
Reduced-intensity conditioning and HLA-matched haemopoietic stem-cell transplantation in patients...
13
Articles www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 1 Reduced-intensity conditioning and HLA-matched haemopoietic stem-cell transplantation in patients with chronic granulomatous disease: a prospective multicentre study Tayfun Güngör, Pierre Teira, Mary Slatter, Georg Stussi, Polina Stepensky, Despina Moshous, Clementien Vermont, Imran Ahmad, Peter J Shaw, José Marcos Telles da Cunha, Paul G Schlegel, Rachel Hough, Anders Fasth, Karim Kentouche, Bernd Gruhn, Juliana F Fernandes, Silvy Lachance, Robbert Bredius, Igor B Resnick, Bernd H Belohradsky, Andrew Gennery, Alain Fischer, H Bobby Gaspar, Urs Schanz, Reinhard Seger, Katharina Rentsch, Paul Veys, Elie Haddad, Michael H Albert*, Moustapha Hassan*, on behalf of the Inborn Errors Working Party of the European Society for Blood and Marrow Transplantation† Summary Background In chronic granulomatous disease allogeneic haemopoietic stem-cell transplantation (HSCT) in adolescents and young adults and patients with high-risk disease is complicated by graft-failure, graft-versus-host disease (GVHD), and transplant-related mortality. We examined the effect of a reduced-intensity conditioning regimen designed to enhance myeloid engraftment and reduce organ toxicity in these patients. Methods This prospective study was done at 16 centres in ten countries worldwide. Patients aged 0–40 years with chronic granulomatous disease were assessed and enrolled at the discretion of individual centres. Reduced-intensity conditioning consisted of high-dose fludarabine (30 mg/m² [infants <9 kg 1∙2 mg/kg]; one dose per day on days –8 to –3), serotherapy (anti-thymocyte globulin [10 mg/kg, one dose per day on days –4 to –1; or thymoglobuline 2·5 mg/kg, one dose per day on days –5 to –3]; or low-dose alemtuzumab [<1 mg/kg on days –8 to –6]), and low-dose (50–72% of myeloablative dose) or targeted busulfan administration (recommended cumulative area under the curve: 45–65 mg/L × h). Busulfan was administered mainly intravenously and exceptionally orally from days –5 to –3. Intravenous busulfan was dosed according to weight-based recommendations and was administered in most centres (ten) twice daily over 4 h. Unmanipulated bone marrow or peripheral blood stem cells from HLA-matched related- donors or HLA-9/10 or HLA-10/10 matched unrelated-donors were infused. The primary endpoints were overall survival and event-free survival (EFS), probabilities of overall survival and EFS at 2 years, incidence of acute and chronic GVHD, achievement of at least 90% myeloid donor chimerism, and incidence of graft failure after at least 6 months of follow-up. Results 56 patients (median age 12∙7 years; IQR 6·8–17·3) with chronic granulomatous disease were enrolled from June 15, 2003, to Dec 15, 2012. 42 patients (75%) had high-risk features (ie, intractable infections and autoinflammation), 25 (45%) were adolescents and young adults (age 14–39 years). 21 HLA-matched related-donor and 35 HLA-matched unrelated-donor transplants were done. Median time to engraftment was 19 days (IQR 16–22) for neutrophils and 21 days (IQR 16–25) for platelets. At median follow-up of 21 months (IQR 13–35) overall survival was 93% (52 of 56) and EFS was 89% (50 of 56). The 2-year probability of overall survival was 96% (95% CI 86∙46–99∙09) and of EFS was 91% (79∙78–96∙17). Graft-failure occurred in 5% (three of 56) of patients. The cumulative incidence of acute GVHD of grade III–IV was 4% (two of 56) and of chronic graft-versus-host disease was 7% (four of 56). Stable (≥90%) myeloid donor chimerism was documented in 52 (93%) surviving patients. Interpretation This reduced-intensity conditioning regimen is safe and efficacious in high-risk patients with chronic granulomatous disease. Funding None. Introduction Chronic granulomatous disease is a rare primary immunodeficiency disorder characterised by functional impairment of the phagocyte NADPH-oxidase complex. NADPH-oxidase is essential for the intracellular and extracellular killing of mainly catalase-positive bacteria, Actinomyces spp, and fungi (eg, Aspergillus spp). 1–4 NADPH-oxidase deficiency also impairs the regulation and termination of proinflammatory cytokine-mediated signals, leading to chronic autoinflammation (eg, granulomatous colitis and progressive granulomatous lung disease). 5–7 Despite the recommended lifelong antibiotic and antimycotic prophylaxis with or without administration of interferon gamma, 4 invasive infections with fungi and bacteria, and abscesses in vital organs regularly Published Online October 23, 2013 http://dx.doi.org/10.1016/ S0140-6736(13)62069-3 See Online/Comment http://dx.doi.org/10.1016/ S0140-6736(13)62144-3 *Contributed equally †Members listed at end of paper University Children’s Hospital, Division of Blood and Marrow Transplantation, Zurich, Switzerland (T Güngör MD, R Seger MD); Centre de Recherche du CHU Sainte-Justine, Département de Pédiatrie, Université de Montréal, Montréal, QC, Canada (P Teira MD, E Haddad MD); Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, UK (M Slatter MBChB, A Gennery MD); University Hospital, Division of Hematology and Blood and Marrow Transplantation, Zürich, Switzerland (U Schanz MD, G Stüssi MD); Hadassah Hebrew University Medical Center, Department of Blood and Marrow Transplantation, Jerusalem, Israel (P Stepensky MD, I B Resnick MD); AP-HP, Hôpital Necker Enfants Malades, Paediatric Immunology, Sorbonne Paris Cité, Université Paris Descartes, Imagine Institute, Paris, France (D Moshous MD, Prof A Fischer MD); Leiden University Medical Center, Department of Paediatrics, Leiden, Netherlands (C Vermont MD, R Bredius MD); Blood and Marrow Transplantation Program, Hôpital Maisonneuve- Rosemont, Université de Montréal, Montréal, QC,
Transcript of Reduced-intensity conditioning and HLA-matched haemopoietic stem-cell transplantation in patients...

Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 1
Reduced-intensity conditioning and HLA-matched haemopoietic stem-cell transplantation in patients with chronic granulomatous disease: a prospective multicentre studyTayfun Güngör, Pierre Teira, Mary Slatter, Georg Stussi, Polina Stepensky, Despina Moshous, Clementien Vermont, Imran Ahmad, Peter J Shaw, José Marcos Telles da Cunha, Paul G Schlegel, Rachel Hough, Anders Fasth, Karim Kentouche, Bernd Gruhn, Juliana F Fernandes, Silvy Lachance, Robbert Bredius, Igor B Resnick, Bernd H Belohradsky, Andrew Gennery, Alain Fischer, H Bobby Gaspar, Urs Schanz, Reinhard Seger, Katharina Rentsch, Paul Veys, Elie Haddad, Michael H Albert*, Moustapha Hassan*, on behalf of the Inborn Errors Working Party of the European Society for Blood and Marrow Transplantation†
SummaryBackground In chronic granulomatous disease allogeneic haemopoietic stem-cell transplantation (HSCT) in adolescents and young adults and patients with high-risk disease is complicated by graft-failure, graft-versus-host disease (GVHD), and transplant-related mortality. We examined the eff ect of a reduced-intensity conditioning regimen designed to enhance myeloid engraftment and reduce organ toxicity in these patients.
Methods This prospective study was done at 16 centres in ten countries worldwide. Patients aged 0–40 years with chronic granulomatous disease were assessed and enrolled at the discretion of individual centres. Reduced-intensity conditioning consisted of high-dose fl udarabine (30 mg/m² [infants <9 kg 1∙2 mg/kg]; one dose per day on days –8 to –3), serotherapy (anti-thymocyte globulin [10 mg/kg, one dose per day on days –4 to –1; or thymoglobuline 2·5 mg/kg, one dose per day on days –5 to –3]; or low-dose alemtuzumab [<1 mg/kg on days –8 to –6]), and low-dose (50–72% of myeloablative dose) or targeted busulfan administration (recommended cumulative area under the curve: 45–65 mg/L × h). Busulfan was administered mainly intravenously and exceptionally orally from days –5 to –3. Intravenous busulfan was dosed according to weight-based recommendations and was administered in most centres (ten) twice daily over 4 h. Unmanipulated bone marrow or peripheral blood stem cells from HLA-matched related-donors or HLA-9/10 or HLA-10/10 matched unrelated-donors were infused. The primary endpoints were overall survival and event-free survival (EFS), probabilities of overall survival and EFS at 2 years, incidence of acute and chronic GVHD, achievement of at least 90% myeloid donor chimerism, and incidence of graft failure after at least 6 months of follow-up.
Results 56 patients (median age 12∙7 years; IQR 6·8–17·3) with chronic granulomatous disease were enrolled from June 15, 2003, to Dec 15, 2012. 42 patients (75%) had high-risk features (ie, intractable infections and autoinfl ammation), 25 (45%) were adolescents and young adults (age 14–39 years). 21 HLA-matched related-donor and 35 HLA-matched unrelated-donor transplants were done. Median time to engraftment was 19 days (IQR 16–22) for neutrophils and 21 days (IQR 16–25) for platelets. At median follow-up of 21 months (IQR 13–35) overall survival was 93% (52 of 56) and EFS was 89% (50 of 56). The 2-year probability of overall survival was 96% (95% CI 86∙46–99∙09) and of EFS was 91% (79∙78–96∙17). Graft-failure occurred in 5% (three of 56) of patients. The cumulative incidence of acute GVHD of grade III–IV was 4% (two of 56) and of chronic graft-versus-host disease was 7% (four of 56). Stable (≥90%) myeloid donor chimerism was documented in 52 (93%) surviving patients.
Interpretation This reduced-intensity conditioning regimen is safe and effi cacious in high-risk patients with chronic granulomatous disease.
Funding None.
IntroductionChronic granulomatous disease is a rare primary immuno defi ciency disorder characterised by functional impairment of the phagocyte NADPH-oxidase complex. NADPH-oxidase is essential for the intracellular and extracellular killing of mainly catalase-positive bacteria, Actinomyces spp, and fungi (eg, Aspergillus spp).1–4 NADPH-oxidase defi ciency also impairs the regulation
and termination of proinfl ammatory cytokine-mediated signals, leading to chronic autoinfl ammation (eg, granulo matous colitis and progressive granulomatous lung disease).5–7
Despite the recommended lifelong antibiotic and anti mycotic prophylaxis with or without administration of interferon gamma,4 invasive infections with fungi and bacteria, and abscesses in vital organs regularly
Published OnlineOctober 23, 2013http://dx.doi.org/10.1016/S0140-6736(13)62069-3
See Online/Commenthttp://dx.doi.org/10.1016/S0140-6736(13)62144-3
*Contributed equally
†Members listed at end of paper
University Children’s Hospital, Division of Blood and Marrow Transplantation, Zurich, Switzerland (T Güngör MD, R Seger MD); Centre de Recherche du CHU Sainte-Justine, Département de Pédiatrie, Université de Montréal, Montréal, QC, Canada (P Teira MD, E Haddad MD); Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, UK (M Slatter MBChB, A Gennery MD); University Hospital, Division of Hematology and Blood and Marrow Transplantation, Zürich, Switzerland (U Schanz MD, G Stüssi MD); Hadassah Hebrew University Medical Center, Department of Blood and Marrow Transplantation, Jerusalem, Israel (P Stepensky MD, I B Resnick MD); AP-HP, Hôpital Necker Enfants Malades, Paediatric Immunology, Sorbonne Paris Cité, Université Paris Descartes, Imagine Institute, Paris, France (D Moshous MD, Prof A Fischer MD); Leiden University Medical Center, Department of Paediatrics, Leiden, Netherlands (C Vermont MD, R Bredius MD); Blood and Marrow Transplantation Program, Hôpital Maisonneuve-Rosemont, Université de Montréal, Montréal, QC,

Articles
2 www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3
contribute to organ dysfunction, impaired quality of life, and mortality. Chronic granulomatous disease has been associated with an annual mortality of 2–5% per year,2 with a worse prognosis in individuals with no NADPH-oxidase activity.8
Allogeneic haemopoietic stem-cell transplantation (HSCT) is able to cure chronic granulomatous disease and to reverse organ dysfunction.9,10 Between 1985 and 2000, patients with chronic granulomatous disease receiving full-dose myeloablative conditioning and mainly HLA-matched related-donor trans plants were shown to have overall survival of 85% (23 of 27) and event-free survival (EFS) of 81% (22 of 27).10 Within the past decade, the results after myeloablative conditioning regimens further improved, especially in children younger than 14 years, even when HLA-matched unrelated-donor11–14 or unrelated cord-blood donor transplants were used.15
High-risk patients with chronic granulomatous disease with intractable infections or autoinfl amma-tion at HSCT and adolescents and young adults (14–39 years) have remained diffi cult to transplant and have increased transplant-related mortality of between 28% and 50%.10–12,16 Eff orts to reduce the toxicity of conditioning were complicated by graft failure, graft-versus-host disease (GVHD), and lethal infections.10,16,17 The study aim was to analyse the eff ect of a reduced-intensity conditioning regimen designed specifi cally to enhance myeloid engraft ment and reduce organ toxicity in patients with mainly high-risk chronic granuloma-tous disease.
MethodsStudy design and participantsWe did this study at 16 centres (university hospitals) in ten countries (Switzerland, Germany, France, the UK, the Netherlands, Sweden, Israel, Australia, Brazil, and Canada). The study was mainly off ered to patients too sick to tolerate myeloablative conditioning or adolescents and young adults, but patients were also enrolled at the discretion of individual centres, mainly on the basis of
absent NADPH-oxidase acitivity or the presence of one of the following criteria: one or more life-threatening infec-tion in the past, non-compliance with antimicrobial prophylaxis, or steroid-dependent autoinfl ammation. There were no prespecifi ed inclusion or exclusion criteria.
The protocol was designed and supervised by the University Children’s Hospital (Zurich, Switzerland) in collaboration with the University Hospital-Huddinge and Karolinska Institute (Stockholm, Sweden). The protocol was reviewed by the Inborn Errors Working Party of the European Society for Blood and Marrow Transplantation, who recommended that it was suitable for high-risk patients with therapy-refractory infections or auto infl ammation and for adolescents and young adults unable to tolerate full myeloablative conditioning. All patients and parents of paediatric patients (<18 years) provided written, informed consent to participate in this study according to the Declaration of Helsinki; adoles-cents older than 12 years also provided written, informed consent. Children younger than 12 years needed the consent of their parents but were informed about the procedure. Sibling family donors were informed about the risks and benefi ts of donation. Parents of sibling donors and sibling adolescents older than 12 years gave written, informed consent to donate. In some coun-tries—eg, Switzerland—local ethics committees had to confi rm and permit donations from paediatric or adoles-cent donors (<18 years) despite confi rmed parental written consent.
ProceduresIn HLA-matched related-donor (sibling) transplants, donor and recipient HLA-matching was confi rmed by HLA-A and HLA-B serology and molecular typing of HLA-DRB1. In HLA-matched unrelated-donor (and HLA-matched related non-sibling donor) trans plants, HLA-matching was confi rmed by molecular four-digit typing (HLA-A, HLA-B, HLA-C, HLA-DRB1, and HLA-DQB1). HLA-matched unrelated donors were defi ned as having an HLA-9/10 or HLA-10/10 match with the recipient. Bone marrow was the recommended stem-cell source. Peripheral blood stem cell (PBSC) donations were accepted when the donor did not want to donate bone marrow.
Before HSCT, ¹⁸F-fl uorodeoxyglucose PET-CT scans and endocoscopic and radiological assessments were done to document the extent and origin of infl ammatory or infectious foci. Patients were defi ned as high risk if they had radiologically and microbiologically proven infection or autoinfl ammation, persisting despite at least 2 months of treatment with appropriate anti-infective or anti-infl ammatory therapy (or both), accom panied by fever of more than 38∙0°C or chronically elevated serum C-reactive protein concentrations (or both). All patients were given supportive care accord ing to local guide lines. Antifungal azoles were dis con tinued at least 4 days before busul-fan administration. Pre-existing steroid treat ment was continued during con ditioning and slowly tapered after
Canada (I Ahmad MD, S Lachance FRCP); Children’s
Hospital, Division of Blood and Marrow Transplantation,
Westmead, Sydney, NSW, Australia (P J Shaw FRACP);
Hospital Albert Einstein, Haematology and
Hematopoietic stem cell transplantation Unit,
Sao Paulo, Brazil (J M Telles da Cunha MD);
University Children’s Hospital, Division of Blood and Marrow
Transplantation, Würzburg, Germany (P G Schlegel MD); University College London Hospitals NHS Foundation
Trust, London, UK (R Hough MD); Department of
Pediatrics, University of Gothenburg, Gothenburg, Sweden (Prof A Fasth MD);
Department of Paediatrics, Jena University Hospital, Jena,
Germany (K Kentouche MD, B Gruhn MD); Instituto da Criança, Universidade de
São Paulo, São Paulo, Brazil (J F Fernandes MD);
Dr von Hauner University Children’s Hospital, Munich,
Germany (M H Albert MD, Prof B Belohradsky MD); Great
Ormond Street Children’s Hospital, Division of Blood and
Marrow Transplantation, London, UK (P Veys FRCP,
Prof H B Gaspar MD); Molecular Immunology Unit; UCL
Institute of Child Health, London, UK (P Veys, H B Gaspar);
University Hospital, Divison of Clinical Chemistry (K Rentsch
PhD), Division of Experimental Cancer Medicine
(Prof M Hassan PhD), KFC, Novum, Laboratory Medicine,
Karolinska University Hospital-Huddinge Stockholm, Sweden;
and Karolinska Institute, Stockholm, Sweden
(Prof M Hassan)
Correspondence to:Dr Tayfun Güngör, Division of
Blood and Marrow Transplantation, University
Children’s Hospital, CH-8032 Zurich, Switzerland
Figure 1: Study fl ow diagram
58 patients enrolled
2 excluded1 alemtuzumab 1·5 mg/kg1 combined alemtuzumab and
ATG-Fresenius administration
56 patients analysed
21 HLA-matched related-donortransplants18 genoidentical sibling
3 phenoidentical related
35 HLA-matched unrelated-donortransplants25 HLA-10/10 matched10 HLA-9/10 matched
Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 3
CGD type
Sex Age at HSCT (years)
Signifi cant pre-existing disease
Complications at time of HSCT
Donor (HLA match)
Stem-cell source
Administered busulfan dose in mg/kg†
Cumulative busulfan AUC (mg/L × h)
CD34+ 10⁶ per kg body weight
TNC 10⁸ per kg bodyweight
Alemtuzumab dose(mg/kg)
rATG dose (mg/kg)
1 CYBB M 0·8 NR Colitis, perianal abscesses
MUD (9/10) PBSC 15·5 (16·0) Yes (33) 9·1 14·0 0·8§ ··
2 CYBB M 1·0 Pulmonary and bone aspergillosis
None MUD BM 14·0 (19·2) Yes (55) 7·0 ·· 0·5 ··
3 CYBB M 1·5 Pulmonary aspergillosis
MAS, intestinal LAP
MUD PBSC 28·0 (19·2) Yes (65) 20·6 16·9 0·6 ··
4* NCF2 F 3·5 Pulmonary aspergillosis, bacillus Calmette-Guérin infection
None MRD BM 13·2 (19·2) No 20·7 10·9 ·· 7·5
5 NCF2 M 3·7 NR Colitis, Burkholderia spp abscess
MUD PBSC 26·4 (19·2) Yes (61) 10·0 ·· 0·6 ··
6 CYBB M 4·4 NR Spondylodiscitis, pulmonary aspergillosis
MRD BM 14·7 (19·2) Yes (59) 4·6 1·2 ·· 7·5
7 CYBB M 4·5 NR Cerebral and pulmonary aspergillosis
MRD BM 15·6 (19·2) Yes (55) 10·0 2·7 ·· 40·0
8 CYBB M 5·1 Thymectomy (granuloma) (at 9 months of age)
Colitis MUD BM 15·7 (17·6) Yes (61) 7·0 1·1 0·5 ··
9* NCF2 M 5·25 NR Colitis, pulmonary infi ltrates
MRD BM 12·8 (17·6) No ·· 4·3 ·· 40·0
10* CYBB M 5·3 Paecilomyces spp liver and bone abscess
None MRD BM 11·0 (17·6) No 11·1 5·4 ·· 7·5
11 NCF1 M 5·5 NR Colitis MUD BM 12·0 (17·6) Yes (56) 6·0 ·· 0·5 ··
12* CYBB M 6·0 Restrictive lung disease
None MRD PBSC 8·0 (17·6) No ·· 27·8 ·· 40·0
13* CYBB M 6·3 Pulmonary actinomycosis
None MUD PBSC 12·8 (17·6) No 11·0 ·· ·· 40·0
14 CYBB M 6·7 NR Colitis MUD (9/10) BM 9·6 (17·6) Yes (42) 0·8 4·7 0·5 ··
15 CYBB M 7·1 Liver abscesses, LAP
Pulmonary aspergillosis
MUD BM 15·4 (15·2) Yes (56) 6·7 0·5 ··
16* NCF1 F 7·2 NR Colitis MUD (9/10) BM 9·5 (15·2) No 2·3 4·2 0·5 ··
17* CYBB M 7·6 NR Colitis, anal fi stula
MUD BM 9·5 (15·2) No 6·1 10·1 0·5 ··
18 CYBB M 8·0 LAP None MUD BM 15·6 (17·6) Yes (53) ·· 10·0 0·5 ··
19 CYBA F 8·1 NR Pulmonary spergillosis
MRD BM 10·5 (15·2) Yes (51) 1·4 3·5 0·5 ··
20 CYBB M 8·5 NR Cervical LAP MRD BM 10·6 (15·2) Yes (60) 4·5 8·8 ·· 40·0
21 CYBB M 9·4 Liver and perirectal abscess
PGLD MUD (9/10) BM 10·6 (15·2) Yes (46) 5·1 4·7 0·5 ··
22 NCF2 M 9·6 Colitis Colitis MUD BM 12·6 (15·2) Yes (55) ·· 1·4 0·5 ··
23 CYBB M 10·0 NR Pulmonary apergillosis, colitis
MRD BM 9·6 (15·2) Yes (46) 9·1 5·2 ·· 7·5
24* NCF1 F 10·1 NR Colitis MRD BM 9·5 (15·2) No 3·7 2·3 0·5 ··
25 CYBB M 11·2 Liver abscess None MUD BM 13·9 (12·8) Yes (57) 3·4 5·3 0·5 ··
26 AR M 11·5 Anal abscess, LAP, colitis
Colitis MUD BM 12·0 (12·8) Yes (60) 2·4 3·4 0·5 ··
27 CYBB M 12·0 Infections with Mycobacteria spp and Salmonella spp
None MUD (9/10) PBSC 9·5 (12·8) Yes (38) 3·5 10·3 0·5 ··
28 AR F 12·5 NR Pulmonary aspergillosis
MUD (9/10) PBSC 8·0 (12·8) Yes (56) 5·0 6·4 0·5 ··
(Continues on next page)

Articles
4 www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3
CGD type
Sex Age at HSCT (years)
Signifi cant pre-existing disease
Complications at time of HSCT
Donor (HLA match)
Stem-cell source
Administered busulfan dose in mg/kg†
Cumulative busulfan AUC (mg/L × h)
CD34+ 10⁶
per kg body weight
TNC 10⁸ per kg body-weight
Alemtuzumab dose(mg/kg)
rATG dose (mg/kg)
(Continued from previous page)
29 CYBB M 12·8 NR Scopulariopsis spp infection (spine and lung)
MUD BM 11·8 (12·8) Yes (49) 3·6 ·· 0·5 ··
30* CYBB M 13·1 NR Pulmonary Neisseria spp infection
MRD BM 8·0 (12·8) No 3·5 ·· ·· 40·0
31* CYBB M 13·9 NR Scedosporium apiospermum pulmary, bone, and brain infection
MRD BM 6·5 (12·8) No 7·8 3·1 0·3 ··
32 CYBB M 14·0 McLeod blood group
Pulmonary aspergillosis, SVC obstruction
MUD PBSC 12·8 (12·8) Yes (65) 6·4 ·· 0·5 ··
33 CYBB M 14·0 Bronchiectasis, perianal abscess
Pulmonary and bone Geosmithia argillacea infection
MUD (9/10) PBSC 11·6 (12·8) Yes (51) ·· 5·9 0·6 ··
34 CYBB M 14·0 NR Pulmonary aspergilllosis
MRD BM 12·0 (12·8) Yes (55) ·· 4·0 ·· 7·5
35 CYBB M 14·1 Liver abscess None MRD BM 9·5 (12·8) Yes (49) 3·5 2·8 ·· 7·5
36 NCF1 F 14·4 NR Colitis, pneumonitis
MRD BM 7·35 (12·8) Yes (59) 7·9 4·7 0·3 ··
37 NCF1 M 14·6 Staphylococcus folliculitis
Staphylococcus folliculitis
MRD BM 6·4 (12·8) Yes (57) 6·4 ·· ·· 7·5
38 NCF1 F 15·0 NR Colitis, PGLD MUD BM 14·0 (12·8) Yes (57) 9·0 ·· 0·5
39 CYBB M 15·5 Splenic abscess, Burkholderia cepacia septicaemia
None MRD BM 9·7 (12·8) Yes (56) 2·8 1·8 ·· 7·5
40 AR F 15·5 Liver abscess, pneumonia
Colitis, rectal stenosis
MUD BM 11·0 (12·8) Yes (61) 2·5 3·5 0·5 ··
41 CYBB M 16·5 NR Colitis MUD BM 6·4 (12·8) Yes (56) 2·5 1·7 0·5 ··
42* CYBA F 16·7 Pulmonary aspergillosis
PGLD MUD (9/10) BM 6·4 (12·8) No 4·4 3·0 0·6 ··
43 AR M 17·5 NR Hepatic and hypophyseal granulomata
MUD (9/10) BM 9·0 (12·8) Yes (51) 3·2 3·7 0·5 ··
44 NCF1 M 18·5 Colitis, post-hemicolectomy
Colitis, renal impairment
MUD BM 11·2 (12·8) Yes (52) ·· 4·2 0·5 ··
45 NCF1 F 18·5 NR Colitis MRD BM 8·0‡ (12·8) Yes (35) 3·5 ·· ·· 40·0
46 CYBB M 18·5 NR Colitis, pulmonary infi ltrates
MUD (9/10) BM 11·2 (12·8) Yes (64) 3·2 ·· 0·6 ··
47 NCF1 M 19·9 NR Liver abscesses, colitis
MUD BM 10·5 (12·8) Yes (49) 3·7 3·9 0·5 ··
48 CYBB M 20·0 NR Colitis, pneumonitis
MUD BM 9·5 (12·8) Yes (41) 2·1 2·4 0·5 ··
49* CYBB M 20·3 NR Pulmonary aspergillosis
MUD PBSC 8·0‡ (12·8) No 5·0 ·· 40·0
50 NCF1 M 21·4 NR Colitis, rectal stenosis
MRD BM 7·0 (12·8) Yes (53) 1·9 3·0 ·· 7·5
51 AR M 22·0 Burkholderia spp sepsis, liver abscess, pulmonary aspergillosis
None MUD PBSC 6·7 (12·8) Yes (53) 6·7 ·· 0·6 ··
52 CYBB M 23·3 Pulmonary actinomycosis
None MRD BM 7·0 (12·8) Yes (30) 2·5 ·· ·· 40·0
(Continues on next page)

Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 5
neutrophil engraft ment. Routine granulo cyte colony-stimu lating factor adminis tration was not given. Mucositis was graded according the WHO classifi cation.18
The reduced-intensity conditioning regimen consisted of immunosuppressive chemotherapy, serotherapy, and low-dose or targeted busulfan administration. Immuno sup pressive chemotherapy consisted of six doses of intra venous fl udarabine 30 mg/m² (infants <9 kg 1∙2 mg/kg; one dose per day on days –8 to –3). Serotherapy in HLA-matched related-donor trans-plants consisted of intravenous rabbit anti-thymocyte globulin (rATG), ATG-Fresenius (Fresenius Biotech, Germany; 10 mg/kg, one dose per day on days –4 to –1), or thymoglobuline (Sanofi -Genzyme, France-USA; 2∙5 mg/kg, one dose per day on days –5 to –3), according to the centre’s preference. In HLA-matched unrelated-donor transplants, low-dose (defi ned as <1 mg/kg) alemtuzumab (0∙5 mg/kg with bone marrow; 0∙6 mg/kg with PBSC or with HLA-9/10 match; on days –8 to –6) was recommended (appendix).
Busulfan was administered mainly intravenously and exceptionally orally from days –5 to –3 with the latest option for administration on day –2. Intravenous busul-fan was dosed according to published weight-based recom mend ations19 and was administered in most centres (ten) twice daily over 4 h.20 Two centres adminis-tered busulfan once daily (3 h infusion),21 and three centres four-times daily (2 h infusions).19
Busulfan plasma concentrations were analysed by high performance liquid or gas chromatography-tandem mass spectrometry at four to six diff erent time points after intravenous or oral administration according to local preference. Pharmacokinetic model ling was done using Win-Nonlin (version 5.2; Pharsight, Mountain View, CA, USA).
For therapeutic drug monitoring (TDM) of busulfan the protocol recommended to target busulfan exposure by adding measured and estimated non-measured single area-under-the-curve (AUC) values to a cumulative AUC of 45–65 mg/L × h, equivalent to 55–75% of the full myeloablative cumulative AUC (80–100 mg/L × h).20,22 According to the regimen of administration (ie, twice daily, once daily, or four-times daily), the AUC after initial busulfan infusions was mainly adjusted to a target AUC of 4∙5–6·0, 9·0–12·0, or 18·0–24·0 mg/L × h, respectively, according to the formula:
Investigators at the Karolinska Institute (Stockholm, Sweden) recalculated busulfan kinetics of all contributing centres (appendix). The diff erence between the total administered busulfan dose and the recommended total weight-based myel oablative busulfan dose was assessed.
For GVHD prophylaxis the protocol recommended adminis tration of calcineurine inhibitors, ciclosporin, or tacrolimus, until day 180, combined with mycophenolate mofetil (1200 mg/m² per day, twice a day from day 0 until day 100).
Chimerism was analysed by karyotyping (fl uorescent in-situ hybridisation analysis), analysis of informative microsatellite DNA sequences, fl ow cytometry (dihydro-rhodamine oxidation assay) or by cytochemical nitroblue tetrazolium assay.
The primary endpoints were overall survival and EFS, probabilities of overall survival and EFS at 2 years, incidence of acute and chronic GVHD, achievement of at least 90% myeloid donor chimerism, and incidence of graft failure after at least 6 months of follow-up. Other
CGD type
Sex Age at HSCT (years)
Signifi cant pre-existing disease
Complications at time of HSCT
Donor (HLA match)
Stem-cell source
Administered busulfan dose in mg/kg†
Cumulative busulfan AUC (mg/L × h)
CD34+ 10⁶
per kg body weight
TNC 10⁸ per kg body-weight
Alemtuzumab dose(mg/kg)
rATG dose (mg/kg)
(Continued from previous page)
53 NCF1 F 24·0 Colitis Colitis, pulmonary infi ltrates
MUD BM 6·5 (12·8) Yes (63) 6·2 4·7 0·5 ··
54 CYBB M 29·2 NR Pulmonary aspergillosis, colitis
MUD BM 8·0‡ (12·8) Yes (45) 3·2 ·· ·· 40·0
55 CYBB M 34·4 NR Pulmonary aspergillosis
MRD BM 8·0‡ (12·8) Yes (41) 3·7 ·· ·· 40·0
56 CYBB M 39·3 Pulmonary aspergillosis
None MUD BM 8·0‡ (12·8) Yes (42) 2·3 ·· ·· 40·0
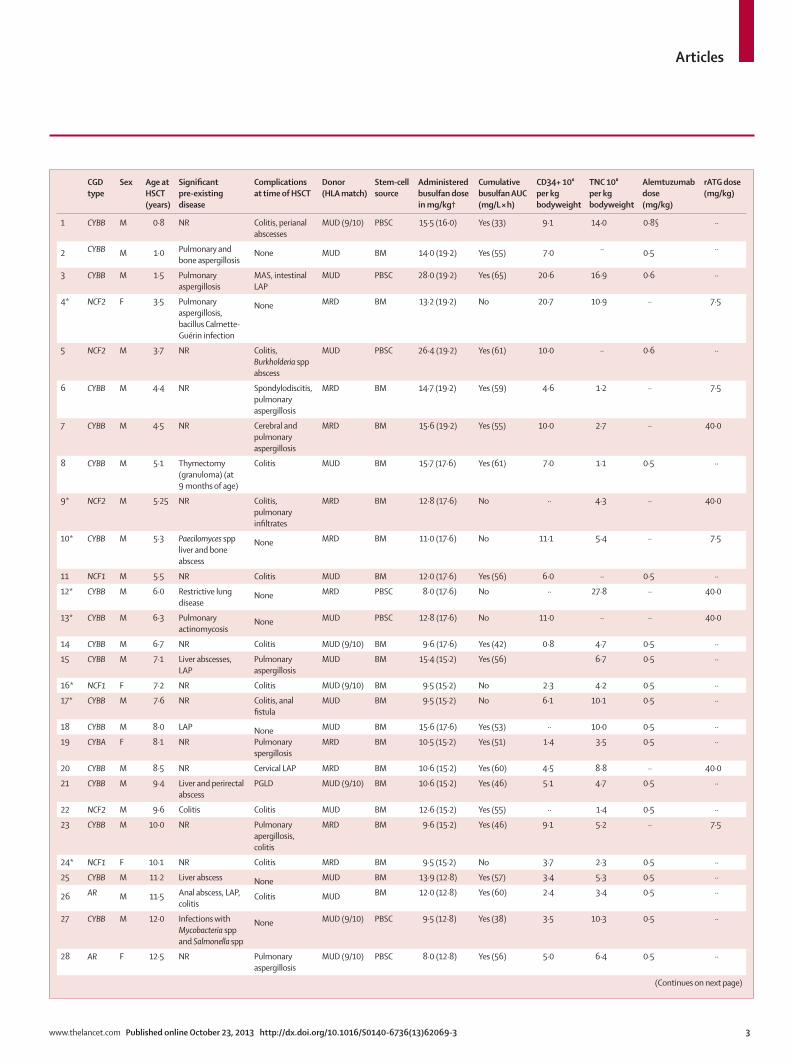
Patients 5, 38, 41, and 45 had residual NADPH-oxidase activity, all other patients had absent NADPH-oxidase activity. AUC=area under the curve. BM=bone marrow. CGD=chronic granulomatous disease. HSCT=haempoietic stem cell transplantation. LAP=lymphadenopathy. PGLD=progressive granulomatous lung disease. PBSC=peripheral blood stem cell. SVC=superior vena cava. MAS=macrophage activation syndrome. MUD=HLA-matched unrelated-donor. MRD=HLA-matched related-donor. NR=not recorded. TDM=therapeutic drug monitoring. TNC=total nucleated cells. rATG=rabbit anti-thymocyte globulin (doses for thymoglobuline 7·5 mg/kg; for ATG-Fresenius 40 mg/kg). *Patients with no TDM. †Total myeloablative busulfan dose based on bodyweight. ‡Patients with oral busulfan. §Higher alemtuzumab dose because of administration of HLA-9/10 matched PBSC (low-dose alemtuzumab <1 mg/kg).
Table 1: Patient and transplant characteristics
adjusted dosedose target AUCmeasured AUC
=×
See Online for appendix

Articles
6 www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3
clinical endpoints were safety of the regimen, resolution of pre-existing morbidity and diff erences of outcome dependent on donor type. Data were collected at last follow-up and reported to the University Children’s Hospital in Zurich. Minimum follow-up was 6 months after HSCT; there were no prespecifi ed follow-up visits, but visits generally occurred at least once every two weeks in the fi rst 6 months.
Statistical analysisOverall survival, EFS, cumulative GVHD incidence, and neutrophil (≥0∙5 × 10⁹/L) and platelet engraftment (≥50 × 10⁹/L) were described by Kaplan-Meier estimates. Gehan-Breslow-Wilcoxon tests, including hazard ratios (HRs) from Mantel-Haenszel analysis, and 95% CI were
applied for the comparison between transplants from HLA-matched related-donor and HLA-matched unrelated-donors. Medians (and IQRs) were used to describe characteristics (ie, age; cell dose; and total, recommended and cumulative AUC) of busulfan administration. We used GraphPad Prism (version 6.0a), Microsoft Excel 2011, and Microsoft Word 2011 for analyses.
Role of the funding sourceThere was no funding source for this study. All authors had access to the clinical and laboratory data. TG, MHA, and MH had full access to detailed busulfan kinetic data. TG had fi nal responsibility for the decision to submit for publication.
ResultsIncluding a pilot phase from June 15, 2003, to Sept 30, 2005, 58 patients were enrolled as per centre preference until Dec 15, 2012. Last follow-up was on July 15, 2013. 56 eligible patients (45 males, 11 females) from 16 centres were analysed (fi gure 1); two patients were excluded for protocol deviations. 34 patients had X-linked (CYBB) chronic granulomatous disease and 22 had autosomal-recessive disease: 11 NCF1, four NCF2, two CYBA, and fi ve molecularly unidentifi ed. All except three patients had non-measurable NADPH-oxidase activity by dihydro-rhodamine oxidation testing. At transplant, 75% (42 of 56) fulfi lled the high-risk defi nition, 25% (14 of 56) were in remission from previous complications. Micro bio logically proven active infections at HSCT were mainly caused by Aspergillus spp (n=11) and less frequently by other pathogens. The main auto infl am matory compli cations at transplant were colitis (n=19) and progressive granulo-matous lung disease (n=3). 13 patients were adults (≥18 years) and 43 were children and adolescents; median age at HSCT was 12∙65 years (IQR 6·8–17·3). 21 patients underwent trans plant from a HLA-matched related-donor (18 sibling donors; three pheno identical related donors) and 35 from a HLA-matched unrelated-donor (25 HLA-10/10 matched; 10 HLA-9/10 matched). 45 patients were infused with bone marrow and 11 with PBSC. The median number of CD34+ haemopoietic stem cells administered was 4∙5 × 10⁶ cells per kg bodyweight (IQR 3·2–7·0); the median number of total nucleated cells was 4∙2 × 10⁸ cells per kg bodyweight (IQR 3·0–6·4; table 1). Three HLA-matched unrelated-donor transplant recipi ents received ATG instead of alemtuzumab and four HLA-matched related-donor transplant recipients had low-dose alemtuzumab (0∙3–0∙5 mg/kg) treatment.
Busulfan was administered twice a day in 29 patients, four-times a day in 24 patients, and once a day in three patients. Busulfan was administered intravenously in 52 patients and orally in four patients. In 44 patients (79%) with available pharmacokinetics, the median cumulative AUC was 55 mg/L × h (IQR 47–59). Eight of 44 patients could only be adjusted below the target with a median cumulative AUC of 39∙5 mg/L × h
Figure 2: Total administered busulfan dose and cumulative AUC(A) Total administered busulfan dose (mg/kg) in 56 patients distributed by age and compared with the recommended total myeloablative weight-based busulfan dose (red line). Six of 56 patients (median age 9 years) showed rapid busulfan excretion and needed 100–146% of the recommended total myeloablative busulfan dose to achieve the target cumulative AUC. (B) Cumulative AUC of busulfan in 44 patients distributed by age. The red area depicts the target submyeloablative cumulative AUC (45–65 mg/L × h), the grey area depicts the full myeloablative AUC (80–100 mg/L × h). Eight of 44 patients could only be adjusted below the target cumulative AUC of 45 mg/L × h (median 39·0 mg/L × h, IQR 33·5–41·8). Patients with primary and secondary graft failure (patients 11 and 48) are depicted with arrows. AUC=area under the curve. HSCT=haemopoietic stem-cell transplantation.
0 5 10 15 20 25 30 35 400
5
10
15
20
25
30A
Tota
l bus
ulfa
n do
se (m
g/kg
)
Age at HSCT (years)
0 5 10 15 20 25 30 35 400
10
20
30
50
70
90
40
60
80
100B
AUC
(mg/
L×h)
Age (years)

Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 7
(IQR 33·5–41·8). In 12 patients with unavailable TDM, reduced total busulfan doses (6∙4–13∙2 mg/kg; median 9∙5) were administered, corresponding to 50–72% of the recom mended total busulfan dose.
In the whole cohort, the median administered total busulfan dose was 10∙5 mg/kg (IQR 8·0–12·8). The median administered total busulfan dose in HLA-matched related-donor transplants constituted 69% (IQR 56–64) and in HLA-matched unrelated-donor transplants 74% (IQR 62–92) of the recommended total busulfan dose. Six outliers in the MUD group (age range 1∙5–15·0 years; median 9 years) showed a rapid busulfan excretion and needed 100–146% of the recommended total busulfan dose to achieve the target cumulative AUC (table 1; fi gure 2).
Conditioning was well tolerated. No sinusoidal obstruc-tion syndrome, interstitial pneumonitis, or mucositis of grade III–IV was identifi ed. Except for one event of transient sudden infl ammatory response syndrome during ATG administration, no events of uncontrollable infl ammatory fl are-up were identifi ed. No granulocyte infusions were administered (table 2).
At a median follow-up of 21 months (IQR 13–35), overall survival was 93% (52 of 56) and EFS was 89% (50 of 56).
The 2-year probability of overall survival was 96% (95% CI 86∙46–99∙09) and of EFS was 91% (79∙78–96∙17).
Analysing HLA-matched related-donor transplants and HLA-matched unrelated-donor transplants separ-ately, the 2-year probability of overall survival was 100% and 94% (79∙03–98∙54), respectively, with HR 1∙91 (95% CI 0∙26–14∙22; p=0·30). The 2-year probability of EFS was 95% (71∙85–99∙34) and 89% (72∙35–95∙55), respectively, (HR 1∙72, 95% CI 0∙38–7∙78; p=0∙31; fi gure 3). Overall transplant-related mortality was 7% (four of 56).
Three patients had early (n=1) or late (n=2) graft failure. Two of them (patients 14 and 48) underwent successful re-HSCT after reduced-intensity conditioning, one with fl udarabine and treosulfan and one with fl udarabine and low-dose total body irradiation, using diff erent HLA-matched unrelated donors. Both patients have fully engrafted and are alive and well. The other patient received low-dose busulfan without TDM and low-dose alemtuzumab (0·3 mg/kg) conditioning before HLA-matched related donor transplantation and had late secondary graft-failure. Because of developing HLA-antibodies after previous granulocyte infusions he
Acute GVHD (overall grade)
Other transplant-related complications
Latest myeloid chimerism (% donor)
Time after trans-plantation of last chimerism (months)
Present status Outcome
4 ·· ·· 100% 23 Alive and well and off immunosuppressants Infection resolved
6 ·· SIRS during conditioning 100% 22 Alive and well and off immunosuppressants Cerebral and pulmonary aspergillosis cured
7 ·· ·· 100% 16 Alive and well and off immunosuppressants Spondylodiscitis and pulmonary aspergillosis resolved
9 ·· CMV viraemia 93% 9 Alive and well and off immunosuppressants Colitis resolved, lung infection resolved
10 ·· ·· 96% 21 Alive and well and off immunosuppressants Cured
12 I ·· 100% 117 Alive and well and off immunosuppressants PGLD resolved
19 ·· Transient red-cell aplasia 95% 29 Alive and well and off immunosuppressants Aspergillosis resolved
20 ·· ·· 91% 30 Alive and well and off immunosuppressants Cervical LAP cured
23 ·· ·· 97% 26 Alive and well and off immunosuppressants Aspergillosis resolved, colitis resolved
24 ·· ·· 100% 28 Alive and well and off immunosuppressants Colitis resolved
30 I ·· 99% 47 Alive and well and off immunosuppressants Pulmonary Neisseria spp infection resolved
31 ·· ·· 92%(day 22)
Secondary graft failure (month 9)
Died during second HSCT (day 10),haemorrhagic shock
Scedosporium apiospermum infection resolved after fi rst HSCT
34 I Transient renal insuffi ciency 100% 9 Alive and well and off immunosuppressants Pulmonary aspergillosis resolved
35 ·· ·· 100% 19 Alive and well and off immunosuppressants Liver abscess resolved
36 ·· ·· 100% 21 Alive and well and off immunosuppressants Colitis resolved, pneumonitis resolved
37 ·· BK virus cystitis 100% 13 Alive and well and off immunosuppressants Staphylococcal infection resolved
39 ·· Lung infection, EBV reactivation
100% 16 Alive and well and off immunosuppressants Lung infection resolved, EBV reactivation resolved without treatment
45 I Cholecystitis 98% 109 Alive and well and off immunosuppressants Colitis cured
50 ·· Rotavirus infection 97% 34 Alive and well and off immunosuppressants Colitis cured, rectal stenosis cured
52 I Renal insuffi ciency, early cessation of ciclosporin
98% 40 Alive and well and off immunosuppressants Fathered a child after HSCT
55 ·· ·· 100% 115 Alive and well and off immunosuppressants Infection resolved, fathered a child after HSCT
Chimerism assessed by fl uorescence in-situ hybridisation or variable number tandem repeat analysis in separated neutrophils or by dihydrorhodamine or nitroblue tetrazolium test. CMV=cytomegalovirus. EBV=Epstein-Barr virus. GVHD=graft-versus-host disease. HSCT=haempoietic stem cell transplantation. LAP=lymphadenopathy. PGLD=progressive granulomatous lung disease. SIRS=sudden infl ammatory response syndrome.
Table 2: Transplant ou tcome after HLA-matched related-donor transplants (n=21)

Articles
8 www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3
needed rituximab therapy and plasmapheresis before retransplantation using myeloablative conditioning and the same donor. He died from haemorrhage 10 days after the second HSCT (table 2).
Neutrophil engraftment occurred after a median of 19 days (IQR 16–22), platelet engraftment occurred after a median of 21 days (16–25). Comparing related-donor and unrelated-donor transplants, median neutrophil (day 18 [15–21] vs day 19 [18–24]) and platelet engraftment (day 21 [15–24] vs day 21 [16–34]) data did not diff er. Figure 4 shows engraftment kinetics and the engraftment probabilities for TDM within target versus TDM below target or no TDM.
Acute GVHD of grade II–IV developed in 11% (six of 56) of patients and of grade III–IV in 4% (two of 56). All these cases occurred in patients given trans-plants from HLA-matched unrelated-donors. The cumu-lative inci dence of severe acute GHVD of grade III–IV did not diff er between related and un related donor groups (p=0∙27).
Three of fi ve patients with acute GVHD of grade II–IV of the skin and gut responded favourably to immuno-suppression with steroids. Steroid-refractory acute GVHD of grade III–IV was encountered in two patients: one died (patient 38) at day 125 after refusal of fur-ther immuno suppressive treatment, the other patient (patient 27) fi rst responded well to extracorporeal photo-pheresis and extend ed immunosuppressive therapy, but relapsed with gut GVHD and died on day 745 from late Epstein-Barr virus-associated lympho proliferation. One adult patient (patient 49) developed chronic GVHD leading to lethal bronchiolitis obliterans at day 187. He had had severe therapy-refractory disseminated lung asper gillosis before HSCT and had received ATG instead of alemtuzumab (table 3). Chronic GVHD in two patients (patients 8 and 42) was limited to the skin and responded to immuno suppression. None of the patients, except one with limited chronic skin GVHD (patient 8), is still under immuno suppressive treatment. The inci dence of chronic GVHD was 0% in the HLA-matched related-donor group
Figure 3: Probabilities of overall survival (OS) and event-free survival (EFS)(A) 2-year OS: 96% (95% CI 86·5–99·1); total OS: 93% (52 of 56). (B) 2-year EFS: 91% (79·8–96·2); total EFS: 89% (50 of 56). (C) 2-year OS for MRD transplants: 100%; 2-year OS for MUD transplants: 94% (95% CI 79·0–98·5). Total OS for MRD transplants: 95% (21 of 22); total OS for MUD 91% (32 of 35). (D) 2-year EFS for MRD transplants: 95% (95% CI 71·8–99·3); 2-year EFS for MUD transplants: 89% (72·3–95·5). Total EFS for MRD transplants: 90% (19 of 21); total EFS for MUD 86% (30 of 35). Event was defi ned as engraftment failure or rejection or death. Vertical line depicts a censored event. MRD=HLA-matched related-donor. MUD=HLA-matched unrelated donor.
Number at risk
0
56
24
24
48
6
72
5
96
4
120
0
0
20
40
60
80
100O
vera
ll su
rviv
al (%
)
A OS
0
56
24
24
48
6
72
5
96
4
120
0
0
20
40
60
80
100
EFS
surv
ival
(%)
B EFS
Number at riskMUDMRD
0
3521
24
1212
48
33
72
23
96
13
120
00
3521
1212
33
23
13
00
Months after HSCT
0
20
40
60
80
100
Ove
rall
surv
ival
(%)
C OS by donor
0 24 48 72 96 120Months after HSCT
0
20
40
60
80
100
EFS
surv
ival
(%)
D EFS by donor
MUDMRD
MUDMRD

Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 9
and 11% (four of 35) in the HLA-matched unrelated-donor group (HR 5∙10; 95% CI 0∙67–38∙80, p=0∙12; tables 2, 3; appendix).
Five patients developed red cell aplasia due to ABO-incompatibility necessitating prolonged erythrocyte trans-fusions until remission 4–6 months after HSCT. Other complications including pancreatitis, cytomegalovirus-viraemia, autoimmune haemolytic anaemia, and Epstein-Barr virus-associated nephrotic syndrome were rare events and responded well to treatment (tables 2, 3).
All surviving patients (93%; 52 of 56) exhibit a stable myeloid donor chimerism of 90% or more and have cleared all infectious and autoinfl ammatory compli-cations. In peripheral blood lymphocytes, donor chimerism ranged between 70% and 100% (data not shown). Two patients fathered children 1 and 3 years after HSCT.
DiscussionIn 56 patients with mainly high-risk chronic granulo-matous disease, reduced-intensity conditioning with high-dose fl udarabine, rATG or low-dose alemtuzumab sero therapy, and low-dose or targeted busulfan adminis-tration followed by HSCT from HLA-matched donors was safe and effi cacious, resulting in overall survival of 93% and EFS of 89%, with no diff erence between transplants from related and unrelated donors. Graft-failure occurred in three patients. The cumulative incidence of acute GVHD of grade III–IV was 4% and of chronic GVHD was 7%. GVHD resolved in all but one surviving patient. Stable (≥90%) myeloid donor chimerism was documented in 93% of surviv ing patients.
There is continuing controversy about indications and optimum timing of allogeneic HSCT in chronic granulomatous disease. Patients with absent NADPH-oxidase activity and predicted poor prognosis have been recommended for early HSCT.4,8,17 Present HSCT indication criteria in children are: one or more life-threatening infection, non-compliance with antimicrobial prophylaxis, or steroid-dependent autoinfl ammation.4 Indication criteria in adolescents and young adults are more diffi cult to apply since organ dysfunction is frequent and transplant-related mortality after HSCT has been high (panel).10,16
Ideally, reduced-intensity conditioning regimens with decreased tissue damage and release of proinfl ammatory cytokines could permit safe transplantation in high-risk patients while preventing long-term sequelae of high-dose chemotherapy (eg, infertility or gonadal failure). Previous eff orts to apply reduced-intensity conditioning regimens in chronic granulomatous disease were complicated by high rates of graft failure and GVHD. Horwitz and colleagues16 treated ten patients with chronic granulomatous disease with a reduced-intensity conditioning protocol consisting of cyclophosphamide, fl udarabine, and ATG-serotherapy followed by T-cell depleted PBSC from HLA-matched related-donors. Two
patients had graft failure; three patients died from transplant-related causes, all of whom were adolescents or young adults. Another reduced-intensity condition-ing regimen, consisting of fl uda rabine, melphalan, and alemtuzumab serotherapy (1 mg/kg)26 resulted in even higher graft failure (three of six patients; unpublished).
Figure 4: Engraftment kinetics(A) Cumulative incidence of neutrophil engraftment (>0·5 × 10⁹/L for 3 consecutive days). Median number of days to neutrophil engraftment was 18·5 for HLA-matched related-donor transplants, and 19·0 for HLA-matched unrelated-donor transplants. (B) Engraftment probability (>90% myeloid donor chimerism) according to busulfan pharmacokinetics: TDM within target (45–65 mg/L × h; n=36) versus TDM below target (30–42 mg/L × h) or no TDM (n=20). (C) Cumulative incidence of platelet engraftment (>50 × 10⁹/L for 3 consecutive days). Median number of days to platelet engraftment was 21 for both HLA-matched related-donor transplants and HLA-matched unrelated-donor transplants. cAUC=cumulative area under the curve. TDM=therapeutic drug monitoring. HSCT=haemopoietic stem-cell transplantation.
0 10 20 30 40 50 600
25
50
75
100
A
Engr
afte
d (%
)Days until >0·5 × 109/L
0 24 48 72 96 1200
20
40
60
80
100
BEv
ent p
roba
bilit
y (%
)
Months after HSCT
0 10 20 30 40 50 600
25
50
75
100
C
Engr
afte
d (%
)
Days until >50 × 109/L
MUDMRD
MUDMRD
TDM (cAUC 45–65 mg/L×h)TDM (cAUC 30–42 mg/L×h) or no TDM

Articles
10 www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3
Slavin and colleagues23 and Jacobson and coworkers24 previously introduced reduced-intensity conditioning protocols for patients with malignant and non-malignant diseases, and we actively searched for ways to improve these protocols. Both reduced-intensity conditioning regimens consisted of fl udarabine, half-dose busulfan, and ATG and were based on a graft-versus-marrow eff ect mediated by unmodifi ed T-cell replete transplants after incomplete myeloablation and the option for donor lymphocyte infusions in case of falling donor chimerism.
In a pilot study, we successfully administered a 2-day shortened Jacobson-protocol consisting of fl udarabine (180 mg/m²), serotherapy with rabbit ATG, and half-dose oral busulfan in three adult patients with high-risk chronic granulomatous disease.25
To further optimise this protocol for children, we introduced TDM of busulfan on the basis of previous
reports27 showing that clearance and exposure variability of busulfan are much higher in children than in adults. Children have been shown to have reduced toxicity and increased effi cacy with TDM (target cumulative AUC 75–80 mg/L per h) after full-myeloablative busulfan-based conditioning.19–21 Jacobson and colleagues24 had previously shown the feasibility of their reduced-intensity conditioning regimen in 13 children with non-malignant diseases. They used TDM for busulfan in three children with a low target cumulative AUC (30–34 mg/L × h); ten children received low doses of busulfan (intravenous 6∙4 mg/kg) without TDM. However, graft failure or vanishing chimerism was a substantial problem in Jacobson’s cohort with 31% (four of 13) receiving stem-cell boosts or second transplants.
In the present study, all (36 of 36) patients whose cumulative AUC of busulfan could be adjusted within a
Acute GVHD (grade)
Chronic GVHD (NIH consensus severity grade)
Other transplant-related complications
Latest myeloid chimerism (% donor)
Time post-HSCT of last chimerism (months)
Present status Outcome
1 I ·· ·· 100% 7 Alive and well and off immunosuppressants Colitis resolved
2 ·· ·· Mucositis 100% 12 Alive and well and off immunosuppressants Cured
3 I ·· ·· 100% 12 Alive and well and off immunosuppressants MAS, intestinal LAP resolved
5 ·· ·· CMV viraemia 95% 23 Alive and well and off immunosuppressants Colitis cured
8 II 1 ·· 100% 16 Alive and well, receiving prednisone 0·15 mg/kg per day
Cured
11 ·· ·· ·· 99% 47 Alive and well and off immunosuppressants Colitis cured
13 ·· ·· ·· >90% 34 Alive and well and off immunosuppressants Infectious foci resolved
14 ·· ·· ·· Primary engraftment failure
NA Alive and well and off immunosuppressants, 23 months after second HSCT (100% donor)
Colitis resolved
15 ·· ·· ·· 100% 9 Alive and well and off immunosuppressants Cured
16 I ·· CMV viraemia, spinal fracture (pre-existing osteopenia)
100% 43 Alive and well and off immunosuppressants Colitis resolved
17 I ·· ·· 100% 31 Alive and well and off immunosuppressants Colitis cured, fi stula healed
18 ·· ·· 100% 7 Alive and well and off immunosuppressants Cured
21 I ·· AIHA 100% 16 Alive and well and off immunosuppressants PFT improved, AIHA resolved (rituximab)
22 ·· ·· ·· 100% 9 Alive and well and off immunosuppressants Cured
25 ·· ·· ·· 97% 34 Alive and well and off immunosuppressants Cured
26 ·· ·· EBV reactivation (after 5 months), AIHA (after 7 months)
100% 16 Alive and well and off immunosuppressants Colitis cured, AIHA resolved (steroids)
27 IV 1 Secondary Scediospermum spp lung and brain abscesses
100% 33 Died (day 745 due to EBV-related PTLD), no response to rituximab and EBV-specifi c T-cell therapy
ECP treatment for GVHDInfections resolved
28 ·· ·· Mild PTLD 100% 42 Alive and well and off immunosuppressants Aspergillosis resolved
29 I ·· ·· 100% 43 Alive and well and off immunosuppressants Fungal infection resolved
32 ·· ·· ·· 100% 11 Alive and well and off immunosuppressants Resolved
33 ·· ·· ·· 100% 8 Alive and well and off immunosuppressants Geosmithia spp infection resolved
38 III··IV ·· ·· 100% 4 Died (day 125) after refusal of immuno-suppressive treatment for acute GVHD
Acute GVHD of skin and gut responding to treatment, PGLD ameliorated
40 II ·· BK cystitis, EBV reactivation (at 6 months)
100% 16 Alive and well and off immunosuppressants Colitis cured, gastric GVHD cured, resolution of stenosis, EBV resolved (rituximab)
41 ·· ·· ·· 100% 35 Alive and well and off immunosuppressants Colitis resolved
(Continues on next page)

Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 11
submyeloablative target range of 45–65 mg/L × h achieved sustained myeloid (≥90%) engraftment. This sub myelo-ablative cumulative AUC was based on experiments by Hassan and colleagues28,29 showing that in cultured human bone marrow and a mouse transplantation model most granulocyte-macrophage colony forming units and CD34+ HSC were inhibited after a busulfan exposure of 45–65 mg/L × h. In our study, two of eight patients whose busulfan exposures could only be adjusted below the target cumulative AUC (patients 14, 48) developed graft failure and needed re-HSCT (fi gure 2B). Despite other potential contributing factors, such as low HSC numbers (patient 14), the practical relevance of this target cumu-lative AUC for engraftment in all age groups was surprising (fi gure 4B). Six paediatric patients needed higher total busulfan doses than recommended to obtain the target submyeloablative cumulative AUC, under-lining the relevance of TDM in children (fi gure 2A, table 1). In our cohort without TDM, one of 12 patients developed secondary graft failure and died after myelo-ablative HSCT 1 year later. The overall rate of graft failure in the present cohort was low (5%; three of 56).
Since most of our cohort had HLA-matched related-donor transplants (including ten HLA-9/10 matched), mainly low-dose alemtuzumab was administered to prevent both severe GVHD and viral reactivation.30 Among the HLA-9/10 matched related-donor transplants, one
Acute GVHD (grade)
Chronic GVHD (NIH consensus severity grade)
Other transplant-related complications
Latest myeloid chimerism (% donor)
Time post-HSCT of last chimerism (months)
Present status Outcome
(Continued from previous page)
42 I 1 Pancreatitis, spinal fracture (pre-existing osteopenia)
100% 48 Alive and well and off immunosuppressants, chronic GVHD resolved
Chronic GVHD, resolvedPFT improved
43 ·· ·· ·· 97% 17 Alive and well and off immunosuppressants Hepatic and hypophyseal granulomata cured
44 ·· ·· ·· 100% 14 Alive and well and off immunosuppressants Cured
46 I ·· ·· 100% 17 Alive and well and off immunosuppressants Colitis cured, pulmonary infi ltrates resolved
47 ·· ·· Transient red-cell aplasia 100% 13 Alive and well and off immunosuppressants Liver abscesses resolved
48 II ·· ·· Second engraftment failure at 5 months
NA Alive and well and off immunosuppressants, 14 months after secomd HSCT (100% donor)
Colitis resolved, pneumonitis resolved
49 II 3 CMV reactivation (donor CMV–, recipient+), pulmonary and gastrointestinal deterioration
100% 5 Died (day 187), respiratory failure In post mortem lung biopsy (no sign of aspergillus or CMV), T-cell mediated lung injury (bronchiolitis obliterans)
51 ·· ·· Transient red cell aplasia 100% 12 Alive and well and off immunosuppressants Cured
53 1 ·· EBV reactivation, nephrotic syndrome
100% 11 Alive and well and off immunosuppressants Colitis cured, lung function improved
54 I ·· ·· 100% 70 Alive and well and off immunosuppressants Aspergillosis resolved, colitis resolved
56 ·· ·· Transient red-cell aplasia 100% 111 Alive and well and off immunosuppressants Infection resolved
Chimerism assessed by fl uorescence in-situ hybridisation or variable number tandem repeat analysis in separated neutrophils or by dihydrorhodamine or nitroblue tetrazolium test. AIHA=autoimmune haemolytic anaemia. CMV=cytomegalovirus. EBV=Epstein-Barr virus. ECP=extracorporeal photopheresis. GVHD=graft-versus-host disease. HSCT=haemtopoietic stem cell transplantation. LAP=lymphadenopathy. MAS=macrophage activation syndrome. NA=not applicable. PFT=pulmonary function test. PGLD=progressive granulomatous lung disease. SIRS=sudden infl ammatory response syndrome.
Table 3: Transplant outcome in HLA-matched unrelated-donor transplant recipients (n=35)
Panel: Research in context
Systematic reviewWe searched PubMed with the terms “chronic granulomatous disease”, “stem cell transplantation”, and “reduced intensity conditioning” for reports in English, French, and German, up to June 25, 2013, and identifi ed several relevant studies.10–12,14–16,23–26 Despite reported overall survival rates of 85%10 after myeloablative conditioning and with matched related-donor transplants, subgroups of patients with intractable infections or autoinfl ammatory complications and adolescents and young adults had high transplant-related mortality of 33% and 36%, respectively.10 Some reports showed improved outcome after myeloablative conditioning regimens and even in unrelated-donor transplants, especially in children with mainly low-risk features;14,15 however, transplant-related mortality in adolescents and young adults remained high11,12 (29–50%). Administration of reduced-intensity conditioning regimens to reduce toxicity had been unsatisfactory, with graft failure of 20% and transplant-related mortality of 30%.16
InterpretationOur reduced-intensity conditioning protocol resulted in reduced toxicity, graft failure, and transplant-related mortality in a prospective cohort of patients with chronic granulomatous disease patients after unmanipulated HLA-matched related-donor or unrelated-donor transplantation. Low-dose or targeted busulfan administration, serotherapy, and high-dose fl udarabine provided sustained myeloid donor engraftment and low occurrence of GVHD in most patients. Overall survival was 93% despite 75% of the present cohort having high-risk features and 45% being adolescents and young adults. Whether long-term sequelae, such as infertility, will also be reduced should be investigated in future studies.

Articles
12 www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3
graft failure occurred, which was cured by re-HSCT, and one death. Despite the low overall occurrence of acute GVHD and viral reactivation, two patients with HLA-matched unrelated-donors (one HLA-10/10 matched bone marrow, one HLA-9/10 matched PBSC) had acute GVHD of grade III–IV, suggesting that the lowest threshold dose of alemtuzumab to prevent severe acute GVHD after HLA-matched unrelated-donor transplants in all cases is probably greater than 0∙5 mg/kg.
The outcomes of HLA-matched unrelated-donor trans-plants in our study (overall survival 91% [32 of 35]; EFS 86% [30 of 35]) compare favourably with two European reports11,12 using full-myeloablative condition ing regi mens and HLA-matched unrelated-donor trans plants for chronic granulomatous disease (overall survival 84%, 16 of 19; EFS 68%, 13 of 19). Transplant-related mortality among adolescent and young adult patients was 29% (two of seven)12 and 50%11 (two of four).
Tewari and colleagues15 used full-myeloablative con-ditioning for paediatric patients with chronic granulo-matous disease and reported overall survival of 100% (12 of 12) and EFS of 83% (ten of 12), compared with 93% (52 of 56) and 89% (50 of 56) in the present study. The 12 children in the US study (aged 8 months to 11∙5 years) had no active infection or autoinfl ammation at HSCT. The cumulative incidences of GVHD (25%, three of 12) and graft failure (17%; two of 12) were higher in the US study than in the present study (7%, four of 56; 5%, three of 56). Major diff erences in serotherapy (fi ve of 15 patients had no serotherapy), stem cell source (eight unrelated cord blood), and toxicity of conditioning might explain these diff erences.15 Martinez and colleagues14 gave seven chil-dren (aged 11 months to 13 years; four with high-risk features) full-myeloablative conditioning, consisting of full-dose busulfan, fl udarabine, cytarabine, and alem tuzu-mab serotherapy (0∙7–2∙4 mg/kg) followed by HLA-10/10 matched unrelated-donor transplantation. Over all survival and EFS were 100% and no patients had acute GVHD of grades II–IV or chronic GVHD. Both these reports14,15 suggest that modern approaches with full-myeloablative regimens might deliver much the same outcomes in selected paediatric patients with chronic granulomatous disease as with the less toxic regimens presented here.
As far as we are aware, this study is the largest analysed series of patients with chronic granulomatous disease treated prospectively with one reduced-intensity con-ditioning regimen. Because of the rarity of the disease the enrolment phase spanned over almost a decade, explaining some variations in the dosing of serotherapy. However, after having shown the effi cacy of the regimen in the sickest and oldest patients, most patients—especially infants and small children—were rapidly enrolled after 2008. Our study is probably subject to some selection bias, because mainly very sick patients and adolescents and young adults deemed to be intolerant to full-myeloablative conditioning were enrolled and only two patients were excluded from the analysis.
Adolescent and young adult patients had very high overall survival and EFS (92% for both; 22 of 24) and low occurrence of acute GVHD of grade III–IV and chronic GVHD (4%, one of 24; and 8%, two of 24). Additionally, two adult patients subsequently fathered children showing that fertility after low-dose or targeted busulfan adminis-tration might be preserved, at least in men. Follow-up studies investigating fertility and pulmonary function are necessary to analyse whether busulfan-associated long-term sequelae will be reduced in all age groups.31
Because of its favourable toxicity and effi cacy profi le, patients with other non-malignant diseases have bene-fi ted from this reduced-intensity conditioning regimen.32 Despite the fi nding that overall survival (90%, nine of ten) and EFS (80%, eight of ten) were excellent among HLA-9/10 matched unrelated-donor transplant recipi-ents, these results are not auto matically trans ferable to transplants from alter native donors such as unrelated cord-blood donors or donors who are less than an HLA-9/10 match. However, pre liminary (unpublished) results of this regimen are promising in unrelated cord-blood transplantation for chronic granulomatous disease with target myeloablative busulfan exposures.ContributorsTG and MHA wrote the report. TG, PV, MH, US, and MHA designed the protocol. TG, RS, PT, EH, MS, AG, US, GS, PGS, IBR, DM, AF, CV, RB, IA, SL, PJS, JMTdC, PGS, RH, KK, BG, JFF, MHA, BHB, PV, and HBG contributed patients and provided clinical and laboratory data and revised and corrected the report. MH and TG calculated and recalculated all busulfan kinetics and cumulative area under the curve. KR analysed the busulfan samples of the Zürich patients in her laboratory. AF and HBG approved and recommended the protocol within the European Society for Blood and Marrow Transplantation Inborn Errors Working Party. US and KK provided data. US provided data that were not used for the analysis because of deviations from the protocol.
Inborn Errors Working Party of the European Society for Blood and Marrow TransplantationAustralia P J Shaw (Children’s Hospital, Division of Blood and Marrow Transplantation, Westmead, Sydney, NSW); C J Fraser (Royal Children’s Hospital, Herston, QLD). Brazil J M Telles da Cunha (Hospital Albert Einstein, Haematology and Haematopoietic Stem Cell Transplantation Unit, São Pãulo); J F Fernandes (Instituto da Criança, Universidade de São Paulo, São Paulo). Canada P Teira, E Haddad (Centre de Recherche du CHU Sainte-Justine, Département de Pédiatrie, Université de Montréal, Montréal, QC); I Ahmad, S Lachance (Blood and Marrow Transplantation Program, Hôpital Maisonneuve-Rosemont, Université de Montréal, QC). France D Moshous, A Fischer (AP-HP, Hôpital Necker Enfants Malades, Paediatric Immunology, Sorbonne Paris Cité, Université Paris Descartes, Imagine Institute, Paris). Germany P G Schlegel (University Children’s Hospital, Division of Blood and Marrow Transplantation, Würzburg); K Kentouche, B Gruhn (Department of Paediatrics, Jena University Hospital, Jena); M Albert, B Belohradsky (Dr von Hauner University Children’s Hospital, Munich); A Wawer (Divison of Pediatric Hematology and Oncology; Children’s Hospital Schwabing, Munich). Israel P Stepensky, I B Resnick (Hadassah Hebrew University Medical Center, Department of Blood and Marrow Transplantation, Jerusalem). Netherlands C Vermont, R Bredius (Leiden University Medical Center, Department of Paediatrics, Leiden). Poland K Kalwak (Wroclaw Medical University, Department of Pediatric Hematology and Oncology and Blood and Marrow Transplantation, Wroclaw). Sweden A Fasth (Department of Pediatrics, University of Gothenburg, Gothenburg); M Hassan (Div of Experimental Cancer Medicine, KFC, Novum, Laboratory Medicine, Karolinska University Hospital-Huddinge, Stockholm; and Karolinska Institute, Stockholm).

Articles
www.thelancet.com Published online October 23, 2013 http://dx.doi.org/10.1016/S0140-6736(13)62069-3 13
Switzerland T Güngör, R Seger (University Children’s Hospital, Division of BMT, Zurich); U Schanz, G Stüssi (University Hospital, Division of Hematology and Blood and Marrow Transplantation, Zurich); K Rentsch (University Hospital, Division of of Clinical Chemistry, Zurich). UK M Slatter, A Gennery (Institute of Cellular Medicine, Newcastle University, Newcastle upon Tyne, Newcastle); R Hough (University College London Hospitals NHS Foundation Trust, London, UK); P Veys, H B Gaspar (Great Ormond Street Children’s Hospital, Division of BMT, London; Molecular Immunology Unit; UCL Institute of Child Health, London). USA U Duff ner (Blood and Bone Marrow Transplant Program, Helen DeVos Children’s Hospital, MI).
Confl icts of interest We declare that we have no confl icts of interest.
AcknowledgmentsWe thank A Wawer (Munich, Germany), C J Fraser (Herston, QLD, Australia), U Duff ner (Michigan, USA), and K Kalwak (Wroclaw, Poland) who provided data that were not used in the study.
References1 van den Berg JM, van Koppen E, Ahlin A, et al. Chronic
granulomatous disease: the European experience. PLoS One 2009; 4: e5234.
2 Winkelstein JA, Marino MC, Johnston RB Jr, et al. Chronic granulomatous disease. Report on a national registry of 368 patients. Medicine (Baltimore) 2000; 79: 155–69.
3 Reichenbach J, Lopatin U, Mahlaoui N, et al. Actinomyces in chronic granulomatous disease: an emerging and unanticipated pathogen. Clin Infect Dis 2009; 49: 1703–10.
4 Seger RA. Advances in the diagnosis and treatment of chronic granulomatous disease. Curr Opin Hematol 2011; 18: 36–41.
5 Meissner F, Seger RA, Moshous D, Fischer A, Reichenbach J, Zychlinsky A. Infl ammasome activation in NADPH oxidase defective mononuclear phagocytes from patients with chronic granulomatous disease. Blood 2010; 116: 1570–73.
6 Deff ert C, Carnesecchi S, Yuan H, et al. Hyperinfl ammation of chronic granulomatous disease is abolished by NOX2 reconstitution in macrophages and dendritic cells. J Pathol 2012; 228: 341–50.
7 Freudenberg F, Wintergerst U, Roesen-Wolff A, et al. Therapeutic strategy in p47-phox defi cient chronic granulomatous disease presenting as infl ammatory bowel disease. J Allergy Clin Immunol 2010; 125: 943–46.
8 Kuhns DB, Alvord WG, Heller T, et al. Residual NADPH oxidase and survival in chronic granulomatous disease. N Engl J Med 2010; 363: 2600–10.
9 The Westminster Hospitals Bone-Marrow Transplant Team. Bone-marrow transplant from an unrelated donor for chronic granulomatous disease. Lancet 1977; 309: 210–13.
10 Seger RA, Gungor T, Belohradsky BH, et al. Treatment of chronic granulomatous disease with myeloablative conditioning and an unmodifi ed hemopoietic allograft: a survey of the European experience, 1985–2000. Blood 2002; 100: 4344–50.
11 Schuetz C, Hoenig M, Gatz S, et al. Hematopoietic stem cell transplantation from matched unrelated donors in chronic granulomatous disease. Immunol Res 2009; 44: 35–41.
12 Soncini E, Slatter MA, Jones LB, et al. Unrelated donor and HLA-identical sibling haematopoietic stem cell transplantation cure chronic granulomatous disease with good long-term outcome and growth. Br J Haematol 2009; 145: 73–83.
13 Honig M, Flegel WA, Schwarz K, et al. Successful hematopoietic stem-cell transplantation in a patient with chronic granulomatous disease and McLeod phenotype sensitized to Kx and K antigens. Bone Marrow Transplant 2010; 45: 209–11.
14 Martinez CA, Shah S, Shearer WT, et al. Excellent survival after sibling or unrelated donor stem cell transplantation for chronic granulomatous disease. J Allergy Clin Immunol 2012; 129: 176–83.
15 Tewari P, Martin PL, Mendizabal A, et al. Myeloablative transplantation using either cord blood or bone marrow leads to immune recovery, high long-term donor chimerism and excellent survival in chronic granulomatous disease. Biol Blood Marrow Transplant 2012; 18: 1368–77.
16 Horwitz ME, Barrett AJ, Brown MR, et al. Treatment of chronic granulomatous disease with nonmyeloablative conditioning and a T-cell-depleted hematopoietic allograft. N Engl J Med 2001; 344: 881–88.
17 Segal BH, Veys P, Malech H, Cowan MJ. Chronic granulomatous disease: lessons from a rare disorder. Biol Blood Marrow Transplant 2011; 17 (suppl 1): S123–31.
18 WHO. Handbook for reporting results of cancer treatment. Geneva: World Health Organization, 1979.
19 Vassal G, Michel G, Esperou H, et al. Prospective validation of a novel IV busulfan fi xed dosing for paediatric patients to improve therapeutic AUC targeting without drug monitoring. Cancer Chemother Pharmacol 2008; 61: 113–23.
20 Malar R, Sjoo F, Rentsch K, Hassan M, Gungor T. Therapeutic drug monitoring is essential for intravenous busulfan therapy in pediatric hematopoietic stem cell recipients. Pediatric Transplantation 2011; 15: 580–88.
21 Bartelink IH, Bredius RG, Ververs TT, et al. Once-daily intravenous busulfan with therapeutic drug monitoring compared to conventional oral busulfan improves survival and engraftment in children undergoing allogeneic stem cell transplantation. Biol Blood Marrow Transplant 2008; 14: 88–98.
22 Olavarria E, Hassan M, Eades A, et al. A phase I/II study of multiple-dose intravenous busulfan as myeloablation prior to stem cell transplantation. Leukemia 2000; 14: 1954–59.
23 Slavin S, Nagler A, Naparstek E, et al. Nonmyeloablative stem cell transplantation and cell therapy as an alternative to conventional bone marrow transplantation with lethal cytoreduction for the treatment of malignant and nonmalignant hematologic diseases. Blood 1998; 91: 756–63.
24 Jacobsohn DA, Duerst R, Tse W, Kletzel M. Reduced intensity haemopoietic stem-cell transplantation for treatment of non-malignant diseases in children. Lancet 2004; 364: 156–62.
25 Gungor T, Halter J, Klink A, et al. Successful low toxicity hematopoietic stem cell transplantation for high-risk adult chronic granulomatous disease patients. Transplantation 2005; 79: 1596–606.
26 Rao K, Amrolia PJ, Jones A, et al. Improved survival after unrelated donor bone marrow transplantation in children with primary immunodefi ciency using a reduced-intensity conditioning regimen. Blood 2005; 105: 879–85.
27 Hassan M, Ljungman P, Bolme P, et al. Busulfan availability. Blood 1994; 84: 2144–50.
28 Hassan Z, Hassan M, Hellstrom-Lindberg E. The pharmacodynamic eff ect of busulfan in the P39 myeloid cell line in vitro. Leukemia 2001; 15: 1240–47.
29 Hassan Z, Hellstrom-Lindberg E, Alsadi S, Edgren M, Hagglund H, Hassan M. The eff ect of modulation of glutathione cellular content on busulphan-induced cytotoxicity on hematopoietic cells in vitro and in vivo. Bone Marrow Transplant 2002; 30: 141–47.
30 Chakraverty R, Orti G, Roughton M, et al. Impact of in vivo alemtuzumab dose before reduced intensity conditioning and HLA-identical sibling stem cell transplantation: pharmacokinetics, GVHD, and immune reconstitution. Blood 2010; 116: 3080–88.
31 Bresters D, van Gils IC, Kollen WJ, et al. High burden of late eff ects after haematopoietic stem cell transplantation in childhood: a single-centre study. Bone Marrow Transplant 2010; 45: 79–85.
32 Gungor T, Albert M, Slatter M, et al. Favourable outcome after reduced-toxicity conditioning with high-dose fl udarabine, serotherapy and low-dose/targeted busulfan in 74 children and adults with non-malignant diseases. Bone Marrow Transplant 2012; 47: S67–68.




















