
Reduced corticomotor excitability and motor skills development in children born preterm
18
J Physiol 590.22 (2012) pp 5827–5844 5827 The Journal of Physiology Neuroscience Reduced corticomotor excitability and motor skills development in children born preterm Julia B. Pitcher 1 , Luke A. Schneider 1 , Nicholas R. Burns 2 , John L. Drysdale 1 , Ryan D. Higgins 1 , Michael C. Ridding 1 , Theodore J. Nettelbeck 2 , Ross R. Haslam 3 and Jeffrey S. Robinson 1 1 Research Centre for Early Origins of Health and Disease, Robinson Institute, School of Paediatrics & Reproductive Health, University of Adelaide, SA 5005, Australia 2 School of Psychology, University of Adelaide, SA 5005, Australia 3 Department of Perinatal Medicine, Women’s and Children’s Hospital, North Adelaide, SA 5006, Australia Key points • Children born preterm commonly experience motor and cognitive difficulties, but the physio- logy underlying this dysfunction is unknown. • We used transcranial magnetic stimulation techniques and age-appropriate assessments of motor skills development to investigate neurodevelopment in 151 children born between 25 and 41 weeks of gestation. • Reduced gestational age at birth was associated with a reduction in corticomotor excitability that persisted in late childhood, poorer development of manual dexterity skills and reduced hemispheric lateralization of hand preference. • We suggest this reduced corticomotor excitability at least partly reflects reduced white matter integrity and functional connectivity in the brain regions subserving movement control. • These findings show that preterm birth, which is increasingly common, impacts neuromotor development and related physiology into adolescence. Whether this altered neurophysiology and motor function persists in adulthood is unknown. Abstract The mechanisms underlying the altered neurodevelopment commonly experienced by children born preterm, but without brain lesions, remain unknown. While individuals born the earliest are at most risk, late preterm children also experience significant motor, cognitive and behavioural dysfunction from school age, and reduced income and educational attainment in adulthood. We used transcranial magnetic stimulation and functional assessments to examine corticomotor development in 151 children without cerebral palsy, aged 10–13 years and born after gestations of 25–41 completed weeks. We hypothesized that motor cortex and corticospinal development are altered in preterm children, which underpins at least some of their motor dysfunction. We report for the first time that every week of reduced gestation is associated with a reduction in corticomotor excitability that remains evident in late childhood. This reduced excitability was associated with poorer motor skill development, particularly manual dexterity. However, child adiposity, sex and socio-economic factors regarding the child’s home environment soon after birth were also powerful influences on development of motor skills. Preterm birth was also associated with reduced left hemisphere lateralization, but without increasing the likelihood of being left handed per se . These corticomotor findings have implications for normal motor C 2012 The Authors. The Journal of Physiology C 2012 The Physiological Society DOI: 10.1113/jphysiol.2012.239269
Transcript of Reduced corticomotor excitability and motor skills development in children born preterm
J Physiol 590.22 (2012) pp 5827–5844 5827
The
Jou
rnal
of
Phys
iolo
gy
Neuroscience Reduced corticomotor excitability and motor skills
development in children born preterm
Julia B. Pitcher1, Luke A. Schneider1, Nicholas R. Burns2, John L. Drysdale1, Ryan D. Higgins1,Michael C. Ridding1, Theodore J. Nettelbeck2, Ross R. Haslam3 and Jeffrey S. Robinson1
1Research Centre for Early Origins of Health and Disease, Robinson Institute, School of Paediatrics & Reproductive Health, University of Adelaide,SA 5005, Australia2School of Psychology, University of Adelaide, SA 5005, Australia3Department of Perinatal Medicine, Women’s and Children’s Hospital, North Adelaide, SA 5006, Australia
Key points
• Children born preterm commonly experience motor and cognitive difficulties, but the physio-logy underlying this dysfunction is unknown.
• We used transcranial magnetic stimulation techniques and age-appropriate assessments ofmotor skills development to investigate neurodevelopment in 151 children born between 25and 41 weeks of gestation.
• Reduced gestational age at birth was associated with a reduction in corticomotor excitabilitythat persisted in late childhood, poorer development of manual dexterity skills and reducedhemispheric lateralization of hand preference.
• We suggest this reduced corticomotor excitability at least partly reflects reduced white matterintegrity and functional connectivity in the brain regions subserving movement control.
• These findings show that preterm birth, which is increasingly common, impacts neuromotordevelopment and related physiology into adolescence. Whether this altered neurophysiologyand motor function persists in adulthood is unknown.
Abstract The mechanisms underlying the altered neurodevelopment commonly experienced bychildren born preterm, but without brain lesions, remain unknown. While individuals born theearliest are at most risk, late preterm children also experience significant motor, cognitive andbehavioural dysfunction from school age, and reduced income and educational attainment inadulthood. We used transcranial magnetic stimulation and functional assessments to examinecorticomotor development in 151 children without cerebral palsy, aged 10–13 years and bornafter gestations of 25–41 completed weeks. We hypothesized that motor cortex and corticospinaldevelopment are altered in preterm children, which underpins at least some of their motordysfunction. We report for the first time that every week of reduced gestation is associated witha reduction in corticomotor excitability that remains evident in late childhood. This reducedexcitability was associated with poorer motor skill development, particularly manual dexterity.However, child adiposity, sex and socio-economic factors regarding the child’s home environmentsoon after birth were also powerful influences on development of motor skills. Preterm birth wasalso associated with reduced left hemisphere lateralization, but without increasing the likelihoodof being left handed per se. These corticomotor findings have implications for normal motor
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society DOI: 10.1113/jphysiol.2012.239269

5828 J. B. Pitcher and others J Physiol 590.22
development, but also raise questions regarding possible longer term consequences of pretermbirth on motor function.
(Received 19 June 2012; accepted after revision 3 September 2012; first published online 10 September 2012)Corresponding author J. B. Pitcher: DX 640-517 Robinson Institute, School of Paediatrics andReproductive Health, University of Adelaide, SA 5005, Australia. Email: [email protected]; URL:http://www.adelaide.edu.au/directory/julia.pitcher
Abbreviations %BF, percentage body fat; BW%, birth weight centile; DTI, diffusion tensor imaging; FA, fractionalanisotropy; GA, completed weeks gestational age; ICF, intracortical facilitation; IRSD, Index of Relative SocialDisadvantage; ISI, interstimulus interval; MABC2, Movement Assessment Battery for Children, version 2; MEP,motor-evoked potential; MRI, magnetic resonance imaging; rMT, resting motor threshold; SICI, short-intervalintracortical inhibition; TMS, transcranial magnetic stimulation.
Introduction
Impaired motor and cognitive development remain thetwo major adverse outcomes of preterm birth despiteadvances in neonatal care (Hack & Fanaroff, 2000). Pre-term birth is defined as one following a pregnancy ofless than 37 completed weeks (or 259 days) of gestation(GA; WHO, 1992). In Australia in 2008, 79% of pre-term infants (or about 7% of all births) were born ‘latepreterm’ between 32 and 36 weeks GA, yet long-termfollow-up studies of outcomes typically confine their focusto the very/extremely preterm (≤32 weeks GA) or verylow birth weight, who accounted for only 21% of pretermbabies (or 1.7% of all births). The statistics are similarin other western countries, and it is now increasinglyrecognized that even late preterm children have a greaterrisk of morbidity and developmental disorders thantheir term-born counterparts, but receive little if anydevelopmental follow-up (Raju et al. 2006; Woythaleret al. 2011). Nevertheless, the few studies examiningdevelopmental outcomes in late preterm children all showan increased risk of motor dysfunction and learningdifficulties at school age (Huddy et al. 2001; Pietz et al.2004; Kirkegaard et al. 2006; Chyi et al. 2008; Morse et al.2009; Woythaler et al. 2011).
Preterm birth between 20 and 37 weeks GA correspondsto a time of rapid cortical growth, particularly in themotor and sensorimotor areas (Eyre et al. 2000; Kapellouet al. 2006; Dubois et al. 2008a). The premature transitionfrom the intrauterine to the extrauterine environmentalters the trajectory and temporal characteristics of braindevelopment, and the earlier the birth, the greater theperturbation from normal growth trajectories (Kapellouet al. 2006). The corticomotor system (including thebrain motor areas and corticospinal tract) is the mostcommon site of brain damage in the prenatal andneonatal periods (Eyre, 2003). An intact corticomotorsystem is indispensable for learning and performingskilled and dextrous movements, particularly of the hands.Even in the absence of focal brain lesions, many pre-term children have reduced regional brain volumes,compromised development of both white and grey matter
and reduced cortical surface area and gyrification, evidentusing magnetic resonance imaging (MRI; Ajayi-Obe et al.2000; Peterson et al. 2000, 2003; Nosarti et al. 2002,2008; Nagy et al. 2003, 2009; Peterson, 2003; Counsell &Boardman, 2005). Critically, these abnormalities remainat least into late adolescence and are present in the majormotor control areas (Peterson et al. 2000, 2003; Nosartiet al. 2002, 2008; Nagy et al. 2003, 2009; Peterson, 2003;van Soelen et al. 2010).
There is increasing evidence that microstructuralabnormalities in cortical development, in particular,underlie many of the cognitive and the more subtle motorsequelae that commonly manifest in preterm children(Ajayi-Obe et al. 2000; Kesler et al. 2004, 2008; Counsellet al. 2008). Diffusion tensor imaging (DTI) studieshave shown that, compared with their term-born peers,preterm children and adolescents have altered neuralconnectivity between brain regions that is associated withreduced white matter integrity (Constable et al. 2008;Miller & Ferriero, 2009; Lubsen et al. 2011). Functionally,these microstructural abnormalities are associated withmotor and cognitive impairments (Constable et al. 2008;Counsell et al. 2008; Ludeman et al. 2008; Mullen et al.2011). However, up to 25% of preterm children whohave apparently normal results on MRI/DTI go on todevelop motor and cognitive dysfunction (Miller et al.2005; Ludeman et al. 2008), suggesting that most currentclinical imaging modalities have limitations in detectingthese microstructural abnormalities.
An alternative approach to investigating the excitabilityand connectivity of cortex is to use transcranial magneticstimulation (TMS), a painless technique that allowsnon-invasive stimulation of the conscious human cortex.When applied at the scalp over the motor cortex regionat sufficient intensity, TMS activates corticospinal outputneurons and results in a response in, for example, thehand muscles on the opposite, or contralateral, side of thebody. This twitch in the muscle, called the motor-evokedpotential (MEP), can be measured using surface electro-des on the skin overlying the muscle. The size and latencyof the MEP reflect the excitability of neurons and impulse
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society
J Physiol 590.22 Preterm birth and corticomotor function 5829
conduction characteristics of the motor cortex, cortico-spinal tract and spinal motor centres in real time.
In this study, we used TMS and surface electro-myography techniques to examine corticomotorexcitability in 10- to 13-year-old children born at25–41 weeks GA. We hypothesized that hithertoundetected alterations in the normal development of themotor areas of the brain and the corticomotor pathwaysunderpin at least some of the motor dysfunction seen inpreterm children and are evident as reduced corticomotorexcitability that is associated with poorer development ofage-appropriate motor skills. To discriminate the effectsof preterm birth from those of suboptimal intrauterinegrowth, we also assessed the effect of birth weightcorrected for gestational age at birth on these outcomes.Preliminary results have been presented elsewhere(Pitcher et al. 2011a,b).
Methods
Ethical approval, participants and recruitment
One hundred and fifty-one children (82 males) andtheir parents/primary care giver gave informed writtenconsent to participate in the study. Gestational age rangedfrom 25 to 41 weeks (34.44 ± 3.52 weeks), and meanuncorrected age at assessment was 155.4 ± 11.15 months(approximately 12 years and 11 months). All childrenborn at ≤37 weeks GA were born at the Women’s andChildren’s Hospital, North Adelaide, Australia betweenJanuary 1996 and December 1997. This participant agegroup was chosen because prevailing evidence indicatesit is the youngest age at which MEPs can be consistentlyevoked in relaxed muscle (Eyre et al. 2000; Fietzek et al.2000; Garvey & Gilbert, 2004). Neonatal intensive care unitfollow-up and labour ward databases were used to identifyand approach prospective children and their families. Inaddition to the exclusion criteria recommended for thesafe use of TMS (Wassermann, 1998; Quintana, 2005),children with known abnormality on perinatal cranialultrasound, known chromosomal or genetic disorders,clearly identified familial or non-familial syndromes(without known chromosomal or genetic defect) andchildren with a physical or intellectual disability andunable to follow simple instructions were excluded.Twenty-nine children were excluded on the basis of theTMS safety screen (not included in the sample of 151).Four children were excluded before protocol completionowing to the presence of ipsilateral responses to trans-cranial magnetic stimulation, which can be developmentalbut may also indicate the presence of a corticospinal tractlesion (Eyre et al. 2001). Five children (two born at term)were taking prescribed methylphenidate (i.e. Ritalin), butall were assessed ‘off’ medication. No children were takingother medications known to alter cortical excitability (e.g.
antidepressants). Term-born children matched for age,sex and ethnicity were recruited from a given pretermchild’s school or classroom. In addition, some controlchildren were also recruited from community newspaperadvertisements. Ethical clearances and approval forthe study were provided by the Child Youth andWomen’s Health Service, University of Adelaide, the SouthAustralian Government Department of Education andChildren’s Services Human Research Ethics Committees,and Catholic Education South Australia. All procedureswere performed in accordance with the Declaration ofHelsinki (2008 revision).
Separate written consent was obtained to access data onchildren’s birth characteristics, including GA and neonatalmorbidities, from the Women’s and Children’s HospitalPerinatal Statistics collection. Maternal anthropometry(height and weight at first antenatal visit), parity andgravity were also recorded. Gestation Related OptimalWeight software (Gardosi & Francis, 2006) was used tocalculate each child’s birth weight relative to their pre-dicted term weight, i.e. their birth weight centile (BW%),and adjusted for maternal size, ethnicity and parity.Socio-economic Indexes for Areas scores were calculatedfor the address each child went home to following theirbirth (1996 National Census), as well as for their currentaddress (2006 National Census).
Protocol
Data for this study were collected as part of thebroader PREMOCODE (Preterm Motor and CognitiveDevelopment) study, for which each child attended at leasttwo assessment visits. Given that the order of assessmentcomponents was randomized within and between sub-jects, some children did not undergo the MovementAssessment Battery for Children, version 2 (MABC2;Henderson et al. 2007) on the same day as the cortico-motor neurophysiology assessment. Of the children whounderwent both assessments on the same day, thecorticomotor assessment was always performed first. Thecharacteristics recorded included the child’s height, weightand percentage body fat (%BF; using bio-impedance).Handedness was determined by calculating the lateralityquotient using the Edinburgh Handedness Inventory(Oldfield, 1971). The inventory provides a measure of anindividual’s preferred hand in performing common tasksof daily living. The resultant scale score is between +1(strongly right hand dominant) and –1 (strongly left handdominant), with a score of zero indicating no hand pre-ference. A score ≥0.4 was considered right handed, ≤−0.4was left handed, and scores between −0.39 and +0.39indicated no hand preference. The MABC2 assessmentswere administered by a physiotherapist with extensivepaediatric experience (J.L.D.). Significant to moderate
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5830 J. B. Pitcher and others J Physiol 590.22
impairment is defined as a total score less than or equalto the fifth centile and mild to moderate impairment as atotal score less than or equal to the 15th centile but greaterthan the fifth centile (Williams et al. 2010; Roberts et al.2011). All assessors were blinded to each child’s GA.
Cortical neurophysiology assessment
Single-pulse TMS and surface electromyography wereused to assess corticomotor excitability in both left andright hemispheres and the respective contralateral cortico-spinal tracts. In 95 children, short-interval intracorticalinhibition (SICI) and intracortical facilitation (ICF) werealso measured. Children sat in an armchair with theirforearms and hands supported. Motor-evoked potentialswere recorded from the index finger abductor muscle, firstdorsal interosseous, of both hands. Adhesive silver–silverchloride electrodes were applied, with the active electrodeover the muscle belly and the inactive electrode overthe metacarpophalangeal joint. Electromyograms (EMGs)were sampled at 5.1 kHz with a laboratory interface(CED 1401; Cambridge Electronic Design, Cambridge,UK), filtered (20 Hz to 1 kHz) and analysed offlineusing commercially available software (Signal version 4;Cambridge Electronic Design). Transcranial magneticsimulation was applied with a 70 mm figure-of-eightstimulating coil, connected to a monophasic Magstim 2002
magnetic stimulator (Magstim Co., Whitland, UK), atthe optimal scalp site, which was determined functionallyusing a ‘hunting’ procedure to find the motor hotspot,i.e. the scalp site where single suprathreshold TMS pulsesproduced the largest amplitude MEPs in the contralateralfirst dorsal interosseous muscle (cf. Rossini et al. 1994).The coil was oriented approximately 45 deg to the sagittalmid-line, so that the current induced in the cortex flowedin a plane perpendicular to the estimated alignment ofthe central sulcus in a posterior-to-anterior direction. Theresting motor threshold (rMT) was determined as thelowest TMS intensity that evoked MEPs of at least 50 μVpeak-to-peak amplitude in the resting first dorsal inter-osseous in five of 10 trials.
Corticomotor stimulus–response curves. Stimulus–response curves were constructed for the corticospinalprojection from the motor cortex of each hemisphere tothe contralateral first dorsal interosseous muscle using theprocedure detailed previously (Pitcher et al. 2003, 2009).Briefly, MEP responses to TMS were recorded at stimulusintensities ranging from below rMT and increasing in 3%steps to either 100% of stimulator output, or to whereMEP amplitude plateaued. Ten TMS pulses were deliveredat each intensity, at an interstimulus interval (ISI) varyingbetween 7 and 8 s, and the mean peak-to-peak amplitudefor each block of 10 MEPs was plotted against stimulus
intensity for each subject. The data were best fitted usingthe Marquardt–Levenberg algorithm for least squaresconvergence using commercially available software(Sigmaplot for Windows 11.0, C© 2008 Systat Software,Inc., Chicago, IL, USA). The resultant five-parametersigmoid is described the following equation:
F = y0 + a(1 + exp
[−x − x0
b
]) ∧ c
where the five parameters are the difference between thesmallest and the largest MEP amplitudes (a), the minimalMEP amplitude (y0), the difference in stimulus intensitiesat 75 and 25% of the maximal MEP amplitude (b), thestimulus intensity required to obtain 50% of the maximalMEP amplitude (x0) and the slope constant (c). Solutionsto the equation to derive the predicted rMT, slope andrate of change of the slope at each stimulus intensity aredetailed elsewhere (Pitcher et al. 2003). The area under thecurve was calculated with Sigmaplot 9.0 software (SystatSoftware Inc.) algorithm, as follows:
Area = yi(xi+1 − xi) +(
1
2
)(yi+1 − yi)(xi+1 − xi)
where y is the stimulus intensity and x is the MEPamplitude at a given intensity. The order in whichthe hemispheres were tested was randomized betweensubjects.
Short-interval intracortical inhibition and facilitation.The SICI at 3 ms ISI and ICF at 10 ms ISI were measuredusing the paired-pulse protocol described previously(Kujirai et al. 1993; Smith et al. 2009). The conditioningstimulus intensity was set at 5% of stimulator output belowactive motor threshold and the test stimulus adjustedto give an MEP of approximately 1.0 mV peak-to-peakamplitude (Ridding et al. 1995; Ziemann et al. 1996).Left and right motor cortices were assessed separately,and the order was randomized between subjects. Thirtystimuli were applied in pseudorandom order, consistingof 10 single pulse test stimuli, 10 paired pulses given atan inhibitory ISI of 3 ms, and 10 paired pulses givenat a facilitatory ISI of 10 ms. The mean peak-to-peakamplitude was measured for each block of 10 MEPs at eachISI and for the test response alone. Inhibited and facilitatedMEPs were expressed for analysis as a percentage of thetest response alone for a given set of conditions.
Data and statistical analysis
Motor-evoked potentials were recorded at high gain, andany with obvious prestimulus EMG were discarded online.Normal distribution and homogeneity of variance of thedata were assessed using the Kolmogorov–Smirnov test
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

J Physiol 590.22 Preterm birth and corticomotor function 5831
and Levene’s statistic, respectively, with GA group as thefactor.
Data were analysed using R statistical analysis freeware(version 2.13.1; http://www.r-project.org/). Measures ofcorticomotor excitability (i.e. right hand rMT and lefthand rMT, the corticomotor curve slope and area) wereexamined both as dependent variables in the primaryanalysis and as explanatory variables. As the rMTs for bothhemispheres were highly correlated (r = 0.83, P ≤ 0.0001,n = 129), only the right hand rMT is reported in theregression analyses of factors influencing MABC2 scores,because this was also the dominant hand for 83% of thechildren. In addition, the models did not significantlydiffer if the left hand rMT was included. Statisticalsignificance was accepted at α = 0.05. All tests were twotailed.
Initial analysis. Gestational age was examined as acontinuous variable (i.e. GA in weeks) and as a categoricalvariable with GA groups as defined by the WorldHealth Organization and others (Tucker & McGuire,2004; Alexander, 2007), i.e. extremely preterm (≤27 weeksGA), very preterm (28–32 weeks GA), late preterm(33–36 weeks) and term (37–41 weeks GA). However, asthere were only seven eligible children in the extremelypreterm group, this group was combined with the very pre-term group to form the early preterm group (≤32 weeksGA). Linear regression modelling was used to determinethe influence of GA (in weeks), BW% and sex on measuresof cortical excitability (including the right hand rMT,left hand rMT, slope and area), intracortical inhibitionand facilitation, and to determine the influence of GA(in weeks), BW% and sex on each of the five dependentvariables, i.e. three MABC2 subscores (manual dexterity,aiming and catching, and balance), the MABC2 total score(MABC2total) and right hand rMT. Likewise, this approachwas used to determine the influence of cortical variableson MABC2total and MABC2 subscores. Univariate analysiswith GA group as the between-subjects factor was used toexamine any differences between the GA groups.
Explanatory variables analysis. Gestational age, BW%and sex were included in all analyses except wherespecifically stated. Explanatory variables were includedin the analysis only if they showed an initial correlationwith the dependent variables. The birth variables includedponderal index, head circumference, Apgar score at1 min, Apgar score at 5 min, singleton or multiple birth,parity, maternal age at child’s birth, maternal bodymass index at first antenatal visit, maternal smokingstatus during pregnancy (non-smoker, stopped duringpregnancy or smoked during pregnancy), and the Indexof Relative Social Disadvantage score of their home atbirth (IRSDbirth). The current variables included the child’s
current height and weight, %BF, laterality quotient, theIRSD score for their current home (IRSDcurrent) and theright hand rMT.
The influences of explanatory variables on MABC2and corticomotor measures were explored using relativeimportance regression modelling. This method allowsquantification of the contribution of each individualregressor (i.e. explanatory variable) to the overall R2
in a multiple regression model (Gromping, 2006). Weused Lindeman, Merenda and Gold’s heuristic approachof averaging over all orderings of regressors in themodel, which allows a more causal interpretation of thevariance allocations of each regressor to the total R2
(Lindeman et al. 1980; Gromping, 2007). Variable groupswere regressed against each of the dependent variables.Variables that accounted for less than around 10% of thevariance explained by the model (i.e. by R2) were removedand the regression repeated until either no variable leftaccounted for <10% of the variance or when removing aminor/non-significant variable did not alter the R2. Thebirth and current variables remaining from these processeswere included in the final regression to determine theexplanatory variables with the most influence on thedependent variable, i.e. the best model.
Results
At birth, both preterm groups had lower BW%, poorerskeletal growth (length and head circumference) andlower ponderal indices and were more likely to be amultiple birth than term-born infants (Table 1). Atassessment, the early preterm children had shorter staturethan the late preterm and term-born groups and tendedto have lower body weight. Interestingly, the meanBW% in those children born at ≤27 weeks GA was83.7 ± 8.2%, compared with 26.8 ± 27.0% in those bornat 28–32 weeks. Apart from BW% and GA, these two sub-groups did not differ significantly when their outcomeswere compared. Child age at assessment was not differentbetween the GA groups.
Effect of sex, GA and BW% on corticomotorexcitability characteristics
Motor thresholds were obtained for at least one hemi-sphere in 138 children and in both hemispheres from 129children. Twelve children chose not to participate in thispart of the study. In seven children, thresholds could beobtained only with target muscle contraction, but this wasnot related to either GA or BW%. Responses could not beobtained from one male (30 weeks GA, BW% < 1). Thisis reflected in the different sample sizes for the variousmotor threshold analyses.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5832 J. B. Pitcher and others J Physiol 590.22
Table 1. Child and maternal characteristics
Early preterm, Late preterm, Term,≤32 weeks GA 33–36 weeks GA 37–41 weeks GA
n Males 21 37 24Females 19 28 22Total 40 65 46
Birth variablesGestational age (weeks) Males 29.7 ± 2.5∗† 34.6 ± 1.1∗ 37.9 ± 1.6
Females 29.8 ± 1.9∗† 35.1 ± 1.0∗ 38.2 ± 1.4Total 29.7 ± 2.2∗† 34.8 ± 1.1∗ 38.0 ± 1.5
Birth weight centile (% term Males 42.2 ± 36.0∗ 36.0 ± 29.5∗ 52.7 ± 31.1optimal weight) Females 33.9 ± 30.7∗ 38.4 ± 34.4∗ 63.9 ± 29.0
Total 37.7 ± 33.0∗ 37.0 ± 31.5∗ 57.9 ± 30.3Length (cm) Males 39.4 ± 3.7∗† 46.5 ± 2.3∗ 48.1 ± 5.3
Females 38.8 ± 3.4∗† 44.8 ± 2.8∗ 49.3 ± 3.1Total 39.1 ± 3.6∗† 45.8 ± 2.6∗ 48.6 ± 4.4
Head circumference (cm) Males 28.1 ± 2.5∗† 32.7 ± 1.7∗ 35.3 ± 4.3Females 27.7 ± 2.4∗† 31.8 ± 2.0∗ 34.2 ± 1.5Total 27.9 ± 2.4∗† 32.3 ± 1.9∗ 34.8 ± 3.4
Ponderal index Males 2.3 ± 0.2∗† 2.4 ± 0.2∗ 3.0 ± 1.3Females 2.2 ± 0.2∗† 2.5 ± 0.2∗ 2.8 ± 0.3Total 2.2 ± 0.2∗† 2.5 ± 0.2∗ 2.9 ± 1.0
Apgar score at 1 min (total score) Males 7.0 ± 1.8 7.9 ± 1.4 8.0 ± 1.3Females 6.1 ± 1.8∗† 7.8 ± 1.8 8.2 ± 1.0Total 6.6 ± 1.8∗† 7.8 ± 1.5 8.1 ± 1.1
Apgar score at 5 min (total score) Males 9.0 ± 1.3 9.1 ± 0.6 9.0 ± 0.7Females 8.3 ± 1.4∗† 9.1 ± 0.8 9.4 ± 0.5Total 8.6 ± 1.4∗† 9.1 ± 0.7 9.2 ± 0.6
Total postnatal days in hospital (n) Males 50.2 ± 33.2∗† 14.0 ± 10.1∗ 5.7 ± 4.3Females 43.6 ± 26.3∗† 9.1 ± 6.2 6.5 ± 6.9Total 47.3 ± 29.9∗† 11.9 ± 9.0 6.1 ± 5.6
Singleton births (n) Males 16 27 22Females 13 18 22%n 72.5%∗ 69.2%∗ 95.7%
Multiple births Males 5 10 2Females 6 10 0%n 27.5%∗ 30.8%∗ 4.3%
Maternal age at time of birth (years) Males 29.8 ± 7.2 31.0 ± 5.8 29.9 ± 4.2Females 28.8 ± 5.4 28.5 ± 5.6 31.4 ± 5.1Total 29.4 ± 6.3 30.0. ± 4.6 30.6 ± 4.6
Maternal height (cm) (prepregnancy Males 1.65 ± 0.07 1.68 ± 0.09 1.64 ± 0.08or first antenatal visit) Females 1.65 ± 0.05∗† 1.60 ± 0.06∗ 1.63 ± 0.06
Total 1.65 ± 0.06 1.64 ± 0.09 1.63 ± 0.07Maternal weight (kg) (prepregnancy Males 61.07 ± 10.3 73.0 ± 23.7 68.1 ± 20.5
or first antenatal visit) Females 68.9 ± 10.8 64.5 ± 17.3 70.3 ± 16.3Total 65.1 ± 11.1 69.1 ± 21.3 69.2 ± 18.4
Parity Males 0.90 ± 1.2 0.81 ± 0.9 1.04 ± 0.91Females 0.79 ± 1.4 0.64 ± 0.8 0.90 ± 1.0Total 0.85 ± 1.3 0.74 ± 0.9 0.98 ± 0.94
Gravida Males 2.3 ± 1.4 2.1 ± 1.2 2.7 ± 1.3Females 2.2 ± 1.6 2.2 ± 1.1 2.5 ± 1.0Total 2.3 ± 1.5 2.1 ± 1.2 2.6 ± 1.2
Current variablesUncorrected age (months) Males 154.5 ± 10.7 156.2 ± 10.6 155.6 ± 11.9
Females 152.6 ± 10.9 156.7 ± 11.5 158.6 ± 11.1Total 153.6 ± 10.7 156.4 ± 10.9 157.0 ± 11.6
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

J Physiol 590.22 Preterm birth and corticomotor function 5833
Table 1. Continued
Early preterm, Late preterm, Term,≤32 weeks GA 33–36 weeks GA 37–41 weeks GA
Child’s height (cm) Males 1.45 ± 0.07† 1.53 ± 0.09 1.48 ± 0.06Females 1.48 ± 0.09∗ 1.48 ± 0.09∗ 1.54 ± 0.09Total 1.46 ± 0.08∗† 1.51 ± 0.09 1.51 ± 0.09
Child’s weight (kg) Males 37.2 ± 8.8† 45.9 ± 10.5 42.3 ± 10.0Females 44.8 ± 11.4 42.3 ± 10.1 49.5 ± 11.7Total 40.8 ± 10.7 44.4 ± 10.4 45.7 ± 11.3
Child’s total body fat (%) Males 15.5 ± 6.3 18.9 ± 6.2 17.6 ± 7.4Females 25.5 ± 8.1 22.4 ± 6.7 24.9 ± 6.6Total 20.2 ± 8.7 20.4 ± 6.6 21.1 ± 7.9
Laterality quotient (–1 = left Males 0.6 ± 0.7 0.7 ± 0.5 0.8 ± 0.4handed, 0 = no preference and
+1 = right handed)Females 0.6 ± 0.7 0.5 ± 0.7 0.8 ± 0.2
Total 0.6 ± 0.7 0.6 ± 0.6 0.8 ± 0.4
Abbreviation: GA, completed weeks gestational age. Data are GA group means ± SD. ∗ Denotes P < 0.05 when compared withthe term group (Tukey’s HSD). † Denotes P < 0.05 when compared with the late preterm group (Tukey’s HSD).
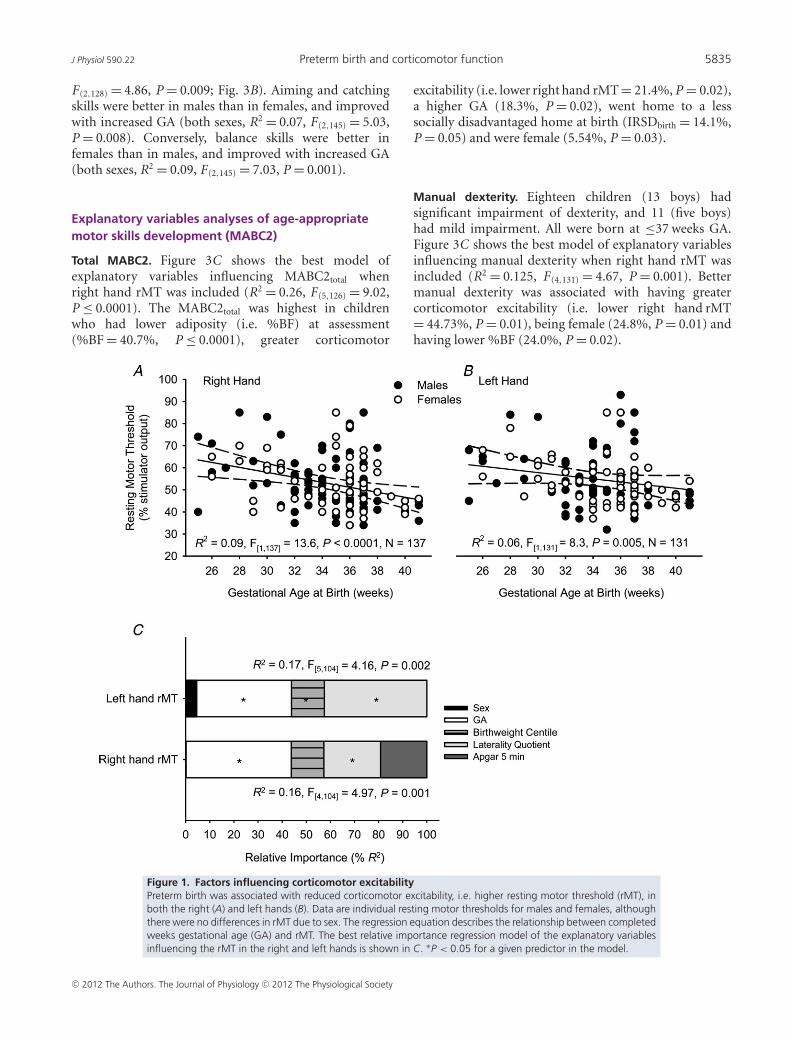
Overall, rMTs were not different when males andfemales were compared (Table 2). Preterm birth waslinearly associated with higher resting motor thresholdsfor the right (R2 = 0.09, F(1,137) = 13.6, P ≤ 0.0001,n = 137; Fig. 1A) and left hands (R2 = 0.06, F(1,131) = 8.3,P = 0.005, n = 131; Fig. 1B). Univariate analyses showeda significant effect of GA group on both right handrMT (F(2,136) = 4.58, P = 0.01) and left hand rMT(F(2,130) = 3.43, P = 0.04), because rMTs in the early pre-term group were higher than those of the late preterm andterm-born groups.
Figure 1C shows the best relative importance regressionmodel of variables explaining right hand rMT (R2 = 0.17,F(5,104) = 4.16, P = 0.002), expressed as the percentageof the total variability explained by the model, i.e.R2 = 0.17 = 100%. A lower right hand rMT was associatedwith a longer gestation (P = 0.02), being more righthanded (i.e. having a laterality quotient closer to +1;P = 0.04), being female, of higher BW% and having ahigher Apgar score at 5 min. Only GA and lateralityquotient were significant at P ≤ 0.05, whereas BW% wasnot (P = 0.09).
Low left hand rMT was associated with being more rightthan left handed (P = 0.01), of longer gestation (P = 0.02)and having a higher BW% (P = 0.02); (Fig. 1C). Sexremained in the final model, but was not significant.
Complete stimulus–response curves could be obtainedfrom the right hands of 76 children and from the left handsof 57 children. Of these, curves for both hands could beobtained from 51 children (30 males). Neither the slopenor the area under the curve was influenced by GA orBW%. A steeper slope and a greater area under the righthand curve was associated with being a female and havinga lower right hand (i.e. left hemisphere) rMT (slope,R2 = 0.11, F(2,76) = 4.72, P = 0.01; and area, R2 = 0.17,
F(2,76) = 7.31, P = 0.001; Fig. 2). However, there were nosimilar findings for the left hand (i.e. right hemisphere).No associations were found to account for differences inthe maximal MEP that could be evoked in either hemi-sphere.
Effect of sex, GA and BW% on intracorticalexcitability characteristics
For 95 children SICI/ICF data were obtained from theleft hemisphere and right hand, for 72 children from theright hemisphere and left hand, and from both hemi-spheres in 70 of these children (Table 2). Data werenot normally distributed, so were logarithmically trans-formed for analysis. Unblinding of the data revealeda negative correlation between active motor thresholdand GA (in weeks; r = −0.31, P = 0.002, n = 95). Inorder to ensure that subjects were being stimulatedat equivalent intensities relative to their active motorthreshold (Orth et al. 2003), the individual conditioningstimulus intensities were expressed as a percentage of activemotor threshold. The conditioning stimulus intensitywas 87.9 ± 2.3% of active motor threshold in early pre-term children, 86.6 ± 2.8% of active motor threshold inlate preterm, and 86.7 ± 2.7% of active motor thresholdin term-born children. One-way ANOVA showed thatthere was no difference in the conditioning stimulusintensity when the GA groups were compared. Neithercovariate analysis with GA (in weeks) nor factor analysisof GA groups showed an effect of preterm birth onSICI. Likewise, ICF was not influenced by either activemotor threshold or GA. However, the data were highlyvariable, and the statistical power of the sample was lessthan 30%.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5834 J. B. Pitcher and others J Physiol 590.22
Table 2. Resting motor thresholds to transcranial magnetic stimulation
Early preterm, Late preterm, Term, 37–41≤32 weeks GA (n) 33–36 weeks GA (n) weeks GA (n)
Right handResting motor threshold (% Males 55.3 ± 13.3∗ (20) 52.5 ± 11.2 (35) 49.2 ± 11.4 (22)
stimulator output) Females 56.7 ± 9.5 (15) 52.8 ± 12.7 (26) 49.0 ± 8.3 (20)Total 56.0 ± 11.4∗ (35) 52.6 ± 11.8 (51) 49.1 ± 10.0 (42)
Active motor threshold (% Males 42.9 ± 9.2 (19) 40.4 ± 8.7 (34) 38.5 ± 10.2 (22)stimulator output) Females 45.5 ± 7.4 (15) 42.7 ± 10.9 (27) 38.7 ± 8.9 (20)
Total 44.0 ± 8.4∗ (34) 41.5 ± 9.8 (61) 38.6 ± 9.5 (42)Area under corticomotor Males 17.2 ± 8.4 (12) 20.3 ± 9.5 (19) 25.1 ± 9.6 (15)
stimulus–response curve Females 28.5 ± 10.8 (8) 33.8 ± 21.4 (11) 24.3 ± 9.2 (12)Total 21.7 ± 10.7 (20) 25.2 ± 16.1 (30) 24.7 ± 9.3 (27)
Curve slope Males 0.22 ± 0.20 (12) 0.17 ± 0.14 (19) 0.23 ± 0.14 (15)Females 0.30 ± 0.19 (8) 0.29 ± 0.17 (11) 0.25 ± 0.19 (12)Total 0.25 ± 0.18 (20) 0.21 ± 0.16 (30) 0.23 ± 0.16 (27)
SICI at 3 ms ISI (% test MEP) Males 49.8 ± 41.7 (14) 42.3 ± 21.3 (23) 34.6 ± 26.8 (14)Females 63.6 ± 61.7 (11) 38.1 ± 30.7 (18) 36.9 ± 23.3 (15)Total 55.9 ± 50.8 (25) 40.5 ± 25.6 (41) 35.8 ± 24.6 (29)
ICF at 10 ms ISI (% test MEP) Males 115.7 ± 48.8 (14) 139.3 ± 78.8 (23) 134.9 ± 67.2 (14)Females 164.1 ± 100.7 (11) 120.6 ± 36.6 (18) 151.5 ± 76.7 (15)Total 137.0 ± 78.2 (25) 131.1 ± 63.8 (41) 143.5 ± 71.5 (29)
Left handResting motor threshold (% Males 55.6 ± 12.1 (20) 55.3 ± 13.8 (35) 51.9 ± 12.1 (22)
stimulator output) Females 58.9 ± 8.7∗ (15) 53.0 ± 12.1 (26) 49.7 ± 6.4 (20)Total 57.2 ± 10.6∗ (35) 54.3 ± 13.1 (61) 50.9 ± 9.8 (42)
Active motor threshold (% Males 43.2 ± 7.9 (17) 43.6 ± 9.9 (33) 38.5 ± 9.7 (21)stimulator output) Females 47.1 ± 7.0 (14) 42.3 ± 9.3 (25) 39.4 ± 6.8 (20)
Total 45.0 ± 7.6∗ (35) 43.1 ± 9.6∗ (61) 38.9 ± 8.3 (42)Area under corticomotor Males 19.1 ± 9.2 (7) 17.8 ± 9.3 (12) 21.7 ± 11.3 (13)
stimulus–response curve Females 21.3 ± 15.3 (5) 35.3 ± 17.5 (10) 16.4 ± 8.5 (10)Total 20.0 ± 11.5 (12) 25.8 ± 16.0 (22) 19.4 ± 10.3 (23)
Curve slope Males 1.03 ± 1.6 (7) 0.19 ± 0.8 (12) 0.17 ± 0.1 (13)Females 0.21 ± 0.1 (5) 0.79 ± 1.3 (10) 0.18 ± 0.2 (10)Total 0.69 ± 1.3 (12) 0.46 ± 0.9 (22) 0.17 ± 0.1 (23)
SICI at 3 ms ISI (% test MEP) Males 27.0 ± 12.4 (9) 46.1 ± 32.1 (21) 47.0 ± 43.0 (11)Females 39.3 ± 23.3 (7) 28.7 ± 16.9 (18) 51.0 ± 30.9 (12)Total 32.3 ± 18.4 (16) 38.1 ± 27.3 (39) 49.1 ± 36.4 (23)
ICF at 10 ms ISI (% test MEP) Males 136.3 ± 57.3 (9) 158.4 ± 98.1 (21) 104.6 ± 57.5 (11)Females 119.1 ± 73.5 (7) 133.3 ± 84.9 (18) 147.5 ± 71.0 (12)Total 128.8 ± 63.2 (16) 146.8 ± 92.0 (39) 127.0 ± 67.1 (23)
Data are GA group means ± SD (number of subjects). Abbreviations: GA, completed weeks gestational age; ICF, intracorticalfacilitation; ISI, interstimulus interval; MEP, motor-evoked potential; SICI, short-interval intracortical inhibition. ∗ Denotes P < 0.05when compared with the term group (Tukey’s HSD).
Effect of sex, GA, BW% and corticomotor excitabilityon age-appropriate motor skills development(MABC2)
One hundred and forty-eight children completed theMABC2 assessment (Table 3). There was no difference inscores due to age (corrected or uncorrected for GA). Elevenchildren (seven boys) had significant impairment and five(two boys) had mild impairment for MABC2total. All wereborn at ≤37 weeks GA. One-way ANOVA showed sexdifferences in the MABC2 subscores, so sex was included
in all regression models. The BW% had no effect oneither MABC2total or subscores. With the exception of rMT,there was no association between any of the corticomotorstimulus–response curve characteristics or SICI/ICF andMABC2total or subscores.
The MABC2total increased with GA (R2 = 0.06,F(1,146) = 7.66, P = 0.006; Fig. 3A). When each sex wasanalysed separately, this association remained statisticallysignificant for males (males only, R2 = 0.06, F(1,79) = 4.83,P = 0.03) but not for females (P = 0.1). Children withlower rMTs had better MABC2total scores (R2 = 0.07,
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society
J Physiol 590.22 Preterm birth and corticomotor function 5835
F(2,128) = 4.86, P = 0.009; Fig. 3B). Aiming and catchingskills were better in males than in females, and improvedwith increased GA (both sexes, R2 = 0.07, F(2,145) = 5.03,P = 0.008). Conversely, balance skills were better infemales than in males, and improved with increased GA(both sexes, R2 = 0.09, F(2,145) = 7.03, P = 0.001).
Explanatory variables analyses of age-appropriatemotor skills development (MABC2)
Total MABC2. Figure 3C shows the best model ofexplanatory variables influencing MABC2total whenright hand rMT was included (R2 = 0.26, F(5,126) = 9.02,P ≤ 0.0001). The MABC2total was highest in childrenwho had lower adiposity (i.e. %BF) at assessment(%BF = 40.7%, P ≤ 0.0001), greater corticomotor
excitability (i.e. lower right hand rMT = 21.4%, P = 0.02),a higher GA (18.3%, P = 0.02), went home to a lesssocially disadvantaged home at birth (IRSDbirth = 14.1%,P = 0.05) and were female (5.54%, P = 0.03).
Manual dexterity. Eighteen children (13 boys) hadsignificant impairment of dexterity, and 11 (five boys)had mild impairment. All were born at ≤37 weeks GA.Figure 3C shows the best model of explanatory variablesinfluencing manual dexterity when right hand rMT wasincluded (R2 = 0.125, F(4,131) = 4.67, P = 0.001). Bettermanual dexterity was associated with having greatercorticomotor excitability (i.e. lower right hand rMT= 44.73%, P = 0.01), being female (24.8%, P = 0.01) andhaving lower %BF (24.0%, P = 0.02).
Figure 1. Factors influencing corticomotor excitabilityPreterm birth was associated with reduced corticomotor excitability, i.e. higher resting motor threshold (rMT), inboth the right (A) and left hands (B). Data are individual resting motor thresholds for males and females, althoughthere were no differences in rMT due to sex. The regression equation describes the relationship between completedweeks gestational age (GA) and rMT. The best relative importance regression model of the explanatory variablesinfluencing the rMT in the right and left hands is shown in C. ∗P < 0.05 for a given predictor in the model.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5836 J. B. Pitcher and others J Physiol 590.22
Aiming and catching skills. Four children (one boy) hadsignificant impairment of aiming and catching skills, andthree (two boys) had mild impairment. All, except one girl(40 weeks GA) with a significant impairment, were born at≤37 weeks GA. Figure 3C shows the best model for aimingand catching skills (R2 = 0.09, F(3,118) = 3.76, P = 0.01).Better aiming and catching skills were associated withhaving a mother with a lower body mass index at thefirst antenatal visit (50.7%, P = 0.02) and a higher GA(35.6%, P = 0.04). Sex was not a significant predictor(13.7%, P = 0.24).
Balance skills. As with aiming and catching skills, cortico-motor excitability had little influence on balance. Tenchildren (six boys) had significant impairment, and nine(eight boys) had mild impairment. All were born at≤37 weeks GA. Figure 3C shows the best model forbalance skill development (R2 = 0.22, F(3,144) = 13.25,P ≤ 0.0001). Superior balance skills were associated withbeing female (43.8%, P ≤ 0.0001), having lower adiposity(39.0%, P ≤ 0.0001) and having a higher GA (17.2%,P = 0.006).
Handedness
Most children were right handed (n = 123, 82.6%), withonly 20 (13%) being left handed and six children (4%)showing no hand preference. While there was only a weaktrend for preterm birth to be associated with being lessstrongly right handed (r = 0.15, P = 0.07, n = 149), allchildren who were either left handed or had no hand pre-ference were born at ≤38 weeks GA. Lateralization wasinfluenced by a child’s right hand rMT (i.e. left hemi-sphere; R2 = 0.09, F(1,128) = 12.50, P = 0.001) but not theleft hand rMT. Children with low rMTs in both hands weremore likely to have a higher laterality quotient, i.e. to bemore right handed. Including predictors such as prenatalexposure to corticosteroids and/or magnesium sulphate,BW%, being a singleton or multiple birth, and the child’ssex failed to account for this finding.
Discussion
The main novel finding of this study is that preterm birthis associated with reduced corticomotor excitability thatpersists in late childhood. Suboptimal fetal growth, evidentas a lower BW%, further contributes independently to
Figure 2. Corticomotor stimulus–responsecurves for males and femalesData are group mean ± SD motor-evokedpotential (MEP) amplitudes for the earlypreterm (A and B), late preterm (C and D) andterm-born groups (E and F). Panels on the left(A, C and E) show data from the lefthemisphere and right hand, while panels onthe right (B, D and F) show data from the righthemisphere and left hand.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

J Physiol 590.22 Preterm birth and corticomotor function 5837
Table 3. Percentile scores for the Movement Assessment Battery for Children, version 2
Early preterm, Late preterm, Term, 37–41≤32 weeks GA 33–36 weeks GA weeks GA
n Males 20 35 24Females 18 27 22Total 38 62 46
Manual dexterity Males 36.8 ± 26.1 34.4 ± 22.3 41.6 ± 24.3Females 32.3 ± 21.5† 53.1 ± 27.4 42.0 ± 25.5Total 34.7 ± 23.8 42.5 ± 26.2 41.8 ± 24.6
Aiming and catching Males 60.8 ± 28.4 74.5 ± 23.8 70.5 ± 28.2Females 49.1 ± 31.4 60.0 ± 27.1 63.4 ± 28.3Total 55.3 ± 30.0 68.2 ± 26.1 67.1 ± 28.1
Balance Males 49.3 ± 34.6 45.5 ± 30.6 62.7 ± 26.7Females 62.5 ± 31.6 67.6 ± 31.2 71.4 ± 28.5Total 55.6 ± 33.5 55.1 ± 32.5 66.9 ± 27.6
Total score Males 46.2 ± 34.1 50.4 ± 26.0 59.8 ± 23.8Females 45.4 ± 26.2 59.4 ± 29.9 60.8 ± 26.8Total 45.8 ± 30.2∗ 54.3 ± 27.9 60.2 ± 25.0
Data are GA group means ± SD. ∗Denotes P < 0.05 when compared with the term group (Tukey’s HSD). † Denotes P < 0.05 whencompared with the late preterm group (Tukey’s HSD).
reduce corticomotor excitability although, unlike GA, thisappears to be confined to the right motor cortex. Whilethe most preterm children have the greatest decrementsin corticomotor excitability, there does not appear to bea ‘critical’ GA after which no further gains in cortico-motor excitability are made (i.e. every week of GA up toapproximately 39–40 weeks is important). While cortico-motor excitability is positively associated with functionalmotor skill development, particularly hand dexterity,other postnatal factors appear to play an important role indetermining the level of motor skills attained.
High corticomotor thresholds in preterm children mayreflect reduced white matter integrity and functionalconnectivity
We speculate that the higher rMTs seen in pretermchildren may reflect, at least in part, persistent reductionsin white matter integrity and functional connectivityin cortico-cortical and/or cortico-thalamic projectionsinvolving the primary motor cortex. In this study, theprimary measure of corticomotor excitability was therMT, which is the lowest TMS intensity required toexcite corticospinal fibres indirectly via excitatory inputfrom cortico-cortical projections and to evoke a smallMEP response in the target muscle (Ziemann, 2004).Excitation of these projections by TMS is also influenced bymembrane voltage-gated sodium channels, because drugsthat inhibit the activity of these channels and modifymembrane excitability increase the rMT (Chen et al. 1997;Ziemann, 2003, 2004). In neurologically healthy adults,the rMT is negatively correlated with the maturation,
myelination and structural integrity of the white matter ofthe primary, premotor and prefrontal cortices, the inter-nal capsule, corpus callosum, corona radiata and cerebralpeduncles (Kloppel et al. 2008). The maturation of whitematter is associated with increasing fractional anisotropy(FA) and a reduction in the apparent diffusion coefficienton DTI (Huppi et al. 1998; for review see Mathur et al.2010); that is, individuals with low rMTs have better whitematter microstructural integrity (i.e. higher FA) in theneuronal networks subserving motor control.
Likewise, higher rMT in preterm children may reflectweaker functional connectivity between the secondary andprimary motor areas (Kloppel et al. 2008). Functionalconnectivity MRI studies indicate that preterm birthdisrupts the normal development of neural connectivitywithin and between cortical regions, even in the absenceof lesions (Smyser et al. 2010, 2011). In preterm infants,the networks contributing to motor and sensory function,auditory and visual processing and language are lessmature and have aberrant connectivity when comparedwith their term-born peers (Smyser et al. 2010). Themechanisms underlying this are not yet clear, althoughwhite matter damage and reduced myelination are knownto affect cortico-cortical and cortico-thalamic connections(Smyser et al. 2010).
A limitation of the study is that MRI facilities werenot available to assist confirmation of the participants’lesion status (neonatal or current) or to investigatewhite matter integrity; however, we think it unlikely thatthe increase in rMT with reduced GA is mainly dueto undiagnosed perinatal lesions. Notwithstanding theinherent limitations, no included participants had anyhistory of abnormal perinatal cranial ultrasound and none
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5838 J. B. Pitcher and others J Physiol 590.22
had either been diagnosed with, or suspected of having,cerebral palsy. Any children with ipsilateral responses toTMS, which might indicate a corticospinal tract lesion(Eyre et al. 2001), were excluded. As stated earlier, however,up to 25% of preterm children who have apparentlynormal results on MRI/DTI go on to develop motorand cognitive dysfunction (Miller et al. 2005; Ludemanet al. 2008). This observation is more consistent withmicrostructural or functional connectivity abnormalities,rather than lesions due to perinatal bleeds per se. It isunlikely that either a greater coil–cortex or scalp–cortexdistance in the preterm children explains their higherrMTs (McConnell et al. 2001; Knecht et al. 2005). Ifanything, the available evidence suggests that the distanceis likely to be shorter in preterm children (Backstrom et al.
2005), and adjustment for this would result in even higherrMTs compared with their term-born peers. There was noevidence that intracortical pathways mediating SICI/ICFare abnormal due to preterm birth, nor responsible forthe effects of GA on rMT. However, given the widespreadcortical microstructural abnormalities seen by others,it seems unlikely that intracortical and/or corticomotorpathways responsible for rMT would be selectively affectedand the cortical networks responsible for mediatingSICI/ICF spared. We would therefore caution against over-interpretation of the SICI/ICF data, particularly given thelow statistical power in the sample. Lastly, there were nodifferences in participants’ age that might explain therelationship. We cannot rule out the possibility that thedevelopment of adult levels of corticomotor excitability
Figure 3. Factors influencing motor skill abilitiesA higher total Movement Assessment Battery for Children, version 2 (MABC2) score was associated with a longergestation (A) and greater corticomotor excitability (B). Data are individual MABC2 percentile scores, GAs and rMTs(right hand). The best relative importance regression model of the explanatory variables influencing total MABC2score and the component subscores is illustrated in C. Abbreviations: BMI, body mass index; IRSD, Index of RelativeSocial Disadvantage. ∗P < 0.05, ∗∗P ≤ 0.0001 for a given predictor in the model.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

J Physiol 590.22 Preterm birth and corticomotor function 5839
is delayed, rather than permanently reduced, in pretermchildren. However, the findings clearly show that thereduced corticomotor excitability has functional effects inchildren well into their school years. While these changesmay seem modest, they are larger than those in childrenwith mild cerebral palsy/periventricular leukomalacia, inwhom a median increase in rMT of 3% stimulator outputcompared with control subjects was reported (Koerteet al. 2010). It is unlikely that the motor areas are theonly cortical regions affected, and reduced excitability inother cortical regions may impair other functions (andtheir development) in, for example, the cognitive andbehavioural domains.
Corticomotor stimulus–response curves
The corticomotor curve slope reflects the size of thecortical representation and the distribution of excitabilitywithin the corticospinal projection (Ridding & Rothwell,1997; Siebner & Rothwell, 2003), while the area under thecurve is generally accepted as a relatively robust overallmeasure of corticomotor output and projection strength(Talelli et al. 2008; Pitcher et al. 2009). Given the cleareffects of reduced GA on rMT, the lack of detectabledifferences due to GA on these stimulus–responsecurve characteristics appears anomalous, because theyare believed to reflect aspects of the integrity and/ormaturation of the cortex and corticomotor projection.However, full curves could be constructed for only abouthalf the children in the sample. This was principally dueto increased rMTs in the preterm children, in whomstimulator output reached maximum before the maximalMEP amplitude was reached. Therefore, the curve dataare representative of higher GA children whose rMT wassufficiently low to allow a full stimulus–response curve tobe constructed, with only limited data from lower GAchildren with higher rMTs, i.e. the children in whomthe curve might be expected to be altered. We wouldadvise future researchers of preterm birth who considerutilizing corticomotor curves to construct them againsta background muscle contraction (which reduces thestimulation threshold to TMS), because resting curvesappear of little value.
Effects of gestation and corticomotor excitability onage-appropriate development of motor skills
Preterm birth was associated with poorer overalldevelopment of age-appropriate motor skills. The mostubiquitous factor in determining motor skill level,however, was the adiposity of the child at assessmentand/or their mother’s adiposity at the first antenatal visit,which were correlated (r = 0.30, P = 0.004). Neither childnor maternal adiposity correlated with GA or BW% of
the child, so the most parsimonious explanation is that,regardless of GA or BW%, high adiposity in the childand/or mother is associated with a lower likelihood ofpractising motor skills regularly, although we offer nodirect evidence to support this.
Reduced corticomotor excitability selectively affectsmanual dexterity skills
Almost 23% of all preterm children in this study had somedegree of manual dexterity impairment. Neither GA norBW% had a direct influence on manual dexterity (Fig. 3A),but low GA and low BW% were both independentlyassociated with reduced corticomotor excitability (i.e.rMT; Fig. 1), which was the most influential factor indetermining dexterity. This is not surprising, given thewell-established critical role of the motor cortex andcorticospinal tract in the dextrous control of the handsand fingers (Porter & Lemon, 1995; Lemon et al. 1998;Lemon, 2008). In children, rMT has been shown tocorrelate inversely with finger tapping speed (Garvey et al.2003). Likewise, Skranes et al. (2007) showed that pre-term adolescents with poor manual dexterity (measuredwith MABC) had reduced white matter development inboth hemispheres, particularly in the posterior limb ofthe internal capsule and the corpus callosum. Diffusiontensor imaging studies of white matter maturation inpreterm neonates commonly report decreased FA andincreased apparent diffusion coefficient values in variouswhite matter regions, particularly the internal capsule andcorpus callosum, and these abnormalities are associatedwith a suboptimal neuromotor outcome (Nagy et al. 2003;Drobyshevsky et al. 2007; Krishnan et al. 2007; Constableet al. 2008; Counsell et al. 2008). When measured in thebrains of preterm adolescents, this decreased FA appearsto be due to fewer and smaller diameter axons, as well aspoorer myelination (Nagy et al. 2003). This is consistentwith our finding that a high rMT was associated witha reduced area under the corticomotor curve and aflatter slope in males, both of which reflect the number,size and degree of myelination of axons in the cortico-motor projection. However, we were not able to show arelationship between manual dexterity and either of thesecorticomotor projection measures.
Aiming, catching and balance skills
Neither aiming and catching nor balance skills wereinfluenced by corticomotor excitability, but 17% of pre-term children were classified as at risk or having impairedbalance skills, and 5% had aiming and catching skillproblems. The reason for this is not clear, althoughthe findings are again consistent with those of Skraneset al. (2007), who found no associations between FA
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5840 J. B. Pitcher and others J Physiol 590.22
values and either balance or aiming and catching skills.A limitation of the present study is that we did not collectphysical activity history data. However, the better balanceskills in the girls and the better aiming and catchingskills in the boys may reflect that these are the types ofmotor skills that they prefer and therefore practise themost. Current participation rate statistics for Australianchildren in this age group support this hypothesis (Sutton,2009; Pink, 2011). This suggests that, while preterm birthmakes acquisition of these skills more difficult, this couldpotentially be ameliorated if the child is assisted to learnand regularly practises the skills.
Fetal growth effects on corticomotor excitability
Few studies of neurodevelopmental outcome after pretermbirth examine GA and BW% separately, although pre-term birth is frequently accompanied by varying degreesof intrauterine growth restriction. The finding that sub-optimal fetal growth (i.e. BW%) adversely affects onlyright corticomotor excitability is consistent with previoussimilar findings by us in young adults (Pitcher et al.2009) and anatomical findings by others in adolescents(Martinussen et al. 2005). The mechanisms underlyingthe association between BW% and cortical developmentof the right hemisphere are not yet clear. However, ourresults show that GA and BW% can have different effectson neurodevelopment, and failure to differentiate theseeffects may contribute to the difficulties inherent in pre-dicting the possible neurodevelopmental outcome for apreterm infant. All children born at ≤27 weeks GA whomet the study entry criteria had a BW% greater than 70%and were less likely to have significant neurological and/orsensorineural impairments than their lower BW% peers.We were not able to determine whether this related to thereasons for their preterm birth (i.e. cervical insufficiencyvs. maternal infection).
Preterm birth and the development of cerebrallateralization
Low GA was associated with a reduction in cerebrallateralization that would normally favour left hemispheredominance. However, while all of the left handed children(or those who showed no hand preference) were bornat ≤38 weeks GA, the prevalence of left handedness/nopreference in the study population (17%) was onlyfractionally higher than that reported in the generalAustralian population (12–15%; Medland et al. 2009).Our findings indicate that development of corticomotorexcitability in both hemispheres is important for thedevelopment of strong motor lateralization. The reasonfor the greater influence of the left hemisphere is notclear. However, it has previously been shown in vivo
that the maturation and gyrification of the left hemi-sphere is delayed with respect to the right, that thisright-greater-than-left hemispheric asymmetry is evidentin preterm infants at birth and is predictive of theirmotor and neurobehavioural scores at term-equivalentage (Dubois et al. 2008a,b). Twin studies suggest that lefthemisphere development is under less genetic control thanthe right and is more vulnerable to an adverse environmentin utero and in early life (Geschwind & Galaburda, 1985;Geschwind et al. 2002). Our data are suggestive of twogroups, one group in which preterm birth has no effecton lateralization and a second group in which reductionsin GA (or an associated pathology) are associated withreduced lateralization towards the left hemisphere thatpersists into late childhood. However, sample sizes in thetens of thousands are required to discriminate betweengenetic and environmental/pathological influences onhandedness (Medland et al. 2009), and the presentstudy was underpowered to explain why some pretermchildren experience less hemispheric lateralization thanothers. Hemispheric motor lateralization and languagelateralization are correlated (Pujol et al. 1999; Knechtet al. 2000), and the failure to develop a dominant hemi-sphere significantly increases the risk of difficulties withlanguage, reading and speech (Orton, 1966; Annett, 1975).Given that up to 50% of preterm children will experienceproblems with motor function, language, reading and/orspeech by school age (Marlow et al. 1993; Bracewell& Marlow, 2002; Chyi et al. 2008), determining whichfactor(s) associated with preterm birth leads to abnormalor reduced development of cerebral lateralization wouldseem to be a major priority for both early identificationand intervention of those children at most risk.
Study limitations
There are a number of limitations of this study. Threehave already been mentioned, namely the lack of MRIdata to confirm the lesion status of our subjects, thelack of physical activity history data and the limitationsof the SICI/ICF data. While detailed perinatal medicalhistories for the most preterm children were available,there was often little information regarding the late pre-term children and the circumstances leading to theirpreterm birth, as many were never admitted to receiveneonatal care. Furthermore, we chose to study across therange of survivable gestations, and the samples size of eachof the gestation groups precluded robust within-groupanalyses of the influence of possible perinatal medicalfactors affecting neurodevelopmental outcomes, evenwhere these data were available. Future studies that areeither larger or that concentrate on a more definedGA range will be required to elucidate the influence ofthese pregnancy-specific and perinatal factors on postnatal
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

J Physiol 590.22 Preterm birth and corticomotor function 5841
neurophysiological and functional motor outcomes morefully. Lastly, the study participant age group correspondswith the onset and/or early stages of puberty, and changesin sex steroid levels are known to modulate cortico-motor excitability and brain maturation (Smith et al. 1999;Herting et al. 2012). We did not determine pubertal stage inthe participants or control for females’ cycle stage (if pre-sent) at cortical assessment, which may have contributedto data variability.
Conclusions
This study has provided the first neurophysiologicalevidence that preterm birth is associated with reducedmotor cortical excitability that remains evident in latechildhood. Functionally, this reduced excitability appearsto affect mainly the development of dextrous use ofthe hands and to reduce hemispheric lateralization.Perhaps most importantly, the findings suggest that, inaddition to GA, BW% and other physiological factors,the socio-economic and psychosocial characteristics ofthe home environment and family a preterm newborngoes home to are critical factors in predicting later motoroutcomes. Larger and prospective studies are required toelucidate the influence of specific preterm birth aetiologieson these outcomes, to confirm whether intracorticalinhibitory and facilitatory networks are altered and todetermine whether the cortical excitability reductions‘catch up’ later in adolescence or persist into adulthood.
References
Ajayi-Obe M, Saeed N, Cowan FM, Rutherford MA & EdwardsAD (2000). Reduced development of cerebral cortex inextremely preterm infants. Lancet 356, 1162–1163.
Alexander GR (2007). Prematurity at birth: determinants,consequences, and geographic variation. In Preterm Birth:Causes, Consequences, and Prevention, ed. Behrman RE &Butler AS. Appendix B, 604-644. National Academies Press(US), Washington, DC.
Annett M (1975). Hand preference and the laterality of cerebralspeech. Cortex 11, 305–328.
Backstrom MC, Kuusela AL, Koivisto AM & Sievanen H(2005). Bone structure and volumetric density in youngadults born prematurely: a peripheral quantitative computedtomography study. Bone 36, 688–693.
Bracewell M & Marlow N (2002). Patterns of motor disabilityin very preterm children. Ment Retard Dev Disabil Res Rev 8,241–248.
Chen R, Samii A, Canos M, Wassermann EM & Hallett M(1997). Effects of phenytoin on cortical excitability inhumans. Neurology 49, 881–883.
Chyi LJ, Lee HC, Hintz SR, Gould JB & Sutcliffe TL (2008).School outcomes of late preterm infants: special needs andchallenges for infants born at 32 to 36 weeks gestation. JPediatr 153, 25–31.
Constable RT, Ment LR, Vohr BR, Kesler SR, Fulbright RK,Lacadie C, Delancy S, Katz KH, Schneider KC, Schafer RJ,Makuch RW & Reiss AR (2008). Prematurely born childrendemonstrate white matter microstructural differences at12 years of age, relative to term control subjects: aninvestigation of group and gender effects. Pediatrics 121,306–316.
Counsell SJ & Boardman JP (2005). Differential brain growthin the infant born preterm: current knowledge and futuredevelopments from brain imaging. Semin Fetal NeonatalMed 10, 403–410.
Counsell SJ, Edwards AD, Chew ATM, Anjari M, Dyet LE,Srinivasan L, Boardman JP, Allsop JM, Hajnal JV,Rutherford MA & Cowan FM (2008). Specific relationsbetween neurodevelopmental abilities and white mattermicrostructure in children born preterm. Brain 131,3201–3208.
Drobyshevsky A, Bregman J, Storey P, Meyer J, Prasad PV,Derrick M, MacKendrick W & Tan S (2007). Serial diffusiontensor imaging detects white matter changes that correlatewith motor outcome in premature infants. Dev Neurosci 29,289–301.
Dubois J, Benders M, Borradori-Tolsa C, Cachia A, Lazeyras F,Ha-Vinh Leuchter R, Sizonenko SV, Warfield SK, Mangin JF& Huppi PS (2008a). Primary cortical folding in the humannewborn: an early marker of later functional development.Brain 131, 2028–2041.
Dubois J, Benders M, Cachia A, Lazeyras F, Ha-Vinh LeuchterR, Sizonenko SV, Borradori-Tolsa C, Mangin JF & Huppi PS(2008b). Mapping the early cortical folding process in thepreterm newborn brain. Cereb Cortex 18,1444–1454.
Eyre JA (2003). Developmental plasticity of the corticospinalsystem. In Plasticity in the Human Brain: Investigations withTranscranial Magetic Brain Stimulation, ed. Boniface S &Ziemann U, pp. 62–89. Cambridge University Press,Cambridge, UK.
Eyre JA, Miller S, Clowry GJ, Conway EA & Watts C (2000).Functional corticospinal projections are establishedprenatally in the human foetus permitting involvement inthe development of spinal motor centres. Brain 123,51–64.
Eyre JA, Taylor JP, Villagra F, Smith M & Miller S (2001).Evidence of activity-dependent withdrawal of corticospinalprojections during human development. Neurology 57,1543–1554.
Fietzek UM, Heinen F, Berweck S, Maute S, Hufschmidt A,Schulte-Monting J, Lucking CH & Korinthenberg R (2000).Development of the corticospinal system and hand motorfunction: central conduction times and motor performancetests. Dev Med Child Neurol 42, 220–227.
Gardosi JO & Francis A (2006). GROW customised centilecalculator, version 5.1. Gestation Network,www.gestation.net.
Garvey MA & Gilbert DL (2004). Transcranial magneticstimulation in children. Eur J Paediatr Neurol 8, 7–19.
Garvey MA, Ziemann U, Bartko JJ, Denckla MB, Barker CA &Wassermann EM (2003). Cortical correlates of neuromotordevelopment in healthy children. Clin Neurophysiol 114,1662–1670.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5842 J. B. Pitcher and others J Physiol 590.22
Geschwind DH, Miller BL, DeCarli C & Carmelli D (2002).Heritability of lobar brain volumes in twins supports geneticmodels of cerebral laterality and handedness. Proc Natl AcadSci USA 99, 3176–3181.
Geschwind N & Galaburda AM (1985). Cerebral lateralization.Biological mechanisms, associations, and pathology: I. Ahypothesis and a program for research. Arch Neurol 42,428–459.
Gromping U (2006). Relative importance for linear regressionin R: the package relaimpo. Journal of Statistical Software 17,1–27.
Gromping U (2007). Estimators of relative importance in linearregression based on variance decomposition. The AmericanStatistician 61, 139–147.
Hack M & Fanaroff AA (2000). Outcomes of children ofextremely low birthweight and gestational age in the 1990s.Semin Neonatol 5, 89–106.
Henderson SE, Sugden DA & Barnett AL (2007). MovementAssessment Battery for Children – Examiners Manual.Pearson Assessment, London.
Herting MM, Maxwell EC, Irvine C & Nagel BJ (2012). Theimpact of sex, puberty, and hormones on white mattermicrostructure in adolescents. Cereb Cortex 22,1979–1992.
Huddy CLJ, Johnson A & Hope PL (2001). Educational andbehavioural problems in babies of 32–35 weeks gestation.Arch Dis Child Fetal Neonatal Ed 85, F23–28.
Huppi PS, Maier SE, Peled S, Zientara GP, Barnes PD, Jolesz FA& Volpe JJ (1998). Microstructural development of humannewborn cerebral white matter assessed in vivo by diffusiontensor magnetic resonance imaging. Pediatr Res 44,584–590.
Kapellou O, Counsell SJ, Kennea N, Dyet L, Saeed N, Stark J,Maalouf E, Duggan P, Ajayi-Obe M, Hajnal J, Allsop JM,Boardman J, Rutherford MA, Cowan F & Edwards AD(2006). Abnormal cortical development after prematurebirth shown by altered allometric scaling of brain growth.PLoS Med 3, e265.
Kesler SR, Ment LR, Vohr B, Pajot SK, Schneider KC,Katz KH, Ebbitt TB, Duncan CC, Makuch RW & ReissAL (2004). Volumetric analysis of regional cerebraldevelopment in preterm children. Pediatr Neurol 31,318–325.
Kesler SR, Reiss AL, Vohr B, Watson C, Schneider KC, Katz KH,Maller-Kesselman J, Silbereis J, Constable RT, Makuch RW& Ment LR (2008). Brain volume reductions within multiplecognitive systems in male preterm children at age twelve. JPediatr 152, 513–520, 520.e1.
Kirkegaard I, Obel C, Hedegaard M & Henriksen TB (2006).gestational age and birth weight in relation to schoolperformance of 10-year-old children: a follow-up study ofchildren born after 32 completed weeks. Pediatrics 118,1600–1606.
Kloppel S, Baumer T, Kroeger J, Koch MA, Buchel C, MunchauA & Siebner HR (2008). The cortical motor threshold reflectsmicrostructural properties of cerebral white matter.NeuroImage 40, 1782–1791.
Knecht S, Drager B, Deppe M, Bobe L, Lohmann H, Floel A,Ringelstein EB & Henningsen H (2000). Handedness andhemispheric language dominance in healthy humans. Brain123, 2512–2518.
Knecht S, Sommer J, Deppe M & Steinstrater O (2005). Scalpposition and efficacy of transcranial magnetic stimulation.Clin Neurophysiol 116, 1988–1993.
Koerte I, Pelavin P, Kirmess B, Fuchs T, Berweck S, LaubenderRP, Borggraefe I, Schroeder S, Danek A, Rummeny C, ReiserM, Kubicki M, Shenton ME, Ertl-Wagner B & Heinen F(2010). Anisotropy of transcallosal motor fibres indicatesfunctional impairment in children with periventricularleukomalacia. Dev Med Child Neurol 53, 179–186.
Krishnan ML, Dyet LE, Boardman JP, Kapellou O, Allsop JM,Cowan F, Edwards AD, Rutherford MA & Counsell SJ(2007). Relationship between white matter apparentdiffusion coefficients in preterm infants at term-equivalentage and developmental outcome at 2 years. Pediatrics 120,e604–e609.
Kujirai T, Caramia MD, Rothwell JC, Day BL, Thompson PD,Ferbert A, Wroe S, Asselman P & Marsden CD (1993).Corticocortical inhibition in human motor cortex. J Physiol471, 501–519.
Lemon RN (2008). Descending pathways in motor control.Annu Rev Neurosci 31, 195–218.
Lemon RN, Baker SN, Davis JA, Kirkwood PA, Maier MA &Yang HS (1998). The importance of thecortico-motoneuronal system for control of grasp. NovartisFound Symp 218, 202–215; discussion 215–208.
Lindeman RH, Merenda PF & Gold RZ (1980). Introduction toBivariate and Multivariate Analysis. Scott, Foresman,Glenview, IL.
Lubsen J, Vohr B, Myers E, Hampson M, Lacadie C, SchneiderKC, Katz KH, Constable RT & Ment LR (2011).Microstructural and functional connectivity in thedeveloping preterm brain. Semin Perinatol 35, 34–43.
Ludeman NA, Berman JI, Wu YW, Jeremy RJ, Kornak J, BarthaAI, Barkovich AJ, Ferriero DM, Henry RG & Glenn OA(2008). Diffusion tensor imaging of the pyramidal tracts ininfants with motor dysfunction. Neurology 71, 1676–1682.
McConnell KA, Nahas Z, Shastri A, Lorberbaum JP, Kozel FA,Bohning DE & George MS (2001). The transcranialmagnetic stimulation motor threshold depends on thedistance from coil to underlying cortex: a replication inhealthy adults comparing two methods of assessing thedistance to cortex. Biol Psychiatry 49, 454–459.
Marlow N, Roberts L & Cooke R (1993). Outcome at 8 years forchildren with birth weights of 1250 g or less. Arch Dis Child68, 286–290.
Martinussen M, Fischl B, Larsson HB, Skranes J, Kulseng S,Vangberg TR, Vik T, Brubakk A-M, Haraldseth O & DaleAM (2005). Cerebral cortex thickness in 15-year-oldadolescents with low birth weight measured by an automatedMRI-based method. Brain 128, 2588–2596.
Mathur AM, Neil JJ & Inder TE (2010). Understanding braininjury and neurodevelopmental disabilities in the preterminfant: the evolving role of advanced magnetic resonanceimaging. Semin Perinatol 34, 57–66.
Medland SE, Duffy DL, Wright MJ, Geffen GM, Hay DA, LevyF, van-Beijsterveldt CEM, Willemsen G, Townsend GC,White V, Hewitt AW, Mackey DA, Bailey JM, Slutske WS,Nyholt DR, Treloar SA, Martin NG & Boomsma DI (2009).Genetic influences on handedness: data from 25,732Australian and Dutch twin families. Neuropsychologia 47,330–337.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

J Physiol 590.22 Preterm birth and corticomotor function 5843
Miller SP & Ferriero DM (2009). From selective vulnerability toconnectivity: insights from newborn brain imaging. TrendsNeurosci 32, 496–505.
Miller SP, Ferriero DM, Leonard C, Piecuch R, Glidden DV,Partridge JC, Perez M, Mukherjee P, Vigneron DB &Barkovich AJ (2005). Early brain injury in prematurenewborns detected with magnetic resonance imaging isassociated with adverse early neurodevelopmental outcome.J Pediatr 147, 609–616.
Morse SB, Zheng H, Tang Y & Roth J (2009). Early school-ageoutcomes of late preterm infants. Pediatrics 123, e622–e629.
Mullen KM, Vohr BR, Katz KH, Schneider KC, Lacadie C,Hampson M, Makuch RW, Reiss AL, Constable RT & MentLR (2011). Preterm birth results in alterations in neuralconnectivity at age 16 years. NeuroImage 54, 2563–2570.
Nagy Z, Ashburner J, Andersson J, Jbabdi S, Draganski B, SkareS, Bohm B, Smedler A-C, Forssberg H & Lagercrantz H(2009). Structural correlates of preterm birth in theadolescent brain. Pediatrics 124, e964–e972.
Nagy Z, Westerburg H, Skare S, Andersson JL, Lilja A,Flodmark O, Fernell E, Holmberg K, Bohm B, Forssberg H,Lagercrantz H & Klingberg T (2003). Preterm children havedisturbances of white matter at 11 years of age as shown bydiffusion tensor imaging. Pediatr Res 54, 672–679.
Nosarti C, Al-Asady MHS, Frangou S, Stewart AL, Rifkin L &Murray RM (2002). Adolescents who were born very pretermhave decreased brain volumes. Brain 125, 1616–1623.
Nosarti C, Giouroukou E, Healy E, Rifkin L, Walshe M,Reichenberg A, Chitnis X, Williams SCR & Murray RM(2008). Grey and white matter distribution in very pretermadolescents mediates neurodevelopmental outcome. Brain131, 205–217.
Oldfield RC (1971). The assessment and analysis of handedness:the Edinburgh inventory. Neuropsychologia 9, 97–113.
Orth M, Snijders AH & Rothwell JC (2003). The variability ofintracortical inhibition and facilitation. Clin Neurophysiol14, 2362–2369.
Orton ST (1966). “Word-Blindness” in School Children andOther Papers on Strephosymbolia (Specific LanguageDisability—Dyslexia) 1925–1946, vol. 2. Orton Society,Pomfret, CT.
Peterson BS (2003). Brain imaging studies of the anatomicaland functional consequences of preterm birth for humanbrain development. Ann N Y Acad Sci 1008, 219–237.
Peterson BS, Anderson AW, Ehrenkranz R, Staib LH, TageldinM, Colson E, Gore JC, Duncan CC, Makuch R & Ment LR(2003). Regional brain volumes and their laterneurodevelopmental correlates in term and preterm infants.Pediatrics 111, 939–948.
Peterson BS, Vohr B, Staib LH, Cannistraci CJ, Dolberg A,Schneider KC, Katz KH, Westerveld M, Sparrow S, AndersonAW, Duncan CC, Makuch RW, Gore JC & Ment LR (2000).Regional brain volume abnormalities and long-termcognitive outcome in preterm infants. JAMA 284,1939–1947.
Pietz J, Peter J, Graf R, Rauterberg-Ruland I, Rupp A,Sontheimer D & Linderkamp O (2004). Physical growth andneurodevelopmental outcome of nonhandicapped low-riskchildren born preterm. Early Hum Dev 79, 131–143.
Pink B (2011). Sport and recreation: a statistical overview.Australian Bureau of Statistics.http://www.abs.gov.au/ausstats/[email protected]/mf/4156.0
Pitcher JB, Ogston KM & Miles TS (2003). Age and sexdifferences in human motor cortex input–outputcharacteristics. J Physiol 546, 605–613.
Pitcher JB, Robertson AL, Cockington RA & Moore VM(2009). Prenatal growth and early postnatal influences onadult motor cortical excitability. Pediatrics 124, e128–e136.
Pitcher JB, Schneider LA, Drysdale JL, Higgins RD, RiddingMC, Burns NR, Nettelbeck TJ, Haslam RR & Robinson JS(2011a). Gestation length and fetal growth have differenteffects on corticospinal excitability and motor skilldevelopment in children. J Dev Orig Health Dis 2,S145–S146.
Pitcher JB, Schneider LA, Drysdale JL, Ridding MC & OwensJA (2011b). Motor system development of the preterm andlow birthweight infant. Clin Perinatol 38, 605–625.
Porter R & Lemon R (1995). Corticospinal Function andVoluntary Movement , Monographs of the PhysiologicalSociety, no. 45, Clarendon Press, Oxford.
Pujol J, Deus J, Losilla JM & Capdevila A (1999). Cerebrallateralization of language in normal left-handed peoplestudied by functional MRI. Neurology 52, 1038–1043.
Quintana H (2005). Transcranial magnetic stimulation inpersons younger than the age of 18. J ECT 21, 88–95.
Raju T, Higgins R, Stark A & Leveno K (2006). Optimizing careand outcome for late-preterm (near-term) infants: asummary of the workshop sponsored by the NationalInstitute of Child Health and Human Development.Pediatrics 118, 1207–1214.
Ridding MC & Rothwell JC (1997). Stimulus/response curvesas a method of measuring motor cortical excitability in man.ElectroencephalogrClin Neurophysiol 105, 340–344.
Ridding MC, Taylor JL & Rothwell JC (1995). The effect ofvoluntary contraction on cortico-cortical inhibition inhuman motor cortex. J Physiol 487, 541–548.
Roberts G, Anderson PJ, Davis N, De Luca C, Cheong J &Doyle LW; Victorian Infant Collaborative Study Group(2011). Developmental coordination disorder in geographiccohorts of 8-year-old children born extremely preterm orextremely low birthweight in the 1990s. Dev Med ChildNeurol 53, 55–60.
Rossini PM, Barker AT, Berardelli A, Caramia MD, Caruso G,Cracco RQ, Dimitrijevic MR, Hallett M, Katayama Y,Lucking CH, Denoordhout ALM, Marsden CD, MurrayNMF, Rothwell JC, Swash M & Tomberg C (1994).Non-invasive electrical and magnetic stimulation of thebrain, spinal cord and roots – basic principles and proceduresfor routine clinical application. Report of an IFCNcommittee. Electroencephalogr Clin Neurophysiol 91, 79–92.
Siebner HR & Rothwell J (2003). Transcranial magneticstimulation: new insights into representational corticalplasticity. Exp Brain Res 148, 1–16.
Skranes J, Vangberg TR, Kulseng S, Indredavik MS, EvensenKAI, Martinussen M, Dale AM, Haraldseth O & BrubakkA-M (2007). Clinical findings and white matterabnormalities seen on diffusion tensor imaging inadolescents with very low birth weight. Brain 130, 654–666.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society

5844 J. B. Pitcher and others J Physiol 590.22
Smith A, Ridding M, Higgins R, Wittert G & Pitcher J (2009).Age-related changes in short-latency motor cortexinhibition. Exp Brain Res 198, 489–500.
Smith MJ, Keel JC, Greenberg BD, Adams LF, Schmidt PJ,Rubinow DA & Wassermann EM (1999). Menstrual cycleeffects on cortical excitability. Neurology 53, 2069–2072.
Smyser CD, Inder TE, Shimony JS, Hill JE, Degnan AJ, SnyderAZ & Neil JJ (2010). Longitudinal analysis of neural networkdevelopment in preterm infants. Cereb Cortex 20,2852–2862.
Smyser CD, Snyder AZ & Neil JJ (2011). Functionalconnectivity MRI in infants: exploration of the functionalorganization of the developing brain. NeuroImage 56,1437–1452.
Sutton T (2009). Children’s participation in cultural and leisureactivities, Australia, 4th edn, Australian Bureau of Statistics.http://www.abs.gov.au/ausstats/[email protected]/mf/4901.0 FederalGovernment.
Talelli P, Waddingham W, Ewas A, Rothwell J & Ward N(2008). The effect of age on task-related modulation ofinterhemispheric balance. Exp Brain Res 186, 59–66.
Tucker J & McGuire W (2004). Epidemiology of preterm birth.BMJ 329, 675–678.
van Soelen ILC, Brouwer RM, Peper JS, van BeijsterveldtTCEM, van Leeuwen M, de Vries LS, Kahn RS, Hulshoff PolHE & Boomsma DI (2010). Effects of gestational age andbirth weight on brain volumes in healthy 9 year-old children.J Pediatr 156, 896–901.
Wassermann EM (1998). Risk and safety of repetitivetranscranial magnetic stimulation: report and suggestedguidelines from the International Workshop on the Safety ofRepetitive Transcranial Magnetic Stimulation, June 5–7,1996. Electroencephalogr Clin Neurophysiol 108, 1–16.
WHO (1992). International Classification of Diseases andRelated Health Problems. World Health Organization,Geneva.
Williams J, Lee KJ & Anderson PJ (2010). Prevalence ofmotor-skill impairment in preterm children who do notdevelop cerebral palsy: a systematic review. Dev Med ChildNeurol 52, 232–237.
Woythaler MA, McCormick MC & Smith VC (2011). Latepreterm infants have worse 24-month neurodevelopmentaloutcomes than term infants. Pediatrics 127, e622–e629.
Ziemann U (2003). Pharmacology of TMS. Suppl ClinNeurophysiol 56, 226–231.
Ziemann U (2004). TMS and drugs. Clin Neurophysiol 115,1717–1729.
Ziemann U, Rothwell JC & Ridding MC (1996). Interactionbetween intracortical inhibition and facilitation in humanmotor cortex. J Physiol 496, 873–881.
Author contributions
J.B.P. conceived the study. J.B.P., N.R.B., T.J.N., M.C.R., R.R.H.and J.S.R. contributed to the design of the experiments. J.B.P.,L.A.S., J.L.D., R.D.H., N.R.B. and R.R.H. collected and analysedthe data. J.B.P., L.A.S., J.L.D., N.R.B., M.C.R., T.J.N., J.S.R.and R.R.H. contributed to the drafting and revisions of themanuscript.
Acknowledgements
We thank Professor Peter Baghurst and Ms Georgia Antonioufor assistance with the patient databases, Dr Michael Stark foradvice on the perinatal clinical histories, Dr Ashleigh Smith forresearch assistance on some of the experiments, and ProfessorsJohn Rothwell and Julie Owens for invaluable discussions andadvice on the manuscript. We wish sincerely to thank themembers of the PREMOCODE study cohort and their familiesfor their generous and tireless voluntary commitment to theproject. This work was supported by grants from the NationalHealth and Medical Research Council of Australia (NH&MRCgrant numbers 565344 to J.B.P. and 299087 to J.B.P.), theSouth Australian Channel 7 Children’s Research Foundation,the Women’s and Children’s Hospital Research Foundation, andthe Faculty of Health Sciences, University of Adelaide. J.B.P. isan M. S. McLeod Trust Research Fellow. M.C.R. is an NH&MRCSenior Research Fellow.
C© 2012 The Authors. The Journal of Physiology C© 2012 The Physiological Society




















