruce, McEwen, 1997. Price of adaptation-allostatic load and its health consequences:
MacArthur studies of successful aging. Archives of Internal Medicine 157, 2259–2269.Shreve-Neiger, Andrea K., Edelstein, Barry A., 2004. Religion and anxiety: a critical review of the literature. Clinical Psychology Review 24, 379–397.Stark, Rodney, Bainbridge, William Sims, 1996. A theory of religion. Rutgers University Press, New Brunswick, NJ.Stark, Rodney, Glock, Charles, 1968. American Piety. University of California Press, Berkeley.Tarakeshwar, Nalini, Pargament, Kenneth I., Annette, Mahoney, 2003. Measures of Hindu pathways: development and preliminary evidence of reliability
and validity. Cultural Diversity and Ethnic Minority Psychology 9, 316–332.Taylor, Robert J., Chatters, Linda M., 1988. Church members as a source of informal social support. Review of Religious Research 30, 193–203.Thoits, Peggy, 1995. Stress, coping, and social support processes: where are we? What next? Journal of Health and Social Behavior 35 (Extra Issue), 53–79.Thoresen, Carl A., Harris, Alex H.S., Luskin, Frederic, 2000. Forgiveness and health: an unanswered question. In: McCullough, M., Pargament, K., Thoresen, C.
(Eds.), Forgiveness: Theory, Research, and Practice. Guilford, New York, pp. 254–280.Tsitsos, William, 2001. Race differences in congregational social service activity. Journal for the Scientific Study of Religion 42, 205–215.Watson, Paul J., Morris, Ronald J., Hood, Ralph W., 1988a. Sin and self-functioning. Part I: Grace, guilt, and self-consciousness. Journal of Psychology and
Theology 16, 254–269.Watson, Paul J., Morris, Ronald J., Hood, Ralph W., 1988b. Sin and self-functioning. Part III: The psychology and ideology of irrational beliefs. Journal of
Psychology and Theology 16, 348–361.Watters, Wendell W., 1992. Deadly doctrine: Health, Illness, and Christian God-Talk. Prometheus Books, Amherst, NY.Williams, Anne, Ware, John, Donald, Cathy, 1981. A model of mental health, life events, and social supports applicable to general populations. Journal of
Health and Social Behavior 22, 324–336.Williams, David R., 1994. The measurement of religion in epidemiologic studies: problems and prospects. In: Levin, J.S. (Ed.), Religion in Aging and Health:
Theoretical Foundations and Methodological Frontiers. Sage, Thousand Oaks, CA, pp. 125–148.Wuthnow, Robert (Ed.), 1994. I Come Away Stronger: How Small Groups are Shaping American Religion. Eerdmans, Grand Rapids, MI.
C.G. Ellison et al. / Social Science Research 38 (2009) 656–667 667