saudi arabia uae, saudi arabia using culture as a cohesive force

Abstracts from the 12th Congress of the InternationalSociety for Organ Donation and ProcurementNovember 21–24, 2013 / Sydney, Australia
130
Conscience-based refusal to participate in donationafter cardiac death (DCD)
Mark Wicclair1,2
1Philosophy, West Virginia University, Morgantown, WV, United States;2Center for Bioethics and Health Law, University of Pittsburgh,Pittsburgh, PA, United States.
While conscientious objection has its historical roots in objections to mil-itary service, a growing number of health professionals have refused toprovide a broad range of goods and services that violate their ethicalbeliefs. Such actions, clearly, can have a major impact on organ dona-tion. Some ICU clinicians, for instance, have objected to participating indonation after cardiac death (DCD) because it is against their con-science. In this presentation, two extreme approaches to managing con-science-based objections to participating in DCD are identified andrejected and a more nuanced middle-ground is proposed.One extreme is “conscience absolutism,” the view that cliniciansshould be exempted from performing any action, including participat-ing in DCD, that is contrary to their conscience. The second extremeis the “incompatibility thesis,” the view that practitioners have an obli-gation to provide any good or service, including participating in DCD,that is legal, professionally accepted, and within the scope of their pro-fessional competence.Neither of these extreme approaches is defensible. Conscience absolut-ism is indefensible because it fails to consider that clinicians haveobligations to patients and their families, other professionals, institutions,and society. The incompatibility thesis is untenable because it fails to ac-knowledge the value of moral integrity, and it presupposes an indefensi-ble conception of clinicians’ professional obligations.An alternative to both extreme approaches is presented. It features thefollowing guidelines: a) Clinicians should provide advance notificationof a conscience-based objection to participating in DCD; b) accommo-dation should not result in a failure to inform surrogates of the DCD op-tion in a timely manner; c) accommodation should not impede orunduly delay DCD; d) accommodation should not impose excessiveburdens on other clinicians, administrators, or institutions.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
131
Legalizing HIV-positive organ donation to HIV-positiverecipients: One giant leap toward addressing organ donationwaiting list burden
Leslie Wolf, Rachel HulkowerCollege of Law, Georgia State University, Atlanta, GA, United States.
In the United States today, over 115,000 patients are waiting for organtransplantation, but, in 2012, only 28,051 organs were transplantedfrom living and deceased donors. The gap between the supply and de-mand continues to grow, while thousands of patients die annuallyawaiting organ transplantation.US laws that ban transplantation of organs from donors who are HIV-infected, even when the recipient is HIV-infected, exacerbate this gap.Such limits may have been necessary early in the HIV/AIDS epidemic,when there were no effective treatments and patients typically diedwithin a year or two of an AIDS diagnosis. Today, however, with accessto effective antiretroviral therapies, people livingwith HIV have life expec-tancies similar to those without HIV and now also add to the number ofpatients awaiting organ transplantation.Eliminating legal barriers to transplantation of organs from HIV-infecteddonors could alleviate the shortage of organs for both HIV-infected andnon-infected transplantation candidates. This would occur by increasingthe pool of organs available to HIV-infected transplantation candidates,moving them off the transplant list, and allocating remaining organs tothose remaining on the list. This presentation will describe the lawsand policies prohibiting organ donation by those who are HIV-infected,the need for and evidence supporting a policy change, and recommendways to accomplish that policy change.
r 27, 2013, Volume 96 Number 10S S165
thorized reproduction of this article is prohibited.

November 27, 2013
132
Changing pattern of death cause and future source
of organs in KoreaWon H Cho1,2, Ui J Park1, Jin S Yu2, Hyeung T Kim1,2
1Department of Surgery, Division of Transplantation, KeimyungUniversity School of Medicine, Daegu, Korea; 2Vitallink Korea,Seoul, Korea.
Required reporting system included in newly revised transplantationlaw increase deceased donor about 20% in recent 2 years. However,nobody can believe this amount of growth in the next year because wealready sense a slowing of growth this year. In order to have a pro-spective possibility of organ donation from deceased donor, nationalstatistics about changing pattern of death cause were reviewed. TheKorea Network of Organ Sharing(KONOS) reported that number of liv-ing donor transplantation is decreasing from 53.3% in 2008 to 50.9%in 2012. Instead, proportion of deceased donor is increased from35.3% to 45.7%.
FIGURE 1.
Among these deceased donor, two most frequent cause of brain deathwere cerebrovascular disease and head trauma by traffic or other ac-cident, which comprised 81.0%. But real problem in recent year is thechanging pattern of death cause which reported by the StatisticsKorea(national statistics). The death rate of cerebrovascular diseaseand head trauma are decreasing definitely and their reducing ratein 2012 are 31.2% and 39.6% compare to 2001. Even we don’t
FIGURE 2.
S166 Supplement to Transplantation NovembeS166 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
use all of the potential donor that developed at hospital right now, weeasily expect the donor from deceased donor will be soon flat or de-creasing. To solve this problem, we actively change our policy to usenon-heart beating donor and aggressively use expanded criteria do-nor which were discarded previously. National consensus aboutchanging the law for removing the life supporting system is also seri-ously considered.
r 27, 2013, Volume 96 Number 10Sr 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
133
An exploration of consent issues in Victorian potential donors
after brain death (DBD) and cardiac death (DCD)Hugh Stephens1, David Pilcher2, Helen Opdam3, Gregory Snell4,Jeffrey Rosenfeld51MBBS/PhD Candidate, Monash University / The Alfred Hospital,Melbourne, Australia; 2Department of Intensive Care, Alfred Hospital,Melbourne, Australia; 3DonateLife Victoria, Melbourne, Australia;4AIRmed Lung Transplant Service, Alfred Hospital, Melbourne,Australia; 5Department of Surgery, Alfred Hospital,Melbourne, Australia.
Background & Aim: Consent remains one of the greatest barriers toincreasing the donor pool [1]. International centres have found familyconsent rates to be associated with brain death status, age, and eth-nicity [2].Methods: From a database of 18,949 deaths occurring in 22 Victorianhospitals between 1 January 2010 and 30 June 2012, we selectedcases where organ donation was discussed with the family or guardian.Examination of patient and family wishes; donor type andwhether dona-tion was successful was completed using univariate analysis.Results: A total of 623 family discussions occurred. Of these, 115 wereunsuitable for donation due to a medical contraindication, were consid-ered unsupportable to facilitate donation or were not ventilated in the6 hours prior to death. There were a total of 175 successful donations(130 DBD donations and 41 DCD donations (n=4 unknown), from 508potential donors, 34%), and one patient survived to discharge (n=4 datamissing). Donation was raised by staff in 73% (n=372) of cases and fam-ily in 24% of cases (n=123). The patient was recorded as a consent onthe organ donation registry in 54 cases out of 256 checks (remaindernot listed). In one of these cases, the family subsequently declined do-nation. Of those not listed on the registry, 45% of families subsequentlyconsented to donation (n=201), with n=242 refusals and n=5 notasked. Family consent was more likely in patients with confirmed orprobable brain death (50% vs 40%, p=0.03), whether the patient diedof non-neurological causes (69% vs 50%, p=0.04) and whether fami-lies initially raised donation (76% vs 42%, p<0.01). This suggests a po-tential lack of understanding from patient families of DCD programs.There was no association with age (p=0.40) or gender (p=0.80).Conclusions: Brain death status, cause of death and who initiallyraised organ donation were factors predicting consent.
References:[1] National Health and Medical Research Council (NHMRC). NationalProtocol for Donation after Cardiac Death. Canberra: Australian Organand Tissue Donation and Transplantation Authority (AOTDA); 2010.[2] Brown, C. V., et al. (2010). “Barriers to obtaining family consent forpotential organ donors.” J Trauma 68(2): 447-451.
Supplement to Transplantation NovembeSupplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
134
Body language of "blood owners" different cultural and legalframeworks need different family approaches in organ request
Masoud MazaheriOrgan Procurement, Emam OPU, Tehran, Iran (Islamic Republic of).
In different countries, different legal systems regulate the whole processof organ donation and transplantation. This legal system has been influ-enced by many historical, traditional and even philosophical local factorsand has always continual dialogue with social forces which representthose factors. The brain-dead’s family interview to request organ dona-tion, where one proposes an emergent request to a still-unbeleiving fam-ily, reveals the hidden internal conflictions and challenges of this legalsystem. In countries like Spain, where the “individual will” is themost de-termining legal factor, the interview takes the shape of an detective mis-sion to discover whether the brain-dead has had any dissagreement withorgan donation in their lifetime or not. On the other hand, in countries in-fluenced by Arabic-Islamic culture (including Iran) the family members’final will is more important than the individual’s and in legal issues suchas organ donation the next-of-kins decision (more specifically, the malerelatives or “blood owners”) is what matters the most. In these countries,the family interview is not as easy and non-challenging as Spain modeland one must struggle to convince a group of male relatives to give per-mission for someone-else organ donation! To do so, the organ procure-ment unit (OPU) coordinators must be aware of all communicative skillsneeded to manage a non-cooperative and heterogen group. To be famil-iar with “body language” is a good weapon in handling family interviewsall over the world, but in a country like Iran, it is very vital and could avoidof many misundertandings and unwanted tensions, and could dramati-cally raise the rate of successful requests for organ donation.
r 27, 2013, Volume 96 Number 10S S167r 27, 2013, Volume 96 Number 10S S167
thorized reproduction of this article is prohibited.

November 27, 2013
135
Getting to 96% family constant rate for organ donationby PEIP method
O. Ghobadi, K. Hadisadegh, S. Abdollahi, M. Mottaghi, M. Moftakhari,A. Jamali, K. NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran(Islamic Republic of).
Introduction: Taking brain dead family consent is one of the most im-portant steps of organ donation process. In spite of extensive socialawareness activities, rate of family consent was still about 32% in Iran.To increase the rate of consent, we started a project named PEIP(Persian educating interviewers’ project) which is presenting here:Methods: 1- We learned brain dead family interview fundamentalsfrom TPM (Transplant Procurement Management) of Spain as one ofthe most successful teams of the world in this subject. 2- By checkingthe causes of family refusal and considering the cultural differences,we adjusted this science with our culture 3- By an interview and examwe selected 6 out of 70 volunteer psychologists. 4- After educatingthese psychologists and our coordinators for brain dead family inter-view we selected the interviewers who could get to the consent rateof more than 60%. 5- The interviewers discussed about their casesand took the others comments every other week and their expertteacher guided them. 6- We changed the interviewer if the first onecould not get the consent in 48 hour. 7- We didn’t give up until gettingthe family consent or until the case had cardiac arrest.Results: Family consent rate increased from %32 to %96.3 onemonth after starting the project and stayed more than 85% until now.The duration of interview needed, decreased from 24 – 72 hours to lessthan 12 hours in 72%, 12-24 hours in 21% and more than 24 hours in7%. Organ retrieval increased from 12 to 27 monthly.Conclusion: Brain dead family interview is a science and with regulareducating the interviewers by experts, consent rate can increase tonear 100%. We advise PEIP to be used in another countries speciallythe ones with similar culture.Keywords: Organ donation, Brain death, family consent
S168 Supplement to Transplantation NovembeS168 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
137
Psychosocial impact of donation process on the living organdonors (FIS project)
Marti Manyalich Vidal1, Ana Menjivar1, Josep Maria Peri1,Xavier Torres1, Eva Oliver2, Nuria Masnou3, Teresa Rangil4,Maribel Delgado5, Antonio Fernandez6, Montserrat Martinez7,Ana Vila8, Chloe Balleste1, Jaume Grau1, Amado Andres5,Ana Zapatero9, Laura Cañas4, Ricardo Lauzurica4, M. Pilar Gracia9,Yolanda Diaz9, Josep Maria Puig91Hospital Clinic of Barcelona, Barcelona, Spain; 2Bellvitge Hospital,Barcelona, Spain; 3Vall d’Hebron Hospital, Barcelona, Spain;4Germans Trias i Pujol Hospital, Barcelona, Spain; 5HospitalUniversitario 12 de Octubre, Madrid, Spain; 6Complejo Universitariode A Coruña, A Coruña, Spain; 7Fundació Puigvert, Barcelona, Spain;8Hospital Sant Joan de Deu, Barcelona, Spain; 9Hospital del Mar,Barcelona, Spain.
Introduction: Living Donation has a positive impact on Living donors(LDs) in terms of their self-estimation and social value. However, an eval-uated risk on their physical and psychosocial outcome is presented. Suchrisk appears to be linearly increased for a longer post donation time.FIS project, 2011-2013, co-founded by European Regional Develop-ment Fund (FEDER), aims to evaluate the psychosocial outcomeand the satisfaction level of Spanish kidney and liver living donors.Objective: To analyze the impact of donation process on the LDsquality of life and psychological well-being and to evaluate the levelof satisfaction received from the process.Methodology: The population includes the LDs who donated in ninetransplant centers all over Spain from year 2000 in continuity.The project is developed in two simultaneous studies:Prospective study- a longitudinal psychosocial follow-up of LDs,assessed in two moments pre and one year post donation.Retrospective study- to evaluate the satisfaction level LDs receivedfrom the donation process. As assessment tool a new version of theEULID (European Living Donation and Public Health) satisfaction sur-vey was designed.The results are introduced in the database surged from EULID project,available on www.eulivingdonor.eu.Results: The centers have adapted the methodology to theircharacteristics and resources. The studies are being developed inde-pendently and currently the project is in the data-analyses phase.Nowadays, there are more than 400 LDs registered; respectively 90%are Kidney LDs and 10% Liver LDs.Out of these approximately 214 LDs are included in the retrospectivestudy and approximately 132 LDs in the prospective study.Conclusion: Changes in the ability to manage or improve life stressorsare fundamental for good psychosocial outcome on LDs. The LDs satis-faction is key point to ensure the overall quality and security of donationprocedures.
r 27, 2013, Volume 96 Number 10Sr 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
138
Correlation between potential donor age and family refusalrates in the State of Rio de Janeiro, Brazil
Janaina Lenzi1, Andreia Assis1, Márcia Ponte1, Priscila Paura2,André Albuquerque2, Rodrigo Sarlo3, Cláudia Araújo5,Eduardo Rocha4,51Family Services, State Organ Procurement Organization, Rio deJaneiro, Brazil; 2Education, State Organ Procurement Organization,Rio de Janeiro, Brazil; 3General Coordination, State OrganProcurement Organization, Rio de Janeiro, Brazil; 4HealthFoundation, State Health Board, Rio de Janeiro, Brazil; 5COPPEAD,Federal University of Rio de Janeiro, Rio de Janeiro, Brazil.
Introduction: It is well known that potential donor (PD) age influencesfamily decision on organ donation. Accepting the death of a child oryoung person often is very difficult and donation rates (DR) may varyaccording to cultural beliefs and general education on organ donation.Studies are contradictory to DR among the elderly. Our study aims toanalyze the influence of age on family refusal, in order to help devel-oping strategies to increase awareness on the subject and trainingof health professionals in charge of interviewing families of PD.Methods: Data from the records of the Rio de Janeiro State Trans-plant Program (PET) from 2011 to 2012 were reviewed and expressedas percentual analysis (%). Family refusal (FR) rates for donationwere organized according to PD’ age group as follows: children(<11), teenagers (12-17), adults (18-64) and seniors (>65).Results: Our data show that in the period studied, among refusals53% were associated to children, 51% to teenagers, 46% to adults,and 55% to senior PD. The main reason for children and teenagerFR were misunderstanding of brain death and fear of body mutilation.These become to have a smaller participation as the potentialdonor age increases. Otherwise, absence of consensus among fam-ily members and first person refusal were the main reasons for FR inelderly PD.Conclusion: Our study shows that FR occurred in over 50% of caseswhen a child, teenager or an elderly PD was involved. This resultreinforces previous research and indicates that young donor age is as-sociated with a reduced probability of donation. Furthermore, this re-search goes further by showing that seniors also have a lowerlikelihood of having their organs donated in RJ, Brazil. This means thathealth care professionals who interview families of PD should betrained to deal with these family questions, using different strategiesaccording to the age of the deceased.
Supplement to Transplantation NovembeSupplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
141
Brain death impairs microcirculation with or without autonomicstorm: an intravital microscopy study with thoracic epiduralanesthesia in rats
Isaac Azevedo Silva, Rafael Simas, Laura Menegat,Cristiano de Jesus Correia, Sueli Gomes Ferreira,Paulina Sannomiya, Luiz Felipe Pinho MoreiraHeart Institute (InCor), University of Sao Paulo Medical School,Sao Paulo, Brazil.
Introduction: Brain death (BD) is associated with hemodynamic in-stability, inflammation and mesenteric hypoperfusion[1]. In a previousstudy, thoracic epidural anesthesia (TEA) blocked the hypertensivecrisis and the hemodynamic instability, without inflammatory responseattenuation[2]. The present study aimed to evaluate the influence ofsympathetic blockade in mesenteric perfusion in brain dead rats.Methods: Male Wistar rats were anesthetized with isoflurane (5-2%)and underwent BD by intracranial catheter insufflation immediately af-ter epidural infusion of bupivacaine (Bupi) or saline. Mean arterialpressure (MAP) was monitored over 3h. The mesenteric microcircula-tion was assessed by intravital microscopy. In the same time point,the expression of mesenteric ICAM-1 was quantified by immunohisto-chemistry and the serum corticosterone level was determined byELISA. Sham-operated rats (SH group) was trepanned only. Resultsare presented as mean±SEM.Results: The autonomic storm was abolished in Bupi group (p<0.001),however, the percentage of perfused mesenteric microvessels was sim-ilar between the study groups and significantly lower than SH (Bupi: 43±6%, saline: 39±7%; SH: 74±6%. p=0.002). The expression of ICAM-1was similar between the study groups (Bupi: 21±5; Saline: 23±8), buthigher than the SH (9±2 mean fluorescence intensity, p<0.001). Serumlevels of corticosterone was lower in Bupi and Saline groups comparedwith SH (p=0.01).Conclusions: TEA with bupivacaine was effective in abolishing theautonomic storm, however, tissue hypoperfusion, elevated expressionof adhesion molecules, and the low serum corticosterone, triggered byBD remained in the animals independently to hemodynamic status.Therefore, inhibition of the hypertensive peak in BD does not improvemesenteric perfusion and does not modulate the endothelial activation.Finnacial Support: FAPESP.
References:[1] Simas, R.; Sannomiya, P.; Cruz, J. W. M. C.; Correia, C. J.; Zanoni,F L; Kase, M.; Menegat, L.; Silva,I. A.; Moreira, L. F. P. Paradoxicaleffects of brain death and associated trauma on rat mesenteric micro-circulation: an intravital microscopic study. Clinics (USP. Impresso)JCR, v. 67, p. 69-75, 2012.[2] Silva, I.A.; Correia, C.J.; Simas, R.; Cruz, J.W.M.C.; Ferreira, S.G.;Zanoni, F.L.; Menegat, L.; Sannomiya, P.; Moreira, L.F.P. Inhibition ofAutonomic Storm by Epidural Anesthesia Does Not Influence CardiacInflammatory Response After Brain Death in Rats. TransplantationProceedings JCR, v. 44, p. 2213-2218, 2012.
r 27, 2013, Volume 96 Number 10S S169r 27, 2013, Volume 96 Number 10S S169
thorized reproduction of this article is prohibited.

November 27, 2013
142
Apnea testing for determination of brain death in childrensupported with veno-arterial ECMO
Thomas A. Nakagawa1, Rima J. Jarrah2, Samuel J. Ajizian3,Swati Agarwal5, Scott C. Copus2Anesthesiology, Wake Forest Baptist Health, Brenner Children’sHospital, Winston-Salem, NC, United States; 1Anesthesiology, WakeForest Baptist Health, Brenner Children’s Hospital, Winston-Salem,NC, United States; 3Anesthesiology, Wake Forest Baptist Health,Brenner Children's Hospital, Winston-Salem, NC, United States;4Pediatrics, Section of Pediatric Critical Care, Inova Fairfax Hospitalfor Children, Falls Church, VA, United States; 5Respiratory Care,Wake Forest Baptist Health, Brenner Children’s Hospital,Winston-Salem, NC, United States.
Introduction: The updated United States guideline for the determina-tion of brain death in infants and children provides important direction forclinicians tasked with determining death.[1] The guideline unfortuantelylacks direction for apnea testing when a patient is supported on extracor-porealmembrane oxygenation (ECMO), as no published literature existsfor this clinical situation.Methods: Retrospective observational case review.Results: Three children ages 5months, 2 years, and 14 years, supportedon veno-arterial (VA) ECMO following cardiopulmonary arrest, developeda neurologic exam consistent with brain death. Apnea testing on VAECMO was successfully performed using the following method:1. PaCO2 was normalized by adjusting ECMO sweep gas flow and
obtaining a baseline arterial blood gas (ABG) analysis.2. Sweep gas FiO2 was increased to 1.0 to provide preoxygenation on VA-ECMO.
3. A flow-inflating bag system with continuous positive airway pressureand FiO2 1.0 was used after removing the patient frommechanical ven-tilation support.
4. Sweep gas flowwas reduced to 0.1 L/min for smaller children and 1.0 L/min for larger children while maintaining sweep gas FiO2 at 1.0. Rate ofPaCO2 rise was monitored using CDI blood parameter monitoring sys-tem and correlated with ABG analysis to confirm PaCO2 level reachedthe recommended threshold to support brain death determination.
In two cases, apnea testing was able to be successfully performed. Inone case, the patient developed hemodynamic instability and hypoxia,and the apnea test was terminated.Conclusions: This pediatric case series describes a method ofconducting apnea testing for children supported with VA ECMO. Weaddress an important clinical scenario that has not been previouslydescribed in children undergoing brain death testing.
Reference:1. Nakagawa TA, Ashwal S, Mathur M, et al. Guidelines for the deter-mination of brain death in infants and children: an update of the 1987Task Force recommendations. Crit Care Med 2011,39(9):2139-2155.
S170 Supplement to Transplantation NovembeS170 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
143
Impact of simultaneous administration of Furosemide andDesmopressin on hypernatremia in brain dead organ donors:A clinical trial
Sahar Sajedi, Katayoun Najafizadeh, Omid Ghobadi, Ali Khalili,Hamid Rashid, Meysam Mojtabaee, Javad GhasemiLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran(Islamic Republic of).
Background: Appropriate brain dead donor management is a critical is-sue and one of the most prominent problems the management team isfacing is fluid and electrolyte disturbances specially hypernatremia. Inthis study we decided to treat hypernatremiawith simultaneous adminis-tration of Desmopressin and furosemide to get advantage of natriureticeffect of Furosemide and water saving effect of Desmopressin. The re-sult expected to be the correction of hypernatremia with smaller amountof fluid.Methods: 45 brain dead donors with hypernatremia were selected anddivided randomly to case and control groups. Every group further di-vided to 3 subgroups according to level of hypernatremia (150-159,160-169 and higher than 170 meq/liter). Water deficit (according to theNa level) plus insensible water loss were calculated and every one hourbeside previous hour urine volume, 10% of calculated fluid was given byIV fluids (half saline for two first subgroups and dextrose water for thirdsubgroup) and 15% by simple water gavage for 3 hours.3 milligrams offurosemide and Desmopressin (0.5 microgram for two first subgroupsand 1microgram for the third subgroup) were added simultaneously onlyin case group.Results: A total of 30 controls and 15 caseswere compared. Mean agewas 34 (6-85 years) which was not significantly different between caseand control groups and 57.8% of donors ware male. Sodium Correctionprogress in 3 hours were significantly different among the groups(p=0.02). Urea correction rate approached close to significance border(p=0.05). There was no significant difference in potassium and creati-nine correction rates.Conclusion: Simultaneous use of Desmopressin and Furosemidecan correct hypernatremia and prerenal azotemia easier and fasterand needs less fluid to be used. This method could be recommendedspecially for lung donor candidates.Keywords: Brain death, hypernatremia, Desmopressin, Furosemide
r 27, 2013, Volume 96 Number 10Sr 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
144
Brain death induces leucopenia and reduction in the number ofbone marrow cells
Julia M. Caliman1, Laura Menegat1, Primavera Borelli2, Rafael Simas1,Luiz F. Ferraz da Silva3, Luiz F. Moreira1, Paulina Sannomiya11University of São Paulo, Sâo Paulo, Brazil; 2Faculty ofPharmaceutical Sciences, University of São Paulo, Sâo Paulo,Brazil; 3Department of Pathology, University of São Paulo MedicalSchool, Sâo Paulo, Brazil.
Introduction: Brain death (BD) is associated with increased inflam-matory response in the different organs. In this study, we evaluatedthe recruitment of bone marrow cells to peripheral blood in rats sub-mitted to BD compared with BD-associated trauma.Methods: Male Wistar rats (250-350g) were anesthetized and me-chanically ventilated. A balloon catheter was placed into intracranialcavity, through trepanation, and quickly inflated to induce BD. Shamoperated rats (SH) were trepanned only. Bone marrow cells wereobtained by flushing the femoral cavity with Iscoves medium 6 hoursthereafter. White blood cell (WBC) counts in the peripheral blood weredetermined at baseline, and after 3 and 6 hours. Total bonemarrow cellsand WBC counts were determined using a hemocytometer. Differentialcounts were performed on smears stained with May-Grunwald Giemsasolution.Results: BD rats exhibited a progressive leucopenia (Baseline: 13171±1377; 3 h: 11086±1779; 6 h: 8300±927 cells/mm3), in contrast withSH group (Baseline: 12863±1283; 3 h: 17013±6186; 6 h: 17353±8286cells/mm3, p=0.012). The leucopenia observed in BD animals was alsoassociated with lower values for neutrophil/lymphocyte ratio in compari-son with the values observed in SH rats at 6 hours (p=0.004). BD ratsshowed a significant reduction in the total number of bone marrow cells(2.8±0.2 x107 cells/mL) compared with SH animals (4.9±0.9 x107 cells/mL, p=0.03), specially due to a significant reduction in the number ofsegmented cells (p=0.03), and lymphocytes (p=0.06). The cellularity re-duced in BD group (p<0,0001).Conclusions: Despite its pro-inflammatory effects, BD itself paradox-ically induced progressive leucopenia and reduction in the number ofbone marrow cells in this experimental model.Grant #2011/22803-2, São Paulo Research Foundation (FAPESP)
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
145
Final report of the Polish multicentre study for evaluationof computed tomographic angiography in the diagnosisof brain death
Romuald Bohatyrewicz1, Marcin Sawicki2, Anna Walecka2,Jerzy Walecki3, Olgierd Rowinski4, Joanna Solek-Pastuszka1,Zenon Czajkowski5, Maciej Zukowski1, Jaroslaw Zylkowski4,Piotr Skrzywanek11, Wojciech Kociemba9, Maciej Guzinski6,Malgorzata Burzynska7, Witold Manko10, Joanna Wojczal81Department of Anaesthesiology and Intensive Therapy, PomeranianMedical University, Szczecin, Poland; 2Department of DiagnosticImaging and Interventional Radiology, Pomeranian Medical University,Szczecin, Poland; 3The Centre of Postgraduate Medical Education,Warsaw, Poland; 42nd Department of Clinical Radiology, MedicalUniversity of Warsaw, Warsaw, Poland; 5Regional Joint Hospital,Szczecin, Poland; 6Department of General Radiology, InterventionalRadiology and Neuroradiology, Wroclaw Medical University, Wroclaw,Poland; 7Department of Anesthesiology and Intensive Therapy,Wroclaw Medical University, Wroclaw, Poland; 8Department ofNeurology, Medical University of Lublin, Lublin, Poland; 9Departmentof Neuroradiology, University of Medical Science, Poznan, Poland;10Department of Anaesthesiology and Intensive Therapy, University ofMedical Science, Poznan, Poland; 11Department of DiagnosticImaging, City Hospital, Poznan, Poland.
Introduction: According to Polish brain death (BD) criteria instituted in2007, confirmatory tests should be used in specific situations such as in-toxication, infratentorial processes, extensive facial damage, in childrenup to one year of age and any case when clinical examination seems tobe inadequate. These tests are often unavailable due to insufficient ac-cess to proper equipment and qualified specialists. Therefore, finding aconfirmatory test, which would be widely available, simple to performand easy to interpret became of fundamental importance. Computed to-mographic angiography (CTA) seemed to be the test of choice for thispurpose because new generation of CT scanners became widely avail-able. Themethod is simple and relatively cheap. Despite of this fact, CTAwas not included in Polish BD criteria because of limited expertise andlack of generally accepted criteria. In this situation, after approval of Bio-ethical Committee we organized Polish national multicentre trial for eval-uation of CTA in the diagnosis of BD.Methods: In 7 cooperating centres, we examined 82 patients, whichfulfilled standard clinical BD criteria. In a first step CTAwas performed,followed by CT perfusion, and finally verified by conventional angiog-raphy. The lack of cerebral blood flow in CTA was defined as the ab-sence of opacification of M4 segments of the middle cerebral artery(M4-MCA) and deep cerebral veins, the same as in criteria of FrenchSociety of Neuroradiology [1].Results: In 76 patients, CTA revealed the absence of opacification ofM4-MCA segments and deep cerebral veins. This met the French di-agnostic criteria of cerebral circulatory arrest. In 62 out of 64 examinedpatients (96.9%), subsequentCT perfusion revealed zero values of cere-bral blood volume and flow in the whole brain. In the remaining 2 casesCT perfusion showed very low values of perfusion parameters in smallcortical regions at the site of decompressive craniectomy. Conventionalangiography confirmed cerebral circulatory arrest in all 82 cases. CTAachieved the sensitivity of 92.7%. Additionally we identified potentialpoints of pitfalls, which will be mentioned in currently elaborated Polishinstruction.Conclusions:1. CTA is a valuable confirmatory test for BD diagnosis.2. Polish instruction will be compatible with French protocol publishedin 2011.
r 27, 2013, Volume 96 Number 10S S171
thorized reproduction of this article is prohibited.

November 27, 2013
The study was supported by a grant from the State Committee for Sci-entific Research of Poland No KBN-N 403 171 137.
Reference:[1] Societe Francaise deNeuroradiologie, Societe Francaise deRadiologie,Agence de la Biomedecine. [Recommendations on diagnostic criteria ofbrain death by the technique of CT angiography]. J. Neuroradiol. 2011.38(1):36-9.
S172 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
146
Role of CT angiography in confirmation of brain death
Subhash Arora, Gopal TaoriIntensive Care, Monash Health, Melbourne, Australia.
Confirmation of brain death requires demonstration of intracranial cir-culatory arrest, especially when clinical assessment is not possibledue to presence of confounding factors. The ANZICS guidelineaccepts conventional 4 vessel cerebral angiography and cerebral per-fusion scintigraphy as “gold standard” to make such diagnosis. How-ever these procedures are disadvantaged by invasiveness, limitedavailability, operator dependence and sometimes substantial delay.Around the world, various other technical aids are used to confirm thediagnosis of brain death. These include somatosensory evoked poten-tial (SSEP), electroencephalography (EEG) and transcranial dopplerultrasonography (TCD). These often yield discordant results necessi-tating interpretation by expert examiners.In recent times, CTangiography (CTA) with CT brain perfusion study, isemerging as a viable alternative and has been licensed for use in somecountries.While the results of studies so far, comparing conventional ce-rebral angiography and CTA with or without CT perfusion favour usingthe later as a rapid method for confirmation of diagnosis of brain death,larger studies are needed to validate their findings further.In our presentation, we describe the various technical aids used to de-termine the diagnosis of brain death, provide information that will beuseful in deciding which of the available techniques to use and com-pare the results of CTangiography available so far with those of otherforms of examination. We also discuss the ethical and practical issuesaround a proposed study comparing CT angiography using a new320-slice CT scanner and conventional cerebral angiography.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
147
A new method to increase brain dead potential donordetection rate
O. Ghobadi, M. Dargahi, M. Hazrati, M. Mazlum, K. NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran(Islamic Republic of).
Background: Brain dead potential donor detection which is one ofthe most important steps of organ donation process has 3 differentmethods: Administrative, Active, Passive. Active method has beenknown the best way for detecting all possible donors. Our OPU in Tehrancovers 112 hospitals. Because it is not practical to have this much in-hospital coordinators, we designed a new project for detecting all possi-ble donors.Methods: 112 hospitals were divided to 4 groups according to thenumber of ICU beds and having the neurosurgery ward. 6 expertnurses were chosen as inspectors. Hospitals were screened by 3complementary methods: PPDDP (Persian potential donor detectionproject), TDDP (Telephone donor detection project), HR (hospital re-porting). A schedule was designed for detection according to the hos-pital group. Inspectors should visit the hospitals in specific timesaccording to the schedule. Telephone detection had to cover the othertimes. Hospital report could be done in any time of the day. Specialforms were designed for: 1-GCS 3 brain dead; 2- GCS 3, not braindead; 3- GCS 4 and 5 and 4- unacceptable donors. Group 1 werefollowed by coordinators, group 2 and 3 were followed by TTDP groupand group 4 were just recorded for statistics.Findings: The rate of detection increased from 50 to 475 per month.Eight out of 40 group 2 and 12 out of 260 group 3 were brain deadin follow up and 6 and 8 were actual donors respectively. 12 out of80 group 1 donated their organs.Conclusion: In the OPUs with high number of hospital, PPDDP is aneffective method to detect all possible donors. This study showed thatclose following the GCS 3 non brain dead and GCS 4, 5 cases arevery important.Keywords: Organ donation, brain death, brain dead donor, detection rate
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
148
Potential pitfalls and problems during implementation ofCT angiography for national brain death diagnosis protocolin Poland
Romuald Bohatyrewicz1, Marcin Sawicki2, Anna Walecka2,Jerzy Walecki3, Olgierd Rowinski4, Joanna Solek-Pastuszka1,Zenon Czajkowski5, Maciej Zukowski1, Jaroslaw Zylkowski4,Piotr Skrzywanek11, Wojciech Kociemba9, Maciej Guzinski6,Malgorzata Burzynska7, Witold Manko10, Joanna Wojczal81Department of Anaesthesiology and Intensive Therapy, PomeranianMedical University, Szczecin, Poland; 2Department of DiagnosticImaging and Interventional Radiology, Pomeranian Medical University,Szczecin, Poland; 3The Centre of Postgraduate Medical Education,Warsaw, Poland; 42nd Department of Clinical Radiology, MedicalUniversity of Warsaw, Warsaw, Poland; 5Regional Joint Hospital,Szczecin, Poland; 6Department of General Radiology, InterventionalRadiology and Neuroradiology, Wroclaw Medical University, Wroclaw,Poland; 7Department of Anesthesiology and Intensive Therapy,Wroclaw Medical University, Wroclaw, Poland; 8Department ofNeurology, Medical University of Lublin, Lublin, Poland; 9Departmentof Neuroradiology, University of Medical Science, Poznań, Poland;10Department of Anaesthesiology and Intensive Therapy, University ofMedical Science, Poznan, Poland; 11Department of DiagnosticImaging, City Hospital, Poznan, Poland.
In 2007, new Polish code of practice reversed brainstem death criteria towhole brain death criteria. At this occasion therewas extensive discussionabout usefulness of CTangiography as a confirmatory test for cessation ofcerebral perfusion. Finally themethodwas not recommended at this occa-sion because of no experience in Poland and lack of widely accepted cri-teria in international literature.Careful analysis of scientific publications was rather confusing. Everycenter elaborated different examination protocol and evaluation crite-ria. Therefore the reports were difficult to compare. Only the FrenchSociety of Neuroradiology published detailed national instructions in2007 and 2011[1].In this situation, after approval of Bioethical Committee we organizedmulticenter trial in order to determine the accuracy of CT angiographyand CT perfusion for the confirmation of BD. Our protocol for CTangiog-raphy was similar to French one and evaluation criteria were the same.The studywas performed in 7 cooperating centers in 122 patients, whichfulfilled standard clinical BD criteria. Unfortunately we had to exclude40 cases because of protocol violations.During the study we organized meetings and discussions concerningprotocols and diagnostic criteria. Finally we identified following poten-tial pitfalls and problems during implementation of CTangiography forBD diagnosis protocol:1. failure to comply with the examination protocol,2. misinterpretation of opacification of the proximal segments of cere-
bral arteries as indicative of persistent cerebral circulation,3. false interpretation of SAH or pseudoSAH sign as real vascular
opacification,4. the apprehension of establishing the diagnosis, which is equivalent
to the declaration of death.Conclusions:1. The introduction of CTangiography to the panel of tests confirming
cerebral circulatory arrest should be preceded by an educationalcampaign with particular emphasis on radiological, neurological,neurosurgical and intensive care community.
2. Instruction, in addition to a detailed methodology should include in-formation about the causes of potential errors and interpretationproblems.
r 27, 2013, Volume 96 Number 10S S173
thorized reproduction of this article is prohibited.

November 27, 2013
The study was supported by a grant from the State Committee for Sci-entific Research of Poland No KBN-N 403 171 137.
Reference:[1] Societe Francaise deNeuroradiologie, Societe Francaise deRadiologie,Agence de la Biomedecine. [Recommendations on diagnostic criteria ofbrain death by the technique of CTangiography]. J. Neuroradiol 2011. 38(1):36-9.
S174 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
151
Auto-resuscitation and circulatory death in potentialorgan donors
David Pilcher1,3, Shena Graham1,2, Hayley Furniss2, Steven Philpot1,3
1Department of Intensive Care Medicine, The Alfred Hospital,Melbourne, Australia; 2DonateLife in Victoria, Melbourne, Australia;3Department of Epidemiology and Preventive Medicine, MonashUniversity, Melbourne, Australia.
Background and Aims: Return of spontaneous circulation (auto-resuscitation) during donation after circulatory death (DCD) has signifi-cant implications, and has been rarely described. The Alfred Hospitalhas a controlled DCD program which mandates a five minute period ofcessation of circulation prior to declaration of death. Our aim was to in-vestigate cases where auto-resuscitation may have occurred in patientsconsidered for DCD, to identify risk factors and highlight processeswhich may assist identification of future episodes.Results: Between 2006 and 2012, 60 patients have undergone con-trolled withdrawal of cardio-respiratory support (WCRS) in the Inten-sive Care Unit in anticipation of DCD. 38 patients (63%) have diedwithin acceptable time frames and become organ donors. There havebeen 2 possible auto-resuscitation episodes. Both patients had non-neurological causes of death.Case one: A 57 year woman with end stage pulmonary fibrosis hadWCRS. Six minutes later, invasive arterial monitoring became unavail-able due to signal alarms. After this no arterial waveform analysiscould be obtained. ECG activity ceased at 8 minutes. After an ab-sence of 3 minutes, ECG activity returned for 3 minutes before perma-nently stopping.Case two: A 41 year old man with extensive spinal, chest, abdominaland pelvic injuries lost ECG and arterial pulsation 5 minutes and 47seconds after WCRS. One minute and 42 seconds later, ECG and ar-terial pulsation returned for a further one minute and 48 seconds be-fore permanently stopping.In both cases, 5 minutes of absence of ECG and arterial pulsatilitywas subsequently observed before death was declared and donationof kidneys proceeded.Conclusions: Auto-resuscitation may be more common in non-neurological DCD cases. These possible auto-resuscitation cases high-light need for accurate monitoring and documentation. We recommendinvasive arterial waveform analysis for all DCD cases.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
152
Donation after cardiac death category II in the emergencydepartment: What is the impact?
Danielle Nijkamp1, Marije Smit2, Marc Seelen3, Bas Bens4,Christina Krikke5, Michiel Erasmus61Surgery, Division of Organ Donation, University Medical CenterGroningen, Groningen, Netherlands; 2Critical Care Medicine,University Medical Center Groningen, Groningen, Netherlands;3Nephrology, University Medical Center Groningen, Groningen,Netherlands; 4Emergency Room, University Medical CenterGroningen, Groningen, Netherlands; 5Surgery, Division of OrganDonation and Transplantation, University Medical Center Groningen,Groningen, Netherlands; 6Cardiothoracic Surgery and LungTransplantation, University Medical Center Groningen,Groningen, Netherlands.
Background: Donation after cardiac death category II (DCD II) in patientsafter unsuccessful cardiac resuscitation could expand the existing donorpool for lung and kidney transplantation.Aim: To assess the size of the potential DCD II donor pool for lung andkidney transplantation in a large university hospital, in which yearly onaverage 20 organ donation procedures are being performed.Methods: A prospective database was retrospectively analyzed toidentify potential DCD II donors among patients who were admittedto the emergency department (ER) from 2010 until 2012. Data on car-diac resuscitation, age, medical history, and national donor registrystatus were collected.Results: In total, 298 patients had out of hospital cardiac arrest; 98(32.8%) died in hospital and met the medical and age inclusion criteriafor both lung (age ≤65) and kidney donation (age ≤50).Forty-two patients (42/98; 42.8%) died in the ER of which 14 (33.3%)could have been both DCD II lung and kidney donor, and 11 (26.2%)only DCD II lung donor.Fifty-three patients (53/98; 54.1%) died in the intensive care unit (ICU)and could have been a DCD III donor. Two out of 53 (3.8%) patientshad a second episode of cardiac arrest and could have been a DCDII donor in the ICU.Three out of 98 (3.1%) patients died in the cardiac catheterization unitand could have been a DCD II lung donor.Conclusions: In three years time in the emergency department of auniversity hospital, 25 patients proved to be potential DCD II lung orkidney donors after unsuccessful resuscitation for cardiac arrest, 2patients proved to be potential DCD II donor in the ICU, and 3 patientsat the cardiac catheterization unit.This programme of lung and kidney donation could be an importantsource of donor organs to expand the existing donor pool by 50%.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
153
A single centre retrospective review of selection criteria fordonation after circulatory death liver transplantation
Georgina E Riddiough1, Michael A Fink1,2, Graham Starkey1,Bao Z Wang1, Adam G Testro1, Paul Gow1, Rhys B Vaughan1,Robert M Jones11Liver Transplant Unit, Austin Hospital, Melbourne, Australia;2Department of Surgery, University of Melbourne,Melbourne, Australia.
Introduction: Ongoing demand for liver transplantation in addition toongoing limited organ availability has led to increased use of organsfrom donation after circulatory death (DCD) donors. Due to concernsover the success of such grafts related to prolonged warm ischaemiatime careful selection of DCD grafts is imperative.Methods: We retrospectively assessed the number of DCD liveroffers made between 1 October 2007 and 7 February 2013. Wereviewed our selection criteria for DCD liver grafts and examinedreasons for declining such livers both immediately and at hepatec-tomy. Data was extracted from our liver transplant database.Results: In total 86 DCD liver offers made to the Austin hospital inVictoria between 1 October 2007 and 7 February 2013. 52% (n = 45)of offers were declined immediately and 47% (n = 40) provisionally ac-cepted, the remaining graft was exported to Queensland. 20% (n = 17)of grafts were transplanted; 9 grafts were declined at hepatectomy(reasons included hypoperfusion [n=2], hepatosteasosis [n=6]; one graftwas declined when intraoperative findings indicated transplantation wasno longer required). Reasons for immediately declining a DCD liver offerwere varied, most commonly donor age>60 years (n=10). In 25 cases acombination of factors such as alcohol consumption, obesity, diabetesmellitus, unknown viral status, down time and abnormal pathologyresults led to immediate graft rejection.Conclusion: One fifth of DCD liver grafts offered to the Austin were fi-nally implanted. In this group of DCD liver transplant recipients 1-yearpatient survival was 82% and 1-year graft survival was 71%.
r 27, 2013, Volume 96 Number 10S S175
thorized reproduction of this article is prohibited.

November 27, 2013
154
The differences between donors after cardiac death anddonors after brain death in 22 Victorian hospitals
Hugh Stephens1, David Pilcher2, Helen Opdam3, Gregory Snell4,Jeffrey Rosenfeld51MBBS/PhD Candidate, Monash University / The Alfred Hospital,Melbourne, Australia; 2Department of Intensive Care, Alfred Hospital,Melbourne, Australia; 3DonateLife Victoria, Melbourne, Australia;4AIRmed Lung Transplant Service, Alfred Hospital, Melbourne,Australia; 5Department of Surgery, Alfred Hospital,Melbourne, Australia.
Background & Aim: Since 2008, donation after cardiac death (DCD)programs across Australia have been increasing the donor poolby providing an alternative pathway to donation after brain death(DBD) [1]. As yet, little research has been conducted comparing thecharacteristics of these two donor types.Methods: We analysed data from the DonateLife Audit database for22 Victorian hospitals from 1 January 2010 through 30 June 2012(n=18,949 deaths) to compare characteristics between donor typesusing ANOVA testing.Results: 140 DBD and 51 DCD successful donors’ data was analysed.There was no significant difference in the proportion of donors that wereDCD compared to DBD across the 3 years studied (p=0.85). No signifi-cant difference was found in age (p=0.20), location of death (p=0.24), orpatient and family wishes (p=0.88, p=0.16 respectively). More DCDdonors were male (75% vs 54%, p=0.01). DCD donors were less likelyto die from a neurological cause of death (p<0.01, although both DBDandDCDdonorsmore commonly died of neurological causes), althoughfor those with neurological causes of death, there was no significant dif-ference between groups (p=0.16). DBD donors more commonly met theDonateLife trigger criteria on admission to the emergency department(32% vs 8%, p<0.01). While more DCD donors came from tertiarycentres (where DCD is facilitated) compared to metropolitan, pediatric,private or regional hospitals, the difference was not significant (p=0.07).Conclusions: DCD donors appear to have different characteristics toDBD donors, particularly regarding cause of death, meeting trigger cri-teria in emergency departments and being male.
Reference:[1] National Health and Medical Research Council (NHMRC). NationalProtocol for Donation after Cardiac Death. Canberra: Australian Organand Tissue Donation and Transplantation Authority (AOTDA); 2010.
S176 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
155
The impact of changing Donation after Cardiac Death criteriaon available potential donors: A study of 22 Victorian hospitals
Hugh Stephens1, David Pilcher2, Helen Opdam3, Gregory Snell4,Jeffrey Rosenfeld51MBBS/PhD Candidate, Monash University / The Alfred Hospital,Melbourne, Australia; 2Department of Intensive Care, Alfred Hospital,Melbourne, Australia; 3DonateLife Victoria, Melbourne, Australia;4AIRmed Lung Transplant Service, Alfred Hospital, Melbourne,Australia; 5Department of Surgery, Alfred Hospital,Melbourne, Australia.
Background: Australian Donation after Cardiac Death (DCD) protocolrequires all potential donors to die within 90 minutes of withdrawal oflife-sustaining therapy and be aged less than 65 years. Internationalcentres have reported favourable outcomes from donors outside thistime limit [1] or from those older than 65 [2].Methods: We analysed a database of 18,949 deaths in Victorianhospitals from 1 January 2010 to 30 June 2012 to determine the im-pact of adjusting these criteria on potential donor numbers. We de-fined a potential donor as a death in ED, ICU or operating theatre,ventilated in the 6 hours prior to death, not having active cancer, un-likely to become brain dead, and having a cardiorespiratory systemsupportable for long enough to facilitate donation.Results: There were 257 potential DCD donors using existingparameters. 89% (n=228) died in ICU, 11% (n=27) in the emergency de-partment and 2 in operating theatre. 42 (16%) subsequently donatedorgans. Increasing the maximum age limit to 70 would result in 71 addi-tional potential donors, and a further 71 were aged 71-75 but were oth-erwise eligible. During the study period, 6 patients donated organsaged 67 to 72, so increasing formal age criteria to 70 or 75 may be al-ready feasible in the Australian context.339 deaths had time until death recorded with (aged under 65). 51%(n=184) died within 30 minutes, 14% (n=52) within 60 and 5.8%(n=21) within 90 minutes (i.e. matched existing criteria). Increasingthe time limit to 120 minutes could provide an additional 11 donors,or 150 minutes a further 18 donors.Conclusions: Modifying age criteria appears to have the most signif-icant impact on increasing the number of potential DCD donors, whilemodifying time to death having a minor effect.
References:[1] Moers C, Leuvenink HGD, Ploeg RJ. Donation after cardiac death:evaluation of revisiting an important donor source. Nephrol Dial Trans-plant. [Editorial Review]. 2010 Mar; 25(3):666-73[2] Frei U, Noeldeke J, Machold-Fabrizii V, Arbogast H, Margreiter R,Fricke L, Voiculescu A, Kliem V, Ebel H, Albert U, Lopau K, SchnuelleP, Nonnast-Daniel B, Pietruck F, Offermann R, Persijn G, BernasconiC. Prospective age-matching in elderly kidney transplant recipients–a5-year analysis of the Eurotransplant Senior Program. Am J Transplant2008; 8(1):50-7.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
156
Development of a competence based training programme forperioperative practitioners undertaking in-situ normothermicregional preservation in DCD donors
John Stirling, Pamela Stenhouse, Graham Johnston,Ian Currie, Gabriel OniscuScottish Organ Retrieval Team, NHS Lothian, Edinburgh,United Kingdom.
Normothermic Regional Perfusion (NRP) is a new approach to DCD or-gan retrieval involving normothermic oxygenated blood perfusion ratherthan cold perfusion. This may improve organ viability and quality and po-tentially increase the number of organs recovered.In Scotland, there is a unifiedmulti-organ retrieval team, the Scottish Or-gan Retrieval Team (SORT). This includes perioperative practitioners re-sponsible for multi-organ perfusion and preservation. Traditionally, thisinvolves hypothermic preservation and packing the organs for cold stor-age. NRP requires greater specialist knowledge of physiology, biochem-istry and organ assessment. In conjunction with the lead clinician for theNRP project, it was identified that the senior perioperative practitionersfrom SORT would undertake an education and training programmefollowed by competence assessment. This was developed in collabora-tion with the practice development team using a Standard OperatingProcedure (SOP). This training programmewas divided into four distinctphases: theoretical learning, practical observation, experiential learningand competence assessment. The theoretical learning component in-cluded education sessions (anatomy, physiology, biochemistry and thecomponents of the console, circuit and pump). Practical observation in-cluded visiting centres using NRP in clinical practice and attending prac-tical workshops. The experiential learning component involved animallabs sessions and repetition of the practical steps laid out in the SOP.The final competence assessment was undertaken once the educationand training components had been completed. The lead clinician for theNRP project carried out the competence assessments. Four practitionershave successfully undergone competence assessment and are involvedwith NRP in clinical practice.This approach could serve as a model for future development in organretrieval and preservation and the expansion of the role of transplanttheatre practitioners.Submitted on behalf of the Scottish Organ retrieval Team (SORT)
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
157
Implementing donation after cardiac death in hospital: barriersand their resolution
Gopal Taori, Subhash Arora, Nicola Stitt, Bridget O'BreeIntensive Care, Monash Health, Melbourne, Australia.
Objective: To report three year experience of successful implementa-tion of donation after cardiac death (DCD) programme in a metropoli-tan teaching hospital.Background: As a part of National reforms agenda for organ and tissuedonation, there has been a significant focus on organ donation byDCD pathway. However hospital based organ donation teams oftenface many difficulties in it's successful implementation. These rangefrom attitudes of the clinical and support staff to logistical problems.Key barriers include a lack of knowledge about DCD, psychologicalbarriers for DCD versus brain death, concerns about whether deathhas been reached, beliefs about saving versus killing patients, trust inthe organ donation team, moving from saving patients to being a dona-tion advocate and concerns with the DCD process particularly timetaken for the process and conflict of interest in assigning priority to man-agement of potential donor versus other critically ill patients.Methods: We describe our experience with regards to changingattitudes towards DCD, overcoming potential barriers and creating op-portunities and strategies for gaining support, which included educationinitiatives, a cultural shift, a consistent DCD protocol separating carefrom recovery, process monitoring, and a strong sense of teamwork.Conclusion: Our findings provide a better understanding of potentialbarriers, critical to the implementation of strategic plans for DCDprogramme in the hospital setting. Communication efforts that are ableto educate healthcare professionals and eliminate misconceptions will in-crease support for DCD. Key to future success requires confident commit-ted and well-trained team.
r 27, 2013, Volume 96 Number 10S S177
thorized reproduction of this article is prohibited.

November 27, 2013
158
Excellence in organ donor coordination at La Raza GeneralHospital of Mexico City during 2013
Cesar Villasenor-Colin, Mariano Hernandez-Dominguez,Marlene Santos-Caballero, Guillermo Careaga-Reyna,Roberto Ortiz-Lerma, Karla Verdiguel, Arturo Robledo-Martinez,Israel Pagola-Quintero, Jaime Zaldivar-Cerverra,Armando Soberanes-HernandezTransplant Surgery, La Raza General Hospital, Mexico City, Mexico.
Introduction: Decisions inOrganDonorCoordinationODCare based onpersonal experience. The reasoning in ODC often obeys a process notsystematic and empiric. A high percentage of the decisions in ODC donot have a scientific solid foundation and it is estimated that less thanthe 20 % are well-founded. The results of ODC should be analysed in re-lation with their importance and application. The recognition of potentialdonors implies the need to count on truthful information provided by the ex-perience in the selection of the optimal multi-organic donors understand-ing that experience is valid when it results in the decrease of errors.Objective: Presenting the evidence of excellence in ODC at La RazaGeneral Hospital during the first six months of the year 2013.Material and Methods: By means of a descriptive and prospectivestudy, there were a total of 156 cases.Results: A total of 48 hearts, 40 livers, 26 kidneys and 48 corneaswere offered; 92 from male and 64 from female.Findings: There were 13 heart transplants, 7 liver transplants, 10 kid-ney transplants and 32 corneal transplants, which consolidates ourhospital as the main transplant centre of excellence at Mexico duringthe first six months of 2013.
S178 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
159
The critical pathway of Deceased Organ Donation inKSA: 2001-2010
Faissal A.M. Shaheen, Besher Al Attar, Abdulla Al Sayyari,Michael Abeleda, Elsayed GadallahMedical Department, Saudi Center for Organ Transplantation,Riyadh, Saudi Arabia.
Objective: Organ transplantation is the best existing method for thetreatment of end-stage organ failure. However, the need for viable or-gan supply limits its progress; thus, we studied the algorithm of pro-cess for deceased heart beating donors with the rate of adapting thecritical pathways of organ donation from possible to potential to eligi-ble to consent and to actual deceased donors (DD) in the kingdom.Methods: A retrospective study comparing the nationwide figures andcomposition of the Critical Pathway of DD cases in a decade from2001-2005 vs. 2006-2010 to Saudi Center for Organ Transplantation(SCOT).Results: The Study showed a remarkable increase in the total number ofPossible Deceased Donor cases from 1827 of 2001-2005 to 2651 (+45%)of 2006-2010. The mean possible case per year in relation to the numberof population for the first half of the decade is 16 PMP as compared to22 PMP in the last 5 years of the decade. The rate of conversion from pos-sible to potential is 63% (1151 and 1674 respectively). Moreover, EligibleDonors ascends its number from 956 to 1336 (+39%) of which270 (28% with 2.2 PMP) and 511 (38% with 4.1PMP) respectively wereconsented for organ donation. The Actual DD for the year 2001-2005was 248 and 453 for the year 2006-2010. As a result, the number of Uti-lized DD organs increased from 244 to 441(+81%) cases.Conclusion: There is a notable increase in the number of PossibleDD reported and consented in the second half of the decade. Thereis also a significant increase in the Actual DD. In relation to this, thevarious strategies being implemented to promote organ donation inevery region of the kingdom are relatively effective in applying the crit-ical pathways of deceased organ donation.
References:• SCOT DATA. Annual Report 2008 – 2010 Ministry of Health, Kingdomof Saudi Arabia. www.scot.org.sa• B.Dominguez-Gil, F.L. Delmonico, F. AM Shaheen, et al. The CriticalPathway for Deceased Donation: 3rd W.H.O Global Consultation onOrgan Donation and Transplantation, March 2010.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
163
A quality of life survey following kidney transplant using agraft after excision of a small tumour
Siva Sundararajan, Luc Delriviere, Bulang HeWestern Australia Liver and Kidney Transplant Service, Sir CharlesGairdner Hospital, Perth, Australia.
Background: It is well recognised that renal transplantation improvesthe quality of life of patients in end stage renal disease (ESRD). Theaim of this study was to investigate the quality of life of renal transplantrecipients who received a tumour resected kidney graft (TRK).Methods: A strategy has been implemented in our transplant ser-vice for using kidney graft after excision of a small renal tumour sinceFebruary 2007. Patients were given the SF-36 questionnaire to as-sess their quality of life pre and post-transplantation. Additional infor-mation regarding concerns about tumour recurrence and whetherthey would choose a TRK transplant again or prefer to stay on dialysiswas obtained. Renal function was also obtained at regular intervals.Results: Twenty-four patients received kidney transplant under thisprogramme. Of them, 20 returned the questionnaire. The mean scoresin all 8 domains of the SF-36 were higher post-transplantation. The dif-ferences were statistically significant. Ninety-five percent of patientswould prefer to have the transplant again. Eighty percent of patients didnot have any significant concerns regarding tumour recurrence. There isno tumour recurrence on median 27 months follow-up. Mean creatininebefore transplantation was 740.55 ± 240.72μmol/L. At 6 months post-transplantation, mean creatinine was 160 ± 69.81μmol/L.Conclusion: Renal transplantation by using tumour resected kidneygrafts result in improved quality of life. Patients prefer transplant tostaying on dialysis and concerns regarding recurrence of tumour areminimal. Kidney transplantation by using the kidneys after excisionof the known tumour is an important novel solution in the context of or-gan shortage with excellent quality of life and biochemical outcomes.
r 27, 2013, Volume 96 Number 10S S179
thorized reproduction of this article is prohibited.

November 27, 2013
165
Outcomes following transplantation: preferences and prioritiesof kidney transplant recipients
Martin Howell1,2, Germaine Wong1,2,4, Allison Tong1,2, John Rose3,Jonathan Craig1,2, Kirsten Howard21Centre for Kidney Research, Westmead, Australia; 2School of PublicHealth, University of Sydney, Sydney, Australia; 3Institute of Transportand Logistics, University of Sydney, Sydney, Australia; 4Centre forTransplant and Renal Reseacrh, Westmead Hospital,Westmead, Australia.
Background: Knowledge of the extent to which recipients would be wil-ling to trade the risk of adverse outcomes for graft survival should betaken into account when considering expansion of the organ donor pool.Aim: To evaluate transplant recipient preferences and trade-offs foradverse outcomes after transplantation.Methods: Kidney transplant recipients were presented a survey thatcontained a list of nine outcomes including; graft survival and the riskof dying before graft failure; serious adverse events; and drug relatedside effects. The survey instrument assessed the participants’ pre-ferences of the best and worst outcomes for each scenario. Thequestionnaires were sent and returned by post or completed on theWeb. Responseswere analysed usingmultinominal logit models to eval-uate relative importance and trade-offs between outcomes. Interviewswere conducted with selected participants to evaluate understandingof the survey.Results: Of the 83 eligible participants, 35 recipients (42%) (35–73years) participated. Graft survival was the most important outcome,followed by cancer, cardiovascular disease and serious infection.Modelling suggested that participants were willing to forgo 4.5 to5 years of graft survival to prevent a 10% increased risk of cancer, car-diovascular disease or serious infection. In contrast participants werewilling to forgo only 2.6 years of graft survival to prevent a 10% in-crease in the risk of dying with a functioning graft.Conclusion: Transplant recipients are willing to accept a high proba-bility of serious outcomes and side effects to maximize graft survival.Aversion of returning to dialysis was reflected in the relatively low im-portance placed on the probability of dying with a functioning graft.
S180 Supplement to Transplantation Novemb
Copyright © 2013 Lippincott Williams & Wilkins. Una
166
The joint impact of donor and recipient parameters on theoutcome of heart transplantation in Germany afterdonor selection
Carl-Ludwig Fischer-Fröhlich1, Irene Schmidtmann3,Marcus Kutschmann2, Sylke R Zeissig3, Nils R Frühauf5,Frank Polster4, Gunter Kirste11Region Baden-Württemberg, Deutsche Stiftung Organtransplatnation,Stuttgart, Germany; 2BQS Institute for Quality and Patient Safety,Düsseldorf, Germany; 3Institute for Medical Biometrics, Epidemiologyand Informatics (IMBEI), Universitätsmedizin der JohannesGutenberg-Universität Mainz, Mainz, Germany; 4DeutscheGesellschaft für Gewebespende gGmbH, Hannover, Germany;5Landesärztekammer Niedersachsen, Hannover, Germany.
Background:Organ shortage in heart-transplantation (HTx) results inincreased use of grafts from donors with substantial risk factors. It isdiscussed controversially which donor characteristics may be detri-mental. Therefore, we evaluated the joint impact of donor and patientrelated risk factors in HTx on patient survival by multiple analysis in anationwide multicenter study after donor selection was carried out.Methods: The research database consists of data concerning heartsdonated and transplanted in Germany between 2006 and 2008 asprovided by Deutsche Stiftung Organtransplantation and the BQS-Institute. Multiple Cox regression (significance level 5%, hazard ratio[95%-CI]) was conducted (n=774, recipient age ≥18 years).Results: Survival was significantly decreased by donor-age (1.021[1.008-1.035] per year), non-traumatic cause of death (1.481 [1.079-2.034]), Troponin >0.1 ng/ml (2.075 [1.473-2.921]), ischemia time(1.197 [1.041-1.373] per hour), recipient-age (1.017 [1.002-1.031]per year) and in recipients with pulmonary vascular resistance ≥320dyn*s*cm-5 (1.761 [1.115-2.781]), with ventilator dependency (3.174[2.211-6.340]) or complex previous heart surgery (1.763 [1.270-2.449]).Conclusion: After donor selection had been conducted, multiple Cox re-gression revealed donor-age, -non-traumatic cause of death, -Troponinand ischemia time aswell as recipient-age, -pulmonary hypertension,-ventilator dependency and -previous complex heart surgery as limitingrisk factors concerning patient survival.
er 27, 2013, Volume 96 Number 10S
uthorized reproduction of this article is prohibited.

November 27, 2013
167
Acute rejection requiring T cell depletive antibodies isassociated with a higher risk of incident cancer afterkidney transplantation
Wai Lim1, Robin Turner2, Jeremy Chapman3, Angela Webster2,3,4,Jonathan Craig2,3,4, Germaine Wong2,3,41Department of Renal Medicine, Sir Charles Gairdner Hospital, Perth,Australia; 2Sydney School of Public Health, University of Sydney,Sydney, Australia; 3Centre for Kidney Research, The Children’sHospital at Westmead, Sydney, Australia; 4Centre for Transplantand Renal Research, Westmead Hospital, Sydney, Australia.
Background: Induction therapy with T cell depletive antibodies is anestablished risk factor for incident cancers, especially post-transplantlympho-proliferative disease (PTLD). However, the relationship be-tween the use of T cell depletive antibodies for rejection (AR-T) andcancer risk after transplantation is unknown. We aimed to determineif AR-T post-transplant was associated with the risk of site specificand overall incident cancers after kidney transplantation.Methods: Using the Australian andNew Zealand Dialysis and TransplantRegistry (ANZDATA), we assessed the association between rejectionstratified by use (AR-T) or non-use (AR) of T cell depletive antibodiesfor all cancers (except for non-melanocytic skin cancers) as well as site-specific cancer incidence using adjusted Cox proportional hazard andcompeting risk models.Results: Over a median follow-up of 4.6 years, 551/7237 (7.6%) kidneytransplant recipients developed incident cancers. Compared with no re-jection, AR-T but not AR was associated with a higher risk of incidentcancer in the adjusted model (HR 1.54, 95%CI 1.51-2.05, p=0.004).There was an excess risk of PTLD in recipients who had experienced re-jection. In the competing risk model, there was an excess risk of incidentcancers in AR-T compared to no rejection or AR groups, particularlybeyond 14-years post-transplant.Conclusion: Acute rejection requiring T cell depletive antibodies is asignificant risk factor for cancers in kidney transplant recipients inde-pendent of competing events such as age and cardiovascular deaths.Strategies to improve cancer surveillance among these recipients whohave experienced rejection requiring T cell depletive antibodies maybe warranted.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
168
Older deceased donor kidneys are associated with anincreased risk of incident cancer in renal transplant recipients
Wai Lim1, Robin Turner2, Jeremy Chapman3, Angela Webster2,3,4,Jonathan Craig2,3,4, Germaine Wong2,3,41Department of Renal Medicine, Sir Charles Gairdner Hospital, Perth,Australia; 2Sydney School of Public Health, University of Sydney,Sydney, Australia; 3Centre for Kidney Research, The Children’sHospital at Westmead, Sydney, Australia; 4Centre for Transplantand Renal Research, Westmead Hospital, Sydney, Australia.
Background: Inflammation has long been associated with the devel-opment of cancer. We hypothesize the greater inflammatory responseassociated with older deceased donor (DD) kidney transplants maycontribute to an increased risk of cancer following kidney transplanta-tion. Our study aims to determine the association between donortypes and the risk of overall incident cancers after transplantation.Methods: Using the Australian and New Zealand Dialysis and Trans-plant Registry (ANZDATA) between 1997 and 2009, we assessed theassociation between donor type and overall cancer incidence usingadjusted Cox proportional hazard models.Results: Over a period follow-up time of 83,535 patient-years, a totalof 563 patients developed cancers. Of the 7,252 renal transplantrecipients, 37%, 6%, 44% and 13% received kidneys from young liv-ing, old living, standard criteria and extended criteria deceased donors(ECD), respectively. There was a significant association between do-nor type and the risk of incident cancer after transplant (p-value fortrend 0.007). Compared with recipients who received young livingdonors (defined as donor age less than 60 years), recipients of ECDkidneys were associated with a greater risk of incident cancer (ad-justed HR 1.49, 95%CI 1.14, 1.95), after adjusted for donor gender, re-cipient characteristics (age, gender, race, cause of end-stage renaldisease, time on dialysis), immunological factors (HLA-mismatches,panel reactive antibodies) and transplant era and initial immunosup-pression. There was no significant difference in the risk of site-specificcancers among the different donor groups.Conclusion: Recipients of ECD kidneys appear to be associated withan increased risk of cancer, independent of recipient age and immu-nosuppression. Strategies to improve cancer surveillance amongrecipients who had received ECD kidneys may be warranted.
r 27, 2013, Volume 96 Number 10S S181
thorized reproduction of this article is prohibited.

November 27, 2013
169
The impact of nosocomial infections for generating an organdonor center of high complexity
Gustavo Melgarejo1Department of Donation Y Transplant, Ips, Asuncion, Paraguay.
Introduction: Paraguay is a country with a population of 6,672,631inhabitants. The Central Hospital of Security Social is the most complexcenter with 68 adult ICU beds. It introduces the concept of hospital coor-dinator in September 2011 with which you start a program of active en-forcement records and cadaveric donors allow us to analyze thestatistics of 2012. The average age of the patients was 51 years. Themain hospital is the first in the country to introduce the model of HospitalTransplant Coordination. The idea is to create strategies to reduce med-ical contraindications and to allow the Hospital of greater complexity ofthe country is also an important source of cadaveric donors.Objective: Prove that hospital infections in patients in critical care,prevents further generation of donor organs.Material and Methods: The statistics are taken as HCIPS records of2012, in Excel format. We performed a retrospective cross-sectionalstudy, which evaluates potential donor cases detected in ICU.Sample:60cases. Inclusion criteria: patients entering a critical carehospitalization period longer than 8 hours. Exclusion criteria: patientswith admission diagnosis of infectious process.Results: The study is evaluated 60 patients. We had 17 cases EVR andKPC infections, 6 cases by virus> Dengue. Other causes are two SLE,Degenerative disease, glioblastoma, and lung cancer. The > cause ofdeath was due to stroke 39 %, 28 % Brain Injury Trauma and other in27% diagnosed with Brain Death 67 %.Period of acquisition of infections was 5 days. Hospital infections com-prise 38% of medical contraindications, which would give a loss of23 Donors cadaveric.Conclusion: Hospital Infections in most cases is the cause of medicalcontraindications to donation, this result in lower number of organ donationIt is important to develop strategies to reduce the incidence of multiresistantbacterial infections.
S182 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
170
Estimating differential renal function using ellipsoidapproximation of renal volume on CT scan
Laura N. Nguyen, Fadi Kamal, Brian BlewDivision of Urology, The Ottawa Hospital/University of Ottawa,Ottawa, ON, Canada.
Background: Living renal donors must undergo extensive medicalinvestigations in order to be approved for the donor program. Amongother testing, this includes both computed tomography (CT) scans toevaluate vascular anatomy and nuclear medicine renal scans to as-sess differential renal function.Extensive research has been done using complex models to calculateprecise radiographic measurement of renal volume on CT in order toestimate differential renal function based on differential renal volumes.Thus, the necessity of the nuclear medicine renal scan can be elimi-nated, reducing the radiographic burden and time commitment of thepotential donor and addressing the ongoing scarcity of the necessaryradionucleotide. However, these models are rarely used as they areoften cost-prohibitive due to the need for proprietary software and theyare labor-intensive for radiologists.Methods: In this study, we examined whether a simplified estima-tion of differential renal volumes based on the ellipsoid formula (renalvolume = πldw/6, where l, d, and w represent three dimensions ofthe kidney) using CT scans, may also adequately estimate differentialrenal function.Results: Charts of 79 consecutive living renal donors were reviewedretrospectively. The differential renal volumes measured on CT scanswere reliable between operators (p<0.05). We found that the volume-based estimations of differential renal volume were in fact correlatedto differential renal function on nuclear medicine scans (r=0.29,p<0.01). We were able to identify the kidney with the greater functionin 53 (67%) of the 79 cases, and in all 8 (100%) of 8 cases in which thedifference in differential renal function was clinically significant (>10%difference between kidneys).Conclusions: Findings support removal of the nuclear medicine scanfrom routine assessment of potential kidney donors without the needfor expensive radiologic software.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
230
Donation after cardiac death following withdrawal ofveno-venous extracorporeal membrane oxygenation
Brett Sampson1,2, Ubbo Wiersema1, Philippa Jones2,Gerry O’Callaghan11Intensive and Critcal Care Unit, Flinders Medical Centre, Adelaide,Australia; 2DonateLife, SA, Australia.
Donation after cardiac death (DCD) has rapidly increased throughoutAustralia in recent years [1,2]. Over the same period there has been in-creased availability of extracorporeal membrane oxygenation (ECMO);a legacy of the 2009 Influenza A (H1N1) pandemic [3,4]. With growingexperience in these two practices, a new pool of potential organ donorsis likely to be realised. In Australia, ECMO is only initiated for severe car-diorespiratory failure when spontaneous recovery is expected, or as abridge to heart (&/or lung) transplantation. Unfortunately, ECMO is notalways lifesaving and sometimes it must be withdrawn to enable endof life care. It is in this cohort of patients that a new pool of potential organdonors may exist. We present a case of a sixty year old man with severecommunity acquired pneumonia, complicated by acute respiratory dis-tress syndrome, who donated both kidneys through DCD after withdrawalof veno-venous ECMO.We discuss how ECMOmight influence the iden-tification of potential organ donors, its impact on the withdrawal of life sus-taining treatments and how it might be used to minimise ischaemic injuryto donated organs. The international practice of initiating veno-arterialECMO after cardiac death, solely to facilitate DCD, is not practiced inAustralia and therefore is not discussed.
References:[1] Sampson BG, O'Callaghan GP, Russ GR: Is donation after cardiacdeath reducing the brain-dead donor pool in Australia? Crit CareResusc. 2013 Mar;15(1):21–7.[2] Opdam H: The rise and rise of donation after cardiac death: a so-lution to the shortfall in organs for transplantation? Crit Care Resusc.2013 Mar;15(1):3–4.[3] Bishop JF, Murnane MP, Owen R. Australia’s winter with the 2009pandemic influenza A (H1N1) virus: N Engl J Med. 2009 Dec 31;361(27):2591–4.[4] ANZIC Influenza Investigators, Webb SA, Pettilä V, Seppelt I et al.Critical care services and 2009 H1N1influenza in Australia and NewZealand: N Engl J Med. 2009 Nov12;361(20):1925–34.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
231
Current situation of donation after cardiac death in Poland
Edyta Skwirczynska-Szalbierz, Adam Nowacki, Marek OstrowskiDepartment of General Surgery and Transplantation, AutonomousPublic Clinical Hospital No. 2 of Pomeranian Medical University,Szczecin, Poland.
The demand for organ donation in Poland is three times greater com-pared to the number of transplant procedures performed in our country.In 2012 there has been 615 donations, which accounted for 16 donorsper 1 million inhabitants (pmp). In Spain this rate exceeded 30. Thereare significant regional differences in the number of harvested organsin Poland. In 2012, in the northwest region there has been 28 donorspmp and in the southern region only 5.8 donors pmp. The deepening or-gan shortage crisis leads inevitably to the increase in the number ofpatients dying while awaiting for organ transplantation. The appropriateutilization of DCD donors seems to be one of the solutions for this crisis.Despite existing regulations there are no separate development strat-egies for DCD donation in Poland. There were no DCD donations inthis country to date.Purpose: To specify the reason for total lack of identification of DCDdonors in the northwest region of Poland despite the highest donationrate in this country.Methods: In 2013 a questionnaire survey was carried out among the staffin intensive care units, cardiology and cardiac surgery departments. Itconsisted of 23 questions divided into 3 sections which tested respondentsfor DCD donation knowledge, respondents’ involvement in the processof DCD identification and asked for suggestions to increase the numberof donations from deceased donors, including DCD donors.Results: 70% of respondents did not know the definition of DCD, 54%deemed that DCD donation is prohibited in Poland, 90% did not knowthe classification of DCD, 75% consider neurological criteria to be suf-ficient for determination of death in organ donation.Conclusions: There is no sufficient knowledge among the hospitalstaff involved in donation process regarding DCD donation.An implementation of appropriate educational and psychologicalworkshops regarding DCD donation is required.
r 27, 2013, Volume 96 Number 10S S183
thorized reproduction of this article is prohibited.

November 27, 2013
232
Extended Criteria Donors (ECD) - expanding the boundariesfor donation after cardiac death
Nicola Stitt1,2, David Pilcher2,3,4, Tim Crozier11Intensive Care Unit, Monash Health, Melbourne, Australia;2Donatelife Victoria, Melbourne, Australia; 3Dept of Intensive Care,The Alfred Hospital, Melbourne, Australia; 4Department ofEpidemiology and Preventative Medicine, Monash University,Melbourne, Australia.
Introduction: The upper age limit for lung donation via the Donationafter Cardiac Death (DCD) pathway has generally been consideredto be 65 years. We report a case of a 73 year old patient who was ableto donate his lungs for transplantation.Case Description: A 73 yr old male ex-smoker was admitted to theIntensive Care Unit (ICU) following an out-of-hospital cardiac arrestdue to myocardial infarction. The likelihood of neurological recoverywas poor and during end of life discussions the family raised the pos-sibility of organ donation with the Intensivist. As he was unlikely toprogress to brain death the only option was the DCD pathway. How-ever current guidelines suggested that he was over the age limit forlungs, liver and kidney donation, with the previous oldest DCD lungdonor being 65 years old.Upon consideration the Intensivist engaged the help of the Nurse Do-nation Specialist who investigated the possibility of donation withDonatelife Victoria (DLV). The initial response received was that hewas too old for DCD. The family were disappointed with this outcome.Further discussions between the Intensivist and Organ Donor Coordi-nator (ODC) at DLV led to another approach to the lung transplantteam for reconsideration.Arterial Blood Gas (ABG) on 100% oxygen. pH 7.35, pCO2 42.3, pO2458, BE -2. Chest X- ray & bronchoscopy were clear. Ventilationrequirements were FiO2 = 0.30, PEEP 10cm, PS 12.*After reviewing the patients’ current condition it was decided that hewould be accepted as potential lung donor.Following withdrawal of life sustaining therapy the patient died peacefullywithin the timeframe required for DCD. This resulted in successful lungdonation, with subsequent successful bilateral lung transplantation.Conclusion: Exploring the possibility of extended criteria donation incarefully selected patients may result in more organs being availablefor transplant.*PEEP: Positive End Expiratory Pressure PS: Pressure Support
S184 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
236
Paediatric donation after cardiac death: The Story of Max
Anne-Maree HolmesNambour Hospital- Intensive care, Nambour Hospital/ DonatlifeQueensland, Nambour, Australia.
Only a small percentage of the organ donor pool is from the paediatricpopulation approximately ten percent of donors were paediatric in2010. Still in the early stages of the introduction of the Donation afterCardiac Death (DCD) process a 3yr old boy MAX was admitted withsevere hypoxia to the Paediatric Intensive care unit with a grossly ab-normal MRI and a GCS of 3. Overtime his parents were given a poorprognosis and unlikely survivability. Discussions moved to focus onwithdrawal of life supporting therapies.Max’s parents introduced the idea of organ and tissue donation. A per-fusion scan showed limited perfusion to the brain. Donation form car-diac death would be the pathway to facilitate max becoming an organdonor.The decision to follow the DCD pathway was easy as Max’s parentswere highly motivated they wanted Max to be able to help other chil-dren and to prevent another family having to deal with the loss of achild. Both the State medical director and the Director of Geneticswere engaged where no reason was found for donation after cardiacdeath not to proceed.With supportive enthusiastic staff we were able to proceed with the do-nation after cardiac death. Many staff had limited or no experience andsop were wary of the process ofDCD but with small educationsessions and support from the donatelife staff everyone worked welland the donation was a success.Max was extubated at 04:19 and death was declared at 04:27. Maxdonated both his kidneys to recipients who now 3 years later are doingwell and his heart valves that were donated have also been used.
References:Australian and New Zealand Intensive Care Society.The ANZICS State-ment on Death and Organ Donation. 3rd ed. Melbourne: ANZICS; 2008.NSW Health. Organ Donation after Cardiac Death: NSW Guidelines.Sydney: NSW Health; 2007.ANZOD Registry Report 2012
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
237
Results of kidney transplantation from controlled donors aftercardio-circulatory death: A single center experience
Hieu LE DINH1, Laurent Weekers2, Catherine Bonvoisin2,Jean-Marie Krzesinski2, Josée Monard3, Arnaud de Roover4,Olivier Detry4, Jean-Paul Squifflet4, Michel Meurisse41University of Medicin Pham Ngoc Thach, Ho Chi Minh city, Viet Nam;2Department of Nephrology, University Hospital of Liège, Liège,Belgium; 3Transplant Coordinator, University Hospital of Liège, Liège,Belgium; 4Department of Abdominal Surgery and Transplantation,University Hospital of Liège, Liège, Belgium.
Background: The aim of this study was to determine results of kidneytransplantation (KT) from controlled donation after cardio-circulatorydeath (DCD). Primary end-points were graft and patient survival, andpost-transplant complications. The influence of delayed graft function(DGF) on graft survival and DGF risk factors were analyzed as sec-ondary end-points.Material and Methods: This is a retrospective mono-center review ofa consecutive series of 94 DCD-KT performed between 2005 and2012. Mean patient follow-up was 33.1 months.Results: Overall and death-censored graft survival rates were 93.6%and 93.6% at 3 months, 89.2% and 93.6% at 1 year, 86% and 91.6%at 3 years, and 78.9% and 91.6% at 5 years, respectively. Main causeof graft loss was patient’s death with a functioning graft. Global patientsurvival rates at the corresponding time points were 97.9%, 93.3%,92%, and 84.8%. No primary non-function grafts. DGF was observedin 36% of all DCD-KT. Renal graft function was suboptimal at hospitaldischarge, but nearly normalized at 3 months. DGF significantly in-creased post-operative length of hospitalization (18.2 ± 5.3 versus13.2 ± 4.1 days, p <0.000) but had no deleterious impact on graftfunction or survival, neither on 3-month acute rejection rate nor onearly post-operative complications (p = ns). However, overall patientsurvival rate in kidney transplants with DGF was significantly lowerthan in those without DGF (p = 0.039). Recipient BMI ≥30 kg/m2
and pre-transplant dialysis duration significantly increased the risk of
FIGURE 1.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
DGF in a multivariate logistic regression analysis (p = 0.036 and p =0.004, respectively).Conclusions: Despite a higher rate of DGF, controlled DCD-KToffersa valuable contribution to the pool of deceased donor kidney grafts,with comparable mid-term results to those procured after brain death.Keywords: brain death, organ preservation, primary graft dysfunc-tion, risk assessment, treatment outcome, warm ischemia.
References:[1] Akoh JA, Denton MD, Bradshaw SB, Rana TA, Walker MB. Earlyresults of a controlled non-heart-beating kidney donor programme.Nephrol Dial Transplant. 2009; 24: 1992–6.[2] Doshi MD, Hunsicker LG. Short- and long-term outcomes with theuse of kidneys and livers donated after cardiac death. Am J Trans-plant. 2007; 7: 122–9.[3] Locke JE, Segev DL, Warren DS, Dominici F, Simpkins CE,Montgomery RA. Outcomes of kidneys from donors after cardiacdeath: implications for allocation and preservation. Am J Transplant.2007; 7: 1797–807.[4] Sudhindran S, Pettigrew GJ, Drain A, et al. Outcome of transplan-tation using kidneys from controlled (Maastricht category 3) non-heart-beating donors. Clin Transplant. 2003; 17: 93–100.[5] Ledinh H, Bonvoisin C, Weekers L, et al. Results of kidney trans-plantation from donors after cardiac death. Transplant Proc. 2010;42: 2407–14.[6] Moers C, Leuvenink HG, Ploeg RJ. Donation after cardiac death:evaluation of revisiting an important donor source. Nephrol Dial Trans-plant. 2010; 25: 666–73.[7] Snoeijs MG, Winkens B, Heemskerk MB, et al. Kidney transplanta-tion from donors after cardiac death: a 25-year experience. Transplan-tation. 2010; 90: 1106–12.[8] Squifflet JP. Why did it take so long to start a non-heart-beating do-nor program in Belgium? Acta Chir Belg. 2006; 106: 485–8.[9] Van Gelder F, Delbouille MH, Vandervennet M, et al. An 11-YearOverview of the Belgian Donor and Transplant Statistics Based ona Consecutive Yearly Data Follow-up and Comparing Two Periods:1997 to 2005 Versus 2006 to 2007. Transplant Proc. 2009; 41: 569–71.[10] Van Gelder F, Delbouille MH, Vandervennet M, et al. Overview ofthe Belgian donor and transplant statistics 2006: results of consecu-tive yearly data follow-up by the Belgian Section of TransplantCoordinators. Transplant Proc. 2007; 39: 2637–9.[11] Ledinh H, Meurisse N, Delbouille MH, et al. Contribution ofDonors After Cardiac Death to the Deceased Donor Pool: 2002 to2009 University of Liege Experience. Transplant Proc. 2010; 42:4369–72.[12] Detry O, Laureys S, Faymonville ME, et al. Organ donation afterphysician-assisted death. Transpl Int. 2008; 21: 915.[13] Ysebaert D, Van BeeumenG, De Greef K, et al. Organ procurementafter euthanasia: Belgian experience. Transplant Proc. 2009; 41: 585–6.[14] Bernat JL, D’Alessandro AM, Port FK, et al. Report of a NationalConference on Donation after cardiac death. Am J Transplant. 2006;6: 281–91.[15] Moers C, Smits JM, Maathuis MH, et al. Machine perfusion or coldstorage in deceased-donor kidney transplantation. N Engl J Med.2009; 360: 7–19.[16] Smits JM, Persijn GG, van Houwelingen HC, Claas FH, Frei U.Evaluation of the Eurotransplant Senior Program. The results of thefirst year. Am J Transplant. 2002; 2: 664–70.[17] Yarlagadda SG, Coca SG, Garg AX, et al. Marked variation in thedefinition and diagnosis of delayed graft function: a systematic review.Nephrol Dial Transplant. 2008; 23: 2995–3003.[18] Houillier P, Froissart M. [Elevated serum creatinine]. Rev Prat.2005; 55: 91–6.[19] Flamant M, Boulanger H, Azar H, Vrtovsnik F. [Plasma creatinine,Cockcroft and MDRD: validity and limitations for evaluation of renalfunction in chronic kidney disease]. Presse Med. 2010; 39: 303–11.[20] Brook NR, White SA, Waller JR, Veitch PS, Nicholson ML. Non-heart beating donor kidneys with delayed graft function have superior
r 27, 2013, Volume 96 Number 10S S185
thorized reproduction of this article is prohibited.

FIGURE 2.
November 27, 2013
graft survival compared with conventional heart-beating donor kidneysthat develop delayed graft function. Am J Transplant. 2003; 3: 614–8.[21] Renkens JJ, Rouflart MM, Christiaans MH, van den Berg-LoonenEM, van Hooff JP, van Heurn LW. Outcome of nonheart-beating donorkidneys with prolonged delayed graft function after transplantation.Am J Transplant. 2005; 5: 2704–9.[22] Kokkinos C, Antcliffe D, Nanidis T, Darzi AW, Tekkis P, Papalois V.Outcome of kidney transplantation from nonheart-beating versusheart-beating cadaveric donors. Transplantation. 2007; 83: 1193–9.[23]Chapman J, Bock A, Dussol B, et al. Follow-up after renal trans-plantation with organs from donors after cardiac death. Transpl Int.2006; 19: 715–9.
S186 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
[24] Keizer KM, de Fijter JW, Haase-Kromwijk BJ, Weimar W. Non-heart-beating donor kidneys in the Netherlands: allocation and out-come of transplantation. Transplantation. 2005; 79: 1195–9.[25] Brook NR, Waller JR, Richardson AC, et al. A report on the activ-ity and clinical outcomes of renal non-heart beating donor transplanta-tion in the United Kingdom. Clin Transplant. 2004; 18: 627–33.[26] Ojo AO, Hanson JA, Meier-Kriesche H, et al. Survival in recipientsof marginal cadaveric donor kidneys compared with other recipients andwait-listed transplant candidates. J Am Soc Nephrol. 2001; 12: 589–97.[27] Snoeijs MG, Schaubel DE, Hene R, et al. Kidneys from donors aftercardiac death provide survival benefit. J Am Soc Nephrol. 2010; 21:1015–21.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
[28] Chudzinski RE, Khwaja K, Teune P, et al. Successful DCD kidneytransplantation using early corticosteroid withdrawal. Am J Transplant.2010; 10: 115–23.[29] Barlow AD, Metcalfe MS, Johari Y, Elwell R, Veitch PS, NicholsonML. Case-matched comparison of long-term results of non-heart beat-ing and heart-beating donor renal transplants. Br J Surg. 2009; 96:685–91.[30] Rudich SM, Kaplan B, Magee JC, et al. Renal transplantationsperformed using non-heart-beating organ donors: going back to thefuture? Transplantation. 2002; 74: 1715–20.[31] Saeb-Parsy K, Kosmoliaptsis V, Sharples LD, et al. Donor typedoes not influence the incidence of major urologic complications afterkidney transplantation. Transplantation. 2010; 90: 1085–90.[32] Droupy S, Blanchet P, Eschwege P, et al. Long-term results of re-nal transplantation using kidneys harvested from non-heartbeatingdonors: a 15-year experience. J Urol. 2003; 169: 28–31.[33] Khairoun M, Baranski AG, van der Boog PJ, Haasnoot A, MallatMJ, Marang-van de Mheen PJ. Urological complications and their im-pact on survival after kidney transplantation from deceased cardiacdeath donors. Transpl Int. 2009; 22: 192–7.[34] Ridgway D, White SA, Nixon M, Carr S, Blanchard K, NicholsonML. Primary endoluminal stenting of transplant renal artery stenosisfrom cadaver and non-heart-beating donor kidneys. Clin Transplant.2006; 20: 394–400.[35] Nicholson ML, Metcalf MS, White SA, et al. Comparison of theresults of renal transplantation from non-heartbeating, conventional,cadaveric and living donors. Kidney International 2000; 58: 2585–91.[36] Kootstra G. The asystolic, or non-heartbeating, donor. Transplan-tation. 1997; 63: 917–21.[37] Wells AC, Rushworth L, Thiru S, et al. Donor kidney disease andtransplant outcome for kidneys donated after cardiac death. Br J Surg.2009; 96: 299–304.[38] D'Alessandro AM, Fernandez LA, Chin LT, et al. Donation aftercardiac death: the University of Wisconsin experience. Ann Trans-plant. 2004; 9: 68–71.[39] Kootstra G, van Heurn E. Non-heartbeating donation of kidneysfor transplantation. Nat Clin Pract Nephrol. 2007; 3: 154–63.[40] Sanchez-Fructuoso AI, Marques M, Prats D, et al. Victims of car-diac arrest occurring outside the hospital: a source of transplantablekidneys. Ann Intern Med. 2006; 145: 157–64.[41] Sanchez-Fructuoso AI, Giorgi M, Barrientos A. Kidney transplan-tation from non–heart-beating donors: a Spanish view. TransplantRev. 2007; 21: 249–54.[42] Cohen B, Smits JM, Haase B, Persijn G, Vanrenterghem Y, Frei U.Expanding the donor pool to increase renal transplantation. NephrolDial Transplant. 2005; 20: 34–41.[43] Brook NR, Nicholson ML. Kidney transplantation from non heart-beating donors. Surgeon. 2003; 1: 311–22.[44] Saidi RF, Bradley J, Greer D, et al. Changing pattern of organ do-nation at a single center: are potential brain dead donors being lost todonation after cardiac death? Am J Transplant. 2010; 10: 2536–40.[45] Watson CJE, Wells AC, Roberts RJ, et al. Cold machine perfusionversus static cold storage of kidneys donated after cardiac death: aUK multicenter randomized controlled trial. Am J Transplant. 2010;10: 1991–9.[46] Wight JP, Chilcott JB, Holmes MW, Brewer N. Pulsatile machineperfusion vs. cold storage of kidneys for transplantation: a rapid andsystematic review. Clin Transplant. 2003; 17: 293–307.47] Schold JD, Kaplan B, Howard RJ, Reed AI, Foley DP, Meier-Kriesche HU. Are we frozen in time? Analysis of the utilization and ef-ficacy of pulsatile perfusion in renal transplantation. Am J Transplant.2005; 5: 1681–8.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
238
A step forward to reduce organ shortage in Malaysia
Farah Salwani muda IsmailFaculty Syariah and Law, Islamic Science University Malaysia, Nilai,Malaysia.
Organ transplantation has always been seen as a miracle in the mod-ern medical world. It is not just the hope that it brings to patients inneed of those precious organs, but it indirectly promotes helpinghands and brotherhood ties to be extended even across totalstrangers. Nevertheless, despite the huge benefit and inspiration thatit brings, a lot of countries including Malaysia suffer from a severeshortage of these donated organs. Supply of organs like kidneys,livers, hearts and many more are scarce, though the demand for it isendlessly shooting high.This problem has been going on for quitesome time and needs to be addressed urgently in an effective man-ner.Therefore, this paper will thoroughly highlight this issue and dis-cuss immediate steps that should be taken by Malaysia, towardseliminating organ shortage through social and legal strategic planning.Suggestions including fully utilizing fatal road accident victims and in-troducing a family support system for new organ pledgers, while stillmaintaining the opting in system will hopefully assist in providingnew frontiers in law and its application, to effectively address andsolve organ shortage issues in Malaysia.
r 27, 2013, Volume 96 Number 10S S187
thorized reproduction of this article is prohibited.

The Cause of Kidney Discharging Frequency (%)
Malignancy or strong suspicion of malignancy in donor body 22,5Poor donor kidney parameters with probability of kidney irreversible injury 22,5Unsatisfactory parameters during machine perfusion 19,7Lack of recipients according to HCV or HBV 8,5Cardiac arrest before organ procurement 5,6Nephrolitiasis 5,6Other 15,5
November 27, 2013
239
Postmortal organ donation in pediatric patients - general aspectsand single center experience
Sivatharsiny Thavarajah1, Nagoud Schukfeh1, Thomas Breidenbach2,Jutta Weiss2, Martin Metzelder1, Carmen Kirchner1, Andreas Paul1,Gernot Kaiser11General-, Visceral- and Transplantsurgery, University HospitalEssen, Essen, Germany; 2Deutsche Stiftung Organspende, Frankfurt,Germany.
Background: In times of urgent need for pediatric transplantationsthe shortage of adequate organs is still challenging. In comparisonto adult transplantations the problem of proper size of the organ is amajor limiting factor in pediatric transplantation. At all there is noage-restriction for organ donation in Germany.Methods: The organ donors after brain death in Germany up to theage of 15 between 2007 and 2012 were analyzed. 2012 there was afurther division into three age groups (< 2 years, 2 – 5 years, 6 – 15years) with evaluation of the number of realized organ donations outof the potential organ donors and the results of the discussions withthe relatives/parents. Additionally we analyzed the pediatric liverstransplanted at our center between 2007 and 2012 independently tothe age of the recipient.Results: The overall percentage of pediatric organ donation was3,2% (2007 – 2012) in Germany. 2012 only 55% of potential pediatricorgan donors became realized as donors, which is significantly lowercomparison to adults (donors > 15 years: 66,4%). The discussionswith the relatives of the potential organ donors lead to a clearly higherrate of refusal for pediatric organ donors (42%) than adult donors(28%). At our center we received 42 livers from pediatric donors(2007 – 2012) with a median age of 5 (range 0 – 15) resulting in prom-ising long-term results.Conclusion: Although children only are a small percentage amongthe potential organ donors, there is a special need for pediatricrecipients. To increase the comparatively low rate of consent in theage group under 16 years, a better education of the relatives as wellas the medical staff seems to be necessary.
S188 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
240
Is there a limit for expanding criteria of kidney donors?How far can we go?
Piotr Domagala, Artur Kwiatkowski, Rafal Kieszek, Michal Wszola,Jakub Drozdowski, Piotr Diuwe, Andrzej Chmura Department ofGeneral Surgery and Transplantology, Medical University of Warsaw,Warszawa, Poland.
Introduction: The lack of organs for transplantation has forced thetransplant community to expand the pool of donors. Using expandedcriteria donor (ECD) organs is one of the strategies for making moretransplants available. Although there are organs that do not fit intodefinition of ECD and remains controversial for transplantation. Theaim of this paper is to report the criteria of discharging kidney fromtransplantation.Patients and Methods: Four hundred and sixteen patients receivedcadaveric renal transplants between January 1, 2010 and June 31,2013. In this time seventy one kidneys were discharged from thetransplantation – thirty eight kidneys (nineteen referred potentialdonors) were disqualified before organ procurement and thirty threekidneys were rejected from transplantation during organ storage. Dataon donors and preservation parameters were collected. Causes of or-gan refusal were analysed.Results: Two the most common causes of kidney rejection from trans-plantation were malignancy or strong suspicion of malignancy in do-nor body as well poor donor kidney parameters with probability ofkidney irreversible injury.
Conclusion: Careful kidney selection is recommended in cases ofexpanded criteria donor kidneys in order to diminish factors that cannegatively affect graft function and survival.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
241
En-bloc kidneys transplanted from infant donors less than 5 kginto school age recipients
Li Zeng, Wen-Yu Zhao, Lei Zhang, You-Hua Zhu, Yu Chen,Fan-Yuan ZhuOrgan Transplantation Institute of PLA, Changzheng Hospital, SecondMilitary Medical University, Shanghai, People’s Republic of China.
Background: Kidney transplantation is currently the best treatmentoption for children with end-stage renal disease. Given the shortageof donor kidneys in China, the use of grafts from deceased infantdonors (weight < 5kg) is a potential approach to expand the donorpool. In this study we reviewed the results of the first cohort of en blockidney transplantation of infant donors to pediatric recipients in ourcenter.Methods: From February, 2012 to March, 2013, four infant en bloc kid-ney transplants in pediatric recipients were performed in our center.The en bloc graft was implanted extraperitoneally in the right iliacfossa. The distal end of the donor aorta was anastomosed end-to-endto the internal iliac artery, while the donor vena cava was anasto-mosed (end-to-side) to the external iliac vein. Both ureters were anas-tomosed individually to the bladder, with the exception of one case, inwhich a donor bladder patch was anastomosed to the bladder. Afterthe operation, the recipients received basiliximab as induction therapyfollowed by tacrolimus andmycophenolic acid for immunosuppression.Prophylactic anticoagulation with heparin was used for the first weekafter transplantation.Results: Recipients included 2 females and 2 males with age rangingfrom 4.6 to 11.6 yr. Donor age ranged from 33 to 56 days with weightranging from 2.5 to 5.0 kg. After a follow up of 2-14 months, patientand graft survivals were 100% and 75% respectively. Complicationsincluded delayed graft function in 1 patient, urine leak in 1, andanticoagulation-related hemorrhage in 1. One graft was lost early fromvascular thrombosis. The remaining 3 recipients had excellent graft func-tion with median serum creatinine of 1.1mg/dL (range, 0.8-1.3mg/dL)at last follow-up.Conclusion: Based on our initial experience, we conclude that favor-able outcomes can be obtained from en bloc transplantation from in-fant donors. The use of this donor population for pediatric recipientsshould be encouraged.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
242
Influence of interleukin 12B, interleukin 16 and interleukin 18genes polimorphisms on delayed graft function and rejectionepisodes in patients after kidney transplantation
Jan Pawlus1, Anita Sierocka1, Karol Tejchman1, Zbigniew Ziętek2,Maciej Romanowski1, Andrzej Pawlik3, Jerzy Sieńko1,Maciej Żukowski4, Kazimierz Ciechanowski5, Marek Ostrowski1,Tadeusz Sulikowski11Department of General Surgery and Transplantation, PomeranianMedical University, Faculty of Medicine, Szczecin, Poland; 2Chair andDepartment of Anatomy, Pomeranian Medical University, Faculty ofMedicine, Szczecin, Poland; 3Department of Experimental andClinical Pharmacology, Pomeranian Medical Uniwersity, Faculty ofMedicine, Szczecin, Poland; 4Clinic of Anaesthesiology and IntensiveCare, Pomeranian Medical University, Faculty of Medicine, Szczecin,Poland; 5Department of Nephrology, Transplantology and InternalMedicine, Pomeranian Medical University, Faculty of medicine,Szczecin, Poland.
Background: Inflammatory mediators have an important role inkidney graft outcomes. The cytokine and chemokine gene poly-morphisms are associated with variable production,activity, expression orligand-receptor affinity[1]. Genetic variation in the DNA sequence of theinterleukin 12B (IL-12B), interleukin 16 (IL-16) and interleukin 18 (IL-18)genes may lead to altered cytokine production and activity. These varia-tions can lead to changes in individual's patient outcome after kidney trans-plantation. That is know,the polymorphisms of interleukins influence oninflammatory diseases, e.g. diabetes, asthma or periodontopathy. Never-theless there were only few publications about their role in kidney graftoutcome [2,3,4].Aim: The aim of this study was to evaluate the correlation between IL-12B, IL-16 and IL-18 genes polimorphisms with graft function (delayedgraft function-DGF) and rejection episodes-acute(AR), chronic(CR).Materials and Methods: 267 (38,6% women, 61,4% men) recipientswere included to the study. The polymerase chain reaction wasused to determine gene polymorphisms of IL-12B(rs3212227), IL-16(4778889), IL-18(rs1946518,rs187238) in serum. Statistical sihnificance(p<0,05) was analised by logit regression (Pearson Chi2, M-L Chi2, Phi,Kendall's test, Gamma test, Spearman Rank R), ANOVA - Tukey's post-hoc test, Odds Ratio (OR)-Chi2 with Yates correction (CI-95%).Results: Regression analysis revealed no significance between AR/DGF/CR and IL-12B (p=,176/p=,328/p=,438), IL-16 (p=,231/p=,784/p=,287), IL-18-rs1946518 (p=,582/p=,279/p=,084), IL-18-rs187238(p=,285/p=,279,p=,303). CR group-AAvsCC genotype (IL-18,rs1946518)OR=2,35 (p=,040).Conclusion: There was no statistical significance between IL-12B,IL-16 and IL-18 gene polimorphisms and kidney graft outcomes aftertransplantation. Presence of AA genotype IL-18 (rs1946518) is con-nected with 2,35 higher risk of CR occurence.Source of Funding: NCN:2013/B/P01/2011/40
References:[1] Nankivell BJ, Alexander SI: Rejection of the kidney allograft.N EnglJ Med 2010, 363: 1451–1462.[2] Trinchieri G, Pflanz S, Kastelein A: The IL-12 family of hetero-dimeric cytokines: new player in the regulation of T cell responses. Im-munity 2003, 19:641–644.[3] Wang S, Diao H, Guan Q, Cruishank WW, Delovitch TL, JevnikarM, Du C: Decreased renal ischemia-reperfusion injury by IL-16 inacti-vation. Kidney Int 2008, 73: 318–326.[4] Wu H, Craft ML, Wang P, Wyburn KR, Chen G, Ma J, Hambly B,Chadbon SJ: IL-18 contributes to renal damage after ischemia-reperfusion. J Am Soc Nephrol 2008, 19:2331–2341.
r 27, 2013, Volume 96 Number 10S S189
thorized reproduction of this article is prohibited.

November 27, 2013
243
Improvement of the system for request for organ donation inbrain death patients
Sakuntala RodmaiCo-ordination Organ Transplant, Sunpasitthiprasong Hospital,Ubonratchatani, Thailand.
Background: The system for request for organ donation in braindeath patients has been in place since 2001. However, a significantnumber of relatives of brain death patients considered potential organdonors were not approached for request for organ donation. In 2001,only 13 from 94 brain death patients completed the organ donation.This may be due to hard workload of critical care units, which mightin turns prevent them from timely notifying an organ donation unitconcerning potential organ donors. We hypothesized that if potentialcandidates for organ donation were approached promptly, the numberand successful rates of organ donation would be improved.Objectives: To increase the rates of organ donation in brain deathpatientsMethods: Between October 2011 and September 2012, attempts toincrease the number and rates of organ donation of brain deathpatients in the Sunpasitthiprasong Hospital, a 1,200-bed regional hos-pital, were taken. This included 1) improving the coordination ofdepartments involved in organ donation procedures, 2) regular morn-ing and afternoon nurse rounds to all critical care units, 3) prompt as-sessment of brain death patients and relevant laboratory test results,4) provision of direct contact to responsible nurses in the organ dona-tion unit, and 5) feedback of the results to stakeholders for further andcontinuous improvement. We compared the numbers and rates of or-gan donation before and after the implementation of the new system.Results: After the implementation of a new system for request for or-gan donation, the number of registered cases of brain deaths in-creased from 94 case in 2011 to 152 case in 2012. The rates oforgan donation increased from 13.8% (13 out of 94 cases) to 23.7%(36 out of 152 cases) in 2011 and 2012, respectively.Discussion: Improvement of the system for request for organ dona-tion in brain death patients through fostering effective co-ordinationand communication between departments and units involved leadsto prompt negotiation with relatives about the possibility of organ do-nation and helps enhance the rates of organ donation. Further impli-cation is to improve the methods to care for subjects with brain death.
S190 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
244
The role of recruitment maneuver in improving the marginallungs donors
Sareh Parto, Shadi Shafaghi,Seyyed Shahabeddin Mohammad Makki, Farahnas Sadeghbeygi,Hamid Reza Khoddami Vishteh, Katayoun NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran (IslamicRepublic of).
Background: Lung transplantation is limited by shortage of suitabledonors. To overcome this problem, Recruitment maneuver have beenused in marginal lungs donors. Recruitment maneuver is a strategyaimed at re-expanding collapsed and edematous lung tissue. Thisstudy was conducted to assess the efficacy of this maneuver on im-proving marginal lungs for transplantation.Methods: All brain-dead donors of Shahid Beheshti University ofMedical Sciences Organ Procurement Unit (SBMU-OPU) of Tehran,Iran were evaluated for lung transplantation from May 2010-2013.Then, those who had marginal donor's criteria (patients with normalChest X Ray or bilateral infiltration and PaO2/FIO2 200-300 mmHg)were selected. The recruitment maneuver was performed and arterialblood gas was obtained before and after maneuver. The recruitmentmaneuver was performed for two hours with pressure control of 25-30 cmH2O and Positive End Expiratory Pressure of 10-15 cmH2O.O2 saturation and patients hemodynamic were checked continuously.Finally patients with normal bronchoscopy and PaO2/FIO2≥300mmHg were considered suitable for lung transplantation.Results: Of 259 brain-dead donors which were assessed for lung do-nation, 45 (17%) had marginal lungs for transplantation. Recruitmentmaneuver which was carried out in all of these cases could increasePaO2 to more than 300 in 14 (31%) which 8 of them weretransplanted. In these patients the mean of PaO2/FIO2 was signifi-cantly increased from 253 to 344 mmHg by recruitment maneuver(P=0.006, Wilcoxon test).Conclusions: The results of this study showed that Recruitment ma-neuver could increase PaO2 more than 300 mmHg and it could con-vert marginal lungs to appropriate ones in one third of brain-deaddonors. So, it is recommended that this maneuver is considered inthe assessment protocol of lungs for donation.Keywords: Marginal donor lungs, Recruitment maneuver, Lungtransplantation
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
246
The Islamic founding principles on organ transplantation andevolution of the collective scholarly Islamic opinion onthe subject
Ruhul KuddusBiology, Utah Valley University, Orem, UT, United States.
Background: Muslims constitute one-fifth of the humanity and a sig-nificant fraction of the organ recipients identify themselves asMuslims. A large fraction of Muslim population is devout but unawareof the religious principles on organ donation and transplantation anddepends on scholars’ (among Sunnis) and imams’ (among Shias)opinions on the matter.Methods: The Qur’an, the authentic Traditions and expert collectiveopinions on the subject were investigated.Results: The founding principles on transplantation medicine are fromthe Qur’an (for example, sacredness of life and the human body, andsome infractions are allowed to preserve life), the Traditions (suchas, sanctity of the corpse, prophet’s allowing of a mutilated male sub-ject transplanting with a prosthetic nose made of noble i.e. forbiddenmetals, and prophet’s forbidding of the use of wigs; etc.) and maslaha(the principles of public interest deduced by the scholars to protect aperson’s religion, life, reason, lineage and property). In general andbriefly, Muslim scholars, particularly the scholars of Indian subconti-nent, initially attempted to establish that organ donation and transplan-tation is prohibited. Thereafter, many Arab and Iranian scholars andMuslim scholars (including those from Indian subcontinent) settled inthe western hemisphere opined that organ donation and transplanta-tion are permitted but organ donation must be a voluntary act of char-ity. Of late, the Iranian scholars (and imams) have recognized that thegovernment but not any private parties may acquire organs for anestablished uniform compensation and equitably distribute the ac-quired organs.Conclusions: The current Islamic working principles on transplanta-tion medicine have remained somewhat transitory, emerging if notconfusing, and detached from the bulk of the Muslim population. Theeffect of such a status on transplantation medicine, particularly on or-gan donation, needed to be investigated.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
247
A questionnaire survey on cognition and intention towards organdonation in driving license holders of mainland China
Lulin Ma1, Lei Zhao1, Lixin Yu2, Tongyi Men27, CHangxi Wang3,Linhui Wang4, Ye Tian5, Yaowen Fu6, Long Liu7, Youhua Zhu8,Xuren Xiao9, Genfu Zhang10, Wei Zhang11, Heng Li12, XiaotongWu13,Shunliang Yang14, Tao Lin15, Huanqing Yang16, Qingguo Zhu17,Jianlin Yuan18, Zhenli Gao19, Wenke Han20, Jun Dong21, Sen Xie22,Ming Cai23, Wujun Xue24, Zhangqun Ye25, Nan Li261Urology, Peking University Third Hospital, Beijing, People’s Republicof China; 2Department of Kidney Transplantation, South HospitalAffiliated to Southern Medical College, Guangzhou, People’s Republicof China; 3Department of Organ Transplantation, the First AffiliatedHospital, Sun Yat-sen University, Guangzhou, People’s Republic ofChina; 4Department of Urology, Shanghai Changhai Hospital Affiliatedto the Second Military Medical University, Shanghai, People’sRepublic of China; 5Department of Urology, Beijing FriendshipHospital, Beijing, People’s Republic of China; 6Department of Urology,the First Hospital of Jilin University, Jilin, People’s Republic of China;7Department of Urology, the General Hospital of Shenyang MilitaryRegion, Shenyang, People’s Republic of China; 8Department ofOrgan Transplantation, Shanghai Changzheng Hospital Affiliated tothe Second Military Medical University, Shanghai, People’s Republicof China; 9Department of Urology, Beijing General Hospital of ArmedPolice Forces, Beijing, People’s Republic of China; 10Department ofUrology, Xinqiao Hospital, the Third Military Medical University,Chongqing, People’s Republic of China; 11Department of Urology,Jiangsu Province Hospital, Nanjing, People’s Republic of China;12Department of Urology, Union Hospital of Tongji Medical College,Wuhan, People’s Republic of China; 13Department of KidneyTransplantation and Dialysis, Second People’s Hospital of ShanxiProvince, Taiyuan, People’s Republic of China; 14Department ofUrology, Fuzhou General Hospital of Nanjing Military Command,Fuzhou, People’s Republic of China; 15Department of Urology, WestChina Hospital of Sichuan University, Chengdu, People’s Republic ofChina; 16Department of Urology, Guangdong General Hospital,Guanzhou, People’s Republic of China; 17Department of Urology, the2nd Affiliated Hospital of Harbin Medical University, Harbin, People’sRepublic of China; 18Department of Urology, Xijing Hospital, theFourth Military Medical University, Xian, People’s Republic of China;19Department of Urology, Yantai Yuhuangding Hospital Affiliated toQingdao University Medical College, Yantai, People’s Republic ofChina; 20Department of Urology, Peking University First Hospital,Beijing, People’s Republic of China; 21Department of Urology, GeneralHospital of Chinese People’s Liberation Army, Beijing, People’sRepublic of China; 22Department of Urology, Wuhan General Hospitalof Guangzhou Military, Wuhan, People’s Republic of China;23Department of Organ Transplantation, the 309th Hospital of ChinesePeople’s Liberation Army, Beijing, People’s Republic of China;24Department of Kidney Transplantation, First Affiliated Hospital ofXi’an Medical University, Xian, People’s Republic of China;25Department of Urology, Tongji Hospital, Tongji Medical College ofHuazhong University of science & technology, Wuhan, People’sRepublic of China; 26Clinical Epidemiology Research Center, PekingUniversity Third Hospital, Beijing, People’s Republic of China;27Department of Urology, Qianfoshan Hospital Affiliated to ShandongUniversity, Jinan, People’s Republic of China.
A questionnaire survey was conducted to investigate the cognition to-wards organ donation, definition of death, transplantation and willing-ness to donate in driving license holders in China. From Jan 2013 to Mar2013, 25,000 questionnaires were distributed to 25 transplant centersin China which were the member units of the Kidney TransplantationGroup of Chinese Urological Association and the survey on local drivinglicense holders was performed by each center randomly. The questionsin the questionnaires included demographic characteristics of respondents
r 27, 2013, Volume 96 Number 10S S191
thorized reproduction of this article is prohibited.

November 27, 2013
aswell as their understanding of kidney transplantation and organ dona-tion and personal willingness. All the questionnaires were collected toPeking University Third Hospital for statistics and the results were ana-lyzed by epidemiology experts. Total 25,000 questionnaires were dis-tributed and 12,807 collected (51.2%).The effective response rate ofquestionnaires was 95.5% (12228/12807). 74.4% respondents approvedvoluntary organ donation, 64.0% advocated organ donation after deathand 48.4% wanted to be volunteers of organ donation. It can be seenfrom the results that most of the respondents approve organ donation,but only less than half wants to be the organ donation volunteers. Thereasons for this are various andmore propagandawill be needed to pro-mote the voluntary organ donation in China.
References:[1] Huang J, Mao Y, Millis JM. Government policy and organ transplan-tation in China [J]. Lancet, 2008, 372(9654):1937–1938.[2] UNOS.OPTN/UNOSTransplantTrends.[EB/OL].http://optn.transplant.hrsa.gov/data/[3] Song YG. Analysis of issues related to organ transplantation [J].Chinese Medical Theory and Practice, 2005, 14(2):199.[4] Huang JF. A key measure to promote the sound development of or-gan transplantation in China-Thoughts on principles of donation aftercardiac death pilot [J]. Chin J Organ Transplant,2011,32(1):1–4.[5] Grewal HP, Willingham DL, Nguyen J, et al. Liver transplantation us-ing controlled donation after cardiac death donors:an analysis of a largesingle-center experience [J]. Liver Transpl,2009,15(9):1028–1035.[6] Ming YZ, Ye QF, Shao MJ, et al. Clinical analysis of 48 cases of kid-ney transplantation from cardiac death donors [J]. J Cent South Univ(Med Sci),2012,37(6):598–605.[7] Xian YX, Chen GD. Advances in DCD donor kidney quality as-sessment and improvement methods [J]. Organ Transplantation,2013, 4(2):113–116.[8] Reich DJ, Mulligan DC, Abt PL, et al. ASTS recommended practiceguidelines for controlled donation after cardiac death organ procure-ment and transplantation [J]. Am J Transplant,2009,9:2004-2011.[9] Wang HY, Béatrice SENEMAUD, Chen ZH. Management andstandards of organ donation and transplantation in France [J]. Chin JTransplant (Electronic Edition), 2012, 6(1):59–64.[10] Hou FZ. Introduction of organ donation and transplantation ad-ministrative system in the United States [J]. Chin J Transplant (Elec-tronic Edition), 2011, 5 (4):330–336.[11] Medical Service Supervision Division of the Ministry of Heath,the People’s Republic of China. Notification of the General Office ofthe Ministry of Heath about launching the donation after cardiacdeath pilot (Attachment1:Classsification of Donation after CardiacDeath in China)[12] Organ Transplantation Association. Guide for donation after cardiacdeath in China [J]. Chin J Organ Transplant, 2010, 31(7):436–437.[13] He XS, Guo ZY. Standardized management to promote the or-derly development of human organ donation in China [J]. Chin JTransplant (Electronic Edition), 2010, 4(1):7–9.[14] Yao Y, Gu JX. Discussion on ethical principles of donation after car-diac death in China [J]. Chinese Medical Ethics, 2012, 25(5):569–571.[15] Yao Y. Ethical reflection and practical exploration on donation aftercardiac death [J]. Medicine and Philosophy, 2012, 33:23–25.[16] Zhang R, Li C, Li ZW, et al. Development status and prospect oftransplantation and donation after cardiac death[J]. Chin J Basesand Clinics in General Surgery,2012,5,19:493–497.[17] Dong Q, Li C, Wang YJ, et al. Feasibility analysis of donation aftercardiac death in China [J]. Chin J Bases and Clinics in General Sur-gery, 2012,5,19:498–501.[18] Wang YJ, Li C, Zhang R. Survey on factors affecting organ dona-tion willingness. Organ Transplantation, 2013, 4(2):75–78.[19] Yin ZK, Yan J. Predicament of donation after cardiac death and itscountermeasures [J]. Medicine and Philosophy, 2012, 33(1A):28–32[20] http://news.sina.com.cn/c/2011-04-26/004522356616.shtml
S192 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
250
Online solicitation of organ donors: An analysis of a living donoronline forum (preliminary findings)
Dominique Martin1, Rebecca Ritte1,21Centre for Health and Society, The University of Melbourne,University of Melbourne, Australia; 2Onemda, VicHealth Koori HealthUnit, The University of Melbourne, University of Melbourne, Australia.
Little is known about the mechanisms by which individuals may solicitor offer organs for transplantation on the internet, despite widespreadrecognition of the ethical concerns raised by online solicitation of unre-lated living organ donors. In this paper, we present the preliminaryfindings of the Online Solicitation of Organ Donors (OSOD) study inthe context of a multinational living donor online forum.Methods: A forum dedicated to communication between potentialdonors and recipients within an international online community web-site with a prohibition on commercial activity was analysed. Publiclypresented personal information was extracted from all threads initiatedduring a six week period (1 June 2013 – 14 July 2013 inclusive). Openlyposted names, usernames, email addresses and phone numbers wereused to trace any further evidence of online activity elsewhere.Results: From a total of 45 individual user profiles identified, four usercategories were defined: offerers (n=20); solicitors (n=20); brokers(n=1) and other (n=4). Approximately 89% of solicitors and offererswere concerned with obtaining or donating livers (n=18) and/or kidneys(n=22). Ten countries were identifiable with 36 of the user profiles; 29%were associated with the USA and 27% with India. Of the offerers, 50%were identified offering their organs in a variety of unrelated internetforums, with at least 7 of the 10 seeking monetary payment.Conclusion: Nominally altruistic organ donation online forums appearto provide a platform for individuals to solicit and offer organs acrossthe world. Participation in such forums is one of the strategies pro-spective organ vendors, buyers and brokers may use to arrange sales.Greater knowledge of these online interactions will inform efforts toprevent harmful practices and assist in the evaluation of illicit organtrade in the international setting.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
251
“Suffering and urgent needs” - online solicitation of Sri Lankankidney donors
Prabhathi Basnayake1, Dominique Martin1, Rebecca Ritte1,21Centre for Health and Society, The University of Melbourne,University of Melbourne, Australia; 2Onemda, VicHealth Koori HealthUnit, The University of Melbourne, University of Melbourne, Australia.
The rising burden of chronic kidney disease in Sri Lanka has led to in-creasing demand for transplantation, with needs predominantly metby living donors. In the setting of widespread reports of organ tradingand an extraordinary national reputation for altruistic corneal donation,the regular solicitation of unrelated kidney donors in online Sri Lankannewspapers raises intriguing questions and serious concerns. We re-port the results of a study of kidney donor solicitation advertisementsin Sri Lankan newspapers published online in Sinhalese and English.We completed a thematic and content analysis of solicitation adver-tisements in 3 online newspapers over a six week period (1 May2013 – 14 June 2013).The analysis of the 15 posted advertisements revealed themes ofsocial and health status; medical urgency; donor qualities; andhealthcare providers. The brief advertisements sought to stimulate in-terest from prospective donors by painting a picture of need, appeal-ing to virtue and providing contact details for further information. Theonline advertisements were consistent with findings from internationalresearch investigating solicitation of organ donors and donors of otherhuman biological materials in a variety of media.Reviewed in the context of current donation policy and practice, ourresults provide some important insights into the challenges and oppor-tunities of organ donor recruitment in Sri Lanka.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
252
Living Donor Observatory (LIDOBS community)
Marti Manyalich1,2, Ana Menjivar2, Xavier Torres2, Josep M. Peri2,Ignacio Revuelta2, Fritz Diekmann2, Constantino Fodevila2,Santiago Sanchez2, David Paredes1,2, Chloë Balleste11School of Medicine, University of Barcelona, Barcelona, Spain;2Hospital Clinic of Barcelona, Barcelona, Spain.
Introduction: LIDOBS is a multidisciplinary community composed byinternational experts on Living Donation interested to join efforts to im-prove the quality of the procedures and to establish international con-sensus in order to protect Living donors’ (LD) health and safetythrough the development of registries and follow-up the living donationimpact on donors’ life.Objective: To promote a High Quality of Living Donation programs of-fering a scientific platform that will help to assure transparency, qualityand safety of the programmes.Methodology:LDs’ protection: by providing detailed information about the process,detecting new ethical dilemmas and being coherent on legislationissues.Registry: Implement a database model for LD registration and dataanalysis. The model is created based on three levels: mandatory,recommended and excellence.Follow-up: Detect the key points for the outcome, donors’ satisfactionand mid to long-term impact of donation process on donor’s quality oflife and their psychological well-being.Research: Continuous scientific researches to identify the bestpractices, to develop quality indicators and make recommendationfor LD safety.Results: On-line database registry: Currently there are more than1600 registered LDs with mandatory data from 19 centres in 13 Euro-pean countries. The actual registry is improving and enhanced withdata from other countries. Such registry will help the research andthe quality of the procedure.LDs assessment/follow-up surveys (tools surged by EULID andELIPSY projects available in several EU languages): LIDOBS enablethe continuity of their application.Conclusion: Promoting LD follow-up and international registrationpractices through research and data analysis, and establishing a con-sensus among professionals will benefit transplant professionals andthe quality of LD programs. The centres that accomplish the LIDOBSrecommendations should be considered as excellence centres.A great gratitude goes to all professionals that were involved in all thestages of the following projects: - ELIPSY project - EULID project - FISproject (Co-founded by European Regional Development FundFEDER).
r 27, 2013, Volume 96 Number 10S S193
thorized reproduction of this article is prohibited.

November 27, 2013
253
Community perspectives on the allocation of deceased donororgans for transplantation: A nominal group study
Michelle Irving1,2, Allison Tong1,2, Stephen Jan3, Alan Cass6,SteveChadban4,5, RichardAllen5, JonathanCraig1,2, GermaineWong2,Kirsten Howard11School of Public Health, University of Sydney, Sydney, Australia;2Centre for Kidney Research, Children's Hospital Westmead,Westmead, Australia; 3The George Institute for global health,Camperdown, Australia; 4Central Clinical School, Bosche Institute,University of Sydney, Sydney, Australia; 5Dept of Renal Medicine, RoyalPrince Alofred Hospital, Camperdown, Australia; 6Menzies School ofHealth Research, Northern Territory, Australia.
Aim: Deceased donated organs are a community held resource yet lit-tle is known about community views on organ allocation. We aimed todetermine community preferences for organ allocation.Methods: Thirteen nominal groups involving 114 participants from thegeneral community were conducted in New South Wales, Victoria,Queensland and South Australia. Participants identified, ranked anddiscussed reasons for factors they believed were influential in theirdecision-making about organ allocation. A mean importance scorewas determined for all the factors. Transcripts were analysed themat-ically to identify reasons for their choices.Results: Medical urgency or need was considered to be the most im-portant factor, followed by ability to survive the surgery. Other factorsranked highly included: time on the waiting list, the age of recipient, lifeexpectancy after transplant and compatibility. Younger participantsvalued time on waiting list; compatibility and lifestyle greater and olderparticipants valued life expectancy after transplant greater. Participantswere relieved that health professional made ultimate decision. We iden-tified three major themes underpinning their preferences for allocation:save and improve as many lives as possible, fairness, and minimisinglost opportunities for patients on the waiting list.Conclusion: The community prioritise medical need, waitlisting time fororgan allocation.While these broadly reflect attributes in the current allo-cation algorithm in Australia, there needs to be amore explicit process ofincorporating community values into organ allocation policies.
S194 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
254
The enlightening lectures to the ordinary people and medicalstuffs about the organ donation on the neurosurgeon’s neutralstandpoint are effective for the futural development of thetransplantation medicine
Shun-ichi YoshikaiDepartment of Neurosurgery, Shin-Kokura Hospital, Kitakyushu, Japan.
The number of the organ donations is quite unsatisfactory and the an-nouncement about the donation is still poor in Japan. One of the majorreasons is that the almost Japanese people including medical doctorshave longstanding misunderstandings about the donation due to thenegative campaigns of the mass media since the first cardiac trans-plantation in 1968 in Japan and also due to the incorrect or maliciousinformation about donation widely spread through the internet. Thetypical misunderstandings are: the donor’s body is brought away formonths or never returns, and the body is cut in pieces at the organextractions, the agreement of the donation is forced and pressed bythe transplantation coordinators, the cost of the transplantation ishuge and the fundraising activities are necessary even in the domestictransplantation etc.. In order to resolve these issues, the Japanesetransplantation academic meetings and networks have tried to an-nounce the correct information, however, the discussions remainstopped at the very beginning issue, the brain death is really anindividual’s death or not. In addition, the emergency room doctors hes-itate the confirmation of the patient’s donor-card possession or theproposal of the option because of their personal prejudices to the or-gan donation. The author is a neurosurgeon with many experiencesof the patients’ cadaveric donations, and has promoted the enlighten-ment activities and published a book especially about the organdonations on a neutral standpoint. For example, the author does notaccept the brain death is the individual’s death medically, however,the author accepts it legally. According to these neutrality and objectiv-ity, the author’s lectures are easily acceptable to the audience. The en-lightening activities do not bring any quick effects, however, it isimportant to educate them to be involved in the organ donation onthe neutrally and objectively.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
255
Are there barriers which prevent family discussion about theirorgan donation wishes?
Mary CampbellNursing, Northern NSW Local Health District, Tweed Heads, Australia.
Background: Organ transplantation is the definitive treatment formany patients with end-stage organ failure. Australia however, has apersistently low donation rate, which results in many Australian’s dyingbefore transplantation.In New South Wales (NSW) in 2011, 31% of families for whom con-sent was requested, declined permission for their loved one to be-come an organ donor. However, evidence suggests that whenfamilies have had a memorable discussion about their organ donationwishes, they are more likely to support their loved ones wish to be-come an organ donor.Aims:1. To identify if barriers exist which prevent or inhibit families from hold-
ing a memorable discussion about their organ donation wishes.2. To identify factors that facilitates organ donation discussions within
families.Methods: Four focus groups were conducted in rural NSW, incorpo-rating a continuum of ages from senior school children to retired seniors.The focus groups included year 10 and 11 students, sterilisationtechnicians employed in the Central Sterilizing Supply Unit (CSSU) ofa local hospital, university lecturers from Southern Cross University(SCU) and members from the University Third Age (U3A).The senior students and the sterilisation technicians had been in-volved in an organ donation education session prior to participating inthe focus group, while the university lecturers and members of U3Ahad not been involved in an educational session prior to participatingin the focus group. The focus group data was transcribed and coded toidentify key themes using an interpretative phenomenology process.Results: The identified barriers were lack of knowledge, geographicaldistribution, hectic pace of family life and age. The findings also showedthat school children and adults were able to initiate family discussionwith ease once they had been involved in an education session.Conclusion: Despite the barriers, family discussions are facilitatedwhen individuals have participated in an education session and giventhe opportunity to ask questions.NSW Organ and Tissue Donation Service,Health Education Train-ing Institute
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
257
Discussing donation: educational DVD resource
Sarah Aranha1, Steve Philpot1,21DonateLife Victoria, Melbourne, Australia; 2Intensive Care Unit,Alfred Health, Melbourne, Australia.
In 2011 DonateLife Victoria (DLV) formed the Communication SkillsWorking Group (CSWG) to develop, implement and evaluate strate-gies within the DLV network to improve the quality of family donationconversations. The group developed a DVD resource to support theprovision of education for health professionals who are involved infamily donation conversations. The resource was designed to assisteducation facilitators who are already skilled and knowledgeable indonation conversations.The DVD contains 16 vignettes showing various elements of the dona-tion conversation, contrasting skilful communication techniques withpoor techniques. The vignettes were partially scripted prior to filmingto ensure that each vignette highlighted one to two key learningpoints. For instance vignette one shows the doctor discussing braindeath with a family using technical jargon, and vignette two showsthe doctor providing the family with more appropriate information byusing simple language. Filming was completed by an external produc-tion company, with members of the CSWG in the role of healthprofessionals and paid actors in the role of family members.The DVD resource is accompanied by a written facilitator’s guidecontaining teaching points, learning objectives and suggested questionsfor participants. The resource has been designed so that each vignettemay be used as a standalone teaching tool, or multiple vignettes maybe used to facilitate a comprehensive organdonation conversationwork-shop. The Australian Organ and Tissue Authority have incorporated theresource into a national training program.The development of this resource was the first project completed bythe CSWG and met its purpose in providing health professionals andeducators with a teaching resource to improve the quality of organ do-nation conversations. It is hoped that this will ensure that families ofpotential organ donors are supported to make an enduring, informedand value-driven decision regarding donation.
r 27, 2013, Volume 96 Number 10S S195
thorized reproduction of this article is prohibited.

November 27, 2013
258
“You say you are doing your job but it feels like so much more…”
An exploration of the intensive care nurse and organ donation
Sharella Robinson, Fiona CoxICU, Alfred, Melbourne, Australia.
The Alfred Intensive Care Unit is a fast paced, dynamic unit. The nurs-ing staff is remarkably adaptable, resilient and work under high levelsof stress. When a life cannot be saved, the focus changes to end of lifecare. Organ and tissue donation offers loved ones the opportunity tosalvage something positive from the tragedy of loss. The bedsidenurse is crucial in supporting families though this process. It is highlycomplex and emotionally taxing, yet so rewarding and a privilege tobe a part of. This study was inspired by the title of the abstract, a state-ment from the wife of a patient who became an organ donor.The role of the bedside nurse in organ donation was explored thoughsurveying ICU nurses. Consisting of 11 questions, the results providedinsight into the perception ICU nurses have of donation and how con-fident they are in this role. The majority of respondents were ClinicalNurse Specialists (CNS) with 5–10 years of ICU experience. It was de-scribed as a “mostly positive” experience with 81% reporting beingcomfortable caring for this patient group. When given a list of wordsto describe the process, Brain Death (BD) donation was describedas respectful, compassionate, rewarding and professional. Donationafter Cardiac Death (DCD) was described as challenging, demandingand emotive. It was evident that the DCD process was more stressfuland confronting. Three quarters of nurses surveyed felt confident insupporting families through this time, the main barriers noted as being“caught up in emotions” and “it’s the questions that throw me….. I feelas their nurse I should have all the answers” as well as a lack of rap-port with family.The survey demonstrated nursing staff developing a bond with theirpatients and loved ones that is unique to organ donation. It oftenbecomes difficult to simply “switch off” emotions. These patients oftenstay with us long after the shift is over. It’s a privilege to be a part of thisprocess, hence why being involved with this special group of patientsis more than just a job.
S196 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
259
Factors influencing on families’ refusal for organ donationin Korea
Jaesook Oh1, Sungae Cheon2, Boosun Park2, Ohyuk Yun2,Jeongrim Lee2, Kyungsook Jang3, Sunhee Kim4, Jongwon Ha5,61Information Education, Korea Organ Donation Agency, Seoul, Korea;2Donation Management, Korea Organ Donation Agency, Seoul,Korea; 3Donation Support, Korea Organ Donation Agency,Seoul, Korea; 4Secretary General, Korea Organ Donation Agnecy,Seoul, Korea; 5President, Korea Organ Donation Agency, Seoul,Korea; 6Department of Surgery, Seoul National University College ofMedicine, Seoul, Korea.
Although the number of deceased donor organ donation is increasingin Korea, we still face many cases of unutilized donors because offamily refusal. Increasing conversion rate is another important way toincrease donor number. We analyzed factors related donors and triedto find out important factors which influence on the donation.Method: Donor records of Korea Organ Donation Agency (KODA)were analyzed. In 2012, 1,126 patients were reported to KODA.Among them, family consent was obtained from 446, and family re-fusal was 343 among eligible donors. Factors of each group such assex, age group (0~19, 20~39, 40~59, more than 60 years old), causesof the brain-death, trauma / non-trauma, marital state, duration of hos-pital stay and region of living were used for analysis. Direct KODA co-ordinator approaches were performed in 216 out of 343 and thesecases were analyzed to see causes of donation refusal. Statisticalanalysis was performed using 2-tailed w2test, t-test and logistic regres-sion analysis (SPSS ver. 18).Results: The agreement from the men showed 1.3 times more thanthat from the women in logistic analysis over the key factors as abovealthough it was not statistically significant. In an age group, it was indi-cated as they get older, the donation also increases to 1.3 times(p=0.014). Family living in Seoul agreed with the organ donation 3 timesmore than that of other area families (p=0.000), and those who have aspouse agreed with the donation 0.35 times lower than the opposite(p=0.000). The causes of the 66 refusal cases (30.6%) were related todisagreement from the rest of the family other than the one who favor-ably consulted first. The 56 cases (25.9%) of the emotional rejection ofthe family come second. The other reasons were the denial of thebrain-death (9.7%), never thought about the donation (8.3%), and beliefin peaceful death (6%).Conclusion: Public education to increase positive support for the de-ceased donor organ donation is important to increase conversion rate.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
260
Providing support to donor families: Evaluation and challenges
Minsun Kang1, Sanghyoung Yoon2, Gahee Kim2, Eunyoung Heo2,Sunny Kim3, Jongwon Ha4,51Management Support Team, Korea Organ Donation Agency, Seoul,Korea; 5Department of Surgery, Seoul National University College ofMedicine, Seoul, Korea; 2Family Care, Korea Organ Donation Agency,Seoul, Korea; 3Chief Operating Officer, Korea Organ DonationAgency, Seoul, Korea; 4President, Korea Organ Donation Agency,Seoul, Korea.
Background and Objective: Various bereavement support programshave been provided through Korea Organ Donation Agency (KODA) toassist families of a brain-dead organ donor. This study aimed to under-stand the decision-making process of donor family members, andevaluate their experience of the organ donation process.Methods: Face-to-face interviews were performed using ten struc-tured questions and four unstructured questions with nineteen familymembers who completed the organ donation process. Informationabout family members’ depression was evaluated using the Centerfor Epidemiological Studies-Depression (CES-D) scale.Results: Thirteen participants (68%) were aware of the possibilityof organ donation and ten families (53%) decided by themselves todonate their deceased relatives’ organs even before they wereapproached to consider it. The process of reasoning behind agreeingto organ donation of the deceased by participants was ‘meaningfuldeath for their relatives’ mostly, and some of them agreed to donateorgans because of either fulfilling the wishes of the deceased or re-ceiving government compensation of funeral costs and the donor’smedical costs. During the organ donation process, ten participants(53%) had felt difficult to understand entire donation process. Overallthe study results indicated that participants were satisfied with the ser-vice provided to them by KODA and twelve participants (63%) were wil-ling to donate their own organs after death. Twelve participants (70%)scored 25 and higher and only five (30%) scored 15 or lower on theCES-D scale, which means that many left experience depression.Conclusion: Most family members felt that they were given enoughinformation to make an informed decision about donation and thestudy results indicated a positive attitude towards the organ donationprocess among family members. However, majority of participants werestruggling with severe or mild depression after donation and thesefindings suggests that developing grieving or counseling programswould be essential throughout and after the donation process.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
261
Longevity of an organ donor coordinator, a personal perspective
Andrew Young, Kelly RogersonDonateLife Victoria, Melbourne, Australia.
Body of Abstract: The role of the organ donor coordinator atDonateLife Victoria (DLV) is a critical component of the organ dona-tion process. The involvement of experienced and efficient organ do-nor coordinator (ODC) is integral to successful organ and tissuedonation outcomes.I have been in this privileged role since July 2007 and believe that therole of the ODC will continue to expand and become even more com-plex. My role over this time has progressed from a case related focusto also leading portfolios that align with the national priorities.During these last 6 years, and more recently, the challenge I find is tomaintain my focus on ensuring organ and tissue cases progress in atimely, effective and professional manner, while also expanding myskills to ensure I remain a valuable team member.My aim with this abstract is to highlight methods and strategies that Ihave found beneficial to ensure my position as an ODC remains satis-fying, from a professional and personal viewpoint while I continue toevolve in an advanced practice nursing role.These strategies include:1. Setting personal goals and recognizing values2. Developing and maintaining relationships with members of the DLV
network3. Regular review of current workload4. Planning and maintaining professional portfolios5. Setting boundaries6. Recognizing that personal ideals and choices do have a profes-
sional impact7. Undertaking professional development opportunitiesThese strategies are completely subjective in nature, however I be-lieve that they may have some relevance for other ODC’s to assistin their own personal development. This can only lead to a more ex-perienced and competent ODC workforce.
r 27, 2013, Volume 96 Number 10S S197
thorized reproduction of this article is prohibited.

November 27, 2013
262
Education, social communication/cooperation with patient
edyta skwirczyńska-szalbierzDepartment of General Surgery and Transplantation, IndependentPublic Clinical Hospital No. 2, Pomeranian Medical University inSzczecin, Szczecin, Poland.
Cooperation is common affair, based on division of mastery and author-ity. Cooperation is not hierarchic. Its mastery is based on knowledge andexperience, which is opposite to mastery based on role or position.In Poland, there is no obligation of having family’s agreement for tak-ing organs from dead relative, because there is obligation of allegedagreement. In practice we are striving to get this agreement. If familyis against transplantation we dissent from taking organs.Positive attitude to medical care results in potential agreement for tak-ing organs from dead relative.The point is to answer the questions:1. Does the way of caring about still living patient, and relation be-
tween doctor and patient’s family has influence on family’s agree-ment for taking organs after death?
2. Does the way of caring about respondents has influence on theiragreement for taking organs?
Research Methods:1. Questionnaire made of 18 questions2. In research participated 173 peopleSummary: Thirty two percent of people are satisfied with level of med-ical care. Majority of them are of the opinion that doctors are treatingthem without expected carefulness. Thirty eight percent believes thatdoctors are capable to stop the therapy to get organs for transplantation.Conclusions: There is necessity to recognize correlation betweencorrect relation doctor-patient, trust gain and reliability of doctor’sopinions. Patient’s conviction that they are well treated may regain be-lief in straightforwardness of doctor’s opinions, less dissatisfaction andcriticism for medical care.
References:[1] W. Kraus Collaboralion in Organizations[2] Ostrowska A.:Doctor patient relationships - new quality. Health Pro-motion. Social Science and Medicine, 2001, 21, 109–121[3] The Cell, Tissue and Organ Recovery, Storage and TransplantationAct 1)2) of July 1st, 2005 (the Official Journal of Acts Dziennik Ustaw05.169.1411, as amended)
S198 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
263
Implementation of educational programs for Russianspeaking countries.
Sergey Trushkov, Janis JushinskisPaul Stradin University Hospital, Department of Transplantation,Riga, Latvia.
There are many large geographical regions speaking the same lan-guage for different historical and political reasons. In European Unionit is English with the main educational programs using this language.The same situation is observed in transplantation, where the moderndestinations in transplantation law, donation aspects, donor family ap-proach, etc. being presented in English.In the former USSR territory Russian was used as international lan-guage and this situation remains in many countries where Russianis more popular than English. At the same time they have big interestin the development of local transplantation programs that needs par-ticipation in education programs in transplantation. Latvian transplan-tation center in cooperation with Riga Stradins University and localauthorities have started educational program in transplantation forRussian speaking countries, which was started as the separatelectures and presentations performed locally and presently processedto specialized educational 7- day program including both theoreticaland practical issues in transplantation. In the result of this educationalprogram presently there are already some changes in Kazakhstan na-tional transplant legislation and deceased donation was started.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
264
The role of trust and hope in organ donation decisions
Holly Northam, Mary Cruickshank, Gylo HercelinskyjDisciplines of Nursing and Midwifery, University of Canberra,Canberra, Australia.
Introduction: Transplantation is the therapy of choice for mostpatients with end stage organ failure; however access to transplanta-tion is limited by the shortage of medically suitable donor organs. In-creasing family agreement to organ donation requests is key toincreasing national and international transplantation rates. Despitewidespread community acceptance of the benefits of donation, lessthan 60% of Australian families will agree to donate their deceasedrelatives’ organs.Objectives: To present findings of a qualitative study designed to ex-amine the factors that contribute to family deceased organ donationfor transplantation decisions.Methods: A PhD study entitled “The factors that influence families todecline organ donation” has been conducted. This project has usedan exploratory case study approach with a qualitative snowball sam-pling recruitment strategy. Following ethics approval, family memberswho had made an organ donation decision for a deceased relativewithin the previous three years were invited to participate in the study.Twenty two participants from nine families were interviewed between2011–2012. The interviews were transcribed and thematic analysiswas performed. The Precaution Adoption Process Model of Decisionmaking was used to propose that trust, hope and deep hope underpinfamily organ donation decisions.Results: Data analysis has revealed strong themes around hope,trust and care for the deceased, the influence of time, information, suf-fering and organs.Conclusion: The findings have implications for consent and non-consentdecisions in both organ and tissue donation circumstances.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
265
The collaborative development of continuing education targetedto funeral professionals delivered by a national professionalassociation.
Jim Mohr, Kim Young, Mathias Haun, Ken LotheringtonOrgans and Tissues, Canadian Blood Services, Ottawa, ON, Canada.
Funeral professionals indicate that 50% of all funerals are pre-planned, presenting a logical opportunity to initiate a donationdiscussion with clients.In 2008, governments gave Canadian Blood Services a mandate fororgan and tissue donation and transplantation to support system per-formance improvement. In 2012 the Funeral Services Association ofCanada (www.fsac.ca) was engaged as a national donation partnerin the development of an on-line donation course targeted to funeralprofessionals to advance donation opportunities and improve relationshipswith recovery organizations.Experts in on-line learning solutions were retained to manage the de-velopment and implementation of the course. The course content wasinformed by a panel of five experts representing funeral home/medicalexaminer liaisons, an eye bank, a tissue bank, a provincial donationorganization and an expert in organ donation. The course was developedover six months and launched June 2013. It has been implementedin both English and French and upon completion of the course par-ticipants can receive Continuing Education Units towards their ongoingfuneral professional education.Module 1 introduces the concept of dual advocacy and provides fu-neral professionals with knowledge and motivation to appropriatelyand positively raise the opportunity for donation during pre-plannedfuneral conversations and to direct clients to provincial donation orga-nizations and donation intent registries to action their wishes or obtainadditional information.Module 2 addresses the surgical aspect of organ and tissue recovery,encourages the development of collaborative working relationshipswith recovery organizations and provides guidance on expected prac-tice of recovery organizations in body reconstruction.Links to all Canadian donation and recovery organizations’ websitesand intent-to-donate registries are provided to facilitate and encour-age communication and relationship development. Each course par-ticipant is asked to complete a course evaluation to compare theirlevel of confidence in discussing organ and tissue donation with clientsbefore and after completing the course.
r 27, 2013, Volume 96 Number 10S S199
thorized reproduction of this article is prohibited.

November 27, 2013
266
Collaborating with medical examiners and coroners toincrease donation
Christina Parsons, Kimberly Young, Jim Mohr, Ken Lotherington,Mathias HaunOrgans and Tissues, Canadian Blood Services, Ottawa, ON, Canada.
Approximately 50% of deaths in Canada occur outside the hospitalenvironment with most falling under medical examiner or coroner juris-diction. In 80% of Canada’s tissue banks, less than 5% of donors areidentified from death investigation cases, identifying a significant op-portunity for improvement.In August 2008, the federal, provincial and territorial (F/P/T) governmentsgave Canadian Blood Services a mandate to work with the tissue dona-tion and transplantation communities to develop leading practices andrecommendations in support of system performance improvement.One national partner organization engaged early on by CanadianBlood Services was the Canadian Conference of Chief Coronersand Chief Medical Examiners, which led to the development of a Ref-erence Manual for Donation for Canadian coroners and medicalexaminers as well as an initiative to implement practical steps to in-crease tissue donations from deaths outside the hospital environment.Canadian Blood Services is facilitating collaborative workshops withmedical examiners and coroners in the Provinces of Manitoba, Ontario,New Brunswick, Saskatchewan and Nova Scotia, and in each provincetissue recovery and organ procurement organizations, pathologists, fu-neral professionals and governments officials are joining these processimprovement workshops, with a goal of increasing the identification andreferral of donors. A panel of Canadian and international tissue bankingand death investigation experts has also been convened to support thisinitiative. The first provincial workshops are taking place in 2013, theothers will follow in 2014.To-date, participants in the provincial workshops have identified sev-eral local opportunities for improvement and are improving or creatingnew functional linkages between organizations to realize more tissuedonations. Knowledge gained through these provincial collaborationswill be detailed in a report and shared with the broader Canadian do-nation community.Medical examiners and coroners can be engaged as key partners tosupport increasing tissue donation from deaths that occur outsidethe hospital.
S200 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
270
Pharmacological conditioning with GTN and Cariporide atcardioplegia activates cardioprotective signaling targetingmitochondria in a model of donor heart preservation
Mark Hicks1,2, Jair Kwan2,4, Ling Gao2, Peter Macdonald2,31Clinical Pharmacology& Toxicology, St Vincent’s Hospital, Darlinghurst,Australia; 2Division of Cardiac Physiology and Transplantation, VictorChang Cardiac Research Institute, Darlinghurst, Australia; 3Heart LungTransplant Unit, St Vincent’s Hospital, Darlinghurst, Australia 4FreeRadical Group, Heart Research Institute, Newtown, Australia.
Background: Storage of donor hearts in cardioplegic solutionssupplemented with agents that mimic ischemic preconditioning en-hanced their post-reperfusion function. The present study examinesthe association of functional recovery produced by glyceryl-trinitrate(GTN), a nitric oxide donor and cariporide, (a sodium-hydrogen ex-change inhibitor), with activation of pro-survival signaling pathways.Methods: After baseline functional measurement, isolated working rathearts were arrested and stored for 6h in either Celsior, Celsiorcontaining 0.1mg/ml GTN, 10μM cariporide or both agents. Afterreperfusion, function was remeasured, then tissue processed for im-munoblotting or histology.Results: Recovery was significantly improved by these supplementsalone or combined (cardiac output 69 vs 20% GTN+cariporide vsCelsior; P<0.05). Necrotic and apoptotic markers in the Celsior grouppost-reperfusion were abolished by GTN, cariporide or both. In-creased phosphorylation of ERK and Bcl2, after reperfusion was seenin groups stored in GTN, cariporide or both along with increasedphospho-STAT3 levels in the GTN/Cariporide group. Inhibition ofSTAT3 phosphorylation blocked recovery. No phospho-Akt increasewas seen in any treatment.Conclusions: Functional cardiac recovery produced by GTN andcariporide was accompanied by activation of signaling pathways con-sistent with mitophagy activation (phosphorylation of ERK and Bcl2[1]), and maintenance of mitochondrial transition pore closure afterreperfusion via the interaction of phospho-STAT3 with cyclophyllin D[2]. Both processes are crucial for functional recovery of the heart afterischemia reperfusion injury.
References:[1] Kang R, Zeh HJ, Lotze MT, Tang D: The beclin 1 network regulatesautophagy and apoptosis. Cell Death Differ 2011, 18: 571–580.[2] Boengler K, Hilfiker-Kleiner D, Heusch G, Schulz R: Inhibition ofmitochondrial transition pore opening by mitochondrial STAT3 and itsrole in myocardial ischemia reperfusion. Basic Res Cardiol 2010,105:771–785.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
272
Is there a limit for expanding criteria of kidney donors? How farcan we go?
Piotr Domagala, Artur Kwiatkowski, Rafal Kieszek, Michal Wszola,Jakub Drozdowski, Piotr Diuwe, Andrzej ChmuraDepartment of General Surgery and Transplantology, MedicalUniveristy of Warsaw, Warsaw, Poland.
Introduction: The lack of organs for transplantation has forced thetransplant community to expand the pool of donors and to use ex-panded criteria donor(ECD) organs. Although there are organs thatdo not fit into definition of ECD and remains controversial for trans-plantation. The aim of this paper is to report the criteria of dischargingkidney from transplantation.Patients and Methods: Four hundred and sixteen patients receivedcadaveric renal transplants between January 1, 2010 and June 31,2013. In this time seventy one nine kidneys were discharged fromthe transplantation – thirty eight kidneys (nineteen referred potentialdonors) were disqualified before organ procurement and thirty threekidneys were rejected from transplantation during organ storage. Dataon donors and preservation parameters were collected. Causes of or-gan refusal were analysed.Results: Two the most common causes of kidney rejection from trans-plantation were malignancy or strong suspicion of malignancy in do-
The cause of kidney discharging Frequency (%)
Malignancy or strong suspicion of malignancy in donor body 22,5Poor donor kidney parameters with probability
of kidney irreversible injury22,5
Unsatisfactory parameters during machine perfusion 19,7Lack of recipients according to HCV or HBV donor infection 8,6Cardiac arrest before organ procurement 5,6Nephrolitiasis 5,6Other 15,5
nor body as well poor donor kidney parameters with probability ofkidney irreversible injury.Conclusion: Careful kidney selection is recommended in cases of ex-panded criteria donor kidneys in order to diminish factors that cannegatively affect graft function and survival.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
273
“Pharmacological conditioning” improves recovery of heartsfrom brain dead rats after prolonged hypothermic storage
Gayathri Kumarasinghe, Ling Gao, Mark Hicks, Aoife Doyle,Padmashree Rao, Arjun Iyer, Alisdair Watson, Andrew Jabbour,Christopher Hayward, Peter MacdonaldCardiac Physiology and Transplantation Laboratory, Victor ChangCardiac Research Institute, Sydney, Australia.
Aim: Cold storage of hearts from brain dead (BD) donors is still themainstay in cardiac transplantation, however ischaemia-reperfusion in-jury (IRI) and primary graft failure (PGF) are significant disadvantages[1]. We found that the addition of ‘conditioning’ agents–Glyceryl trinitrate(GTN), Erythropoietin (EPO) and Zoniporide (ZON) to standard preser-vation solutions attenuates IRI in rat hearts[2–4]. We aimed to test theirefficacy under conditions of BD and prolonged cold storage.Methods: Male Lewis rats were subjected to BD by inflation of a sub-dural embolectomy catheter. Invasive haemodynamic changes weremeasured in BD and sham groups. Cardiac output (CO) was thenassessed on an isolated working heart model (IWHM) and heartsarrested and preserved in 4°C using either Celsior preservation solu-tion for 1, 3 or 6 hours, or Celsior supplemented with GTN, EPO andZON for 3 or 6 hours (n=6 each sub-group). Post-storage CO wasreassessed on an IWHM.Results: Hearts from BD rats showed inferior recovery of CO com-pared with shams. Supplementing Celsior preservation solution withGTN+EPO+ZON significantly improved CO in hearts from BD rats.
Conclusion: Pharmacological conditioning agents GTN, EPO & ZONsignificantly improve recovery of hearts from BD rats after prolongedcold storage. This shows promising potential for application in clinicalcardiac transplantation.
References:[1] Iyer A, Kumarasinghe G, Hicks M, Watson A, Gao L, Doyle A,Keogh A, Hayward C, Kotlyar E, Dhital K, Granger E, Jansz P, PyeR, Spratt P, Macdonald PS. Primary graft failure after heart transplan-tation. J Transplantation. 2011;2011:175768. doi: 10.1155/2011/175768. Epub 2011 Aug 1[2] Watson AJ, Gao L, Sun L, Tsun J, Jabbour A, Ru Qiu M, Jansz PC,Hicks M, Macdonald PS. Enhanced preservation of the rat heart afterprolonged hypothermic ischemia with Erythropoietin-supplementedCelsior solution. J Heart Lung Transplant 2013. 32 (6):633–40[3] Gao L, Tsun J, Sun L, Kwan J, Watson A, Macdonald PS, Hicks M.Critical role of STAT3 pathway in cardioprotective efficacy ofZoniporide in a model of myocardial preservation – the rat isolatedworking heart. Br J Pharmacol 2011 Feb;162(3):633–47[4] Hicks M, Hing A, Gao L, Ryan J, Macdonald PS. Organ preserva-tion. Methods Mol Biol. 2006;333:331–74
r 27, 2013, Volume 96 Number 10S S201
thorized reproduction of this article is prohibited.

November 27, 2013
274
The I Now Know (iNK) PROjECT- a pilot education program andvideo competition to engage secondary schools students tocreate a one minute video that reflects their perception andunderstanding of organ and tissue donation
Annie Jarvie-Cross, Catherine ChanterNurse Donation Specialist, Northeast Health, Wangaratta, Victoria,Australia.
As part of the Victorian DonateLife Rural Special Interest Group(RSIG), Nurse Donation Specialist (NDS) from Northeast healthWangaratta (NHW) were successful in attaining a Grant from theCanberra DonateLife Authority. To promote community awareness ofOrgan and tissue donation for DonateLife 2013.Utilizing the 2013 theme “Make you wishes count”, NHW NDS initi-ated an innovative pilot project to engage young adults to increasetheir awareness of organ and tissue donation. The I Now Know (iNK)PROjECT - education program and video competition was conceptual-ized and developed by the NHW NDS as part of a collaborative engage-ment involving three regional secondary schools.Eligibility to enter the competition saw 350 students participate in ed-ucation sessions based on “The Last Race” education package en-dorsed by DonateLife. Students were invited to create a one minutevideo about their perceptions and understanding on any aspect of or-gan and tissue donation and how they would share their thoughts.Evaluations by the students written on DonateLife postcards werephotographed for The iNK PROjECT face book page. A total of 50students elected to submit, producing 19 individual or group videosfor judging.A judging DVD was collated for a panel of seventeen national andstate DonateLife representatives as well as the NHW executive andregional community leaders. Winners were selected using a specificjudging criteria based questionnaire developed by the NDS using sur-vey monkey as a response tool.Funding provided the platform for the Awards Event, prizes andDonateLife branded photo booths. Over 500 students viewed the win-ning videos that were also featured in television news coverage. Suc-cess of the project has not only been measured by the high standardand quality of the videos, but in the ongoing community engagementand requests for further activities and discussions about Organ andTissue Donation.DonateLife
S202 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
275
Transplanting the transplanted
Andree Gould, Mary Lynch, Nicola Fletcher, Sarah Kelley, Kylie Monk,Sarah Markham, Rebecca Reid, Marie Schaumann, Melissa SmithDonateLife WA, DonateLife WA, Perth, Australia.
Presented is a case of a successful donation of a previouslytransplanted kidney.Mr X. was a 60 year old male who unfortunately had a catastrophic in-tracranial haemorrhage which despite treatment resulted in progres-sion to brain death. During conversations of prognosis and pooroutcome his family raised the potential for organ donation. He had re-ceived a kidney transplant 7 years previously from a living relative forpolycystic renal disease.While it is accepted that a transplant recipient can be an organ donorthe question arose – which organs could we consider for donation?During investigation and consideration for organ donation it was deter-mined that the gentleman’s heart was not medically suitable due to hiscardiac history. His lungs were not medically suitable due to poor ox-ygenation and infection. His liver was not medically suitable due tothe presence of multiple hepatic cysts and his pancreas was declineddue to his complex medical history. The organ considered medicallysuitable for donation was his previously transplanted kidney.In this paper we outline the challenges to achieve a successful dona-tion outcome in this case, including consent from the original living do-nor and tissue typing considerations.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
276
Scoping study into the potential eye and tissue donor pool at theRoyal Melbourne Hospital
Martin Dutch1,2, Tracey Mackay21Emergency Department, Royal Melbourne Hospital, Melbourne,Australia; 2Organ and Tissue Donation Team, Royal MelbourneHospital, Melbourne, Australia.
Introduction: Eye and Tissue donation has the capacity to signifi-cantly improve the quality of life for recipients, and in some cases isa live saving intervention. Improvements in public health have seena reduction in the amount of banked tissue from traditional coronialsources. Non-Coronial eye and tissue donations are thus an increas-ingly important source for tissue within the state of Victoria, Australia.Methods: The Royal Melbourne Hospital (RMH) is a tertiary, teaching,referral hospital that provides general medical, surgical and specialistservices A retrospective scoping study was undertaken to analyse thesize of the potential, isolated eye and tissue donor pool within RMH.The last 5 years of hospital deaths were electronically reviewed. Foreach in hospital death, all separations which occurred over the pre-ceding 5 years were screened using International Classification ofDisease codes. Cases were screened positive for potential eye or tis-sue donation if they met both age criteria (<80yrs), and had no recordof specific exclusion diagnoses. Results: Between 2008–2012, 5,091patients died in the hospital. Deaths most commonly occurred in theICU and pallative care wards. Approximately 32% of all deaths occured“in hours” (M-F, 8am-4pm). The screening tool identified 2231 potentialisolated eye donors, and 930 potential isolated tissue donors. A randomselection of identified patients were audited (n=24). The positive predic-tive value (PPV) for the eye screening tool was 71%, the PPV for the tis-sue screening tool was 25%. Discussion: Each year over 1000 patientsdie at the RMH. The screening tool identified 9 eye, and 4 tissue poten-tial donors/wk. An in hours, eye and tissue donor referral program, witha consent rate of 50%, could realise approximately 50 eye donors and7 tissue donors each year. This increased, non-coronial source of tissuecould significantly bolster banked tissue stores.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
277
Improving Corneal Referrals from Palliative Care Services
Nigel Palk1, Margaret Philpott21DonateLife SA, Adelaide, Australia; 2Eye Bank of South Australia,Flinders Medical Centre, Adelaide, Australia.
Eye donation gives many people the opportunity upon death to be-come organ donors, even when collecting solid organs is not an optiondue to age or other factors. Families are often under great stress whentheir loved one dies. They may be unable to make clear decisions oreven remember a previous conversation about donation (1). We pro-pose that if stronger links are established with Adelaide’s metropolitanpalliative care services, more referrals will be made to the Eye Bankprior to death. The referrals will allow more informed decisions to bemade by the family, including the patient. Palliative care services inAustralia had a 50% increase in admissions from 2001 to 2010. Nearlyhalf the admissions were people over the age of 75 and 85% of thosewere admitted to public hospitals (2).The increased number of referrals to the Eye Bank over the last twoyears suggests that eye donation education aimed at palliative carenursing staff and allied health workers is effective.We are developing an easy-to-understand guide on the facilitation ofcorneal donation in the setting of palliative care. The guide will includethe contraindications to eye donation, common questions and answers,and a sticker that is placed in the case notes after the initial referral iden-tifying the patient as a potential eye donor. Through the guide and a sim-plified referral process, we expect to see an increase in palliative carereferrals to the Eye Bank.We believe that approaching palliative care services for eye donationwill decrease the need for ‘cold calls’ to families. This improvement willbe the result of an increasing number of palliative care donors, theirpotential incorporation into the Advance Care Directive, the empower-ment of patients and families, and the further education of palliativecare staff.
References:[1] Verbal &WorthWhite paper 2013 http://www.verbleworthverble.com/wp-content/uploads/2013/04/Framing-the-Donation-Question3.pdf[2] Palliative Care Services in Australia Report 2012 http://www.aihw.gov.au/WorkArea/DownloadAsset.aspx?id=10737423346
r 27, 2013, Volume 96 Number 10S S203
thorized reproduction of this article is prohibited.

November 27, 2013
278
Graphical approach in the risk factor analysis for the death withfunctioning graft in kidney transplantation from Japaneseregistry data
Makiko Mieno1, Takashi Yagisawa2, Kenji Yuzawa3, Shiro Takahara41Department of Medical Informatics, Center for Information, JichiMedical University, Shimotsuke, Japan; 2Division of Renal Surgeryand Transplantation, Department of Urology, Jichi Medical University,Shimotsuke, Japan; 3Department of Transplant Surgery, NationalHospital Organization Mito Medical Center, Ibaraki, Japan;4Department of Advanced Technology for Transplantation, OsakaUniversity Graduate School of Medicine, Suita, Japan.
Background: Death with functioning graft has been a common causeof graft failure in kidney transplantation. We investigated the impact ofthe risk factors associated with the death with functioning graft or theother competing causes of graft failure graphically.Methods: By using the kidney transplantation registry data in Japan from1992 to 2009, we analyzed first-time kidney-only adult (20-year-oldor more) transplants: 9,203 living donor transplants and 2,616 deceaseddonor transplants. The recipient’s sex, recipient’s age, donor’s age, thenumber of HLA-mismatches, pre-transplant dialysis, primary cause ofend-stage renal disease (specifically, diabetes or not) and the year ofthe transplantation performed were examined for living donor transplants.The warm ischemia time and the total ischemia time were also includedfor deceased donor transplants analysis. We examined possibly non-linearrelation between the covariates and outcome, such as the hazard ratioof the competing events, non-parametrically with restricted cubic splineswith extended Cox regression analysis.Results: For death with functioning graft, older recipient and longerpre-transplant dialysis were the significant risk factors (the importanceof recipient's factor), whereas for the other causes of graft failure, malerecipient, older donor, increasing HLA mismatches and longer ische-mia time were more important (relatively donor’s factor).Conclusion: When calculating the graft survival, the difference be-tween the death with functioning graft and the other causes of graftloss should be considered, and graphical approach might help well.
S204 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
279
Challenges and progress of eye banking in Bangladesh
Mir RahmanEye Bank, Chittagong Eye Infirmary and Training Complex (CEITC),Chittagong, Bangladesh.
Introduction: In Bangladesh, thousands of people suffer from cornealdiseases and await corneal transplantation. Eye banks throughout thecountry are working towards collecting donor cornea to reduce corneablindness. Though the eye donation program is not yet popular inBangladesh, eye banks have been trying to maintain standard prac-tice of cornea collection since inception.Objective: Understanding the challenges of eye banking system inBangladesh with primary focus on the functioning of eye banks. Thiswill also include the willingness of eye donation, donor selection crite-ria, quantity of quality cornea and follow up procedure of corneatransplantation.Method: In the history of almost a decade, eye banking system haschanged significantly in terms of collection of quality corneas, preser-vation system, cornea distribution policy and follow up procedure ofthe patient.Results: The Eye Banking Pilot Project in 2004 has set the standardsfor quality cornea collection, processing and preservation system, fol-low up of cornea distribution in Bangladesh. The Project has devel-oped skilled manpower, technical lab, SOP and has also initiatededucational program, grief counseling.Conclusions: With elaborate and efficient planning for grief counsel-ing and public awareness program on eye donation, the numbers ofcornea donation in Bangladesh are likely to increase significantly. Suf-ficient financial and technical support from donor side can help to facesuch eye banking challenges in Bangladesh.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
281
Prognostic impact of kidney volume and early kidney resistanceindex on graft and patient survival in 1-year observation
Anita Sierocka1, Jan Pawlus1, Karol Tejchman1, Maciej Romanowski1,Jerzy Sieńko1, Maciej Żukowski3, Kazimierz Ciechanowski2,Aleksander Falkowski4, Marek Ostrowski1, Tadeusz Sulikowski11Department of General Surgery and Transplantation, PomeranianMedical University, Szczecin, Poland; 2Department of Nephrology,Transplantology and Internal Medicine, Pomeranian MedicalUniversity, Faculty of Medicine, Szczecin, Poland; 3Clinic ofAnaesthesiology and Intensive Care, Pomeranian Medical University,Faculty of Medicine, Szczecin, Poland; 4II Department of RadiologicalDiagnostics, Pomeranian Medical University, Faculty of Medicine,Szczecin, Poland.
Background: Resistance index (RI) is measured by Doppler sonogra-phy during the early posttransplant period. RI reflects vascular sus-ceptibility connected with interstitial kidney oedema. RI>0,8 isidentified as a powerfull predictor for worse kidney function [1,2,3].Kidney graft volume seems to have importance in a matter of adjustingnumber of active nephrons to the recipient. However mentioned corre-lation was confirmed by only a few publications [4]. There are alloca-tion protocols which includes adjusting kidney mass to the bodyweight of the recipient, neverthelles those procedures seem not tohave sufficient scientific confirmation.Aim: The aim of this study was to evaluate the correlation betweenkidney volume as well as early kidney resistance index (RI) and graftoutcome and patient survival.Material and methods: 66 recipients were included to the study. Kid-ney volume was determined before graft implantation, RI was mea-sured in the first day after surgery. Statistical analysis was performedto adjust for demographic and clinical variables. Statistical signifi-cance was analised with T-Student test and Spearman-R correlation(p<0,05).Results: Kidney volume (Vk) was correlated with graft function, acuterejection episodes (AR), eGFR and graft survival with no statisticalsignificance. We observed statistical significance between Vk and di-uresis 1 month after transplantation (Tx) (p=.01). There was signifi-cant correlation between RI and DGF (p=.02), AR (p=.02), diuresisduring 1 week after Tx (p<.05), creatinine during 1 month after Tx(p<.05) and eGFR 3 month after Tx (p=.0009).Conclusion: Vk has no influence on graft function. HigherRI values in theearly post-transplant period are correlated with higher DGF occurence,higher AR episodes occurence 1 year after Tx, higher creatinine serumconcentration 1 month after TX, lower eGFR 3 month after Tx.Source of Funding: NCN:2013/B/P01/2011/40
References:[1] Kolonko A, Chudek J, Zejda JE, Więcek A: Impact of early kidneyresistance index on kidney graft and patient survival during 5-yearfollow-up. Nephrol Dial Transplant 2012; 27:1225-1231.[2] Knemann R, Frank D, Brendenburg UM, Heussen N, Takahama J,Krüger T, Riehl J, Floege J: Prognostic impact of renal arterial resis-tance index upon renal allograft survival: the time point matters.Nephrol Dial Transplant 2012; 27: 3958-3963.[3] Bigé N, Lévy P, Callard P, Faiutuch JM, Chigot V, Jousselin V,Rouco P, Poffa JJ: Renal arterial resistance index is associated withsevere histological changes and poor renal outcome during chronickidney disease. Nephrol DIal Transplant 2006, 21:2916-2920.[4] Hugen CM, Polcari AJ, Faroog AV, Fitzgerald MP, Holt DR, MilnerJE: Size does matter: donor renal volume predicts recipient functionfollowing live donor renal transplantation. The Journal of Urology2011, 185:605-609.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
r 27, 2013, Volume 96 Number 10S S205
thorized reproduction of this article is prohibited.
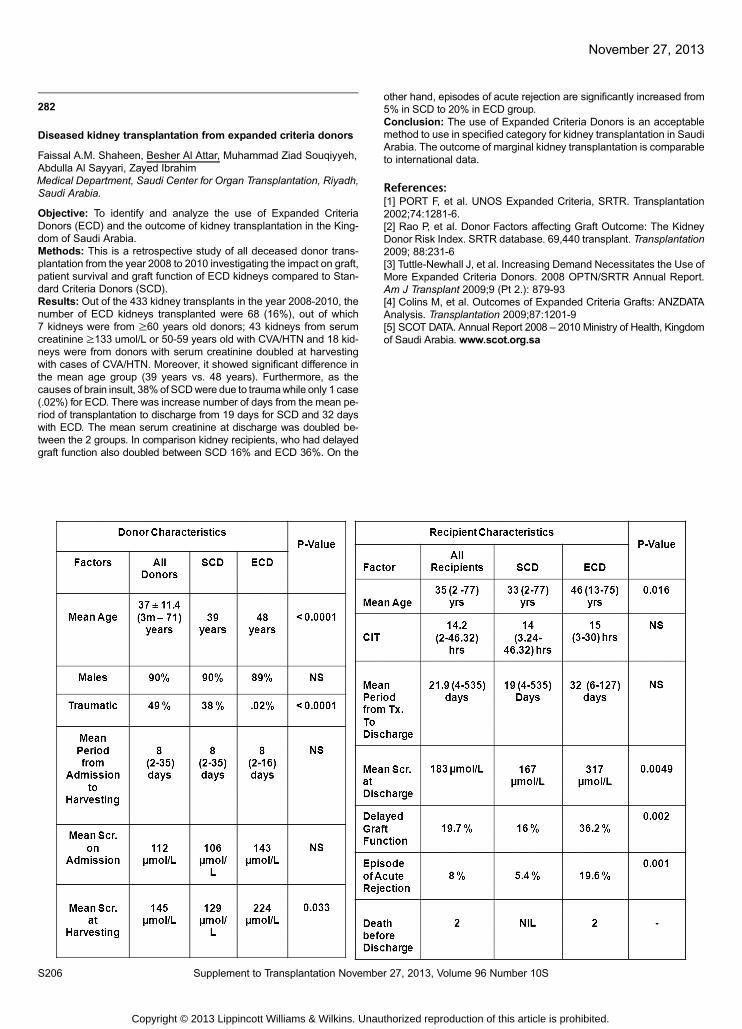
November 27, 2013
282
Diseased kidney transplantation from expanded criteria donors
Faissal A.M. Shaheen, Besher Al Attar, Muhammad Ziad Souqiyyeh,Abdulla Al Sayyari, Zayed IbrahimMedical Department, Saudi Center for Organ Transplantation, Riyadh,Saudi Arabia.
Objective: To identify and analyze the use of Expanded CriteriaDonors (ECD) and the outcome of kidney transplantation in the King-dom of Saudi Arabia.Methods: This is a retrospective study of all deceased donor trans-plantation from the year 2008 to 2010 investigating the impact on graft,patient survival and graft function of ECD kidneys compared to Stan-dard Criteria Donors (SCD).Results: Out of the 433 kidney transplants in the year 2008-2010, thenumber of ECD kidneys transplanted were 68 (16%), out of which7 kidneys were from ≥60 years old donors; 43 kidneys from serumcreatinine ≥133 umol/L or 50-59 years old with CVA/HTN and 18 kid-neys were from donors with serum creatinine doubled at harvestingwith cases of CVA/HTN. Moreover, it showed significant difference inthe mean age group (39 years vs. 48 years). Furthermore, as thecauses of brain insult, 38%of SCDwere due to traumawhile only 1 case(.02%) for ECD. There was increase number of days from the mean pe-riod of transplantation to discharge from 19 days for SCD and 32 dayswith ECD. The mean serum creatinine at discharge was doubled be-tween the 2 groups. In comparison kidney recipients, who had delayedgraft function also doubled between SCD 16% and ECD 36%. On the
S206 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
other hand, episodes of acute rejection are significantly increased from5% in SCD to 20% in ECD group.Conclusion: The use of Expanded Criteria Donors is an acceptablemethod to use in specified category for kidney transplantation in SaudiArabia. The outcome of marginal kidney transplantation is comparableto international data.
References:[1] PORT F, et al. UNOS Expanded Criteria, SRTR. Transplantation2002;74:1281-6.[2] Rao P, et al. Donor Factors affecting Graft Outcome: The KidneyDonor Risk Index. SRTR database. 69,440 transplant. Transplantation2009; 88:231-6[3] Tuttle-Newhall J, et al. Increasing Demand Necessitates the Use ofMore Expanded Criteria Donors. 2008 OPTN/SRTR Annual Report.Am J Transplant 2009;9 (Pt 2.): 879-93[4] Colins M, et al. Outcomes of Expanded Criteria Grafts: ANZDATAAnalysis. Transplantation 2009;87:1201-9[5] SCOT DATA. Annual Report 2008 – 2010 Ministry of Health, Kingdomof Saudi Arabia. www.scot.org.sa
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
283
Increased donor rates - the hidden impact oncoordination workload
Victoria Dale1, Jessica Amsden1, Kelly Rogerson1, David Pilcher2,31DonateLife, Melbourne, Australia; 2Department of Intensive Care,The Alfred Hospital, Prahran, Australia; 3Department of Epidemiologyand Preventative Medicine, Monash University, Melbourne, Australia.
Background: Since the implementation of the National Health Re-form in 2009, Victoria has seen a 63% increase in donation cases(to December 2012). Strategies utilised to achieve this include educa-tion around donor identification, communication training, and broaden-ing of the donor pool. These strategies have led to increased referralsto organ donor coordinators (ODCs), and the impact of this increasedworkload has not been measured.Objective: Our aim was to describe the number and duration ofreferrals to DonateLife Victoria in July 2011 - June 2013, and to deter-mine the relative proportion of these, which led to attendance of anODC at a hospital to facilitate actual or intended donation.Methods: The number of referrals and the time spent on each wereextracted from the DonateLife Victoria referral database. Trends overtime were analysed.
Results: Over the 2 year period, there were 664 referrals, which in-curred a total duration of 677 hours (average 1.01 hours per referral).1. 43% (285/664) of referrals resulted in an ODC hospital attendance2. Referrals which led to an attendance had a longer duration than
those where there was no hospital attendance (<P=0.001).3. The average number of referrals/month was 284. A rise was seen from 17 in the July-September(1st quarter) 2011 to
36 in the Mar-June 2013 (last quarter), which is equivalent to 3 ad-ditional referrals every 2 months (P<0.001).
5. There has been a trend to a reduction in the proportion of referralswhich have led to ODC hospital attendances from 54% in the firstquarter to 37% in the final quarter (P=0.054).
Conclusion: There has been an increase in referrals over the past2 years which reflects increased awareness and a desire to checkmedical suitability in patients who would not have previously been re-ferred. This results in a significant increase in workload associatedwith initial referrals, and should be considered when planning servicedelivery models.
r 27, 2013, Volume 96 Number 10S S207
thorized reproduction of this article is prohibited.

November 27, 2013
284
Oral history and a history trip - tools supporting transition: TheSouth Australian Organ Donation Agency (SAODA) to DonateLifeSouth Australia (DLSA)
Sally Tideman1, Tim Dalmau2, Johanna Kijas31DonateLife, DonateLife South Australia, SA, Australia; 2DalmauNetwork, Brisbane, Australia; 3Kijas Histories, Lismore, Australia.
With the introduction of a ‘World’s Best Practice Approach to Organand Tissue Donation for Australia’ DLSA acknowledged that the re-form brought with it complex change and transition challenges. TheState Medical Director held the view that leaders within the organisa-tion had the responsibility to ensure staff were skilled and supportedthrough the change, transition and into the future. The theoreticalmodels of organisational psychology and the academic body of workon ‘followership’ and ‘leadership’ ignited by Grint 2006 [1] underpinthe DLSA attention to organisational development and to sustaininga high- performing clinical service for optimising all aspects of organdonation for transplantation.During four years of sector reform in Australia DLSA has used andreported on a range of organisational development ‘tools’ including:- Values in Action- Totems, Taboos and Repetitive Interactions- Behaviourally Specific Feedback- The Six Circle LensTwo additional tools used by DLSA in the ongoing development pro-gram ‘Change Conversations’ are described. The foundation is inthe fields of history, story-telling and psychology and share the princi-ple that the act of sharing information builds stronger relationships andaids in forming a stronger identity.The first, ‘The SAOrgan Donation Oral History Project ‘ used the skillsof an historian Dr Kijas, to interview and record the oral testimony [2] ofindividuals closest to the establishment and development of SAODAthrough to DLSA.The second, ‘The History Trip’ enabled staff to recall events thatsymbolised (more than any other event) the essence of ‘who we areand why we are here’as DLSA.In conclusion the additional tools described brought context and clarityto the identity and the future of DLSA.
References:[1] Grint K:Followership:the anvil of leadership, in Grint K, Jupp,J(eds), Beyond Command.London:HMSO[2] Perk R, Thomson A eds.,: The Oral History Reader London:Routledge, 2003
S208 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
285
Donor evaluation for lung transplantation in Iran
Sareh Parto, Seyyed Shahabeddin Mohammad Makki,Shadi Shafaghi, Abolghasem Daneshvar, Kambiz Sheykhi,Hamid Reza Khoddami Vishteh, Masoureh Vahdati,Katayoun NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran(Islamic Republic of).
Introduction: Transplantation has evolved as the treatment of choicefor many patients with end-stage organ disease. But it is limited by theavailability of transplantable donor lungs. So, assessment of lungs inbrain dead donors is very important. The aim of this study was to as-sess the lungs of brain dead donors in Masih Daneshvari organ pro-curement unit which is one of the most active ones in the Middle East.Materials & Methods: This prospective study was performed on all ofbrain dead donors who were transferred to this center from May 2010to 2013. Evaluation was carried out in 4 steps including history takingand physical examination, chest-x-ray (CXR), O2 challenge test andbronchoscopy. Finally, patients with normal CXR, normal bronchos-copy and PaO2/FIO2≥300 mmHg were considered as standardcandidates for lung transplantation.Result: From 259 brain-dead donors 162 were males (63%), meanage of 32.5±15.1 years. The most common cause of brain death wasTrauma (46%). 17% of cases had chest trauma according to history,physical examination and/or chest x ray. 43% of donors had history ofsmoking more than 20 packs per year and 49% had turbid trachealsecretion. Abnormal CXR in 64%, abnormal bronchoscopy in 50%and PaO2/FIO2 more than 300 mmHg in 25% of all cases have beenreported.Conclusion: Findings of this study showed that the majority of caseshad unsuitable lungs (81.5%). This study illustrate that lung is as avery damageable organ in brain dead cases. So, it is recommendedthat strategies like use of methylprednisolone, endotracheal suctioning,changing the position, antibiotic therapy if necessary and recruitmentmaneuver in potential brain dead donors has an essential role in improv-ing lungs donors which reducing the number of inadequate donor lungs,increasing the overall donor pool and organ availability.Keywords: Lung evaluation, Brain dead donors, Lung transplantation
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
286
Main causes of lung transplant mortality in Iran
Shadi Shafaghi, Seyyed Shahabeddin Mohammad Makki,Sareh Parto, Majid Marjani, Kambiz Sheikhy, Tahereh Parsa,Hamid Reza Khoddami Vishteh, Katayoun NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran(Islamic Republic of ).
Introduction: Lung transplantation is an effective treatment for a vari-ety of end-stage lung diseases. Although transplant can significantlyimprove the quality of life and prolong survival, complex complicationsmay result in morbidity and mortality especially in learning curve of acenter. The recognition and early treatment of these complications isimportant for optimizing outcomes. This article provides an overviewof the causes that led to mortality in Masih Daneshvari Hospital lungtransplant patients.Method: In this retrospective study, all complications of 67 patientswho were transplanted during 2000 and 2013 were collected and maincauses of early and late mortality categorized into 4 groups: 1. hemo-dynamic instability, 2. Any kind of infections (bacterial, fungal and viralinfection), 3. Any type of rejection (acute and/or chronic) and 4. others.Result: In this study 56% of mortality was early (during 3 weeks aftertransplant) and 44% was late. Early mortality causes were hemody-namic instability in 68% of patients, acute bacterial and/or fungal and/or viral infection in 20%, pulmonary emboli in 4% and other causes in8%. Infection made 42%, rejection 38%, hemodynamic instability 5%and other causes 15% of all causes of late mortality.Conclusion: Recognition of these main factors for lung transplant mor-tality, and decision making directed to prevent these complications, maylead to reduce morbidity and mortality in patients who have undergonelung transplant. Early hemodynamic instability as one of the mainreasons of early mortality in our center needs changes in peri-operativeprotocols, especially selection of patients in better condition and also us-ing different instruments like extra corporeal membrane oxygenation(ECMO) to manage intraoperative complications. High infection rate (es-pecially fungal and bacterial resistant infections) needs serious consid-eration and may also more aggressive anti-fungal therapies even forprophylaxis regimen.Keywords: Lung transplantation, Mortality cause, Infection,Rejection, Hemodynamic instability
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
287
13 Years of lung transplantation in Iran: Experience of theNational Research Institute of Tuberculosis and Lung Diseases
Shadi Shafaghi1, Seyyed Shahabeddin Mohammad Makki1,Abolghasem Daneshvar1, Shideh Dabir1, Majid Marjani2, Sareh Parto1,Zahra Ansari1, Kambiz Sheikhy3, Hamid Reza Khoddami Vishteh1,Katayoun Najafizadeh11Lung Transplantation Research Center, Masih DaneshvariHospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran(Islamic Republic of); 3Tracheal Diseases Research Center,National Research Institute of Tuberculosis and Lung Diseases(NRITLD), Shahid Beheshti University of Medical Sciences, Tehran,Iran; 2Mycobacteriology Research Center, Masih DaneshvariHospital, Shaheed Beheshti University of Medical Sciences,Tehran, Iran.
Introduction: Lung transplantation is the ultimate treatment in manypatients with advanced stages of pulmonary disease. Complexity, lackof donors, lack of specialized centers and cost of the procedure aresome problems for its expansion. This study was conducted to de-scribe our 12-year center experience in lung transplantation.Materials and Methods: We used the database of lung transplanta-tion research center of Masih Daneshvari Hospital, Tehran, Iran andextracted all cases of lung transplantation during 2000-2013 periods.Masih Daneshvari Hospital is a university based hospital and the re-ferral center for lung transplantation. We analyzed the survival of thepatients using life table and Kaplan-Meier method.Results: Lung transplantation undergone in 67 patients that one ofthem was re-transplantation, and heart lung transplantation in one pa-tient during this period. Fifty one patients (76%) were male and themean age was 34±13 yr. The causes of transplantation were pulmo-nary fibrosis (45%), bronchiectasis (22%), COPD (15%), cystic fibro-sis (11%), and others (7%). Lung transplantation was double-sidedin 38 (57%) and single-sided in 29 (43%) patients. One and three-yearsurvivals of the lung transplanted patients were 51% and 40%, andthe mean and median of patients’ survival were 44 and 22 months, re-spectively. In patients who were alive after two weeks of transplanta-tion, one and three-year survivals were 68% and 56% and the meanand median of patients’ survival were 61 and 67months, respectively.Discussion: Although lung transplant is a complex procedure, ourexperiences show that it can be performed in developing countriessuch as Iran. According to our previous report, the survival of ourpatients improved gradually mainly due to long term post-operationfollow up alongside other factors such as better candidate selection,improvement of experiences of our surgeons, using ECMO and higherstandards of patients management at time of transplantation.Keywords: Lung transplantation, Pulmonary fibrosis, COPD,Bronchiectasis, Cystic fibrosis, Survival
r 27, 2013, Volume 96 Number 10S S209
thorized reproduction of this article is prohibited.

November 27, 2013
290
Awareness and knowledge of eye and tissue donationamongst emergency department registered nurses
Bridget O’Bree, Nina Mao, Nicola StittMonash Health, Melbourne, Australia.
Introduction: Monash Health (MH), which is Victoria’s largest healthservice, has experienced a threefold increase in organ donation sincethe implementation of the national reform agenda in 2009. Howevereye and tissue donation has not seen the same increases especiallyfrom the Emergency Departments (ED). MH has three ED’s withinthe organisation.Objectives: To determine the level of awareness and knowledge ofeye and tissue donation in order to meet the learning needs of RN’sfrom the ED’s within MH.Methods: The survey was developed and consisted of ten componentswith an overall total of 20 questions. It was sent to all ED nursing staff viaemail. A total of 75 responses were received during the two weeks thesurvey was open, which was a 24% response rate. One ED had a re-sponse rate of 49%.Results: A total of 91% of respondents were supportive of eye and tis-sue donation. The majority of respondents (93%) thought that lessthan 50% of the Australian population were willing to become eyeand tissue donors, with over half of respondents (63%) believing thatless than 25% of the Australian population were willing to becomeeye and tissue donors. The majority of nurses (84%) were comfortablesupporting grieving families and felt the most appropriate time to raisethe subject of eye and tissue donation with the family was during end-of-life care discussions (76%). Over half (57%) did not feel they hadthe necessary skills and knowledge to introduce tissue donation to afamily nor did they feel competent to explain tissue donation to a family(64%), although the majority (76%) felt comfortable to notify the appro-priate personnel or agency when a potential donor was identified.Conclusions: RNs working in ED were supportive of eye and tissuedonation and were comfortable notify the appropriate personnel oragency when a potential donor was identified. The ED RNs were notcomfortable to converse with a family about eye and tissue donation.
S210 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
291
Corneal donation, when 1 + 1 = 3
Andrew Young1, Prema Finn, Graeme Pollock, Kelly Rogerson1
DonateLife Victoria, Melbourne, Australia.
Body of Abstract: Corneal donation is an important transplant proce-dure which restores eyesight to people with severally effected vision.The value of a solid organ donor in facilitating this for a number of trans-plant recipients will be a focus of this presentation. Our focus is on theinitial setting where a gentleman died as a result of a severe neurologicalinjury. His family were approached and consent to the donation of hiseye tissue for the purpose of both research and transplantation.The donation highlights how the generosity of the families’ consent ledto a successful donation outcome for 5 recipients related to this eyetissue alone. This included 3 recipients who required urgent cornealtransplants and 2 recipients who received scleral transplants.Relevant details which will be covered include:1. why there were 3 recipients;2. how 2 corneas were able to be donated to 3 recipients;3. recipient outcome;4. informing the family of this outcome;5. family opinion of this outcome;6. long term recipient outcomes;7. learnings for donor coordinators and Lions scientists and surgeons.The surgical technicality/techniques of obtaining 3 transplants from asingle cornea will be discussed, highlighting the use of both the ante-rior and posterior keraoplasty from a single cornea.This outcome resulted in improved quality of life for these 3 cornealrecipients. All cases were deemed emergencies/urgent cases, withtight associated time frames which is unusual for this type of trans-plantation. Two of these recipients had severely impaired vision whilethe third recipient had suffered an acute eye injury. This recipient wasat significant risk of losing his eyesight without this precious trans-plant. His surgery went extremely well and the risk of him losing hiseyesight was averted by this corneal transplant.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
292
Time Delays in the organ allocation process a South Australianperspective
Renee Chambers, Tricia WilliamsDonateLife SA, DonateLife SA, Adelaide, Australia.
The organ donation process is a complex task with multiple clinical andlogistical components that require time critical coordination if the processis to proceed smoothly [1]. Organ donation can take on average 16 to24 hours with the biggest proportion of time taken for the allocation oforgans. Anecdotally there was a perception that transplant teams werecausing delays in the organ allocation process by not adhering to thenominated times as outlined in the Transplant Society of Australia andNew Zealand, Consensus Statement onEligibility Criteria and AllocationProtocols to accept or decline organ offers [2]. As a continual quality im-provement activity DonateLife SA, identified a need to examine thelength of time taken for the organ allocation process. The review wasparticularly focused on the length of time transplant teams deliberatedprior to acceptance or decline of an organ offer and how often agreed or-gan offer response times were not observed. This would determine abaseline for future practice improvements.DonateLife SA undertook an audit of all organ donor case files for a12month period to establish if transplant teamswere delaying the organoffering process by accepting or declining an offer outside the nominatedtime frames. Forty six donor case files were reviewed, with a total of305 organ offers made. Responses outside the nominated time framesfor organ offers ranged from 6-9% for kidneys, 10% for pancreas, 13%for lungs, 19% for heart, 25% for livers, and 45% for heart and lungs.In conclusion, non-adherence to agreed criteria has had a demon-strated impact on organ donation timelines with flow-on effects forfamilies, clinicians (Intensive Care Units, Theatres, retrieval teams)Intensive Care Units bed utilisation and the overall cost associatedwith organ procurement.
References:[1] Aldea A, Lopez B, Moreno A, Riano D and Valls A 2001, “A MultiAgent System for Organ Transplant Co-ordination’, Artificial Intelli-gence in Medicine, 2101, pp. 413-416.[2] Organ Transplantation from Deceased Donors 2012, ConsensusStatement on Eligibility Criteria and Allocation Protocols, Version1.2, 16th May, Transplant Society of Australia and New Zealand, Aus-tralian Government, Organ and Tissue Authority, viewed 9 July 2013,http://www.tsanz.com.au/organallocationprotocols/.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
296
Process mapping the donation pathway: What can we learn?
Kelly RogersonDonateLife Victoria, Carlton, Australia.
Organ donation has increased by 85% in Victoria since the implemen-tation of the National health reform in 2009. The services providedhave evolved and the care of the donor and family form an essentialfocus in facilitating the family’s wishes. Staffing models have changedto meet the increasing demands and to enable service delivery. Pro-cess mapping was used to document (or review) the donation processand activities from a quality and risk perspective to ensure consistentand robust practice.Over the last eighteen months, the DonateLife Victoria team led by thenursing workforce have process mapped both pathways by which anindividual can donate their organs and tissues. While process map-ping is not new, understanding the nuances and practices that haveevolved to ensure donation proceeds and capturing them in a timeline,is new. Some initial work was undertaken during the Donation collab-orative in 2007, but this work no longer reflects the practices of today.The early outcomes of the mapping identified clear changes in prac-tice that would benefit both the staff involved and overall donation pro-cess. As the mapping process evolved, significant changes in practicehave been implemented, documented and evaluated.A positive outcome of this work has been the ability to capture thecomplexity of the donation process. Areas which were initially identi-fied as minor have evolved into areas of great cost savings and risk re-duction. The benefits of taking the time to reflect and review theactivities of your service can lead to cultural, budgetary and risk reduc-tion benefits.
r 27, 2013, Volume 96 Number 10S S211
thorized reproduction of this article is prohibited.

November 27, 2013
297
Admission to intensive care for consideration of organdonation in Australia and New Zealand
Andrew P Melville1, David V Pilcher1,2,3, Joanna Mitropoulos1,Steve J Philpot1,31Intensive Care Unit, Alfred Hospital, Melbourne, Australia;2Australian & New Zealand Intensive Care Society (ANZICS) Centrefor Outcome and Resource Evaluation, Melbourne, Australia;3Department of Epidemiology and Preventive Medicine, MonashUniversity, Melbourne, Australia.
Background: ICU admission for consideration of organ donationremains controversial in some contexts. Limited data is available onthe frequency and outcomes of this practice.Aim: To define epidemiology of patients admitted to ICU for consider-ation of organ donation and identify factors associated with outcome.Methods: Retrospective analysis of data from the Australian and NewZealand Intensive Care Society Adult Patient Database between 2007and 2012.Results: Between 2007 and 2012, there were 467 admissions to ICU forconsideration of organ donation (0.08% of total ICU admissions), andthese numbers are increasing, with 118 in 2012.Median length of ICU staywas 25.7 hours (IQR 15.3-41.9). The most common diagnosis was intra-cerebral haemorrhage. Hospital mortality was 97.2%. 9 patients (1.9%)were discharged home and 4 (0.9%) to a chronic care or rehab facility.No data was available on the proportion that became organ donors.Factors independently associated with survival were increasing age (OR1.05, 95% CI 1.01–1.10, p=0.012), not being intubated and ventilated(OR 8.1, 95% CI 2.2-29.8, p=0.002) and non-neurological diagnoses(OR 14.2, 95% CI 3.8–53.4, p<0.0001).Discussion: Admission to ICU for consideration of organ donation is an un-common but increasing occurrence and most patients die. Non-neurologicaldiagnoses were associated with survival.Conclusion: More work is required to establish the accuracy of theseresults and extent of possible data error. Survival may represent a fail-ure to identify patients appropriately and assessment of events duringICU stay and functional status of survivors is needed.
S212 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
298
Donors and reason behind decline in transplantation:Oman experience
Isa Al Salmi, Abdul Massieh YoussefRenal Medicine, Royal Hospital, Muscat, Oman.
Objectives: Relatives of patients with endstage kidney disease(ESKD) are generally very willing to get their loved well a kidney trans-plant. Relatives as Kidney donors are worked up thoroughly to ensurethe best care given for both donor and recipient. We will evaluate thereasons for decline to go ahead with kidney donation.Method:We review all cases that being worked up for the period from2009 till 2012 to evaluate the reasons for decline to go ahead with kid-ney donation. All cases attend the kidney donor clinic as the main ser-vice for the country for people interested to undergo transplantation.Kidney donor clinic worked every day and provide all type of clinicalcare and investigational procedures.Results: The number of new cases worked up as kidney donors, fortheir relatives who suffer with ESKD, has increased progressively from116 on 2009 to 132 case in 2012. Similarly, the number of recipients withESKD cases worked up for kidney transplant has increased from 60cases in 2009 to 80 cases during 2012. However, the number of trans-plant done at the hospital was 23 on 2009 and only 14 cases in 2012.The drop of number of cases that have been transplanted does not goin parallel to the number of cases and donor that been worked up.In fact, the transplanted cases decrease significantly from 2009 to2012 by almost 50%. In parallel, the cases of commercial transplanta-tion continued at a high rate. Out of all the total number of 483 cases,74 cases went ahead with their donation. One hundred and fifty twoout of 483 (31%) declined because of medical reasons. Almost 20%changed their mind to go ahead with transplantation.Conclusion: Few cases of all worked up go ahead with their donationprocess. There are many reasons including medical but social reasonplay a major part. Similarly, easy access to commercial transplantationplays a major effect as well. In addition, lack of national cadavericprograme contributes significantly to this matter.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
299
Extending the search for the missed potential organ donor:A six-month audit of deaths in a large Australianteaching hospital
Jonathan Gatward, Michael O’Leary, Myra SgorbiniIntensive Care Service, Royal Prince Alfred Hospital,Sydney, Australia.
The DonateLife Audit (DLA) is a review of all deaths that occurred in theIntensive Care Unit (ICU) and Emergency Department (ED) of selectedNew SouthWales hospitals, and those who died due to an irrecoverablebrain injury within 24 hours of leaving these areas, tomeasure organ do-nation (OD) activity. A 6 month retrospective audit of all in-hospitaldeaths was conducted at Sydney’s Royal Prince Alfred Hospital to es-tablish whether potential organ donors were being missed by the DLA.Neonates and patients with oncological diagnosis, for palliative care,failed resuscitation in ED and over 80 years were excluded from a totalnumber of 429 deaths. The remaining 119 deaths were subdivided byage: 65 years and under (41/119) and over 65 years (78/119). ThreeOD Specialists reviewed the deaths and found that nearly half of alldeaths (58/119) and the majority of deaths under 65 years (31/41) oc-curred in ICU with only a small proportion dying in ED (6/119). Over 65swere deemed not medically suitable (NMS) if they had a non-neurologicaldiagnosis (57/119). Of the 21 patients over 65 yearswith a neurological di-agnosis, 12 were NMS, 1 was assessed for OD and 7 were set aside forfurther discussion. Of the 12 patients under 65 years with a neurologicaldiagnosis, 3 were NMS and 9 were assessed for OD (resulting in 3donors). Of 29 patients with a non-neurological diagnosis, 25 were NMS,1 was assessed for OD and 2 were set aside for further discussion. The9 identified patients were discussed at a multidisciplinary meeting of ODexperts. It was decided that 1 ICU patient should have been consideredfor OD, but the remaining 8 patients would not have been considered forOD for various valid reasons.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
300
IMPETRO: The IMProvEmentTs in Live ORgan DOnationsproject in South Auckland
Mark Marshall, Denise Beechey, Michael Lam Po TangRenal Services, Counties Manukau DHB, Auckland, New Zealand.
Counties Manukau DHB serves South Auckland with a high prevalenceof indigenous peoples (NZ Maori & Pasifika). This group have a dispro-portionately higher rate of End Stage Kidney Disease and lower rate ofkidney transplantation, unexplained by medical co-morbidities. Theyalso have greater social deprivation and lower literacy skills. Barriers totransplantation/organ donation include: access to understandable infor-mation, lack of cultural skills in health providers, over-emphasis on dial-ysis decision-making, and insufficient resources/operational support forwork-up.The IMPETRO Study is a joint venture with the Kidney SocietyAuckland, a patient support group. It aims to increase live kidney do-nation rates in South Auckland over 3 years using a multi-facetedhealth service delivery improvement project to educate, encourageand facilitate live donation.Interventions include:Development of culturally- and health literacy-appropriate educationalresources on live kidney transplantation and organ donation.Local implementation of a “Home & Kidney first” policy to focus ontransplantation (& home therapies) as the treatment of choice.Formation of culture-specific health educators aimed at building indi-vidual and Whaanau health literacy skills.Development of a community engagement framework aimed at com-munity/religious leaders as well as specific communities through edu-cational sessions.Development of an educational programme aimed at primary careproviders to enable them to support patients and donors.Year 1(2013) of the project involves the development of the resourceslisted above with year 2 and 3 being the implementation period.The primary outcome is the number of potential live kidney donorswho offer, and the main secondary outcome, the number who convertinto successful donation. Subgroup analyses of outcomes in indigenousgroups will be conducted. Initial results are expected in late 2014.
r 27, 2013, Volume 96 Number 10S S213
thorized reproduction of this article is prohibited.

November 27, 2013
301
Analysis of reasons for family refusal on organ donation in theState of Rio de Janeiro, Brazil
Janaina Lenzi1, Andreia Assis1, Márcia Ponte1, Priscila Paura2,André Albuquerque2, Rodrigo Sarlo3, Cláudia Araújo5,Eduardo Rocha4,51Family Services, State Organ Procurement Organization, Rio deJaneiro, Brazil; 2Education, State Organ Procurement Organization,Rio de Janeiro, Brazil; 5COPPEAD, Federal University of Rio deJaneiro, Rio de Janeiro, Brazil; 3General Coordination, State OrganProcurement Organization, Rio de Janeiro, Brazil; 4HealthFoundation, State Health Board, Rio de Janeiro, Brazil.
Introduction: Family Refusal (FR) to organ donation is well-known asa major barrier to transplantation worldwide. In recent years we ob-served a drop in FR rates in the State of Rio de Janeiro (RJ). Compar-ing 2011 to 2012, FR went from 51.9% to 44%. Our study aims toanalyze FR in this region of Brazil in order to formulate strategies forpublic awareness, as well as to improve interviewers’ qualification.Methods: Donation interviews occurring in 2011 and 2012 werereviewed and reasons for FR were classified in the following catego-ries: first person refusal (FPR), family misunderstanding of brain death(FMBD), lack of familial consensus (LFC), religion issues (RI), others(O) and unknown reason (UR). Data were extracted from the Trans-plant State Program data base and are expressed as percentage (%).Results: Respectively in 2011 // 2012, the reasons for FR were: LFC21% // 25%, FPR 19% // 14%, FMBD 14% // 23%, RI 6% // 3%, O 8%// 10% and UR 32// 25%.Conclusion: Our numbers indicates that the main reasons for FRwere FPR, FMBD and LFC as shown in previous research by others.In our series, religion issues were not identified as an important rea-son for FR in RJ. Noteworthy is the large number of cases of FR forUR, which clearly demonstrates a need for educational efforts towardthe health care team, in order to identify and clarify families’ reasons.Findings related to LFC and FPR point to the importance of previousdiscussing the subject with the society in order to decrease the conflictand the emotional instability of families at the decision-making mo-ment. Furthermore, considering FMBD, it is important that bereavedfamilies have a better understanding of what brain death means. It’sdifficult for members of a family to understand and accept brain deathif there is miscommunication with physicians and nurses. Therefore,these themes should be the focus of awareness campaigns andreinforced in the training of health professionals.
S214 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
302
Profile of family member responsible for organ and tissuedonation in the State of Rio de Janeiro
Andreia Assis1, Janaina Lenzi1, Márcia Ponte1, Priscila Paura2,André Albuquerque2, Rodrigo Sarlo3, Cláudia Araújo5,Eduardo Rocha4,51Family Services, State Organ Procurement Organization, Rio deJaneiro, Brazil; 2Education, State Organ Procurement Organization,Rio de Janeiro, Brazil; 3General Coordination, State OrganProcurement Organization, Rio de Janeiro, Brazil; 4HealthFoundation, State Health Board, Rio de Janeiro, Brazil; 5COPPEAD,Federal University of Rio de Janeiro, Rio de Janeiro, Brazil.
Introduction: In Brazil, there is a shortage of organs to be donatedand study the profile of families who consent to donation may help toincrease the number of transplantations. In this sense, this study aimsto investigate the gender and degree of kinship of who authorizes thedonation in Rio de Janeiro (RJ), in order to improve the communica-tion strategy with families of potential donors. There is no consensuson the influence of gender on the decision to donate or not to donatean organ of a family member. According to Breitkopf (2009), womenare more likely to consent to donation than are men. On the otherhand, Morais et al. (2012) analyzed Brazilian families of potentialdonors who did not choose to donate organs in the period from Janu-ary 1997 to December 2004 and the results indicated that most familymembers responsible for refusing donation were women; regardingthe degree of kinship, the family members were offspring (34%),spouses (25%), parents (23%) or siblings (18%).Methods: Analysis of the donation rates by gender and kinship of thefamily member responsible for authorizing donation. Data were col-lected from medical records of the donors filed at the Transplant StateProgram for the year of 2012.Results: Women were responsible for 55.46% of consent for organdonation of the family member, of which 33.33% were mothers,27.78% daughters, 23.81% spouses or partners, and 15.08% sisters.Conclusion: These results differ from the findings of Morais et al.(2012), whose data were from 1997 to 2004, and suggest that, inRio de Janeiro, women have an important role in the process of organdonation since they are more likely to consent to donation. Therefore,the findings highlight that women may serve as an excellent bridge be-tween healthcare providers and families to increase the number ofdonations in Rio.
References:[1] Breitkopf, C.R. (2009). Attitudes, beliefs and behaviors surroundingorgan donation among Hispanic women. Current Opinion in OrganTransplantation, 14(2): 191–195.[2] Morais et al. (2012). Families Who Previously Refused Organ Do-nation Would Agree to Donate in a New Situation: A Cross-sectionalStudy. Transplantation Proceedings, 44: 2268–2271.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
303
Development of Facts & Tips sheets for point-of-care medicalsuitability assessment for the potential organ donor
Carrie Alvaro, Alice Coulson, Leslie Johnson, Trevor Rock,Adam Roshan, Deborah Verran, McKay LeighDonateLife, NSW Organ and Tissue Donation Service,Sydney, Australia.
Despite a significant increase in organ donation, the disparity betweenorgan supply and demand continues to grow. This disproportion andchanging of donor demographics has led to reassessing thresholdsfor acceptable risk and to re-consider the use of organs from donorswith characteristics once thought to preclude donation. During thepast 5 years, the proportion of extended criteria donors (ECD) inNSW has increased 2-fold.To address this issue and to encourage the referral of ECDs, DonateLifeNew South Wales (NSW) has developed 20 Facts and Tip Sheets. TheTip Sheets have been developed since November 2012 as a point-of-care tool for donation clinicians to provide them with a brief overview ofmedical conditions known to require further evaluation for donation suit-ability. Topics cover a vast range including congenital disorders, malig-nancies and infectious risks. Specific to the Tip Sheets are ‘red-flagalerts’ and special investigations required to assist with the assessmentof medical suitability. The Fact Sheets have been developed to assistwith implementation into the wider hospital community.All donation specialists (medical and nursing) within NSW have beenprovided with the Facts and Tip Sheets for point-of-care use as well asbeing a resource reference tool. The Facts and Tip Sheets can also beaccessed from the DonateLife Portal.To date, there have been at least 10 incidences where the Tip Sheetswere used. In all of these cases they were used as an adjunct to assistwith the determination of donor suitability for organ donation.In conclusion this new information tool has provided staff with a soundscientific rationale for enabling the final decisions made relating to theassessment of donor suitability. It is planned for DonateLife NSW tocontinue to develop additional Facts & Tips Sheets.
Reference:ANZOD Registry Report 2010
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
305
Progressing towards an Asian Transplant Registry - Indiantransplant registries can show the way forward
Sunil ShroffMOHAN Foundation, Chennai, India.
National or regional Transplant registries have distinct advantages inlooking at various parameters of graft outcomes both in short and longterm. In Asian sub-continent very little effort has been made in thisfront. The UNOS and Euro-transplant registry have over the years setthe benchmark for the western countries. We in Asia are dependent onthese registries for all our information related to transplants and theiroutcomes. Efforts have been made in the past to form an Asian trans-plant registry but this has failed to live up to its expectations. With Inter-net becoming easily available and with no shortage of knowledgeablemanpower in our sub-continent it is time to start our efforts in the direc-tion of creating a viable transplant registry for the Asian region. Therehave been some efforts in China, Japan, Singapore and Taiwan in thisdirection but no long term strategy has been formulated. In this respecttwo organisations in India have made significant progress in this direc-tion and can offer valuable inputs in making the dream of Asian Trans-plant registry a reality. The Indian Society of Organ Transplantationformed a national registry [1] and has fast track data and a full versionavailable. MOHAN Foundation (an NGO) has to helped with state trans-plant registries for deceased donation and transplantation [2]. Theseregistries are fully functional and will be demonstrated (Fig.1). An Asianfast track model would be presented too for adoption by the Asian Trans-plant Society.
References:[1] www.transplantindia.com[2] www.tnos.org
r 27, 2013, Volume 96 Number 10S S215
thorized reproduction of this article is prohibited.

November 27, 2013
306
Creating sustainable and consistent community engagementthrough corporate outreach and the development ofeffective partnerships
Simone McMahonOrgan Donation & Transplant Foundation of WA, Perth, Australia.
Title: Creating sustainable and consistent community engagement throughcorporate outreach and the development of effective partnershipsBackground: Effective community engagement strategies play an in-tegral part in encouraging family discussion and raising communityawareness about organ and tissue donation, directly impacting on do-nation and consent rates.In 2008 Simone McMahon AM founded the Organ Donation & Trans-plant Foundation of WA (ODAT) as a result of returning from aWinstonChurchill Fellowship. As part of the fellowship, she travelled to the US,UK and Spain where she studied the Internationals models of organand tissue donation and the educational and promotional strategiesused to increase organ and tissue donation awareness and commu-nity engagement.As a result of findings from this Fellowship, in 2009 ODATestablishedthe “Workplace Partnerships for Life Program”
Aim of the Workplace Partnerships for Life Program1. To provide encouragement and support to employers in educating
their staff about the life-saving and life-enhancing benefits of organand tissue donation.
2. To facilitate in the dissemination of accurate information about or-gan and tissue donation via workplaces.
Outline Summary: This program provides employers of WAworkplaceswith access to accurate information required to enable their staff to makean informed decision about donation for themselves or their loved ones.This is achieved through;
1. Appointment of Project Officer2. Onsite Education Seminars3. Networking Events4. eNewsletterSince its establishment 2009, this corporate outreach program hasevolved to become a proven successful mechanism in building part-nerships and creating sustainable and consistent community engage-ment reaching over 10,000 employees within its first year.Acknowledgements:TheOrgan andTissueAuthority andDonateLifeWA
S216 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
310
Over 1,400 DCD organs transplanted in 18 years: An effectiveorgan procurement organization's DCD program increases thedonor pool
Howard M. Nathan, Richard D. Hasz, John D. Abrams,Sharon M. West, Michael J. Moritz, MDGift of Life Donor Program, Philadelphia, PA, United States.
Aim: Demonstrate an effective DCD program increases organ donorpool & provides lifesaving transplants to those on the waiting list.Methods: A single OPO, multi-center study evaluating the recovery &utilization of DCD donor organs. Ongoing hospital education on earlyreferral & DCD protocols were initiated prior to DCD donor recoveries.Transplant outcomes were evaluated using the Kaplan-Meier method.Results: Since implementation of its DCD program (Jun 1995 - Dec2012), OPO has procured 806 DCD organ donors. DCDs increasedthe donor pool by 13% resulting in the transplant of 1,468 organs.Mean donor age was 39 yrs (r=0.5-76). Mean time from donorextubation to cross-clamp, or warm ischemic time (WIT), for kidneystransplanted (n=1,272) was 32 minutes (r=2-214). Mean WIT for liverstransplanted (n=175) was 19 minutes (r=2-69). Of the 806 DCDorgan donors, 658 (82%) were Maastricht Category 3; 74 were Cate-gory 2; & 74 were Category 4. Kidney ATN rate was 46% & kidneygraft survival was 86% at 1 yr, 75% at 3 yrs & 64% at 5 yrs. Livergraft survival was 72% at 1 yr, 63% at 3 yrs & 56% at 5 yrs.
Conclusion: An effective DCD program and clinical practice can leadto an increase in the availability of transplantable organs. Properlyimplemented OPO donor referral protocols can result in an increasein procurement of DCD organ donors. Further research should beconsidered to identify ways to increase DCD liver, lung and pancreaseutilization.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
311
One OPO’s 17 year experience with uncontrolled DCD donors
Richard D. Hasz, Howard M. Nathan, John D. Abrams,Sharon M. West, Michael J. Moritz, MDGift of Life Donor Program, Philadelphia, PA, United States.
Aim: To show that uncontrolled DCD organ donation can lead to suc-cessful retrieval of tx organs & to evaluate kidney & liver tx outcomesfor recipients of organs from uncontrolled donorsMethods: Single OPO, multi-center retrospective study evaluating theprocurement and utilization of organs from uncontrolled DCD donors.Graft survival was evaluated using the Kaplan-Meir method.Results: Between 1996 and 2012, 290 kidneys, 33 livers & 3pancreata were recovered for tx from 148 uncontrolled DCD donorsresulting in the tx of 198 kidneys, 12 livers, and 2 pancreata. Meandonor age was 31 yrs (r=05-76). Mean warm ischemic time (WIT) of66 mins (r=9-214) for the 74 Maastricht Category (MC) II donors wassignificantly higher than the mean WIT of 45 mins (r=2-177) for the74 brain dead donors recovered subsequent to unexpected arrest(MC IV). Kidney utilization rate was 65% for MC II donors and was72% for MC IV donors and the liver utilization rate was 58% forMC II donors and 24% for MC IV donors. The ATN rate for kidneyrecipients was not significantly different between the 2 categories(53% ATN rate for MC II & a 56% ATN for MC IV). Kidney graft survivalfor MC IV was 86% at 6 mos, 80% at 1 yr, 72% at 3 yrs and 61% at5 yrs. Kidney graft survival for MC II was 80% at 6 mos, 74% at 1 yr,65% at 3 yrs and 59% at 5 yrs. Of the 7 livers txd from MC II, 6 failedwithin 60 days of tx and the 7th functioned for 12 years, 7 mos post-tx.Of the 5 livers txd from MCIV, 3 failed within 65 days of tx and 2 arefunctioning at 11 yrs and 5 yrs post-tx.Conclusion: Uncontrolled DCDs provide acceptable kidney graft sur-vival outcomes and represnt a pool of organs that should be pursuedfor transplantation. Results from the small number of liver tx aredisappointing.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
312
What is the potential source of heart allografts from Donationafter Circulatory Death (DCD) donors?
Arjun Iyer1,2, Ben Wan2, Gayathri Kumarasinghe1,2,Michelle Harkess1,Bronwyn Levvey3, Greg Snell3, Paul Jansz1, Emily Granger1,Phil Spratt1, Kumud Dhital1,2, Allan Glanville1, Peter Macdonald1,21Heart Lung Transplant Unit, St Vincent's Hospital, Darlinghurst,Australia; 2Heart Transplantation Lab, Victor Chang Cardiac ResearchInstitute, Darlinghurst, Australia; 3Lung Transplant Service, AlfredHospital, Melbourne, Australia.
Aim: Heart Transplantation (Tx) remains the gold standard treatmentof ESHF, however is limited by the shortage of donor cardiac allograftavailability. Our group has been investigating the viability of heartsfrom DCD donors, and have demonstrated recovery of hearts post30 minutes warm ischaemic time (WIT) in pre-clinical studies. In thisreview, we aim to investigate the potential increase in available heartallografts for Tx from DCD donors.Methods: We retrospectively reviewed the DCD donor database forLung Tx across the two highest volume transplant institutions inAustralia & New Zealand (St Vincent’s Hospital, Sydney & The AlfredHospital, Melbourne). Inclusion criteria were WIT ≤30 minutes, donorage <50, and donor inotropes (Noradrenaline (NA)<0.2 mcg/kg/min),being evaluated between 2007 and 2013.Results: 115 DCD lung donors were reviewed between November2007 and April 2013. During this period, 38/115 (33%) DCD donorsmet the criteria of age <50 & WIT ≤30 minutes. This amounts to anadditional 7 donors per year, or a 17% increase in donors (38/223 heartTx at the 2 institutions during this period). Inotrope data was availablefor St Vincent’s Hospital DCD donors. Incorporating donor NA dose<0.2 mcg/kg/min, there were 11/39 DCD donors suitable for heart dona-tion. At this institution, this amounts to an additional 9% (11/122) ofdonors for cardiac Tx.Conclusion: Based on this review of the data, viable cardiac allograftsfromDCD donors may allow an increase in heart Tx by up to 17%, a sig-nificant increase especially considering the 10%mortality on the waitinglist. This review was limited to DCD accepted lung donors, thereforelikely to be underestimating the potential – evaluation of the entire (allorgans) DCD pool is underway to gauge the true potential.
r 27, 2013, Volume 96 Number 10S S217
thorized reproduction of this article is prohibited.

November 27, 2013
313
Case report of cardiac allografts retrieved from Human Donationafter Circulatory Death (DCD) donors - assessment on ex vivoOrgan Care System
Arjun Iyer1,2, Ling Gao1, Mark Hicks1, Padmashree Rao1, Ben Wan1,Gayathri Kumarasinghe1,2, Andrew Jabbour1,2, Anders Aneman4,Michael O’Leary6, Arvind Rajamani8, Matthew MacPartlin10,Peter Saul11, Gordon Flynn7, Andrew Cheng9, Dani Goh12,Ray Raper5,Suhel Al Soufi3, Emily Granger2, Paul Jansz2, Phil Spratt2,Kumud Dhital1,2, Peter Macdonald1,21Heart Transplantation Lab, Victor Chang Cardiac Research Institute,Darlinghurst, Australia; 2Heart Lung Transplant Unit, St Vincent’sHospital, Darlinghurst, Australia; 3Intensive Care Unit, St Vincent’sHospital, Darlinghurst, Australia; 4Intensive Care Unit, Liverpool Hospital,Liverpool, Australia; 5Intensive Care Unit, Royal North Shore Hospital,St Leonards, Australia; 6Intensive Care Unit, Royal Prince Alfred Hospital,Camperdown, Australia; 7Intensive Care Unit, Prince ofWales, Randwick,Australia; 8Intensive Care Unit, Nepean Hospital, Kingswood, Australia;9Intensive Care Unit, St George Hospital, Kogarah, Australia; 10IntensiveCare Unit, Wollongong Hospital, Wollongong, Australia; 11Intensive CareUnit, John Hunter Hospital, New Lambton Heights, Australia; 12IntensiveCare Unit, Westmead Hospital, Westmead, Australia.
Aim: Hearts from DCD donors are not used clinically due to concern ofwarm ischaemic (WI) injury. Our preclinical studies have shown that, us-ing pharmacological post-conditioning and ex vivo normothermic perfu-sion, WI times (WIT) of ≤30 minutes demonstrate good recovery. Wereport the first two cases of cardiac allograft resuscitation from humanDCD donors using this strategy.Methods: Donor 01was a 62 y.omalewithGuillain Barre Syndrome.WIT(b/w extubation & organ preservation) was 32 mins. Donor 2 was a 39 y.omale, with hypoxic encephalopathy. Hewas declared brain death (BD), butsubsequently was exposed to 30 minutes WIT for the study. Hearts wereflushed with Celsior solution supplemented with post-conditioning agents,before being cannulated and reperfused on aTransmedicsOCSdevice for7-8 hrs of beating heart assessment - functional, metabolic & biochemicalparameters were evaluated with hearts in resting mode for 4 hrs, & work-ing mode for 3 hrs.Results: During resting perfusion, heart 1 had favourable lactateprofiles (lactate extraction) suggestive of viable myocardium. Heart 2had adverse lactate profiles (lactate production) suggestive of ischaemicmyocardium. In a loaded working state, undergoing a left atrial pressurechallenge, heart 1 functioned better than heart 2 (figure 1 - cardiac out-put & generated pressure). The inferiority of Heart 2 was likely the resultof dual BD & DCD insult, decreased post-conditioning activation, and anundiagnosed patent foramen ovale (PFO).Conclusion: We report the first 2 DCD human hearts recovered onthe Transmedics OCS. Despite not being ideal donors for DCD heartdonation (donor 1 – age>50, WIT>30 mins; Donor 2 – BD+DCD, &PFO), both demonstrated viability & the potential for DCD cardiacallografts. Further studies of ideal criteria DCD donors are underway.
S218 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
314
Draft copy more than 20% increase in deceased-donor organprocurement and transplantation activity following the use ofDonation after Cardiac Death: Single centre experience
Hieu LE DINH1, Josée Monard2, Marie-Hélène Delbouille2,Marie-France Hans2, Laurent Weekers3, Catherine Bonvoisin3,Jean-Marie Krzesinski3, Jean Joris4, Séverine Lauwick4,Abdour Kaba4, Pierre Damas5, Didier Ledoux5, Arnaud de Roover5,Pierre Honoré5, Olivier Detry5, Jean-Paul Squifflet5, Michel Meurisse51University of Medicin Pham Ngoc Thach, Ho Chi Minh city, Viet Nam;2Transplant Coordinators, University Hospital of Liège, Liège,Belgium; 3Department of Nephrology, University Hospital of Liège,Liège, Belgium; 4Department of Anesthesia and Intensive CareMedicine, University Hospital of Liège, Liège, Belgium; 5Departmentof Abdominal Surgery and Transplantation, University Hospital ofLiège, Liège, Belgium.
Background: We evaluated organ procurement and transplant activ-ity from controlled donation after cardiac death (DCD) at our institutionover an 11-year period in order to determine whether this program in-fluenced the transplant program and donation after brain death (DBD)activity.Material and Methods: Deceased donor (DD) procurement and trans-plant data were prospectively collected in a local database for retrospec-tive review.Results: There was an increasing trend in the potential and actualDCD number over time. Mean conversion rate turning potential into ef-fective donors was 47.3%. DCD accounted for 21.9% of the DD poolover 11 years. Mean donor age was 54.6 years (3-83). Donors ≥60years old made up 44.1% of the DCD pool. Among referred donors,reasons for non-donation were medical contra-indications (33.7%)and family refusals (19%). Mean organ yield per DCD donor was 2.3organs. Mean total warm ischemia time was 19.5 min (6-39).The number of DCD kidney and liver transplants has progressivelyrisen over time. DCD- KT and LT represented 23.7% and 24.2% ofthe DD kidney and liver pool, respectively, over 11 years. The DBD re-trieval and transplant activity increased during the same time period.In 2012, 17 DCD and 37 DBD procurements were performed in Liègeregion with a little >1 million habitants.Conclusions: The implementation of the DCD program at our institu-tion enlarged the DD pool and did not compromise the development ofDBD programs. The potential DCD pool is still underused and appearsas a valuable donor source for transplantation.Keywords: brain death, cardiac death, deceased donors, organ pro-curement, kidney transplantation, liver transplantation
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
Supplement to Transplantation Nov
Copyright © 2013 Lippincott Williams & Wilkins.
References:[1] Ledinh H, Bonvoisin C, Weekers L, et al. Results of kidney trans-plantation from donors after cardiac death. Transplant Proc. 2010;42: 2407-14.[2] Le Dinh H, de Roover A, Kaba A, et al. Donation after cardio-circulatory death liver transplantation. World J Gastroenterol 2012;18: 4491-506.[3] Salvalaggio PR, Davies DB, Fernandez LA, Kaufman DB. Out-comes of pancreas transplantation in the United States using cardiac-death donors. Am J Transplant. 2006; 6: 1059-65.[4] Muthusamy AS, Mumford L, Hudson A, Fuggle SV, Friend PJ. Pan-creas transplantation from donors after circulatory death from theUnited kingdom. Am J Transplant. 2012; 12: 2150-6.[5] Mason DP, Brown CR, Murthy SC, et al. Growing single-center ex-perience with lung transplantation using donation after cardiac death.The Annals of thoracic surgery. 2012; 94: 406-11; discussion 11-2.[6] Brook NR, Nicholson ML. Kidney transplantation from non heart-beating donors. Surgeon. 2003; 1: 311-22.[7] Cohen B, Smits JM, Haase B, Persijn G, Vanrenterghem Y, Frei U.Expanding the donor pool to increase renal transplantation. NephrolDial Transplant. 2005; 20: 34-41.[8] Summers DM, Counter C, Johnson RJ, Murphy PG, NeubergerJM, Bradley JA. Is the increase in DCD organ donors in the UnitedKingdom contributing to a decline in DBD donors? Transplantation.2010; 90: 1506-10.[9] Squifflet JP. Why did it take so long to start a non-heart-beatingdonor program in Belgium? Acta Chir Belg. 2006; 106: 485-8.[10] Le Dinh H. Extending Donor Pool with Donation after CardiacDeath in Kidney and Liver Transplantation: What is the Price to Pay?Faculty of Medicine. University of Liège, Liège - Belgium, 2012: 206pages, http://orbi.ulg.ac.be/handle/2268/139275.[11] Detry O, Le Dinh H, Noterdaeme T, et al. Categories of donationafter cardiocirculatory death. Transplant Proc. 2012; 44: 1189-95.[12] Colloque Liégeois de Coopération (CLIC) - Don d’Organes. http://www.nicolas-sottiaux.be/ULG/ULG.html. Centre Hospitalier Universitairede Liège, Liège - Belgique, 2011 et 2012.[13] Kootstra G, Kievit J, Nederstigt A. Organ donors: heartbeatingand non-heartbeating. World J Surg. 2002; 26: 181-4.[14] Matesanz R, Marazuela R, Dominguez-Gil B, Coll E, Mahillo B, dela Rosa G. The 40 donors per million population plan: an action planfor improvement of organ donation and transplantation in Spain.Transplant Proc. 2009; 41: 3453-6.[15] Kootstra G, van Heurn E. Non-heartbeating donation of kidneysfor transplantation. Nat Clin Pract Nephrol. 2007; 3: 154-63.[16] Lamy FX, Atinault A, Thuong M. [Organ procurement in France:new challenges]. Presse Med. 2013; 42: 295-308.[17] Dominguez-Gil B, Haase-Kromwijk B, Van Leiden H, et al. Currentsituation of donation after circulatory death in European countries.Transpl Int. 2011; 24: 676-86.[18] Saidi RF, Bradley J, Greer D, et al. Changing pattern of organ do-nation at a single center: are potential brain dead donors being lost todonation after cardiac death? Am J Transplant. 2010; 10: 2536-40.[19] Moers C, Leuvenink HG, Ploeg RJ. Donation after cardiac death:evaluation of revisiting an important donor source. Nephrol Dial Trans-plant. 2010; 25: 666-73.[20] Terasaki PI, Cho YW, Cecka JM. Strategy for eliminating the kid-ney shortage. Clin Transplant. 1997: 265-7.
embe
Unau
[21] Chaib E, Massad E. The potential impact of using donations aftercardiac death on the liver transplantation program and waiting list inthe state of Sao Paulo, Brazil. Liver Transplant. 2008; 14: 1732-6.[22] Noterdaeme T, Detry O, Hans MF, et al. What is the potential in-crease in the heart graft pool by cardiac donation after circulatorydeath? Transpl Int. 2013; 26: 61-6.
r 27, 2013, Volume 96 Number 10S S219
thorized reproduction of this article is prohibited.

November 27, 2013
315
Uncontrolled donors with controlled reperfusion: Reliablerecourse of kidney transplantation
Andrey Skvortsov, Denis Kuzmin, Alexey Tutin, Alexey Kutenkov,Irina Ulyankina, Alexey Ananyev, Igor Loginov, Oleg ReznikDepartment of Transplantation and Organ Donation, Saint-PetersburgI. I. Dzhanelidze Research Institute of Emergency Medicine,Saint-Petersburg, Russian Federation.
Background: The global critical organ shortage leads to use of kidneyfrom the donors after sudden cardiac death, or uncontrolled donors(UDCDs). The purpose of our clinical investigationwas to define the clin-ical applicability of kidney obtained from UDCDs and resuscitated byextracorporal perfusion technology in situ after 60 minutes of asystole.Methods: Between 2009 and 2012, organ procurement service of StPetersburg, Russia, performed the transplantation of kidneys (KTx)obtained from 23 UDCDs. All donors died as ICU patients after suddenirreversible cardiac arrest and failed cardiopulmonary resuscitation.Themean warm ischemic time, or asystole (WIT) was 61.3±3.8minutes.For kidney resuscitation was employed the subnormothermic (27-32˚C)extracorporeal isolated abdominal perfusion with thrombolytics (Strepto-kinase) and leukocyte depletion by a leukofilter. The outcome of theextracorporeal perfusion resuscitated kidneys transplanted into 46recipients was compared with outcome of 92 KTx from 74 brain deathdonors (BDDs).Results: Immediate functioning of kidney grafts was observed in 23 ofthe 46 cases; there was no one PGNF. Only 8 episodes of rejectionwere observed to the end of first year after surgery (17.4%), and27 episodes of acute cellular rejection at the end of the twelfth monthin group from BDD (29.3%). The actuarial 1-year graft survival ratewas 95.7% (n=44) in UDCD group, 93.5% (n=86) in BDD group. Themean creatinine level at the end of the first year of observation was0.113±0.003 mmol/l (UDCD), 0.115±0.004 mmol/l (BDD).
FIGURE 1. Common schemeof donor’s procedures. 1:Death of patientafter sudden irreversible cardiac arrest; 2: documentation by hospitaltransplant coordinator; 3: initiation of contact with regional transplantcoordinator; 4: arrival of medical vehicle with perfusion and surgicalteam from local OPO; 5: surgical access to femoral vessels andcatheterization of donor by procurement team; 6: performing of warmextracorporeal perfusion; 7: possible addition to described protocol -verification of organ quality after explantation in OPO.
Conclusions: Kidneys from uncontrolled deceased donors with criticallyprolongedwarm ischemic time could be successfully used for transplanta-tion if the resuscitation perfusion procedure in situ is implemented in organprocurement protocol. This approach could substantially expand the poolof the organ donors.
S220 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
316
SEUSA Program, an international collaborative strategy toincrease deceased organ donor activity
Maria Paula Gómez Gómez1, Martí Manyalich1, Xavier Guasch1,José Manuel García Buitron2, Antonio Fernández2, Lesley Roberts3,José Ignacio Sánchez4, Antoine Stephan5, Farida Younan5,Francesco Paolo Schena61DTI Foundation, Barcelona, Spain; 2Juan Canalejo Hospital, ACoruña, Spain; 3National Organ Transplant Unit (NOTU), Port ofSpain, Trinidad and Tobago; 4Regional Coordination ofTransplantations of Aragon, Zaragoza, Spain; 5National Organizationfor Organ and Tissue Donation and Transplantation (NOOTDT),Beirut, Lebanon; 6Apulia Transplant Regional Center, AziendaOspedaliero-Universitaria Policlinico di Bari, Bari, Italy.
Objective: The SEUSA is a program to improve the organ donationand transplant system based on the best practices of the Spanish, Eu-ropean and USA models. The objective of the present study is to col-lect evidence of the effectiveness of the SEUSA increasing thedeceased organ donation from the experience of implementation inthree regions, the South of Italy (La Puglia), Lebanon and Trinidadand Tobago.Method: The SEUSA includes: 1) Diagnose of the organ donation andtransplantation activity through the “Organ Donation Diagnosis Sur-vey” (ODDS); 2) Establishment of the Transplant Procurement Man-agement Team; 3) Implementation of the “Deceased Alert System”
(DAS); 4) Application of the “Essential in Organ Donation” (EOD)and 5) Hospital Audit. Monthly monitoring meetings to make neededadjustments based on the specific characteristics of the country aredone. The program also contributes with the definition of specific eco-nomic funds direct to the procurement system.Results: SEUSA-Apulia started in 2007 and after three years of im-plementation, comparing to the data from the three previous years ofthe project (2005-2006-2007) we found an increase of 36.5% of braindeath diagnose (83 vs. 113.3) and the total number of donors in-creased to 47% (89 vs. 131). SEUSA-Lebanon started in 2009. Sofar, SEUSA has increased Lebanon’s donation rate from 0 to 2.5PMP and it has been possible to implement the cornea donation pro-gram, obtaining 90 cornea donors. SEUSA-Trinidad and Tobago iscurrently being implemented and started on July 2010. During the firstyear of DAS 161 alerts of possible DBD and DCD happened, fromthem 17 Brain death were diagnosed.Conclusion: The SEUSA has contributed to the improvement of theorgan donation/transplant system in the three regions. In addition, itmay represent an example of valuable and replicable strategy to ame-liorate organ and tissue activity in other countries.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
317
Meeting donor management goals maximizes organrecovery in children
Thomas Nakagawa1, Susan Galbraith2, Jim Quetschenbach3,Ginger DeLario31Anesthesiology, Wake Forest Baptist Health, Winston-Salem, NC,United States; 2LifeShare of the Carolinas, Charlotte, NC, UnitedStates; 3Carolina Donor Services, Durham, NC, United States.
Introduction: There is a clear need to reduce the gap betweendonors and patients awaiting transplant.Achieving donor management goals (DMGs) results in more organstransplanted per donor (OTPD) in adults. We sought to determine ifmeeting DMGs in pediatric donors resulted in more OTPD in additionto other factors that might influence organ recovery and transplantation.Methods: Data from 2 Organ Procurement Organizations (OPO) wereretrospectively reviewed from 2007 through 2012 for pediatric donorsage 0–18 years meeting brain death criteria. The time period corre-sponds with implementation of electronic medical record systems withineach organization. DMGs included: systolic blood pressure appropriatefor age, central venous pressure 4-12 cm H2O, arterial pH 7.3-7.5,PaO2>80 mm Hg on FiO2≤.4, serum Na+ ≤160 meq/L, serum glu-cose <200 mg/dL, single vasopressor agent at low dose, and urineoutput 0.5-7 cc/kg/hour in the 4 hours prior to recovery. We reviewednumber of organs recovered, transplanted, discarded and organs usedfor research.Results: 148 brain dead pediatric donors had 673 organs recoveredfor transplantation. 605 organs were transplanted (4.09 OTPD). 102donors had 4.39 OTPD when >80% of the DMGs were achieved.46 donors had 3.37 OTPD when <80% of the DMGs were met.24 organs were discarded and 42 organs were used for research. Sur-gical damage or damage to organs due to traumatic cause of deathoccurred in 2 cases. Medical examiner restriction (thoracic organsonly) occurred in 4 cases resulting in 8 organs not recovered for trans-plant. Discarded organs occurred more frequently in donors <1 yearof age despite exhausting match runs and, in most cases, werepancreata. The youngest brain dead donor was 9 days old (2 organsrecovered). A total of 29 donors were <1 year of age.Conclusions:Meeting >80%of DMG’s before organ recovery in childrenresulted in more OTPD. Other factors influencing organ recovery and or-gan transplanted included donor age and medical examiner restriction.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
318
Evidence-based guideline for the hormone modulation of theadult brain-dead organ donor: Vasopressin, corticosteroids andthyroid hormones use
Vilma Inés Brunetti1, Pablo Centeno2, Ernesto Germán Monteagudo2,Rogelio Matías Anchorena21Laboratory, HZGA Simplemente Evita, Gonzalez Catàn, Argentina;2Intensive Care Unit, HZGA Simplemente Evita, GonzalezCatán, Argentina.
Background: There is disagreement about the best hormone treat-ment indicated for the brain-dead (BD) organ donor (OD), maybe be-cause there is no high-quality guideline published.Aims and Objectives: Establishing hormone modulation strategiesto optimize: circulatory function, organ procurement, graft survival,benefits and costs. These outcomes were used to formulate PICOquestions for every hormonal treatment. Target population: BD peopleand possibly OD older than 14 years old, in intensive care units. Targetgroup: OD manager physicians.Methods: Systematic literature search in PubMed using keywords ofthe PICO questions added to a Google search of the references ofinterest. FLCritica 1.1.1 (Osteba) was used for the critical appraisalof literature. Evidence grading system, and grading system for recom-mendations: SIGN. Agreement method: nominal group.Brief Summary of Key Recommendations: We recommend admin-istering methilprednisolone (1 gr bolus) soon after BD, repeatingdoses every 24 hours, recommendation grade (RG): A. Both in caseof haemodynamic impairment (HI) or diabetes insipidus (DI), we rec-ommend using vasopressin (AVP) as first choice, RG: B, starting with1 U bolus, followed by infusion (maximum dose: 2.4 U/h), RG: D. Wesuggest using norepinephrine as a second choice to treat HI, RG: B.We suggest using desmopressin as a second choice to treat DI or toenhance AVP use, RG: D. We suggest treating hypernatremia, RG:D. We do not recommend the use of thyroid hormones.Implementation and Monitoring of Guideline: Several indicatorswere developed for monitoring the described outcomes. A check listand a quick consult guideline stands out. Update: every 2 years.External assessment by using the AGREE instrument. Domainscores: each of the six are independently above 80 %.Conclusions: The present guideline simplifies the access to databased on evidence which might improve the standardizing criteriaand outcomes.
r 27, 2013, Volume 96 Number 10S S221
thorized reproduction of this article is prohibited.

November 27, 2013
319
Heart donation in Japan before and after revision of JapaneseTransplantation Act
Norihide Fukushima1, Minoru Ono2, Yoshikatsu Saiki3,Takeshi Nakatani4, Satoshi Saito5, Suguru Kubota6, Juntaro Ashikari71Department of Therapeutics for End-Stage Organ Dysfunction,Osaka University, Suita, Japan; 2Department of CardiothoracicSurgery, Tokyo University, Tokyo, Japan; 3Department ofCardiovascular Surgery, Tohoku University, Sendai, Japan;4Department of Transplantation, National Cardiovasuclar Center,Suita, Japan; 5Department of Cardiovascular Surgery, TokyoWomen’s Medical College, Tokyo, Japan; 6Department ofCardiovacular Surgery, Hokkaido University, Sapporo, Japan;7Head Quarter, Japan Organ Transplant Network, Tokyo, Japan.
After revision of Organ Transplant Act in July 2010, brain dead organdonation increased from 13 to 45 in a year and heart donation in-creased. The purpose of this study is to review consecutive 163 braindead heart donors to evaluate our special strategies to identify andmanage organ donors.Method: Consecutive 163 brain dead heart donors since the Act wasissued were reviewed. While 69 heart donations were performed be-tween October 1997 and July 2010 before revision of the Act, 97 heartdonations were done for 3 years after revision.Donor Evaluation and Management System: Since November in2002, special transplant management doctors were sent to donorhospitals in order to assess donor’s organ function and to identifywhich organ could be transplanted. They also intensively cared thedonor to stabilize hemodynamics and to improve cardiac function byintravenously giving anti-diuretic hormone and pulmonary toileting bybroncho-fiberscope.Results: A mean donor age of heart donor was increased from 41.0 to43.9 years. Especially 11 hearts from a donor older than 60 years weretransplanted successfully. Before revision, the cause of death was 37 incerebrovascular disease (SAH 34, stroke 1, bleeding 2), 18 in headtrauma, 13 in asphyxia, and 2 in post-resuscitation brain damage. Afterrevision, that was 49 in cerebrovascular disease (SAH 37, stroke 2,bleeding 16 and other 4), 17 in head trauma, 10 in asphyxia, and 11 inpost-resuscitation brain damage. 58 donors had a history of cardiac ar-rest. 58 required high dose of cathecholamine drip infusion. Only onerecipients died of primary graft dysfunction (PGD). Patient survival rateafter heart Tx at 3 years was not different before and after revision ofthe Act (95.2 % vs 94.2%).Conclusion: Although donor age was increased and donor who diedof cerebral bleeding or post-resuscitation after the revision of Act, theoutcome after heart transplantation was not changed.
S222 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
320
Deceased donor transplantation programme in AndhraPradesh - a Southeastern State in a developing country India
Swarnalatha GuditiNephrology, Nizam’s Institute of Medical Sciences, Punjagutta,Hyderabad, India.
In developing country like India the prevalence of end stage organ diseaseis increasing due to shift in health related problems from communicablediseases to chronic diseases. Though transplantation has been in practicein India for more than 3 decades, it has been grossly inadequate in termsof actual numbers, due to a shortage of resources and organs. The onlysolution for the shortage of organs is deceased donor transplantation.Globally, Spain has highest rate of deceased donor transplantationrate of 32 per million population per year. The deceased donor trans-plantation in USA is 20.7 per million population per year, Europe 15.9per million populations per year and Asia 1.1 per million population peryear. Deceased donor transplantation rate in India is 0.08 per millionpopulation that accounts to 2 % of total transplantation.In India the Human Organs Transplantation Act, was enacted in 1994with the objective of promoting and regulating the transplantation ofhuman organs like kidney, liver and heart - both live as well as de-ceased donor. There was no significant increase in deceaseddonortransplantation over the past two decades for various reasons. Indiafollows “opt in” system and brain death declaration is not mandatory.Andhra Pradesh is one of the 28 states of India, situated on the country'ssoutheastern coast. It is India's fourth largest state by area and fifth larg-est by population. Government of Andhra Pradesh, considering theshortage of organs and increasing burden of end stage organ failure inthe state, has come up with a Government Order1 called “Jeevandan”to streamline the procedure for facilitating and regulating the cadavertransplantations on an end-to-end basis. Theword “Jeevanadan”means“to donate life.”Wepresent our experience of deceased donor transplan-tation programme initiated by government of Andhra Pradesh, India.Jeevandan program practically came into force from 1st January 2013.Since the inception of deceased donor transplantation (Jeevandan) pro-gram in the Andhra Pradesh, there have been 23 deceased donations.Male donors were 16 and female 7:; female to male ratio being 1: 2.28.The mean age of deceased donors was 33.88 years (range 8 to 72). Fif-teen (65.12%) donors were educated and 8 (34.78%) were uneducated.Most common Blood group was B positive in 11 (47.82%) donorsfollowed by A positive andOpositive in 5 (21.73%) donors each. ABpos-itive bllod group was in 2 (8.69%) donors only. Total 102 organs were re-trieved from 23 deceased donors; 41 kidneys, 20 livers, 22 heart valves18 corneas and 1 lung.Total deceased donor renal transplantations during this period were 41.Out of 23 donors, Kidneys were not utilized from 2 donors; as one donorhad chronic kidney disease with serum creatinine of 4.5 mg/dl and otherdonor was 72 year old female with hypertension, diabetic and had dia-betic nephropathy. Both the kidneys from a 8 year old male donor wereplaced in single recipient. Mean age of renal recipients was 41.35 years(range 13 to 63). There were 12 females and 29 males, female to maleratio being 1:2.41. Among deceased donor renal transplant recipients,B positive blood group was most common, seen in 19(46.34%) followedby O positive in 10 (24.39%) A positive in 8 (18.51%) and AB in 4(9.75%) recipients. Among 41 renal transplant recipients eleven patients(26.82%) had delayed graft function. One (2.43%) patient underwentgraft nephrectomy due to candida fungal infection. One (2.43%) patientdeveloped humoral mediated rejection which responded to plasmaphe-resis and rituxibmab therapy and one (2.43%) patient expired due to in-fection. Graft function in rest of the renal transplant recipients was goodwith mean serum creatinine of 1.45mg/dl.Submitted on be half of Government of Andhra Pradesh, India
Reference:G.O.MS.NO. 184 HM&FW (M1) Department, dated 16-08-2010, Gov-ernment of Andhra Pradesh, India
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
321
Organ donor screening by serology and NAT allows immediatediagnosis of blood-borne viruses and safer use of organs fromincreased risk donors
Chee Choy Kok1, Cristina Baleriola2, Sanghamitra Ray3,Peter Robertson4, William Rawlinson51Microbiology, South eastern Area Laboratory Services, Randwick,Australia; 2Microbiology, South Eastern Area Laboratory Services,Randwick, Australia; 3Microbiology, South eastern Area LaboratoryServices, Randwick, Australia; 4Microbiology, South Eastern AreaLaboratory Services, Randwick, Australia; 5Microbiology, SouthEastern Area Laboratory Services, Randwick, Australia.
Serology and nucleic acid test (NAT) screening for HBV, HCV and HIVare key steps to prevent blood-borne-virus (BBV) transmission from or-gan donors. We assessed optimal use of NAT in the solid organ trans-plant setting for 4 years through evaluation of requests and results forNATand serology testing in routine and increased risk donors (IRD).Review of NAT and serology results for donor screening from October2009 to July 2013 showed NATwas performed on a total of 422 donors;100 performed prospectively while 322 performed retrospectively. Therewere 295 organs (3.0 organs/donor) retrieved from IRD and 1,121organs retrieved from 322 average-risk donors (3.5 organs/donor).NAT screening of 42 serology positive (1 HIVAb+, 11 HCVAb+, 30 HBVHBcAb or HBsAg+) donors resulted in transplantation of 67 additionalorgans that without NAT screening would either have not been used orused with restrictions. The NAT assays demonstrated the HIV donorwas NAT positive, the HCV donors were 9/11 NAT positive, and theHBV donors were 3/30 NAT positive. Of the HBV donors, 27/30 wereHBcAb positive and 0/27 NAT positive, and 3/30 HBsAg with 3/3 NATpositive. Donors accepted for transplantation were HIV 0/1, HCV 3/11(all of whom were NAT positive and transplanted into HCV RNA positiverecipients) and 19/27 HBcAb positive donors transplanted. Mosttransplanted organs with positive serology and negative NATwere fromHBcAb positive donors (n=19 donors with 63 organs transplanted) and4 organs retrieved from 3 HCV positive donors.The availability of a 24/7 NAT screening service for organ donorsprovides diagnosis within 8 hours of blood delivery. This enabled theuse of organs from donors with positive serology but inactive viral infec-tion and donors with false positive serology results. This algorithmallowed use of organs from IRD with safer expansion of the donor pool.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
325
Information sources, donation knowledge and attitudestowards transplant recipients in Australia
Melissa Hyde, Suzanne ChambersBehavioural Basis of Health, Griffith Health Institute, Griffith University,Mt Gravatt, No, Australia.
Background: Knowledge is linked consistently with organ donationattitudes, willingness, and consent. Negative information about dona-tion and the recipients of donation can affect public opinion and dona-tion willingness. However, it is unclear which information sources aremost important in forming knowledge, particularly in Australia wherelittle prior research exists. In this regard, we aimed to identify informa-tion sources that may inform Australian’s organ donation knowledgeand attitudes towards transplant recipients.Methods: 1487 Australian residents aged 18 years or older completedan online survey. Self-reported knowledge, information sources, andattitudes toward transplant recipients were assessed.Results: Participants felt fairly well informed about organ donation; partic-ularly if they registered donation wishes, were female and older. Over halfreported their driver’s license, news on TV, and discussion with family/friends, as donation information sources. However, information sourcescontributing to knowledge were personal experience, online, hospital,Government campaign, discussion with family/friends, Medicare, doctor’ssurgery, and the newspaper. Differences based on registration status, sex,and age, were found. Discussion with family/friends and movies/TVshows, as well as not having seen information in a newspaper or doctor’ssurgery, contributed to positive attitudes towards recipients; although thevariance explained was small.Conclusion: People felt more informed by personal, medical, and gov-ernment information sources compared tomassmedia. Family discussionwas not only a common information source but also contributed signifi-cantly and positively to both donation knowledge and attitudes towardsrecipients. Further exploration of information sources contributing to youngmale’s donation knowledge and community attitudes toward transplantrecipients is needed.
r 27, 2013, Volume 96 Number 10S S223
thorized reproduction of this article is prohibited.

November 27, 2013
326
Creation of a donation after circulatory death (DCD) training DVD
Kathryn Coumans2, Helen Opdam1, Nicole Gauthier1,Elizabeth Treasure11DonateLife Victoria, Melbourne, Australia; 2Barwon Health,Geelong, Australia.
DonateLife Victoria (DLV) has developed a unique model for the imple-mentation of donation after circulatory death (DCD). With support fromthe DonateLife Victoria Agency, hospital donation specialist staff de-velop a local DCD protocol and undertake other activities such as edu-cation of ICU and operating theatre personnel and run a mock DCDcase. This process achieves engagement of key hospital stakeholdersand provides strong local ownership by clinical staff, vital for subsequentsuccess in undertaking DCD.Twelve hospitals in the metropolitan and greater Melbourne area cur-rently have active DCD programs, with the aim now to expand DCD ca-pability to include rural and smaller Victorian hospitals. DLV identified alack of resource material for training staff specifically in DCD donation,and wanted to fill this gap.Wewill demonstrate howa group of dedicatedprofessionals were able to create a DVD of a mock DCD case for usewithin Victoria and nationally to train staff with no or minimal exposureto DCD.The process of creating the video included:1. Formation of a DCD DVD working group consisting of DLV Agency
and hospital staff, transplant surgeons, operating theatre staff, and afilmmaker
2. Identifying target audience information needs and key elements of theDCD process
3. Developing a script which accurately illustrates the organ donation pro-cess from the first family conversation to the family viewing after surgery
4. Casting roles using members of the working group and actors5. Undertaking the filming at Geelong Hospital within the ICU and operat-
ing theatre6. Review and editing of scenes with the film companyConclusion: The DCD DVD working group has successfully createda high quality training resource available to educate hospital staff inVictoria and Australia about the DCD process. The resource achievesthe goal of providing clear, accurate and relevant information to staff inan engaging way.Source of Funding: DonateLife Victoria
S224 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
327
Effects of a modified education program in organdonation in Norway
Käthe Meyer1,2, Ingebjørg Kvangarsnes1,2, Pål Foyn Jørgensen1,2,Per Arne Bakkan1,2, Urs Christen1,2, Stein Foss1,1,21Transplantation, Oslo University hospital, Oslo, Norway; 2Norwegianresource group for organ donation, Oslo, Norway.
Background: Competence in the organ donor process is known to beessential for high rates in organ donation, low refusal rate and organsavailable for transplantation. Two Norwegian surveys investigating inten-sive care personnel’s knowledge and attitudes revealed a deficiency incommunicative skills and cognition of the organ donor process. The ed-ucational program, organised as a two days seminar by the NorwegianResource Group for Organ Donation (Norod), did not fulfil physicians’and nurses’ perceived needs.Method and materials: In 2009 we initiated a modification of our pro-gram. A revised program with uniform lectures focusing on communi-cation training was introduced in 2011.Concomitantly we started systematically evaluation. An evaluationform was filled in by the participants at the end of each seminar. Theitems covered all lectures and the learning effect employing a Likert-like scale as well as an evaluation in own words. The results wereanalysed by frequency, and the previous and present program werecompared by t-test. The written evaluation was assessed by text anal-ysis to describe participants’ opinions about the program and theirsuggestions for improvement.Results: A total of 275 participants evaluated the seminars. Theparticipants in the present education program scored high on mostthemes, mean 4.18-4.74 (range1-5), and the learning effect was higherin the present than in the previous program. More interactive lectureswere requested and the communication training was much appreciated.The donation rate has increased from 21.14 pmp in 2009 till 23.27 pmpin 2012. In the same period the refusal rate declined from 26 % to 17%.Conclusion: Participants of the Norod seminars seemedmore satisfiedwith the new educational program.Wewill continue to refine the programand highlight the interactive educational method.Modifications of the do-nor hospitals educational program according to reported needs may in-crease the donation rate significantly.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
328
Analysis of social awareness of organ donation in thesecondary school population in Galicia
Jacinto Sanchez-Ibañez1, Marta Alvarez Vazquez1,Encarnacion Bouzas Caamaño1, Anton Fernandez Garcia2,Maria Valentina Fernandez Lopez2, Enrique Alemparte Pardavila31Regional Transplant Coordination, Galician health Service, Santiagode Compostela, Spain; 2Hospital Transplant Coordination Office,Complejo Hospitalario universitario A Coruña, A Coruña, Spain;3Hospital Transplant Coordination Unit, Complejo HospitalarioPontevedra, Pontevedra, Spain.
Introduction: The family refusal rate in Galicia is traditionally higherthan that of Spain as a whole. To change this attitude it is importantto work with the young population in school. We analyse the resultsof a program designed by the Transplant Coordination Office in Galiciato introduce organ donation to students over 14 years old.Material and Methods: From 2007 until June 2013, 531 talks weregiven at schools in Galicia by hospital transplant coordinators togetherwith organ recipients about all aspects of donation and transplanta-tion. We analysed the answers to the five questions included in thequestionnaire given out at the end of each talk.Results: 27,850 students attended the talks. The mean age was 17.3 ±4.4 years old; 56.7%were female and 43.3%male. Q1:Would you like tobe transplanted? Yes: females 97.4% vs males 94.1% (p=0.000). Q2:Will you donate your organs? Yes: females 89.2% vs males 81.2%(p=0.000); population of the municipality >10,000 inhabitants (86.2%) vs<10,000 (83,8%) (p=0.000); students >15 years old (86.2%) vs <15(84,4%) (p=0,001). Q3: Would you donate the organs of a relativewho doesn’t manifest his or her wish in life? Yes: females 46.6% vsmales 43.3% (p=0.000); population of the municipality >10,000inhabitants (45.9%) vs <10,000 (42.4%) (p=0.000); students >15 yearsold (46.5%) vs <15 (41,6%) (p=0.000). Q4: Will you respect a relative’sdecision to donate? Yes: females 98.3% vs males 96.1% (p=0.000);population of the municipality > 10,000 inhabitants (97.5%) vs <10,000(96.7%) (p=0.002); students >15 years old (97.6%) vs <15 (96.8%)(p=0.000). Q5: Is brain death the death of the person? No difference be-tween genders, greater acceptance when the population >10.000 (69%) vs<10,000 (63.5%) (p=0.000) and when the age is >15 years old (69.2%) vs<15 (64.1%) (p=0.000). The mean score for student assessment of thetalks was 8.5/10.Conclusion: After the talks we observed a positive attitude towardsdonation, although the understanding of the concept of brain deathshows room for improvement. We observed differences according togender, age, and population of the municipality.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
329
Training course in donation for hospital nursing staff in Galicia:Analysis and results before and after the course
Jacinto Sanchez-Ibañez1, Marta Alvarez Vazquez1,Encarnacion Bouzas Caamaño1, Carlos Leon Vara Perez2,Juan Cortes Cañones3, Maria Isabel Alvarez Dieguez4,Francisco Garcia Novio5, Luis Amador Barciela21Regional Transplant Coordination, Galician health Service, Santiagode Compostela, Spain; 2Hospital Transplant Coordination Unit,Complejo Hospitalario Universitario Vigo, Vigo, Spain; 3HospitalTransplant Coordination Unit, Complejo Hospitalario Ourense,Ourense, Spain; 4Hospital Transplant Coordination Unit, ComplejoHospitalario Ferrol, Ferrol, Spain; 5Hospital Transplant CoordinationUnit, Complejo Hospitalario Lugo, Lugo, Spain.
Background: The level of knowledge of donation and transplantationtogether with that of hospital nursing staff awareness is crucial in im-proving the positive atmosphere around donation.Aim:We designed in Galicia training courses for nursing staff in all thehospitals authorized for donation and compared their knowledge ofand attitude to the donation and transplantation process before and af-ter the course.Material and Methods: 55 accredited courses were held between2008 and the 1 of June 2013. A questionnaire was completed beforeand after the course and the answers were analyzed. The variablesstudied were: gender, age, type of hospital (only procurement or pro-curement and transplant); type of unit (donor’s unit or not)Results: 1,697 health professionals took part in the courses, of whom75.8% completed the questionnaire before and after the course.95.7% were female and 4.3% male. The average age was 41.8 years(S.D. 9.3 years).. 96.5% of the participants had a positive attitude be-fore the course. Before the course 61.7% recognized the diagnosis ofbrain death as the death of the patient, this figure rising to 95.6%(p<0,000) after the course. Before the course only 49,5% were familiarwith Spanish legislation on consent, changing after the course to89.8% (p<0.000). The most appropriate moment to talk about dona-tion was recognized before the course by 80,4% of participants, andafterwards by 93.9% (p<0,000).Conclusion: Hospital staff’s awareness in donation is important toavoid misunderstandings with relatives and to create a positive envi-ronment. The results show that training courses for hospital nursingstaff should be part of any action plan.
r 27, 2013, Volume 96 Number 10S S225
thorized reproduction of this article is prohibited.

November 27, 2013
330
The influence of Transplant Procurement Management(TPM) training program in organ and tissue donationand transplantation
Tyler R. Harrison1, Melania G. Istrate2, Susan E. Morgan1,Gloria Paez2, Maria Paula Gomez2, Quan Zhou1, Ricard Valero2,3,Marti Manyalich2,31Brian Lamb School of Communication, Purdue University, WestLafayette, IN, United States; 2TPM-DTI Foundation, Barcelona, Spain;3Hospital Clínic de Barcelona, Barcelona, Spain.
Background: Training on organ donation/ transplantation (D&T) is rel-evant for transplantation improvement [1]. TPM has been providingtraining on organ D&T [2-3] in compliance with the agreed profes-sional requirements.Methods: Considering that micro level change practices can havemacro level influences, a survey was developed assessing the impactof training on development of policies, practice, career choices, lead-ership, and knowledge dissemination. Thus a new type of evaluationwas designed focusing on how different groups perceive trainingbenefits. It was translated into five languages (Spanish, English, Ital-ian, French, and Portuguese). Individuals who participated in TPMtraining courses were sent a recruitment letter and link to an onlinesurvey. Additionally, links were posted on Facebook and handed outat organ donation meetings and congresses. Potential participantsand key individuals were asked to forward the link to individuals activein D&T. Respondents were required to rate on a scale of 1-5 (1- no in-fluence and 5- a great deal of influence) the influence of trainings on12 items to answer the following Research question: What is the per-ceived influence of specialized training programs on career, collabora-tion, and skills in D&T?. Institutional review boards at the University ofBarcelona and Purdue University (USA) approved the study.Results: 1102 participants agreed to take the survey, 87% reported par-ticipating in a TPM course, out of which 95% selected TPM courses asmost influential. Specifically, 98% reported influence on knowledge[score 4.45/5], 93% on technical [4.15] and communication [4.14] skills,89% on attitude toward D&T [4.08], 92% on motivation to work [4.23],91% on desire to innovate [3.98], 87% and 79% on ability to changeD&T practices [3.85] and policies [3.51], respectively.Conclusion: Participation in TPM training courses has positive per-ceived benefits.
References:[1] Manyalich M, Guasch X, Paez G, Valero R, Istrate M and theETPOD partner consortium: ETPOD (European Training Program onOrgan Donation): a successful training program to improve organ do-nation. Transpl Int 2013 Apr;26(4):373-84[2] Communication from the Commission. Action plan on Organ Donation andTransplantation (2009-2015): Strengthened Cooperation between MemberStates. Available at: http://ec.europa.eu/health/ph_threats/human_substance/oc_organs/docs/organs_action_en.pdf (last review 16 July 2013).[3] Paez G, Valero R, Manyalich M. Training of health care students andprofessionals: a pivotal element in the process of optimal organ donationawareness and professionalization. Transpl Proc 2009; 41: 2025.
S226 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
335
Estimating differential renal function using ellipsoidapproximation of renal volume on CT scan
Laura Nguyen, Fadi Kamal, Brian BlewUniversity of Ottawa/The Ottawa Hospital, Ottawa, ON, Canada.
Background: Living renal donors must undergo extensive medicalinvestigations in order to be approved for the donor program. Amongother testing, this includes both computed tomography (CT) scans toevaluate vascular anatomy and nuclear medicine renal scans to as-sess for differential renal function.Complexmodels have been used to calculate precise radiographicmea-surement of renal volume on CT to estimate differential renal functionbased on differential renal volumes. Thus, the necessity of the nuclearmedicine renal scan can be eliminated, reducing the radiographic bur-den and time commitment of the potential donor and addressing the on-going scarcity of necessary radionucleotides. However, these modelsare rarely used as they are often cost-prohibitive due to the need for pro-prietary software and they are labor-intensive for radiologists.Methods: We examined whether a simplified estimation of differentialrenal volumes based on the ellipsoid formula (renal volume = πldw/6,where l, d, and w represent dimensions of the kidney) using CT scans,may also adequately estimate differential renal function.Results: Consecutive living renal donors were reviewed retrospectively(n=79). The volume-based estimations of differential renal volume werecorrelated to differential renal function on nuclear medicine scans(r=0.29, p<0.01). We were able to identify the kidney with the greaterfunction in 53 (67%) of the 79 cases, and in all 8 (100%) of 8 cases inwhich the difference in differential renal function was clinically significant(>10% difference between kidneys).Conclusions: These findings support removal of the nuclear medi-cine scan from routine assessment of potential kidney donors withoutthe need for expensive radiologic software. Further research lookingspecifically at potential donors with clinically significant differential re-nal function between kidneys is required to confirm our findings.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
336
Use of kidneys with small renal tumors for transplantation:Potential benefits of organ recycling for high-riskdialysis patients
Yoshihide Ogawa1, Keimei Kojima2, Rensuke Mannami2,Makoto Mannami2, Keiichi Kitajima3, Mitsuo Nishi4, Hisaaki Afuso5,Seiichi Ito6, Naoki Mituhata61Urology, Tokyo-West Tokushukai Hospital, Akishima, Japan;2Urology, Uwajima Tokushukai Hospital, Uwajima, Japan; 3Urology,Kagoshima Tokushukai Hospital, Kagoshima, Japan; 4Urology, SaintMartin's Hospital, Sakaide, Japan; 5Urology, Chubu TokushukaiHospital, Okinawa, Japan; 6Urology, Kure Kyosai, Kure, Japan.
Objectives: Buell, Mannami, Nicol, Masquera, and He respectivelyreported 14, 8, 31, 7, and 19 transplant cases using kidneys after re-section of RCC. Donor-transmitted renal cell carcinoma in transplantis unavoidable but guidelines were issued to optimize organ usage.To balance the risk of dying on dialysis against cancer transmission,high-risk recipients are suggested best to deserve the procedure. Uti-lizing these discarded kidneys may help to suppress the rise of organtrafficking and transplant tourism. Therefore, we performed a prospec-tive open trial that utilizes resected kidneys for transplant into third-party recipients after restoration.Subjects and Methods: Our clinical trial (stage 1 and 2) consisted of 5cases each has been completed after one year of follow-up. Donorswere recruited from 6 donor-harvesting hospitals and subsequently se-lected from among patientswho opted to undergo nephrectomy for smallRCC (<4 cm) after extensive discussion of other treatment modalities.The recipient selection wasmainly based on ABO compatibility and clin-ical scores, and immunological data (PRA and HLA mismatch) wereadded to the selection criteria in the extended trial (stage 2).Results: In the stages1 and 2, five male patients and 3 male & 2 fe-male patients were the donors with T1a RCC, respectively. Thenephrometry RENAL scores for their renal tumors were of low andmoderate complexity. A total of 56 dialysis patients and 76 patientswere enrolled as candidate recipients for the stages 1 and 2, respec-tively. Five recipients aged 47–66 and 46–65 years were selected ineither stage 1 or 2, respectively. Two recipients had a history of kidneytransplant in each stage. Four recipients in each stage have experi-enced rejection so far and the latest serum creatinine levels rangefrom 1.10 to 5.55 mg/dl without recurrence of RCC after 17 to 43months of follow-up.Conclusions: Restored kidney transplant led to achieving good renalfunction without recurrence of RCC at 17–43 months. The procedureappears technically demanding, however, with expertise hands selectedcandidates can benefit from accepting these discarded kidneys.
References:[1] Buell JF, Hanaway MJ, Thomas M, Munda R, Alloway RR, FirstMR, Woodle ES. Donor kidneys with small renal cell cancers: can theybe transplanted? Transplant Proc. 2005 Mar;37(2):581–2.[2] Mannami M, Mannami R, Mitsuhata N, Nishi M, Tsutsumi Y, NanbaK, Fujita SLast resort for renal transplant recipients, ‘restored kidneys’from living donors/patients. Am J Transplant. 2008 Apr;8(4):811–8.[3] Nicol DL, Preston JM, Wall DR, Griffin AD, Campbell SB, Isbel NM,Hawley CM, Johnson DW. Kidneys from patients with small renaltumours: a novel source of kidneys for transplantation. BJU Int. 2008Jul;102(2):188–92[4] Musquera M, Perez M, Peri L, et al Kidneys from donors with inci-dental renal tumors: should they be considered acceptable option fortransplantation? Transplantation 2013 Feb 14[5] He B, Mitchell A, Lim W, Delriviere L. Restore kidney graft from urologistreferrals for renal transplant. 24th Int Congr Transpl Society July 19, 2012,Berlin, Germany (Transplantation: 27 November 2012 - Volume 94 - Issue -p 1093
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
337
Australian Supporting Leave for Living Organ Donors ‘‘Scheme”An innovative example of successful advocacy
Luke Toy1, Tim Mathew2, Anne Wilson3, Marie Ludlow2
1Kidney Health Australia, Canberra, Australia; 2Kidney HealthAustralia, Adelaide, Australia; 3Kidney Health Australia,Melbourne, Australia.
Every year in Australia more than 200 healthy people undergo an inva-sive, voluntary surgical procedure to become a live kidney donor. Thosewilling to donate a kidney are subjected to a number of out of pocketexpenses for the cost of the procedure. In addition, some are unable tosecure paid leave from their employment, compounding their financialsituation or presenting a potential reason to withdraw from the proce-dure. Australian live donors are characterised by a significant under-rep-resentation in the lower socio-economic quintiles.Financial hardship for live donors is an issue that KidneyHealth Australiahas been advocating for, both on behalf of and with, living donors, thosewith kidney disease, their families and carers. On 7 April 2013 the Fed-eral Minister for Health announced with Kidney Health Australia, a twoyear pilot of a ‘Supporting Leave for Living Organ Donors’ Scheme.The pilot commenced on 1 July 2013, covering live kidney and partialliver donations.The Scheme is not an incentive to donate, but is designed to help sup-port those people who wish to donate but cannot afford to due to lossof income. By extension it will assist to offset the financial stress on thedonor’s family. Under the initiative, people who are employed or self-employed can, with the support of their employer, seek reimbursementof up to the minimum wage rate per week, for a period of six weeks, in-cluding time off taken for both work-up periods and recovery.The success of the Scheme depends on a comprehensive communica-tion, media and support strategy to ensure potential donors andrecipients, their employers, and hospital staff are confident in accessingthe Scheme. Although modelling suggests the Scheme may pay for it-self over time, the strongest justification is its potential in correctingthe current burdens borne by live donors.
r 27, 2013, Volume 96 Number 10S S227
thorized reproduction of this article is prohibited.

November 27, 2013
338
Hypertension does not negatively impact post living kidneydonor residual GFR
Hatem Amer1, Hisham Elsherbini1, Harini Chakkera2, Andrew Rule11Nephrology and Hypertension and The William J von LiebigTransplant Center, Mayo Clinic, Rochester, MN, United States;2Transplant Medicine, Mayo Clinic Arizona, Scottsdale, AZ,United States.
Introduction: Hypertension is considered a contraindication to live kid-ney donation by some centers. The objective of this study was to examinethe impact of pre-existing hypertension on post donation renal function.Methods: We studied 902 living kidney donors who donated at ourcenter. Renal function was assessed at the time of evaluation byiothalamate clearance. Blood pressure was measured by in officemeasurements as well as automated ambulatory blood pressure mon-itoring. Hypertension was defined as a previous diagnosis with ongo-ing antihypertensive therapy at the time of evaluation and/or averageawake ambulatory blood pressure >135/85 mmHg. Our centeraccepts donors with mild hypertension controlled by a single agentwith or without a diuretic. Post donation renal function was measuredby repeat iothalamate clearance post donation. Residual GFR was de-fined as (Post Donation GFR/Pre donation GFR)*100. Higher numb-ers indicating greater post nephrectomy compensation.Results: 789 (87.5%) of donors were normotensive (NT) and 113(12.5%) were hypertensive donors. Hypertensive donor were older55.1±9.1 vs. 43.8±10.8 years p<0.001. Equal proportion of females56% vs. 58% p=0.6 and Caucasian race 95% vs. 97% p 0.2 (hyper-tensive vs. normotensive respectively). For all donors, residual GFRafter donation was 65.2±11.8% of pre donation levels. Age was thestrongest predictor of lower residual renal function −0.12 per yearp=0.017. Hypertensive donors had lower residual GFR 62±14 vs. 66±11%p 0.03. Adjusted for age there was no difference p=0.15. Nocturnal dip-ping status could be assessed in 845 donors. 62% were dippers(>=10% decrease in systolic blood pressure during sleep), 37% non-dippers and 1%were reverse dippers (nocturnal increase in blood pres-sure). Dipping status did not have an impact on residual GFR.Conclusion: Mild hypertension that is treated by a simple antihyper-tensive regimen did not have a negative impact on the compensatoryincreased function of the remaining kidney.
S228 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
339
Living kidney donor assessment: Challenges, uncertainties andcontroversies among transplant nephrologists and surgeons
Allison Tong1,2, Jeremy Chapman3, Germaine Wong1,2,3,Jonathan Craig1,21Sydney School of Public Health, The University of Sydney, Sydney,Australia; 2Centre for Kidney Research, The Children's Hospital atWestmead, Sydney, Australia; 3Centre for Transplant and RenalResearch, Westmead Hospital, Sydney, Australia.
Background: The assessment of living kidney donors presents uniqueethical challenges and complex psychosocial implications. This studyaimed to ascertain the perspectives of transplant nephrologists andsurgeons on living kidney donor assessment.Methods: Semi-structured, face-to-face interviews were conductedwith 110 transplant nephrologists and surgeons from 43 transplantunits in 12 countries from Europe, Australasia, and North America.Results: The challenge of defining acceptable risk to the donor wascentral to five themes identified (Figure): burden of responsibility(personal accountability, policing morality, democratic decision mak-ing, meeting legal obligations, optimizing outcomes and innovation,relinquished control); medical protectiveness (prognostic uncertainty,scepticism of donor risk perception, avoidance of undue coercion, concernsfor dubious motivations and coercion, safeguard donor well-being,ethical information disclosure); respecting donor autonomy (facilitateinformed-decision making, concede to donor risk acceptance, benefitof the doubt, donor mandate to maintain health, acceptable altruism);driving ideologies (preserving equity, championing living donation,cognisance of anti-paternalism); and contextual pressures (evolving do-nor demographic, resource limitations).
Conclusions: Living kidney donor assessment involves complexinteractions between safeguarding the donors’ welfare and respecting theirautonomy. In our opinion, authoritative and well-described transplant unitandpublic policy positions thatmakeexplicit the considerationswhichareof-ten implicit, may reduce the uncertainty within which donors are assessed.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
340
Assessment of potential renal donors using principles of theAmsterdam Forum: A single centre review
Andrew Emerson, Lincoln Dealtry, Philip O’Connell,Henry Pleass, Jeremy ChapmanWestmead Hospital, Westmead, Australia.
We reviewed the reasons for living renal donor exclusion at our centrefollowing implementation of recommendations for assessment madeat the Amsterdam forum. A retrospective audit was therefore under-taken of all 577 potential renal donors considered by our centre be-tween 6 April 2004 and 20 September 2012. Potential renal donorswere 18-70 years of age, and were all assessed to have an altruisticmotivation for donating, and being able to consent for the procedure.Results: 53 donors were rejected for non-medical reasons and 186for medical reasons. The three most common single criteria reasonsfor donor exclusion were HLA sensitisation/incompatibility (15%), im-paired renal function (13%) and impaired glucose tolerance (10%).Hypertension was the most common reason for donor exclusion whenpaired with other assessment criteria. There was an equal gender bal-ance with 52% of actual donors being female. Assessed first degreerelatives were less likely to proceed to donation than more distantrelatives and spouses.Conclusions: Introduction of the paired kidney exchange programand approaches to transplantation of ABO incompatible kidneys mayreduce donor exclusion by 15%, but data on long term follow up ofdonors with marginal medical criteria for acceptance will be requiredbefore liberalising acceptance criteria could be considered.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
400
Organ donation and transplantation - in the focus betweenmedicine, ethics and law
Helmut Arbogast1, Hans Neft2, Detlef Bösebeck31Department of Surgery, University of Munich, Munich, Germany;2Bavarian State Ministry of Health, Government of Bavaria, Munich,Germany; 3Deutsche Stiftung Organtransplantation, Berlin, Germany.
Introduction:With the aim of increasing the awareness for the neces-sity of organ donation and transplantation, in November 2001, in coop-eration between the Transplant Centre of the University of Munich, theBavarian State Ministries of Social Affairs, Education and Health andthe German Foundation of Organ Transplantation (DSO), an educa-tional project for schools was launched.Materials and Methods: After first promising events with intensediscussionswith students age 16 to 18, before graduation from high school,we expanded the invitations to junior high school students and introducedspecial events for teachers, which we see as effective multiplicators of theeducational contents. The activity, scheduled for approximately 4.5 hours,begins with a display of the legal basics of organ donation and transplan-tation, followed by a vivid interactive presentation of the work of the organprocurement organisationDSO, endingwith a quiz. A representative of thetransplant centre demonstrates the milestones of transplantation, initiallyin a historical, chronologic way. Interposed are personal presentations oftransplanted patients. The audience gets emotionally involved, by listeningto their mostly touching fate on the waiting list, but also by their successfultransplant story. Ethical questions related to the topic of organ donationand transplantation form a final discourse at the end of the clinical presen-tation. A 20-minute movie summarizing the tasks of the Eurotransplantfoundation is completing the event.Results: Meanwhile, in 110 performances, issued monthly duringschooldays, more than 6.000 students andmore than 500 teachers havebeen involved. The excellent feedback for this event is mirrored in thefirst “price for enhancing organ donation”, awarded by the GermanTransplant Society (DTG), in 2005 Its attraction is uncompromised, evenin its 12th year after launching the activity, stressed by the fact of themonthly events being booked out already at the beginning of the new year.Additionally, the most important topics are available in PDF format,intended for download for teachers and use in their classrooms, thus fur-ther spreading the open discussion about organ donation and transplanta-tion. Occasional participation of celebrities, politicians and broadcastersfurther enhance the attractivity of the event.Conclusions: The project presented demonstrates a promising way,how to deal with a frequently tabooed, ethically explosive topic, by in-formation without indoctrination and thus leads to a positive reso-nance in favor of organ donation and transplantation, and promotesthe evolution of students into responsible individuals.
r 27, 2013, Volume 96 Number 10S S229
thorized reproduction of this article is prohibited.

November 27, 2013
401
The motivation of organ donation among college studentsin the United States
Ruhul Kuddus1, Reza Sanati-Mehrizy2, Afsaneh Minaie21Biology, Utah Valley University, Orem, UT, United States;2Computer Science, Utah Valley University, Orem, UT, United States.
Background: Majority of the patients waiting for an organ is waitingfor a kidney. Living persons can safely donate a kidney and donationof a kidney by about 1% of the adult population would completely elim-inate kidney shortage. Current laws of the western nations allow organdonation only as a charity and prohibit compensation. We investigatedcomprehension and concerns of college students towards charitableand compensated organ donation.Methods: A 40-question survey approved by the Institutional ReviewBoard was conducted to collect the data. The respondents werestudents of biological sciences. The data was tabulated and analyzed.Results: The participants (n=320) include 47% males, 53% females,47% Caucasian and 53% other races, 44%married and 56% unmarriedor divorced with an annual household income of <30,000. 48 % of theparticipants had at least one person in the family with some healthcareneeds and 22% of the participants had a family member or a friendwho is waiting for an organ or had an organ transplanted. 95% of therespondents support organ donation but most have little or no idea ofthe current system of organ procurement and distribution. 48% of theparticipants thought that transplantation benefits organ recipients and39% believed that the donors should be compensated in some form.64%of the participants thought that compensationwould increase organdonation. Opinion of the participants on the ethical issues of compen-sated organ donation, organ theft rumors, brain death issues, organ har-vest from comatose patients and from prisoners and organ harvest in thedeveloping countries have been analyzed. Correlation of age, sex, eth-nic background and other aspects of the participants with their motiva-tion to organ donation are currently being analyzed.Conclusions: A large fraction of young participants supports com-pensated organ donation and considers that compensation will in-crease organ donation.
S230 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
417
International Registry in Organ Donation and Transplantation
Martí Manyalich2, Maria Paula Gómez Gómez1,Blanca Pérez Gavalda11DTI Foundation, Barcelona, Spain; 2Hospital Clínic de Barcelona,Barcelona, Spain.
Background: IRODaT is the first registry in this field, which containsstatistics of deceased/living donors and transplants. Out of the 105countries with organ donation or transplantation activity, 86 nationalreporters submit data to IRODaT during 15 years.Methods: IRODaT is a friendly, easy to use database. Reporters intro-duce the figures of their countries directly to the webpage. Experts vali-date and update the data. IRODaT staff process the information andproduce different materials to meet users’ needs and requirements. In-ternet users’ also may consult information by IRODaTwebsite.Results: During the first six month of 2013 IRODaT collected the2012 year data from more than 56 countries. Information on donationand transplantation activity is analyzed and it is noticed an improved ofthe actual deceased donor rates in some countries around the world(see Fig 1). The great numbers are detected in Finland, which its rateincreases from 17,3 in 2011 to 20.5 pmp in 2012. Belgium, increase from29.3 pmp in 2011 to 32.9 pmp in 2012; Estonia had 19.4 in 2011 and24.3 pmp in 2012, and finally the most significant rise is located inSlovenia, which increase from 15.5 pmp in 2011 to 23 pmp in 2012.
Conclusions: IRODaT is able to provide statistics within a shorttimeframe, based on a worldwide network of experts involved in organdonation and transplantation. The data have proved to be of an extremevalue to scientific programs, social and governmental bodies.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
418
Development and the global diffusion of transplantation activities
Sarah White1,2, Richard Hirth1,2,3, Beatriz Mahillo4,Beatriz Dominguez-Gil4, Mar Carmona4, Marina Alvarez4,Jose Ramon Núñez4, Rafael Matesanz4, Francis Delmonico5,6,Alan Leichtman1,21Department of Medicine, Division of Nephrology, University ofMichigan, Ann Arbor, MI, United States; 2Kidney Epidemiology andCost Center, University of Michigan, Ann Arbor, MI, United States;3Department of Health Management and Policy, School of PublicHealth, University of Michigan, Ann Arbor, MI, United States;4Organización Nacional de Trasplantes, Madrid, Spain;5The Transplantation Society, Montreal, QC, Canada;6Department of Surgery, Harvard University, Boston, MA,United States.
Background:Organ transplantation is now a global practice, performedacross high- to low-income countries. The interaction between eco-nomic, technical, socio-cultural, administrative and/or political factors in-fluencing supply and demand, and the diffusion of transplantationtechnology has not been investigated in detail.Materials and Methods: Data were obtained from the Global Obser-vatory on Donation and Transplantation, World Bank, World HealthOrganization, and the World Values Survey. Two models were fitted:a logit model in which the dependent variable was any reported organtransplantation activity from 2006-2011, and a linear regression modelin which the dependent variable was the log-transformed rate of solidorgan transplantation in 2011.Results: In amultivariate logit model, education (index combining yearsof schooling, secondary/tertiary enrollment; odds ratio [OR] per standarddeviation [SD] increase=9.2, 95%CI 1.9 - 43.2), private sector indicators(index combining ease of doing business, logistics performance;OR=12.5, 95% CI 2.5 - 63.6), and life expectancy (OR=3.2, 95% CI0.84 - 12.3) were positively associated, and mortality from cardiovascu-lar disease and diabetes (ages 30-70) negatively associated (OR=0.3,95% CI 0.1 - 1.1), with the existence of any transplantation activity after ad-justment for population size. In amultivariate linear regressionmodel, healthexpenditure from external sources >5% (b= -1.4, 95% CI -2.0 - -0.8), rateof scientific publications (b=0.9, 95% CI 0.5 - 1.2), and values orientation(self-expression vs. survival, b=0.5, 95% CI 0.1 - 0.9) were significantpredictors of volume.Conclusion: Economic development per se is not the principal deter-minant of transplantation availability: instead, uptake of transplanta-tion was predicted by educational attainment, health outcomes, andprivate sector indicators. Higher transplant volumes were predictedby self-sufficiency with respect to health resources, scientific researchoutput, and values orientation emphasizing quality of life and altruism.A limitation of this analysis is the inability to consider all possiblefactors influencing the availability of transplantation, in particular theimpact of regional/international cooperation.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
419
The analysis of discarded deceased organs in KSA
Faissal A.M. Shaheen, Besher Al Attar, Abdulla Al Sayyari,Mohamed Kamal, Michael AbeledaMedical Department, Saudi Center for Organ Transplantation,Riyadh, Saudi Arabia.
Objective: To evaluate the rate and causes of unused organs in ten-year period.Methods: A retrospective study was done during the period of 2000-2009, comprising the eligible, the actual, the utilized deceased organdonor cases and consented not harvested cases. Organs involvewere kidneys, livers and hearts.Results: From the total of 4227 reported cases as Possible DeceasedDonors (DD), 2162 (51.1%) were approached for organ donation afterdeclaration of Death, and 702 (32.5%) were consented for organ dona-tion with 635 (90.5%) harvested, while 67 (9.5%) were rejected. Fromthe 635 actual cases, 98%were consented for kidney donation includingcases from organ sharing program with GCC countries and Spain.There were 1066 kidneys retrieved locally, 1009(94.7%) of them wereutilized, and 57 (5.3%) were not used. All in all, 653 (93%) cases wereeligible for liver donation, 249 (38.1%) of which were rejected for utilizingmainly due to hypernatremia and elevated liver enzymes, 422 (64.6%)cases were harvested while 323(76.5% from the harvested cases) wereutilized with 99 (23.5%) unused. There were 596 (84.9%) eligible forheart donation with only 84 (14.1%) were used as whole heart and296 used as a source for valves.
r 27, 2013, Volume 96 Number 10S S231
thorized reproduction of this article is prohibited.

November 27, 2013
Conclusion: The rate of rejection to harvest were 10.13% for kidneys,34.41% for liver and 36.92% for heart, mainly as a result of the donorqualities, while the rate of unused organ after harvesting is around19.14%, usually due to characteristics itself. Still, we could lessenthe rate of rejection by preventing technical reasons and the muchneeded improvement in the area of donor management.
Keywords: Deceased Donors, Unused Organs, Rejection Rate,Saudi Arabia
References:[1] Int J Org Transplant Med 2012; Vol. 3 (4)
[2] Rao P. et. al. Donor Factors affecting Graft Outcome: the KidneyDonor Risk Index.[3] SRTR database 69,440 transplant. Transplantation 2009; 88:231-6[4] Tuttle-Newhall J. et.al., Increasing Demand Necessitates the Useof More Expanded Criteria Donors. 2008 OPTN/SRTR Annual Report[5] SCOT DATA. Annual Report 2008-2010 Ministry of Health, Kingdomof Saudi Arabia. www.scot.org.sa
S232 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
420
Living Donor Registry (LIDOBS Community)
Ana Menjivar2, Xavier Torres2, Josep M. Peri2, Ignacio Revuelta2,Fritz Diekmann2, Constantino Fondevila2, Santiago Sanchez2,David Paredes1,2, Chloe Balleste1, Marti Manyalich1,21School of Medicine, University of Barcelona, Barcelona, Spain;2Hospital Clinic of Barcelona, Barcelona, Spain.
Introduction: Nowadays, there is no any central database for LivingDonation practices in Europe. Living Donor Observatory (LIDOBS) amultidisciplinary team of international experts in the field, is concernedinto developing a central database for these practices.Such registry will ensure a rich resource of information for Europeantransplant community and will be very useful for all the centers apply-ing Living donors (LDs) practices.Objective: To develop an on-line simplified registry model for LDs withcentral database reports to an international level.Methods: LIDOBS registry use the database created previously dur-ing EULID project (European Donation and Public Health) and testedfor EULID participating countries.The registry data are classified in three levels:1st Transparency: Include the mandatory data.2nd Security: Include the recommended data of clinical pre and postdonation parameters.3rd Quality of donation programs: Include excellence data representingthe quality of donation programs. All these data are collected by the appli-cation of the questionnaires for LD satisfaction and psychosocial follow-up.Results: LIDOBS registry is active and being used for the researchprojects European and Spanish that LIDOBS group is running out.Currently there are more than 1600 registered LDs with mandatory datafrom 19 centers in 13 European countries. 1461 out of these are KidneyLDs and 162 are liver LDs. This divergence is due to the superiority innumber and operative centers for Kidney LDs programs.Conclusions: An online database is useful to simplify the registrationand analysis processes, increasing the quality of the disposable infor-mation on LDs as well increasing the quality of the programs.All registries offer the opportunity to promote results and experienceson donation and transplantation activity development.A great gratitude goes to all the professionals from all the participantcentres that were involved in the following projects: ELIPSY projectEULID project FIS project (co-founded by European Regional Devel-opment Fund FEDER).
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
421
Patients’ attitudes towards living kidney donation: Systematicreview and thematic synthesis of qualitative research
Camilla S. Hanson1,2, Steven Chadban3, Jeremy R. Chapman2,4,Jonathan C. Craig1,2, Germaine Wong1,2,4, Allison Tong1,21Sydney School of Public Health, The University of Sydney, Sydney,Australia; 2Centre for Kidney Research, The Children’s Hospital atWestmead, Sydney, Australia; 3Transplantation, Royal Prince AlfredHospital, Sydney, Australia; 4Centre for Transplant and RenalResearch, Westmead Hospital, Sydney, Australia.
Living donor kidney transplantation can offer optimal clinical outcomesfor recipients compared with dialysis or deceased donor transplants.However, decision-making can be complex for patients, given themedical and psychosocial risks to donors. This study aimed to de-scribe the beliefs, attitudes, and expectations of patients with chronickidney disease (CKD) towards living kidney donation. We conducteda systematic review of qualitative studies of patients’ attitudes towardsliving kidney donation using a comprehensive literature search to Feb-ruary 2013. Thematic synthesis was used to analyse the findings.Thirty-seven studies involving 1732 patients with CKD (stages 1–5) wereincluded. We identified five major themes: prioritising health (better graftsurvival, urgency and desperation, resuming normal life, accepting risk,active self-advocacy); burden of responsibility (jeopardising donor health,anticipated donor regret, fear of graft failure, donor inconvenience); sen-sitive and cautious communication (donor initiation, respectful communi-cation, decisional pressure, donor unsuitability, lacking self-efficacy,emotional vulnerability); shifting relationship dynamics (strengthenedbonds, tension and conflict, unrelenting indebtedness, maintainingself-reliance, renegotiating relationship roles); and support structures(religious altruism, family loyalty, limited professional support).Patients believed a living kidney donation could offer a lifesavingtreatment with minimal medical risk to themselves or donors. How-ever, patients felt accountable for potential adverse outcomes likegraft failure and donor health complications, and feared their donorwould regret their decision to donate. Initiating discussions with po-tential donors was emotionally challenging for patients. Clarifying,validating and addressing these concerns, coupled with educationand psychosocial support can empower patients to make informeddecisions about living kidney donation.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
422
European living donor psychosocial follow-up (Elipsy Project)
Marti Manyalich1, Ana Menjivar2, Ingela Ferhman-Ekholm3,Christian Hiesse4, Leonidio Dias5, Christina Papachristou7,Niclas Kvarnström3, Levent Yucetin, Xavier Torres2, Josep M. Peri2,Inês Carvalho2, Fritz Diekmann2, Ignacio Revuelta2, David Paredes2,Constantino Fondevila2, Entela Kondo21School of Medecine, University of Barcelona, Barcelona, Spain;2Hospital Clinic of Barcelona, Barcelona, Spain; 3KarolinskaUniversitetssjukhuset, Stockholm, Sweden; 4Hôpital Foch, Paris,France; 5Centro Hospitalar do Porto, Porto, Portugal; 6CharitéUniversity Hospital Berlin, Berlin, Germany; 7Medical ParkAntalya Hospital Complex, Antalya, Turkey.
Introduction: ELIPSY project, co-funding by EAHC aims to develop acommon methodology for EU countries to assess/follow-up the psy-chosocial sphere of Living Donor (LD).Objective: To contribute guaranteeing high quality living organ dona-tion programs, by creating a follow-up model for LDs psychologicalwell-being, Quality Of Life (QOL) and the impact of recipients’ out-come on the donor and donors’ perception of donation process.Methodology:Working tasks:1. Current psychosocial follow-up practices: LD’s assessment/follow-up
methodology among partner’s centers.2. Donor follow-up methodology: Evaluate the psychosocial well-being,
QOLof LDbefore andafter donation and the impact of donation process.3. Recipient follow-up: Design a recipient follow-up methodology to
correlate recipients’ outcome with the LDs psychosocial sphere.
Studies:
1. Prospective: Assessing short-term outcome (percentage of changebetween pre-donation and one year after) of LDs to detect andcharacterize worsening of psychosocial status.
2. Retrospective: Identifying long-term impact (up to five years) of livingdonation and recipient/graft outcome in LDs psychosocial sphere.
Results: Survey about current psychosocial assessment/follow-uppractices was conducted in 52 centres from 10 countries. Resultsshow no consensus among the centres.Prospective study shows no changes in the psychosocial outcome of87 LDs assessed before and after donation, within the range ofhealthy general population.Retrospective study shows no significant differences in the psychoso-cial outcome of 302 assessed LDs compare to the healthy generalpopulation.Conclusions: LDs assessed by ELIPSY methodology go well both atshort and long term follow-up.ELIPSY project contributes for the harmonization of LDs psychosocialfollow-up practices promoting high quality LD programs.A great acknowledgement goes to all the professionals from the sixparticipants centers that were involved in all the stages of the project.
r 27, 2013, Volume 96 Number 10S S233
thorized reproduction of this article is prohibited.

November 27, 2013
423
Mortality in patients with potential living donor liver awaitingliver transplantation
Hussien Elsiesy, Rania Alarieh, Zohor Mubaraki, Faisal Abaalkhail,Almoutaz Hashim, Hamad Albahili, Waleed Alhamoudi,Mohamed AlsebayelLiver transplantation, KFSH&RC, Riyadh, Saudi Arabia.
Background: Living donor liver transplantation has the advantage ofavoiding the long waiting time for cadaveric liver transplantation withpossibility of decreasing mortality before liver transplantation.Objective: To identify the mortality in patients with decompensatedcirrhosis with potential living donor during the evaluation process forboth donors and recipients before liver transplantation.Methods: We retrospectively reviewed our records for patients withliver cirrhosis requiring liver transplantation that has a potential donor,the number of donors evaluated for each candidate, the mortality dur-ing the evaluation process either related to complication of liver dis-ease or progression of hepatocellular carcinoma (HCC).Results: Out of 370 liver cirrhosis patients with potential living donorfor liver transplantation, 102 died (27.6%), 79 died related to complica-tion of liver disease and 23 related to HCC progression.The mortality increased as the number of donors evaluated increase,it was 27.6% for patients with one or two donors (86 out of4=311),37% for patients with 3 donors evaluated (13 out of 35), and 50% withfive or seven donors evaluated (2 out of 4). We do not have a MELDlimit for living donor and patients with MELD >25 are discussed incase to case bases, and the donor work up time from 2 to 18 days (av-erage 10 days).Conclusion: The mortality is high in patients with potential living do-nor liver transplantation, with increase in mortality as the number ofpotential donors increase.This may be explained by the time needed for the donor evaluation aswell as late referral.King Faisal Liver Group
Reference:None
S234 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
424
A prospective audit of 50 retrievals in 12 months by a singlesurgeon: The good, the bad and the ugly
Henry Pleass, Lawrence Yuen, Vincent Lam, Brendan Ryan,Wayne Hawthorne, Richard AllenWestmead, Westmead Hospital, Sydney, Australia.
Over a 12 month period all deceased organ donor procedures performedby a single surgeon were prospectively recorded. In total 50 deceased do-nor procedures were attempted during this time.Of these 38 were brain dead donors (DBD) and 12 were DCD donors.Looking at the DBD donors more closely only 1 was a Kidney only do-nor, the other 37 being multi organ procedures. 6 Livers were split insitu in addition to kidney and Pancreas retrieval. There were 19 LiverKidney retrievals, 7 Liver Kidney Pancreas and 2 Liver only retrievalswhere the kidneys had no suitable recipients. 4 livers were deemedunusable because of either severe steatosis or fibrosis (11%).There were 12 DCD donors and of these, only 2 failed to progress dur-ing the 60 minute time frame. 2 DCD donors were deemed suitableLiver donors although only 1 was subsequently transplanted. The re-mainder was Kidney DCD donors, with or without Lung retrieval.Over 12 months no Livers were deemed unusable because of retrieval in-jury. All split Liver procedures resulted in the Transplantation of both anadult and child in each case. Only 1 kidney was deemed untransplantablebecause of an intimal tear within the renal artery, although the kidney itselfhad been well perfused in the donor.In conclusion deceased donor procedures remain complex, largelymulti organ and mainly DBD donors within NSW. As only 1 procedurewas a Kidney only donor during this study period, this has costimplications for providing a skilled readily available retrieval service,capable of retrieving all abdominal organs and splitting Livers to max-imise organ utilisation. This remains a vast and largely untapped train-ing opportunity for surgeons within NSW. Organ quality is fed back tothe retrieval surgeon by way of an organ retrieval report form, filled outby the recipient surgeon. These forms are reviewed in NSW, by thestate Transplant Advisory Committee and also by the Deceased donororgan procurement service committee to ensure optimum outcomesand the prevention of iatrogenic organ injury.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
425
A review of perioperative staffing and competence levels fornational organ retrieval teams in the United Kingdom
John Stirling, Ian CurrieScottish Organ Retrieval Team, NHS Lothian, Edinburgh,United Kingdom.
Organ retrieval from cadaveric donors in the United Kingdom is under-taken by National Organ Retrieval (NORS) teams. Organ preservationtechniques are developing rapidly, with new technologies includingNormothermic Regional Preservation and ex-situ normothermic pres-ervation now emerging into clinical practice. Currently organ preserva-tion is often undertaken by Specialist Nurses in Organ Donation whoalready have significant other commitments during the organ retrievalprocess. Increased complexity in surgical retrieval and organ preser-vation requires highly trained individuals working to a national compe-tence framework to undertake these roles. As workload increases,and roles become more complex, Specialist Practitioners in OrganRetrieval and Transplantation are emerging. Adequate staffing numbersand competence levels are critical for quality in organ retrieval and preser-vation. The staffing levels recommended in theNORSstandards fall belowthat required by the Association for Perioperative Practice. Additionally,new competencies need to be developed to support staff from differentdisciplines that are developing specialist knowledge in organ retrievaland preservation. The composition and competence levels of NORSteams should therefore be reviewed to ensure cadaveric organ donors re-ceive the same level of care as other patients in the operating room.Submitted on behalf of the Scottish Organ Retrieval Team
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
430
Donor action per Vital-Link in Korea
Soon KimSurgery, Yonsei University Health System, Seoul, Korea.
Since the establishment of government driven organ donation network(KONOS) and deceased donor organ transplantation Acts for organ trans-plantation in 2000, the patients on deceased organ donor waiting list wereincreased more than 6 folds for the last decade in Korea. To increase thenumbers of deceased organ donor per sophisticate donor action and pub-lic education, the members of “The Korean Society for Transplantation”embarked Vital-Link Korea in October, 2009. After then, Vital-Link Koreahadmade a lot of efforts for publishing books and booklets relevant to organdonationand transplantation for public educationaswell as hostedmanydo-mestic and international forums to establish a solid supporting system in or-gan and tissue transplantations in Korea. Per the effort of Vital-Link Korea,we had 2nd renewed version of deceased donor organ transplantationActs inMay, 2010 andwe had 409 deceased organ donors in 2012whencompared to 261 in 2009 and 52 in 2000.
r 27, 2013, Volume 96 Number 10S S235
thorized reproduction of this article is prohibited.

November 27, 2013
431
Changes of public recognition for organ donation in Korea
Kyung Sook Jang1, Eun Joo Lee2, Han Duk Jung3, Sun Hee Kim2,Jon Won Ha5,61Donation Support Deptartment, Korea Organ Donation Agency(KODA), Seoul, Korea; 2Public Relations Department, Korea OrganDonation Agency, Seoul, Korea; 3Division of Donation SupportDirector, Korean Network for Organ Sharing, Korean Center forDisease Control, Seoul, Korea; 4Chief Operating Officer, Korea OrganDonation Agency, Seoul, Korea; 5Department of Surgery, SeoulNational University College of Medicine, seoul, Korea; 6President,Korea Organ Donation Agency, Seoul, Korea.
To increase the organ donation, public awareness for brain death and or-gan donation is important. We analyzed survey data to find out what isthe effective public promotion method and direction.Method: Two surveys were performed in 2009 (1,346 answers) and2012 (1,002 answers) including donor family, medical professionals,and general public. The proportion of general public was more in 2012.Result: Knowing the concept of organ donation increased mildly (from93.4% to 97%). However, the proportion of having only basic knowledgeof organ donationwas 62.1% in 2009, which increased to 73.8% in 2012.Those who know the whole procedure of organ donation also increasedfrom 3.3% to 23.2%. Most of information was obtained through TVand itwas more in 2012 (from 84.6% to 89.4%). Information posted in hospital(31.1%), friends and colleagues (29.2%), newspapers (24.5%), and in-ternet (14.6%) followed next in 2012. However, dependence on newspa-per decreased from 35.1% in 2009 and hospital information was anothermajor source of information in 2012.Conclusion: Ratio of people with full knowledge on organ donationand its process increased 20%, which reflects the effect of public ed-ucation as well as medical professional education. General public ac-quire information mainly via TV, the strategy to use multimedia such asTV and newspapers should be developed.
S236 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
432
Characteristics and preliminary determinants of family consentregarding organ donation from 4 Melbourne hospitals
Claudia Marck1, Sandra Neate2, Michelle Skinner3,Bernadine Dwyer3, Tracey Weiland1, George Jelinek11Emergency Practice Innovation Centre, St Vincent's Hospital,Melbourne, Australia; 2Emergency Department, St Vincent's Hospital,Melbourne, Australia; 3DonateLife Victoria, Melbourne, Australia.
Family consent rates for deceased organ donation (OD) are below60% in Australia[1]. To better understand the experiences and decisionmaking process when next of kin (NOK) of potential donors are askedto consent for OD we are collecting data from 4 hospitals in Melbournewith the aim of interviewing 30-40 NOK. Data is collected if OD wasdiscussed with the NOK of a potential donor, except for cases wheredonation was considered unlikely to proceed due to lack of medicalsuitability or the patient was unlikely to die in the required timeframefor donation after cardiac death (DCD). NOK receive information aboutthe study 6 weeks after the death and are invited to participate byphone 2 weeks later. Data collection is ongoing, but preliminary analy-sis shows that of the 108 potential donors identified for inclusion in thestudy, 59% were eligible for DCD, most were identified in the ICU(83%), 61 were male and the median age at death was 59 years. Ofthe 53% (57) where consent for OD from NOK was obtained, 7 were“intended donors”, organ retrieval did not commence; 10 were “plannedDCD”, DCD did not occur; and 40 were “organ donors” of which 35%DCD donors. 51 were “non-consent” where the NOK declined consent,of which 70% potential DCD donors. Consent was not related to gender,age, or religiosity, but was significantly related to country of birth, withthose born in Asia or Oceania less likely to consent (8%) compared tothose born in Europe (55%) or Australia (68%, p=0.001). Non-Englishspeaking families were also less likely to consent for OD compared toEnglish speaking (8% vs 61% p<0.001). Of those 63 invited, 35 agreed(including 12 non-consenting NOK) to be interviewed to explore theirexperiences and decision making related to the consenting and OD(qualitative data presented elsewhere). Interviews took place on aver-age 91 days after the death. Additional data collection and analysis willprovide further understanding of factors related to family consent.
Reference:[1] Opdam, H.I. andW. Silvester: Potential for organ donation in Victoria:an audit of hospital deaths. Med J Aust 2006, 185(5): 250-254.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
433
Introducing simulation training to improve the organdonation conversation
Ellie McCann, Jonathan GatwardNSW Organ and Tissue Donation Service, Sydney, Australia.
Simulation training within a protected learning environment providesunique opportunities for clinicians to rehearse realistic clinical scenariosand actively participate in role playing within a team setting. Key to thesimulation learning experience is a facilitated debriefing session whereexamples of good practice and areas for improvement are discussed.Together, these processes trigger ongoing reflection about participants’knowledge, skills and attitudes.We developed a simulation course to consolidate skills acquired fromthe National Education Program, as part of the overall training re-quired to become a Designated Requestor: the specially trained clini-cian that will conduct the sensitive organ donation conversation andprovide information and support to families considering the opportu-nity to donate.Our course gives participants the opportunity to rehearse, review and re-flect on the difficult ‘family conversation’ in a simulation setting, usingprofessional actors. The aim of the course is to increase participants’confidence in undertaking the family conversation in clinical practiceand to better support families through the decision making process.Real scenarios are used with professional actors in the role of familymembers. The debriefing process is led by qualified experts and utilisesvideo review and feedback from the actors, both ‘in’ and ‘out-of-character’.This program was piloted in 2012 and formally commenced in January2013. To date, one pilot and five training sessions have been conductedwith 35 participants. Further sessions are scheduled for 2013 and it isanticipated that the program will continue to develop beyond this time.Evaluations have been overwhelmingly positive with 70% of participantsrating the training as outstanding, with requests to provide it regularly asa ‘refresher’ course.Our presentation will highlight the value of simulation training in improv-ing end of life conversations including those involving organ donations.The Royal Prince Alfred Hospital, Sydney
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
434
ETPOD dissemination: The transferability of a successfulEuropean training program
Gloria Paez1, Marti Manyalich1,2, Xavier Guasch3, Ricard Valero1,2,Melania G. Istrate11TPM-DTI Foundation, Barcelona, Spain; 2Hospital Clínic deBarcelona, Barcelona, Spain; 3Hospital de la Plana, Villarreal, Spain.
Background: The European Training Program on Organ Donation(ETPOD) is a successful educational initiative addressing 3 different pro-fessional levels in organ donation that achieved a significant improve-ment in both numbers of utilized donors and organs recovered [1]. Onetraining program developed is “Training for Trainers” that aims at provid-ing key donation professionals with the skills required to replicate the“Essentials in Organ Donation Training seminars” (EOD).Objectives: The aim of this study is to ensure the continuity and trans-ferability of the ETPOD training program, disseminate the educationaltools created and analyze dissemination impact.Methods: A dissemination strategy was developed to ensure ETPODcontinuity and transferability. Due to its successful outcomes, ETPODparticipants were encouraged to continue the implementation of EODs.Moreover, participants from 22 countries, belonging to the European Trans-plant Network (ETN) and the Mediterranean Transplant Network (MTN),benefitted from Training for Trainers Programs and implemented EODs.The impact of ETPOD results reached non-participating countries anddue to its feasibility, new organizations expressed their interest to im-plement the training program in their countries.A database was created (http://www.etpod-dissemination.eu) to followup the EODs carried out.Results: Since 2009whenETPOD finished, a total of 172 EODseminarshavebeen carried out and8477 healthcare professionals trained as follow-ing: 71 EODs and 4223 professionals trained by ETPOD participants,98 EODs and 4195 professionals trained in the ETN and MTN countries,3 EODs and 59 professionals trained by Life's Donor, São Paulo, Brazil.Conclusions: ETPOD, a successful training that produced significantimprovements in organ donation, has been continued reaching out ahigh number of professionals worldwide.
Reference:[1] Manyalich M, Guasch X, Paez G, Valero R, Istrate M and theETPOD partner consortium: ETPOD (European Training Program onOrgan Donation): a successful training program to improve organ do-nation. Transpl Int 2013 Apr;26(4):373–84
r 27, 2013, Volume 96 Number 10S S237
thorized reproduction of this article is prohibited.

November 27, 2013
435
Create an interactive eLearning portal to increase staffknowledge and understanding of the organ and tissuedonation process.
Karli Brkljacic1, Kelly Rogerson2, Nicola Stitt1,21Intensive Care Unit, Monash Health, Melbourne, Australia;2Donatelife Victoria, Melbourne, Australia.
Introduction: A key activity of the Australian Organ and Tissue Au-thority (The Authority) 2009 health reform was employing specialistdonation staff (SDS) dedicated to improving organ and tissue donationprocesses in hospitals. Monash Health (MH) which is Victoria’s largesthealth service has experienced a threefold increase in Organ donationsince the implementation. Alternative methods of education deliveryhave eventuated to meet staff need. The paper reports on the devel-opment of an E Learning Portal to deliver interactive accessible edu-cation to staff.Methods: SDS utilised a strong knowledge base, and linked with an ex-ternal IT consultant to place clinical knowledge in a usable interactive for-mat. Four modules were proposed by the SDS. The first was theNational Clinical (GIVE) trigger. This module was launched in February2012.The GIVE Trigger is used in all Emergency Departments and In-tensive Care units to identify potential donors. This was subsequentlyfollowed by the second module, Eye and Tissue donation, which waslaunched in October 2012. This module was designed for all medicaland nursing staff.Results: 1000 MH staffs have completed the online modules. Organand tissue donation recognition, approach and consent rates are atan all-time high for the organisation which can be partly attributed toan increased awareness and understanding formed from the E Learn-ing portal.Conclusions: Due to the success of the E Learning Portal in MH,Donatelife Victoria has engaged with the SDS to launch both modulesacross Victoria and New South Wales. E learning activities are nowstrategic activities at a National Level.
S238 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
436
How eLearning is utilized to augment the classroom trainingof donation professionals
Robert J. Norden, Cherry P. Wise, Theresa A. Daly,Patricia A. Mulvania, Howard M. NathanGift of Life Institute, Philadelphia, PA, United States.
Background: For nearly ten years, an international training institutefor donation professionals has offered interdisciplinary resources forskill-based learning. Recognizing that its training audience is increas-ingly digital-native, the institute offers eLearning—a tool that providesanywhere, anytime instruction over the web—to augment its tradi-tional classroom-based model.Aim: By offering eLearning as a tool to provide fundamental conceptsprior to classroom training, instructors can better manage time to en-gage learners through skill-building and problem-solving.Results: Since July 2012, eLearning has been utilized in five separateon-site trainings, resulting in classroom sessions more focused on practi-cal application. Facilitators spend significantly less time lecturing andmoreon deepening the understanding of complex donation-related issues. Astestament to the effectiveness of eLearning, of the 54 participants whoresponded to a survey, 89% stated they Strongly Agree/Agree that theyWould like to seemore eLearningmodules in the future; 9%Neither Agreeor Disagree; 2% Disagree. When the same learners were asked if theyWould recommend these modules to others, 91% either Strongly Agree/Agree and 9% Neither Agree or Disagree.Materials and Method: Toestablishabase knowledgeamongparticipantsprior to classroom training, the institute offers 15 self-directed modules on do-nation-related topics. Tomaximize learner engagement, instruction is providedthrough text, audio, and video. Knowledge checks and a final assessment areused to gauge comprehension, with results documented in a learning man-agement system.Conclusion: In addition to the inherent benefits of providing on-demandtraining and the ability for learners to revisit training topics on an ongoing,as-needed basis, eLearning offers classroom participants with moreskill-practice and problem-solving opportunities.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
437
One OPO’s experience using online role-play tool to increasedonation professionals’ skill and confidence level in leadingfamily conversations for organ donation
Theresa A. Daly1, Patricia Mulvania2, Robert Norden1,Howard Nathan11Gift of Life Institute, Philadelphia, PA, United States; 2Gift of LifeDonor Program, Philadelphia, PA, United States.
Background: Int’l training institute uses medical school online role-play tool to augment donation professionals (DP) family donation con-versation (FDC) training, provide focused feedback and improve skilland confidence. Training institute offered tool to OPO to do same withits DPs and assess for ongoing use.Aim: Increase skill and confidence levels of DPs leading FDCs as re-search indicates improved DP confidence in leading FDCs is associ-ated w/higher authorization rates.[1]Materials and Methods: Tool offered opportunity for interactive skillspractice and to assess, coach and improve staff judgment andcommunications skills. OPO leadership trialed use of tool to augmentworkshop training and increase skill and confidence through one-on-one remediation.Results: Initial feedback from coaches, leadership and DPs was pos-itive and indicated improved skill and confidence levels. When DPswere asked about impact on confidence levels leading FDCs AFTERusing tool, 80% said Very Good-Good; 80% reported Extremely toVery Satisfied when asked to rate his/her experience using the tool;and 80% reported the feedback received from the coach was Ex-tremely to Very Valuable. The OPO determined tool important enoughto integrate into existing formal training program. Tool will be used fororientation sign off, annual training, improvement plan and staffrequested practice. It is too early to measure impact on long term au-thorization rates.Conclusion: Research indicates that higher confidence levels leadinga FDC correlate to higher authorization rates. Confidence comes fromexperience and practice. OPOs are challenged to provide adequateone-on-one training opportunities to strengthen skill and build confi-dence. [1] Based on a survey of initial use of the online role-play tool,confidence levels in leading family donation conversations increasedand the OPO is formally integrating this tool into its training with ex-pectation that it will contribute to long term increased skill and autho-rization rates.
Reference:[1] Siminoff L, Gordon N, Hewlett J, Arnold R: Factors influencing fam-ilies’ consent for donation of solid organs for transplantation. JAMA2001, 286(1):71-77.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
438
Trial of education program of in-hospital coordinators in Japan
Norihide Fukushima1, Setsuko Konaka1, Mayumi Yasuhira21Department of Therapeutics for End-Stage Organ Dysfunction,Osaka University, Suita, Japan; 2West Japan Branch, Japan OrganTransplant Netwrok, Osaka, Japan.
Objectives: Although the Japanese Organ Transplant Act was revisedin 2010 and brain dead organ donation increased from 13 to 45 casesin a year, the number was still extremely smaller than other developedcountries. In these circumstances, In-Hp Cos may play great roles in in-creasing organ donation andmaking procurement procedure smooth. Inthe present study, our Education Program of In-HpCos is described andthe future of education program of In-Hp Cos in Japan is discussed.Materials and Methods: In May 2012, our Department started the Ed-ucation Program of In-Hp Cos. In the first semester, two-hour lecture areprovided every two weeks for 5 months to 10 to 20 In-Hp-Cos. Most ofthem are working near Osaka. In the second semester, twenty lectureswere provided for continuous three days to 32 In Hp Cos. Two third ofthem are working far from Osaka,The topics of lectures are history of Organ transplantation in Japan andin the world, the current status of organ donation and transplantation inJapan, the social regulation of organ donation, care of transplantrecipients, overall procedures of organ donation (brain dead and dona-tion after cardiac death), the role of In-Hp Co, donor family care, and do-nor indications, and donor assessment and management. There arealso simulation of organ donation process inwhich every participant playtheir special role and group discussion of family care.Results: Regards to opinion survey of participants after the program,most of participantswere satisfiedwith the program, topics and duration.Asmost of them are not a full-time In-Hp, they prefer to attend 3-day pro-gram. Although not so many organ donations have not been performedin hospital in which the participants are working, many participants arenow working main In-Hp Cos and establishing their own organ donationsystem in their hospital.Conclusions: To establish organ procurement system and increaseorgan donation, In-Hp Cos have great roles in Japan. However, nonewas a full-time In-Hp Cos and most In-Hp Cos required more profes-sional education. This program may help to establish systematic edu-cation program for each occupation in Japan.
r 27, 2013, Volume 96 Number 10S S239
thorized reproduction of this article is prohibited.

November 27, 2013
445
Potential and evolution of organ donation in Galicia(Spain) 2006-2011
Jacinto Sanchez-Ibañez, Marta Alvarez Vazquez,Encarnacion Bouzas CaamañoRegional Transplant Coordination, Galician health Service, Santiagode Compostela, Spain.
Aim: To describe the potential for donation in Galicia and to study itsevolution in the last 6 years,Material and methods: We analyzed all ICU deaths (ICUDs) from2006-2011, specifically all with intracranial diseases (ICDs) that candevelop brain death (BD), their evolution to BD and to donor. We eval-uated the age impact and the cause of death in the total number ofBDs and organ donors.Results:We analyzed 9,280 ICUDs where we knew the cause of death(98.7% of the total number of ICUDs from all the authorized hospitals).27.4% died from ICDs, of whom 37.8% developed BD, 52.8% of thesefinally becoming organ donors. The median age of ICUDs was 71 yearsold, 68 years old for the ICDs. The most frequent causes of death in theICD group were cerebrovascular accident (59.2%), non traffic braintrauma (15.2%) and anoxia (14.4%). During 2006-2011 the ICUD per-centage decreased by 11%, ICDs decreased by 12.8%, especially cere-brovascular accident and traffic brain trauma. Nevertheless the totalnumber of BDs and donors has been maintained. The median age ofICUDs and ICDs was maintained but BD increased from 61 to 71 yearsold and actual donors from 58 to 60 years old. These figures variedslightly between hospital with or without neurosurgery but the trendwas the same.Conclusion: ICUDs is decreasing progressively, including from ICDsin all the hospitals. Nevertheless the total number of BDs and organdonors remain constant, probably due to the ongoing improvementin the work done by hospital transplant coordinators.
S240 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
446
Educational efforts impacting on critical care staff's attitudestowards donation: Donor action data from Korea and Japan
Beatrice Pelleriaux1, Jongwon Ha2, Tomonori Hasegawa3,Jacqueline Smits4, Leo Roels11Donor Action Foundation, Linden, Belgium; 2Korea Organ DonationAgency, Seoul, Korea; 3Toho University School of Medicine, Tokyo,Japan; 4Eurotransplant International Foundation,Leiden, Netherlands.
Background: Critical Care (CC) staff’s attitudes towards donation varybetween professional categories, hospitals and countries, depending,amongst other co-factors, on educational efforts, and, hence, may influ-ence donation rates.Methods: 17,860 Donor Action (DA) Hospital Attitude Survey (HAS)questionnaires (Korea: n=1,454, Japan: n=16,406), collected betweenJanuary 1, 2010 and December 31, 2012, were entered into the DAdatabase to compare CC staff’s attitudes towards donation as wellas their confidence levels with donation related tasks and their trainingneeds. In Korea, a governmentally supported educational program byskilled transplant coordinators (81 training sessions in 27 hospitals)preceded this survey.Results: General support for donation was higher amongst Koreanmedical/nursing (M/N) staff (87.3%) compared to their Japanesecolleagues (73.1%, P <.0001). Whilst 52.3% of Korean M/N staff woulddonate their own organs, only 41% of Japanese colleagues would doso (P<.0001). In Japan, 22.3%ofM/N staff would object to donating theirrelative’s organs, versus only 15.4% in Korea (P<.0001). Confidencelevels with referring a potential donor, explaining brain death (BD) or in-troducing the subject of donation were 66.9, 48.3 and 31.7% respec-tively amongst Korean staff, against only 9.5, 2.9 and 2.6% in Japan(P<.0001). BD was accepted as a valid determination of death by84.6% of medical and 63.3% of nursing staff in Korea, versus only60.9 and 32.9% in Japan (P<.0001). In Korea, 27% of medical and17% of nursing staff on average had received specific training on organdonation related issues vs. only 6.5 and 4.5% in Japan (P<.01).Conclusions: Data presented suggests a strong correlation betweenself-reported attitudes, skills and confidence levels and specific educa-tion received in 2 neighbouring Asian countries with an otherwise com-parable socio-economic, technical level and religious background.Further investigations to understand the subtle cultural disparities thatmay explain diverging relationships amongst CC and transplantprofessionals may help to adapt and export the ‘Korean model’ oftargeted training of CC staff to other Asian countries and will ultimatelyincrease donation rates in these countries.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
448
Kidney transplantation from donors with acute kidney failurereceiving haemofiltration.
Jo Sanders1, Hayley Furniss1, Helen Opdam1, Daryl Jones1,21DonateLife Victoria, DonateLife, Carlton, Australia; 2Intensive CareUnit, Austin Health, Heidelberg, Australia.
Acute kidney failure (AKF) is common in critically ill patients but gen-erally resolves with non invasive treatment. Some patients may re-quire haemofiltration to ensure adequate renal function during theacute kidney impairment episode. More than 90% of acute renal fail-ure resolves with resolution of critical illness. Despite this, kidneysfrom potential donors with renal impairment have traditionally beenconsidered unsuitable for transplantation due to the concern of poorrenal recovery and function post transplantation.We aim to report the Victorian experience of facilitating cadaveric donationin patients with established acute kidney failure requiring haemofiltration,to demonstrate that such donations can result in successful kidney trans-plantation. A retrospective analysis of all organ donors from 2008 to 1st
July 2013 was undertaken to identify the number and outcomes, of renaldonations in the context of acute kidney failure.625 donors were reviewed, identifying 293 who had at least one epi-sode of oliguria (oliguria = <20ml/hr UO) throughout admission. Ofthese oliguric donors, eight donors were identified to have receivedhaemofiltration for renal impairment treatment during their hospital admis-sion prior to donating their kidneys. Fifteen successful kidney transplantsresulted, with one kidney not transplantable due to surgical complications.The kidney recipients were followed up for one year to five years posttransplant and have shown favourable outcomes.As there is a widening gap between the number of patients needingkidney transplantation and number of kidneys available for transplan-tation, strategies should be developed to expand the kidney donorpool. We have demonstrated that utilising kidneys from deceaseddonors with established AKF requiring haemofiltrtion should be con-sidered as one strategy to overcome the current shortage of kidneys.
FIGURE 1.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
450
A 17 year summary of one OPO's changing pool ofpotential donors
Gweneth O'Shaughnessy, Sharon West, Richard Hasz,Howard M. NathanGift of Life Donor Program, Philadelphia, PA, United States.
Purpose: Study characterizes one organ procurement organization’s(OPO) evolving donor demographics and donation outcomes over a17 year period of time.Methods: Characterizing donor demographics and donation outcomesallows the OPO to understand its pool of potential donors, and alignstrategies/resources. Characteristics examined: cause of death, mecha-nism of death, ethnicity, gender, and age. Outcomes examined: organreferrals, potential donors, actual donors (brain dead and donors aftercirculatory death), and conversion rates (actual donors as a percentageof potential donors).Results: Organ referrals among anoxic patients increased from 24%(200) of total referrals to 57% (2093) in 2012. In 1995, anoxic potentialdonors represented 15% of the donor pool vs 44% of the donor pool in2012. Organ donors in the anoxic pool increased from 12% (27) of to-tal donors in 1995 to 41% (171) in 2012. DCD donors represented46% of all DCD donors in 2012 (n = 65). The primary mechanism ofinjury was cardiovascular (50% in 1995; 71% in 2012). Conversionrates are higher in the ‘other’ cause of death category.
r 27, 2013, Volume 96 Number 10S S241
thorized reproduction of this article is prohibited.
Conclusion: There has been a dramatic increase in the overall volume ofreferrals, potential, and donors in the anoxic population. These patientsare typically cared for in medical/cardiac intensive care units (ICUs) vsother ICUs. To ensure that there is an optimal donation process in place,OPOs should evaluate the impact of shifting hospital development (HD)staffing resources to these areas. Although conversion rates in the anoxicdonor pool improved to 50%, other strategies should be considered to im-prove consent and conversion.

November 27, 2013
452
Family perspectives on organ and tissue donation fortransplantation: Thematic synthesis of qualitative studies
Angelique Ralph1,2, Jeremy Chapman3, Jonathan Gillis4,Jonathan Craig1,2, Phyllis Butow5, Kirsten Howard1,Michelle Irving1,2, Bernadet Sutanto1,2, Allison Tong1,21Sydney School of Public Health, The University of Sydney, Sydney,Australia; 2Centre for Kidney Research, The Children’s Hospital atWestmead, Sydney, Australia; 3Centre for Transplant and RenalResearch, Westmead Hospital, Sydney, Australia; 4Centre for Values,Ethics and Law in Medicine, The University of Sydney, Sydney,Australia; 5Centre for Medical Psychology & Evidence-basedDecision-making, The University of Sydney, Sydney, Australia.
Background: A contributing factor to the critical shortage of de-ceased organ donors is family refusal to give consent, or veto a priordecision of the donor. We aimed to describe the beliefs and views ofdonor families on organ and tissue donation.Methods: We conducted a systematic review and synthesis of qualitativestudies on family perspectives on organ and tissue donation for transplan-tation. Electronic databases were searched to September 2012.Results: Thirty-four studies involving 1,035 participants were included.We identified seven themes: comprehension of unexpected death (in-cluding sub-themes of accepting finality of life, ambiguity of brain death);finding meaning in donation (altruism, letting the donor live on, fulfilling amoral obligation, easing grief); fear and suspicion (financial motivations,unwanted responsibility of death, medical mistrust); decisional conflict(pressured decision-making, family involvement and consensus, internaldissonance, adhering to religious beliefs); vulnerability (valuing sensitiv-ity and rapport, overwhelmed and disempowered); respecting the donor(honouring the donor wishes, preserving body integrity); and needingclosure (appreciating acknowledgement, regret over refusal, unresolveddecisional uncertainty, feeling dismissed).Conclusions: Bereaved families can derive emotional benefit from the“lifesaving” act of donation but also report a sense of uncertainty aboutdeath and the donation process, vulnerability, an acute emotional andcognitive burden, and pre- and post-decisional dissonance. Educationand counselling strategies are needed to help families understand andaccept death in the context of donation, address anxieties about organprocurement, foster trust in the donation process, resolve insecuritiesand tensions in their decision-making, and gain a sense of closure afterdonation. This may improve family experiences and decision making inorgan donation.
S242 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
453
Facilitating donation after circulatory death subsequent towithdrawal of extracorporeal membrane oxygenation support
Alice Coulson1, Hazel Christine1, Carrie Alvaro1, Robert Herkes1,21NSW Organ and Tissue Donation Service, Sydney, Australia;2Intensive Care Services, Royal Prince Alfred Hospital,Sydney, Australia.
Patients dependent on extracorporeal membrane oxygenation (ECMO)for cardio-respiratory support are rarely considered for donation after cir-culatory death following agreement towithdraw treatment. In NSW,man-agement of these potential organ donors typically involves complexmedical suitability assessment and logistical planning for withdrawal oftreatment.The referral database at the NSW Organ and Tissue Donation Servicewas reviewed from 2007 to 2013. Five ECMO-dependent patients wereidentified. Four patients were supported with veno-venous ECMO forrespiratory failure and the other with veno-arterial ECMO for cardiac fail-ure from idiopathic cardiomyopathy.Consent for organ donation was obtained in four cases. The family de-clined donation in the remaining case. Of those consented hospital lengthof stay ranged from 8 to 60 days, and ECMO duration ranged from 12 to43 days. Unexpectedly, the patient supported with veno-arterial ECMOdid not die within the required sixty minutes. The remaining three casessuccessfully donated kidneys, resulting in six kidneys being available fortransplantation. Liver donation was considered in two of the donors butwas ultimately not possible due to timeframes within which the patientsdied. Medical suitability determination in all cases required thorough eval-uation of admission history and multiprofessional consultation, includingtransplant professionals.The logistics of ceasing ECMO as part of withdrawing treatment are com-plex. While the process of withdrawing treatment remains the responsibil-ity of the treating Intensive Care team, collaboration and guidance fromdonation and retrieval staff was required to ensure that management ofthe cannulae and circuit did not inhibit organ retrieval.Patients dependent on ECMO for cardiorespiratory support can be suc-cessful kidney donors with thorough assessment of suitability and col-laborative planning of withdrawal and retrieval. Liver donation may befeasible, but cessation of ECMOwas not consistent with a rapid progres-sion to death making retrieval of the liver possible.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
460
State-wide organ donation project of Western Australia
Teik Oh, Bruce PowellDonateLife WA, Perth, Australia.
The OTA Australia identified six strategic priorities. DonateLife WAembarked on a project to implement the first: Develop a clinical gover-nance framework to support and guide DonateLife Network staff in theprovision of quality organ and tissue donation services within thebroader health system.SWOT analysis explored possibilities for new initiatives, and a plan,the “State-wide Organ Donation Project” was conceived. This parentproject begets projects (below) to be developed, all with one goal -to improve organ donation services in WA.Projects: A framework of the process state-wide, agreed to by all keystakeholders, standardises and clarifies step-by-step interactions to im-prove communications, ownership, and responsibilities, thus minimisingmisunderstandings and subsequent loss of organ donation opportunities.Organ donation is relevant to all health sectors in the State but onlythree major metropolitan hospitals undertake organ retrieval. Engage-ment of regional general hospitals in the State to retrieve organs willbenefit the donation rate and engage health care professionals out-side the metropolitan area.Collaboration with community groups in partnerships in fund raising,education, and PR ventures aims to increase public awareness of or-gan donation and raise funds for projects to be undertaken.Although all health professionals support organ donation, the supportis not comprehensive. Engagement of key medical professionals withcloser ties to DonateLife WA, is envisaged with a Council of Expertsthat is a resource to promote clinical interactions. More frequentworkshops related to Medical ADAPT are intended to inform juniorICU and ED doctors about the importance of organ donation.Desirable outcomes are increased involvement of regional centresand Teaching Hospital doctors, increased referral and consent rates,improved awareness of organ donation in the WA community, and bet-ter data capture.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
461
The importance of sound management and organizationalculture in donation and transplantation: A single center organprocurement organization experience in the US
Joseph Ferreira, Simon Keith, John st John, Dr. John Ham,Karen Hess, Kathy Crabtree, Barry Grace, Carrie DeeseNevada Donor Network, Las Vegas, NV, United States.
Introduction: The Nevada Donor Network (NDN) is federally desig-nated by the US Department of Health and Human Services as the Or-ganProcurementOrganization (OPO)which covers approximately 80%ofthe total population in the State of Nevada. The NDN coverage area iscomprised of a population of approximately 2.1 million people accordingto the 2012 census report. In June of 2011, NDNwas declared as a “Mem-ber Not in Good Standing” by theOrgan Procurement and TransplantationNetwork/United Network for Organ Sharing (OPTN/UNOS) based on aregulatory peer review process which revealed underperformance andcompliance violations.Methods: The Board of Directors of NDN took decisive action basedon these findings and recruited new leadership to transform the cul-ture of the organization. The culture deployed by the new leadershipwas based on a blend of sound management principles and entrepre-neurial concepts from the private sector of business.Results: During the second quarter of 2012, the organization beganto experience significant growth in organ donation. In 2011, prior tothe cultural changes by new management, the organization recoveredorgans for transplantation from 53 donors. This equates to 25 donorsper million population which ranked NDN 30th out of the 58 OPOsin the US. In 2012, the number of donors recovered increased to75 which translates to 36 donors per million population which improvedNDN’s ranking to 12th out of the 58 OPOs. Year to date in 2013, NDNhas recovered organs from 56 donors. This equates to 53 donors permillion which ranks NDN 1st out of the 58 OPOs in the US.Conclusion: The resultant increase in the number of donors per mil-lion population at NDN denotes the importance of effective leadershipand organizational culture in the donation mission. It also emphasizesthe value of regulatory oversight and peer review of the OPTN/UNOSin the US to maximize OPO performance.Submitted on behalf of the entire team at Nevada Donor Network andour community partners in Nevada for their hard work and dedicationwhich led to these results.
r 27, 2013, Volume 96 Number 10S S243
thorized reproduction of this article is prohibited.

November 27, 2013
462
Doha Donation Accord (DDA) on the trail of the Declaration ofIstanbul (DOI): A local implementation of an internationalframework to improve organ donation and combatcommercialism
Riadh A. Fadhil, Hanan Alkuwari, Yousef Almaslamani,Abdalla Alansari, Hassan Almaliki, Hatem Khalaf, Omar AliQatar Organ Donation Center & Qatar Center for Organ Transplantation,Hamad Medical Corporation, Doha, Qatar.
Qatar is a small Gulf state of 1.7million multicultural society(1), RenalTransplantation in Qatar started 1986, but the number of transplantsremained low because of lack of donors that pushed most of theESRD patients to seek commercial transplantation abroad and returnback with high complications and mortality(2,3). All liver transplan-tations average 15/year, used to be done abroad.In order to combat commercial transplantation and to develop organdonation and transplantation, HMC the main tertiary health care facil-ity adopted the recommendations of DOI and WHO guiding principles,and extracted what is compatible from the Qatari laws and regulationsto launch the DDA in 2010 (4,5,6,7).The Principles of the DDA include; Equity & Fairness in access toorgans, Extra care of Donors and recipients, community education,development of Donor Registry. And no financial incentives to donorsor families, instead it is a community focused removal of disincentivesscheme with the leaders' inspirational vision that poor and underpriv-ileged communities will donate organs if they sense fairness, respect,dignity and freedom to donate(8).Since the implementation of the DDA early 2011 There has been in-crease in the consents rate gradually to 3/year in 2010, and to 1 or2/month since January 2013, seekers of transplant abroad dropped69% in 2012, 80 % of the native ESRD ready for transplantation haveregistered for transplant in Doha, Kidney transplants done abroad tothose done in Qatar decreased tremendously in 2012 to 1/1 as com-pared to 30/1 in 2008.No liver transplantation done abroad since April2012, While four successful Liver transplantations were done in HMCso far.Conclusion: DDA has succeeded to increase organ donation, and de-velop transplantation, We recommend it to countries that have compa-rable demography and socioeconomic status. local factors should betaken in consideration in implementing the DOI recommendations.
References:[1] Population statistics: http://www.qsa.gov.qa/eng/PopulationStructure.htm[2] Riadh A.S. Fadhil, y.moslemani, A.Alansari, O.Alani. The outcomeof commercial kidney transplantation : A Qatari study on preoperativeand post-transplant follow –up records of patients having commercialrenal transplantation abroad. Transplantation Journal July 27,2008.volume 86. Number 2S.[3] Riadh A.S. Fadhil, H.Althani, Y. Almaslamani, O.Alani. TrichosporonFungal Arteritis Causing Rupture of Vascular Anastamosis After Com-mercial Kidney Transplantation: A Case Report and Review of Litera-ture. Transplantation Proceedings, (2011) 43, 657–659[4] Organ trafficking and transplant tourism and commercialism: theDeclaration of Istanbul. The Lancet, Volume 372, Issue 9632, Pages5–6, 5 July 2008[5] WHO Guiding Principles on Human cell, Tissue and Organ Trans-plantation. Transplantation. 2010 Aug 15;90(3):229–33[6] Qatari Organ Donation and transplantation Law 21/1997 in http://www.gcc-legal.org/MojPortalPublic/LawAsPDF.aspx?opt&country=3&LawID=2838[7] http://www.qatarembassy.net/Qatar_Labour_Law.asp[8] http://odc.hamad.qa/en/how_to_become_a_donor/doha_donation_accord/doha_donation_accord.aspx
S244 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
463
Organ donation in different health regions inRio de Janeiro State
Priscila Paura1, Rodrigo Sarlo4, Janaína Lenzi3, Andreia Assis3,André Albuquerque1, Tereza Guimarães1, Claudia Araújo2,Eduardo Rocha11Education, Transplant State Program, Rio de Janeiro, Brazil;2COPPEAD, UFRJ, Rio de Janeiro, Brazil; 3Family Coordination,Transplant State Program, Rio de Janeiro, Brazil; 4GeneralCoordination, Transplant State Program, Rio de Janeiro, Brazil.
Introduction: The State of Rio de Janeiro (RJ) has 16 million in-habitants and had a significant increase in the number of actualdonations (AD = 176%) in the last 3 years. This increase was boththrough the number of brain death notifications (BDN = 38%) andthe rate of effectiveness (RE = 93%). This study analyzed the resultsof the RJ, to support performance management strategies consideringthe different health regions. Methods: This was a retrospective studyfrom 2011–2012. Data were collected in reports of BDN from Trans-plant State Program (PET-RJ) and analyzed by health regions. Thenumbers of BDN and AD were computed per million population(pmp) and RE in percentage (%). Results: The RJ received 559(35 pmp) and 693 (43.4 pmp) BDN, respectively, in 2011 and 2012.Of these, 121 (8 pmp) and 221 (13.4 pmp) resulted in AD. Thedata in the North and Central South regions were: decreasedBDN (37–22 // 50–25 pmp) and AD (9–8 // 15–10 pmp), but an in-crease in RE (25–37 // 30-40%), both RE higher than the state(31%). Metropolitan and Lagos regions increased BDN by 38 to49 and 10 to 27 pmp, AD by 8 to 15 and 0 to 8 pmp, RE by 21 to30 and 0 to 28%, however the MR’s RE has some raise and asLR, despite having considerable proportional performance whencompared to the last year, was still below the average of RJ(31%). There was a reduction of BDN in the Middle Paraíba(29–26 pmp), nevertheless had better numbers than State’s AD(9–12 pmp) and RE (31-46%). The Northwest region also de-creased the BDN (33–24 pmp) and AD (27–21 pmp), but had asuperior RE (82-86%). The Serrana Region has improved theBDN (17–23 pmp), but remains at low RE (33-19%). Conclusion:Regional differences point to the need of different action plansaddressing educational and logistical aspects, especially inregions with high BDN, but low AD. Also, the regions which stillshowed low BDN and AD, need to intensify training in variousstages of organ donation.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
464
Success and challenges of deceased donation andtransplantation
Sunil Shroff, Sumana Navin, Lalitha Raghuram, Pallavi KumarMOHAN Foundation, Chennai, India.
India started deceased donation programme after its law acceptedbrain death as form of death in 1995. The programme has been slowto take off, however significant strides have been made in a few statesin the country and these success stories could be duplicated in otherregions. Six of the 28 states have done better than rest in promotingthe programme and have done 90% of the deceased donations in last17 years. Similar is the state with corneal donations and of 45,000donations last year. The current donation rate in India still remains be-low 1 per million population however 2012 was a landmark year for theprogramme with almost 196 donations (Fig.1) in the country. The suc-cessful model of the state of Tamil Nadu which has a donation ratethat is 10 times the national average could be duplicated in some ofthe other states provided the state government works together withother stake holders such as public, private hospitals and NGO’s. Theoverall potential of deceased donation is extremely high as the num-ber of fatal deaths due to road traffic accidents every year exceeds140,000 and head injury occurs in over 60% of such deaths. The cur-rent donation rate, if pushed to 3 per million, would take care of all thecurrent requirements of organs. The recent amendments bringing inthe required request law to ask for organs in event of brain deathand compulsory appointment of transplant coordinator may give therequired momentum to the programme.
FIGURE 1. Deceased donation transplantations in India
State
No. ofDeceasedDonors Kidney Liver Heart Lung Pancreas
SmallIntestine Total
Tamil Nadu 83 148 80 16 8 0 0 252Maharashtra 29 49 19 0 0 0 0 68Karnataka 17 32 13 1 0 0 0 46Andhra
Pradesh13 21 12 2 1 1 0 37
Kerala 12 24 2 0 0 0 0 26Gujarat 18 30 16 0 0 0 0 46Delhi – NCR 12 24 6 0 0 0 1 31Punjab 12 24 0 0 0 0 0 24Total 196 346 147 19 9 1 1 530
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
465
A critical discourse analysis of the introduction of an embedded,dedicated nursing role supporting organ and tissue donation inVictoria, Australia
Damien W. Hurrell1, Kathleen Tori21Nurse Donation Specialist, Medical & Critical Care Services, BendigoHealth, Bendigo, Victoria, Australia; 2Lecturer/Emergency NursePractitioner, Department of Rural Nursing and Midwifery, Rural HealthSchool, Faculty of Health Sciences, Latrobe University, Bendigo,Victoria, Australia.
Background: As part of Australian Organ and Tissue Donation (OTD)reforms introduced in 2009, embedded, dedicated nursing roles (ini-tially titled Hospital Senior Nurse, Organ and Tissue Donation (HSNOTD);since renamed Nurse Donation Specialist (NDS)) with responsibility forsupporting OTD were created in 76 Australian hospitals. There is littleinformation in the professional literature about these roles and theirspecific responsibilities.Method: Documents such as position descriptions, codes of conduct,training materials, evaluation templates, government policy documents,acts of parliament, scholarly publications and media articles were col-lected and analysed using Critical Discourse Analysis.Results: HSNOTD roles were introduced into a complex system ofAustralian Organ and Tissue Donation stakeholders including a newlyestablished national authority, established state level government de-partments and non-government authorities, local general health services,transplant services, advocacy groups, and persons who had received orwere waiting for organ and tissue transplants. This complex contextresulted in multiple lines of formal and informal responsibility and account-ability. HSNOTD responsibilities included auditing, professional and com-munity education, policy development and implementation, and supportof donation processes and donor families. Emphasis on various responsi-bilities varied between different stakeholder groups.Conclusion: This study describes the context for and responsibilitiesof the HSNOTD as envisioned in the available documents establishingthe role. Further studies are required to explore aspects of the rolesuch as the challenges faced during the implementation of the roleand strategies used to overcome them, development and evolutionof the roles since implementation, and differences between the evolvedroles in different contexts.
r 27, 2013, Volume 96 Number 10S S245
thorized reproduction of this article is prohibited.

November 27, 2013
466
Organ donation: New hope through the expectedamendment in Germany?
Gernot M. Kaiser1, Radunz Sonia1, Ulrike Wirges2, Andreas Paul1,Matthias Heuer11General, Visceral and Transplantation Surgery, University HospitalEssen, Essen, Germany; 2Region Northrhinr-Westphalia, DSO,Essen, Germany.
Introduction: The current organ donor shortage in Germany results inthe death of 1,000 patients on the transplant waiting list every year. Inresponse, a recent amendment to the German Transplant Act aimingto increase donor rates was passed in 2012. The objective of thisstudy was to collect and evaluate data on the public's attitude towardorgan donation prior to the amendment.Methods: A survey on the subject of organ donation was conducted in2011 among clients of a public pharmacy in a major city in the federalstate North Rhine-Westphalia, Germany. Data regarding gender, age,health behavior and attitude toward the amendment were collectedand analyzed in comparison to whether or not the individual pos-sessed an organ donor card.Results: A total of 1,485 questionnaires were evaluated. Of those sur-veyed, only 14.1% had an organ donor card. No statistically significantassociations between gender (p-value 0.3045), age (p-value 0.1453)and the possession of a donor card were observed. 72.5% of res-pondents stated that they appreciated the expected amendment,and in the case of implementation, 83.4% would obtain an organ do-nor card.Discussion: The future success of transplantation medicine relies onan increase in the public's overall willingness to donate organs. Edu-cating the public and ensuring transparency in transplantation medi-cine are necessary to achieve higher donation rates. It remains to beseen whether the amendment to the German Transplantation Act willbring the desired results. At the very least, the measure signifies ac-tion to address the organ donor shortage.
S246 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
467
Regional variation in organ donation in Saudi Arabia
Hussien Elsiesy, Mohamed Al Sebayel, Almoataz Hashim,Waleed Al-hamoudi Al-hamoudi, Hamad Albahili,Faisal Abaalkhail AbaalkhailLiver transplantation, KFSH&RC, Riyadh, Saudi Arabia.
Background and Aim: Cadaveric organ donation started in 1986, outof 8820 cases reported, 4661 cases documented, and 1384 donorsharvested since the program inception until the end of 2011, with con-version rate of 29.7%. There is marked regional variation in organ do-nation among different region of Saudi Arabia. Our aim is to study thereasons for this variation in order to improve organ donation in areasof low donation rate.Method: Saudi Center for organ transplantation (SCOT) data for ca-daveric organ donation from 2006–2011 detailing the number of casesreported, documented, consented and harvested, as well as the distri-bution by region (central 29.4% of the total population Saudi Arabia,western 32%, eastern 15%, northern 8%, southern 15.6%). The num-ber of contributing ICU stratified by size of ICU and the region wasalso reviewed.The overall donation rate as well as the percentage of harvested casesper region as well as the conversion rate (harvested/Documented)was reviewed.Results: Between 2006–2011, 448 cases procured form Saudi Arabia,of which 343 where procured for central region representing 76.5%coming from 30 out of 97 contributing ICU's (31%), the eastern regioncame second with 49 cases (11%) followed by the western region with35 cases (7.8%) while northern and southern region had 12 and 9 cases(2.7&2%) respectively. The conversion rate followed a similar trend.This is related to the presence of active mobile donor team in Riyadh(the capital) as well as active transplant centers.Conclusion: There is marked variation with regards of contribution toorgan donation in different regions in Saudi Arabia from 2% in thesouthern area to 76.5% in central area. This is related to the presenceof active mobile donor team in the central region. A similar trend to-wards increasing number of cases and conversion rate was observedin the eastern region after having a new mobile donor team. We sug-gest that having active well trained mobile donor team in each regionwill increase the number of cadaveric donor at least 3 folds in the next3–5 years.Keywords: Cadaveric organ donation, Regional variation, Donor teamKing Faisal Liver Group
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
468
In-house coordination for organ donation - single centerexperience in a pilot project in Germany
Gernot M. Kaiser1, Claas Baier2, Sonia Radunz1, Holger Krauss3,Andreas Paul11General, Visceral and Transplantation Surgery, University HospitalEssen, Essen, Germany; 2Administration, University Hospital Essen,Essen, Germany; 3NRW, DSO, Essen, Germany.
The most urgent challenge for solid organ transplantation in Germanyis the shortage of organs. Recent data demonstrate a consistently lowdonation rate in Germany (less than 15 organ donors per million) com-pared to the rest of the world. In an effort to increase donation rates,some federal states mandated that hospitals install transplantationofficers to coordinate, evaluate, and enhance the donation and trans-plant processes.In 2009 the German Foundation for Organ Transplantation (DSO)implemented the so called “In-house Coordination Project,” whichincludes retrospective, quarterly, IT-based case analyses of all de-ceased patients with primary or secondary brain injury in regard tothe organ donation process. From 2006 to 2008 an analysis of poten-tial organ donors was performed in our hospital using a time consum-ing, complex method that of questionnaires, hand-written patient files,and the hospital IT documentation system (standard method). Analy-ses in the In-house Coordination Project are instead carried out by aproprietary semi-automated IT Tool called Transplant Check, whichuses easily accessible standard data records of the hospital control-ling and accounting unit. The aim of our study is to compare the resultsof the standard method and Transplant Check in detecting and evalu-ating potential donors. To do so, the same period of time (2006 to2008) was re-evaluated using the IT Tool.In the comparison of both investigation methods during the same timeperiod, Transplant Check was able to record significantly more patientswho fulfilled the criteria for inclusion (641 vs. 424). The methodsdisplayed a wide overlap, apart from 22 patients who were only re-corded by the standard method (see figure 1). In these cases, the ac-companying brain injury diagnosis was not recorded in the controllingand accounting unit data records due to little relative clinical signifi-cance. None of the 22 patients fulfilled the criteria for brain death.The IT Tool detected a greater number of deaths, which includedthose who eventually became organ donors and who qualified as po-tential donors. Therefore, Transplant Check is an easy to use, reliable,and valid tool for evaluating donor potential in a maximum care hospi-tal. Therefore from 2010 on, analyses were performed exclusively withTransplant Check.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
480
Interventions to increase willingness for deceased organdonation: A systematic review
Andrew Li1,2, Michelle Irving1,2, Stephen Jan3, Germaine Wong2,Kirsten Howard11School of Public Health, University of Sydney, Sydney, Australia;2Centre for Kidney Research, The Children's Hospital at Westmead,Sydney, Australia; 3The George Institute for Global Health, Sydney,Australia.
Aims: The shortage of deceased donor organs for transplantationmay be explained by community unwillingness to donate. We aimedto evaluate the effectiveness of interventions to increase willingnessfor deceased organ donation.Methods: Medline, Embase, PsycINFO and CINAHL were searchedto December 2012 for analytic studies that evaluated any interventiontargeting the willingness of the general public to become solid organdonors after death. Risk of bias was assessed, and data was collectedfor rates of registration and intention to donate. A descriptive synthesisof the results was undertaken, and where possible, the results werecompared quantitatively.Results: 46 studies were included and incorporated over 50 000participants. Interventions varied greatly in their approaches, e.g. advertis-ing, community partnerships, educational materials and structured educa-tional interventions. Most studies exhibited a low or unclear risk of bias.Due to the heterogeneity in participants, methods and outcomemetrics,no one approach could be definitively identified as the most effective.However, a greater general trend towards significant increases in intentionto donate was seen in interventions that included emotive componentsand/or interpersonal contactwith participants, andagreater general trend to-wards significant increases in registration rates was seen in interventionsthat included interpersonal contact with participants.Conclusion: Interventions to increase community willingness for de-ceased organ donation varied in their approach and effectiveness,with no one approach definitively emerging as the most effective, al-though it seems that interventions that include emotive componentsand/or interpersonal contact with individuals or groups may help in-crease willingness for deceased organ donation.
r 27, 2013, Volume 96 Number 10S S247
thorized reproduction of this article is prohibited.

November 27, 2013
481
Edutainment on nursing students by “One’s Gift of Life to Many”Programme
Methikar PrapthanawatchOrgan Donation Centre, Thai Red Cross Society, Bangkok, Thailand.
Introduction: Nowadays organ shortage is a crucial obstacle for or-gan and tissue transplantation in Thailand. “One’s Gift of Life to Many”Programme is a programme for organ and tissue donation which iscreated by the Organ Donation Centre Thai Red Cross Society. Ithas been done continuously for 15 years in various activities in orderto enhance knowledge and correct missed understanding and rein-force positive attitudes about organ and tissue donation.Material and Method: This is a retrospective descriptive analysis of“One’s Gift of Life to Many” Programme from 2010-2013. We orga-nized activities such as walk rally in order to give knowledge about or-gan and tissue donation, brain dead criteria, transplantation andcoordination to nursing students. Participants were divided into groups.Each group had activities as they rotated to each knowledge stations.Awards or points were given to participants.Results: After nursing students finished the edutainment activities,they understood and had good attitude towards organ donation. Afterthe 1st programme in 2010 nursing student became donor pledgers38 (20.88%) from 182. The 2nd programmes in 2011 turned nursingstudents to be donor pledgers 215 (54.99%) from 391. In 2012 wegot donor pledgers 207 (64.29%) from 322. And this year, 2013 therewere donor pledgers 242 (65.41%) from 370. Totally there are donorpledgers 702 (55.19%) from 1,265.Discussion: The superstitious misconception must be clarified by ap-propriate discussion by scientific facts and religious doctrine. “One’sGift of Life to Many” Programme has been organized for 4th year nurs-ing students that will be in medical team and play major role in the na-tional health care system. They can provide accurate information tocreate awareness, understanding and good attitudes towards organdonation.sz.On behalf of The Organ Donation Centre Thai Red Cross Society
S248 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
482
Master in donation and transplantation of organs, tissues andcells: The second edition results
Chloë Ballesté1,2, Ricard Valero1,2, David Paredes1, Gloria Páez2,Ana Menjívar, Melania Istrate2, Martí Manyalich1,21Surgery Department, School of Medecine, University of Barcelona,Barcelona, Spain; 2Transplant Procurement Management, Donationand Transplantation Institute, Barcelona, Spain.
Introduction: The Master´s degree in Donation & Transplantation oforgans, tissues and cells is offered by the University of Barcelona.Its second edition was held during years 2011-2012. The Master’sdegree was structured in 3 common modules: Research in donation,Research in organ transplantation, Research in tissues, cells & hema-topoietic progenitor’s transplants and 2 specialized: Research & Pro-fessional Path.Objectives: Evaluate the efficiency of the teaching programmethrough student’s feedback analyses.Methodology: We evaluated following aspects: experience and moti-vation of the students; participation; material´s content; way of pre-senting; way of running question/answer minutes; personal benefitsfrom the participation in the class.Results: Participant’s profile: 28 participants, with a heterogeneouscultural and professional profile background; 12 Medical Doctors, 12Nurses, 1Biologists, 1 Bacteriologists and 1 Pharmacists. All of themdid graduate. Internal subjects evaluations: The evaluation showedthe following scores: Content of the materials (4,40±0.28); presenta-tion (4,37±0.34); Questions/answers minutes (4,41±0.29);Personalbenefits (4,10±0.29) On- line results: Online learning system wasused. The evaluation was a summary of student activities and thetasks fulfilled by them. Research projects: Divided in 2 different fields:Research & Investigation (48% of the participants) and ProfessionalPractice (42 % of the participants). 100% of the participants fulfilledthe study on time. All were considered as adequate by the ad-hoctribunal.Conclusions: This Master offers the possibility to enlarge knowledges and skills of a large number of foreign professionals providingthem with an official degree, known in the scientific and academiccommunity. This programme achieved the expectations.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
483
Community attitudes towards the provision of informationregarding organ & tissue donation & end of life care in criticalcare waiting rooms
Carol Woeltjes1, Shena Graham1, Belinda Heasman1,Joanne Matchado2, David Pilcher1,3, Asim Shah1, Steve Philpot1,31ICU, The Alfred Hospital, Melbourne, Australia; 2Patient and FamilyServices, The Alfred Hospital, Melbourne, Australia; 3Department ofEpidemiology and Preventive Medicine, Monash University,Melbourne, Australia.
Introduction: Limited literature exists relating to the acceptability andimpact of providing information on organ and tissue donation, deathand end of life care in Intensive Care Unit (ICU) waiting rooms. Pres-ently no such information is provided in the ICU waiting room at TheAlfred Hospital. Our aim was to determine attitudes to provision of in-formation about death and organ donation amongst family membersof patients who have previously been admitted to ICU.Method: Family members of patients who had been admitted to ICUwere identified from the ICU database. Potential participants werecontacted by telephone. Those who agreed to participate were thensent a questionnaire regarding acceptability, usefulness and appropri-ateness of information about death and organ donation, if it weremade available in the ICU waiting room.Results: 161 families were contacted by telephone of whom 100agreed to participate in the survey. Reasons for non-participation in-cluded: not contactable (n=34, 21.1%); excluded for both no responseand English being a second language (n=62, 38.5%); “wished to moveon” and “limited experience of ICU waiting room” (n=33, 20.5%). Pre-liminary analysis of the first 10 of 59 surveys returned, suggest that9/10 respondents thought it was acceptable to have information aboutorgan and tissue donation and all 10 thought it appropriate to have in-formation about death in the ICU waiting room.Conclusion: If responses to this survey reflect general public opinion,it is likely that future provision of information about death and organdonation within the ICU waiting room will be acceptable to familymembers of patients. Further analysis of all surveys is required to con-firm these findings. If information is provided, its impact will beassessed in a future study.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
484
Successful international collaboration improves family donationconversations resulting in 29% increase in organ donations.
Patricia Mulvania1, Cherry Wise1, Yael Cass2, Eva Mehakovic2,Theresa A. Daly1, Howard Nathan1, Robert Norden11Gift of Life Institute, Philadelphia, PA, United States; 2Organ & TissueAuthority, Canberra, Australia.
Background: A country’s donation leaders concluded that to increaseorgan donations, health professionals (HPs) conducting family dona-tion conversations (FDC) required support & training. An int’l traininginstitute w/programs based on proven results was engaged to createand implement customized training program to influence change inFDC practice & culture.Aim: Increase donation rates by developing & implementing custom-ized, self-sustaining training program to enhance HP’s FDC practices.Provide training & communications skills to lead FDC, support familiesto make enduring decisions & influence HPs to adopt practice as FDCcultural norm.Materials and Methods: Planning meetings assured thoughtful devel-opment and customization. To gain support and determine program suit-ability, two 1-day pilot trainings were provided to 45 donation leaders in2011. Training was further customized w/emphasis on creating changethat would achieve/sustain desired results. Comprehensive nat’l trainingplan was implemented over 18 months. Eighteen 2-day FDC trainingworkshops were held in 8 cities w/492 participants. Program evaluationsand debriefings showed distinct shifts in perspectives and enthusiasm toimplement new process. Between 2012-2013, instructor programwas de-veloped to transition training facilitation. Training institute remains involvedin development and training to build and sustain skill and expertise.Results: Total organ donors 2011-337; Jan-June 2013-216; on pacefor 432, represents 29% increase.Conclusion: When existing donation conversation processes do notyield desired results, change is needed. Integration of another or-ganization’s process poses distinct challenges; however, thoughtfulcollaboration, sensitive to cultural aspects and family care, communi-cation and donation practices, can result in successful training thatshifts perspectives, provides new skills and achieves/sustains an in-crease in organ donation rates.
r 27, 2013, Volume 96 Number 10S S249
thorized reproduction of this article is prohibited.

November 27, 2013
486
The Robyn Hookes Shield: An organ and tissue donationcommunity education event in regional Victoria, Australia
Damien W. HurrellNurse Donation Specialist, Medical & Critical Care Services, BendigoHealth, Bendigo, Victoria, Australia.
Background: DonateLife week is Australia’s annual organ and tissuedonation awareness week, held annually towards the end of February.As community education is an important part of the role of Nurse Do-nation Specialists in Australia, Nurse Donation Specialists in regionalareas have since 2009 staged events to raise awareness of organ andtissue donation during the week.Method: A cricket match between a team of transplant recipients fromthe Australian Transplant Cricket Club and an invited team, comprisingcommunity members, local celebrities, and state and international rep-resentative cricketers was staged in Bendigo, a regional city in Victo-ria, Australia, on February 24, 2013: the first day of DonateLifeWeek. The teams competed for the Robyn Hookes Shield, named inhonour of the wife of David Hookes, an international cricketer who do-nated his organs after his death in 2004. Multiple strategies were usedto generate interest in the match, which was free to attend, and lever-age that interest into communicating the key organ and tissuemessages of DonateLife Week.Results: The two teams played a close and exciting match on a veryhot day in front of a crowd of over 300 people. Over 120 radioadvertisements, 5 radio interviews, local television news coverage,multiple local press stories and a radio broadcast of the match on acommunity radio station increased the reach of the event, andhundreds of posters and flyers containing key messages were distrib-uted. Trained organ and tissue donation volunteers and healthprofessionals provided information and merchandise to attendees,while fun, non-cricket related activities ensured the event had broadappeal to the community. Lessons for the future include ensuringtasks are distributed amongst multiple staff, everything must bechecked at least twice, and strategies to attract celebrities to play.Conclusion: The inaugural Robyn Hookes Shield was a successfulcommunity education event, with significant potential to grow into thefuture.This Project was funded by a DonateLife Community Education Grantfrom the Australian Commonwealth; a community grant from theCity of Greater Bendigo, and sponsorships from a number of localbusinesses.
S250 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
487
A systematic review of family influence on consentdecisions for deceased organ donation
Melissa Hyde1, Suzanne Chambers1, Jason Siegel21Behavioural Basis of Health, Griffith Health Institute, GriffithUniversity, Mt Gravatt, Australia; 2School of Behavioral andOrganizational Sciences, Claremont Graduate University, Claremont,CA, United States.
Family typically have the final say as to whether their loved one’sorgans are donated. However, the extent to which research has con-sidered family influence on consent decisions for donation is unclear.A framework including family attitude, family norm, and family efficacywas developed to describe evidence of family influence on consentdecisions in two contexts: 1) prior to a critical incident via a donor reg-istry or family discussion, and 2) at the time of a loved one’s death. Ev-idence for family attitude, norm, and efficacy on consent decisions wasdescribed and compared across contexts. Medline and PsycINFOwere searched for peer-reviewed articles published in English after1st January 1970 and prior to 31st December 2012. Inclusion criteriawere: individuals eligible to consent to donation via a donor register orfamily discussion, and/or family asked to consent to donate a lovedone’s organs/tissue for transplantation from countries with opt-in con-sent systems; and focused on deceased donation for transplantation;and discussed family influence on consent decisions. 47 articles metall criteria and considered family influence on consent decisions fordonation prior to a critical incident (n = 19) and for a deceased lovedone (n = 28). Studies were mostly quantitative, cross-sectional, usedconvenience samples, conducted in the United States, and publishedfrom 2001 onwards. Although understudied and rarely the primary fo-cus of studies reviewed, there was some evidence for family influenceon consent decisions. However, evidence was indirect; more oftenreported family influence on decision-making at the time of loved one’sdeath; and was more consistent for family attitude and norms thanefficacy. A future focus on family influence more broadly is neededincluding family attitudes towards communicating consent; the dis-crepancy between perceived and actual family reaction; and family ca-pabilities (e.g. communication style).
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
488
Exploring next-of-kin perceptions of optimal strategiesto request family consent for organ donation in ahypothetical scenario
Melissa Hyde1, Renata Meuter21Behavioural Basis of Health, Griffith Health Institute, Griffith Univer-sity, Mt Gravatt, Australia; 2School of Psychology and Counselling,Queensland University of Technology, Kelvin Grove, Australia.
Next-of-kin refusal for donation is a key factor preventing recovery oforgans. Conversations with Organ Procurement (Donor) Coordinators(OPCs)/health professionals can impact on next-of-kin consent. Whilecommon consent gaining strategies have been identified, it is less wellknown whether next-of-kin find these strategies acceptable. Identify-ing optimal request strategies may ultimately improve the request pro-cess and subsequent family consent rates. We used a scenariobased-study conducted in a non-clinical setting to explore potentialdonor families’ likelihood of consent to and perceived acceptability of12 strategies which are used by OPCs/health professionals to requestorgan donation. A convenience sample of 163 participants completedan online survey containing one of four scenarios manipulating next-of-kin’s prior knowledge of their loved one’s donation wishes (wishesknown/unknown) and the sex of their loved one (Mother/Father). UsingMANOVA we explored differences in participants’ ratings of consentand acceptability of request strategies across scenarios. There weresignificant differences in consent and acceptability ratings based onprior knowledge of loved one’s donation wishes only (not across thefour scenarios). Strategies least likely to gain consent or acceptanceincluded mentioning well known others who support donation (wishesunknown), making next-of-kin aware their parent needs an autopsy,and explaining the donation process. Strategies most likely to gainconsent and acceptance included informing next-of-kin their parenthad joined the donor register and ask for permission (wishes un-known) or support (wishes known) to donate. Consent and accep-tance of request strategies may vary based on next-of-kin’s priorknowledge of their loved one’s donation wishes. Optimal request strat-egies tailored to next-of-kin’s prior knowledge of loved one’s donationwishes may facilitate consent.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
495
Hospital model development donor in a public hospitalin Argentina
Pablo Centeno1,2, Matias Anchorena1,2, Julian Juarez1,2,Marco Flores1,2, Matias Willig1,2, Leonardo Del Rio1,2, Adrian Tarditti2,Mariana Casalins1,21HZGA Simplemente Evita, Gonzalez Catàn, Argentina; 2CUCAIBA,INCUCAI, Buenos Aires, Argentina.
Because efforts to increase organ and tissue donation in Argentina,growth in donation rate has increased slowly but steadily in recentyears. However, it is observed that not all health centers participatingin the activity and that most of those who develop donor policies tendto complete a cycle of increase, plateau, decline and disappearance inthe generation of donors. This cycle lasts about five years.A medium-complexity hospital located in an area of extreme povertyand history contrary to the donation has developed a program basedon quality of care, collaboration with the bereaved family, speciallytrained human resources and focus in the intensive care unit as thekey to detect potencial donnors.The result was:
r 27, 2013, Volume 96 Number 10S S251
thorized reproduction of this article is prohibited.

November 27, 2013
Continuous increase in organ and tissue donation in the last ten years.[1] Annual donors fivefold in ten years, while growth in the country wasfifty percent.Negative to donation rate less than 3% in last two years (In the sameperiod, national rate was close to 35%) [1]Loss of donors due to missed detections close to 10%, including car-diac arrest deceased. The estimated national rate of missed detectionis over 50% for potential beating heart donors and over 90% for postcardiac arrest.Supporting these results over time despite a turnover of health per-sonnel for a period of ten years, maximizing donation rate the last four.These results have led the national procurement and transplantationto use (the Catan’s Model) as a role model for the rest of the country’sinstitutions.
Reference:National Information System of Procurement and Transplantation ofthe Republic Argentina.https://cresi.incucai.gov.ar/IniciarCresiFromSintra.do
S252 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
496
Family approach - retrospective analysis of 6617 donationrequests
Franz Schaub1, Carl-Ludwig Fischer-Froehlich1, Guenter Kirste21Deutsche Stiftung Organstransplantation (DSO), Frankfurt am Main,Germany; 2Universitätsklinik Freiburg, Freiburg, Germany.
Introduction: The German Transplantation-Legislation was modifiedin November 2012 with promoting voluntary decision of people aboutorgan donation. Despite the current national transplantation-scandal,citizens have a positive attitude towards organ donation. Even thoughthe law now requires every citizen to enter their decision about organdonations in the minutes, the decedent’s written consent is missingmost of times. Therefore donor families have to be approached aboutthis specific issue. Thereby the refusal rate of 40% exceeds the onesof other countries. It was evaluated which factors might influence con-sent rate beyond personal decisions during donation requests.Methods: 6.617 documented donation requests between the years2009 and 2011 were analysed for factors that could influence thedecisions beyond personal values.Results: The decedent’s was often unknown (67.4%) and then thefamily’s decision was based on assumptions about the patient’s will.This resulted in 4.097 (61.9%) consents and 2.520 (38.1%) refusals.4.669 (70.6%) of these donation-requests were done by the physicianin charge only and 1.948 (29.4%) with a coordinator present addition-ally. Predictive (p<0.001) for consent were the presence of a speciallytrained transplantation coordinator and the timing of the request for or-gan donation (especially when the donation request was initiated inthe time period when measures for certifying death by neurologic cri-teria were started, p<0.001).Conclusion: There is a big difference between the attitude displayedin surveys and the real rate of consent to organ donation. The majorchallenge is that improved caregiving of donor family members is re-quired. Donation requests should be done by trained physician as wellas coordinators. Waiting until the finalized certification of brain deathmay not be appropriate nowadays: A transparent description of all de-tail contributes to build up a therapeutic relation to donor families andthis allows them to have a proper timeframe for a stable decisionabout organ donation.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
497
Web-net tool based and nationwide system for referring andmonitoring serious adverse events and reactions in the area oforgan transplantation
Jarosław Czerwiński1,3, Piotr Kaliciński2, Roman Danielewicz1,31Dep. of Surgical and Transplant Nursing, Medical University ofWarsaw. Poltransplant, Warsaw, Poland; 2Dep. of Pediatric andTransplant Surgery, Children's Memorial Health Institute, Warsaw,Poland; 3Polish Transplant Coordinating Center, Poltransplant,Warsaw, Poland.
Following Directive 2010/53/UE serious adverse events (SAEs) andreactions (SARs) alerting system in the area of organ transplantationwas implemented in Poland on technical basis of web-net platformconnecting all transplant centers.Substantial issue of this system, distinctly problematic and widelydiscussed among professionals and decision makers was the catalogof events and reactions must be referred.Finally constructed catalog consists of:1. Events related to organ recipients: transplantation from the donorwith incomplete or incorrect characteristic, transplantation of organ af-ter abnormal or too long preservation, absence of valid potentialrecipient’s plasma for cross-match, organ transplantation from a donorwith a viral infection (unrelated to the rules of allocation), severe anduncontrolled bacterial, fungal or protozoan infection, transplantationform a donor with cancer, unintentional transplantation from a donorwith non-identical or incompatible blood group ABO.2. Reactions related to organ recipients: resignation from transplanta-tion due to organ damage at the time of donation, storage and implan-tation, transmission from a donor viral infection (unrelated to the rulesof allocation), organ lost due to the absence of proper recipient, trans-mission of cancer, never function of the graft, recipient’s death within30 days after transplantation or during the initial hospitalization graftloss within 30 days of transplantation or during the initial hospitaliza-tion, HIV transmission from the donor, severe bacterial, fungal, or pro-tozoan infection.3. Events related to living organ donor: organ procurement from thedonor with incomplete or incorrect characteristic.4. Reactions related to living organ donor: serious health consequen-ces (illness, serious complications) in the donor associated with thedonation.In the year of 2012 the total number of 51 SARs and 6 SAEs wasdocumented in the system with regards of 1653 totally transplantedorgans.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
498
System of donor hospital transplant coordinators maintainedand financed by national transplant organization improvesdonation rates, but it is effective only in a half of hospitals
Jarosław Czerwiński1,2, Teresa Danek2, Adam Parulski3,Monika Trujnara4, Roman Danielewicz1,21Dep. of Surgical and Transplant Nursing, Medical University ofWarsaw. Poltransplant, Warsaw, Poland; 2Polish TransplantCoordinating Center, Poltransplant, Warsaw, Poland; 3Dep. ofCardiosurgery, The Cardinal Stefan Wyszyński Institute of Cardiology,Warsaw, Poland; 4Dep. of Anaesthesiology and Intensive Care,Międzyleski Specialistic Hospital, warsaw, Poland.
Coordinators in the number of 218 trained professionals (134 doctorsand 84 nurses) are employed by Poltransplant in 200 hospitals (ca50% of total number of hospitals with potential of donation). Thisresulted, after 21 months of work, compared to 21 month period priorto their employment in changes of the following hospital donationindicators:� Increasing the number of reported potential deceased donors by 27%� Increasing the number of actual deceased organ donors by 24%� increasing the percentage of multiorgan donation from 54% to 56%� increasing the number of transplanted organs by 20%� increasing the percentage of family refusals to donation from 8.5%to 9.3%� reducing the rate of utilized organs per actual donor from 2.65 to2.57
The desired effect of the employment of hospital donor coordinators toimprove organ procurement rates was reached in 102 (51%) hospitals;in this group there were hospitals where there was no pre-employmentdonations and they took place after the employment, where the num-ber of donations has increased or remained the previous level. In 98(49%) hospitals had no procurements before or after the employmentof coordinators, were before hiring them, but there was no after or thenumber of actual donors has decreased. Pronounced effect was ob-served in hospitals:� located in regions with low baseline rate of donation (59%)� academic hospitals (63%) and multi-profile hospitals in large cities (77%)� hospitals, where a team of two coordinators was set up (67%)� hospitals for adults (52%)� hospitals, where doctors were assigned coordinators (55%)
The annual formal analysis of activity of donor hospital coordinatorsgives to national transplant organization a rational basis for their em-ployment taking into account the characteristics of hospitals and thecharacteristics of hospital coordination team.
r 27, 2013, Volume 96 Number 10S S253
thorized reproduction of this article is prohibited.

November 27, 2013
499
Argentine training program for transplant coordinators in theframework of presumed consent
Rogelio M Anchorena1,2, Ricardo Ibar1, Carlos Soratti1,Alejandro Yankowsky1, Maria E Barone1, Martin Torres1,Roxana Fontana1, Alberto Maceira1, Adriana Carballa1,Hector Iudicsissa1, Rodrigo Salas1, Monica Juarez1, Vilma Brunetti21National Institute for Organ Donation and Transplantation INCUCAI,Buenos Aires, Argentina; 2Hospital Simplemente Evita, GonzalezCatan, Argentina.
Background: In recent years, Argentina improved the donation rate.Reached in 2012 15.7 donors PMP, however the family interview is amajor and critical point in this process. Since 2006 in Argentina hasbeen incorporated presumed consent in the law. This changed theway of doing the family interview. In this framework should be priori-tized the donor decision upon the family decision. It was necessarydevelop tools to train transplant coordinators. In 2011 began the “Ar-gentine training program for transplant coordinators in the frameworkof presumed consent ”.Material and Method: National System of Procurement and Trans-plantation in Argentina (SINTRA) collects one hundred percent ofthe donation process including family interview data. 115 pro-fessionals were trained divided into four theoretical and practicalcourses. By SINTRA analyzed the results of interviews before and af-ter training.Results: There was a statistically significant impact on communica-tion processes, decreasing the chance that the result is negative(OR: 0.55, 95% CI: 0.39 to 0.78, p = 0.00045).The study evidence a individually improvement in the family interviewafter training (p=0.0059).Conclusion: Communication after training for the use of presumedconsent showed a statistically significant reduction of the risk of neg-ative results during the family interview with a consequent increasein the number of donors.
S254 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
500
Deciding to donate a family member's organs: What factors aremost important to the community? Results of a best-worstscaling study
Kirsten Howard1, Stephen Jan2, John M. Rose3, Michelle Irving1,4,Germaine Wong1,4, Allison Tong1,4, Jonathan C. Craig1,4,Steven Chadban5,6, Richard D. Allen6, Alan Cass2,71School of Public Health, University of Sydney, Sydney, Australia;2The George Institute for International Health, Sydney, Australia;3Institute for Transport and Logistics Studies, University of Sydney,Sydney, Australia; 4Centre for Kidney Research, The Children'sHospital Westmead, Westmead, Australia; 5Central Clinical School,Bosch Institute, University of Sydney, Sydney, Australia; 6Departmentof Renal Medicine, Royal Prince Alfred Hospital, Sydney, Australia;7Menzies School of Health Research, Casuarina, Australia.
Background: Despite broad public support for organ donation, thereis a chronic shortage of deceased donor organs. The final decision onorgan donation is made by donor’s families. We aimed to identify thekey factors influencing decisions to donate a family member’s organs.Methods: A best-worst-scaling method was used where policies/services are described by factors presented with varying levels. Commu-nity respondents were recruited from an existing internet panel; quotasampling ensured they were broadly representative of the adult Australianage distribution. Participants answered 30 online scenarios presentingeight factors (Table1), and chose, in each, the factor that made themmostlikely, and least likely, to agree to donate their family member’s organs.Using MNL regression we calculated: the importance of each factor,and the contribution each factor made to overall utility of a policy.Results: There were 2002 respondents with a mean age of 44.9(range18-84); 51.9% were female. The importance ranking of attributesis shown below (Table1), with knowing a family member’s preferenceranked highest. The largest gains in overall utility of a policy could beachieved from: knowing a family member’s preferences, by telling thefamily how death is defined, by giving family priority for organs in the fu-ture, and provision of direct payments. There were some differencesin the valuation of attributes with respondent age, with respondents<50 yrs valuing financial mechanisms more highly than older people.Conclusions: Knowing a family member’s wishes about donation wasthe most important factor. Conversely, less important attributes suchas funeral expense reimbursement and direct payments contributedpositively to overall policy utility, suggesting the Australian public isopen to donation policies that include financial mechanisms.
TABLE 1.
Factors presented
Factorimportance
score
Rankimportance of
factor
Overall impactof factor levelson utility of
policy
Rank ofutilityimpact
Whether you know familymembers preferences
1.057 1 3.800 1
Whether family receive adirect payment
0.412 2 0.885 4
Who discusses organdonation with family
0.333 3 0.683 7
How death is defined 0.310 4 1.610 2Whether family receive
priority for organs in thefuture
0.157 5 0.914 3
Whether family receivereimbursement offuneral expenses
0.132 6 0.832 5
Whether you are toldanything about therecipient
0.116 7 0.526 8
Whether there is anyformal acknowledgementof donation (base factor)
0 8 0.816 6
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

TABLE 1.
Factorimportance
Rankimportance
Overall impact offactor levelson utility of
Rank ofutility
November 27, 2013
501
Becoming an organ donor - what are the most influential factorsfor the general community when considering deceased organdonation? A nominal group study
Michelle Irving1,2, Allison Tong1,2, Stephen Jan3, Alan Cass6,Steve Chadban4,5, Richard Allen5, Jonathan Craig1,2,Germaine Wong2, Kirsten Howard11School of Public Health, University of Sydney, Sydney, Australia;2Centre for Kidney Research, Children's Hospital Westmead,Westmead, Australia; 3The George Institute, Camperdown, Australia;4Central Clinical School, Bosche Institute, University of Sydney,University of Sydney, Australia; 5Dept of Renal Medicine, Royal PrinceAlfred Hospital, Camperdown, Australia; 6Menzies School of HealthResearch, Northern Territory, Australia.
Aim: The observed donation rate in Australia appears substantiallylower than the high level of community support for the principle of or-gan donation would suggest. We aimed to identify factors perceivedby the community to be influential on their willingness to register asa deceased organ donor.Methods: Thirteen community nominal groups involving 114 participantsfrom the general community were conducted in New South Wales, Vic-toria, Queensland and South Australia. Participants identified, ranked anddiscussed reasons for factors they believed were important in decision-making about organ donation. A mean importance score was de-termined for all the factors. Transcripts were analysed thematicallyto identify reasons for their choices.Results: 38 factors were identified with “saving life” being the highestranked. Secondly, families should not be able to veto the decision todonate. Highly ranked factors also included clarity about the consentprocess, that families should not be able to overrule an individual’spreference, the benefits of organ donation for the recipients, the organdonation process and benefits of positive media coverage. Youngerparticipants particularly indicated that compulsory choice or opt-outconsent systems were acceptable and older groups viewed incentivessuch as the payment of funeral expenses quite favourably. Themesunderpinning their choices included; core beliefs, external and emo-tional influences and the need for a simpler consent system.Conclusion: The general community tends to hold a complex range ofpersonal reasons for becoming organ donors. Continuation and expan-sion of current community education is recommended and should in-clude: organ donation procedure, consent process and recipientbenefits. A policy review may be undertaken with community input re-garding potential incentives and families’ power to veto prior decisions.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
502
I'd register, but I've never been asked! Key factors influencingdecisions about whether to register as an organ donor
Kirsten Howard1, Stephen Jan2, John M. Rose3, Michelle Irving1,4,Germaine Wong1,4, Allison Tong1,4, Jonathan C. Craig1,4,Steven Chadban5,6, Richard D. Allen6, Alan Cass2,71School of Public Health, University of Sydney, Sydney, Australia;2The George Institute for International Health, Sydney, Australia; 3In-stitute for Transport and Logistics Studies, University of Sydney,Sydney, Australia; 4Centre for Kidney Research, The Children's Hos-pital Westmead, Westmead, Australia; 5Central Clinical School, BoschInstitute, University of Sydney, Sydney, Australia; 6Department ofRenal Medicine, Royal Prince Alfred Hopspital, Sydney, Australia;7Menzies School of Health Research, Casuarina, Australia.
Background: Despite broad public support for organ donation, thereis a chronic shortage of deceased donor organs. We aimed to identifythe key factors that would influence the decision about whether to reg-ister as an organ donorMethods: A best-worst-scaling method was used where policies/services are described by factors presented with varying levels. Com-munity respondents were recruited from an existing internet panel;quota sampling ensured they were broadly representative of the adultAustralian age distribution. Participants answered 30 online scenariospresenting 9 factors (Table1), and chose, in each, the factor that madethem most likely, and least likely, to register to be a donor. Using MNLregression we calculated: the importance of each factor, and the con-tribution each factor made to overall utility of a policyResults: There were 2041 respondents with a mean age of 45.4(range18-87); 51.8% were female. The importance ranking of attributesis shown below (Table1), with the type of consent system rankinghighest. The largest gains in overall utility of a policy could be achievedfrom: reimbursement of funeral expenses, family priority in the future,how death is defined and direct payment mechanisms. There weresome differences in the valuation of attribute levels with respondent
Factors presented score of factor policy impact
How donationis registered(consent system)
1.308 1 0.484 9
Whether family areable to overruledecision
1.021 2 0.743 5
How often you needto register/ confirm
0.545 3 0.720 7
How easy it is to registerdonation intent
0.484 4 0.516 8
Whether a directpayment is madeto your family
0.449 5 1.554 4
How death is defined 0.227 6 1.597 3Whether family
receive priorityin future
0.164 7 1.723 2
Whether reimbursementof funeral expensesis provided
0.073 8 1.817 1
Whether there is anyformal recognitionof donation
0 9 0.724 6
r 27, 2013, Volume 96 Number 10S S255
thorized reproduction of this article is prohibited.

November 27, 2013
age, for example respondents <50yrs valuing financial mechanismsmore highly than older people.Conclusions: How donation intent is registered (ie the consent sys-tem in place) and the extent of family overrule were valued highly, aswas ease of registration. Interestingly, less important attributes suchas possible incentive mechanisms (funeral expense reimbursement,direct payment and family priority) all significantly contributed posi-tively to overall policy utility, suggesting the Australian public isopen to donation policies that include incentives, including financialmechanisms.
S256 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
503
Donor organ shortage crisis: A case study review of aneconomic-incentive system
Mohamed Al Sebayel1, A Al Enazi, R Sabbagh, T Al Aqeel,M Al Enazi, Hamad Al Bahili1, Hussien Elsiesy11Liver transplantation, KFSH&RC, Riyadh, Saudi Arabia.
Introduction and Background: Gross disparity between organ de-mand and supply created a profound negative impact on organ trans-plantation. Organ supply system depends on altruistic non-coercivedonation (ADS). Desperate demand for organs and the need to com-bat organ trafficking, transplant tourism and human exploitation haveresulted in the search for effective alternatives. Financial incentivesare one of them. Its feasibility is debatable as it relates to medical, eth-ical and economic dimensions.In Riyadh, Saudi Arabia, organ shortage was approach by Incentive-based procurement system (IBPS) applied by Mobile Donor ActionTeam (MDAT). Aggressive approach towards incentives for donors'families and health workers was associated with a threefold increasein donation rate.The aim is to provide a qualitative review of a five-year IBPS and to as-sess medical, ethical, religious, cultural and economic issues thathave, and may impact the system and to make recommendations tothe transplant community and health authority in KSA and elsewhereregarding the transferability of the system and areas for furtherresearch.Method Is qualitative. Review of documents was used to create a chronolog-ical audit and to shape interviewquestions. Samplingwas purposeful and inclu-sive of MDAT members. Semi-structured interviews were conducted. Findingswere subjected to thematic analysis.Result Documents reflected evolution of MDAT. The essence of MDAT isfield work and liberal use of financial incentive resulting in 3 fold increase indonation rate. MDAT members believed that IBPS is the reason behind thisincrease. Moreover, IBPS has been acceptable from moral, ethical and re-ligious aspects with high degree of professional satisfaction.Discussion Theoretical assumptions doubted the feasibility of IBPS. Thisreal-life experience with IBPS proved the contrary. The findings may be ap-plicable only to the setting in Riyadh, KSA. Further research is needed toexplore its transferability to other settings.Conclusion IBPS can be an alternative to ADS and should be piloted indifferent settings.
King Faisal Liver Group.
Reference: None
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
504
Rewarming to subnormothermia for DCD liver graftwith machine perfusion preservation in pigs
Naoto Matsuno1,3, Hiromichi Obara1, Toshihiko Hirano2,Kiyoko Kubota3, Masako Fujiyama3, Shin Enosawa31Mechanical Engineering, Tokyo Metropolitan University, Tokyo,Japan; 2Clinical Pharmachology, Tokyo Unversity of Pharmacy and lifeSicience, Tokyo, Japan; 3Transplantaton and innovative surgery,National Center for Child Health and Development, Tokyo, Japan.
Utilization of grafts from donors after cardiac death (DCD) wouldgreatly contribute to the expansion of the donor organ pool. However,the implementation of such a strategy requires the development of novelpreservation methods to recover from changes due to warm ischemia.To assess potential methods and effect, livers procured after 60 minutesof warm ischemic time (WIT) were perfused and preserved.Methods: Porcine livers were perfused with newly developed machineperfusion (MP) system. The livers were perfused with modify UW-gluconate(UW-G) or amino solution(JPS). Euro-ollins (EC) was usedfor simple cold storage (CS). All grafts were procured after acute hemor-rhagic shock and ventilator off. Group 1 (n=4): grafts were procured afterWIT of 0 min and preserved with CS for 2 hrs. and hypothermic MP(HMP) with UW-G for 2 hrsas a positive control.. Group 2 (n=4): graftswere procured with WITof 60 min and preserved with CS for 2 hrs andHMP with JPS for 2hrs. Group 3 (n=5): preserved with CS for 2 hrsand rewarming up to 25°C by MP with JPS for 2hrs. The preserved livergrafts were transplanted orthotopicaly.Results: The release rate of AST, ALTand LDH in perfusate as the dif-ference from initial value during MP maintained as low in Group 3. Theserum ASTand LDH levels in 2 hr after reperfusion were significantlylower in Group 1 and 3 than in Group 2, (AST; 596.0, 1203,3 and535.5 IU/L, LDH;637.5, 1417.2, and 778.2 IU/Lin each group,). Histo-logically, the necrosis of hepatocytes were less severe in Group 3.Survival rate with good postop. in Group 1 and3 was 3/4 and 3/5 re-spectively, but 0/4 in Group 2.Conclusion: Rewarming up to subnormothermia iby MP is expectedto facilitate the recovery and resuscitating function of DCD liver grafts.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
505
Safety and feasibility of modified histidine-tryptophan-ketoglutarate solution for liver preservation prior transplantation
Gernot M. Kaiser1, Matthias Heuer1, Renate Reinhardt1,Guntje Kneiseler2, Hideo Baba3, Phillip Würzinger1, Ursula Rauen4,Andreas Paul1, Thomas Minor1General, Visceral and Transplantation Surgery, University HospitalEssen, Essen, Germany; 2Gastroenterology and Hepatology,University Hospital Essen, Essen, Germany; 3Pathology, UniversityHospital Essen, Essen, Germany; 4Institute of Pysiological Chemistry,University Duisburg-Essen, Essen, Germany; 5Surgical ResearchDivision, University Clinic of Surgery, Bonn, Germany.
Cold storage is still a major concern in liver transplantation. Previousanimal studies pointed out better results for a modified Histidine-Tryp-tophan-Ketoglutarate solution (HTK) in heart, lung and kidney trans-plantation compared to previously used HTK. Aim of this study is todemonstrate safety and feasibility of the modified HTK solution in alarge animal model.20 female swine were randomized into two groups (n=10) each with 5donors and 5 recipients. The solution used for each transplant wasblinded and randomized to modified HTK and standard HTK as controlgroup. Liver transplantations were performed with all anastomoses inan end-to-end fashion. Anesthesia was maintained by intravenous ad-ministration of fentanyl and propofol continuously. In each swine theobservation period was 7 days, immunosuppression applied as cyclo-sporine A (8,5mg/kg BW/d) and prednisolone (500 mg intraoperativesingle dose).Liver transplantations was performed after a mean cold ischemic timeof 307±10 minutes. Mean warm ischemic time was 23.2±2.9 minutes.Mean total surgery time was 225±39 minutes. There were no signifi-cant differences in cold ischemic time (p=0,88), warm ischemic time(p=0,69), time of surgery (p=0,98), donor weight (p=0,69) and recipi-ent weight (p=0,81) between the both groups. All animals survived 7days after operation, although one swine in the standard HTK groupshowed secondary dysfunction of the transplanted liver. Laboratoryanalysis demonstrated a tendency to improved liver function or lessreperfusion injury, but no significant differences between the groups.On POD 7 the Quick´s value in the test group was 116.6±5.6 (controlgroup 82.2±37.9; p=0.08); mean serum creatinine was 1.03±0.22(control group 2.54±1.73; p=0.09). Partial thromboplastin time, serumbilirubin, alanine transaminase, cholinesterase and μ-GTwere equal.Orthotopic liver transplantations seems to be feasible and safe usingthe modified HTK solution due to first results of this in this large animalmodel. The advantages of the modified solution shown for otherorgans and in rat liver transplantation could not be reproduced, possi-bly due to the small number of animals in our study.Further evaluationin clinical setting seems to be justified to confirm the positive resultsshown in previous studies.
r 27, 2013, Volume 96 Number 10S S257
thorized reproduction of this article is prohibited.

November 27, 2013
506
Normothermic extracorporeal perfusion of porcine and humanliver following donation after cardiac death
Michael A. Fink1,4, Rinaldo Bellomo2, Bruno Marino3,Graham Starkey4,Bao-Zhong Wang4, Nan Zhu4, Satoshi Suzuki2, Shane Houston2,Glenn Eastwood2, Paolo Calzavacca2, Neil Glassford,Brenton Chambers5, Alison Skene6, Antoine G. Schneider2,Daryl Jones2, Andrew Hilton2, Helen Opdam7, Stephen Warrillow2,Nicole Gauthier7, Lynne Johnson8, Robert M. Jones41Department of Surgery, Austin Hospital, The University of Melbourne,Melbourne, Australia; 2Department of Intensive Care, AustinHospital, Melbourne, Australia; 3Perfusion Services, Austin Hospital,Melbourne, Australia; 4Liver Transplant Unit, Austin Hospital,Melbourne, Australia; 5Faculty of Veterinary Science, The Universityof Melbourne, Melbourne, Australia; 6Department of AnatomicalPathology, Austin Hospital, Melbourne, Australia; 7DonateLifeVictoria, Melbourne, Australia; 8Department of Radiology, AustinHospital, Melbourne, Australia.
Donation after cardiac death (DCD) has increased the pool of potentialdonors for liver transplantation. However, DCD livers are at increasedrisk of primary graft dysfunction and biliary tract ischaemia. Normo-thermic extracorporeal liver perfusion (NELP) may increase the abilityto protect, evaluate and transplant DCD livers. Proof-of-conceptexperiments using a DCD model in the pig and in a discarded DCDhuman liver were performed to assess the short-term (3–4 hours) fea-sibility, histological effects and functional efficacy of NELP. Using ex-tracorporeal membrane oxygenation, parenteral nutrition, separatehepatic artery and portal vein perfusion, and physiological perfusionpressures, we achieved NELP and evidence of function (bile produc-tion, paracetamol removal, maintenance of normal ammonia and lac-tate levels) for 4 hours in the pig livers subjected to 15 and 30 minutesof cardiac arrest before explantation and for 3 hours in the human liver.There was essentially normal liver and biliary tract histology after8 hours perfusion. Our experiments justify further investigations ofthe feasibility and efficacy of human DCD liver preservation by ex-vivoperfusion.
S258 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
507
A donor whole blood-based perfusate provides superiorpreservation of myocardial function during ex vivo heartperfusion
Christopher W. White1,2, Paul Mundt1, Yun Li2, Devin Hasanally2,Bo Xiang2, Rakesh C. Arora1,2, Trevor W. Lee3, Amir Ravandi2,Ganghong Tian4, Larry Hryshko2, Darren H. Freed1,21Cardiac Surgery, University of Manitoba, Winnipeg, MB, Canada;2Institute of Cardiovascular Sciences, University of Manitoba,Winnipeg, MB, Canada; 3Department of Anesthesia and PerioperativeMedicine, University of Manitoba, Winnipeg, MB, Canada; 4NationalResearch Council Institute for Biodiagnostics, Winnipeg, MB, Canada.
Background: Discarded hearts from brain-dead and DCD donorsrepresent unutilized organs for transplantation; however, demonstra-tion of adequate function prior to transplant is necessary. Ex vivo heartperfusion (EVHP) facilitates such functional assessment. We soughtto determine what type of oxygen carrier provides superior preserva-tion of myocardial function during EVHP.Methods: 27 pig hearts were procured and underwent EVHP for6 hours. Hearts were allocated to 4 groups according to the composi-tion of the perfusate solution. Donor red blood cell concentrate (RBC,N=6), donor whole blood (RBC+Plasma, N=6), an acellular hemoglo-bin based oxygen carrier (HBOC, N=8), or HBOC plus donor plasma(HBOC+Plasma, N=7) were added to STEEN solution to achieve a
FIGURE 1. Left ventricular diastolic function as assessed by the end-diastolic pressure volume relationship at 1 (T1), 3 (T3), and 5 (T5)hours of ex vivo heart perfusion.
FIGURE 2. Average fold-change in 83 oxidized phosphatidylcholinecompounds released into the perfusate over the 6-hour ex vivo heartperfusion interval.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
hemoglobin concentration of 40 g/L. Myocardial function was assessedin working mode using pressure-volume loop analysis. Oxidative stresswas assessed through quantification of oxidized phosphatidylcholine(OxPC) compounds using mass spectrometry. Myocardial energeticswas assessed using magnetic resonance spectroscopy.Results: A hemoglobin concentration of 40 g/L preserved myocardialenergetics. Systolic function was comparable between treatmentgroups. Diastolic function was assessed using the end-diastolic pres-sure-volume relationship (EDPVR) and was superior in RBC+Plasmahearts at 1, 3, and 5-hours of EVHP (Figure 1). Donor plasma reducedthe generation of OxPC compounds (Figure 2) and the developmentof myocardial edema in HBOC perfused hearts (HBOC+Plasma9.8±1.7 vs. HBOC 16.3±1.9 grams/hr, p=0.03) but not in RBC perfusedhearts (RBC+Plasma 6.6±0.9 vs. RBC 6.6±1.2 grams/hr, p=0.98).Conclusion: During EVHP a hemoglobin concentration of 40 g/Lpreserves myocardial energetics. Donor plasma minimizes oxidativestress and the development of myocardial edema, and a donor wholeblood-based solution (RBC+Plasma) provides superior preservationof diastolic function.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
508
Clinical experience supplementing celsior preservation solutionwith pro-survival kinase agents glyceryl trinitrate anderythropoietin demonstrates excellent myocardial recovery postcardiac transplantation
Gayathri Kumarasinghe1,2, Arjun Iyer1,2, Alasdair Watson1,2,Mark Hicks2, Ling Gao2, Aoife Doyle2, Padmashree Rao2,Anne Keogh1,2, Christopher Hayward1,2, Eugene Kotlyar1,Andrew Jabbour1,2, Emily Granger1, Kumud Dhital1,2, Paul Jansz1,Phillip Spratt1, Peter Macdonald1,21Heart and Lung Transplant Unit, St. Vincent's Hospital, Sydney,Australia; 2Cardiac Physiology and Transplant Laboratory, VictorChang Cardiac Research Institute, Sydney, Australia.
Aim: Primary graft failure (PGF) is the leading cause of early morbidity andmortality in cardiac transplantation[1].We have shown in animalmodels thatmyocardial recovery is significantly improvedby supplementingpreservationsolutions with pro-survival kinase agents that reduce ischaemia-reperfusioninjury[2,3].We translated these findings into clinic practice by supplementingCelsior solution with two agents glyceryl trinitrate (G) and erythropoietin (E)and report our findings.Methods: Cardiac transplants performed in our institution since June2010 used Celsior+G+E for cardioplegia and hypothermic storage.Donor and recipient baseline data, ischaemic time and post-transplantoutcomes were retrospectively compared with historical controlswhere hearts were procured using Celsior alone.Results: Celsior+G+E was used for 51 transplants (June 2010-February2013), and Celsior alone was used for 104 transplants (March 2005-June2010). There was increased use of left ventricular assist devices (LVADs)and a trend towards higher numbers of marginal donors in the Celsior+G+E group. Therewas a trend towards reducedPGF (lower use ofmechan-ical circulatory assist devices) and improved survival in this group.
r 27, 2013, Volume 96 Number 10S S259
thorized reproduction of this article is prohibited.

November 27, 2013
Conclusion: Despite increasing use of marginal donors and LVADs,supplementing Celsior with glyceryl trinitrate and erythropoietin allowsexcellent recovery of donor hearts.
References:[1] Iyer A, Kumarasinghe G, Hicks M, Watson A, Gao L, Doyle A,Keogh A, Hayward C, Kotlyar E, Dhital K, Granger E, Jansz P, Pye R,Spratt P, Macdonald PS. Primary graft failure after heart transplanta-tion. J Transplantation. 2011;2011:175768. doi: 10.1155/2011/175768.Epub 2011 Aug 1[2] Watson AJ, Gao L, Sun L, Tsun J, Jabbour A, Ru Qiu M, Jansz PC,Hicks M, Macdonald PS. Enhanced preservation of the rat heart afterprolonged hypothermic ischemia with Erythropoietin-supplementedCelsior solution. J Heart Lung Transplant 2013. 32 (6):633–40[3] Watson AJ, Gao L, Sun L, Tsun J, Doyle A, Faddy S, Jabbour A,Orr Y, Dhital K, Hicks M, Jansz PC, Macdonald PS. Enhanced preser-vation of pig cardiac allografts by combining erythropoietin with Glyc-eryl trinitrate and Zoniporide. Am J Transplant 2013. 13(7): 1676–87
S260 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
509
Prolonged Ex-Situ perfusion: Twelve hours of heart perfusion
Benjamin Bryner2, Alvaro Rojas-Peña1,2, Yao Nie2, Cory Toomasian2,Robert Bartlett2, Martin Bocks2,3, Gabe Owens2,31General Surgery-Section of Transplantation, University of Michigan,Ann Arbor, MI, United States; 2General Surgery-Extracorporel LifeSupport Laboratory, University of Michigan, Ann Arbor, MI, UnitedStates; 3Pediatric and Cardiology, University of Michigan CongenitalHeart Center, Ann Arbor, MI, United States.
Background: Ex situ organ perfusion can extend time before trans-plant, expand the donor pool, and allow for optimization of donororgans.Methods: Forty-kilogram swine are used as heart and blood donors.The swine’s blood is centrifuged, and perfusate is created byreconstituting erythrocytes and plasma (leukocytes are discarded)with a target hemoglobin of 3–4 mg/dL. The perfusion circuit includesa membrane oxygenator, heat exchanger, collapsible rotary pump,pressure-release valve, and bubble trap (figure 1). Perfusate entersthe aortic root at a goal pressure of 50-55mmHg, and drains passivelyinto the reservoir. Once the heart is rewarmed, it is defibrillated to re-store sinus rhythm, but is not continually paced. A portion of the per-fusate is exchanged hourly to dilute out metabolic byproducts. Asampling catheter is placed in the coronary sinus, and EKG leadsare placed in the myocardium. Perfusion pressure, flow, temperature,and blood gas measurements are monitored. Experiments wereended when resistance rose above a critical threshold, or at 12 hours.Results:We perfused nine hearts ex situ at body temperature (37-39°C) and two at room temperature. Initial pathology results showedpatchy hemorrhage within the myocardium, prompting us to decreasethe target perfusion pressure in later experiments from 65mmHg to55mmHg. The room-temperature hearts were perfused for 7 and8.5 hours; the normothermic hearts for 9–12 hours. Normothermiawas necessary for hearts to regain sinus rhythm (fig 2); this did notoccur at lower temperatures despite defibrillation. Despite regularchanges of perfusate, lactate increased significantly by the end of
FIGURE 1. Ex-situ Heart Perfusion System.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
the perfusion in most experiments. Mean weight gain was 17% overthe course of perfusion.Conclusion: Perfusion of a swine heart for 12 hours with maintenanceof sinus rhythm is feasible.
FIGURE 2. Ex-situ Heart Perfusion -EKG.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
510
Ex-Situ Limb Perfusion System: 24hr preservation of limbs
Alvaro Rojas-Peña1,2, Benjamin Bryner2, Yao Nie2, Cory Toomasian2,Jeffrey Punch1,2, Robert Bartlett2, Kagan Ozer2,31General Surgery-Section of Transplantation, University of Michigan,Ann Arbor, MI, United States; 2General Surgery-Extracorporel LifeSupport Laboratory, University of Michigan, Ann Arbor, MI, UnitedStates; 3Orthopaedic Surgery, University Michigan, Ann Arbor, MI,United States.
Limbs used for transplantation or re-implantation are cold stored for6-9hr before re-attachment. However, anaerobic metabolism wasteproducts are released after reperfusion affecting recipient outcomes.The goal of this study was to develop and test a 25°C ex-situ limbperfusion system (ELiPS) that improves limb viability prior to trans-plantation in a porcine model.Methods: Control group (n=2), limbs were amputated, flushed andcold-stored for 9-12hr, then transplanted. Study group (n=6), limbswere attached to ELiPS for 24hr using pressure-controlled perfusion(80-90mmHg) with a blood-derived perfusate (plasma + 10%RBC,no WBC) then transplanted. Reperfusion was monitored (12hr) inanesthetized recipients. ELiPS settings, perfusate gases and response
FIGURE 1. Ex-situ Limb Perfusion System.
FIGURE 2. Transplanted Limbafter 24hr of Ex-situ Perfusion in a PorcineModel.
r 27, 2013, Volume 96 Number 10S S261
thorized reproduction of this article is prohibited.

November 27, 2013
to neuro-muscular stimuli were monitored. Biopsies were taken forhistology.Results: Successful 24hr ELiPS was feasible in the study group. Allparameters were normal at the end of ELiPS, except for lac-tate=12.8±1.4mmol/L (normal <2mmol/L). Average limb vascular re-sistance=1.3±0.27mmHg/(mL/min) –normal=<1mmHg/(mL/min)-.Throughout 12hr of transplantation, lactate levels in the recipient werenormal, and response to neuro-muscular stimuli was positive in 40%of the limbs in the study group, compared to 0% in the control group.Weight gain at the end of reperfusion was >15% from baseline inthe control group, compared to <10% in the study group.Conclusion: 24hr ELiPS perfusion, followed by transplantation is fea-sible in this animal model. Lactate levels increased throughout ELiPS,but normalized after reattachment. Future directions include, addinghemodialysis to the ELiPS (lactate clearance), perfusate oncotic pres-sure (edema) and long-term sterility.
S262 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
511
Intermediate xeno host reverses the viability ofsmall for size liver graft in rodent
Yinghua Tian1, Thomas Fehr2, Achim Weber3, Bostjan Humar1,Rolf Graf1, Pierre-Alain Clavien11Department of Visceral and Transplantation Surgery, UniversityHospital of Zürich, Zürich, Switzerland; 2Department of Nephrology,University Hospital of Zürich, Zürich, Switzerland; 3Department ofPathology, University Hospital of Zürich, Zürich, Switzerland.
Background: Living related liver transplantation is a prevalent choicefor end stage liver disease patient due to the shortage of the organ do-nor. However, the small for size liver graft syndrome impedes the op-eration, results in unexpected outcome of increasing morbidity andmortality.Hypotheses: Small for size liver graft is able to regenerate rapidly inan intermediate Xeno host; consequently the enlarged liver graft mightbe re-harvested and implanted back to final recipient of original donorspecies hence reverses the small for size syndrome.Methods: 30% liver graft was harvested from C57/B6 mouse, andthen auxiliary orthotopic transplanted into Lewis rat; Tacrolimus wasapplied as suppressant; liver grafts were harvested at 2nd, 7th days af-ter transplantation. The weight of graft was measured before and aftertransplantation, diverse tests were performed for the investigation.Results: The recipient rats were all survived till harvesting days. Theweight of the liver graft was increased significantly both at 2 and 7 daysafter surgery. The hepatocytes of the grafts showed the mitosis andactive proliferation in H&E, PCNA and Ki-67 staining at 2 days aftertransplantation. The histology showed some lymph cells infiltration inhepatic portal track and sinusoids at 7 days. IL-6, TNF-a, HGF ele-vated differently in liver graft and rat liver. Anti-rat CD3 staining waspositive in mouse liver grafts of 2 and 7 day’s postoperatively, butanti-CD68 staining displayed negative result.Conclusion: Small for size liver graft of mouse is able to regenerate inrat. The volume of the small liver graft was increased significantly aftertransplantation. Acute rejection was not observed by FK-506 treat-ment. Regeneration of liver graft and host residual liver were activatedthrough their own regenerating pathway separately. Rat T cells infil-trated in mouse liver graft postoperatively, but Kupffer cell not.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
512
Predictors of early graft loss in donation after circulatorydeath liver transplantation
Georgina E Riddiough1, Michael A Fink1,2, Graham Starkey1,Boa Z Wang1, Paul Gow1, Adam G Testro1, Rhys B Vaughan1,Robert M Jones11Liver Transplant Unit, Austin Hospital, Melbourne, Australia;2Department of Surgery, University of Melbourne,Melbourne, Australia.
Introduction: Liver transplantation using grafts from donation aftercirculatory death (DCD) donors has been shown to result in inferioroutcomes. The identification of controllable factors that can predictgraft loss is crucial and could positively impact graft and patientoutcome.Methods: We retrospectively collected data for all DCD livertransplants performed at this centre. We compared DCD liver graftsfunctioning > 1month with those grafts that were lost (including dueto patient death) ≤ 1month follow-up with regard to donor and recipi-ent variables. Donor variables assessed included age, cause of death,donor risk index, use of antemortem heparin, time from extubation toperfusion, time from systolic blood pressure ≤ 50mmHg to perfusion,interstate offer and cold ischaemia time. Recipient factors assessedincluded age, MELD score, TSANZ listing status, medical status andventilatory support.Results: Between 1 October 2007 and 31 December 2012 16 DCDliver transplants were performed. Graft loss by 1 month follow-up oc-curred in 31% (n=5). Factors which significantly increased the risk ofearly graft loss included not giving antemortem heparin (p=0.049),time from systolic blood pressure ≤ 50mmHg to perfusion greaterthan 15 mins (p=0.037), cold ischaemia time > 420mins (p=0.049), in-terstate donor offer (p=0.025), ventilatory support (p=0.025) and recip-ient listed TSANZ status 1 (p=0.025).Conclusion: Controllable factors such as the administration of ante-mortem heparin, warm ischaemia time, cold ischaemia time and recipi-ent selection can influence graft outcome in DCD liver transplantation.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
515
Organs transplanted per donor: Our experience in Japan
Juntaro Ashikari, Setsuko Konaka, Kikuo NomotoJapan Organ Transplant Network, Tokyo, Japan.
Since the Organ Transplant Act has been enacted in Japan in 1997,we have had 220 donations after brain death (DBD), resulting in 961recipients receiving the transplants and 1,156 organs transplantedas of May 2013.As the number of DBD per million population (PMP) is very low (0.35),we have attempted to maximize the utilization of organs transplantedper donor (OTPD).The donor age was 46.2 plus minus 14.1. The male/female ratio was123/97. The causes of death were cerebral vascular 60.0%, anoxia21.4%, head trauma 17.7%, CNS tumor 0.5%, other 0.5%. The dura-tion from hospital admission to organ recovery were 8.4 plus minus8.9 days. From the 220 donors, 161 hearts (73.2%), 251 lungs (countin single lungs, 57.0%), 174 livers (79.1%), 156 pancreas (70.9%),401 kidneys (91.1%), 13 small intestines (5.9%) were transplanted.The OTPD were average 5.3 plus minus 1.7, median 5.Three major factors that are thought to have influenced the OTPD areaggressive donor evaluation and donor management by designatedmedical consultants, aggressive placements of the expanded criteriadonor (ECD) organs by the Japan Organ Transplant Network, and ag-gressive utilization of the ECD organs by the transplant centers.Despite the utilization of ECD organs, our five year survival rates wereheart 95.4%, lung 70.5%, liver 78.2%, pancreas 69.1%, kidney 74.5%,and small intestine 72.2%.As the numbers of DBD are limited in Japan, we have maximized theOTPD by aggressive donor evaluation, donor management, place-ment of organs and utilization by the transplant centers.
r 27, 2013, Volume 96 Number 10S S263
thorized reproduction of this article is prohibited.

November 27, 2013
516
Kidney transplantation using donors over 60 years of age inrecipients older than 60 in Argentina
Liliana Bisigniano1, Victor Fernandez1, Viviana Tagliafichi1,Daniela Hansen Krogh2, Carlos Soratti31Cientific and Technical Direction, INCUCAI, Buenos Aires, Argentina;2Informatic Apartment, INCUCAI, Buenos Aires, Argentina;3Presidence, INCUCAI, Buenos Aires, Argentina.
Objective: To analyze results after implementation of kidney trans-plantation program using donors over 60 years of age in recipientsolder than 60 in Argentina.Material and Methods: We analyzed patients who underwent trans-plantation between December 13, 2010 and March 30, 2013. Thesepatients were included in a special distribution list, and also remainedin the general kidney waiting list. This was a study of descriptive statis-tics; and included measurements of frequency and distribution asmean, median and proportions. This report shows both patient andgraft survival curves obtained by the Kaplan-Meier method.Results: Between December 13, 2010 and March 30, 2013; 271transplants were performed in patients over 60 years of age usingkidneys from donors older than 60. The mean donor age was 64.44years, while the recipient´s mean age was 66.26 years old. Thecauses of death of the donors included Cerebral Vascular Accident(83%), head trauma (14%) and other causes (3%). One hundred nine-teen (119) kidneys were obtained by multiorgan retrieval and 152 bymonorganic retrieval. As for the cold ischemia time (CIT) the medianwas 21.67 hours (8.92-47.08). The Cross Match was less than 20 in265 patients, between 30 and 50 in 4 patients, and above 50 in 2patients. The leading cause of chronic renal failure (CRF) was un-known in 27% of the cases, followed by nephroangiosclerosis (23%),and diabetic nephropathy (20%) as the third cause. Time on waitinglist to transplantation was a median of 1.19 years, with a minimum of0.03 to a maximum of 10.08 years. As for the time between inclusionin the program and transplantation the median was 66.46 days, with aminimum of 1 day and a maximum of 523 days. The distribution of theplace where the patient was to transplant allocation was a median of 7with a minimum of 1 and a maximum of 115. Two hundred seventy sixof a total of three hundred sixteen organs procured were implantedand 40 (13%) were non accepted. The leading causes of none accep-tance were macroscopic alterations (16), prolonged CIT (11), biopsy(7) and absence of an appropriate recipient (6). Most donors camefrom Buenos Aires and the federal district. However, the second prov-ince with the largest number of recipients was Santa Fe, Buenos Aireswas the first one and the federal district the third one. Patient survivalrates at 30 and 365 days were 96% and 76.3% and 95.2% and 72.3%for graft survival respectively.Conclusions: The average age of both donors and recipients wassimilar. The most common cause of death was stroke. 59% of dona-tions were monoorganic retrieval procedures. The median CITwas sim-ilar to that of the general list. The median allocation order rate (7) washigher than the national rate (4). Time on waiting list to transplant wasshorter than the national average time. The average stay in the programwas less than 3 months. The provincial and regional distribution rateamounted to 70%. Patient and graft survival rates were not statisticallysignificant as for differences with those patients over sixty years of agewho received an organ from donors under the age of sixty.
S264 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
517
Making difficult choices: Community preferences forallocation of donor organs
Kirsten Howard1, Stephen Jan2, John M. Rose3, Michelle Irving1,4,Germaine Wong1,4, Allison Tong1,4, Jonathan C. Craig1,4,Steven Chadban5,6, Richard D. Allen6, Alan Cass71School of Public Health, University of Sydney, Sydney, Australia;2The George Institute for International Health, Sydney, Australia;3Institute for Transport and Logistics Studies, University of Sydney,Sydney, Australia; 4Centre for Kidney Research, The Children'sHospital Westmead, Westmead, Australia; 5Central Clinical School,Bosch Institute, University of Sydney, Sydney, Australia; 6Departmentof Renal Medicine, Royal Prince Alfred Hospital, Sydney, Australia;7Menzies School of Health Research, Casuarina, Australia.
Background: The demand for organs for transplant far exceeds sup-ply. Organs for transplant can be viewed as a community held re-source, but little is known about community preferences for how theyshould be allocated. We used discrete choice methods to assesscommunity preferences for organ allocation.Methods: Community respondents answered 30 scenarios eachpresenting two hypothetical patients, indicating which patient shouldreceive a transplant if only one organ was available. Patients were de-scribed by factors such as age, sex, number of previous transplants,time on waiting list, pre- and post- transplant life-expectancy, pre-and post- transplant quality of life (QOL).Results: There were 2051 respondents with a mean age of 44(range18-83); 51% were female. Compared to a patient aged 40,younger patients were given higher preference, while older patientswere less preferred. Family members being registered as donors,the patient having caring responsibilities, and spending a longer timeon waiting lists all increased priority. Patients with lower pre-transplantlife-expectancy and lower pre-transplant QOL were given a higherpreference (need); as were patients who had a higher post-transplantlife-expectancy and a higher post-transplant QOL (capacity to benefitor utility). Lower pre-transplant life-expectancy was however, valuedmore highly than increased post-transplant life-expectancy. When LEand QOL were combined into quality adjusted life years (QALYs) therewas a higher preference for giving organs to patients with lower pre-transplant QALYs, compared to higher post-transplant QALYs withone fewer pre-transplant QALY requiring an extra 2.12 post-transplantQALYs to compensate for the loss.Conclusions: Many factors considered in current organ allocationalgorithms are consistent with community preferences. Lower pre-transplant life expectancy and QALYs (which can be thought of as‘need’) were more important than higher post-transplant life expec-tancy or QALYs. This suggests that whilst there is a current movetoward allocation algorithms favouring high life expectancy after trans-plant (utility), emphasis also ought to be given to ‘need’ as measuredby pre-transplant life expectancy and quality adjusted life expectancy.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
518
Validation of risk models for allocation by survivalbenefit in liver transplantation
Michael A Fink1,2, Graham Starkey2, Bao-Zhong Wang2,Peter W Angus2, Paul J Gow2, Adam G Testro2, Robert M Jones1,21Department of Surgery, Austin Hospital, The University of Melbourne,Melbourne, Australia; 2Liver Transplant Unit, Austin Hospital,Melbourne, Australia.
The imbalance between demand for and supply of organs makes ra-tioning of available organs inevitable. Appropriate allocation of this lim-ited resource is essential to maximise the clinical impact oftransplantation. One approach that has been developed is allocationby survival benefit of transplantation over waiting. The liver transplantmodels developed by Schaubel et al. [1] were validated in a single cen-tre. The waiting list model was evaluated in patients on the waiting liston 1st January and 1st July each year from 2000 to 2012 (n = 758).The post transplantation recipient and donor models were evaluatedin patients transplanted from 1/1/2000 to 31/12/2012 (n = 497).Patients were grouped according to hazard ratio for each model andsurvival rates were compared using log rank. The waiting list modelstratified patient survival on the waiting list (P<0.001) and predictedthe survival of low risk patients well, although it did not differentiatewell between higher risk patients. The donor risk model stratified posttransplantation survival well (P = 0.019). The recipient risk modelstratified post transplantation survival (P = 0.004), although thepatients predicted to be at greatest risk (HR > 3) in fact had a low riskof post-transplantation graft loss (87% 5-year graft survival). Riskmodels can enable evaluation of allocation by survival benefit, butcontinued exploration, refinement and validation of allocation modelsand estimation of impact on survival is required.
TABLE 1
Waiting
Reference:[1] Schaubel DE, Guidinger MK, Biggins SW et al: Survival benefit-based deceased-donor liver allocation. Am J Transpl 2009, 9:970–981.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
519
Would eplet matching change the allocation of deceased donorkidneys to unsensitised renal transplant recipients?
Hung Do Nguyen1, Germaine Wong2, Sam Fidler3, Lloyd D'Orsogna3,Wai Lim1
1Department of Renal Medicine, Sir Charles Gairdner Hospital, Perth,Australia; 2Centre for Kidney Research, Sydney University andWestmead Hospital, Sydney, Australia; 3Clinical ImmunologyDepartment, Royal Perth Hospital, Perth, Australia.
Background: It is suggested that donor/recipient matching at the struc-tural epitope level (i.e. amino acid sequence known as eplets)may betterpredict rejection, graft survival and development of anti-human leukocyteantigen (HLA) antibodies compared to broad HLA-antigen matching fol-lowing kidney transplantation. Broad antigen mismatch with 0–2 epletmismatches identified using HLAMatchmaker is considered an accept-able mismatch (AM) at the structural level.Aim: To determine whether the inclusion of AM would change the al-location of deceased donor kidneys to unsensitized recipients inWestern Australia (WA).Methods: Unsensitized (defined as panel reactive antibodies ≤20%)renal transplant recipients who had received deceased-donor kidneysin WA from January to December 2011 were included. Allocationscores and rankings were recalculated for historical matches with in-clusion of AM to determine potential reductions in waiting time.Results:We identified 420 pairs (47 recipients). Results are shown inTable 1. If AM were considered, 34% (16/47) of patients would haveimproved to levels 1–4 ranking with 28% (15/47) being offered a kid-ney, reducing waiting time by a mean (SD) of 15 (10) months.Conclusions: Inclusion of AM in the allocation of deceased-donorkidneys would reduce the waiting time for up to 30% of unsensitisedrecipients.
HLA-A(pairs)
HLA-B(pairs)
HLA-DR(pairs)
Level 1-4Rank
(patients)
KidneyOffer
(patients)
timereduction,months
(mean [SD])
HLAMatchmaker(0-2 eplet mm)
47 87 8 16 13 15 [10]
r 27, 2013, Volume 96 Number 10S S265
thorized reproduction of this article is prohibited.

November 27, 2013
520
Modelling the benefits and costs of integrating an acceptableHLA mismatch allocation model for highly-sensitised patients
Hung Do Nguyen1, Germaine Wong2,3, Kirsten Howard2,Frans Claas4, Jonathan Craig2,3, Samantha Fidler5,Lloyd D’Orsogna5, Jeremy Chapman3, Ashley Irish6,Paolo Ferrari7, Frank Christiansen5, Wai Lim1
1Department of Renal Medicine, Sir Charles Gairdner Hospital, Perth,Australia; 2Sydney School of Public Health, The University of Sydney,Sydney, Australia; 3Centre for Kidney Research, The Children’sHospital at Westmead & Centre for Transplant and Renal Research,Westmead Hospital, Sydney, Australia; 4Eurotransplant ReferenceLaboratory, Department Immunohematology and Blood Transfusion,Leiden University Medical Centre, Leiden, Netherlands; 5Departmentof Clinical Immunology, Royal Perth Hospital, Perth, Australia;6Department of Renal Medicine, Royal Perth Hospital, Sydney,Australia; 7Department of Renal Medicine, Fremantle Hospital, Perth,Australia.
Background: The Eurotransplant acceptable mismatch program hasimproved transplantation access for highly-sensitised recipients. How-ever, the benefits and costs of implementing such a program remainunknown.Methods: Using decision analytical modelling, we compared the averagewaiting time for transplantation, overall survival gains (in life-years andquality-adjusted life-years gained) and costs of integrating an acceptablemismatch allocation model compared with the current deceased-donorkidney allocation model in Australia.Results: Acceptable mismatches were identified in 12 of 28 (43%)highly-sensitised recipients using HLAMatchmaker. Inclusion of accept-ablemismatches in the current allocation model improved the transplan-tation access for 4 (14%) highly-sensitised recipients, with an averagereduction in waiting time of 34 months (from 86 to 52 months). Com-pared with the current allocation model, incorporating an acceptablemismatch allocation model achieved an overall lifetime gain of 0.034quality-adjusted life-years and savings ofover $4,000per highly-sensitisedpatient, with a small consequential loss of 0.005 quality-adjusted life-yearsand extra costs of $800 for every reallocated patient.Conclusions: Despite modest overall health gains, application of anacceptable mismatch allocation model is an equitable approach to im-prove transplantation access for highly-sensitised transplant candidateswithout compromising the overall health benefits among the otherpatients on the deceased-donor waitlist in Australia.
S266 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
521
Kidney transplantation from deceased donors with terminalcreatinine > 3.0
Richard D. Hasz, Howard M. Nathan, Sharon M. WestGift of Life Donor Program, Philadelphia, PA, United States.
Purpose: Demonstrate that kidneys from donors with creatinine ≥ 3.0can be utilized for transplantation.Method: Analysis of organ donors recovered over an 18-year period(January 1995- December 2012) was performed. Kidney utilization &transplant outcomes were evaluated for donors with terminal creati-nine ≥ 3.0 from whom at least one kidney was recovered with intentto transplant. Kidney graft survival was evaluated at 6 months, 1 yr,3 yrs and 5 yrs post-transplant using the Kaplan-Meier method.Result: 6,392 organ donors were recovered during the study period &397 (6.21%) had a terminal creatinine ≥ 3.0. Of the 5,908 kidneydonors recovered, 208 (3.52%) had terminal creatinine ≥ 3.0. A totalof 410 kidneys were recovered and 233 (57%) were utilized for trans-plant from these donors. The mean donor age for kidney donors withhigh terminal creatinine was 37 yrs (r = 6–80) & the mean donorage for organ donors that did not become kidney donors was 50 yrs(r = 0.25–78). The ATN rate was 61% and median graft survival was6.4 years, with 90% graft survival at 6 months, 87% at 1 yr, 71% at3 yrs and 61% at 5 yrs. Kidney recovery & utilization by terminal creati-nine is summarized below.
Conclusion: Donors with creatinine ≥ 3.0 have a higher ATN rate butacceptable graft survival and warrant further evaluation & should notnecessarily be eliminated from the limited renal donor pool. Evaluationof donor age & terminal creatinine can assist in donor selection.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
522
The outcome of renal transplants engrafting grafts from dcddonors and risk factors for the long-term graft survival - a singlecenter experience during the three decades -
Kiyotaka Hoshinaga1, Mamoru Kusaka1, Yusuke Kubota1,Hitomi Sasaki1, Naohiko Fukami1, Masashi Takenaka1, Taihei Itoh2,Takashi Kenmochi2, Ryoichi Shiroki11Urology, Fujita Health University, Toyoake, Japan; 2TransplantSurgery, Fujita Health University, Toyoake, Japan.
Introduction: In recent years, it is known that kidneys procured fromdonors after cardiac death (DCD) have a potential to expand the donorpool. In this study, the posttransplant outcome of renal allografts re-covered from DCD donors is investigated and the risk factors affectingthe renal prognoses were analyzed.Study subjects: From April 1979 to Dec. 2012, 535 kidneys were re-trieved from 270 DCD donors at our center, using in situ regionalcooling technique. Only 49 (9.2%) grafts were discarded and 443transplanted between 1983 and 2011 were enrolled in this study.The age of the donors and recipients ranged from 0.7 to 75 (mean;47.6 years) and from 7 to 72 (mean; 41.7 years), respectively. Thewarm ischemic time (WIT) ranged from 1 to 71 minutes (mean;11.7). The serum creatinine level before cardiac arrest ranged from0.4 to 5.4 mg/dl (mean; 1.49). All the patients were treated withimmunotherapy consisting of calcineurin inhibitos, steroid and others.For the statistical analysis, Kaplan-Meier method and Log-rank testwere used.Results:Following renal transplants, primary non-function was noted in 27(6.5%), immediate function (IF) in 58 (13.1%), and delayed graft functionin 358 (80.9%). The 1, 3, 5, and 10 year patient survival rates were97.0%, 92.1%, 90.0%, and 82.9%, respectively. The 1, 3, 5, and 10 yeargraft survival rates were 86.1%, 75.6%, 68.5%, and 52.8%, respectively.The significant risk factors for the long-term graft survival were the donorage, cause of death (CVA), donor hypertension and WIT.Conclusion: Kidneys procured from DCD donors had good renalfunction as well as excellent long term graft survival, when in situ re-gional cooling technique was applied. DCD donors should be the ex-cellent resources of deceased donor renal grafts, and they shouldhave a great potential to expand the donor pool in the era of severe or-gan shortage.Transplant Surgery
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
523
Evaluation of patients who are referred to lungtransplant clinic in Iran
Shadi Shafaghi, Sareh Parto, Seyyed ShahabeddinMohammad Makki, Hamid Reza Khoddami Vishteh, Fariba Ghorbani,Katayoun NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran (IslamicRepublic of).
Background: Although lung transplantation is a lifesaving option insome end stage lung diseases, it’s outcome is highly dependent to re-cipient selection and management in lung transplant waiting list. Weconducted this study to evaluate referred patient’s condition to lungtransplant clinic.Methods: We evaluated 960 visited patients in our transplant clinic,as one of the most active transplant center in Iran in 2012, for theirgeneral condition, body mass index (BMI), heart assessment and es-pecially pulmonary artery pressure (PAP), socioeconomic status andcompliance to treatment.Findings: Although %41 of referred patients were suitable for trans-plant, 22% were referred early and 37% were unsuitable for transplan-tation. They were considered unsuitable because of severely highPAP in 33%, severe deconditioning and low BMI in 21%, too old fortransplant in 16 %, very poor socioeconomic status of 15% and nothaving enough compliance to follow the treatment in 8%. Pleural thick-ening was dramatically significant in 7% of the patients, that oursurgeons didn’t accept them for transplant.Conclusion: Most Patients referred for lung transplant were in poorcondition because of late referring for transplantation and not havinga suitable rehabilitation. Establishing the rehabilitation program in dif-ferent parts of the country and informing the pulmonologists about thereferral criteria and better management of the patients with end stagelung disease are essential.Keywords: Lung transplantation, End stage lung disease, Transplan-tation waiting list, Transplantation clinic
r 27, 2013, Volume 96 Number 10S S267
thorized reproduction of this article is prohibited.

November 27, 2013
618
Single center experience in lung transplantation usingextended donors versus standard donors
Dewei Ren1, Brian Bruckner1, Tadashi Motomura1,Limael Rodriguez3,Thomas Kaleekal2, Soma Jyothula2, Saverio LaFrancesca1,Scott Scheinin1, Matthias Loebe11DeBakey Heart and Vascular Surgery Departmenta, HoustonMethodist Hospital, Houston, TX, United States; 2Division ofPulmonary Medicine, Department of Medicineb, Houston MethodistHospital, Houston, TX, United States; 3Department of Surgery, St.Luke’s Memorial Hospita, Ponce, PR, United States.
Background: Currently a shortage of donor lungs remains the mostimportant limitation to lung transplantation. Short-term and long-termeffects of lung transplants with extended donors are not well known.This study evaluated the outcome of recipients of lungs from extendeddonors in our program.Methods:Weperformed a retrospective analysis of 492 consecutive lungtransplants at our institution from January 2007 through September 2012.Recipients were divided into two groups, standard donor (SD) or extendeddonor (ED). ED was defined as having one of the following criteria: donorage> 55 years, pulmonary contusion, pulmonary inflammation, smoking20 pack/year, duration of ventilation longer than 5 days, purulent secretionsor inflammation at bronchoscopy, PO2 < 300 on FiO2 100%, Chest X-ray/CT indicate infiltration, Localized emphysema. The primary end point was30-day, 6-month and 12-month mortality. Survival data were calculated byKaplan-Meier analysis with the Log-Rank test.Results: Of 492 double/single lung transplants done, 156(31.7 %)were from ED. The two groups were evenly matched in recipientage, sex and BMI. ED group had 62 elderly donors (mean 59.3 yearsold, range 55-70); 50 smokers; 51 intubation>5 days; 26 all others. Pri-mary diagnoses and double or single lung transplant were not signifi-cantly different between two groups. The 30-day mortality for SD was18(5.4%) of 336 versus 16(10.3 %) of 156 for ED (P=0.049). The six-month mortality for SD was 37(11%) of 336 versus 32(20.5%) of 156for ED (P=0.018). The 12-month mortality for SD was 49(14.6%)of 336 versus 37 (23.7 %) of 156 for ED. The 30-day, 6-month and12-month mortality for SD versus ED if smoker lungs were excludedwas not statistically significant (p=0.42, 0.067, 0.11).Conclusions: The result of this analysis showed inferior outcomesfrom ED with heavy smoking history. Donor age > 55 years, intubationtime and mild lung contusion had no significant effect on postoperativesurvival.
S268 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
619
Exchange of best practices: Standardization of abdominalorgan procurement surgery
Christina C Krikke1, Sijbrand SH Hofker1, Jeannette J de Graauw5,Andre AG Baranski2, Paul OP Gobee3, Sandor SS Mihaly4,Rutger RJ Ploeg1,6, Bernadette BJJM Haase-Kromwijk5,Candide C Font-Sala71Surgery, University Medical Center, Groningen, Netherlands;2Surgery, University Medical Center, Leiden, Netherlands; 3Pathology,University Medical Center, Leiden, Netherlands; 4Organ procurement,HNBTS-OCO, Budapest, Hungary; 5Dutch Transplant Foundation,Leiden, Netherlands; 6Transplant Surgery, University of Oxford,Oxford, United Kingdom; 7WP 6, ACCORD, Paris, France.
Background: Considering the growing organ demand worldwide, it ismandatory to optimise organ procurement and training of surgeons in or-der to reduce injury of organs during procurement and increase the qual-ity of transplanted organs. In the Netherlands a complete trajectory fromtraining of surgeons in procurement surgery to the quality assessment ofthe procured organs was implemented in 2010. This mandatory trajec-tory comprises three training and certificationmodules: E-learning, train-ing-on-the-job and aMasterclass. A national committee of supervisors ofthe procurement teams and policymakers of the Dutch Transplant Foun-dation has been established tomonitor the 32 surgeons that started withthe curriculum and to further improve the quality of the procured organs.Methods/Material: Thanks to the ACCORD Joint Action project(Achieving Comprehensive Coordination in Organ Donation), co-funded under the European Commission Health Programme, threetwinning activities to exchange best practices between countries arebeing overseen by France. The Dutch trajectory is being adaptedand implemented in Hungary, as one of these twinning activities.Results: The E-learning was tested by a panel of 6 Hungarian surgeonsand 56 surgeons from the United Kingdom and was accredited in July2013 by the European Accreditation Council for Continuing Medical Ed-ucation of the European Union of Medical Specialist. As a pilot phase forfuture national training, 6 Hungarian surgeons from the SemmelweisUniversity are being trained: they already fulfilled their E-learning, train-ing on the job activities are progressing, and a Masterclass in Hungaryis programmed in 01/2014.Conclusion: There is great potential for sharing best practices andespecially to export this standardized training in organ procurementsurgery to other European countries and even broader, with the finalaim to provide a national training to all countries lacking one and to im-prove quality and safety criteria of donated organsAll participants woud like to thank the European Commission forfunding.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

All Kidneys AKI kidneys only
November 27, 2013
620
Time to donate: The relationship between the time fromdeclaration of brain death to procurement of organs on livertransplant allograft outcomes
Nudrat Rashid1, Oran Rigby2, Myra Sgorbini31Intensive Care Unit, Nepean Hospital, Sydney, Australia; 2TraumaServices, Wagga Base Hospital, Wagga, Australia; 3Intensive CareService, Royal Prince Alfred Hospital, Sydney, Australia.
Initial poor graft function (IPGF) following orthotopic liver transplanta-tion (OLTx) is important in prognostication of recipient outcome. A ret-rospective study was conducted at Sydney’s Royal Prince AlfredHospital (RPAH) of 47 adult patients who underwent OLTx in 2010from brain dead donors. The aim of this study was to determine if timefrom declaration of brain death to organ procurement is a risk factor forIPGF. Data was obtained from medical records maintained by the Aus-tralian National Liver Transplant Unit based at RPAH and by accessingthe databases kept by the Australia and New Zealand Liver TransplantRegistry as well as data held by the Australia and New Zealand OrganDonation Registry. We studied the incidence of IPGF and analysedmatched donor parameters to graft outcomes. IPGF was definedbased on an aspartate aminotransferase (AST) or an alanine amino-transferase (ALT) of >1500U/ml on two consecutive measurementswithin the first 72 hours after OLTx, with an elevation lasting for48 hours. Results show that IPGF occurred in 4 of the 47 patientsand there was no significant difference in the mean duration of timefrom declaration of brain death to organ procurement (15.5 +/- 2.9hours in IPGF group versus 16.2 +/- 9.2 hours in non-IPGF group,P=0.619). The occurrence of IPGF in the recipient was associatedwith a significant increased length of stay in the intensive care unit(20.3 +/- 12.8 hours versus 6.4 +/- 5.6 hours, P=0.003). The incidenceof IPGF in this study (8.5%) was low as compared to other reports inthe literature of up to 23%. The lack of a significant effect may beexplained by the fact that this was a relatively small study and there-fore underpowered. Additional research is required to further delineatedonor factors that contribute to initial poor graft functions after OLTx.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
621
Deceased donors with severe acute kidney injury - A potentialsource to expand the donor pool
Adyr Moss, Raymond Heilman, Nitin Katariya, David Mulligan,Winston Hewitt, Ramesh Battra, Hasan Khamash, Harini Chakkera,Jana Huskey, Maxwell Smith, Kunam ReddyTransplant Center, Mayo Clinic Arizona, Arizona, AZ, United States.
Background: Our aim was to determine the outcome of transplantingkidneys from selected donors with severe AKI.Methods: We selected all patients receiving single organ deceaseddonor kidney transplant at our center transplanted between June2004 and October 2012. AKI donor was defined as a donor terminalCr > 2.0. Donor data was obtained from UNET. The acute kidney injurynetwork criteria (AKIN) were used to stage the severity of the AKI inthe donor (stage 1 to 3 with 3 requiring Cr 3 times baseline elevationor increase Cr ≥ 4 or urine output < 0.3 ml/kg for > 24 hours or anuria >12 hours). Continuous variables are given as mean± 1 SD.Results: There were 104 in the AKI group and 501 in the non AKIgroup. Baseline characteristics were similar, except AKI group hadlonger cold ischemia time (19.8±7.8 vs. 15.6±7.2, p<0.0001), weremore likely to be male (76% vs. 57%, p=0.02). HLA mismatch washigher in the AKI group (4.1±1.7 vs. 3.6±2.0, p=0.03). Characteristicsof the donors in the AKI group: peak Cr 4.02±1.84, terminal Cr 3.53±1.62, oligoanuric in 39%, renal replacement therapy in 10%. Pulsatilepump was used more often in the AKI group (61% vs. 23%,p<0.0001). Delayed graft function (DGF) was more frequent in theAKI group (69% vs. 27%, p<0.0001). The Cr at 1 week was higherin the AKI group (4.26±2.18 vs. 2.66±1.95, p<0.0001) but Cr andeGFR at 1 year (yr) were similar. 1 yr protocol biopsy (Bx) findingswere not significantly different. Actuarial graft survival was similar at1 and 3 yr (AKI 92% and 88%, non AKI 92% and 86%). For the AKIgroup, the kidneys from donors with AKIN stage 3 were more likelyto have DGF and a higher Cr at 1 week, but eGFR and Bx findingsat 1 yr were similar (table).
Non AKI donor(n=501)
All AKI donors(n=104) P
AKIN <3(n=32)
AKIN 3(n=64) P
DGF 27% 69% <0.0001 50% 78% 0.03Cr 1 week 2.66±1.95 4.26±2.18 <0.0001 3.47±2.20 4.65±2.08 0.01Cr 1 month 1.72±1.02 1.84±1.22 0.32 1.85± 1.57 1.84± 1.01 0.97eGFR 1 year 60.0±22.6
(n=328)60.2±21.9(n=54)
0.94 58.1±21.8(n=20)
60.7±20.5(n=29)
0.70
Banff ci>1 on1 yr Bx
30% (n=264) 40% (n=43) 0.23 36% (n=11) 38% (n=26) 1.0
Conclusion: Kidneys from AKI donors, including carefully selecteddonors with severe AKI, have similar outcomes to non AKI donorkidneys. More liberal use of these organs will help relieve the organshortage.
r 27, 2013, Volume 96 Number 10S S269
thorized reproduction of this article is prohibited.

November 27, 2013
622
Osteoporosis in lung transplant candidates in Iran:predisposing factors
Meysam Mojtabaie, Shadi Shafaghi,Seyyed Shahabeddin Mohammad Makki, Fariba Ghorbani,Sareh Parto, Hamid Reza Khoddami Vishteh, Katayoun NajafizadehLung Transplantation Research Center, Masih Daneshvari Hospital,Shahid Beheshti University of Medical Sciences, Tehran, Iran (IslamicRepublic of).
Background: It has been previously shown that end stage lung dis-ease is associated with osteoporosis and also post-transplantoutcomes are affected by this situation. Due to higher prevalence ofosteoporosis in our general population we decided to determine rela-tionship between osteoporosis and lung transplant candidates possi-ble predisposing factors.Methods: Bone mineral densitometry (BMD) was conducted by usingdual energy X-ray absorptiometry in patients who were candidate forlung transplantation during 2009 and 2012. BMD was reported forlumbar spine (LS) and femoral neck (FN) densitometry. Patient demo-graphics, spirometry and 6 minutes walking test (6mwt) results wererecorded and analyzed by logistic regression analysis.Results: In this study 108 patients were evaluated, 22 with emphy-sema, 35 with bronchiectasis, 46 with idiopathic pulmonary fibrosis(IPF) and 5 with primary pulmonary hypertension (PPH). Mean agewas 40.7 ± 11.7 year. Overall, 43.5% of patients had osteoporosis(Hip or Spine-Tscore > -2.5 SD). Mean T score and SD were -1.87and 1.52 for lumbar spine and -1.98 and 1.40 for femoral neck. 38patients (35.2%) were osteoporotic and 46 of them (42.6%) wereosteopenic in femoral neck. Meanwile 33 patients (30.6%) were oste-oporotic and 50 of them (46.3%) were osteopenic in lumbar spine andapproximately 25% of patients in both groups had normal BMD. Meandistance in 6MWTwas 275 ±94.5 meters which founded to be corre-lated with osteoporosis (p=0.021). Osteoporosis also founded to becorrelated with body mass index (BMI) (r=0.472, p=0.001 for femoralneck, r=0.311 and p=0.01 for lumbar spine) and had no associationwith disease diagnosis, sex, age, and pulmonary function test.Conclusion: Bone densitometry is correlated with BMI and also thedistance in 6MW that means patient conditioning. This studyemphasizes the importance of rehabilitation and nutrition for endstage lung disorders.Keywords: Osteoprosis, Lung transplantation waiting list
S270 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
625
Good samaritan kidney donation: A comparative studybetween New Zealand and Australia
Kusam Nagi, Moohambika Srinivasan, Piyumi B. Lekamlage,Katrina A. BramstedtBond University School of Medicine, Gold Coast, Australia.
Australia and New Zealand are trans-Tasman neighbours who share aBritish colonial heritage, but the similarities end when the topic turns toliving organ donation. We conducted a comparative study of the ratesof Good Samaritan [altruistic] Kidney Donation and living donation (ingeneral) in Australia and New Zealand. Data was sourced fromANZDATA. In the Oceania region, New Zealand pioneered the firstGood Samaritan donation in 1998, with Australia following with theirfirst Good Samaritan donation six years later, in 2004. Our analysisshows New Zealand outpacing Australia in the rates of both Good Sa-maritan kidney donation (statistically significant) and living donation ingeneral (not statistically significant). We pose three reasons for thedisparity: 1. Website content analysis finds that every New Zealandhospital which offers Good Samaritan donation mentions “unrelated”or “altruistic” donation on their website (kappa 0.78; 3 raters) whereasonly 2 of 15 Australian hospitals offering this procedure mention suchon their website (prior study)[1]; 2. Since 2005, New Zealand has of-fered a financial safety net for living donors, namely, up to 12 weeksnon-taxable financial assistance due to lost income and/or extrachildcare costs, whereas Australia introduced a financial assistanceplan only recently (July 2013, 6 weeks taxable paid leave); 3. UnlikeAustralia, with its numerous states, territories and policies, NewZealand is not carved into jurisdictional segments with multiple poli-cies on donation, lending to a more streamlined approach. Only timewill tell if the Australian paid leave program will have a significant im-pact on living donation rates. A national Australian policy on Good Sa-maritan donation could potentially have a positive impact and shouldbe trialled as a pilot. Additionally, enhancing the content of Australianhospital websites might also raise community awareness about GoodSamaritan donation.
Reference:[1] Bramstedt KA, Dave S. The silence of Good Samaritan kidney do-nation in Australia: a survey of hospital websites. Clin Transplant2013, 27:E244-8.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
626
Value adding information distribution to a distributed networkof organ donation professionals via content curation
Deborah Verran, Tim Kreukniet, Jonathan GillisDonateLife Network, Canberra, Australia.
Introduction:One of the challenges of meeting the information needsof healthcare professionals is being able to stream appropriate con-tent to them. Content curation is one method via which informationcan be distilled along with being value added prior to distribution.Methods: A strategy was developed for streaming information fromthe relevant academic literature to the DonateLife network acrossAustralia. This involved the development of a portal on an informationtechnology platform. Onto this site selected curated articles would beplaced on a regular basis. The content curation was performed by aprofessional with expertise in organ donation aided by the medicaldirector.Results: The portal went live initially in November 2012. Following aninitial introductory phase site metrics are now being monitored. Cu-rated commentary on a total of 27 published articles has been posted.The majority of articles are related to organ donation alone (54%), oron both organ donation and transplantation (28%). Categories ofarticles include scientific reports 41%, topic reviews 22%, qualitativeliterature 22%, guidelines 7.5% and case reports 7.5%. The most fre-quent topics for postings are donation after cardiac death 30%, donormanagement/selection 18.5%, surveying attitudes on organ donation18.5%, donor infection 15% and other 18%. Statistics for the site fora 4 month period have revealed a total of 330 page views via 90unique visitors, averaging approximately 2 page views per day.Conclusions: It is possible via both content curation and informationtechnology to stream value added information to a distributed organdonation network. The type of information being streamed reflectsthe current needs and trends in organ donation. Preliminary metricsreveal moderate engagement with the tool by the network members.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
627
Education and strategy: Aligning the focus to increaseparticpant engagement
Rohit D’Costa1,2, Kelly Rogerson21ICU, Royal Melbourne Hospital, Parkville, Australia; 2DonateLifeVictoria, Carlton, Australia.
The Victorian DonateLife Network (DLV network) employs 23 medicalspecialists and over 50 nursing specialists and donor co-ordinators.Professional development meetings have been held regularly sincenetwork formation focusing on audit of missed potential donation op-portunities within hospitals. In 2012 an education working group withrepresentation from across the DLV network was formed with the in-tention of developing, implementing and evaluating education strategiesto ensure alignment with DonateLife national strategic priorities[1].The group decided to adapt and re-format the network meetings.Themes were planned for each meeting with reference to the nationalpriorities, e.g. “eye and tissue donation”, “marginal and high riskdonors” or “culturally and linguistically diverse potential donors”. Dy-namic methods of delivering material were used such as moderated“hypothetical” case discussions with participation from transplant sec-tor panellists, presentations from Victorian researchers involved incutting-edge transplantation research and case presentations fromnetwork staff. It was strongly felt that presentation of cases for auditshould remain a core feature of each session.A web-based survey of staff response was undertaken 6 months postimplementation of the changes with 10 questions posed (a combina-tion of Likert scored and nominal data). With 61% (38/62) of eligiblestaff responding (we excluded education working group members),we found strong support for the thematic format of the meetings (87% pos-itive response) and the structure of themeetings in terms of interactive vs di-dactic presentation (71% positive response). Discussion of cases in theaudit at these meetings was felt to be beneficial by 79% of respondents,underlining the importance of maintaining this component at the core ofthe meetings. Overall the majority (70%) of respondents felt that themeetings “meet [their] educational needs” and it is planned that the workinggroup will continue to evaluate and adapt the programme to ensure this.
Reference:[1] Accessed at: http://www.donatelife.gov.au/the-authority/national-reform-agenda-/strategic-priorities
r 27, 2013, Volume 96 Number 10S S271
thorized reproduction of this article is prohibited.

November 27, 2013
628
The development and facilitation of an organ donationeducation workshop for perioperative nurses
Paula Lyons, Jo Sanders, Leanne McEvoyDonateLife Victoria, DonateLife, Carlton, Australia.
The role of the perioperative nurse is essential to the success of theorgan retrieval process and dignified care of the donor. From the liter-ature and anecdotal evidence, it was identified in 2011 that manyperioperative nurses found their role in organ retrieval emotionallyand professionally challenging. In response, a theatre specific work-shop was planned at DonateLife in Victoria, with a focus on providingeducation, support strategies and networking opportunities.A full day workshop was trialled in October 2011 with content specificto the role of the perioperative nurse, a comprehensive overview of thedonation process, and donor family and recipient experiences. Topicsincluded brain death declaration, dealing with death in the operatingsuite and perioperative nurses presenting on their experiences withorgan donation. Group sessions highlighted local organisationaland cultural challenges and corresponding support strategies. 32perioperative nurses attended from a variety of Victorian metropolitanand regional centres.Participant evaluations were overwhelming positive with results statingthe workshop filled a significant gap in education and support inthis challenging area of practice. 100% of attendees stated they wouldrecommend the workshop to their colleagues. Due to participantevaluations, registration demand and support from Victorian operatingtheatres, the theatre specific workshop has been facilitated quarterlyat DonateLife Victoria. This workshop has highlighted the need forcomprehensive theatre specific education in local hospitals and in-formed the facilitation of local workshops by the DonateLife network.An organ donation education workshop specific for perioperativenurses can successfully inform and support perioperative nursesthrough the organ donation process. This workshop has assisted Vic-torian nurses to be prepared, supported and comfortable in their rolein organ retrieval.
S272 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
629
Interpreting in end of life and organ and tissue donationconversations - a DVD to guide and support interpreters, medical,nursing, social work and pastoral care staff involved in theseconversations.
Monica DowlingOrgan and Tissue Donation, Northern Health, Melbourne, Australia.
In all end of life and organ donation family conversations specific train-ing of medical and nursing staff is considered essential. Interpretersare asked to deliver the healthcare professional’s very challengingand often emotive discussions to grieving families without any specifictraining, or even awareness of the orientation of these conversations.Interpreters involved in end of life and organ donation situations needto feel supported in their role, to be familiar with the terms andconcepts associated with end of life and organ donation, to have someunderstanding of the organ donation process and to have consideredtheir own attitudes to, and assumptions about end of life and organdonation.This DVD highlights the multiple conversations on end of life and or-gan donation that occur in the emergency department and in the inten-sive care unit: 1) Breaking bad news to a Turkish family in theEmergency Department. 2) Discussing futility of treatment and with-drawal with a Chinese family in the Intensive Care Unit. 3) Completingthe personal questionnaire with an Arabic family eliciting donor infor-mation on lifestyle, drug and sexual history. 4) Obtaining consentand discussing the organ donation process with an Italian family resid-ing overseas using the Skype medium. A number of culturally andlinguistically diverse (CALD) actors portray families participating inthese conversations. Segments of difficult and sensitive conversationsare highlighted eliciting a range of family responses. Experiencedinterpreters provide tips on the successful and effective utilization ofthe interpreter when conducting face to face conversations andconversations through the Skype medium. Information on end of lifeand organ donation processes is provided in a logical and contextualformat. A menu option allows for the DVD to be played in its entiretyor for each scenario to be played individually.Project funded by a Commonwealth Government grant
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
630
Addressing stigma and engaging orthodox religiouscommunities around organ and tissue donation.
Lyn Phillipson1, Karen Larsen-Truong1, Sandra Jones1, Leissa Pitts2,Miriam Nonu3, Marilisa Filippi3, Anica Petkovski2,Helen Tsalidis2, Zaga Trkulja21Centre for Health Initiatives, University of Wollongong, Wollongong,Australia; 2Multicultural Health Service, Illawarra Shoalhaven LocalHealth District, Wollongong, NSW, Australia; 3Organ and TissueDonor Co-ordination, Illawarra Shoalhaven Local Health District,Wollongong, NSW, Australia.
In Australia, people from culturally and linguistically diverse back-grounds are less likely to have held memorable family discussion ormade decisions about organ and tissue donation. Formative researchconducted in 2011 with members of the Macedonian, Serbian andGreek Orthodox religious communities in the Illawarra-Shoalhavenhighlighted the significant barriers to discussing and making an in-formed decision. In response to identified needs, an integrated socialmarketing program including ‘testimonial-style’ resources, informationbooths, educational forums (involving religious leaders, medicalexperts and testimony) and a media campaign were conducted.Importantly, resources and events targeted the specific concerns ofthe communities and provided opportunities to discuss and raisequestions in a supportive environment. Results from a survey evalua-tion (n=182) showed that more than 90% of all respondents agreedthat the educational resources answered their questions and that theyhad a better understanding of the views of other community membersabout organ and tissue donation. Most Macedonian (77.6%), Greek(94.3%) and Serbian (97.6%) respondents felt that they also had abetter understanding of the views of the Orthodox Church. Almost allMacedonian (98.6%), Greek (100%) and Serbian (97.7%) respondentsfelt that they were more aware of the benefits of organ and tissue dona-tion and importantly, 50% of Macedonian, 63.8% of Greek and 39.5% ofSerbian respondents had discussed their views about organ and tissuedonation with their family at the end of the program. Overall, the projectwas able to translate results from research into a resources and activitieswhich promoted greater awareness and family discussion within com-munities who previously considered the topic taboo. The project alsoadds to the evidence base required to understand and address the spe-cific needs of Orthodox religious communities in regard to the promotionof organ and tissue donation.This project was conducted as a partnership between the Universityof Wollongong and the Illawarra Shoalhavan Local Health District. Itwas funded by a grant from the Commonwealth Organ and TissueAuthority.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
636
Driving data up, driving data down: One’s experience utilizingdashboards, scorecards and reports to increase organ andtissue donation
Sharon West, Richard Hasz, Howard NathanGift of Life Donor Program, Philadelphia, PA, United States.
Aim: To create a data driven culture through the development and useof automated reporting tools to increase organ and tissue donation.Methods: Between June 2007 and June 2013, a set of customizedautomated reporting tools including five dashboards with over 50drill-down reports, sorting and filtering functions and six cascadingscorecards were developed to provide all clinical staff with access todata to monitor and evaluate performance relative to established goalsand peer performance. Departmental and individual goals related tocritical metrics in the referral, evaluation, consent and recovery of po-tential organ and tissue donors are established and re-evaluated byOPO leadership through an ongoing strategic planning process. Allclinical staff have close to real-time access to relevant performancedata and receive feedback related to their performance at least on amonthly basis through individualized scorecards. Managers utilizedashboards on a daily basis to make decisions and monitor and dis-cuss performance. Overall procurement between July 2006 and June2007 (pre-implementation) was compared to overall procurement be-tween July 2012 and June 2013 (post-implementation).Results: The number of organ donors recovered increased by 21%from 366 to 444, the number of organs transplanted increased by17% from 970 to 1134, the number of musculoskeletal donors recov-ered increased by 95% from 628 to 1225 and the number of corneadonors recovered increased by 86% from 1271 to 2360.Conclusion: Reporting tools providing employees throughout theOPO timely access to relevant performance data is critical to meetinggoals and establishing a data-driven culture of accountability.
r 27, 2013, Volume 96 Number 10S S273
thorized reproduction of this article is prohibited.

November 27, 2013
637
Organ Donation European Quality System - ODEQuS Project
Martí Manyalich1, Xavier Guasch2, Maria Paula Gomez3,Gloria Paez4, Luciana Teixeira41School of Medicine, University of Barcelona, Barcelona, Spain;2Intensive Care Unit, Hospital de La Plana, Vilarreal, Spain; 3DTIFoundation, Barcelona, Spain; 4Transplant ProcurementManagement, Barcelona, Spain.
Background: Differences in the number of organ donors amonghospitals cannot be explained only by the number of ICU beds or neu-rologic patients treated. The figures obtained are influenced by the or-ganizational structure of donation process and how efficient it is.ODEQUS is a three years project (October 2010-September 2013) co-financed by the European Agency for Health and Consumers(EAHC20091108) which aims to define a methodology to evaluatethe organ procurement performance at hospital level.Methods: ODEQUS specific objectives are to identify Quality Criteria(QC) and to develop Quality Indicators (QI) in 3 types of organ dona-tion: after Brain Death, after Cardiac Death and Living Donation.Those tools will be useful for hospitals self-assessment as well asfor developing an international auditing model.In order to do so, a consortium has been established involving 14 as-sociated partners from Austria, Croatia, France, Germany, Italy,Poland, Portugal, Romania, Spain, Sweden and United Kingdom,and 5 collaborating partners from Greece, Hungary, Malta, Sloveniaand Turkey.Afterwards, the project has been established in three steps:1. Design of a survey about the use of quality tools in a wide sample of
European hospitals.2. Development of QC and QI by the project experts. The main fields
considered have been organizational structures, clinical proceduresand outcomes.
3. Elaboration of an evaluation system to test the QI in Europeanhospitals.
Moreover, two types of training have been designed and performed:one concerns the development of QC and QI, while another is focusedon how to use evaluation tools.Results: The project has achieved so far to identify 130 Quality Crite-ria and develop 30 Quality Indicators. Those indicators have beentested in 12 European hospitals by means of internal and externalevaluations.ODEQUS Consortium
S274 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
638
A survey on hospital attitude in Korea by usingdonor action program
hyunjin kang1, Minyoung Chu4, Hyunjin Park4, Jaesook Oh3,Song Lee1, Kyungsook Jang1, Jongwon Ha2,51External Cooperation Team, Korea Organ Donation Agency, Seoul,Korea; 2Department of Surgery, Seoul National University College ofMedicine, Seoul, Korea; 3Information Education Team, Korea OrganDonation Agency, Seoul, Korea; 4Donor Mangement Team, KoreaOrgan Donation Agency, Seoul, Korea; 5President, Korea OrganDonation Agency, Seoul, Korea.
Background and Aim: To activate brain death organ donation, Koreahas introduced DAP (Donor Action Program) in Europe to 9 hospitalsas the first pilot application and in 2012 KODA (Korea Organ DonationAgency) introduced DAP in full. Accordingly, this study is to providebasic materials for activities of KODA as an organ procurement orga-nization and the improvement of brain death organ donation.Material and Methods: Survey questionnaires were distributed to 417staffs in 9 DAP hospitals in 2009, and 1035 staffs in 22 hospitals in2012 to compare and analyze their perception, attitude and knowl-edge level on organ donation.Results: The subjects were 53 doctors (12.7%), 328 nurses (78.7%)in 2009, and 258 doctors (25%) and 647 nurses (62.6%) in 2012. Re-garding organ and tissue donation, 87.3% agreed in 2009, and 87.6%in 2012, which shows there has not been a big change. The intentionto donate their own organs increased a little bit from 50.5% in 2009 to52.8% in 2012. Relating with the intention to donate organs of family,the response that they would donate organs with the agreement ofthe family before death did not show change as 60.4% in 2010 and60.0% in 2012, while the response that they have intention to donateeven without the agreement of the family when they were alive in-creased from 2.9% in 2010 to 5.6% in 2012. On the other hand, tothe question if they decide the donation of organs based on the inten-tion of family, positive answers increased dramatically from 39.9% in2010 to 83.5% in 2012. Regarding the consideration of brain deathas death, positive answers increased remarkably from 56.7% in2010 to 72.5% in 2012. Regarding whether they can talk about organdonation freely, positive answers increased a little from 66.7% in 2010to 77.0% in 2012. However, the response that they would not care in-creased a little from 11.5% in 2010 to 13.2% in 2012. Regarding theexperience in training program related to donation, positive answersincreased a lot from 8.0% in 2010 to 28.8% in 2012, and even in edu-cational program on brain death positive answers increased a lot from6.1% in 2010 to 18.0% in 2012.Conclusion: Although the experience of medical professionals in ed-ucational programs on organ donation increased remarkably from2009 to 2012, the positive perception and agreement have not beenincreased much regardless of increased educational opportunities.However, perceptions on the judgment of brain death as death and in-tention to donate organs of family members are changed positively. Di-versified education should be performed for medical professionals toshift the paradigm of medical professionals on organ donations.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
639
Understanding family decisions regarding organ donation
Sandra Neate1,3, Michelle Skinner5, Claudia Marck2,George Jelinek2,3,Tracey Weiland2,3, Bernadine Dwyer6, Bernadette HIckey41Emergency Department, St Vincent's Hospital Melbourne,Melbourne, Australia; 2Emergency Practice Innovation Centre, StVincent's Hospital, Melbourne, Australia; 3Department of Medicine,University of Melbourne, Melbourne, Australia; 4Intensive Care Unit,St Vincent's Hospital, Melbourne, Australia; 5DonateLife Victoria,Melbourne, Australia; 6Australian Organ and Tissue Authority,Canberra, Australia.
Aim: To assist an understanding of factors influencing familydecisions about organ donation (OD).Methods: Face to face or telephone interviews with one or moremembers of families asked to consider OD. Purposive sampling en-sured representation by families who consented to and declined dona-tion. Qualitative exploration of families’ experiences of the request,decision-making and process around OD. Interviews were audio-recorded, transcribed and thematic analysis identified issues impor-tant to participants.Results: Eligible families who had been asked to consider OD fromfour Melbourne hospitals were invited to participate. Families ofintended organ donors, organ donors and families who declined dona-tion were interviewed. Reasons for consenting to donation included:prior discussion regarding or knowledge of loved one’s wishes; dona-tion was consistent with loved one’s values; wanting something goodto come from a tragic situation; and understanding the rareness ofthe opportunity to donate. Reasons for declining OD included: no priordiscussion regarding or knowledge of loved one’s wishes; knowingloved one did not wish to donate; cultural/religious reasons; prolongedtime to donation/wanting it all to be over; not realising the decisionneeded to be made rapidly; too much to take in; not wanting to putthe deceased through anything more; specific aspects of the conver-sation; and OD being raised “too early”. Several families noted an in-fluence of the donation conversation on their ultimate decision.Conclusion: Conversations about OD, and other events or experiencesin the hospital, can influence family decisions regarding OD. Knowledgeof the factors influencing families’decisionsmay assist those conductingdonation conversations.The authors wish to acknowledge the contributions of Dr HelenOpdam, Dr Rohit D’Costa; Dr Sam Radford, Dr Forbes McGain andthe Nurse Donation Specialists of St Vincent’s, Royal Melbourne,Austin and Western Hospitals Melbourne.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
640
Marked improvement of potential donor recognition with theimplementation of a donor action program in Korea
Hyunjin Kang1, Minhwa Kim3, Eunkyong Jang3, Jaesook Oh2,Song Lee1, Kyungsook Jang6, Sunhee Kim7, Jongwon Ha4,51External Cooperation Team, Korea Organ Donation Agency, Seoul,Korea; 2Information Education Team, Korea Organ Donation Agency,Seoul, Korea; 3Donor Management Team, Korea Organ DonationTeam, Seoul, Korea; 4Department of Surgery, Seoul NationalUniversity College of Medicine, Seoul, Korea; 5President, KoreaOrgan Donation Agency, Seoul, Korea; 6Donation Support DeptDirector, Korea Organ Donation Agency, Seoul, Korea; 7Chiefoperating officer, Korea Organ Donation Agency, Seoul, Korea.
Background: Although deceased organ donations increase with newsystem, the gap between supply and demand keeps widening moreand more. Therefore, to improve organ donation from deceaseddonors, we started donor action program (DAP) in collaboration withthe Donor Action Foundation. We tried to find out which step is a weakpoint among organ donation steps and whether the DAP improvedthat step.Methods: Memorandum of understanding (MOU) was made with 27hospitals about the Donor Action Program in 2012, this study reviewedand analyzed the medical records of a total of 2027 deaths consistedof 1355 (66%) who died before the MOU and 672 (44%) who died afterthe MOU.Results: Of the entire analyzed deaths, 30% (617 out of 2027) werepotential donors, of whom 33% (203 out of 617) were identified asdonors, of whom 33% (67 out of 203) had agreed and 64 completeddonation. We identified potential donors of 31% before the agreementand 29% after the agreement. Recognized potential donors by doctorswere 26% before the agreement and 48% after the agreement. As forthe region‐based rate of recognition, it increased from 28% before theagreement to 44% after the agreement in the region 1, from 7% to72 % in the region 2, and from 30% to 47% in the region 3. Recogni-tion rate with respect to the sizes of the agreeing hospitals, therewas no significant difference according to the number of beds and itwas around 57%.Conclusion: We have achieved an increase in the recognition ratewith a short‐term application of the Donor Action Program. In orderto increase the rate of deceased donor organ donation, continued ed-ucation of medical staffs and development of strategy to improve con-sent rate are necessary.
r 27, 2013, Volume 96 Number 10S S275
thorized reproduction of this article is prohibited.

November 27, 2013
646
Donating organs? OK, "But tissues? Hmm" Any suggestion toimprove the situation?
Beatrice Pelleriaux1, Jacqueline Smits2, Leo Roels11Donor Action Foundation, Linden, Belgium; 2EurotransplantInternational Foundation, Leiden, Netherlands.
Background: Whilst there is growing evidence of a relatively strongsupport for organ donation amongst Critical Care (CC) professionalsin Europe, little is known about CCs’ related attitudes, self-reportedconfidence levels and skills with regard to tissue donation.Methodology: A total of 18,532 Donor Action (DA) Hospital AttitudeSurvey (HAS) questionnaires, collected in 6 European countries(Belgium: n=5226, Finland: n=619, France: n=7620, Italy: n=1807,Luxembourg: n=212, Switzerland: n=3048) between January 1, 2006and December 31, 2012, were entered into the DA System Databaseto compare CC medical (n=3201) and nursing (n=13,218) staffs’attitudes, self-reported confidence levels and donation related skillswith regard to organ and tissue donation.Results: Average general positive attitudes to donation varied between96.2% amongst medical and 91.4% of nursing staff (P<.0001). Whilst92.1% of medical and 83.9% of nursing staff would donate their ownorgans after death, willingness to donate tissues decreased to 88.5%and 76.4% respectively (p<.0001). Comfort levels with introducing thesubject of organ vs. tissue donation varied significantly between medical(65.1 % vs. 52.8% (p<.0001)) and nursing staff (31.9% vs. 26.3%(p<.0001)). Medical staff felt more comfortable with obtaining consent fororgan donation than for tissue donation (59.2%vs. 48.7%, p=.0038). Med-ical staff’s self-reported competence levels with obtaining consent werehigher for organs (62.4%) than for tissues (59.3%, p<.01). On average,26.4%ofmedical and 14.6%of nursing staff reported to have received ap-propriate training (p<.0001), whilst 38.9 vs. 51.5% expressed their needfor further specific training (p<.0001).Conclusions: Data presented demonstrates significant differences inCCs’ attitudes, self-reported confidence levels and skills related to or-gan and tissue donation. Further research on why nursing staff haslower positive attitudes and skills levels compared to medical staff willbe necessary. As demonstrated by the educational needs expressedby medical and nursing staff, both organ and tissue donation couldbenefit from further investing in tailored organ and tissue related train-ing efforts.
S276 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
648
Challenges of implementing a donation service in rural andremote Australia
Nichalas Nuttall1, Lee Wood2, Kelly Anstey2, Dianne Stephens21Organ and Tssue Donation Service, Metro South Health,Woolloongabba, Australia; 2DonateLife NT, Northern TerritoryDepartment of Health, Darwin, Australia.
Eye and tissue banks are established in the five mainland states andin the Australian Capital Territory. The Northern Territory has 233 000people spread over 1.3 million square kilometres. Organ Donationprograms have been implemented in the two larger centres in Darwinand Alice Springs, but the Territory, the country’s third largest jurisdic-tion does not have the population to develop its own tissue bank. in2011 DonateLife Northern Territory formed a partnership withQueensland Eye Bank in Brisbane, 3400 km to the south-east to facil-itate an eye donation program in the Northern Territory. The projectuncovered some unique challenges such as:1. Before a patient can be considered for donation, an airline schedule
must be consulted to determine if timelines can be met if donation isto be undertaken.
2. No federal legislation overiding state legislation (e.g. The USA'sUniform Anatomical Gift Act), thereby complicating the donationprocess where donor assessment, consent and tissue recoveryoccurs under Northern Territory legislation and processing, assess-ment, storage and allocation of the tissue occurs under the aus-pices of Queensland legislation.
3. The legislative instruments are not necessarily compatible.4. The travelling time of tissue restricts the number of patients that can
donate eye tissue (by reducing recovery time-lines) compared withpatients in metropolitan Brisbane.
Nevertheless the project phase is almost complete with only servicelevel agreements to be signed before implementation can occur. Bythe time this paper is presented, the program should have com-menced and the first patients should have been able to donate eye tis-sue for transplantation.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
650
Fact not fiction, unifying Australian wide tissue andeye donation data is possible.
Lauren Bell, Kylie HurstANZDATA and ANZOD Registry, Adelaide, Australia.
Objectives: To consolidate Australian tissue and eye data to produceconcise aggregate reporting on unique donors, donations, recipientsand grafts transplanted.Methods: In 2012, the Australian and New Zealand Organ DonorRegistry (ANZOD) in collaboration with the Australian Organ and Tis-sue Authority (AOTA) and Australian tissue banks, initiated a pilot proj-ect for retrospective reporting of 2012 tissue donations. All partiesagreed upon collection of a minimum dataset and prospective datacollection with the creation of a web-based application and databaseto enable concise aggregate reporting.Results: All Australian tissue donation agencies contributed 2012data. Upon review, duplicate counts in donor and donation numbersraised concern. ANZOD identified common data entry errors and for-mulated data cleansing mechanisms to strengthen data integrity andinclude in a web-based unique identification application. The 2012 pi-lot enumerated 3,843 individual tissue donors and 3,978 donations(95.0% musculoskeletal; 2.3% cardiovascular; 2.7% skin). Datadiscrepancies indicated further action was required to guarantee dataquality from initial tissue collection to utilisation.Conclusion: Australian wide tissue donor and donation data was suc-cessfully consolidated for 2012, although areas of erroneous datawere identified. Cleansing mechanisms were introduced to addresserrors and strengthen data integrity. Consolidation continues for2013 data, modified data collection is now capturing total of notifiedgrafts implanted and notified graft recipients for the Australian tissuesector. Continued collaborationwith theEyeBankAssociation of AustraliaandNewZealand (EBAANZ) will allow eye donor and recipient data to un-dergo similar cleansing mechanisms currently performed on tissue data.Ultimately continued refinement of data collection will accurately identifythe supply and demand of the Australian eye and tissue sector.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
802
Cooperation with patient.
Edyta Skwirczy’nska-SzalbierzDepartment of General Surgery and Transplantation, IndependentPublic Clinical Hospital No. 2, Pomeranian Medical University inSzczecin, szczecin, Poland.
In Poland, there is no obligation of having family’s agreement for tak-ing organs from dead relative, because there is obligation of allegedagreement. In practice we are striving to get this agreement. If familyis against transplantation we dissent from taking organs.Positive attitude to medical care results in potential agreement for tak-ing organs from dead relative.The point is to answer the questions:1. Does the way of caring about still living patient, and relation be-
tween doctor and patient’s family has influence on family’s agree-ment for taking organs after death?
2. Does the way of caring about respondents has influence on theiragreement for taking organs?
Research Methods: Questionnaire made of 18 questions. In researchparticipated 173 people.Summary: Thirty two percent of people are satisfied with level of med-ical care. Majority of them are of the opinion that doctors are treatingthem without expected carefulness. Thirty eight percent believes thatdoctors are capable to stop the therapy to get organs for transplantation.Conclusions: There is necessity to recognize correlation betweencorrect relation doctor – patient, trust gain and reliability of doctor’sopinions. Patient’s conviction that they are well treated may regain be-lieve in straightforwardness of doctor’s opinions, less dissatisfactionand criticism for medical care.
Reference:[1] The Cell, Tissue and Organ Recovery, Storage and TransplantationAct 1)2) of July 1st, 2005 (the Official Journal of Acts Dziennik Ustaw05.169.1411, as amended).
r 27, 2013, Volume 96 Number 10S S277
thorized reproduction of this article is prohibited.

November 27, 2013
804
Disqualification of a haemodynamically functional heart withLQTS syndrome - unjustified organ loss?
Romuald Bohatyrewicz1, Maciej Zukowski1,Carl Ludwig Fisher-Froelich2, Maria Wujtewicz3, Radoslaw Owczuk3,Joanna Pastuszka-Solek1, Jowita Biernawska1, Agnieszka Zienciuk4,Antoni Ottowicz3, Katarzyna Kotfis1, Anna Milecka51Department of Anaesthesiology and Intensive Therapy, PomeranianMedical University, Szczecin, Poland; 2Region Baden-Wuerttemberg,Deutsche Stiftung Organtransplanation, Stuttgart, Germany;3Department of Anaesthesiology and Intensive Therapy, MedicalUniversity of Gdansk, Gdansk, Poland; 4Department of Cardiologyand Electrotherapy, Medical University of Gdansk, Gdansk, Poland;5Regional Transplant Coordination Center, Medical University ofGdansk, Gdansk, Poland.
Long QT syndrome (LQTS) is a genetically determined ion channeldisorder. It might be the reason of severe ventricular arrhythmias lead-ing to sudden cardiac death. Early introduction of cardiopulmonary re-suscitation may effect in a restoration of efficient circulation in somecases, however brain death due to anoxia is possible.Case Report: 19 year old female suffered from recurrent syncopalattacks. She was admitted to the hospital following cardiac arrest athome in a mechanism of ventricular fibrillation. During in-hospitaltreatment an episode of the pulseless electrical activity with a shortepisode of nonsustained polymorphic ventricular tachycardia was ob-served. All brain stem reflexes slowly disappeared except for residualrespiratory drive, which persisted until day 17th. On 19th day patientwas declared brain dead. Predonation echocardiography showednormal heart contractility - EF 55%. She was heamodynamically sta-ble, RR-120/80mmHg, HR-106/min, without catecholamine infusion.Kidneys, corneas and aortal homograft were harvested. Heart wasnot transplanted due to suspicion of LQTS. Genetic studies, com-pleted later, confirmed polymorphism KCNH2 gene and all familywas included to program of sudden cardiac death prevention.We presume that LQTS in brain dead patients as a result of cardiacarrest might be unexpectedly frequent, especially in a group of youn-ger donors. Brain death may be the result of brain hypoxia after car-diac arrest in some cases and mechanical injuries due to syncopesin the others.Current guidelines of the ISHLT do not recommend to transplanthearts with intractable ventricular arrhythmias [1]. LQTS obviouslydoes not lead to intractable arrhythmias if earlier recognized and prop-erly treated. So far, at least one case of unplanned but successful“LQTS heart” transplantation with subsequent ICD implantation hasalready been reported [2]. Probably many more were performed with-out such knowledge. The authors of above mentioned publicationwould accept such heart for really sick patient [dr M. Shehata - per-sonal information].Conclusions:1. Transplantation of “LQTS hearts” with concomitant LCD implanta-tion may be considered after proper risk benefit assessment in specialcases.2. The clear opinion of the ISHLT concerning acceptance of “LQTSheart donors” is needed.
References:[1] Costanzo MR et al. The International Society of Heart and LungsTransplantation Guidelines of the Care of Heart TransplantationRecipients. J Heart Lung Transplant 2010;29:914–956.[2] Liu T, Shehata M, Chang D, et al. Prolonged QTand cardiac arrestafter heart transplantation: inherited or acquired? J Electrocardiol2011 44(3):350-2.
S278 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
805
Successful managed care applied in organ donationin “La Raza General Hospital” of Mexico City.
Cesar Villasenor-Colin, Mariano Hernandez Dominguez,Marlene Santos-Caballero, Guillermo Careaga-reyna,Arturo Robledo-Martinez, Israel Pagola-Quintero,Jaime Zaldivar-Cervera, Armando Soberanes-HernandezTrasplant Surgery, Centro Medico Nacional La Raza Imss, MexicoCity, Mexico.
Introduction: The term Managed Care (MC) describes a varied col-lection of techniques to reduce the cost. In the worldwide literaturethere is a minimum of related publications for Managed care appliedin organ donation.Objective: Presenting the first fruits of the successful managed careprogram applied in organ donation in “La Raza General Hospital”(LRGH) of Mexico City.Material and Methods: By means of a descriptive prospective studythe first data of the implementation of the MC program in LRGH fromJuly 01, 2012 to June 30, 2013 are analysed (one year).Results: By the new MC program, were driven a total of 175 CadavericOrgan Donations, originating successfully 56 (32%) Renal Transplants,10 (5.72%) Liver Transplants, 21 (12 %) Heart Transplants and 88(50.28%) Corneal Transplants.Findings: The implementation of some points of the MC system inLRHG by means of the application of multiple mechanisms as healtheconomics toward the medical staff, patients and relatives in agree-ment to the characteristics of Mexican Law is controversy, but thereis not experience in direct implementation in organ donation of highcomplexity as well as the final impact in the process. The MC systemrelated with the handling of the cadaveric donor with brain death Re-nal, Liver, Heart and Corneal multi-organic donor successful pro-cesses implicates revision of the strategies of other transplantgroups with less revenue-yielding results.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.

November 27, 2013
806
A study in surgical errors during organ retrieval
Sandhya Mendon1, Michael Fink1,2, Helen Opdam1,3, Robert Jones1,41Department of Surgery, Austin Health, University of Melbourne,Australia; 2Consultant Surgeon, Liver Transplant Unit Victoria;3Intensive care Specialist, Austin Health, Victorian Medical Director ofOrgan and Tissue Donation, DonateLife; 4Director, Liver TransplantUnit Victoria.
Surgical problems during organ retrieval may cause complications inthe transplant recipient and these surgical problems may result inthe complete loss of donor organs. As the practice of organ donationhas grown rapidly in the last decade, our goal is to interpret thesefindings to improve surgical awareness for a better recipient organoutcome.From the transplants made between January 2011 and March 2013 atotal of 223 donors were studied. This study involved donor reportsfrom DonateLife Victoria of 689 organs which included 64 Hearts,109 Lungs, 119 Livers, 30 Pancreas, 367 kidneys. Corresponding or-gan retrieval report forms were also analysed.Surgical problems were classified into the following categories:1. Surgical problems observed by donor surgeon2. Surgical problems observed by the recipient surgeon3. Surgical problems leading to organ loss4. Level of the retrieving surgeon5. Time of surgery of retrieving and transplantingSurgical problems recorded during this 27 month time period were;non-identified abnormal anatomy (2.90%), damaged vein (1.02%),damaged artery (1.60%), damaged ureter (0.73%), damaged organ(0.15%), non-identified pathology (0.73%), paperwork and packaging(3.92%) and organs discarded (0.6%).It was observed that the error rate was slightly high (2.3%) in detectingaberrant anatomy when the procedures were performed by fellowsand hence Consultants should be present during retrieval proceduresto identify abnormal anatomy and errors.Organ retrieval is prone to surgical problems. Especially in a system oforgan transport, consistent reporting of surgical problems and qualityassurance is needed to maintain and to improve surgical quality.
Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
807
The general surgeon as a kidney donation coordinator,a model of certainty, experience in the general hospital La Razaof Mexico City.
Cesar Villasenor-Colin, Mariano Hernandez-Dominguez,Marlene Santos-Caballero, Arturo Robledo-Martinez,Israel Pagola-Quintero, Jaime Zaldivar-Cervera,Armando Soberanes-HernandezTransplant Surgery, La Raza General Hospital, Mexico City, Mexico.
Introduction: In a Cadaveric Kidney Transplant, the coordinator takescare of the organization of the whole process, existing principally two:the donation coordinator (in charge of the detection and care of the pa-tient that has lost his life as well as of talking with the family to facilitatethe donation) and the transplant coordinator (in charge of organizationand logistics, among the assessment of the potentially viable organsand tissues, as the best way of taking them to the final implantation'splace), both working on complete harmony. In Mexico, most of the do-nation and transplant coordinators are nursing staff criticizing thesurgeons as donation and transplant coordinators.Objective: Presenting the experience of a General Surgeon as Kid-ney Donor and Transplant Coordinator at “La Raza General Hospital”of Mexico City.Material and Methods: They were analysed the total of cadaveric kid-ney transplants during July 01, 2011 to June 30, 2013 under the coor-dination of a General Surgeon.Results: In the course, under the coordination of a General Surgeon,took effect 103 successful kidney cadaveric transplants, 61 male and42 female. 14 rejections of potential donors showed up only.Findings: The low kidney donation rate leads to contemplate theneed of a professional General Surgeon principally at the moment ofhaving the first contact with the family of the donor.
r 27, 2013, Volume 96 Number 10S S279
thorized reproduction of this article is prohibited.

November 27, 2013
808
Expert decision support systems in cadaveric organ donationat La Raza General Hospital of Mexico City
Cesar Villasenor-Colin, Mariano Hernandez-Dominguez,Marlene Santos-Caballero, Guillermo Careaga-Reyna,Roberto Ortiz-Lerma, Karla Verdiguel, Arturo Robledo-Martinez,Israel Pagola-Quintero, Jaime Zaldivar-Cervera,Armando Soberanes-HernandezTransplant Surgery, La Raza General Hospital, Mexico City, Mexico.
Introduction:When the knowledge on a theme is distributed betweenseveral people, the Expert Decision Support System (EDSS) is thebest way of using the combined knowledge as in cadaveric organ do-nation (COD).Materials and Methods: By a descriptive-prospective-observationalstudy, cadaveric organ donations were analysed from July 01, 2012to June 30, 2013 at La Raza General Hospital (LRGH) of Mexico City.EDSS was implemented in the selection, attainment and multi-organicprocuration of patients with encephalic death firstly defining the
S280 Supplement to Transplantation Novembe
Copyright © 2013 Lippincott Williams & Wilkins. Unau
problems in terms that were specific and reasonably acceptable forall the members of the team where all the participating members con-tributed establishing models and parameters.Results: By means of the implementation of the EDSS managed toincrement the organ donation at LRGH as compared with the prioryear. Taking effect 88 Corneal Transplants, 10 Liver Transplants, 56Kidney Transplants and 21 Heart Transplants, all originating of COD.Managed to avoid sessile discussion between LRGH members to de-fend own positions, avoiding waste of time and achieving always spe-cific agreements accepted by all with positive attitude in front of thepresented problems.Discussion: The main advantage of the EDSS has two aspects: first,it is not necessary for the LRGH members to have experience onthings such like symbolic analogies and second, the decisions for con-sent do not require the total agreement of all LRGH members, al-though the decision should be acceptable for all, if it is not, it meansthat the whole information has not been considered completely andit takes more discussion, which implies the utilization of methodologyfor elaboration and implantation with systematization of activities. TheEDSS enabled the increment in the number of COD without decreasein the quality of results.
r 27, 2013, Volume 96 Number 10S
thorized reproduction of this article is prohibited.
Copyright © 2022 FDOKUMEN