Recent National and Regional Drug Reforms in Sweden
15
Terms and Conditions for Use of PDF The provision of PDFs for authors' personal use is subject to the following Terms & Conditions: The PDF provided is protected by copyright. All rights not specifically granted in these Terms & Conditions are expressly reserved. Printing and storage is for scholarly research and educational and personal use. Any copyright or other notices or disclaimers must not be removed, obscured or modified. The PDF may not be posted on an open-access website (including personal and university sites). The PDF may be used as follows: • to make copies of the article for your own personal use, including for your own classroom teaching use (this includes posting on a closed website for exclusive use by course students); • to make copies and distribute copies (including through e-mail) of the article to research colleagues, for the personal use by such colleagues (but not commercially or systematically, e.g. via an e-mail list or list serve); • to present the article at a meeting or conference and to distribute copies of such paper or article to the delegates attending the meeting; • to include the article in full or in part in a thesis or dissertation (provided that this is not to be published commercially). This material is the copyright of the original publisher. Unauthorised copying and distribution is prohibited. 2008, Vol. 26, No. 7 (pp. 537-550) ISSN: 1170-7690 Current Opinion Swedish Drug Reforms and Pharmaceutical Companies
-
Upload
strathclyde -
Category
Documents
-
view
1 -
download
0
Transcript of Recent National and Regional Drug Reforms in Sweden
Terms and Conditions for Use of PDF
The provision of PDFs for authors' personal use is subject to the following Terms & Conditions: The PDF provided is protected by copyright. All rights not specifically granted in these Terms & Conditions are expressly reserved. Printing and storage is for scholarly research and educational and personal use. Any copyright or other notices or disclaimers must not be removed, obscured or modified. The PDF may not be posted on an open-access website (including personal and university sites). The PDF may be used as follows: • to make copies of the article for your own personal use, including for your own classroom teaching use (this includes posting on a closed website for exclusive use by course students); • to make copies and distribute copies (including through e-mail) of the article to research colleagues, for the personal use by such colleagues (but not commercially or systematically, e.g. via an e-mail list or list serve); • to present the article at a meeting or conference and to distribute copies of such paper or article to the delegates attending the meeting; • to include the article in full or in part in a thesis or dissertation (provided that this is not to be published commercially).
This material is the copyright of the original publisher. Unauthorised copying and distribution is prohibited.
2008, Vol. 26, No. 7 (pp. 537-550)
ISSN: 1170-7690
Current OpinionSwedish Drug Reforms and Pharmaceutical Companies
Pharmacoeconomics 2008; 26 (7): 537-550CURRENT OPINION 1170-7690/08/0007-0537/$48.00/0
2008 Adis Data Information BV. All rights reserved.
Recent National and Regional DrugReforms in SwedenImplications for Pharmaceutical Companies in Europe
Bjorn Wettermark,1,2 Brian Godman,3 Karolina Andersson,4 Lars L. Gustafsson,1,2
Alan Haycox5 and Vittorio Bertele′3
1 Division of Clinical Pharmacology, Department of Laboratory Medicine, Karolinska Institute,Stockholm, Sweden
2 Department of Drug Management and Informatics, Stockholm County Council,Stockholm, Sweden
3 Institute for Pharmacological Research ‘Mario Negri’, Milan, Italy4 Nordic School of Public Health, Goteborg, Sweden5 University of Liverpool Management School, Liverpool, UK
With an aging population and increased prevalence of chronic diseases, such asAbstractobesity and diabetes mellitus, drug reforms are needed across Europe to ensure thecontinued provision of comprehensive healthcare. It is also a challenge, with thelimited resources available, to fund new innovative drugs that significantlyimprove patient health.
Recent national and regional reforms in Sweden have moderated the rate ofincrease in drug expenditure, despite increased volumes of drug use and thelaunch of new, expensive drugs. National reforms include the adoption of eco-nomic principles when assessing the value and subsequent reimbursement of newand existing drugs, as well as reforms to obtain low prices for generic drugs.Regional reforms aim to encourage the rational use of medicines through theestablishment of drug and therapeutic committees, development of guidelines,academic detailing, continuous benchmarking of prescribing patterns, and finan-cial incentives.
Some of these reforms provide examples to other European countries, whilstothers duplicate existing measures. As such, we believe other European countriescan benefit from an analysis of the Swedish reforms. We believe the pharmaceuti-cal industry can also benefit from this analysis by working with key regionalpayers involved with developing and implementing the reforms as they moderateand refine their future activities, including finding acceptable ways of introducingnew expensive drugs.
There are 21 regional county councils (herein 1998.[1,2,4] Between 2002 and 2005, counties werereferred to as counties) in Sweden, with Stockholm responsible for the costs of excessive use of drugsCounty Council and Vastra Gotaland (incorporating exceeding national targets, although there was aGoteborg) being two of the largest, accounting for generous risk-sharing model with the govern-approximately 40% of the total population (3.5 mil- ment.[3,5] Since 2005, counties have had the opportu-lion of 9 million).[1-3] Drug budgets have been de- nity to levy additional taxes, if needed, to addresscentralized to the counties to a varying extent since budget deficits.

538 Wettermark et al.
Despite a number of reforms, total pharmaceuti- 1. Methodology of Reviewcal expenditure grew significantly in Sweden duringthe 1990s and early 2000s, at an average annual rate A thorough review of the literature concerningof approximately 10%.[2,4,6,7] This growth was driv- the Swedish reforms was undertaken using MED-en by new, expensive drugs[2,5] such as oncology LINE and PubMed and the following keywords:drugs and immunosuppressants,[8] and increased Sweden, pharmaceuticals, drugs, reimbursement, re-volumes of drug use for the treatment of chronic forms, generics, costs, cost controls, cost savingsdiseases,[2] with volumes almost doubling between and cost effectiveness.1986 and 2002.[9] As a result, drug costs rose from This search was supplemented by published pa-approximately 9% of healthcare expenditure in 1990 pers known to the authors that eluded the initial listto approximately 15% in the early 2000s,[3,5] before of possible papers, including PhD theses (B. Wet-
termark and K. Andersson). Additionally, an in-moderating to 12.3% in 2004.[7] Total expenditureternet search of pertinent websites was conducted,on drugs in Sweden (including patient copaymentincluding those of the Organisation for Economicand over-the-counter drugs) is now more than halfCooperation and Development (OECD), Cochraneof the total cost of running primary healthcare. InCollaboration, LFN (Lakemedelsformansnamndenview of this, since 2000 there has been renewed– Swedish Pharmaceutical Benefits Board), SBUfocus on containing drug costs, particularly among(the Swedish Council on Technology Assessment inregional payers, to ensure continued provision ofHealth Care) and the Swedish Federation of Countycomprehensive healthcare.Councils. Internal county documents known to the
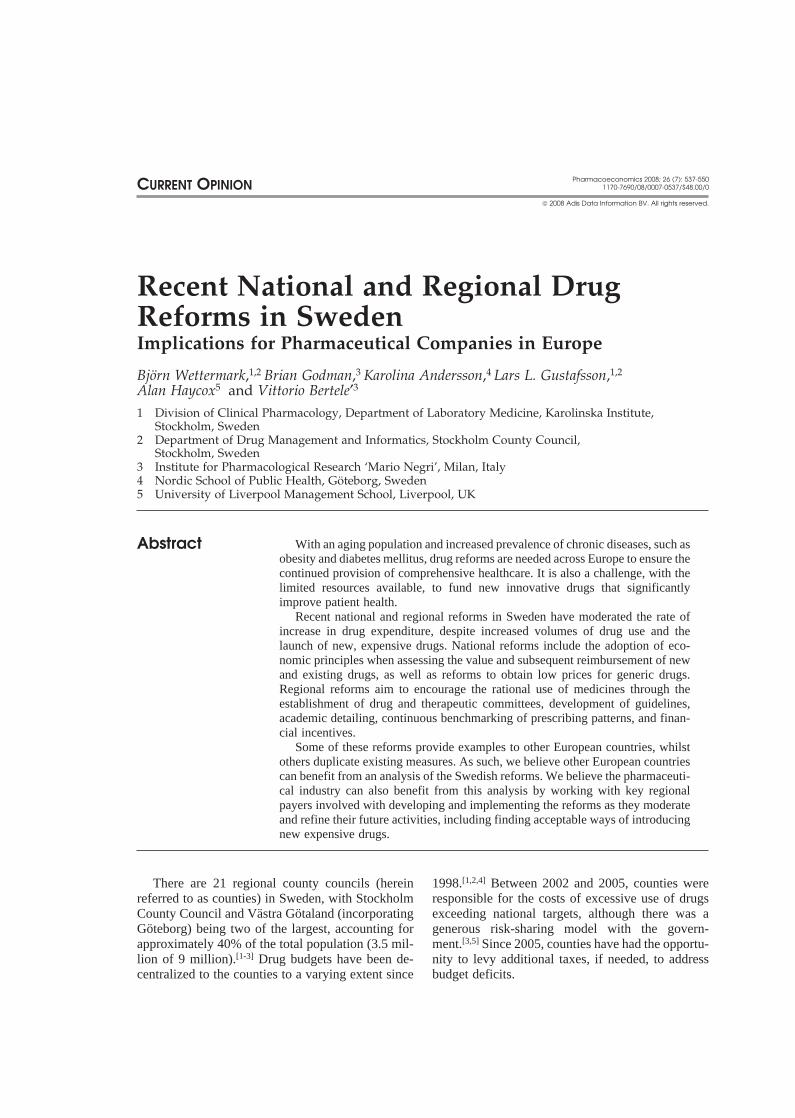
The resultant reforms have moderated the growth authors (B. Wettermark and L. Gustafsson) werein pharmaceutical expenditure to between 1% and added and supplemented with knowledge of ongo-3% per annum from 2003 to 2006,[1,7,10] despite drug ing reforms in other EU countries as part of a PhDuse volumes growing between 1% and 3.5% per thesis (B. Godman) and as part of general activitiesannum since 2002 (figure 1).[10]
(V. Bertele′ and A. Haycox), along with feedbackfrom key stakeholder groups in Sweden (ApoteketThis article describes the myriad of recent drugAB [National Corporation of Swedish Pharmacies]reforms in Sweden, with a particular focus on theand the LFN). Costs related to Sweden have beenimplications of the Swedish model for other Europ-presented in Swedish kronor (SEK) throughout theean countries and pharmaceutical companies in thepaper (€1 = SEK9.4; 1 February 2008 value).future. The effects of the various reforms have to be
Calculations on the annual increase in total drugviewed in tandem because it is difficult to isolateexpenditure were derived from data on total pharma-their individual impacts, which have also been exac-ceutical costs in recent years documented in publica-erbated by the launch of new, expensive, innovativetions[1,7,10] and from data supplied by Apoteket AB .drugs in recent years. However, these new drugs hadThe data on the annual increase in drug use volumesonly a limited impact on sales in 2003 and 2004;[1]
were derived from data supplied by Apoteket AB.[10]although this is changing, particularly in the hospital
The paper is not an evaluation of the impact ofsetting.individual drug reforms, as these are difficult torobustly calculate, nor an evaluation of the quality ofthe published papers on this subject, using for in-stance criteria used by the Cochrane Collabora-tion.[11] The intention of this paper is to provide athorough compilation of various recent national andregional drug reforms instigated in Sweden. Weacknowledge some of the referenced papers arefrom internal non-peer-reviewed sources. We haveincluded these to provide insight into current ap-proaches, their rationale and impact, where docu-
6
5
4
1998
3
2
1
1999 2000 2001 2002
Year
2003 2004 2005 20060
7
Tota
l D
DD
s (
bill
ion)
Fig. 1. Total volume of drug use in Sweden from 1998 to 2006.[10]
DDDs = defined daily doses.
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

Swedish Drug Reforms and Pharmaceutical Companies 539
mented by actual payers involved in the develop- Alongside this, there is a comprehensive techni-ment and implementation of these changes. In addi- cal support system in Sweden that enables pharma-tion, we have acknowledged data deficiencies cies to continually stock the cheapest product, withalongside ongoing activities to address these. As prices reviewed at least twice a month by thesuch, we believe the findings and discussion will be LFN.[12,14] This is facilitated by the fact that there isof interest to all stakeholders in the field of pharma- only one national pharmacy chain in Sweden –ceutical care, including other European countries Apoteket AB,[2,5] which is owned by, and reportsand innovative pharmaceutical companies, as they directly to, the government. In view of this, origina-adapt to the requirements of cost-effective use of tor prices must be similar to current generic prices ordrugs for all patients. else the product will have a very limited sales vol-
ume.2. Ongoing National and Regional As a result of these initiatives and characteristics,Drug Reforms price competition has been marked in high-volume
areas such as antidepressants, proton pump inhibi-Major drug reforms introduced nationally and tors (PPIs) and antihypertensives, leading to low
regionally in Sweden in recent years include mea- retail prices for generics.[15] For example, on a de-sures to encourage low prices for generics and to fined-daily-dose (DDD) basis, the current price ofobtain low prices for existing products in a class or generic simvastatin is 93% below pre-patent expiryrelated classes. In addition, reforms have been intro- prices, citalopram is 85% below and omeprazole isduced to encourage the rational use of medicines, 78% below (November 2007 values).[16] Overall,particularly at a regional level. since generic substitution was introduced, generic
prices have decreased by an average of 40%.[7,15]
2.1 Low Prices for Generics Whilst it is difficult to accurately determine theimpact of these reforms and measures, the LFNThe generic market in Sweden is characterizedestimated accumulated savings of €700 millionby free pricing, although a reimbursement level isfrom 2002 to the end of 2005.[14] The low pricesapplied corresponding to the price of the cheapestobtained for generics have also significantly impact-product.[7,12] In addition, from 1 October 2002, thereed on pharmaceutical prices generally, with somehas been mandatory generic substitution of inter-authors documenting overall price reductions ofchangeable products at pharmacies, with the cheap-5–6%,[7] whilst others estimate greater reduc-est product dispensed unless the following situationstions.[15] In any event, pharmaceutical prices areapply:[1,12,13]
envisaged to fall still further once all 49 classes of• the prescriber indicates that the drug should notmedicines on the market have been reviewed by thebe substituted on medical grounds;LFN as part of its ongoing value-based pricing pro-• substitution is allowed to be restricted for reasonsject (see following section).such as differences in taste for oral solutions or
divided tablets;2.2 Low Prices for Existing Products in a Class
• the patient is willing to pay the difference in priceor Related Classes
for a more expensive brand or branded generic.A recent survey showed that the proportion of The LFN is currently reassessing the value of
prescriptions where substitution was not allowed by nearly 2000 medicines already included in the reim-the prescriber was low, at only 1–8% across a range bursement scheme.[2,7,17] The objective of these re-of products.[12] This was helped by several high- views, which started in October 2002, is to make thevolume brand products losing their patent, offering most efficient use of resources. This will beconsiderable savings alongside budget devolu- achieved through deciding the future reimbursementtion.[4,6] Substitution has also been well accepted by status of each drug, especially as more standardpatients,[12] with patients rarely resisting substitution drugs become available as generics. This is in lineunless, for instance, prices for originator brand prod- with economic theory to cancel funding for pharma-ucts are similar to the generic price.[12] ceuticals that are no longer seen as cost effective,
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

540 Wettermark et al.
and to transfer the released resources to fund tech- be reimbursed, with prices similar to parallel-im-ported products.nologies, including new drugs, that enhance the
level of health gain efficiently.[18] The philosophy in The review for drugs against disease caused bySweden is similar to the philosophy behind refer- acid stomach (a disease area accounting forence-pricing approaches in other EU countries, e.g. SEK891 million in 2005, with PPIs dominating) wasGermany[19] and Italy.[20] published in April 2006.[22] The LFN concluded all
PPIs have the same therapeutic effect, with theThe use of cost-effectiveness analyses in the LFNexception of esomeprazole, which at higher dosesreviews has been limited by the lack of head-to-headgives a better outcome in the treatment of heartburncomparisons.[1] However, it is unlikely these analy-with oesophageal reflux.[22,23] However, a range ofses would have been performed if companies be-PPIs is still needed, as patients can react differentlylieved the efficacy and safety of their new drugsto a drug, although this needs to be balanced againstwere similar to existing, less expensive standards.costs. As a result, a price premium of up to 25%
The LFN has divided existing medicines into 49 versus generic omeprazole was considered accept-groups, based on their Anatomical Therapeutic able for the remaining patent-protected PPIs to beChemical (ATC) classification.[17] The first four re- reimbursed.views are completed and published. The overall
Some companies were prepared to lower theirsales of the remaining groups are dictating theirprices, but others were not. In view of this, the LFNsequence for review. The future evaluations willstated in April 2006 that only generic omeprazole,focus on drugs to treat depression, hyperlipidaemia,pantoprazole and esomeprazole Helicobacter pyloripain and diabetes mellitus.[17]
combination package with antibacterials for eradica-Each review is concluded with the publication of tion of H. pylori should be fully reimbursed, with
a final report that suggests which products should partial reimbursement for esomeprazole and mis-continue to be reimbursed in all or some popula- oprostol, the latter only for the prevention of ulcerstions, based on their costs and effectiveness.[16]
caused by NSAIDs.[22] There should be no reim-Companies and the counties have 5 weeks to res- bursement for the remaining PPIs, histaminepond to the draft, with identified products delisted H2-antagonists and antacids.[22] However, a numberwithin 3 months.[17] The LFN’s decision is instigat- of manufacturers complained at the time, and theed immediately to help conserve resources, even if courts are still reviewing the situation.manufacturers want to appeal. However, the courts This economic philosophy has continued in thecan decide to grant an ‘inhibition’ during their delib- LFN’s review of medicines to treat asthma, cough,erations, which means pertinent products will still chronic obstructive pulmonary disease and cysticbe reimbursed until the final judgement has been fibrosis,[24] as well as medicines to lower bloodmade. pressure.[25] In its review of respiratory products, the
The first review was on migraine products.[21] It LFN delisted cough medicines because it believes itfocused on the triptans, as they accounted for 93% is unreasonable to reimburse medicines that haveof the total SEK340 million in 2004 spent on mi- only limited efficacy and are used to treat short-termgraine products and 70% of the spend on oral tab- conditions with only relatively minor discomfort.lets. As the literature review showed no single The resources released can be used to fund moretriptan had a sufficiently superior clinical advantage serious conditions.[24] Four asthma treatments wereversus other triptans, the LFN concluded that the delisted from 1 October 2007, including theophyl-original branded sumatriptan 100 mg product should lines for maintenance treatment, as they were con-be delisted, as a premium was still sought. The brand sidered to be not cost effective compared with newerequivalent should still be reimbursed as Glaxo- medicines.[24] Mometasone furoate is currently sub-SmithKline lowered its price to 42% below that of ject to a court decision, with the LFN looking tothe original branded sumatriptan. Naratriptan delist it because it is 60–70% more expensive than2.5 mg will also be reimbursed, with its price re- current drugs with similar efficacy.[24] However,duced by 14%.[1,21] The remaining triptans will also long-acting bronchodilators are still reimbursed, de-
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

Swedish Drug Reforms and Pharmaceutical Companies 541
spite higher acquisition costs than short-acting bron- since the late 1960s, but became obligatory inchodilators, because health economic studies have 1997.[1,6,26,27] Their overall aims[1,26,27] are as fol-demonstrated their cost effectiveness.[24] Tiotropium lows:is also still reimbursed despite higher acquisition • promote the rational use of drugs at all levels ofcosts than ipratropium, for similar reasons.[24] Fol- the healthcare system through developing guide-lowing the review of medicines to lower blood pres- lines, continuous professional education, andsure, several ACE inhibitors and calcium channel feedback on prescribing patterns;antagonists alone or in combination have either been • provide independent information on drugs to bal-delisted or reimbursement limited because of con- ance against the activities of the pharmaceuticalcerns with their value versus current drugs. All industry and to inform the public;angiotensin receptor antagonists are now only reim- • provide county administration with expertise onbursed in patients intolerant to ACE inhibitors or as the quality of drug use, drug procurement andan addition to ACE inhibitors in view of their high distribution, and also develop policy documentsacquisition costs versus generic ACE inhibitors.[25] and initiate strategies to enhance the rational use
Savings from these various initiatives may be of drugs.substantial. It is estimated that savings from the Interconnecting measures include the productionreview of triptan prices will be approximately of regional guidelines, academic detailing, bench-SEK42 million per year from 2005.[1,21] This is marking, prescribing targets and incentives.sufficient to treat another 63 000 migraine patients, Academic detailing has been an established prac-endorsing the value of this pricing approach for tice to influence prescribing in Sweden and otherexisting drugs.[21] The LFN envisaged savings up to countries for a number of years.[28,29] O’Brien eta maximum of SEK175 million per year[22] or al.,[30] in their review for the Cochrane Collabora-€20 million per year from the review of PPI tion, advocated it as a promising approach to modi-prices[14] and up to SEK40 million per year from full fying behaviour. Prescribing targets and incentiveimplementation of the review of prices for respira- schemes have also been used in the UK amongtory products[24] once the court cases have been Primary Care Trusts (PCTs) to help control pharma-resolved. The LFN also expects savings will corre- ceutical costs.[29,31] They have also been used inspond to over SEK400 million per year from imple- other European countries, including Germany.[6,32]
mentation of the antihypertensive review.[25] This The Stockholm County Council therapeuticincludes SEK250 million per year from restricting guidelines for rational drug therapy are called theangiotensin receptor antagonist prescribing. ‘Wise Drug list’.[26,27,33] The list contains around 240
This economic approach will continue for the first-line drugs for common diseases and incorpo-remaining 45 groups, with the savings redirected to rates the concept of therapeutic ladders or guide-improve the care of patients, which will include the lines.[33,34] This list and guidelines are decided afterfunding of new expensive innovative drugs. recommendations from 23 expert groups and after
consultations with five local DTCs in Stockholm’s2.3 Rational Use of Prescription Medicines at metropolitan region, involving over 300 physiciansa Regional Level and a substantial number of clinical pharmacolo-
gists, pharmacists and various stakeholders. TheThe reforms to encourage rational use of pre-recommendations are based on the following:[26,27]scription medicines at a regional level have gathered• medical efficacy and safety – based on availablepace with drug budgets now fully devolved to the
evidence (evidence-based medicine [EBM] crite-counties and, from 2005, the counties have beenria);able to levy additional taxes if they are necessary to
• pharmaceutical suitability – formulations,address budget deficits. All counties have now intro-strengths and pharmacokinetic properties;duced a variety of interconnecting measures to en-
hance rational prescribing. This follows the wide- • efficiency – the cheapest drug is chosen whenspread instigation of Drug and Therapeutic Commit- two pharmaceutical preparations have identicaltees (DTCs). DTCs have been operating in Sweden efficacy and safety;
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

542 Wettermark et al.
• experience – recommended drugs should gener- cians and pharmaceutical advisers is provided, ifally have been on the market for at least 2 years; required, to enhance the rational use of drugs.more recent drugs are included if, under EBM The cost of providing these profiles and feedbackrules, they improve care; is estimated by one of the authors (B. Wettermark)
• environmental aspects – an increasingly impor- to be far lower than the drug cost savings achievedtant consideration,[35] especially if drugs have through regular feedback, with preliminary esti-similar safety and efficacy profiles as well as mates suggesting that every percentage increase insimilar costs. adherence to the guidelines produces average annual
savings of more than SEK30 000 per GP.[39]There is also a separate patient version of theWise Drug List in Stockholm[36] to facilitate patient- One main criticism of the DU90% methodologydoctor communication surrounding the guidelines is that it does not link drug use to a diagnosis. It onlyand as a means of enhancing adherence. monitors to what extent the drugs prescribed are
those included in the guidelines, providing only aThere have been concerns regarding the limitedraw assessment of prescribing quality. However, theuse of health economic data in decision makingmethodology has been found useful to stimulateamong the counties, with costs principally focusingdiscussions around the guidelines and, hence, in-on drug acquisition costs.[1] This has been exacer-crease adherence.[34,38,40,41] The methodology alsobated by the counties now being fully responsiblehelps identify major problem areas to review infor their drug budgets and that the LFN does notmore detail. There are also concerns that followingconsider the budget impact of new drugs in itsthe guidelines may negatively impact on care de-deliberations;[7] consequently, this situation is un-spite the robust methodology involved. However,likely to change in the short term.preliminary data from 25 primary healthcare centresAlong with the published guidelines, there is also(PHCs) in southern Stockholm did not demonstratea computerized information and feedback system inany difference in the outcome for patients withStockholm called Janus[34,37] to help with the ration-hypertension (blood pressure targets reached) oral use of medicines. This system contains details ofdiabetes (glycosylated haemoglobin [HbA1c]) underthe Wise Drug List, current county guidelines, eval-control) with different levels of guidelines adher-uations of new drugs, alerts for drug-drug interac-ence,[42] suggesting high adherence rates do result intions, pre-written prescriptions for recommendedsavings without negatively affecting patient out-drugs and cost data.[37]
comes. Nevertheless, further studies need to beThe main benchmark tool used by the Stockholmundertaken before robust conclusions can be made.County Council is the drug utilization 90%
Allocating indicative prescribing budgets has(DU90%) methodology.[34,38] This methodology in-been used in some counties to help control drugcludes two indicators: (i) the number of differentexpenditures,[6,43] along with providing prescribingdrugs prescribed by an individual GP, a hospitalsupport systems and information on good-qualityspecialist or all doctors in a practice during a definedprescribing. For instance, the southernmost county,period, and (ii) the overall adherence to the guide-Scania, accompanied budget devolution with infor-lines recommended by the county (measured as themation campaigns and visits from pharmacists toproportion of DDDs prescribed that include drugs inimprove adherence to published guidelines, such asthe county guidelines).[34,38] The rationale behindthose for HMG-CoA reductase inhibitors (sta-these indicators is that high-quality prescribing im-tins).[44] However, the results have been variable andplies the use of only a limited number of drugs withmay depend on whether, for instance, health centresevidence-based documentation. Typically, of a totalhad already instigated measures to enhance rationalof around 300 drugs prescribed by GPs, about 90prescribing prior to devolving budget responsibili-substances should account for 90% of the volumety[4] or whether targeted physicians have controlprescribed.[34] Monthly updates of performance ac-over all the costs of drugs prescribed.[6]cording to these indicators for each individual physi-
cian or practice are now available on the internet Stockholm County Council has addressed these(protected with passwords). Feedback from physi- issues by using financial incentives to reward
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

Swedish Drug Reforms and Pharmaceutical Companies 543
achievement of target drug budgets and guideline ‘demand re-allocation’ to more expensive brandadherence targets.[38] Currently, 139 of 164 PHCs products in the class. Interestingly, the targets set byare involved in this incentive scheme, which also Stockholm County Council for high-profile areas,includes each practice writing an annual report on such as PPIs, statins and renin-angiotensin drugs,their quality of prescribing, incorporating a self- are less stringent than those seen, for instance,assessment evaluation of their current prescribing among the most efficient PCTs in the UK.[31]
behaviour, areas for improvement, and ongoing sys- Other ongoing reforms in Stockholm and Swedentems for orchestrating the introduction of new medi- include the development of quality indicators, whichcines. In 2006, Stockholm County Council spent are available to the public, with incentives linked toSEK20 million of its total budget on incentives for targets. However, this system is not as extensive asthe 139 PHCs participating in the scheme, with the Quality and Outcome Framework measures inpayment per practice varying depending on their the UK.[47] It is too early to undertake an analysis ofperformance. As an example, a PHC with six GPs its impact, although its importance will grow, cer-and an adherence to the DTC guidelines of 88% tainly in Stockholm.received a payment of SEK174 000.[39]
Adherence to DTC guidelines and prescribingOverall, guideline adherence has continuously targets is no doubt helped by restricted contact be-
increased among Stockholm GPs over the past few tween physicians and pharmaceutical representa-years with regular feedback and incentive schemes. tives in Sweden.[7] In Stockholm, for instance, anyAn 82% adherence rate (using DU90% methodolo- contact is forbidden for public-sector physicians.[7]
gy) was achieved in primary healthcare inOctober–December 2006, 3 percentage units higher
2.4 Limiting Reimbursement of Drugs Wherethan the corresponding period in 2005.[39,45] TheThere are Concerns about Valueaverage adherence has increased substantially over
the last 10 years, although historical comparisonsare difficult because of annual changes in guideline The LFN was established in Sweden in Octoberrecommendations.[40] As a result, this methodology 2002 to toughen pricing and reimbursement deci-is likely to grow, although further research is still sions for new and existing drugs in ambulatory careneeded to validate the preliminary findings on the (community and outpatients).[2,7,14] Its role includesoverall costs and outcomes of this approach. delisting or refusing reimbursement where there are
concerns about the value of a product. Prior to this,To further conserve resources, counties have alsopractically all new medicines were reimbursed instarted establishing prescribing targets in high-pro-Sweden,[6,14] apart from inexpensive drugs for thefile disease areas, along with prescribing guide-treatment of less severe conditions, such as hair loss,lines.[46] For instance, Stockholm County Councilsmoking cessation and some cough suppressantshas established targets for all ambulatory and outpa-and expectorants.[5]tient care physicians for the percentage of statins
prescribed as generic simvastatin (>80%), the per- Sweden was one of the first European countriescentage of PPIs prescribed as generic omeprazole to use economic evaluations in reimbursement deci-(>80%) and the percentage of renin-angiotensin sion making.[48] This has continued with the LFNdrugs prescribed as ACE inhibitors (>75%).[45] The basing its reimbursement decisions for new drugs onprescribing targets were developed and decided by the overall cost effectiveness of the drugs versusthe DTC after intense consultations and reviews current standards in all relevant patient groups or inamong physicians and medical opinion leaders to subpopulations.[1] This involves reviewing, for in-enhance efficiency without compromising patient stance, the incremental cost per QALY for the newcare. This robust methodological approach also drug.[1,7,49] A societal perspective is allowed for inhelped with the implementation and ongoing devel- the calculations, which is unusual in Europe.[7] Real-opment of the targets. However, there has not as yet life outcome and cost-effectiveness data are alsobeen any cost-effectiveness analysis of this reform requested, to support continued reimbursementincluding the positive consequences of reducing when there are concerns about value.[1]
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

544 Wettermark et al.
Table I. Examples of new products approved by the LFN with conditions and/or restrictions for reimbursement[1,14,57]
Product Conditions and restriction criteria for new products in Sweden
Efalizumab Additional data on the impact of the drug on the quality of life and cost effectiveness vs othertreatments for moderate to severe psoriasis in real life was requested to support continuedreimbursement
Insulin detemir Only initially reimbursed for patients with type 1 and not type 2 diabetes mellitus (this decision wasreversed on 19 June 2007 following a change in the label, and the documentation is now similar tothat provided by the manufacturer of insulin glargine)
Orlistat Only reimbursed for patients with type 2 diabetes and a BMI of at least 28 kg/m2; alternatively BMI>35 kg/m2
Rimonabant Only recommended in patients with a BMI >35 kg/m2; alternatively in patients with a BMI of >28 kg/m2 together with type 2 diabetes and/or dyslipidaemia
Risperidone long-acting injection Additional data on the impact of the drug on hospitalizations and quality of life was requested to(Risperdal a, Consta) support continued reimbursement
Rosuvastatin Only reimbursed in patients not achieving target lipid levels with generic simvastatin
Teriparatide Restricted to second-line use in patients with previous fractures unable to tolerate bisphosphonates.First-line treatment only for patients with a very low bone density (T-score less than –3) who havehad more than two previous fractures and are at very high risk for new fractures
a The use of trade names is for product identification purposes only and does not imply endorsement.
BMI = body mass index; LFN = Lakemedelsformansnamnden – Swedish Pharmaceutical Benefits Board.
The LFN has not set any cost per QALY cut-off effective versus the generic alternatives avail-levels for reimbursement decisions as it believes able.[1]
there are different cut-off levels for different dis- • In 2006, 4 of 40 (10%) new chemical entityeases.[7] In addition, companies will try and set (NCE) applications were not approved for reim-prices for new products just under the limit, i.e. bursement. However, the manufacturers are cur-trying to ‘play the system’,[7] which may mean pay- rently appealing against two of the decisions.ing higher prices in reality. Alongside this, any limit
This figure does not include the eight applica-will need to rise with inflation, requiring constant
tions that were withdrawn by the manufacturersadjustment, with limits continually being challengedbefore final publication because they were awareby manufacturers, as seen in the UK with newa negative decision was imminent. In addition,cancer drugs.[50] This approach is different from thatover 20% of the NCEs received restricted reim-of the UK National Institute for Health and Clinicalbursement only.[55] All new formulations, indica-Excellence (NICE). Whilst there is no absolute costtions and generics were reimbursed.[55]
per QALY threshold to guide decision making,[51] inreality NICE, with a few exceptions, approves fund- • In 2007, five new applications (10%) were de-ing for new technologies with a cost per QALY less nied reimbursement with restricted reimburse-than £30 000 per year.[52-54] ment given to 11 applications.[56]
The new approach of the LFN is reflected in the Examples of limited reimbursement and/or con-following outcomes: ditions for reimbursement in cases where the LFN
was concerned about the value of new drugs in all• The LFN approved 94% of applications in 2003,approved indications are shown in table I.with a significant number being for new generic
preparations.[2] The LFN subsequently requires manufacturers toprovide information on the restrictions in their mar-• Between October 2002 and March 2005, the LFNketing[1] and data showing the reimbursement re-denied reimbursement for 13 (12%) new drugsstrictions are being applied in practice. This is doneand gave limited or conditional reimbursement tothrough prescription volume data[1] as well as spe-a further 12 (11%).[1,7] Reasons for denials in-cific studies capturing clinical data from medicalcluded the cost effectiveness of the new product
was not proven and the new product was not cost records.
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

Swedish Drug Reforms and Pharmaceutical Companies 545
2.5 Regional Activities to Limit the Utilization counties. This is being addressed through initiativesof New Expensive Drugs with Limited Value to more tightly control diffusion and by counties
forming cooperatives to enhance their bargainingpower.Counties such as Stockholm undertake their own
Counties can also ask the LFN to approach manu-independent studies for drugs used in hospitals (andfacturers for a price reduction if volumes of newthus not reimbursed by the LFN) and for certaindrugs are growing significantly greater than expec-drugs used in ambulatory care where the LFN hasted. This option has yet to be implemented; how-limited the reimbursement. These studies are alsoever, it is likely to be an increasing considerationseen as important tools with which to implementwith the continued launch of new expensive drugs.regional guidelines and monitor important quality
aspects, such as outcomes and adverse events, e.g. inStockholm the appropriateness of prescribing new 3. Discussion and Implicationsanti-obesity drugs is being monitored alongsidetheir impact on body mass index, adverse drug reac- The myriad of reforms recently introduced intions and patient compliance/persistence.[58,59] Inter- Sweden have helped to moderate the annual increaseventions are planned if prescribing is outside of in drug expenditure despite increased volumes ofagreed guidelines. This trend is likely to grow with drug use (figure 1). However, it has been difficult tocontinued pressure on county resources. compute the impact of individual reforms against a
Alongside this, counties can further restrict the background of increasing volumes of drug use andprescribing of a new community drug after LFN the launch of new, more expensive drugs. This is thedeliberations when they are still concerned about the greatest weakness of this article from an empiricalvalue of the drug. For instance, counties may only perspective. However, we believe the greatest indi-include the drug as a third- or fourth-line treatment vidual impact has been made by the reforms insti-in their guidelines or recommend it is prescribed gating mandatory generic substitution coupled withonly in exceptional circumstances. Such steps may online systems and incentives to drive down thebe required because the LFN does not explicitly price of generics and, as a result, overall prices in theconsider the budget impact of new drugs in its class.[15] We also acknowledge that a number ofdeliberations,[7] instead concentrating on the overall references for the current article are from internalcost effectiveness of new drugs.[1,49] This conflict non-peer-reviewed sources.between national decision making and regional/lo- The Swedish drug reforms we have described,cal budget responsibility mirrors the state of affairs which centre on economic principles, mirror somewith PCTs in the UK, which has been highlighted of those initiated in other European countries, whilstrecently with the situation regarding the funding of others are novel, providing examples to other coun-trastuzumab for early-stage breast cancer.[54] tries faced with similar concerns. This is already
Manufacturers can elect, if they wish, not to happening, as witnessed by the Office of Fair Trad-include their new drug in the reimbursement system. ing (OFT) using the pricing reforms for PPIs inThis may be the case if manufacturers want to Sweden to develop a value-based pricing policy forconfine new expensive drugs to hospital-only use, drugs in the UK.[53,60] In addition, both Germany andavoiding close scrutiny by the LFN. Counties are the UK have recently instigated marketplace re-starting to address this anomaly in view of recent forms to drive down the cost of generic drugs,[60-62]
resource implications through discussing usage and no doubt facilitated by the experiences in Sweden.discounts with the manufacturers before launch[7,23] In view of this, analysis of the drug reforms inand by introducing prescribing restrictions. This is Sweden, their rationale, impact and future directionstarting to happen with new oncology treatments; should be of interest to other European countrieshowever, no agreements have as yet been finalized. introducing further measures to help control drug
Discounts obtained for hospital sales are still costs and release resources to fund increased drugrelatively small at only approximately 8–10%,[7] and volumes and new, expensive drugs. The analysisare limited by the purchasing power of individual should also be of interest to pharmaceutical compa-
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

546 Wettermark et al.
nies seeking to effectively address the implications Italy, Poland and Sweden,[13,60,64] and with patientsof current reforms, including stricter reimbursement reluctant to pay any difference,[12,65] preferring low-controls for new, expensive drugs, to enhance fund- er priced alternatives. The only exceptions are Ger-ing. many (where originator brand prices are still typical-
ly higher than generic prices, although they fall onceWe believe the implications of the reforms can begeneric drugs are available) and the UK. This maydivided into four main areas:well change in the UK if the OFT proposals are• likely prices for generics in the future and corre-accepted.[53,60]sponding implications for originator brand
prices;
• potential prices for products in a class or related 3.2 Prices for Related Products as Standardclasses as more standard drugs become available Drugs Become Genericsas generics;
• activities to address demand measures, such as The transparent method of value-based pricing inprescribing guidelines, academic detailing, tar- Sweden, especially for the PPIs, for existing patentgets and incentives; products in a class or related class once standard
• activities to enhance funding of new products as drugs become available as generics provides an ex-restrictions grow. ample to other countries looking to introduce similar
reforms, in view of the potential savings. These3.1 Prices for Generics in the Future and savings can be used to fund improved care of pa-Implications for Originator Brand Prices tients with chronic diseases and new, innovative
drugs.The low prices for some generics in Sweden at
This current system in Sweden compares wellonly 10–20% of the originator brand price mirror thewith the more complex reference price calculationssituation in the UK following recent marketplacein Germany and Italy.[60]
changes, with prices in the UK falling on average byPharmaceutical companies can ensure existing32.4% in 2005 versus previous years,[62] with some
and new products are excluded from current refer-products, such as generic simvastatin, now less thanence classes by providing robust comparative clin-2% of the originator price.[63] In France, genericsical data showing a significant improvement inmust now be priced at least 50% below the originalhealth gain (efficacy, safety, quality of life) for theirbrand price for reimbursement.[60,64] This trend fordrug versus current standard drugs in the class in alllower prices for generic drugs will continue as EUpatient groups or subpopulations.countries learn from each other, with generics be-
Pharmaceutical companies need to be aware thatcoming an indispensable part of healthcare. As asubsequent prescribing will increasingly be moni-result, pharmaceutical companies should anticipatetored by regional payers as decentralized budgetsthat generic drug prices will be a maximum of onlyevolve. This is starting to happen in Stockholm,30% of the originator brand price unless there arebuilding on the experiences with anti-obesity drugslimited volumes, and that prices will likely fall asand the review of DU90% prescribing profiles.competition grows. Greater competition can be ex-
pected with increased volumes due to greater pre- However, care must be taken in Sweden andscribing of generic drugs as a result of guidelines other EU countries to ensure that there are sufficientand prescribing targets. In line with this, we are incentives to attract manufacturers to launch alterna-likely to see more generic companies operating tives in each class, to compensate for inter-patientacross Europe, with the growing EU market further variation.[1] This was the basis behind the OFTdriving down prices. proposal for a 50% premium for interchangeable
products in a class or related classes,[53] which mayOriginator brand prices must fall accordingly towell become the benchmark for countries newlyretain market share, with generic prices typicallyseeking to introduce reference pricing that providesbecoming the reference price for the particulara calculation point for pharmaceutical companies.chemical entity, as is the case in Austria, France,
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

Swedish Drug Reforms and Pharmaceutical Companies 547
The alternative to this is the instigation of rebates ed in regional guidelines by providing robust com-and price cuts for all medicines to help governments parative clinical trial data, as previously men-and insurance companies control pharmaceutical ex- tioned.[26,27] Non-inferiority and placebo-controlledpenditure, as seen, for instance, in France and Ita- (with no active comparator arm) studies are of limit-ly.[20,23,66] This is less transparent, and requests to ed value,[68,69] and there are also increasing concernscontinually lower prices may be more detrimental to with regard to using composite measures that caninnovative companies. mislead, especially where no benefit has been
shown against individual outcome measures.[70]
Other important data include budget impact data,3.3 Activities to Address Demand Measuresespecially concerning drug costs; comparative costIncluding Guidelines, Targets and Incentiveseffectiveness will be helpful in the future. Data onthe environmental impact of drugs will grow inThe multi-layer strategy implemented by Stock-importance, building on the experiences in Stock-holm County Council to help limit the prescribing ofholm.community drugs to an agreed list mirrors activities
As the power of regional groups grows and repre-seen in other European countries, such as France,sentative activity becomes increasingly restricted,Germany and the UK.pharmaceutical companies should aim to approachCurrently, there are very few consistent modelskey personnel in national and regional bodies direct-across countries in Europe to enhance the rationally with this information first, rather than lobbyinguse of drugs and to provide balance against compa-politicians and using direct marketing to promoteny marketing activities. This is in sharp contrast toproducts to physicians.the strict models in place for drug approval and for
conducting clinical drug trials. This is being ad-dressed across Europe; consequently, the Stockholm 3.4 Activities to Enhance Funding of Newexperience can provide future direction to other Products as Restrictions GrowEuropean countries as well as to pharmaceuticalcompanies. Enhancing the rational use of drugs also Increasingly, pharmaceutical companies need toreduces potential misuse or overuse of medicines, accept that there will be growing restrictions on thewhich is a current key WHO strategic target.[67] use of new, expensive products, especially as more
Pharmaceutical companies can enhance their standard agents lose their patent protection and be-chances of having current and new products includ- come available as generic versions. Strategies will
Table II. Potential pharmaceutical company activities to enhance funding and use of new drugs
Provide robust phase III clinical trial data in all relevant and meaningful patient populations with appropriate and well arguedcomparators in line with EBM principles
Build meaningful improvements in outcomes into phase III hypotheses ascertained from discussions with all key stakeholder groups(these could include meaningful improvements in quality-of-life measures to assist with QALY calculations; this requirement will grow,especially because some previous trials have had insufficient power to show meaningful improvements, e.g. only 3% of recent trials ofdrugs for schizophrenia had enough power to show a 20% improvement in the mental state of patients[68])
Resist placebo-controlled (with no active comparator arm) and non-inferiority trials (such trials make comparisons difficult, delayingpotential reimbursement and regional authorization. They may also result in new drugs being launched that, in reality, turn out to beless safe and/or effective than current standard agents, which is not in the best interests of patients, physicians or payers[68])
Provide data to reduce uncertainty for economic models, including budget impact models (this can be undertaken by including outcomerather than surrogate data in phase III trials, especially where surrogate markers are not validated predictors of therapeutic outcomes.[68]
For example, in solid tumours, an evaluation of anticancer drugs approved by the EMEA between 1995 and 2004 showed a meanincreased survival of only 1.5 months, where reported, despite significant improvements in response rates and time-to-progression/progression-free-survival times[71])
Provide both budget impact data as well as cost per QALY data for all patient populations and potential subpopulations
Accept prescribing restrictions, rebates and follow-up activities where there are concerns with value (rebates and/or price reductions, forexample, where prescribing volumes exceed agreed limits; follow-up activities can include help with instigating patient databases tomonitor adverse effects and outcomes in designated patients, and review of reimbursement and prescribing restriction levels asknowledge grows)
EBM = evidence-based medicine; EMEA = the European Agency for the Evaluation of Medicinal Products.
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

548 Wettermark et al.
include increased monitoring of drug use against References1. Anell A, Persson U. Reimbursement and clinical guidelines foragreed strict protocols of care. Alongside this, phar-
pharmaceuticals in Sweden: do health-economic evaluationsmaceutical companies will need to accept that tradi- support decision making? Eur J Health Econ 2005; 50: 274-9tional marketing approaches, including direct con- 2. Glenngard AH, Hjalte F, Svensson M, et al. Health systems in
transition. Copenhagen: WHO Regional Office for Europe, ontact with physicians and lobbying of politicians,behalf of the European Observatory on Health Systems and
needs to be superseded by provision of robust data to Policies, 20053. Anell A. Swedish healthcare under pressure. Health Econ 2005;key national and regional expert groups, following
14: S237-S54predetermined rules to provide information and evi-4. Granlund D, Rudholm N, Wikstrom M. Fixed budgets as a cost
dence. These approaches will ensure that new drugs containment measure for pharmaceuticals. Eur J Health Econ2006; 7: 37-45are introduced effectively to patients following evi-
5. Lundkvist J. Pricing and reimbursement of drugs in Sweden.dence-based criteria and will release valuable com-Eur J Health Econ 2002; 3: 66-70
pany resources that can be redirected towards R&D 6. Bergstrom G, Karlberg I. Decentralized responsibility for costsof outpatient prescription pharmaceuticals in Sweden: assess-activities.ment of models for decentralized financing of subsidies from aIn line with ongoing reforms, we believe that management perspective. Health Policy 2007; 81: 358-67
there are several activities that pharmaceutical com- 7. Moise P, Docteur E. Pharmaceutical pricing and reimbursementin Sweden. 2007 Sep 13 (OECD health working papers no.:panies can undertake to enhance funding and use of28) [online]. Available from URL: http://www.olis.oecd.org/
new, expensive drugs regionally and nationally; olis/2007doc.nsf/FREDATCORPLOOK/NT00002E52/$FILE/JT03231887.pdf [Accessed 2008 Feb 2]these are contained in table II.
8. Gerdtham UG, Lundin D. Why did drug spending increaseduring the 1990s? A decomposition based on Swedish data.
4. Conclusions Pharmacoeconomics 2004; 22: 29-429. Andersson K, Petzold MG, Sonesson C, et al. Do policy changes
in the pharmaceutical reimbursement schedule affect drugWe believe our description and analysis of theexpenditures? Interrupted time series analysis of cost, volumereforms in Sweden and the suggested implications and cost per volume trends in Sweden 1986–2002. HealthPolicy 2006; 79: 231-43of these reforms, coupled with details of similar
10. The National Corporation of Swedish Pharmacies, Apoteketreforms in other European countries, should be ofAB, Statistikenheten, Stockholm FDB. Sales data; supplied
interest to other European countries and innovative 2007 Jun 11. (Data on file)11. Aaserud M, Dahlgren AT, Kosters JP, et al. Pharmaceuticalpharmaceutical companies as they remodel their
policies: effects of reference pricing, other pricing, andactivities to meet future requirements. This is espe- purchasing policies. Cochrane Database Syst Rev 2006; (2):cially of interest as national and regional European CD005979
12. Andersson K, Sonesson C, Petzold M, et al. What are thepayers will need to instigate further reforms to en-obstacles to generic substitution? An assessment of the beha-sure the continued provision of comprehensive viour of prescribers, patients and pharmacies during the firstyear of generic substitution in Sweden. Pharmacoepidemiolhealthcare, including the funding of new, expensiveDrug Saf 2005; 14: 341-8drugs, without raising taxes and/or premiums. How-
13. Act (2002:160) on pharmaceutical benefits, etc. Solna: Pharma-ever, we accept our analysis can not identify the ceuticals Benefits Board, 2002 [online]. Available from URL:
http://www.lfn.se/upload/English/ENG_Act_2002-160.pdfimpact of individual drug reforms.[Accessed 2007 Jan 19]Addressing a number of the issues raised may 14. The Swedish pharmaceutical reimbursement system. Solna:
also lead to shorter times between market authoriza- Pharmaceuticals Benefits Board, 2007 Jan [online]. Availablefrom URL: http://www.lfn.se/upload/Bakgrundsmaterial/swetion and reimbursement and/or funding of newdish_pharmaceutical_reimbursement_system_070122.pdf
drugs, which will be an increasing issue.[72] This will [Accessed 2007 Mar 5]15. Engstrom A, Jacob J, Lundin D. Sharp drop in prices after thebe in the best interests of all stakeholder groups.
introduction of generic substitution. Solna: PharmaceuticalsBenefits Board, 2006 [online]. Available from URL: http://
Acknowledgements www.lfn.se/upload/Pressmeddelanden/generiskt_utbyte_engelsk_061010.pdf [Accessed 2007 Mar 5]
The authors wish to acknowledge Elisabet Torell from 16. The National Corporation of Swedish Pharmacies – ApoteketAB, Statistikenheten, Stockholm, Sweden. Data on prices; dataApoteket AB for help in providing drug sales and volumesupplied 2007 Dec 17. (Data on file)data and Niklas Hedberg from LFN for his helpful comments
17. Working guidelines for the pharmaceutical reimbursement re-regarding LFN activities. This study was in part supported byview. Solna: Pharmaceuticals Benefits Board, 2006. Refer-funds from the Karolinska Institute. ence: 1023/2003 [online]. Available from URL: http://
The authors have no conflicts of interest that are directly www.lfn.se/upload/Genomgangen/GLS_060815_guidelinesrelevant to the content of this review. _english.pdf [Accessed 2007 Mar 12]
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

Swedish Drug Reforms and Pharmaceutical Companies 549
18. Cohen J, Stolk E, Niezen M. The increasingly complex fourth profiles at a primary healthcare centre in Stockholm, Sweden.hurdle for pharmaceuticals. Pharmacoeconomics 2007; 25 (9): Qual Prim Care 2004; 12: 225-34727-34 35. Larsson DG, de Petro C, Paxeus N. Effluent from drug manufac-
tures contains extremely high levels of pharmaceuticals. J Haz-19. Schreyogg J, Henke K-D, Busse R. Managing pharmaceuticalard Mater 2007; 148 (3): 751-5regulation in Germany [discussion paper 2004/6]. Berlin:
Technische Universitat Berlin, Fakultat Wirtschaft und Man- 36. Kloka Listen: patient version [in Swedish]. Stockholm Countyagement, 2004 Council, Regional Drug & Therapeutics Committee, 2007
[online]. Available from URL: http://www.janusinfo.se/20. Rocchi F, Addis A, Martini N, et al. Current national initiativesimcms/servlet/GetDoc?meta_id=8943 [Accessed 2007 Novabout drug policies and cost control in Europe: the Italy13]example. J Ambulatory Care Manage 2004; 27: 127-31
37. Eliasson M, Bastholm P, Forsberg P, et al. Janus computerised21. Hedberg N, Ramsberg J. The review of medicines used forprescribing system provides pharmacological knowledge attreating migraine: a summary. Solna: Pharmaceuticals Bene-point of care: design, development and proof of concept. Eur Jfits Board, 2006 [online]. Available from URL: http://Clin Pharmacol 2006; 62: 251-8www.lfn.se/upload/Bakgrundsmaterial/migraine_review
_summary.pdf [Accessed 2007 Mar 5] 38. Wettermark B, Pehrsson A, Jinnerot D, et al. Drug utilisation90% profiles: a useful tool for quality assessment of prescrib-22. Wessling A, Lundin D. The review of drugs against diseaseing in primary health care in Stockholm. Pharmacoepidemiolcaused by acid stomach: a summary. Solna: PharmaceuticalsDrug Saf 2003; 12: 499-510Benefits Board, 2006 [online]. Available from URL: http://
www.lfn.se/upload/genomgangen/engelsk_sammanfattning_ 39. Almkvist H, Bergman U, Edlert M, et al. Quality report –magsyra_slutgiltig.pdf [Accessed 2007 Mar 5] Stockholm County Council’s incentive schemes for drug pre-
scribing in primary healthcare [in Swedish]. Lakartidningen.23. Office of Fair Trading (UK). The pharmaceutical price regula-In Presstion system: an OFT study. Annexe K: international survey of
pharmaceutical pricing and reimbursement schemes. London: 40. Wettermark B. Drug utilization 90%: using aggregate drugThe Office of Fair Trading, 2007 [online]. Available from statistics for the quality assessment of prescribing. Stockholm:URL: http://www.oft.gov.uk/shared_oft/reports/comp_policy/ Repro Print, AB, 2004oft885k.pdf [Accessed 2007 Mar 6] 41. Wettermark B, Haglund K, Gustafsson LL, et al. A study of
24. Hugosson K, Engstrom A. Review of medicines against asthma, adherence to drug recommendations by providing feedback ofCOPD, and coughs: a summary. Solna: Pharmaceuticals Bene- outpatient prescribing patters to hospital specialists. Pharma-fits Board, 2007 [online]. Available from URL: http:// coepidemiol Drug Saf 2005; 14: 579-88www.lfn.se/upload/Genomgangen/GLS_asthma_summary_ 42. Wettermark B. Internal report produced for Stockholm County070829.pdf [Accessed 2007 Nov 12] Council on outcomes following adherence to county guide-
25. Hedberg N, Jacob J. A review of medicines for lowering blood lines [internal report]. Stockholm: Stockholm County Council,pressure: a summary. Solna: Pharmaceuticals Benefits Board, 2007 Mar2008 [online]. Available from URL: http://www.lfn.se/upload/ 43. Jansson S, Anell A. The impact of decentralised drug-budgets inGenomgangen/Summary%20Hypertension_080221.pdf [Ac- Sweden: a survey of physicians’ attitudes towards costs andcessed 2008 17 Mar] cost-effectiveness. Health Policy 2006 May; 76: 299-311
26. Gustafsson LL. Drug and Therapeutic Committees: concept, 44. Ohlsson H, Merlo J. Understanding the effects of a decentralisedexperience and capacity to improve use of drugs. Stockholm: budget on physicians’ compliance with guidelines for statin2005 Jan [online]. Available from URL: http://www.janusin prescription: a multilevel methodological approach. BMCfo.se/imcms/servlet/GetDoc?.meta_id=7148 [Accessed 2007 Health Serv Res 2007; 7: 68Mar 5] 45. Janus [online]. Available from URL: http://www.janusinfo.se/
27. Sjoqvist F, Bergman U, Dahl ML, et al. Drug and therapeutics imcms/servlet/GetDoc?meta_id=10148e [Accessed 2007 Marcommittees: a Swedish experience. WHO Drug Information 5]2002; 16: 207-13 46. Wettermark B, Tomson G, Bergman U. Quality indicators for
28. Stalsby Lundborg C, Hensjo LO, Gustafsson LL. “Academic drug prescribing: the situation in Sweden [in Swedish]. Lakar-drug detailing”: from project to practice in a Swedish urban tidningen 2006; 103: 3607-11area. Eur J Clin Pharmacol 1997; 52: 167-72 47. Smith PC, York N. Quality incentives: the case of UK general
29. Mason A, Towse A, Drummond M, et al. Influencing prescrib- practitioners. Health Affairs 2004; 23 (1): 112-8ing in a primary care led NHS. London: OHE Publications, 48. McGuire A, Drummond M, Rutten F. Reimbursement of phar-2002 maceuticals in the European Union in ‘Regulating pharmaceu-
30. O’Brien MA, Oxman AD, Davis DA, et al. Educational out- ticals in Europe: striving for efficiency, equity and quality’.reach visits: effects on professional practice and health care Maidenhead, Berkshire: McGraw-Hill Education, 2004outcomes. Cochrane Database Syst Rev 1997; (4): CD000409 49. General guidelines for economic evaluations from the Pharma-
ceutical Benefits Board (LFNAR 2003:2). Solna: Pharmaceu-31. Beishon J, McBride T, Scharaschkin S, et al. Prescribing coststicals Benefits Board, 2003 [online]. Available from URL:in primary care. London: National Audit Office, 2007 May 18http://www.lfn.se/upload/English/ENG_lfnar2003-eng.pdf[online]. Available from URL: http://www.nao.org.uk/publi[Accessed 2007 Mar 5]cations/nao_reports/06-07/0607454.pdf [Accessed 2007 May
21] 50. Hoey R. Experts disagree over NICE’s approach for assessingdrugs. Lancet 2007; 370: 643-432. Sturm H, Austvoll-Dahlgren A, Aaserud M, et al. Pharmaceuti-
cal policies: effects of financial incentives for prescribers. 51. Rawlins M, Culyer A. National Institute for Clinical ExcellenceCochrane Database Syst Rev 2007; (3): CD006731 and its value judgements. BMJ 2004; 329: 224-7
33. Kloka Listen: physician version [in Swedish]. Stockholm 52. Wells J, Cheong-Leen C. NICE appraisals should be everyone’sCounty Council, Regional Drug & Therapeutics Committee, business. BMJ 2007; 334: 936-82007 [online]. Available from URL: http://www.janusinfo.se/ 53. Office of Fair Trading (UK). The pharmaceutical price regula-klokalistan/external/baselist.asp [Accessed 2007 Nov 13] tion system: an OFT study. London: OFT 2007 Feb [online].
34. Wettermark B, Nyman K, Bergman U. Five years’ experience of Available from URL: http://www.oft.gov.uk/shared_oft/repquality assurance and feedback with individual prescribing orts/comp_policy/oft885.pdf [Accessed 2007 Mar 6]
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)

550 Wettermark et al.
54. Barrett A, Roques T, Small M, et al. How much will herceptin Pharmaceutical Care and Pharmacoeconomics, 2006 [online].really cost? BMJ 2006, 20 Available from URL: http://www.egagenerics.com/doc/sim
oens-report_2006-04.pdf [Accessed 2006 Oct 16]55. The Swedish Pharmaceutical Benefits Board (LFN) 2006 annu-al report [in Swedish; online]. Available from URL: http:// 65. Atella V, Schafheutle E, Noyce P, et al. Affordability of medi-www.lfn.se/upload/Om_oss/arsredovisning_2006.pdf [Ac- cines and patients’ cost-reducing behaviour: empirical evi-cessed 2006 Jun 25] dence based on SUR estimates from Italy and UK. Appl Health
56. The Swedish Pharmaceutical Benefits Board (LFN) 2007 annu- Econ Health Policy 2005; 4: 23-35al report [in Swedish; online]. Available from URL: http:// 66. Le Pen C. The drug budget silo mentality: the French case.www.lfn.se/upload/Om_oss/Arsredovisning%20layoutad%20 Value Health 2003; 6 Suppl. 1: S10-9080328.pdf [Accessed 2008 Feb 27]
67. WHO medicines strategy 2004–2007 [online]. Available from57. Sweden approves Acomplia reimbursement. Scrip 2006 Nov 13:URL: http://www.who.int/publications [Accessed 2007 OctS0094020610]
58. IRIS: introduction of Rimonabant in Stockholm [project plan:68. Garattini S, Bertele V. How can we regulate medicines better.2007-04-03]. Stockholm: Stockholm County Council, 2007
BMJ 2007; 335: 803-559. Wettermark B, Raaschou P, Forslund T, et al. Fortsattafragetecken kring bantningsmedlet rimonabant. Lakartidn- 69. Garattini S, Bertele V. Non-inferiority trials are unethical be-ingen 2007; 51: 3879-81 cause they disregard patients’ interests. Lancet 2007; 370:
1875-760. Godman B, Haycox A, Schwabe U, et al. Having your cake andeating it: Office of Fair Trading proposal for funding new 70. Lapostolle F, Catineau J, Lapandry C, et al. Endpoints in studiesdrugs to benefit patients and innovative companies. Pharmaco- on myocardial infarction. Lancet 2007; 369: 1430economics 2008; 26 (2): 91-8
71. Apolone G, Joppi R, Bertele V, et al. Ten years of marketing61. Rabbata S. The legislation on saving of drug costs is effective approvals of anticancer drugs in Europe: regulatory policy and
[in German]. Dtsch Arzteblatt 2007; 104: A308 guidance documents need to find a balance between different62. Office of Fair Trading (UK). The pharmaceutical price regula- pressures. Br J Cancer 2005; 93: 504-9
tion system: an OFT study. Annexe A: market for prescription72. Lundkvist J, Jonsson B, Rehnberg C. The costs and benefits ofpharmaceuticals in the NHS. London: The Office of Fair
regulations for reimbursement of new drugs. Health PolicyTrading, 2007 [online]. Available from URL: http://www.2006; 79: 337-4oft.gov.uk/shared_oft/reports/comp_policy/oft885a.pdf [Ac-
cessed 2007 Mar 6]63. UK NHS Business Services Authority electronic drug tariff
Correspondence: Brian Godman, Institute for Pharmacologi-2007 [online]. Available from URL: http://www.ppa.org.uk/cal Research ‘Mario Negri’, Via La Masa 19, 20156 Milano,edt/March_2008/mindex.htm [Accessed 2008 24 Mar]Italy.64. Simoens S, De Coster S. Sustaining generic markets in Europe.
Leuven: Katholieke Universiteit Leuven, Research Centre for E-mail: [email protected]
2008 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2008; 26 (7)