“The Moriscos in Morocco: From Granadan Emigration to the Hornacheros of Salé”
Upload
independentCategory
view
1download
0
American Journal of Transplantation 2007; 7: 2020–2030Blackwell Munksgaard
C© 2007 The AuthorsJournal compilation C© 2007 The American Society of
Transplantation and the American Society of Transplant Surgeons
doi: 10.1111/j.1600-6143.2007.01879.xBrief Communication
Emigration from the British Isles to SoutheasternSpain: A Study of Attitudes TowardOrgan Donation
A. Rıosa,b,∗, P. Cascalesa,b, L. Martıneza,b,
J. Sanchezc, N. Jarvisa, P. Parrillaa
and P. Ramıreza,b
aDepartamento de Cirugıa. Hospital Universitario Virgende la Arrixaca, El Palmar, Servicio Murciano de Salud,MurciabCoordinacion Regional de Trasplantes de la ComunidadAutonoma de Murcia, Consejerıa de Sanidad, MurciacAsociacion de Ayuda al Enfermo Renal (ADAER), Murcia∗Corresponding author: Antonio Rıos,[email protected]
Southeastern Spain is a cosmopolitan area wherethere is a growing British and Irish population. Theobjective is to analyze the attitude toward organ do-nation among British and Irish citizens living in south-eastern Spain. A sample was taken stratified accordingto a respondent’s country of origin (n = 1700) betweenNovember 2005 and April 2006. Attitude was evalu-ated using a validated questionnaire, which was self-administered and completed anonymously. A sampleof 2000 Spanish citizens was used as a control group.The survey completion rate was 95% (n = 1611). Atti-tude toward donation is favorable in 72% (n = 1155)of respondents with 8% (n = 122) against and 20%(n = 334) undecided. Attitude is more favorable thanin the control group (72% vs. 63%; p < 0.0001). Thefollowing factors influence this attitude: (1) attitudetoward the donation of a family member’s organs (OR= 4.891); (2) having discussed the matter of organ do-nation within the family (OR = 2.513); (3) a willingnessto accept an autopsy if it were necessary (OR = 1.706);(4) having no concern about the mutilation of the de-ceased donor (OR = 3.294); (5) having a partner whois in favor of donation (OR = 2.786) and (6) a respon-dent’s belief that he or she might need a transplant inthe future (OR = 2.243). The attitude of this populationis more positive than in the native Spanish populationand is determined by many psychosocial factors.
Key words: Attitude, British, cadaver, family, generalpopulation, Irish, organ donation, Spain psychosocialfactors
Received 25 December 2006, revised 21 April 2007 andaccepted for publication 26 April 2007
Introduction
Organ transplantation has become more efficient and of-fers increasingly more favorable life conditions (1). It is onlylimited by the shortage of organs available for carrying outthis technique (2). In order to increase the number of trans-plant organs it is necessary to take action in different areas,both within organizations (3) and on the social conscience(4–6).
Currently, immigration is a frequent and growing phe-nomenon in Western European society given its great eco-nomic development. This fact is having an effect on theworld of transplantation, because there is an increasingnumber of patients who are foreign nationals on the trans-plant waiting list (7), and requests for organs from nonna-tive families is also occurring (8).
In Spain, this notable increase in the foreign populationis creating a new social and demographic reality in thewhole country. Moreover, there is not just a nonnativepopulation from poor countries but given its climate andthe services on offer; in certain areas the number of resi-dents from developed countries has increased, especiallyfrom the British Isles and Germany, places where thedeceased organ donation rates are much lower than inSpain. This development, together with the new politi-cal and social European reality, involving the implementa-tion of new European Union freedom of movement laws,makes the population flows between member countrieseasier and simpler. This has changed southeastern Spaininto a cosmopolitan area in which the population originat-ing from the British Isles is increasing and is perfectly in-tegrated into the social structure. What is more, airlinecompanies have created a network of flights in all the lo-cal airports that connect this area with the whole of theBritish Isles every day, with different flights and at a lowcost.
The objectives of this study are to: (1) find out the na-ture of attitude toward the donation of one’s own or-gans in the population aged over 15 years in our RegionalCommunity born anywhere in the British Isles and (2)to analyze the psychosocial variables that influence thisattitude.
2020

British People in Spain and Organ Donation
Materials and Methods
Study population
A random sample was taken of the population aged ≥15 years who residein the Autonomous Regional Community of Murcia in southeastern Spainand who were born anywhere in the British Isles. This sample was strati-fied by the respondents’ nationality (n = 1700). The sample was stratifiedby age and sex for each nationality and according to the available data. Inorder to find out about the population with these characteristics, we stud-ied the most recent census of inhabitants in our Regional Community inwhich there is a record of the legal population born in the British Isles. Thismunicipal census corresponds to the year 2003 (total population: 1,269,230inhabitants) and the British/Irish population living here permanently com-prises of 3,464 people (http://www.ine.es/inebase/cgi/axi). In addition, inhousing estates created in the last 10 years in different areas of the coast,there is normally a population of 15,000 inhabitants from the British Islesaccording to the private companies that manage these housing estates.Such a population in each municipality tends to be located in specific areasor housing estates, making it easy to locate this population. The margin oferror at a confidence level of 95.5% (2 sigmas), K = 2, was estimated to bee ± 1.91 for the whole sample, p = q = 0.5.
Data collection procedure
The instrument used to measure attitude was a questionnaire validated inour geographical area (4–6) (see Annex 1). A pilot study was carried outbetween May and August of 2005 involving a random sample, in order toconfirm and validate the questionnaire in this population sub-group. Theonly problem encountered was the language in certain sub-groups so thatone questionnaire was used in Spanish and another in English.
This questionnaire was self-administered and completed anonymously (3–5min were necessary for it to be completed in person), and the whole pro-cess was supervised by collaborators from the Regional transplant Center(five professionals who were previously trained and they carried out thestudy between November 2005 and April 2006). To carry out the study thecollaborators went to the areas where the British and Irish tend to reside.
Variables analyzed
The attitude toward the donation of one’s own organs was studied as a de-pendent variable. The following were analyzed as independent variables: (1)social-personal factors [age, sex, marital status, having descendents, levelof education and a respondent’s place of origin in the British Isles where therespondent is native]; (2) knowledge about organ donation and transplanta-tion [previous experience of organ donation and transplantation; knowledgeof the concept of brain death; a respondent’s belief that he or she mightneed a transplant in the future]; (3) social interaction variables [a partner’sattitude toward organ donation and transplantation; family discussion aboutorgan donation and transplantation; and attitude toward the donation of theorgans of a family member if it had to be decided]; (4) pro-social behavior [at-titude toward participation in voluntary type pro-social activities]; (5) factorsrelated to religion [a respondent’s religion; and knowledge of the attitude ofa respondents religion toward organ donation and transplantation] and (6)variables about attitude toward the body [attitude toward corpse cremation,corpse burial and carrying out an autopsy if it were necessary and concernabout the mutilation of the body after donation].
Control group
A random sample of 2000 citizens aged >15 years of the native populationof our regional Community was taken as a control group. This group wasstratified by age, sex and geographical location (7). In such a group, attitudetoward the donation of a respondent’s own solid organs was evaluatedusing the same questionnaire: attitude was favorable in 63% of cases (n =
1274), unfavorable in 31% (n = 620) and 6% (n = 106) were undecided. InTables 1 and 2 there is a summary of the bivariate and multivariate statisticalanalysis of the control group.
Statistical analysis
The data were stored on a database and analyzed using the SPSS 11.0 sta-tistical package. Student’s t-test and the v 2 test were used for the analysisof data. Fischer’s exact test was applied when the contingency tables hadcells with an expected frequency of <5. In order to determine and evaluatethe multiple risks, a logistic regression analysis was applied using the vari-ables that were statistically significant in the bivariate analysis. Values of p< 0.05 were considered to be statistically significant.
Results
Attitude toward organ donation
The questionnaire completion rate was 95% (n = 1611).The 89 cases, which did not complete the questionnaire,comprised 57 respondents who directly refused to respondalleging a lack of time; 15 who refused to complete the sur-vey because ‘it was about organ donation and transplanta-tion’ and the remaining 17 were nonvalid questionnaires.
Attitude toward the donation of one’s own solid organsis favorable in 72% of respondents (n = 1155). The mainreasons given for this favorable attitude are: (1) to avoidthe useless destruction of organs (49%; n = 571); (2) reci-procity, in other words doing for others what we would liketo be done for ourselves (38%; n = 442) and (3) consideringit to be a moral duty (33%; n = 386).
Of the rest, attitude is against in 8% (n = 122) and 20%(n = 334) are undecided. Most do not given any reasonfor such an attitude (n = 257; 56%), and among thosewho give a reason, the most common is fear of mutilationof the corpse 15% (n = 68), wanting to leave the deadin peace 12% (n = 56), and fear of apparent death whenorgan donation takes place 11% (n = 48).
In comparison with the Spanish control group we find thatattitude toward organ donation is more favorable amongresidents of British and Irish origin (72% vs. 63%; p <
0.0001). What is more, among those who are not in favor,it is noteworthy that the percentage of the population thatis undecided is much higher than in the control group (20%vs. 6%), as seen in Figure 1.
Socio-personal variables
There is a similar mean age among those who are in fa-vor and not in favor of donation (45 vs. 43 years; p =0.141). However when we analyze the sample accordingto age group, there is a less favorable attitude among theyoungest respondents (between 15 and 34 years 66% arein favor; 35–49 years 72% are in favor and >50 years 75%are in favor). With respect to sex, attitude is more favorableamong British and Irish women than among men (74% vs.69%; p = 0.012). There is also an association between
American Journal of Transplantation 2007; 7: 2020–2030 2021

Rıos et al.
Table 1: Summary of the influence of different variables on the opinion toward the donation of one’s own organs in the control group
Variable Favorable attitude Unfavorable attitude p
Socio-personal variablesMean age: 45 ± 13 years <35 years >50 years <0.001Sex – – N.S.Marital status Single Married, widowed <0.001Municipality 20–50,000 > = 250,000 <0.001
100–250,000Level of Education Secondary Literate or less <0.001Profession – – N.S.Descendents No Yes <0.001
Variables of knowledge about ODTPrevious experience of ODT Yes No <0.001Knowledge about needs – – N.S.Knowledge about brain death Yes No <0.01
Variables of social interactionKnowledge of a partner’s attitude Yes No <0.001Family discussion about ODT Yes, favorable Not known <0.001
AgainstVariables of pro-social behavior
∗Attitude toward blood donation Yes, usually willing to donate Refusal <0.001Attitude toward pro-social activities Yes, usually willing to participate Refusal <0.001
Religious variablesReligious attitude Agnostic Practicing Catholic <0.001Knowledge of the opinion of the Church – – N.S.
Variables of opinion about the bodyCremation Yes No <0.001Burial – – N.S.Autopsy – – N.S.Concern about mutilation after donation No Yes <0.01
∗This question is only included in the control group questionnaire.ODT = Organ donation and transplantation.
the respondent’s attitude and his or her marital status (p =0.012) and having descendents (p = 0.006) (Table 1).
Finally, there are no differences according to the respon-dent’s level of education (p = 0.575), nor according to therespondent’s original country (p = 0.176). For example,77% of those respondents from the Republic of Irelandare in favor compared to 71% in favor in the UK. More-over, within the UK, attitude toward donation is similar re-gardless of the country of origin. In this respect, there is afavorable attitude among 73% of the northern Irish, among73% of the Scottish, among 76% of the Welsh and among70% of the English (p = 0.416). The most numerous groupof respondents is from England, and there are no differ-ences according to the part of England from which theycome, so that the attitude among those from the Northis 72%, among those from the Midlands 72% and amongthose from the south it is 73% (p = 0.957). As shown inFigures 2 and 3, the percentages in favor of donation aresimilar between the different nations and also according tothe different counties from which they come.
Variables of knowledge about organ donation
The respondents who have had previous experience of thematter, through family members and friends, have a morefavorable attitude than those who have not (82% vs. 69%;
p < 0.001). There is also an association between attitudeand knowledge of the concept of brain death (p = 0.191)(Table 3). Thus, those who know of this concept and whoaccept it are more in favor than those who do not equatebrain death with actual death or those who do not under-stand the concept (77% vs. 68% and 67% respectively;p < 0.001).
It is worth noting that only 8% of respondents (n = 126)consider that they might need a transplant for themselvesin the future. However, this factor is significantly associatedwith attitude toward donation, in such a way that thosewho believe that they would need one are in favor in 87%of cases, those who do not are in favor in 68%, and thosewho are undecided in 71% (p < 0.001).
Social interaction variables
Regarding social interaction variables, it has been foundthat those respondents who had previously discussed thematter of organ donation and transplantation within thefamily have a more positive attitude (85% vs. 53%; p <
0.001). Within the family, the opinion of a respondent’spartner toward donation is very important. Thus, when thepartner is in favor, 86% of respondents are in favor, whilstwhen they are against this percentage decreases to 56%(p < 0.001) (Table 4).
2022 American Journal of Transplantation 2007; 7: 2020–2030

British People in Spain and Organ Donation
Table 2: Variables associated with the donation of one’s own solid organs in the control group (Multivariate study)
Variable Regression coefficient (b) Standard error Odds ratio (CI) p
Age15–34 years (n = 840) 135–49 years (n = 460) –0.40345 0.3498 0.83 (1.67–0.41)≥50 years (n = 700) –0.7949 0.1987 0.45 (0.67–0.3) 0.002
Level of education<Secondary (n = 1114) 1≥Secondary (n = 884) 0.6432 0.2196 1.78 (2.76–1.15) 0.006
Previous experienceNo (n = 1388) 1Yes (n = 611) 0.2989 0.0652 2.02 (2.30–1.77) 0.001
Knowledge of the concept of BDNo (n = 972) 1Yes (n = 1028) 0.9121 0.1012 1.4 (1.71–1.14) 0.013
Knowledge of partner’s attitudeNot known (n = 556) 1Yes, against (n = 129) –0.9110 0.5185 0.9 (2.53–0.32)Yes, favorable (n = 853) 0.6284 0.0281 2.6 (2.75–2.45)No partner (n = 412) 0.3007 0.6219 1.8 (6.2–0.52) 0.002
Blood donationNo (n = 727) 1Yes (n = 1244) 0.6491 0.2811 3 (5.26–1.7) < 0.001
Pro-social attitudeNo (n = 529) 1Yes (n = 1450) 0.6100 0.1002 1.6 (1.95–1.31) 0.017
In favor of cremationNo (n = 1342) 1Yes (n = 658) 0.5919 0.0744 1.8 (2.11–1.55) < 0.001
DK/NA = Does not know/ No answer; ODT = Organ donation and transplantation; BD = brain death.
It has been seen that those who are in favor of the donationof a deceased family member’s organs are more in favorof the donation of their own organs (84%), than those whoare not (29%) and those who are undecided (44%) (p <
0.001).
Variables of pro-social activity
The respondents who usually participate in pro-social vol-untary type or social help activities, or who are willing toparticipate in them, have a more favorable attitude than
Figure 1: Attitude toward the donation of
one’s own organs in the study group and
the control group.
those who do not [76% and 74% vs. 63% respectively; p< 0.001] (Table 4).
Variables of religion
Regarding religious activity there are some differences:those who believe in a religion that is other than Catholic orAnglican-Protestant have a less favorable attitude (59% vs.70% and 72%, respectively). Moreover, those who statethat they are atheist-agnostic are more in favor (77%) thanthose with a religion (p = 0.010). It must be emphasized
American Journal of Transplantation 2007; 7: 2020–2030 2023

Rıos et al.
Figure 2: Favorable attitude toward the
donation of one’s own organs in the dif-
ferent countries of the British Isles.
that among those who state that they are religious, only30% know that their religion is in favor of donation, andknowing that their religion is in favor is clearly associatedto an attitude in favor of donation compared to those whobelieve that their religion is against or who do not know theopinion of their religion (80% vs. 25% and 67%, respec-tively) (Table 5).
Variables of attitude about the body
With respect to variables about attitude toward manipula-tion of the corpse various associations have been found. Inthis respect, those respondents who are willing to acceptcremation of the body after death are more in favor of or-gan donation than those who are not (75% vs. 65%; p <
0.001). Similarly, attitude is more favorable among thosewho would be willing to have an autopsy carried out upondeath if it were necessary (81% vs. 67%; p < 0.001). Re-garding attitude according to whether burial of the bodyis preferred or not, attitude is more favorable toward or-gan donation among those who prefer options other thanburial, although this is not a statistically significant relation-ship (p = 0.066). As shown in Table 5, fear of mutilationafter donation or uncertainty when faced with this situa-tion make attitude toward donation less favorable than itis among those who do not report any fear about suchpossible mutilation (49% and 50% vs. 84%; p<0.001).
Multivariate analysis
The following variables persist as independent variables af-fecting attitude toward the donation of one’s own organs:(1) attitude toward the donation of a family member’s or-gans (Odds Ratio = 4.891 if it is favorable and OR = 0.432if it is not favorable); (2) having discussed the matter of or-gan donation and transplantation within the family (OR =2.513); (3) a willingness to have an autopsy carried out if itwere necessary (OR = 1.706); (4) having no concern aboutmutilation of the deceased donor after death (OR = 3.294);(5) having a partner who is in favor of organ donation andtransplantation (OR = 2.786) and (6) a respondent’s beliefthat he or she might need a transplant in the future (OR =2.243) (Table 6).
Discussion
There are fully developed transplant programs in the vastmajority of European countries. However, it has been seenthat donation rates in these countries are very disparate(12). These differences have been attributed, among otherfactors, mainly to cultural differences (9). However, al-though populational studies about attitude toward organdonation (10–11) provide disparate acceptance rates ac-cording to the country, there are generally favorable atti-tudes in different European countries, with rates rangingfrom between 65% and 90%.
2024 American Journal of Transplantation 2007; 7: 2020–2030

British People in Spain and Organ Donation
Figure 3: Favorable attitude toward the donation of one’s own organs in the different countries of the British Isles and in different
English counties.
Our study challenges this theory where the differences arejustified by cultural factors, at least in Spain and the BritishIsles. In this way we can see that the attitude toward or-gan donation among British and Irish citizens who cometo reside in southeastern Spain is more favorable than thatpreviously described in our native population. Moreover,various respondents have only been living in our Commu-nity for a short time, which makes it difficult to think of achange in mentality just because of living in Spain. All ofthis means that in the same country, with the same organprocurement system, the donation rates among Spanishcitizens and British or Irish residents in Spain are very simi-lar, as shown by the data of the National Transplant Organi-zation (13). With this same attitude, the real donation ratesin the British Isles are lower than Spanish rates (11,14–16).Therefore, the differences between donation rates in Spainand the British Isles, assuming that the British/Irish andSpanish populations are equally generous, must be found
mainly at a structural and institutional level. In this respect,the Spanish model is currently the one that has proven tobe most efficient (16) and because of this it is being copiedby many countries. However, other factors should be con-sidered (legislation, institutional and political support, etc)(17). In the UK professionals related to transplantation arein favor of a change in the donation system in order toincrease the donation rate (18,19). In this respect, somestudies in English-speaking communities suggest that theproblem is the system and that when changes were made(similar to those of the Spanish model) there was an in-crease in the donation rate.
In Spain a coordination system has been achieved that hasobtained high rates of donation and if we want to reducedonation refusals action should be taken at the level of thegeneral public (3,12). The situation of awareness of thegeneral public is the same, or better, among citizens from
American Journal of Transplantation 2007; 7: 2020–2030 2025

Rıos et al.
Table 3: Socio-personal, knowledge about donation and transplantation and social interaction variables that influence attitude towarddonation
Favorable attitude Unfavorable attitudeVariable (n = 1155; 72%) (n = 456; 28%) p
Socio-personal variablesMean age: 45 ± 13 years 45 ± 13 43 ± 15 0.141
Age (groups)15–34 years (n = 365) 241 (21%) 124 (28%) 0.009
35–49 years (n = 556) 398 (35%) 158 (36%)≥50 years (n = 654) 491 (44%) 163 (37%)DK/NA (n = 36) 25 11
SexMale (n = 718) 492 (43%) 226 (50%) 0.012
Female (n = 881) 654 (57%) 227 (50%)DK/NA (n = 12) 9 3
Marital statusSingle (n = 234) 234 (20%) 126 (28%) 0.012
Separated/divorced (n = 161) 119 (10%) 42 (9%)Married (n = 1048) 773 (68%) 275 (61%)Widowed (n = 30) 20 (2%) 10 (2%)DK/NA (n = 12) 9 3
DescendentsYes (n = 1117) 823 (72%) 294 (65%) 0.006
No (n = 487) 326 (28%) 161 (35%)DK/NA (n = 7) 6 1
Level of educationNo education (n = 120) 90 (12%) 30 (11%) 0.575Primary (n = 30) 24 (3%) 6 (2%)Secondary (n = 469) 337 (45%) 132 (50%)University (n = 387) 291 (39%) 96 (36%)DK/NA (n = 605) 413 192
Country of originUnited Kingdom (n = 1497) 1067 (92%) 430 (94%) 0.176Republic of Ireland (n = 114) 88 (8%) 26 (6%)
Country of United Kingdom∗Northern Ireland (n = 180) 131 (12%) 49 (11%) 0.416Scotland (n = 327) 237 (22%) 90 (21%)Wales (n = 126) 96 (9%) 30 (7%)England (n = 864) 603 (57%) 261 (61%)
Area of England where native∗∗North (n = 301) 217 (40%) 84 (41%) 0.957Midlands (n = 161) 116 (21%) 45 (22%)South (n = 286) 209 (39%) 77 (37%)DK/NA (n = 116) 61 55
Variables of knowledge about ODTPrevious experience of ODT
No (n = 1283) 890 (78%) 393 (87%) <0.001
Yes (n = 310) 254 (22%) 56 (13%)DK/NA (n = 18) 11 7
Knowledge of the concept of brain deathWrong concept (n = 240) 162 (15%) 78 (18%) <0.001
Concept known (n = 692) 538 (49%) 158 (36%)Concept not known (n = 605) 405 (37%) 200 (46%)DK/NA (n = 74) 54 20
A respondent’s belief thathe or she might need a transplant
Yes (n = 126) 110 (10%) 16 (4%) <0.001
No (n = 216) 146 (13%) 70 (16%)Not sure (n = 1209) 859 (77%) 350 (80%)DK/NA (n = 60) 40 20
∗ Only 1497 respondents are from the UK.∗∗ Only with the 864 respondents from England.DK/NA = Does not know/ No answer; ODT = Organ donation and transplantation.
2026 American Journal of Transplantation 2007; 7: 2020–2030

British People in Spain and Organ Donation
Table 4: Variables of social interaction and pro-social activity variables that influence attitude toward donation
Favorable attitude Unfavorable attitudeVariable (n = 1155; 72%) (n = 456; 28%) p
Social interaction variablesKnowledge of a partner’s attitude
Yes, favorable (n = 804) 693 (62%) 111 (26%) <0.001
Not known (n = 448) 245 (22%) 203 (47%)Yes, against (n = 100) 56 (5%) 44 (10%)I do not have a partner (n = 194) 120 (11%) 74 (17%)DK/NA (n = 65) 41 24
Family discussion about ODT:No (n = 657) 310 (69%) <0.001
Yes (n = 935) 138 (31%)DK/NA (n = 19) 8
Donation of a family member’s organs:Yes (n = 1165) 980 (85%) 185 (41%) <0.001
No (n = 122) 35 (3%) 87 (19%)Not sure (n = 316) 138 (12%) 178 (40%)DK/NA (n = 8) 2 60
Variables of Pro-social activityParticipation in pro-social activity (Voluntary):
Yes (n = 459) 348 (32%) 111 (26%) <0.001
No, nor will I (n = 400) 252 (23%) 148 (34%)No, but I would like to (n = 664) 490 (45%) 174 (40%)DK/NA (n = 88) 65 23
DK/NA = Does not know/ No answer; ODT = Organ donation and transplantation.
the British Isles; therefore, the donation rates of Britishand Irish citizens when they reside in Spain are similar tothose of Spanish citizens and much higher than in theiroriginal countries (12,13). In our country, when donation isconsidered among British and Irish citizens, the thinkingis the same as with the Spanish, and no special treatmentis required. Perhaps one of the most important points isthe language, because when a request is made for dona-tion, at such a critical time for the family, it is essentialto have a perfect level of communication if we want toachieve good results. In our study it was fundamental tohave the questionnaire translated into English in order forit to be completed, which shows the importance of the lan-guage factor. However, because English is a language fre-quently used among health care professionals from aroundthe world this problem is less important.
Perhaps there is a nuance in our study: that the populationthat travels to Spain from the British Isles is a ‘wealthy’population group, so that it is possible that this is a moreselect group that might be more in favor. However, it isunlikely that by coincidence these respondents who travelto Spain have a more favorable attitude toward donation,whilst in other countries where there are many British andIrish citizens this is not the case. Moreover, as shown inTables 3–5 the respondents are elderly people, with a lowlevel of education, etc. that are classic factors in peoplewho are against organ donation.
Finally, an analysis of the psychosocial profile shows thatmost factors described in western populational studies oc-cur in our study group. It is worth noting that there is
uniformity in the attitude toward donation independentlyof the country of origin or even the county, as seen inFigures 1 and 2. On the other hand, there are differencesaccording to sex, with a greater predisposition to donateamong women than men. This is important, especially ifwe take into account that British and Irish society is not sopatriarchal as Spanish society.
Factors such as previous experience of donation and/ortransplantation, that is, the fact of knowing a neighbor, fam-ily member or friend who has had a transplant (21,23), andparticipation in pro-social activities or being in favor of par-ticipating in them favor positive attitudes toward donation.It is clear that donation is part of an altruistic concept of life,like collaboration in pro-social activities (6,22); therefore,solidarity and moral duty are often indicated as reasons forbeing in favor of donation.
Knowledge of the concept of brain death, a classic factorrelated to attitude toward donation (4–6) is a significantfactor in this subgroup. However, contrary to other studies(6) this does not persist as an independent factor. In thisrespect it should be emphasized that nearly half of therespondents accept that this is the death of an individual,which might explain why fear of apparent death does notfigure as one of the main reasons for not being in favor ofdonation, whilst in other studies it is the main reason (4–6).
The most important factors detected in this population ofBritish and Irish origin that persist in the multivariate anal-ysis are mainly related to two aspects: the family and han-dling of the corpse. At the level of the family it has been
American Journal of Transplantation 2007; 7: 2020–2030 2027
Rıos et al.
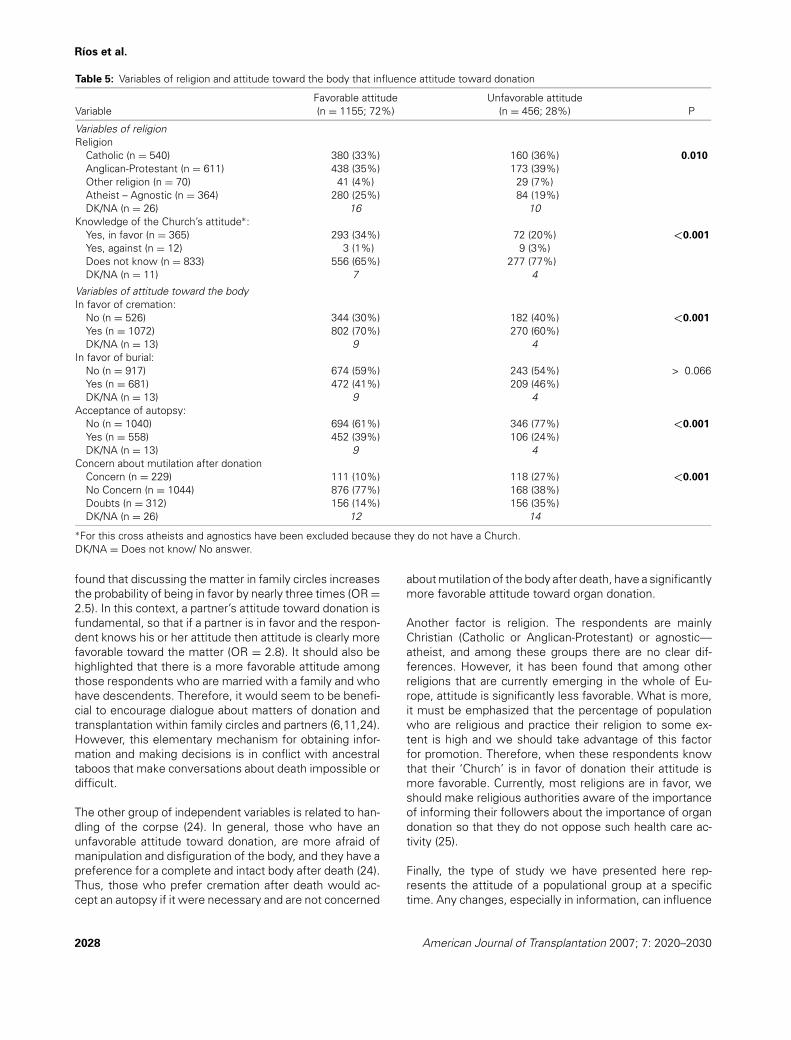
Table 5: Variables of religion and attitude toward the body that influence attitude toward donation
Favorable attitude Unfavorable attitudeVariable (n = 1155; 72%) (n = 456; 28%) P
Variables of religionReligion
Catholic (n = 540) 380 (33%) 160 (36%) 0.010
Anglican-Protestant (n = 611) 438 (35%) 173 (39%)Other religion (n = 70) 41 (4%) 29 (7%)Atheist – Agnostic (n = 364) 280 (25%) 84 (19%)DK/NA (n = 26) 16 10
Knowledge of the Church’s attitude∗:Yes, in favor (n = 365) 293 (34%) 72 (20%) <0.001
Yes, against (n = 12) 3 (1%) 9 (3%)Does not know (n = 833) 556 (65%) 277 (77%)DK/NA (n = 11) 7 4
Variables of attitude toward the bodyIn favor of cremation:
No (n = 526) 344 (30%) 182 (40%) <0.001
Yes (n = 1072) 802 (70%) 270 (60%)DK/NA (n = 13) 9 4
In favor of burial:No (n = 917) 674 (59%) 243 (54%) > 0.066Yes (n = 681) 472 (41%) 209 (46%)DK/NA (n = 13) 9 4
Acceptance of autopsy:No (n = 1040) 694 (61%) 346 (77%) <0.001
Yes (n = 558) 452 (39%) 106 (24%)DK/NA (n = 13) 9 4
Concern about mutilation after donationConcern (n = 229) 111 (10%) 118 (27%) <0.001
No Concern (n = 1044) 876 (77%) 168 (38%)Doubts (n = 312) 156 (14%) 156 (35%)DK/NA (n = 26) 12 14
∗For this cross atheists and agnostics have been excluded because they do not have a Church.DK/NA = Does not know/ No answer.
found that discussing the matter in family circles increasesthe probability of being in favor by nearly three times (OR =2.5). In this context, a partner’s attitude toward donation isfundamental, so that if a partner is in favor and the respon-dent knows his or her attitude then attitude is clearly morefavorable toward the matter (OR = 2.8). It should also behighlighted that there is a more favorable attitude amongthose respondents who are married with a family and whohave descendents. Therefore, it would seem to be benefi-cial to encourage dialogue about matters of donation andtransplantation within family circles and partners (6,11,24).However, this elementary mechanism for obtaining infor-mation and making decisions is in conflict with ancestraltaboos that make conversations about death impossible ordifficult.
The other group of independent variables is related to han-dling of the corpse (24). In general, those who have anunfavorable attitude toward donation, are more afraid ofmanipulation and disfiguration of the body, and they have apreference for a complete and intact body after death (24).Thus, those who prefer cremation after death would ac-cept an autopsy if it were necessary and are not concerned
about mutilation of the body after death, have a significantlymore favorable attitude toward organ donation.
Another factor is religion. The respondents are mainlyChristian (Catholic or Anglican-Protestant) or agnostic—atheist, and among these groups there are no clear dif-ferences. However, it has been found that among otherreligions that are currently emerging in the whole of Eu-rope, attitude is significantly less favorable. What is more,it must be emphasized that the percentage of populationwho are religious and practice their religion to some ex-tent is high and we should take advantage of this factorfor promotion. Therefore, when these respondents knowthat their ‘Church’ is in favor of donation their attitude ismore favorable. Currently, most religions are in favor, weshould make religious authorities aware of the importanceof informing their followers about the importance of organdonation so that they do not oppose such health care ac-tivity (25).
Finally, the type of study we have presented here rep-resents the attitude of a populational group at a specifictime. Any changes, especially in information, can influence
2028 American Journal of Transplantation 2007; 7: 2020–2030

British People in Spain and Organ Donation
Table 6: Variables that influence attitude toward deceased donor organ donation (Logistic regression multivariate analysis)
Regression StandardVariable coefficient (b) error Odds Ratio (CI) p
Donation of a family member’s organs:Doubts (n = 316) 1.587 0.184 1Yes (n = 1165) –0.840 0.325 4.891 (3.411–7.014) <0.001
No (n = 122) 0.432 (0.228–0.816) 0.010Family discussion about ODT:
No (n = 657) 0.921 0.176 1Yes (n = 935) 2.513 (1.779–3.546) <0.001
Acceptance of autopsy:No (n = 1040) 0.535 0.184 1Yes (n = 558) 1.706 (1.190–2.445) 0.004
Concern about mutilation after donationNot sure (n = 312) 0.166 0.240 1Concern (n = 229) 1.192 0.193 1.181 (0.737–1.891) 0.414No concern (n = 1044) 3.294 (2.255–4.812) <0.001
Knowledge of partner’s attitude:No partner (n = 194) 1.025 0.296 1Yes, favorable (n = 804) 0.153 0.285 2.786 (1.560–4.975) 0.001
Not known (n = 448) 0.079 0.388 1.165 (0.666–2.038) 0.591Yes, against (n = 100) 1.082 (0.505–2.318) 0.839
Belief that one might need a transplant:Not sure (n = 1209) 0.808 0.362 1Yes (n = 126) –0.320 0.230 2.243 (1.104–4.560) 0.026
No (n = 216) 0.726 (0.462–1.140) 0.164
changes in this attitude. What is more, although attitudeand opinion are not quite the same, this study determinesattitude using an opinion questionnaire (21). These stud-ies are carried out in this way because attitude is under-stood to mean the willingness to respond in an evalua-tive way (emotional, cognitive or behavioral) when pre-sented with a certain object and that this can expressedthrough language as a certain opinion toward a matter.Consequently, we believe as other authors (21) that opin-ions and attitudes are variables that interact with eachother. Therefore, one of the most important elements in achange of attitude, in this case social, is the prior change ofopinion.
To conclude, the attitude toward organ donation of Britishand Irish citizens who usually reside in southeastern Spainis more positive than in the native Spanish population andis determined by many psychosocial factors, mainly relatedto the family and to attitude toward the manipulation of thebody.
References
1. Ramırez P, Mejıas D, Miras M et al. Valoracion del estado de saludy calidad de vida de pacientes sometidos a trasplante de hıgado.Cir Esp 1999; 66: 203–207.
2. Cantarovich F. Improvement in organ shortage through education.Transplantation 2002; 73: 1844–1846.
3. Miranda B, Fernandez M, de Felipe C, Naya M, Gonzalez JM,Matesanz R. Organ donation in Spain. Nephrol Dial Transplant1999; 14(Suppl 3): 15–21
4. Conesa C, Rıos Zambudio A, Ramırez P, Canteras M, RodrıguezMM, Parrilla P. Socio-personal profile of teenagers opposedto organ donation. Nephrol Dial Transplant 2004; 19: 1269–1275.
5. Conesa C, Rıos A, Ramırez P et al. Psychosocial profile in favor oforgan donation. Transplant Proc 2003; 35: 1276–1281.
6. Conesa C, Rıos A, Ramırez P, Canteras M, Rodrıguez MM, ParrillaP. Estudio multivariante de los factores psicosociales que influyenen la actitud poblacional hacia la donacion de organos. Nefrologıa2005; 25: 684–697.
7. Clark TJ, Richards NT, Adu D, Michael J. Increased prevalence ofdialysis dependent renal failure in ethnic minorities in the WestMidlans. Nephrol Dial Transplant 1993; 8: 146–148.
8. Roderick PJ, Jones I, Raleigh VS, McGeown M, Mallick N. Pop-ulation need for renal transplantation therapy in Thames regions:Ethnic dimension. Br Med J 1994; 309: 1111–1114.
9. Fleischhauer K, Hermeren G, Holm S et al. Comparative reporton transplantation and relevant ethical problems in five Europeancountries, and some reflections on Japan. Transpl Int 2000; 13:266–275.
10. Gross T, Martinoli S, Spagnoli G, Badia F, Malacrida R. Attitudesand behavior of young European adults towards the donation oforgans-a call for better information. Am J Transplant 2001; 1: 74–81.
11. Keggie J. Public attitudes towards organ transplantation in theUnited Kingdom. EDTNA ERCA J 1996; 22: 18–20.
12. Organizacion Nacional deTrasplantes. Memoria de actividadesONT 2005 (1a parte). Rev Esp Traspl 2006; 14.
13. http://www.ont.msc.es/ (Last consult 4 April 2007)14. Wakeford RE, Stepney R. Obstacles to organ donation. Br J Surg
1989; 76: 435–439.15. Randhawa G. Developing culturally competent renal services in
the United Kingdom: Tackling inequalities in health. TransplantProc 2003; 35: 21–23.
American Journal of Transplantation 2007; 7: 2020–2030 2029
Rıos et al.
16. Keggie J. Public attitudes towards organ transplantation in theUnited Kingdom. EDNTNA ERCA J 1996; 22: 18–20.
17. Matesanz R. Cadaveric organ donation: Comparison of legislationin various countries of Europe. Nephrol Dial Transplant 1998; 13:1632–1635.
18. Francome C, Bryant C, Dunne M. Opting out scheme for donorshas support in Britain. BMJ 1995; 310: 1404.
19. Rudge CJ. Transplantation of organs: Natural limitations, possiblesolutions–a UK perspective. Transplant Proc 2003; 35: 1149–1150.
20. Sade RM, Kay N, Pitzer S, Drake P, Baliga P, Haines S. Increasingorgan donation: A successful new concept. Transplantation 2002;74: 1142–1146.
21. Martınez JM, Martın A, Lopez Jorge S. La opinion publica espanola
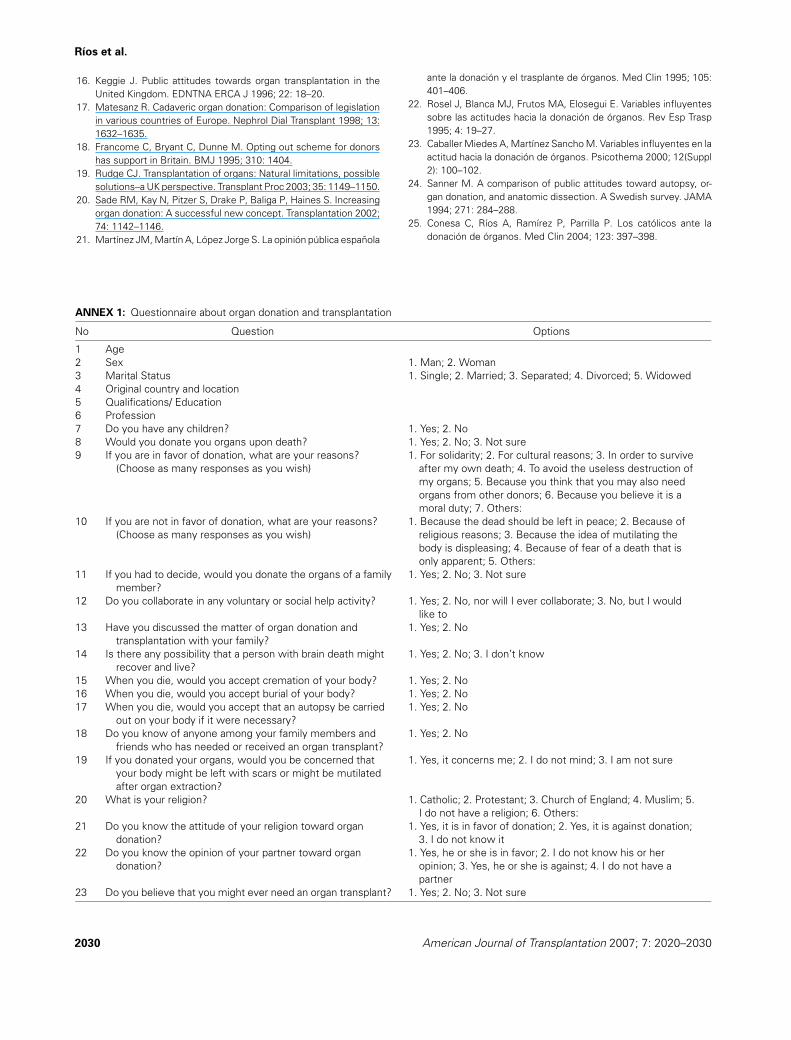
ANNEX 1: Questionnaire about organ donation and transplantation
No Question Options
1 Age2 Sex 1. Man; 2. Woman3 Marital Status 1. Single; 2. Married; 3. Separated; 4. Divorced; 5. Widowed4 Original country and location5 Qualifications/ Education6 Profession7 Do you have any children? 1. Yes; 2. No8 Would you donate you organs upon death? 1. Yes; 2. No; 3. Not sure9 If you are in favor of donation, what are your reasons?
(Choose as many responses as you wish)1. For solidarity; 2. For cultural reasons; 3. In order to survive
after my own death; 4. To avoid the useless destruction ofmy organs; 5. Because you think that you may also needorgans from other donors; 6. Because you believe it is amoral duty; 7. Others:
10 If you are not in favor of donation, what are your reasons?(Choose as many responses as you wish)
1. Because the dead should be left in peace; 2. Because ofreligious reasons; 3. Because the idea of mutilating thebody is displeasing; 4. Because of fear of a death that isonly apparent; 5. Others:
11 If you had to decide, would you donate the organs of a familymember?
1. Yes; 2. No; 3. Not sure
12 Do you collaborate in any voluntary or social help activity? 1. Yes; 2. No, nor will I ever collaborate; 3. No, but I wouldlike to
13 Have you discussed the matter of organ donation andtransplantation with your family?
1. Yes; 2. No
14 Is there any possibility that a person with brain death mightrecover and live?
1. Yes; 2. No; 3. I don’t know
15 When you die, would you accept cremation of your body? 1. Yes; 2. No16 When you die, would you accept burial of your body? 1. Yes; 2. No17 When you die, would you accept that an autopsy be carried
out on your body if it were necessary?1. Yes; 2. No
18 Do you know of anyone among your family members andfriends who has needed or received an organ transplant?
1. Yes; 2. No
19 If you donated your organs, would you be concerned thatyour body might be left with scars or might be mutilatedafter organ extraction?
1. Yes, it concerns me; 2. I do not mind; 3. I am not sure
20 What is your religion? 1. Catholic; 2. Protestant; 3. Church of England; 4. Muslim; 5.I do not have a religion; 6. Others:
21 Do you know the attitude of your religion toward organdonation?
1. Yes, it is in favor of donation; 2. Yes, it is against donation;3. I do not know it
22 Do you know the opinion of your partner toward organdonation?
1. Yes, he or she is in favor; 2. I do not know his or heropinion; 3. Yes, he or she is against; 4. I do not have apartner
23 Do you believe that you might ever need an organ transplant? 1. Yes; 2. No; 3. Not sure
ante la donacion y el trasplante de organos. Med Clin 1995; 105:401–406.
22. Rosel J, Blanca MJ, Frutos MA, Elosegui E. Variables influyentessobre las actitudes hacia la donacion de organos. Rev Esp Trasp1995; 4: 19–27.
23. Caballer Miedes A, Martınez Sancho M. Variables influyentes en laactitud hacia la donacion de organos. Psicothema 2000; 12(Suppl2): 100–102.
24. Sanner M. A comparison of public attitudes toward autopsy, or-gan donation, and anatomic dissection. A Swedish survey. JAMA1994; 271: 284–288.
25. Conesa C, Rıos A, Ramırez P, Parrilla P. Los catolicos ante ladonacion de organos. Med Clin 2004; 123: 397–398.
2030 American Journal of Transplantation 2007; 7: 2020–2030
Copyright © 2022 FDOKUMEN